
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1002/34. The contractual start date was in June 2010. The final report began editorial review in July 2012 and was accepted for publication in November 2012. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors' report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen's Printer and Controller of HMSO 2013. This work was produced by Coombs et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Increasing pressure from technological developments and changes in legislation and government policy has meant that change can be regarded as a continuous feature of the contemporary health-care environment. 1 The ability of health-care managers or organisations to adapt and respond to change engendered by these stimuli is vital if they are to succeed in such an environment. Whether at the level of the individual or the organisation, change typically involves not only the learning of new behaviours, ideas or practices, but also giving up, or abandoning, some established ones. Despite both of these elements being equally important to change, there has been a significantly greater academic focus on processes of learning and acquiring new knowledge and practices than on processes of abandoning or giving up established knowledge and practices. 2 The objective of this study is to make a contribution to addressing this neglect through undertaking a detailed examination of individual-level processes of abandoning or giving up knowledge, which is more formally defined as unlearning.
The concept of individual unlearning
The capability to unlearn is important as the inability to give up or abandon knowledge, values, beliefs and/or practices can produce a rigidity in thinking and acting, and can create a blinkered outlook, limiting a health-care manager's or organisation's adaptability. 3 This can occur when existing views are never questioned or challenged, for example through the use of ‘defensive routines’. 4 The inability to question what may have been successful organisational norms, values, practices and knowledge can create what have been referred to as ‘competency traps’,5 in which useful competencies become outdated through never being challenged, revised or abandoned. Thus, the ability of health-care managers or organisations to unlearn established knowledge, behaviours or values can be a significant catalyst to and facilitator of change.
The analysis developed in this report builds from and extends the work of Tsang and Zahra,2 who developed a conceptual analysis of organisational-level unlearning processes. Tsang and Zahra 2 concluded their article by suggesting which areas of knowledge on unlearning are still limited and which require development (p. 1454). One key area where knowledge is particularly limited is the dynamics and character of individual-level processes of unlearning, and how they connect to and interact with organisational learning and unlearning. Individual-level processes of unlearning represent a neglected topic in an under-researched field, in which analysis has been relatively limited. Our concern here is to take a first step towards addressing this gap in knowledge.
Rushmer and Davies6 argue that distinctions can be made between three separate types of individual unlearning. The first type of individual unlearning that they identify, which they label fading, refers to the slow gradual process of unlearning that can occur over time, when particular skills and capabilities are forgotten through a lack of usage. This form of unlearning is typically not experienced as being significant or challenging for people, and because of the gradual way that it occurs people may not be conscious that they are experiencing it. The second type of individual unlearning identified by Rushmer and Davies is labelled wiping. This represents a more significant, deliberate and conscious form of unlearning. Wiping is a form of unlearning focused relatively narrowly on a particular practice, or activity, in which a person consciously unlearns through making deliberate efforts to give up a particular way of thinking/acting, as a precursor to changing these beliefs/practices. Rushmer and Davies argue that this process of unlearning may be initiated by some external catalyst, such as a change initiative, which places demands on people to change their ways of working and/or thinking. The third form of individual unlearning identified by Rushmer and Davies is deep unlearning. Deep unlearning represents a radical form of unlearning that typically occurs rapidly and unexpectedly, and is experienced by people as significant as it brings into question some basic assumptions and values. Because of these characteristics this form of unlearning can produce significant emotions (fear, confusion, etc.) in the people who experience it. Rushmer and Davies argue that some external catalyst, such as an event whose characteristics or outcomes are unexpected, initiates deep unlearning. A key difference between this form of individual unlearning and wiping is the speed at which the change is made and the emotional impact associated with the experience. Deep unlearning is argued to be a fast process involving high emotional impact for the individual experiencing the unlearning.
Context of the study
The central focus of this study was on examining the extent to which health-care managers engage in processes of individual unlearning. A typical catalyst for individual unlearning is processes of change that require the adaptation of working practices. 2 The pace of change in the NHS in recent years has been significant. For example, Greener7 talked about how the ‘pace and scope of change’ was ‘intense’ (p. 206). Thus, as a result of the amount of ongoing change in the NHS, all health-care managers are likely to have experiences of individual unlearning, in which they have had to adapt their work practices and routines as a result of change. Further, individual unlearning may also be experienced by health-care managers who have undergone a significant role transition, such as would happen when a clinician moves into a managerial role. For example, a clinician moving into a clinical management position may need to adapt the way he or she uses knowledge to act and make decisions, as anecdotal evidence suggests that clinical and managerial decision-making processes are underpinned and supported by different knowledge bases. Clinicians moving into managerial roles thus arguably need to engage in processes of individual unlearning to effectively adapt how they act and make decisions in the new managerial roles they occupy. The lack of research on the topic of individual unlearning means that there is a limited understanding of how frequently health-care managers experience it or the type of events/circumstances that trigger it. Therefore, in this study we also investigated the triggers to individual unlearning with all participating health-care managers.
This research was also concerned with understanding the barriers to and enablers of individual unlearning that exist. Although individual unlearning has the potential to be an important component in the processes of learning and change, research suggests that there are many barriers to unlearning at both the individual and the team/organisational level, which means that learning from mistakes, failure and crisis often does not happen. 8 Similar observations can be made regarding enablers to individual unlearning. For example, Becker9 argues that, to enable staff to have a positive attitude to change and consequently to unlearning, managers need to demonstrate commitment, make the case for change, involve staff in planning and provide reassurance. Other examples of enablers include having secure but challenging conversations with trusted colleagues,6 and the informal support of colleagues and managers9,10 and mentors. 10 The small amount of research on unlearning6 and learning from failure that has been carried out in the health sector suggests that this is a work context in which the barriers and enablers to unlearning can be significant. However, our understanding of the key barriers to and enablers of different forms of unlearning remains sketchy.
Existing research also suggests that NHS managers with clinical and non-clinical backgrounds may have a different approach to issues such as accountability, use of guidelines and finance. It has been argued that these differences are a result of each discipline's training, beliefs and experiences. 11 Similarly, there is evidence to suggest that clinicians and managers have different priorities concerning health-care delivery: clinicians tend to prioritise patient care, whereas managers focus more on cost. 12 Research by Guven-Uslu13 suggests that these different mindsets influence how managers with a clinical background are likely to approach decision-making compared with those without clinical experience. Given the increased emphasis that is being given to encouraging clinicians into leadership and managerial roles,14 these different mindsets are likely to become increasingly more significant to the efficient running of the NHS. Therefore, the individual unlearning processes associated with significant change, such as changes in role, may also have implications for the way that health-care managers review and reflect on their decision-making processes, and ultimately how they make future decisions.
Thus, there is a need for more research to understand the nature of individual unlearning in the health-care environment. The main aims of this study were to examine whether or not health-care managers engage in processes of individual unlearning, and the individual- and/or organisational-level barriers that may inhibit effective unlearning and learning from occurring or facilitate it. It also explored the implications of individual unlearning for managerial decision-making in the health service.
This study investigates these aims through an examination and synthesis of the academic literature concerning the processes of individual unlearning, and capturing and analysing health-care managers' experiences of individual unlearning. The study utilised a case study approach, investigating experiences of unlearning in two different types of NHS trust (an acute trust and a mental health trust). A case study-based approach represents a suitable methodology for the investigation of individual unlearning because, as outlined, individual unlearning is a relatively neglected and unexplored aspect of learning and change processes, and qualitative case studies provide an effective way to conduct exploratory research, which can give rich, qualitative insights into managers' experiences of individual unlearning. 15,16
Within each organisation, the main source of data was face-to-face, one-to-one, semistructured, qualitative interviews with a range of health-care middle managers. The purposive sample participants varied in terms of clinical/non-clinical background, type of department/unit and length of time as a manager. A total of 29 health-care managers were interviewed across both sites, which captured a total of 57 episodes of unlearning and 28 episodes of fading. The participants were also invited to attend a workshop to hear about initial findings and to comment on those findings.
Contributions
Although this original exploratory study is relatively small in scale, with the data drawn from 29 health-care managers from two NHS trusts, it still provides a number of important contributions. First, we have developed the concept of individual unlearning. We argue that individual unlearning is a distinctive type of learning, involving a conscious decision to give up knowledge, values or behaviours. However, this abandoned knowledge is not permanently lost but put to one side, and it remains retrievable for future use. Using this conceptualisation of unlearning, we argue that the category of fading proposed by Rushmer and Davies6 is more akin to a process of unintentional forgetting rather than unlearning. Indeed, fading may not enter individuals' consciousnesses unless they are invited to identify lost skills or capabilities. Therefore, as unlearning requires conscious and intentional action, it is questionable whether or not fading can be conceptualised as unlearning.
Second, we conceptualise two distinct types of individual unlearning and their differentiating features and dynamics. The first type of unlearning (behavioural) is triggered by a deliberate process of change that has been externally imposed. We argue that behavioural unlearning has a bidirectional relationship with organisational change and that an individual's attitude to change may shape his or her attitude to unlearning. A significant weakness in the unlearning literature is its neglect of people's attitudes to unlearning, an area that must be considered when attempting to understand individual behavioural-type unlearning processes. The second type of individual unlearning (cognitive) is triggered by an unexpected external event that questions some basic assumptions of the individual. We argue that it is important to recognise that the cognitive unlearning process is emotionally challenging, but may not occur suddenly or produce an instant change in behaviour.
Third, we develop a new typology that distinguishes between four separate types of individual unlearning, as shown in Table 1. Previous research on unlearning6 proposes that each type of individual unlearning is linked to a different type of catalyst. Thus, using Rushmer and Davies'6 labels, change events are the catalyst for wiping (behavioural unlearning), whereas individual experiences are the catalyst for deep unlearning (cognitive unlearning). However, during the course of data collection it became apparent that this distinction between catalysts was questionable, as the catalysts for both wiping and deep unlearning included both individual experiences and change events. Thus, our analysis suggested that, although the distinction between unlearning types was useful, as was the distinction between types of catalyst, Rushmer and Davies' typology could be improved through a recognition that specific catalysts were not associated with each type of unlearning. This led us to reconceptualise their typology (see Table 1). This was carried out by combining Rushmer and Davies' two types of unlearning, which results in a typology that distinguishes between four separate types of individual unlearning.
In addition, with two exceptions,6,17 the literature on this topic defines unlearning as the conscious and intentional abandoning of skills, behaviours and values, whereas fading equates to forgetting and is unconscious and unintentional (see Chapter 2, Types of individual unlearning and the nature of individual unlearning processes, Fading). De Holan and Phillips18 take this further by distinguishing between memory loss or accidental forgetting and unlearning, which is intentional. In our view, lack of conscious action means that fading is more akin to unintentional forgetting than unlearning, hence the exclusion of fading from the typology.
| Catalyst of unlearning | Type of unlearning | |
|---|---|---|
| Behavioural unlearning (wiping) | Cognitive unlearning (deep unlearning) | |
| Individual experience | Behavioural unlearning initiated by individual experience | Cognitive unlearning initiated by individual experience |
| Change event | Behavioural unlearning initiated by change event | Cognitive unlearning initiated by change event |
Another way in which we reconceptualised Rushmer and Davies' typology6 was by relabelling wiping as behavioural unlearning and deep unlearning as cognitive unlearning. The reason for doing this was to create labels for the unlearning types that were more explicit and clear regarding what was being unlearned, as supported by our empirical data analysis. In this new typology, ‘behavioural unlearning’ refers to the individual unlearning of specific behaviours such as practices, activities or routines, which have no (or limited) impact on people's underlying knowledge, values and assumptions. As in Rushmer and Davies' model,6 behavioural unlearning, like wiping, does not have a significant affective impact. Deep unlearning, which is relabelled ‘cognitive unlearning’, is emotionally charged as it involves giving up or abandoning more deeply held knowledge, values and assumptions. In making this distinction, we further found that, although behavioural unlearning may be restricted to this domain, cognitive unlearning is likely to be accompanied by or lead to behavioural unlearning. However, it must be emphasised that the typology was developed from the data analysis and informed by a review of the relevant literature and that Rushmer and Davies' unlearning typology was the initial perspective utilised to differentiate between different types of unlearning.
Fourth, our study also considers the influence of unlearning on health-care managers' decision-making, a variable that has not been examined in other unlearning studies. Our study provides evidence to suggest that individual unlearning can impact on some health-care managers' decision-making processes. This impact involves managers moving away from an idea imposition process of decision-making to a discovery-led process of decision-making. The discovery-led process has been argued in the literature to be more successful and, therefore, the findings from this study suggest that there may be a relationship between health-care managers who engage with individual unlearning and improvements in decision-making.
Fifth, our study involved a type of research data not previously utilised in this domain – qualitative interview data – which give insights into how individual health-care managers understand the changes that their unlearning experiences have produced.
Structure of the report
In the following chapter we review in more detail the literature concerning unlearning. The chapter clarifies and develops the unlearning concept before reviewing the academic literature on unlearning. The types of individual unlearning are discussed along with the nature of the individual unlearning process. The chapter also provides a summary of recent change in the NHS, which provides the context for the study. The chapter concludes with the research questions that the study investigated.
Chapter 3 discusses the key methodological considerations for the study. The choice of research strategy, selection of case study sites and processes of data collection and analysis are explained. The chapter also provides a description of the case study sites.
Chapter 4 presents the findings of the study and reflects on the research objectives presented at the end of Chapter 2. It is divided into six main sections. Episodes of individual unlearning and fading describes the nature of unlearning and fading episodes and the ways in which health-care managers experience unlearning and fading. Barriers to individual unlearning and Enablers of individual unlearning and fading report, respectively, the barriers to and enablers of unlearning and fading that were identified by participants. The impact of individual unlearning and fading on managers' decision-making reports the influence of individual unlearning on decision-making and the changes that participants had made in relation to the different types of unlearning experienced. The influence of health-care setting and professional background on health-care managers' individual unlearning and fading reports the analysis examining whether health-care context or the professional background of participants differentiated participants' experiences of individual unlearning and fading. Finally, Workshop findings provides a summary of the key findings from the workshop conducted at each case study site.
Chapter 5 discusses the key findings of the report in relation to the study research objectives and the existing literature. It also provides a discussion of the relationship between learning, unlearning and change that became evident during the course of the study. Finally, conclusions, limitations, recommendations for future research and implications for practice are presented in Chapter 6.
Chapter 2 Background
Introduction
This chapter draws on a range of literature to suggest that the process of individual unlearning may have particular features. The analysis of individual unlearning presented here is based on a review of the contemporary academic literature on unlearning, but to help address themes that are relatively unexamined by this literature it also draws on a wider body of work on learning and change. After the chapter unpacks and defines the concept of unlearning, it presents the details of the literature search that was conducted. Following this is a large section that differentiates between two different types of individual unlearning, and which suggests that each type of individual unlearning may have its own distinctive features and dynamics. The final two sections summarise recent changes in the UK health-care sector and present the research questions of the study.
Clarifying and developing the unlearning concept
Thus far, ‘unlearning’ has been very broadly defined as abandoning or giving up knowledge, ideas or behaviours. This is in contrast to ‘learning’, which has been defined as increasing one's capacity to take effective action through the addition of new skills or knowledge. 19 However, to fully understand the concept of unlearning it is necessary to define it in greater detail. Although unlearning can be traced back to the 1950s, until recently it has been largely neglected in the literature on learning and knowledge management. Akgün et al. 20 trace the origins of unlearning to literature on learning and cognitive psychology published in the 1950s and 1960s. Another perspective on unlearning emerged in the 1950s, which explored ‘unlearning . . . the inherent dominative mode’ in relation to Western thinking about the ‘other’ (p. 376). 21 The ‘other’ referred to how people in the West view people or perspectives they regard as non-Western. Unlearning in this context concerned Westerners trying to think beyond their own perspective to take account of others. 21 Indeed, some educational literature22 applied Williams'21 meaning to understand how trainee teachers could unlearn their attitudes to ethnic minority and working-class young people. Similarly, Mavin et al. 23 utilise unlearning in the same sense and suggest that an unlearning process is necessary to challenge the unquestioned and unchallenged gender-blind and male-biased character of the academic business and management literature.
In the business and management literature unlearning tends to be linked to one or more of organisational learning, change and memory,2,8,9,20 knowledge management24,25 or human resource management. 26 However, some authors draw on more than one discipline, relate unlearning to individuals and/or groups and locate the concept in the disciplines of education and learning2,22,27 or psychology. 26
If unlearning involves the giving up or abandonment of knowledge, values or behaviours, it needs to be acknowledged that this can happen both unconsciously and deliberately. The unconscious or accidental giving up of something is typically referred to as forgetting, as it occurs over time through particular knowledge or behaviours becoming unused and eventually forgotten. 6,17 This process of forgetting contrasts with deliberate unlearning, which involves a process of consciously choosing to abandon or give up particular knowledge, values or behaviours. As with Tsang and Zahra,2 the assumption here is that unlearning is a conscious and intentional process and, as such, is distinct from forgetting. De Holan and Phillips18 agree about the deliberate nature of unlearning, although they do not distinguish in the same way as others between forgetting and unlearning. Indeed, for them, ‘managed unlearning’ is one of four modes of forgetting old knowledge.
A second area of difference in the unlearning literature relates to whether or not the knowledge or behaviours being given up are obsolete, outdated and in some way inferior to new knowledge or behaviours that are subsequently acquired. As highlighted in Table 2, a number of articles make this assumption. 24,28,29 Thus, for example, Srithika and Bhattacharyya28 define organisational unlearning as ‘the identification or removal of ineffective or obsolete knowledge’ (p. 68). However, making such a value judgement regarding the inferiority of the knowledge to be abandoned is unnecessarily restrictive and judgemental. Thus, similar to Tsang and Zahra,2 we suggest that it is more appropriate to define unlearning simply as abandoning or giving up knowledge or behaviours without making any judgement on the status of the knowledge or behaviours being unlearned.
In considering individual unlearning, an issue that is typically neglected is what happens to the knowledge or behaviours that people unlearn. It is important to acknowledge that what is unlearned is not permanently lost by people such that they are unable to think or act in the way that they had done previously. Arguably, the only ways that particular capabilities could become permanently lost are through some type of medical or neurological intervention (drugs, surgery, etc.), through developing an illness or having an accident (such as having a stroke or a car accident that results in brain injury) or through lack of use over a long time period. Thus, the type of deliberate individual unlearning considered here does not involve the permanent loss of something, but instead involves a person putting particular values, knowledge or behaviours ‘to the side’ and consciously choosing not to continue using them. Thus, individual unlearning in this sense is not necessarily permanent because, either consciously or unconsciously, people may at some point in the future begin to reuse that which they had previously abandoned or unlearned. An example of this would be when someone changed how he or she undertook a task by returning to do it in a way that had been previously abandoned.
The final issue in developing the concept of unlearning is how it is relates to learning. Tsang and Zahra2 consider that unlearning may precede learning, occur simultaneously with learning or occur independently of learning. However, the dominant perspective regarding the relationship between the sequencing of unlearning and learning is that unlearning is a unique stage and is a prerequisite to, and a precursor of, learning. 20,26,30–32 For example, Cegarra-Navarro et al. 30 define unlearning as ‘the elimination of obsolete knowledge’, which is regarded as a necessary precursor to learning, or ‘the creation and absorption of new knowledge’ (p. 901). However, an alternative way to conceptualise the relationship between unlearning and learning is to consider unlearning as a distinctive type of learning. 33 This is the perspective utilised by Argyris and Schön,34 who argued that ‘we may also speak of the particular kind of learning that consists of “unlearning”: acquiring information that leads to subtracting something (an obsolete strategy, for example) from an organisation’s existing store of knowledge’ (pp. 3–4).
In summary, in examining individual unlearning this section suggests that individual unlearning should be conceptualised as a distinctive type of learning. It involves a conscious process of choosing to give up knowledge, values or behaviours. No value judgement should be made regarding the value or status of what is abandoned, and that what is unlearned is not permanently lost to people and may be utilised again at some point in the future.
Reviewing the academic literature on unlearning
Although Tsang and Zahra2 conducted a partial review of the unlearning literature, their central focus was organisational-level unlearning rather than individual unlearning. Their review identified 34 separate pieces of work. However, they do not specify the boundaries of the search that was conducted to produce this list, with it including book chapters and journal articles published over a wide time frame.
Because of the multidisciplinary nature of the interest in the topics of learning and unlearning, we searched several management (Business Source Complete, Emerald), psychological (PsycINFO), health (MEDLINE) and education [Education Resources Information Center (ERIC)] electronic databases for English-language articles that were published between January 2000 and March 2012. We searched for articles that had ‘unlearning’ in the title, abstract or keywords. Additionally, we searched for articles on ‘abandoning behaviour or knowledge’ and ‘giving up behaviour or knowledge’. This search generated over 330 articles. From these sources we concentrated on those published in peer-reviewed scientific journals, leaving 261 articles. After removing duplicate search results we examined the abstracts of these articles and excluded studies that reported on animal-based, psychological or memory experiments. We also excluded personal viewpoint and unreferenced opinion articles, leaving approximately 100 articles. After a first round of reading of the collected articles, we selected those articles that investigated the topic of unlearning, either theoretically or empirically. This led to the exclusion of articles that used the term ‘unlearning’ in the abstract or title, but which were not fundamentally concerned with investigating it as a topic. Although the focus in this article is fundamentally on individual-level unlearning, our initial review included all articles on unlearning, whether they were focused on individual-, team- or organisational-level unlearning (see Tables 2 and 3). We also searched the reference lists of all sources collected and performed citation searches, which resulted in the addition of several relevant articles.
A total of 34 articles2,3,6,9,10,20,22–26,28–32,37–49 were identified for analysis (Table 2). An initial observation from the list is that < 35 relevant articles were identified in a time period of over 10 years, which highlights the extent to which the concept of unlearning is neglected and underdeveloped. This neglect is in stark contrast to the considerable level of interest in the topic of learning since the mid-1990s. 5,35,36
In terms of how the literature defines unlearning (see Table 2, column 2), although many authors develop their own particular form of words, what is noticeable about the way that unlearning is defined (also found to be the case by Tsang and Zahra2) is the striking degree of homogeneity that exists. What is common to these definitions is that unlearning involves ‘abandoning’, ‘eliminating’, ‘rejecting’, ‘discarding’ or ‘giving up’ something – with that something being particular values, assumptions, knowledge or behaviour at the individual level, and knowledge, assumptions or routines at the organisational level.
In terms of the type of unlearning examined, as Table 3 highlights, there has been a greater focus on organisational or group or team unlearning (21 articles2,3,20,23,24,26,28,31,37,40,42–44,46,47,50–54) than on individual-level unlearning (16 articles6,9,10,22,23,25,26,29,30,32,37–39,41,45,48). In this context, group or organisational unlearning, as with organisational learning, refers to norms, assumptions, behaviours and routines that are collectively shared and understood. 20,24 Although a few articles look at multiple levels of unlearning,37 or the inter-relationship between different levels of unlearning,38 the vast majority of articles focus on one level of unlearning alone.
| Author | Definition of unlearning | Topic | Details of empirical study |
|---|---|---|---|
| Cegarra-Navarro et al.39 | Unlearning defined as ‘the changing of beliefs, norms, values, procedures and routines’ (p. 234) | How organisational context can counteract the negative effects of counterknowledge and facilitate individual unlearning | Survey of 164 small- and medium-sized enterprises in the Spanish construction industry |
| Wong et al.40 | Presents multiple definitions used by others – no clear definition | Develops and tests conceptual model to study effect of unlearning on the relationship between organisational learning and organisational success | Survey of 200 professionals in consultant offices and contractor firms in Hong Kong |
| Cegarra-Navarro et al.41 | No formal definition of unlearning | How organisational context facilitates individual unlearning of technology knowledge in a health-care environment | Survey of 117 nurse managers and medical managers |
| Cegarra-Navarro et al.42 | No formal definition of unlearning | How organisational context facilitates unlearning and influences organisational performance | Survey of 263 Spanish metal industry firms |
| Lee43 | Team unlearning defined as ‘ability . . . to change beliefs and routines to address rapidly changing environments’ (p. 1843) | Studies role of challenge and hindrance stressors on team unlearning | Survey of 200 new product development teams based in three science parks in Taiwan |
| Lee and Sukoco44 | Organisational unlearning defined as ‘actively reviewing and breaking down the organisation's long-held routines, assumptions, and beliefs’ (p. 412) | Studies role of team reflexivity and team stress on unlearning and product innovation | Survey of 200 new product development teams based in three science parks in Taiwan |
| Low45 | Presents multiple definitions used by others – no clear definition | Explores the antecedents of individual unlearning | Three focus groups with a total of 25 educators |
| Pighin and Marzona46 | Unlearning defined as ‘throwing away concepts learnt in the past to give space for possible new learning’ (p. 59) | Examines role of unlearning for business process re-engineering based on the reorganisation of information systems | Single case study |
| Zahra et al.47 | Uses Tsang and Zahra's2 definition of organisational unlearning: ‘the discarding of old routines to make way for new ones, if any’ (p. 324) | How organisational context may influence unlearning and entrepreneurial capability | None – conceptual article |
| Becker9 | ‘A process of releasing old ways’ (p. 252) | Examines factors that facilitate and inhibit unlearning during a change process | Survey of people involved in change in one Australian company |
| Casillas et al.24 | Organisational unlearning defined as per Cegarra-Navarro and Mayo37 as eliminating ‘ineffective and obsolete knowledge and routines’ (pp. 162–3) | How organisational unlearning affects internationalisation | Survey of 103 Spanish small- and medium-sized enterprises |
| Cegarra-Navarro et al.30 | Individual unlearning defined as ‘the elimination of obsolete knowledge’, which is regarded as a necessary precursor to learning (‘the creation and absorption of new knowledge’) (p. 901) | How organisational context facilitates individual unlearning | Semistructured interviews with nine staff in a Spanish regional hospital |
| Cegarra-Navarro et al.48 | Individual unlearning defined as in Cegarra-Navarro et al.30 | How unlearning affects knowledge of the business environment | Survey of 127 Spanish hospitality companies |
| Conner22 | Unlearning defined as ‘any time when prospective teachers describe instances or ways in which they come to recognize and rethink previously held views and attitudes’ (p. 1171) | Role of unlearning in changing perspectives and attitudes of low-income urban youth | Interviews with and survey of 21 prospective educators |
| Yildiz and Fey49 | Use Tsang and Zahra's2 definition of organisational unlearning: ‘the discarding of old routines to make way for new ones, if any’ (p. 450) | Develops theoretical model regarding the role of organisational unlearning in knowledge transfer processes | None – conceptual article |
| Srithika and Bhattacharyya28 | Organisational unlearning defined as the ‘identification and removal of ineffective or obsolete knowledge’ (p. 68) | How appreciative inquiry (a particular type of organisational development intervention) can facilitate the process of organisational unlearning | None – conceptual article |
| Becker10 | Presents multiple definitions used by others – no clear definition | Examines factors that facilitate and inhibit unlearning during a change process | Qualitative case studies of change in three Australian companies (23 interviews) |
| Tsang and Zahra2 | Organisational unlearning defined as ‘the discarding of old routines to make way for new ones, if any’ (p. 1437) | Developing understanding of the concept of organisational unlearning | None – literature review |
| Tsang50 | Organisational unlearning defined as ‘the discarding of old routines to make way for new ones’ (p. 7) (does not have the ‘if any’ element of definition in Tsang and Zahra2) | How organisational unlearning affects knowledge transfer processes | Interview-based study of a number of technology transfer joint venture initiatives |
| Akgün et al.51 | Unlearning defined as ‘changes in beliefs and routines in the organisation’ (p. 207) | How environmental turbulence affects team unlearning and team unlearning affects team performance | Survey of 197 firms in north-east region of the USA |
| Akgün et al.20 | Individual and organisational unlearning defined as ‘eliminating memory’ (p. 797) | Develops understanding of the unlearning concept through linking it to the literature on change and organisational memory | None – conceptual article |
| Fotaki31 | Unlearning defined as ‘the absence of in-depth questioning of predominant paradigms’ (p. 1063) | Lack of learning by UK and Swedish governments in relation to patient choice regarding health care | None – conceptual article |
| Rebernic and Sirec29 | Abandoning ‘obsolete tacit knowledge’ (p. 406) | The problems and challenges related to managing and unlearning tacit knowledge | None – conceptual article |
| Cegarra-Navarro and Sanchez-Polo38 | Definition of individual unlearning not clearly specified | The effect that individual unlearning had on organisational relearning | Survey of 130 small- and medium-sized enterprises in the Spanish telecommunications sector |
| Cegarra-Navarro and Dewhurst25 | Individual unlearning defined as a ‘process in which obsolete and misleading knowledge is rejected’ (p. 50) | How organisational context facilitates individual unlearning | Survey of 139 Spanish optometrists |
| Akgün et al.3 | Team unlearning defined as ‘changes in beliefs and routines’ (p. 73) | How the business environment affects team unlearning, as well as some consequences of this | Survey of 319 new product development teams in the USA |
| Becker et al.26 | Unlearning defined as ‘the process by which individuals and organisations acknowledge and release prior learning (including assumptions and mental frameworks) in order to accommodate new information and behaviours’ (p. 610) | The extent to which different types of organisation take account of unlearning in human resource development interventions | Survey of 70 Australian human resource and operational managers |
| Cegarra-Navarro and Moya37 | Individual unlearning defined as ‘the capacity of individuals to reflect on their performance in order to identify and promote actions that will result in improved performance’ (p. 162) | How individual and group unlearning contribute to organisational performance | Survey of 139 Spanish optometrists |
| Rushmer and Davies6 | Individual unlearning defined as ‘getting people to stop doing things’ (p. 10) | Developing the concept of unlearning by examining processes of unlearning and distinguishing between different types of unlearning | None – conceptual article |
| Rampersad52 | No formal definition of unlearning | Developing analysis that regards change as fundamentally involving learning and unlearning | None – conceptual article |
| Mavin et al.23 | Defines unlearning as ‘raising and challenging taken for granted assumptions’ (p. 572) | The ‘gender-blind’ and male-biased nature of management education | None – conceptual article |
| Sheaffer and Mano-Negrin53 | Defines unlearning as ‘systematically rethinking and overhauling prescribed procedures, programmes, policies, and strategies underlying flexible corporate vision’ (p. 581) | Assesses the extent to which companies' unlearning capability predicts their crisis preparedness | Survey of 130 chief executive officers or vice-presidents for human resource management in Israeli firms |
| Sinkula54 | Organisational unlearning defined as ‘process by which firms eliminate old logics and make room for new ones’ (p. 255) | Develops a conceptual model to map how organisational unlearning is linked to organisational performance | None – conceptual article |
| MacDonald32 | Transformative unlearning regarded as a complex, challenging and lengthy process; about giving up established practices/knowledge/assumptions that may be linked to sense of identity | Develops understanding of the character, dynamics and emotional challenges of ‘transformative unlearning’ | Detailed reflection on personal experience |
| Author | Individual or organisational unlearning | Aspect of unlearning examined (antecedent, process or consequences) |
|---|---|---|
| Cegarra-Navarro et al.39 | Individual | Antecedent |
| Wong et al.40 | Organisational | Consequences |
| Cegarra-Navarro et al.41 | Individual | Antecedent |
| Cegarra-Navarro et al.42 | Organisational | Antecedent |
| Lee43 | Team | Antecedent |
| Lee and Sukoco44 | Organisational | Antecedent |
| Low45 | Individual | Antecedent |
| Pighin and Marzona46 | Organisational | Antecedent |
| Zahra et al.47 | Organisational | Antecedent |
| Becker9 | Individual | Antecedent |
| Casillas et al.24 | Organisational | Consequences |
| Cegarra-Navarro et al.30 | Individual | Antecedent |
| Cegarra-Navarro et al.48 | Individual | Consequences |
| Conner22 | Individual | Antecedent |
| Yildiz and Fey49 | Organisational | Consequences |
| Srithika and Bhattacharyya28 | Organisational | Process |
| Becker10 | Individual | Antecedent |
| Tsang and Zahra2 | Organisational | Process |
| Tsang50 | Organisational | Consequences |
| Akgün et al.51 | Team | Antecedent and consequences |
| Akgün et al.20 | Organisational | Antecedent and process/types of unlearning |
| Fotaki31 | Organisational | Consequences |
| Rebernic and Sirec29 | Individual | Consequences |
| Cegarra-Navarro and Sanchez-Polo38 | Individual | Consequences |
| Cegarra-Navarro and Dewhurst25 | Individual | Antecedent |
| Akgün et al.3 | Team | Antecedents and consequences |
| Becker et al.26 | Individual and organisational | Antecedent |
| Cegarra-Navarro and Moya37 | Individual and team/group | Consequences |
| Rushmer and Davies6 | Individual | Process/types of unlearning |
| Rampersad52 | Organisational | Process |
| Mavin et al.23 | Individual and group | Consequences |
| Sheaffer and Mano-Negrin53 | Organisational | Antecedent |
| Sinkula54 | Organisational | Consequences |
| MacDonald32 | Individual | Process |
Another difference in the focus of the reviewed articles was whether they examined the antecedents, process or consequences of unlearning. The largest proportion of articles (n = 183,9,10,20,22,25,26,30,39,41–47,53) examined the antecedents of unlearning, with unlearning facilitated by the organisational context,9,25,30 environmental turbulence51 and organisational size. 26 A total of 133,23,24,29,31,37,38,40,48–51 of the reviewed articles examined the consequences of unlearning, with unlearning argued to be related to a diverse range of processes and outcomes including knowledge transfer processes,49,50 processes of internationalisation,24 the non-academic impact of academic scholarship,33 organisational performance37,54 and health-care policies. 31 Finally, only 62,6,20,28,32,52 of the 34 articles examined the character and dynamics of unlearning processes.
Table 3 also reveals that of the 34 articles reviewed only two6,32 focused on individual processes of unlearning. These are the articles by Rushmer and Davies6 and MacDonald. 32 Further, of these two only MacDonald32 presents any empirical evidence, which was a reflection on personal experience. Thus, to say that there is a conceptual and empirical gap in knowledge with regard to the process of individual unlearning is an understatement.
The following utilises the work of MacDonald32 and Rushmer and Davies6, as well as some other literature on learning and change, to consider the character and dynamics of the process of individual unlearning. In so doing it is suggested that distinctions can be made between different types of individual unlearning.
Types of individual unlearning and the nature of individual unlearning processes
As has been outlined thus far, distinctions can be made between individual- and organisational-level unlearning, and between the unlearning of values/assumptions, beliefs, skills, knowledge and/or behaviours. A number of authors go beyond these distinctions to construct distinctive categories of unlearning. 6,51,54 For example, Akgün et al. 51 develop a typology that links differences in the nature of the business environment to the character of organisational unlearning. Sinkula54 on the other hand distinguishes between the unlearning of axiomatic knowledge and the unlearning of procedural knowledge. Here, axiomatic knowledge is defined as fundamental unquestioned beliefs and values, and procedural knowledge is considered to be equivalent to Argyris and Schön's34 concept of ‘theory in use’, referring to the tacit knowledge that shapes the way that people act.
However, the categorisation proposed by Rushmer and Davies6 is the most relevant to individual unlearning as they propose a useful distinction between three possible separate and distinctive types of individual unlearning: fading, wiping and deep unlearning (Table 4). Each type of unlearning is argued to differ in respect of catalyst, intentionality, speed and impact. First, fading or routine unlearning occurs gradually over time through lack of use. It is regarded as neither significant nor challenging for people. Indeed, fading may not enter individuals' consciousness unless they are invited to identify lost skills or capabilities.
| Category | Fading | Wiping | Deep unlearning |
|---|---|---|---|
| Catalyst | Lack of use | Imposed change event | Unexpected individual experience |
| Level/type of impact on individual (identity, values, knowledge, behaviour) | Minor and unproblematic | Mainly behavioural, but may involve abandoning knowledge | Typically significant – not only behaviour/knowledge questioned but also values and/or identity |
| Speed of unlearning | Slow | Variable, but not necessarily sudden | Sudden |
| Extent of emotional impact/challenge | Minimal | Variable, but not necessarily significant | Typically significant |
Wiping is the second category of individual unlearning identified by Rushmer and Davies. 6 The catalyst for wiping is a change initiative external to the person. Wiping can be defined as a process of unlearning that results from a deliberate process of change that has been externally imposed, for example a change initiative or a change in job role. Wiping is deliberate, conscious and more significant than fading, and is typically focused on a relatively narrow practice or activity, with a person consciously making deliberate attempts to give up a particular way of thinking and acting as a precursor to changing his or her beliefs and practices.
Parallels between wiping and categories of unlearning developed by other authors can be discerned. For example, wiping is similar to ceasing a particular behaviour and making incremental change8 and to intentional forgetting of new or existing knowledge. 18 The notion of wiping is reinforced and extended by other categories such as ‘operational level unlearning’, whereby performance routines (enacted by individuals) and ostensive routines (codified systems) are discarded as a result of evolutionary, continuous, incremental change. 2 Wiping is also similar to ‘adjustive unlearning’, in which incremental changes in beliefs are accompanied by fundamental changes in routine, and to ‘operative unlearning’, which involves small-scale changes in beliefs and routines. 51
The third category of individual unlearning proposed by Rushmer and Davies6 is deep unlearning. This radical form of unlearning is argued to occur rapidly as a result of an external event whose characteristics and/or outcomes are unexpected, and which bring into question some basic assumptions. Characteristically, it has a significant impact on the individuals who experience it, leading them to question their values and beliefs, and possibly their frame of reference. As a consequence, deep unlearning may be accompanied by challenging emotions such as anxiety, fear and confusion. Thus, in contrast to wiping, deep unlearning is more likely to involve the unlearning of values and assumptions.
Like wiping, the notion of deep unlearning is echoed elsewhere. Baumard and Starbuck8 talk about challenging core beliefs and Tsang and Zahra2 characterise deep unlearning as discarding values and norms as a result of episodic, discontinuous change. Deep unlearning is also similar to reinventive unlearning and formative unlearning identified by Akgün et al. 20,51 Reinventive unlearning occurs when an organisation changes both beliefs and routines in response to a changing and highly unpredictable environment, whereas formative unlearning occurs when new beliefs structures are combined with incremental routine change. Finally, there are similarities between deep unlearning and what MacDonald32 defines as transformative unlearning (see Deep unlearning).
Finally, linking back to the idea that unlearning represents a distinctive type of learning, it can be suggested that, although wiping has parallels with single-loop learning (incremental learning or change in which basic assumptions remain unchallenged), deep unlearning can be equated more with double-loop learning (learning or change in which existing assumptions and values are questioned and reflected on).
The above definitions and descriptions provide only a brief overview of the general character of fading, wiping and deep unlearning processes. Thus, to develop a fuller understanding of the dynamics and character of the processes of fading, wiping and deep unlearning it is necessary to consider them in more detail. The definitions suggest that there are significant differences between the ways that people experience and understand fading, wiping and deep unlearning, and in the process dynamics of fading, wiping and deep unlearning. Therefore, it is useful to consider each separately, which is presented in the following three subsections.
Fading
Rushmer and Davies6 argue that unlearning could be considered as a process that will automatically occur when the factors that sustain the original learning are removed. Schein55 refers to unlearning as the forgetting curve, which suggests that some past learning will simply fade away over time. Rushmer and Davies6 propose that, with simple behavioural actions, this passive replacement can be seen as moving down the unlearning curve. They give an example of a health-care professional comprehending a new, altered, mandatory health form. The professional may first puzzle over the new layout and in completing the form may make errors through an erroneous habitual response. However, Rushmer and Davies argue that, as the health-care professional continues to complete the form, familiarity and confidence are gained with the new layout. The old way of completing the form recedes, discomfort and previous expectations fade and forgetting takes place.
However, as unlearning requires conscious and intentional action it is questionable whether or not fading should be conceptualised as unlearning. A lack of conscious action suggests that fading is more akin to a process of unintentional forgetting, rather than unlearning. Even authors who use the term ‘forgetting’ in their definitions of unlearning18,30 identify intentionality or purposefulness as defining characteristics of unlearning. We could not find any other studies that conceptualise passive unlearning, possibly because of the difficulty of investigating the concept. Without longitudinal study it would be very hard to gather data on learning that had been unintentionally forgotten, as by definition the participant could struggle to identify it. For this study we decided to continue to use the fading category for the purposes of empirical testing and fulfilling our original project proposal. This allowed us to examine the concept of fading and the value of this element in Rushmer and Davies'6 categorisation.
Wiping
In terms of the relationship between unlearning and change, the dominant perspective in the unlearning literature is that unlearning is a facilitator of change. 2,9,10,23,31,38,50 Although this may be true in relation to wiping (see Table 4), it also needs to be acknowledged that the relationship works in the opposite direction, with external change acting as the prime catalyst for wiping. Thus, in the context of wiping, the primary reason why people engage in unlearning is because it is perceived as being a necessary element of a specific organisational change initiative. This is articulated explicitly in a textbook on change,56 which, in talking about the importance of change for contemporary organisations, says that ‘people are being required to unlearn old ways and develop new competencies’ (p. 7).
Although much of the unlearning literature suggests that the relationship between unlearning and change is close, it has considered only unlearning as being a facilitator of change and has not examined the relationship between unlearning and change in any detail. Consequently, the literature provides limited insight into how change can be a facilitator of wiping, or how individuals experience the character and dynamics of the process of wiping.
The most useful article for considering the bidirectional relationship between unlearning/wiping and change is the conceptual article by Akgün et al. 20 In talking about the relationship between unlearning and change it refers explicitly to Lewin's57 three-stage model of change. This very simplified and much criticised model of change suggests that change happens through the sequential processes of unfreezing, change and refreezing (see Akgün et al.,20 pp. 800–1; Hayes,56 p. 52). Akgün et al. assume that unlearning and learning together constitute the second stage in Lewin's model. This conceptualisation of the wiping/change relationship, with unlearning being at the centre of change, highlights the bidirectional nature of the change/wiping relationship. However, the focus of Akgün et al.'s20 article is on organisational-level unlearning/wiping and, thus, it does not provide insights into the character and dynamics of individual-level unlearning/wiping.
Tsang and Zahra2 also examine the relationship between learning, unlearning and organisational change. They distinguish between different types of change (continuous and episodic) and suggest that each type of change will involve a distinctive form of unlearning. They define continuous change as change that is incremental and gradual in character. By contrast, episodic change is typically discontinuous and infrequent and is greater in scope than continuous change. Episodic change can also be linked to a process of double-loop learning in which basic assumptions are challenged. Thus, in relation to the types of unlearning considered here, continuous change can be linked more to wiping, whereas episodic change can be linked more to deep unlearning.
As wiping is so closely inter-related with processes of organisational change, it is useful to refer to some change-related concepts. In this context, if organisational change provides the catalyst for wiping/unlearning, people's attitude to unlearning is likely to be closely linked to and virtually inseparable from their attitude to the change process that precipitated it. Thus, if people do not regard the changes being undertaken as favourable they are unlikely to have a positive attitude to any unlearning that flows from the change. Equally, if the opposite is the case and people do regard change as necessary and important, they are likely to have a more positive attitude to any unlearning it precipitates. Although Tsang50 does not explicitly use the concept of resistance to change, the reluctance to unlearn and learn that he found in relation to the knowledge transfer processes that were examined can be argued to constitute resistance to change.
The concept of resistance to change is useful when considering people's attitudes to change and unlearning. The change literature suggests that, because of the uncertainty caused by change, resistance is common. A key theme in the change literature is concerned with anticipating, managing and minimising any potential resistance to change. 56 Although some of the unlearning literature touches on the topic of resistance to change,47,52 people's attitudes to unlearning are neglected. This neglect may be because of the assumption that people will embrace wiping-type unlearning relatively willingly. However, this assumption represents an important omission because people's attitude to unlearning is likely to be shaped by their attitude to change. Thus, to understand the character and dynamics of individual-level wiping-type unlearning processes it is fundamentally necessary to take account of people's attitudes to the changes that precipitated them.
Deep unlearning
In examining how individuals experience deep unlearning and the process through which it unfolds, few of the unlearning articles reviewed are relevant. Of the six articles2,6,20,28,32,52 that focus on the process of unlearning (see Table 3), only two examined processes of deep unlearning,6,32 with the other four concerned with individual and organisational unlearning, which is more equivalent to wiping. In tentatively outlining a model for the dynamics of the process of deep unlearning this section draws on MacDonald's32 empirical and conceptual work and links it with some wider, relevant literature on learning.
MacDonald32 suggests that the process of what she labels ‘transformative unlearning’, which has much in common with deep unlearning, has three distinctive but overlapping steps. The key features of transformative unlearning that resonate with deep unlearning are that it involves questioning, reflecting on and giving up some core values, assumptions, knowledge and practices, and also that this process is deeply emotional and challenging for people to undertake. Similar to the mainstream perspective in the unlearning literature, MacDonald conceptualises unlearning as a necessary precursor to learning, and that both together are interlinked components of change. Finally, the catalyst for transformative unlearning is a process of change that brings a person's pre-existing values, assumptions knowledge and practices into question.
The first stage in MacDonald's model is receptiveness, in which a person accepts the possibility that there are perspectives and viewpoints that challenge his or her assumptions and that he or she is prepared to consider these perspectives. Following this is the second stage of recognition, which is the process through which a person acknowledges the veracity of these alternative viewpoints, and the limitations that exist in his or her own perspectives. Finally is the process of grieving, which she suggests is the emotional core of transformative unlearning, whereby a person comes to terms with ‘the loss of prior ways of seeing – the loss of fundamental assumptions which until now had brought certainty and security’ (p. 174). It is only after these three stages of the transformative unlearning process have been undertaken that a person is able to effectively change and learn new assumptions, knowledge and practices.
MacDonald's32 model can be illustrated by summarising the example she uses, which involves her own experiences as a practising nurse in relation to changes in the recommended sleeping position for infants following research on cot death, or sudden infant death syndrome (SIDS). In the 1970s and 1980s, the generally accepted and unquestioned practice was that babies were put to sleep in the prone position (lying on their front with the head to the side). This was a practice that MacDonald not only recommended to young mothers but also used with her own children. However, research in the early 1990s into the causes of SIDS suggested that putting infants to sleep in a supine position (lying on the back or side) reduced the risk of SIDS. Being aware of and reading this research represented the process of receptivity for MacDonald. However, this process was not quick or easy as it challenged ideas and practices she had taken for granted her whole working life. As more research emerged in the early to mid-1990s on the causes of SIDS, and as MacDonald read more of it, she entered the recognition phase in which she started to accept the validity of the new perspective on infant sleeping positions and began to accept the need to change her own assumptions and practices. This process was facilitated by dialogue with other nurses who were also going through the same process. However, before she was able to comfortably and fully accept the need for this change, MacDonald suggests that it was necessary to go through a process of grieving in which she came to terms with the fact that current research and advice suggested that her previous knowledge and practices had their limitations. This was argued to be the most emotional aspect of the unlearning process as it ‘touched the emotional core of my identity as a nurse’ (p. 174). As with the process of recognition, this process of grieving was facilitated by dialogue and communication with others.
Although this model of the process of transformative unlearning has resonances with Rushmer and Davies'6 concept of deep unlearning, it also differs from it in two key respects. First, the catalyst for transformative unlearning was external change rather than some specific incident or experience. Second, a more significant difference was the timescale over which transformative unlearning occurred. Although Rushmer and Davies suggest that deep unlearning involves a sudden and rapid realisation of the need for change, and an equally sudden process of change, in MacDonald's model transformative unlearning was a slow process that occurred over a period of years. As both transformative and deep unlearning involve the emotionally challenging process of unlearning fundamental assumptions and values, they represent comparable forms of unlearning. However, what MacDonald's perspective highlights is that not all deep unlearning occurs through the sort of sudden Archimedean epiphany which produces an instantaneous change in behaviour. Although particular events may lead people to question their values and assumptions, it may take more time for behavioural change to follow.
Two other process models of learning from the learning literature also have potential relevance to understanding the character of deep unlearning processes. First is Garud et al.'s58 narrative model for learning from what they call ‘unusual experiences’. Unusual experiences are defined as ‘situations that bear little or no resemblance to the types of experiences that have occurred in the past’ (p. 587). Although Garud et al. talk of learning rather than unlearning, there is the potential that, in making sense of unusual experiences, people's assumptions, values and practices may be brought into question and a process of individual unlearning may be undertaken, in which certain values and/or behaviours are abandoned and changed. However, although the narrative model that they develop for how people make sense of unusual experiences may have some relevance to understanding the dynamics of individual unlearning processes, a major limitation of their framework is the lack of consideration given to emotional issues. Despite acknowledging that making sense of unusual experiences involves reflecting on basic assumptions, and that dialogue with others in doing so may result in contrasting perspectives, issues of emotion are not considered. For this reason, Garud et al.'s model is not considered appropriate for understanding the dynamics of the process of deep unlearning.
A final very general model that is relevant for understanding the process of deep unlearning, which has some synergy with MacDonald's model, is the process of organisational inquiry outlined by Argyris and Schön,34 which takes inspiration from the work of the pragmatist philosopher John Dewey. Similar to deep unlearning, and Garud et al.'s58 unusual experiences, the catalyst for a process of inquiry is the experience of doubt, which is defined as the experience of a ‘problematic situation’, triggered by a mismatch between the expected results of action and the results actually achieved. Such experiences, they argue, inhibit continued action and encourage a process of reflection/inquiry aimed at resolving the doubt. Thus, the start of this process of inquiry can be considered equivalent to the initial stage of receptiveness in MacDonald's32 model, with the objective of resolving the sense of doubt that has been experienced, providing the primary catalyst to this receptiveness. The process of inquiry outlined by Argyris and Schön34 is relatively generic and lacking in detail but it involves combining reflection and action as well as an active process of dialogue with others. The ultimate aim of this process of inquiry is doubt resolution, whereby the mismatch that was experienced is made sense of. Arguably, this process of inquiry is equivalent to both the receptiveness and the grieving stages of MacDonald's model. Once the process of inquiry has resulted in the doubt that was experienced being resolved, this makes it possible for learning and change to occur, whereby people adapt their knowledge and actions to take account of the recently experienced mismatch.
Overall, therefore, MacDonald's three-stage model of dealing with transformative unlearning provides a useful template for understanding how people experience and make sense of what is referred to here as deep unlearning. However, as the only empirical illustration of this model is MacDonald's reflections on her own experience, further research is necessary to empirically test and evaluate this model before its validity can be established. As has been revealed by reviewing the literature on individual unlearning types, change can feature as the catalyst to individual unlearning and unlearning can trigger further change. Therefore, the following section briefly reviews the literature concerning individual-level transitions in change theory.
Reviewing the literature concerning individual-level transitions in change theory
When examining individual attitudes to and experiences of change there are two main literatures of relevance: resistance to change and emotion/attitude to change. The following reviews each of these literatures and considers how they may relate to individual unlearning.
Organisational change has been studied from many perspectives with the use of many methods. 59 In their literature review, Armenakis and Bedeian60 identified five themes in the change literature: content issues, which deal with the substance and nature of a particular change; contextual issues, which deal with forces and issues that exist in an organisation's internal and external environment; process issues, which examine the actions taken to implement change; criterion issues, which focus on outcomes from organisational change efforts; and affective and behavioural reactions to change. It is the last category that is of most interest to this study.
Resistance to change is a concept that is frequently discussed in conjunction with the unfreezing stage of Lewin's57 change model. It is often presented as a negative barrier to change, defined as a restraining force acting to maintain the current state of equilibrium. 61 Traditional approaches to resistance to change frame compliant behaviours as non-resistant and non-desirable behaviours as resistant. The early solution presented to overcome resistance was to increase employee participation. 62 However, Lawrence63 argued that this was an oversimplified solution to resistance and that change had both technical and social characteristics. It was a lack of attention to the latter that often led to resistance to change. Lawrence's view was that attitudes were important in how managers think about resistance to change and that expecting resistance to change from employees often delivered resistance.
In his review of the literature Foster59 observes that other scholars have conceptualised resistance to change as an emotional reaction rather than a purely behavioural one. For example, Argyris and Schön64 discussed resistance in terms of defensive routines and frustration, and Kanter65 refers to feelings of uncertainty and loss of control in understanding individual responses to change. Klarner et al. 66 argue that the literature concerning emotions during change can be divided into two parts. First, some studies in change management focus on employee behaviour as a result of emotions evoked during change. Second, other studies have used psychological stage models to explain the relationship between emotions and employee behaviour during change. Both of these parts are considered briefly below.
It has been argued that emotion drives the adaptive behaviour of employees in response to change. 67 This adaptive behaviour involves learning new strategies and being resilient to setbacks. 68 Several studies have considered the behavioural outcomes of employees who show either positive or negative emotions. It has been argued that failure to emotionally adapt to change leads to resistance among employees. 69 For example, resistance can lead to withholding of participation during change events. By contrast, Avey et al. 68 found that positive emotions could help individuals cope and could create support for the change. Positive emotions were found to increase the level of commitment and emotional engagement to the organisation, even in times of disruption. 70 However, Piderit71 has argued that dichotomising individual responses to change as either altogether negative or altogether positive is an unhelpful oversimplification. Piderit71 proposes that conceptualising resistance to change as multidimensional would help account for the possibility of ambivalence or mixed feelings towards change, and presents a tripartite attitudinal model of resistance to change that includes three components: emotional (affective), intentional (behavioural) and cognitive. She concludes that the term ‘resistance to change’ is inaccurate and unhelpful, and does not provide the best framework for understanding organisational change implementation. Ford et al. 72 add that, by assuming that resistance is necessarily bad, change agents have missed potential contributions that could help build awareness and momentum and eliminate unnecessary or counterproductive elements, increasing the likelihood of successful implementation of change. Both Piderit71 and Foster59 conclude that studies at the individual level would be better served using the term ‘response to change’. Further, Klarner et al. 66 argue that studies on emotions during change treat change as a snapshot event but would be better served by characterising change as a process, with the result that emotions could evolve during change. Klarner et al. 66 add that studies often focus on single change but neglect to consider the repetitive nature of change that occurs in many organisations and that emotion should also be examined as a continual construct.
Studies in human resource management and organisational behaviour have also attempted to use psychological stage models to explain the relationship between triggers for employee emotions, coping behaviours and change outcomes. 66 It has been argued that the trigger for the change process can produce strong emotions as well as the change itself. 73 Other studies have looked at the relationship between employee emotions and coping behaviour during change. Smith and Lazarus74 advocate psychological appraisal theory to explain this relationship, with the employee engaging with an appraisal process that considers the implications of the change for his or her personal goals and well-being. The appraisal process shapes the individual emotional response, which is translated into specific coping behaviour. These coping strategies can influence the organisational change outcome. 75 Positive employee emotions towards change can increase engagement, affecting the emotions of other team members. 76 By contrast, resistance to change is demonstrated by disengagement, which can hamper effective change. 68 Klarner et al. 66 contend that these stage models suffer from the same deficiencies as those of change management studies that have examined emotion. The studies tend to consider emotions as either positive or negative rather than considering multiple possible emotions during change. They treat change as a snapshot event and fail to consider how emotions may evolve during a change process, with different events during a change process triggering different emotions. Consequently, they call for more studies that consider the evolving character of emotions during a change process, as well as studies that consider employees' emotions during repeated change.
Reflecting on the literature presented in this section suggests synergies between individual unlearning and individual transitions from change. Several studies have proposed that a catalyst to unlearning can be an organisational change event. 2,6 Therefore, individual unlearning may be part of the adaptive behaviour process that employees experience as a result of change. Employees may be required to give up or abandon some previous strategies or knowledge as well as learning new ones, and this abandonment may trigger strong emotions. MacDonald32 argues that the unlearning process can involve giving up some core values, assumptions, knowledge and practices, which can be challenging and deeply emotional for people to undertake. Similarly, studies of individual transitions during change have found that employees report feelings of uncertainty, loss of control and frustration and enact defensive routines. 64,65 Positive emotions have been found to increase commitment and engagement with change, but may also demonstrate an increased willingness to engage with individual unlearning, seeing it as an opportunity to refresh old thinking and knowledge. Therefore, it is possible that employee emotions during change may also influence their engagement with unlearning processes, which may explain how employees respond and adapt to change.
Emotion has also been linked to decision-making processes, the main outcome of interest for this study, and the following section reviews the decision-making literature in relation to individual unlearning.
Reviewing the academic literature on decision-making
In reviewing the literature concerning individual decision-making and decision-making processes we examined the learning, knowledge management and organisational behaviour fields. By searching for literature published from 2005 we identified 29 articles that considered learning and decision-making in the article title, but we found none of these articles to be directly relevant to this study. Similarly, since 2005, 11 articles had been published that included knowledge management and decision-making in their titles, but these also did not provide any further insights for this study. Neither field provided any new material regarding unlearning and decision-making. However, searches in the organisational behaviour field were more successful, especially concerning work psychology, which is most relevant to this study because of its focus on the individual. Consequently, the following discussion draws heavily from this discipline.
Much of the work psychology literature on decision-making has considered how individuals deviate from strictly ‘rational’ processes, with ‘rationality’ defined as choosing the option that has the highest expected value among those options available to the individual. 77 However, this definition assumes that all other things are equal, and Tetlock78 has argued that in different circumstances individuals may have different motives and goals for a decision and that the attractiveness and utility of certain decisions is subjective to individuals' perceptions of these possible outcomes. Arnold77 states that there are many different strategies for decision-making, such as evaluating options using a very limited range of important criteria, or searching for an option that an individual considers to be good enough. This latter approach has been termed ‘satisficing’ and can be contrasted to ‘maximising’ in which a thorough search is made for the best possible option. Arnold77 argues that a satisficing strategy may be suitable if a person does not have time and/or the ability to use a more thorough approach. Frisch and Clemen79 argue that, although attention to the perceived attractiveness and utility of a decision outcome is useful, attention should also be given to the early stages of the decision-making process. In particular, they argue that to understand decision-making well it is important to consider consequentialism (the expected personal consequences of making a decision), thorough structuring (considering more than one option and the likely consequences) and compensation (the trade-offs between one benefit and another from making different decisions). These three influences on decision-making highlight the key role of information processing in the decision-making process.
There are several different aspects to information processing in decision-making such as attitudes to uncertainty and risk, gains compared with losses and framing of information. Although these aspects are relevant to decision-making we identified four areas that may have particular significance for individual unlearning and process management decision-making. The first of these areas was the role of emotion, action and inaction. Isen80 provides evidence to suggest that individuals who are experiencing positive emotion are able to be more creative and are more able to process information than those who are not. However, it appears that positive emotion can also lead individuals to be unrealistically optimistic about future events and outcomes. 81 Further, individuals seem likely to consider future emotions when making decisions and, in particular, the emotion of regret. It is argued that individuals regret actions more than inactions, probably because the consequences from actions are more tangible. In line with these results, Baron82 found that worries concerning future regrets encouraged inaction over action. This may suggest that managers could choose not to abandon certain behaviours or knowledge even if they feel that they are outdated or not well suited to the current environment if the alternative is a step into the unknown.
The second area was escalation of commitment. This phenomenon is now well established77 and emphasises that, if a decision is made freely and explicitly, the individual making it is committed to it and retrospectively seeks to find reasons to justify his or her rationale for making it. McCarthy et al. 83 report evidence of this escalation of commitment in some managerial decisions. This phenomenon is important for managerial decision-making because laboratory experiments have shown that, when decisions are reported to individuals as unsuccessful, they will feel compelled to continue to support their decision in the belief that they will ultimately prove that their wisdom was correct. Simonson and Staw84 investigated how to counter this compulsion and found that decision-makers who set advance minimum outcome levels were less likely to pursue the course of action if the minimum outcome had not been reached than decision-makers who had not specified a minimum outcome level. Escalation of commitment was also reduced if decision-makers were told that it was the quality of the decision-making process that would be evaluated, not the outcomes achieved (which in any case may be beyond the control of the decision-maker). Such strategies may have value to managers when assessing the quality and effectiveness of their decision-making by providing indicators of when existing decision-making practices should be reviewed and potentially abandoned.
The third area was heuristics. Heuristics are rules of thumb that people use to simplify information processing and decision-making. 77 In their seminal work, Tversky and Kahneman85 identified three common heuristics. The ‘representativeness’ heuristic refers to when an individual judges something purely according to how representative it appears of a particular category, regardless of the probability of it actually belonging to that category. For example, if an individual encounters three medical students who are all aggressive and demanding, the individual may conclude that all medical students are aggressive and demanding, regardless of the probability of this actually being the case. The ‘anchoring bias’ heuristic refers to a person's failure to change his or her views as much as he or she should in the light of new information, for example the difficulty an interviewer may have in dislodging the first impression of a candidate over the course of an interview. The ‘availability’ heuristic concerns a person's tendency to consider an event more probable if it can be easily imagined than if it cannot. For example, after seeing news reports about redundancies in local government, a manager in the NHS may believe that he or she is in danger of being made redundant, regardless of whether or not there is any genuine risk in their sector. Such rules can therefore skew individual decision-making processes and risk poorly founded decisions being implemented. The process of unlearning may provide opportunities for managers to become aware of the influence of heuristics on their decision-making processes, abandoning old rules in favour of more structured information-gathering procedures, enabling more objective decision-making.
Finally, the fourth and final area in which information processing can affect decision-making was evidence-based management. Evidence-based management is defined by Briner et al. 86 as follows:
Evidence based-management is about making decisions through the conscientious, explicit and judicious use of four sources of information: practitioner expertise and judgement, evidence from the local context, a critical evaluation of the best available research evidence, and the perspectives of those people who might be affected by the decision.
p. 19
They argue that evidence-based management is a relatively new concept, although the use of research evidence to help make managerial decisions is well established. Reay et al. 87 observe that many of the calls for the increased use of evidence-based management reference the more mature discussions in the medical and health-care literatures, which promote the use of the ‘best available evidence’ in medical decision-making.
There is still considerable debate concerning the value of evidence-based management for improved decision-making. In the review of the literature by Reay et al.,87 it was found that much of the existing research lacks strong evidence from which to draw conclusions. Reay et al. 87 also concluded that research had so far failed to provide clear evidence to determine whether or not employing evidence-based management improved organisational performance. There is also debate concerning what constitutes suitable ‘evidence’ on which to base management decisions. Evidence-based medicine draws heavily on evidence gathered using rigorous methods such as systematic reviews and randomised controlled trials. However, Briner et al. 86 caution against following a blind adoption of a big science perspective that privileges randomised controlled trials and meta-analyses above all other kinds of research evidence. This is partly because of a lack of systematic reviews in management or organisational studies for managers to draw on, but also, as Walshe and Rundall88 note, because the constrained, contested and political nature of many managerial decisions may make the application of research evidence difficult for managers, even when it is available.
A further dimension that has attracted growing attention in evidence-based medicine research has been investigating how to effectively translate research findings to practice settings. Reay et al. 87 argue that this area of research, known as knowledge translation, has potential as a model for evidence-based management. Knowledge translation research in health care focuses on understanding how complex interventions, based on research evidence and involving multiple providers, recipients and organisations, can be implemented. What has become clear from knowledge translation research is that the existence of evidence is critical but not sufficient to guide action. Despite the existence of evidence to support a particular behaviour change, Kitson et al. 89 found that changing practitioner behaviour remained difficult. Reay et al. 87 believe that innovative and creative methods are required to bring evidence to managers to overcome barriers to change. Consequently, it is possible that the inability of a manager to engage with processes of unlearning may help to explain why some managers resist changing or abandoning established behaviours and practices, despite the availability of evidence to support the change.
Furthermore, the shortage of systematic management research evidence compared with medical research evidence, and the increased political and constrained aspects of management decision-making, may mean that clinicians moving into managerial roles are not able to translate established evidence-based medicine practices into effective strategies for management decision-making. Walshe and Rundall90 highlight the divide between the biomedical and the social science evidence bases that clinicians and managers are likely to draw on. One is experimental, replicable and generalisable and the other is non-replicable and contextual. As a result, clinicians who become health-care managers may feel that they have to abandon or give up their established views of what constitutes reliable evidence and learn to use new forms of evidence for their decision-making. This type of change is illustrated by recent work investigating the use of evidence in NHS commissioning processes. 90 Swan et al. 90 concluded that commissioners needed to view evidence as something that is coproduced rather than being purely external and independent. For example, they argue that knowledge of the local context may be just as relevant as the latest research-based findings or policy guidance. They also argue that commissioners needed to recognise the limits of medical and scientific models for effective management decision-making and that evidence-based medicine templates could not be simply transferred to management decision-making processes.
The decision-making process
Several authors have proposed various conceptualisations of decision-making processes. For example, Briner et al. 86 suggest that an evidence-based management process could comprise five steps. First is the manager's attempt to define or state the problem or issue. Second, having stated the problem, internal organisational evidence is collected to check the problem relevance and validity, leading to a reformulation of the problem as necessary. Third, external evidence from published research about the problem is identified and critically appraised. Fourth, the views of stakeholders and those likely to be affected by the decision are considered along with ethical considerations. Fifth, having critically appraised all of these sources of information, a decision is made that attempts to take into account these four sources of information. Alternative conceptualisations of a decision-making process have been presented by several authors although, as Nutt91 observes, these conceptualisations differ significantly, which makes integration of the findings difficult. For example, Dean and Sharfman92 classify the decision-making process through procedural features of rationality, political behaviour and flexibility. Others focus on coalition formation and decision-maker attributes such as tolerance for ambiguity, uncertainty or risk aversion. 93 However, Nutt91 argues that, although these studies are helpful, they do not explain how decisions were made.
To address this weakness, Nutt91 compared four different types of decision processes to investigate their adoption, value and duration. First, based on interpretive studies, Nutt argues that decision-makers cater to the interests of powerful stakeholders by looking for ready-made solutions that they can support. These solutions provide a clear course of action leading to an outcome that can easily be visualised, a process called ‘idea imposition’. Second, by contrast, the literature calls for decision-makers to gather intelligence about their needs, discover and evaluate options according to their benefits, and implement the chosen decision by working with relevant interest groups. This process is called ‘discovery’ because it calls for learning about possibilities. Nutt also investigates two hybrid processes to decision-making. If an idea presented in an idea imposition process seems ill advised then the decision-maker might change to a ‘redevelopment’ process to find a replacement. If a discovery process throws up an ‘emergent opportunity’ then the discovery process may be abandoned if the opportunity seems beneficial.
Nutt91 found compelling evidence to support the discovery process model of decision-making with little empirical support for the idea imposition process. He also found that the discovery process was more successful than either of the hybrid approaches. Nutt concludes that the sequencing and steps in decision-making matter. The most important steps include to investigate needs, conduct a sensitive stakeholder implementation and set a direction. Further, these steps should be conducted early in the decision-making process. There was an emphasis on logical and political rationality with expectations needing to be set and politics managed early in the process. Decision-makers who preferred idea imposition seem to be keen for action, the motivation for a quick solution being motivated by pragmatics and fear. However, Nutt argues that such quick fixes can create a trap that limits search and discourages knowledgeable people from offering ideas. In addition, the opportunity can be seen as a personal idea, raising questions about the decision-makers' motives and requiring the rapid action to be delayed while the decision-maker formulates a defence.
The attractiveness of remedy-driven solutions that seem compelling may be due, in part, to a decision-maker's desire to remove ambiguity. By following this path, sources of ambiguity are swept away, giving temporary relief but stopping the search for intelligence and alternatives. The approach also distracts decision-makers away from contemplating their needs, and draws decision-makers to document their ideas and the stakeholder response. Nutt91 concludes that accepting ambiguity is a necessary motivator to effectively address difficult and troubling issues. This transition may well be an important aspect for managers who have moved from clinical roles with established evidence-based decision-making practices into managerial roles that have a less well-defined evidence base and involve higher levels of ambiguity. Managers in these roles may initially adopt idea imposition as a process of decision-making to remove the ambiguity associated with their new positions. If, as Nutt's research suggests, this method of decision-making proves unsuccessful, this experience may act as a catalyst for unlearning this approach and adopting a more discovery-orientated approach. As a key antecedent of individual unlearning has been found to be change at an individual, an organisational or a policy level, the following section reviews recent major changes in the NHS to provide a contextual background to the study.
Recent changes in the National Health Service
Over the last 40 years, significant organisational changes have taken place in the NHS. Major reforms in, for example, general practitioner (GP) fund holding, NHS organisations moving to trust status, governance management and patient involvement have meant that staff frequently experience major structural and organisational transformations. The introduction of ‘formal’ management positions into the NHS followed the Griffith Report in 1983. 94 In addition to recommending the introduction of general managers into health authorities, the report also focused on specific management training for NHS staff, particularly for those with a medical background. 95 Since the Griffith Report, changes in the health service have been accompanied by the introduction of many formal management positions. Managers from both clinical and non-clinical backgrounds now occupy many of the crucial senior roles within the health service, bringing about local organisational change and reform.
The pace of change in the NHS has continued to be significant in recent years. For example, Greener7 talked about how the ‘pace and scope of change’ was ‘intense’ (p. 206). Most recently, the introduction of the health and social care reforms for the NHS in England in 2012–13 will require many NHS staff to further adapt in their roles and responsibilities. In summary, the reforms have meant that almost every GP practice across England has joined with neighbouring surgeries to form clinical commissioning groups (CCGs). The 152 local NHS primary care trusts (PCTs) that managed most of the NHS budget in England have merged at a senior managerial level to form 51 clusters. Some staff will stay on after PCTs are abolished in 2013 in organisations that will continue to advise the new GP-led groups on how to plan and buy health care. A new NHS Commissioning Board that was established in shadow form in October 2011 will undertake specialised care that needs to be planned at a national level. Below the board will be four regional hubs and then beyond that 50 local offices. From 1 April 2013, strategic health authorities and PCTs will be abolished, and the CCGs and National Board will take on their full functions. 96,97
Thus, it is anticipated that, because of the amount of ongoing change in the NHS, all health-care managers are likely to have experiences of unlearning processes such as Rushmer and Davies'6 categories of wiping and fading in which they have had to adapt their work practices and routines as a result of change. Rushmer and Davies' category of deep unlearning on the other hand may be experienced by health-care managers who have undergone a significant role transition, such as would happen when a clinician moved into a managerial role. Thus, it is possible that processes of deep unlearning may be more evident in managers who have undergone such transitions. To examine these aspects in more detail we developed the following research questions for the study.
Research questions
The overall research aim of this project was to empirically investigate the extent to which health-care managers engage in processes of individual unlearning and the barriers that exist to them doing so. This is important because it will improve our understanding of how managers make decisions and will help provide relevant support and training for those involved in running the health service. An addition was made to the second research question from the outset of the project to investigate enablers as well as barriers to unlearning. This change was made to ensure that the study captured a full understanding of the factors influencing health-care managers' unlearning processes.
The specific research questions investigated were:
-
To what extent do health-care managers engage with the process of unlearning and what impact does the engagement with this process have on health-care managers' decision-making?
-
What are the barriers and enablers that influence the engagement of health-care managers with the process of unlearning?
-
To what extent does the health-care setting affect the level of engagement with the process of unlearning by health-care managers?
Having provided a comprehensive review of the literature and provided a brief summary of the key changes in the NHS that were being implemented at the time of data collection, in Chapter 3 we explain the methods adopted for the study and the process of data collection and analysis.
Chapter 3 Methods
This chapter describes the research process and the methods used to collect, analyse and interpret data. It opens with a description of the organisation of the study and the role of the steering group, before outlining the research strategy, the selection of the case study sites and process of gaining ethical approval. Next, the process of data collection is explained, which includes the pilot interviews, the participant recruitment process at each site, a discussion of recruitment problems and a description of the participants who were interviewed. The purpose and content of the workshops is then described, followed by an explanation of the data analysis techniques employed for the study. The chapter closes with a description of each case study site.
Organisation of the study
Coombs took overall responsibility for the management of the study, with support from Hislop and Holland. Coombs had experience in undertaking health-care management research projects using multisite case studies and managing research associates. Hislop provided the project with subject area expertise and project management support for Coombs and managed the data collection and analysis. Holland managed the liaison with NHS trusts, contributed to the data analysis and facilitated the workshops. A research associate, Bosley, was appointed and commenced work in January 2011. In late 2011, Bosley was appointed to a lectureship at the School of Business and Economics, Loughborough University, Loughborough, UK. A new research associate, Manful, was appointed on a secondment from the Loughborough University Centre of Research into Social Policy and commenced work in January 2012. It was agreed that Bosley would remain part of the research team to ensure continuity for the project and because unlearning was a research interest that Bosley wished to follow. The project team had monthly meetings to monitor progress and additional regular supervisory meetings with the research associate.
Project steering group
A steering group comprising a director of governance, a patient safety lead and two academics was established early in the project. Meetings were chaired by a senior lecturer in the School of Business and Economics, Loughborough University, who has extensive research experience in the health-care sector. The steering group met on three occasions: June 2011, December 2011 and May 2012. Terms of reference (see Appendix 2) were discussed and agreed at the first meeting in June 2011. Group members provided useful comments and advice on a range of topics including the draft literature review, findings from the pilot study and emergent findings from the main study, and draft Service Delivery and Organisation programme reports. They advised on the conduct of the workshops and dissemination of findings, and suggested relevant literature that might aid interpretation of the data. Project team members attended all meetings and took account of the valuable comments and advice provided by the group.
Choice of research strategy
Unlearning is a relatively neglected and unexplored aspect of learning and change processes. A case study-based approach was identified as a suitable method because qualitative case studies provide an effective way to conduct exploratory research that can generate rich, qualitative insights into managers' experiences of unlearning. 15,16 Given the limited literature on and knowledge of the concept of unlearning, the case study design enabled an inductive approach to theory-building rather than seeking to test theoretical hypotheses. The intention was to investigate the experiences of unlearning in three different types of NHS trust (an acute trust, a PCT and a mental health trust) to explore the extent to which the organisational context affects unlearning. The reason for choosing these three types of context is that they represent some of the most important and common organisational types that the managers being investigated work in.
Unlike some case study designs, the research does not draw on a range of different data sources but focuses on individual interviewees' experiences of episodes of unlearning. In other words, the unit of analysis is the episode of unlearning experienced by the individual manager rather than the individual manager or case study site, both of which provide a context for comparison. For example, it was possible to compare experiences of episodes of unlearning between managers with clinical backgrounds and those with non-clinical backgrounds, and also between managers working in acute health-care environments and those working in mental health-care environments. Our main source of data was the individuals themselves, who provided descriptions of their job roles, immediate work context and the barriers and facilitators of unlearning, some of which related to the department, NHS trust or wider policy context. We justified this on the grounds that our interest was individual rather than organisational unlearning, which can be illuminated only through one-to-one interviews.
Selection of case study sites
The intention was to recruit an acute trust, a mental health trust and a PCT. Given that participation involved 14 managers being released for 1 hour to be interviewed, a key criterion for inclusion was securing senior management support and willingness to commit some resource to assist in recruitment. Holland used her NHS contacts to identify interested NHS trusts and to secure initial written agreement to take part. The acute and mental health trusts were identified relatively quickly using this approach, but the PCT that initially agreed to participate later withdrew. The engagement of another PCT was secured in March 2011 but, as described in Recruitment at site C: primary care trust/clinical commissioning group, recruitment at this site failed to generate any participants. Consequently, the results of the study are based on two rather than three case study sites.
Ethical approval
Loughborough University gave ethical approval for the conduct of the exploratory interviews on 29 March 2011. The main study did not require approval from the University Ethical Advisory Committee because it was subject to NHS ethical clearance. Application for NHS ethical approval and NHS R&D clearance was made through the Integrated Research Application System. Notification of clearance by the National Research Ethics Service Committee [. . .] Proportionate Review Sub-Committee was received on 10 May 2011. (The name of committee was not included to ensure anonymity.) The following documents were provided to the committee along with the completed NHS ethics application form:
-
summary CVs for the chief investigators
-
letter of invitation to participants, participant information sheet (PIS), consent form, interview schedule, pre-interview questionnaire, examples of unlearning
-
transcriber's confidentiality agreement
-
letters from the sponsor and funder, professional indemnity and employers' liability certificates
-
the protocol, summary flow chart of the protocol, referees' assessment form and comments on the research proposal.
Application for NHS R&D clearance was handled through the Co-ordinated System for Gaining NHS Permission (CSP). Documents submitted for this stage were the research protocol, summary flow chart of the protocol, letter from the funder, summary interview schedule and pre-interview questionnaire. Permissions were secured from case site B on 9 June 2011, from case site A on 15 June 2011 and from case site C on 24 November 2011.
Data collection
Data were collected through one-to-one semistructured interviews with health-care managers. A semistructured approach enabled the interviewees to respond to the researcher's questions using their own words and to introduce and discuss new topics, issues and experiences that they deemed appropriate. 98
Interviews were framed by a topic guide that was informed by a typology of unlearning proposed by Rushmer and Davies6 and used critical incident technique. 99 Interviewees were invited to identify specific incidents of unlearning and fading that they regarded as significant and could clearly recall, along with identifiable antecedents and consequences. They were invited to identify one incident each of fading (the gradual forgetting of skills/capabilities no longer required), wiping (deliberate efforts to unlearn specific beliefs and/or behaviours) and deep unlearning (sudden and unexpected unlearning that challenges deeply held beliefs and assumptions). Using Kemppainen's100 three-component approach, questions were asked about the circumstances and context of the incident being discussed, the specific details of how they experienced and remembered the incident being examined and their understanding of the consequences or outcomes resulting from the incident.
Pilot interviews
To test the topic guide, nine formative, exploratory interviews were conducted with health-care managers who were or had recently been studying part-time on Masters programmes in Medical Management and Healthcare Governance in the School of Business and Economics at Loughborough University. These interviews took place between the end of March and early May 2011. All participants were sent an information sheet, an interview schedule and examples of the different types of unlearning in advance of the interview. All were invited to complete a pre-interview questionnaire providing background about their previous work and qualifications, although not all did this. All gave either written consent or oral consent, which was digitally recorded before beginning the interview.
The pilot interviews showed that the research documentation worked satisfactorily but also drew our attention to the need for participants to have an opportunity to discuss the concept of unlearning and to read the documentation in advance of the interview. The interviewer also gained from the experience by developing skills and supplementary questions to tease out unlearning experiences from the interviewees.
Recruitment of interviewees for the main study
The research team identified and worked with a key contact and human resources manager at each site. The key contacts were sent a briefing sheet about the project (see Appendix 3) and then the principal investigator and research associate arranged to meet with the contact and a human resources manager. At this meeting the aims and time frame of the project were explained, any questions and issues were addressed and the most appropriate method or methods of recruitment were identified. During the revisions to the original project proposal it was identified by the Department of Health through the Health Services and Delivery Research (HS&DR) programme that the employer of NHS staff who participated in the study should be compensated for the loss of staff resources. Consequently, a payment of £141 per 1-hour interview was offered to each case study site. This figure was based on the rate used in clinical trials to calculate a doctor's time. The payment was not passed directly to participants. The key contact and human resources manager helped the research team identify the target group and the most effective method of recruitment. For this reason, different recruitment strategies were used at different sites.
Inclusion criteria
We envisaged that health-care managers who may have had to adapt their work practices and routines as a result of policy changes, responded to new research on clinical effectiveness or undergone a significant role transition, such as moving from a clinical to a managerial role, were most likely to be found in middle management roles. Therefore, for the main study, the aim was to identify a purposive sample of 14 middle managers at each case study site. Given the definitional issues surrounding the term ‘middle manager’ and different usage in different organisational structures, the research team acted on the advice of the steering group and sought managers working at Agenda for Change bands seven and eight. Thus, participants needed to (1) be working at Agenda for Change bands seven or eight or be GPs or consultants; (2) have some managerial responsibilities that involved making decisions about the use and allocation of resources, such as staff and/or finances, data collection and management or service delivery; (3) be able to identify and be willing to talk about their experiences of unlearning; and (4) be willing to complete the pre-interview questionnaire, participate in an interview of approximately 1 hour in length and give informed written consent to the conditions of participation.
Recruitment at site A: mental health trust
On the advice of the site contact, two researchers attended a scheduled managers' forum in July 2011. The researchers discussed the project informally with interested managers and distributed letters of invitation (see Appendix 4) and the PIS (see Appendix 5). Delegates were invited to leave contact details if they were interested in participating in the project or to contact the researchers after the event. Those who expressed an interest were subsequently contacted for further information about their roles and responsibilities in order to select those who most closely met the inclusion criteria and to ensure maximum variance. Managers who met the criteria were sent further documentation: the interview topic guide (see Appendix 6), examples of unlearning (see Appendix 7), a consent form (see Appendix 8) and the pre-interview questionnaire (see Appendix 9). Documentation assured participants that their identities would be protected and that nothing they said would be reported in a way that could be traced to them. The pre-interview questionnaire collected basic data such as contact details, job title, band role description and previous jobs held. Participants were invited to read the questions and examples in advance of the interview to identify examples from their own experience, and to complete and return the questionnaire. The consent form was sent for their information: signed consent was taken at the beginning of each interview after the participant had had the opportunity to ask questions.
As doctors did not attend the managers' forum, an e-mail [drafted by the researcher and amended by the clinical studies officer (CSO) at site A] was sent by the CSO to four psychiatrists identified as having managerial responsibilities. They were invited to contact the researcher if they were interested in being interviewed and the researcher sent the PIS and letter of invitation to those who wished to participate. Those who continued to express an interest in participating and committed to be interviewed were sent the further documentation. These two strategies resulted in the successful recruitment of 15 middle managers and consultants.
Recruitment at site B: acute trust
The director of human resources and the local contact circulated an e-mail with the PIS and letter of invitation to the relevant group of managers, inviting them to contact the researcher within 2 weeks if they wished to be considered as participants. Those who responded to the researcher were then sent the interview topic guide, examples of unlearning, a consent form and the pre-interview questionnaire. They were invited to read the questions and examples in advance of the interview to identify examples from their own experience, and to complete and return the questionnaire. The consent form was sent for their information as signed consent was taken at the beginning of each interview. Potential participants were informed that the researcher would contact them again with potential interview dates once the directors of human resources and governance had identified dates when a suitable room for the conduct of the interview could be secured. To protect confidentiality, the researcher did not inform the directors of the names or roles of participants. In total, 14 volunteers were recruited using this approach.
Recruitment at site C: primary care trust/clinical commissioning group
The recruitment method used at this site was similar to that deployed at site B. The human resources manager and local contact were sent an e-mail invitation, the PIS and a letter of invitation to managers working at Agenda for Change bands seven and eight in the CCG, public health and the local PCT cluster, and to some GPs involved in the CCG. A reminder was circulated to the same group in January 2012. However, neither invitation generated any interest from relevant managers.
We discussed the lack of interest from participants with our site contact and the HS&DR programme manager. The programme manager took advice from a HS&DR scientific advisor, who recommended contacting the local hub of the primary care research network (PCRN), principal investigators with recent experience of successfully accessing primary care middle managers for National Institute for Health Research (NIHR) projects and individuals in local universities with links to site C. All three strategies were employed and, although helpful responses were provided, the PCRN and local university routes proved unsuccessful. The final recommended approach from experienced principal investigators and one that was also identified by our key contact was to attempt to make face-to-face contact with potential participants, such as attending a CCG development meeting to ‘sell’ the project and encourage participation. We requested this opportunity through our contact but unfortunately no response was forthcoming from the CCG. At this point our recruitment and data collection from a PCT was already overdue by 2 months and, following discussion with the HS&DR programme manager, it was decided that there would be no further attempts to collect data from the primary care sector.
Reflections on the recruitment experience and implications for the study
One of the requests from the HS&DR programme manager and scientific advisor was that a summary of our recruitment experience was provided to share learning with other projects. There were several possible reasons for the lack of participation at site C. First, the pool of potential participants was much smaller (109) in comparison with the other two sites (about 250 participants at case site A and 400 participants at case site B). Second, we were unable to arrange a meeting with our contact and the human resources manager until October 2011 and full NHS permissions were not secured at this site until November 2011. Consequently, the first invitation to participate was not circulated until the beginning of December, when recipients may have been preoccupied with other concerns or taking leave. Third, at the time of sending out invitations to participate the NHS primary care sector was experiencing considerable change with the move from PCTs to CCGs. Our key contact indicated that several potential groups of managers at site C had either recently changed role or moved to a new organisational structure or completely new organisation. In addition, some managers were also uncertain about their long-term job security. It is possible that many of our target group were focused on preparing for these changes and, therefore, may have been unwilling to participate in additional tasks such as research interviews.
Reflecting on our experiences across all three sites, three observations can be made. First, having a good relationship with key contacts in each site was vital in enabling the opportunity to access potential participants. Second, arranging NHS permissions can take several months; although this was achieved quite quickly at sites A and B, site C took considerably longer. Third, to encourage interest in the project and participation, taking opportunities to present the project face-to-face with potential participants was extremely effective. This observation is supported by our own experiences at site A and also by the experiences of principal investigators with recent success in recruiting primary care middle managers for their NIHR projects.
The original participant recruitment target was 42 health-care middle managers across three sites, that is, 14 interviewees per site. In the event, 15 health-care managers volunteered and were interviewed at site A and 14 at site B, giving a total of 29 managers. Although the data collection met our intended target at both sites, data analysis indicates that the data were short of saturation. It is likely that if more managers had been recruited a wider variety of examples may have been found. However, this was an original exploratory study and the sample size reflects the preliminary aspect of the investigation.
Collecting data from three different organisational contexts was intended to allow analysis of the extent to which these organisational contexts affected unlearning. The reason for choosing these three types of context is that they represented some of the most important and common organisational types that the managers being investigated worked in. As a result of the lack of representation from the primary care sector, this study was not able to analyse the extent to which the primary care context affects unlearning in comparison with the acute or mental health contexts. However, because data were still captured from two different organisational contexts, the third research question can still be examined. In addition, although the significant organisational and structural change in the primary care sector at the time of data collection (2011–12) indicates that this sector would be a valuable context in which to study unlearning, it is possible that participants would not have had sufficient time in their new roles to be able to comment on their unlearning experiences. Further investigation of the role of unlearning in the primary care sector in 2013–14 may be of particular value to complement the findings of this study.
Description of participants
At each site we aimed to maximise variance. In other words, we aimed to include interviewees from a wide range of directorates and units, occupying a variety of roles, and to include a mix of those with and without a clinical background. The sample was therefore varied in terms of occupation, management/clinical mix and job role.
Of the final sample, 12 managers were working at band seven, 14 were working at band eight and 3 were consultants and, therefore, not subject to Agenda for Change banding. The sample included 6 men and 23 women. To ensure anonymity of excerpts of the interview quotes, we categorised the interviewees into three job groups (Table 5):
-
manager: manager with no clinical background or function
-
manager (clinical background): manager with clinical background, but with no clinical function
-
clinical manager: manager with clinical background who has clinical and managerial function.
| Job group | Example job titles |
|---|---|
| Manager | Facilities manager, laboratory manager, information manager, performance manager, project assurance manager |
| Manager (clinical background) | Risk manager, project manager, leadership development manager |
| Clinical manager | Senior charge nurse, consultant, senior research nurse, specialist physiotherapist, ward manager |
Interviews took place between 4 August 2011 and 13 October 2011. Each lasted between 45 and 73 minutes with the average length being 60 minutes. The research associate conducted the majority of the interviews (26 interviews) and the two other researchers conducted the other three interviews. Two researchers were present at eight of the interviews to ensure the validity of the interview schedule and rigour in data collection. Interviews were digitally recorded after participants had given written consent. Recordings were fully transcribed. Participants who requested a copy of the interview transcript were sent one. All were invited to attend a workshop to hear about initial findings and to comment on those findings. Taking part in the interview did not commit participants to attending a workshop. Participants and case study contacts were promised a summary of the final report and a web link to the full report.
Workshops
The final part of the project was to conduct feedback workshops with interviewees from the participating sites. The aim of the workshops was to provide an opportunity for additional data gathering. The workshops had three main objectives: to feed back preliminary results from the study; to gather participants' views on the preliminary findings; and to discuss the practical implications of the findings with participants in terms of how the information could be used within the sites. Each workshop was attended by the principal investigator (Coombs), workshop facilitator (Holland) and Bosley (site A) or Hislop (site B). Hislop and Bosley captured the key points from each workshop on flip charts that were transcribed for analysis.
The feedback workshops were held on the 15 March 2012 and 12 March 2012 in sites A and B respectively. All interviewees were invited to attend the session at their site. In addition, after discussion with our key contacts at both sites, a number of additional staff who were interested in the study but who had not participated in the interviews were invited to attend the workshops. These staff included middle managers, research managers and, at site B, senior trust management. Nine health-care managers, including three health-care managers who did not participate in the interviews, attended the workshop at site A. At site B there were 20 participants, including 11 health-care managers who did not participate in the interviews.
Data analysis
Data analysis followed the three concurrent activities identified by Miles and Huberman101 of data reduction, data display and conclusion drawing/verification (p. 10). Both deductive and inductive approaches were used. A deductive approach was used initially to reduce the data. A coding frame was developed based on the research questions and concepts being examined and applied to the data collected in the exploratory interviews. The research team subsequently tested the coding frame with each member independently coding two transcripts selected from the corpus of the data and comparing and discussing their coding decisions with the whole team. This led to a further iteration and additional testing of the coding frame.
To promote consistency the research associate coded all transcripts. The research associate used an inductive approach to code findings from the interview data. Thus, she added further codes and split and spliced codes as she worked on new transcripts. Team members reviewed coding and conducted periodic queries in NVivo 10 (QSR International, Southport, UK) to test and validate coding decisions.
Using the software package facilitated the coding process, enabling the research associate to compare and revisit codes during the coding process and thus ensure consistent application and identify codes that could be split or spliced. NVivo also enabled quick retrieval and comparison of data segments allocated the same code and the construction of conceptually ordered displays (data display). Such displays or matrices enabled the researchers to study the variables in more depth and generate more explanatory power. The matrices were created through a series of iterative steps, with initial drafts created by the research associate with the initial and subsequent drafts reviewed and discussed by the project team. This approach ensured consistency and validity when categorising data such as the nature of unlearning episodes, barriers, enablers and impact on decision-making processes. As the draft matrices were often large and covered several pages, an example of part of a draft matrix is shown in Table 6.
The data from the workshops were analysed using content analysis to derive the key themes that emerged from the meetings. Because of the method of data collection, the level of analysis of the workshop data was largely descriptive, but it does provide some interesting additional perspectives for the study.
| Subcategory | Description of category | Sources | Example |
|---|---|---|---|
| Assumptions | Examples of deep unlearning that is in relation to things taken for granted | 8 | 3.10 ‘And I suppose sort of giving up this belief that clinicians are always right because clinicians often aren't right actually and clinicians can be very rigid in their way of thinking’ |
| 3.11 ‘I suppose maybe the sort of unlearning is being willing to let go of the assumption that the way we've always done things clinically is right and be willing to think about it and I think there are some things that are right, but you've got to think about it and you've got to think about, even if they are right, can it be done in a different way. And it may be giving up the belief that as a clinician you're always right and that the bigger picture is that clinicians might not be completely right’ | |||
| Attitude | Examples of deep unlearning that is in regards to feelings in relation to work event | 6 | 3.12 ‘I came from a private sector where you did have those conversations and I've learnt not to have them because they've not been supported by HR. This could be my unlearning, couldn't it, because I came from a very performance managed organisation in [. . .] and came into the NHS and you didn't have those sorts of conversations and nobody worried about how you were acting or performing in your role and, you know, if you got on with your manager that was fine. There is no negotiation to be had with that person, so that's got to be [. . .] forgotten in this situation. Yeah’ |
Description of case study sites
Data about the case study sites were gathered from NHS trust websites, annual reports and informal discussions with site contacts. Data from these sources were used to construct the case study descriptions. As the case study sites (like other NHS trusts) were subject to considerable change during the study period, it was difficult to construct accounts that accurately represented them. The site descriptions are intended to provide the reader with sufficient detail to make sense of the findings while protecting the anonymity of the participating NHS trusts.
Description of site A: mental health trust
Site A is a NHS foundation trust located in the Midlands employing more than 2400 staff, with approximately 350 staff holding managerial responsibilities. The trust provides mental health, substance misuse, learning disability and children's services. At the time of the interviews, one of the initiatives that the trust had introduced was the Releasing Time to Care Productive Care Pathway programme. This was a formal process in which staff teams, with the help of a facilitator, identified ways of changing the way that they do things, including ward structure and work space, to release time for more interaction with patients. The trust had also introduced organisational changes that had resulted in some tiers of staff being removed, placing some staff at risk of redundancy.
Description of site B: acute trust
Site B is a NHS acute foundation trust located in the north of England. It employed more than 3500 staff with close to 400 staff holding managerial responsibilities. The trust was established in 2005. In 2011 it took over local and some countywide community-based services. The trust provides a full range of general acute secondary care hospital services through a clinical business unit structure. The services include medical services, surgical services, obstetrics, emergency medicine, diagnostics, community and integrated care, theatres, anaesthetics, sterile services and critical care. There was structural organisational change at the time of the interviews at this site. Three new directorates were created with new directors appointed, resulting in more devolved decision-making. However, as it was a small organisation, all directors at the trust had operational as well as corporate roles. The organisational restructuring also resulted in the loss of some managerial posts.
Having summarised the research design, methods, approach to data analysis and case study site descriptions adopted for the study, in Chapter 4 we present the findings from the data analysis.
Chapter 4 Results
As stated in the introduction, although we used Rushmer and Davies'6 unlearning typology as the initial perspective to differentiate between different types of individual unlearning, we were able to develop a new typology from the data analysis. This new typology of individual unlearning distinguishes between four separate types of individual unlearning that can be triggered by either individual experiences or change events. For clarity, the new typology is repeated in Table 7. We have not included fading in the new typology as the data supported our interpretation from the literature that fading does not include a deliberate and conscious action, which we believe is necessary for unlearning to occur. Therefore, the findings related to fading are provided in a separate section after the findings related to individual unlearning.
In reconceptualising Rushmer and Davies' typology we also relabelled wiping as behavioural unlearning, and deep unlearning as cognitive unlearning to create labels for the unlearning types that were more explicit and clear regarding what was being unlearnt. Behavioural unlearning refers to the individual unlearning of specific behaviours such as practices, activities or routines, which has no (or limited) impact on people's underlying knowledge, values and assumptions. Deep unlearning, which is relabelled ‘cognitive unlearning’, is emotionally charged as it involves giving up or abandoning more deeply held knowledge, values and assumptions.
| Catalyst of unlearning | Type of unlearning | |
|---|---|---|
| Behavioural unlearning (wiping) | Cognitive unlearning (deep unlearning) | |
| Individual experience | Behavioural unlearning initiated by individual experience | Cognitive unlearning initiated by individual experience |
| Change event | Behavioural unlearning initiated by change event | Cognitive unlearning initiated by change event |
In the following six sections we present the findings of the study using the labels of behavioural unlearning and cognitive unlearning to clearly show the empirical support for this new conceptualisation of unlearning. We include the empirical findings concerning fading in this structure to illustrate why fading is not included in the new conceptualisation. This labelling also allows the reader to easily cross-reference the discussion provided in Chapter 5 to the empirical findings. The structure of the findings has been chosen to ensure a direct fit with the research questions for the study. This enables a wider understanding to be extracted from the individual experiences of unlearning reported by participants and therefore provides insights from the data in a form that can help inform organisational- and policy-level responses.
Episodes of individual unlearning and fading
The first research question for this study was to investigate the extent to which health-care managers engaged with the process of individual unlearning. This section reports how individual experiences or change events resulted in participants experiencing behavioural and cognitive unlearning. Also in this section we present examples of responses relating to episodes of fading. From the interview data we identified 85 episodes of individual unlearning and fading: 29 behavioural unlearning episodes, 28 cognitive unlearning episodes and 28 fading episodes. Based on the new unlearning typology, Table 8 provides a summary of the types of knowledge that had been unlearnt by participants in the study. The table shows that the types of knowledge reported as being unlearnt by participants were varied, with the most common knowledge unlearnt being concerned with procedures and practices for both behavioural and cognitive unlearning. These episodes are reported in more detail in the following sections before considering episodes of fading.
| Trigger | Behavioural unlearning | Cognitive unlearning |
|---|---|---|
| Individual experience |
|
|
| Change event |
|
|
Behavioural unlearning episodes
Participants identified relatively few examples of behavioural unlearning triggered by individual experiences. The most frequently mentioned catalyst involved a change in job role that was initiated by the individual. This trigger tended to lead to unlearning of procedures and practices. For example, one participant explained how moving into a new role resulted in a change in his daily structured tasks. The new role meant that the participant had to unlearn his previous management style, no longer interacting with staff and service users on a daily basis and having direct control, and develop a more influencing and strategic perspective with less structured focus on specific operational activities. He explained:
So the sense was suddenly all the things I'm used to doing in my daily structure [had disappeared]. The biggest one was as an operational manager my day's pretty well structured for me. [. . .] I suddenly moved into a setting where that whole skill set, particularly of managing staff and processes were now simply not needed. [. . .] When I was operationally managing young people's services I was out there negotiating with commissioners and in one sense I was [. . .] much more making things happen as to change and talking back with the staff trying to get the way we do things changed. So I was . . . in a different way I was more directly affecting change. Here it's at a subtler level [that I'm part of]. In one sense I'm just part of making a system work.
Manager, A1
By contrast, several different types of change event were identified that led to behavioural unlearning. The main types of change event catalyst identified were changes in organisational structure, often resulting in an imposed change in role, the introduction of new policies and changing guidelines for reporting. These change events also resulted in staff having to unlearn existing procedures and practices. For example, as a result of organisational restructuring a participant moved from an emergency department to a medical outpatient area. The change meant that she had to unlearn the variety and quick responsive style of working required in the emergency department for a more controlled and predictable environment. She commented:
I suppose the whole concept of outpatient work and starting at, you know, 8 o'clock in the morning and they'll be leaving at 5 o'clock I really found very difficult to get my head round when the sort of rat race almost in emergency medicine is very diverse. So it took me a while I think to feel as though I was able to support them in those areas constructively [. . .] I suppose what I had to give up was the fact that I had to learn a new set of things and relinquish some of the time and energy that I would put into the emergency department.
Clinical manager, B12
A second example is provided by another participant who explained that organisational restructuring had resulted in her role changing from managing a single ward to managing multiple wards and the associated additional staff. She had to relinquish control of her ward and abandon the personal relationships she had with her previous team and focus more on the strategic needs of the service, patients and staff. A clinical manager who recalled how organisational change provided the opportunity to work with a new team on a new ward provided a further example. The change meant that she had the opportunity to abandon old practices in favour of more person-centred care. She commented:
I was fortunate enough to be ward sister on a ward that was closing in one of the old asylums and moving that ward or the new version of that ward into a local community hospital and because we were not only moving sites but we were having a newly put together team with some older staff that were on the old ward but we had a lot of new people coming in as well, it was an opportunity to actually start afresh really. So I think in terms of unlearning I did quite a lot of that in the planning stage really because what I was trying to do was discard the old, traditional, institutional behaviour, particularly in looking at the patient stay and what that could look like and should look like. So I was trying to discard all that that I'd sort of learnt over the previous 10 or 15 years and start again from scratch to make it more person-centred – and this was before anybody talked about person-centred care. But in actually doing that the first thing it created for me was a need to change shift patterns – actually start the morning shift or the day shifts a little bit later because what that actually did was give the patients a lie-in by half an hour.
Clinical manager, A7
Participants also mentioned the introduction of new policies as a catalyst for unlearning existing policies and procedures. Examples mentioned by participants included changes in national policies regarding appraisals, resulting in a need to abandon old appraisal systems that had been developed at the trust, and adapting to new commissioning arrangements. New commissioning policies meant that the method of recording contacts changed from block contracts to costing each activity individually. This change required the participant to give up her existing way of measuring contacts and learn a new method. She explained:
I think some of it may be around how we count activity and all of a sudden the commissioners want to commission slightly differently. So perhaps we were on a block contract once and now we're on a cost per case contract, so you have to parcel away the block contract thinking where activity isn't as important. It is, but it isn't and now you have to suddenly think it is, but if they change back to a block contract, which they have in one of these cases this year, you suddenly have to be doing all of that thinking back again. [. . .] They want us to record contacts with the carer when the topic of conversation is the patient, but not contacts with the carer where it's talking about the carer themselves. That isn't counting to our activity anymore whereas it did. We were treating the whole of the family rather than just the patient and now we've got to change to be treating the patient.
Manager, A2
The requirement to implement new policies and guidelines resulted in some participants with training responsibilities having to unlearn how they approached their training. For example, one participant commented that changes in hand hygiene policy meant training guidelines had to be altered to reflect the emphasis on using alcohol-based rubs, and that this required changes in how the training was delivered. Further, changes in policies are often accompanied by new reporting guidelines leading to unlearning. One participant narrated her experience when the National Cleaning Specification was introduced in 2004. As a result, the participant had to abandon her previous reporting format that focused solely on the cost of services, adjusting to include more strategic and operational information to report to the management board. She explained the process:
The biggest change for us was the implementation of the National Cleaning Specification back in 2004 [. . .] Before that, [. . .], as far as cleaning was concerned [. . .] you were looking at cutting all the corners to save and also provide a quality service. [. . .] it was a big learning curve to go from being a service that nobody was bothered about [. . .] to all of a sudden actually we were on the Boards, you know, and when the Board met they were actually interested in what you were doing. [. . .] It was that type of thing, down to that detail, right down to the whole management. It's a 90-page document, every single one of it, down to what policies you've got to have. We had to have strategic cleaning policies, you had to have operational, you had to have cleaning groups.
Manager, A6
Cognitive unlearning episodes
The majority of participants reported episodes of cognitive unlearning being triggered by individual experiences. The most common experience was clinical incidents, with job role changes, clinical investigations and organisational changes also being mentioned. Clinical incidents resulted in several participants commenting that their beliefs and views regarding the delivery of care had been challenged and changed as a result of the incident. For example, a manager recalled two deaths on her ward that made her realise that incidents could happen irrespective of the processes and systems put in place to reduce harm. As a result, she has continually attempted to influence other staff members to be vigilant to ensure patient safety. Similarly, another manager explained how a suicide on a ward she was responsible for made her change her assumptions regarding the risk of a patient hanging him/herself. The manager's unlearning centred on the perception that the measures that had been put in place to reduce the risk of a patient using a ligature to hang himself or herself were sufficient. The incident demonstrated the extreme measures that some people will take to end their lives and caused the manager to unlearn her original perception of a safe ward environment. She explained:
We had a very tragic death where a patient on one of those wards hung himself on a wardrobe door. [. . .] So it was a really rude awakening because we'd assumed previously that all the work we'd done on curtain rails and window bars and everything had really addressed and reduced the risk of anybody hanging themselves using a ligature, was nil, and it made us . . . well, it made me look very differently at the environment and we did an awful lot of work on reassessing that particular ward to completely obliterate any ligature risks. [. . .] We just hadn't realised the potential or the extremes that some people could go to if they wanted to take their own life. So it really made us look very differently at the environment and we made a huge number of changes.
Manager (clinical background), A14
As well as changing beliefs regarding the delivery of care, episodes of cognitive unlearning also included unlearning views and perceptions of participants' work environment. More specifically, several managers reported that being the subject of a clinical investigation had caused them to reassess their perceptions of their colleagues. For example, one participant commented that during the investigation she was surprised that her colleagues were not willing to support her defence. The participant believed that this lack of support was due to a desire from her colleagues to avoid also being blamed for the incident. Another manager who was unhappy about a change in his working arrangements provided a similar example. He spoke to a senior manager who made it clear that the decision would not be changed and that challenging the decision was unlikely to improve the situation. The manager believed that this experience resulted in him unlearning his desire to always follow his personal principles and instead being more pragmatic in some situations. A clinical manager reported a further example of unlearning views of the work environment. The manager explained how he had to abandon his assumption that all medical services were easily accessible after moving from a regional health organisation with access to many services to a smaller unit with limited facilities. He explained:
I came here from like a big hospital. The previous one was like a big regional centre and this one is a small unit compared to that because there we were like 12 consultants and here we are 2 or 3, so . . . And what happened when I initially came – there was a patient we did an angiogram on who had a renal problem as well. [. . .] the [CAT] lab here was just established 4 years ago, so there was no sort of protocol and it was just as and when on a needs basis. [. . .] I had thought that this was commonplace that everything was in place that the patient gets a kidney test after so many days and then, you know, the results come to me and then, you know . . . But obviously there was no protocol here, so I was a bit, you know, shocked. [. . .] I think giving up or unlearning would be my thought process that everything else was in place whereas it wasn't. Obviously if you're a smaller hospital and the [CAT] lab is just, you know, a few years old, these things are not quite in place.
Clinical manager, B6
The third category of cognitive unlearning triggered by an individual experience involved the abandoning of previous perceptions of management priorities. Both episodes identified were reported by participants to be triggered by a change in job role and moving into a senior management position. For example, one manager gave up her assumptions that members of the trust board were not concerned with the best interest of patients when she changed her role. In the new role she realised that the care of patients was considered equally as important as ensuring the cost-effectiveness of the services provided. She reflected on the process of giving up her previous views, commenting:
I was very much [for the] patient – it doesn't matter how much it costs or what's the implication, they should always come first – where I sort of had to have that shift of, ‘Hold on a minute. I recognise that we've got to meet those targets on that [as well].’
Manager, A3
A second episode involved slightly different circumstances, with the manager joining the NHS from the private sector. Initially she found that the senior managers in the NHS were not as focused on performance management as she had encountered in her role in the private sector. This required the manager to abandon her previous style of management and adapt to the culture in the NHS, where she felt staff performance issues were not confronted in the same way.
Fewer episodes of cognitive unlearning triggered by a change event were identified by participants than episodes triggered by individual experiences. The type of change event most commonly mentioned involved organisational restructuring and associated role changes, which led to perceptions of management issues being unlearnt. For example, one manager commented that, because of organisational changes, she had now become responsible for managing the annual leave rota. The manager explained that the new responsibility had meant that she had to abandon her perception that she would always be able to keep her staff happy and be liked, in preference to prioritising the effective delivery of the service. She explained her change of attitude:
Annual leave is the part of my job that I really don't like being responsible for because it's a bit of a nightmare because the way our rotas work [. . .] about a couple of months ago there was definitely a reaction where someone had asked for annual leave at very short notice and I just couldn't do it. There was no way and I fully explained why, but this wasn't good enough for the person and yeah, they didn't really talk to me for a couple of days and I just kind of felt . . . I was very annoyed by that [. . .] That was the real point where I thought, ‘Right, some of this role and responsibility as a team leader isn't going to make you popular all the time’, and that was a real changing point for me.
Clinical manager, B1
Managers who had taken on more responsibilities as a result of role change from organisational restructuring reported two further episodes of cognitive unlearning. In these episodes the beliefs and attitudes that were unlearnt were associated with procedures and practices. For example, one manager commented that she had to abandon her informal approach to addressing staff issues after organisational restructuring split health and social services within her trust. The clinical manager commented that she had to adopt more formal procedures requiring more documentation to maintain clear and agreed communication. She explained the change, commenting:
I think this is where I wanted to pick up on the split with social services. For as long as I can remember we have worked as one service. [. . .] You have to unlearn, you have to put to one side the mechanisms for working that you've been very used to doing. Like I said to you, I could just pop in to one of my colleagues, very informal, very quick, very easy. [. . .] I now do process notes for individual conversations that I have with staff and that was something that I learnt very clearly.
Clinical manager, A15
Fading episodes
The vast majority of fading episodes identified by participants were triggered by changes in job functions. Other triggers that were identified included developments in technology and policy changes. The nature of the fading most commonly involved the forgetting of specific skills. For example, one manager commented that she felt that her in-class teaching skills had faded because of her role change and lack of use. She commented:
I used to do a lot of in-class work but I've not been in class for a long, long time. It just doesn't fall into my remit at the moment.
Manager, A11
Similar comments were made by participants regarding a lack of use of technology or new developments in technology that would require the updating of their skills. For example, managers commented:
I think learning an IT system and learning to use an IT system is one that can fade with no use. So if you have to do a task once in a blue moon on an IT system you would know how to do it and if you did it repeatedly you just do it naturally, but if you leave it for 6 months or you leave it for a year it's faded away and you have to relearn it.
Manager, A2
I suppose drafting things is entirely different on a computer to what you used to have to do when you were writing essays, but also just the ability to write for any length of time I can't do it anymore, it makes my hand hurt.
Manager, B11
I think we've lost that a bit just because of the technologies now around and so much of it is on-line that you can search for things quite quickly in terms of just a different skill. But yeah, I think that's probably what's lost. So yeah, your search skills obviously have to develop and how you search.
Manager, A13
When discussing episodes of fading it became clear that participants struggled to identify examples of skills and knowledge that had faded. None of the participants who identified fading episodes gave any indication that they had made a conscious decision to intentionally forget the skills and knowledge. This suggests that the examples of fading that our participants provided were more akin to forgetting than to individual unlearning as conceptualised in this study. They also frequently framed their examples in terms of the length of time it would take them to recover a skill, such as performing a previous task on an updated IT system. Some participants also commented that, although they were confident that they would not perform to the same standard as previously, they also felt that they still held some residual knowledge. Consequently, it was difficult to gauge the degree of fading that participants were reporting.
Summary of episodes of individual unlearning and fading
The analysis of behavioural and cognitive unlearning and fading episodes has shown that health-care managers frequently experience unlearning and that unlearning can take a variety of different forms. It was noticeable that the catalysts were often closely related to the knowledge being unlearnt, particularly regarding behavioural unlearning. For example, new procedures and practices, reporting guidelines or training guidelines often required the unlearning of previous procedures, reporting or training methods. In addition, changes in job role, either imposed from an external change event or instigated by the individual, was a frequently mentioned trigger for both forms of unlearning and fading. Finally, the nature of unlearning episodes described by managers illustrates the greater emotional impact associated with many cognitive unlearning episodes compared with behavioural unlearning, and the greater challenge of coming to terms with the need to abandon previous beliefs or knowledge. Having considered the catalysts and types of behaviour and knowledge that either have been unlearnt or have faded, the following section reports the barriers to unlearning identified by participants.
Barriers to individual unlearning
The second research question of this study focused on investigating the barriers and enablers that influenced health-care managers' level of engagement with the process of unlearning. This section addresses the first part of that question. Overall, participants mentioned 36 examples of barriers encountered during episodes of behavioural unlearning, but mentioned fewer examples of barriers encountered during cognitive unlearning episodes (n = 19). Some participants mentioned more than one barrier to their unlearning or fading episode, which is why the number of barriers identified is greater than the number of unlearning episodes described in the previous section. Table 9 shows that the most common forms of barrier identified were staff resistance to changes in practice, personal behaviour, lack of management support, high workloads and organisational culture. Other barriers that were mentioned included financial constraints and job insecurity. In addition, we also identified 13 examples of barriers to fading, the most common of which was the ability to recall past knowledge and experience. The following explains the nature of the barriers identified by participants and the types of unlearning they were associated with, before considering barriers to fading.
| Number of episodes | |||
|---|---|---|---|
| Trigger | Barrier | Behavioural unlearning | Cognitive unlearning |
| Individual experience | Personal behaviour | 11 | |
| Change event | Staff resistance to changes in practice | 10 | 7 |
| Lack of management support | 7 | 3 | |
| High workload | 3 | 3 | |
| Organisational culture | 0 | 6 | |
| Financial constraints | 3 | 0 | |
| Job insecurity | 2 | 0 | |
| Total | 36 | 19 | |
Staff resistance to changes in practice
The most frequently identified barrier mentioned by participants was the resistance of other staff to changes in practice. This barrier was most commonly mentioned in relation to behavioural unlearning episodes. In general terms, the unlearning episode that the health-care manager had experienced would result in a desire to implement a new practice. However, this change would often require other staff to also adopt the new practice, which is the point when resistance was encountered, thereby also inhibiting the manager's ability to change to the new behaviour. For example, a clinical manager commented that during the process of abandoning previous hand-washing protocols to newly adopted alcohol rubs she found that some community nurses were reluctant to adapt to the new practice. She observed that:
Some of the nursing staff, I'd say more in community settings were resistant. For them trying to make the link between preventing and spreading infection and what they were doing is always a difficult one. They see themselves as being less clinical, less hands-on and that's a significant part of our service actually, so it was much easier in wards than it was in community teams.
Clinical manager, A10
Staff resistance to new practice was also mentioned as a barrier to cognitive unlearning for some managers. For example, one manager commented that one particular new way of working that she had wanted to implement was to ensure that staff were more engaged with procedures and practices. This change required staff to be more involved and to provide feedback on new procedures, but the lack of engagement from staff meant that the manager found it difficult to implement the new way of working. She shared her frustrations saying:
I'm trying to feed back to anybody and everybody that would listen and never getting any feedback. So that was a real barrier and I just tried different ways that I could do it, but never really getting any feedback at all as to is this is the right way, is this the wrong way, what can we do differently? So that really was a definite barrier [to unlearning].
Manager (clinical background), B8
Personal behaviour
The second most frequently mentioned barrier to unlearning was participants' own personal behaviour, although this barrier was mentioned only in relation to behavioural unlearning episodes and particularly those episodes triggered by an individual experience. Managers mentioned a variety of different examples as they reflected on their personality traits. For example, a lack of confidence in a new job and the associated required knowledge inhibited one manager from abandoning her old ways of working. Another manager explained a similar example involving a change in job role, but in this case framed her barrier to unlearning as the challenge of giving up complete control when delegating tasks. She explained her behaviour:
I'm quite a perfectionist probably and I'm a completer [. . .], so I quite like having everything tidy and sorted [. . .] I think the thing about delegating I suppose and trusting other people probably to do it the way you want. [. . .] It's probably just my personality, isn't it, as opposed to the job necessarily. But yeah. Or sometimes accepting that something's been done maybe not quite how you would do it, but it's good enough, so just let it go. [. . .] I don't want to feel the wrath of somebody higher up in the organisation, [. . .] So I suppose what I feel is a top-down pressure that makes me think that I can't let mistakes happen, so I've got to [be in] control.
Manager, B11
Another manager also considered her personality type to be a barrier to unlearning. She recognised that she had a strong desire to always get on well with her staff and that this could compromise her decision-making, as some decisions would not be well received. Therefore, she needed to unlearn her view that she could always be ‘friends’ with her staff and her personality made this change challenging. She stated:
Me myself, if I'm completely honest. Yeah because, as I said, there's always that part of me that wants to be liked and unfortunately, being management doesn't always work with that and I'm actually not here to be their friend; I'm here to make sure that the practice within the unit and the safety within the unit is as good as it can be and that's what I'm here to do.
Manager, B4
Other examples mentioned by participants included the challenge of completely unlearning behaviour that had become ingrained over a long period of time. They suggested that some people would find the change of behaviour easier to adapt to than others. Another clinical manager added that she felt that she had some difficulties in embracing change and the associated behavioural unlearning, as the benefits of new practices were often not without their drawbacks. She explained that these drawbacks provided a concern that further changes were likely and that some elements of previous practice would be needed again in the future.
Lack of management support
The lack of support from immediate managers was also identified by participants as being a barrier to both behavioural and cognitive unlearning. For example, a manager commented that although he had moved to a new role he was not being protected from ongoing demands from his previous role, restricting his behavioural unlearning. Another manager explained that when she wished to abandon a previous behaviour the controlling style of her senior manager and associated lack of support inhibited her making the change. She explained her opinion:
[There was a] person who was senior to me who had a skill set and way of behaving that was alien to me. [Their] poor leadership and managerial ability and communication deficits on a personal level and a lack of valuing what many people in the organisation were doing and a very controlling way of managing people [meant I couldn't make the change I wanted].
Manager (clinical background), A12
Lack of management support was also mentioned in relation to cognitive unlearning episodes. A clinical manager explained that although she had support at board level this was not continued at lower levels, which inhibited her ability to introduce the new changes.
High workloads
Heavy workload was another factor mentioned by several managers as a barrier to both behavioural and cognitive unlearning. For one manager the high workload generated by her department's clinical priorities tended to be a barrier to her adapting to her managerial roles. Although her role change required her to work in a new strategic way, attempting to unlearn the need to think only about operational demands, she found that the nature of the clinical work that her department provided required her to retain this way of working. She explained:
The things that have got in my way always are the clinical priority of the department. So, you know, I'd plan to go to a meeting or to do something or spend some time there and for whatever reason things would go disastrously wrong in the department and I'd have to say, ‘I can't. I have to go back. Clinical priority. This is going on and this supersedes it really because of patients.’ So I suppose it's the conflict of clinical areas.
Clinical manager, B12
When discussing barriers to cognitive unlearning, high workloads were also mentioned. For example, a clinical manager commented that, following a change in role, although she wished to change her habits to apply more formal processes for communication between her staff, the volume of work she encountered meant that she had little time to implement this new way of working and thinking. She stated:
Just the sheer number of staff and volume of work. I mean I went from getting maybe 30 e-mails a day to getting on a good day it was about 80 and a lot of them were just what I call navel fluff. You know, it's just somebody going, ‘I really ought to tell somebody about this’, ping, and sending it off into the ether and that you didn't really need to know about. So you could go through and maybe 30% of it was like that, but the rest of it was, ‘I have to do something about this today’, and that was just not do-able. You know, you could just sit and have your computer tell you what to do all day, let alone what is in your diary.
Clinical manager, A15
Organisational culture
When discussing barriers to cognitive unlearning a number of participants suggested that they found that the organisational culture held by certain groups acted as a barrier to unlearning old mindsets. This challenge was best illustrated by a clinical manager who explained how the clinical mindset found among clinicians was difficult to change unless they had been involved in training programmes that were designed to introduce new ways of thinking. She stated:
Yeah, you get into that culture of, you know, we're clinicians and we do the clinical thing. Yeah, the culture, the clinical side of it, the colleagues who haven't experienced the mentorship programme that I have, so trying to get that over to them without appearing like a mad woman.
Clinical manager, B10
This barrier is also likely to be closely related to staff resistance to change mentioned earlier, the two barriers combining to slow the implementation of new ways of working or thinking. Ultimately, these factors are thought to also act as a barrier to managers' personal cognitive unlearning, because of the pressure to continue with old practices or thought processes.
Financial constraints
Barriers to behavioural unlearning episodes were also identified in the form of financial limitations that challenged the implementation of new ways of working. For example, when discussing the new changes in hand-washing protocols a clinical manager commented that the cost of moving to new alcohol-based rubs presented an initial problem. Therefore, being able to fully implement the unlearning was made more difficult. She explained:
Cost was a concern actually. For all a little bottle of hand rub costs about 60 pence, when you start to multiply that up into [. . .] and giving everyone one and replacing it frequently there was a lot of concern about cost in doing this. They weren't funded to do this. This had to come out of an existing pot of money. So that was also a ‘So where's the money coming from, [. . .]?’ conversation, which is a frequent part of my job. So yes, that was a bit of a barrier.
Clinical manager, A10
Job insecurity
A further barrier mentioned in relation to behavioural unlearning was staff concerns over their job security associated with new ways of working. A manager illustrated this point by explaining that it was difficult to embrace new ways of behaving and working and abandon old behaviours when either their own role or the roles of their peers could be threatened by removing old activities. The manager commented:
I suppose the thing that drives some of that is the external influences from the Department of Health around transformational change, cost improvements [. . .] it will have to impact on staffing and that's pretty difficult to work with [new] programmes [. . .] when you're in that environment where people are feeling threatened around, you know, ‘Will I be able to pay my rent next week?’ You know, it's as real as that. There's a huge amount of movement in the organisation of staff being put at risk and then moved to a different area.
Manager (clinical background), A12
Barriers to fading
When discussing episodes of fading participants mentioned barriers only in terms of well-established skills that had often been developed from lots of experience and repetition. Managers also tended to refer to core skills and knowledge being retained, but no longer being able to recall more specific skills or recent developments, meaning that their previous skills would be outdated. For example, a clinical manager commented:
I mean if I had to go and do quite a complicated, aseptic technique dressing I'd feel confident as if I did it every day and that's perhaps because it's maybe not so invasive so there's not so much can go wrong, but it's also something that's perhaps more embedded in me because I've done it for so many years and it became a core part of my job.
Clinical manager, A7
However, she admitted that changes in technology associated with other procedures meant that she would have to update some skills. She continued:
Things like taking blood pressure, for instance – yeah, I still know how to do it, but it's different equipment now. It's new-fangled and so I'd need to use it quite a bit more before it became second nature to me.
Similar comments were made by another manager who felt that, although she would not have the latest skills in some aspects of work, she would still be able to recall some fundamental aspects. She added:
If there was a wound dressing to do, I would have some core knowledge and competency about wounds, [. . .], but I might not know the most up-to-date application of a particular dressing. So I would have the wherewithal to look that up and know, but the core thing about how you care for a wound and wound healing, nutrition, all that I would know. So the core thing's there, but what I've lost is what's current.
Manager (clinical background), A12
A manager who was a former clinician mentioned a related aspect to the barrier to fading of being ableto recall skills and knowledge. She said that in some situations in her current role it was important for her to recall her knowledge of clinical practice, for example when assessing a clinical risk situation. Consequently, the need to occasionally reuse her clinical knowledge acted as a barrier to it fading. She stated:
So there were some things that I sort of did transfer, but a lot of the actual clinical skills I just don't have a use . . . no, I don't have a use for now, but I suppose they're still there. Some basic knowledge is there and I use that when I'm sort of assessing some sort of clinical risk in a clinical environment, but I'm not in a clinical environment now.
Manager (clinical background), A14
Summary of barriers to individual unlearning and fading
Participants reported personal behaviour as the only barrier to behavioural unlearning triggered by an individual experience. More specifically, lack of confidence, reluctance to delegate, desire to be liked and habits were identified as obstacles to setting aside particular ways of acting. In contrast, participants identified several barriers to behavioural unlearning triggered by a change event; all of these barriers were external to the individuals who experienced the unlearning episode. Participants reported staff resistance to changes in practice, lack of management support, high workload and financial constraints limiting the implementation of new practices and staff concern about job security as barriers to this type of unlearning.
All reported barriers to both types of cognitive unlearning were external to the individual who experienced unlearning. Personal behaviour was the only reported barrier to unlearning triggered by an individual experience. External barriers to cognitive unlearning triggered by a change event were identified as staff resistance to changes in practice, organisational culture and high workload. In other words, other people (managers or staff), culture or work context were most commonly perceived as barriers to cognitive unlearning. This may suggest participants' perceived lack of power or autonomy to implement the changes required as part of the unlearning process.
Staff resistance to change, lack of management support and high workload were identified as barriers common to both cognitive and behavioural unlearning triggered by a change event. However, organisational culture was identified as a barrier specific to cognitive unlearning triggered by a change event, whereas financial constraints and job insecurity were regarded as barriers specific to behavioural unlearning triggered by a change event.
As noted above, skills and knowledge, even those infrequently used, were perceived as too well entrenched to be forgotten. In other words, the barriers to unintentional forgetting (i.e. fading) are specific to the individual. Having considered the barriers to unlearning and fading, in the following section we examine enablers of unlearning.
Enablers of individual unlearning and fading
This section examines the factors that managers perceived enabled them to engage with the process of unlearning or fading. With the exception of one factor, all of the enablers mentioned by participants could facilitate either behavioural or cognitive unlearning. As was the case when discussing barriers, participants often identified multiple enablers to particular unlearning episodes, resulting in a higher number of enablers than individual unlearning episodes. As shown in Table 10, a total of 48 and 49 examples of enablers of behavioural and cognitive unlearning were identified respectively.
| Number of episodes | |||
|---|---|---|---|
| Trigger | Enabler | Behavioural unlearning | Cognitive unlearning |
| Individual experience | Personal skills and attitudes | 16 | 11 |
| Leadership and networks | 9 | 14 | |
| Support from specific individuals | 11 | 11 | |
| Change event | Management support | 3 | 5 |
| Wider pressure to improve the service | 6 | 2 | |
| Training opportunities | 2 | 2 | |
| Change in work circumstances | 1 | 1 | |
| Changes in policies and procedures | 0 | 3 | |
| Totals | 48 | 49 | |
By contrast, participants identified a greater variety of enablers facilitating fading episodes. Participants identified 32 examples of enablers for fading, the most common being the nature of the current job role, introduction of new practices and knowledge, development in technology and infrequent use of skills.
Personal skills and attitudes
Personal skills and attitudes towards change and exposure to new ideas were mentioned by 27 participants as factors that enabled them to unlearn. A variety of different examples were provided by participants, such as a willingness to place oneself into new, challenging roles, or acknowledging a personal interest in a particular skill or approach that enabled behavioural unlearning. For example, a manager explained how regular changes in role as her career progressed had given her experience in adapting to new knowledge and unlearning old ways of thinking and behaving. She stated:
I felt like I'd got a lot of integrity to do that because of my previous roles in the organisation as a ward sister, charge nurse for many years and then subsequently matron, clinical manager. You know, I'd worked across the whole organisation, so that was really helpful. [. . .] I felt competent because of the investment of what I'd put in around exposing myself to experiential learning, theory and having a broad kind of 360 overview of the components [. . .] There were some personal skills that definitely helped me around being able to work out of a comfort zone, having resilience in challenging difficult times of sustained periods. The [. . .] ability to critically analyse and face difficult, not nice information really and deal with challenging situations, having negotiating skills [. . .] listening skills . . . all of that comes together, doesn't it, when you've got to do something like that.
Manager (clinical background), A12
Similarly, another manager acknowledged that she enjoyed using technology and that this had helped with her adjustment to a new way of working. She added:
Mean I personally from a purely personal point of view [. . .] I personally think having an electronic system for this and for data audit and monitoring is a good idea and I'm quite happy with that. [. . .] I think just from a sort of geeky point of view I'm quite happy working with technology.
Clinical manager, B7
Personal attitudes were also identified as a key enabler for cognitive unlearning. The nature of these attitudes also varied depending on the circumstances of the unlearning episode being described, such as a desire for further career development and opportunity, or having high levels of compassion or empathy when dealing with difficult situations, such as disciplinary procedures. However, one particular example demonstrates the emotional aspect of cognitive unlearning, and how that can act as a motivator to unlearn. A manager explained that, after experiencing one particularly difficult situation with a member of staff who she thought she had a good relationship with, the emotional pain and upset she felt following that experience served as a strong motivator to act differently in the future and unlearn her previous way of thinking. She commented:
What I would say looking back on it and generalising is that it was the negative stuff that you think, ‘That hurt. I'm not going to do that again.’ And when I say hurt I mean things like, ‘That was difficult. That didn't work well. That didn't have a positive outcome.’ So you learn from the negativity to adapt what you do and adapt your approach and think, ‘Well okay, I'll do that differently.’
Clinical manager, A15
Leadership and networks
The second main category of enablers of both behavioural and cognitive unlearning involved the influence of leadership from specific individuals and established networks. For example, the leadership exhibited by a senior nursing team in ensuring the implementation of changes in infection control enabled one manager to experience behavioural unlearning. She described the influence by saying:
I would say at the time that the leadership of the senior nursing team who sort of stood firm and said, ‘We're doing this’, the Director of Nursing was very, ‘This isn't up for debate. This will happen.’ [. . .] It is now what we do, but we needed that sort of visible leadership and the matron role was key around delivering a lot of the infection control.
Clinical manager, A10
Similarly, having feedback from senior managers resulted in behavioural unlearning for another manager who was trying to effect change. The experience boosted her confidence and she stated that feedback from senior managers helped her shape some projects. She stated:
Also conversations in terms of obviously going to these people, senior managers and saying, ‘This is what needs to happen. This is what needs to change’, and getting feedback from those in terms of the way it should be going. [. . .] And I was going to these people to seek advice. So there was a bit of feedback from there.
Manager (clinical background), B8
The opportunity to draw on established networks was also described as an enabling factor for behavioural unlearning after taking on a new role. One manager commented that, although having changed roles and therefore having to unlearn old operational control behaviour and adopt new influencing techniques, her knowledge of the networks within the trust enabled her to embrace her new way of working effectively. She stated:
Some of my former sort of networks obviously was still there, [. . .] Interestingly, I know most of the trust. I know most of the clinical staff in the trust because I've been around a long time and I cover a lot of areas. So I know all the team bases and so on, so I did know people I could call on [. . .] so what I did was get onto some of those committees, some by invitation and some I sort of turned up at and sort of managed to get myself invited to [. . .] So I got onto some of the new committees which gave me access to some of the topics that I was dealing with.
Manager, A5
Support from other individuals through networks and mentoring was also identified as an important enabler for cognitive unlearning. For example, participants commented that having good relationships within networks helped in ensuring people attended meeting and training sessions for implementing change. In addition, support from other colleagues who acted as intermediaries could also help to boost the motivation to cognitively unlearn. For example, a manager said:
There were other people who were willing to put the case forward on our behalf – you know, other committees and things that I belong to. You know, sort of like people who are on the Research Committee, which I belong to, they were quite willing and the Junior Doctors' Training Committee, they were all quite willing to write to this Director and put forward a case for needing and did in fact two or three of them. So that was nice. That was supportive that people valued the service enough to put pen to paper and try and support it.
Manager, A13
Similarly, networking with other managers also gave participants a wider appreciation of their own management experiences, which helped the cognitive unlearning process. A manager commented:
I think something that maybe was helpful was we did have a sort of peer meeting with all the other service managers once a fortnight and through observation and discussion of the way that they worked and how they addressed things, [. . .] So maybe with hindsight I used that more and I learnt and unlearnt from that more than I actually gave it credit for at the time. [. . .] There would maybe be HR issues that would come up and they'd maybe talk about difficulties that they were having with particular staff and I'd sort of think, ‘Oh, so this maybe isn't as bad as I think it is’, [. . .] So that was a useful forum, but I wouldn't say it was a particular person. It was several people.
Clinical manager, A15
Support from specific individuals
As well as general support from networks, it was noticeable that in several interviews participants referred to specific individuals whom they felt had made a significant difference to either their behavioural or their cognitive unlearning. These individuals varied considerably, from particular staff members at the NHS Institute for Innovation and Improvement to shared secondments, mentors, line managers and family. For example, when discussing a behavioural unlearning episode a manager stated that:
I was extremely supported by the NHS Institute and a particular person there who was so supportive around us being a mental health showcase for the UK in the way that we approached the programme and they have continued to work with us in a really positive way. So that was really helpful.
Manager (clinical background), A12
Another manager added:
So I got a secondment with somebody that I'd worked with on and off over the previous 10 years, but didn't see as a very close friend, but really became a very good ally, very supportive and I learnt a lot from her, which surprised me, I have to say.
Manager, A11
Support from specific line managers or a family member was mentioned by several managers when discussing cognitive unlearning. One manager explained how a senior manager had acted in a mentoring role, enabling her to change role and facilitate her unlearning. She explained:
I've been using as a bit of a mentor. He identified this opportunity for me – that's the secondment – and sort of talked to me about it and facilitated my move here and so I've been using him as the coach/the mentor when I needed that information, that learning from him.
Manager, A2
Another manager commented on the important influence that a close family member had on his decision to change role. He stated:
My wife, [. . .] she was very supportive and I think she now knows that this post is coming up and obviously we're expecting as well, so she was very supportive and saying, ‘No, go for the job. You need a change. You want a change. You want to get out of what you're doing and move forward.’ So she's been very supportive and that's been fantastic. And without her there . . . you know, if we weren't together I may have made a different decision and said, ‘No, stuff it, I'll challenge it’, which would have been the wrong decision I think. It wouldn't have been positive at all. So yeah, that was very helpful.
Manager, B5
Management support
Closely related to the previous category, a further category of enablers of both types of unlearning mentioned by participants was management support. However, in these examples, the references made by participants were to more general support rather than support from specific individuals. For example, when speaking about behavioural unlearning, a manager commented that if an idea was likely to result in improvement of services then management support was readily forthcoming. He gave this example:
We were really riding a crest of a wave and everything we put in for we won – [. . .]. You could go and say [to management], ‘I've got this idea. It's going to cost us, but I've got this idea’, and it'd be, ‘Right, what are the cost implications? What would we get from it?’
Manager, A3
Another respondent had the view that changes were encouraged by management to save cost and improve services and in so doing supported cognitive unlearning processes. A manager narrated his experience in lobbying management to introduce changes by saying:
I mean I think obviously you have to speak to management in a way to try and, you know, get your message across and I simply told them that, you know, if these things keep happening people will sue you and cost you even more. So they saw my point and, you know, they have helped me [. . .], I mean money is a big factor as always in the NHS, but I think they realised that things couldn't carry on the way they were because if complaints keep rising, then obviously something has to give and I think they realised. So the management were supportive I would say in the end.
Clinical manager, B6
We also found examples from the interview data which suggested that the introduction of new policies supported by management could also enable cognitive unlearning. For example, when discussing the change to a more performance-managed way of working and the challenge that this would present to established organisational culture, a manager commented on the support provided by the human resource managers. This support was reflected in recognition of the need to provide managers with more training and development regarding conflict and challenge, which the new management approach was likely to create. A manager said:
Now we're starting to be performance managed, to be managed to deliver what we need to deliver and so all of a sudden the culture's changing and when people aren't doing their job you've got to tackle it. [. . .] in the leadership forums because they're starting . . . they're starting to teach coaching so that you can nurture somebody along, but they're also starting to think about confrontation and difficult conflict management type things as well. So yeah. HR are being supportive.
Manager, A2
Wider pressure to improve the service
A further category of enabler that was mentioned by several participants regarding unlearning was a wider pressure to improve the service provided, often motivated by a desire for efficiency savings or cost-cutting because of the challenging wider economic environment. One manager encapsulated the situation by explaining that financial pressures had prompted many managers to reflect on current practices and look for new ways of working, leading to behavioural unlearning. She stated:
I realise and recognise that we're in a situation economically let alone just within the health service, but generally economically that we have to think of different ways of working. We have to look at different . . . changing the way we work.
Manager, A3
Similarly, another manager added that in his view the pressure to improve efficiency had enabled him to cognitively unlearn and move to a style of management that was more coaching orientated. He believed that this new management style would increase the likelihood of encouraging his staff to find new and more efficient ways of working. He stated:
I don't think it would have changed if it hadn't been because of the efficiency argument. [. . .] We've had external facilitation talking to us about coaching and so far a lot of the examples [of coaching] have been on a one-to-one basis or a small group basis.
Clinical manager, A8
Additional enablers
Three other categories of unlearning enablers were identified from the interview data, although these were less frequently mentioned. The first was training opportunities, and in particular the environment they provided for reflection and discussion. For example, referring to a cognitive unlearning episode from the introduction of a new approach to contracting services a manager commented that:
It was a good environment for doing that. It was a very safe and secure environment. We'd done a reasonable amount of work around about . . . not team building, but just developing confidences and contracting and set some good contracting, so it gave us a good, secure base for discussion and there were some really strong discussions.
Clinical manager, B10
The second category was changes in work circumstances. In two unlearning episodes, changes in staffing levels because of illness or staff shortages served as enablers to unlearning. For example, one manager experienced behavioural unlearning the day before she went on annual leave when senior managers asked her to urgently analyse some data at short notice; to complete the analysis the manager had to abandon the way she used to work by delegating tasks. This experience prompted the manager to continue delegating in subsequent situations. She narrated her actions:
Well, the timing of it was actually it happened the last day before I was due to go on leave for a week. [. . .] in a way that was good because I had to delegate the first bit of it which was, you know, we had all this data about the patients and somebody had to go through and understand what the data was saying and understand what measures we should be looking at within this data and stuff. And so I had to delegate that to one of my staff.
Manager, B11
The third category was changes in policies and procedures, which was mentioned in relation to three unlearning episodes. For example, a nurse recalled how she had been involved in a clinical trial that examined the use of aspirin in the treatment of heart disease. She noticed the significant improvement in patients who were given aspirin compared with those who were not. This information has been reflected in new policies regarding the treatment of heart disease, which she explained prompted her to be more reflective on existing practices. She stated:
There were a lot more clinical trials going on. [. . .] The trial that changed the way we look at heart disease, which is, you know, the trial that looked at aspirin, I was actually on. You know, we took part in that trial in our coronary care unit and recruited patients to that and they stopped the trial 3 months in because the group that didn't get the aspirin had so much worse outcomes [than when] they added aspirin in. So it was all really exciting stuff going on. So yeah, the environment was very much supportive of it and then when I came back here we'd moved on here, so there was still more going on and more asking.
Clinical manager, B2
Enablers of fading
Overall, participants provided 32 examples of factors that enabled fading. It was possible to place the enablers of fading episodes into four main categories. These categories were very similar to the barrier categories discussed in Barriers to fading and included the nature of the current job role, new practices or knowledge, developments in technology and infrequent use.
The most common enabler to fading that was mentioned by managers was a change in job role that resulted in some skills no longer being performed. For example, for one participant, being in a more senior managerial role meant that she no longer worked with detailed finance sheets. As a result, she felt that she did not analyse budgets to the same detailed extent that she had previously. She commented:
Now I get my finance sheet through monthly from my finance management accountant that's got, you know, the progress against budget each month and I don't scrutinise it in the way that I might have done [. . .] I leave that to our finance department now. [. . .] Probably because I haven't got the time. I haven't got the time to do it to be honest. So a requirement for me in my role is to make sure that we're spending against the budget and we're not going over budget, so I just look at that each month and don't necessarily go into all of the other elements.
Manager (clinical background), B9
Similarly, another manager explained how his career path to become a manager had meant that technical skills he had needed in previous roles were no longer used. He stated:
To become a manager in pathology you tend to be a scientist and then you progress through to become a manager where actually you're not doing any technical work and you lose those sorts of skills which is a necessity, but you still have the background knowledge that you refer to on a regular basis, but actually the doing sort of skills, the microscopy skills and those sorts of things that you're actually not using on a frequent basis.
Manager, B5
New practices or knowledge from scientific advancement in health care leading to changes in clinical practice were also reported as enabling fading. The new guidelines and policies that result from this advancement could render previous knowledge obsolete. Several participants explained that they were no longer confident that they could perform some activities because of changes in clinical practice. For example, a clinical manager commented:
There'd probably be a fair amount of apprehension because I would naturally think that I'm very out of date. So although it probably hasn't changed that much, I would have to go back and read up a bit and ring people and probably speak to the fracture clinic and just check out how we do things because how we position an ankle, for example, probably hasn't changed that much, but there might be something around extra support for part of a joint for example that I would feel well out of touch with.
Clinical manager, A10
Closely related to the previous category, developments in technology were also mentioned as an enabler to fading of skills. For instance, one manager acknowledged that she would need help in using infusion pumps as the machines had been upgraded. She stated:
Some of the machines that they use in nursing, some of the infusion pumps and things, I probably would need an update on how to use those, but I don't feel like I'd say I wouldn't do it now because of the infusion machines. I'd go and I'd say, ‘Just give me an update on this infusion machine’ because, you know, the principle's the same and it's just got different buttons for doing different things.
Clinical manager, B2
Finally, infrequent use of a particular skill was also identified as a enabler to loss of skills in four fading episodes. A manager gave the example of how some of her computer skills had faded because of a lack of use. She explained:
I think learning an IT system and learning to use an IT system is one that can fade with no use. So if you have to do a task once in a blue moon on an IT system you would know how to do it and if you did it repeatedly you just do it naturally, but if you leave it for 6 months or you leave it for a year it's faded away and you have to relearn it.
Manager, A2
Summary of enablers of individual unlearning and fading
Our data indicate that, with one exception, the same factors enabled behavioural and cognitive unlearning, with the most common enablers being personal skills and attitudes, leadership and networks, and support from specific people. Less frequently mentioned were wider pressure to improve the service, management support, training opportunities and changes in work circumstances. Changes in policies and procedures was the only enabler specific to cognitive unlearning. No single enabler was identified as specific to behavioural unlearning.
However, enablers of unlearning triggered by individual experiences differed from enablers of unlearning triggered by change events. Personal skills and attitudes, leadership and networks, and specific individuals enabled unlearning triggered by individual experiences. Participants identified specific personal qualities such as resilience, compassion towards colleagues, confidence gained through experience and interpersonal and communication skills as helping them to give up particular ways of thinking and acting. Leaders, senior managers, line managers and colleagues also helped by providing advice, feedback and support and acting as role models. Specific individuals – within and outside the workplace – were identified as providing support, encouragement and effective supervision.
Five enablers of unlearning triggered by a change event were identified: management support, pressure to improve services, training, changes in work circumstances and changes in policies and procedures. Not surprisingly, management support tended to be enabling when participants sought to improve services or save money. Interestingly, what initially might be seen as negative situations, such as staff shortages and cost-cutting, were sometimes seen as enabling participants to give up particular ways of acting when this meant taking on more responsibility or introducing new ways of working.
External change and infrequent use of particular skills were the main enablers of fading. Participants referred to loss of front-line skills and knowledge as they took on managerial responsibilities, and to new knowledge, practices and technology as changes that enabled them to forget technical or clinical skills and knowledge, or to discard obsolete knowledge.
Having reviewed the findings regarding the triggers and nature of unlearning and fading episodes and the barriers to and enablers of the unlearning process and fading, in the following section we focus on the impact that unlearning and fading can have on managers' decision-making.
The impact of individual unlearning and fading on managers' decision-making
In this section we illustrate how the process of individual unlearning can impact on health-care managers' decision-making. Table 11 provides a summary of the types of impact on decision-making that participants identified. From the data analysis 30 examples of changes in decision-making were identified of which 19 were related to individual unlearning triggered by change events and 11 were related to unlearning episodes triggered by individual experiences. Six participants did not give any examples of how the individual unlearning process had impacted on their decision-making. From the data we identify that the process that leads to each unlearning type results in different changes in decision-making. Behavioural unlearning resulted in more collective and decisive decision-making, adaptation of management style and more effective reporting plans. Engagement with cognitive unlearning resulted in more rational decision-making, a more negotiative management style, changes in attitudes towards work and changes in procedures.
| Trigger | Behavioural unlearning | Cognitive unlearning |
|---|---|---|
| Individual experience |
|
|
| Change event |
|
|
None of the participants was able to provide an example of fading having an impact on their decision-making. This is likely to be because of the difficult nature of investigating the fading concept as it requires participants to recall examples that they have, by definition, forgotten and then attempt to recall whether or not this forgotten knowledge or behaviour altered their decision-making processes.
The following sections present examples of decision-making changes related to each individual unlearning type according to the trigger (individual experience or change event) associated with the unlearning.
The impact of behavioural unlearning on managers' decision-making
We identified three types of change in decision-making as a result of managers experiencing behavioural unlearning triggered by individual experience: more collective decision-making, more decisive decision-making and new staff management practices.
In three episodes of behavioural unlearning participants explained that they had changed their approach to making decisions from making individual decisions to making a concerted effort to get greater involvement from other people or groups. The managers felt that making this new approach increased the likelihood of the decisions being accepted by all interested groups and reduced the level of resistance to new ways of working. For example, a clinical manager explained how she felt that she had changed her decision-making approach after engaging with unlearning:
I would now look to gather a number of key areas and work on a showcase principle where I'd engage certain people and we'd embed it properly. Properly test, properly implement, seek a lot of feedback so that we got the buy-in from those clinicians across all spectrums not just ‘The nurses are doing it, so it's fine.’ It's got to be everyone doing it and I would showcase and roll it rather than ‘You will, you will.’ I would probably have a bit of a project team beforehand as well and that's part of what have changed as an organisation as well, but I would get my key people assembled first to help me do that influence and persuade and convince before we set out with it.
Clinical manager, A10
Another manager shared a similar experience explaining that in her role as a manager on a ward she had to interact with a wide range of different clinical professions. To enact change with such a diverse group she found that she also had to change her management style to become more collective in her decision-making. She stated:
When you run a ward you still oversee the work that the rehab assistants do, you work very closely with the occupational therapists, the nursing staff, the doctors. [. . .] I think it has because now when I make a decision it doesn't just affect one small area of the team; it affects the whole team and sometimes I have found it hard to make decisions, especially when people have challenged them [. . .] I've introduced quite a lot of new systems and any time I've introduced it we've had a trial period, we've all come back together and had a chat about it but, you know, it's very different because I'm just very aware that it affects everyone [. . .] I always do it as far as I can with full backing, but sometimes people don't like change and if they're a bit kind of set in their routine it is hard to get people to come on board, so I've had to learn new skills of how to show things in a positive light and persuade people that the outcome will be worth it. So yeah, I've found that quite challenging, but that's part of my role that I've really enjoyed.
Clinical manager, B1
Two participants felt that having experienced unlearning they had changed their decision-making to become more decisive. Each case was slightly different. In the first example, a manager explained that having experienced severe pressure at work her unlearning episode had been to change how she managed her time at work. The manager explained that as a result she was now a lot firmer in her decision-making and would be less inclined to automatically say ‘yes’ to requests. She explained:
The difference is now that I do say no. I'm very strict with myself in terms of the hours that I work. Yeah, some days I work a long day. Tuesday I worked a 12-hour day, but already in my diary that time is booked to take off again next week. So it's about looking after myself. Short term I can put the time and effort in, but I need to give myself time to catch my breath and I am getting quite confident now at saying to people, ‘I'm sorry if you want that tomorrow. Unless you don't want something else today you can't have it. You know, let's negotiate or get somebody else to do it’, and not accept ridiculous sort of demands and deadlines that it's just easy to get in, especially if it's something that had you got the time you might quite enjoy doing. So it's those sort of lessons that I've had to teach myself and of course now I'm quite evangelical about it.
Clinical manager, A7
By contrast, another manager explained that her unlearning experience had encouraged her to move away from constantly looking for advice and asking for feedback on choices in her management decision-making. Her experience gave her the confidence to be more bold and directive. She explained:
Before I would ask a lot of people a lot of different things and say, ‘What do you think about this? What do you think about this?’ and this time I've actually said, ‘Well no, I need to make this change because of this reason and this reason’ and therefore I put the wheels in place and we just got on and did it and I suppose in conjunction with the clinical lead because obviously it was to do with that as well and instead of like talking to 120 different people and asking permission . . . I think that's the difference. It was that whole asking permission, ‘Is it okay if I do this?’ Instead I said, ‘Well I'm going to do it. This is my job role and actually this is what I'm going to do and we're going to put it in place.’ So I suppose it's the asking for permission thing that I've stopped doing now, much to the relief of my matron.
Manager, B4
In one case a participant felt that her experience of behavioural unlearning had resulted in a change in how she approached her staffing-related decisions. The manager explained that her unlearning episode had resulted in her thinking of new ways to ensure that her staff were more productive and focused on improving the patient experience. As a result, the manager now employs a more participative and empowering approach to staff management, encouraging her staff to think of new ways of working and how these new ways can benefit patient care. She commented:
I think the issue for me is about saying to the staff, ‘Let's look at time management for you.’ If we're running about doing all this and we're not engaging with the patients as much as we can, then it's going to make things worse, so what we've tried to turn on its head is – and again it's through the Productive Programme – ‘Where we save time are we putting that back into the patients?’ [. . .] So empowering them a bit more and, you know, they'll be doing activities with the patients now today.
Clinical manager, A9
Behavioural unlearning that was triggered by a change event was identified as impacting on managers' decision-making in 10 episodes. The change in decision-making involved either adapting previous approaches to managing or implementing better reporting plans. For example, one participant explained how she had gained more confidence and assertiveness after implementing a large project, unlearning her previous cautious behaviour. The manager was now more inclined to embrace a structured and strategic approach to her management. In another example, a manager experienced unlearning from a change in role which meant that she had to be more strategic in focus, giving up some operational control. As a result, the manager explained that she had to delegate more tasks, which was a change from her previous ‘hands-on’ management style. She commented:
I mean I suppose allowing my staff to do things that they should be doing anyway frees up my time to do the more sort of strategic things or, you know, the thinking about the future type things which ultimately, I suppose, is good for me personally in terms of developing myself and the role.
Manager, B11
In three other behavioural unlearning episodes we identified that engagement with the process of unlearning resulted in improved reporting plans or frameworks for making decisions. For example, a manager explained that her unlearning experience had highlighted the need for effective planning and one outcome of this new approach was the development of an improved workforce plan for the trust.
The impact of cognitive unlearning on managers' decision-making
From the data, two changes in decision-making were evident from engagement with cognitive unlearning triggered by individual experience. In four episodes we categorised the change as a more rational, evidence-based approach to decision-making. In one further episode the change referred to the adoption of a more negotiating style of management.
The cognitive unlearning episodes leading to more rational decision-making tended to involve the participant having a bad experience, or having difficultly in defending a decision because of a lack of information to support the decision that he or she had made. Consequently, the managers concerned had moved to a core documented and data-driven approach to their decision-making. For example, one manager commented that, rather than basing decisions on her experience and sense of staff views, she now made a more conscious effort to capture that information in a more formalised way. She stated:
I make decisions knowing that I've listened to and thought about people's views much more extensively than previously. So when I'm talking now at a board or some committee meeting, I always was grounded in reality, but I now have the evidence for being grounded in reality because I've recorded it. So I can say, ‘Well, when I met with the patient group, when I met with the carer group, when I met with the health-care assistants, this is what they told us.’ And I use a lot more of that information in reporting.
Manager (clinical background), A12
In an second example, a manager explained that the experience of not being able to agree a desired retirement plan with a member of staff and the difficulties that resulted from that situation resulted in her being more strict in the way she followed regulations when discussing retirement plans. She stated:
I think the other thing that I do differently – just comparing the two instances – is that I'm less flexible. So you know in the first instance I said to you that she came to me and we had a discussion. With the second member of staff I was telling her, you know, ‘There's this process, there's that process. We need to get around those before I can make a decision with you.’ I think what I would now do in hindsight is I'd say, ‘Right, I'm going to send it in now, but I'm going to have to say that you can't have it and you can reapply in 12 months.’
Clinical manager, A15
The second type of change in decision-making that was identified was moving to a more negotiation-orientated style. The participant explained that his cognitive unlearning experience of trying to introduce new ways of working and the resistance that he encountered had made him focus on changing the way he managed discussions regarding new change. His approach was to focus on areas of agreement and emphasise the positive aspects and make areas of disagreement appear less significant. He explained:
Then you have to say, ‘Well okay, but what do you think we need to do then? How are we going to . . .?’ And usually sort of by taking that sort of coaching style . . . The other thing that I've tried to adopt is people seem very much against what it is that you've got to do. ‘Let's see what we can agree on first. What do we agree on? Let's not talk about what we disagree on, but let's . . .’. Usually you agree on 80% or 90% of stuff, don't you? If we're in agreement 80–90% of the way, let's look at this. We've got 10, let's have a look at it. It shrinks a lot of the grief out of the situation where people think, well actually [. . .] what I'm trying to do and what they're trying to do is preserve what's good and improve on what's good.
Clinical manager, A8
Cognitive unlearning triggered by change events also resulted in two types of change in decision-making. The most common change was a change of participants' attitude towards work, but two participants gave examples regarding changes in procedures. The changes in attitude towards work and therefore decision-making varied across participants. For example, a manager explained that she had become more critical and analytical in her decision-making. She commented:
I suppose in a broad way I don't take everything at face value. I don't think I ever have, but I think now more so. I look for the unexpected and perhaps pick up on smaller things and see the significance of smaller things that previously I would have just dismissed. I think I've got more of a critical eye for detail and can see the potential of perhaps where things could go wrong and take that more seriously. Rather than saying, ‘Well, it's a one in a million chance’, I say, ‘Yeah, but we need to do something about it because we can't take that risk.’ So perhaps in that way.
Manager (clinical background), A14
By contrast, another manager commented that her attitude had changed since moving from the private sector to the NHS because she was not able to achieve her personal targets in the same way, now having to rely on less timely information. She stated:
I'm having to do some work myself that I wouldn't naturally have expected and it's testing my [. . .] attitude because I like to deliver the best I can and I will deliver to a timetable. Because of my project management style that if I say I'll do something by then, I'll do it by then because that keeps everything else running in line and I've now had to go to two meetings and I haven't had what I would have wanted to give at that meeting [. . .] that isn't my style and so it's not been comfortable.
Manager, A2
A further example was prompted by a manager's cognitive unlearning experience from changing to a more influencing role in the trust, no longer having direct control. Consequently, the manager explained that she had to recognise that her decisions and recommendations would not always be followed. She said:
The problem is that from a hierarchical point of view the ultimate decision doesn't always come down to me; it will come from the clinician, consultant doctor in charge of the care for that patient. So it's difficult really. You can advise them. You can say, ‘Well look, my opinion is . . . ’ and, in fairness, people take these things on board, but ultimately I wouldn't have a lot of influence over that kind of thing and so I would just say to people, you know, ‘if we're doing this, then we're going to do it and to the best of our ability really’.
Clinical manager, B7
Two participants commented that the changes they had made in their decision-making as a result of experiencing cognitive unlearning were related to how they made decisions regarding procedures and organised their staff. For example, a manager explained that she had altered the management structure within two teams to ensure that the same service would be delivered but that the delivery was no longer reliant on individual staff members.
Summary of impact of unlearning on managers' decision-making
The analysis presented demonstrates that engaging with unlearning does seem to have some impact on the decision-making of health-care managers. The precise nature of the change varies quite considerably based on the examples provided by managers. In some aspects the cases were contrasting. For example, some managers moved to more decisive decision-making, whereas others adopted more negotiative or collective approaches. This variation seems to be driven by the particular circumstances of an individual's unlearning episode rather than the type of trigger or unlearning that was undertaken. However, in each case it appears that having engaged with the unlearning process the participants felt that they had made improvements in their decision-making, and that they were able to work in a more effective way, for them personally and/or in their organisational role.
The influence of health-care setting and professional background on health-care managers' individual unlearning and fading
The third research question of this study was to investigate whether or not the health-care setting of managers influenced their level of engagement with the process of unlearning. Therefore, the interview data were analysed to assess whether or not there were any significant differences between data collected from different case study sites in terms of unlearning episode type, enablers and barriers. In addition, we were also interested to examine whether or not there was any empirical evidence of health-care managers' professional background influencing their level of engagement with unlearning. The following sections present the results of our analysis regarding each of these questions.
Health-care setting
Table 12 provides a comparison of the data collected from the two case study sites. What is apparent from this table is the similarity of experiences of health-care managers at both sites. Participants at both sites reported very similar levels of experience of each unlearning type and also the type of knowledge that was unlearnt. The data also revealed that, with the exception of financial constraints, the same barriers to unlearning were mentioned by managers at both sites. The greatest contrast between the sites was in lack of management support, which was mentioned in relation to only two episodes of unlearning at site B compared with eight episodes at site A. This suggests that participants perceived managers at site A to be less supportive, although it is not clear whether or not the absence of this barrier at site B is confirmation that managers at this site were more supportive. The same pattern was repeated regarding the enablers identified by participants at each site, with the exception of changes in policies and procedures, which was identified only by participants from site A.
Similarly consistent themes were identified when health-care managers' experiences of fading were compared between the two case study sites, as shown in Table 13. Although there were some minor differences between the cases, we could not clearly identify any consistent patterns of response which would indicate that the health-care settings considered in this study were influencing health-care managers' experiences of fading.
| Number of episodes | ||
|---|---|---|
| Aspect of unlearning | Site A: mental health trust | Site B: acute trust |
| Unlearning type | ||
| Behavioural unlearning – individual experience | 3 | 3 |
| Behavioural unlearning – change event | 12 | 11 |
| Cognitive unlearning – individual experience | 8 | 9 |
| Cognitive unlearning – change event | 6 | 5 |
| Types of knowledge unlearnt | ||
| Procedures and policies | 10 | 12 |
| Training guidelines | 5 | 2 |
| Reporting guidelines | 1 | 1 |
| Assumptions of management priorities | 1 | 1 |
| Training approach | 2 | 1 |
| Views on delivery | 5 | 4 |
| Views on work environment | 2 | 4 |
| Attitude towards management issues | 4 | 2 |
| Barriers to unlearning | ||
| Personal behaviour | 5 | 6 |
| Financial constraints | 3 | 0 |
| Job insecurity | 1 | 1 |
| Lack of management support | 8 | 2 |
| Staff resistance to changes in practice | 9 | 8 |
| High workload | 4 | 2 |
| Organisational culture | 3 | 3 |
| Enablers of unlearning | ||
| Personal skills and attitudes | 14 | 13 |
| Leadership and networks | 11 | 12 |
| Support from specific individuals | 12 | 10 |
| Wider pressure to improve the service | 4 | 4 |
| Management support | 5 | 3 |
| Training opportunities | 1 | 3 |
| Changes in work circumstances | 1 | 1 |
| Changes in policies and procedures | 3 | 0 |
| Number of episodes | ||
|---|---|---|
| Aspects of fading | Site A: mental health trust | Site B: acute trust |
| Fading type | ||
| Knowledge | 7 | 8 |
| Skills | 7 | 6 |
| Barriers to fading | ||
| Ability to recall | 3 | 0 |
| Experience | 6 | 4 |
| Enablers of fading | ||
| Infrequent use | 3 | 1 |
| Developments in technology | 3 | 2 |
| New practices or knowledge | 2 | 6 |
| Nature of current job role | 7 | 8 |
The findings from the comparative analysis suggest that health-care setting, at least in terms of mental health compared with acute trusts, does not seem to influence whether or not health-care managers engage with unlearning. However, it should also be acknowledged that these two types of NHS trust compared with other health-care organisations in the NHS are relatively similar in terms of their structure and manner in which they deliver care (e.g. ward based). These similarities may explain the relatively consistent findings in this study when assessing the influence of organisational setting. It is possible that different health-care settings may reveal different levels of engagement with unlearning of health-care managers. This study did attempt to collect data from managers working in a primary care setting; however, data collection was unsuccessful at the planned third site (see Chapter 3, Recruitment at site C: primary care trust/clinical commissioning group) and, as a result, this study is unable to provide further insights in this respect. This limitation is revisited in the recommendations for future research (see Chapter 6, Research agenda).
Professional background
As stated earlier in this report, anecdotal evidence suggests that clinical and managerial decision-making processes are underpinned and supported by different knowledge bases. Crilly et al. 102 argue that:
The professional and scientific culture of doctors stands in contrast with the world of managers. Doctors are aligned with the quantitative and positivistic nature of biomedical research where clinical decisions may be codified. Managers' decisions depend on pragmatism and subjectivity rather than research which is more often qualitative and in any case is perceived as contingent and not readily generalisable.
p. 145
Thus, clinicians moving into managerial roles arguably need to engage in processes of unlearning to effectively adapt how they act and make decisions in the new managerial roles they occupy. Therefore, the data were analysed to investigate whether or not there were any clear differences in the unlearning experiences of participants that could be attributed to their professional background, that is, were managers who were formerly clinicians more likely to experience unlearning than managers with no clinical background because of the potentially greater change in their knowledge base having changed role.
Participants in the study had three distinct professional backgrounds. We had five respondents who were managers with a clinical background but who had no current clinical role, 11 managers with no clinical background and 13 managers with a clinical background and a current clinical role. For comparison, the participants were spilt into two groups: managers with no clinical background and managers with a clinical background. The total number in each group was 11 and 18 respectively.
Table 14 compares both groups of managers and their responses regarding different aspects of unlearning. Examining the different experiences of unlearning between the two groups indicates that managers with no clinical background were more likely to experience behavioural unlearning triggered by individual experience, whereas managers with a clinical background were more likely to experience behavioural unlearning from a change event. This may indicate that managers with a clinical background are more likely to change their behaviour from external factors such as the introduction of policies, whereas individual experiences are more likely to lead to behaviour change for managers without a clinical background. However, regarding cognitive unlearning there were less clear differences between the two groups, both experiencing relatively similar amounts of cognitive unlearning.
Examining the other aspects of unlearning such as the type of knowledge that was unlearnt, barriers and enablers generated few clear differences between the groups. Both groups of managers most frequently unlearnt procedures and practices, which may reflect the frequent changes in policy and enhancements to health-care practice that characterise the NHS. Managers with a clinical background mentioned staff resistance to change as a barrier to unlearning more frequently than managers without a clinical background. However, this contrast may be due to the nature of their current role and the staff who they work with rather than being explained by the managers' professional background.
| Number of episodes | ||
|---|---|---|
| Aspects of unlearning | Managers with no clinical background (n = 11) | Managers with a clinical background (n = 18) |
| Unlearning type | ||
| Behavioural unlearning – individual experience | 8 | 5 |
| Behavioural unlearning – change event | 3 | 13 |
| Cognitive unlearning – individual experience | 6 | 11 |
| Cognitive unlearning – change event | 5 | 6 |
| Types of knowledge unlearnt | ||
| Procedures and practices | 7 | 14 |
| Training guidelines | 4 | 3 |
| Reporting guidelines | 1 | 1 |
| Assumptions of management priorities | 2 | 0 |
| Private sector work values | 1 | 0 |
| Training approach | 1 | 2 |
| Views on delivery | 2 | 7 |
| Views on work environment | 2 | 4 |
| Attitude towards management issues | 2 | 4 |
| Barriers to unlearning | ||
| Personal behaviour | 6 | 5 |
| Financial constraints | 2 | 1 |
| Job insecurity | 0 | 2 |
| Lack of management support | 6 | 4 |
| Staff resistance to changes in practice | 4 | 13 |
| High workload | 2 | 4 |
| Organisational culture | 2 | 4 |
| Enablers of unlearning | ||
| Personal skills and attitudes | 9 | 18 |
| Support from specific individuals | 9 | 13 |
| Leadership and networks | 8 | 15 |
| Wider pressure to improve the service | 2 | 6 |
| Management support | 3 | 5 |
| Training opportunities | 0 | 4 |
| Changes in policies and procedures | 1 | 2 |
| Changes in work circumstances | 2 | 0 |
Regarding enablers to unlearning, both groups frequently cited personal skills and attitudes and support from specific individuals.
Regarding experience of fading episodes, the interview data reveal that there is little difference between the two groups (Table 15).
| Number of episodes | ||
|---|---|---|
| Aspects of fading | Managers with no clinical background (n = 11) | Managers with a clinical background (n = 18) |
| Fading type | ||
| Knowledge | 5 | 9 |
| Skills | 6 | 8 |
| Barriers to fading | ||
| Ability to recall | 2 | 1 |
| Experience | 5 | 5 |
| Enablers of fading | ||
| Infrequent use | 3 | 1 |
| Developments in technology | 2 | 2 |
| New practices or knowledge | 1 | 7 |
| Nature of current job role | 7 | 9 |
Interestingly, although we expected managers moving from clinical to managerial roles to be more likely than managers with no clinical background to have skills that they no longer used, both groups were able to cite situations in which skills or knowledge had been forgotten. However, managers with a clinical background referred to new knowledge and skills as an enabler for fading, which could be a result of their greater change in knowledge base from a role transition. However, overall, the data provide little evidence to suggest that professional background is a strong differentiator for the level of fading experienced by health-care managers. Having presented the findings from the analysis of the interview data, in the following section of this chapter we report the findings from the workshop conducted at each case study site.
Workshop findings
An important aspect of our original project plan was to undertake a feedback workshop at each of our case study sites. The workshop objectives were to feed back preliminary results from the study, to gather participants' views on the preliminary findings and to discuss the practical implications of the results with participants in terms of how the information could be used within the sites. Details of the administration of the workshops and participants are provided in Chapter 3.
Content of the workshops
Some of the workshop participants had not participated in the research interviews. Consequently, the workshops began with a brief explanation of unlearning. The participants were then asked to form small groups and identify situations in which they believed they had abandoned or given up existing behaviour or knowledge. These examples were fed back to the group and captured on a flip chart. The preliminary findings of the study were then presented to the group. After an opportunity for clarification of the findings, the participants were asked to return to their small groups to discuss the implications of the findings and to consider how this information could be used within their work and organisation. These observations were also captured using flip charts. The following section describes the key themes that emerged from the two workshops.
Themes emerging from the workshops
Three main themes emerged across the two workshops when discussing individual unlearning experiences. The most common situation, in line with our interview results, was individual unlearning as a result of role change. Changes in job role were triggered by a range of factors including organisational restructuring, reductions in staffing levels or moving from a clinical role into a managerial capacity. Participants commented that as a result of a change in job role they had needed to change their approaches to delegation, by more ‘letting go’ of tasks and actions, abandoning specialist clinical knowledge to work in broader roles and changing communication strategies. Abandoning the use of paper-based systems in favour of electronic systems such as electronic calendars was also cited as an example of unlearning at both sites. In site B, participants emphasised that a key requirement for unlearning of previous manual practices was to fully trust the new IT systems and the data held on them. The third theme raised at both sites was changes in organisation, which had meant that some staff were having to unlearn their way of thinking about the services that the NHS trust provided. For example, organisational changes at site A had meant that the NHS trust now covered new geographical areas and was responsible for new services. Similarly, in site B, a participant commented that, as this NHS trust also acquired new and diverse services, there was a need to change how the NHS trust was understood and conceptualised. There was a need for staff to unlearn that the NHS trust was solely focused on providing care in a hospital environment.
When considering the implications of the preliminary findings of the study participants in both workshops focused on the emotional aspect of the unlearning process. Participants spoke of a sense of grieving or bereavement from giving up a behaviour or knowledge. This sadness was considered to be particularly common when staff had given up methods or knowledge that they were familiar with and attached to, and did not wish to discard. Further, feelings of annoyance and resentment were also mentioned, especially when the individual unlearning had been as a result of an imposed change. It was also emphasised that previous experience of unlearning did not reduce the sense of grief or sadness that staff felt from new unlearning episodes prompted by further change initiatives.
Workshop participants in site A added that experiences of having to give up roles could be influencing staff sickness and stress levels but that once individuals had completed the unlearning process they were more likely to be able to accept and reframe the experience in a positive way. Having time to reflect and getting feedback on what knowledge or behaviour needed to be unlearnt and what skills and knowledge could be transferred into the new role were also considered important. Workshop participants in site B added that the way that people responded to change and associated unlearning was likely to vary between individuals and that different individuals may unlearn at different speeds. Successful unlearning was thought to require staff to be adaptable. Further, there was an observation that there may be a difference between staff unlearning in their behaviour but not necessarily their thinking. For example, some staff might behave as if they have unlearned and changed, but this behavioural change might mask how they really feel, that is, that the old established routines were acceptable and did not need to change. Consequently, participants at site A suggested that there was a need to support and reinforce the unlearning process during change initiatives to stop staff ‘going back to the old ways’.
In terms of possible actions that could be taken within the sites, both groups of workshop participants felt that the findings emphasised the importance of focusing on the needs of individual staff during change and individual unlearning. In particular, participants felt that a greater understanding and recognition of the emotional impact and grieving that were associated with some unlearning experiences would help staff with the transition to abandoning former roles, methods or knowledge. Workshop participants at site B thought that one way that this could be achieved would be through increased consultation with staff before, during and especially after change projects, to monitor how staff feelings evolve as change and unlearning take place. In addition, workshop participants at site A were keen for senior managers at their trust to be aware of the study's findings. They also suggested that the development of models or frameworks could help clinical staff who move to managerial roles.
Summary of findings
This chapter has presented the findings from our analysis of our interviews with health-care managers at two case study sites and the findings from workshops conducted at both sites. The previous sections have shown that health-care managers who participated in this study engaged with both forms of individual unlearning and fading. The engagement with individual unlearning was triggered through either an individual experience or a change event and in some cases these triggers were similar. For example, a change in role could be initiated by an individual or by a wider organisational change. Participants also referred to the greater emotional impact often associated with cognitive unlearning than with behavioural unlearning, and this was a strong theme that also came from the workshops. There was little evidence to indicate that health-care setting or professional background had a strong influence over whether or not health-care managers participating in this study engaged with individual unlearning. However, the small sample size and similar characteristics of the two case study organisations must be kept in mind when considering this finding.
Participants identified a variety of barriers to individual unlearning and there was some evidence of a possible relationship between the trigger that initiated the individual unlearning and managing the associated barrier. For example, if the trigger was an individual learning episode, managers may need support in building confidence, the challenging of their need to be liked, relinquishing control and breaking habits. On the other hand, if unlearning was triggered by a change event, some action may be needed at an organisational level, for example to encourage senior management support and address concerns about workload and job insecurity.
With one exception the same factors enabled behavioural and cognitive unlearning. Overall, personal skills, attitudes and relationships were more commonly cited than organisational enablers such as policies, procedures and work circumstances. More enablers were identified in relation to individual unlearning triggered by individual experiences than in relation to unlearning triggered by change events.
The findings also suggest that engaging with individual unlearning did seem to have some impact on the decision-making of health-care managers who participated in this study, although the nature of the impact seems to vary depending on an individual's circumstances. However, a positive finding was the associated improvement that managers inferred having engaged with individual unlearning. In several cases participants felt that the effect of individual unlearning on their decision-making was that they were able to work in a more effective way, for them personally and/or in their organisational role.
Fading episodes were often triggered by a change in role and resulted in the forgetting of particular skills or knowledge. However, many participants felt that they could still recall some core knowledge associated with tasks and it was specific details that had most commonly been forgotten. In addition, no participants indicated that they had made a conscious action to forget particular skills or knowledge; these specific details had simply faded from memory. This was reflected in the barriers and enablers that were identified, with reference being made to the ability to recall (barrier) and ingrained experience (barrier) or external change (enabler) and infrequent use (enabler) when discussing episodes of fading. We found no evidence of fading having an impact on participating health-care managers' decision-making. However, this may also be partly a reflection of the challenge of capturing this possible change for participants, as it requires them to remember skills that they had forgotten. Similarly, for both types of unlearning, we did not find strong evidence to suggest that health-care setting or the professional background of participants could differentiate experiences of fading, although this finding is also subject to the same limitations. The following chapter discusses these findings in more detail and in reference to the existing literature regarding unlearning.
Chapter 5 Discussion
The discussion of our empirical findings is organised into five separate sections. The first section looks at the first part of the first research question, the extent to which health-care managers engaged with processes of individual unlearning and fading. The second section focuses on the second research question, the barriers to and enablers of individual unlearning and fading that were identified in the research. The third section examines the second part of the first research question, the impact of individual unlearning and fading on managerial decision-making. The fourth section then examines the final research question, the impact that the health-care setting had on managerial experiences of individual unlearning and fading. The final section of the discussion considers a topic that was not one of the project's research questions but which emerged during the course of the project: the relationship between individual unlearning, learning and change.
The extent to which individual unlearning and fading occurred and the nature of individual unlearning experiences
This section focuses on the first part of the first research question of the project, the extent to which health-care managers engage in unlearning. It is divided into two parts with the first part analysing the data related to behavioural and cognitive unlearning and the second part examining fading.
The extent to which health-care managers engage in behavioural and cognitive unlearning
Chapter 4 gave detailed insights into the nature and frequency of each type of individual unlearning (see Episodes of individual unlearning and fading). The discussion here shifts focus to take a more high-level and analytical perspective, which attempts to provide an explanation for the overall pattern of individual unlearning episodes that were uncovered in the research. At the most high-level perspective, the numbers of each type of individual unlearning that was discovered are summarised in Table 16.
In terms of the absolute number of individual unlearning episodes discovered, the fact that 57 examples of behavioural and cognitive unlearning were revealed in interviews with 29 health-care managers suggests that unlearning is relatively common among our participants, with catalysts for these episodes being both specific individual experiences and organisation-wide change events (see more discussion below).
| Number of episodes | |||
|---|---|---|---|
| Trigger | Behavioural unlearning | Cognitive unlearning | Total |
| Individual experience | 6 | 17 | 30 |
| Change event | 23 | 11 | 27 |
| Total | 29 | 28 | 57 |
These data show broad similarities in the numbers of different types of individual unlearning reported, that is, 29 episodes of behavioural unlearning and 28 episodes of cognitive unlearning. Further, in terms of catalysts, of the 57 unlearning episodes that were reported, the catalyst for each was as likely to be a change event as it was an individual experience. This pattern in terms of catalysts can be explained with reference to the nature of the work context that interviewees operated in. Thus, in the context of both NHS trusts examined, people had to deal with and respond to a significant number of different organisational-level change events (such as expansion of the NHS trust's services and the internal restructuring of service provision). However, the fact that their work typically involved the direct provision of health care meant that they simultaneously had to deal with significant individual experiences on a regular basis, such as patient deaths or unexpected developments in treatment.
One small difference in the patterns of unlearning episodes revealed by the data in Table 16 is that the catalyst for cognitive unlearning episodes was more likely to be an individual experience (17 episodes) than a change event (11 episodes). The fact that change events were more likely to result in behavioural unlearning (23 episodes) than cognitive unlearning (11 episodes) suggests that the change events that people experienced were more likely to involve changing working practices than more significant changes in managers' knowledge, values or assumptions. Thus, although managers experienced a significant amount of change, and this provided a catalyst to individual unlearning, it was more likely to be behavioural than cognitive unlearning that managers experienced. The nature of the behavioural unlearning examples provided by managers also suggests that behavioural unlearning can be linked to subsequent single-loop learning involving continuous corrective or adaptive action. This would be in contrast to double-loop learning, which may be more likely to occur following cognitive unlearning as it involves episodic modification of underlying processes or generative learning. 102
One issue that we were interested in was the extent to which managers' professional background affected the extent to which they experienced individual unlearning. More specifically, we were interested in whether or not managers who had a clinical background undertook individual unlearning more than managers with no clinical background. With respect to cognitive and behavioural unlearning we did see some differences (see Chapter 4, Professional background); however, as these data revealed, there was no consistent pattern across the different types of individual unlearning. Thus, although with behavioural unlearning initiated by an individual experience, managers with no clinical background were more likely to experience individual unlearning than managers with a clinical background, the opposite pattern was identified with behavioural unlearning initiated by a change event. Further, in relation to cognitive unlearning a third pattern was found, with the extent to which managers experience individual unlearning being relatively similar for those with clinical and non-clinical backgrounds. We suspect that people's specific roles and responsibilities rather than their background may shape the extent to which they engage in individual unlearning, and are exposed to catalysts to individual unlearning. However, further research analysis is necessary to establish this.
The extent to which health-care managers engage in fading
As noted in Chapter 2 (see Fading), although the literature suggested that fading equates to forgetting and is not conceptualised as unlearning, we wished to find out if this understanding was supported by empirical research. The participants identified 28 examples of fading. In most cases fading related to skills and knowledge that had fallen into disuse because of a change in job role. Loss of technical or front-line skills was associated with gaining managerial responsibilities and moving away from or reducing time spent on operational duties. In other words, most examples of fading arose as a result of change affecting individuals, with fewer examples resulting from external changes such as new technology or a change in policy. Some participants no longer used particular skills and knowledge because changes in clinical practice or technology rendered them obsolete, rather than because the knowledge or skills themselves had faded. Although limited, the data support the characterisation of fading as minor, slow and without emotional charge. 6 However, the sections on barriers to and enablers of fading show that in most instances participants did not think that their skills and knowledge had been totally lost. Indeed, some thought that skills gained early in their careers and/or used very frequently in their front-line role had been internalised and were still accessible to them.
The barriers to and enablers of individual unlearning and fading
As noted in Chapter 2, the literature focuses on organisational unlearning and the antecedents of unlearning, identifying unlearning as facilitated by organisational context,9 environmental turbulence3,51 and organisational size. 26 Only one article32 explores the process of individual unlearning and in so doing identifies receptiveness and recognition as necessary conditions for unlearning to take place. Antecedents – pre-existing conditions that enable or prevent the unlearning from beginning – may be the same as or distinct from the enablers of or barriers to the unlearning process. Less attention has been given to the latter, although some studies offer relevant insights from empirical studies. 9,10 As discussed in Chapter 2, when antecedents equate to ‘triggers’ (individual experiences or change events that initiate individual unlearning) they are integral to the definitions of the different types of unlearning that we have identified. However, the discussion that follows considers enablers and barriers in relation to both initiating and engaging in the process of individual unlearning and fading.
Comparison with the literature on barriers to unlearning
As shown in Chapter 2, the empirical studies that address the barriers to unlearning are limited in terms of relevance, quality and empirical basis, or they focus on organisational – as opposed to individual – unlearning. As the literature does not distinguish between specific types of unlearning, the discussion considers the barriers to individual unlearning in general rather in relation to the four categories described in the typology.
Like Becker,9,10 our study showed that barriers to individual unlearning could be individual (personal behaviour) or organisational (e.g. lack of management support, high workload, organisational culture). Whereas Becker10 refers to individuals' discomfort with change and unlearning (i.e. an aspect of personality) as a barrier to unlearning, our study identified behavioural barriers such as reluctance to delegate and habit. Negativity,45 anxiety about change9 and being an expert or having in-depth knowledge10 did not emerge as barriers for our participants. This does not mean that they were not experienced as barriers, rather that participants did not recall or wish to discuss them as such. Interestingly, participants' reported difficulty in forgetting skills and knowledge embedded through experience and training suggests that expertise may have been a barrier to fading, even if not recognised as affecting intentional and conscious attempts to unlearn.
Organisational barriers to unlearning mentioned in the literature, including poor history of managing change, strategies and processes that lag behind change,9 structure and size,10 low staff turnover and strong organisational memory,26 were largely absent in the accounts of our participants. However, like Becker's participants,10 the health service managers in our study referred to culture, staff resistance and lack of management support as barriers. Financial constraints, high workload and concerns about job security might, in the current climate and the context of the NHS, be perceived as barriers or hindrance stressors. 43 It seems that our participants focused on more proximate factors that impact on their daily lives rather than the wider organisational context.
Comparison with the literature on enablers of unlearning
The limitations of the literature in respect to barriers noted above largely apply to enablers as well, although literature about unlearning in the health sector6,32 and research into unlearning in new product teams3 add useful insights.
Our findings and those reported in the literature can be broadly divided into individual and organisational enablers. Organisational antecedents or triggers of individual unlearning identified in our study were changes in work circumstances, policies and procedure, and pressure to improve services and make savings. To some extent these findings support the published literature, which reports enablers of unlearning as work context,43 environmental turbulence,3 and mandatory and discontinuous change. 10 For example, challenge stressors that provide enabling work contexts,43 namely responsibility, complex tasks, deadlines and high workload, are likely to have been features of the contexts of our participants' individual unlearning. However, our participants regarded high workload as a barrier to individual unlearning. Weak organisational memory and high staff turnover identified by Becker et al. 26 as enablers of unlearning were not mentioned by our participants.
As noted in Chapter 2 (see Recent changes in the NHS), change in the NHS is intense in terms of pace and scope. The environment within which it operates can be described as turbulent in the sense of being subject to rapid and unpredictable change. 3 According to these authors, turbulence enables team unlearning by exposing inadequate mental models and routines and causing teams to change their beliefs and routines. Reference in our study to change at the local level and in the wider context suggests that our participants might share this view.
The organisational enablers – leadership and networks – identified by our participants may provide a supportive unlearning environment. The literature is more specific about management action that enables unlearning. According to Becker,9 to enable staff to have a positive attitude to change and consequently to unlearning, managers need to demonstrate commitment, make the case for change, involve staff in planning and provide reassurance. Both our participants and published research9 identified training as an enabler of individual unlearning.
Support from specific individuals featured in our study, enabling health-care managers' unlearning through providing feedback, support, advice and role modelling. Such comments are reflected in the literature, which refers to the informal support of colleagues and managers9,10 and mentors,10 and having secure but challenging conversations with trusted colleagues. 6
In terms of individual enablers, health-care managers in our study reported that their skills and attitudes helped them to unlearn, a finding that in general terms is supported by the existing literature. Specific attitudes referenced in the literature, but not mentioned by our participants, include having a positive attitude towards change,9,10 being receptive to other perspectives and recognising their veracity,32 being open-minded and lacking emotional attachment to a particular way of thinking45 and having a willingness to be vulnerable and tolerant of feeling inadequate or embarrassed or losing status. 6 However, there may be closer parallels than at first sight as confidence, which was mentioned in our study as an enabler, may underpin such attitudes. Becker10 also refers to individual experiences that promote openness and lack of attachment: being in post or in the employing organisation for a short time, having broad rather than in-depth knowledge and being accustomed to learning through involvement in training and development.
The main skill that our participants identified as supporting their individual unlearning was communication, a viewpoint supported by the literature, which talks about the value of questioning45 and listening6,45 along with the ability to discern what needs to be unlearnt6 and to come to terms with the loss of previous ways of seeing and of fundamental assumptions. 32 It seems likely that the positive attributes that enabled individuals to unlearn also assisted them in building supportive relationships that further supported their individual unlearning. In other words, the different sets of enablers are likely to interact and reinforce one another.
The impact of individual unlearning and fading on managerial decision-making
An important aspect of our study was investigating the extent to which managers' experiences of unlearning impacted on their decision-making. In general terms, as outlined in Chapter 4 (see The impact of individual unlearning and fading on managers' decision-making), we did find some evidence that health-care managers' individual unlearning experiences impacted on the way that they made decisions, although there was no evidence of fading having an impact. However, it should be noted that our participants often had difficulty relating their unlearning and fading experiences to specific changes in their decision-making processes. Out of the 85 episodes of unlearning and fading, we were able to identify only 30 examples of changes in decision-making, none of which was linked to fading episodes. Consequently, we can offer only relatively tentative insights concerning the relationship between unlearning and health-care managers' decision-making. Before reflecting on these findings, this section begins by looking back at the literature review on unlearning that was presented in Chapter 2 to highlight the nature of the contribution to this literature that our empirical data make.
As outlined in Table 3, of the 34 articles on unlearning that were reviewed, 13 examined the consequences of unlearning. Of these 13, five were conceptual articles and only eight presented original empirical data on the outcomes or consequences of unlearning. Furthermore, of these eight articles, only three examined individual unlearning. 37,38,48 In all three articles the empirical data presented are taken from survey-based studies and no qualitative data are used; thus, there are very few empirical data on the consequences of individual-level unlearning.
Therefore, our exploratory empirical findings on the impact of individual unlearning on managers' decision-making processes make a contribution to knowledge in two respects. First, our study involves a type of research data not previously utilised in this domain – qualitative interview data that give insights into how individual managers understand the changes that their unlearning experiences have produced. Second, it also looks at a variable – managerial decision-making – that has also not been examined in other unlearning studies.
The analysis of our research data found that the likelihood of people's unlearning experiences producing changes in the way that they made decisions was typically the same for all types of unlearning examined. Thus, for both types of behavioural unlearning and for cognitive unlearning initiated by a change event, changes in managers' decision-making behaviours were identified in approximately 50% of cases. The exception to this pattern was cognitive unlearning initiated by an individual experience, for which changes in health-care managers' decision-making were identified in just under one-third of episodes. A possible reason for this is that change is less likely with this type of unlearning because of the combined effect of it being a challenging type of unlearning (cognitive) and the individualised nature of it. The individual aspect means that people typically experience it in isolation from others and may have limited opportunities to share their experiences with others and learn from them.
Changing focus to look at the type of changes in decision-making that were identified, a number of observations can be made. First, although the decision-making changes that people reported undertaking were described as being positive, in general terms the scale of the changes undertaken was relatively small and incremental. For none of the unlearning episodes examined could it be said that they produced a radical transformation in the way that people thought or acted. Thus, a typical example of the scale of change in decision-making that people's unlearning experiences produced was when one manager reported taking more account of the fact that there were limitations to his ability to make decisions because of the constraints placed on him by more senior colleagues. This is in line with the observations of Walshe and Rundall88 that managerial decision-making is often more politicised and constrained than decision-making in medical practice.
In broad terms, the types of changes in decision-making that were identified can be grouped into two primary categories. The first concerns changes in how people consulted and communicated with colleagues regarding the implementation of change (such as adaptations of participants' management styles aimed at getting more involvement and commitment to change, and consulting with a wider range of people before making decisions). The second concerns the processes of planning and information seeking that are undertaken before decisions are made (labelled as more rational decision-making and better reporting plans).
These experiences suggest that the changes that managers were making in their decision-making practices as a result of individual unlearning experiences, such as collecting evidence from a variety of sources, critically appraising that information and considering the views of stakeholders, are in line with the steps prescribed by Briner et al. 86 for adopting evidence-based management. However, there was little evidence from our participants that external published research was being regularly integrated into these decision processes, the information tending to be gathered from within the organisation. Furthermore, both categories suggest that participants' unlearning experiences had caused them to reflect on their decision-making processes and move away from practices that were akin to idea imposition to more discovery-orientated approaches. 91 After the unlearning experience, some participants appear inclined to adopt a more systematic gathering of information to learn about possibilities and to understand stakeholder views and perceptions.
However, there was one exception to this trend, with one manager reporting that she had moved away from a heavily consultative discovery approach to a more decisive idea imposition-based approach (see quote on p. 57, paragraph 5). This was in reference to a situation in which the change was imposed from an external policy request that was required to be implemented. In this case, it appears that the manager thought that she had been consulting excessively with stakeholders regarding change that was non-negotiable. The participant's comments suggest that this change in style had been effective, although it is not clear whether this was purely due to the specific circumstances of the change required or that the consultation aspect of the discovery approach can be over applied.
However, overall, the broad message from our exploratory findings is that the experience of unlearning seems to encourage the adoption of more organised approaches to searching for and collecting information and stakeholder opinions and critically evaluating this information for decision-making. This suggests a move towards the discovery process of decision-making, which Nutt91 has demonstrated to be more successful than other decision-making processes.
The extent to which the health-care setting affects health-care managers' engagement with individual unlearning and fading
As the findings indicate, managers at the acute and mental health NHS trust sites engaged in both types of individual unlearning and reported experiencing fading. Managers at both sites reported unlearning policies and procedures most commonly. Overall, there was little difference between what was unlearnt at the different sites, suggesting that the organisational characteristics of the two case study NHS trusts did not affect either the level of engagement in individual unlearning or the nature of individual unlearning for our participants.
Barriers to individual unlearning were largely the same at both sites, although financial constraints were reported only by managers at the mental health NHS trust and lack of management support was identified by a larger number of managers at this site than at the acute NHS trust. Enablers were also much the same at both sites and the number of times that particular enablers were cited was similar. However, only managers at the mental health NHS trust reported changes in policies and procedure as enabling individual unlearning. New practices or knowledge was mentioned as an enabler of fading by more managers at the acute NHS trust than at the mental health NHS trust.
Our findings suggest that lack of management support rather than the type of NHS trust may explain the limited differences in barriers to and enablers of individual unlearning experienced by our participants. Alternatively, the differences may be due to the different lengths of time since the NHS trusts acquired foundation trust status. At the time of the interviews the acute NHS trust had had foundation trust status for more than 6 years, whereas the mental health trust had had foundation trust status for less than 2 years. As a result, managers at the latter site may have been subject to a greater degree of change in a short time frame than those at the acute site. Having said that, at the time of the interviews both sites had recently acquired new community services and the acute NHS trust was undergoing an internal restructuring. However, it should also be acknowledged that these two types of NHS trust compared with other health-care organisations in the NHS are relatively similar in terms of their structure and manner in which they deliver care (e.g. ward based). These similarities may explain the relatively consistent findings in this study when assessing the influence of organisational setting. This issue will be revisited in the conclusions of the report and the research agenda.
The relationship between learning, individual unlearning and change
This was not a topic that the study explicitly aimed to examine. However, it is a topic that emerged as being of interest at various points throughout the study, largely because of some of the challenges of data collection and data analysis that occurred, which encouraged the research team to reflect on this topic. There is scope to make a potentially significant contribution to knowledge regarding the inter-relationship both between learning and unlearning and between unlearning and change for two reasons. First, our analysis challenges the dominant way in which the relationship between these topics is conceptualised in the unlearning literature. Second, we were able to collect rich data on people's experiences of unlearning, which gave good empirical insights into the nature of individual unlearning processes (which, as outlined previously in Chapter 2, Reviewing the academic literature on unlearning, is a neglected topic in the unlearning literature) and which helped shed light on the relationship between learning, unlearning and change.
One of the key challenges experienced both during data collection, in conducting the interviews, and during data analysis, when research data were being coded in NVivo, was the close relationship between learning, unlearning and change. These concepts were so inter-related that it was difficult to tease them apart and separate them. For example, in terms of data collection, when we asked managers to describe their unlearning experiences, they often started by talking about their experiences of change, and only on detailed probing revealed information on unlearning. We argue that these challenges do not relate to any limitations in our data collection or analysis skills but instead say something about the intrinsic nature of the relationship between individual unlearning, learning and change. In considering these issues, this section is divided into two parts, with the first considering the relationship between learning and individual unlearning, and the second considering the relationship between individual unlearning and change. Further, these discussions link back to Chapter 2 (Reviewing the academic literature on unlearning and Types of individual unlearning and the nature of individual unlearning processes) where discussion on these topics has already been undertaken.
Individual unlearning and learning
As was outlined in Chapter 2, Reviewing the academic literature on unlearning, the consensus in the unlearning literature regarding the relationship between unlearning and learning is that they represent two separate and distinct processes which occur independently, and that typically unlearning is a precursor to learning (see, for example, Becker et al.,26 Cegarra-Navarro et al. 30). In contrast to this, and following Antonacopoulou33 and Argyris and Schön,34 we argue that unlearning should be conceptualised instead as a specific type of learning that is concerned with the process of subtracting, abandoning or stopping some established practices, knowledge or values.
Building from this, the collection and analysis of our empirical data point towards two important inter-related features of the relationship between individual unlearning and learning that challenge the mainstream perspective on unlearning and learning. First, individual unlearning does not occur before learning and, second, processes of learning and individual unlearning are not clearly distinct. Instead, processes of individual unlearning (abandoning/giving up established practices or ideas) and learning (the development of new practices or knowledge) typically occur virtually simultaneously. This can be illustrated by linking back to a couple of the unlearning episodes presented in previous sections. First, consider the last example of cognitive unlearning initiated by a change event presented in Chapter 4, Cognitive unlearning episodes on p. 41. In this case the individual unlearning involved giving up an informal and undocumented method of communicating with colleagues in related services. However, from the way that the participant describes her experiences, this individual unlearning happened simultaneously with the learning of a new, more formalised style of communicating with colleagues. Second, the same is visible in the second example of cognitive unlearning initiated by an individual experience presented in Chapter 4, Cognitive unlearning episodes on p. 40. In this case, the catalyst to individual unlearning was an unexpected tragic event, when a patient managed to kill himself by hanging. In this case, what was unlearnt was the assumption that the patient's room was safe. This individual unlearning resulted in learning, through the reassessment of patient safety, which produced a number of changes in the organisation of patients' rooms. However, the individual unlearning and learning arguably occurred virtually at the same time, and from the perspective of the participant they were not distinct and separate processes. Although people may find it hard to distinguish between individual unlearning and learning, and both processes may be inter-related and occur in parallel, it is still useful conceptually to distinguish between individual unlearning and learning as individual unlearning does arguably represent a distinct form and type of learning.
Individual unlearning and change
This section considers the relationship between individual unlearning and change. This discussion links to what was outlined in Chapter 2, Types of individual unlearning and the nature of individual unlearning processes, where this topic was initially examined. In the unlearning literature it is generally acknowledged that in different circumstances change can be a trigger for individual unlearning, and also that unlearning can be a catalyst for and facilitator of change. However, there are very few empirical studies of the relationship between change and individual unlearning. Two articles that examine the relationship between change and unlearning in reasonable detail are those by Akgün et al. 20 and Tsang and Zahra. 2 However, both of these articles are purely conceptual. Furthermore, Tsang and Zahra's2 main contribution regarding the relationship between unlearning and change is to suggest that different types of change are linked to different types of unlearning, with them distinguishing between small-scale incremental/continuous change and large-scale episodic/discontinuous change. However, they provide limited insights into the sequencing and ordering of the relationship between unlearning and change. A weakness of Akgün et al.'s20 analysis is that it is linked to Lewin's57 oversimplistic and much criticised model of change.
There are three empirical studies of unlearning that do consider the topic of change. First are two articles by Becker. 9,10 Both articles consider change to be a catalyst to and precursor of individual unlearning and present a range of evidence to highlight what aspects of organisational change processes facilitated and inhibited unlearning. The other empirical article on this topic is by Tsang,50 which suggests that change is a precursor of unlearning and also that unlearning may facilitate and inhibit subsequent change. In this case, the initial change was a merger between companies, which required one site to implement new work practices. Here, the unlearning related to the giving up of established work practices and routines. The extent to which this occurred was argued to be subsequently linked to the extent to which work practices were modified. Thus, the merger represented the initial change event, which facilitated the unlearning, with the nature of unlearning then impacting on the way in which work practices changed.
In linking our empirical findings to this topic it is necessary to distinguish between and separately discuss the four types of individual unlearning, as the relationship between change and unlearning varies depending on the type of catalyst. The unlearning types reported in this study that fit most closely with Tsang's50 findings are the two types of unlearning for which the catalyst was an organisational change event. With these types of individual unlearning, the relationship between change and unlearning was similar to that identified by Tsang, with both change acting as an initial catalyst for individual unlearning and unlearning processes affecting subsequent change. This pattern of change–unlearning–change is visible in most of these unlearning episodes. To illustrate this, consider the example in Chapter 4, Behavioural unlearning episodes on p. 39, paragraphs 1 and 2. In this case the initial changes that provided the catalyst to individual unlearning included the physical relocation of the ward, the reorganisation of the ward staffing and the change in priorities regarding patient care. These changes resulted in unlearning regarding how patient care was understood. As the relevant quotation highlights, this individual unlearning then resulted in subsequent changes being made to work practices to reflect the new patient care priorities, which included the reorganisation of staff shift patterns. As well as being in line with Tsang's work this example also suggests that the participant had positive emotions about the change event, viewing the change as an opportunity to improve practice and patient care. Bakker et al. 76 report that positive emotions can increase engagement and affect the emotions of other team members. This reinforcement may have helped the manager abandon previous ways of working and implement the new practices and behaviour, which required personal changes by both the manager and the staff working on the ward.
Although this analysis suggests that processes of individual unlearning and change have a bidirectional relationship and are closely inter-related, the analytical advantage of making use of the concept of unlearning is that it allows the different aspects of change processes to be teased apart and separated. It also suggests that individual unlearning is an integral part of the process of adaptive behaviour that is triggered in response to change events. Thus, the empirical data on the individual unlearning episodes initiated by organisational-level change events that we identified have provided detailed qualitative insights into the complex relationship that exists between change and individual unlearning.
The focus now shifts to the two types of individual unlearning that were initiated by individual experience rather than change events. With these types of individual unlearning the relationship between unlearning and change was slightly different. However, with these types of individual unlearning a distinction can be made between two types of individual experience. The data analysis suggests that a distinction can be made between individual experiences that are related to (personal-level) change processes and individual experiences that involve sudden and unexpected events. With the first type of individual experience, the individual-level change was typically a promotion or role change. Our data suggest that this type of individual-level change is relatively common, partly because both of the NHS trusts examined were undertaking significant processes of organisational restructuring as our study was conducted. With this type of individual unlearning catalyst, the relationship between unlearning and change was similar to that described earlier in relation to unlearning initiated by organisational-level changes. Thus, the relationship between individual unlearning and change was bidirectional, with managers' individual changes (promotions, etc.) facilitating individual unlearning and this individual unlearning then subsequently leading to subsequent learning and change.
With individual unlearning for which the catalyst was an unexpected individual experience (such as the patient death discussed earlier), the relationship between individual unlearning and change was quite different and somewhat simpler. With this type of individual unlearning the relationship with change was unidirectional, with the unexpected event precipitating individual unlearning and these unlearning experiences precipitating subsequent change.
Overall, therefore, the empirical data collected have provided detailed insights into the complex relationship between individual unlearning and change, highlighting their close inter-relationship. Our analysis also suggests that the relationship between individual unlearning and change also varied depending on the particular type of catalyst that initiated the unlearning.
Chapter 6 Conclusions
This exploratory study sought to investigate whether or not health-care managers engaged with processes of unlearning and fading and the impact that the unlearning and fading may have had on their decision-making. We collected qualitative data on 85 episodes of unlearning and fading from 29 middle managers working in two NHS settings: an acute trust and a mental health trust. Although our findings add to the limited literature regarding individual unlearning and fading and provide some important new insights regarding the types of unlearning that health-care managers who participated in this study experienced, the exploratory and relatively small-scale aspects of this study should be noted when drawing conclusions. Specifically, the findings are based on a limited range of case study sites and the data fell short of saturation levels. The study investigated three research questions and the findings of the study are considered in relation to each of these questions in the following sections.
To what extent do health-care managers engage with the process of unlearning and what impact does the engagement with this process have on health-care managers' decision-making?
The findings demonstrate that the health-care managers who participated in this study engaged with unlearning processes although the form and circumstances of the unlearning varied. The findings of the study were conceptualised into two distinct types of individual unlearning experienced by participating health-care managers. The first was behavioural unlearning, which was triggered by a deliberate process of change that had been externally imposed. The second was cognitive unlearning, which was triggered by an unexpected external event that questioned some basic assumptions of the individual. We have added further refinement to this conceptualisation by developing a new typology, which distinguishes between four separate types of individual unlearning.
The findings indicate that 57 episodes of individual unlearning were identified by the 29 health-care managers who participated in the study. All participating health-care managers were able to identify at least one unlearning episode. The most common individual unlearning type was behavioural unlearning triggered by a change event (23 episodes), followed by cognitive unlearning triggered by an individual experience (17 episodes). The least common individual unlearning type was behavioural unlearning triggered by an individual experience (six episodes) (see Table 8). These findings give some indication of the extent to which our participants engaged with processes of unlearning. However, we are not able to generalise from these findings to health-care managers working in other settings in the NHS, although we also have no reason to believe that our findings are atypical.
The findings suggest that engaging in processes of individual unlearning did impact on decision-making for some participating health-care managers, with 30 examples of decision-making changes identified from 57 unlearning episodes. However, some managers found it difficult to clearly identify examples of changes to decision-making that were a result of individual unlearning experiences and six participants did not give any examples of impact on decision-making. The difficulty that some participants encountered is probably due to a lack of awareness at the time of unlearning and not easily associating changes in decision-making as an obvious outcome. Acknowledging this limitation, the findings show that after engaging with individual unlearning several managers moved away from idea imposition approaches to decision-making in favour of more discovery-focused approaches. Particular changes involved more systematic and formalised procedures for collecting and documenting information, and greater consideration of stakeholder views and perceptions when formulating and implementing decisions. Research suggests that discovery-orientated approaches to decision-making processes are more successful than idea-imposed processes. 91 Consequently, it is likely that these managers have improved the effectiveness of their decision-making by engaging with unlearning processes.
What are the barriers and enablers that influence the engagement of health-care managers with the process of unlearning?
Participants mentioned 36 examples of barriers encountered during episodes of behavioural unlearning, but mentioned fewer examples of barriers encountered during cognitive unlearning episodes (n = 19). The most common forms of barrier identified were staff resistance to changes in practice, personal behaviour, lack of management support, high workload and organisational culture. Other barriers that were mentioned included financial constraints and job insecurity. In addition, we also identified 13 examples of barriers to fading, the most common being the ability to recall past knowledge and experience. Our findings show that barriers to individual unlearning could be individual or organisational. These barriers could influence either the individual unlearning process or the implementation of the new ways of working or behaving that the unlearning process required for full implementation by the individual. For example, an individual's personal behaviour may act as a barrier to adopting a better work–life balance because of his or her desire to maintain control and resist delegating tasks. However, a lack of support from managers to devolve decision-making to more junior members of a team, or team members not wishing to take responsibility for decision-making, may also prevent an individual from abandoning his or her old ways of working. Of course, in the latter case, it is possible that the person has engaged with unlearning but has been unable to implement the outcome of this unlearning experience. Further research is required to fully unpick the relationship between individual unlearning and barriers to unlearning processes.
A further aspect of unlearning that is worth noting in relation to barriers to individual unlearning is the variation in emotional impact between the types of unlearning reported by study participants. In particular, the cognitive unlearning experience often involved high emotional strain and appeared to be associated with feelings of sadness and grieving. Although the catalyst for the cognitive unlearning may be a relatively sudden change or event, the associated emotional adjustment and process of unlearning may take a considerable amount of time. In addition, our workshop findings suggest that this emotional impact does not reduce, even if the individual has experience of previous cognitive unlearning episodes. Studies of individual transitions during change have shown that employees often find change to be a deeply emotional process that can engender a sense of uncertainty, frustration and defensive routines. 63,64 These responses are often interpreted as ‘resistance to change’; however, our findings suggest that they may also be associated with some types of individual unlearning. Consequently, it is important that change agents do not immediately interpret these types of emotional response to change as non-desirable58 but recognise that they are likely to be the early signs of employees giving up old practices in order to adapt to new knowledge or behaviours.
Support networks, usually in the form of particular individuals, seemed to be important in helping individual managers when experiencing this change, with less reference to organisational support mechanisms. This reflects the individual and personal nature of the cognitive unlearning experience, but may also indicate a lack of sufficiently individualised organisational support mechanisms. Participants from our workshops also suggested that more continuous support may be required after change events, both to ensure that the unlearning is successfully embedded and to help the emotional transition for the staff concerned. Emotion has been identified as an important aspect influencing information processing for decision-making. Individuals who are experiencing positive emotion have been found to be more able to process information and be creative than those who are not. 80 Therefore, it is possible that a health-care manager experiencing cognitive unlearning that triggers negative emotion could find his or her decision-making processes impaired.
Regarding the enabling factors for individual unlearning, a total of 48 and 49 examples of enablers of behavioural and cognitive unlearning were identified respectively. With the exception of one factor (changes in policies and procedures), all of the enablers mentioned by participants could facilitate either behavioural or cognitive unlearning. The most common enablers were personal skills and attitudes, leadership and networks and support from specific individuals, all of which are supported in general terms by the literature. Becker9 argues that, to enable staff to have a positive attitude to change and consequently to unlearning, managers need to demonstrate commitment, make the case for change, involve staff in planning and provide reassurance. Overall, the main skill that our participants identified as supporting their unlearning was communication, a viewpoint supported by the literature, which talks about the value of questioning45 and listening6,45 along with the ability to discern what needs to be unlearnt6 and to come to terms with the loss of previous ways of seeing and of fundamental assumptions. 32 It seems likely that the positive attributes that enabled individuals to unlearn also assisted them in building supportive relationships that further supported their unlearning. In other words, the different sets of enablers are likely to interact and reinforce one another. These recommendations echo some of the key aspects advocated by Briner et al. 86 for evidence-based management, so the promotion of these activities by senior managers may help in providing role models for effective decision-making practices coupled with a supportive and more receptive environment for individual unlearning by health-care managers.
To what extent does the health-care setting affect the level of engagement with the process of unlearning by health-care managers?
This study also attempted to investigate the influence of health-care setting on individual unlearning experiences of health-care managers. The study had planned to address this question by comparing individual unlearning experiences of managers across three different case study sites (acute, mental health and primary care trusts). However, the extent to which this question could be fully addressed by the findings was limited by not being able to recruit any participants from the primary care site. Consequently, the comparison of experiences could be made only between two case study sites. Further, as our study was concerned with individual experiences of unlearning rather than organisational unlearning, our findings are limited in the degree to which they can be generalised to other health-care managers within each case study, as well as to other health-care settings. Despite these limitations the study did find some interesting results.
The findings showed that participants at both sites reported very similar levels of experience of each unlearning type and also of the types of knowledge that were unlearnt. This was also the case for barriers to and enablers of unlearning. Similarly, consistent themes were identified for fading. These similarities suggest that the type of NHS trust did not influence the level of engagement in unlearning or the nature of what was unlearnt. However, it could also be argued that the relative similarity of these two trusts in terms of their organisational structures may also explain the consistency of findings. Consequently, as noted in the research agenda later in this chapter, further research is required to investigate individual unlearning in a wider variety of health-care settings to establish whether or not there are context-specific aspects to health-care managers' unlearning experiences.
Limitations of the study
Although this study makes some important contributions, it is subject to a number of limitations that should be kept in mind when considering the findings and conclusions. First, the exploratory nature of the study means that, although the findings provide a useful foundation for future research in specific aspects and impacts of unlearning, the study is limited in the depth of insight that it can provide in terms of specific aspects of unlearning processes and the extent to which they occur among health-care managers across different health-care settings.
Second, it is acknowledged that this is a relatively small-scale study involving a small number of participants drawn from two NHS trusts. The original plan for the study involved data collection at a third site in a primary care setting, but, unfortunately, recruitment of participants for the study was unsuccessful at this site (see Chapter 3, Recruitment at site C: primary care trust/clinical commissioning group). Consequently, the loss of the primary care site limited the degree of contextual influence that could be examined in the study and the findings are therefore limited with respect to their generalisability to health-care managers working in other health-care settings.
Third, we found the process of eliciting the details of the unlearning experience from participants to be challenging. During the interviews, participants would often begin by and return to talking about change processes rather than the specific types of knowledge and behaviours that they had given up or abandoned as a result of experiencing a change event or individual experience. We dealt with this challenge through careful probing and follow-up questions during the interviews and also by two or more members of the project team reviewing potentially ambiguous examples during the data analysis to achieve an agreed interpretation. However, it is possible that the distinction between change event comments and references to unlearning could have been interpreted differently.
Fourth, because of the relatively low numbers of participants in our study, the findings provide limited insights regarding the extent to which managers engage with processes of unlearning and the impact on their decision-making. This exploratory study does show the extent to which our study participants engaged with unlearning processes and suggests that further research would be valuable to assess wider levels of engagement by health-care managers in other health-care settings. Similarly, this study's findings are helpful as they indicate that there may well be a relationship between unlearning and health-care managers' decision-making processes; however, this relationship would also benefit from further research to fully understand the precise nature of the relationship. Acknowledging the limitations of this original exploratory study highlights a number of specific areas where further research would be valuable.
Fifth, the study was able to provide only limited insights into the nature of fading, although the empirical data do provide evidence that fading should not be conceptualised as a type of individual unlearning. The study participants had difficulty recalling examples of skills and knowledge that they had forgotten. A longitudinal data collection strategy may be more effective at capturing the process of forgetting, which was outside the scope of this study.
Research agenda
-
The investigation of a greater number of health-care managers' experiences of unlearning in a wider range of settings is necessary to establish the significance of health-care setting for individual unlearning experiences and provide greater generalisability to the findings of this study. In particular, extending this study to investigate the role of unlearning in the primary care sector in 2013–14 would be of value to explore health-care managers' unlearning experiences in relation to the significant structural and organisational change they will have recently experienced.
-
The findings of this study indicate that there is a relationship between individual unlearning and health-care managers' decision-making. However, the precise nature of this relationship requires further investigation. In addition, several of our participants found it challenging to identify changes in decision-making as a result of unlearning, probably because they did not consider this relationship at the time. A new study that asks health-care managers to identify and record episodes of unlearning over a 6-month period and after each episode to identify resultant changes in decision-making may be more effective for investigating this relationship.
-
The data suggest that change of one type or another (individual-level role change and organisational-level structural change) is a catalyst for unlearning, and also that (further) organisational-level change may result from people unlearning and learning. However, further research on both aspects of this relationship is necessary to more fully understand the dynamic interaction between change and unlearning. For example, one (untested) suggestion by Tsang and Zahra2 was that different types of organisational change event might result in different types of unlearning. Thus, in further investigating this topic it would be useful to be sensitive to both the specific type of change that precedes the unlearning episode and the type of unlearning that results from such changes.
-
For practitioners, further understanding of the character and dynamics of individual unlearning processes would be valuable. This understanding may help to identify likely causes of resistance to change and organisational structures and employers' actions that may (inadvertently) present barriers to unlearning and therefore barriers to achieving desired change. Recognising employees' attitudes to change will provide an indication of how receptive they are likely to be to new change events that require them to abandon previous knowledge or ways of working. Furthermore, a better understanding of the process of individual unlearning will also enable practitioners to have more realistic expectations regarding the impact of a change process, and the likely time required for new practices and procedures to become embedded.
In-depth qualitative research would be the most suitable to explore this complex phenomenon, in a range of contexts and environments. In particular, as the time between the catalyst for individual unlearning and changes in attitudes or behaviour may vary in duration, longitudinal studies that involve participants recording changes in their behaviour and attitudes in research diaries could be of particular value. This approach would also enable the study of inhibitors of and facilitators to individual unlearning and their relationship with the different stages of the unlearning process.
Implications for practice
As a result of our study we are able to offer three tentative implications for practice. However, when considering these suggestions the small data set and exploratory nature of this study should be kept in mind.
-
The individual unlearning experiences of our participants (in their view) led to improvements in some participants' decision-making processes. These improvements involved greater and more formalised information searching and gathering, critical appraisal of this information and a consideration of stakeholder views and perceptions of possible options. These changes are all in line with what is prescribed in the literature for adopting evidence-based management decision-making processes.
-
People may find it hard to distinguish between unlearning (abandoning/giving up established practices or ideas) and learning (the development of new practices or knowledge) as these processes typically occur virtually simultaneously. Training programmes designed to support change may need to actively acknowledge and address participants' abandonment of existing knowledge and behaviours as well as concentrating on explaining and delivering new knowledge and desired behaviours.
-
Individual unlearning can be triggered by change events or individual experiences and unlearning may lead to further change. The period of transition to new ways of working or thinking may stretch beyond initial change-related training. During this period managers could benefit from ongoing informal feedback, support, advice and role modelling from colleagues, managers and mentors to support both the individual's well-being and embed the new knowledge and/or behaviours. Individuals who experience unlearning may also generate new ideas and opportunities for further changes and possible improvements in their own ways of working or the functioning of their team or department.
Acknowledgements
We are particularly grateful to our research participants who gave up their time to participate in our study. We would also like to thank our key contacts at each of our case study sites for their efforts in helping the recruitment of research participants, the members of our steering group for their valuable advice and the HS&DR programme team for their prompt and helpful responses to our queries during the project.
This report presents independent research commissioned by the NIHR. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, NIHR, NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC), HS&DR programme or Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors or those of the NHS, NIHR, NETSCC, HS&DR programme or Department of Health. This project was funded by the NIHR HS&DR programme (project number 09/1002/34).
Contribution of authors
Dr Crispin Coombs (Senior Lecturer in Information Systems) led the study, participated in the fieldwork and analysis, contributed to the writing of the literature review, methods and conclusions and provided overall editorial support for the entire report.
Dr Donald Hislop (Senior Lecturer in Human Resource Management and Organisational Behaviour) participated in the fieldwork, led the writing of the literature review and discussion sections and provided input to the analysis.
Dr Julie Holland (Director of the Glendonbrook Centre for Enterprise Education) facilitated access to the case study sites and designed and delivered the workshops.
Dr Sara Bosley (Lecturer in Human Resource Management and Organisational Behaviour) was appointed as the project's research associate for the first 12 months of the study. Dr Bosley contributed to a number of areas including the literature review and methodology and discussion sections of the report. Dr Bosley also conducted the majority of the research interviews and developed the qualitative coding scheme for the analysis.
Dr Esmeranda Manful (Research Associate) was appointed as the project's research associate for the final 6 months of the study, following Dr Bosley's change in role. Dr Manful undertook and wrote the analysis sections of the report.
Disclaimer
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Burnes B. Kurt Lewin and complexity theories: back to the future. J Change Manag 2004;4:309-25. http://dx.doi.org/10.1080/1469701042000303811.
- Tsang E, Zahra S. Organizational unlearning. Hum Relat 2008;61:1435-62. http://dx.doi.org/10.1177/0018726708095710.
- Akgün A, Lynn G, Byrne J. Antecedents and consequences of unlearning in new product development teams. J Prod Innovat Manag 2006;23:73-88. http://dx.doi.org/10.1111/j.1540-5885.2005.00182.x.
- Tranfield D, Duberley J, Smith S, Musson G, Stokes P. Organisational learning – it's just routine. Manag Decis 2000;38:253-60. http://dx.doi.org/10.1108/00251740010326315.
- Shipton H. Confusion or cohesion? Towards a typology for organizational learning research. Int J Manag Rev 2006;8:233-52. http://dx.doi.org/10.1111/j.1468-2370.2006.00129.x.
- Rushmer R, Davies H. Unlearning in healthcare: nature, importance and painful lessons. Qual Saf Health Care 2004;13:10-5.
- Greener I. Decision making in a time of significant reform: managing in the NH. Admin Soc 2008;40:194-210. http://dx.doi.org/10.1177/0095399707312829.
- Baumard P, Starbuck W. Learning from failures: why it may not happen. Long Range Plann 2005;38:281-98. http://dx.doi.org/10.1016/j.lrp.2005.03.004.
- Becker K. Facilitating unlearning during implementation of new technology. J Organ Change Manag 2010;23:251-68. http://dx.doi.org/10.1108/09534811011049590.
- Becker K. Unlearning as a driver of sustainable change and innovation: three Australian case studies. Int J Technol Manag 2008;42:89-106. http://dx.doi.org/10.1504/IJTM.2008.018062.
- Degeling P, Maxwell S, Kennedy J, Coyle B. Medicine, management, and modernisation: a ‘danse macabre'. BMJ 2003;326:649-52. http://dx.doi.org/10.1136/bmj.326.7390.649.
- Nicolini D, Powell J, Conville P, Martinez-Solano L. Managing knowledge in the healthcare sector. Int J Manag Rev 2008;10:245-63. http://dx.doi.org/10.1111/j.1468-2370.2007.00219.x.
- Guven-Uslu P. Uses of performance metrics in clinical and managerial networks. Publ Money Manag 2006;26:95-100. http://dx.doi.org/10.1111/j.1467-9302.2006.00507.x.
- High quality care for all – NHS next stage review final report. London: Department of Health; 2008.
- Hartley J, Cassell C, Symon G. Essential guide to qualitative methods in organizational research. London: Sage; 2004.
- Berg B. Qualitative research methods for the social sciences. Boston, MA: Pearson; 2007.
- Coles M, Masters A. Retraining and long-term unemployment in a model of unlearning by not doing. Eur Econ Rev 2000;44:1801-22. http://dx.doi.org/10.1016/S0014-2921(99)00005-7.
- De Holan P, Phillips N. Remembrance of things past? The dynamics of organizational forgetting. Manag Sci 2004;50:1603-13.
- Kim DH. The link between individual and organizational learning. Sloan Manag Rev 1993;35:37-50. http://dx.doi.org/10.1016/B978-0-7506-9850-4.50006-3.
- Akgün A, Byrne J, Lynn G, Keskin H. Organizational unlearning as changes in beliefs and routines in organizations. J Organ Change Manag 2007;20:794-812. http://dx.doi.org/10.1108/09534810710831028.
- Williams R. Culture and society 1780–1959. London: Chatto and Windus; 1959.
- Conner JO. Learning to unlearn: how a service-learning project can help teacher candidates to reframe urban students. Teach Teach Educ 2010;26:1170-7. http://dx.doi.org/10.1016/j.tate.2010.02.001.
- Mavin S, Bryans P, Waring T. Unlearning gender blindness: new directions in management education. Manag Decis 2004;42:565-78. http://dx.doi.org/10.1108/00251740410522287.
- Casillas J, Acedo F, Barbero J. Learning, unlearning and internationalisation: evidence from the pre-export phase. Int J Inform Manag 2010;30:162-73. http://dx.doi.org/10.1016/j.ijinfomgt.2009.07.005.
- Cegarra-Navarro J, Dewhurst F. Linking shared organizational context and relational capital through unlearning: an initial empirical investigation in SMEs. Learn Organ 2006;13:49-62. http://dx.doi.org/10.1108/09696470610639121.
- Becker K, Hyland P, Acutt B. Considering unlearning in HRD practices: an Australian study. J Eur Indust Train 2006;30:608-21. http://dx.doi.org/10.1108/03090590610712278.
- Dean B. Learning from prescribing errors. Qual Saf Health Care 2002;11:258-60. http://dx.doi.org/10.1136/qhc.11.3.258.
- Srithika T, Bhattacharyya S. Facilitating organizational unlearning using appreciative inquiry as an intervention. Vikalpa 2009;34:67-7.
- Rebernic M, Sirec K. Fostering innovation by unlearning tacit knowledge. Kybernetes 2007;36:406-19. http://dx.doi.org/10.1108/03684920710747039.
- Cegarra-Navarro J, Wensley A, Sanchez-Polo M. An application of the hospital-in-the-home unlearning context. Soc Work Health Care 2010;49:895-918. http://dx.doi.org/10.1080/00981389.2010.506410.
- Fotaki M. Patient choice in healthcare in England and Sweden: quasi-market and back to market? A comparative analysis of failure in unlearning. Public Admin 2007;85:1059-75. http://dx.doi.org/10.1111/j.1467-9299.2007.00682.x.
- MacDonald G. Transformative unlearning: safety, discernment and communities of learning. Nurs Inq 2002;9:170-8. http://dx.doi.org/10.1046/j.1440-1800.2002.00150.x.
- Antonacopoulou E. Impact and scholarship: unlearning and practising to co-create actionable knowledge. Manag Learn 2009;40:421-30. http://dx.doi.org/10.1177/1350507609336708.
- Argyris C, Schön D. Organizational learning II: theory, method, and practice. Reading, MA: Addison-Wesley; 1996.
- Easterby-Smith M. Disciplines of organizational learning: contributions and critique. Hum Relat 1997;50:1085-113. http://dx.doi.org/10.1177/001872679705000903.
- Scarbrough H, Swan J. Explaining the diffusion of knowledge management. Br J Manag 2001;12:3-12. http://dx.doi.org/10.1111/1467-8551.00182.
- Cegarra-Navarro J, Moya B. Business performance management and unlearning process. Knowl Process Manag 2005;13:161-70.
- Cegarra-Navarro J, Sanchez-Polo M. Linking unlearning and relational capital through organizational relearning. Int J Hum Resour Dev Manag 2007;7:37-52.
- Cegarra-Navarro J, Eldridge S, Sanchez ALG. How an unlearning context can help managers overcome the negative effects of counter-knowledge. J Manag Organ 2012;18:231-46. http://dx.doi.org/10.5172/jmo.2012.18.2.231.
- Wong PSP, Cheung SO, Yiu RLY, Hardie M. The unlearning dimension of organizational learning in construction projects. Int J Proj Manag 2012;30:94-104. http://dx.doi.org/10.1016/j.ijproman.2011.04.001.
- Cegarra-Navarro J, Cepeda-Carrion G, Eldridge S. Balancing technology and physician–patient knowledge through an unlearning context. Int J Inform Manag 2011;31:420-7. http://dx.doi.org/10.1016/j.ijinfomgt.2010.12.006.
- Cegarra-Navarro J, Sánchez-Vidal ME, Cegarra-Leiva D. Balancing exploration and exploitation of knowledge through an unlearning context: an empirical investigation in SMEs. Manag Decis 2011;49:1099-119. http://dx.doi.org/10.1108/00251741111151163.
- Lee LT. The effects of challenge and hindrance stressors on unlearning and NPD success: the moderating role of team conflict. Afr J Bus Manag 2011;5:1843-56.
- Lee LT, Sukoco BM. Reflexivity, stress, and unlearning in the new product development team: the moderating effect of procedural justice. R Manag 2011;41:410-23. http://dx.doi.org/10.1111/j.1467-9310.2011.00645.x.
- Low PKC. Must we unlearn to learn well. Educ Res 2011;2:1801-9.
- Pighin M, Marzona A. Unlearning/relearning in processes of business information systems innovation. J Inform Organ Sci 2011;35:59-72.
- Zahra SA, Abdelgawad SG, Tsang EWK. Emerging multinationals venturing into developed economies: implications for learning, unlearning, and entrepreneurial capability. J Manag Inq 2011;20:323-30. http://dx.doi.org/10.1177/1056492611408266.
- Cegarra-Navarro J, Eldridge S, Martinez-Martinez A. Managing environmental knowledge through unlearning in Spanish hospitality companies. J Environ Psychol 2010;30:249-57. http://dx.doi.org/10.1016/j.jenvp.2009.11.009.
- Yildiz H, Fey C. Compatibility and unlearning in knowledge transfer in mergers and acquisitions. Scand J Manag 2010;26:448-56. http://dx.doi.org/10.1016/j.scaman.2010.09.010.
- Tsang E. Transferring knowledge to acquisition joint ventures: an organizational unlearning perspective. Manag Learn 2008;39:5-20. http://dx.doi.org/10.1177/1350507607085169.
- Akgün A, Byrne J, Lynn G, Keskin H. New product development in turbulent environments: impact of improvisation and unlearning on new product development. J Eng Tech Manag 2007;24:203-30. http://dx.doi.org/10.1016/j.jengtecman.2007.05.008.
- Rampersad H. Learning and unlearning in accordance with organizational change. Organ Dev J 2004;22:43-60.
- Sheaffer Z, Mano-Negrin R. Executives' orientations as indicators of crisis management policies and practices. J Manag Stud 2003;40:573-606. http://dx.doi.org/10.1111/1467-6486.00351.
- Sinkula J. Market-based success, organizational routines, and unlearning. J Bus Ind Market 2002;17:253-69. http://dx.doi.org/10.1108/08858620210431660.
- Schein E. Organizational culture and leadership. San Francisco, CA: Jossey Bass; 1985.
- Hayes J. The theory and practice of change management. Basingstoke: Palgrave; 2002.
- Lewin K, Cartwright Dorwin. Field theory in social science: selected theoretical papers. New York, NY: Harper Bros; 1951.
- Garud R, Dunbar R, Bartel C. Dealing with unusual experiences: a narrative perspective on organizational learning. Organ Sci 2011;22:587-60. http://dx.doi.org/10.1287/orsc.1100.0536.
- Foster RD. Resistance, justice, and commitment to change. Hum Resource Dev Q 2010;21:3-39. http://dx.doi.org/10.1002/hrdq.20035.
- Armenakis AA, Bedeian AG. Organizational change: a review of theory and research in the 1990s. J Manag 1999;25:293-315. http://dx.doi.org/10.1016/S0149-2063(99)00004-5.
- Dent EB, Goldberg SG. Challenging ‘resistance to change'. J Appl Behav Sci 1999;35:25-41. http://dx.doi.org/10.1177/0021886399351003.
- Coch L, French JRP. Overcoming resistance to change. Hum Relat 1948;1:512-32. http://dx.doi.org/10.1177/001872674800100408.
- Lawrence PR. How to deal with resistance to change. Harv Bus Rev 1954;32:49-57. http://dx.doi.org/10.1097/00043764-197005000-00027.
- Argyris C, Schön D. Organizational learning: a theory of action approach. Reading, MA: Addision Wesley; 1978.
- Kanter RM. Managing the human side of change. Manag Rev 1985;74:52-6.
- Klarner P, By RT, Diefenbach T. Employee emotions during organizational change – towards a new research agenda. Scand J Manag 2011;27:332-40. http://dx.doi.org/10.1016/j.scaman.2011.06.002.
- Scherer KR. What are emotions? And how can they be measured. Soc Sci Inform 2005;44:695-729. http://dx.doi.org/10.1177/0539018405058216.
- Avey JB, Wernsing TS, Luthans F. Can positive employees help positive organizational change? Impact of psychological capital and emotions on relevant attitudes and behaviors. J Appl Behav Sci 2008;44:48-70. http://dx.doi.org/10.1177/0021886307311470.
- Spiker B. Making change stick. Ind Week 1994;243.
- Staw BM, Barsade SG. Affect and managerial performance: a test of the sadder-but-wiser vs. happier-and-smarter hypotheses. Admin Sci Q 1993;38:304-31. http://dx.doi.org/10.2307/2393415.
- Piderit SK. Rethinking resistance and recognizing ambivalence: a multidimensional view of attitudes toward an organizational change. Acad Manag Rev 2000;25:783-94. http://dx.doi.org/10.2307/259206.
- Ford JD, Ford LW, D’Amelio A. Resistance to change: the rest of the story. Acad Manag Rev 2008;33:362-77. http://dx.doi.org/10.5465/AMR.2008.31193235.
- Fox S, Amichai-Hamburger Y. The power of emotional appeals in promoting organizational change programs. Acad Manag Exec 2001;15:84-9. http://dx.doi.org/10.5465/AME.2001.5897664.
- Smith CA, Lazarus RS. Appraisal components, core relational themes, and the emotions. Cognit Emot 1993;7:233-69. http://dx.doi.org/10.1080/02699939308409189.
- Paterson JM, Härtel CEJ. An integrated affective and cognitive model to explain employees' responses to downsizing. I. Managing Emotions in the Workplace n.d.
- Bakker AB, van Emmerik H, Euwema MC. Crossover of burnout and engagement in work teams. Work Occup 2006;33:464-89. http://dx.doi.org/10.1177/0730888406291310.
- Arnold J. Work psychology: understanding human behaviour in the workplace. Harlow: Pearson Education; 2005.
- Tetlock PE. The impact of accountability on judgment and choice: toward a social contingency model. Adv Exp Soc Psychol 1992;25:331-76. http://dx.doi.org/10.1016/S0065-2601(08)60287-7.
- Frisch D, Clemen RT. Beyond expected utility: rethinking behavioral decision research. Psychol Bull 1994;116. http://dx.doi.org/10.1037//0033-2909.116.1.46.
- Isen AM, Lewis M, Haviland JM. Handbook of emotions. New York, NY: Guilford Press; 1993.
- Nygren TE, Isen AM, Taylor PJ, Dulin J. The influence of positive affect on the decision rule in risk situations: focus on outcome (and especially avoidance of loss) rather than probability. Organ Behav Hum Decis Process 1996;66:59-72. http://dx.doi.org/10.1006/obhd.1996.0038.
- Baron J. Nonconsequentialist decisions. Behav Brain Sci 1994;17:1-10. http://dx.doi.org/10.1017/S0140525X0003301X.
- McCarthy AM, Schoorman FD, Cooper AC. Reinvestment decisions by entrepreneurs: rational decision-making or escalation of commitment. J Bus Vent 1993;8:9-24. http://dx.doi.org/10.1016/0883-9026(93)90008-S.
- Simonson I, Staw BM. Deescalation strategies: a comparison of techniques for reducing commitment to losing courses of action. J Appl Psychol 1992;77. http://dx.doi.org/10.1037//0021-9010.77.4.419.
- Tversky A, Kahneman D. Judgment under uncertainty: heuristics and biases. Science 1974;185:1124-31. http://dx.doi.org/10.1126/science.185.4157.1124.
- Briner RB, Denyer D, Rousseau DM. Evidence-based management: concept cleanup time. Acad Manag Perspect 2009;23:19-32. http://dx.doi.org/10.5465/AMP.2009.45590138.
- Reay T, Berta W, Kohn MK. What's the evidence on evidence-based management. Acad Manag Perspect 2009;23:5-18. http://dx.doi.org/10.5465/AMP.2009.45590137.
- Walshe K, Rundall TG. Evidence-based management: from theory to practice in health care. Milbank Q 2001;79:429-57. http://dx.doi.org/10.1111/1468-0009.00214.
- Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care 1998;7:149-58. http://dx.doi.org/10.1136/qshc.7.3.149.
- Swan J, Clarke A, Nicolini D, Powell J, Scarbrough H, Roginski C, et al. Evidence in Management Decisions (EMD) – Advancing Knowledge Utilization in Healthcare Management 2012.
- Nutt PC. Investigating the success of decision making processes. J Manag Stud 2008;45:425-55. http://dx.doi.org/10.1111/j.1467-6486.2007.00756.x.
- Dean JW, Sharfman MP. Does decision process matter? A study of strategic decision-making effectiveness. Acad Manag J 1996;39:368-92. http://dx.doi.org/10.2307/256784.
- Poole MS, Van de Ven AH. Handbook of organizational change and innovation. Oxford: Oxford University Press; 2004.
- Griffiths R. NHS management inquiry. London: HMSO; 1983.
- Davies P. The Griffiths report: 25 years on. Health Serv J 2009. www.hsj.co.uk/resource-centre/best-practice/the-griffiths-report-25-years-on/5001481.article (accessed 25 May 2012).
- Jeffreys B. NHS Changes: The Picture Now 2012. www.bbc.co.uk/news/health-16986808 (accessed 25 May 2012).
- Triggle N. Analysis: What Next for the NHS? 2012. www.bbc.co.uk/news/health-17448838 (accessed 25 May 2012).
- King N, Horrocks C. Interviews in qualitative research. London: Sage; 2009.
- Chell E, Cassell C, Symon G. Essential guide to qualitative methods in organizational research. London: Sage; 2004.
- Kemppainen J. The critical incident technique and nursing care quality research. J Adv Nurs 2000;32:1264-71. http://dx.doi.org/10.1046/j.1365-2648.2000.01597.x.
- Miles MB, Huberman AM. Qualitative data analysis: an expanded sourcebook. London: Sage Publications; 1994.
- Crilly T, Jashapara A, Ferlie E. Research Utilization and Knowledge Mobilisation: A Scoping Review of the Literature 2010.
Appendix 1 Protocol
Full title of project: The Role of Unlearning in Healthcare Managers' Decision Making
Proposed duration (in months): 18
Proposed start date: 01 Jan 2011
Aims and objectives
The overall research aim of this project is to empirically investigate the extent to which healthcare managers engage in processes of unlearning, and the barriers that exist to them doing so. This is important because it will improve our understanding of how managers make decisions and will help provide relevant support and training for those involved in running the health service.
In addressing this aim the following specific research questions will be investigated:
-
To what extent do healthcare managers engage with the process of unlearning and what impact does the engagement with this process have on healthcare manager decision making?
-
What are the barriers that prevent healthcare managers engaging with the process of unlearning?
-
To what extent does the healthcare setting (acute care, mental health care or primary care) affect the level of engagement with the process of unlearning by healthcare managers?
Link to SDO call on research utilisation and knowledge mobilisation by healthcare managers
This research proposal responds directly to the main primary research topic area ‘the contribution of “unlearning” in managers' use of research and other forms of knowledge’ in the SDO call on research utilisation and knowledge mobilisation by healthcare managers. It addresses the increasing interest in understanding the mechanisms that encourage or reduce the adoption of new interventions such as clinical research or management practice. Unlearning may impact on the extent to which knowledge is used or transferred by managers. Old knowledge may need to be unlearnt before new knowledge can be learnt and applied to management decision making. If healthcare managers fail to unlearn existing practice, this may act as a barrier to knowledge flow and implementation. This study will explore managers' use of research and existing knowledge and how this relates to managers' own decision making through analysis of the process of unlearning.
Background
The concept of unlearning (a deliberate process of reflection which results in ‘giving up’ some existing knowledge which is deemed to be outdated) is closely linked to processes of learning and change. Fundamentally, for change to occur unlearning must happen, as people need to acknowledge the limitations of existing knowledge/practice, be prepared to ‘give up’ such knowledge and adapt their knowledge/practice by actively learning and developing new ways of working/thinking. Thus, unlearning is arguably a necessary precursor to processes of learning (Akgünet al2007). Despite this, the concept of unlearning is under-utilised and poorly understood both in the general literature on learning and knowledge management (Hislop 2009), and also in the literature on learning in the health sector (Crillyet al2009, Rushmer & Davies 2004). This project will thus contribute to developing a greater understanding of this aspect of knowledge management and learning processes.
Rushmer & Davies (2004) argue that distinctions can be made between three separate types of unlearning which vary in a number of ways, most importantly their degree of significance. One type of unlearning they identify, which they label fading, refers to the slow gradual process of unlearning that can occur over time, where particular skills and capabilities are forgotten through a lack of usage. This form of unlearning is typically not experienced as being significant or challenging for people, and due to the gradual way it occurs, people may not be conscious they are experiencing it.
The second type of unlearning identified by Rushmer & Davies (2004) is labelled wiping. This represents a more significant, deliberate and conscious form of unlearning. Wiping is a form of unlearning focussed relatively narrowly on a particular practice, or activity, where a person consciously unlearns through making deliberate efforts to give up a particular way of thinking/acting, as a pre-cursor to changing these beliefs/practices. This process of unlearning may be initiated by some external catalyst, such as a change initiative, which places demands on people to change their ways of working and/or thinking. An example of wiping in a clinical-managerial context would be someone deliberately changing a work procedure for deciding how and when patients are to be discharged from hospital.
The third form of unlearning identified by Rushmer & Davies is deep unlearning. Deep unlearning represents a radical form of unlearning which typically occurs rapidly and unexpectedly, and is experienced by people as significant as it brings into question some basic assumptions and values. Due to these characteristics this form of unlearning can produce significant emotions (fear, confusion etc.) in the people who experience it. Typically, deep unlearning is initiated by some external catalyst, such as an event whose characteristics or outcomes are unexpected. An example of deep unlearning, gained from conversations with healthcare managers studying at Loughborough was a sudden change a manager made in the way they communicated with their staff when consulting about important ward management decisions. The person concerned switched from consultation by e-mail, to making a significantly greater use of face-to-face interactions when consulting people, after it was found that there were problems and discontent among clinical staff when they were consulted only by e-mail. A key difference between this example and the wiping example, was the speed at which the change was made, and the emotional impact associated with the experience, the manager describing the experience as being ‘burned’ due to the discontent that arose among her staff and the difficult atmosphere that ensued.
Thus, Rushmer & Davies' three types of unlearning can be distinguished from each other in a number of ways including their:
-
Level of significance, with fading having a low level of significance to people, and deep unlearning a high level of significance.
-
Scope, or breadth, with wiping and fading typically having a narrow scope, being limited to particular, specific skills or practices, whereas deep unlearning may have a broader scope, due to the questioning of basic assumptions and values it involves.
-
Speed, with fading happening relatively slowly and gradually, while deep unlearning typically happens rapidly.
-
Catalyst, with wiping being a deliberate and conscious process of unlearning (typically in response to some external change), whereas both fading and deep unlearning are instead initiated by unexpected external events or the lack of use of particular skills and capabilities.
-
Emotional impact/consequences, with fading being experiences as having a limited emotional impact, while deep unlearning can have a significant emotional impact for people.
One of the main aims of this research is to examine the extent to which healthcare managers undertake all three forms of unlearning (research question 1). A typical catalyst for all forms of unlearning are processes of change that require the adaptation of working practices (Tsang & Zahra 2008). The pace of change in the NHS in recent years has been significant. For example, Greener, (2008, p. 206), talked about how the ‘pace and scope of change’ was, ‘intense’. Tsang & Zahra (2008) suggest that different types of unlearning may be associated with particular forms of change, distinguishing between continuous and episodic change. With continuous change, which is small-scale, evolutionary and occurs on a day-to-day basis, unlearning is likely to take the form of wiping and fading. For episodic change (which is large-scale rapid change) unlearning is likely to take the form of deep unlearning. Thus, it is anticipated that due to the amount of ongoing change in the NHS, all healthcare managers are likely to have experiences of processes of wiping and fading, where they have had to adapt their work practices and routines as a result of change. Deep unlearning on the other hand may be experienced by healthcare managers who have undergone a significant role transition, such as would happen when a clinician moved into a managerial role. Thus, it is possible that processes of deep unlearning may be more evident in managers who have undergone such transitions.
A possible example of this process of deep unlearning generated by a significant role transition is the experience of change for a clinician moving into a clinical-management position, due to the challenges clinicians who have moved into management roles are likely to face. One challenge is the need to adapt the way they use knowledge to act and make decisions, as somewhat anecdotal evidence suggests that clinical and managerial decision-making processes are underpinned and supported by different knowledge bases. Thus, Crillyet al(2009, p. 145) argue that, ‘the professional and scientific culture of doctors stands in contrast with the world of managers. Doctors are aligned with the quantitative and positivistic nature of biomedical research where clinical decisions may be codified. Managers' decisions depend on pragmatism and subjectivity rather than research which is more often qualitative and in any case is perceived as contingent and not readily generalisable.’
Clinicians moving into managerial roles thus arguably need to engage in processes of unlearning to effectively adapt how they act and make decisions in the new managerial roles they occupy. Thus, it is anticipated that processes of deep unlearning are more likely to be experienced by managers who have undergone any type of significant role transition.
While we anticipate that clinical managers may be more likely than the non-clinical managers to experience deep unlearning, we will also look for evidence of deep unlearning in the interviews with all healthcare managers. As deep unlearning is triggered by unexpected external events it may be that healthcare managers have experienced it sometime in carrying out their work, despite not having made the type of disciplinary transition that clinical-managers have. The lack of research on the topic of unlearning means that there is a limited understanding of how frequently people experience it, or the type of events/circumstances that trigger it. Thus, examining all forms of unlearning with every interviewee allows comparisons to be made between clinical and non-clinical managers, and will also give insights into the extent to which both experience unlearning (research question 1).
This research is also concerned with understanding the barriers to unlearning that exist. While unlearning has the potential to be an important component in the processes of learning and change, research suggests that there are many barriers to unlearning, which means that learning from mistakes, failure and crisis often does not happen (Baumard & Starbuck 2005). Barriers to unlearning exist at both individual and team/organisational levels. The small amount of research on unlearning (Rushmer & Davies 2004) and learning from failure that has been done in the health sector suggests that this is a work context where the barriers to unlearning can be significant. Further, this research suggests that in such contexts both individual level barriers (concern about negative consequences/sanctions from admitting mistakes, and a preference for local/contextual knowledge) and organisational level barriers (a culture where admitting to mistakes isn't encouraged) can be causes of unlearning (Dean 2002) (research question 2). Through interviewing healthcare managers in three distinct organisational contexts (acute care, mental health care and primary care) we will investigate the extent to which organisational level barriers to unlearning are shaped by the work context (Research question 3).
The central focus of this project is on examining the extent to which the managers interviewed engage in processes of unlearning, and the individual and/or organisational level barriers which may be inhibiting effective unlearning and learning from occurring. Thus the focus of this project is distinctive from that of other SDO funded projects, which are more focussed on inter-personal processes (such as Swan's study of the ‘co-production’ of knowledge – SDO/244/2008, and Dopson's study on the motivation of health managers to use knowledge – SDO/242/2008).
This research will make a number of practical contributions to policy and practice in the NHS. Most fundamentally, it will advance knowledge on a neglected aspect of the processes of change and learning. By examining unlearning, and the barriers to achieving it that exist, the research can help develop a greater understanding of what may be an important barrier to change. In practical terms, this knowledge can be used to help facilitate processes of change and learning through addressing the barriers to unlearning that are identified. A second contribution to policy and practice in the NHS is that the research will shed light on some of the challenges to learning and decision-making faced by healthcare managers. This knowledge can thus be used to develop ways to better support healthcare managers. In terms of healthcare managers' decision making the findings of this study can be used to address the barriers to learning from mistakes and failure, thereby improving the learning process which should enable better decisions to be made in the future.
Need
This project meets and contributes to the needs of the NHS. Improving our understanding of how managers make decisions will help us provide relevant support and training for those involved in running the health service. Improving management performance will in turn lead to better delivery of services and ultimately improved patient care. The study has the potential to generate new knowledge in the area unlearning and will be of direct value to trust boards and those who provide training and support for NHS managers (e.g. HR departments, Institute of Innovation & Improvement and external training providers such as universities).
Existing research suggests that NHS managers with clinical and non-clinical backgrounds may have a different approach to issues such as accountability, use of guidelines and finance. It has been argued that these differences are a result of each discipline's training, beliefs and experiences (Degelinget al., 2003). Similarly, there is evidence to suggest that clinicians and managers have different priorities concerning healthcare delivery: clinicians tend to prioritise patient care whereas managers focus more on cost (Nicoliniet al., 2008). Research by Guven-Uslu (2006) suggests that these different mindsets influence how managers with a clinical background are likely to approach decision making compared to those without clinical experience. Given the increased emphasis that is being given to encouraging clinicians into leadership and managerial roles (Darzi, 2008) these different mindsets are likely to become increasingly more significant to the efficient running of the NHS. Clearly, both cost and high quality patient care are key considerations for healthcare delivery and getting the best balance between these two issues is important for the NHS especially in the current and likely future economic conditions. However, achieving this balance may be difficult for NHS trusts when their managers come from different backgrounds and may be influenced by their existing knowledge, training, beliefs and experiences on which they rely when making decisions.
For example, due to their structured evidence based clinical training, managers with a clinical background may find it difficult to challenge management practice because there is often no evidence based knowledge supported by hard data and publications to support their management decision making. Anecdotal evidence from our own medical management programme indicates that clinicians find management challenging because there is often no clearly defined management protocol to follow, compared to clinical practice which has a comprehensive evidence base. Discarding obsolete knowledge (unlearning) may be an alien concept to many clinicians who may consider hoarding explicit clinical knowledge as essential when dealing with the diagnosis and treatment of disease. The concept of doing things differently, particularly in a clinical setting, may be unfamiliar or frowned upon because of the unsafe consequences a poor medical decision can have. When this approach is applied to a management situation, organisational unlearning may be prevented.
Similarly, non-clinical managers may find the unlearning processes challenging when faced with, for example, resource and cost perspective issues. They may be instinctively resource led in their decision making and have a strong desire to improve the quality of data, or gather comparative data on which to make numerically based decisions. Without a direct involvement in patient care, this group may find it harder to develop a more ‘needs led’ approach to decision making.
This study will investigate the role of unlearning in healthcare managers' decision making. It will also explore the implications of unlearning for managerial decision making in the health service.
Methods
Context
To empirically investigate the unlearning undertaken by healthcare managers this project will utilise a multiple case study approach, investigating experiences of unlearning in three different types of NHS trust (an acute trust, a primary care trust and a mental health trust). Conducting research in these different organisational contexts allows analysis of the extent to which the organisational contexts affects unlearning (research question 3). The reason for choosing these three types of context is that they represent some of the most important and common organisational types that the managers being investigated work in. A case study based approach represents a suitable methodology for the investigation of unlearning because, as outlined, unlearning is a relatively neglected and unexplored aspect of learning and change processes, and qualitative case studies provide an effective way to conduct exploratory research which can give rich, qualitative insights into managers' experiences of unlearning (Berg 2004, Hartley 2004).
Expressions of interest have been received from The Harrogate and District NHS Foundation Trust, Derbyshire Mental Health Services NHS Trust and Leeds Primary Care Trust. We have also received expressions of interest from other trusts and we have included these in our contingency plans should one of our named trusts decide not to participate.
Data Collection
One-to-one semi-structured interviews
Within each organisation, the main source of data will be face-to-face, one-to-one semi-structured, qualitative interviews with a range of healthcare managers. The research is fundamentally concerned with how the managers being investigated experience and make sense of the need to unlearn and adapt their approaches to decision making. Qualitative, semi-structured interviews provide an appropriate method for the collection of data on this topic, as they allow interviewees to articulate their experiences in their own words, and provide a mechanism via which interviewees can respond to issues raised by researchers, as well as introducing and discussing new topics, issues and experiences that they deem appropriate (King & Horrocks 2009). Further, qualitative interviews have been used effectively for the investigation of unlearning in a number of contexts such as in response to international joint ventures (de Holan & Phillips 2004, Tsang 2008) and in response to organisational change initiatives (Tranfield et al. 2000).
Sampling
In each of the 3 case study Trusts 14 interviews will be conducted with healthcare managers (total n = 42) – see Table 1: The Sample. We envisage that healthcare managers that may have had to adapt their work practices and routines as a result of policy changes, responded to new research on clinical effectiveness or undergone a significant role transition, such as moving from a clinical to a managerial role are most likely to be found in middle management roles. Given the definitional issues surrounding the term ‘Middle Manager’ and different usage in different organisational structures, the actual selection will be informed by exploring these issues at each case study site. Interviewees will be purposively sampled and drawn in consultation with the Human Resources Directorates and key case study contacts with the aim of maximising variance, i.e. interviewees from a wide range of directorate and units occupying and variety of comparable roles across the three trusts. We will also sample interviewees with different levels of clinical background to ensure we have captured a full range of managers in all participating organisations.
| NHS Acute Trust | NHS Mental Health Trust | NHS Primary Care Trust |
|---|---|---|
| Middle Managers | Middle Managers | Middle Managers |
| One-to-one, face-to-face semi-structured interviews n = 42 | ||
| Healthcare managers n = 14 | Healthcare managers n = 14 | Healthcare managers n = 14 |
| e.g. Clinical Director, General Manager | e.g. Associate Director of Services, General Manager | e.g. Practice Performance Manager, Business Manager |
Each interview will last approximately one hour and will be tape recorded (with consent) and fully transcribed. Conducting interviews with both groups will make it possible to establish the typical values, knowledge and decision making criterion of managers, and also study the extent to which healthcare managers feel they need to unlearn and adapt the way they make decisions and the type of knowledge they draw on in carrying out their managerial responsibilities.
Interview technique
A critical incident technique will be used in these interviews. Critical incident interviews examine specific activities and incidents which interviewees experience as significant, which they have good recall of, and which they believe have particular, identifiable antecedents and consequences (Chell 2004). It is argued to be a useful technique for exploring events/processes which people may experience as significant and/or difficult (Kemppainen 2000). There are a number of reasons why critical incident interviews represent an appropriate interview method for examining people's experiences of unlearning. Firstly, it is a technique that has been used both in the healthcare context (Kemppainen 2000), and for the investigation of learning by entrepreneurs – see Cope & Watts 2000. Secondly, the literature suggests that the way people experience unlearning and especially deep unlearning, (the latter often being triggered quickly and unexpectedly due to particular events and is associated with intense emotional feelings); fits closely with what constitutes a critical incident (see Rushmer & Davies 2004).
All three types of unlearning will be investigated: fading (the gradual forgetting of skills/capabilities no longer required), wiping (deliberate efforts to unlearn specific belief and/or behaviours) and deep unlearning (sudden and unexpected unlearning which challenges deeply held beliefs and assumptions) in the interviews using the critical incident methodology. Each type of unlearning will be explored separately, and will be explained to interviewees via the use of a combination of layman's terms and relevant examples.
It is anticipated that managers will have experience of wiping and fading via the need to adapt behaviour in response to change initiatives. Thus, in exploring this type of unlearning interviewees will be asked to think about specific, recent change initiatives and any changes that they are individually required to implement. In terms of deep unlearning, interviewees will be asked to discuss and reflect upon specific decision making episodes that they experienced as difficult and which challenged some of their fundamental beliefs.
In examining the interviewee's experiences of unlearning use will be made of Kemppainen's (2000) three component approach, with questions being asked about firstly the circumstances and context of the incident being discussed, secondly, the specific details of how they experienced and remembered the incident being examined, and thirdly, their understanding of the consequences or outcomes resulting from the incident. For all interviews a briefing sheet would be provided to participants in advance of meeting face-to-face to try and prime recall of relevant specific incidents and collect basic demographic data. It is envisaged this briefing sheet would promote reflection and reduce the length of the interview. An indicative outline structure for the interviews is presented in Appendix 1.
Pilot interviews
Prior to the completion of the research interviews in the case study organisations, eight formative, exploratory interviews will be conducted, to test the research instrument. These interviewees will not be drawn from the case study organisations, and will be recruited from cohorts of healthcare managers who are studying part time in our department. The primary purpose of these interviews will be to test and refine the interview schedule, to ensure that unlearning is explained and illustrated in a way that is understandable to interviewees.
Analysis of data
As the project will generate a large volume of data in the form of interview transcripts to be analysed the analysis will follow the three concurrent activities identified by Miles & Huberman, (1994, p. 10) of data reduction, data display and conclusion drawing/verification. This approach is necessary to ensure that the researcher does not become overloaded from unreduced data transcripts and their information processing abilities impaired (Faust, 1982).
The analysis and coding of the data will be done both deductively and inductively. A deductive approach will be used to initially code the data using codes related to the research questions and concepts being examined (data reduction). Initial coding of the data will be done by the research assistant, but to ensure reliability of the data coding process, all three investigators will be independently code a selection of interview transcripts, with the RA and investigators then comparing their coding templates. The exploratory nature of the research also means that an element of inductive analysis is also appropriate, to allow unexpected findings to emerge from the data. Thus, the initial coding framework will be revised and adapted through a process of inductive analysis that will involve both the researcher and the three investigators. N'Vivo software will be used to facilitate the data coding process. The data will then be presented in a series of conceptually ordered displays (data display) in order to study the variables in more depth and generate more explanatory power. A thematic conceptual matrix will be developed for each case to study the manifestation of unlearning and learning and examine the facilitators and inhibitors directly related to the process of unlearning and learning.
Workshops
A key part of the projects methodology will to carry out feedback workshops with interviewees from participating organisations, where preliminary findings will be presented. Input from participants from these workshops will be used to review and discuss the practical implications of the findings. These insights will be used to provide further richness to the findings presented in the final reports to the SDO and participating organisations and in conference articles, and practitioner and academic publications.
Collective research effort – contribution to research utilisation
It is envisaged that the findings from this study will provide a number of important contributions. It will identify the importance of the process of unlearning for healthcare managers and the barriers to this process. These findings should provide insights and recommendations in terms of new issues to address for managers in terms of their awareness of their current decision making processes and how these could be improved. It should also provide useful information on the importance of unlearning that could be used to enhance and refine future management training courses for managers. Unlearning is likely to be a key precursor that needs to be successfully completed before managers are able to improve their use of knowledge and may influence their motivations to use knowledge and evidence in decision-making. Therefore the findings of this study will also complement and enhance the understanding of management decision making in the NHS that is being developed from current SDO projects (e.g. Swan's study of the ‘co-production’ of knowledge – SDO/244/2008, and Dopson's study of the factors which influence the motivation of health managers to use knowledge – SDO/242/2008).
After reporting to the SDO, initial dissemination of findings must be to the people best placed to use them. Firstly, we plan to share our findings with participants, senior managers and the boards of each participating NHS Trust. This will take the form of two stages. Once data analysis is complete, we will share our finding in a workshop format allowing participants to feedback on our findings and discuss their practical applications and implications. Once this stage is complete, a summary report will be made available to the participating NHS trusts.
Once the research findings have been shared with the participating NHS trusts we will then disseminate the findings in two domains. Firstly, the findings will be disseminated to a practitioner-oriented audience, both through presenting articles at relevant conferences (such as the annual Institute of Healthcare Managers conference), and also publishing articles and papers in practitioner-oriented journals (such as the Health Service Journal).
Secondly, we will disseminate the findings of our research to the academic community through presenting articles at conferences and also publishing articles in a range of relevant journals. The extent to which the concept of unlearning is neglected and under-utilised means that there is scope to make a potentially significant contribution to knowledge. The focus of our research means that the findings are relevant to a number of different academic domains, including healthcare, knowledge management, and business/management. Thus, we will present research data, and publish articles in all three domains. Examples of relevant conferences we will present our findings at include the British Association of Medical Managers Conference, the Organisational Learning, Knowledge and Capabilities conference, and the British Academy of Management conference. Examples of relevant journals we will target publications at include the Journal of Health Services Research and Policy, Health Services Management Research and the Journal of Knowledge Management.
Following the Darzi Report (2008), shifting managerial power and control of resource allocation back to clinical professionals is being encouraged in the health service. As a result, management training programmes run by the NHS and a growing number of universities must accommodate the training needs of healthcare managers. Changing the decision making processes of NHS managers will be challenging and will be best addressed by management training, coaching and mentoring. If the findings of our study show that unlearning is an important precursor to learning, we will incorporate this insight into our healthcare management training programmes at Loughborough University. This will enable us to have an immediate direct impact on NHS managers' decision making in the NHS. Understanding how healthcare managers unlearn could influence significantly the future style and content of management training programmes. We will therefore disseminate our findings to internal NHS training providers (e.g. Institute of Innovation & Improvement) and relevant universities.
Plan of investigation and timeline
Table 2 provides a detailed summary of the project plan of investigation and also indicates when the progress reports of the project will be available. It is anticipated that the start date of the project should give sufficient time to advertise and recruit a research associate so that they will be in post for the start of the project. In addition to the details provided below, there will be monthly project team meetings and more frequent supervisory meeting with the research associate.
Approval by Ethics Committees
We will gain informed consent from our research subjects. They will be guaranteed individual anonymity in terms of not being individually identified in written material and confidentiality in that interview transcripts will only be viewed by the research team and will be held in a secure and anonymised form. More generally, data will be held in accordance with the Data Protection Act. It will be necessary to apply for NHS Research Ethical Committee (REC) approval and subsequently to obtain Honorary Contracts to enable researchers to interview in the case study sites. Following consultation with RECs associated with participating trusts, we have confirmed that approval is needed from one REC only. We will therefore submit our proposal to Trent Research Ethics Committee (Appointing Authority – East Midlands Strategic Health Authority).
Project management
Coombs will take overall responsibility for the management of study, with support from Hislop and Holland. Coombs has experience in undertaking healthcare management research projects using multi-site case studies and managing research associates. Hislop will provide the project with subject area expertise, project management support for Coombs and will manage the data collection and analysis. Holland will manage the liaison with NHS trusts, contribute to the data analysis and facilitate the workshops. In addition a research associate will be appointed for the project term who will be responsible for the data collection, analysis and drafting the final report. Coombs, Hislop and Holland will be involved in the pilot interviews and at least the first two interviews of the main study with each case study trust. The presence of two interviewers for these interviews will ensure the validity of the interview schedule and rigour in data collection. All members of the research team will contribute to the overall dissemination of the project's findings as described in Section 0. The project team will have meetings every month to monitor progress and will have additional regular supervisory meetings with the research associate.
Service users/public involvement
As this study is specifically focused on the role of unlearning in NHS managers' decision making, and having reviewed the INVOLVE documentation, we do not anticipate that service users or the public will be able to usefully contribute to the study's research objectives. Consequently, we do not propose to include service users or the public in this study.
Expertise and justification of support required
The members of the team that will undertake the study bring a complementary range of skills and expertise to the project. Coombs and Hislop are both experienced researchers having conducted several qualitative research studies. Coombs has an established track record of healthcare research having held Department of Health, DTI, ESRC and Society of Radiographers grants and previously worked for the NHS Modernisation Agency Clinical Governance Support Team as a researcher. Hislop has been researching and writing on the topic of knowledge management for the last decade and has published academic work on unlearning. Hislop has strong experience of research project management having held grants from the British Academy, EPSRC, ESRC and White Rose Trust. Holland, is an expert in work-based learning, knowledge management and management education for clinical staff, and has recently been instrumental in developing and delivering the University's MSc in Medical Management which is aimed at clinicians working as clinical managers within the health service. Holland has previously studied learning and its effect on job control and decision making and the role of daily learning for problem solving in SMEs and has held grants from the East Midlands Development Agency. Previously, Holland was Director of the East Midlands NHS Innovation Hub, the knowledge transfer management and commercialisation office for primary and secondary care NHS trusts and therefore also provides expert knowledge of practical healthcare management issues and key NHS contacts to the project.
FIGURE 1.
Flow diagram for project.
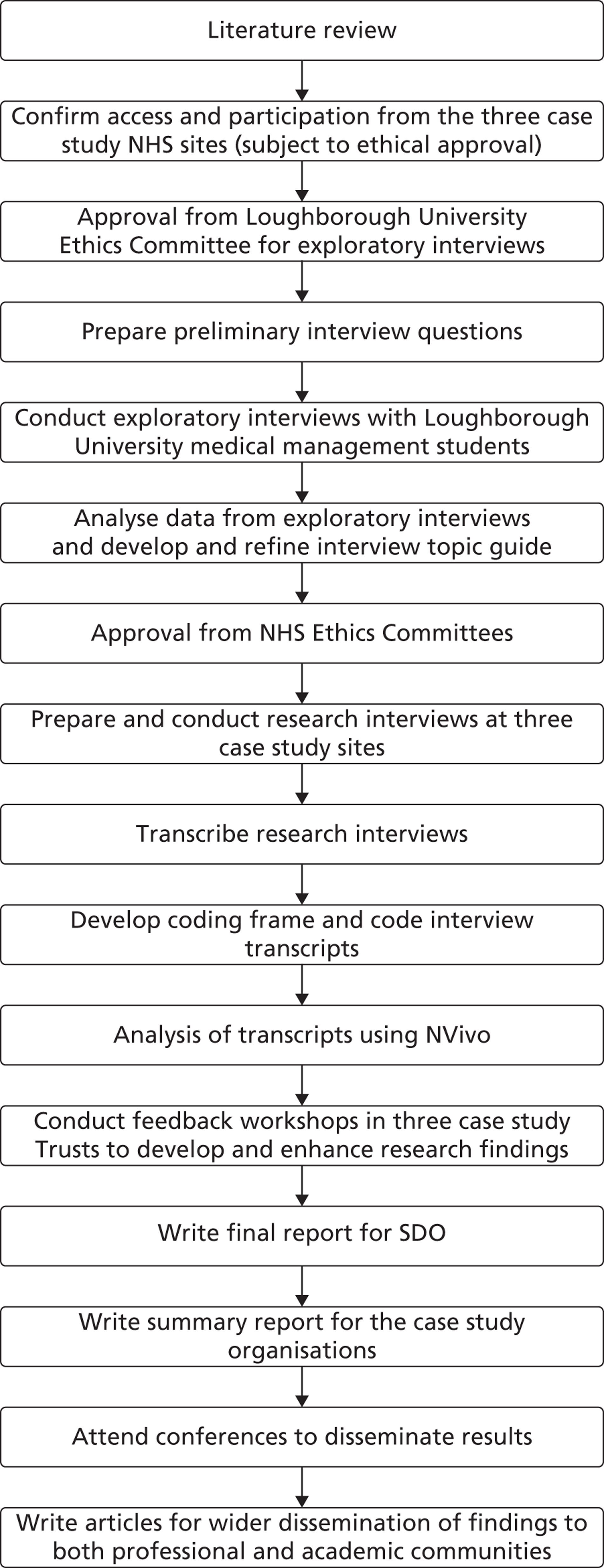
Recent relevant publications for Coombs, Chief Investigator
- Coombs C.R., Arnold J., Loan Clarke J., Bosley S., Martin C. “Allied Health Professionals' Intention to Work for the NHS: A Study of Stayers, Leavers and Returners'”,. Health Services Management Research n.d.
- Coombs C.R., Arnold J., Loan Clarke J., Wilkinson A.J., Park J., Preston D. Improving the Recruitment and Return of Nurses and Allied Health Professionals: A Quantitative Study. Health Services Management Research 2007;20:22-36.
- Arnold J., Loan Clarke J., Coombs C.R., Wilkinson A.J., Park J., Preston D. How well can the Theory of Planned Behavior Account for Occupational Intentions?. Journal of Vocational Behavior 2006;69:374-90.
- Coombs C.R., Park J.R., Loan Clarke J., Arnold J., Preston D., Wilkinson A.J. Perceptions of Radiography and the National Health Service: A Qualitative Study. Radiography 2003;9:109-22.
- Park J.R., Coombs C.R., Wilkinson A.J., Loan Clarke J., Arnold J., Preston D. Attractiveness of Physiotherapy in the National Health Service as a Career Choice: Qualitative Study. Physiotherapy 2003;89:575-83.
- Arnold J., Coombs C.R., Wilkinson A.J., Loan Clarke J., Park J., Preston D. Corporate Images of the United Kingdom National Health Service: Implications for the Recruitment and Retention of Nursing and Allied Profession Staff. Corporate Reputation Review 2003;6:223-38.
References
- Akgün A., Byrne J., Lynn G., Keskin H. Organizational Unlearning as Changes in Beliefs and Routines in Organizations. Journal of Organizational Change Management 2007;20:794-812.
- Baumard P., Starbuck W. Learning from Failures: Why it May Not Happen. Long Range Planning 2005;38:281-98.
- Berg B. Qualitative research methods for the social sciences. Boston, Mass: Pearson; 2007.
- Chell E., Cassell, Symon. Essential Guide to Qualitative Methods in Organizational Research. Sage; 2004.
- Cope J., Watts G. Learning by Doing – An Exploration of Experience, Critical Incidents and Reflection in Entrepreneurial Learning. International Journal of Entrepreneurial Behaviour and Research 2000;6:104-2.
- Crilly, Jashapara, Ferlie. Research Utilization and Knowledge Mobilisation: A Scoping Study. SDO; 2009.
- De Holan P., Phillips N. Remembrance of Things Past? The Dynamics of Organizational Forgetting. Management Science 2004;50:1603-1.
- Dean B. Learning from Prescribing Errors. Quality and Safety in Healthcare 2002;11:258-60.
- Degeling P., Maxwell S., Kennedy J., Coyle B. Medicine, management, and modernisation: a “danse macabre”?. BMJ 2003;326:649-52.
- Faust D. A needed component in prescriptions for science: Empirical knowledge of human cognitive limitations. Knowledge: Creation, Diffusion, Utilisation 1982;3:555-70.
- Greener I. Decision Making in a Time of Significant Reform: Managing in the NHS. Administration and Society 2008;40:194-210.
- Guven-Uslu P. Uses of Performance Metrics in Clinical and Managerial Networks. Public Money and Management 2006;95.
- Hartley J., Cassell C., Symon G. Essential Guide to Qualitative Methods in Organizational Research. London: Sage; 2004.
- Hislop D. Knowledge Management in Organizations: A Critical Introduction. Oxford University Press; 2009.
- Kemppainen J. The Critical Incident Technique and Nursing Care Quality Research. Journal of Advanced Nursing 2000;32:1264-71.
- King N., Horrocks C. Interviews in Qualitative Research. London: Sage; 2009.
- Miles M.B., Huberman A.M. Qualitative Data Analysis: An Expanded Sourcebook. London: Sage Publications; 1994.
- Nicolini D., Powell J., Conville P., Martinez-Solano L. Managing Knowledge in the Healthcare Sector. A Review. International Journal of Management Reviews 2008;10:245-63.
- High Quality Care For All – NHS Next Stage Review Final Report. 2008.
- Rushmer R., Davies H. Unlearning in Healthcare: Nature, Importance and Painful Lessons. Quality and Safety in Healthcare 2004;13:10-5.
- Tranfield D., Duberley J., Smith S., Musson G., Stokes P. Organisational Learning – It's Just Routine!. Management Decision 2000;38:253-60.
- Tsang E. Transferring Knowledge to Acquisition Joint Ventures: An organizational Unlearning Perspective. Management Learning 2008;39:5-20.
- Tsang E., Zahra S. Organizational Unlearning. Human Relations 2008;61:1435-62.
Appendix 1 Outline interview schedule
PRE-INTERVIEW BRIEFING SHEET
Explanation of purpose of interview & research
Non-technical description of unlearning supported by examples of each type of unlearning
Preliminary Questions
-
Age
-
Gender
-
Job title
-
Length of time in current role
INTERVIEW SCHEDULE
Contextual Details On Interviewees
-
Work/career history
-
Disciplinary background/training
-
Self-label/identity
-
How long had managerial responsibilities
-
Extent to which had formal training in management
-
Description of normal decision making process for routine decisions
Contextual Details on Work Environment
-
Size and characteristics of hospital/trust worked
-
Size and characteristics of immediate work context – department
-
Character of work done in department
Critical Incident Element
-
Experiences of need for unlearning/change in decision making processes/behaviours
-
Use the below question structure to explore and examine each of three models of unlearning separately with interviewees. Explain each mode of unlearning via use of relevant illustrations/examples.
-
Circumstances
-
Describe context/cause/catalyst to decision making process being described
-
Why was a decision necessary?
-
Why were you responsible for making this decision?
-
Who else was involved in making this decision?
-
Describe issue requiring decision – complexity, how many people involved/affected . . . .
-
-
Process of Decision Making
-
Why was the decision easy/difficult?
-
What emotions were experienced by you and did they affect your decision making?
-
Process undertaken in making decision
-
What sources of knowledge consulted (if any)?
-
What people consulted (if any)?
-
-
Outcomes
-
What were the consequences of the decision making event for you – change beliefs/behaviours? (significantly?)
-
What were the consequences of the decision making event for others?
-
What was the consequence of the decision making event for your organisation?
-
Appendix 2 Steering group terms of reference
The Role of Unlearning in Healthcare Managers' Decision Making Steering Group Terms of Reference
Author: Dr Sara Bosley, Research Associate, The School of Business and Economics, Loughborough University.
Date: 14 June 2011
Version number: Version 2 agreed
Purpose
This document describes the terms of reference, membership and methods of communication for the Steering Group for the research project, ‘The Role of Unlearning in Healthcare Managers' Decision making’.
Background
The aim of the research project is to empirically investigate the extent to which healthcare managers engage in processes of unlearning, the barriers that prevent and the enablers that promote their engagement in unlearning.
The concept of unlearning (a deliberate process of reflection which results in ‘giving up’ some existing knowledge) is closely linked to processes of learning and change. For change to occur unlearning must happen, as people need to acknowledge the limitations of existing knowledge/practice, be prepared to ‘give up’ such knowledge and adapt their knowledge/practice by actively learning and developing new ways of working/thinking.
This topic is important because it will improve our understanding of how managers make decisions and will help provide relevant support and training for those involved in running the health service.
The project will address the following specific research questions:
-
To what extent do healthcare managers engage with the process of unlearning and what impact does the engagement with this process have on healthcare manager decision making?
-
What are the barriers that prevent healthcare managers engaging with the process of unlearning?
-
To what extent does the healthcare setting (acute care, mental health care or primary care) affect the level of engagement with the process of unlearning by healthcare managers?
Terms of Reference
-
To comment and advise on the progress of the project.
-
To comment and advise on the research process, early findings and draft reports.
-
To ensure that the research team adheres to the research protocol.
-
To consider any new information of relevance to the research question.
-
To suggest relevant literature.
-
To provide detailed comment on any extension requests or substantial changes to protocol.
Membership
Chair: John Loan-Clarke (Senior Lecturer, School of Business and Economics, Loughborough University)
| Anne Lawson, Director of Governance | Harrogate and District NHS Foundation Trust |
| Professor Kate Robinson, Non-executive Director of Milton Keynes Hospital NHS Foundation Trust and University of Bedfordshire | Milton Keynes Hospital NHS Foundation Trust |
| Dr Rosemary Rushmer, Senior Lecturer in Knowledge Exchange and Organisational Learning in Public Policy and Health | School of Medicine and Health, Wolfson Research Institution |
| Tina Worth, Patient Safety Lead | Milton Keynes Hospital NHS Foundation Trust |
| Research Team members from the School of Business and Economics, Loughborough University: | |
|---|---|
| Dr Crispin Coombs, Principal Investigator | |
| Dr Donald Hislop, Co-investigator | |
| Dr Julie Holland, Co-investigator | |
| Dr Sara Bosley, Research Associate | |
Meetings
Three meetings will be held over the course of the project. These will be scheduled to proceed the timing of reports submitted to the NIHR SDO i.e. in June 2011, December 2011 and June 2012. The precise dates and timing of the meetings will be agreed between the research team and Steering Group members. Meetings will take place in the School of Business and Economics at Loughborough University.
Communications
Communications between meetings will be conducted by e-mail. To reduce the burdens on Steering Group members, such communications will be kept to a minimum and mainly comprise documentation and reports sent to members prior to Steering Group meetings. On occasion, additional advice on specific issues will be sought from members between meetings.
Appendix 3 Briefing sheet
The Role of Unlearning in Healthcare Managers' Decision Making
This project runs for 18 months and is funded by the National Institute for Health Research Service and Delivery Organisation. The Chief Investigator on the project is Dr Crispin Coombs, and Co-Investigators are Dr Donald Hislop and Dr Julie Holland, and the Research Associate is Dr Sara Bosley. The project is based in Loughborough University's School of Business and Economics.
Aims and objectives
The overall research aim of this project is to empirically investigate the extent to which healthcare managers engage in processes of unlearning, the barriers that prevent and the enablers that promote their engagement in unlearning. This topic is important because it will improve our understanding of how managers make decisions and will help provide relevant support and training for those involved in running the health service.
In addressing this aim the following specific research questions will be investigated:
-
To what extent do healthcare managers engage with the process of unlearning and what impact does the engagement with this process have on healthcare manager decision making?
-
What are the barriers that prevent healthcare managers engaging with the process of unlearning?
-
What are the enablers that promote healthcare managers' engagement with unlearning?
-
To what extent does the healthcare setting (acute care, mental health care or primary care) affect the level of engagement with the process of unlearning by healthcare managers?
Background
The concept of unlearning (a deliberate process of reflection which results in ‘giving up’ some existing knowledge deemed to be out-dated) is closely linked to processes of learning and change. Fundamentally, for change to occur unlearning must happen, as people need to acknowledge the limitations of existing knowledge/practice, be prepared to ‘give up’ such knowledge and adapt their knowledge/practice by actively learning and developing new ways of working/thinking. Thus, unlearning is arguably a necessary precursor to processes of learning (Akgünet al2007). Despite this, the concept of unlearning is under-utilised and poorly understood, both in the general literature on learning and knowledge management (Hislop, 2009), and also in the literature on learning in the health sector (Crillyet al2009; Rushmer & Davies 2004). This project will thus contribute to developing a greater understanding of this aspect of knowledge management and learning processes.
This research is also concerned with understanding the barriers to unlearning that exist. While unlearning has the potential to be an important component in the processes of learning and change, research suggests that there are many barriers to unlearning, which means that learning from mistakes, failure and crisis often does not happen (Baumard & Starbuck 2005). Barriers to unlearning exist at both individual and team/organisational levels. The small amount of research on unlearning (Rushmer & Davies 2004) and learning from failure that has been done in the health sector suggests that this is a work context where the barriers to unlearning can be significant. Further, this research suggests that in such contexts both individual level barriers (concern about negative consequences/sanctions from admitting mistakes, and a preference for local/contextual knowledge) and organisational level barriers (a culture where admitting to mistakes isn't encouraged) can be causes of unlearning (Dean, 2002).
However, the heath-care literature suggests that individual factors and contextual features may enable unlearning. To some extent enablers mirror barriers. For example, having an open culture, identifying root causes of errors and establishing systems that provide feedback to those involved in errors (Dean, 2002). More specifically an organisation may need to develop an ‘unlearning context’ (Cegarra-Navarroet al2010) which enables individuals to examine their perception and interpretation of situations, to change routines and to consolidate emergent understanding. In order to do this, individuals need the capacity to reflect on new ways of acting, to tolerate embarrassment, risk and threats to status (Rushmer & Davies, 2004).
Research Method
To empirically investigate the unlearning undertaken by healthcare managers this project will utilise a multiple case study approach, investigating experiences of unlearning in three different types of NHS trust (an acute trust, a primary care trust/Clinical Commissioning Group and a mental health trust). Conducting research in these different organisational contexts allows analysis of the extent to which the organisational contexts affects unlearning (research question 4). The reason for choosing these three types of context is that they represent some of the most important and common organisational types that the managers being investigated work in. A case study based approach represents a suitable methodology for the investigation of unlearning because, as outlined, unlearning is a relatively neglected and unexplored aspect of learning and change processes, and qualitative case studies provide an effective way to conduct exploratory research which can give rich, qualitative insights into managers' experiences of unlearning (Berg 2007; Hartley 2004).
Within each organisation, the main source of data will be face-to-face, one-to-one semi-structured, qualitative interviews with a range of healthcare managers. In each of the 3 case study Trusts 14 interviews will be conducted with healthcare managers. The research is fundamentally concerned with how the managers being investigated experience and make sense of the need to unlearn and adapt their approaches to decision making. Qualitative, semi-structured interviews provide an appropriate method for the collection of data on this topic, as they allow interviewees to articulate their experiences in their own words, and provide a mechanism via which interviewees can respond to issues raised by researchers, as well as introducing and discussing new topics, issues and experiences that they deem appropriate (King & Horrocks, 2009).
Case studies
At each case study site, the research team will recruit a sample of middle managers who vary in terms of clinical/background, type of department/unit and length of time as a manager.
To be included participants need to:
-
be middle managers. We expect the sample to comprise mainly Agenda for Change grade 7/8 staff, along GPs involved in the shadow Clinical Commissioning Group;
-
have some managerial responsibilities that involve making decisions about the use and allocation of resources, including staff and/or finances, data collection and management, service delivery etc.
-
be able to identify and be willing to talk about their experiences of unlearning; and
-
be willing to complete the pre-interview questionnaire, participate in an interview of approximately one hour in length and to give informed, written consent.
The research team will work with Human Resource Managers (HRMs) to identify the most appropriate group of managers to invite to participate in the project and the most effective way of engaging and recruiting them. The proposed recruitment process is as follows, but is open to discussion with HRMs:
-
The researcher, Sara Bosley, will provide HRMs with an invitation and a Participant Information Sheet to be sent by e-mail to potential participants.
-
If they are happy to do so, HR staff will send the e-mail and Participant Information Sheet to potential participants. They may also be requested to send a reminder if the initial e-mail generates limited interest.
-
Those managers who are interested will be invited to reply to Sara Bosley by e-mail or phone.
-
Sara will provide them with more information about the project and respond to any questions.
-
Managers who volunteer to take part will be invited to complete a pre-interview questionnaire giving their current job title, employing organisation, clinical background and previous job titles. They will be invited to return the questionnaire as an e-mail attachment (password protected if they wish) before the interview and to give e-mail consent about the use of the data they provide in the questionnaire. They may return their completed questionnaire by post or at the interview, should they wish to do so.
-
An interview date, time and venue will be agreed between the researcher and participant. We anticipate conducting the interviews at the participants' place of work unless they choose an alternative venue.
-
The researcher will send to participants the main interview questions, examples of unlearning and a consent form before the interview.
-
Before the interview starts, participants will have an opportunity to ask more questions and will be invited to sign the consent form.
After the interview, participants will be offered a copy of the interview transcript. They will be invited to attend a workshop in the spring of 2012 to hear about initial findings and to comment on those findings. However, taking part in the interview does not commit them to attending a workshop. Participants and case study contacts will be sent a summary of the final report and a web link to the full report.
References
- Akgün A., Byrne J., Lynn G., Keskin H. Organisational Unlearning as Changes in Beliefs and Routines in Organisations. Journal of Organisational Change Management 2007;20:794-812.
- Baumard P., Starbuck W. Learning from Failures: Why it May Not Happen. Long Range Planning 2005;38:281-98.
- Berg B. Qualitative research methods for the social sciences. Boston, Mass: Pearson; 2007.
- Cegarra-Navarro J-G., Wensley A.K.P., Sanchez-Polo M-T. An application of the Hospital in- the-home unlearning context. Social Work in Health Care 2010;29:895-918.
- Crilly T., Jashapara A., Ferlie E. Research Utilisation & Knowledge Mobilisation: A scoping review. London: HMSO; 2010.
- Dean B. Learning from Prescribing Errors. Quality and Safety in Healthcare 2002;11:258-60.
- Hartley J., Cassell C., Symon G. Essential Guide to Qualitative Methods in Organisational Research. London: Sage; 2004.
- Hislop D. Knowledge Management in Organisations: A Critical Introduction. Oxford University Press; 2009.
- King N., Horrocks C. Interviews in Qualitative Research. London: Sage; 2009.
- Rushmer R., Davies H. Unlearning in Healthcare: Nature, Importance and Painful Lessons. Quality and Safety in Healthcare 2004;13:10-5.
Appendix 4 Letter of invitation
Project title: Healthcare managers' decision making
Dear Healthcare Manager
I am writing to invite you to take part in a research study exploring healthcare managers' experiences of abandoning established ways of thinking and acting (unlearning), and how this affects their decision making. The study will help us better understand the processes of change, learning and decision making. We will use this knowledge to make suggestions about how healthcare managers can be better supported.
We are approaching you because of your position as a manager within one of the Trusts that has agreed to be a case site study. Taking part will involve completing a short pre-interview questionnaire and being interviewed for about one hour. In the interview we will ask you about:
-
Your work context
-
Your job role and responsibilities
-
Occasions when you abandoned some aspect or aspects of the way you act and think
-
Skills and knowledge that you once used but no longer use
Please read the attached Participant Information Sheet and then contact the researcher, Sara Bosley, if you are interested. Expressing an interest does not commit you to taking part. You can reach Sara by email on s.l.c.bosley@lboro.ac.uk or by phone on 01509 223177. Sara will tell you more about the study and answer any questions you may have. You can then decide if you would like to be considered for inclusion in the study.
Best wishes
Dr Crispin Coombs
Chief Investigator
Appendix 5 Participant information sheet
Healthcare Managers' Decision Making
We would like to invite you to take part in our research study. Before you decide, we would like you to understand why the research is being done and what taking part would mean for you. One of our team will go through the information sheet with you and answer any questions you have.
What is the purpose of the study?
We are exploring healthcare managers' experiences of abandoning established ways of thinking and acting (unlearning), and how this affects their decision making. You may have had such experiences when you have adapted to changes in the health service or in your role, or as a result of moving between Trusts. We are also interested in the barriers that limit the process of abandoning established ways of thinking and acting, and the enablers that promote engagement with this process.
We are undertaking this study to help us better understand the processes of change, learning and decision making. We will use this knowledge to make suggestions about how healthcare managers can be better supported.
Why have I been invited?
We are approaching you because of your position as a manager within one of the Trusts we have identified as case study sites. We are looking for: middle managers (probably on Agenda for Change grade 7) and GPs involved in a shadow GP consortium who have some managerial responsibilities that involve making decisions about the use and coordination of resources including staff and/or finances. Human Resource Staff in your NHS Trust have advised us that you meet our criteria. To participate, you will also need to have some experience of unlearning and be willing to talk about your experiences. We will interview 14 managers from this Trust/GP consortium, and 14 from each of the other two case study sites we have selected. We would like to include managers with different backgrounds and from different departments and units. In the unlikely event of attracting too many managers with a similar background and/or from the same department, we may not be able to include you. If this is the case, we will let you.
Do I have to take part?
It is up to you to decide to join the study. The research team will explain the study and you will have an opportunity to ask questions before you make a decision.
If you agree to take part, we will invite you to sign a consent form. You will be free to withdraw at any time, without giving a reason. If you withdraw from the study, we will seek your permission to use the data collected up to the time of your withdrawal.
What will happen if I take part?
We will invite you to take part in an interview. Before the interview, we will send you a short questionnaire, a list of the main questions we will ask you and examples of the types of experiences we would like you to tell us about.
The interview will start with a few questions about your immediate work context, your job and your managerial responsibilities. I will then ask you to talk about two occasions since you have been a since when you abandoned some aspect of the way you think and act. And finally, I will ask you about any skills or knowledge that you once used in your daily life but no longer use.
The interview will last for approximately one hour and be conducted at your workplace, unless you choose an alternative venue. Interviews will be held between July and December 2011. The time and date of the interview will be agreed between you and the researcher, Sara Bosley.
Your interview will (with your consent) be digitally recorded and transcribed. The research team will analyse the data by identifying themes in your responses and those of other participants. We will look for different types of unlearning, the impact of giving up established ways of thinking and acting, what makes it difficult and what makes it easier to give up established ways of thinking and acting.
You will also be invited to attend a workshop in spring 2012 to hear about our preliminary findings, to comment on them and to suggest practical implications for healthcare managers and their training.
Expenses and payment
We are unable to pay you and we hope that you will not incur any expenses. However, we will give your Trust £141 as an acknowledgment of the time commitment of your participation in the study.
What do I have to do?
If you are interested in taking part, please email the researcher, Dr Sara Bosley (s.l.c.bosley@lboro.ac.uk). Sara will then phone or email you (according to your preference) to explain the project and answer any questions you may have. If you decide to take part and give initial consent by email, she will arrange a mutually convenient place and time to conduct the interview. She will also send you:
-
a short pre-interview questionnaire
-
a consent form, which we will invite you to sign on the day of the interview
-
a list of the main questions we would like to ask you in the interview
-
some examples of abandoning established ways of thinking and acting to help you identify some of your own experiences that you would be willing to discuss with us.
What are the possible disadvantages of taking part?
You will need to spend a short time preparing for the interview by completing the pre-interview questionnaire and thinking about the experiences you would like to talk about at the interview. The interview itself will take approximately an hour. You will also be invited to attend a workshop in spring 2012. The workshop will be held within your Trust and last for about 2 hours. You do not need to attend this workshop, but we would value your input at this stage.
We don't think there are any other disadvantages, although some people feel emotional when they talk about change and their experiences of giving up established ways of thinking and acting. If you are affected in this way, the researcher will handle the discussion sensitively and give you an opportunity to have a break or to end the interview if you wish. If you need further support after the interview, you can contact the counselling service identified at the end of this information sheet.
What are the possible benefits of taking part?
The interview will give you an opportunity to reflect on your learning, your management practices and the way you make decisions. Taking part in the workshop will give you an opportunity to comment on our research findings and the implications for healthcare managers' training.
Will my taking part in the study be kept confidential?
Yes. All information collected about you during the course of the research will be kept strictly confidential and in compliance with the Data Protection Act.
We will only collect data about you directly from you. We will do this by inviting you to complete a short pre-interview questionnaire and by interviewing you. In the unlikely event of you losing capacity after completing the pre-interview questionnaire or during the interview, the data that we have collected up to that point will be destroyed and not used in the study.
The recordings and transcripts of your interview will stored using an identification number, and not under your name or specific job title. Paper copies of your interview data and your personal data (name and contact details) will be stored securely in a locked filing cabinet accessible only by members of the research team. Your personal data will be stored separately from your interview data. All electronic data will be stored on password protected computers accessible only by the research team. Personal data will be retained for up to 3 years and interview data for 10 years, after which it will be destroyed.
Transcribers who are not directly employed by the university will be required to sign a confidentiality agreement. Recordings will be password protected and transferred between the researcher and the transcriber using secure mail. Transcripts will be returned by the transcriber as password protected electronic files. The transcriber will not have access to any of your personal data. You may have a copy of the transcript of your interview and comment on it if you wish.
You will not be identifiable in any reports and articles that result from our study. If we need to refer to your job role, we will use generic terms not your actual job title.
What if there is a problem?
If you have a concern about any aspect of this study, please speak to the researcher, Dr Sara Bosley, tel: 01509 223176; email: s.l.c.bosley@lboro.ac.uk or the Principal Investigator, Dr Crispin Coombs, tel: 01509 228835; email: c.r.coombs@lboro.ac.uk. They will be happy to respond to your questions.
If you remain unhappy and wish to complain formally, you can do this by contacting, Loughborough University's Research Policy Officer, Zoe Stockdale, tel: 01509 222423; email: z.c.stockdale@lboro.ac.uk.
What will happen to the results of the research study?
We will write a report for the funder, the National Institute for Health Research, Service and Delivery Organisation. We will send a summary of this report and the weblink to the full report to the case study sites and to you individually. We will share findings more widely by writing articles for academic and practitioner journals and by attending conferences.
Who is organising and funding the research?
The research is being organised and sponsored by Loughborough University and funded by The National Institute for Health Research, Service and Delivery Organisation.
Who has reviewed the study?
All research in the NHS is looked at by independent group of people, called a Research Ethics Committee, to protect your interests. This study has been reviewed and given favourable opinion by ______________Research Ethics Committee.
Further information and contact details
-
For information about this research project, please contact:
Dr Sara Bosley, Research Associate: 01509 223176; email: s.l.c.bosley@lboro.ac.uk or Dr Crispin Coombs, Chief Investigator, tel: 01509 228835; email: c.r.coombs@lboro.ac.uk. You can also find out more by looking at The National Institute for Health Research, Service and Delivery Organisation's website: www.sdo.nihr.ac.uk/projdetails.php?ref=09-1002-34#
-
For counselling and support, please contact [to be complete with guidance from each of the case study sites].
Thank you for reading this information
Appendix 6 Interview topic guide
Interview Schedule Healthcare managers' decision making
Instructions and prompts for the interviewer are in italics.
Introduction: check participant has received and read project information. Go through the information sheet and answer questions. Talk through consent form, and gain permission to record. Ask participant to sign the consent form. If the interviewee has completed a pre-interview questionnaire, refer to this to prompt responses to Q2.
Introduction
Thank you for agreeing to be interviewed for this study. In our discussion today, I would like us to focus on four topics. First, I'd like to ask you some questions about your job and your managerial responsibilities. Next, I'd like to ask you about your immediate work context. Then I will ask you to identify and describe two occasions while you have been a manager when you abandoned some aspect of the way you think and act. Finally, I will ask you if you can identify any skill or knowledge that you once used in your daily life but no longer use.
-
First, some questions about your job role and your managerial responsibilities
-
Please describe your current job role(s) and responsibilities.
Approximately what proportion of your time do you spend on your managerial responsibilities (as opposed to clinical responsibilities)?
What sorts of decisions are you responsible for? Eg budgets, line managing staff, planning, information/data selection and editing.
How (if at all) have recent changes (eg govt policy, restructuring, efficiency/cost savings) affected your role?
-
What (if any) had formal management training have you undertaken?
Explore the type, length, level of training; the provider; and interviewees' perception of usefulness of training.
-
Which aspects of your work do you most identify with?
How would you describe yourself professionally?
-
-
Now, some questions about your immediate work context
-
Please tell me about the size of the department/team/practice you are responsible for? (eg number of beds, patients, staff, budget)
-
How would you describe the work of your department/immediate work context?
How (if at all) have recent changes (eg govt policy, restructuring, efficiency/cost savings) affected your department/the Trust?
-
-
Next I am going ask you to identify an occasion in your time as a manager when you abandoned some aspect or aspects of the way you act and think. I am interested in an experience that came about because of an (external), planned change such as a new initiative ( procedure ) or a new system.
Please can you think of a situation that made you stop and think or a situation when you hit a brick wall or had to do things differently or set aside previous learning.
-
a. Please describe the event that led to you giving up (or setting aside) some aspects of the way you think and act.
What happened? Who was involved? How did you feel?
-
b. What were the circumstances leading up to this event?
What was the context? What was the catalyst or trigger?
-
c. What did you think? What did you do? How was this different from your usual way of thinking and acting? What unlearning did this involve? What did you stop doing or thinking? What decisions did you have to make?
-
d. How challenging was this situation for you? How did you feel? How do you think your emotional responses affected your approach to this situation?
-
e. What/Who helped you to give up the way you usually think and act?
Explore internal (attitudes, previous experiences) and external (culture, role of other staff and managers)
-
f. What/who made it difficult to give up the way you usually think and act?
Explore internal (attitudes, fears) and external (culture, role of other staff and managers)
-
g. How did giving up particular ways of thinking and acting affect you?
(What were the benefits?
What were the risks?)
-
h. In what ways do you think this experience affected your decision making as a healthcare manager?
Eg used different sources of information; gave different weighting to different sources of evidence/information; more independent/collective decisions.
-
i. How did this experience affect other people?
Consider the affect on clinical and managerial staff, patients and others, and whether or not they abandoned some aspects of the way they think and act.
-
j. How did this experience affect your organisation/the NHS?
How did the organisation benefit from your experience? How (if at all) were you able to share the lessons of this experience?
(What risks did the organisation incur as a result of this experience?)
-
-
Now, I would like you to describe another type of experience which led you to quite suddenly abandon some aspect of aspects of the way you act and think. I am interested in a specific incident or experience that had a significant impact on the way you feel and on your values and beliefs. I am going to ask you similar questions to those I asked about the experience you have just described.
Repeat the same series of questions as above.
-
To finish, I would like to ask you about skills or knowledge that you once used, but no longer use.
-
What skill or type of knowledge have you used in the past but you no longer use?
-
What are the main reasons that you no longer use this skill or knowledge?
(How did you come to lose /give up this skill/knowledge)
-
What (if any) skills or knowledge do you use its place?
-
In terms of your decision making, what is the effect of no longer using this skill or knowledge?
-
Is there anything else that you would like to say about your experiences of abandoning established ways of acting and thinking?
Thank the participant.
Check that she/he is OK and pass on information about support/counselling services if necessary.
Ask if she/he would like a transcript.
Explain what happens next and how the information will be used.
Appendix 7 Examples of unlearning
Examples of abandoning established ways of acting and thinking
Healthcare managers' decision making
We are interested in finding out about your experiences of abandoning established ways of thinking and acting. You may have such experiences when you adapted to new situations, roles, locations or systems or when you gained new information. Changing jobs or responsibilities, moving between employers, trusts or partnerships, or experiencing restructuring or new policy priorities may have led you to abandon particular ways of thinking and acting.
We think that there are three different types of abandoning established ways of thinking and acting. The first involves deliberately giving up a particular activity or way of doing something. This may happen gradually as you learn or as you are required to do things differently. Abandoning an activity or way of doing things usually happens because of an external, planned event or change, or new knowledge. Changes such as the introduction of a new initiative, system, procedure or evidence may result in you giving up a particular way of doing things.
The second type of abandoning happens suddenly and unexpectedly, and as a result of an external, unpredicted event or incident. It affects not just what you do and the way you do it but also the way you think and what matters to you. A serious untoward incident, for example, may affect your assumptions and beliefs. Because of this, such experiences may be quite emotional.
A third type is when you forget or no longer use a particular skill or piece of knowledge through lack of use. This may happen as you adapt to new technology or when you change roles, for example. You may not be very conscious of the process at the time, but on reflection realise that you have given up a particular way of doing things or lost a skill.
In the interview, we will ask you to identify and describe occasions when you experienced these different types of abandoning. The following examples will help you do this.
Abandoning an activity or way of doing things
A new procedure for deciding how and when patients are discharged is introduced into your hospital by senior managers. In order to implement the new procedure effectively, you decide to delegate the oversight of the discharge process to a more junior member.
Pressure from the Government and patient demand require you to change current practice of the prescribing anti-depressants and decide how your PCT or Practice-based Commissioning Group can cost-effectively provide other options such as talking therapies and prescriptions for exercise.
Abandoning beliefs and ways of thinking
Having previously worked solely as a clinician, your role changes so that you are required to spend 50% of your time on managerial tasks. You are expected to make quick management decisions (e.g. about finance or human resources), with limited information about the implications of your decisions and little empirical evidence about likely outcomes. These decisions challenge your beliefs about risk and uncertainty.
The death of a patient in the surgery waiting room shocks and disturbs staff and other patients. The event requires an investigation which has to be handled very sensitively and involves you in reassessing your assumptions about how patient share information with reception staff, your staff's ability to handle difficult situations and the practice's approach to onsite risk and safety.
Abandoning skills or knowledge through lack of use
The introduction of computers means that many of you are less skilled at writing manually or at spelling.
New electronic systems may mean that you make less use of informal personal contacts to find information or organise treatments, and make more use of online sources and systems. As a consequence you may forget how you previously went about doing these things before the technology was available.
Identifying your own experiences of unlearning
Clinical events may result in unlearning approaches to managerial decision making. When you are thinking about your own experiences of unlearning, please focus on managerial, rather than clinical decisions even if your unlearning was triggered by a clinical event.
Appendix 8 Participant consent form
Case study site number:
Study number: 09/1002/34
Participant Id number:
CONSENT FORM
Please read this form carefully and ask the researcher if you have any questions. Then initial each box and then sign and date the form. You have the right to change your mind at any time, including after you have signed this form.
Title of Project:
The Role of Unlearning in Healthcare managers' decision making
| Name of Researchers: Sara Bosley, Crispin Coombs, Donald Hislop and Julie Holland | Please initial box |
|---|---|
| 1. I have read and understand the information sheet (version 3) dated 27-07-11 for the above study. I have had the opportunity to consider the information, ask questions and I have had these answered satisfactorily. | □ |
| 2. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving any reason. | □ |
| 3. I agree to take part in the above study. | □ |
| 4. I am willing for my interview to be digitally recorded. | □ |
| 5. I am willing for what I say to be used in reports and articles written as a result of this study, provided it is not linked to me in anyway. | □ |
| ____________________ | ____________ | _____________________ |
| Name of Participant | Date | Signature |
| ____________________ | ____________ | _____________________ |
| Researcher | Date | Signature |
Appendix 9 Pre-interview questionnaire
The Role of Unlearning in Healthcare managers' decision making
Introduction
Thank you for agreeing to be interviewed for our research project. During the interview we will ask you about your job, your managerial responsibilities and your experiences of abandoning established ways of thinking and acting. We are sending another document with this questionnaire that gives examples of the types of experiences we are interested in discussing with you at the interview. Please read these examples and use them to help you to identify some experiences of your own that you can speak about at the interview.
For more information about the research, please refer to the participant information sheet and the interview schedule. If you would like to discuss the research with a member of the team, please contact Sara Bosley (Research Associate) at s.l.c.bosley@lboro.ac.uk; tel 01509 223176.
It would be very helpful if you could complete the following questionnaire and return to us before your interview. This information will provide us with some background information about you and save time in the interview itself. Information about returning the questionnaire is given at the end. We will not use your name or contact details in our study and we will anonymise all the information you give us. By returning this questionnaire you are giving us consent to use the information you provide in this study.
Part one: Name and contact information
| Name | |
| Job title(s) | |
| If you have two jobs, please give both | |
| Agenda for Change band or other | |
| Employing organisation | |
| Eg NHS Trust/PCT/GP Consortia/GP partnership | |
| Work phone number | |
| Work email address | |
| Date |
Part Two: Academic and Professional Qualifications
| 1) Do you hold a degree? | Yes/No |
| Please insert delete as appropriate | |
| 2) If you answered Yes, what was the subject of your first degree? | |
| 3) Please list the titles of any other degrees and professional qualifications you hold and the date when you gained this qualification. | |
| Qualification | Date |
|---|---|
Part Three: Current Job Role and Career
4) What are your main responsibilities in your current job?
5) What other jobs have you done?
Please record the titles and approximate dates of any substantial jobs have had in the table overleaf. You do not have to list all the jobs you have done or give a full CV.
| Job title | Dates |
|---|---|
Please save this with your name as part of the document title and return it to s.l.c.bosley@lboro.ac.uk or by post to Sara Bosley, Research Associate, School of Business and Economics, Loughborough University, Loughborough, Leicestershire LE11 3TU. If you wish to password-protect your questionnaire before emailing it, please let Sara know your password in a separate email or by phone (01509 223176). If you prefer not to send the questionnaire in advance of the interview, please give it to the researcher on day of the interview. Thank you for your assistance.
List of abbreviations
- CCG
- clinical commissioning group
- CSO
- clinical studies officer
- GP
- general practitioner
- HS&DR
- Health Services and Delivery Research
- NIHR
- National Institute for Health Research
- PCRN
- primary care research network
- PCT
- primary care trust
- PIS
- participant information sheet
- SIDS
- sudden infant death syndrome
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.