

Notes
Article history
The research reported in this issue of the journal was funded by the HSDR programme or one of its preceding programmes as project number 16/52/04. The contractual start date was in December 2017. The final report began editorial review in March 2021 and was accepted for publication in October 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HSDR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
Copyright © 2022 Waring et al. This work was produced by Waring et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2022 Waring et al.
Chapter 1 Introduction
The context: the politics of major system change
The implementation of change in health and care systems is notoriously difficult. 1–4 Change processes are often protracted and wasteful of scarce resources, and can result in variable, dysfunctional or unintended outcomes. Research within the field of implementation science, together with complementary insights from political science, management studies and organisational sociology, shows that a vast array of contextual and procedural factors influence change processes, including the availability and distribution of resources, incentives and opportunities, local cultures, regulatory pressures, leadership styles, communication patterns, public opposition and professional attitudes. 3–11
Although sometimes overlooked within implementation frameworks or subsumed within other contextual factors, a large body of social science research shows that change processes can be significantly complicated by the ‘micropolitics’ or ‘organisational politics’ of care services. 3,4,12–14 This is the idea that people often hold different and competing preferences and interests about change, which become manifest through particular behaviours or strategies as people seek to influence (or resist) the change process in line with their preferences and interests. 4,15,16 It also recognises that organisations are shaped by informal lines of power and influence, in the form of cliques or networks, which function alongside more formal structures of authority. This is exemplified by the abilities of health-care professionals to subvert or corrupt change that is seen as challenging their underlying interests or institutional jurisdiction. 12,16–20
Reflecting on these ideas, Langley and Denis12 describe how the micropolitics of health-care improvement stem from competing value systems that can lead to conflict around change processes. They suggest that change often involves winners and losers, and, therefore, it is important to consider the distribution of benefits and costs that influence how people respond to change. Further highlighting the political challenge of health-care improvement, Bate et al. 3 describe the importance of ‘. . . securing stakeholder buy-in and engagement, dealing with conflict and resistance, building change relationships, and agreeing and committing to a common agenda for improvement’. 3 Bate et al. 3 also describe the importance of ‘politically credible leaders’ who can broker between competing interest groups and manage political processes.
To clarify our understanding of ‘organisational politics’ or ‘micropolitics’, it is important to acknowledge that this study is concerned less with the formal or big ‘P’ politics of government policy-making, statutory institutions or formal governance structures, and more concerned with the informal or small ‘p’ politics of interpersonal influence, ‘soft power’ or the localised strategies that shape the everyday organisation of care. It is accepted that these two domains are interconnected and, in many ways, overlap. For example, political decisions made during formal policy processes frame the microlevel politics of policy implementation. At the same time, it is important to recognise that micropolitical behaviours are not confined to the local level of policy implementation but also exist in the ‘corridors of power’ in the ‘heart’ of policy-making. For this study, however, the primary methodological and analytical focus is the micropolitics located in the local and regional organisation and governance of services, rather than the national arena of policy-making (accepting that these two perspectives are clearly connected).
Taking stock of these ideas, the study investigated how health and care leaders can and do address the political challenge of change, by focusing in particular on the distinct skills, strategies and actions that are required to recognise and mediate the interests and behaviours that underlie the organisational politics of health service change. Although designated ‘leaders’ clearly have a significant role in this regard, for example chief executives or clinical directors, the study focused more broadly on change ‘leadership’ or the idea that change is a process undertaken by many ‘change agents’ working together in a distributed or co-ordinated way,21 rather than necessarily by a designated leader or role-holder. For this reason, this study was concerned with producing a more explicit and empirically developed understanding of the political skills, strategies or actions used by people as they seek to engender (or stymie) change.
In developing its focus, the study considered the distinct political challenges of implementing large-scale change or ‘major system change’ within health and care services. 9,22 If research suggests that the implementation of change within organisations is complicated by ‘organisational politics’, it can be reasonably assumed that the implementation of change across multiple interconnected organisations is likely to be even more complicated by ‘system politics’. Major system change has become a prominent feature of contemporary health-care reform as policy-makers try to redesign services in more co-ordinated ways to better meet the needs of people and communities. 9,23,24 In broad terms, this involves changing the way that multiple care organisations work together to provide a more integrated care service, to improve care outcomes, to share and optimise scarce resources and to realise aggregate health benefits for communities. Although there is no agreed definition, Best et al. 9 suggest ‘large-system transformation’ might be understood as:
. . . interventions aimed at coordinated, systemwide change affecting multiple organizations and care providers, with the goal of significant improvements in the efficiency of health care delivery, the quality of patient care, and the population-level patient outcomes.
Best et al. 9
In other words, large-scale transformation involves changing not only the way that individual organisations work, but also the distribution of roles and responsibilities among multiple organisations and how these organisations work together as a complex interconnected system. Prominent cases of major system change include, for example, the reconfiguration of specialist services for cardiac, stroke or major trauma care and, more recently, the introduction of regional Sustainability and Transformation Partnerships (STPs) across the English NHS. 10,22,25–27
As might be expected, the implementation of major system change can be challenging and involves co-ordinating a complex system of relationships and interdependencies. There is growing recognition that the implementation of change, especially large-scale change, rarely happens in a linear or planned way; rather, the dynamic properties of most complex systems mean that change happens in unpredictable and unintended ways. 28 Such complexity requires particular forms of ‘system leadership’ capable of dealing with the dynamic demands of care systems. In their review of the literature of large-scale service transformation, Best et al. 9 propose five ‘simple rules’ for change:
-
Engage individuals at all levels, with senior leaders shaping the vision while distributing the responsibilities for change to individuals and teams.
-
Establish continuous feedback loops through validated measures that allow for collective reassurance.
-
Attend to history and draw on learning opportunities from similar processes.
-
Engage physicians through facilitation, incentives and alignment with regulatory systems.
-
Involve patients and families as the ultimate beneficiaries of change, as opportunities for learning and to validate change.
These ‘rules’ speak to the ‘micropolitics’ of major system change, but they do not offer a developed or specific account of how ‘system politics’ affect change processes nor what system leaders can do about it.
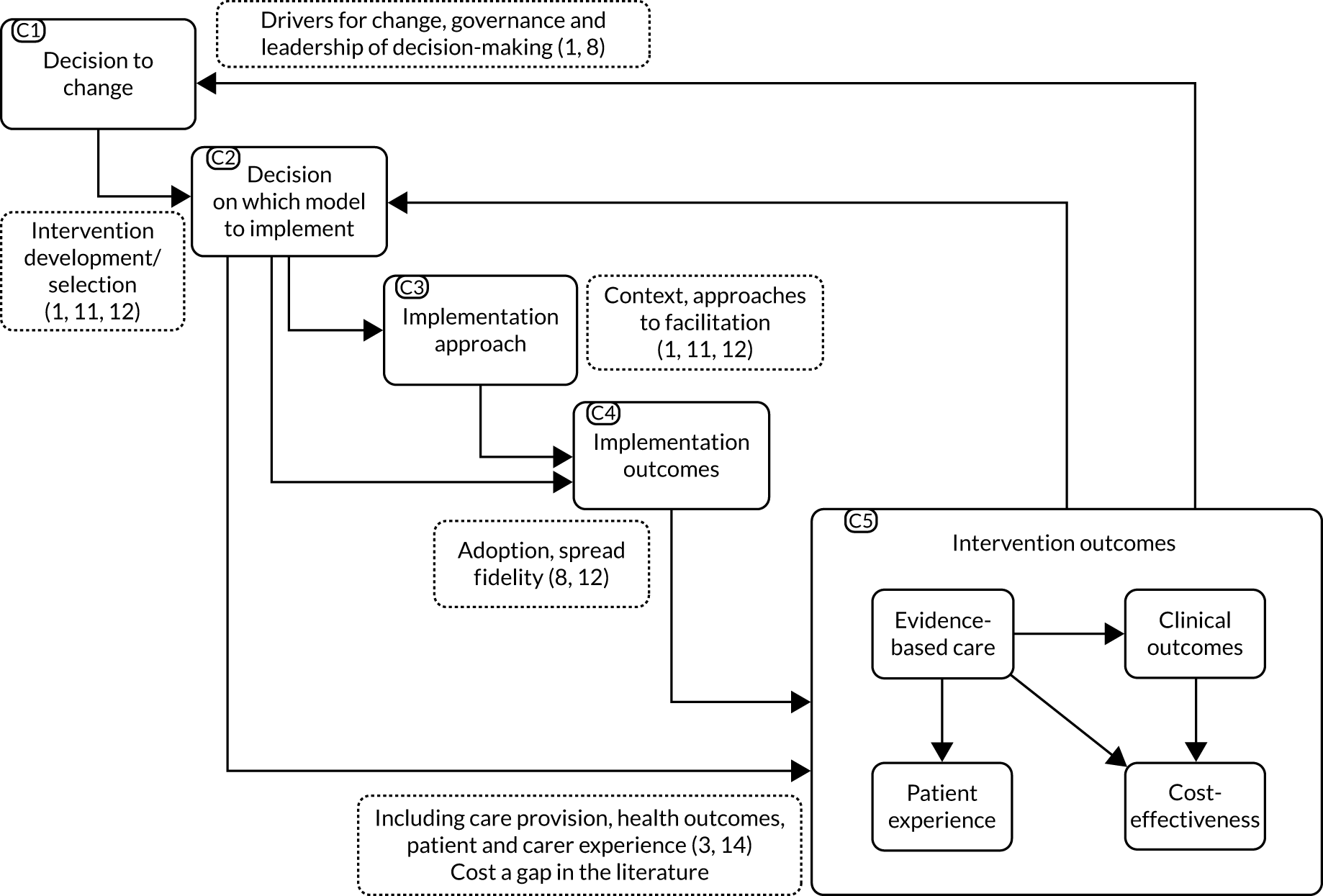
The application of these ideas to the reconfiguration of strokes services elaborates the challenges faced by system leaders. 2,22,29 In particular, Fulop et al. 2 examine the implementation of change across a series of linked stages (Figure 1), in which the implementation process ultimately shapes the implementation outcomes. Significantly, each stage represents a particular site for decision-making around which actors often disagree and, hence, each stage becomes a site for ‘system politics’ and political action. This research shows how the different approaches taken by leaders to reconcile competing preferences and priorities influence the resultant configuration of change and outcomes for patients.
FIGURE 1.
Implementation model with key decision points. Reproduced with permission from Fulop et al. 2 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
A recent review of the literature on major system change identified a number of underdeveloped dimensions in the mainstream literature. 30 Of relevance here, the review identified the hidden politics of system change, in which issues of ideology and power are elided through an emphasis on technical evidence and planning. Building on this idea, there is a need for more direct and developed consideration of the way that ‘system politics’ shape the implementation of system change and the scope for leaders to manage with and through these politics.
As noted above, STPs are a prominent contemporary example of major system change. 27 They grew out of a long-standing agenda for more integrated care, especially between the health-care and the social care sectors. The need for integration has, arguably, accelerated following the Health and Social Care Act31 of 2012, which saw continuing calls for service integration but also increased fragmentation, with the emphasis on market mechanisms and the dissolution of regional-level strategic bodies for service planning. 32 In 2014, the NHS Five Year Forward View25 set out a renewed vision for integrated care, describing health-care systems that were centred on patients, people and communities. The ‘new models of care’ emphasised the role of primary care and encouraged multicare providers to expand services and tackle difficult issues. 25 By 2015, collaborative groups were invited to form ‘Vanguards’ to expedite the formation of these new care models and, drawing on the experiences of the Vanguards, the report Delivering the Forward View: NHS Planning Guidance27 introduced the idea of STPs to lead the development of regional-level service integration. The main themes addressed by the 44 STPs include redesigning primary care, prevention and early intervention, improving mental health, improving productivity, workforce development, changing the role of acute and community hospitals, and enhanced integration of health care and social care.
As with any form of major system change, the implementation of STPs has been complicated and constrained by a range of factors. 33 A significant issue has been the ambiguity of the statutory basis of the STPs, especially their position and function within (or rather, in-between) the prevailing NHS and social care regulatory landscape. STPs have relied on so-called ‘system leadership’ to nurture and guide collaboration among various regional organisations and bodies. Additional complications, which further add to the political challenges of change, include the extent and forms of public, professional and patient involvement, especially where STP plans have been developed at considerable pace. 34 For this reason, the continuing evolution of STPs, and now integrated care systems (ICSs), provides a prominent focus for investigating both the ‘system politics’ of change and the political skills, strategies and actions needed to engender change.
The challenges and opportunities of organisational politics
This study was informed by a well-developed, but also fragmented, literature on ‘organisational politics’ found across management studies, organisational sociology, social psychology, and public policy and management. Across these disciplines, it has long been recognised that organisations are complex ‘political arenas’ in which actors utilise a variety of interpersonal strategies to advance their personal or organisational interests. 35–44 In their influential analysis of bureaucratic organisations, Crozier and Freidberg45 challenged the assumption that order is realised through hierarchical structures, arguing instead that actors within a ‘relational system’ utilise various strategies to influence the organisation of work.
Influenced by pluralist political theories,46 organisational scholars have developed an extensive body of research demonstrating the strategies and tactics used by organisational actors when seeking to maximise their personal or professional interests in the organisation of work. 36,38,40,42,47 These interests often come to light during periods of change, when the distribution of roles and resources is disrupted. 4,47,48 Mintzberg39,44 describes how these interests are expressed through various ‘political games’ or strategies, such as ‘alliance-building’, ‘budgeting’ or ‘insurgency’. As suggested by Clegg et al. ,49 ‘strategy, once conceived, struggles to come into being through the processes of micro-politics’. Kotter and Schlesinger48 note that strategic change is often difficult because people fear that it will threaten established ways of working and vested interests. For this reason, managers need to pay closer attention to the interests that drive organisational politics and the resultant lack of trust that forms between ‘camps’. In overcoming these politics, they suggest that managers need to educate employees and communicate the rationale for change; engage and involve people in change processes; and, if necessary, find the inducements and incentives to secure support. Such ideas provide the foundations for Kotter’s eight-step approach for realising episodic change. 50 Although organisational politics can be seen as self-serving (so-called Machiavellian) behaviour, a growing body of research shows that it can have a more constructive influence. 41 For example, the competing interests of stakeholders need not result in destructive conflict, but can be a source of innovation as people forge a degree of shared understanding out of their differences. 51,52
Research within the field of management studies suggests that, given the inherently political character of organisations, those people leading strategic change should develop and use particular political ‘strategies’, ‘behaviours’ and ‘skills’. Political skills enable leaders, first, to recognise and understand conflicting interests within the workplace and, then, to mediate those interests and build constructive coalitions in support of desired change. For Pfeffer,38 political skill involves ‘strategies’ to control the agenda, build coalitions and use experts; the use of ‘language’ to frame ideas and persuade others; and the control of ‘resources’. 38 As described in Chapter 3, the concept of political skill has been developed substantially by the US scholar Gerald Ferris and colleagues,53 among others,51 who describe it as a person’s:
. . . ability to effectively understand others at work, and use such knowledge to influence others to act in ways that enhances one’s personal and/or organizational objectives.
Ferris et al. 53
This is specified along the dimensions of ‘social astuteness’, ‘interpersonal influence’, ‘networking ability’ and ‘apparent sincerity’ to explain how individuals can influence others to realise their personal or organisational goals. The idea that leaders can develop and use political skill when seeking to implement organisational change was the primary point of departure for this study. Specifically, the study aimed to understand how health and care leaders can acquire, develop and use such skills for the implementation of major system change. Before developing this focus, it is important to briefly acknowledge wider debates on politics and power that further inform this study and provide the basis for lines of analysis that differ from the more mainstream ideas found in management studies.
Clarifying the concepts of organisational politics and power
It is far beyond the scope of this report to summarise the extensive literature on social power. However, the close connection between the terms ‘politics’ and ‘power’ requires some clarification, especially given that the terms are often used together in the wider health services research and policy literature. As noted, these terms are typically used to refer to forms of influence and power that operate beyond the statutory or formal institutions of government or policy-making, and instead focus on the informal relations of influence and power that are dispersed throughout and across the organisation of public services. 54 For some, micropolitics is a form of ‘soft’ interpersonal power,35,37,42 whereas for others it reflects ‘deeper’ ideological or structural interests. 17,55,56 For the purpose of this report, four perspectives are highlighted as relevant to the study of organisational politics in health and care services.
The first perspective treats power as an individualised resource or behavioural capability that usually resides within an individual and that is enacted over others through episodic forms of influence, persuasion or coercion. This can be through direct interpersonal influence or indirect forms of agenda setting or opportunity framing. This view is common within the predominant conceptualisations of political skill found within the management studies literature,53,57 in which ‘person A’ influences ‘person B’ based on their political skills. The second view develops this episodic viewpoint by attending not only to the capabilities or skills of individuals, but also, more importantly, to the relational interplay between social actors. From this point of view, social life is organised through the ‘interactive order’ that emerges from the relational patterns through which people make sense of themselves and others. 58–61 The third perspective focuses on the relative position of actors within a wider social field of relations. 62,63 This recognises that people hold variable and unequal positions within social settings, which is reflected, for example, in their access to certain roles, resources and relations, and also their acquired preferences, dispositions or viewpoints. These condition or shape a social actor’s inclination and opportunities to act or engage in both change processes and organisational politics. This dispositional power is derived less from an individual’s skills or abilities and more from the structured opportunities to act reflective of their acquired dispositions and forms of social, cultural economic and symbolic capital. 63 The fourth perspective sees power as more systemic, ideological or discursive. Rather than residing in people, power flows through the relationships between people, and these structured relationships are reflective of broader structural interests or ideological imperatives. On one level, this represents a hegemonic form of power55 in which actors may not be entirely conscious of the interests that structure their lives. On another level, it suggests that the ‘micropolitics’ of everyday life are shaped or constituted by broader social and political discourses that are manifest in bodies of knowledge, social institutions and other apparatus of governing. 64
These different perspectives span the structure/agency divide within the social sciences for which, at extremes, research emphasises either the voluntaristic behaviours of autonomous actors or the determinism of social structures, institutions and ideologies. 65 Without reducing analysis to either structure or agency, this study developed an integrative view of organisational politics in which the different forms of power and influence co-exist across different analytical dimensions while still being connected and influencing each other, and without reducing analysis to one over the other. For the study of health-care organisation, this means paying attention to the structural interests that shape health policies,17 the institutionalised forms of power associated with certain professions,66 and the prevailing biomedical and economic rationalities that constitute modern health care. 67 It also means recognising that health-care professionals not only engage in interpersonal relations from the discursively constituted social positions within the field of health-care organisation, but also can act both within and beyond these positions in their day-to-day episodic interactions and negotiations with others. 68,69
It is worth recognising from the outset that, although the literature on organisational politics often recognises that power and influence operate across and between multiple dimensions, the literature of political skill and, to some extent, political astuteness tends to focus on the more behavioural aspects of political influence. That is, it focuses on the capacity for individuals to exert influence over others, typically based on their particular skills or abilities. Although this influence is seen as inherently relational and interactive, the unit of analysis often remains the individual, which means that the contribution or contingencies of wider social and ideological factors can be downplayed or overlooked. This study took the concepts of political skill and astuteness as its primary conceptual and analytical focus because these afforded a discrete empirical focus from which to contribute to the health services research literature on the implementation of change, and also because they offered a more focused and practical basis for informing leadership development. This meant, however, that some of the wider conceptions of power and politics were not directly or explicitly operationalised or applied in the conduct or reporting of this study, primarily for the purpose of analytical clarity.
The need: acquiring and developing political skill
With growing recognition that the implementation of change in health-care services is complicated by organisational politics, there is commensurate interest in the need for health and care leaders to acquire and use political skills to better understand and navigate these politics. To some extent, these ideas appear to be shaped by the wider management literature, but there remains a significant lack of research and theory considering what political issues are involved in the implementation of major system change and what types of political skill or ‘political astuteness’ are required to manage ‘system politics’. Such evidence could then inform existing leadership development programmes or offer a more critical analysis of system change.
The pedagogical literature on workforce development suggests that the acquisition and development of leadership skills occur through a combination of at least three forms of learning. 70 First, through participation in formal education and training programmes, in which abstract concepts or methods are taught in the classroom or simulated environments. Second, through mentoring, coaching and action-learning in which learners are guided through individual and group reflection on ‘real-world’ challenges. 71 Third, through experiential and reflective learning in the context of taking actions in relation to ‘real-world’ situations. 72 To date, however, there has been limited research on how health and care leaders acquire and develop political skill or astuteness. Research suggests that formal training and real-world experience are both important. Hartley et al. ’s73 research with public managers in the UK, Australia and New Zealand finds that political skills are often acquired in a haphazard and sometimes painful manner. More evidence is required to both understand and meet the development needs of current and future leaders to acquire and use political skill (or astuteness) when leading major systems change.
In the English NHS, a number of established leadership programmes aim to enhance the capabilities of the health-care workforce to implement strategic change. The NHS Leadership Qualities Framework,74 developed in the mid-2000s, describes 15 aspects of leadership clustered around ‘personal qualities’, ‘setting direction’ and ‘delivering the service’. 74 This framework recognised the importance of ‘political astuteness’ in terms of (1) the capacity to understand the climate and culture of the organisation; (2) knowing who the key influencers are and how to involve them; (3) being attuned to national and local strategies; and (4) understanding the interconnected role of leadership. 74 The subsequent Healthcare Leadership Model75 included nine dimensions and again highlighted the need for leaders to understand the culture and politics of health care, including the informal chain of command. This suggests ‘successful innovation involves the exercise of political astuteness’ (© NHS Leadership Academy, 2013),75 including the cultivation of relationships and the building of coalitions among competing interests. However, the more recent NHS framework for improvement and leadership development – Developing People: Improving Care76 – gives less explicit attention to the importance of political skill. In various places, these capabilities are addressed in relation to ‘system leadership’, which involves building relationships and shared goals across organisational boundaries to help implement new service models. However, there is limited recognition of the need for service leaders to manage both the formal and the informal politics of health-care and social care services when implementing strategic change.
Although political skill is acknowledged across these frameworks, there is little evidence about how it is best acquired or how it can contribute to effective change. Many of the attributes are poorly specified or subsumed within other broader behavioural competencies. Even when there is explicit reference to political astuteness, there is limited evidence on which these qualities are based, and no explanation about how the concept has been adapted to the NHS context. With the pressing need to implement major strategic changes across the NHS, especially efforts to better integrate care services, there is a need to better understand the acquisition and contribution of political skill and to use that knowledge to inform the design and content of new learning and recruitment resources for service leaders and other change agents.
Study aims and objectives
The overall aim of this study was to produce a new empirical and theoretical understanding of the acquisition, use and contribution of leadership with ‘political astuteness’, specifically in the implementation of major health system change, from which to inform the co-design of materials and resources for the training, development and recruitment of current and future service leaders.
The study had six objectives:
-
identify key theories and frameworks of political astuteness within the social science literature and apply these to recent evidence of health system change to understand how service leaders can constructively create a ‘receptive context’ for change
-
understand the perceptions, experiences and reported practices of service leaders, and other change agents, about their acquisition and use of political astuteness in the implementation of health system change, taking into account differences in professional background, age, gender, ethnicity, geopolitical context and change context
-
understand how recent recipients of NHS leadership programmes think about, have acquired and make use of political astuteness to inform the development of new training resources
-
revise existing theoretical models of political skill and astuteness with reference to the wider social, cultural and relational context of health system change, from which to develop new theoretical propositions
-
investigate how political astuteness is used constructively by service leaders to create a ‘receptive context’ for implementing major health system change
-
work with providers of NHS leadership training, NHS recruitment agencies and patient and public involvement (PPI) groups to co-design recruitment and learning materials that support the acquisition, use and development of political astuteness for existing and future health-care leaders.
Structure of the report
The report is structured as follows. Chapter 2 describes the study design and methods. The following four chapters describe each of the study’s workstreams, including the findings of the two narrative reviews (see Chapter 3), the findings of the interview study (see Chapter 4), the findings of the in-depth case study research (see Chapter 5) and the development and co-design of learning resources and materials (see Chapter 6). Chapter 7 returns to the original research aims to make the final conclusions.
Chapter 2 Research design and methods
Introduction
This chapter describes the research design and methods used to address the study aims and objectives. It draws heavily from, and elaborates on, the published study protocol77 and also describes the challenges and changes in study design and practice encountered over the course of the study. The study comprised four linked work packages (WPs), each addressing a particular research objective. The findings produced through these activities are presented and discussed in subsequent chapters.
Work package 1: narrative reviews of the literature
The purpose of WP1 was to carry out two literature reviews: the first to identify key theories and frameworks of political skill, and associated terms, within the wider social science literature, and the second to apply the learning from this review to the health services research literature to understand how service leaders use such skills to create a ‘receptive context’ for change.
Review 1: a ‘review of reviews’
A preliminary scoping review showed that a number of recent systematic literature reviews on the concept of political skill had been published in the last 10 years. 43 For this reason, a ‘review of reviews’78 was carried out to (1) identify and synthesise the main theories and frameworks, (2) clarify the conceptual and theoretical assumptions informing these frameworks, (3) identify the different methodological approaches and (4) determine how political skill is both acquired and used in different strategic contexts.
Search specification and strategy
The preliminary scoping review found that the study of political skill can involve a range of closely related terms and concepts, such as ‘astuteness’, ‘intelligence’, ‘nous’ and ‘savvy’. Candidate search terms were reviewed in consultation with experts in the fields of organisational studies, public management, political science and sociology, as well as through the analysis of recently published reviews. The selected search terms and Boolean operators were ‘political skill’ or ‘political astuteness’ or ‘political savvy’ or ‘political acumen’ or ‘political nous’ or ‘political intelligence’ or ‘political leadership’ and ‘systematic review’ or ‘narrative review’ or ‘synthesis’ or ‘review’. These terms were used to search the following databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL) Plus, Google Scholar (Google Inc., Mountain View, CA, USA), MEDLINE® (National Library of Medicine, Bethesda, MD, USA), ProQuest® (ProQuest LLC, Ann Arbor, MI, USA) Social Science, PsycInfo® (American Psychological Association, Washington, DC, USA), PubMed® (National Library of Medicine), Scopus® (Elsevier, Amsterdam, the Netherlands) and Web of Science™ [Clarivate Analytics, Philadelphia, PA, USA; including Conference Proceedings Citation Index – Science (Clarivate Analytics)]. Finally, study advisors recommended manual searches of journals, including Academy of Management Review, International Journal of Management Reviews, Organisation Science and Political Quarterly.
Extraction and analysis
In total, the searches identified 303 sources (after duplicates were removed). These were screened (title and abstract review) by Jenelle Clarke, Simon Bishop and Justin Waring, excluding 275 sources. In line with our study design, for papers to be included they needed to relate directly to the concepts of political skill, astuteness or an associated term, as outlined above. Given that this was designed as a review of reviews, it excluded all primary research papers or empirical studies and included only narrative or systematic reviews of these concepts. Although the inclusion criteria may appear broad, in practice the searches returned a majority of studies that did not relate specifically to the theoretical concept of political skill or related concepts, and many cases addressed more general notions of politics or did not represent reviews of the literature. Three authors (JW, JC and SB) reviewed all of the titles and abstracts, made comments on a spreadsheet and met in person to go over the results. Two authors (JC and JW) independently reviewed 28 articles, excluding a further 10. Independent selections were reviewed and disagreements were deliberated (with SB). Selected publications were extracted and summarised using a standardised template, including authors, date, review method, number of sources, inclusion criteria, quality assessment, disciplinary perspective, theoretical background, empirical focus and review themes or findings (see Appendix 1). 79
Given the diversity of disciplinary, theoretical and methodological approaches within the literature, a narrative synthesis approach was taken to describe and interpret the main themes. 79 This involved a close reading of selected papers to summarise relevant themes and subthemes and, importantly, to interpret the reviews in terms of their contribution to prevailing disciplines, theories or debates.
Review 2: a review of ‘political skill’ in health services research
The second review aimed to understand how the concept of ‘political skill’ or associated concepts have been used in the health services research literature, especially research investigating the implementation of organisational and system change. The review investigated (1) how the concept is defined and operationalised in the health service research, (2) what methods of enquiry are used to study political skill, (3) what the concept contributes to the study of organisational change in health services and (4) to what extent the concept offers distinct or novel analytical insight into the wider social science literature. Unlike the first review, this was inclusive of primary sources and was not limited to review papers.
Search strategy
Search terms were identified in consultation with expert advisors in the fields of health services research, public policy and management, organisational studies and medical sociology. The search terms and Boolean operators were ‘political skill’ or ‘political astuteness’ or ‘political savvy’ or ‘political acumen’ or ‘political nous’ or ‘socio-political intelligence’ or ‘political leadership’ and ‘health’ or ‘healthcare’ or ‘health service’ or ‘health policy’ or ‘health policies’. A systematic literature search was undertaken using seven databases: MEDLINE, Web of Science, PsycINFO, ProQuest Social Science, PubMed, CINAHL Plus and Scopus. The searches were run between October and November 2018.
Selection criteria included any study written in English that described or applied the concept of political skill (or related terms) within a health-care context, including empirical and theoretical papers and prominent grey literature. No time restrictions were applied. Manual searches were carried out of identified bibliographies for further sources and literature recommended by domain-relevant experts (see Appendix 2).
Extraction and analysis
In total, 1718 records were identified (after duplicates were removed). Jenelle Clarke, Simon Bishop and Justin Waring independently screened the results (titles and abstract review), excluding 837 papers. Two authors (JC and JW) independently reviewed 96 articles (full text), excluding a further 35, with 62 identified for inclusion; disagreements were deliberated with Simon Bishop.
A standardised template was used to summarise and extract relevant data. 79 Characteristics included the full citation, method of study, disciplinary perspective, theoretical background, phenomenon of interest with regard to the change agenda or political issues, context for the study, methodological position, analytical approach, key findings, interpretation and explanation related to the study of change, and theoretical contribution. Narrative analysis of the papers was conducted thematically, with particular attention to how the concept of political skill has been used to explain health-care change.
Work package 2: narrative interview study
The purpose of the interview study was to investigate the perceptions, experiences and reported practices of service leaders and other change agents (broadly defined as people involved in leading the change process) about the acquisition and use of political skill in the implementation of health system change, taking into account differences in professional background; sociodemographic factors, such as age, gender and ethnicity; the geopolitical context; and the change context.
Methodological approach
The interview study followed a narrative approach to investigate how people experience and make sense of their lives in the form of stories. 80,81 The telling of stories involves organising experiences in ways that make them comprehensible to the narrator and the audience through forms of ‘emplotment’, that is, when events are connected together in a way that conveys meaning and order. These stories reveal underlying assumptions, beliefs and values. The interpretation of these stores surfaces the meanings that actors hold while still recognising that these stories are being told to a particular ‘audience’ for a given purpose. 80–84
Sampling and recruitment
Sampling aimed to investigate service leaders’ experiences of acquiring and using political skill within and across different care sectors (health and social care), organisational types (primary care, acute and community), strategic and operational arenas (senior management and delivery teams), professional backgrounds (medicine, nursing and pharmacy), career stage and regional contexts. A purposive sampling approach was adopted in which participants were recruited on the basis of exploring one or more of these differences. 85 In addition, people were recruited who were currently participating or had recently participated in leadership training programmes, to investigate how aspects of political skill are addressed in current training programmes.
An initial sampling frame was populated by members of the research team based on existing research connections and knowledge of prominent service leaders and professional representatives. In addition, opportunistic sampling of service leaders occurred during research engagement activities, for example conference attendance. Over 80 people were identified, all of whom were categorised to inform representative sampling decisions in terms of their professional background, occupational role, organisational affiliation and geographical location. All of the identified people were contacted in writing to seek their participation, resulting in 50 participants.
Two strategies were used to identify and recruit people enrolled on, or who had recently completed, leadership training programmes. First, and following attendance at the 2018 Health Services Research UK annual conference, contact was made with the professional network for NHS leadership and management trainees, who issued an invitation on behalf of the study to over 40 people, from whom five people were recruited. Second, the academic leads for two postgraduate leadership development programmes distributed a similar letter of invitation to their respective learner cohorts. This resulted in three people agreeing to participate in interview, while eight learners from one programme offered to take part in a focus group. In total, 16 ‘trainees’ were recruited.
In total, 66 people participated in either qualitative interviews (n = 58) or a focus group (n = 8). In terms of demographic composition, the sample included 37 females and 29 males: 59 were white British, four were Asian or British Asian and three were black or black British. In terms of career experience, the sample was categorised into three groups: 10 people with < 10 years of experience, 23 people with 11–20 years of experience and 33 people with > 20 years of experience. It was not possible to determine the career length for 12 participants because the information was not given or they had multiple career changes. Of the 16 ‘trainees’ recruited for interview or a focus group, six were within the first 10 years of their career, with the other 10 being in established professional positions (eight in quality improvement and two in general management).
Participants were recruited from different health and care settings, although the majority were based in the acute hospital setting. Five were significantly involved in STP leadership and had ‘dual roles’ both with their primary NHS employer and in the management of a STP. Three people were recruited from the social care sector and one from the police services on the basis of having a significant role in health-care planning (Tables 1 and 2).
| Role | Participants (n) |
|---|---|
| Regional-level director | 3 |
| Quality/service improvement | 18 |
| External relations/communications | 1 |
| Local authority management | 2 |
| Primary care leadership | 1 |
| Medical leadership (hospital/regional) | 5 |
| Management (general) | 17 |
| Nursing leadership | 6 |
| Research leadership | 2 |
| Patient/public | 3 |
| Voluntary | 5 |
| Police leadership | 1 |
| Non-executive | 3 |
| National-level leader | 3 |
| National-level service improvement | 4 |
| Total | 66a |
| Setting/sector | Participants (n) |
|---|---|
| Acute or specialist hospital | 30 (n = 2 also STP) |
| Primary care | 1 |
| Specialist service network | 3 |
| Research | 5 |
| Quality improvement agency | 5 |
| Commissioning | 3 (n = 1 also STP) |
| Ambulance | 1 |
| Local authority/social care | 3 |
| STP (employed by other organisation) | 5 (n = 3 dual roles) |
| National (NHS England/Improvement) | 4 |
| Voluntary sector | 5 |
| Police | 1 |
| Public representative/organisation | 3 |
| Medical trainee | 3 |
| Total | 66a |
Data collection
Narrative interviews invited participants to reflect on and talk about their experiences of organisational politics and political skill in the context of their involvement in health service change. A preliminary interview topic guide was developed to mirror the research objectives. This was piloted independently by three of the study team with the first seven participants, with feedback provided by the participants leading to revision of the topic guide (see Appendix 3). A total of 48 interviews were carried out face to face at a location chosen by the participants and 18 interviews were carried out over the telephone. All interviews were recorded with the consent of participants and transcribed verbatim.
Data analysis and reflections
Narrative analysis aimed to interpret how participants make sense of their experiences through story-telling, linking individual accounts to shared systems of meaning and cultures. Narratives were ‘read’ for their content (what they talk about) and form (how they talk it). An important reflection is that many participants appeared to see the interview exchange itself as a ‘political act’, and forms of attribution bias were clearly present in the narratives. Importantly, the narrative approach is less concerned with determining the ‘facts’ of a given situation and more with the perceptions and meanings of participants. For Josselson,82 this requires a degree of suspicion on the part of the researcher to interpret meanings or assumptions that might be disguised or layered under more explicit statements.
In practical terms, data analysis followed a ‘step-wise’ approach to interpretative data analysis. 86–88 This involved (1) familiarisation with data through close reading, (2) generating initial codes through the systematic tagging of data, (3) constant comparison of codes to assure internal coherence, (4) axial coding to identify second-order codes and to elaborate overarching themes, and (5) reviewing themes in the light of the wider literature.
Data analysis started with all members of the study team closely reading at least two transcripts to identify ‘interesting’ narratives of political skill to guide subsequent coding. Three members of the team (JW, BR and SB) then coded the data through close reading and open coding of transcripts. Codes were subject to regular review to clarify interpretation and internal consistency. ‘Second-order’ codes were developed incrementally through the categorisation and grouping of codes. These were then further aggregated in the form of overarching themes. In these later stages, themes were simultaneously related back to the research literature to confirm or challenge existing research and theory. Overall, in excess of 100 detailed stories were identified that described experiences of organisational politics and examples of political skill.
Work package 3: in-depth qualitative case studies
The purpose of WP3 was to investigate how political skill is used constructively when implementing major system change. This involved applying and refining concepts and propositions developed through the preceding WPs to the study of political skill ‘in action’.
Methodological considerations
Work package 3 involved a qualitative case study approach. Case study research aims to produce a detailed description and analysis of a given ‘case’, which in many studies is representative of a broader phenomenon, but in others can be a rare, extreme or deviant case. 89,90 For health services research, case studies are especially relevant when seeking to understand how policy interventions are implemented in real-world settings. 91 Case study research is especially suited to the study of organisational politics because it provides fine-grained contextual understanding of how people interact and influence each other over time. 92
The initial study design proposed taking an ethnographic case study approach, with the aim of producing an immersive interpretative account of change processes. 93–95 It was recognised early within the study, however, that it would be challenging to carry out sustained in-depth fieldwork across multiple subcase study sites (i.e. the anticipated nine change projects). Specifically, the ability of two field researchers, even with the support of the wider study team, to carry out immersive longitudinal field observations tracking the ongoing development of nine different cases became unfeasible, even when field work was staggered across different time periods. The scheduling of field work was further complicated and compressed by the challenges and delays of case recruitment. For this reason, research was informed by the methodological principles of ethnography, especially developing an in-depth and interpretative understanding, but with greater reliance on time-limited observations of key events and greater use of interview and documentary data. 96
Sustainability and Transformation Partnership selection and recruitment
The study was designed to investigate change within three regional STPs as prominent examples of major system change. Given that STPs are made up of diverse portfolios of system change, the study intended to focus on three ‘subcases’ or system change ‘projects’ within each selected STP.
A preliminary desk review of all 44 STPs (completed during proposal development) identified key STP characteristics in leadership arrangements, strategic priorities and thematic areas for system change, such as urgent care, integrated care and mental health. Based on this desk review, three ‘candidate’ STPs were purposively selected during the initial application stage from Greater London and the Midlands to investigate differences in (1) geographical location and profile (demographic make-up, number of cities/towns and urban/rural features); (2) the number of large and specialist service providers; and (3) the profile of service transformation projects (with the intention of exploring both similar and different initiatives across the regions). Although these three sites were initially supportive of participating in the research, two of these later withdrew support and the research experienced significant challenges in recruitment, leading to both delays and variation in sampling and selection, the reasons for which are indicative of the organisational politics of health and care systems.
First, it was often difficult to determine where approvals should be sought within the STP governance structures and which body had statutory responsibility to approve research participation. Even when senior STP leaders were supportive of the research, managers from constituent NHS organisations could be less supportive, or vice versa. Although project teams or middle-level STP leaders were often supportive of the research, it took as long as 6 months to work through the various governance layers to find the group to authorise the research. Second, two of the candidate STPs experienced unanticipated changes in senior leadership, making it difficult to secure access. With one STP, the research team had many meetings with senior leaders over a 6-month period and eventually gained approval from the executive group; however, three members of this group then left their posts and the newly appointed leaders withdrew support for the study on the grounds that the recent leadership changes were ‘too sensitive’. Third, although STP leaders were highly interested in the study focus, they were often apprehensive about bringing to light ‘sensitive’ political issues during ‘live’ transformation processes. These recruitment challenges speak directly to the organisational politics of the STP agenda.
Given these challenges, STP recruitment was protracted and challenging. Following the planned approach, three candidate sites were approached through existing research networks, for example the National Institute for Health and Care Research (NIHR) Collaborations for Leadership in Applied Health Research and Care (CLAHRCs).
After 6 months of discussions with STP leaders, two of these candidate sites withdrew support: one because of the aforementioned leadership changes and the other because of perceived political sensitivities. After nearly 6 months of discussions, one site in the Midlands agreed to participate. Another candidate site in Greater London was approached and, following another 6 months of negotiations, approval was granted. In parallel, all STPs in the Midland regions were contacted in writing to invite them to participate. Following a further 6 months of discussions, one STP agreed to participate. Because of the challenges around recruitment of STPs, case study data collection was delayed by over 6 months in two sites and by over 1 year in the other. The recruited STPs’ case study sites are summarised in Table 3, and the STP regions have been given pseudonyms to protect the anonymity of participating sites. Shortly after commencing fieldwork with this third site, field research was paused because of the COVID-19 pandemic (the impact of this is discussed in The impact of the COVID-19 pandemic).
| Regional characteristics | STP case 1 (Blue) | STP case 2 (Green) | STP case 3 (Red) |
|---|---|---|---|
| Population | 1.2 million | 1.1 million | 1 million |
| Geographical footprint | Three medium-sized towns (c. 150,000 people) and villages, on edge of Greater London | One medium-sized city (c. 350,000), several towns and rural villages. Areas of high deprivation and wealth | One medium-sized city (c. 250,000), several large settlements (c. 100,000) and numerous smaller villages. Mix of dense urban and sparsely populated rural areas. Areas of high deprivation and low wealth |
| Demographic features | 0.7% among the most deprived in the UK. Predominantly white population, around 90%, which is higher than the average in the UK, but there is also an established traveller population | One-third of the population is an ethnic minority. Life expectancy is lower than the UK average. Substantial inequality. Problems with access to care and variety of quality of care. Large number of people dying from long-term conditions | Around 97% white British in the county but diverse cultural population in the main city. Ten-year gap in life expectancy between most deprived and most affluent areas. Rising ageing population. Over 20 areas in the county are among the poorest in the UK |
| NHS trusts | Six, including ambulance | Four, including ambulance | Five, including ambulance |
| Commissioning bodies | One merged CCG | Six CCGs then one merged CCG | One merged CCG |
| Primary care networks | 24 | 20 | 15 |
| Other NHS services | Community health social enterprise | Community health services social enterprise | Private community interest company |
| Local authorities | 1 | 2 | 2 |
| Strategic objectives |
|
|
|
| Programme priorities |
|
|
|
Subcase transformation project: selection
The study design proposed to select three ‘subcases’ of system change within each selected STP. This was based on the assumption that the politics of system change would vary between the more ‘strategic arenas’ of high-level STP leadership and the more ‘operational arenas’ of system change. Informed by the preliminary desk review, common system transformation domains were identified, including urgent care, health and social care integration, and resource prioritisation. However, during STP recruitment, senior leaders asked the research team to focus on transformation projects that they regarded as priority issues, which were accepted as subcases on the basis of being a necessary compromise to support research access. Nevertheless, the selection of subcases took into account the difference in the focus of transformation, especially whether they were focused on the strategic or the operational levels of change, and how each project contributed to the overarching STP priorities. As described below, each subcase offered a distinct analytical focus for the study.
The recruited STPs’ subcase study areas are summarised in Table 4. Study names have been modified to protect the anonymity of teams.
| STP case 1 (Blue) | STP case 2 (Green) | STP case 3 (Red) | ||||||
|---|---|---|---|---|---|---|---|---|
| Transformation project focus | STP system architecture plan | Integration of primary and acute service | Integration of specialist pharmacy services | Merger of CCGs | Prioritisation for urgent care transform | Implementing personal health budgets | STP vision and mission | Workforce development |
| STP level | Strategic | Thematic programme | Operational project team | Strategic | Thematic programme | Operational project team | Strategic | Strategic |
| STP domain | Children’s, families and maternity | Placed/locality services | Medicines | Commissioning | Urgent care | Mental health | STP wide | STP wide |
| Analytical focus | Sharing vision and resources | Organisational (vertical) integration | Professional (horizontal) integration | Consultation processes | Mediating competing priorities | Reading the political landscape | Mediating interests | Sustaining change |
Selection and recruitment of individual participants
The recruitment of individual participants was also purposive, based primarily on a person’s direct or indirect involvement in system change and with the intention of exploring variations within and across project activities. 85 Participants were identified and recruited through three techniques. First, a review was undertaken of publicly available STP documentation that identified people involved in STP governance and project management, that is from organograms. Second, people were identified as potential participants during observational research, that is based on involvement in project work. Third, participants recommended speaking with others to pursue particular lines of enquiry as a form of ‘snowball’ sampling. All participants were provided with the study participant information sheet and gave written consent.
The study protocol anticipated recruiting representatives of patient groups involved in and affected by the proposed service transformations. A surprising finding was the limited involvement of patient or public groups in ‘day-to-day’ project activities. Most projects involved some formal public or patient representative from a recognised charity or advocacy group, and most of these people participated in the study. However, there was little wider service user or public engagement, which then limited the scope to involve such people in the research.
The impact of the COVID-19 pandemic
It is important to acknowledge the impact of the COVID-19 pandemic on fieldwork. By the end of February 2020, data collection at the Greater London STP (Blue) was nearing completion and data collection at one Midlands STP (Green) was progressing well, with two subcase studies completed and the third under way. The second Midlands STP (Red) had agreed to participate and data collection was under way with senior system leaders and introductory meetings had been held with project teams. Following the introduction of the first UK ‘lockdown’ in March 2020, and in accordance with NIHR guidance, data collection for WP3 was paused, with activity focused on completing data analysis and preparing WP4.
At this time, it was decided to conclude data collection with the Greater London site. The Midlands STPs were contacted to discuss the ‘pause’ and to agree ways to restart the research in due course. One month into the pause, the research team was contacted by the lead of the project team for personal health budgets (STP Green) with the news that this project had been terminated. They reported that, owing to the pandemic, funding for the initiative was no longer available and members of the project team had returned to their primary ‘jobs’ to respond to COVID-19. Sufficient data had been collected up this point to provide important learning about the challenges of project set-up, from which a case report was developed. This concluded data collection at the first Midlands STP (Green).
Following the end of the first lockdown, the second Midlands STP (Red) was contacted to discuss recommencing the study. At this time, it was communicated that data collection could not recommence until the autumn owing to a backlog of work and new challenges associated with the pandemic. Further contact was made with the STP in early September to discuss data collection. At this time, the ‘cancer care’ project team indicated that they could no longer take part in the study owing to excessive work demands. Data collection with the ‘transforming the patient journey’ and ‘workforce development’ project teams was rescheduled for October to December. By the time that data collection was about to recommence, there was an increase in COVID-19 cases and hospital admissions and, subsequently, in November, a second lockdown. At this point, the ‘patient journey’ project team withdrew from the study owing to unprecedented work demand. The overarching STP leadership agreed to continue involvement in the research with the ‘workforce development’ and ‘system architecture’ project teams. However, as a result of the second lockdown and additional pressures on the service, data collection was further delayed and relied primarily on remote interviews carried out between December 2020 and February 2021. One of the advantages of in-depth qualitative work is that it enables collection of a large number of data in various forms and, therefore, when data collection was possible, there is sufficient data to meet the study objectives.
Data collection
The in-depth case study research involved a combination of qualitative methods, including semistructured interviews and group interviews, focused observations and shadowing, ‘in site’ ethnographic interviews and documentary analysis.
Interviews and focus group
Semistructured interviews were the primary method of data collection. Consistent with WP2, these took a narrative approach with the aim of exploring participants’ reflective experiences of change processes. Unlike the preceding WP, these interviews were able to explore multiple participants’ perspectives of a shared issue, thereby enabling greater understanding of the relational interplay between people. An interview topic guide was used to ensure that broadly common themes were investigated, but with considerable scope to allow participants to shape the conversation. The topic guide was designed based on the thematic findings of WP2, examining (1) the controversies of change; (2) the people involved and their interests; (3) the political skills, strategies and actions; and (4) the settlements.
As described above, interviews were carried out with people involved in ‘high-level’ STP governance and more operational system change. A small number of participants were interviewed on more than one occasion to investigate their experiences of change over time. With the restrictions brought about by COVID-19, the majority of later interviews were carried out using video-conferencing. With the time constraints owing to the pandemic, focus groups with the senior members of the second Midlands (Red) STP were organised to investigate change over time. In total, 73 people took part in 83 interviews (Table 5).
| STP case 1 (Blue) | STP case 2 (Green) | STP case 3 (Red) | |
|---|---|---|---|
| Strategic STP leadership |
|
|
|
| Project team 1 | Integrated ‘place’:
|
Urgent care:
|
Workforce development:
|
| Project team 2 | Medicines optimisation:
|
‘Personalised’ mental health care:
|
|
| Project team 3 | ‘New-born’ project
|
CCG reconfiguration
|
|
| Total | n = 26 participants | n = 32 participants (n = 40 interviews) | n = 15 participants (n = 17 interviews) |
Observations and ‘in situ’ interviews
Non-participant observations were carried out to develop in-depth understanding of the politics and political skill of system change. As described above, it was impractical to carry out in-depth participant observations across multiple case study projects. Instead, a more focused approach was taken, in which field researchers observed a sample of key senior leadership meetings for each STP and transformation project team. These observations focused on understanding how controversial issues were manifest in group settings, how people acted and interacted in relation to these issues and, in particular, the political skills and strategies used to influence change. The observations enabled the identification of people who could be invited to participate in an interview.
As part of the observations, many people were engaged in informal ‘in situ’ conversations about change processes. These took place within meetings, but more often in post-meeting discussions. These ethnographic-style interviews were useful for clarifying observations. In addition, five people agreed to be shadowed as part of their project work. This involved spending sustained periods of time with an individual while they participated in project meetings, met with other individuals or discussed key elements of the change process. These observations were usually arranged to take place before or after a scheduled project meeting, and lasted between 2 and 4 hours. In total, 23 meetings were observed over 49 hours (Table 6). As noted above, the impact of the pandemic meant that direct observations were not possible for much of the data collection for STP 3, with almost complete reliance on online technologies for data collection. Although such technology facilitated data collection for interviews and workshops, it reduced the scope for first-hand observations of both formal meetings and the more opportunistic in situ observations usually available in field research. For this reason, STP 3 has relatively less of this type of data to inform analysis.
| STP case 1 (Blue) | STP case 2 (Green) | STP case 3 (Red) | |
|---|---|---|---|
| Strategic STP leadership | Four STP board meetings (8 hours) | One STP board meeting (1 hour) | Two project meetings (2 hours) |
| Project team 1 | Integrated ‘place’
|
Urgent care
|
Workforce development
|
| Project team 2 | Medicines optimisation
|
Mental health
|
|
| Project team 3 | Maternity and new-born project
|
CCG reconfiguration
|
|
| Total | 11 meetings (22 hours) | 14 meetings (22 hours) | Three meetings (5 hours) |
Documentary data collection
Data collection involved collecting a large number of documentary and online sources for each STP and project team. Documentary sources provided important contextual understanding for each case study to inform sampling decisions, as well as primary data about how system change processes were reported, from which aspects of organisational politics could be ‘read’.
Desk research was carried out for each candidate and selected STP case study sites. This involved the collection and review of online documentary resources and other publicly available materials, including:
-
public strategy documents
-
public information provided in websites
-
public information available in downloaded documents
-
organograms
-
public information videos.
When research access was secured, additional documentary information was requested from project leads, including:
-
project plans and proposals
-
logic models
-
meeting agenda and minutes.
Data analysis
Data analysis involved three complementary approaches that moved from ‘within’-case to ‘cross’-case analysis, and then re-engaging with the analysis that was undertaken in preceding WPs.
First, data from each case study STP and transformation project were analysed with the intention of producing individual case reports. As with earlier WPs, an empirically grounded and interpretative approach was followed. 86–88,95 Specifically, case study data were open coded and summarised by Justin Waring and Bridget Roe by identifying common and distinct features: project/service focus, project maturity, project team members and stakeholders, significant issues or controversies, observed or reported actions and interactions, and project outcomes.
Second, a ‘rich’ descriptive account was produced for each STP and subcase. Following Stake,89 case reports were organised to give (1) an entry ‘vignette’ to set the scene and provide relevant background information, (2) a narrative account of the case that described the people involved and issues addressed, (3) a detailed account of the key or defining issues of the case, and (4) assertions or interpretations of the account relevant to the study objectives. In preparing these case reports, the thematic analysis from the preceding interview study was used to inform analysis in terms of the ‘controversies’, ‘protagonists’ and, in particular, the types and forms of ‘skills, behaviours and practice’. Data analysis showed that each transformation project experienced a range of political controversies, but that each was defined by a small number of key controversies at different stages of the change process.
The third stage involved cross-case analysis with the aim of identifying and explaining common and unique features,85,90 specifically how certain types and patterns of political skill were used around particular controversies. Preliminary cross-case analysis involved comparative ‘process mapping’ to understand how each case evolved over time, comparing ‘where’, ‘when’ and ‘why’ events occurred, ‘who’ was involved and ‘what’ they did. 90 From this, a ‘composite’ synthesis was developed of the ‘system change processes’, building on the existing literature on major system change. 2 Each case report was then reanalysed to illustrate a significant controversy within this composite picture of system change (see Chapter 5, Figure 9). For instance, some case reports illustrate the political issues experienced earlier in project planning or prioritisation, whereas others illustrate issues experienced later in project implementation or closure.
Work package 4: co-design learning materials and resources
The purpose of WP4 was to co-design learning and recruitment materials that support the acquisition and development of political skill and astuteness for health-care leaders. WP4 involved a number of linked activities informed by the earlier WPs.
Activity 1: a review of the literature on the acquisition and development of political skill
Activity 1 was undertaken as part of WP1 and involved a review of the literature to identify and summarise research on the acquisition and development of political skill. The selected review papers were further analysed to identify and categorise the methods and approaches for supporting the acquisition and development of political skill. In addition, a manual search was undertaken of prominent textbooks and monographs on political skill and leadership development (that would have been missed in the earlier search). This resulted in a total of 24 research papers and five monographs. The review summarised the main methods of acquiring and developing political skill, the pedagogic features of these methods, and the reported positive and negative features in terms of delivery, experience and learning.
Activity 2: qualitative interviews with service leaders
Activity 2 was undertaken as part of WP2 and involved carrying out narrative interviews with health and care leaders to understand their experiences of acquiring and developing political skill over their careers. As reported above, 66 participants took part in these interviews, including 16 people who were undertaking or had recently undertaken formal leadership education or training. All participants were invited to reflect on significant learning events and situations, including formal training and more everyday encounters. Participants were also invited to offer recommendations for how future leaders might learn and develop these skills.
Activity 3: a pragmatic review of training and development literature
Activity 3 involved a pragmatic review of frameworks, tools and learning resources that are specifically designed to support the acquisition and development of political skill or related capabilities. This review involved a pragmatic search of well-established leadership development agencies, university courses, professional press and other leadership development frameworks.
The pragmatic review started by carrying out interviews with four experts in leadership development to discuss the emerging study findings and to understand how current leadership programmes address the theme of political skill. Informed by these interviews, an online search was carried out of health and care leadership development agencies, including the NHS Leadership Academy (Leeds, UK), The King’s Fund (London, UK), The Health Foundation (London, UK) and the Institute for Health Improvement (Boston, MA, USA), and the online archives of agencies, such as the NHS Institute for Innovation and Improvement (Coventry, UK). An additional online search was undertaken of commercial and non-commercial leadership development frameworks, including sources in the field of international development.
The identified frameworks, tools and resources were reviewed and categorised by Bridget Roe and Justin Waring, summarising (1) the express purpose of each tool or resource, (2) the originating source or underpinning theory, (3) key constructs about pedagogy or change, (4) the method of delivery and (5) the evidence base. Practical considerations were also recorded, such as the time needed for delivery, acceptability and actual or potential adaptation. A shortlist of candidate approaches and tools was created based on (1) the clarity and relevance of pedagogy, that is do they have a developed understanding or theory of learning; (2) alignment with the study’s empirical themes; and (3) feedback and recommendations from the preliminary workshops. The candidate list was then further reviewed and deliberated with study advisors in the light of the study findings.
Activity 4: workshops
Activity 4 involved facilitating a series of workshops to iteratively develop learning resources and materials. The workshops were initially planned to take place after the completion of data collection; however, following discussion with the study’s scientific committee, the workshops were configured to take place alongside the early WPs to inform the extrapolation of learning.
An initial set of three workshops was carried out in conjunction with WP1 to explore the perceived learning needs for health-care leaders to acquire and develop political skill and to consider how existing leadership programmes address these needs. An ‘educator workshop’ took place that involved seven people recruited through university networks, including representatives from Health Education England and the NHS Leadership Academy, three university-based providers of leadership education and two workforce development leaders from different NHS trusts. This workshop focused on the contribution of existing leadership development frameworks to service leaders’ acquisition of political skill. A ‘practitioner’ workshop was carried out with 12 health service leaders working in the area of quality improvement, who were recruited through a regional quality improvement network. This workshop explored participants’ understanding of organisational politics and recommendations about how political skills could be addressed in leadership development programmes. An ‘expert advisor’ workshop was carried out with four research experts (including organisational studies, public policy and management, and leadership research) and four relatively senior NHS executives to develop a greater understanding of the conceptual aspects of organisational politics and political skill. All three workshops were recorded and transcribed verbatim.
A fourth workshop was carried out in conjunction with WP2 to clarify the emerging analysis from the interview study. This workshop was organised as a dedicated session of a national Q Community knowledge exchange event. The Q Community is a network of people who are actively engaged in improving the quality of care services. It is supported by The Health Foundation, in conjunction with NHS England, and hosts various developmental events. The study team were invited to facilitate a workshop on ‘Harnessing Political Astuteness’ at a Q Community event on 13 November 2019. Nearly 60 delegates participated in the workshop, which explored their views about organisational politics, the impact on service improvement and how people can learn to use political skills in improvement work. These views were recorded through the use of flip charts, Post-It® notes (3M, Saint Paul, MN, USA) and other verbal summaries.
A fifth workshop was organised to review and appraise the shortlist of ‘candidate’ tools and resources that had been identified through the pragmatic scoping review of leadership development frameworks. Workshop participants included five specialists in knowledge exchange, capacity development and implementation science, who were recruited through the NIHR CLAHRC infrastructure. Participants were asked to review the identified tools and to consider their relevance and application to health-care services. Through this workshop, the candidate list of learning tools and resources was appraised, with recommendations offered on how the tools and resources could be adapted for use with health and care leaders. In addition, the workshop discussed the design, content and use of a complementary ‘workbook’.
A final series of four co-design workshops was carried out after the completion of primary data collection, which aimed to iteratively develop, pilot and appraise candidate learning resources and materials. Co-design has a relatively long history97 and has had a significant influence in health policy-making, research and service improvement. 98 In broad terms, this rests on the idea that the users and beneficiaries of a given service, product or research activity should be involved in its design, specification and application for it to be more meaningful, relevant and legitimate to these communities. 99 The four workshops were carried out with different learner communities or groups to understand whether they were better suited to different audiences or change agendas. Two workshops were organised with STP project teams (recruited following participation in WP3). One workshop was carried out with a regional Healthwatch organisation on the basis that the organisation explicitly aims to promote community and patient perspectives in decision-making. Furthermore, although being a recognised part of the health and care system, these organisations are unlike statutory care providers and, therefore, offer a distinct opportunity for testing the learning materials. In addition, one workshop was organised as an ‘open’ public invite for any person involved in managing or leading health service change, but without the expectation that participants would be working on the same change agenda; this, therefore, offered insight into whether or not the learning materials can be used by a heterogenous group. All workshops lasted 3 hours and were facilitated by study team members via Zoom (Zoom Video Communications, San Jose, CA, USA) because of the COVID-19 pandemic restrictions. Each workshop involved between 7 and 15 participants.
A structured co-design approach100 was used for the workshops, with clearly defined organisational groups working on discrete change projects, but not for the ‘open’ workshop. First, the project leads and other team members were invited to a pre-workshop planning meeting to discuss their learning needs, clarify their change project, share their preferences for the organisation of the workshop and identify any potential ‘sensitivities’ that should be considered. Second, the learning resources and activities were revised in accordance with the bespoke requests and feedback from project teams. Third, the learning tools and resources were delivered through the workshop. Fourth, immediately after the completion of the workshop, participants were invited to give feedback on the meaningfulness, relevance and application of the learning resources and tools to their change project. Finally, 2–3 weeks after the workshop, the project lead and other participants were invited to give further reflective feedback on the relevance and use of the materials for their ongoing activities. The ‘open-invite’ workshop did not involve the pre- and post-workshop activities because participants were not working on a shared project, but participants were invited to give immediate feedback.
Activity 5: recruitment workshop/interviews
The final activity involved carrying our four semistructured interviews with people working in NHS human resources (HR) management and talent management. The interviews explored how current recruitment practices assess the political skills of applicants for employment or promotion. This included further appraisal of the study findings and candidate learning resources, with recommendations for how the tools and resources could be adapted for use by HR managers, that is as selection tools or situation-based activities to assess candidate understanding of organisational politics. This led to the development of a question topic guide for use during recruitment interviews.
Research ethics approvals
The study received favourable ethics approval from the University of Nottingham Research Ethics Committee (Business School Committee).
Project oversight
The study team was supported by a Scientific Steering Committee, which was chaired by Dame Stella Manzie. The committee met at three time points to coincide with the three initial WPs, but the final meeting was cancelled owing to the COVID-19 pandemic. Members of the committee provided critical insight and guidance at other times to support recruitment and methodological challenges.
Public and patient involvement
The project was supported by a PPI group, which was co-ordinated by Clare Ramshaw with the support of Anthony Chuter. In particular, both provided ongoing advice and guidance from study design to writing up, meeting with members of the research team on a regular basis, and also contributed to the Study Scientific Committee. The study was also supported by a wider network of representatives from community and third-sector organisations to help with the translation of study findings and development of learning resources. This included, for example, a regional Healthwatch organisation and volunteer groups in the area of mental health. As noted above, there was not extensive PPI involvement in data collection and analysis. This was because the primary focus of the study was on the experiences and practices of service leaders or those involved in implementing change, and the study found that public and community groups had limited involvement in leading or contributing to such change processes. In most cases, such public involvement was limited to ‘official’ or ‘designated’ public advisors, most of whom were involved in the study as interview participants. As described above, public involvement in WP5 was also facilitated through the facilitation of a public co-design workshop and through organising a co-design workshop with a regional Healthwatch organisation.
Conclusion
Notwithstanding the significant recruitment difficulties and the challenges brought about by the COVID-19 pandemic, the majority of the planned research activities, as set out in the study proposal, were completed. In total, the study reviewed over 100 articles; carried out 138 semistructured interviews; carried out qualitative research with three STPs, including eight (of nine) in-depth case studies of system change; and engaged 112 people in workshop activities. The limitations of the study are reviewed in Chapter 7, together with recommendations for future research.
Chapter 3 Narrative synthesis of research on political skill as applied to health and care services
Parts of this chapter have been reproduced from Clarke et al. 101 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Introduction
This chapter addresses the research objective to identify key theories and frameworks on political skill and related concepts, and to understand how these have been, or could be, applied to the analysis of change in health and care systems. This took the form of two linked narrative reviews that provided the theoretical and empirical foundations for subsequent research. As described in Chapter 2, the first review was a ‘review of reviews’ to describe the main theoretical perspectives, clarify conceptual debates and constructs, and specify available methods for researching political skill. The second review applied the learning from the first review to the health services research literature to understand how existing theories and concepts have informed health services research and to identify potential outstanding research questions for future study. This second review has since been published and this chapter draws on this publication. 101 The chapter presents the main findings from each review.
Review 1: political skill – a review of reviews
The purpose of the ‘review of reviews’ was to identify and synthesise the main frameworks and theories of political skill and the associated concepts; to clarify the empirical, conceptual and theoretical assumptions on which these frameworks are based; to understand how political skill can contribute to organisational change; and to identify potential gaps within or extensions to the existing literature.
Review findings
Conceptual terms and definitions
For the majority of review papers (i.e. 12/18), the concept of ‘political skill’ is associated with the research of Ferris et al. 53 who define this as:
[T]he ability to effectively understand others at work, and to use this understanding to influence others to act in ways that enhance one’s personal and/or organizational objectives.
Ferris et al. 53
A range of extensions to this concept are described in the form of generalised traits or developed attributes, which provide the analytical constructs for observational and experimental research. 43,53,57,102–112 For example, Perrewé et al. ,104 collaborators of Ferris et al. ,53 offer a variation of the above:
Political skill is characterized by social perceptiveness and the ability to adjust one’s behavior to different and changing situational needs to influence others.
Perrewé et al. 104
Political skill is typically described as a form of interpersonal influence that is distinct from, but may overlap with, more formal forms of influence and authority. 53 As discussed below, the dominance of this conceptualisation is significant because it stems from a particular approach to studying organisational politics largely informed by small-group psychology.
For many reviews, the concept of ‘political skill’ was framed by a particular understanding of ‘organisational politics’ that is largely derived from the seminal works of Cyert and March,36 Pfeffer38 and Mintzberg. 40 These authors have contributed to the idea that organisations can be seen as ‘political arenas’ in which actors engage in political ‘games’ to obtain their self-interested goals or interests. 39 Pfeffer37 describes political skill less in terms of skills and abilities, and more in terms of the use of ‘strategies’ to control agendas, build coalitions and use experts; the use of ‘language’ to persuade others; and the control of ‘resources’. 37
Although ‘political skill’ is the most frequently cited term, a number of other concepts are also used to describe how organisational leaders, or other change agents, affect change in the context of organisational politics. These include ‘social astuteness’, ‘impression management’, ‘emotional intelligence’, ‘social learning’ and ‘political will’. 43,112 These represent complementary concepts, but the reviews consistently described these as distinct from ‘political skill’. The variety, frequency and influence of these different terms within the literature is significant because it suggests, first, that the research field does not have clear boundaries and, second, that there remain important theoretical differences underpinning the literature. It might be suggested, for example, that concepts centring on the term ‘skill’ tend to emphasise personal attributes or capabilities, those dealing with ‘will’ are concerned with motivation or intent and those dealing with ‘intelligence’ suggest a higher-order quality associated with learning towards more developed capabilities. There is an important conceptual distinction between skill and capability (in terms of potential) and behaviour and action (in terms of enactment), which often varies according to the context or situation.
Such terminological and conceptual differences are described by Manzie and Hartley,113 for whom terms such as political ‘savvy’, ‘nous’ and ‘antennae’ describe the skills, knowledge and judgements exercised by leaders when dealing with stakeholders' competing preferences, agendas and interests. This review offers an alternative to the Ferris concept53 of political skill and goes beyond a focus on individual attributes to more explicitly recognise the interplay between individual and context. Manzie and Hartley113 offer the concept of ‘political astuteness’ as:
. . . a set of skills, knowledge and judgements about the interests, goals and values of stakeholders and how to exercise leadership in ways which take account of diverse and competing interests among stakeholders.
Manzie and Hartley113
The terms ‘political skill’ and ‘political astuteness’ have similarities. It might be suggested that the term ‘astuteness’ emphasises attributes and qualities that are associated with an individual’s perceptive understanding, awareness and insight about a given ‘political’ context and their ability to operate and effect change in this environment, whereas ‘skill’ could be viewed as focusing more on an individual’s abilities or competencies to effect change.
Disciplinary and theoretical perspectives
Few of the review papers were explicit about the underpinning disciplinary or theoretical perspectives. In most cases, this was inferred from the wider literature cited in background sections of the reviews or from the journal publication title. The majority of review papers are located within the broad field of social psychology, work psychology, organisational psychology and management science (17/18). Some reviews were located in the broader field of ‘organisational behaviour’, with overlaps to other disciplinary influences, such as sociology, politics and philosophy. 112,114 Some made reference to the field of ‘leadership studies’, especially when leaders’ use of political skill was contrasted with notions of charismatic, transformational and distributed leadership. 57,115 A more recent strand of research has applied the concept of political skill to the disciplinary field of ‘public policy and management’, expanding the focus to include wider contextual issues. 73,113 An unexpected finding, and one that is particularly relevant to this study, is that a highly general and untheorised concept of political skill has been used within the field of ‘nursing studies’ for over 40 years and predates the more recent upsurge of interest in organisational psychology and management science. 102,116
Constructs, dimensions and traits
All reviews described political skill through a range of constructs, dimensions and traits. As noted, the majority utilised the multidimensional framework of ‘political skill’ developed by Ferris et al. 53,57 This conceptualises political skill along four dimensions:
-
social astuteness – being diligently observant of others and keenly perceptive of even subtle social situations and, thus, adjusting their behaviours accordingly72,107
-
interpersonal influence – the ability to produce desired changes in other people through using a subtle, convincing style to exercise influence103,107,117
-
networking ability – access to information, resources and other assets based on a person’s social networks and relationships, including the ability to identify and build relations with other people with useful resources and to build connections among others107
-
apparent sincerity – perceived as possessing a high degree of integrity and sincerity to the extent that individuals trust them because their actions are not perceived to be manipulative. 72,107
These dimensions provide the foundational constructs for many empirical studies, which, in most cases, involve quantitative measures (surveys) of individual political skill, which are then analysed to demonstrate associations and corelations with various individual, group and organisational outcomes.
The concept of ‘political astuteness’, as proposed by Hartley et al. ,73,113,118 offers an alternative to the work of Ferris et al. ,53 including the following dimensions:
-
personal skills – to exercise self-awareness and self-control
-
interpersonal skills – to influence the thinking and behaviours of others, even in the absence of formal authority
-
reading people and situations – to think about the dynamics that can occur when stakeholders come together and recognising wider social systems and processes
-
building alignment and alliances – promoting collaboration or alignment when there are different interests and motives
-
strategy direction and scanning – having a sense of the organisation’s purpose and thinking about the long-term factors that may affect the organisation.
The review also found that many papers use a number of more generalised or unspecified terms, phrases and concepts to elaborate the features of political skill,43,102,106,113,119,120 and, although these can, to some extent, explain or extend the dimensions provided by Ferris et al. ,53 few were really linked to a specific theoretical construct. The more common terms are mapped onto the Ferris constructs (Table 7).
| Social astuteness | Interpersonal influence | Networking ability | Apparent sincerity |
|---|---|---|---|
| Affable | Able to influence others | Has own resource supply (something to offer) | Humble |
| Handles stress well | Manipulation | Proactive | Trustworthy |
| Identifies opportunities | Empowers subordinates | Perseverant | Accountable |
| Adjusts behaviour to fit in | Goal-setting | Cognitive and social capital | Disguises personal motives |
| Reads others and interactions well | Use of unobtrusive power | ||
| Self-confident | Persuasion | ||
| Understands needs of others | Mastery over others | ||
| Uses social environment for own and organisational goals | |||
| Uses less emotional expenditure | |||
| Self-motivated | |||
| Resilient | |||
| Hardy |
Mechanism and outcomes
All reviews tend to describe political skill as making positive, sometimes necessary, contributions to the implementation of strategic change. Much of the literature applies the Ferris et al. 53 constructs to predict and explain variability in individual, group or organisational performance. A preliminary observation is that all reviews describe (or assume) ‘political skill’ as being an attribute or quality of an individual, which is used or enacted through their interactions with others. Although this body of research recognises that interpersonal influence is often manifest through group dynamics, the primary analytical focus is on the individual and their capacity or skill to enact this influence, rather than the wider group dynamics. For this reason, the mechanisms of change are grounded ‘in’ the individual and realised ‘through’ their interpersonal relationships with others. However, few reviews explain the interaction between these causal properties or attributes, for example how ‘interpersonal influence’ relates to ‘networking ability’. In seeking to clarify or develop a heuristic model, it could be suggested the Ferris et al. 53 concept offers a more linear view of the dimensions of political skill (Figure 2), which can be summarised through the following propositional logic:
-
Heuristic proposition of political skill53 – to enhance one’s personal or organisational objectives through influence with others requires (1) social awareness to understand opportunities for change and to develop a realistic plan, in which actors can use (2) networking abilities to access resources and information in support of this plan, alongside their use of (3) interpersonal influence to realise the implementation of their plan, while at same time presenting their (4) apparent sincerity to ensure that people do not feel that they are being manipulated.

The Hartley et al. 52,113 concept of political astuteness offers a different propositional logic and a more dynamic view of how the dimensions of political astuteness interact and contribute to how a person seeks to understand and align interests (Figure 3):
-
Heuristic proposition of political astuteness – to achieve the desired outcomes through aligning diverse interests and securing consent requires (1) strategic direction and scanning to understand and articulate the organisation’s strategic goal, and in parallel (2) the ability to read people and situations to understand the barriers to and drivers of change, which then informs (3) the use of interpersonal influence and (4) the ability to build alliances to realise strategic goals, while drawing on (5) personal skill to manage the perception of others.
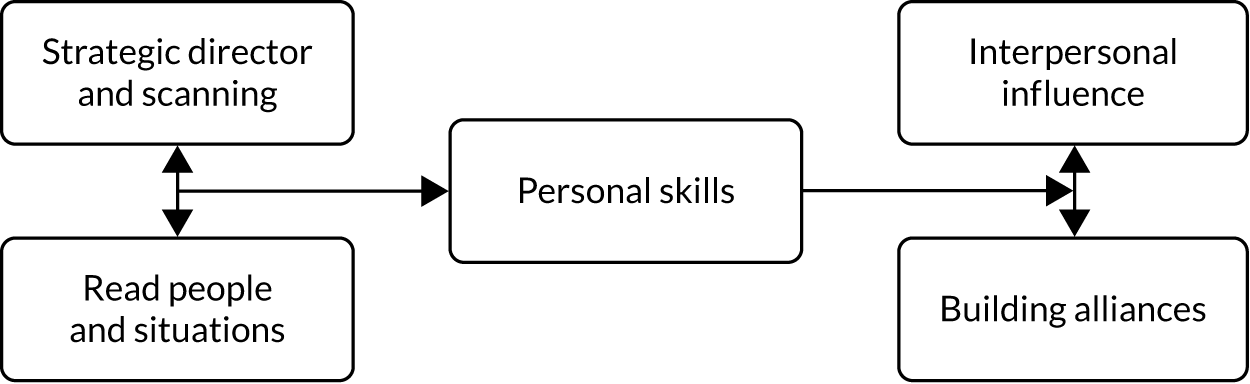
A number of reviews describe aggregated statistical associations and correlations between measures of political skill (as an independent variable) and different individual, interpersonal or organisational outcomes (as dependent variables). For example, individuals ‘high’ in political skill experience the following effects/outcomes:
-
high levels of team cohesion and team success120
-
trust and confidence in others120
-
interactions with enthusiasm and confidence110
-
positive and high levels of job performance/success (but not salary)43
-
high levels of job satisfaction110
-
low levels of workplace stress43
-
affects teams through evaluating and planning activities, uses effective communication, manages conflict and facilitates group cohesion111
-
enhances both leaders and followers, leading to better outcomes. 112
At the individual level, the reviews suggest that those with high degrees of political skill tend to have higher levels of self-efficacy, job satisfaction and career success and lower levels of stress. 57,102,107,114,120 The reviews also show that political skill is self-perpetuating, so that those individuals successful in using their political skill become more successful and continue to use these skills. At the interpersonal level, the reviews show that those with high degrees of political skill are more capable of influencing and persuading others. 43,109,110,113 This influence is manifest, for example, through the ability to create and articulate a vision, motivate others, build trusting relationships, win the confidence of others, foster positive and high-quality relationships, mobilise rewards and incentives, negotiate differences and manage conflict. 102,110,113 Interpersonal influence produces advantage for the individual with political skill, and is shown to contribute to both group and organisational performance. At the group or team level, the review papers show that those with high degrees of political skill tend to be able to foster team cohesion and strong interpersonal relationships, especially through articulating shared goals, managing interpersonal conflict and supporting team development. 102,106,110,113
A relatively small number of reviews make reference to the contexts within which political skill is situated. 102,113 The majority of studies appear to draw on data from the private sector, or they do not state the specific context, but these rarely elaborate the particular contextual features or how these vary between sector or business. The exception to this is the literature on ‘political astuteness’ that looks at civil servants,54,113 and also Montalvo,102 who explores the health-care setting through the political skill of nurses. In summary, the literature tends to describe political skill or associated terms as a highly individualised set of traits and qualities that are enacted through interpersonal influence to affect change around individuals, groups and organisations.
Discussion
The ‘review of reviews’ found that political skill, as defined by Ferris et al. ,53 is the predominant concept for describing how individuals influence others and implement change in the context of organisational politics. The Ferris et al. 53 concept comprises four well-developed and empirically validated constructs (social astuteness, interpersonal influence, networking ability and apparent sincerity) that provide the basis for a large body of research, and is positively associated with different individual, interpersonal, group and organisational outcomes. The literature tends to present political skill, as informed by Ferris et al. ,53 as highly individualised skills, attributes or traits that are manifested through interpersonal relationships. 53 In contrast, research on political astuteness offers an alternative conceptualisation, especially for addressing the interplay between the individual and their context, moving beyond internalised skills to think more about the relational behaviours and forms of influence. 113 Furthermore, the vast majority of primary sources described in the reviews were quantitative in design,107,110,121 involving statistical analysis of an individual’s degree of political skill in relation to team and organisational performance. 111 Some reviews do refer to qualitative interview studies, but few offer detailed ethnographic studies, with the exception being the textbook by Buchanan and Badham. 41
Through this ‘review of reviews’, we identified a number of conceptual features from which there is potential to develop additional and complementary lines of analysis. First, it is important to disentangle the idea of skills and capabilities (as a form of ‘potential’ residing within individuals) from behaviours and actions (as enacted skill in a relational or social context). The existing literature seems to conflate these two aspects so that political skill is seen as both the underlying capability for influence and, simultaneously, the behaviour of influence. Moreover, skill or capability is largely described as residing within the individual, whereas the behaviours and actions are typically manifest through interaction in the given context. Arguably, these represent subtly different aspects of the broader phenomena of engaging in organisational politics.
Second, it is important to develop a more interactional and contextual understanding of political skill and behaviour as being manifest through interpersonal relationships. Much of the existing literature seems to present a unilateral view that ‘Person A’ (with political skill) exerts influence over ‘Person B’ (without reference to their political skill). However, it is important to recognise that all actors will have some form and degree of political skill and all will be influencing one another throughout their interactions, whether intentional or not. This suggests a more dynamic and interdependent notion of political skill and interaction, in which the moves and counter moves of different actors shape the political environment. More significantly, however, it could be argued that the unit of analysis could be extended beyond the individuals and their skills to the relationship between individuals and groups.
Third, and stemming from the above, the enactment of political skill and behaviour is inherently situated and context specific; this is something that the identified reviews appeared to overlook. For this reason, in one encounter a person may appear to have high degrees of political skill and behavioural influence over others, but in other situations the same person may appear to have relatively limited forms of skill and influence, either because the situation presents different challenges or because the people in this particular situation have greater levels of skill than those in the previous situation. In other words, a person’s political skill is relative to the relational and situational context. Taking this line further, it suggests, therefore, that when analysing political skills and behaviours, perhaps more attention is needed to the context and relational dynamics than to the individual.
Review 2: political skill and health service change – a narrative review
The purpose of the second review was to understand how the concept of ‘political skill’ or the associated concepts are used in the health services research literature to analyse and explain the implementation of organisational and system change. Unlike the above ‘review of reviews’, this review was inclusive of primary sources and was not limited to review papers. It was acknowledged from the outset, however, that, although many studies talk explicitly about ‘health-care politics’ and ‘organisational politics’, they are often less explicit about the concept of ‘political skill’. For this reason, a challenge in conducting this review was determining whether research was dealing with political skill or related concepts, or the broader phenomena of organisational politics and power.
Review findings
Summary of the literature
The review found that the health services research literature is structured along four lines when deploying the concept of political skill, each reflecting different policy and professional contexts that have been the focus of research over the last four decades (Table 8).
| Domain | Time period | Papers (n) | Definition of political skill | Main methods | Empirical topics and themes | Interpretative analysis |
|---|---|---|---|---|---|---|
| Nursing | 1970–2017 | 35 |
|
Conceptual, surveys, some interviews, some ethnographies | Focus on nurses developing and using political skill or astuteness to secure greater influence in an organisation, or more often to engage and have influence in legislative process | The concept of political skill linked to the macropolitics of the nursing profession, especially the professionalisation and politicising agendas of US nursing. Some focus on workplace informal politics |
| Health-care managers | 1979–2018 | 9 |
|
Conceptual, surveys, some interviews | Focus on how hospital managers (can) use political skill or other forms of interpersonal influence to implement organisation change, with some attention given to external policy relations | The concept of political skill linked to the informal politics of organisational change and broader politics of management reform, especially the difficulties of managing change in contexts of professional resistance |
| Other health professionals (physicians and including public health) | 1991–2017 | 13 |
|
Conceptual, surveys, interviews | Focus on how non-nursing professionals use political skill to influence organisation of work, especially in policy-making processes, and through the professional leadership acting ‘politically’ | The concept of political skill seems to have been transferred from nursing with a focus on interpersonal influence or macroinfluence on policy processes, dealing with professional dominance and more often influencing policy decisions |
| System leadership | 1998–2016 | 5 |
|
Surveys, interviews, ethnographies | Focus on how system leaders understand and manage competing interests in the implementation of large-scale system change | The concept is aligned closely with ‘system leadership’ and reflects broader shifts in analysis from managers to leaders and a single organisation to a system |
Emerging in the 1970s, the first literature domain deals with nurse leaders’ use of political skill when seeking to influence formal policy processes. 116 This literature reflects broader goals to enhance the professional status of nursing. From the 1980s, the second literature domain deals with the use of political skill by health service administrators, managers and leaders in the implementation of organisational change. This literature coincides with the broader managerialisation of health-care services throughout the 1980s, and shows growing influence of theories derived from management studies. 122 Earlier articles utilise a general and untheorised concept of political skill, but from the 1990s papers draw more explicitly on the work of Ferris et al. 53 The third (more dispersed) literature domain deals with the use of political skill by other (non-nursing) sections of the health-care workforce in the implementation of change. 123 This mirrors earlier research in nursing, and over time the work of Ferris et al. 53 again becomes more prominent. The fourth, and more recent, literature domain deals with the use of political skill in the context of current debates on ‘system leadership’. 22 Various concepts aligned with political skill are used in this research, rather than political skill itself, describing how leaders work with the competing interests of multiple stakeholders located within and across different organisational and occupational boundaries. This thematic review does not emphasise any particular prior theorisation of political skill, but does acknowledge when included research papers do draw on a particular conceptualisation.
Thematic analysis
Personal performance
A small number of research papers describe political skill as a form of personal competency and self-efficacy that is strongly associated with enhanced personal performance and career development. 102,124–127 These tend to focus on nurse administrators and leaders and use a relatively generalised (non-defined) notion of political skill, but over time this line of research has been increasingly informed by the work of Ferris et al. 53 For example, Montalvo’s102 integrative review of the nursing literature describes political skill as a form of personal mastery for navigating interpersonal relationships and influencing group dynamics in the workplace. This is associated with personal resilience, accumulated influence and career progression. The theme of resilience, coping and survival in the face of competing interests is also discussed in the parallel literature on hospital managers. Taylor124 describes the importance of managers’ self-awareness or knowing one’s capabilities in the context of prevailing lines of power. Similarly, Young126 describes the importance of laboratory managers developing personal routines and political styles to deal with the political behaviours of others. Whitman et al. ’s128 surveys of nurse supervisors found that political skill can act as a self-regulatory mechanism to discourage supervisors from adopting assertive and abusive behaviours. This theme, therefore, deals with the personal and psychological aspects of political skill, showing how these relate to other forms of interpersonal and organisational influence when implementing change.
Contextual awareness
A substantial theme within the literature describes political skill in terms of health service leaders’ ability to understand the prevailing ‘political context’ of their service environment. 123,124,129–132 Three linked aspects of such contextual understanding are described. The first is to understand the prevailing ‘lines of power’ manifested among different stakeholders, especially understanding the influential or dominant groups. 123,124,132 The second describes leaders’ ability to understand the underlying interests or motivations of these groups. 124,130 As an example, Taylor124 considers how health managers must engage with the interests of wider community groups, especially when building networks around a change agenda. The third aspect is to determine how best to respond to or manage the prevailing political context when seeking to implement change, that is to draw support from some groups and manage the resistance of others. For instance, Berger129 examines the need for social workers to gain awareness of power and politics within a hospital organisation to exert influence over patient management, particularly during discharge planning.
As above, research before the 1990s offers a relatively atheoretical, descriptive view of nurse leaders’ and hospital managers’ ability to ‘read situations’ and assess ‘lines of power’, whereas more recent research is more explicitly informed by Ferris et al. ’s53 idea of ‘social astuteness’ or similar concepts of ‘situational awareness’ drawn from the public management and organisational psychology literature.
Interpersonal influence
Nearly all studies describe political skill as involving interpersonal influence, but this is especially the case for those articles that deploy the Ferris et al. 53 concept. 102,132 These papers tend to focus on a given person’s ability to use particular interpersonal skills to influence others in a given change context. For example, Smaltz et al. 132 discuss how chief information officers need to use ‘political savvy’ in terms of their ability to ‘negotiate, influence and persuade’ colleagues to engage with new information technologies. Interpersonal influence is described in a number of slightly different ways, such as persuasion, negotiation and coercion. 102,123,133,134 However, studies rarely elaborate or theorise the specific types, features or boundaries of interpersonal influence.
The more recent literature on ‘system leadership’ highlights the importance of transformational and distributed leadership when seeking to influence others. Turner et al. ’s22 study of major system change describes the importance of balancing an assertive or directive approach with an inclusive and delegated approach as two complementary approaches to interpersonal influence. 22 Although this literature focuses on different occupational relations (e.g. managers influencing doctors) and contexts (e.g. the implementation of information technology innovations), the underlying conceptualisation of interpersonal influence tends to treat it as an individual skill or ability, rather than a shared collective or occupational quality.
Stakeholder engagement and network building
The literature describes political skill as a broader form of stakeholder engagement and network building. This is associated with the ability to understand and mediate stakeholders’ competing interests to engage them positively with a given change agenda. McAuliffe et al. ’s135 study of health system change highlights the importance of stakeholder engagement as an element of more general change management activities, in which health-care leaders need to clarify the purpose, scope and timing of change in ways that align with the prevailing expectations of stakeholders. It also relates to the more general literature on the importance of communication strategies, but, again, the literature is very general in its description of these engagement and communication strategies, offering little in the way of detail on style or techniques that might be used with different professional groups. Mateo et al. 134 and Rafferty and Traynor136 describe the importance of nurse leaders’ information processing (and stewardship), especially for communicating national policy changes in local service contexts. Wilber and Coberly137 similarly describe the importance of doctors’ different communication skills when working with internal and external stakeholders. Turner et al. 22 also highlight the importance of using information systems and feedback loops to maintain stakeholder engagement during change processes.
The ubiquity of communication and engagement strategies in health-care management in general, and change management in particular, might account for the relative lack of empirical detail in the literature. Although the wider health services research literature shows growing sophistication in its analysis of communication strategies, it is not explicitly associated with political skill. More recent research further demonstrates the importance of building networks and alliances at the interorganisational level in the context of system change22,124,138 and the associated challenges of aligning competing interests across organisational or sectoral boundaries. This includes reconciling differences both among health-care organisations, such as in the centralisation of stroke services,22 and, increasingly, among health and social care organisations. 129
Influence on policy processes
Finally, and extending beyond the organisational arena, a significant early strand of research describes how political skill can facilitate improved influence on formal policy processes. 139 This is exemplified by the seminal work of Clark116 that set out an operational definition of nurses’ ‘political astuteness’: their participation in formal democratic voting processes, membership of political bodies, understanding of formal political institutions and processes, and use of channels to engage in policy decision-making. This research seeks to advance the professional status and position of nursing, vis-à-vis other professional groups in policy-making processes. Subsequent research has developed the work of Clark,116 such as Byrd et al. 140 who use the Political Astuteness Inventory to examine nursing students’ awareness of policy processes, and outside nursing, Wilber and Coberly137 examine how gerontologists use political astuteness to advocate for more engagement in legislation and policy. Significantly, this literature talks of political skill as a form of ‘upwards’ influence on formal policy processes, rather than influence in more local organisational processes.
Discussion
The review found that over the last four decades concepts such as political astuteness, skill and savvy have been most applied and developed within the nursing field, including notable conceptual articles that predate much of the organisational studies literature116 and review articles that summarise nurses’ use of political skill to influence policy-making and organisational change. 102,139 Looking beyond nursing, the concept of political skill is used to describe how hospital managers, other health professionals and, more recently, system leaders seek to introduce organisational or interorganisational change. 134 What unites many, but not all, of these studies is the idea that leaders need to develop and deploy political skill because of the perceived dominance of other health-care professionals, who are often presented as resistant to change. Sometimes, political skill appears to be a strategy to counter the informal ‘power’ of the medical profession.
The review also showed how the conceptualisation of political skill and associated terms within the health services research literature vary considerably and that there is limited definitional or conceptual agreement. Much of the earlier research, especially in nursing, uses terms such as ‘political astuteness’ and ‘political skill’ in a largely descriptive and generalised way with limited theoretical underpinning. 116 Subsequent research has been enhanced by concepts drawn from management studies, but it is only with the later use of Ferris et al. ’s53 concept that a clear and distinct concept of political skill has informed research. 102,131,139 For this reason, there is a noticeable shift from a relatively ‘loose’ descriptive concept to a ‘tight’ analytical concept. Although this shift results in enhanced descriptive and analytical clarity, it risks marginalising certain aspects in favour of others. The five aspects of political skill presented in this review (personal performance, contextual awareness, interpersonal influence, stakeholder engagement and network building, and policy influence) are directly comparable to the work of Ferris et al. ,53 but they also highlight factors beyond individual skills in ways that more explicitly address the wider organisational context of health-care services. 53
The review also found that the research evidence underpinning these different conceptualisations varies considerably. There is more descriptive evidence on the importance of leaders’ ‘contextual awareness’, ‘stakeholder engagement’ and effective ‘communication’. However, the evidence base appears relatively underdeveloped for ‘interpersonal influence’, especially as there is little empirical or analytical detail about the form of this influence beyond relatively general accounts of negotiation, persuasion and coercion.
As with the wider social science literature, the health services research literature rarely explores the interconnections between the different aspects of political skill. For instance, individuals’ use of ‘stakeholder engagement’ appears to be collapsed alongside building ‘networks and alliances’; however, these might better be thought of as two related, but distinct, processes that require different skills. Even those studies that drew explicitly on the framework of Ferris et al. 53 tended to treat the different dimensions of political skill as relatively discrete variables, with only a small number of papers elaborating the interconnections between the constituent parts of political skill. One example is Montalvo’s102 integrative review that shows political skill as operating first through ‘the self’, then through influence on ‘others’ and then on the performance of the ‘organisation’.
This review provides a foundation for exploring the connections, relationships and dependences between these themes in the form of a more integrative conceptual heuristic (Figure 4). Specifically, the literature suggests a close connection or interplay between ‘personal performance’ and ‘contextual awareness’, in that leaders need to effectively understand their own skills and capabilities relative to existing lines of power. This provides the orientation and basis for ‘interpersonal influence’, in terms of understanding who to influence and how to influence them. In turn, such influence extends from the individual to the group level through ‘stakeholder engagement’ and, in parallel, ‘network building’, which provides the basis for co-ordinated and collective ‘organisational change’, often in the context of opposition. Moreover, stakeholder engagement and networking can provide positive feedback loops for enhancing interpersonal influence with other stakeholders. Finally, and somewhat tangentially, the literature also suggests that leaders can also seek to use political skill to engage in more formal ‘policy influence’, perhaps to reinforce the more informal forms of political skill.
It is important to acknowledge the wider health services and social science literature that describes the micropolitics of health-care organisation and delivery, but which was not included in this review because it rarely deploys the concept of political skill, or an associated term. This includes, for example, a long tradition of research on the negotiated order of health-care organisation that focuses on the interactive dimension. 69,141–143 In addition, more critical and interpretative perspectives bring to the fore the influence of prevailing structural interests and ideological forces on the local manifestations of change, such as the divergent agendas around professionalism and managerialism. 16,56 Importantly, this literature demonstrates the importance of looking beyond individual skills and capabilities to understand the social and cultural context of ‘political action’, together with more explicit recognition of the structural inequalities that frame organisational politics related, for instance, to issues such as profession, gender, ethnicity or class. As such, a significant limitation of this review was the exclusion of many seminal and influential texts in the field of health-care policy and politics, such as Alford’s Healthcare Politics17 or Klein’s The New Politics of the NHS: From Creation to Reinvention. 144
FIGURE 4.
Conceptual heuristic of political skill derived from the narrative review.

Second, the relational dimension recognises the limits of taking an individualised approach and, by implication, directs attention to the collective dimensions of organisational politics and political action. Although individuals might have certain forms and degrees of political skill (following the dominant Ferris et al. 53 approach) from which to effect change, it might be suggested that in complex organisations and systems the range of political challenges and conflicts that have an impact on the implementation of change will require more than the skills and competencies of a given individual. That is, they are likely to need groups of people with complementary skills and abilities. Moreover, change processes occur over time and space, involving multiple interlinked stages. For this reason, it is more likely that multiple actors with complementary skills or abilities will be involved in implementing change, as suggested by research on social movements. 10,145 In other words, there is a need to move beyond the focus on the individual change agent or transformational leader to think about more distributed forms of political skill and action. 22
Third, a more relational and social view of organisational politics highlights the idea that political activities are structured or organised according to shared (and divergent) cultural meanings, norms and beliefs. These ideas represent an important departure from mainstream thinking on political skill, because they bring to the fore the idea that people engage in organisational politics from different positions of status and power. 63 Therefore, for example, some groups within an organisation may be relatively privileged by formal authority or professional background, which conditions both the need to act politically and what type of political actions they might take. Those that are less privileged by the established order might have a different need or inclination to act politically and might also need to use certain skills, or rather strategies, because of their particular access to resources, roles or relationships, which are a reflection of their social position. 26 As such, there is a need to look beyond the political skills of individuals, to understand the political actions and interactions of people who are embedded in broader fields of social relations and inequality.
Fourth, the mainstream approaches to political skill tend to suggest that people use their skills to influence others with the aim of obtaining their self-interested goals, often in terms of career enhancement, personal status enhancement or group performance. Within the health services research literature, there is greater appreciation of the way that political skill might stem from professional interests in the context of service change. 16 However, there is relatively limited appreciation that political skill or political action might be shaped by deeper, even subconscious, beliefs, interests and agendas. In the health and care sector there has been longstanding interest in the relative power of professional groups within the division of labour, in which attempts to promote or resist change have been interpreted as strategies to articulate deeper collective interests. 66 As noted above, such studies talk indirectly to the idea of political skill or practice, but nevertheless surface the underlying dynamics of power that shape care services. Extending this line of thinking, greater attention is needed to connections between individual or collective political action and the interests and agendas that inform or guide them.
Finally, the reviews show that almost all of the existing literature deals with political skill at the intraorganisational level. Within the wider social science literature, there is a tendency to focus on what might be termed ‘office politics’ between workers. The seminal work of Pfeffer38 and Mintzberg40 locates political skill in a context of broader strategic change and, further still, Hartley and Fletcher54 locate political astuteness in the context of political systems. However, there is a paucity of research dealing with political skill at the interorganisational or system level. This is highly relevant to contemporary health and care reforms that seek to reconfigure the organisation and delivery of care at the ‘system’ level. Furthermore, when change is planned or occurs outside formal organisational authority structures, as in the case of system change, social actors often need to draw on interpersonal influence or political skill to realise change in the absence of formal role authority. For this reason, system change offers an important site for developing new theoretical understanding of interorganisational politics and political practice.
Chapter 4 Narratives of political skill, strategy and action
Introduction
This chapter reports the findings of the narrative interview study that investigated the perceptions, experiences and reported practices of acquiring and using political skill in the implementation of health and care system change. This chapter describes the types and forms of political skill or, as explained below, the ‘skills, strategies and actions’ used by leaders in the context of different change agendas, and the experiences of acquiring and developing political skills are reported in Chapter 6. The interview study was informed by the findings of the preceding literature reviews described in Chapter 3 and focused on a number of underdeveloped issues. First, how participation in organisational politics involves context-specific strategies and dynamic forms of (inter)action over and above individual skill or capabilities. Second, how political strategies and actions are conditioned by actors’ social position within the wider structures and cultures of care organisations. Third, how organisational politics could be manifest through group actions as much as individual behaviours.
Narratives of political skills, behaviours and actions
In excess of 100 detailed stories were provided, covering a range of prominent reform agendas, including microlevel changes in care delivery (e.g. new technologies and roles or teamwork arrangements); workforce reconfiguration and service transformation (e.g. staffing/rostering changes, care pathway design or ward management); organisational or management change (e.g. budgetary planning, strategic development and culture change); interorganisational system transformation (e.g. integration projects between health care and social care); and changes associated with macrolevel policy or regulation (e.g. commissioning and dissolution of Strategic Health Authorities).
Although there were substantive and stylistic variations between participants’ narratives, a number of common features were identified. As a result of the types of interview questions asked, narratives tended to focus on a given event or change process that was in some sense regarded as controversial. The terms ‘controversial’ and ‘controversy’ are used to highlight how health-care ‘politics’ is commonly described in terms of differing views and preferences of stakeholders, rather than the inherent features of a given change agenda. To illustrate, a quality improvement initiative in one setting could be seen as uncontroversial because all people shared the view that it is important, whereas the same intervention in another setting could be controversial because people hold divergent views, which might reflect deeper fault lines or agendas of this workplace.
When introducing a given controversy, participants would ‘set the scene’ by describing the local political landscape in terms of the prevailing authority structures, lines of power, professional agendas and organisational priorities. This scene setting was important for identifying the underlying sources of influence and power, as well as the local cultures that conditioned a given change process and shaped responses to change. When elaborating the substance of the event, participants usually focused on the actions (or roles) played by key people or protagonists who held competing preferences and agendas, and which guided their actions, interactions and reactions. These preferences and agendas could be a source of both cohesion and discord in the sense that they could unite or divide people around a given change agenda. Through focusing on the activities and strategies of these protagonists, participants elaborated different types and forms of political skill, which are the main focus of this chapter. As explained below, participants’ accounts went beyond describing individualised skills and competencies, detailing instead more nuanced, situational and contingent instances of political skill, strategy and action that were manifest in the context-specific and turn-taking interactions. This distinction is important because it emphasises a conceptual difference between a ‘skill’ as some form of acquired capability or potential to engage in political behaviour, a ‘strategy’ as the judgement and acquired insight from which to make decisions about how to use these skills in a given context, and the ‘actions’ of engaging in political behaviour, especially through interacting with others.
A preliminary observation is that political skills, strategies and actions were rarely described in formulaic or systematic ways. Although participants might have presented their narratives in relatively linear or sequential stages, there was little sense that people use a predetermined or ‘worked out’ combination of actions to bring about an expected outcome. Instead, organisational politics were presented as highly dynamic, contingent and iterative, involving high degrees of trial and error and adaptation in the context of relational feedback. This chapter proceeds by describing these ‘skills, strategies and actions’ across five thematic categories (Table 9). A limited number of illustrative quotations are provided in the chapter and more extensive extracts of data organised according to the thematic coding are provided in Appendix 4.
| Theme | Dimensions |
|---|---|
| Self and interpersonal style | Self-awareness, self-belief and self-reflection |
| Resilience and perseverance | |
| Emotional intelligence | |
| Interpersonal style | |
| Strategic thinking | Understanding the broader political landscape |
| Reading the local political landscape | |
| Defining and redefining problems and solutions | |
| Understanding what is possible and what is a priority | |
| Communication and engagement | Active listening |
| Asking questions | |
| Opening up dialogue | |
| Framing strategies | |
| Rhetorical strategies and resources | |
| Empowering and delegating | |
| Networks and networking | Identifying and appraising networks |
| Access to personal and professional networks | |
| Fostering and mobilising networks | |
| Creating alignments | |
| Identifying and using key people | |
| Relational strategies and tactics | Dealing with ‘egos’ |
| Negotiating and dealing with powerful groups | |
| Manipulating | |
| Engaging with formal organisational structures |
Self and interpersonal style
The first theme describes the personal and interpersonal qualities that are commonly associated with political skill and action. These qualities were commonly described as the foundations for more strategic and tactical forms of action; for example, the ability to be (and be seen as) ‘assertive’ or ‘authentic’ was linked to other forms of action, such as ‘building relationships’. For many, these personal qualities were based on the principles of ‘reflective practice’ or, in broader terms, self-awareness or the capacity to realistically appraise one’s own abilities relative to others and in a given situational context:
So it’s about me knowing who I am, and I suppose if I know who I am, I am more likely to understand other people, and have empathy for other people, so maybe emotional intelligence, linked in with leadership, but I think that they overlap because of that motivation, that drive and determination, that self-awareness, that being open to feedback, because if you’re comfortable with yourself, and knowing your own strengths and weaknesses, then actually that’s fine, and appreciating that we’ve all got that but then within a team, trying to play to everybody’s strengths.
WP2-37
Many participants described the importance of ‘self-belief’. This was described in three ways: first, with participants’ belief in their personal motives or intent for acting politically, that is ‘doing the right thing’; second, with participants having confidence in their own abilities, that is they have the ‘right skills’; and third, with participants believing that they will succeed despite resistance, that is ‘being resilient’. Alignment between these different aspects would create the conditions for engaging in politics, whereas a misalignment could, for some, discourage political action: I want to do the right thing but I do not have the skills to deal with a given issue.
Participants described organisational change as a drawn-out process, in which leaders often needed to ‘play the long game’, ‘stay the course’ or wait for the ‘windows of opportunity’. In some cases, change was depicted as a ‘war of attrition’, in which personal and emotional losses had to be weathered. Accordingly, being resilient and having perseverance were seen as essential personal qualities for engaging in organisational politics.
Participants described a discrete set of personal qualities related to understanding and managing their emotions, what might also be labelled as ‘emotional intelligence’. 146 First, it was described as important to effectively appraise the emotional mood surrounding a given change agenda, which relates closely to the ability to read the political landscape (see Strategic awareness and thinking). This suggests that change (and the response to change) not only is a matter of rationality or evidence-based decision-making, but also involves understanding people’s deeply held beliefs, values and emotions. For this reason, change often involves anticipating for emotional responses to change:
So, it’s being aware of your own personality, again, which comes back to emotional intelligence, it comes back to your political influence small ‘p’ because of your interpersonal influence, and the skills that you have, in your toolkit, to be able to influence someone.
WP2-37
Second, participants talked about managing the presentation of their own emotions. The ability to appear empathetic with those struggling with change, for example, was seen to be important for maintaining positive relationships and minimising resistance. In other ways, limiting one’s emotional responses could project a more professional demeanour to show that a person was above or not influenced by emotional considerations. In this sense, the self-regulation of emotion was described as a strategy for managing the responses of stakeholders that was based on the ability to listen to and understand the emotions of others.
Although self-awareness and self-belief are primarily concerned with how participants think about themselves, such talk demonstrates the importance of understanding how to present one’s self with others when seeking to influence these others. In various ways, participants described displaying appropriate forms of physical, interpersonal and emotional behaviour that reflected their self-belief and commitment to change while being responsive to the expectations of others. For this reason, effective leaders were sometimes described as ‘chameleon-like’, in that they could change their presentation to align with the expectations of audiences. Accordingly, those with relatively fixed or entrenched demeanours were often seen as inflexible:
So you look at it, you then just sort of adapt your style and it’s, and is it your body language, because then you’re thinking, OK I was getting quite comfortable here, just listening, but actually I’m in the work mode and this person has only got half an hour and I’ve only got that amount of time, to influence them, for the first time, but as I say, it’s about being able to continue and to develop that relationship.
WP2-37
The ability to manage presentational style could involve, for example, using the ‘right’ language or dressing in an ‘appropriate’ way. As an illustration, one participant talked about not being seen as ‘too managerial’ when engaging with clinical groups, whereas others ‘talked up’ their clinical background to enhance their standing with front-line clinicians. However, there seemed to be a balancing act with how much one could alter one’s representational style because of the risk of being seen as inauthentic.
Looking closer at these representational styles, the majority of participants talked about the importance of having, or being seen as having, ‘integrity’. In slightly different ways, this involved being honest and faithful to one’s own beliefs and values, as well as the shared values of the health and care service (which were somewhat more variable). In other ways, people talked of being transparent and not seeking to deceive others. Participants offered cautionary accounts of co-workers whom they regarded as manipulative, inauthentic or lacking integrity.
Some participants elaborated this as having an ‘authentic’ style. This was described as being honest to one’s self and being ‘genuine’ in relationships with others, or not cultivating a presentational style for the purposes of influence. Caution is needed in interpreting this idea of authenticity because there remains a possibility of creating an authentic style with the intention of influencing others, which could be inauthentic:
. . . got to be yourself haven’t you, and celebrate yourself. And that’s where the sensitivity . . . and understand how other people might experience you. And for good and bad, and I think just understand that and own it.
WP2-65
In other ways, and not always consistent with the idea of integrity, participants talked about being ‘charismatic’. There were many accounts of leaders using their personal charisma to inspire others. This seemed especially prominent among medical groups in which charismatic leadership tropes were aligned with mastery of shared symbolic markers around clinical reputation:
It’s that charisma bit around actually they generally look like they’re quite interesting people and they’ve got a certain presence around them, I think they tend to be more yeah skilful, political operators in that respect in that they can get on with a lot of people and they can get a lot of people to work around a similar cause.
WP2-9-D
Another example of interpersonal style was associated with being ‘diplomatic’ or being attentive to, and considerate of, the diverse interests of different stakeholders. Although this diplomacy relates to a vast range of political skills and strategies that are described below, the key point here is the ability to cultivate and project a diplomatic style:
What he did, he navigated some very bumpy political waters and I think kind of, I’m sure had to bite his tongue for a lot of things. Because I guess effectively he had a number of brownie points and he knew he needed to play them when he needed to play them, would be my thought.
WP2-65
By contrast, participants talked about a more ‘assertive’ or directive interpersonal style that involved, for example, standing up to dominant or powerful groups and challenging inappropriate behaviours. What seemed important, however, was knowing when to be more assertive through assessing the context and anticipating the response of others:
It’s really important to be articulate, be assertive and I think what comes with experience, and I didn’t have this when I started off as a nurse director, is just taking time to really understand others’ perspectives because I think I was probably a bit bombastic and I knew what was right because I was the nurse director and I knew what patients needed, so I think that I needed to just moderate my approach a bit.
WP2-5-D
Strategic awareness and thinking
The second theme describes how participation in organisational politics requires forms of ‘strategic awareness and thinking’ for understanding the local political context, formulating realistic goals and plans for change, and selecting the corresponding ‘tactics’ for realising these plans. As with the other themes, the aspects associated with strategic thinking do not fall into neat categories, but rather illustrate clusters of qualities that are linked to other aspects of political action.
Many participants described the need to ‘see the big picture’ or to understand the wider economic, organisational and political context of health service change. This included the broader (big ‘P’) political landscape of national policy priorities, regulatory requirements and wider resource issues that set the context for the local organisational politics. For a small minority of participants, direct exposure to, and involvement in, formal political settings afforded developed understanding of the skills used by politicians in engaging with different stakeholders:
Working at a national level, working for a regulator, there are massive politics, with a big ‘P’ and a small ‘p’ because you’re so close to Westminster that actually your chief exec[utive] is meeting with the Secretary of State every Monday morning, that feels very real when you work in an arm’s length body and then of course because there are several arm’s length bodies working in the national health and care system there are big politics between them all, so I, so the experience of working with, in that environment was fascinating because you’re getting, well you’re getting very interesting dynamics between very senior people.
WP2-35
Participants talked about ‘understanding the history’ of health service reform, especially the changing political ideas that have shaped policies and the historical conditions that enable or constrain certain types of change. 9 Some participants talked of ‘learning from the past’ to avoid common pitfalls, such as the engrained challenges to integrating health care and social care or the challenges of regulating medical practice. In common ways, these views suggest that those leading change need to trace both the historical roots and the development of the given intervention and, at the same time, appreciate the history of similar events within the local context that might condition how a given change is received:
Be able to look at the wider picture . . . I did that when I was doing that job to go really wide and bring it down. . . . so I think you need to have an appreciation of the macro picture.
WP2-4
A connected form of strategic awareness is understanding the local political landscape that surrounds a given change agenda. Most participants talked, for example, about recognising the prevailing ‘lines of power’ within care services, from the formal governance structures to the informal lines of power that shape day-to-day care delivery. The formal governance systems of the NHS were widely described as exhibiting high degrees of complexity and incoherence that could drive change in some areas but inhibit change in others. Understanding the governance landscape and appreciating what financial, clinical or regulatory ‘buttons’ to press were seen as essential skills for navigating formal authority structures.
Some participants talked, for example, of navigating the formal ‘chain of command’ when seeking to gain authorisation and funding for proposed change initiatives:
So many departments, teams, organisations and the conflicts between them, in terms of understanding what the whole system needs but knowing what the regulatory landscape requires of them, within their particular silo, or within their particular department, or unit, or whatever it was.
WP2-63
Almost all participants described how formal governance arrangements were complicated by informal lines of power and influence that, in some ways, appeared to shape the day-to-day organisation of care more than formal requirements. Participants talked, for example, of understanding how ‘influential individuals’ and ‘dominant cliques’ regularly complicated change processes. Doctors were commonly seen to resist change that challenged established ways of working or undermined professional status; however, other occupational groups were also highlighted as acting politically to either block or promote certain types of change, especially nurses, managers and patient advocacy groups. Participants’ narratives often foregrounded a significant ‘other’ as acting politically to complicate change or maintain established ways of working to safeguard some position or interests that they held. However, the narratives also suggested that informal influence was not always aligned with a specific professional group, but could vary according to the issue at hand. That is, some issues saw professional groups working together to promote change, whereas other issues would see the same professionals as opposing factions. Part of understanding the local political landscape, therefore, involved understanding these ‘dynamic lines of power’ and recognising that political actions are not fixed according to unilateral or bilateral relationships, but rather they function through highly dynamic multilateral relations:
When they [doctors] go with an idea into the trust they have to wade through all the levels of treacle and in doing so they either find a way of circumnavigating the system to get what they want, because they’re used to getting what they want or they’ll just do it anyway and bear the consequences.
WP2-3
Participants also described the importance of ‘seeing the hidden agendas’ and ‘recognising when people are acting politically’. This was often more difficult for participants to articulate and seemed to rely on past experiences of working with certain people, that is knowing what they typically aim to achieve, or reflecting on the ongoing processes of change to assess the ulterior motives of those one is working with. It seemed to be that more experienced participants were more able to describe how underlying agendas motivate individuals and groups to engage in political behaviours:
You do need to be able to recognise when people are using their political skill to their own ends and potentially negatively and I think that’s something that you need your sort of antennae out for because there’s certainly people who do do that.
WP2-8
Many participants talked about more generalised forms of strategic thinking. One example was with the need for leaders to articulate ‘clarity of purpose’ when initiating change. However, participants described how effective political action involved not only understanding the problems and solutions driving change, but also, more significantly, the ability to ‘define and redefine’ these problems and solutions in ways that aligned with the prevailing political landscape and with the interests of stakeholders. This aspect of strategic thinking links closely with the communication skills of framing (see Communication and engagement). Linked to this, it was described as important to have a ‘realistic understanding of what is possible’ or what is likely to be successful given the prevailing political landscape. Many reflected on how planned changes were unsuccessful because they had not fully appreciated the opposition of certain groups. As some described, it was important not to waste political credibility on changes that were unlikely to be successful:
. . . that was a challenge, because obviously the clinical side of the team were very blunt in terms of this is how it will be. And there’s more considerations that we had to take into account, in terms of cost, in terms of resources, and a need, as an organisation to develop our own strategy and would make it a bit more sustainable and fit for purpose, going forwards.
WP2-62
Communication and engagement
The vast majority of participants described communication and engagement skills as key to engaging in organisational politics, which linked to leaders’ ability to both understand and read the local landscape and influence others and reshape the political landscape. The techniques of communication and engagement are well described in the social science literature, and this section, therefore, focuses on those aspects that participants described as especially significant in relation to organisational political and political action.
The ‘art of listening’ was widely regarded as a key to effective communication in general, and political action in particular. Active listening seemed to offer at least three contributions to political action. First, it enabled leaders to better understand the concerns and hopes of individuals involved in, or affected by, change, so that change processes could be tailored or presented in ways to be received more positively (see also below). Second, and moving beyond individuals or groups, active listening was key to reading the local political landscape, especially understanding the lines of power and the likely areas of support and resistance. Third, the practice of listening, or giving the impression of listening, had an additional symbolic function of showing that a leader has shown interest in the concerns of others and that being heard could provide the basis for ongoing and respectful engagement:
Oh, absolutely listen, but really, really demonstrate your listening. Don’t just pretend and pay lip service to it. If you are asking somebody to give you their view, their advice, their expertise then absolutely listen to them and take notice. Don’t think that you know it all and you can do it all better. Ask the people that really know and that really understand and really take notice of it. Really, really listening, I think really listening. . . . People are a valuable asset and people are under a lot of stress and not helped if you’re in an environment where you’ve got all the conflict and problem. I think you learn, you look for the opportunities.
WP2-3
Complementing these listening skills is the ability to ask probing questions as a way to better read and understand stakeholders’ preferences and their likely reactions to change, and, in turn, to adapt one’s strategies. A number of participants talked, for example, about the strategic use of naive questions, especially when working with new teams or organisations, as a means of exploring how others make sense of their local context and probing (with the perception of naivety) the assumptions that underpin this context. In more duplicitous ways, asking the ‘right’ question was described as demonstrating shared understanding or empathy for the concerns of others, whether or not this was actually the case. In other words, the dual tactics of active listening and asking questions could function as symbolic and presentational strategies of engagement over and above attending to the information provided by stakeholders:
And also, a bit of naivety just to ask stupid questions is very handy.
WP2-36
A number of participants talked about the importance of not being too directive, but rather being facilitative of two-way conversations and opening up dialogue with and, importantly, among different groups. This could make a number of important contributions to mediating organisational politics. First, it enabled leaders to better understand stakeholders’ different interests, especially to identify mutual areas of interest from which to build alliances. Second, dialogue was seen as creating opportunities for stakeholders to express their concerns, especially their fears and hopes for change, thereby creating a platform for engagement. Third, by opening up dialogue and building connections between stakeholders, it became possible to find ways of empowering people and sharing (or even delegating) responsibilities as a major driver for progressing change. A related engagement strategy was allowing others to ‘shape the agenda’ or giving people the impression that they were shaping the agenda. For some participants, this was seen as a more ‘inclusive approach to change’ that ensured that the best ideas or ‘collective wisdom’ shaped the formulation and implementation of change:
The longer I’ve done it or perhaps in some of the more senior roles is it matters less and less what you think and I think you probably achieve more if you’re prepared to relinquish your own control and that’s more than just delegation. That’s not just about having a team of people that you can give jobs to it’s about being prepared to hear something that’s different to your original plan and acknowledge that that might be a better way of doing it or it might be the more successful route to follow.
WP2-8
When some participants talked about ceding authority as a form of engagement, there was often an implied assumption that control could be reclaimed, which suggests that perhaps allowing others to shape the agenda was a more complex and manipulative strategy than sometimes implied. This type of engagement strategy created an illusion of influence, usually in the context of seeking to engage relatively powerful groups who ‘need to feel they are in charge’:
I grow whatever they’ve brought to the table, I have the skill set to do that, then bring them back to the table and you’ve got something tangible to show, because they’ve built it they’ve owned it. They then own it and because they own it they implement it.
WP2-2
In a variety of ways, participants talked about the importance of presenting proposals for change in ways that would be positively received by stakeholders or, more significantly, in ways that could motivate their active participation in change processes. These ideas speak to the concept of ‘framing’, which in the wider social science literature is used to describe how the presentation of an event or situation can influence how an audience makes sense of and reacts to this event. Frames act like ‘frames of reference’ or ‘cognitive schema’ that influence how people filter, perceive and comprehend a situation,147 and, therefore, are potent in shaping reactions to change. 148
A common way that participants talked about such framing was in terms of ‘selling’ a vision of change that would secure the ‘buy-in’ of stakeholders by aligning with the underlying interests and agendas. This involved, first, determining the prevailing interests or concerns of stakeholders before constructing and articulating a relevant set of ideas about how a proposed change initiative would address or align with their agendas:
I mean selling people, staff, the public, whoever, on the list of options you’ve put in front of them, if it is indeed a list. So it’s a question of . . . it’s stopping people coming back and saying, ‘Oh, actually we should do this instead’. ‘Oh you shouldn’t do that, you should do this’.
WP2-2
In a related way, participants talked of presenting change in ways that not only aligned with or addressed the interests of stakeholders, but also, more significantly, influenced or modified how people understood and reacted to the need for change. This involved more complex and dynamic forms of ‘persuasion’, in which leaders sought to subtly alter the prevailing views of stakeholders by presenting more compelling or convincing ideas about why change was needed. Effective framing required the ability to ‘speak multiple languages’ and to understand the relevant ‘priorities and trigger points’ that will elicit the support of stakeholders. Similarly, framing required knowing what ‘not’ to say and to rerepresent ideas or facts in ways that would appeal to stakeholders:
. . . how can I suss out where I need to influence you? What’s the trigger? Like you said ‘Oh can I?’, so it’s always [chuckling], it sounds awful. It is always being aware, of the other person and what, therefore, what’s right for their organisation?
WP2-37
It’s not that you’re being deliberately devious or withholding information. It’s just you have to learn what’s appropriate and what individuals want to know. And what they don’t want to know. So that . . . having that support is essential, crucial, vital.
WP2-41
Another way that participants talked about their framing activities was through the use of particular ‘rhetorical devices’ or strategies, that is stylistic techniques for the organisation and the presentation of arguments with the explicit intention of eliciting a desired reaction. These rhetorical techniques were often linked to particular ‘resources’ (sources of information, evidence or policy) that had certain appeal or relevance to stakeholders:
I think it’s about persuading people that your way is the right way but everyone knows it’s there . . . but one prefers to use influence and argument and logic and empathy and all that, that’s my preferred style of working whereas when one works, as you’re describing, laterally or upwards you’ve got to use relationships . . .
WP2-31
One approach was the rhetorical ‘use of data’ to justify change, typically based on the idea that such data were objective or independent. The use of data appeals primarily to the logical reasoning or sensibilities of stakeholders as the basis of persuasion. The most prominent examples of this were the use of clinical evidence to engage medical specialists and the use of financial data to persuade those with budgetary responsibilities. There were noteworthy differences, however, in terms of what participants regarded as ‘robust data’, reflective of their professional background or organisational role:
The only thing I can do is be very clear about the numbers, and then, from now on, I keep . . . I will develop very, very clear charts and graphs because I think she might understand a picture, and just keep, ‘this is what we’re doing, this is what we’re doing, this is what we’re doing’.
WP2-4
Another approach was the ‘use of authority figures’ or the use of those with recognised credibility to endorse change or, in some instances, to persuade others of the need for change. In this sense, authority figures could symbolically represent and legitimise change based on their own standing and reputation, often when the primary leader of change was in some sense lacking in credibility with a given community. For this reason, it seemed that these change leaders reflected on the limits of their own position (self-awareness), while also having a developed understanding of what types of people have credibility with certain audiences (again, drawn from the ability to listen and understand):
There’s always probably someone else who can say it for you. So let them say it for you and then you don’t get all the hassle that goes with it, but it’s been said, the message is there, you don’t have to be the fall guy.
WP2-10
Participants also talked about using the ‘patient perspective’ or ‘voice’ as a powerful basis of justifying change, persuading others and countering opposition. Many described how a ‘good patient story’ could be more influential in communicating an idea than an abundance of financial or clinical data. For some participants, direct patient involvement in service planning was seen to be important for ensuring that service improvements were organised in the interests of patients, rather than in line with the assumptions of professionals and managers; however, some participants reflected that such patient involvement could be used in more contrived and purposeful ways to counter the views of others:
It’s helping people to see all the time that what we’re doing is the best for the patients and the pathways and that actually it’s not around shifting services, moving services, stopping services, it’s around pulling those services to work together in one system.
WP2-3
Networks and networking skills
In various ways, participants talked about the importance of social connections, group memberships or other instances of networks as facilitating, and being the vehicle for, change. Participants describe these networks in three common ways. First, it was widely recognised that the pre-existing political landscape of health-care organisation was shaped by professional or interpersonal networks. Second, networks could provide key resources (e.g. people, finances and intelligence) when seeking to formulate or implement change. Third, the creation and mobilisation of networks could help to co-ordinate change activities and counter opposition. These networking skills strongly related to other forms of political action, from strategic thinking and awareness of the local context to communication and engagement activities.
Elaborating these ideas, participants described the importance of identifying and understanding the configuration of stakeholder networks that might positively or negatively affect change. As part of reading the political landscape, this involved a complementary set of relational skills that in many ways resembled the common elements of ‘stakeholder analysis’. 149,150 For example, participants described identifying the different interest groups around an issue, understanding the interests that united and divided them, anticipating the responses to change, appraising their influence, and recognising what resources and support they might offer:
. . . as I say in broader terms, I think that understanding relationships, understanding power, understanding interests, understanding stakeholders, those are all political skills and they’re all absolutely crucial to this job.
WP2-46
A number of participants talked about their membership of, or access to, such networks. These took two different, but arguably overlapping, forms. The first was access to personal informal networks in the form of connections with influential people or peers who could provide access, support or influence. A number of participants in senior management roles talked, for example, about their peer networks among senior managers working in hospitals. These peer networks provide confidential support and reflective insight when leading change projects, including access to ‘influential people’ or help to ‘work through’ challenging decisions. Some participants described these connections as a source of intelligence to gauge the likely critical pathways to change. In other ways, peer networks could be used as a form of ‘proxy-influence’, in which influential people would represent a person in a setting in which they have limited standing:
So if you build up lots of friendships in an organisation and lots of collaborators then you can make things happen. If you don’t life can be very, very hard. And processes are meant to irradiate that variance but they often don’t because people can use a process to their own end and that can be problematic.
WP-29
A second type of network was associated with membership of well-defined professional groupings, in the form of ‘professional networks’. Perhaps unsurprisingly, the majority of these participants were medical doctors whose professional networks were often developed through specialist training or employment within the same organisation, and which provided a strong source of professional identification, peer support and solidarity in the face of change. Less prominent were similar networks for nurses and other health-care professionals. In other ways, participants talked about the importance of fostering and mobilising networks around particular change programmes. These were often presented as ‘alliances’ among people who shared aspirations for change.
Arguably, networking skills are not unique to how people participate in organisational politics, but are relatively common to general forms of strategic management. The activities described resembled many of the steps identified in the wider literature151 and included (1) identifying key people within the local environment; (2) understanding the interests that unite people in a common cause; (3) using relational skills for engaging and enrolling groups in networks; (4) co-ordinating skills for bringing people together; and (5) using skills related to managing conflict and difference within nascent networks. However, participants described network building as a highly iterative and contingent process, with many false starts and overlapping tasks that relied on complementary communication and engagement skills, for example leaders need to frame change programmes with different stakeholders. For many participants, building and mobilising networks was an important strategy for counteracting the influence of established groups or networks that are resistant to change:
. . . so, yeah, I think, 90% of what we do is about brokering conversations between people about trying to find a way to bring people together and to bind them around a common goal and almost being a counsellor between two folk, enabling them to speak.
WP2-63
Part of the skill of building networks is creating alignments between different stakeholders in the form of ‘common ground’. In many instances, common interests were framed in terms of improving the well-being of patients or local communities. Participants also talked of ‘creating win–wins’ so that all parties felt that they were benefiting from a given change and, therefore, felt compelled to join a collective approach. In another way, the skill of network building was ensuring that the potential losers saw some wider benefit from change or at least some form of ‘compensation’ to motivate their involvement.
Participants also talked about creating alignments through identifying ‘common enemies’. This was much less explicit, but it seemed that, as part of their framing strategies, leaders could characterise a group in negative terms as a means of galvanising support. To some extent, this seemed to reflect deeper cultural differences or ‘fault lines’ between hospital departments or health and social care sectors, and stemmed from underlying notions of ‘them and us’.
Another aspect of network building involved drawing on ‘key people’ to help to co-ordinate and champion group activities. As one person suggested, ‘a lot of the times we target people for things that we need doing’ (WP2–1). As mentioned above, participants talked of using ‘authority figures’ to endorse change and, in a similar way, some talked about recruiting ‘champions’ who could advocate for change within areas in which a project leader might have limited influence. One important, but largely under valued, example was the role of the ‘first-follower’ or the individual who supports an emerging network:
. . . that’s really important and having a safe group of people that you can do that with be they in your work situation or ideally some sort of action-learning group that you can draw on, someone that you can pick up the [tele]phone to where you can reflect.
WP2-35
Relational strategies and tactics with ‘difficult’ groups
The final theme describes the relational strategies and interpersonal skills used, in concert with the above strategies and actions, in more direct instances of interpersonal influence. These represent a relatively discrete set of skills that in many ways deal with the ‘sharp end’ of organisational politics, especially the ‘face-to-face’ encounters, with influence and persuasion, as well as coping with resistance and hostility.
Many participants spoke about dealing with ‘prominent’ individuals or ‘egos’ who had significant sway among clinical teams and could often be outspoken opponents of change. These people tended to benefit from high standing within their professional community and workplace, and were often presented as defending the status quo or advocating for certain types of change that would safeguard ‘their’ professional standing (when ‘their’ could be personal or professional). These prominent people were the focal point for resistance around which others coalesced. For this reason, it was seen to be necessary to deal with these people. The most common approach was to open up dialogue and actively listen to such people (as described above), but less as a strategy of listening and learning and more to give the impression of engagement and to win them over. It was seen as important to pinpoint the particular interests that mattered and find ways to allay their concerns (or at least to give the impression of this):
We had to go and smooth some egos. I remember having to go to one of our trauma units. There was myself, the medical lead and the chief operating officer of the hospital who met with a senior doctor and thinking that we were meeting with the senior doctor, but when we got there we were met with a barrage of the senior doctor plus his team, I think. There was something around smoothing the ruffled feathers.
WP2-3
When seeking to influence powerful people and groups, participants also talked about the purposeful strategy of empowering others. In some ways, empowering stakeholders was a way of reducing or containing conflict by enrolling recalcitrant groups within change processes, even if this was in only a superficial way. That said, some participants described their leadership style as explicitly facilitative, with the aim of supporting others to become more skilled and capable of implementing change for themselves, thereby suggesting a less manipulative view of empowerment:
. . . very much delegating and working to people’s strengths . . . encouraging others to take the lead, ensuring what happens is right rather than who decides what happens. So it’s terribly important that the right thing happens rather than them looking to the boss.
WP2-38
The ability to delegate tasks and empower others was seen to be part of a dynamic strategy. On the one hand, it was presented as a way of securing the involvement and commitment of stakeholders through encouraging them to shape or own change processes in ways that reflected their interest. On the other hand, these delegation strategies were useful for distributing tasks to key actors or opinion leaders based within clinical teams or communities with whom leaders might have limited influence.
More experienced participants talked of the importance of ‘confronting and challenging’ influential individuals who repeatedly blocked change. Before attempting this, it seemed to be important to both determine ‘the red lines’ or critical issues that needed to be achieved and ‘[pick] their battles’ so as not to expend political energy on lost causes. Significantly, the capacity to challenge and influence people and groups was clearly predicated on a person’s self-determination and, importantly, formal position or status within the workplace. For this reason, it was more common for senior managers to talk of challenging powerful clinicians:
[It’s] being able to stand up and say ‘I think you’re wrong, and this is why’, is just as important as you know, being authentic and all of that, so it’s like the thing about [inaudible] is quite uncomfortable, so like being uncomfortable is not something we like doing, because it’s uncertainty.
WP2-1
Nearly all participants talked of strategies and tactics for negotiating with different people. Effective negotiation skills were informed by the complementary skills and behaviours described above, especially the ability to listen and understand the stakeholders’ preferences and the ability to frame change in persuasive or compelling ways. The negotiation tactics that were used tended to fall into one of two approaches. One approach was to identify trade-offs and ‘deals’ that would satisfy the expectations of a given group as part of an overarching engagement strategy. This might involve, for example, offering additional staffing resources, finances or access to technologies for participating in a new service model. In this regard, it seemed to be important to first determine what the other party wanted in return for their support and then to secure this item as part of a ‘trade’. Another approach was to offer ‘compensation’ when change negatively affected a group as a way of maintaining their support. In general, these negotiating skills were described as highly interactive, involving ‘offers and counter-offers’. Importantly, these interactions were rarely part of the formal change process, but rather were conducted through ‘informal channels’, possibly with a view to protect the reputation or ‘face’ of both parties:
I think there’s a lot of what you would call back stage or behind-the-scenes conversations, so building, firstly trying to build relationships with peers . . . to say ‘OK this is happening to me, I’m raising it’, and they would go ‘yeah, I had one of those, but I’ve just tried to deal with that,’ you would build a coalition.
WP2-47
In other ways, participants described interpersonal influence as being manipulative. When reflecting on their career, for example, some participants recounted instances in which they had felt unduly pressured into accepting a situation that was not necessarily in their interest. Significantly, participants with more developed and senior careers reflected on how they had used techniques to influence and manipulate people when seeking to introduce change. For some participants, these activities were self-serving and reflected personal career ambitions, whereas others described how they were commonly used as part of other engagement strategies, especially when empowering others. Although many participants recognised that forms of manipulation were widely used in the health sector, and that manipulation was arguably a key part of political behaviours, few actually endorsed or admitted to using forms of manipulation. This may illustrate their attribution bias or desire to present a positive impression with the interviewers:
In the organisation you get very politically astute people who . . . I would . . . yes. Calling it ‘political astuteness’ in these people is a euphemism for being manipulative . . . that is knowing how to play the system to get their own way . . . What’s good for them, for their careers . . .
WP2-41
Although interpersonal and relational tactics were typically described as operating through informal channels, some participants highlighted the interdependencies with the more formal organisational structures and processes. An important point to make is that the scope to use more formal organisational processes is inherently conditioned by a person’s formal role and authority within an organisation. Many narratives described the need to ‘move between the formal and informal domains’ of managing change, which inevitably involved understanding how best to work within the formal structures and when to move into the more informal realm. This could occur, for example, when ‘hard’ formal authority could be used by those in authority to block change:
What’s the bureaucracy you have to step through to be able to talk to. So at that point in time it was still very hierarchical. There’s still degrees about there now. I don’t think it’s as bad but back in 2007–8 when this all started to emerge for me you weren’t allowed to go speak to without going through the chain of command otherwise that tended to upset a lot of people.
WP2-63
Interestingly, participants also said that effective political action could involve ‘creating formal structures’ to help to implement or sustain change. For example, some participants talked about drawing on formal authority to stipulate or enact change, while others described how their ‘formal’ control of resources could be used to create incentives and inducements to win over difficult groups:
I think there’s something about, forming formal structures. Often being straightforward personalities, I think being fair and firm so whatever it is . . . I know it’s really dull but it’s not really dull is it?
WP2-65
Discussion
Thematic analysis of participants’ narratives resulted in five broad categories: ‘self-style’, ‘strategic thinking’, ‘communication and engagement’, ‘networks and networking’ and ‘relational strategies and tactics’. It could be argued that such ‘skills, strategies and action’ are relatively common to more general models or frameworks of ‘change management’ or ‘strategic leadership’.
To some extent, these themes are similar to the conceptualisation of ‘political skill’ developed through the work of Ferris et al. 53 and Manzie and Hartley’s113 concept of ‘political astuteness’ (Figure 5). ‘Self and style’ focuses on the personal qualities of leaders that can be seen as similar to Ferris et al. ’s53’ concept of ‘interpersonal influence’ (personal style during interactions), ‘apparent sincerity’ (being seen as honest and genuine) and, to some extent, ‘social astuteness’ (awareness of self in relation to others), but it also describes a range of additional qualities related to ‘self-awareness’ and ‘perseverance’ that are closer to the qualities described by Manzie and Hartley’s113 notion of ‘personal skill’. The theme of ‘strategic thinking’ relates to the Ferris concepts53 of ‘social astuteness’ as well as ‘reading situations’, but it also suggests a more forward-looking and iterative type of strategic planning in the context of unfolding events that is found in Manzie and Hartley’s113 ‘strategic thinking’. For the study participants, the theme of ‘communication and engagement’ was by far the most important and prominent, involving the ability to listen and learn and to influence and persuade. It is arguably the case that such communication skills are embedded within many of the constructs provided by Ferris et al. 53 (interpersonal influence) and Manzie and Hartley113 (interpersonal skill), but subsuming them in this way and not treating them as analytically distinct downplays the significance of communication as a form of political action. One of the most direct areas of read-across between the study findings and the existing concepts is in the area of ‘networks and networking’, which relates to Ferris et al. ’s53 ‘networking ability’ and Manzie and Hartley’s113 ‘building alignment and alliances’. The study narratives offer a more nuanced view of networks that resembles the types of activities associated with social movements and, importantly, demonstrates the collective dimensions of political action. Finally, the ‘relational strategies and tactics’ described in this study relate closely with Ferris et al. ’s53 idea of ‘interpersonal influence’, ‘networking ability’ and, to some extent, ‘apparent sincerity’, and the Manzie and Hartley113 construct of ‘interpersonal skill’. As described above, these tactics were often embedded within, or emerged in parallel to, other activities, but were often concerned with dealing with especially difficult or powerful stakeholders. The narrative study departs more noticeably from the Ferris et al. 53 concept with regard to an explicit theme of ‘apparent sincerity’. Although participants describe the importance of presenting a particular persona or style and being seen as sincere, it appeared to be less of a distinct strategy and more something that was embedded in other aspects of political action. Furthermore, participants were at pains to say that it was not enough to ‘appear’ authentic: rather, leaders needed to be authentic.
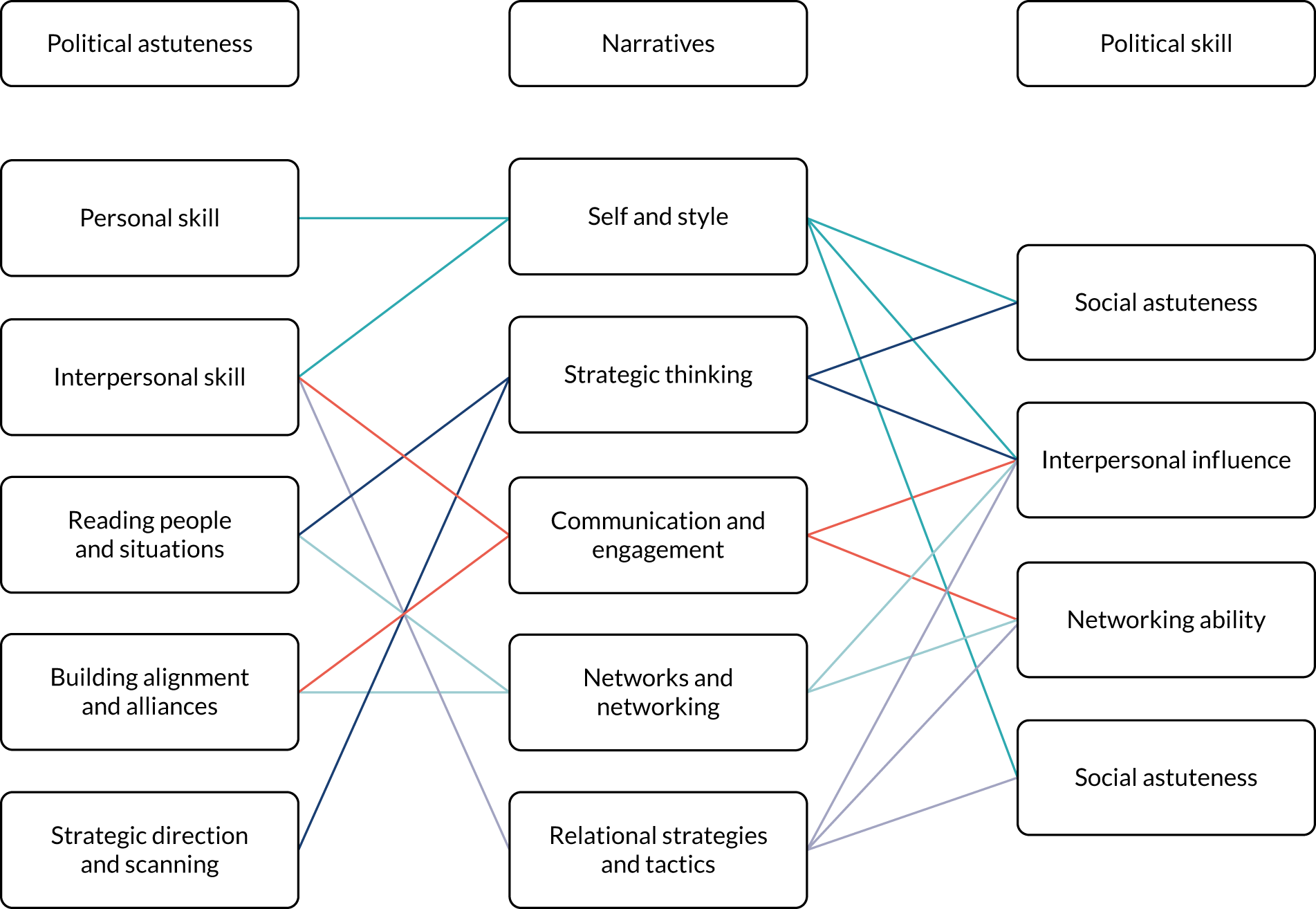
The study departed from the work of Ferris et al. 53 and other writers on political skill in two more fundamental ways. The first was to question and go beyond the relatively narrow and individualised view of political skill that appears to dominate much of the management literature. 43 As discussed in Chapter 3, this wider literature tends to focus on the psychological capabilities and behavioural skills of leaders to engage in interpersonal influence with the goal of realising personal or organisational goals. In other words, the focus is typically on the relational skills of Person A to influence Person B. This narrative study revealed a more complex and contingent understanding of organisational politics, which involves highly complex patterns of action, interaction and counteraction or interlocking constellations of political action in which multiple actors are seeking to influence one another. This is not to say that the wider literature is ignorant of this aspect of organisational politics, but by focusing primarily on individual skills and capabilities, analysis invariably focuses on individuals or interacting sets of individuals rather than the character of the interactions or constellations of interactions. In widening the unit of analysis, it is possible to analyse the interplay between the individual, the interactive order and the social context as distinct but linked ontologies. As an illustration, the interactive order of turn-taking and game-like exchanges continually shapes how interacting actors see themselves in relation to others, leading to microlevel adjustments in their actions. 59 The scope to recognise, reflect and adjust to the interactive order is in part shaped by a person’s psychology and personality, but also their social position enabling them to draw on wider social roles, rules and resources. 152 In other words, some people were able to engage in organisational politics not only because they had a better appreciation of the landscape or interpersonal skills, but also because they were members of a given professional community, had access to social, cultural or economic resources, and could draw on broader forms of social influence and power beyond the formal authority of the organisation.
Elaborating this idea, participants’ narratives repeatedly showed how a person’s social position shaped or conditioned their willingness and capacity to engage in organisational politics in terms of their experience, professional background, gender and other sociodemographic differences. The most obvious factors were career stage and level, and professional background. Specifically, those with more years of service and in senior professional or managerial levels were more appreciative of, and willing to engage in, political action (see Chapter 6 for further analysis of participants’ acquisition of political skill). It was also the case that some older participants, who described themselves as being towards the end of their career, had different perceptions of risk, with some indicating that they had little to lose from making political mistakes. In other ways, political action was also described as gendered. 153 Some female participants saw political behaviour as associated with more masculine behavioural traits, especially when it was associated with negative forms of manipulation and bullying. A small number of participants talked of a type of ‘boys’ club’, in which informal forms of influence were held by a small number of male leaders. Although the study did not explicitly focus on differences in ethnicity, our sample did seek to include diversity of health and care leaders from whom to analyse potential differences. Interestingly, participants rarely discussed how ethnicity could be a factor in influencing or conditioning an actor’s political behaviour. One noteworthy contribution was with regard to the influence of religious beliefs and faith in guiding a participant’s behaviour in terms of moral expectations. There is certainly more scope to look in closer detail into the role of such sociodemographic differences in conditioning political behaviour.
The further contribution to the literature was through offering greater insight into the interests and agendas that motivated political action. Within the mainstream literature, political skill is motivated by the desire to realise relatively narrow personal or organisational interests, often for career advancement or competitive gain. This study found that multiple and, sometimes, unclear interests shape the ways in which health and care actors engage in political activities. The study focused primarily on participants’ experiences of implementing organisational or system change and, for this reason, most narratives talked about the purpose or goal of such reforms, at least in the preliminary elements of their accounts. Looking closer at these narratives, participants were motivated to engage in political activities for a number of deeper reasons that complemented, or even contradicted, the particular change agenda. By far the most common reason for engaging in political action was to improve the organisation and delivery of care for local people and patients. The majority of participants invoked patient benefit or public good as guiding their actions. It is arguably the case, however, that invoking such ideals is itself a political strategy, that is for legitimising an agenda; however, notwithstanding this possibility, it seems to be that almost all participants saw their actions as ultimately driven by improving patient care, as also identified by Montalvo. 102 Looking closer at participants’ narratives, a significant reason for engaging in political action was because of the constraints of formal organisational processes and the institutional power of health and care professionals to resist or subvert change. This, again, highlights the dynamic and interactive aspect of political action, inasmuch as the political strategies used by some leaders to counter the dominance of certain professionals lead in turn to these professionals utilising a distinct set of strategies to counteract the strategies of managers as a type of political game. This suggests that deeper ideals and interests around the organisation and governance of health and care services also guide political actions, especially when they relate to professional groups. Furthermore, some participants seemed to speak to even deeper political agendas, especially around the values of the NHS and where there were concerns about the involvement of private sector organisations in service delivery. It seemed, therefore, that interests operated at a more superficial or overt level, often related to patient benefit, and also at a deeper and unspoken level related to personal or professional influence and power. It was also the case that some participants were perceived as holding multiple positions at one time, for example saying one thing but meaning another.
By moving the analysis beyond the individuals, their narrow interests and their skills at interpersonal influence, the narrative study showed how participating in organisational politics or (inter)acting politically was a highly dynamic, iterative and context-specific activity. The study found that political action rarely occurs in a linear or formulaic way, that is when a given combination of skills produces certain outcomes. Rather, the skills, strategies and actions of interlocking constellations of actors are highly dynamic, contingent on the pattern of interactions and context specific. For example, the implementation of a given change initiative, such as a new cancer pathway, in one organisation might involve a particular set of challenges and corresponding strategies to address the different interests of stakeholders, whereas the same change initiative in another setting could be described in radically different ways. Elaborating this idea, participants talked about how change processes were often complicated by organisational politics, leading to various types of dead ends or false starts, and requiring leaders to go back several steps, to restart or even abandon change. In such instances, participants talked about testing out different approaches as a form of trial and error, further suggesting that participating in, and managing, organisational politics is difficult to prescribe or pre-empt in any formulaic way. This, therefore, confounds the idea of a typology or ‘playbook’ for effective political behaviour, but rather suggests a context-specific set of thematic options that need to be considered for different types of controversies.
That said, participants’ accounts of organisational change did often resemble more general frameworks of ‘change management’ and ‘strategic leadership’ with common steps and activities. 50 It could be suggested that ‘political skills, strategies and action’ are a subset or distinct type of more generalised leadership capabilities, but it remains important to consider that engaging in political action might not be limited to leadership and it can be concerned with maintaining the status quo as much as implementing change. Moreover, people can be motivated or guided by agendas that run far deeper than a given change initiative. Although participants’ accounts of organisational politics and politics action were highly dynamic and contingent, it remains possible to identify a number of commonly described types and forms at different stages of the change process. For example, in the preliminary stages of ‘project planning’, participants talked about the importance of strategic thinking, especially needing to read the local landscape, identify the individuals or groups that might be supportive or resistant to change and determine what change was feasible given the historical context of change, which, in turn, involved communication skills for asking questions and listening to the stakeholders, as well as drawing on informal networks. In the stages of ‘project specification and initiation’, participants mentioned supplementary forms of strategic thinking to redefine the problems facing local stakeholders in ways that supported the implementation of a given initiative as a solution. These contributed to the construction and articulation of particular communicative frames to shape how stakeholders perceive and interpret change, in ways that would encourage their support and involvement. During periods of ‘project executive and implementation’, participants talked about drawing on the networks to recruit champions or figureheads to support engagement with difficult or hard-to-reach groups, and complementary networking skills to create supportive groups or communities around change initiatives. Through each of these stages, leaders also talked about the importance of dealing, negotiating or managing difficult individuals, through either interpersonal tactics or building collective pressures. In addition, all activities seemed to be premised on the personal qualities and style of leaders in terms of how they understood themselves in relation to others, their personal resilience and coping strategies, and their ability to adapt to resistance or setbacks. Although participants described highly dynamic patterns of political skills, strategies and action around context-specific controversies and political landscapes, the narratives also suggest the tentative foundations for a new or revised understanding of political skill (Figure 6).
FIGURE 6.
Illustration of political skills, strategies and actions in the change process.
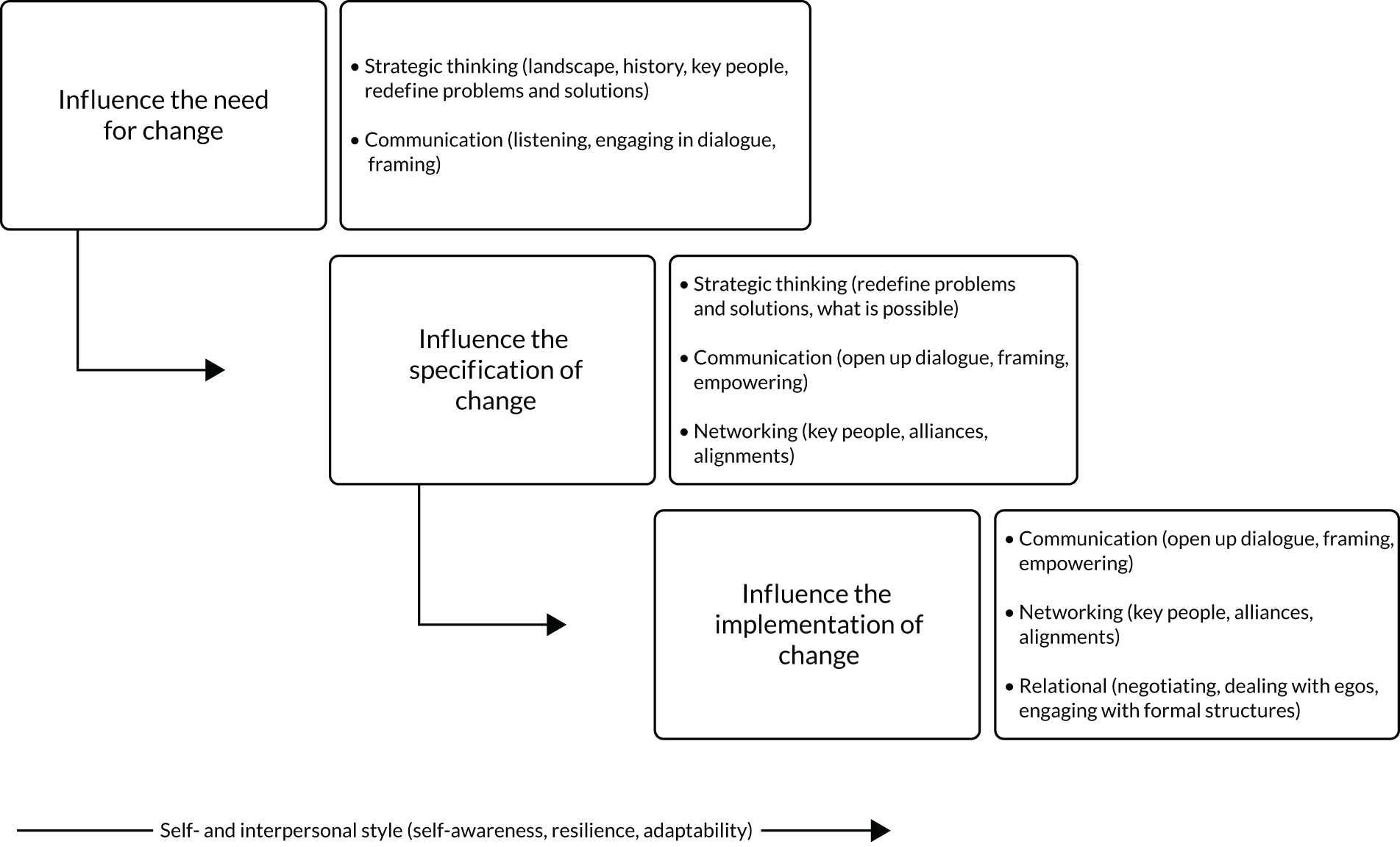
Chapter 5 The politics and political skill of major system change: qualitative case studies of Sustainability and Transformation Plans
Introduction
This chapter reports on the findings of the in-depth qualitative case study research with three STPs. The research aimed to investigate how political skills, strategies and actions are used constructively by service leaders to create a ‘receptive context’ for implementing major health system change. When the interview study investigated the reflective narratives of individual participants about health services change, this WP investigated ‘real-time’ cases of system change that took into account the experiences of multiple actors, together with their actions and interactions, around particular change processes and over time; specifically, the ongoing implementation of three STPs between 2018 and 2021. As well as offering rich contextual analysis of political skill ‘in action’, this chapter also serves to develop understanding of the types and forms of political action that take place at different stages of the change process. In addition, it examines change at the regional care system level in England, thereby offering a new level of understanding of the political skills, strategies and actions used at both the organisational and the interorganisational levels.
Descriptive overview of Sustainability and Transformation Partnership governance and system transformation
Politics and political skill are influenced by context; therefore, it is first important to outline the broad context of the three STP case studies. Although there were clear differences in the organisational structures, governance arrangements and transformation plans for each STP, there were common features that, arguably, stemmed from national-level guidance as set out by NHS England and pre-existing NHS governance and commissioning arrangements. 25,27,31 It is useful to summarise these common structures and lines of accountability between organising units to contextualise subsequent case descriptions and analyses (Figure 7 and Table 10).
FIGURE 7.
Illustration of main STP governance structures.

| Organisational unit | Main roles and responsibilities | Membership |
|---|---|---|
| STP board | Responsible for determining the overarching strategic vision and mission of the STP, including setting the thematic priorities and deliverables of system change, authorising major transformation programmes, developing collaboration agreements, redefining the overall ‘system architecture’ and overseeing system-wide performance | The senior leaders of regional health and care organisations, including commissioners, NHS provider organisations, local authorities, social care, police and emergency services, third-sector organisations; public and patient group representations; professional representation; and operational managers drawn from executive group |
| STP core or executive group (including communications and engagement group) | Responsible for the operational development and implementation of the STP strategy and plan, including authorising, overseeing and co-ordinating the programme of work; providing support for collaborative interorganisational working; and providing financial assurance | Senior- and middle-level managers and other clinical leaders either seconded from or acting as representatives of main health and care provider organisations and commissioners, as listed above. Usually appointed by a STP board |
| Locality/areas partnership groups | Subgroup of the main STP board providing more locality or place-based leadership and oversight of service transformation, co-ordinating with both the core group and the programme boards | Senior service leaders and managers of the main health and care provider organisations and commissioners, within the given locality area |
| Thematic programme board | Responsible for formulating, identifying, prioritising, authorising and reviewing transformation ‘projects’ in discrete service areas (e.g. cancer, children’s, dementia, mental health and urgent care); co-ordinating between the STP board and the area partnerships and specific change projects | Professional and managerial representatives of the given thematic service area, public and patient representation, and representation from the core STP group, including project management support, CCG representatives, and service provider representatives |
| Project teams | Responsible for specifying, managing and implementing system transformation project within (or across) a given programme area | Variable, but usually clinical and managerial representatives from a given service area, as well as public or patient representation, and with project management support from the core STP group |
Model of system transformation
Comparative analysis across case study data led to the creation of an aggregate or a composite model of major system change, with specific reference to STPs (Figure 8). The composite model presents a sequence of linked activities and tasks that are grouped in stages. To some extent, this model resembles many of the ‘change management’ frameworks found in the wider management literature and also the implementation models of major system change developed through health services research. 2 The model developed through this study is different from these in that it focuses on those common and prominent stages in which political controversies, and hence political action, were found to have a significant bearing on system transformation.
FIGURE 8.
Composite model and analytical framework of STP transformation.
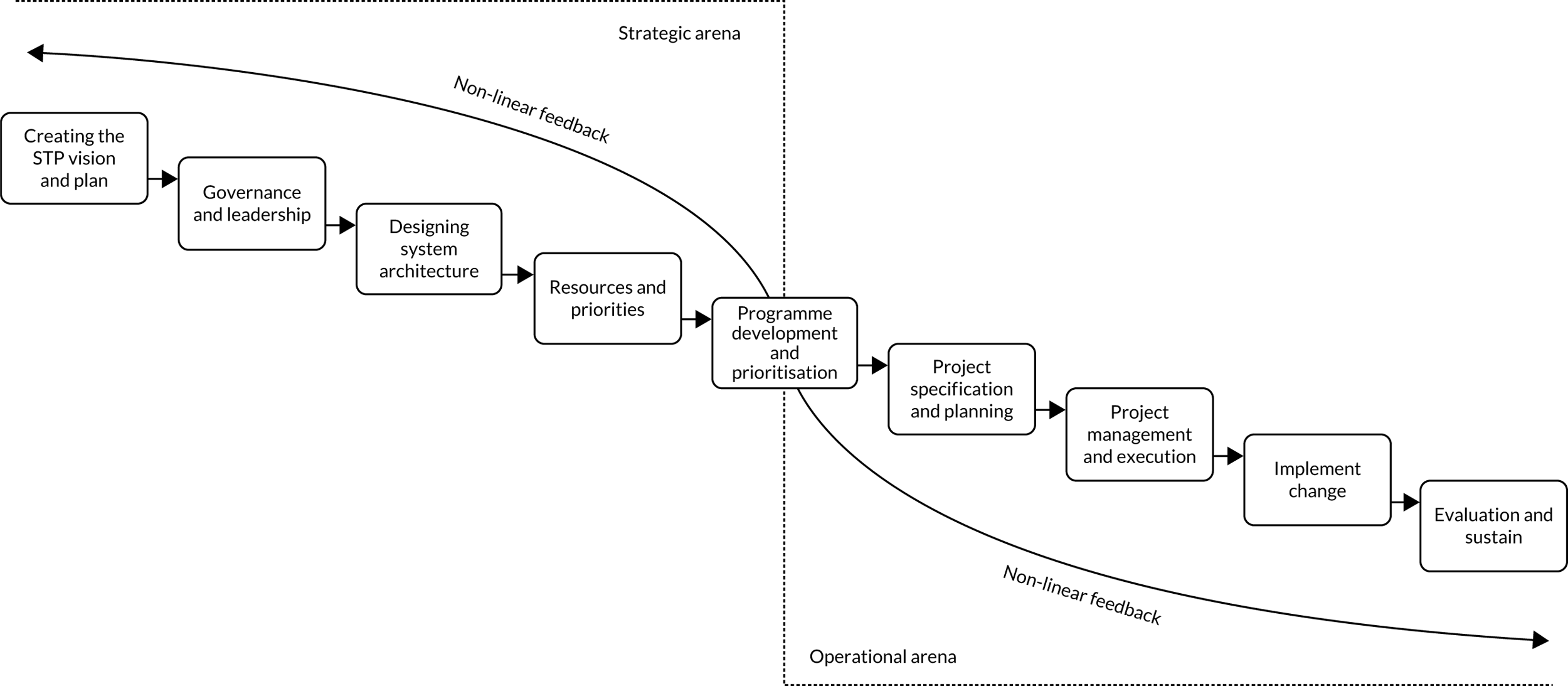
Drawing on Hartley and Bennington,154 the composite model distinguishes between those activities and controversies found in the ‘strategic arena’ of each STP and those activities and controversies found in the more ‘operational arena’ of service transformation. Controversies experienced in the ‘strategic arena’ tended to be associated with the organisation and work of the STP board, the STP executive group, the locality partnership boards and the thematic programme boards. These tended to centre on, for example, the STP vision, governance arrangements, system redesign and interagency work, prioritisation of change and resource management. Controversies experienced in the ‘operational arena’ tended to focus on the connections between the thematic programme boards, the individual transformation projects, to some extent the STP executive group (in its more operational capacity) and, indirectly, front-line care services. These tended to focus on aspects of project specification, planning and implementation, and often reflected commonplace stages of change management. As the model suggests, an interface between the strategic and the operational arenas is depicted through the work of the thematic programme board that translated overarching STP priorities into more specific programmes of service transformation in the form of individual transformation projects.
The composite model suggests a sequential view of major system change and, to some extent, the study findings do show that change unfolded through interlinked stages, when, for example, decisions deliberated and reached at an earlier stage would set in train a series of subsequent activities. However, the model also recognises that the implementation of change in complex systems rarely happens in a planned or linear way28 and, consistent with existing research on major system change,2,9,22 each case study project experienced many ‘detours’, ‘false starts’ and ‘dead ends’ that required teams to return to earlier stages to resolve an underlying controversy before restarting or abandoning an aspect of change. These events were often the consequence of political issues experienced at each stage or because of issues not resolved at a preceding stage.
This composite model provides the framework for analysing the ‘system politics’ and, importantly, the political skills, strategies and actions of implementing major system change. Table 11 summarises the main political controversies observed or reported within each stage across the case studies. Below, more detailed analysis is given of the ways that political skills, strategies and actions were used to resolve (or not) these controversies, drawing on the findings of an exemplar empirical case study to illustrate how political skills, strategies and actions are used by different groups to resolve (or perpetuate) these controversies. By drawing together the findings from the individual case studies, the chapter develops a synthesis or composite picture of major system change that brings to light the main controversies and protagonists, and political skills, strategies and actions. It is important to note that at least two of the subcase study projects did not result in successful change.
| Transformation Stage | Focus | Main controversies |
|---|---|---|
| Creating the STP vision | Agreeing the overarching STP purpose and strategy for population health improvement through a programme of system transformation, focusing on the values, vision and key objectives |
|
| Governance and leadership | Determining the governance structure of the STP in terms of authority and accountability structures, leadership and management roles, as part of the overarching organisation and governance of system transformation |
|
| System architecture plan | Developing and articulating a ‘blueprint’ for system change that reflects the overarching vision, takes account of broader policy changes, reflects emerging evidence of successful integration and respects the continuing obligations of constituent organisations |
|
| Resource management and priority setting | Agreeing how financial, human and other resources will be shared or pooled within the STP and determining the priorities for resource allocation in the context of existing service commitments and STP objectives |
|
| Programme development and prioritisation | Developing the specific objectives, priorities and programme of work for system transformation in a given area, including the identification and selection of transformation projects, supporting individual project teams, and sharing lessons across projects |
|
| Project specification and planning | Developing the proposal or business case for a specific transformation project, planning the anticipated project road map and implementation process, and identifying and securing necessary resources |
|
| Project management and execution | Forming the project team, allocating roles and responsibilities, agreeing a schedule of activities and deliverables, and reporting on progress |
|
| Implementing change | Implementing the given system transformation project in real-world service contexts, as either a pilot project or a fully-fledged service transformation project |
|
| Evaluation and sustainability | Developing evidence of the change process and outcomes, identifying resources and mechanisms to sustain the change, and sharing lessons with similar service areas |
|
Illustrations of the political skill, strategy and action of major system change
The chapter now draws on the findings of individual case studies to illustrate the types of political skills, actions and strategies used to resolve one or more of the political controversies experienced during the implementation of major system change. As shown in Figure 9, the illustrative case broadly corresponds to one or two of the key stages identified in the composite model; the alignment between the specific stages and the case reports is not exact because the boundaries between these stages are typically fluid, that is when preceding decisions continue to influence a given issue and the decisions reached at one stage affect future stages.
FIGURE 9.
Mapping the illustrative case to the composite model of system change.
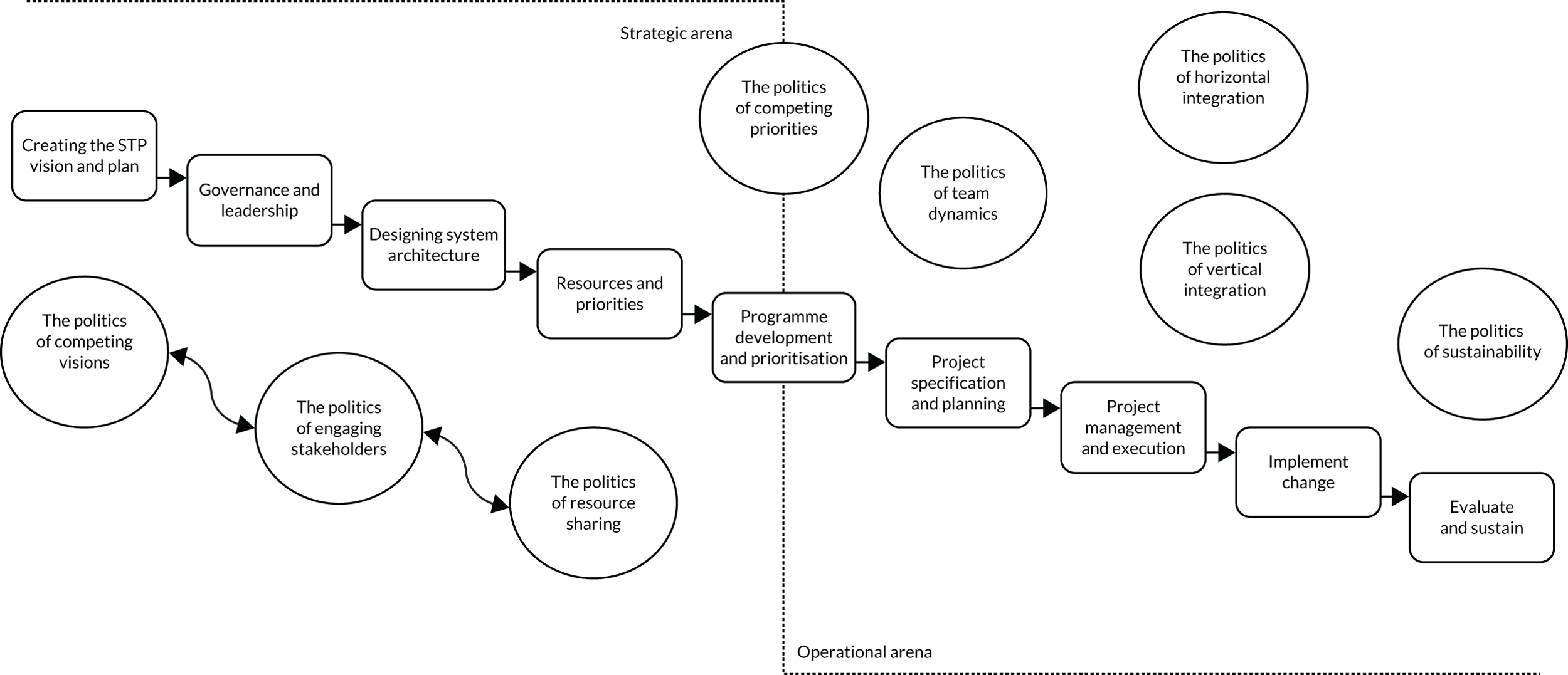
Illustration 1: the politics of competing visions for regional system transformation
Case one focuses on the challenge of creating a shared vision or sense of purpose for what a given STP aims to achieve in the overarching ‘strategic arena’. The diversity of constituent groups and complex governance arrangements meant that it was often difficult to establish a shared sense of purpose that all relevant stakeholders could align with or work towards. Most participants described the purpose of the STPs as a positive development for health and care system reform; however, beyond the broad ‘headlines’ around more place-based integration, STP plans could easily be interpreted as too broad and imprecise or as reflecting the narrow views of relatively dominant regional actors. In two STP case studies, determining and articulating a coherent and inclusive vision of change was an initial, and to some extent ongoing, hurdle in the transformation process that brought to light a key focus for political controversy.
This case describes how one ‘core’ STP executive group worked to craft, articulate and reinforce a shared vision of system change that reflected the overarching goals set out by the STP board and could provide a coherent sense of purpose and orientation for local project teams involved in implementing change. The case focuses on the changing strategy of this core executive group in its relationship with regional stakeholders and its attempt to move from a focus on managing the ‘harder’ aspects of system governance to a focus on the ‘softer’ side of values and purpose, which would better secure stakeholder buy-in for change.
A significant feature of the ‘core’ group’s approach was their commitment to self-reflection (or group reflection) in terms of their position in the system and contribution to system transformation. In terms of ‘self-reflection’, this included a, somewhat paradoxical, view of their liminal position within the care system, that is operating between statutory organisations and having little formal authority, and yet at the same time having delegated authority from the senior STP leader to authorise, co-ordinate and oversee system change initiatives. For this reason, much of their early activities focused on establishing workable governance arrangements that clarified their position, rather than the more symbolic or values-based aspects of change:
We are in a precarious position. We are a small team and we don’t really fit anywhere, but we are responsible for making sure the plans are taken forward.
Field notes: STP project lead
In taking forward the STP plans, the group further reflected that regional stakeholders often held different views about what system change aimed to achieve. As members of the core group reflected, regional stakeholders might easily embrace the broad principles of system change; however, when this this had an impact on their finances or service levels, the prospect of system change became problematic:
They might think system change is important in their hearts but not necessarily in their heads.
STP leader
It was through such reflective understanding about both their role in the system and the difficulties of securing stakeholder buy-in that members of the executive ‘core’ group recognised the need to change their approach and refocus their efforts away from managing the administrative structures to determining and articulating a shared sense of vision and purpose that stakeholders could more easily align with and support. The core group discussed how regional partners had distinct interpretations of system change, which were shaped by their particular service context and recent history of funding. For example, it was suggested that the view of system change held by local government partners was shaped by their prevailing financial constraints and service pressures, and the party-political priorities of formal political leaders. By contrast, commissioners were seen as understanding system change as a potential opportunity for cost saving and efficiencies. For this reason, it was necessary to create a new ‘system view’ in which stakeholders recognised that by ‘individually giving up a little, we gained a lot more as a system’ (STP lead).
In crafting a vision for system change, the executive group focused on four linked communicative and framing elements. The first was to be clear about ‘the who’ and ‘the why’ of change, specifically to foreground the health needs of local people and communities as the ultimate beneficiaries of system change:
We have got to remind people why we are doing this. The people of [place] deserve a better care service.
Field notes: organisational development lead
Linked to this, the second element was to emphasise the values and moral imperative for system change, by being more explicit about the normative standards of doing the right thing for patients. The third element was to be clear about ‘how’ system change would meet these needs and deliver the desired improvements. A prominent idea discussed among the core group was the need to ‘help’ (or encourage) stakeholders to ‘see the big picture’, especially the idea that by ‘giving up a little we can achieve more important and far-reaching improvements in the long run’ (STP lead). The fourth element was a focus on language and using the words and terms that speak to the different stakeholders. On one level, this related to selecting and using appropriate routine service data to demonstrate particular problems, and on another level drawing on powerful patient narratives to justify the vision. For example, recent innovations in the integration of community and care home services were widely described in terms of the impact on patient experience and well-being.
In reinforcing this recreated vision, the group highlighted the continuing role of formal governance structures to reinforce and (re-)incentivise engagement in system change. In particular, the vision was aligned with new commissioning arrangements that similarly took a regional perspective, together with longer-term plans to develop the STP into integrated care systems with enhanced statutory responsibilities for system change. In other ways, the executive group promoted the vision of the system by working more closely with public and community groups to reinforce the values and benefits of system working. This included, for example, partnering with prominent sports clubs, employers and voluntary groups to contribute to directly supporting change through hosting community events, and also being vocal in their support for more systems working:
We have been working with [team name] for a few years now as part of our community outreach programmes. They have helped us organise and deliver events and they have helped us get the message out in ways that probably makes more sense to the people of [place].
Field notes: project team lead
By reflecting on their position and activities to date, especially recognising the limits of their influence, the executive group worked to reframe the vision of the STP in ways that focused more on the symbolic or normative aspects of system change rather than on system governance. This was framed through alignment with both national and local priorities, especially the needs of local communities, and it was reinforced, somewhat paradoxically, through re-emphasising the changing role of formal governance structures (Box 1).
-
Reflection on ‘track record’ and own position within the system.
-
Understanding the different views and perspectives.
-
Framing strategies to align stakeholder perspectives.
-
Aligning vision with formal governance structures.
-
Careful use of language to appeal to particular stakeholders.
Illustration 2: the politics of stakeholder engagement in system transformation
This second case focuses on the politics of stakeholder involvement in the design and transformation of ‘system architecture’, specifically the reconfiguration of regional care commissioning. All three STP cases talked of changing the overarching ‘architecture’ or ‘design’ of their care system, which usually referred to reconfiguring the prevailing organisation of services and distribution of resources held by individual organisations, so that they better addressed the needs of local communities. As illustrated above, a key challenge of any system transformation process is securing the meaningful involvement of stakeholders across the stages: the design, specification and implementation. National guidance suggests that, alongside patients and the public stakeholders, ‘clinicians should determine and drive the case for change, based on best available evidence’155 (contains public sector information licensed under the Open Government Licence v3.0). By ensuring that change processes are shaped by stakeholder involvement, change can be expected to have greater relevance and, importantly, legitimacy with such stakeholders.
This case illustrates the politics of engaging clinicians in system change. It focuses on one STP’s experience in reconfiguring its multiple commissioning organisations into a single regional body [Clinical Commissioning Group (CCG)] that mirrors the footprint of the overarching STP with the goal of offering more strategic system-wide commissioning. This case examines how system leaders from the STP and CCGs engaged general practitioners (GPs) in this process. This case focuses on the interactions between, on the one hand, CCG leaders and the ‘engagement group’ within the STP and, on the other hand, GP leaders and representatives from across the region.
It was reported that managers from the region’s multiple CCGs started planning for a type of merger in the early days of formulating the STP and, significantly, long before any consultation strategy was considered. For CCG and STP leaders, change seemed inevitable and aligned with national policies and, therefore, the rationale of stakeholder engagement was less about co-designing change and more about securing support. Although CCG managers talked of undertaking preliminary engagement activities, it seemed that these activities involved largely informal conversations with GP leaders:
. . . you can’t swim against the tide . . . staying as we are would not directly align with the national direction for the NHS . . . We need to operate at a ‘system’ level across the entire geographical area.
Field interview
A more formal engagement strategy was developed that included (1) the preparation and dissemination of a proposal document; (2) a website and communication campaign directed to local GPs, patient groups and third-sector groups; and (3) an online survey with public and professional representations. GP stakeholders raised questions about this approach, describing it as relatively superficial or at best ‘information giving’, which led to an extended consultation plan, including (4) public engagement events or ‘town hall’ meetings, (5) focus groups with stakeholder groups and (6) a ‘listening exercise’ with GP representatives from across the CCG areas.
The communication and framing of both ‘system change’ and the engagement strategy seemed to be concerned with giving the impression of an inclusive and legitimate decision-making process.
The framing strategy focused in particular on the anticipated benefits both to the wider public and to clinicians and clinical leaders, such as saved clinical time, stronger clinical voice and reduced management. This could be further seen in the idea that there would be a series of ‘must-haves’ whatever the outcomes of the engagement process, which included strong clinical leadership. However, a contrasting policy narrative was that change was part of a bigger agenda, so there is little point in opposing it.
The reactions of GPs were directed at the details of both the proposal and the engagement processes. Some GPs actively questioned key procedural aspects of the overall decision-making process in public meetings, seeing decision-making processes as a fait accompli. For example, a number argued that senior CCG managers had effectively agreed the proposal long before the consultation was planned. The majority of our interviewed GPs described the decision as ‘top-down’ and the consultation processes as ‘tokenistic’ and a ‘rubber-stamping exercise’; such views underpinned a shared concern not with the substance of reform but with the way that change was being introduced:
If they had done [the consultation exercise] before they merged the governing bodies it would have looked more like a consultation and less like a foregone event.
GP1
It’s been too little too late. We’ve been told that it’s happening but we’re not told that we could have a vote on it till very recently.
GP4
They haven’t . . . the consultations were a couple evenings . . . most GPs are too busy to attend in the evenings . . . anything you put on in an evening is not going to engage people.
GP5
Despite this, the majority of GPs involved in the study described the proposed merger as having both administrative and clinical advantages. In particular, it was suggested that the new CCG arrangements could lead to more strategic commissioning, especially for planning services at the regional level and for countering the dominance of NHS trusts in determining service models:
The CCGs will become more of a strategic commissioner . . . if it works it’ll be fantastic.
GP8
. . . it will give a more strategic overview of the system and CCGs with a smaller footprint will have a small voice. A larger CCG will have greater power as they are negotiating on behalf of a large population. . . . The larger commissioner might have more power over the large hospital than we have.
GP9
Some GPs raised concerns about the proposed changes, illustrating this with counter arguments and rhetorical framings. One common view was that change was motivated less to improve decision-making, strengthen clinical voice or improve care outcomes, as implied, and more to reduce administrative duplication and create more standardised models of work. Others argued that regional commissioning could neglect and, over time, diminish the expertise of local commissioning processes. Challenging the message set out by CCG leaders, GPs saw reduced opportunities for their involvement in commissioning, or at best clinical leadership being tokenistic. The response from many GPs was that they would not actively engage in the new commissioning arrangements and that they would instead invest their energies in new clinical leadership roles within their GP practices or primary care networks (Box 2). For this reason, parallel system changes facilitated disengagement and diverted professional attention away from commissioning:
It’s a distraction from health care. Our jobs stay the same but it’s just rearranging the deck chairs on the Titanic.
GP2
There are other ways we can bring about the needed changes in care . . . the PCNs [primary care networks] should become much more focused on the needs of local communities.
GP3
-
Information-giving (problematic).
-
Listening and engagement activities (tokenistic).
-
Framing strategies focusing on clinical issues.
-
Public criticism (as response by GPs).
-
Disengagement (as response by GPs).
Illustration 3: the politics of sharing resources for new system architecture
Case three focuses on the combined challenges of redesigning ‘system architecture’ and, by implication, encouraging system actors to share resources (e.g. staff, finances and buildings) to enable more integrated ways of working. As with the other STPs, system redesign involved, for example, redistributing roles and responsibilities, merging organisations, replacing organisations, and changing the boundaries and connections between organisations. Each of these represented a site (or microsite) for the broader politics of system change, especially when it involved sharing or redistributing scarce or specialist resources.
This case illustrates the challenges of sharing resources when redesigning children’s services, family services and maternity services within one STP. The intention of the new architecture plan was to create more integrated and holistic care for children and families in the early years of life. The proposed plan comprised a programme of transformation projects that involved the redistribution of hospital and community maternity services and the creation of multiagency regional ‘hubs’, which required the distribution of roles and resources among hospital and community services, as well as primary care and local authority care services.
As above, an initial controversy was with the vision of system change. Although the overall idea of integrating a more seamless service was understood, it was difficult for all stakeholders to share an understanding of what change would look like, how stakeholders would work at different levels and where responsibilities lay. It was also unclear how individual transformation projects, some of which preceded the idea of system reconfiguration, would fit with the new model of care:
But, you know, ah, but we’re in it together. Ah, no, but we’re not. So there’s still this push/pull about are we in it together or aren’t we in it together? What are you responsible for? What aren’t you responsible for?
Clinical lead
A significant complication related to the allocation and sharing of financial and physical resources. In terms of financial resources, a major issue related to how new ways of working would align with prevailing financial governance systems. Although commissioners were broadly supportive of a new integrated model, there was uncertainty about how proposed services should be commissioned, especially in terms of who would control the resources in this multiagency framework. The second related to the control of physical estates, for example hospital buildings, because the proposed system architecture plan involved introducing new community ‘hubs’ located in NHS and local authority venues, but on the basis of shared responsibility. This highlighted additional complications, such as the infection control requirements of different care sectors:
We’ve been round to all the (STP) locality meetings and had discussions at their boards but I don’t know whether we’ve progressed it anywhere really. I don’t think it’s moved. It’s still the same issue. Where is the money coming from? It’s difficult.
Clinical lead
. . . it is quite different you know, in terms of the traditional way of delivering hospital services and I think, support, and more looking at how we shifted from the funding from kind of the community providers into the voluntary sector to do some of that intervention.
Project manager
The approach taken by system leaders, comprising members of the STP executive group, the locality partnership group and the thematic programme board, was seemingly unplanned and messy. Based on a history of interagency tensions, the change process became protracted and riven with conflict, with little overarching strategy or immediate success. For example, the Child and Adolescent Mental Health Services felt marginalised by the ‘saintly’ maternity services. One of the first strategies adopted by the executive group was to open up dialogue with constituent organisations with the dual aims of listening to their concerns about the prevailing model of care and, simultaneously, encouraging them to recognise the potential benefits of system change. This led some stakeholders to feel that they had come up with the rationale of system change rather than it being imposed. As part of these engagement activities, leaders also talked of developing a better understanding of the interests and agendas of regional actors, especially around the control of resources and the tensions between hospital- and community-based services:
It’s just building up that . . . I suppose if I was working in an office I’d have a better relationship with them, or a worse one. Depends. It’s all about personality at the end of the day . . . It’s just building that rapport up with the person that’s leading the project and I suppose it’s about telling them . . . you know, because everything’s to do with performance reporting or performance management, you’ve got to take out the fact that I’m not there to beat them with a stick, you know it’s beneficial for me and the person running the project to get the information that I need to help them run that project.
Project manager
A subgroup of system leaders, drawn from one of the region’s children’s and family services, proactively worked to mediate the tensions between regional organisations about the redistribution of roles and resources. Building on the above, this involved fostering dialogue among local organisations so that they could better understand their respective priorities and explore how differences could be resolved through a systems approach. On a personal level, leaders recognised that the situation was complex and emphasised the importance of persevering in fostering mutual understanding. Interestingly, some participants described how system leaders adopted a particular style that perhaps reflected the ‘maternal’ character of their profession, in that they sought to defuse conflict, promote a calm approach and nurture a supportive environment:
. . . it feels like you could not have ridden this sort of tide if you need everything very orderly and in a box, kind of thing, because it just feels so unlike that at the moment. We’re constantly adapting to whatever the next thing is.
Project manager
Although progress was made in resolving local tensions, system leaders opted to contract a management consultant to facilitate the co-design of the new system architecture plan. This highlighted three significant turning points. First, leaders recognised and advocated for a co-design approach so that stakeholders could see and feel that change was based on an open and deliberative approach. Second, the employment of an external consultant perhaps suggests that local leaders recognised their lack of specialist skills in co-design methods. The third turning point was the importance of being seen as neutral or not embroiled in local politics:
. . . the local authority has funded a management consultant who’s working with the senior teams, so we had a workshop last Friday. We’ve got a workshop again tomorrow. So it’s moving at quite a pace developing and thinking around what would integration look like? What’s the [unclear] culture? . . . What type of roles should be integrated? What functions are definitely one or the other?
Clinical leader
Through this process, participants described how a ‘bottom-up’ approach to system change emerged that reflected the local interests of stakeholders and emerging evidence of effective system change; however, to some extent, the eventual model of system change continued to reflect the outlined specification previously set out by system leaders (Box 3).
-
Open up dialogue.
-
Actively listen to concerns.
-
Foster shared understanding.
-
Utilise a supportive style.
-
Personal perseverance.
-
Recognise limits of approach.
-
Engage specialist support.
-
Use co-development method.
Illustration 4: the politics of competing priorities for transformation
The STP programme boards appeared to function in the middle of the STP structures, working to translate the broad strategic plan for system change into a more specific programme of change within discrete service areas, for example maternity or mental health, that would then be operationalised by individual project or transformation teams. An initial task faced by these programme boards was the elaboration of the overarching aims for system change and population health improvement into specific and operational priorities for change. This case illustration describes the experiences of one urgent care programme board as it worked to determine its strategic priorities. This case highlights the political skills, strategies and actions of the designated programme lead (PL) in working with others to identify, mediate and reconcile competing viewpoints and preferences.
In setting the context for group discussions, the PLs would often restate the ‘big picture’ of system change, rearticulating the expectations from the STP and promoting shared values or a sense of purpose for system change. They also worked to ‘open up dialogue’ and debate among board members to explore the problems and issues facing urgent care, especially by encouraging stakeholders from outside the acute hospital sector to contribute to the analysis of the challenges facing urgent care, such as primary, community and mental health services. This helped to create a more nuanced and shared understanding of the issues from which subsequent proposals for change could be appraised:
It’s about being inclusive . . . so people can feel engaged and inspired . . . I know how difficult it can be to try to force people, doctors, to accept change and it has to feel that it is driven by the community.
Field interview
As deliberations continued, the PL tasked opposing groupings to develop and evidence their priorities and proposals for system change. This involved drawing on the expertise of the CCG representatives (as people more accustomed to reviewing business cases) and the STP management representatives (as people with insight into other programme themes) to articulate the expectations and requirements of these proposals. This strategy of ‘delegation’ seemed to pause or defuse debate by suggesting that ‘more work was needed’ to understand and evidence the issue before carrying on with deliberations. It also enabled the PL to identify nascent project teams around shared interests and to continue the strategy of delegation. In reviewing these proposals, the PL often advocated the importance of ‘data-driven decision-making’ or establishing a robust set of measures on the urgent care system from which to identify system challenges, prioritise change and, in time, evaluate improvement. This was presented as a more objective and technical basis of prioritisation than relying on group debate within the programme board:
The PL asks the lead for the ‘Street Care’ project [name changed] to give an update of the development of the proposal. The Street Care lead [from the community mental health team] reports that he has been in contact with the police service community liaison and mental health leads, and also the ambulance services, to identify potential sources of data. The PL asked how they intended to use the data, to which the project lead talked about better understanding the numbers of people needing primary care in public spaces.
Field notes
When dealing with conflicting perspectives, the PL seemed skilled at keeping people ‘at the table’ or discouraging their disengagement from the process. It was described how the PL met with people ‘outside the meeting’ to defuse disagreements, reconcile differences or find inducements that would maintain their involvement:
It’s so important to find the things that will keep them interested, it doesn’t always have to be more resource or pandering to their egos, it is better when it’s about the issues that really matter to the service and communities.
PL
In seeking to move beyond conflict, the PL seemed to adopt a strategy of ‘sufficient consensus’. This involved developing some degree of collective consent for a given priority and transformation project that the PL would then authorise with additional support from the STP management representative and the CCG lead. Although this gave the appearance of enhanced deliberation and inclusive decision-making, it still seemed to suggest that authority mainly rested with a smaller group of people who, however, still needed the involvement and support of the wider group of stakeholders.
One reading of this was that the PL was committed to a more deliberative and democratic approach to decision-making that would lead to greater legitimacy and commitment among system stakeholders. However, a more critical interpretation of these activities suggests a slightly different set of political intentions, skills and activities. First, the PL seemed to use their opening remarks on the ‘big picture’ to frame or ‘set the agenda’ for debate around which a common viewpoint could be engendered. Second, this initial framing had the effect of also positioning the PL in a relatively distinct position to other board members in that they had a more developed understanding of the ‘big picture’ because of their involvement in ‘higher-level’ strategic decision-making. Third, the PL was able to better understand the areas of alignment and disagreement, which informed their subsequent engagement activities. Fourth, the deliberative process gave participants a sense of having influence on the decision-making process, even if they did not (Box 4).
-
Set the agenda.
-
Open up dialogue.
-
Foster shared understanding.
-
Look to evidence issue.
-
Delegate tasks.
-
Informal interpersonal influence.
-
Work towards sufficient consensus.
Illustration 5: the politics of team dynamics and (mis-)reading the political context
All STP transformation projects needed, in some sense, to appraise the political context of designing and implementing change. A small number of teams engaged in more explicit discussions and assessments of the lines of power and competing interests that would probably have an impact on their project work. Most teams, however, seemed to engage in more ad hoc and informal discussions about such issues, and often relied on implicit assumptions that were not clearly shared by other team members. This case illustrates the dilemmas faced by one project team as it worked through the different ways that its team members ‘read’ and made sense of the diverse and competing interests among wider stakeholders.
The case focuses on a project team that aimed to introduce personal health budgets (PHBs) for people diagnosed with personality disorder. The broad rationale for the project was to enable people diagnosed with personality disorder to identify and acquire more personalised support to meet their psychological needs and, in turn, to reduce the demand on acute mental health services. This project team comprised six people: the deputy chief nurse from a mental health NHS trust (who acted as project lead), a senior medical representative from the same trust, a STP lead for personalised care (seconded from one of the region’s CCGs), a representative for mental health commissioning from another CCG, a representative from the local authority adult mental health service and a representative from a patient advocacy group. It became clear during their initial project meetings that these team members held differing views about the levels of support or interest among wider system stakeholders for this initiative.
Differences in how project team members appraised the preference and views of the wider care system shaped both how the project team members worked together and how they worked with external stakeholders. It was clear that these differences in understanding within the project team stemmed from team members’ primary affiliation or role in the wider system of care. For this reason, the case elaborates a key internal political challenge for multiagency project teams that stems from their reading of the external political landscape:
Unlocking funding is the challenge, when you get down to it, everyone saying, well social care are saying the funding should come of the trust, and the trust is overspent and it’s running out of beds. So, we have got to make argument that if we spend a little bit more we could bring that overspend down . . . If we can overspend . . . but on things that are helpful for people that is better than spending on private providers out of area.
Project lead
Specifically, project team members appeared to ‘read the local political environment’ in two contrasting ways. Those from the NHS trust saw the main obstacles to introducing PHBs to be a lack of understanding among front-line health and social care staff about the potential benefits to patients, and relatedly their lack of ability to assess patients as requiring PHBs and supporting them to make use of their enhanced financial autonomy. For these team members, it was imperative that community health and social care teams were supportive of the scheme and able to fully support its implementation with patients:
Clinical, strategical and vision it is absolutely the right thing to do . . . But internally, I haven’t got the trust to identify any funding, something has come via the CCG for a small number of patients. Whilst the money seems to be the block, I don’t really think it is, I think it is the resource in terms of capacity and frontline [NHS] staff to engage with it. We want to try it as proof of concept.
Medical representative
By contrast, team members from the STP PHB team, the local authority and the patient advocacy group saw specialists and leaders from the acute NHS trust (and to a lesser extent the CCGs) to be the primary obstacles to change. This coalition of team members held the strong view that the NHS trust would oppose the introduction of PHBs because it would potentially divert patients and resources from the acute statutory sector. In other words, local organisations for which representatives were not only part of the project team but also leading the project team were seen as the primary barriers to change:
It’s not that they don’t understand personal budgets. It’s that they don’t really want them in their [emphasis] clinical service. They see it as diverting resources.
PHB lead
The project team’s differing perceptions and viewpoints underscored a lack of shared purpose and, more significantly, complicated team dynamics. Several team members described team meetings as disorderly and disrespectful, with people talking over each other and not being prepared to listen to different perspectives:
I have never been in a team like it. Everyone just talked over each other, there is no dialogue.
Project lead
A major internal political challenge was to reconcile these differences and to establish a shared sense of purpose. This involved, for example, agreeing to take part in a series of team-building activities to improve interpersonal relationships and fostering more open dialogue outside formal team meetings to explore team members’ different perceptions of the issues facing mental health services.
In parallel, the PHB lead took a more proactive, unilateral or ‘breakaway’ role in moving forward project work, without the direct or full involvement of all team members. This could be described as a patient-centred engagement strategy that aimed to work directly with service users to test and develop the evidence for the new service model; this is evidence that could then be used to persuade both internal and external stakeholders. This involved three strands of activity. The first strand of activity was to carry out a preliminary assessment with patient representative groups of the anticipated needs and benefits of PHB, especially what types and levels of services might be wanted by people, that is to gather the patient perspective. The second strand of activity was to undertake a short evaluation of the PHB scheme for a small community of people with a diagnosis of personality disorder, that is to develop the evidence. The third strand of activity was the formation of a small patient representative group to champion the implementation and use of PHBs among relevant service user groups but also to represent the experiences of patients with key strategic decision-makers:
We know PHBs work for other communities, and we really need to find the evidence that they can work for people with personality disorder. We need to show the outcomes for people can be better and that there are potential savings to the system.
Field note: PHB lead
Despite these activities, the PHB project was paused and then discontinued because of system pressures brought about by the COVID-19 pandemic. One reason given was that it would be difficult for people to access non-statutory services during lockdown conditions and another reason was that project team members needed to return to their primary clinical or organisational duties during the pandemic. However, another reading could be that the pandemic provided the rationale or a changed context to close down a potential innovation that, according to the PHB lead, was not a priority or well received by prominent actors in the regional care system (Box 5).
-
Main political skills, strategies and actions.
-
Open up dialogue and foster shared understanding.
-
Unilateral action.
-
Develop and utilise patient perspective.
-
Develop evidence.
-
Identify and recruit advocates.
It is not clear whether or not these contributed positively to change owing to wider contextual factors.
Illustration 6: the politics of implementing integrated acute and primary care services
Each case study STP had plans to introduce more integrated ways of organising and delivering services. Such integration is typically premised on the idea that existing models of service organisation can be fragmented, wasteful of scarce resources and poorly suited to address the complex care needs of people and communities. For this reason, the integration of care aims to achieve more high-quality patient-centred care, as well as resource savings through supporting care providers to work in more co-ordinated ways.
One prominent model of integration is when multiple health and care service provider organisations involved in the delivery of different aspects of care within a given new locality are brought together into a single, more streamlined and co-ordinated, entity. In practice, this involves creating a layer of operational and financial governance to oversee and co-ordinate the activities of primary, secondary, community and social care organisations, including new ‘vertical’ lines of accountability and co-ordination, as well as new ‘horizontal’ pathways for care delivery.
This illustrative case focuses on the political controversies surrounding the introduction of a new locality partnership organisation that aimed, in broad terms, to provide referral processes and continuity of care, as well as other forms of functional integration of non-clinical administration, such as information systems, by bringing together a large NHS (acute) trust, a GP federation (of multiple GP practices), local authority social care providers, and private and third-sector care providers. Significantly, this resembled a form of ‘vertical’ integration in which one organisation (the NHS trust) was designated to oversee and manage the overarching ‘supply chain’ of locality care pathways from referral to hospital care to community care, with the anticipated benefits of reducing transaction costs and streamlining interdependent ‘production’ processes. This case study is important because it reflects the awareness, skills and groundwork that is required to understand and deal with divergent interests and move the change from a position of impasse to a position of agreed objectives and outcomes. In addition, the case is interesting because it shows that the groundwork is both ‘front stage’ and ‘back stage’.
The primary issue faced by the project team (comprising service leaders from the STP executive, the local CCG, the NHS trust and GP federation) was a breakdown in relations between local GPs and the NHS trust when the integration was proposed by the STP. Despite a positive history of close working between primary and secondary care providers, the planned integration appeared to fracture this working relationship and destabilise the balance of power in the locality. GPs perceived that the proposed arrangement gave too much influence and power to the NHS trust:
. . . and it really quickly became apparent that nobody was on the same page, you know, there was no agreement about what the priorities were, they, the contract actually wasn’t that good, there weren’t many safeguarding measures in it, so we didn’t know what was going on in the services. Letting the contract to the acute provider, put the acute provider very much in the driving seat. And there was . . . I suppose within 6 months, it was really apparent that the GPs were . . . all on the same page about what they were going to deliver and how they were going to do that, and there was some big falling outs, big arguments.
Senior STP leader
A number of GP leaders argued strongly that hospital managers did not understand the value of primary care and that there was a risk that many of the advances made in primary care could be lost if services were transferred back to the hospital sector. GPs also saw such change as having a negative impact on their finances that were dependent in part from providing certain services. Such tensions were manifest in interpersonal behaviours in project team meetings in which, for example, there was clear confrontational and accusatory behaviour, with stakeholders unable to agree priorities and becoming distracted in their arguments as they debated preferred governance arrangements. In many instances, these debates reinforced sectoral boundaries and identities.
In taking a new approach (or changing tack), the project team decided to appoint an independent chairperson who could help to mediate relationships from an impartial standpoint, while also appointing a new project lead (a CCG finance director) who was able to ‘wear two hats’ and understand the details of contracting and procurement across the primary and secondary care boundary. Working together, in a conjoint way, these project leads talked with local stakeholders about the importance of seeing the longer-term benefits of change and persevering to resolve the tensions in the relationship between GPs and the trust. This involved adopting a more open and deliberative approach to stakeholder engagement, in which representatives were encouraged to ‘see the world from the other’s perspective’. This seemed to play on reading and empathising with the heated emotions that stakeholders had around change, for example understanding their fears:
[S]ome of it’s been about developing relationships and alliances . . . getting a better, clearer, shared understanding across the different stakeholders about the current situation and what the facts are and what the evidence is, and what needs to change.
New project lead
As part of these activities, the leaders targeted key people of influence from the respective organisations to develop a better understanding of their particular interests and concerns to devise targeted solutions that could win their support. This involved exploring forms of change that would benefit all parties through negotiated forms of ‘give-and-take’ or identifying ‘win–wins’, such as creating more flexible joint contracts for GPs. It was reported that these influential people worked ‘behind the scenes’ to build more trusting and collaborative ways of working among stakeholders. One prominent example was to encourage stakeholders to recognise that defunding social care or primary care would ultimately have a knock-on effect of increasing demand on emergency services; therefore, it is in the acute trust’s interests to maintain support for community services. The subsequent endorsement and support of these people helped to consolidate group deliberations. The learning from these activities was then brought back to subsequent project meetings to inform decision-making and often counter the views of recalcitrant groups:
. . . and it won’t necessarily always be around even the main board table. There are sub-boards and there are other things out there . . . So we don’t get hung up on the mechanics.
GP representative
The study also found that the project leaders were open about their capacity to use more formal authority structures to enforce change in the absence of finding agreement. Although reluctant to use this option, leaders from the CCG talked of using their financial controls to take services away from the trust and either find alternative secondary care providers or explore the potential for more primary care provision. This type of ‘nuclear option’ was rarely used but mention of it seemed to refocus the attention of the NHS trust leaders by demonstrating the underlying lines of formal authority and the inherent interdependencies:
. . . in terms of leverage, then that acute trust knows that, the commissioner is prepared to take another chunk out of it if it doesn’t behave.
STP senior leader
Over time, the barriers to integration were overcome by a combination of strategies concerned with relationships and alliances, communication, and self and style. The element of neutrality of the network chairperson seemed to be important to gain trust and they used a personal style that helped to push beyond the controversies with an empathetic but emphatic approach (Box 6).
-
Appraisal of the political landscape.
-
Use of empathy and emotional intelligence to break down boundaries.
-
Foster shared understanding of shared or interdependent problems.
-
Development of conjoint and impartial leadership.
-
Behind-the-scenes activities.
-
Networking.
-
Targeting key people.
-
Evidence gathering.
-
Using formal authority.
Illustration 7: the politics of implementing integrated specialist services across acute and community boundaries
Following the above case, this illustrative case focuses on a different example of integration that involved drawing together specialists from the same profession but based in different organisations and locations into a single integrated provider organisation. Specifically, this case focuses on the experiences of one STP project team that was established to develop and test the integration of pharmacy services that were previously distributed (and poorly co-ordinated) across multiple hospital and community settings. This example of integration resembles a form of ‘horizontal’ integration in which multiple similar functions or specialists are brought together as a regional-level service. This was part of a national scheme to integrate NHS pharmacy services and medicines optimisation,156 with the aim of ensuring that patients get the most benefit from their medicines, especially for people with complex conditions requiring multiple medicines, while also controlling expenditure on medicines and the additional costs associated with poor adherence and risk. In practical terms, the newly integrated services involved establishing a single pharmacy leadership team for medicines optimisation across the STP region and integrating pharmacy expertise in local services to support, for example, antibiotic stewardship, patient adherence and prescribing practice.
A challenge faced by this integration project was how to create a shared understanding of the value and benefits of local-level service integration, especially when local stakeholders might prefer or benefit from customary models of service delivery or have concerns about the ulterior motives for change. Such tensions were exacerbated by a history of service fragmentation, manifest in both different service delivery models and the corresponding allocation and control of resources. For example, pharmacists in hospital and community settings were accustomed to different work routines, information systems and levels of interprofessional working. One significant area of tension was with the relative financial burden of medicines management. It was reported that the use of block contracts to fund pharmacy services in the acute hospital setting enabled the discounting of medicines for hospital patients, but once a patient moved to a community setting such discounting did not apply and the financial burden of medicines management had to be covered in the budgets of community hospitals and primary care:
. . . supposed to be working together, but there will still be the financial directors of organisations that will want to maintain their books and balance the books. So there is still that financial tension which has an impact, as well as workload issues that get passed across. So that integrating primary, secondary the politics is to do with finance, their contracts, workload, and negotiating with drug pharma[ceutical] companies.
GP lead
For this reason, the project team had to devise a new funding model that would share the risk and benefits across multiple organisations to deliver more integrated medicines management. For service leaders, this key first step made possible subsequent changes by offering a sense of fairness and enabling more collaborative working:
So having the funding which was exactly what it was designed to do was to give them the head space to think about what they needed to do and coming together as a group and really working.
Community pharmacist
There were further tensions around the allocation of distributed leadership roles within a new integrated pharmacy service, especially whether hospital or community pharmacists would have a greater influence on decision-making. For example, individual NHS trusts were anxious about losing a portion of their pharmacists’ time to the new system-wide model of working, resulting in a need to backfill their time in the hospital. Moreover, chief pharmacists from individual trusts were critical of being made subordinate to peers who have acquired leadership roles within the STP; for this reason, ensuring some elevated or senior status for the hospital pharmacist community was seen as necessary as a kind of recognition and compensation for new ways of working:
I think that having the new chief pharmacist in the hospitals has really helped. There was a . . . there was a sort of us and them going on before, because the providers were separate from the commissioners. There was a wall between them and that was the way it was all set up but now of course it is all integration.
Project lead
An additional complication was the persistence of technical, functional and cultural differences in the working practices of hospital and community pharmacists, especially the character and depth of the relationships that they developed with other clinical groups and understanding the logistics of working and different population needs. The project team, therefore, needed to secure the active involvement of pharmacy leaders and pharmacists working across the hospital and community sectors, and also the support of the organisations within which they worked:
At this point I re-established informally the leaders from all the partner organisations . . . We starting meeting, and we just started discussing what bits of work would be beneficial from the pharmacy perspective to . . . work on collaboratively . . . And so we’ve built up the relationships again, and we did actually agree on some key areas that would be beneficial to work on collaboratively.
Project lead
The early stages of project activity demonstrated the prevailing tensions within the landscape. This was evident through the marked lack of engagement of certain hospital providers and when representatives did attend project meetings it was observed that interactions among pharmacists and the STP lead were often ‘awkward’, with pharmacists often voicing concerns about their changed role. Perhaps more significant were the breakdowns in relations manifest in the silences and refusal to give consent to proposals. In other words, political action can involve inaction and withdrawal as much as active opposition.
In seeking to reconcile these tensions, the project leaders reflected on the range of system representatives involved in project planning and also the wider engagement work. In particular, it was decided to involve additional pharmacy leaders who could speak to the different roles and responsibilities of pharmacists across the wider care system, not just hospital and community services. It was also thought to be important to utilise existing connections to invite more independent (non-pharmacy) perspectives from across the care system to help to contextualise the pharmacy viewpoint and help stakeholders to see the bigger picture. On the one hand, participants talked of putting the patient perspective at the centre of the conversations and guiding the strategy, and on the other hand they also talked of the absence of medical involvement that was seen by some as dominating conversations:
. . . you can talk about how, well if we can work better together as a group and you may lose a little bit and we may lose a little bit. We work together and in an altruistic way it’s better for patients, it might be more efficient, some losers, some gainers, that kind of approach, give and take approach, and our negotiations can occur in that fashion.
GP leader
Through changing the range of people involved in project planning and implementation, the project team were able to develop a more fine-tuned understanding of the common and diverse pressures across the system and, importantly, were able to foster corresponding shared understanding among regional stakeholders. Building on this new insight, project leaders set about devising a revised communication strategy that incorporated the various concerns and aspirations into a clear and consistent vision around which there was a large degree of consensus. In particular, service leaders emphasised the big picture and greater good, framing strategies that meant an acceptance of losing some aspects of pharmacy work for the greater benefit of the system and patients.
That said, some degree of opposition remained, especially in the allocation of new system-wide leadership roles for pharmacists and how changes would negatively affect the day-to-day work of some hospital and community pharmacists. The main responses to these concerns were, in the first instance, to identify and promote ‘win–win’ situations that demonstrated the overall benefits to individual service organisations even when they might not appear of particular benefit. For example, pharmacy leaders emphasised how the proposed initiative would have collective benefits for the profession, especially for raising its profile in the division of labour, offering greater autonomy to pharmacists and ensuring that it played a more direct and ongoing role in new models of working. Another strategy was to develop forms of compensation to placate vocal resistance to change. For example, a number of pharmacists expressed concerns about the allocation of new leadership roles and responsibilities, but seemed to be appeased by being offered a new peer-pharmacist role to help coach and support other pharmacists (Box 7).
-
Broaden stakeholder engagement.
-
Utilise developed and familiar connections.
-
Use patient perspective.
-
Foster shared understanding.
-
Clear vision with broad consensus.
-
Create win–wins.
-
Offer compensation.
Illustration 8: the politics of sustainability in workforce development
Case eight focuses on the political challenges of sustaining and extending transformation activities beyond the initial project work. It focuses on the experience of one STP project team leading a portfolio of organisational and workforce development activities across the region. This initially had a very specific remit to facilitate joint health-care and social care apprenticeships to address skills shortages in these areas and then evolved to include workforce development activities to support integrated and interprofessional working across the system. Over a 2-year period, the project team developed a series of targeted and system-wide workforce initiatives, but often with variable levels of engagement with regional stakeholders in health-care and social care sectors. Furthermore, financial support for this project team was always time limited or project limited and stemmed from multiple sources, including STP funds and financial support from individual NHS organisations or external bodies, such as Health Education England. A major challenge for the project team, therefore, has been to develop longer-term change initiatives and secure their position within the system landscape, especially given that they were required to seek refinancing on an annual basis or to secure external funding:
The real problem is the lack of longer-term funding so we can put together a more substantial programme of workforce development and offer people a kind of pathway for career progress.
Field note: workforce lead
The case brings to light the challenges of a new, small team building sustainable collaborations with larger, more hierarchical stakeholder organisations. The experiences of the project team bring to light the key issues of stakeholder engagement and funding as having an impact on the sustainability of change. Team members reflected that their work was not always valued by stakeholder organisations, and even when senior leaders talked about the importance of a ‘systems approach’ to workforce development, too often middle managers within individual organisations would continue to develop internal activities rather than engage in the STP projects. Reflecting on these challenges, team members described variable levels of support. Some small organisations were more positively engaged in and supportive of the work, whereas other, larger, NHS trusts would be less engaged and act more unilaterally in disengaging with the project team and using their own financial resources to develop internal and bespoke programmes. There were added complications about where resources were managed and who was accountable for project team activities, which meant that some stakeholders saw project work as being aligned with certain sectors rather than others. Even when funding was secured from an external agency, it often led to relatively short-term project-focused engagement rather than more sustained collaboration. One team member suggested that individual organisations were fearful of the system-wide approach being taken by the project team because they saw it as threatening their own roles and responsibilities. Other organisations did not feel the need to collaborate and were happy with their own ‘in-house’ activities. The project lead reflected on that need to constantly justify what they do and to ‘sell themselves’:
The [STP] board is very supportive and seems to understand how a workforce programme could go alongside new service models or the shift of services to the community, but the workforce leads in the individual trusts can only see what their organisation needs and so they allocate the budgets in ways that support them.
Project lead
In seeking to establish a more sustainable basis for their activities, the team showed clear signs of collective self-reflection by appraising their success and struggles and considering their image and reputation in the wider system (i.e. why did they keep needing to justify their worth). They also considered whether or not they had the appropriate people and groups involved in the wider project activities, especially on standing committees. They also identified key people in a small number of prominent organisations as ‘blocking’ their progress through not engaging in system-wide development programmes and communicating opportunities within their organisations:
We needed the time to reflect as a team and share our experiences of trying to work in the system and recognise what does and what doesn’t seem to.
Field note: workforce team member
For this reason, a dual strategy was developed to better engage more senior system leaders and to better demonstrate their contribution to the overarching STP agenda by building on projects that had been successful. This involved working with more supportive organisations to evidence their success stories to ‘convince the unconvinced’. They also described working more closely with influential individuals who could promote their work and widening their communication activities to reach those leaders who might not hear about their work because of the negative role played by middle managers and HR leads within individual organisations:
We have tried to build the evidence across a number of levels. So showing how what we do can contribute to how services work in their own right and how they can work better together. There are some obvious indicators around staff retention but the key is to show the clinical improvements and potential for costs savings.
Project lead
As part of their new engagement strategy, the project team described working within the less-engaged partner organisations to encourage them to determine the system-wide priorities that might foster their future involvement, but which could also be used as a way to hold them to account for future funding obligations (Box 8).
-
Collective self-reflection.
-
Critical appraisal of landscape and individuals blocking change.
-
Engage senior system leaders and other influential figures.
-
Evidence success stories.
-
Build networks of support.
-
Engage difficult groups in priority setting.
Discussion
Each of the above illustrative cases offers understanding of the ‘system politics’ and political skills, strategies and actions involved in implementing major system change within health and care services. Presented together as a composite analysis of change, the stages and activities described resemble many of the common step-wise models of change management. However, the study findings build on, and contribute to, such models in a number of novel ways. First, the study foregrounds the political controversies or struggles experienced during change as the primary focus of analysis, rather than the anticipated or prescriptive stages of change. As noted by Clegg et al. ,49 ‘strategy, once conceived, struggles to come into being through the processes of micro-politics’. Second, the study shows how the political controversies do not necessarily arise at particular or fixed stages in the change process, but rather they can occur at the intersection or point of transition between more stages, that is where the design of system architecture and resource sharing connect. For this reason, political controversies are more fluid and dynamic, operating in the spaces between the stages of more change models, and in many ways defining the overall change process. Third, and extending the idea of politics being dynamic, it seems to be that controversies experienced during one stage can have downstream implications (both positive and negative) for the politics at other stages depending on how these are resolved, while still recognising that change is far from linear and involves many feedback loops and ‘dead ends’ requiring adjustments in the preceding stages of the change process. This is especially the case when change activities are tightly coupled or interdependent, which in this study was more common in the ‘strategic domain’ than in the ‘operational domain’. Strategic activities for establishing a vision, engaging stakeholders, determining the system design and sharing resources were found to be more interdependent, in which adjustments in one element would require accommodations in another because they collectively set the broad agenda for system transformation. By contrast, individual transformation projects were often managed as relatively discrete or independent activities, although it is clearly the case that many change projects interacted with others and that activities in one stage of the change process, for example project specification, could both influence and be influenced by later stages in project management and execution, that is requiring later adjustments in project specification. Fourth, the study recognises the contextual contingencies that shape the political controversies of change and how these are (or are not) resolved through the political skills, strategies and action of local actors. That is, each STP case was characterised by a particular configuration of actors, a local history of change and prevailing lines of power and influence that shaped how the controversies manifest themselves and how they are resolved (or not). A significant aspect of system leaders’ political astuteness was in many ways understanding these contextual contingencies to orientate themselves, devise realistic plans for change and know how to influence established lines of power.
Mapping the illustrative cases to the earlier model to develop an aggregate analysis of change (see Figure 9), it is possible to identify the particular controversies and common skills, strategies and actions at the different stages of system change (Table 12).
| Transformation stage(s) | Case illustration | Controversies | Skills, strategies and actions |
|---|---|---|---|
| Creating the STP vision and plan (and system governance and leadership) | The politics of competing visions |
|
|
| System architecture (and system governance and leadership) | The politics of stakeholder engagement |
|
|
|
Creating the STP vision and plan, resources and priorities System architecture |
The politics of resource sharing |
|
|
|
Programme development and prioritisation (Project specification) |
The politics of competing priorities |
|
|
|
Project specification and planning (Project management) |
The politics of team dynamics |
|
|
|
Project management and execution Implementing change |
The politics of vertical integration |
|
|
|
Project management and execution Implementing change |
The politics of horizontal integration |
|
|
| Evaluation and sustainability | The politics of sustainability in workforce development |
|
|
Thematic cross-case analysis
Cross-case analysis supports the identification of a number of common themes and issues that characterise and contextualise how political skills, strategies and actions are used in the formulation and implementation of major system change. These represent significant empirical and conceptual contributions to the existing literature on organisational politics and political skill as found in the wider social science and health services research literature.
System politics as liminal, necessary and problematic
The case studies show that, in many instances, the politics of ‘system change’ are broadly similar to the (more widely researched) politics of organisational change, that is the competing interests and agendas of actors. However, in some key ways politics takes on a relatively distinct form at the interorganisational level. The main feature of ‘system politics’ is that it is manifest between organisational structures and, therefore, outside (and often in opposition to) prevailing formal authority structures. This is especially the case within the STP landscape in which system leaders sought to develop authority structures for system working but which still lacked a statutory basis, and at the same time were often required to comply with existing governance arrangements at the organisational level. In the light of this challenge, many of the controversies identified relate to defining visions and plans for system change, determining priorities and implementing system transformations in the absence of formal authority structures or formal/legal decision-making processes. This means that system leaders and other system actors need to function beyond and between formal authority structures when political skills, strategies and actions become the primary basis of resolving system politics and shaping system working.
System politics as dynamic (often unanticipated) context-specific political challenges
The case studies supported the findings of the narrative interview study, specifically that system politics and the associated political strategies and actions that influence how these controversies are played out are highly dynamic and context specific. Correspondingly, they can often be poorly anticipated or planned for by local actors. As noted, it is not always clear whether or not a change initiative will become a political controversy in itself; rather, it is the way that local actors interpret and respond to both the initiative and, importantly, the other actors involved in or affected by a given initiative that determines whether or not it will become a political issue. In some STPs, the integration of specialist community services into a new multidisciplinary team was relatively uncontroversial because, for example, local actors had a history of working together and shared aspirations for service change, whereas in another STP the same type of initiative would become a key controversy as there was a history of difficult working relations and competing values about community services. This highlights the important of history and path dependency in the implementation of change. Furthermore, the consequent actions and reactions to change can either exacerbate tensions or sustain positive working. For this reason, it seems important not only to understand the specific features of a change initiative, but also to attend to local history and to understand the receptive context as being the underlying driver of system politics.
Constellations of interacting actors simultaneously engaged in political action
Further supporting the findings of the interview study, it was rarely the case that system politics or organisational politics were manifest in the manner of Person A using their political skills to exert influence over Person B, which often seems to be suggested within the wider literature. Rather, the case studies suggest that around each controversy a particular constellation of interacting actors influence each other, both intentionally and inadvertently, as they seek to shape the implementation of change. Moreover, the direction of influence is not unilateral or even bilateral: rather, all actors are in some way engaged in a multilateral game of politics. Importantly, the strategies and actions of one person or group are inherently influenced by the actions, reactions and counteractions of others, and when those indirectly involved (the audience) are also constantly responding to the politics of change as manifest in the interactions between others. For this reason, it is difficult to offer a prescribed or formulaic view of political skill that might denote, for instance, ‘in Situation X, Person A should attempt behavioural influence with Person B through utilising skills x, y, and z . . .’. Rather, this study suggests a more contingent view of understanding the context-specific challenges as being manifest in these constellations of interactive political action, and where arguably the main overriding strategy is to read the political landscape, recognise that it is dynamic and sometimes volatile, and reflect on the action and interactions with others, before then determining how best to engage.
Individual and collective dynamics
Developing the above, the study showed how participation in system politics was more than an individual activity (i.e. when one person interacts with others); instead it was more often a conjoint or team activity. Many of the project teams studied in this research brought together multiple actors with distinct but complementary political skills and ways of acting that they could draw on as a co-ordinated, but often implicit, form of political action. As illustrated above, this might involve combining one person’s political awareness and strategic thinking with another’s network of connections and another’s communication skills. The study further suggests that it is unlikely that one person could realistically develop and utilise the full range of political skills, strategies and actions to understand and mediate the system politics investigated in this study given the diversity of stakeholders involved. In addition, the scope for an individual from one care setting to engage with, influence and have credibility with those from another care setting is often limited, which in the context of interorganisational or system working can constrain the capacity of a given leader to have system-wide influence. For this reason, the study suggests that effective participation in organisational and system politics is more of a ‘team sport’. Although the organisational studies literature tends to describe individuals as using political skill, this may stem from the fact that this research tends to focus on interpersonal influence and group psychology, rather than the intergroup or interorganisational levels. As this study shows, system politics often stems from the different ways people and groups made sense of and valued system change.
The horizontal, vertical and diagonal directions of system politics
The study found that the dynamics of system politics operate at, and interact across, horizontal and vertical directions of influence. The horizontal line describes the forms of political interaction observed between individuals, groups or organisations operating at the same level, that is profession–profession or department–department. At this level, system politics is often focused on the distribution and control of resources or activities or work related, for example, to a given care pathway or service. The vertical line describes the forms of political actions observed between, for instance, the ‘strategic’ arena of senior leadership and the ‘operational’ arena of service organisation and delivery. At this level, system politics is typically focused on the ‘top-down’ influence of decision-makers to formulate and implement change (often in concert with formal authority structures), the bottom-up influence of front-line clinicians to inform, shape or contest change, and further the mediating role of middle-level actors to resolve the tensions between the levels. What becomes empirically and theoretically significant, therefore, are the different skills, strategies and actions used by actors at these different levels. Moreover, and adding to the dynamic complexity described above, the horizontal and vertical dimensions are in constant interplay, suggesting that the diagonal lines of politics are perhaps the most significant, that is moving across horizontal and vertical simultaneously. As an illustration, a proposed service transformation may reconfigure the horizontal working relationship between two or more professionals, prompting corresponding negotiations around the allocation of resources and work. In seeking to resolve these tensions, actors may engage in vertical forms of political action to seek support from or influence senior level decision-makers.
The interplay between formal big ‘P’ politics and informal small ‘p’ politics
The study found that almost all examples of small ‘p’ informal politics were, in some way, triggered or framed by wider big ‘P’ formal policy and politics. The primary focus of this study was the informal aspects of interpersonal politics, micropolitics or organisational politics, but the changes that studies and narratives provided were consistently framed by the influence of more formal national policy-making, statutory requirements, regulatory systems and party politics. As noted, some participants suggested that exposure to, and familiarity with, the formal political realm enhanced one’s informal political skills, through offering insight into the interplay between the two realms and also the understanding of the skills and strategies used by politicians. The interplay between the two realms was especially significant for senior system leaders in their role as translators of national requirements and statutory obligations. However, the study also found that other system actors would often draw on formal political processes and policies to justify or counter less formal forms of political skill and action. In other ways, participants described how constant change within the formal political realm could easily undermine or derail local level changes, which seemed to nullify specific controversies but leave behind the legacy of informal disagreements or alliances.
Social position and political action
The study shows how participation in system or organisational politics is enabled or shaped not only by the particular skills or competencies of a given individual, but also by their social position and status within the wider social context. The term ‘social position’ is used to recognise that social actors within a given field of activity hold different positions relative to one another, and that these positions reflect variable preferences and opportunities to act relative to others within the same field of activity. Differences in social position, therefore, relate to the social status, influence and power of actors in a system of social relations. These variations in social position are typically a reflection of acquired social resources or capital, the institutionalised distribution of social rules, roles and resources, and the prevailing interests and ideologies that shape a given field of activity. In short, some people are both more inclined to and have greater potential to engage (and succeed) in organisational politics because of their acquired social resources, institutionalised social roles or ideological commitments. For example, medical professionals have long been recognised as powerful institutional actors in the health-care field because of their acquired expertise, associated networks and political connections, the institutionalised status of professionalism and the ideological dominance of biomedicine within modern society. For this reason, some actors were able to engage more successfully in system politics because they had significant social roles (as well as formal authority positions), enhanced access to social connections and specialist forms of knowledge, and because of other sociodemographic differences. In particular, the social position of certain specialists and professions was found to be important in determining how political controversies played out or were resolved. It would be wrong, however, to assume that because of their social position such groups inevitably dominated or marginalised others (although this could be the case); rather, their dominant position meant that less influential others needed to utilise particular types of political skill and action as means of countering such institutional dominance. This means that marginal or non-dominant actors arguably need to engage in particular forms of political action, such as building coalitions and developing new evidence, to challenge the dominance. For this reason, social position should not only be interpreted as some actors being more or less able to engage in political action, but also as actors need to develop and utilise different types of political action because of their social position.
Gender, ethnicity and age
A particular aspect of social position relates to the influence of sociodemographic differences. Although gender and ethnicity differences were not observed to have a major impact on the change processes studied in this research, it was notable that the majority of project-level, thematic-level and STP executive roles were occupied by women, while the more senior leadership roles on STP governance were more mixed, with some being more dominated by men. In addition, many but not all of the senior professional leadership roles were occupied by men. Although not a prominent theme in the cross-case analysis, some participants talked of political skill in terms of more masculine and negative terms, such as using ‘bully-boy’ tactics. It was also the case that different political strategies and actions were observed and reported in terms of gender. Some female service leaders were described by participants as taking a gendered approach to leadership in the style of being ‘nurturing’ or ‘maternal’, whereas one (female) participant talked about female leaders using gendered and sexualised tactics to influence men. The key point to recognise, however, is that the inclination and opportunities to participate in organisational politics are in some sense gendered and this shapes the types or styles of political action that are used.
Conclusion
This chapter has presented illustrative case examples from the in-depth qualitative case study research to demonstrate how political skills, strategies and actions can contribute to the implementation of major system change. It presents a composite model of change processes and shows how particular sets of political actions are used by different actors around particular controversies. The research findings suggest that it is difficult to establish a prescriptive ‘play-book’ or formula of political skills to be deployed in certain circumstances, primarily because system politics are typically context specific and contingent on the specific constellation of interacting actors pursuing various interests and agendas. That said, the study did find that controversies of system change were associated with relatively common and prominent instances of political skill, strategy and action (Table 13). Moreover, the study highlights the importance of having a developed strategic understanding of the wider landscape, the overarching change process and the likely protagonists, so that, when required, strategies and actions can be adapted accordingly. It also seems important that system leaders have self-belief and perseverance to maintain a commitment to change in the face of opposition.
| System change focus | Prominent skills, strategies and actions |
|---|---|
| Strategic ‘system’ vision and plan |
|
| Sharing ‘system’ resources |
|
| Determining ‘system’ priorities |
|
| Team dynamics across the ‘system’ |
|
| Implementing ‘system’ change |
|
Chapter 6 Learning materials and resources for the acquisition and development of political skills, strategies and actions
Introduction
This chapter reports the findings and outcomes of activities that were undertaken as part of WP4, which address the objective to co-design learning materials and recruitment resources to support health and care leaders to acquire and develop forms of political skill. Although there are many leadership programmes for health and care professionals that, to a greater or lesser extent, deal with issues of organisational politics, to our knowledge, few programmes give exclusive and evidence-based attention to the development and use of political skill when seeking to implement change. The activities reported in this chapter address this gap. The five activities that make up WP4 draw directly on the learning from previous WPs, with three of the activities being undertaken as part of these earlier stages, that is literature reviews and interviews, whereas other activities were carried out exclusively as part of WP4, that is the workshops. Together, the different activities bring together the new findings from the literature review and new qualitative research, and through a series of workshops contribute to the iterative development of learning materials.
Literature on the acquisition and development of political skill
The literature on the acquisition and development of political skill is dispersed across a number of disciplines, including health services research, nursing, management and psychology. The literature review focuses on three main modes of learning: (1) ‘experiential learning’ in practice settings, (2) reflecting on practice through ‘mentoring and executive coaching’, and (3) formal training.
Experiential learning
Experiential learning involves acquiring and developing skills through direct involvement in real-world or situated activities in which people ‘learn through doing’. 157,158 Skills are moulded through ‘hands-on’ experience and leaders gradually develop the competencies or ‘know-how’ to read situations, understand stakeholders and learn resilience. 43,159 The experiential development of political skill can be haphazard and costly and mistakes can be damaging, with Hartley et al. 73 showing that many skills and qualities are acquired and honed through ‘trial and error’. 73 Others72,159 suggest that people can be more proactive in their learning in the form of either self-reflection or self-monitoring. The concept of experiential learning has traditionally been associated with reflective learning through practical activity;160,161 however, within the political skill literature, it aligns more with ideas of cognitive or ‘personal learning’, for which knowledge is seen as an entity and the person as ‘a personal container’ of knowledge. 72,159
Mentoring and coaching
Mentoring and coaching feature prominently in the literature. 72 Mentors can support mentees to ‘reflect on practice’ and develop new ways of behaving. 72,131 Research suggests that mentors can provide timely feedback, read situations and understand prevailing power structures. 131 In general, mentoring is described to lead to increased political skill and job performance and the ability to appear sincere and influence others. 159 Mentoring programmes that include Ferris et al. ’s53 concept of political skill have also helped nurses to reach more senior positions. 131
Mentoring is a two-way exchange that is often initiated by the mentee;114 this means that some form of political skill is needed to initiate a mentoring relationship. 162 The workplace learning literature also suggests that mentees can benefit from multiple dispersed mentors to address different aspects or challenges of their workplace. 163
Mentoring can be particularly useful for female leaders. Mainiero’s153 study on female managers found that women need political skills to ‘break the glass ceiling’153 and to overcome the deep-rooted cultures and norms that can stymie career progression. Although women do benefit from mentors, they often lack them owing to bias in the workplace, and men who mentor women can be put off by the reaction of other male colleagues. 162
There is less material in the literature about executive coaching. Generally, coaching is seen as only one approach to skill development and tends to focus on psychological and behavioural enhancements. 71,159,164 Perrewé and Nelson162 note that executive coaching increases ‘understanding and psychological awareness’162 and builds important relationships. 162 In the grey literature, executive coaching programmes directly and indirectly engage with the concept of political skill through components such as ‘developing interpersonal relationships’. 165 The NHS Leadership Academy offers executive coaching with the aim of developing the trainee’s understanding of work teams. 166 Barriers to coaching are often highlighted, particularly expense and exclusivity. 159
Formal training programmes
There is evidence that formal training can support increased awareness of organisational politics and the development of political skill. 167,168 Furthermore, training programmes can supplement workplace learning and mentoring158 and are considered useful for aspiring leaders. 169 Training sessions legitimise a way to talk about organisational politics and encourage dialogue about ‘thorny issues’. 170 Group-based training sessions are seen as especially important for resolving real-life problems, with a focus on developing shared strategies for change. 170 An important caveat for formal development is that psychological safety is needed and some programmes have failed because of a lack of attention in this regard. 159 In terms of the format of training sessions, some authors recommend a blend of learning methods. For example, Ferris et al. 159 suggest bringing organisational politics to life using drama-based approaches. However, formal training programmes are often competency based (demonstrating learning of prescribed skills and abilities) and do not always show how the skills should be applied in a dynamic context. 171 As previously noted, formal provision is especially important for women, one reason being that they are more likely to view organisational politics negatively. 162
Summary
The evidence on the acquisition of political skills is sparse and diverse. Many studies continue to see some people as ‘naturally’ gifted or capable of engaging in political behaviour,43 whereas others suggest that such skills can be learnt and honed through experience, mentoring and training. Arguably, these two positions can be reconciled by the idea that some people more readily develop political skill because of their innate ‘talent’, whereas for others skill development requires more effort in explicit learning. Although political skill is acknowledged across prominent health-care leadership frameworks, there is little evidence of how it is best acquired or contributes to health-care change. Many of the attributes are poorly specified or are subsumed within other behavioural competencies. Even when there is explicit reference to political skill, there is limited theory on which these qualities are based and there is no explanation about how the concept has been adapted to the NHS context.
Narrative interviews on the acquisition and development of political skill
This section examines how interview participants involved in WP2 reflected on their acquisition and development of political skill. Consistent with the wider literature, participants differentiated between more experiential learning, personalised development and formal training.
Experiential learning
Almost all participants described their growing awareness of organisational politics and their acquisition of political skill as stemming from experiential learning or involvement in specific ‘events’, ‘projects’ or ‘placements’. These experiences provided the basis for learning about the political landscape and the political behaviours of others and, importantly, for reflective understanding of their own attitudes, beliefs and behaviours in relation to others:
So I was the lead director for [the trust’s] division and I remember going into [the] station once and putting across a proposal that I thought was quite sensible and the PTR, the paramedic team leader, at the coffee break said you’ll never get that through here because this is going on and you need to know the background here and actually it’s something about understanding the politics of that station or that division, so what are those other things that are going on . . .
WP2-5-D
Participants’ involvement in these situations varied according to career stage. Early career participants described these situations as novel and significant, often because this was the first time that organisational politics were encountered. For a number of participants, these early career encounters focused on a role model and ‘watching them in action’. These role models tended to be senior or more experienced leaders who provided a template on which to model behaviour at different stages of their careers. As well as ‘positive’ role models, some participants talked about ‘negative’ role models or people whose behaviour they would not want to emulate, such as the politically naive or those who often offended others or made mistakes. By contrast, more senior participants talked of honing their skills through ongoing participation in change projects.
Nearly all participants talked about ‘seminal moments’ that brought organisational politics and political skill to the fore of their attention and provided the impetus for reflection learning and personal development. A number described these moments as not only novel but also personally challenging, emotional or embarrassing. Some saw these situations as exposing their naivety or lack of judgement, which prompted personal development expectations. Many of these seminal events were described as errors of judgement, behavioural mistakes or other forms of faux pas that contravened expected behaviours.
Participants also talked about other significant experiences as enhancing their awareness of organisational politics. In particular, working in or across multiple organisational settings was seen as beneficial for highlighting subtle differences in informal organisational politics that might otherwise be taken for granted. Certain types of care settings were described as especially ‘rich’ in experiential learning because of their underlying political character, such as working in specialist hospitals. Those who had worked in both ‘health’ and ‘social care’ settings talked of their enhanced understanding of the different financial and national political pressures, which, in turn, made some more able to work across these boundaries:
Being in different sectors, that in itself, opens up your mind to different ways of working and obviously the people within those sectors, have got different experiences and the training and development opportunities that I have been on, formally.
WP2-37
A relatively small number of participants talked about learning through exposure to formal (big P) politics and political processes. A number of participants had previously worked, for example, as civil servants in the central or local government, some participants had undertaken leadership placements with central government agencies and other participants had been seconded as specialist advisors to government departments, policy committees and regulatory bodies. These participants saw such exposure as helping to develop their skills for when they returned to their usual leadership or clinical roles within the health and care sectors. Further sources of experiential learning came from participants’ past experience of working in non-health-care or public service sectors, through either the third sector or private industry. Those with experience in industry mentioned with some surprise that staff within the NHS often appeared unaware or naive about the influence of office or organisational politics, despite it being such an obvious feature of the health and care sector.
Mentoring and coaching
As above, many participants talked of role models helping them to understand and navigate organisational politics. Some of these mentoring relationships were relatively formal, established as part of a training initiative or induction programme, whereas others were more informal, dynamic or issue based, being formed through pre-existing connections or when a line manager had mediated a mentoring relationship to assist with a given issue or career stage, for example a promotion application:
I’ve been really fortunate with mentors, unofficial mentors, official mentors, role models, [name] was one of them. And some other key people that I’ve developed relationships with that have helped me and people that I’ve looked up to and seen how they work and tried to emulate that myself.
WP2-4-M-p
Of interest here, participants described the benefits of mentors in three overlapping ways. The first was orientating or understanding the political landscape. This included, for example, explaining the power dynamics in a given service or helping to anticipate political issues. The second was developing connections within the organisation. This involved a mentor making a preliminary introduction on behalf of the individual or endorsing their involvement in a given activity. The third was creating a ‘safe space’ for personal reflection and to offer ‘constructive criticism’. In most cases, these interactions were seen as developmental, allowing for exploration and reflection on events and possible actions. This was especially the case for participants who felt that they had made a political ‘faux pas’ or had met significant resistance to a piece of their work. These interactions tended to be described as informal and confidential, with a view of helping the participant to reflect on their behaviour and think of alternative strategies.
Although less common, a number of participants also talked of receiving ‘coaching’. There seemed to be two different approaches to coaching. The first might be termed ‘executive coaching’ and was described by a relatively small group of senior-level participants, for example chief executives, and was arranged on a private or ad hoc basis to provide confidential and independent guidance around key leadership issues. The second might be termed ‘placement coaching’ and was provided to participants as part of their formal leadership development. In some ways, participants talked of their coaches in similar ways to mentors, but with a focus on planning and rehearsing different scenarios in advance of taking action. In most cases, coaching seemed narrower in focus than mentoring, being focused more on self-reflective personal development:
Coaching can be very good. And to be fair, I’ve personally had a more I think, use out of coaching, and I know certain colleagues have certainly found coaching really useful. And in a way, all the coaches largely actually only self-reflect back individuals, back their style and their approach, and how they work, but sometimes that’s quite useful.
WP2-45-Cl
Formal training
The majority of participants had undertaken some kind of formal leadership or management training over the course of their career. Many participants had completed, or were still enrolled in, national management training programmes, others had completed specialist postgraduate programmes in clinical leadership, a few completed a Master’s degree in business/administration, and many had attended short courses on leadership development. Despite the widespread experience of formal training, it was striking that only a small number of participants (< 15) talked of receiving formal training in the areas of organisational politics and political skill.
A small number of participants talked positively about their experience of an interactive workshop on organisational politics that was provided as part of their enrolment on a national leadership programme. This was facilitated by an academic researcher and involved a mixture of structured teaching and group work in which participants applied concepts related to organisational politics to their work experiences. Although positively received, they also questioned whether or not, at their career stage, they had sufficient first-hand experience to fully appreciate these issues or to relate concepts to their work context:
[We] had some kind of training in how to frame problems, change, help develop people’s thinking in certain ways . . . it was really new to me and it made so much sense and it was, it was like a relief that somebody was naming power and politics. I was doing it before, but I was doing it unconsciously and I was doing it based on my own personality and wit and my nature, but once I could put something, I could see that people had been talking about this and the normalisation I think is really important. It takes so much guilt away.
WP2-47
A small number of participants talked about attending bespoke training on ‘the politics of organisational change’ (or with similar themes) that had been designed by external ‘organisational development’ consultants to address their employing organisation’s priorities for change. Such workshops introduced common ideas related to organisational politics and encouraged participants to apply these to their own work. Some of the memorable or prominent ideas that were described included, for example, Baddley and James’s167 characterisation of political skill in terms of animal metaphors. Such training was experienced positively because the broader theme of organisational politics continued to be under-recognised and underdeveloped within more established learning curricula, for example when political issues were subsumed within such themes as culture change or change management. In other words, training recognised the importance of the issue and gave permission for participants to talk about organisational politics, which was especially important for people working on a shared change project:
. . . was really powerful is that we have 18 people as a cohort and you get to discuss politics and power openly, you can discuss the use of things and gives you the courage to go and test that.
WP2-47
Overall, formal learning programmes did provide participants with an important opportunity for reflection and learning about organisational politics outside the ‘classroom’. A number of participants talked about their involvement in ‘action-learning’ sets, in which they could bring ‘live’ issues to their learning group for structured and facilitated deconstruction, reflection and action-planning. In addition, participants talked of the benefits of sharing experiences with other learners in and around structured learning activities in the form of peer support.
Summary
Study participants saw merit in formal training activities to structure or guide their learning, but also the importance of experiential learning around real-world challenges to focus their learning. These activities could be supported by aligning mentorship and peer networks with formal training, that is when ‘classroom’ learning is supplemented with additional mentoring.
Participants’ recommendations for formal training suggested that the topic of organisational politics could be introduced early within foundational professional education, that is during undergraduate clinical training, and especially as people start to develop a management or leadership career pathway. It was further suggested that formal learning could be graduated, moving from ‘context-free’ core ideas to more ‘context-specific’ practical strategies to reflect the likely challenges faced by leaders at different career stages. At later career stages, more bespoke and tailored training was preferred in the form of organisational or professional development, with action-learning that was aligned more directly with the real-world challenges to help to build consensus on issues and demands faced by leaders. Such structured learning can be complemented with in-service mentoring, coaching and peer learning. For study participants, the most preferred approach was for a trusted and typically more experienced person to take the individual ‘under their wing’, especially around specific operational or strategic activities.
Workshops on learning needs and opportunities
An initial set of workshops was carried out with three groups to clarify the learning needs and opportunities of health and care leaders: ‘practitioners’, ‘educators’ and ‘scientific experts’. The workshops provided slightly different, but also many overlapping, views on (1) the real-world needs for political skill, (2) the existing and potential approaches to skill development, and (3) the link between theory and practice (Table 14).
| Theme | Feedback |
|---|---|
| Real-world challenges |
|
| Developmental opportunities |
|
| Theory and practice |
|
A further workshop was carried out with members of the Q Community to both clarify the emerging findings from the interview study and explore participants’ perceptions of learning needs and opportunities. The learning from this workshop is summarised in terms of participants’ views about the content or focus of training, the methods of development and other recommendations (Table 15).
| Theme | Feedback |
|---|---|
| Content of training |
|
| Training suggestions |
|
| Further ideas and recommendations |
|
The main recommendations identified from these preliminary workshops include closer linking of theory and practice, so that abstract concepts can be made real; a combined approach that links formal training with real-world action-learning; more interprofessional or project training opportunities; and the need to go beyond existing training programmes.
Scoping review of training and development tools
The purpose of this review was to identify candidate frameworks, resources and tools for supporting practitioners and leaders to acquire, develop and apply political skills or related qualities. This pragmatic review focused on identifying and appraising available leadership development and training resources that could be adapted in the light of the study findings and through co-design workshops with stakeholder groups.
Frameworks were identified from three distinct literatures. First, the academic change management literature offered an extensive range of frameworks, from long-term strategic planning to more operational project management. Prominent examples include, for example, ‘force field analysis’, ‘SWOT’ (strengths weakness opportunities threats), ‘PESTLE’ (political, economic, social, technological, legal, environmental) and ‘stakeholder analysis’. 49,50,150 Second, a number of prominent and highly influential frameworks were identified in the international development literature that explicitly address issues of politics and political skill when working to implement public service change. This included, for example, the UK Department for International Development’s ‘Drivers for Change’ framework172,173 and the Swedish International Development Agency’s ‘Power Analysis’ approach. 174 From this literature, a number of highly developed toolkits were found to be especially relevant to the study of organisational politics, such as the ‘Power Cube’ and the ‘Power Matrix’. 175 Third, from the leadership development literature, a number of frameworks were identified that support the acquisition and development of political skills for organisational leaders. These range from psychological- or personality-based frameworks for appraising an individual’s leadership capabilities to general models of change management. A number of these frameworks were developed, tested and promoted by the prominent health leadership agencies, such as the NHS Modernisation Agency, NHS Institute for Innovation and Improvement and The King’s Fund. 176 Many of these leadership frameworks address, in broad terms, an individual’s skills and capabilities for understanding the ‘interpersonal’ and ‘cultural’ context, but only a small number deal explicitly with issues of politics, such as the ‘Perception of Politics Scale’177 and the ‘Political Skill Inventory’. 178
Based on this review, a ‘candidate’ list of frameworks, resources and tools was identified as being potentially relevant to health services leaders’ acquisition and development of political skill. This list took into account (1) the express purpose of each tool or resource, (2) the underpinning theory, (3) the pedagogic approach and (4) the evidence base. It is noteworthy that the candidate list included more resources that addressed the landscape and stakeholders, in which there were many similar or overlapping resources to draw on, but there were fewer resources dealing with leaders’ use of political skill. The candidate resources were then reviewed and adapted in the light of learning from study findings and preliminary workshops. Specifically, the resources and tools were mapped against, and then adapted according to, how they supported learners to understand change as a process or ‘journey’; to appraise their local political ‘landscape’; to identify and profile the relevant ‘protagonists’ or stakeholders; and to develop and use corresponding ‘political skills, strategies and actions’ (Table 16).
| Theme | Tool or technique | Rationale |
|---|---|---|
| Change as a journey | Adapted from the NIHR A Guide to Implementing Change179 | Participants’ narratives demonstrate that change is experienced as a journey. This tool asks questions such as ‘what is your destination?’ and focuses on ‘what challenges lie ahead?’ and ‘what people, resources and activities will you need?’. This encourages learners to develop a specific project plan focused on the ‘political road ahead’ |
| Thinking about your landscape | Adapted from Jarrett’s The 4 Types of Organisational Politics180 | This is a relatively well-known resource that asks learners to appraise and categorise their local political context in terms of ‘sources of power’ and ‘where political activity takes place’ leading to four types of political landscapes: weeds, woods, high ground and rocks. As indicated by study findings, users tend to find this relatively easy to use and applicable to multiple settings |
| Understanding your stakeholders | Combining and adapting three different techniques: |
|
| Understanding and using political skills, strategies and actions | Adapted from Ferris et al.’s178 PSI and drawn from the novel study findings | The PSI offers an analysis of individual levels of political skill along the four dimensions, which can be adapted to act as a personal reflective tool. The HeLPA study findings can also be used to offer empirical insight and case examples of skills, strategies and actions. The emphasis in this section is around group deliberation and planning in relation to different stakeholders |
The adaptation of candidate resources took three forms. First, relatively generic change management tools, such as stakeholder analysis, were adapted so that they more directly spoke to the theme of organisational politics and reflected the idea that stakeholders hold different agendas. Second, more specialised frameworks that specifically deal with organisational politics and political skill were adapted so that they were more directly relevant to the health and care context rather than, for example, international development. Third, when there was an absence of developed resources, new tools were proposed based on the study findings. These candidate tools were further reviewed through a co-design workshop with study advisors.
The candidate list of learning resources was presented and appraised with a workshop comprising five specialists in leadership development, capacity building, knowledge exchange and implementation science, recruited through the NIHR CLAHRC (now Applied Research Collaboration) infrastructure. This workshop also considered options for the structure and facilitation of training events. The feedback from this workshop was generally positive about the candidate lists, with a number of specific and general recommendations provided. The first was that some of the symbolic representations of the political landscape and protagonists, for example characterising a person as a ‘fox’ or ‘donkey’,167 could be viewed negatively by some participants. The main recommendation was to discuss the relevance of these ideas with potential learners and to stress that they are figurative, not realistic, representations. The second was that some participants might not be familiar with general stakeholder analysis and this could consume considerable time within the learning workshops. For this reason, it was recommended that the early stages of stakeholder analysis could be completed as ‘pre-work’ in advance of the learning workshops. The third related to the overall structure and facilitation of the learning events, especially the need to create a ‘safe space’ for open discussion around potentially sensitive issues. It was recommended that facilitators use the workshop introduction to establish the credibility and independence of the facilitators and the ‘ground rules’ for group discussion. In addition, there were useful recommendations about the use of language and presentation, especially the removal of terms that could be seen as ‘too academic’. Finally, the group helped with the co-design of a complementary ‘workbook’ to support learners prior, during and after the learning event. Based on these recommendations, further changes were made to the learning resources and workbook (see Report Supplementary Material 1).
Through this review process, a package of resources was drafted for piloting, appraisal and co-design with health and care leaders. These were organised as four themes, with corresponding tools and techniques (see Table 16).
Co-design workshops to test and appraise learning resources
As described in Chapter 2, four workshops were carried out to pilot and refine the candidate learning resources, with people and groups actively involved in managing or contributing to change processes. Two workshops were carried out with STP-based project teams involved in implementing transformation projects. One workshop was organised at a regional Healthwatch organisation to understand the relevance of the resources to agencies representing public and community interests, and one workshop was organised as an ‘open’ event for individuals from multiple organisations but without working on a shared or common change agenda. As described, a co-design approach, in which representatives from each group participated in specifying and adapting the programme of learning activities, was used for all but the ‘open’ workshop. This chapter now summarises the main feedback and learning from the four co-design workshops at which the candidate resources were piloted.
Before detailing specific feedback and recommendations on the workshop activities, a number of overarching learning points can be identified. First, the workshops appeared to function better with organisations or teams working on a shared project. This not only seemed to help teams to develop a deeper or more developed understanding of the political issues that they face, from the perspectives of multiple team members, but also seemed to enhance the quality of team dynamics, especially through bringing to light subtly different understandings of the purpose of, and challenges faced by, the team. By contrast, the ‘open’ workshop with a mixed group of participants working on different change initiatives did not have the clarity of shared focus or depth of analysis. Second, it is important to engage participant representatives in pre-workshop co-design to clarify the purpose of their given change project, to understand the existing team dynamics, to identify sensitive issues and to specify desired learning outcomes. This pre-workshop engagement can involve reviewing candidate activities, emphasising some tasks over others and agreeing the schedule and arrangement for the workshop. Third, the co-design activities with the Healthwatch organisation showed that there are important design considerations when using the tools with third-sector or community-facing organisations, that is not care provider organisations. The feedback from this activity indicated that it was important to make significant changes in language and terminology; for example, participants were unclear about concepts such as ‘organisational politics’, and tended to see these as relating to more formal policy or political processes, rather than informal forms of influence and power. Similarly, participant feedback suggested that technical terms, such as ‘political skill’, were inappropriate and confusing, and rather the workshop should focus on notions of ‘engagement’ and ‘influence’. Such feedback led to the production of a distinct programme of activities and a redesigned slide deck.
Understanding change as a journey
This introductory section or activity aims to encourage participants (who share a common change agenda) to think about their change initiative as a process or journey and to invite team members to reflect on the potential political challenges or controversies faced in this journey. This activity was adapted from the NIHR Guide to Implementing Change. 179 This activity is suitable only for groups or project teams working on a shared change project and is not feasible for the ‘open’ workshop given the diversity of change issues, although more general group discussion about change processes can be facilitated in ‘open’ workshops.
Based on feedback from each workshop’s project team leaders (as part of the co-design process), participants were asked to complete ‘pre work’ in the form of developing or sharing a ‘plan on a page’ or similar diagram to summarise their change project, thereby reducing the length of the workshop. In the workshop itself, a project representative then delivered a brief overview of the project, with reference to the ‘plan on a page’, followed by group reflection and discussion on the political controversies. In practice, group discussion was facilitated through the ‘chat’ function in Zoom, but this could also be facilitated through other in-person activities. When participants identified multiple controversies, further discussion was facilitated to identify the ‘key’ issues that were complicating change, again encouraging use of the ‘chat’ function. It would also be possible to close this activity with a deliberated ‘voting exercise’, whereby the participants select the most pressing (urgent) and significant (important) issues that will then become the focus of subsequent group activities.
Participants’ feedback indicated that they generally welcomed the opportunity to discuss with their co-workers the common and divergent expectations for their shared change project. In particular, it was described as surfacing differences within the groups that had hitherto been unnoticed, or an opportunity to question the ‘official’ narrative of change. However, it was also reported that the success of this activity was dependent on the skills of independent facilitation and the willingness of the designated team leaders to engage with divergent views.
Understanding the landscape
The next section of the workshop invited participants to further analyse their political landscape using Jarrett’s180 conceptual matrix of the four types of organisational politics. This matrix characterises organisational environments according to their ‘levels of political activity’ (individual/organisational) and ‘sources of power’ (informal/formal), resulting in four ideal-type settings (weeds, woods, high ground and rocks). 180 Applying this matrix to the health sector, the facilitators used relevant examples drawn from the earlier WPs and emphasised that the political landscape of the health and care sector is highly dynamic across both time and space, especially in the context of system change.
In all workshops, this activity was facilitated as an open plenary discussion. For the workshops with STP project teams, participants were encouraged to reflect on the features of their political landscape that would have an impact on their change processes. For the ‘open’ workshop, participants were invited to reflect on the relevance of these ideas to their individual work contexts and to discuss the common and divergent issues, thereby sharing experiences across participants. For the Healthwatch workshop, the decision was made not to undertake this activity because feedback from the pre-workshop co-design meetings indicated that it was potentially not relevant to public and community groups and possibly too technical or jargonistic.
Reflecting on the use of this tool, some participants struggled with applying the matrix to their particular environment, primarily because it was felt that the health sector could not be defined as one type of landscape (of four). This was addressed in the workshops by encouraging participants to discuss what types or forms of political activity predominated at different times and places, and to recognise the connections between different political environments, for example how decisions in health care impact on decisions in social care. Further feedback suggested, however, that the ideas raised by the use of the Jarrett matrix180 could have been discussed without the use of the four ideal types or categories. The main recommendation was that group discussion could deepen appreciation of the issues, but this required facilitation with developed understanding of the health and social care context to reduce the constraints of the matrix typology.
Understanding stakeholders
This section of the workshops invited workshop participants to identify and appraise the stakeholders relevant to their change agenda. This activity was developed through adapting relatively commonplace stakeholder analysis frameworks,150 as well as more specialist tools aimed at characterising stakeholder types as ‘political animals’167 and also tools to help identify stakeholders’ underlying interests and agendas in terms of the ‘what’s in it for them’ framework. 176
Feedback from the pre-workshop meetings indicated that the two STP project teams had already completed basic stakeholder analysis and they would prefer to revisit this as part of their ‘pre work’, thereby affording more time in the workshops for in-depth stakeholder analysis. By contrast, pre-workshop co-design activities with the Healthwatch organisation indicated that they would prefer to dedicate more time to all aspects of the stakeholder analysis and the ways that different stakeholders could be influenced. In all but one workshop, participants were allocated into ‘breakout groups’ to work through the resources, with the support of a facilitator, leading to the identification and analysis of the key stakeholders. The findings were then shared in plenary discussion to surface common and divergent views.
For the ‘open’ workshop, this session was introduced with a general discussion of the ‘political animal’ concepts, and participants were then invited to discuss in open plenary the actions or responses that such stakeholders might be expected to take with regard to a given change project. For this reason, the workshop surfaced breadth of understanding of the different stakeholders, but less depth than the workshops with discrete project teams.
Feedback indicated that the stakeholder activities were positively received by the project team workshops. They seemed to provide focused and in-depth analysis of key people or groups, especially their particular interests and agendas, from which to devise relevant strategies to manage these stakeholders. Participants of the ‘open’ workshop also seemed to welcome the ideas but reflected that it was something that they would carry out after the event in subsequent project work, because there was limited scope in the workshop to carry out the depth of analysis. A key finding from this activity was the importance of expert facilitation to explain and support the use of the frameworks and tools for stakeholder analysis. In addition, post-workshop feedback suggested that it would be useful to simplify the activity and reduce the reporting back, thereby giving people more time for discussion, but it was also felt to be important not to oversimplify the process.
Understanding and using political skills, strategies and actions
This activity was informed, in part, by the political skills inventory (PSI) developed by Ferris et al. ,178 with the intention that it could be used to foster individual and group critical reflection about the acquisition and use of political skill. In addition, the workshop made use of empirical findings from the HeLPA (Healthcare Leaders’ use of Political Acuteness) study to offer real-world case examples of how political skills, strategies and actions can be used to mediate the local political landscape as a prompt for group reflection and forward planning.
One prominent developmental tool that was identified as part of the scoping review was the PSI developed by Ferris et al. 178 This is a self-completion survey to appraise an individual’s political skill, which could be used as part of a self-reflective exercise. The PSI was reviewed with the expert workshops (see Co-design workshops to test and appraise learning resources) and also with workshop participants as part of the pre-workshop co-design activities. Although the expert panel was broadly supportive of this tool, workshop participants suggested that it was too similar to an academic personality survey and that they were unsure if it would contribute to group learning. It was also recommended that the survey should be distributed and returned in advance of the workshop, with anonymised group feedback offered to foster this group reflection. Despite following this recommendation, it was found that a very small percentage of workshop participants (< 20%) completed and returned the survey, which rendered group discussion unfeasible. For this reason, the PSI was not used directly in the workshops.
Instead, this section of the workshops involved facilitating a discussion among participants about the key strategies and activities that could be used to manage the interests and agendas of different stakeholders (who had been identified and analysed in the previous activity). This ensured a degree of continuity between earlier sections of the workshop and helped participants to build up a more developed understanding of ‘political strategies in context’. For example, workshop discussion was purposefully directed towards addressing the outcomes of the ‘what’s in it for them’ activity, in terms of targeted strategies, negotiation tactics and interpersonal skills with different stakeholders. Importantly, this section of the workshops was informed more directly by the study findings from preceding WPs, including a review of the reported (WP2) and observed (WP3) ‘political skills, strategies and actions’ of service leaders. These findings were then used to prompt discussion and forward planning by workshop participants. This facilitated section was concluded by inviting participants to develop an ‘action plan’, drawing on the materials in the workbook. This section of the workshop was difficult to address in the ‘open’ workshop because of the diverse change issues being discussed by participants.
Feedback from this activity was mixed. Participants broadly described it as the most novel and forward-looking stage of the workshop, especially because it was directed towards formulating strategies to manage organisational politics. However, participants were apprehensive about completing the PSI in advance of the workshop (see Co-design workshops to test and appraise learning resources) and found the application of study findings to specific change contexts to be challenging. The two STP project teams requested a follow-up workshop to focus explicitly on the strategies for dealing with different stakeholders and managing organisational politics. Further feedback suggested that the study findings could have been used to inform a ‘scenario-planning’ or ‘foresight’ exercise in which different tactics were discussed in terms of the anticipated outcomes. Overall, the feedback from participants was that the workshops ended ‘just as the difficult issues’ were being addressed, suggesting a rebalancing of the content with greater emphasis on the action plans, rather than landscape analysis, together with greater use of pre-work via the workbook to inform workshop discussion.
Summary
The co-design workshop, together with preceding activities, informed the development of a package of learning resources and activities and a workbook, together with two slide-decks, one for team development (see Report Supplementary Material 2) and one for third-sector organisations (see Report Supplementary Material 3), with an accompanying facilitator’s guide (see Report Supplementary Material 4).
A significant finding from the co-design workshops was that the package of resources and activities was much better suited to the developmental needs of project teams working on specific change projects, rather than individuals enrolled on or participating in an ‘open’ workshop. Feedback showed, for example, that project teams were able to directly apply the ideas and learning activities to a real-world, practical issue; moreover, this issue was also shared by the group, providing a basis for team-based action-learning. This further reinforced the idea that the development of political skills, strategies and actions is perhaps best targeted at groups, rather than individuals, in which complementary capabilities are distributed and shared among team members. It also demonstrates the importance of understanding and addressing organisational politics as highly context-specific phenomena, involving particular political landscapes and protagonists, further suggesting the relevance of action-learning approaches rather than more abstract or generic learning.
The human resources management perspective
Interviews were also carried out with five people involved in NHS HR management, workforce planning and talent management to understand how the political skills of applicants for employment or promotion are currently appraised. The interviews found a mixed picture. It was reported that the recruitment and promotion of middle- and senior-level managers, as well as clinical leaders, explicitly assessed for aspects of political skills or more generalised qualities related to political ‘nous’ and ‘intelligence’. This would usually be part of a wider competency-based assessment, rather than a distinct or explicit political skills assessment, and there was no indication that formal frameworks and tools were routinely used in recruitment processes. The main method of undertaking such assessment was interview questions, but it was suggested that some form of scenario or situational exercise could be used as part of the assessment process. One participant reflected that, from their experience, some NHS trusts were probably better at addressing these issues more explicitly than others, especially for senior-level appointments.
It was further reported that for junior and earlier career recruits, political skill or related qualities were rarely assessed in any formal or informal way. More significantly, those with expertise in medical staffing also noted that the recruitment of doctors, including recruitment in medical-management roles, rarely assessed a person’s political skills or similar qualities. Although participants noted marked variations in doctors’ political awareness or skill, it was reported that those in senior-level roles tended to have acquired these skills over their career and that it was often implicitly accepted that they would be effective at managing the ‘politics’ associated with their medical colleagues.
Participants were unable to recall or describe any formal tools and frameworks that were used for assessing political skill in assessment and recruitment, but welcomed the possibility of using such resources. A further issue discussed in the interviews was that it would be necessary for the person administering such resources to have, in themselves, some degree of political nous, either for facilitating scenario exercises or for appraising individual responses to direct questioning.
Through reviewing both the thematic study findings (e.g. political landscape, controversies, protagonists and skills) and the candidate development frameworks (see Table 16) and tools, these study participants contributed to the development of a draft interview topic guide for use during recruitment interviews (see Report Supplementary Material 5). This topic guide focuses on different scenarios in which leaders might expect to deal with organisational politics, with each scenario addressing a different level of seniority and complexity (departmental, organisational and system change). It is entirely possible for recruiters to devise other scenarios relevant to their organisation. Using a given scenario as the focus, the recruiter can then use the interview to investigate a candidate’s level of political awareness and skill through four directed questions addressing (1) their assessment of the given political landscape, (2) their ability to identify key stakeholders, (3) their appraisal of stakeholders’ interests and agendas, and (4) their strategies and approaches for engaging and influencing stakeholders. The guide also offers a checklist for what a positive or strong response might include.
Conclusion
This chapter explained the development of a package of learning resources and materials to support health-care leaders’ acquisition and development of political skills, strategies and actions. The resultant tools draw on the empirical findings from the preceding three WPs to adapt pre-existing frameworks and tools, as well as developing novel resources, workbooks and a facilitation guide. Through the co-design workshops, these have been tested and revised.
Chapter 7 Conclusion and research implications
Introduction
Change is a near-constant feature of health and care services across the world. The COVID-19 pandemic shows how change can be rapid and profound in times of unprecedent crisis, but often change is protracted and difficult. This is especially the case when change is planned at the ‘system’ level; that is, when change is intentionally concerned with reconfiguring how multiple organisations work together to provide care services, requiring change both within and among these organisations. Research on the implementation of this ‘major system change’ shows how many factors complicate change processes,2,9,22,26 with growing attention to the role of ‘organisational politics’.
With the growing recognition that implementation of change in health-care services is often complicated by organisational politics, there is commensurate interest in the need for health and care leaders to acquire and use ‘political skill’ or ‘political astuteness’ to better understand and navigate these politics. These ideas appear to be shaped by the wider management literature on organisational politics and political skill;43 however, there remains a significant lack of research and theory considering what political issues are involved in the implementation of major system change and what types of political skill (or, as we suggest, action) are required to manage this ‘system politics’. This research set out to investigate the politics and political skills of health services change, specifically major system change, with the intention of producing evidence to inform the development of leadership development programmes. This concluding chapter draws together the main findings of the study and looks forward at the future research agenda and the opportunities for leadership development.
Aims and objectives
The overall aim of this study was to produce a new empirical and theoretical understanding of the acquisition, use and contribution of leadership with ‘political astuteness’, specifically in the implementation of major health system change, from which to inform the co-design of materials and resources for the recruitment, training and development of current and future service leaders.
The study had six objectives:
-
identify key theories and frameworks of political astuteness within the social science literature and apply these to recent evidence of health system change to understand how service leaders can constructively create a ‘receptive context’ for change
-
understand the perceptions, experiences and reported practices of service leaders, and other change agents, about their acquisition and use of political astuteness in the implementation of health system change, taking into account differences in professional background, age, gender, ethnicity, geopolitical context and change context
-
understand how recent recipients of NHS leadership programmes think about, have acquired and make use of political astuteness to inform the development of new training resources
-
revise existing theoretical models of political skill and astuteness with reference to the wider social, cultural and relational context of health system change, from which to develop new theoretical propositions
-
investigate how political astuteness is used constructively by service leaders to create a ‘receptive context’ for implementing major health system change
-
work with providers of NHS leadership training, NHS recruitment agencies and PPI groups to co-design recruitment and learning materials that support the acquisition, use and development of political astuteness for existing and future health-care leaders.
This chapter now shows how the research findings address each of the research questions, integrating evidence from across the WPs and making links with the existing research literature, while also identifying key learning and action points, where relevant.
Objective 1
Objective 1 was to identify key theories and frameworks of political astuteness within the social science literature and apply these to recent evidence of health system change to understand how service leaders can constructively create a ‘receptive context’ for change.
Chapter 3 reports the findings of two systematic narrative reviews. The first reviewed the wider social science literature on the concept of political skill and the second reviewed the health services research literature on the application of these concepts to the study of health services change. The first review shows that a number of key frameworks and theories of political skill and astuteness have dominated contemporary organisational and management research. In particular, the concept of political skill developed by Ferris et al. 53 was identified as the most prominent approach to describing and explaining how leaders and other change agents can influence others to realise their personal or organisational objectives. This comprises four dimensions: social astuteness, interpersonal influence, networking ability and apparent sincerity. The first review also identified the concept of ‘political astuteness’ as an alternative approach to studying how people seek to understand and mediate competing interests when seeking to realise certain goals. 54
The second review applied the findings of the first review to the health services research literature, showing that concepts, such as political acuity, astuteness and skill, have a relatively long history, especially in the area of nursing research. Although such terms have often been used in a relatively ‘loose’ or general way, in recent years the concept of political skill drawn from Ferris et al. 53 has become more common, leading to a more ‘tight’ or specific understanding. These have been applied primarily with regard to the nursing profession’s involvement in service change,102 but also with regard to other professional and managerial groups.
The reviews elaborate a critique of the existing literature, especially the Ferris et al. 53 model, which is interpreted as emphasising personal skills and behavioural capabilities43 while potentially downplaying the relational and social context of people engaging in political action. 169 The reviews note important distinctions between a person’s underlying skills or capabilities, the application of these skills in the form of behaviours and actions, the idea that other people will also have such skills and engage in corresponding behaviours, and that such interactions take place within a given context. Taken together, these broaden the focus beyond skills to including actions and interactions and context, thereby calling for closer attention to the interactive and relational dynamics of political action, rather than individualised political skills. By taking an inclusive approach, the narrative review suggests that ‘political action’ is operationalised along a number of interconnected dimensions, including personal performance, contextual understanding, interpersonal influence, stakeholder engagement, networking, organisational change and policy influence. In many ways, this mirrors many of the features set out by the likes of Ferris et al. 53 and Manzie and Hartley,113 but it also indicates other aspects, especially policy influence. Moreover, the review provided the basis for elaborating the linkages between these dimensions as the basis for a heuristic framework to inform subsequent empirical research (see Figure 4).
Objective 2
Objective 2 was to understand the perceptions, experiences and reported practices of service leaders, and other change agents, about their acquisition and use of political astuteness in the implementation of health system change, taking into account differences in professional background, age, gender, ethnicity, geopolitical context and change context.
Chapter 4 reports the findings of the narrative interview study that investigated how health and care leaders perceive, experience and talk about their acquisition and use of political skill in the implementation of health system change. This was informed by the preceding literature reviews and focused on the use of political skill in managing the ‘politics of change’. The study found that participants talked about ‘organisational politics’ and political behaviours (and skills) in a number of common ways. The narrative interviews showed that people tend to think and talk about organisational politics with reference to a wider ‘political landscape’ in terms of historical precedents and prevailing relations of power, within which they experience particular ‘controversies’ or disagreements. As part of explaining these controversies, leaders focus on the role and positions taken by different stakeholders or ‘protagonists’ who hold different preferences or interests for change, and, in turn, the narratives describe the ‘political skills, strategies and actions’ used by these protagonists when seeking to influence the organisation of care. These political skills, strategies and actions were analysed along five dimensions (see Table 9).
Participants’ narratives broadly reflect the prevailing concepts of political skill and astuteness, but they depart empirically and conceptually in four important ways. First, the findings problematise the relatively narrow and individualised view of political skill, revealing instead a more complex and contingent understanding of organisational politics that involves complex patterns of action, interaction and counteraction. The findings suggest that it is useful to see organisational politics as involving interlocking constellations of political action in which multiple actors are seeking to influence one another. Second, the findings demonstrate the importance of a person’s social position in shaping their inclination, opportunities and approach to political action. 152 In particular, career experience and professional background were significant factors conditioning political action. Third, the findings show the importance of understanding political skill and action as a group or collective activity, rather than individual, whereby multiple people work together in complementary ways and with complementary skills to influence the organisation of care. Finally, the study offers insight into the interests and agendas that motivate political action. Within the mainstream literature, political skill is motivated by the desire to realise relatively narrow personal or organisational interests,43 yet study participants’ participation saw organisational politics as framed in terms of improving patient care or public health, in addition to deeper concerns about the allocation of roles and responsibilities. 181
Participants’ narratives also suggest that political action varies at different stages of the change process. Although there was no clear formula of skills to be used at a given time or with a given group, it was possible to identify more common sets of action at different stages of the change process (see Figure 7). These provided the foundations of subsequent in-depth empirical case research. The findings of acquisition and training were reported in Chapter 6 and are addressed further below.
Objective 3
Objective 3 was to understand how recent recipients of NHS leadership programmes think about, have acquired and make use of political astuteness to inform the development of new training resources.
As part of the narrative interview study, all participants, including recent recipients of leadership development programmes, were asked to reflect on the acquisition and development of their political skill. For the recipients of training, the questions focused on the perceived contributions of current training programmes. The study identified three prominent methods of acquiring and developing political skill and related leadership qualities, comprising experiential learning, mentoring and coaching, and formal training. In different ways, these each contribute to the development and refinement of political skills, strategies and actions. Experiential learning was by far the most prominent method of skill development, especially through participating in difficult change initiatives, learning from role models and, importantly, learning from mistakes. Mentoring and coaching were also seen as important, especially as supporting reflection on experienced events and situations and forward planning, and also for helping to connect more formal or classroom learning with the real world of health services change. Although mentors and role models were common to many participants, coaching seemed to be more common to more experienced and senior participants. Formal training activities had a mixed reception. Many described how leadership development could neglect issues of organisational politics or subsumed these within broader aspects of strategic change. When people had experienced specialist or dedicated training on organisational politics and political skill, it was seen as important for this to be grounded in real-world events, not abstract theory, and to be able to take learning back to the shopfloor. The main learning from the interviews was that action-based learning with expert facilitation and mentoring was the preferred method of acquiring and developing political skill.
Objective 4
Objective 4 was to revise existing theoretical models of political skill and astuteness with reference to the wider social, cultural and relational context of health system change from which to develop new theoretical propositions.
The predominant conceptualisation of political skill, both in the wider social science literature and in the health services research literature, is associated with the work of Ferris et al. ,53 and is largely informed by work or organisational psychology. Based on the findings of the literature reviews and the interview study, a number of additional lines of enquiry and conceptual analysis were identified as having potential for expanding this predominant approach and providing the basis for subsequent empirical research.
The first line of development is that, in practice, organisational politics involves multiple people engaging in interconnected and parallel lines of activity that go beyond the idea of individual skills, and focuses instead on the interactive order of organisational politics. To expand this point, people have varying types and degrees of skill in the form of personal capabilities to do something, but these skills come into operation only in highly specific interactive contexts. This involves the formulation and enactment of particular context-specific strategies that align available skills with the given contextual challenge, often in the form of other actors or groups who are themselves entering into an interactive exchange with certain capabilities and skills. 59 For this reason, these skills and strategies come into operational and empirical existence through meaningful action and interactive study, in which the interactive feedback or responses from others requires ongoing microlevel adjustments in the strategy and actions of multiple actors. 59,61 As elaborated below, the interactive dimension ultimately defines the character of organisational politics. The study suggests, therefore, that it is important to explore the interplay between skills (capabilities), strategies (plans) and actions (doings) as the basis of participating in or mediating organisational politics. This means that the unit of analysis can be moved from the actor (and their skills) to the relationships and interactions between multiple actors. 61 The interview study showed that people talked about organisational politics as involving constellations of interdependent and interacting actors. The iterative and recursive turn-taking interactions among people define the reality of organisational politics.
The second line of development extends the first by suggesting that political action is rarely an individual behaviour of a given leader of change; rather, political action is a highly co-ordinated and collective activity. In many instances, political action involves multiple people working together as an alliance to counter the influence of other alliances. This clearly resonates with research on social movements10,182 and, more recently, field theory,62 which describe the important contribution of social groups working in co-ordinated ways to challenge, create and defend social institutions. Moreover, the study suggests that by viewing political action as a collective process it becomes possible to understand how political skills and actions are distributed and co-ordinated across different people within a group. Relating these ideas to the leadership literature, it further reinforces the view that organisation and reorganisation of public and health-care services is dependent less on the transformational vision and capabilities of heroic leaders, but more on the distributed and shared practices of leadership by multiple actors. 21 Collective leadership involved co-ordinating across distributed assets and capabilities through an emergent social process,21 which in the case of this study centred on the co-ordinated political capabilities and resources of multiple actors.
The third line more explicitly acknowledges that people do not engage in organisational politics, either individually or as a group, from equal starting positions. Rather, people occupy variable ‘social positions’ relative to one other that reflect different inclinations and opportunities (or dispositions) to engage in political action. 63,152 In particular, relatively powerful or influential people tend to be privileged by the prevailing distribution of resources, rules and relationships, meaning that their willingness and need to engage in organisational politics, as well as their strategies and actions, will be markedly different from those who are less privileged. For example, non-dominant actors might be expected to use strategies and actions that challenge and undermine the position of those in more dominant positions. 26
The final line of enquiry is less theoretical and more substantive in focus. The existing literature tends to deal with politics and political skill within organisation settings. However, contemporary public service reforms, especially in the field of health and social care, increasingly involve implementing change among and within organisations. What becomes further significant about this aspect of interorganisational change is that those leading change often lack the formal authority associated with a given organisational role, and more often need to rely on forms of political skill to enact influence beyond authority. 22 For this reason, more attention is need to ‘system politics’.
Objective 5
Objective 5 was to investigate how political astuteness is used constructively by service leaders to create a ‘receptive context’ for implementing major health system change.
The in-depth case study research with three STPs showed how ‘system politics’ is manifest in the implementation of system change. In the aggregate and comparative analysis of individual cases, the study shows that the stages of implementing change are associated with particular types of political controversy or disagreement operating across the strategic and operational domains. Moreover, it shows how these controversies and, importantly, the resolution of these controversies are associated with certain types and forms of political skill, strategy and action. The study shows how there is little in the way of a formula or prescribed set of skills, strategies or actions for engaging in system politics; rather, it is highly contingency based and iterative. In fact, the case studies showed how precarious and complicated system change can be, with many false starts and failed activities.
With specific reference to the theoretical and empirical gaps outlined above, the research further demonstrates how ‘system politics’ was manifest through highly dynamic and context-specific challenges that required individuals, but more often groups and teams, to make situated assessments and test out various approaches to understanding and influencing their stakeholders. Of particular note, system politics seemed to play out across vertical and horizontal dimensions, simultaneously. The horizontal dimension describes the forms of political interaction observed between individuals, groups or organisations operating at the same level, that is profession–profession or department–department. The vertical dimension describes the forms of political actions observed between, for instance, the ‘strategic’ arena of senior leadership and the ‘operational’ arena of service organisation and delivery. At this level, system politics is typically focused on the ‘top-down’ influence of decision-makers to formulate and implement change (often in concert with formal authority structures); the bottom-up influence of front-line clinicians to inform, shape or contest change; and further the mediating role of middle-level actors to resolve the tensions between the levels.
The composite analysis or synthesis of case findings suggests that certain configurations of skills, strategies and actions were more prominent at certain stages of the change process than others, recognising that these stages often overlapped and involved dynamic feedback and recursive change (see Table 13).
Objective 6
Objective 6 was to work with providers of NHS leadership training, NHS recruitment agencies and PPI groups to co-design recruitment and learning materials that support the acquisition, use and development of political astuteness for existing and future health-care leaders.
The findings of the literature reviews and qualitative studies were deliberated through a series of workshops with the intention of co-designing a package of learning resources and materials. The initial workshops focused on deepening the understanding of the learning needs and opportunities, whereas later workshops reviewed and co-designed ‘candidate’ resources. The findings of the reviews and qualitative research suggested that a relatively structured, even formal, approach to leadership development would be beneficial, but also that this should be directed towards real-world issues and ideally involve action-learning by people and teams working on a shared issue, rather than focusing primarily on theory and prescriptive guidance. The later workshops collaborated with different system change project teams to plan, test and appraise the package of learning resources, leading to feedback and iterative changes. Based on this learning, the study produced (1) a slide deck of structured activities and tools to be used during facilitated workshops, which can be adapted in consultation with teams to suit learning needs; (2) a facilitator guide to explain how the workshops and resources can be planned, adapted and used; and (3) a workbook for use before, during and after the workshop. These resources could also be used by NHS recruitment bodies to support the appraisal of candidates through structured assessment activities.
Deviations from study design and study limitations
The overall study adhered closely to the proposed design and methods. There were, however, a number of notable deviations and limitations, all of which are discussed in Chapter 2.
A significant challenge was recruitment of STPs for in-depth case study research as part of WP3. Although early engagement with three STPs was positive, recruitment processes were protracted and involved extensive discussion, especially around appropriate governance approvals. The challenge of securing the necessary approvals for carrying out research in the STP landscape stemmed from a lack of understanding within STP leadership about where statutory responsibility rested in this system context. It was also the case that leadership changes in the STP complicated the recruitment of one initial candidate site, from which feedback indicated that the political sensitivities of such change were so great that it would be unwise, or lacking in political astuteness, to make them the focus of empirical research. In terms of learning for future research, one possibility is that reframing or presenting the research in terms of the broader challenges of ‘strategic change’ might have avoided some of the anxieties associated with the term ‘political skill’. Taking this approach, the study could have examined the broader processes of change from which to study political skills and behaviours inductively, but then this might have also risked the analytical focus and clarity of the intended study. More significantly, presenting the study in ways that are not authentic or consistent with the funded study purpose raises ethics concerns around the potential to deceive participants, especially because research documentation, that is the participant information sheets, require an overview of the study purpose, methods and anticipated outcomes. The challenges of recruitment created significant delays in data collection, which, when combined with the COVID-19 pandemic, resulted in the recruitment of one less subcase study than planned. Moreover, the selection of subcase studies needed to be more pragmatic and opportunistic to secure the participation of STPs, rather than following a prescribed sampling framework.
The second challenge and point of deviation resulted from the COVID-19 pandemic. As well as creating delays in data collection and causing the withdrawal of study participants, it also required changes in the approach to data collection, including significant constraints on the ability to carry out observational field research. Specifically, data collection with the third case study STP relied almost exclusively on virtual online data collection methods through video conferencing (Zoom). Although there remain debates about the quality of data gathered through online technologies, there is growing consensus that they have significant practical benefits, can enhance inclusion and are cost-effective. 183 That said, the reliance on online technologies for data collection significantly constrained the opportunities for supplementary data collection that usually occur during and alongside field observations, such as the opportunity to observe pre- and post-meeting discussions or to ask in situ questions of participants to clarify or probe their understanding of events.
The third limitation relates to the recruitment of public and patient representatives around specific change projects. The intention of the original study design was to understand how patients and community groups were engaged in and experienced change processes, together with their views about the politics and impact of change. A significant study finding was that relatively few service users or community groups were directly involved in ongoing STP change projects. It was usual for formal bodies, such as Healthwatch, to have representatives in strategic STP planning and for additional PPI or service user representatives to be engaged in more operational project management; however, direct patient or community involvement was limited. Most of the people and community representatives involved in the STP case studies did participate in the research, but overall there was limited opportunity to engage wider public and patient groups in the research, especially when system change had only limited impact on the direct delivery of patient care, as was the case for many ‘system architecture’ projects.
A final limitation of the study was its primary focus on the concepts of ‘political skill’ and ‘political astuteness’ in its theoretical framing and in the subsequent reviews of the literature. The over-riding premise of the study, as informed by the existing literature, was that the implementation of change in health-care services is often complicated by political controversies or challenges,3 and that those leading change can benefit from developing and using particular political skills, strategies and actions to recognise and deal with these challenges. The literature searches carried out as part of WP1 reviewed the wider social science literature and then health services literatures to establish the main theoretical perspectives and current evidence on the concept of ‘political skill’ and related terms. It is noted, however, that if the study had taken a broader view of politics in health-care settings and focused less exclusively on concepts such as political skill and political astuteness, it would have engaged with a much wider social science and policy literature dealing more broadly with forms of politics and political behaviours, even when they are not always conceptualised in these terms. The main risk of taking this approach is that it could have detracted from a more focused study and analysis of political skills, strategies and behaviours, but the opportunity now exists to relate the findings of this study to this wider literature.
Future research
In terms of future research, three main opportunities are identified:
-
Further test and revise the produced learning resources.
The study concludes with a package of resources that have been developed and co-designed through a series of workshops, but there is scope to more formally appraise these as contributing to the acquisition and use of political skills, strategies and action. This could include more short-term development research to further refine the materials, as well as more longitudinal cohort research that explores the impact of the learning on service change and career progression.
-
Understand how COVID-19 and other major events change system politics and create new political issues.
The research found that the pandemic altered the political landscape of the health and care system, with many radical innovations seemingly introduced at pace, which in the past might have been more protracted and contested. In particular, it seemed that strategic change was being shaped more strongly by top-down government authority that ‘cut through’ some of the more customary lines of power at the local level. This is often common in crisis management responses to major disasters and societal problems. 184 New questions can now be posed as to whether or not the changes in the political landscape will endure beyond the pandemic and whether or not, in the context of pandemic recovery, a new set of distinct political controversies will emerge that require different skills, strategies and behaviours. There is, therefore, potential for further qualitative research to understand how system politics has changed in the context of the pandemic and to what effect.
-
How system politics will change as new statutory bodies are formed around the ICS agenda.
Shortly before the research came to its conclusion, policies detailed the next stage in the development of regional care system integration, with the expectation that STPs evolve into ICSs. This also includes the possibility that ICSs will become regional-level statutory bodies to lead system change, in many ways acting like the former Strategic Health Authorities. These new governance arrangements also have the potential to transform the political landscape of the care system, especially as they introduce more formal authority structures that perhaps change the role of actors to use forms of political astuteness when leading change beyond the structures of formal authority. For this reason, there is future potential to investigate how these proposed reforms will transform ‘system politics’ and how more formal structures will change the contribution of political astuteness in system change.
-
Comparative research across multiple public service sectors.
The study focused almost exclusively on the English NHS, although some local authority and third-sector representatives were involved in individual case studies sites. With growing emphasis on health and social care integration, there is clearly scope for research that more explicitly compares the distinct micropolitical contexts of these sectors and how they interact during such integration processes. There is also scope for further research to compare the experiences of change management across other public services domains, such as local authorities, police services, transport and education, thereby developing a broader and comparative understanding of the role of political skills and astuteness within and across public service areas. 54
Acknowledgements
The study team would like to thank the Scientific Steering Committee, chaired by Dame Stella Manzi, and the Patient and Public Engagement group, co-ordinated by Clare Ramshaw and Anthony Chuter.
The study team also acknowledge the support of Will Warburton from the Health Foundation who helped co-design and facilitate one of the co-design workshops.
The study team is extremely grateful to all of the study participants, especially the service leaders and clinicians who participated in the in-depth case study research during the period of the COVID-19 pandemic.
Contributions of authors
Professor Justin Waring (https://orcid.org/0000-0003-1459-5896) (University of Birmingham) led the project, was first author of the final report and participated in all aspects of study design, data collection and analysis, and writing of the final report.
Dr Simon Bishop (https://orcid.org/0000-0001-8527-7081) (University of Nottingham) was the second author of the final report, co-designed the study and contributed to all aspects of data collection and analysis and writing of the final report.
Dr Jenelle Clarke (https://orcid.org/0000-0002-2061-9287) (University of Birmingham) was the third author of the final report, co-designed the study, contributed to data collection and analysis of WP1 and WP2, and contributed to the writing of the final report.
Professor Mark Exworthy (https://orcid.org/0000-0003-4791-7513) (University of Birmingham) was the fourth author of the final report, co-designed the study, contributed to data collection and analysis of WP2, and contributed to the writing of the final report.
Professor Naomi J Fulop (https://orcid.org/0000-0001-5306-6140) (University College London) was the fifth author of the final report, co-designed the study and contributed to the writing of the final report.
Professor Jean Hartley (https://orcid.org/0000-0002-9488-1894) (The Open University) was the sixth author of the final report, co-designed the study, contributed to data collection and analysis of WP1 and WP2, and contributed to the writing of the final report.
Dr Angus IG Ramsay (https://orcid.org/0000-0002-4446-6916) (University College London) was the seventh author of the final report, co-designed the study, contributed to data collection and analysis of WP2, and contributed to the writing of the final report.
Dr Georgia Black (https://orcid.org/0000-0003-2676-5071) (University College London) was the eighth author of the final report, contributed to data collection and analysis of WP3, and contributed to the writing of the final report.
Dr Bridget Roe (https://orcid.org/0000-0002-2625-9315) was the ninth author of the final report; contributed to data collection and analysis of WP2, WP3 and WP4; and contributed to the writing of the final report.
Publications
Waring J, Bishop S, Clarke J, Exworthy M, Fulop NJ, Hartley J, Ramsay AI. Healthcare leadership with political acuteness (HeLPA): a qualitative study of how service leaders understand and mediate the informal ‘power and politics’ of major health system change. BMC Health Serv Res 2018;18:1–10.
Clarke JM, Waring J, Bishop S, Hartley J, Exworthy M, Fulop NJ, et al. The contribution of political skill to the implementation of health services change: a systematic review and narrative synthesis. BMC Health Serv Res 2021;21:1–15.
Waring J, Bishop S, Black G, Clarke J, Exworthy M, Fulop N, et al. Understand the political skills and behaviours for leading the implementation of health services change: a qualitative interview study. Int J Heath Policy Manag 2022; in press.
Data-sharing statement
Data can be obtained from the corresponding author in such a way that safeguards the confidentiality and anonymity of participants and organisations. All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care.
References
- Massey L, Williams S. Implementing change: the perspective of NHS change agents. Leadersh Organ Dev J 2006;27:667-81. https://doi.org/10.1108/01437730610709282.
- Fulop NJ, Ramsay AI, Perry C, Boaden RJ, McKevitt C, Rudd AG, et al. Explaining outcomes in major system change: a qualitative study of implementing centralised acute stroke services in two large metropolitan regions in England. Implement Sci 2016;11. https://doi.org/10.1186/s13012-016-0445-z.
- Bate P, Mendel P, Robert G. Organizing for Quality: The Improvement Journeys of Leading Hospitals in Europe and the United States. Oxford: Radcliffe Publishing; 2007.
- Pettigrew AM, Ferlie E, McKee L. Shaping Strategic Change. London: SAGE Publications Ltd; 1992.
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009;4. https://doi.org/10.1186/1748-5908-4-50.
- Kitson AL, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A. Evaluating the successful implementation of evidence into practice using the PARiHS framework: theoretical and practical challenges. Implement Sci 2008;3. https://doi.org/10.1186/1748-5908-3-1.
- Bate P. Perspectives On Context. Context Is Everything. London: The Health Foundation; 2014.
- Greenhalgh T, Humphrey C, Hughes J, Macfarlane F, Butler C, Pawson R. How do you modernize a health service? A realist evaluation of whole-scale transformation in London. Milbank Q 2009;87:391-416. https://doi.org/10.1111/j.1468-0009.2009.00562.x.
- Best A, Greenhalgh T, Lewis S, Saul JE, Carroll S, Bitz J. Large-system transformation in health care: a realist review. Milbank Q 2012;90:421-56. https://doi.org/10.1111/j.1468-0009.2012.00670.x.
- Waring J, Crompton A. A ‘movement for improvement’? A qualitative study of the adoption of social movement strategies in the implementation of a quality improvement campaign. Sociol Health Illn 2017;39:1083-99. https://doi.org/10.1111/1467-9566.12560.
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 2004;82:581-629. https://doi.org/10.1111/j.0887-378X.2004.00325.x.
- Langley A, Denis JL. Beyond evidence: the micropolitics of improvement. BMJ Qual Saf 2011;20:i43-6. https://doi.org/10.1136/bmjqs.2010.046482.
- Rogers L, De Brún A, Birken SA, Davies C, McAuliffe E. The micropolitics of implementation; a qualitative study exploring the impact of power, authority, and influence when implementing change in healthcare teams. BMC Health Serv Res 2020;20. https://doi.org/10.1186/s12913-020-05905-z.
- Waring JJ, Bishop S. Lean healthcare: rhetoric, ritual and resistance. Soc Sci Med 2010;71:1332-40. https://doi.org/10.1016/j.socscimed.2010.06.028.
- Gale N, Dowswell G, Greenfield S, Marshall T. Street-level diplomacy? Communicative and adaptive work at the front line of implementing public health policies in primary care. Soc Sci Med 2017;177:9-18. https://doi.org/10.1016/j.socscimed.2017.01.046.
- Waring J, Currie G. Managing expert knowledge: organizational challenges and managerial futures for the UK medical profession. Organ Stud 2009;30:755-78. https://doi.org/10.1177/0170840609104819.
- Alford R. Health Care Politics. Chicago, IL: University of Chicago Press; 1975.
- Davies HTO, Harrison S. Trends in doctor-manager relationships. BMJ 2003;326:646-9. https://doi.org/10.1136/bmj.326.7390.646.
- Harrison S. New labour, modernisation and the medical labour process. Labour 2002;32:465-85. https://doi.org/10.1017/S0047279402006694.
- Lozeau D, Langley A, Denis JL. The corruption of managerial techniques by organizations. Hum Relations 2002;55:537-64. https://doi.org/10.1177/0018726702055005427.
- Denis JL, Langley A, Sergi V. Leadership in the plural. Acad Manag Ann 2012;6:211-83. https://doi.org/10.5465/19416520.2012.667612.
- Turner S, Ramsay A, Perry C, Boaden R, McKevitt C, Morris S, et al. Lessons for major system change: centralization of stroke services in two metropolitan areas of England. J Health Serv Res Policy 2016;21:156-65. https://doi.org/10.1177/1355819615626189.
- Hunter DJ, Erskine J, Small A, McGovern T, Hicks C, Whitty P, et al. Doing transformational change in the English NHS in the context of ‘big bang’ redisorganisation findings from the north east transformation system. J Heal Organ Manag 2015;29:10-24. https://doi.org/10.1108/JHOM-01-2014-0019.
- World Health Organization (WHO) . Leading Health System Transformation to the Next Level 2017.
- Department of Health and Social Care (DHSC) . Five Year Forward View 2014.
- Waring J, Crompton A. The struggles for (and of) network management: an ethnographic study of non-dominant policy actors in the English healthcare system. Public Manag Rev 2020;22:297-315. https://doi.org/10.1080/14719037.2019.1588360.
- Department of Health and Social Care (DHSC) . Delivering the Forward View: NHS Planning Guidance 2016.
- Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: a theoretical and empirical analysis of systems change. BMC Med 2018;16. https://doi.org/10.1186/s12916-018-1057-z.
- Fraser A, Baeza JI, Boaz A. ‘Holding the line’: a qualitative study of the role of evidence in early phase decision-making in the reconfiguration of stroke services in London. Health Res Policy Syst 2017;15. https://doi.org/10.1186/s12961-017-0207-7.
- Jones L, Fraser A, Stewart E. Exploring the neglected and hidden dimensions of large-scale healthcare change. Sociol Health Illn 2019;41:1221-35. https://doi.org/10.1111/1467-9566.12923.
- Great Britain . Health and Social Care Act 2012 2012.
- Exworthy M, Mannion R, Exworthy M, Mannion R, Powell M. Dismantling the NHS?. Bristol: Policy Press; 2016.
- Alderwick H, Ham C. Sustainability and transformation plans for the NHS in England: what do they say and what happens next?. BMJ 2017;356. https://doi.org/10.1136/bmj.j1541.
- Martin GP, Carter P, Dent M. Major health service transformation and the public voice: conflict, challenge or complicity?. J Health Serv Res Policy 2018;23:28-35. https://doi.org/10.1177/1355819617728530.
- Burns T. Micropolitics: mechanisms of institutional change. Adm Sci Q 1961;55:257-81. https://doi.org/10.2307/2390703.
- Cyert R, March J. A Behavioral Theory of the Firm. London: Wiley–Blackwell; 1992.
- Pfeffer J. Managing with Power: Politics and Influence in Organizations. Boston, MA: Harvard Business School; 1994.
- Pfeffer J. Power in Organizations. London: Pitman; 1981.
- Mintzberg H, Shafritz J, Ott S, Jang Y. Classics of Organizational Theory. London: Cengage Learning; 2015.
- Mintzberg H. Power in and Around Organizations. London: Prentice Hall; 1983.
- Buchanan D, Badham R. Power, Politics, and Organizational Change. London: SAGE Publications Ltd; 2020.
- Mayes BT, Allen RW. Toward a definition of organizational politics. Acad Manag Rev 1977;2:672-8. https://doi.org/10.5465/amr.1977.4406753.
- Kimura T. A review of political skill: current research trend and directions for future research. Int J Manag Rev 2015;17:312-32. https://doi.org/10.1111/ijmr.12041.
- Mintzberg H. The organization as political arena. J Manag Stud 1985;22:133-54. https://doi.org/10.1111/j.1467-6486.1985.tb00069.x.
- Crozier M, Friedberg E. Actors and Systems: The Politics of Collective Action. Chicago, IL: University of Chicago Press; 1980.
- Dahl RA. Pluralism revisited. Comp Polit 1978;10. https://doi.org/10.2307/421645.
- Pettigrew AM. The Politics of Organizational Decision-Making. London: Tavistock Press; 1973.
- Kotter JP, Schlesinger LA. Choosing strategies for change. Harv Bus Rev 1979;57:106-14.
- Clegg S, Carter C, Kornberger M, Schweitzer J. Strategy: Theory and Practice. London: SAGE Publications Ltd; 2011.
- Kotter JP. Leading Change. Boston, MA: Harvard Business School; 2012.
- Hartley J, Sancino A, Bennister M, Resodihardjo SL. Leadership for public value: political astuteness as a conceptual link. Public Adm 2019;97:239-49. https://doi.org/10.1111/padm.12597.
- Hartley J, Alford J, Hughes O, Yates S. Public value and political astuteness in the work of public managers: the art of the possible. Public Adm 2015;93:195-211. https://doi.org/10.1111/padm.12125.
- Ferris GR, Treadway DC, Perrewé PL, Brouer RL, Douglas C, Lux S. Political skill in organizations. J Manage 2007;33:290-32. https://doi.org/10.1177/0149206307300813.
- Hartley J, Fletcher C. Leadership Perspectives. London: Palgrave Macmillan UK; 2008.
- Lukes S. Power: A Radical View. Basingstoke: Palgrave Macmillan UK; 2005.
- Harrison S, McDonald R. The Politics of Healthcare in Britain. London: SAGE Publications Ltd; 2007.
- Ferris GR, Perrewé PL, Daniels SR, Lawong D, Holmes JJ. Social influence and politics in organizational research. J Leadersh Organ Stud 2017;24:5-19. https://doi.org/10.1177/1548051816656003.
- Goffman E. The Presentation of the Self in Everyday Life. London: Penguin; 1990.
- Goffman E. Strategic Interaction. Oxford: Blackwell UK; 1970.
- Blumer H. Symbolic Interaction. Berkeley, CA: University of California Press; 1986.
- Emirbayer M. Manifesto for a relational sociology. Am J Sociol 1997;103:281-317. https://doi.org/10.1086/231209.
- Fligstein N, McAdam D. Toward a general theory of strategic action fields. Sociol Theory 2011;29:1-26. https://doi.org/10.1111/j.1467-9558.2010.01385.x.
- Bourdieu P. Outline of a Theory of Practice. Cambridge: Cambridge University Press; 1977.
- Foucault M. Power/Knowledge. London: Harvester Wheatsheaf; 1980.
- Clegg S. Frameworks of Power. London: SAGE Publications Ltd; 1993.
- Freidson E. The Profession of Medicine. Chicago, IL: University of Chicago Press; 1970.
- Foucault M. The Birth of the Clinic. London: Vintage; 1994.
- Svensson R. The interplay between doctors and nurses – a negotiated order perspective. Sociol Heal Illn 1996;18:379-98. https://doi.org/10.1111/1467-9566.ep10934735.
- Allen D. The nursing-medical boundary: a negotiated order?. Sociol Health Illn 2008;19:498-520. https://doi.org/10.1111/j.1467-9566.1997.tb00415.x.
- Freeman R. Epistemological bricolage: how practitioners make sense of learning. Adm Soc 2007;4:476-96. https://doi.org/10.1177/0095399707301857.
- Chopin S, Danish S, Seers A, Hook J. Effects of mentoring on the development of leadership self-efficacy and political skill. J Leadersh Stud 2012;6:17-32. https://doi.org/10.1002/jls.21253.
- Blass F, Ferris G. Leader reputation: the role of mentoring, political skill, contextual learning, and adaptation. Hum Resour Manage 2007;46:5-19. https://doi.org/10.1002/hrm.20142.
- Hartley J, Alford J, Hughes O, Yates S. Leading with Political Astuteness: A Study of Public Managers in Australia, New Zealand and the United Kingdom. Australia and New Zealand. London: Chartered Management Institute; 2013.
- NHS Leadership Centre . NHS Leadership Qualities Framework 2002.
- NHS Leadership Academy . Healthcare Leadership Model 2013.
- NHS Improvement . Developing People: Improving Care 2016.
- Waring J, Bishop S, Clarke J, Exworthy M, Fulop NJ, Hartley J, et al. Healthcare leadership with political astuteness (HeLPA): a qualitative study of how service leaders understand and mediate the informal ‘power and politics’ of major health system change. BMC Health Serv Res 2018;18. https://doi.org/10.1186/s12913-018-3728-z.
- Noble H, Smith J. Reviewing the literature: choosing a review design. Evid Based Nurs 2018;21:39-41. https://doi.org/10.1136/eb-2018-102895.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: Final Report. ESRC Methods Programme 2006.
- Barthes R. An introduction to the structural analysis of narrative. JSTOR 2016;6:237-72. https://doi.org/10.2307/468419.
- Czarniawska B. Narratives in Social Science Research. London: SAGE Publications Ltd; 2004.
- Josselson R, Wertz F. Five Ways of Doing Qualitative Analysis: Phenomenological Psychology, Grounded Theory, Discourse Analysis, Narrative Research, and Intuitive Inquiry. London: Guildford Press; 2011.
- Kvale S. Doing Interviews. London: SAGE Publications Ltd; 2008.
- Wengraf T. Qualitative Research Interviewing: Biographic Narrative and Semi-Structured Methods. London: SAGE Publications Ltd; 2001.
- Miles M, Huberman A. Qualitative Data Analysis. London: SAGE Publications Ltd; 1994.
- Gibbs G. Analysing Qualitative Data. London: SAGE Publications Ltd; 2018.
- Silverman D. Interpreting Qualitative Data. London: SAGE Publications Ltd; 2015.
- Strauss A, Corbin J. Grounded Theory in Practice. London: SAGE Publications Ltd; 1997.
- Stake R. The Art of Case Study Research. London: SAGE Publications Ltd; 1995.
- Yin R. Case Study Research and Applications. London: SAGE Publications Ltd; 2018.
- Keen J, Pope C, Mays N. Qualitative Research in Health Care. London: Blackwell; 2006.
- Buchanan D, Vigoda-Gadot E, Drory A. Handbook of Organizational Politics. Cheltenham: Edward Elgar; 2016.
- Atkinson P. For Ethnography. London: SAGE Publications Ltd; 2014.
- Charmaz K, Olesen V. Ethnographic research in medical sociology: its foci and distinctive contributions. Sociological Methods Res 1997;25:452-94. https://doi.org/10.1177/0049124197025004004.
- Fetterman D. Ethnography: Step-by-Step. London: SAGE Publications Ltd; 2019.
- Vindrola-Padros C, Vindrola-Padros B. Quick and dirty? A systematic review of the use of rapid ethnographies in healthcare organisation and delivery. BMJ Qual Saf 2018;27:321-30. https://doi.org/10.1136/bmjqs-2017-007226.
- Bevir M, Needham C, Waring J. Inside co-production: ruling, resistance, and practice. Soc Policy Adm 2019;53:197-202. https://doi.org/10.1111/spol.12483.
- Robert G, Donetto S, Williams O, Loeffler E. The Palgrave Handbook of Co-Production of Public Services and Outcomes. London: Palgrave; 2021.
- Osborne S, Radnor Z, Strokosch K. Co-production and the co-creation of value in public services: a suitable case for treatment?. Public Manag Rev 2016;18:639-53. https://doi.org/10.1080/14719037.2015.1111927.
- Steen M, Manschot M, DeKoning N. Benefits of co-design in service design projects. Int J Des 2011;5:53-60.
- Clarke JM, Waring J, Bishop S, Hartley J, Exworthy M, Fulop NJ, et al. The contribution of political skill to the implementation of health services change: a systematic review and narrative synthesis. BMC Health Serv Res 2021;21. https://doi.org/10.1186/s12913-021-06272-z.
- Montalvo W. Political skill and its relevance to nursing: an integrative review. J Nurs Adm 2015;45:377-83. https://doi.org/10.1097/NNA.0000000000000218.
- Harris J, Maher L, Ferris G, Vigoda-Gadot E, Drory A. Handbook of Organizational Politics: Looking Back and to the Future. Cheltenham: Edwards Elgar; 2016.
- Perrewé PL, Zellars KL, Rossi AM, Ferris GR, Kacmar CJ, Liu Y, et al. Political skill: an antidote in the role overload-strain relationship. J Occup Health Psychol 2005;10:239-50. https://doi.org/10.1037/1076-8998.10.3.239.
- Drory A, Romm T. The definition of organizational politics: a review. Hum Relations 1990;43:1133-54. https://doi.org/10.1177/001872679004301106.
- Ashraf F, Zahid Iqbal M. A research agenda on the leaders political intelligence for effective change management. Afr J Bus Manag 2011;5:5798-806.
- Bing MN, Davison HK, Minor I, Novicevic MM, Frink DD. The prediction of task and contextual performance by political skill: a meta-analysis and moderator test. J Vocat Behav 2011;79:563-77. https://doi.org/10.1016/j.jvb.2011.02.006.
- Bolino MC, Kacmar KM, Turnley WH, Gilstrap JB. A multi-level review of impression management motives and behaviors. J Manage 2008;34:1080-109. https://doi.org/10.1177/0149206308324325.
- Ferris GR, Kane RE, Summers JK, Munyon TP. Psychological and physiological health and well-being implications of political skill: toward a multi-mediation organizing framework. Res Occup Stress Well Being 2011;9:63-107. https://doi.org/10.1108/S1479-3555(2011)0000009007.
- Munyon TP, Summers JK, Thompson KM, Ferris GR. Political skill and work outcomes: a theoretical extension, meta-analytic investigation, and agenda for the future. Pers Psychol 2015;68:143-84. https://doi.org/10.1111/peps.12066.
- Treadway DC, Douglas C, Ellen B, Summers J, Ferris G, Riggio T, et al. Leader Interpersonal and Influence Skills. London: Routledge; 2014.
- Treadway D, Bentley J, Williams L, Wallace A, Day D. The Oxford Handbook of Leadership and Organizations. Oxford: Oxford University Press; 2014.
- Manzie S, Hartley J. Dancing on Ice: Leadership with Political Astuteness Be Senior Public Servants in the UK. Milton Keynes: The Open University Business School; 2013.
- Usman M, Fan L, Anwar-ul-haq M. Political skill and career success: a review and directions for future research. J Innov Sustain 2016;7:39-46. https://doi.org/10.24212/2179-3565.2016v7i1p39-46.
- Ashraf F, Iqbal MZ. A research agenda on the leaders’ political intelligence for effective change management. African J Bus Manag 2011;5:5798-806.
- Clark MJ. Community Nursing. Reston: Prentice-Hall; 1984.
- Leary M. Self-Presentation: Impression Management and Interpersonal Behaviour. Boulder, CO: Westview Press; 1995.
- Hartley J. Politics and Political Astuteness in Leadership. London: Routledge; 2016.
- Bolino M, Long D, Turnley W. Impression management in organizations: critical questions, answers, and areas for future research. Annu Rev Organ Psychol Organ Behav 2016;3:377-406. https://doi.org/10.1146/annurev-orgpsych-041015-062337.
- Blickle G, Ferris GR, Munyon TP, Momm T. A multi-source, multi-study investigation of job performance prediction by political skill. Appl Psychol 2011;60:449-74. https://doi.org/10.1111/j.1464-0597.2011.00443.x.
- Ferris G, Blickle G, Schneider P, Kramer J, Zettler I, Solga J, et al. Political skill construct and criterion-related validation: a two-study investigation. J Manag Psychol 2008;23:744-71. https://doi.org/10.1108/02683940810896321.
- Brown SG. Identifying and Prioritizing Political Values and Skills Essential in Influencing Public Policy: A Component of the Political Socialization of Baccalaureate Nursing Students 1990.
- Crow SM, Hartman SJ. Improving the political skills of health care supervisors. Health Care Superv 1996;14:35-41.
- Taylor B. The political role of the health services executive. Healthc Manag Forum 1989;2:26-33. https://doi.org/10.1016/S0840-4704(10)61409-3.
- Lussier RN. Developing power and political skills. Clin Lab Manage Rev 1990;4:409-13.
- Young S. Developing your political skills. Clin Lab Manag Rev 1989;3:100-2.
- Carroll TL. Leadership skills and attributes of women and nurse executives: challenges for the 21st century. Nurs Adm Q 2005;29:146-53. https://doi.org/10.1097/00006216-200504000-00009.
- Whitman MV, Halbesleben JRB, Shanine KK. Psychological entitlement and abusive supervision. Health Care Manage Rev 2013;38:248-57. https://doi.org/10.1097/HMR.0b013e3182678fe7.
- Berger CS. Enhancing social work influence in the hospital: identifying sources of power. Soc Work Health Care 1990;15:77-93. https://doi.org/10.1300/j010v15n02_07.
- Gilson L. Everyday politics and the leadership of health policy implementation. Health Syst Reform 2016;2:187-93. https://doi.org/10.1080/23288604.2016.1217367.
- Montalvo W, Byrne MW. Mentoring nurses in political skill to navigate organizational politics. Nurs Res Pract 2016;2016. https://doi.org/10.1155/2016/3975634.
- Smaltz DH, Sambamurthy V, Agarwal R. The antecedents of CIO role effectiveness in organizations: an empirical study in the healthcare sector. IEEE Trans Eng Manag 2006;53:207-22. https://doi.org/10.1109/TEM.2006.872248.
- Berger CS. Enhancing social work influence in the hospital. Soc Work Health Care 1991;15:77-93. https://doi.org/10.1300/J010v15n02_07.
- Mateo MA, Frusti DK, Newton C. Management skills in an era of shifting paradigms. Semin Nurse Manag 1997;5:10-7.
- McAuliffe E, O’Brien T, Coghlan D, Albers Mohrman S, (Rami) Shani AB. Organizing for Sustainable Health Care. Bingley: Emerald Group Publishing Ltd; 2012.
- Rafferty AM, Traynor M. Context, convergence and contingency: political leadership for nursing. J Nurs Manag 2004;12:258-65. https://doi.org/10.1111/j.1365-2834.2004.00481.x.
- Wilber K, Coberly S. Competency requirements for policy gerontologists. J Aging Soc Policy 1991;3:51-69. https://doi.org/10.1300/J031v03n03_05.
- Greer SL, Lillvis DF. Beyond leadership: political strategies for coordination in health policies. Health Policy 2014;116:12-7. https://doi.org/10.1016/j.healthpol.2014.01.019.
- Benton DC, Al Maaitah R, Gharaibeh M. An integrative review of pursing policy and political competence. Int Nurs Rev 2017;64:135-45. https://doi.org/10.1111/inr.12275.
- Byrd ME, Costello J, Gremel K, Schwager J, Blanchette L, Malloy TE. Political astuteness of baccalaureate nursing students following an active learning experience in health policy. Public Health Nurs 2012;29:433-43. https://doi.org/10.1111/j.1525-1446.2012.01032.x.
- Strauss A. Work and the division of labor. Sociol Q 1985;26:1-19. https://doi.org/10.1111/j.1533-8525.1985.tb00212.x.
- Strauss A, Schatzman L, Bucher R, Ehrlich D, Sabshin M, Freidson E. The Hospital in Modern Society. New York, NY: Free Press; 1963.
- Day R, Day JV. A review of the current state of negotiated order theory: an appreciation and a critique. Sociological Q 1977;18:126-42. https://doi.org/10.1111/j.1533-8525.1977.tb02165.x.
- Klein R. The New Politics of the NHS: From Creation to Reinvention. Oxford: Radcliffe Publishing; 2010.
- Waring J, Currie G, Crompton A, Bishop S. An exploratory study of knowledge brokering in hospital settings: facilitating knowledge sharing and learning for patient safety?. Soc Sci Med 2013;98:79-86. https://doi.org/10.1016/j.socscimed.2013.08.037.
- Goleman D, Boyatzis RE. Emotional Intelligence Has 12 Elements. Which Do You Need to Work On? 2017. https://hbr.org/2017/02/emotional-intelligence-has-12-elements-which-do-you-need-to-work-on (accessed 9 February 2022).
- Goffman E. Frame Analysis. London: North Eastern; 1974.
- Benford R, Snow D. Framing processes and social movements: an overview and assessment. Annu Rev Sociol 2000;26:611-39. https://doi.org/10.1146/annurev.soc.26.1.611.
- Ramirez R, Buckles D. Cultivating Peace. Conflict and Collaboration in Natural Resource Management. Washington, DC: International Development Research Centre; 1999.
- Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy Plan 2000;15:239-46. https://doi.org/10.1093/heapol/15.3.239.
- McGuire M. Managing networks: propositions on what managers do and why they do it. Public Adm Rev 2002;62:599-60. https://doi.org/10.1111/1540-6210.00240.
- Battilana J. Agency and institutions: the enabling role of individuals’ social position. Organization 2006;13:653-76. https://doi.org/10.1177/1350508406067008.
- Mainiero LA. On breaking the glass ceiling: the political seasoning of powerful women executives. Organ Dyn 1994;22:5-20. https://doi.org/10.1016/0090-2616(94)90075-2.
- Hartley J, Benington J. Leadership for Healthcare. Bristol: Policy Press; 2010.
- NHS England . Planning, Assuring and Delivering Service Change for Patients 2018.
- NHS England . Integrating NHS Pharmacy and Medicines Optimisation into Sustainability &Amp; Transformation Partnerships and Integrated Care Systems 2018.
- Lankau M, Scandura T. An investigation of personal learning in mentoring relationships: content, antecedents, and consequences. Acad Manag J 2002;45:779-90. https://doi.org/10.5465/3069311.
- Doldor E. From politically naïve to politically mature: conceptualizing leaders’ political maturation journey. Br J Manag 2017;28:666-86. https://doi.org/10.1111/1467-8551.12219.
- Ferris GR, Anthony WP, Kolodinsky RW, Gilmore DC, Harvey MG, Wankel C, et al. Rethinking Management Education for the 21st Century. Greenwich, CT: Information Age Publishing; 2002.
- Schon DA. The Reflective Practitioner: How Professionals Think in Action. New York, NY: Basic Books; 1983.
- Kolb D. Experiential Learning: Experience as the Source of Learning and Development. Englewood Cliffs: Prentice-Hall; 1984.
- Perrewé PL, Nelson D. Gender and career success: the facilitative role of political skill. Organ Dyn 2004;33:366-78. https://doi.org/10.1016/j.orgdyn.2004.09.004.
- Marsick W, Watkins K, O’Connor B, Malloch M, Cairns L, Evans K. The SAGE Handbook of Workplace Learning. London: SAGE Publications Ltd; 2013.
- Crosby BC, Bryson JM. Integrative leadership and the creation and maintenance of cross-sector collaborations. Leadersh Q 2010;21:211-30. https://doi.org/10.1016/j.leaqua.2010.01.003.
- West of England Coaching and Counselling. Coaching and Counselling 2020.
- NHS Leadership Academy . Coaching and Mentoring 2012.
- Baddeley S, James K. Owl, fox, donkey or sheep: political skills for managers. Manag Educ Dev 1987;18:3-19. https://doi.org/10.1177/135050768701800101.
- Primomo J. Changes in political astuteness after a health systems and policy course. Nurse Educ 2007;32:260-4. https://doi.org/10.1097/01.NNE.0000299480.54506.44.
- Oerder K, Blickle G, Summers JK. How work context and age shape political skill. J Manag Psychol 2014;29:582-99. https://doi.org/10.1108/JMP-01-2013-0004.
- James K. Leadership in Context: Lessons from New Leadership Theory and Current Leadership Development Practice. London: The King’s Fund; 2011.
- Bolden R, Casebeer A, Harrison A, Mark A. Innovations In Healthcare: A Reality Check. London: Palgrave Macmillan UK; 2006.
- Department for International Development (DFID) . Drivers for Change Paper 1: What Does Drivers for Change Mean for DFID 2003.
- Vogel I. Review of the Use of ‘Theory of Change’ in International Development Review Report 2012.
- Pettit J. Power Analysis: A Practical Guide. Stockholm: Swedish International Development Agency; 2018.
- Gaventa J, Pettit J. Powercube: Understanding Power for Social Change n.d. www.powercube.net (accessed 3 March 2022).
- NHS Institute for Innovation and Improvement . Improvement Leaders’ Guide. Managing the Human Dimensions of Change. Personal and Organisational Development 2005.
- Kacmar K, Carlson D. Further validation of the perceptions of politics scale (POPS): a multiple sample investigation. J Manage 1997;35:627-58. https://doi.org/10.1177/014920639702300502.
- Ferris GR, Treadway DC, Kolodinsky R, Hochwarter WA, Kacmar C, Douglas C, et al. Development and validation of the political skill inventory. J Manage 2005;31:136-52. https://doi.org/10.1177/0149206304271386.
- Roe B, Rowley E, Seymour A. A Guide to Implementing Change. London: Collaboration for Leadership in Applied Health Research and Care East Midlands; 2014.
- Jarrett M. The 4 Types of Organizational Politics. Harvard Business Review; 2017.
- Currie G, Lockett A, Finn R, Martin G, Waring J. Institutional work to maintain professional power: recreating the model of medical professionalism. Organ Stud 2012;33:937-62. https://doi.org/10.1177/0170840612445116.
- Brown P, Zavestoski S. Social movements in health: an introduction. Sociol Health Illn 2004;26:679-94. https://doi.org/10.1111/j.0141-9889.2004.00413.x.
- Lobe B, Morgan D, Hoffman KA. Qualitative data collection in an era of social distancing. Int J Qual Methods 2020;19. https://doi.org/10.1177/1609406920937875.
- Boin A, Hart P, Stern E, Sundelius B. The Politics of Crisis Management. Cambridge: Cambridge University Press; 2016.
Appendix 1 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for the ‘review of reviews’
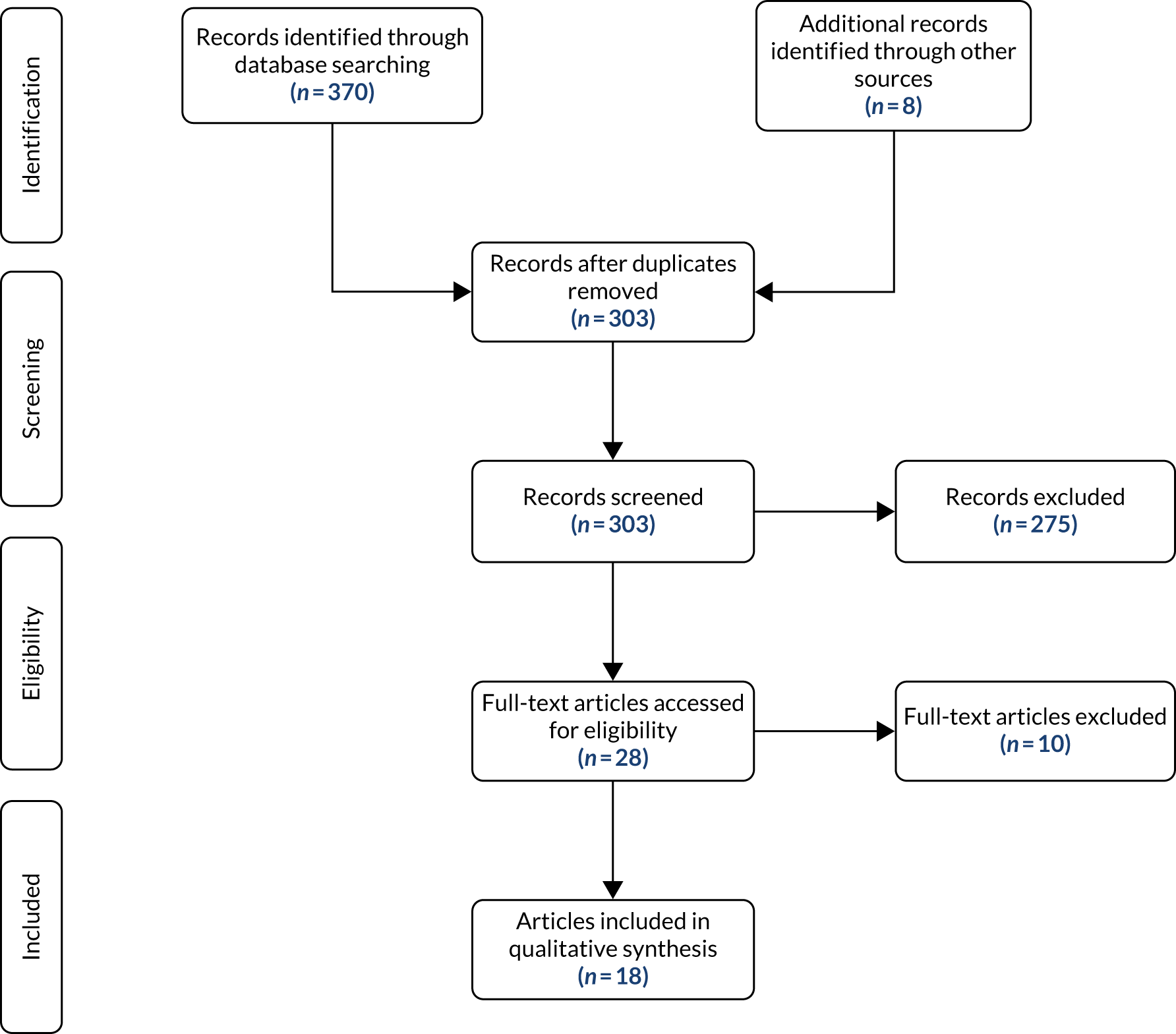
Appendix 2 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for the review of health services research literature

Appendix 3 Interview topic guide
General HeLPA interview topic guide
[Draft v1.6]
This is designed as a general topic/prompt guide for use with health service managers or leaders. The questions are illustrative prompts and the expectation is that they will be adapted to reflect the circumstances and responses of individual participants.
General points
Try to encourage participants to be reflective and think back over career; ask for specific examples, events or situations; but make it clear that we do not assume there is always right or wrong answer, rather people’s experience might be unclear or ambiguous.
The interview is divided into three sections: (a) the organisational politics of the health and care system exploring how they understand the environment they work within, (b) political skill and astuteness and its forms within the health and care system, and (c) how political skill or astuteness is acquired.
Biographical questions:
-
Can we start by asking a few questions about your career background, the roles you have held and your current role?
-
What have been the main motivating ambitions in your career to date?
-
How long have you been in your current role?
-
What are the main responsibilities in your current role?
A. Organisational politics
Our questions are concerned with your experiences of what is often termed ‘organisational politics’ or small ‘p’ politics, and how people operate and manage in the context of these politics:
-
Looking over your career, can you describe a particular situation, event or project where organisational politics had a significant bearing?
-
– How was the politics manifest – what was the issue?
-
– Who did what – what positions were taken?
-
– How did the event unfold – what interactions took place?
-
– What impact did it have?
-
(It is very useful for us to have specific case studies and it illuminates the discussion considerably. We will anonymise anything you tell us and if we quote you directly you will be asked to ‘clear’ the quote.)
-
Reflecting on [the specific case] and/or other experiences, how would you define ‘organisational politics’ – what are the key features?
-
When thinking about the organisations you have worked in, what are the key organisational issues, controversies or debates at the focus of organisational politics?
-
Do some people or groups seem to act more ‘politically’ than others?
-
– What characterises these people (role/gender/age/etc.)
-
– How are they received by yourself or others in the workplace?
-
– Why do they do it?
-
-
Are different types of political behaviour found in different NHS contexts, for example in the front-line workplace, or working with commissioners or interacting with policy-makers? [Again, use previous example.]
-
As well as thinking about politics within organisations, is there a form of politics that exists at the interorganisational or system level, for example commissioners or regulators?
-
– What are the key political issues or debates?
-
– Who are the main protagonists?
-
-
Do people talk openly about organisational politics, or do you feel that it is something we don’t openly recognise?
-
– Why do you think people don’t talk about it?
-
– Or where and when do people tend to talk about it?
-
-
In your view, does organisational politics and political behaviour have a negative or constructive influence on how services are organised [example of each]?
-
What do the terms political skill, astuteness or savvy mean to you?
-
From your experiences, what would you see as the key attributes or qualities?
-
Reflecting on your career, when do you think you became aware of organisational politics? Was there a time or event that brought it to the fore?
-
Do you see yourself as acting politically? Can you give an example from your career, maybe in relation to a project? If not, why not?
B. Acquisition
Our final set of questions looks at how you or others acquire and develop the skills to act politically. (May already have been followed up in relation to earlier questions.)
-
Looking back over your career, how have you developed your political awareness and skill?
-
Have there been key events or episodes that you would see as learning points – expand?
-
How have mentors or leaders helped you develop your political skill?
-
Have you received any formal training in this area?
-
How have mistakes in the process of change or management helped you learn about organisational politics?
-
What would you recommend for future service leaders?
Appendix 4 Thematic coding framework with illustrative data extracts from the interview study
| Main themes | Subtheme | Code | Illustrative data extract |
|---|---|---|---|
| Self and interpersonal style | Self-awareness, self-belief and self-reflection | Self-awareness | So it’s about me knowing who I am, and I suppose if I know who I am, I am more likely to understand other people, and have empathy for other people, so maybe emotional intelligence, linked in with leadership, but I think that they overlap because of that motivation, that drive and determination, that self-awareness, that being open to feedback, because if you’re comfortable with yourself, and knowing your own strengths and weaknesses, then actually that’s fine, and appreciating that we’ve all got that but then within a team, trying to play to everybody’s strengthsWP2-37. . . becoming the deputy of this place [name] was a big step up for me and I suddenly found myself being the boss and I didn’t know how to be that person to be honest and I, so actually learning to be myself in a different role was hugely challenging and the source of some considerable self-doubt . . . I’ve, I think one of my strengths, and I’ve got many weaknesses, is I’m reasonably good at reading situations of people and that’s a hugely helpful skill where one, to a degree, abstracts one’s self from the heat and burden of the situation and you’re very expert on what’s going on here.WP2-31 |
| Self-belief | . . . and there are choices you don’t have to make about how you act in order to try to improve that and make a difference to that in a way that allows you to keep your integrity and trying to do something in the interests of patients and the organisation while recognising that other people are defending their own interests . . .WP2-47If you let something psych you out then you’re likely to fail whereas if you look at it as, well this is a challenge, it needs a steady approach or whatever or I need a bit of help from some friends and it’s no bad thing to ask for some help . . .WP2-38-P. . . don’t get me wrong, we’re all dispensable . . . I think my position helped and I knew what I was talking about . . . I wasn’t just saying things for the sake of it, I knew I was measured and actually I was loyal to the trust. So, I was not . . . I was supportive of the trust, I represented them appropriately in meetings, and then I think you can be heard, can’t you? The difficult things you’re saying can be heard in a way that potentially if you are a . . . have limited . . . if you can’t . . . if you’re all contained and they’re effectively just wanting to shout fire because you’re scared of it, then actually people don’t listen and why would they really? To be honest. So, in a way it was interesting to do. I found myself acting . . .WP2-65 | ||
| Self-reflection | Yeah and I think the other thing you need to do is understand self. So absolutely understand yourself and be challenged about that and therefore understand how others perceive you, because that’s key to being political isn’t it? If you think you’re one thing, but others see you as something else [chuckling], that’s a problem, and therefore how you tailor your behaviours, your responses, your communication, to different audiences. So if you know, I’m seen as quite blunt, as quite direct and sometimes quite cold, because I like to get on with things, I like to put my head down, I don’t want to be interrupted, I’m busy, people might interpret that, as oh God, she’s not approachable and that’s how people perceive youWP2-10I think really helpful to have a safe place and the important thing is safe where one can say look this is what I think is going on, have you got any ideas and then what you’re doing is you’re crowdsourcing amongst a small group of trusted mates who essentially as participants in these groups often become tutors, an opportunity essentially for reflection as well as getting ideasWP2-31So I think, what I think my experience working in a national role is that you, we probably ended up taking more reflective time, trying to interpret and make sense of what was going on than in organisational politics that are at an NHS trust level, I think you just got on with itWP2-35 | ||
| Resilience and perseverance | Staying the course | I think you have to be resilient as well, you need to not take things personally which is quite a tension really because you’re using a lot of personal skills to sell but then you can’t take any negativity personally. So yeah it’s having a . . . I think you need to have, well be politically astuteWP2-4. . . it’s just about making sure that you very proactively engage and you’re not scared about being knocked back and failing because sometimes people don’t want to take you onWP2-5-D | |
| Emotional intelligence | Empathy and reading the climate | So, it’s being aware of your own personality, again, which comes back to emotional intelligence, it comes back to your political influence small ‘p’ because of your interpersonal influence, and the skills that you have, in your toolkit, to be able to influence someoneWP2-37 | |
| Understanding the emotions of change | . . . skilled political operators are very good at, often quite good at promotion of things but very good at emotional intelligence and understanding what people need from different situations and reading the room and there’s nothing better than sitting back watching sometimes when somebody’s like that because you can just see what they’re doing and it is definitely something that people must, I don’t know how much of it is innate, I don’t know how much of it is learnt, but some people are just very good at doing that and I think they understand how different people need different things from situations that they’re inWP2-9-D | ||
| Managing own emotions | . . . think there’s something very important about building support, so there’s the listening skills, the awareness of others’ viewpoints, empathy, being able to take account of where other people are, being able to cope with the unpleasantness that comes and being able to expect that and being able to separate the personal and professional which I think has helped when things, when you frame things in, if you think about in particular, so framing things in terms of what you’re there to do, why you’re, why does this organisation existWP2-47 | ||
| Personal style | Chameleon like | There was one particular episode where . . . I had to go to all the professional bodies . . . and one person came back and was really going at it and I sat there and I thought, you know when you feel quite defensive, but I didn’t, I sat on my hands and just think right so just go back calm, show that you trust them, thank them, do the stuff that inside you’re thinking it’s alright for you sitting, but then others came back and went ‘you really dealt with that well because you could feel the’ . . . so I think it shows about integrity, it shows about the ability to manage what might be in someone’s headWP2-32-AD. . . ones where it feels clunky and difficult and awkward and you’ve got to mind your P’s and Q’s and sometimes it’s just through being more formal but it’s not, the formality isn’t it, there can be formal and facilitative and enabling but they can also be informal and just either going nowhere or quite uncomfortable. I think part of it is building those relationships and I think certainly one of the ideas is trying to always for example make the emails fairly friendly rather than absolutely bold as it were, it only takes a couple of words not much effort really but just to make that slight bit of difference in the way you communicate with somebody so you’re a human being rather than just a computerised response to somethingWP2-34-DSo you look at it, you then just sort of adapt your style and it’s, and is it your body language, because then you’re thinking, OK, I was getting quite comfortable here, just listening, but actually I’m in the work mode and this person has only got half an hour and I’ve only got that amount of time, to influence them, for the first time, but as I say, it’s about being able to continue and to develop that relationshipWP2-37 | |
| Integrity | . . . got to be yourself haven’t you, and celebrate yourself. And that’s where the sensitivity . . . and understand how other people might experience you. And for good and bad, and I think just understand that and own itWP2-65. . . to be authentic and actually you’ve got, I’ve got to live with myself, and I will only do things that I know are right and proper, and that at the end of the day I can put my hand on my heart, and even if something wasn’t quite right, it was done with the best of intent, and it wasn’t a call, to be malicious or anything like thatWP2-37The term I would use is smiling assassin, is that sometimes I’ve worked with people who have tried to appear authentic and sincere, but you can see through it, so I actually, I disagree with the . . . I mean I think it’s true, I mean if you think you’re a supreme actor then maybe you can get away with it, but I think ultimately if you’re not authentic then something will let you down and your true self will be revealedWP2-35 | ||
| Charismatic | It’s that charisma bit around actually they generally look like they’re quite interesting people and they’ve got a certain presence around them, I think they tend to be more yeah skillful, political operators in that respect in that they can get on with a lot of people and they can get a lot of people to work around a similar causeWP2-9-DThere are certain people, our previous chief exec[utive] and the current one . . . he could schmooze a room, everybody loved him, well most people loved him and he could make you feel valued, you might have had 10 minutes, but you felt he was listening and he valued and he was really interested in what you were doing and he could remember people’s names, it’s about that personal touch, he’d remember your nameWP2-34 | ||
| Diplomatic | . . . would be, diplomatic to ensure that people continue to be engaged and continue to work together. We bring an awful lot of characters together in the network and I work really hard to keep them on board. It might be that we get something in and it might be a difficult email to write and I will be really measured and careful with the use of language and with how I write it to maintain and retain engagement. I work really hard not to disengage, not to cause disengagement because as soon as you start to lose people, you’ve lost something big haven’t you?WP2-35. . . what he did, he navigated some very bumpy political waters and I think kind of, I’m sure had to bite his tongue for a lot of things. Because I guess effectively he had a number of brownie points and he knew he needed to play them when he needed to play them, would be my thoughtWP2-65 | ||
| Assertive | I’m not saying that I never use the steamroller approach, I wouldn’t say it’s very frequent but there are times when you have to say sorry but this has to happen in this way. I think as long as you can justify why you’re being so directive then that’s fine and I think it’s about understanding why you know if you’ve tried the collaborative approach and it’s not working why is that, what are the background issues that people are putting barriers up, is it because they don’t understand the outcome that you’re trying to get to, is it because they don’t fundamentally agree with it. There are times when we do have quite difficult conversations particularly with our staff as to why we’ve taken a certain course of action because fundamentally people come into social care because they want to help peopleWP2-7. . . it’s really important to be articulate, be assertive and I think what comes with experience, and I didn’t have this when I started off as a nurse director, is just taking time to really understand others’ perspectives because I think I was probably a bit bombastic and I knew what was right because I was the nurse director and I knew what patients needed, so I think that I needed to just moderate my approach a bitWP2-5-D | ||
| Strategic thinking | Understanding the broader political landscape | Understanding history | The whole experience of working with a chair[person] who, quite rightly, can make or break you as an individual operator as well as being hugely important in terms of setting the climate for the organisation and representing the organisation to the outside world, nobody prepares you for that and so that was a very seminal set of experiences for me and I think there’s a correlation between the amount of pain one feels and the amount of leadership development one experiencesWP2-31I think there are more people in trusts and in NHS organisations who need to stop thinking that political is a dirty word, and start embracing the fact that they are operating within a political system and understand that and you know, oh God, they are so risk adverse, that anything that could be seen as political, and that’s part of the reason for my argument about the NHS is a political football, because I think they believe . . . wholly wrongly that somehow or another that political always conflicts with party political, which it doesn’t and that there’s an illegitimacy of political discussion in the NHS and my argument is no, the whole NHS is a political construct, and if you don’t understand that you can’t run it properlyWP2-46 |
| Seeing the big picture | Be able to look at the wider picture . . . I did that when I was doing that job to go really wide and bring it down . . . so I think you need to have an appreciation of the macro pictureWP2-4I think by recognising the broader context in which you’re operating and that health doesn’t begin and end at the doors to the hospital as we said, I think having a slightly broader range of people on your board in terms of your non-exec[utive] directors, I think developing that relationship with local government, because then inevitably some of the cultures will begin to you know, not an enormous amount, but there’ll be a little bit sort of leakage of the cultures backwards and forwardsWP2-39 | ||
| Understanding the system | So many, many layers of I suppose political issues, that you had to be aware of, from the individual’s perspective, because of their background, because it had to be disadvantaged, what does disadvantaged mean? And then you have the layer of administration, and the organisation, political overview that actually might not translate from London to what’s happening in [here – name removed], because the landscape is different and it’s about how things were shared, communication, it comes back to communication, creativity and your own motivation . . . to translate some of the excellent practices, that are, have been used elsewhere in the country, but to make them relevant to what’s happening within our small environmentWP2-37[Should have] paid much more attention to the politics up front, actually, and explored what could we possibly know about what we were stepping into for all of those different domains before we actually went live in terms of bringing those people together. Although we knew it was likely to be political I don’t think enough attention was given to the upfront analysis of what that might look like before we actually went to the first meeting for that group to then start to explore what were some of the sticky issuesWP2-63 | ||
| Interface between big ‘P’ and small ‘p’ | It was very fractured at that point in time and that’s quite late in the day to discover that, when you’re actually sat in the House of Lords in a meeting room to discover that there’s all these issues and subcurrents going on that weren’t apparent, so there was a lack of preparedness on our partWP2-63Working at a national level, working for a regulator, there are massive politics, with a big ‘P’ and a small ‘p’ because you’re so close to Westminster that actually your chief exec[utive] is meeting with the Secretary of State every Monday morning, that feels very real when you work in an arm’s length body and then of course because there are several arm’s length bodies working in the national health and care system there are big politics between them all, so I, so the experience of working with, in that environment was fascinating because you’re getting, well you’re getting very interesting dynamics between very senior people in those organisations and often those are personality clashes and differences of philosophy and approach, but they’re dressed up as being well this is just the way the [agency] works or this is just the way [agency] worksWP2-35If I offer myself as a case study, in that when I’ve had the opportunity of working with capital P politicians, special advisors and the whole political machine and firstly one establishes, one hopes high trust relationships with colleagues operating in that space. Secondly, one understands the mechanics of the execution of power and the deployment of power and that then is internalised as part of one’s natural operating system. So one understands how policy is made which is usually product, a requirement for speech and the whole series of projects . . . the politicians make in terms of which announcements are made and there’s a skill in promoting particular projects so that they’re oven ready so to speak for deployment in a speech depending on who’s going to make it. One’s got to be lucky as well, money’s got to be available otherwise. So I think in terms of the individual, individuals have the opportunity and in my case the privilege of operating quite close to the centre of proximity to power, political power, have the opportunity to become more fluent in how it’s used . . .WP2-31 | ||
| Reading the local political landscape | Lines of power and influence | So it’s about trying to detach yourself from the situation, and think about so what is the situation I’m in here? It might even be preparing a talk to other people about what is the situation I’m in here, to really try and understand something of the reality of that situationWP2-36So many departments, teams, organisations and the conflicts between them, in terms of understanding what the whole system needs but knowing what the regulatory landscape requires of them, within their particular silo, or within their particular department, or unit, or whatever it wasWP2-63 | |
| Influential groups | Ah, because when you’re talking about the situation, you’re necessarily talking, it’s a matter of opinion, opinions will vary, and there will be different artists, and it will inevitably be a complex situation. It’s fundamentally unknown in its entirety, you have to accept that you don’t know enough about the situation, you will never know enough about the situation, but you might be able to get some insight and understanding of the situation that you’re in. But unless you’re prepared to connect that to the question about, what’s my part in this, then you can’t do anything to affect the situation. You can examine what’s my part in it, whether you’ve done nothing or whether you’ve been overbearing or whatever, then you can begin to. And what’s my part in it, well I would argue, and I think this is where you can think about this politically too, it’s your part in it is always to do with what you are co-creating with the other people in the situation with you. So in other words it’s always in the relationship that you hold with the other players who are part of this situation. And that for me is the bit where you can, that always is political because it’s relational. So it’s about power, it’s about how we’re creating the world togetherWP2-36The key challenge is to actually understand why people that you interact with are doing what they’re doing and to really try to get to know what their drivers are, what are the things that cause them anxiety every dayWP2-43 | ||
| Multilateral forces | When they [doctors] go with an idea into the trust they have to wade through all the levels of treacle and in doing so they either find a way of circumnavigating the system to get what they want, because they’re used to getting what they want or they’ll just do it anyway and bear the consequencesWP2-3When you have a meeting where there might [be] an element of dissent and people are stirring up for a bit of a conflict or refusing to do something. It’s no, why should we do that?WP2-3. . . it’s just your classic, they came in and they fired the guns of the clinical lead, because people tend to think clinicians can get away with something, to land their point, and [name] basically managed very, very impressively to say to them, ‘You’re not saying that, I’m not accepting the points you made, they’re not technically correct and I want a, I’m not just going to gloss over this, I want a formal apology’WP2-6 | ||
| Recognising when people are being political | You do need to be able to recognise when people are using their political skill to their own ends and potentially negatively and I think that’s something that you need your sort of antennae out for because there’s certainly people who do do thatWP2-8I don’t often get these hidden agendas, I find it hard to work out sometimes, what is it they mean, just say it. Because I think, I’m a straightforward person, I say it as it is, I don’t say one thing and mean something else. So I hope that people are clear when they’re having a conversation with me, exactly what I meanWP2-10 | ||
| Understanding what is possible and what is a priority | Scope for change | Sometimes I guess you’d have to take a short-term loss, but we’re not going to win on this one? But hopefully, for a longer-term gain, we might win something bigger . . . a good example would be things like when we’ve had things like the control target, so many, many organisations fought with the control target, a lot. We didn’t and we had a very difficult control target, but basically we went with many, many conversations. In the end we said no, we’ll agree to that, but we want support for doing this, this and this, on the stuffWP2-45 | |
| Prioritising | That was a challenge, because obviously the clinical side of the team were very blunt in terms of this is how it will be. And there’s more considerations that we had to take into account, in terms of cost, in terms of resources, and a need, as an organisation to develop our own strategy and would make it a bit more sustainable and fit for purpose, going forwardsWP2-62. . . it also needed an understanding of the timescales. That’s not to say I wasn’t frustrated, I thought it took far too bloody long, but sometimes I think one of the other things you can bring to people is an understanding that if there are political players involved, they will have a whole range of different things that will, and actually your timescale doesn’t fit with their timescale, and you need to understand that but you also need to understand how to get yourself into the position, where you’re rather higher up their list of to dos, then you previously would beWP2-46 | ||
| Defining the problem, purpose or solution | Clarity of purpose | I’ve always been interested in matching all those things up and looking at the wider picture to then bring it, develop things and bring it through to the front line. That was how I did things and that always gave it some leverage and validation with whatever level across the organisation, if you hang it on those sort of external driversWP2-4 | |
| (Re)defining problems and solutions | Finding out a bit about people before you go in. Understanding what the clinical area is about . . . And then kind of know the subject matter really well so I wouldn’t . . . I’d make sure that I understood the benefits of the guideline, the evidence and sit down and talk to the managers around the benefits of doing that, firstlyWP2-4It’s not that you’re being deliberately devious or withholding information. It’s just you have to learn what’s appropriate and what individuals want to know. And what they don’t want to know. So that . . . having that support is essential, crucial, vitalWP2-41I think skilled up, skilled political operators are very good at, often quite good at promotion of things . . . understanding what people need from different situations and reading the room and there’s nothing better than sitting back watching sometimes when somebody’s like that because you can just see what they’re doing and it is definitely something that people must doWP2-9Now you can imagine [unclear] the politics with a big ‘P’ and a small ‘p’ between 13 national organisations . . . really, really challenging. So what we had to do was get quite . . . We had to work at different levels, so we had to make sure that the senior people were on board, but actually really to do the day job, the ins and outs of actually producing a policy and strategy document like that we needed to create a virtual team of people who worked horizontally at the same level as us across those other organisations. So I think, when I say tactical it’s like, again you, if you’re setting out on a piece of work like that it’s working out yeah that you’ve got to work at several different levels and you have to influence differently, so we made sure we had, for example, two senior responsible officers, one from one organisation, one from the other and that was quite carefully chosen to make sure that we had closeness to them and that they, that, I suppose that the power was shared in some wayWP2-35 | ||
| Communication and engagement | Actively listening to others | Listening and responding to concerns | I think it’s knowing your audience. On one level it’s, I understand, the people you work with and the people you interact with from outside the NHS, how they would react to something. How you could make something more palatable perhaps, or, I think, on another level it’s understanding your role as an NHS employee and what you’re expected to do, and how things might look to the publicWP2-2Oh, absolutely listen, but really, really demonstrate your listening. Don’t just pretend and pay lip service to it. If you are asking somebody to give you their view, their advice, their expertise then absolutely listen to them and take notice. Don’t think that you know it all and you can do it all better. Ask the people that really know and that really understand and really take notice of it. Really, really listening, I think really listening . . . People are a valuable asset and people are under a lot of stress and not helped if you’re in an environment where you’ve got all the conflict and problem. I think you learn, you look for the opportunitiesWP2-3Yes I mean first of all identifying it was the issue, it was, you know, when you’re leading something, you’ve got people working on the various project streams for you, they’re reporting into you, you’re having your meetings and you think everything’s going swimmingly and then you just can’t, you get the objections that are coming forward, the noise in the background, and you say what’s all this about?WP2-43 |
| Facilitating others to listen and understand | Listening [is] a huge thing, absolutely. Listening and giving time for people to pause and reflect, ‘cause I have a habit of jumping in a bit too quickly and filling in the blanks . . . going away for 2 or 3 weeks, thinking about it, coming back, and not being worried that you haven’t heard anything yet; allowing people time and space to think about it and really getting under the skin of what’s going on for them because it takes a long time to build trust with a new group and that work needed a lot of trust, given where some of them were particularlyWP2-63So, we did it as collective learning. So that was my approach to trying to rationalise and deal with their objections, by pushing the objection back to them and asking them to explain why?WP2-43 | ||
| Asking questions | Sense-checking | It gave us an opportunity to explore what that loss looked like and what are you fearful of, and how do we mitigate that? So we’d get this fear of change but is all of this real? Is some of this perceived? Is some of this misinformed? We started to explore what that meant for those different groups. So, give me your ideal view of what would that look like? How does it affect all of these peopleWP3-63 | |
| Naive questions | And also, a bit of naivety just to ask stupid questions is very handyWP2-36I think when you’re coming in from outside you haven’t got that inside knowledge, you’re much more likely to blunder into something without meaning to, to put your foot in it but equally there is also power in coming from outside because you can, particularly if you stick to quite a coaching style, you can ask naive coaching questions which then bring the issue into the room in a way that you couldn’t do when you know the systemWP2-40 | ||
| Opening up dialogue | . . . that most people aren’t interested in that at the beginning. You have to open it up. You have people that will say to you look, I just want to come in and do the job that I’m being paid for, and then I want to go home. And they’re the difficult ones in terms of how do you work with them? And I used to do it by physically taking people to show them things out of the building. Get them to meet other organisations that have nothing to do with the organisation or the product, or the service that you’re offeringWP2-39. . . also recognising that other people’s motivations are different to yours, so again being prepared to open up those conversations with others about what matters to them . . . We have to create an environment where those clinicians want to come to the tableWP2-3. . . trying to create a safe psychological space for some difficult conversations. That was the approach that we took really early on. We made a conscious effort to say what is it that ultimately we’re all here to try and achieveWP2-63 | ||
| Allowing others to shape the agenda | Inclusive approach | The longer I’ve done it or perhaps in some of the more senior roles is it matters less and less what you think and I think you probably achieve more if you’re prepared to relinquish your own control and that’s more than just delegation. That’s not just about having a team of people that you can give jobs to it’s about being prepared to hear something that’s different to your original plan and acknowledge that that might be a better way of doing it or it might be the more successful route to followWP2-8It helps, you see things from different perspectives and things get done the right way, particularly if it’s about actually, whether it’s clients or staff, their actual experience. And I think to do that requires letting go of aspects of power and control, it needs the right structure where it’s not even that it isWP2-65 | |
| Feeling in charge (but not) | You become more politically astute, I mean be willing to walk in others’ shoes, be willing to understand what others can contribute and don’t be so fixed on well we’re the big teaching hospital and we’ve always done it this way and we’ll always do it that way, it’s actually being open to others helping us to iterate what we doWP2-35I grow whatever they’ve brought to the table, I have the skill set to do that, then bring them back to the table and you’ve got something tangible to show, because they’ve built it they’ve owned it. They then own it and because they own it they implement itWP2-2 | ||
| Framing strategies | Selling | I mean selling people, staff, the public, whoever, on the list of options you’ve put in front of them, if it is indeed a list. So it’s a question of . . . it’s stopping people coming back and saying, ‘Oh, actually we should do this instead’. ‘Oh you shouldn’t do that, you should do this’WP2-2What were the real burning issues that were causing difficulties for folks, both working in that system and delivering the care and receiving the care? We focused interest on three words: harm, waste, delays. We really simplified itWP2-63So if I’m sitting down with the director of finance I need to understand their agenda you know, what does that person see as important? What will swing it for them? Is it about reducing length of stay because their internal costs per case will go down for example? So OK, OK I’ve got all that clinical evidence I need to just tell them that they’ll be in a day lessWP2-8There’s a learning cycle to go through then, that says ‘How do I make this interesting?’, how do you actually engage these people and that was when we started to really dissect what were the issues behind what we were trying to tackle and really take it back to. So if we’re dealing with, say for instance we’ve got a problem, this is specific issues, say we’ve got a travelling community, living in [place], and there’s a particular situation [a lot of background noise at this point], the vulnerable members of the [place] population that have been preyed upon by members of the travelling community who are doing bogus visits and stealing from those people. Well you suddenly find that those vulnerable people are the same vulnerable people that the fire service want to get involved in, with certain trips and falls and they’re also the same vulnerable people that they want to put smoke alarms into their houses and then you find that actually these are the people that the health service are having extended services into their communityWP2-43 | |
| Persuading | . . . how can I suss out where I need to influence you? What’s the trigger? Like you said, ‘Oh can I?’, so it’s always [chuckling], it sounds awful. It is always being aware, of the other person and what, therefore, what’s right for their organisation?WP2-37. . . the skills that you need in [unclear] are influencing skills to be able to explain to somebody else what the issues are and see if they’ll help you and I think if you’re, if you don’t approach that in the right way then I think that’s when it becomes very difficult. So I think it’s about just having enough skill and understanding to be able to work with different people and individualsWP2-9I think it’s about persuading people that your way is the right way but everyone knows it’s there . . . but one prefers to use influence and argument and logic and empathy and all that, that’s my preferred style of working whereas when one works, as you’re describing, laterally or upwards you’ve got to use relationships . . .WP2-31 | ||
| Multilingual | The conversation I might have with the director of finance about a situation might be really quite different to the conversation and the language I might use working with the medical director. That doesn’t mean to say that the medical director and the director of finance are both motivated by giving high-quality care, they probably both care about that, but in terms of what the finance director needs to achieve in his job and what will make sense to him, sometimes the information needs to be presented with a slightly different slant on it or with a, the way I would present something might be more about the numbers, whereas if I was working with the medical director it might involve something else. So there’s something about having an awareness of what other people’s motivators are, but also what their jobWP2-35I don’t think sometimes people understand the sensitivity of the language that they use. They don’t know how that, they don’t get how that lands with people, in the way that politicians do, because they’ve been on the receiving end and they know what people think when a certain, you know. So if you say reconfiguration, people here, think closureWP2-46 | ||
| What ‘not’ to say | Knowing when to act, with whom, how, in what forum and being really, really careful with your choices and really deliberate with your choices and that seems essential to me and then there’s obviously all the good stuff about just building situations that or describe things, articulate things in ways that persuade people and being assertive when you need to beWP2-47It becomes almost like what . . . hardly a better way of describing this, but almost how can you get to a point where you almost deal with the other members, and say right, we’re going to test it here, but we are doing to do in other areas, and can we sell a narrative?WP2-45It’s not that you’re being deliberately devious or withholding information. It’s just you have to learn what’s appropriate and what individuals want to know. And what they don’t want to know. So that . . . having that support is essential, crucial, vitalWP2-41 | ||
| Rhetorical strategies and resources | Data | The only thing I can do is be very clear about the numbers, and then, from now on, I keep . . . I will develop very, very clear charts and graphs because I think she might understand a picture, and just keep, ‘this is what we’re doing, this is what we’re doing, this is what we’re doing’WP2-4‘So OK, so let me tell you about the statistics’, if you’re thinking that person is really into statistics. So you look at it, you then just sort of adapt your styleWP2-37Absolutely doing homework, absolutely knowing your stuff inside out, being able to answer questions at a drop of a hat, being able to give data, because what commissioners will ask you is, they’ll just [tele]phone you up and say ‘Right what’s the status on x?’, and they’ll expect you to know it, yeah off the top of your head, yeah they will, and if you don’t know it then, you have to get back to them quickly, making sure that you’re assured that you know what is happening in your organisation and we’ve seen organisations fail haven’t we, when they get board assurance, but the front line are doing something completely different. So it is making sure that you’ve got that confidence throughout the trust, so yeah being prepared, knowing your stuff, having the dataWP2-10The only thing I can do is be very clear about the numbers, and then, from now on, I keep . . . I will develop very, very clear charts and graphs because I think she might understand a picture, and just keep, ‘this is what we’re doing, this is what we’re doing, this is what we’re doing’. And have the finance team on board. That’s the only thing I can doWP2-41 | |
| Authority figures | . . . there’s always probably someone else who can say it for you. So let them say it for you and then you don’t get all the hassle that goes with it, but it’s been said, the message is there, you don’t have to be the fall guyWP2-10I e-mailed the director of nursing at [trust] which hadn’t even seen her because she’s the top of the tree and I was at the bottom of the tree and just really outline what my ambition was and I think because I asked and I was boldWP2-5They are still championing the work but that has been down to two or three key individuals. If it hadn’t have been for them the alliance would definitely have flounderedWP2-63Depending on how senior you are and what your relationships are like, sometimes that’s easier said than done, and I think for a lot of staff, that’s why I’m very interested in models of collective leadership and how you distribute leadershipWP2-35So by building some peer based coalitions and then tactically thinking, OK, who else could I bring into this conversation beyond the individual that’s blocking this and doesn’t want to acknowledge the scale of the problem, but being quite thoughtful about how you doWP2-47 | ||
| Patient perspective | . . . it also took pulling notes, it took some basics like rather than just looking at what the data on the computer was telling us, actually pulling the sets of notes and really looking underneath and saying well actually what’s happened to these patients and what delays are happening and actually really holding the mirror up for the clinical team in a supportive way, but actually working with the clinical team to pull the mirror up and say actually there’s some things would could do better here aren’t there, there are some things we could try doing differently, so we needed to find a way of unlocking it, but it required a combination of different tactics with different staff membersWP2-35. . . rather than the important thing being that service users share power on the same committees and stuff like that it’s actually about the relationship between us and service users so that we are, we both value the other as it were in it. So it’s not the angry service user saying we’ve got rotten services make something better and it’s not us saying service users we haven’t got much money this is what we’re going to do for you it’s us working together to take those problems on together and produce something together in a way that means we have a relationship where each respects where the others coming from and enjoys working together reallyWP2-34It can be as overt as actually cynically getting a patient or service user into the room, into the conversation. And it, kind of goes back to that sort of missed targeting. Sort of saying which is . . . if you get a patient in the room, you’ll know what they want, and what they expectWP2-1It’s helping people to see all the time that what we’re doing is the best for the patients and the pathways and that actually it’s not around shifting services, moving services, stopping services, it’s around pulling those services to work together in one systemWP2-3 | ||
| Empowering and delegating | Coaching | It’s a different way that you lead, you have to, it’s facilitating and coaching, not this is how you’re going to do it and everybody’s going to do it the same. So showcasing the small seeds of innovation tells people what’s in it for themWP2-32 | |
| Containing conflict | Clinical engagement I think is a problem at different levels. I did a lot of fact finding around engaging clinicians in the leadership and management of the NHS and I discovered that really there’s either engaged doctor or the reluctant manager in effect. What I discovered was that we try and make senior clinicians take on the role of managementWP2-3. . . very much delegating and working to people’s strengths . . . encouraging others to take the lead ensuring what happens is right rather than who decides what happens. So it’s terribly important that the right thing happens rather than them looking to the bossWP2-38 | ||
| Delegating to commit | I work really hard not to disengage, not to cause disengagement because as soon as you start to lose people, you’ve lost something big haven’t you? I think I work really hard with the people skills, to keep people on board to maintain the engagement, so that’s where my diplomatic skills really come inWP2-3 | ||
| Networks and networking skills | Identifying and appraising stakeholder networks | . . . as I say in broader terms, I think that understanding relationships, understanding power, understanding interests, understanding stakeholders, those are all political skills and they’re all absolutely crucial to this jobWP2-46So and we had quite a long run in to that, and there I would have said that actually political skills and activity like recognising who were likely to be the, in the broad community and the broad political system, who were likely to be the people that were concerned about it? Who were likely to be the people that we therefore needed to communicate with? The fact that you had to build a relationship in advance of asking them to do something. The relationships that I had anyway, that enabled me a way in and way of talking with people, common language and understandingWP2-46, emphasis added | |
| Access to professional networks | Professional networks as resource | I know I’m well respected by senior clinicians and I know it in lots of ways because I’ve had it reflected back to me and also my best friends are senior clinicians. Some of those best friends I have been identified to look after their children should they not be here. That means I’ve got really good relationships with them. In actual fact if I look at my friendship set there are few that sit outside being senior cliniciansWP2-3Clinicians have recognised the benefit of using the network in a political environment to get what they want, or to push through what they want, or to get something they want implemented. In a way that probably is politic isn’t it? It’s the politics of learning that you’ve got this big tool that you can use to your benefitWP2-3 | |
| Peer networks as support | I’ve got to know some chief executives in the health authorities very well. The one in [place] I got to know, I mean, that wasn’t a failing trust, but I got to know [name] very well. And actually, we worked together very well to do things which helped the reputation of the council, and it helped the reputation of the hospital. And there’s a big arts centre there, and they’d got into trouble, and [name] had enough trust in me, he said, ‘Look, we need some really good people on the board now, I’d like you to join the board because we’ve got to turn it round’ . . . And that sort of thing, you know, we became good professional friends. In [place] I worked very closely with two chief executives who were trying to reshape the image of [place]. And I was helpful to them and they were helpful to us. But they also knew loads of things I didn’t know which, you know, you could go to them and say, ‘Look, I can’t understand what’s going on’. ‘Ah, don’t do that, do that. The person you need to influence is so and so, the person you need to not annoy is so and so. And this thing’s untouchable. This is what the population of this area wants’WP2-24So if you build up lots of friendships in an organisation and lots of collaborators then you can make things happen. If you don’t life can be very, very hard. And processes are meant to irradiate that variance but they often don’t because people can use a process to their own end and that can be problematicWP-29 | ||
| Building and mobilising networks | Building support | So by building some peer-based coalitions and then tactically thinking OK who else could I bring into this conversation beyond the individual that’s blocking this and doesn’t want to acknowledge the scale of the problem, but being quite thoughtful about how you do that rather than, not in a big front stage way of standing up in a meeting and going this place is rotten and you’re rotten and all this sort of thing, but actually just gently building that coalition to move it from an individual problem to an organisational oneWP2-47We engaged them in the creation of some films about patient stories, we upped the engagement and comm[unication]s that they were doing around that and we made a compelling case for commissioners toWP2-40 | |
| Relationship management | You know my successes have been built more on actually developing relationships with people and actually getting them to understand my agenda but also understanding their agenda and actually looking at what’s the common ground and how can we both win or partly win by working together. So my approach is much more around building relationships with people and I think you can be successful whether you have the steamroller approach or the collaboration approach and I prefer the collaboration. I’ve seen people who steamroll all the time and it affects how people view them, it certainly affects whether people want to work with them or not . . .WP2-7. . . at the time I didn’t realise I was learning it, but one learns a repertoire of relational skills I think which when you work in an organisation for which you’re responsible you need, but you don’t need them as forcefully because, not that I like to think I use, well I hope I don’t use this very often, one’s got positional power which is very rarely used, but everyone knows it’s there . . . but one prefers to use influence and argument and logic and empathy and all that, that’s my preferred style of working whereas when one works, as you’re describing, laterally or upwards you’ve got to use relationshipsWP2-31. . . so, yeah, I think, 90% of what we do is about brokering conversations between people about trying to find a way to bring people together and to bind them around a common goal and almost being a counsellor between two folk, enabling them to speakWP2-63 | ||
| Alliances to counter resistance | . . . relationships with the CCGs is very, very hard . . . you’re not working with them every day. And because they’re the other side of the fence. They are your commissioners . . . That’s a whole other area of skill development that is . . . well, that would take you a lot of time to really work your way in to a CCG, and figure out who’s who, where’s the power in that organisationWP2-41My real skills in my role is that I bring together the clinical expertise. They understand the pathways, they under the issues to do with the patients, but I’m able to bring them together and find a way to enable them to cross pollinate, to share best practice, to do all the things that they do that are of benefitWP2-3. . . that it’s actually about the relationship between us and service users so that we are, we both value the other as it were in it. So it’s not the angry service user saying we’ve got rotten services make something better and it’s not us saying service users we haven’t got much money this is what we’re going to do for you it’s us working together to take those problems on together and produce something together in a way that means we have a relationship where each respects where the others coming from and enjoys working together reallyWP2-34We had to work at different levels, so we had to make sure that the senior people were on board, but actually really to do the day job, the ins and outs of actually producing a policy and strategy document like that we needed to create a virtual team of people who worked horizontally at the same level as us across those other organisations. So I think, when I say tactical it’s like, again you, if you’re setting out on a piece of work like that it’s working out yeah that you’ve got to work at several different levels and you have to influence differently, so we made sure we had, for example, two senior responsible officers, one from one organisation, one from the other and that was quite carefully chosen to make sure that we had . . .WP2-35 | ||
| Creating alignments | Common ground | I tend to, you know my successes have been built more on actually developing relationships with people and actually getting them to understand my agenda but also understanding their agenda and actually looking at what’s the common ground and how can we both win or partly win by working together. So my approach is much more around building relationships with peopleWP2-7 | |
| Aligning divergent interests | We’d agreed a set a working principles. We’d agreed a set of design principles for the way we were going to approach things and we’d just . . . from the summit we’d already got three asks from the group of folk that had been involved with that. One was to form the alliance in the first place and then it was to look at a charter. What are the 10 things that would make a real difference that everybody could sign up to, then the mobilisation campaign, so we had a focus, which helped. It was trying to get people on board for that focusWP2-63 | ||
| Win wins | I think when you’re implementing changes you see it a lot more because there’s an element of how to create win–win situations because if you go into something and there’s clearly going to be a loser there that’s not going to, depending on them and how they’re going to manage it, that’s generally not going to work is it? So it’s about understanding who they are and what their issues are, but I certainly think if you, if you underestimate that particular group of people you’ll come a cropperWP2-3I think just helping people to see that it wasn’t loss, but it was gain almost, and that it’s the bigger picture, not the personal. Sometimes people take it personally don’t they that it’s their service and it’s their whatever, but actually when they see the benefits for the patients and you actually give them the statistics of the survival rates etc., then it helps them to start to see that it might workWP2-3 | ||
| Identifying and using key people | Authority figures | . . . there’s a fear that things will move to the centre and that therefore the periphery hospitals might not, not that they’re as important but they might just have a fear really. I think it’s around managing the politics that are involved in that. We still have politics in the relationships and part of my job is smoothing that. It’s helping people to see all the time that what we’re doing is the best for the patients and the pathways and that actually it’s not around shifting services, moving services, stopping services, it’s around pulling those services to work together in one systemWP2-3If you knew the right person they could unlock doors. If you spoke using the right frame to the right people then you could unlock doors, but nobody ever sits you down and takes you through that stuff so you kind of learn accidentally, I think, rather than you learn in a meaningful way how to navigate some of that system and the use of different frames and understanding people’s perspectives and the lengths through which they’re looking at the worldWP2-63 | |
| Champions | By feeding information into them that excites them about where they’re going, and that can be done in lots of different ways. You can give them experiences. You can open their minds to the way that things are going or moving. You can create opportunities for people to get to know each other within an organisation, and learn from each other. You can identify skills that are required that you can match then to the way forward. And let people recognise that there is a big world which is changingWP2-39The other thing is having champions, so lots of people talk about oh you’ve got to have a project champion lovely but one person on their own can’t do anything so you’ve got to have champions and they’ve got to be at every level within the organisation. So whether it’s the CEO [chief executive officer] who knows about it, he probably won’t do that much about it but he knows about it and if it comes up to him he will more than likely be a supporter if he knows about it but then you’ve got to have the clinical champion . . . But I mean my real message to any leader is to do things that excite people about the business they’re in, the organisation they’re in. And then how do you do that, and how do you make it work? And they become the champions of the organisation that’s working thereWP2-39 | ||
| Facilitators | That’s really important and having a safe group of people that you can do that with be they in your work situation or ideally some sort of action-learning group that you can draw on, someone that you can pick up the phone to where you can reflectWP2-35I think that I was a bit naive about how much time you have to invest building solid relationships in order to get the best outcome or the outcomes you want really I supposeWP2-5 | ||
| Relational strategies and interpersonal skills | Dealing with egos | Smoothing egos | We had to go and smooth some egos. I remember having to go to one of our trauma units. There was myself, the medical lead and the chief operating officer of the hospital who met with a senior doctor and thinking that we were meeting with the senior doctor, but when we got there we were met with a barrage of the senior doctor plus his team, I think. There was something around smoothing the ruffled feathersWP2-3If I suss out that OK this is somebody who’s old school and he or she, needs to have their ego muscled, then you just do it. It’s like, you adapt your style to suit the receiver, but its being aware that you have to and that you can’t take that same approach each time. For example, in this role, I would go out with a presentation, written on the back of, so these all things that I should be saying, that I designed myself, there we go, I wouldn’t think of going through that with somebody, because how can I suss out where I need to influence you?WP2-37 |
| Challenging authority | Don’t be afraid to sometimes challenge the status quo. Now that’s hard and dependent on what level, well depending on how senior you are and what your relationships are like, sometimes that’s easier said than done and I think for a lot of staffWP2-35[It’s] being able to stand up and say ‘I think you’re wrong, and this is why’, is just as important as you know, being authentic and all of that, so it’s like the thing about [inaudible] is quite uncomfortable, so like being uncomfortable is not something we like doing, because it’s uncertaintyWP2-1 | ||
| Negotiating and dealing with powerful groups | Trades and deals | . . . but then you don’t have direct responsibility for those people. So the skills that you need in these case are influencing skills to be able to explain to somebody else what the issues are and see if they’ll help you and I think if you’re, if you don’t approach that in the right way then I think that’s when it becomes very difficult. So I think it’s about just having enough skill and understanding to be able to work with different people and individualsWP2-9I think there’s a lot of what you would call back stage or behind-the-scenes conversations, so building, firstly trying to build relationships with peers . . . to say OK this is happening to me, I’m raising it and they would go yeah, I had one of those, but I’ve just tried to deal with that, you would build a coalitionWP2-47We’re looking to build new hospitals, so that’s really difficult to find the finances for it, but essentially we’re going into conversations saying right, if you agree that, now you’re going to support us properly, and that’s not . . . and that’s opened up some conversations that I don’t think we would have easily got into in kind of other waysWP2-45 | |
| Manipulation | In the organisation you get very politically astute people who . . . I would . . . yes. Calling it ‘political astuteness’ in these people is a euphemism for being manipulative . . . that is knowing how to play the system to get their own way . . . What’s good for them, for their careers . . . So you get career climbers who are usually obvious in the way that they behave in certain meetings because they make a beeline to speak to the person with the most power in the room at the end of the meeting [chuckles] tell them, how brilliant they are, and how much they enjoyed the meeting, and also sort of massage their egos, and will present themselves in this light of, ‘see I’ve done this, and I did that, and I knew that, and I’ve done that for you, and perhaps we could talk about that at another . . . outside of this meeting. What do you think?’. And you can see they’re career climbingWP2-41People don’t like the idea that they’re being manipulated anyway do they or that they are manipulating, but I don’t think people always know (a) that they’re doing it or (b) that it’s being done to them, so actually if those two, if in their head those two things are synonymous then that is a problem, but actually a lot of the time it happens anyway because it’s about how you engage with peopleWP2-9Is about lying and it’s about presenting a face onto things that isn’t real . . . So apparent sincerity and authenticity . . . is important and yeah they draw on many things that I don’t care about that I actually have demonstrated to people that I do care about and actually I don’t really, I’m just trying to get my own way . . .WP2-43 | ||
| Using organisational structures, processes and resources | Using the rules | What’s the bureaucracy you have to step through to be able to talk to. So at that point in time it was still very hierarchical. There’s still degrees about there now. I don’t think it’s as bad but back in 2007–08 when this all started to emerge for me you weren’t allowed to go speak to without going through the chain of command otherwise that tended to upset a lot of peopleWP2-63That’s why I’m very interested in models of collective leadership and how you distribute leadership because I think we work in a very hierarchical system and in a hierarchical system it’s very difficult to challenge if you’re at the earlier level in your career or more junior in the structure or whatever term we want to use and what’s really important to me is how do you distribute the responsibility for leadership so that actually you are engaging other voicesWP2-35 | |
| Following the rules | I worked hard at making sure I developed very solid relationships with the non-exec[utive] directors on the boards and also the other exec[utive]s so I was able to say, ‘look I need this to go through, can I talk to you a bit before we go in’, so I might talk to the medical director to say look this is why it’s really important and almost pave the wayWP2-5I will expect people to meet deadlines, I’ll set deadlines for myself that I have to stick to and in terms of priorities, planning, all this kind of thing and they’re also all the things that need to get doneWP2-42 | ||
| Creating the rules | I think there’s something about, forming formal structures. Often being straightforward personalities, I think being fair and firm so whatever it is . . . I know it’s really dull but it’s not really dull is it?WP2-65I’m a natural organiser, I think that’s where my strengths lie. I think I was never sure whether I was in charge bossy, or just a really good organiser. I have a skill in being able to organise and see and do, so my skills are around systems and processorsWP2-3 | ||
List of abbreviations
- CCG
- Clinical Commissioning Group
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- GP
- general practitioner
- HeLPA
- Healthcare Leaders’ use of Political Acuteness
- HR
- human resources
- ICS
- integrated care system
- NIHR
- National Institute for Health and Care Research
- PHB
- personal health budget
- PL
- programme lead
- PPI
- patient and public involvement
- PSI
- political skills inventory
- STP
- Sustainability and Transformation Partnership
- WP
- work package
Notes
-
System leadership: developing and using political skill – workbook
-
System leadership: developing and using political skill – slide deck for team development
-
System leadership: developing and using political skill – facilitator’s guide
-
Political awareness and skill: recruitment interview topic guide
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/FFCI3260).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.