
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1002/14. The contractual start date was in October 2010. The final report began editorial review in December 2012 and was accepted for publication in May 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2013. This work was produced by Salway et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background and rationale
Although the volume of enquiry into the mobilisation and utilisation of research evidence within the health sector is growing rapidly, there remain important gaps in our understanding about which strategies work to encourage greater and more appropriate use of research evidence and how and why specific approaches might work. In particular, our understanding of knowledge utilisation processes within the policy context is far weaker than our understanding of knowledge utilisation processes within the clinical practice environment. 1 The current project responded to this gap in understanding by exploring the health-care commissioning cycle – an increasingly powerful determinant of the health services on offer and the care that patients receive – and by explicitly focusing on an area that has so far been overlooked, namely the mobilisation and utilisation of evidence relating to ethnic diversity and inequality.
The study’s broader goal was to support the commissioning of health services that better meet the needs of black and minority ethnic (BME) people and thereby help reduce ethnic inequalities in health-care access, experiences and health outcomes.
The project was novel and ambitious in bringing together three complex and contested areas of investigation: ethnicity, evidence use and commissioning. We found no previous studies that had sought to engage in detail with this particular focus, but instead drew on a wide range of related literature that explores particular aspects of this arena.
Ethnic diversity and inequality in health and health care
England has long been recognised as a multiethnic society and the diversity of the population is growing rapidly both in terms of the range of ethnic identities represented and the proportion of the population who identify as other than white British (around 20% of the total population in the 2011 census2). Ethnicity is a complex and contested ‘biosocial’ concept, a form of group identity that draws on notions of shared origins or ancestry, but which commonly invokes aspects of sociopolitical hierarchy as well as cultural commonality and shared biological features. 3 Ethnic identity influences the health of individuals and groups through a variety of mechanisms including direct and indirect discrimination; differential access to health-promoting resources; cultural practices; migration; and some genetic or biological factors. 4 Not surprisingly, therefore, mortality and morbidity patterns across ethnic groups are complex. Nevertheless, substantial evidence indicates that minority ethnic groups suffer disadvantage across a range of indicators. 4,5 Furthermore, a large body of evidence documents lower satisfaction with health services among minority groups than among the white British majority6,7 as well as poorer access,8–10 poorer quality of care and worse outcomes in several areas of service provision. 11–13 Inaccessible services, unmet need, poor patient–provider communication, inappropriate diagnoses and treatment, and negative service experiences remain common. 14,15 Therefore, rather than mitigating the disadvantages that many minority ethnic people experience in wider society, health services may often make things worse.
Despite a significant volume of national policy and guidance over many years, as well as several focused initiatives, progress towards health-care services that effectively meet ethnically diverse needs has been disappointing. 16 The Commission for Equality and Human Rights’ [previously the Commission for Racial Equality (CRE)] formal investigation into the Department of Health (DH), and Nigel Crisp’s 10-point action plan response,17 highlighted the need for significant improvement in this area.
Earlier research has sought to illuminate the factors operating at organisational and individual level that support or hamper progress towards cultural competence within health-care organisations. Several studies highlight the way in which education and training programmes designed to address gaps in professional knowledge require wider, systems-based approaches to achieve desired shifts in practice. Kripalani et al. 18 notes the importance of clear support from senior staff in terms of signifying priority and modelling desired behaviour; Yamada and Brekke19 identify the need for attention to organisational factors influencing practice; and Shapiro et al. 20 suggest that practice-based learning and models of good practice are needed alongside training courses. These findings point to the embedded nature of practitioner assumptions and behaviours and the need to challenge ‘tacit knowledge’ through new learning that is context specific, has a link to action and is informed by experience. 21 Other research highlights the significance of systems in the development of culturally relevant interventions and the importance of practitioner self-awareness. 19
Analyses that situate the formulation of health-care policy and practice within the wider sociocultural context of contemporary Britain are also helpful. It has been argued that UK policy relating to ethnic diversity lacks coherence and suggests at best ambivalence towards minority ethnic groups and uncertainty regarding the form that multicultural Britain should take. 22,23 Atkin and Chattoo24 argue that strategies for addressing disadvantage in health-care provision are undermined as providers and managers struggle to reconcile conflicting messages regarding minority ethnic populations and their needs and entitlements. It is increasingly argued that progress towards more culturally competent health services requires practitioners and organisations to examine value bases; expose stereotypes, prejudices and ethnocentrism; challenge power relationships and oppressive practices; and work in true partnership. 25 It is noteworthy, however, that, although such models often emphasise the importance of community consultation and local intelligence data, they are commonly silent on the role of other types of evidence, including research evidence. Similarly, recent policy documents and initiatives aimed at supporting commissioners and managers to address ethnic diversity and inequality pay little attention to how research and other types of evidence might be mobilised and utilised in this endeavour (see, for example, materials from Race for Health26,27).
Evidence use in health-care policy and practice
The study’s premise was that progress towards better services for minority ethnic populations is, at least in part, hampered by limited and inappropriate evidence use. Better use of research evidence alongside other types of evidence and knowledge should help to overcome persistent shortcomings in the design and delivery of health care for our ethnically diverse population. However, there is a need to understand more about the current patterns of evidence use, the barriers to and supports for the mobilisation and utilisation of evidence of different types, and how the critical and effective use of evidence might be enhanced.
The growing body of studies exploring knowledge mobilisation and utilisation within the health policy-making arena, some with an explicit focus on health inequalities, provided some useful insights to inform our enquiry. Much of this work draws on broader theoretical perspectives that view policy-making as a process of collective interaction between diverse stakeholders, in which both the identification of, and responses to, problems are viewed as socially situated and constructed. 28–30 These contributions highlight the distinctive nature of evidence utilisation in policy formation (at both strategic and service design levels) compared with the clinical practice context. 1,31 Kelly and Swann32 note the way in which evidence syntheses within public health can offer only ‘scientifically plausible frameworks for action’ (p. 270) and not prescriptions for specific intervention, as decision-making requires judgements based on knowledge of local context, including prevailing practices, organisational structures and commitment and engagement of key actors. Similarly, Elliot and Popay’s33 investigation of evidence use by NHS managers revealed that research was felt to offer clarity and to contribute to decision-making, but rarely to provide simple, clear-cut answers. Other work confirms that health-care policy-makers work with a ‘mixed economy’ of evidence, piecing together information from diverse sources in their decision-making. 1,34
Blackman et al. 35 look particularly at policy-making related to health inequalities and identify this area as a ‘wicked problem’ that cuts across traditional organisational boundaries and whose complexity limits the scope of evidence-based action. ‘Wicked problems’ tend to carry with them greater scope for debate around what should be done and how it should be achieved and more room for disagreement on what counts as robust and relevant evidence. They suggest that policy-making in relation to ‘wicked problems’ tends to be less a technical exercise and more a process of dialogue and argument with power relationships clearly in evidence. Exworthy et al. 36 highlight similar factors that may complicate the knowledge-into-action process relating to the health inequalities agenda, including the multiplicity of agencies and the diffuse nature of responsibility. Although this past research exploring the utilisation of evidence within the health inequalities context is an important backdrop to the present study, there is a need for enquiry that specifically focuses on ethnic diversity and inequality. Mir and Tovey’s37 study begins to explore these issues and shows that whether managers act on research and other knowledge is shaped by resources, organisational culture and particularly the absence of substantial disincentives. However, there is a need for further systematic study, particularly because of the significant additional issues that arise in terms of the generation and application of a research evidence base in this area.
Past work has highlighted some of the current inadequacies in availability of evidence relating to ethnicity and health. The poor collection, analysis and reporting of service-level ethnic monitoring data has been identified as a particular impediment to action for several decades,38,39 although there has been recent notable progress in some service areas. 40 A lack of evidence about specific ways in which practice guidelines should be modified to improve health outcomes for minority ethnic populations19,41 and omission of these populations from studies of evidence-based treatments42 have been highlighted. The lack of evidence on the efficacy and cost-effectiveness of cultural competence interventions may result in these being seen as an extra burden, particularly in the context of staff shortages and financial restrictions. 43 The need for better mobilisation of evidence to improve understanding of the links between ethnicity and health among health-care managers and practitioners has also been repeatedly highlighted. 44 As the volume of research on ethnicity and health expands, so too do concerns regarding quality, its potential role in stereotyping and stigmatising ethnic minorities, and its limited benefit to minority ethnic populations. 45 Critically appraising and applying research evidence on ethnicity and health presents significant challenges and demands particular competencies. 3 Issues include the need to interrogate conceptualisations of ethnicity that erroneously present ethnic ‘groups’ as stable or discrete entities and/or fail to address its multifaceted nature; question whether research adequately addresses the concerns of minority ethnic people; recognise the limited analytical potential offered by crude administrative ethnic categorisation; and carefully consider how evidence can best be synthesised across contexts when concepts and categorisations vary widely. 46,47 Clearly, then, there are some significant challenges relating to both the quantity and quality of available evidence that are likely to impact importantly on how managers access and apply evidence relating to ethnic diversity and inequality. To date, these have not been explored in any detail.
Related work in the broad area of health inequalities highlights a number of factors related to the characteristics of research evidence and research products that have relevance to the focus of the present study. Exworthy et al. 36 suggest that the multifactorial nature of inequalities, the paucity of evidence of effective interventions and the need for upstream and long-term investments all complicate the knowledge-into-action cycle in health inequalities policy. Pettigrew et al. 1 found that policy-makers charged with the health inequalities agenda commonly perceive the lack of locally relevant evidence and evidence on the distributional effects of interventions to be problematic. More generally, Greenhalgh et al.’s48 major review of innovation diffusion in health-care organisations identifies a number of key attributes of successful innovation that are rarely applicable to the evidence base on ethnic diversity and inequality, including evidence of clear benefits and cost-effectiveness, low complexity, ease of adaptation and low risk or uncertainty. Indeed, utilisation of the research evidence relating to ethnic diversity and inequality is likely to be compromised by the predominance of grey literature, the lack of evaluative studies, the lack of studies that consider the distributional effects of interventions by ethnicity and the lack of consideration of ethnicity within influential evidence syntheses [e.g. Cochrane reviews, National Institute for Health and Care Excellence (NICE) guidance]. 19
Notwithstanding weaknesses in the evidence base that need to be filled, there is nevertheless a substantial body of evidence of the scale and nature of the health disadvantage suffered by BME groups, as well as evidence that identifies generic ways in which health services could be modified to better meet the needs of minority ethnic patients (such as the provision of adequate interpretation facilities and enhanced cultural competence among health-care providers). 49,50 Furthermore, in some service/disease areas the quality of the research evidence base could lend itself to more specific, instrumental use by commissioners in pursuit of improved outcomes for minority ethnic groups, such as evidence-based diabetes interventions. 51 However, although a growing number of studies seek to identify factors that shape whether research evidence impacts on policy or practice,30,52 to date none has specifically engaged with the issue of ethnic diversity and inequality. More needs to be understood regarding the factors that support or inhibit the use of evidence in this context, including how evidence is presented and conveyed to decision-makers; what is regarded as evidence or knowledge; how the quality and relevance of evidence is assessed; when evidence is regarded as necessary; how easily evidence of different types can be accessed, appraised, synthesised and adapted to the local context; and how decision-making is achieved in the face of significant evidence gaps.
Commissioning
The term ‘commissioning’ is peculiar to the UK health system, with terms such as ‘strategic purchasing’ or ‘planning and funding’ used elsewhere. A useful definition of commissioning is provided by Woodin:53 ‘the set of linked activities required to assess the healthcare needs of a population, specify the services required to meet those needs within a strategic framework, secure those services, monitor and evaluate the outcomes’ (p. 203). Since 2002, primary care trusts (PCTs) have had responsibility for commissioning most local health services, including primary care and public health interventions, with some specialist services and national programmes being commissioned at regional or national level. The election of the coalition government in 2010 has been followed by radical restructuring of the NHS, with clinical commissioning groups [CCGs, led by general practitioners (GPs) with support from other clinicians and commissioning managers] now taking up the reins for most local health-care commissioning. Despite these changes, a continued aspiration for an enhanced role of commissioning in reshaping health services is clearly evident. Government policy continues to emphasise the proactive and strategic nature of commissioning, which should involve both transformational (reshaping the configuration of services) and transactional (custodianship of the budget, contract monitoring) elements. 54 The government’s aspiration for an evidence-driven commissioning infrastructure that drives up the quality and efficiency of health services is clearly evident in the QIPP (Quality, Innovation, Productivity and Prevention) transformational programme, with its range of resources to assist commissioners in their role, including comparative expenditure data, benchmarking of quality indicators and a growing number of detailed disease-focused commissioning toolkits. Key competencies for commissioners increasingly place knowledge management centre stage. World-class commissioning (WCC) competencies included critically mobilising and utilising research and best practice evidence; effectively garnering local intelligence and promoting engagement to assess needs; and turning information into knowledge and action for service reconfiguration that improves access, quality and outcomes. 55 And although the language of WCC has been shelved with the change in government, more recent policy guidance continues to highlight the central role of evidence and ‘intelligence’. 54 The role of public health in the commissioning cycle, particularly through the profiling of health needs of local populations and the synthesising of wider research evidence, is recognised as important,56 and public health teams are expected to continue to provide a ‘core offer’ to CCGs in support of health-care commissioning even once they have been relocated to local authorities.
As such, commissioning remains a key arena within which the mobilisation and utilisation of evidence of different types takes place, with the potential to importantly impact on the shape and content of health-care services. 57 To date, however, commissioning has received relatively little attention within health services research, and evidence use within commissioning has not been explored in any depth. Early investigation by the King’s Fund58 suggested that a lack of timely and high-quality information undermined effective practice-based commissioning. McCafferty et al. 59 explored the development and implementation of WCC and concluded that inappropriate and poor-quality data, a lack of robust information systems and a lack of capacity to generate data and interpret knowledge were considerable obstacles. McDermott et al. 60 looked at the commissioning of stop-smoking services and found that evidence-based guidelines on effective interventions were inconsistently drawn on by commissioners and that in fact services were often not specified by commissioners in very much detail. Clearly, these few studies paint only a very partial picture of evidence use within commissioning, and none has focused on the needs of multiethnic populations.
Goal, aims and objectives
Although research to date has helped to describe the complexity of the processes involved in, and the very wide range of factors that can act as barriers to, evidence mobilisation and utilisation,48,52,61 as yet little has been done to identify effective routes to shaping or enhancing the process in real-life policy-making contexts. There is a need to move towards identifying routes of intervention to effectively shift embedded values, beliefs, structures and practices that serve to undermine the contribution of evidence. The present study aimed to contribute to this general need and to generate specific understanding in an important area that has not to date been the focus of enquiry.
Goal
To support the commissioning of health services that better meet the needs of BME patients and thereby help reduce ethnic inequalities in health-care experiences and health outcomes.
Aim
To enhance the critical use of research evidence alongside other forms of knowledge by managers within the PCT commissioning cycle.
Objectives
Theoretical
-
To develop a theoretical model of knowledge utilisation that explicates the emotional, ideological and political dimensions through the example of ethnic diversity and inequality.
-
To contribute to the theoretical literature that addresses mechanisms for enhancing the critical use of research evidence by managers in complex decision-making environments.
-
To contribute to the theoretical literature that addresses mechanisms for enhancing the cultural competence of health-care services by integrating an understanding of the role of knowledge(s) mobilisation.
Empirical
-
To describe, across a range of commissioning contexts, how managers seek out, appraise and apply research evidence relating to ethnic diversity and inequality alongside other forms of knowledge.
-
To identify factors (at evidence, individual and contextual levels and their interfaces) that support or inhibit the critical and effective use of research evidence within the commissioning cycle and thereby identify promising routes of intervention.
Operational
-
To develop practical diagnostic, evaluative and change management tools for use by individual managers, teams and organisations to (1) assess and promote critical reflection on current competencies and practice with respect to utilisation of evidence on ethnic diversity and inequality, (2) identify actions to strengthen competencies and good practice and (3) support specific elements of the knowledge utilisation process.
-
To educate researchers and research funders regarding the current limitations of the evidence base and how they might generate research products that are more appropriate and accessible for managers charged with the task of commissioning services for multiethnic populations.
-
To strengthen links between university researchers and managers and contribute to the development of a shared commitment to enhancing research evidence utilisation for enhanced organisational performance.
Chapter 2 Methodology and methods
Conceptual framework
Recent reviews have highlighted the diverse streams of theoretical literature on knowledge utilisation processes. 52,62 They also call for more research within health-care contexts to draw on these traditions and thereby become more explicitly theory based. 48,63
Recent work that seeks to integrate micro-, meso- and macro-level conceptual frameworks and articulate the interplay between these levels is also useful here. 48 So too are frameworks that emphasise the complex and contested nature of research evidence as well as the messy, diverse and convoluted pathways that often link research evidence to policy-making and practice. In this, Davies et al.’s64 notion of ‘knowledge interaction’ is attractive as it captures the way that multiple actors engage with varied sources of evidence to craft policy-making within the context of competing drivers. Empirical work based on such holistic models seems more likely to identify fruitful avenues for intervention to enhance effective evidence use, particularly compared with that focusing on pieces of the jigsaw in a more piecemeal fashion. We therefore conceptualised evidence mobilisation and evidence utilisation within the commissioning cycle as resulting from dynamic interactions between diverse evidence sources alongside variation in individual agency and organisational rules, structures and processes. This was further situated within the wider health-care setting and its current restructuring agenda, themselves situated within the broader sociopolitical context of multicultural Britain.
Within this comprehensive multilayered framework, our focus on ethnic diversity and inequality demands that we foreground four specific issues. First, we draw on Weiss’s65 insights regarding the varied ways in which research evidence might emerge and be used within policy-making: as empirical findings (be they direct or instrumental), as ideas or challenges to current thinking (i.e. conceptually) or as briefs or arguments for action (be these persuasive or symbolic). We also recognise the often inherently contested and political nature of research and other evidence relating to ethnic diversity and inequality. Reviews of past work suggest that the direct use of evidence in policy-making is generally the exception rather than the norm. 66,67 They also note the limited progress that has been made to date in modifying services to meet the needs of BME populations. 44 For these reasons we were particularly mindful of the potential importance of the indirect influences of evidence.
Second, at the level of individual actors and their interface with knowledge sources, we draw on sociocognitive perspectives68,69 that emphasise the importance of the ‘thinking subject’ and the ‘mental models’ that guide people’s ‘sense-making’. Although the crucial role of policy-makers as receptors of knowledge is widely recognised,30,69 sociocognitive models look beyond technical skills and resources to values, assumptions and worldviews. We suggest that the ways in which individual commissioners understand the nature of ethnicity and associated inequalities will be central to how they seek out, appraise and apply different types of knowledge within their work. These perspectives fit closely with the work of Hunter,70 Husband71 and Gunaratnam and Lewis,72 all of whom highlight the need to explore the ‘felt dimension’ of health-care policy-making and practice within the multiethnic, post-Macpherson setting. As Hunter70 argues, in exploring the role of those in policy-making positions, we must ‘consider these individuals as emotional as well as relational actors’ (p. 150). For example, professional anxiety and uncertainty about cultural competence can be disempowering to professionals and detrimental to care. 73
Third, within the organisational context, we seek to expose the taken-for-granted ‘ways of being and doing’ that operate and how these interact with research and other forms of evidence. We view the health system and health-care organisations not just as mechanical structures that provide health care but rather as culturally embedded and politically contingent,74 as purveyors of wider societal norms and values. 75 These ideas fit with Lam’s76 notion of ‘social embeddedness’ – the recognition of the interconnections between individual managers (micro), their organisational context (meso) and the wider societal context (macro) within which these operate. This means that, although evidence utilisation processes might be characterised as anarchic and unpredictable, there are nevertheless ‘deep structures’, including racialised hierarchies, that shape and constrain these processes in persistent ways.
Fourth, within the layer of the wider context, we pay particular attention to the influence of stakeholders beyond commissioning organisations, particularly service users, the public and their representatives. Given commissioning’s strong generic focus on consultation and ‘knowing communities’, and our particular focus on ethnic equality, we seek to understand not only the ways in which these external stakeholders represent additional, perhaps conflicting, sources of knowledge (such as patient preferences, or public notions of entitlements), but also the ways in which they access, appraise, interpret and present research evidence to the commissioning tasks independently.
Notwithstanding our choice of a multilayered theoretical model that is sufficiently sophisticated to allow understanding of the complex processes of evidence mobilisation and utilisation, our underlying assumptions are that these processes can be understood; causes and effects can be identified; and steps can be taken to modify these processes to build on strengths and mitigate weaknesses.
Methodological overview
The theoretical framework outlined in the previous section, together with our review of the relevant empirical literature presented in Chapter 1, directed our methodological approach in a number of ways.
First, we adopted an explicit integrated knowledge translation model for the conduct of the study,77 bringing university researchers and PCT managers to work together in a collaborative team throughout the entire research process: developing research questions, shaping methodology, generating and interpreting data and disseminating findings in accessible formats. Past work has indicated that sustained and intense interaction between users and researchers increases the likelihood that research findings will be utilised. 78 Given the complex and potentially challenging focus of the present study, such collaborative working was deemed crucial to ensure that the project was successfully completed and had both reach and impact.
Second, we adopted a broad and inclusive understanding of ‘evidence’ and did not seek to offer respondents any kind of definition. We also recognised that ‘research evidence’ comes in many different guises and might perform many different tasks that are potentially useful within commissioning for multiethnic populations. These could include alerting commissioners to issues for consideration; describing patterns of ill health by ethnicity; explaining the underlying causes of differentials between ethnic groups in key outcomes; evaluating the effectiveness of alternative approaches to reducing ethnic inequalities; developing appropriate indicators for monitoring service implementation; and so on. As there remain significant gaps in the research evidence base relating to ethnicity and health (see Chapter 1), and as the commissioning task inevitably involves identifying approaches that are feasible and acceptable within a specific local context, we also recognised that many other sources of evidence would feature heavily within commissioning work. We therefore chose not to draw any clear distinction between the concepts of ‘knowledge’ and ‘evidence’ and to view research as just one source within a complex ‘mixed economy’ of knowledge. 1,34 During data generation we allowed respondents to be guided by their own mental models of ‘evidence’ and ‘knowledge’ and to use a range of related terms – such as ‘data’, ‘information’, ‘intelligence’ and ‘insight’ – as they saw fit.
Third, we combined detailed case study investigation in particular sites with key informant interviews and workshops that engaged with a wider spread of respondents. The case study approach excels at understanding complex, multifactorial real-life situations and allowing the integration of data on a number of levels alongside a detailed contextual analysis of events and relationships. 79,80 This type of approach was needed to capture the dynamics of the whole system, allowing the examination of individual and institutional actors and exploring their values, ways of working and skill sets in relation to evidence. Respondent narratives were seen both as a representation of the personal attitudes and perspectives held by each set of key actors and as a window into the complex processes operating within the commissioning arena. Nevertheless, combining interviews with observational and documentary evidence was important to develop a more holistic picture than is possible from interviews alone. Meanwhile, the use of broader data-generation methods before and after the case study work allowed us to engage with a wide range of commissioning contexts in order to generalise theoretical understanding and develop research products with wider relevance and transferability.
Fourth, we aimed to describe how well research evidence was being used, not just whether it was used at all. Given our focus on improving the cultural competence of health-care provision for BME groups, the ultimate test of how well research evidence is used is whether it leads to modifications in policy and practice that improve levels of access and satisfaction and service outcomes for minority ethnic users. Tracing the use of evidence to such outcomes or benefits was, however, beyond the scope of the current study. Instead, we examined the intermediate steps in this process, looking at whether and how commissioners and other actors within the commissioning arena accessed varied sources of evidence; critically appraised and selected evidence; synthesised evidence across sources and methods; adapted and presented evidence in appropriate formats; integrated research evidence with other knowledge sources; explicitly articulated assumptions, priorities and values underlying the assessment of different knowledge sources; and translated syntheses of integrated knowledge into commissioning products and processes (such as service specifications, business cases, care pathway models, tenders, provider contracts and performance management indicators).
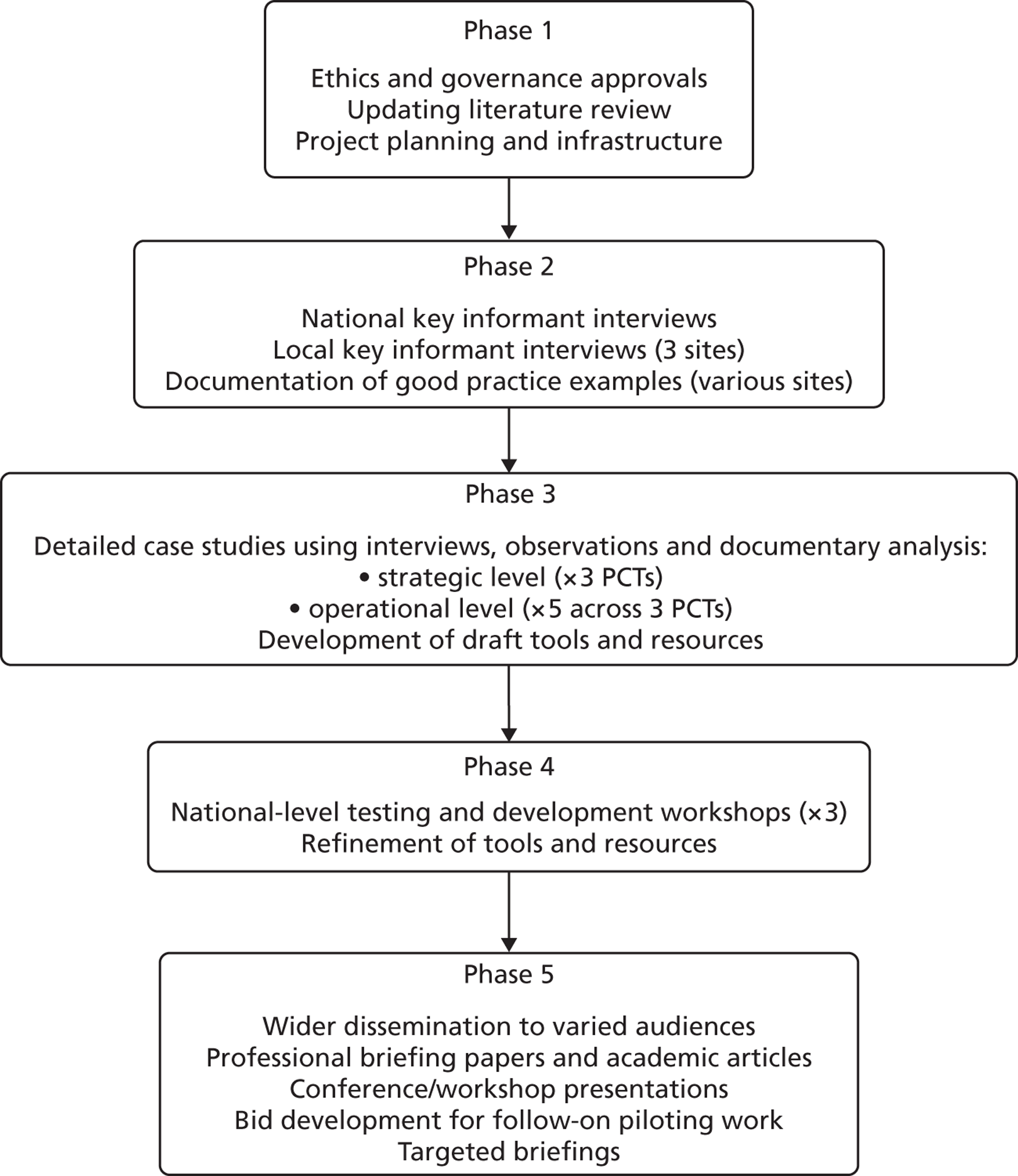
Figure 1 illustrates the five phases of the project.
FIGURE 1.
Project phases.
Research questions
Three broad research questions were identified to guide the empirical components of the study. Each broad research question was broken down into a set of more detailed questions that indicated our intention to explore five inter-related ‘levels’ that make up the evidence mobilisation and utilisation process: evidence, individual managers, commissioning teams, organisational settings and the wider context.
Research question 1: how does a focus on ethnic diversity and inequality shape the knowledge mobilisation and utilisation process within the health services commissioning context?
-
What characteristics of research evidence relating to ethnic diversity and inequality influence how it is received by managers (e.g. source, method, (un)certainty, relevance, concepts/theory)?
-
What mental models of ‘how research evidence should be used’ are managers working with?
-
To what extent is the accessing and application of information relating to ethnic diversity and inequality part and parcel of broader evidence-gathering exercises for commissioning or rather a distinct exercise?
-
What factors prompt managers to seek out research (and other types of evidence) relating to ethnic diversity and inequality (e.g. policy directives, new priorities, external audit, stakeholder inputs, signs of service failure)?
Research question 2: how does organisational context shape the mobilisation and utilisation of knowledge relating to ethnic diversity and inequality?
-
How often, and at what stages, do managers apply research evidence relating to ethnic diversity and inequality in their commissioning tasks?
-
How are commissioning teams constituted and organised? How does this impact on evidence use?
-
Who is seen as holding expertise and insight in relation to ethnic diversity and inequality? Why?
-
To what extent do PCT commissioning organisations have explicit models, structures, processes and objectives that support the mobilisation and utilisation of evidence? Do these consider ethnic diversity?
-
In what ways does managerial behaviour support and encourage, or deter, the explicit consideration of research evidence relating to ethnic diversity and inequality within commissioning teams?
-
In what ways do the available infrastructure and resources support and encourage, or deter, the explicit consideration of evidence relating to ethnic diversity and inequality within commissioning teams?
-
How do national, regional and organisational policy priorities inter-relate to shape the mobilisation and utilisation of evidence in this area?
Research question 3: how can individual, team and organisational competencies be effectively enhanced to support the critical use of research evidence for the commissioning of services that better meet the needs of a multiethnic population?
-
How competent are managers to (1) identify and access, (2) critically appraise and synthesise and (3) adapt and apply evidence relating to ethnic diversity and inequality?
-
What expectations do managers have of, and what problems do they encounter with, the evidence base?
-
What individual-level factors facilitate or hinder the mobilisation and utilisation of research evidence in this area (e.g. knowledge/awareness, skills and experience, ‘mental maps’, autonomy, authority, personal biography)?
-
What areas of capacity development would likely improve the individual- and team-level competencies required for the mobilisation and utilisation of research evidence relating to ethnic diversity and inequality?
-
How does research (and other) evidence relating to ethnic diversity and inequality currently find its way into the commissioning process – through which actors and which routes? How can these be supported?
-
Who are the key actors and what are the key organisational settings and processes that present barriers against enhanced mobilisation and utilisation of evidence?
-
What factors in the wider societal and broader NHS context must be buffered against, or can be drawn on, to support the routine, critical use of research evidence in commissioning for multiethnic populations?
-
What characteristics of the form, content and delivery of interventions in support of enhanced mobilisation and utilisation of research evidence are likely to increase relevance and utility?
Phase 1 development
Literature review
Before the start of the project an extensive literature review was undertaken to guide the development and methodology of the project. It was important for this to cover not only academic papers and research, but also national policies, guidelines and toolkits relating to commissioning, evidence use and ethnicity. This was updated throughout the project and a RefWorks® (version 2.0; ProQuest LLC, Ann Arbor, MI, USA) database maintained. Considering the evolving nature of the NHS commissioning infrastructure during the period of this study, the research team also attempted to keep up to date with articles in the media, policy directives and information from colleagues.
Project teams
The project was a collaborative endeavour involving two universities and three PCTs. Each PCT had one mid-level manager assigned to the project as a co-researcher and one senior staff member designated as a champion for the project. The champions and one of the co-researchers were engaged in the development of the initial proposal, identifying the research questions and shaping the study design alongside the academic researchers. The named co-researchers in two of the sites were unable to take up the role on the project, a reflection of NHS restructuring and the long time between proposal development and funding. However, once the project was under way, two new co-researchers were appointed and all three co-researchers subsequently engaged in all aspects of the project work alongside the university researchers, including the national-level work (phases 2 and 4) and local case study work (phase 3) that focused on their own organisations. The champions were also engaged in the project, particularly in one of the sites, although their senior roles necessarily meant that they did not have day-to-day involvement, providing input instead at key junctures of the project.
To assist in the development and delivery of the project, three project teams were created to manage and guide the research. The project management group comprised university researchers and PCT-based co-researchers. This group met regularly to design research tools, co-ordinate data collection, provide updates on emerging themes and findings, complete analysis and produce project outputs. This was also the core operational research team, with most members directly engaged in data generation, analysis and reporting. The research team included individuals identifying as white British, British Pakistani and Pakistani, both male and female, across both the academic and PCT researchers. Team reflections during the course of the project did not reveal any significant concerns regarding the influence of researcher ethnicity on the data generated. We did, however, wonder whether the significance of racism might have been more salient had we had a more ethnically diverse research team.
The project advisory group had a wider strategic role in guiding the development, analysis and outputs of the project and linking the project to relevant developments. The group met three times during the project period. This group was formed of senior academics engaged in health inequality and ethnicity at a national level, as well as senior stakeholders from the partner PCTs and individuals from the NHS and third sector with extensive experience of commissioning and health-care policy.
Finally, a user guidance group was convened, comprising representatives from community organisations and third-sector providers engaged specifically with ethnicity and health. Although the end-users of the project are considered to be commissioning managers and other stakeholders involved in health-care commissioning rather than service users, input from organisations directly involved in representing and providing services for minority ethnic communities was considered important. This helped to ground the project towards improving service delivery and prevent the findings from becoming too abstracted. Organisations and individuals were chosen who had previously been engaged in commissioning and who were able to share experiences from service provider and user perspectives.
Selection of primary care trust study sites
Three PCTs were recruited as partner organisations for the study. The intention was that these organisations would form the sites for the in-depth case study work and engage in the project as full partners – in keeping with our integrated knowledge translation model. 77 The PCTs were therefore chosen on the basis of both theoretical and practical considerations. It was important for the sites to reflect a degree of variation in relation to our topic of focus, but it was also important that the organisations would be active partners, willing to invest staff time and engage in reflection on the study findings and their implications for policy and practice. Sites were therefore chosen across South and West Yorkshire where the research team already had strong ties to practice and where relevant work was already under way. A regional focus was also felt to offer the possibility of useful sharing and learning between PCTs. The sites were chosen to have PCTs covering urban areas with significant but contrasting minority ethnic populations, where it was anticipated that there might be a variety of commissioning activities as well as available data and a range of awareness on ethnicity-specific issues. Sheffield, Leeds and Bradford were chosen as sites that fit these criteria, each with different ethnic demographics and organisational structures for health and social care.
Bradford, with its history of immigration from the Indian subcontinent, has long recognised itself as a multiethnic city, with 36% of its population identifying themselves as belonging to an ethnic group other than the white British majority in the 2011 census. 2 In contrast, Sheffield and Leeds had much smaller minority ethnic populations of around 19% and their public services have only recently started to engage seriously with the needs of these communities. Nevertheless, all three cities have experienced high levels of inward migration in recent years and now have well-established as well as newer minority communities. At the time of the study design, all three PCTs were engaged in achieving WCC targets and engaged in work on meeting the needs of BME groups, and all had staff members who were willing and interested to actively engage in shaping the project.
During the study period, Bradford and Airedale PCT and Leeds PCT clustered to form NHS Airedale, Bradford and Leeds. As this initially had little impact on day-to-day commissioning work, the restructuring did not reduce the amount of relevant work being undertaken. However, it did provide opportunities for co-researchers to contrast and reflect on different organisational practices as their functions and management structures were amalgamated.
Although the PCTs formed the focal point of the research, we also explored partnership working and engaged with other key stakeholders across the three cities, including local authorities and third-sector provider organisations.
NHS restructuring
Between the submission of the project proposal to funders and the commencement of the project in October 2010, the new coalition government released their White Paper81 on the NHS, which became the Health and Social Care Act 201282 in March of that year. During this long period of debate, in which the Bill was substantially redrafted, there was great uncertainty as to how the NHS would be restructured. However, it was clear from an early stage that commissioning structures would change significantly.
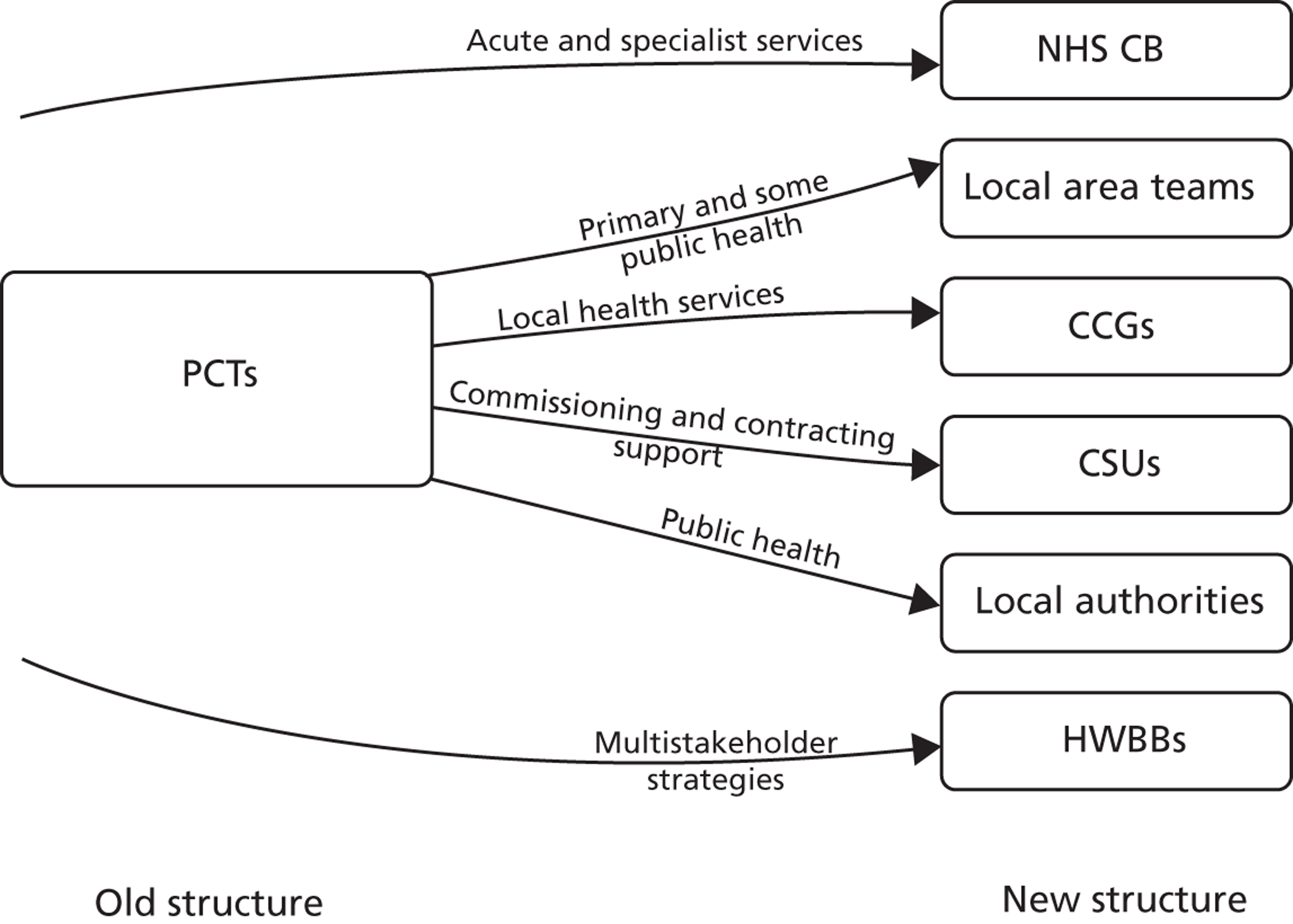
Central to this was the abolition of PCTs and the establishment of CCGs led by GPs with support from other clinicians. Although some former PCT staff transferred their employment directly to the new CCGs as commissioning managers, others transferred to separate commissioning support units (CSUs), providing commissioning and contracting support to the CCGs. Meanwhile, the public health function of PCTs was transferred to local authorities. Strategic health authorities were also abolished, with a new national body called the NHS Commissioning Board (NHS CB) established with responsibility for commissioning primary care and specialist health services through a network of local offices. Health and well-being boards (HWBBs) were established as local partnerships bringing together the CCGs, local authority, patient and public representatives and other stakeholders as the primary mechanism for setting local health and well-being strategies (Figure 2).
FIGURE 2.
Simplified representation of role shifts from PCTs to new organisations in post-2010 commissioning structures.
Despite these emerging changes, the project retained its focus on PCTs and continued to pursue the original set of research questions, as it was agreed with the Health Services and Delivery Research programme that they retained relevance and value regardless of how commissioning work might be organised in the new NHS. However, three adjustments were made to our methodology. First, explicit questions were added to the key informant interviews to elicit respondents’ opinions and concerns about how evidence and minority ethnic health would be considered in the new commissioning arrangements. Second, the project team deliberately devoted less time in the case study work to comprehensively documenting existing structures within and across the local organisations, focusing instead on functions and processes that were likely to persist following structural transition. Third, we extended our original plan for phase 2 to include the documentation of a number of ‘good practice’ examples. Fourth, the project team kept up to date with developments and designed the analysis and outputs to reflect the changing structures, aiming to ensure that findings were framed in a way that would be applicable, and provide guidance, to the new commissioning teams.
Ethics and governance
Ethical approval was obtained from Nottingham Research Ethics Committee 2 and specific research permission was gained from each of the PCTs that were the main focus of the study. Standard procedures for ensuring informed consent and protection of research data were maintained. The main area of concern related to the difficulty of ensuring complete anonymity given that the identity of the case study sites would be public knowledge – a common issue in this type of health services research. During consent, participants were given the option to review any use of quotes from their interview before publication, or to express their right to have their contributions attributed to them.
Pilot interviews
Before undertaking the main data collection, as described below, a series of informal pilot interviews (n = 6) were undertaken with experts in the field of health-care policy and/or health inequalities. The interviews were very loosely structured and aimed to generate ideas about how the phase 2 interviews might best be structured, complementing the literature review work. These interviews suggested the need to adopt an open-ended and wide-ranging approach to generation of the main data, rather than focusing too narrowly on issues relating to ethnic diversity and inequality. This was felt to be important for three reasons: first, to allow respondents the opportunity to shape their responses and highlight the issues that they felt to be important, particularly because the pilot interviews suggested (and the later fieldwork confirmed) that many commissioning actors do not have a particular interest or expertise in ethnic equality issues; second, to ensure that any claims made for factors operating in relation to our focus on ethnic diversity and inequality were informed by an understanding of factors that shape (and, importantly, constrain) evidence use and commissioning work more generally; and third, pilot interviews alerted us to the potential danger that our findings and subsequent tools could lack relevance to and credibility for end-users unless they were well grounded in a broader understanding of day-to-day commissioning realities.
Phase 2 methods
The purpose of phase 2 was threefold: (1) to gain insights, from a broad range of perspectives, into the key characteristics that facilitate or hamper progress towards evidence utilisation in pursuit of reduced ethnic health inequalities (particularly as these relate to the wider sociopolitical setting and the health policy context); (2) to document elements of good practice that illustrate how progress on this agenda can be made (particularly as there were widespread concerns about loss of expertise and learning during transition); and (3) to inform the shape and focus of the phase 3 case studies.
National key informant interviews
Interviews with selected informants aimed to collect a broad range of perspectives on key characteristics relating to NHS management, the research evidence base, the PCT commissioning context and the wider sociopolitical setting that facilitate or hamper progress towards evidence utilisation in pursuit of reduced ethnic health inequalities. In-depth qualitative interviews with experts have been used successfully to examine the structure and functioning of health-care policy-making at national levels83 and, specifically, to examine evidence use in health. 84
Sampling
Respondents were selected for their broad experience and associated ability to provide a rich perspective on the evidence–practice interface within health-care policy-making. Most also had a particular interest or expertise in equality and diversity (E&D) or health inequalities issues. Respondents recruited included senior staff working in DH directorates, strategic health authorities, public health observatories, national third-sector policy-focused stakeholder organisations and universities.
Participants were identified initially by networks of association with the research team and project advisory group members. Snowball sampling85 was used to expand the number of participants by asking interviewees for recommendations of other key informants who the research team should contact. The aim was to interview around 20 national key informants. Respondents were contacted by e-mail and/or by telephone, informing them about the project and providing them with a participant information sheet. There was a high participation rate, with only three people declining to participate because of the pressure of work.
Data generation
A semistructured interview guide was prepared to assist the different researchers in covering a similar range of topics in each interview while still allowing for opportunistic and individual-specific questions. The topics included in the guide covered professional background and experience; commissioning structures, networks and processes; the impact of commissioning; the role of evidence and knowledge in commissioning; barriers to and opportunities for commissioning to address ethnic health inequalities; and how participants anticipated the new commissioning structures might impact on their work and the field.
The team followed Hunter’s70 advice regarding the use of reflexive, narrative approaches that emphasise dialogue within the research context, as ‘prior and on-going relationships with professional participants make it difficult and indeed undesirable for researchers to maintain silence’ (p. 149). This assisted in accessing more implicit understandings and discussion of sensitive topics that might not easily have been articulated within the interview setting. In following the COREQ (COnsolidated criteria for REporting Qualitative research) guidelines for qualitative research,86 interviewers were encouraged to reflect on their position and relationship with the interviewee, and how this might impact on how participants reflected on each of the questions posed.
Most interviews were audio recorded with the respondents’ consent and these recordings were transcribed verbatim by a professional transcriber with substantial experience in NHS research. All identifiable names and places were subsequently anonymised within these transcripts.
Basic profile information about each interviewee’s current and previous roles, experience, age group, sex and ethnicity were recorded. Participants also indicated whether they wished quotes taken from their interviews to be anonymised or attributed, and if they wished to see the context of any quotes used in project reports before publication. This information was collated into a database (Microsoft Access 2010; Microsoft Corporation, Redmond, WA, USA), with each interviewee given an anonymised code.
To provide context and permit reflexivity for these interviews, interviewers also prepared a short memo immediately after each interview to record the location and any interruptions that might have impeded discussions; their perceptions on key messages and the flow of the interview; whether participants were hesitant to discuss any particular topics; and any pre-existing relationship between the interviewer and interviewee. This contextual information was considered during analysis to record factors that might affect how the interview was interpreted, and to provide background to other researchers who were not present during the interview.
Good practice examples
During the pilot interviews, concern was expressed that cuts and efficiency savings to the NHS, particularly to PCTs, were leading to reductions in capacity amongst E&D staff and the potential for loss of learning and experience in meeting the needs of minority ethnic health populations. We therefore undertook to select and profile 10 examples of promising practice on how evidence had been used to inform commissioning for specific projects on minority ethnic health. The aim of this strand of work was to capture the expertise and experience of staff involved in overcoming specific barriers in this area and to collect positive examples of how projects had been moved forward to completion. Researchers used interviews with key staff alongside documentary analysis to develop a brief narrative of how each piece of work had been undertaken, and to identify any transferable learning on how evidence on ethnicity might best be used to influence commissioning.
A purposeful sample of examples from different areas of health work was selected following recommendations of good practice from key informant interviews and an open call for suggestions on the minority-ethnic-health JISCMail network (see www.jiscmail.ac.uk/lists/minority-ethnic-health.html). A copy of the good practice guide can be found on the project website (see www.eeic.org.uk/mcs).
Local key informant interviews
In addition to the national-level interviews, a number of key informants were identified and interviewed during phase 2 in each of the three focused case study sites. These interviews generated similar data regarding the wider policy and organisational context of commissioning work and formed an essential first step in the case study work. As such, they provided background information and identified areas that would provide examples of ongoing commissioning work. Engaging with local stakeholders early on during the project also proved very useful for establishing the later phases of the project.
Sampling
Respondents were selected on the basis of their extensive local experience and ability to provide a broad perspective on local structures and processes as well as on national level drivers and context. The PCT co-researchers were particularly important in identifying potential respondents. The response rate was high and the final sample included senior and mid-level staff from various directorates within the three PCTs, the local authorities and third-sector organisations.
Data generation
Data generation employed the same topic guide as for the national-level interviews although more emphasis was given to eliciting local examples and illustrations of the wider policy context. Again, the majority of interviews were recorded and transcribed verbatim.
Phase 3 methods
In contrast to some case study designs, we did not select our study sites, or our operational case study examples within these sites, to be exemplars of good practice in terms of research utilisation. Given the emergent nature of commissioning practices, particularly in relation to ethnic diversity and equality issues, such an approach was neither feasible nor appropriate. Instead, the case studies were intended to provide sufficient variation to be able to compare and contrast commonalities and differences and thereby gain analytical purchase.
Case studies
To further explore and extend thematic findings from the key informant interview stage, detailed case studies were undertaken over several months to examine commissioning in depth. A case study approach allows for the examination of behaviours and phenomena while explicitly embedding exploration within a specific context. 87 A suite of data collection methods was used, including participant observation, interviews, and documentary analysis to collect data at operational group, individual and strategic levels. In our original protocol we stated the intention to convene formal focus group discussions with commissioning staff. However, in practice this proved difficult as respondents’ work commitments made it difficult to identify extended periods of time when they could come together for the research and consequently they preferred us to piggyback our data generation onto their existing work schedules. This meant that we opted for more observational periods, although we also engaged in some guided group discussions, particularly around emerging findings, allowing for useful respondent validation.
Observational work often adopted an ‘observer as participant’ model88 in which researchers were present in commissioning meetings as part of a team, asking prompting questions and, in some cases, engaging and contributing to discussions when relevant. Participants were regularly reminded of the researcher’s role as a research observer. Individual participant interviews allowed the questioning of commissioning actors away from group settings and provided important background information that was not available from observing operational group meetings. Interpretive documentary analysis89 was employed to identify and synthesise key themes from relevant documents. This analytical approach enabled us to identify different layers of explicit and implicit meaning within these documents and link these to themes from the interviews and observational work. Drawing on the experience of researchers focusing on diversity and equality issues, we sought to ‘follow documents around’90 and tap into both official and private discourses to uncover taken-for-granted ‘rules’ and convoluted pathways of influence. As such, the formal data-generation methods were complemented by many informal opportunities and by regular reflection on the part of PCT co-researchers.
Strategic and operational case study foci
In line with Black’s31 distinction between ‘governance policy-making’ (i.e. the level at which strategic agendas are set) and ‘administrative policy-making’ (i.e. the operational level), the case study work engaged with both distinct levels of commissioning activity. Therefore, the operational-level case studies profiled a condition- or issue-specific commissioning work stream, whereas the strategic-level case studies examined commissioning work undertaken by senior staff and strategic groups.
Local participants from the key informant phase were asked to suggest areas of ongoing commissioning that, although not necessarily ‘best practice’ in terms of evidence use or consideration of ethnicity, might illuminate common practices, barriers or enablers. The ongoing NHS restructuring meant that options for observing active commissioning work were reduced. Nevertheless, relevant areas of commissioning were identified at each site and case study work was completed as originally planned (see Chapters 4 and 5).
Data generation
Once each case study area had been identified and the teams therein had consented to involvement in the project, researchers, co-researchers and some participants undertook informal mapping exercises to identify key actors, partners and processes involved in the work. A timeline for each case study was produced as a prompting tool and to show how individuals, agendas and partnerships had changed over time, leading to the current structure of commissioning work.
Individual interviews used the same procedures detailed earlier for key informant interviews but employed a revised topic guide that enabled the collection of more specific detail while still allowing cross-comparison with earlier phases of data collection.
As noted above, observational work was undertaken in both formal and informal settings, with researchers participating to a greater or lesser extent in the ongoing discussions and interactions. In the case of the more formal observational sessions, including meetings of groups and teams, the researchers took detailed written notes during and immediately after each observation period, using a standard template. The template prompted the researcher to record information relating to commissioning processes in general, as well as evidence use and ethnicity (see Appendix 2). Whenever possible, direct verbatim quotations by participants were noted alongside a more general description of the interactions and discussion, and relevant supporting material (such as documents circulated before, during or after the meeting) was compiled alongside the observational notes. Relevant information provided by the more informal observational opportunities, such as witnessing corridor conversations, was recorded by the researchers at suitable opportunities using a series of research memos, again using the same thematic codes to organise the material.
Interpretive documentary analysis was conducted on items presented or discussed at meetings and other background reports and materials using a standard template (see Appendix 2). These reports/materials were given to researchers by members of the group or accessed online when applicable. Although relevant documents varied in each case study, strategic documents included:
-
minutes of board meetings/strategic team meetings
-
strategic statements and organisational aims/values
-
joint strategic needs assessments (JSNAs) and other needs assessments
-
evidence presented/utilised
-
research and development plans or policy
-
health inequality action plans
-
national policy documents
-
policy-level equality impact assessments.
Templates used across the case study work prompted researchers to be alert to a range of relevant factors and processes, including how evidence was presented as part of the process (including consideration of its source and how it was received), who raised issues of ethnicity (and how related debates were framed), who was taking responsibility for evidence and ethnicity and how commissioning was changing (see Appendix 2).
Analysis, synthesis and integration of data
Key informant interviews
An ongoing process of analysis was used involving a coding scheme developed and iteratively adjusted during the first interview period, based on theory-derived topics and concepts from pilot interviews. This analysis schema was piloted and refined by all researchers and PCT-based co-researchers in dedicated workshops used to clarify themes and ensure consistent coding across the sites and researchers (see Appendix 2).
Microsoft Excel and Access were used to organise these codes (around 120 grouped into 10 broader themes) into a practicable framework,91 with summary descriptions and direct quotes extracted and used to populate the codes for each interview. This approach allowed researchers to read a topic-by-topic summary of each interview by reading the framework horizontally, or examine a particular coded theme by reading vertically across all of the interviews to explore commonalities and contrasts.
Coding of transcripts was undertaken by the team member who conducted the interview, with around 20% of transcripts checked by a second member of the team to ensure that themes and codes were being completed consistently. The two researchers with most capacity on the project read the coding for all transcripts. After transcription and coding were completed, team members engaged in a series of analysis workshops to discuss, challenge and refine interpretations.
Case studies
Producing an integrated analysis of the rich data generated through the range of methods used in the diverse case study was challenging both practically and theoretically. Data from the interviews, documentary analyses and observational work were all systematically organised and indexed against the coding framework that was developed for the key informant interviews. Regular analysis sessions were held involving university researchers and PCT co-researchers to engage in the inductive and interpretive identification and testing of emerging themes. Internal briefing documents were prepared and circulated during the generation and refinement of theory to ensure transparent links between data and emerging claims (see Appendix 2 for an illustration of the theme document used to link phase 2 emerging findings to the phase 3 work). In line with the theoretical model described earlier, the overarching approach to the analysis was informed by critical ethnographic perspectives, in that we attempted to synthesise the traditional ethnographic focus on the subjective meanings and beliefs of respondents with the insights gained from a broader structural analysis. 92
Analysis of case study material was first carried out at a ‘within-case’ level. The researcher/co-researcher pairs who had undertaken the bulk of data generation in each site worked together to produce the analysis. Detailed narrative templates were prepared separately for both the strategic- and operational-level case studies conducted at each site, detailing the holistic ‘story’ of each of these case studies. Following this stage, thematic templates were next prepared for each case study. The focus here was on integrating, and triangulating, data across each of the domains of analysis (evidence, individual, team, organisation and wider context) in order to describe the diverse factors that shaped evidence utilisation and to identify any enabling factors that support evidence use. Appendix 2 includes the templates that were used for the operational-level case studies by way of illustration; similar templates were also used systematically for the strategic-level work.
Once templates had been completed for the within-case analyses we moved on to the cross-case analysis. This involved a systematic comparison across the three sites to identify relational and substantive patterns. Cross-case analysis work was initiated through a series of face-to-face team workshops in which a structured process of review and reflection on the case-specific templates was followed. The standard templates encouraged all researchers to interrogate their material against a common analytical framework and allowed team members to readily engage with the claims and supporting materials emerging from all three study sites. Subsequently, draft integrated analysis documents were produced and an iterative process of review and refinement involving all research team members was used to draw the data together across the sites into a more general set of claims and findings.
Tools development
A key project aim was to develop a series of tools and resources to support the critical and effective use of evidence on ethnic diversity and inequality within commissioning. Tools development was firmly grounded in the research findings and also involved structured inputs from potential end-users. Chapter 7 provides an overview of some of these tools and details the process of tools development.
Chapter 3 The wider context: findings from national key informant interviews
Introduction
This chapter draws on the 19 national-level key informant interviews, detailed in Table 1. These interviews were expected to generate information in response to research questions 1 and 3, detailed below, with a particular focus on the wider policy context and organisational factors that direct and shape commissioning work, and the place of evidence use within this arena.
| Characteristics | National key informants |
|---|---|
| Sector/organisationa | Two DH, two senior GPs, two strategic health authority, two academics, two public health observatory, one local government (LGID), eight national third sector |
| Sex | Nine female, 10 male |
| Ethnicity | Nine white British, 10 other |
| Total | 19 |
Research question 1: how does a focus on ethnic diversity and inequality shape the knowledge mobilisation and utilisation process within the health services commissioning context?
-
What factors prompt managers to seek out research (and other types of evidence) relating to ethnic diversity and inequality?
-
To what extent is the accessing and application of information relating to ethnic diversity and inequality part and parcel of broader evidence-gathering exercises for commissioning or rather a distinct exercise?
-
What characteristics of research evidence relating to ethnic diversity and inequality influence how it is received by managers?
Research question 3: how can individual, team and organisational competencies effectively be enhanced to support critical use of research evidence for the commissioning of services that better meet the needs of our multiethnic population?
-
What factors in the wider societal and broader NHS context shape the routine, critical use of research evidence in commissioning for multiethnic populations?
-
How does research (and other) evidence relating to ethnic diversity and inequality currently find its way into the commissioning process – through which actors and which routes?
-
Who are the key actors and what are the key organisational settings and processes that present barriers against enhanced mobilisation and utilisation of evidence?
The bulk of this chapter is devoted to describing these wider contextual issues. However, in practice, many of the key informants also offered important insights into micro-level factors operating at the level of individuals and teams. We have noted these where relevant, although most were explored in greater detail through the case study work, which is presented in Chapters 4 and 5.
As noted in Chapter 2, our data collection did not focus narrowly on patterns of ethnicity evidence use but also solicited a wider range of information on commissioning structures and processes, and evidence use more generally. Key informant interviews were therefore loosely structured to allow respondents the opportunity to shape their responses and highlight the issues that they felt to be important. In particular, we did not offer any precise definition of ‘evidence’ but encouraged respondents to think broadly about the varied types of evidence (or knowledge) that play a part in commissioning work, with formal research evidence being just one aspect of this bigger picture.
Exploring generic commissioning drivers, structures and processes was important as these were likely to fundamentally shape the demand for evidence of different types as well as the access to, and use of, evidence within commissioning work. Further, an understanding of the more generic landscape was felt to be important in ensuring that any claims made for factors operating in relation to our focus on ethnic diversity and inequality were informed by an understanding of processes that shape and constrain evidence use in commissioning work more generally.
For this reason the findings in the present chapter are organised into three main sections: general findings relating to (1) evidence-informed commissioning and (2) ethnic diversity and inequality within English health-care policy and practice, followed by findings relating more specifically to (3) use of evidence on ethnic diversity and inequality in commissioning. Although research evidence did feature in respondents’ narratives, they also discussed a wide range of other types of evidence, reflecting the fact that these may often feature more prominently within commissioning work.
Respondents have been identified by their current broad role and sector but most had varied backgrounds giving them experience of different aspects of commissioning and evidence mobilisation processes. People in director-level roles have been identified as ‘senior managers’. More specific titles have been avoided to preserve anonymity.
Evidence-informed health-care commissioning: rhetoric and reality
What is health-care commissioning? What kinds of models are used?
The key informants varied in how closely they had been involved in commissioning work, yet all had sufficient exposure to commissioning organisations to provide useful commentary on the general features of commissioning structures and processes.
All respondents recognised commissioning as a complex set of activities, the intention of which is to shape health services to better meet population health needs:
I think, my sense is that commissioning actually covers a lot of different sorts of activities, but broadly speaking it’s the process of understanding the health needs of a population, and planning and procuring services to meet those needs. But within that, you know, there’s a lot of different sorts of functions, and different kind of patterns about how that might be carried out.
Third-sector manager and analyst
However, the consensus was that there was wide variation in the ways in which PCTs have been organised and commissioning work has been achieved in practice. Some respondents drew distinctions between PCT and local authority commissioning, but most felt that there was also important variability in approach and quality within each of these commissioning arenas.
To an extent, such variability might be considered to reflect an appropriately responsive system, in that no single model of commissioning might be suitable for all circumstances. Nevertheless, there was also a sense in the respondents’ reports that there remains a lack of clarity in terms of what ‘good commissioning’ might look like and significant contestation of roles and responsibilities within the commissioning arena. Moreover, although all respondents felt that commissioning should be an important lever for health-care redesign and improvement, most also expressed the feeling that the transformational potential of commissioning remains largely unrealised. For this reason it is important to examine the scope of variation described, with three distinct inter-related areas of variation evident.
First, respondents felt that there was important variation in the extent to which people in commissioning roles saw their job as one of transforming services to better meet needs as opposed to ensuring robust control of contracts and budgets (the so-called ‘transactional’ elements). Our respondents indicated that they felt that the former aspects were very important but were, in practice, not always emphasised:
I guess a broader role of bringing in, you know, not just the evidence, but . . . more widely [thinking] about the problems and how they would be resolved and what other bits of the system would be part of that. I think that’s what many of us would think was meant by ‘commissioning’. But then, you know, meeting people who have that ‘commissioner’ in their title, they, you know, often had a more contractual focus with the organisations, in terms of, you know, what would be delivered, and how it would be performance monitored.
Public health observatory senior manager and analyst
Second, respondents suggested that there was substantial variation in people’s understandings regarding the extent to which commissioning should be carried out exclusively by people formally identified as ‘commissioners’ rather than a diverse range of stakeholders being actively engaged (in assessing need, reviewing provision, identifying viable solutions and monitoring this process of ongoing improvement). Whether and how such diverse stakeholder working might be organised and managed in commissioning practices appears to vary widely:
It’s kind of, yeah, I suppose sort of two different views on what it is. Is the commissioning what commissioners do, in terms of tighter contractual type . . . of development, or is it, is it a broad role of a lot of people in the system?
Public health observatory senior manager and analyst
Third, respondents highlighted variation in opinions and practice regarding the extent to which commissioners and commissioning can, and should, contribute to the identification and implementation of service solutions, rather than focusing solely on the clear specification of outcomes required (so-called ‘black box’ commissioning). In other words, there appeared to be a lack of clarity in terms of where the boundaries of responsibility for different elements of service improvement might lie:
From talking to the voluntary sector in particular, they say their commissioners are not really particularly interested in that [service specification], it’s very much more about, well, how many people have you seen, is that in line with what we’ve asked you to see, and things. But actually understanding a bit more about what intervention is used and why it’s effective or not effective.
Third-sector senior manager
Commissioning is a fantastically blunt tool . . . quite a lot of commissioning is about bean counting . . . counting patients in, patients out.
Public health observatory senior manager
Notwithstanding this apparent variation in orientations to commissioning, respondents identified a range of more systemic factors that they felt made transformational commissioning difficult. Many respondents drew attention to the centrality of the relationships between PCTs and NHS provider trusts. They highlighted the greater political power of the provider organisations and the limited room for manoeuvre that this afforded commissioners whose budgets were felt to be (predominantly) tied up in large historical contracts and who often have no alternative source of provision:
I think the second big issue, which is a pertinent one, is really the momentum of the historical contracts . . . you know, a lot of what the commissioners are doing is almost working at the margins. Where you’ve got extra resources you can have a discussion about how they’re best deployed. Obviously most of the resources are in a basic set of core contracts to provide a hospital with an accident and emergency department, medicine and surgery and that kind of thing.
Public health observatory senior manager and analyst
I don’t think it works in a consistent, sustainable way anyway, because we’ve been pretty much, I think, commissioning the same [services] and we’ve very rarely decommissioned anything. So as commissioners – mental health services is a classic – it feels like we need to tear up the whole thing and start again. So . . . I think the whole thing isn’t working. The way that we describe it theoretically in the NHS . . . In theory that’s the way to do it, but in reality I don’t think it works anyway.
Strategic health authority senior manager
Some respondents drew attention to the inherent tensions and complexities in the system and particularly the lack of clarity around how a market-inspired model of commissioning should function in practice:
But [commissioning’s] origins have come out, you know, have come out of the purchaser–provider split, and I’m not sure how well thought through, in a sense there’s quite a lot of theoretical work about how providers ought to behave in a [market] You know, the model is an essentially market model, which is that you split the purchaser and the provider apart, and we kind of, there’s a model for how providers ought to behave, you know, faced with these incentives, but there seems to be much less work on what the incentive, you know, what should be driving commissioners or purchasers to do a good job.
Third-sector manager and analyst
What drives commissioning?
Across the board respondents felt that the major driver for commissioning action was currently a financial one. Some respondents noted that, although it was often considered to be taboo to explicitly discuss health-care rationing (with concepts of efficiency and value for money being seen as more palatable), a drive to cut costs did in fact underpin most work. Respondents noted that the prompt for PCT transformational work often resulted from national comparative data that indicated spend was high in a particular area, or national directives concerning ways of improving value and cutting costs:
You know, so in that sense the, often the driver of the commissioning is financial rather than more to do with the clinical and quality type issues. So that these things become a sort of add on to the contract, but you know, maybe almost irrelevant if somebody’s saying well you know, you need 5% efficiency savings this year.
Public health observatory senior manager and analyst
Several respondents also referred to the quality agenda and NHS Outcomes Frameworks93 as being influential in directing commissioning energy and resources.
That said, the key informants also felt that those national agendas that focused on other issues could be very influential in directing the work of PCTs. This is because PCTs were felt to be ‘obedient’ in this regard, such that national priorities would even take precedence over local needs and divert commissioning resource away from other work:
I mean if there is a national agenda on a certain something, vascular health checks programme is a clear example. No one had heard of that until three years ago . . . suddenly that became a key priority nationally and the PCTs were tasked to deliver that, and they then develop different models of delivering that within the PCT, and it’s suddenly happening.
GP/academic
Respondents acknowledged that the health inequalities agenda was prominent in health policy rhetoric, but felt that in practice this was not a major driver and remained a marginal concern within the commissioning work of most PCTs, where it was often equated with the work of the public health team within the PCT. One respondent used a football analogy, referring to public health commissioning as ‘minor league’ compared with the bulk of the PCT’s ‘premiership commissioning’ for primary and secondary care. Respondents noted the predominant focus of PCT activity on patients and service users – whether through a concern to curb demand or raise quality standards – and felt that this meant that the wider population, and inequalities in service access, are rarely a focus of attention for health-care commissioners.
Evidence use in commissioning
Most of the key informants expressed the opinion that evidence should be central to the commissioning process and that a wide range of evidence sources must be drawn on and synthesised to inform strong commissioning work, with formal research evidence being just part of this picture.
However, there was general agreement that, in practice, systematic and effective use of evidence was not routine. Respondents were aware of good examples in which commissioners had adopted a systematic and rigorous approach to mobilising and synthesising diverse sources of evidence to inform decisions, but noted that this was usually in response to a clear policy or local driver (e.g. an individual funding request) and that external assistance is often sought in undertaking this kind of more detailed work:
PCTs have got a record of delving into the evidence when they need to, certainly for making decisions about, you know, whether drugs are cost-effective or not, you know, there can be quite systematic reviews [of the evidence] that PCTs do.
Third-sector manager and analyst
Respondents felt that the variability in evidence use was in part explained by limited commissioning resource. They felt that commissioning work was often rushed and linked to annual cycles and budgets, and there was simply a lack of capacity to look carefully at each issue or draw on diverse evidence sources. This was felt to be contributing to a tendency to maintain existing patterns of purchasing rather than seeking to redesign services.
However, in addition to resource constraints, respondents highlighted the ways in which commissioners’ approaches to finding and using evidence are shaped by other factors. Respondents tended to agree that certain types of information and evidence are more prominent and more routinely used within commissioning than others, in particular those types of evidence that relate to costs, which appeared to reflect the prominence of financial drivers:
PCTs have large information departments and they link to their local public health observatories and they make use of data sets like the compendium . . . All the programme budgeting stuff, that looks at outcomes in relation to spend.
Third-sector manager and analyst
Some respondents expressed concern that there was sometimes very selective use of evidence on the part of commissioners, with evidence being used to provide support for decisions that have already been taken, rather than being used to inform understanding of an issue and thereafter guide an appropriate response. They also highlighted the political nature of commissioning and the way in which decisions can often be influenced by vocal interest groups – as one respondent put it, ‘whoever shouts loudest’ – rather than by a balanced review of the available evidence:
Evidence is not, you know, politically neutral, it either emphasises something, or you know, sort of backs up, you know, something that somebody believes anyway, or contradicts it, and therefore it’s, you know, it’s evaluated in that particular way. And one of the issues I think when you’re looking at things critically is that . . . sometimes you’re just looking for evidence to back up your point of view, as opposed to looking at everything out there, and I think that’s a big sort of issue as well around sort of commissioning.
Third-sector senior manager
In relation to research evidence, respondents generally felt that commissioners were most heavily reliant on national guidance and other forms of synthesised evidence, and that many commissioners did not access primary research evidence. Indeed, respondents referred to the process by which research evidence informed commissioning as both ‘ad hoc’ and ‘precarious’:
[It depends upon] people with a bee in their bonnet . . . in terms of the evidence bubbling up through other routes, that’s kind of a bit of a precarious thing.
Public health observatory senior manager and analyst
In some cases, respondents felt that this reflected the fact that commissioners were working on areas about which they knew very little. Research evidence was more likely to be drawn on either when particular researchers had built up a strong relationship with commissioners and were conducting research locally or when clinicians were engaged in the commissioning process, as these clinicians were considered more likely to be well versed in the evidence base relating to their area of expertise.
Further, several respondents felt that there was a need for commissioners, and the commissioning process, to expand and extend what counts as evidence and to recognise the value of different types of information and insight. In particular, these respondents were concerned that insight from patient experience and public consultation might potentially be very useful in improving services yet was not commonly drawn on in a systematic fashion to influence the commissioning process:
I mean there was a process about what is counted as evidence, and then what is published, you know, sort of a key thing. What is valued as evidence as well, and of course the value of evidence that is not random controlled trials.
Third-sector senior manager
Some respondents pointed to the lack of standards around good evidence use in commissioning. Several also felt that there was substantial variation in the skills and interests of different commissioning actors – variation that affected how evidence was brought into the commissioning process. Appraisal and synthesis skills were highlighted as particularly important for commissioners given the wide range of relevant information and the challenge of translating national guidance into local-level action. Yet these skills (appraisal and synthesis) were felt to be lacking and were often not recognised as a core requirement for commissioners. Some respondents also noted that, when commissioning teams are constituted to ensure representation of organisations or professional groups rather than skill sets, expertise in evidence-related skills can end up lacking. On this, respondent narratives suggested that commissioning organisations and teams rarely have assigned ongoing roles and responsibilities to identify or generate relevant evidence and channel it into the appropriate part of the commissioning process. Instead, evidence generation and evidence mobilisation appear to occur more as discrete, allocated pieces of work. For instance, a focused needs assessment may be commissioned from an external research company or a literature review may be undertaken by a specialty registrar in public health based at a PCT for part of their training:
They usually ask us [third sector/GP researcher] for the evidence . . . That’s an area that definitely commissioners do not have much expertise in, that I’m aware of anyway. There may be some PCTs who have evidence synthesis officers or something, but that’s something that we have spoken to our commissioners about [needing in future structures].
GP/academic
What we find is that commissioners are not very good at using evidence and understanding the different kinds of evidence that there are.
Third-sector senior manager
Some respondents also expressed concern that PCTs tended to use consultants for various elements of the evidence-gathering and synthesising tasks rather than developing these skills and subsequent in-depth understanding in-house. Consultants appear to be used regularly for a range of evidence-related tasks, including needs assessments, community consultation and insight work, research evidence syntheses, projection work and economic modelling:
I’ve always been sceptical where people sort of contract out a needs assessment, because it seems to me that has to be done by the commissioner, because they have to internalise that knowledge in order to be able to, over the next few years, commission those services better. They need to know everybody that’s involved on the provider side. They need to know the sort of broader population understanding.
Public health observatory senior manager and analyst
Respondents also highlighted the fragmented nature of commissioning work, so that evidence skills, even if available within organisations, often sit within silos and are not necessarily brought to bear where needed:
The bits of the process don’t always link together . . . the people who are perhaps particularly interested in evidence about best treatments, and you know, data about numbers and projections and things, are often within public health, are often not integral to the people who call themselves commissioners . . . so there may be good knowledge about evidence, but it’s not playing in at the right place at the right time to change contracts.
Public health observatory senior manager and analyst
Innovation through commissioning
Commissioning was not generally considered to be an important source of innovation by our respondents. Commissioners were often characterised as risk averse:
So if I give you the commissioners’ perspective, you know, at the end of the day we’re accountable for public money. I have to visibly show how I’ve spent it. New things are very uncomfortable.
GP
Commissioners were also felt to be distant from the realities of service delivery, making them unlikely to identify opportunities for innovation:
Examples of innovation are there, but these are despite rather than because of the system.
Third-sector senior manager
These observations linked closely to respondents’ opinions that ‘strong commissioning’ – commissioning that actually transforms services to better meet needs – has to involve a wide range of stakeholders. Several respondents highlighted the importance of having clinicians and other front-line practitioners closely engaged with the commissioning process. These respondents felt that this was essential to ensure adequate understanding of the realities of delivering the service and that health-care practitioners with this understanding were therefore more often a source of innovation. They also noted that, even when the impetus for change comes from commissioners, providers have to be committed to the innovation for it to happen:
There was an end of life care [project] . . . it worked with the palliative care commissioners and also with heart failure nurses, so it was a carers’ organisation . . . but they worked really well with commissioners, and also they had really self-critical evaluation about what difference they made . . . and it influenced the strategic plan around palliative care, because the commissioner was involved from the beginning, in fact they were joint bidders.
Third-sector senior manager
Some respondents also felt that innovation is more likely when the commissioning process draws in the public and potential users of the service in a meaningful way:
So the local authority absolutely threw a fit right at the beginning, saying, you know, ‘what do you mean you’re going to put a mental health unit in the xxx?’ And then slowly as we’ve got them on board, then we’ve got the local authority on board . . . And it only got off the ground, and that design only worked because it was the public who asked for it.
GP/ex-senior commissioner
A couple of respondents identified a further characteristic of commissioning work that they felt often undermined the potential for innovation, namely the failure to carefully evaluate service redesigns. These respondents felt that commissioners tended to focus on ‘bottom-line’ outcomes rather than generating learning through unpacking the processes and understanding what did and did not work as anticipated.
Nevertheless, some respondents did feel that PCT commissioning was improving, and that progress was being made, at least in some areas, towards more responsive and impactful commissioning that took population health needs as the focal point:
In terms of structural thinking I think PCTs were a really good invention; they were bringing public health down to a local level, using that to inform commissioning process, really having responsibility for linking in with primary care providers. I think there was a lot of potential there . . . innovative thinking . . . I do see that that would have come in time.
Third-sector senior manager
Ethnic diversity and inequality in English health-care policy and practice
Marginalisation
An important theme within the key informant interviews was that attention to ethnic diversity and inequality remains a marginal concern within English national health-care policy:
I always say that people don’t get discriminated any more, the equality and inclusion agenda gets the discrimination . . . it’s the area itself that gets the discrimination, that gets less resources, that gets the less importance . . . Which of [the] agendas do you think is going to be keeping people awake at night time? It will not be the inclusion agenda. It will be QIPP and commissioning and providing. So there is a hierarchy in the importance of areas within the NHS.
Strategic health authority senior manager
There was some disagreement between respondents in terms of whether there had been any progress during the period of the Labour government (1997–2010), with some feeling that real progress had been made within the DH and central policy during this time and others suggesting that there had never been genuine commitment from the top to make this a core policy driver. Nonetheless, respondents agreed that other priorities and agendas tended to take precedence and they drew attention to the ways in which equalities work could be presented as conflicting with, rather than aligned to, other priorities:
They don’t have to be, but in this modern world where senior decision makers don’t understand the equality inclusion agenda, and often some of them don’t believe in that agenda, then it becomes conflicting, yes, it’s one or the other.
Strategic health authority senior manager
Several respondents drew attention to the apparent synergies between the quality agenda and equalities issues but noted that in practice there was very little connection at national or trust level. One respondent had spent time reviewing quality accounts across a large number of trusts and found that they had been prepared with little or no reference to equalities issues. Others explained the need to convince people working on quality issues of the relevance of taking an equalities focus:
If you look at quality one of the big features in and around that is around patient experience. How can you get patient experience right if you’re not disaggregating and getting the patient experience, whether qualitative or quantitative, of all the different groups that are using those services? I think for those people leading on quality, until you start talking about all of that, they don’t really get it at all, they just really see it as ‘oh E&D, that doesn’t really apply to us’. But actually you can’t really achieve quality for everybody unless you achieve equality in that process.
Strategic health authority senior manager
[QIPP] has a financial component in it, but to be interrogating that in terms of equality as opposed to just quality, no. It was not part of the package.
Third-sector senior manager
Several respondents also highlighted the way in which the national health inequalities agenda has lacked adequate reference to ethnicity, opting to understand inequalities primarily in terms of differences between geographical areas and socioeconomic groups:
Every review of health inequalities has excluded ethnicity. The previous one said they couldn’t do it because the data wasn’t good enough. Now the data’s good enough . . . [but] until there is some sort of ‘must do’, ‘have to do’, I think we are not going to [do it].
Public health observatory senior manager
I said repeatedly that it was completely unhelpful that the previous policy agenda had health inequalities here and the equality agenda here [indicates with hands wide apart]. So the equality agenda was formulated in terms of the law and fairness and justice and non-discrimination and so on, whereas the health inequalities agenda was coming from a different perspective.
Third-sector manager and analyst
The only exception to this picture of marginalisation was in relation to mental health work, in which several respondents highlighted significant national policy drivers to understand and tackle ethnic inequalities. However, even in relation to mental health, some respondents felt that progress had been disappointing and that gains on the ground had not been matched by system-wide changes to mainstream ethnic inequality within commissioning work.
Respondents felt that this general lack of strong direction from national policy-makers was often reflected at the local level in the behaviour of PCTs. They felt that in most PCTs there was no sign that attention to ethnic diversity and inequality was embedded within the main commissioning processes. Some respondents felt that attention to ethnic diversity and inequality had largely been confined to an internal human resources issue, or had taken on a very narrow legal compliance focus within PCTs, rather than being a fundamental part of knowing and responding to the health needs of the local population. One respondent even referred to a ‘get out of jail free card’ to signify the way in which PCTs showcased a one-off project focusing on ethnic inequality issues, in lieu of being able to demonstrate a consistent and embedded approach to this axis of inequality.
I think locally it still remains a very Cinderella issue I think for many groups, for many areas . . . I think overall it’s probably still not that high on people’s radar, is it?
Third-sector manager and analyst
I think because we’re still moving from what is a very white Anglo-centric approach to health care to recognising difference as part of our community, rather than something that if we’ve got time and leisure we’ll deal with.
Third-sector senior manager
PCTs seem to have interpreted a lot of this, a lot of them have tried to meet the legal duties, you know . . . you know, the action was taken to write equalities schemes, and comply with the law, and . . . there was almost a sort of disconnect, you know, inequalities, the racial and ethnic inequalities really related to writing a race equality scheme, at the time. But actually, if you really, you know, a PCT that was doing something about this would have its public health people kind of, you know, embedded and immersed in that whole agenda, and not its human resources, you know, legal people, who were writing this document.
Third-sector manager and analyst
Importantly, several respondents highlighted the fact that there had never been any performance management focused on ethnic (or other) equalities-related outcomes. Respondents noted that this meant that the work had not been a ‘must do’ and that, in the target-driven culture of the NHS, this absence of either a carrot or a stick had served to keep the issue at the margins:
There is a prior problem here, which goes back to the regulation side. If this isn’t monitored, as you know, a national priority, then most people are not going to worry about it are they?
Third-sector manager and analyst
We measure everything else within the NHS. We’ve got targets; over the top most of the time. But around this agenda, we’ve never really had measurement.
Strategic health authority senior manager
Some respondents noted significant variation in the extent to which ethnic inequality is taken seriously in commissioning organisations. However, respondents felt that this gulf had not changed much over time and that there could well be slippage backwards in the future, with organisations becoming less attentive to this issue:
I think you’ve got a big continuum haven’t you from the people who are engaged, switched on and fairly active in this area, right through to the other end, to people who say ‘what?’ And that’s always been there, because that’s one of the things I’m struck by, is over the last ten years, it’s always been . . . one or two proactive [places] like that, and there’s all these others where there is less happening. Why has that whole curve not shifted over time? It doesn’t seem to have.
Third-sector senior manager
Ignorance, ambivalence and obstruction at senior level
Some key informants suggested that the marginalisation of the ethnic equality agenda within the DH and the NHS could be explained in part by ambivalence and complacency on the part of senior leaders and in part by their need to prioritise action within a host of competing agendas. As one respondent put it, there are ‘many distractions’. Thus, some respondents drew attention to senior policy-makers who they felt were not convinced that important ethnic inequalities exist, or who they felt believed that such issues are already understood and dealt with without the need for specific measures:
So I think there’s something around people not seeing it, not seeing it as important.
GP
Decision makers who feel that we already have a fair society, that we already have an equal world, that we already have a very civilised society, so therefore all this inclusion and equality resources that we’re putting in is political correctness gone mad.
Strategic health authority senior manager
In London, in many places, my sense is that there is a belief that – of course we’re commissioning for BME needs . . . we have been doing that for years, so what’s your problem?!
Third-sector senior manager
Other respondents felt that the default position within the DH and much of the NHS is simply to overlook the relevance of this dimension:
Nobody in the Department of Health thinks about it. I think the information centre is all in different bits so they don’t necessarily join up on this. I wish I could think that there was a conspiracy theory – I just think it’s default.
Third-sector manager and analyst
I go to meetings so many times and I’m the only black face there. And I know this issue of equality is happening but nobody raises it. They just try to ignore it. And so you do raise it, people like me have to raise it, because if nobody else will, I always will. But it shouldn’t have to be that way.
Strategic health authority senior manager
However, some respondents also drew attention to more active forms of obstruction and undermining that they felt were linked to the protection of professional boundaries, vested interests and the contestation of minority ethnic entitlement and representation:
It [race equality] is divorced because people have got a monopoly on health inequalities. Those people who are working in it don’t want the inclusion and equality agenda to be anywhere near it because they’re protecting their own jobs, their own little power houses. That’s what it is, the reality of it from my experience, that’s what I think . . . Otherwise actually inclusion and health inequalities fit very nicely together. It’s a natural fit.
Strategic health authority senior manager
The other dimension where the local authority’s involved . . . is [where] you start to get into a political dimension about who ‘our people’ are, and you know, where we should be focusing resources on, on local people, you know and that, and that, there’s a risk that . . . local people can actually be, you know, stereotyping that as, someone who was born and bred in the area . . . and all these other groups are kind of not necessarily local.
Public health observatory senior manager
Most respondents also identified a lack of comfort in raising issues related to race and ethnicity that served to silence discussion and further marginalise the agenda. Respondents noted that people could often be fearful and perceive the topic as politically sensitive and complex, with the result that they would try to avoid it:
I think it’s uncomfortable, because, and part of it’s around what we view as politically correct and not politically correct . . . otherwise we’d be talking about it quite openly. There is an element of, it’s a bit of a taboo subject.
GP/ex-senior commissioner
There was certainly a degree of concern about either stereotyping or, you know, sort of representing communities in particular difficult ways . . . and so it’s one thing to be aware of the background, it’s another thing to say certain things up front and out loud.
Local authority consultant
They had a race equality review as part of being a Race for Health PCT, but nobody would talk about race equality in the room, we were with their board, all the senior people . . . The local authority and the PCT are absolutely – it’s the same in XX – absolutely terrified that there’ll be a backlash if they focus on BME communities.
Strategic health authority senior manager
Notwithstanding possible variation in the underlying attitudes and perspectives that might characterise particular actors’ avoidance of or obstruction towards the ethnic equality agenda, key informants felt that a lack of senior leadership and an absence of concern regarding ethnic inequalities were common across PCTs: ‘Very rarely do we get key players at a senior level pushing this agenda’ (strategic health authority senior manager).
Lack of infrastructure and resources
Respondents felt that the ethnic equality agenda lacked adequate infrastructure and resources at national and local levels. They pointed out that central initiatives that could be helpful, for instance the NHS Equality and Diversity Council, were not effectively connected to what happens on the ground within PCTs.
At the level of local PCTs, respondents noted the varied location and number of staff within each organisation who had an E&D role and responsibility. This was felt to usually be a small resource that was isolated from core commissioning work. Some commented that it was rare to have senior posts devoted to this agenda and contrasted the limited investment in this area of work with the investment in agendas with greater legitimacy. Moreover, respondents felt that there was often a heavy dependence on just one or two people within organisations, often individuals of minority ethnic identity themselves, who were tasked with pursuing this agenda and acting as spokespersons for very diverse communities. Respondents referred to such staff ‘battling’ alone and becoming frustrated and exhausted:
One person appointed on equality to make that happen is very demanding. It’s draining. It won’t happen . . . We would never expect QIPP to be done on a part-time or voluntary basis.
Strategic health authority senior manager
Elsewhere, some respondents noted the reliance on unpaid community representatives to provide relevant input to commissioning processes. Meanwhile, respondents also felt that PCT structures and processes rarely linked E&D activities effectively into other elements of the organisation and did not hold staff members elsewhere to account on this agenda. For example, equality strategies and equality impact assessments, although useful in theory, were identified as often being tick-box exercises that were not linked to action:
How are the priorities, as set out in the Single Equality Scheme, linked back to the strategic plans of that organisation? Most of the time they sit out in a vacuum and most of the time the priorities set out in the Single Equality Scheme don’t even feature anywhere near any of the strategic business plans at all.
Strategic health authority senior manager
Lack of confidence and competence among commissioners
A further important theme highlighted by key informants related to the lack of confidence and competence to address ethnic diversity and inequality among commissioning staff. Respondents felt that in some PCTs the lack of diversity within the workforce and the lack of connection to issues of inequality contributed to low levels of both confidence and understanding. They were also concerned that PCTs had been quick to cut engagement and equality posts in ongoing restructuring, thereby removing people who might have otherwise contributed a sustained understanding of minority ethnic needs and experiences.
As before, respondents noted that external consultants were often being called in from outside, so that expertise and resources tend not to be mainstreamed or embedded. And again, there was felt to be a tendency for PCTs to assume that members of staff from ethnic minority backgrounds would provide the necessary source of insight and would champion this agenda. Yet this went hand in hand with substantial reluctance on the part of some BME professionals to take on the mantle of this role (in part as a result of the marginalisation and exhaustion experienced by others, as described earlier). Elsewhere, some key informants reported a general unwillingness, both in themselves or amongst colleagues, to consistently raise the issue of ethnic inequality when other people did not, primarily because they were concerned that they might be perceived to be conflating personal and professional issues. Respondents also noted that, although public health might be considered the natural home for inequalities work within PCTs, this did not necessarily translate into a consistent and careful consideration of ethnic inequality amongst public health staff, this instead being highly dependent on individual confidence, expertise and interests.
Respondents also felt that commissioners could often hold unsophisticated understandings around ethnicity and often had a tendency to stereotype rather than recognise intragroup heterogeneity and changes in group needs, aspirations and experiences over time. These respondents worried that commissioners essentially tended to blame minority ethnic people themselves for poor access or poor experiences rather than considering potential limitations of the services on offer. As such, these commissioners were felt to equate responding to minority ethnic needs with the need for additional resources and/or special services:
So some people [commissioners] are a bit wary of going to certain groupings . . . [I’m thinking of] a very well educated executive who wouldn’t be willing to go to any of these, any of these meetings [with the Somali community] . . . I suppose internally within the system we’ve stereotyped what groups ask for, so what’s happened is actually without going out they’ve just assumed it’s going to be an angry mob.
GP/ex-senior commissioner
At the same time, however, respondents acknowledged the ways in which understanding and responding to ethnic inequalities can be complex and challenging. In this, they pointed to the need for greater support and direction at national level to equip commissioners to respond appropriately to these complexities and challenges.
Nonetheless, respondents’ narratives suggest that the lack of a wider supportive context means that there is no particular impetus for commissioning managers or their teams to recognise or address their low levels of understanding, confidence and competence, and no clear penalties for failing to do so: ‘People don’t know what they don’t know and so avoid it altogether’ (DH senior consultant).
Competing ways of making the case
Reading across and between the key informant interviews revealed the varied and conflicting ways in which the need for attention to ethnic diversity and inequality within health-care policy and practice is framed by different actors.
Interestingly, most respondents felt that focusing on legal duties had not been productive, serving instead simply to reinforce a compliance or ‘tick-box’ mentality rather than encouraging people to take ownership and enthusiastic action. Moreover, although some argued that social justice and discrimination provides the only legitimate frame of reference, others found this focus to be unhelpful and off-putting, and some even felt that framing the issue always in terms of inequality was potentially stigmatising and disempowering for minority groups: ‘The moment you raise the race agenda, people back off because they’re scared’ (third-sector manager and analyst).
Some respondents were particularly concerned about focusing on racial discrimination within the health service, which they felt had been overplayed and had served to alienate key actors who needed to be persuaded to work towards the same objectives rather than defending their (in)action. Others also argued that a predominant focus on racism, particularly within the mental health service arena, had diverted attention away from understanding a wider range of factors that might also contribute to higher levels of ill health amongst minority ethnic populations, including wider social disadvantage.
Elsewhere, some of the key informants talked about people strategically aligning the agenda with the ‘flavour of the month’, and worried that this made equalities work vulnerable to short-termism and threatened longer-term gains:
Equality and fairness on its own is an important area, and those leaders who lose that, lose a very fundamental thing. You can’t pick and choose equality and fairness into different areas. Human rights and fairness is a given for everybody. It’s the cornerstone for any business . . . It should be because it’s the right and the fundamental thing to do . . . It doesn’t have to be linked with QIPP. It needs to stand on its own as a priority. Let QIPP come to human rights and equality and inclusion area.
Strategic health authority senior manager
However, others argued the case that equality was genuinely an integral part of quality and efficiency issues and wanted to see a greater effort to position it more closely with these agendas regardless of their recent emergence as topical drivers of commissioning practice. This was felt to be part and parcel of mainstreaming inequalities work within, and aligning it to, core processes: ‘[We need to have] equalities embedded in the boring stuff that people feel they had to do, because that’s the way that people accept it as part of the institutional framework’ (NHS manager).
However, some examples of respondents’ aspirations for such alignment used language that did not necessarily serve to focus attention on ethnic health inequalities:
We aligned it [diversity and equality] with world-class commissioning . . . if you look at the competencies they apply to any commissioner really . . . So competency 5 was about knowing your population and the health needs of your population. Competency 3 was about partnership and how you’re engaging at a local level and all those.
Strategic health authority senior manager
Perhaps unsurprisingly, some respondents also pointed to the need to ensure that arguments for paying greater attention to minority ethnic needs were framed in terms of cost savings and/or efficiency:
What happens is things are pulled, because financially our situation has changed, and so therefore the priority is to take things off the table, and it becomes a bit of a soft target.
GP/ex-senior commissioner
If the condition is leading to increased cost, admission rates, referral rates, then we won’t have to give them any evidence, they’ve got that evidence and those are key priority areas for them, to reduce admission rates, reduce referral rates.
GP/academic
Several of our key informants were themselves aware of the potential conflicts between, for instance, arguments based on potential cost savings and those focused on issues of social justice, and felt that progress could be (and had been) undermined by advocates pulling in different directions. Some argued instead for the need to use a variety of arguments – as one respondent said, ‘to pump on all sides’ (third-sector senior manager) – to increase action on this agenda.
Enhancing health care for minority ethnic people: a role for commissioning?
Most of the key informants we spoke to considered commissioning to have a key role to play in improving health care for minority ethnic people and tackling ethnic inequalities:
Our philosophy and approach round the whole equalities agenda, because it really does need to sit in the heart of commissioning, and that’s half your battle over once you get the commissioning end of it right.
Strategic health authority senior manager
Although recognising that there are issues with providers around race equality, the real lever for change lies within commissioning.
Third-sector senior manager
Two aspects of understanding and addressing ethnic diversity and inequality highlighted by respondents seem particularly tied to the commissioning role. First is the importance of understanding the health needs of the whole population, including the needs of those people who are not already accessing services. Second is the need to address shortfalls in the ability of current provider organisations to deliver the types of services that are required to meet diverse needs, that is, the need to ‘develop the market’.
Although respondents saw commissioning as a real lever for improvement, they also recognised that significant progress still needs to be made, and that commissioners have hitherto rarely pushed the agenda. Some key informants felt that provider organisations, particularly committed health-care practitioners or third-sector organisations, were most often the current source of innovation around meeting minority needs: ‘This comes back to a committed clinician identifying a need and doing something about it’ (third-sector senior manager).
Although respondents identified some PCTs that had achieved a more embedded approach to considering and addressing ethnic diversity and inequality, they generally felt that their responses had been piecemeal – being characterised by passionate individuals and short-lived projects, or being prompted by some kind of serious problem rather than being proactive and sustained:
The whole of this needs to feature right the way through that [commissioning cycle], so right from identifying needs. So you identify a particular need, you then find the right providers to commission that and then build into the requirements what it is that you want them to specifically do. Whereas, at the moment, we don’t . . . We kind of commission whatever service and just commission it for the whole population but not really set any requirements for different parts of our population that might need to access that service or experience that service in a particular way.
Strategic health authority senior manager
Use of evidence on ethnic diversity and inequality in commissioning: current patterns and influences
Patterns of evidence use
Most respondents argued that evidence use should be a big part of effective commissioning for multiethnic populations and that a wide range of complementary evidence sources were useful at different stages of the commissioning cycle:
There’s information at all sorts of levels. There is the demographic stuff, just knowing who’s living in your patch . . . the epidemiological information . . . the health observatory work and other sources, what that means in potential need for services . . . But then there also needs to be the opportunity to engage with representatives of local communities . . . where commissioners actually listen to what is being said about what is needed.
Third-sector senior manager
However, perhaps reflecting the wider marginalisation of the ethnic equality agenda, and the patchy use of evidence more generally described above, all respondents felt that in practice there was often very limited use of evidence on ethnic diversity and inequality within commissioning work.
In terms of understanding population health needs and identifying gaps in provision, most respondents emphasised the central importance of good ethnic monitoring data, particularly in primary care, as this was felt to offer a population-level ethnic profile.
Some respondents also drew attention to the potential of JSNAs to widen the focus of commissioning beyond those who already engage with services to those with unmet need. Nonetheless, these respondents raised concerns about the current lack of adequate depth of JSNAs in relation to minority ethnic communities and their weak connection to either strategy or action: ‘What we found from that evaluation [looking across a region] was that JSNAs themselves don’t disaggregate [population groups]’ (strategic health authority senior manager).
As before, respondents were often aware of examples of good practice, for instance when special pieces of needs assessment work had been commissioned by PCTs, but felt that these were usually the exception rather than the rule:
What they did was set up their own engine around patient profiling and they supported their GP practices. I think they’ve got well over 50% now of GP practices or more who are doing the patient profiling, and they’re not just doing it by ethnicity.
Third-sector manager and analyst
In relation to identifying solutions and procuring services, key informants thought that it was rare for service specifications to include detail on how services should address ethnic diversity or tackle inequalities. One respondent felt that, even when commissioners were aware of the need for service providers to address ethnic inequalities, it would be unusual for commissioners to compile evidence around potential service responses or to use such information to inform the service specification, with one respondent noting that this would be considered ‘a nicety not a necessity’ (GP respondent with extensive past commissioning experience).
Respondents felt that practitioner experience and insight could be important both in flagging up problems and in identifying viable routes of intervention to improve services for minority ethnic people. Key informants gave examples of clinicians raising issues and pushing for appropriate responses, and also of some PCTs that had facilitated inputs into the commissioning process from community development workers, thereby gleaning important insights about unmet need and poor service experiences. But once again, respondents often felt that these aspects generally needed further strengthening.
Finally, in terms of monitoring performance and prompting further improvement through the analysis of service processes and outcomes, respondents gave few examples of contracts, key performance indicators (KPIs) or performance review mechanisms being used to generate information on service performance in relation to different ethnic groups. Several participants regarded evidence of patient experience, whether generated through qualitative or quantitative data sources, as an important potential source of information. Nonetheless, they felt that this evidence was often not drawn on by commissioners, and was rarely disaggregated by ethnic group. Indeed, even when respondents described initiatives to commission new services that met the needs of an ethnically diverse patient population, it was rare for these to also include provision for monitoring against ethnicity-specific outcomes:
So, the thing about ethnic minorities, making sure there’s stuff in there [in contracts] about equality, doing equity audits, using interpreters and so on. But then I think it’s worth doing, because you know, most professionals will take on-board those things, but on the other hand there’s almost never the capacity to actually monitor whether that’s really happened in practice . . . so monitoring is very unsophisticated.
Public health observatory senior manager
Gaps in data and evidence
The key informants identified a range of issues relating to the quality and quantity of available evidence on ethnic diversity and inequality that contributed to the low levels of usage described above.
First, most respondents highlighted the absence of a detailed consideration of minority ethnic needs within many influential policy documents, such as National Service Frameworks (see www.nhs.uk/nhsengland/nsf/Pages/Nationalserviceframeworks.aspx). Second, many respondents highlighted the persistent poor quality of ethnic monitoring/patient profiling data within service settings, and particularly within primary care. Third, many respondents felt that there was still little evidence on how services should be shaped to address ethnic diversity and inequalities. One respondent described this situation as ‘scandalous’, arguing that the academic public health community had failed to provide an adequate steer for commissioners on ‘what works’ to reduce minority ethnic disadvantage (as well as other health inequalities). Several respondents noted that, in the absence of alternatives, commissioners predominantly drew on national syntheses of evidence, such as those produced by NICE, and that these include very little detail on how to shape services for minority ethnic populations. Fourth, respondents pointed to the lack of all-important information on the cost-effectiveness of interventions/service modifications, something they argued was essential in the current climate of cost-cutting to build appropriate business cases for selective dis- and reinvestment.
Notwithstanding the gaps in the evidence base, key informants also felt that commissioners could often be guilty of overlooking potentially important sources of evidence or assuming that there was a lack of evidence when this was patently not the case. For instance, some respondents pointed out that ethnic monitoring data is often more complete than might be imagined and that there are strategies that can be used to work around incomplete data and produce useful information. Yet they felt that commissioners frequently did not request such data from provider organisations. Indeed, the general failure on the part of commissioners to ask such questions of the data that were available was highlighted by several respondents:
What we found was the commissioners were really, really weak on setting these requirements in terms of this cycle for the providers. When we went to talk to the providers, the providers were saying actually we’ve got loads of data and evidence that we collect but the commissioners never asked for it around ethnicity.
Strategic health authority senior manager
Some respondents also noted the many missed opportunities for generating evidence through the careful piloting of innovative interventions. They felt that too many initiatives aimed at addressing minority ethnic disadvantage were short-lived and remained unevaluated, so that lessons were neither learnt within the organisation nor shared more widely. Some respondents also felt that commissioners were too reluctant to seek out and learn from interventions developed and tested elsewhere; in the words of one respondent, there is a culture of ‘if it’s not made here then it doesn’t fit’ (third-sector senior manager). Similarly, they felt that too few commissioners drew on national data and research evidence to inform their local picture:
I think most of the time people don’t know how to use the national published research at all, and I think if you look at commissioning . . . I think there’s a lot of work to be done with the commissioning teams . . . I think there’s a major issue about their capability and competence to be able to use [evidence].
Strategic health authority senior manager
Many of the key informants felt that commissioners were not generally good at drawing on the expertise of, and insight from, third-sector organisations or service users and members of the public from minority ethnic communities, to fill gaps in their understanding of need or identify viable solutions:
There are many sources and we need to look beyond the kind of NHS sources as well, because there are lots of third sector organisations, both regionally and nationally or locally that might be working with some of the groups that have far better information about their communities on certain health issues, but we’re not really gathering that. Even when they’re coming to us as the advocates or the activists through their local interest networks or whatever and giving us that information, is it making the journey into commissioning for example? I think there are serious question marks about that.
Strategic health authority senior manager
Well in central XX we have no XX service, and there’s no patient there coming forward, because they’re not as coordinated, they can’t speak the language, they can’t articulate very well what their needs are, and so therefore they can’t really, they have very little advocacy, and so you have that disparity which plays out in the system too . . . you’ve already silenced the voices if that makes sense, of a lot of ethnic minority groups, because they don’t understand the system, and they have very few people who represent them in the system.
GP/ex-senior commissioner
In addition to missed opportunities to draw in relevant evidence, some key informants bemoaned the lack of a push from commissioners to improve processes of data collection, analysis and reporting. In particular, respondents noted the persistent lack of commissioner pressure for better ethnic monitoring: ‘I think the London Strategic Health Authority actually set targets for their PCTs and GPs to roll out ethnicity recording. But . . . it’s always been patchy’ (third-sector manager and analyst).
Some felt that continued scepticism about the value of ethnic monitoring among some practitioners and commissioners tended to hamper progress. In contrast, others felt that it reflected a basic lack of will power to prioritise this area, or even suggested an intentional resistance to collecting and reporting these data:
The lack of data is actually kind of a useful shield for people to do nothing with as well, so you know, the fact that we haven’t put ethnicity high up in any of this is because there hasn’t been data, it’s not in anyone’s interest to have data, because then, then you might see something you have to fix.
Third-sector manager and analyst
Conceptual and practical challenges
In addition to their more general observations on the quality and quantity of evidence relating to ethnic diversity and inequality, the key informant interviews highlighted a number of important challenges that are encountered in generating and mobilising evidence on ethnic diversity and inequality.
First, respondents noted a range of challenges relating to describing patterns of health and health care by ethnicity, including high levels of population turnover and the need for regular updating; a lack of enumeration of smaller ethnic groups rendering them invisible in quantitative data; and heterogeneity within ethnic categories and the need for more detailed breakdowns (such as by age, language competency, migration status or religion).
Second, some key informants identified a range of complexities relating to commissioners’ broader understanding of poor access, poor experiences and poor outcomes for minority ethnic people; and particularly the importance of unpacking the underlying causes to identify potential interventions that might be prescribed by commissioners. For instance, key informants highlighted the complex relationships between minority ethnic identity and low socioeconomic status, and between minority ethnic identity and migrant status:
All the things that come with low socioeconomic status, are a factor in it, but . . . there’s various aspects to culture and language and other things, you know, entangled with this . . . you know, you’ll need to think about the two things at the same time, but conceptually it’s quite tricky . . . but I think this is a real problem . . . because I think unless that gets, you know, straightened out it is very difficult for people to know what they think they’re doing, and understand ‘what is this problem we’re trying to solve here?’
Third-sector manager and analyst
Third, the interviews highlighted challenges in relation to identifying effective responses to unmet need and inequalities. Respondents noted a lack of guidance on how findings on the effectiveness of interventions should be translated across different contexts, and the need to weigh up the pros and cons of specialist service responses compared with the pros and cons of efforts to accommodate diverse needs within mainstream services. Some respondents also felt that it was difficult for commissioners to establish feasible approaches to monitoring service outcomes by ethnicity and thereby determine the degree of success of service modifications.
More generally, several respondents alerted us to the need for work that more clearly identified standards and expectations around commissioning services to meet diverse needs and address inequalities. They felt that pockets of innovation and progress often existed in isolation, and that more sharing of lessons learned was needed to establish common understandings and encourage more consistent attention to these: ‘You know, the idea of what good practice would look like, I think that is a question worth bottoming out’ (third-sector manager and analyst).
Mobilising evidence for improved services
There were somewhat mixed views among the key informants in relation to how important the generation and application of evidence might be to the goal of improving service access, experiences and outcomes for minority ethnic people.
Some respondents recognised the increasingly strong discourse around evidence-based policy-making and felt that a lack of data and evidence on ethnic diversity and inequality presented a major obstacle to action. As mentioned earlier, respondents were concerned about the absence of detail on minority ethnic health needs, particularly in JSNAs, which they felt undermined efforts to make progress in this area; as one respondent said, ‘you’ve lost at first base’ (strategic health authority senior manager). Likewise, respondents felt that the limited evidence on effective interventional strategies to address ethnic inequalities was a major impediment to action in the current climate:
I think part of it [lack of attention] is due to lack of information . . . a lot of the data on access to services and so on just isn’t there by ethnicity.
Third-sector manager and analyst
Because that’s the other thing that then inhibits people, is saying, ‘OK, so you’ve told me what the problem is, let’s do something about it’, ‘oh well let’s do an evidence based response to this’, and of course you’re back in the woods again, because you don’t know necessarily what’s going to work.
Third-sector manager and analyst
These respondents also emphasised the importance of rigorous evidence use, arguing that poor analysis leads to inappropriate responses. Some even accused other stakeholders of ‘muddled thinking’ and questioned the extent to which programmes of work aimed at tackling ethnic inequalities – such as Delivering Race Equality94 and Pacesetters95 – had been sufficiently ‘evidence based’:
You do the epidemiology and guide your prioritisation and your actions on that basis, rather than just treating people as a homogenous group of black or Asian people, do you know what I mean? I think sometimes the race agenda didn’t do itself any favours by taking that kind of victim role all the time . . . So I think if you really want to tackle the problem you need to do your diagnostic properly and scientifically. I think that’s really what I’m saying. We need to bring science to it.
Third-sector manager and analyst
In contrast, other respondents, although acknowledging the contribution of data and research evidence, questioned whether weaknesses in this area were really the most significant obstacles to progress towards improved services:
It just feels like some of it, it’s not rocket science to find out what’s happening with some of the black and Asian communities [in town X] . . . I could have told them that at the age of ten, some of it. But yet, nothing significantly – we’ve been doing things at the edges, tinkering at the edges . . . the Asian population is huge [in town X] . . . Yet in terms of commissioning and targeted interventions of that community, it’s still not . . . you know. It’s the same in Y; any community you look at.
Strategic health authority senior manager
Selective research, selective thinking. For example, if they want to progress on, say, diabetes within the Asian community, or infant mortality amongst Pakistani women, there’s enough information out there that tells us exactly where the issues are, where the concerns and the problems are. What stops people doing that? . . . There isn’t that passion to make things happen for that particular group.
Strategic health authority senior manager
Linked to this awareness of other, more systemic factors blocking action towards improved services, several respondents talked about the need to connect decision-makers to the issues and felt that evidence needed to play a role in this, acting in an influential rather than a purely instrumental way. A combination of personal stories alongside hard facts was thought to be particularly powerful here, with one respondent describing a ‘pincer movement’ to influence key decision-makers, bringing together national statistics showing the scale of an issue with an authentic personal narrative, so that the ‘light bulb goes on’ (third-sector senior manager).
Respondents also emphasised the need for ongoing engagement and persistence, as audiences are often not already primed and progress is likely to be slow:
Just evidence to show that, how badly people are dealing with a particular issue, that needs to be almost a starting point.
Public health observatory senior manager
I think part of the challenge really for a lot of, and especially with the new GP commissioners, is getting them to understand that there might be a problem here.
Third-sector manager and analyst
Respondents also talked about the importance of the credibility of the evidence and its bearer, and the significance of using peer networks – particularly among clinicians – to effectively mobilise evidence. They felt that different audiences were comfortable with, and valued, different types of evidence (particularly whether this was qualitative or quantitative evidence) but that many commissioners recognised the need for instrumental, ‘how to’ evidence most readily:
GP/academic: I think they need statistics, in terms of if there is a problem in access, in referrals, you know, in high referrals, low referrals, mortality, I think you need to have evidence, you need, only then will someone start looking at it, if you don’t have any evidence they will say, ‘Well what, there doesn’t seem to be a problem’.
Interviewer: And particularly the quantitative evidence?
GP/academic: Yes, so much so.
Commissioners want some information, but mostly solutions with a business case.
NHS manager
Perhaps of particular significance in this area, respondents expressed concern that evidence brought to commissioning relating to minority ethnic health needs and potential solutions is often subjected to higher quality standards than that required for other issues: ‘The proof that is required for commissioning mainstream services is of a far lower level than the proof that is required for commissioning specialist services’ (third-sector senior manager).
Although respondents recognised that the current financial climate meant that any proposal would be likely to be challenged, they felt that there were two key additional factors that meant there was usually closer scrutiny of ethnicity-related evidence. First, responses to ethnic inequalities are often constructed as new and additional to, rather than as improving the quality of, existing services. Second, commissioners are usually distant from these communities, lack understanding of their needs and are fearful of taking risks. One respondent noted that these factors together tended to raise significant obstacles to action on inequalities with ‘people waiting for the evidence base for years’ (GP).
Chapter 4 Commissioning in practice: organisational structures and cultures
Introduction
As described in Chapter 2, the case study work was intended to provide an in-depth look at commissioning practice at strategic and operational levels, involving the integration of data on a number of levels and providing a detailed contextual analysis of actions and relationships. Although the case studies provided further data of relevance for research questions 1 and 3, they were particularly intended to focus on research question 2.
Research question 2: how does organisational context shape the mobilisation and utilisation of knowledge relating to ethnic diversity and inequality?
-
How often, and at what stages, do managers apply research evidence relating to ethnic diversity and inequality in their commissioning tasks?
-
How are commissioning teams constituted and organised? How does this impact on evidence use?
-
Who is seen as holding expertise and insight in relation to ethnic diversity and inequality? Why?
-
To what extent do PCT commissioning organisations have explicit models, structures, processes and objectives that support the mobilisation and utilisation of evidence? Do these consider ethnic diversity?
-
In what ways does managerial behaviour support and encourage, or deter, the explicit consideration of research evidence relating to ethnic diversity and inequality within commissioning teams?
-
In what ways do the available infrastructure and resources support and encourage, or deter, the explicit consideration of evidence relating to ethnic diversity and inequality within commissioning teams?
-
How do national, regional and organisational policy priorities inter-relate to shape the mobilisation and utilisation of evidence in this area?
Although the data collection activities were nominally undertaken as part of either the strategic-level or the operational-level case studies in each study site, in practice there was overlap in the material generated. For instance, many of the interviews conducted for the operational-level case studies also provided rich insights into the wider workings of the organisations, whereas observation of strategic-level meetings revealed information not only about organisational priorities and structures but also about how individual actors might exert their own agency in responding to them. Therefore, although the findings are organised into two chapters – Chapters 4 and 5, with the current chapter focusing on organisational-level structures and cultures – we draw across the range of data generated as appropriate.
The case study work provided confirmatory evidence in support of many of the themes highlighted by the key informant interviews, and gave more detailed illustration of how these factors played out within the operational settings of the three PCTs. In addition, this stage of the project provided further insight into how commissioning work is achieved in practice, and in particular the factors operating at different levels to shape and constrain the use of research and other forms of evidence in commissioning in general as well as in relation to ethnic diversity and inequality.
We therefore take the key themes highlighted from the key informant interviews in Chapter 3 as a starting point and use summary tables to illustrate the ways in which the case study materials support or refute each of these, providing selective commentary to highlight additional themes not previously highlighted by the key informants.
Descriptive overview of the three case study sites
As described in Chapter 2, our case study work was centred on three PCTs: NHS Sheffield, NHS Bradford and Airedale and NHS Leeds. The case study sites were selected on both practical and theoretical grounds, providing both the possibility for fruitful networking and learning across the partner organisations and the opportunity to observe commissioning practice within a range of contexts. Table 2 provides a sketch of these three PCTs, illustrating some important commonalities and differences.
| Site characteristics | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) |
|---|---|---|---|
| Size of population served (approximate) | 550,000 | 530,000 | 750,000 |
| Ethnic profile of population (2011 census estimates2) | 19.2% non-white British | 36.1% non-white British | 18.9% non-white British |
| Largest enumerated minority ethnic groups | Pakistani/British Pakistani, Indian/British Indian, white other, Chinese | Pakistani/British Pakistani, white other, Indian/British Indian, Bangladeshi/British Bangladeshi | Pakistani/British Pakistani, Indian/British Indian, black British |
| No. of staff (2011 NHS staff survey96) | 309 | 400 | 478 |
| % of workforce not white British (2011 NHS staff survey96) | 9 | 15 | 11 |
| No. of NHS provider trusts (excluding ambulance) | 3 | 3 | 3 |
| Sole commissioner for NHS trusts | No | Yes | Yes |
| No. of emergent CCGs (as at December 2012) | 1 | 3 | 3 |
| Structural changes during project period | None | Clustered with case study 3, October 2012 | Clustered with case study 2, October 2012 |
| WCC 2010 overall score (out of 200) | 166 | 157 | 120 |
| WCC 2010 competency 5: manage knowledge (out of 12) | 9 | 9 | 5 |
| Research activity | Strong; established partnerships with universities | Strong | Developing rather than established |
| CLAHRC engagement | Yes, strong involvement | Yes, strong involvement | Yes, but weak and very recent |
| E&D staff | 0.4FTE, Grade 8a | 1FTE, Grade 8a | 1FTE, Grade 8a; 0.35FTE Grade 8b; administrator 0.5FTE, band 4 |
| E&D structures | Corporate Equality and Human Rights Group, meets monthly | Reporting to Governance and Risk Board Committee | E&D Steering Group link via chair to Cluster Board |
| Member of Race for Health | No | Yes | Yes |
| Engaged in Pacesetters programme | Yes | Yes | Yes |
| Engaged in Innov897 (diverse leadership) | No | Yes | Yes |
Table 3 provides a summary of the strategic-level data collection activities undertaken in each of the three sites. In each case the bulk of our data collection involved individuals and groups working within the PCTs, but, recognising the importance of partnership working and joint commissioning arrangements, we also engaged with relevant individuals and groups within the local authorities, particularly social care commissioners, as well as managers within NHS provider trusts and the third sector.
| Data phase | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) |
|---|---|---|---|
| Key informant interviews completed in phase 2 | Three PCT commissioning managers (one senior), three public health managers, three local authority commissioning managers, one GP, two third-sector managers | Three PCT commissioning managers (one senior), one public health consultant, one local authority commissioning manager, one GP | Two PCT commissioning managers, two local authority commissioning managers, one third sector manager, one public health consultant, two PCT Information officers, one GP |
| Key informant interviews completed in phase 3 | One NHS commissioning manager (senior), one public health practitioner, one non-NHS commissioner (senior), one third-sector manager, one provider trust E&D lead (EDS focus), one public health intelligence manager | Three NHS commissioning managers (two senior), one public health practitioner, five E&D leads | One GP, one E&D lead, two NHS commissioning manager, three senior NHS managers |
| Total no. of interviews | 18 (13 white British; eight male) | 15 (12 white British; five male) | 16 (16 white British; nine male) |
| Observational work | Corporate Equality & Human Rights Group (seven meetings), Health Inequalities Board (nine meetings), EDS implementation (one workshop) | Strategic health authority workshop on EDS (one), EDS planning and grading meetings (six), Equality Group meetings (six), Innov8 research project meetings (five) | E&D Steering Group (one meeting), JSNA equality impact assessment meeting (one), EDS planning and grading meetings (two) |
| Total no. of hours | 35 | 42 | 30 |
| Documentary analysis | Core docs: JSNA 2010; Achieving Balanced Health (Corporate
Plan); Health Inequalities Action Plan; draft BME commissioning
strategy; EDS grading documents; Equality Objectives;
Commissioning for Quality Others: service specifications; needs assessments; business cases; communities of interest report; action plans |
Core docs: JSNA 2011; EDS grading documents; national EDS guidance; EDS panel minutes; Equality Objectives; patient survey equalities data; Innov8 Charter; Innov8 precursor reports; research report drafts, final reports, minutes from meetings, literature review | Core docs: JSNA 2011; Fairness Scheme (single equality scheme);
Innov8 Charter; Single Integrated Plan Development 2011/12;
Patient and Public Involvement Strategy; WCC report; Corporate
Communications and Engagement Strategy; Leeds City Priority
Plan; Health and Wellbeing Board report; reports to Scrutiny
Board; Public Sector Equality Duty information; E&D Steering
Group: terms of reference and minutes; equality impact
assessments; board reports; BME health report Other: service specifications, needs assessments, business cases |
| Total no. of documents | 30+ | 70+ | 30 |
| Other | Frequent interaction with commissioning staff through honorary post; frequent reflection by co-researcher; feedback events after phase 2 | Frequent reflection by co-researcher; feedback meeting after phase 2 | Co-researcher membership of E&D Steering Group; regular reflection by two co-researchers; feedback event after phase 2 |
| Reflections on data volume and quality | Large volume; detailed interviews; good opportunities to observe; potential for slight public health bias as strongest links there | Small number of third-sector interviewees but strong third-sector involvement in Equality Group meetings. Detailed investigation of EDS process provides useful lens; restructuring limited observation of other strategic-level work | Detailed interviews; limited third-sector interviews but good sense of relevant BME third-sector activity through informal links of researcher/co-researcher |
Case study work began in each site in phase 2, with a series of key informant interviews with individuals identified as having wide experience of commissioning work within their own cities. In phase 3 we employed a range of methods including interviews, structured observations and documentary review to enhance our understanding of strategic-level work in each site. The focus here was on understanding the organisational structures and cultures operating within the three PCTs to shape commissioning work. Opportunities for data collection varied across the sites, reflecting different structures and networks, but multiple points of contact were used in all three sites to ensure a range of perspectives. In addition, the implementation of the Equality Delivery System98 and the production of Equality Objectives took place during the study period and were investigated across all three sites. Further, the co-researchers engaged in regular structured reflection, completing reflective diaries or debriefing exercises with the university researchers, across the whole study period.
Commissioning aims, organisation and impact
Table 4 illustrates that many of the general themes relating to health-care commissioning highlighted in the national key informant data in Chapter 3 were reiterated in our strategic-level case study work.
| Themes from national key informant interviews | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) | Between-case comparisons |
|---|---|---|---|---|
| Financial drivers dominate | ✓ History of overspend; consistent message across organisation | ✗ History of sound financial management; current focus on QIPP | ✓ Financial drivers mainly combined with government priorities | ∞ Consistent current focus but more recent in case studies 2 and 3 |
| Department of Health-led quality agenda a secondary driver | ✓ Large team and infrastructure; consistent message and visible commitment across organisation | ✓ Large team, often described as carrying out risk management; somewhat isolated | ? Visible infrastructure but not prominent in interviews | ✓ Confirmed across all three sites; national agenda reflected in local-level resources and activity |
| Other national agendas and targets also prompt local action | ✓ Response to health visitor target clear
illustration ∞ Not all agendas get response |
✓ National targets consume energies | ✓ National targets are key levers for local action | ✓ Confirmed across all three sites but ‘obedience’ of PCTs to national drivers variable |
| Many commissioners see contract management (transactional work) as main responsibility | ✗ Clear transformational orientation and explicit aspiration | ✓ Contracting and performance management been key focus; one interviewee talked of ‘bean counting’ | ✗ Clear transformational orientation and explicit aspiration | ∞ Despite limited impact, many commissioners do hold a transformational model |
| Needs assessment not linking to commissioning action; limited impact on service reshaping; innovation often provider led | ✓ Widely expressed sentiment. Observations confirm many
areas have no active commissioning ∞ But redesign projects and ongoing programmes and PCGs |
∞ Observations support; MSP introduced to encourage transformational work but largely abandoned as ‘too much on top of the day job’ | ✓ Generally true; individual knowledge of area and
motivation important ∞ ICTs and service redesigns aim to be transformational |
∞ Confirmed across all three sites but case study 2 much weaker transformational focus than case study 1 or 3 |
| Commissioning organisations lack power in relationships with NHS provider trusts | ✓ Consistently reported; ‘there are no
levers’ ∞ Dissenting voices outside PCT, e.g. ‘weak commissioning’ |
∞ Observation suggests this is true; not perceived this way at strategic level | ✗ Not perceived this way at strategic level; commissioners control membership of decision-making groups | ∞ Divergent perspectives; provider–commissioner relationships operate on many levels, some are productive |
| Involvement of wider stakeholders important to commissioning but variable in practice | ✓ Strong self-image of partnership working but varied models in practice | ✓ Strong self-image of partnership working but varied models in practice | ✓ Lots of stakeholder involvement/consultation around JSNA but variable in other areas | ✓ Comparison across sites confirms variability; indications of increasing partnership work, particularly around JSNA |
| Public health input to commissioning work important but variable in practice | ✓ A ‘matrix’ organisation with public health visible and influential in health-care commissioning | ✗ Public health role mainly seen as needs assessment and commissioning public health services | ∞ Seen as key actors in commissioning process; variable in practice | ✓ Comparison across sites confirms variability in how public health input is both sought and valued |
| PPI important to commissioning but limited in practice | ✓ High-level consultation; public
relations ∞ Some commissioning areas have sustained good PPI |
✓ High-level consultation; public
relations ∞ Some commissioning areas have sustained good PPI |
∞ Good PPI engagement in some areas but limited input into actual commissioning | ✓ Confirmed across all three sites. Rhetoric of PPI not reflected in influence on commissioning |
In particular, the strong focus on curbing expenditure, particularly through reducing secondary care usage, and the dominance of national drivers, particularly around quality and the NHS Outcomes Framework,93 were clearly evident. Importantly, however, there was evidence to suggest that not all national drivers and targets are responded to with the same degree of senior-level direction and co-ordinated action across the organisation. Differential organisational responses appear to relate to perceptions of both achievability and accountability, with the following questions being raised: Is the target reasonable? Is this really within our remit and responsibility? How closely are we being monitored on this area of performance?
The case studies provided confirmation that commissioning has had limited impact on reshaping health-care provision and that needs assessment work and commissioning action are not as closely connected as they should be. Nevertheless, we found an explicitly transformational aspiration in two of the three study sites, at both organisational and individual level, and the third had begun work to move towards a more transformational approach. The case study work added to our understanding of factors that limit transformational potential by illustrating the fragmented way in which commissioning work is organised and delivered. We found that transformational projects tended to be undertaken in relative isolation from each other, focusing on particular disease pathways or service areas, often working within fixed ‘envelopes’ of spend. This often appeared to be a pragmatic way of managing many competing demands and vested interests both within and outside the PCT, as well as negotiating some degree of change within elements of existing service configurations perceived to be fixed. Key actors were well aware of these limitations and there were some attempts under way to take a more holistic approach – to pool budgets and address the interplay of different elements of service provision in the form of larger programmes of transformational work. Importantly, there was also variation across the three sites in the extent to which commissioning options were perceived to be constrained by powerful NHS provider trusts.
The three PCTs were structured and organised quite differently. In two of the three PCTs there was a stronger internal sense of the whole organisation being a ‘commissioning organisation’, whereas in the third there appeared to be a more disjointed approach with separate teams not necessarily having a clear sense of their work contributing to the broader commissioning agenda. The role of public health within health-care commissioning varied significantly. When public health was closely engaged across the commissioning cycle and not confined to needs assessment, a strong population perspective and inequalities focus (although not necessarily ethnicity focus) was evident, again chiming with the earlier key informant reports. However, even when public health was well integrated into the core health-care commissioning work, there were evident tensions, with public health priorities at times being seen as conflicting with other drivers, and some public health staff expressing the feeling that they had to battle to have their objectives reflected in strategies and provider contracts. (Respondents have been identified by their current organisation and broad role. More specific job titles and case study site have been avoided to preserve anonymity.)
But if you talk to people in strategy they’ll, they’ll talk about public health as the biggest financial leak that there is, do you know what I mean? Because it’s sort of like we can’t afford what public health want, public health drive all of this, you know . . . woolly stuff that we can’t afford. You know what I mean, and that’s, you’ve got to understand that there’s always those different perspectives, so there’s XX there going well we need more, we need health checks rolled out, we need this, we need that, we need all of these health improvement workers doing all of this lovely woolly work and taking people out on walks to make them healthy and stuff, and we’re here sort of going we can’t meet our A&E [accident and emergency] targets because we can’t afford the doctors and we’re struggling with contract neg . . . It’s the balance, you know, XX is there with his performance, we need to be performing, what do we need to do to up performance.
PCT commissioning manager
In relation to involvement of wider stakeholders and patients and the public within commissioning, the case studies found that these elements were recognised as important across the three sites but not yet operationalised effectively.
In addition to the themes in Table 4, the case study work also revealed the importance of local drivers and the challenge of responding to national directives within the context of local priorities and opportunities:
There tends to be top-down directives around what services should look like and a lot of obviously NICE guidance and so on. As well as that we would, you know, draw on for that, so it’s to oversee the commissioning cycle within [the city], but in that, in the context of national policy and priorities, and local policy and priorities, because obviously we have different, you know, configurations of service, and particular opportunities to improve things locally which aren’t so nationally determined. But, so in terms of that commissioning cycle it’s about understanding the needs, understanding how we’re currently meeting those needs with our current models of service, how we might improve those, reviewing the performance . . . we do have quite a big focus on outcomes . . . so we regularly would look at key indicators that we’re responsible for, some of which we have, you know, national targets for, others we’ve determined local targets.
PCT senior public health commissioner
Organisational structures and influences on ethnic diversity and inequality work
As illustrated in Table 5, the case study work tended to confirm and further illuminate the organisational structural and cultural factors identified by the national key informants as barriers to attention to ethnic diversity and inequality. The consistent message was that this remains a marginal, poorly resourced and, at times, contested agenda within commissioning.
| Themes from national key informant interviews | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) | Between-case comparisons |
|---|---|---|---|---|
| Lack of direction from strategic health authority or DH; no performance management; few supportive policy documents or structures | ✓ Respondents reported weak strategic health authority leadership on equality | ✓ Local work to establish EDS in spite of weak direction from strategic health authority and DH. Past good work built on national drivers, e.g. Delivering Race Equality | ∞ Strategic health authority not prominent; focus on sign-off of top-level strategic plans, no reference to equality. But key strategic health authority role in Innov8 | ∞ Where national policy is explicit, local champions strive to use it influentially. Regional and national champions important |
| Ambivalence and lack of leadership from the top | ✓ No leadership during project; active obstruction also evident; complacency | ✓ Seen as good at race equality externally but
complacency ∞ Waning leadership over time |
✓ Little organisational ownership of this agenda | ∞ Confirmed in all three sites. EDS may offer useful framework to engender greater support |
| Not embedded in structures and processes; no reward or sanction; equality impact assessments ineffectual; rare exceptions | ✓ Brief mention in top-level strategic documents but
consistently absent elsewhere. Equality impact assessments
‘tick box’ not linked to action ∞ Loss of accountability over time |
✓ Generally not mentioned explicitly, no focus in
contracting work. Equality impact assessments not
transformational ∞ Evidence of reduced attention over time |
✓ Senior staff statements of importance not reflected in consistent action or processes. Inconsistent equality impact assessment use; perceived to be outdated | ∞ Confirmed across all three sites. Past gains can be
lost with changes in senior leadership and new top-down
drivers ∞ EDS may hold promise |
| Marginalisation from other agendas with greater resource and infrastructure | ✓ Equality absent from quality documents; patchy attention in health inequalities work | ✓ Expertise seen as situated in E&D team and called on in ad hoc way when needed | ✓ E&D/inequality is seen as an add on, not core | ∞ Attitudes, arguments and strategies that sideline vary across settings |
| ‘Race’ and racism are taboo | ✓ Very rarely mentioned | ✓ ‘Community cohesion’ agenda avoids ‘race’; concerns about sensitivity and stereotyping | ✓ Very rarely mentioned | ∞ Confirmed in all three sites, but local discourses of ethnic diversity and inequality vary |
| Discourses question legitimacy; construct as special, costly, additional | ✓ Minority ethnic groups constructed as problematic, ‘hard to reach’, costly | ∞ ‘Special’ attention seen as unnecessary; presumed already embedded in work | ∞ Discourses present colour-blind approach, i.e. services for all; discourses of (il)legitimacy | ∞ Comparisons across sites confirmed and expanded range of obstructive discourses |
| E&D resource variable; often limited and isolated; senior appointments unusual | ✓ Very low E&D investment; E&D group not formally linked to other workstreams | ✓ E&D resource adequate and committed but reduced and poorly networked within organisation | ∞ E&D resources available but limited ownership and communication at senior levels | ∞ Individual skills, confidence and approach of E&D staff can compensate |
| Consultants often used rather than building in-house expertise | ∞ Some evidence of this but also exceptions | ✗ In-house capacity built; despite losses, West Yorkshire CSU has more capacity than elsewhere | ∞ Some evidence of this but also exceptions | ∞ Examples found but also in-house expertise that can be better utilised |
| Lack of staff diversity; lack of connection to the issues | ✓ Particularly at upper levels; lack of challenge by communities or third sector | ✓ Glass ceiling at Grade 6; BME staff network challenged cases but not organisation culture | ✓ Agenda driven by staff from white backgrounds; more diversity in short E&D projects | ✓ Confirmed in all three sites |
| Lack of overarching strategies or structures to link piecemeal projects or support ‘champions’ | ✓ Past effort at BME strategy not endorsed by PCT; isolated good practice not shared | ✓ Isolated projects; no well-established partnerships for race equality | ✓ Project-based work on BME communities; no overall strategy on inclusion/inequality | ✓ Confirmed in all three sites; reflects ambivalence and marginalisation |
The lack of direction from the DH and strategic health authorities, and a lack of senior local leadership on this agenda, was confirmed in all three sites. In particular, the absence of any kind of performance management was clearly reflected at local PCT level. In contrast to the highly developed infrastructures for monitoring quality and finances, the E&D resource was found to be low (particularly in case study 1) and poorly connected to these other strands of work. Importantly, in all three sites respondent reports and our observations confirmed that equality impact assessments were often poorly carried out, were detached from core commissioning processes and lacked impact or follow-up work:
What they tended to do was say, ‘OK, we’ve done our impact assessments, they’re on the website, that’s it, we’ve done it’. Whereas for me, if people, organisations really understood what impact assessment is about, it’s about a process.
PCT E&D manager
We’d been doing equality impact assessments without any sort of external input.
PCT E&D manager
We have had a process of equality impact assessments, but it was a fairly feeble process, it felt like, because I remember, in that there was no real follow-through.
PCT senior public health commissioner
Key documents, such as those relating to quality assurance, were found to lack any mention of equality. Furthermore, in all three sites we found poor specification of ethnicity within health inequalities strategies and targets.
In the absence of systematic and regular reviews of performance against equality standards, attention to ethnic diversity and inequality issues was largely found to be reliant on the interest and commitment of particular individuals (as discussed in Chapter 5). However, focused work was occasionally prompted by local patterns of service use by minority ethnic people, particularly those that were perceived to be problematic. Even more rarely, important aggregate outcome indicators were affected by rates within minority ethnic groups. One example of this was high infant mortality rates among the Pakistani population, prompting particular attention by public health commissioners. However, it should be noted that there were significant concerns among local stakeholders in two of the sites regarding the nature and adequacy of the response to this issue.
Looking across the three sites also confirmed that a range of obstructive discourses were in operation, with attention to ethnic diversity and inequality at times being explicitly blocked or undermined and at times being overlooked or sidelined by arguments that construct such a focus as unnecessary, inappropriate or too difficult. For instance, in one site a detailed strategy document focusing on the health and social care needs of ‘BME adults’ was prepared by mid-level staff from both the PCT and the local authority who had E&D as part of their role, but it was never officially adopted by the PCT despite considerable efforts to lobby senior leaders. Another example of obstruction found in two of the sites was the expressed need to focus on other equality groups and the implicit or explicit suggestion that sufficient focus had already been given to ethnic inequality issues. Importantly, evidence from all three sites confirmed the importance of strong leadership, with past gains being lost when senior staff committed to the agenda had left the organisation or moved roles because of restructuring.
An unhelpful reliance on external consultants to undertake ethnic diversity and equality work was seen but did not appear to be as much of a problem as the lack of structures and processes to connect in-house expertise to core commissioning functions. However, there were isolated pockets of good practice and a willingness at an individual level to enhance skills and confidence in this area, potential opportunities that largely remained unsupported by the wider organisational context. Nevertheless, in all three sites a lack of ethnic diversity among staff was evident, particularly at higher levels, and respondents felt that this undermined a more consistent focus on this agenda.
Despite this generally rather gloomy picture, our investigation of the Equality Delivery System and the Innov8 diverse leadership programme did suggest some potential avenues for progress towards a more enabling strategic environment, and these are discussed in more detail in Chapter 6.
Organisational structures and influences on evidence use generally
Table 6 confirms that the following themes from the national key informant interviews were clearly reflected in the case studies:
-
data use on spend and quality indicators was supported by strong internal infrastructures
-
public health involvement in commissioning tended to enhance the use of evidence (particularly population-level data)
-
there were clear expectations that commissioners would be aware of, and their work would reflect, national-level synthesised research evidence in the form of NICE guidance and policy documents, and there were processes in place to support this (e.g. regular circulation of new documents)
-
there were few structures or processes that routinely connected commissioning activity to primary research evidence
-
there was a lack of local evidence generation or sharing through the evaluation of interventions or service redesigns.
| Themes from national key informant interviews | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) | Between-case comparisons |
|---|---|---|---|---|
| Lack of structures/processes to guide evidence use or ensure standards | ✓ Diffuse responsibility; no standards, checklists | ✓ Diffuse responsibility; no standards, checklists | ✓ Disjointed approach to data generation; no processes to synthesise | ∞ Broader issue of poor information management revealed across all three sites |
| Limited resources/time constrains evidence use | ∞ Reported, but commissioning resource not
budgeted ? Main constraint external deadlines |
✗ Fractured evidence journeys reported as main block | ✓ Feeling of local data overload and lack of resource to turn into information | ∞ Other factors may be more significant than lack of resources |
| Selective evidence use tolerated; ‘policy-based evidence making’ | ✓ Examples of selective use observed and
reported ∞ Can be uncomfortable |
✓ Examples of selective use observed and reported | ? Not explicitly mentioned or observed | ∞ Evident across all three sites, but can clash with mental models of appropriate evidence use |
| Strong infrastructure to support data use on spend and quality markers | ✓ Large dedicated resource for quality; skilled performance team; regular reporting systems | ✓ Large resource dedicated to quality indicators, payment by results, etc. | ? Visible infrastructure but not mentioned by respondents | ✓ Confirmed across all three sites |
| Public health involvement enhances evidence use | ✓ Public health provides skills and extra
resource ∞ Public health skills variable |
✓ Yes, but inputs variable here, public health more remote | ✓ GP interviews confirmed public health importance in evidence use | ✓ Confirmed across all three sites |
| National synthesised research (e.g. NICE) core to process | ✓ Clear expectation; mentioned in contracts | ✓ NICE and DH guidance often cited | ✓ Lots of reference to NICE guidance; visible prompt to redesign work | ✓ Confirmed across all three sites; processes to support |
| Lack of routine trawling or use of primary research | ✓ Generally true | ✓ Generally true | ✓ Generally true | ✓ Confirmed across all three sites |
| Needs assessments not well connected to other stages of commissioning cycle | ∞ Widely reported but efforts under way to change this | ✓ Fractured evidence journeys, silo working | ∞ Variable, dependent on individuals involved, some good examples found | ∞ Evident across all three sites, but some good examples and efforts to improve |
| Narrow organisational understandings of what counts as evidence | ✗ Wide range used; no explicit line on what evidence
counts ∞ Stricter criteria used to block investment at times |
∞ Qualitative evidence and patient stories not well valued but attitudes changing | ✗ Wide range used; national and local data and service user experience | ∞ Understandings of evidence vary between and within organisations; not generally debated and no explicit standards/agreements |
| Evidence skills not highly valued in commissioners | ✗ Public health data/analysis input valued; productive partnerships with researchers | ✓ Public health distant from health-care commissioning; other skills valued more in commissioners | ✗ Public health input valued; recent relationships with researchers, inconsistent across commissioning areas | ∞ Varied picture; evidence skills valued but structures and processes do not always ensure they are drawn in |
| Lack of evaluative approach to transformational work | ✓ Confirmed bottom-line focus; lack of reflective culture | ✓ Few examples of transformational work; lack of reflective culture | ∞ Some examples found; personal interest prompts | ✓ Confirmed all three sites; missed learning opportunities. |
The following quotes from a local key informant clearly illustrate the contrasting organisational support and expectations around the mobilisation of nationally synthesised evidence compared with other, primary research evidence:
So we have a mechanism in this organisation for circulating and distributing new evidence that’s published, so our library service sends a daily bulletin around every day that says NICE have just published this, this has just come from the department, you know, whatever it might be . . . so that’s one mechanism, which is kind of very much a kind of top-down stuff . . . It’s kind of, the purpose of NICE is to make sure that we’re, we, commissioners and providers, are informed of research, which tends to be very clinical research, doesn’t it, the NICE stuff . . . the guidance and appraisals and new technology, all that stuff comes into the organisation. And that tends to be well-implemented I think, because there’s a clear route, we keep track of the NICE stuff that’s been published, and we have a mechanism for keeping track of how it’s been implemented. So the quality team will do that, and they will ask providers to report on their implementation of the guidance that affects them.
PCT senior commissioning manager
How well we use kind of research from other sources is probably more variable I think, and it’s part of everybody’s jobs, like H or S or whatever, as, you know, as the strategy managers, to keep abreast of what’s happening. And of course it’s part of professional clinicians’ jobs and service managers’ jobs to do the same, and that might involve subscribing to stuff, or, which might be more like specific alerts perhaps rather than magazines . . . So S will see stuff that I never see, and about her areas of interest. And of course the same with the GPs now, because again as clinicians and particularly sort of clinical leaders, it’s part of what they, they need to do.
PCT senior commissioning manager
Interestingly, although respondents often mentioned a lack of time and resource to read or compile primary research evidence, we also observed that some relevant in-house resources, such as literature search facilities and data analysts, were at times underutilised. Furthermore, it appeared that the actions constituting the commissioning process were not clearly prescribed, with many commissioning managers making independent decisions about how to use their time, suggesting that the lack of time for engagement with research (and other evidence) may reflect the perceived greater importance of other activities. However, there was also evidence that yearly cycles of activity and tight deadlines (a more general constraint on commissioning work) could prevent commissioning managers from feeling that they had time to regularly compile and review research (and other) evidence.
Also, it is important to note that we found no sign of any structures or processes to guide evidence use or ensure standards around the access, appraisal, synthesis or application of evidence of different types within the commissioning cycle. Thus, although it was clear that the PCTs had explicit governance arrangements for approving commissioning decisions and resource allocation, often involving structured business case templates and committee review, these did not include any explicit checklists on what types of evidence should have been drawn on or how they should be appraised or synthesised. Our observation of pieces of commissioning work further confirmed the lack of guidance to individual commissioners in terms of what evidence should be garnered and used in their work, and the consequent idiosyncrasy in how tasks were accomplished in practice.
Some themes from the national key informant interviews were importantly elaborated, or even refuted, by the case study work. First, although some key informants suggested that evidence skills are not valued in commissioners, we tended to find a more nuanced picture in our PCTs. Thus, although it was true to say that the evidence skills of health-care commissioning managers were very mixed and that this was not generally seen as a core skill, each of the three organisations had established working structures that aimed to ensure that evidence skills fed into the commissioning process effectively, although it was unclear how well these worked in practice:
It feels more like a push than a pull to me, at the moment, in terms of what I’m delivering [as a data analyst], but I’m Mr Ad Hoc in a way, a lot of what I do is kind of spur of the moment, somebody asks for something and I deliver that information, rather than be strategic or planned approaches.
PCT information officer
The data-analytical skills of both public health intelligence and performance management teams seemed to be particularly valued and drawn on extensively. Clearly, it should be recognised that the commissioning process demands a very wide range of skills and competencies and these are unlikely to be present in any one individual. So, for example, we found public health staff in lead commissioning roles who were skilled evidence users but felt ill-equipped to effectively manage contract negotiations, as well as strategic managers who had the opposite skill mix. Similarly, the case study work tended to suggest a more positive picture than the key informant interviews with regard to the range of evidence sources that are recognised by commissioning organisations.
Notwithstanding the fact that the actual impact on commissioning decisions was still felt to be limited, we found that in two of the sites there was organisational support for drawing in varied types of evidence, particularly patient experiences, which links closely with the national quality agenda. It was also noticeable, for example, in relation to the JSNA that work to enhance the inclusion of qualitative, experience-rich evidence had recently been started in two of the sites. Nevertheless, it was clear that understandings of what counts as evidence remain variable and fluid within organisations, and that there was little by way of guidance or standards on how different evidence sources should be weighted or integrated.
A further important theme highlighted by some of the national key informants was the selective use of evidence to support decisions already made rather than to inform such decisions. Respondent reports and observational work confirmed instances of this type of evidence use across two of the three sites. For example, the selective use of evidence to construct internal business cases was widely recognised. However, it is important to note that this type of evidence use was recognised as not being ideal and seemed to conflict with the mental models of how evidence should be used for many involved in commissioning:
I’m personally not convinced that we are that systematic with the assessment of evidence and evidence base, I would suspect that, there’s a, there’s occasional, if not more than occasional, use of selective evidence to make the argument.
PCT senior commissioning manager
[Reflecting on a piece of needs assessment work] It was nice to do, you know, and to really understand the issue, because it did feel a bit like oh, well actually we’re going to look and see what the issue is and then work out what to do about it, which felt like the right way around, you know, sometimes things go round in different ways, don’t they?
PCT public health practitioner/commissioner
A final important finding from the case study work was the generally poor management of knowledge and evidence within these commissioning organisations. We found that a lot of knowledge was personal rather than collective, and that evidence generated internally could have a narrow audience and a short life (although this was not always the case). This seemed to reflect both practical obstacles, including limited physical and computer-based storage space, and a tendency towards silo working, a lack of reflective culture and an absence of processes to prompt documentation and evidence compilation. It was interesting to note that the NHS restructuring prompted the production of various legacy documents that detailed work programmes in ways that were rare to find previously.
Organisational structures and influences on ethnicity evidence use
Clearly, many of the factors operating at organisational level to shape general evidence use are also relevant when the focus is on ethnic diversity and inequality. In addition, however, the key informant interviews and case study work suggest some factors that have particular significance for this area of work, as well as some additional themes that may be specific to evidence use on ethnicity. Table 7 highlights how these factors were reflected across the three case study sites.
| Themes from national key informant interviews | Case study 1 (Sheffield) | Case study 2 (Bradford and Airedale) | Case study 3 (Leeds) | Between-case comparisons |
|---|---|---|---|---|
| Commissioning organisations lack ethnic profiling for their populations | ✓ Reliant on census for population profile (plus some use of other data, e.g. schools) | ✗ Significant improvements in primary care ethnic monitoring; yet to inform commissioning | ✓ Remains poor; Mosaic software (Mosaic Origins, Experian, Nottingham, UK) provides demographic data, not linked to health | ✓ Confirmed across all three sites, despite some progress in case study 2 |
| JSNA process and products lack detail on ethnicity (potentially undermines agenda) | ✓ Limited detail in 2010 | ✓ Limited detail in 2011 ∞ Work under way to improve this for all equality groups |
✓ Limited detail in 2010 ∞ Recognised but limited efforts to improve |
✓ Confirmed across all three sites, but signs of improvement |
| Service specifications not expected to detail ethnicity | ✓ Standard templates include general statements
only ∞ Rare exceptions give more detail |
✓ Generally true, except for targeted services | ✓ Generally true; specifications and pathways view users as homogeneous | ✓ Confirmed across all three sites; such detail seen as inappropriate/too difficult |
| Systems for performance monitoring not used to examine ethnic inequality | ✓ Generally true ∞ Rare exceptions, found in third-sector contracts |
✓ Generally true; data for staff by ethnicity published, but no action to reduce inequalities | ✓ Generally true ∞ Rare exceptions |
∞ Confirmed across all three sites; several factors limit active monitoring by ethnicity |
| Structures do not draw in practitioner insights on BME needs effectively | ✓ No prominent clinicians driving this
locally ∞ Some well-informed practitioners, but not regularly engaged |
✓ Generally true to date; may be changing in CCGs where GP leads focused on inequalities and ethnicity | ✓ Generally true to date; third-sector providers not
engaged ∞ Innov8 work seeks to address this but isolated example |
∞ Confirmed across all three sites; some exceptions; signs of interest among some clinicians in emergent CCGs in all three sites |
| User engagement approaches fail to represent ethnic minorities | ✓ Generally true; no effective BME partnership for
health ∞ Good examples do not ripple out |
∞ Generally true; no effective BME partnership for health; poor solidarity among local communities; efforts to improve | ✓ Generally true; minority engagement limited to particular projects when considered relevant | ∞ Confirmed across all three sites; range of factors block meaningful engagement |
| Few systems/processes within PCTs to draw in relevant data and evidence on ethnicity | ✓ Lack of systematic approach means variable sets of evidence fed into commissioning | ✓ Managers completing equality impact assessments often cited lack of evidence as a barrier | ✓ Data officer resource exists but ad hoc use dependent on individual interest | ∞ A number of inter-related factors hamper use of wide range of evidence; E&D work not expected to be evidence driven |
| Decision-makers demand higher quality threshold for ethnicity evidence | ✓ Some respondents reported witnessing this tendency | ? Not directly reported by respondents; fits with co-researcher experience | ✓ Reported by some respondents | ✓ Findings tend to confirm but warrants greater investigation |
| Commissioning organisations do not push for improvement in ethnicity data/evidence even when gaps known | ✓ Poor primary care data recognised for years; inability
to disaggregate service data regularly reported ∞ Some commissioner-led research |
✗ E&D work to improve GP ethnicity recording successful | ✓ True in most areas; reliance on providers to make
improvements to service data ∞ Some commissioner-led research to fill knowledge gaps |
∞ Commissioner-pushed initiatives are found but need to link to core work so that data are actually used |
The case studies confirmed that currently all three organisations were operating with an inadequate demographic and health profile of their local populations by ethnicity. There were, however, signs that work was under way in all three sites with an explicit focus on improving data, apparently prompted by the legal duty in the Equality Act 201099 to identify and publish equality information and objectives. It remains to be seen whether these initiatives will lead to greater collection and utilisation of such data within commissioning, as past progress on ethnic monitoring in primary care in one site had not yet resulted in such a shift, highlighting the need for complementary work to increase the demand for evidence on ethnicity:
The reason why we’ve got no decent monitoring is because either people don’t think it’s relevant, it’s not important, or they’re afraid to ask, nor do the commissioners require it I expect, they say that they do . . . [but] there’s no consequences, no one cares, I think that, in the same way that if you don’t put your accounts in, year on year, then you should have the auditors crawling on your back, I believe that you should not only have your ethnicity data and your basic demographics in, but you should also be able to chart and show and demonstrate progress.
Third-sector manager
There was wide variation across and within the three PCTs in terms of the extent to which practitioners and clinicians were regularly engaged in commissioning work, with some examples of strong, ongoing engagement. However, in all three sites we observed and heard reports of missed opportunities to draw valuable insights from practitioners and clinicians into the commissioning process relating to the needs of minority ethnic people. Although this is clearly a wider issue, there was evidence to suggest that a failure to use such provider insight may be a particular problem when there is a large social distance between commissioners and service users. The third-sector and community organisation representatives who we spoke to felt that they struggled to find a way to inform the commissioning processes and sometimes described instances in which evidence that they had presented to commissioners had been contested or was not valued. At the same time, some commissioners expressed doubts about the representativeness of particular community groups or worried that community forums were dominated by a narrow range of people, and could therefore be dissuaded from drawing on evidence from such sources.
It seems that such organisations may often be in the difficult position of having to play the multiple roles of advocate, knowledge bearer and potential provider of services to minority ethnic communities, with consequent concerns about vested interests being raised by commissioners.
More generally, there were concerns that structures did not effectively connect PCT staff working at community level with more senior decision-makers, so that their knowledge remains outside the commissioning arena. The Innov8 (described in Chapter 5) work taking place in one case study site was an explicit attempt to address this shortcoming in the field of mental health.
The case studies also tended to confirm the failure of PCT structures and processes to ensure good representation of minority ethnic people within consultation and engagement initiatives, despite a few notable exceptions. There was little evidence of the PCTs firmly accepting their responsibility for ensuring such representation, with no significant investment in this area (as has been the case in some places, reported by the key informants) and commissioning staff at times openly contesting whether it was their job to ensure such input. It was also apparent that in two of the three sites there was poor coherence at community level, with no active partnership for health among the ‘BME’ third sector, meaning that there was a weak and inconsistent challenge to commissioners to achieve better representation and address unmet needs in BME communities. Although some individual members of commissioning staff were working to improve the situation, they did not appear to receive organisational support for this.
As noted above, the case studies revealed few structures and processes to support commissioners’ access to, and use of, research evidence in general, with a heavy reliance on national policy and guidance documents. Although clearly this will mean that a large amount of potentially relevant evidence is overlooked across the board, this lack of connection to primary research may be particularly problematic for work on ethnic diversity and inequality as national guidance often does not include detail on this area and the evidence base remains new and rapidly evolving. We found little sign that use of national resources such as NHS Evidence & Ethnicity (recently discontinued) or the NHS Northwest Health Equality Library Portal (HELP) (see www.help.northwest.nhs.uk/; accessed January 2013) were promoted within the organisations, although some individuals did take their own initiative.
A further important theme highlighted by the case studies was that E&D work has not, to date, generally been expected to be evidence driven. Individuals with an E&D remit, who might raise pertinent questions regarding minority ethnic access to and experiences of services, commonly did not have strong evidence skills themselves and were not necessarily able to draw these in from other parts of the organisation. It seems possible that this situation will change in those areas where the Equality Delivery System is taken seriously (as described further in Chapter 6).
A further area confirmed by the case study work was the lack of detail included in service specifications, or contracts, regarding how services should be configured and delivered to ensure that the needs of patients and users are adequately met regardless of ethnicity. We found that there was no organisational expectation of such detail and that documents tended to include only very general statements about making services accessible to all groups of people and ensuring absence of discrimination. This tendency to limit detail in service specifications was not peculiar to ethnicity and seemed to relate to concerns about the amount of work involved to draw up detailed specifications; the danger of restricting the commissioners’ room for manoeuvre if the service was required to respond to new issues; and the complexity of monitoring contracts against a large number of requirements. Documentary review of several service specifications was carried out and, although some did specify generally that services should be ‘appropriate and meet the needs of the diverse local population’, these factors were not described in any detail nor included as measurable outcomes or performance targets.
As also noted by some of the key informants, there was a lack of clarity at the organisational level around commissioner and provider responsibilities to find service solutions and ensure effective implementation. Despite variation in the extent to which individual commissioners worked actively to support the improved delivery of services to minority ethnic people (as described further in Chapter 5), there was evidence of uncertainty about the commissioning role in questioning the performance of large provider trusts in this area, particularly when this related to behaviours and competency of staff. These factors clearly relate fundamentally to how the content and process of commissioning work is understood and operationalised within different organisations. Again, although this is a general issue, the implications of contested roles in relation to finding effective service models may be particularly important for our focus on ethnic inequalities, for which there are few tried and tested approaches and an absence of national standards or guidance.
A final important theme related to the tendency for decisions-makers to demand a higher standard of evidence when the focus was on minority ethnic health needs, again something that was noted by the national key informants. Although this was in part related to the wider organisational cultures and structures that marginalised attention to ethnic inequality, we discuss this more in Chapter 5 as its significance in blocking action also seemed to relate closely to the agency of individuals.
Chapter 5 Commissioning in practice: individuals, teams, activities
Introduction
Chapter 4 drew on the case study work to highlight key structures and processes at the organisational level that shape the use of evidence on ethnic diversity and inequality in commissioning. Here, we turn to look more closely at individuals and teams, drawing on the case studies to describe patterns of evidence use in different aspects of commissioning work and how these are influenced by characteristics of individuals, teams and the evidence base itself. We aimed not only to determine whether evidence on ethnicity was being used, but also to assess how well evidence was used, considering the following aspects:
-
accessing appropriate sources
-
critical appraisal and selection of appropriate evidence (rigour, relevance, bias, transferability)
-
synthesis of evidence across sources and methods
-
adaptation and presentation of evidence in appropriate formats
-
explicit articulation of assumptions, priorities and values underlying the weighing up of different knowledge sources
-
the translation of integrated knowledge synthesis into commissioning products and processes (such as service specifications, business cases, tenders, provider contracts and performance management tools).
We also draw links to the wider context described in Chapters 3 and 4 to illustrate how the understandings and behaviours of individuals and teams are influenced by these cultural and structural factors.
Description of the operational case studies
As noted in Chapter 4, although our case study work was nominally divided into strategic or operational, in practice this distinction was not clear-cut. We therefore describe here the data generation that constituted the operational case studies, but the findings that follow also draw heavily from the interviews and observations that were conducted as part of the strategic-level work (detailed in Chapter 4). Furthermore, interviews that were conducted as part of the operational work often yielded information that was wide-ranging, with interviewees providing a great deal of detail and examples from other aspects of their commissioning work. This was valuable because, although the operational case study work provided an in-depth picture of particular projects and pathways, the strategic-level work allowed us to look more broadly across the organisations, something that was important in terms of identifying pockets of good practice in what remained a marginal area of interest for these commissioning organisations.
Box 1 provides a narrative description of the five operational case studies that were conducted and Table 8 details the data generation that made up each of these.
This case study explored a piece of public health-led commissioning work focused on increasing the proportion of women who ‘book early’ (by 12 weeks) once they know that they are pregnant. The original impetus for the work can be traced back to Maternity Matters,100 and early booking remained a nationally monitored indicator for PCTs at the time of the fieldwork. Work to understand and address late booking was ongoing over a number of years within this case study site, with the indicator being regularly monitored. A number of distinct, but linked, pieces of evidence generation and utilisation work were undertaken in support of this, including an equity audit, insight work and development of a maternity communications plan. The work included an inconsistent focus on ethnic diversity and inequality, with some clear efforts to address this dimension but also several obstacles. At the time of the case study, this work sat within the Infant Mortality Action Plan, monitored by a multiprofessional Planning & Commissioning Group, involving commissioners, providers and user representation.
Accident and emergencyThis case study explored a series of activities that were undertaken as part of the commissioning organisation’s efforts to reduce inappropriate use of A&E services. The overall impetus for these work streams was a QIPP strategic focus on reducing unscheduled care. However, in practice, the case study found that the individual pieces of work were not necessarily well co-ordinated or clearly monitored within the umbrella of the QIPP programme. Some of the activities were public health led whereas some were led by health-care commissioning managers and others had close involvement of GPs through the practice-based commissioning consortia. The generation and utilisation of different types of evidence was clearly evident, with examples of detailed analysis of performance data; qualitative insight work; review of practice experiences elsewhere in the country; literature review and evidence synthesis; and small-scale local research. However, at the time of the research there was a lack of any systematic process to co-ordinate progress or to share learning. There was little consideration of the relevance of ethnic diversity and inequality within this work area.
Case study site 2 Maternal and child healthThis case study explored the evidence journey involved in a piece of project work focused on maternity services. The project aimed to use service user experience evidence, gathered from a series of focus groups with BME women (and one with men) who had used local maternity services, to improve services. The project leader tried to use different commissioning structures and processes to influence change. The case study explored the process of evidence generation, the content of the evidence that was generated, how it was mobilised and received, and the various factors that acted as obstacles to it informing service development.
Case study site 3 Innov8Although the Innov8 Charter was studied as a strategic case study, the project also followed the work of a research project conducted under the Innov8 framework. This aimed to provide a ‘diverse leader’ with the opportunity to lead a significant piece of work, gaining management experience and developing networks with senior leaders. The research project explored the specific contribution of BME staff to mental health services, by interviewing and conducting surveys with white and non-white staff engaged in delivering mental health care. The case study followed the progress of the project, through the data collection phase and production and launch of the final report, with a member of the research team being invited to be part of the steering group. The case study explored how evidence on a specific BME issue was collected, conceptualised and packaged, with the aim of eventually seeing how it was received within the organisation, and if it would impact on commissioning. The case study also explored the contribution of Innov8, how the research project was ‘commissioned’ and barriers that members of the steering group had encountered in trying to improve mental health services for minority ethnic users.
Cardiac rehabilitationThe focus of this case study was the redesign of the cardiac heart failure service, part of a larger redesign of cardiac services overseen by the Cardiac Re-design Steering Group. The work was based around the National Service Framework for coronary heart disease101 as well as national targets for quality and accessibility of services. A local needs assessment had been conducted by a previous commissioner linked to cardiac rehabilitation. The process involved a wide range of stakeholders, including commissioners, providers, clinicians and GPs, but with limited user input. The case study work involved observing the steering group for several months and included a large number of interviews with stakeholders and document analysis of evidence presented at the group and national guidance. Outputs created by the group, including a pack for GPs detailing the cardiac pathway, were also examined for content on minority ethnic needs. A specific focus was the low availability of ethnicity-specific information and how the limited data available impacted on the planning work.
| Data phase | Case study site 1 | Case study site 2 | Case study site 3 |
|---|---|---|---|
| Interviews | Early booking: one PCT commissioning manager (senior), two
public health commissioner/manager, one public health
practitioner (twice), one provider manager, one third-sector
manager, one user representative A&E: one public health practitioner, one public health trainee, one NHS commissioning manager |
Maternity focus groups: one NHS commissioning manager, one third-sector manager | Innov8: one senior PCT manager, one external consultant, one
senior trust manager, one project leader Cardiac rehabilitation: one NHS commissioning manager, two GPs, two practitioners, four provider managers, one third-sector provider |
| Total no. of interviews | Early booking: seven (six white British, one
male) A&E: three (two white British, no males) |
Maternity focus groups: two white British, no males | Innov8: four (three white British, no males) Cardiac rehabilitation: 10 (eight white British, seven males) |
| Observational work | Early booking: Planning & Commissioning Group (five
meetings), community-level consultation (one event), stakeholder
events (three events) A&E: informal observation/discussion only |
Maternity focus groups: Children’s Network meeting (commissioners and providers), Children’s, Maternity and Newborn Commissioning Board meeting, Maternity Services Liaison Committee meetings (three) | Innov8: research project steering group meetings
(five) Cardiac rehabilitation: observation sessions Heart Failure Task Group and Cardiac Re-design Steering Group (five), cardiac rehabilitation training (one event) |
| Total no. of hours | Early booking: 25 A&E: informal only |
Maternity focus groups: 12 | Innov8: 10 Cardiac rehabilitation: 12 |
| Document analysis | Early booking: core documents – Maternity
Matters commissioning toolkit; equity audit;
insight report; other docs – service specification;
action plans; marketing materials A&E: insight report; QIPP bids; paper to unscheduled care network |
Maternity focus groups: minutes of meetings; terms of reference of different groups | Innov8: minutes of meetings; literature review; draft and final
reports; Innov8 Charter; e-mail correspondence and
queries Cardiac rehabilitation: NICE guidelines; health needs assessments; equity impact assessment; service specifications; JSNA |
| Total no. of documents | Early booking: 20+ A&E: six |
Maternity focus groups: 10 | Innov8: 14 Cardiac: 10 |
| Other | Frequent interaction with commissioning staff through honorary post; frequent reflection by co-researcher; feedback discussion on case study findings | Frequent reflection by co-researcher | Frequent interaction with commissioning staff through related research projects; frequent reflection by co-researcher |
| Data volume and quality | A&E work more limited; good range and quality for early booking | Somewhat limited | Good range and quality for cardiac rehabilitation; Innov8 research a much smaller project but good coverage |
Evidence use across the commissioning cycle
The case study work tended to confirm many of the overarching themes from the key informant interviews relating to patterns of evidence use both in general and in relation to ethnic diversity and inequality in particular. Several of these patterns clearly reflect the wider organisational structures and processes described in Chapter 4.
However, the case studies also provided much greater insight into the workings of commissioning teams and the behaviours of individual commissioners. This allowed us to understand in greater detail the varied influences that lay behind observed practices. The case study work also revealed significant variation within and across the PCTs in the ways that individuals and teams demanded, accessed and used evidence of different types, including that relating to ethnicity. This variability illustrates the idiosyncratic nature of much commissioning work and the way in which individuals exercised their own agency. Nevertheless, some consistent obstacles to evidence use were also highlighted.
As the following quote illustrates, the job of specifying and procuring health-care services that respond to local need while also meeting national directives to both improve quality and reduce costs was seen as a huge challenge by most commissioning staff. Although this national policy and guidance was seen to provide important direction, it also had recognised limitations. In common with other research, we found that commissioners work with a diverse range of evidence to inform decisions and prompt action, mobilising different sources at different points in the commissioning cycle. Reflecting on a discussion session between practitioners and commissioners aimed at identifying possible ways to improve a service, one respondent noted that:
I don’t think in that particular instance we kind of said ‘so what does NICE tell us about outpatient care?’ or whatever, but that was probably because we knew that NICE doesn’t tell us anything about outpatient care. I mean NICE tends to give us clinical guidance, which might give us pathways, it might describe what interventions work best for depression and what doesn’t and so on, it almost certainly doesn’t tell you much about how many CPNS [cardiopulmonary nurse specialists] you really need to look after a population of half a million people or, you know, or how they’re best organised or whatever . . . We had some of that [operational guidance] with the National Service Frameworks, which did attempt to pull together evidence and best practice and so on . . . So there was a kind of a top-down, this is what the evidence tells us that you should need, and that was an attempt to kind of reduce variability in services . . . In some instances we then get into a debate with the department . . . you know, we’ve got a service but there isn’t actually that level of demand! [Now] there’s a load of quality standards that are published by the department, or are being published . . . they don’t help with QIPP, they tell us that a service should do this, this, this and this and that’s kind of part of the nature of the NHS where on the one hand you’ve got the pressure to reduce spend, and on the other hand you’ve got pressure to increase standards, so it’s kind of like you’re being pulled in two directions.
PCT senior commissioning manager
Table 9 draws across the case study work to provide an overview of the varied types of evidence that we found being used across the commissioning cycle, both in general and also in relation to ethnic diversity and inequality. The table divides the commissioning job into three phases: assessing needs and identifying gaps; prioritising action and finding solutions; and monitoring performance and evaluation.
| Evidence source/type | Assessing needs and identifying gaps | Prioritising action and finding solutions | Monitoring and evaluation |
|---|---|---|---|
| Population-based demographic and health data (including primary care ethnic monitoring) | ✓✓✓ Considerable local production of
health profiling in JSNAs and focused needs assessments; public
health observatory data often used by public
health ✗ Health outcome data rarely disaggregated by ethnicity |
✗ Fragmentation; poor link to commissioning action
currently; analysis often remains at the descriptive
level ✗ Data unavailable by ethnicity |
✓✓ For public health outcomes ✓ Very few outcomes defined by ethnic group (e.g. infant mortality) |
| Service use data; locally and nationally produced indicators | ✓✓ Not always well linked to outcomes; primary
care data underutilised ✗ Ethnic monitoring data often incomplete or unused |
✓✓ Indicators of poor service performance prompt
action ✗ Data unavailable or not demanded by ethnicity |
✓✓✓ Large infrastructure and regular
monitoring of key indicators ✓ Rarely disaggregated by ethnic group; some examples |
| Detailed process analysis of how services function in practice | ✗ Not found as part of needs assessments | ✗ Rare to find commissioners using ‘plan–do–study–act’-type development cycles | ✗ Rare to look in detail; bottom-line
focus ✗ No examples found of evaluations focused on diversity and equality |
| Patient, user and carer input | ✓✓ Some examples; not always demanded by
commissioners ✓ A few areas of provision seek out BME user input |
✓ User/carer input valued; impact on service shaping and
priorities less obvious ✓ A few areas of provision seek out BME user input |
✓✓ Some examples; not completely
embedded ✓ A few areas of provision seek out BME user input |
| Community consultation | ✓✓ Increasing use of ‘story’ and
experience in JSNAs ✓ Under-representation of BME but some good examples |
✓ Rare examples in which decisions highly political; some with BME focus | ✓ Rare examples ✗ No examples found with BME focus |
| Practitioner/clinician experiential knowledge | ✓✓ Seen where strong provider engagement in
commissioning ✓ Some examples of ethnicity focus but valuable insights overlooked |
✓✓✓ Informal and formal inputs
prominent ✓ Some examples of ethnicity focus but valuable insights overlooked |
✓ Mainly informal; not consistently demanded
here ✗ No examples found when focused on ethnicity |
| Examples of good practice from elsewhere | ✗ Not found (could possibly inform needs assessment questions or help to fill gaps if similar profile to local population) | ✓✓✓ Popular source of guidance for
commissioners ✓ Some examples found for ethnicity focus |
✓ May be drawn on to identify appropriate
indicators ✗ No examples found with focus on ethnicity |
| Own research/insight work (commissioned or in-house) | ✓✓ Several examples found, some focused on BME needs, e.g. gypsy and traveller census work; stroke awareness insight work | ✓ Some use in service design but less obvious than in
needs assessment ✗ No examples found with focus on ethnicity |
✓ Some commissioned evaluations; questionable
transparency ✗ No examples found with focus on ethnicity |
| Other local primary research | ✓ Examples found, some focused on BME needs, but irregular use | ✗ Not found; could be used in theory | ✗ Not found; could be used in theory |
| Primary research conducted elsewhere | ✓ Accessed irregularly ✓ Very rare use for ethnicity; transferability issues raised |
✓ A few examples of review and synthesis work; often
with public health input ✓ Rare examples on ethnicity |
✗ Not found; could be used in theory |
| Synthesised evidence in national policy documents | ✓✓ Examples found ✓ A few examples focused on BME needs found; mobilised by ‘champions’ |
✓✓✓ Important source of guidance for
commissioners but requires local adaptation ✓ Rarely detailed on ethnicity |
✓ May be drawn on to identify appropriate
indicators ✗ No examples found with focus on ethnicity |
| Commissioner expert knowledge | ✓ May be used when local knowledge; sometimes BME focused but rare | ✓✓ Often used when other evidence
lacking ✓ Rare BME focus; mobilised by ‘champions’ |
✓ May influence what counts as success
criteria ✗ Rarely BME focused |
| Other | ✓ National and local data may be combined to produce estimates when local evidence incomplete, including for ethnicity | ✓ Political pressure can prompt action, in some cases on BME issues | ✗ Not found |
We identify a range of different evidence sources and use different symbols to indicate how commonly we found each type of evidence being used within the three phases of work. These indicators are provided for both evidence use in general and evidence use relating to ethnic diversity and inequality for each source of evidence, thereby flagging up any areas where there were noticeable differences. The table has been populated by drawing from direct observations, respondent reports and documentary analysis.
The following sections provide further illustrations of these patterns of evidence use, with a particular focus on whether and how evidence on ethnic diversity and inequality was being used.
Assessing health needs and identifying gaps
Case study respondents in all areas identified needs assessment as a core element of commissioning, especially when public health was closely involved in commissioning work. We found several examples of focused needs assessment work as well as investment of resource, particularly from public health, in the more holistic JSNAs. Population-level demographic and health data were important components of needs assessments, as were service use data, although the latter seemed to feature more clearly in focused needs assessments than JSNAs. There was also evidence of community-level and service user consultation feeding into needs assessment documents.
We also found examples of very detailed work that brought together local and national data and reviews of published research to build a detailed picture of local need in the context of the wider evidence base on a particular area. These pieces of work often seemed to be prompted by a particular individual’s interest and were often supported by additional resource. Furthermore, there were many examples in which such analysis would have been helpful but was not undertaken.
In terms of assessing health needs across different ethnic groups, as already noted, this was often severely hampered by an absence of population- or service-level data disaggregated by ethnicity. The lack of such basic descriptive data was reflective of the low organisational priority given to understanding and addressing ethnic inequalities, suggesting a mutually reinforcing cycle. However, the lack of data was clearly recognised and felt to be frustrating by some commissioners: ‘We need to get our data gathering around ethnicity improved. You can’t redesign or reprioritise services if you don’t know who’s coming through the chuffing door’ (PCT public health practitioner/commissioner).
The case studies also confirmed that good minority ethnic representation was often not achieved in community- and service-level consultations that were intended to inform needs assessments. For instance, the Maternity Service Liaison Committee in both case studies in which it was examined had struggled over a long period of time to ensure the engagement of minority ethnic women.
However, there were some examples in which needs assessments included ethnic breakdowns of quantitative data and we also found examples of commissioners initiating a range of strategies to plug gaps and draw in a range of complementary evidence (Box 2). These creative approaches are promising; however, they appeared to be highly dependent on individual skills and interests and were not often shared widely within or outside the organisations.
The early booking maternity work included an equity audit, in which rates of late booking were presented by ethnic group as well as by geography, and a piece of commissioned insight work focused on understanding the needs of ‘hard-to-reach’ groups, including several minority ethnic communities.
The strategic case study work in one site identified a piece of work that had involved the use of national-level data on levels of heart disease from the Health Survey for England, census estimates of the local ethnic profile and local service statistics to examine possible unmet need and unequal access to cardiac revascularisation among Pakistani people.
The health needs assessment undertaken as part of the cardiac rehabilitation work combined national guidance and data on low use of cardiac rehabilitation by people with learning disabilities and South Asian populations with local data on deprivation to examine underuse of this service locally by people from these populations.
A public health commissioning manager had commissioned detailed insight work to understand needs and service experiences of minority ethnic groups around smoking cessation services.
Furthermore, there were two common areas of weakness. First, there was often uncritical use of ethnic categories. Even in projects that had an explicit ethnicity or equalities focus, we found that the broad category ‘black and minority ethnic’ was employed without any justification and it was rare to find any discussion of why particular ethnic categories had been used or what their strengths or limitations might be. Second was the failure to go beyond basic descriptions of health or service use patterns by ethnic group to explore the factors explaining any observed differences.
Designing service responses and prioritising action
Many respondents noted that prioritisation often took place at a very high level of generality and that there was often a weak link between health needs assessment and the areas that were prioritised for focused commissioning attention. Rather than population health profiles and community consultation evidence, the sources that featured heavily at the prioritisation stage tended to reflect the strong drivers and infrastructure around the quality and efficiency agendas. At the operational level we found benchmarking data on expenditure and quality being regularly used to identify areas that might warrant closer commissioning scrutiny and possibly yield savings:
Some of the other work that I do is on a sort of benchmarking basis around areas that we might have a higher level of commissioning activity in, and we may want to readdress with our providers to look at efficiencies and drive forward change in the ways we’re delivering services, NHS services. So I’m heavily involved in QIPP, which you may have heard of so that’s really about looking at our NHS comparative data or other national benchmarking data, looking at where we overperform in activity terms and overspend NHS resources on secondary care services.
PCT commissioning manager
Similarly, the organisational importance attached to adherence to government policy was reflected in regular use among the commissioning managers who we interviewed and observed of synthesised research in the form of NICE guidance and policy documents:
Yes, it would be the policy, definitely the policy, so it’s very much that overview.
PCT commissioning manager
It’s synthesis of evidence from around the place . . . on the basis of what the literature tells us, and systematic reviews, evidence base reviews, NICE guidance, other guidance from other authorities like NICE and so on, so a whole range of things like that, trying to bring those sorts of things into the commissioning process.
PCT senior public health commissioner
However, as illustrated in the quote in Evidence use across the commissioning cycle on p. 67, commissioners found national policy to be often lacking in guidance on how to shape service responses at a local level. We found commissioners drawing heavily on the experiential knowledge of local practitioners and clinicians, as well as practice examples from elsewhere, for evidence of how services might be shaped effectively to achieve improvements (usually defined in terms of national quality markers and cost saving).
In the context of an innovative reconfiguration of children’s mental health services, we recorded the following comments:
Interviewer: So would that, would you say that that came from the commissioning side of things, or from the provider?
PCT commissioning manager: No, it came from the provider, from the clinicians and from education. You know, coming round the table together and saying can we do anything differently . . . So, the process of bringing people together is stimulated by commissioners, but actually the solutions come from, you know, came from the clinicians.
Drawing in practitioner experiential evidence (sometimes called expert knowledge) happened in many ways, both formal and informal, as well as ongoing and more ad hoc. For example, the early booking work was based within a Maternal and Child Health Planning and Commissioning Group that included senior practitioners from midwifery, health visiting and general practice who were formal group members and who regularly offered their insights into how services were functioning and how new directives from the DH, or local issues, might best be responded to. In contrast, the following quote illustrates a one-off focused effort to access practitioner expert knowledge using external resource:
It appears that we have a considerable number of more people in secondary care mental health services than our comparators, which suggests that community mental health teams are maybe not discharging people as often as they, or as soon as they should, or that GPs are referring more people than other places do . . . We talked to our lead GPs on mental health services a couple of months back, got them in a room with the clinical directors from the Care Trust, had a conversation about so what do we think they could do differently, and it didn’t get us anywhere which was a bit disappointing, yeah. So we’ve, we kind of thought we needed some expert help in, in getting ideas, so we’ve commissioned this company to talk to 20 or 30 GPs about their perceptions of mental health services, the scope for service improvement, and in particular identify areas where we do things inefficiently or we do things that we needn’t and that kind of thing.
PCT senior commissioning manager
Examples from other PCTs of how services had been configured were a popular source of evidence on what service solutions might look like. In some cases commissioners identified regional and national networks that were a useful route to information on how other people were shaping services, but in other cases access to such practice learning seemed to be much more ad hoc:
The other forum I use is the regional commissioning network, so it’s sort of like do we know anything, has anybody else done any work around this. Yeah, we’ve got a good, because we’ve got a children’s regional commissioning network meeting. It’s one of the meetings I do go to, because it is useful for exactly that, you know, so and so’s just done a service redesign and might have a specification that she can share with me and it will . . . you know what I mean, I’ve got a starting point rather than a completely blank page in front of me.
PCT commissioning manager
I think Google is the most rapid way to find out what’s out there and then through doing more research on the internet, unpick that. And it is, it’s literally through Google.
Local authority commissioning manager
Despite efforts to engage patients and the public in commissioning, respondents recognised that service user views were often not gathered early enough in the process but more commonly as part of a consultation process after decisions had already been made, meaning that they had little influence on the process of service design. Consultation with service users on the heart failure pathway occurred after the pathway had been agreed. Within the commissioning group there was recognition by members that they could be criticised if this consultation was not undertaken, but the value of such input was also contested by some group members on the basis that clinical expertise was, in their opinion, the most important factor in the design of the pathway.
Furthermore, there could be conflicts between different types of evidence. For example, one respondent noted that complementary therapies that are not shown to be effective by empirical research nevertheless receive very positive service user feedback, thereby creating challenges to synthesising disparate evidence sources.
In general we found few examples of primary research evidence being accessed and used systematically to inform service solutions. Individual commissioners were found to use research evidence at times, with some respondents mentioning particular researchers whose reports and papers they would regularly access and others identifying particular research studies that had influenced their work, but in general this use seemed to be very individualised. This seemed to reflect the lack of structures mentioned in Chapter 4 and the tendency for evidence mobilisation to be seen as a diffuse responsibility, something that everyone should be doing but with little guidance on what this should involve in practice. However, there were exceptions. We identified a number of more comprehensive and systematic pieces of work in which research evidence was reviewed and synthesised alongside other types of evidence to inform the design of services (e.g. a review of parenting support interventions and a review of self-management approaches).
In keeping with comments from some of the national key informants, there was evidence to suggest that local research could be particularly influential. We observed commissioning groups inviting local researchers to attend their meetings to present their work and taking time to discuss the findings from other local studies. Some respondents also talked about influential research during the interviews, again tending to cite local work most often.
As already noted in Chapter 4, it was rare for evidence of ethnic inequalities to be the prompt for focused commissioning attention. However, there were some examples. For instance, across all three sites there was ongoing public health-led work to address the issue of genetic risk associated with consanguineous marriage. Importantly, this is one of the rare examples in which heightened risk among a particular minority group is actually reflected in the overall level of a key national outcome indicator – infant mortality – although it should be noted that the commissioning response was considered to be inappropriately narrow by some local stakeholders. Another example was late presentation for diagnosis of human immunodeficiency virus infection in black African men, an issue that had been flagged up by the specialist provider service and taken on by the commissioner as an area needing development.
We also found examples in which commissioning attention became directed towards the needs of minority ethnic people when their use of health services was perceived to be inappropriate or problematic. In the absence of routine monitoring of service use by ethnicity in our case study sites, it often appeared to be provider intelligence that prompted commissioner attention:
I mean the Slovak community suck up our health visiting resource in the north of the city, and we know that, but there’s nothing you can do about that, because they have particularly high needs. You know, so it’s not like we can sort of say well . . . well you can’t say anything, can you, you’ve just got to respond to it. But to try and get some of the information to truly understand it, because they’re such a transient population it’s almost like they’re not still enough long enough to know whether that’s what we’re counting or if we’re double counting, if we count the move there, and it’s just, I don’t think we’ve got a clue picture of it at all.
PCT commissioning manager
Occasionally, evidence brought by third-sector or community organisations of unmet need among minority ethnic groups had also been the prompt for commissioning action.
In terms of the shaping of services, it was also rare to find commissioners drawing on research or other evidence relating to ethnic diversity and inequality. In some cases commissioners seemed simply to overlook this dimension, viewing service users as a homogeneous group and adopting a ‘one size fits all’ approach to specifying services, as clearly recognised by some of our respondents and confirmed by our documentary review of multiple service specifications:
I think – this is how I perceive what we’ve commissioned in the past, is a sort of flat service assuming that everybody’s going to access it in the same way, not particularly looking at other groups and whether everyone does have equal access once you’ve set it up.
PCT senior commissioning manager
In other cases, commissioners seemed to recognise the potential relevance of specifying the service in relation to different needs, but lacked access to the required evidence to inform a detailed specification. In still other cases, however, there appeared to be a withholding of detail that could have been specified on the basis of available evidence. Although this tendency to limit detail in service specifications was not peculiar to ethnicity, the lack of detail is likely to be particularly problematic when providers lack other sources of guidance on how to ensure that diverse needs are met. It was particularly noticeable that, even in areas of service development where there is strong evidence of both important ethnic inequalities and effective interventional approaches that might be specified by commissioners, such as diabetes management, detail on ethnicity remained lacking.
Practitioner expert knowledge seemed to be less regularly drawn on to inform service responses relating to minority ethnic needs than to inform services more generally, and there were signs of important missed opportunities in this regard. In particular, third-sector organisations that might have important insights were not generally routinely included in commissioning forums, and respondents from such organisations talked about struggling to find routes to get their evidence into commissioning processes. The exception to this was the Innov8 research case study, which specifically focused on the contribution of BME practitioners and included input from third-sector providers. However, this issue had clearly been identified as a gap in the current processes of generating understanding of need and identifying service responses and it remains to be seen whether this project can have an impact beyond the individuals directly involved.
It was also rare to find examples of commissioned research or insight work focused on identifying approaches to improving services for minority ethnic populations, with these tending to focus more often on minority communities themselves and being restricted to the needs assessment phase.
We found few examples of commissioners drawing on published research evidence on ethnic diversity and inequality to inform service designs and specifications, but there were some examples of this and in other cases commissioners clearly wanted access to better evidence on effective interventions. One public health commissioner was particularly keen that the current project should produce evidence digests as part of the package of tools as she expressed great frustration at not being able to easily access evidence on successful interventions for minority ethnic populations:
What you are challenging me with today is about how do we use that [evidence], but if the evidence isn’t there, or it’s not sufficiently orientated to me or my services to which I have some remit, then there’s a disconnect, a complete disconnect, and how can we bridge some of that?
PCT senior public health commissioner
Monitoring and evaluating services and service changes
As already noted, we found that commissioners regularly accessed locally and nationally produced performance indicators relating to spend and quality to monitor the performance of the services they commission:
You know, we’ve just had a meeting with XX, the contract manager and everybody, and basically really beat them up about C-section rates and said you’ve got to do something . . . and we are going to work with you on it and we’re going to point out the fact that we’re benchmarking high on this and we’re not happy with the rates and we want to see a reduction.
PCT commissioning manager
There was also some evidence of commissioners drawing on user and carer experience data to assess the quality of services, although this was clearly not completely embedded and varied in terms of detail and frequency. Further, it was not always clear what action resulted from reviews of this type of evidence. For instance, the Maternal and Child Health Planning and Commissioning Group in one site funded an annual survey of maternity users by an independent local group and the findings of this were shared and discussed, but it was more difficult to see how these were brought together with other evidence sources to really evaluate the current provision and feed into service developments.
It was rare to find commissioners generating or accessing any detailed process information on how services function, or undertaking any kind of process evaluation, even when detailed redesign work had been undertaken. In the A&E case study, one area of activity involved the analysis of routine data sets to identify individual patients who were high users of A&E departments followed by individual GP practices identifying and introducing a range of initiatives aimed at reducing usage (e.g. leaflet campaigns and recall of high users). After a period of follow-up, data on the overall trend of A&E usage across different parts of the city were presented to the unscheduled care network. Although the data suggested a smaller rise in A&E use in those areas of the city where there had been these new initiatives than elsewhere, there was agreement that no causal link could be drawn. There was no investigation of how the interventions had operated in practice. This meant missed opportunities to generate important local implementation evidence that could inform further service improvement, a limitation recognised by some of the managers involved in the work. We did identify a number of external evaluations that had been commissioned to examine particular programmes of work or clusters of interventions, although in some cases local stakeholders raised questions about how transparent these had been and whether commissioners were really interested to learn about things that did not work well or rather just wanted to hear the so-called ‘good news stories’.
In the main, neither quantitative nor qualitative sources of evidence on service performance were broken down by ethnicity. It was rare to find that commissioners had included ethnic-specific KPIs or used Commissioning for Quality and Innovation (CQUIN) to define areas of service improvement for minority ethnic groups, through which the generation of ethnic-specific monitoring data could have been prompted:
And in the health visiting specification we haven’t got anything, any, we haven’t got any kind of KPIs around ethnic inequalities, so you know, we may, or may not be entirely following through on, you know, on these things in the areas where we could.
PCT senior public health commissioner
It was more common for community and third-sector organisations than NHS trusts to be required by commissioners to record and report service-level data by ethnicity, but even these data were not often drawn on to inform service improvement. Some respondents felt that the general failure to evaluate service modifications was a particular problem in relation to interventions targeted at minority ethnic populations, many of which were funded by short-term pots of money. Respondents identified important missed opportunities to develop local learning and confidence about how to address minority needs. They felt that the lack of such evaluative evidence – which might show indications of progress made, even if bottom-line measures took much longer to impact – tended to perpetuate unhelpful perceptions that ‘nothing works’ and communities are ‘hard to reach’.
However, it is again important to note those rare instances of good practice in which particular commissioners had taken the initiative to undertake service evaluation and monitoring work with a particular focus on minority ethnic communities and service users (Box 3).
In one site routine service monitoring work in a particular service area included a breakdown of quantitative service data by ethnicity and also qualitative focus group discussions with users and community members. This work highlighted the under-representation of Chinese people in the service and some particular unmet needs of South Asian women. Commissioners used this information to include explicit detail in subsequent service specifications about how the service should address these particular needs, although recognised the need for further development work to gain better inclusion for the Chinese community.
Influences on mobilisation and utilisation of evidence on ethnic diversity and inequality
Chapter 4 described in some detail the organisational cultural and structural factors that shaped evidence use in the case study PCTs. Here we identify factors operating at the more micro level, exploring individual, team and evidence-related factors that support or constrain evidence use. We focus here on use of evidence on ethnic diversity and inequality and, although some of the issues may be more generic, highlight those that seem to have particular relevance for this area of work. As the overwhelming picture was one of limited and inconsistent use, we focus here primarily on the barriers. However, Chapter 6 draws together findings across the study to suggest potential enabling factors.
Demand for evidence
The case study work suggested a number of factors that operated to produce a low demand for evidence on ethnic diversity and inequality within the commissioning organisations that we studied. In many cases commissioners simply did not think about the relevance of considering ethnicity in their work, reflecting the wider marginalisation of this agenda, and therefore did not demand evidence at any stage of the commissioning cycle.
In other cases commissioning staff were aware of the potential relevance of ethnicity, but a range of obstructive attitudes undermined their tendency to seek out evidence. The wider ambivalence towards addressing ethnic inequality at policy and organisational levels was reflected in some individual commissioners who expressed uncertainty about the legitimacy of giving attention to this issue, and questioned whether it would be construed as ‘privileging’ minorities over other sections of the population. Another prominent theme was the fear of getting it wrong, with commissioners opting not to pursue the issue rather than engage in work that was perceived to be complex and sensitive:
People’s awareness of the issues is very variable . . . some people struggle . . . And to be able to write about ethnicity, people can be a bit sensitive about it. Am I writing it the right way? Am I using the right terminology?
PCT senior public health commissioner
There was also evidence that some commissioners made assumptions about the additional cost that they felt would necessarily be involved in commissioning services that took minority ethnic needs into consideration and therefore chose not to demand evidence even of need. This perception was linked closely to the assumption that responses to minority ethnic health needs necessarily involve separate and additional services, rather than recognising the scope for existing services to be made more responsive:
There’s a mindset that says if we do anything for BME communities that’s on top of what we already do, rather than what we already do should incorporate the needs of BME communities.
Local authority manager
So I always feel there’s this ginormous tension between how do we do the best for the most, against balancing up how much do we then pull off to spend a proportionally more amount of money and time targeting a group which they might have greater needs, but it might take three times more money per head to actually get the same numbers of people through the door, and you’re always measured then on numbers through the door.
PCT public health practitioner/commissioner
We found that in some cases commissioners assumed that data or evidence were unavailable rather than exploring whether this was really the case or putting in place measures to improve the data that were being collected. Importantly, provider organisations noted that they often had data and evidence that were not demanded by commissioners. There were also assumptions that a general focus on health inequalities would mean that ethnic inequality was taken care of:
I would like to say it’s core business, you know, mainstream, I mean health inequalities certainly is and we certainly have a, you know, fairly strong understanding, I think I would say across the board that a dimension of health inequality is ethnicity. So, I would think that everyone round that table would have quite a developed understanding of that. [For instance] with the CAF [Common Assessment Framework] we focus on vulnerable families. We’d know that there would be more families from Pakistani, Bangladeshi, African Caribbean community with CAFs so you would be addressing that vulnerability, but we’re not looking at it [ethnicity explicitly], and to be honest I don’t know if they would have the data where they could tell us that anyway, you would hope they might do.
PCT senior public health commissioner
Finally, we found that some commissioners made assumptions about other members of staff – particularly E&D staff, but also sometimes staff of a minority ethnic background – being responsible for ensuring adequate consideration of this agenda, again reflecting the fact that attention to ethnicity is not part and parcel of understanding and meeting population health needs.
Given the wider organisational contexts that did not reward good work or sanction work that overlooked this dimension, there were few challenges to attitudes and beliefs that undermined a demand for evidence on ethnicity. Indeed, a perception among individual commissioners that focusing on ethnicity was not perceived to be relevant among their managers could reinforce their belief that such efforts were illegitimate. Further, a general lack of guidance in terms of what commissioners might be expected to do to ensure adequate understanding of, and responses to, ethnically diverse needs, and the lack of sharing of good practice within and between organisations, appear to perpetuate these attitudes and beliefs. Where national drivers did exist for more concerted work on this agenda, they were found to be important prompts. For example, the equity audit carried out as part of the early booking case study was prompted by a recommendation in Maternity Matters. 100 Similarly, the need to address under-representation of South Asian coronary heart disease patients in cardiac rehabilitation services was highlighted in NICE guidance and prompted the local health needs assessment work observed in one site. The Equality Delivery System had also acted as a national driver that highlighted many gaps in the understanding of health needs for minority ethnic communities, and was actively engaged with in two out of the three sites.
Accessing and sharing relevant evidence
The case study work suggested a number of factors operating at the micro level that were important in facilitating or constraining access to relevant evidence on ethnicity within the commissioning arena.
A key theme here was the centrality of the relationship between commissioners and providers. We found that, in many instances, accessing relevant evidence to inform commissioning action was highly dependent on a co-operative commissioner–provider relationship. In the case of large NHS provider trusts, commissioners could find it difficult to enforce the provision of necessary information within the context of large contracts with many competing demands (Box 4).
In one case study site commissioners struggled for over a year to secure data from the NHS provider trust needed to inform a particular area of service development. A number of factors appeared to contribute to this delay, including changes to database systems and competing priorities. However, a lack of support from provider-side managers also clearly presented an obstacle. In contrast to other areas of work where these same individuals provided extensive support to commissioners in both service monitoring and development, their lack of ‘alliance’ on this issue undermined the ability of the commissioners to make progress.
In some cases, providers were observed to advocate on behalf of minority ethnic needs, bringing evidence to commissioners to challenge the omission of issues or the misspecification of need:
Here, in XX, even though it’s 90 something per cent black and ethnic minority, in terms of a need analysis for breastfeeding, there isn’t, that it’s so good, the breastfeeding rates, so somebody could say well you don’t need a breastfeeding peer support worker in XX at all, and then we would fight to say no, we do need it, because we know the issues whereby people will stop or people will come out of hospital bottle feeding unless a breastfeeding peer support worker’s supporting them.
Third-sector manager
However, as discussed in Chapter 4, evidence from third-sector providers could also be contested and rejected by commissioners, particularly if it challenged pre-existing decisions, a reflection of their relative lack of power within the commissioning arena.
More generally, we found that some commissioners lacked the time and/or confidence to pursue areas of service development focused on the needs of minority ethnic people and looked to providers for co-operation and support in mobilising the necessary evidence. If not forthcoming, they would invest their energies elsewhere.
That said, there was evidence of uncertainty and contestation around commissioner and provider responsibilities to find service solutions and ensure effective implementation. There was wide variation in the extent to which commissioners worked actively with provider organisations to mobilise evidence of different types in support of improved delivery of services to minority ethnic people. Although some commissioners were clearly instrumental in shaping service responses, others seemed to view finding solutions as beyond their remit, looking instead to providers for this input:
I wouldn’t see it as just up to us to do that [find the solutions], it’s up to the service that’s operating to do some of that work and that development work. There’s a fair amount of evidence out there.
PCT senior public health commissioner
At times commissioners expressed discomfort at raising issues relating to ethnic inequalities, particularly if these related to the behaviour and performance of health-care staff within large NHS trusts, questioning whether it was appropriate for commissioners to ‘interfere’ in these areas. Interestingly, however, we found both commissioning and providing managers who expressed frustration at the unwillingness of the other party to devote time to finding solutions to ethnic inequalities. As the following quote suggests, commissioning efforts to access evidence and inform service development for minority ethnic people will often be overtaken by other priorities unless there is good co-operation from providers:
PCT commissioning manager: We tried to do one [CQUIN] on CAMHS [Child and Adolescent Mental Health Services] . . . we tried to do something around [ensuring] the level of activity was appropriate to the ethnicity profile within the locality team and the configuration but they just wouldn’t have it, they just would not go there at all, it’s just too hard, it was too difficult. Because they can’t achieve it, and I know exactly why, because what it takes is it takes a provider going out there and getting the people in, so it takes a provider taking responsibility for the mental health care of children in the city, instead of providing what comes in through the door and what’s on my waiting list . . . yeah, ‘we need extra resource to do that, it would take a lot of targeting and interventions, there would be a reluctance and there’s a cultural difference in terms of understanding treatment, family therapy and family interventions aren’t accepted by a lot of these ethnic groups’. You know, there was a raft of excuses. So you know, you get to the point where you sort of think well if family intervention and family therapy is not accepted what else are we doing, you know, is there an alternative to family therapy then, that, you know, these groups of people accept so we ensure that their mental health needs are treated?
Interviewer: So to what extent can the commissioner’s role sort of extend to seeking some of those solutions, you know?
PCT commissioning manager: Yes, yes, if you want to drive change, but it’s how hard you want to press some of the buttons and the priorities, the overall priorities because I suppose in CAMHS for me at the minute it’s reducing waiting times . . . a waiting list reduction initiative is a major priority, so therefore looking at things like access for ethnic minority groups is less of a priority, you know what, and that’s awful but it’s the harsh reality around targeting resources, and when I say targeting resources it’s commissioning resources as well as . . . so that’s the tricky one.
A further important theme was the extent to which commissioners and other stakeholders, or evidence bearers, were networked. There appeared to be many missed opportunities for relevant evidence to inform the commissioning process. For example, we found instances in both maternal and child health case studies in which highly relevant local research evidence was not brought to the attention of commissioners or was only discovered by chance. Some commissioners expressed the feeling that they were not part of networks that shared research evidence in the way that clinicians and managers working in provider trusts often were. In part, this may reflect the more generalist nature of some commissioners, but it also seemed to reflect a need for more deliberative inclusion of commissioning organisations within collaborative structures through which evidence circulates, such as Collaboration for Leadership in Applied Health Research and Care (CLAHRC) networks. Evidence and data on ethnicity held by other agencies, particularly local authorities, that could inform needs assessment work were not always accessed by health-care commissioners. For example, in one case study site an interview with a commissioning manager for young people and families revealed that complete self-reported ethnicity data were available for all children and their parents in the region, which had never been used by the health sector to improve its population ethnic profile, which was based on crude estimates. However, this situation seems to be improving to some extent, with JSNAs becoming increasingly collaborative efforts.
It was also evident that there were missed opportunities for sharing within PCTs themselves, with isolated pockets of good practice being common and internally generated evidence not being shared very widely. In one case study site there had been significant improvement over time in ethnic monitoring in general practice, but we could not find evidence of a single case of these data being used by commissioners.
Using evidence critically and effectively
In relation to commissioners’ confidence and competence to use evidence on ethnic diversity and inequality critically and effectively, three important themes were prominent.
First, there was evidence to suggest that unsophisticated understandings of ethnicity and its links to health could lead to partial and inappropriate use of evidence as well as a failure to adequately appraise the quality of different evidence sources. We found commissioners failing to ask appropriate questions of particular evidence sources (such as whether patterns of service use varied within ethnic groups by sex or migration status). We also noted that commissioners could overlook the relevance of some sources of evidence and give undue emphasis to particular pieces of evidence that fitted with their mental models of how ethnicity impacts on health and health-care experiences and/or what constitutes appropriate service responses (Box 5).
In one case study site, insight work conducted early on during a piece of service improvement clearly indicated that poor service experiences, and particularly poor provider–user communication, were part of a cluster of factors that deterred some minority ethnic people from using services. However, over the course of the work this evidence received very little attention, with the focus being placed more on educating the public about the importance of service uptake, an approach that seemed to fit well with a mental model of ‘hard-to-reach’ groups who needed to become more familiar with the local health system. Although the ensuing work may have addressed some of the obstacles to access, it appeared to be informed by a partial reading of the available evidence.
Although some respondents clearly recognised the complex and contested nature of ethnicity – for example raising questions in the interviews about the adequacy of ethnic categories or the need to understand the inter-relationships between ethnicity and religion or the role of discrimination in minority experiences – these respondents were few in number. Interviews with many more commissioning staff suggested a lack of reflection on these issues and a tendency to foreground culture and language as the defining elements of ethnicity and to downplay structural disadvantage and discrimination. Furthermore, we witnessed very little open discussion of such conceptual issues within commissioning arenas aside from those that were prompted by the feedback of our own study findings.
Second, we found that many commissioners had low levels of competence in appraisal, synthesis and integration skills. Synthesising evidence from a wide range of sources is clearly challenging and, as noted by the key informant respondents, some significant additional complexities arise when the focus is on minority ethnic health issues. Nevertheless, various tools exist for helping with evidence appraisal and approaches have also been developed for plugging evidence gaps, working with incomplete data and integrating evidence across a range of sources. It was rare to find people who were aware of, and confident to use, such tools and approaches. Individual interest and expertise were the key factors determining whether or not such techniques were employed to make more effective use of available evidence. It was particularly noticeable that E&D leads, who might otherwise champion these issues, often lacked the skills, experience and confidence to mobilise and synthesise evidence effectively.
This brings us to a further key theme, the importance of being able to mobilise evidence in influential ways to make progress on ethnic inequalities. Echoing the observations of some of the national key informants represented in Chapter 3, several respondents in the case study work expressed the opinion that decision-makers demanded a higher standard of evidence when the focus was on addressing ethnic diversity and inequality. Observational work also suggested that key actors could at times draw on a ‘hierarchy of evidence’ mental model, whether implicitly or explicitly, to block action on ethnic inequality. Commissioning managers seeking to introduce a new service or bring about improvements to an existing service generally had to leverage resource to fund the proposed changes. This involved commissioning managers (or sometimes stakeholders from provider organisations or community groups) negotiating for reallocation of resources within a fixed envelope of spend; ‘bidding’ internally for investment (e.g. by making an invest-to-save proposal to a QIPP programme); or perhaps submitting an application to an external source of funding designed to encourage innovation. Regardless of who was making this case, respondents often reported that it was challenging to prepare a strong business case in the face of incomplete local data and very limited evidence on the cost-effectiveness of proposed interventions. The importance of packaging and communicating evidence was clearly important to securing decision-makers’ support for proposals. Some individuals seemed to be much more confident about, and influential in, using evidence in this way. For instance, we found a few examples in which incomplete data had been mobilised effectively by commissioners to gain investment for development work on ethnic minority issues. On the other hand, we also observed a case in which personal clinical experience was used to trump NICE guidance on drug use for African Caribbean cardiac patients and thereby block consideration of ethnic difference within the pathway work. The ability to use evidence influentially also linked closely to skills in conceptualising ethnicity clearly, and appraising and synthesising evidence effectively, as it was common for proposals to be challenged on the basis of issues such as small numbers; representativeness; inappropriate ethnic categories; lack of disaggregation of data into subgroups; questionable transferability of findings to the local context; and insufficient detail on the underlying causes of observed differences, and whether these causes were really something that health-care commissioners could and should do something about.
Chapter 6 Enabling factors and opportunities
Introduction
This chapter draws from findings across all phases of the research, including the key informant interviews, the main case studies and the good practice examples. It aims to identify factors that encouraged critical and effective use of evidence on ethnic diversity and inequality within the commissioning process. This synthesis will contribute to answering research question 2 (How might individual, team and organisational competencies be effectively enhanced to support critical use of research evidence for the commissioning of services that better meet the needs of a multi-ethnic population?) and also one of the main empirical objectives [to identify factors (at evidence, individual and contextual levels and their interfaces) that support or inhibit the critical and effective use of research evidence within the PCT commissioning cycle and thereby identify promising routes of intervention].
Enabling themes
The previous chapters have highlighted a range of obstacles that acted to inhibit the mobilisation and utilisation of evidence on ethnicity within commissioning work. These factors operated through:
-
a low demand for evidence on ethnic diversity and inequality
-
important gaps in the evidence and missed opportunities to access available evidence
-
uncritical and ineffective use of evidence within commissioning.
The first of these was particularly important as it tended to perpetuate the second two.
Broadly speaking we saw progress towards better commissioning for minority ethnic populations where people were mobilising evidence in such a way that attention to ethnic diversity and inequality was legitimised and promoted; and uncertainty around problems and solutions was reduced, thereby increasing the confidence of stakeholders to act. The first of these often involved people using evidence in influential ways, paying careful attention to presentation and argument, and seeking to align their objectives with core organisational drivers. The agency of individuals was particularly striking, often producing innovative work despite (rather than because of) the wider organisational contexts that did not support a focus on minority ethnic needs. Other cross-cutting themes that seemed important were finding creative approaches to filling evidence gaps and taking an incremental approach to improving data quality and quantity, rather than being blocked by inadequate evidence.
Findings across the full range of the study’s diverse sources of evidence indicated that progress on this agenda required action at three levels: creating an enabling environment, empowering wider stakeholders to support and challenge commissioners (particularly by bringing evidence into the commissioning arena) and equipping commissioners with skills and confidence to access and use evidence appropriately.
Creating an enabling environment within commissioning organisations
Leadership
The research data indicated that strong leadership on ethnic inequalities was a key enabler, especially in ensuring that attention to ethnicity was mainstreamed and good work was prioritised and shared across the organisation.
It doesn’t matter how brilliant, innovative, courageous, forward-looking operational folk are, they can only make a difference in a small corner of the world. If you’ve got good leadership then there’s an opportunity for those innovative beings to flourish and for what they’re doing to be extended into other areas of the organisation.
Third-sector senior manager
As earlier sections of this report identified ‘silo working’ and a lack of knowledge-sharing or practice-sharing across and within NHS organisations, it was key to have senior guidance that not only recognised ethnic inequalities in health as a major issue but also facilitated joint work and goal-setting across departments. This was particularly key in information-sharing, as human resources, engagement officers, service providers and public health all had useful evidence on ethnicity. And awareness of different data sources, and the signposting of relevant information from disparate departments, requires input from managers with a strategic role across all of these areas.
Some respondents felt that having leaders who personally empathised with and fearlessly championed the agenda was a key enabler:
If you’re a decision maker but you, say, have an adopted black son or a daughter and that son or daughter goes through racism, discrimination, unfairness in society, then that decision maker is actually affected by that because there is a link. What makes him or her change their views on fairness in the workplace is because there’s somebody at home reminding them about those things that are happening. But if you don’t have anybody like that at home or in the workplace, which often aren’t there, then you become in a very bubble world of fairness that exists, but the experience of people who are visible minorities and women and gay people and others is completely different to the decision makers.
Strategic health authority senior manager
This perception was echoed by those participants who described how a new chief executive had changed workplace culture on inequalities by being open about his own disability. This openness legitimised attention to this and all other areas of potential disadvantage, making them visible within the organisational culture. Indeed, one of the key factors in the Innov8 Charter was to promote diverse leadership for this very reason: a sense that people from a range of backgrounds drew on different, marginalised experiences, away from the ‘bubble of fairness’, and that different experience was the most important thing to bring to leadership roles: ‘There’s no point recruiting, you know, different leaders, if what you’re saying to them is we expect you to behave like us, and we expect you not to share what makes you who you are’ (PCT senior manager).
The Innov8 programme also argued that there was a strong business case for increasing the diversity of leaders, highlighting the ability of leaders with different backgrounds to consider different solutions to problems, and offer more effective solutions by being able to better understand and empathise with disadvantaged communities.
However, respondents also expressed the feeling that leadership on this agenda did not need to come solely from the senior level but was essential at a range of different levels to maintain project momentum through the many challenges:
It comes down to leadership. I don’t mean just necessary chief executive or whatever, but you know if you get, if you get a strong public health group, or in some cases it’s a strong patient and public involved PPI [patient and public involvement] lead, it’s a strong character that knows the importance of this stuff and will rattle cages to make sure that it gets done.
DH senior manager
Committed individuals and dedicated staff
The most critical enabling factor observed during the research project was the role of individuals with a deep understanding of, and commitment to, the race equality agenda. Regardless of seniority or role, these individuals became significant drivers for change. Sometimes these individuals were from external third-sector or community organisations, but often they were internal staff with a specific E&D remit (particularly E&D leads based within the PCTs): ‘The equality teams tend to be very passionate, doing it for their personal, moral, you know, values’ (commissioning group chair).
The E&D leads, either in provider trusts or PCTs, were often the lead actors in the good practice examples that we documented. Furthermore, our observations on the implementation of the Equality Delivery System in two out of the three case study sites confirmed the central role of effective E&D staff in making the Equality Delivery System productive. The Equality Delivery System example explicitly demonstrated, across each of the three case study sites, that those organisations with the most E&D staff produced the most in-depth assessments, drew from more sources of evidence and had the best engagement processes. It was also evident that when E&D leads were placed at more senior levels/bands they gained greater autonomy, allowing them to allocate their time more dynamically to issues that they identified as being critical, even in those organisations that generally provided little direction on important equality issues. This finding supports the recommendations of the Competency Framework for Equality and Diversity Leadership (a strategic document produced as part of the Equality Delivery System), which call for E&D roles to be placed at senior levels/bands.
At the same time there was some evidence that having specific roles and responsibilities for equality (or, ideally, for minority ethnic health issues in particular) can be a powerful organisational enabler. These roles permit networks, deep(er) engagement and specific skills to develop:
Often PCTs had particular race equality leads, and I think having somebody with that remit in their job title was really important, and a lot of innovation and good work, and it’s often about relationship, isn’t it, so having somebody you know to link in with works for the community group and works for the lead as well in the PCT, because over time they build up these sort of relationships with people, so they know about an organisation, they know what they’re trying to achieve, and they know what they’ve been achieving year on year, so at least there’s the dialogue going on.
Third-sector senior manager
Yet another key enabler observed was having staff with a community and/or equality role embedded and well networked within the organisation, rather than having such work contracted out to external groups or consultants:
The community development workers . . . were placed within the primary care trust rather than the voluntary sector, that has helped, so they are based with the PCT there, so they are a core part of the group. I guess they’ve been able to engage with the strategic staff a lot better than some of the other areas who might have been outside of the PCT and outside of health services.
Third-sector senior manager
Many of our research respondents also felt strongly about the need for the workforce of commissioning organisations to be ethnically diverse and to reflect the communities for whom they made decisions. Again, this was felt to increase the likelihood that commissioning staff would understand the need for dedicated work to engage with ethnic diversity and inequality and thereby prompt the demand for evidence production and utilisation:
That’s why having an organisation that reflects the communities that we serve is a very, very important part of it, because if they reflect the community they serve then people who are actually at the decision making process know what it’s like to be a woman, know what it’s like to be Black, know what it’s like to be a gay person. That thinking, that experience is brought into the decision making of what is important, what are the priorities.
Strategic health authority senior manager
Supportive and productive networks
As well as having committed staff within commissioning organisations, networking was identified as an important enabler. In particular, organisational investment in communities of practice – particularly to support and connect E&D and other staff who can otherwise become isolated when working on this agenda – was felt to be very helpful. The value of communities of practice was demonstrated most clearly in the case study work, from which a powerful network of E&D leads was identified in one of the study sites: ‘I think that’s one of the things I’ve really really found useful, and I don’t think I’ve realized how much until we’ve not met for a while, because it’s quite an isolating job being head of equality’ (commissioning group chair).
Previously, the individuals in these networks had had few opportunities for joint working. However, by setting up regular meetings they were able to raise common concerns and scale up solutions that had worked in one provider trust across the whole city. This led to a common approach for equality monitoring of complaints and to the sharing of resources for community outreach events, saving a great deal of time and duplication across provider trusts.
Communities of practice were also clearly beneficial for commissioners wanting to find solutions to equality-related issues. Here, informal networks with other commissioners, including those working on other clinical areas in other PCTs, had facilitated information-sharing and greater awareness of successful interventions:
We used to have regional networks until very recently . . . I wouldn’t say it’s perfect, but yes, I could call on colleagues and say ‘have you done anything on; it doesn’t look like our service is hitting this community. I know you’ve got a similar community. What have you done?’
PCT senior public health commissioner
Importantly, however, national, regional and organisational support for such networks is currently in decline. Nonetheless, as well as these formal/institutional networks, informal networks and interpersonal relationships can also be important enablers. These informal networks, both within and between organisations, ensured that commissioners were well informed about issues and sources of information. They also ensured that commissioners had ‘allies’ who they could draw on to increase support when tackling minority ethnic issues that would otherwise have been marginalised with senior decision-makers:
I have to be honest with you, individual relationships really matter. I have seen a lot of decisions are made in corridors and at tables, I’ve been a part of those, I’m sat outside saying look I need your support on this when we go in there and it’s happened, not just because of the relationship, it’s because they know that it will benefit us, but we have had a pre-meeting before going into the meeting so you’re more privy to the stuff than before.
Local authority senior commissioning manager
Although often personalised, another aim of the Innov8 programme is to foster and support networks between ‘diverse’ members of staff and thereby provide opportunities for such individuals to take the lead on small pieces of work for the first time. This was the case in the Innov8 research project in which the leader of the work had gained opportunities through Innov8 to work directly with the chief executive and senior project managers for the first time.
Incorporating ethnicity into national agendas and routine processes
As previous chapters have noted, ethnic inequalities are rarely a major agenda within the NHS. However, we found that progress on this agenda was more likely when actors engaged with core priorities and processes, and sought to integrate attention to ethnic health issues within these other core areas. This was particularly evident during the period of this study, when budget cuts and efficiency challenges led to little ‘new’ commissioning. For example, much of the work observed in the operational case studies followed the redesign of existing clinical pathways, providing an opportunity to ensure that services were being equitable. One good practice example involved a project for enhancing stroke awareness that had grown from a national agenda (promoting the ‘act FAST’ message) and tailoring this message to meet a local need amongst minority ethnic communities.
Meanwhile, compliance with legal duties was an issue that was often raised by participants to ensure that the NHS was paying due regard to equality issues. By drawing on the nine protected characteristics in the Equality Act 2010,99 the Equality Delivery System was an important part of the NHS response to meeting its public sector duty, with Equality Delivery System outcomes leading to Equality Objectives set by each PCT. However, the Equality Delivery System process demonstrated that evidencing disadvantaged service delivery amongst one or more minority groups was often difficult to achieve because data on service use and users’ experiences were often not disaggregated by ethnic group. This process was nevertheless positive in that it highlighted gaps in the data and prompted the setting of targets to improve data collection and disaggregation in each of the sites for the next iteration of the Equality Delivery System.
Elsewhere, commissioners and activists had to be creative to identify suitable mechanisms for enhancing attention to minority ethnic issues. Where services were not meeting the needs of minority ethnic users, the QIPP programme could be argued as delivering a poor-quality service to these groups. It might also be argued as leading to potential inefficiencies if unmet need was likely to have been leading to late diagnosis and treatment. Indeed, because cost saving was a common concern for commissioning organisations during the period in which this research study took place, it was good to see that some individuals had had considerable success by acknowledging the need for efficiency and developing business cases that successfully demonstrated how a better understanding of the needs of minority communities could lead to more efficient resource use:
I worked with some of the managers there, listen to what they had to say, what their reservations were, what their priorities were, but then after observation I worked with them to show them how we could fill those four beds or not fill those four beds, whatever the priority was, by ensuring that we’re doing the equality proofing, because we can prevent people from filling those beds so it will cost you low, that’s why we need to do this. So it’s very important then to relate it back to what is meaningful to other managers who may not have equalities as their priority.
Third-sector senior manager
Another scheme that had been used successfully to address ethnic inequalities was the Quality and Outcomes Framework (QOF)102 payment by results system for primary care. One PCT had used a local QOF outcome to successfully encourage GP surgeries to improve the ethnic monitoring of their patients. In another example one GP surgery that worked specifically with asylum seekers and ethnic minorities persuaded the PCT to develop a QOF indicator that would allow them to meet the specific needs of their service user populations:
So they managed to negotiate with the primary care trust about, back in 2004, 2005, for a modified QOF . . . where payments were made for them delivering services better aligned for them, so providing TB [tuberculosis] service screening, or providing new entrants screening, and the points were awarded for that, rather than our standard measures of cancer care and what not, which were less common in this group.
GP
Here, a provider had worked with the commissioners to ensure that they were able to provide appropriate additional services without the need to specify, or tender for, an additional service, an arrangement that was beneficial to both parties.
In both cases improving the monitoring of access to, and outcomes of, services disaggregated by ethnicity was part and parcel of service improvement. As such, this illustrates the importance of incremental and integrative approaches to improving the evidence base for commissioning.
Looking to the future, several respondents suggested potential opportunities for embedding attention to ethnic inequality within emerging commissioning structures. In particular, there were hopes that commissioners would be more accountable to local communities through the health and wellbeing boards, and that stronger JSNAs and more co-ordinated work would help to address the wider social and economic determinants as a result of the move to local authorities of public health. At the same, however, they noted that a national policy context that had been further weakened could continue to undermine progress towards a more enabling environment in the future.
Empowering wider stakeholders: partnerships and networks
Although commissioners need to be asking the right questions about ethnic diversity and inequality, they cannot be expected to have all the answers. There is therefore a need to more effectively bring in a wider group of stakeholders. Stakeholders who are important knowledge bearers in relation to understanding and addressing ethnic inequalities can both challenge and support commissioners (in a role that respondents identified as ‘critical friends’ or even ‘external agitators’).
Progress was more likely when commissioners effectively drew from a wide variety of stakeholders and engaged them as partners and co-producers. One of the few commonalities in the examples of good practice that we documented was that they all described the development of a cross-disciplinary team. This was clearly a critical factor for success. With regards to evidence in particular, a team with a variety of backgrounds tends to draw from a much wider evidence base, including, for example, information from surveillance and demographic data from public health, providers’ service use data and service experience stories from community engagement workers.
Key informants and actors in the main case studies that we examined were rarely aware of any national infrastructure to support knowledge generation, synthesis and mobilisation. For this reason they found it necessary and beneficial to draw on local skill sets. There was certainly a gulf (i.e. a large ‘social distance’) between decision-makers and service users. There was also limited time available to most commissioners to ‘do’ service user or community engagement. For these reasons, joint working between providers and commissioners is essential to bridge the gap between commissioners and users and to ground decision-making in front-line experiences.
Provider–commissioner relationships
As discussed in previous chapters, there was substantial evidence of uncertainty and contestation around the role boundaries of, and relationships between, providers and commissioners. Many respondents expressed the sentiment that relationships were difficult to manage and tended to undermine progress towards better services: ‘The model is an essentially market model, which is that you split the purchaser and the provider apart’ (third-sector manager and analyst).
However, many felt that the most productive work was achieved when relationships between commissioners and providers, especially the larger provider trusts, allowed both organisations to input into service specifications and outcomes. Provider staff – particularly clinicians and practitioner managers – were concerned with more than simply delivering a contract; they often had a genuine desire to improve equitable service delivery and held invaluable knowledge and front-line experience of feasible solutions:
I have really good links with clinical colleagues delivering the services that we’re talking about, so it’s not like I just sit in a room and say ok, this is all the data, let me just think up a service. It isn’t like that. It’s very much a partnership approach to a lot of this with clinical colleagues, with providers, with other stakeholders. I jointly commission quite a lot, particularly older people’s mental health services, so myself and a colleague in the council sit down together and jointly put together commissioning plans. Again, they bring different evidence to the table; they see things sometimes from quite a different perspective which is really quite refreshing sometimes.
NHS senior commissioning manager
Respondents were also sometimes concerned that pressure on commissioners to act as impartial buyers of services in an open market system limited the opportunities for co-working with potential providers to develop better solutions. Case study respondents and the good practice examples detailed several situations in which deep relationships between commissioners and providers had led to innovative services being trialled, such as those in mental health, thereby generating important new evidence of what works best to meet diverse needs: ‘That’s what I think the job of commissioners is, and commissioners are there to help the market, and then to help build the market’ (third-sector manager). This was especially apparent when community-based service providers that worked with minority ethnic communities had been commissioned for targeted services, particularly in mental health.
Clinician buy-in
Getting clinician involvement in all stages of the commissioning process helped strengthen the acceptability and adoption of new and revised services. Clinicians, especially GPs and consultants, were seen as having a large degree of autonomy. They also preferred to take direction from other people with a clinical background: ‘I think if you come from primary care, so again it’s almost like coming from within, and you’re trying to sell the package back to your peers, there’s much more of a buy-in there, really’ (GP).
Specific examples raised by respondents around ethnic monitoring in primary care emphasised the importance of getting clinicians to understand the need for attention to be paid to minority ethnic health issues. Again, all of the examples of good practice that we documented involved teams of commissioners and clinical staff or managers. By integrating both ‘sides’ during the service planning and development phase, they were able to ensure that both understood the issues and the need for interventions. This was also recognised by respondents as a critical part of the successful commissioning process:
There was a combination of the consultant, the, not consultant, medical director, being able to trek his way around the practices, on a peer basis, to sort of push them, you know, ‘this isn’t good enough for us, is it’, sort of thing rather than it being a big stick from somewhere else . . . If you can actually get general practice to see it as ‘our problem’, rather than ‘you’re telling us to do this, but we need more money’, it’s a different world.
Third-sector senior manager
Respondents speculated on the likely prospects for evidence-based commissioning for minority ethnic populations once GPs led the emergent CCGs. Our respondents were generally doubtful that GP commissioners could, or would, take any clearer action on ethnic health inequalities in the near future. They expressed concern that many GP commissioners lacked the necessary skills and experience to engage with relevant sources of evidence. They were also concerned that the immediate concern of GPs would be with the transactional aspects of commissioning and that they would have little time for transformational work. Meanwhile, concerns were expressed that GPs might have low levels of engagement, and poor relationships, with local authority and third-sector organisations. Efforts were under way at the time of this study by champions for this agenda to engage with the new commissioners and to seek to increase their understanding of why it is important and fits closely with their own priorities for better-quality patient care. Furthermore, there were signs that some commissioning GPs’ professional identities, clinical expertise and awareness of local needs might actually help enable them to bring about positive change.
Researchers/academics
There were several examples cited by key informants in which researchers had contributed to commissioning by providing evidence or local research on minority ethnic health issues. However, such work had been most productive when academics were well known to the service group using the findings and were prepared to engage in person:
If academics come along to talk about things, I think people do sit up and listen in a way that perhaps someone else just sort of saying you know, ‘there’s a paper here that says we should do this’, is less, is less powerful.
Public health observatory senior manager and analyst
Professional networks to share evidence between researchers and commissioners, such as CLAHRC networks, were active in each of the study sites. However, respondents had varying degrees of exposure to evidence through these networks. Several respondents noted that evidence was most useful when packaged in brief, easy-to-read formats. They made it clear that they did not have the time to read long academic journal articles or conduct extensive literature reviews.
Collaborations were also most productive when academics had made the effort to reach out to relevant service groups, explain their research in person, make links to actions and possible interventions and establish longer-term relationships to allow a process of inquiry to develop. For example, in the vitamin D mini-case study (see www.eeic.org.uk/mcs/vitd), personal networks with clinicians had not only helped identify the deficiency but also led to subsequent local qualitative research with Somali patients. This revealed dietary patterns that were compounding low vitamin D intake.
User and community involvement
Although user and community engagement is a strong and increasing agenda across the NHS, ensuring representation from across minority ethnic groups was a significant challenge. Engagement worked best when it was an integral part of the whole commissioning cycle, rather than taking the ‘tokenistic’ approval of plans for service improvement that had already been completed. One good practice example on stroke awareness involved engagement from the very start of the process to identify how best to develop messages specifically tailored for minority ethnic communities. This example used a ‘social marketing’ approach at the start of the process. This ensured that specific, evidence-based, solutions were considered from the outset:
I mean a good example where things have worked well has involved social marketing and insight work with communities, so we understand what the issues are for them, what the barriers are to using services are, what their views about health are and so on.
PCT senior public health commissioner
Respondents, particularly those from third-sector organisations but also many commissioners, noted the risks of engagement ‘fatigue’, in which the same well-known people from particular communities were asked for input on all of the service redesign work under way. Cross-sector working in this area was rare, but very successful when it was carried out, minimising resources and frustration from participants:
There’s not one method to talk to everybody. You have to build relationships with people . . . But I think we need to do things differently in terms of jointly doing engagement. So rather than the organisation A, B and C all doing it differently, it may be that A, B and C should do it collectively, and have a database of what you learn shared between three of you. So rather than certain groups being bombarded with A, B and C, they go in one. Because if there is fewer organisations, or organisations with less capacity, you can’t be seeing all these organisations who wanted information from you, who in your experience have done nothing with it.
PCT commissioning manager
In addition, wide cross-sector collaboration on engagement brought unexpected benefits to commissioners in different organisations:
The fire service spoke at one of our consultation events around health . . . but he said the most important thing for him is community engagement and the cross-sector working. Usually you wouldn’t expect for somebody who’s doing a health consultation for the fire service to be there, but he does it, so you know putting in fire alarms is a prevention of health . . . trying to prevent people from smoking would actually have an impact on their health but also actually stop them having a fire.
Third-sector senior manager
However, first commissioners needed to understand the benefits of including evidence from consultation with minority ethnic groups. And, as with providers, the power relationship between commissioners and community groups needed careful consideration. Engagement was clearly most useful when it had a constructive focus, and for this to happen commissioners needed to be open and not defensive:
We arranged for about twelve, maybe fourteen, local community groups to host a meeting with four or five commissioners from elsewhere in the country . . . That, for the majority of commissioners who participated was a life-changing event, because for the first time they didn’t feel they were going to meet with local communities to defend what they’d been doing, they didn’t feel they were going there to be attacked for what they’d not been doing, they didn’t feel that they were going there and people were going to be asking for loads of money that they didn’t have – it was just an opportunity for them to listen and to hear. The impact of that was that when they got back to their local areas they set up similar ways of consulting with local communities.
Third-sector senior manager
Yet to establish these productive engagement opportunities, considerable investment needed to be made in establishing relationships with groups who actually understood the commissioning process: ‘So yes, it may want a time commitment, consulting with local communities, building those relationships, but it’s not just a one-off. You build that relationship and that then becomes an on-going resource to the commissioners’ (third-sector senior manager).
This was seen operationally in the Equality Delivery System case study, in which one site had invested a great deal of time and resource in developing an equality group to consult on issues across the provider and commissioner trusts. This investment paid off by providing an established and well-briefed group for Equality Delivery System community engagement, with participants trusting the process, understanding the goals of the group and participating constructively as knowledge bearers. Commissioners who developed meaningful engagement with minority ethnic communities were able to gain evidence on health needs, test ideas for interventions and gain legitimacy for commissioning decisions.
Skills and confidence in using evidence on ethnicity
Despite significant evidence gaps, there were several examples in which data had been successfully brought together from different sources to create sufficient evidence to inform careful commissioning decisions. Frequently this was achieved by combining local and national data and/or research. For example, estimating the demand for cardiac services across a diverse urban area could be achieved by looking at national data on the prevalence of cardiac conditions by ethnicity and extrapolating these prevalence data to the local area by combining with local demographic information.
However, it was clear from talking to respondents that many commissioners lacked the skills to perform this kind of data analysis and integration. Sources of support for commissioners under these circumstances were often unclear or absent. This was especially true for E&D leads who were often expected to lead work in this area and not only lacked the data analysis skills required but also received little in the way of support. Yet some simple, creative solutions were nonetheless found (Box 6).
One E&D lead with very little statistical experience created a simple spreadsheet in Excel that took data from a publicly available GP satisfaction survey and compiled individual-level GP practice scores to provide a picture of local satisfaction by ethnicity. This information was presented in a succinct and meaningful way and was fed into the Equality Delivery System. This led the strategic health authority to fund a further data analysis exercise to break down information from national GP and hospital patient surveys by protected group.
This highlights another necessary skill that commissioners require: the ability and willingness to ask the right questions of the data. Many respondents, including data analysts, felt that there were plenty of data available that were (or could be) disaggregated by ethnicity, yet commissioners were largely unaware that these data were available or did not ask for the data to be presented in this way. Increasing the demand by commissioners for such disaggregated evidence, as detailed in earlier sections, was seen as a key critical first step. But to ensure that these data were influential to the commissioning process, they then need to be formatted and presented in an appropriate way.
In the stroke awareness good practice example, the findings of the social marketing exercise were collected as qualitative information, that is, as stories and quotes from participants. To present this information to the board responsible for deciding whether to commission further work, the team had to condense all of these rich data into a few brief bullet points, summary statistics and a matrix table of the key issues for a 10-minute presentation. By carefully considering the commissioning audience, and making the qualitative findings concise enough to be understood by a largely clinical audience, the data were made influential and supported the next phase of the project. Clearly this skill is needed by a wide variety of stakeholders who wish to feed into the commissioning process.
Earlier chapters have highlighted uncertain and unhelpful understandings of ethnicity among some commissioning actors. This suggests the need for interventions that would increase conceptual clarity and confidence to engage with these issues. We did not find any concrete examples of enablers in this area during the study period. But it was clear that within each of the study sites there was untapped expertise within the organisations that could have been shared more widely to enhance confidence and competence.
Chapter 7 Development of tools and resources
Introduction
This chapter outlines the development of a suite of tools and guides, based on the findings of the project. These tools are designed to help organisations at the policy level to understand minority ethnic health issues; enable actors in the commissioning process to better utilise evidence around minority ethnic populations; and also encourage wider participation in commissioning, from providers, service users and community representatives.
As such, the aim of the tool and resource development was to address research question 3 (How can individual, team and organisational competencies be effectively enhanced to support critical use of research evidence for the commissioning of services that better meet the needs of a multiethnic population?).
Tool and resource development also aimed to meet one of the key objectives outlined in the original research proposal, namely to develop practical diagnostic, evaluative and change management tools for use by individual managers, teams and organisations that aim to assist these to (1) assess and promote critical reflection on current competencies and practice with respect to utilisation of evidence on ethnic diversity and inequality; (2) identify actions to strengthen competencies and good practice; and (3) support specific elements of the knowledge utilisation process.
The preceding chapters have provided a rich description of current patterns of evidence use relating to ethnic diversity and inequality within commissioning organisations, as well as highlighting a number of key obstacles to, and enablers of, a more critical and systematic use of evidence in these contexts. These findings informed the focus and content of the tools and resources, identifying a number of critical gaps which, if addressed, might improve commissioning practice in this area. In particular, the critical gaps included:
-
increasing commissioner demand for evidence
-
making the case for considering ethnic inequalities
-
increasing confidence and addressing uncertainty on ethnicity
-
making best use of available data
-
developing service specifications and outcome measures specific to ethnicity.
In addition to these gaps, the key informant interviews and case studies provided insights into the wider organisational structures and cultures of commissioning organisations and the day-to-day realities of commissioning work. These insights informed our thinking around how interventions, such as tools, aimed at enhancing evidence use in this area might be received. For this reason we generated relevant data both through direct questioning of respondents regarding their preferences and working practices, and through the observational and documentary work in which people were directly using or were unaware of key resources. Many of the key themes emerging from the interviews, observations and documentary research have already been touched on in earlier chapters. However, it is worth providing further detail here of those findings that are directly relevant to the process of developing tools and resources.
Meanwhile, the project team was aware of a large number of existing tools and resources that were already available to commissioners and health-care practitioners, and wanted to ensure that any outputs from the present project would complement and draw inspiration from, rather than duplicate, existing tools and resources. Data collection therefore included compiling an inventory of existing tools and resources to inform the development of the outputs intended to be useful to the present project’s target audiences.
Draft tools were then presented at a series of national workshops so that potential users could evaluate and critique the tools in draft form and suggest suitable improvements and amendments. These workshops also generated valuable information on how we might ensure that toolkits and resources will actually be used and on the most appropriate format(s) for these audiences.
Perceptions and utilisation of existing tools and resources in commissioning: findings from the key informant interviews and case study work
Perceptions from interviews on existing tools
Respondents from the key informant interviews were asked if there were any specific tools or guides in their area of work that they were aware of and/or had already used. They were also asked what formats they would find most useful for such tools and their general perceptions of toolkits relating to commissioning, evidence use and ethnicity.
Respondents were aware of a large number of existing toolkits but, in general, questioned their usefulness. More than one respondent felt that toolkits were rarely used and tended to ‘sit on the shelf’, and many people felt that there were already more than enough (if not too many) available:
People [are] snowed under with toolkits – I think it’s almost like the latest buzz word, oh here’s a toolkit, everything’s going to be OK now.
PCT senior commissioning manager
There are 101 commissioning toolkits around already.
PCT public health practitioner/commissioner
Many others questioned the need for toolkits for commissioning, either because they did not believe that they were useful in practice – ‘I can’t say I’ve ever seen a really good toolkit for commissioning’ (PCT senior commissioning manager) – or because they felt that, particularly with regard to commissioning for multiethnic populations, a deeper level of change and understanding was needed first:
I don’t want toolkits and guidance, speaking frankly with you, that’s not what’s going to change the culture . . . The connection to equality is not through guidance and toolkits; the connection to equality is through people.
Strategic health authority senior manager
I’m not sure that it’s toolkits that we actually need, I think it’s actual people to record the information in the first place.
PCT public health practitioner/commissioner
However, some respondents had found toolkits to be useful and provided guidance on how to ensure that they would be used, in particular stressing the importance of brevity. As noted in the previous chapters, it was unusual for commissioners to have dedicated time to engage with research, especially on what were seen to be marginal issues, and respondents felt that the best tools and sources of information were therefore the shortest: ‘You’re going to get somebody who will say “yes, I’ve got ten seconds to read this” – bang . . . Two- or three-sided evidence summaries which are backed up with full reports’ (PCT commissioning manager).
Additionally, participants emphasised the importance of getting the format of such tools right, highlighting their experience of the importance of optimum presentation to maximise impact:
We spent three grand to tidy it up into a booklet, give the book away, all of a sudden it receives currency around the NHS . . . the work didn’t change, what we did was exactly the same as what had been evaluated before, putting it into a glossy cover, and with some pictures on it . . . gave it currency.
Third-sector manager
[A website] needs to be actively managed, so it’s not just a static portal, but it’s somewhere where people will keep coming back, you’ve got to keep refreshing it.
DH manager
Finally, there were notable recommendations for the content of the tools:
What would work for me almost an FAQ [frequently asked questions] or a questions and answers document about if you’re commissioning in an area where you think you have different health needs which are due to ethnicity, these are the questions you should be answering and asking.
PCT senior commissioning manager
It needs to include a cost-effectiveness bit in it. Because a lot of those toolkits don’t.
PCT senior public health commissioner
Largely these findings mirror the advice provided by previous research in this area, which highlights the importance of succinct evidence, with Brocklehurst and Liabo advocating ‘evidence nuggets’ or short briefings to share information. 103
Examples of the use of tools and resources from case studies
In general, the case studies did not reveal many examples of toolkits actually being used by commissioning staff. Amongst these few examples, in the Equality Delivery System case study there was a process guide that had been developed by the DH, which contained a grading manual that provided some examples of the sorts of activities that would be indicative of each of the four grades. However, several respondents found the guide unhelpful or even confusing, describing it as verbose and the examples as poor, so that there was little evidence of it actually being used during the Equality Delivery System process.
Case study work also revealed other issues with tools and guides. For example, they were felt to have a short shelf life as frequent changes to organisational structures and priorities made them quickly lose their relevance. Some respondents noted that there was often a need for some kind of external driver to get people to take the time to formally use a tool or a toolkit. This was true of the many guides developed as part of the WCC agenda, an initiative that had itself lost momentum even before the recent commissioning restructure. In the maternity case studies, toolkits that had been produced alongside Maternity Matters100 were no longer in use.
Two other aspects of guides and tools were also highlighted: first, that their use varies between and within organisations, so their impact was varied and difficult to measure; and, second, that some organisations customise or adapt tools for their own needs.
Finally, case study work identified variation in awareness of national-level tools and in the tools used in individual organisations. When tools, even nationally produced ones, are used or altered, there was little evidence of feedback to the tool producers or of sharing experiences of using/adapting these with other organisations. There was therefore limited sharing of valuable real-world experience. The tools produced for the WCC agenda were hosted on an intranet site that was rarely used by staff, one respondent noting that, although visible at first (on the main page of the website), the tools quickly became difficult to find, and general awareness of these was low. Another case study respondent, who was not aware of several of the tools suggested by the interviewer, commented, ‘I think these tools are often very useful but they are time-consuming and we only complete them when “required” to’ (workshop attendee).
Draft tool development
The process of translating the research findings into tools and resources that had relevance and utility to key stakeholders was an iterative one. Indeed, it is a process that remains ongoing at the time of writing this report, involving all members of the research team and the project advisory group. From early on in the project, the research team began to map emergent findings from preliminary interviews, observations and documentary analyses to possible opportunities for tool development, particularly thinking about the content, format, audience and context of use appropriate for each finding. Figure 3 illustrates the type of ‘logic framework’ that was used to think through these connections.
FIGURE 3.
Example ‘logic framework’ linking research findings to draft tool development. Note: circles indicate the tools that were developed in draft form for piloting in the workshops.
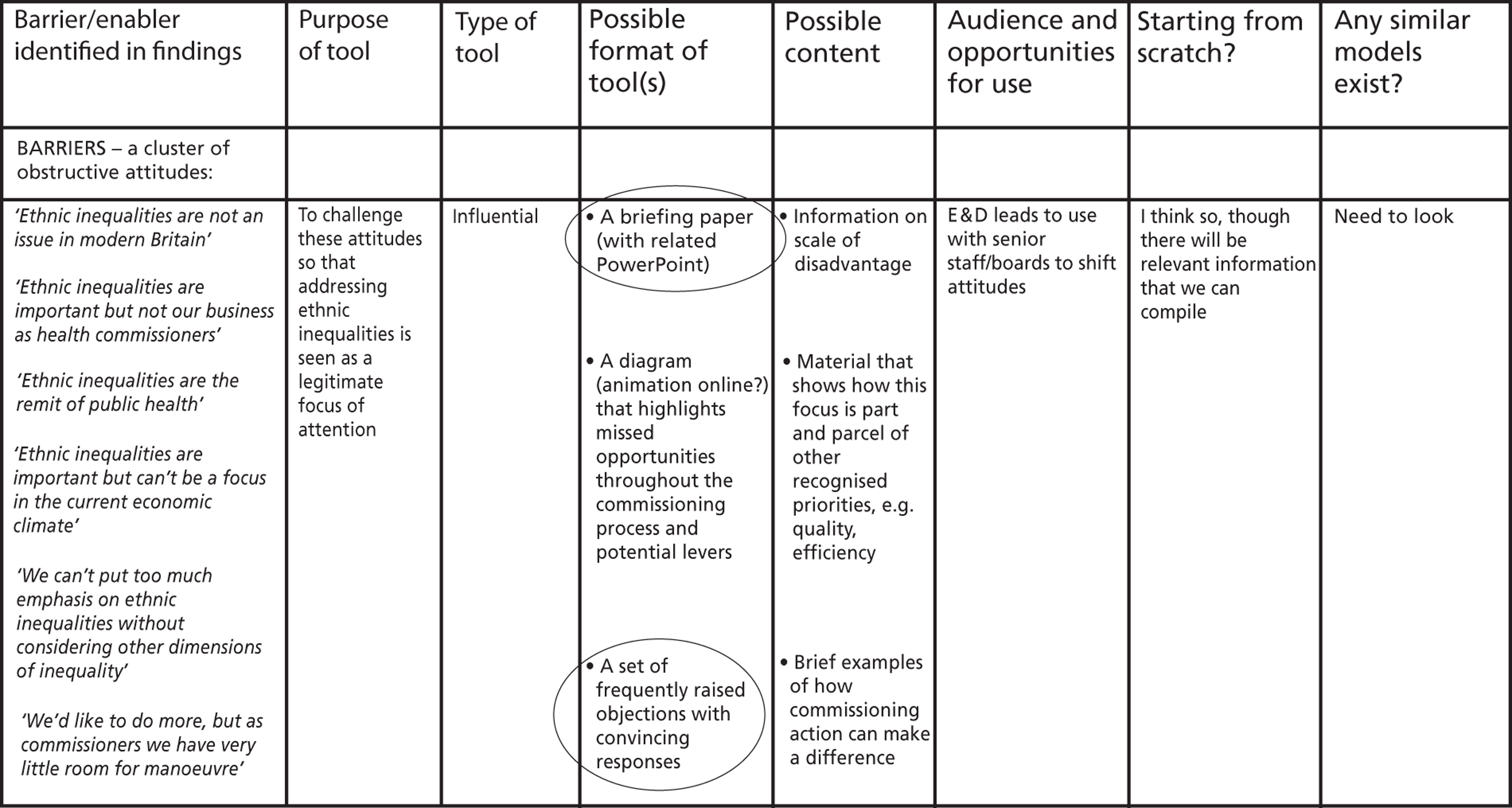
Various internal documents were then produced by the research team, outlining possible tools and resources, and these were shared at team meetings for comment and feedback from colleagues and project advisory group members. Co-researchers in particular were able to provide ongoing commentary on the structures and processes operating within their organisations that would shape the reception and likely impact of any tools or interventions. Examples of styles and formats of tools from other sectors were collected, drafts were developed and presentations of potential tools were given at a number of forums to gain input from likely end-users.
At the final project advisory group meeting, a presentation was made to group members of a draft strategy for tool development. This was then reworked following their comments and suggestions. More detailed plans and drafts were shared with wider team members, particularly co-researchers, who were able to comment on the applicability of individual tools to different practice contexts.
Identifying audiences
The research findings tended to confirm the importance of viewing commissioning as an arena within which varied stakeholders can make an important contribution, rather than as the preserve of a narrow set of actors formally designated ‘commissioners’. The findings also revealed shortcomings in the extent to which this wider audience of stakeholders – with their wide range of important skills, resources and evidence – were being effectively engaged in the commissioning process. For example, E&D leads often had extensive experience of, and evidence to share on, minority ethnic health issues but were infrequently involved with commissioning. For these reasons the project team decided that tools and outputs should be relevant to as wide an audience as possible, not least to facilitate the inclusion of this diverse range of stakeholders.
Key informant interviews revealed how many of the ‘success stories’ on minority ethnic health had been advanced by ‘champions’, individuals with deep commitment to and understanding of the agenda. Yet the interviews also revealed that these individuals were not necessarily those with power and influence in the commissioning process. We therefore viewed people as ‘champions’, regardless of whether they fulfilled specific roles within NHS organisations or were external ‘activists’. These people were a key resource to empower others and thereby strengthen any opportunities to improve confidence and understanding of the commissioning process. Tools for this group were focused on building on their own experience, expertise and commitment by helping them draw from the skills and resources of other actors.
Senior members of staff, especially chief executives or board members of provider trusts, PCTs and CCGs, were also seen to be a key target for tools as our research generally showed a lack of senior commitment and understanding of ethnic inequalities in health. For this audience, tools needed to be especially brief, quickly make a strategic case for mainstreaming attention to minority ethnic health and link this into wider agendas such as legal duties and QIPP. Given the difficulty of attracting this audience to in-person workshops, it was decided that the tool development workshops should focus on other target audiences at this stage.
Finally, our findings highlighted a lack of depth in the extent of community engagement undertaken by commissioners, with many commissioning organisations taking an arm’s-length approach. Although demonstrating the benefits to commissioners of including community representatives and service users from minority ethnic groups was one important part of the potential solution to this issue, it was also apparent from our work with both commissioners and community organisations themselves that many community representatives found the commissioning process confusing and/or lacked confidence in how to engage. Tools for strengthening community organisations’ capacity to become involved would therefore need to address the current gap between commissioning and community engagement, and ensure that groups had the confidence and skills to provide meaningful engagement so that it would then take a beneficial form for commissioners. However, tools for this audience need to assume little or no previous understanding of the commissioning process, and be promoted through different networks from those targeting NHS staff.
Establishing the scope of potential tools and resources
Drawing on the study findings we identified three broad ways in which the tools and resources that we developed needed to be able to operate:
-
influencing (challenging) key actors
-
clarifying thinking and raising confidence
-
supporting action to overcome challenges.
Influential tools and resources to challenge and increase attention to ethnic diversity and inequality within the commissioning arena
A key gap identified by our study was a general lack of understanding about why minority ethnic health issues needed attention. For this reason, a ‘Making the case’ tool was needed to guide actors through the basics as a critical first step.
Such a tool also needed to have the effect of increasing demand for evidence on ethnic diversity and inequality within commissioning processes, thereby contributing to improved quality and quantity of evidence use.
Thinking tools and resources that increase understanding and confidence to address ethnic diversity and inequality
Our research findings highlighted the level of confidence and knowledge needed to understand and respond to ethnic diversity and inequality. In particular, there was evidence that discussion and debate were often uncomfortable and ill-informed, so that misconceptions and low confidence were often perpetuated.
To tackle this, all tools and resources developed had to recognise that some actors would be starting with a basic level of understanding and could not assume any previous knowledge. There was clearly a need to repeatedly spell out what ethnicity is, how ethnicity relates to health and health care and what this might imply when commissioning health and social care services. To assist this it was decided to prepare a series of brief ‘Thinking clearly’ documents to provide clarity on some of the common areas of confusion, such as:
-
what is ethnicity?
-
how does ethnicity impact on health?
-
what are the links between ethnicity, deprivation and health?
-
making sense of health inequalities and ethnic equality work
-
understanding ethnicity and religion
-
understanding ethnicity and migration.
Again, it was felt to be important that such tools have the effect of increasing demand for evidence as people gain confidence to tackle the issues, and equipping people to be better able to appraise and synthesise relevant evidence sources.
‘How to’ tools to support stakeholders to generate, find and use evidence of different types within the commissioning arena
The project identified a general lack of resource and experience in all stages of identifying, analysing, assessing and utilising evidence and data – a problem that was not limited to, but was especially acute for, evidence regarding minority ethnic communities. To support evidence-based commissioning in this area, the team wanted to provide guidance to increase confidence in using evidence and drawing on the expertise of staff with experience of accessing and using data. In particular, it was considered important for commissioners and analysts to be aware of sources of evidence that were already available and to be able to ask the right questions of the data.
However, the project findings also clearly illustrated the many missed opportunities within commissioning work to introduce evidence. Understandings of commissioning tended to follow particular organisational conceptualisations, language, templates and procedures. Understanding these, and helping commissioners see how minority ethnic inequalities can be tackled in their existing structures, was therefore key, as was making tools available that are aligned with current representations of commissioning. This would help a wider number of people identify opportunities to engage with the commissioning process, bringing specialist knowledge and evidence on minority ethnic health to the table.
At the same time, the findings of our project and earlier work highlighted the many challenges faced when trying to locate and apply evidence on ethnic diversity and inequality, such as low levels of awareness of possible sources of evidence, concerns about the quality of ethnic monitoring data and lack of confidence in appraising evidence. However, the research also identified a range of strategies used by commissioners to deal with these issues, which suggested that sharing these strategies through practical tools would be beneficial.
Perhaps unsurprisingly, then, a very wide range of possible tools and resources were identified through the course of the project within this ‘How to’ category, including guidance on how to improve the collection and analysis of ethnic monitoring data and tools to support the development of effective business cases.
Format
Feedback from participants had established that tools should be brief and targeted to ensure that they would actually be utilised. The aim was thus to create a linked suite of brief tools that were modular, in that people could select or be guided to the most appropriate tool for their need and follow up with additional tools if further guidance was required. Adopting this approach would also need to include links to tools developed by other groups, to reduce duplication and ensure that the limited resources available to the project team were focused on the most critical gaps.
The project team identified a number of existing guides or toolkits in this area, either on minority ethnic health issues per se or on more general, yet relevant, areas of commissioning. These had been produced by professional bodies (e.g. NHS Confederation, Royal College of General Practitioners), third-sector organisations with a health or an ethnicity remit (e.g. King’s Fund, Afiya Trust) or individual NHS trusts or the DH itself.
Discussions within the team, and examples from other authors, resulted in the identification of a number of different approaches to formatting exercises for the toolkits in addition to those specified in the project proposal. These included diagnostic, evaluative and change management tools for individuals, teams and workflows, in a variety of formats, such as grading exercises, discussion exercises, structured questions and checklists.
Signposting to, and complementing, other resources
As noted above, the project did not set out to generate the resources necessary to cover the huge wealth of issues identified in the project’s research, particularly those that constituted more generic organisational barriers, or those that affected health inequalities more broadly. In addition, scoping exercises had identified a number of ostensibly effective tools and guides that were already available on ethnicity, commissioning or evidence use. As relatively few respondents seemed aware of, or were using, these resources, it made sense to include signposting to these in the new tools developed by the present project.
Therefore, the project team felt that promoting these resources would be useful to commissioning, and integrating the existing resources in the new tools would allow actors to address a wider range of knowledge and skills than could be tackled with the resources available to the project. It was also suggested that the research project website should provide a selected library of resources for commissioners to draw on, which would help them to understand and mainstream attention to minority ethnic health. However, rather than being standalone resources, it was decided that, where possible, the project’s tools should be designed to link directly to other relevant guides.
At the same time, the project team had engaged with a number of different stakeholders who were themselves engaged in the process of developing tools or resources and who were keen to use input from our research project. This was desirable, not only to prevent duplication of activity, but also to ensure that outputs were promoted through more varied networks. Three ongoing tool development projects fall into this co-production category: a tool for completing equality impact assessments being developed by the West Yorkshire CSU (formerly staff from the PCT); the development of a guide for commissioners on the Equality Delivery System by a multidisciplinary team in Luton; and engagement with the DH in which a list of suitable tools for enhanced JSNAs is being populated.
Tool development workshops
Method and approach
For the tool development workshops a specific range of tools was developed, selected on the basis that they would work as time-limited workshop-based exercises, fall within the expertise of the research team and cover topics not currently targeted by existing resources. On this basis it was decided that feedback on those briefing resources that were not intended to be interactive, such as the ‘Thinking clearly’ guides, would be better collected outside of the workshops.
For the sake of the workshops it was necessary to create exercises for each tool to stimulate discussion, while ensuring that participants with different roles and experiences could work together and anticipate how the tools would work in practice. Fictional scenarios were therefore created for each tool, enabling group members to focus on the utility of the tool within research-based contexts derived from case studies to ensure that they raised realistic issues, particularly those that the tools were specifically designed to address.
Three full-day workshops in Sheffield, Leicester and London were organised in November 2012 to provide opportunities for generating and collecting feedback on draft tools during their development and to increase the likely utility and impact of these proposed outputs.
It was planned for each event to have up to 20 participants, with exercises based on the tools designed to stimulate small group work based on commissioning, evidence use and minority ethnic health issues. It was stressed in the invitation that the workshops would be interactive and would involve draft tools and exercises that would be revised as a result of feedback provided by participants during the day.
In total, six draft tools/guides were selected for presentation in these workshops:
-
Sheffield – ‘Making the case’, ‘Service specification’
-
Leicester – ‘Stakeholder analysis’, ‘Evidence mobilisation’
-
London – ‘JSNA interrogation’, ‘Service specification and improvement’ (revised).
The service specification tool was trialled a second time at the London workshop after being reworked following feedback received at the Sheffield workshop.
Participants were also given a brief overview of all of the tools that the project intended to produce so that they could get a sense of the complete suite of tools and identify any gaps they saw in their coverage. In addition to the six above, this suite included a brief presentation of the ‘Thinking clearly’ and ‘How to’ guides and the co-produced equality impact assessment and Equality Delivery System tools. At each of the workshops the ‘Frequently raised objections’ tool was also presented and used as a guide to completing the workshop exercises, particularly the ‘Making the case’ and ‘Stakeholder analysis’ tools.
Workshop participants
The initial intention was to invite participants to the workshops who represented a wide variety of stakeholders and, by holding events outside the case study areas, explore experiences of participants based in other regions, which might be useful in testing the generalisability of the tools. Each workshop was promoted through a range of channels, including targeted e-mails to key individuals and invitations disseminated through a variety of professional networks.
During online registration for the workshops, participants were asked a series of questions about their current experiences of tools and resources, which organisations they felt provided useful tools and their opinions regarding the most useful formats of such tools. In addition, a number of potential topics and audiences for toolkits were presented and respondents were asked how important each one of these might be to themselves or their colleagues.
In total, 52 people registered to attend one of the three workshops and 38 were able to attend on the day. Table 10 gives an overview of the organisations and roles represented by those registering and attending who completed the online form.
| Organisation/role | Registered | Attended |
|---|---|---|
| Organisation | ||
| PCT | 10 | 7 |
| NHS provider | 7 | 3 |
| CCG | 3 | 3 |
| Department of Health | 3 | 2 |
| Council/local authority | 3 | 1 |
| Third sector | 22 | 11 |
| Academic | 10 | 8 |
| Job role | ||
| Commissioning manager | 8 | 4 |
| Research/analysis | 16 | 14 |
| E&D or community engagement | 14 | 9 |
| Service delivery/management | 11 | 7 |
| Other manager | 9 | 3 |
As intended, the participants had a variety of roles and were from a range of organisations, although there was a higher than expected number of people representing third-sector organisations (as either service providers or representing a community or condition) and fewer than anticipated with a direct role as a commissioner. Particular efforts were made to engage with CCG commissioners, a key audience for future tools.
Format and feedback collection
Each workshop presented two draft tools and involved group work exercises based on them. The workshops provided hands-on time with each of the tools and extensive time for feedback and discussion. Each exercise was approximately an hour long, with an additional 30 minutes allocated for verbal feedback, which was collected by project team members acting as facilitators. Facilitators also made notes during the exercises to record how participants were engaging with each tool and to identify any areas in each exercise that appeared unclear.
A written template sheet for comments was also provided, asking participants to reflect on both good and bad parts of each tool/exercise and to suggest improvements and potential audiences. These were collected and transcribed following each workshop. In addition, 45 minutes was allotted at the end of the day for more general feedback on the suite of tools, those parts of the workshop that had worked well and general suggestions for improvements.
Workshop feedback
General reflection on tools
In the online pre-workshop survey, participants agreed that tools should be made available online, with simplicity, speed and brevity commonly cited desirable characteristics. Respondents also mentioned the importance of having web-based tools that were interactive and easy to navigate but which could be downloaded and printed for use in group situations. Ease of use and non-technical language were also seen as important, to ensure that tools were flexible and useful to a wide audience.
Few respondents were aware of other toolkits focusing on ethnic inequality in commissioning that they would recommend, with ‘None that I feel do the job particularly well’ being a common refrain. And although many respondents mentioned tools or reports with which they had been involved that would be relevant to minority ethnic health issues, none mentioned any involving evidence use or commissioning.
Although the survey question asking participants to rate the importance of developing particular tools had a small sample size, it still showed a clear trend regarding those areas in which more support was felt to be warranted. Figure 4 displays these data, with tools that ‘help find data’ and ‘understand minority ethnic health issues’ having the highest ranking, needs that fit well with the issues highlighted in our earlier research findings.
FIGURE 4.
Importance of developing specific tools: pre-workshop online survey (n = 52).
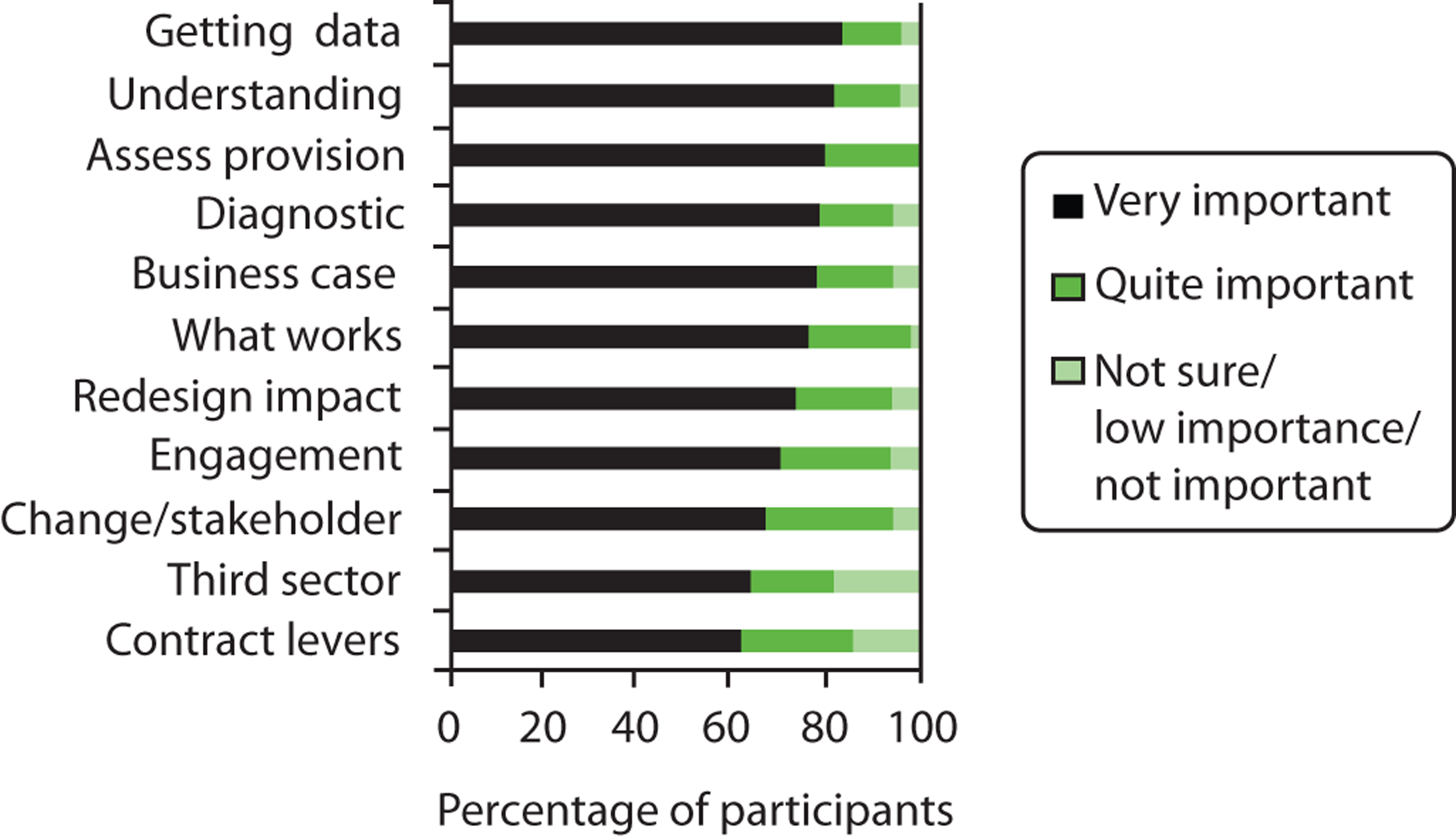
Most surprising from these results was the relatively low priority given to tools designed to increase community engagement and the participation of third-sector providers and representatives in the commissioning process. Indeed, these were the only two tools for which votes of low importance were recorded. However, our research findings also found a low prioritisation of wider engagement amongst many commissioners, and this finding is probably reflected by a lack of awareness of the benefits and/or importance of including minority ethnic groups in commissioning, or perhaps the belief that there were already many tools addressing this issue, even if they are not currently well used. Clearly all tools have to make a convincing case for their use and have to be promoted to actors who might not necessarily be aware of gaps in their current ways of working. Not all of the tools listed in the survey had been drafted for testing at the workshops, but the pre-workshop survey data helped the team choose tools that either were a high priority or would need to be well promoted to persuade actors that they were useful.
Tool- and resource-specific feedback
Making the case
The aim of this specific tool was to increase the confidence of people to raise minority ethnic health issues by creating a PowerPoint slide template that could be presented to a senior board meeting or a team engaged with commissioning work. The tool is designed to be customised, offering slots in which local data on the population and evidence from specific health services can be inserted.
The tool consisted of a presentation given by one of the research team followed by an exercise in which the participants were asked to share questions that a senior board at a CCG might ask to challenge a focus on ethnicity. This was used to feed into a presentation of the frequently raised objections tool.
Respondents engaged well with the tool and suggested other situations in which the presentation would be useful. They also had a number of constructive suggestions for improvement, feeling that the slides outlining reasons for considering ethnicity and health should be made ‘punchier’ and should directly make a ‘What’s in it for me?’ argument to the audience. Most responses were related to two main concerns, the first over how to make the case for the ethnicity-in-commissioning agenda itself and the second over how best to present data/evidence in support of this agenda.
Participants shared a good many experiences of having evidence or data challenged and suggested that the tool also needed to have pointers to good sources of national and local data and needed to encourage people to be prepared for such challenges and know their evidence well. In feedback forms, participants felt that the tool would be useful for a wider audience than anticipated, including CCG and commissioner boards, service providers, activists, public health consultants and E&D leads.
In feedback the flexibility of the tool was also praised but again it was stressed that it should be made shorter, simpler and ‘punchier’ and that there should also be a one-sided sheet of summary bullet points, summarising the importance of considering minority ethnic health issues. Meanwhile, there was a concern that finding local sources of evidence on services could be difficult and that this would depend on the availability of expertise in finding and packaging suitable data sources. To tackle this issue there should be clear links from this tool to the evidence mobilisation tool, which was specifically designed to facilitate evidence access and use.
Stakeholder analysis
The stakeholder analysis tool was developed to help individuals/teams with a specific piece of work in mind to consider the different actors who they might need to convince in the complex networks of NHS organisations. In this the tool aimed to identify what useful resources and skills different individuals would bring and how they might be persuaded that addressing minority ethnic health issues would be beneficial to their own work and agendas. Although the tool drew on standard stakeholder analysis approaches, it incorporated insights from our research around the particular types of perspectives that are held by actors in the commissioning agenda and how they can support or hamper work on this agenda.
Different exercises were drafted for the workshop and these were intended to be followed as a series. However, early feedback from co-researchers indicated that it was unrealistic to expect people to have sufficient time to invest in such a tool and in the end only two different exercises were trialled in the workshop. As before, a hypothetical scenario was used, but one that was based on the project’s maternity case study so that it dealt with genuine, real-world issues.
The first part comprised an ‘in their shoes’ exercise in which participants were given a series of ‘personas’ – people with different roles in the scenario, including head of the service, E&D lead and the commissioner and chief executive of the trust. Based on a short profile, participants were asked to answer a series of questions for each persona, to help them anticipate how each could contribute to the scenario and anticipate possible objections and to persuade them that the project would meet their own objectives. They were also provided with a short version of the frequently raised objections tool (see Frequently raised objections tool) to help them think through this exercise.
Feedback for this section of the tool was very positive, with pairs of participants quickly engaging with the profiles and identifying parallels with their own work and experience.
The second part of the tool comprised a mapping exercise in which participants were encouraged to identify/map the people who they would want to engage with, their parent organisations and any linkages between individuals and/or institutions. This was intended to help users of the tool consider all of the people and all of the resources available to them and the best avenues for contacting each potential actor. For a number of reasons this exercise proved to be more difficult for the workshop participants. As a hypothetical example it was difficult to imagine a wider network of actors; participants were concerned that they did not understand all of the structures in the new commissioning arrangements; some participants mentioned local examples of partnerships that other participants were unfamiliar with; and, without listing all of the potential actors first, participants found it difficult to map out connections between them.
Although it was clear to the facilitators that both groups struggled with this exercise, the workshop participants still gave positive feedback on the potential utility of a mapping tool. They felt that it would be useful in a real-life situation (particularly with a team) and that the exercise had helped them think of the ‘big picture’ and ‘outside the normal boundaries’. It was also suggested that the mapping could focus more broadly on flows of knowledge and evidence rather than on actors and organisations.
One participant did express concern that maps of services can be very time-consuming to produce and can quickly become obsolete. However, as part of a suite of tools with individuals choosing exercises that are useful to them, there was general enthusiasm for this mapping exercise, especially as the tool itself could be used for wider inequality issues and to encourage partnership working in this area. The latter was particularly meaningful given the finding from our case studies and interviews that individuals often feel that they have to work on their own with little support.
Specifying service models and driving up service standards
The aim of this tool was twofold: first, to raise awareness of the content of contracts and service specifications that guide service delivery; and, second, to show experienced commissioners how familiar service specifications and standards can be adjusted to incorporate considerations about health issues for minority ethnic populations.
Participants were given a short presentation on the exercise by a member of the research team followed by details of a scenario based around the redesign of a diabetes management service (in which a particular minority ethnic group had been found to have poorer than average outcomes). Working in groups, participants were asked to think through what factors might explain these poor outcomes and what further information might be needed/helpful for identifying possible actions. This acted as a preliminary stage to a subsequent exercise in which groups of participants could choose whether they would opt to design a new complementary service targeted specifically at this ethnic group or change the specifications of the existing service to improve or extend its impact on that ethnic group.
In the first of these exercises, participants were given a copy of the actual template used for service specifications and were encouraged to use this to flesh out an appropriate service that could be put out to tender. The exercise also included the key organisational objectives that need to be considered, such as quality, patient satisfaction and safety.
In the second of the exercises, participants were given an example of existing contract performance indicators (e.g. ‘the existence of an annual audit’) and were asked to consider how they would make these indicators more specific to ensure that the provider was actually meeting the needs of this minority ethnic group.
To help with both of these exercises, an A3 sheet listing common issues that had been identified during the research phase of the project was shared with workshop participants; this included examples of how service specifications (e.g. those on ‘access’ and ‘engagement’) could be specified in more detail to help address specific issues.
Feedback from the first workshop indicated that, although the objectives of this tool were felt to be useful, the layout of the exercise was too complicated. This was therefore subsequently improved for use again in the London workshop. Nonetheless, there was very strong enthusiasm for the prompting sheet, with suggestions at both workshops that it should be offered as a tool in its own right and/or produced as a wall poster.
Because of the technical nature of the tool, most individual feedback sheets suggested that the exercise was more suitable for commissioners, especially those based in CCGs. However, there was substantial enthusiasm from third-sector providers represented at the workshop who had worked with similar specifications. These participants noted that the exercise had helped them to better understand the commissioner’s side of the process, and was an eye-opener for organisations that had not been closely involved in commissioning before.
The argument that provider–commissioner co-operation might be helpful when developing service specifications was raised at both workshops and again resonates with the findings from the research component of the project.
Following the second iteration of the exercise, there remained some concerns that the tool might need to be more succinct and easy to read. However, it is worth noting that the use of a hypothetical scenario in the workshops added to the complexity of the exercise; in practice, it is envisaged that the tool will be used by experienced teams working on an actual commissioning area, removing the need for any ‘complicated’ or unfamiliar scenario.
Evidence mobilisation
This tool was designed to help teams and individuals mobilise available sources of evidence on minority ethnic health issues for use in commissioning. This was identified as a key weakness of current commissioning practice in the findings of the research component of the project, alongside a general lack of awareness of potential data sources, a lack of confidence in dealing with health data and examples of success being dependant on evidence being packaged in the right format for the audience.
The exercise in the workshop began with a presentation on the importance of using information to help understand ethnic health inequalities and on using evidence to support actions to tackle these inequalities by packaging it in appropriate formats and prescribing solutions. Five brief pieces of evidence, each reduced to a single side of paper, were circulated to each group, with one participant required to read and present one source to the rest of the group. The examples comprised a mix of fabricated data and real-world research evidence and provided a variety of quantitative demographic, service use, disease-specific and qualitative data.
The scenario chosen was based on smoking cessation services for minority ethnic groups, an example that was again taken from the research component of our project. Participants were asked to appraise and format the available evidence to specify, and make the case for, a specific service for one or more minority ethnic groups. The first part of the exercise involved participants working as a group to decide which sources of evidence might indicate inequality, which might explain any inequality, which might identify potential remedial actions and what other information they would want to have before presenting a service specification proposal to commissioners.
In the second exercise participants worked in the same groups to use the evidence identified in the first section to justify a new service specification, how the service would best be presented to fund holders (i.e. by listing the key messages included in this presentation) and how the data might best be packaged and delivered for the audience.
Although the first exercise proved to be easier for those with experience of using health service data than for those without, having just one participant read each source of evidence helped the groups digest a lot of information quickly, the relevant aspects of which they could then share with the whole of their group. Several workshop participants commented that this was a good approach for sharing out work when there was a lot of information to get through in a limited amount of time.
The second part of the exercise was felt by participants to be particularly engaging and, with prompting from facilitators, all of the groups moved on from imagining innovative interventions to planning interesting ways of packaging the data and developing strong messages on potential improvements in service quality and potential cost savings.
Individual participant feedback forms suggested that participants appreciated how well the two parts of the exercise followed on from each other and thereby led to the development of tangible outputs. However, many participants expressed concern that the best element of the exercise was actually working as a group and that there were often few opportunities for doing this in their work. It was also apparent that the exercise would also benefit from links to other tools from the project, especially the stakeholder analysis and service specification tools, to encourage participants to consider how they might better meet the strategic objectives of the organisation. It would also usefully link to other existing resources that help people access and appraise evidence sources.
Joint strategic needs assessment interrogation tool
As with the stakeholder analysis tool, a number of different exercises had been drafted around the focus of appraising the evidence presented in a local JSNA to identify weaknesses or gaps in describing unmet needs and inequalities in minority ethnic health. These were based, in particular, on issues raised during a workshop on JSNAs and ethnicity that the team had organised and facilitated as part of a series of feedback/respondent validation exercises that were conducted throughout the project period. The workshop included a team of people involved with JSNAs in the three study sites. The aim of this tool would be either to help authors of JSNAs ensure that they were considering ethnicity in their work or to help individuals and community organisations with an interest in minority ethnic health to challenge existing JSNAs.
For the workshop it was decided to use a brief grading exercise in which participants were put into two groups and given an example chapter from two real JSNAs to grade. These chapters were selected for their different approaches to describing ethnicity and their differing levels of detail. Eleven questions were used to generate a RAG (red, amber, green) rating based on how well the workshop participants felt that the JSNA had met each of the criteria. This exercise was designed as much to test the concept of using such a rating system as it was to test the JSNA-related nature of the exercise.
An initial problem with this workshop exercise was the amount of time it took each group to read the example JSNA chapter. However, the subsequent questions provided a good structure for examining the chapter and provoked a good deal of debate in the workshop groups about how well each of the criteria had been met.
Despite varied previous experience of JSNAs, the ranking exercise seemed simple enough for all to engage with, indicating that this is likely to be a useful tool for groups not normally engaged in the development of JSNAs.
Feedback was generally positive, with constructive suggestions focusing on reordering the questions and/or putting these into stand-alone modular sections to make them easier to follow and allow different levels of depth within whatever time is available. As for the ranking exercise, participants were fully engaged but subsequently suggested that four grades rather than three would work better, with a fourth grade to score ‘absence of evidence’. This was felt to be the case for many of the criteria, and this fourth rank was felt to offer more differentiation at the lower levels of compliance.
However, participants voiced concerns that the exercise did not lead to obvious actions and expressed a desire for the tool to be able to make recommendations and include examples of ‘gold standard’ JSNAs. It was also suggested that the tool might be helpfully linked to other existing resources or sources of evidence so that it offered help to those writing JSNAs.
Frequently raised objections tool
This was not presented as a separate exercise in the three workshops but as a tool that supported a number of the other tools, in particular the making the case and stakeholder analysis tools. Nonetheless, it was also intended to be useful as a stand-alone tool.
This tool was designed to help actors anticipate a range of common objections that are raised when minority ethnic health issues are presented to a range of health professionals. These included concerns that there were no resources to deal with the issue, that it was unfair to pay attention to one ethnic group over another and that there was not enough data to justify interventions. The aim of the tool was to help those working on this agenda to suggest responses/answers to these objections based on examples that participants had presented during the research interviews or case studies as well as their wider experience.
Workshop participants expressed a lot of enthusiasm for this tool. In the exercises at the two workshops on making the case and stakeholder analysis, in which the tool was used for support, they were asked to list any objections that they had heard raised in their own work, or any additional objections to, addressing ethnic inequalities in health. The idea resonated well with participants and most of the objections that they raised were already covered in the draft tool. Participants liked the fact that examples had been taken from participant interviews as this gave them authenticity and they also appreciated the comprehensiveness of the full list. It was even suggested that the tool could be presented in a ‘bingo card’ format, for users to cross out objections that they had heard raised in their work.
Redrafting process
The feedback from the workshops provided a wealth of views on the content and format of the tools and related resources that the project team could use to revise and improve them. Following the workshops, minor changes suggested by participants were made before placing the tools in a complete form on the project website, which was then disseminated to workshop participants. The intention of this process was to show that feedback had been taken on board while allowing a quick turnaround so that participants could examine the tools in depth in their own time and start using them in their own work.
All of the tools were made available with an explicit note that they were still in draft form and that comments and feedback were still being solicited from website visitors and tool readers/users. As many of the workshop participants expressed considerable enthusiasm about sharing the tools with colleagues, and given that a number of potential workshop attendees were keen to feed back comments on the tools, this approach (i.e. early web-based dissemination in draft form) aimed to access a wider audience for critical feedback. A cut-off for further feedback was set in spring 2013 and after this date the tools were revised in light of these contributions.
Other resources and next steps
A cross-sector review of effective knowledge transfer activities104 noted that the best knowledge transfer interventions did not have any one particular format but used an effective mode of delivery. The review recommended reminders, incentives, peer review, marketing and educational interventions as the most effective means of knowledge transfer. To this end, interactive follow-on work was felt to be crucial for ensuring the successful utilisation and impact of the project’s tools and resources.
Funding has therefore been secured to finalise the suite of tools developed and piloted by the project, including the ‘co-produced’, ‘Thinking clearly’ and ‘How to’ guides. These project outputs will then be disseminated further through master classes and bespoke in-practice support to commissioning teams.
Workshop participants expressed substantial interest in being involved in this work and it is intended that this will link in with wider health commissioning professional development training and support offered by Sheffield Hallam University. It will also draw on the networks developed through the workshops, as many participants were keen for assistance in this area.
This dissemination phase will collect further feedback on how well the tools work in real-life commissioning situations, before they are ultimately finalised. Hopefully there will be opportunities to both guide the use of the tools with a facilitator and establish how well the tools can be used on their own, as well as identifying where further guidance would be helpful and/or is required.
Although it may not be feasible to take a longitudinal approach to this dissemination phase (i.e. examining how this impacts on the delivery of services after the commissioning process is completed), it is hoped that there will be opportunities to engage with short pieces of commissioning work that can be followed through to completion.
Piloting dissemination will both refine and lend credibility to the tools in a commissioning environment that is still emerging and will allow the tools to be offered as ‘tried and tested’ with comments and feedback attached from end-users. Following on from this, it will be important to ensure greater awareness of the available outputs. This will be achieved primarily through professional networks and through existing relationships developed by the project team, such as local and regional CLAHRC groups.
Further details of the tools and the workshops are available at www.eeic.org.uk.
Chapter 8 Discussion
Introduction
This chapter brings together our research findings in relation to the overarching questions that the study was designed to explore. We attempt to interpret these findings in the context of existing literature in three key areas: knowledge mobilisation and utilisation within the health policy-making arena; the characteristics of evidence related to diversity and inequality; and factors involved in achieving cultural competence within health-care organisations.
Strengths and limitations
The study generates new empirical understandings of the factors that shape the effective utilisation of evidence relating to ethnic diversity and inequality and identifies promising routes of intervention to enhance such use. Findings are based on a wide range of data and in-depth analysis of evidence from national key informants as well as detailed case studies of three NHS commissioning organisations with a regional focus. We have validated findings at three national workshops, seeking to test our claims with a wider range of people with experience of commissioning in different contexts.
Nevertheless, we may have overlooked some important dimensions of our research questions; in particular, we found it harder to identify enablers of effective use of evidence in this area than barriers. It is possible that including a case study of an organisation that had achieved greater mainstreaming of the ethnic diversity agenda could have added to our understanding of enabling factors. That said, our findings from national respondents suggest that the organisations that we studied are likely to share much in common with organisations from other places.
The study was conducted during a period in which there was fundamental restructuring of NHS commissioning structures and processes. This resulted in some difficulties in gathering data and it is possible that the ongoing process may have influenced respondents to reflect more negatively on current practices and future expectations than would otherwise have been the case. However, we would hope that this potential influence on our results has been balanced by the fact that data were gathered over a 2-year time period and included observational and documentary evidence in addition to the views of interviewees.
Knowledge mobilisation, ethnic diversity and inequality
Our findings suggest that the mobilisation and use of evidence on ethnic diversity and inequality shares many of the same characteristics as knowledge mobilisation and utilisation in general. At the same time, specific features of evidence on ethnicity influence its potential to be effectively utilised and create an additional layer of complexity to the knowledge mobilisation process.
Generic issues affecting knowledge mobilisation
Key competencies for commissioners place knowledge management centre stage and include critically mobilising and utilising research and best practice evidence; effectively garnering local intelligence and promoting engagement to assess needs; and turning information into knowledge and action for service reconfiguration that improves access, quality and outcomes. 54,55 Commissioners are expected to be transformational rather than transactional, encouraging innovation and ambition to serve those in greatest need.
Our findings confirm that commissioners often work with a ‘mixed economy’ of evidence, piecing together information from diverse sources in their decision-making. 1,34 However, they may lack clarity on how to appraise, weight or synthesise these various sources and there appears to be little active debate on what constitutes good practice in this regard. The absence of such skills suggests that evidence is unlikely to be effectively mobilised to inform commissioning processes and is perhaps more likely to be used selectively to justify decisions that have been influenced by other factors.
In terms of the ‘mental models’ that guide people’s sense-making,67,68 we found awareness among our respondents of the need to use evidence in influential ways, but also widespread recognition that this is not common in practice. The use of evidence to inform transformational shaping of service provision is often constrained by perceptions that limit the commissioning role to specifying desired outcomes that are subsequently monitored. It is less common to find commissioning being seen as an arena in which collaborative partnerships with providers and other relevant stakeholders help decide what outcomes are needed and how these might be achieved (although some commissioners do hold this aspiration).
In addition to these generic characteristics, however, our findings highlight a range of additional contextual factors operating in relation to evidence on ethnic diversity and inequality. These indicate that, although policy-makers may have a crucial role as receptors of knowledge,25,69 sociocognitive models that look beyond technical skills and resources to values, assumptions and worldviews are also important to consider. Our findings suggest that the ways in which individual commissioners understand the nature of ethnicity and associated inequalities are central to how they seek out, appraise and apply different types of knowledge within their work. These specific issues are outlined in the following section.
Mobilising evidence on ethnic diversity and inequality
Our findings indicate that accessing and making use of information relating to ethnic diversity and inequality is generally not part and parcel of broader evidence-gathering exercises for commissioning and is frequently overlooked. Attention to this kind of evidence is most often dependent on the interests and expertise of individual actors and consequently remains a distinct exercise, with resulting knowledge not being widely shared.
National policy directives, although rarely specific to ethnic inequality, can be influential in prompting attention to research and other evidence on ethnic diversity and inequality, and can provide helpful levers for actors who wish to address ethnic health inequalities. At all of our sites, for example, the external audit linked to infant mortality reviews prompted requests for data on birth outcomes and ethnicity and a focus on initiatives aimed at reducing ethnic health inequalities. Although there has been investment by the DH in initiatives such as Race for Health and Pacesetters, which aimed to improve the commissioning of health services to address the needs of minority ethnic populations, there has to date been poor articulation of the role that commissioners should play in effectively bringing evidence to bear on such commissioning decisions. Furthermore, this kind of national leadership is not consistent or strategic, suggesting that the interests and expertise of individual policy actors are key factors at national as well as local levels. Furthermore, a heavy reliance on synthesised evidence from national sources, such as the DH or NICE, is problematic when this contains no details on ethnicity.
Evidence linked to service failures, such as poor take-up of provision, low levels of satisfaction or poor health outcomes for particular ethnic populations, is less often a prompt to action for commissioners. Our findings demonstrate that routine performance monitoring systems within services do not often include a focus on ethnic equality, or indeed any dimension of equality, and commissioners themselves rarely request that such data be collected. When such data are available they can, however, play a similar role to national evidence overviews and provide a platform from which individual actors can seek to influence commissioning decisions.
We found that the competency of those involved in commissioning to (1) identify and access, (2) critically appraise and synthesise and (3) adapt and apply evidence relating to ethnic diversity and inequality was very variable and, as with commissioning in general, we identified some significant skills gaps. In some cases creative approaches to fill evidence gaps are found, such as combining national quantitative data with local qualitative feedback to highlight unmet need; however, such approaches need to be more widely shared within commissioning organisations.
Hunter70 argues that, in exploring the role of those in policy-making positions, we must ‘consider these individuals as emotional as well as relational actors’ (p. 150). For example, professional anxiety and uncertainty about how to achieve cultural competence is disempowering to professionals and detrimental to care. 49 Our findings highlight the absence of action within strategic and operational commissioning processes and structures that would dispel such uncertainty. Furthermore, there is little or no challenge to conceptual models of commissioning that perceive a focus on particular ethnic groups as ‘privileging’ these populations or unnecessarily specifying communities that are felt to be already included within a generic framework for ‘the whole population’. As our findings highlight, such approaches serve to reinforce social exclusion and maintain or exacerbate health inequalities experienced by minority ethnic groups. There is consequently a need for tools that improve understanding of ethnicity and its relationship to health, which often remains unsophisticated and problematic.
We found that the limited range and quality of the available evidence on ethnic diversity and inequality is often a barrier to actors who do wish to engage with the field of ethnic health inequalities. At the same time, gaps in the data from service providers are sometimes imagined rather than real and there is the potential for existing data on ethnicity, which may exist but not be requested, to be analysed in ways that could helpfully inform commissioning decisions.
Respondents often expressed a desire for evidence about how to reduce ethnic health inequalities rather than more research about what these were, and our findings confirm that intervention studies is an area on which research on ethnicity and health needs to focus, as highlighted elsewhere. 44 High-quality evaluations exploring effectiveness and costs are important for transformational commissioning in the area of ethnic health inequalities. Although evidence from local sources on ‘what works’ may be valued for its contextual relevance, it is vulnerable to being contested in terms of its credibility, particularly if put forward by third-sector organisations who may be seen as unrepresentative of those whom they purport to advocate for, or as having vested interests in, promoting work in this area.
Organisational context and evidence on ethnic diversity and inequality
At both strategic and service design levels commissioning decision-making may be seen as a process of collective interaction between diverse stakeholders that is socially situated and constructed. 28–30 Our findings confirm that policy-making is constructed within the context of competing drivers64 and decision-making is heavily influenced by local and national context, including prevailing practices, organisational structures and the commitment and engagement of key actors. 32 Within this context our findings highlight marginalisation of the agenda on improving services for minority ethnic people and consequently little support from organisational structures or cultures for evidence mobilisation and utilisation relating to ethnic diversity and inequality.
Generic organisational constraints
We found patchy and inconsistent application of evidence at all stages of the commissioning cycle alongside isolated examples of comprehensive and effective evidence mobilisation and use. Public health staff are important actors in relation to needs assessment activity; however, the fragmented nature of commissioning work may mean that their skills are not routinely utilised. In addition, the skills needed for other aspects of evidence mobilisation and use, such as the identification and synthesis of data from diverse sources, may not be well represented across a commissioning organisation and these aspects are therefore often neglected. The routine use of evidence in commissioning appears to be constrained by an absence of staff with specific evidence mobilisation roles, and commissioning models, structures and processes do not currently support the routine generation and use of evidence as an indispensable aspect of decision-making. The general sense from our data is therefore of idiosyncratic and unstable practices linked to an absence of organisational expectations or support for knowledge mobilisation.
Although a ‘transformation agenda’ was articulated by strategic managers at all three of our sites, this appeared to be focused on a narrow range of service areas; in other areas the absence of this focus – through incentives or penalties for such work – made narrowly transactional approaches to commissioning more likely. In general, low priority appears to be afforded to the use of evidence as a commissioning activity, indicated by constraints linked to organisational culture and practice: lack of time, resources and skills to carry out such activity; silo working; and some commissioners having poor knowledge of the service area for which they have responsibility. Our findings suggest that, in the current climate, access to and use of relevant evidence to support a transformation agenda, such as evaluations of service redesigns, is secondary to other internal processes that focus on cost saving within short timescales.
The context for use of evidence on ethnic diversity and inequality
We found efforts to establish teams that encompassed a range of perspectives and skills, such as integrated commissioning teams and planning and commissioning groups. However, valued attributes for such teams rarely ensure the presence of individuals with an understanding of evidence relating to minority ethnic health needs. When good practice on evidence use exists this does not tend to have content relevant to ethnic health needs. Although some of our respondents recognised their own limited expertise and indicated willingness to develop their capacity in relation to these issues, there was little encouragement or incentive from key drivers to do so and no mechanisms for accountability that would support their aspirations, particularly in the context of tight deadlines and a pressured environment. Managerial priorities largely deter consideration of evidence relating to ethnic diversity and inequality within commissioning teams by a practice of omission; there is no reward or sanction for attention to such evidence and no challenge to those who perceive that this consideration complicates matters further than necessary.
Our findings highlight various missed opportunities to consider such evidence within the available resources and infrastructure, such as the quality and transformation agenda, in which there is the potential for considerable overlap with addressing unmet need in minority ethnic communities. Our findings confirm that neglect of the dimension of ethnicity within the national health inequalities agenda appears to have had a major adverse impact on meeting unmet need within minority ethnic populations, as argued elsewhere. 105,106 There appears to be a clear interplay between how these agenda are conceptualised at national, regional and organisational levels in terms of policy priorities. Although some key actors recognise the potential to align these more, the general picture is one of omission, ambivalence and marginalisation at national level. This is unsurprisingly reflected at organisational level, resulting in low demand for this type of evidence. Interest in and use of evidence relating to ethnic health inequalities is unlikely when such issues are not raised and questions that need answers are not asked.
Expertise in and insight into ethnic health inequalities is thus not considered a general concern and our findings show that this responsibility is often concentrated within staff in E&D roles, on whom there may be heavy reliance not only to provide understanding of such inequalities but also to ensure that commissioners meet legal obligations. Third-sector organisations, which are often utilised to engage with groups perceived as ‘hard to reach’ (or ‘easy to ignore’), are not necessarily recognised as holding expertise and at times their insight may be questioned. BME staff members may be assumed to have such expertise and some report resisting responsibility for ethnic health inequalities when this is neglected in terms of commissioning priorities. The view that aligning oneself with a marginalised issue is likely to impact on one’s position within the organisation in general is perhaps understandable; however, it also contributes to the continued marginalisation of evidence in this area.
Given the significance of individual interest and expertise in generating attention to evidence on ethnic health inequalities outlined earlier, who is involved in commissioning is of crucial importance. Our findings indicate constraints on the ability and capacity of those most likely to promote such evidence to be involved in commissioning processes and structures. Staff in E&D posts may be accorded a narrow focus in terms of their remit and are not embedded in the structures and processes that routinely contribute to commissioning decisions. Their influence on commissioning consequently appears to be ad hoc and dependent on pre-existing relationships. The poor representation of people from minority ethnic communities at all stages of the commissioning cycle is also a key factor influencing the low priority and fragmented nature of attention afforded to evidence on ethnic diversity and inequality. Although we found some positive examples of user input, in which extended and meaningful engagement of minority ethnic patient representatives had occurred, this was neither consistent nor normal practice.
Our findings also highlight wide variation in the extent to which third-sector providers, where expertise in engaging with minority ethnic communities is most likely to be found,107 are regularly engaged in commissioning teams. Examples of service users or organisations that represent their interests prompting managers to seek out and use evidence were rare; individuals or groups working within minority communities did not often have the capacity or resources to effectively engage with evidence sources or commissioning structures in ways that could significantly influence decision-making. Most significantly, membership of commissioning groups was not representative of minority ethnic populations, limiting the extent to which members’ individual expertise and knowledge of evidence on ethnic health inequalities could inform work undertaken and making performance management in this area unlikely. Thus, more often than not, commissioning structures appear to reflect and maintain the more general social exclusion of minority ethnic communities, reinforcing the status quo rather than modelling the social change needed to reduce exclusion and inequalities. 108
Such contexts, in which key actors may have little knowledge or understanding of the need to address ethnic inequalities, can help explain why higher standards of evidence are often required for small-scale service developments to meet the needs of minority ethnic communities than for multimillion pound contracts to large providers. Those who argue for such development may be required to produce robust evidence that demonstrates unmet need and a business case showing cost-effectiveness, which is often impossible given the gaps in existing evidence on ethnic diversity and inequality. An evidence-based culture can thus not only undermine progress towards reducing ethnic health inequalities but also mask the underlying factors that cause commissioners to be risk averse in this area of activity.
Enhancing the use of evidence in commissioning for multiethnic populations
Our focus in this study was on assessing the use of evidence in commissioning and its relationship to improving the cultural competence of health-care provision for minority ethnic groups. We therefore seek to describe how well evidence on ethnicity, diversity and inequality is being used as well as whether it is used at all. In the following sections we identify specific areas in which our findings suggest that support for knowledge mobilisation on ethnic health inequalities is likely to be helpful, either to individuals involved in the commissioning process or to the development of enabling organisational contexts.
Individual and team-level support
At the level of individuals involved in commissioning our findings suggest that knowledge, awareness, skills and experience, the ‘mental models’ of commissioning used and personal background are all likely to facilitate or hinder the mobilisation and utilisation of evidence on ethnic health inequalities. A strong theme in our data was the high dependence on individual interest, commitment and capacity to engage with this agenda. Although this may be linked to organisational context and team dynamics it also requires attention in its own right, given that many individuals were championing the issue of ethnic health inequalities despite low levels of organisational interest and others felt poorly equipped to engage with this agenda.
Our findings suggest that increased awareness of the relevance and importance of ethnic health inequalities would improve conceptual understandings of both the commissioning role and the relationship between ethnicity and health. This kind of support could help increase the demand for evidence on ethnic diversity and inequality. There is also a need to increase awareness of the different sources from which existing evidence may be available. Support for skills in synthesising, critically appraising, packaging and presenting evidence is also necessary as these skills appear crucial to mobilising evidence use in terms of commissioning action that could reduce ethnic inequalities in health-care access, satisfaction and outcomes.
The need to increase and enhance the routes through which evidence relating to ethnic diversity and inequality currently finds its way into the commissioning process is also suggested by our findings. These are currently ad hoc and precarious and receive little attention. Support to develop structures that facilitate regular inputs from important actors, such as practitioners, third-sector organisations, user and carer groups and academics, is likely to increase access to the important sources of insight and ideas for innovation that they can bring. Strategies for developing long-term relationships are needed along with ways of engaging that empower these actors as critical friends or external agitators so that they can confidently bring evidence to the commissioning arena.
Current barriers to mobilising and using evidence on ethnic diversity and inequality exist at both individual and organisational levels. Our findings highlight a lack of leadership in terms of a low demand for such evidence and failure to recognise its relevance. This is particularly significant in key, well-resourced areas of commissioning activity. More clarity about how commissioners could be expected to link ethnic health inequalities with mainstream activity is needed, along with good practice examples demonstrating what service models should look like in relation to minority ethnic needs and how these can be achieved. Support for organisational activity must crucially come through national drivers, which dominate the commissioning agenda and which are not often defined in relation to ethnicity.
Once demand for evidence is generated, support is also required to deal with problems that exist with the evidence base that is currently available and expectations about what this should deliver. Creative approaches to dealing with evidence gaps and incomplete data need to be disseminated widely and should draw on mainstream commissioning practices, which may sometimes face similar problems. For example, an incremental approach to data gathering using audit procedures, observed at one of our case study sites, appears to be a promising approach for dealing with the current gaps in ethnic data monitoring. Strategies for overcoming and dealing with a lack of evidence on effective interventions and a lack of cost-effectiveness studies are also required as well as guidance on how to synthesise different sources of evidence on ethnic diversity and inequality, and how to translate findings from one context to another. For example, our findings suggest that combining evidence from national data sets with very local qualitative evidence can be helpful in addressing the need for credibility alongside a preference for data that take account of local contexts.
Support at organisational and national level
Organisational legitimacy for work on ethnic diversity and inequality and an enabling environment appear to be of fundamental importance to the mobilisation and use of evidence in this area. The routine, critical use of research evidence in commissioning for multiethnic populations is currently hampered by national drivers that reflect poor understanding and consequent ambivalence towards ethnic health inequalities. Our findings show that strategies for linking mainstream activity with work to reduce ethnic health inequalities do exist, but require more dissemination and further development. Wider societal discourses that question the entitlements of minority ethnic people or seek to silence discussions of ‘race’ and racism can also prevent attention being given to the significant body of evidence on ethnic health inequalities. Effective responses to these challenges need to be formulated and disseminated to support individuals faced with such barriers, thereby reducing their impact and supporting alternative discourses that focus on equity and social justice.
An enabling environment is characterised by senior commitment to reducing ethnic health inequalities, reflected in strategic frameworks, service specifications and monitoring processes that specifically address this issue. Our findings suggest that the Equality Delivery System may have the potential to provide the strategic framework within which such legitimacy can be expressed if it is explicitly adopted and promoted by senior executives within commissioning organisations.
The capacity to draw effectively on a range of evidence on ethnic diversity and inequality appears most likely to develop when organisations resource senior-level appointments dedicated to providing a continuous in-depth focus on this area of activity. Our findings also suggest that capacity to understand and generate evidence on ethnic diversity and inequality is more likely within the context of a diverse workforce that represents the populations it serves. We found that access to a broad spectrum of evidence is made possible through collaboration with wide, cross-disciplinary groups of relevant stakeholders, including those who may challenge existing practices. A constructive and open approach and investment in long-term engagement with such groups is most often found to support the co-production of knowledge that leads to innovative approaches and adaptations of existing levers.
Pooling capacity through networks and regular meetings of E&D staff within and between organisations enables information sharing, for example about successful interventions. These structures can also support cross-sector work and avoid duplicate activity generating evidence from the same sources. Informal networks and relationships also appear to be important in terms of improving access to different sources of information, and developing ‘allies’ that can increase support from senior decision-makers.
We found that the ability and confidence to package evidence in ways that are credible and meaningful is important in terms of influencing those involved in commissioning to adopt an ethnicity focus. This kind of influential use of evidence is likely to feed back into, and reinforce, the organisational legitimacy of this agenda, potentially leading to further resource allocation.
The need for easy access to a diverse range of qualitative and quantitative, nationally and locally produced evidence and synthesis briefings that increase understanding of, and commitment to, reducing ethnic health inequalities is also suggested by our findings. These would need to be presented in ways that inform and influence individuals, commissioning groups and policy-makers at local and national levels. Support to understand what kinds of data on ethnicity would be meaningful in particular contexts is also necessary, given the complex underlying causes of ethnic health inequalities and the need to target resources in areas that are likely to make most difference.
Principles for effective evidence mobilisation
The findings presented above suggest the following key principles for effective mobilisation of evidence on ethnic diversity and inequality in the commissioning process.
Increasing demand for evidence on ethnic diversity and inequality
-
Encourage an understanding of commissioning that focuses on meeting heath needs rather than transactional approaches and that embeds a requirement to address health inequalities and population diversity.
-
Show political will and commitment by establishing senior leadership roles and incentives for commissioners to mobilise evidence on these issues within all areas of commissioning activity.
-
Ensure that attention to ethnic diversity and inequality is addressed in well-resourced areas of commissioning activity, such as that stimulated by national initiatives and drivers.
-
Link to national-level support that provides guidance and promotes consistency and good practice amongst commissioners in diverse geographical and service areas.
-
Provide standards and models for service specifications that include targets and measures relating to ethnic diversity and inequality.
Increasing access to varied sources of relevant evidence
-
Create a local infrastructure that supports information sharing, pooling of expertise and cross-sector work for those working in this area of activity.
-
Promote the active contribution of knowledge from a wide range of stakeholders, including E&D staff, minority ethnic service users/carers and organisations that represent their interests, and academics with relevant expertise.
-
Encourage an incremental approach to filling data and evidence gaps, using audit processes, service specifications and research as tools to support this development.
-
Seek out evidence that would support a transformational approach to service provision in areas in which current configurations are unlikely to reduce ethnic health inequalities.
-
Develop, pilot and evaluate interventions that produce evidence on what works to reduce ethnic health inequalities where this is not currently available.
-
Provide incentives and resources to disseminate good practice locally and nationally and use a wide range of networks and dissemination routes to achieve this.
Enhancing confidence and competence to use evidence critically and systematically
-
Expect E&D work to be evidence based and to provide opportunities to upskill staff specialising in this area and to link them more effectively to evidence experts.
-
Expect all commissioning staff to understand the importance of meeting minority ethnic needs and provide opportunities for staff to gain the necessary skills and experience to work confidently and competently in this area.
-
Establish routes to wider commissioning activity through which commissioners can seek out creative approaches to problems with current evidence on ethnicity.
-
Work to overcome fragmented, isolated activity by bringing together different pieces of work in this area under a strategic framework such as the Equality Delivery System, and showcase and reward such work.
A number of the areas for support outlined above have been addressed through the development of tools for use by individual managers, teams and organisations to enhance performance in this area (see http://research.shu.ac.uk/eeic/index.html). Further research will aim to explore the use of the tools in practice to support further their refinement.
Relevance of findings to emerging structures
Clearly, the commissioning context within which the present study was undertaken is changing substantially. Nevertheless, the findings outlined above are likely to have relevance for the new structures and actors as the obstacles identified appear to be long-standing and deeply embedded within UK health policy- and practice-making. Our respondents highlighted a number of opportunities and risks in terms of future prospects for evidence-based commissioning for multiethnic populations. First, they expressed concern that many GP commissioners lack the necessary skills and experience to engage with relevant sources of evidence and that their immediate concern would be with the transactional aspects of commissioning with little time for transformational work. Concerns were also expressed that GPs will have low levels of engagement and poor relationships with local authority colleagues and third-sector organisations. The cumulative effect of these potential limitations confirms suggestions that GP commissioning may have little impact beyond primary care109 and indicates that health and wellbeing boards may struggle to achieve cross-sectional commitment to ethnicity and equalities work.
Nevertheless, some respondents suggested a number of potential opportunities for action on health inequalities presented by the emerging structures. In particular, there were hopes for greater accountability of commissioners to local communities through the health and wellbeing boards as well as stronger JSNAs and more co-ordinated work to address wider social and economic determinants resulting from the move of public health to local authorities. Further, several respondents were optimistic that, although likely to be patchy, some CCGs would take ethnic and other inequalities seriously, and that commissioning GPs’ professional identities, clinical expertise and awareness of local needs would enable them to bring about positive change despite a weaker national policy context. Our findings suggest that the individual agency of GPs committed to reducing health inequalities and the ability of CCGs to develop effective partnerships with relevant interest groups will be key to determining whether GP-led commissioning emerges as an effective mechanism for addressing ethnic health inequalities.
Conclusion
We have drawn on diverse streams of existing literature to help our interpretation of how knowledge is utilised and to generate better understanding of the factors that shape current use of evidence relating to ethnic diversity and inequality. Our findings highlight and confirm the complex and contested nature of knowledge and the messy, diverse and convoluted pathways that may link evidence to policy- or practice-making. 48,64 The study demonstrates that knowledge mobilisation and utilisation within the commissioning cycle occurs in the context of dynamic interactions between individual agency, organisational rules, structures and processes, and the wider health-care setting with its current restructuring agenda, all situated within the broader sociopolitical context of multicultural Britain.
Our findings highlight support for previous critiques of PCT progress on health inequalities110–112 and the need for improvement on the PCT commissioning era. Although there are pockets of good practice, and developing skills, the general picture is of limited organisational engagement and low priority. This study highlights the need for specific guidance, standards and models relating to commissioning for a multiethnic population alongside incentives and resources to generate and disseminate creative approaches to problems with current evidence. A more comprehensive infrastructure is also required to facilitate and support access to evidence on ethnic diversity and inequality and to promote networks that would support those working on this agenda. Perhaps most importantly, there is a need for greater political will and commitment to promote practice that focuses on reducing ethnic health inequalities at all stages of the commissioning cycle.
Acknowledgements
The authors thank all of the research participants for their generosity. We also thank the members of the project advisory group and user guidance group, John Beech, Mark Exworthy, Mark Johnson, Ruth Thorlby, Mark Gamsu, Bunny McCullough, Chris Bentley, Liddy Goyder, Ade Adebajo, Udi Archibong, Parveen Ali, Pia Bruhn, Jeremy Wight, Ali Jan Haider, James Gunn, Touchstone, the Sheffield BME Network, Mubarak Ismail and Malcolm Whitfield for various and valuable support to the project.
Contribution of authors
All authors (Sarah Salway, Daniel Turner, Ghazala Mir, Bushara Bostan, Lynne Carter, John Skinner, Kate Gerrish and George Ellison) engaged in study design, data analysis, interpretation and report writing.
All authors except Kate Gerrish and George Ellison also engaged in primary data generation.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Pettigrew M, Whitehead M, Macintyre S, Fraham H, Egan M. Evidence for public health policy in inequalities: 1: the reality according to policymakers. J Epidemiol Commun Health 2004;58:811-16. http://dx.doi.org/10.1136/jech.2003.015289.
- Ethnicity and National Identity in England and Wales 2011. London: ONS; 2012.
- Salway S, Ellison G, Gerrish K, Lacey A. The Research Process in Nursing. Oxford: Wiley-Blackwell; 2009.
- Nazroo J. The Health of Britain’s Ethnic Minorities. London: Policy Press; 1997.
- Gill PS, Kai J, Bhopal RS, Wild S, Stevens A, Raftery J, et al. Health Care Needs Assessment: The Epidemiologically Based Needs Assessment Reviews. Abingdon: Radcliffe Medical Press; 2007.
- Report on Self-Reported Experience of Patients from Black and Minority Ethnic Groups. London: HMSO; 2008.
- Lakhani M. No Patient Left Behind: How Can We Ensure World Class Primary Care for Black and Minority Ethnic People?. London: Department of Health; 2008.
- Crozier A, McNeill A. Mapping Black and Minority Ethnic Tobacco Prevention Resources. London: Department of Health; 2003.
- Webb R, Richardson J, Esmail A, Pickles A. Uptake for cervical screening by ethnicity and place-of-birth: a population based cross-sectional study. J Public Health 2004;2:293-6. http://dx.doi.org/10.1093/pubmed/fdh128.
- Survey of South Asian People with Diabetes 2006: Access to Healthcare Services at a Glance. London: Diabetes UK; 2007.
- Rhodes P, Nocon A. A problem of communication? Diabetes care among Bangladeshi people in Bradford. Health Soc Care Commun 2003;11:45-54. http://dx.doi.org/10.1046/j.1365-2524.2003.00398.x.
- Lewis G. The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers’ Lives: Reviewing Maternal Deaths to Make Motherhood Safer – 2003–2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH; 2007.
- Kai J. Safety and achieving equality amid diversity in healthcare. Brit J Gen Pract 2007;57:774-6.
- Chau R. Health Experiences of Chinese People in the UK. London: Race Equality Foundation; 2008.
- Moriarty J. The Health and Social Care Experiences of Black and Minority Ethnic Older People. London: Race Equality Foundation; 2008.
- Culley L, Dyson S, Culley L, Dyson S. Ethnicity and Nursing Practice. Basingstoke: Palgrave; 2001.
- Race Equality Action Plan. London: Department of Health; 2004.
- Kripalani S, Bussey-Jones J, Katz M, Genao I. A prescription for cultural competence in medical education. J Gen Intern Med 2006;21:1116-20. http://dx.doi.org/10.1111/j.1525-1497.2006.00557.x.
- Yamada AM, Brekke JS. Addressing mental health disparities through clinical competence not just cultural competence: the need for assessment of sociocultural issues in the delivery of evidence-based psychosocial rehabilitation services. Clin Psychol Rev 2008;28:1386-99. http://dx.doi.org/10.1016/j.cpr.2008.07.006.
- Shapiro J, Lie D, Gutierrez D, Zhuang G. ‘That never would have occurred to me’: a qualitative study of medical students’ views of a cultural competence curriculum. BMC Med Educ 2006;26.
- Russell J, Greenhalgh T, Boynton P, Rigby M. Soft networks for bridging the gap between research and practice: illuminative evaluation of CHAIN. BMJ 2004;32:2-7. http://dx.doi.org/10.1136/bmj.328.7449.1174.
- Ahmad WIU. ‘Race’ and Health in Contemporary Britain. Buckingham: Open University Press; 1993.
- Culley L. Transcending transculturalism? Race, ethnicity and health-care. Nurs Inq 2006;13:144-53.
- Atkin K, Chattoo S. The dilemmas of providing welfare in an ethnically diverse state: seeking reconciliation in the role of a ‘reflexive practitioner’. Policy Polit 2007;35:377-93. http://dx.doi.org/10.1332/030557307781571632.
- Papadopolous I, Tilki M, Lees S. Promoting cultural competence in healthcare through a research-based intervention in the UK. Diversity Health Soc Care 2004;1:107-15.
- Race for Health . Towards Race Equality in Health: A Guide to Policy and Good Practice n.d. www.raceforhealth.org/storage/files/Race_for_Health_Commissioning_Guide.pdf (accessed July 2009).
- Race for Health . Leading Action on Race Equality and Health: A Guide to What We n.d. www.raceforhealth.org/news/archive/2009/10/16/nhs_leaders_tackle_race_equality_in_health_at_london_summit (accessed November 2009).
- Yanow D. How does a policy mean? Interpreting policy and organizational actions. Washington, DC: Georgetown University Press; 1996.
- Colebatch HK. Policy analysis, policy practice and political science. Aust J Public Admin 2005;64:14-23. http://dx.doi.org/10.1111/j.1467-8500.2005.00448.x.
- Hanney S, Gonzalez-Block M, Buxton M, Kogan M. The utilisation of health research in policy-making: concepts, examples and methods of assessment. Health Res Policy Syst 2003;1. www.health-policy-systems.com/content/1/1/2 (accessed October 2013).
- Black N. Evidence based policy: proceed with care. BMJ 2001;323:275-9. http://dx.doi.org/10.1136/bmj.323.7307.275.
- Kelly M, Swann C. Evidence into practice and health inequalities. Health Educ 2004;104:269-71. http://dx.doi.org/10.1108/09654280410560514.
- Elliot H, Popay J. How are policy makers using evidence? Models of research utilisation and local NHS policy-making. J Epidemiol Commun Health 2000;54:461-8. http://dx.doi.org/10.1136/jech.54.6.461.
- Whitehead M, Pettigrew M, Graham H, Macintyre S, Bambra C, Egan M. Evidence for public health policy on inequalities: 2: assembling the evidence jigsaw. J Epidemiol Commun Health 2004;58:817-21. http://dx.doi.org/10.1136/jech.2003.015297.
- Blackman T, Greene A, Hunter DJ, McKee L, Elliott E, Harrington B, et al. Performance assessment and wicked problems: the case of health inequalities. Public Policy Admin 2006;21:66-80. http://dx.doi.org/10.1177/095207670602100206.
- Exworthy M, Bindman A, Davies H, Washington E. Evidence into policy and practice? Measuring the progress of US and UK policies to tackle disparities and inequalities in US and UK health and healthcare. Milbank Q 2006;84:75-109.
- Mir G, Tovey P. Cultural competency: professional action and South Asian carers. J Manag Med 2002;16:7-19. http://dx.doi.org/10.1108/02689230210428599.
- Connelly N. Ethnic record keeping and monitoring in service delivery. London: Policy Studies Institute; 1988.
- Aspinall PJ, Anionwu E. The role of ethnic monitoring in mainstreaming race equality and the modernization of the NHS: a neglected agenda?. Crit Public Health 2002;12:1-15. http://dx.doi.org/10.1080/09581590110113277.
- Iqbal G, Gumber A, Johnson MRD, Szczepura A, Wilson S, Dunn JA. Divers Health Care. 2009.
- Chen E, Kakkad D, Balzano J. Multicultural competence and evidence-based practice in group therapy. J Clin Psychol 2008;64:1261-78. http://dx.doi.org/10.1002/jclp.20533.
- Whaley AL, Davis KE. Cultural competence and evidence-based practice in mental health services – a complementary perspective. Am Psychol 2007;62:563-74. http://dx.doi.org/10.1037/0003-066X.62.6.563.
- Engebretson J, Mahoney J, Carlson ED. Cultural competence in the era of evidence-based practice. J Prof Nurs 2008;24:172-8. http://dx.doi.org/10.1016/j.profnurs.2007.10.012.
- Mir G, Salway S, Kai J, Karlsen S, Bhopal R, Ellison GT, et al. Principles for research on ethnicity and health: the Leeds Consensus Statement. Eur J Public Health 2013;23:504-10. doi:10.1093/eurpub/cks028.
- Gunaratnam Y, Douglas J, Earle S, Handsley S, Lloyd C, Spurr S. A Reader in Promoting Public Health: Challenge and Controversy. Basingstoke: Palgrave; 2007.
- Bradby H. Describing ethnicity in health research. Ethn Health 2003;8:5-13. http://dx.doi.org/10.1080/13557850303555.
- Gerrish K. Researching ethnic diversity in the British NHS: methodological and practical concerns. J Adv Nurs 2000;31:918-25. http://dx.doi.org/10.1046/j.1365-2648.2000.01357.x.
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organisations: systematic review and recommendations. Milbank Q 2004;82:581-629.
- Kai J, Beavan J, Faull C, Dodson L, Gill P, Beighton A. Professional uncertainty and disempowerment responding to ethnic diversity in health care: a qualitative study. PLoS Med 2007;4. doi:10.1371/journal.pmed.0040323.
- Betancourt JR, Green AR, Carrillo JE, Park ER. Cultural competence and health care disparities: key perspectives and trends. Health Aff (Millwood) 2005;24:499-505. http://dx.doi.org/10.1377/hlthaff.24.2.499.
- Bellary S, O’Hare JP, Raymond NT, Gumber A, Mughal S, Szczepura A, et al. Enhanced diabetes care to patients of south Asian ethnic origin (the United Kingdom Asian Diabetes Study): a cluster randomised controlled trial. Lancet 2008;371:1769-76. http://dx.doi.org/10.1016/S0140-6736(08)60764-3.
- Susawad P. Knowledge Translation: Introduction to Models, Strategies and Measures. Austin, TX: National Center for the Dissemination of Disability Research; 2007.
- Smith J, Woodin J, Walshe K, Smith J. Healthcare Management. Maidenhead: Open University Press; 2006.
- NHS Commissioning Board . Developing Commissioning Support: Towards Service 2012. www.commissioningboard.nhs.uk/files/2012/01/NHSCBA-02–2012–8-Guidance-Developing-commissioning-support-Towards-service-excellence.pdf (accessed December 2012).
- Department of Health . World Class Commissioning: Vision 2007. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_080956 (accessed December 2012).
- NHS Networks . Developing a Public Health Commissioning Network (PHCN) for England 2009. www.nks.nhs.uk/commissioningnet/A4%20flyer%20Jan%2009.pdf (accessed July 2009).
- Baker R, Tang MY. The role of research in helping general practice commission efficient healthcare. Lond J Prim Care 2011;4:27-32.
- Practice Based Commissioning: from Good Idea to Effective Practice. London: King’s Fund; 2007.
- McCafferty S, Williams I, Hunter D, Robinson S, Donaldson C, Bate A. Implementing world class commissioning competencies. J Health Serv Res Policy 2012;17:40-8. http://dx.doi.org/10.1258/jhsrp.2011.011104.
- McDermott MS, Thomson H, West R, Kenyon JA, McEwen A. Translating evidence-based guidelines into practice: a survey of practices of commissioners and managers of the English stop smoking services. BMC Health Serv Res 2012;12. http://dx.doi.org/10.1186/1472-6963-12-121.
- Mitton C, Adair C, McKenzie E, Patten SB, Perry BW. Knowledge transfer and exchange: review and synthesis of the literature. Milbank Q 2007;85:729-68. http://dx.doi.org/10.1111/j.1468-0009.2007.00506.x.
- Crilly T, Jashapara A, Ferlie E. Research Utilisation and Knowledge Mobilisation: a Scoping Review of the Literature. Draft report to SDO. London: Department of Health; 2009.
- Eccles M, Armstrong D, Baker R, Cleary K, Davies H, Davies S, et al. An implementation research agenda. Implement Sci 2009;4. http://dx.doi.org/10.1186/1748-5908-4-18.
- Davies H, Nutley S, Walter I. Why ‘knowledge transfer’ is misconceived for applied social research. J Health Serv Res Policy 2008;13:188-90. http://dx.doi.org/10.1258/jhsrp.2008.008055.
- Weiss C. The many meanings of research utilization. Public Admin Rev 1979;39:426-31. http://dx.doi.org/10.2307/3109916.
- Davies H, Nutley S, Smith P. What Works? Evidence-based Policy and Practice in Public Services. Bristol: Policy Press; 2000.
- Dunn W. Measuring knowledge use: creation, diffusion, utilisation. Knowledge 1983;5:120-33.
- Ringberg T, Reiglen M. Towards a socio-cognitive approach to knowledge transfer. J Manag Stud 2008;45:912-35. http://dx.doi.org/10.1111/j.1467-6486.2007.00757.x.
- Landry R, Amara N, Lamari M. Climbing the ladder of research utilization: evidence from social science research. Sci Commun 2001;22:396-422. http://dx.doi.org/10.1177/1075547001022004003.
- Hunter S. Negotiating professional and social voices in research principles and practice. J Soc Work Pract 2005;19:149-62. http://dx.doi.org/10.1080/02650530500144709.
- Husband C, Ahmed WIU, Atkin K. ‘Race’ and Community Care. Milton Keynes: Open University Press; 1996.
- Gunaratnam Y, Lewis G. Racialising emotional labour and emotionalising racialised labour: anger, fear and shame in social welfare. J Soc Work Pract 2001;15:131-48. http://dx.doi.org/10.1080/02650530120090593.
- Kai J, Beavan J, Faull C, Dodson L, Gill P, Beighton A. Professional uncertainty and disempowerment responding to ethnic diversity in health care: a qualitative study. PLoS Med n.d.;2007. doi:10.1371/journal.pmed.0040323.
- Freedman L. Achieving the MDGs: health systems as core social institutions. Development 2005;48:19-24. http://dx.doi.org/10.1057/palgrave.development.1100107.
- Gilson L. Trust and development of health care as a social institution. Soc Sci Med 2003;56:1453-68. http://dx.doi.org/10.1016/S0277-9536(02)00142-9.
- Lam A. Embedded firms, embedded knowledge: problems of collaboration and knowledge transfer in global cooperative ventures. Organ Stud 1997;18:973-96. http://dx.doi.org/10.1177/017084069701800604.
- Knowledge Translation within the Research Cycle. Ottawa, ON: Canadian Institutes of Health Research; 2007.
- Landry R, Lamari M, Amara N. The extent and determinants of the utilization of university research in government agencies. Public Admin Rev 2003;63:192-205. http://dx.doi.org/10.1111/1540-6210.00279.
- Keen J, Pope C, Mays N. Qualitative Research in Health Care. Oxford: Blackwell; 2006.
- Flyvbjerg B. Five misunderstandings about case-study research. Qual Inq 2006;12:219-45. http://dx.doi.org/10.1177/1077800405284363.
- Equity and Excellence: Liberating the NHS. London: Department of Health; 2010.
- London: The Stationery Office; 2012.
- Berndtson K, Daid T, Tracy CS, Bhan A, Cohen ER, Upshur RE, et al. Grand challenges in global health: ethical, social, and cultural issues based on key informant perspectives. PLoS Med 2007;4. doi:10.1371/journal.pmed.0040268.
- Lavis J, Oxman A, Moynihan R, Paulsen E. Evidence-informed health policy 3: interviews with the directors of organisations that support the use of research evidence. Implement Sci 2008;3.
- Noy C. Sampling knowledge: the hermeneutics of snowball sampling in qualitative research. Int J Soc Res Meth 2008;11:327-44. http://dx.doi.org/10.1080/13645570701401305.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. http://dx.doi.org/10.1093/intqhc/mzm042.
- Hartley J, Cassel C, Symon G. Essential Guide to Qualitative Methods in Organizational Research. London: Sage; 2004.
- Burgess RG, Burgess RG. Strategies of Educational Research: Qualitative Methods. Philadelphia, PA: Falmer Press; 1985.
- Abbott S, Shaw S, Elston J. Comparative analysis of health policy implementation. Pol Stud 2004;25:259-66.
- Ahmed S. You end up doing the document rather than doing the doing: diversity, race equality and the politics of documentation. Ethnic Racial Stud 2007;30:590-609. http://dx.doi.org/10.1080/01419870701356015.
- Swallow V, Newton J. How to manage and display qualitative data using ‘Framework’ and Microsoft Excel. J Clin Nurs 2003;12:610-12. http://dx.doi.org/10.1046/j.1365-2702.2003.00728.x.
- Wainwright D. Can sociological research be qualitative, critical and valid?. Qual Rep 1997;3. www.nova.edu/ssss/QR/QR3–2/wain.html (accessed November 2009).
- NHS Outcomes Framework 2012 to 2013. London: Department of Health; 2011.
- Delivering Race Equality in Mental Health Care: an Action Plan. London: Department of Health; 2005.
- Department of Health . About the Pacesetters Programme 2010. http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Managingyourorganisation/Workforce/Equalityanddiversity/Pacesetters/DH_078778 (accessed October 2013).
- Picker Institute . Staff Survey 2011 – Detailed Spreadsheets n.d. www.nhsstaffsurveys.com/Page/1022/Past-Results/Staff-Survey-2011-Detailed-Spreadsheets/ (accessed October 2013).
- Yorkshire and the Humber NHS . Innov8 Charter 2011. http://yh.hee.nhs.uk/files/2013/06/Innov8-Charter-Sept11-Final-version.docx (accessed October 2013).
- The Equality Delivery System. London: Department of Health; 2010.
- Equality Act 2010. London: The Stationery Office; 2010.
- Maternity Matters: Choice, Access and Continuity of Care in a Safe Service. London: Department of Health; 2007.
- National Service Framework: Coronary Heart Disease. London: Department of Health; 2000.
- National Institute for Health and Care Excellence . About the Quality and Outcomes Framework 2013. www.nice.org.uk/aboutnice/qof (accessed October 2013).
- Brocklehurst N, Liabo K. Evidence nuggets: promoting evidence-based practice. Commun Pract 2004;77:371-5.
- Walter I, Nutley S, Davies H. Research Impact: a Cross Sector Review. St Andrews: University of St Andrews, Research Unit for Research Utilisation; 2003.
- Salway S, Nazroo J, Mir G, . Fair society, healthy lives: a missed opportunity to address ethnic inequalities in health. BMJ 2010. http://171.66.124.147/cgi/eletters/340/feb09_1/c684#234369 (accessed 14 November 2013).
- Ingleby D. Ethnicity, migration and the ‘social determinants of health’ agenda. Psychosoc Interv 2012;21:331-41.
- Mir G, Sheikh A. ‘Fasting and prayer don’t concern the doctors . . . they don’t even know what it is’: communication, decision-making and perceived social relations of Pakistani Muslim patients with long-term illnesses. Ethnic Health 2010;15:327-42. http://dx.doi.org/10.1080/13557851003624273.
- Lorant V, Bhopal RS. Ethnicity, socio-economic status and health research: insights from and implications of Charles Tilly’s theory of durable inequality. J Epidemiol Commun Health 2011;65:671-5. http://dx.doi.org/10.1136/jech.2010.116418.
- Smith J, Mays N. GP led commissioning: time for a cool appraisal. BMJ 2012;344. http://dx.doi.org/10.1136/bmj.e980.
- Smith J, Curry N, Dixon A, Jones L. Understanding New Labour’s Market Reforms of the English NHS. London: King’s Fund; 2011.
- Allen P. A socio-legal and economic analysis of contracting in the NHS internal market using a case study of contracting for district nursing. Soc Sci Med 2002;54:255-66. http://dx.doi.org/10.1016/S0277-9536(01)00025-9.
- Bravo Vergel Y, Ferguson B. Difficult commissioning choices: lessons from English primary care trusts. J Health Serv Res Policy 2006;11:150-4.
Appendix 1 Protocol
1st October 2010
Towards equitable commissioning for our multiethnic society: understanding and enhancing the critical utilisation of evidence by strategic commissioners and public health managers
Aims and objectives
Goal: To support the commissioning of health services that better meet the needs of black and minority ethnic patients and thereby help reduce ethnic inequalities in healthcare experiences and health outcomes.
Aim: To enhance the critical use of research evidence alongside other forms of knowledge by managers within the PCT commissioning cycle.
Objectives:
Theoretical:
-
To develop a theoretical model of knowledge utilisation that explicates the emotional, ideological and political dimensions through the example of ethnic diversity and inequality.
-
To contribute to the theoretical literature that addresses mechanisms for enhancing the critical use of research evidence by managers in complex decision-making environments.
-
To contribute to the theoretical literature that addresses mechanisms for enhancing the cultural competence of healthcare services by integrating an understanding of the role of knowledge(s) mobilisation.
Empirical:
-
To describe, across a range of commissioning contexts, how managers seek out, appraise and apply research evidence relating to ethnic diversity and inequality alongside other forms of knowledge.
-
To identify factors (at evidence, individual and contextual levels and their interfaces) that support or inhibit the critical and effective use of research evidence within the commissioning cycle and thereby identify promising routes of intervention.
Operational:
-
To develop practical diagnostic, evaluative and change management tools for use by individual managers, teams and organisations to (i) assess and promote critical reflection on current competencies and practice with respect to utilisation of evidence on ethnic diversity and inequality, (ii) identify actions to strengthen competencies and good practice and (iii) support specific elements of the knowledge utilisation process.
-
To educate researchers and research funders regarding the current limitations of the evidence base and how they might generate research products that are more appropriate and accessible for managers charged with the task of commissioning services for multiethnic populations.
-
To strengthen links between university researchers and managers and contribute to the development of a shared commitment to enhancing research evidence utilisation for enhanced organisational performance.
Background
While the volume of enquiry into the mobilisation and utilisation of research evidence within the health sector is growing rapidly, there remain important gaps in our understanding about which strategies work to encourage better use of research evidence and how and why specific approaches might work. In particular, our understanding of knowledge utilisation processes within the policy context is far weaker than for the clinical practice environment (Pettigrew et al, 2004). The current project responds to this gap in our understanding by exploring the PCT commissioning cycle – an increasingly powerful determinant of the NHS services on offer and the care that patients receive - and by explicitly focusing on an area that has so far been overlooked, namely the mobilisation and utilisation of evidence relating to ethnic inequalities in health. While no prior studies have engaged with our specific area of focus, we identify three bodies of work that can be drawn upon and integrated to identify fruitful new avenues of investigation.
First, a growing body of studies explores knowledge mobilisation and utilisation within the health policy-making arena, and some take an explicit focus on health inequalities. Much of this work draws on broader theoretical perspectives that view policy making as a process of collective interaction between diverse stake-holders in which both the identification of, and responses to, problems, are viewed as socially situated and constructed (Yanow 1996; Colebatch, 2005; Hanney et al. 2003). These contributions highlight the distinctive nature of evidence utilisation in policy formation (at both strategic and service-design levels) when compared to the clinical practice context (Black 2001; Pettigrew et al., 2004). Kelly and Swann (2004) note the way in which evidence syntheses within public health can only offer ‘scientifically plausible frameworks for action’ (p270) and not prescriptions for specific intervention, since decision-making requires judgements based on knowledge of local context including prevailing practices, organisational structures, commitment and engagement of key actors. Similarly, Elliot and Popay’s (2000) investigation of evidence use by NHS managers revealed that research was felt to offer clarity and to contribute to decision-making but rarely to provide simple, clear-cut answers. Other work confirms that healthcare policy-makers work with a ‘mixed economy’ of evidence, piecing together information from diverse sources in their decision-making (Pettigrew et al., 2004; Whitehead et al., 2004).
Blackman et al. (2006) look particularly at policy-making related to health inequalities and identify this area as a ‘wicked problem’ that cuts across traditional organisational boundaries and whose complexity limits the scope of evidence-based action. ‘Wicked problems’ tend to carry with them greater scope for debate around what should be done and how it should be achieved and more room for disagreement on what counts as robust and relevant evidence. They suggest that policy-making in relation to ‘wicked problems’ tends to be less a technical exercise and more a process of dialogue and argument with power relationships clearly in evidence. Exworthy et al., (2006) highlight similar factors that may complicate the knowledge-into-action process relating to the health inequalities agenda, including the multiplicity of agencies and the diffuse nature of responsibility. While this past research exploring the utilisation of evidence within the health inequalities context is an important backdrop to the present study, there is a need for enquiry that specifically focuses on ethnic diversity and inequality. Mir and Tovey’s (2002) study begins to explore these issues and shows that whether managers act upon research and other knowledge is shaped by resources, organisational culture and particularly the absence of substantial disincentives. There is a need for further systematic study of the factors that hamper or facilitate the effective utilisation of research evidence relating to ethnic diversity and inequality, particularly because of the significant additional issues that arise in terms of the generation and application of a research evidence base in this area and also because of the embedded nature of racial discrimination within UK society.
Turning first to the consider the research evidence base, work that engages with the ethics and science of researching ethnicity and health is pertinent but has yet to be integrated with research that explores the role of the characteristics of research evidence within utilisation processes. As the volume of research on ethnicity and health expands, so too do concerns regarding quality, its potential role in stereotyping and stigmatising ethnic minorities, and its limited benefit to minority ethnic populations (Gunaratnam, 2007). Critically appraising and applying research evidence on ethnicity and health presents significant challenges and demands particular competencies (Salway and Ellison, 2009). Issues include the need to: interrogate conceptualisations of ethnicity that erroneously present ethnic ‘groups’ as stable, discrete entities and/or fail to address its multifaceted nature; question whether research adequately addresses the concerns of minority ethnic people; recognise the limited analytical potential offered by crude administrative ethnic categorisation; and carefully consider how evidence can best be synthesised across contexts when concepts and categorisations vary widely (Bradby, 2003; Gerrish, 2000; Morning, 2008). These issues are likely to impact importantly on how managers use research evidence relating to ethnic diversity and inequality, though to-date this has not been explored.
Related work in the broad area of health inequalities highlights a number of factors related to the characteristics of research evidence and research products that have relevance to the focus of the present study. Exworthy et al., (2006) suggest that the multifactorial nature of inequalities, the paucity of evidence of effective interventions and the need for upstream and long-term investments all complicate the knowledge-into-action cycle in health inequalities policy. Pettigrew et al. (2004) found that policy-makers charged with the health inequalities agenda commonly perceive the lack of locally relevant evidence and evidence on the distributional effects of interventions to be problematic. More generally, Greenahalgh et al. ’s (2004) major review of innovation diffusion in healthcare organisations identifies a number of key attributes of successful innovation that are rarely applicable to the evidence base on ethnic diversity and inequality including: evidence of clear benefits and cost-effectiveness; low complexity; ease of adaptation and low risk or uncertainty. Indeed, utilisation of the research evidence relating to ethnic diversity and inequality is likely to be compromised by: the predominance of grey literature; the lack of evaluative studies; the lack of studies that consider the distributional effects of interventions by ethnicity; and the lack of consideration of ethnicity within influential evidence syntheses (e.g. Cochrane reviews, NICE guidelance) (Yamanda and Brekke, 2008).
Notwithstanding weaknesses in the evidence base that need to be filled, there is nevertheless a substantial body of evidence that highlights the scale and nature of the health disadvantage suffered by black and minority ethnic groups, as well as evidence that identifies generic ways in which health services could be modified to better meet the needs of minority ethnic patients (such as the provision of adequate interpretation facilities and enhanced cultural competence among healthcare providers, (Kai et al., 2007; Betancourt et al., 2005)). Furthermore, in some service/disease areas the quality of the research evidence base could lend itself to more specific, instrumental use by commissioners in pursuit of improved outcomes for minority ethnic groups such as evidence-based diabetes interventions (Bellary et al 2008). However, while many studies have identified factors that shape whether such research evidence impacts upon policy or practice (Hanney et al., 2003; Susawad, 2007), none have specifically engaged with the issue of ethnic diversity and inequality. More needs to be understood regarding the factors that support or inhibit the use of evidence in this context including: how evidence is presented and conveyed to decision-makers; what is regarded as evidence or knowledge; how the quality and relevance of knowledge is assessed; when evidence is regarded as necessary; how easily evidence can be accessed, appraised, synthesised and integrated with other knowledge so that it can be adapted to the local context; and how decision-making is achieved in the absence of adequate research evidence.
Finally, our study is informed by, and seeks to further develop, the body of work that explores factors involved in achieving cultural competence within healthcare organisations. Attempts to translate knowledge about ‘cultural competence’ into improved healthcare experiences and outcomes for black and minority ethnic patients have most often adopted either training/education or evidence-based practice approaches. To-date, there has been no investigation of how research evidence informs policy-making or the commissioning of services for multiethnic populations. Nevertheless, past studies of training/education or evidence-based practice approaches do offer some useful insights.
Several studies highlight the way in which education and training programmes designed to address gaps in professional knowledge require wider, systems-based approaches to achieve desired shifts in practice. Kripalani (2006) notes the importance of clear support from senior staff in terms of signifying priority and modelling desired behaviour, Yamada and Brekke (2008) identify the need for attention to organisational factors influencing practice, and Shapiro et al. (2006) suggest that practice-based learning and models of good practice are needed alongside training courses. These findings point to the embedded nature of practitioner assumptions and behaviours and the need to challenge ‘tacit knowledge’ through new learning that is context-specific, has a link to action and is informed by experience (Russell et al., 2004).
An evidence based practice (EBP) approach to developing culturally competent services has combined best available research evidence with clinical expertise in the context of individual client characteristics. This approach has drawn on research highlighting the significance of systems in the development of culturally relevant interventions and the importance of practitioner self-awareness (Yamada and Brekke, 2008). EBP efforts are hampered, however, by a lack of evidence about specific ways in which practice guidelines should be modified to improve health outcomes for minority ethnic populations (Chen et al., 2008; Yamada and Brekke 2008) and omission of these populations from studies of evidence-based treatments (Whaley and Davis, 2007). The lack of evidence on the efficacy and cost effectiveness of cultural competence interventions may result in these being seen as an extra burden, particularly in the context of staff shortages and financial restrictions (Engebretson et al., 2008).
In addition to the above work, there is a large body of research that explores ‘cultural competence’ within healthcare from an organisational development perspective without engaging specifically in an exploration of the mobilisation and utilisation of research evidence. Analyses that situate the formulation of healthcare policy and practice within the wider sociocultural context of contemporary Britain are helpful. Despite sustained attention, UK policy relating to ethnic diversity lacks coherence and suggests at best ambivalence towards minority ethnic groups and dissensus regarding the form that multicultural Britain should take (Ahmad 1993; Culley, 2006). Two significant wings of policy and legislation – relating to immigration control and citizenship on the one hand, and to racial equality on the other – conflict (Hepple, 1992). Atkin and Chattoo (2007) argue that strategies for addressing disadvantage in healthcare provision are undermined as providers and managers struggle to reconcile these conflicting messages regarding minority ethnic populations; their needs and entitlements. It is increasingly argued that progress towards more culturally competent health services requires practitioners and organisations to: examine value bases; expose stereotypes, prejudices and ethnocentrism; challenge power relationships and oppressive practices; and work in true partnership (Papadopolous et al., 2004). It is noteworthy, however, that while such models often emphasise the importance of community consultation and local intelligence data, they are commonly silent on the role of research evidence (Dreaschlin, 2007). Similarly, recent policy documents and initiatives aimed at supporting commissioners and managers to address ethnic diversity and inequality pay little attention to how research evidence might be mobilised and utilised in this endeavour (Race for Health, n.d.; Race for Health, 2009). This is particularly surprising given the significant recent investments and initiatives aimed at fostering an evidence based approach to tackling ethnic inequalities, including the Ethnicity & Health specialist library of NHS Evidence. The present study seeks to address these important gaps.
While research to-date has helped to describe the complexity of the processes involved in, and the very wide range of factors that can act as barriers to, the knowledge utilisation process (Greenhalgh et al., 2004; Mitton et al., 2007; Susawad, 2007), as yet little has been done to identify effective routes to shaping or enhancing the process in real-life policy-making contexts. There is a need to move towards identifying effective areas for intervention – so-called ‘weak points’ – where intervention can effectively shift embedded values, beliefs, structures and practices that serve to undermine the contribution of research evidence. The present study aims to contribute to this general need and to generate specific understanding in an important area that has not to-date been the focus of enquiry.
Need
The study’s focus on enhancing critical use of evidence in the commissioning process aims to enhance the quality, acceptability and effectiveness of services for minority ethnic communities, which comprise 13% of the population of England (in terms of those identifying as other than ‘White British’ in the 2001 Census). Mortality and morbidity patterns are complex, however substantial evidence indicates that minority ethnic groups suffer significant disadvantage across a range of indicators (Nazroo, 1997; Natarajan, 2004; Gill et al., 2007) as well as lower satisfaction with services (e.g. DH/HCC, 2008). The study will support managers to utilise evidence to improve commissioning and delivery of healthcare that effectively serves the needs of minority ethnic people, an area in which progress has been limited to-date (Culley and Dyson, 2001). Better use of evidence will help to overcome persistent problems relating to ineffective and insensitive patient–provider interactions, inappropriate constellation and design of services, inequitable allocation of resources and ethnocentric and oppressive cultures of care, that have been documented across a variety of service settings (e.g. Singh and Newburn 2000; Bhui et al., 2007). The research products will have pertinence to the increasing ‘ethnic diversity’ of the UK population considering both persistent disadvantage among established minority communities alongside the differing health needs of new migrant populations. The study therefore responds to the Commission for Equality and Human Rights’ (previously the CRE) formal investigation into the Department of Health, and Nigel Crisp’s 10-point action plan response, which highlight the need for significant improvement in this area.
Past policy intentions to tackle ethnic health inequalities have been undermined by competing priorities and diffuse locations of responsibility. However, recent policy developments and NHS reforms signal the alignment of efficiency and equity principles (including the NHS Constitution, DH, 2009; High Quality Care for All, DH, 2004; and World Class Commissioning, DH, 2007) and create new opportunities for evidence-driven commissioning by primary care trusts (PCTs) (King’s Fund, 2007). Key competencies for today’s PCT commissioners place knowledge management centre stage and include: critically mobilising and utilising research and best practice evidence; effectively garnering local intelligence and promoting engagement to assess needs; turning information into knowledge and action for service reconfiguration that improves access, quality and outcomes (DH/Commissioning, 2007). Commissioners are to be transformatory, rather than transactional, encouraging innovation and ambition to serve those in greatest need. The role of public health teams in the commissioning cycle, via both profiling local populations and synthesising wider research evidence, is gaining importance (PHCN, 2009). At the same time, Practice Based Commissioning (PBC) is increasingly promoted as a way to ensure that practitioner experience and insight effectively inform the design and delivery of services. Practice Based Commissioning consortia are intended to articulate population needs and identify innovative solutions to delivering better care and increased patient choice more efficiently. While World Class Commissioning and PBC present important opportunities, it is clear that they also demand significant development in competencies and infrastructure, particularly in relation to the mobilisation and utilisation of evidence. For instance, early investigation by the King’s Fund (2007a) suggests that a lack of timely and high quality information currently undermines effective PBC. The current project responds to the needs of this emergent commissioning environment by seeking to enhance PCT managers’ critical use of evidence in their task of commissioning services for multiethnic populations.
Enhancing the utilisation of evidence is particularly pertinent to the task of tackling ethnic inequalities in health. As well as better ethnic monitoring at local level, there is a need for better understanding of ethnic inequalities in health – their nature, causes and potential solutions – among those responsible for commissioning services (Aspinall and Anionwu, 2002; King’s Fund 2007b; Yorkshire & Humber SHA, 2009). Furthermore, while there has been significant investment by DH in initiatives aimed at improving the commissioning of health services that address the needs of minority ethnic populations (for instance Race for Health and Pacesetters), there has to-date been poor articulation of the role that research evidence should play or how commissioners should be supported to effectively bring research evidence to bear on such commissioning decisions. This project extends and links several strands of ongoing collaborative work focused on knowledge translation, intelligent commissioning and ethnic diversity and inequality between university researchers and PCTs. The research focus has been jointly identified and responds to expressed needs among NHS managers. Recent events indicate a high level of interest in this area nationwide (King’s Fund, 2007b; Yorkshire & Humber SHA, 2009), so that the project will have relevance to current and future priorities of PCT managers both regionally and nationally. The project will generate new empirical and theoretical understanding of the factors that shape effective utilisation of evidence relating to ethnic diversity and inequality and identify promising routes of intervention to enhance such use. The project will then use this new knowledge to design specific tools to enhance performance in this area, for use by individual managers, teams and organisations. Managers in Public Health, Workforce and Corporate Development as well as Commissioning Directorates are particularly likely to benefit from these outputs. The study addresses the SDO’s core aims through its focus on improving practice in the organisation and delivery of health care for minority ethnic communities in the UK and contributes an added dimension to theoretical knowledge to the knowledge utilisation literature. By generating new knowledge about the way that managers perceive and utilise evidence on ethic diversity and inequality within the PCT commissioning cycle, and developing tools which help to apply this knowledge, the project represents good value for money. Further, by linking to the NIHR CLAHRC programme, the project’s tools will be taken forward into pilots to test their impact on commissioning practice and outcomes.
Methods
Study focus
The focus of the study is the mobilisation and utilisation of research evidence within the health services commissioning cycle. Rather than taking as our starting point a discrete package of research evidence or a new innovation, we seek to understand how research is drawn upon and used within the everyday context of commissioning. In addition, we focus on research evidence that relates to ethnic diversity and inequality and examine whether, how and why this is brought to bear on the commissioning of healthcare services for multiethnic populations.
We adopt an explicit Integrated Knowledge Translation model for the conduct of the study (CIHR, 2007), bringing university researchers and PCT managers together in a collaborative team across the entire research process, to develop research questions, shape methodology, generate and interpret data and disseminate findings in accessible formats. Past work has indicated that sustained and intense interaction between users and researchers increases the likelihood that findings are utilised (Landry, Lamari and Amara, 2003). Given the complex and potentially challenging focus of the present study, such collaborative working is crucial to ensure the project’s impact. PCT managers have contributed to the development of the proposal and preliminary work has confirmed the project’s relevance to these and other stakeholders.
Theoretical framework
Recent reviews highlight the diverse streams of theoretical literature that may inform enquiry into knowledge utilisation processes (Crilly, Jashapara and Ferlie, 2009; Susawad,2007) and call for research within healthcare contexts to draw on these traditions and become more clearly theory-based (Greenhalgh et al. 2004; Eccles et al., 2009).
Recent work that seeks to integrate micro-, meso- and macro-level conceptual frameworks and to articulate the interplay between these layers is useful (such as Greenhalgh et al.’s (2004) review on the diffusion of innovations). So too are frameworks that emphasise the complex and contested nature of research knowledge and the messy, diverse and convoluted pathways that may link research evidence to policy or practice-making. Davies et al.’s (2008) notion of ‘knowledge interaction’ is attractive since it captures the way in which the application of research evidence involves multiple actors engaging with varied knowledge sources to craft policy-making within the context of competing drivers. Empirical work based on such holistic models seems more likely to identify fruitful avenues for intervention to enhance effective evidence use than those that focus on particular pieces of the jigsaw in a more piecemeal fashion. We therefore conceptualise knowledge mobilisation and utilisation within the commissioning cycle as resulting from dynamic interactions between individual agency, organisational rules, structures and processes, and the wider healthcare setting with its current restructuring agenda, all situated within the broader socio-political context of multicultural Britain.
Within this comprehensive framework, our focus on ethnic diversity and inequality demands that we foreground four particular aspects. First, we draw on Weiss’s (1979) insights regarding the varied ways in which research might appear and be used within policy-making: as empirical findings (direct or instrumental); as ideas or challenges to current thinking (conceptual); or as briefs or arguments for action (persuasive/symbolic). We also recognise the often inherently contested and political nature of research evidence relating to ethnic diversity and inequality and that the characteristics of research evidence must be explicitly considered within our theoretical framework. Given that reviews of past work suggest that the direct use of evidence in policy making is in general the exception rather than the norm (Davies, Nutley and Smith, 2000), and the limited progress that has to-date been made in modifying services to meet the needs of black and minority ethnic populations, we give particular attention to elucidating the indirect influences of research evidence.
Second, at the level of individual actors and their interface with knowledge sources, we draw on socio-cognitive perspectives (Dunn, 1983; Ringberg and Reichlen, 2008) that emphasise the importance of the ‘thinking subject’ and the ‘mental models’ that guide people’s sense-making. While the crucial role of policy-makers as receptors of knowledge is widely recognised (Landry, Amara and Lamari, 2001; Hanney et al.; 2003), socio-cognitive models look beyond technical skills and resources to values, assumptions and worldviews. We suggest that the ways in which individual commissioners understand the nature of ethnicity and associated inequalities will be central to how they seek out, appraise and apply different types of knowledge within their work. These perspectives fit closely with the work of Hunter (2005), Husband (1996) and Gunaratnam and Lewis (2001) who highlight the need to explore the ‘felt dimension’ of healthcare policy and practice-making within the multiethnic, post-Macpherson setting. As Hunter (2005, 150) argues, in exploring the role of those in policy-making positions, we must ‘consider these individuals as emotional as well as relational actors.’ For example, professional anxiety and uncertainty about cultural competence is disempowering to professionals and detrimental to care (Kai 2007).
Third, within the organisational context, we adopt a critical awareness of power and seek to expose the taken-for-granted ‘ways of being and doing’ that operate and how these interact with research evidence. We view the health system and healthcare organisations as not just mechanical structures that provide healthcare but rather as culturally embedded and politically contingent (Freedman, 2005), as ‘purveyors of a wider set of societal norms and values’ (Gilson, 2003, 143). These ideas fit with Lam’s (1997) notion of ‘social embeddedness’ – the recognition of the inter-connections between individual managers (micro), their organisational context (meso) and the wider societal context (macro) within which these operate. This means that although knowledge utilisation processes are characterised as anarchic and unpredictable, there are nevertheless ‘deep structures’ – in this case racialised hierarchies – that shape and constrain in persistent ways.
Fourth, within the wider context layer, we pay particular attention to the influence of stakeholders beyond the commissioning organisations, particularly patients and the public and their representatives. Given the strong focus on consultation and ‘knowing communities’ of World Class Commissioning in general, and ethnic equality guidance in particular, we seek to understand not only the ways in which these individuals and groups represent additional, perhaps conflicting, sources of knowledge (for instance patient preferences, or public opinion regarding entitlements), but also the ways in which they access, appraise, interpret and present research evidence to the commissioning tasks independently.
Notwithstanding our choice of a multilayered theoretical model that is sufficiently sophisticated to allow understanding of the complex processes of knowledge utilisation, our underlying assumption is that knowledge utilisation processes can be understood, that certain causes and effects can be identified, and that steps can be taken to modify these processes – building on strengths and mitigating weaknesses.
Overall approach
This theoretical framework directs our methodological approach in a number of ways.
-
We combine detailed case study investigation of three commissioning organisations with broader data generation methods that allow us to engage with a wide range of commissioning contexts and managers in order to generalise theoretical understanding and develop research products that have wider relevance and transferablity.
-
We employ a case study approach that excels at understanding complex, multivariate real-life situations allowing the integration of data on a number of levels and detailed contextual analysis of events and relationships (Keen, 2006; Flyvbjerg, 2006).
-
Within the case studies we follow Innvær et al.’s (2002) recommendation to combine documentary review and interviewing, but go beyond this to incorporate naturalistic observation and reflective diaries. Drawing on the experience of researchers focusing on diversity and equality issues, we will ‘follow documents around’ (Ahmed, 2007) and tap into both official and private discourses in order to uncover taken-for-granted ‘rules’ and convoluted pathways of influence.
-
We engage in the co-production of knowledge between university researchers and PCT managers.
-
We focus on identifying factors that facilitate or hamper critical and effective use of research evidence, with a view to using these insights in the development of supportive tools that can help to enhance managerial practice in this regard.
-
We seek to describe how well research evidence is being used, not just whether it is used at all.
Given our focus on improving the cultural competence of healthcare provision for black and minority ethnic groups, the ultimate test of how well research evidence is used is whether it leads to policy and practice modifications that improve levels of satisfaction and service outcomes for minority ethnic patients. Tracing the use of evidence to such outcomes or benefits is beyond the scope of the current study. Instead our focus is on assessing the intermediate steps in this process. Past research suggests that we should examine: accessing appropriate sources; critical appraisal and selection of appropriate evidence (rigour, relevance, bias, transferability); synthesis of evidence across sources and methods; adaptation and presentation of evidence in appropriate formats; effective integration of research evidence with other knowledge sources; explicit articulation of assumptions, priorities and values underlying the weighing up of different knowledge sources; and the translation of integrated knowledge synthesis into commissioning and benchmarking tools, products and processes (such as: service specifications, business cases, business models, service specifications, care pathway models, tenders, provider contracts, performance management tools, and quality and standards monitoring tools). Though the importance of each of these elements may vary depending on whether research evidence is being used instrumentally, conceptually or influentially, they are nevertheless likely to be of relevance across the board. Our Phase One Key Informant Interviews and preparatory work for the Case Studies (see below) will be used to refine our indicators of ‘good use’ across these steps so that they are meaningful to the stakeholders involved and relevant data can be accessed to illuminate how well these dimensions are being achieved in practice.
Research questions
We identify below the three broad research questions that guide the empirical components of the study. Each broad research question is followed a set of more detailed questions that illustrate the range of issues that are likely to be relevant and that indicate our intention to explore five inter-related ‘levels’ – evidence, individual managers, commissioning team, organisational setting and wider context – that make up the knowledge mobilisation and utilisation process.
RQ1: How does a focus on ethnic diversity and inequality shape the knowledge mobilisation and utilisation process within the health services commissioning context?
-
What characteristics of research evidence relating to ethnic diversity and inequality influence how it is received by managers? (e.g. source; method, (un)certainty; relevance; concepts/theory);
-
What mental models of ‘how research evidence should be used’ are managers working with?
-
To what extent is the accessing and application of information relating to ethnic diversity and inequality part-and-parcel of broader evidence gathering exercises for commissioning, or rather a distinct exercise?
-
What factors prompt managers to seek out research (and other types of evidence) relating to ethnic diversity and inequality? (policy directives, new priorities, external audit, stakeholder inputs, signs of service failure etc.)
RQ2: How does organisational context shape the mobilisation and utilisation of knowledge relating to ethnic diversity and inequality?
-
How often, and at what stages, do managers apply research evidence relating to ethnic diversity and inequality in their commissioning tasks?
-
How are commissioning teams constituted and organised? How does this impact upon evidence use?
-
Who is seen as holding expertise and insight in relation to ethnic diversity and inequality? Why?
-
To what extent do PCT commissioning organisations have explicit models, structures, processes and objectives that support the mobilisation and utilisation of evidence? Do these consider ethnic diversity?
-
In what ways does managerial behaviour support and encourage, or deter, the explicit consideration of research evidence relating to ethnic diversity and inequality within commissioning teams?
-
In what ways do the available infrastructure and resources support and encourage, or deter, the explicit consideration of evidence relating to ethnic diversity and inequality within commissioning teams?
-
How do national, regional and organisational policy priorities inter-relate to shape the mobilisation and utilisation of evidence in this area?
RQ3: How can individual, team and organisational competencies be effectively enhanced to support critical use of research evidence for the commissioning of services that better meet the needs of a multiethnic population?
-
How competent are managers to (i) identify and access, (ii) critically appraise and synthesise; (iii) adapt and apply, evidence relating to ethnic diversity and inequality?
-
What expectations do managers have of, and what problems do they encounter with, the evidence base?
-
What individual level factors facilitate or hinder the mobilisation and utilisation of research evidence in this area (knowledge/awareness; skills and experience; ‘mental maps’; autonomy; authority; personal biography)?
-
What areas of capacity development would likely improve the individual and team-level competencies required for the mobilisation and utilisation of research evidence relating to ethnic diversity and inequality?
-
How does research (and other) evidence relating to ethnic diversity and inequality currently find its way into the commissioning process; via which actors and which routes? How can these be supported?
-
Who are the key actors and what are the key organisational settings and processes that present barriers against enhanced mobilisation and utilisation of evidence?
-
What factors in the wider societal and broader NHS context must be buffered against, or can be drawn upon, to support the routine, critical use of research evidence in commissioning for multiethnic populations?
-
What characteristics of the form, content and delivery of interventions in support of enhanced mobilisation and utilisation of research evidence are likely to increase relevance and utility?
Research phases, methods and links to research questions
Preparatory work: Prior to the official start of the project the following tasks will be initiated if funding is confirmed from SDO: applications for ethics and governance clearance, recruitment of the full-time researcher and Advisory and User Guidance Group establishment.
Phase 1 (Oct–Dec 2010): Preparatory work; ethics and governance approvals; team building; literature up-dating; researcher induction. Literature reviewing and updating will focus particularly on new evidence relating to the form and content of interventions that have been shown to be effective at enhancing evidence utilisation in policy-making settings and will thereby contribute towards answering RQ3 above. Meeting of the Project Advisory Group and the User Guidance Group. Towards the end of this phase an internal briefing paper will be written to clearly articulate the conceptual framework and methodological approach guiding the project.
Phase 2 (Jan–Jun 2011): Expert Interviews (N = 30–40) The purpose of Phase 2 is threefold (i) to gain, from a broad range of perspectives, insights into the key characteristics (relating particularly to the research evidence base, the PCT commissioning context, and the wider socio-political setting) that facilitate or hamper progress towards evidence utilisation in pursuit of reduced ethnic health inequalities, and thereby contribute to answering RQs 1 and 3 above; (ii) to document elements of good practice that have been developed during the PCT commissioning period that are valuable to preserve and promote as we move forward into new commissioning structures; and (iii) to inform the shape and focus of the Phase 3 case studies. Expert, in-depth interviews are well-suited to gaining insights into the structure and functioning of particular, complex environments (Berndtson et al. , 2007) and recent studies have confirmed the usefulness of gaining expert opinion regarding the research–practice interface in relation to health inequalities (Lavis et al., 2008). An initial sample of 10–15 respondents will be identified through professional networks and contacts including those of our Project Advisory Group and the CLAHRC initiative. Subsequently, a modified snowball approach will be used in which respondents will be asked to recommend individuals who can offer particular perspectives. The main inclusion criteria will be that respondents are able to provide a detailed perspective on the evidence–practice interface within healthcare policy making. Different respondents will have differing expertise, but we will seek to recruit respondents who can provide rich description of: the PCT and newly evolving commissioning environment; the ethnic diversity and equality agenda; the research evidence base, its quality, accessibility and utility; and PPI. Respondents are likely to include: PCT managers involved in commissioning; managers within central DH directorates; Leads for specific relevant initiatives (such as DRE and Race for Health); clinicians actively involved in PBC; academics (particularly those involved with KT initiatives); SHA staff with a diversity and equality remit; and third sector stakeholder representatives (such as King’s Fund, Race Equality Foundation and local BME networks). Respondents will also be mixed in terms of their seniority, gender and ethnicity. Respondents will be contacted by email and, if necessary, by follow-up phone call. Following full consent, respondents will be asked to complete a short online questionnaire to capture background information. Respondents will then be invited to participate in a loosely structured interview either face-to-face or by telephone at their convenience. The interview guide (which will need to be prepared prior to ethics approval) will be piloted and refined prior to the first interview and this will ensure that the main topics of interest are covered while not rigidly determining the direction of the interview. Interviewees will be asked to comment on the role of research evidence alongside other forms of knowledge within the commissioning cycle and specifically in relation to tackling ethnic inequalities in health; factors that support or inhibit research evidence utilisation in this area; ways of supporting better use and examples of good practice; and issues that are poorly understood and would warrant further attention.
In addition to the Key Informant interviews, a small number (4–6) of ‘mini case studies’ will also be completed in Phase 2 with the intention of capturing information about instances of ‘good practice’ in relation to commissioning specific services for multiethnic populations. The rationale for these is that at a time of major restructuring of commissioning infrastructure there is a danger that elements of innovation and effective working in this area may be lost. Potential case studies will be identified through professional networks, and we anticipate a mix of local case studies (Sheffield/Leeds/Bradford) and some further afield. For each mini case study we will interview 2–3 key actors, either individually or as a group, and also review relevant documentation. Case study respondents will be asked to contribute general information similar to that sought from the Key Informants, but will also provide information specific to their own field of practice, describing how they have addressed the issue of commissioning for a multiethnic population, how various types of information have been brought to bear on this task, and the barriers and facilitators to the use of evidence, as well as other factors that may have supported or hindered an explicit focus on ethnic diversity and inequality.
Subject to consent, interviews will be tape-recorded. Interviews will be transcribed in full and soon after the interviews researchers will prepare detailed, holistic memos to record observations on the interview process as well as capture overarching themes. Ongoing reflection and aggregation of the interview memos will allow the research team to identify when data saturation is achieved. We anticipate 30–40 interviews, conducted by the Researcher, SS, GM and PCT co-researchers. Following completion and transcription of around 20 interviews, the Researcher (with support from SS) will establish a project database using the qualitative analysis package Nvivo which is ideal for managing large quantities of qualitative material and coordinating analysis across teams of researchers. Data analysis will follow an inductive, interpretive approach combining holistic, contextual analysis and indexing (Mason, 2005). In practice this means that interview transcripts will be subjected to both line-by-line coding and holistic ‘narrative’ analysis. The coding scheme will be developed for use through an iterative process involving line-by-line blind coding of a sub-sample of transcripts by several members of the research team, comparison, refinement and annotation. Once finalised, the coding structure will then be applied to all the interview transcripts and, through multiple ‘search-and-retrieve’ actions, information from across the range of respondents will be brought together for further theme building. This ‘code and compile’ approach will be complemented by the detailed memo writing for each interview which will use a consistent guideline in which themes running through each narrative, contextual information, and more interpretive comments (for instance regarding inconsistency or obvious omissions) will be noted. The Researcher and SS will lead the development of the analysis approach, but will work closely with GM and the PCT co-researchers to co-produce the final presentation of themes and claims. The findings from this phase of the study will be written up as a journal paper and a shorter briefing note. An internal project workshop involving all co-applicants will also be held to discuss the findings and identify key issues for shaping the case studies.
Phase 3 (Jul 2011–Mar 2012): In-depth Case Studies of 3 commissioning organisations serving Leeds, Sheffield and Bradford. Involving a minimum of: 36 in-depth individual interviews; 15 focus group discussions; 60 naturalistic observation periods; 45 documentary analyses across the three sites combined.
In contrast to some case study designs, we have not selected our case study sites to be exemplars of good practice in terms of research utilisation. Given the emergent nature of commissioning practices, particularly in relation to ethnic diversity and equality issues, such an approach would not be feasible or appropriate. Instead, we have selected our sites with the intention of providing sufficient variation to be able to compare and contrast commonalities and differences and thereby gain analytical purchase, but also to engender cross-fertilisation of ideas and mutual learning across the sites.
We have therefore opted for a regional focus and within this to include three PCTs and related commissioning organisations that – by virtue of serving populations with diverse ethnic profiles and having distinct organisational approaches – offer sufficient variety to support the generation of findings that will have transferability to a wide range of commissioning settings. Bradford, with its history of immigration from the Indian sub-continent, has long recognised itself as a multiethnic city and 24% of its population identified as belonging to an ethnic group other than the majority White British in the 2001 census. In contrast, Sheffield and Leeds had much smaller minority ethnic populations at the 2001 census – around 10% – and their public services have only more recently engaged seriously with the needs of these communities. Despite this, Sheffield is home to some long-established minority ethnic groups, including the Yemeni and Somali communities, and the Leeds population includes significant concentrations of Pakistani and Indian groups as well as smaller minorities such as Turkish and gypsies and travellers with particular unmet health needs. All three cities have experienced high levels of in-migration in recent years and now have both well-established and newer minority communities, with the pace of ethnic diversification being particularly marked in Sheffield. The choice of case study sites also offers the potential for exploring issues related to commissioning services for individuals and groups with varied migration statuses, socioeconomic resources and health profiles.
Importantly, all three PCTs have engaged in significant recent work related to achieving World Class Commissioning and to meeting the needs of black and minority ethnic groups, so that the current study has pertinence. NHS Sheffield has recently undergone a knowledge management review and is currently examining the ways in which qualitative evidence, and particularly patient experience data, can be effectively integrated with other forms of evidence. In addition, a recent Audit Commission review of health inequalities progress has prompted new work on BME populations. Both Leeds and Bradford & Airedale are members of Race for Health. Relevant initiatives in Leeds include the commissioning of community development workers through third sector organisations with a specific remit to consult with BME communities to feed knowledge into the commissioning cycle. In Bradford a number of commissioning areas are currently under review from an E&D perspective and there are several examples of innovative service design and delivery to meet minority ethnic needs. Not surprisingly, there are important differences in emphasis and approach between the three PCTs and related commissioning organisations in relation to issues of ethnic diversity and equality and these will ensure that a range of minority ethnic communities and related concerns will be explored during the case study work. For instance, it is likely that in Leeds some attention will be given to gypsies and travellers since this is a current focus, in Sheffield economic migrants and the Somali community are potential ‘groups’ of focus, while in Bradford we would aim to explore issues relating both to the well-established and very large Pakistani community as well as to a smaller, newer community.
Over a nine month period, the research team will work intensively across the three sites employing a range of methods. During the course of the case studies, the PCT co-researchers will act as Key Informants for their organisational contexts, playing the combined role of guide, assistant, interpreter and historian (Burgess, 1985). It is important to note that, in line with our Integrated KT approach, the details of data generation will be developed in consultation with stakeholders in each city and that the draft description below is based on preliminary discussions regarding what would be feasible and effective at generating the required data.
Given the current uncertainty regarding the shape of commissioning organisations of the future, we can not specify precisely what the case study units will consist of at this time. However, our intention is to focus on organisational units that are likely to have longevity so that study findings are perceived to be meaningful for commissioners as they move forward with work within the emerging structures. In each commissioning organisation, data generation will focus at two levels, using Black’s (2001) typology these are: [I] ‘Governance policy-making’, that is, the strategic, agenda-setting level, and [II] ‘Administrative policy-making’, that is the operational level, at which two focused areas will be identified for each organisation. The operational commissioning areas of focus (which may be defined by disease or service/care pathway) will be selected in consultation with stakeholders since it will be important to produce findings that are pertinent and timely. These are likely to be areas identified within existing commissioning plans as in need of service improvement, extension or redesign. However, priority will be given to areas for which the research evidence base is relatively rich in relation to minority ethnic needs and effective service interventions (e.g. diabetes, mental health). We will also seek diversity in terms of how the commissioning teams are constituted, and in particular the role that different directorates, including public health, play within these teams.
In each commissioning organisation, for both level [I] – agenda-setting and [II] – operational commissioning, data generation will begin with a comprehensive mapping of people, processes and partners (including identification of the timeline and cycle of activities and stakeholder analysis); essential given the diverse and evolving structures. Exploration at both levels will also include in each organisation: participatory workshops, documentary analysis, focus group discussions, in-depth follow-up work with 2–3 key managers (sequential interviews and naturalistic observation) and consultation exercises with BME forum/user groups.
We anticipate using participatory workshops early on during the case studies to gain a broad understanding of prevailing practices and competencies within teams and the organisations. These will employ prompting techniques that integrate and extend diagnostic tools developed for assessing research capacity (e.g. ARC for CLAHRC, Sarre & Cooke, 2009) and race equality or cultural competence (e.g. Mir 2008; Department of Health 2004; Dreaschlin, 1999; CRE’s SHA Race Equality Performance Framework, 2004). These will generate data that will begin to address RQ1 and 2 above, particularly relating to commissioning teams and organisational setting.
Interpretive documentary analysis (Abbott, Shaw and Elston, 2004) will be employed to identify and synthesise key themes from relevant documents. This analytical approach will enable us to identify different layers of explicit and implicit meaning. The identification and selection of relevant documents will be guided by the PCT co-researchers and other managers/commissioners. At the ‘governance/agenda setting’ level these are likely to include: JSNAs, Commissioning Strategies; Health Inequality Action Plans, Race Equality Strategies, Research & Development Strategies; broad level Equality Impact Assessments, external evaluations, relevant meeting minutes and background briefing documents that trace the origins and evolution of key strategy documents. We will explore: how key issues are framed and what knowledge sources have informed the articulation of these issues; what assumptions exist regarding the desirability or necessity of change and the possible routes of intervention and what knowledge(s) have informed these; who are the key stakeholders and what knowledge(s) they bring. At the operational level, we anticipate looking for signs that ethnic diversity and equality issues have been considered at a general level (e.g. do service specifications include interpretation/language support requirements, is monitoring data to be collected by ethnic group, are expected outcomes clearly specified with respect to ethnicity?) as well as in more specific ways (e.g. do service specifications stipulate particular models of care that have been shown to be more effective than standard approaches for minority ethnic populations?). Where these are evident, investigation will seek to explore the prompts to such inclusion and the possible role of different types of knowledge. Where these are not evident, investigation will focus on the reasons for absence. Templates will be designed to guide document review, though these will not be rigidly prescriptive. Documentary analysis will be carried out side-by-side with the interviews and group discussions (see below) so that we can develop a detailed understanding of the factors that fed into the production of these documents and subsequently how these documents circulate and impact practice. The documentary analyses will particularly generate data that will address RQ1 and also RQ2 in relation to commissioning teams, organisational setting and wider context.
In-depth follow-up work will take place with 2–3 key managers for the strategy level and each of the operational levels within each commissioning organisation involving sequential interviews and naturalistic observation (shadowing) in order to understand more about the individual factors that shape evidence use in this area. We follow Hunter’s (2005) advice to use reflexive, narrative approaches emphasising dialogue within the research context (since ‘prior and ongoing relationships with professional participants make it difficult and indeed undesirable for researchers to maintain silence’ (p149) in order to access more implicit understandings and discuss sensitive topics that might not easily be articulated within the interview setting. This element of data generation will particularly address RQs 2 and 3 providing rich information relating to individual managers, and commissioning teams as well as enabling refinement of emerging claims relating to the influences of organisational setting and wider context.
Focus group discussions will be held with senior managers and commissioning teams, two each if possible, part-way through each case study period. In addition to open-ended question prompts, a variety of prompting tools may be used including: problem tree exercises, vignettes, and ranking exercises. The design and focus of the group discussions will be informed by ongoing analysis so that they are used purposively to generate data to test emerging claims. These discussions will particularly aim to generate data that address RQ2 in relation to commissioning teams, organisational setting and wider context as well as RQ3.
In addition to the varied data generation activities with NHS managers, group discussions will be held with relevant representatives of BME populations and other stakeholders (e.g. PBC consortia) that have a significant role in the commissioning cycle. These discussions will provide information in support of answering RQ3 particularly in relation to the wider context and how this can help or hinder individual and organisational change.
Producing an integrated analysis of rich data generated through these diverse methods is clearly challenging both practically and theoretically. SS and GM, who will be closely involved in data generation across all three case studies, are both experienced in handling large quantities of qualitative data, as are KG and SN who will contribute to this stage of the study. The research team will use Nvivo to systematically organise and index materials from each of the data generation methods described above. As with Phase 2, analysis will combine ‘code and retrieve’ approaches across the data sources with holistic memo writing for each data source. Reflective journals will also be kept using a standard format by SS, GM, the Researcher and PCT Co-researchers. Regular analysis sessions will engage researchers and PCT managers in the inductive and interpretive identification and testing of emerging themes and ensure the ongoing iterative co-production of knowledge that is both credible and relevant to the end-users. Visual and diagrammatic methods of organising data will be used alongside text-based methods (e.g. using software Inspiration) and the generation and refinement of theory will be carefully documented to ensure transparent links between data and claims. In line with the theoretical model described above, the overarching approach to the analyses is informed by critical ethnographic perspectives in that we attempt to synthesise the traditional ethnographic focus on subjective meanings and beliefs of respondents with the insights gained from a broader structural analysis (Wainwright, 1997). While we give a central place to the ways in which managers describe their commissioning roles and their experiences of working within their organisations, we consider that such accounts require situating within an understanding of the broader socio-political structures that constrain and direct the behaviours of individual actors. In this way our approach can be seen to be ‘grounded’ in the emic perspectives of our respondents, but also guided by the theoretical perspectives outlined above.
Analysis of case study material from each site will first be conducted at a ‘within-case’ level. The focus will be on integrating, and triangulating, data across the domains of analysis (evidence, individual, team, organisation and wider context) in order to holistically describe the factors that shape evidence utilisation and to identify promising routes of intervention in support of more effective evidence use. Analysis approaches will include ‘process-tracing’ whereby data are integrated across sources to elucidate intervening processes and the exploration of implicit and explicit ‘predictions’ that should be observed if emerging claims are defensible. As Mahoney (2007) argues, detailed case studies of this type can provide substantial leverage for causal inference and, by virtue of developing rich contextualized knowledge, decrease the likelihood of overlooking key variables or mis-specifying the interrelations among factors of interest. Each case study will result in an internal project paper that will inform the development of the draft managerial/organisational tools, as well as feed into the cross-case analysis (see below). Tools development will begin towards the end of case study 1 and be ongoing throughout the case study period and into Phase 4.
When descriptions and explanations are complete for the within-case analyses we will move on to cross-case analysis, that is, the systematic comparison across the three sites to identify relational and substantive patterns. Such cross-case analysis is appropriate since the project aims to generate theory, and also practical tools, that can have applicability to a wider universe of commissioning contexts. While recognising the need for caution regarding the potential limits to extrapolation beyond the case study sites, we concur with Mahoney (2007) that good quality case study work can provide a strong position from which to make suggestions about the kind of modifications that might be necessary to extend causal theories to other settings. Initial cross-case analysis work will be conducted by the Researcher, SS and GM, followed by a participatory workshop including all the co-applicants and other interested managers in order to integrate findings across the settings and shape the form and content of research products including the supportive tools.
Phase 4 (June 2011–July 2012): Tools development, refinement and Testing and Development Workshops
This Phase overlaps with Phase 3 in that as case study work proceeds the team will start to develop potential tools and to seek feedback from respondents. Part way through this phase, SS, GM, the Researcher and the PCT Co-researchers will work together to further develop these supportive tools for use by managers and commissioning organisations, as well as to develop the format and materials for the Testing & Development Workshops. These draft tools and workshop materials will be circulated to all team members for input and will be discussed in Advisory and User Guidance Group meetings.
Three national-level Testing & Development Workshops will be facilitated. These events constitute a further round of data generation, analysis and synthesis, and not merely an opportunity to disseminate findings from the prior phases. The intention of these workshops is to test and further develop the explanatory models emerging from Phases 2 and 3 and to refine the practical, supportive tools in order to take account of stakeholders’ concerns and priorities and to maximise their transferability to a wide range of commissioning contexts. This Phase of the study thereby contributes data towards answering both RQ2 and RQ3 and directly feeds into the refinement of the practical tools that flow from the empirical and theoretical insights generated. Potential participants will be identified via professional networks including: the CLAHRCs, the NHS Institute for Innovation and Improvement and the Public Health Commissioning Network. Participants will be PCT managers involved in commissioning. Each workshop will include around 20 participants and we will seek to recruit diverse sample of participants in terms of the size and geographical location of their organisations, age, seniority, ethnicity and area of expertise. Additional participants will be included from key stakeholder groups that input into commissioning decisions relating to black and minority ethnic health including service user representatives from local LINks. Participants will be expected to have detailed knowledge and experience of the commissioning cycle within their organisation. All participants will be expected to complete preparatory work prior to the workshops which will include the completion of a short online questionnaire and a reflexive exercise based on the findings from Phases 2 and 3. This background information will then be drawn on in the workshop exercises. The workshops will be carefully facilitated and comprehensively documented so that the insights from these events can be effectively integrated with the data gathered through the earlier phases. Other recent work has successfully used similar ‘Think Tank’ approaches to generate understanding in the field of KT (Pettigrew et al., 2004).
Phase 5 (overlapping with Phase 4: Mar–Sept 2012): Wider dissemination and follow-on work
Team members will engage in writing for academic publications and delivery of dissemination seminars at stages throughout the project period. In addition, we allocate three months at the end of the project for completion of additional academic outputs and conference attendance (subject to conference timing, of course). Phase 5 will also put in place vehicles for increasing the sustainable impact of the project via the preparation of protocols for the piloting of the supportive tools within CLAHRC (SY) lead by KG and SS and promotion via ETN and other networks.
Collective research effort
Contribution to knowledge
This study begins to build a body of research knowledge about how commissioners and managers respond to the significant unmet health need among minority ethnic communities, and specifically how commissioners can be supported to better use evidence in decision-making. Such research is currently missing from the UK evidence base and from the NIHR SDO programme. The project will make both an empirical and a theoretical contribution, innovatively integrating ideas across usually disparate strands of work.
Specifically, the project will generate new knowledge regarding: how managers source, appraise and integrate different forms of knowledge regarding the needs and entitlements of minority ethnic populations, as well as managers’ potential responses to these demands; how strategic commissioners operate in the face of limited evidence including whether and how they seek to generate evidence or otherwise inform decisions; whether the commissioning of services for minority ethnic needs are disproportionately affected by poor evidence; and how personal attributes, identities and competencies of managers inter-relate with organisational contexts, and the wider socio-political context, in the appraisal and application of different types of knowledge. The project will integrate empirical findings and theoretical insights to identify promising routes of intervention in support of more effective evidence use.
Reaching multiple audiences; maximising reach:
The project will contribute significant outputs in a range of formats aimed at reaching the diverse set of stakeholders with interests in this area. The project will develop a comprehensive website to provide easy access to all project outputs. Team members will be active across the project life in delivering seminars, workshops and sharing work-in-progress to maximise project impact. Wide-ranging networks and complementary disciplinary and professional associations will increase the project’s reach.
Our primary audience is managers at various levels of seniority who contribute to the process of commissioning health services for multi-ethnic populations. Our Integrated KT model is well-suited to the development of research products that are accessible, appropriate and impactful. Preliminary team work has highlighted the need to identify and target not just the end-users of the research products, but the senior managers who shape organisational processes and structures and therefore determine whether or not such innovations are adopted and sustained. Working in partnership, NHS managers and university researchers will identify the key people and processes that need to be targeted in order to effect change; the appropriate language, style and content of research products; and the routes to introduction that are likely to be successful.
The project will also link closely to the NIHR CLAHRCs regionally and nationally, thereby capitalising on opportunities for mutual learning and dissemination. Several team members are associated with CLAHRC work and the present project is borne out of synergistic links with this programme. The project will also make use of relevant networks and organisations including: the Ethnicity Training Network; Minority Ethnic Health jiscmail (large virtual network); and Race for Health. We also intend to link with the NHS Institute for Innovation and Improvement at Warwick University that produces tools and resources to support commissioners and the Public Health Commissioning Network. The Project Advisory Group (see below) will ensure opportunities to enhance the usefulness and relevance of the research, to contribute to the collective research effort and to disseminate effectively to all stakeholders are maximised.
Our secondary audience is the research community, including researchers and the funders of research. The project will highlight the current inadequacies in the evidence base in terms of informing effective commissioning for black and minority ethnic populations. We aim to prompt more researchers to make their research inclusive of, and appropriate to, the health needs of minoritised groups. For researchers already working in the field of ethnic inequalities, the project will increase awareness of the barriers and facilitators to utilisation of research findings in this area. The project will provide a greater appreciation of the focus, content and format of research studies and products that are likely to make an impact; as well as give insights into the factors that might help to build relationships with commissioners that can enhance the contribution of research evidence to tackling ethnic inequalities in health.
Specific research products and outputs:
– A suite of practical diagnostic, evaluative and change management tools that can be used by individual managers, teams and organisations to (i) assess and promote critical reflection on current competencies and practice with respect to mobilisation and utilisation of evidence on ethnic diversity and inequality, (ii) identify actions to strengthen competencies and good practice and (iii) support specific elements of the knowledge utilisation process. We intend to build on existing tools (across knowledge utilisation, organisational development and cultural competence) to develop new products that respond specifically to (i) the emergent commissioning context, and (ii) the complexity and challenges associated with evidence utilisation relating to ethnic diversity and inequality. Without wishing to pre-empt the findings of the study, which we expect to shape both the content and the format of the tools, as well as provide insights as to the key actors and processes that need to be targeted, we provide some indication here of the likely form that these tools may take. The final tool design will also be informed by the wider evidence base on effective intervention to enhance evidence use.
The diagnostic tools are likely to focus on assessing the readiness and capability of individual commissioners and teams to mobilise and critically utilise appropriate evidence relating to ethnic diversity and inequality within the commissioning cycle. These may take the form of text-based checklists or questionnaires linked to a hierarchy of descriptive statements that characterise different ‘levels’ of competence and good practice to which the individual or team might aspire. These tools might use a similar format to that adopted for the ARC for CLAHRC tool (Sarre & Cooke, 2009) or the CRE’s SHA Race Equality Performance Framework (CRE, 2004). We envisage that such tools would be made available for self-directed use by individuals and teams via download from our project website. In addition, however, it may be that a package of materials is developed for use as a facilitated workshop and that this would form part of the Phase 5 piloting activities.
The evaluative and supportive tools are likely to be designed to follow on from the diagnostic tools to allow individuals and teams to identify more clearly those aspects of their competence and current practice that are strengths and should be supported and areas in need of further improvement, while being flexible enough to be applicable to diverse commissioning contexts. We envisage text-based tools that comprise prompting questions and issues for reflection as well as illustrative case stories (derived from our empirical data) that bring to life potential strengths, weaknesses, opportunities and threats that commissioners may face in this area. As in the case of the diagnostic tools, it is likely that the evaluative tools would be prepared in a self-directed format for use by individuals and teams via download from the project website, as well as in the format of a package of materials for use as a facilitated workshop, again likely to be piloted in Phase 5 (which extends beyond the life of this funded project).
These evaluative tools would help individuals and teams identify which of a linked set of supportive learning and development tools they might benefit from (as well as guide engagement with the change management tools mentioned below). Here we envisage the production of a number of tools designed to support commissioners in specific aspects of the knowledge mobilisation and utilisation process as it applies to ethnic diversity and inequality. Possible topics include: sourcing evidence on ethnicity and health; assessing the relevance of research evidence from national sources or other regions to local circumstances; developing an economic argument for investments in equitable services; and working with researchers to generate useful knowledge. The format of the supportive tools is likely to be web-based and interactive, allowing flexible engagement with the material as-and-when needed. The tools are likely to be made up of ‘nuggets’ of learning points tailored towards the realities of the commissioning cycle (perhaps similar in form to the ‘evidence nuggets’ found effective by Brocklehurst and Liabo 2004), self-assessment tests that allow users to assess their own understanding and competence, and guidance checklists to remind commissioners of key points during their working day. In this way, these tools may be similar to the ‘intervention packages’ described by Nieva et al. (2005). Topics will be prioritised to address those issues identified through the study as presenting the greatest impediments to evidence mobilisation and utilisation.
The change management tools will seek to support managers in bringing about the necessary shifts in thinking and behaviour to embed new practices that enhance the critical mobilisation and utilisation of research evidence relating to ethnic diversity and inequality within the commissioning cycle. We expect our empirical work to generate substantial insight into the factors at organisational setting and wider context level that can support or hinder the routine best use of research evidence in this area and anticipate using this material to generate hypothetical scenarios that illustrate the issues that can arise and effective ways to negotiate them, similar to those presented by Iles and Cranfield (2004). It is likely that such scenarios would be combined with prompting questions, templates and checklists that would enable managers to develop and deliver an action plan aimed at enhancing the critical use of evidence within the commissioning of services for multiethnic populations. Again, we envisage that such tools will be produced in the form of a web-based self-directed analysis and planning resource, but that in addition we would produce materials for facilitated workshops and possibly learning set activities, since the process of change is likely to extend over a period of several months. Careful consideration will be given to the form of these tools, how these tools are administered, and who they seek to engage with. These issues will be explored during Phase 4 (as well as with our Project Advisory Group) and may result in the development of networks of individuals across the country who are working, and mutually supporting, shifts in commissioning practice in this area.
Depending on the findings from Phase 4, it may be that we aim to consolidate all the materials into a comprehensive tool-kit that would guide managers through the diagnostic, evaluative and change management stages in an integrated way. Alternatively, a more flexible set of tools may be warranted that is more responsive to the differing starting points of individuals and teams who may wish to engage with the materials.
– Briefing Papers for NHS managers. University researchers will work in close collaboration with the NHS co-researchers to produce a series of Briefing Papers to disseminate the newly generated knowledge to peers regionally and nationally. These will be carefully designed and may be modelled on ‘evidence nuggets’ (Brocklehurst and Liabo, 2004).
– High quality, peer-reviewed journal articles. We expect to publish at least 5 papers in high quality journals, including open access journals, across public health; management science; implementation science; sociology; and health services research. All co-applicants will contribute to these outputs.
– Seminars and conference presentations. SS, GM, the Researcher and PCT Co-researchers will all engage in dissemination of work-in-progress during the life of the project, seeking opportunities regionally and nationally to engage with researchers and PCT research users. In addition, we have budgeted for attendance at two national conferences towards the end of the project. We anticipate presenting at the UKPHA conference, but, given the likelihood of new, NHS commissioning-focused conferences, we will decide on the most appropriate forums for our work in light of the available opportunities at the time. KG is a member of the International Knowledge Utilisation Colloquium and will take the opportunity to present findings from the study at annual meetings of this influential group.
Follow-on work – extending project impact:
CLAHRC (SY): The managerial and organisational tools developed by the project will subsequently be piloted in the NIHR CLAHRC South Yorkshire as follow on activity supported by existing funding from the CLAHRC. A total of 4 PCTs, including NHS Sheffield, are partners in the CLAHRC SY. Drawing upon the joint expertise of CLAHRC SY implementation themes on knowledge translation (lead KG) and evidence-based commissioning (lead MW) research products will be trialled and evaluated with strategic commissioners and managers from these PCTs. After piloting, the research products will be shared more widely across the other 8 NIHR CLAHRCs. KG as implementation lead for the SY CLAHRC has excellent links with the implementation leads of the remaining CLAHRCs to support this activity. Workshops will be hosted linked to CLAHRCs located in areas with an ethnically diverse population, for example Manchester, Leeds, Leicester, Birmingham, North London. This activity will be supported by CLAHRC (SY) funds and will occur following completion of the proposed project.
Ethnicity Training Network: ETN will also be an important conduit for the research products. The theoretical and empirical knowledge generated will be used refine the strategies and model of knowledge transfer currently used within ETN’s programme of work. In addition, the ETN will be an important route through which to promote and disseminate study findings and tools through its network of around 2,000 members, many of whom are leads for diversity within NHS settings.
Canadian links: Several team members have ongoing collaborative links with researchers and policy-makers in Canada, including: Gina Higginbottom, Canada Research Chair in Ethnicity & Health, University of Alberta; Zubia Mumtaz, Assistant Professor, School of Public Health, University of Alberta; Carole Estabrooks, Professor and Canada Research Chair in Knowledge Translation, University of Alberta; Jacqueline Tetroe, Senior Advisor Knowledge Translation, Canadian Institutes of Health Research. We would welcome the opportunity to extend the project focus to include comparative work in Canada should this be possible via the SDO programme.
Outcomes:
Tools developed from the study will enhance PCT managers’ and commissioners’ ability to draw on research evidence relating to ethnicity in health decision-making at both strategic and operational levels. Findings will support academics to draw on new knowledge about how to increase the impact of research on ethnic diversity and where to focus their efforts. The study will also equip Local LINks and service users with the knowledge to draw on the existing evidence base in lobbying for improved service provision and for research that fills current gaps in knowledge via the commissioning process.
Approval by ethics committees
Governance approval will be sought from all participating PCTs. The project will need ethics approval from the NHS Research Ethics system for phases 2–4.
Project management
Involving quite a large team engaged in a wide array of activities across several organisations, the project will require strong management structures and a high level of effective communication to be successful. SS will be the project manager and will design and employ formal project planning and management proformas. A wikispace will be established as a repository for all project documents and as a medium for within-team consultation and consultation with the PAG. Brief monthly progress reports will be prepared by SS and the Researcher to indicate progress against clearly identified activities and outcomes and distributed to all team members. More detailed 6-monthly progress reports will be prepared in accordance with SDO reporting requirements. SS, the Researcher, KG, SN and MW will be co-located at Sheffield Hallam University. Weekly contact will be maintained with GM and the PCT Co-researchers across the life of the project. Regular team meetings will bring all co-applicants together at critical junctures and teleconferences will also be used to ensure close communication. All meetings will have clear agendas, objectives and minutes/action points. The project builds on past successful working relationships and we do not anticipate communication or management problems.
Project Advisory Group
A Project Advisory Group including academics, statutory and third sector managers, practitioners and policy-makers will be convened to provide guidance to the study and to ensure that connections are made to other relevant work. Membership will include people with expertise across: knowledge translation; equality and diversity; organisational transformation; PPI and commissioning. The group will meet face-to-face three times at critical junctures in the research cycle. Additional email communication and wikispace posting of material will maintain engagement and input across the project life. The following individuals have expressed interest in being part of this group: Professor Helen Hally, National Director – Race for Health; Dr Mark Exworthy, Reader in Public Management and Policy and Director, Centre for Public Services Organisations (CPSO) and Deputy Director, Institute of Leadership & Management in Health (ILMH), Royal Holloway, London; Dr Peter Aspinall, Reader in Population Health, University of Kent, Research Advisor, NHS National Institute for Health Research: Research Design Service SE and Honorary Special Advisor, London Health Observatory; Dr Ruth Thorlby, Fellow in Health Policy, King’s Fund; Lynda Brooks, National Programme Director, NHS Equality Delivery Team, Workforce Directorate, ‘Everyone Counts’; Judy Carrivick, Health Inequalities Manager (Vulnerable Groups), NHS Leeds; Ronny Flynn, Director of Health and Housing, Race Equality Foundation; Mark Gamsu, Programme Director, Health Inequalities and Local Improvement, Department of Health; Dr. Elizabeth Goyder, Reader in Public Health ScHARR University of Sheffield and Theme Lead for Inequalities Implementation Theme, CLAHRC (SY); Dr Ade Adebajo, Consultant Rheumatologist, Patient and Public Involvement Lead, NIHR CLAHRC South Yorkshire; Professor Christine Godfrey, Head of Department, Department of Health Sciences, University of York and Addictions lead for LYBRA CLAHRC and Professor Uduak Archibong, Professor of Diversity & Director Centre for Inclusion and Diversity, University of Bradford.
Service users/public involvement
The project’s approach is underpinned by the belief that the active involvement of service users and the public is central to the endeavour of conducting high quality research that has the potential to contribute to positive change. The project team members have extensive experience of user involvement in research and strong links with user-groups. Sheffield Hallam University is a leading institution in the field of user involvement in research and service design (http://research.shu.ac.uk/chscr/user-involvement/) with strong links to INVOLVE. Preparatory work for this proposal has included consultation with individuals and groups representing the needs of black and minority ethnic communities and confirmed the appropriateness of a two-pronged approach:
First, we will convene a User Guidance Group that will meet three times during the course of the project to provide advice on the direction of the study and to offer user perspectives on the emerging findings. Provision is made within the budget to ensure meaningful contribution from all participants including: interpreting facilities for non-English speakers; honoraria; travel and carer expenses; and appropriate venues and formats for events. The group will include individual service users and members of the public as well as representatives of the LINk organisations and BME-focused patient/user groups in Sheffield, Leeds and Bradford. The following organisations and individuals have expressed interest in being part of this group: Melvyn Newton, Project manager, Bradford LINk; Jim Kerr, Leeds LINk Equality & Diversity Group; Jon Beech, Co-ordinator Community Development & East Leeds Health For All, Touchstone, Leeds; Hardeep Pabla, Service Manager, Breakthrough – f.k.a. Sheffield Black Drugs Service and Sheffield BME Network; Mike Smith, Chair, Sheffield LINk; Blake Williamson, Governing Board member, Sheffield LINk; Mubarak Ismail, Governing Board member, Sheffield LINk.
Second, the case studies will each include three open-ended group discussions with service users and representatives from minority ethnic communities. Again, there will be provision for non-English speakers and events will be organised with guidance from local people to ensure effective and meaningful participation.
Expertise and justification of support required
Sarah Salway will be the project manager, coordinating the inputs of all team members (including a full time researcher) and liaising with project partners. She will also provide overall academic direction, integrating the specialist inputs from other team members into the project design and implementation. SS will engage closely in data collection, analysis and translation activities. With a background in sociology and public health SS has been CI on numerous large research projects and is an experienced project manager. SS has extensive experience in conducting qualitative research and has previously used all of the methods to be employed in the current project. Recent relevant work includes: organisational analysis and community consultation to enhance the cultural competence of South Yorkshire Eating Disorder Association’s service offer; Research capacity development (commissioning, conduct and application) in the area of ethnicity and health for NHS Sheffield; and work on the scientific and ethical rigour of public policy-relevant research into race/ethnicity (funded by the Joseph Rowntree Foundation). The project builds on past collaborative work with NHS Sheffield and NHS Bradford & Airedale and links to her role within the CLAHRC (SY) Inequalities Implementation Theme. SS will contribute 40% FTE across the life of the project.
Ghazala Mir will contribute 20% FTE across the life of the project (this translates into 44 days per annum). GM has contributed to the study design and will work closely with SS over the course of the project. During Phase 2 GM will support recruitment and data collection for expert interviews and work with the Researcher and SS to develop the coding scheme for analysing data and to produce the final presentation of themes. She will also contribute to a journal paper and briefing note from this phase and to the internal project workshop to identify key issues for shaping case studies. In Phase 3 she will lead the in-depth Case Study on NHS Leeds and ensure a comprehensive mapping of people, processes and partners. She will organise and work with others to facilitate participatory workshops, documentary analysis, focus group discussions, in-depth follow-up work with 2–3 key managers (sequential interviews and naturalistic observation) and consultation exercises with BME forum/user groups. She will work with SS and other members of the research team to analyse data from this phase and contribute a reflective journal and further data from regular analysis sessions with co-researchers/PCT managers. She will support SS and the Researcher to carry out cross-case analysis work to integrate findings across the settings. In Phases 3 and 4 she will help shape the form and content of research products including the supportive tools and the protocols and workshops for testing and further developing these.
Kate Gerrish will contribute 5% FTE (11 days per annum) across the project period, providing ongoing support to the operationalisation of the Integrated KT approach and to the links between the project and the CLAHRCs across the country. KG’s focused input (with estimated days) in year one will relate to: ethics/governance (1); team building workshop (1); interview guide development (1); analysis workshop for key informant interviews (1); conceptual paper (1); design of case study methods (2); case study data collection (2); analysis of case study data (2); and in year 2 will relate to: case study data collection (2); analysis of case study data (2); design and orchestration of the Phase 4 Testing and Development workshops (5); tools development (2).
Susan Nancarrow will contribute 5% FTE across the project period (11 days per annum). SN will provide specialist input on university–NHS partnership working and translating research findings relating to professional and organisational practices into effective tools to enhance performance. SN’s focused input (with estimated days) in year one will relate to: team building workshop (1); team building visits (2); analysis workshop for key informant interviews (1); conceptual paper (1); design of case study methods (2); case study data collection (2); analysis of case study data (2) ; and in year 2 will relate to: case study data collection (2); analysis of case study data (2); tools development (5); Phase 4 Testing and Development workshops (2).
Malcolm Whitfield will contribute 2% FTE (4–5 days per annum). MW brings specialist knowledge of the PCT commissioning and management context and in his role as non-Executive director of NHS Sheffield and Board of Sheffield First Partnership for Health & Wellbeing he will champion the project and identify opportunities for effective translation of study findings. MW’s focused input (with estimated days) in year one will relate to: team building workshop (1); key informant identification (0.5); key informant interview guide development (0.5); analysis workshop for key informant interviews (1) design of case study methods (2); and in year 2 will relate to: case study analysis (1); tools development (2); Phase 4 Testing and Development workshops (2).
George Ellison will contribute 2% FTE (4–5 days per annum). GE will provide specialist input on: the generation and application of research evidence relating to ethnic diversity; critical appraisal and synthesis skills; and developing supportive tools for managers. GE’s focused input (with estimated days) in year one will relate to: team building workshop (1); key informant identification (0.5); conceptual paper (1); analysis workshop for key informant interviews (1); design of case study methods (1.5); and in year 2 will relate to: tools development (4); Phase 4 Testing and Development workshops (1).
Note: All the academic partners will contribute time to the production of academic journal articles and conference presentations over-and-above the time budgeted in the proposal since this is considered to be part of their core academic activity.
John Skinner, Lynne Carter and a Sharon Moore will each play the role of co-researcher and facilitator within each PCT. These individuals will contribute 10% FTE (22 days per annum) and be closely involved in all phases of the project, but will play a particular role in designing and conducting the case study within their own organisation and in facilitating mutual learning across the organisations. These individuals will contribute the design of the practical tools and also to the production of the briefing papers for NHS managers.
Ali Jan Haider, Jeremy Wight and Jane Westmoreland are not costed within the budget but will champion the project within their own organisations ensuring that case study work can proceed smoothly and that opportunities for translating study findings into action are maximised. AH will facilitate the contribution of NHS B&A and provide specialist input on partnership working. JW will facilitate the contribution of NHS Sheffield and provide specialist input on the public health contribution to commissioning. JM will facilitate the contribution of NHS Leeds. We have not included costs for the time of these senior managers in the budget since they each consider support to the project to fall within their wider, senior leadership roles.
Researcher: A suitably skilled and experienced post-doctoral researcher will be recruited to work 100% FTE on the project under the guidance and mentoring of Sarah Salway. This researcher will be involved in all stages of the design and implementation of the study and will undertake a large portion of the data generation and analysis alongside SS, GM and the PCT co-researchers. The researcher will be involved in all project outputs.
Non-staff costs are kept to a minimum.
We request costs for rail travel and limited overnight stays where this is efficient for the research team associated with conducting the expert interviews and case studies. We also request travel costs for advisory and user group meetings and for participants at the testing and development workshops (Phase 4). We cost attendance for 2 people each at 2 national conferences as part of our dissemination strategy. We identify the UKPHA conference but will identify the other conference depending on what is available during the second year of the project since there are several relevant ad hoc conferences being convened each year. In all cases team members will book train travel in advance so that fares are cheaper.
The project will largely be supported by the equipment already available to the university and PCT co-applicants. We request 4 digital recorders – one each for the PCT co-researchers and one for the fulltime researcher – for the recording of interviews and group discussions, as well as observational oral note-taking during the case studies. SS and GM already have digital recorders at their disposal and the appropriate software for downloading recorded material. Data analysis software (Inspiration and Nvivo) is not requested as this is already available at SHU.
We request modest costs for refreshments for the advisory and user group meetings and for the Phase 4 testing and development workshops. Room costs are not requested and we will seek to use university or PCT premises free of charge.
Transcription and translation costs (for the BME user group discussions) are included for Phases 2 and 3 on the basis of past experience of realistic costs for high quality work.
We cost 50 hours of support from a web-designer at £40 per hour to enable the design and maintenance of both an external facing website and an internal wikispace for project communication.
To enable rapid access to project findings we include the costs of publishing two papers in BioMed Central open-access journals.
In accordance with INVOLVE guidelines we cost a £50 per person per half-day meeting as honorarium for involvement in User Guidance Group meetings.
Plan of investigation and timeline
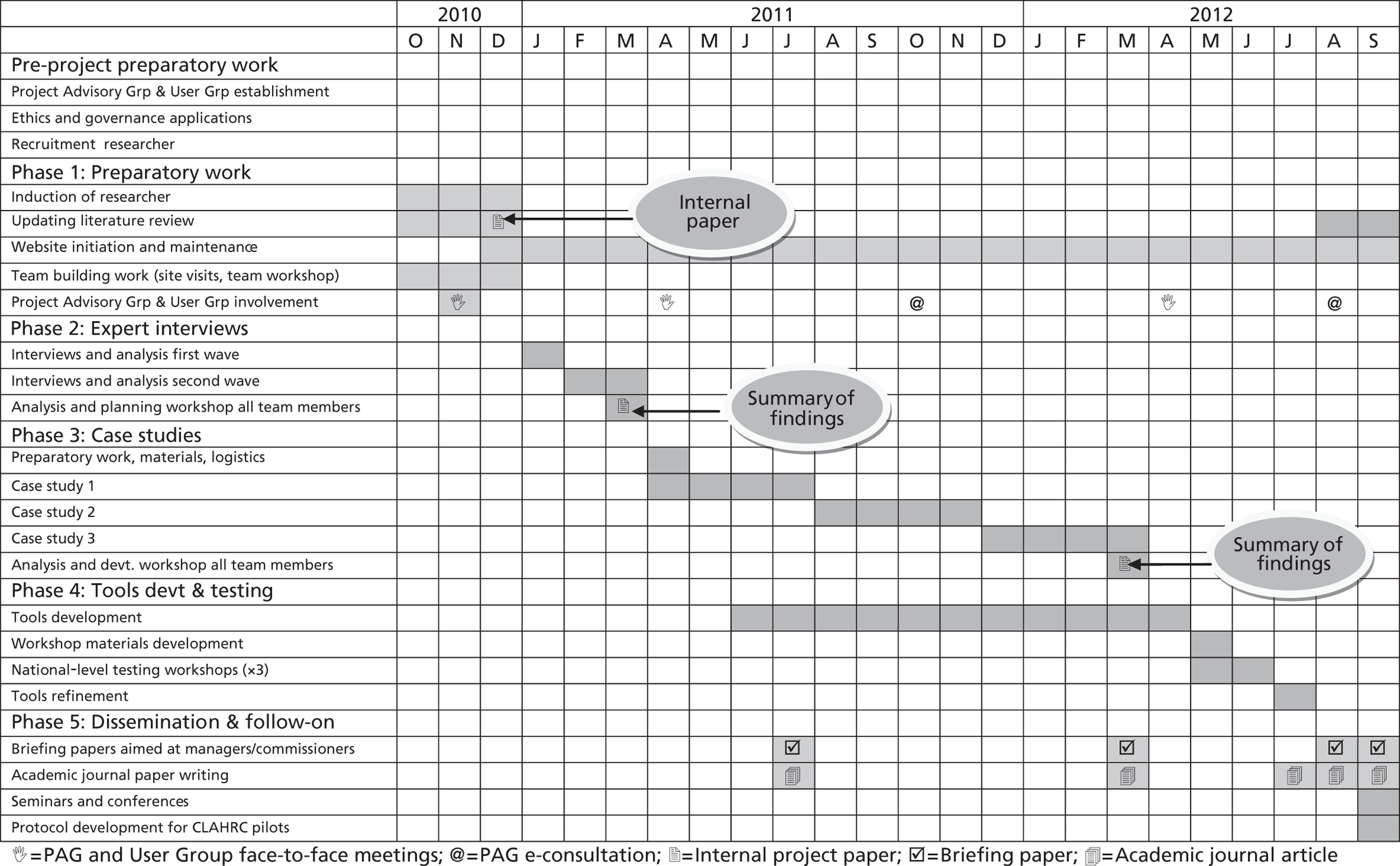
Appendix 2 Selected research tools
List of abbreviations
- A&E
- accident and emergency
- BME
- black and minority ethnic
- CCG
- clinical commissioning group
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- CQUIN
- Commissioning for Quality and Innovation
- CRE
- Commission for Racial Equality
- CSU
- commissioning support unit
- DH
- Department of Health
- E&D
- equality and diversity
- GP
- general practitioner
- HWBB
- health and well-being board
- JSNA
- joint strategic needs assessment
- KPI
- key performance indicator
- NHS CB
- NHS Commissioning Board
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- PCT
- primary care trust
- QIPP
- Quality, Innovation, Productivity and Prevention
- QOF
- Quality and Outcomes Framework
- WCC
- world-class commissioning