
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1002/29. The contractual start date was in September 2010. The final report began editorial review in March 2013 and was accepted for publication in September 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Bresnen et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background to the research
Understanding how managers in the NHS access and use management knowledge to help improve organisational processes and so promote better service delivery is of pressing importance in health-care research. 1–3 Given the expectations we have of managers in the NHS to improve performance in the face of constant pressures for change, and the grave consequences of poor management,4 it is important to know that managers are at the leading edge of thinking in management theory and research. For this, it is key to understand how managers access ideas that can improve health-care delivery and are able to translate these effectively into a health-care setting.
Yet, despite a good deal of research that has begun to look in-depth at how managers in the NHS perform their roles, we have only limited understanding of how managers access management knowledge, how they interpret it and how they adapt and apply it in their own health-care settings. 5 There is also very little research that has tried to understand how the use of management knowledge relates to managers’ individual learning and development, how this ties in with their own development as ‘professional’ managers among different communities across the NHS. 6,7 Similarly, we know relatively little about how the organisational setting itself influences the ways in which managers access, make sense of, select, adapt and apply relevant management knowledge. 8
This research sets out to fill these gaps by exploring how middle managers in the NHS access knowledge and learning from various sources to apply, develop and improve management practice. In doing so, it recognises that there are different groups within management that have their own needs and perspectives and that draw upon different types of management knowledge (e.g. operational, financial), that management knowledge itself is often the subject of considerable debate (particularly when transferred from different contexts, such as manufacturing industry) and that managers are part of wider communities and networks of practice (NoPs) within the NHS and beyond that influence approaches to professional training and development.
Aims and objectives
The aim of the research is to investigate how NHS middle managers encounter and apply management knowledge and to examine the factors [particularly organisational context, career background and NoPs/communities of practice (CoPs)] that facilitate or impede the acceptance of new management knowledge and its integration with practice in health-care settings. Following on from this are three specific objectives:
-
to establish how occupational background and career influence knowledge receptivity, knowledge sharing and learning among health-care managers
-
to examine how relevant CoPs enable or obstruct knowledge sharing and learning
-
to ascertain which mechanisms are effective in supporting knowledge receptivity, knowledge sharing and learning/unlearning within and across such communities.
The research therefore emphasises the importance of understanding flows of management knowledge and learning as heavily influenced by the social and organisational context within which managers and their work are embedded. 8,9 These contextual influences – namely, their background and career development, the organisational settings in which managers operate, and the networks and communities to which they belong – are expected to have an important effect on the ways in which managers access and use management knowledge and how they apply it to their management practices.
Research context
Managerial capacity development is considered integral to the UK government’s strategy for implementing programmatic change connected to public service modernisation,10 particularly within the modern NHS. Reform in the NHS has closely reflected some broader trends in the private economy as market-based and performance management incentives have been introduced and competition has increased. 11 The emergence of new public management in public sector restructuring has led to changing demands on the managerial workforce. 6,7,12,13 Findings from such studies have been echoed in recent NHS research that has reported huge growth in the complexity of managers’ work owing to increased outsourcing and the need to deal with outside organisations, privatised hotel and cleaning services, private hospitals and private finance initiative companies. 14–16 At the same time, the devolution of authority and the flattening of hierarchies has given managers wider spans of control and broader responsibilities. 17–19
Coping with, and excelling within, these conditions requires the capacity of health-care managers to engage with, interpret, adapt and support the implementation of innovations and other advances in research. 20,21 Improving this capacity relies then on a clear understanding of the dynamics of knowledge flow at an individual and collective level and the social, political and professional landscape within which knowledge flows associated with management learning take place.
There has been, in the last decade, a renewed interest in how health-care organisations manage or mobilise knowledge, reflected in active debates on evidence-based medicine and evidence-based management. 1,22 This research has been given some impetus by studies such as the Cooksey review of publicly funded research into health care in 2006, which identified substantial ‘cultural, institutional and financial barriers to translating research into practice’ (p. 4, © Crown copyright 2006, A Review of UK Health Research Funding). 2 While a significant amount of research has been conducted into policy-makers and their relationship with new clinical and medical innovations,3,21 there is a pressing need for more research into the uptake of management research and innovative practice by NHS health-care managers and how this relates to their professional development as managers. 4 Moreover, there is a need to understand better how managers access and use knowledge in the context of wider NoPs and CoPs that operate at a more meso level and which are associated with the existence of relevant professional and personal networks. These not only provide access to different sources and types of knowledge and learning, but also help shape how managers make sense of and apply that knowledge and learning to the health-care context. 23,24
Locating health-care management
To identify these knowledge and learning processes accurately, there is a need to unpack further the notion of middle management. This is particularly so in the health-care sector, given the diversity of operational and functional groups and roles found within the NHS as well as the diversity of routes into NHS management.
Middle managers are traditionally a difficult cadre to define, as boundaries between levels of hierarchy in contemporary organisations are frequently unclear and demarcation is often ambiguous. 19,25,26 For the purposes of this study, middle managers were defined inductively as ‘people identified as such within the organisation, provided that they were part of a clear chain of management and involved in the delivery of an end service, being responsible for at least two subordinate levels within the hierarchy, and with at least one superior between them and the organisational executive.’ (p. 639). 25 This approach allows for a more contextualised understanding of the exact location and nature of middle management in the organisations studied, in contrast with an alternative approach that may tend to impose a more abstract definition on the data from the outset.
This definition also enabled us to attempt to encapsulate a broad range of health-care managers, with diverse professional, clinical and/or managerial experience and training, different career trajectories and varied managerial roles and responsibilities. It also enabled us to explore the distributed nature of management in health care27 as well as focus in on the levels at which conceptions of management and leadership may intertwine. 28 While it is important to somehow capture systematically such diversity, at the same time it is important to be able to pragmatically differentiate between distinct managerial cohorts for study. As will be explored in Chapter 2 , to do this we developed an initial taxonomy of management cohorts within the NHS that provided us with a framework for capturing and categorising the diversity of NHS middle managers that we could then refine more inductively as we moved into the empirical stages of the research.
Given the diversity within middle management, there is a need to understand not only the distinct perspectives on knowledge and practice that these differences may give rise to, but also the ways in which contextual factors and practices at an organisational level may combine to impact on orientations towards management knowledge within the managerial cadre.
To understand the flow, translation and utilisation of managerial knowledge into practice in the NHS, we adopted an approach that was sensitive not only to the complexities (and contested nature) of that managerial knowledge base itself, but also to the socially constituted and situated nature of knowledge and learning. That is, the research approach paid particular attention to the ways in which the translation of managerial knowledge into practice is strongly influenced by that particular context. 29–31
For example, while the provision of bespoke management training through the nationally provided NHS Graduate Management Training Scheme (GMTS) provides some collective socialisation for NHS managers, previous educational and employment history, foundational professional affiliations and function-specific training programmes promote quite substantial differences in the orientation towards knowledge of NHS managers. 21,32 Furthermore, such differences in interest and perspective highlight the potential importance of power relations as they relate to flows of knowledge and learning occurring within and between managerial groups. 33–35 As the managerial knowledge base is continually contested and debated,4,36 it becomes important to recognise that the acquisition and use of such knowledge to effect change is not necessarily neutral in its effect.
Knowledge, networks, community and identity
Research into flows of knowledge and learning through and between groups has evolved significantly in recent years from earlier, more mechanistic models that tended to stress knowledge codification37 and that treated knowledge (including management knowledge) as an object or commodity that could readily be transferred from one setting to another. 38 Advances in this area draw inspiration instead from understandings of knowledge flows as socially constructed processes,39 which are inevitably shaped by social and power relations within organisations and across wider communities. 40,41
Of particular value here are the insights generated from the CoPs literature. 42–44 CoPs link individuals and groups with shared interests and professions and provide the networks of social and professional relationships within which information and experiences are shared and, through which, learning and professional identity develop. Lave and Wenger42 refer to the socialisation processes involved in becoming part of a CoP as legitimate peripheral participation and make strong connections between the situated learning that occurs as individuals engage in joint practice and the development of professional identity. Importantly, therefore, CoPs can extend within and/or beyond organisational/functional boundaries to encompass the wider networks of professional relationships within which individuals are embedded. 9 In some cases, of course, these can become formalised and institutionalised in what we would recognise as clearly demarcated professions which are able to achieve occupational closure providing accreditation based on a distinct and accepted body of knowledge. 45
Consequently, understanding how CoPs – whether institutionalised or not – promote knowledge sharing and learning prompts one to seek to understand not only the barriers and enablers of knowledge sharing which reside in organisational cultures and subcultures,35 but also how processes of knowledge sharing, knowledge diffusion and learning occur within wider networks of knowledge and practice and how these processes, in turn, relate to the ongoing development and transformation of managerial and professional practice and identity. 9,46,47
Within the NHS, flows of management knowledge into practice are also inevitably affected by the socialisation associated with induction into, and progression within, the various communities that constitute the managerial cadre. Although a number of researchers have applied practice-based perspectives to explore these distinct epistemic communities in health-care management and their impact on the development or implementation of cross-cutting initiatives,48–50 so far there has been little attempt made to focus on the reproduction of knowledge and transmission of learning through and between the various CoPs found within NHS middle management. Divisions within health-care management that mirror political and epistemic differences between policy makers and various professional communities have been well recorded. 23,32 Yet comparatively little attention has been directed towards exploring how such differences influence processes of knowledge and learning associated with the translation of management knowledge into practice, via distinct patterns of socialisation and learning associated with the immersion of managers in differentiated managerial and professional activity.
The various (cross-cutting) NoPs within which managers are embedded are likely to affect, in complex ways, their knowledge sharing and learning and, through these, their managerial identity and orientations. So, for example, research on the constant interaction between NHS managers and colleagues in various clinical domains frequently highlights significant differences in perspective on the nature of knowledge or evidence informing practice. 1,22 These professional/occupational boundaries, in which two or more professional groups are engaged in joint practice, and the mechanisms used to translate knowledge at such boundaries, have a significant effect on the knowledge base of managers and their ability to influence practice across the organisation, and more widely. 35,46,48,49 Therefore, they constitute important knowledge and learning processes that can only be properly understood by inductively tracing the effects of such cross–cutting NoPs and CoPs on the accessing, appropriation, mobilisation, translation and use of managerial knowledge and how this shapes, and is shaped by, the development of managerial identity. 42,51
Research approach
An emphasis on understanding the effects of context requires an approach that can capture the subtleties of how different groups of managers go about accessing and using management knowledge in their everyday work. Not only does this suggest a very qualitative approach to data collection and analysis (examined further in Chapter 2 ), it also points to the value of a comparative case study approach that allows for the in-depth examination of important similarities and differences between, and within, cases and managerial communities. 52–54
The study examined middle managers within and across three types of NHS trust (located in England). Three trusts were selected to provide quite distinct cases with regard to the diversity of services provided and, consequently, the knowledge requirements faced by managers and the networks likely to be available to them.
To capture differences across managerial groups in each trust, a selection framework was developed in the early stages of the project that was refined as the project developed and which allowed us to differentiate between cohorts of managers that could be selected in each trust on the basis of their managerial and clinical orientation. This framework was used as the basis for the selection of managerial respondents in the main empirical part of the study. The derivation, refinement and application of the model are explained fully in Chapter 2 .
Patient and Public Involvement was not a feature of this study as it concerned and required only interviews and interaction with health-care managers concerning their management responsibilities.
Report structure
The rest of this report is structured as follows.
In Chapter 2 we explain the methodology of the research, outlining the epistemological basis of our approach, the logic behind the choice of case studies and managerial groups for our study and the detailed qualitative research methods that we used to collect, code and analyse the data from interviews and observations.
Chapter 3 sets the scene for the analysis of the data by examining the institutional and organisational context for the research, exploring management within the sector as a whole in a changing institutional context. After that, we drill down into an outline description of each of the three trusts and an assessment of the organisational contexts affecting management, knowledge and learning at each of them.
Chapters 4–6 then constitute the main set of findings, which are ordered according to three main themes: management, knowledge and networks. An explanation of the derivation and use of this schematic is presented at the end of Chapter 3 . In each chapter, we present the data from the interviews and observations to surface and analyse the key themes and issues identified by different groups of managers across, and within, the three trusts.
Chapter 7 discusses the main findings of the research. Despite a great deal of (sometimes unexpected) similarity in the themes identified and accounts given across the trusts and groups of managers, our analysis also allows us to identify some important differences (both obvious and more nuanced) between the trusts and managerial groups. This leads to a short final concluding Chapter 8 in which we present our conclusions and recommendations.
Chapter 2 Research methodology
General approach to the research
In this chapter, we outline and explain the methodology used to conduct the research. The chapter is developed in four parts that consider the general approach to the research and underpinning epistemology, the design of the study (including the selection of cases and identification of managerial cohorts), the research process and schedule of activities, and the methods of data collection and analysis used.
As noted in Chapter 1 , this research project aimed to investigate how NHS managers encounter and apply new management knowledge, examining the organisational and extra-organisational factors that facilitate or impede the acceptance of new management knowledge and its integration with practice in health-care settings. As such, there were three specific questions addressed in the course of our research:
-
How do occupational background and careers influence knowledge receptivity, knowledge sharing and learning among health-care managers?
-
How do relevant CoPs enable/obstruct knowledge sharing and learning?
-
What mechanisms are effective in supporting knowledge receptivity, knowledge sharing and learning/unlearning within and across such communities?
Before we outline and explain the design of the study and the detailed methods used to gather data to address these questions, it is important to say something about the general approach to the research and its underpinning epistemology as the research reported here departs significantly from approaches to research that rely on orthodox quantitative analysis based on statistical generalisation or experimental design.
Research philosophy and methodological choices
This study takes up an interpretivist qualitative methodology, underscored by a broadly constructivist epistemology, which contends that realities are socially constructed, the product of individual interpretations and meanings, intersubjective relations and the affordances and limitations of particular social and historical conditions. Accordingly, research that seeks to understand particular realities, such as the knowledge mobilisation of middle managers in the NHS, begins with the assumption that terms such as middle manager and knowledge are socially defined. Therefore, our research attempts to explore a range of interpretations of specific phenomena on the part of individuals, the relations in which they are embedded and the social forces that shape, and are shaped by, these interpretations and relations.
Research of this kind therefore attempts to place individuals at the centre of the analysis and explores the relations, connections and broader social forces within which individuals are embedded. The overall aim is to produce an analysis that is meaningful to individuals within these types of situations, while also remaining sensitive to changing social and political forces. This last point is particularly relevant to the context of the current study. The launch of the government white paper directed at ‘Liberating the NHS’55 (© Crown Copyright 2010, Equity and Excellence: Liberating the NHS) appeared at the time of our investigation, contributing to a highly salient political climate for health care and its management. This was a context in which, in Burrell and Morgan’s terms,56 conditions could arguably be characterised as much by ‘change, conflict, disintegration and coercion’ (p. 13) as by ‘stability, integration, coordination and consensus’ (p.16). The sociological context therefore reflects forces of ‘radical change’ rather more than ‘regulation’ (p. 16). 56
Our adoption of the comparative case study method in this study reflects this broad epistemological perspective of phenomenology. Following Silverman,57 this contends that sociology should be concerned with the phenomenological understanding, rather than positivist measurement of behaviour, as it is the meanings ascribed to phenomena that define social reality rather than social reality being self-evident through inspection. Social reality does not somehow reside outside of people’s perceptions, but instead is constituted intersubjectively. The inference is that people can adjust and even change meanings through social interaction. Explanations of social action therefore need to take account of the meanings that those participating attach to actions. For Silverman,57 social researchers should build their theories on foundations that view reality as being socially constructed, sustained and changed. In the study of organisations, he argued that the social actor should be at the centre of the analytical stage, for it is crucial that researchers understand subjective and intersubjective meanings if they are to understand the significance of organisational actions. This puts an emphasis on a view of the social world as processual, in which organisational actors interpret the situation in which they find themselves and act in ways that are meaningful to them. It also requires interpretive, qualitative methods that can tap into action at the level of meaning.
The comparative case study method54 adopted here draws on interpretive ethnography, which is a qualitative approach and set of methods directed at understanding cultural phenomena that, in turn, reflect the system of meanings guiding the actions of a social group – in our case, health-care managers. This method also contends that research participants’ perceptions of social reality are themselves theoretical constructs. While participants’ constructs are more directly connected with lived experience58 than the researchers’, they remain, nevertheless, subjective constructions of social reality.
In remaining cognisant of the changing political context experienced by managers in this study, we understand that participants’ reconstructions are embedded within particular policy narratives, which, in turn, are embedded within a particular social order. Implicit in the understanding of management as a socially constructed phenomenon is the understanding that particular constructions of management promote the reproduction of particular social and economic relations. Therefore, the attempt made through fieldwork is to present an integrated perspective of context, arguing that external factors are a fundamental part of the internal composition of the local domain and should be recognised as such – even at the most micro level of interaction.
Design of the study
In developing such research, it can be argued that our attempt to understand the effects of differences in organisational and community context on how managers use managerial knowledge requires a research strategy that allows depth of analysis as well as breadth of application. This suggests the need for a comparative case study approach that is able to examine, using in-depth qualitative methods, the practices of managers – but in a way that is also sensitive to important differences in context (both organisational and institutional).
A comparative case study approach has proven to be a powerful methodology, particularly for allowing the direct application of research findings to their practical context and also for helping understand the issues involved in complex organisational settings. 53 It is particularly important when, as the previous discussion suggests, it is difficult to separate out analysis of the phenomenon of interest from its context. 52 Research into health-care organisations has, of course, made particular use of the case study method to explore complex network-based interactions amongst managers and clinicians. 48,54
Sample of organisations
A comparative case study approach was adopted by focusing attention on studying middle managers within and across three very different types of NHS trust. These three trusts were selected to provide quite distinct cases with regard to the diversity of services provided and, consequently, the knowledge requirements faced by managers and the networks likely to be available to them. The three trusts studied were all based in the north-west of England and consisted of a foundation acute trust, a foundation care trust (mental health and community services) and a foundation tertiary/specialist trust.
Our expectation on commencing the research was that each trust context would be distinct with regard to the knowledge requirements faced by managers and the networks likely to be available to them. Our assumption was that this would be reflected in several characteristics that differentiate these types of trust, including their geographical spread, the number of locations from which services are provided, the diversity of services provided and the number of organisations purchasing services from them. More specifically:
-
Acute trust, which offers a wide range of acute services centralised mainly in one location and covering a fairly limited (local) geographical area. Service contracts are likely to originate largely with one commissioner. Knowledge networks are likely to be available to managers according to specialism.
-
Care trust, which delivers a diverse range of mental health and community services with operations distributed in many locations over a large (regional) geographical area. Multiple purchasers are likely from both health and social care. Knowledge networks are likely to reflect a more limited range of specialisms.
-
Specialist trust, which offers a limited range of specialist services mainly from one central location to patients spread across a very wide (regional and national) geographical area. The trust has to contract with multiple purchasers. Knowledge networks are more likely to be focused on the particular specialism.
A summary of these characteristics can be seen in Table 1 .
| Type of trust | Diversity of services | Area coverage | Number of purchasers | Number of locations | Nature of patient contact | Managerial knowledge networks |
|---|---|---|---|---|---|---|
| Acute | High | Low | Low | Low | Mixed | Varied according to specialism |
| Care | High | High | Medium | High | Cyclic | Limited specialisms |
| Specialist | Low | High | High | Low | Episodic | Focused specialism |
The categorisation of each trust in this table is necessarily very broad, highlighting factors which were relatively objective and identifiable and which may be expected to have an impact on issues of relevance to the study. However, this categorisation was also largely a priori, inferred and set out in the research project design in advance of detailed empirical work in each trust (the exceptions were the two bold areas for which original expectations that the care trust would rate medium were revised to high ratings following initial investigations). A key priority in the research was to establish empirically which aspects of context, both historical and immediate, impacted most directly on operations and activity in each trust. This is the focus of Chapter 3 , in which we provide a more fine-grained analysis of the salient aspects of the organisational context in each trust and also indicate the most pressing current concerns for managers at each organisation, drawing directly upon the perceptions of our interviewees.
Identifying managerial cohorts
As was noted in Chapter 1 , management in the NHS is highly complex, consisting of groups with very distinctive professional orientations and knowledge bases. 59 The dependence on management and markets to drive health care reform has meant that a range of hybrid managerial roles have emerged that require combinations of clinical expertise, public administration and business acumen. 60 Furthermore, there is little standardisation of role titles between and even within trusts, and few people with managerial responsibility actually carry the formal title of manager. 61 As a consequence, the identification of distinct cohorts of managers is a difficult problem in a setting as complex as the NHS.
We set out to include middle managers across the three types of trust, to be selected on the basis of important expected differences in the community of middle managers who work in these organisations and in the managerial activities and challenges that they face. Our intention was to understand the effects of differences amongst communities of NHS managers (in terms of sources of managerial knowledge, knowledge utilisation and learning processes). Therefore, it was important to be able to develop a systematic framework for the identification and selection of managers.
Our NHS Management Model, which broadly differentiates between three general categories of manager – functional, general and clinical – and which includes within it more precise indications of the locations of particular managerial roles, is presented in Figure 1 .
FIGURE 1.
NHS Management Model (final version).
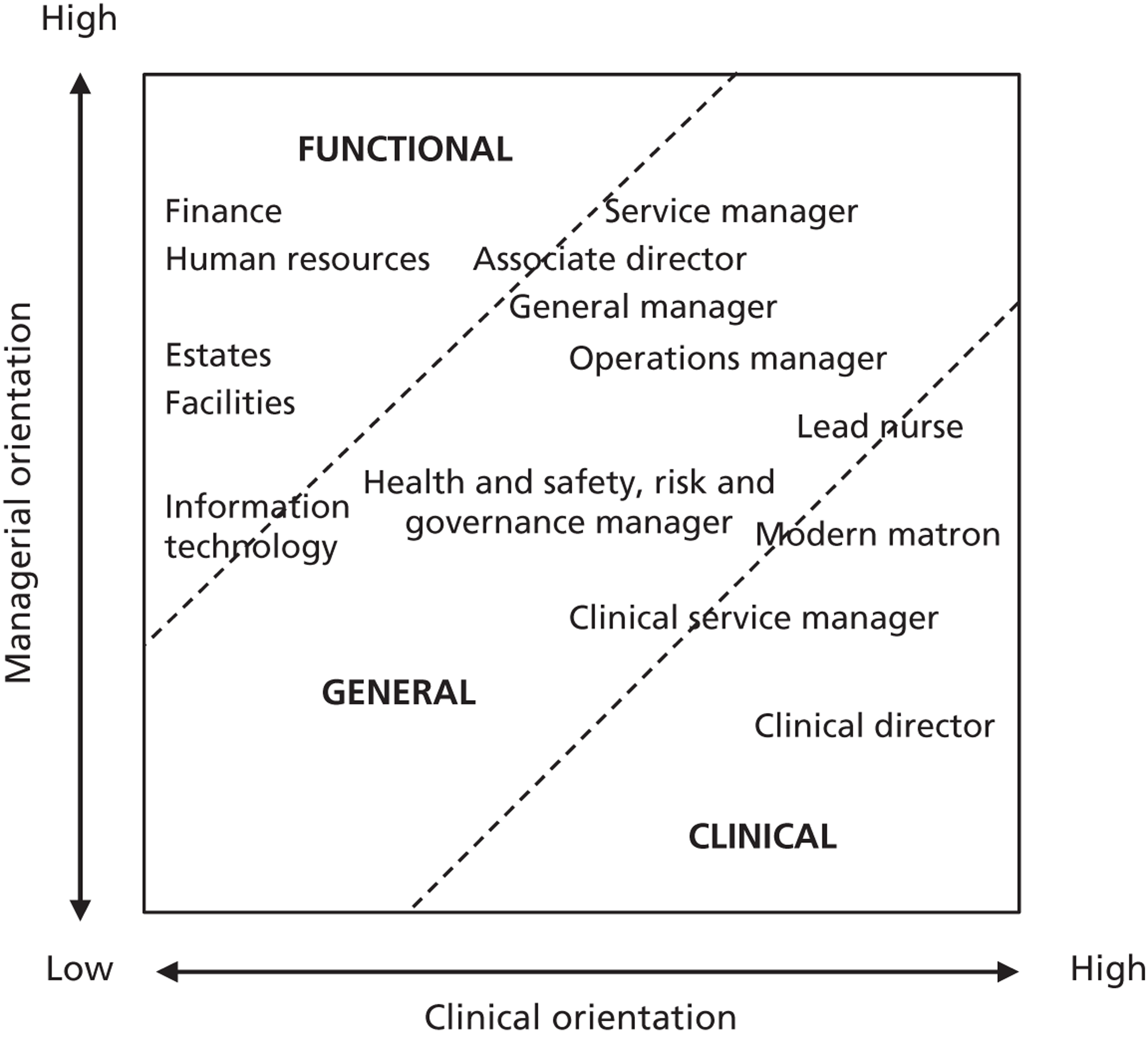
This model was the result of the development and refinement of an initial framework that had attempted to differentiate between managerial groups on the basis of their qualifications and experience. It was arrived at through interviews and meetings with advisory group members and other key informants from across the sector in the early phase of the research. The model goes further than the original framework in recognising the interconnectedness of managerial and clinical orientations (especially among some general managers), as well as the often blurred boundaries between managerial groups.
Using this framework, it was possible, in principle, to locate particular managerial roles in terms of the expected combination of clinical and managerial orientation, which may of course reflect and represent very different patterns of managerial and clinical training/experience. Pragmatically, this would also enable us to construct a sample of interviewees in each organisation that we were confident covered the diversity of middle management in each trust in a balanced manner and which we hoped and expected would be clearly recognisable to potential participants in the study. Of course, our interviewees were not types or categories but real individuals, hence the precise combination of background, experience, training and inclination of each particular interviewee was likely to vary significantly, as might be expected. The focus of the empirical analysis was to explore this in some considerable detail.
Research process and schedule of activities
The research project was scheduled to last 28 months and our original plan of investigation saw the research organised into four main stages or phases: project initiation, phase 1 empirical work, phase 2 empirical work and write-up. These phases are captured in the project flow chart in Appendix 1 and are summarised below.
Project initiation
This phase lasted 5 months and involved the appointment of the research associate and establishment of an advisory group, an extensive literature search, identification and contact with key informants for interview, detailed design of research protocols and the securing of ethical approval.
Phase 1: key informant interviews
The first empirical phase of the study (months 6–12) involved face-to-face or telephone interviews with a variety of key informants, selected to provide overviews of the key challenges and problems facing managers at a local, regional and national level in locating, interpreting and applying knowledge and learning.
The advisory group included six external members (including the lead collaborator or their representative from each trust) who were among the key informants who were interviewed. Interviewees during this stage also included a number of figures of national and regional prominence, including those associated with:
-
NHS employers
-
NHS Confederation
-
The King’s Fund
-
regional strategic health authority (SHA)
-
regional leadership academies
-
participating trusts.
These interviews generally lasted approximately an hour and were structured around a set of broad questions (see Appendix 2 ) regarding:
-
NHS trust contexts (appropriateness of choices and categorisations)
-
framework for selection of managerial cohorts (validity, suitability)
-
encounters/events (to observe management knowledge processes in action)
-
current changes and possible effects
-
management knowledge and learning
-
human resources (HR) practices
-
organisation, systems and practices.
Interviews were conducted by at least two members of the research team, they were recorded and transcribed and notes were also taken.
They allowed a detailed picture to be built up of the background, capabilities and orientation towards management knowledge of diverse groups of managers, as well as providing further background sources on the policy/practitioner context of the research. As already suggested, they also represented the first stages in the coproduction62 of the research framework and research instruments, by contributing significantly to the validation/refinement of the framework for trust and participant selection.
During this phase, the first advisory group meeting was also held in order to help steer the design of the study (by further validating the frameworks being developed) and to assist with the identification of appropriate managerial cohorts. Advisory group members were also prompted to identify and discuss with the research team appropriate managers for interview and key events to observe. Trust participants on the advisory group were also able to identify common interests and concerns across each trust as well as important differences in the use and exploitation of managerial knowledge.
Phase 2: ethnographic study via interviews and non-participant observation
Phase 2 represented the main empirical component of the research (months 9–24) and combined semistructured interviews with selected cohorts of managers with ethnographic observation methods. Data collection was phased over a rolling programme of research over a period of about a year at each trust. Details of interviewing and observation methods and processes, as well as the coding and analysis of the data, are explained in greater detail in Methods of data collection and analysis.
Write-up
The final stage of the research (months 24–28) involved further analysis of the empirical material and activity leading to the production of this final report. During this phase, a second advisory group meeting was held, at which emergent findings were presented and discussed. Following this, separate research symposia were held at each of the three trusts where the results of the research were presented and discussed with managers who had participated in the research. This enabled the results to be further validated and also fed directly back into practice.
Selection of phase 2 interviewees
The second phase of the study required the selection of a limited number of participants from identifiable groups of managers – clinical, general and functional – who could exemplify the range in each group. By selecting individuals from each group or cohort, it would then be possible to explore important sources of similarity and difference both within and between each trust. To capture this qualitative variation, a purposive, non-random sample of approximately eight managers was identified for each of the three cohorts of managers in each of the three participating trusts, yielding a total target sample size of around 72 managers across the three trusts who would be interviewed during the main fieldwork phase (in the event, 68 were actually interviewed).
Access to potential participants was arranged through each trust’s lead collaborator and HR department. In the early stages of research, the research team worked with lead collaborators to identify potential interviewees among the managers. Selections were made on the basis of meeting the need to generate sufficient numbers of interviews in each broad group (clinical, general and functional) while allowing some variation in their work position and context (e.g. different clinical/functional specialism or service operations). It also became clear that managerial grade was a useful proxy indicator of middle management status. In the event, most of those managers interviewed had salaries that were in grades 8a–8d (the exceptions were one grade 7 manager, four grade 9 managers and five who were on the consultants scale).
Once potential candidates for interview were identified, they were contacted by e-mail via the trust’s HR department and asked if they would be willing to be contacted by a member of the research team to establish their willingness to participate. The initial e-mail contact had been drafted by the researchers and included outline details of the research. Contact details of managers who agreed were then passed on from the HR department and they were contacted directly and provided with full information about the research, including an invitation letter, participant information sheet, project summary document and consent form (see Appendices 3–6 ). As part of the process of obtaining consent, managers were guaranteed that any information they gave would be kept confidential. There was also a guarantee of anonymity in the use of any examples and quotes from interviews. Consequently, the interview data presented in this report have been anonymised and pseudonyms are used to protect the identity of respondents. Managers were given time to confirm whether or not they wanted to participate and, if there was agreement, interviews were arranged in situ at the manager’s convenience, at which time consent forms were signed.
The final sample consisted of a total of 68 interviewees across the three trusts. Details of the sample of managers, including information about their distribution and response rates with regard to numbers willing to participate, are presented in Table 2.
| Trust | Clinical managers | Functional managers | General managers | Declined/did not respond | Total participantsa |
|---|---|---|---|---|---|
| Acute | 5 | 7 | 8 | 4 | 20 |
| Care | 7 | 6 | 12 | 10 | 25 |
| Specialist | 6 | 8 | 9 | 10 | 23 |
| Total | 18 | 21 | 29 | 24 | 68 |
Character of phase 2 sample
The gender and age distribution of the 68 managers interviewed are summarised and compared by trust and managerial group in Table 3 .
| Trust | Clinical | Functional | General |
|---|---|---|---|
| Acute | 3 male, 2 female | 4 male, 3 female | 3 male, 5 female |
| Care | 3 male, 4 female | 3 male, 3 female | 3 male, 9 female |
| Specialist | 2 male, 4 female | 3 male, 5 female | 4 male, 5 female |
| Total | 18 | 21 | 29 |
There was a relatively even gender spread, apart from a concentration of female general managers in the care trust. The distribution of managers by age was also relatively even across the trusts, although the age profile of managers in the care trust was a little higher and of those in the specialist trust a little lower ( Table 4 ).
| Trust | 18–30 years | 30–40 years | 40–50 years | 50–60 years | 60 + years |
|---|---|---|---|---|---|
| Acute | 2 | 4 | 10 | 4 | – |
| Care | 1 | 4 | 13 | 7 | – |
| Specialist | 2 | 9 | 9 | 2 | 1 |
| Total | 5 | 17 | 32 | 13 | 1 |
Most of those interviewed (64, 94%) were white British, with the remaining four (6%) being Asian British and male (two in the care trust and one in each of the other trusts).
Table 5 shows the average time that managers had spent in their current post, their current organisation, in the NHS more generally and also outside the sector.
| Trust | In post | In organisation | In NHS | Outside NHS |
|---|---|---|---|---|
| Acute | 2.30 | 4.86 | 17.25 | 4.83 |
| Care | 3.87 | 11.71 | 22.34 | 3.03 |
| Specialist | 3.02 | 9.09 | 14.41 | 6.70 |
The greatest longevity of employment in both the organisation and NHS was found amongst managers interviewed in the care trust (where many had worked for long periods prior to trust status and reorganisation). Those with considerable experience outside the sector were found mainly in functional management roles and also amongst clinical and general management staff who had worked in private health care. Other distinctive and quantifiable features of experience, including educational qualifications and training received, will be explored in Chapter 5 .
Methods of data collection and analysis
The methodological strategy was that the research would make use of a qualitative mixed-method approach that combined a primary emphasis on semistructured interviews with ethnographic observation methods, so as to get as complete as possible a picture of the engagement of cohorts of managers with their networks and communities.
Qualitative methods such as these are well suited to exploring the workings of CoPs, both within and outside organisations, and have been used effectively to illuminate the dynamics of organisational relationships between managers and staff63 as well as between staff and patients. 64
Interviews at each trust were carried out by two members of the research team – one of the principal investigators (who focused on that particular trust and who took the lead in questioning) and the research associate (who covered interviews at all three trusts to ensure consistency and comparability).
The interview followed a semistructured format based on a set of questions and detailed prompts that ranged across seven key thematic areas (see Appendix 7 ):
-
Background information: including age, gender, managerial role and grade, educational and professional qualifications, professional background and length of experience in the NHS, the trust and the role.
-
Occupation/career: including current position and role, educational background and career path and entry into the organisation/role.
-
Leadership/management: including current responsibilities, conceptions of management and leadership and views on the occupational/professional status of management groups.
-
Knowledge: including managerial skills needed, formal and informal sources of knowledge and learning, and organisational mechanisms in support of knowledge and learning.
-
Networks: including internal and external networks, their nature, purpose, scope and mode of operation and individual networking activity.
-
Organisational context: including factors enabling/hindering knowledge work and barriers and enablers of communication (e.g. structural and spatial aspects of work organisation, technology, HR policies and practices).
-
Change: including sector/organisational changes affecting knowledge and learning processes, the personal impact of change and future career aspirations.
Interviews lasted between 1 and 2 hours (the majority lasting around 1.5 hours) and all were recorded and transcribed. Including interviews from phase 1, the result was a primary data set that consisted of a 139 hours of recording and over 924,000 words!
Phase 2 non-participant observations
When possible and appropriate, meetings and other forms of event or encounter at each trust were also observed when these managers were involved and knowledge processes would be expected to be most critical (this was with the explicit agreement of those managers and others present). The aim was to underpin the analysis by supplementing interview-based accounts of knowledge processes with observation of the reality of how management knowledge was accessed, used and shared in practice. It would also allow the research team to gather more in-depth understanding of how management knowledge and management processes were related and allow the follow-up of key themes and issues identified in interviews. It therefore also allowed the introduction of a more longitudinal element to the research.
A number of events were observed, including management meetings and training events and these are listed in Appendix 8 , along with the thematic guide used for the ethnographic encounters (see Appendix 9 ).
Standard note-taking by those members of the research team present, structured broadly by the thematic guide to ensure consistency, formed the main means of capturing action in these events and management meetings and these were transferred to electronic format. In addition, observational elements were included through field note summaries produced by each member of the research team before and after the interviews that aimed to capture general observations and impressions. Table 6 provides an overall summary of data collection across the two phases of research, including the time spent in observations.
| Data source | Interviews (formal recorded) | Interviews (informal) | Observations |
|---|---|---|---|
| Key informants | 13 | 0 | 3 hours over 3 days |
| Acute trust | 20 | 0 | 18 hours over 6 days |
| Care trust | 25 | 13 | 22 hours over 9 days |
| Specialist trust | 23 | 6 | 11 hours over 2 days |
| Totals | 81 | 19 | 54 hours over 20 days |
The rich detail obtained from the observations did not lend itself to coding or presentation in the same way as the interview data did, and this detailed background information was used instead to help contextualise the interview data and/or to provide confirmatory information for points raised or claims made in interviews (e.g. about decision-making or management training processes – see illustrative examples in Chapter 7 ). Consequently, the observation data were used more implicitly and/or illustratively to support the analysis and were not subject to the same coding or analytical techniques as the interview data.
Data coding and analysis
All the data collected were transcribed, collated and stored centrally for coding and analysis using NVivo 9 (QSR International, Warrington, UK) qualitative data analysis software. The development of the coding framework for the semistructured interviews that made up the greater part of the data set relied on a schema combining open and axial coding methods, which aimed to combine inductive and deductive logics in line with the construction of grounded theory. 65
Following the completion of the first set of semistructured interviews, three interview transcripts were chosen and were independently coded by each member of the research team. The research team then met in order to compare the coded transcripts so as to construct a basic list of coding categories. These categories were then structured into broad themes (management/leadership, knowledge, networks, organisation and personal), reflecting the research questions, the structure of the interviews and extant relevant classificatory schemas from the management literature. This resulted in the creation of an axial framework against which transcripts could then be coded.
The coding for each case was undertaken by the members of the research team responsible for data collection in that site, which capitalised on the tacit understandings each had gained through data collection. A smaller selection of transcripts were analysed by another member of the group in order to check interpretation and to improve inter-rater reliability. Additionally, regular meetings of the research team were held to discuss the emerging analysis, explore contradictions and disagreements and develop consensus. Throughout analysis, the coding framework remained open to the inclusion of additional categories or deletion/combination of nodes.
Once coding was complete, each team member selected one theme to explore the findings in more detail, drawing out comparisons and distinctions between the three trusts and the three management groups. The thematic analysis and interpretation of the data proceeded largely inductively, with each theme being explored using the structure provided by the coding framework (and being informed by observations in the field) while, at the same time, being shaped by the overarching research questions concerned with management knowledge and learning processes. Although individual team members were responsible for developing the thematic analysis, the process was an iterative one, with regular team meetings, presentations and comments on drafts being used to ensure accuracy and consistency of interpretation.
Themes, rather than cases, were used to organise further analysis and data presentation, as preliminary analysis of the emerging findings at each case through the later fieldwork and early coding stages clearly indicated that there was a good deal of consistency in responses across the interviews regarding the central themes of management, knowledge and networking. At the same time, however, it was clear that there were important differences between the cases that had effects on management activities and knowledge and learning processes (e.g. in the experiences of formal management training and development and the extent of networking activity). Consequently, while the preliminary analysis was case based (coinciding with the phased ending of fieldwork at each case), this gave way to further analysis which was more thematically driven.
However, comparative case analysis was also still important and this was retained through case narratives that described the context for the main findings and through the examination of significant differences (sometimes very obvious, but often quite subtle and nuanced) that were explored within each theme. The steps taken here to strike a balance between thematic analysis and rich case narrative are consistent with those normally expected in, and recommended for, qualitative case study research. 53 Preliminary results of this secondary analysis were also shared with the Advisory Group and then further developed through the feedback sessions held at each participating trust. Each team member then took responsibility for the final write-up of his or her theme, which culminated in the writing of this final report.
An important point to note is that some of the data presented in the next four chapters make use of the technical capabilities of NVivo to create quantitative summaries of each qualitatively coded data (represented in bar charts and pie charts). Unless otherwise indicated, the numbers given along the x-axis of each of the bar charts (and in segments of the pie charts) are frequency counts, indicating the number of times a specific theme or category was referred to by respondents in interviews. Although this proved to be a very useful way of identifying starting points for the preliminary and further analysis of the data, it is important to note that the frequency with which particular themes and issues were discussed by a particular group, or within a particular trust, does not necessarily correspond to the frequency with which managers engaged in or experienced this behaviour, or to particular outcomes. So, for example, frequent discussion of training might signify many different things, including its value, its absence or its inadequacy. Nevertheless, it does provide a useful entrée into the thematic analysis, flag up some basic but interesting points about presence or absence of a discourse and, perhaps, reflect to some extent managerial norms and key features of their cultural, organisational and professional environment. However, understanding these in detail requires us to look beyond these basic quantitative signifiers into the qualitative analysis that forms the bulk of each chapter.
Presentation of empirical data
Having explained the methodology and detailed research methods involved in our study, Chapter 3 turns to an exploration of the wider context in which the managers we interviewed were operating. This is partly informed by our wider literature search, but also by early findings and observations from phase 1 interviews and discussions with the Advisory Group, trust representatives and other academics and practitioners in the field.
The aim of Chapter 3 is to give an overview of the organisational context of management/leadership within the NHS, before drilling down into a summary full description of each of the three trusts and then into presenting summary data about the particular managerial cohorts and individual managers involved in their study.
The three chapters that follow then address, in turn, each of the three major themes of the research that emerged from the coding and analysis of the data, namely management/leadership (see Chapter 4 ), knowledge (see Chapter 5 ) and networks (see Chapter 6 ). After that, in Chapter 7 , we revisit what the data have to say about the research questions set out at the start of this chapter.
Chapter 3 The institutional and organisational context for National Health Service management
Introduction
Middle managers play a vital role in large organisations, co-ordinating activity between the upper and lower organisational reaches and across various departments, translating broader policy/strategy into operational outcomes and frequently serving as a key repository of organisational memory. 66,67 However, middle managers also represent one of the least contentious targets of restructuring, particularly reductions in headcount which attempt to avoid impacting the front-line of operations. 17,19 In this context, it is unsurprising that management represents an identity few find desirable, and that even those with the responsibility of managing repudiate the management part of their role68 – with, we argue, significant repercussions for managerial work.
It may be argued that these wider tensions impinge even more acutely on middle managers in the NHS. 25,30,69 Reforms introduced by the coalition government in 2010 to increase efficiency emphasise the importance of removing around half of management costs in the NHS. 55 Although many aspects of the reforms have been subject to intense debate, there has been remarkably little negative reaction to the proposed cuts in management costs. This lack of public outcry can be accounted for as resulting from negative characterisations of NHS middle managers, casting them as petty bureaucrats, and descriptions of the NHS as a whole as burdened by a growing, unproductive and even obstructive management cadre. 69,70,71 To understand the nature of management in the current NHS, it is essential to situate NHS management as an activity and a formal role in some historical context.
The aim of this chapter is to outline the context in which the study took place and we do this in four parts. First, we provide an overview of the institutional context for management in the NHS, in terms of broad policy and more specifically in terms of impact on NHS management. Second, we complement this overview with a brief exploration of the training and development of managers and leaders within this context, taking into account the impact of contemporary changes within the sector. Third, having selected out case studies, we examine the specific organisational context of the three participating organisations in detail, again in light of these ongoing changes, in order to elaborate key organisational characteristics and to examine points of difference and similarity to inform the research analysis. Fourth, having developed our management selection framework in the previous chapter, we outline characteristics of the sample of managers selected for in-depth interview and compare and contrast their demographic characteristics.
The institutional context of the study
The NHS has been undergoing regular and radical reform over the last 40 years. These reforms have involved structural changes, reorganisation and adjustments to management arrangements. There have been general moves towards marketisation and business-like functioning. These changes have had striking effects on management practice, professional values and service organisation and delivery in the NHS as a whole and in the English context in particular, which is the focus of this research. This section provides an overview of government policy as it affects NHS management; for fuller accounts of NHS policy see Harrison and McDonald72 and Klein. 73
Changing policy and management context
Table 7 indicates several periods of change mapped against major policy initiatives. Administrative arrangements for the NHS remained relatively stable in the period between nationalisation and the introduction of general management following the Griffiths Report. 74 The 1980s and 1990s saw government health policy that emphasised the importance of specific managerial roles to improve efficiencies as part of a number of NHS reorganisations. The NHS Management Inquiry by Roy Griffiths, Chairman of Sainsbury’s supermarket, effectively abolished consensus management in favour of general management and provided the structural arrangement for a rational management system. 80 As a result of Griffiths’ recommendations, the following management reforms took place: appointment of general managers, introduction of management budgets, value for money reforms and management training and education. General managers from inside and outside the NHS were to be in place in hospitals and health authorities by the end of 1985. Management budgets were to be introduced alongside greater financial controls. Savings arising from these reforms were to be returned to improving services for patients and the NHS Training Authority was established in order to extend management training, especially for doctors. 74 Doctors were to become more closely involved in financial matters and budgeting.
| Period | Major change(s) | Policy initiative |
|---|---|---|
| 1948–82 | Public administration | Nationalisation of health |
| 1974 NHS reorganisation | ||
| 1983–97 | General management | Griffiths Report (1983)74 |
| Quasi-markets | NHS and Community Care Act (1990)75 | |
| 1997–2007 | Business management | New NHS: Modern, Dependable (1997)76 |
| Reform | NHS Plan (2000)77 | |
| Foundation trusts | Community Health and Standards (2004)78 | |
| 2008–13 | Leadership | Darzi Review (2008)79 |
| Structural reform | Liberating the NHS (2010)55 |
The 1989 white paper ‘Working for Patients’81 passed into law as the NHS and Community Care Act in 1990. 75 This act introduced an (internal) quasi-market for health care by encouraging services to split along purchaser [health authority and some general practitioners (GPs)] and provider (acute, mental health, ambulance and community) lines. Purchasers were given budgets to buy health care from providers. Providers became NHS trusts (independent organisations with their own management teams), and it was envisaged that these trusts would then compete with each other to provide services to the purchasers. Between 1991 and 1995, all providers became NHS trusts and GPs could hold budgets (GP fund holding) to purchase care for their patients from the NHS or private providers. Some GP fund-holders were able to accelerate care for their patients, leading to accusations of an emerging two-tier health system. 73 As well as attempting to increase managerial control of services, these changes were also designed to introduce competition and a business culture.
Although these quasi-market institutions were originally abandoned by the New Labour government of 1997, these early experiences may have paved the way for market-orientated changes in the coming years. This period saw unprecedented change involving the formation and dissolution and rearrangement of structures and responsibilities of NHS authorities and trusts. The white paper ‘The New NHS: Modern, Dependable’76 saw the abolition of the internal market and dismantling of GP fund holding. This was an era of centralised management of the NHS as one organisation. It involved target setting intended to reduce waiting times and improve access to services and the introduction of a star rating system for NHS organisations. Organisations were rated by the newly established Commission for Health Improvement (CHI). Although national targets were subsequently abandoned, along with the star rating system, priorities continued to be indicated through the annual Operating Framework for the NHS that was published each year. The National Institute for Health and Care Excellence (NICE) was created to make decisions on the adoption of treatments. These two institutions (CHI and NICE) took control of areas previously controlled by the medical profession. Decisions about suitable treatments were now being made by NICE and clinical governance was being carried out by the CHI.
The NHS Plan77 in 2000 described a 10-year plan for the NHS and National Service Frameworks described service standards for areas such as mental health and cardiac care. Decades of under-spending on health care meant that England had notably poor health outcomes compared with other developed nations. In 2000, Tony Blair promised to increase health spending to European levels. This meant a rise from 6.6% (1999/2000) to 9% of gross domestic product (2005/6). 77 Although the targets and associated penalties were initially successful in reducing waiting times, increasingly disturbing behaviours linked to intense centralised control preceded a radical change in direction towards decentralisation and the readoption of market-based reforms. These included the promotion of patient choice and competition between providers as well as allowing for organisations based on not-for-profit structures – NHS foundation trusts (FTs).
The first wave of FTs came into being in 2004. At the same time, the previous system of block contracts to service providers was replaced by a new funding system called Payment by Results. This system was aimed at reducing waiting times by targeting payments towards specific treatments and, thus, providing a powerful incentive for trusts to direct activity towards areas of greatest need. In addition, it allowed for private providers to claim payments for services provided in independent treatment centres. GP incentives to provide additional services outside of hospital were provided for through the Quality Outcomes Framework. The 2008 review entitled High Quality Care for All (NHS Next Stage Review Final Report)79 set out the second 10-year plan for the NHS, although it was rapidly displaced by the unfolding financial crisis and the change of government in 2010. The review laid out plans to increase patient choice, to improve public health provision and to extend the role of doctors as managerial leaders.
This frequent and substantial institutional change over recent decades has continued through the course of the project to have striking effects on management practice, professional values and service organisation and delivery in the NHS as a whole. Moves towards the decentralised control of NHS organisations, with increasing numbers of hospitals becoming FTs, and efforts to increase patient choice and competition between health provider organisations, have relied on NHS management for delivery. Managers have thus been given increasing responsibility for implementing health service reforms,55 providing the links between those planning and organising services and those providing services to patients while at the same time bearing the brunt of the efficiencies implied by the reforms.
Consequences for managers and management
Between 2000 and 2009, amid these changes, the NHS workforce grew by around 30%. Across this period, figures for the number of managers and senior managers rose from 2.7% (full-time equivalent) in 2000 (n = 24,253) to 3.4% in 2009 (n = 40,094),82 remaining broadly in line with figures for most other developed countries. 83 Since 2010, employment in the NHS has been falling, and recent reductions in NHS staffing numbers generally have been more than matched by reductions in the total numbers of managers. Figures from 2012 show the proportion of managers at 3.2%, suggesting that policy reforms targeted at reducing management costs might be beginning to bite. 84 In all likelihood, managerial numbers will continue to decrease in subsequent years as middle managers are targeted in health reforms aimed at reducing management costs. This comes at a time when effective organisational co-ordination will be central to maintaining safety during a period of reduced investment.
As well as the increased demands for management resulting from higher staffing levels, other recent institutional changes that have generated additional management workloads include:
-
moving to service line management
-
applying for FT status
-
achieving national performance standards
-
payment by results, changing to tariffs, fines
-
the Quality, Innovation, Productivity and Prevention agenda
-
creation of clinical commissioning groups (CCGs)
-
changing regulatory, auditing and accreditation regimes
-
making £20B savings by 2015. 69
The new coalition government of 2010 brought health policy full circle by proposing the removal of management layers to improve efficiency. The white paper ‘Equity and Excellence: Liberating the NHS’55 proposed to deliver the 45% reduction in management costs by delayering the NHS, abolishing 151 primary care trusts (PCTs) and 10 SHAs. The Health and Social Care Act85 in 2012 took the changes further by reducing the emphasis on GPs as commissioners and providing for private sector commissioning. The impact of this across the NHS is still emerging, but through the period of study the immediate consequences were widespread uncertainty, exacerbated by the ongoing and substantial pressures to reduce costs significantly, year on year, while at the same time maintaining service quality. Achieving this with often reduced staff numbers, particularly reduced number of managers, as attempts were made to avoid reductions in ‘front-line’ staffing levels (i.e. doctors and nurses) led to a widespread experience of severe work intensification among NHS managers, described elsewhere as ‘normalised intensity’. 86
In this section, we have charted political change, influential government policies and consequent institutional and cultural changes involving management of the NHS from its inception to date. Since the start of this research project, the landscape has continued to change substantially. There have been three notable landmarks, acute financial pressures (the so-called ‘Nicholson Challenge’ to make savings of £20B over 5 years), major structural reforms (Health and Social Care Act, 2012)85 and expected changes to professional/managerial configurations emerging from the Francis Report. 4 In Management and leadership development in the NHS, we explore the professional development challenges facing managers in the sector and the initiatives taken to develop managerial and leadership capabilities.
Management and leadership development in the NHS
Since the first intake of the NHS Management Training Scheme in September 1956, the content, location and impact of management and later leadership development in the NHS has undergone regular transformation ( Table 8 ). Although terminology has changed, the core aim of these programmes remains consistent: in 1955, the aim was to provide the NHS with ‘well-trained administrators who would be competent to fill senior administrative posts in years to come’87 (p. 37, © Queen’s Printer and Controller of HMSO 2012, Talent Management in the NHS Managerial Workforce). In 2012, the newly formed NHS Leadership Academy set out as its aim to equip managers from across the different professional backgrounds in health care with the skills needed for leading and improving their organisations in ways that were still consistent with the values of the NHS. 88
| Year of commencement | Key management training programme | Agency responsible |
|---|---|---|
| 1956 | Management Training Scheme | Regional Staffing Officers (RSO) |
| National Staff Committee for Administrative and Clerical Staff (NSCA&C) | ||
| Standing Committee on Management Education and Training (SCMET) | ||
| 1983 | National Management Training Scheme | NHS Training Authority |
| 1986 | GMTS | |
| 1993 | National Management Training Scheme | NHS Training Directorate |
| National management development programme | ||
| 2002 | GMTS | NHS Leadership Centre |
| Breaking Through | ||
| Gateway to Leadership | ||
| 2009 | Top Leaders | NHS Leadership Council |
| Emerging Leaders | ||
| Inclusion | ||
| Clinical Leadership | ||
| Board Development | ||
| 2012 | Foundation programme (award: post-graduate diploma) | NHS Leadership Academy |
| Mid-career programme (award: masters degree) | ||
| Executive/senior leadership programme (peer assessed) |
In the intervening period, the responsibility for producing these administrators, managers and, latterly, leaders has oscillated between the regions and more central NHS bodies. There has also been a notable shift in the basis of professionalisation of NHS managers represented by the shift in terminology from administration, to management and then to leadership. 28,89 Before exploring these very different orientations in greater depth in Chapter 4 , it is useful to note briefly this shifting emphasis in management training and development initiatives.
The NHS Management Graduate Training Scheme (MGTS) broadly retains the structure set up in 1986, combining formal education [leading to a Master of Science (MSc)] with a rotaring series of placements and internships in NHS organisations that give prospective managers direct experience of a range of health-care management situations together with formalised education and training. Other than the MGTS, most of the important current management/leadership development programmes were established as part of the Modernisation Agenda in the early 2000s, including initiatives promoting diversity in management, including Breaking Through (for black and minority ethnic employees), Gateway to Leadership (to develop senior managers from outside the NHS) and the Athena Programme for Executive Women. Such initiatives were underpinned by the creation of the Leadership Qualities Framework (LQF) in 2004 by the NHS Leadership Centre. Details of these programmes are summarised in Appendix 10 .
In 2009, the Department of Health published Inspiring Leaders. 90 Reflecting the strategy set out in The Operating Framework for the NHS in England 2008/09,91 the Inspiring Leaders report explicitly devolved responsibility for leadership development to regional employers, requiring SHAs to produce talent and leadership plans by the end of July 2009. In line with the principle of subsidiarity, these plans were to be cascaded down to the local and individual level, guided by the overarching activities of the newly formed NHS Leadership Council.
Any potential impact of this was, however, curtailed by the change of government and the Health and Social Care Act of 2012,85 which set in train the abolition of the bodies charged with overseeing leadership development. 92 The new arrangement to ensure continuity in this area took the form of the replacement of the short-lived NHS Leadership Council followed by a new NHS Leadership Academy (formed in April 2012). The principle of subsidiarity, whereby responsibility for leadership development would be cascaded down to regional and local organisations, was rejected. Instead, the NHS Leadership Academy was formed (1) to ensure a more centralised strategy, reducing duplication, fragmentation and discontinuity by providing a single national structure for leadership development and (2) to set in place a more bottom-up approach to development by giving employers ‘greater autonomy and accountability for planning and developing the workforce’55 (p. 40, © Crown Copyright 2010, Equity and Excellence: Liberating the NHS). The intention was to ensure that an integrated national approach was established that made better use of resources by rationalising and standardising what had previously been very localised and fragmented training for leadership. 88
The NHS Leadership Academy sets as one of its primary tasks the need to professionalise leadership in health care. Associated with this would be greater expectations of health-care managers to be more proactive in taking responsibility for performance. 88 Citing recent research reports,93 wider academic research and widely cited instances from the private sector (e.g. General Electric), the NHS Leadership Academy briefing makes strong claims regarding the ability of leadership to make a significant difference to the performance and outcomes of organisations. Although still at an early stage of development, the Leadership Academy has set out three core programmes that are to be established:
-
The foundation-level programme is aimed at aspiring leaders with some experience of managing people and leads to a postgraduate certificate.
-
The mid-career programme is aimed at those who manage team leaders, for example, and who seek a broader leadership role. This programme leads to a Masters degree.
-
The senior leadership programme is preparation for an executive, national or other senior leadership role. There is no formal qualification; instead, individualised, bespoke programmes will include academic support, coaching, peer review, self-management and self-direction.
If we also consider the managerial framework developed in Chapter 2 , it is clear that, quite apart from these general initiatives, managers face a considerable variety of forms of formal education, training and development associated with their distinct career pathways into management. 80,94 A well-established pathway of clinical training and development is likely to underpin not only medical staff who move into management positions (and medical science staff), but also nurses and allied health professionals (AHPs), whose development into management roles is likely to take a more experiential learning route. 95–97 Similarly, many functional experts are likely to follow quite distinct paths of professionalisation (e.g. in finance, HR, marketing, law) that may or may not coincide exactly with health service experience or with progression into health-care management roles. 31,32 General managers in health care are, of course, expected to be a more diverse group in terms of their background, training and experience. 98 The question becomes, ‘How do different types of manager in different types of trust access and develop their management knowledge base in order to help them become effective managers?’.
The case study trusts: organisational context
The first step is to identify some of the key contextual features of each of the trusts as they influenced and informed management issues, actions and concerns. The answers to phase 2 interview questions asked about ‘organisational context’ and ‘change’ yielded a set of coded factors that were identified by the respondents as important.
The factors relating to organisational context were:
-
Charity: the impact of any charity related to the trust, its strategic influence/importance and financial contribution.
-
Clinical activity: references to specific clinical area(s) or specialism(s) of the trust.
-
Commercial activity: references either to strategic commitments or to actual financial contribution.
-
Finance: references to the financial status of the trust, either positive or negative in tone.
-
Foundation trust status: references to its impact, typically in terms of governance or strategic direction.
-
Human resource management: reference to HR issues and the make-up of the workforce.
-
Patient population: reference to the patient profile with particular implications for practice.
-
Research activity: impact of research activity within the trust, in shaping priorities or financial or other contributions.
-
Size: references to the trust’s absolute or relative size, including the impact of any organisational resizing.
The incidence of discussion of particular factors in the interviews at each trust is summarised in Figure 2 . As may be expected, in each trust a different set of factors were identified as salient contextual issues; moreover, some trusts appear to be high-context organisations, in which interviewees regularly highlighted the unusual or distinctive aspects of the context in their accounts. In others, specifically the acute trust, explanations were rarely framed in this way.
FIGURE 2.
Contextual factors by trust.
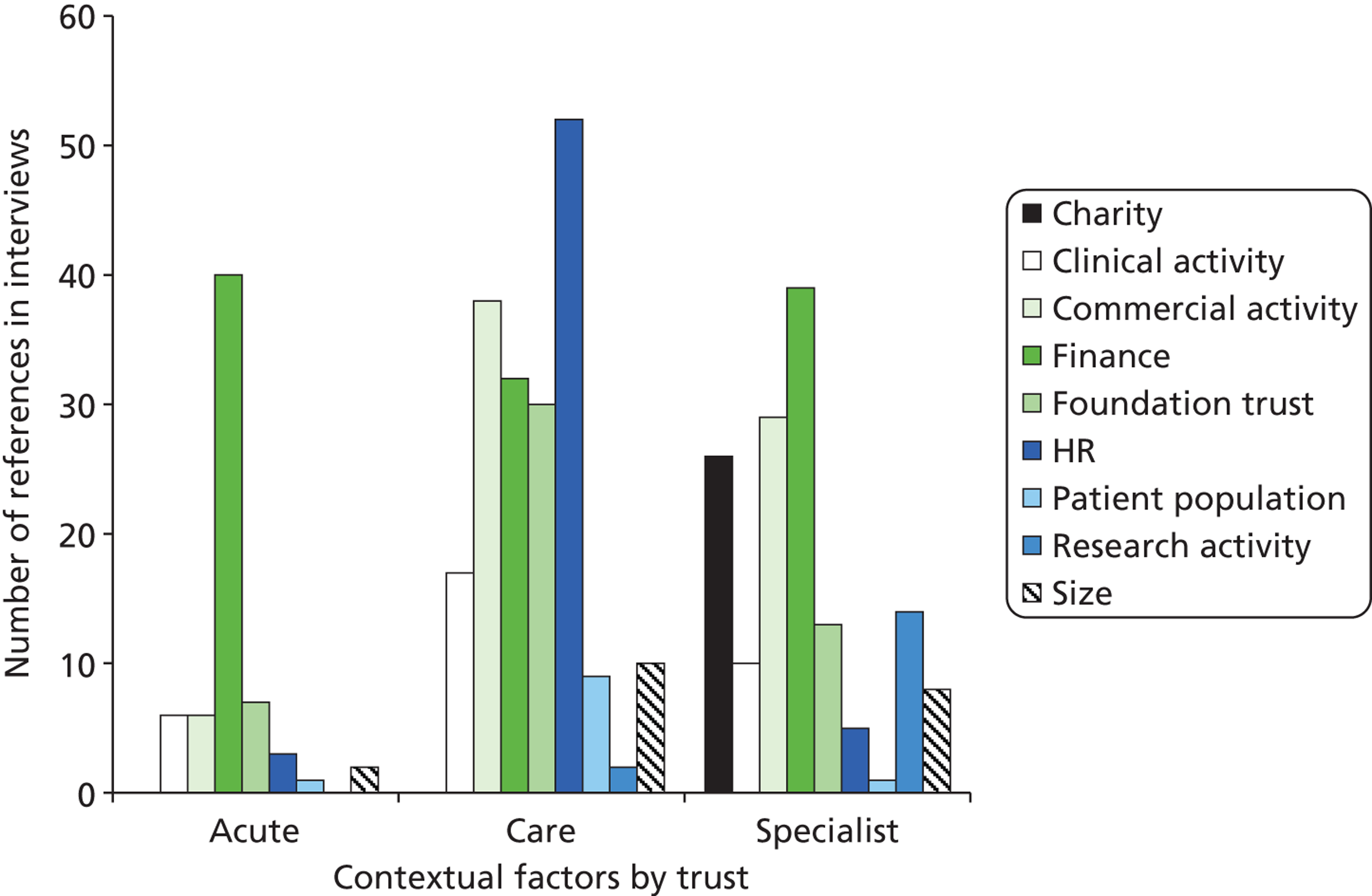
The factors identified related to change were:
-
Competition: the impact of increased competition on the trust and the individual.
-
Growth: opportunities and pressures resulting from the expansion of the organisation, the service area or the department in question.
-
Policy reform: changes resulting from government or Department of Health policy, typically relating to either the ‘Nicholson challenge’ (the requirement to save £20B by 2015) or the reforms set in place by the Health and Social Care Act (2012). 85
-
Organisational restructuring: the opportunities or challenges resulting from local restructuring, either intraorganisational or through mergers and successful tendering to run additional services.
The incidence of these themes in interviews at each trust is summarised in Figure 3 . As with the contextual factors, there were significant differences between the trusts in what interviewees saw as important aspects of change, and also in the extent to which they raised any concerns at all about change and its implications for them and their organisation.
FIGURE 3.
Aspects of change by trust.
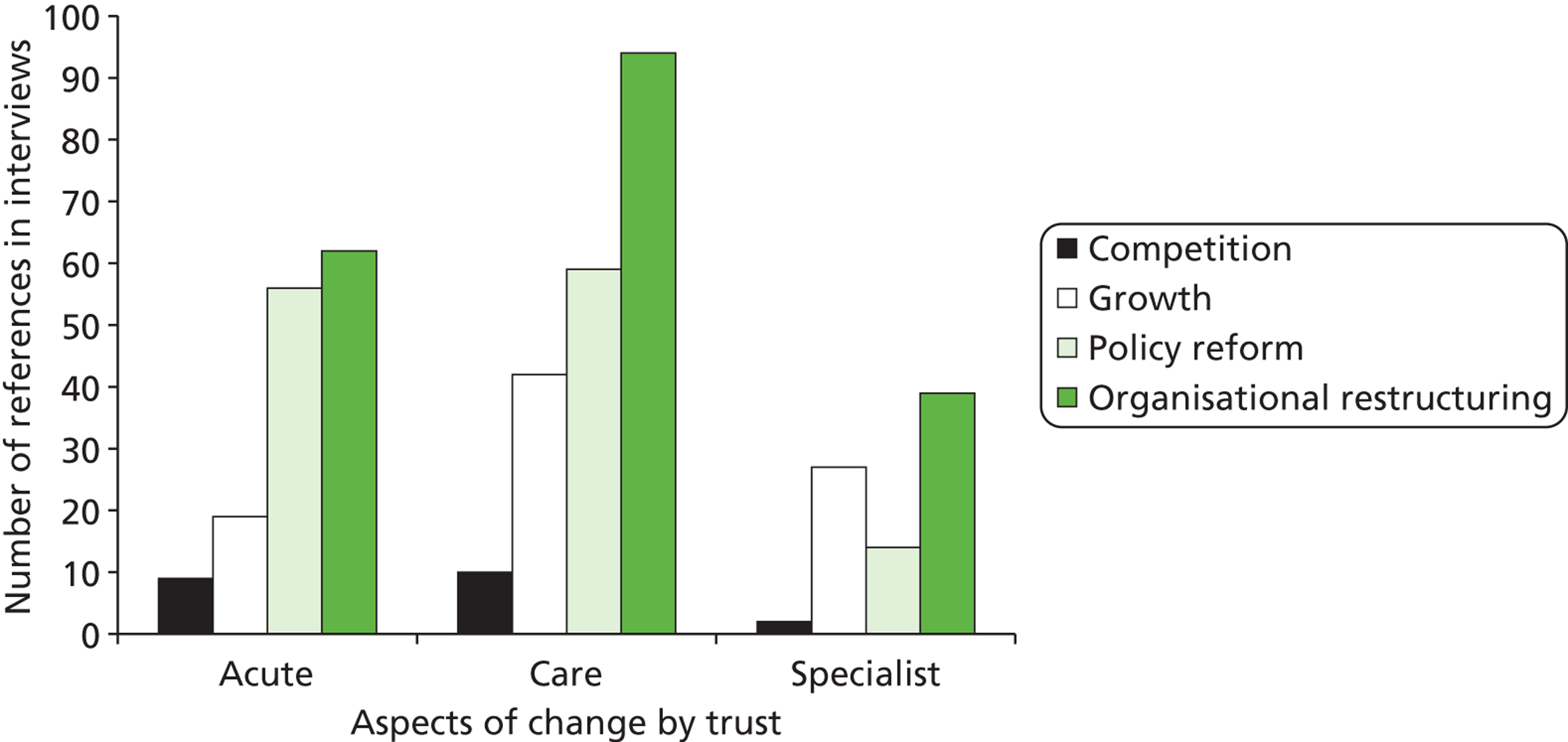
The remainder of this chapter delves more deeply into the aspects of context and change of relevance to each of the trusts. A summary of the key points that will emerge from that discussion is presented in Table 9 .
| Feature | Acute trust | Care trust | Specialist trust |
|---|---|---|---|
| Workforce | 5700 | 5500 | 2500 |
| Turnover | £275M | £230M | £170M |
| Spatial/geographical | Largely single site, some off-site community services | Extremely dispersed geographically | Largely single-site divided by main road, some outreach |
| Cultural | Divided by business group as well as between clinicians and management | Each region has a different culture, substantial effort put in by headquarters to co-ordinate | Largely unitary culture owing to size, some insularity within trust |
| Hierarchy | Relatively flat but evidence of status consciousness | Fragmented, efforts by headquarters and HR to co-ordinate/control | More managerial layers than other trusts |
| Clinical–managerial relations | Managers attempt to manage clinicians as source of tensions | Managers typically are clinicians | Managers attempt to influence clinicians from subordinate role |
| Performance management | Objective set and clearly communicated by board. Commitment to enact disciplinaries | Regime seen as inflexible and a little punitive. HR blamed, although most recognise external forces at play | Increased since acquired FT status |
| Competition | Seen as threat and undermining local collaborative relationships | Seen as opportunity, strong track record of bidding for contracts and generating income | Use of outreach to pre-empt takeover threat and some concerns about external providers |
Acute trust
The largest of our three trusts, Acute, was one of the first FTs established and was primarily focused around a large district general hospital (DGH) originally opened in the early 1900s. It is based in a medium-sized town in northern England and, with 5700 employees, it represents one of the major local employers. The hospital treats around 500,000 patients a year, has over 50 wards and has an annual budget of around £275M.
During the course of the project, the trust expanded by taking on responsibility for community health-care services for a local area. Community services now accounts for a third of the trust workforce and a fifth of its income. Apart from community services provision, the trust is almost entirely located on a single suburban site, with the original buildings the centre of a mesh of new expansions and extensions added over nearly a century. Trust senior managers are located at the heart of the oldest buildings, while large sections of administration are located in 1960s’ offices on the outskirts of the grounds.
Culturally, there was a strong impression of a highly managed trust, in the sense that there was a strong bureaucratic structure supported by explicit corporate strategy driving rigorous performance management, which did not necessarily result in harmonious relationships between clinicians and management. Historically, there had been a stable senior management team at the trust, although various changes undermined this throughout the course of the project. Across the same period, Monitor downgraded the financial risk rating for the hospital from 4 to 3 and the governance risk rating increased from amber to red, indicating increased pressures across the trust.
More generally, Acute was consistently regarded by interviewees as having clear strategic direction, thorough systems of governance and a generally formal and corporate style. This was captured in a typical comment from Felix, a functional manager:
I’d describe Acute as business-like, a lot more business-like. When I came I was, like, wow, it’s run like a business and that’s a cliché, but (my previous trusts) felt amateurish, just bumbling along and ‘yeah, all right, we spent 2 million pounds more than we should do, oh dear’ type of thing. But here it’s a lot more joined up and a lot more business-like, and a lot more intelligent. I think the trust board, there’s a lot of intelligent people on that a lot of the execs are good people to work with and interesting people to work with, with good ideas. And it [percolates down], absolutely.
However, other accounts challenged this picture of corporate efficiency, pointing to a number of disruptions in the senior management team due to departures and long-term absences, and reflected by the changing status of the trust in the eyes of Monitor. One clinical manager, Bethany, captured well the growing levels of uncertainty at the trust:
The trust is in difficulty and the SHA aren’t stepping in, our chief exec’s on long term sick. Everybody’s acting up and shuffling around. Massive issues, Monitor are going to step in, this, that and the other; why aren’t they doing anything; are they waiting for us to fall over and in will come somebody else? [laugh] I don’t know. Interesting times.
Compared with the other two trusts, staff at Acute made very little direct reference to contextual factors relating to the organisation in their account of practices or indeed the particular challenges facing the organisation impacting on them, with the significant exception of finance ( Figure 4 ). One explanation for this would be that it was not seen internally as particularly distinctive, that it represented a standard, traditional DGH, a typical organisation in the modern NHS and financial pressures are experienced across the NHS at present.
FIGURE 4.
Contextual factors at acute trust: number of interview references.
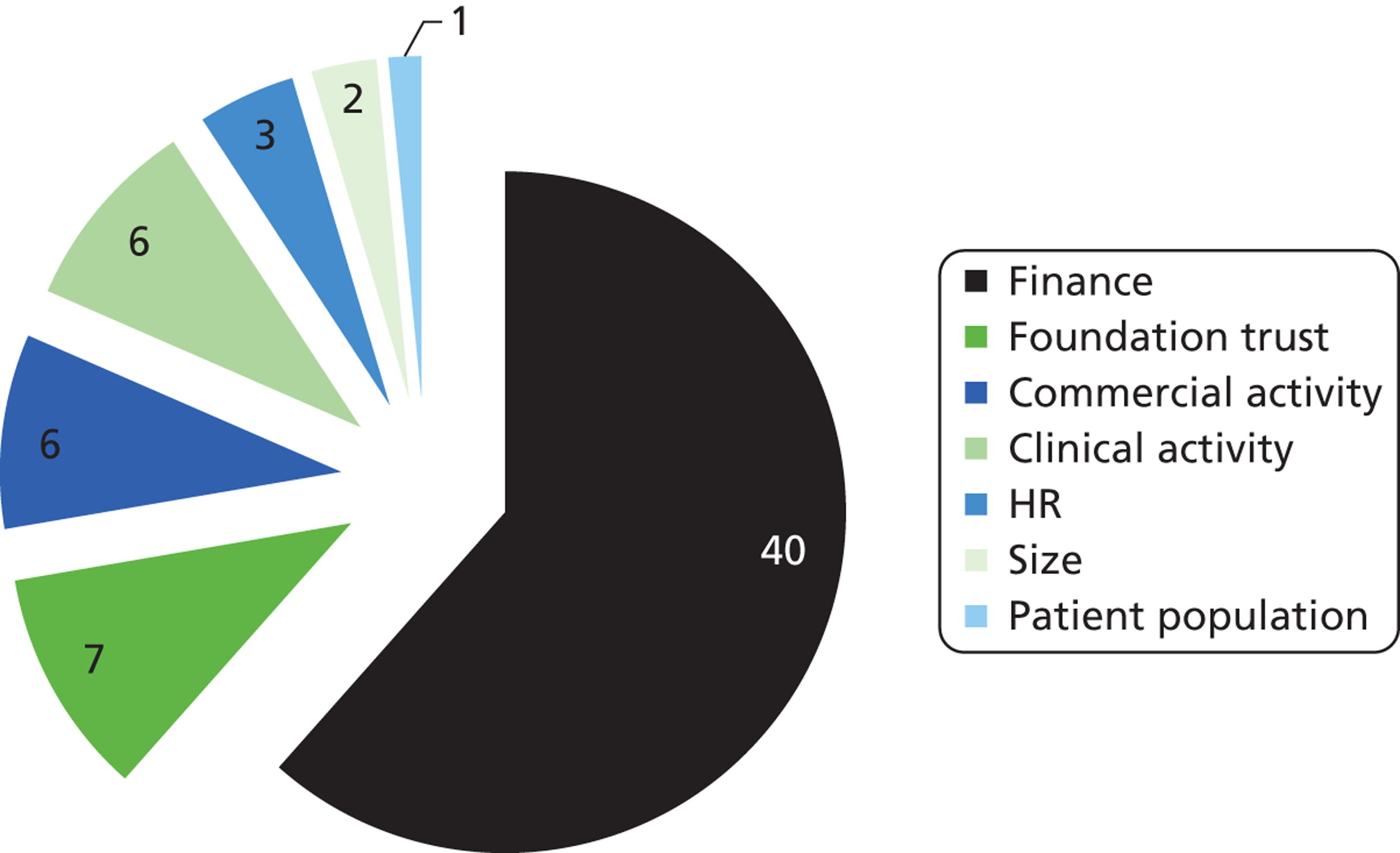
Discussions of financial pressure pervaded most interviews at the acute trust. Staff were accustomed to the policy of not replacing colleagues who left and sharing the work, and it was noticeable how many staff in the trust, when asked to define their responsibilities, were acting up or covering two or more positions. The immediate consequence across the board was a palpable intensification of work:
It’s hard, every day, every week seems harder, it feels like wading through treacle (. . .) It’s a lot tighter now. I mean I’m not saying we didn’t work hard before, but it’s really, really pressurised now and there’s not a minute to spare.
Felix, functional, Acute
The process of adapting to demands for more radical change was not helped by the relatively poor relations between management and consultants in the trust:
Most clinicians just want to stick the blinkers on, turn up to their clinic and their theatre list and whatever little audit they’re doing at the time, or whatever service they’re trying to develop, they just want to blinkers on and do that and be left alone and, I think, the problem is, there’s a big ugly truth out there, which is, the NHS can’t stay the way it is, you know, it’s got to change and if you’re going to be in a successful hospital, it’s going to be a hospital that adapts to that change by streamlining services, liaising with others and some services going, some being dropped elsewhere, hospitals closing.
Brian, clinical, Acute
The need to share ownership of the financial challenge between clinicians and management, although by no means unique to the acute trust, did pose particular difficulties, which became more intractable as it became apparent that trimming budgets would not be sufficient and more fundamental rethinking and redesign of clinical services would be necessary. A common theme in accounts was that the trust had saved as much as it could through trimming small percentages from individual budgets through non-replacement of staff and extracting more work from individuals. The challenge of achieving the scale of savings demanded was seen to require creative, strategic action, but the intensity of operational demands often prevented this kind of long-term innovation on service delivery:
We’re too busy staring in the mirror about current problems, and we’re not going to deliver 15 million pounds’ worth of savings to deliver this year. And you can find maybe half of that by working harder and cutting corners and stuff, but at least the other half of that’s going to have to come from doing things radically differently, transformational work.
Greg, general, Acute
For others, the scale of the necessary savings resulted in a kind of fatalism, as in the case of Ramesh, a clinical manager:
The amount of cost savings they’re expecting, it cannot be done at a business group level, full stop. So I’ve analysed it and thought about it and from my thinking and understanding. So that actually takes away the pressure completely, because the scale of financial thing they need can only happen at wide scale organisational changes, i.e. organisations merging or much more transformational change across the health economy.
Ramesh, clinical, Acute
For most, however, maintaining a safe service while delivering savings represented the most pressing concern, now and into the foreseeable future.
Other than finance, only three aspects of the organisation were mentioned with any regularity – FT status and commercial and clinical activity – and then only by barely a quarter of the 20 managers interviewed. Given this difficulty in articulating what made Acute distinctive, there is a need to avoid overinterpreting the few attempts by interviewees to describe other relevant contextual factors. Several interviewees made reference to the impact of FT status in the organisation, typically using this to account for the stability in strategic direction and leadership in this trust compared with other DGHs nearby, or emphasising the professional business culture and clear lines of accountability through the trust brought in by FT governance:
Foundation trusts are so much more business focused and whilst it isn’t about profit at any extent above patient care, it is about trying to look at business decisions on things and not just let things go as they always have been really. It is about looking at getting the best for your money and about linking it all to quality a lot more and making people think about things really.
Jessica, functional, Acute
In the background, the major reorganisation implied by the acquisition of new community services and their integration with the trust as a whole and with the existing community services run by Acute was a pressing issue, particularly for those most directly concerned. For those in community services joining the organisation, there were frequent complaints that they were being absorbed by a larger, bureaucratic organisation with little interest in their own established way of working (through, for instance, multiprofessional teams).
There’s an element of our business group feel as though we’re having to jump through Acute’s hoops and we’re having to take on things that we actually might feel are a backward step. ‘Well, we did that ten years ago and we didn’t think it was a good idea, and that’s why we went through this process and came out here’. And an element of frustration, ‘Why can’t Acute see that actually, this is a much better way of doing it?’
Gloria, general, Acute
Instead, the integration process was perceived to involve primarily forcing the new services to comply with procedures that were inappropriate or counterproductive for their work. Integration and efficiencies of scale through merging elements of community services were nonetheless a key element in the cost-savings programme envisaged here.
Looking ahead, the most pressing concerns for the trust related to the impact of the ongoing reforms within the NHS and, related to these, internal restructuring and reorganisation within the trust itself. The ever-present demands for cost savings, the shift to CCG commissioning and, in particular, the drive towards diversity of supply and enhanced supplier competition, which was frequently interpreted as meaning the engagement of any willing provider, exercised the minds of many interviewees at the acute trust.
Care trust
The second largest trust studied, care trust, provides mental health and community services across a mixed urban and rural region. The trust was formed through a merger of various mental health services in the region in the early 2000s and became a FT in the late 2000s. It expanded substantially throughout the course of the project, taking on services in various neighbouring boroughs. By the end of the project, it provided services to over one million residents across an area covered by several acute trust providers and working in partnership with several local authorities. Although the trust recently expanded into community services, our research access focused on those parts of the trusts dedicated to mental health services (although the impact of this expansion and the reorganisation was an important feature of many of the accounts and clearly had an impact across the organisation).
Growth and restructuring had gradually, over the last decade, brought together, in one organisation, several different services, in different locations and across different service levels and sectors. The incorporation of community services, which occurred during the course of the study and which almost doubled the organisation’s size, suggested that this was a pattern that was set to continue. Experiences of restructuring varied in different parts of the trust. One of the most recent restructuring processes involved the bringing together of four of the main service directorates areas in one division, with a single service director. This change was perceived to have been successful, owing partly to the popularity of the new service director, but also to the opportunities it afforded for exchange and collaboration within the trust and for heralding a shift to a less directive culture:
Before the change in management, it was very command and control. It was almost like if you didn’t have your deadline met at least three days before, you knew there would be serious trouble . . . and now you meet your deadline, when your deadline comes, you do it the day before, yeah. You get reminders but the work still gets done, which I think is interesting. But it gets done without you feeling kind of anxious and therefore I think you produce a better piece of work.
Heather, general, Care
Reform, as with finance, was as important at care trust as elsewhere. However, here there was more of an impetus created by the threat of competition. This threat was felt in the more commercially orientated services in the trust, with their distinctive requirements for commissioning and collaboration. Although these services were an important source of income for the trust, managers’ fears related to the intensified threat from any willing provider. Many in these services feared that private and third-sector organisations could take away large parts of their business:
The basic principles [of care are the same] but the actual interventions are different and the commercial world we live in is massively different. (. . .) The first DGH, district general hospital has gone to a private provider, but that’s hard getting a DGH off an NHS trust . . . and it’s the same thing with mental health. It’s a very specialised, very specific industry. The stuff around the edges, the private providers and the voluntary sector providers are a little bit more geared up for, so it makes us very exposed; and things like forensic services, it makes them very exposed as well. So we do have to have quite a different outlook.
Kerry, general, Care
Given the distinctive nature and development of the care trust described above, it is perhaps not surprising that it faced its own particular challenges and had its own narrative of change. Central to these challenges and narrative were the tensions inherent in efforts being made to centralise and standardise processes and rationalise service delivery across an organisation that was very fragmented (geographically and structurally) and in which there was little sense of a cohesive culture, despite efforts by the centre to promote one that encouraged more business-like qualities and a more entrepreneurial approach. Despite there being a quite complex mixture of medical and psychological specialisms, here there was much less of a structural divide between clinical and managerial groups as most of those in general management positions were from clinical backgrounds.
In interviews, staff within the care trust referred to a range of contextual factors ( Figure 5 ), namely HR (largely referring to the distinctive character of the workforce), commercial activity, finance, FT status (a little more negatively than in the other two trusts) and clinical area/patients (not to a great degree, but more than in the other trusts).
FIGURE 5.
Contextual factors at care trust: number of interview references.
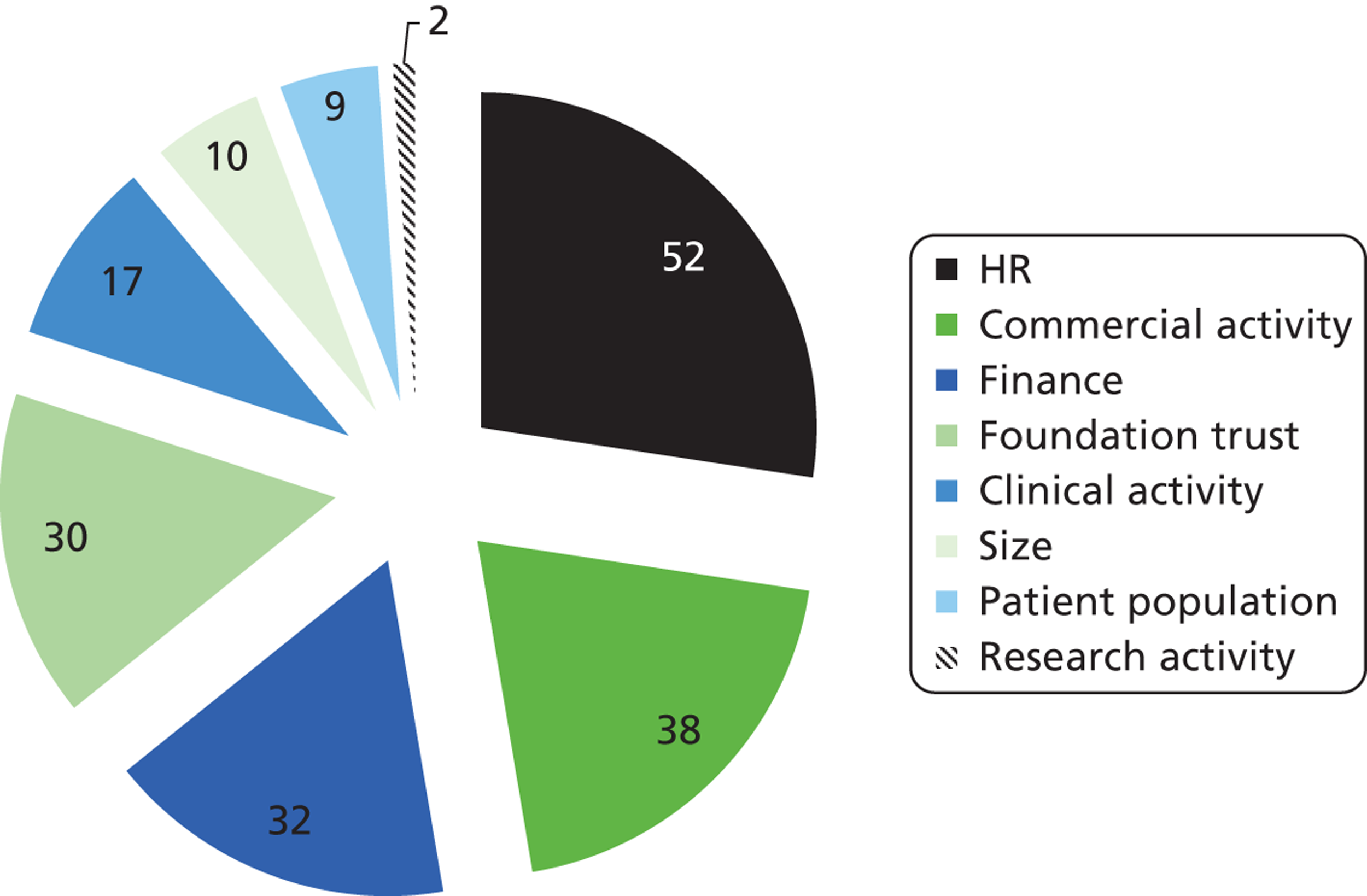
The contextual factors that were of particular importance in the care trust were largely related to the two prominent features of its recent development: growth through the acquisition of geographically and culturally diverse services, and the attempted integration and centralisation of these services.
The focus on HR was in part due to its prominence in these processes of integration and in part to recent problems within the HR department itself. As a function, HR at Care is organised centrally, with business partners attached to particular service groups and areas. Therefore, as a function it straddles the central/peripheral divide of the trust, responsible for many of the challenges faced in integrating the workforce and developing standard practices. The consensus both from within HR and from other parts of the organisation was that it had not coped with recent challenges well, having been left (after the loss of a director) with no senior management representation and lower levels of staffing owing to downgrading and delayering.
The commercial activity of the trust is located in specific service areas which have a mixture of secondary and tertiary services and which have distinctive requirements regarding commissioning and collaboration. Psychological services, rehabilitation services and drug and alcohol services are all services which are external facing and require interaction with a multitude of services across different sectors such as social care, the prison service and the third sector. These services also have a distinctive commissioning landscape, with regular competitive tendering of services and closer day-to-day relations with commissioners (particularly in drug and alcohol services), in which target-focused performance management is intense:
We are massively visible to our commissioners in a way that the mental health service aren’t . . . My commissioners know the name of my staff, they are in and out of our buildings . . . It can be quite adversarial and I think that one of the problems that we have had in the past is the trust standpoint can make that very adversarial . . .
Kerry, general, Care
As this excerpt makes clear, these services have a character which is distinct from what was conventionally seen as the main business of the trust in traditional mental health services and which was contrasted by some with the more localised and insular nature of these traditional services, which were considered to have less of a commercial orientation and little, if any, external network collaboration.
Finance was as important here as it was in the other two trusts, for much the same reasons. The recent financial pressures were of great concern across the trust and this was felt more acutely in some areas than in others. The more commercially orientated services were less fearful of financial pressures from the trust as they were an important part of the trust’s business and central to its growth strategy. However, there was the fear of the increasing external competition.
Foundation trust status was again related to the history of growth and reintegration. Many of the individuals interviewed in this study had been attached to their local services for a decade or more; membership of the care trust followed by FT status were comparatively recent events. Many individuals spoke of the difficulties faced in processes of integration and assimilation and, when this was specifically related to FT status, there was some ambivalence from peripheral services about the more rational and intensified financial accountability and business sense of the trust. This ambivalence was often expressed through a somewhat reluctant recognition of the purpose and benefits of greater rationality in these areas, combined, though, with a sense of culture shock:
I think Care’s very financially driven but I think that’s FT land. That was the biggest change for me culturally . . . Two things are finance and serving effective services – so the regulation and finance. And I guess once you understand that, anything that you’re presenting you can present to them in that way, so you’ve boxed those two key issues off and then you’ve got the audience there.
Harriet, general, Care
Finally, the relative importance of the clinical work and patient population, as compared with the other two trusts, introduced something of an intriguing aspect of the care trust as a therapeutic organisation. The vast majority of the staff we interviewed had some kind of clinical background and they regularly related to their managerial work via their clinical orientation. As suggested by the comparative tables we devised to compare the trusts in the early stages of the study, there was something related to the long-term, cyclical nature of patient relations in the care trust that brought a strong relational quality to the activity of management, which many individuals drew on in their constructions of work-identity narratives:
I think most people that have been in nursing or other professions and end up in management miss what they went in for, which was speaking to patients, spending time with patients . . . I’ve had very little clinical time over the past four years so it’s been a real shift in that respect and I think sometimes when I’m feeling a bit disillusioned with the job . . . I just go and spend some time on the wards with the patients and then it makes you realise that you’re not very hard off really compared to the majority of people on those wards, so that’s a good eye-opener. I think most people in the caring profession genuinely want to come in and help people and I don’t think that’s changed.
Luke, general, Care
This characterisation was expressed throughout the trust. Not only did it go some way to unifying the otherwise somewhat distinct and disparate parts of the organisation, it also fed into the receptivity towards particular forms of management knowledge and development, as will be seen in Chapter 5 .
Specialist trust
Finally, the specialist trust included in the research project was the smallest of the three organisations, with around 2500 staff serving a regional population of around 3 million. The trust is based around a hospital formed at the end of the 19th century and has specialised since its inception in a particular group of diseases. It is prominent in its field at national and international levels, a quarter of its patients being referred from outside the local region. Its annual revenue is around £270M, benefiting from both a substantial and prominent charity and a substantial amount of research activity, supported by strong links to a local university. During the period of research, the trust was undergoing some internal restructuring, combining two divisions into one, but otherwise the narrative at the trust was largely one of growth building on success. Monitor ratings for the trust were consistently high throughout the research project and had been so historically.
The specialist trust was universally described as a highly distinctive health-care organisation, typically in terms of its rather elite status both locally and nationally, and often these descriptions cited the strong brand of the trust, the outstanding clinicians and world-leading research taking place within the organisation as well as the highly effective charity associated with the organisation ( Figure 6 ). Given the specialist focus at this trust, it was surprising how infrequently the clinical activity or the specific demands of the patient population were cited to account for practices here.
FIGURE 6.
Contextual factors at specialist trust: number of interview references.
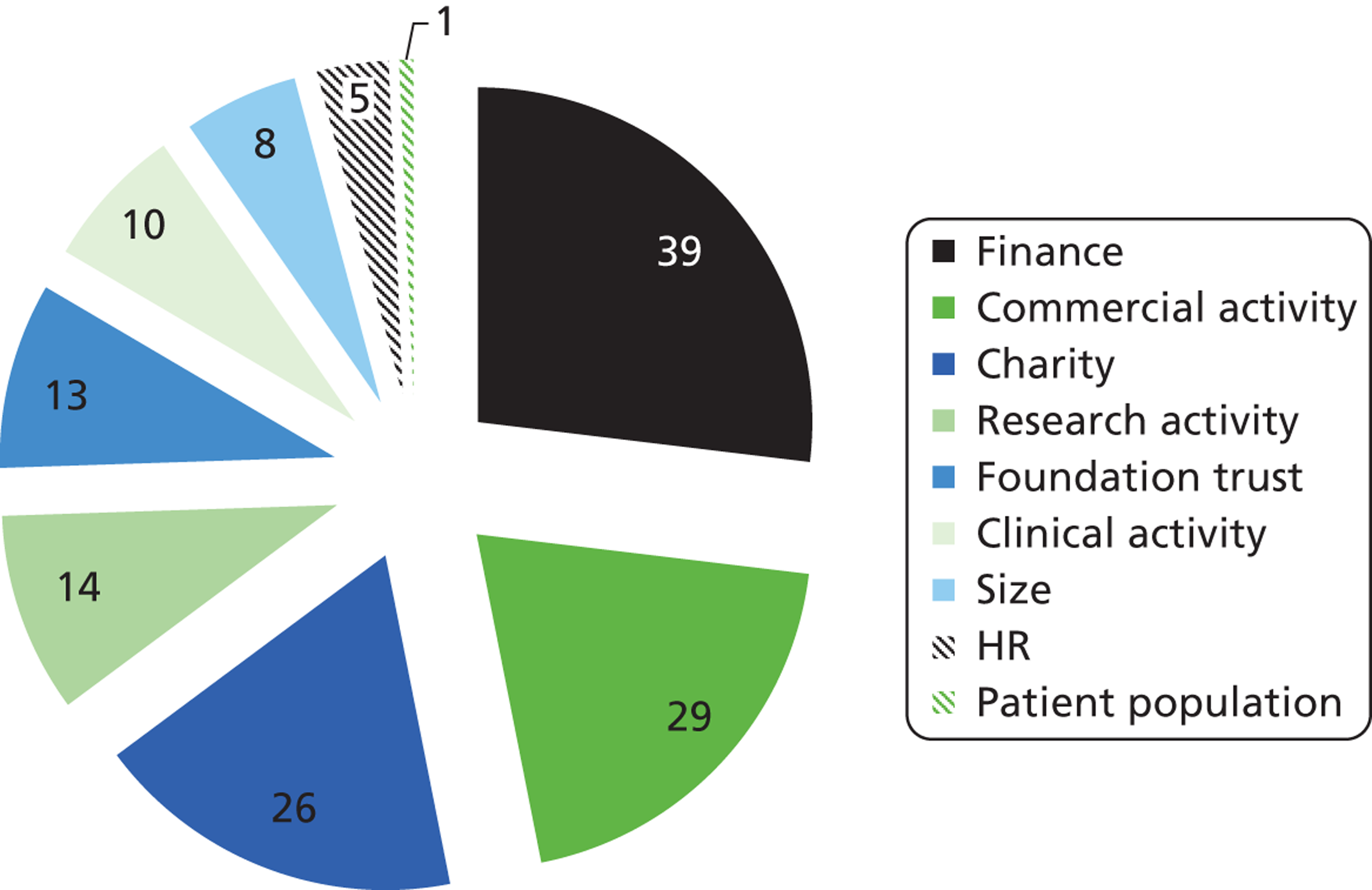
Most described the specialist trust as a rewarding place to work in many respects. This was summarised effectively by a general manager, Becky;
You would be mental to leave the job here and go and work (elsewhere). And everybody (. . .) knows the grass is no greener. So we do tend to retain managers and keep people here for quite some time, because it is a nice place to work. Although everybody’s faced with financial difficulties it is a nice place to work – small hospital, friendly hospital, a good ethos and good outcomes. There are things that we can celebrate, there are a lot of successes. Whereas I know that doesn’t feel that way at some of the other big acute trusts.
Becky, general, Specialist
Across the trust, most staff interviewed evinced a fierce pride about working for such a prestigious institution.
Go and talk to the people down there. We are the best. We want to be the best. We’re going to stay the best. With regards the NHS overall, I can’t really comment because I’ve only ever worked here, right. But I think if a lot of the philosophies that are adopted here, were adopted elsewhere, possibly the NHS might be in a bit better position.
Adrian, functional, Specialist
Although interviewees frequently discussed financial issues and there were pressures to make savings, often quite considerable, most were entirely aware that the trust did not face the same financial pressures experienced at other trusts. The financial health of the trust was physically apparent across the site: substantial building programmes were under way and the high quality of build was clear from the furniture, décor and surroundings in most part of the main hospital, including the offices for senior management and consultants. The administration and management blocks were of a significantly poorer standard, with cramped offices and some departments being located in rather flimsy prefabricated units. The trust was located on a single site, although there was a geographical separation between the management offices and the rest of the hospital with some divisive consequences, which staff made efforts to overcome.
Many staff pointed to the adoption of FT status around 5 years previously as resulting in clearer communication and systems of accountability through the divisions. The organisational culture at the specialist trust was generally represented as proactive, with a clear strategic direction cascaded effectively through the organisation and an effective professional relationship between management and clinicians, with an implicit understanding that both were in some sense at the top of their fields. A number of general managers at the trust mentioned the particular challenge of managing the body of consultants at this trust, who, it was suggested, were less willing to be managed because of their very high status in their clinical fields. There was, however, a clear understanding here that clinical leadership took priority, which perhaps accounts for the relative success described here in securing clinical engagement in difficult areas such as cost-saving through service redesign (in contrast to experiences at the acute trust).
Over the last 12 to 18 months, the message is out there and it now it does feel like it is everyone’s responsibility. So when we have a bi-weekly financial review group meeting here, which looks at efficiencies, there is always clinical engagement, medical engagement on there, and they always attend.
Danielle, functional, Specialist
Interestingly, however, discussions of efficiency savings and financial pressure here were of a different flavour to those encountered in the other trust. Specifically, there was awareness that the trust was relatively affluent and that the savings were largely about protecting the surplus and, thus, maintaining strong Monitor ratings.
Overall, the strength of the culture at the specialist trust was referred to frequently in interviews, explained in part by some as a consequence of the minimal turnover of staff mentioned above and in the fierce pride many displayed about working for such a prestigious institution. However, several respondents highlighted the dangers of this internal cohesion, in potentially creating an institutionalised mind-set and a complacent insularity at the trust, which staff had to deliberately challenge by forming external connections.
Staff at the specialist trust had less to say on the challenges caused by broader change than staff in the other two trusts, appearing to face the future with some equanimity. In discussions of change and its ramifications for the specialist trust, the most remarkable item was how little staff in the trust had to say here, relative to staff in the other trusts (see Figure 6 ). Consideration of possible avenues for growth, including an increased interest in possible commercial ventures and partnerships with private or third-sector organisations, and some debate over the long-term implications of merging two clinical divisions, dominated the discussion. The challenge of competition was almost entirely disregarded, reflecting the trust’s national reputation in its field of specialisation (this was other than some speculation that private-sector companies could undercut the trust in the provision of some basic services).
When pressed on future challenges for the trust, the most threatening scenario most could envisage was the remote possibility that a larger trust may attempt to take over the specialist trust. Avoiding this was frequently linked to efforts of the specialist trust to expand its footprint through outreach, providing specialist services to, and through, other trusts in the area, often located on the premises of the neighbouring trust but using the specialist trust’s branding. In principle, this was seen as not only a means to increase the apparent size of the trust and so fend off other trusts interested in acquisition, but also a strategy of collaborating as an alternative to competing with local trusts. In practice, the competitive tensions and wider financial landscape often challenged such attempts at local co-operation given pressures to reduce costs elsewhere:
We have got really good relationships with some trusts we (provide specialist services to) and some of them are very shaky relationships because they’re in a position financially perhaps aren’t as good as we are so they need to claw an income from whatever they can get so the negotiation is ‘No we’re not paying for that, yes we are paying for that and we will provide this service ourselves maybe.’
Hannah, general, Specialist
Overall, a very consistent picture was painted of the trust – one that emphasised its relative financial security due to charity and research income and supplemented by sophisticated commercial operations working effectively to support high-quality specialist care.
Summary
This chapter has explored the institutional and organisational context within which management knowledge and learning occurs and highlighted key features of that context, its impact on management work and on the knowledge base required to perform management. Chapters 4–6 present the data and analysis based on the three main sets of factors that helped shape the interview process and that were highlighted through the coding of the data: management, knowledge and networks. Each of these themes will be addressed in turn in a distinct chapter, in which the impact of the wider institutional context as well as variation in organisational conditions will also be taken into account.
Chapter 4 Management
Introduction
For me . . . a leader is someone that is very visionary, innovative . . . they’re the people who can sit in a room and come up with something that nobody else can think about. You take people with you, you get people on board, you take them with you but you’re not frightened of making that decision that needs to be made that’s not the consensus or the popular decision . . . As a manager . . . you just tell people what to do . . . I guess managers just manage don’t they?
Ellen, functional, Specialist
The quote above indicates the marked difference in importance placed on management and leadership by many interviewees, reflecting the changing wider discourse examined in Chapter 3 associated with new public management (NPM). Of particular relevance here for health care is the notion that NPM is part of a broader discourse of new managerialism,99 which is conceived as a shift in organisational control away from the established professions towards more managerial forms of regulation and control. 7 Given the historical power and influence of the medical profession within health-care organisations,100 it is perhaps not surprising that this purported shift has received a great deal of research attention. 27,28,60 However, it also bears on a number of important themes in our research concerning the experience of being a manager in health care. These relate to the importance of managerial identity in understanding management practice, how middle management work and leadership are related, what these processes mean for managing the professional–managerial divide and the professionalisation of management itself in the NHS. Of particular interest to us here is the notion of hybridisation 36,60 with professionals moving into management and managers becoming professionals amid the shifting distinctions between different kinds of professional/managerial work.
Managing identities
Key to an understanding of being a manager is an understanding not only of the day-to-day performance of management work, but also of the relation of individual managers to the organisations and institutions they work in and from which they draw meaning in an attempt to construct particular work identity narratives. 101 These narratives are of particular importance to this study, with its focus on individual career trajectories, occupational socialisation and professional identity.
The maintenance of a coherent and stable work identity narrative for managers is challenged by the ‘ambiguity, obscurity and linguistic muddle surrounding the meaning of management itself’,102 which creates a highly diverse and often contradictory set of meanings through which narratives are constructed. This challenge has been represented as antagonisms 101 – requiring, for example, managers to be emotionally detached and emotionally engaged at the same time and caring for business while caring for people. As will be seen, these antagonisms are clearly relevant in the contemporary health-care management context and are likely to have important implications for management responsibilities.
Narratives are also shaped by organisational and institutional conditions. The social conditions in health care under NPM are composed of networks of public and private organisations, bound by contracts, within competitive, market-style relations. 80,103 In this context, managerial work may be less a technical exercise in the application of rules and procedures and more about managing relationships. Whether or not this promotes more of an emphasis on hard business skills or soft social skills (or some combination), it does suggest a greater intrusion of identity regulation into hitherto unchartered internal depths. 104,105 In other words, are managers more liberated by marketisation or do they find their identities more tightly regulated and constrained?106
Middle management
As previously noted, one of the headlines of the most recent changes in health policy was that around 45% of management was to be removed. Historically, it is middle management that has been the most disadvantaged through such organisational change,107 with those remaining often facing intensified work. 86
The delayering of middle management often goes hand in hand with its denigration, reinforced socially by stereotypical portrayals of middle management. As one study reporting nurse attitudes to management noted, managers were seen as ‘aloof’, ‘smarmy’, ‘shifty’, ‘yes-men’, who used the ‘old boy network’, had ‘slept or crept their way up’, were ‘invisible at ward level’ and ‘hostile to patient care’. 108 It is difficult to see how such social stigmatisation would not feed into the self-concepts of managers. 109 As Merali71 also found: ‘the majority of the managers [in that study] were convinced that the general public believed that doctors and nurses were the only professionals in the NHS who are motivated by a desire to serve/provide care to society’. 71
Middle managers in health care may experience a distinct lack of credibility as they lack the influence of more senior directors and are distanced from the clinical frontline. They can find themselves in an ambiguous and fragile occupational space somewhere between ‘board and ward’, with only a somewhat abstracted ‘belief in the NHS’ or ‘public sector ethos’ to which to tether their work identity. 102
It may be then that the recent valorisation of leadership in the NHS context70,89 provides a way for middle managers to develop their role and identity in more positive, constructive and even heroic ways. 110 Learmonth argues that the rhetorical shift from management (which itself conveyed in its time more status and authority than administrator) to leadership is an attempt to replace the ‘more ebullient and less bureaucratic image’ associated with the former. 89 At the same time, it is perhaps a term that is likely to hold some currency with the medical profession (which provides clinical leadership).
The question becomes, ‘To what extent are the two – leadership and management – separate or synonymous functions as managers presumably need to combine (managing) targets and operations with (leading) staff and change?’. In addition, to what extent does the shift to a discourse of leadership allow for the observation that it is the work of middle managers in negotiating local engagement and implementing new processes that drives change?31 Furthermore, is ‘driving’ less in keeping with middle managers’ ‘semi-autonomous’ roles, when research suggests they may act more as ‘facilitators’ rather than directors of change?26
Managers and professionals
A third and related set of questions concerns the changing nature of the relationship between managers and professionals and what this means for their relationships, as well as for managerial professionalisation. O’Reilly and Reed28 argue that leadership constitutes a distinctive change narrative in the current NHS context that brings together aspects of both managerialism and professionalism. This hybridisation is an important notion for the present study, as will be seen.
Management as a technical practice has long been seen as at odds with the interests of other professional groups that may dominate what Mintzberg111 might define as the professional bureaucracies in which they both work, as professionals are more able to establish closure around their own expertise, whereas managers are not. 36,45 Conventionally, this is a model which fits health care very well, with the medical profession being one of the oldest and most influential professional groups. 100 Indeed, the resistance to new managerial initiatives by the medical profession is a common theme of health-care research. 48,50,112
Nevertheless, many such studies have noted that ‘professional intransigence’112 has perhaps only slowed the inevitable encroachment of managerial logic into health-care organisations – most obviously perhaps through the financial rationalisation of medical decision-making and the increasing demands placed on health-care professionals to respond to government targets. This hybridisation of work in health care has, therefore, muddied the conventional distinctions between professional and managerial work, with a good deal of research focusing on the changing work identity narratives of nurses and their transformation into ‘managerialist professionals’113 and ‘boundary spanners’. 50
In this more complex and nuanced context of ‘organised professionalism’114,115 in health care, research has focused on the power plays at work among the more integrated manager professionals, the tensions underlying idealised notions of ‘distributed leadership’27 and the relative ‘strategic contributions’ made by different groups of managers. 26
According to Brooks,113 nurses have used managerial discourses to sure up their own professionalism, an argument that contains an irony given that managers themselves have never been able to do the same. 36 Such a strategy also underlines the importance of clinical credibility both for constructing a stable work-identity and for developing greater professional autonomy (as well as enhancing job security). The argument also prompts the questioning of exactly what is meant by professionalism in this context. If clinical credibility is the main difference between the professional claims of nurses and non-clinical managers, then this resembles a form of ‘status’ rather than ‘occupational’ professionalism,36 tied to the local conditions of particular organisations. To what extent, then, does this form a basis for wider projects of professionalisation the occupational group of managers as a whole?116
To explore these themes, we now move to our empirical examination of the case data, exploring, in turn, management and leadership, the clinical–managerial interface and implications for management responsibilities and skills.
Management and leadership
As noted above, the definition and distinction of management and leadership has been a topic of investigation in the management literature for some time and has also been frequently discussed in relation to health care. The relative seniority of participants in this study meant that this topic was important to explore as we imagined that in practice these skills would be interlinked and often embodied in the same person. However, the most striking pattern in responses to questions about management and leadership was the conception, held by the vast majority of participants, that they were best understood as separate functions: the former more about achieving stability and the latter more about change. Furthermore, in the majority of cases, there was a clear valorisation of leadership and a clear denigration of management.
The following excerpts demonstrate this pattern of response and through them we can begin to draw out some of the consequences of such a fixed conception:
I would definitely see management and leadership as different. I think management I see as more of the nuts and bolts, day-to-day, getting tasks done. I see leadership as inspiring people, driving them forward, making them want to come to work, empowering them to use their initiative.
Felix, functional, Acute
Having drawn this sharp distinction, the same respondent goes on to describe a further set of implications:
You can’t teach leadership. Management you can read it in a book and you can teach me how to manage someone and do their appraisal and manage poor performance and that sort of thing. But leadership, you can’t really learn leadership, it’s in there somewhere and you have to find it and bring it out.
Felix, functional, Acute
Understanding leadership as an internal, possibly innate, set of attributes implies that it is something embodied within individuals rather than easily codified and shared, or developed formally. This creates challenges for knowledge mobilisation and development, which is one of the themes to be discussed further in Chapter 5 . Such an individualised conception also creates challenges for such things as succession planning:
Yes, I think management of people is getting people to do their job, and to ensure that they do the job well. And it doesn’t necessarily have to be people, you could be managing other things. Whereas leadership, I see as someone who would have more of an inspirational role, someone who would motivate, probably a larger number of people as well. I think [the Director]’s position, certainly, has more leadership than mine, in that you’re presenting to a number of people, you’re delivering your strategy, you’re telling them where you want to be. Whereas management, if I think of the lower levels of management, those that manage, say, five or six of the trade staff, the junior . . . lower management . . . there isn’t that much leadership in their positions. I see it as a sort of higher role.
Christopher, functional, Acute
In the above excerpt, there is first of all a split created between management and leadership, here understood as different roles and people. There is also the conceptual divide between the content of these roles, with management understood to be ‘getting people to do their job’ while leadership is seen more as ‘someone who would motivate’. Interestingly this excerpt also draws a distinction in terms of seniority, with leadership seen as residing towards the top of the hierarchy. This stands in contrast to more progressive models of ‘democratic’, ‘transformational’ and ‘distributed leadership’. 27
Building on previous work by Kotter,117 Table 10 summarises some of the key consistent dichotomies that our respondents highlighted in the sizeable amount of qualitative data that constituted discussion in our interviews about perceptions of management and leadership.
| Management | Leadership |
|---|---|
| Nuts and bolts | Visionary |
| Following policies, procedures, processes | Make decisions |
| Day to day | Long term |
| Can read it in a book | Cannot be taught |
| Improved through (standard) training and development experiences | Natural born, charismatic though enhanced through self-awareness training |
| Sat behind a desk | Being dynamic |
| Getting people to do their jobs | Helping people see why they do what they do |
| Very specific skill set | Influencing/inspiring people |
| Safe services from standardisation | Improve services by taking risks |
| Focus on task | Focus on strategy |
| Bureaucratic | Heroic |
| Unpleasant | Dynamic |
| Enacted practices | Embodied qualities |
Although there were some important differences in how leadership and management were understood and related to one another, what was remarkable was the surprisingly high degree of consistency across the trusts and across managerial groups in how respondents viewed leadership and management in these terms, and the absence of any clear and systematic relationship to factors such as age or training.
Although many of the characteristics of management undoubtedly fulfil important functions in health care, for example paying attention to detail, following policies and procedures exactly and having highly specialised skills, it was clear too that there was a preference for leadership over management. Descriptions of leadership qualities included seemingly extraordinary powers of vision and influence. In contrast, management was portrayed as a dull, procedural function that involved following policies and procedures, focusing on tasks and getting the day-to-day ‘nuts and bolts’ (Felix, functional, Acute) of the job done well.
I see a manager more as a kind of functional keep the show on the road type job, and I’d say that [is] probably more what I am or how I perceive myself. I think leadership is much more about being out there, being visionary and taking teams with you and less of the kind of mundane day-to-day stuff.
Sarah, general, Acute
There are consequences of this conception both in the denigration of management as a function and also in the valorisation of leadership as something mystical and heroic. As noted by Rost,118 caricaturing one group as good and another group as bad establishes sets of assumptions through which bounded communities can be formed. The fact that clinical managers were more inclined to present themselves as leaders rather than managers demonstrates the relations between conceptions of self and social identity in groups that can, in turn, impede interaction and knowledge sharing between groups. Furthermore, the denigration of management undermines the importance of management as a function, reinforcing the view implied in the following quote (and echoed by other interviewees) that the NHS was overmanaged and underled:
The NHS . . . has got a lot of managers, it’s just the way it is . . . because, you know, everything’s in teams and little pockets and things wouldn’t be successful if there wasn’t someone steering in the right direction (. . .) But I don’t think there’s as many leaders in the NHS. I’d say a leader is someone who sticks their head above a bit more and really pushes things forward . . . There’s lots of people managing in the NHS.
Thomas, functional, Specialist
Khurana119 has critiqued what he has referred to as the ‘quasi-religious belief in the powers of charismatic leaders’, arguing that this overlooks more important and essential social and economic determinants of organisational success. Other critics of the ‘superleader’ concept66,67 argue that in organisations facing continual change and reform, it is middle management that is responsible for achieving the balance between change and continuity.
Although there was a surprising uniformity among participants regarding this management/leadership dualism, this view was not unanimously held, and there was a small minority of participants who presented a contrasting position based on leaders ‘getting [their] hands dirty’:
I think this leadership is a very amorphous kind of notion that is very difficult to pin down and therefore very difficult to achieve (. . .) I think that leadership is often projected as vision and strategy and actually I think a lot of leadership is about getting your hands dirty with everybody else and not sitting there and going, well you all do it . . . So it is a kind of a lead by example, rather than just thinking up a fancy strategy and waiting for everybody who has got a day job to have to do it.
Kerry, general, Care
Even when such a conscious self-positioning was not evident, several participants reflected on their own practices in relation to management and leadership and would often draw on the same notion:
I think the way you prove you’re a leader in this role is by leading by example, by sorting things out that are quite difficult to sort out, by being on the ward, by being present, by mucking in, by showing that you’re able to.
Luke, general, Care
However, the question was also raised of whether or not organisations would be receptive to more transformative and democratic ideals of management and leadership:
My total ideal would be if I was working with a whole bunch of managers who actually thought that the hierarchy was upside down and that they were working for their team and that their job was to make their team the best and the most productive and to have the best employment experience they could, not that they’re large and in charge and telling people what to do (. . .) and I don’t think that that’s necessarily entirely acceptable here by any stretch of the imagination. It’s a very directional type of organisation with leadership from the front rather than from behind. So for me I feel I have to operate in that mode more than I probably want to because that’s what’s expected. You’re expected to get in the front and lead the services.
Ruth, functional, Care
In the excerpt above, Ruth uses what she sees as the rigid and conventional ideal of leading from the front to suggest that this may not be the best way to integrate organisational transformation and individual development.
These points reveal a tension at the interface between leadership understood as heroic, risk-taking and visionary, and what were often felt to be dominant organisational strategies and imperatives. Placed as they were immediately beneath divisional directors and board members, participants in this study often found themselves as leader–managers having to face simultaneously in two directions:
That operational manager role is the interface between the organisation and the ground level staff and, I think, that it’s really important to be a strong leader for your practitioners, so that they know they can discuss issues, that are challenging to them, without it feeling punitive or exposing. They need to feel safe to be able to think about their practice. So, you need to create that. But, equally, you need to be mindful of what the organisation is requiring and what the organisation might think about some of that practice and some of the changes that the organisation tries to impose.
Gabrielle, general, Care
Some differentiation between clinical and non-clinical orientations is hinted at here, and this will be picked up in The clinical–managerial interface. However, it also suggests a rather different skill set than one might associate with the visionary superleader:
I think, that’s one of the key skills, really, is buffering and understanding enough about both systems to know when you can ignore something and when you, absolutely, need to let your team, you know, kick them up the backside.
Gabrielle, general, Care
Although Gabrielle does refer to the need for active performance management, this is seen to require a softer skill set involving empathy and emotional intelligence, with the intent of reconciling two potentially incongruous perspectives. Regardless of the softness of the approach, the excerpt does underline the importance of reinforcing accountability – an approach more forcefully stated by Kerry:
I have a couple of phrases I switch between depending on which way the wind is blowing, but one is, ‘by any means necessary.’ So if there is a job to be done, actually we have to get the job done. And that’s the other one: ‘the job is to get the job done’, not some airy fairy idea about well this is my preferred management style. I don’t care, you take the public money, you do the job that’s in front of you.
Kerry, general, Care
Again, this echoes the point about leaders getting their hands dirty, but it also shows some frustration at the emphasis on the soft approach to management leadership. As this excerpt continues, Kerry returns to an interrogation of the concept of leadership and the misperceptions it can create further down the hierarchy:
I think if you were to go the next layer down, they have this idea of leadership which doesn’t involve doing the job that they are doing now and actually my view is you’re doing that job that you’re doing now and a bit more – it’s not a trade-off. When you move up the ladder what you always do is just join at the bottom of the higher food chain . . . I’m at the bottom of a much more senior food chain than my managers, so it goes like that. And I have much less autonomy than they do.
Kerry, general, Care
Her sophisticated take on power in organisations and its implications for leadership found an echo in the words of another general manager at the care trust (Heather), who commented that ‘the higher you climb the less air you breathe’.
The actual experience of being a leader–manager at this level appears to contrast with the almost universally held understanding of management and leadership as a duality. Although practice-based reflections can obviously reveal more nuance within and between this duality, these still tend to be overshadowed by the idealisation of one over the other. The struggle of middle management can here be described as doing as much as possible to avoid doing one’s job in a managerial fashion, while always holding oneself, and one’s staff, to account.
This analysis now moves to consider a further layer of complexity for management and leadership within a health-care context, in the attempted integration of distinct professional and managerial groups.
The clinical–managerial interface
As noted in Chapter 1 , the relationship between clinical and managerial groups within the NHS has been extensively researched and written about, and most of this research suggests that it is an inherently problematic relationship. We do not seek to fundamentally displace this assumption, as the majority of interview comments relating to this interface made clear reference to continuing problems. However, with the diversity of our sample, we are able to add some important nuances to understanding the interplay between these groups, as well as identify different organisational strategies taken to manage the interface.
As almost half of our sample of managers had some kind of clinical background, we will conclude this section by building on work on ‘hybrid’ managers26 and their distinct positioning in relation to competing domains. Although the interface will be returned to in the analyses of management knowledge and networks in Chapters 5 and 6 , here an exploration of the interface is situated within the discussions about being a manager–leader in the three trusts.
The following extract creates an impression of a normalised tension and the use of humour implies a resignation to it as a fact of life.
Consultants hate managers. We don’t do anything do we? (. . .) I am sure some of the staff think I don’t do anything. I don’t think the junior staff realise the responsibility that we do have certainly. I have joked that I am going on holiday for a week and we’ll get one of the Band 5’s to step in for me for a week, just to see how it feels.
Belinda, general, Acute
Each organisation in this study recognised the fundamental tension that could exist between clinicians and managers. However, notable within our data set were the differences found in the nature and subtleties of this relationship across the three trusts and the different means developed at each trust to cope with and manage the interface. Some of these were the result of an overt strategy and some had developed more by accident than by design.
In Acute, perceptions were of a unified and influential body of medical consultants resistant to what was thought to be a business-oriented organisation. Historically, this tension had been managed via a combination of charismatic and command-and-control leadership. At the time we were researching the trust, however, there was a period of transition at the top (as noted in Chapter 3 ). One of the responses to this period of change was to redesign the clinical managerial structure at the sub-board level, creating two new positions of associate director and associate medical director, who would sit between divisional heads and the board. On the clinical side, this was an attempt to try to attach some greater status and credibility to the medical management role:
Doctors train to be doctors, they don’t train to be managers and actually there’s very few of them start aspiring to be managers . . . Unfortunately, the medical management has been seen as a poisoned chalice that someone has to do their stint at all too often and there’s not much to draw people into it . . . I think, that’s a shame, but . . . most people train to be doctors. They don’t train to be managers . . . I don’t think we’re alone, as a trust, in that.
Brian, clinical, Acute
By giving medical managers responsibility for groups of consultant outside their own profession, this redesign could also be seen as an attempt to counter some of the silo effects of professionalism, by drawing doctors away from their core clinical interests and moving them more towards a managerial agenda:
. . . it’s trying to draw doctors into the senior management roles, because, in all honesty, up until now, even at clinical director level, there’s been a quite serious disengagement from the real mechanics of senior management within the trust.
Brian, clinical, Acute
However, one of the unintended effects of this was to create tensions between the new associate medical directors and the consultants they were now asked to manage:
We work very closely together and the thought of surgeons being managed by anaesthetists or anaesthetists being managed by a surgeon is a bit abhorrent to a lot of people and it will just be interesting to see how it evolves, you know, I had to use all my diplomacy skills, I thought, managing 32 relatively likeminded anaesthetists. Trying to manage surgeons as an anaesthetist – particularly if I fundamentally disagree with what they’re saying, or what they’re refusing to do – may prove quite challenging and, I think, that will be my big challenge, if I’m honest . . . I think it’s going to be quite difficult to get that role, because I’ll have to support the surgeons, to some extent. I can’t just oppose everything they want, otherwise they’ll just see me as being the enemy.
Brian, clinical, Acute
Promoting the associate director from a divisional operational remit to this new interfacing role was also an attempt to create a sense of clinical/managerial synergy:
With me being associate medical director for surgery and him being associate director for surgery, we should be standing shoulder to shoulder and I should be there to support his ideas, maybe mould him a little bit if I think there are problems. Try and help him find the way forward. But I would see it as really needing to almost act in synergy with each other and I hope that’s what I will bring in this new role.
Brian, clinical, Acute
In Care, there was not the same perception of a unified body of consultants, possibly owing to the diversity of specialisms and geographical spread of the organisation. Instead, the potential for clinical resistance to organisational aims came more from a local–central tension. As explained in Chapter 3 , the trust had grown over time by bringing in more and more local services. While we did not get the sense that this had been an unwelcome or predatory series of acquisitions, there nevertheless existed tensions between local autonomy and increasing central control.
One of the ways in which the care trust presented itself as an organisation was through the rhetoric of clinical leadership. In our sample, there seemed to be a good deal of reality to this rhetoric: > 90% of participants in this trust had a clinical background and, beyond this, many still had some kind of clinical input, even if this was mainly in an advisory capacity. One of the effects of this policy was to create a group of senior managers who had grown up through the ranks to become service managers overseeing their locality or operational managers with a remit across the whole trust. This tended to lead to the buffering positions described above, as managers had a dual commitment to their clinical area and to the organisation. Perhaps unsurprisingly, we found some diversity in the experiences of this potentially demanding role, which was also the personal embodiment of the clinical–managerial interface.
So managing staff is very much influenced by the need to try and understand where they’re at and try and reassure them that I’m on their side as much as I can be, not against them, and will support them as much as I can and I’ll roll my sleeves up and do work with them. And I will only whip them [chuckles] if they make me. And then I’ll turn into my father who used to say to me as a child, ‘this is going to hurt me more than it hurts you,’ when he would be ever so disappointed with me and he’d have to hit me or threaten to hit me. He’d say, ‘this is going to hurt me more than it hurts you,’ and I’d go, in my head . . . ’No it won’t!’. [laughs]
Laura, general, Care
In relating her managerial work to parenting, Laura creates a nurturing work narrative that demonstrates something of the therapeutic character of the care trust, reflecting the emotional work of boundary-spanning roles. 101
As the two contrasting excerpts below demonstrate, emotional work could be experienced in a variety of ways. It could be seen as very restrictive, leaving managers without the ability to act or move freely:
It still feels at times, quite isolating, because I guess the role of a senior manager is that you have to make very difficult decisions. Some quite harsh decisions at times. And people are looking at you to make those decisions for them, which I think, that’s obviously a big challenge, to do that. But also, I’ve got to, with the managers that sit below me, encourage them to also make difficult decisions as well, and actually not to apportion the blame, that it’s just my decision.
Heather, general, Care
The response to such restriction in the above excerpt is to try and ‘distribute’27 management and leadership responsibilities among lower levels of staff. For others, however, making difficult decisions could mean less restriction and more opportunity:
I moved into a senior management role and (. . .) we had two failing services . . . So we had both residential services, both subject to external reviews (. . .) and it was a case of ‘this service is failing we need to put a turnaround team in, will you head that up?’ (. . .) I had a new services manager (. . .) he’d had a poor experience in the NHS previously into a job that he knew nothing about (. . .) It was a real tough time for us initially (. . .) But the good thing is there’s only one way to go and you’ve nothing to lose have you when you take on failing services? So it gave us both quite a lot of opportunities.
Harriet, general, Care
Finally, the specialist trust was described as having a powerful and influential body of consultants, who were generally recognised as being at the top of their fields, but also a strong managerial culture and commercial orientation that was led from the top and communicated clearly throughout the organisation. Therefore, there existed a powerful group of consultants and, when compared with the other two organisations, a powerful countervailing group of managers as well.
With its relatively financially solvent position, Specialist managed this potential clash through a multilayered senior clinical and management team structure, which moved beyond what might be called the conventional triumvirate of consultant–nurse–manager72 to introduce an additional layer of middle management between divisional director and service manager: one general manager (at grade 8d or 9) to be more externally focused, partnering with the clinical director, and one deputy general manager (at grade 8b or 8c) to partner with the lead nurses, be more internally focused in managing day-to-day divisional operations as well as oversee the work of service managers (at grade 8a or 8b).
At the acute trust, these responsibilities were combined in the single role of the associate director and, as will be seen in Chapter 5 , this tended to crowd out the strategic and externally focused aspects of their role, in favour of operational demands. Although the deputy general manager and the service managers at Specialist did describe themselves in similarly inward-looking and insular terms, the overall strategic direction of the trust had both senior managerial and clinical input, which led to a mutual respect in the relations between clinical director and general manager and helped create an organisation that combined clinical and managerial leadership. While the job of the deputy general and service managers was more akin to the conventional relationship of consultants to managers, this was in an organisational context in which there was a considerable degree of satisfaction among all occupational groups. As one of the deputy general managers stated:
It’s about bringing people with you, especially when they’re people that are highly intelligent. I do try to encourage these people to work with me rather than feel they’re being told; I don’t think they respond too well to that. And certainly the service managers are very good at engaging with them.
Gavin, general, Specialist
Interviews revealed a shared sense of confidence that, although there were challenges, these were not insurmountable and that everyone was essentially pulling in the same direction. Rather than a sense of conflict and mistrust, there was clear recognition of the strategic advantages to be gained from this mutual dependency and respect.
This was not about eradicating the divide but about making the divide manageable based on an appropriate structuring and sense of mutual respect. Some of the most important skills of the job were to do with managing relations and personalities, an aspect that will be turned to next.
Management responsibilities and skills
I’m tempted to boil it down into three things (. . .) Some clinical experience, some clinical understanding of the work (. . .) Some ability to understand data and number crunching, waiting times and think about capacity and throughput (. . .) And that’s the other area, managing staff, leadership of staff (. . .) in a way that combines the ability to whip staff up into a passionate frenzy to get them engaged to do their job, and also whip them when they don’t.
Laura, general, Care
As authors such as Handy120,121 and Mintzberg111,122 have noted, management is more complex than may be conventionally understood and is made up of a diverse set of tasks, responsibilities, competencies, skills and dispositions, of which leadership may just be one. By organising our own classificatory schema around this understanding, we have attempted here to draw out and describe some of this complexity, as it is significant for our later discussions of the knowledge required and networks accessed.
The conventional understanding of management and leadership that the majority of our participants subscribed to (explored earlier in Management and leadership) was seldom consistent with the array of responsibilities, skills and knowledge bases that many participants went on to describe in detail that preoccupied them in their day-to-day work of just managing.
Responses to questions about day-to-day roles and responsibilities were coded according to several distinct areas of responsibility that emerged: line, budget, operational, functional, clinical, strategic, research, education and professional. The amount of attention directed to these areas in the interviews is represented in Figure 7 , which again charts the frequency with that themes were addressed.
FIGURE 7.
Management roles and responsibilities: number of interview references.
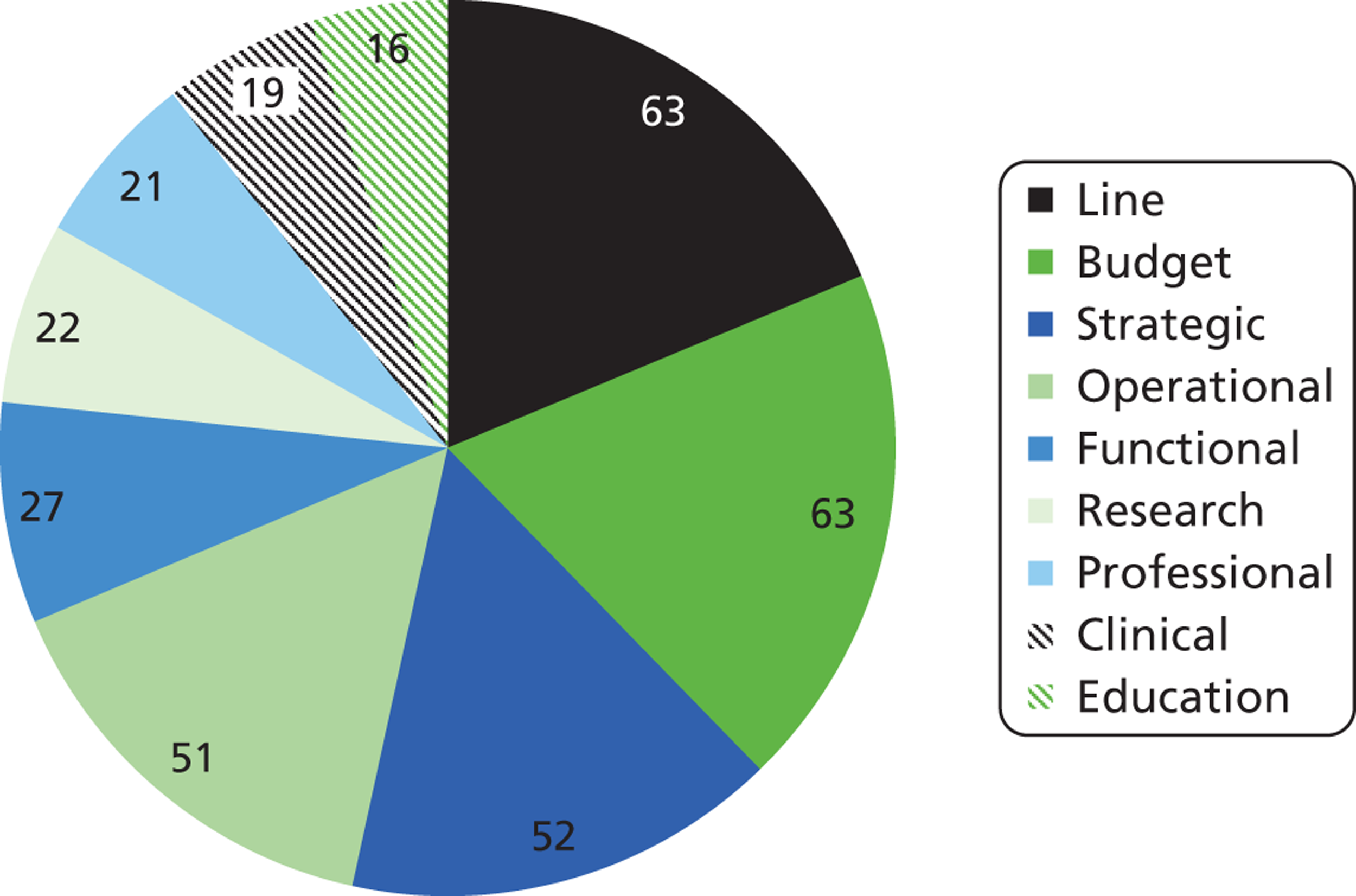
Out of our total sample of 68 interviewees, the vast majority had line, budget, strategic and operational managerial responsibilities and a range of responsibilities in other areas. One thing that emerged clearly from the interviews was the considerable number of individuals who had multiple responsibilities. Looking at this more closely, 55 respondents referred at length to at least four of these areas and 30 referred to five or more.
Comparing management groups, the clinical group experienced the greatest diversity of responsibilities, as they were more likely to be involved in clinical, education, professional and research management. The responsibilities of functional managers were not surprisingly more narrowly defined, given their task and knowledge specificity and more limited operational roles.
Knowledge domains will be explored further in Chapter 5 . Suffice to say that there were clear differences in the three managerial groups with respect to their knowledge base. Clinical managers, which included doctors, nurses and AHPs, all had the secure backing of a significant amount of specialist training, both pre and post registration. As their knowledge base also constituted the main business of their organisation, these groups had professional and organisational security. This was also the case with some functional managers, notably accountants, whose professional knowledge base and status were both more established and secure. With the increasing hold that finance has in health-care organisations,72 their professional security and influence was unlikely to be diminished and more likely to be enhanced [this was not necessarily the case of course for other functional groups such as HR, information technology (IT) and estates]. In contrast, general managers do not have the same specificity of knowledge or associated networks of professional support, knowledge and representation. 36 Consequently, they struggle to achieve the security that comes with closure around their occupational domain. 45
What will be explored more here are the variety of skills that manager–leaders in our study described as being associated with their jobs and important in dealing with the pressures brought about by increasing responsibilities, normalised intensity and a context in which management was increasingly denigrated while leadership was increasingly valorised. 28
As previously noted, Mintzberg’s influential work on management suggests that, in practice, it consists of varied and complex combination of responsibilities and skills. 122 Mintzberg122 identified 10 areas, which he divided into three sets of roles ( Table 11 ).
| Management activity | Managerial role |
|---|---|
| Interpersonal | Leader |
| Figurehead | |
| Liaison | |
| Decisional | Monitor |
| Disseminator | |
| Spokesperson | |
| Informational | Entrepreneur |
| Disturbance handler | |
| Resource allocator | |
| Negotiator |
To make sense of our own data on management skills, we began coding with this schema. However, respondents’ descriptions of managerial skill requirements rarely cleanly broke down into such a list of competencies and technical skills. Instead, the identification of skills would range across a wide and disparate set of strategies, styles and aspirations – a set of values rather than of competencies. By digging further, we were able to uncover sets of skills leading out of these. However, before describing these, it is worth first focusing on the means by which participants moved from conceptions and aspirations to concrete skills, as this also demonstrates our analytical path in moving from Mintzberg’s conceptual categories to the concrete skills that evoke them.
Many participants seemed more comfortable with the language of ‘style’ (Emma, functional, Care) in moving towards more concrete descriptions of management and leadership:
I guess the things that are really important to me that translate into style . . . are what I would consider . . . fairly old-fashioned values. So honesty, integrity and trust.
Emma, functional, Care
I think if you haven’t got a vision then other people might struggle to have that vision. At [another trust] where I worked before, the staff knew [what the vision was and] they knew because I communicated it. The first day I was there I [got] everybody together and [told] them what I’m about.
Oliver, clinical, Acute
The two excerpts above demonstrate the attempt to draw a set of values into an approach to managing or leading a situation or staff group. Interestingly, although both excerpts refer to the importance of open communication, there are very different value sets underlying this, fostering integrity and getting other people in line with a vision.
Vision was one of the things commonly held as one of the essential differences between management and leadership. At the same time, however, simply having a vision was not enough; there needed to be practical management techniques associated with achieving that vision:
I think one of the things that happens a lot in the NHS is it is lots of talk and lots of paper and lots of strategy. My view is that anybody can write strategy, it’s very easy. We all know what we’d like things to look like. The difficulty and the challenge is how you get that into the real world, so that affects the lived experience (. . .) I think that’s where the magic happens and that’s where the challenge is and that’s how we have to work . . . So you have to look at what kind of staff you have, you have to look at all your recruitment and how that happens and make sure you get the right people in the right place. I believe very strongly you have to try and engage people with a vision so people know which way they’re going.
Beth, general, Care
Perhaps not surprisingly, given these kind of aspirations, the skill sets themselves were varied and did not always fit easily into one or other category. Through our initial coding, we found that there were skills that either combined one or more of the three types of role (e.g. project management), or were tied to a specific occupational domain (e.g. finance). Alternatively, there were more ubiquitous skills that seemed to warrant their own category (e.g. communication). These were added to our list of categories to produce the range and distribution of management skills referred to by participants and summarised in Figure 8 .
FIGURE 8.
Management skills: number of interview references.
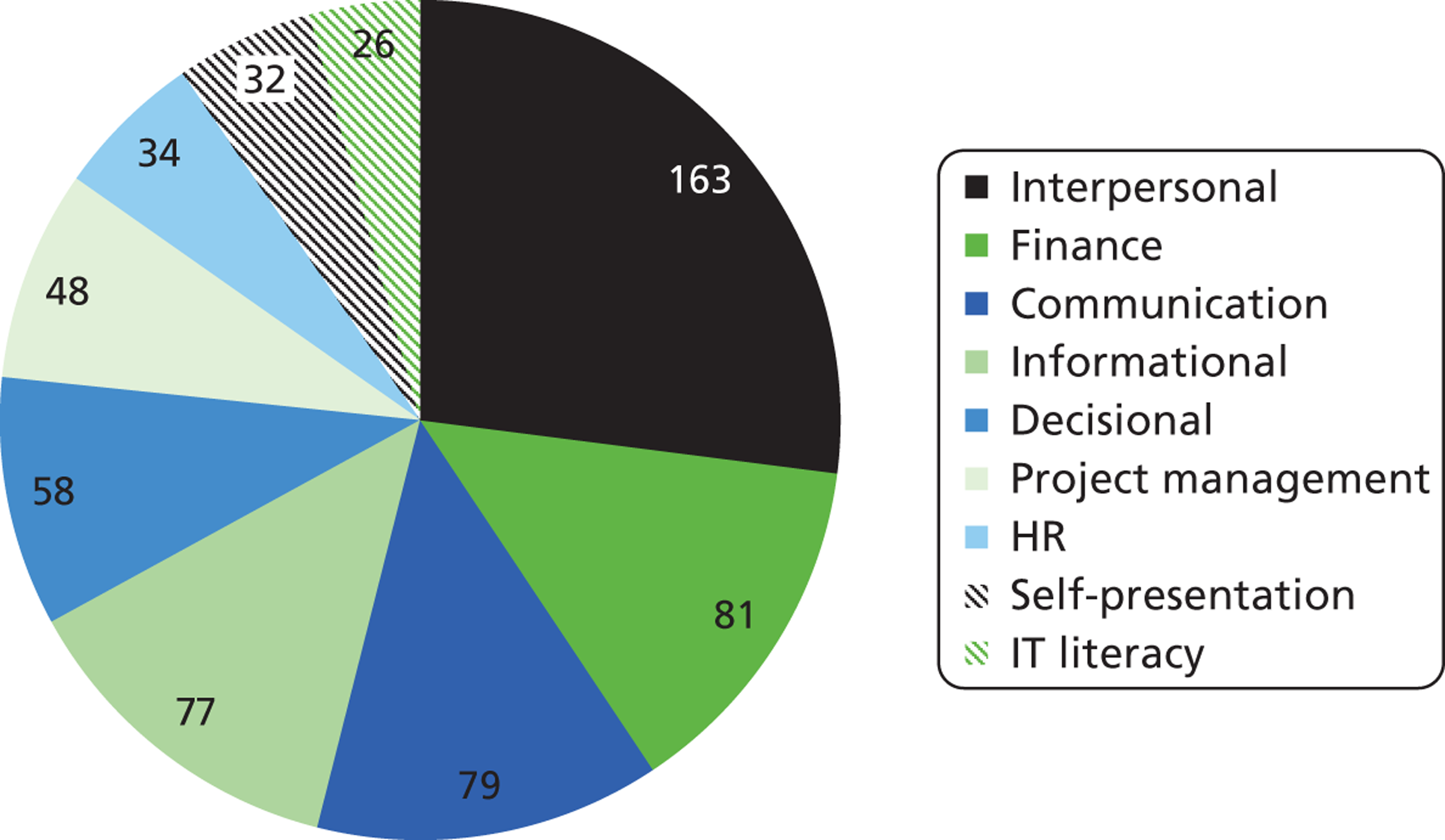
As the preceding discussion of strategies and styles suggests, there was a great deal of conceptual complexity and subtlety in the explanations given in each of these areas, creating a very rich and heterogeneous data set.
Across nearly all the categories there was a strong emphasis placed on the importance of soft personal and relational skills, which were consistently seen as of greater importance than the harder technical knowledge associated with some skills. The view was that the latter could be more easily developed than the former (a theme explored further in Chapter 5 ). The major exception to this was in the finance category, the second biggest category of discussion here, which underlined the importance attached to having the ability to deal with numbers, budgets and balance sheets in order to succeed in management in modern NHS organisations.
The emphasis on the interpersonal category clearly demonstrates the importance attached to soft skills. This was the biggest category by some considerable way and encapsulated a range of relational skills which individuals valued, sometimes in fostering a working environment that reflected their values and sometimes, more instrumentally, in being an effective means of getting the job done. There were also some important differences in the organisational contexts that had a bearing on the relational skills required and used.
Across all three organisations, individuals talked about the importance of fostering and maintaining relationships. As described in the following excerpt, this was something that was seen as particularly important in a sector in which you cannot always rely on there being an explicit technical process to follow:
There’s no contractual relationships with us. It’s purely relationship and commitment and that’s one of the key features (. . .) a lot of what we deliver is based on relationships and commitment to having shared vision and to wanting to get that and not, actually, a service-level agreement or a contract (. . .) I think it requires that commitment to long term maintenance of relationships and constantly keeping them up to date, even if there’s nothing happening, even if things are going OK. Just maintaining contact, keeping that dialogue, keeping the vision there.
Gabrielle, general, Care
Organisational distinctions did begin to emerge in the extent to which dealing effectively with relationships was considered an end in itself, as opposed to being considered necessary for the achievement of specific goals. The care trust provided some of the best examples of individuals emphasising the importance of developing relationships as an end in itself:
I think it’s really important for you to know your staff . . . people will say that their personal lives don’t matter, but it’s totally part and parcel. If you’re doing a longitudinal job, you know, if you’re doing a 20-year job, you can’t forget that there is an absolute part to people, human beings, you’re going to have that. That’s so important.
Hasin, general, Care
The following account from the acute trust still retains some of the quality of Hasin’s ideal, while also beginning to tie this to particular goals:
The one thing I’ve always tried to do is remember the little things about people. It’s the tiny little things that matter. That, even if everything is going really badly and it’s really busy, if you just remember some of the small things . . . people will remember them and you’ll get people far more on side by doing things like that.
Jessica, functional, Acute
In contrast, in the specialist trust, the nature of the organisation’s strategy and environment put a considerable premium on the value of relationship building, articulated as knowing the right person at the right time:
One of the skills you need to build up really quickly is knowing who the important people are and who does what . . . so when you have got a problem, especially in finance, you know who to pick the phone up to. So that’s one of the things that I kind of tried to focus on . . . in the first two or three months – is just figure out who was who in the organisation, how things worked really.
Thomas, functional, Specialist
Across all three trusts, the importance of interpersonal skills was a crucial element in dealing with the inherent tensions between managerial and clinical groups, as the following quote indicates:
You’re caught in between . . . [With] medics here, I can’t go and walk into one and say can you do clinic tomorrow because I’m telling you. They’ll say ‘on your bike’. They’ll say who are you, a manager, coming in to tell me . . . It’s about how you get across here’s what’s happening: quite a lot of pressure, what the impact will be, would it be possible for you to look at doing something about it, and then seeing what options come forward. It’s taking that approach. So influencing is the key aspect of it. I think having awareness of what’s going on or an overview . . . at my level and beyond you can’t get into all and every detail because then you’ll miss something at that end or that end.
Pavak, general, Specialist
What this demonstrates is the interaction that occurs between many of the different categories of skills. While this may be expected in relation to softer skills, what we also found was the importance of combining the two sets of skills: hard and soft. That is, it’s in part about ‘knowing your stuff’ (Hasin, general, Care) but also it’s about knowing how to get it across. Figure 9 tries to capture this degree of interaction between the skill sets that emerged in the connections made by our interviewees when considering the range of skills required.
FIGURE 9.
Management skills interactions.
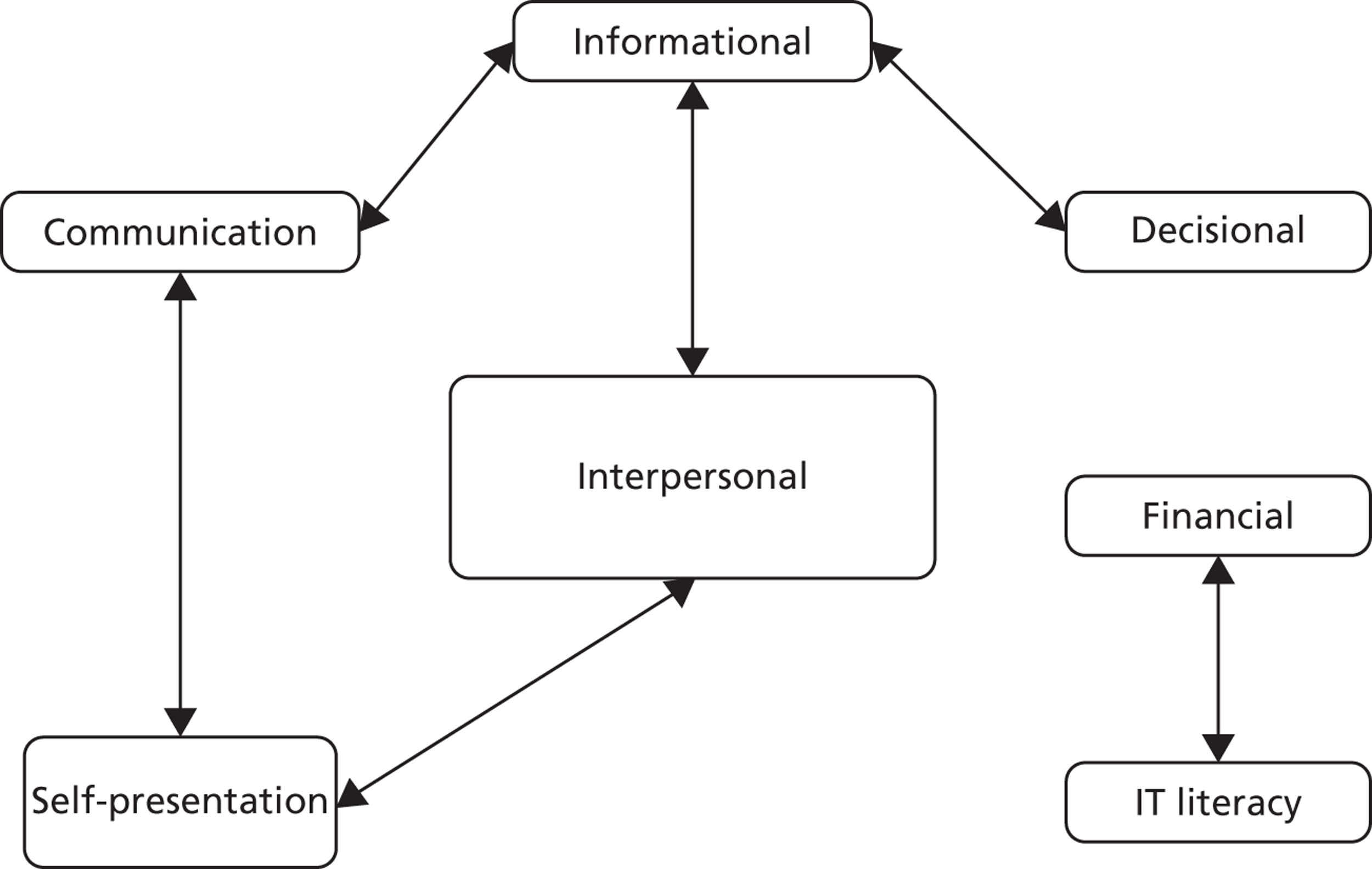
Summary
The analysis in this chapter has set out to explore issues related to the distinction between management and leadership, the challenges of overcoming the clinical–management divide and the pressures faced by middle managers, set within a wider and changing institutional context that, in turn, raises questions about the changing basis of managerial work and professionalisation associated with new public management and leadership discourses.
The tensions and contradictions identified in how management and leadership are articulated and inter-related, how different strategies emerge for managing the interface between clinicians and managers and what changing conditions mean for the diversity and complexity of middle management (both as an occupational group and in terms of their diverse managerial responsibilities) are taken further in Chapter 5 , which examines the knowledge base accessed and used by these managers.
Chapter 5 Knowledge
Introduction
As will be seen, the backgrounds and careers of those managers who were interviewed varied enormously and reflected the wide range of variation generally found in managerial career trajectories across health care. 69,94 What was perhaps most striking was the degree of consistency right across the board in how management knowledge and management learning processes were approached and made sense of. This consistency was apparent, despite there being considerable variation in time spent in the sector/trust, clinical/managerial background and levels of clinical experience and orientation, differences in formal qualifications and experience of formal management training and development.
Aspects of knowledge
In what follows, variations and differences found across the three trusts and the three managerial cohorts are highlighted. What emerges is a consistent set of findings regarding the difficulties of translating and embedding more abstract management knowledge into heath-care settings, the dominant influence of home-grown management knowledge embedded in systems and practices, the importance of managerial experience and the embodiment of management knowledge and the potential value, but also limitations, of formal training and development as ways of imparting management knowledge and cementing management learning.
In elaborating these points, this chapter follows a structure relying on a framework ( Figure 10 ) that provides a useful heuristic method for exploring the mobilisation and utilisation of management knowledge by managers. It does so by combining together consideration of the different forms of knowledge they may represent and how they relate to different forms of learning.
FIGURE 10.
Forms of knowledge and modes of learning.
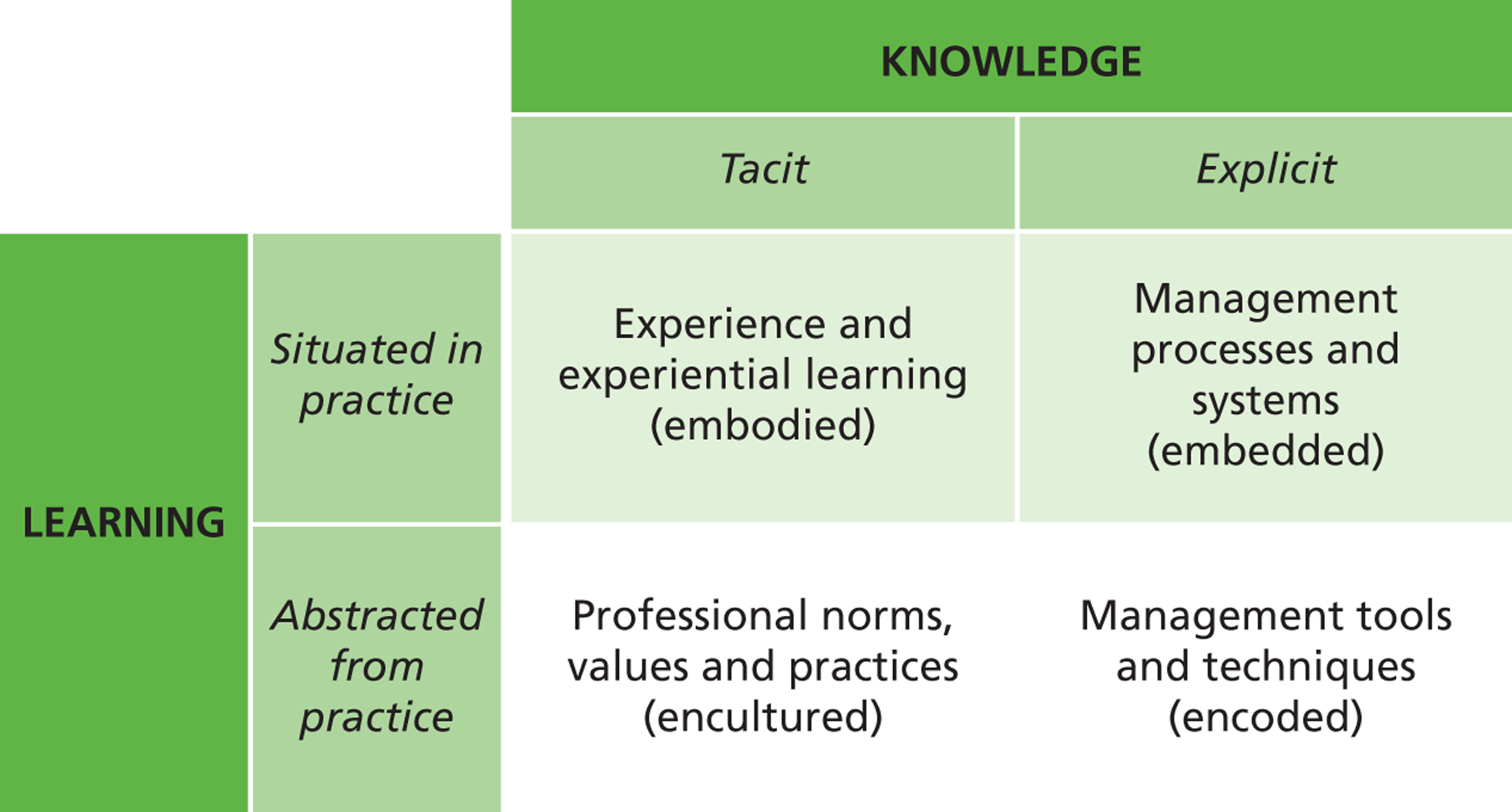
Along the horizontal axis (forms of knowledge), it is possible to make a classical differentiation between explicit and more tacit forms of (management) knowledge. Although it can be argued that the two forms of knowledge are in practice mutually constitutive,123 separating them out like this does allow one to highlight differences between more explicit, codified forms of knowledge and those that are more dependent on individual action/cognition and social interaction. 124 In turn, this helps in bringing out some of the challenges of socialisation, externalisation, combination and internalisation involved in attempting to translate one form of knowledge and understanding into another. 37
Along the vertical axis, it is possible to differentiate between more abstract forms of learning and learning that is more situated in practice. Contemporary thinking on knowledge sharing and learning in organisations tends to take a more practice-based view of these processes, which emphasises the socially situated nature of knowledge and the importance of learning or ‘knowing’ through social interaction in CoPs. 9,42 Making this distinction can help bring out some of the important differences and interactions that can occur when one considers the challenges of translating meaning and transforming practice based on the types of knowledge and learning involved and how they relate to practice. 29,35
Combining the two dimensions together allows us to focus on very distinct sets and bases of managerial know-how. Following Blackler’s ideas125 about different forms of knowledge and how they relate to practice (and to appropriate modes of organisation), we identified four primary types of knowledge that were clearly important in our analysis: that which encultured in the professional norms, values and practices of (institutionally accredited) managers, that which embedded in local management systems and processes, that which is encoded in more abstract management knowledge and associated tools and techniques, and that which is embodied in the skill sets of individuals. The interactions between these four forms of knowledge are complex and are explored in the following four sections. The rest of this chapter follows the fourfold logic suggested by this framework and finishes with a fifth major section that also examines relationships with formal management training and development processes.
Professional norms, values and practices (encultured knowledge)
Given the stress noted in Chapter 4 regarding the more routine aspects of management, a key challenge facing management across all the three trusts (as well as more widely within the health-care sector) is in establishing a clear, distinct and coherent knowledge base that could provide the basis for greater influence and managerial effectiveness.
You almost need to like learn little bits of everything. So, you know, you need to understand how like a nurse rota works and things like that. But equally, you know, when a surgeon goes in to do a complex procedure, broadly what he’s doing kind of thing, so you can understand the time pressures, how many people are in there, what they’re doing . . . so you’re not ever an expert in anything.
Thomas, functional, Specialist
Studies of professionals and professionalisation have long recognised the difficulty faced by management in laying claims to professional status around a distinct body of knowledge. 36 Management within health care is certainly no exception, and it was clear that it had its own distinct requirements that made it difficult to rely on more general forms of management expertise.
You need a good clinical understanding of the work, and I think that’s important because the whole idea that a manager’s a manager and you manage a carpet factory then you manage a day hospital I don’t think it’s the same. Because I think you need to understand the business, and it’s quite different, health.
Leo, clinical, Care
However, before we look at the ways in which attempts were made to constitute, mobilise and use management knowledge in the trusts we investigated, it is important to consider the direct and indirect consequences of managers having to work with, through and around the more dominant discourses associated, first, with clinical knowledge and expertise and, second, with other influential knowledge bases (notably, finance).
The influence of clinical knowledge
One of the obvious consequences, which has already been explored in Chapter 4 , was the perceived need to engage with clinicians and to bridge the clinical–managerial divide. Chapter 4 identified the various ways in which attempts were made to bridge this gap and how it took different forms (structural, relational, personal) within the three trusts. With regard to knowledge, the key need for managers was to establish credibility in the eyes of clinicians, and often this could only effectively be achieved through mobilising individuals’ interpersonal skills and/or their own clinical experience.
In the specialist trust, this divide was more pronounced and bridging it tended to rely more on relational skills:
I think the key is to build up relationships with clinicians . . . Because if you can’t approach them in a certain way . . . then you’ve failed. If you can’t get them on side, you can’t do your job. And that takes years to build up that relationship properly. It takes a long time . . . They don’t trust you, they see you as a manager. And until they realise that you’re actually working with them instead of against them, it makes your job very difficult.
Joanna, general, Specialist
This could lead to key individuals performing critical boundary-spanning roles:
From the engagement point of view, the management consultants saw me as a way in, because I knew the consultants, I knew a lot of the medics, a lot of the senior team at the trust. I could get in and deliver their message without it being all management spiel.
Becky, general, Specialist
In contrast, in the care trust, personally embodied clinical knowledge was considered more important:
I’ve been in a number of meetings with consultants who’ve said well, we can’t do that, clinically that wouldn’t be viable. But I’ve done it or other people have done it . . . If I go into a room as a business manager they just see the label. But I’ve lived and breathed their culture so I understand it
Glen, clinical, Care
In both cases, however, the form of management knowledge applied was likely to be strongly influenced by the norms and expectations associated with the dominant clinical discourse that effectively drew upon a well-established, coherent and institutionally legitimised knowledge base. So, for example, concepts such as diagnosis and prescription could be a general way of understanding that would shape perceptions of managerial problems and would feed into management know-how. Consider, for example, the following explicit account and the presumption it contains about reliable and valid forms of knowledge:
I don’t think I need my clinical background to do my job, what I think is that as an AHP the way that we have practised absolutely influences the way I work and perform as a manager . . . As a physiotherapist . . . I would go and I would meet a patient, and I would assess them. And then have a conversation with them about what the treatment options are . . . and then treat. And then at the end of it, are you better or not? . . . And those are actually fundamental principles that I apply in my role now. So we assess a situation . . . What is the problem . . . what are our options? Okay, how are we going to take this forward? . . . We’ll treat or we’ll implement the change that we need to implement, and do it, but we need to review it. And is it better or not?
Melissa, general, Acute
Such encultured understandings may, in turn, prove difficult to counteract, meaning that managers may choose to, or have to, conform to expectations about what constitutes an appropriate epistemology of knowledge in order to create convincing and credible arguments. In turn, this was very likely to shape the nature of management knowledge mobilised in practice.
The influence of specialist knowledge
Management knowledge is also likely to be significantly influenced by other influential discourses. In management more generally, the power of the logic and language of accounting and finance to shape management discourse has long been recognised. 126 Again, health care is no exception. Indeed, what was apparent from those interviewed was how natural and normalised the emphasis on finance had become and how this shaped perceptions and processes of managerial work. For example:
The NHS does not live in a benign helpful background any more [where you are taught] about values and about clinical delivery and about how you set up a ward. That’s not what our managers do any more. Our managers have to figure out how to write bids or how to be in meetings with commissioners and come out with a good result or what happens when you get an enormous budget cut that you can do nothing about and you’ve got 10 more staff than you’ve got money for.
Kerry, general, Care
Not only does this changing context influence the balance of management skills required (as explored in Chapter 4 ), it also shapes perceptions of the important underlying knowledge base and criteria for approaching management problem-solving and decision-making situations:
One of the best pieces of management advice I ever got was get the money right, if you don’t get the money right nothing else ever works because you spend the whole time trying to get the money right. As soon as you get the money right you can concentrate on the clinical services.
Kerry, general, Care
At the same time, it was clear that there was some effort of translation required in applying financial (and also HR) management principles and practices directly to the health-care sector. As Matthew, a finance manager at the specialist trust, put it, ’The whole basis of finances are different.’ Similarly:
Up till recently, our head of finance was even new into the NHS – he came from KPMG – so he had workings with the health service but didn’t really understand community services; and it was quite a steep learning curve for him to understand it wasn’t just about making cuts and stopping. You had to understand the implications that that would have on the services that were delivered and how clinicians operate.
Hugh, general, Acute
The question then becomes how other forms of management knowledge that are somehow accessed, mobilised and used in health care may be shaped by such strongly encultured understandings and counter-acting pressures.
Management tools and techniques (encoded knowledge)
Explicit references to established and codified systems of management knowledge, which were consciously drawn upon in an attempt to apply them to the sector, were comparatively rare. Clinicians inevitably referred rather less to management knowledge per se than to the importance of relevant clinical expertise. Functional managers naturally drew upon their own expert knowledge in the routine performance of their work (e.g. accounts, IT protocols). Similarly, there were instances in which more general management activities, such as process mapping or strategic modelling, were drawn upon by individuals keen to apply what they saw as relevant generic management tools and techniques to make sense of management problems. Referring, for example, to ‘some of the tools of trade . . . like the “Boston Box” ’, Emma noted:
I have to say, I love frameworks and tools and techniques . . . My old team used to laugh because they used to say, Emma wants to put everything in a box. But I suppose it’s just the way my brain works, it helps me think things through if I can use some sort of tool to start to work an issue through, and categorise things. And that’s my way of making sense of it.
Emma, functional, Care
At the same time, there were limits to how easily such strategic techniques trickled down into day-to-day management activity:
If you’re doing a full developmental day with a team, then I would absolutely use some tools to help them take through. But in terms of day-to-day management of my team . . . problem solving, it’s probably far more intuitive. I’m not constantly . . . doing a SWOT [strengths, weaknesses, opportunities, threats] analysis of everything.
Emma, functional, Care
The sources of such knowledge are considered later in this chapter and the networks used to access knowledge and learning in these areas are considered in the next. What is perhaps worth noting here is that the adoption and use of management tools and techniques tended to be either more implicit in the skills and knowledge being applied by specialist management groups (especially clinical, functional) or more directly influenced instead by internal home-grown management processes and practices.
Explicit reference was made by some, particularly at the acute trust, to attempts made to import and apply lean thinking principles to the sector. At the time of research, the heyday of these initiatives had perhaps passed and the clear message from those interviewed was that, although applying lean principles could be beneficial, application had been patchy owing to significant problems experienced in embedding the initiatives in practice. At the same time, however, it was possible to make use of lean thinking to encourage different ways of acting, provided they were not packaged as such:
We had an all-day event yesterday with the new community teams . . . about how we can amalgamate and transform these teams. And really what we did in that day was effectively Lean, in the sense that it was value stream mapping; we were going through, looking for elements of waste . . . but it was never packaged as that. We didn’t do half a day on the Toyota management system before we went into that. You know, it was just the way we did it.
Greg, general, Acute
Management processes and systems (embedded knowledge)
It was also clear that there could be a strong self-referential bias that acted as a constraint on the direct import of management knowledge and ideas into practice:
The other phrase that is used a lot here is ‘Don’t reinvent the wheel’, so if another NHS trust has done something, well let’s just do that. Let’s copy what they’ve done. Let’s use their papers and their process, rather than ‘Is that the best way?’.
Christian, functional, Acute
Research elsewhere has demonstrated that importing established best practices across health-care organisations is by no means a straightforward exercise, as those practices still need to be properly embedded in the local context and, in the process, contend with existing interest groups and their practices. 30 However, what is nicely crystallised in the above quote from Christian is the privileging of home-grown management systems and practices that may owe some debt to a wider, more diffuse management knowledge base, but which are shaped and driven more by local practical conditions and constraints. The following quote nicely captures the emphasis on cure rather than prevention this could reinforce:
I’m trying to bring in the ideas of concepts of service improvement, because the other thing here I would say is people identify that there’s a problem and they jump straight to solutions . . . It’s the natural thing to do. What I’m trying to get them to do is saying well, hang on a minute, why have we got the problem? They don’t answer that, they put sticking plasters on things all the time. Another plaster, another plaster, and the problem is never resolved properly because you never understand why we’ve got a problem in the first place
Melissa, general, Acute
The institutional requirements on trusts to meet expected standards of care and to do this according to expected performance standards [as defined by Care and Quality Commission (CQC), Monitor, etc.] was principal among these conditions and constraints. This emphasis on monitoring of levels of care and performance had clear consequences not only for the balance and focus of managerial effort, but also for the primacy attached to locally situated management knowledge that was embedded in systems and processes (as opposed to more abstract management ideas and practices). For example:
We already have integrated psychological services, we already have a really, really high standard of quality. We’ve implemented a thing called CAPA, which is a Choice and Partnership Approach, to manage our demand and capacity and, within that, comes the need for very clear pathways, review, constant review, flexibility of services, listening to what users want . . . We’re perceived, within the directorate, as being quite structured, quite robust and a lot of those principles fit with the IAT [interauthority transfer] principles, particularly CAPA, the separation of an assessment and a treatment process and making sure it’s evidence based, and meaningful, and collaborative.
Gabrielle, general, Care
It was clear that external institutional pressures, to the extent that they required more recording and reporting of information about performance in relation to targets, predisposed the trusts to apply and/or develop management systems and procedures that were geared towards standardisation and formalisation of process. As such, they could reinforce a more bureaucratic tendency in managerial work:
We still have to evidence that the quality of care that you are providing is at a level that the PCT don’t want to de-commission this service. So without saying unless you do it we’re not going to have money for your team any more, therefore you are going to be out of a job . . . [the] messages that we try to get across to them, actually this is about protecting the organisation by providing this information. It’s just the nature of the world . . . you all have to be able to evidence what you’re doing.
Carl, functional, Care
This did not necessarily mean that the organisations were seen as acting overall less flexibly. At the care trust, for example, a clear distinction was drawn between the imperatives of what Mintzberg111 might define as the machine bureaucracy operating within the organisation’s administrative core111 and the greater degree of flexibility and responsiveness found at the executive level.
However, it did mean that pressures towards standardisation could work against attempts to develop distinct management practice targeted at the needs of particular parts of the organisation:
The organisation needs you to be able to tick their boxes, so being able to understand their must-dos and their must-haves and their givens, the data stuff – if you can pay attention to that and translate your activity into that in a comprehensible way that, that can carry you a long way.
Laura, general, Care
It also meant that one of the continuing challenges facing all of the trusts we looked at was the tension that existed between corporate attempts to standardise and rationalise processes and practices and the more localised, situated and embodied practices that managers continued to try to adopt within their own parts of the organisation.
Experience and experiential learning (embodied knowledge)
The value of managerial and clinical experience
A very consistent view held across the sample was that experience really mattered:
I’ve been on lots of courses, when we were on the training scheme we did lots of courses in leadership and management and weeks away doing it, and I never really learnt anything. And it’s not until you start doing it. I think it’s like driving a car, until you actually do it you’re not going to learn it and it’s learning from your mistakes and all that sort of thing.
Felix, functional, Acute
Managers’ career and job experiences varied considerably, and it was not always direct managerial experience that was of importance; clinical experience was also important.
Table 12 delineates those with clinical/nursing occupational backgrounds in each of the three groups across each of the trusts and shows information about their clinical qualifications.
| Trust | Cohort | Numbers with clinical backgrounds | Clinical qualifications (or PhD) |
|---|---|---|---|
| Acute | Clinical, n = 5 | 2 doctors | 2 MDs |
| 2 nurses | 2 RGNsa | ||
| 1 scientist | 1 PhD | ||
| Functional, n = 7 | 1 nurse | 1 RGN | |
| General, n = 8 | 1 nurse | 1 SRN | |
| 4 AHPs | – | ||
| Care | Clinical, n = 7 | 2 doctors | 2 MDs |
| 3 nurses | 2 RGNs + 1 RMN | ||
| 2 AHPs | – | ||
| Functional, n = 6 | – | – | |
| General, n = 12 | 10 nurses | 7 RMNs + 3 RGNsa | |
| 2 social workers | – | ||
| Specialist | Clinical, n = 6 | 1 doctor | 1 MD |
| 3 nurses | 3 RGNsa | ||
| 1 AHP | – | ||
| 1 scientist | 1 PhD | ||
| Functional, n = 8 | 1 scientist | 1 PhD | |
| General, n = 9 | 3 nurses | 1 BSc + 2 RGNs | |
| 2 scientists | – | ||
| Total | 68 | 42 | 31 |
Of the total of 68, a large proportion of managers across the trusts came from a clinical or clinical-related background. Of these, most had the relevant medical or nursing professional qualifications and the latter were largely registered general nurses, state registered nurses or registered mental nurses. There were a small number with the newer degrees in nursing in addition to other nursing qualifications. The exceptions were AHPs, social workers and some of the medical scientists. Clinical experience and qualifications were obviously concentrated among the clinical manager cohorts, but there was also a preponderance of those with clinical experience and qualifications among the three general management cohorts, particularly at the care trust.
Among managers at the care trust, in particular, clinical experience was considered a vital part of the knowledge base brought to bear on management problems:
I’ve grown up through the ranks if you like and I’ve had that experience as a clinician, as a student nurse, as a senior member of staff, so I’ve gained that experience and I think that’s what’s helped me grow into this position and be reasonably okay at it. But without that I feel myself that I wouldn’t have been able to achieve where I’m at because I think you miss a real sound foundation to becoming a manager.
Kate, general, Care
Moreover, this was often considered as something that easily overshadowed any more indirect or more generalised managerial experience that might be drawn upon:
I feel having the clinical background has been a real advantage. Because you can see it’s not just about a process, a management style, a service, you look at things in a very different perspective when you’ve been hands on. You’ve been on that ward, you’ve delivered treatment, you’ve delivered patient care. You’ve had that interaction with the patient.
Becky, general, Specialist
Indeed, it could be frustrating for managers if their clinical experience and expertise was not explicitly recognised:
I keep reminding the team that I am a physio . . . Some of the junior staff that have never worked with me in that role, you know, they forget that they can come to me for that kind of advice and support and they see me as ‘the manager’.
Gloria, general, Acute
Interestingly, the opposite also applied and introduced a constraint for some; for example, Hannah at the specialist trust felt she was not taken seriously as a nurse ‘acting up’.
The importance of experiential learning
However, the process of experiential learning was not necessarily associated with a smooth journey that gave managers great opportunities for reflective learning. Indeed, many of those interviewed had experienced enormous changes, challenges and transitions in the path to reaching their current position. Such management career development was even, in a few cases, an unintended consequence of the frequent reforms and reorganisations occurring within health care (that left jobs redefined, recombined or open to competitive application). Managerial experience and skills could also be developed and honed by the relatively few managers willing and able to harness new management initiatives that gave them opportunities for learning and capability development. Conscious career development was comparatively rare and what was more apparent was a degree of manoeuvring around the changes that were going on at the management level.
Muddling through also typified a good deal of the managerial learning involved in the development of skills. General and clinical managers, in particular, tended to emphasise the level of trial and error associated with learning how to do their jobs:
Most of it, in all honesty, is muddling your way through a problem and finding a solution that works and thinking, well, actually, you know, with hindsight, that worked
Brian, clinical, Acute
Many also stressed, some quite positively, the importance of managers being stretched outside of their ‘comfort zone’ (Nancy, clinical, Acute):
I’m trying to [take] my Band 7s . . . out of their comfort zone a little bit, so I’ve rotated them all, as much as they’re all kicking and screaming, and it was a bit of a nightmare to start with; they’ve all done each other’s wards because there was some very insular people there, and that’s helped. But equally what I tend to do is, as I’m doing things with [their] consent.
Nancy, clinical, Acute
However, what is also evident in these quotes (and many others across the sample) is that not only were these tendencies a reflection of the often sporadic nature of day-to-day managerial work,122 they were also a consequence of the real constraints and demands on managers’ time that were a result of resource limitations and pressures on managers to deliver in the context of highly fluid organisational conditions.
Moreover, the general tenor of the accounts suggested that, to a large extent, those requirements had become internalised as the normal way of managing in such complex, changing and resource limited conditions. Managerial learning was taking place but it was as much about learning to cope without sufficient time and resources as it was about being able to use time and resources more effectively.
Learning from others
An important aspect of developing managerial knowledge and skills was the social learning that occurred through interaction with, and observation of, others. 9
Formal ways in which this occurred involved established mentoring and coaching relationships with senior colleagues. Although mentoring and coaching was highly valued by some of the managers we spoke to, it was clear that there were limits to the extent to which managers were able to access and make use of that type of support. Formal coaching, in particular, was more limited an experience and did attract some scepticism. When managers had an established relationship with chosen mentors, considerable value was often placed on the guidance, knowledge and support that came from that relationship:
Everyone in the senior finance team have got a coach who comes in once a month for each of us. And we spend an hour with him, and I was actually with him yesterday, and I found it really useful, it’s really good.
Felix, functional, Acute
It was recognised that the more general guidance and support provided by mentors did not necessarily directly help managers in their day-to-day work. However, it did help them to deal with the sense of isolation that could be experienced in their work and with the development of knowledge and skills that were seen as important for coping with day-to-day challenges as well as wider career development.
More importantly, perhaps, was the extent to which managers may not have access to such relationships. This could be for a variety of reasons, including individual predispositions to mentoring/coaching, the lack of availability of senior staff to act as mentors, difficulties experienced in finding the time to be able to focus on developing close relationships and lapses in the mentoring relationship as staff moved on from the organisation.
Informal social learning was equally apparent and, again, depending on individual predilection and opportunity, managers identified a variety of ways in which they learned implicitly from each other, including their direct observation of management actions and conscious role modelling the behaviour of other (effective) managers:
My manager is a real business manager, she’s got a real business head on her, and it’s interesting to learn from her, because she’s a radiographer by background. She does think completely differently to me, but I think we actually complement each other quite well. I’ve learnt an awful lot from her.
Belinda, general, Acute
The general point here is that learning how to be a manager was strongly influenced by social aspects and by the socialisation processes involved. When that occurred in a setting involving relatively intense ongoing interaction within and between managerial groups, it could provide important opportunities for managers to develop their skill sets through the sharing of tacit understandings. However, at the same time, it also meant that there was an implicit dependence on there being the available managerial role models:
I’ve probably learnt more about how not to manage and lead in management than I have about the other stuff. I’ve seen very few role models so far in the NHS who I would say, ‘God, I want to manage like that’.
Becky, general, Specialist
When opportunities for such intense interaction were more limited, it tended to foster a greater reliance on more formal means of passing on knowledge and learning (e.g. courses) that may not translate so easily and directly into practice. Although the weak ties these relied on127 may help open up managers to a wider potential range of knowledge and influences, it was clearly the strong ties needed to share tacit understandings that were more highly valued.
Evaluating experience and experiential learning
Whatever the precise source of knowledge and learning, there were a number of obvious, but also very important, benefits that came from experience and the experiential learning that came with managers learning-by-doing. Clearly, the very situated nature of learning-by-doing and drawing upon experience enabled managers to deal very practically with the problems and issues they faced and encouraged the very direct application of acquired skills and tacit understandings to the solution of immediate operational and practical problems. Although managers’ experiences may not be directly comparable to the situation at hand, it was more likely that past learning could be extrapolated to current needs and that localised solutions to problems could be found that were well grounded in experience. However, there were also a number of downsides (some of which have already been alluded to) that reflect an over-reliance on the embodied skills of individual managers and the situated learning taking place within their immediate operational context ( Table 13 ).
| Advantages | Disadvantages |
|---|---|
| Enables very practical, situated knowledge and learning | Makes it difficult to codify and generalise (‘sticky’ knowledge) |
| Makes the best use of people’s skills and experiences | Depends a lot on people’s skills, experiences and longevity |
| Tends to emphasise operational needs | Can crowd out the time available for strategising |
| Encourages localised learning focusing on existing solutions | Search for new solutions depends on individual orientations/networks |
Looking at these in turn, first it was quite clear that the highly practical and situated nature of knowledge and learning at the same time made it difficult for organisations that were trying to externalise knowledge and learning as well as codify and disseminate it across the organisation.
I wouldn’t envy somebody coming in and trying to do my role. I don’t think they’d be able to do my role the way I do it . . . unless they came from within and they had that kind of exposure and that knowledge, it would be very, very difficult to do. And, as I say, that might be for the greater good. They might bring a different approach to dealing with the requirements and the priorities of the organisation. I’m not saying that the way I do it is perfect
Ian, functional, Specialist
A good example of this was given in the reliance on the care trust and the comparatively small number of managers in particular parts of the trust that had built up a successful track record in writing tenders. Although this was considered an increasingly important activity for the trust to engage with (and, therefore, a skill that needed to be developed amongst its managers), a continued reliance on the expertise of those individuals ensured that the knowledge remained with them and proved difficult to capture and generalise. The knowledge had become ‘sticky’128 or difficult to extract and apply elsewhere, and this was reinforced by the emphasis on the embodied and embrained skills of those individuals seen as possessing the relevant know-how. Other examples of such ‘sticky’ knowledge were encountered elsewhere, particularly in the knowledge brought to bear by clinicians and certain functional specialists, but also in relation to more generalist and tacit management skills (particularly at the care trust, in which the operational units were more differentiated).
Second, and related to the first point, the retention and transmission of such knowledge was highly dependent on the people’s longevity in the organisation. In other words, the organisation’s collective memory and its impact on longer-term organisational learning and capability development could largely depend on the embodied/embrained knowledge and skills of particular individuals:
[I’ve got] to the point now where the knowledge I’ve got of the organisation is scary to be honest. Not just from knowing the people but knowing the services, knowing the interlinks and the dependencies and how reliant they are for infrastructure and if this fails what does that mean? It’s not something you could necessarily teach somebody. You couldn’t sit down and say, ‘Right. I want to give you all of this knowledge.’
Ian, functional, Specialist
When continuity and staff retention occur, this may not be a problem, although it does raise some important questions regarding one of the consequences of contemporary changes and their impact on management knowledge.
Third, an overemphasis on the immediate operational needs and demands was, in the view of some of those interviewed, clearly a major constraint on the development of more strategic management. This has been looked at in Chapter 4 as a constraint on leadership activity and will not be examined further here. The clear implication, however, is that there exists the danger of self-reinforcing tendencies to privilege operational needs over the strategising behaviour among managers. One consequence of this may be the reinforcement of ‘single loop’ learning,129 geared to the solution of problems on a ‘management by exception’ basis, as opposed to the ‘double loop’ or ‘triple loop’ learning that questions underlying assumptions about existing ways of operating and deciding which are important for effective organisational learning. 130 It is also worth noting that constraints on learning could not only result from pressing operational needs, but also be a consequence of organisational success, as was the case, to some extent, with the specialist trust.
Formal management training and development – views and prospects
You can go on management courses till the cows come home, can’t you, but you can either manage or you can’t, and I think a lot of it does come from experience and your own personality . . . I know managers who have been on PhDs and everything, but they can’t manage to save their lives. They know the theory but they just can’t do it.
Belinda, general, Acute
Given the emphasis on experience, it is perhaps not surprising that there were very mixed views expressed about the logic and value of various forms of formal management training and development, including the value for management knowledge and learning development of educational qualifications, the graduate training scheme, training associated with continued professional development and wider formal career development initiatives within the sector (such as the Gateway to Leadership, Aspiring Directors, Breaking Through and Athena programmes).
Educational qualifications and professional accreditation
Table 14 details the full range of non-clinical formal educational qualifications of the three cohorts across the three trusts.
| Trust | Cohort | Non-clinical health degrees | Management degrees | Other degrees | PgDip health (management) | MSc health (management) |
|---|---|---|---|---|---|---|
| Acute | Clinical, n = 5 | 1 | (1) | 1 (1a) | ||
| Functional, n = 7 | 1 | 4 | (3) | 1 (3) | ||
| General, n = 8 | 2 | 1 | 1 | 4 | 4 (1a) | |
| Care | Clinical, n = 7 | 3 | 2 | 3 (1) | 4 | |
| Functional, n = 6 | 1 | 2 | (3) | 1 (1) | ||
| General, n = 12 | 1 | 1 | 4 (3) | 4 | ||
| Specialist | Clinical, n = 6 | 2 | 1 (1) | 2 (1) | ||
| Functional, n = 8 | 1 | 1 | 5 | 1 (2) | 1 (2a) | |
| General, n = 9 | 1 | 2 | 2 | 1 (2) | 1 (2a) | |
| Total | 68 | 11 | 7 | 16 | 14 (16) | 19 (11) |
In addition to clinical qualifications (see Table 12 ), there were also quite a large number of managers who had non-clinical degrees and further degree qualifications. Table 14 inevitably includes some double counting of those with multiple qualifications (although it does not include additional professional qualifications).
Management educational qualifications were obviously far less prevalent across the board than clinical or health-related formal qualifications (particularly when one includes the figures for clinical qualifications from Table 12 ). However, approximately one-quarter of managers had some type of formal management educational qualification [usually postgraduate diploma or MSc/Master of Business Administration (MBA)]. Clinical groups were less likely to have non-clinical or non-health qualifications and functional managers were those most likely to have degrees unrelated to health, while at the same time having more management educational qualifications. However, it was also interesting to see how prevalent formal management educational qualifications were amongst general managers at both the acute and care trusts. At the specialist trust, they were comparatively rare (although one general manager did have a MBA).
If we first consider educational qualifications, these were clearly of necessity for those on clinical as well as some specialist functional career pathways in providing not only the technical knowledge and skills base but also the accreditation needed to practise. For those in managerial positions (including those managing in clinical and functional areas), educational qualifications may have been necessary but were clearly insufficient to provide the practical grounding needed for managers to perform their work effectively.
There was a time when a degree was really valuable, and a management qualification was really important. But gradually, we’ve realised that, having a management qualification or being an NHS management trainee, does not necessarily equip you to be a manager. It’s the clinical experience that equips you to be a manager . . . Managers that come without the clinical experience . . . don’t really progress.
Hasin, general, Care
Among general managers, there were a large number encountered who held educational qualifications in clinical or clinically oriented knowledge domains. These were considered important in helping provide the bedrock of technical understanding that enabled managers to communicate effectively with their teams and, in particular, to engage appropriately with clinicians:
If you’ve got that clinical background it is a major advantage. There’s managers within my business group – our theatre manager and some of the heads of nursing – [that] are more clinical based. I quite often find that they do have a massive advantage [as] they’ve got that clinical knowledge.
Stewart, general, Acute
Rarely, however, were general managers encountered who had undertaken and achieved explicitly managerial qualifications at degree or postgraduate degree level. The exceptions were some specialist functional managers whose academic grounding will inevitably have encompassed some management or business-related subjects:
From an HR perspective then, in terms of managing a team, there’s an expectation, certainly at this level, that you’ve done a CIPD [Chartered Institute for Personnel Development] qualification, which gives you sort of the good grounding in theory, I suppose, around management practice.
Theresa, functional, Care
At the same time, it was also made explicit how the continued absence of formal educational qualifications could act as a barrier to the further development of managers into more senior positions. Partly, this reflected the perceived need to fill particular gaps in managers’ knowledge base. But another important reason given was the perceived importance of achieving appropriate accreditation for pursuing managerial careers.
[In] the transition from nurse to manager, it’s getting that confidence to be able to challenge evidence, data, financial, systems. You’ve got to be quite confident in those to be able to challenge those, and I guess going through a formal MSc in public health helped me to develop that skill set.
Roxanne, general, Acute
Again, and interestingly, it was only exceptionally that such qualifications should be explicitly management focused (such as the MBA, for example). Educational development through more health-specific or clinically orientated MSc programmes was still the norm. In addition, this tended to reflect the importance attached to the development of analytical skills applied to a health-care context as opposed to the generic management skills that were often emphasised as being important for the job, but which were more commonly felt could be developed through experience and training.
The MSc did just elevate me clinically to a higher level, which is everything a masters is supposed to do, so that was around critical thinking, being able to understand and utilise research and to develop evidence-based practice.
Leo, clinical, Care
The following account, for example, highlights the usefulness of further study for developing an understanding of management in the health-care context through developing research and analytical skills needed for examining evidence.
The masters in research I took was a pivotal moment in my education and training. It’s when I first understood . . . what research and evidence really means, and how critical it is to try and critique research.
Ross, general, Care
The Graduate Management Training Scheme
Not surprisingly perhaps, the juxtaposition that occurred in other accounts about the limits of formal education as opposed to the value of experience was reflected in a fairly consistent pattern of opinion about the GMTS. Although highly regarded for the grounding it gave graduates, it was not considered as valuable in giving graduates the hands-on experience that they ultimately needed to manage. Views on the GMTS were expressed from more than just the eight managers (five from the acute and three from the specialist trust) who had come through that route. For example:
I’ve worked with a number of graduates now, probably four or five in my time. I’ve got one who was very, very good and he’s sat next door in there now as one of my senior managers, because he seemed to be able to do what a lot of the graduate trainees couldn’t, and that was communicate with other human beings. A lot of them seem to not be able to do that, I don’t why.
Greg, general, Acute
On the other hand, it was seen as extremely useful in helping prospective managers gain a wider range of experiences of their organisation and of the sector than other progressing through alternative career paths:
One of the big things they tell you pretty much on day one is that one of the main focuses on the graduate scheme is networking . . . We attended loads of events where there’d be directors of finance there, chief execs, and . . . you’re encouraged to network . . . It’s like a skill that you can’t really learn, it’s just a case of doing it. So that was one thing that we were fortunate enough to get the opportunity to do.
Thomas, functional, Specialist
This socialisation into networking was particularly the case for those in functional specialist areas (finance, HR, estates, IT), who perhaps relied more heavily on the network of professional contacts they were able to develop and who shared a common orientation to the health-care sector.
Formal training and development
I think I’ve learned more on the job than anywhere else. And often the two didn’t really meet up with each other because there are times you are managing the situation and you think, now what did I learn on that management course? . . . Maybe that just says something about the quality of the courses I’ve been on? But I don’t know . . . It would be great to have something that you could go away to, and would help you, quickly with all these skills.
Robert, clinical, Care
Managers across the three trusts had access to a range of formal training and development opportunities that often encompassed more technical or administrative aspects of managerial work, such as health and safety or IT training, as well as those aspects concerned more directly with the managerial challenges they faced, e.g. interpersonal skills development or leadership training. Uptake of such opportunities also varied considerably.
An attempt was made to categorise the level of formal management training experienced by managers in their careers. Based on lengthy responses to questions about their background, training and experience, respondents were categorised as having received minimal training (i.e. none or only very occasional), some training (sporadic or regular, if not frequent and intense) or substantial training (frequent and intense periods of training). Figures 11 and 12 show the numbers of managers in each category, by trust and by management group, respectively. As Figure 11 indicates, most managers across the trusts had received some, or a substantial amount of, formal management training (although this varied significantly in terms of content and level). On balance, there had been a greater intensity of management training at the acute trust.
FIGURE 11.
Levels of formal training by trust.
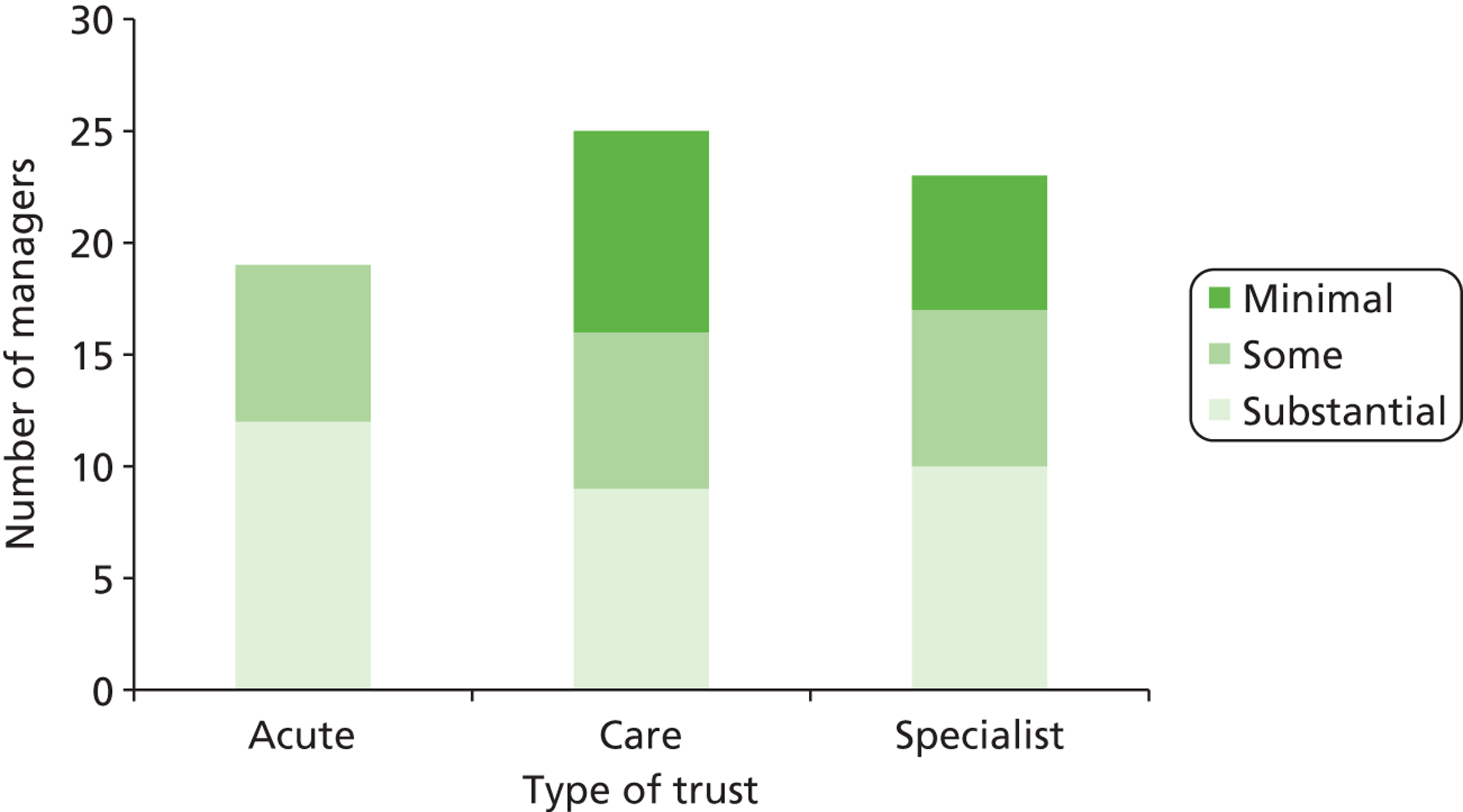
FIGURE 12.
Levels of formal training by management group.
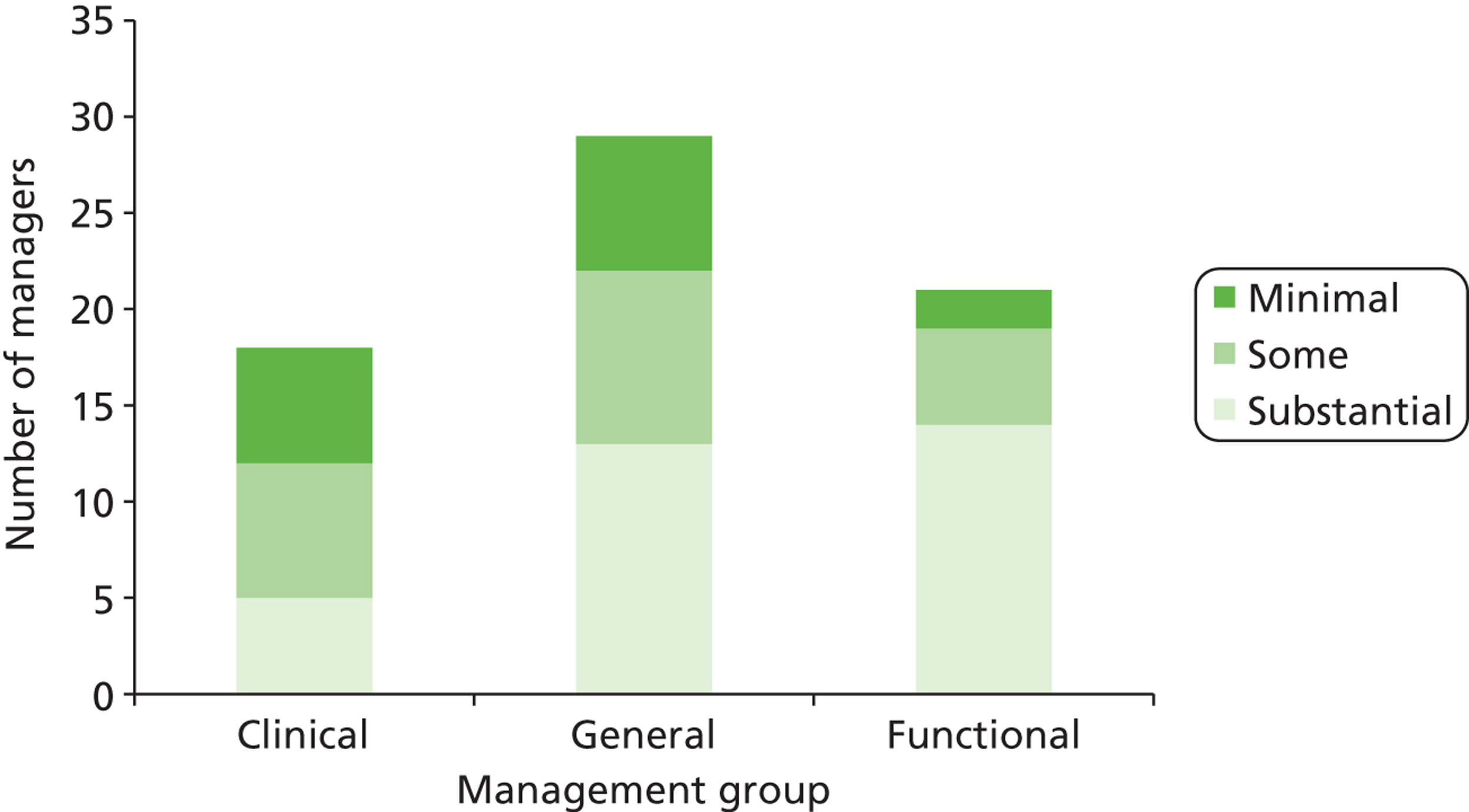
Figure 12 further indicates that the greater numbers experiencing minimal management training were mainly found among general managers at the care trust (plus some clinicians at both the care and specialist trusts). Figure 12 also suggests a greater intensity of management training was found overall among functional managers.
Evaluating formal training?
Table 15 summarises some of the main themes that emerged, again expressed as juxtaposed advantages and disadvantages of training. Each of these themes and their main implications will be explained and examined in turn.
| Advantage | Disadvantage |
|---|---|
| Critical for developing/updating professional knowledge and skills | Can be more concerned with routine knowledge requirements |
| Opportunities for sharing knowledge and networking with peers | Difficult to synchronise with managerial career development needs |
| Value of action learning sets | Limitations of formal learning as detached from practice |
| Allows time for reflection away from daily pressures | Difficult to find the time to take up training opportunities |
| Value placed on individual development and self-awareness techniques (e.g. Myers–Briggs) | Less of a connection with formal, abstract tools and techniques (e.g. lean principles, process mapping) |
First, there was clearly a good deal of importance attached to training that was considered vital in developing or updating professionally related technical skills, particularly, of course, for those in the clinical domain, but also among some functional specialists (e.g. new accounting practices or regulatory requirements). However, for general managers, such technical training tended to relate to what were perceived as the more mundane aspects of their work, as identified in the discussion in Chapter 4 . A lot of training across the trusts was considered very positively, with many comments being made about the general good quality of training experienced.
However, it was also clear that such training did tend to cater predominantly for the more routine knowledge requirements of the job and that, for general and functional managers alike, this could make it much less valuable than direct experience.
For clinical managers in particular, this could be very unattractive:
I’ve been delivering some health and safety and reporting training to the consultants and have actually set up proper dates for them now . . . You get the odd one who will come, but certainly not surgical – sorry, lords and masters. They forget that they’re managers as well, they’re consultants, and they are managers of a team and that’s something I remind them of with the health and safety law what their responsibilities are.
Hayley, functional, Specialist
Second, a strong emphasis was placed in virtually all of the interviews on the importance of having training that was very practical and applied. This was most clearly expressed in the value placed on training activity that made use of action learning sets and associated project/case assignments, as well as more interactive learning such as that connected with role-play:
The trust put on a senior manager training course . . . that was a week away for senior managers. It was really good, it was excellent, a week’s training where we looked at the theory around leadership and management styles, different ways of working. I got a lot out of that week . . . I had a couple of people in the service [who] were really challenging to manage, really difficult. And part of the training was they brought actors in and you gave the scenario to the actor and then you came in and you had to do the role play around it . . . I learnt such a lot from that process about what I was doing and how that wasn’t particularly helpful . . . I found that I was able to transfer that learning to other situations as well.
Jocelyn, general, Care
However, it was also apparent that there was value placed on particular sorts of training experienced that focused on developing self-awareness and teamworking. One particularly striking example was in the singling out for praise of training based on the use of personality assessment using the Myers–Briggs indicator. Respondents who had undertaken this training across the acute trust and (particularly) the care trust were highly enthusiastic about the use of this tool in training to help develop greater self-awareness and perceptions of others:
I’ve known what my Myers–Briggs profile is for quite some time, but one of the things that we did do on the first part of [the course] . . . was a real in-depth look at Myers–Briggs. And when you were pushed to extremes of pressure how it flipped. And that was really insightful because although there’s lots of theory attached to it I could relate and think, do you know, I do do that. So I got a lot from that particular session, and again it was about more self-awareness.
Melissa, general, Acute
Receptivity in the care trust could have reflected the trust’s fundamental orientation towards care and personal issues. Of course, the course may also have been particularly inspiring! However, it is also likely that it reflected the emphasis on the personal embodiment of skills that come out strongly from across this analysis and to which the respondents could clearly relate. In other words, the approach was rather more based on understanding the whole person as opposed to the impersonal check-listing of distinct management competencies.
Back in 2001, we had a five-day course away from services, and it was the best course ever because it was very much around emotional intelligence and growing with emotional intelligence. I did what you call the MBTI [Myers–Briggs Type Indicator] stuff . . . and it was fantastic, it was absolutely fantastic. Because I got to learn about my colleagues, I got to learn about how people can be at work, why people are the way they are at work. I got to learn about a range of leadership styles; how to apply them, when to apply them. And the best bit is, I got to learn about myself, which was really important.
Hasin, general, Care
Although this focus on practicality, engagement and practical application seems fairly obvious and understandable, it did have something of a downside. When the focus was on potentially less routine knowledge and learning, for example in training on lean thinking or other more generic management practices, the danger was that it could be seen as less directly and practically relevant and transferable to the immediate work situation. It could easily reinforce a tendency to value what was perceived as directly relevant training at the expense of training that might seem more esoteric and theoretical:
When I went to the lectures, I just thought, what am I doing here, because I didn’t understand all the jargon at all. Then when I spoke to the tutor and said, generic questions aren’t going to help me. Can I make it specific to this new role? So she used to set assignment questions specific to the nurse consultant role to help me develop that.
Beryl, clinical, Specialist
As in any training or learning situation, the challenge is to enable the development of insights and learning that is a fusion of new ideas related to practical circumstances and needs. The danger here, particularly when more mundane training requirements are important, is the potential for reinforcing a training regime that emphasises activity that is manifestly practical at the expense of activity that requires a greater degree of reflection.
Indeed, and as a third theme, many of those interviewed placed considerable value on the prime opportunity that training presented to allow time for reflection away from the daily pressures of work. The downside was that it was often difficult to allow for training in busy schedules and managers often had to go out of their way to make time to make the best use of training opportunities. For some general managers in particularly busy operational roles, this proved to be too challenging and difficult a task, with the result that training opportunities may be missed or rarely taken up.
I think the opportunities are there within the organisation if you want them. I think if you really want to push on and you really want to expose yourself to as much training and development as you want, then there are opportunities there to do that. I think one of the biggest hindrances to that is that once you’re actually in a post, the day-to-day grind of doing your day-to-day job [makes it] difficult to find that time to be able to remove yourself from the position for maybe two, three days or whatever . . . You almost have to force yourself to try and do that if you want to continue learning and development.
Stewart, general, Acute
Fourth, there was clear indication of the importance of social factors and the opportunity that training gave to participants to network with their peers and to share experiences, knowledge and learning. Again, managerial networking is covered more thoroughly in the next chapter. The main point to note here is that not only was this seen as an important potential benefit of training undertaken, it was also seen as one that was particularly difficult to achieve given the challenge of synchronising management training and development with the career needs of middle managers. The following quote explains the irony fairly clearly and concisely:
When you’re doing a management course that tells you how to manage staff or gives you the theory about managing staff, it’s really difficult without having practised in HR. It’s kind of like catch 22 almost . . . You need the experience to apply the learning, but you . . . need the learning . . . to do the job.
Theresa, functional, Care
In other words, it was clear from the interviews that it was extremely difficult for managers, at the level of seniority that we were talking to, to find appropriate training opportunities that aligned with their managerial needs and career development trajectory. For example:
Theory was something I’d got in my head but I hadn’t got the experience necessarily to be able to apply it, and other periods where I’d got experience that I really could have done with some more formal development to work out how best to use that.
Ruth, functional, Care
Together these factors suggest that training opportunities provided some potential for the very profound development of management knowledge and learning. However, there were real tensions in the ways in which training was oriented and how it was delivered and received. Quite apart from the more practical issues associated with the value of particular sessions or types of training and the difficulties in scheduling them into busy managerial schedules, there are clearly challenges in developing training programmes that are seen as suited to middle management development and that provide the timely opportunities seen as necessary to help develop the social interaction and practically applied reflective learning that managers felt was highly desirable and could help them become effective and reflective managers. 131,132
This last set of comments contrasted with the more favourable experiences generally reported by many of those who had managed to secure places on wider leadership developmental programmes (such as Aspiring Directors, Gateway to Leadership, Breaking Through and Athena). Although issue of substance and synchronisation with current career needs could still be seen as an issue, access to such programmes was generally considered as providing valuable opportunities for networking and, for some, an inspiring entrée into the domain of leadership.
It [included] four days of assessments, which was quite tiring actually. Just four consecutive days of being observed and watched in group exercises, individual things, every psychometric test you could possibly imagine in the world, and then . . . they worked with you on a personal development plan to meet the development areas, and then we got coaching to follow that up and we also established a network from the group . . . We were staying away together as well. But that was brilliant and I think had quite an impact on my career after that.
Ruth, functional, Care
Perhaps not surprisingly, this could create an impression of selectivity, overemphasis on self-presentation and style and a divorce from what was considered the real work of management for those who had experienced people’s involvement on the programme only second hand. Consequently, although seen as positive and valuable experiences, such programmes did attract some scepticism.
Summary
The chapter has explored the different forms of knowledge available to, and accessed by, managers in our study and related these to the different processes of learning. It has emphasised a distinction between knowledge and learning that was more codified and abstract (and so difficult to translate into practice or into shared meanings) and that was more tacit and situated (which was more salient and immediate, if less generalisable and transferable). Along the way, the discussion has hinted at the important part played by networking in these processes, and it is to this theme that we turn next.
Chapter 6 Networks and networking
Introduction
If you just look around a trust like this, you’ve got people with experience in practically everything and anything you can think of, but we don’t use it. We don’t, because of our failure to network with one another and use other people’s skills and knowledge and understanding, we just don’t use it. You’ve got all these people with all this knowledge and we don’t use it, and we don’t manage to tap into it. And it’s something about we’re so busy trying to keep afloat that we just don’t look forward.
Greg, general, Acute
The quote above indicates the latent potential within the NHS, in terms of breadth and depth of knowledge and experience, both clinical and managerial, and the frustration felt when this potential goes unfulfilled. This third main aspect of the study addresses the issue of networks and networking, a theme that complements and connects the preceding discussions of management/leadership and knowledge. Network relationships are the predominant way that knowledge and understanding are shared in a large and diverse meta-organisation such as the NHS. Networks, in a more formal sense, have also been seen as the organisational solution to providing an integrated service across organisational and professional boundaries, through the establishment of managed networks connecting fields of practice or patient pathways. As a consequence, there has been substantial interest in recent years among health-care management researchers regarding network organisations, network analysis and also in related concepts, including CoPs and social capital.
This chapter will set out the insights emerging from this study relating to networks and networking. To do this, it is important from the outset to establish our understanding of networks and networking and how this relates to other standard concepts and approaches in this field. The specific networks identified, discussed and observed in the study will then be described and categorised, before addressing the deeper question of how and why health-care managers network.
Understanding networks in health care
Social, managerial and organisational research has adopted the concept of the network with some relish in the late 20th century. In his book The Rise of the Network Society, Castells argues that networks ‘constitute the new social morphology of our societies’133 (p. 500) and points to the new recognition of the vital importance of knowledge and knowledge flows across all aspects of society, business and culture. The particular strengths of the network as a highly dynamic and (in principle) open system of inter-related nodes lie in the fluidity of this phenomenon, capable of rapid expansion or adaptation. The model of the network has been used to represent and analyse a vast array of social phenomena: as methodological tools to understand the functioning of communities and society,134 as designs for new and more effective organisations,135 as the solution to the failings of markets and bureaucracy136 and as models to account for the vital flows of knowledge within and between contexts, organisations and communities. 9
Networks, as discussed here, also bear many similarities to the widely discussed ‘community of practice’,42 referring to delimited groups of practitioners bound by communal relationships, shared understandings of the world and the joint enterprise or mission of the community. 43 In particular, CoPs are locations where members learn collectively and are at the same time socialised into a common way of thinking and acting through frequent and face-to-face social interactions. In this way, CoPs serve to enhance knowledge sharing and knowledge creation among members, but also serve to inhibit knowledge exchange and learning between CoPs, owing to epistemic and social boundaries. 48,137
Although some of the networks identified below (see Table 16 ) share a number of characteristics with CoPs, most are less cohesive, consisting of relatively weak links and more distant or infrequent interactions, closer perhaps to the notion of NoPs. 138 Both CoPs and NoPs have had some significant impact in health-care research and practice,99,139,140 principally in the deliberate formation of managed clinical networks such as those constituting ‘linked groups of health professionals and organisations from primary, secondary and tertiary care working in a coordinated manner, unconstrained by existing professional and (organisational) boundaries to ensure equitable provision of high quality effective services’141 (p. 63).
A key analytical concept widely adopted in this field is that of social capital, frequently drawn upon to focus on the characteristics of the individual within the network, rather than the network itself, and at times used to ascribe a value to the individual in terms of their social connectedness. Social capital defined as ‘the sum of the actual and potential resources embedded within, available through, and derived from the network of relationships possessed by an individual or social unit’142 (p. 243). The value of this concept is summarised effectively by Burt, who argues that:
Social capital explains how people do better because they are somehow better connected with other people. Certain people are connected to certain others, trusting certain others, obligated to support certain others, dependent on exchange with certain others. One’s position in the structure of these exchanges can be an asset in its own right.
Burt,143 p. 4
Analysing the extent to which individuals are embedded in networks and the ways in which they rely on networks to help them to achieve any of a number of goals implies a consideration of their social capital. The danger, however, of prioritising social capital is that the notion of capital prioritises the economic aspects of social relationships, and frames these primarily in terms of ‘economic exchange, possession and organisational effectiveness’144 (p. 236) while neglecting the less instrumental reasons why individuals forge relationships (including for emotional closeness, affirmation of self and identity, or the reassurance of belonging in a community). For this reason, social capital is not the primary way in which we have approached networks and networking in this study. Although we are attentive to the impact of networks in terms of individual and organisational effectiveness, we do not assume a priori that this is the sole purpose or predominant consequence of networks.
Rather than identifying networks in advance and exploring their nature and use, the approach adopted in this study was to ask individual practitioners themselves about their network relationships, emphasising a broad rather than a narrow scope of enquiry. In this way, the aim is to avoid the widespread assumption in health management literature, noted by Ferlie et al. ,139 that managed networks are those most worthy of investigation. 139 As a consequence, the analysis avoids a preoccupation with formal, structured, closed and centralised networks, and incorporates analysis of informal, loose, open and flat or distributed networks, such as friendship and affinity groupings, or highly dispersed communities bound by ‘weak ties’. 127
Similarly, the research does not adopt a sociometric approach to networks, attempting to quantify network relationships by measuring the frequency and duration of contact (as implied by social network analysis, for instance). The approach adopted here focuses less on counting and measuring the incidence of networks and instead on an understanding of the ‘situated and contextual quality of relationships’144 (p. 236) in terms of the significance and nature of networks and the specific practices of networking undertaken by our interviewees.
Varieties of networks
As a consequence of the methodological approach adopted, a wide range and variety of networks were identified and explored through the interviews and the ethnographic encounters. Table 16 summarises the main categories of network discussed and analysed through the study.
| Nature of network | Description |
|---|---|
| Academic/scientific | Links to universities, research or scientific bodies |
| Alumni | Connections made through participation in a specific training or educational programme which persist beyond end of programme |
| Peer/cohort | Relationships formed with others who joined this (or another) organisation at the same time |
| Commercial/third sector | Links to private sector organisations or charities |
| Elite | Connections to senior decision-makers, within the trust/organisation or at a regional/national level |
| Functional specialist | Relationship or collectivities bound by a shared work specialism |
| Government | Relationships with individuals within regional or national government |
| Managerial | Relationships between groups of managers, including both occupational networks and more operational groups |
| Mentor | One-to-one relationships with a formal or informal mentor, typically but not necessarily outside the organisation |
| NHS | Connections to individuals in other NHS organisations, including the Department of Health, SHAs/PCTs, GPs/CCGs, etc. |
| Operational/clinical | Day-to-day relationships typically formed through the day-to-day execution of responsibilities |
| Personal | Friendships, non-work relationships, family connections, etc. |
| Professional | Links with general or health-specific formal professional bodies, in accounting, HR, facilities, health and safety, etc. |
| Public sector | Non-governmental public connections, with for instance schools, legal bodies (e.g. coroners), prisons, armed forces |
| Political | Networks specifically cultivated to develop influence, typically diverse in composition, hence not captured by other categories |
The networks identified may, themselves, be differentiated along a number of different dimensions, such as the degree of co-ordination, strictures on membership, the way in which the network was formed and its location within or across organisational boundaries ( Table 17 ). With few exceptions, each of these categories contained a diverse set of actual networks; for instance, alumni networks ranged from the formal (prescribed action learning sets) to the informal (loose affiliations of friends who socialised together); elite networks may be highly instrumental, built on engineered introductions and self-promotion, or relatively organic, resulting from a shared interest or a genuinely accidental social connection. A small minority of categories were largely homogeneous: personal networks were generally organic, informal, loose and external in scope, while most professional networks were closed and relatively formal. Nonetheless, the dimensions provided a means to differentiate particular networks and also to identify similarities between networks that, on the surface, were very different in composition and nature.
| Dimension | From | To |
|---|---|---|
| Structure | Formal | Informal |
| Co-ordination | Tight | Loose |
| Membership | Closed | Open |
| Formation | Instrumental | Organic |
| Position | Internal to organisation | External to organisation |
Overall, most frequent reference was made to external networks by interviewees in the care trust, reflecting the multiple connections between different primary, secondary and community health bodies. Markedly fewer references to networks of any kind, internal or external, were made within the acute trust, reflecting the overall size of the organisation and perhaps, in part, a more functional organisational structure compared with the fluidity of service delivery in the care trust. In terms of the pattern of networks discussed by the three management groups, it was unsurprising to see the functional managers relying most heavily on their professional or functional specialist networks and enjoying connections to some powerful elite networks, either through these professional associations or by their representation of a professional area at board level. To a lesser degree, clinical managers also retained important networks through their clinical or scientific professional associations; in some cases this was clearly active and highly committed (in the case of medical directors, for example), in other cases this was more latent (membership of a nursing body retained as a career to fall back on, or a way to retain clinical legitimacy when managing clinicians). While the background or formation of some general managers enabled them to participate in clinical or professional networks, they would more typically rely on networks established through day-to-day operations, which were necessarily less formal and less enduring owing to the disruptions of normal organisational change. A substantial number of the general managers spoke with feeling of the perceptible absence of supportive networks in their role, compared with their clinical and functional peers.
Who networks and why?
Analysis of the interviews revealed four motives for networking, although discussion of each varied substantially between trust and between management group. The key motives were:
-
networking for knowledge
-
networking for support
-
networking for career advancement
-
networking for influence.
In terms of frequency, it seems that, overwhelmingly, the main purpose of networking among our interviewees was to acquire knowledge. Over half of the references to networking motives related specifically to knowledge acquisition, either actively or passively ( Figure 13 ). A sizeable minority (25%) of references discussed the value of their network connections in providing personal and emotional support. A smaller proportion (14%) discussed the value of networking in terms of their career management and the smallest proportion (9%) explicitly discussed networking in order to influence policy, decisions or behaviour in or beyond their organisation.
FIGURE 13.
Networking motives: number of interview references.
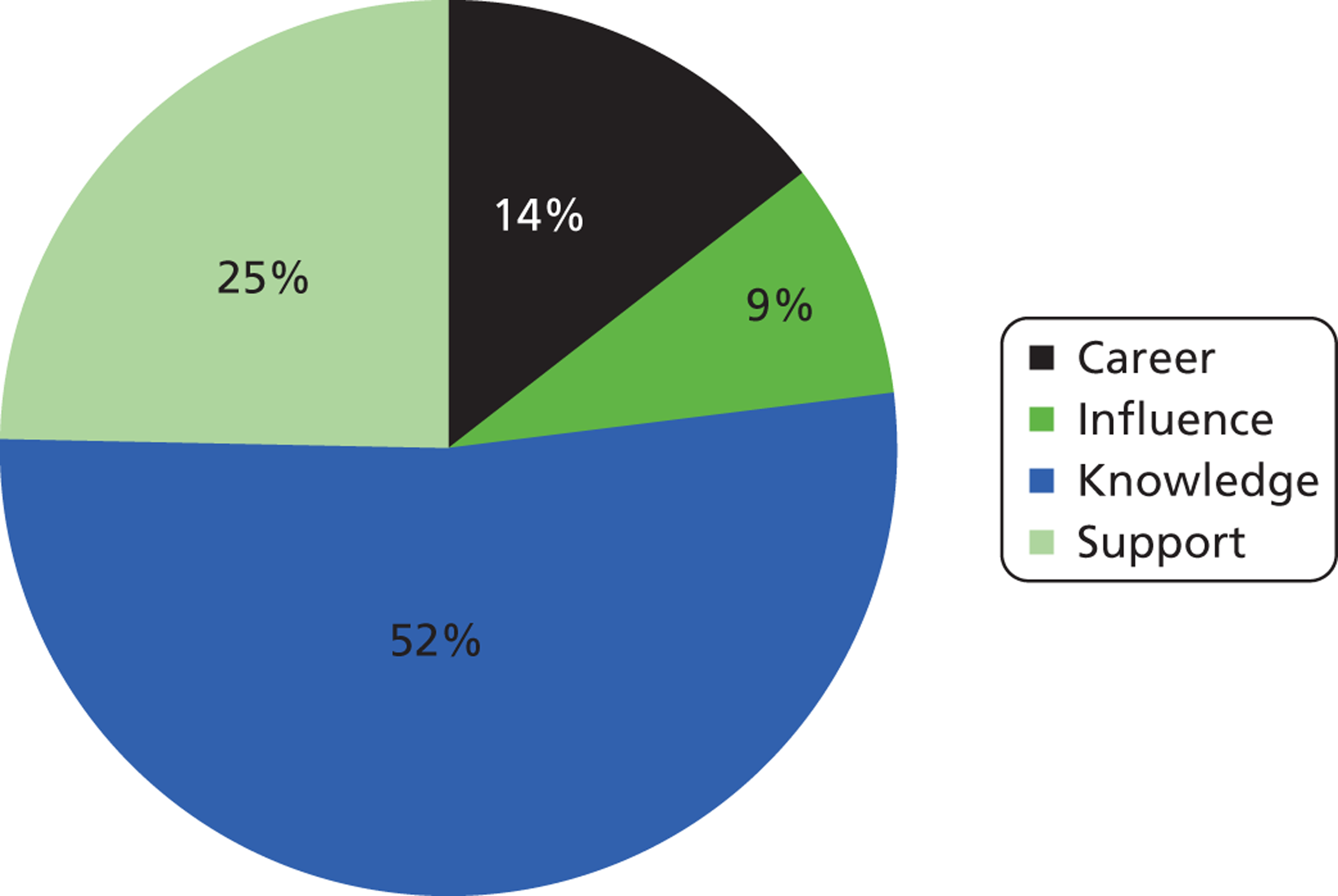
Discussion of each of these motives varied significantly between trusts ( Figure 14 ) (for instance, managers at the care trust were substantially more likely to discuss networking for support than managers in the other two trusts) and also by management group ( Figure 15 ) (e.g. managers with a clinical background were significantly more likely to refer to networking for knowledge than other managers).
FIGURE 14.
Networking motives by trust.
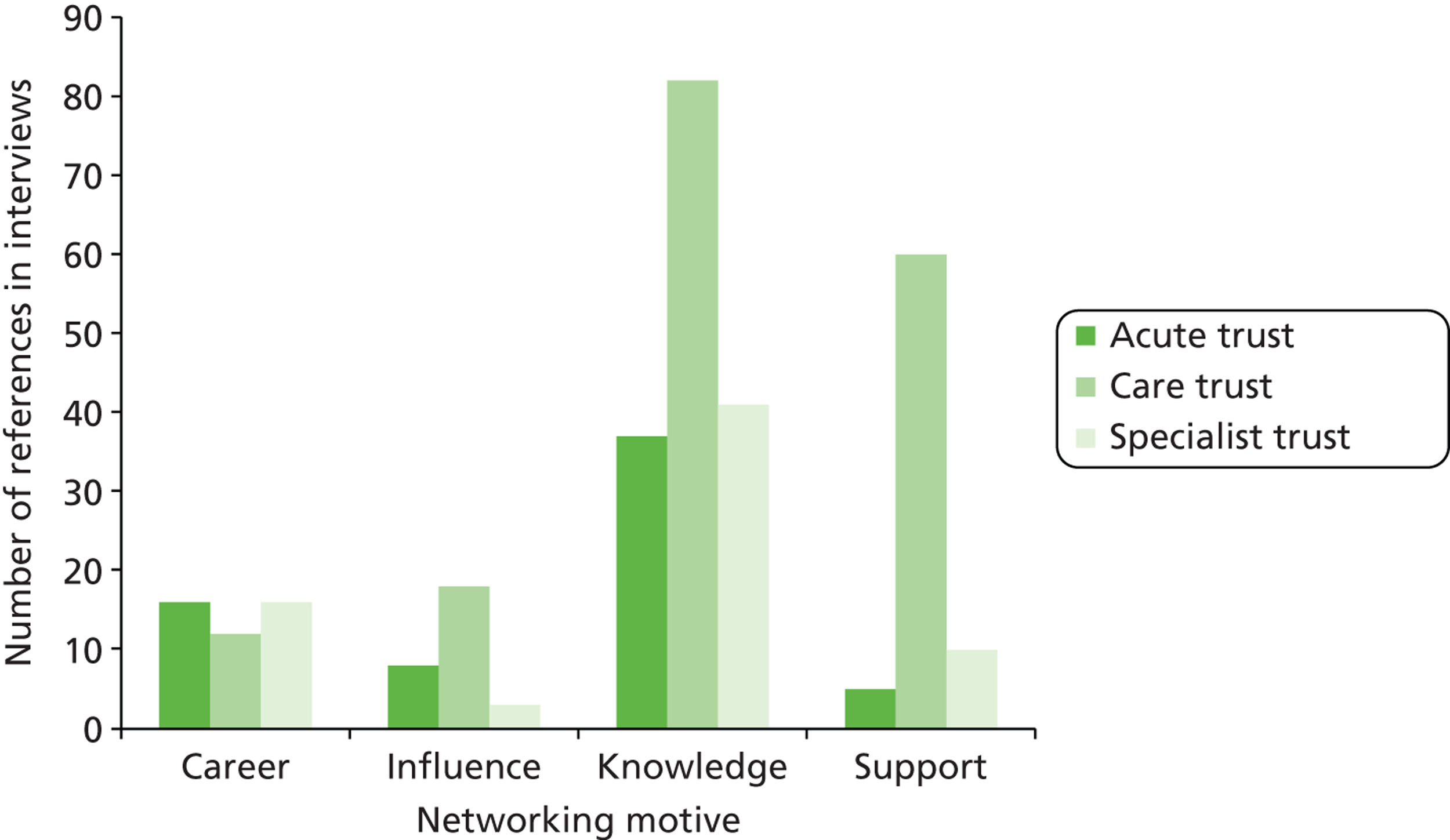
FIGURE 15.
Networking motives by management group.
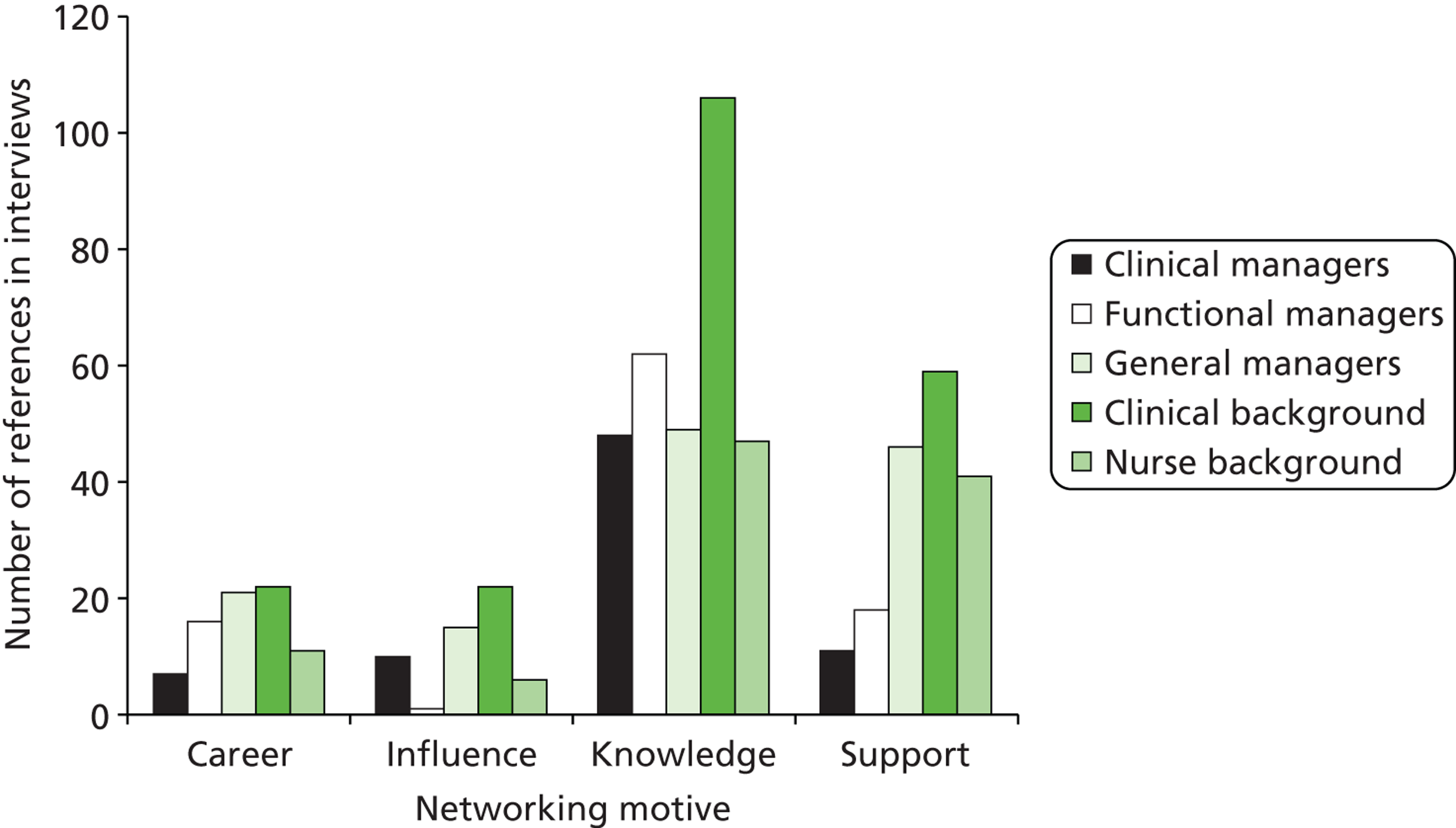
A striking difference also emerged between male and female managers. Male managers were twice as likely as female managers to discuss networking for career or influence, while female managers were more likely to mention networks as a source of personal support ( Figure 16 ; note that figures are normalised to take into account proportion of respondents of each gender).
FIGURE 16.
Networking motives by gender.
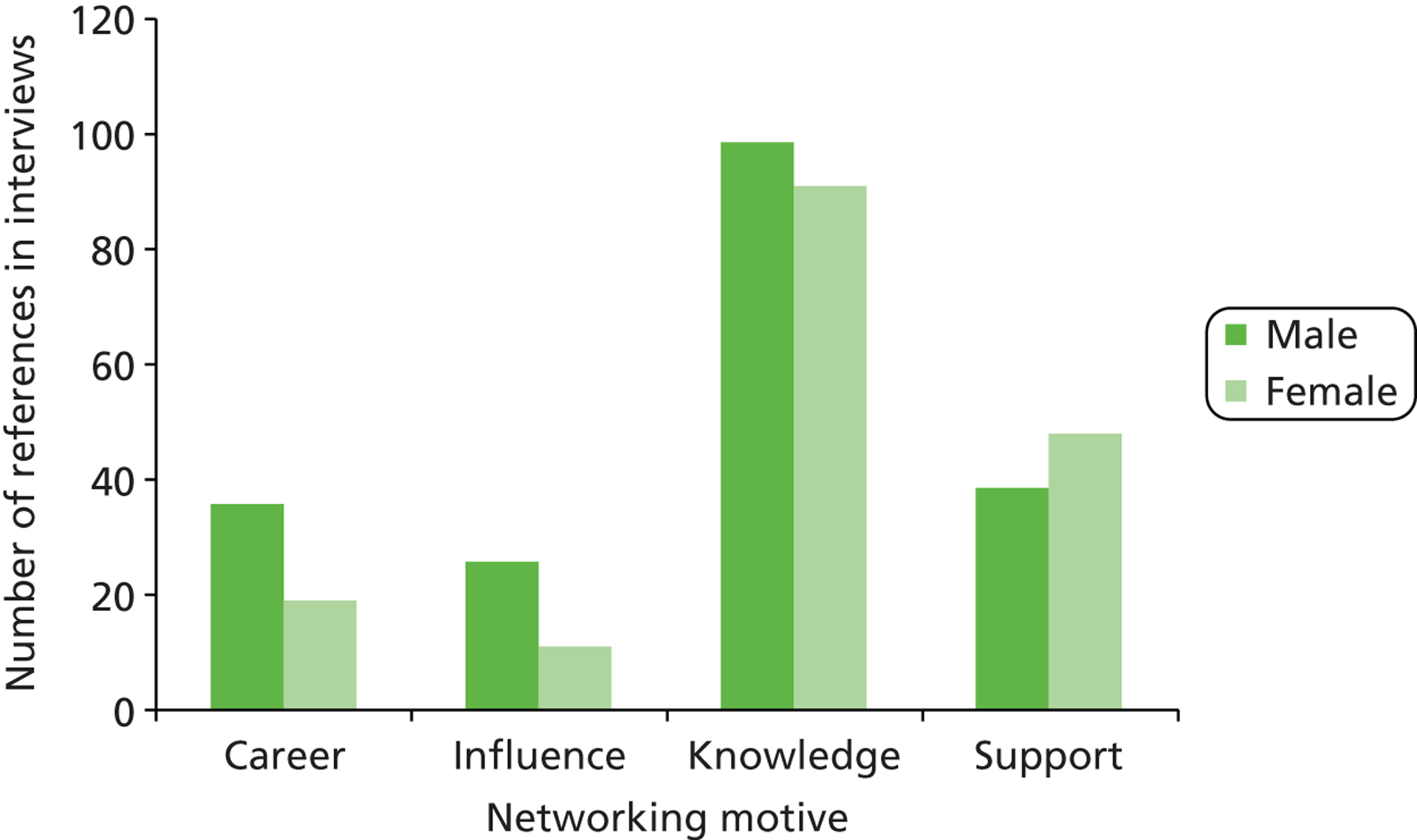
Before discussing these motives in detail, it is important to reiterate the point that the frequency with which each motive was discussed by a particular group, or within a particular trust, does not necessarily equate to the frequency with which individuals engaged in this behaviour, or even the importance of this behaviour to them. Critically, interviewees may have discussed only motives that they felt it to be legitimate to discuss in their particular organisation or environment. This may particularly have affected discussions of networking for support or networking for career. However, rather than this representing a limitation, this constitutes one of the strengths of the qualitative research methodology. The frequency with which each motive was discussed provides insight not only into the practices and orientation of each interviewee but also, inevitably, reflects to some degree the norms of their cultural, organisational and professional environment and their socialisation to abide by such norms. This theme will be expanded on as we deal with each particular dimension of networking.
Networking for knowledge
The primary purpose of networking, for almost all managers interviewed, was to acquire or share knowledge. This was widely discussed across all three trusts and all management groups and mentioned with particular regularity by managers with some clinical background. There were, however, significant differences in how this was understood or practiced, a key distinction existing between passive and active networking for knowledge. Passive networking for knowledge largely related to partaking in events, or membership of formal or informal groups, networks or associations in order to be broadly informed about new or potential changes in policy, to scan a community for new ideas that may be transferable or to learn lessons from failed initiatives elsewhere. We refer to this more passive activity as peripheral awareness, primarily to differentiate it from the more active networking for knowledge discussed below.
The secret is always having the ability to look over the garden fence and see what’s happening in somebody else’s garden. Because that’s the only way you learn. And you might learn something you don’t want to learn. You know what I mean, you might see something you don’t want to see. But also, from all this variety, as I’ve said before, why reinvent the wheel, why do it?
Adrian, functional, Specialist
Active networking for knowledge we refer to as problem-solving. Here, interviewees discuss the value of networks and networking in terms of providing a resource for the pursuit of intentional enquiries or searches for information in order to fix a particular challenge or problem faced in everyday practice. This targeted problem-solving networking was typically related more closely to networks based around a particular specialism, operational or clinical networks. In many cases, such networks are specifically formed to facilitate such activities:
The clinical leaders’ network tends to start off with a sort of a general presentation and then you’ll get into your area networks, so there’d be perhaps (Town A, B and C) might sit as a sort of subgroup within the network and then you’d bounce off your problems from your colleagues and sort of see whether you could learn anything from others’ experiences.
Hugh, general, Acute
Similarly, various specialist functional networks, dedicated to particular occupational or professional groups such as finance or HR management, take advantage of the size of the NHS to maximise learning opportunities:
We only meet once a year, and we go round the table, at the end of the meeting, and it might be what we’re doing here. And then you might say, ‘Well, I’ve got a problem with so-and-so’, and this guy over here will say, ‘Well, hang on, I did that last year’. And it’s all very informal, but it doesn’t half bring it out.
Adrian, functional, Specialist
Less formal, structured problem-solving networks include the action learning sets established on many development programmes. Those formed during the NHS GMTS were highlighted by a number of interviewees, building on the strong group relationships formed during extended training and induction programmes:
I mean, I still stay in touch pretty much weekly with probably 15 others (from the GMTS) . . . If there’s a problem, we’ll put it out there, you know, e-mail it out. Yeah, so there is . . . I’d say that is one of my key networks.
Thomas, functional, Specialist
This knowledge sharing is, therefore, supported strongly by the establishment of trust and underpinned frequently by long-term personal relationships and affiliations outside the work environment. One interviewee captured this well, describing a relationship established on a training programme in which a conversation about child care challenges provided the basis for a personal relationship with tangible benefits for work-related knowledge sharing:
My ‘challenging situation’ (discussed at a leadership course) was my 5-year-old at home at bedtime, but it felt a safe environment to have those discussions. And actually, the lady that ran the course, I e-mailed her three nights after and said, ‘You know, I tried X, Y and Z and, you know, woohoo, it’s working!’ kind of thing. And I’ve now got an e-mail relationship with this lady that, if I did have a problem in work, I’d find it really easy to just pick up the phone and say ‘Jacqueline, you know, I’ve tried this, what do you think?’ Rather than an outside agency or a consultancy that once they’ve gone, they’ve gone.
Gloria, general, Acute
Although, in principle, networking for knowledge is the most instrumental and practical mode of networking, it frequently has a complementary relationship with other, less pragmatic, modes of networking, an issue that is returned to in Complementarity of networking.
Networking for support
Networking for support represented the second most cited motive for forming and maintaining networks: the reliance on such relationships for emotional reassurance, personal validation, consolation, or for the expression of feelings outside of the immediate work context. The incidence of this theme was noteworthy, as it was mentioned by almost half of those interviewed but was especially common in the care trust and relatively rare in the acute trust. This substantial variation may result from the perceived legitimacy of such therapeutic discourses in care settings and the relative formality of the culture at the acute trust, where such discussions may be seen as inappropriate and, thus, may not fully reflect the actual incidence of this form of networking. Discussions of networking for support were also complicated at times by the reluctance of some interviewees to define such relationships as a network; these were friendships, often long-standing personal relationships that may be quite separate from their job role and, for some, perceiving these as a network attributed an instrumentality to them that seemed inappropriate.
What was striking was the importance attached to such networks. Managers frequently discussed how difficult it would be to survive in a pressurised and often emotionally challenging role without a strong support network, which may include current or former colleagues, friends, family members or more formal and explicit arrangements with mentors, peers, members of action learning sets, etc.
We meet weekly, we talk about what’s going on or we have a moan about something, but often it’s helpful just to have a moan about something with someone that you’re comfortable to do that, rather than it becoming winding you up (. . .) Sometimes it’s like damn . . . and she’ll say, what are you getting worried and stressed about that for? (. . .) I have gone have you heard what they’ve done! But she just kind of goes, it will all get sorted and yes I just kind of . . . we bring each other down at times.
Carl, functional, Care
Descriptions of this form of networking ranged from the clearly emotional [as a safe place for venting emotions or to ‘have a moan’ (Carl, functional, Care) outside the work context, as a relationship which enabled someone to remain grounded] to the more functional (as a kind of informal coaching, or a place to get objective comment on your decisions and actions). However, this distinction was not a clear one, reinforcing the importance of relational attributes such as trust and interpersonal understanding for effective knowledge sharing or meaningful advice. Equally, some descriptions emphasised the performative benefits of this emotional support, as enhancing their own resilience and, therefore, their ability to do the job well, or stay in the job at all.
Frequently, networking for support was mentioned as a secondary issue in interviews, as something beneficial for the individual but less important than the acquisition of knowledge to improve practice. Many represented networking for support as a positive, perhaps unintentional, by-product of more formal networking (for knowledge, for example). In many situations, such relationships formed as a result of joint participation in a training or development programme, but often extending beyond the specific goals or scope of the programme itself.
Going back to the Athena course, that has been invaluable because it’s not only making the connection and networking to start with and meeting up and speaking to each other. At any point at any time I can think ‘oh god I’m not really sure about this.’ Gemma in Bedford, she might have an idea about that. And I know, as we all do, that we can just e-mail each other, ring each other and that’s really beneficial. I think it’s really important. Some days it could be just ‘oh god I’m having a crap day.’ It could be just an offload, but it’s at the right level. I couldn’t do that to my matrons, although I have great relationships with my matrons it wouldn’t be appropriate. And equally you don’t want to go to your divisional director. It’s about professional pride, not because I don’t get on with them.
Nina, clinical, Specialist
Often, the importance of external networks (separate from the organisation or immediate working surroundings) was stressed, given the need for confidentiality and to maintain a professional bearing with work colleagues:
I think that no matter how well you think you’ve set your network up and what have you, I think that there are occasions when you can feel quite isolated in a trust as big as this. And you can’t imagine who you could go to and just actually say that without it escalating into something that’s really taken out of all proportions.
Elena, general, Care
Broadly, it seems, this aspect of networking is frequently ignored or under-represented in research in this area, but is one that a substantial number of managers interviewed find invaluable, given the increasing tensions and pressures of their everyday roles.
Networking for career advancement
The role of networking in supporting the career advancement of managers was discussed by just less than one-third of those interviewed. For this form of networking, the need to be informed about new opportunities and openings co-existed with the perceived importance of being known by key decision-makers. Given the diversity of positions, organisations and career structures, it was noticeable that this was cited consistently across all three trusts and across all management groups. A number of interviewees also pointed to the emphasis placed on encouraging this mode of networking by key management and leadership development programmes in the NHS:
One of the big things they tell you pretty much on day one is that one of the main focuses on the Graduate Scheme is networking. So . . . we attended loads of events where there’d be sort of like the directors of finance there, chief execs, and you know, it was always kind of like you’re encouraged to network.
Thomas, functional, Specialist
Networking for career development was practised either collectively or individually. Collectively, career networking typically relied on membership of particular communities or participation at key events, such as research conferences or senior training programmes, whereby a manager could raise her or his profile and establish a personal reputation, while at the same time making personal connections to individuals.
I came and talked about my involvement in lean methodology within the trust and how we’d made some powerful changes that lead to some high-quality impacts within the services. So I presented here, and then following that was kind of networked into the organisation, and then they created a job and approached me to apply.
Glen, clinical, Care
Individually, career networking normally builds on some kind of formal or informal mentorship arrangement. Several interviewees were quite open on the importance of approaching career networking tactically, to ensure mentoring connections are made with influential individuals and with a long-term career strategy in mind.
I was very keen to come back to this organisation after the training scheme. And as a ploy, as a tactic in me trying to do that my mentor whilst I was on the training scheme was X, who’s now the acting chief exec here. And I kept my contacts from when I was working here previously, and then obviously heard that there was a new Associate Director that was coming into this business group and I arranged to meet with him fairly early on as well. So certainly having that network and the training scheme, drumming it into you to make sure that you network with as many people as possible, I think that’s true in one sense, but I think it’s also about networking with the right people at the right time, and it’s just picking your opportunities and just being a little bit cute about who you speak to and who you make your networks with really.
Stewart, general, Acute
Similar to the notion of networking for support, there is often a sensitivity to suggestions that this may be behaviour that is in some sense inauthentic, instrumental or even manipulative. Several interviewees expressed deep reservations over the perceived need to network for career advancement, or discomfort engaging with what they understood as self-promotional or inauthentic behaviour:
There’s a lot of people on this course that ask a question for question’s sake and they do the mingling on the tables at dinner. Every time they got up to ask a question, they’d get up just to say their name and say where they came from. (. . .) Well I found it uncomfortable – I wouldn’t do that. And even though I’ve been here 3 years, that’s not what I would do. I still find it strange now.
Danielle, functional, Specialist
Reflecting this sensitivity, several interviewees who described themselves as engaging in career networking deny that their career progression is dependent on their social capital, or argue that any career networking was marginal in its impact, or that their own networking itself was unintentional or not strategic:
I was interested in the work-life balance thing (. . .) and he recommended X (as a mentor), who’s the Director here [laugh]. Yeah, so I had quite a long relationship with him. It was very much like me and him. It’s not – I didn’t get this job because of that, I’m pretty confident of that [laugh]. He’s told me that, and if you’ve met him, he’s not the sort of bloke who’d lie about that.
Thomas, functional, Specialist
Particularly for those who had joined the NHS mid-career or in their late career, the importance of career networking is perceived as an impediment to their career progression:
My colleagues that have been in the organisation with the NHS for 20 years plus, because they’ve moved around jobs they’ve, you know, people they trained with they’re also now directors of nursing somewhere else, so because they’ve grown up in the NHS. (They’ve accrued that kind of network anyway?) And I haven’t!
Hugh, general, Acute
Importantly, career networking has value not just for the individual but for the group or organisation, in that some interviews described how their strong networks enabled them to identify and attract higher quality recruits:
You need a network, you can’t function without a network (. . .) I’ve got a lot more from doing things and building up those networks. It’s like the graduate trainees, I’ve had a lot who’ve ended up here, in years past, without even me actually applying, because they know that the training they’ll get is the right training and they know that I’ll look after them (. . .) If you look at it another way, and this sounds quite cold, I’ve got a free member of staff for three years, virtually, who is going to add value to the organisation who, ultimately, could be a permanent member of staff and that’s just from spending a little time networking.
Jessica, functional, Acute
Overall, this particular practice was highly valued, despite deep ambivalence about the practice in some quarters and a widespread recognition among those who engaged in career networking that it required sophisticated interpersonal skills to enact successfully.
Networking for influence
The specific use of networking in order to secure some influence over a decision or behaviour in another organisational location was the least common outcome or intention of networking in the study, mentioned by only 11 interviewees. However, those interviewees frequently spoke at some length and detail about this approach to networking, particularly within the care trust where service delivery was more fragmented and thus more reliant on networks of connections than in the other trusts.
Networking for influence was typically undertaken deliberately, consciously and strategically, and those who described themselves as networking for influence typically emphasised this as vitally important, for themselves and often for their field/area of activity/division. Ross, a general manager in the care trust, epitomised this approach:
Networks, they’re fundamental to me. They’re absolutely the actual core of how I approach my work (. . .) It’s not just some kind of pleasurable experience, I engage with a network approach to management, because I think it gives you the best chances of delivering things.
Ross, general, Care
In terms of networking practices, a broad distinction could be made between networking based on a reciprocal exchange of favours and a broader attempt to push or represent a particular agenda through links with senior management, key role-holders or influential external parties. Hence, one interviewee (Ross, general, Care) summarised both of these as parallel activities, describing part of his approach as building reciprocal favours, or ‘just scratching each other’s back’ and another as strategically representing a set of interests (‘having a cup of tea with the chief exec, it’s purely about me making sure he doesn’t forget about the agenda here’). In each case, this involved deliberately maintaining a list of useful and influential contacts across a wide network. Others mentioned that it was important that they knew how they could get around the organisation and who, among their peers, to contact for information, advice and influence.
Many of those who engaged in networking for influence were passionate about its importance and contrasted their activity here with other colleagues who were politically naive and, therefore, less effective as a manager. So, for instance, Christian (general, Acute) described his role in enhancing the political skills of staff in his area:
X sent a guy to me a while ago who was new, and she said to him, ‘You just don’t get politics. You don’t know how to operate.’ So sent him to spend some time with me to talk through how to play the game here – it’s the same where you work and the same where everybody works.
Christian, general, Acute
Effective networking for influence relies partially on a particular understanding of organisations and relationships, a specific set of interpersonal skills to effectively build up influence and, crucially, time in the field, as all involved describe the process of building up contacts as one which is lengthy and time-consuming.
Complementarity of networking
It is important to note that although these motives were identifiably distinctive, in the actual practice of networking – introducing oneself to a colleague, forwarding on an e-mail, attending a conference – individuals may be driven by a combination of motives and indeed the same activity may result in a combination of outcomes which do not fit neatly into any one of the categories described above.
For instance, interviewees described personal relationships outside their organisation that they found valuable for personal support in times of stress, but also mentioned that these personal networks also provided knowledge (in the form of advice) as well as reassurance or comfort. Similarly, many mentor relationships were primarily seen as focused on knowledge acquisition, learning from the experience of a more senior manager, but these relationships often led to offers of employment or at least information about vacant posts and recommendations that the mentee may wish to apply. Therefore, in various ways, the four motives for networking are inter-related in that they complement and support each other ( Figure 17 ).
FIGURE 17.
Complementary motives for networking.
A number of these complementarities appeared particularly key in the accounts of managers. First, several identified a strong overlap between networking for support and for knowledge:
I have a colleague from X, kind of a mutual mentor that I’ve carried on all these years, because I left there in 2006, and so we meet up every couple of months. But that’s not about solving specific problems. That’s about just getting through it. I mean the whole period of the organisational restructure in here I value very much having someone, like you say, a confidante, that I could just say how it really was and how awful it was (. . .) and yeah, she put in various different ideas and suggestions which was food for thought, but that’s my own kind of deliberately set up mechanism for doing that.
Ruth, functional, Care
What is striking here is the underpinning trust relationship that is formed as the two colleagues become mutual confidantes and informal counsellors, but also how this process enables more informed and insightful advice to be offered, based on a deep mutual understanding of each other’s personalities and respective situations. Similarly, interviewees discussed the potential complementarity between networking for support and influence, again based on the establishment of a personal relationship of trust, explaining how doing a favour for a previous service user provided an opening to ask for a testimonial for their service:
That’s the kind of example of just scratching each other’s backs and things that develop out of relationships. He wouldn’t have had that conversation with me unless he knew me. I wouldn’t have had that conversation with him. Even though my directorate was, you know, scrabbling around, desperate for testimonials, I wouldn’t have been able to get that unless I’d had that relationship with this guy.
Ross, general, Care
A similar complementarity relationship, between support and career networking, implicitly underpins many mentoring relationships, for which it is difficult to draw a hard and fast line between a personal relationship of coaching and counselling and a more strategic and political relationship with a senior colleague initiated to raise profile and generate career opportunities.
A more pragmatic complementarity would connect networking for knowledge and for influence. In the account from Carl below, the organic continuity between these two activities is explained, underpinned by an implied and established mutual interest:
So this guidance came out, this lady at (another trust) was party to this information before I was, she called me up, said ‘have you seen this?’ ‘No, I haven’t seen it’ – sent it across, we had a bit of discussion about it ‘what should we do about this?’ ‘Well, shall we put a united response back to the SHA on this?’ ‘Yes a good idea’. We’ll do that kind of thing.
Carl, functional, Care
Similarly, a complementarity is often observed between networking for knowledge and for career progression, with the former being the overt motivation and the latter being an unspoken yet deliberate by-product of the relationship.
Sometimes you learn just as much through experience, talking to those people, as you do the sort of formal training. It’s that networking thing as well, isn’t it, once you’re out there doing these things it’s who you know, because you never know when you might meet them in an interview room . . .
Hugh, general, Acute
Finally, although not frequently discussed, there were occasions when a complementarity was illustrated between networking for career and for influence. An example was the case of Justine in the care trust, who discussed using her strong connection with board members to make a case for taking on a contract in a new area for the trust, after which Justine herself was chosen to head up the new service, a significant enhancement of her management responsibilities in the trust.
Overall, the motivations or, indeed, the eventual outcomes of networking are not necessarily pure; managers engage in networking for a complex variety of reasons, network relationships change and often mature over time, and individuals often find the benefits of networking are wider than initially expected. Critically, though, there are various synergies between networking activities that encourage a broader conception of networking and its collective benefits, individually and organisationally.
Challenges to networking
Across these overlapping and interconnected motivations for networking, a number of issues are raised consistently as obstacles to effective networking and, by implication, as obstacles to effective performance and career development. In particular, time pressure, competitive tensions and the practical challenge of building, managing and benefiting from networks represent the most substantial difficulties faced.
The most consistently cited challenge to networking of all kinds is time pressure and intensive work demands. The issue of work intensification and stress was raised as a theme by over two-thirds of those interviewed, and often discussed at some length. The impact of the substantial (and often increasing) pressure of work on the ability to network was substantial and felt especially acutely when managers attempted to engage in the less formal networking, such as establishing a relationship with a mentor, or maintaining learning sets after the completion of a training programme:
We had learning sets with, you know, people from similar roles, backgrounds, et cetera, which I found really, really useful. The minute that, that programme finished and we tried to carry those on, it lasted about a month. And everybody got subsumed again into their daily grind. (. . .) I make a commitment that I’m going to start doing that again. And then the next time I look up, it’s been 6 months and I’ve just been sat in the office and never left the hospital. And it’s terrible; really terrible how that happens. We just all get totally consumed by our individual organisation’s problems.
Greg, general, Acute
Other, more formal, networks such as professional associations and practice-related networks also had their effectiveness undermined by the difficulty in maintaining active engagement levels:
There is the allied health professional network but it’s not always that well attended. Everybody is under such huge pressure now, there is just no time to do anything
Belinda, general, Acute
I find that (the clinical networks) are out there but fitting it into the day job, you know? It’s about managing how you fit everything in. The first thing that goes, rightly or wrongly, is yourself; (. . .) if your diary’s full and you’re desperate for an appointment, well, oh, yeah, cancel the network meetings
Hugh, general, Acute
There are a lot of events that (the professional body) hold as well, but I have to say to be honest I’ve only been to a few because I can’t seem to get out at the minute.
Danielle, functional, Specialist
In practice, and with little immediate prospect of a significant decrease in work intensity, the challenge, even for those convinced by the importance of networking, is to maintain a balance so as to protect this long-term activity in the face of more immediate work demands.
Networking with a focus is absolutely essential, that kind of going and learning and bringing the learning back, going and looking, absolutely essential, we don’t do enough of that. There is a balance to be struck about how you create the capacity to do that and the spin-offs that can be learnt from that versus the number crunching, the day-to-day grind meeting, the must-dos, keeping the front door open and not taking your eye off that ball.
Laura, general, Care
The potential for knowledge exchange through networks is most clearly impeded by the presence of competitive tensions between trusts. This obstacle was affirmed by a number of interviewees across the trusts, but particularly among general and functional managers and most frequently in the acute and care trusts:
When we meet, we are directorate managers, same level, but also, we are working for a foundation trust. A foundation trust has to survive as its own, as a business. And that’s the dark side to the NHS, I guess, but that’s what FTs have to do. And so there is a sharing of information but titrated sharing of information, should I say, is a better way of putting that. Because some of it is service sensitive, business sensitive. So some information you would share, some you wouldn’t. (There are certain) constraints on the free flow of information, definitely.
Hasin, general, Care
The barriers described here related not only to information of a commercially sensitive nature, as might be expected, but also to knowledge that was not clearly confidential, such as lessons learned from experience in a particular area, guidance on good practices or even information on future developments which were not widely announced.
At one extreme, this may be seen to constitute a complete barrier to network formation between particular groups or organisations:
Basically, I don’t network with them because they are the competition! So I can’t ring them up and say, ‘Oh, I’m doing this business case . . .’ I don’t feel able to.
Graham, functional, Care
A common means to balance this tension between the necessity of networking and the danger of knowledge sharing in a competitive context relates to the ‘titrated sharing of information’ discussed earlier by Hasin (general, Care). In practice, this involves a careful selectivity in terms of what can be discussed at the expense of a fuller and more effective knowledge-sharing process.
So here, when you’re in a foundation trust and you’re surrounded by other foundation trusts, there’s not a huge willingness to work together as organisations, because you’re in direct competition. So you probably find less that people would get together and discuss the issues and the problems they’re having, their risks, when you’re in direct competition. I’m seeing (colleagues at another trust) tomorrow afternoon, we’re going to have a conversation about a couple of things we might be able to work together on. And then we’re going to avoid a conversation about all the other issues that we’ve got because, you know, that could result in difficulty. So that doesn’t help, I don’t think. You would hope we’d all be mature enough to have those conversations but I think it just doesn’t work.
Greg, general, Acute
Elsewhere, these formal competitive tensions appear to be more stratified, presenting more rigid barriers to formal requests to knowledge sharing, but allowing a freer exchange of information through managerial tiers in which personal networks have been established.
I would say we were permanently in direct competition with a fairly large trust (nearby). When we look where we are on some sort of report it will be like ‘Oh my God where are they?’ (. . .) And yet we’ll go to a conference at the end of the month and we will all go out and have way too much to drink together. So I know that I can ring their head of X up and say, ‘can you just send me a copy of your policy?’ and they’ll send it me. Interestingly a little bit lower than that level that isn’t there (. . .) The ward sister asked a similar ward sister over there for their document – not a hope! ‘No I haven’t got it’!
Bridget, functional, Acute
A final, and more individual, obstacle to networking lay in the personal discomfort in engaging in networking and, for some, their lack of the often sophisticated interpersonal skills necessary to network effectively. A strong injunction to network was a message clearly received by a significant minority of managers, particularly those who had attended formal management/leadership training programmes:
What came through (on the course) was they were saying network, network, network. That’s it. That is what it’s about.
Pavak, general, Specialist
However, a number of interviewees spoke at length about their personal distaste at this activity, because they were uncomfortable with the instrumentality implicit in networking, particularly for career or influence, sycophancy, or inauthentic behaviour. Many expressed their unwillingness or inability to engage in ‘brown-nosing’ or ‘sucking up to’ senior or influential colleagues within or outside the organisation (Felix, functional, Acute), even when encouraged to do this:
I found it uncomfortable – I wouldn’t do that. And even though I’ve been here 3 years, that’s not what I would do. I still find it strange now.
Danielle, functional, Specialist
However, several interviewees who expressed this discomfort went on to say that they had later come to recognise the value and importance of networking and that they had eventually overcome their qualms in this regard:
When you first start (on the graduate training scheme) they go on about networking and you can’t . . . I remember thinking I can’t be bothered. And it just seemed to me like, forgive my terminology because I can’t think of any way else to describe it, but brownnosing people. It just felt like that to me. But as you mature which I did when I started, you realise how important it is.
Felix, functional, Acute
Although networking is often a form of socialisation for managers, it is clear that managers were notequally socialised into engaging in networking activity, over time accepting its apparent importance or inevitability and attempting to suppress their disinclination or compensate through the development of networking skills.
The networked manager and the isolated manager
Many of those interviewed are committed and self-conscious networkers, able and willing to speak at length about their networking strategies and practices and often able to identify the benefits of their networking for their own effectiveness and for their organisation. As noted, many of these have been effectively socialised as a networked manager through training programmes, advice and encouragement from leaders and mentors and through their established membership of professional and clinical associations and groups.
The challenge for the networked managers is typically how to engage in this activity in a way that appears natural rather than instrumental, avoiding the appearance of manipulative or self-serving behaviour. The line in particular between instrumental and organic networking is difficult to draw, in part because frequently instrumental networking is only effective if it presented as natural networking. Networking frequently fails when the instrumental intent in forming a relationship is explicit, as described by one interviewee:
One colleague (. . .) seemed as though she was just using, and that’s not the way to get a relationship or whatever. So you meet someone, you’re not asking for a job the next week or whatever. It’s more about keeping contact, what things are going wrong.
Pavak, general, Specialist
The obvious inference is that most effective networked managers present themselves as skilled social performers who can network deliberately and strategically with a focus on a goal while ensuring that this appears both authentic and natural. There are also occasions, such as formal networking events, when all participants engage in networking based openly on mutual benefit and, for example, knowledge sharing. The consequence of this may be the formation of goal-orientated networks that provide mutual benefit.
Alongside the challenge of networks, there is the particular issue of isolates – those individuals and groups who lack the requisite connections to acquire knowledge, influence actions, forge careers and build supportive relationships. The particular subgroup of managers who most commonly described themselves as lacking in networks was general managers. Roles such as the service manager suffered particularly from a combination of intensity of work pressure, infrequency of contact with managers in similar positions, an absence of a standard training route into the role that may form cohort relationships and a lack of dedicated formal networks to share knowledge and best practice. The damaging impact of this, in terms of the challenge of acquiring knowledge, building career, representing their interests and building support networks, was particularly noticeable among this group.
There is frequently a perception that the isolation of particular groups of managers, in terms of their lack of networks, is not a particular concern of the trusts themselves. Specifically, this isolation is often seen to be a personal rather than an organisational issue and the employing organisation is seen to be predominantly focused on the output rather than the activity of management:
I don’t think the trust is massively interested in any of that; what the trust is interested in is that you deliver. They’re not interested in you as an individual, not interested in how you get, not only support, but how you get technical help.
Beth, general, Care
However, the comparative absence of network opportunities, as well as a question mark over the ability of wider, more institutionalised managerial networks to provide a basis for knowledge sharing and learning,139,140 does raise important questions about what opportunities organisations might be missing to benefit from this aspect of management development.
Summary
The study suggests four broad reasons for networking: for knowledge, for support, for career development and for influence. These motives may overlap and synergies exist between particular approaches to networking. At the same time, a range of particular issues impedes or undermines networking within the modern NHS. We discuss these in detail before concluding by reviewing the importance of networking in the sector and the distinctive way that the various management groups attempt to form, and benefit from, networks to enhance their effectiveness and resilience as managers.
Chapter 7 Discussion
Introduction
This research set out to investigate how NHS managers encounter and apply new management knowledge, examining the organisational and extra-organisational factors that facilitate or impede the acceptance of new management knowledge and its integration with practice in health-care settings.
The previous three chapters have presented the main emerging themes from the data collected across the trusts and attempted to draw out the main findings in relation to each of those main themes (management, knowledge and networks). Considered together with the contextual similarities and differences highlighted and explored in Chapter 3 , these three sets of data and analysis have yielded some important insights into the nature of managerial work in the sector, how this is changing and with what implications for the knowledge base and networks that managers draw upon.
The aim of the current chapter is to crystallise those insights around the three central research questions pursued in this study. We use those questions to provide a threefold structure for the discussion of findings this chapter. Conclusions can then be drawn about what the findings mean for the challenges of mobilising and using management knowledge within the sector and recommendations can be made about what health-care organisations can do to effectively respond to those challenges.
1. How do occupational backgrounds and careers affect knowledge receptivity, sharing and learning?
The samples of managers consisted of very diverse groups of managers with a wide range of educational qualifications and diverse personal experiences. Capturing and analysing the often lengthy career narratives of those managers through interviews gave us a clear sense of where critical sources of variation and difference were to be found. Nevertheless, those experiences did tend to converge around one of a small number of well-established professional or occupational career trajectories, as reflected in the model.
Clinical managers
Clinical managers placed a lot of emphasis on the clinical aspect of their professional identity, which was forged through their educational and professional qualification and associated continued professional development. Among clinical managers, there was quite a sharp distinction between the ‘accidental’ managers – those whose clinical career path had led them (usually unexpectedly, not by design or inclination) into management positions, found more among medics and at the acute and specialist trusts – and the ‘reluctant but resourceful managers’20 – those for whom management responsibilities were an inevitable (and often not desirable) next step in the development of their career, found more amongst those with nursing backgrounds and, in particular, at the care trust.
For both of these groups, the clinical frame of reference was still a very strong one. For the accidental managers, receptivity towards management responsibilities and ideas was much more of an exception than the rule. Although there were some clinicians whose orientations were more towards management processes (e.g. the psychologists at the care trust) and some who saw themselves in a hybrid, bridging or translational role (e.g. particular clinical directors at the specialist or acute trusts), management activity still tended to be seen as an adjunct to a largely clinical professional role.
For the reluctant managers, although clinical experience was still important in shaping views about managing, there was a greater degree of acceptance, if not necessarily internalisation, of management practices and management thinking. Managers of this type (often with nursing backgrounds) would typically draw upon and value the more experiential learning they had experienced as clinicians and proto-managers in charge of wards and were also well attuned to the challenges faced in bridging the clinical–managerial divide. As such, the analysis appeared to offer some support for the idea that management knowledge, albeit quite localised and informally developed, could offer some support for those from clinical backgrounds attempting to harness managerial knowledge to further a professionalisation project based on a mixture of clinical and managerial knowledge and experience. 113
There were a few, notably exceptional, cases of clinical managers who were rather less accidental and reluctant than their counterparts and who were not only more receptive to management thinking generally, but also more enthusiastic than many in accessing and using more imported, commodified forms of management knowledge in pursuit of their management aspirations (e.g. Nina at the specialist trust, who had become a manager via the Athena programme, and Nancy at the acute trust, who had a MBA).
However, these exceptions aside, for the most part, neither group of clinical managers was receptive or responsive to more abstract and commodified managerial knowledge and practices (or in turn willing and able to transmit them to others). These knowledge bases generally neither matched the clinical requirements of managers with a strong clinical/scientific frame of reference nor met the requirements of those managers from a clinical background steeped in experiential learning and for whom translation into management practice they could relate to and use immediately was a sine qua non. In general, a historical and often continuing reluctance to take part in formal management or leadership development was evident, in part owing to scepticism regarding their value and in part because their legitimacy in their role depended primarily on their clinical experience and expertise and not their management knowledge.
General managers
General managers had reached their positions through a varied set of routes. The most common denominator was some level of clinical experience, combined with some level of qualification related to health care or health-care management, although many did have some formal management postgraduate qualifications and training (especially at the acute and care trusts) as well as plenty of direct managerial experience.
Management experience was, however, still quite varied although what was fairly consistent was the comparative absence of wider (i.e. outside the sector) management experience and pure general management qualifications. Fewer than half of the general managers had some experience of working in the private sector and, in several of these cases, they had rather limited experience. Only in a very few cases did this appear to consciously shape thinking about the nature of management and management challenges in health care. Most often, the distinctiveness of managing in a health-care environment was emphasised. Experience in the NHS (especially clinical experience) was what characterised how managers in this group had developed their skills, particularly among the sizeable group of hybrid managers found among those who had entered management from a nursing background (these were particularly prevalent at the care trust).
The diversity of managerial circumstances and challenges this group faced was highly reminiscent of the sorts of differences in management practice that have traditionally made it very difficult for general managers anywhere to forge a strong professional identity around a distinct body of knowledge. Managerial responsibilities were not only diverse but also lacked any real commonality across the trusts. This was particularly the case given the wide disparity in organisational characteristics not only between, but also within, each trust and the very different pressures and trajectories for change that they faced. So, although there was certainly a good deal of consensus around the nature of general management responsibilities (the challenges of dealing with clinicians, the intensity of work in terms of volume and speed) and associated key management skills (especially the emphasis on generic interpersonal skills), the practical contexts in which these general managerial skills were developed and applied and the managerial challenges they needed to meet were very different.
Moreover, as noted in Chapter 3 , there were also significant differences between the trusts in terms of their perceptions of financial and other pressures, structural and organisational divisions faced, patterns of interprofessional conflict negotiated and experiences of stability or change, etc. Thus, for general managers in the acute trust, the principal challenge was frequently the need to bridge the entrenched divide between management and clinicians, whereas for general managers in the care trust, all of whom shared a clinical background, concerns focused on the difficulty of integrating practice across a diverse and fragmented organisation.
This emphasis on the more home-grown development of management knowledge and skills was reinforced by the strongly held perception that experience was the most important way of developing the expertise and learning required to perform managerial work. Consequently, the development of managerial careers in situ and in very particular localised clinical and organisational domains could tend to reinforce a reproduction of managerial knowledge and practice that was driven rather more by immediate organisational needs and management challenges than by attempts to access and apply more abstract management knowledge and learning or to generalise learning from experiences elsewhere in the organisation. This could, in some circumstances, lead to difficulties in spreading knowledge and learning from certain parts of the organisation to others. On the other hand, it did create conditions in which a form of professionalisation could develop that was based on ‘responsibilisation’, or the status conferred on particular individuals and groups by virtue of their expertise in dealing with key local problems in their local situation. 116
The comparative absence of wider networks for general managers to access readily and to draw upon different forms of knowledge also reinforced the likelihood that the existing ways of operating and managing would become self-reinforcing. In other words, managers were not only focused on responding to local managerial challenges but were also more isolated than the other two groups from sources of knowledge and learning potentially accessed through networks of peers, not only outside the organisation (where competitive conditions could constrain open dialogue anyway) but also within the organisation (where operational conditions were likely to be quite different).
Functional managers
These were the groups that varied most widely in their professional orientation and status, depending, of course, on their particular occupational specialism. For these managers, career development depended on the nature and extent of professionalisation (in institutional terms) of the professional development pathway associated with their discipline. For some, this was quite established and formalised and involved expected levels of intense formal education and training leading to recognised professional qualifications (e.g. finance managers and also some specialists in HR and estates). For others, whose discipline was less professionally institutionalised, the nature and intensity of formal education and training was clearly less formal and intense and career pathways were sometimes more diffuse or ill-defined (e.g. specialists in marketing and IT).
By the same token, functional managers were the group most predisposed and receptive to formalised and generic management knowledge, albeit knowledge that was likely to reflect the particular nature and requirements of their specific role, rather than general management practice (such as Chartered Institute for Personnel Development courses on aspects of people management in the case of HR managers). In turn, their knowledge base often directly constituted the knowledge and expertise deemed essential by general managers, as was the case for finance and HR. General managers’ work was often explicitly focused on financial aspects and they commonly relied heavily on HR support and saw implicit HR activity as an important aspect of their role and responsibilities. Other forms of knowledge either generally underpinned the activities of general managers (e.g. the contributions of IT and marketing specialists), or represented a more distinct and separate knowledge and practice domain (as was the case, for example, with estates management). What was interesting about this group was the extent to which certain knowledge bases of functional managers constituted some of the important aspects of managerial work (and was recognised as such by general managers).
As a group, functional managers also tended to be more highly networked and made much wider professional networks, which allowed them to interact with colleagues elsewhere more regularly. Most belonged to formal professional associations, as did a number of the clinical managers, although they varied greatly in their activity, ranging from regular and proactive participation in formal events and other activities to merely remaining on a mailing list. At one level, this reflected the wider range of professional connections they depended on to develop their careers, knowledge base and learning. At another level, it was perhaps necessary for those managers to avoid becoming too enveloped by immediate trust conditions and concerns. This does not mean that the occupational mobility of functional managers was such as to make them look beyond the health-care sector for future career development opportunities, although there were one or two exceptions who did talk about other possibilities beyond health care. However, there were some differences between organisations suggesting some within-sector occupational mobility. For instance, although there was a much greater degree of longevity and commitment at the specialist trust (owing to its prestige) and the care trust (owing to the strength of local ties), there was much less evidence of this at the acute trust.
2. How do communities of practice enable/construct knowledge sharing and learning?
Communities of practice may or may not be associated with particular formal professional groupings, but membership of a CoP typically involves an immersion in the practices of that community and developing one’s identity as a practitioner and learning from within, rather than about, that practice. The role of CoPs may be framed in terms of the local or cosmopolitan orientation of the practitioner,145,146 their propensity to search and adapt knowledge from beyond their organisational setting (from a professional association, for example) and the location of their reference groups as part of a wider community. Therefore, in principle, membership of a CoP should enable extra-organisational learning and arguably the transfer of this knowledge within an organisation.
At the same time, the benefits of learning associated with CoPs are often gained at the expense of difficulties encountered when more than one CoP, with quite different epistemic practices, need to interact. For this reason, the question was broadened in practice to cover not only CoPs but a broader range of networks drawn upon by managers for knowledge sharing and learning as well as a varied range of motives, as discussed in Chapter 6 . A distinction may immediately be made between those groups that enjoyed the most extensive networked relationships, primarily clinical and functional managers, and the relative lack of networks in the case of most, but not all, general managers.
In addition, there were important differences that should be noted between the organisations. In the more fluid and fragmented care trust, engaged in multiple joint initiatives with a range of other agencies (in local government, social services, etc.), managers reported numerous and varied network connections. However, in the acute trust, owing in part to its size, physical concentration and functional organisational structure, fewer and less diverse networks were reported overall.
The obvious primary distinction here was between those located within the two broad but very distinct communities of clinician managers and general managers. The clinical–managerial divide has been explored in great detail elsewhere but was also clearly an important issue in the managerial work at the trusts we researched and an issue that posed particular challenges for knowledge sharing between clinicians and managers, frequently exacerbated by an underlying epistemic division between these communities. As discussed in Chapter 4 , there was an interesting variation in both the nature of the divide and in the means employed to bridge that divide across the trusts.
In the acute and specialist trusts, there was perceived to be much more of a barrier between the two communities which needed to be overcome and the mechanisms used in both cases were essentially structural – making changes to the hierarchy in order to build bridges between clinicians and managers. In the specialist case, managers also emphasised the importance of enhancing their persuasion skills through establishing clinical credibility and emphasising relational skills. In the care trust, this credibility and a more direct form of communication was more personally embodied through the (clinical) experience and skill sets of managers. While this personal embodiment of the clinical–managerial divide for such hybrid managers may have led to better opportunities for the translation of knowledge and meaning across medical and managerial CoPs, it did, however, also often cause discomfort for the managers concerned (who struggled with balancing their clinical and managerial identities) and, as others have also noted, in bridging the gap between ‘board and ward’. 20,26,31
If we drill down further, at one level, the diversity among managerial groups explored here clearly works against the idea of sharing knowledge and learning through a unified managerial CoP within health care. Managerial groups clearly had very diverse and distinct bodies of knowledge that they drew upon and often connected with very distinct networks of practitioners. This was particularly true of those with distinct functional backgrounds (i.e. finance, HR managers), but was also the case when considering the very diverse knowledge bases represented among both clinical and general managerial groups (e.g. clinicians, psychologists and AHPs had their own distinct clinical networks and managers were much less professionally networked, but connected with very distinct operational groups).
At another level, there were quite strong connections that linked managerial groups through their engagement in common practices of management at each of the trusts. Carlile35 draws a distinction between the translation required to generate common meanings across the semantic boundaries that separate different specialist groups with different understandings and the transformation required to generate new shared practices that transcend the pragmatic boundaries that separate groups with different interests as well as orientations. What was evident here was that the challenge was in creating shared practices that overcame not only the semantic boundary but also the pragmatic boundary in ways that fused clinical and managerial needs and orientations. Carlile35 and others (e.g. Boland and Tenkasi46) tend to emphasise the role of boundary objects in helping achieve this transformation, although other mechanisms such as boundary spanning may be just as important.
Taking three contrasting examples may serve to clarify the challenge of knowledge mobilisation and transformation of practice. Attempts to transplant abstract and codified forms of management knowledge often faced difficulty in that they lacked an appropriate point of reference within health care that would make them seem relevant and applicable to both those attempting to engineer changes and those being subjected to the efforts. For example, while there was plenty of discussion about the principles of lean thinking, there was clearly a good deal of scepticism directed towards the application of such abstract bodies of knowledge into the particular conditions of health care. Moreover, not only was this a result of very real concerns about the purpose and intent behind such initiatives (given pressures for savings in the current context), as the scepticism of even those advocating change illustrated, there were clear problems identified and experienced in translating such ideas into the health-care context.
Interestingly, not only did these problems relate to the practical difficulties of incorporating them in practice, they also related to the problems experienced in legitimising the knowledge and practice they represented. It was an absence of legitimacy as much as the practical challenges of translation that made it difficult to make them become more accepted and taken for granted. 147,148 In other words, there was a clear need to overcome perceptions not only of their lack of suitability but also their lack of acceptability. When more effort was made to be subtle and flexible in the use of such tools and techniques and engage through what we depicted as a ‘generative dance’29 that sought to marry codified knowledge with tacit forms of knowing, then there was perhaps scope for overcoming these barriers of suitability and acceptability. Otherwise, there were clear problems in translating such codified forms of knowledge into practice.
On the other hand, more localised forms of knowledge associated with formulating responses to reporting requirements (such as responses to CQC, etc.) were far more readily transferred. Despite the diverse contexts faced by general managers, what knowledge was shared typically related to management practices and the knowledge and learning associated with them developed to meet wider organisational demands (e.g. for standardisation) and/or national institutional needs (e.g. reporting requirements). Such knowledge was fundamentally situated in local management practice but was reproduced through the passing on of knowledge and learning by groups of managers working in situ (and often in relative isolation, both organisationally and physically, from their peers). The problem here, however, was that the forms of knowledge they represented and gave rise to were those forms of knowledge that emphasised standardisation and routinisation of processes centred around fairly bureaucratic requirements. These were precisely the forms of knowledge that, although transferred relatively easily, were antithetical both to the sort of strategic thinking that managers felt was in danger of being crowded out by routine and to forms of learning that would rely less on ‘knowledge redundancy’124 (important though this is for compliance and risk management) and more on creative and innovative thinking.
A third and more experiential form of learning in contrast to those mentioned above shows both the value but also limitations of a much more person-centred approach to management learning and development that contrasts with a more impersonal approach that is commonly associated with using standard metrics for assessing competency development. Particularly at the care trust, but also at the acute and specialist trusts, managers spoke enormously positively about the use of self-awareness training based on personality assessment frameworks, and the Myers–Briggs indicator in particular, as something that had real value for them in assessing their own performance and development needs, as well as judging the characteristics and needs of others within their teams. The point here is that, while such methods demonstrated the power that a standardised set of development tools might have to encourage reflective learning, they also tended to reinforce the idea that the important sources of knowledge and processes of learning were those that were personally embodied and developed experientially. In other words, there needed to be a strong intuitive connection, preferably highly situated in practice, for the effects of more commodified forms of knowledge embedded in management tools and techniques to have the desired learning effects. Inevitably, however, such personalised forms of learning, although they depended on accepted tools and techniques to act as a catalyst, ultimately relied on the translation into practice of tacit understandings developed by individual managers.
3. Which mechanisms support knowledge receptivity, sharing and learning?
Considering the mechanisms that support (or hinder) knowledge receptivity, knowledge sharing and learning, there was a good deal of attention directed in the analysis to human resource management and other organisational factors as well as to extra-organisational factors and conditions.
With regard to HR practices, internally, organisations had in place many of the formal prerequisites one would expect to find for enabling managers to access, mobilise and use management knowledge. With regard to training and development programmes, there were generally positive views expressed about levels and types of training that were available to managers across all organisations. This consistent message is striking given the different approaches to management and leadership training between the trusts, whether delivered on site and in house (in the acute and care trusts) or left to the individual to choose and supported financially subject to a case being made (specialist trust). Our own observations of a training programme at the care trust (for band 7 managers) gave an impression of a good deal of receptivity among the managers regarding the opportunity it gave them to compare their experiences and share their management problems with peers in an environment that gave them time and space away from the office to reflect, and which used a facilitated highly interactive group of activities, including exercise case work and action learning sets.
On the other hand, it was clear that pressures of day-to-day work coupled with immediate operational demands (particularly for general managers) and a preference for very directly relevant, practical training, combined with the emphasis on experience, often introduced an element of scepticism for middle managers (especially general managers). It also meant that training inevitably tended to be very practically oriented to operational needs, as opposed to initiatives associated with longer-term organisational learning and development, for example. The absence of suitable leadership development opportunities geared specifically to the needs of middle managers often also meant a lack of synchronisation between those opportunities available and their needs at particular points of managerial careers. Externally, some very formalised programmes, such as Aspiring Directors, were, of course, available, used and valued. However, these were accessed by only a few and there was a clear sense that these programmes were for these selected few.
Again, networks were important for knowledge sharing and learning, as well as for support; however, it was as interesting to see what they did not enable as much as what they did encourage. Internally, a focus on operational challenges and day-to-day needs meant that connections were much more operationally focused in nature and centred around standard communication and reporting mechanisms. These could take very different forms: direct observation of comparable monthly management meetings in the acute and care trusts, for example, showed a very clear cultural differentiation between the more formal way of working observed at the acute trust compared with a more informal way of working at the care trust. However, the agendas and outcomes were very similar and they shared a common focus on formalised processes of knowledge sharing and communication driven by performance reporting requirements (as opposed to more informal opportunities for knowledge sharing and learning). Contacts were, of course, available to managers across each trust; however, it was noticeable how consistently these were activated more in the interests of formal reporting/communicating or specific managerial problem solving, rather than as more generalised avenues for general knowledge sharing and support.
Externally, there were differences across the trusts and managerial groups noted in Chapter 6 in their access to external professional or other networks and in their propensity to engage in networking activity. What emerged as a clear overall finding was the relative isolation of many non-specialist and general managers from more widely based sources of knowledge and support through clearly definable and well established NoPs, whether formal or informal. Clinical and functional groups benefited more in this regard. For general managers, their operational demands could tend to create more inward-looking tendencies149 by creating more of a propensity to look inside the organisation for help with knowledge important for problem solving and decision-making. Efforts to look outside the organisation were due not only to the lack of opportunities but also to constraints that emerged as a result of competition and commercial pressures that inhibited knowledge exchange and learning. At the same time, however, managers only comparatively rarely felt comfortable with active networking and, apart from the very explicit recommendation to network found in major development programmes, there was comparatively little explicit organisational support for such activity. Strong ties associated with internal teamworking and tacit sharing of knowledge were, understandably, emphasised rather more than the weaker ties that may allow access to wider sources of knowledge. 127
Other internal mechanisms, such as material conditions and IT support, have not been the focus of discussion so far as they were not seen as crucially important factors in enabling or inhibiting knowledge receptivity, sharing and learning. Technology was considered, for the most part, appropriate and adequate. Research on knowledge sharing and learning processes has long seen technology as a facilitating, rather than determining, factor and has emphasised instead the importance of understanding the importance of the relationship between technological and social aspects of knowledge flows within organisations associated with learning. 150 In this research, the clear message was that technology was not an issue and that information and communication technologies (ICTs) were largely appropriate to the task of enabling knowledge and learning to be spread and shared.
We do have generally fairly good flows of knowledge and information. I’m not sure we’re strong enough at learning the lessons from them and feeding it back and seeing behavioural cultural change in practice. But electronic wise I think we’ve got so much more we can do.
Glen, clinical, Care
Consequently, there was a feeling that owing to social and organisational factors, the full benefits of IT were not perhaps being realised in some instances. There were, however, pockets of highly active (often widely networked) individuals and groups that took full advantage of the wider sources of knowledge and information opened up. System integration could also be an issue (e.g. in the care trust), but was not considered a major impediment to knowledge sharing and learning. However, this finding does at least emphasise the limitations of relying on technological ‘fixes’ to enhance knowledge sharing and learning among CoPs and NoPs. 151
However, returning to issues related to context and managerial role, it was clear that the aspects of institutional and organisation context and their effects on managerial roles, responsibilities and career development explored earlier did have an important bearing on the enabling of knowledge sharing and learning. Although these features cannot easily be considered as mechanisms as such, they are important aspects of the structure and culture of management in conditions of change that have a profound bearing on the generation of managerial knowledge and learning associated with their continuing professional development.
Interwoven through this analysis has been a consideration of the organisational factors (particularly structural differentiation, clinical–management interaction, centralisation–formalisation tendencies and pressures due to change) that have combined with institutional/policy driven aspects (greater demands on managers and greater regulation and control) to shape the ways in which managers see their professional development and role, how this relates to their experience base, knowledge and networks and how they respond to the associated challenges. In doing so, we have explored some of the major similarities and differences between the trusts and their varied impact on different managerial groups. That analysis will not be repeated here.
However, it is important to note that, in our analysis, many of those factors have been shown to have an often unintended and sometimes subtle and insidious effect on managers’ ability to be receptive to knowledge and to engage appropriately in knowledge sharing and learning within their organisations and across the sector and to develop appropriate NoPs and CoPs. In particular, the research brings into question not only the idea that developing knowledge sharing and learning across CoPs is difficult when these communities are so diverse and disparate and the networks they rely on so sporadic (and often truncated), but also that organisational processes can, if not considered carefully, have the unintended effects of reinforcing some of the problems faced by managers in accessing and mobilising wider sources of managerial knowledge and learning, if too much of an inward-looking approach is encouraged. For the sector as a whole, there are clear implications, such as the challenges created in developing a managerial cadre that is both valued for the management skills and responsibilities they draw upon and enact, while at the same time being given sufficient opportunity for marrying these skills with more indeterminate leadership skills in the interests of professional, personal and organisational development.
This chapter has sought to summarise and discuss the main findings of the research and, in doing so, has attempted to address the main objectives pursued in the research. The next and final chapter of our report will draw upon the findings presented to draw out the main conclusions and recommendations from the research.
Chapter 8 Conclusion and recommendations
In exploring how managers in health care encounter and apply management knowledge, our study has focused on three main aspects: management and leadership in the health-care context, knowledge, knowledge mobilisation and learning processes, and NoPs and CoPs. In this final chapter, we summarise our main conclusions in each of these areas, preceding this with a consideration of the effects of organisational and managerial diversity, before turning to assess the limitations and implications for future research and, finally, drawing out the recommendations from our study.
Effects of organisational and managerial diversity
The study was designed to enable analytical generalisation reflecting the diversity in the range of trusts within the NHS and across the range of employees in the NHS charged with management responsibilities.
To capture organisational diversity, three case study organisations were chosen: an acute trust, a care trust and a specialist trust. Our assumption was that these trusts would vary in terms of geographical spread, the number of locations from which services are provided, the diversity of services provided and the number of organisations purchasing services from them. Empirically, these presumed differences were confirmed, although two of the three trusts did undergo substantial changes during the course of the research. However, contextual influences are not merely objective forces acting on organisations: their impact is moderated by individual and collective perception and interpretation in each case. Therefore, a core element of our study was to identify organisational factors and aspects of change which interviewees themselves saw as impacting most powerfully on management practice and knowledge sharing. Collectively, these differences provided a detailed and complex picture of the context within which our managers operated and represented a key element in developing our empirical and thematic analysis.
Managerial diversity was equally important, particularly in the light of the contested nature of management (and leadership) in the NHS discussed in Chapters 3 and 4 . A key objective was to ensure that the study fully captured the distributed nature of the management and leadership in the modern NHS and avoided a too simplistic and misleading dichotomy between management and clinicians.
To ensure that this happened in a structured and meaningful way, a model of management in the NHS was developed and refined, based around a continuum of clinical and managerial training and experience (see Figure 1 ). The main purpose of this model was to guide us in the recruitment of research participants in each trust, using purposive and non-random samples to differentiate between broad clusters of clinical, general and functional managers in each trust. As with the selection of case studies, these differences were necessarily broad-brush, but the empirical research was then used to reveal the substantial richness and complexity encapsulated within this simple model. Nonetheless, these three broad management groups, alongside the three case study organisations, did provide a valuable analytical tool in our empirical and thematic analysis. Therefore, the model itself represents a novel feature and direct deliverable from our research as it provides a tool that allows us to differentiate between these three managerial groups.
Management and leadership in the health-care context
As noted in the discussion in Chapter 1 , the study of management in health-care organisations faces a number of theoretical and empirical challenges, one of which is to work with the complex relationship between management and leadership, a theme that has been explored at long length in academic and practitioner literatures. 27,28,89 This distinction typically contrasts visionary, strategic and transformative leadership, with a more procedural, operational and bureaucratic approach to management. 28
Within the NHS, the management/leadership distinction is probably more sharply defined and has greater palpable weight and political significance than in many other sectors, for the reasons outlined in Chapter 4 . In particular, historical tensions between management and clinical professions result in an ongoing suspicion of (and resistance to) management both as a function and as a cadre. Our analysis of health-care management, therefore, recognises the evolution of terminology in the NHS, in the first instance in the privileging of management over administration, and more recently in moves to celebrate leadership, including clinical leadership, over management. 70,89
The consequence is a complex and delicate ontological landscape, in which many NHS employees who manage will, for a variety of reasons, be reluctant or conflicted over the title ‘manager’ and indeed may not recognise their practice as ‘managing’, typically identifying instead with the role of leader and the practice of leadership. To address management effectively, paying full recognition to its political complexity in this context, our approach in this study was to address management inductively: as a question, informed by extant research on management and leadership within the NHS, and more widely. The first aim of our empirical research was to draw out and differentiate understandings of management and leadership as understood and practised by respondents in our study, rather than imposing meaning externally. The result is a more complicated and contested, but nevertheless richer, picture of management in our subject organisations, as understood, practised and articulated by managers both formally and informally.
This mapping out of meanings of management in our study, assisted through the development of our selection framework for managers (see Figure 1 ), led to two key findings from our research. First, management in the NHS is not only a heterogeneous activity, but also a heterogeneous identity, in that it is distributed among a wide range of occupational groups (classified by ourselves into the aggregate categories of clinical, general and functional), which draw upon highly diverse sources of knowledge, learning and experience and who interact through very diverse and open distinct networks of interaction and CoPs. Second, in this milieu, it is general managers who face the greatest challenge in sharpening their sense of professional identity based around a distinct and coherent managerial knowledge base.
Knowledge, knowledge mobilisation and learning
To examine these knowledge processes further, the report drew upon a classical differentiation between explicit and tacit forms of (management) knowledge and between abstract learning and learning that is situated in practice. This enables us to distinguish between four primary types of knowledge in our study:125
-
knowledge encultured in the norms, values and practices of managers
-
knowledge embedded in local management systems and processes
-
knowledge encoded in management tools and techniques
-
knowledge embodied in the skill sets of individuals.
In turn, this system helps to draw out the challenges involved in attempting to mobilise knowledge between contexts and to abstract it from, and translate it into, practice, through processes of socialisation, externalisation, combination and internalisation. 37 As a consequence, our study focused substantially on issues of knowledge translation, of putting encoded knowledge such as lean thinking into practice, for instance. Equally, however, there was the challenge of translating local and embodied solutions and innovations into generalisable and transferable knowledge. Similarly, this focus enabled the identification of particular barriers and gaps in this mobilisation process. A particular theme of interest in light of this framing was the role of formal training and development in management and its impact and importance when compared with other, more experiential modes of learning.
Although focused on management knowledge, the elephant in the room throughout our discussions has been the particularly influential body of professional knowledge associated with clinicians, against which managerial knowledge and understanding are often juxtaposed. It was therefore necessary to pay attention to the ways in which management knowledge was perceived to be in competition with, or judged against, medical bodies of knowledge in the process of collective decision-making, for example. At the same time, as many of our managers were simultaneously, or formerly, clinicians, the performance of their role often relied as much on their clinical or other professional knowledge and experience (and the credibility it gave them) as it did on their managerial know-how.
Taking these two aspects together points to a third key finding to emerge from the research, namely the strong tendency for managerial knowledge, particularly that harnessed by general managers, to be more home grown (situated in local practices) and experiential. Local pressures associated with trust reporting and management requirements combined with the hegemony of clinical know-how and the influence of a financial discourse tended to create a strong reliance on local and experiential knowledge (notwithstanding the potential value of alternative, external forms of knowledge and learning).
Although our theoretical framing was substantially informed by contemporary thinking on knowledge sharing and learning, which emphasises the socially situated nature of knowledge, it also emphasises the importance of learning or knowing through social interaction in NoPs and CoPs and this is what we turn to next as the third of our major themes.
Networks and communities of practice
An understanding of flows of knowledge requires an insight into the nature and dynamics of the networks and communities within which practitioners are located, opening up a consideration of the various NoPs and CoPs to which managers may belong, their role and organisation, the relationship between the interactions they enable (or constrain) and associated processes of socialisation and learning (or exclusion and non-learning).
Despite the value of the substantial literature on CoPs that highlights the interpenetration of socialisation and knowledge-sharing processes, we also recognise the limitations of too exclusive a focus on this type of arrangement. 151 Membership of a CoP revolves around shared narratives of experience, shared paradigmatic modes of analysis and shared modes of representation. 46 Although CoPs are typically defined as closely related groups of practitioners who develop and share common understandings through frequent and close interaction, we aimed to remain sensitive to the variety of groups and communities to which managers may belong and to potential interplays between them. Therefore, we focus on a broader and more extensive concept of networks, a concept which allows for a greater diversity in terms of their degree of co-ordination and cohesion, strictures on membership, the ways in which they are formed and their location within or across organisational boundaries. To be clear, several of the networks examined empirically in the study do indeed display the cohesion of a CoP, but many are significantly more informal, loose, open and flat or distributed networks, which nonetheless play a key role in knowledge mobilisation and socialisation for the managers in our study.
To capture the meaning and significance of these networks, we set out to discover what networks exist, how they function and what purpose they serve for the managers in each trust. In other words, the process was an inductive one of ascertaining the network connections of salience and importance to managers, rather than a narrow but more constrained focus on formal, closed or centralised networks and, especially, those with a highly performative focus on narrow instrumental goals. Through this flexibility, we were able to explore the diverse range of inter-related purposes served by networks, including not only knowledge acquisition but also career advancement, influencing policy and practice, and personal/emotional support. We examined these outcomes in terms of both individual and organisational benefits, cognisant of recent and on-going debates on the value of social capital but, again, without reducing networks and the activity of forging relationships to narrowly instrumental motives.
Perhaps the key general finding to emerge in this respect was the challenges faced by general managers in being able to access fully and be actively engaged with wider networks of professionals (not only across trusts but within them too). Not only did this mean that general managers had less opportunity to gain potentially valuable knowledge and support, but also that it tended to reinforce any reliance on local and experiential knowledge, adding to any inward-looking tendencies.
Limitations and directions for future research
Our research has lent strong support to the framework developed in Figure 1 as a means of differentiating between relatively distinct managerial groups and the quite different NoPs and CoPs they tend to engage with. It has also demonstrated the value of situating analysis of management knowledge mobilisation and utilisation in the context of the particular organisational conditions and challenges facing those diverse managerial groups. However, that very complexity and diversity also inevitably creates limitations for how qualitative research is able to tap into the processes concerned.
One obvious limitation is in the restriction in the range of case organisations to three types of trust. The research has adopted standard and accepted protocols for case study design and selection that emphasise the importance of choosing cases that show variation in key conditions (in this research, expected variation in managerial knowledge networks) and which rely on analytical, rather than statistical, generalisability to extrapolate findings to different types of setting. 52,53 Consequently, it becomes possible to conclude, for example, that challenges to management networking may equally be found in other highly differentiated forms of trust. However, the importance of a holistic understanding of case conditions and their effects also alerts one to the possibility that different constellations of conditions may create different outcomes in other types of trust. Only by extending the research systematically to consider all potential types of trust would it be possible to conclude that the range of likely conditions are fully captured in the research design.
Second, a similar limitation is in the number and range of participants included in the research. Again, the research has applied small-scale purposive sampling, rather than large-scale random sampling methods to systematically select participants for interview. As such, the findings are inevitably restricted to the range of experiences and conditions faced by the selected group of managers. The qualitative nature of the study has allowed us to choose our participants carefully in order to ensure an appropriate range of respondents and then to examine their experiences in considerable depth. Moreover, respondents have also effectively acted as key informants on the issues faced by managers generally and we have been able to augment interview data with direct observation of management practices. However, there is clearly scope here for more extended research that explores the issues raised through larger-scale systematic or random sampling of respondents both within and across trusts. This could be based on the use of the framework of management types developed in our study.
Third, the ethnographic study of the managers, their access to knowledge sources and their involvement in networks is also inevitably constrained by the resources available to conduct such research in the depth that would be required to get a complete picture of managerial knowledge mobilisation and utilisation. The data obtained have provided rich insights into the ways in which different managers access, share and use managerial knowledge and how this relates to diverse organisational and professional circumstances. However, each of these networks of interaction in which specific groups of managers are involved is worthy of study in their own right. Studying wider networks of activity has been beyond the scope of the current study, as the emphasis has been on managers’ perceptions. Consequently, there is clearly further scope for exploring in greater depth any or all of the networks of interaction that involve the managers we studied (and others) effectively in their own right. Research of this type may employ similar ethnographic methods, but could also use more quantitative techniques, such as social network analysis. This research has signposted areas in which further research may reveal important details about the structure and dynamics of such networks of interaction, knowledge creation and sharing, but has not been able to capture these in full.
Fourth, the ethnographic element of the research has been important in helping to understand and situate management knowledge and learning processes in practice. But there is more that could be done to extend this type of work to get deeper insights into these processes. Resource constraints meant that it was not possible to extend this aspect of the work fully, for example through extended periods of stay or shadowing of managers or tracking interaction further into external NoPs and interaction. Selection of managerial events and encounters to observe also means that a standard criticism of ethnography (that findings from observations are inevitably restricted to what is observed) apply to this research as well. More extended ethnographic study is one way to build on the insights from this study to get further insights into the processes involved.
Last but not least, recent changes to the relationships between primary and secondary health care pose a number of further important potential questions about the nature, sources and application of management knowledge in a changing health-care environment. The scope of this research has not extended to primary-care organisations, so there is a need for further research to explore management knowledge and learning processes in the primary-care domain as well as in the changing interface between secondary and primary care.
Recommendations
There are seven general recommendations that emerge from the research, each of which has a number of implications for practice at, variously, national, regional or trust level. These are particularly in the realm of management training and development, but also encompass steps that trusts and other agencies might take to improve the structural context within which managers work and are embedded.
-
Value management as well as leadership. The research points to a widespread tendency to denigrate management in favour of heroic conceptions of leadership. There are benefits to be gained from a clearer recognition of the contribution of effective management and the necessity of explicitly presenting management and leadership as equal partners in managing complex and changing organisations.
-
Leadership training and development programmes (e.g. via the NHS Leadership Academy) need to ensure that the development of leadership takes account of the complex relationship between leadership skills and management practice on the ground.
-
Such programmes also need to balance an emphasis on leadership with continued attention to the importance of management skills (especially leadership-related skills, such as interpersonal communication).
-
Local trust training and development programmes can help maximise the transferability of context-specific leadership training to management practice by ensuring that analysis of leadership challenges and solutions continue to be firmly situated in management problem-solving and decision-making scenarios.
-
-
Balance experiential learning. The research indicates that the challenge of codifying and translating management knowledge leads to an over-reliance on experience and localised, situated knowledge and/or a tendency to privilege other forms of knowledge, such as clinical or financial. The evidence underlines the value of networks and other social modes of engagement to overcome these epistemic boundaries and assist the circulation of knowledge.
-
Training and development programmes provided at trust level need to ensure a balance of emphasis on learning from experience with the use of more codified systems of knowledge that can effectively challenge received wisdom and accepted practices.
-
Trusts need to be aware of the need to capture and share knowledge and learning that may be localised in specific parts of the organisation (e.g. tender bidding skills), such knowledge may be particularly important to generalise across trusts in the light of recent changes to the organisation of primary, secondary and tertiary health-care provision.
-
-
Facilitate clinical–managerial relations. The challenge of managing the relationship between clinical and managerial communities is pervasive across health-care organisations. Our trusts each adopted distinct structural, relational or personally embodied means to manage this relationship, each reflecting their organisational contexts. The research suggests that there is no universal solution and that trusts need to tailor their approaches to manage this divide.
-
Trusts need to carefully consider how they attempt to bridge the clinical–managerial divide and tailor their approaches to achieving this to match the specific context of interaction (e.g. by combining structural adjustments with the relational skills of key individuals for whom status differentials are high, or by relying on embodied experience when there is more of a blending of clinical and managerial orientations).
-
National leadership programmes should be considered as an opportunity for cultivating networked interaction between distinct types of managerial groups (especially clinical and general). This approach would encourage development of shared perspectives between the CoPs on the use and application of specific types of managerial knowledge.
-
There may also be opportunities for trusts to develop mechanisms for such networked interaction focused on management issues and solutions at a more local level, provided that they occur away from immediate operational pressures. Such initiatives may be particularly important in the context of significant recent changes in the relationship between secondary and primary care.
-
-
Enable reflective learning. In the light of the evidence on translation gaps in health-care organisations, our research suggests that receptivity to management knowledge, and the innovative or creative use of this knowledge, is enhanced by training and development that allows space and time for reflection and knowledge translation. This applies across all managerial groups, but especially to general managers.
-
Middle managers, especially those in general management positions, need more access to leadership development and training opportunities that are better synchronised with the demands of their role and the stage of their career. There is currently a gap in the more strategic (as opposed to operational) training opportunities that tie in with middle managers’ needs.
-
Wider (national) leadership training programmes can help bridge that gap, provided that the knowledge base they impart (e.g. lean thinking, strategic analysis) is not abstracted from health-care practice but used instead in a more heuristic way to inform analysis of health-care management problems.
-
Trusts also need to find ways of giving middle managers time out from busy schedules to take up any opportunities afforded by more advanced training and development programmes that are based on such reflective learning processes.
-
-
Encourage strong network ties. The research indicates that networking for knowledge acquisition/sharing, support, career development and influence are closely inter-related. Therefore, recognition of the embeddedness of knowledge processes in social networks points to the importance of supporting the formation of strong network ties to enhance knowledge sharing and learning.
-
Opportunities provided for networking through national leadership development programmes are recognised as valuable but can also be sporadic or limited in their availability. More could be done to encourage continued interaction through these networks at a regional or local level following core programme activities.
-
Recognition needs to be given (in national and more local training programmes) to the importance and benefits of both formal and informal networks of interaction as sources of knowledge and support for managers and how specific mechanisms for middle managers may help significantly (e.g. mentoring).
-
-
Extend general management networks. Given the evidence pertaining to isolation and inward-looking tendencies among general management groups in health care, trusts may consider the advantages of providing greater opportunities for internal and external networking to assist knowledge sharing and learning.
-
Initiatives at national, regional or individual trust level need to recognise that networked interaction among managers, when it occurs, does so largely within the distinct CoPs associated with general, clinical and functional managerial groups (as opposed to there being one distinct and coherent CoP).
-
External (regional, area) networks of managers could be actively cultivated (either by individual trusts or through intertrust collaboration). These external networks should be focused on particular knowledge and learning themes (e.g. aspects of management best practice), as opposed to being driven primarily by operational requirements.
-
Trusts that are highly differentiated (geographically, organisationally, professionally) may benefit particularly from taking their own internal networking initiatives that have the dual advantage of helping managers share best practice as well as improving organisational integration.
-
Trusts faced with recent challenges associated with changes in secondary/primary care may find managerial networking of increased relevance and importance to the achievement of their goals.
-
-
Strengthen professional communities of practice through leadership development. The research underlines the challenges posed by the extreme diversity of managers’ responsibilities and skills owing to task and organisational differentiation and the fragmentation this creates within managerial CoPs. This supports the value of a widely available management and leadership development programme that meets the needs of the whole spread of middle managers more effectively.
-
National leadership development programmes should continue to build on the networking opportunities they offer and networking skill development they aspire to provide.
-
In addition, such programmes should also build on the potential they offer for greater collective development and further institutionalisation of a distinct body of health-care management knowledge and practice.
-
Acknowledgements
We are grateful to NIHR Health Services and Delivery Research (HS&DR) programme for funding this project and to all of the participants and key informants who generously gave their time and insights throughout this study. We would like, in particular, to thank the research co-ordinators at each trust who did so much to facilitate the empirical access and to enrich our understanding of the dynamics at play within each trust and more widely. We hope the report proves both interesting and useful to all of those who contributed. We also extend our thanks to Jo Lowe for her vital administrative and organisational support through a large part of the project.
We would also like to thank our Advisory Group for their invaluable advice. The board consisted of representatives from each of the three trusts participating in the research, plus:
Ruth Boaden, Professor of Service Operations Management, Manchester Business School.
Maxine Robertson, Professor of Innovation and Organisation, Queen Mary University of London.
Dean Royles, Director, NHS Employers.
Contributions of authors
Mike Bresnen, Professor of Organisation Studies, provided project leadership and was the lead for the care trust and knowledge theme.
Damian Hodgson, Senior Lecturer in Organisational Analysis, provided project management and was the lead for the specialist trust and networks theme.
Simon Bailey, Research Associate, carried out the literature review, fieldwork, fieldwork organisation and organised liaisons with trusts. He was also the lead for the management theme.
Paula Hyde, Senior Lecturer in Leadership, was joint-lead for the acute trust and lead for the NHS and organisation context.
John Hassard, Professor of Organisational Analysis, was joint-lead for the acute trust and lead for the methodology.
Project outputs and publications
Conference papers (refereed)
Bailey S, Bresnen M, Hodgson D, Hyde P, Hassard J. CoPs and Robbers: Making and Taking Management in UK Healthcare. Submitted to Academy of Management, Orlando, FL, USA, 9–13 August 2013.
Bailey S, Bresnen M, Hodgson D, Hyde P, Hassard J. CoPs and robbers: making and taking management in UK healthcare. In Bridging Continents, Cultures and World Views, 29th EGOS Colloquium (subtheme 26), Montreal, Canada; 4–6 July 2013.
Hyde P, Hodgson D, Bresnen M, Bailey S, Hassard J. Bridging or breaching knowledge domains in a changing context? Discourses and practices of management and leadership in healthcare. In Bridging Continents, Cultures and World Views, 29th EGOS Colloquium (subtheme 26), Montreal, Canada, 4–6 July 2013.
Bresnen M, Hyde P, Hodgson D, Bailey S, Hassard J. Enabling Managers to Emerge as Leaders? Exploring Changing Patterns of Healthcare Management in the UK. Submitted to Democratising Management, European Academy of Management, Galatasaray University, Istanbul, Turkey, 26–29 June 2013.
Bailey S, Bresnen M, Hodgson D, Hyde P, Hassard, J. ConDem-ing communities: where to for social learning theories amid resurgent politics of individualism? In Ethnographic Horizons in Times of Turbulence, 2012 Ethnography Symposium, University of Liverpool.
Academic workshop presentations (invited)
Bresnen M, Hodgson D, Hyde P, Hassard J, Bailey S. Being a manager, becoming a professional? Exploring the use of management knowledge across communities of practice in healthcare organisations. In Management Knowledge and Practice in Healthcare, Service Delivery Organisation (SDO)-Funded Workshop, Manchester Business School, 14 November 2011.
Bresnen M, Hodgson D, Hyde P, Hassard J. Being a manager, becoming a professional? Exploring the use of management knowledge across communities of practice in healthcare organisations. In NETSCC SDO Welcome Meeting, University of Southampton, 26 November 2010.
Presentations at practitioner conferences and workshops
Bresnen M, Hodgson D, Hyde P, Hassard J, Bailey S. Being a manager, becoming a professional? Exploring the use of management knowledge across communities of practice in healthcare organisations. In New Forms of Healthcare Management, Health Workforce Research Network, Manchester Business School, 14 June 2011.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Walshe K, Rundall TG. Evidence-based management: from theory to practice in health care. Milbank Q 2001;79:429-57. http://dx.doi.org/10.1111/1468-0009.00214.
- Cooksey D. A Review of UK Health Research Funding. London: The Stationery Office; 2006.
- Swan J, Clarke A, Nicolini D, Powell J, Scarbrough H, Roginski C, et al. Evidence in Management Decisions: Advancing Knowledge Utilization In Healthcare Management. Final Report. London: NIHR Service Delivery and Organisation Programme; 2012.
- Francis R. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry. London: HMSO; 2013.
- Crilly T, Jashapara A, Ferlie E. Research Utilisation and Knowledge Mobilisation: A Scoping Review of the Literature. London: NIHR Service Delivery and Organisation Programme; 2009.
- McKee L, Ferlie E, Hyde P. Organizing and Reorganising: Power and Change in Health Care Organizations. London: Palgrave Macmillan; 2008.
- Kirkpatrick I, Ackroyd S, Walker R. The New Managerialism and Public Service Professions. London: Palgrave; 2005.
- Dopson S, Fitzgerald L, Ferlie E. Understanding change and innovation in healthcare settings: reconceptualizing the active role of context. J Change Manag 2008;8:213-31. http://dx.doi.org/10.1080/14697010802133577.
- Brown J, Duguid P. Knowledge and organization: a social-practice perspective. Organ Sci 2001;12:198-213. http://dx.doi.org/10.1287/orsc.12.2.198.10116.
- Health Strategy Review: Analytical Report. London: Cabinet Office; 2002.
- The UK Government’s Approach to Public Service Reform: A Discussion Paper. London: Cabinet Office; 2006.
- Carter B, Fairbrother P, Butler T, Savage M. Social Change and the Middle Classes. London: University College London Press; 1995.
- Morris J, Farrell C. The ‘post-bureaucratic’ public sector organization. New organizational forms and HRM in ten UK public sector organizations. Int J Hum Resource Manag 2007;18:1575-88. http://dx.doi.org/10.1080/09585190701570544.
- Marchington M, Grimshaw D, Rubery J, Willmott H. Fragmenting Work: Blurring Organizational Boundaries and Disordering Hierarchies. Oxford: Oxford University Press; 2004.
- Ezzamel M, Morris J, Smith JA. Accounting for New Organizational Forms: The Case of Subcontracting and Outsourcing. London: CIMA; 2005.
- Boaden R, Marchington M, Hyde P, Harris C, Sparrow P, Pass S, et al. The Process of Engagement and Alignment: Improving Health Through HRM. London: CIPD; 2008.
- Cascio W. Responsible Restructuring: Creative and Profitable Alternatives to Layoffs. San Francisco, CA: Berrett-Koehler; 2002.
- Cascio W. Strategies for responsible restructuring. Acad Manag Exec 2002;16:80-91. http://dx.doi.org/10.5465/AME.2002.8540331.
- Hassard J, McCann L, Morris J. Managing in the Modern Corporation. Cambridge: Cambridge University Press; 2009.
- Currie G. Reluctant but resourceful middle managers: the case of nurses in the NHS. J Nurs Manag 2006;14:5-12. http://dx.doi.org/10.1111/j.1365-2934.2005.00613.x.
- Fitzgerald L, Ferlie E, Wood M, Hawkins C. Interlocking interactions, the diffusion of innovations in healthcare. Hum Relat 2002;55:1429-49.
- Pfeffer J, Sutton RI. Hard Facts, Dangerous Half-Truths and Total Nonsense: Profiting from Evidence-Based Management. Boston, MA: Harvard Business School Press; 2006.
- Bate P, Robert G. Knowledge management and communities of practice in the private sector: lessons for modernizing the national health service in England and Wales. Public Adm 2002;80:643-63. http://dx.doi.org/10.1111/1467-9299.00322.
- Gabbay J, Le May A. Practice-based Evidence for Healthcare: Clinical Mindlines. London: Routledge; 2011.
- McConville T. Devolved HRM responsibilities, middle-managers and role dissonance. Personnel Rev 2006;35:637-53. http://dx.doi.org/10.1108/00483480610702700.
- Currie G, Procter S. The antecedents of middle managers’ strategic contribution: the case of a professional bureaucracy. J Manag Stud 2005;42:1325-56. http://dx.doi.org/10.1111/j.1467-6486.2005.00546.x.
- Buchanan D, Addicot R, Fitzgerald L, Ferlie E, Baeza J. Nobody in charge: distributed change agency in healthcare. Hum Relat 2007;60:1065-90. http://dx.doi.org/10.1177/0018726707081158.
- O’Reilly D, Reed M. The grit in the oyster: professionalism, managerialism and leaderism as discourses of UK public services modernization. Organ Stud 2011;32:1079-101. http://dx.doi.org/10.1177/0170840611416742.
- Cook S, Brown J. Bridging epistemologies: the generative dance between organizational knowledge and organizational knowing. Organ Sci 1999;10:381-400. http://dx.doi.org/10.1287/orsc.10.4.381.
- Newell S, Edelman L, Scarbrough H, Swan J, Bresnen M. ‘Best practice’ development and transfer in the NHS: the importance of process as well as product knowledge. Health Serv Manag Res 2003;16:1-12. http://dx.doi.org/10.1258/095148403762539095.
- Dopson S, Fitzgerald L. The role of the middle manager in the implementation of evidence-based health care. J Nurs Manag 2006;14:43-51. http://dx.doi.org/10.1111/j.1365-2934.2005.00612.x.
- Hyde P, Braithwaite J, Hyde P, Pope C. Culture and Climate in Health Care Organizations. London: Palgrave; 2009.
- Contu A, Willmott H. Re-embedding situatedness: the importance of power relations in learning theory. Organ Sci 2003;14:283-96. http://dx.doi.org/10.1287/orsc.14.3.283.15167.
- Roberts J. Limits to communities of practice. J Manag Stud 2006;43:623-39. http://dx.doi.org/10.1111/j.1467-6486.2006.00618.x.
- Carlile P. Transferring, translating, and transforming: an integrative framework for managing knowledge across boundaries. Organ Sci 2004;15:555-68. http://dx.doi.org/10.1287/orsc.1040.0094.
- Reed M, Anthony P. Professionalizing management and managing professionalization: British management in the 1980s. J Manag Stud 1992;29:591-613. http://dx.doi.org/10.1111/j.1467-6486.1992.tb00680.x.
- Nonaka I, Takeuchi I. The Knowledge Creating Organization. Oxford: Oxford University Press; 1995.
- Gourlay S. Conceptualizing knowledge creation: a critique of Nonaka’s theory. J Manag Stud 2006;43:1415-36. http://dx.doi.org/10.1111/j.1467-6486.2006.00637.x.
- Van De Ven A. Central problems in the management of innovation. Manag Sci 1986;32:590-607. http://dx.doi.org/10.1287/mnsc.32.5.590.
- Newell S, Robertson M, Scarbrough H, Swan J. Managing Knowledge Work. London: Palgrave; 2002.
- Alvesson M, Karreman D. Odd couple: making sense of the curious concept of knowledge management. J Manag Stud 2001;38:995-1018. http://dx.doi.org/10.1111/1467-6486.00269.
- Lave J, Wenger E. Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge University Press; 1991.
- Wenger E. Communities of Practice: Learning, Meaning and Identity. Cambridge: Cambridge University Press; 1998.
- Wenger E. Communities of practice and social learning systems. Organization 2000;7:225-46. http://dx.doi.org/10.1177/135050840072002.
- Abbott A. The System of Professions: Essay on the Division of Expert Labour. Chicago: University of Chicago Press; 1988.
- Boland R, Tenkasi R. Perspective making and perspective taking in communities of knowing. Organ Sci 1995;6:350-72. http://dx.doi.org/10.1287/orsc.6.4.350.
- Wenger E, McDermott R, Snyder W. Cultivating Communities of Practice: A Guide to Managing Knowledge. Boston, MA: Harvard Business School Press; 2002.
- Ferlie E, Fitzgerald L, Wood M, Hawkins C. The nonspread of innovations: the mediating role of professionals. Acad Manag J 2005;48:117-34. http://dx.doi.org/10.5465/AMJ.2005.15993150.
- Swan J, Bresnen M, Newell S, Robertson M. The object of knowledge: the role of objects in biomedical innovation. Hum Relat 2007;60:1809-37. http://dx.doi.org/10.1177/0018726707084915.
- Currie G, Finn R, Martin G. Accounting for the ‘dark side’ of new organizational forms: the case of healthcare professionals. Hum Relat 2008;61:539-64. http://dx.doi.org/10.1177/0018726708091018.
- Watson TJ. In Search of Management: Culture, Chaos and Control in Managerial Work. London; New York, NY: Routledge; 1994.
- Yin RK. Case Study Research: Design and Methods. Beverly Hills, CA: Sage; 1984.
- Eisenhardt KM, Graebner ME. Theory building from cases: opportunities and challenges. Acad Manag J 2007;50:25-32. http://dx.doi.org/10.5465/AMJ.2007.24160888.
- Fitzgerald L, Dopson S, Buchanan D, Bryman A. Handbook of Organizational Research Methods. London: Sage; 2009.
- Equity and Excellence: Liberating the NHS. Cm 7881. London: The Stationery Office; 2010.
- Burrell G, Morgan G. Social Paradigms and Organizational Analysis: Elements of the Sociology of Corporate Life. London: Heinemann; 1979.
- Silverman D. The Theory of Organizations. London: Heinemann; 1970.
- Geertz C. The Interpretation of Cultures: Selected Essays by Clifford Geertz. New York, NY: Basic Books; 1973.
- Hyde P, McBride A, Walshe K, Smith J. Healthcare Management. Maidenhead: Open University Press; 2011.
- Kippist L, Fitzgerald A. Organisational professional conflict and hybrid clinician managers. J Health Organ Manag 2009;23:642-55. http://dx.doi.org/10.1108/14777260911001653.
- Hyde P, Granter E, Hassard J, McCann L, Morris J. Roles and Behaviours of Middle and Junior Managers: Managing New Organizational Forms of Healthcare. Final Report 2013.
- Beech N, MacIntosh R, MacLean D. Dialogues between academics and practitioners: the role of generative dialogic encounters. Organ Stud 2010;31:1341-67. http://dx.doi.org/10.1177/0170840610374396.
- Hyde P, Thomas A. Organisational defences revisited: systems and contexts. J Manag Psychol 2002;17:408-21. http://dx.doi.org/10.1108/02683940210432646.
- Hyde P, Davies H. Service design, culture and performance: collusion and co-production in health care. Hum Relat 2004;57:1407-26. http://dx.doi.org/10.1177/0018726704049415.
- Strauss A, Corbin JM. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park, CA: Sage; 1990.
- Huy Q. In praise of middle managers. Harvard Business Rev 2001;79:72-9.
- Huy Q. Emotional balancing of organizational continuity and radical change: the contribution of middle managers. Adm Sci Q 2002;47:31-69. http://dx.doi.org/10.2307/3094890.
- Brocklehurst M, Grey C, Sturdy A. Management: the work that dares not speak its name. Manag Learn 2009;41:7-19. http://dx.doi.org/10.1177/1350507609347590.
- Buchanan D, Denyer D, Jaina J, Kelliher C, Moore C, Parry E, et al. How Do They Manage? A Qualitative Study of the Realities of Middle and Front Line Management Work in Healthcare. Final Report 2013.
- The Future of Leadership and Management in the NHS: No More Heroes. London: The King’s Fund; 2011.
- Merali F. NHS managers’ views of their culture and their public image: the implications for NHS reforms. Int J Public Sector Manag 2003;16:549-63. http://dx.doi.org/10.1108/09513550310500409.
- Harrison S, McDonald R. The Politics of Healthcare in Britain. London: Sage; 2008.
- Klein R. The New Politics of the NHS: From Creation to Reinvention. Oxford: Radcliffe Publishing; 2010.
- Griffiths R. Report of NHS Management Inquiry. London: Department of Health and Social Security; 1983.
- NHS and Community Care Act. London: HMSO; 1990.
- The New NHS: Modern, Dependable Cmnd 3807. London: HMSO; 1997.
- NHS Plan: A Plan For Investment. London: HMSO; 2000.
- Health and Social Care (Community Health and Standards) Act 2003. London: The Stationery Office; 2003.
- High Quality Care for All (NHS Next Stage Review Final Report): Darzi Report Cmnd 7432. London: HMSO; 2008.
- Exworthy M, Macfarlane F, Willmott M. NHS Management: 60 Years in Transition. London: Nuffield Trust; 2009.
- Working for Patients. Cm 555. London: HMSO; 1989.
- NHS Hospital and Community Services Non-Medical Staff England 1999–2009. London: The NHS Information Centre; 2010.
- Working Together for Health. Geneva: World Health Organization; 2006.
- NHS Workforce: Summary of staff in the NHS: Results from September 2011 Census. London: The NHS Information Centre; 2012.
- Health and Social Care Act. London: HMSO; 2012.
- McCann L, Morris J, Hassard J. Normalized intensity: the new labour process of middle management. J Manag Stud 2008;42:343-71. http://dx.doi.org/10.1111/j.1467-6486.2007.00762.x.
- Powell M, Durose J, Duberley J, Exworthy M, Fewtrell C, MacFarlane F, et al. Talent Management in the NHS Managerial Workforce. Final Report. London: NIHR NETSCC Health Services and Delivery Research; 2012.
- NHS Leadership Academy . Why Do We Need the NHS Leadership Academy Core Programmes? n.d. www.leadershipacademy.nhs.uk (accessed February 2013).
- Learmonth M. Doing things with words: the case of ‘management’ and ‘administration’. Public Adm 2005;83:617-37. http://dx.doi.org/10.1111/j.0033-3298.2005.00465.x.
- Department of Health . Inspiring Leaders: Leadership for Quality 2009. http://webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_093407.pdf (accessed 1 March 2014).
- Department of Health . The Operating Framework for the NHS in England 2008 09 2007. http://webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_081271.pdf (accessed 1 March 2014).
- NHS Institute for Innovation and Improvement . About the NHS Institute n.d. www.institute.nhs.uk/organisation/about_nhsi/about_the_nhs_institute.html (accessed February 2013).
- Nicolson P, Rowland E, Lokman P, Fox R, Gabriel Y, Heffernan K, et al. Leadership and Better Patient Care: Managing in the NHS. Final Report. London: NIHR NETSCC Health Services and Delivery Research; 2011.
- Walshe K, Smith J. Healthcare Management. Maidenhead: Open University Press; 2011.
- Ham C, Dickinson H. Engaging Doctors in Leadership: A Review of the Literature. Coventry: The NHS Institute for Innovation and Improvement; 2007.
- Llewellyn S. ‘Two-way windows’: clinicians as medical managers. Organ Stud 2001;22:593-62. http://dx.doi.org/10.1177/0170840601224003.
- Forbes T, Hallier J, Kelly L. Doctors as managers: investors and reluctants in a dual role. Health Serv Manag Res 2004;17:167-76. http://dx.doi.org/10.1258/0951484041485638.
- Hyde P, Granter E, McCann L, Hassard J, Dickinson H, Mannion R. The Reform of Health Care: Shaping, Adapting and Resisting Policy Developments. London: Palgrave; 2011.
- Osborne D, Gaebler T. Reinventing Government: How the Entrepreneurial Spirit is Transforming the Public Sector. New York, NY: Penguin; 1993.
- Friedson E. The Profession of Medicine. New York, NY: Dodd, Mead; 1970.
- Clarke C, Brown A, Hope-Hailey V. Working identities? Antagonistic discursive resources and managerial identity. Hum Relat 2009;62:323-52. http://dx.doi.org/10.1177/0018726708101040.
- Thomas R, Linstead A. Losing the plot? Middle managers and identity. Organization 2002;9:71-93. http://dx.doi.org/10.1177/1350508402009001356.
- Ferlie E, Pettigrew A. Managing through networks: some issues and implications for the NHS. Br J Manag 1996;7:S81-99. http://dx.doi.org/10.1111/j.1467-8551.1996.tb00149.x.
- Alvesson M, Willmott H. Identity regulation as organizational control: producing the appropriate individual. J Manag Stud 2002;39:619-44. http://dx.doi.org/10.1111/1467-6486.00305.
- Miller P, Rose N. Governing the Present: Administering Economic, Social and Personal Life. London: Polity Press; 2008.
- Du Gay P, Salaman G, Rees B. The conduct of management and the management of conduct: contemporary managerial discourse and the constitution of the ‘competent’ manager. J Manag Stud 1996;33:263-82.
- Grey C. ‘We are All Managers Now’; ‘We Always Were’: on the development and demise of management. J Manag Stud 1999;36:561-85. http://dx.doi.org/10.1111/1467-6486.00149.
- McCartney S, Berman Brown R, Bell L. Professionals in health care: perceptions of managers. J Manag Med 1993;7:48-55. http://dx.doi.org/10.1108/eb060566.
- Preston D, Loan-Clarke J. The NHS manager: a view from the bridge. J Manag Med 2000;14:100-8. http://dx.doi.org/10.1108/02689230010346411.
- Alimo-Metcalfe B, Lawler J. Leadership development in UK companies at the beginning of the twenty-first century: Lessons for the NHS?. J Manag Med 2001;15:387-404. http://dx.doi.org/10.1108/EUM0000000006185.
- Mintzberg H. The Structuring of Organizations. Englewood Cliffs, NJ: Prentice-Hall; 1979.
- Currie G, Brown A. A narratological approach to understanding processes of organizing in a UK hospital. Hum Relat 2003;56:563-86. http://dx.doi.org/10.1177/0018726703056005003.
- Brooks I. Managerialist professionalism: the destruction of a non-conforming subculture. Br J Manag 1999;10:41-52. http://dx.doi.org/10.1111/1467-8551.00110.
- Noordegraaf M. Remaking professionals? How associations and professional education connect professionalism and organizations. Curr Sociol 2011;59:465-88. http://dx.doi.org/10.1177/0011392111402716.
- Noordegraaf M. Risky business: How professionals and professional fields (must) deal with organizational issues. Organ Stud 2011;32:1349-71. http://dx.doi.org/10.1177/0170840611416748.
- Grey C. Management as a technical practice: professionalisation or responsibilization?. Syst Pract 1997;10:703-25.
- Kotter J. A Force for Change: How Leadership Differs from Management. New York, NY: The Free Press; 1990.
- Rost J. Leadership for the Twenty-First Century. Westport, CT: Praeger/Greenwood; 1991.
- Khurana R. The curse of the superstar CEO. Harvard Business Rev n.d.;80:1-10.
- Handy C. Understanding Organizations. London: Penguin; 1993.
- Handy C. Gods of Management. London: Souvenir; 2009.
- Mintzberg H. The manager’s job: folklore and fact. Harvard Business Rev 1975;53:49-61.
- Tsoukas H. The firm as a distributed knowledge system: a constructionist approach. Strat Manag J 1996;17:11-25.
- Spender JC. Organizational knowledge, learning and memory: three concepts in search of a theory. J Organ Change Manag 1996;9:63-78. http://dx.doi.org/10.1108/09534819610156813.
- Blackler F. Knowledge, knowledge work and organizations: an overview and interpretation. Organ Stud 1995;16:1021-46. http://dx.doi.org/10.1177/017084069501600605.
- Armstrong P. The rise of accounting controls in British capitalist enterprises. Account Organ Soc 1987;12:415-36. http://dx.doi.org/10.1016/0361-3682(87)90029-8.
- Granovetter M. The strength of weak ties. Am J Sociol 1973;78:1360-80. http://dx.doi.org/10.1086/225469.
- Szulanski G. Exploring internal stickiness: Impediments to the transfer of best practice within the firm. Strat Manag J 1996;17:27-43.
- Argyris C. Double loop learning in organizations. Harvard Business Rev 1977;55:115-25.
- Senge PM. The Fifth Discipline: The Art and Practice of the Learning Organization. London: Random House; 1990.
- Schön D. The Reflective Practitioner: How Professionals Think in Action. New York, NY: Basic Books; 1983.
- Reynolds M. Reflection and critical reflection in management learning. Manag Learn 1998;29:183-200. http://dx.doi.org/10.1177/1350507698292004.
- Castells M. The Rise of the Network Society. Oxford: Blackwell Publishers; 1996.
- Putnam RD. Bowling Alone: The Collapse And Revival Of American Community. New York, NY: Simon & Schuster; 2001.
- Miles RE, Snow CC. Network organizations: new concepts for new forms. California Manag Rev 1986;28:62-73.
- Powell WW. Neither market nor hierarchy: network forms of organization. Res Organ Behav 1990;12:295-336.
- Swan J, Scarbrough H, Robertson M. The construction of ‘communities of practice’ in the management of innovation. Manag Learn 2002;33:477-96. http://dx.doi.org/10.1177/1350507602334005.
- Agterberg M, Van Den Hooff B, Huysman M, Soekijad M. Keeping the wheels turning: the dynamics of managing networks of practice. J Manag Stud 2010;47:85-108. http://dx.doi.org/10.1111/j.1467-6486.2009.00867.x.
- Ferlie E, Fitzgerald L, McGivern G, Dopson S, Exworthy M. Networks in Health Care: A Comparative Study of Their Management, Impact and Performance. London: HMSO; 2010.
- Addicott R, McGivern G, Ferlie E. The distortion of a managerial technique? The case of clinical networks in UK health care. Br J Manag 2007;18:93-105. http://dx.doi.org/10.1111/j.1467-8551.2006.00494.x.
- Edwards N. Clinical networks. BMJ 2002;324. http://dx.doi.org/10.1136/bmj.324.7329.63.
- Nahapiet J, Ghoshal S. Social capital, intellectual capital, and the organizational advantage. Acad Manag Rev 1998;23:242-66. http://dx.doi.org/10.2307/259373.
- Burt R. Brokerage and Closure. Oxford: Oxford University Press; 2005.
- Anderson-Gough F, Grey C, Robson K. Professionals, networking and the networked professional. Res Sociol Organ 2006;24:231-56. http://dx.doi.org/10.1016/S0733-558X(06)24009-6.
- Gouldner AW. Cosmopolitans and locals: toward an analysis of latent social roles – I. Adm Sci Q 1957;2:281-306. http://dx.doi.org/10.2307/2391000.
- Gouldner AW. Cosmopolitans and locals: toward an analysis of latent social roles – II. Adm Sci Q 1958;2:444-80. http://dx.doi.org/10.2307/2390795.
- McNulty T. Reengineering as knowledge management: a case of change in UK healthcare. Manag Learn 2002;33:439-58. http://dx.doi.org/10.1177/1350507602334003.
- Waring J, Bishop S. Lean healthcare: rhetoric, ritual, resistance. Soc Sci Med 2010;71:1332-40. http://dx.doi.org/10.1016/j.socscimed.2010.06.028.
- Uzzi B. Social structure and competition in interfirm networks: the paradox of embeddedness. Adm Sci Q 1997;42:35-67. http://dx.doi.org/10.2307/2393808.
- Newell S, Robertson M, Scarbrough H, Swan J. Managing Knowledge Work and Innovation. London: Palgrave Macmillan; 2009.
- Amin A, Roberts J. Knowing in action: beyond communities of practice. Res Policy 2008;37:353-69. http://dx.doi.org/10.1016/j.respol.2007.11.003.
Appendix 1 Project flow chart
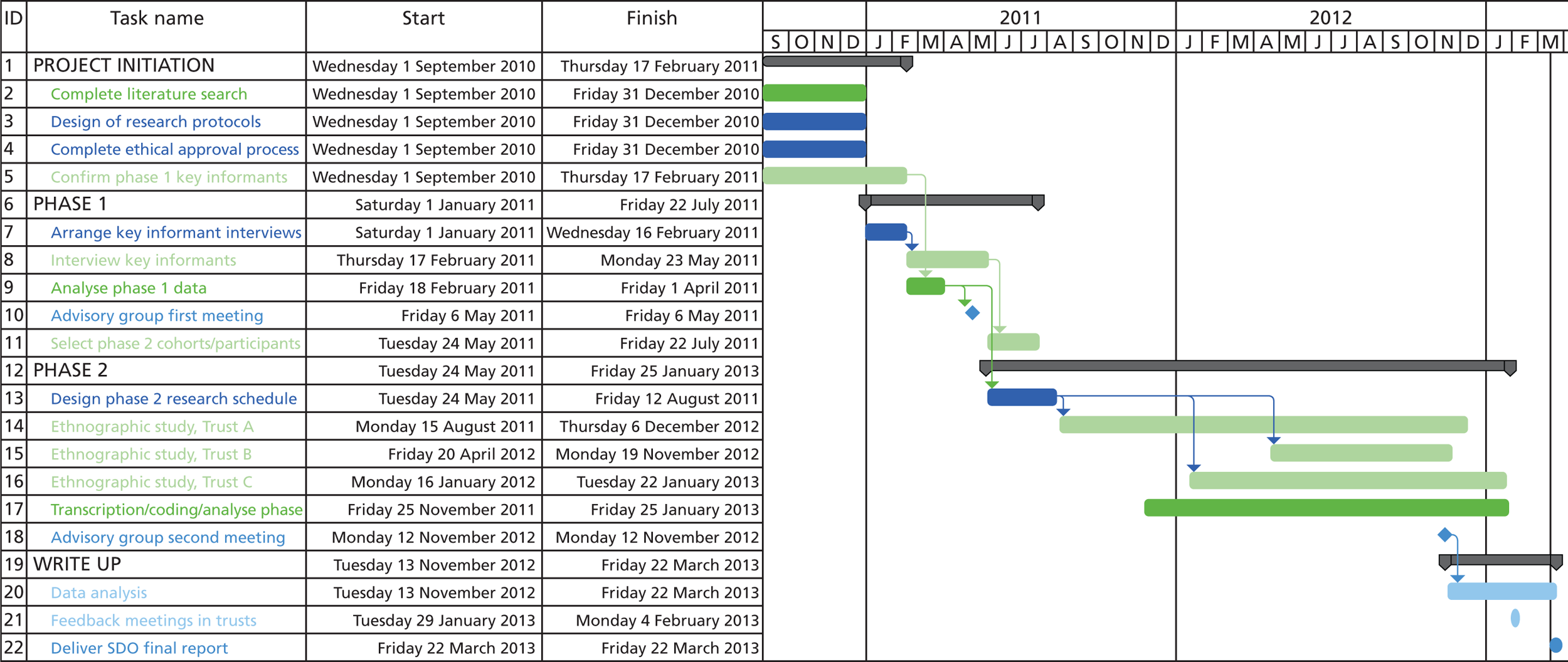
Appendix 2 Phase 1 key informant interview schedule
| Themes/questions |
|---|
| 1. NHS trust contexts |
| How well does the type of trust framework reflect key differences between the trusts in terms of management groups and the challenges they face? Where/how might it need refining? |
| How much differentiation and interdependence might we expect to find amongst managerial groups within each type of trust? |
| 2. Framework for selection of managerial cohorts |
| How good/appropriate is it for defining managerial groups? Where/how might it need refining? |
| Are any or all of these management groups connected in with broader (organisational, regional, national) networks and communities of practice (including professional associations)? Are there distinct professional identities? How might this affect how we define these management groups? |
| How much differentiation and integration might we expect to find amongst these groups? How much coordination of work, communication and knowledge sharing? |
| How might we apply this selection framework to identify cohorts in each case? Which groups and individuals can we identify in each cohort in each trust? |
| 3. Encounters/events |
| What local encounters/events might be suitable for observing management interactions connected to flows of knowledge and learning? |
| What regional/national encounters/events might be suitable for observing management interactions connected to flows of knowledge and learning? |
| 4. Current changes and possible effects |
| How might changing conditions (e.g. policy changes) affect how the trusts are organised (and how we compare and contrast them), how management groups are defined/demarcated and what events/encounters might be relevant to observe? |
| 5. Management knowledge and learning |
| Preliminary thoughts on what types of knowledge and learning managers in these groups tend to apply to their everyday work? How might this be affected by their background, experience, professional development and personal or professional networks? |
| 6. HR practices |
| Preliminary thoughts on whether and how HR systems and practices in individual trusts (e.g. recruitment, selection, training and development) might enable or hinder flows of knowledge and learning within and between managerial groups? |
| 7. Organisation, systems and practices |
| Preliminary thoughts on whether and how other organisational practices in individual trusts (e.g. division of work, ICT support available) might enable or hinder flows of knowledge and learning within and between managerial groups? |
Appendix 3 Invitation letter
Appendix 4 Participant information sheet
Appendix 5 Project summary document
Project summary, version 1, 28 May 2010
Being a manager, becoming a professional? Exploring the use of management knowledge across communities of practice in health-care organisations
Research context
Given the expectations we have of managers in the NHS to improve performance and the constant pressures for change they face, it is important to know that managers are able to access the leading edge knowledge that they need and that management ideas that can improve health-care delivery are readily accessible and able to be effectively translated into a healthcare setting.
Yet, despite a good deal of research that has begun to look in-depth at how managers in the NHS perform their roles, we have only limited understanding of how managers access management knowledge, interpret it and seek to adapt and apply it in their healthcare settings.
There is also very little research that has tried to understand how the use of management knowledge relates to managers’ individual learning and development, how this ties in with their development as ‘professional’ managers within their particular health-care setting and how that setting itself (and the wider community of practice of which they are a part) influences the ways in which managers have access to, make sense of, select and apply relevant management knowledge.
Aims and objectives
This research sets out to fill these gaps in our understanding by exploring how middle managers in the NHS use knowledge and learning from various sources to apply to develop and improve management practice.
In doing so, it recognises that there are different groups within management that have their own needs and perspectives and that draw upon different types of management knowledge, that management knowledge itself is often the subject of considerable debate (particularly when transferred from other contexts), that organizational practices (e.g. human resource management) can be important in facilitating or inhibiting the acceptance and application of management knowledge, and that managers are part of a wider community of practitioners within the NHS and beyond that influence approaches to professional training and development.
The specific questions/objectives to be addressed in this research project are:
-
How do occupational background and careers influence knowledge receptivity, knowledge sharing and learning among healthcare managers?
-
How do relevant communities of practice enable/obstruct knowledge sharing and learning?
-
What mechanisms are effective in supporting knowledge receptivity, knowledge sharing and learning/unlearning within and across such communities?
Methods
After the initial exploratory and detailed design phases of the research, the main empirical part of the study will involve in-depth research on selected cohorts of managers within three distinct types of NHS Trust (one Foundation Acute Trust, one Tertiary Specialist Hospital and one Mental Health Trust).
Interviews will be used to explore managers’ actual career development experiences and to gauge where, how and why managers acquire their practical managerial knowledge and how it translates into everyday management practices and experiences.
Managers will also be observed at key events where managerial knowledge is acquired, shared or otherwise used (e.g. meetings, workshops and conferences, training events).
An Advisory Group consisting of representatives from the three trusts involved as well as others from across the health sector will be established to help guide the research.
Research findings will be fed back directly to the participants at each trust and also via a Research Symposium held towards the end of the project that will involve representatives from across the trusts.
Outcomes and benefits
The research will produce findings that can be generalised to similar types of trusts operating elsewhere and which are sensitive to the conditions influencing different groups of managers facing different conditions and challenges.
Practical suggestions and recommendations for health-care practitioners and policy makers will be made concerning how to develop training and development for managers in ways that improves their access to and use of appropriate management knowledge and how to identify and deal with barriers to using appropriate knowledge that may arise from existing management practices and features of the health-care setting in which they operate.
The research results will be disseminated widely (and anonymously) through research reports, presentations and publications (in both health-care management and general management outlets).
Participants
| Project partners | Research Team |
|---|---|
| Manchester Business School | Prof Mike Bresnen |
| NIHR Service Delivery Organisation | Dr Damian Hodgson |
| Acute Trust | Dr Paula Hyde |
| Specialist Trust | Prof John Hassard |
| Care Trust | Dr Simon Bailey |
Funding body: NIHR Service Delivery Organisation (SDO)
Research period: September 2010 to December 2012
Contact: xxxxxxxxxxx@xxxxxxxxx
Appendix 6 Consent form
Appendix 7 Phase 2 interview schedule
-
Occupation/Career:
-
Current role and responsibilities, place in organisation
-
Educational background, career path
-
Induction/socialisation into organisation/current role
-
-
Leadership/Management:
-
Current managerial/leadership responsibilities
-
Understanding of management/leadership as a function
-
Conception of management as professional group
-
-
Knowledge:
-
Skills/knowledge necessary to carry out managerial/leadership responsibilities
-
Skill/knowledge development:
-
formal
-
informal
-
-
Organisational mechanisms which support skill/knowledge development (ICT, HR . . .)
-
-
Networks:
-
Networks used in resolving managerial/leadership challenges.
-
Nature of different networks:
-
purpose, scope, membership, formality, cohesion, media
-
establishment, governance and lifespan
-
-
Inter-network activities: conflict/cooperation, governance, impact
-
-
Organisational Context:
-
Organisational role in helping/hindering knowledge work
-
Organisational barriers to knowledge communication
-
Knowledge receptivity of organisation
-
-
Change:
-
Changes occurring which affect knowledge & learning
-
Personal account of changes and impacts
-
Personal and organisational future
-
Appendix 8 Full list of network events observed
| Name of network event | Key organisations involved | Date | Informal/formal | Internal/external | Type |
|---|---|---|---|---|---|
| Future of Education | NHS employers | 23 February 2011 | Formal | External | Webinar |
| The Engaging Manager | NHS employers | 27 February 2011 | Formal | External | Webinar |
| Team Leader Programme | Care | 30 October 2012 | Formal | Internal | Training |
| Patient Experience Group | Acute | 14 November 2012 | Formal | Internal | Meeting |
| End of Life Workshop | Care and Acute | 20 November 2012 | Formal | External | Network |
| Team Leader Programme | Care | 21 November 2012 | Formal | Internal | Training |
| Audit and Research Group | Care | 26 November 2012 | Formal | Internal | Meeting |
| Divisional Integrated Governance Group | Care | 28 November 2012 | Formal | Internal | Meeting |
| End of Life Workshop | Care and Acute | 29 November 2012 | Both | External | Network |
| End of Life Workshop | Care and Acute | 4 January 2012 | Both | External | Network |
| End of Life Managers Briefing | Care and Acute | 10 January 2012 | Formal | External | Network |
| Research Nurse Network | Specialist | 12 December 2012 | Formal | External | Network |
| Divisional Board Meeting | Specialist | 18 December 2012 | Formal | Internal | Meeting |
| Leadership Development Consultation | Care | 19 December 2012 | Both | Internal | Training |
| Shared Leadership Day | Acute | 8 February 2013 | Informal | Internal | Training |
Appendix 9 Thematic guide for observations
Date – time – trust – location
Context
-
Network name and type (internal, external, formal, informal, operational, training, etc.)
-
Who is attending, numbers, occupational types, grades, who is facilitating/chairing, is there a mixture of groups – clinical/managerial?
-
What is the agenda, how formal is the atmosphere: relationships, uniforms, informal chat, breaks?
Knowledge
-
What kind of knowledge bases or skill sets are used?
-
Are they tacit, commodified?
-
What kind of language is used?
-
What kind of knowledge is required to participate – is this made explicit?
-
Management
-
How is management and management knowledge articulated?
-
What does it mean to be a manager in this situation?
-
Peer groups, professionals, negotiators, compromisers, performance managers, technical specialists.
-
-
Power
-
What are the implicit rules of participation?
-
Who is talking most, are there dominant groups?
-
Who sits where, how is space used?
-
Is hierarchy/authority/status apparent?
-
Organisation
-
How does the organisation present itself?
-
How is it received, is there any feedback?
-
Appendix 10 Key NHS leadership training programmes
| Programme | NHS GMTS | Breaking through | Athena programme for executive women | Gateway to leadership |
|---|---|---|---|---|
| Provider | The King’s Fund | Hay Group | The King’s Fund | The King’s Fund |
| Structure | Structured NHS work placements with a range of education and development opportunities provided via a range of respected academic, professional and personal development providers, built around the NHS Leadership Qualities Framework covering a range of personal, cognitive and social qualities, 15 qualities arranged in three clusters: personal qualities, setting direction and delivering the service | Top Talent: 18-month programme, during which time the participants secure a placement that will enable them to gain the experience required to perform successfully at senior level. Transformational Leadership Programme: intense 5-week programme (spread over 6 months), aims to equip participants to develop into transformational leaders and encourages discussion about barriers or apparent barriers that challenge BME staff in the NHS. In addition, Towards Strategies for Success, 1-day course for BME men and women (separately) | Four modules over a period of 4–6 months plus two one-to-one executive coaching sessions with Athena programme directors | 25 days’ development over a 2-year period. This includes executive coaching, peer action learning sets and a 15-day modular residential development programme |
|
||||
|
||||
|
||||
|
||||
| Plus one-to-one executive coaching and learning sets | ||||
| Networking | Action learning sets, encouraged to secure mentor, meetings with senior managers, chief executives, etc. | Top talent: coaching, action learning sets, mentoring during secondment | Peer learning sets, presentations/meetings with senior managers, chief executives, etc. | Mentoring, 360-degree feedback, learning account, peer learning sets, meetings with senior managers, chief executives, etc. |
| Inception | 1986 (in current form) | 2003, relaunched in 2007 | 2004 | 2002 |
List of abbreviations
- AHP
- allied health professional
- CCG
- clinical commissioning group
- CHI
- Commission for Health Improvement
- CoP
- community of practice
- CQC
- Care and Quality Commission
- DGH
- district general hospital
- FT
- foundation trust
- GMTS
- Graduate Management Training Scheme
- GP
- general practitioner
- HR
- human resources
- ICT
- information and communication technology
- IT
- information technology
- MBA
- Master of Business Administration
- MSc
- Master of Science
- NICE
- National Institute for Health and Care Excellence
- NoP
- network of practice
- PCT
- primary care trust
- SDO
- Service Delivery Organisation
- SHA
- strategic health authority