
Notes
Article history
The research reported in this issue of the journal was funded by the EME programme as project number 09/150/28. The contractual start date was in June 2011. The final report began editorial review in January 2015 and was accepted for publication in March 2016. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The EME editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Keith R Abrams reports personal fees from Roche, Novartis, AstraZeneca, Janssen, Astellas, Lilly, GlaxoSmithKline, Allergan, Association of the British Pharmaceutical Industry and NICE International, and reports grants from European Union – European Federation of Pharmaceutical Industries and Associations (EU-EFPIA) and was partially supported as a National Institute for Health Research Senior Investigator during the course of this study (NF-SI-0512-10159). Gerry P McCann reports grants from Servier and Menarini International.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Nazir et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Ischaemic heart disease is a leading cause of morbidity and mortality worldwide, with more than 100,000 patients presenting with ST-elevation myocardial infarction (STEMI) in the UK each year. 1 Timely delivered primary percutaneous coronary intervention (PPCI) has become the primary reperfusion therapy for STEMI in the USA and Europe. 2 However, this interventional technique has not abolished the unpredictable phenomenon of no-reflow and the underappreciated, but potentially equally important, syndrome of abnormal epicardial-microvascular obstruction (MVO).
Microvascular obstruction describes abnormal tissue perfusion and/or coronary blood flow despite normal patency of the infarct-related artery (IRA). 3 This can result in persistent myocardial injury and necrosis through interacting processes. Distal microembolisation of thrombus and plaque debris, activation of the inflammatory cascade, neutrophil plugging, toxic free-radical generation and capillary obstruction by intraluminal (endothelial protrusion by cell swelling and cellular infiltrate rich in red blood cells, platelets and granulocytes) and extraluminal (compression from surrounding oedematous myocytes) mechanisms promote poor perfusion and irreversible injury to potentially viable myocytes. 3–10 These ultrastructural and functional changes result in a spectrum of MVO that, as detected by cardiac magnetic resonance (CMR) imaging, manifests in up to 70% of patients with STEMI treated with PPCI. 11–17 Although the incidence of MVO varies between studies, presumably because of a combination of modifiable and non-modifiable patient-related factors, its presence been reported to be associated with major adverse cardiac event (MACE) rates of up to 30% at 1 month and 60% at 12 months. 12
Manual thrombectomy has been shown to improve angiographic microvascular flow irrespective of the presence of visible thrombus18 and to reduce infarct size and preserve microvascular integrity assessed by CMR imaging,19 leading to improved left ventricular (LV) function and tissue perfusion assessed by myocardial contrast echocardiography (MCE). 20 However, there is conflicting evidence whether this leads to overall improved clinical outcomes, although the large ongoing TOTAL trial [randomized trial of routine aspiration ThrOmbecTomy with percutaneous coronary intervention (PCI) versus PCI ALone in patients with ST-elevation myocardial infarction undergoing primary PCI] will provide further insights. 21–27 Glycoprotein IIb/IIIa (GPIIbIIIa) inhibitors further reduce infarct size and improve markers of microvascular perfusion in STEMI patients undergoing PPCI. 28–30 Bivalirudin has been shown in the ACUITY (Acute Catheterization and Urgent Intervention Triage strategY)31 and HORIZONS-AMI (Harmonizing Outcomes with RevascularIZatiON and Stents in Acute Myocardial Infarction)32 trials to provide similar efficacy with less bleeding and even reduced mortality compared with unfractionated heparin plus GPIIbIIIa receptor inhibitors in high-risk patients undergoing PPCI. However, residual mortality and subsequent MACE rates suggest that there is room for improvement even in those patients who do not demonstrate slow-flow or no-reflow angiographically.
Basic understanding of the MVO process has led to the evolution of several treatment regimens designed to improve outcome, including the use of vasodilators,33–41 albeit mostly in clinical trials. Of these, sodium nitroprusside (SNP)13,42–49 and adenosine44,50–62 and their effects on attenuating or preventing MVO have been the most studied. The randomised controlled trials of adenosine and SNP in PPCI are presented in Appendix 1. Adenosine, aside from being a potent vasodilator,63 may have additional benefits because of its pleiotropic effects: the anti-inflammatory action of adenosine is well recognised64,65 and its ability to block the neutrophil-mediated processes that promote MVO may explain the reduction in reperfusion injury seen with intracoronary (IC) adenosine in canine infarct models. 66 Similarly, SNP, a direct nitric oxide (NO) donor that requires no intracellular metabolism,67 utilises NO’s multiple vascular functions. These include vasodilatation of arterioles, inhibition of platelet adhesion and anti-inflammatory activity,68 which effectively reduce no-reflow in animal reperfusion injury models. 69,70 SNP and adenosine have, in some trials, demonstrated a favourable improvement in electrocardiographic and angiographic markers of microvascular perfusion, as well as improvements in short-term MACE rates. 42,44,55,71 The randomised and placebo-controlled Acute Myocardial Infarction STudy of ADenosine (AMISTAD)-II trial sought to determine the benefits of adenosine in 2118 patients presenting within 12 hours of onset of anterior STEMI treated with thrombolysis (60%) or PPCI (40%). 59 Infarct size and adverse clinical events were reduced in a subgroup who received a higher (70 µg/kg/minute) dose of adenosine and in those reperfused within 3 hours of symptom onset. This trial, although the largest to date, has a number of limitations in addition to the mixed reperfusion strategy cohort: (1) adenosine was administered by intravenous infusion after the PPCI, (2) infarct size was measured relatively late after presentation in only 11% of patients and by technetium-99m sestamibi single-photon emission computed tomography (SPECT), which may underestimate infarct size compared with CMR imaging, and (3) no measure of myocardial salvage was obtained. Overall, the AMISTAD-II study appears not to be applicable in the modern PPCI era.
The effects of adenosine on the coronary microcirculation during STEMI have been assessed using CMR imaging in only one previous study. Desmet et al. 51 assessed whether IC administration of adenosine, distal to the occlusion site and immediately before initial balloon inflation, resulted in increased myocardial salvage and decreased MVO compared with placebo on CMR imaging at 48–72 hours post PPCI in 112 patients. They reported no significant difference in myocardial salvage between the two groups (41.3% vs. 47.8%; p = 0.52). MVO extent, angiographic markers of reperfusion and infarct size at 4 months were also similar in both groups. Interestingly, the authors reported a statistically significant benefit in favour of adenosine in patients with Thrombolysis in Myocardial Infarction (TIMI) flow grade (TFG) 2–3 pre PPCI. This suggested that establishing flow prior to adenosine delivery was beneficial and perhaps necessary for the drug to have a clinical effect. As thrombectomy was not performed in this study, it is possible that adenosine may have been ineffective because of a combination of its short half-life and failure to reach the distal vascular bed. In addition, more patients had an anterior myocardial infarction (MI) in the adenosine group (48% vs. 33%). Anterior STEMI is known to be associated with larger infarct sizes, reduced myocardial salvage and increased LV remodelling. 72 Moreover, the spontaneous reperfusion rate was high (28%) in this study, evident as TFG 2–3 prior to PPCI. The placebo group had almost twice as many patients with established TFG 2–3 prior to PPCI and this is known to be associated with higher myocardial salvage and reduced infarct size. Finally, the expression of MVO indexed to the area at risk (AAR) rather than infarct size or total LV mass has not been described previously in the evidence base and is unexplained in this study.
Although benefits have been shown for both adenosine and SNP in smaller trials, the results of such studies have been largely conflicting and hence there is currently no consensus on the value of routine administration of adjunctive pharmacotherapeutic agents to prevent or reduce MVO. In fact, a recent Cochrane review73 found that adenosine, when given as an adjunct during PPCI, did not reduce all-cause mortality, non-fatal MI or the incidence of angiographic no-reflow. However, the authors conceded that the evidence base was limited and highlighted the need for further research with larger high-quality trials. Heterogeneity in trial design (small numbers of participants, suboptimal drug dosages, inadequate antiplatelet therapy and variably chosen end points often lacking imaging confirmation of MVO and infarct size) has resulted in contradictory outcome data that may not be clinically applicable. Consequently, there is divergent clinical practice, even within institutions. Furthermore, the incidence of no-reflow/MVO remains difficult to predict on coronary angiography alone. It could be argued that, given the strong relationship between MVO and prognosis, prophylactic prevention of MVO should be considered in all patients presenting with STEMI, irrespective of the thrombus burden, with delivery of agents theoretically able to reduce MVO.
The failure of some previous randomised clinical trials to show a reduction in MVO may in part be related to factors other than clinical efficacy. The lack of a sensitive imaging modality to detect MVO and the failure to deliver vasoactive agents close to the microvascular bed may potentially have reduced their therapeutic impact.
We therefore designed the REperfusion Facilitated by LOcal adjunctive therapy in ST-Elevation Myocardial Infarction (REFLO-STEMI) study to evaluate whether adjunctive adenosine or SNP, administered in two doses (the first optimally delivered by distal IC injection following thrombectomy), would be effective in preventing MVO and reducing infarct size, as determined using the sensitive measure of CMR imaging, in patients undergoing PPCI for STEMI. 74
Chapter 2 Research objectives
The original research objective of the REFLO-STEMI trial was to determine whether IC adenosine and/or SNP reduces CMR-measured infarct size (% total left ventricular end-diastolic mass; %LVM) at 48–72 hours post PPCI.
Secondary questions were as follows.
-
What is the expected size of effect of both SNP and adenosine on MVO (incidence and absolute reduction in MVO as %LVM)?
-
What is the CMR incidence and extent of MVO (%LVM) at 48–72 hours post PPCI?
-
What is the impact of the study drugs on the CMR-measured myocardial salvage index (MSI), haemorrhage, left ventricular ejection fraction (LVEF) and volumes in the acute stage?
-
Does administration of IC adenosine and/or SNP reduce angiographic markers of MVO?
-
What is the incidence of angiographic slow-flow/no-reflow after PPCI with the three different management strategies?
-
Is there a difference in the incidence of complete (> 70%), and degree of, ST-segment resolution (STR) between the three treatment arms?
-
Do the study agents affect overall MACE rates and their components at 6 months, namely death, need for target lesion revascularisation, recurrent MI, severe heart failure and cerebrovascular event?
Chapter 3 Methods
Study design
The REFLO-STEMI trial was a multicentre randomised controlled open-label clinical trial undertaken in four regional cardiac centres in the UK. All patients presenting within 6 hours of symptom onset of STEMI, who were suitable for reperfusion by PPCI and had a baseline corrected QT interval (QTc) of < 450 milliseconds on admission electrocardiography (to limit the risk from the possible QT prolongation effect of the study drugs), were provisionally eligible to participate in the study. TFG 0–1 in the IRA and no flow-limiting bystander disease (i.e. no stenosis ≥ 70% in non-IRAs) were prerequisites for randomisation. Full eligibility criteria are provided in Table 1. Following verbal consent (also referred to as assent75,76), patients were randomised 1 : 1 : 1 to adjunctive IC adenosine, SNP or control (standard PPCI alone) by a member of the research team using a dedicated 24/7 computerised telephone service (provided by the Sealed Envelope Ltd, London, UK) with stratification by (1) symptoms to balloon of < 3 hours or ≥ 3 hours and (2) anterior infarction or not.
| Inclusion criteria | Exclusion criteria |
|---|---|
|
|
In all cases PPCI was performed in line with accepted practice with transradial or femoral arterial access using 6 and 7 Fr sheaths. Patients were pretreated with dual antiplatelet therapy with aspirin (300-mg loading dose and 75 mg/day maintenance dose) and prasugrel (60-mg loading dose and 10 mg/day maintenance dose)77,78 or ticagrelor (180-mg loading dose and maintenance dose of 90 mg twice daily), given for up to 12 months. 79–81 Bivalirudin was administered to all patients (0.75-mg/kg bolus plus infusion of 1.75 mg/kg/hour) [as was standard practice then, i.e. prior to the HEAT-PPCI (How Effective are Antithrombotic Therapies in Primary Percutaneous Coronary Intervention) trial82] in the absence of specific contraindication, with dose reduction for renal insufficiency, and was discontinued at the completion of PPCI (but could have been continued for 4 hours if clinically indicated). For patients randomised to an intervention arm, following manual thrombectomy and thorough flushing of the catheter the first drug dose (adenosine 1 mg or SNP 250 µg) was injected as distally as possible via the thrombus aspiration catheter. Immediately following stent deployment, and providing a repeat measure of QTc was < 450 milliseconds and remained < 60 milliseconds above the baseline value, the second drug dose (1 mg of adenosine if the IRA was the right coronary artery (RCA); otherwise, 2 mg of adenosine or 250 µg of SNP) was given by slow injection (> 1 minute) via the guide catheter. Administering the second drug dose distal to the stent via the thrombectomy catheter had been considered in the trial planning phase but the risk associated with crossing the stent with the thrombectomy catheter was thought to outweigh the benefit of distal drug delivery.
The electrocardiogram (ECG) was recorded and retained at each angiography time point. The degree of STR was determined from 12-lead ECGs acquired pre and post PPCI and categorised as complete (> 70%), partial (30–70%) or no (< 30%) STR. 17,83 The maximal sum of ST-segment elevation, measured 60 milliseconds after the J point, was calculated from three contiguous leads in the infarct territory.
Angiographic images were acquired at 30 frames per second with long acquisitions (to visualise the venous phase in contrast passage) in orthogonal views before intervention and after stenting (at the time of the final/optimal angiographic result) to enable determination of angiographic markers of MVO offline at a core laboratory (Newcastle University); TIMI myocardial perfusion grade (TMPG) was assessed visually as previously described84,85 (Table 2). Digital quantification of myocardial perfusion or ‘blush’ was performed using QuBE (Quantitative Blush Evaluator) version 1.0 software (University of Groningen, the Netherlands);86 corrected TIMI frame count (cTFC) was calculated as the number of cine frames needed for the dye to reach standardised distal landmarks, to objectively evaluate coronary blood flow as a continuous variable. 87,88 The final TFG < 3 (Table 3) was also taken to represent angiographic MVO post PPCI. 89 Thrombus score was reported according to TIMI criteria (Table 4). 90 A list of angiographic markers of MVO assessed is provided in Table 5.
| TMPG | Definition |
|---|---|
| 0 | Failure of dye to enter the microvasculature |
| 1 | Dye slowly enters but fails to exit the microvasculature |
| 2 | Delayed entry and exit of dye from the microvasculature |
| 3 | Normal entry and exit of dye from the microvasculature |
| TFG | Definition |
|---|---|
| 0 | No perfusion |
| 1 | Penetration without perfusion |
| 2 | Partial perfusion |
| 3 | Complete perfusion |
| TIMI thrombus score | Definition |
|---|---|
| 0 | No characteristics of thrombus |
| 1 | Possible thrombus, as reduced contrast density, haziness, irregular lesion contour or a smooth convex ‘meniscus’ at the site of total occlusion suggestive but not diagnostic of thrombus |
| 2 | Definite thrombus, with greatest dimensions less than half vessel diameter |
| 3 | Definite thrombus, greatest linear dimension greater than half but less than two vessel diameters |
| 4 | Definite thrombus, largest dimension greater than two vessel diameters |
| 5 | Total occlusion |
| Type of outcome measure | Outcome measure |
|---|---|
| CMR imaging parameters |
|
| Angiographic markers of MVO | |
| Electrocardiography | |
| Echocardiography |
|
| Subanalyses |
|
Following the PPCI procedure, and when clinically stable, patients were provided with a detailed patient information leaflet and were then asked for written informed consent to continue participation in the trial. A 20% dropout rate (high allowance because of the CMR imaging component) between PPCI and CMR imaging was allowed for. Studies on informed consent in acute MI patients have suggested that oral information is far better received, processed and recalled by patients than written information. 92,93 In the ISIS-4 (Fourth International Study of Infarct Survival) patient cohort, 95% of participants recalled receiving the oral information whereas only 37% recalled receiving the written consent form. 92 Furthermore, only 18% of 346 patients prospectively studied reported reading the patient information sheet before providing or refusing consent to participate in the Hirulog and Early Reperfusion or Occlusion (HERO)-2 acute MI trial. 93 Of particular note is that patients who gave consent were more likely to report good or partial understanding of the written material than those who refused consent. This raises the possibility of selection bias at the time of consent. Consequently, we believe that verbal explanation of a trial may be a more effective and valuable source of information than a written consent form in the emergent situation of STEMI, when treatment must be provided without undue delay. This approach has also been successfully used in two recent STEMI trials. 75,76
Blood samples were drawn at baseline and at 4, 12 and 24 hours after PPCI for cardiac enzyme [creatine kinase MB isoenzyme (CK-MB) and troponin] estimation and pre discharge for N-terminal pro-brain natriuretic peptide (NT-proBNP) estimation. Electrocardiographic recording was undertaken at 90 minutes, 24 hours and pre discharge. All patients were commenced on a beta-blocker, angiotensin-converting enzyme (ACE) inhibitor and high-dose statin in addition to dual antiplatelet therapy, unless contraindicated, according to international guidelines. 1
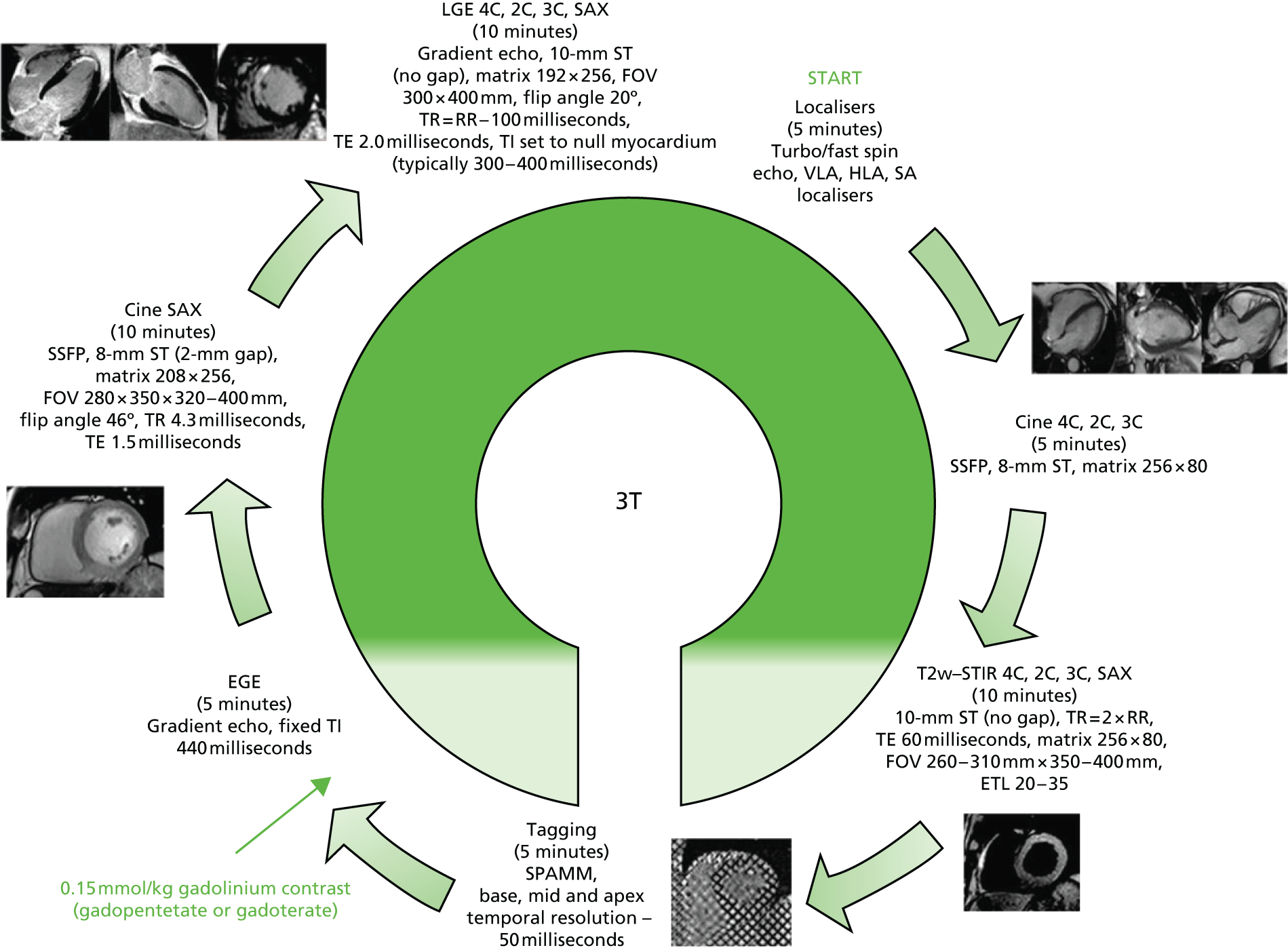
Patients underwent CMR imaging at 48–72 hours after presentation with STEMI on a 3.0-T scanner with retrospective electrocardiographic gating and dedicated cardiac receiver coils at each of the four participating centres (Figure 1) to provide the primary end point. 94,95 Prior to contrast administration, T2-weighted short-tau inversion recovery (T2w-STIR) imaging with coil signal intensity correction was performed in long-axis (LAX) views and contiguous short-axis (SAX) slices covering the entire left ventricle to assess for oedema (AAR). Three SAX (base, mid and apical) tagged images were acquired using a prospectively gated spatial modulation of magnetisation (SPAMM) gradient-echo sequence. Early gadolinium enhancement (EGE) imaging was acquired 1–3 minutes after administration of 0.15 mmol/kg of gadolinium-DTPA (diethylenetriamine penta-acetic acid) (Magnevist®; Bayer) using a single-shot inversion-recovery gradient-echo sequence. Functional assessment of LVEF and LV volumes and mass was according to current standards with the use of a steady-state free precession (SSFP) cine pulse sequence covering the whole left ventricle with 8–12 contiguous SAX slices. Late gadolinium enhancement (LGE) imaging96 was then performed in LAX (two-/three-/four-chamber) views and contiguous SAX slices covering the whole left ventricle. LGE images were acquired 10–15 minutes post contrast using a segmented inversion-recovery gradient-echo sequence. The inversion time was progressively adjusted to null unaffected myocardium. The full study outcome measures are listed in Table 5.
FIGURE 1.
Cardiac magnetic resonance imaging protocol. 2C, 3C, 4C, two-, three- and four-chamber LAX views. EGE, early gadolinium enhancement; ETL, echo train length; FOV, field of view; HLA, horizontal long axis; RR, ECG RR interval; SA, short axis; SPAM, spatial modulation of magnetisation; SSFP, steady-state free precession; ST, slice thickness; TE, echo time; TI, inversion time; TR, repetition time; VLA, vertical long axis.
Cardiac magnetic resonance analysis, blinded to patient details, was undertaken in a central core lab (University of Leicester) using cmr42 software (Circle Cardiovascular Imaging, Calgary, AB, Canada). Anonymised CMR images were graded for image quality before analysis using a 4-point scale (4 = excellent, 3 = good, 2 = moderate and 1 = non-analysable). Endocardial and epicardial borders were manually contoured on contiguous SAX LV slices, excluding papillary muscles, trabeculae and blood-pool artefact, for LV volumetric, AAR and infarct size analyses. Infarct was identified as enhancement on LGE images and quantified using the full-width half-maximum (FWHM) technique. 97 MVO was defined (and quantified) as hypoenhancement within infarcted myocardium, as determined from LGE images, and was included in the total infarct size. Myocardial oedema was quantified using semi-automatic thresholding, defining AAR as enhancement within myocardium of signal intensity > 2 standard deviations (SDs) above that of a region of interest contoured in remote myocardium. Hypoenhanced areas within the AAR were regarded as intramyocardial haemorrhage (IMH). The MSI was calculated as 100 × [(AAR – infarct size)/AAR]. Infarct size, MVO, AAR and IMH were expressed as %LVM and LV volumes were indexed to body surface area. Intra- and interobserver variability is reported for the primary outcome measure. The tagging data will be analysed as a separate substudy and presented in a separate publication.
All patients were followed up for at least 1 month following randomisation and throughout the course of the study until the last patient recruited to the trial had completed the 1-month follow-up. Median follow-up is reported. Patients were also flagged with the Office for National Statistics to ensure capture of mortality data. Most adverse events were expected as recognised complications of STEMI or the revascularisation procedure. Such events were recorded for the evaluation of outcome measures and for safety monitoring. Definitions of important adverse events are provided in Table 6. Investigators were required to notify the co-ordinating centre (University Hospitals of Leicester NHS Trust, UK) within 24 hours if any of the following adverse events occurred: death; a serious deterioration in a patient’s health that resulted in a life-threatening injury or illness; an event resulting in permanent impairment of a body structure or function; an event resulting in medical or surgical intervention to prevent permanent impairment to a body structure or function; or an event prolonging inpatient hospitalisation. On receipt of notification of any trial adverse or clinical event, the co-ordinating centre requested additional details specific to the nature of the event and carefully monitored the episode. A clinical events committee was established to review and adjudicate key trial adverse events, blinded to patient details and treatment allocation, using original source documents.
| Adverse event | Definition |
|---|---|
| Cardiogenic shock | Systolic blood pressure < 90 mmHg for at least 30 minutes (or the need for supportive measures to maintain a systolic blood pressure of > 90 mmHg) in the presence of a heart rate of > 60 beats/minute in association with signs of end-organ hypoperfusion (cold extremities, low urinary output of < 30 ml/hour and/or mental confusion) |
| MI | MI was defined differently in specific clinical situations in this trial. The European Society of Cardiology (ESC) and American College of Cardiology (ACC) criteria for acute, evolving or recent MI were applied98 |
| Reinfarction | Further chest pain during the index admission lasting > 20 minutes accompanied by new electrocardiographic changes (new Q waves > 0.04 seconds or ST-segment elevation > 0.1 mV in two leads for > 30 minutes), further enzyme rise or both |
| Recurrent MI | A ≥ 20% rise in the value of the biomarker measured serially 6–12 hours apart, provided the absolute value was greater than the 99th percentile upper reference limit. For patients who died and for whom no cardiac markers were obtained, the presence of new ST-segment elevation and new chest pain would meet criteria for MI |
| Contrast-induced nephropathy | A 25% increase in serum creatinine concentration from the baseline value or an absolute increase of at least 0.5 mg/dl (44.2 µmol/l), appearing within 48 hours of administration of contrast media and maintained for 2–5 days99–101 |
| Cerebrovascular events | Stroke was defined as a new focal neurological deficit of presumed vascular aetiology persisting for > 24 hours combined with a neurological imaging study that did not indicate a different aetiology. Transient ischaemic attack was any focal ischaemic neurological deficit of abrupt onset, which resolved completely within 24 hours |
| Severe heart failure | Early heart failure: any new-onset cardiogenic shock or heart failure occurring after randomisation and during the index admission with radiographic evidence of pulmonary oedema requiring intravenous diuretic therapy. Late heart failure: admission to hospital for treatment for documented New York Heart Association (NYHA) class III or IV heart failure |
| Major bleeding | Defined according to the TIMI criteria as fatal bleeding, any intracranial bleeding or clinically overt signs of haemorrhage associated with a drop in haemoglobin of ≥ 50 g/l |
Statistical methods
Demographics are presented and values of infarct size and MVO are summarised, both overall and by treatment group. The distribution of continuous variables, including infarct size, was investigated and when found to be non-normally distributed was log-transformed prior to analysis. Normally distributed continuous variables were expressed as mean ± SD and compared using linear mixed models. Non-normally distributed data were presented as median (25th–75th quartiles) and compared using non-parametric methods such as the Mann–Whitney or the Kruskal–Wallis test.
Primary analysis was by intention to treat (ITT) with a secondary analysis by treatment received, that is, per protocol. Patients entering into the study but not completing the CMR imaging continued to be followed up for MACEs on an ITT basis. For continuous outcomes, including infarct size, t-tests were used to compare means between groups; comparison between the groups for categorical outcomes was undertaken using chi-squared tests. Each drug was compared with the control (i.e. adenosine vs. control and SNP vs. control). Multivariable analysis using linear regression took into consideration possible confounders such as sex, age and other comorbidities. The major confounders of location of infarct (anterior/non-anterior) and time from symptom onset to reperfusion were addressed by the stratified randomisation process. Other important confounders, such as collateral blood flow to the infarct territory determined by the Rentrop score,98 were assessed in the statistical analysis using a forward selection procedure using a statistical significance level of 5%.
Secondary end point analysis employed time-to-event Cox proportional hazards regression models to investigate potentially important predictors of first MACE (both at 30 days and at the end of the study) and obtain unadjusted and adjusted hazard ratios (HRs) together with 95% confidence intervals (CIs) for adenosine compared with control and SNP compared with control. Further analyses investigating the incremental benefit of infarct size in predicting first MACE at 30 days used Cox proportional hazards regression models to derive a linear predictor, which was then summarised using a receiver operating characteristic curve together with the area under the curve and 95% CI.
Sample size
Sample size was based on previous observations of a significant correlation between the extent of CMR-measured MVO and infarct size (which on average is 20% of LVM as detected by CMR imaging after PPCI). 17 As there were no available data regarding the incidence of MVO with the study drugs assessed by CMR imaging, and because of the wealth of published data on infarct size following PPCI, we chose infarct size as the primary end point of the trial. Infarct size is a powerful predictor of ventricular function, adverse LV remodelling and short- to medium-term clinical outcome. 14,16,17,102–114 Furthermore, new infarct size of 4% of LVM has been shown to be associated with adverse prognosis in patients with coronary artery disease undergoing revascularization-related injury. 115 To detect a reduction in infarct size from 20% to 15% of LVM, assuming a SD of 10%,19,105,111,112,116–120 α of 0.05, two-tailed, 80% power and a drop-out rate of 20% between PPCI and CMR, 80 subjects per group (240 in total) were required. It should be noted that the original sample size was set at 297 patients (99 in each group) based on 90% power. There were many challenges during the recruitment phase, which was difficult for this study. Consequently, we approached the funding body for an extension to the trial with an associated request for additional funding. Unfortunately the request was denied and, hence, to deliver a meaningful trial, the power and sample size of the study were reduced. However, our statistician, and the National Institute for Health Research (NIHR) study progress review body, felt that the reduction in power from 90% to 80% would not affect the final results.
Patient and public involvement
As this grant application went through a fast-track application there was limited time to involve service users. However, the study was presented to the patient and public involvement (PPI) group of the NIHR Leicester Cardiovascular Biomedical Research Unit and was welcomed. A layperson from the public volunteered to join the Trial Steering Committee (TSC) and regularly attended meetings. Co-investigators spoke at regional PPI meetings about active CMR studies and heart disease, including the REFLO-STEMI trial.
Patients who were recruited to the study were given the opportunity to have a one-to-one meeting following their CMR imaging to discuss their CMR and angiographic images. They also had the opportunity to ask any questions that they had in a relaxed atmosphere, which was well received and appreciated.
Once the study results have been published the study will be presented at our local and regional PPI meetings to help disseminate the findings.
Study organisation
This project was funded by the Medical Research Council (MRC) through the Efficacy and Mechanism Evaluation (EME) Board (project number 09/150/28) and managed by the NIHR on behalf of the MRC–NIHR partnership. The trial sponsor was the University Hospitals of Leicester NHS Trust. Trial support was provided by the Leicester Clinical Trials Unit [UK Clinical Research Collaboration (UKCRC) ID 43], which was responsible for database provision, data management and statistical analysis. The study was overseen by a TSC, with an independent chairperson and two additional independent members. Safety data (particularly unexpected adverse events and protocol violations) were scrutinised by an independent Data and Safety Monitoring Board (DSMB), who reported back to the TSC. The DSMB assessed whether adverse events were complications of study treatments or expected consequences of having a STEMI. The DSMB had the remit to terminate the study early in the presence of trial safety concerns; members convened when 115 patients had been recruited and at the end of recruitment. The DSMB remained satisfied that the study was conducted appropriately and found no cause for concern regarding safety.
Chapter 4 Results
Recruitment
The REFLO-STEMI trial began recruitment on 25 October 2011. In total, 247 patients were randomised (last patient recruited on 8 April 2014). The study completed at the end of June 2014 (Figure 2). A total of 222 patients (89.9%) consented to CMR imaging post PPCI, although only 207 patients (83.8%) had CMR imaging attempted, with further attrition during the scan (because of claustrophobia or musculoskeletal discomfort) resulting in 197 patients (79.8%) completing CMR imaging for the primary outcome measure of CMR-derived infarct size.
FIGURE 2.
Study recruitment flow chart. CABG, coronary artery bypass graft; CTO, chronic total occlusion; LCA, left coronary artery; POBA, plain old balloon angioplasty. Patients who died during the follow-up period were deemed to have completed follow-up and hence, ‘Follow-up completed’ includes deaths.

Interim analysis
An interim analysis of the CMR imaging data after 50 patients had been recruited was intended at the outset. However, this could not be undertaken because, for various logistical reasons, the clinical fellow responsible for the day-to-day running of the trial was not in place when recruitment began and then had to be trained to an appropriate standard of practice. The recruitment phase of the study had progressed considerably and hence it was no longer appropriate to perform an interim analysis of the CMR imaging data. An interim safety analysis evaluating adverse events was performed and submitted to the DSMB during this period.
Baseline characteristics
Baseline characteristics for randomised patients and those completing CMR imaging by treatment allocation are presented in Table 7. There were no differences in characteristics between those who were randomised and those who completed the CMR imaging. Groups were generally well matched. A reduced incidence of hypercholesterolaemia and statin use was observed in the control group (standard PPCI without adjunctive pharmacotherapy). There was also a trend towards a greater incidence of diabetes in the SNP treatment arm. Groups were well matched for infarct territory and, in particular, for anterior MI (randomisation stratified) and the remaining baseline characteristics, with no other statistically significant differences between the groups.
| Characteristics | Adenosine | SNP | Control | p-value | ||||
|---|---|---|---|---|---|---|---|---|
| All (n = 82) | With CMR data (n = 63) | All (n = 79) | With CMR data (n = 69) | All (n = 86) | With CMR data (n = 65) | All | With CMR data | |
| Clinical | ||||||||
| Age (years) | 57.9 ± 12.8 | 56.4 ± 12.3 | 60.5 ± 13.0 | 59.3 ± 12.5 | 59.5 ± 11.2 | 60.0 ± 10.8 | 0.406 | 0.192 |
| Male | 65/82 (79.3) | 52/63 (82.5) | 66/79 (83.5) | 59/69 (85.5) | 64/86 (74.4) | 50/65 (76.9) | 0.355 | 0.429 |
| Hypertension | 23/82 (28.0) | 14/63 (22.2) | 26/79 (32.9) | 23/69 (33.3) | 22/86 (25.6) | 16/65 (24.6) | 0.574 | 0.313 |
| Current smoking | 47/82 (57.3) | 39/63 (61.9) | 41/79 (51.9) | 37/69 (53.6) | 45/86 (52.3) | 31/65 (47.7) | 0.332 | 0.238 |
| Diabetes | 6/82 (7.3) | 3/63 (4.8) | 12/79 (15.2) | 10/69 (14.5) | 9/86 (10.5) | 4/65 (6.2) | 0.274 | 0.095 |
| Hypercholesterolaemia | 17/82 (20.7) | 15/63 (23.8) | 23/79 (29.1) | 17/69 (24.6) | 11/86 (12.8) | 6/65 (9.2) | 0.035 | 0.042 |
| Previous MI | 0/81 (0) | 0/63 (0) | 3/79 (3.8) | 3/69 (4.3) | 3/86 (3.5) | 2/65 (3.1) | 0.219 | 0.268 |
| Previous PCI | 0/82 (0) | 0/63 (0) | 3/79 (3.8) | 3/69 (4.3) | 2/86 (2.3) | 1/65 (1.5) | 0.225 | 0.197 |
| Killip class > 1 | 3/82 (3.7) | 2/63 (3.2) | 4/79 (5.1) | 3/69 (4.3) | 4/86 (4.7) | 3/65 (4.6) | 0.905 | 0.908 |
| Total ischaemia time (minutes) | 159 (124–221) | 155 (121–221) | 150 (122–201) | 150 (121–205) | 145 (105–196) | 141 (106–188) | 0.169 | 0.209 |
| BMI (kg/m2) | 27.5 (25.0–30.1) | 27.5 (25.1–32.1) | 26.1 (24.3–30.8) | 26.8 (24.7–31.0) | 27.3 (24.4–30.6) | 27.3 (25.1–30.7) | 0.659 | 0.833 |
| SBP (mmHg) | 137.5 ± 25.1 | 136.2 ± 25.4 | 133.0 ± 23.4 | 132.9 ± 23.3 | 135.1 ± 23.3 | 136.2 ± 23.5 | 0.505 | 0.663 |
| DBP (mmHg) | 86.6 ± 19.2 | 86.0 ± 18.8 | 81.8 ± 16.4 | 82.3 ± 16.4 | 80.5 ± 17.0 | 80.6 ± 17.8 | 0.067 | 0.215 |
| Heart rate (beats/minute) | 74.0 ± 17.3 | 72.8 ± 18.8 | 71.9 ± 14.8 | 72.3 ± 14.9 | 71.2 ± 14.6 | 71.3 ± 14.7 | 0.487 | 0.878 |
| Cr clearance (ml/minute/1.73 m2) | 98.1 ± 28.1 | 101.6 ± 26.4 | 93.4 ± 29.1 | 93.8 ± 30.0 | 92.7 ± 25.6 | 93.9 ± 26.1 | 0.401 | 0.190 |
| Medication on admission | ||||||||
| Beta-blocker | 6/82 (7.3) | 4/63 (6.3) | 6/79 (7.6) | 6/69 (8.7) | 6/86 (7.0) | 3/65 (4.6) | 0.988 | 0.633 |
| ACE inhibitor/A2RB | 14/82 (17.1) | 7/63 (11.1) | 17/79 (21.5) | 16/69 (23.2) | 13/86 (15.1) | 12/65 (18.5) | 0.549 | 0.190 |
| Statin | 17/82 (20.7) | 14/63 (22.2) | 25/79 (31.6) | 19/69 (27.5) | 13/86 (15.1) | 7/65 (10.8) | 0.036 | 0.049 |
| IRA | ||||||||
| LAD – proximal | 19/82 (23.2) | 11/63 (17.5) | 18/79 (22.8) | 16/69 (23.2) | 20/86 (23.3) | 15/65 (23.1) | 0.997 | 0.663 |
| LAD – other | 13/82 (15.9) | 12/63 (19.0) | 15/79 (19.0) | 12/69 (17.4) | 14/86 (16.3) | 12/65 (18.5) | 0.848 | 0.969 |
| LCX | 10/82 (12.2) | 6/63 (9.5) | 13/79 (16.5) | 13/69 (18.8) | 18/86 (20.9) | 12/65 (18.5) | 0.314 | 0.259 |
| RCA | 40/82 (48.8) | 34/63 (54.0) | 33/79 (41.8) | 28/69 (40.6) | 34/86 (39.5) | 26/65 (40.0) | 0.455 | 0.197 |
| TFG | ||||||||
| 0–1 | 80/81 (98.8) | 61/62 (98.4) | 72/79 (91.1) | 63/69 (91.3) | 83/86 (96.5) | 62/65 (95.4) | 0.057 | 0.180 |
| 2 | 1/81 (1.2) | 1/62 (1.6) | 5/79 (6.3) | 5/69 (7.2) | 1/86 (1.2) | 1/65 (1.5) | 0.078 | 0.124 |
| 3 | 0/81 (0.0) | 0/62 (0.0) | 2/79 (2.5) | 1/69 (1.4) | 2/86 (2.3) | 2/65 (3.1) | 0.367 | 0.368 |
| Thrombus score | ||||||||
| 4–5 | 75/81 (92.6) | 57/62 (91.9) | 72/79 (91.1) | 64/69 (92.8) | 81/86 (94.2) | 60/65 (92.3) | 0.754 | 0.985 |
Angiography and primary percutaneous coronary intervention details
A high use of radial vascular access is noted in this contemporary PPCI study (Table 8). Thrombectomy was mandated as a precursor to drug delivery and the slightly lower thrombectomy use observed in the control arm was not statistically significant. Drug-eluting stent use was uniformly high across groups, in keeping with a contemporary study. The median length of stented segment was similar in all groups and ranged from 23 to 26 mm.
| Characteristics | Adenosine (all subjects) (n = 82) | SNP (all subjects) (n = 79) | Control (all subjects) (n = 86) | p-valueb | p-valuec |
|---|---|---|---|---|---|
| Procedural data | |||||
| Femoral approach | 12 (14.6) | 9 (11.4) | 7 (8.1) | 0.184 | 0.481 |
| Radial approach | 70 (85.4) | 70 (88.6) | 79 (91.9) | 0.184 | 0.481 |
| Thrombectomy | 81 (98.8) | 75 (98.7)d | 80 (93.0) | 0.118 | 0.122 |
| DES implantation | 73 (89.0) | 72 (91.1) | 81 (94.2) | 0.226 | 0.452 |
| Number of stents, median (IQR) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.613 | 0.790 |
| Diameter of stented segment (mm), median (IQR) | 3.5 (3.0–3.5) | 3.5 (3.0–3.5) | 3.0 (3.0–3.5) | 0.465 | 0.649 |
| Length of stented segment (mm), median (IQR) | 26.0 (18.0–39.0) | 23.0 (18.0–38.0) | 24.0 (18.0–34.5) | 0.585 | 0.833 |
| Intraprocedural complications | |||||
| Transient AV block not requiring pacing | 7 (8.5) | 2 (2.5) | 10 (11.6) | 0.507 | 0.034 |
| AV block requiring pacing | 2 (2.4) | 1 (1.3) | 0 (0.0) | 0.237 | 0.479 |
| Transient hypotension not requiring vasopressor drugs or IABP | 5 (6.1) | 13 (16.5) | 5 (5.8) | 0.938 | 0.028 |
| Hypotension requiring vasopressor drugs or IABP | 5 (6.1) | 3 (3.8) | 6 (7.0) | 0.818 | 0.499 |
| Ventricular tachycardia/fibrillation | 5 (6.1) | 3 (3.8) | 5 (5.8) | 0.938 | 0.722 |
Intraprocedural complications were similar across all groups. However, the incidence of transient atrioventricular (AV) block not requiring pacing was greater in the control arm. There was a low incidence of AV block requiring pacing in this study (2.4% vs. 1.3% vs. 0% in the adenosine, SNP and control arms, respectively). A significantly higher rate of transient hypotension (not requiring vasopressor or intra-aortic balloon-pump support) was observed in the SNP arm (p = 0.028). Other complications were as expected as a consequence of STEMI and were similar across the groups.
Angiographic, electrocardiographic and enzymatic assessment of myocardial injury
The incidence of angiographic slow-flow/no-reflow (TFG < 3 or final visual TMPG 0–1) was low and similar across the groups and was consistent with the quantitative angiographic [myocardial blush grade (MBG) and cTFC] and electrocardiographic (STR > 70%) assessment of microvascular tissue perfusion (Table 9). There were no statistically significant differences between these markers of MVO post PPCI.
| Characteristics | Adenosine (all subjects) (n = 82) | SNP (all subjects) (n = 79) | Control (all subjects) (n = 86) | p-valueb | p-valuec |
|---|---|---|---|---|---|
| Angiographic | |||||
| Final TFG < 3 | 4 (4.9) | 6 (7.6) | 3 (3.5) | 0.652 | 0.313 |
| Final TMPG 0–1 | 0 (0.0) | 1 (1.3) | 1 (1.2) | 0.327 | 1.000 |
| Quantitative MBG | 10.0 (7.0–14.0) | 11.0 (7.0–17.8) | 12.0 (8.0–17.0) | 0.144 | 0.481 |
| Final cTFC | 14.0 (9.0–20.0) | 14.0 (10.0–21.0) | 15.0 (10.0–22.0) | 0.457 | 0.928 |
| Electrocardiographic | |||||
| Baseline maximal sum of ST-segment elevation | 9.0 (6.0–12.0) | 9.0 (5.0–13.0) | 9.0 (5.0–13.0) | 0.931 | 0.686 |
| Post-PPCI maximal sum of ST-segment elevation | 2.0 (0.0–5.0) | 2.0 (0.0–5.0) | 2.0 (0.0–4.0) | 0.684 | 0.472 |
| STR > 70% | 56 (68.3) | 48 (60.8) | 56 (65.1) | 0.662 | 0.562 |
| Enzymatic | |||||
| Peak CK (mg/dl) | 1559 (601–2804) | 1171 (430–2259) | 1336 (511–2632) | 0.601 | 0.393 |
There was no statistically significant difference in enzymatic infarct size represented by peak creatine kinase (CK) between the groups.
Cardiac magnetic resonance imaging assessment of myocardial injury
Cardiac magnetic resonance imaging characteristics of the study population are presented by treatment arm in Table 10. There was no statistically significant difference in the primary outcome measure of unadjusted infarct size (%LVM) between the adenosine- or SNP-facilitated PPCI groups and the control group. On multivariable regression analysis, adjusting for significant confounders, there was a trend towards a significant increase in mean infarct size in the adenosine group (mean difference 2.73, 95% CI –0.18 to 5.64; p = 0.066) compared with the control group. This was not seen in the SNP group.
| Characteristics | Adenosine | SNP | Control | p-valueb | p-valuec |
|---|---|---|---|---|---|
| Scar assessmentd | n = 63 | n = 69 | n = 65 | ||
| Infarct size (%LVM) | 10.1 (4.7–16.2) | 10.0 (4.2–15.8) | 8.3 (1.9–14.0) | 0.062 | 0.160 |
| Microvascular injury | n = 63 | n = 69 | n = 65 | ||
| Presence of IMH, n/N (%) | 20/38 (52.6) | 19/43 (44.2) | 16/38 (42.1) | 0.358 | 0.850 |
| Presence of early MVO, n/N (%) | 41/60 (68.3) | 42/59 (71.2) | 38/63 (60.3) | 0.452 | 0.254 |
| Presence of late MVO, n/N (%) | 43/63 (68.3) | 52/69 (75.4) | 37/65 (56.9) | 0.205 | 0.029 |
| Early MVO (%LVM) | 1.2 (0.0–5.2), n = 60/82 | 1.0 (0.0–5.0), n = 59/79 | 1.4 (0.0–4.3), n = 63/86 | 0.637 | 0.770 |
| Late MVO (%LVM) | 1.0 (0.0–3.7) | 0.6 (0.0–2.4) | 0.3 (0.0–2.8) | 0.205 | 0.244 |
| Salvage | n = 34 | n = 38 | n = 37 | ||
| AAR (%LVM) | 30.6 ± 12.2 | 34.7 ± 14.4 | 30.3 ± 11.5 | 0.907 | 0.152 |
| MSI (%) | 60.2 ± 23.3 | 63.6 ± 24.7 | 67.5 ± 23.3 | 0.188 | 0.477 |
| Function and volumes | n = 63 | n = 71 | n = 68 | ||
| LVEDVI (ml/m2) | 91.3 ± 16.1 | 87.0 ± 16.9 | 84.4 ± 14.6 | 0.011 | 0.336 |
| LVESVI (ml/m2) | 52.3 ± 13.8 | 49.1 ± 12.7 | 46.1 ± 11.6 | 0.006 | 0.155 |
| LVMI (g/m2) | 59.1 ± 11.5 | 56.0 ± 11.2 | 53.6 ± 9.2 | 0.003 | 0.174 |
| LVEF (%) | 43.2 ± 7.9 | 43.9 ± 6.5 | 45.7 ± 8.0 | 0.080 | 0.165 |
Microvascular obstruction was present on LGE images (late MVO) in 67% of patients. The presence of late MVO was significantly higher in the SNP arm than in the control arm (75.4% vs. 56.9%; p = 0.029). However, there was no statistically significant difference in quantitative late MVO between the two groups (p = 0.244). Quantitatively, late MVO also appeared higher in the adenosine-treated arm than in the control arm, although, again, this was not statistically significant. Other CMR parameters of microvascular injury were similar between the groups. For both early and late MVO none of the potential confounders was identified as being of statistical importance by the forward selection procedure.
An increase in LV volumes was observed in the adenosine arm compared with the control arm and this was accompanied by a borderline significant reduction in ejection fraction. LV volumes and function were similar in the SNP-treated and control arms.
Diagnostic quality T2w-STIR (oedema) imaging, required for AAR estimation and derivation of MSI, was obtainable in only 109 patients (55%). In patients who had oedema assessed, there was no significant difference between the groups in myocardial salvage.
Echocardiography
Echocardiography was performed at 3 months in 108 subjects (44%) (n = 44 adenosine group, n = 30 SNP group, n = 34 control group). The ejection fraction [%, median, interquartile range (IQR)] was significantly higher in the control arm (58.5, 54.5–64.0) than in the adenosine arm (53.5, 41.3–60.0; p = 0.010) and the SNP arm (51.5, 45.0–61.0; p = 0.015).
Clinical outcomes
Patients were followed up for a median of 6 months. In total, 232 patients (94%) completed follow-up (four patients died before follow-up was completed, four patients withdrew consent, five patients refused follow-up and two patients were lost to follow-up). An overview of clinical events is presented in Table 11. There was a significant increase in MACEs in patients undergoing adenosine-facilitated PPCI compared with control patients, driven by heart failure, at 30 days (HR 5.39, 95% CI 1.18 to 24.60; log-rank p = 0.04) and 6 months (HR 6.53, 95% CI 1.46 to 29.2; log-rank p = 0.01) post randomisation. There was no statistically significant difference in bleeding between groups and the low bleeding event rate is consistent with the use of predominantly radial vascular access and bivalirudin in this study.
| Characteristics | Adenosine (all subjects) (n = 82) | SNP (all subjects) (n = 79) | Control (all subjects) (n = 86) | p-valueb | p-valuec |
|---|---|---|---|---|---|
| First event | |||||
| MACE | 12 (14.6) | 5 (6.3) | 2 (2.3) | 0.01 | 0.261 |
| Death | 1 (1.2) | 1 (1.3) | 0 (0.0) | 0.488 | 0.479 |
| CVE | 1 (1.2) | 1 (1.3) | 0 (0.0) | 0.488 | 0.479 |
| MI | 2 (2.4) | 1 (1.3) | 1 (1.2) | 0.614 | 1.000 |
| HF | 8 (9.8) | 2 (2.5) | 1 (1.2) | 0.016 | 0.607 |
| TLR | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 | 1.000 |
| Composite of death, MI and HF | 11 (13.4) | 4 (5.1) | 2 (2.3) | 0.009 | 0.428 |
| Number of patients with > 1 event | 3 (3.7) | 1 (1.3) | 1 (1.2) | 0.359 | 1.000 |
| Bleeding | |||||
| All bleeding | 4 (4.9) | 2 (2.5) | 5 (5.8) | 1.000 | 0.446 |
| Fatal bleeding | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 | 1.000 |
Kaplan–Meier graphs of time to first MACE are shown in Figure 3. When adjusted for confounders (age, sex, diabetes, anterior MI, ischaemia time and Rentrop score), the observed effect remains, with similar HRs and log-rank p = 0.018 at 30 days and p = 0.01 at 6 months (see Table 14).
FIGURE 3.
Kaplan–Meier graphs showing clinical outcome in the three treatment arms at 30 days and 6 months (ITT). (a) Time to first MACE within 30 days; and (b) time to first MACE (median follow-up 6 months).


Per-protocol analysis
We observed a high rate of failed study drug delivery in the adenosine and SNP arms (Table 12). Almost one in five patients randomised to drug-facilitated PPCI did not receive the second dose of the study drug post stent deployment as a result of an increased QTc following the first dose. Consequently, secondary analysis per protocol was performed (Table 13)
| Reason study drug not administered | n (%) |
|---|---|
| First dose | N = 161 |
| Hypotension | 3 (1.9) |
| Unable to cross lesion | 3 (1.9) |
| Coronary dissection | 1 (0.6) |
| Total | 7 (4.3) |
| Second dose | N = 155 |
| Prolonged or > 60-millisecond increase in QTc | 30 (19.4) |
| Coronary dissection | 1 (0.6) |
| Ventricular fibrillation | 1 (0.6) |
| No stent deployed | 1 (0.6) |
| Other SAE (operator decision) | 1 (0.6) |
| Total | 34 (21.9) |
| Either first or second dose | N = 161 |
| Prolonged or > 60-millisecond increase in QTc | 30 (18.6) |
| Hypotension | 3 (1.9) |
| Unable to cross lesion | 3 (1.9) |
| Coronary dissection | 2 (1.2) |
| Ventricular fibrillation | 1 (0.6) |
| No stent deployed | 1 (0.6) |
| Other SAE (operator decision) | 1 (0.6) |
| Total | 41 (25.5) |
| Characteristics | Adenosine (N = 66) | SNP (N = 53) | Control (N = 86) | p-valueb | p-valuec |
|---|---|---|---|---|---|
| Angiographic | |||||
| Quantitative MBG | 11.0 (7.0–14.0) | 11.0 (7.0–15.0) | 12.0 (8.0–17.0) | 0.165 | 0.134 |
| Final cTFC | 14.0 (9.0–21.0) | 15.0 (10.0–21.0) | 15.0 (10.0–22.0) | 0.639 | 0.909 |
| Echocardiographic | |||||
| LVEF (3 months) (%) | 53.0 (40.0–60.0) | 54.0 (45.0–61.0) | 58.5 (54.5–64.0) | 0.006 | 0.038 |
| Electrocardiographic | |||||
| STR > 70%, n (%) | 46 (69.7) | 28 (52.8) | 56 (65.1) | 0.604 | 0.158 |
| Enzymatic | |||||
| Peak CK (mg/dl) | 1664 (788–2886) | 1333 (578–2247) | 1336 (511–2632) | 0.253 | 0.387 |
| CMR data | |||||
| Function and volumes | n = 52 | n = 48 | n = 68 | ||
| LVEDVI (ml/m2) | 91.4 ± 14.1 | 87.3 ± 16.3 | 84.4 ± 14.6 | 0.009 | 0.304 |
| LVESVI (ml/m2) | 52.7 ± 11.6 | 49.0 ± 12.6 | 46.1 ± 11.6 | 0.003 | 0.203 |
| LVMI (g/m2) | 59.9 ± 11.5 | 56.7 ± 11.4 | 53.6 ± 9.2 | 0.001 | 0.109 |
| LVEF (%) | 42.5 ± 7.2 | 44.3 ± 6.8 | 45.7 ± 8.0 | 0.029 | 0.332 |
| Salvage | n = 30 | n = 26 | n = 37 | ||
| AAR (%LVM) | 31.6 ± 10.9 | 34.7 ± 14.4 | 30.3 ± 11.5 | 0.639 | 0.147 |
| MSI (%) | 59.0 ± 22.1 | 63.6 ± 24.7 | 67.5 ± 23.3 | 0.134 | 0.544 |
| Microvascular injury | n = 52 | n = 47 | n = 65 | ||
| Presence of IMH, n/N (%) | 19/33 (57.6) | 14/30 (46.7) | 16/38 (42.1) | 0.238 | 0.807 |
| Presence of early MVO, n/N (%) | 35/49 (71.4) | 31/42 (73.8) | 38/63 (60.3) | 0.238 | 0.208 |
| Presence of late MVO, n/N (%) | 38/52 (73.1) | 37/47 (78.7) | 37/65 (56.9) | 0.083 | 0.025 |
| Early MVO (%LVM) | 1.6 (0.0–5.3), n = 49/66 | 0.9 (0.0–3.3), n = 42/53 | 1.4 (0.0–4.3), n = 63/86 | 0.506 | 0.960 |
| Late MVO (%LVM) | 1.2 (0.0–3.7) | 0.6 (0.0–2.3) | 0.3 (0.0–2.8) | 0.106 | 0.345 |
| Scar assessment | n = 52 | n = 47 | n = 65 | ||
| Infarct size (%LVM)d | 12.0 (4.8–16.5) | 10.0 (7.3–13.8) | 8.3 (1.9–14.0) | 0.031 | 0.088 |
| First event, n (%) | N = 66 | N = 53 | N = 86 | ||
| MACE | 10 (15.2) | 3 (5.7) | 2 (2.3) | 0.005 | 0.369 |
| Death | 0 (0.0) | 1 (1.9) | 0 (0.0) | 1.000 | 0.381 |
| CVE | 1 (1.5) | 1 (1.9) | 0 (0.0) | 0.434 | 0.381 |
| MI | 2 (3.0) | 0 (0.0) | 1 (1.2) | 0.580 | 1.000 |
| HF | 7 (10.6) | 1 (1.9) | 1 (1.2) | 0.021 | 1.000 |
| TLR | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 | 1.000 |
| Composite of death, MI and HF | 9 (13.6) | 2 (3.8) | 2 (2.3) | 0.010 | 0.636 |
Patients in the adenosine arm who received both doses of the study drug per protocol had an even stronger statistically significant signal of harm in CMR parameters than patients in the control arm. Infarct size was increased in adenosine-treated patients compared with control patients (p = 0.031) and increased LV volumes and a reduced ejection fraction were also observed in the adenosine arm.
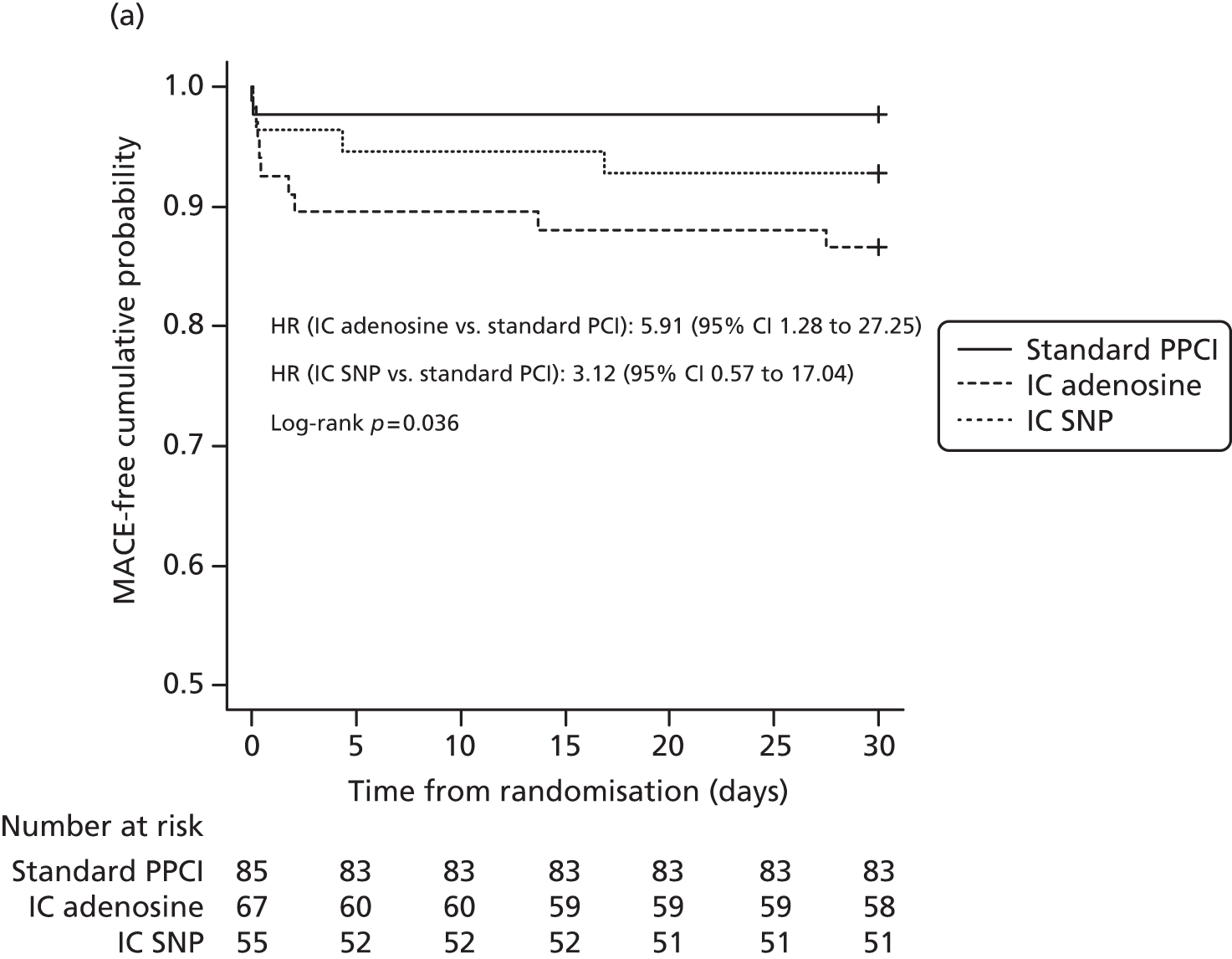
Considering only patients who received both doses of the study drug and plotting Kaplan–Meier graphs for time to first MACE again shows a statistically significantly increased HR for adenosine-facilitated PPCI compared with the control at 30 days (HR 5.91, 95% CI 1.28 to 27.25; log-rank p = 0.036) and 6 months (HR 7.31, 95% CI 1.62 to 33.0; log-rank p = 0.008) post randomisation (Figure 4).
FIGURE 4.
Kaplan–Meier graphs showing clinical outcome in the three treatment arms at 30 days and 6 months in patients treated per protocol. (a) Time to first MACE within 30 days; and (b) time to first MACE (median follow-up 6 months).

Survival analysis demonstrated a clear signal of increased hazard with adenosine-facilitated PPCI compared with the control (Table 14). Our clinical outcome data are consistent with the CMR imaging data (increased LV volumes, reduced ejection fraction and increased infarct size), which together suggest possible adverse LV remodelling with adenosine treatment leading to worse clinical outcomes than with standard PPCI (control).
| Analysis | Adjusted or unadjusted | Comparison | HR | 95% CI | p-value | Log-rank p-value |
|---|---|---|---|---|---|---|
| First MACE within 30 days | ||||||
| ITT | Unadjusted | Adenosine vs. control | 5.39 | 1.18 to 24.60 | 0.03 | 0.04 |
| SNP vs. control | 2.75 | 0.53 to 14.16 | 0.2 | |||
| Adjusteda | Adenosine vs. control | 5.24 | 1.13 to 24.33 | 0.03 | 0.018 | |
| SNP vs. control | 2.36 | 0.45 to 12.40 | 0.3 | |||
| Per protocol | Unadjusted | Adenosine vs. control | 5.91 | 1.28 to 27.25 | 0.02 | 0.036 |
| SNP vs. control | 3.12 | 0.57 to 17.04 | 0.2 | |||
| Adjusteda | Adenosine vs. control | 5.76 | 1.21 to 27.35 | 0.03 | 0.1 | |
| SNP vs. control | 2.94 | 0.52 to 16.60 | 0.2 | |||
| First MACE after 6 months’ median follow-up | ||||||
| ITT | Unadjusted | Adenosine vs. control | 6.53 | 1.46 to 29.20 | 0.01 | 0.01 |
| SNP vs. control | 2.76 | 0.53 to 14.21 | 0.2 | |||
| Adjusteda | Adenosine vs. control | 6.54 | 1.45 to 29.64 | 0.01 | 0.01 | |
| SNP vs. control | 2.53 | 0.48 to 13.24 | 0.3 | |||
| Per protocol | Unadjusted | Adenosine vs. control | 7.31 | 1.62 to 33.00 | 0.01 | 0.008 |
| SNP vs. control | 3.14 | 0.57 to 17.13 | 0.2 | |||
| Adjusteda | Adenosine vs. control | 7.32 | 1.59 to 33.59 | 0.01 | 0.05 | |
| SNP vs. control | 3.20 | 0.57 to 18.01 | 0.2 | |||
Chapter 5 Discussion
The REFLO-STEMI trial was designed to test whether adjunctive pharmacotherapy with adenosine and/or SNP could reduce the extent of myocardial injury (infarct size and MVO) as measured by the sensitive CMR surrogate markers and, additionally, as a secondary end point, improve clinical outcome. In the introduction the theoretical case for benefit of these agents was made. There is good basic science and preclinical evidence that both drugs have the potential to attenuate the MVO process. The REFLO-STEMI study is the first study to combine what are considered appropriate drug dosages, delivered optimally to the site of maximal benefit, with the use of CMR imaging to robustly measure reperfusion success and scar size in a group of patients treated with a contemporary reperfusion strategy. The study was powered accordingly to deliver a definitive answer to the question of whether these agents can reduce infarct size. Additional measures of myocardial perfusion (angiographic and electrocardiographic) and early clinical outcome data provide further insight into the potential role of prophylactic adjunctive pharmacotherapy administered universally for STEMI patients.
The trial was designed to ensure that account was taken of potential safety parameters. Thus, prolongation of the QTc after the first dose resulted in the second dose not being given in 19% of patients. This had some impact on the numbers in the two groups who completed the treatment strategy, with only 66 of 82 (80%) patients in the adenosine group receiving both doses and only 53 of 79 (67%) patients in the SNP group receiving both doses. All results are therefore presented as ITT analyses, as per the statistical analysis plan, but also as per-protocol analyses.
Baseline characteristics and procedural detail
The groups were well matched in terms of baseline demographics in the trial overall and in those who completed the CMR scan (see Table 7). There tended to be more diabetic patients in the SNP group but this was not significant. There was a significant excess of patients with hypercholesterolaemia in both treatment groups compared with the control group and to be expected a greater use of statins in these patients. There were no differences between the groups in important potential confounders such as age, site of infarct and total ischaemic time. As per the inclusion criteria most patients had TFG 0–1 at first angiography.
In keeping with a study undertaken in expert centres there was a high rate of use of the radial approach and a very high rate of drug-eluting stent usage, consistent with contemporary practice. Thrombectomy was mandated as the device was subsequently used for local delivery of the drug and so the rate of thrombectomy was high in each group. It is interesting to note that mean stent length was 23–26 mm. Intraprocedural complications are shown in Table 8. We expected there to be a high incidence of AV block in the adenosine group but this was higher (albeit not requiring pacing) in the control group. We suspect that this is because of the natural incidence of AV block in such patients and we should note that a proportion of the adenosine and SNP patients did not receive a second dose. Even so, this cannot be the cause of the findings and so they must be regarded as a play of chance. Transient hypotension not requiring resuscitative therapy was significantly higher in the SNP group and this may be a more expected finding given the profound vasodilating properties of SNP.
Angiographic and electrocardiographic outcomes
Again, in keeping with a study undertaken in high-volume expert centres, the number of participants with a final TFG of < 3 was in single digits (see Table 9). Importantly, despite the basic science and observational data,46,63,66,121–127 there was no difference in this or other markers of microvascular blood flow (final TMPG, quantitative MBG, final cTFC) between the treatment groups or between either treatment group and the control group. This is consistent with some42,44,51,52 but not all44,53,60,61,128,129 randomised trials. Similarly, a surrogate marker of flow (resolution of ECG peak elevation to > 70%) was seen to be similar in all three groups and was relatively high at 68.3%, 60.8% and 65.1% compared with previous studies,44,51–53,129 probably reflecting the fact that recruitment was limited to those with a time from symptoms to presentation of ≤ 6 hours. All of these markers are of course surrogates of flow and infarct size that are less sensitive than our chosen end point.
Primary end point: infarct size and other cardiac magnetic resonance imaging markers of reperfusion injury
Of the trial population, 20% of patients did not undergo the CMR assessment. The main reasons for exclusion were early repatriation to a secondary care hospital (before CMR assessment could be undertaken), lack of consent and patients being too unwell. Those completing the CMR assessment had similar characteristics to those not completing the assessment (see Table 7).
The main finding was that there was no significant difference in infarct size between the groups, although when the results were adjusted for infarct location there was a borderline significant increase in infarct size in the adenosine group compared with the control group. Certainly, neither drug reduced infarct size. Additionally, there was no decrease in MSI, early MVO or late MVO, indicating a lack of efficacy of adenosine and SNP in terms of preventing reperfusion injury. These results are consistent with those of the only other randomised trial that included CMR imaging;51 this trial also did not show any benefit of high-dose IC adenosine. It is interesting to note that the adenosine-treated patients had increased myocardial volumes and a non-significant trend towards a reduced ejection fraction compared with the control group. The per-protocol analysis actually showed that patients who received both doses of adenosine had an increased infarct size, increased LV volumes and a reduced ejection fraction (also seen on follow-up echocardiography) on CMR imaging compared with the control group, which suggests not only a lack of efficacy but also potential adverse effects on reperfusion.
Clinical outcomes
Clinical events were included in the study as an important safety consideration but the trial was not powered to detect clinically meaningful differences in MACEs between groups. However, clinical outcome was incidentally found to be significantly worse for the adenosine group than the control group (see Table 11), largely driven by increased early heart failure events. Although this finding may have occurred by chance and was not shown in previous trials, the HR is high, it fits with the infarct size measures being increased and is consistent whether assessed in ITT or in per-protocol analysis, at 1 and 6 months’ follow-up and after adjustment for potential confounding variables (age, sex, ischaemia time, diabetes, anterior MI or not and Rentrop score). Taken together with the CMR findings, the results suggest that using adenosine to protect against MVO and its potential clinical consequence not only fails to do so but may also in fact have significant clinical adverse outcomes. This finding of an adverse effect of adenosine remains difficult to explain. One possible explanation is that ischaemia already induces high levels of endogenous adenosine51,130 and that further doses, particularly high doses, have no additional benefits and possibly detrimental effects because of distal embolisation, hypotension and bradycardia, although we did not see any significant differences in these parameters in this study. The finding is hypothesis generating. High-dose IC adenosine should not be used in the setting of PPCI to prevent reperfusion injury. Whether this applies to IC adenosine given for angiographic clear no-reflow remains contentious, as the risk/benefit ratio may be different.
Limitations
The study was open label and this may have influenced the management of patients, particularly at the time of PPCI; however, the primary outcome was assessed on blinded CMR scans. A major limitation of T2w-STIR imaging for AAR is that the sequence is prone to artefacts and oedema may not be discernible. In one previous study T2w-STIR identified only 64% of culprit arteries in 54 acute STEMI patients and the AAR was less than the amount of LGE in 30% of patients. 131 In our recently published CMR substudy of CvLPRIT (Complete versus culprit-Lesion only PRimary PCI Trial), the AAR was only quantifiable in 75% of the 203 patients who completed the baseline CMR assessment at 1.5T. 132 In this study, using 3.0T CMR with greater field inhomogeneity and the early scanning of patients post STEMI, diagnostic quality T2w-STIR imaging was obtainable in only 55% of patients who completed the CMR assessment. In at least one other multicentre trial with core laboratory analysis, T2w imaging obtained an even lower rate of analysable images for oedema (≈50%) than we have reported. 133 Although issues with T2w-STIR are well recognised,134 in multicentre trials this sequence is still frequently used as the newer T1 and T2 mapping sequences, which appear to be more robust for AAR detection, are not widely available. However, given the importance of the MSI in the comparison of therapies in STEMI, such sequences should be used in future studies.
A mechanistic substudy evaluating periprocedural platelet activity was planned but had to be abandoned because of a lack of sufficient data (partly because of staffing issues including staff pregnancy) to make any significant scientific statement.
The trial assessed whether or not MVO could be attenuated prior to PPCI and our negative results do not imply that SNP and adenosine are ineffective if no-reflow occurs post PPCI.
Recommendations for research
Studies undertaken in the modern PPCI era have collectively shown a failure of therapies underpinned by an extensive body of positive experimental data to prophylactically reduce MVO or infarct size. Future trials could perhaps focus on limiting reperfusion injury when angiographic slow-flow/no-reflow is encountered, utilising robust end points as in our study.
The MSI measures reperfusion success and predicts prognosis post STEMI. 103 The MSI requires accurate assessment of myocardial oedema and AAR. Oedema is typically imaged on pre-contrast T2w-STIR imaging, as used in our study, but its use is hampered by its susceptibility to artefacts. 135 We note that there was a failure rate of 45% in achieving accurate oedema assessment in our study. This may have been exacerbated by the use of 3.0T CMR imaging in our study but nonetheless should caution the general MRI community against using T2w-STIR for routine oedema assessment following STEMI. Pre-contrast T1 mapping on CMR may be superior to T2w-STIR for the identification of reversible myocardial injury and prediction of functional recovery in acute MI. 136 Using the former technique to detect myocardial oedema and evaluate CMR surrogate markers of myocardial injury in future studies may also reduce the sample sizes required137 and this should perhaps be the first-choice CMR imaging technique for assessing AAR and MSI post STEMI in future trials.
Chapter 6 Conclusions
The REFLO-STEMI trial was a well-designed trial that tested two drugs, adenosine and SNP, in appropriate doses and delivered locally, using a sensitive marker (CMR imaging) of the potential impact of these drugs on flow and therefore infarct size. If these drugs were beneficial this trial should have shown it. There was no demonstrated efficacy with either drug, a finding that will inform the interventional community. Indeed, we will ask the community to note the adverse effects in the adenosine group. Outcomes after PPCI are still far from optimal and this was an attempt to see whether adjunctive pharmacotherapy delivered optimally would improve outcomes. As such, it was an important and worthy, albeit challenging, study.
We conclude that neither adenosine nor SNP reduce infarct size or reperfusion injury when administered during PPCI treatment of STEMI. Furthermore, use of high-dose adenosine in STEMI may cause cardiac toxicity and worsen clinical outcome. Current STEMI guidelines advocate the use of adenosine in established angiographic MVO (slow-flow/no-reflow) and clinicians frequently give repeated doses of adenosine in this setting. Our results should strongly discourage clinicians from using cumulatively high doses of IC adenosine during PPCI to prevent reperfusion injury.
Acknowledgements
We are grateful to the NIHR for their support and patience during at times a difficult trial. Logistical issues strove to prevent us completing the study, which although negative should be regarded as a robust answer to an often-asked clinical science question. The study was sponsored by the University Hospitals of Leicester NHS Trust. GPM was supported by a NIHR postdoctoral fellowship. We also acknowledge the contribution of the following as TSC members – Professor Bob Wilcox (chairperson), Dr Peter Ludman, Dr Jim Nolan, Mr Gerry Thompson (lay member), Lorraine Shipley (trial manager) and Dr David Hetmanski (sponsor) – and the DSMB members – Professor Jennifer Adgey (chairperson), Dr Ian BA Menown, Dr Mazhar Khan and Mr Cathal Walsh (statistics). The support nurses and particularly the patients also warrant our gratitude.
Contributions of authors
Sheraz A Nazir prepared the final report, which all authors read and approved.
Sheraz A Nazir, Jamal N Khan, John P Greenwood, Daniel J Blackman, Vijay Kunadian, Martin Been and Anthony H Gershlick were responsible for patient recruitment.
Islam Z Mahmoud, Gerry P McCann and Anthony H Gershlick conceived the idea for the study.
Sheraz A Nazir, Islam Z Mahmoud, John P Greenwood, Daniel J Blackman, Gerry P McCann and Anthony H Gershlick designed the study and developed protocols.
Vijay Kunadian was responsible for analysing all angiograms.
Sheraz A Nazir and Keith R Abrams performed all statistical analyses.
Robert Wilcox chaired the TSC and AA Jennifer Adgey chaired the DSMB.
Islam Z Mahmoud, John P Greenwood, Daniel J Blackman, Keith R Abrams, Gerry P McCann and Anthony H Gershlick prepared the funding application.
Sheraz A Nazir and Gerry P McCann were responsible for all CMR analyses.
John P Greenwood, Daniel J Blackman, Keith R Abrams, Gerry P McCann and Anthony H Gershlick also had TSC membership.
Publication
Nazir SA, Khan JN, Mahmoud IZ, Greenwood JP, Blackman DJ, Kunadian V, et al. Strategies to attenuate micro-vascular obstruction during P-PCI: the randomized reperfusion facillitated by local adjunctive therapy in ST-elevation myocardial infarction trial. Eur Heart J 2016;37:1910–19.
Data sharing statement
All available trial data can be obtained by request to the corresponding author.
Disclaimers
This report presents independent research. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the MRC, NETSCC, the EME programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the EME programme or the Department of Health.
References
- Steg PG, James SK, Atar D, Badano LP, Blömstrom-Lundqvist C, . Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology . ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012;33:2569-619. http://dx.doi.org/10.1093/eurheartj/ehs215.
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361:13-20. http://dx.doi.org/10.1016/S0140-6736(03)12113-7.
- Kloner RA, Ganote CE, Jennings RB. The ‘no-reflow’ phenomenon after temporary coronary occlusion in the dog. J Clin Invest 1974;54:1496-508. http://dx.doi.org/10.1172/JCI107898.
- Braunwald E, Kloner RA. Myocardial reperfusion: a double-edged sword?. J Clin Invest 1985;76:1713-19. http://dx.doi.org/10.1172/JCI112160.
- Harlan JM. Leukocyte–endothelial interactions. Blood 1985;65:513-25.
- McCord JM. Oxygen-derived free radicals in postischemic tissue injury. N Engl J Med 1985;312:159-63. http://dx.doi.org/10.1056/NEJM198501173120305.
- Engler R, Covell JW. Granulocytes cause reperfusion ventricular dysfunction after 15-minute ischemia in the dog. Circ Res 1987;61:20-8. http://dx.doi.org/10.1161/01.RES.61.1.20.
- Topol EJ, Yadav JS. Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation 2000;101:570-80. http://dx.doi.org/10.1161/01.CIR.101.5.570.
- Gersh BJ. Optimal management of acute myocardial infarction at the dawn of the next millennium. Am Heart J 1999;138:S188-202. http://dx.doi.org/10.1016/S0002-8703(99)70342-X.
- Kotani J, Nanto S, Mintz GS, Kitakaze M, Ohara T, Morozumi T, et al. Plaque gruel of atheromatous coronary lesion may contribute to the no-reflow phenomenon in patients with acute coronary syndrome. Circulation 2002;106:1672-7. http://dx.doi.org/10.1161/01.CIR.0000030189.27175.4E.
- Araszkiewicz A, Grajek S, Lesiak M, Prech M, Pyda M, Janus M, et al. Effect of impaired myocardial reperfusion on left ventricular remodeling in patients with anterior wall acute myocardial infarction treated with primary coronary intervention. Am J Cardiol 2006;98:725-8. http://dx.doi.org/10.1016/j.amjcard.2006.04.009.
- Galiuto L, Lombardo A, Maseri A, Santoro L, Porto I, Cianflone D, et al. Temporal evolution and functional outcome of no reflow: sustained and spontaneously reversible patterns following successful coronary recanalisation. Heart 2003;89:731-7. http://dx.doi.org/10.1136/heart.89.7.731.
- Rezkalla SH, Dharmashankar KC, Abdalrahman IB, Kloner RA. No-reflow phenomenon following percutaneous coronary intervention for acute myocardial infarction: incidence, outcome, and effect of pharmacologic therapy. J Interv Cardiol 2010;23:429-36. http://dx.doi.org/10.1111/j.1540-8183.2010.00561.x.
- Wu KC, Zerhouni EA, Judd RM, Lugo-Olivieri CH, Barouch LA, Schulman SP, et al. Prognostic significance of microvascular obstruction by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 1998;97:765-72. http://dx.doi.org/10.1161/01.CIR.97.8.765.
- Wu KC, Kim RJ, Bluemke DA, Rochitte CE, Zerhouni EA, Becker LC, et al. Quantification and time course of microvascular obstruction by contrast-enhanced echocardiography and magnetic resonance imaging following acute myocardial infarction and reperfusion. J Am Coll Cardiol 1998;32:1756-64. http://dx.doi.org/10.1016/S0735-1097(98)00429-X.
- Hombach V, Grebe O, Merkle N, Waldenmaier S, Höher M, Kochs M, et al. Sequelae of acute myocardial infarction regarding cardiac structure and function and their prognostic significance as assessed by magnetic resonance imaging. Eur Heart J 2005;26:549-57. http://dx.doi.org/10.1093/eurheartj/ehi147.
- Nijveldt R, Beek AM, Hirsch A, Stoel MG, Hofman MB, Umans VA, et al. Functional recovery after acute myocardial infarction: comparison between angiography, electrocardiography, and cardiovascular magnetic resonance measures of microvascular injury. J Am Coll Cardiol 2008;52:181-9. http://dx.doi.org/10.1016/j.jacc.2008.04.006.
- Vlaar PJ, Svilaas T, van der Horst IC, Diercks GF, Fokkema ML, de Smet BJ, et al. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS): a 1-year follow-up study. Lancet 2008;371:1915-20. http://dx.doi.org/10.1016/S0140-6736(08)60833-8.
- Sardella G, Mancone M, Bucciarelli-Ducci C, Agati L, Scardala R, Carbone I, et al. Thrombus aspiration during primary percutaneous coronary intervention improves myocardial reperfusion and reduces infarct size: the EXPIRA (thrombectomy with export catheter in infarct-related artery during primary percutaneous coronary intervention) prospective, randomized trial. J Am Coll Cardiol 2009;53:309-15. http://dx.doi.org/10.1016/j.jacc.2008.10.017.
- Liistro F, Grotti S, Angioli P, Falsini G, Ducci K, Baldassarre S, et al. Impact of thrombus aspiration on myocardial tissue reperfusion and left ventricular functional recovery and remodeling after primary angioplasty. Circ Cardiovasc Interv 2009;2:376-83. http://dx.doi.org/10.1161/CIRCINTERVENTIONS.109.852665.
- Stone GW, Maehara A, Witzenbichler B, Godlewski J, Parise H, Dambrink J-HE, et al. Intracoronary abciximab and aspiration thrombectomy in patients with large anterior myocardial infarction: the INFUSE-AMI randomized trial. JAMA 2012;307:1817-26. http://dx.doi.org/10.1001/jama.2012.421.
- Dudek D, Mielecki W, Burzotta F, Gasior M, Witkowski A, Horvath IG, et al. Thrombus aspiration followed by direct stenting: a novel strategy of primary percutaneous coronary intervention in ST-segment elevation myocardial infarction. Results of the Polish-Italian-Hungarian randomized thrombectomy trial (PIHRATE trial). Am Heart J 2010;160:966-72. http://dx.doi.org/10.1016/j.ahj.2010.07.024.
- Frobert O, Lagerqvist B, Olivecrona GK, Omerovic E, Gudnason T, Maeng M, et al. Thrombus aspiration during ST-segment elevation myocardial infarction. N Engl J Med 2013;369:1587-97. http://dx.doi.org/10.1056/NEJMoa1308789.
- Tomassini F, Gagnor A, Montali N, Gambino A, Bollati M, Infantino V, et al. Impact of thrombus aspiration during primary percutaneous coronary intervention in cardiogenic shock complicating ST-segment elevation myocardial infarction. Cardiovasc Revasc Med 2013;14:307-10. http://dx.doi.org/10.1016/j.carrev.2013.08.006.
- Kumbhani DJ, Bavry AA, Desai MY, Bangalore S, Bhatt DL. Role of aspiration and mechanical thrombectomy in patients with acute myocardial infarction undergoing primary angioplasty: an updated meta-analysis of randomized trials. J Am Coll Cardiol 2013;62:1409-18. http://dx.doi.org/10.1016/j.jacc.2013.04.025.
- De Luca G, Navarese EP, Suryapranata H. A meta-analytic overview of thrombectomy during primary angioplasty. Int J Cardiol 2013;166:606-12. http://dx.doi.org/10.1016/j.ijcard.2011.11.102.
- Jolly SS, Cairns J, Yusuf S, Meeks B, Shestakovska O, Thabane L, et al. Design and rationale of the TOTAL trial: a randomized trial of routine aspiration thrombectomy with percutaneous coronary intervention (PCI) versus PCI alone in patients with ST-elevation myocardial infarction undergoing primary PCI. Am Heart J 2014;167:315-21. http://dx.doi.org/10.1016/j.ahj.2013.12.002.
- Thiele H, Schindler K, Friedenberger J, Eitel I, Fürnau G, Grebe E, et al. Intracoronary compared with intravenous bolus abciximab application in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention: the randomized Leipzig immediate percutaneous coronary intervention abciximab IV versus IC in ST-elevation myocardial infarction trial. Circulation 2008;118:49-57. http://dx.doi.org/10.1161/CIRCULATIONAHA.107.747642.
- Bartorelli AL, Trabattoni D, Galli S, Grancini L, Cozzi S, Ravagnani P. Successful dissolution of occlusive coronary thrombus with local administration of abciximab during PTCA. Catheter Cardiovasc Interv 1999;48:211-13. http://dx.doi.org/10.1002/(SICI)1522-726X(199910)48:2<211::AID-CCD20>3.0.CO;2-V.
- Kakkar AK, Moustapha A, Hanley HG, Weiss M, Caldito G, Misra P, et al. Comparison of intracoronary vs. intravenous administration of abciximab in coronary stenting. Catheter Cardiovasc Interv 2004;61:31-4. http://dx.doi.org/10.1002/ccd.10730.
- Stone GW, McLaurin BT, Cox DA, Bertrand ME, Lincoff AM, Moses JW, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med 2006;355:2203-16. http://dx.doi.org/10.1056/NEJMoa062437.
- Stone GW, Witzenbichler B, Guagliumi G, Peruga JZ, Brodie BR, Dudek D, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med 2008;358:2218-30. http://dx.doi.org/10.1056/NEJMoa0708191.
- Ishihara M, Sato H, Tateishi H, Kawagoe T, Shimatani Y, Kurisu S, et al. Attenuation of the no-reflow phenomenon after coronary angioplasty for acute myocardial infarction with intracoronary papaverine. Am Heart J 1996;132:959-63. http://dx.doi.org/10.1016/S0002-8703(96)90005-8.
- Kaplan BM, Benzuly KH, Kinn JW, Bowers TR, Tilli FV, Grines CL, et al. Treatment of no-reflow in degenerated saphenous vein graft interventions: comparison of intracoronary verapamil and nitroglycerin. Cathet Cardiovasc Diagn 1996;39:113-18. http://dx.doi.org/10.1002/(SICI)1097-0304(199610)39:2<113::AID-CCD1>3.0.CO;2-I.
- Kloner RA, Alker KJ. The effect of streptokinase on intramyocardial hemorrhage, infarct size, and the no-reflow phenomenon during coronary reperfusion. Circulation 1984;70:513-21. http://dx.doi.org/10.1161/01.CIR.70.3.513.
- Werner GS, Lang K, Kuehnert H, Figulla HR. Intracoronary verapamil for reversal of no-reflow during coronary angioplasty for acute myocardial infarction. Catheter Cardiovasc Interv 2002;57:444-51. http://dx.doi.org/10.1002/ccd.10375.
- Weyrens FJ, Mooney J, Lesser J, Mooney MR. Intracoronary diltiazem for microvascular spasm after interventional therapy. Am J Cardiol 1995;75:849-50. http://dx.doi.org/10.1016/S0002-9149(99)80430-5.
- Rawitscher D, Levin TN, Cohen I, Feldman T. Rapid reversal of no-reflow using abciximab after coronary device intervention. Cathet Cardiovasc Diagn 1997;42:187-90. http://dx.doi.org/10.1002/(SICI)1097-0304(199710)42:2<187::AID-CCD20>3.0.CO;2-K.
- Skelding KA, Goldstein JA, Mehta L, Pica MC, O’Neill WW. Resolution of refractory no-reflow with intracoronary epinephrine. Catheter Cardiovasc Interv 2002;57:305-9. http://dx.doi.org/10.1002/ccd.10303.
- Ota S, Nishikawa H, Takeuchi M, Nakajima K, Nakamura T, Okamoto S, et al. Impact of nicorandil to prevent reperfusion injury in patients with acute myocardial infarction: Sigmart Multicenter Angioplasty Revascularization Trial (SMART). Circ J 2006;70:1099-104. http://dx.doi.org/10.1253/circj.70.1099.
- Kunadian V, Zorkun C, Williams SP, Biller LH, Palmer AM, Ogando KJ, et al. Intracoronary pharmacotherapy in the management of coronary microvascular dysfunction. J Thromb Thrombolysis 2008;26:234-42. http://dx.doi.org/10.1007/s11239-008-0276-0.
- Amit G, Cafri C, Yaroslavtsev S, Fuchs S, Paltiel O, Abu-Ful A, et al. Intracoronary nitroprusside for the prevention of the no-reflow phenomenon after primary percutaneous coronary intervention in acute myocardial infarction. A randomized, double-blind, placebo-controlled clinical trial. Am Heart J 2006;152. http://dx.doi.org/10.1016/j.ahj.2006.05.010.
- Kobatake R, Sato T, Fujiwara Y, Sunami H, Yoshioka R, Ikeda T, et al. Comparison of the effects of nitroprusside versus nicorandil on the slow/no-reflow phenomenon during coronary interventions for acute myocardial infarction. Heart Vessels 2011;26:379-84. http://dx.doi.org/10.1007/s00380-010-0065-5.
- Niccoli G, Rigattieri S, De Vita MR, Valgimigli M, Corvo P, Fabbiocchi F, et al. Open-label, randomized, placebo-controlled evaluation of intracoronary adenosine or nitroprusside after thrombus aspiration during primary percutaneous coronary intervention for the prevention of microvascular obstruction in acute myocardial infarction: the REOPEN-AMI study (Intracoronary Nitroprusside Versus Adenosine in Acute Myocardial Infarction). JACC Cardiovasc Interv 2013;6:580-9. http://dx.doi.org/10.1016/j.jcin.2013.02.009.
- Parikh KH, Chag MC, Shah KJ, Shah UG, Baxi HA, Chandarana AH, et al. Intracoronary boluses of adenosine and sodium nitroprusside in combination reverses slow/no-reflow during angioplasty: a clinical scenario of ischemic preconditioning. Can J Physiol Pharmacol 2007;85:476-82. http://dx.doi.org/10.1139/Y07-013.
- Pasceri V, Pristipino C, Pelliccia F, Granatelli A, Speciale G, Roncella A, et al. Effects of the nitric oxide donor nitroprusside on no-reflow phenomenon during coronary interventions for acute myocardial infarction. Am J Cardiol 2005;95:1358-61. http://dx.doi.org/10.1016/j.amjcard.2005.01.082.
- Shinozaki N, Ichinose H, Yahikozawa K, Shimada H, Hoshino K. Selective intracoronary administration of nitroprusside before balloon dilatation prevents slow reflow during percutaneous coronary intervention in patients with acute myocardial infarction. Int Heart J 2007;48:423-33. http://dx.doi.org/10.1536/ihj.48.423.
- Wang HJ, Lo PH, Lin JJ, Lee H, Hung JS. Treatment of slow/no-reflow phenomenon with intracoronary nitroprusside injection in primary coronary intervention for acute myocardial infarction. Catheter Cardiovasc Interv 2004;63:171-6. http://dx.doi.org/10.1002/ccd.20149.
- Youssef AA, Wu CJ, Hang CL, Cheng CI, Yang CH, Chen CJ, et al. Impact of percusurge device conjugative with intracoronary administration of nitroprusside on no-reflow phenomenon following primary percutaneous coronary intervention. Circ J 2006;70:1538-42. http://dx.doi.org/10.1253/circj.70.1538.
- Claeys MJ, Bosmans J, De Ceuninck M, Beunis A, Vergauwen W, Vorlat A, et al. Effect of intracoronary adenosine infusion during coronary intervention on myocardial reperfusion injury in patients with acute myocardial infarction. Am J Cardiol 2004;94:9-13. http://dx.doi.org/10.1016/j.amjcard.2004.03.021.
- Desmet W, Bogaert J, Dubois C, Sinnaeve P, Adriaenssens T, Pappas C, et al. High-dose intracoronary adenosine for myocardial salvage in patients with acute ST-segment elevation myocardial infarction. Eur Heart J 2011;32:867-77. http://dx.doi.org/10.1093/eurheartj/ehq492.
- Fokkema ML, Vlaar PJ, Vogelzang M, Gu YL, Kampinga MA, de Smet BJ, et al. Effect of high-dose intracoronary adenosine administration during primary percutaneous coronary intervention in acute myocardial infarction: a randomized controlled trial. Circ Cardiovasc Interv 2009;2:323-9. http://dx.doi.org/10.1161/CIRCINTERVENTIONS.109.858977.109.858977.
- Grygier M, Araszkiewicz A, Lesiak M, Janus M, Kowal J, Skorupski W, et al. New method of intracoronary adenosine injection to prevent microvascular reperfusion injury in patients with acute myocardial infarction undergoing percutaneous coronary intervention. Am J Cardiol 2011;107:1131-5. http://dx.doi.org/10.1016/j.amjcard.2010.12.010.
- Mahaffey KW, Puma JA, Barbagelata NA, DiCarli MF, Leesar MA, Browne KF, et al. Adenosine as an adjunct to thrombolytic therapy for acute myocardial infarction: results of a multicenter, randomized, placebo-controlled trial: the Acute Myocardial Infarction STudy of ADenosine (AMISTAD) trial. J Am Coll Cardiol 1999;34:1711-20. http://dx.doi.org/10.1016/S0735-1097(99)00418-0.
- Marzilli M, Orsini E, Marraccini P, Testa R. Beneficial effects of intracoronary adenosine as an adjunct to primary angioplasty in acute myocardial infarction. Circulation 2000;101:2154-9. http://dx.doi.org/10.1161/01.CIR.101.18.2154.
- Micari A, Belcik TA, Balcells EA, Powers E, Wei K, Kaul S, et al. Improvement in microvascular reflow and reduction of infarct size with adenosine in patients undergoing primary coronary stenting. Am J Cardiol 2005;96:1410-15. http://dx.doi.org/10.1016/j.amjcard.2005.06.090.
- Petronio AS, De Carlo M, Ciabatti N, Amoroso G, Limbruno U, Palagi C, et al. Left ventricular remodeling after primary coronary angioplasty in patients treated with abciximab or intracoronary adenosine. Am Heart J 2005;150. http://dx.doi.org/10.1016/j.ahj.2005.07.012.
- Quintana M, Hjemdahl P, Sollevi A, Kahan T, Edner M, Rehnqvist N, et al. Left ventricular function and cardiovascular events following adjuvant therapy with adenosine in acute myocardial infarction treated with thrombolysis, results of the ATTenuation by Adenosine of Cardiac Complications (ATTACC) study. Eur J Clin Pharmacol 2003;59:1-9.
- Ross AM, Gibbons RJ, Stone GW, Kloner RA, Alexander RW. A randomized, double-blinded, placebo-controlled multicenter trial of adenosine as an adjunct to reperfusion in the treatment of acute myocardial infarction (AMISTAD-II). J Am Coll Cardiol 2005;45:1775-80. http://dx.doi.org/10.1016/j.jacc.2005.02.061.
- Stoel MG, Marques KM, de Cock CC, Bronzwaer JG, von Birgelen C, Zijlstra F. High dose adenosine for suboptimal myocardial reperfusion after primary PCI: a randomized placebo-controlled pilot study. Catheter Cardiovasc Interv 2008;71:283-9. http://dx.doi.org/10.1002/ccd.21334.
- Zhang H, Tian NL, Hu ZY, Wang F, Chen L, Zhang YJ, et al. Three hours continuous injection of adenosine improved left ventricular function and infarct size in patients with ST-segment elevation myocardial infarction. Chin Med J 2012;125:1713-19.
- Vijayalakshmi K, Whittaker VJ, Kunadian B, Graham J, Wright RA, Hall JA, et al. Prospective, randomised, controlled trial to study the effect of intracoronary injection of verapamil and adenosine on coronary blood flow during percutaneous coronary intervention in patients with acute coronary syndromes. Heart 2006;92:1278-84. http://dx.doi.org/10.1136/hrt.2005.075077.
- Berne RM. The role of adenosine in the regulation of coronary blood flow. Circ Res 1980;47:807-13. http://dx.doi.org/10.1161/01.RES.47.6.807.
- Ernst PB, Garrison JC, Thompson LF. Much ado about adenosine: adenosine synthesis and function in regulatory T cell biology. J Immunol 2010;185:1993-8. http://dx.doi.org/10.4049/jimmunol.1000108.
- Linden J. Molecular approach to adenosine receptors: receptor-mediated mechanisms of tissue protection. Ann Rev Pharmacol Toxicol 2001;41:775-87. http://dx.doi.org/10.1146/annurev.pharmtox.41.1.775.
- Olafsson B, Forman MB, Puett DW, Pou A, Cates CU, Friesinger GC, et al. Reduction of reperfusion injury in the canine preparation by intracoronary adenosine: importance of the endothelium and the no-reflow phenomenon. Circulation 1987;76:1135-45. http://dx.doi.org/10.1161/01.CIR.76.5.1135.
- Bates JN, Baker MT, Guerra R, Harrison DG. Nitric oxide generation from nitroprusside by vascular tissue. Evidence that reduction of the nitroprusside anion and cyanide loss are required. Biochem Pharmacol 1991;42:S157-65. http://dx.doi.org/10.1016/0006-2952(91)90406-U.
- Gavin JB, Maxwell L, Edgar SG. Microvascular involvement in cardiac pathology. J Mol Cell Cardiol 1998;30:2531-40. http://dx.doi.org/10.1006/jmcc.1998.0824.
- Pemberton M, Anderson GL, Barker JH. Characterization of microvascular vasoconstriction following ischemia/reperfusion in skeletal muscle using videomicroscopy. Microsurgery 1996;17:9-16. http://dx.doi.org/10.1002/(SICI)1098-2752(1996)17:1<9::AID-MICR2>3.0.CO;2-K.
- Wang WZ, Anderson G, Fleming JT, Peter FW, Franken RJ, Acland RD, et al. Lack of nitric oxide contributes to vasospasm during ischemia/reperfusion injury. Plast Reconstructr Surg 1997;99:1099-108. http://dx.doi.org/10.1097/00006534-199704000-00028.
- Kloner RA, Forman MB, Gibbons RJ, Ross AM, Alexander RW, Stone GW. Impact of time to therapy and reperfusion modality on the efficacy of adenosine in acute myocardial infarction: the AMISTAD-2 trial. Eur Heart J 2006;27:2400-5. http://dx.doi.org/10.1093/eurheartj/ehl094.
- Masci PG, Ganame J, Francone M, Desmet W, Lorenzoni V, Iacucci I, et al. Relationship between location and size of myocardial infarction and their reciprocal influences on post-infarction left ventricular remodelling. Eur Heart J 2011;32:1640-8. http://dx.doi.org/10.1093/eurheartj/ehr064.
- Aung Naing K, Li L, Su Q, Wu T. Adenosine and verapamil for no-reflow during primary percutaneous coronary intervention in people with acute myocardial infarction. Cochrane Database Syst Rev 2013;6. http://dx.doi.org/10.1002/14651858.cd009503.pub2.
- Nazir SA, Khan JN, Mahmoud IZ, Greenwood JP, Blackman DJ, Kunadian V, et al. The REFLO-STEMI trial comparing intracoronary adenosine, sodium nitroprusside and standard therapy for the attenuation of infarct size and microvascular obstruction during primary percutaneous coronary intervention: study protocol for a randomised controlled trial. Trials 2014;15. http://dx.doi.org/10.1186/1745-6215-15-371.
- Kelly DJ, McCann GP, Blackman D, Curzen NP, Dalby M, Greenwood JP, et al. Complete Versus culprit-Lesion only PRimary PCI Trial (CVLPRIT): a multicentre trial testing management strategies when multivessel disease is detected at the time of primary PCI: rationale and design. Eurointervention 2013;8:1190-8. http://dx.doi.org/10.4244/EIJV8I10A183.
- Armstrong PW, Gershlick AH, Goldstein P, Wilcox R, Danays T, Lambert Y, et al. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med 2013;368:1379-87. http://dx.doi.org/10.1056/NEJMoa1301092.
- Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007;357:2001-15. http://dx.doi.org/10.1056/NEJMoa0706482.
- Prasugrel for the Treatment of Acute Coronary Syndromes with Percutaneous Coronary Intervention. NICE Technology Appraisal Guidance TA182. London: NICE; 2009.
- James S, Akerblom A, Cannon CP, Emanuelsson H, Husted S, Katus H, et al. Comparison of ticagrelor, the first reversible oral P2Y(12) receptor antagonist, with clopidogrel in patients with acute coronary syndromes: rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial. Am Heart J 2009;157:599-605. http://dx.doi.org/10.1016/j.ahj.2009.01.003.
- European Society of Cardiology . ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting With ST-Segment Elevation 2012. www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/Guidelines_AMI_STEMI.pdf (accessed 15 January 2014).
- Ticagrelor for the Treatment of Acute Coronary Syndromes. London: NICE; 2011.
- Shahzad A, Kemp I, Mars C, Wilson K, Roome C, Cooper R, et al. Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention (HEAT-PPCI): an open-label, single centre, randomised controlled trial. Lancet 2014;384:1849-58. http://dx.doi.org/10.1016/S0140-6736(14)60924-7.
- Schroder R, Dissmann R, Bruggemann T, Wegscheider K, Linderer T, Tebbe U, et al. Extent of early ST segment elevation resolution: a simple but strong predictor of outcome in patients with acute myocardial infarction. J Am Coll Cardiol 1994;24:384-91. http://dx.doi.org/10.1016/0735-1097(94)90292-5.
- Gibson CM, Cannon CP, Murphy SA, Ryan KA, Mesley R, Marble SJ, et al. Relationship of TIMI myocardial perfusion grade to mortality after administration of thrombolytic drugs. Circulation 2000;101:125-30. http://dx.doi.org/10.1161/01.CIR.101.2.125.
- Gibson CM, Cannon CP, Murphy SA, Marble SJ, Barron HV, Braunwald E, et al. Relationship of the TIMI myocardial perfusion grades, flow grades, frame count, and percutaneous coronary intervention to long-term outcomes after thrombolytic administration in acute myocardial infarction. Circulation 2002;105:1909-13. http://dx.doi.org/10.1161/01.CIR.0000014683.52177.B5.
- Vogelzang M, Vlaar PJ, Svilaas T, Amo D, Nijsten MW, Zijlstra F. Computer-assisted myocardial blush quantification after percutaneous coronary angioplasty for acute myocardial infarction: a substudy from the TAPAS trial. Eur Heart J 2009;30:594-9. http://dx.doi.org/10.1093/eurheartj/ehn542.
- Gibson CM, Cannon CP, Daley WL, Dodge JT, Alexander B, Marble SJ, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation 1996;93:879-88. http://dx.doi.org/10.1161/01.CIR.93.5.879.
- Kunadian V, Harrigan C, Zorkun C, Palmer AM, Ogando KJ, Biller LH, et al. Use of the TIMI frame count in the assessment of coronary artery blood flow and microvascular function over the past 15 years. J Thromb Thrombolysis 2009;27:316-28. http://dx.doi.org/10.1007/s11239-008-0220-3.
- The Thrombolysis in Myocardial Infarction (TIMI) trial . Phase I findings. TIMI study group. N Engl J Med 1985;312:932-6. http://dx.doi.org/10.1056/NEJM198504043121435.
- Gibson CM, de Lemos JA, Murphy SA, Marble SJ, McCabe CH, Cannon CP, et al. Combination therapy with abciximab reduces angiographically evident thrombus in acute myocardial infarction: a TIMI 14 substudy. Circulation 2001;103:2550-4. http://dx.doi.org/10.1161/01.CIR.103.21.2550.
- van’t Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ, Zijlstra F. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Zwolle Myocardial Infarction Study Group. Circulation 1998;97:2302-6. http://dx.doi.org/10.1161/01.CIR.97.23.2302.
- Yuval R, Halon DA, Merdler A, Khader N, Karkabi B, Uziel K, et al. Patient comprehension and reaction to participating in a double-blind randomized clinical trial (ISIS-4) in acute myocardial infarction. Arch Intern Med 2000;160:1142-6. http://dx.doi.org/10.1001/archinte.160.8.1142.
- Williams BF, French JK, White HD. HERO-2 consent substudy investigators . Informed consent during the clinical emergency of acute myocardial infarction (HERO-2 consent substudy): a prospective observational study. Lancet 2003;361:918-22. http://dx.doi.org/10.1016/S0140-6736(03)12773-0.
- Ibrahim T, Hackl T, Nekolla SG, Breuer M, Feldmair M, Schömig A. Acute myocardial infarction: serial cardiac MR imaging shows a decrease in delayed enhancement of the myocardium during the 1st week after reperfusion. Radiology 2010;254:88-97. http://dx.doi.org/10.1148/radiol.09090660.
- Albert TSE, Kim RJ, Judd RM. Assessment of no-reflow regions using cardiac MRI. Basic Res Cardiol 2006;101:383-90. http://dx.doi.org/10.1007/s00395-006-0617-0.
- Tilak GS, Hsu LY, Hoyt RF, Arai AE, Aletras AH. In vivo T2-weighted magnetic resonance imaging can accurately determine the ischemic area at risk for 2-day-old nonreperfused myocardial infarction. Invest Radiol 2008;43:7-15. http://dx.doi.org/10.1097/RLI.0b013e3181558822.
- Flett AS, Hasleton J, Cook C, Hausenloy D, Quarta G, Ariti C, et al. Evaluation of techniques for the quantification of myocardial scar of differing etiology using cardiac magnetic resonance. JACC Cardiovasc Imaging 2011;4:150-6. http://dx.doi.org/10.1016/j.jcmg.2010.11.015.
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. Third universal definition of myocardial infarction. Eur Heart J 2012;33:2551-67. http://dx.doi.org/10.1093/eurheartj/ehs184.
- Reed MD, Bell D. Clinical pharmacology of bivalirudin. Pharmacotherapy 2002;22:105S-11S. http://dx.doi.org/10.1592/phco.22.10.105S.33616.
- Cortese B, Picchi A, Micheli A, Limbruno U. Intracoronary bivalirudin for no reflow reversal: a second chance to treat this disorder?. J Thromb Thrombolysis 2009;28:74-6. http://dx.doi.org/10.1007/s11239-008-0243-9.
- Bertomeu-Gonzalez V, Bodi V, Sanchis J, Nunez J, Lopez-Lereu MP, Pena G, et al. Limitations of myocardial blush grade in the evaluation of myocardial perfusion in patients with acute myocardial infarction and TIMI grade 3 flow. Rev Esp Cardiol 2006;59:575-81. http://dx.doi.org/10.1016/s1885-5857(07)60008-5.
- Bello D, Einhorn A, Kaushal R, Kenchaiah S, Raney A, Fieno D, et al. Cardiac magnetic resonance imaging: infarct size is an independent predictor of mortality in patients with coronary artery disease. Magn Reson Imaging 2011;29:50-6. http://dx.doi.org/10.1016/j.mri.2010.03.031.
- Eitel I, Desch S, de Waha S, Fuernau G, Gutberlet M, Schuler G, et al. Long-term prognostic value of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. Heart 2011;97:2038-45. http://dx.doi.org/10.1136/heartjnl-2011-300098.
- Ezekowitz JA, Armstrong PW, Granger CB, Theroux P, Stebbins A, Kim RJ, et al. Predicting chronic left ventricular dysfunction 90 days after ST-segment elevation myocardial infarction: an assessment of pexelizumab in acute myocardial infarction (APEX-AMI) substudy. Am Heart J 2010;160:272-8. http://dx.doi.org/10.1016/j.ahj.2010.05.035.
- Ganame J, Messalli G, Dymarkowski S, Rademakers FE, Desmet W, Van de Werf F, et al. Impact of myocardial haemorrhage on left ventricular function and remodelling in patients with reperfused acute myocardial infarction. Eur Heart J 2009;30:1440-9. http://dx.doi.org/10.1093/eurheartj/ehp093.
- Gerber BL. Accuracy of contrast-enhanced magnetic resonance imaging in predicting improvement of regional myocardial function in patients after acute myocardial infarction. Circulation 2002;106:1083-9. http://dx.doi.org/10.1161/01.CIR.0000027818.15792.1E.
- Kelle S, Roes SD, Klein C, Kokocinski T, de Roos A, Fleck E, et al. Prognostic value of myocardial infarct size and contractile reserve using magnetic resonance imaging. J Am Coll Cardiol 2009;54:1770-7. http://dx.doi.org/10.1016/j.jacc.2009.07.027.
- Klem I, Shah DJ, White RD, Pennell DJ, van Rossum AC, Regenfus M, et al. Prognostic value of routine cardiac magnetic resonance assessment of left ventricular ejection fraction and myocardial damage: an international, multicenter study. Circ Cardiovasc Imaging 2011;4:610-19. http://dx.doi.org/10.1161/CIRCIMAGING.111.964965.
- Kwong RY, Chan AK, Brown KA, Chan CW, Reynolds HG, Tsang S, et al. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. Circulation 2006;113:2733-43. http://dx.doi.org/10.1161/CIRCULATIONAHA.105.570648.
- Larose E, Rodes-Cabau J, Pibarot P, Rinfret S, Proulx G, Nguyen CM, et al. Predicting late myocardial recovery and outcomes in the early hours of ST-segment elevation myocardial infarction traditional measures compared with microvascular obstruction, salvaged myocardium, and necrosis characteristics by cardiovascular magnetic resonance. J Am Coll Cardiol 2010;55:2459-69. http://dx.doi.org/10.1016/j.jacc.2010.02.033.
- Lund GK, Stork A, Muellerleile K, Bansmann MP, Schlichting U, Mu M, et al. Prediction of left ventricular remodeling and analysis of infarct resorption in patients with reperfused myocardial infarcts by using contrast-enhanced MR imaging. Radiology 2007;245:95-104. http://dx.doi.org/10.1148/radiol.2451061219.
- Wu E, Ortiz JT, Tejedor P, Lee DC, Kansal P, Carr JC, et al. Infarct size by contrast enhanced cardiac magnetic resonance is a stronger predictor of outcomes than left ventricular ejection fraction or end-systolic volume index: prospective cohort study. Heart 2008;94:730-6. http://dx.doi.org/10.1136/hrt.2007.122622.
- Lonborg J, Vejlstrup N, Kelbaek H, Holmvang L, Jorgensen E, Helqvist S, et al. Final infarct size measured by cardiovascular magnetic resonance in patients with ST elevation myocardial infarction predicts long-term clinical outcome: an observational study. Eur Heart J Cardiovasc Imaging 2013;14:387-95. http://dx.doi.org/10.1093/ehjci/jes271.
- Izquierdo M, Ruiz-Granell R, Bonanad C, Chaustre F, Gomez C, Ferrero A, et al. Value of early cardiovascular magnetic resonance for the prediction of adverse arrhythmic cardiac events after a first noncomplicated ST-segment-elevation myocardial infarction. Circ Cardiovasc Imaging 2013;6:755-61. http://dx.doi.org/10.1161/CIRCIMAGING.113.000702.
- Rahimi K, Banning AP, Cheng ASH, Pegg TJ, Karamitsos TD, Channon KM, et al. Prognostic value of coronary revascularisation-related myocardial injury: a cardiac magnetic resonance imaging study. Heart 2009;95:1937-43. http://dx.doi.org/10.1136/hrt.2009.173302.
- Nijveldt R, Beek AM, Hofman MB, Umans VA, Algra PR, Spreeuwenberg MD, et al. Late gadolinium-enhanced cardiovascular magnetic resonance evaluation of infarct size and microvascular obstruction in optimally treated patients after acute myocardial infarction. J Cardiovasc Magn Reson 2007;9:765-70. http://dx.doi.org/10.1080/10976640701545008.
- Beek AM, Nijveldt R, van Rossum AC. Intramyocardial hemorrhage and microvascular obstruction after primary percutaneous coronary intervention. Int J Cardiovasc Imaging 2010;26:49-55. http://dx.doi.org/10.1007/s10554-009-9499-1.
- Masci PG, Ganame J, Strata E, Desmet W, Aquaro GD, Dymarkowski S, et al. Myocardial salvage by CMR correlates with LV remodeling and early ST-segment resolution in acute myocardial infarction. JACC Cardiovasc Imaging 2010;3:45-51. http://dx.doi.org/10.1016/j.jcmg.2009.06.016.
- Hahn J-Y, Song YB, Gwon H-C, Choe YH, Kim JH, Sung J, et al. Relation of left ventricular infarct transmurality and infarct size after primary percutaneous coronary angioplasty to time from symptom onset to balloon inflation. Am J Cardiol 2008;102:1163-9. http://dx.doi.org/10.1016/j.amjcard.2008.06.042.
- Nijveldt R, van der Vleuten PA, Hirsch A, Beek AM, Tio RA, Tijssen JGP, et al. Early electrocardiographic findings and MR imaging-verified microvascular injury and myocardial infarct size. JACC Cardiovasc Imaging 2009;2:1187-94. http://dx.doi.org/10.1016/j.jcmg.2009.06.008.
- Humphrey SM, Seelye RN, Gavin JB. The influence of adenosine on the no-reflow phenomenon in anoxic and ischaemic hearts. Pathology 1982;14:129-33. http://dx.doi.org/10.3109/00313028209061285.
- Cronstein BN, Levin RI, Belanoff J, Weissmann G, Hirschhorn R. Adenosine: an endogenous inhibitor of neutrophil-mediated injury to endothelial cells. J Clin Invest 1986;78:760-70. http://dx.doi.org/10.1172/JCI112638.
- Babbitt DG, Virmani R, Forman MB. Intracoronary adenosine administered after reperfusion limits vascular injury after prolonged ischemia in the canine model. Circulation 1989;80:1388-99. http://dx.doi.org/10.1161/01.CIR.80.5.1388.
- Gruber HE, Hoffer ME, McAllister DR, Laikind PK, Lane TA, Schmid-Schoenbein GW, et al. Increased adenosine concentration in blood from ischemic myocardium by aica riboside. Effects on flow, granulocytes, and injury. Circulation 1989;80:1400-11. http://dx.doi.org/10.1161/01.CIR.80.5.1400.
- Hanna GP, Yhip P, Fujise K, Schroth GW, Rosales OR, Anderson HV, et al. Intracoronary adenosine administered during rotational atherectomy of complex lesions in native coronary arteries reduces the incidence of no-reflow phenomenon. Catheter Cardiovasc Interv 1999;48:275-8. http://dx.doi.org/10.1002/(SICI)1522-726X(199911)48:3<275::AID-CCD8>3.0.CO;2-M.
- Barcin C, Denktas AE, Lennon RJ, Hammes L, Higano ST, Holmes DR, et al. Comparison of combination therapy of adenosine and nitroprusside with adenosine alone in the treatment of angiographic no-reflow phenomenon. Catheter Cardiovasc Interv 2004;61:484-91. http://dx.doi.org/10.1002/ccd.20010.
- Hillegass WB, Dean NA, Liao L, Rhinehart RG, Myers PR. Treatment of no-reflow and impaired flow with the nitric oxide donor nitroprusside following percutaneous coronary interventions: initial human clinical experience. J Am Coll Cardiol 2001;37:1335-43. http://dx.doi.org/10.1016/S0735-1097(01)01138-X.
- Pan W, Wang LF, Yu JH, Fan Y, Yang SS, Zhou LJ, et al. Intracoronary nitroprusside in the prevention of the no-reflow phenomenon in acute myocardial infarction. Chin Med J 2009;122:2718-23.
- Zhao YJ, Fu XH, Ma XX, Wang DY, Dong QL, Wang YB, et al. Intracoronary fixed dose of nitroprusside via thrombus aspiration catheter for the prevention of the no-reflow phenomenon following primary percutaneous coronary intervention in acute myocardial infarction. Exp Ther Med 2013;6:479-84. http://dx.doi.org/10.3892/etm.2013.1139.
- Rubio R, Berne RM, Katori M. Release of adenosine in reactive hyperemia of the dog heart. Am J Physiol 1969;216:56-62.
- Payne AR, Casey M, McClure J, McGeoch R, Murphy A, Woodward R, et al. Bright-blood T2-weighted MRI has higher diagnostic accuracy than dark-blood short tau inversion recovery MRI for detection of acute myocardial infarction and for assessment of the ischemic area at risk and myocardial salvage. Circ Cardiovasc Imaging 2011;4:210-19. http://dx.doi.org/10.1161/CIRCIMAGING.110.960450.
- McCann GP, Khan JN, Greenwood JP, Nazir S, Dalby M, Curzen N, et al. Complete versus lesion-only primary PCI: the randomized cardiovascular MR CVLPRIT substudy. J Am Coll Cardiol 2015;66:2713-24. http://dx.doi.org/10.1016/j.jacc.2015.09.099.
- Siddiqi N, Neil C, Bruce M, MacLennan G, Cotton S, Papadopoulou S, et al. Intravenous sodium nitrite in acute ST-elevation myocardial infarction: a randomized controlled trial (NIAMI). Eur Heart J 2014;35:1255-62. http://dx.doi.org/10.1093/eurheartj/ehu096.
- Raman SV, Ambrosio G. T2-cardiac magnetic resonance: has Elvis left the building?. Circ Cardiovasc Imaging 2011;4:198-200. http://dx.doi.org/10.1161/CIRCIMAGING.111.965343.
- Ferreira VM, Piechnik SK, Dall’Armellina E, Karamitsos TD, Francis JM, Choudhury RP, et al. Non-contrast T1-mapping detects acute myocardial edema with high diagnostic accuracy: a comparison to T2-weighted cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2012;14. http://dx.doi.org/10.1186/1532-429X-14-42.
- Dall’Armellina E, Piechnik SK, Ferreira VM, Si QL, Robson MD, Francis JM, et al. Cardiovascular magnetic resonance by non contrast T1-mapping allows assessment of severity of injury in acute myocardial infarction. J Cardiovasc Magn Reson 2012;14. http://dx.doi.org/10.1186/1532-429X-14-15.
- Nazir SA, Khan JN, McCann GP. Free breathing motion-corrected T1 mapping for robust assessment of myocardial injury post myocardial infarction. Int J Cardiovasc Imaging 2015;31:123-4. http://dx.doi.org/10.1007/s10554-014-0500-2.
Appendix 1 Main randomised controlled trials investigating the role of adenosine and sodium nitroprusside in attenuating or preventing microvascular obstruction in ST-elevation myocardial infarction treated with primary percutaneous coronary intervention
| Study/author | Year | Main inclusion/exclusion | Number of patients (n given study drug/total N) | Age (years), mean; time to PPCI (minutes), median | Dose administered | Mode of drug delivery | Primary outcome(s)a | Secondary outcome(s)a | Main findingsa | Main limitations |
|---|---|---|---|---|---|---|---|---|---|---|
| Adenosine | ||||||||||
| Niccoli et al.44 | 2013 | Symptom onset < 12 hours before enrolment; TFG 0–1 in IRA pre PCI; ‘rescue’ PCI; excluded LBBB | 80/240 | 63; 278 | 120-µg rapid bolus then 2 mg over 2 minutes | Selective IC | STR > 70% | TFG; MBG; 30-day MACE | ↑ STR; ↑ MBG; ↓ TFC | No direct assessment of IS/MVO |
| Zhang et al.61 | 2012 | Symptom onset < 12 hours before enrolment; ‘new’ LBBB; TIMI 0–3; excluded MVD | 59/90 | 63; 279 | 50 or 70 µg/kg/minute | i.v. infusion (3 hours) | IS (SPECT) | TFG; MBG; incidence NR; LV function; MACE at 6 months | ↓ IS (at 6 months); ↑ MBG; ↓ NR | No CMR imaging – IS may be underestimated by SPECT; IS only in 60%; MSI not assessed; no reported use of TA or GPIIbIIIa inhibitors |
| Desmet et al.51 | 2011 | Symptom onset < 12 hours before enrolment; ‘new’ LBBB; TFG 0–3 | 56/110 | 61; 215 (150–296) and 193 (150–305) for adenosine and placebo, respectivelyb | 4 mg | Selective IC | MSI and MVO (CMR) | TFG; TFC; MBG; STR; 30-day and 1-year MACE | No benefit | No routine TA; no details on IS data; assessed ‘early’ rather than ‘late’ MVO; no stratified randomisation: more anterior MIs in adenosine arm and ↑ (almost double) spontaneous reperfusion rate in control arm |
| Grygier et al.53 | 2011 | Symptom onset < 6 hours before enrolment; TFG 0–2 | 35/70 | 65; 249 | LCA 2 mg; RCA 1 mg | IC via guide catheter | MBG; STR | TFG; TFC; 30-day MACE | ↑ MBG; ↑ STR; ↓ MACE | No imaging assessment of IS; no routine TA |
| Fokemma et al.52 | 2009 | Symptom onset < 12 hours before enrolment; TFG 0–3; included MVD | 226/448 | 62; 180 (130–288) and 165 (125–255) for adenosine and placebo, respectivelyb | 2 × 120 µg | IC via guide catheter | Residual STD | STR; MBG, TFG; IS (enzymatic); 30-day MACE | No benefit | No imaging assessment of IS; low drug dose injected proximally via guide catheter |
| Stoel et al.60 | 2008 | STR < 70% and persistent ST ↑ post PPCI with TFG 2–3 and < 30% residual stenosis | 27/49 | 67; 220 | 60 mg | Selective IC (over 5–10 minutes) | STR | TFC; MBG; 1-year MACE | ↑ STR; ↑ MBG; ↓ TFC | Preselected patients with suboptimal reperfusion success; no imaging assessment of IS; no TA; shorter ischaemic time in adenosine arm; no ITT analysis reported |
| Micari et al.56 | 2005 | Symptom onset < 6 hours before enrolment; excluded if previous MI | 14/30 | 57; 292 | 50 or 70 µg/kg/minute | i.v. infusion (3 hours) | MSI | MBV in AAR | ↑ MSI, ↑ MBV | IS and AAR assessed by MCE; no TA; low study numbers; used anterior MI patients from AMISTAD-II59 |
| Petronio et al.57 | 2005 | Symptom onset < 6 hours before enrolment; TFG 0–1; included MVD | 30/90 | 59; 179 | 4 mg | Selective IC | LV remodelling (LVEDV ≥ 20% on echo) at 6 months | Angiographic NR; TFC; ΔLVEDV | Improved angiographic results but no ↓ prevalence of remodelling | No direct IS assessment; selection bias (‘alternate’ randomisation); allowed use of other vasoactive drugs if NR occurred |
| Marzilli et al.55 | 2000 | Symptom onset < 3 hours before enrolment; TFG 0–2; included MVD | 27/54 | 60; 116 | 4 mg | Selective IC | Feasibility; safety; TFG | LV function; in-hospital clinical events | Well tolerated, feasible; ↑ flow, ↑ ventricular function, ↓ incidence NR | As for ATTACC;58 no outpatient follow-up |
| SNP | ||||||||||
| Zhao et al.129 | 2013 | Symptom onset < 12 hours before enrolment; TFG 0–2; age ≤ 75 years | 80/162 | 63; 345 | 100-µg rapid bolus | Selective IC | TFC; MBG; STR > 70% | TFG; LVEF (echo); MACE at 6 months | ↓ TFC; ↑ STR; ↑ MBG; ↑ LVEF | No imaging assessment of IS |
| Niccoli et al.44 | 2013 | Symptom onset < 12 hours before enrolment; TFG 0–1; ‘rescue’ PCI; excluded LBBB | 80/240 | 63; 278 | 60-µg rapid bolus then 100 µg over 2 minutes | Selective IC | STR > 70% | TFG; MBG; 30-day MACE | No benefit | See above; Low dose SNP; more anterior MIs in SNP arm; ECG surrogate for IS |
| Pan et al.128 | 2009 | Symptom onset < 12 hours before enrolment; TFG 0–3 | 46/92 | 53; 492 | 100-µg bolus; repeated after 5 minutes if TFG < 3 | Selective IC | TFG; TFC; MCE parameters | Plasma Hs-CRP and NT-proBNP; MACE at 6 months | ↑ TFG; ↓ TFC; ↓ MACE; improved MCE parameters | No direct imaging assessment of IS/MSI; TA at operator discretion (63%) |
| Parikh et al.45 | 2007 | High-risk ACS; TIMI 0–2 | 26/75 | 55; N/A | 50-µg bolus SNP ± 12-µg bolus adenosine | IC via guide catheter | TFG; MBG (visual) | MACE at 6 months | Combination of adenosine + SNP ↑ TFG, ↑ MBG and ↓ MACE vs. adenosine alone | Included non-STEMI ACS patients; no ‘SNP only’ arm; fewer high-risk lesions and greater prevalence of triple-vessel disease (possible preconditioning effect) in combination arm |
| Amit et al.42 | 2006 | Symptom onset < 12 hours before enrolment; TFG 0–2; excluded LBBB | 48/98 | 62; 202 (146–311) and 240 (146–325) for SNP and placebo, respectivelyb | 60 µg | Selective IC | TFC; STR > 70% | TFG; MBG; MACE (TLR, MI or death) at 6 months | No ↓ TFC or MBG but ↓ MACE | No IS assessment; underpowered; no TA; only 45% received GPIIbIIIa inhibitor |
List of abbreviations
- AAR
- area at risk
- ACE
- angiotensin-converting enzyme
- AMISTAD
- Acute Myocardial Infarction STudy of ADenosine
- AV
- atrioventricular
- CI
- confidence interval
- CK
- creatine kinase
- CMR
- cardiac magnetic resonance
- cTFC
- corrected TIMI frame count
- DSMB
- Data and Safety Monitoring Board
- ECG
- electrocardiogram
- GPIIbIIIa
- glycoprotein IIb/IIIa
- HR
- hazard ratio
- IC
- intracoronary
- IMH
- intramyocardial haemorrhage
- IQR
- interquartile range
- IRA
- infarct-related artery
- ITT
- intention to treat
- LAX
- long axis
- LGE
- late gadolinium enhancement
- LV
- left ventricular
- LVEF
- left ventricular ejection fraction
- LVM
- total left ventricular end-diastolic mass
- MACE
- major adverse cardiac event
- MBG
- myocardial blush grade
- MCE
- myocardial contrast echocardiography
- MI
- myocardial infarction
- MRC
- Medical Research Council
- MSI
- myocardial salvage index
- MVO
- microvascular obstruction
- NIHR
- National Institute for Health Research
- NO
- nitric oxide
- NT-proBNP
- N-terminal pro-brain natriuretic peptide
- PCI
- percutaneous coronary intervention
- PPCI
- primary percutaneous coronary intervention
- PPI
- patient and public involvement
- QTc
- corrected QT interval
- QuBE
- Quantitative Blush Evaluator
- RCA
- right coronary artery
- SAX
- short axis
- SD
- standard deviation
- SNP
- sodium nitroprusside
- SPECT
- sestamibi single-photon emission computed tomography
- STEMI
- ST-elevation myocardial infarction
- STR
- ST-segment resolution
- T2w
- T2-weighted
- T2w-STIR
- T2-weighted short-tau inversion recovery
- TFG
- TIMI flow grade
- TIMI
- Thrombolysis in Myocardial Infarction
- TMPG
- TIMI myocardial perfusion grade
- TSC
- Trial Steering Committee