

Notes
Article history
The research reported in this issue of the journal was funded by the HSDR programme or one of its preceding programmes as project number 16/116/25. The contractual start date was in May 2018. The final report began editorial review in March 2021 and was accepted for publication in July 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HSDR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
Copyright © 2022 Jones et al. This work was produced by Jones et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2022 Jones et al.
Chapter 1 Introduction and background
Introduction
The overall aim of this study is to better understand the introduction of a new role in NHS England that is designed to support workers to speak up about ‘anything that gets in the way of providing good care’ (© National Guardian’s Office. Contains public sector information licensed under the Open Government Licence v3.0). 1 These roles are called Freedom to Speak Up Guardians (FTSUGs). We were interested to find out how FTSUG roles are being implemented in acute trusts and mental health trusts and whether or not FTSUGs are helping workers to ‘speak up’ about their concerns.
Background to ‘speaking up’ in the NHS
Employees who ‘speak up’ or ‘raise concerns’ about problems with health-care services have traditionally been referred to as ‘whistleblowers’. The terms whistleblowing/whistleblower, raising concerns and ‘speaking up’ are commonly and interchangeably used in the health-care literature, policy and the media. This report refers to speaking up and raising concerns, referring to whistleblowing and its derivatives only where others use those terms.
Although speaking up makes an important contribution to delivering safe care, NHS workers who raise concerns have not always been listened to or treated well. 2 The public inquiry into appalling patient care failings at Mid Staffordshire NHS Foundation Trust, eponymously referred to as the ‘Francis Report’,3 found that workers’ concerns were often ignored, and that those speaking up were mistreated by colleagues. The report also concluded that the unnecessary and avoidable suffering of patients was primarily caused by serious failure on the part of the trust board, who ‘did not listen sufficiently to its patients and staff or ensure the correction of deficiencies brought to the Trust’s attention’ (© The Stationery Office. Contains public sector information licensed under the Open Government Licence v3.0). 3
The issues identified in the Francis Report, however, were not unique to Mid Staffordshire or isolated to the early 2000s. Since the 1960s, several reports and inquiries4 have described the difficulties experienced by health-care workers attempting to speak up and how the many and varied concerns raised were missed, misunderstood or ignored by those responsible for assuring safety and quality across the NHS. 5,6 The failure to listen to and protect workers speaking up has been described by the House of Commons Health Select Committee as a stain on the reputation of the NHS. 7 Nonetheless, these issues are not exclusively found in the NHS because health-care employees globally report mistreatment and indifference as a result of raising concerns. 8–10
The introduction of Freedom to Speak Up Guardians
The events at Mid Staffordshire had a profound impact on health-care policy in England. 11 One of the many government responses to the Francis Report was the commissioning of a review of culture and practice around raising concerns in the NHS, the Freedom To Speak Up (FTSU) review, also referred to as the ‘Francis Review’. 12 The review refers to speaking up as a patient safety issue and confirmed many of the worries previously identified, finding widespread reluctance to speak up among some workers, rooted in a sense of futility. It also refers consistently to the detriment experienced by some who raise concerns and outlines that concerns raised about workplace incivility should be viewed as patient safety issues:
. . . wherever there is a reference to ‘raising concerns’, ‘speaking up’ or ‘whistleblowing’ it should be considered to refer to the raising of a concern relevant to safety or the integrity of the system. I include in this concerns about oppressive behaviour or bullying and dysfunctional working relationships, which I consider to be safety issues.
Francis12 © Francis R, 2015. Contains public sector information licensed under the Open Government Licence v2.0
In addressing these significant challenges, the FTSU review set out 20 principles to guide the development of ‘a consistent approach to raising concerns . . . whilst leaving scope for flexibility for organisations to adapt them to their own circumstances’ (© Francis R, 2015. Contains public sector information licensed under the Open Government Licence v2.0). 12 A single ‘overarching Principle’ states that every NHS organisation should ‘foster a culture of safety and learning in which all staff feel safe to raise concerns’ (© Francis R, 2015. Contains public sector information licensed under the Open Government Licence v2.0). 12
Principle 11 (‘Support’) proposed the introduction of the flagship FTSUG role in all NHS England trusts and foundation trusts, supported by the National Guardian for Freedom to Speak Up and the National Guardian’s Office (NGO) (see The role of the National Guardian’s Office). The FTSUG role was founded on three interlinked objectives to ensure that:
-
NHS employees are not victimised for raising concerns
-
speaking up is part of the normal routine business of any well-led NHS organisation
-
NHS organisations, both individually and collectively, learn from employees who speak up.
The FTSU review12 further proposed that the responsibility for driving, maintaining and monitoring progress in effecting culture change rested with the board. Responsibilities were outlined for a designated non-executive director (NED) and executive lead for FTSU, which ensured that support was available to all workers speaking up, and facilitated open discussions, reflective practice and shared ownership of problems and solutions.
Implementing the review’s proposals, the government mandated that each organisation providing health care in England should appoint one or more Guardian13 to act as a point of contact for anyone with ‘a concern about risk, malpractice or wrongdoing (they) think is harming the service’ (© NHS Improvement, 2016. Contains public sector information licensed under the Open Government Licence v3.0). 14 FTSUG roles had to be funded from organisations’ own resources, with the NGO funded via a centrally allocated budget of £950,000 per annum. At commencement of data collection for this project (October 2018), over 500 FTSUGs had been appointed.
The FTSU review12 clearly states a preference for flexibility in the role’s implementation and local adaptations to fit with each organisation’s perceived needs. A universal job description, which was produced by the NGO for the FTSUG role,15 provided numerous and broad guidance, expectations, principles and outcomes for the role. The job description is discussed and analysed in detail in Chapters 4–6.
In broad terms, the role of the FTSUG is intended to be an independent, impartial and objective role, serving as a highly visible contact for any worker with a concern, while also ensuring that concerns are responded to appropriately. The independence of FTSUGs is a recurring theme in many of the NGO’s documents and guidance; however, this refers to cultivating independence of thought, and from the hierarchy within the NHS trusts, rather than in procedural terms. For example, the guidance stresses that FTSUGs should function within existing procedures and processes, serving as an additional route only where concerns raised through the organisation’s existing channels do not gain traction. 14 However, FTSUGs are also entrusted to open a line of communication between workers, senior managers and the board, offering a route to speaking up outside the direct line management and formal human resources (HR) options. Having to navigate these discipline-specific, professional and procedural boundaries places the FTSUG in a potentially precarious position. FTSUGs are also potentially vulnerable as employees of organisations that they must hold to account when practices are contrary to the Francis vision12 of open and transparent culture in which speaking up is a consistent and normalised feature of everyday practice.
The role of the National Guardian’s Office
The NGO was established in April 2016 as an independent non-statutory body that was tasked with normalising speaking up and leading effective cultural change, but was not concerned with historical cases and the instigation of speak-up investigations. The NGO is jointly sponsored by the Care Quality Commission (CQC), NHS England and NHS Improvement, and its Accountability and Liaison Board includes senior representatives from the sponsoring bodies. Three years after its establishment, additional funding was allocated to the NGO to support its work to integrate FTSU in primary care, including the appointment of regional leads to spearhead this work.
The NGO provides resources for Guardians and the organisations in which they are situated; for example, guidance on recording cases and reporting data for Guardians,16 and FTSU guidance for boards. 17 Training materials and events for Guardians are also disseminated, in addition to national guidelines on FTSU training for organisations. The NGO also arranges an annual FTSU conference and co-ordinates regional FTSUG networks. Data, annual reports, survey reports, responses to consultations and other publications are archived on the NGO’s website. The NGO also obtains feedback from FTSUGs on its own performance. Respondents to the 2019 Guardian’s survey18 were asked to rate how supportive they perceived the NGO to be, on a scale ranging from zero (‘not at all’) to 10 (‘fully’). The average score was 6.5, indicating that perceptions of support had dropped from the previous year’s score of 7.1.
In June 2017, a 12-month pilot scheme for case reviews was undertaken by the NGO, during which the NGO considered referrals for case reviews by current and former workers in NHS trusts and foundation trusts who were unsatisfied with speaking-up procedures and response to concerns. Following a review, the trusts involved were expected to implement the recommended improvements, which would then be monitored by the regulators. Publication of the findings encouraged learning to be shared across the FTSUG network, which many Guardians interviewed in work package (WP) 2 described as useful. Following an evaluation of the pilot scheme, the case review process seems set to continue.
Measuring and monitoring speaking up in the NHS
As is discussed at length in Chapter 4, FTSUGs submit non-identifiable data to the NGO about speaking up in their organisation. Data are collated every 3 months and are published in the NGO’s annual report. The 2019/20 report19 indicated that 16,199 FTSU cases were raised with Guardians, an increase from 12,244 cases in the previous year. Many concerns (23%) included an element of patient safety/quality, while 36% included an element of bullying/harassment.
In addition, the NGO, working with NHS England, devised a ‘FTSU Index’, which was described as a ‘key metric’20 by which organisations can monitor their FTSU culture, comparisons can be made between trusts and good practice can be shared. The FTSU Index is a compound measure that is calculated as the mean of responses to four questions from the previous year’s NHS staff survey, rounded to one decimal place. The index has risen nationally from 75.5% in 2015 to 78.7% in 2019, leading the NGO to declare that the NHS has much to celebrate. 20 The index is utilised by the NGO as an indicator of potential areas of good practice and concern on matters of FTSU culture in organisations. Information is shared with stakeholders, including CQC, NHS England and NHS Improvement, to inform various aspects of their work to normalise speaking up. FTSU is also inspected within the CQC ‘Well Led’ domain; those trusts exhibiting higher scores on the index are more likely to be rated ‘good’ or ‘outstanding’ by the CQC.
However, drawing meaningful comparisons and definitive conclusions from FTSU data is fraught with difficulties. Despite NGO guidance, the collection of FTSU data is beset with problems of accuracy and consistency, as discussed in Chapter 4. There is also a fundamental question, possibly unanswerable, of what a rise or fall in the number of speak-up cases realistically signifies. Caution is also advisable regarding the contribution of FTSUG roles to upwards or downwards trends in data when we consider that this novel role was implemented locally without specific requirements over delimitation of remit, responsibilities and accountability structures. A further degree of localness is added because speaking up is highly situational and context dependent, and the work of FTSUGs is superimposed on to existing organisational procedures and protocols. These inherent issues could be positive in the sense that FTSU’s adaptation to the local environment, interwoven practices and operational contingencies could allow the Guardian role to evolve alongside the necessary changes in organisational culture. However, as an unprecedented intervention in the context of the NHS, or health-care internationally, and having no requirement for uniformity, the implementation of the Guardian role was always likely to vary across England.
Report structure
In Chapter 2, the aims and objectives are presented alongside the methods used to address these. Chapter 3 presents a literature review of speak-up interventions in health care. The results of telephone interviews undertaken with FTSUGs regarding the implementation of the role are presented in Chapter 4, which subsequently contributed to the design of data collection in case sites. In-depth exploration of the implementation and work of FTSUGs and the impact of FTSU more generally are presented in the findings from six case site reports in Chapter 5, and cross-case findings in Chapter 6, both drawing on non-participant observations, analysis of documents and interviews with FTSUGs and FTSU stakeholders. Finally, we summarise and discuss our findings and present our conclusions in Chapter 7.
Chapter 2 Methods
This chapter reports the study aims and objectives, the research questions and the methodological approach used to address these. The aims of the study were twofold: (1) to map varying approaches to implementing and configuring FTSUG roles in acute and mental health trusts, and (2) to gain insights into benefits and drawbacks of different FTSUG implementation models on speaking up and responding to workers’ concerns.
The study objectives were to:
-
assess the scale and scope of the deployment and work of FTSUGs
-
assess how the work of FTSUGs is organised and operationalised alongside other relevant roles with responsibilities for workers’ concerns
-
evaluate the comparative effectiveness of different types of FTSUG roles in supporting ‘Freedom to Speak Up’
-
identify barriers to, facilitators of and unintended consequences associated with the implementation of FTSUG roles.
Finally, the following research questions were addressed:
-
How are FTSUGs being variously deployed, managed and held accountable for their work?
-
How is the work of FTSUGs defined and negotiated in relation to the work of others who also deal with workers’ concerns?
-
Do different implementation models for the FTSUG role affect the ‘Freedom to Speak Up’, both in the ways that workers raise concerns and in how these concerns are responded to?
Overview of theoretical approaches and work packages
This section opens with a discussion of the theoretical frameworks that informed the study’s design, followed by a detailed overview of the relevant WPs. For the purposes of this investigation, we conceptualise the FTSUG role as a complex intervention. 21 Complex interventions are conventionally defined as difficult to implement because they consist of several interacting and interlocking components spanning a number of organisational levels, from the macro level (national policy organisations and regulators) to the meso level (individual trusts) and the micro level (individual employees, teams and wards/units). 22 These organisational levels have also been described as ‘nested’, simultaneously sitting above and below (and interacting with) other systems of different scale. 23
Given the complex nature of the FTSUG role and the contexts within which the role was implemented, as outlined in Chapter 1, Normalisation Process Theory (NPT) offered an appropriate framework to guide the study. 24,25 NPT assists researchers to identify factors that promote or inhibit the routine incorporation of complex interventions, such as FTSUGs, into everyday practice. NPT consists of four main components, or generative mechanisms, that help to identify the social processes underpinning the implementation of complex interventions (Table 1). 25
| NPT generative mechanism | Explanation of the mechanism and how it may be enacted in the context of FTSUG work |
|---|---|
| Coherence or sense-making | Sense-making work undertaken individually and collectively to operationalise the FTSUG role. The ‘success’ of this depends on the perceived workability and integration of the various elements of the new role into everyday practice |
| Cognitive participation | The incorporation of FTSUGs within the workplace depends on relevant individuals’ capacity to resource, cooperate and co-ordinate their actions |
| Collective action | The FTSUG role will be more disposed towards normalisation into practice if there is individual and collective intention and commitment to operationalising the role in practice |
| Reflexive monitoring | The appraisal work that people do to assess and understand the ways that the FTSUG role affect them and others around them |
In simple terms, NPT proposes that practices are embedded in social contexts as the result of people working, individually and collectively, to implement them. For example, if those involved in the implementation of FTSUGs can identify coherent arguments for adopting the role, are engaged in the process of implementation, are able to adapt their work processes to utilise FTSUGs (or FTSUGs adapt to fit in with existing practices) and judge FTSUGs to be valuable once they are in use, then FTSUGs are more likely to become embedded in routine practice. The introduction of FTSUGs cannot, therefore, be considered a discrete intervention that works in the same way regardless of the organisational context. Instead, FTSUG roles are likely to be designed and used in different ways depending on prevailing institutional arrangements.
A limitation of NPT is that it does not (and cannot) cover all phenomena of interest. 25 Accordingly, we also draw on insights from other relevant theories, such as the Consolidated Framework for Implementation Research (CFIR). 26 The CFIR provides terms and definitions for constructs that allow researchers to clearly and consistently articulate factors that potentially affect implementation outcomes. Particularly useful are CFIR insights into the influence of factors from the outer setting (e.g. policy or regulatory recommendations) and how they are often mediated through changes in the inner setting of organisations, such as changes in personnel or resources that affect, positively or negatively, the implementation of the FTSUG role implementation.
Work package 2: telephone interviews with Freedom to Speak Up Guardians working in acute hospital and mental health trusts
Work package 2 addressed the research aims, objectives and questions by providing an in-depth understanding and national picture of how FTSUGs are selected/recruited, deployed and organised within their organisations. To this end, we conducted semistructured telephone interviews (n = 87) with FTSUGs working in acute hospital trusts and mental health trusts. Participants were asked the same set of questions about their variable characteristics, such as their age, sex and nature of employment (e.g. hours allocated), as well as the work systems within which they were embedded. FTSUGs were also asked how they monitored FTSU within their organisation, such as the staff group and the demographics of those speaking up, and whether or not workers experience detriment following speaking up. The questions were informed by the findings of the literature review and existing concepts that had influenced some of our previous work on this subject (see standalone document 1 WP2 interview schedule; see https://fundingawards.nihr.ac.uk/award/16/116/25/#/documentation). 2,4,27–29 For example, interview questions regarding the coherence and clarity of new work processes and boundaries, the monitoring of change, and the availability of resources to support the implementation were informed by the literature review.
Freedom to Speak Up Guardians were identified and purposively sampled from the NGO register of FTSUGs. Initial contact with FTSUGs was made by e-mail and a telephone interview was arranged with those volunteering to participate. FTSUGs were recruited from each of the 10 (at the time) NHS England regions (see standalone document 2; see https://fundingawards.nihr.ac.uk/award/16/116/25/#/documentation) and worked in the following type and size of trusts:
-
23 out of 54 mental health trusts in existence at the time
-
64 out of 135 acute trusts in existence at the time
-
42 from small organisations (< 5000 staff)
-
35 from medium organisations (5000–10,000 staff)
-
10 from large organisations (> 10,000 staff).
We also interviewed FTSUGs from organisations with different CQC overall ratings, as shown in Table 2, which also shows the numbers of FTSUGs contacted, a 34% overall response rate and that a large percentage of FTSUGs responding were interviewed.
| WP2 recruitment stage | CQC rating, n (%) | Total, n (%) | |||
|---|---|---|---|---|---|
| Outstanding | Good | Requires improvement | Inadequate | ||
| Contacted | 36 | 123 | 82 | 14 | 255 |
| Responded | 15 (42) | 55 (45) | 29 (35) | 8 (57) | 107 (42) |
| Interviewed | 14 (39) | 44 (36) | 23 (28) | 6 (43) | 87 (34) |
Interviews were audio-recorded, which allowed subsequent review to clarify any confusion or inaccuracy. Data analysis, which was aided by NVivo 12 software (QSR International, Warrington, UK), took place concurrently with data collection. Initially, descriptive statistics and bar charts were produced to help to visualise the ‘shape’ of the data, for example summarising categorical variables, such as sex and professional background. These steps helped to identify interesting or anomalous features and proved useful in generating cross-tabulations of the relationships between these characteristics and other variables.
Thematic qualitative analysis, which followed a recognised six-step process,30 proceeded with in-depth familiarisation of the interview transcripts followed by inductive coding and thematic analysis, which identified the range of respondents’ views about their experiences of organisational commitment to the role, including barriers to and enablers of role normalisation. FTSUGs’ accounts of their work were also situated within the NPT generative mechanisms (see Table 1), generating insights that were revisited during case studies.
Once data were grouped into qualitative themes, we revisited the quantitative findings to establish whether a theme (or its dimensions) applied to only a particular group or whether it was a more general theme. Implications for fieldwork in WP3, such as the emergence of issues or problems that were not initially anticipated, were discussed and our field methods were modified accordingly. For example, we became increasingly aware that many FTSUGs were employed in substantive roles that they undertook alongside the FTSUG role. Fieldwork was, therefore, arranged to minimise researchers’ exposure to sensitive or confidential information unrelated to the project.
Methodological rigour was ensured through standard procedures of reflexivity, transparency and auditability. 31 Initial coding and emergent themes were developed within and then across the two teams based in Cardiff and London. Research associates at each site (JB and CB) individually undertook the initial analysis, overseen by the chief investigator (AJ) and Mary Adams and Jill Maben, who reviewed a further proportion of all transcripts to ensure inter-rater consistency/reliability. Emergent and final themes were regularly discussed and agreed with all members of the research team during three-weekly team meetings (face to face initially and online following COVID-19 workplace and travel restrictions). Additional insights into emergent findings were provided by public involvement members and the project advisory group (PAG), thus ensuring rigour was maximised at each step of analysis and across the data set.
Work package 3: six organisational case studies
We purposefully sampled four acute trusts and two mental health trusts, initially identifying potential case study sites from our analysis of WP2 data. However, although we contacted several trusts from each CQC band and different ‘types’ of FTSUGs (full time, part time and undertaking another role or not), ultimately we could recruit only trusts that volunteered to take part. Eight trusts agreed to take part. An additional seven trusts expressed an interest but did not participate, citing organisational pressures, or following further discussion with senior colleagues. Following consultation with the PAG, the final six sites were selected because they provided a range of CQC ratings, sizes and types of FTSUGs deployed (e.g. part or full-time), which best addressed the research aims and objectives.
Three months were spent at each case site shadowing FTSUGs, followed by 1 month undertaking preliminary within-case and tentative cross-case consolidation. Case sites were divided equally between Carys Banks and Joanne Blake, who undertook the large majority of data collection and were supported and supervised by Mary Adams, Aled Jones and Jill Maben, who also undertook visits to case sites and undertook short periods of observations. Three-weekly online whole-team meetings provided Carys Banks and Joanne Blake with the opportunity to present updated progress reports to other team members and to compare and contrast case site activities and the overall management of data collection. Case studies focused on exploring whether or not and how the role had been normalised alongside other local roles and initiatives overlapping with FTSU, in addition to understanding how FTSUGs were working in relation to their social and physical settings. CQC inspection reports and the NGO ‘Speak-Up Index’ provided useful historical and contemporary insights into speaking-up cultures within organisations. Planning for the case studies also drew on the findings of the literature review (see Chapter 3), especially the key finding that the implementation of speaking-up interventions is best understood within the wider context that they occur.
Purposive sampling was again used within the case sites to identify key informants, documents and stakeholders who were involved in the oversight and delivery of the FTSUG role, and any related speak-up initiatives. Prior to data collection, an initial visit to each site was arranged with the FTSUG to discuss plans for data collection, including how the FTSUG’s activities could be shadowed without the researcher’s presence being intrusive. With this in mind, an activity planning document (see Appendix 1) was completed in conjunction with the FTSUG, including information on FTSU-relevant events/meetings and key individuals who may subsequently be recruited for interview.
An initial 2-week introductory and orientation period helped to establish rapport with FTSUGs and other staff, and enabled an early sense of the Guardian’s work and FTSU in each organisation. Thereafter, data were concurrently generated at two sites using the following methods:
-
Overt non-participant observations of:
-
the FTSUG role in practice, for example delivering ‘speaking-up’ training and advice to workers, participating in walk-rounds and attending meetings within the trust (e.g. board meetings and operational meetings)
-
face-to-face meetings and/or telephone or e-mail activities with workers wanting to speak-up or with workers who had already spoken up to the FTSUG
-
meetings to review concerns with colleagues, such as line managers and NED/executive leads for FTSU.
-
-
Descriptive free-text fieldnotes were recorded during and/or following each observation event, either while in the field or soon after being in the field. These were written up in Microsoft Word® (Microsoft Corporation, Redmond, WA, USA) and collated at the completion of data collection at each site alongside relevant documentation, and summarised prior to analysis to identify the most relevant content in relation to FTSU.
-
Relevant organisational policies, internal communications and reports carried out by FTSUGs were recorded.
-
Trust board reports on concerns raised by workers were also collected.
-
Semistructured interviews were conducted with the following individuals:
-
FTSUGs – two interviews: one when fieldwork commenced and one towards the end of the data collection period
-
employees who had raised concerns via the FTSU service
-
key stakeholders closely involved in the implementation and ongoing deployment of the FTSUG role, including board members, executives, NEDs, directors or assistant directors of HR, organisational development (OD) and staff-side chairpersons
-
employees who had not spoken-up to the FTSUG.
-
Up to 20 interviews at each site were tentatively predicted, with the final number (Table 3) being slightly short of this. The final number of interviewees (n = 109) tallies with our purposive sampling strategy, which meant that the data saturation point was reached when key participants (listed above) at each case site were interviewed. We were very encouraged by the range of staff at all sites who dedicated time for the interviews, often despite very busy schedules. The data generated proved to be rich and contributed greatly to our understanding of the implementation of the role.
| Case sites (n) | ||||||
|---|---|---|---|---|---|---|
| Albany | Olympia | Montgomery | Columbus | Providence | Concord | |
| Number of interviews undertaken | 19 | 18 | 19 | 18 | 16 | 19 |
Central to our conduct throughout the study was sensitivity to the demands of the FTSUG role and the potential for the researchers’ presence to influence speaking up by workers. During observation periods, the researcher removed themselves if it appeared that the FTSUG was being approached by someone with a concern or if the FTSUG or employee requested that the researcher withdraw (see Research ethics). The main objective during observations was for the researcher’s presence to be unobtrusive and to alter practices as little as possible.
Although the data collection phase is presented here separately from data analysis, in practice the two phases were intertwined. A software package (NVivo 12) assisted with the storage of transcribed interviews and other documents, as well as the thematic analysis of data in a process underpinned by the same approach to methodological rigour outlined in Work package 2: telephone interviews with Freedom to Speak Up Guardians working in acute hospital and mental health trusts. An inductive ‘data condensation’28 process, foreshadowed by research aims/objectives/questions, was used to select, focus, simplify and abstract data from the range of field data and interview transcripts. Each case study was individually analysed prior to cross-case analysis. To integrate and aggregate findings across cases, a series of NPT thematic charts were developed for each case study. Further exploration of the charted themes was then undertaken to map and understand the range of views and experiences across each site. Established theory and research into speaking up and organisational culture, in addition to our own expertise and the perspectives from the PAG/patient and public involvement (PPI) team members, all contributed to the interpretation of the qualitative findings.
Telephone interviews with national stakeholders (n = 7)
Semistructured telephone interviews were undertaken by Daniel Kelly and Aled Jones with national stakeholders. These individuals were purposively sampled from roles and organisations involved on a national level in establishing, liaising with or oversight of the FTSUG initiative, or had worked in organisations that had a direct interest in FTSU (e.g. trade unions or patient safety campaign groups). Individuals were initially identified from organisational webpages or from previous contact with or awareness of the research team and PAG members. If agreeing to participate, interviewees were recruited and interviewed and the data analysed in the same manner as described in WP2.
Research ethics
All study work packages were approved by the School of Healthcare Studies, Cardiff University, Research Ethics Committee reference HCARE/14082018.
Patient and public involvement in the research
From the outset, PPI was integral to the development, design and overall conduct of this project, shaped by the awareness that PPI involvement should be both meaningful and relevant. A group of four PPI members initially participated during the study design phase. Two of the PPI group continued to contribute directly to all WPs throughout the study via the PAG and other activities, such as the following:
-
contributing to preparation for data collection and data analysis activities, such as reviewing emerging findings and development of later findings
-
informing the preparation and accessibility of dissemination materials
-
participating in future workshops and other dissemination events and activities, such as authoring and providing a PPI perspective to training materials for NHS employees
-
playing a significant role in setting future research priorities and, overall, helping us to not lose sight of why the research is important and how the research might positively influence practices from a PPI perspective.
Details of the PPI and PAG members can be found in the Acknowledgements.
Summary
This chapter has set out the research design and the approaches taken towards data generation and analysis, which were underpinned by NPT. The empirical elements of the study were set across two phases: WP2 comprised telephone interviews with FTSUGs working in acute trusts and mental health trusts in England, and WP3 comprised six in-depth case studies of the implementation of FTSUGs at four acute trusts and two mental health trusts. Input from relevant external stakeholders was interwoven throughout in the form of contributions by PPI members and a dedicated PAG.
Chapter 3 Literature review
Introduction
A systematic narrative review of the literature was conducted for two purposes:
-
to identify and examine international research reporting on strategies or interventions promoting ‘speaking up’ practices in the workplace
-
to critically appraise and map key concepts and tensions to inform the development of research tools and to inform interpretation of primary research findings.
A version of the review was published in January 2021. 32
Review question and methodology
The review question was ‘What workplace strategies and/or interventions have been implemented to promote speaking up by health-care employees?’. Consistent with the study’s theoretical orientations (see Chapter 2), the review was underpinned by recent writing on complex adaptive systems in health care. 33,34 A previous scoping review35 identified that this topic area embraces diverse theories and methods across numerous contexts and is, therefore, unsuitable for systematic review approaches involving the formal weighting of independent bodies of evidence. Instead, an acknowledged and widely used systematic narrative review approach was used to ‘tell the story’ from within the literature36 and to deepen the understanding of the review question by interpretation and critique. 37
Searching and screening
Searches were undertaken to include findings on studies of international speak-up interventions designed for workers in all areas of health-care practice and all health-care settings, including education. Grey literature, statutory interventions and regulatory interventions were not reviewed because they were unlikely to contain empirical research reporting the outcomes of speak-up interventions in the workplace (Box 1 gives further information on search terms and inclusion/exclusion criteria).
-
Speak*-up OR ‘Speak* up’ AND employee* OR staff OR student* AND train*OR teach* OR educat* OR evaluat* OR implement* OR interven* OR tools OR strateg* OR “pilot test*” OR ‘pilot-test*’
-
Whistle-blow* OR Whistleblow* OR whistle
-
‘raising concerns’ OR ‘raise concerns’
-
‘employ* voice’
-
‘voice concerns’ or ‘voicing concerns’
Databases used: MEDLINE, PsycINFO, EMBASE™ (Elsevier, Amsterdam, the Netherlands), Social Policy and Practice, ASSIA and Web of Science™ (Clarivate Analytics, Philadelphia, PA, USA).
Inclusion and exclusion criteriaInclusion criteria: English-language journal articles published in 2008–18 inclusive, reporting any empirical research on interventions designed to promote speaking up or improve teamwork, communication or work culture where speaking up was identified as an outcome.
Exclusion criteria: editorials, reviews, theoretical papers, methodological papers, discussion papers and anything not published in English. Books, book chapters, theses, conference papers and any empirical papers were all excluded where there were no data reported.
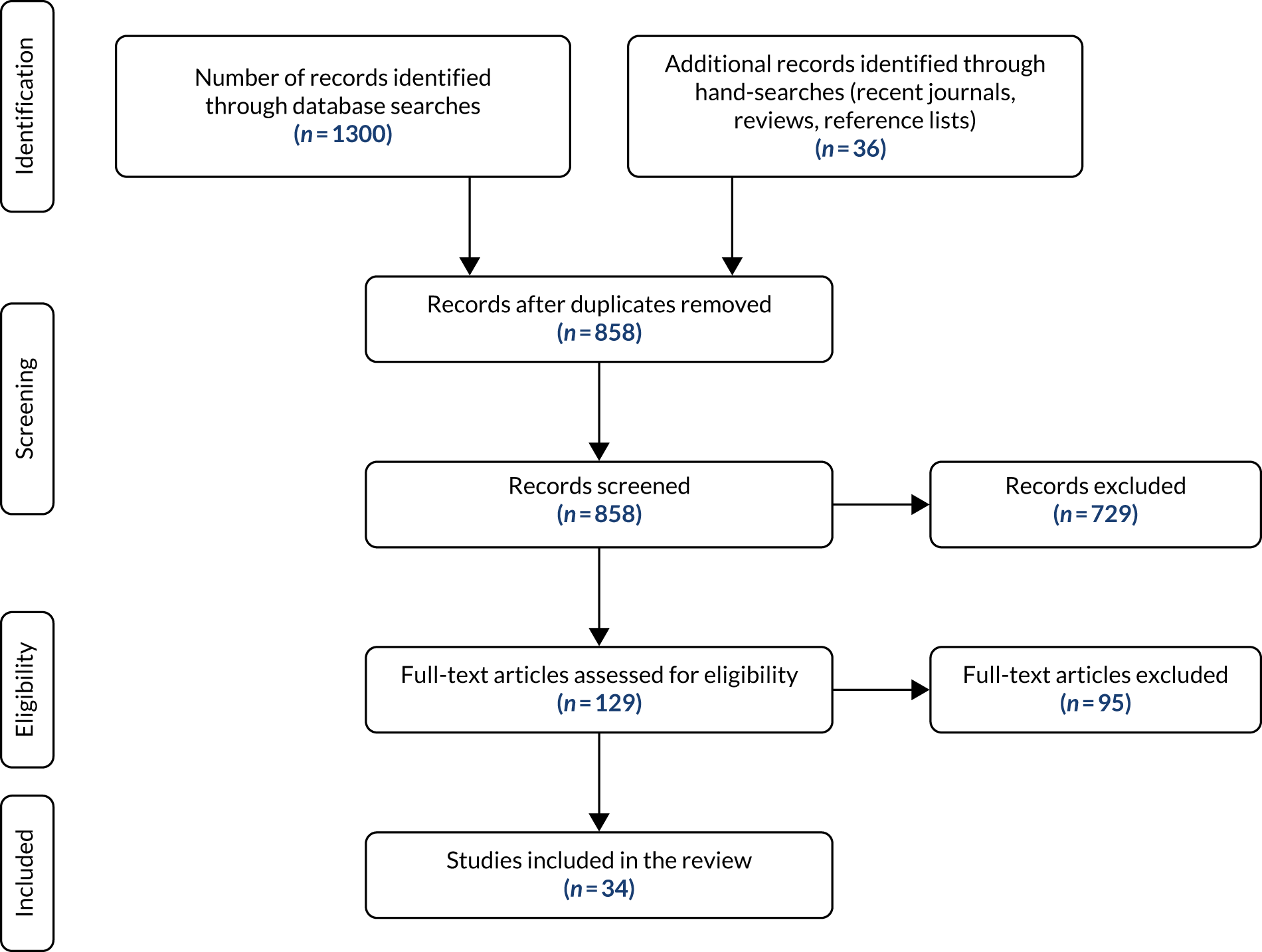
The searches identified 1300 citations, with a further 36 records identified via searches of reference lists or search updates. After eliminating 478 duplicates, the titles and abstracts of 858 records were screened for relevance by Aled Jones and Joanne Blake. Of these, 729 were excluded because they did not meet the inclusion criteria (e.g. editorials or viewpoint articles rather than empirical research), leaving 129 articles for full-text review. Following full-text review, a total of 34 papers were included in the final review, as shown in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart (Figure 1). Joanne Blake and Aled Jones undertook data extraction, which enabled data analysis and synthesis (see the following section).
FIGURE 1.
The PRISMA flow chart of the paper screening process.
Data analysis
The team’s prior experiences of researching the topic area and undertaking narrative reviews38,39 indicated that an inclusive review of the research would help to identify a range of evidence that best represented the complexities and ambiguities associated with the topic. Although the emphasis was mostly on including rather than excluding papers, the relevant Critical Appraisal Skills Programme frameworks guided the appraisal of papers and resulted in the exclusion of some studies owing to a lack of key information, such as research ethics approvals or data analysis approaches. The review findings were subsequently themed and synthesised by Joanne Blake and Aled Jones, with particular reference to authors’ accounts of the effectiveness of interventions and contextual factors, such as implementation barriers or facilitators. Other members of the team critically reviewed and contributed to the iterative process of identifying themes and synthesising the literature.
The remainder of this chapter describes the types of study design and interventions reported. This is followed by interpretation and synthesis of the findings, taking into account contextual factors40 identified within the studies that influence (for better or for worse) the implementation of employee speaking-up initiatives.
Results
The final 34 publications originated from Europe, Asia and North America, comprising studies using quantitative (n = 23), qualitative (n = 5) and mixed-method (n = 6) methodologies. Three types of intervention feature in the included papers: educational initiatives (n = 5), workplace/workforce training initiatives (n = 17) and workplace initiatives (not involving formal or overt training, or educational input) (n = 12). Interventions were designed as either ‘stand-alone’, focusing on only improving the act of speaking up,41–59 or ‘bundled’ initiatives,60–72 in which speaking up was targeted within a multifaceted intervention aimed at improving teamworking62 or clinical protocols65 (Table 4).
| Type of intervention | Methodology | Total | ||
|---|---|---|---|---|
| Quantitative | Qualitative | Mixed methods | ||
| Educational initiatives: speak-up learning interventions undertaken within universities with undergraduate students | 3 | 0 | 2 | 5 |
| Workplace initiatives: interventions undertaken within workplaces not involving formal training or educational input | 6 | 5 | 1 | 12 |
| Workplace/workforce training initiatives: mostly voluntary, occasionally mandatory enrolment of employees onto formal training courses, often involving simulated practices and/or teamworking interventions | 14 | 0 | 3 | 17 |
| Total | 23 | 5 | 6 | 34 |
Quantitative approaches were as follows:
-
randomised controlled trials of speak-up interventions, for example simulations41,42 and training programmes60
-
quasi-experiments of speak-up educational interventions for registered nurses and health-care students43,61
-
post-course surveys following safety communication training62 and a speaking-up action exercise44
-
pre- and post-implementation surveys of interventions, including executive walk rounds (EWRs);45–50 various team-based communication tools for use by trauma resuscitation teams, by interventional ultrasound teams, by theatre/anaesthesia teams and during infection prevention practices,51–54,63–67 and an educational intervention and an educational course for nursing students. 68
Qualitative approaches were as follows:
-
interdisciplinary team development using focus group interviews and auto-ethnography55
-
communication and decision-making using observation, audio-recorded meetings and individual interviews69
-
infection prevention using individual interviews70
Mixed-methods approaches were as follows:
-
speak-up teaching and learning activities using a survey, a focus group and individual interviews58
-
a patient safety course for medical students using a survey and written vignettes71
-
an intervention to prevent faculty mistreatment of medical students in learning environments using surveys and focus groups72
-
workplace patient safety initiatives using qualitative interviews, observations and surveys,59,73 including routine hospital data. 74
The following sections discuss indicative conclusions about the effectiveness (or otherwise) of the interventions. Given the large array of interacting and emergent factors that influence whether or not interventions in complex systems are successfully implemented, it is unsurprising that the studies reviewed could not be apportioned into a neat binary of effective or ineffective interventions. 33,34 Instead, the effectiveness of most of the interventions reviewed was indeterminate, that is, some aspects of an intervention resulted in the desired changes but other aspects did not. As a number of others have recently noted,75–77 the success or failure of interventions within complex adaptive systems is rarely ‘all or nothing’; more typically, interventions are partially fulfilled. Based on these insights and informed by narrative reviewing guidance,36 we divide the results into an overview of interventions that were effective, ineffective or indeterminate, followed by a section that synthesises the results to draw new insights and conclusions based on the body of evidence.
Intervention effectiveness
There was significant variation between papers on whether or not and how intervention effectiveness was defined. Some studies lacked pre-implementation baseline measures,44,62 whereas others evaluated effectiveness from self-reported perceptions of intervention participants. 46,50,53 Notably, few studies evaluated change in speaking-up practices within clinical practice contexts, with the majority of interventions undertaken in simulated clinical environments or classrooms.
Many studies reported inconclusive results, and no specific characteristics of interventions and implementation approaches were associated with more positive implementation outcomes. The heterogeneous nature of the interventions and outcomes measured contributed significantly to this. However, in those studies reporting only positive outcomes, it was notable that several involved interventions informed by and targeting multidisciplinary teamworking,42,63–66 although two studies were undertaken with uni-disciplinary teams. 43,72 Although the details of the intervention design are not fully discussed by the study authors, these findings echo previous studies that suggest that increased multidisciplinarity in planning and decision-making is positively associated with successful implementation. 26 A summary of the type and design of the interventions and their overall effectiveness is presented in Table 5, and these are further discussed in the following thematic overview and cross-study synthesis of researchers’ explanations of why, or how, their speak-up interventions were implemented successfully (or not).
| Intervention type | Description | Summary of findings |
|---|---|---|
| Effective interventions | ||
| Workplace/workforce training (standalone) | Team-based communication or teamwork improvement training (with content including ‘speaking up’ skills)63–66 | Pre- and post-implementation survey: statistically significant changes in likelihood to speak up scores |
| Assertiveness-based team training course vs. effective team training course42 | Pre- and post-implementation survey: statistically significant changes in likelihood to speak up scores with assertiveness-based team training | |
| Small-group, multifaceted educational intervention (including personal reflection and peer-support – nursing workforce)43 | Statistically significant change in mean speaking up scores (‘post test’) | |
| Educational (bundle) | Awareness-raising of medical students about processes for speaking up and handling concerns about mistreatment by faculty members during clinical placement plus system for anonymous reporting with timely response and awareness-raising of all participants in learning environment (e.g. administrators and faculty members)72 | Self-reported awareness of speaking up policies and procedures increased from 67% to 100%; stigma of speaking up declined but fear of reprisal remained a major concern for students |
| Indeterminate/partially effective interventions | ||
| Workplace (stand-alone interventions) | Staff forum for team members to speak up about safety concerns69 | Reported success in only 7 out of 25 sites. Difference explained by key leader (physician or practice manager) of the intervention: their engagement in the improvement project and their encouragement/discouragement of discussions within the teams |
| Structured hospital ward-based team debriefing policy (to encourage speaking up about clinical and administrative challenges)55 | Reported increase in confidence that the team could speak up and concerns aired; however, some areas of speaking up were ‘off limits’ (e.g. disputes over legitimacy of some concerns and delving into performance of another team member) | |
| Surgical checklist (as intraoperative communication tool during surgery)67 | Nurses and anaesthesiologists surveyed were significantly more likely to speak up to team members with this tool. However, follow-up interviews raised concerns with perceived intimidation in teams and the possibility of non-deployment of checklists by surgeons not supportive of intervention | |
| EWRs as a means of improving speaking up between senior leaders and ward staff45–50,56,57,78 (developed by the IHI in the early 2000s) | EWRs were intended to provide a structured opportunity for staff to directly communicate concerns during executive visits to clinical areas. Some evaluations noted that staff felt more at ease when discussing errors and reporting safety concerns.46,47,50 Collection of 6 years of longitudinal data by one study50 showed a marked increase from 30% to 90.5% of EWR participants agreeing that their reporting of incidents had increased, and that 96% of issues raised were resolved. Concerns about the fidelity of the IHI model have been reported,57 with some studies unclear about the benefits of local adaptations or derivations from the IHI EWR model. Deviations may result in a culture of ‘checking up’, rather than listening to staff speaking-up about their concerns.57 Some studies report the limited engagement of senior management in the intervention, and with the concerns of front-line staff47 | |
| Workplace (bundled) | Hospital-based, infection-risk prevention initiative including speaking up fostered by interdisciplinary and collaborative adverse event investigations and by interdisciplinary care work (e.g. patient rounds)70 | There were more speaking-up opportunities in hospitals with better infection prevention outcomes (where retrospective learning events were seen as collaborative rather than interrogative). Especially for nurses, interdisciplinary care processes facilitated speaking up where physicians valued collaborative, interdisciplinary care interventions |
| Hospital intervention to improve workplace culture and speaking up (interventions included workshops, forums and online resources)74 | Significant changes in ‘culture scores’ across all hospitals (baseline to 24-months later). Four out of 10 hospitals had no statistically significant or marked qualitative changes in culture. Staff in the six (out of 10) hospitals in which changes were significant reported no fear in speaking up; there were greater decreases in mean risk-standardised mortality rates in these organisations | |
| Patient safety training for medical interns and staff (error communication technique training, presentations by senior staff on their own speaking-up experiences), including speaking-up training to senior team members52 | Post-training self-rated scores of interns showed significant improvement in knowledge and attitudes; no reported effects on behaviours | |
| ‘Empowerment’ workshops for nurses (with specific content on speaking up)60 | Post training, self-reported scores indicated improvements in ‘communication openness’; views of punitive response to errors did not change significantly | |
| ‘Ethical Action Exercise’ with third-year medical students; tasked with one speaking-up intervention during clinical placement44 | Of 111 students completing the exercise, 86% found speaking up difficult. A total of 12 students reported negative reactions | |
| Educational (blended) | Didactic and varied interactive classroom programme for students in professional training (social work) to support students to speak up more to staff during clinical placements plus prompt card to guide students on a six-step speaking-up approach58 | Post-course interviews showed self-reported increase in confidence and support of the prompt card, but the six-step speaking-up approach was expected to be too difficult to implement in practice |
| Ineffective interventions | ||
| Workplace/workforce training (standalone) | ‘Conversational skills’ improvement workshop with anaesthesiologists41 | No significant differences between intervention and control group subjects. Speaking-up behaviours deeply rooted and difficult to change by education alone |
| Educational (standalone) | Inter-professional (undergraduate) training using ‘Crucial Conversations’ to promote psychological safety during error disclosure61 | Ineffective, significantly as a result of ‘negative attitudes towards such inter-professional conversations’61 |
Thematic overview and synthesis of the factors affecting the implementation of interventions
Undertaking thematic analysis within a narrative review entails working with and reflecting directly on the main ideas and conclusions across studies. These will now be discussed under the following themes: Theme 1: workplace culture – hierarchical and interdisciplinary factors and the implementation of speak-up interventions, and Theme 2: Psychological safety and the implementation of speak-up interventions.
Theme 1: workplace culture – hierarchical and interdisciplinary factors and the implementation of speak-up interventions
Definitions of workplace culture routinely refer to an organisation’s hierarchical form(s); its division of labour by organisational locations, departments, units, the sets of roles, tasks and jobs, and the technologies used. 79 It is widely accepted, therefore, that any attempt at nurturing a culture of speaking up in the workplace has to take into account wider organisational factors, including the inter-related issues of workplace histories, power, norms and hierarchies. 27 Indeed, the implementation of speak-up interventions was often explained by researchers as being contingent on the enduring and mostly adverse influence of pre-existing workplace cultures, hierarchies and interdisciplinary tensions.
For example, Balasubramanian et al. 69 described how lead physicians and office managers, who are accustomed to chairing and managing team meetings, refused to relinquish control of meetings to subordinate colleagues during workshops that were designed to encourage speaking up about workplace problems. As a result, team members who attempted to introduce discussion in a less hierarchically mediated way eventually ‘gave up in the face of this tag team opposition’. 69 Even in teams in which lead physicians encouraged team-led discussion, airing problems that might be perceived as encroaching into a physician’s territory were proscribed. Similar interdisciplinary and hierarchical tensions were described by others,55 who explained that regardless of a general sense that ‘things had changed for the better’,55 deeply rooted hierarchical and cross-disciplinary tensions persisted, which resulted in certain clinical concerns, such as clinicians’ performance, remaining off-limits.
A further hierarchical issue that was identified as both an enabler of and a barrier to successful implementation of speak-up initiatives was the perceived support of medical leaders for the intervention. 51,53,55,63,69,70 Robbins and McAlearney70 described how nurses were more likely to implement a speaking-up intervention when physicians ‘clearly valued and encouraged this input’. 70 Ironically, it seems that entrenched interprofessional, hierarchical and cultural attitudes within organisations were insoluble barriers to the successful implementation of interventions designed to tackle such attitudes.
Although workplace cultures and hierarchies were often invoked as contextual explanations for unsuccessful implementation and intervention outcomes, researchers rarely considered pre-existing cultural and hierarchical issues within the wider society. There were, however, two notable exceptions.
Roh et al. 71 described how Korean national culture proved an insurmountable barrier to medical students speaking up about senior doctors’ transgressions. National cultural norms strongly reinforced workplace hierarchies where ‘less powerful people expect their superior to tell them what to do, with dependency on many formal rules or informal customs’. 71 Unsurprisingly, following an educational intervention, low confidence in speaking up to seniors persisted among students, possibly resulting from students ‘feeling confused or even shocked’71 because implementation of the educational package challenged long-standing national cultural norms. Similarly, Oliver et al. 58 acknowledged that the design of their educational programme had not reflected how ‘structural inequalities faced by students of non-hegemonic identities influenced the difficulty of speaking-up’. 58 As one student commented, ‘I am a racialized young woman, and a difficult conversation is just different for me than it is for a cisgendered white male’. 58
There is a dearth of literature focusing on the influence of wider societal intolerances, such as racism or homophobia, on speaking up within health care. This is particularly relevant given the heightened social awareness of barriers to speaking up owing to international social justice movements, such as ‘Black Lives Matter’ and ‘#metoo’. With the exception of the two studies discussed above,58,71 researchers position workplace cultures as existing in isolation from broader societal culture. However, they are not alone, as disregarding the dynamic interplay between the wider socioeconomic-political system and the local organisational setting is a known limitation of many studies and systematic reviews. 40,80 Similarly, others conclude that national cultures have a greater impact than organisational cultures on policy implementation and innovation, but are ‘often overlooked’. 81 Furthermore, although health-care teams often consist of workers from multiple ethnic and cultural backgrounds, the question of speaking up within culturally diverse teams is also overlooked in the literature.
Not representing this level of interconnectivity can threaten the transferability of research findings and of policy recommendations in the future. As a result, future research and reviews should provide detailed descriptions of the context(s) and setting(s) in which studies are carried out and acknowledge the potential for setting–context interplay.
Theme 2: psychological safety and the implementation of speak-up interventions
Psychological safety, an important and conceptually sound construct that is often cited within health policy82 and organisational learning literature, is defined as ‘a sense of confidence that the team will not embarrass, reject, or punish someone for speaking-up’, stemming ‘from mutual respect and trust among team members’. 82 A prevailing ‘theory of change’ in the studies reviewed was that the implementation of speak-up interventions would enhance psychological safety, which would result in more staff raising concerns. 41,47,49,50,55,61,63–65,72 However, not all studies proceeded to report the direct effects of their interventions on psychological safety and speaking up. Of those that did,47,49,55,69 the majority reported improved psychological safety in terms of colleagues’ confidence to speak up, while others had little effect41 or more variable success. 42
Negative repercussions for psychological safety were reported when interventions created an expectation of mutual respect among staff, only for this not to materialise. This was particularly apparent in the EWR literature,56,57,71 in which promises made by senior leaders to respond to the concerns of front-line employees were subsequently broken.
The results of some studies41,51,53,55,58,63,69–71,74 also expose a more intricate relationship between psychological safety and mutual respect. For example, ensuring or enhancing mutual respect between workplace colleagues is a prerequisite of psychological safety,82 which unsurprisingly was regularly targeted by many interventions. However, mutual collegial respect can sometimes unintentionally evolve into a barrier to speaking up when manifested as a form of deference to colleagues, based on long-standing professional hierarchical norms or sociocultural customs. 41,51,53,55,58,63,69–71,74
To summarise, we do not question the premise that psychological safety and related values, such as mutual respect, are fundamentally important in optimising conditions for speaking up. However, those designing and implementing interventions to enhance psychological safety need to be cognisant of a fine line between mutual respect and less helpful deference between colleagues, and the difficulties of finding the ‘sweet-spot’ of neither too much nor too little mutual respect.
Discussion
This review demonstrates that health-care researchers internationally are attempting to address difficulties that are associated with speaking up in health care. A disparate range of research designs, academic and professional disciplines, and perspectives informed the studies, including medicine, nursing, social work, human factors, sociology and psychology. Some significant limitations were identified across the papers reviewed. For example, there was very little evidence of researchers critically reviewing and building on extant studies when preparing and designing new projects, with many of the flaws of previous study designs being overlooked. Similarly, researchers rarely placed their findings within broader local, national or transnational policies and contexts. The body of knowledge is, therefore, piecemeal and limited in impact.
The small-scale nature of most studies may be explained by the fact that research funding was seldom declared. Relatively poorly funded research can also result in implementation studies that often fall short of truly understanding how complex socioprofessional systems work. 33 This is evident in many of the papers reviewed, which reflect implicit mechanistic or cognitive-rationalist assumptions about the nature of speaking up. Researchers consistently overlooked how otherwise well-conceived individual components of training interventions (e.g. improved communication skills) are often usurped in practice by complex inter-relationships with pre-existing contextual issues, such as sociocultural relationships, workplace hierarchies and perceptions of speaking up.
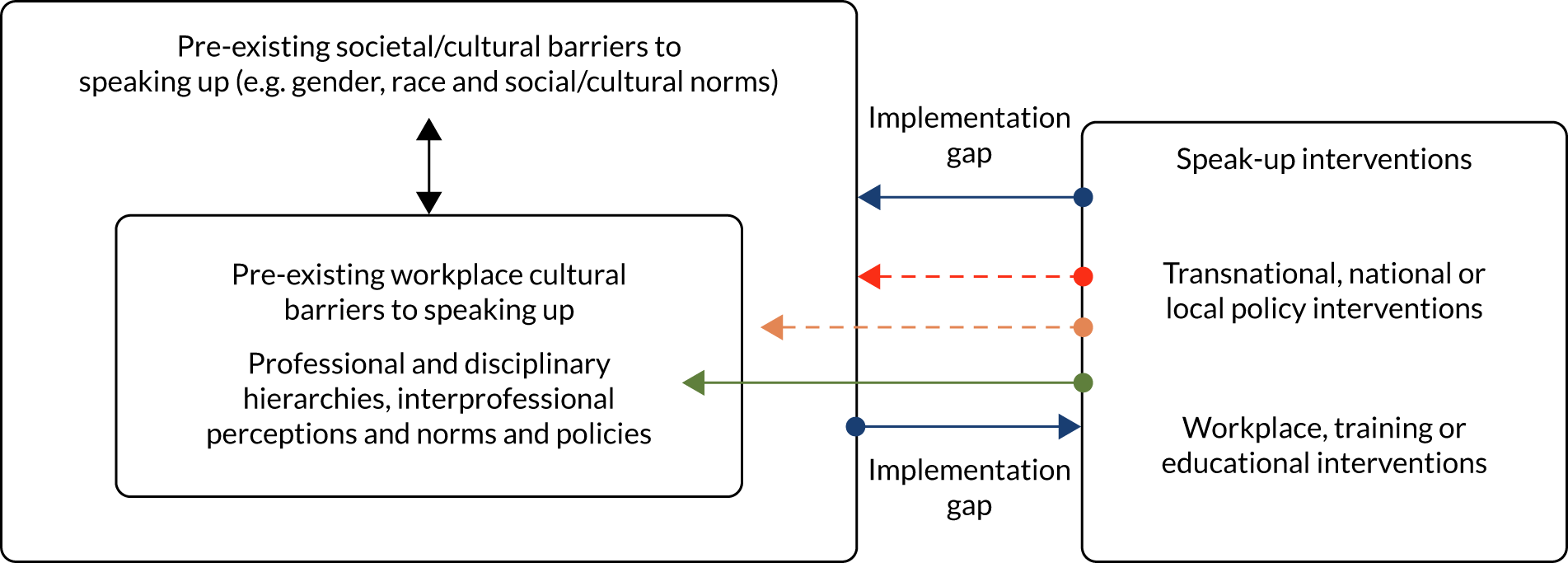
Figure 2, informed by complex systems thinking perspectives and implementation models such as the CFIR,26 presents a nuanced and intersectional model of the forces described that speak-up interventions had to contend with. The model takes into account pre-existing and entrenched inner forces (workplace barriers) and outer sociocultural forces, many of which are present in the NHS and relevant to the implementation of FTSUGs. An intersectional approach refers to the complex ways in which multiple issues (e.g. race, sex and cultural norms) routinely interact to influence everyday experiences of people receiving and working within health care. 83
FIGURE 2.
Iterative model of intersectionality of pre-existing workplace and societal barriers to and their effects on speak-up interventions. This model takes account of the intersectionality of pre-existing societal and workplace culture, which forms a formidable barrier (blue arrows) to the implementation of speak-up interventions in practice. Some interventions successfully bridge the gap (green arrow), others bridge but the effect is variable or weak (amber arrow) and others fail to bridge the gap (red arrow).
There are few certainties within the complex realities of modern health-care practices;84 however, a significant theme in the literature is the global pervasiveness and dominance of workplace cultures that were inimical to speaking-up interventions. Implementing speak-up interventions was reported as immensely challenging work in the USA, Republic of Korea, Islamic Republic of Iran, Canada and England. Regardless of their location, health-care researchers and policy-makers who are interested in improving employee’s freedom to speak up will have to overcome pre-existing complex societal and workplace norms, which are often long standing in nature.
To the best of our knowledge, this narrative review is the first to locate the evidence within broader health systems and a policy context, and to adopt a complex systems perspective that is currently lacking within systematic review literature. 40 Doing so results in a better understanding of ‘speaking up’ as an action that has emergent and dynamic properties within a ‘messy’ system, rather than as fixed entities and stable properties. We problematise certain aspects of psychological safety that have been left unexplored in other reviews;85 in particular, we discuss the concept of mutual respect and how the closely related issue of deference can be a significant barrier to speaking up. Furthermore, we have shown how the complex interplay between societal/cultural values and societal/cultural norms affect speak-up intervention, although this was largely unexplored within the evidence reviewed.
-
Additional academic papers may have been published during the long process of peer reviewing and publishing this report.
-
Studies were conducted in higher-income countries, and the factors influencing speaking up may be different in lower- and middle-income countries.
-
The papers reviewed were published in English-language journals, excluding studies published in other languages.
-
The search strategy may have missed relevant studies that used different sets of terms or different words in the title or abstract.
Summary and conclusions
While noting the limitations of the review (Box 2), the review presents a critical overview of factors that could assist policy-makers and researchers when developing interventions to support speaking up in the health-care workforce. We recommend that future developments are based on a meaningful collaboration between a range of stakeholders from diverse cultural backgrounds and workplaces, including researchers, policy-makers, service users and practitioners. One enabler of meaningful collaborative working is adequate research and development funding to properly resource various stakeholders, meetings and equipment. We also recommend, therefore, that speaking-up research (and related engagement and research impact activities) be prioritised in the allocation of research funding.
Recommendations for future research include the need to consolidate and build on existing knowledge and to better situate studies within complex local and national contexts and culturally diverse workforces. In addition, more studies of speaking up in health care within low- and middle-income countries would address a significant gap in the literature and provide better understanding and solutions to meet the demands therein. Our review findings can facilitate the implementation of new policies as it surfaces conditions that may counter efforts to create more open speak-up cultures in health care. However, there is unlikely to be a one-size-fits-all approach to creating such a culture.
Chapter 4 Telephone interviews with Freedom to Speak Up Guardians
This is the first of three chapters presenting empirical findings. This opening chapter focuses on findings from national telephone interviews undertaken with FTSUGs (also referred to as Guardians), followed by findings from in-depth case studies (see Chapter 5) and a final chapter consisting of cross-case findings (see Chapter 6).
The following research objectives are addressed in this chapter:
-
assess the scale and scope of the deployment and work of FTSUGs
-
assess how the work of FTSUGs is organised and operationalised alongside other relevant local and national roles with responsibilities for managing concerns
-
identify barriers to, facilitators of and unintended consequences associated with the implementation of FTSUG role.
As outlined more fully in Chapter 2, interviews (n = 87) were undertaken with Guardians working in acute trusts and mental health trusts across NHS England. The following sections provide insights into the demographic details of the FTSUGs interviewed, how they were appointed and the effects of implementation decisions, particularly regarding time and resource allocations, on the work of FTSUGs. The availability of resources is considered to be a tangible and an immediate indicator of organisational commitment and readiness to implement an intervention. Indeed, the level of dedicated resources is positively associated with implementation, but is not necessarily sufficient to guarantee success. 26 Being unprepared or unrealistic about the effort required to implement change has also been shown to demotivate and anger staff. 86
Freedom to Speak Up Guardian: one title, many roles
The age, ethnicity and sex of the Guardians who were interviewed closely mirror the NGO annual survey results,18 with Guardians mostly consisting of white women (n = 75) aged 45–64 years (n = 58) (see Appendix 2). Although the FTSUGs who were interviewed ranged from entry-grade professionals (band 5: £25,000–30,000) on the NHS ‘Agenda for Change’ pay scale to very senior managers (earning > £100,000 with board-level responsibilities), most Guardians (n = 44) interviewed were working at middle-ranking management bands 7 and 8a.
Surprisingly, given the extensive and challenging remit of the FTSUG role, as outlined in Chapter 1, the majority of Guardians (n = 55) who were interviewed were allocated ≤ 2 days to undertake the role, with most allocated ≤ 1 day (n = 44); only 11 out of 87 worked as full-time Guardians (see Appendix 3). Furthermore, most Guardians (n = 59) undertook the FTSUG role alongside a range of clinical (e.g. nurse specialist, radiographer and physiotherapist) or non-clinical (e.g. HR or OD practitioner) roles, whom we refer to as ‘adjunct’ FTSUGs. The remaining 28 Guardians who were interviewed occupied no other role within the trust and were appointed as part-time or full-time FTSUGs; we refer to them as ‘stand-alone’ Guardians.
From the outset, it is clear that there is much variation in terms of both those undertaking the role (their seniority, disciplines and skills) and the implementation decisions related to the role. At one extreme of implementation variation are the full-time ‘stand-alone’ FTSUGs, who are supported (as will be demonstrated later in the chapter) by administrative staff, external supervision and an independent budget. At the other extreme is the ‘adjunct FTSUGs’, who are allocated no time, or any supporting resource, while undertaking the role alongside a substantive full-time role.
The effects of such implementation variation on the practical fulfilment of the role are considerable, and an attempt to unpick this is the focus of much of this report. Nevertheless, a fundamental point to consider at this stage of the report is that the role title ‘Guardian/FTSUG’ has rather inexact and ‘fuzzy boundaries’,87 which makes precise ‘like-for-like’ comparisons across trusts difficult. The origins of such variation are embedded within the FTSU report,12 which offers little implementation guidance for trusts other than ‘Boards should decide what is appropriate for their organisation’ (© Francis R, 2015. Contains public sector information licensed under the Open Government Licence v2.0). 12 The assumption that trust boards know what is ‘appropriate for their organisations’ requires further scrutiny given the evidence that points to significant contrast between NHS senior managers’ perceptions of raising concerns and the problematic realities encountered by workers. 88
The following extracts from the telephone interviews demonstrate that pre-implementation decisions within some trusts were often poorly thought-out or were based on assumptions that proved unsustainable once the FTSUG role was implemented:
Implementing the role was a bit of a kneejerk reaction. Not enough thought went into although full of good intentions. Lots more work than expected and not enough time to do it.
r64
When I started I was told by senior management to expect only one or two concerns a year. In reality the number is very different.
r08
Although the NGO produced guidance for the FTSUG role,15–17 which is discussed at length in Chapter 6, the prevailing approach adopted during the role’s implementation was for boards to decide what was appropriate. Throughout this chapter, and elsewhere in the report, we return to the various NGO guidance as we track the implementation of the FTSUG role through different local organisational structures, systems and processes.
To summarise, there was little in the way of shared understanding and coherence across trusts about how to implement the role. Variations in time and banding allocated to the role could be the result of some boards carefully and optimally tailoring the role to fit the conditions ‘deemed appropriate for their organisation’. However, there is also evidence of knee-jerk implementation of the role and unrealistic expectations, with marked differences in implementation across organisations of similar size, function and CQC rating. Nonetheless, the majority of trusts believed that it was feasible and appropriate to appoint one person, allocated little or no extra time alongside a substantive role, to address the challenging prospect of supporting cases of speaking up, while simultaneously building a trust-wide culture of openness. The following comment neatly summarises the views of many FTSUGs:
Speaking-up is couched as an issue and solution which concerns organisational culture but it’s certainly not possible for one individual to change culture of one organisation that is part of a complex system.
r06
Selection and appointment of Guardians
Ensuring the careful selection and appointment of FTSUGs would appear to be particularly important, given the contested nature and long-standing problems of speaking up in the NHS and the ambitious culture change remit associated with the new role. The only reference made to selecting and appointing FTSUGs in the FTSU review, however, states that the person should be appointed by the organisation’s chief executive officer (CEO) to act in a genuinely independent capacity.
Trusts chose very different approaches to appointing Guardians, varying from open and democratic approaches to closed and obscure selection processes that favoured those already known to decision-makers. Most Guardians (n = 54, 62%) were appointed following a formal and competitive recruitment process, culminating in a selection interview:
I applied following an external advert. It was the most stringent process and toughest interview I’ve ever been through. Very senior people interviewing.
r36
Some trusts deployed a democratic/participative recruitment process that involved employees in initial recruitment decisions, such as the following process in which employees’ views also informed implementation decision-making:
Staff were asked did they want an internal candidate, did they want it bolted-on to an existing role or to be a substantive role. The board agreed to go with whatever decision was made, which was an externally appointed person in a full-time role.
r33
Interestingly, whenever the broader workforce was consulted, their decision was for a full-time FTSUG role to be externally advertised and appointed following a formal interview process. On each of these occasions, an external applicant was appointed.
By contrast, other trusts (n = 33, 38%) opted to appoint Guardians via closed, informal and opaque recruitment processes, often following a personal approach from a senior manager or a board member:
The trust secretary suggested I submit an expression of interest. I then met with them and the board chair and they offered me the role.
r85
I created the job following a discussion with the CEO. I wrote the job description and was seconded to set up the role and remained when it became a substantive post.
r45
Several respondents reported being ‘tapped on the shoulder’ (r32) as a direct result of their current or previous roles within the organisation. Those working in ‘patient complaints’ or ‘staff liaison’ roles were often approached because they were regarded as offering ‘a good fit, they said I was already talking confidentially to staff and raising concerns with senior managers’ (r74).
Others described how they were informed when interviewed for a substantive role or soon after appointment that the remit of their new role included being the Guardian. A newly appointed director of nursing explained that she was unexpectedly ‘advised that I was the Guardian on my second day’ (r35). Importantly, none of these unexpected and retrospective appointments was allocated any time to undertake the role.
There were no discernible patterns based on type of trust (acute or mental health) or on differences in trust size or CQC ratings. For example, a trust rated as inadequate and another rated as outstanding both appointed FTSUGs through closed processes. It is questionable whether or not the ‘good fit’ argument is sufficient justification for trusts to embark on restrictive recruitment processes that deny others the opportunity to apply for the role. Given that FTSUGs generally and those interviewed primarily identify as being of white ethnicity, it is also important to note that ethnic minority groups are likely to be disadvantaged in any organisation that relies on informal recruitment methods. 89 Furthermore, according to recent analysis,90 only 8% of NHS chief executives and chairpersons (who are often involved in FTSUG recruitment) are from ethnic minority communities, who make up 19% of the workforce. The potential significance of this can be seen in research findings that suggest that executives and managers commonly identify and sponsor the cases of demographically similar individuals, thereby facilitating their career progression and conserving rather than disrupting existing workplace culture. 89
Effects of implementation decisions on the Freedom to Speak Up Guardian role
Building on the above findings, the following sections discuss how FTSUGs undertake the role in the light of trust’s resource implementation decisions, especially time allocation. Realising that most FTSUGs were allocated little time to undertake such a potentially complex role, we asked Guardians whether or not they felt able to fulfil the requirements of the role. Most felt that they fully (n = 25) or mostly (n = 28) met the role’s requirements in the time allocated (Table 6).
| Time allocated | Guardians’ self-assessments: meeting the role requirement (N = 87), n | |||
|---|---|---|---|---|
| Fully (n = 24) | Mostly (n = 28) | Partially (n = 24) | Not (n = 11) | |
| 0–1 day (n = 44) | 11 | 13 | 12 | 8 |
| 2–3 days (n = 28) | 6 | 10 | 10 | 2 |
| 4–5 days (n = 15) | 7 | 5 | 2 | 1 |
Given that completely unbiased self-assessments are unattainable,91 Table 6 is illustrative of the perceptions of FTSUGs rather than a definitive analysis of role fulfilment. We also recognise that some Guardians may have been reluctant to say that they were unable to fulfil the role’s requirements. Most described being fully, or mostly, able to undertake the role in the time allocated, including 54% of Guardians who were allocated ≤ 1 day. We now discuss how some Guardians managed the seemingly impossible task of fully undertaking the role by deploying workaround behaviours that temporarily compensated for a range of workplace issues and implementation decisions, such as insufficient time and poor work design. 92 Some of the following extracts include the time allocated to the role, type of trust and type of Guardian role, where relevant and possible without compromising participants’ anonymity.
Discretionary working and ‘flexing’
Discretionary work effort is a term used to define employees working unpaid overtime and/or working more intensively at times of high demand. 93,94 For example, the interpersonally challenging and unpredictable nature of Guardians’ work meant that contracted hours were often exceeded to fit around the workers’ needs:
I’m employed 3 days a week but actually work 4 and a half mostly. It’s difficult to know when a call might come but I make myself available to meet people when and wherever they want.
r51, acute trust, stand-alone FTSUG
At the moment I work more like 4 days but only paid for 3. They may talk for an hour, they might want to talk for two. You can’t say sorry not today, you have to sit and listen.
r52, mental health trust, stand-alone FTSUG
Adjunct Guardians managed the unpredictability of speaking up by ‘flexing’ or redistributing time from their substantive roles when they were required to:
Two days a week as a Guardian, although I often do more. CEO says it’s OK if the role takes more than 2 days a week as speaking up is a priority.
r43, mental health trust, 2 days per week
Four hours a week is simply not enough. Inevitably my substantive job takes a backseat. It has been extremely difficult. Cases take many hours and days. My clinical work has to be backfilled within the team and my managerial aspects take a back seat. Flexing can get fraught at times for us all but it’s just about do-able.
r90, acute trust, 0.5 days per week
Workarounds deployed by FTSUGs were clearly useful in addressing immediate demand but, characteristic of workarounds more generally, flexing was not a ‘cost-neutral’ strategy because it resulted in tangible deleterious effects on Guardians’ substantive roles and their colleagues’ workloads, which itself required flexing to cover the insufficient time allocated to some FTSUGs. Flexing was also described as unsustainable and unsatisfactory. The quotation ‘I end up doing two jobs badly’ (r08, mental health trust, adjunct FTSUG 1 day per week) is a sobering summation of the experiences of many adjunct FTSUGs, which proved too much for some:
The trust has had a larger response to the role than anticipated. I don’t have enough time to dedicate to the Guardian role which sadly means I am resigning as my clinical role has to take priority.
r54, acute trust, adjunct FTSUG 1 day per week
The findings that FTSUGs routinely resort to workarounds, and are expected and enabled to do so, raises additional questions about whether or not trusts fully considered and understand the demands of the FTSUG role. Some trusts were clearly unprepared for the unmet need for speaking up within their workforce, with pre-implementation assessments of the time required for the role proving to be considerably misaligned with the realities of undertaking the role.
Gaps between organisational rhetoric and reality were also exposed, including in the case of the CEO who claimed to prioritise speaking up yet allocated only 2 days per week for an adjunct Guardian (r43, mental health trust, 2 days per week); this was a leadership decision that shifted the burden of ensuring that sufficient time was given for the role onto the Guardian and other colleagues. The sustainability of adjunct FTSUG roles is uncertain, considering the potential deleterious effect of workarounds on Guardians’ performance of substantive roles and their colleagues who are covering, and the longer-term effects of pressurised working on FTSUGs and FTSU within their organisations.
Finally, although the term ‘discretionary work effort’ usefully captures how FTSUGs meet their role demands, the term ‘discretionary’ does suggest that these efforts are optional and voluntary. In reality, FTSUGs often had no choice but to exert the additional effort required, and line managers and senior organisational figures appeared to have designed and enabled the role to operate in this way. However, despite some of the considerable limitations outlined above, the following section demonstrates that certain benefits could result from the adjunct FTSUG role.
‘The roles work hand in hand’
The skills, experience and ‘know-how’ garnered by adjunct FTSUGs in their substantive roles were described as transferable to and enhancing of the FTSUG role in a number of ways:
I understand what it’s like to be a manager and dealing with complaints. I navigate the organisation easily, I know the stories of the organisation and its history. The role and my experience is respected.
r48, mental health trust, stand-alone FTSUG 2 days per week
Furthermore, when the operational scope of a substantive role overlapped with the remit of a Guardian, these resulted in beneficial synergies for adjunct FTSUGs:
I advise on equality issues and receive incident reports and reports of bullying and harassment which I might not see as a Guardian. This allows me to triangulate information, identify hotspots and explore areas where there are issues. The roles work hand in hand.
r58, acute trust, adjunct FTSUG 2.5 days per week
Similarly, many adjunct FTSUGs described how being a clinician bestowed the Guardian role with additional credibility when clinical concerns were raised.
However, some Guardians presented a less certain picture, in which the benefits of an adjunct role were counterbalanced by drawbacks; for example, where seniority or prior organisational experiences and overlapping roles in some instances could ‘be the absolute advantage or the disadvantage’ (r34, mental health trust, FTSUG 0 days per week):
Some individuals feel I am too senior to approach with a concern. It’s tricky because my other role provides access to senior individuals in the organisation. Where more junior Guardians struggle with getting a response from managers it isn’t an issue for me.
r34, mental health trust, FTSUG 0 days per week
There are several benefits associated with the appointment of adjunct FTSUGs. Organisational capital and networks accrued in their substantive roles, often described in terms of credibility, authority and respect, are redeployed to the benefit of undertaking the FTSUG role. Meetings and information of importance and relevance to FTSU are accessible where they may not otherwise be. These beneficial overlaps may seem to be the intended consequences of the informal, closed and opaque internal recruitment processes detailed above, in which trusts recruit employees whose existing roles, attributes and skills complement the FTSUG role. However, some of the claimed benefits are ambiguous; clinical credibility was often allied to a demanding clinical workload, a combination that proved unsustainable for some alongside the unpredictable and time-consuming FTSUG role. Similarly, an adjunct FTSUG whose senior role enabled access to meetings or individuals who were inaccessible to more junior Guardians also described how the same senior role was viewed by some as an insurmountable hierarchical barrier to speaking up. Likewise, the credibility of FTSUGs appointed with little or no transparency may well be tarnished within the organisation.
To summarise, the findings earlier in this chapter established that labels, such as ‘part-time’ or ‘full-time’ FTSUGs, are only partially useful in understanding the implementation and deployment of the role. For example, part-time and adjunct Guardians routinely rely on workarounds, such as discretionary working or ‘flexing’, to create the additional time required in practice to accomplish their work. In some cases, workarounds are utilised, as they typically are in the NHS, as informal, occasional and temporary measures to manage variable demand. 92 However, many adjunct FTSUGs, often in senior management roles, are deployed by trusts with no time allocated to the role, meaning that such workarounds are often not discretionary or occasional but are expected and normalised: ‘hard-wired’ into the implementation of the FTSUG role.
Many trusts, therefore, have chosen to implement one of the most significant workforce initiatives in the history of the NHS by allocating it minimal time and little other resource. These limitations are circumnavigated by many FTSUGs who deploy short-term workarounds. Several others describe workarounds that have become routinised and detrimental to Guardians’ ability to fulfil the role, their well-being and, in the case of adjunct FTSUGs, the microsystems within which their substantive role operates. Furthermore, the following section demonstrates that workaround strategies were not always successful in releasing sufficient time to meet the various demands of the role.
Guardians’ work left undone
The NGO’s job description for FTSUGs15 specifies that the ‘purpose’ of FTSUG is to ensure that:
-
workers are supported in speaking up
-
barriers to speaking up are addressed
-
a positive culture of speaking up is fostered
-
issues raised are used as opportunities for learning and improvement.
However, Guardians consistently described having insufficient time to fully undertake all aspects of the role. Consequently, the term ‘work left undone’ is adapted from the existing literature95 to refer to any aspect of the Guardian’s work that is delayed and/or omitted either in part or in whole. The notion of FTSUG work left undone is further discussed in the following three overlapping themes: ‘difficult to keep up’, ‘I’m just being reactive’ and ‘managing workload through restricting role visibility’.
‘Difficult to keep up’
Some Guardians described general difficulty in addressing several aspects of the role, including providing timely responses to speaking up, promoting awareness of FTSU and monitoring the progression of cases. The unpredictable nature and demand of speaking-up work described earlier is also highlighted in the second extract:
I’m not always available to respond or follow up on cases and that’s with me working more than the allocated 2 days a week. It’s also difficult to keep up with wider speak-up agenda.
r48, mental health trust, stand-alone FTSUG 2 days per week
I often feel overwhelmed, it’s difficult to keep up with managing and tracking concerns and strategy work. I’m very stretched and need more time to do the role effectively. I will prioritise managing and handling concerns over everything else. Some concerns take little time, but sometimes I can be speaking with individuals for half a day.
r66, acute trust, stand-alone FTSUG 2 days per week
‘I’m just being reactive’
Guardians who reported having little or no time to undertake the role often described their mode of operation as ‘reactive’, rather than ‘proactive’:
I’m just being reactive and unable to triangulate data and promote the role as there’s just no time to think.
r35, acute trust, adjunct FTSUG 0 days per week
I only get a snapshot but if I had more time my understanding would grow. I quite often know there’s more to a case, but it’s complex and difficult to explore every case. I can’t access the big picture.
r29, acute trust, stand-alone FTSUG 2.5 days per week
Guardians were frustrated with time scarcity and were aware that reactive working limited their opportunities to generate a ‘big picture’ understanding of speaking up. Several FTSUGs also doubted the longer-term sustainability of a role that routinely relied on discretionary work efforts:
Lack of time is a big barrier to keeping up with wider speak-up issues. It’s often down to me burning the midnight oil. It’s not sustainable as it’s very dependent on me carrying on in this way, which is unlikely.
r48, mental health trust, stand-alone FTSUG 2 days per week
A key purpose of the FTSUG role is to actively foster an open workplace culture in which workers feel safe to speak up. However, two activities stood out in the Guardians’ descriptions of work left undone that are important in fostering an open learning culture: triangulating FTSU concerns with other data sources and increasing awareness of speaking up through staff engagement activities:
Being full time would give me time to triangulate data. That could lead to more awareness-raising and targeting specific staff meetings, events, generally increasing the role’s visibility.
r47, mental health trust, adjunct FTSUG 3.5 days per week
I manage to get everything done that is needed. However, I can see how the role could be full time. With more time comes more exposure for the role and the more concerns I would capture.
r38, acute trust, adjunct FTSUG 2.5 days per week
The FTSUGs repeatedly discussed having insufficient time available to raise the role’s visibility, and how not doing so could result in fewer workers speaking up. Furthermore, the following section demonstrates that some FTSUGs intentionally restricted their visibility within the trust because they feared being unable to manage any concomitant increase in workload owing to time scarcity.
Managing workload through restricting role visibility
Although some time-pressed FTSUGs managed to occasionally undertake activities related to raising awareness of the role and to speaking up more generally, others decided to not ‘generate business’ that they knew that they were unable to manage:
I have made no effort to advertise the role and generate business as there is no time to do this or to deal with the concerns had I triggered more interest in staff.
r53, medium acute trust, adjunct FTSUG 0 days per week
Guardians also described operationalising a modified version of the NGO’s job description by organising their work into a hierarchy of primary and secondary priorities. Primary priorities, which were undertaken by all FTSUGs, relate to their perception of the role’s core purpose, amounting to receiving and responding concerns. Secondary priorities were described as ‘other’ tasks and activities that were undertaken only when time allowed and were left undone when time was scarce. These included activities such as generating a positive culture and learning from speaking-up cases (further discussed in Monitoring and learning from speaking up).
In summary, important aspects of the role were left undone when FTSUGs were allocated insufficient time to fully undertake all aspects of the role, which could have deleterious consequences on speaking up in trusts. The impression generated, therefore, is of partial or inconsistent implementation of key elements of the job description within many trusts.
Budgets and workspaces
Although time was identified as the most important resource for undertaking the role, other essential resources identified included having a budget and a dedicated workspace. Although attempts to foster a FTSU culture were often thwarted by a lack of time, some Guardians did undertake a range of marketing and communication activities. Although some promotional activity was largely resource neutral, such as the use of Twitter (Twitter, Inc., San Francisco, CA, USA; www.twitter.com) as a publicising tool, some promotional activities and materials (e.g. pens, balloons and reusable cups) required funding. Having independent access to a budget was, therefore, identified by many FTSUGs as important in itself, as well as being an affirmative indicator of autonomy from formal management structures:
I have a small budget that I manage myself to attend events and purchasing publicity things which has helped with setting up the role and also creates a healthy distance from my line manager.
r03
I have a small budget of about £4K [£4000] a year to purchase promotional materials and attend events. Having autonomy to use resources is important for how the role looks in the trust.
r9
Others described experiences that were demoralising, with little managerial support when submitting budgetary requests, which in one instance led to the furtive diversion of funds from other budgets to supplement the Guardian role:
Unfortunately, it is difficult to get leaflets printed. When I ask for a budget code they just ignore me. It takes me months to get this code.
r89
A designated budget would be great for badges, posters, pens. Unfortunately and annoyingly my requests are often turned down so I actually sneakily supplement my Guardian work through my other role’s budget.
r31
The lack of a dedicated workspace for FTSUGs was described by many as a threat to confidentiality and privacy, a potential deterrent to speaking up and a further source of frustration for Guardians:
Things would be much better if I had my own office. I have to use a quiet room or a seminar room, but these can’t be relied on. Confidentiality is a worry and having no space could be inhibiting speaking up.
r88
The biggest barrier is not having a space to see people. I have been asking but to no avail. I’ve been seeing people all over the place. One of the last straws which triggered my resignation was when I was stood outside in the rain talking to someone about their concern and I thought ‘what on earth are you doing?’.
r25
However, not all Guardians were in favour of having an office allocated, or at least not when the office was located near to the trust’s executives:
It was initially discussed that I would have an office on the executive corridor but I said this was not appropriate. Can you imagine a little band 2 going there to speak up? I said no way.
r83
Many of the difficulties recounted by Guardians were related to a lack of space and place to undertake their work. Sociologists who study organisational spaces have long held that matters of who has space, how much and who can move where are intimately connected with constructing symbolic meaning and working practices, ‘silently communicating widely understood messages about bureaucratic status, social status and inequality’. 96 The lack of a dedicated workspace led to FTSUG resignations and itinerant working practices, including hosting clandestine meetings and telephone calls at the margins of organisations or in public spaces inappropriate for sensitive interactions (rainy car parks, coffee shops, corridors and libraries). Underlying many Guardians’ frustrations were concerns that the lack of physical space signified that the trust did not sufficiently value the role.
However, two separate yet related issues create complexities and subsequent difficulties for the physical positioning of Guardians. First, the historical perception of speaking up as a risky, morally dubious and taboo act and the need, therefore, for a space within which speaking-up activities can be cloistered without fear of exposure and retribution. 97–100 Second, some FTSUGs were reluctant to be situated on the ‘executive corridor’ for fear that this symbolised too close an association or exposure to senior leaders that could taint Guardians’ independence and workers’ perception of a safe space.
The notion of tainted work is relevant in many ways to FTSUG implementation. Kreiner et al. 101 figuratively describe how dealing with tainted aspects of work constitutes marginalised and ‘dirty work’. These terms resonate with aspects of Guardians’ work that can be considered socially and morally tainted owing to their proximity to what has sometimes been regarded as stigmatised activity (speaking up). Virtually all occupations, including those considered high prestige, are associated with at least some dirty work some of the time, resulting in dirty work being considered a necessary evil in society. However, too close an association with dirty work can mean that some workers are marginalised by organisational decision-makers and face difficulties accessing organisational resources and influence, which further render their work as low status, undervalued and invisible. 102 Clearly, allocating a dedicated working space for FTSUGs that sensitively addresses these complex demands is not easy, but should not be regarded as unmanageable or a rationale to allocate no space.
A lonely and stressful job for some
As highlighted in earlier sections, time-limited FTSUGs undertook compensatory workarounds that negatively affected some aspects of undertaking the role. This section describes how time limitations also affected FTSUG well-being and resilience. A further possible indicator of dirty work and marginalisation was that the FTSUG roles were often enacted in isolation, with Guardians frequently reporting the role as ‘lonely’ with little or no supervision or support for Guardians to discuss their work concerns:
I enjoy the role, it’s a great job, but the role is very lonely and stressful. No one calls me because they’re happy, they call because they’re distressed and need support. My organisation has put in place some psychological support, but because of confidentiality of the role it is very lonely. The NGO should put more guidance out with respect to how trusts can support Guardians. When you have had three or four calls in a row with people crying for an hour and an half on the phone, it is hard to get yourself together again afterwards.
r12
I have a therapist provided by the trust as it is so hard to listen to the difficult stories that we are told. We don’t have anywhere to offload and it can be a lonely place. If I didn’t have a therapist I would have walked away about a year ago. Nobody comes with good issues, everybody comes with a massive issue and once they unravel you can’t stop someone from speaking. But it seems to fall on deaf ears with the NGO.
r73
Experiences strongly suggest that, even where organisations provide support, Guardians remain lonely and emotionally vulnerable as a result of the substantial demands made on them. On the whole, Guardians described receiving little support from the trust or nationally (from the NGO) to cope with a clearly stressful and emotionally demanding role. The following extracts similarly reiterate the impact of the role on FTSUGs’ well-being, with sleeplessness, migraines and stress frequently referred to during interviews:
We are expected to listen to lot of sensitive stuff, to take a lot of stuff on board and then have to carry that. There’s a lot of pressure to keep things quiet and confidential. We have to manage our own stress and well-being. A lot of staff members will want to speak just to feel better or will ask for advice. It’s a bit like counselling, but there’s no one offering that to me. It’s mentally exhausting and I’m worried I won’t be in the right mental state to deal with something more serious should that happen. I would like support from NGO or something external to unload my stress safely without any vested interests. No one is interested in my health and well-being. Sometimes I feel too stressed to sleep and the stress seeps into the rest of my life.
r36
The director has not been supportive. I have experienced isolation and bullying from other staff which has been very distressing. I’ve also experienced migraines and I failed a course I was taking. I do not feel that I can continue to be a Guardian when I know what happens when you do speak up. I’ve been labelled a troublemaker.
r86
There is little literature about the individual experiences of those who are responsible within organisations for supporting victims of bullying and harassment, and for resolving often harrowing and long-standing concerns. This is a significant gap in the literature, and of particular relevance here given the frequency with which FTSUGs are called on to undertake both of these responsibilities. FTSUGs also have to frequently acknowledge sometimes traumatic events or information that can become detrimental over time at an emotional level, and magnified when they are also expected to support others.
The extent of role-related stress experienced by FTSUGs is troubling and raises potentially significant short- and longer-term issues. For example, in the short term, Guardians described how consistent exposure to (di)stress reduced their ability to function and respond to concerns. In the longer term, the individual harm to and the potential turnover of Guardians owing to unmanageable levels of stress create challenges for retaining Guardians in the role.
Summary
The level of resource invested in FTSUGs varied considerably across trusts, which, in turn, often resulted in extreme variations in the FTSUG role being undertaken. Variations were seen in the time allocated to the role (zero hours to full time) and the availability of other resources, such as office space and budgets. Most FTSUGs interviewed could be described, from an organisational and workplace perspective, as destitute: time-poor and mostly deprived of budgets, space and other resources. Of concern is that many FTSUGs described how the lack of available resources negatively affected the number of workers speaking up. Guardians also gave clear examples of being unable to monitor and learn from speaking-up cases, in addition to not developing the role or promoting FTSU culture. It is important to remember, therefore, that, in addition to the variances in recording data discussed in the following sections, the published data of rates at which workers speak up to FTSUGs may also be significantly affected by the resources allocated to the FTSUG role, rather than being read as unfettered measures of speaking-up activity or a broader sense of FTSU culture within a trust.
Counting and recording speaking-up data
The NGO’s guidance on recording cases and reporting data16 states that FTSUGs ‘are required to record all cases of speaking-up that are raised to them . . . in a consistent and systematic way’ (original emphasis) (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16 Numerous FTSUGs followed the guidance closely, which they found to be ‘clear, coherent and very helpful’ (r7):
I count everything whether it comes to me by e-mail, text, phone call or bumping into someone in the corridor. They are all counted and reported every quarter to the NGO including signposting to others.
r36
However, Guardians’ practices often diverged from national guidance. By contrast to the extract above, ‘signposting’ concerns to other processes (such as diverting concerns to a grievance process within Human Resources) was not counted by some Guardians, while others counted only those cases that they considered to be ‘proper’ concerns:
I do not record signposting, a phone call or a chat in the corridor. I will record cases when people properly offload, when something takes time to address. If I recorded everything I would run out of time so it’s only when I’ve got a loop to close that I record it as a proper concern.
r73
The only concerns I recognise as a proper case is what I end up working on. If I counted everything this would skew the figures. Anything that is signposted to others I bat away and don’t count them.
r47
The FTSUGs were, thus, making various individual judgements about what ‘counts’ as a concern. Not all concerns were considered as having equal weighting, with many Guardians keen to ensure the primacy of patient safety concerns:
The NGO are too prescriptive about categorising concerns. I know some will count everything but minor issues like car parking is not something the NGO should know about. I deal with it but it doesn’t get counted. If I recorded those things as a concern then it would have the same weighting as a patient safety issue, which isn’t right.
r51
I know some Guardians would count every concern even if it was a light not working properly. That is where I think the NGO is wrong and not reflecting the true patient safety essence of what we should be doing.
r05
Despite considerable unease that counting all concerns could misrepresent what FTSUGs considered to be the essential (patient safety) meaning of their work, care was needed when deciding what constituted a ‘minor issue’:
I never push anyone away and always thank them for coming. They’re more likely to trust you if something bigger comes up in the future. If the culture is right staff will speak up. Even if someone takes the time to help someone with a mundane concern, that creates a better culture, it’s all interlinked. A concern was raised about air con where I felt the person may have been testing me with a minor issue and indeed they came back later with something serious. Another was when a shredder was reported to me as broken and when I explored I found a bigger issue as confidential information was left lying around the room. You can’t be too quick to dismiss things.
r46
There were also difficulties when applying the NGO’s counting guidance that ‘each individual speaking-up through the Guardian route should be counted as a separate case even if they are speaking-up about the same issue, together or separately’ (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16 Most of the FTSUGs who were interviewed did not comply with the guidance because they (again) thought that it risked ‘over-inflating the numbers of concerns’ (r77):
The NGO wants every single concern to be reported as a separate case. This doesn’t make sense. I had 10–12 different people raising concerns about the same thing which I counted as a single concern.
r02
Despite the NGO’s attempts to establish consistency through codifying the process of counting and recording concerns, FTSUGs described deeply held reservations about a process that was too open to interpretation and difficult to generate meaningful comparisons across trusts:
My greatest criticism so far of the NGO is that they need to develop a national reporting system as the categories and what to report is currently too subjective. Practically it means we are not always comparing like with like.
r01
Similar issues of subjectivity and robustness of data produced and published are further discussed in the following section.
Counting bullying and harassment
NHS workers’ contributions to the FTSU review12 drew attention to two types of pervasive bullying and harassment behaviours that inhibit speaking up: bullying and harassment that occur as a direct consequence of workers speaking up, and the more prevalent incidents of bullying and harassment that contribute to creating a hostile workplace culture that is ill-disposed to speaking up. FTSU data published by the NGO18 show that bullying and harassment remains a major issue within the NHS, with a consistently larger number of speaking-up cases categorised by FTSUGs as ‘bullying and harassment’ than ‘patient safety’. This was further reinforced during our interviews:
Bullying and harassment is the top number of cases every quarter. I do get patient safety concerns but not as much as I should or as often as you would think.
r52
Guardians described NGO guidance16 regarding recording and categorising incidents of bullying and harassment as reductive and unclear, and the process as overly open to interpretation, all of which affected the quality and accuracy of data:
I feel that the guidance and data collected by NGO is not useful in regard to bullying and harassment. I feel we are all reporting it very differently so I am not sure the collation of that information is as accurate as it could be.
r21
The majority of cases would be what we class as bullying and harassment . . . but the definition of the categories, I don’t know what constitutes bullying and harassment, is it down to what the person feels it is? I don’t know.
r34
Some FTSUGs expressed surprise and discontent about dealing with the large number of bullying concerns because these ‘incorrectly’ detracted from what they considered to be the intended patient safety remit of the role:
I thought this role was about patient safety post mid staffs. But most concerns are bullying and harassment not patient safety. B&H [bullying and harassment] such a big thing and is such a cultural thing, people raise it more than anything else.
r54
I feel bullying and harassment has incorrectly taken over the role. The role is there for patient safety, although I acknowledge team bullying can impact on patient safety.
r22
Although there was no evidence that FTSUGs did not count some bullying and harassment concerns, as in the preceding section’s example of Guardians counting only what they considered ‘proper’ concerns, there was the same sense that bullying and harassment concerns somehow overshadowed, ‘skewed’ or misrepresented the intended patient safety nature of their work.
Summary
Our findings suggest that NGO guidance on counting concerns was welcomed and adhered to by FTSUGs, but also that many Guardians significantly adapted the guidance to fit with their notions of what constituted meaningful and ‘proper’ concerns. As a result, their subsequent practices differed markedly from the guidance (Table 7).
| NGO guidance16 | FTSUG modifications |
|---|---|
| FTSUGs are consistently and systematically ‘required to record all cases of speaking-up that are raised to them’16 (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0) | Some FTSUGs count only what are considered ‘proper concerns’. This can mean (1) FTSUGs record only when they ‘work on’ a concern, and often do not include counting concerns that are signposted to others or raised via corridor conversations; and (2) insufficiently ‘weighty’ concerns are not counted and patient safety concerns prioritised. This ensures that FTSU figures are not skewed and maintain the primacy of patient safety, rather than incidental issues, such as car parking |
| Each individual speaking-up through the Guardian route should be counted as a separate case even if they are speaking up about the same issue, together or separately16© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0 | Some FTSUGs count the same concern originating from a team as one concern rather individual concerns |
In summary, a number of salient points arise from this analysis. One of the most challenging tasks in monitoring the safety and quality of health care is distinguishing irrelevant noise from important signals that ought to be attended to. 5 A practical issue that FTSUGs are grappling with is that the role’s introduction has generated a large amount of information or ‘noise’ within the organisation, which can overwhelm FTSUGs’ often meagre resources and leave potentially important signals routinely undetected, misunderstood or not addressed. We show, for example, how FTSUGs adapt guidance on how to count and categorise speak-up cases in an attempt to preserve their scarce time for what they perceive as ‘proper concerns’. Similarly, others ‘bat away’ seemingly lesser concerns that require only signposting, whereas others respond to and ‘count everything’.
In NPT parlance (see Chapter 2), these repertoires of common practices are a confluence of sense-making (coherence) and workability: FTSUGs modify the NGO’s definition of a countable concern to cohere with what Guardians deem to be a ‘proper concern’ and, in so doing, manage and more accurately capture their workload. Although subjectively modifying the guidance on what counts as a concern benefits individual FTSUGs, doing so is clearly problematic in terms of the validity and reliability of the NGO’s quarterly and annual FTSU reports. Differences between FTSUGs in how they count concerns may be one explanation for the wide variation in concerns reported across otherwise comparable trusts. Subjective counting practices also raise questions about whether the number and types of concerns are actually an accurate barometer of FTSU culture within and across trusts, or may instead be more representative of what some FTSUGs consider to be a ‘proper concern’.
Monitoring and learning from speaking up
Concerns raised to a Guardian have the potential to facilitate organisational learning and to generate a culture in which workers feel free to speak up. The NGO acknowledges that Guardians alone cannot be responsible for tapping into this learning potential. Their guidance document for NHS boards17 suggests that boards should ensure that FTSUGs have access to data that ‘enable Guardians to triangulate speaking-up issues and proactively identify patterns, trends and potential areas of concerns’ (© NHS Improvement, 2019. Contains public sector information licensed under the Open Government Licence v3.0). 17 Furthermore, the NGO’s education and training guide for FTSUGs103 stipulates that FTSUGs should be competent in ‘analysis and identification of trends. . .and interpreting data’ (© National Guardian Freedom to Speak Up, 2018. Contains public sector information licensed under the Open Government Licence v3.0). 103 The following sections explore the practical ways in which Guardians collect and analyse data for patterns and trends, which generates learning from FTSU data.
‘I’m always looking for trends, cold and hot spots’
Several interview participants described how they analysed the issues identified within a single speak-up case, in addition to triangulating data across several cases and other sources of data:
My ears prick up when I suddenly receive a concern about bullying from somewhere that is usually quiet. I will look at their incident reports, complaints and staff turnover and benchmark patient safety issues which I collate using a heatmap approach. Any potential problems will trigger a quality-of-care summit led by the CEO and an independent NED. I will also look at the quarterly and biannual committees. The long view is helpful for identifying culture underneath issues.
r01, adjunct FTSUG 0 days per week
It is noteworthy that the above adjunct FTSUG, allocated zero hours for the role, has a substantive role within organisational learning, which echoes our earlier findings about the ‘added value’ of some adjunct FTSUG appointments. However, it was not only adjunct FTSUGs who triangulated speaking-up data to directly trigger change within organisations. Other FTSUGs also embodied a problem-sensing11 approach to their work, heading off issues before they become serious problems and mobilising the involvement of those at the ‘blunt end’ (senior managers and HR) and ‘sharp end’ (clinical teams and individuals).
Triangulating information about who was speaking up and/or where within the organisation (‘hot spots’) or not (‘cold spots’) also led to useful interventions, such as Guardians engaging with seldom-heard or difficult-to-reach workforce groups:
I’m always looking for trends in cold and hot spots. I had a high number of contacts from one area and the themes were very similar. I wrote to board members with my analysis and asked them to intervene which they acted on. But there are also quieter areas. We realised porters haven’t access to PCs [personal computers] so they miss e-mails. I have now developed a one-page poster for speaking up resulting in a number of concerns raised by porters and changes made to service.
r04, full-time FTSUG
Not many concerns received from estates and facilities so I do a lot of proactive work there. Junior doctors are difficult to access, they are a bit of a work in progress. I now do an induction session for them, but no regular access. Consultants won’t let me in as they don’t understand what my role is and then don’t understand the importance of me speaking to them.
r50, adjunct FTSUG 3 days per week
It is rare that estates and facility workers are considered to share similar workforce characteristics to doctors, but these extracts provide an insight into the breadth of work and the challenges facing Guardians. Both of these workforce groups were consistently described as being less likely to speak up, albeit for different reasons. Estates and facilities workers were ‘hard-to-reach’ because they were not routinely provided with NHS e-mail addresses and/or PCs [personal computers], which Guardians regularly used to communicate with the workforce. Difficulties reaching junior doctors were described as a more complex and self-perpetuating ‘access’ and comprehension/legitimacy issue, which was difficult to crack owing to restrictions imposed by gatekeepers (consultants). However, Guardians reported substantial progress when they were able to directly engage with these groups (see also the quotation from ‘r04’ above):
We had zero concerns from medics when I first started but now they raise concerns since going to junior doctors meetings.
r38, acute trust, adjunct FTSUG 2.5 days per week
External events could, however, undermine FTSUGs’ work and expose the fragility of psychological safety within organisations. For example, Guardians referred to the damaging fallout following national media coverage of the poor treatment by NHS senior managers and regulators of two junior doctors (Dr Hadiza Bawa-Garba and Dr Chris Day). Negative perceptions and distrust in the FTSUG role occurred despite the lack of involvement of Guardians in either of these cases:
Recently met with consultants and junior doctors to increase my zero visibility with them. It was the most challenging session I’ve had as a Guardian. Lots of mistrust coming from the Bawa-Garba case.
r29, FTSUG 2.5 days per week
We have good spread of concerns from cleaners to senior managers. Doctors aren’t coming to me though. The Bawa-Garba and Chris Day case has not helped. There’s nothing an organisation can do to stop perceptions being changed by this.
r02, FTSUG 2 days per week
Limited learning from concerns
The following data further support the earlier identified difficulties caused by time scarcity and that, for some FTSUGs, ‘work left undone’ also extends to aspects of data analysis and triangulation for learning and improvement purposes:
To be honest I don’t have time to use this information meaningfully. I think I know where the gaps are but have no capacity to further analyse and act on this information.
r08, mental health trust, adjunct FTSUG 1 day per week
I know there are some groups that undoubtedly speak up less but I have no time to act. Further analysing this will have to wait another year.
r70, adjunct FTSUG 2 days per week
Other FTSUGs were generally less curious about and proactive in their analysis of speak-up data:
I send quarterly data to the NGO and share with HR who monitors ethnicity, staff group and division. I don’t personally monitor anything and haven’t needed to explore this sort of information yet.
r10, adjunct FTSUG 0 days per week
Although all of the FTSUGs who were interviewed presented the number and types of concerns raised at board meetings and submitted quarterly data to the NGO, many trusts and FTSU stakeholders (such as executive and non-executive leads and FTSUG line managers) seemed not to routinely expect or demand any further detailed analyses of FTSU data. Rather than implementing a FTSU strategy that normalised an environment of continuous and rigorous reflexive inquiry of FTSU data, many trusts adopted a contrasting position of ‘normalised incuriosity’ towards FTSU, as identified in recent studies of organisational cultures of openness in the NHS. 6 The following section further explores the notion of incuriosity, drawing specifically on FTSUGs’ descriptions of the protected characteristics, particularly race and ethnicity, of those speaking up.
‘Further demographic data’: understanding speaking up in ethnicity and minority groups
As previously discussed, the NGO guidance on recording cases and reporting data16 requires Guardians to collect and submit quarterly data on speaking-up cases (Table 8). The guidance also details a range of ‘additional items’ that ‘could be recorded’ when Guardians request feedback from those speaking up following the closure of a case (see Table 8).
| The following items will be requested from trusts and foundation trusts on a quarterly basisa | What else to record?b |
|---|---|
|
There is a range of information that could be recorded for each case that you deal with . . . additional items are likely to include:
|
The following sections report that some Guardians opted to collect and utilise to good effect ‘additional items’ of demographic data, mostly race, sex and ethnicity data [often referred to by Guardians as ‘BME (black and minority ethnic) data’], with a smaller number of Guardians collecting data on workers’ sexual orientation and disability. The FTSU review12 also commonly refers to the term BME, as does NGO guidance while also occasionally referring to BAME (black, Asian and minority ethnic). We are aware of and sympathetic to the limitations and criticisms of both of these terms and acronyms,104 but mostly refer to the term BME in this report for consistency with those that we are studying.
In some instances, collecting and analysing demographic data resulted in significant improvements in communication and engagement with minority groups, as well as FTSUGs advocating for data-led changes at the board level:
I was anecdotally concerned about BME and vulnerable groups. Then the data showed they were not coming forward so I am currently working with equality and diversity leads. I also developed my own groups and forums for BME and disability and ensure that I share the data with them.
r46
As a result of my concerns about local data I met with equality and diversity leads. We agreed to work together to encourage those with protected characteristics to speak-up. I recognise they face additional barriers so I have also asked for FTSU to be added to the terms of reference for the BME network in the trust, and I now attend the LGBTQ [lesbian, gay, bisexual, transgender and queer] network. I have highlighted in board’s report that they need to improve targeting and reach to groups with protected characteristics.
r52
However, most of the Guardians who were interviewed opted to not request additional demographic details from those speaking up; the many and various reasons for this decision and how this affects FTSU is the focus of the following sections.
‘The NGO doesn’t ask for ethnicity’
Several Guardians did not collect ‘ethnicity data’ because they believed that they ‘are not required to by the NGO’ (r51):
The NGO doesn’t ask for ethnicity data so I don’t keep up with it and don’t use it in my work currently.
r36
The following Guardian collected ethnicity data, but only after seeking the NGO’s permission to do so:
Ethnicity yes I started to collect this data once I got permission from NGO to collate this data.
r62
It is worth remembering that the NGO guidance suggests that collecting ‘further demographic data’ may be useful. Nowhere does the guidance state that ethnicity data should not be collected because they are ‘not required’ or that ‘permission’ to do so is required. However, the NGO’s labelling of some demographic data as ‘additional’, and thus not requiring quarterly reporting (and subsequently not published by the NGO), has clearly, but unintentionally, influenced many Guardians to not collect data that other FTSUGs have demonstrated to be enormously valuable in improving the voice of minority workforce groups. It is also worth noting, given the earlier sections outlining the pervasiveness of bullying and harassment concerns raised with FTSUGs, that there are direct and inextricable links between workplace bullying and harassment and discriminatory behaviours. 105
‘It doesn’t feel right to ask about this’
All trusts provided several different channels for workers to speak up to FTSUGs about their concerns, such as a dedicated e-mail address and/or telephone line. Although face-to-face meetings were sometimes arranged following initial contact, Guardians mostly responded to concerns via e-mail or telephone. This mode of ‘remote’ working was often linked to organisational decisions during the implementation of the FTSUG role. For example, for those Guardians who were allocated ≤ 1 day per week to undertake the role in an organisation consisting of thousands of workers dispersed over several sites, communicating via e-mail or telephone was an effective time management strategy and the only viable communication option. However, telephone or e-mail communication was also described as a significant obstacle to interaction; in particular, the process of enquiring about ethnicity was described as uncomfortable, difficult, or inappropriate:
Ethnicity data, no not collecting yet. I have looked at doing so but asking such questions doesn’t always naturally fit into a conversation, particularly over the phone. There is no comfortable way of figuring it out.
r8
I don’t collect this information but have thought about it. I know BME and other vulnerable groups are disproportionately put off speaking up. But it’s difficult as a lot of communication is over the phone or e-mail so I don’t ask. On the phone people are often in tears and over e-mail I feel it sometimes takes people a lot of effort just to give me a phone number. So it doesn’t feel appropriate to ask.
r46
Feelings of inappropriateness or discomfort were not only discussed in the context of telephone or e-mail communication. Guardians also described how asking about ethnicity and disability triggered feelings of discomfort and inappropriateness when meeting workers ‘in person’:
It doesn’t feel right to ask about this when people come to me, I’m sure it’s the last thing they want.
r5
Lots of emotional issues when I meet with people. Asking questions about ethnicity and disability is inappropriate.
r31
Other Guardians explained how those speaking up may be intimidated or ‘put off’ when asked about ethnicity and other protected characteristics:
I think it can be intimidating to ask about ethnicity. I don’t think people like it.
r35
Why is it necessary to ask all these questions? It can be intrusive and a little bit tricky because if you start asking these questions people are put off.
r85
Such commonly held apprehensions were based on Guardian’s perceptions and feelings (‘I think’, ‘I am a bit worried’ and ‘I have thought’) of how others from minority communities may react, rather than recounting actual experiences of adverse feedback from those speaking up.
Indifference, questionable motives and misplaced concerns about confidentiality
Some Guardians demonstrated an indifference and questioned the utility of ethnicity and diversity data:
In my area BME is not a huge group so the data wouldn’t be that useful and isn’t included in my breakdown of numbers or in my reports.
r33
I don’t collect diversity and ethnicity data and in fact I’m afraid to say that I don’t even know what percentage of ethnicity there is in the organisation.
r55
These answers were somewhat surprising given the significant concerns about the poor treatment often experienced by BME communities who speak up in the NHS. 106 The following extracts demonstrate what we have termed ‘questionable motives’, where Guardians portray collecting ethnicity data as a ‘box ticking’ (r42) exercise or amounting to breaching a ‘fundamental belief’ (r70) in equality that, although commendable, is out of kilter with the experiences of many individuals working in the NHS who identify as belonging to minority groups:
I use information to identify trends but haven’t looked at ethnicity. Our trust at the moment is very much into the Windrush generation. It feels like there’s a lot of box ticking, almost forcefully pushing message of equality and diversity almost to the exception of white British. That’s how it feels working here, and it comes from a real range of people.
r42
I don’t monitor ethnicity because I act out of the fundamental belief that people should be treated equally and I just wouldn’t treat anybody differently.
r70
Sensitivities relating to protecting confidentiality and anonymity of those speaking up were also frequently discussed as a reason for not requesting information about ethnicity:
If I collected data on ethnicity the staff member raising concern would become easily identifiable this would compromise their anonymity to others. Some units are so small which is why I am trying to protect the staff. I think it’s a good thing that this sort of data is not collected.
r47
Guardians were rightly concerned with protecting the identities of those wishing to speak up. However, the resulting decisions that were made by some Guardians to not collect ethnicity data seem misguided and their anxieties disproportionate to the actual risk of disclosing identities, given that such data when analysed and shared can generate improvements while still protecting individuals’ identities. Examples of this are provided earlier in this section and in the following extract:
Ethnicity is not easy, people may not want to disclose ethnicity or gender as they want things to be treated confidentially and ethnicity or gender can sometimes give things away. But you just have to go carefully. I ask their permission before revealing ethnicity. I also collate this data in a bigger picture report to board or committees, but in smaller reports it can be difficult to hide things and not always appropriate to report specifics.
r48
This useful example demonstrates how ethnicity data can be utilised in a number of ways that remain sensitive to the circumstances and preferences of the person speaking up. The accrued benefits from sensitively collecting the information supported by a clear rationale for doing so can outweigh the manageable risks to confidentiality or to interactional rapport.
Finally, the NGO guidance on counting concerns states that ‘feedback should be obtained when a case is closed’ and that this ‘may be the best time to give individuals the opportunity to provide additional information’, such as protected characteristics (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16 Guardians often discussed that feedback forms were frequently not returned, stating ‘no feedback received yet’ (r25) or that ‘only 33 out of 89 people fed back to me’ (r70).
Furthermore, delaying the collection of protected characteristics data until ‘a case is closed’ is potentially problematic when managing cases. Although concealing protected characteristics may allay the risks of FTSUGs and others succumbing to residual or unconscious biases, doing so denies access to information that may have an important bearing on understanding and responding to FTSU cases. In short, protected characteristics information should not be considered to be ‘feedback’ but instead should be seen as important ‘feed-forward’ information. The rationale for requesting the information should be communicated clearly and sensitively, and the data handled in accordance with the preferences of the person speaking up and in a manner that minimises any risks to detriment.
In summary, the FTSU review12 identified significant barriers to speaking up experienced by NHS workers from BME communities, which the COVID-19 pandemic recently revealed to be still commonplace for many. 107 Given the findings of the review,12 it is surprising that the NGO guidance does not mandatorily require FTSUGs to report race/ethnicity characteristics of those speaking up. Instead, race (as well as disability, sex and sexuality) is identified as ‘further demographic details’, a form of optional information that ‘could be recorded’ at the Guardian’s discretion. Some FTSUGs heeded this suggestion and used demographic details to meaningfully give voice to minority groups. Most FTSUGs interviewed, however, did not collect this information and their explanations for not doing so were wide-ranging. The NGO’s decision to delineate data about ethnicity, sex and disability as ‘additional’, rather than essential, was a justification and refrain used by many FTSUGs, who explained that they did not collect these data because the NGO guidance ‘did not ask’ or request them to do so.
In contrast to the small number of FTSUGs interviewed who collected and utilised such data, the majority simplified the task of data collection to meet a ‘satisficing’ (satisfactorily sufficing) criterion, which adequately fulfilled the minimum requirements of the NGO’s data requests rather than optimising data collection opportunities to better understand speaking up. Doing so, however, is not inconsequential because it denies, at a very fundamental level, that race/ethnicity issues (and issues of, for example, disability or sexuality) are significantly relevant to understanding speaking up within the NHS. It also assumes that those speaking up have the same experiences in the same contexts regardless of obvious differences in personal characteristics. It also appears to demonstrate a specific form of historical ignorance, embedded in wilful blindness and/or deafness2 to the multiple reports and surveys that describe the mistreatment and fear experienced by workers from minority communities who speak up.
This is potentially problematic on a number of levels. First, the decision by the NGO, FTSUGs and trusts to not prioritise the collection of data from minority groups potentially perpetuates unconscious bias and power dynamics in organisations in ways that legitimise and privilege the interests of the majority and their capacity to set the terms of intraorganisational relationships. 89 In addition, most FTSUG reports to a board consist of only the data ‘required’ by the NGO, which often results in trust boards being insulated from ‘additional’ information that may challenge, for example, their racial or gendered understandings. 108
The NGO guidance is, therefore, best understood as an important ‘generative document’,109 which influences how other documents are constructed and conveys the conceptual boundaries within which Guardians and notable others (e.g. trust boards, the NGO/NHS England and the government) analyse and comprehend FTSU data in the NHS. However, although it is important to consider the NGO guidance as more than a passive resource, it does not completely determine the work of all FTSUGs. Words may be conveyed by text, but meaning, interpretation and decisions are ultimately undertaken by human actors. 109
Decisions taken by most FTSUGs to communicate remotely by e-mail and telephone conversations, rather than in person, are inextricably linked to resourcing decisions at a trust level, especially the allocations of protected time and working space for the role. However, Guardians describe how remote modes of communication severely constrain interactions with those speaking up, where topics that are perceived as sensitive or emotional are avoided. Although Guardians’ intentions are often well intended, constrained interactions create blind spots given that complex issues are unexamined, reduced or (re)constructed into a manageable set of concerns, which nevertheless still meet the minimum expectations of the NGO quarterly speak-up reports.
In terms of race and ethnicity, the active avoidance of difficult conversations is reminiscent of some ideas aligned with the concept of white fragility,108 which has attracted interest recently within the NHS. 110,111 Importantly in this case, being white is conceptualised as a ‘constellation of processes and practices rather than as a discrete entity (i.e. skin color [sic] alone)’. 108 White fragility is a state in which minimum amounts of racial stress become intolerable and trigger a range of defensive moves, including fear, silence and avoiding/leaving the stress-inducing situation. These behaviours, in turn, ‘function to reinstate white racial equilibrium’. 108 Although not without their critics, DiAngelo108 concludes that the white insistence for racial comfort ensures that structural inequalities that may be caused by historical racism are not tackled.
The NGO’s decision to make it optional, and not compulsory, to collect ethnicity data and include such data in quarterly reports inadvertently signalled that these data are less important than other data that must be reported. This was an unintentional yet significant driver of why many trusts and FTSUGs, who are often time pressed, do not engage authentically with data and wider issues relating to race and ethnicity. This guaranteed that any misinformation within trusts about speaking up within minority communities continued to circulate unabated. Importantly, white fragility is not always manifested in overt ways; silence, inaction and withdrawal are also potential indicators of fragility. Questions of who speaks, who does not speak, when and for how long and with what emotional valence ‘are all keys to understanding the relational patterns that hold oppression in place’. 108 Guardians seemed to be unprepared for dealing with difficult conversations and the issues arising from them, which in the context of remote communications and time constraints meant that they frequently opted to not engage with such issues.
Monitoring detriment
Numerous government inquiries, reports and research findings from the UK and elsewhere have described the costs borne by those speaking up in health care. The FTSU review12 gathered ‘harrowing’ testimony from workers who had experienced reprisals, resulting in deterioration of their emotional and physical well-being, detriment to their professional standing and career progression, and financial hardship. Given these serious and long-standing concerns, it is unsurprising that the NGO guidance on counting cases instructs Guardians to record the number of cases where ‘an individual feels they have suffered detriment as a result of speaking-up’16 and where a case reveals elements of detriment these should be recorded ‘even if the individual bringing the case does not identify detriment’ (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16 The same document describes detriment as ‘any treatment which is disadvantageous and/or demeaning and may include being ostracised, given unfavourable shifts, being overlooked for promotion, moved from a team, etc. (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16
The NGO’s 2019 annual report19 described detriment occurring in 5% of the 12,244 cases handled by FTSUGs; however, as discussed in the previous section, the Guardians whom we interviewed often did not receive feedback from those speaking up. Furthermore, according to recent data published by the NGO, only 45% of Guardians (n = 592) agree with the statement that ‘people in my organisation do not suffer detriment as a result of speaking-up’ (© National Guardian’s Office, 2020. Contains public sector information licensed under the Open Government Licence v3.0). 18 In response to our question ‘Do workers suffer detriment as a result of speaking up?’, 68% (n = 59) of Guardians stated yes, with 32% (n = 28) replying no.
There is a notable discrepancy, therefore, between the numbers of Guardians agreeing that detriment occurs within their organisation (68% in our interviews, 55% in the NGO survey) and the number of actual cases where detriment was identified via feedback (5% in the 2019 NGO annual report). The following sections offer further insights into how Guardians count and respond to incidents of detriment and provide a window into workers’ distressing experiences of dealing with colleagues’ reprisals within the workplace.
‘I have had zero response to this’
Some of the Guardians who were interviewed clearly stated that they closely monitored whether or not those speaking up had experienced detriment and, as a result of doing so, were confident that detriment had not occurred:
Our culture would very much support people if they suffered detriment. If detriment did ever happen, which it has not, it would be immediately escalated to board level. A non-executive for speaking up takes a direct interest in all cases so that is the level at which the trust is involved, which I find very supportive and a clear demonstration of commitment.
r84
Not yet, up until last month where a colleague said they were unsure of whether staff thought slightly differently of them since they spoke up.
r46
The final data extract touches on the interplay of perception and subjectivity, which play an important role in shaping individuals’ experiences of speaking up and their deliberations over whether or not detriment has been experienced. This question of perception will be returned to in a later subsection (see ‘In the eyes of the beholder’: perception, subjectivity and detriment). The strategy employed by many Guardians and trusts more generally is to communicate a commitment to protect workers from detriment and that retribution against those speaking up will not be tolerated. However, as the following section demonstrates, this does little to change the perception of many that speaking up is a risky undertaking.
‘Lots of people are scared’
Given the past victimisation of NHS workers speaking up, it was unsurprising that many Guardians described colleagues’ fear of retribution as a real and significant barrier to speaking up:
Fear is definitely there for sure. The fear is that people will suffer because some staff have suffered negative experiences in the past when raising concerns.
r01
Some Guardians actively addressed workers’ fear of retribution, again demonstrating how collecting and analysing data led to actions that resulted in meaningful change for workers:
To try and increase confidence I target areas where data tells me few people have raised concerns. I inform them that I provide confidential feedback sessions for people who speak-up and reinforce that they will not experience detriment. That’s worked well and resulted in change without anyone feeling too vulnerable. Feedback from staff has been very good, one said it had been life changing.
r26
However, many Guardians indicated that workers suffered detriment as a direct result of speaking up; the following sections provide insights into several shocking and unpleasant episodes.
‘It clearly was a punishment for speaking up’
Raising concerns to line managers (or to a lead clinician or tutor) is the initial course of action recommended within the Freedom to Speak Up: Raising Concerns (Whistleblowing) Policy for the NHS. 14 If this is not possible, or does not resolve the concern, workers are then recommended to contact FTSUGs. However, several Guardians described detriment occurring to workers who followed the recommended course of action of first speaking up to management about their concerns:
Someone came to me after they had spoken up to their line manager. It was a ward manager critical of the lack of consultant cover and serious patient safety concerns. However, senior management decided to move them into a different role. I and the trade union got involved and we prepared to pursue a grievance. However, management offered a reinstatement and an apology but this has taken time to implement. The ward staff were so demoralised and angry that some of them left as they really valued the ward manager. So, it is not possible to reinstate to the original position because it has completely changed. Who would want to go back there?
r85
Yes, people do suffer negative consequences but this occurs after they speak up elsewhere, usually to the manager. People have been passed over for promotions, turned down for leave, bullying behaviours worsened since they have spoken up.
r60
The following extracts show that reprisals occur (and recur) even when Guardians are involved at the outset of a concern:
Recently someone spoke to me about the behaviour of a team member. They’d not raised it to their manager, so I went to the director and conversations were had. But the person who raised concerns left her e-mail open and someone forwarded correspondence she had with me, printed it out and then gave the correspondence to the person the concern was about, leading to a nasty confrontation. This is currently under formal investigation.
r35
The very first person who spoke up to me suffered negative consequences. She resigned and went to employment tribunal but then dropped it at the last minute. Someone else I am supporting has also had an awful experience after speaking up, it’s just been a real battle. She was well supported by her clinical director and me but her peers, the other doctors and nursing staff, made her working life very difficult. This individual has done nothing but do the right thing. It is wrong and harmful but she has got a label now that she will grass.
r91
Although speaking up in the NHS, via a Guardian or otherwise, continues to be risky and harmful to the careers and well-being of some, it is clear that Guardians are a vital source of support and remedy when detriment occurs:
I had a case where time off in-lieu was imposed counter to the agreed policy. I had supported this person’s concern and it clearly was a punishment for speaking up. So I told the manager that the behaviour bordered on victimisation and asked her to re-instate the time off in-lieu. But it wasn’t the manager it was the deputy who did that, and the manager agreed with me, so it was easy to resolve that.
r22
A concern was raised about someone senior in the organisation who somehow found out who had spoken up. The person speaking up was then ostracised within the department and found it very difficult to continue. But the director of workforce and I managed to secure her a post in another part of the organisation. But people frequently leave saying ‘I can’t stand this any more’ and I often get told that ‘if I did not have you to come to, I would have just left’.
r50
Much of the literature on inadequate or inappropriate organisational responses to speaking up focuses on how deficient organisational learning (concepts such as ‘organisational disregard’, including the ‘deaf effect’ and ‘organisational blindness’2) has led to recurring patient safety failures. Existing literature also suggests that workers’ perceptions of organisational tardiness, or complete lack of response to their concerns, is a key barrier to future workplace speaking up. 112 Interestingly, the final extract above and the following extract demonstrate a seldom explored issue in health care, namely that a lack of managerial or organisational response to concerns can also be perceived by workers as a detrimental act that prompts their exit from the organisation:
No one has come to me saying they’ve suffered detriment directly as a result of speaking up. But I see a type of detriment when people come to me who are at the end of the line, stressed and about to resign because they have already spoken up and nothing happens.
r20
These extracts and others clearly demonstrate the formidable task facing FTSUGs, whose remit includes building a psychologically safe culture of openness in the NHS. FTSUGs describe protecting workers from the detrimental consequences of speaking up as a ‘real battle’ with line managers, senior employees and team colleagues who seek to expose and ‘punish’ those speaking up. Unfounded suspicions and negative perceptions of FTSUGs’ trustworthiness abound and are difficult to overturn, as demonstrated earlier in the section where national coverage of the detriment experienced by two junior doctors undermined the Guardian’s efforts to engage with this workforce group. However, FTSUGs also describe successfully collaborating with cognate colleagues in the trade unions, as well as directors and managers who seek to protect those speaking up from unwarranted harm.
‘In the eyes of the beholder’: perception, subjectivity and detriment
The NGO acknowledges that determining whether or not detriment has occurred can be a subjective process that is open to competing perspectives, recommending that Guardians record details of detriment ‘even if the individual bringing the case does not identify detriment’ (© National Guardian’s Office, 2021. Contains public sector information licensed under the Open Government Licence v3.0). 16 The following extract demonstrates the complexities of determining whether or not individual’s claims of detriment were reasonable:
Detriment is difficult because I guess this is in the eyes of the beholder. I know of two people who left after speaking up but their reasons for leaving were also as a result of additional things happening outside of work. They decided to leave rather than work through the resolution. I don’t think they left solely because of the detriment. It is and can be a stressful time and these people did not have the energy to commit to the issue. In their home-life balance, their home took priority. I don’t think there was a detriment although I don’t know that for definite as I didn’t receive feedback.
r80
The extract above yields a couple of useful insights. First, the experiences outlined are analogous to those recounted in earlier extracts, in which the process of speaking up is erosive for the individual, resulting in concerns being abandoned or withdrawn because those speaking up were frequently devoid of ‘the energy to commit’. Second, our earlier identified limitations concerning the lack of feedback are supported further because the Guardian is clearly uncertain whether or not detriment occurred. The following extracts provide further evidence of the sometimes-contested nature of detriment:
Yes people have said they have experienced detriment. That’s their perception and who would I be to challenge that. We had someone who had spoken up having their holiday cancelled. I went to the manager to get clarification. They explained that the person didn’t request their holiday until the very last minute and they couldn’t sign off as the ward needed covering. I concluded that this was the manager doing their job as opposed to the person suffering detriment.
r48
A member of staff felt they suffered detriment because they were moved after speaking up. I looked into it but they had to be moved temporarily because they mentioned during the case having an issue which stopped them responding to patients properly. They were not safe to care for patients but now it’s been addressed they are due back on the ward. But they still think they were moved because they spoke up.
r71
Although changing someone’s leave or working location can be an act of retaliation within the NHS, the above actions, once fully investigated, were deemed by FTSUGs to be reasonable steps in ensuring patient safety.
Chapter summary and conclusions
This chapter has provided detailed insights into the implementation, deployment and work of FTSUGs, which are discussed via the theoretical ‘lenses’ outlined in Chapter 2. In so doing, barriers to, facilitators of and unintended consequences relating to the implementation of FTSUGs have also been identified and analysed.
The 87 Guardians who were interviewed collectively portrayed wide variability in how the role had been implemented, resourced and deployed by organisations. The role title ‘Freedom to Speak Up Guardian’ is, therefore, best considered as an umbrella term, covering the multiple versions of the role that exist simultaneously across England and within the regions. Any comparisons of Guardians’ effectiveness and/or of the FTSU performance of a trust are likely to be possible or meaningful only when this variability is properly accounted for and factored alongside the numerous other variables that affect speaking up.
In NPT terms, a lack of shared coherence or sensemaking within trusts of the current demand for speaking up, and the aims, objectives and expected benefits of a FTSUG, explained many of the suboptimal implementation decisions made. The experiences of the FTSUGs who were interviewed suggest that most trusts underestimated both the resources required by FTSUGs and (relatedly) the unmet need for speaking up within their workforce. The roots of such misaligned coherence, in part, lie in the absence of detailed specification issued to trusts about the appointment, responsibilities and accountabilities of the role’s introduction to the NHS. However, it is also striking that, given the freedom to choose how to implement the FTSUG role, most trusts opted to invest minimal resources into an initiative that was described at its commencement as potentially making a ‘huge contribution’12 to the NHS. A potentially notable backdrop of significance, not directly addressed in this study, was the economic pressures within NHS England when the FTSUG role was first introduced.
Pre-implementation and early implementation decisions were consequential for the way that the FTSUG role was realised in practice. The lens of NPT brought into focus the problematic issues of operationalising routine and everyday aspects of the FTSUG role and how they often overlapped with early decisions about resource allocation. For example, delayed or limited responses by FTSUGs to cases, a lack of awareness-raising or culture-improving activities and/or Guardians’ being restricted to telephone or e-mail interactions were common where resources, especially time, were limited or non-existent. Such problems also negatively affected another area of implementation, identified within NPT as reflexive monitoring, or the appraisal work that is undertaken to understand how a new set of practices are embedded within an organisation and the effects of these practices on others. In this case, the lack of resources had an impact on data gathering and the limited analysis of data, and/or in generating meaningful organisational learning. The literature review in Chapter 3 found that workers became disillusioned when organisational leaders failed to deliver on their promises to listen and respond to concerns, while other studies demonstrated that delayed or ineffective responses to concerns deter workers from speaking up in the future. 112 In view of the underlying mistrust and scepticism experienced by some FTSUGs, these issues may result in damaging delays to or reversal of FTSU culture change and a situation in which insufficient allocation of resources is misinterpreted as a problematic culture of speaking up within the workforce. These points are further developed, especially from a NPT perspective, in Chapters 5 and 6. Improvements in the response rates and/or quality of feedback to FTSUGs from those speaking up is essential to enable a full understanding of the realities of speaking up within their organisations.
The FTSUGs were faced with limited resources, seemingly unexpected demand and a caseload consisting of a large number of concerns about bullying and harassment, which led them to resort to a variety of compensatory and discretionary strategies in an attempt to best manage their workload. For example, we identified a number of workarounds deployed by FTSUGs that proved temporarily beneficial in meeting the role’s demands in most cases, but were unsustainable in the longer term. Guardians also reported having to prioritise certain aspects of the role, describing a reactive mode of working (i.e. reacting to concerns as they are raised and deadlines for compiling data returns and reports) at the expense of proactive working (culture building and triangulating data were often aspects of the work that were left fully or partially undone). Unsurprisingly, the question of the role’s sustainability was raised by many FTSUGs, especially in the light of the role’s potential to impair the FTSUGs’ well-being.
The implementation process also shows signs of being ‘historically ignorant’. For example, implementation decisions made within trusts and guidance/recommendations for practice produced at a national level demonstrate little evidence of learning from past events, which clearly showed that speaking up in the NHS could result in personal and professional detriment, especially so for those from minority communities.
Chapter 5 Case study results: understanding the implementation of Freedom to Speak Up Guardians in practice and national stakeholder interviews
In this work package, we took a closer look at the implementation of the FTSUG role in practice in six case study sites. The following research questions, aims and objectives are primarily addressed.
Research questions
How is the work of FTSUGs defined and negotiated in relation to the work of others who also deal with employee concerns and patient safety at local and national levels?
Research aims
The research aim was to generate evidence of the extent to which the FTSUG role has been ‘normalised’ in organisations.
Research objectives
To assess how the work of FTSUGs is organised and operationalised alongside other relevant local and national roles with responsibilities for managing concerns.
Case study sites and methods
The six case sites were four acute trusts and two mental health trusts (Table 9), which were purposefully sampled and the names anonymised and assigned pseudonyms (US state capitals). Further details of each case site are provided prior to the individual case site analysis.
| Characteristic | Albany | Olympia | Montgomery | Columbus | Providence | Concord |
|---|---|---|---|---|---|---|
| Size and location |
|
|
|
|
|
|
| Type |
|
|
|
|
|
|
| CQC (overall and well-led rating) |
|
|
|
|
|
|
| Type of FTSUG |
|
|
|
|
|
|
A full account of our case study methods is provided in Chapter 2, but, to summarise, we collected non-participant observational data and organisational documents relevant to FTSU activities and meetings. In addition, 109 semistructured interviews were undertaken with a range of organisational stakeholders key to the implementation of the FTSUG role, including Guardians, executives and non-executives, directors and managers. We also interviewed workers who had or had not spoken up to the Guardian (see Appendix 4 for all case study interview schedules).
These rich data were subjected to within and cross-case thematic analysis, informed by Damschroder’s implementation framework26 and the NPT model24 (see Chapter 2), focusing on the influence of organisational characteristics and key stakeholders on the implementation of FTSU and the FTSUG role within trusts. The distinctive and dynamic nature of inter-relationships within each case site and their unique effects on implementation decision-making reinforce the findings discussed in Chapter 4, which concluded that the FTSUG role cannot be conceived of nationally as a single entity, creating challenges when considering like-for-like comparison.
The following section describes how the FTSUG role was shaped by historical events within each trust, also providing an introductory understanding of context and setting at the pre-implementation phase, before we present a fuller analysis of the role’s early and ongoing implementation at each case site.
Organisational legacies that shaped the pre-implementation phase
Developing an understanding of how prior events and circumstances shape current organisational contexts and events is important when evaluating the implementation of complex interventions. 33 The idea of the ‘critical juncture’ (and synonyms, such as ‘turning point’) and the underpinning logic of historical causation113,114 are particularly relevant here. Historical events were invoked as ‘touchstones’ during interviews, used to frame and determine the relative value of FTSU generally and the introduction of the Guardian role specifically. For example, the narratives of key organisational stakeholders (e.g. a FTSU executive and NED leads, a CEO and board members) in each of the case sites identified past moments of far-reaching significance that informed the course of FTSUG implementation. Seen through this lens, the implementation of the FTSUG role unfolds as contingent on a temporally bounded sequence of events and interactions. 115
It is important to note that, despite our reference to causation and contingency, our position is that prior events do not solely or fully shape the direction of FTSUG implementation. Nonetheless, historical events clearly informed the ongoing sensemaking25 work within trusts, often underpinning collective understanding and coherence about the purpose and potential value of the FTSUG role. For example, stakeholders at Albany and Olympia recounted challenging events, which took place approximately a decade beforehand, that shaped formal and informal organisational narratives and strategies within which FTSU was implemented.
In Albany, the significant historical event was an internal report into a serious patient safety failure. In turn, this led to a concerted and successful organisational strategy founded on principles of continuous improvement, which the Guardian was described by the CEO as being ‘immersed’ within. Olympia’s critical juncture, according to the trust’s CEO, was the time when the trust was ranked near the bottom of the NHS England staff engagement table. Since then, organisational leaders have invested significant resource in communicating with staff and identifying shared organisational values to inform staff engagement and trust strategies. A senior leader described the Guardian as ‘embodying’ the principles of this engagement approach. Both trusts, therefore, reinforced a narrative arc of ‘lessons learned’ following suboptimal performance, framing the implementation of FTSU as embedded within previous episodes of suboptimal performance to the extent of appointing FTSUGs who were clearly aligned with ongoing changes.
Concord’s critical juncture was also prompted by feedback that reported it was failing on several aspects of patient and staff outcomes. However, in this instance the feedback was a publicly reported judgement of the organisation’s failure in the form of a very critical CQC inspection rating. Concord’s recent organisational history was, consequently, best understood as occurring over two epochs, namely the time before and the time after the CQC inspection report. Prior to the report’s publication, rudimentary preparations to implement the FTSUG role were under way, although Concord was the least prepared of the six case sites, having achieved little by way of a collective or coherent vision for how the role fitted into the trust. The CQC report resulted in workers’ morale plummeting, acute escalation of a pre-existing ‘atmosphere of blame’ (as described by the FTSU NED) and wide-ranging structural and personnel changes. Most of the key stakeholders involved in early discussions about implementing FTSU soon left the trust, with only one being in post when we undertook the case study (although their departure was also imminent). As the case site analysis demonstrates, plans to develop and embed the FTSUG role into the trust’s working practices were disrupted, often despite the Guardian’s best attempts.
Montgomery and Columbus’s key historical frame of reference was their legacy of successful innovation and performance, including a recent history of winning regional and national awards for clinical improvements and leadership. Continuing this tradition of leading and improving through innovation was a significant contributory factor to decisions made during the pre-implementation and early implementation phases of FTSUG. For example, both trusts had drawn lessons from the 2013 Francis Report12 and launched ‘in-house’ speak-up initiatives prior to the 2015 FTSU Review3 recommendations and the subsequent obligation to appoint Guardians. The initiative in Columbus pre-dated the Francis Review by at least 2 years, whereas Montgomery’s was launched approximately 6 months prior to the full details of the FTSUG role being published. A board member at Columbus pointed out (twice) during interview that they were ‘probably one of the first’ organisations nationally to appoint a Guardian-like figure. The FTSUG roles in both trusts were merged into the pre-existing speak-up initiatives and their constituent structures and processes.
Key stakeholders in Providence explained how the trust’s understanding of speaking up had been shaped by learning from the Mid Staffordshire Inquiry. 3 A pattern emerged in which new speaking-up policies and practices were launched in the wake of the initial Francis Report and then subsequently adapted following the Francis Review. More recently, a modernisation of the trust’s structures, personnel and operational philosophy heralded a new era in which changes were driven from within, rather than in response to external prompts. For example, the rebranding and re-envisaging of HR as the ‘Directorate of People’ and the appointment of a director whose background was in OD, not in HR, led to significant changes to how the FTSUG role was understood and deployed.
The in-depth cross-case analysis and findings will be fully explored in the next chapter. However, on the whole, all trusts, apart from Concord, demonstrated a progressive trajectory of change, in which speaking-up strategy and interventions (including those pre-dating the FTSUG role) were developed collaboratively and agreed on by senior stakeholders, and subsequent effects measured and reviewed. Concord was initially on a similar pathway, with progression stalling and regressing following the CQC report. Key internal stakeholders at the pre-implementation and early implementation stages were similar across trusts, with directors of HR/people, FTSU NEDs and executives, staff-side representatives, chairpersons and chief executives all featuring prominently in decision-making. We also saw complex interaction between events originating in the outer setting (e.g. regulatory or policy imperatives) and decisions in the inner setting of trusts. 26 For example, in Albany’s case, an outstanding CQC inspection rating motivated leaders towards maintaining and furthering a culture of patient safety and improvement, efforts that the FTSUG implementation was aligned with. By contrast, Concord’s CQC inspection ratings led to immense internal disruption, fuelling a pre-existing culture of blame and resulting in FTSUG implementation paralysis as senior leaders and FTSUG stakeholders vacated the organisation and their replacements took time to orientate to troubled surroundings.
Case study: Albany (Box 3)
Type of trust: Mental Health Foundation Trust providing a wide range of inpatient and community services.
Size and location of trust: medium; inner large city. Approximately 5000 staff based at over 100 locations.
CQC overall and well-led rating: outstanding/outstanding.
Speak Up Index and number of concerns Q3 2018/19 to Q2 2019/2020: Speak Up Index 2019 and 2020 were well above the national average – 101 concerns reported to NGO over 12 months (data from only three-quarters reported).
FTSUG pseudonym and details of FTSUG role and type of appointment: Delia; full-time stand-alone FTSUG; band 8b. Internal candidate, competitively appointed from a senior clinical role and project management.
Line manager: chief nurse/executive lead for FTSU.
Key implementation stakeholders: chief executive, FTSU NED, chief nurse and staff-side chairperson.
Guiding implementation principles: FTSU embedded within a continuous improvement organisational philosophy and maintaining recent track record of high performance. Learning from past while reflecting on the present, genuine attempts to be ‘problem-sensing’ at senior/board level. Guardian appointed as someone who aligns with organisational commitment to improvement.
Albany had implemented formal mechanisms for speaking up prior to the introduction of the FTSUG role, including access to trade union officials, a trust-confidential ‘concerns mailbox’ and a ‘whistleblowing’ policy, although these were used infrequently by staff. A FTSUG was not immediately deployed when required; instead a decision was taken to observe how other organisations recruited and deployed FTSUGs before finalising the role’s implementation. The CEO considered the FTSUG role to be a ‘huge opportunity to provide as much intelligence as possible’, enabling senior leaders ‘to look for where there are issues or problems’ (CEO, Albany). Such a problem-sensing11 approach ensured that a trust that was rated ‘outstanding’ remained alert to failure; this was a rating that was described as a ‘burden’ by the CEO, who believed it could lead to organisational complacency and a loss of focus on key issues.
Kate (NED) was a key influencer during the pre-implementation phase, having attended an information day at the then newly created NGO and gained insights into early implementation elsewhere. Kate then wrote a board report suggesting ideas for the implementation of the FTSUG role, which she explained ‘the execs then made it happen’. Kate was subsequently appointed as the FTSU NED and remained a key strategic actor in FTSUG recruitment and deployment decisions. This included consulting with Albany’s workforce committee on how the role should work alongside trade unions and HR. Besides determining the role’s boundaries, pre-implementation decisions included providing protected time for the role and ensuring that the role holder had autonomy and confidence to ‘manage upwards . . . go to very senior people and say difficult things’ (CEO).
The Guardian (Delia), an existing employee at Albany with a clinical and project management background, was appointed via a recruitment process open to internal and external candidates. She was initially deployed as an adjunct FTSUG for 2.5 days per week, with an equal amount of time allocated to a project management role. Delia was described by the CEO as possessing the desired attributes and being ‘immersed in improvement methodology’. Appointing an individual who had previously demonstrated confidence and competence in the language and techniques of improvement seemed to be important in ensuring that FTSU was seamlessly embedded into Albany’s working practices and organisational norms.
To summarise, there were limited pre-Francis speak-up mechanisms and processes in Albany. The trust was relatively late in implementing the FTSUG role, but this delay was strategically shrewd rather than an indicator of resistance or apathy towards FTSU. Being a late adopter allowed Albany to review implementation progress in other trusts, which, alongside consultations with key individuals and committees, informed the pre-implementation decision-making process that was led by a NED and closely supported by the executive team.
The following sections focus on the role’s ongoing implementation in relation to existing roles, structures and processes. It becomes clear that shared sense-making about the role’s remit, value and purpose identified at pre-implementation and early implementation stages were continually subjected to scrutiny and reflection, which, in turn, fed into adaptations made to the Guardian role. This interweaving of reflexivity, sense-making and ongoing implementation decision-making is well captured by the FTSU executive lead, who stated that:
We are continually reviewing . . . so has this made a difference? If it hadn’t, is it because we haven’t implemented it in the right way? And if it has, great but then do we need more, the same or something different?
FTSU executive lead
‘The real implementation’
Although senior leaders had purposefully forged a shared understanding of the role, it soon became clear following Delia’s appointment that pre-implementation efforts had not adequately prepared the trust for the realities of undertaking the role. A stakeholder involved in pre-implementation preparations stated that ‘in retrospect we’d not given it enough thought in terms of the real implementation and what was needed to make the role an effective entity’.
Some of the issues experienced during implementation at Albany were commonplace in many other trusts. For example, as discussed earlier (see Chapter 4), the FTSUG had to respond to significantly more bullying and harassment concerns than patient safety concerns, with stakeholders sharing the commonly held view that ‘bullying isn’t really what the role came about for’ (board member). These concerns were a ‘bit of a surprise’ (staff-side chairperson) to those involved in pre-implementation planning and sense-making, and resulted in practical and jurisdictional difficulties between the FTSUG, trade unions and HR. A point of interest, given Albany’s pre-eminent reputation as an ‘outstanding’ trust built on the ethos of continuous improvement, was that bullying and harassment behaviours and/or staff dissatisfaction often resulted from constant ‘organisational change and relationships. Perhaps getting things done, regardless of how you get things done’ (board member). Given the relationship identified between transgressive behaviours and continuous improvement, the high proportion of bullying and harassment concerns raised with the Guardian continued unabated throughout the case study period.
None of the parties had anticipated or prepared for a Guardian role that dealt mostly with staff-on-staff behavioural transgressions, and the frequent contacts and tensions associated with such cases. The implementation of the FTSUG role disrupted previously accepted working practices, where HR and trade union processes were historically deployed to deal with bullying and harassment concerns. Matters reached a critical point when Delia accompanied those speaking up to meetings with HR and trade unions, at which she seemingly appeared to advocate for those who had spoken up. These actions were considered a breach of boundaries by trade unions, HR and those closely involved in managing and supporting the FTSUG role. An executive explained that ‘when Delia first started, she kind of struggled. We had to say your role is to take a concern to the manager and not get involved like a union rep[resentative] . . . stay independent’. A similar view from another executive stated that ‘it took a bit of working out. She had to be a bit more disciplined about the boundaries of who does what’.
Although Delia may have struggled initially, the extent and intensity of cases related to workers’ behaviours had caught everyone out. The required rebalancing was described by Delia as a process of reflecting and acting on helpful feedback, which prompted a reconsideration of boundaries and resulted in a fuller understanding of the role:
I now realise why I was getting a defensive response from managers. I’ve learnt that I also have to support them and my focus can’t be too much on the staff raising concerns as it’s not one-way traffic. It helped that I met with HR and others to discuss how best to work together to get the right outcome for the person speaking up.
Each party hastily reset their early assumptions about the role and sought a workable solution that maintained trade unions’ and HR’s positioning as the initial points of contact for workers wishing to speak up about bullying concerns. Delia noticeably delineated the remit of the FTSUG role during staff induction events, as well as recommending trade union membership. Delia clearly communicated that Guardians are there for guidance and do not function as trade unions or HR:
I would recommend you all to join a union. They can help you to understand processes and support you. I will guide staff through processes, but I won’t sit in meetings or represent staff, which is why I always advocate staff joining a union. If it’s about interpersonal dynamics or bullying then I will signpost you to HR.
Delia
The staff-side chairperson reported that this approach had resulted in increased referrals to trade unions.
Resourcing Freedom to Speak Up and the challenges of continuous improvement
As was the case for many other FTSUGs (see Chapter 4), the time initially allocated for Delia to undertake the role was insufficient to undertake all aspects of the role:
Both roles were demanding full-time hours. I was often working until 2 a.m. and feeling pressure in the new role. I was just firefighting and couldn’t really think beyond reacting to cases.
Delia
Delia further explained how the stress of undertaking the FTSUG role ‘wasn’t good for me in terms of my health and well-being’. In response to these challenges, a variety of useful support mechanisms were introduced that helped Delia to talk about her experiences, such as the allocation of a coach and regular supervision/debriefing. In addition, 12 months following appointment, Delia’s hours were increased to full time:
I couldn’t have continued without additional time. I listed what I was doing and how much time it took. My business case for increased hours was then approved.
Although Albany’s leaders had underestimated the time required to undertake the role, they rectified the situation before Delia’s workload became critical (albeit not long before). Delia described how the increased hours provided additional ‘headspace’ to manage concerns and to plan a longer-term FTSU strategy.
Additional time was not, however, a panacea for all of the issues experienced. First, investing additional time into strategising and raising the profile of the FTSUG role generated further demands on Delia’s time, often in the form of attending and presenting at a wide variety of trust and regional FTSUG meetings. Echoing the earlier discussion of the impact of change management on Delia’s workload, there were further indications that Albany’s focus on improvement and expansion contributed to the challenges experienced. For example, Albany had recently taken over the running of less-successful services elsewhere in the region, stretching the geographical and operational boundaries that Delia had to cover. A board member described how ‘as we grew, we started to notice there were spikes in speaking-up activity at some of our new services where there was transformation happening’.
As a result, the benefits of the additional hours and ‘headspace’ could be lost to one of the many diary or travel commitments. Responding to concerns would often be squeezed into tight gaps between meetings or during the numerous journeys on foot, car or public transport across a densely populated inner city. FTSU users commented that Delia was very conscientious in her role, but that at times she appeared ‘far removed from the process, took time to respond’ (SU02); another reflected that ‘I got a sense she was very split in terms of role demands and the trust’s really huge geographical spread’ (SU05). In addition, although aligning FTSU with a quality improvement (QI) approach was an important strategic intention, this was later deemed to be operationally difficult by Delia, who, even following an increase in hours, stated that ‘QI is always a good way of making improvements but at the moment I don’t know whether I have the capacity, but it’s a real desire’.
Frustrated ambitions: creating a sustainable long-term model for speaking up
As Albany expanded and FTSU became established, Delia developed a strategy to future-proof FTSU by introducing a network of six ambassadors who were tasked with raising awareness of speaking up within their local settings and signposting those with concerns to the appropriate processes. As a solitary FTSUG who was spread increasingly thinly, ambassadors potentially offered Delia a degree of respite and a sustainable future model for FTSUG. However, despite Delia investing much effort and hope into the ambassador role, change proved frustratingly difficult to deliver. Although senior stakeholders were in general agreement with an awareness-raising role of ambassadors, their solution to meet growing demand was to ensure that managers were functioning as the first contact point for workers wishing to speak up:
We need to actively promote speaking up with managers, because Delia could never do it by herself. Even if we gave her all the ambassadors she would still struggle. Instead, we need staff to see managers saying ‘Please talk to me. And if you can’t talk to me, we have got freedom to speak up’.
Executive
Delia and senior stakeholders, therefore, agreed that a future sustainable model of FTSU required increased involvement and support of others, but disagreed on who should provide this support. Senior stakeholders’ preference for the increased involvement of managers as a first point of contact was consistent with NHS policy recommendations for normalising speaking up as an activity primarily dealt with, as far as reasonably possible, by those in close proximity to the issue. 14 Resourcing ambassadors and operational/boundary uncertainties were also proving difficult:
We are grappling with releasing time, backfill but also how ambassadors actually work. It is unresolved at the moment.
Executive
Delia was reluctant to rely more on managers, a position that was deeply rooted in her fundamental understanding of speaking up as often requiring a more complex and separate approach to management processes; this was an activity which, to some extent, required ‘guarding’ from management. For example, she described the reactions of ‘middle managers’ to FTSU as ‘mixed’ and focused on the needs of managers, rather than on the person speaking up. She recounted many experiences in which managers did not engage with or felt threatened by concerns, or overly focused on the individual character or the personal history of those speaking up. Managers, therefore, frequently adopted a different approach and logic to workers’ concerns that was incompatible with FTSU. The situation had reached a difficult impasse during our fieldwork, with Delia visibly upset and in a reflective mood during the final week of fieldwork:
Over time I’ve just become so frustrated with it, I’ve lost a bit of motivation as it feels like I’ve been on the case of ambassadors forever. It’s not good, because one of my visions is really to develop the role beyond myself. That’s all I wanted to do, but resistance sometimes can knock you down. I’ll be honest, I feel tired with chasing and not getting the response, I can’t give up because that’s just what the job is, isn’t it?
Summary
Despite pre-implementation planning, initial difficulties were experienced in embedding the FTSUG role into existing processes and ways of working, which led senior FTSU stakeholders (NED, executive lead and CEO) to instruct the Guardian to alter her working practices. Given the unprecedented nature of the role, this was unsurprising, and there was much about the implementation that was praiseworthy. Albany’s leadership team had clearly adopted a mature, reflexive and shared sense of responsibility for the role’s implementation. This included successfully amending some of their shared initial assumptions about the workability of the role and initial resource decisions (e.g. doubling Delia’s working hours and recruiting a part-time administrative assistant for FTSU). Delia was well connected to and supported by the leadership team. In addition, the relationship with senior leaders was respectful and ‘psychologically safe’ enough for Delia to be described by Erica (CEO) as having ‘pushed back quite confidently’ on a number of occasions.
Within 18 months of implementation, the role was, therefore, relatively well set. Delia was ambitious for the role and her own future, being increasingly invited to high-profile events and meetings within the trust and regionally. There was a desire to plan ahead, based on the shared recognition that even a well-resourced Guardian (Delia was one of the best resourced of the 87 FTSUGs involved in the study) required further support to grow and sustain FTSU in an ever-expanding organisation. However, service expansion, the demands of continuous improvement and the conduct of change management were at the core of many concerns. The exact details of the future configuration of the FTSU Guardian and ambassadors, and the role of managers, were proving difficult and contentious within Albany and was the only area, albeit significant, where there were palpable difficulties with the ongoing implementation of the role. Table 10 provides a brief summary overview of the main findings from Albany, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | Overarching organisational philosophy informed senior leaders and FTSUG collaborative working and shared understanding of the role. Emergence of individual differences in understanding of future and sustainable model for FTSU |
| Collective action: operational work to enact the role | Sense-making and resource investment resulted in FTSUG integration into operational strategies and decision-making. Early boundary tensions resolved by robust but supportive feedback. Questions remain about future operational configuration |
| Cognitive participation: relational work to build and sustain new practices | Initial sense-making and early reorganisation of FTSUG boundaries ensured ongoing co-operation and commitment of stakeholders to FTSUG. Middle managers identified as source of ongoing resistance |
| Reflexive monitoring: appraisal work to assess and understand new practices | Frequent appraisal of data and experiences providing rationale for, and modifications to, FTSUG’s resources, practice and effectiveness |
Case study: Olympia (Box 4)
Type of trust: mental health and learning disabilities foundation trust providing a wide range of inpatient and community services.
Size and location of trust: small; urban and rural locality. Approximately 2300 staff across 39 locations.
CQC overall and well-led rating: good/good.
Speak-up Index and number of concerns Q3 2018/19 to Q2 2019/20: Speak Up Index 2019 and 2020 were well above the national average – 84 concerns reported to NGO over 12 months.
FTSUG pseudonym and details of FTSUG role and type of appointment: Rachel; part-time stand-alone FTSUG; band 8d. Internal closed appointment from a senior corporate role.
Line manager: chief nurse/FTSU executive lead.
Key implementation stakeholders: chief executive, NED, chief nurse and Guardian.
Guiding implementation principles: Guardian in her former senior manager role closely involved in writing the job description. FTSU strategy aligned with ‘staff engagement’ and ‘people management’ initiatives and continuous improvement ethos. Guardian known to, and worked closely with, the board prior to appointment, but also respected as representing staff interests.
There appeared to be no formal mechanisms for speaking up within Olympia that pre-dated the FTSUG role, with a low trade union presence. The CEO articulated that pre-implementation decisions about FTSU and the Guardian role were only ‘one component of a whole range of people management strategies . . . to set the organisation on a path towards continuous improvement’. The path referred to by the CEO could be tracked back ‘to at least 2008 when we were about the third worst rated trust in the country for staff experience. Now we are in the top half a dozen’. Such was the progress being made that the FTSUG role was not initially welcomed:
Because it was imposed on by the outside there is a natural inclination just to sabotage it. We were already doing these things. We didn’t need an externally defined role.
CEO
Several interviewees positioned FTSU as contributing to a larger strategy of staff engagement and continuous improvement; for example, a prominent director in FTSUG implementation described the key function of FTSU as ‘identifying key improvement themes which come through people’s stories’.
Olympia was unique among the case sites in that the FTSUG (Rachel), who at that time was a senior manager, was closely involved in the pre-implementation. Rachel initially alerted trust leaders to the role after attending a workshop, describing how ‘I was ready for a change and thought the role might be of interest to me’. Rachel subsequently wrote the job specification and presented it to the trust executive committee, which triggered the recruitment process overseen by the deputy CEO and a director.
The decision to appoint Rachel, a senior leader who had worked closely with senior stakeholders and was key to establishing the FTSUG role, was not considered risky by the senior leaders interviewed. The view of many was that the process of appointment was openly contested (one other person interviewed for the role) and that Rachel’s outstanding personal characteristics and professional experiences legitimated her appointment:
She had a reputation with front-line staff for being approachable and quite credible . . . we also knew that she wasn’t really afraid of the hierarchy. We thought the best chance of success was her mixture of approachability and passion for helping staff, and also her seniority of experience.
Board member
Rachel’s involvement as a principal figure in pre-implementation decision-making about the FTSUG role is, however, impossible to separate from subsequent recruitment and deployment decisions. For example, the hours and banding allocated for the role accorded fully with Rachel’s previous banding and her time availability. The following sections untangle and track the unfolding implementation of the role in terms of how Rachel’s work was enacted and accomplished.
Being organised and prioritising independence
Olympia’s leaders clearly valued and trusted Rachel’s judgement, skills and experience from her time as a senior manager. Stakeholders shared a sense of faith that Rachel ‘just knows’ how to prepare for and enact the role:
She is absolutely capable of operating at such a senior level, she just knows what she needs to do and how she wants to do it . . . therefore she comes to me rarely.
Deputy CEO and line manager
Decisions made during the early and ongoing implementation were, therefore, predominantly Rachel’s:
I just literally read all the documents, thought about what staff want and really just doing the whole job without very much support or guidance.
Although clearly experienced, capable and committed, there was a sense that Rachel was heavily relied on by leaders to ‘just do the whole job’. With only 2 days per week allocated to the role, Rachel clearly and coherently managed her work, explaining that the ‘primary parts of the role’ were supporting workers who speak up, clearly recording the concern and ensuring that the concern was appropriately responded to by colleagues. This amounted to ‘70% of the role’, with the remaining time allocated to ‘the admin’, including preparing board reports, the NGO quarterly data returns and, when possible, promoting FTSU, especially to new workers and outlying areas of the trust.
Rachel’s experience, tenacity and skills as a former director of HR underpinned how the role was operationalised and understood. One FTSU user, Beatrice, described how Rachel had ‘hit a bit of a brick wall’ after taking the concern directly to a senior manager but nevertheless ‘she was marching forward to get some tangible feedback’ (SU03). The methodical distribution and processing of work within the time available reflected her experience of successfully leading a large department and workload. Similarly, Rachel’s management of concerns was impressive, underpinned by a spreadsheet referred to as ‘the tracker’:
That tracker is really important to me, everything gets updated and closed however long that might take . . . helps me to be tenacious.
Prior experiences also shaped how Rachel understood and managed concerns; here she reflects on how some FTSUGs are sidetracked by the emotions of speaking up:
Having been a senior manager I am always aware that another version of the truth can emerge once you speak to others. This makes me sound a bit cold, but I wonder if some Guardians get a bit too wrapped up in the emotion and all the issues of the person, rather than doing really what their role is, which is getting management to take that on and action it. This wouldn’t be the right job for someone who gets upset too often.
An awareness that concerns were seldom uncomplicated enabled containment and management of emotions and the avoidance of costly (in terms of time and effort) distractions from delivering the role’s requirements. However, although the containment of emotions was somewhat explained in terms of efficiency, it fell short of emotional distancing or ‘coldness’, as our feedback from those who had used Olympia’s FTSUG service allied to our observations of Rachel’s interactions demonstrating a Guardian who was ‘business-like’, effective yet empathic. For example, one worker described Rachel as being ‘really supportive’ (SU01) and related how she had been encouraged to seek support from Rachel, who had ‘stood out at induction . . . I remembered her face and voice. She said if there’s ever a situation, you ring, and I just remember her’.
Observations (fieldnotes from 25 June 2019) also demonstrated Rachel’s skill in recognising and appreciating different perspectives on concerns, especially understanding concerns as embedded within complex operational contexts and relationships. Although other FTSUGs also successfully negotiated similar organisational complexities and balancing acts, they did so as a result of hard-won experiences as a Guardian, rather than, as in Rachel’s case, by drawing on pre-existing experiences.
Another notable difference was that, unlike many other Guardians interviewed, Rachel rarely attended trust strategy meetings or participated in job interview panels, staff networking groups or meetings related to patient safety or adverse events. Fundamentally, the decision to not attend meetings (other than board meetings) was closely related to Rachel’s need for stringent time management. However, senior stakeholders’ views also contributed significantly: they claimed that Rachel not attending meetings would ensure that ‘she is not too overly involved and needs to hold an independent space’ (director) and ‘remains completely independent of structures’ (board member).
The role’s independence was clearly and rightly valued, while circumscribing the role to addressing concerns and ‘concerns admin’ ensured that workers speaking up were well supported. However, the need to manage scarce time and the maintenance of independence narrowed the potential of FTSU in Olympia; few opportunities were taken, for example, to raise awareness of FTSU or to triangulate speaking-up data with other sources of organisational intelligence. The flipside of striving for the role to remain completely independent of organisational structures was that the FTSUG was rather remote and solitary within the organisation.
This manifested itself operationally (discussed further in the next section) and at a personal level because, despite being highly experienced, capable and well respected throughout the organisation, Rachel often reflected on the loneliness of the role (fieldnotes, 12 June 2019). Rachel also described positive aspects of the role, stating ‘I have had more thanks in this job in 2 years than I ever had as a senior manager. I know I’m appreciated by staff’, and there was as awareness that senior colleagues were supportive, although Rachel reflected that seriously challenging senior leaders ‘feels a bit scary and could mean being out of a job within a year’ (fieldnotes, 16 July 2019).
Freedom to Speak Up’s contribution at an organisational level
Although senior leaders and managers valued the Guardian once implemented, there was also a sense that senior stakeholders’ initial reservations affected ongoing implementation. For example, the CEO explained that ‘we were quite ambivalent that it [FTSUG] would add anything’ and the role was largely described as ‘additional to other approaches such as QI and staff engagement’ (director of governance). The extent to which FTSU additionally contributed to organisational improvement efforts was, however, questionable. Rachel explained significant difficulties generating improvement themes from FTSU cases because ‘most things are very personal and don’t necessarily go across teams’.
As previously discussed, Rachel’s engagement at organisation-wide fora was largely restricted to appearances at quarterly board meetings, at which she delivered a FTSUG report. Rachel also explained that the board ‘certainly monitor concerns from a quant[itative] perspective so I am expected every quarter to at least have double figures of speaking up’. Given this, and the importance of boards in the governance of patient safety,28,116 we were interested in a better understanding of the FTSUG report and related interactions at board meetings.
The overall tone of communication during the board meeting was formal and respectful. The FTSU report functioned to provide reassurance, with board members exhibiting low levels of reflection, support or challenge to the report. Unsurprisingly, a common topic within the report was the number of FTSU cases within Olympia and comparisons with previous quarters and national data. Interestingly, despite the board’s expectation of an increased number of concerns, the report showed that the number of concerns had ‘reduced slightly’ in the current quarter; however, earlier in the report, the same number was described as ‘broadly consistent’ with the previous quarter. The report’s conclusion served to reassure potentially alarmed board members that, nonetheless, rates had increased annually and ‘remain at a high level compared to similar NHS trusts’ (Trust Board Report, June 2019).
Reinforcing our earlier point about the limited influence of FTSU on organisational learning, the FTSU report’s ‘Learning and next steps’ section outlined a series of seemingly unconnected single cases of concerns that were themed as being ‘about staff experience’. These cases could alternatively and perhaps more accurately have been categorised in a number of different ways, such as workplace culture or patient safety. Framing these concerns as ‘staff experience’, however, usefully ensured FTSU’s alignment with the CEO’s and other senior stakeholders’ narratives, which positioned FTSU as an ‘additional’ contribution to Olympia’s established staff engagement improvement journey. However, FTSU’s contribution to organisational improvement efforts was not a feature of the board meeting and was rarely discussed, or viewed, throughout the course of our fieldwork.
In addition, of relevance was the decision by board members to discuss FTSU in the ‘public’ board meeting, rather than in the closed private meeting. A director explains further:
The tension we have wrestled with is the importance of Rachel reporting to the board meeting in public. That’s what being open and honest means. But clearly seeing a report in public inevitably carries a different dimension to providing a report in private. When reporting publicly we need to make sure we don’t undermine or worry people. We try to make sure that we are dealing honestly and openly about difficult issues, but not sensationalising or overly sanitising them either.
Director
The tone (respectful) and content (reassuring) of the board report might, therefore, be better understood in terms of senior leaders’ deliberations about the public nature of the proceedings and anxieties of being too critical and possibly threatening Olympia’s recent (and much cherished by executives) progress with staff engagement and organisational reputation. On the basis of the (albeit single) board meeting and report analysed here, the question of balance between sensationalising and sanitising seems to have somewhat tipped in favour of sanitising. In the context of managing a public meeting and image-related pressures, this may well be a prudent course of action; however, a workplace culture that genuinely values the freedom to speak up is surely dependent on creating psychologically safe interactions whether they occur in open or closed settings.
We do not claim that the Guardian and the board inappropriately interpreted or minimised workers’ concerns. However, Rachel’s limited working hours, non-attendance at trust meetings and committees, and the rather sanitised board meetings resulted in infrequent opportunities for robust, yet safe, discussion with senior stakeholders about workers’ concerns and FTSU strategy in its own right, as opposed to being a subsidiary activity of staff engagement.
Summary
Rachel, in her previous senior management role, instigated pre-implementation discussions with senior leaders and executives as a precursor to the introduction of the FTSUG role. Although some senior colleagues described themselves as ambivalent and resentful about the top-down imposition of the role, Rachel was instructed to write the job description for the role that she was subsequently appointed to. The board unanimously agreed that Rachel should be appointed FTSUG owing to her experience and relevant background and ‘know-how’ to do the job.
Rachel, as instructed to do so by the board, embedded the role within existing organisational improvement and staff engagement strategies, and was closely bounded by the 2 days per week that she chose to work. This resulted in relationships with the board remaining healthy and respectful, as well as allowing efficient management of speaking-up cases. However, the nascent FTSU culture was, at times, partially or completely overshadowed by these pre-existing organisational strategies, senior individuals’ doubts and the pursuit of independence that tipped into detachment. In addition, ensuring that the Guardian was sufficiently independent of organisational hierarchies and structures appeared, at times, to isolate FTSU from organisational processes.
Although the implementation of the role met the needs identified of senior stakeholders, there was also a sense that the role’s implementation was underpinned by an approach where ‘function followed form’. That is, role implementation was primarily and closely bounded by what worked for Rachel (i.e. time availability, skill set and capacity) and was informed by senior stakeholders’ ambivalence based on preconceptions about the role’s limitations. There seemed to be little consideration of how the role should be resourced and implemented to address the FTSU needs of workers. The perception of successful implementation of the FTSUG was, therefore, heavily dependent on the role fitting within, rather than disrupting, these initial parameters. Whereas other trusts continuously reflected and questioned their implementation of FTSUGs, leading to a change in approach and/or resources, there was little evidence of such reflective and critical monitoring of progress at Olympia. Trust stakeholders are entitled to be satisfied with implementation and there is much to suggest that FTSU functions well in Olympia, albeit without unleashing the full potential and scope of the role. Table 11 provides a brief summary overview of the main findings from Olympia, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | Role’s collective coherence framed by (1) senior stakeholders’ ambivalence towards ‘top-down’ introduction of FTSU, (2) the requirement that FTSU fitted into organisational staff engagement and improvement strategies and (3) the need to fit role with Guardian’s time availability and skill set. The role was conceived as a mechanism to promote not challenge organisational norms and priorities |
| Collective action: operational work to enact the role | FTSU operationally enacted in an efficient but rather limited way, focusing mainly on managing concerns as they arose. Little operationalisation of the culture change aspect of the role. Operationally, FTSU was secondary to senior leaders’ preferred strategies around staff engagement |
| Cognitive participation: relational work to build and sustain new practices | Relational work undertaken by a skilled and confident FTSUG who drew on long experience of the organisation to navigate the role’s introduction. FTSU embedded well into the organisation generally |
| Reflexive monitoring: appraisal work to assess and understand new practices | Infrequent appraisal of data and experiences, seldom triangulated with other data sources or seen as a genuine safety initiative. The role has progressed unchanged since initial introduction. There is much that goes well, and this seems to satisfy stakeholders. But little consideration of whether or not the full potential of the role is realised |
Case study: Montgomery (Box 5)
Type of trust: integrated foundation trust providing a range of hospital, intermediate and community health-care and social care.
Size and location of trust: medium; urban outskirts of large inner city. Approximately 7000 staff across several sites.
CQC overall and well-led rating: outstanding/outstanding.
Speak Up Index and number of concerns Q3 2018/19 to Q2 2019/20: speak-up index 2019 below national average and 2020 marginally above national average – 22 concerns reported to NGO.
FTSUG pseudonym and details of FTSUG role and type of appointment: Karen; part-time (6 hours per week) adjunct FTSUG alongside a busy substantive clinical role; band 7. Internal appointment, former FTSUG Champion.
Line manager: senior Guardian with responsibility for FTSU across several hospitals in the region.
Key implementation stakeholders: senior Guardian, chief nurse/FTSU executive lead, director of patient safety and director of HR.
Guiding implementation principles: in-house speaking-up initiative launched months prior to national FTSUG roll-out. FTSUG role embedded within in-house initiative and processes largely positioned FTSU as a signposting and communications role owing to confidence in robust existing processes.
In 2015, after a concern was raised about a senior member of staff, the director of patient safety (David) identified potential barriers to and the lack of a meaningful mechanism for workers to speak up, with staff perceiving that when faced with concerns ‘organisational leaders would circle the wagons and look after their own’. David and Isabel (chief nurse and FTSU executive lead) subsequently appointed a senior medical clinician (Catherine) to develop and launch an ‘in-house’ initiative to support staff to speak up. Catherine was selected because she had previously led award-winning changes to clinical services at Montgomery, informed by QI approaches. Isabel explained that appointing Catherine to lead the in-house initiative was also a strategic move ‘to get medical staff engaged and to realise that the concerns of a porter or health-care assistant is as valid as yours. Catherine was outstanding and just flew with it’. The director of HR was also a key influencer at this stage, described by Catherine as a ‘fantastically helpful springboard for ideas’.
These four senior stakeholders collectively agreed that the guiding principle of Montgomery’s in-house speak-up initiative was that all workers, regardless of status, should initially try to resolve their concern by speaking up directly to the person causing the concern. Where that proved ineffective, or not possible, workers were signposted to utilise existing internal mechanisms for raising concerns and reporting (e.g. incident reporting processes or contacting a line manager). If the concern remained unresolved, workers were then signposted to contact Catherine, who would intervene to seek a satisfactory outcome to the concern. This final step was referred to by many as a ‘safety net’, operating when all other avenues had been exhausted or were considered unsuitable. Triggering the safety net signalled, therefore, that one or more response mechanism was ineffective and acted as a cue for Catherine to deploy a QI approach that would ‘beef up process so they are fit for purpose’ (Catherine).
A communications strategy to raise awareness of speaking up was also deployed, including the use of posters, screensavers and an e-bulletin. The ‘in-house’ initiative was launched in early 2016 when the FTSUG role and the NGO were still being formed, although Catherine explained that they realised that the proposed FTSUG role was ‘going to be more or less the same type of thing we were doing’.
As further details about the FTSUG role emerged during 2016, these were progressively merged into the in-house speak-up initiative. The terms FTSU and FTSUG were adopted, and Catherine was appointed the first FTSUG (4 hours per week, a non-competitive appointment mandated by David). However, the logo, colour scheme and design for the in-house initiative were mostly retained on posters, for example, rather than adopting the national FTSU branding. The decision to implement the in-house initiative, rather than delaying in the light of the imminent introduction of the national FTSU initiative, was symbolic of the team’s confidence and indicative of an organisational culture that valued leadership, innovation and distinctiveness. The fact that the in-house branding was retained when FTSU/FTSUG was later mandated across the NHS was a further sign of self-confidence and the desire to retain Montgomery’s distinctiveness.
Montgomery then embarked on a period of substantial and rapid expansion, including taking over trusts in the region that were poorly performing. In January 2018, Catherine assumed additional and demanding responsibilities as a director overseeing FTSU for each of Montgomery’s trusts, prompting Helen’s appointment as the FTSUG for Montgomery. There were no other applicants for the role and Helen was recruited without interview. Prior to becoming the FTSUG, Helen had been assisting Catherine as a voluntary FTSU ‘Champion’, who had been deployed to help raise awareness of, and signpost relevant concerns to, the Guardian. Helen described how she was initially attracted to the Guardian role as it was ‘very much around supporting staff to raise concerns about patient safety’. However, as was commonplace for almost all Guardians, Helen reported that ‘the majority of concerns are bullying and harassment or toxic cultures’.
The role was an adjunct to Helen’s substantive role as a busy, full-time, band 7 clinician. Following a handover period, Helen continued to deliver Montgomery’s pre-existing vision of FTSU, largely based on the in-house signposting initiative. The appointment of a new Guardian was, therefore, mostly a case of ‘business as usual’ rather than an opportunity to review and reset priorities. One small change saw an increase in the time allocated from 4 to 6 hours per week, with the additional hours earmarked for increasing communications with workers via social media activity or publishing a FTSU newsletter and posters.
Box 6 exhibits an extract from an updated ‘How to’ poster displayed across the trust, illustrating a four-step approach that was core to Montgomery’s FTSU strategy, including reference later in step 4 to contacting the trust’s Guardian. The information was particularly orientated towards safety concerns and professional workers (i.e. those practising as a regulated workforce), with little specifically targeted information for other workers (non-regulated). There is also no acknowledgement of concerns about cultural or behavioural transgressions, despite these being the issues most frequently raised with the FTSUG.
Step 1: can you tackle the issue yourself there and then? A firm polite challenge can work well.
Step 2: using existing systems in place at Montgomery, for example incident report form, or escalate to a manager or educator.
Step 3: if you feel unable to do this or have not had a satisfactory outcome, you can speak to someone who is independent of this process.
Step 4: such as trust’s confidential call line and the trust speak-up Guardian.
REMEMBER
Professional code of conduct; consult the trust’s ‘Concerns Reporting Procedure’ for further details on how to raise concerns.
The Trust will not tolerate the harassment or victimisation of anyone raising genuine concerns.
To recap, the pre-implementation and early implementation stages saw the FTSUG role being absorbed within a pre-existing ‘home-grown’ initiative, which marginally predated the mandatory introduction of the FTSUG role. With only 6 hours per week allocated for the Guardian role, it was critically important to the workability of the FTSUG role that Montgomery’s workers followed a four-step approach to speaking up, with the FTSUG functioning as a ‘safety net’ to capture any concerns that were not addressed by the initial three steps. It was also critically important, in terms of managing the FTSUG workload, that one of the initial three steps resulted in a satisfactory response to the worker’s concerns and, where this was not the case, that identified shortcomings were rectified by a QI approach. The following sections present common themes from the data that explore the ongoing implementation of the role in the light of these early guiding principles.
Freedom to speak up within a system
In common with other senior leaders, the FTSU executive lead summarised Montgomery’s ‘safety net’ approach as the FTSUG ‘operating within, not in parallel to the wider system’. The small number of concerns dealt with by the FTSUG (four per quarter on average, up to the time of data collection) was, therefore, considered to be indicative that the signposting system approach to FTSU was operating as intended.
However, several interviewees described how HR was not operating optimally within Montgomery, which was problematic given that many concerns raised to the Guardian related to HR and were then directly signposted back into HR or required HR’s involvement in some way. An executive explained that ‘HR could be better. They are taking too long over investigations and feedback’. Delays within HR processing were also identified by other senior managers, such as a case that was stalled for 2 years awaiting HR resolution ‘going in a circular motion . . . HR kept batting it back to different line managers, nothing would happen and then the Guardian would chase and we were back to square one again with HR’. Others reported a ‘big mistrust’ of HR within Montgomery, perceived by workers as ‘not impartial’ (i.e. siding with managers when concerns were raised) and that delays in responding to concerns deterred speaking up.
Other indicators suggest that workers had been wary of speaking up for some time, such as the trust’s below national average speak-up index scores between 2015 and the time of fieldwork in 2019. Senior staff described how the staff at the trust were shocked by these results and the realisation that workers feeling safe to speak up may be ‘be a bit of a red herring’ (fieldnotes 1 November 19). Further potential signs of unmet need within the workforce included the FTSUG undertaking a ‘walk round’ to raise awareness of FTSU on wards but being unexpectedly swamped with a large number of concerns on the first two wards, necessitating the cancellation of plans to visit more wards.
The workers’ mistrust of HR, the above-mentioned ‘circular motion’ of unresolved cases languishing between HR and managers and the lower-than-average index scores suggest an alternative interpretation to the one that was assumed by senior leaders for the small numbers speaking up. Instead of small numbers indicating that the four-step system was working optimally, where the FTSUG safety net is not triggered because concerns are satisfactorily dealt with elsewhere, the small numbers of speaking-up cases could reflect workers concerns about a timely response from and the trustworthiness of HR, which have been identified in the literature as strongly deterring workplace speaking up. 112 We observed one meeting between the FTSUG and a worker who was considering speaking up about a manager’s uncivil behaviour; they explained that HR’s likely involvement in the case was a barrier to speaking-up: ‘my manager knows senior people in HR and it would get back to him’.
In fairness, senior leaders at pre- and early implementation stages were aware that systems may require ‘beefing up’ and there was some evidence of system improvements during the ongoing implementation of FTSU. A senior executive described being prompted by Catherine’s feedback to have a ‘conversation with the head of HR and set a priority about training the HR office to make sure that they were more aligned to Freedom to Speak Up’. Furthermore, senior HR managers were working with other executive leads to further align HR, patient safety and FTSU.
However, despite the support of many senior leaders, there was an impression 3 years into the merged in-house/FTSUG initiative that change was slow in materialising, culminating in a heartfelt plea by a senior FTSU stakeholder at a board meeting (fieldnotes 30 September 2019), requesting the board’s support in ensuring that concerns were resolved more rapidly. The plea was supported by a senior executive and seconded by another, who also made an emotive speech about the importance and value of the FTSUG, while thanking Catherine for her leadership.
It was interesting to note that it was the interface between FTSU and HR (and to some extent middle managers) that was the main focus for reflection and planned change, rather than appraising the practices of the FTSUG initiative itself. Both senior leaders who were operationally closest to the FTSUG role were largely of the view that the role and processes, with the exception of HR, were working sufficiently well and in little need of change, despite evidence suggesting that some adaptation to the role may have been beneficial, as discussed in the following section.
Time allocation
The 6 hours per week allocated to Helen for undertaking the FTSUG role, although in line with many FTSUGs across England, was the smallest number of hours allocated across all of our case sites. Although the hours had increased from the initial 4 hours per week, we were struck by the significant difficulties that Helen outlined when describing balancing her busy clinical role with the FTSUG role, which were reminiscent of many of the telephone interviews reported earlier:
I’m almost switching hats hour by hour and it’s a real juggling of roles. I don’t think the role is sustainable in this way.
Helen
Time scarcity limited Helen’s opportunities to engage with workers and raise awareness of the role in person. The opportunity to be ‘more proactive’ was a common refrain of many time-limited FTSUGs, echoed here by Helen:
It’s great to have screensavers and electronic newsletters but you also need to be a face as well, don’t you? You have to be more than just a poster. But that comes down to time. At least a 50/50 split with my other role is needed but I don’t think others agree.
Helen
The FTSU executive lead shared Helen’s view, stating that ‘6 hours is not enough for the role’. Evidence that workers responded well when she undertook ward visits compounded Helen’s frustrations. In one such case, Helen visited ward staff who had raised concerns directly to an external body, further suggesting that the four-step process did not always operate smoothly. Helen’s visit resulted in an important exchange of information between workers and managers around barriers to speaking up internally.
Others were, however, not persuaded by the case for additional hours. One senior manager, who was initially unaware of Helen’s time allocation during interview, was nonetheless of the opinion that 6 hours per week was ‘generous’ given that the Guardian provided a ‘support service’. The same senior manager was also adamant that workers trusted the system and other reporting systems were working well, which, along with some staff groups having a ‘culture of not being bothered’, explained the small number of concerns.
Helen was correct in her instinct that some FTSU stakeholders would not agree with her assessment of requiring additional time:
I think the hours allocated reflect the work being done. The task is purely to market the service, advertise, and see cases through. There has been an extra push on comms, writing a blog and things like that. But that is included in the hours. The structure is there, the governance is there . . . it is now just running with it.
FTSU stakeholder
The presentation at the board meeting (as discussed in Freedom to Speak Up within a system) and interview data detailing difficulties with HR and staffs’ reluctance to speak up are at odds with the above claim that the ‘structure’ was in place and the FTSUG role was merely a case of ‘just running with it’. Even if FTSU structures and processes were in place, it was clear that an underpinning workplace culture consistent with FTSU was yet to fully develop.
This depiction of FTSU as a mostly technocratic and transactional activity, simply requiring structures and processes for information exchange to run smoothly, is at odds with the complex realities of culture change and speaking up that Helen had to deal with. For example, it seems to overlook the time-consuming yet rewarding work in learning from concerns that many Guardians dutifully undertake, including Helen who would engage with others (when time allowed or when she exceeded her contracted hours) to triangulate concerns with governance and workforce senior managers.
Summary
There is plentiful evidence that senior leaders at Montgomery were committed to the principles of supporting workers to speak up, although the provision of time and resources for the role was by far the lowest of all case study sites and one of the lowest in our data set. Collaborative working across senior stakeholders supported the emergence of a coherent strategic vision and an in-house speak-up initiative predating national requirements. The success of the initiative, within which FTSU was subsequently merged, hinged on assumptions about the optimal performance of the ‘four-step system’ and communications (‘comms’), and on workers’ perceptions that the system is trusted and responsive. Senior leaders’ faith in the system’s performance and in a QI approach to address emergent shortcomings underpinned their decisions to appoint an adjunct FTSUG, who was allocated only 6 hours per week alongside a busy clinical role.
However, the data challenge these assumptions. Limitations of a ‘comms’-only and transactional approach to raising awareness and information-giving about FTSU were identified. Helen’s infrequent visits to clinical areas showed that workers responded positively to the physical presence of the FTSUG. The visits also strongly suggested that workers wanted to speak up but that they clearly were not doing so via the FTSUG system. The FTSUG and FTSU executive lead both agreed that the role’s function, profile and sustainability would benefit from additional time. Furthermore, data collected by and the experiences of the FTSUG, national data and our own data strongly suggested that the system supporting FTSU was not performing optimally. The centrally important functions of HR were proving problematic, leading to long delays in resolving concerns and compounding workers’ anxieties about trust.
There was evidence that HR’s shortcomings were in the process of being addressed; however, despite these known issues, cases continued to be referred to HR and to languish. Although HR were closely involved in the pre-implementation sense-making phase, it seems that the processes and realities of handling concerns were routinely more problematic than initially imagined and were resistant to QI. However, some key stakeholders remained adamant that the FTSUG role did not require more time, despite significant evidence that workers’ needs could be better met. Although it seemed feasible to continue with an adapted and improved version of FTSU as originally conceived, some leaders seemed unable, or perhaps disinclined, to recognise clear indications that their initial assumptions had been superseded by the realities of implementing this complex role. Table 12 provides a brief summary overview of the main findings from Montgomery, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | Most workers’ concerns were believed to be addressed via existing organisational processes and mechanisms (but often were not). Minimal resourcing of FTSUG role was, therefore, required. QI deployed to address shortcomings as they arose. Evidence of emerging divergence in sense-making around FTSUG time allocation |
| Collective action: operational work to enact the role | The FTSUG role operationalised as a ‘safety-net’ (that should be rarely deployed) and producer/deliverer of ‘comms’. Most of the operational work relating to concerns being redirected back into the system and monitored by FTSU. Lack of FTSUG time meant direct contact with workers infrequent, culture building unable to be prioritised |
| Cognitive participation: relational work to build and sustain new practices | Relational work interfacing with HR problematic, but identified and being addressed. Despite the emergence of divergent sense-making, relational work remained mostly productive |
| Reflexive monitoring: appraisal work to assess and understand new practices | The role has progressed largely unchanged since initial introduction, despite the existence and awareness of multiple sources of evidence/views that the initial role as implemented might benefit from modifications and further resources |
Case study: Columbus (Box 7)
Type of trust: integrated foundation trust providing a range of hospital, intermediate and community health-care and social care.
Size and location of trust: large, dense inner city. Approximately 16,200 staff across two main hospital sites and several community sites.
CQC overall and well-led rating: good/outstanding.
Speak Up Index (national average 2018 78.1%; 2019 78.7%): Speak Up Index 2019 and 2020 well above national average.
Number of concerns Q3 2018/19 to Q2 2019/20: 223 concerns reported to the NGO.
FTSUG pseudonym and details of FTSUG role and type of appointment: Charlie; full-time stand-alone, band 8a. Internal appointment.
Line manager: chief nurse/FTSU executive lead.
Key implementation stakeholders: chief nurse/FTSU executive lead, NED, staff-side lead and chief people officer.
Guiding implementation principles: FTSUG added to and improved pre-existing speak-up initiative. The role was stringently implemented to signpost concerns into pre-existing structures and processes, especially relating to HR and staff-side boundaries. Implementation increasingly informed by and shaped organisational cultural initiatives.
The Francis Report in 2013 was an external trigger for Columbus to undertake a series of ‘listening exercises’ with workers, led by the chief nurse (Sheryl), to better understand any barriers to or facilitators of speaking up. As a result of this activity, Columbus launched an employee speaking-up initiative in 2015, which comprised a confidential e-mail service, external speak-up telephone line and a large network of speak-up ‘Champions’ situated across the organisation. This early initiative was a clear signal of organisational commitment to learn the lessons of the Francis Reports and confidence to be at the forefront of change nationally.
With the emergence of the Guardian role, the pre-existing initiative was completely subsumed within FTSU. The transition process was again led by Sheryl, who established a formal working group consisting of the then director of HR, a NED (Suki) and the staff-side lead. Interviews and documents indicate that channels of communication between the working group and other organisational stakeholders were open from the start, including communication with the CEO and the board, who were regularly updated (and approved) of the working group’s progress. During this transitional period, considerable effort was invested into generating a shared coherence of the FTSUG role’s position and remit. The transition group’s preparation also included a number of calls with the NGO to further clarify national FTSU guidance, described as ‘very haphazard’ by a working group member. These calls signified the group’s commitment to establishing external and internal coherence about the role, and further reflected the trust’s sense of assured self-confidence in liaising directly with national bodies.
Sheryl explained that the working group agreed that the role required someone with ‘authority and gravitas’, who felt ‘confident to talk to whoever in the organisation’. The culmination of several weeks’ interaction resulted in the working group agreeing clear boundaries and the remit for the FTSUG role:
. . . number one is signposting, number two we deployed it as speaking up for patient safety. Everyone understood their role and the Guardian understood that anything HR and employment based like bullying or pay is outside their remit.
FTSU working group member
Suki was initially appointed the FTSUG, working 1 day per week, and was supported by a deputy Guardian (Charlie) who had worked in Columbus in a clinical role for a number of years, with Sheryl appointed the FTSU executive lead. However, following the publication of NHS guidance117 detailing expectations regarding resources and positioning of the FTSUG role, alongside internal insights that the role required the allocation of more time to function effectively, Charlie was appointed (following interview) as a full-time FTSUG, with Suki appointed the FTSU NED. The trust’s strong financial position, which was referred to in a number of interviews with senior stakeholders, was intrinsic to the successful re-evaluation of the role, ensuring that sufficient resources were mobilised to support a full-time role at band 8a (uplifted from the original band 7 allocated), in addition to Charlie having her own budget and access to office space on the executive floor.
These changes were framed as delivering on the working group’s pre-implementation vision of an independent FTSUG who had access to senior leaders. To this end, the physical positioning of the role alongside senior management was considered symbolically important by Suki, while Sheryl described Charlie as ‘approachable to all in the organisation’. Data collected during fieldwork suggest that this pre-implementation conception of the role was translated into practice. Charlie’s clinical credibility and approachability was foregrounded on FTSU promotional material (wearing a uniform), somewhat distancing the role from too close an association with corporate or managerial functions. FTSU service users (SU1, SU3) described how promotional material had been helpful in alerting them to the existence of the FTSUG and how they viewed Charlie as approachable and having influence with but functioning independently of management. The CEO also stated that Charlie has raised issues directly to him, facilitated by their physical proximity.
To summarise, several resources were deployed to support speaking up that predated the Francis Review and its requirements by some months. These existing resources were subsequently and fully rebranded to ensure consistency with the mandatory introduction of the FTSUG role. A transitional working group agreed and demarcated the remit and boundaries within which FTSUG operated and undertook deliberations with key internal and external stakeholders. Considerations concerning the interface of the FTSUG with trade unions and HR were at the fore, and the role’s signposting remit was agreed. It was made abundantly clear to the Guardian that any involvement in employment issues would be regarded as an unwelcome breach of existing boundaries and encroachment into territory occupied by trade unions and HR. The following sections consider these pre-implementation and early implementation assumptions as the FTSUG role became further established.
Practically navigating boundaries and remits
As the FTSUG role progressively became embedded, several issues challenged stakeholders’ assumptions that underpinned pre-implementation and early implementation decisions demarcating the boundaries of the FTSUG role. First, as was the case nationally, a large majority of cases that were raised related to non-patient safety issues. A FTSU working group member was ‘surprised that 79% of the speak-up cases are about employment issues’, despite stakeholders’ shared coherence and a well-resourced communications campaign emphasising FTSU as a patient safety initiative.
Charlie described how patient safety concerns were often complex but straightforward to resolve, as actions that improved the safety of patients were relatively unambiguous and uncontested by workers. By contrast, the large numbers of ‘employment issues’ triggered frequent, complex, lengthy and occasionally acrimonious boundary skirmishes between the FTSUG, HR, managers and trade unions. As a senior stakeholder explained:
Boundaries became a bit blurred . . . a feeling that individuals were overstepping their mark, it got a bit tetchy and tense. The Guardian got involved in trade union or HR matters. Someone got disciplined, they didn’t like it so they phone the Guardian. Charlie then tried to unpick the HR processes to change the outcome. We’ve had a few of those. That is not the job of the Guardian. Others are accountable for HR process and that’s their responsibility. Questions also whether the Guardian was basically representing staff which raises the question of why bother paying union fees etc.
Senior stakeholder
Other senior stakeholders also described how the originally agreed boundaries were breached and the role became ‘far too operational, too involved . . . taking cases on not signposting’. However, Charlie’s ‘hands-on’ approach was a reflection of the complexities and tensions inherent within many of the HR/employment issues raised. Workers also had few other means of support, as a frequent concern raised ‘with monotonous regularity is that staff have no idea who their line manager is, let alone a relationship with them’ (FTSU advocate interview).
The complex realities of working as a FTSUG had, therefore, confounded pre-implementation assumptions and processes designed to establish and protect traditional organisational boundaries and divisions of labour. The early and ongoing implementation issues experienced at Columbus, however, not only were a case of misaligned process or communications but also were symptomatic of complex relationships and historical-cultural matters that we now further consider.
First, Sheryl (chief nurse/FTSU executive lead), who had long generated and maintained a high profile with workers across the trust, was described by a board member as ‘representing old-fashioned matron values, gets out there among people. She knows all the nurses’ bloody birthdays and sends them a card [laughs]’. As the lead of Columbus’s pre-Francis speak-up initiative, Sheryl explained her approach as ‘a very visible fixer. I’ve always been the first port-of-call for staff in the organisation whoever they are’. Being a ‘fixer’ may have created unintended and unsustainable expectations of the Guardian, as Sheryl further clarifies:
The rate and type of concerns could be about me and the fact that my office has a reputation for responding to whatever concerns staff have and that’s been linked to the Guardian role.
Sheryl
Second, with a very large percentage of the many concerns raised annually relating to employment and behavioural issues, the implementation of the FTSUG role also seemed to address a substantial level of unmet HR need at Columbus. An executive referred to the opening of ‘Pandora’s Box’ as a result of FTSU challenging a range of long-tolerated suboptimal working practices within management and HR. This included workers speaking up about unresolved employment concerns ‘that had been going on in HR for years and years . . . Charlie can’t do much about it. It’s hard and she feels frustrated’ (executive). Feedback received by Charlie also suggested that workers perceived her as ‘trustworthy and a safe person, they come to me as an alternative to avoid other routes like HR and line management’.
Although aware of boundary tensions and stakeholders’ claims that she became ‘too involved’, Charlie viewed many of the HR, employment and behavioural concerns as the legitimate business of a Guardian. Such an example of a breakdown in coherence between Charlie and senior stakeholders was a speak-up case resulting from the uncivil conduct of a senior doctor towards colleagues. The case was subsequently managed as a HR issue, although Charlie considered her ongoing involvement as relevant and appropriate given that the incident signalled a problematic workplace culture. Charlie was aware that issues could linger and fester ‘because HR systems here aren’t perfect’.
Charlie cited the Francis Review as rationale for her ongoing involvement with cases, particularly the fact that Guardians are deployed to protect and support workers’ interests as they progress through bureaucratic, sometimes cold-hearted and contentious, organisational processes. Charlie’s description of the ‘massive mental and emotional drain of dealing with such cases’ demonstrates that such support work was not blithely offered. Charlie’s rationale and motives for ongoing involvement with cases was, however, at odds with stakeholders’ perceptions of the motives of FTSU (collectively, not only Charlie) as underpinned by strategic ambitions, a ‘move into others’ territory . . . they are trying to expand FTSU’ (FTSU stakeholder), which occasionally resulted in ‘tanks on the lawn, you’re on my turf moments’ (executive).
Charlie described how the ‘organisation pushing me’ to signpost more readily and lessen involvement was having the desired effect. There remained, however, a lingering sense that the process of maintaining boundaries remained somewhat combative, rather than consensual. Charlie described gradually submitting to organisational requirements and the exacting effects of several months of emotional turmoil, incessant work and high levels of personal commitment:
In the past something horrendous would be reported and I’d really feel it and get involved. Now I just feel really numb I don’t feel like I’m being as compassionate. I’m happy not to be involved because I’m probably burnt out more than I used to be.
Charlie
Ongoing reflection and learning
Although differences in understanding and clashes occurred throughout the FTSUG implementation period, stakeholders reported that contentious issues were frequently debated, rather than suppressed or glossed over. An executive described that:
Charlie frequently tells me she is frustrated at times with my team, we’ve had some frank exchanges. I know she has had similar conversations with others. But there is mutual respect, trust and desire to make this work. We now work very well but it’s not all cosy cooking. She holds us all to account regardless of hierarchy, which is how it should be.
Executive
These open and robust discussions were a continuation of the collaborative approach, initiated and led by Sheryl at the pre-implementation and early implementation phases, which had normalised the sharing of information between stakeholders. Robust openness and ongoing reflection were emblematic of the organisation’s pursuit of continuous service improvement, as reflected in the following extract from an interview with a senior executive:
Charlie and FTSU are making great progress. But we’ve got to think a little bit about the future organisation . . . reflect on the way we’re orientated at the moment for versus how we may want to run and improve FTSU in the future.
Senior executive
Furthermore, senior leaders (led by OD) at Columbus had latterly introduced a ‘Culture and staff experience steering group’ for sharing intelligence and insights from FTSU, HR, staff-side, OD and occupational health. The group informed the trust’s work, while also preventing potentially unproductive duplication, boundary overlaps and transgressions. The increasing collaboration between Charlie and OD was symptomatic of an evolving interface between FTSU and organisational cultural initiatives. Although Charlie admitted that ‘OD came quite late in the game for me’, ongoing collaboration included utilising FTSU data and experiences to inform ‘cultural interventions which create the conditions for people to feel safe speaking up locally’ (OD worker).
Given the embryonic nature of the FTSUG role in Columbus and nationally, Charlie actively pursed opportunities for ‘soft’ reflective learning and triangulating FTSU concerns with ‘hard’ data, a developmental learning process that had ‘helped me to find my feet. None of what we now know is given to you at the start’. Capitalising on the valuable and occasionally painful learning gleaned over the implementation journey was core to Charlie’s functioning as both a Guardian and an influential figure regionally. Learning from concerns was set to remain a core activity of FTSU in Columbus. By the completion of fieldwork, a full-time band 5 information officer for FTSU had been appointed, in addition to an existing administrative officer, to further triangulate FTSU data with other organisational metrics, such as staff surveys and workforce data. Increased and robust data analysis dovetailed well with Charlie’s burgeoning collaboration with OD in terms of developing workforce culture interventions and, furthermore, ensured that Columbus remained at the forefront of speaking-up innovation.
Summary
A speak-up initiative, significantly pre-dating the Francis Review, provided useful groundwork for FTSUG role implementation. The role’s introduction attracted little resistance at the pre-implementation and early implementation phases, which was a time characterised by interdisciplinary collaboration and the emergence of shared coherence via an implementation working group. However, as the role became increasingly embedded into Columbus’s working practices, the FTSUG’s handling of bullying/behavioural concerns triggered disciplinary and professional boundary tensions. HR and trade unions were particularly intermittently hostile to FTSU, protective of their disciplinary territory and defensive about the service limitations surfaced by the concerns raised to the FTSUG.
However, although some of the pre-implementation assumptions and remit-setting for the role were not fully thought through, the underlying ethos of collaboration enabled robust and open conversations between stakeholders, which prevented tensions destabilising the role’s implementation. Charlie’s handling of FTSU concerns was continually reviewed and reinforced to contain boundary encroachments and to ensure that stakeholders’ existing organisational remit was maintained and protected. Ongoing co-operation in dealing with FTSU concerns between HR, trade unions and the Guardian was commonplace, albeit mostly undertaken according to the terms dictated by HR and trade unions. Despite initial and occasional ongoing tensions, concerns were managed and organisational learning was a clear priority and vigorously pursued by Charlie. In addition, not all boundaries were defensive; the boundary interface between FTSU and OD was increasingly open and fruitful, with the Guardian’s work complementing and enhancing OD initiatives, rather than being perceived as a threat.
Given that the FTSUG role was often the focus of these tensions, this had a cumulative effect on Charlie’s ability to perform the role optimally and empathically, although the organisation supported her and FTSU more generally with an impressive level of resource and individual psychological support in the form of supervision and counselling. Having built impressively on existing initiatives and undergone a difficult, yet productive, early implementation phase, FTSU at Columbus seemed well positioned to further enhance its reputation as making a positive contribution to learning and improving patient safety and workforce well-being. Table 13 provides a brief summary of the main findings from Columbus, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | Speaking up was a long-standing organisational priority with meaningful pre-Francis attempts to support staff to speak up. FTSU was fully embraced and implemented with significant increased resource. Shared coherence that FTSUG activity should not encroach on the work of existing organisational stakeholders, although this occasionally caused tension with the FTSU core ethos of protecting workers |
| Collective action: operational work to enact the role | FTSUGs instructed and reminded to operate within rigid boundaries. Although workers were supported, any ongoing FTSUG input into concerns was minimal. However, the FTSUG operated effectively at a strategic and organisational level, especially in terms of ensuring organisational learning and future workforce developments |
| Cognitive participation: relational work to build and sustain new practices | Following early and significant tensions, there was mostly collegiate and collaborative relationships between stakeholders. Discussions were robust but mostly psychologically safe, although at times the FTSUG’s considerable resilience was dented |
| Reflexive monitoring: appraisal work to assess and understand new practices | The role was consistently scrutinised by senior stakeholders and change introduced when necessary. Data were rigorously analysed and triangulated with a genuine desire to learn from concerns and build a culture of speaking up |
Case study: Providence (Box 8)
Type of trust: acute foundation trust providing a wide range of hospital and diagnostic services.
Size and location of trust: medium; inner (small) city location. Over 4500 staff based in one main hospital site and local outpatient/same-day services at community hospitals.
CQC overall and well-led rating: good/good.
Speak Up Index and number of concerns Q3 2018/19 to Q2 2019/20: Speak Up Index 2019, below national average; 2020 equal to national average; 51 concerns reported to NGO, data from only three quarters.
FTSUG pseudonym and details of FTSUG role and type of appointment: Hannah; stand-alone FTSUG allocated 3 days, band 7. Internal appointment from clinical post.
Line manager: Deputy Director of People.
Key implementation figures: Director for People/FTSU executive lead; Deputy Director of People; CEO.
Guiding implementation principles: current iteration of FTSUG strongly guided by principles of independence, collegial yet constructive critical appraisal of cases and workplace culture more generally. FTSU strategy centralised around supporting FTSUG to support workers’ concerns and open workplace culture.
Since 2013, whistleblowing and speaking-up processes in Providence had been consistently reviewed and adapted. As Table 14 outlines, a pattern of external policy factors prompted internal appraisal and sense-making activities between 2013 and 2016. Senior leaders from HR, the staff-side chairperson and a NED collaborated throughout these review activities, which were requested by and reported to the board, who also approved the subsequent modifications. The appraisals analysed various ‘soft’ and ‘hard’ data sources, such as e-mail and telephone support-line usage, the numbers of concerns raised by workers and their experiences of doing so.
| Year | Triggering event | Organisational response |
|---|---|---|
| 2013 | External: publication of Francis Report and ‘After Francis’ Government response | Whistleblowing policy updated. Confidential telephone and e-mail lines launched. Communications campaign to raise awareness of new resources |
| 2015 (FTSUG version 1) | External: publication of Francis FTSU Review | Internal evaluation of speaking up presented to board. ‘Concerns review group’ (senior HR manager, NED and staff-side chairperson) established to review FTSU and implement Guardian role. Four ‘divisional’ Guardians (no time allocated) and joint FTSU executive leads appointed |
| 2016 (FTSUG version 2) | External: NGO publishes FTSUG job description | HR director, staff-side chairperson and a NED review and change FTSU implementation. One day per week adjunct FTSUG appointed, three of the other original FTSUGs in supporting roles. FTSU located and line managed within HR |
| 2018 (FTSUG version 3) | Internal: FTSUG departs. External whistleblowing events bypass FTSU processes. Raquel appointed as Director for People and new FTSU Executive Lead | The FTSUG’s departure and external whistleblowing triggered a review of processes and the FTSUG role. New FTSUG appointed (stand-alone, 3 days per week) and a discernible shift under new FTSU executive lead: aligning FTSU with staff engagement and organisational culture initiative |
Three different versions of the FTSUG role were implemented between 2015 and 2018. Initially, in response to the FTSU review, the role was undertaken by four FTSUGs, who worked in different divisions within Providence, with the aim of offering workers a choice of Guardians. Members of the executive team approached individuals directly to undertake the FTSUG role. However, the FTSUGs were allocated no time for the role and were largely tasked with undertaking awareness-raising and promotional events, with few concerns being raised.
Version 2 was implemented in 2016 following the NGO’s publication of the FTSUG job description, which recommended ‘ring-fenced’ time for FTSUGs. 15 One of the four original FTSUGs was appointed as lead Guardian, with the other three Guardians assuming supporting FTSUG roles. The lead guardian was allocated 1 day per week for the role, alongside their busy band 7 clinical role. The medical director and director of nursing and midwifery operated as joint FTSU executive leads. The FTSUG was located and line managed within HR.
The case study was undertaken during version 3 of the FTSUG role, which was a substantially different FTSUG role from the previous versions. Notably, the source of these changes was internal, rather than external, triggered by the following events:
-
the FTSUG role becoming vacant
-
staff whistleblowing to external agencies, avoiding contact with the FTSUG owing to concerns about the confidentiality of the FTSU service
-
Raquel being appointed as Director for People and the new FTSU executive lead.
Version 3 of the role also consisted of a number of key operational changes, including an open recruitment process, the adoption of a stand-alone FTSUG model, rather than an adjunct FTSUG, and increased time for the role (3 days per week, from 1 day per week). Hannah was appointed the FTSUG at band 6 from a clinical role within Providence. She had no previous involvement in FTSU and was line managed by the Deputy Director of People (Delyth). These significant alterations to the FTSU role were intrinsically linked to key internal operational changes occurring within Providence in 2018, which are further explored in the next section.
Internal change and a new Freedom to Speak Up Guardian role
Particularly noteworthy in the recent history of FTSUG implementation in Providence was the restructuring and renaming of HR into the ‘Directorate of People’, in parallel with the appointment of Raquel as the new Director for People and the FTSU executive lead. Raquel’s appointment signalled a marked change in strategic direction within Providence. With a strong track record of leading organisational culture change in non-health-care sectors and more recently the NHS, Raquel explained that she had ‘absolutely no background in HR. The organisation deliberately appointed me because they wanted somebody who was a bit different’. Redesigning and more fully resourcing the FTSUG role was a priority for Raquel, especially so to realise the role’s untapped potential for culture change:
It’s a culture change role as much as supporting staff to raise concerns. There was just no chance that somebody could do that in a day-a-week. It needed to be a dedicated post rather than somebody flitting in and out.
Raquel
With this in mind, Raquel and Delyth undertook a review of FTSU in 2018. Delyth explained that she reviewed the job description and ‘sought national advice about how others had done it’. A further departure from previous ways of working was that no other organisational stakeholders directly contributed to decision-making about version 3 of the FTSUG role. Raquel and Delyth were united in their understanding and desire for change, a sequence of events that Delyth summarised as ‘we just made the decision that these changes were the right thing for the organisation’.
Proposed changes were, however, discussed with stakeholders (such as the staff-side chairperson) and approved, and were subsequently monitored by the board. In addition, the CEO participated in the FTSUG interview panel and further reinforced the view that, given preceding events, Hannah’s appointment was a critical juncture as ‘she brought something new to the role. It was important we got the right type of person . . . that staff trusted the individual and the process’.
Changes in sense-making and relational working can also be explained by Raquel and Delyth’s awareness of workforce discontent following the apparent internal disclosure of information related to two FTSU cases in 2016. The exact nature of these events was unclear during our study, with Hannah (FTSUG) describing only a vague awareness of ‘some confidentiality breach, something happened that made people feel unsure about Freedom to Speak Up and unsafe to talk’. However, the effects on the workforce were tangible and ensuring that the ‘new’ FTSUG role was insulated from these historical events became vital.
To recap, since the Francis Report in 2013, Providence had consistently and decisively reviewed its provision of structures and processes to support workers to speak up. However, despite best intentions, the initial two versions of the FTSUG role did not flourish and, if anything, FTSU culture at Providence deteriorated in the first 2 years. Implementation decisions around the current FTSUG were contingent on the previous iteration’s perceived failure in protecting both organisational reputation and workers’ trust in FTSU. A radically different approach to FTSU and the Guardian role was therefore deployed, which was untarnished by association with the past and underpinned by the appointment of Raquel, who, along with Delyth, recalibrated sense-making around speaking up and its contribution to the organisation. The emergence of Hannah, Delyth and Raquel as a FTSU triumvirate reflected a deliberate and bold organisational strategy to reset FTSU strategy at Providence, which was supported by the CEO. The following section explores prevalent themes since the launch of the reconstituted FTSUG role.
Emergence of the ‘new’ Freedom to Speak Up Guardian role: developing sense-making, relationships and independence
Given the troubled history of and workers’ reservations about FTSU, it was particularly important that the relaunched Guardian role displayed a significant degree of independence and autonomy from organisational leaders. This was especially the case given that the role was closely associated with and developed by two senior leaders (Raquel and Delyth), who worked closely with HR and the board. However, whereas other organisations argued that the role was developed and shaped by the FTSUG, albeit within predefined and rigid processes and structures, Hannah indisputably drew her own role boundaries. This was enabled by leaders giving Hannah space, guidance and confidence, which lent much-needed credibility to claims of FTSUG independence. For example, although Raquel and Delyth supported and worked closely with Hannah, several other factors ensured that Hannah’s operationalisation of the FTSUG role was informed and enhanced by the views and experiences of others.
First, although Hannah was line managed by Delyth, the CEO highlighted the independence and autonomy of the FTSUG role, explaining that ‘Hannah sits outside our normal management hierarchy on purpose and takes the opportunity to have frank conversations with me and the Chair’. On a similar note, highlighting collegiality rather than hierarchy, Delyth viewed her relationship with Hannah as a ‘trusted colleague . . . bit like a confidante’ rather than a line manager, stating ‘I wouldn’t be so daft quite frankly to try and tell her how do deal with cases’.
Regular monthly meetings with the CEO and (separately) the chairperson proved useful in developing supportive relationships between Hannah and senior executives, with the chairperson suggesting that ‘Hannah understands that I am a very safe place for bad news’. Hannah shared this view and thought that the chairperson and CEO, in addition to meetings with others, such as the staff-side lead, provided insights and guidance that added to her sense-making about the function and remit of the role. Furthermore, the meetings conveyed legitimacy to the FTSUG role, which was visible to workers. An executive, for example, felt that some spoke up to Hannah because they know ‘the Guardian has CEO’s ear’, a view that was shared by the CEO, who stated that ‘people know that Hannah sees me every month and they think, hang on a minute, FTSU is important enough for the boss to give access to Hannah once a month’.
Interactions with senior stakeholders were also key to Hannah’s orientation to and understanding of the organisation more generally. This was particularly important given that, unlike many FTSUGs, Hannah had little prior experience of managerial concepts and strategy, explaining ‘I needed to learn a new language. People were talking about comms and I was like “what’s comms?” ’. Indeed, Hannah became aware of the role only when a colleague alerted her to the FTSUG job advert.
Hannah was, however, also aware of the dangers of overassimilation into organisational structures and relationships, and endeavoured to preserve and capitalise on the advantages that being a relative ‘newcomer’ bestowed. Hannah’s unfamiliarity with the corporate hierarchical structures ensured that she acted independently by ‘not getting tied-up in trust relationships and politics . . . otherwise I could feel more protection for, or more alliance with the trust’. Identifying and aligning the role with the NGO strategy and the values within the Francis Review allowed Hannah ‘to remind [her]self of where the role sits’. Hannah also resisted any involvement in investigating concerns, but maintained close contact with the person speaking up and obtained feedback on their progress and outcomes:
There’s a phrase used clinically that pain is what the person says it is. I kind of operate from that rationale, I view the concern as what they say it is . . . I will protect them in that process. That’s the role, full stop.
Hannah
The FTSUG service users whom we interviewed clearly endorsed the trust’s approach to the Guardian role and Hannah’s trustworthiness:
It’s positive that the organisation believes in the role sufficiently that it is stand alone and we don’t make someone do it in addition to the day job.
SU02
Hannah actually believes in the values of the role and it’s a completely different experience from speaking up at my previous trust, which was farcical.
SU04
You have to trust someone to be able to disclose potentially sensitive situations, and yeah, I felt she was a very approachable person.
SU01
An increasing number of invitations to meetings was also regarded as a potential distraction from Hannah’s unerring focus on supporting workers. It is unsurprising, therefore, that the notion of ‘fresh eyes’ is referred to in several interviews, a phrase that was emblematic of Providence’s approach to implementing version 3 of the Guardian role. This shared acknowledgement of newness and transition was not limited to describing Hannah’s appointment, but was also prevalent in descriptions of Delyth and Raquel’s involvement in FTSU. However, although there was some evidence that workers had a growing awareness of a transition to a new FTSU model, the extract below demonstrates that changing workers’ historical perceptions would take time:
I don’t think people know what Freedom to Speak Up is yet. Someone said to me today, that people still don’t trust the service and I thought, oh gosh that’s really interesting.
Hannah
Summary
The initial implementation of the FTSUG role in Providence, which was collectively agreed on by senior stakeholders, resulted in an unexpected and unwelcome deterioration in speak-up culture. Resetting the FTSUG role was, therefore, critically important, and the current version benefited from the allocation of increased resources, a fresh strategic vision driven by the FTSU executive lead and line manager, and regular interaction between the Guardian, CEO and chairperson.
While other Guardians were very familiar with and immersed within their trust’s working practices and were often appointed as a result of working within them, Hannah’s appointment was enhanced by her having little prior involvement or, indeed, insight into Providence’s corporate/managerial practices, customs and culture. Once appointed, Hannah invested time and thought about the maintenance of an ‘arm’s length’ approach to the role and the trust. She was closely aligned with and supported by senior stakeholders, yet also productively independent.
It was, however, too early to conclude whether or not Hannah’s appointment and the trust’s ‘fresh eyes’ strategy was having the desired positive effect. Some indications and feedback were positive: the number of concerns had risen and informal feedback was positive. However, attributing any direct causal relationship is unwise, and there were still some in Providence who had difficulty trusting FTSU and felt that speaking up was fundamentally a risky act. However, it is undeniable that the current FTSU strategy had established a refreshingly different approach, with the Guardian ensconced as a ‘critical friend’ who was affiliated to the organisation and stakeholders, but also as detached as practicably possible from organisational structures, processes and the potentially complex relationships therein. Table 15 provides a brief summary overview of the main findings from Providence, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | FTSU was an organisational priority. There was a recent shift in sense-making towards FTSU as a culture-building initiative that required more resources and independence from organisational structures and relationships, rather than embedded within them |
| Collective action: operational work to enact the role | Clear operational processes in situ. The FTSUG remit clearly focused on supporting workers throughout the handling of the concern, with little involvement in case handling. Deliberate limits on operational scope imposed and agreed by FTSUG and stakeholders to preserve FTSU independence |
| Cognitive participation: relational work to build and sustain new practices | Relational work was collegial, yet constructively critical. Operational limits result in clear lines of relational work, ensuring that FTSUG remains focused on supporting the concern rather than the trust’s/stakeholders’ interests |
| Reflexive monitoring: appraisal work to assess and understand new practices | FTSU strategy has undergone consistent and robust monitoring and appraisal, resulting in significant change. Appraisal is ongoing featuring formal analyses of data and informal reflective discussions with senior leaders |
Case study: Concord (Box 9)
Type of trust: acute foundation trust providing a wide range of hospital and diagnostic services.
Size and location of trust: small; urban location. Over 3300 staff based in two hospital sites providing emergency acute and specialist services.
CQC overall and well-led rating: requires improvement/requires improvement.
Speak Up Index and number of concerns Q3 2018/19 to Q2 2019/20: Speak Up Index 2019, both below national average; 72 concerns reported to NGO.
FTSUG pseudonym and details of FTSUG role and type of appointment: Carly; stand-alone FTSUG allocated 2 days, band 8a. Internal appointment from a clinical post.
Line manager: Director for People.
Key stakeholder figures: Director for People/FTSU executive lead, staff-side lead.
Guiding implementation principles: initial implementation embedded within HR with little by way of FTSU guiding strategy. Since critical CQC report ongoing implementation principles mostly absent; role has thus lacked coherent remit and strategy.
There appeared to be little in terms of a pre-Francis Review organisational strategy or associated resource to support speaking up in Concord, beyond the customary access to trade unions and HR. However, the critical CQC inspection rating in mid-2018 resulted in the replacement of many of the senior leaders who were in post during the pre-implementation phase of the FTSUG role. An executive who was appointed following the CQC report outlined the severely critical nature of the CQC inspection findings:
Systems and processes weren’t in place. How we investigate and learn from incidents, none of that’s been done properly. Basic things like board governance and the governance within divisions. Basic standards of care not being done properly. Chaos. It’s a nice place to work, but people have been here a very long time. They don’t see things . . . they have no idea of what good looks like.
Executive
The trust was also beset by debt and underinvestment, resulting in an estate described as ‘crumbling’. Repair costs were estimated to be £250M, equal to the total annual operating budget for the organisation. Decaying buildings and wards were described by another executive as ‘appalling, they’re awful environments for staff and patients . . . if our staff feel rubbish that’s a patient safety issue’.
Another executive voiced a common theme that was identified during fieldwork, explaining that environmental contingencies normalised poor working conditions at Concord, which blinded many to the consequences of their actions or inactions:
It’s quite hard when things have been that way for a long time for staff to actually see it and recognise that actually this is unacceptable and glossing over it results in bigger problems.
Executive
One original initiator of the FTSUG role remained in post during fieldwork, although the departure of the Director of People/FTSU executive lead was also imminent and was described by a colleague as ‘currently winding down’ (fieldnotes, 21 January 2020). The FTSU executive lead identified a prevailing blame culture within the organisation as a key challenge to implementing a FTSUG, which, unsurprisingly, resulted in ‘a kind of reticence to tackle issues’. A culture of blame and the sightlessness and/or sense of helplessness resulting from chronically poor working conditions were significant barriers to speaking up.
Compared with the other case studies, there was little pre-implementation preparation or forward planning undertaken for the FTSUG role. A board member explained how they were mostly informed of implementation actions, rather than directly contributing to them:
We were all told after they employed someone what their remit was. The execs were paying lip service, I would say it’s almost a tick box exercise.
Board member
The Director of People’s preference was to recruit a FTSUG who had a clinical background, thus representing the largest staff group in the trust that was ‘normally not afraid to speak truth to power’. The initial FTSUG recruitment process generated no applicants. A second recruitment process, supported by increased advertising of the vacancy and directed at clinical staff, eventually resulted in the appointment of Carly as a part-time (2 days per week, band 8a) stand-alone FTSUG in January 2017. Carly described the interview, which was undertaken by a panel featuring three executives, as ‘a grilling’. Carly, who was considering retirement or changing from her specialist clinical role in Concord, explained being very hesitant when initially applying for and then undertaking the role. This was due, in part, to her awareness that the organisation had planned little for how FTSU would evolve or unfold. Carly agreed to take on the role only when the trust approved her request to work 2 days per week, the maximum hours that Carly was prepared to work.
Carly’s line manager embarked on integrating FTSU into existing processes within the ‘People Directorate’, which was mostly referred to as ‘HR’ within Concord. Workers broadly associated the FTSUG with a HR role, which had implications for the Guardian, which will be discussed later. Early deliberations about how to triangulate FTSU data with various other data sources, such as adverse incident reporting, was also facilitated.
Frequent meetings between Carly and the FTSU executive lead became the norm, alongside less frequent, but nonetheless regular, meetings with the CEO. Carly and the FTSU NED also delivered speak-up training for other NEDs, who became active supporters of FTSU across the organisation. As a result, the FTSUG role became ‘increasingly integrated into the organisational workings’ (FTSU executive lead), while Carly also liaised closely with the FTSU NED, who described their relationship with Carly and the FTSU executive lead as an ‘important triangle based on trust’. Carly frequently described being well supported by both FTSU leads.
Despite a slow early implementation period, there were indications that momentum was building around FTSU. Plans for a longer-term FTSU strategy, focusing on further data triangulation and concerns about bullying and harassment, were being discussed when the critical CQC inspection report was published in mid-2018. The report proved to be a turning point for FTSU within Concord. Many of the initial FTSU stakeholders left the trust and, although they were eventually replaced, a significant amount of the trust’s energy and resource was diverted to addressing a number of remedial actions required by CQC. Progress with developing and implementing a longer-term FTSU strategy faltered significantly. Consequently, as the following sections demonstrate, the Guardian role and FTSU more generally struggled to be integrated into Concord’s working practices as a coherent presence amid an organisational climate and culture that was described by a board member as ‘bleak’.
‘Mixed-up’ sense-making
A number of interviews described a lack of collective sense-making about the function and remit of the FTSUG role, a situation described as ‘mixed-up thinking’ by an executive. From the outset, a very high proportion of FTSU cases raised to Carly related to bullying, harassment and incivility between staff (as was the case nationally). One FTSU service user explained that clinical areas were particularly regarded as a toxic working environment:
. . . on the wards it is much more, the level of bullying it’s like in your face.
SU01
The FTSU executive lead viewed such ‘behavioural issues’ as beyond the remit and relevance of the FTSUG role and advised Carly to focus on promoting the FTSUG role as a patient safety initiative. Carly and the staff-side lead, however, strongly disagreed and openly promoted the role as supporting speaking up by staff about all/any concerns. Carly explained that, given the context of distrust within the workforce and a further deterioration in a workplace culture of blame since the CQC report, hearing workers’ concerns regardless of the issue would generate trust in the role and may, in turn, encourage further concerns to be disclosed. The staff-side lead also promoted the role as ‘being there for staff who wanted to speak up confidentially about bullying’. This supportive aspect of the role was deemed to be particularly important by a board member, who described aggressive and uncivil conduct between managers, directors and executives:
Endemic . . . I saw a director screaming at a car park attendant because the office was closed for lunch. ‘Do you know who I am’ sort of thing. The language here is generally aggressive, people in meetings saying ‘just effing do it’ to managers and then managers go off and speak the same to staff.
Furthermore, senior stakeholders who were appointed within the preceding 12 months disagreed with how Carly was undertaking the role. Having worked closely with Guardians elsewhere, they were surprised and confused somewhat by the FTSU approach that was adopted in Concord. One senior stakeholder described how FTSU was:
. . . reasonably embedded, but the relevant question is whether the right thing is being embedded . . . Carly does practical solutions rather than signposting and supporting. She singlehandedly addressed an issue in one area but then it actually meant that the department were not supported in solving their own issues.
Similarly, another senior stakeholder stated that ‘I’m confused and not quite sure I or Carly know what her role is’ after Carly provided the senior stakeholder with information about a concern, in addition to ‘basically operational advice which I didn’t really warm to, to be honest’. Later in the same interview, the senior stakeholder explained that the concern, in addition to others raised by Carly, had not been raised by workers but had resulted from Carly ‘literally walking around the hospital and observing’, echoing a description offered by a board member about Carly’s actions:
. . . doing a lot of wandering around and sitting in corners watching. People thought she was there to catch them out. ‘Spying on us’ they told me.
Board member
Although colleagues were reassured that the FTSUG’s intentions were to better understand culture and working conditions, there remained a perception that the role was an unwelcome extension of management or HR.
Carly explained, however, that visiting and ‘hanging around’ hospital sites was a strategic decision, which was approved by the FTSU executive lead, that had resulted in useful exchanges with workers:
I’m there to increase visibility, see what is happening especially where HR are aware of problems. People have spoken to me because I have been in the right place at the right time.
Carly
There was clearly a lack of shared coherence and agreed boundaries to guide the FTSUG role. In the absence of coherent strategic direction, Carly adopted a trouble-shooting and solution-focused approach to the role, which was often at odds with others’ experiences and expectations of the FTSUG role and somewhat contrary to the role’s principles outlined within the Francis Review. Taking decisive actions and resolving concerns without consultation with stakeholders suggests that the ‘just effing do it’ culture, discussed earlier, may also have influenced Carly’s decision-making. Nevertheless, any attempts to communicate an understanding of the Guardian’s role and place within a coherent and wider organisational FTSU strategy had clearly bypassed colleagues working at all levels within Concord. These insights are further developed in the next section.
‘What is this?’: vagueness and conflict in the absence of guidance
The absence of formalised and agreed processes and coherent guidance to shape the role’s operation resulted in tensions and significant disruption between senior staff. This is captured in the following extract, in which a senior FTSU stakeholder describes how they expressed their frustration to the FTSU executive lead following an e-mail exchange with Carly:
I said to them I don’t even understand what this is. What flow chart am I using? I need to know what policy I’m working with. Is this genuinely speaking up? I didn’t get much back as the FTSU lead is literally leaving but I have flagged it with his interim replacement.
Executive
The absence of an overarching FTSU strategy and process seemed to also limit the dissemination and analysis of FTSU data. Interviews confirmed that the absence of in-depth data analysis, or triangulation with other data sets, was known to senior stakeholders. The same stakeholders, however, also acknowledged that they had not addressed these known limitations. For example, months following an appointment to a role that they described as having ‘a learning from incidents portfolio’, a senior clinician described having very limited knowledge of FTSU data analysis and whether or not FTSU had resulted in any service improvements. In reply to our question of whether or not they had expressed concerns to the FTSU executive lead or Carly, they stated that:
To be honest we’ve got plenty of other things going on other to me sorting this out as well . . . I haven’t even thought of saying this is different from what I have seen elsewhere. But Carly is very committed.
However, this was not simply the case of relative newcomers being overwhelmed with work. Other employees who had worked at Concord for a number of years also conceded to knowing little about the analysis or improvement capability of FTSU data and to have not reflected on the matter:
Talking to you now and thinking about it, the data and its uses should be something I should see and know about.
Board member
It is perhaps unsurprising, therefore, that Carly described feeling dislocated and unsupported by senior leaders:
No executive takes this role seriously apart from FTSU Lead and one of the directors. Senior exec[utive]s just look at me blankly . . . I am not able to say yet that learning is happening at board and that changes have been made.
Adding to the impression of dislocation between Carly and senior colleagues was that senior colleagues’ perception of Carly’s work was somewhat mismatched with the practical and operational realities of undertaking the FTSUG role. For example, Carly described facing ‘most resistance in the role from managers’, especially when attempting to achieve timely responses and closure of concerns.
As noted earlier, some senior leaders had expressed concerns during interviews about the time that Carly invested in ‘wandering around’ hospital sites. During our fieldwork, an alternative characterisation to the ‘wandering Guardian’ presented itself, one in which Carly was frequently compelled to visit several operational areas to unblock concerns that had long languished on senior and/or middle managers’ desks. While shadowing Carly during such visits, we witnessed how achieving progress with a concern took considerable time and required physical endeavour and mental fortitude: walking significant distances, locating avoidant individuals in their offices or catching people in corridors, standing in front of them and being frank about what was needed.
Several interviewees praised Carly’s commitment and passion, which were also observed during fieldwork observations and FTSUG shadowing undertaken at Concord. Furthermore, Carly had waited for over 12 months to be allocated a dedicated office space to work within, by which time she had occupied an empty office space that still contained the previous occupant’s property, located on a remote and unkempt corridor adjacent to the main hospital building. All of this contributed to a frenetic and occasionally chaotic atmosphere to Carly’s working week, which comfortably exceeded the 15 hours allocated.
Summary
The early and ongoing phases of FTSUG role implementation at Concord overlapped with the publication of a critical CQC report, resulting in the replacement of senior role holders, significant structural reorganisation and a distinct deterioration in workers’ morale. This tumultuous transitional process offers an immediate and compelling explanation for the apparent breakdown in individual and shared understanding of the FTSUG role. However, the issues that led to Concord’s critical inspection, such as underinvestment, unacceptable working conditions and an ineffective and toxic workplace culture, did not appear overnight. Instead, these were long-standing issues that had a chronically damaging effect on the organisation and, ironically, had an impact on contemporary improvement efforts, including the Guardian’s implementation. For example, unlike all other case sites, Concord had developed no pre-existing speak-up processes, structures or initiatives in response to the Francis Report. The later publication of the Francis Review similarly triggered little action other than the appointment of the FTSUG, a role that was implemented without an overarching collective understanding of or strategy for FTSU, with few processes and boundaries to guide practices.
The sense of connection or after-effect from past actions or inactions to contemporaneous events was, therefore, ever present. The incomplete preparation and sense-making during the pre-implementation and early implementation phases was highly consequential for the ongoing implementation and deployment of FTSUG, as belated attempts to establish a FTSU strategy and process once Carly had been appointed were completely derailed by the necessary and all-embracing response to the CQC inspection.
Although encouraged and broadly supported by the FTSU executive lead, Carly implemented the role with little guidance or resource and without collective understanding, which, when added to the churn of senior staff, resulted in differing perspectives regarding the role’s remit and function at all levels of the organisation, from board to wards. Senior stakeholders were understandably and considerably distracted by the remedial actions required in response to the CQC’s report. However, their disengagement and incuriosity about all aspects of FTSU and the Guardian role specifically was surprising, especially given that a well-functioning FTSU system is positively evaluated by CQC inspectors. The FTSU executive lead’s departure coincided with the final weeks of fieldwork and noticeably left the FTSUG role further isolated within Concord, with Carly admitting that ‘I still need to find out who is my replacement line manager’, followed, half-jokingly, by ‘and if I need to find another job!’. Table 16 provides a brief summary overview of the main findings from Concord, as informed by NPT.
| NPT constructs | Case site summary of NPT construct |
|---|---|
| Coherence: sense-making work, individually and collectively | Minimal initial coherence work prior to FTSUG appointment. Thereafter, emerging coherence of FTSU as a patient safety/culture-building role derailed by CQC report. FTSU mostly lacking in shared coherence |
| Collective action: operational work to enact the role | Strategy vacuum/lack of collective coherence resulted in an isolated FTSUG enacting the role in a way that others did not understand or agree with. Local ‘just effing do it’ culture shaped a ‘problem-solving’ approach |
| Cognitive participation: relational work to build and sustain new practices | Relational work largely focused on responding to those speaking up and ensuring that avoidant managers responded to concerns. Minimal culture building to normalise speaking up across the organisation. Strained relations with newly appointed senior leaders |
| Reflexive monitoring: appraisal work to assess and understand new practices | Focused narrowly on counting concerns and presenting biannually to the board. Guardian was motivated and enthusiastic to embed reflection and learning but had little support from the board to translate enthusiasm into meaningful monitoring processes |
National stakeholder interviews
Interviews with national stakeholders about FTSUG implementation provided insights that were additional to, and possibly less invested than, the insights of those already interviewed, who work more closely and directly with FTSUGs. The seven interviews occurred between May and August 2020, and offered an opportunity for participants to reflect on their own experiences of the FTSUG role, the early findings of the study and the effect of the COVID-19 pandemic on FTSUGs. Two prominent and somewhat overlapping themes, ‘scratching the surface’ and ‘expectation management’, were identified during analysis, and are now discussed further.
Scratching the surface
A prominent theme across the interview data was the notion that FTSUGs were only ‘scratching the surface’ (SH1: workplace culture/policy expert) of workplace culture, rather than instigating meaningful change across trusts and the health-care system more generally. For example, some felt that trusts had implemented ‘a title rather than a role, they’ve not been as useful as we thought they might be’ (SH2: trade union legal advisor). This view was shared by others, with phrases such as ‘tick box implementation’ (SH7: third-sector campaign manager) used in relation to trusts that appointed a FTSUG without demonstrating significant commitment to, or providing sufficient resources to effect, culture change. There was a view that the appointment of large numbers of FTSUGs should not be mistaken as confirmatory evidence of deep culture change:
Just because there’s a vast number, doesn’t mean they are dealing with the climate. It could be that the more Guardians there are the more surface you’ll scratch.
SH1
Achieving change beyond the surface level was dependent on senior staff members within trusts being comfortable ‘with the idea of being challenged, not comfort-seeking all the time’ (SH4: national policy role). All of those who were interviewed broadly agreed with the premise that appointing a Guardian was, in itself, unlikely to trigger meaningful change. However, some of those interviewed described that that the presence of FTSUGs in the NHS was a step in the right direction. For example, interviewee SH4 (national policy role) explained that ‘appointing at least one Guardian in every NHS trust is excellent and in that respect I’d say it has met expectations’. A complementary view was that ‘after Mid Staffs we had to start somewhere and disrupt. Allowing local decision-making about implementation meant that appointments have taken off’ (SH6: national policy role).
Although the large number of concerns raised nationally was roundly welcomed, the NGO, trusts and FTSUGs were yet to convince national stakeholders that they had fully grasped the question of what a larger or smaller number of concerns actually represented, a shared view that is captured in the following extract:
I think the National Guardian and trusts have found that extracting meaning can be difficult. What does one concern or 10 actually mean? Annual increases mean what exactly?
SH5
Stakeholders’ perceptions that FTSUGs were yet to be established beyond the surface level of organisations were further reinforced when FTSUGs were redeployed into other roles during the COVID-19 pandemic:
At a very poignant moment when staff were more reluctant to speak up they should have been most active and noticeable.
SH1
We just didn’t see FTSUGs get involved with PPE [personal protective equipment] and BME concerns.
SH3
Expectation management
Building on some of the above insights, national stakeholders were also clear that expectations regarding the FTSUG role required managing and grounding in the realities of what was possible for one or a small number of Guardians to achieve:
Guardians can’t be the only way of improving speaking up. It can’t be all things to all people.
SH4
This was always intended as a cultural initiative where Guardians were one amongst many actions to improve speaking up. No one envisaged they would be tasked to singlehandedly carry speaking up and often while doing their own jobs.
SH6
As was the case with our earlier interviews, adequately supporting and resourcing Guardians was identified by national stakeholders as key to achieving the ambitious aims that were outlined in the FTSU Review. Some aspects of the role (e.g. line management and banding) were considered relevant for local, rather than national, decision-making. However, the issues of time and resource allocation and FTSUG well-being were consistently identified as key implementation issues requiring firm national implementation guidance, rather than trust-level decision-making. Reflecting earlier comments about the integrity and meaning of data collection, several stakeholders thought that a nationally agreed and co-ordinated online reporting system for Guardians was long overdue and would assist organisations to more fully analyse and track data.
To summarise, national stakeholders were of the view that, although the FTSUG initiative was to be welcomed and that appointing FTSUGs had raised awareness of speaking up, FTSUGs were yet to make a noticeable impact on workplace culture and speaking up in the NHS. Furthermore, local and national FTSU stakeholders were yet to satisfactorily address fundamental questions about the usefulness and meaning of FTSU data. Some of the overstated expectations associated with introducing the Guardian role were unrealistic, especially where implementation followed a ‘tick-box’ approach, which lacked insufficient resourcing, planning and an accurate assessment of the challenges and opportunities of introducing the freedom to speak up.
Chapter 6 Cross-case integration and discussion
This chapter draws together findings from across the six case sites in relation to the research aims, objectives and questions outlined in Chapter 2. In accordance with the aims and objectives, our cross-case analysis draws on multiple sources of data and is informed by the NPT and CFIR typologies. We particularly focus on the impact of implementation and deployment decisions on the realities of undertaking the FTSUG role. In doing so, we also embark on broader reflections of what our findings suggest about the challenges and opportunities for the future implementation and deployment of the FTSUG role. The research questions are then returned to in Chapter 7, where they are answered more directly and concisely, alongside key implications for practice, research and policy.
The CFIR’s overarching typology for implementation science suggests that interventions can be conceptualised as having ‘core components’ (essential and indispensable elements of the intervention) and an ‘adaptable periphery’ (adaptable elements, structures and systems related to the intervention and organisation into which it is being implemented). 26,118 It is notable that the FTSUG role is an intervention that has only one core component, namely that trusts are contractually compelled to implement the role. All other components of the intervention are adaptable (see Chapters 4 and 5), rather than core. The FTSUG job description15 provides a useful example because it presents trusts with non-binding and somewhat loosely explained ‘role expectations’, rather than a set of ‘hard core’ role components to implement.
Assessing implementation fidelity, which is defined as the extent to which ‘hard core’ or irreducible elements of the intervention have been implemented,119 is, therefore, deemed to be not particularly helpful or practicably possible. Instead, we opted to analyse multiple sources of data to rate the congruence that we perceived to exist between the implementation decisions made at each case site and the non-binding and somewhat loosely explained FTSUG role expectations, as outlined in Table 17.
| Role expectations | Summary of explanatory information from FTSUG job description |
|---|---|
| Appointing the FTSUG | Appointments should take into account the needs of workers and be made fairly, openly and transparently |
| Resourcing the role | FTSUGs should be supported with the resources they need, including ring-fenced time, to ensure that they meet the needs of workers |
| Senior leaders and executives | FTSUGs regularly meet in person with and report to senior leaders, including the CEO with meaningful reporting at board level |
| Operate independently | FTSUGs should operate impartially and objectively, while working in partnership with individuals, groups and the senior leadership team |
| Supporting workers to speak up | FTSUGs are responsible for ensuring that workers have access to training and knowledge, especially groups facing particular barriers to speaking up. Communicate regularly across the trust about their role and speaking up. Impact of these communications is measured |
| Information from speaking up used to learn and improve | Information triangulated with intelligence from other sources, such as patient safety, staff experience and service quality, and used to inform organisational learning and development |
| Case management | Cases recorded according to NGO guidance and cases managed effectively, fairly and transparently. Workers speaking-up are thanked and do not suffer detriment |
Congruence ratings (CRs) proved to be very useful summary indicators that triggered both within-case and cross-case insights, leading to analysis and synthesis of the potential effects of variances in implementation on the FTSUG role (Table 18). There are three congruence ratings (CRs):
-
CR = 2 – high degree of congruence between implementation decisions and FTSU role expectations
-
CR = 1 – an intermediate degree of congruence between implementation decisions and FTSU role expectations
-
CR = 0 – where there was no perceived congruence between implementation decisions and FTSU role expectations.
| Role expectations | Sub-component | Case sites and CQC well-led rating | Cross-case | |||||
|---|---|---|---|---|---|---|---|---|
| Albany: outstanding | Olympia: good | Montgomery: outstanding | Columbus: outstanding | Providence: good | Concord: requires improvement | |||
| Appointing FTSUG | Transparency | 2 | 0 | 2 | 2 | 2 | 2 | 10/12 |
| Resourcing the role | Time allocated | 2 | 1 | 0 | 2 | 1 | 1 | 7/12 |
| Resources allocated | 2 | 0 | 1 | 2 | 1 | 0 | 6/12 | |
| Senior leaders and executives | Board reporting and senior leader engagement | 2 | 2 | 1 | 2 | 1 | 0 | 8/12 |
| Operate independently | FTSU objectivity | 1 | 1 | 1 | 1 | 2 | 0 | 6/12 |
| Supporting workers to speak up | Policies and processes | 2 | 2 | 2 | 2 | 1 | 0 | 9/12 |
| Comms and engagement | 1 | 1 | 1 | 2 | 0 | 1 | 6/12 | |
| Learning and improving | FTSU data and experiences linked to improvement | 2 | 1 | 1 | 2 | 1 | 0 | 7/12 |
| Handling and managing cases | Support, resolution and follow-up | 1 | 2 | 1 | 1 | 2 | 1 | 8/12 |
| Total congruence per trust | > 11 high; 6–11 medium; < 6 low | 15/18 | 10/18 | 10/18 | 16/18 | 11/18 | 5/18 | 67/108 |
| Speak-up Index (2020) | Above national average 2; average 1; below average 0 | 2 | 2 | 1 | 2 | 0 | 0 | |
| Concerns recorded | Q3 2018/19–Q2 2019/2020 | 101 | 84 | 22 | 223 | 51a | 72a | |
The rows in Table 18 display CRs for each FTSUG role expectation at each case site, in addition to a cross-case total CR (final column). For example, ‘Resourcing the role’ includes the expectation that FTSUGs are allocated adequate and ‘ring-fenced time to ensure that they meet the needs of workers’ (contains public sector information licensed under the Open Government Licence v3.0). 15 A rating of 2 (high congruence) was assigned where a full-time FTSUG was implemented, a rating of 1 (partial congruence) was assigned where a FTSUG was implemented for 2–4 days per week and a rating of 0 (low or no congruence) was assigned where the FTSUG was implemented ≤ 1 day per week. Likewise, CRs for the ‘Senior leaders and executives’ categories were assigned as follows:
-
CR = 2 – direct and meaningful engagement between the FTSUG and multiple organisational leaders (e.g. directors of patient safety, HR/People, OD, medicine and nursing) and where FTSUG reports directly to the board and FTSU is critically and expansively discussed
-
CR = 1 – more limited contact (in frequency and number of individuals) between FTSUG and senior leaders and/or where the FTSUG may not attend and/or FTSU is a perfunctory item at board
-
CR = 0 – very limited or no contact with any senior leaders and/or where the FTSUG may not attend and/or FTSU is a perfunctory item or not discussed at the board meetings.
The columns in Table 18 show each individual trust’s congruence with each role expectation, culminating in a CR total for each case study site. The FTSU Index score and numbers of concerns provide further context. The final column (cross-case) is an indicator of congruence across sites. It is also important to note, as per the overall objective of this project, that CRs reflect trust implementation decision-making, rather than FTSUG performance.
In line with our stated research aims and objectives, the following sections demonstrate that the notion of congruence viewed through a NPT lens helps to further explain the effects of underlying decisions and processes on implementation, while also identifying factors that seem to be important in successful implementation of the role across cases. 120
Comparing congruence with role expectations between trusts: Normalisation Process Theory-inspired insights
Concord had the least congruence between FTSUG role expectations and implementation decisions (CR = 5), with Columbus (CR = 16) and Albany (CR = 15) demonstrating the most congruence. Some of the different CRs between these three sites are explained in Table 19 and are further discussed below in relation to the other three sites: Montgomery, Olympia and Providence.
| Role expectations | ||||
|---|---|---|---|---|
| Resources allocated | Policies support speaking up | Board reporting and leaders’ engagement | Learning and improvement | |
| Columbus and Albany: all expectations allocated CR = 2 (high congruence) | Administrative support, work space allocated, external supervision and support, abundant promotional material | Clear policies and processes to support FTSU driven by organisational strategy established at the outset | Some conflict between FTSU stakeholders, but discussions mostly constructive and respectful. Board interested and engaged with FTSU data | FTSUG data and experiences regularly reviewed and contributed to improvements in FTSU and collaborative improvement/cultural initiatives |
| Concord: all expectations allocated CR = 0 (low/no congruence) | No administrative support, formally allocated office space or external support/debriefing. Limited comms resources | Policies and processes unclear and lacking in coherent strategic direction | Little support and engagement from stakeholders and board. Discussions could often be undermining and hostile towards FTSUG | Review of data limited and no interface with FTSU improvements or culture-building initiatives |
Interpreted through a NPT lens, Table 19 establishes that FTSU stakeholders in Albany and Columbus responded positively during the pre-implementation and early implementation phases to a clear sense of what they were contractually required to do (FTSU coherence: see Table 19, column 3). As the implementation unfolded, their subsequent responses to this (their collective action: see Table 19, columns 4 and 5) were monitored and measured against the expectations of internal and external observers (reflexive monitoring: see Table 19, column 5). Allocating adequate resources (see Table 19, column 2) was an integral component of enabling and supporting these mechanisms. Increased resourcing at Columbus and Albany as the implementation unfolded (e.g. significant uplift in FTSUG hours, appointing FTSU support staff) was a by-product of actively monitoring the role’s ongoing effectiveness in relation to the shared understanding of the role’s potential contribution to the organisation. In Concord, pre-implementation, early or ongoing sense-making and reflexive monitoring were not evident and resources were limited for FTSUG implementation.
Establishing collective coherence was an important element as a necessary precursor to collective participation, monitoring and action, and, therefore, in creating a receptive FTSU ‘implementation climate’ in Albany and Columbia. Implementation climate is defined by Damschroder et al. 26 as the shared receptivity of involved individuals to an intervention. Importantly, receptivity and climate are both enhanced by adequate resources and the extent to which policies, procedures and related relationships support the implementation. In addition, our analysis suggests that the process and climate of implementation in these sites was also enhanced by various feedback loops prompting learning and adaptation as the implementation unfolded (both sites CR = 2 for learning and improvement). The implementation in Albany and Columbus could, therefore, be characterised as non-linear and interacting dynamically with factors that emerged as the FTSUG role became embedded.
By contrast, the implementation climate in Concord was characterised by a lack of shared receptivity, with minimal resourcing (see Table 19, column 2) and a lack of coherence, supportive relationships, policies and monitoring (see Table 19, columns 3–5). Pre-existing and extremely challenging contextual issues, allied (and possibly contributing) to the absence of pre-implementation and minimal early-implementation sense-making and a related leadership vacuum, derailed the implementation of the FTSUG role. Relational work (cognitive participation) with senior leaders (CR = 0) was particularly unproductive: a characteristic that seemed deeply entrenched in the culture of the organisation. This even extended to those recently appointed to senior roles being critical of FTSU, but with no related attempts to resolve obvious implementation problems (CR = 0 for learning and improvement), individually or collectively. For this reason, the implementation climate for FTSU was extremely unconducive to change, despite (or perhaps because of) major change occurring elsewhere in the trust.
Normalisation Process Theory helps us to draw out, as others have previously shown,120,121 that each normalisation mechanism works not through an aggregate effect of individual parts but because parts link together to form social systems that promote the embedding of interventions. For example, there is obvious synergy present when clear and collectively coherent FTSU processes and strategies co-exist with supportive/robust boundaries and relationships and monitoring.
The implementation of the FTSUG role at Olympia and Montgomery further reinforces these insights. For example, both trusts produced coherent FTSU processes and policies, but this coherence co-existed with deficits in resourcing the role, relational disputes and/or limitations to reflexive monitoring of FTSU performance. FTSU implementation in Providence similarly demonstrated strengths in relation to certain role expectations, such as achieving an effective balance of close engagement with, but also operational independence from, senior leaders (CR = 2). However, FTSU implementation paid less attention to other expectations, such as ensuring that FTSU data and monitoring processes for speaking up fed into service improvement and organisational learning (CR = 1). Implementation of the FTSUG role at these trusts can, therefore, be characterised as less dynamic and responsive to feedback mechanisms. Although these three trusts established coherence early in the implementation process, this overshadowed or occurred at the expense of some other activities. There was a sense that some FTSU stakeholders in Montgomery and Olympia were reluctant to question how the role was initially specified and understood, despite emergent feedback that some aspects of the role were not functioning optimally. In Providence, the significant sense-making effort invested in implementing an independent FTSUG and FTSU system had occurred somewhat at the expense of embedding the role into improvement and learning mechanisms or promotional activities.
These insights also resonate with our literature review findings (see Chapter 3), in which certain interventions were considered partially or fully ineffective when researchers conceptualised speaking up as consisting of unconnected individual actions, rather a system of interconnected parts; for example, communication training was introduced to improve raising concerns by workers, with no related efforts to improve the way that concerns were responded to by managers.
In summary, Figure 3 maps differences and similarities in the implementation of the FTSUG role in terms of NPT mechanisms across sites. Columbus and Albany are shown to have closely grouped NPT mechanisms, which are also in dynamic interaction (signified by the central four-way arrow). Implementation elsewhere is characterised by more fractured grouping, with some implementation mechanisms working closely (e.g. coherence and relational work in Olympia and Montgomery) and other aspects of implementation mapped as less connected and embedded. In Concord’s case, the mechanisms are disconnected, reflecting the troubled implementation of the role.
FIGURE 3.
Mapping similarities and differences in NPT mechanisms across sites.
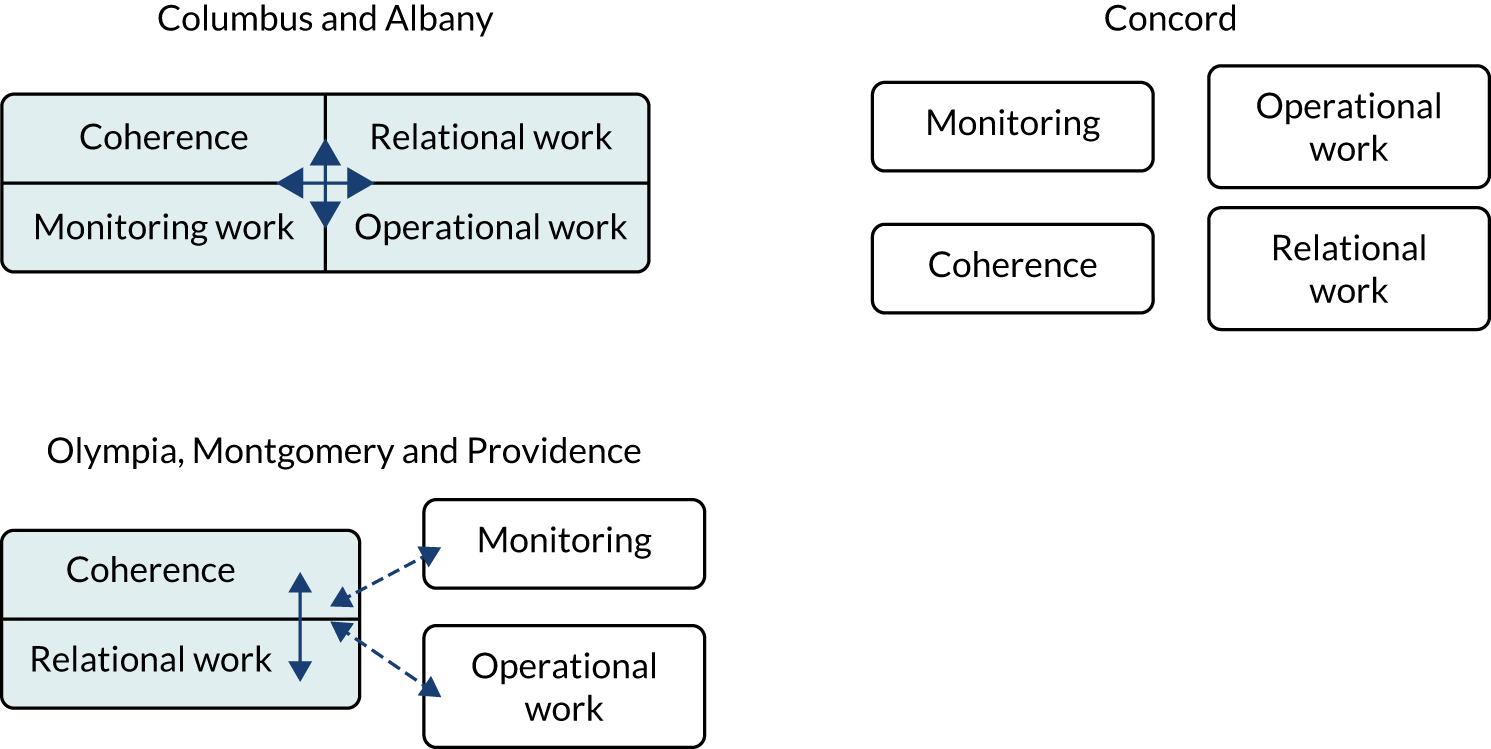
The significant influence of resources and reflexive monitoring
Resources allocated to the FTSUG role are further considered here given their significant impact on implementation. Compared with the other four case sites, Columbus and Albany invested significantly more resource (CR = 2) in supporting FTSU and their Guardians. In addition to investing in full-time FTSUG roles, other resources that were made available at initial implementation or added later included employing FTSU administrative assistants and a data analyst, purchasing a wide range of FTSU promotional material (e.g. mugs, cups and pens) and procuring sessional supervision and debriefing sessions for the FTSUGs with an external counsellor, among other things.
As noted in the preceding section, many of these resources were invested in response to monitoring (CR = 2) the role’s ongoing implementation, for example the provision of administrative support in the light of the unexpected and increasing demand of FTSU administration or counselling for Guardians in response to the emotionally exhausting work. Providence had also, to a lesser extent (CR = 1), augmented FTSUG resource, increasing the allocated hours from 1 to 3 days per week and allocating a dedicated workspace, as a direct response of monitoring earlier versions of the role.
Echoing our WP2 findings on the frustrating effects of time/resource scarcity on FTSUGs’ work, increased resources extended the Guardians’ capacity to undertake more proactive working (e.g. raising awareness of FTSU, culture building and triangulating data) rather than being restricted to reactive working (e.g. responding/supporting and documenting concerns). This is demonstrated in Figure 4 as a positive, ‘virtuous’, loop: reflexive monitoring led to the identification of operational gaps in provision, and this, allied with the availability of additional resources, led to the deployment of FTSUGs who more fully met the expectations of the role, including increased capacity to undertake more reflexive monitoring.
FIGURE 4.
Positive/virtuous feedback loop in Albany and Columbus.
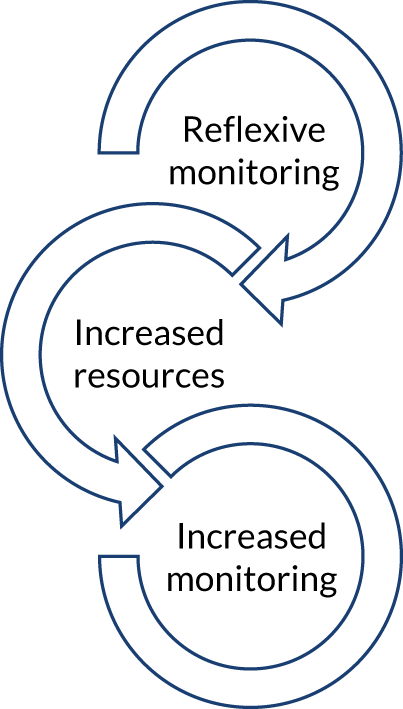
It is worth recalling that central funding was not made available to trusts to support the introduction of FTSU. This may have been particularly telling for resourcing decisions during the implementation of FTSU in Concord (CR = 0 for resourcing, CR = 1 for time). Dire financial circumstances and an estate that was undersized and unfit and in which office or meeting spaces were at a premium were instrumental in creating practical difficulties for the FTSUG and a broader context of low workforce moral and scarce innovation.
Although Montgomery had allocated an additional 2 hours per week to the FTSUG role (increasing the total to 6 hours per week, CR = 0), it along with Olympia and Concord, had maintained the status quo since implementation, and pre-implementation and early implementation resource assumptions and decisions remained largely intact. As was discussed in detail in Chapter 5, there were issues with reflexive monitoring, learning and improving (CR = 1) of the FTSU role in each of the sites that were potentially problematic.
For example, the decision by FTSU decision-makers not to increase FTSU resources in Montgomery was underpinned by the rationale that an optimal FTSU process would result in a small number of concerns being raised with the Guardian, thus obviating the need to increase FTSUG hours. As detailed in the case study, however, despite one confirmatory indicator (small numbers of concerns raised), FTSU decision-makers within Montgomery were also aware of evidence suggesting that the FTSU process was not functioning optimally or resourced adequately. Despite this, key decision-makers maintained that role reconfiguration was not required.
Similarly, in Olympia, although the FTSUG role was implemented as a role embedded within staff engagement and service improvement, our evidence (including the view of the Guardian) suggested that the role seemed to have minimal input into these areas; despite this, FTSU stakeholders insisted differently. Monitoring at both sites seemed to operate mostly to reassure stakeholders that their initial implementation decisions remained correct, rather than prompting a robust review based on the realities of undertaking the role.
Freedom to operate independently: a case of interdependence and independence?
The FTSUG job description highlights the ‘expectation’ that the role should ‘operate independently, impartially and objectively, while working in partnership with individuals and groups throughout their organisation, including senior leadership’ (contains public sector information licensed under the Open Government Licence v3.0). 15 The extent to which an employee, who is embedded, remunerated and managed within an organisation’s managerial structures and processes, can fully ‘operate independently, impartially and objectively’ is a question that is beyond the remit of this project to fully answer. However, our case study data provide useful insights into some tensions inherent to implementing a FTSUG who can operate independently. ‘Operating independently’ was allocated a CR score of 1 across most case sites, with the exception of Providence (CR = 2) and Concord (CR = 0).
It is useful to briefly reflect on certain features of the implementation of the FTSUG role at Providence that resulted in the allocation of the highest CR for this role expectation. For example, the appointment of a Guardian with little prior experience of corporate roles, strategy and organisational management contrasted with the Guardians who were appointed at the other sites. This point will be expanded on below. In addition, the Guardian in Providence was encouraged by key FTSU stakeholders to align the role with the recommendations published in the NGO’s guidance and the FTSU review’s ethos. These FTSU tenets, and the FTSUG’s understanding of them, acted as a metaphorical compass for the Guardian to navigate the many interdependencies, boundaries and complexities intrinsic to the FTSUG role. They also served to remind the FTSUG of the potential dangers of too much ‘alliance’ (a phrase used by the Guardian) with the trust at the cost of undermining the interests of those speaking up and the perceived legitimacy and independence of the role within the broader workforce.
We do not claim that other FTSUGs were not also guided by similar principles. However, notable at other case sites was the extent to which Guardians had to counterbalance the ethos of the FTSU role with competing organisational strategies and senior leaders’ expectations. For example, the FTSUGs in Albany, Olympia, Montgomery and Columbus operated, to varying degrees, within narrow role boundaries and organisational expectations originating from pre- and early-implementation coherence-setting activities. Corrective steps were taken by stakeholders to ensure that FTSUGs operated within organisational expectations to maintain, rather than disrupt, existing relationships and disciplinary boundaries. FTSUGs at Albany and Concord were, however, compelled periodically to disrupt these boundaries and relationships, but the resulting stress and conflict had a telling effect on both Guardians’ well-being, who described symptoms akin to burnout. FTSUGs at Olympia and Montgomery were less disruptive and, as discussed in the preceding section, the role was largely unchanged from how it was conceived in these trusts.
Other implementation factors that could weaken claims of the FTSUGs’ independence were the various prior associations between Guardians and FTSU stakeholders:
-
In Montgomery and Columbus, the FTSUGs previously held supporting FTSUG roles (both were previously FTSU Champions).
-
In Albany and Columbus, the FTSUGs had previously worked closely with senior organisational leaders as project managers.
-
In Olympus, the FTSUG previously occupied a senior management role, during which she wrote the FTSUG role specification and led initial discussions about the role’s introduction with senior leaders.
Each of the above FTSUGs, for different reasons, was known to organisational leaders and familiar with organisational expectations and boundaries. All were also fluent in the dialect of organisational strategy, improvement and project management. Again, we are keen to stress that we do not claim that such prior association renders these FTSUGs as lacking in independence or objectivity. However, the accounts of FTSU stakeholders were inconsistent; on the one hand they described wanting to appoint Guardians who could independently and robustly represent the workforce, but on the other hand known ‘insiders’ accustomed to the organisation’s ways of working were appointed.
It was evident that there were benefits to this ‘insider-ness’ and prior exposure and immersion to organisational processes and members, including Guardians being considered as a known and trusted person by workers in the organisation. It was evident that FTSUGs capitalised on their in-group knowledge of the distinctive language, behaviours and organisational rituals used by the people who FTSU interfaced with, which resulted in Guardians being privy to informal discussions and insider information beneficial to the work of FTSU. However, although building cohesive and strong connections with a variety of organisational stakeholders is an essential skill for a FTSUG, caution is needed to ensure that group dynamics do not inhibit the expression of dissenting views and, in doing so, undermine the delivery of safe care. 28 Reflexive monitoring can ensure that ‘insider-ness’ does not result in unquestioning acceptance of tacit understandings and business as usual, which could easily tip insider-ness towards groupthink, such that a sense of loyalty means group members avoid raising controversial issues. 122
Some of these points are surfaced when we further consider the FTSUG at Providence, which offers an interesting contrast to the discussion of insider-ness. Prior to being appointed, the Guardian was unacquainted with individuals working at the managerial and/or executive level and was unfamiliar with the various taken-for-granted language and concepts used during interactions at this level (describing having to learn a new language and having to clarify the meaning of the term ‘comms’ during a meeting). As a result, the FTSUG negotiated boundaries and relationships with key stakeholders on their own terms, independent of prior associations and relationships, which may restrict as well as enhance interactions.
In the case of Concord’s FTSUG, as has often been described in this report, there was no strategic direction or planning to guide FTSUG implementation. However, similar to Providence’s Guardian, being a clinician prior to appointment provided useful distance from the potential complications of previous associations with senior stakeholders and strategies. It could be argued, therefore, that the lack of prior association, the ‘light touch’ and inconsistent contact with senior leaders and the low-level organisational expectations meant that Concord’s Guardian was well positioned to operate independently and objectively. To some extent there was independence of action, with the Guardian ensuring that many concerns were managed effectively despite the considerable challenges identified in the preceding chapter. However, the lack of strategy and guidance for FTSU increasingly rendered the Guardian isolated from organisational overview, resulting in the development of operational practices that were revealed as problematic only when the Guardian interacted with recently appointed senior leaders who had worked with FTSUGs elsewhere.
Figure 5 summarises the preceding discussion of the independence–dependence/insider–outsider dynamic. The notion of independence is represented here on the x-axis, which indicates the extent to which FTSU issues were aligned with NGO and Francis Review expectations and principles or, alternatively, where FTSU principles could be intermittently overshadowed by organisational strategic priorities. The insider–outsider dynamic on the y-axis represents the extent of a Guardian’s prior associations with organisational stakeholders, processes and structures. An insider’s awareness could avail the FTSUG role of potentially valuable insights and opportunities, but the appointment of outsiders offered a fresh perspective on taken-for-granted working practices and expectations, which were more openly questioned and challenged. The positioning of FTSU at each trust is further discussed below, with brief reference to the CR for the ‘operating independently’ role expectation.
FIGURE 5.
The position of FTSU within case site trusts on the independence–dependence/insider–outsider dynamic. a, Concord’s position represents the Guardian’s status as a relative outsider, but also indicates that FTSU sits beyond the x-axis parameters, being simultaneously adrift of organisational strategy within Concord, as well as functioning outside most of the Francis Review’s/NGO’s expectations (CR = 0).
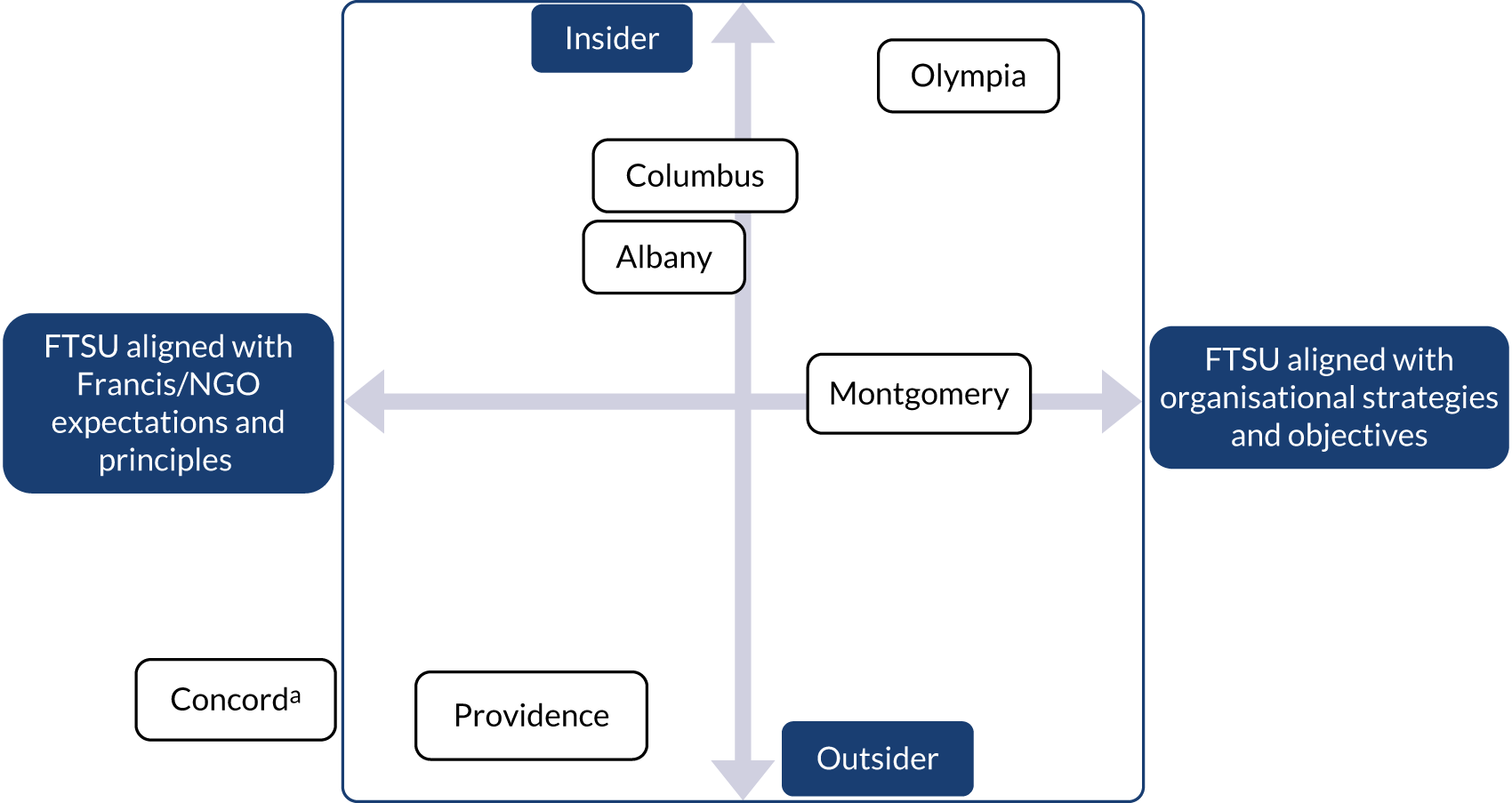
Providence is positioned with reference to a FTSUG who was an outsider in terms of prior associations, but also in relation to resisting close involvement in organisational or strategic initiatives that could be considered somewhat peripheral to FTSU and the interests of workers speaking up. FTSU at Providence was, therefore, strategically aligned with and practically guided by FTSU principles, with supportive line management and executive input that focused on maintaining the Guardian’s independent positioning (CR = 2).
Freedom to speak up at Albany and Columbus straddled the border between organisational priorities and expectations and FTSU principles and expectations. Guardians at both trusts had prior associations with senior stakeholders and strategic programmes before their appointment. Both were also heavily involved in a range of strategic and organisational initiatives following appointment, some of which at times appeared tangential to FTSU and would result in increased work pressures and time scarcity. Although there were indisputable benefits from involvement with organisational actors and broader strategies, FTSU principles could at times be blurred by prevailing organisational interests (both CR = 1).
Montgomery’s FTSUG positioning reflects being a relative outsider through working mostly in a clinical role, but also prior association with the FTSU programme as a Champion (CR = 1). FTSU more generally was closely aligned with organisational strategies and objectives, to the point that organisational priorities overshadowed FTSU expectations and the optimal working of the Guardian. Finally, Olympia’s (CR = 0) position reflects the FTSUG’s close and long-standing working relationships with senior organisational stakeholders and FTSU planning prior to implementation. In addition, FTSU principles, at times, struggled to gain legitimacy and independent strategic footing, being co-opted into senior leaders’ pre-existing organisational priorities rather than FTSU being represented as a key strategic imperative in its own right.
In keeping with our earlier discussion of dynamic contexts and the interplay of various factors within implementation settings, the labels of insider/outsider and aligned/not aligned should be understood as representing dynamic rather than static positions. It is not our intention to present these as binary labels that ‘freeze’ the position of FTSU and FTSUGs within trusts. Instead, we believe that it is rare within organisations for any individual to consistently remain an insider, and few remain complete outsiders. Our data have also shown how turbulent forces, triggered by internal and external events, can result in fluctuating positions along these dynamics on a daily or weekly basis, which adds enormous stresses and pressures on to FTSUGs. All FTSUGs, at times, are drawn away from FTSU principles by the strong pull and push of internal relationships, expectations and boundaries. At other times, Guardians successfully resist these internal forces (some more so than others) to productively pursue a FTSU-focused agenda of actions. External forces, such as the priorities of regulators, the NGO or national policy initiatives in response to exigent issues, such the COVID-19 pandemic, can similarly pull FTSU and FTSUGs in directions that are not always compatible with original FTSUG role expectations.
Identifying, monitoring and reflecting on these forces are key. Such increased awareness may help to forecast and possibly prevent forces pulling and pushing FTSUGs to positions that are incompatible with role expectations. Reflection by Guardians and others in the organisation using a simple tool, such as seen in Figure 5, may increase learning about stabilising forces, that is the forces that resist the displacement of FTSU and FTSUGs to positions in which they are less prevalent within the organisation or lose visibility completely.
To summarise, the FTSUG role expectations within the NGO’s job description explain that FTSUGs should operate independently, while also ‘working in partnership with individuals and groups, including senior leadership teams’ (contains public sector information licensed under the Open Government Licence v3.0). 15 This section has provided original insights into some of the difficulties and possibilities presented by FTSUGs working in partnership with others. The section shows that FTSUGs are skilled in undertaking aspects of partnership working, but also that partnership working can result in difficulties, especially when partners’ positions and views are unyielding to the views of Guardians and the principles of FTSU. Working independently and in partnership is a tricky undertaking for FTSUGs, and a process that organisational partners have to be ready and willing to participate in.
Optimal conditions for implementation of the Freedom to Speak Up Guardian role
Our study offers insights into features of implementation that seem consistently conducive with the wider ambitions of the FTSU Review and the FTSUG role. These insights stem from the careful attention invested during analysis to the interactions between coherence, relationships, operational decisions and reflexive monitoring during the process of implementation. The literature review, the breadth of our sampling and our reflexive within-case and cross-case analysis (see Chapters 5 and 6) reinforce our confidence in the rigour and transferability of our findings.
Optimal implementation has six interlinked components: (1) early, collaborative and coherent strategy congruent with the values of FTSU fosters the implementation of (2) policies and robust yet supportive practices (3) informed by frequent and reflexive monitoring of FTSU implementation, which is (4) underpinned by sufficient time and resource allocation, leads to (5) a positive implementation climate, which is best placed to engender sustainable FTSU culture and the well-being of a FTSUG.
Although the first four steps can occur simultaneously, the early establishment of a collaborative and coherent strategy for FTSU and the Guardian role set the context that fostered agreement about and alignment of productive policies, supportive practices and ongoing reflexive monitoring of the implementation. However, as the role is progressively embedded and implemented, reflexive monitoring emerges as being key to ensuring that implementation remains embedded within the values and expectations of FTSU, rather than becoming overly co-opted or lost to senior leaders or organisational priorities that may not be congruent with these values. Given the stressful nature of Guardians’ work, monitoring should also be extended to ensuring their well-being. Underpinning all of the above is sufficient resourcing to enable FTSUGs to undertake proactive practices that support speaking up, to build and maintain productive relationships with key stakeholders, and to collect and triangulate data to monitor FTSU across the organisation. Resources should also be allocated to ensure the personal and professional development of the FTSUG.
The self-reflection exercise demonstrated in Table 20 could be utilised by all trusts to review the current standing of the role’s implementation. Figure 5 could also be utilised during the exercise to plot and discuss the current positioning of the FTSUG and the forces that fix or challenge this position. Such reflective exercises are important because they reinforce the fact that FTSUG role implementation does not end when it is introduced into practice; in many ways, the introduction of the role into practice heralds the beginning, not the end, of the process.
| Key implementation climate statements | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| 1. Strategy is agreed, coherent and congruent with the values of FTSU | |||||
| 2. Policies and practices are robust and congruent with the values of FTSU: from the ‘board to ward’ | |||||
| 3. Reflexive monitoring of FTSU implementation and the FTSUG role is frequent, detailed and underpinned by curiosity about a range of ‘soft’ and ‘hard’ data sources | |||||
| 4. FTSUG believes that there is sufficient time and resource allocated to the role | |||||
| 5. The FTSUG role is currently supported and implemented in a way that protects the well-being of the FTSUG | |||||
| Implementation climate score (total of 1 + 2 + 3 + 4 + 5) |
The exercise in Table 20 could be completed each quarter alongside the NGO’s data return: trusts score their degree of agreement with each statement, from 0 (low) to 4 (high). The exercise should be a collaborative and reflexive process undertaken over ‘360 degrees’ by all FTSU stakeholders before totals are reviewed. Such an exercise can elicit constructive and reflexive conversations based on experiences and data, not preconceived ideas or assumptions about how the implementation of the FTSUG role has progressed, or not. It is clear from our data that many FTSUGs currently lack such a reflexive mechanism to trigger discussion and self-awareness with FTSU stakeholders.
Many of these factors mirror the NGO expectations for the FTSUG role, although documents, such as the job description that we have frequently referred to, are devoid of detail and a clear, coherent explanation (or ‘theory of change’) why all of the above factors are important, both individually, and perhaps even more so, collectively. It is the interconnectedness of these implementation factors that provides strength to the foundations and the structures that are required to fully implement this challenging role.
Chapter 7 Conclusion and research implications
In this final chapter, we return to the research objectives that were set out in Chapter 1. We present a narrative summary of our findings and identify implications for practitioners, policy-makers and future researchers under each objective in turn. Finally, we consider the strengths and limitations of the study.
Research objective 1: assess the scale and scope of the deployment and work of Freedom to Speak Up Guardians
Although all organisations had appointed FTSUGs soon after being notified of the requirement to do so, our findings in Chapters 4 and 5 painted a mixed picture, revealing wide variability in how the role had been implemented, resourced and deployed. We could discern no apparent pattern according to type of trust (acute or mental health), size (large or small) or CQC rating. We concluded that such was the variability in the implementation of the role that the FTSUG title is best considered as an umbrella term, covering the multiple versions of the role that exist simultaneously within each region and also across England.
Most trusts underestimated both the resources required by FTSUGs and (relatedly) the unmet need for speaking up within their workforce. The roots of such disparity lay in the absence of detailed specifications issued to trusts to guide the role’s introduction. However, it is striking that, given the freedom to choose how to implement the FTSUG role, most trusts opted to invest minimal resources to support the role’s implementation. Alarmingly, many FTSUGs clearly identified how the lack of available resources, especially time scarcity, directly and negatively affected their ability to respond to concerns, analyse and learn from speaking-up data, and, more generally, the extent to which FTSUGs developed their role and FTSU culture adequately and effectively. These may all negatively impact on workers’ intentions to speak up. Furthermore, undertaking such a complex and demanding role often resulted in Guardians experiencing significant levels of stress and emotional upheaval which led to deterioration in their psychological and physical well-being. This raises questions about the long-term sustainability of the role, especially in trusts that invest little resource in the role and where there is little specific psychological support for FTSUGs (as was often the case).
It is also striking that Guardians often felt unable to or simply did not raise these issues with FTSU stakeholders, or felt ignored when they did. This is partly explained by FTSUGs, trusts and the NGO equating the Guardian’s worth with the numbers of concerns raised, which is regarded as the primary indicator of FTSU culture. Trusts, the NGO and FTSUGs need to address this over-reliance on monitoring FTSU through counting: knowing the number of concerns raised is a necessary but not sufficient condition for understanding FTSU within trusts.
Reflexive monitoring of the ongoing implementation of the role by all FTSU stakeholders is, therefore, fundamentally important to ensuring that FTSU is properly resourced and undertaken in a way that is consistent with the Francis Review’s focus on protecting workers who speak up, ensuring learning from speaking up and promoting a culture in which workers feel free to speak up without fear of detriment.
Key actions
-
The following minimum resource requirements are required to ensure Guardians’ well-being and an implementation addressing all aspects of the role:
-
full-time position
-
allocated a budget
-
dedicated psychological support
-
access to a dedicated space to undertake their work.
-
-
Trusts that do not meet these minimum requirements should provide a clear assessment and rationale for their decision-making. Rather than FTSUGs presenting a business case to increase the hours/resources allocated, trusts need to justify why FTSUGs are not allocated full-time hours and appropriate resources.
-
CQC should evaluate the resourcing of the FTSUG role as part of the well-led inspection framework questions relating to a culture of high-quality, sustainable care (key line of enquiry W3).
-
Self-assessment of the climate of ongoing implementation/deployment of FTSUGs and the extent to which it is aligned with FTSU principles/expectations should be undertaken using the tools outlined in Chapter 6. The assessment should involve a range of stakeholders, including unions and patient groups.
Research objective 2: assess how the work of Freedom to Speak Up Guardians is organised and operationalised alongside other relevant roles with responsibilities for workers’ concerns
The variability in the role, outlined in research objective 1 above, also extended to how the role was organised and operationalised alongside other roles with responsibilities for concerns. FTSUGs were variously located and subsequently line manged within HR or OD, service improvement, or patient safety teams. Many were located within a corporate/executive infrastructure, for example with office space allocated alongside executive and/or corporate management teams and line managed by a chief executive or other executive board members (e.g. chief nurse). There were both positives and negatives to each of these locations; for example, being closely located within HR provided useful opportunities for shared learning, but could also raise questions about the independence of Guardians. Similarly, close association with executives afforded the role a certain amount of legitimacy and kudos, but also risked tarnishing FTSUGs’ credibility and independence through the appearance of being overly aligned with the interests of organisational leaders.
One of the key determinants of the extent to which the FTSUG role was operationalised into the everyday working of trusts was the degree of curiosity shown by trusts towards FTSU. Curious trusts, especially FTSU stakeholders (e.g. FTSU executive and non-executive leads, chairpersons, CEOs, directors/executives and staff-side leads), demonstrated a problem-sensing approach to FTSU and the Guardian role, consistently undertaking reflexive monitoring of the contribution of speaking up to the organisation and normalising rigorous analysis of FTSU data and triangulating with various other data sources. Demonstrable benefits of curiosity included improving the experiences of minority communities and workers who may otherwise be seldom heard from, alongside learning that fed into service improvements, including updating and improving the Guardian role. Curiosity also normalised an environment in which Guardians probed and enquired beyond established disciplinary boundaries and routine ways of working.
By contrast, where incuriosity was normalised, FTSUGs often worked within restrictive boundaries and practices in which senior leaders were disengaged and limited data were collected and ‘reported’, rather than analysed, triangulated and integrated, into routine organisational processes of reflection and improvement. The intrinsic curiosity of the Guardian, FTSU stakeholders and others with a remit for concerns was more important than the physical positioning of a FTSUG on an executive corridor or whether or not the CEO’s door was ‘open’. Positioning alongside and ‘access’ to leaders were often lauded as indicators of acceptance and a positive FTSU culture, but could be present in trusts in which FTSU contributed little to organisational actions and leaders’ behaviours seldom extended beyond the ‘laminated values’123 emblazoned on walls and web pages.
Key actions
-
Curiosity (in the form of reflexive monitoring and a problem-sensing approach to FTSU) should be recognised as a barometer of FTSU culture and assessed and addressed quarterly via the FTSU climate 360° self-assessment tool outlined in Table 20.
-
Positioning/location of the FTSUG should not be overly interpreted as meaningful in isolation. Being personally acknowledged and accepted by senior leaders is a necessary but not sufficient factor in establishing a robust relationship based on a clear data-driven and problem-sensing understanding of the FTSUG role and FTSU more generally.
-
Meaningful support for the FTSUG should include a clear commitment by senior leaders to open and psychologically safe exploration of all aspects of the FTSUG role.
Research objective 3: identify barriers to, facilitators of and unintended consequences associated with the implementation of Freedom to Speak Up Guardian roles
Many of these points and actions have been foreshadowed earlier in the chapter. To avoid overly repeating material, this section summarises the main facilitators of and barriers to the implementation of FTSUG roles, alongside key actions, where relevant:
-
Facilitators –
-
Agreed and coherent strategy that is congruent with the values of FTSU, which should be regularly reflexively monitored (every quarter) and adjusted as ongoing implementation and sustainability of the Guardian role is reviewed.
-
FTSU stakeholders, the FTSUG and relevant others adopt a problem-sensing approach to speaking up.
-
Adequate resourcing to enable all aspects of the role to be undertaken, rather than a selective or partial implementation approach. Resources should enable both reactive (managing and responding to concerns and routine data requests) and proactive (raising the profile of FTSU, data triangulation, FTSU outreach activities) working practices.
-
Trusts should optimise FTSUG performance by regularly assessing and maintaining the well-being of the FTSUG. Key actions for trusts include resourcing debriefing and restorative supervision for FTSUGs, from relevant individuals internally and/or via external individuals/agencies. FTSU resourcing, including access to well-being resources, should be a focus of CQC well-led inspection criteria.
-
-
Barriers –
-
Embedding FTSUGs within organisational strategies and traditional ways of working to the extent that FTSU is compromised by organisational demands, rather than meeting workers’ needs.
-
Recruiting FTSUGs who have prior close working relationships with senior individuals and organisational strategies to the extent that this may undermine FTSUG independence.
-
A form of retrograde and collective amnesia in that trusts and policy-makers appear to disregard or forget details of events in the NHS that occurred before the development of this role, for example detriment experienced by workers following speaking up.
-
Insufficient resources (scarcity of time, administrative support, budget for promotional activities and access to supervision).
-
NGO guidance currently allows too much FTSUG/trust interpretation, which undermines the accuracy and robustness of FTSU data collection and monitoring of concerns. Furthermore, guidance suggesting that the collection of ‘feedback’ (including key professional and personal characteristics) should follow the closure of cases significantly limits access to and use of potentially valuable data for the ongoing management and understanding of concerns.
-
FTSUG lacking an understanding of data anonymity and confidentiality and the use of data to generate reflection and learning; this should be addressed through training and clear best practice examples of the collection and use of potentially sensitive data.
-
Metrics, such as the number of concerns or the speak-up index ratings, are considered as the only indicators of FTSU culture and performance and are considered in isolation to other sources of data.
-
-
Unintended consequences –
-
The large and unexpected numbers of FTSU concerns raised to Guardians relating to unprofessional behaviours among colleagues, for example bullying, harassment and incivility. FTSUGs expressed deep frustrations that what they considered to be a mostly patient safety role was instead addressing significant unmet demand resulting from under-resourced and/or poorly executed HR processes and related issues.
-
NGO guidance and national publication of selected FTSU data resulting in certain types of data collection by FTSUGs not being undertaken or deemed as not required (e.g. ethnicity and protected characteristics data), or certain types of concerns not being deemed or counted as ‘proper’.
-
Celebrating annual increases in speaking-up cases has driven a perception that ‘more is better’ and perversely incentivises some trusts to seek increased quarterly numbers of concerns. However, there is a poor understanding generally of what more (or fewer) cases actually mean. Fewer cases in some trusts may well be cause for celebration.
-
When adjunct FTSUGs were allocated insufficient time, there was a ‘knock-on’ effect on their colleagues, who were burdened with increased work when covering for FTSUG colleagues.
-
Key actions
-
Freedom to Speak Up Guardian implementation should be sufficiently resourced to enable both reactive (managing and responding to concerns and routine data requests) and proactive (raising profile of FTSU, data triangulation and FTSU ‘outreach’ activities) working practices.
-
The NGO’s guidance on collecting FTSU data, monitoring concerns and gathering feedback from those speaking up is to be significantly tightened to reduce FTSUGs’ and trusts’ variable approaches to data collection and interpretation. A clear and national FTSU data reporting system should be introduced.
-
Freedom to Speak Up Guardians’ understanding of data anonymity and confidentiality and the use of data to generate reflection and learning should be addressed through training and clear best-practice examples.
-
Debriefing and restorative supervision for FTSUGs should be mandatory.
-
Sufficient FTSU resourcing, including access to well-being resources, should be a focus of CQC well-led inspection criteria.
-
The NGO and other national leaders need to counter the perception that (when counting concerns) ‘more is better’, which perversely incentivises some trusts to seek increased quarterly numbers of concerns. An open discussion and better understanding of what more (or fewer) cases actually mean should be promoted.
-
Trusts and CQC/NGO should review the ‘knock-on’ effect on adjunct FTSUGs’ colleagues, who are often burdened with increased work when covering for FTSUGs.
Research objective 4: evaluate the comparative effectiveness of different types of Freedom to Speak Up Guardian roles in supporting ‘freedom to speak up’
Our findings suggest that organisational histories and critical junctures were important in pre- and early-implementation decision-making. Some FTSUGs benefited, in terms of role effectiveness, when the introduction of the Guardian role was a continuation of work that had been commenced prior to the Francis Review. These early initiatives were prompted by specific internal events or by the realisation, especially following the Mid Staffordshire Inquiry, that improvements to speaking up in the NHS were long overdue. However, early gains in normalising a speak-up culture could be reversed, or derailed completely, by subsequent internal or external events. Similarly, organisations that may have initially delayed implementing or had a troubled early implementation could make rapid gains once early difficulties were navigated. The path to creating a culture of speaking up can be long and circuitous, seldom direct and linear.
Any direct comparisons of Guardians’ performance and effectiveness between trusts are unwise and fraught with difficulties owing to the marked variability in approaches to implementation, various organisational histories and unpredictable contemporary events, and diverse local interpretation of NGO guidance on counting and reporting concerns. However, FTSUGs were more likely to be effective when they were adequately resourced, supported by a clear and coherent strategy, and supported by policy that reinforced FTSU principles and was underpinned by an approach to monitoring and data that stimulated robust and transparent discussion of FTSU priorities, including future directions for the role.
Key actions
-
Trusts should closely track FTSUG implementation and FTSU culture over time and adapt in response to changes in the organisation and key FTSU stakeholders, and broader societal expectations and change. Current perceptions of implementation effectiveness are no guarantee of future effectiveness.
-
Comparisons of FTSUG performance or comparison of FTSU culture should fully consider local implementation and organisational factors to avoid reaching unhelpful and potentially misleading conclusions.
Strengths and limitations of the study
Strengths of the study include that this is, to the best of our knowledge, the first study to investigate the practices of FTSUGs within their workplaces. The study is also a rare insight into how speak-up concerns are managed and ‘processed’ within a health-care system. The complex interactions, interdependencies and associated emotional turmoil have, to date, largely been communicated and understood through the specific lenses and requirements of government/regulatory bodies or public inquiries, rather than subjected to robust independent research.
A further strength is the depth and richness of the data collected, including the analysis of 206 interviews alongside approximately 240 hours of observations and a large archive of organisational documents. It is also noteworthy that the nuanced data and associated insights and observations were generated from individuals and contexts ranging from ‘board to ward’. Collectively, these make a significant contribution to the understanding of the implementation of this internationally novel role, in addition to more broadly reflecting the current state of speaking up in NHS England.
As with all research projects, it is important to acknowledge the limitations of the study. First, the participants interviewed were self-selected. It is plausible that those interviewed represented organisations that were more receptive of FTSU/FTSUGs. Similarly, a related limitation is that some of the interview responses may have been viewed as ‘socially desirable’ and, therefore, may not always represent respondents’ true perceptions. Nevertheless, the balance of both positive and negative experiences conveyed by Guardians and others during interviews suggests that participants were not overly biased by considerations of social desirability. Furthermore, although WP2 is limited to interview accounts of FTSUGs’ views, prolonged periods of fieldwork during WP3 case studies (involving the collection of observational and documentary data, in addition to interviews with a range of stakeholders) provided a richer understanding and a balance to the views captured during interviews.
In WP3, although we purposively sampled volunteering trusts according to criteria such as size and location of the trust, CQC rating and type of FTSUG recruited (adjunct or standalone), there may be some important contextual factors that we were unable to select, and we cannot state categorically that our findings are necessarily generalisable to all acute trusts and mental health trusts in England or beyond. More longitudinal case studies may have uncovered additional or even, possibly, contradictory findings. Nevertheless, we are reasonably confident that the data collected are sufficiently deep and diverse to enable us to uncover important aspects of FTSU and the FTSUG role that are transferable to hospital trusts more generally.
Recommendations for research
The following recommendations for future research are considered to be of equal priority:
-
There is value in undertaking a similar study in non-hospital settings and where peripatetic working is commonplace, such as in ambulance services and in primary care settings.
-
The role of HR and ‘middle managers’ in the management of concerns is an area requiring further research, especially regarding the management of concerns relating to unprofessional and transgressive behaviours, which often led to practical difficulties, boundary conflicts and suboptimal learning from concerns.
-
Studies of the speaking-up experiences of minority communities and ‘seldom-heard’ workforce groups are a priority requirement.
-
Devolved administrations in Scotland and Wales have adopted different approaches to speaking up. Research undertaken in these contexts would offer valuable comparative insights and lessons for speaking up in systems designed in broadly similar ways and guided by similar, or the same, legislation, regulation and principles of care.
-
Studies of the Guardian role ≥ 5 years post implementation will provide an understanding of the medium-term impact of the role and further understanding of the links between pre- and early-implementation decisions and the longer-term sustainability of the role and well-being of Guardians.
Acknowledgements
We extend our thanks to all who participated in the study and to the members of the Project Advisory Group. We are also grateful to Project Administrator Claire Simpson for her contribution and support and Deborah Edwards for advice on conducting literature searching and screening.
Contributions of authors
Aled Jones (https://orcid.org/0000-0002-2921-8236) (Professor of Patient Safety and Healthcare Quality) designed the study, provided overall direction, conducted the narrative literature review, collected and analysed data and drafted sections of the report.
Jill Maben OBE (https://orcid.org/0000-0002-6168-0455) (Professor of Health Services Research and Nursing) designed the study, contributed to the narrative literature review, collected and analysed data and reviewed the report.
Mary Adams (https://orcid.org/0000-0003-1276-617X) (Senior Research Fellow) designed the study, contributed to the narrative literature review, collected and analysed data, drafted sections of the report and reviewed the report.
Russell Mannion (https://orcid.org/0000-0002-0680-8049) (Professor Health Systems) designed the study, contributed to the narrative literature review, analysed data and reviewed the report.
Carys Banks (https://orcid.org/0000-0002-5212-6217) (Research Fellow) collected and analysed data, drafted sections of the report and reviewed the report.
Joanne Blake (Research Associate) conducted the narrative literature review and collected and analysed data.
Kathleen Job (https://orcid.org/0000-0001-9959-2111) (Research Associate) analysed data, drafted sections of the report and reviewed the report.
Daniel Kelly OBE (https://orcid.org/0000-0002-1847-0655) (Professor of Nursing Research) designed the study, contributed to the narrative literature review, collected and analysed data, drafted sections of the report and reviewed the report.
Publications
Jones A, Blake J, Adams M, Kelly D, Mannion R, Maben J. Interventions promoting employee ‘speaking-up’ within healthcare workplaces: a systematic narrative review of the international literature. Health Policy 2021;125:375–84.
Jones A, Blake J, Banks C, Adams M, Kelly D, Mannion R, Maben J. Speaking up about bullying and harassment in healthcare: reflections following the introduction of an innovative ‘speak up’ role in NHS England. In Montgomery A, van der Doef M, Panagopoulou E, Leiter MP, editors. Connecting Healthcare Worker Well-Being, Patient Safety and Organisational Change: The Triple Challenge. Berlin: Springer; 2020. pp. 145–61.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review. Exclusive use will be retained until the publication of major outputs.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care.
References
- National Guardian Freedom to Speak Up . What Is Speaking Up? n.d. www.nationalguardian.org.uk (accessed 21 January 2021).
- Jones A, Kelly D. Deafening silence? Time to reconsider whether organisations are silent or deaf when things go wrong. BMJ Qual Saf 2014;23:709-13. https://doi.org/10.1136/bmjqs-2013-002718.
- Mid Staffordshire NHS Foundation Trust Public Inquiry . Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry 2013.
- Mannion R, Blenkinsopp J, Powell M, McHale J, Millar R, Snowden N, et al. Understanding the knowledge gaps in whistleblowing and speaking up in healthcare: narrative review of the research literature and formal inquiries, a legal analysis and stakeholder interviews. Health Serv Deliv Res 2018;6. https://doi.org/10.3310/hsdr06300.
- Macrae C. Early warnings, weak signals and learning from healthcare disasters. BMJ Qual Saf 2014;23:440-5. https://doi.org/10.1136/bmjqs-2013-002685.
- Martin GP, Chew S, Dixon-Woods M. Senior stakeholder views on policies to foster a culture of openness in the English National Health Service: a qualitative interview study. J R Soc Med 2019;112:153-9. https://doi.org/10.1177/0141076818815509.
- House of Commons Health Committee . Complaints and Raising Concerns 2015. https://publications.parliament.uk/pa/cm201415/cmselect/cmhealth/350/350.pdf (accessed 21 January 2021).
- Fasterling B, Brown A, Lewis D, Moberly R, Vandekerckhove W. International Handbook on Whistleblowing Research. Cheltenham: Edward Elgar Publishing; 2014.
- Lewis D, D’Angelo A, Clarke L. Industrial relations and the management of whistleblowing after the Francis report: what can be learned from the evidence?. Ind Relat J 2015;46:312-27. https://doi.org/10.1111/irj.12106.
- Black LM. Tragedy into policy: a quantitative study of nurses’ attitudes toward patient advocacy activities. Am J Nurs 2011;111:26-35. https://doi.org/10.1097/01.NAJ.0000398537.06542.c0.
- Dixon-Woods M, Baker R, Charles K, Dawson J, Jerzembek G, Martin G, et al. Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study. BMJ Qual Saf 2014;23:106-15. https://doi.org/10.1136/bmjqs-2013-001947.
- Francis R. Freedom to Speak Up. An Independent Review into Creating an Open and Honest Reporting Culture in the NHS 2015. http://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf (accessed 31 May 2022).
- Department of Health and Social Care (DHSC) . Learning Not Blaming: Response to 3 Reports on Patient Safety 2015.
- NHS Improvement and NHS England . Freedom to Speak Up: Raising Concerns (Whistleblowing) Policy for the NHS 2016.
- National Guardian Freedom to Speak Up . Freedom to Speak Up Guardian Job Description 2018.
- National Guardian’s Office . Recording Cases and Reporting Data. Guidance for Freedom to Speak Up Guardians 2021.
- NHS Improvement and NHS England . Guidance for Boards on Freedom to Speak Up in NHS Trusts and NHS Foundation Trusts 2019.
- National Guardian’s Office . Freedom to Speak Up Guardian Survey 2019 2020.
- National Guardian’s Office . Annual Report 2019 2020.
- National Guardian’s Office . Freedom to Speak Up Index Report 2020 2020.
- Øvretveit J. Understanding the conditions for improvement: research to discover which context influences affect improvement success. BMJ Qual Saf 2011;20:i18-23. https://doi.org/10.1136/bmjqs.2010.045955.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Hannigan B. Connections and consequences in complex systems: insights from a case study of the emergence and local impact of crisis resolution and home treatment services. Soc Sci Med 2013;93:212-19. https://doi.org/10.1016/j.socscimed.2011.12.044.
- Murray E, Treweek S, Pope C, MacFarlane A, Ballini L, Dowrick C, et al. Normalisation process theory: a framework for developing, evaluating and implementing complex interventions. BMC Med 2010;8. https://doi.org/10.1186/1741-7015-8-63.
- May C. Towards a general theory of implementation. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-18.
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009;4. https://doi.org/10.1186/1748-5908-4-50.
- Jones A, Kelly D. Whistle-blowing and workplace culture in older peoples’ care: qualitative insights from the healthcare and social care workforce. Sociol Health Illn 2014;36:986-1002. https://doi.org/10.1111/1467-9566.12137.
- Mannion R, Freeman T, Millar R, Davies H. Effective board governance of safe care: a (theoretically underpinned) cross-sectioned examination of the breadth and depth of relationships through national quantitative surveys and in-depth qualitative case studies. Health Serv Deliv Res 2016;4. https://doi.org/10.3310/hsdr04040.
- Mannion R, Davies HT. Cultures of silence and cultures of voice: the role of whistleblowing in healthcare organisations. Int J Health Policy Manag 2015;4:503-5. https://doi.org/10.15171/ijhpm.2015.120.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Jones A, Bugge C. Improving understanding and rigour through triangulation: an exemplar based on patient participation in interaction. J Adv Nurs 2006;55:612-21. https://doi.org/10.1111/j.1365-2648.2006.03953.x.
- Jones A, Blake J, Adams M, Kelly D, Mannion R, Maben J. Interventions promoting employee ‘speaking-up’ within healthcare workplaces: a systematic narrative review of the international literature. Health Policy 2021;125:375-84. https://doi.org/10.1016/j.healthpol.2020.12.016.
- Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: a theoretical and empirical analysis of systems change. BMC Med 2018;16. https://doi.org/10.1186/s12916-018-1057-z.
- Davidoff F. Understanding contexts: how explanatory theories can help. Implement Sci 2019;14. https://doi.org/10.1186/s13012-019-0872-8.
- Kelly D, Jones A. When care is needed: the role of whistleblowing in promoting best standards from an individual and organizational perspective. Qual Ageing Older Adults 2013;14:180-91. https://doi.org/10.1108/QAOA-05-2013-0010.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme 2006. www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed 3 June 2022).
- Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews?. Eur J Clin Invest 2018;48. https://doi.org/10.1111/eci.12931.
- Jones A, Hannigan B, Coffey M, Simpson A. Traditions of research in community mental health care planning and care coordination: a systematic meta-narrative review of the literature. PLOS One 2018;13. https://doi.org/10.1371/journal.pone.0198427.
- Millar R, Mannion R, Freeman T, Davies HT. Hospital board oversight of quality and patient safety: a narrative review and synthesis of recent empirical research. Milbank Q 2013;91:738-70. https://doi.org/10.1111/1468-0009.12032.
- Booth A, Moore G, Flemming K, Garside R, Rollins N, Tunçalp Ö, et al. Taking account of context in systematic reviews and guidelines considering a complexity perspective. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000840.
- Raemer DB, Kolbe M, Minehart RD, Rudolph JW, Pian-Smith MC. Improving anesthesiologists’ ability to speak up in the operating room: a randomized controlled experiment of a simulation-based intervention and a qualitative analysis of hurdles and enablers. Acad Med 2016;91:530-9. https://doi.org/10.1097/ACM.0000000000001033.
- Weiss M, Kolbe M, Grote G, Spahn DR, Grande B. Why didn’t you say something? Effects of after-event reviews on voice behaviour and hierarchy beliefs in multi-professional action teams. Eur J Work Organ Psychol 2017;26:66-80. https://doi.org/10.1080/1359432X.2016.1208652.
- Sayre MM, McNeese-Smith D, Leach LS, Phillips LR. An educational intervention to increase ‘speaking-up’ behaviors in nurses and improve patient safety. J Nurs Care Qual 2012;27:154-60. https://doi.org/10.1097/NCQ.0b013e318241d9ff.
- Dwyer J, Faber-Langendoen K. Speaking up: an ethical action exercise. Acad Med J Assoc Am Med Coll 2018;93:602-5. https://doi.org/10.1097/ACM.0000000000002047.
- Thomas EJ, Sexton JB, Neilands TB, Frankel A, Helmreich RL. The effect of executive walk rounds on nurse safety climate attitudes: a randomized trial of clinical units. BMC Health Serv Res 2005;5. https://doi.org/10.1186/1472-6963-5-28.
- Zimmerman R, Ip I, Daniels C, Smith T, Shaver J. An evaluation of patient safety leadership walkarounds. Heal Q 2008;11:16-20. https://doi.org/10.12927/hcq.2008.19643.
- Frankel A, Grillo SP, Pittman M, Thomas EJ, Horowitz L, Page M, et al. Revealing and resolving patient safety defects: the impact of leadership WalkRounds on frontline caregiver assessments of patient safety. Health Serv Res 2008;43:2050-66. https://doi.org/10.1111/j.1475-6773.2008.00878.x.
- Tucker AL, Singer SJ. The effectiveness of management-by-walking-around: a randomized field study. Prod Oper Manag 2015;24:253-71. https://doi.org/10.1111/poms.12226.
- Pronovost PJ, Weast B, Bishop K, Paine L, Griffith R, Rosenstein BJ, et al. Senior executive adopt-a-work unit: a model for safety improvement. Jt Comm J Qual Saf 2004;30:59-68. https://doi.org/10.1016/S1549-3741(04)30007-9.
- Lim RB, Ng BB, Ng KM. Evaluation of the patient safety Leadership Walkabout programme of a hospital in Singapore. Singapore Med J 2014;55:78-83. https://doi.org/10.11622/smedj.2014019.
- Columbus AB, Castillo-Angeles M, Berry WR, Haider AH, Salim A, Havens JM. An evidence-based intraoperative communication tool for emergency general surgery: a pilot study. J Surg Res 2018;228:281-9. https://doi.org/10.1016/j.jss.2018.03.007.
- O’Connor P, Byrne D, O’Dea A, McVeigh TP, Kerin MJ. ‘Excuse Me:’ teaching interns to speak up. Jt Comm J Qual Patient Saf 2013;39:426-31. https://doi.org/10.1016/S1553-7250(13)39056-4.
- Ginsburg L, Bain L. The evaluation of a multifaceted intervention to promote ‘speaking up’ and strengthen interprofessional teamwork climate perceptions. J Interprof Care 2017;31:207-17. https://doi.org/10.1080/13561820.2016.1249280.
- Pian-Smith MC, Simon R, Minehart RD, Podraza M, Rudolph J, Walzer T, et al. Teaching residents the two-challenge rule: a simulation-based approach to improve education and patient safety. Simul Healthc 2009;4:84-91. https://doi.org/10.1097/SIH.0b013e31818cffd3.
- Pannick S, Archer S, Johnston MJ, Beveridge I, Long SJ, Athanasiou T, et al. Translating concerns into action: a detailed qualitative evaluation of an interdisciplinary intervention on medical wards. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-014401.
- Rotteau L, Shojania KG, Webster F. ‘I think we should just listen and get out’: a qualitative exploration of views and experiences of Patient Safety Walkrounds. BMJ Qual Saf 2014;23:823-9. https://doi.org/10.1136/bmjqs-2012-001706.
- Martin G, Ozieranski P, Willars J, Charles K, Minion J, McKee L, et al. Walkrounds in practice: corrupting or enhancing a quality improvement intervention? A qualitative study. Jt Comm J Qual Patient Saf 2014;40:303-10. https://doi.org/10.1016/S1553-7250(14)40040-0.
- Oliver C, Jones E, Rayner A, Penner J, Jamieson A. Teaching social work students to speak up. Soc Work Educ 2017;36:702-14. https://doi.org/10.1080/02615479.2017.1305348.
- Benning A, Ghaleb M, Suokas A, Dixon-Woods M, Dawson J, Barber N, et al. Large scale organisational intervention to improve patient safety in four UK hospitals: mixed method evaluation. BMJ 2011;342. https://doi.org/10.1136/bmj.d195.
- Amiri M, Khademian Z, Nikandish R. The effect of nurse empowerment educational program on patient safety culture: a randomized controlled trial [published online ahead of print July 3 2018]. BMC Med Educ 2018. https://doi.org/10.1186/s12909-018-1255-6.
- Delisle M, Grymonpre R, Whitley R, Wirtzfeld D. Crucial conversations: an interprofessional learning opportunity for senior healthcare students. J Interprof Care 2016;30:777-86. https://doi.org/10.1080/13561820.2016.1215971.
- Johnson HL, Kimsey D. Patient safety: break the silence. AORN J 2012;95:591-60. https://doi.org/10.1016/j.aorn.2012.03.002.
- Gupta RT, Sexton JB, Milne J, Frush DP. Practice and quality improvement: successful implementation of TeamSTEPPS tools into an academic interventional ultrasound practice. AJR Am J Roentgenol 2015;204:105-10. https://doi.org/10.2214/AJR.14.12775.
- Hughes KM, Benenson RS, Krichten AE, Clancy KD, Ryan JP, Hammond C. A crew resource management program tailored to trauma resuscitation improves team behavior and communication. J Am Coll Surg 2014;219:545-51. https://doi.org/10.1016/j.jamcollsurg.2014.03.049.
- Hanson D. Reducing central line-associated bloodstream infection rates in the context of a caring-healing environment: a patient safety program evaluation. J Infus Nurs 2017;40:101-10. https://doi.org/10.1097/NAN.0000000000000212.
- Stewart-Parker E, Galloway R, Vig S. S-TEAMS: a truly multiprofessional course focusing on nontechnical skills to improve patient safety in the operating theater. J Surg Educ 2017;74:137-44. https://doi.org/10.1016/j.jsurg.2016.06.020.
- Savage C, Gaffney FA, Hussain-Alkhateeb L, Olsson Ackheim P, Henricson G, Antoniadou I, et al. Safer paediatric surgical teams: a 5-year evaluation of crew resource management implementation and outcomes. Int J Qual Health Care 2017;29:853-60. https://doi.org/10.1093/intqhc/mzx113.
- Kent L, Anderson G, Ciocca R, Shanks L, Enlow M. Effects of a senior practicum course on nursing students’ confidence in speaking up for patient safety. J Nurs Educ 2015;54:12-5. https://doi.org/10.3928/01484834-20150218-04.
- Balasubramanian BA, Chase SM, Nutting PA, Cohen DJ, Strickland PA, Crosson JC, et al. Using Learning Teams for Reflective Adaptation (ULTRA): insights from a team-based change management strategy in primary care. Ann Fam Med 2010;8:425-32. https://doi.org/10.1370/afm.1159.
- Robbins J, McAlearney AS. Encouraging employees to speak up to prevent infections: opportunities to leverage quality improvement and care management processes. Am J Infect Control 2016;44:1224-30. https://doi.org/10.1016/j.ajic.2016.03.007.
- Roh H, Park SJ, Kim T. Patient safety education to change medical students’ attitudes and sense of responsibility. Med Teach 2015;37:908-14. https://doi.org/10.3109/0142159X.2014.970988.
- Fleit HB, Iuli RJ, Fischel JE, Lu WH, Chandran L. A model of influences on the clinical learning environment: the case for change at one U.S. medical school. BMC Med Educ 2017;17. https://doi.org/10.1186/s12909-017-0900-9.
- White MC, Peterschmidt J, Callahan J, Fitzgerald JE, Close KL. Interval follow up of a 4-day pilot program to implement the WHO surgical safety checklist at a Congolese hospital. Global Health 2017;13. https://doi.org/10.1186/s12992-017-0266-0.
- Curry LA, Brault MA, Linnander EL, McNatt Z, Brewster AL, Cherlin E, et al. Influencing organisational culture to improve hospital performance in care of patients with acute myocardial infarction: a mixed-methods intervention study. BMJ Qual Saf 2018;27:207-17. https://doi.org/10.1136/bmjqs-2017-006989.
- Peters D, Adam T, Alonge O, Agyepong I, Tran N. Implementation research: what it is and how to do it. BMJ 2013;347.
- Hudson B, Hunter D, Peckham S. Policy failure and the policy-implementation gap: can policy support programs help?. Policy Des Pract 2019;2:1-14. https://doi.org/10.1080/25741292.2018.1540378.
- McConnell A. What is policy failure? A primer to help navigate the maze. Public Policy Adm 2015;30:221-42. https://doi.org/10.1177/0952076714565416.
- Pronovost P, Weast B, Rosenstein B, Sexton JB, Holzmueller CG, Paine L, et al. Implementing and validating a comprehensive unit-based safety program. J Patient Saf 2005;1:33-40. https://doi.org/10.1097/01209203-200503000-00008.
- Myers DJ, Nyce JM, Dekker SW. Setting culture apart: distinguishing culture from behavior and social structure in safety and injury research. Accid Anal Prev 2014;68:25-9. https://doi.org/10.1016/j.aap.2013.12.010.
- Noyes J, Booth A, Moore G, Flemming K, Tunçalp Ö, Shakibazadeh E. Synthesising quantitative and qualitative evidence to inform guidelines on complex interventions: clarifying the purposes, designs and outlining some methods. BMJ Glob Health 2019;4. https://doi.org/10.1136/bmjgh-2018-000893.
- Bonello M, Morris J, Azzopardi Muscat N. The role of national culture in shaping health workforce collaboration: lessons learned from a case study on attitudes to interprofessional education in Malta. Health Policy 2018;122:1063-9. https://doi.org/10.1016/j.healthpol.2018.06.013.
- Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q 1999;44:350-83. https://doi.org/10.2307/2666999.
- Corus C, Saatcioglu B. An intersectionality framework for transformative services research. Serv Ind J 2015;35:415-29. https://doi.org/10.1080/02642069.2015.1015522.
- Braithwaite J. Changing how we think about healthcare improvement. BMJ 2018;361. https://doi.org/10.1136/bmj.k2014.
- O’Donovan R, McAuliffe E. A systematic review exploring the content and outcomes of interventions to improve psychological safety, speaking up and voice behaviour. BMC Health Serv Res 2020;20. https://doi.org/10.1186/s12913-020-4931-2.
- Vaughn VM, Saint S, Krein SL, Forman JH, Meddings J, Ameling J, et al. Characteristics of healthcare organisations struggling to improve quality: results from a systematic review of qualitative studies. BMJ Qual Saf 2019;28:74-8. https://doi.org/10.1136/bmjqs-2017-007573.
- Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift. BMC Med 2018;16. https://doi.org/10.1186/s12916-018-1089-4.
- Cleary SR, Doyle KE. Whistleblowing need not occur if internal voices are heard: from deaf effect to hearer courage: comment on ‘Cultures of Silence and Cultures of Voice: The Role of Whistleblowing in Healthcare Organisations’. Int J Health Policy Manag 2016;5:59-61. https://doi.org/10.15171/ijhpm.2015.177.
- Ogbonna E. The uneasy alliance of organisational culture and equal opportunities for ethnic minority groups: a British example. Hum Resour Manag J 2019;29:309-27. https://doi.org/10.1111/1748-8583.12227.
- NHS Confederation . Chairs and Non-Executives in the NHS: The Need for Diverse Leadership 2019.
- Karpen SC. The social psychology of biased self-assessment. Am J Pharm Educ 2018;82. https://doi.org/10.5688/ajpe6299.
- Debono DS, Greenfield D, Travaglia JF, Long JC, Black D, Johnson J, et al. Nurses’ workarounds in acute healthcare settings: a scoping review. BMC Health Serv Res 2013;13. https://doi.org/10.1186/1472-6963-13-175.
- Felstead A, Green F, Grimshaw D, Fagan C, Hebson G, Tavora I. Making Work More Equal. A New Labour Market Segmentation Approach. Manchester: Manchester University Press; 2017.
- NHS Employers . Guide to Engagement for Line Managers 2020.
- Ball JE, Murrells T, Rafferty AM, Morrow E, Griffiths P. ‘Care left undone’ during nursing shifts: associations with workload and perceived quality of care. BMJ Qual Saf 2014;23:116-25. https://doi.org/10.1136/bmjqs-2012-001767.
- Halford S. ‘Towards a Sociology of Organizational Space’. Sociol Res Online 2004;9:13-28. https://doi.org/10.5153/sro.885.
- Barnsteiner J, Disch J. Creating a fair and just culture in schools of nursing. Am J Nurs 2017;117:42-8. https://doi.org/10.1097/01.NAJ.0000526747.84173.97.
- Ahern K. Institutional betrayal and gaslighting: why whistle-blowers are so traumatized. J Perinat Neonatal Nurs 2018;32:59-65. https://doi.org/10.1097/JPN.0000000000000306.
- Bjørkelo B, Macko M. The stigma of reporting wrongdoing at work: when doing right is perceived as wrong. Pol Psychol Bull 2012;43:70-5. https://doi.org/10.2478/v10059-012-0008-3.
- Stein M. The lost good self: why the whistleblower is hated and stigmatized. Organ Stud 2019;42:1167-86. https://doi.org/10.1177/0170840619880565.
- Kreiner GE, Ashforth BE, Sluss DM. Identity dynamics in occupational dirty work: integrating social identity and system justification perspectives. Organ Sci 2006;17:619-36. https://doi.org/10.1287/orsc.1060.0208.
- Di Fabio A, Palazzeschi L. Marginalization and precariat: the challenge of intensifying life construction intervention. Front Psychol 2016;7. https://doi.org/10.3389/fpsyg.2016.00444.
- National Guardian Freedom to Speak Up . Guardian Education and Training Guide 2018. www.cqc.org.uk/sites/default/files/20180419_ngo_education_training_guide.pdf (accessed 22 May 2022).
- Bunglawala Z. Please, don’t Call Me BAME or BME! 2019. https://civilservice.blog.gov.uk/2019/07/08/please-dont-call-me-bame-or-bme/ (accessed 10 May 2020).
- Lewis D, Glambek M, Hoel H, Einarsen SV, Hoel H, Zapf D, et al. Bullying and Harassment in the Workplace. Boca Raton, FL: CRC Press; 2020.
- Kline R, Somra G. Difference Matters: The Impact of Ethnicity on Speaking Up. London: National Guardian’s Office; 2021.
- NHS Confederation . The Impact of COVID-19 on BME Communities and Health and Care Staff. Member Briefing 2020. www.nhsconfed.org/publications/impact-covid-19-bme-communities-and-health-and-care-staff (accessed 16 June 2022).
- DiAngelo R. White fragility. Int J Crit Pedagogy 2011;3:54-70.
- Prior L. Using Documents in Social Research. London: SAGE Publications Ltd; 2003.
- Birmingham Women’s and Children’s NHS Foundation Trust . Black Lives Matter – an Open Letter from Our Trust Chairman and Acting Chief Executive n.d. https://bwc.nhs.uk/news/black-lives-matter-an-open-letter-from-our-trust-chairman-and-acting-chief-executive-2848/ (accessed 31 May 2022).
- Benjamin A. Dear White People in the UK – NHS Senior Leadership Onboarding and Support n.d. https://archive.ph/OxXQg (accessed 31 May 2022).
- Rauwolf P, Jones A. Exploring the utility of internal whistleblowing in healthcare via agent-based models. BMJ Open 2019;9. https://doi.org/10.1136/bmjopen-2018-021705.
- Hannigan B, Evans N. Critical junctures in health and social care: service user experiences, work and system connections. Soc Theory Health 2013;11:428-44. https://doi.org/10.1057/sth.2013.16.
- Capoccia G, Fiorestos O, Falleti TG, Sheingate A. The Oxford Handbook of Historical Institutionalism. Oxford, UK: Oxford University Press; 2016.
- Greener I. The potential of path dependence in political studies. Politics 2005;25:62-7. https://doi.org/10.1111/j.1467-9256.2005.00230.x.
- Jones A, Lankshear A, Kelly D. Giving voice to quality and safety matters at board level: a qualitative study of the experiences of executive nurses working in England and Wales. Int J Nurs Stud 2016;59:169-76. https://doi.org/10.1016/j.ijnurstu.2016.04.007.
- NHS England and NHS Improvement . Guidance for Boards on Freedom to Speak Up in NHS Trusts and NHS Foundation Trusts 2019.
- Maben J, Taylor C, Dawson J, Leamy M, McCarthy I, Reynolds E, et al. A realist informed mixed methods evaluation of Schwartz Center Rounds® in England. Health Serv Deliv Res 2018;6. https://doi.org/10.3310/hsdr06370.
- Pearson ML, Wu S, Schaefer J, Bonomi AE, Shortell SM, Mendel PJ, et al. Assessing the implementation of the chronic care model in quality improvement collaboratives. Health Serv Res 2005;40:978-96. https://doi.org/10.1111/j.1475-6773.2005.00397.x.
- Johnson MJ, May CR. Promoting professional behaviour change in healthcare: what interventions work, and why? A theory-led overview of systematic reviews. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-008592.
- May CR, Johnson M, Finch T. Implementation, context and complexity. Implement Sci 2016;11. https://doi.org/10.1186/s13012-016-0506-3.
- Mannion R, Thompson C. Systematic biases in group decision-making: implications for patient safety. Int J Qual Health Care 2014;26:606-12. https://doi.org/10.1093/intqhc/mzu083.
- Samuriwo R, Hannigan B, Pattison S, Todd A. Values in Health and Social Care: An Introductory Workbook. London: Jessica Kingsley Publishers; 2018.
Appendix 1 Work package 3: activity planning tables at case sites
| Date and time of meeting/visit/event etc. | Location | Meeting title and/or brief overview of activity |
|---|---|---|
| Potential interviewee – may overlap e.g. line manager may have another role | Notes and relevant contact details |
|---|---|
| 1. Chief executive | |
| 2. NED lead for speaking up | |
| 3. Executive lead for speaking up | |
| 4. Board secretary | |
| 5. Nursing director | Or nominated deputy |
| 6. Medical director | Or nominated deputy |
| 7. Therapies director | Or nominated deputy |
| 8. HR director | Or nominated deputy |
| 9. Quality lead | |
| 10. Patient safety lead | |
| 11. Estates director/manager | Also admin staff, catering etc. – i.e. support/ancillary staff not clinical |
| 12. Guardian’s line manager | |
| 13. Staff-side chairperson trade unions lead | Possibly more than one person |
| 14. Employees speaking up via Guardian | |
| 15. Champions, associates |
Appendix 2 Demographic details of Freedom to Speak Up Guardians who were interviewed
| Characteristic | Total (n) |
|---|---|
| Sex | |
| Male | 18 |
| Female | 69 |
| Age range (years) | |
| 18–24 | 0 |
| 25–34 | 5 |
| 35–44 | 21 |
| 45–54 | 35 |
| 55–64 | 23 |
| ≥ 65 | 3 |
| Ethnicity | |
| White | 75 |
| Black | 7 |
| Asian | 3 |
| Mixed | 2 |
Appendix 3 Time allocated to the Freedom to Speak Up Guardian role and ‘Agenda for Change’ banding of Freedom to Speak Up Guardian role occupant
| Agenda for Change banding | Time allocation | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 days | 0.5 days | 1 day | 2 days | 2.5 days | 3 days | 3.5 days | 4 days | 5 days | ||
| 5 | 1 | 1 | 2 | |||||||
| 6 | 1 | 3 | 1 | 1 | 6 | |||||
| 7 | 1 | 1 | 4 | 7 | 3 | 6 | 1 | 2 | 4 | 29 |
| 8a | 2 | 1 | 3 | 3 | 1 | 2 | 3 | 15 | ||
| 8b | 2 | 1 | 1 | 1 | 1 | 1 | 7 | |||
| 8c | 4 | 2 | 1 | 1 | 8 | |||||
| 8d | 3 | 1 | 1 | 5 | ||||||
| 9 | 1 | 1 | 2 | |||||||
| Very senior management | 1 | 1 | 2 | |||||||
| Other | 2 | 3 | 3 | 1 | 2 | 11 | ||||
| Total (% of sample) | 19 | 10 | 21 | 15 | 6 | 9 | 2 | 5 | 13 | |
Appendix 4 Interview schedules for work package 3 participants
Glossary
- Adjunct Freedom to Speak Up Guardian
- Those undertaking the Freedom to Speak Up Guardian role alongside another role. Cf. Stand-alone Freedom to Speak Up Guardian.
- Banding
- The NHS pay system that covers all staff except doctors, dentists and very senior managers. Each of the nine pay bands has a number of pay points. Staff will normally progress to the next pay point annually until they reach the top of the pay band. Pay ranges from £18,005 (the bottom of band 1 to £104,927 (the top of band 9).
- Board (trust board)
- A body with overall responsibility for the activity, integrity and strategy of the trust (accountable to the NHS Trust Development Authority and the Secretary of State for Health and Social Care).
- Care Quality Commission
- The organisation that monitors, inspects and regulates health-care services (e.g. hospitals, general practices and care homes) to make sure that they meet fundamental standards of quality and safety.
- Care Quality Commission overall inspection ratings
- Following inspection by the Care Quality Commission, health and social care services are awarded one of four possible ratings, namely outstanding, good, requires improvement and inadequate.
- Care Quality Commission well-led inspection rating
- A rating of the leadership, management and governance of the organisation ensuring that it provides high-quality care that is based around individual needs, encourages learning and innovation, and promotes an open and fair culture.
- Comfort-seeking
- A term used to describe managers who limit their purview to reassurances from limited sources that systems are compliant with regulatory standards, policy or guidance. Cf. Problem-sensing.
- Critical juncture
- A term often used in the analysis of institutions to signify events and developments in the past, generally concentrated in a relatively short period, that had a crucial impact on outcomes later in time (synonym: turning point).
- Foundation trust
- A trust that has a greater degree of managerial and financial autonomy than a standard NHS trust (see also Trust).
- Francis Report
- The report of the inquiry into the care provided by Mid Staffordshire NHS Foundation Trust between January 2005 and March 2009.
- Francis Review
- Also referred to as the Freedom to Speak Up review, an independent review published in 2015 into creating an open and honest reporting culture in the NHS. Commissioned by the Secretary of State for Health in response to the Francis Report.
- Freedom to Speak Up Ambassador/Freedom to Speak Up Champion
- A volunteer role dedicated to encouraging and offering rudimentary guidance to staff raising concerns. The role’s remit varies greatly across trusts, with some Champions assuming aspects of the Freedom to Speak Up Guardian’s remit.
- Freedom to Speak Up Executive Lead
- An executive director tasked with responsibility for freedom to speak up.
- Freedom to Speak Up Index
- A compound measure first published in 2019 by NHS England and the National Guardian’s Office combining the responses to four questions from the NHS staff survey. These questions relate to whether or not staff feel knowledgeable, secure and encouraged to speak up and whether or not they would be treated fairly after an incident. The index is used by organisations to monitor speaking-up culture in the NHS.
- Freedom to Speak Up Non-executive Director
- A designated non-executive director tasked with responsibility for freedom to speak up.
- Intranet
- A private internet network accessible only to an organisation’s staff.
- Problem-sensing
- A term used to describe managers and senior leaders who seek out issues and concerns, drawing on a wide range of hard data and soft intelligence. Cf. Comfort-seeking.
- Purposive sampling
- A non-probability sampling technique whereby the sample is selected for inclusion based on specific criteria (e.g. undertaking a role closely associated with speaking up).
- Staff-side chairperson
- The lead person representing the interface between the various unions, and sometimes recognised professional bodies, within an organisation. Staff-side chairpersons and committees operate differently in each organisation, but they mostly link with other workplace committees (including the board) and meet with employer representatives to ensure that workers’ voices are heard.
- Stand-alone Freedom to Speak Up Guardian
- Those whose sole role in the organisation is as a Freedom to Speak Up Guardian. Cf. Adjunct Freedom to Speak Up Guardian.
- Trust
- A body that manages hospitals or community services. An NHS trust may be responsible for managing one or many hospitals or community services, and can manage both hospitals and community services.
- Worker
- An individual who works for an NHS organisation. The term applies also to agency workers, temporary workers, students and volunteers.
List of abbreviations
- BAME
- black, Asian and minority ethnic
- BME
- black and minority ethnic
- CEO
- chief executive officer
- CFIR
- Consolidated Framework for Implementation Research
- CQC
- Care Quality Commission
- CR
- congruence rating
- EWR
- executive work round
- FTSU
- Freedom to Speak Up
- FTSUG
- Freedom to Speak Up Guardian
- HR
- human resources
- NED
- non-executive director
- NGO
- National Guardian’s Office
- NPT
- Normalisation Process Theory
- OD
- organisational development
- PAG
- project advisory group
- PPI
- patient and public involvement
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QI
- quality improvement
- WP
- work package