
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 10/2000/40. The contractual start date was in January 2012. The final report began editorial review in October 2013 and was accepted for publication in April 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Gavin et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
What is complex regional pain syndrome?
Complex regional pain syndrome (CRPS) is difficult to diagnose and is characterised by burning pain in one or more limbs, swelling, and temperature and colour changes, with 15–20% of patients developing long-term disability. 1 The cause is unknown and there is currently no cure. It has an incidence of 5.46–26.2 per 100,000 person-years. 2 For those patients whose symptoms do not spontaneously resolve within the first year, long-term residual symptoms or impairment are common. Treatment is palliative rather than curative and so focuses on improving function. CRPS can be both distressing and debilitating and have a considerable impact on the lives of both the person with CRPS and those closest to them. 3
What is the impact of complex regional pain syndrome?
Impact on person
Complex regional pain syndrome can have a negative impact on the physical, emotional, social and financial aspects of patients’ lives. 4 CRPS pain is often invisible and is difficult to explain to family, friends and colleagues. In addition, patients are faced with the frustration of no longer being able to do the things they used to and can lose their sense of identity. Furthermore, patients have reported that their health-care professionals lacked knowledge of CRPS as a condition and this is a source of considerable frustration. 4
Impact on carer
A study on the carer experience of CRPS demonstrated that they were disappointed to discover that CRPS was not well known or understood by health professionals. 5 Furthermore, obtaining information from the internet, which often displayed ‘worst-case scenario’ accounts and pictures, created uncertainty and anxiety about how CRPS might progress and what it meant for the future of their relative or friend. It has been suggested that providing relatives with better information might have the added benefit of improving the situation for the patient. 6 The way in which significant others respond to the person with CRPS can have an impact on the person’s illness experience. 7 Furthermore, there is a growing body of research which suggests that chronic illness may have profound effects on the well spouse. 8
Current NHS policy and practice
Multidisciplinary rehabilitation (including psychological interventions) is recommended for the management of CRPS. 9 Patients in the UK may be referred to an inpatient programme at the Royal National Hospital for Rheumatic Diseases (RNHRD) in Bath. This is the only specialist inpatient programme for people with CRPS in the UK. The programme at the RNHRD is multidisciplinary, with a focus on physical rehabilitation (including physiotherapy, occupational therapy and hydrotherapy) and also includes sessions with health and clinical psychologists. Because treatment is palliative rather than curative, the main objective is to improve function and to encourage self-management. Implementation of skills developed on the inpatient programme (i.e. adherence to advice) is essential in order to lessen the impact that CRPS has on patients’ lives. Furthermore, active participation in the treatment process by the person with CRPS is essential for successful rehabilitation. 10 Online support can complement the rehabilitation process.
Coping with complex regional pain syndrome
The relationship between social support and physical and psychological well-being is well documented and includes positive adjustment and coping with illness,11 increased positive health behaviours12 and decreased physical disability. 7,13
Online support
Online support communities (also known as online support groups, online discussion groups or online support forums) are a type of virtual community in which people can discuss a common health issue. Virtual communities are identifiable as groups of people who discuss matters of mutual concern. 14 The proliferation of mutual support groups in Western countries in the 1990s was part of a larger social movement of self-help organisations for people affected by a variety of chronic diseases and stressful life circumstances whose needs had not been fully addressed by traditional health-care interventions. 15 This trend has been repeated in cyberspace, where the number of internet sites devoted to a wide range of social and health issues has grown. 16 Many of these sites enable people suffering from a particular health condition to share their experiences, offer advice when it is sought and provide emotional and practical support, as well as receiving benefits in kind.
Online support forums are internet sites where individuals write messages to one another which can stimulate discussion as other individuals read and respond to the messages. They can be open where anyone can read, post or respond to messages. Some discussions are hidden from public view and in order to read or participate individuals must register with the site and obtain a password to gain access. Most web forums have a hierarchical, tree-like structure. 17 The top level usually has an index page comprising several boards that are organised thematically into sections. Each of these boards provides an area where members can join in with a particular topic of discussion. Within each board, discussions are organised into threads. These are groups of related messages where a member starts a new discussion by posting an initial message asking a question, requesting advice or describing an experience. Other members can contribute by posting replies, and these replies often generate additional responses of their own.
Online discussion forums are increasingly used by patients as a source of information, advice and psychological support for health-related issues. While face-to-face support groups provide members with the opportunity to help each other, online forums provide similar opportunities, but also open up the possibility for discussing taboo topics and forms of self-expression that are often unavailable offline. 18 There is growing evidence that forum participation can have a positive impact, for example reduced sense of isolation, increased self-efficacy and reduced anxiety. 19 Of particular importance is the development of a shared group identity and, consequently, the validation of members’ thoughts, feelings and experiences. 18,20,21 It should be noted that many of the benefits of online support are contingent on the anonymity afforded by many online forums. Typically, members use pseudonyms that reveal little, if any, identifying information. Increasingly, social network sites such as Facebook (www.facebook.com) are being used to create online health communities for health-related support, such as the Facebook CRPS community. However, many such social networking sites are ‘nonymous’; that is, they are anchored environments, with member profiles usually including identifying information such as name, location and affiliations (such as university or work), with one’s social network ‘friends’ often having some connection to each other’s offline lives.
A growing number of studies have focused on exploring how online support group members communicate with each other, in order to identify potentially therapeutic processes which may be active within an online setting. 22,23 In particular, it is argued that the exchange of social support between group members is especially beneficial. 19,24 Social support has been described as ‘a social network’s provision of psychological and material resources intended to benefit an individual’s ability to cope with stress’. 25 A number of qualitative studies have sought to explore the ways in which social support may be provided by members of online support groups. For example, Coulson26 examined a sample of messages posted to an online support group discussion forum for individuals living with irritable bowel syndrome. The results revealed both informational and emotional support to be particularly prevalent in this online context.
Five main categories of support-intended communication behaviours have been identified: emotional support (communicating love, concern or empathy), information support (providing information or advice), esteem support (communicating respect and confidence in abilities), network support (communicating belonging to a group of persons with similar concerns or experiences) and tangible assistance (providing, or offering to provide, goods or services), each subsuming a number of subcategories. 22,27 This typology has been successfully adapted and used in the qualitative analysis of messages posted to other health-related online support groups. 19,24
A developing sense of community often found in online forum participation can also provide elements of support. 28 Of particular importance is the development of a shared group identity and, consequently, the validation of patients’ thoughts, feelings and experiences. This has been demonstrated in relation to a range of commonly misunderstood health conditions, including self-harm, eating disorders, infertility, human immunodeficiency virus (HIV)/(acquired immunodeficiency syndrome (AIDS) and CRPS. 18,20 Moreover, for those with a chronic pain condition, the online world offers an easily accessible form of support.
Online support for complex regional pain syndrome
Online social support may be particularly important for CRPS patients. Perceived social support helps to reduce depression, negative moods and feelings of anger, and can also reduce the level of pain experienced the following day. 29 Support can be accessed at any time of the day or night30 without any barriers that might be associated with travelling to a face-to-face support group. 31 The anonymity of the internet makes it easier to discuss sensitive or embarrassing topics32 and may aid individuals in obtaining support for rare or debilitating illnesses. 31 However, there are also disadvantages. Online communities can be used only by individuals who have access to a computer, the internet, and the computer skills needed to use them,31 and can produce large volumes of messages that may be time-consuming to read,31 which could pose difficulties if using a computer for long periods of time exacerbates an existing medical condition such as a pain disorder.
People with CRPS often find themselves becoming socially isolated and withdrawn because their ability to participate in social and recreational activities is affected,33 and it can leave them with a greatly reduced network through which they can obtain support. 34 This means that social support received over the internet may be particularly beneficial to individuals who suffer from CRPS. The means by which a supportive environment develops is likely to rely upon the development of a shared group identity. This is particularly relevant for those with CRPS because loss of identity is one of the issues which motivate people to seek support.
The importance of online support for people with CRPS is evidenced by our own experience, whereby a patient group at a national referral centre for patients with CRPS in the UK expressed a need for online support to complement the hospital-based services already provided. Previously, there was an interactive forum for people with CRPS (known as ‘RSD UK’); however, this had closed. Many people with CRPS, in consultation with one of the authors in her role as CRPS health psychologist, mentioned that they missed this source of support and hoped to have such a forum resurrected. At that time, people with CRPS who were being treated at the RNHRD were able to join an independently run peer-support group for people with CRPS (crps@themin), which was a static resource providing information and downloadable text resources but with no capacity for online interaction.
Collaborative writing
To date, all research in this area has been conducted retrospectively on pre-established message boards. None have created a board from scratch and/or charted the development of support over time. Furthermore, the bulk of online support has been restricted to ‘traditional’ online systems (such as online forums) and not made use of more recent web technologies designed to encourage collaborative writing and the sharing of feelings, experiences and information. Blogging technologies have moved online self-expression and commentary forward, with the creation of sets of personal web pages that encourage a reaction from an invisible audience. Wikis are more community-centred technologies that were invented about 10 years ago. They originated to support collaborative document production and are, in essence, web pages with an edit button. However, some have been extended to incorporate personal blogs and, critically for this proposal, discussion spaces. MediaWiki is the most well known example, as it is the platform on which Wikipedia runs and has been designed to encourage people to get involved and has the effect of surfacing community roles and behavioural norms. 35 The productions of community members include not only the equivalent of an expository web page but also the discussion behind it. The discussion is quite unlike other online forums because it is editable, or ‘mutable’, in the same way as the web page. 36
Summary
In summary, our own and others’ previous research has shown that participating in online forums can be beneficial in terms of online support. While we expected these processes to develop naturally in the online support forum, this project aimed to develop support further by asking members to participate in a structured collaborative writing activity intended to help them construct a positive collective identity.
Chapter 2 Aims and objectives
This project had two objectives:
-
To set up a peer-support online forum in order to identify the nature of support provided and to explore its development over time.
-
To facilitate the development of social processes implicated in psychological support by applying a technological innovation known as a wiki.
This was intended to facilitate the exploration of the following questions:
-
What constitutes support in newly developed online interactions?
-
How does the process of giving and receiving support online evolve?
-
Can the combination of an online forum and a collaborative writing task increase support as well as a sense of psychological and physical well-being relative to an online forum alone?
Chapter 3 Methods
Design
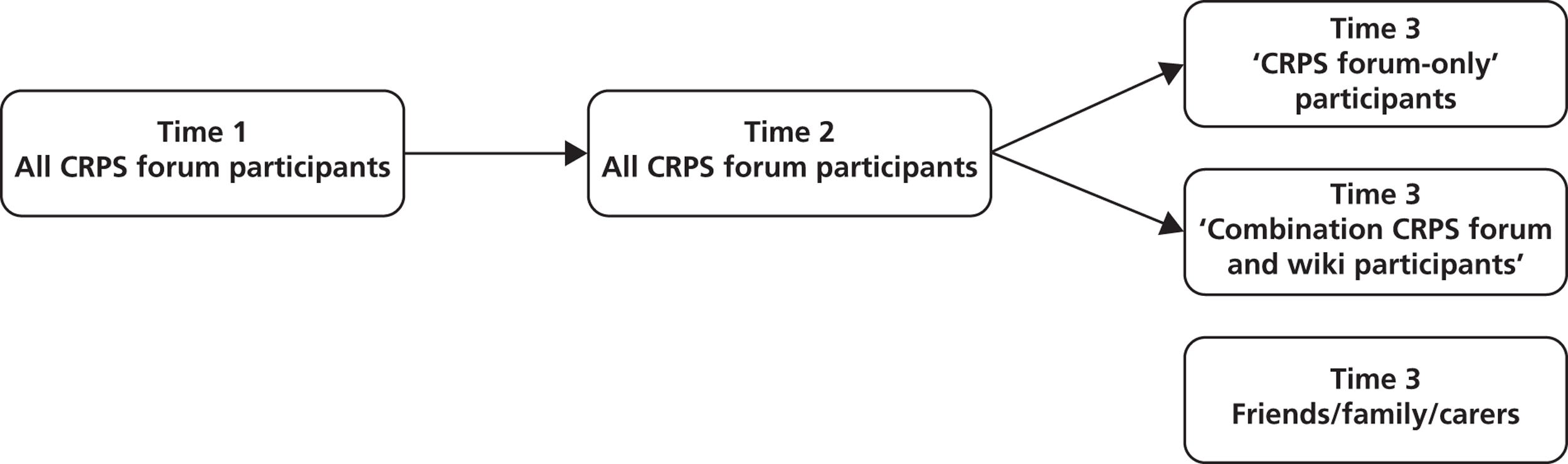
We adopted a three-phase mixed-methods approach to this study (Figure 1). In phase, 1 an online forum for people with CRPS was developed and all members of crps@themin were invited to join, subject to agreeing to the moderation policy we developed in anticipation of this work (see Appendix 1). Phase 2 commenced after 3 months, when we introduced a collaborative writing task designed to run alongside the forum. In this task, forum members were invited to coconstruct a web page presenting CRPS in a way that they felt addressed the misconceptions around the condition. This was to be modelled on the Wikipedia page (http://en.wikipedia.org/wiki/Complex_regional_pain_syndrome) for the same condition, which had been written by experts and so lacked the voice of the person with CRPS. The intention behind the task, therefore, was to address this gap and ensure that the point of view of people with CRPS themselves was represented. In phase 3, the completed information resource was made available to forum members, their friends, family and carers.
FIGURE 1.
Three-phase approach.
Steering committee
All phases of this study were guided by a steering committee, which met at the beginning of the project and then 1 month prior to the beginning of each new element of the study. In addition to the named researchers, the steering committee included an expert patient, a research nurse with CRPS experience and a learning technology officer. The members of the steering committee saw drafts of the individual papers and presentations that comprise this report.
Sampling and recruitment
Initially, participants for phases 1 and 2 were drawn from a convenience sample consisting of members of crps@themin. Crps@themin was an independent support group formed by and for those who have been diagnosed as having CRPS and who have completed, or are currently undergoing, the rehabilitation programme run by the RNHRD. It changed its name to CRPS-UK and was subsequently suspended for much of our research study because the volunteers running the site were struggling to manage their commitments in addition to coping with their own CRPS. CRPS-UK has recently been relaunched (12 October 2013) in a limited capacity as a static website with the intention of introducing a Facebook site. Each year, the RNHRD sees approximately 80–100 new CRPS patients, all of whom are informed of the existence of the patient-run support group. This support group’s website functioned as a static online information resource, rather than an interactive forum. The commencement of the project was announced via a flyer (see Appendix 2) which was sent to all members of crps@themin inviting them to participate. Those who responded were sent an e-mail explaining the study and providing a link to the forum (see Appendix 3). Recruitment dropped off after the first month, and a further notice was posted on the CRPS-UK website (a more interactive off-shoot of the now-defunct crps@themin), and recruitment activities broadened to target a CRPS Facebook group and a Twitter (www.twitter.com) feed used by CRPS UK members. In phase 3, it was intended that participants would recruit family and friends to give feedback on the information resource. It is difficult to ascertain how many potential participants have seen our invitation because we targeted members of CRPS@themin and used a snowballing technique that included Facebook and Twitter.
All forum posts were collected for analysis; that is, they were copied from the forum into a Microsoft Word document (Microsoft Corporation, Redmond, WA, USA) in preparation for analysis. This method of data capture is one which has been used in a variety of other online contexts. 18
Addressing the research questions
In summary, the research was designed to answer the following three questions.
Research question 1: what constitutes support in newly developed online interactions?
First, a thematic analysis was conducted on all ‘introductory posts’ (i.e. the first post by each active forum member) in the first 5 months of the forum’s operation. The aim was to explore the role of first posts in the development of a supportive community, in terms of both forum content and tone.
Research question 2: how does the process of giving and receiving support online evolve?
Second, a content analysis was conducted on all forum posts in the main body of the forum posted during the first 9 months of the forum’s operation. This allowed us to explore whether or not elements of support were present and whether or not they changed over time. This analysis used the Social Support Behavior Code (SSBC),22,27,37 which codes for five categories of social support (informational, emotional, esteem, network and tangible).
Research question 3: can the combination of an online forum and a collaborative writing task increase support as well as a sense of psychological and physical well-being relative to an online forum alone?
Data were collected at three points. Baseline data were collected at time 1 from new members as they registered for the forum. Time 2 data were sought from forum participants after 3 months of forum activity and time 3 data 3 months later.
The survey (see Appendix 4) was designed to measure their experience of CRPS and of the support available. It consisted of initial background questions on the use of the internet, experience in other off- and online support groups, and a number of other self-report questionnaires on psychosocial well-being and support. 38–45
Data were entered into a SPSS database (version 20; IBM Corporation, Armonk, NY, USA) and analysed using descriptive statistics – the aim was to identify any trends over time, rather than searching for statistical significance. It became apparent that sampling issues prevented us from addressing fully the longitudinal aspects of forum use. Specifically, it proved difficult, in spite of considerable efforts on the part of the investigators, to keep the response levels sufficiently high across all three data collection points to permit reliable longitudinal comparisons, or to compare those who participated in the forum only with those who participated in the forum and contributed to the collaborative writing task. Our subsequent qualitative analyses, therefore, included longitudinal changes in support where relevant, for example by focusing on first posts and their impact on the long-term development of the forum, and noting changes to the types of support requested and provided over time.
Evaluating the trustworthiness of qualitative analysis
The process by which the quality of qualitative research can be assessed has been widely debated and it has been acknowledged as typically less straightforward than that employed for quantitative work. 46 The relevance of traditionally positivist terms such as ‘reliability’ and ‘validity’ has been questioned, and the term ‘trustworthiness’ has been suggested as being more appropriate. 46 With this in mind, Yardley47 and Rolfe48 both emphasise the importance of the following principles when conducting high-quality qualitative work: sensitivity to context; commitment and rigour; transparency and coherence; and impact and importance.
Similarly, Mason49 suggests that researchers should demonstrate the trustworthiness of their work by showing that:
Data generation and analysis have not only been appropriate to the research questions, but also thorough, careful, honest and accurate (as distinct from true or correct – terms which many qualitative researchers would, of course, wish to reject). At the very least this means that you must satisfy yourself and others that you have not invented or misrepresented your data, or been careless and slipshod in your recording and analysis of data.
p. 188
Phase 1: the forum
The members
The forum was launched at the CRPS-UK patient-led conference at the RNHRD, Bath (2012). As recruitment dropped off after the first 2 months, a further notice was posted on the CRPS UK website, and recruitment activities were broadened to target a CRPS Facebook group and a Twitter feed used by CRPS UK members. As a result, the number of members increased substantially. After running for 6 months, there were 62 forum members, 29 threads and 217 topics on the forum. This exceeded our target of 50 members (Table 1).
| Month | Members, n | Threads, n | Posts, n |
|---|---|---|---|
| 0 | 15 | NA | NA |
| 1 | 22 | 18 | 107 |
| 2 | 26 | 19 | 116 |
| 3 | 46 | 23 | 172 |
| 4 | 49 | 24 | 187 |
| 5 | 60 | 29 | 217 |
| 6 | 62 | 29 | 217 |
On the advice of the steering committee and forum users, a Facebook community was created and forum participants were invited to ‘like’ the page. Each fortnight, one of the researchers posted a message on the Facebook page reminding members of the forum. This extra facility was requested by users as a way of linking the page to their more routine social networking activities.
The anonymous nature of the internet meant that demographic information about participants was limited. It was possible to obtain some information about the 26 members by examining the self-disclosed content of postings. Sex was available for all participants, comprising seven males (26.9%) and 19 females (73.1%). Age was available for nine participants, ranging from 20 to 54 years with a mean age of 35.6 years. Number of years since diagnosis was available for 14 participants, ranging from 5 months to 10 years with a mean duration of 3.9 years. However, the difficulties involved in diagnosing CRPS meant that some participants were diagnosed immediately while others reported suffering from symptoms for up to 12 years prior to diagnosis. All participants lived in the UK, with the exception of one former UK resident now living in New Zealand. It was important to the study that participants were UK-based as the implications of our findings are targeted towards the NHS, and the UK context more broadly. We therefore targeted UK-based groups and social media.
The forum
The CRPS web forum used in this study was a closed, password-protected online community with no external access. Individuals had to agree to the rules of the forum (see Appendix 5) to join the project and to register with a username and password before they could access the forum and view messages posted by other individuals. All members were informed during the registration procedure that the forum was part of a research project and they gave full informed consent to their forum postings being used anonymously for research purposes. The welcome page reminded members of the forum etiquette, the fact that it was a research project and that the space was theirs to make of what they would (see Appendices 6 and 7).
The forum was divided into four distinct message boards under the broad heading ‘a place to discuss all things CRPS in the UK’. When the forum was launched, there were three boards: ‘welcome’, ‘your thoughts and experiences’, and ‘is the forum working for you?’. A fourth board (‘raise awareness of CRPS’) was added after 6 months to launch the collaborative writing task. The boards ‘raise awareness of CRPS’ and ‘is the forum working for you?’ contained a small number of threads and messages, with discussions that were primarily initiated by two of the researchers and our technical support officer. The other two boards, ‘welcome’ and ‘your thoughts and experiences’, contained a larger number of threads and messages, and discussions were primarily initiated by members who were CRPS patients. The four boards were created, named and described by the researchers in consultation with the steering committee. The forum administrators (i.e. the researchers) posted the first message on each board by way of introduction and to encourage members to begin posting. After this initial post, the researchers did not contribute any further posts to the three original boards. All threads and topics were initiated by the members themselves, and the forum was allowed to develop organically. Table 2 shows the board names and the initial posts describing them to forum members.
| Name | First post |
|---|---|
| Welcome | If you are new here (just registered with the forum), please tell us something about yourself in this section. Write as much or as little as you like, maybe how you discovered CRPS and how you are living with it |
| Your thoughts and experiences | Here is a space for you to discover the thoughts and experiences of other people living with chronic regional pain syndrome |
| Is the forum working for you? | Here’s where you have the opportunity to share your thoughts about the forum with the research team and the other members of the site. What’s working for you? What isn’t working? Or is there anything else you’d like to tell us? |
| Raise awareness of CRPS | People with CRPS said they wanted somewhere they could tell others what it was like to live with CRPS. Based on your ideas we have started an information resource. Each thread is targeted at different audiences and we need your help to fill in the details |
The analyses of support (see Chapters 4 and 5) are based on messages posted in the ‘your thoughts and experiences’ and ‘welcome’ boards, as these boards are where the majority of member interactions occurred and they represent the thoughts, feelings and experiences of online forum members with CRPS, rather than being led by the researchers. The collaborative writing task was based in part on messages posted on the ‘raise awareness of CRPS’ board. The number of messages posted per month on each of the two member-led boards is shown in Table 3. The majority of forum activity occurred within the first 6 months after launch, with 215 out of 232 messages (92.7%) being posted during this period. Only 17 messages (7.3%) were posted during the second 6 months from December 2012 to May 2013.
| Month and year | ‘Welcome’ board, n | ‘Your thoughts and experiences’ board, n | Total, N |
|---|---|---|---|
| March 2012 | 1 | 0 | 1 |
| June 2012 | 16 | 68 | 84 |
| July 2012 | 6 | 18 | 24 |
| August 2012 | 3 | 1 | 4 |
| September 2012 | 12 | 16 | 28 |
| October 2012 | 26 | 25 | 51 |
| November 2012 | 7 | 16 | 23 |
| December 2012 | 5 | 1 | 6 |
| January 2013 | 0 | 6 | 6 |
| February 2013 | 0 | 1 | 1 |
| March 2013 | 0 | 1 | 1 |
| April 2013 | 0 | 1 | 1 |
| May 2013 | 0 | 2 | 2 |
| Total | 76 | 156 | 232 |
Figure 2 shows a screenshot of one of the boards and Figure 3 shows a screenshot of two example posts.
FIGURE 2.
Screenshot of the ‘your thoughts and experiences’ board.
FIGURE 3.
Screenshot of two example posts.
Phases 2 and 3: patient-generated information resource
In the second phase of the study, we planned to invite a subset of participants to create a wiki-like page explaining CRPS to friends, family and carers, the medical community and the wider public. However, phase 2 of the study was delayed due to two unexpected influxes of participants. As discussed above, recruitment to the forum slowed after the first month. In response, a further notice was posted on the CRPS UK website, and recruitment activities broadened to target a CRPS Facebook group and a Twitter feed used by CRPS UK members. As a result, the number of members increased substantially (see Table 1). Therefore, the launch of time 2 data collection and the collaborative writing task was delayed by 6 weeks in order to allow new members to settle into the site before adding the shared writing activity. During this 6-week period, however, there was a second influx of new members, with numbers increasing from 62 to 111. This coincided with the temporary suspension of a large online CRPS support community, CRPS UK, due to the resignation of the site co-ordinator. Monitoring of the posts indicated that this second increase in members did not result in an increase in activity on the forum. Our technical officer (TO) then discovered that only one of the second set of new members was a real person and that the forum had been hacked. A person or persons cracked our Captcha (a type of challenge-response test used in computing to ensure that the response is not generated by a computer) and created their own user accounts. Owing to the fact that all of our forum pages were protected, the hackers were unable to edit or create any linked pages or post on the forum. Our TO removed the suspect members and further secured the site. The clean-up of the site, and increased security, led to another delay of 1 month. During the clean-up process, the forum was closed for approximately 6 days.
Once we launched the writing task, although members were supportive and excited about the end product, they were reluctant to be the first to post their thoughts about the proposed content. We discuss in Chapter 6 how we overcame this obstacle.
Ethical considerations
The CRPS support group around which this study was based is independent of the NHS, and therefore the study did not require NHS ethics approval. The project needed approval from the University of Bath Psychology Ethics committee only. The chairperson of Central Bristol Research Ethics Committee (REC) has confirmed that the project does not require review by a NHS REC. Fully informed consent was sought from all participants at every stage of this study. As this was in part an observational study of user engagement, users were informed that we would be analysing their discussions.
Consent was sought from all participants prior to taking part. They were informed that they could withdraw at any time, but that their data up until the point of withdrawal would be kept and analysed by the researchers. We anticipated this would be done online, but were prepared that, should this not be feasible, a paper consent form would be sent out via the site moderator.
Moderation, anonymity and confidentiality of online wiki and forum participants
Use of the site was subject to the same terms and conditions that are in force for the online resources provided by NHS Choices. These terms and conditions are intended to safeguard members from inadvertently exposing themselves to the risk of criminality, such as identity theft. They further protect those who run the site from prosecution in the case of the illegality of actions its users might carry out by clearly debarring any form of activity that might be in breach of criminal or civil law. We additionally made clear that the content created by users should not be read or used as any form of officially sanctioned health advice.
Contributions to the community site were moderated by broadly the same set of rules that govern contributions to the NHS Choices communities. Moderation was undertaken by members of the research team on a rotating basis. In joining the wiki and/or the forum, participants agreed to abide by the terms and conditions that we outlined in our protocol and, as such, we did not envisage moderating being an onerous task. All team members were trained to undertake these editing actions by the technical support person. It was intended that future moderation would be undertaken by members of the (now-defunct) crps@themin. We planned to train them to moderate, and to be confident that they could train others to do so. This would ensure that they would have the skills to moderate the forum themselves, and to create accounts for new members.
We did not intend to remove any contributions on the grounds that they promoted a particular health perspective. However, we planned to remove contributions, and retain the option to bar the relevant contributor, if there was clear evidence that the contribution was offensive. This was not a situation that arose.
Users were free to use their own names; however, they were required to maintain the anonymity of any friends, family or health-care professionals who they discussed. If members failed to do this, the relevant identities would have been edited out of the online text and the member reminded of their obligation to respect third parties. The general recommendation that was clearly visible on the site was that any medical queries should be directed to the participants’ own general practitioner (GP).
Anonymity and confidentiality of focus group participants
As friends/family were to be recruited via the person they support, they would have had knowledge of each other’s participation in the study. This was made explicit in the recruitment materials and on the consent sheet.
Chapter 4 Developing a supportive online community
Introduction
As outlined in Chapter 1, the means by which a supportive environment develops is likely to rely upon the development of a shared group identity. This is particularly relevant for those with CRPS because loss of identity is one of the issues that motivate people to seek support. Schwämmlein and Wodziecki50 recently highlighted the role that initial self-presentation plays in establishing a shared group identity online. Self-presentation generally is recognised as playing an important role in the development of online communities, enabling initiation of interactions, development of relationships and access to information. While research tends to focus on issues of privacy and anonymity in self-presentation,51 the importance of ‘initial self-presentation’ in online communities has recently been highlighted. Schwämmlein and Wodziecki50 demonstrated that the nature of the information provided in member profiles reflects the type of community and personal goals of group members. In particular, these initial forms of self-presentation distinguish between common-bond and common-identity communities.
Common-bond communities are defined by interpersonal relations among the members, who are encouraged to connect with each other. In contrast, common-identity communities are defined by a common topic or interest and support their members in performing a common task or working towards a common goal. While the former community is based on interpersonal attraction, the latter is based on social identification. The current study extends the work of Schwämmlein and Wodziecki50 by examining another form of initial self-presentation: first posts by members of a newly formed online support forum for people with CRPS.
In this chapter, we report on phase 1 of the study. This was the phase where the online forum was developed and people with CRPS invited to join. We monitored their interactions for 5 months. We encouraged members to make the forum their own. This enabled us to monitor the type of community that was evolving. Introductory (first) posts from phase 1 were cut and pasted from the forum into a Microsoft Word document. The posts were then thematically analysed according to the principles detailed by Braun and Clark. 52 Thematic analysis allows common themes and salient issues to be identified across a data set; the technique was, thus, considered particularly appropriate to the aims of the present study. We also report on the qualitative responses to the surveys completed at time 1 and time 2. Briefly, the process of analysis was as follows:
-
Familiarising self with the data: reading and rereading the posts, highlighting ideas for coding/themes.
-
Generating initial codes: organising the data into meaningful groups. The data set was worked through systematically and attention paid specifically to data items that might form the basis of repeated patterns (themes) across the data set.
-
Searching for themes: sorting the different codes into potential themes and collating all of the relevant coded extracts within the identified themes. Relationships between codes, between themes and between different levels of themes were identified.
-
Reviewing themes: ensuring that data within themes cohered together meaningfully and that the distinctions between themes were clear.
-
Defining and naming themes: identifying the ‘essence’ of what each theme was about and determining clearly what aspect of the data each theme captured.
The posts were initially coded by a member of the research team (KR), but in order to reduce researcher bias and optimise the trustworthiness of the analysis, a sample was independently coded by two other members of the team (JG and the research assistant). Coding initially involved attaching descriptive labels to discrete instances in the posts (e.g. ‘Took about 3 or so years to diagnose’ was labelled ‘diagnosis’). As coding progressed, more analytical categories were identified which served to integrate the aforementioned descriptive categories [e.g. the participants’ references to their diagnosis experience(s) were encapsulated by the category ‘journey to diagnosis’]. The three researchers then reviewed their analyses and agreed on themes. No substantial differences were found during the comparison. The final themes were chosen on the basis of the salience of the theme in the posts, rather than on the basis of prevalence of the theme alone. In line with the recommendations made by Braun and Clarke,52 it was considered good practice to make transparent the theoretical framework in which the analysis was conducted at the onset of the work. Unlike many qualitative analysis techniques, thematic analysis is not tied to a particular theoretical position and can thus be used within numerous theoretical frameworks, all of which bring with them different assumptions about the nature of data and what they represent in terms of ‘reality’. The present analysis was conducted in an essentialist/realist framework, which aims to report on the experience, meanings and reality of participants. Themes were, therefore, identified at the semantic level, i.e. within the explicit or surface meaning of the data.
Results
Twenty-three first posts were made in phase 1. Four posts were analysed separately because they contained no introductory information or preamble; instead, they sought advice, offered information, or sought sponsorship or volunteers. Following a thematic analysis of the remaining 19 posts, five themes were identified.
A standard format was quickly established by users as a means of introducing themselves: real name, age and ‘journey to diagnosis’. Indeed, ‘journey to diagnosis’ was a key theme, involving onset of symptoms, the quest for medical explanations, misdiagnoses, misunderstandings and multiple attempts at treatment, all of which contributed to a sense of frustration and exhaustion. The presentation of this journey served to legitimise their right both to membership and to speak on the site. Four other key themes comprised ‘treatment’, where they shared their experiences of different medications, and physical and psychological therapies; ‘contact with health professionals’, where they detailed both positive and negative experiences of interactions with the health-care community; ‘looking for the positives’, where they explicitly reframed their experiences in order to find the positives, and, in doing so, to shape the tone of the forum; and ‘hobbies’, which detailed both loss in terms of activities they could no longer perform and gain in terms of finding a means of engaging in these activities, albeit in modified form. All extracts from the first posts are presented verbatim, and therefore the original typographical and spelling errors are retained.
Journey to diagnosis
The theme ‘journey to diagnosis’ involved describing the onset of symptoms, the quest for medical explanations, misdiagnoses, misunderstandings and multiple attempts at treatment, all of which contributed to a sense of frustration and exhaustion. The presentation of this journey served both to legitimise their right to membership and to speak on the site. Fourteen participants referred to their diagnosis journey in their first posts.
There was a sense that participants were disappointed with, but reluctantly accepting of, the length of time it took to get diagnosed. This is a typical experience of those with CRPS because CRPS is diagnosed when all other explanations have been excluded. 53 This takes time and causes huge amounts of uncertainty for those undergoing the tests.
[I] got diagnosed in April this year [. . .] after an ankle injury 5 yr’s ago which kept recurring
Forum member 8
I’ve had CRPS in my right foot for must be about 7 years now if not longer. Took about 3 or so years to diagnose as I’m one of the odd ones that didn’t have surgery or any obvious injury to cause my CRPS.
Forum member 1
The lack of an explanation for their painful symptoms causes those affected to doubt themselves, not least because many report being told that it is possible that the pain is ‘all in their head’, in other words health-care professionals suggest that the symptoms might be psychosomatic in nature. There was a sense of relief when participants finally got their diagnosis and so had confirmation that CRPS was, in fact, not psychosomatic.
I was diagnosed with CRPS/RSD [reflex sympathetic dystrophy] in January after years of misdiagnosis and been fobbed off that it was psychosomatic (which is on my medical notes from a few years ago [. . .] finding out what it finally was was a relief in so far as it finally had a name and wasn’t all in my mind
Forum member 3
The experience of not being believed was very destructive, but the chance to share their ‘journey’ enabled those posting to see that others had had similar experiences and that they were, therefore, not alone. This recognition of similarity helped confirm that CRPS was ‘real’ and that they were ‘not mad’. They were able to find an instant means of bonding with one another through sharing their joint experiences of adversity.
Treatment
Participants shared their experiences of different medications, and physical and psychological therapies. Fourteen referred to treatment in their first post. Sharing this factual information as part of their introductory post allowed participants to demonstrate the legitimacy of their diagnosis and enabled them to share their frustration at how much medication they had been prescribed and how little it helped.
I am on 800 mg × 3 neurontin and 50 mg amitriptyline plus all the rest, I am currently 5 weeks through a pain management programme with 3 more sessions to attend. I am having real problems with my scs [spinal cord stimulator]. This is my second scs as I burned out the first in 5 months (it was supposed to last 5 years)
Forum member 17
The list of illness I suffer is rediculas [sic] and the list of medication even longer.
Forum member 5
Discussions of treatment typically included complex medical terminology, reference to specific pharmaceuticals, and dosages. It was taken for granted that other members would share an understanding of such terms, and ‘insider knowledge’. There was a sense of disappointment that the health-care system was unable to cure them or to take away their pain and in fact many of the treatments tried had to be discontinued for various reasons.
[I] have been on all the normal meds at various dosages, I’ve also tried Capsicum cream, have done 5 physio sessions and 3 acupuncture sessions. Physio was stopped because there was no improvement and acupuncture got stop because 90% of the needles put in hurt me and I had such a ‘strong’ reaction during & after each session
Forum member 8
Some of those posting decided to stop their medication on the basis that they were in pain whether or not they were on the medication. Therefore, it was better to be off the medication, still in pain but free of side effects.
Currently don’t receive any treatment or medication for it, I gave up trying the painkillers after them just causing side effects with no positive effects but have tried a few in the past and had physio for a while
Forum member 1
Contact with health-care professionals
This theme was expressed in one of two polarised ways: negative versus positive experiences. Ten referred to health-care professionals in their first post. Disappointment at the lack of knowledge and understanding of CRPS evidenced by the health-care profession was expressed. In particular, participants reported not being believed, being ‘manhandled’ and receiving conflicting advice:
I was referred to the [clinic] pain consultant, who I refuse to go back and see him after him summarising the consultation with ‘I’ve seen more people in more pain, you have to get over it. Physio will work & you need an x-ray.’ I still haven’t had the x-ray.
Forum member 8
I had to wait 3 months for an appointment. Meanwhile during the 3 months my physio was handling my foot in a rough way and the pain, ohh I still remember how excruciating the pain was.
Forum member 4
However, the posts were not overwhelmingly negative; there were balancing posts from those who expressed the relief they had felt on finding a health-care professional who listened to them, believed them and reassured them about their symptoms. As a consequence, these participants had their doubts and fears smoothed away. Mostly, these positive experiences were framed in terms of ‘good luck’: it was lucky that the physiotherapist noticed the symptoms, it was lucky a health-care professional had recognised the symptoms of CRPS, and it was lucky to be referred to a health-care professional who knew something about CRPS.
I was fortunate that my physio noticed the symptoms and told me to inform the consultant at the fracture clinic
Forum member 4
I was lucky to be diagnosed relatively early – after 6 months – thanks to my hydrotherapist at the [hospital]
Forum member 6
Looking for the positive
‘Looking for the positive’ was evidenced by participants explicitly reframing their experiences in a positive way. This does not mean that participants did not mention negative experiences; rather, after they had done so, they were careful to add a positive spin to their post. The aim was to give a realistic account of their experiences, without being too depressing. One effect of this approach was to develop a positive tone to the forum. Ten focused on the positive in their first post. In the first quote below, forum member 5 engaged in downwards comparison and found solace in the fact that although CRPS was very difficult to live with, it was not a life-threatening condition, and so she was able to see her children grow, an option not available to those with a terminal illness. Forum member 9 referred to suicidal ideation and how he actively made an effort to find the positive. In doing so, he found a means of directing his energy and attention outwards and created a new role for himself. Those who focused on the positive tended to turn their thinking around and to focus their attention outwards:
[A]s bad as it gets I thank god I’m here because it could have been so different I may not have been alive to see my gorgeous children grow up go to uni and get joe jobs have good partners and have good lives so in some respects think myself lucky
Forum member 5
I hit rock bottom and considered suicide, but then decided I’d got a fantastic wife, kids and friends and instead I am going to work towards seeing up a charity with the aim of educating medical professionals about CRPS and how the sufferers should be treated and raise funds for research in the hope that a cure can be found
Forum member 9
Forum member 18 wrote about the battle he experienced as he tried to come to terms with the limitations and difficulty of living with CRPS. He did not shy away from the fact that CRPS is a ‘horrid’ condition, but also wrote about the process of reaching acceptance, and in so doing, found more healthy ways to cope with and manage living with CRPS:
However, despite all this, I find that now 10 years down the line I have accepted that I have this horrid condition and that my life will no longer be the same so have stopped looking at life from the aspect of things I cannot do and now look at what I can do as an achievement. I have stopped chasing new appointments with doctors looking for a cure as there won’t be one. I have accepted that I am in pain every day and it is about managing the pain and not letting the pain manage you. With this new outlook I am now happy again and no longer think that life is useless
Forum member 18
Others took a confrontational stance towards CRPS and made the decision not to bow to the limitations that CRPS brings. One means of doing this was to adjust one’s expectations about what is and is not possible. Adapting goals, as in the example below, allowed participants to maintain normality:
I’m not going to allow THIS to take away any more of my life. I now have goals, sensible goals
Forum member 2
Finally, throughout the posts, participants demonstrated their sense of humour and made it clear that this was an important coping strategy. In spite of the difficulties they were facing, keeping a sense of humour enabled them to keep a sense of themselves:
I have kept my good sense of humour and always try to keep positive; I am still me – just with a painful dysfunctional arm!
Forum member 6
Hobbies
Participants detailed loss in terms of activities they could no longer perform, but also wrote about finding a means of engaging in their chosen activities albeit in modified form, or indeed of finding new hobbies. Ten mentioned hobbies in their first post.
I’m getting involved in wheelchair basketball and wheelchair fencing
Forum member 10
Mention of an outside interest served to demonstrate that they were more than just ‘CRPS’. CRPS is not life-threatening, but it is life-changing. This can bring a difficult period of adjustment, with a tendency to focus on the elements of one’s life which have been lost. Finding a hobby is more than finding something to do; it is about finding out what you can do given your limitations, and finding you are able to do something can boost confidence hugely. There was recognition in these first posts that similarities between members were being identified. In the post below, this is exemplified by the phrase ‘like all of you’. This participant positioned herself as similar to others on the message board. She had been able to read their posts and recognise elements of her own experience in them.
Like all of you, it has totally changed my life which I have to admit I struggled with enormously up until May when I found tandem cycling
Forum member 16
Some of those posting had found new hobbies because it was no longer possible to engage in their pre-CRPS activities, or they had adjusted the way in which they engaged with their original activities. One participant, who could no longer play rugby, was actively looking to try other sports that would enable him to keep his upper body in condition. Another had adapted the way in which she rode her horse so that she could continue to engage in a pastime she was passionate about:
My surgeon 5 years ago said ‘I will get you back on the rugby field’ – no chance of that now! Looking in to trying new sports – kayaking – use my upper body – but I would love to try wheelchair basketball.
Forum member 19
I used to be a really good horse rider and I have my own horses. I was never going to give up riding, so I have learnt to ride side saddle on 1 of my horses. This has now opened many doors for me and I am trying to work towards the Para Olympics in 4 years time.
Forum member 12
Another reason to seek a new hobby was to aid the physical rehabilitation. Taking up a new interest which requires particular movements means that the individual will have to practise these movements in order to be able to engage with the hobby. This can act as a powerful motivator to continue with physiotherapy exercises, something which is hard to do when working on your own without a physiotherapist giving instructions and, in a sense, making the individual do the exercises. Completing the exercises in the course of an activity can be more meaningful. This is best exemplified in the quote below from a participant who had taken up art. She was increasing dexterity and movement through engaging with her hobby. This became positively reinforcing and increased the likelihood of this person continuing to engage with the exercises:
Now after 10 years I am trying to get my life back and have taken up a new hobbie, I am trying out art even though I cannot use my right hand and am right handed. It is getting more controlled movement in my non-dominant hand and has been the best thing I have done.
Forum member 18
Qualitative data: time 1 and time 2
Surveys were administered at time 1 and time 2. Because so few participants completed the surveys (n = 15 at time 1 and n = 4 at time 2), we report here on the qualitative data that were collected in response to the final question, which invited participants to share anything else they thought we should know in order to better understand how the participants coped with CRPS. Thematic analysis of the responses identified four master themes: ‘symptoms of CRPS’, ‘understanding CRPS’, ‘support’ and ‘impact of CRPS’.
Symptoms of complex regional pain syndrome
This theme encapsulates responses that were focused around the participant’s symptoms of CRPS and how they alleviated the symptoms. Within this theme, they mentioned aspects such as seeking out warmth, rest and keeping movement in the affected limb.
This isn’t always easy, due to tiredness or lack of concentration. I make endless lists, of jobs that need doing.
Female 3
I’ve kept going, started using the affected limb normally again once I was diagnosed and discovered that by not doing so would cause it to worsen
Female
Each participant tended to focus on one symptom of CRPS in particular and the issues this caused them in their everyday lives. This was followed with how they dealt with that key symptom. The participants who talked about additional symptoms tended to mention either common ones, for example tiredness because of the pain, or unexpected ones such as memory loss.
Understanding complex regional pain syndrome
Particular reference was made to symptoms often being misunderstood or forgotten by others. Participants talked about how little other people knew about CRPS. The gaps in knowledge were identified predominantly within research, government agencies and family members.
I lost my marriage of 26yrs due to lack of understanding or tolerance by my ex-husband
Female 5
For some of the participants, the lack of understanding about CRPS had implications for their personal life, such as losing partners or having struggles with family and friends. The lack of awareness or understanding of CRPS meant that the participants reported significant others becoming distant or unable to maintain relationships.
The lack of awareness was also described as being displayed by the medical profession:
The treatment I have received from many GP’s and Hospital staff has either been excellent (they want to learn about the condition) or atrocious my CRPS hasn’t even been mentioned at handover and didn’t want to know about it.
Male 2
Participants either reported that their care went above expectation and CRPS was taken very seriously, or reported that those who were treating them were uninformed or unwilling to consider CRPS as an option.
Support
Many participants felt that they were insufficiently supported, and often reported feeling isolated.
My CRPS has ruined my life, everything is centred around it, taking tablets etc, how tired I am, how frightened I am. do not want to go out where there are large crowds. Ruined my homelife, not just for me but for all my family, and to realise that it’s upsetting the whole house is so upsetting. Amputate, take it away remove it. . .. . .. give me back my old life.
Female 2
For many participants, CRPS appeared to decrease the social life that they had once had. This was the strongest theme talked about by the participants; it appeared that the pain or symptoms were almost manageable, yet by managing the symptoms their social network deteriorated.
Possibly as a consequence of this, many participants reported seeking social support in the form of online interaction. This was considered to be a safer alternative to socialising in the real world, where people could be unpredictable. Using the internet in this manner enabled participants to rebuild connections with others.
I have found Twitter invaluable to cope with my CRPS when I have been awake at 3am. I suffer greatly from pain related insomnia. There is always someone around the world who will be awake with you to chat and generally distract you from the pain.
Female 8
Impact of complex regional pain syndrome
The final master theme, ‘impact of CRPS’, focuses on how participants dealt with CRPS after diagnosis. Participants talked about how they had tried to cope with the impact of CRPS.
I’ve carried on with life and am trying my hardest to do what I want to do and not let CRPS stop me, even if I’m in agony at the end of the day; at least I have something to show for the pain
Female 6
They tended to separate themselves from their diagnosis and talked about CRPS as something that was actively fighting against them. They framed achievements in terms of battling through the barriers that they faced as a result of CRPS, rather than as decreasing the symptoms.
My pain does not change, only my tolerance does.
Female 7
Summary
The main focus of participants’ free comments was their social network. Many reported losses in this area, predominantly through the loss of friends and everyday socialising; a few participants commented that their families had also suffered, with some reporting marriage collapse as a result of CRPS. Although some participants found new avenues for socialising via the internet, it was clear that this did not replace what they had lost prior to diagnosis. What the comments highlighted was the widespread impact that CRPS had; it affected not only the participant’s jobs or careers, but also those of the people who the participants relied upon for support.
Discussion
In this chapter, we have presented our preliminary analyses exploring the process by which a supportive community developed. Specifically, we explored the role of first posts in the development of a supportive online community and presented the thematic analysis of the free-text sections of the surveys conducted. In doing so, we have identified what participants considered both relevant and appropriate to share when joining the forum, and in this way have begun to address the question of how a supportive online community develops.
On joining, members took the opportunity to establish a ‘common-identity’ community. 50 This was established via three types of information-sharing evidenced in members’ initial self-presentations: ‘journey to diagnosis’, ‘treatment’ and ‘contact with health-care professionals’ were a means of demonstrating to other members the posters’ right to membership of the forum. These three types of information established a common experience of the route to diagnosis, the types of treatment and the kinds of interactions with health-care professionals that they had experienced. Together, these three themes might serve to create a developing sense of social identification and enhance the chance of being accepted by the community. 54 This, in turn, could foster commitment and attraction among the group,55 and, through the development of group identification, foster support and engagement with the group. 56
The remaining two types of information (‘looking for the positive’ and ‘hobbies’) were a means of establishing the tone of the forum. Although it was acceptable to write about negative experiences in a first post, and to note the struggles and obstacles that had been placed in one’s way, there was an explicit attempt in the posts (through gentle humour or overt positive framing) to proactively look for the positive in the posters’ (difficult) situation. Consistent with the establishment of a common-bond community, this latter set of themes served to establish interpersonal relations and to encourage members to connect at a more personal level. There was no attempt to hide how difficult it was to live with CRPS, but effort was directed towards ensuring that posts had a positive tone. Hiding the reality of CRPS is something that occurs often in the offline world, with individuals fearful of becoming a burden or of being negatively perceived. 53 The forum provided members with an opportunity to be honest about how they were really feeling; the perceived need for pretence was not evident in their posts. Belonging to a group of people with similar experiences gave permission to ‘tell it how it really is’.
It is important to point out that we have not looked at interactions between those posting. We are mindful of the fact that those who joined the forum soon after its launch and starting posting at that time were likely to have ‘set the tone’ of the forum and so may have influenced the way in which subsequent members structured their own first posts. It is, therefore, not surprising that we found a marked consistency in the style and content of these first posts. The next chapter examines the types of support exhibited between members.
Chapter 5 Results: types of online support found on the forum
Introduction
A content analysis was conducted on all forum posts in the ‘welcome’ and ‘your thoughts and experiences’ boards in order to explore whether or not elements of support were present and whether or not they changed over time.
Data collection
All messages posted on both boards were selected and downloaded for analysis, covering the 12-month period between launching the forum on 1 June 2012 and data collection taking place on 31 May 2013. The data consisted of 79 messages (two threads) from the ‘welcome’ board and 157 messages (20 threads) from the ‘your thoughts and experiences’ board. Duplicate messages were removed, leaving an overall total of 232 messages for analysis. Messages were copied and pasted into a Microsoft Word document, where the messages were converted into plain-text format. This removed tables and other formatting features from the web forum, while retaining textual features such as spacing, punctuation and the use of abbreviations. The majority of forum activity occurred within the first 6 months after launch, with 215 out of 232 messages (92.7%) being posted during this period. Only 17 messages (7.3%) were posted during the second 6 months from December 2012 to May 2013. At this stage, most activity on the forum was occurring in the ‘raise awareness of CRPS’ board (see Chapter 6).
A total of 27 unique usernames were identified in the data set, comprising 26 members together with one administrator who was involved in running the project. The number of messages posted by each participant ranged from 1 to 53, with a median of three. Seven out of 26 participants (26.9%) posted only a single message in the forum. An additional 13 participants (50%) were also low-frequency posters, who all posted fewer than the mean number of messages. The remaining six participants (23.1%) were high-frequency posters, who together wrote 184 out of 232 messages (79.3%) posted to the forum.
The number of threads created by each participant ranged from none to four, with a median of zero threads started by each participant. Fourteen out of 26 participants (53.8%) did not create any new threads of their own. These participants only contributed to discussions that had previously been initiated by other members, responding to existing postings within the forum. Twelve out of 21 threads (57.1%) were created by the six high-frequency posters who also wrote the majority of forum messages. This indicates that this small group were core members of central importance to the forum, as they were responsible for the majority of threads and postings.
Analysis
Content analysis was used to examine the social support content of messages, using deductive (top-down) analysis to code the data into existing social support categories derived from the SSBC. 27,37 The SSBC was originally developed to assess the frequency of face-to-face supportive behaviours between spousal couples. This taxonomy was used to guide the analysis of messages in order to explore the occurrence of support-intended communication behaviours that fall into five main categories: emotional support (communicating love, concern or empathy), information support (providing information or advice), esteem support (communicating respect and confidence in abilities), network support (communicating belonging to a group of persons with similar concerns or experiences) and tangible assistance (providing, or offering to provide, goods or services). Each of these five categories can be divided into a number of subcategories (Table 4) and our analysis looked for instances of 22 subcategories in total. This taxonomy has been successfully adapted and used in the qualitative analysis of messages posted to other health-related online support groups. 19,24 This study uses Coulson and Greenwood’s22 adaptation, as shown in Table 4.
| Support type | Definition |
|---|---|
| Informational support | |
| Advice | Provides ideas or suggestions for action |
| Referral | Refers the recipient to other sources of information or help |
| Situation appraisal | Helps reassess or redefine the situation faced by the recipient |
| Teaching | Offers detailed information, facts or news |
| Emotional support | |
| Relationship | Conveys the importance of closeness |
| Physical affection | Offers physical contact, such as hugs and kisses |
| Confidentiality | Keeps the recipient’s problem in confidence |
| Sympathy | Sorrow or regret for the situation faced by the recipient |
| Understanding/empathy | Expressions of understanding of the situation or discloses similar experience in a way that conveys understanding |
| Encouragement | Provides the recipient with hope and confidence |
| Prayer | Offers prayer for the recipient |
| Esteem support | |
| Compliment | Says positive things about the recipient |
| Validation | Provides agreement with the views of the recipient |
| Relief of blame | Alleviates any feelings of guilt the recipient has about the situation |
| Network support | |
| Access | Provides the recipient with access to new people |
| Presence | Offers to be there |
| Companions | Reminds recipient that there are others who share similar experiences and are available |
| Tangible aid | |
| Loan | Lend money to the recipient |
| Direct task | Offers to do a direct task |
| Indirect task | Offers to take over a task from the recipient while they are stressed |
| Active participation | Offers to join the recipient in an activity |
| Willingness | Offers or expressions of willingness to help |
Using a deductive approach, data were coded in units of whole messages rather than using smaller units such as individual sentences, making it possible to identify the number of forum postings that fell within each social support category. Whole posts were analysed, rather than individual sentences within posts. If two or more categories of social support were present in a message, it was assigned to all relevant categories rather than labelling it with one category only. After each message had been several times to identify and label all instances of social support, the number of labels was counted to identify how many postings fell within each support category.
The content analysis was undertaken by NC together with a PhD student who has extensive experience of online support data coding. Each coder read and reread the data set independently, and using the coding framework (see Table 4), rated each message according to whether or not each of the five main types of social support was present. At this stage of the data analysis, there was agreement for 224 out of 232 (96.5%) of the messages. In the eight messages that were ambiguous, the coders discussed the nature of the ambiguity and this was easily resolved. Therefore, the 232 messages received 100% agreement in terms of the five main categories.
In terms of the social support subtypes, both coders reviewed all 232 messages and coded whether or not each subtype was present for (a) the requests and (b) what was offered. In terms of the analysis of social support requests, reliability was established by calculating Cohen’s kappa and this revealed an excellent level of agreement (κ = 0.92). Similarly, for the analysis of social support provision, inter-rater reliability was very good (κ = 0.87).
Results
Two types of analyses were conducted. The first looked at requests for social support and the second looked at the type of support offered. Requests for social support occurred infrequently on the forum, occurring in only 15.5% of posts. Support was frequently offered, however, occurring in 88.8% of posts.
Social support requests
Support requests were present in 36 out of 232 messages (15.5%). In the ‘welcome’ board, 13 out of 76 messages (17.1%) contained requests for support, while in the ‘your thoughts and experiences’ board, 23 out of 156 messages (14.7%) contained requests for support. The number of requests for each category of social support is shown in Table 5. Note that subcategories that were not mentioned have been removed from the table. As can be seen, the most frequent category was requests for informational support (8.6%), followed by requests for network support (2.6%) and tangible aid (2.6%), with emotional (1.7%) and esteem support (1.3%) being the least frequently requested.
| Support type | ‘Welcome’ board, n (%) | ‘Your thoughts and experiences’ board, n (%) | Overall, N (%) |
|---|---|---|---|
| Informational support | 7 (9.2) | 13 (8.3) | 20 (8.6) |
| Advice | 6 (7.9) | 11 (7.1) | 17 (7.3) |
| Teaching | 1 (1.3) | 2 (1.3) | 3 (1.3) |
| Emotional support | 1 (1.3) | 3 (1.9) | 4 (1.7) |
| Relationship | 0 (0.0) | 1 (0.6) | 1 (0.4) |
| Understanding/empathy | 1 (1.3) | 2 (1.3) | 3 (1.3) |
| Esteem support | 1 (1.3) | 2 (1.3) | 3 (1.3) |
| Validation | 1 (1.3) | 2 (1.3) | 3 (1.3) |
| Network support | 5 (6.6) | 1 (0.6) | 6 (2.6) |
| Access | 1 (1.3) | 0 (0.0) | 1 (0.4) |
| Companions | 4 (5.3) | 1 (0.6) | 5 (2.2) |
| Tangible aid | 1 (1.3) | 5 (3.2) | 6 (2.6) |
| Direct task | 1 (1.3) | 5 (3.2) | 6 (2.6) |
Informational requests
Requests for informational support were present in 8.6% of postings. Only two subcategories of informational support were requested: advice and teaching.
Advice
Informational requests concerning advice were often focused on how to cope with the challenges and difficulties of living with CRPS on a daily basis. For example, several members requested advice on how to cope with temperature sensitivity:
Anyone got tips on desensitising to cold?
Welcome board, thread 1, message 53
There were also discussions about the impact of CRPS on employment opportunities. One member described her frustration over the loss of her previous career and asked:
If anyone out there knows of any ‘Home-working’ opportunities that are reliable – I would love to know!
Welcome board, thread 1, message 19
The lack of public awareness and understanding of CRPS was a common theme running through many threads and phases of the study, and led to some explicit requests from other forum members. One member, for example, asked for advice about medical alert bracelets, asking:
What do others carry and what info?
Your thoughts and experiences board, thread 6, message 1
Teaching
Informational requests related to the subcategory of teaching support often took the form of requests for factual information. During a discussion about work assessments and eligibility for disability benefits, one member requested statistical information regarding how many CRPS patients are inappropriately judged as being fit for work despite the debilitating nature of their illness:
I would like to know how many more crps patients are been denied DLA [Disability Living Allowance] and ESA [Employment and Support Allowance] support criteria by the dwp [Department for Work and Pensions] and atos [a health-care organisation providing independent assessment on behalf of the DWP] and forced in to the work capability groups
Your thoughts and experiences board, thread 16, message 1
Requests of this type were not limited purely to information about CRPS. For example, one member described having problems reading and replying to private messages, and asked if group members could teach them how to use the forum’s personal messaging facility, saying:
I think you sent me a message to my inbox which I now can’t find to reply. Am I being thick or is it obvious how to access inbox messages? When I read it I was on my mobile but now I am on the laptop it seems my inbox (which incidently I didn’t know existed) has disappeared. Heeeeeeeelllllpppp!!!
Welcome board, thread 1, message 60
Emotional requests
Requests for emotional support were present in 1.7% of postings. Only two subcategories of emotional support were requested: relationship and understanding/empathy.
Relationship
There was only one relationship request observed in the two threads, and this involved asking other members to share information about their daily lives as a way of encouraging a sense of closeness among the group:
I thought I’d start a thread where we could talk about our days, what we’ve been up to, how things have been etc. . . . So I’ll start
Your thoughts and experiences board, thread 4, message 1
Understanding/empathy
Understanding/empathy requests expressed concerns about the difficulties of living with a debilitating and untreatable illness like CRPS, and fears for what the future may hold. For example, one member commented:
I just have had enough twenty years sept since the car accident I had that started all my problems off was and i just dot think I can face another year let alone twenty
Your thoughts and experiences board, thread 7, message 1
Esteem requests
Requests for esteem support were present in 1.3% of postings, representing only the single subcategory of validation.
Validation
Typically, validation requests involved asking other members to share common experiences of CRPS-related difficulties. One member, for example, described lying in bed and being unable to sleep because of pain, and asked:
Anyone else struggle with sleeping?
Your thoughts and experiences board, thread 14, message 1
Another member talked about her problems with feeling cold one moment and then hot the next, saying:
My core temperature crashes to 35 degrees and then Like a switch I am boiling hot and sweating. Does anyone else have full body temperature changes
Welcome board, thread 1, message 53
Network requests
Requests for network support were present in 2.6% of postings. Only two subcategories of network support were requested: access and companions.
Access
Only one access request was found in the data. During a discussion about music and how playing an instrument helped to maintain dexterity in a CRPS-affected hand, a member asked if anyone else in the area needed a piano player, jokingly saying:
if anyone needs a wonky-armed piano player, whose left hand boogie-woogie has seen better days, please give me a shout!
Welcome board, thread 1, message 19
Companions
Companions requests typically asked about the possibility of meeting others who lived in the same geographical area or who were experiencing similar challenges.
I’m in Kilkeel in Co. Down, N Ireland and would be interested in being in touch with fellow sufferers
Welcome board, thread 1, message 49
Tangible aid requests
Only one subcategory of tangible aid was requested: direct task.
Direct task
Direct task requests typically asked board members to do something directly related to the poster’s situation. One member described having problems convincing his care manager that installing a bath at his home would be more beneficial than having a wet-floor shower room, and asked if group members knew of any evidence that might help to support his case:
Has anyone got any links or information sources or even personal experiences that I can print off to take to all of these people, to assist in my fight
Your thoughts and experiences board, thread 9, message 1
Similarly, during a discussion about educating health professionals to increase their awareness and understanding of CRPS, a member asked for help in obtaining CRPS statistics:
How would I find out roughly how many CRPS sufferers are there are in the uk. And whether there are geographic hotspots. Because this could identify the areas that have the least knowledge and most knowledge of CRPS
Your thoughts and experiences board, thread 1, message 15
Social support offered
Social support was present in a high proportion of forum postings. In the ‘welcome’ board, 75 out of 76 messages (98.7%) were found to contain some form of social support. In the ‘your thoughts and experiences’ board, 131 out of 156 messages (84.0%) contained social support. Group members most frequently offered emotional support (72.8%), followed by informational support (36.2%) and esteem support (30.2%), with network support and tangible aid (7.8%) less frequently offered (2.6%). Table 6 shows the number of forum postings in each category of social support. Note that those not mentioned are not included in the table.
| Support type | ‘Welcome’ board, n (%) | ‘Your thoughts and experiences’ board, n (%) | Overall, N (%) |
|---|---|---|---|
| Informational support | 24 (31.6) | 60 (38.5) | 84 (36.2) |
| Advice | 11 (14.5) | 43 (27.6) | 54 (23.3) |
| Referral | 4 (5.3) | 4 (2.6) | 8 (3.4) |
| Situation appraisal | 10 (13.2) | 17 (10.9) | 27 (11.6) |
| Teaching | 3 (3.9) | 8 (5.1) | 11 (4.7) |
| Emotional support | 68 (89.5) | 101 (64.7) | 169 (72.8) |
| Relationship | 10 (13.2) | 2 (1.3) | 12 (5.2) |
| Physical affection | 19 (25.0) | 12 (7.7) | 31 (13.4) |
| Sympathy | 2 (2.6) | 4 (2.6) | 6 (2.6) |
| Understanding/empathy | 57 (75.0) | 94 (60.3) | 151 (65.1) |
| Encouragement | 14 (18.4) | 20 (12.8) | 34 (14.7) |
| Esteem support | 25 (32.9) | 45 (28.8) | 70 (30.2) |
| Compliment | 13 (17.1) | 12 (7.7) | 25 (10.8) |
| Validation | 14 (18.4) | 37 (23.7) | 51 (22.0) |
| Network support | 10 (13.2) | 8 (5.1) | 18 (7.8) |
| Access | 1 (0.0) | 0 (0.0) | 1 (0.4) |
| Presence | 5 (0.1) | 5 (3.2) | 10 (4.3) |
| Companions | 4 (0.1) | 3 (1.9) | 7 (3.0) |
| Tangible aid | 3 (3.9) | 3 (1.9) | 6 (2.6) |
| Direct task | 2 (2.6) | 2 (1.3) | 4 (1.7) |
| Indirect task | 0 (0.0) | 1 (0.6) | 1 (0.4) |
| Willingness | 1 (1.3) | 0 (0.0) | 1 (0.4) |
Emotional support
Emotional support was present in 72.8% of postings. Five of the seven subcategories were present in the data: relationship, physical affection, sympathy, understanding/empathy and encouragement. There were no examples of prayer or confidentiality.
Understanding/empathy
Understanding/empathy messages were the most common type of emotional support identified. Members used a high level of self-disclosure to share their stories, talk about their medical histories and how they came to be diagnosed with CRPS, and discuss the difficult and complex issues involved in living with this debilitating illness. Others showed their understanding by disclosing similar information about themselves, after which the member who wrote the initial message would often post subsequent replies giving further information. This led to a shared understanding that was expressed through a high level of empathy. In an exchange that was typical of this process, a new member introduced herself by posting the following message:
Hello! Am not sure if I am writing this in the right place – but here goes! I have CRPS in my left arm following a broken humerus in January 2011. It extends from my left shoulder to fingertips – and yes, I am left handed! I was lucky to be diagnosed relatively early – after 6 months – thanks to my hydrotherapist at the RUH. I was really grateful for this – as other people were telling me that I wasn’t trying hard enough etc, even though I couldn’t move my arm, shoulder and hand . . .! I also tried to keep my fingers moving as much as possible right from the beginning – my arm and hand were really swollen and I was worried it would all seize up. I play the piano so kept doing exercises with my hand – I’m sure this helped a lot
Welcome board, thread 1, message 19
She quickly received a reply from another member who expressed her understanding by comparing the original poster’s experiences with her own:
Hi [name], and welcome, Im your other half lol!! Mine is in my right hand up to my shoulder and yep Im right handed too. Wow how lucky were you to be diagnosed that quick. Im not a piano player, but many many years ago I could play the bagpipes, and thats something, as Ive no ties to Scotland, and Im a born and bred Londoner
Welcome board, thread 1, message 20
This led the first poster to disclose additional details about her experiences, as illustrated in this reply:
Perhaps we could do a weird duet with our musical skills haha!! I’ve never tried bagpipes – my only link with Scotland is that I enjoy porridge for breakfast! – though I’ve had a go on quite a few different instruments . . . I’m a bit frustrated now because I keep trying to play my flute – couldn’t play properly before, but having great difficulties now – and can’t put my fingers on guitar frets any more, perhaps we should start a band and team up with people with spare hands lol!
Welcome board, thread 1, message 21
Members often expressed appreciation about these exchanges, as this quote illustrates:
Thank you for your response. It gives me much hope hearing others story’s
Welcome board, thread 1, message 34
Encouragement
Encouragement messages expressed hope to members, attempted to boost their confidence about achieving personal goals, and encouraged them to continue with therapeutic treatments and other activities. The importance of hope was particularly evident when one member talked in detail about her complex CRPS-related problems and her fears that she would not be able to regain control over her life. She immediately received a reply encouraging her not to give up or lose hope, saying:
Hopefully things will start to fall into place for you and don’t give up, keep going as best you can
Welcome board, thread 1, message 6
Similarly, a member spoke of her determination to walk without the aid of sticks or crutches, and received a reply that said:
I fully believe that you will achieve your goal
Welcome board, thread 1, message 8
During a discussion about hydrotherapy, when a member said that things went well until he left the water and spent the following 3 days in agony, others encouraged him to continue:
Stick to the hydrotherapy it is good for us I guess
Your thoughts and experiences board, thread 8, message 4
I find hydrotherapy really helps and so much easier to do exercises in the water than on land
Your thoughts and experiences board, thread 8, message 6
Sporting activities also received a lot of encouragement:
Am really pleased to hear that you have found an alternative way to ride your horse & keep enjoying it
Welcome board, thread 1, message 38
Physical affection
Physical affection was conveyed through written messages due to the text-based nature of online communities:
Gentle hugs.xx
Welcome board, thread 1, message 13
Warm hugs to you all
Welcome board, thread 2, message 1
Relationship
Relationship messages expressed the importance of closeness within the online community:
it is so lovely to see everyone supporting each other on here. It is a great idea to have a site where we can chat to others who truly understand what it is like to live with CRPS
Welcome board, thread 1, message 46
Isnt strange that we live so close, with quite a lot in common, and when all this started I felt so alone, and ‘its only me, know one else understands’, so from that the forum has been a great idea
Your thoughts and experiences board, thread 18, message 19
I’m really pleased to see this forum, it helps to know there are lots of people in similar circumstances – not that I’d wish this on anyone, but I’m sure everyone knows what I mean
Welcome board, thread 1, message 49
Sympathy
Sympathy messages expressed sorrow for the pain and distress experienced by the recipient, with a particular focus on diagnosis, symptoms and CRPS-related limitations on the type of activities that members can perform. For example, when one member explained that she had experienced 7 years of agony, distress and worsening symptoms before receiving a CRPS diagnosis, a member replied:
I am sorry it took you so long to be diagnosed
Your thoughts and experiences board, thread 18, message 12
Informational support
Informational support was present in 36.2% of postings. All four subcategories were present in the data: advice, referral, situation appraisal and teaching.
Advice
Advice messages typically offered suggestions for how to cope with CRPS and manage the impact of the illness on daily life. Members urged each other to continue using limbs, joints and other bodily areas that had been affected by CRPS, rather than avoiding using them because of the pain. This is illustrated in the following quote, which was written in reply to a woman with CRPS in her lower leg and foot:
Even though you have not been given physio help I would suggest that you keep your foot as mobile as you can
Welcome board, thread 1, message 29
Members sometimes suggested using occupational therapy such as knitting to keep CRPS-affected hands active; for example:
An OT [occupational therapist] at [hospital] gave me knitting needles as a therapy, my left hand has to work first to get my right hand working, and would you believe it, it works
Welcome board, thread 1, message 3
Medication was often discussed on the forum, with members providing advice about both the advantages and the disadvantages of taking medications:
If taking pills helps with mobility then I personally would keep taking them
Your thoughts and experiences board, thread 1, message 6
I will advise you though, don’t just stop taking them! I did a few months ago and ended up having to start them again as I felt all over the place and couldn’t drive etc. . . . I ran out over xmas so had no choice but it took a good few weeks at least for them to get out my system
Your thoughts and experiences board, thread 19, message 2
Situation appraisal
Situation appraisal messages helped members to reassess their situation, putting things into a more positive perspective. For some members, being diagnosed with CRPS was a significant breakthrough:
I’ve lived with this for the last 7 1/2 years and wow to be told that it wasnt in my head was such a relief and that I was normal (ish) was such a relief. From a small bang on the arm, my/our quality of life has been so badly affected, and even though I thought it was only affecting me I didnt realise how badly it was affecting the rest of the family
Welcome board, thread 1, message 3
Many messages featuring this type of support urged forum members to stay focused on the positive aspects of their lives:
as bad as it gets I thank god I’m here because it could have been so different I may not have been alive to see my gorgeous children grow up go to uni and get joe jobs have good partners and have good lives so in some respects think myself lucky
Welcome board, thread 1, message 12
Finally, messages containing this subcategory of support encouraged members to understand their situation by stressing the importance of setting achievable goals:
im not going to allow THIS to take away any more of my life. I now have goals, sensible goals
Welcome board, thread 1, message 3
Teaching
There were two broad types of teaching messages. The first is factual information regarding CRPS.
CRPS pain can improve within one year after the injury, but if it is still unchanged after 12 months (longstanding CRPS), then it will often not improve at all. Longstanding CRPS affects about 1 in 5,000 people in the UK
Your thoughts and experiences board, thread 1, message 21
I do think some people read far too much into this kinda thing and I’m not sure it always has a positive effect on people/their illness. [. . .] My theory is, if it hasn’t been published by a reputable source (such as Arthritis Research UK, NHS etc. . . .) then there is a potential for the info to be unresearched or not evidenced based
Your thoughts and experiences board, thread 13, message 12
The second type of teaching involved instructions for using the forum, for example how to use the personal messaging facility of the forum:
Go to the top of page and click on “mem cp” scroll down and “pm” is listed . . . not sure how well it works, we had trouble with txt ect, went for old fashioned e-mail in the end
Welcome board, thread 1, message 64
Referral
Referral messages directed members to other sources of information. Most referrals were to internet sites and charity organisations that might be able to provide additional knowledge and information.
If you don’t already have leaflets, the Arthritis Research site has the info from their’s online I think, it’s a pretty good one and is the one my rheumatology department have on the condition
Your thoughts and experiences board, thread 6, message 3
There are hospitals that specialise in CRPS dotted around the country. I personally attend one in [location name] and can not praise them highly enough
Welcome board, thread 1, message 29
Esteem support
Esteem support was present in 30.2% of postings. Two of the three subcategories were present in the data: validation and compliment.
Validation
Over one-fifth of the messages posted in these two threads were validation, in which one member expressed agreement with the feelings or assessments of other group members regarding their CRPS. When members expressed fears that they were moaning and saying too much on the forum, others would often post reminders that it was important to be able to express themselves and talk openly about their feelings.
you go on as long as you like, Ive had a good whinge on here
Welcome board, thread 1, message 13
A member who did not know what to do after she was refused a referral to a specialist centre was told:
You need to be taken seriously
Welcome board, thread 1, message 29
Compliment
Compliment messages expressed positive things about the recipient and what they have achieved despite suffering from CRPS. For example, a complimentary message was sent to a forum member who mentioned that she was preparing for possible inclusion in the Paralympics:
Good luck with the Paracycling assessment, what your doing is fantastic
Welcome board, thread 1, message 62
Similarly, when a member bought an electric wheelchair and was able to follow a cliff path to the beach for the first time in years, she received the following complimentary message:
congrats on your freedom, it makes each day an easier day lol
Your thoughts and experiences board, thread 18, message 10
Network support
Network support was present in 7.8% of postings. Two subcategories were present in the data: presence and companions.
Presence
Presence messages provided support by offering ‘to be there’ for the recipient, often in response to new members’ first posts:
welcome to the forum, where hopefully we can all help and be supportive to you
Welcome board, thread 1, message 69
Companions
Companions messages reminded members that they were not alone and that other forum members shared similar backgrounds and experiences. For example, in the following message, one member explained the importance of being able to talk to others who also have CRPS and have been through similar experiences.
I have a family support network and friends that are supportive but even so the only people that really understand are people that have the same condition
Welcome board, thread 1, message 14
Tangible aid
Tangible aid was present in only 2.6% of postings. Three of the five subcategories were present in the data, although they were very few examples of each: four messages included support by way of a direct task (e.g. ‘I will try and research some more into the cold’), and there was one message each offering an indirect task (‘I am not sure how to find out how many people have CRPS in the UK however I will try and do some research’) and willingness to provide help (‘if I can help in anyway’).
Discussion
Requests for social support were infrequent, with only 15.5% of messages explicitly requesting some sort of support. In contrast, almost 90% (88.8%) of messages offered some form of support. More specifically, the most frequent type of support offered was ‘emotional’, with nearly three-quarters of posts (72.8%) containing offers of such support. By far the most important subcategory of emotional support was understanding/empathy, which was present in over 65% of the posts.
On the whole, there were strong levels of empathy, validation and advice displayed on this forum. Our previous research showed that validation and understanding were two of the most influential elements in facilitating the development of a supportive community. 18,53 From this point of view, we can conclude that, at least in the first 6 months of operation, our CRPS forum did indeed develop successfully as a supportive environment for people with CRPS.
It is important to note the types of support that were not (or were rarely) present in forum messages. There were relatively few offers of ‘network support’ (7.8%) or ‘tangible aid’ (2.6%). One possible explanation for this absence is that, although adapted for the online context, some categories of support measured by the SSBC were simply impractical for this particular virtual community, which was geographically spread, with members who have real-world physical disabilities. Future research could explore the relative balance and impact of offline physical support and online emotional support.
Chapter 6 User involvement and developing the collaborative resource
User involvement
People living with CRPS have been involved throughout this research, from inception and design to implementation and analysis. The initial idea for the study arose from interactions between KR (chief investigator) and patients in her practice role. It was clear that patients wanted a space where they could share their experiences with one another, as well as seek and provide support for each other. In the past there had been another CRPS message board,34 but this had been disbanded because the person running it could no longer co-ordinate the site on her own. Although patients appreciated and liked the existing site, they were not willing to help with the administration of it. A static website had been developed by the patient support group then known as crps@themin, and as a team we mooted the idea of a new interactive site being set up which crps@themin could take over on completion of the study, should the site be well received. This idea was positively received by the small group running crps@themin.
Design strategy: user value versus management outcomes
Our approach to the foundation of an active new interactive site owes to the user-centred design tradition in human–computer interaction (HCI). The ‘paradigm’ of the technology acceptance model (TAM) originated in the 1980s to address the problem of ‘active’ uptake of existing fixed and pre-determined information systems in commercial settings. 57 It was based on Fishbein and Ajzen’s58 theory of rational action, assuming that ‘intentions to use’ predict active behaviour. TAM’s simple assertion is that the combination of perceived usefulness and perceived ease of use is sufficient to account for ‘intention to use’. In advocating user-centred design, Gould and Lewis59 argued that the creation of a useful and easy-to-use computer system is subject to a very different dynamic. It depends on an early and continual focus on users; empirical measurement of usage; and a commitment to react and reformulate interactions on a similarly continuous basis. In the context of this project, it is very important to be clear about the meaning of our ‘users’. The TAM paradigm is premised on a performance concept of utility at work and is aimed at practicing managers where use is typically mandated. Users might refer to any potential beneficiary of the use of a system, including users of data derived from primary usage. In HCI, a ‘user’ is a person who actually interacts with an interactive system. Gould and Lewis originated this approach as a reaction to the many failed attempts to ‘get it right first time’, and development work that was driven by sets of management requirements rather than genuine user needs. In the context of an interactive system for a health community, the key elements that might constitute TAM utility are likely to be a poor fit for the values of our users. Holden and Karsh,60 in a critical review of the application of TAM to health information technology, argue that both perceived utility and perceived ease of use may be ‘drastically different’ with health-care culture and social influences that are simply absent from commercial settings.
As we developed our research strategy, we involved crps@themin in all decisions. Consequently, the ‘perceived utility’ was not a matter that applied to an innovation in service of anyone other than our users themselves. Although as researchers our own use was also a factor, we took a strong view that our own role must be deprecated in favour of people living with CRPS. Olson and Olson,61 in review, identify facilities for users to establish common ground, and with the potential for mutual understanding, as well as a mode of interaction that is loosely coupled as key determinants of success. To this end, a member of crps@themin agreed to join our steering group. She played an active role throughout the course of this research and has been an invaluable sounding board at times when ethical and practical issues have arisen. Furthermore, the research itself has involved people who were living with CRPS themselves. All phases of the study have involved them actively cocreating the forum and the wiki resource.
Developing the collaborative resource
The second phase of the study was designed to involve a subset of participants who would create a wiki-like page explaining CRPS from the perspective of a person living with CRPS to complement the existing wiki page written by health-care professionals.
Once we launched the writing task, although members were supportive and excited about the end product, they were reluctant to be the first to post their thoughts about the proposed content. After consultation with the steering group, we approached those members for whom we had e-mail details and invited them to contribute their thoughts anonymously via us. We were then able to collate the suggestions and post their ideas in the form of a rudimentary draft of the information resource. We posted this draft in a new board entitled ‘raise awareness of CRPS’, which contained threads corresponding to six ‘target audiences’ and suggested topics that had been identified by an analysis of users’ forum posts and e-mails. This approach created a safer start point, and discussion subsequently picked up.
We were then able to collate the suggestions and post them in the form of a rudimentary draft of the information resource describing CRPS to the outside world. This was posted on the site and opened for discussion and modification by forum members. Members remained reticent to post their thoughts openly, but some sent the team feedback via e-mails to the research assistant.
Our original plan had been to thematically analyse the construction of this coauthored text (online comments, amendments, deletions and discussions), with the aim being to identify how participants worked collaboratively to reach consensus about what to include on their wiki page. However, participants had not wished to engage with the task in this manner and so did not engage in discussions among themselves; instead, they simply added their suggestions to the resource or e-mailed the team directly to request that their suggestions be included.
As a consequence, although we have not been able to conduct the planned analysis, we have been able to analyse the forum posts and e-mails that ultimately formed the basis of this task, and have completed a thematic analysis of these data in a manner consistent with our original plans. This analysis has facilitated the development of the cocreated wiki page and to the suite of cocreated leaflets that are currently in draft format.
Extending the wiki resource
The team recognised the potential to extend the wiki resource by developing a suite of leaflets that could be downloaded and used by people with CRPS. We used the information from the wiki page developed in phase 2 in conjunction with an analysis of conversations that had been held on the forum, and designed three leaflets that were essentially written from the point of view of people with CRPS for health professionals, friends and family and employers. These draft leaflets (see Appendices 8, 9 and 10) were piloted at a patient-run conference on 12 October 2013. Fifty patients attended the conference, all of whom received copies of the draft leaflets and a feedback sheet. Sixteen provided feedback, which was overwhelmingly positive and constructive. General comments included:
These leaflets will be a great asset and take away that jumble of explanation you find yourself in so often
Thank you for representing us and for the above leaflets
Brilliant leaflets – am sure they will raise awareness and understanding. Thank you
Could you produce a pdf copy of each in black and white as well as colour – easier/cheaper to print
All the leaflets are a good form of information for everyone from health professionals to employers. Mainly employers – they have no idea what CRPS is at all and are too keen to dismiss or discriminate the employee
Constructive suggestions for improving the various leaflets were also made.
For the health professionals’ leaflet:
Love the mantra ‘move it, love it, touch it’ – perhaps include it in the other leaflets too
Make the patient feel like they are not alone
Under resources, put the website for CRPS professionals so that they can network and find out how to get advice
I think you should give more options to referral than Bath i.e. Liverpool (is there anywhere else?)
For the friends and family leaflet:
Could you add in the ways in which to help: wheat bags. Tens machine [a transcutaneous electrical nerve stimulation machine that can be used as an alternative to painkilling medication]. Desensitisation with different substances e.g. rice, play dough, custard powder mix etc? Include ideas like swimming, RDA [Riding for the Disabled Association] riding, distraction, board games, wii games (fun whilst moving?)
Could you put the CRPS mantra section that is in the health professionals leaflet in the friends and family leaflet, even if it is just the bit about touching the affected area?
Looks a bit boring, could do with more colours and pictures. Budapest criteria not really relevant, would be better with a better description of CRPS and more ways to help the person with CRPS instead
Not sure about the picture, but does show pain! Good information about CRPS showing CRPS is real! To believe the sufferers that they are experiencing real pain sensitivity etc
For the employers’ leaflet:
Extreme hot or cold can affect CRPS so don’t sit them near draughty doors. Allow 5 mins earlier for breaks to avoid the rush of staff/busyness in corridors. Allow them to use wheat bags, tens
People with CRPS should be given the chance to work from home. Suitable furniture should be supplied for DSE [display screen equipment] use
There is nothing about getting the employer to consider a more suitable role in the organisation, how sufferers can get fatigue, lack of concentration. Employers need to listen as it is such an individual condition – mention everyone is different
Really good. Employers perhaps need to make allowances if an employee has to take time off due to pain, but could suggest flexi-time? Work from home should always be an option if the work is suitable. At the same time, employees should be accountable and work to the best of their ability
The team are currently incorporating these suggestions into the draft leaflets, which will ‘go live’ once this task has been completed. The delegates at the patient-led conference wanted this to happen as soon as possible. This is an example of 360° feedback, whereby the online interactions among people with CRPS led to the development of the leaflets which have been piloted with another group of people living with CRPS.
Chapter 7 Discussion and conclusions
Aims
In this project, we set up a peer-support online forum in order to identify the nature of support provided and to explore its development over time. We then introduced a collaborative writing task to the forum to facilitate further the development of social processes implicated in psychological support. This was intended to facilitate the exploration of the three questions: (1) What constitutes support in newly developed online interactions? (2) How does the process of giving and receiving support online evolve? (3) Can the combination of an online forum and a collaborative writing task increase support as well as a sense of psychological and physical well-being relative to an online forum alone?
How the protocol altered during the research process
We followed the protocol closely up until phase 3. At this time point, participants had disengaged from the forum and had been reluctant to engage in the writing task. This had a number of implications:
-
It was impossible to collect time 3 survey data. Furthermore, the responses to the time 1 and 2 survey had been poor, which meant that comparisons would be meaningless.
-
A comparison of forum-only and forum-plus-wiki participants was not feasible as the writing task remained part of the forum due to participants’ reluctance to write the wiki page themselves.
-
The wiki page remained in draft format and was never completed to a sufficient level for sharing more widely.
-
The lack of engagement with the writing task combined with the disengagement with the forum meant that it was not possible recruit friends and family to take part in online focus groups about their perception of the wiki.
In order to overcome the problem of lack of engagement (which began after the hacking event), we instituted a number of different strategies to try to re-engage the participants. We realised that participants were reluctant to be the first to write their thoughts about their condition in what was to become a formal wiki page. In order to get the ball rolling, we e-mailed members privately to ask them to indicate what issues they would like to see included on the wiki page. In addition, we analysed forum posts to identify issues that seemed to be of prime importance to members, which we integrated with the e-mail replies into a draft wiki page. We then shared the draft wiki page with the forum members and invited them to edit, add and comment on this. Using this iterative process generated some positive responses. However, the members did not fully engage and the wiki page remained in draft format.
The process of analysing the forum posts led to a recognition among the research team that there was enough information on the forum to generate an alternative resource which would address the patients’ concern that was the original driver for this piece of research: namely, that ‘others’ did not understand CRPS and that the voice of the person with CRPS was missing from what information was available. The team, therefore, developed a suite of leaflets written by people with CRPS for health-care professionals, friends and family and employers (see Chapter 5). Although not an intended outcome, this is one with a potentially large impact. The leaflets were piloted at a recent conference held by people with CRPS for people with CRPS and these comments were incorporated. The leaflets are now available online (https://sites.google.com/site/drkarenrodham/crps/crps-downloadable-docs) and have been circulated via the CRPS-UK e-mail list. A journal article discussing this as a useful process and outcome in its own right is currently in preparation.
What constitutes support in newly developed online interactions?
As we concluded in the previous chapter, few members of the forum explicitly requested social support, but many offered it. Perhaps joining the forum was a request for support in and of itself. Indeed, nearly 90% of posts contained some form of social support. Support was constituted here in a number of ways. In terms of types of social support offered in the community, emotional support (in particular empathy and understanding) was the most prevalent. Posts offering validation and advice were also well represented in the forum. This support was offered in what appeared to be a strong, supportive community. From the outset, there was evidence of both common-identity and common-bond community development on the forum, which was in first posts as well as in the types of support offered in the first 12 months of forum activity.
One of the unique features of online support, compared with support offered face to face, is that it facilitates the discussion of taboo topics. 18 The forum analysed here did indeed open up such discussions. Specifically, it provided a safe space to criticise the health profession without fear of jeopardising future treatment options. The discussion of this ‘taboo’ topic dominated first posts and played a leading role in the establishment of a common-identity community. The topic formed the basis of many of the common experiences shared on the site, as well as generating much of the empathy and validation offered to fellow forum members. Related to this, hiding the reality of CRPS is something that is common in the offline world, with individuals fearful of becoming a burden or of being negatively perceived. 53 The forum provided members with an opportunity to be honest about how they were really feeling and the perceived need for pretence was not evident in their posts. Belonging to a group of people with similar experiences gave permission to ‘tell it how it really is.’
In the real world, people with CRPS can feel disempowered as they are able to engage less and less in activities that, prior to CRPS, were their norm. 53 They feel that they are a burden, and withdraw socially. 33 The online environment created by members of this forum provided an opportunity for them to reach out and offer support to others in a similar position, in effect helping them to re-engage with the wider world.
How does the process of giving and receiving support online evolve?
In Chapter 3, we presented a table showing how the membership, threads and posts evolved over time (see Table 1). The site was steadily increasing in membership and discussion up until the point that it was hacked. As mentioned in Chapter 3, we were forced to temporarily shut down the site while we unravelled who was and was not a bona fide member. After the site was reopened, use tailed off markedly. We had also intended to collect quantitative data at three time points to measure changes in support. Response rates were so low that statistical analysis of these data would have been meaningless and we therefore reported on the qualitative free text that was shared by participants at the end of the survey.
Nonetheless, one of the unique features of this study was that we were able to investigate the development of a supportive online community from its inception. That is, we were able to investigate this online community from the very first post. Indeed, in Chapter 4, we presented thematic analysis of these first posts, and their role in establishing a common-identity community and in setting the tone of the forum. Specifically, a community based on a common identity was established via three types of information sharing evident in initial self-presentations: the journey to diagnosis, treatment, and contact with care professionals. Each was a means of establishing a ‘right to membership’ of the group,21 thereby enhancing the possibility of members being accepted by the group and laying the foundations for the development of a sense of social identification. 54 We have shown that, during the early stages of the forum, the members set up a space that had an over-riding positive, open and supportive tone. These first posts also served to establish a common bond between users of the forum. Specifically sharing the struggles and obstacles they faced served to emphasise the similarities in their respective offline situations, thereby creating a common connection.
The elements of a common-bond and common-identity community, once established in initial posts, continued to shape forum interactions throughout the 12 months of forum activity. For example, two key subcategories of support involved validation of thoughts and feelings and expressions of understanding and empathy. Such forms of support strengthened members’ ‘right to belong’,21 while further contributing to the development of a growing common identity. Similarly, in terms of tone, there was a continued and explicit emphasis on ‘looking for the positive’ throughout forum posts. For example, many of the messages under the subcategory of encouragement related to overcoming obstacles, and in particular to successfully finding alternative hobbies or interests to replace ones curtailed by CRPS. Indeed, hobbies and sporting interests featured heavily in first posts, continued to feature throughout forum interactions, and were related to several types of support (e.g. validation, situation reappraisal and understanding/empathy).
It should be noted that, on the surface, participation on the forum appears to have been low, with just 6 of the 62 members posing 79.3% of the forum messages. However, this is line with comparable forums. 62 Indeed, ‘lurking’, or the act of reading but seldom publicly contributing to an online group, can be supportive in its own right. 63 Further research is needed to explore this passive form of engagement with health-related online support communities.
In summary, these analyses demonstrate that online support can evolve quickly, but the newly formed community can also erode quickly. In this respect, the hacking of our forum was actually very informative. It exemplified this process, but was not a situation that we as researchers could have anticipated or engineered. Indeed, it would have been unethical for us to do so. The demise of the forum in this way highlights the fragility of newly formed online communities and could offer some insight into why previous user-led/-run CRPS communities have folded.
Can the combination of an online forum and a collaborative writing task increase support as well as a sense of psychological and physical well-being relative to an online forum alone?
For a variety of reasons, we were unable to address this question fully. Because we were watching a forum grow organically, we made the decision not to assign participants to different groups. Instead, we gave all members the option of contributing to the collaborative writing task. We expected to be able to compare those who accepted the invitation with those who did not. However, the response to our invitation was ‘all or nothing’: either they contributed to both the forum and the writing task or they stopped participating in the forum and did not contribute to the writing task. This did not allow us to compare across conditions. Moreover, the writing task was launched just prior to the hacking event, after which usage of the forum markedly dropped off. It was, therefore, not possible to compare support before and after the introduction of the writing task. Similarly, it was not possible to collect the quantitative data further, limiting our ability to compare across time and task.
Ethical lessons
We made a decision to take a laissez-faire approach to moderating the forum. This was done with the intention of allowing the members of the forum to self-manage. From a research perspective, this was necessary to allow us to watch the unfettered evolution of support; any interference from the research team would have influenced the interactions taking place on the board. In taking this stance we were able to honour our ethos as researchers. However, from a practitioner perspective there is another ethos at work: to intervene if distress is detected. Although it is true that researchers have a responsibility to ‘do no harm’, they would be perhaps more comfortable with the presence of caveats which explained that the forum was not a medical forum and any health concerns were to have been addressed to the participants’ own GPs and not to the forum. One particular issue highlighted the tensions that exist between these subtle differences in researcher and practitioner ethics.
Several months into the study, a member of the research team (researcher 1) noticed that a member of the forum had posted a comment about not coping. Although the post suggested that this individual was very depressed and potentially suicidal, none of the other members of the community had responded. Another member of the research team (researcher 2) outlined a number of options in an e-mail to the rest of the team, and concluded with the following suggestion:
So what to do? It seems a real shame that there is no reply to this message. Our laissez-faire philosophy suggests that it is a community matter and we should do nothing. A bit like natural selection, members who can’t hack it wither away leaving only those who can thrive in this environment. But this isn’t natural selection. It is an attempt to foster the development of a supportive community. So I think it sets a poor precedent. [. . .] If we do intervene, it could be with a post under our existing identities or we could ask [computer technician] to create a fake account so it doesn’t look as though we are descending from upon high. [. . .] I shall ask [computer technician] to create an androgenous dummy account called ‘Alex’ that we could use for this purpose. So what do you think?
Researcher 1 responds positively to this suggestion, and this triggers researcher 3 to write:
Sorry – coming into this late – but
Noooooooooooooooooooooooooooooooooooooooooooooooooooooooo!!!
We cannot deceive people and let them think someone real is helping them – that’s completely unethical and I cannot be party to it. It is the sort of thing that could completely explode in our faces.
This example raises a number of issues. Most obviously, when and how should a researcher intervene? Researchers need to balance several conflicting interests: the objectivity of scientific research, their effect on the dynamics of the group and ensuring the safety of participants. As noted above, the multifaceted nature of online research ethics also brings to the fore the potential conflict between researcher and practitioner ethics. Thankfully, this was a moot point, as we discovered through our steering group member that the distressed participant had in fact been replied to in a separate Facebook page with an overlapping community that was not part of our study. Future researchers who set up their own forum need to consider not just ethical issues but also legal and moral responsibilities towards the participants. This is particularly important in health settings where research and practice responsibilities can become blurred. It is, therefore, of paramount importance to ensure that participant expectations are carefully managed from the start (e.g. explaining that the forum is not a source of 24-hour professional support).
Implications and future research
It is clear that it is no longer feasible to investigate online supportive communities or outpatient support in isolation. Patients provide and receive support via a number of online environments simultaneously, and online supportive communities are spread across multiple sites and multimedia platforms. For example, some of the members of our CRPS online forum were also familiar with each other through their interactions in Facebook and Twitter CRPS-related groups. Rather than think in terms of a support community existing in a single, bounded online space, it is more realistic to think in terms of ‘networked communities’, operating across several discrete but overlapping online settings.
Forums seem ‘old-fashioned’ as more and more online support is being set up by user groups (e.g. CRPS-UK) on social network sites such as Facebook. Would participants be as willing to discuss their condition ‘like it is’ in an online environment shared by members of their online social networks, which might include family and friends? Our study indicates that a seemingly ‘old-fashioned’ platform (i.e. a standalone online forum) was conducive to the development of a supportive community, albeit one that proved to be fragile. The implication is that those planning to set up an online supportive community should not automatically turn to the newest technologies or the latest trends in social networking, but should instead consider their membership, the issues those members might discuss, and, therefore, the type of online platform most suited to these goals. This leads to a number of questions:
-
How does the type of support offered in a number of online platforms (e.g. forums, Twitter, Facebook) compare? Does the support differ by type? Does support evolve differently depending on the platform?
-
Could it be that the closed nature of the community in our study meant that people felt safe and, therefore, happy to talk online? Would we necessarily get the same results in a forum that was in the public domain? Theory suggests that perceived privacy is helpful; this is worth exploring in the future.
-
How does online engagement and interaction impact on offline interactions with family, friends and health professionals? How might it empower people to take ownership of their health and CRPS?
As the focus of much of this research would be on social media, future research needs innovative approaches adapted from media psychology, computer science and communication fields that go beyond controlled studies of self-contained and researcher-led websites. For example, internet-mapping techniques64 could be used to investigate the content and interconnectedness of formal and informal health-related websites and online communities. Participants of health-related forums or social networking sites could be interviewed while using a laptop with internet access and be asked to browse the web and show the sites, images and videos that they talk about and access regularly. Focus could include participants’ own websites (e.g. Facebook pages and Twitter feeds), and their posted stories, photos, videos and friendship networks, particularly those which involve the target health condition. These interviews could be recorded by digital video, allowing a visual record of the use of the laptop alongside the discussions between the researcher and the participants. Such research would enable a greater understanding of patient engagement with multiple and interconnecting websites, social media and networks.
Finally, when joining the forum, a standard format was quickly established as a means of members introducing themselves: real name, age and ‘journey to diagnosis’. Indeed, ‘journey to diagnosis’ was a key theme throughout forum posts, and involved onset of symptoms, the quest for medical explanations, misdiagnoses, misunderstandings and multiple attempts at treatment, all of which contributed to a sense of frustration and exhaustion among forum members. As discussed in Chapter 4, the presentation of this journey served to legitimise their right both to membership and to speak on the site. Other key themes included ‘treatment’, where members shared their experiences of different medications, and physical and psychological therapies, and ‘contact with health professionals’, where they detailed both positive and negative experiences of interactions with the health-care community. The fact that these themes were of such importance to this community has implications for other people living with CRPS as well as for clinicians. As noted in the introduction, CRPS is a condition diagnosed by exclusion, which can be a lengthy process. Clinicians need to be aware of the impact of this (often) long journey to diagnosis and the frustration that this engenders. This is particularly important in light of research demonstrating that frustration can impede engagement with therapy. 65 Forum posts indicate that forum users feel that their experiences were not heard by health-care professionals. Therefore, encouraging health-care professionals to actively listen to patients’ experiences, rather than medicalising the frustration, will foster a more productive partnership.
Final reflections
The over-riding barrier to our attempt to answer our third research question was the unexpected disengagement from our participants. This was especially surprising given that this project was a response to a patient-expressed need. This lack of engagement is, however, an extremely interesting finding in its own right and as a consequence of our attempts to re-engage participants we began to understand the challenges faced when dealing with patient use of multimedia settings. We suggest there were four potential explanations for the reduced engagement in our forum:
-
Our site was hacked and had to be suspended while we addressed the problem, and possibly at that point lost its momentum.
-
The wiki platform was ‘clunky’ and not user friendly. By this we mean that, unlike other more commonly used social media, such as Facebook or Twitter, the wiki platform was not intuitive to use, and the process of engaging with it lacked familiarity; moreover, it was not part of members’ social networking routine (see next point).
-
Participants were members of a variety of other forms of social media and so had other, more established means of communication, which many used in addition to, and often in preference to, our platform.
-
Participants were reluctant to voice their opinions concerning the content of the writing task; just because our participants were confident and experienced at writing in one public context (e.g. their own Facebook pages) did not mean that they would feel confident about doing so in other online contexts, particularly when the aim is to produce a more permanent record of their experiences.
This is a valuable lesson for any health professional or organisation considering setting up interactive online health initiatives. To keep the site running and to keep it safe (from hackers and other unwanted guests) was expensive and time-consuming. Even with our team skills we could not prevent the hacking event. Those thinking of setting up a site might consider how best to use existing social media that is both familiar to patients and already part of their e-routine. Moreover, this technology is free to harness and does not require dedicated technical staff to set up and maintain; nonetheless, it will require consideration of the ethical responsibilities.
Acknowledgements
We would like to thank our research participants who took part in our online forum, and especially those who gave up their time to contribute to the writing of the online resource. We would also like to thank the members of our steering committee (Julie Weymouth, Sharon Grieve and our technical officer Martin Post) for their advice and support. We are particularly grateful to Julie Weymouth for her invaluable help in recruitment, and for her advice as expert patient. We would also like to thank Hannah Heath, our research assistant.
Contributions of authors
Dr Jeff Gavin (Lecturer in Psychology) codesigned and led the study, conducted the analysis of first posts, and led the write-up of the report.
Dr Karen Rodham (Senior Lecturer in Psychology) contributed to the design of the study, facilitated access to participants, conducted the analyses of first posts and members’ feedback, and contributed to the writing of the entire report. She has been a practising health psychologist since 2006 and until December 2013 led the CRPS Psychology Centre at the Royal Mineral Hospital for Rheumatic Diseases, Bath.
Dr Neil Coulson (Associate Professor of Health Psychology) contributed to the design of the study, led the content analysis of forum posts, contributed to the literature review and conclusions, and provided overall editorial support for the entire report.
Dr Leon Watts (Lecturer in Computer Science) contributed to the literature review, creation and management of the forum, and provided support in writing the report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
Publications
Rodham K, Gavin, J, Coulson N, Watts L, Heath H. Let me introduce myself: the role of first posts in establishing a common-identity community in an online support forum. Conference on Social Psychology and Social Harmony, Beijing, China, 24–26 May 2013.
Unpublished
Smedley J, Coulson N, Gavin J, Rodham K, Watts L. Online social support for Complex Regional Pain Syndrome: a content analysis of support exchanges within a newly launched discussion forum. Comput Hum Behav 2014; in review.
References
- Geertzen JHB, Dijkstra PU, van-Sonderon EL, Goothoff JW, ten Duis HJ, Elsma WH. Relationship between impairment, disability and handicap in reflex sympathetic dystrophy patients: a long-term follow-up study. Clin Rehabil 1998;22:402-12. http://dx.doi.org/10.1191/026921598676761735.
- Sandroni P, Benrud-Larson LM, McClelland RL, Low PA. Complex regional pain syndrome type I: incidence and prevalence in Olmsted County, a population-based study. Pain 2003;103:199-207. http://dx.doi.org/10.1016/S0304-3959(03)00065-4.
- Kelmer M, Furnée CA. The impact of chronic pain on life in the household. J Pain Symptom Manag 2002;23:433-41. http://dx.doi.org/10.1016/S0885-3924(02)00386-X.
- Rodham K. Adapting to Life with Complex Regional Pain Syndrome: A Booklet for People with CRPS. Bath: Royal National Hospital for Rheumatic Diseases NHS Foundation Trust; 2009.
- Lauder A, McCabe C, Rodham K, Norris E. An exploration of the support person’s perceptions and experiences of complex regional pain syndrome and the rehabilitation process. Musculoskel Care 2011;9:169-79.
- Sverker A, Östlund G, Hallert C, Hensing G. Sharing life with a gluten-intolerant person: the perspective of close relatives. J Hum Nutr Diet 2007;20:412-22. http://dx.doi.org/10.1111/j.1365-277X.2007.00815.x.
- Beugnot S. Pain Beliefs, Coping, and Social Support As Predictions of Physical and Psychological Adjustment in Chronic Pain Patients 2001.
- Maugham K, Heyman B, Matthews M. In the shadow of risk: how men cope with a partner’s gynaecological cancer. Int J Nurs Stud 2002;39:27-34. http://dx.doi.org/10.1016/S0020-7489(01)00004-9.
- Harden RN, Swan M, King A, Costa B, Barthel J. Treatment of complex regional pain syndrome: functional restoration. Clin J Pain 2006;22:420-4. http://dx.doi.org/10.1097/01.ajp.0000194280.74379.48.
- Bruehl S, Chung OY. Psychological and behavioral aspects of complex regional pain syndrome management. Clin J Pain 2006;22:430-48. http://dx.doi.org/10.1097/01.ajp.0000194282.82002.79.
- Holland KD, Holahan CK. The relation of social support and coping to positive adaptation to breast cancer. Psychol Health 2003;18:15-29. http://dx.doi.org/10.1080/0887044031000080656.
- Franks MM, Stephens M, Rook KS, Franklin BA, Keteyian SJ, Artinian NT. Spouses’ provision of health-related support and control to patients participating in cardiac rehabilitation. J Fam Psychol 2006;20:311-18. http://dx.doi.org/10.1037/0893-3200.20.2.311.
- Gaede BM, Majeke SJ, Modeste RR, Naidoo JR, Titus MJ, Uys LR. Social support and heath behaviour in women living with HIV in KwaZulu-Natal. Sahara J 2006;3:362-8. http://dx.doi.org/10.1080/17290376.2006.9724862.
- Preece J. Empathic communities: balancing emotional and factual communication. Interact Comput 1999;12:66-77. http://dx.doi.org/10.1016/S0953-5438(98)00056-3.
- Chien WT, Chan S, Morrissey J, Thompson D. Effectiveness of a mutual support group for families of patients with schizophrenia. J Adv Nurs 2005;51:595-608. http://dx.doi.org/10.1111/j.1365-2648.2005.03545.x.
- Rodham K, Gavin J, Miles M. I hear, I listen and I care: a qualitative investigation into the function of a self-harm message board. Suicide Life Threat Behav 2007;37:422-30. http://dx.doi.org/10.1521/suli.2007.37.4.422.
- Holtz P, Kronberger N, Wagner W. Analyzing internet forums: a practical guide. J Media Psychol 2012;24:55-66. http://dx.doi.org/10.1027/1864-1105/a000062.
- Adams J, Rodham K, Gavin J. Investigating the ‘self’ in deliberate self-harm. Qual Health Res 2005;15:1293-309. http://dx.doi.org/10.1177/1049732305281761.
- Coulson N, Buchanan H, Aubeeluck A. Social support in cyberspace: a content analysis of communication with a Huntington’s disease online support group. Patient Educ Couns 2007;19:162-9.
- Mo PKH, Coulson NS. Exploring the communication of social support within virtual communities: a content analysis of messages posted to an online HIV/AIDS support group. Cyberpsychol Behav 2008;11:371-4. http://dx.doi.org/10.1089/cpb.2007.0118.
- Riley S, Rodham K, Gavin J. Doing weight pro-ana and recovery identities in cyberspace. J Community Appl Soc 2009;19:348-59. http://dx.doi.org/10.1002/casp.1022.
- Coulson NS, Greenwood N. Families affected by childhood cancer: an analysis of the provision of social support within online support groups. Child Care Health Develop 2012;38:870-7. http://dx.doi.org/10.1111/j.1365-2214.2011.01316.x.
- Perron B. Online support for caregivers of people with a mental illness. Psychiatr Rehabil J 2002;26:70-7. http://dx.doi.org/10.2975/26.2002.70.77.
- Braithwaite DO, Waldron VR, Finn J. Communication of social support in computer-mediated groups for people with disabilities. Health Commun 1999;11:123-51. http://dx.doi.org/10.1207/s15327027hc1102_2.
- Cohen S. Social relationships and health. Am Psychol 2004;59:676-84. http://dx.doi.org/10.1037/0003-066X.59.8.676.
- Coulson N. Receiving social support online: an analysis of a computer-mediated support group for individuals living with irritable bowel syndrome. Cyberpsychol Behav 2005;8:580-4. http://dx.doi.org/10.1089/cpb.2005.8.580.
- Cutrona CE, Suhr J. Controllability of stressful events and satisfaction with spouse support behaviours. Commun Res 1992;19:154-74. http://dx.doi.org/10.1177/009365092019002002.
- Gavin J, Rodham K, Poyer H. The presentation of ‘pro-anorexia’ in online group interactions. Qual Health Res 2008;18:325-33. http://dx.doi.org/10.1177/1049732307311640.
- Feldman SI, Downey G, Schaffer-Neitz R. Pain, negative mood, and perceived support in chronic pain patients: a daily diary study of people with reflex sympathetic dystrophy syndrome. J Consult Clin Psych 1999;67:776-85. http://dx.doi.org/10.1037/0022-006X.67.5.776.
- Malik SH, Coulson NS. Computer-mediated infertility support groups: an exploratory study of online experiences. Patient Educ Couns 2008;73:105-13. http://dx.doi.org/10.1016/j.pec.2008.05.024.
- White M, Dorman SM. Receiving social support online: implications for health education. Health Educ Res 2001;16:693-707. http://dx.doi.org/10.1093/her/16.6.693.
- Coulson NS, Knibb RC. Coping with food allergy: exploring the role of the online support group. Cyberpsychol Behav 2007;10:145-8. http://dx.doi.org/10.1089/cpb.2006.9978.
- Galer BS, Henderson J, Perander J, Jensen MP. Course of symptoms and quality of life measurement in complex regional pain syndrome: a pilot survey. J Pain Symptom Manag 2000;20:286-92. http://dx.doi.org/10.1016/S0885-3924(00)00183-4.
- Rodham K, McCabe C, Pilkington M, Regan L. Coping with chronic complex regional pain syndrome: advice from patients for patients. Chronic Illn 2013;9:29-42. http://dx.doi.org/10.1177/1742395312450178.
- Butler B, Joyce E, Pike J. Don’t Look Now, But We’ve Created a Bureaucracy: The Nature and Roles of Policies and Rules in Wikipedia n.d.:1101-10.
- Billings M, Watts L. Understanding Dispute Resolution Online: Using Text to Reflect Personal and Substantive Issues in Conflict n.d.:1447-56.
- Cutrona CE, Suhr JA, Burleson BR, Albrecht TL, Sarason AG. Communication of Social Support: Messages, Interactions, Relationships, and Community. Thousand Oaks, CA: Sage; 1994.
- Carvers CS. You want to measure coping but your protocol’s too long: consider the brief COPE. Int J Behav Med 1997;4:92-100. http://dx.doi.org/10.1207/s15327558ijbm0401_6.
- Melzack R. The short-form McGill pain questionnaire. Pain 1987;30:191-7. http://dx.doi.org/10.1016/0304-3959(87)91074-8.
- Ruta DA, Garratt AM, Leng M, Russell, IT, McDonald LM. A new approach to the measurement of quality of life: the patient generated index. Med Care 1994;32:1109-26. http://dx.doi.org/10.1097/00005650-199411000-00004.
- Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self mastery and self esteem): a re-evaluation of the life orientation test. J Pers Soc 1994;67:1063-78. http://dx.doi.org/10.1037/0022-3514.67.6.1063.
- Scheier MF, Wrosch, C, Baum A, Cohen, S, Matire LM, Matthews KA. The life engagement test: assessing purpose in life. J Behav Med 2006;29:291-8. http://dx.doi.org/10.1007/s10865-005-9044-1.
- Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med 1991;32:705-14. http://dx.doi.org/10.1016/0277-9536(91)90150-B.
- Zhang Y. Development and validation of an internet use attitude scale. Comput Educ 2007;49:243-53. http://dx.doi.org/10.1016/j.compedu.2005.05.005.
- Zigmond AS, Smith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70. http://dx.doi.org/10.1111/j.1600-0447.1983.tb09716.x.
- Rodham K, Fox F, Doran N. Exploring analytical trustworthiness and the process of teaching consensus in interpretive phenomenological analysis: lost in transcription. Int J Soc Res Method 2013;16:1-13. http://dx.doi.org/10.1080/13645579.2013.852368.
- Yardley L, Smith JA. Qualitative Psychology: A Practical Guide to Methods. London: Sage; 2008.
- Rolfe G. Validity, trustworthiness and rigour: quality and the idea of qualitative research. J Adv Nurs 2006;53:304-10. http://dx.doi.org/10.1111/j.1365-2648.2006.03727.x.
- Mason J. Qualitative Researching. London: Sage; 2012.
- Schwämmlein E, Wodzicki K. What to tell about me? Self-presentation in online communities. J Comput-Mediat Comm 2012;17:387-40. http://dx.doi.org/10.1111/j.1083-6101.2012.01582.x.
- Boyd D. Social network sites: public, private or what?. Knowledge Tree 2007;13:1-7.
- Braun V, Clark V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. http://dx.doi.org/10.1191/1478088706qp063oa.
- Rodham K, McCabe C, Blake D. Seeking support: an interpretative phenomenological analysis of an Internet message board for people with complex regional pain syndrome. Psychol Health 2009;24:619-34. http://dx.doi.org/10.1080/08870440802563245.
- Klein O, Spears R, Reicher S. Social identity performance: extending the strategic side of SIDE. Pers Soc Psychol Rev 2007;11:28-45. http://dx.doi.org/10.1177/1088868306294588.
- Lieberman MA, Wizlenberg A, Golant M, Di Minno M. The impact of group competition on internet support groups: homogeneous versus heterogeneous Parkinson’s groups. Group Dyn 2005;9:239-50. http://dx.doi.org/10.1037/1089-2699.9.4.239.
- Chiu M, Hsu MH, Wang ETG. Understanding knowledge sharing in virtual communities: an integration of social capital and cognitive theories. Decis Support Syst 2006;42:1872-88. http://dx.doi.org/10.1016/j.dss.2006.04.001.
- Venkatesh V, Morris MG, Davis GB, Davis FD. User acceptance of information technology: toward a unified view. MISQ 2003;27:425-78.
- Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975.
- Gould JD, Lewis C. Designing for usability: key principles and what designers think. Commun ACM 1985;28:300-11. http://dx.doi.org/10.1145/3166.3170.
- Holden RJ, Karsh B-T. The technology acceptance model: its past and its future in health care. J Biomed Informatics 2010;43:159-72. http://dx.doi.org/10.1016/j.jbi.2009.07.002.
- Olson GM, Olson JS. Distance matters. Hum Comput 2000;15:139-78.
- Preece J, Nonnecke B, Andrews D. The top five reasons for lurking: improving community experiences for everyone. Comput Hum Behav 2004;20:201-23. http://dx.doi.org/10.1016/j.chb.2003.10.015.
- Han JY, Hou J, Kim E, Gustafson DH. Lurking as an active participation process: a longitudinal investigation of engagement with an online cancer support group. Health Commun 2014;26:1-13.
- Rogers R, Marres N. Landscaping climate change: a mapping technique for understanding science and technology debates on the world wide web. Public Understand Sci 2000;9:141-63. http://dx.doi.org/10.1088/0963-6625/9/2/304.
- Dow C, Roche PA, Ziebland S. Talk of frustration in the narrative of people with chronic pain. Chronic Illn 2012;8:176-91. http://dx.doi.org/10.1177/1742395312443692.
Appendix 1 Moderation policy
Moderation, anonymity and confidentiality of online wiki and forum participants
Use of the site will be subject to the same terms and conditions that are in force for the online resources provided by NHS Choices (http://talk.nhs.uk/terms/houserules.aspx). These terms and conditions are intended to safeguard members from inadvertently exposing themselves to the risk of criminality, such as identity theft. They further protect those who run the site from prosecution in the case of the illegality of actions its users might carry out by clearly debarring any form of activity that might be in breach of criminal or civil law. We shall additionally make clear that the content that users create should not be read or used as any form of officially sanctioned health advice. Contributions to the community site will be moderated by broadly the same set of rules that govern contributions to the NHS Choices communities. Moderation will be undertaken by members of the research team on a rotating basis. We will check the site on a twice daily basis, first thing in the morning and last thing in the afternoon. In joining the wiki and/or the forum, participants agree to abide by the terms and conditions we outlined in our protocol and as such we do not envisage moderating being an onerous task. All team members will be trained to undertake these editing actions by the technical support person. Future moderation will be undertaken by members of crps@themin. They will be both trained to moderate, and in turn to train others to moderate. This will ensure that they will have the skills to moderate the forum themselves, and to create accounts for new members. NC has experience at providing such training and will lead this phase of the project.
We do not intend to remove any contributions on the grounds that they promote a particular health perspective. However, we would remove contributions and retain the option to bar the relevant contributor, in the case that there is clear evidence that the contribution was offensive. Users will be free to use their own names, however they will be required to maintain the anonymity of any friends, family or health-care professionals that they might discuss. If and when members fail to do this, the relevant identities will be edited out of the online text and the member reminded of their obligation to respect third parties.
Appendix 2 Project flyer
Appendix 3 Welcome e-mail
Appendix 4 The survey
Appendix 5 Rule agreement form
By signing up to access this site, also known as the CRPS Community Space, you agree to use the site subject to the terms and conditions stated on this page. We have tried to keep them short and direct but may need to change them from time to time as we learn about how best to support the activities of members of the site.
Signing up means that you become a member of the site. Postings or other information you encounter on the site will have been created by other members and hence should have been created by people who have also agreed to these terms and conditions.
The spirit of this site is one of informal help and personal support for people whose lives are affected by CRPS. So by signing up you agree to read and contribute to the site in a way that you believe is important to your understanding and experience of CRPS. You do so with a reasonable expectation of being treated fairly by others and with reasonable care in your treatment of others.
These terms and conditions are intended to safeguard you and other members of the site from inadvertantly exposing yourselves to the risk of criminality, such as identity theft. They are also intended to help protect those who run the site from prosecution in the case of illegality of action its users might carry out by clearly debarring any form of activity that might be in breach of criminal or civil law.
The content of messages or other information that you encounter on this site is entirely the responsibility of those who posted it. Under no circumstances should you treat anything you read or see on the site as officially sanctioned health or legal advice. We trust that the information you encounter has been provided in good faith but we cannot be held responsible if it is inaccurate or misleading and so results in physical, mental, financial or other forms of loss or damage.
Unfortunately, previous experience tells us that from time to time some people or third party organisations will attempt to profit from or actively damage the site for their own ends. We cannot guarantee the safety of the information on the site because new forms of threat and abuse of online forums and websites are constantly being invented. Consequently, by signing up you agree to adhere to the following rules.
-
You must at all times act in a manner that is lawful.
-
You must respect the opinions and experiences of other members of this site.
-
You must not post your address, financial or other legal identity information on this site.
-
You must not post your address, financial or other legal identity information of other people or organisations on this site.
-
You must not attempt to profit from your use of the site through sale or promotion of goods or services.
-
You must not abuse or insult fellow members of the site, or threaten or bully other members of the site.
-
You must not create or transmit any offensive, obscene or indecent images, data or other material.
-
You must not create or transmit materal which is confidential or copyrighted to others.
-
You must not carry out activities that corrupt or destroy other members’ data, including their messages.
We hope and trust that you find your membership of this site to be a positive experience as you confront your own personal challenges in living with CRPS.
Appendix 6 Recruitment e-mail
Appendix 7 Welcome page
Welcome to the CRPS Community Space.
This free site has been created for people who are living with CRPS as a space to talk to one another about anything that matters in their lives. It is intended to be a space (or venue) through which you can connect to other people affected by CRPS and we hope that over time it will be a valuable and support space for you.
Your site, your thoughts
This site is for people with CRPS. It is for you to use as you see fit within the bounds of UK law and the terms of the user agreement you made when you registered to join it.
Respect one another
CRPS does not discriminate among those it strikes. You will know that CRPS affects people from all walks of life, in all circumstances, all races, all religions, and all political affiliations. Please respect one another. We do not moderate anything that you post to the forum in advance. This is a matter of principle for this project. So you should feel free to write whatever you want to but do not defame, slander or incite hatred. If disputes about the appropriateness of your postings arise, and they cannot be resolved by those involved, we shall make a binding decision on the matter and leave or delete accordingly. Remember the terms of the user agreement that you committed to when you signed up to join the site. If you break the terms of the agreement, we will delete your posts and your account will be suspended.
Research project
This CRPS online community has also been developed as part of a research project being conducted by the University of Bath and the University of Nottingham. Our aim is to explore how technology can be used to support the ongoing needs of individuals living with CRPS. Our goal is to share the positives – and to learn from the negatives – so that people who face challenges like CRPS can do so with more confidence and mutual support in the future. Your thoughts and experiences throughout this project are therefore incredibly valuable and we look forward to hearing from you going forward.
How information will be used
All the text on this site will be stored for the purposes of the research we are carrying out. However, we shall anonymise this information such that you will not be identifiable in any reports or presentations we, as researchers, may make as a result of the project.
We shall not use your postings or contact details in any way for advertising or other commercial purposes and will only use them for the purposes of research and understanding your online experience. We shall however contact you by e-mail from time to time to ask you to fill in an online questionnaire about your current CRPS situation and what you think of the forum. You do not have to complete one of these online questionnaires to stay a member of the online community but the more people who volunteer to do so will help us build a better picture of how, if at all, online communities such as this CRPS space, might help people like you. You can also share your thoughts and feedback about the forum by posting about it or contacting the research team (details below). We are always very keen to hear from you about your experience of the CRPS online community space.
User agreement
By signing up to access this site, also known as the CRPS Community Space, you agree to use the site subject to the terms and conditions stated on this page. We have tried to keep them short and direct but may need to change them from time to time as we learn about how best to support the activities of members of the site.
Signing up means that you become a member of this site. Postings or other information you encounter on the site will have been created by other members and hence should have been created by people who have also agreed to these terms and conditions.
The spirit of this site is one of informal help and personal support for people whose lives are affected by CRPS. So by signing up, you agree to read and contribute to the site in a way that you believe is important to your understanding and experience of CRPS. You do so with a reasonable expectation of being treated fairly by others and with reasonable care in your treatment of others.
These terms and conditions are intended to safeguard you and other members of the site from inadvertently exposing yourselves to the risk of criminality, such as identity theft. They are also intended to help protect those who run the site from prosecution in the case of the illegality of actions its users might carry out by clearly debarring any form of activity that might be in breach of criminal or civil law.
The content of messages or other information that you encounter on this site is entirely the responsibility of those who posted it. Under no circumstances should you treat anything you read or see on the site as officially sanctioned health or legal advice. We trust that the information you encounter has been provided in good faith but we cannot be held responsible if it is inaccurate or misleading and so results in physical mental, financial or other forms of loss or damage.
Unfortunately, previous experience tells us that from time to time some people or third party organisations will attempt to profit from or actively damage the site for their own ends. We cannot guarantee the safety of the information on the site because new forms of threat and abuse of online forums and website are constantly being invented. Consequently, by signing up you agree to adhere to the following rules:
-
You must at all times act in a manner that is lawful.
-
You must respect the opinions and experiences of other members of this site.
-
You must not post your address, financial or other legal identity information on this site.
-
You must not post the address, financial or other legal identity information of other people or organisations on this site.
-
You must not attempt to profit from your use of the site through sale or promotion of goods or services.
-
You must not abuse or insult fellow members of the site, or threaten or bully other members of the site.
-
You must not create or transmit any offensive, obscene or indecent images, data or other material.
-
You must not create or transmit material which is confidential or copyrighted to others.
-
You must not carry out activities that corrupt or destroy other members’ data, including their messages.
We hope and trust that you find your membership of this site to be a positive experience as you confront your own personal challenges in living with CRPS.
Appendix 8 Health professionals’ leaflet
Appendix 9 Friends and family leaflet
Appendix 10 Employers’ leaflet
List of abbreviations
- CRPS
- complex regional pain syndrome
- GP
- general practitioner
- HCI
- human–computer interaction
- lol
- laugh out loud
- REC
- research ethics committee
- RNHRD
- Royal National Hospital for Rheumatic Diseases
- SSBC
- Social Support Behavior Code
- TAM
- technology acceptance model
- TO
- technical officer