
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1809/1073. The contractual start date was in November 2009. The final report began editorial review in July 2013 and was accepted for publication in December 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Lockett et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Over recent years with the provision of new funding streams, translational research initiatives have become increasingly important to health-care research in Europe, Canada, the UK and the USA. 1–3 In the UK, the National Institute for Health Research (NIHR) has invested £450M over 5 years to establish five comprehensive and seven specialist biomedical research centres (BRCs), alongside five accredited academic health science centres (AHSCs). 4 Similar initiatives have already been established in the USA, including a consortium of 60 multidisciplinary research centres known as clinical and translational science centres. These were set up to enable collaboration between clinical and basic science and provide training in clinical research. 5
The ‘bench to bedside’ rhetoric has, therefore, seen the creation of research centres and a growth in knowledge in basic sciences and clinical medicine. The role of the translation of knowledge in improving patient care has been strongly argued for ‘effective translation of the new knowledge, mechanisms, and techniques generated by advances in basic science research into new approaches for prevention, diagnosis, and treatment of disease is essential for improving health’. 6
The increasing importance of understanding the knowledge translation (KT) process has led to the identification of two translational gaps. The first gap addresses the translation of ideas from basic and clinical research into the development of new health technologies, products and approaches to the treatment of illness and disease. The second translational gap (T2) focuses on the implementation of these technologies, products, and services in clinical practice. Funded by the NIHR, nine Collaborations for Leadership in Applied Health Research and Care (CLAHRCs) aim to bring together universities and their surrounding NHS organisations to test new treatments and new ways of working. CLAHRCs were seen as a unique way of strengthening collaborations between universities and local NHS organisations. Importantly, they aimed to address the ‘second gap in translation’ as identified by Sir David Cooksey in A Review of UK Health Research Funding. 7
The policy intention is that CLAHRCs have three key interlinked functions: (1) conducting high-quality applied health research, (2) implementing the findings from research in clinical practice and (3) increasing the capacity of NHS organisations to engage with and apply research. The CLAHRCs are regionally focused, and their agendas are determined by partner organisations and the health-care needs of their geographical areas. While mandated by policy, CLAHRCs were regarded by the NIHR as experimental in nature during their inception, with considerable variation allowed for their structures and processes. Academic research and clinical practice were blended in different ways. For example, social sciences were variably integrated into CLAHRC plans, which included engagement with business schools. There were also differences in the disease emphases of CLAHRCs, and the clinical disciplines involved, both medical and non-medical. Overall, all CLAHRCs focused on translational research around long-term conditions.
Institutional entrepreneurship and Collaborations for Leadership in Applied Health Research and Care
The ‘translation gap’ between academic research and routine practice in health-care provision is a longstanding global problem8,9 which has given rise to a plethora of translational health research interventions, for example, in the USA, the Veterans Health Administration’s Integrated Health and Research System,10 American Quality Enhancement Research Initiative, and Clinical Translational Science Centres;5 in Canada, the Canadian Health Services Research Foundation;11 and in the Netherlands, the Dutch Academic Collaborative Centres for Public Health. 12 As described above, England has followed suit with investment in BRCs, biomedical research units (BRUs), AHSCs, academic health science networks (AHSNs) and CLAHRCs,4 the last of which we focus on.
Translational initiatives are positioned in a landscape governed by multiple institutional forces from professions with different priorities and values. Academics, for example, are required to meet the academic credentials that underpin their legitimacy and credibility, and clinicians are tasked with translating research into practice to improve patient care. These two professions must, therefore, collaborate successfully to ensure that research is effectively implemented into practice and patient care is improved. However, the paradigm of translational research that underpins translational and collaborative initiatives has not sufficiently considered or reflected the complex realities of these different professional environments.
Existing studies highlight that the uptake of evidence into practice is more complex13 and that the translation of evidence-based innovation is a non-linear process overshadowed by cultural changes and political forces which are intertwined across various organisational and professional boundaries. 14 Such translational initiatives are challenging because they seek to bring together and bridge two institutional worlds, health care and academia, with different structures, cultures and norms. 15,16 Furthermore, Martin et al. 17 have highlighted the role of differences in institutionalised power that can facilitate resistance to policy. Furthermore, Albert et al. 18 offer insights into the particularities of different research practices in the health domain in Canada suggesting that the interaction between different actors in the translational field is affected by an actor’s position and affected by epistemic culture and what constitutes as legitimate science.
Translational initiatives pose a potential space for conflict between different actors, who may interpret such ventures in different ways, resulting in varying practices, systems and ultimately outputs. We consider these conflicts that are nested in the T2 to be institutional in nature. Research, therefore, is required to understand how to support the translation of clinical research into practice where such spaces host knowledge that is multidisciplinary and requires different communities to interact, including clinical scientists and social scientists. 18,19 As CLAHRCs are tasked with overcoming such institutional problems of translating research into practice, through reshaping existing institutions that frame KT, they are an ideal platform to examine such important institutional issues.
To examine the work undertaken by CLAHRC actors to encourage institutional change in promoting CLAHRCs, we have drawn on the emerging theory of institutional entrepreneurship, a subtheme within neo-institutional theory. Drawing on the work of Lockett et al. ,20 based on a recent Department of Health (DH)-funded study of mainstreaming genetics innovation,21 we argue that the theory of institutional entrepreneurship is an important tool for understanding change in health care.
Our focus is on identifying and analysing the actions of the institutional entrepreneurs (IEs) in developing and implementing the CLAHRCs. Consistent with the emphasis on the need for a broad perspective on institutional working by institutional entrepreneurship research,22,23 and the NIHR Service Delivery and Organisation’s (SDO) [now encompassed within NIHR Health Services and Delivery Research (HSDR) programme] call to pay closer attention to the involvement of a wider array of field-level actors and activities;24 and with the introduction of the CLAHRCs, we view institutional entrepreneurship as transcending any one specific role. IEs may be drawn from a range of different stakeholder groups including CLAHRC directors, scientific programme managers, commissioners, clinicians and service users. A broad perspective on institutional work (IW) enables us to encompass internal and external organisational issues both within and across the NHS and universities.
Employing the concept of institutional entrepreneurship to the CLAHRC initiative, the proposed aims of our report were:
-
to provide a formative evaluation of CLAHRCs in relation to the generation of applied research, and the impact on practice and capacity building across CLAHRCs as they were envisaged and enacted
-
to apply institutional theory to identify and examine the challenges facing CLAHRCs
-
to apply the concept of institutional entrepreneurship to make a theoretically informed analysis of how to engender and sustain the translation and exchange of research knowledge into service facing innovation in CLAHRCs.
Feedback and engagement with user groups
Engagement with CLAHRC stakeholder groups was a major objective of our research (see Chapter 3). At all stages of our research process, we engaged with stakeholders, from the shaping our original application for funding of the research through to the final writing of this report. The major forms of engagement were as follows:
-
Scientific and stakeholders’ advisory panel (SSAP). This group was able to meet only twice during the research process as a result of problems in scheduling meetings. The meeting of the SSAP ensured that scientific and user input were garnered into the research direction and interpretation of emerging research findings. Moreover, members of the SSAP were consulted via e-mail and telephone as issues arose outside formal meetings. This included discussions around the findings and analysis of the research, where feedback was sought and subsequently fed into the report.
-
Feedback to or from collaborating sites. Formal and informal feedback sessions were conducted at four of the research sites, through the direct reporting of research findings to CLAHRC directors and deputies, on an ongoing basis. In addition, a number of workshops and presentation events were held in six different CLAHRCs (with as many as five meetings in one CLAHRC) to feed back our results to the wider CLAHRC communities in each region, including advisory boards, learning events and stakeholder boards. All of the feedback sessions enabled us to validate our emerging findings and to provide new learning for those involved.
-
Feedback at CLAHRC directors’ meetings. In addition to individual feedback to individual CLAHRCs, feedback sessions were conducted at periodic CLAHRC directors meetings and wider CLAHRC-wide events. Again, these sessions enabled us to validate our emerging findings and to provide new learning for those involved.
-
National workshop. A 1-day national workshop was conducted in November 2012 to disseminate findings and obtain feedback on our emerging findings. The event included a panel discussion of the emerging results, with the panel comprising four current directors and one ex-director of a CLAHRC.
Report structure
Chapter 2 provides a narrative synthesis of the key concepts related to (1) KT in health care and (2) institutional entrepreneurship. From our synthesis of the literature on KT in health care we conclude that the extant research is under-institutionalised in nature, which motivates our review of the institutional entrepreneurship literature.
In Chapter 3 we present our methodological approach, which encompasses issues of data collection and data analyses. Specifically, we present our mixed methods outlining our approach to qualitative case studies and social network analysis (SNA), and our overarching model of institutional entrepreneurship in CLAHRCs.
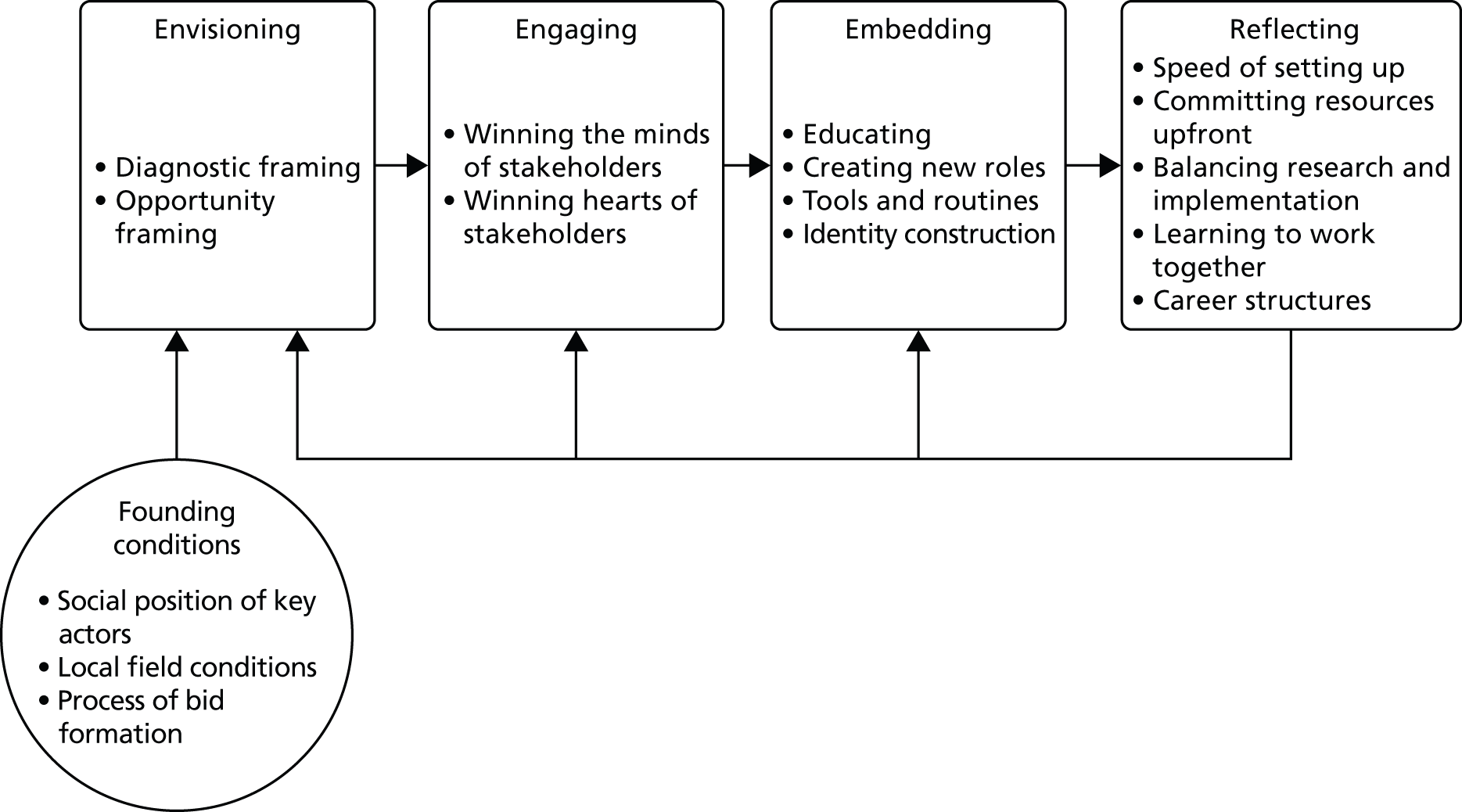
In Chapter 4 we outline the founding conditions of each of the CLAHRCs. Building on the tradition of Pettigrew et al. ,25 whose work on strategic change in health care highlighted the importance of history and context, we examine the social positions of the key actors involved in attempting to engage in institutional change, the local field conditions in terms of the extent to which there was pre-existing activity in the local region, and whether the bid formation involved a collective or more autonomous process. Importantly, we argue that it is the founding conditions that shape the local context and influence the nature of institutional change.
Chapters 5–7 outline three distinct phases of institutional entrepreneurship work: envisaging, engaging and embedding. Envisaging (see Chapter 5) relates to the important first stage in any change process in which actors formed an ‘embryonic’ vision, based on the interplay between themselves and the context in which they are situated. 26 Engaging (see Chapter 6) relates to the mobilisation of support from the IEs’ allies27,28 and the cultivation of co-operation and strategic alliances. 29–31 Embedding (see Chapter 7) involved the education of actors both within the CLAHRC and in practice with the skills and knowledge-based tools needed to support the creation of the new institution. 32,33
In Chapters 8 and 9 we examine how CLAHRC actors changed their patterns of interaction over time and, then, reflected on the effectiveness of their work. In Chapter 9 we draw on our SNA, based on the data collected in two survey waves in 2011 (wave I) and 2013 (wave II), to examine how successfully different CLAHRC actors bridged the divide between research and practice and the extent to which the patterns of interaction changed over time. In Chapter 10, we examine how the actors who managed and led the projects reflected on the way CLAHRCs were set up and run, and how they sought to rebalance the activities necessary to improve translation initiatives.
In the penultimate chapter we link our findings back to the KT literature. Here, we present our development of five schematic archetypes of KT. The archetypes are not representative of all the characteristics of one particular CLAHRC partnership, but rather a culmination of distinctive strategies used by CLAHRC entities into an archetype. Finally, in Chapter 11, we present the conclusions from our study.
Chapter 2 Literature: knowledge translation in health care and institutional entrepreneurship
In this chapter we provide a narrative synthesis of the literatures relating to (1) KT in health care and (2) institutional entrepreneurship. We dovetail both syntheses in one chapter as we conclude from our review of the KT in health-care literature that the main conclusions are under-institutionalised in nature, which motivates a synthesis of the institutional entrepreneurship literature.
The KT and health-care literature is characterised by a burgeoning number of articles, a number of which provide exhaustive reviews (e.g. Dopson and Fitzgerald,34 Graham et al. ,35 Mitton et al. ,36 Kitson et al. 9). Given the presence of exhaustive reviews, and as our intention is to employ the literature in this chapter as a means of framing our research, we present an overview that highlights and grounds key debates in the literature. To inform this review, we used Google Scholar, EBSCOhost and Science Direct databases to do a number of searches across relevant literature streams (from November 2009 to April 2010). For example, we did a forward citation of Weiss,37 a seminal paper on research utilisation in the KT field to build our understanding of the conceptual landscape of the KT field. 38 We selected and retrieved 75 scholarly papers from over 400 articles. Three researchers knowledgeable in the field then developed a conceptual map working iteratively between the research papers. Using the references from retrieved papers (original research, review and policy papers), we looked for additional papers that might help further develop and clarify our conceptual development of KT. Rather than seeking to be exhaustive our goal was to synthesise and be integrative.
In contrast to the literature on KT and health care, the literature on institutional entrepreneurship is still in its relative infancy. 39 As such, there is no real formal body of evidence to synthesise; rather, there is an emerging collection of studies that focus on the role of individual (and collections of individuals) agency in promoting institutional change. Consistent with our approach for the KT and health-care synthesis, we used Google Scholar, EBSCOhost and Science Direct databases to do a number of searches across relevant literature streams. We identified 35 main scholarly papers that have informed the emerging debate on institutional entrepreneurship; using the references from retrieved papers (original research, review and policy papers), we looked for additional papers that might help further develop and clarify our conceptual development of institutional entrepreneurship. Rather than seeking to be exhaustive, our goal was to synthesise and be integrative.
In performing both syntheses, our intention was to delineate the main concepts and constructs to be employed when analysing the qualitative data. The advantage of such an approach is that it enables a theoretically informed analysis of the data, thereby avoiding the pitfall of mere data description.
Knowledge translation in health care
A critical concern with KT is that advances in research knowledge can take years to be implemented into practice, and change realised. Given the pace of innovation and research in the health-care field, this ‘knowledge gap’ has generated significant attention within health-care research and policy, and has been the subject of numerous reports7,40 editorials commentaries2,41 and papers. 42,43 Thus, managers, clinicians and researchers are finding themselves increasingly called on to actively participate in the process of KT. This interdisciplinary field draws heavily on perspectives from clinical epidemiology, but also integrates scholarship from innovation studies, management, psychology, public health and sociology. 44 Given the increasing attention on KT in health care, it is important that scholarship crosses disciplinary boundaries and taps into existing resources, so that concepts do not have to be ‘reinvented’ in neighbouring fields. In the section Institutional theory and institutional entrepreneurship we argue that institutional theory provides helpful analytical concepts with which to understand the disciplinary knowledge silos and contrast ways of organising for knowledge production and its application.
A number of models and theories have been developed to overcome the barrier of translating knowledge between research and practice. We review three dominant approaches used in addressing the KT gap. 38,45 Given the burgeoning number of articles in this area, our purpose was not to provide an exhaustive review (which can be found elsewhere)26,27,38,39 but rather an overview that highlights and grounds key debates in the literature.
Linear and unidirectional models
Early conceptualisations of the knowledge–practice gap frequently used the term ‘research utilisation’,37 a term that remains popular in the USA. 46 The early knowledge-driven and problem-solving models conceptualised the process as a linear, unidirectional and passive flow of information from research to practice or vice versa. 37 The ‘knowledge-driven model’ was used mostly within the natural sciences, including the medical fields. The model assumed that basic research would progress to applied research and eventually lead to development stages, such as a new medicine or technology and then find application in the realm of practice. 37 Nonetheless, as highlighted by Mosteller,47 200 years elapsed between the discovery and adoption by the British Navy of a cure for scurvy, which emphasises the difficulty of knowledge ‘moving’ from research into practice. Thus, the passive view of KT has become increasingly questioned.
Although early models of KT accounted for the various modes of relations between research and practice, they generally did not consider the role of normative differences in knowledge flow. Subsequent research proposed a ‘two-communities’ model to highlight cultural differences among academics and practitioners, which was seen to be a major constraint to knowledge transfer or exchange. 48 Although these models emphasised the cultural incommensurability of the professional domains in the process of knowledge exchange between the two worlds, they did little to bridge the KT gap between research and practice. 49
The evidence-based medicine (EBM) movement in the 1990s further highlighted the ongoing concern of the slow uptake of research findings into the domains of health and medical practice. Originating at McMaster University in Canada, EBM sought to maximise the efficiency of medical practice by adopting a more rationally ordered means of predicting health outcomes and organising service provision. This model of medical practice organised knowledge into levels of rational validity, and used double-blind randomised control trials (RCTs), which were considered the most trustworthy forms of explicit medical knowledge as they are based on statistical inference. 50 Though grounded in epidemiology, linear models of KT drew ideas from innovation diffusion studies and technology transfer.
An important premise of EBM was that many clinicians were also researchers and, therefore, familiar with medical science literature, which enabled clinicians to make use of ongoing research updates. This modern, rational approach to formalising and disseminating explicit components of medical knowledge sat alongside the political narrative of medical learning and government policy concerns with the accountability and efficiency of health-care provision. 51,52 The predominant emphasis of EBM was to expect and anticipate that clinical practitioners would initiate the search for knowledge based on their professional motivation to provide the best possible care.
Interactional models with bidirectional knowledge flows
Interactional models developed by the Canadian Institute for Health Research (CIHR) highlighted the social nature of learning and the need for engagement between individuals from research, decision (or policy)-makers and clinical practice communities. 2,53 This view argued for the relevance of new research knowledge as research findings were often conceived as ‘square pegs that need to be fitted into a round hole’. 54 Instead of viewing knowledge flow as a linear process whereby decision-makers would seek out and use knowledge to inform their practice, researchers and those tasked with producing knowledge were encouraged to consider how they could actively facilitate the use of knowledge from research.
This view of bridging the research–practice gap emphasised the two-way nature of knowledge flow and the need for active engagement. The conceptual focus shifted to the process of interaction and collaboration and away from diffusion. Drawing on management and sociology scholarship, the roles of ‘knowledge brokers’ and ‘absorptive capacity’ have been emphasised. For example, Mitton et al. 55 identified that interactively engaging key champions was an important factor for successful ‘knowledge-transfer and exchange’. Others2,56 identified the importance of opportunities for building long-term relationships and highlighted the KT process as cyclical and iterative.
While the EBM logic of efficiency reconciled variations involved in problem selection and analysis, further developments of the knowledge exchange literature recognised and reconciled cultural differences through a symmetrical and reciprocal interaction of researchers and practitioners. 57,58 In particular, ongoing interactions between researchers and practitioners were identified as critical to knowledge use in practice2 and often involved the role of knowledge brokers in knowledge exchange. Other literature has also identified the importance of opportunities for building long-term relationships in enabling knowledge exchange activities. 59,60
A further concept – ‘knowledge linkage and exchange’ – has been developed as a model for the Canadian Health Service Research Foundation. This model suggested that knowledge generation and use is cyclical and that, at different stages in the knowledge translation process, effort needs to be expended in linking knowledge with potential users. The linkage and exchange activities could be conceptualised as either the researchers ‘pushing’ the knowledge out towards decision-makers in the practice communities, or as ‘pulling’ activities, whereby decision-makers initiate the linkage process.
The term ‘knowledge translation’, with a strong emphasis on impact, was also introduced by the CIHR in 2000. The CIHR61 stated that the process of KT included knowledge dissemination, communication, technology transfer, ethical context, knowledge management, knowledge utilisation, a two-way exchange process between researchers and those who apply knowledge, implementation research and the development of consensus guidelines. Rather than emphasising discrete events whereby ‘links and knowledge exchange’ could occur, an ongoing dynamic that reshaped knowledge and its meaning for the various stakeholders affected was highlighted. 62
The World Health Organization then adapted the CIHR’s definition to ‘the synthesis, exchange, and application of knowledge by relevant stakeholders to accelerate the benefits of global and local innovation in strengthening health systems and improving people’s health’40 (p. 2). The National Institute on Disability and Rehabilitation Research (NIDRR), based in the USA, also adopted and extended the use of the term KT by developing a working definition in its long-range plan for 2005–9. 63 In this light, KT has been an important step towards the recognition of the linkages between diverse communities and constitutes a key assumption in Baumbusch et al. ’s57 ‘collaborative model’ of KT. As emphasised by Harvey et al. ,56 a collaborative model of KT defines accountability regarding roles in relation to KT activity, reciprocity and respect for one another’s knowledge as important for the KT process.
In explaining the notion of reciprocity, Baumbusch et al. 57 made a brief reference to the mutual negotiation of meaning and power. However, the authors did not account for the processes through which these negotiations could be enacted in practice. Moreover, the intricacies of failures to establish common meanings and the rise of conflict over meaning, although crucial in understanding how knowledge is created and legitimated, are absent from their analysis. Although the current emphasis on highly collaborative notions of engagement and reciprocal exchange are increasingly common in the health services KT literature, it is interesting to note that models evaluating the success of KT programmes continue to focus on more linear and quantitative approaches. 64–66
Multilevel implementation research
In recent years, the complexity of changing clinical and organisational practices has oriented health services research to more explicitly include broader contextual features of practice and organisations into their analysis. 67,68 This perspective draws on the fields of change management and service improvement. While a number of scholars focus their discussions around the term ‘implementation science’,43,44,69 the terms ‘KT’ and ‘knowledge exchange’ continue to be used extensively, with overlapping definitions. The launch of the new online open-access journal Implementation Science in 2006 has consolidated a growing body of knowledge around what scholars term ‘implementation research’. In their initial editorial, Eccles and Mittman41 suggested that ‘implementation research is the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice’ and called for papers which include more details around the context and developmental process of moving research knowledge into practice.
While interactional models included the context as an important component, the analytical focus has predominantly been on the interaction and relationships between individuals and groups. Yet Keith et al. 64 highlighted ‘the real-world clinical environment is more susceptible to contextual factors than is the controlled research environment in which interventions are often designed’. As such, there is increasing focus on developing organisational readiness, capacity and capabilities. Wensing et al. ,70 for example, have argued for the importance of tailored implementation, and made the assumption that, in practice, innovations can be successful if they effectively address the most important determinants of practice for improvement in a targeted setting. Furthermore, Wensing et al. 70 have argued that ‘systematic tailoring entails three key steps: identification of the determinants of health-care practice, designing implementation interventions appropriate to the determinants, and application and assessment of implementation interventions that are tailored to the identified determinants’.
Eccles et al. 69 have argued for wider use of theory in implementation research, both for intervention development and for evaluations of intervention effectiveness. By contrast, Oxman et al. 71 have argued for a pragmatic and empirical approach, where pragmatic models specified a list of potentially relevant factors, but did not embed these in a comprehensive theoretical framework. Wensing et al. 70 (p. 2) also note that ‘although tailoring implementation interventions to determinants of practice seems logical and has received growing attention, research evidence that tailored strategies are substantially more effective than other approaches is lacking’.
Chamberlain et al. 72 have set out a model for understanding the stages of implementation completion (SIC), based on Feldstein et al. ’s73 Practical, Robust Implementation and Sustainability Model (PRISM). The SIC model was developed to measure the progression through the stages of implementation in an evidence-based programme in the context of a RCT. Alongside other models, references to, and discussions of, the Promoting Action on Research Implementation in Health Services (PARIHS) 2004 framework were widespread. 74 The aim of the PARIHS framework was to ‘present successful research implementation as a function of the relationships among evidence, context, and facilitation . . . [which] have a dynamic, simultaneous relationship’75 (p. 289).
In addition to context, evolving implementation research literature has increasingly questioned the epistemological nature of knowledge. 76 As Ward et al. 77 noted, KT literature has, to date, largely assumed a rational, technical view of the problem and has not developed discussion on the nature of knowledge. Harvey et al. 56 divided evidence (as knowledge) into three types (theoretical, empirical and experiential) and called for the use of all three types. This gave experiential evidence a greater role than it had typically held in biomedical sciences. Harvey et al. 56 argued that: ‘Given the inherent complexity and context dependent nature of the implementation process, as well as the insufficiency of empirical evidence about implementation, it becomes impractical to prioritise one type of knowledge over the others.’ (p. 4). 56 In contrast to earlier KT concepts where the critical knowledge was encapsulated as objective and professionally defined research outputs, the current shift towards a more inclusive and expansive evaluation of knowledge begins to acknowledge a wider distribution of relevant expertise.
Conclusions
In summary, the KT literature has largely focused on the individual-level learning and clinical encounter, although with a view to influence a large population of clinical decision-makers. While the level of the individual is important in the health-care industry, as health encounters often occur on a one-to-one basis, recent work has increasingly emphasised the social nature of KT and the need to engage in long-term relationships with bilateral communication processes in order to generate changes in decision-makers’ practices. Furthermore, understanding the context and diverse types of knowledge have been found to be increasingly important in influencing behavioural change.
Based on our reading of the KT literature, we suggest that there is a greater need to attenuate to the importance of context in shaping KT in health care. Following the lead of Pettigrew et al. ,25 we suggest that much research on strategic change is ahistorical and does not take account of context. Importantly, the role of the reshaping of context in influencing KT has implications for the promotion of effective and sustainable KT beyond resource deployment. In the next section we examine the issue of context, and how actors may seek to engage in reshaping context in a manner that promotes KT, drawing on a synthesis of the literatures of institutional theory and institutional entrepreneurship.
Institutional theory and institutional entrepreneurship
As outlined in Chapter 1, we frame the T2 as being institutional in nature. Based on our review of the literature on KT in health care, we argue that many of the models of KT are under-institutionalised and, as such, fail to account for important institutional constraints that shape actors’ work in closing the T2. In this chapter we review the literature on institutional entrepreneurship and frame the discussion within the broader literature on institutional theory and IW.
Traditionally, institutional theory had developed to provide insight into how deeply embedded beliefs, roles and patterns of interaction could structure social practice and compel individuals and organisations into forms of conformity. 78,79 In particular, it has been used to explain how exogenous institutional forces structure organisational processes. For Scott80 these consisted of three elements or pillars: regulative elements, consisting of formal rules, laws and public policies; normative elements, including norms, conventions and practices; and cognitive elements comprising beliefs and understandings as well as scripts and schemas. 81–83
Institutional theory had particular resonance in the study of organisational change and continuity. Organisations are located in organisational fields, which are characterised as clusters of organisations and occupations whose boundaries, identities, and interactions are defined and stabilised by shared institutions. 80 Seen in this way, institutions are resilient social structures, sometimes enshrined in law, that specify field rules, membership, and the appropriate behaviour of its constituents. 84 The more developed a field, the more likely institutions will have become entrenched. A mature field will tend to have a stable membership with a strong mutual understanding of which organisations occupy the field,80,85 and organisational forms will converge to be consistent with the field’s institutions. 78
Field characteristics
Fields are more than just an aggregate of organisational players, and consist of ‘distinctive’ ‘rules of the game’, relational networks, and resource distributions that differentiate multiple levels of actors and models for action’ (p. 251). 86 Fields may be characterised by the presence of multiple institutions or institutional logics. 84,87–89 These fields can have multiple field constituents who are ‘often armed with opposing perspectives rather than with common rhetoric’ and, so, institutional change ‘may more resemble institutional war than isomorphic dialogue’ (p. 352). 90
Pluralistic fields provide actors with the raw materials to challenge existing practices as they are confronted by competing logics and present new potential ways of working that are outside the dominant template. 84,91 Recent work has investigated the diversity in organisations’ responses to the guiding principles of overlapping logics. For example, Greenwood et al. 92 noted the variations in organisational responses to the competing logics of ‘family’ compared with ‘markets’ in different regions across Spain. In doing so they identified how internal organisational factors as well as the local environment shaped individual responses to contradictions in their institutional environment.
We propose that CLAHRCs are located within the overlapping fields of higher education and health care, giving rise to a pluralistic field structure that provides fertile ground in which institutional change may be possible. The pluralistic field means that CLAHRCs faced an institutional landscape of diffuse power structures and divergent objectives, arising from competing institutions, both at the macro and micro level.
Historically, within each health-care region there typically exist one or more teaching hospitals, two or more primary care trusts (PCTs) and a strategic health authority (SHA). However, during the funding period of CLAHRCs, the Health and Social Care Act 201293 replaced PCTs and SHAs with clinical commissioning groups. Historically, NHS organisations formed links with higher education institutions (HEIs) most notably through HEIs’ medical schools. Furthermore, medical schools have been charged with the tripartite mission of excellence in research, education and practice. However, there are strong institutional forces that make the accomplishment of the tripartite mission challenging. Specifically, regulatory/coercive, normative and mimetic forces within the health-care sector impact upon cultural–cognitive processes that underpin knowledge sharing across organisational and professional boundaries. 15
At the macro level, the government sets public policy and creates regulatory institutions for many public sector organisations. A particular issue is that government set performance indicators and priorities can cause the activity of organisations in health care and higher education to diverge, leading to the separation of research and practice. 15
The macro-level regulatory environment in the field of health care has been under considerable flux for the last few years. At present, the NHS is currently in the final year of transition to the new commissioning and management system. In enacting this change, NHS leaders have been required to respond to three inter-related challenges: (1) the need to maintain strong performance on finance and service quality, (2) the need to address the difficult changes to service provision required to meet the quality, innovation, productivity and prevention challenge in the medium term, and (3) the need to complete the transition to the new delivery system set out in Liberating the NHS. 94
At a macro level, HEIs are subject to a centrally driven set of performance measures. In the higher education sector the Research Excellence Framework (REF), previously the Research Assessment Exercise, frames academic activity as ranked within a UK level. This is largely based on research outputs in the form of academic publications (weighted at 60%), with the environment (weighted at 20%) and the impact of research (weighted at 20%) accounting for the remainder. University medical schools, similar to hospitals, are ranked within the UK in a publicly available league table according to their national research rating. Funding varies with research ratings. Crucially, these form part of the basis for the department’s reputation, with an indirect effect on attracting further research income and student numbers. The overall effect appears to be one that enhances, rather than dilutes, boundaries between health care and higher education. Arguably, the explicit tripartite agenda of NHS and HEI organisations has become less pronounced.
Academic research and clinical practice have become unbundled, to the possible detriment of patient care: ‘The strategies for patient care and research are pointing in different directions and driving the integrated ethos into history unless we strive for its preservation’ (p. 38). 95 At an organisational level, Currie and Suholminova15 have suggested that mimetic forces have buttressed the divergence that stems from what can be called ‘coercive pressures’. Organisations tend to imitate the practices of their most successful peers so that, for instance, universities seek to pursue more laboratory-based research, in line with high performers in academia globally.
At the level of the professions, the process of professionalisation has undermined the sense of a tripartite mission. The tendency towards increasing specialisation – and, thus, divergence – in the career paths between clinical researchers and clinical practitioners has acted to pull apart the worlds of research and practice. 15 One consequence of divergent career paths is that medical consultants and aspiring professors are now unlikely to develop a shared perspective on a given problem that is necessary for an effective knowledge exchange across the professional divide. The opportunities for integration of academic research and clinical practice, fostered under the ‘old’ climate of a tripartite mission, are likely to be lost with the decoupling of research and practice, which will have detrimental effects on patient care. Similarly, the rise of professions allied to medicine and the rise in the status of various categories of professionals in the health-care field more generally (vis-à-vis the traditionally high-status hospital consultants), have also contributed to the strengthening of normative pressures operating on those groups and, thus, a further divergence in perspectives between them. Again, mimetic pressures, which have resulted in professional associations and educational institutions following the lead of the most prominent peer organisations, have added to the normative pressures.
Finally, the picture is complicated further by the internal stratification of professions. For example, within HEIs, academics are not a homogeneous group; rather, Becher and Trowler96 have referred to them as being organised into their own tribes seeking to defend and enhance their own territories. Hence, important differences in norms and customs may further drive apart the tripartite mission, whereby different professional groups (inter- and intraprofessionally defined) clash over issues such as epistemology, ontology, methodology, etc. Such stratification is more pronounced in the clinical world, where elite professionals engage in IW when faced with changes in the health landscape and are likely to maintain pre-existing arrangements. 97
Institutional entrepreneurship
The literature on institutional entrepreneurship emerged in response to the strong determinism of institutional theory, which characterised institutional change as largely exogenous. Although organisational fields are structured, and institutional forces influence actors’ behaviours, endogenous struggles between actors still occur in relation to resources and relative positions of power. 98 The literature on institutional entrepreneurship focused on the nature of these struggles and how actors may seek to influence institutional arrangements in order to enhance their position and promote interests which they value. 27,99–101
Institutional entrepreneurs are defined as organised actors who envisage new institutional configurations as a means of advancing interests they value highly, yet are often suppressed by extant logics. 102 These new configurations may be realised through the creation of new institutions or the transformation of existing ones. 27,86,102 The work undertaken by IEs can be diverse, but is inevitably political and contingent on prevailing forms of legitimacy and power. 86
Research suggests that not all individuals or groups may be equally adept at engaging in institutional entrepreneurship. 27,102 Key to an actor’s scope to envisage and enact change is his or her social position, or location within the pre-existing institutional configuration, in terms of their access to resources, participations in activities, formal roles and legitimated identities. 103
In linking the concepts of field and social position, we argue that a given field can be conceptualised as a structured system of social positions, each with interests and opportunities,104 from which actors compete to promote their vision of future states of the world. 98 Social positions are defined in terms of the capital (economic, cultural, social and symbolic) endowments that underpin them and the associated relationships with other field members. 105 These social positions shape actors’ outlook, perceptions, motivation and ultimately their ability to enact institutional change. 106
A key debate for scholars of institutional entrepreneurship has been concerned with the distinction between central and peripheral social positions in a field in terms of their influence on actors’ IW. The distinction between central and peripheral social positions recognises both the differing capacities of actors to establish and sustain institutional arrangements in line with their own interests and their degree of embeddedness in a field. 107,108 Those who occupy central social positions, with the authority and connections to compel change, are arguably best placed to engender an institutional transformation. Conversely, those who occupy peripheral social positions are arguably less able to engender institutional change. The empirical evidence, however, attests to a more complex picture. 24,82,108–113
A number of studies, focusing on a range of different fields including health care and open-source software, have found that instead actors located in peripheral social positions are most likely to bring about institutional change. 25,87,102 Actors located in peripheral social positions are the most disadvantaged by current institutions and, so, will be more able to see the faults, alternatives and ways around living according to institutional expectations. 114,115 Seo and Creed116 have suggested that peripheral organisations are also more likely to be exposed to the contradictions in the current institution, especially when facing pluralistic fields. Therefore, actors and organisations in peripheral social positions will be exposed to alternative fields and, consequently, come into contact with alternative logics and/or ideas, which may help instigate change. 109
In contrast, actors in central social positions that are more privileged by existing institutions may be least likely to promote institutional change. The argument is that: ‘Although central, dominant actors may be able to champion institutional change, they appear unlikely to come up with novel ideas or to pursue change because they are deeply embedded in – and advantaged by – existing institutions’ (p. 199). 117 There are instances in which centrally positioned actors have been seen to promote change; however, they appear to occur when some movement in the wider environment has meant that the current institutions are not fully aligned with the dominant actors’ interests. 28,108,118–120 Greenwood and Suddaby108 examined changes initiated at the centre of the mature field of large accounting firms. In particular, the leading firms sought regulatory changes in order to expand the range of services they offered, in response to demand from clients. Rao et al. 121 examined centre-led change in relation to the rise of nouvelle cuisine, which arrived from restaurants at the top of the French culinary hierarchy. In both examples, although the change promoted was significant, it further cemented the actors’ dominant field position.
Institutional work for entrepreneurship and maintenance
In this review, we highlight the importance of the work of IEs, but also that, in general, a range of different actors may undertake IW. Lawrence and Suddaby22 suggested that IW is a more general category of embedded agency than institutional entrepreneurship, used to describe any ‘intelligent situated institutional action’ (p. 219) of individuals and organisations ‘aimed at creating, maintaining and disrupting institutions’ (p 215). 22 The myriad, day-to-day instances of agency that, ‘although aimed at affecting the institutional order, represent a complex mélange of forms of agency–successful and not, simultaneously radical and conservative, strategic and emotional, full of compromises, and rife with unintended consequences’ (p. 52),122 are missing from accounts of institutional entrepreneurship.
Although the literature on institutional entrepreneurship implies that institutions generally remain stable unless remoulded by a motivated actor, the literature on IW focuses on how actors across a field are continually engaged in the partial re-enactment of routines and practices that may ultimately lead to field-level dynamism, but may also result in the strengthening of existing institutional arrangements. 123 As Lawrence et al. 122 stated, institutions are continued by ‘the everyday getting by of individuals and groups who reproduce their roles, rites and rituals at the same time that they challenge, modify, and disrupt them’ (p. 57). 122 To this end, we argue that institutional entrepreneurship can be seen as one specific type of IW that divergently challenges aspects of the prevailing institutional order with the aim of establishing new institutions in place of old. The development of the concept of IW, therefore, appears to be an important move in presenting a more balanced account of agency within institutions.
Furthermore, there is a risk of the misclassification of the nature of the IW undertaken. Currie et al. 97 suggested that the maintenance of an institutional status quo by elite actors may be more than an act of mere resistance or maintenance. Rather, Currie et al. 97 have argued that elite professionals combine elements of IW such as ‘theorising’ and ‘defining’ in a more creative manner than is presented by the types of IW categorised as maintenance by Lawrence and Suddaby. 22 Powerful actors (re)generate or (re)create institutional arrangements in the face of external threats, in a way that can enhance, not merely maintain, their position. In essence, the elite actors are engaging less in change resistance and more in positive action through IW to shape the change trajectory to ensure continued professional dominance. Consequently, we argue that IW to maintain professional elite status is likely to encompass a wider variety of IW than previously categorised by Lawrence and Suddaby. 22 We observed types of IW for maintenance that Lawrence and Suddaby22 associated with creating institutions.
Based on the above, we suggest that actors are continuously engaged in a struggle to (re)shape the institutional landscape in a manner that promotes the interests that they value highly. The willingness and ability of actors to engage in a process of (re)shaping institutions, however, will vary across actors and institutional fields. In addition, we suggest that the nature of the IW (for maintenance and/or entrepreneurship) will vary by actor and field.
Conclusions
We conclude that the field of CLAHRCs is pluralistic in nature and spans the institutions of the NHS and HEIs. As such, CLAHRCs provided a fertile ground for actors to expose and explore institutional contradictions in promoting institutional change. In addition, drawing on the emerging literature on institutional entrepreneurship we argue that IW for entrepreneurship and/or maintenance will be influenced by the antecedents of the nature of the field, and the social position within it, in which the actor is located. To date, however, there has been a dearth of research that has focused on comparisons of institutional actors within a common institutional field, and how their different subject positions may shape their work for institutional entrepreneurship and/or maintenance. We suggest, therefore, that it is important to examine the work of all institutional actors, located in a range of social positions in a field, and how their work may either promote or hinder institutional change.
Chapter 3 Methods and data
In this chapter, we outline out the research methods we employed, and in doing so, discuss our approach to data collection and data analysis. The study gained ethics approval from the Leicestershire, Northamptonshire and Rutland Research Ethics Committee 2 (reference number: 10/H0402/6). In addition, we worked to authenticate our work, as documented in our study protocol, by holding advisory boards, and feeding back to CLAHRC directors regularly, where we presented our emerging findings and discussed issues with the study as we progressed.
First, we outline our approach to qualitative methods, explaining the multistage nature of our research process across the CLAHRC case study sites. Second, we outline the social network methods of data collection and analysis, which complemented the qualitative case study work.
Qualitative methods
We employed a qualitative, induction-driven research design to enable contextualisation, vivid description and an appreciation of subjective views. 124,125 Drawing on institutional theory, with a specific focus on institutional entrepreneurship and IW, we examine the work of a range of different institutional actors as they engage in the CLAHRC initiative. In conducting our research, we employed a multiple case study format as it enabled a more robust basis for theory building,126 and often yielded more accurate and generalisable explanations than single case studies. 127
Qualitative data collection
Our research strategy involved collecting data from three sources: (1) archival data, (2) interview data and (3) observational field notes. In so doing, we sought to strengthen our ideas by triangulating our sources of evidence. 128 As with Pettigrew et al. ,25 the research adopted a longitudinal strategy across comparative cases, which encompassed the three data sources over a period of 4 years (2009–13).
First, documentation was collected, such as initial CLAHRC bids (where possible), annual reports, study protocols, corporate publicity material and minutes of operational and CLAHRC board meetings. In Gephart’s terms, we developed ‘a substantial archival residue’ (p. 1469)129 from the different published sources. All interviews, observational, and documentary material were collated into a case study database, and were organised on a case-by-case basis.
Second, we embarked on a two-stage process of conducting primary data. Data presented in this report encompass the 174 qualitative interviews which took place during the mobilisation phase of CLAHRCs and include a number of bid documents developed prior to the launch of CLAHRCs in late 2008. Overall, 104 interviews were carried out in the first exploratory phase across all nine CLAHRCs. In the second phase of data collection across four in-depth comparative cases, a further 70 interviews were carried out. These second-phase in-depth CLAHRCs were chosen based on the following criteria: variation in antecedent conditions (e.g. site based on existing translational activity or greenfield site) and the social position of the CLAHRC director (NHS or HEI as main employer, clinical or social scientist). The indicative interview schedules are presented in Appendix 1, which were employed as interview prompts. In reality, the discussion engendered in the interviews encompassed much more than is indicated on the interview schedules.
Staff central to the initiatives were interviewed, including CLAHRC senior managers (both HEI and NHS employees, clinical and social scientists), theme leads (clinical scientists and social scientists), researchers, other NHS staff involved in CLAHRCs, such as senior NHS managers represented on the CLAHRC boards and clinicians seconded to work on CLAHRC studies. Given that our theoretical focus was to examine the process of institutional entrepreneurship in CLAHRCs, our interviewees were largely drawn from middle and senior management levels in CLAHRCs and their partner organisations. We did so because such actors were mandated with attempting to enact institutional change.
Our interest lay in examining the motivations of different actors to get involved with the CLAHRC initiative, what they were seeking to achieve and why, and to what extent they thought that they were be able to achieve their aims. The focus of the interviews was broad, but encompassed questions about lead actors’ backgrounds, disposition towards change and vision for CLAHRCs during bid development.
All interviewees and participants of observed meetings were presented with details on the nature of the project and were required to complete a consent form before the interview and/or observation began. As such, the relationship between the researcher and the respondent was made clear at all times. The research was subject to strict NHS research governance and ethical guidelines, and gained ethical approval. Interviews were semistructured in nature, were openly recorded and each lasted between 45 minutes and 2 hours. All interviews were fully transcribed. Interviewing stopped when we reached a point of theoretical saturation – when interviews were only adding marginally to our knowledge. 130
Third, we supplemented the archival and interview data with over 100 hours of site-specific and programme-wide observations. We spent extensive time carrying out observational work, involving attendance at key meetings, workshops, presentations and other educational events. In terms of CLAHRC sites, we undertook observations in six of the nine CLAHRCs. The observation guide is presented in Appendix 1.
At educational events, for example, one or two of the research team would present feedback and facilitate discussion, while a third member of the research team did not participate but observed and took notes with an emphasis on CLAHRC vision and background of participants. The research team attended three CLAHRC directors’ meetings of around half a day in length, facilitated two cross-CLAHRC educational events and gave individualised feedback to four of the CLAHRCs on at least two occasions each. Members of the team were able to attend a range of different intra- and inter-CLAHRC events, involving the CLAHRCs’ senior leadership teams for each case. During the observations, the researchers took detailed notes and then wrote up a more expansive commentary post observation, in which they reflected on what they had witnessed. The notes were written up on the day the visit took place. 131 In collecting the observational data, we were keen to reflect on how the nature of interaction involved by the researchers may have influenced the nature of data we collected.
Qualitative data analysis
Data analysis was iterative and undertaken in an inductive manner, but was informed by key concepts in the literature. 132,133 Each interview transcript, set of observational notes and archival document was read several times, generating and coding themes according to both issues identified in the literature and features of the data that emerged inductively. Analysis was conducted with the assistance of NVivo 8 (QSR International Pty Ltd, Doncaster, VIC, Australia).
Our data analysis involved three stages. Across all stages, two members of the authorial team who had conducted the fieldwork undertook initial coding of the data. In advance of the analysis, we assembled all of the documents, interview transcripts and field notes for each of the cases into a single data file. This enabled us to share data across the research team. In order to understand the complexity of each project,134 we coded the data on a within-case basis. 132 We began by analysing the data collected in stage one, involving all nine CLAHRCs, with a focus on the initial founding conditions of the nine CLAHRCs and their models for closing the T2. We then analysed the four in-depth cases, where we focused on examining how the CLAHRCs were introduced over time.
Across both stages of analysis, we began with a fine-grained reading of the data. 135 After inductively creating a list of first-order codes from the case evidence, we consolidated all of our codes across the nine and four cases, and progressed with axial coding, structuring the data into second-order concepts and more general aggregate dimensions. 136 In doing so, we engaged in deductive reasoning whereby we linked our inductive codes with existing concepts and frameworks. 137 Although we accept that our accounts are one of many potential interpretations,137 we worked in two ways to ensure that we did not retrospectively fit the data to service our theorising. 138 First, we triangulated between data types. Second, we triangulated across analysts with one member, remaining independent of the data, able to challenge and interrogate the coders’ knowledge and interpretations. 139 Our coding was based on interview and archival data, and we included codes in our work only if we had at least four archival and/or interview sources for each of our cases where relevant. The observational data were employed to contextualise and corroborate the interview and archival coding.
In order to avoid identification of individuals or CLAHRC cases, we reveal the social position of the interview respondent only. To define their specific role in a CLAHRC (e.g. director, etc.) would pinpoint the respondent and organisation in question. The process through which we classified actors by their social positions is outlined in Chapter 4. Our approach aligns with our research protocol following ethics approvals, and a need for particular sensitivity given ongoing CLAHRC refinancing.
Consistent with the preceding point, in presenting our qualitative analysis we do not draw explicitly on our observational data, as many of these data (1) were not intended for public consumption, i.e. were a commentary of others; (2) were highly personal views that were communicated in confidence; or (3) revealed the details of meetings, etc., which may risk revealing the identity of respondents. As such, we drew exclusively on data from formal interviews in the text, but employed the observational data as a means of informing our analysis.
We began by examining the founding conditions for each of the nine CLAHRCs in terms of the local institutional conditions, the social positions of the main actors involved and the nature of the process through which the CLAHRC bid was developed, the analysis for which is presented in Chapter 4. Founding conditions constitute a key concept in institutional entrepreneurship theory, which are used to explain variation of institutional entrepreneurship work and outcomes.
The next stage was to take the data for the nine CLAHRCs and examine how the founding conditions shaped the IW undertaken by the CLAHRC actors. We identified distinct theoretical categories of IW that was undertaken, across the nine cases initially, and then in the four in-depth cases following the later-stage developments. All of the different forms of IW relate to the process of enacting institutional entrepreneurship for institutional change. The themes were developed inductively through first-order coding, which then progressed to axial coding, working back and forward between the data and theory, as outlined above. First, this work was related to the way in which actors interpreted the CLAHRC mission and responded accordingly, as shaped by the founding conditions. We termed this work the ‘envisaging’, which we defined as the process through which actors developed an ‘embryonic’ vision of change, based on the interplay between themselves and the context in which they are situated. 26 This work is presented in Chapter 5. Second, was the work that actors undertook in signing up stakeholders of the CLAHRC, which we term ‘engaging’ and present in Chapter 6. Third, was the work around the sustaining of the CLAHRCs, which we term ‘embedding’ and present in Chapter 7. Finally, there was a distinct area of IW that involved the rethinking of initial decisions and learning from the process of establishing the CLAHRCs, which we term ‘reflecting’, and is presented in Chapter 9. All of the different themes are expanded on in the introduction sections to the relevant chapters. Across these different areas of IW, we were able to identify distinct differences in the nature of the work undertaken by actors, as shaped by the institutional antecedents of the local institutional context and the social position of the actors involved.
The final stage of our analyses involved re-examining our data to understand the temporal sequencing of the theoretical categories of IW and the nature of relationships between them. As is common in process-based studies, it is difficult to establish whether or not a process is entirely linear;140 however, we present the second-order codes in the temporal sequence in which they generally emerged in the case histories. Employing both inductive and deductive reasoning, and travelling back and forth between data and theory, we aimed to develop an understanding of how an actor’s social position shaped the envisaging process. 125,132,135 Our emerging theoretical arguments were based on the interplay between theory and data, drawing on both within-case and cross-case analysis. 141 Based on our analysis of the temporal sequencing of the different forms of IW to promote KT we developed a process-based model of institutional entrepreneurship as presented in Figure 1.
FIGURE 1.
A process model of institutional entrepreneurship.
In addition, and based on the work of the different IEs, we identified five different archetype models that were employed by actors to try to close the T2. In Chapter 10 we explore those models and the issues arising from each. In doing so, we emphasise that the models do not represent any one CLAHRC, but rather the elements of the different models that may be exhibited in any CLAHRC.
Patient and public involvement in the research
Patient and public involvement (PPI) in the CLAHRCs was not a theme which we focused on in the project. We recognise, however, that PPI is important to inform and contribute to research,142–144 especially where translational research is concerned. 145 In terms of PPI in the project, two service users were consulted (we use the pseudonyms service user 1 and service user 2), who were ‘experts’ in two different long-term health conditions and were both familiar with CLAHRCs. One service user was consulted at the start of the project to discuss, clarify and provide feedback on our initial thoughts of CLAHRCs. A second service user was consulted for their opinion on the methods employed, specifically on the selection of the four in-depth CLAHRCs and the appropriateness of the interviewees. The second service user was consulted again towards the end of the project for their feedback on the findings of the work and on any further avenues the project should consider taking.
At the start of the project, a discussion took place with service user 1 to discuss and refine our initial thoughts of the CLAHRCs and the view that CLAHRCs were set up differently reflecting the social position of the IEs and focal actors. Service user 1 was asked his view on how CLAHRCs were set up, their mission and the balance between research and implementation:
Each theme is supposed to have a research element and the research element is then supposed to translate into practice through the commissioning of services. Those services should have, research and implementation and both should be brought together and users should be part of that too. That is my understanding of really what the CLAHRC mission is.
Service user 1
Following this initial consultation with service user 1, we proceeded to carry out the data collection across all of the nine CLAHRCs. In choosing the four in-depth CLAHRCs, we consulted service user 2 on his views on the selection of the in-depth CLAHRCs.
I think that it is good picking the different CLAHRCs, and talking to the different directors and other main people, it will provide interesting variations.
Service user 2
Furthermore, service user 2 advised us to consider questioning interviewees on the mission of CLAHRCs and how they were rolled out. His view was that CLAHRCs were led by many ‘powerful researchers’, and that CLAHRCs were ‘to some degree all about research’ – a finding that emerged from the data.
As we began to structure our findings, we consulted service user 2 to discuss and validate the findings. This enabled us to organise the research findings and draw out important points. One of the findings discussed with service user 2 was the variation across CLAHRCs, particularly in relation to the balance between research and implementation.
CLAHRCs talk about getting research quicker into practice but as your findings found not all achieved that. And that’s what I thought CLAHRCs were for, we do the research and then we get it into practice quicker than normal research.
Service user 2
Consulting two service users on different aspects of our research enabled us to think about issues more broadly, refine preliminary results and organise our findings more appropriately. Furthermore, PPI during the project helped us to frame practical recommendations for CLAHRCs and provided useful insights into future avenues of research, specifically around PPI in translational initiatives.
Social network analysis
We complemented our in-depth qualitative research by employing a SNA of the development CLAHRC actors’ ego networks of interaction over two points in time, for the four in-depth sites. Our SNA complemented our in-depth qualitative case studies through providing quantitative evidence as to the extent to which CLAHRCs had enabled the new patterns of working to bridge the T2.
Ego networks relate to an individual actor’s network of relationships and enable us to examine variation across actors’ networks, with a particular focus on the extent to which they bridge the research–practice divide. We examined actors’ ego networks at two points in time: (1) early on in the development of CLAHRCs, and (2) during the run-up to CLAHRC refinancing. In doing so we wanted to gain insights into actors’ ego networks across all levels of the CLAHRC, including those actors engaged in senior and more front-line roles.
To carry out the SNA, we used a web-based sociometric survey [Network Genie146 (Tanglewood Research, Inc., Greensboro, NC, USA)] to capture actors’ personal characteristics and networks, which was e-mailed to a list of CLAHRC staff as agreed with the directors (or deputy directors) of the four CLAHRCs. Each actor was then sent a link to the survey, and we then followed up with a number of additional reminder e-mails. Network Genie enables us to ask actors (the egos) about the people they interact with (the alters). The questionnaire is automatically generated by each actor based on the names they select of people they interact with. The number of names provided for each CLAHRC ranged from 35 to 48, and included actors from a range of different roles including CLAHRC senior managers (both HEI and NHS employees, clinical and social scientists), theme leads (clinical scientists and social scientists) and other NHS staff involved in CLAHRCs, including secondees and researchers. We present an abridged version of the SNA instrument in Appendix 1 because of the problems of presenting a web-based survey.
The first wave of data collection in 2011 (wave I) produced 81 complete responses and the second wave, in 2013, (wave II) produced 86 responses. Sample sizes for each of the four CLAHRCs are presented in Table 1. In wave I we asked actors to outline their networks and patterns of interaction at the inception of CLAHRCs, to capture actors’ actual ego networks as CLAHRCs were first established (i.e. looking backwards). In wave II, we captured actors’ current ego networks (at the end of CLAHRCs 5 years of funding).
| CLAHRC | Survey | |
|---|---|---|
| Wave I | Wave II | |
| CLAHRC A | 22 | 20 |
| CLAHRC B | 17 | 27 |
| CLAHRC C | 27 | 23 |
| CLAHRC D | 15 | 16 |
| Total | 81 | 86 |
Our aim was to examine how individuals’ professional characteristics influenced the four different outcome measures of social interaction for understanding the KT processes in CLAHRCs: (1) formation of networks across academics and clinicians, (2) integration of decision-making practices among CLAHRC academics and clinicians, (3) formation of networks across members of research and implementation themes, and (4) formation of networks across members of clinical and non-clinical departments involved in CLAHRC.
The professional characteristics we focused on were the respondents’ professional background (i.e. academic or clinical), their professional status (i.e. senior vs. junior), the status of professionals in an actor’s ego network, the number of professionals in their network with whom the respondent had not worked with before joining the CLAHRC and the number of professional connections from the same professional category.
Social network research has tended to focus on whole networks, and the extent to which actors find themselves in social structures characterised by dense, reciprocal, transitive or strong ties. These approaches may tell us some interesting things about the entire network and its substructure, but they do not tell us very much about the opportunities and constraints facing individuals. Thus, to understand the variation in the behaviour of individuals, we need to take a closer look at their local circumstances. Describing the variation across individuals in the way they are embedded in local social structures is the goal of the analysis of ego networks.
We collected actors’ ego network data using Network Genie, which asks actors (the egos) about the people they interact with [in our case for the purposes of KT (the alters)]. The typical way to generate ego network data is to create an exhaustive list of alters with whom the respondent has some type of relationship. Termed a name generator, the respondent was asked to list alters who occupy certain social roles, those with whom he/she shares interactions, or those with whom he/she exchanges resources. This approach is used in many classic studies of ego networks. 147
To analyse the SNA data, we employed regression analysis and bivariate analyses where we were limited by sample size. Our analysis consisted of cross-sectional regression models for both waves of data collection independently, thereby providing two snapshots of patterns of interaction. In addition, we conducted longitudinal analyses for the changes in behaviour over time. Specifically, we explored the effects of CLAHRC participants’ professional and organisational characteristics on the change in the measures of the bridging of academic–practitioner networking and decision-making gap, and the formation of connections among members of research and implementation themes and members of clinical and non-clinical departments. The criterion change over time in all cases is measured as the difference between criterion scores in waves II and I (CChange = Cwave II − Cwave I).
We drew on and adopted SNA and in-depth qualitative research to explore institutional entrepreneurship across the different CLAHRCs in facilitating KT. In the following chapters we present our findings, beginning with the founding conditions of CLAHRCs.
Chapter 4 Founding conditions of the Collaborations for Leadership in Applied Health Research and Care
In this chapter we focus on the founding conditions of the nine CLAHRCs. In doing so, we have drawn on the seminal work of Pettigrew et al. 25 that highlighted the importance of context and receptivity for the type of strategic change envisaged by policy-makers in funding CLAHRCs. An important point raised by Pettigrew et al. 25 was that much research on strategic change has been ahistorical. To understand possibilities for future strategic change, we need to understand past patterns of change and stability, which includes consideration of the local context, as well as the national context.
We examined the importance of actors as situated in their local context by drawing on the concept of institutional entrepreneurship. 39 Specifically, we have cast senior CLAHRC leaders as IEs and examined how their position in the structural context of translational interventions impacted on early strategic decisions in bid development. Although organisational fields are in some sense structured by institutional forces, struggles still occur between different stakeholders in relation to resources and social action, and these have the capacity to recreate, and even change, institutionalised practices. Institutional entrepreneurship has focused on the nature of these struggles and how actors seek to influence existing and emerging institutional configurations. 19,88,90,91
Drawing on our literature review of institutional entrepreneurship, and IW more broadly, we have focused on the social positions of the main actors, and how the local-level field conditions played out in each of the localities. Here, in terms of the local institutional context, we identified important differences relating to the partner institutions and the extent to which the CLAHRC was based on new or existing activity (a distinction we term ‘greenfield’ vs. ‘brownfield’). And, finally, how both of the above shaped the initial bid formation process in terms of the extent to which it was an individualistic or collective process. As we will develop later, the important differences in founding conditions shaped the resulting nature of the CLAHRC that was envisaged, and enacted though the work around engaging, embedding, and reflecting.
Social positions of key actors
The CLAHRCs were established to bridge a pluralistic institutional field, spanning both research and practice. As such, the social positions of the main players in each of the nine CLAHRCs varied and shaped how they viewed the CLAHRC initiative. However, a clean categorisation of actors’ social positions, in terms of their primary role or employer, is complex, particularly for clinical academics, which were the largest group of interviewees. In analysing our data it became clear to us that roles were often shared or hybrid in nature, and actors tended to have a dominant orientation, towards the institutions of HEI or the NHS.
Clinical academics were employed by the HEI or the NHS partner and, at times, held joint positions in both research and clinical practice, medical practice and therapy. The data suggest that clinical academics, despite their employer or whether or not they held a joint position, exhibited a dominant orientation towards either research (HEI) or practice (NHS), which was most likely a reflection of their professional backgrounds and the associated norms and values linked to this.
A number of those interviewed were NHS-based researchers but were employed by the HEI, whereas others were employed by the NHS but were part of research projects led by the HEI. In such cases, their dominant orientation towards research or practice was usually linked to the researchers’ CLAHRC role and associated activity rather than the institution they were employed by and in some cases even their professional background.
Finally, a number of people were seconded from the HEI to the NHS or from the NHS to work for CLAHRC in a different role. For example, one interviewee working in clinical practice had been seconded to work as a manager in CLAHRC from the NHS and, in another case, an academic from the HEI partner was seconded to work in the CLAHRC as a manager for the duration of CLAHRC. At times, these arrangements were part of the financial agreements resulting from the interpretation of matched funding by CLAHRC actors. The data, however, suggest that CLAHRC managers were largely NHS-facing because of the nature of their role in CLAHRCs.
Based on the discussion above, we suggest that it is important to combine an actor’s primary role and their dominant orientation to be able to classify actors by their social positions. While acknowledging the diverse professional backgrounds and employment arrangements of those involved in CLAHRCs, and to retain anonymity of those involved, we broadly categorised those interviewed into the following positions:
-
Clinical academic – dominant orientation towards HEI (research).
-
Clinical academic – dominant orientation towards NHS (practice: medical or therapy).
-
Social science academic – may be located in a business school or health sciences department. To retain anonymity we have called these actors social science academics and did not state if they are located in a business school or health sciences department.
-
CLAHRC managers – (not influenced by who they are employed by, as some are seconded from either the NHS or the HEI to work for CLAHRC).
-
Knowledge broker, implementation lead, practitioner researcher or researcher – enacted a hybrid role so that they could act as translators across different epistemic communities in the HEI and NHS.
-
Other – engineering academics.
For the purposes of analytical parsimony in the remainder of Social positions of key actors, we collapsed the seven categories into three main generic social positions: HEI-facing clinical academic, NHS-facing clinical academic and non-clinical actor. We did so because our data suggested that the vast majority of actors were broadly clinical academics [including HEI (research)-facing clinical academics and NHS (practice)-facing clinical academics]. The non-clinical CLAHRC actors encompassed social science academics, engineering academics, knowledge brokers, researchers (largely those employed at a junior and mid-career level for the duration of CLAHRCs) practitioners and managers.
Higher education institution-facing clinical academics
In general terms, HEI-facing clinical academics, although they may have held dual appointments, faced institutional requirements, such as the production of publications and the raising of research income. For such actors, there was a clear incentive to get involved, as CLAHRCs provided them with the opportunity to raise research income. Such a position was attractive to those who had not traditionally secured large NIHR (and other medical funding body) grants, and also to others who aspired to enter the same arena.
I ran the research here at a teaching hospital and quite simply the call came out for academic health science centres of the future as it was called [. . .] It was for centres that had not previously accrued vast amounts of NIHR money, it was for centres that were ready to go, in other words that had research that was ready to make the step change.
Clinical science academic, HEI-facing, case F
Although the CLAHRCs were intended for new, implementation-focused research, for many HEI-facing clinical academics the CLAHRC bid aligned with academics’ existing work. As many HEI-facing academics had projects seeking funding, from their social position the CLAHRC initiative presented them with a new funding source.
So I’ve been involved in lots of projects but the CLAHRC funding gave us the opportunity to fund two studies that we had wanted to do for a long time but we probably wouldn’t have perhaps had access to such a big pot of money. So it was an opportunity really, to develop some ideas that I’ve been batting around for some years.
Clinical science academic 3, HEI-facing, case I
In numerous ways, the opportunity for the funding of existing research projects provided an opportunity for HEI-facing clinical academics to align their current research interests with the CLAHRC. Consequently, there was a significant degree of opportunism for some actors, as CLAHRCs were a suitable vehicle to fund existing work and extend their work as clinical science academics. Many of the CLAHRCs undertook large research projects led by HEI-facing clinical science academics whose research interests were mirrored in the way the CLAHRC was set up and the research carried out.
Arguably, the problem of creating an incentive for HEI-facing clinical academics to interpret CLAHRCs as being similar to a collection of large grant applications was reinforced by the fact that the deliverables of traditional academic outputs were interpreted as being at the centre of the CLAHRC application process. As one CLAHRC manager commented:
I think we have had a reasonable amount of freedom to try and deliver what it is that I think CLAHRCs were set up to do. The brief itself was not the most clear of documents in terms of deliverables: What is it that CLAHRCs are meant to deliver? Tackling the second gap in translation could be interpreted in a million different ways, it doesn’t actually tell you what it is you need to deliver. [My view is that] we are being asked to deliver on traditional academic outputs.
CLAHRC manager, CLAHRC I
Directors who were HEI-facing clinical academics were more likely to interpret the CLAHRC mission through the lens of academic scholarship. In doing so, their focus of attention was largely drawn towards the need to deliver against the metrics of academic publications and research income, as enshrined in performance management structures in the HEI sector rather than in NIHR performance indicators for CLAHRCs.
NHS-facing clinical academics
The CLAHRC directors who were more NHS-facing engaged with the CLAHRC initiative from a different social position. For example, one CLAHRC was led by a NHS-facing clinical science academic with an established track record of managing and delivering change management programmes in the NHS and, as such, interpreted the brief differently from HEI-facing clinical academics.
Why did I get involved? Well I am a clinician by background. I have done a lot of ‘change’ in health-care work, change at a variety of levels of the years including two national change programmes, and they both suffered from the fact that evaluation wasn’t built into the programmes from the beginning.
Clinical science academic, NHS-facing, case D
Here, the focus was on using the CLAHRC as a means of engaging in change management in the NHS, but doing so with a mandate to evaluate the process in order to learn from the experience. This is an interesting distinction from the practice of many of the HEI-facing clinical science academics who had interpreted the CLAHRC bid as a funding opportunity to engage in clinical research, rather than an implementation opportunity. For a number of NHS-facing clinical academics, this was about using any form of evidence to improve practice, and then monitoring how implementation is done.
In my line of work we use RCTs when we want them to stop something happening or to start something happening. RCTs we definitely need, but I just don’t think an RCT is the only way, it can’t be the only solution and it isn’t the way change happens in all of the rest of the real world, you know Microsoft, IBM (International Business Machines Corporation), you name it, they don’t do an RCT and then decide that that is the way forward, they may use evidence but then they decide what to implement and they monitor the implementation.
Clinical science academic, NHS-facing, case D
In addition to a focus on improving practice, the above quote indicates that, in parallel with many of the HEI-facing clinical academics above, the CLAHRC project presented for NHS-facing clinical academics an interesting opportunity to align their interests with funding and work around implementation and health-care improvement.
Before the CLAHRC bids came along I was already working with XX to try and set up a centre for health-care improvement and delivery . . . then the bid came up so we said ‘well that is what we wanted to do; how do we make what we wanted to do meet the needs of this bid?’
Clinical science academic, NHS-facing, case D
This highlights the importance of the antecedent conditions to the CLAHRC that framed the way CLAHRC bids developed. The NHS-facing clinical academics were seen to bring an understanding of what was required in practice in terms of the implementation of specific areas of research, to then help align the rigorous research conducted by HEIs and implement the research back into clinical practice.
The idea of very explicitly trying to use the methodological understanding to inform clinical practice as well as using clinical practice to somewhat change the way I did research was very fruitful.
Clinical science academic 1, NHS-facing, case G
The NHS-facing clinical academics understood the importance of clinical and health services research, but emphasised the need to apply and embed the research into clinical practice. For the NHS-facing clinical academics the emphasis was on changing practice, not with driving academic profile.
My leadership model is not to drive the academic profile because actually they don’t need that [. . .] When the call for CLAHRCs was announced my vision was to create a platform for world class health services research, that had its application in the [local] health economy, but which was driven by an academic partnership between the small but strong group in health services in the [university partners] which arguably has, certainly in the UK, a portfolio of health services research.
Clinical science academic 1, NHS-facing, case H
In summary, as documented in the previous section, NHS-facing clinical academics were more likely than their HEI-facing counterparts to view CLAHRCs as a means to promote service delivery. For NHS-facing clinical academics, the importance of research stemmed from what it could do to enhance service delivery.
Non-clinical actors
Actors who lay outside the mainstream clinical academics were largely social science academics from business schools, health science departments and engineering departments. In deciding how to allocate the funding in the CLAHRC, one social scientist commented that:
It was like a bun fight. The usual suspects are there fighting their corner for the research income, to continue their current projects, and I needed them on the bid to get the money from the NIHR. Once they’ve got what they want, trying to get them to act in a CLAHRC-type manner is very difficult.
Social science academic 2, case E
Many of the non-clinical actors held a strong perception that they were the outsiders in the CLAHRCs. As non-clinical actors who did not conform to the clinical academics’ gold standard of RCTs for research, their approaches were often viewed as being rather ‘woolly’ by some clinical academics. Although in a number of cases business schools were well integrated into CLAHRCs, as well as engineering and health sciences schools, this was not always a comfortable relationship.
Social science academics brought expertise to clinical settings around the diffusion of innovations, KT and understanding organisational behaviour and change management – all crucial to bridging the implementation gap. However, different academic disciplines hold distinctive research models and assumptions about the nature of research and the way in which it should be implemented. NHS-facing clinical academics were concerned with improving clinical care through the implementation of existing research and HEI clinical academics tended to be more research oriented using the CLAHRC as a funding stream to carry out new research.
What is interesting is working with those clinical researchers who know an awful lot about their subject, who are really, in some cases, really cottoning on to the idea that there is something about evidence based how to do as well as evidence based what to do.
Social science academic 3, case C
In general, social science academics viewed the implementation gap as a complex KT problem and focused on ‘how’ to implement research into practice. Furthermore, social science academics examined the context in which evidence-based innovation is implemented, which is often non-linear, unpredictable and dependent on a number of interconnected social processes and professional networks. Behavioural change and lessons around organisational change were identified as important to social science academics. This suggests that success for CLAHRCs involved understanding interactions between research and practice, and between different academics’ communities, in order to harness the positive synergies from interactions between different groups.
There are different levels and there is stuff about how to change behaviour and organisational change, and bringing all those things together is challenging. It is not just about the research themes and the products that they produce, it is research and implementation.
Social science academic 3, case C
We note that two CLAHRCs were originally led by social science academics and that, in one of these at least, the envisaging of CLAHRC differed from that seen in CLAHRCs led by clinical science academics. This was clear from the way the CLAHRC was set up, incorporating a large number of knowledge brokers, and the distinct focus on KT initiatives from the start. We suggest that, and as we will outline in the next chapter, actors located in more social science- and/or engineering-facing roles were more likely than their clinical science counterparts to view the T2 as being an organisational or systems-level problem.
The danger is that we could spend all of our time convincing academics to move closer to practice, and for practitioners to engage more in research, but that will all be for nothing if we cannot embedded the changes at a system level. Without system[-]level change we may able to ‘turn a few heads’ and get people to ‘act in a CLAHRC-type way’ while we are resourcing them. But what happens when the money stops?
Social science academic 2, case E
Although CLAHRCs set out to bridge the divide between academics and practitioners, the different epistemic academic communities (e.g. clinical and social science interests) at times resulted in tensions in interpreting the CLAHRC mission and the way in which it was envisaged by those central to CLAHRCs. We discuss this further in Chapter 9 with respect to reflecting on CLAHRCs.
Overall, based on the discussion of social positions, we can see that there is variation in terms of who the main actors were and their location in the field. We suggest that the different social positions shaped the ‘cognitive context’, in terms of both orientation and agency, of how different actors envisaged the CLAHRC initiative. 148
The local field conditions
The local field conditions helped shape the way in which CLAHRCs were founded. This meant that pre-existing relationships with NHS partners, academics and other organisations, as well as projects, played a role during the putting together of each CLAHRC’s bid. CLAHRCs were seen as a well-resourced opportunity to fund existing research and networks, and were used pragmatically to build on existing research and expertise in both research and clinical practice. It was important to leverage existing, more mature research for translation to be effective but also possible. Furthermore, academics often viewed the CLAHRC as an ideal opportunity to showcase their academic expertise.
There is a combination of that which is pragmatic, it fits, it is a worthy candidate for this resource, but the resource isn’t likely to be wasted because it is building on a heritage and foundation of good quality science and that is important. It is also a strategic view as well on the part of [director] and a senior group of influential pro-vice chancellors.
Social science academic, case H
In one CLAHRC, such antecedent conditions included strong service user networks, but this might be characterised as unusual (we noted that all CLAHRC leaders claimed strong user networks in bids, although, interestingly, they did not commonly privilege this in their interview accounts).
When we set up our original research unit pre CLAHRC, it included people interested in involving patients in research design. We also had a very longstanding patient organisation that was well funded. The net result is that patient–public involvement is not as new in our CLAHRC as others.
Clinical science academic 1, NHS-facing, case G
Accordingly, in the next sections we focus on the pre-existing relationships that were most influential as CLAHRC founding conditions.
Pre-existing relationships and networks: higher educational institution – NHS
In a number of regions there were strong pre-existing relationships that spanned both the HEIs, which cut across different departments and local NHS organisations. Where these relationships were well established, they enabled actors in the region to quickly mobilise other individuals and also to co-ordinate existing activity behind the bid, thereby enabling the CLAHRC to ‘hit the ground running’. Senior actors, mainly clinical academics, both HEI- and NHS-facing, had strong connections in the HEI and NHS and were able to use these networks to mobilise groups together during the bid process.
In terms of research what we did was we found that there were people with similar research interests that ran across the NHS and the university that weren’t represented by a department so what we do is we form an institute of health sciences, a research network. Then this network then meant that when the bid came along to form a CLAHRC the opportunity was there because we had a readymade network and we were already working in partnership with the NHS and we already had clinical themes.
Clinical science academic 1, HEI-facing, case C
That many CLAHRCs focused on existing relationships was also encouraged by the short time frame in which the application had to be put together. There was only a limited time period for actors to build a coalition of people and then to write the bid. Therefore, those central to this process drew on existing networks and relationships to locate research projects.
I think you have to recognise that there was a fairly rapid assembly of a group of academics who come from different backgrounds and perspectives and that you bring your own historical personal baggage to these things.
Clinician, case I
For one applicant, the writing of the bid was deemed to be straightforward because the remit of the CLAHRC fitted exactly what it had been doing in the local region.
It is one of the easiest grant applications I have ever written, it wrote itself because we had done a lot of ground work. The ideal way of scaling up that ground work and the theory into great application and implementation was through CLAHRC, they were asking for the sort of things we wanted to do anyway.
Clinical science academic 4, HEI-facing, case C
Pre-existing relationships were considered to be an advantage in the formation of CLAHRCs, particularly where they spanned HEI and NHS organisations. In one region, the existence of a joint institute between a HEI and a NHS organisation was ideally suited to the CLAHRC call.
[the institute] is . . . clinically facing, [doing] applied, relevant research and that is why we were originally set up. It happened that we were at that end of the research spectrum between the pure and the applied, there are other areas of research strengths but they were not very good at applied if you like.
Social science academic 1, case E
As such, pre-existing activity and relationships across the CLAHRCs helped in the formation of the CLAHRC model enabling the extension of existing research. However, in drawing on existing relationships actors also ran the risk of constraining CLAHRCs’ activities in the future.
Basically if I am very honest it was going to be an extension of where we got to with existing research before we run out of funding for doing it . . .
Clinical science academic 2, HEI-facing, case C
In a number of cases some CLAHRC actors were concerned by the fact that the founding of their CLAHRC had been significantly influenced by the need to plug funding gaps for existing research projects.
[. . .] basically the CLAHRC was set up, the academics got together and said ‘Oh what projects have we got that we want to get funded?’ and then put those projects in with the bid and they’ve got the funding for them and then just gone ahead and done them.
CLAHRC management 1, case I
Rather than a new fresh CLAHRC initiative, in a number of cases, some actors viewed that the reliance on existing relationships, particularly research strengths, meant that the CLAHRCs were captured by certain vested interests. We develop this idea in the next section.
Brownfield compared with greenfield sites
As outlined above, CLAHRCs were shaped by current activity. This can be understood through the terms ‘brownfield’ and ‘greenfield’. Brownfield applies to CLAHRC bids that were built on existing activity and greenfield describes bids that were shaped around new activities. In developing CLAHRC bids, it was common for actors to first look at pre-existing research activity in their region.
We started with what we have got on the shelf. Then we looked at what are we good at. So we were looking for well-developed projects. And [one clinical science academic] was working in this area, had the programme grant that had not been funded but had received very good feedback [. . .] So that is where we started with the projects and how we ‘chose’ what got into the CLAHRC projects.
Clinical science academic 1, HEI-facing, case B
The CLAHRC funding provided an opportunity for failed research bids to be funded and the continuation of existing research projects. However, all actors acknowledged that the research needed to have a greater focus on implementation and the dissemination of the research findings than was common in standard models of research funding.
Although perceived as necessary to mobilise engagement for the CLAHRC bid, in what was described as a short space of time for bidding, the presence of existing activity and networks acted as a cognitive constraint on some actors in terms of how they conceived the CLAHRC initiative. Specifically, basing the CLAHRC on existing activity ran the risk of actors interpreting the CLAHRC as simply a large research grant led by people who operated within pre-existing relationships and networks and who were already engaged in applied research.
The CLAHRC partly feels a bit like a programme grant in that we’re allowed to sort of do that development work, they’re all these sorts of straight RCTs. So I don’t think that was alien for us, a lot of us are involved in a whole variety of different programme grants. And in many ways, CLAHRC just feels like a massive extra large programme grant in a way.
Clinical science academic 5, HEI-facing, case C
There was clear acknowledgement that encouraging HEI-facing clinical academics to think more along the lines of CLAHRCs than traditional large-scale grants was a real challenge.
So we didn’t [referring to programme/theme leads] realise that this was a different type of research. So we have had to move down the scale towards the more applied side of research. Though we still have a way to go, and still needing to move away from the removed researcher who is primarily assessed on their ability to produce valid results and publish in high-quality journals.
Clinical science academic 1, HEI-facing, case B
As we will return to later in this report, the integration of existing research projects into the founding of CLAHRCs created specific issues around managing the mindsets of specific individuals in terms of the uniqueness of CLAHRCs. The issues were particularly pronounced where funding for the projects were allocated during the bid formation. However, research projects that were required to put the bid together at the start led to more traditional research-focused projects, which would later lead into implementation.
Most of the money being allocated to named projects before the actual funding came in and the CLAHRC started. So that was pretty much set in stone, so that was kind of difficult to change. There wasn’t really much scope to start a CLAHRC process of engagement and then designing and sort of funding projects through that; it was all pretty much done before. I think a lot of that was to do with the fact that was a very short cycle of trying to get a bid in. And so to get partners on board I think we had to allocate funding to them, so they could then bring those partners together.
CLAHRC management 1, case I
The use of brownfield sites ran the risk of shaping the path along which the CLAHRCs unfolded, which later constrained the discretion of CLAHRC directors.
We didn’t involve the business school or other areas and I think if we had done that, then it might have been easier to have a different type of model where for example you had a more kind of engagement process to start with and then allocating money afterwards.
CLAHRC management 1, case I
Where the CLAHRC was developed as more of a greenfield site, with less focus around existing activity and relationships, this had a different effect on how the CLAHRC was conceived. For example, there was less consideration about how the different elements of existing activity could be integrated into a coherent package of CLAHRC activities. Instead, the question was framed more in terms of ‘what do we want to do?’.
The CLAHRC came along as an opportunity and we all tossed around a fair number of ideas at that time about what we would do, so we are almost going back to where we were before CLAHRC and saying ‘well what do we now need to do’.
Clinical science academic, NHS-facing, case D
By not drawing on established relationships and activity in the region, senior actors started with more of a blank sheet of paper in envisaging their model of a CLAHRC. In one CLAHRC, after funding was secured, the model was one of trying to embed themselves into existing activity in the region. This shifted the focus of CLAHRC activity to the local needs in which the CLAHRC would eventually operate. However, developing the CLAHRC as a more greenfield operation brought with it a number of risks.
People didn’t really know where we were coming from, so the job of getting them on board, and the job of building a consensus for that would be much tougher, and it’s had variable results.
CLAHRC management 1, case D
The process of bid formation
The process of bid formation differed across CLAHRCs, particularly in relation to the extent to which the process was a collective one managed across a range of different actors. In the majority of cases the initial bid was written employing a collective approach, at least in the initial stages of bid construction. In other cases, a much smaller group of individuals wrote the bid, which was more of an autonomous approach. We suggest that the nature of the bid formation process was shaped by the social position of the local actors and the local-level field conditions.
The most common approach to bid formation was collective in nature, and was driven by a number of factors, including the status of the CLAHRC director in relation to other ‘big players’ in the locality, the extent to which there were pre-existing relationships between HEIs and NHS in the locality, and the level of existing activity that could be encompassed as CLAHRC activity.
There were people that were brought in because it was clear that we had to focus on the applied clinical research and we basically tried to include the people that had a very strong track record.
Clinical science academic 1, HEI-facing, case I
It was common that, in each region, a range of meetings were held, which brought together key actors from HEIs and the NHS over a period of 9 months leading up to the bid. In some cases, as well as pre-existing relationships and activity in the local landscape, there were also existing structures and groups that automatically fed into the CLAHRC bid, making the bid process smoother.
We had a readymade group and structure for creating the connections that were necessary to do this bid and immediately mobilising that through the institute that already had a facilitated infrastructure.
Clinical science academic 1, HEI-facing, case C
An important factor in the promotion of the collective process was that many HEI-facing clinical academics were attracted by the amount of research funding on offer, which provided them with the incentive to engage in a process to ensure that ‘their research projects’ were included in the collective formation of the CLAHRC. Furthermore, during the bid-writing process it was natural for those leading the CLAHRCs to look internally to what their strengths were and the needs of the local population and health landscape, and then structure the bid around these areas. Many HEI-facing clinical academics leading the CLAHRCs mobilised other clinical academics together to integrate research projects into the bid.
In some CLAHRCs and in the beginning at the bidding process, the director would ask certain people if they could put together a research project. At times research projects were already in the pipeline or were already running, so they would just put those ideas forward.
CLAHRC management 1, case I
In particular, we note that many HEI-facing clinical academics had a vested interested in ensuring that their research projects were part of the CLAHRC bids and, for this reason, sought to influence the process of bid formation in their favour. Their ability to shape the bid-writing process was influenced by the extent to which the lead bid writers perceived that they needed the ‘big name’ HEI-facing clinical academics on the bid in order to demonstrate research excellence to the NIHR.
In a number of regions there were well-established relationships across HIE and NHS organisations, which in some cases involved existing hybrid organisational forms. In regions where well-established relationships were present, gaining early involvement of NHS partner organisations was straightforward, particularly when the NHS organisations were deemed to be ‘research savvy’. In the absence of such relationships, HEI-facing clinical academics found it more challenging to engage with the NHS partners during the bid processes because there were differences in opinion about what the CLAHRC was set up to achieve. These differences reflected common issues arising from the T2.
The more autonomous process of the CLAHRC bid formation was less common. This type was associated with the strong social position of the CLAHRC director, either in his or her local region or nationally, and a lower level of vested interests stemming from pre-existing relationships and existing activity in the local region.
The director has an excellent reputation in terms of the national collaborative of programmes. He has a lot of respect locally from both medical and managerial staff and executive staff. We’ve been given quite a lot of freedom to get on with it, partly because of the trust and the respect that people have for the director [. . .].
CLAHRC management 1, case D
In the case below, the actor was able to act with relative autonomy because of his position in the region and, also, because there was limited interference from HEI clinical academics.
Having a good strong director makes a big difference, someone with gravitas and breadth, someone who can broker relations and so I particularly enjoy working with the director.
Clinical science academic 4, HEI-facing, case C
Under such conditions, a small number of CLAHRC directors were able to lead the bid formation process in a less collective manner.
I mean generally it was me and the director saying about decisions being made and stuff, I think at the beginning no one else quite understood what we were doing. They liked the sound of it or they liked bits of it, there were bits of it they felt comfortable with but no one got the whole picture.
CLAHRC management, case D
As a result, and as we will develop in the next chapter, the resulting envisaged model of CLAHRCs was significantly different to that seen in other CLAHRCs.
Conclusion
In terms of the founding conditions, we have highlighted the importance of (1) the social positions of the main IE actors; (2) the local field conditions in terms of the extent to which the CLAHRC was being developed as a brownfield development or was more greenfield in nature, and the existing relationships between NHS and HEI organisations in the local region; and (3) the resulting influence of the actors’ social positions and the local field context on the degree to which the bid formation was an autonomous or a collective process.
Our research suggests that actors’ social position shape their relationship with the local region in which they are embedded. 149,150 Actors’ social position is important because it influences both their perception of the local context105 and their ability to influence others. 101 In terms of an actor’s social position, we concluded the following. First, HEI-facing clinical academics were generally more likely to view the CLAHRC initiative as another opportunity to gain income to fund their research activities. Given that HEIs often privileged academic publications and research income over other forms of performance indicators, such as research impact indicators, this approach is logical for many HEI-facing clinical academics. Second, NHS-facing clinical academics were more likely to view CLAHRCs as a means to promote service delivery. For NHS-facing clinical academics, the importance of research stemmed from what it could do to enhance service delivery. And, finally, non-clinical actors, including social science academics located in business schools and health sciences departments, health services researchers and engineering academics, sought to use theories and concepts of KT to bridge the implementation gap. However, this group commonly viewed the CLAHRC as a means of generating and testing of academic theory about KT.
In terms of the local field conditions, the presence of pre-existing relationships that spanned HEI and NHS organisations meant that a greater number of actors could be drawn together to develop the CLAHRC bid in a short space of time. In addition, the nature of the local field conditions also shaped who was involved in the bid formation stage. Both the presence of pre-existing relationships and activity shaped the extent to which the CLAHRC bid was developed in an individualistic or collective manner. Where there were pre-existing relationships and activity, the development of the CLAHRC was carried out in a collective manner, and more actors, with their vested interests, were involved. In contrast, where there were fewer pre-existing relationships and less activity, and particularly where the lead actor occupied a powerful social position, the bid formation process was more autonomous in nature, and the resulting CLAHRC was more of a pure de novo activity.
In examining the founding conditions of each of the nine CLAHRCs, attention was drawn to the extent to which the founding conditions may engender ‘lock-in’ towards distinctive ways of conceiving and mobilising CLAHRCs, as evident in the diagnostic and prognostic framing within the envisaging processes. This is discussed in the next chapter.
Chapter 5 Envisaging the Collaborations for Leadership in Applied Health Research and Care
In the previous chapter, we examined the founding conditions of each of the nine CLAHRCs. We suggest that the founding conditions provide the ‘cognitive context’148 through which actors make sense of the world in responding to the call for CLAHRCs to develop a model for closing the T2. Envisaging has been highlighted as the important first stage in any change process in which actors form a vision of the change they want to enact, which is based on the interplay between themselves and the context in which they are situated. 26
Envisaging renders visible the often subconscious views that influence attitudes and behaviours, and enables us to understand the relationships between the objective field (here, funding opportunities) and actors’ subjective views on the potential for change (their ‘envisaging’). Individuals frame problems and propose changes in routines that are grounded in their perspectives as members of distinct and different professional communities and backgrounds. 151 Frameworks, or schemata of interpretation, enable the individual to derive meaning and to locate, perceive, identify, and label events they experience. We identified two main envisaging activities: diagnostic framing and prognostic framing. Diagnostic framing is the process through which actors identify and diagnose the source of the problem affecting current practice and assign blame. 152 Prognostic framing involves generating potential solutions that can be promoted as being superior to a previous arrangement, thereby delegitimising existing institutional arrangements and those supported by opponents,152,153 and legitimating to stakeholders the new form of practice. 154,155
In examining the nine CLAHRCs we found significant variation in the way in which the different actors envisaged their CLAHRCs, in terms of both diagnostic and prognostic framing. The point was succinctly made by one actor:
Well I think that one of the things we discussed at the time is that absolutely we are accountable to the NIHR. There is a lot of money and you have got to have accountability and you have got to report to them, but it is almost equally important to our local partners because at the end of the day, if we tick every box for the NIHR, but our local NHS partners aren’t happy then we have failed completely because the CLAHRC is set up to leave that legacy and that infrastructure.
CLAHRC management, case H
In the following sections we examine the different ways and degrees to which the main actors engaged in diagnostic and prognostic framing. We then relate the nature of envisaging back to the founding conditions of the CLAHRCs. In our analysis we present the main themes and recognise that there may be divergent framing within any CLAHRC depending on the main actors involved. The different frames are, therefore, related to broad groups of actors.
Diagnostic framing
Some actors’ diagnosis of the problem that CLAHRCs were required to solve was the closing of the T2 and they shaped their bid accordingly. However, for others, there was limited engagement with diagnostic framing, as they saw the CLAHRC as another programme grant.
From my perspective, what I think CLAHRCs are for is not necessarily what all the other senior academics in this CLAHRC or other CLAHRCs that I have spoken to think they are for. Some people I think, some senior academics I know that are involved with CLAHRC seem to think they are rather like programme grants and they get down to their theme and they think ‘I am just going to do it because it is applied health research and it is good for the NHS’. I think, myself, my reading of the CLAHRC is that the themes ought to all be replaceable because they are vehicles for doing something else, the research is a vehicle for doing something else.
Clinical science academic 2, NHS-facing, case H
It was interesting to observe that there was heterogeneity in terms of the way in which actors constructed the problem. We identified three dimensions of their diagnostic frames, which we will discuss below. It is important to note, however, that the dimensions presented are not mutually exclusive.
What is the problem and who defines it?
In addition to the translational problem, actors also highlighted the issue of who defines the problem and its meaning to different actors. For example, the problem could be defined by a number of different actors, ranging from the end user of the service, to the person who is delivering the service, to the commissioner of the service. This changed depending on whether clinical academics were HEI- or NHS-facing, but also across different clinical domains, and whether actors were therapy or medically oriented. Clinical academics who were practice facing tended to define the translational problem more in terms of improving patient care through improving services rather than focusing on generating new research. CLAHRCs were seen as a vehicle to take evidence and implement into clinical work to improve services:
I think the services we have are very caring and would do anything, but I think we just don’t have that culture and I guess what I see myself as doing is trying to sow that seed of having that kind of culture in practice so that therapists actually understand about putting this evidence in practice and understand that we need to include so many people and we need to take the evidence and implement it in our work and getting it working and accepting that there will always be limitations.
Clinical science academic, NHS-facing, case E
Furthermore, many CLAHRC actors highlighted problem definition as key to being able to more easily ‘translate the findings of research into practice’, through the development of a more engaged and receptive audience for the knowledge. It can be argued that by engaging practitioners and users in the problem definition, researchers will be more able to incorporate an agenda of practice, enhancing the relevance of their work to practice. In this regard, the issue of who defines the problem neatly aligns with the more translational diagnostic frame highlighted above.
Our NHS partners want to see the researchers bring them something that they have already done so that they can perhaps reply with the need, but the researchers will tell you that in order for them to get off the ground and align themselves with the NHS they need to know at the very start. So you have got this tangle of misunderstandings and it is almost a self-fulfilling prophecy where the NHS want to see something and the researchers don’t want to do anything in case it is not what the NHS need and so on and so forth.
CLAHRC manager, case H
For others, however, the issue of who defines the problem was much more significant and challenged some of the assumptions of the KT model. A number of actors argued that there was a degree of commonality of what was done across the research and practice divide, but that what was missing was an agreement of what the fundamental KT problem was. One CLAHRC director displaced the concept of KT to focus instead on the problem itself:
Knowledge translation is a really bad idea. In my view the formulation of the problem is the problem. Start with the problem and work backwards. [. . .] Telling them [clinicians] about the research is a pretty kind of thankless task. I don’t like the phrase knowledge translation, because what is needed is not knowledge translation, it’s about starting with the person who is going to make the decision and then working with them to understand how they can narrow the bounds of their uncertainties by using what is out there.
Clinical science academic 1, NHS-facing, case G
The argument was that the problem was not really about how we get knowledge to move across groups or epistemic boundaries, but instead the problem was about clearly defining the issue itself, starting from practice:
The problem is not an epistemic one, it’s about pragmatism . . . the old fashioned idea about the separation between knowing and doing; that’s the problem. We need to start with the problem and work backwards, and we may look everywhere for different sources of knowledge.
Clinical science academic 1, NHS-facing, case G
A similar position was adopted by another NHS-facing CLAHRC, in which the term KT was also disliked. Rather than focus on translating knowledge, it was important to focus on generating user relevant knowledge though processes of implementation.
I would start by disagreeing with the concept of knowledge implementation/translation. I guess the whole of our CLAHRC approach challenges that. It’s about creating ‘knowledge through doing’. We can only learn what works in the real world through doing things. And that doesn’t mean you can’t take knowledge from elsewhere, but you need to assess how valid is that evidence or how real is that evidence.
CLAHRC management 1, case D
How can we translate evidence?
One view of the translation gap was that current practice is inefficient in using existing research. Rather than starting by conducting more research that could be better translated into practice, according to this view, it is important to place a greater emphasis on using existing evidence and adopting a problem-solving approach to clinical questions. Poor communication was identified by one clinical science academic as a key barrier to the use of research:
The problem is one of making our research more accessible to practice. If we are to close the second translation gap we need to make sure that they use our evidence more, and one way of doing that is making sure we communicate it to them in a way that they can more easily understand it and therefore use it. Translation occurs when I write and they read.
Clinical science academic, HEI-facing, case A
The problem of a lack of receptivity for existing research delayed the uptake of research in certain clinical domains. To some extent, not only organisational affiliation, but also the clinical discipline, impacted the envisaging of CLAHRC mission. For example, an academic with a background in therapy viewed the CLAHRC mission as an opportunity to expand clinical domains.
We know from lots of literature reviews and surveys that therapists don’t read anything other than their own professional journal. They don’t like looking anywhere else for any evidence. I am always banging on about reviewing the literature outside your own profession to inform your practice, but that doesn’t happen and it still doesn’t happen.
Clinical science academic, NHS-facing, case E
We note that the ‘translational perspective’ dominant diagnostic frame fitted well with actors who were drawn from more research-oriented social positions. A number of actors argued that the ‘translational perspective’ reflected the way in which the CLAHRC funding process was organised, which focused on a discourse of ‘translating evidence into practice’. As one social science academic commented:
CLAHRCs are a product of backroom decision-making where the flavour of the day was the ‘translation of evidence into practice’ is the problem; and have been rather captured by the notion that ‘translation’ is the problem.
Social science academic 2, case E
As we will outline below, other actors diagnostically framed the problem facing CLAHRCs in a different way, but there was a dominant steer from the commissioning process to use the ‘translational perspective’ to shape their CLAHRC bids. For example, one NHS-facing clinical academic spoke of tensions between different perspectives being evident at the stage of the commissioning of the bids and in the interview process during the CLAHRC bidding process:
[. . ] we saw ourselves as trying to address that problem: the problem of clinical variation not the problem of translation. The discussions in the committee were quite quickly pushed by the officials towards translation. But a number of people on the committee [. . .] were keen to force the discussion back to saying that that is not the question, the question is ‘how do we provide best health care?’
Clinical science academic 1, NHS-facing, case G
Consequently, a number of actors questioned the very idea of a translation gap, arguing that defining the CLAHRC mission as being to close the T2 misses the point. As outlined in the previous section, discussions of translation tended to ignore the issue of what is the problem and who defines it, which some actors saw as the key issue facing CLAHRCs.
Of course translation is important and I do agree that there is a moral imperative to use the evidence that you have. We cannot lose sight of the fact that the areas where there is evidence are often decided by rather idiosyncratic priority setting by academics. [. . .] I don’t think that the CLAHRC is just about the second translational gap at all, it’s much more complicated than that. How I would characterise it, in terms of my own research, is that I try to do research that answers questions of real significance for the people who are trying to use research – people who make decisions at every level from policy to individual people who have to decide whether they will use an intervention or not.
Clinical science academic 1, NHS-facing, case G
Individual compared with organisational/system-level problem
The third dimension of diagnostic framing was whether the problem lay at the level of the individual or at a more organisational or systems level. The vast majority of CLAHRC actors viewed the challenge facing CLAHRCs as one of changing individual actors’ behaviours. We suggest that this focus is aligned with clinical academics’ model of ‘curing the patient that faces them.’ In envisaging CLAHRCs, a small number of actors diagnosed the problem as being at a more organisational or systems level. Such actors were more likely to be located in social sciences- and/or engineering-facing roles:
The problem CLAHRCs are there to solve are system-level problems. The danger is that we could spend all of our time convincing academics to move closer to practice, and for practitioners to engage more in research, but that will all be for nothing if we cannot embed the changes at a system level. Without system-level change we may able to ‘turn a few heads’ and get people to ‘act in a CLAHRC-type way’ while we are resourcing the CLAHRCs. But what happens when the money stops?
Social science academic 2, case E
The focus on an organisational/systems-level approach is based on the diagnosis that even if one can change peoples’ behaviour within a specific CLAHRC project, actors are more likely to revert to convention once they leave the project; institutional forces will continue to orient actors’ behaviour towards the dominant institutions they face and that any change in behaviour will arguably be only temporary in nature. In order to embed behavioural change, the challenge is how CLAHRC behaviour can become sustainable while independent of financial incentives. This position was echoed by a NHS-facing CLAHRC director in a comment about the role of resources in the CLAHRC project:
We shouldn’t be thinking about how we find second translation gap solving work. We can’t keep asking for more financial resource as this may be the problem itself . . . We need to think ‘how can we do this with no additional financial resource?’
Clinical science academic, NHS-facing, case D
Arguably, if CLAHRCs are successful in embedding change in local health-care systems there would be no need for CLAHRCs. This position was made by a NHS senior manager chairing a CLAHRC:
This is not about academics just getting their research grants. It’s about leadership, and CLAHRC reaching the parts that we don’t normally reach. To do so we need to build capacity for innovation so that we sustain change.
NHS senior manager, case E
We note that the NHS senior manager above was one of the few CLAHRC leaders to highlight its importance in sustaining any translational gains through capacity building.
Whether actors diagnosed the problem facing CLAHRCs as being located at an individual level or at an organisational/systems level had important implications for the way in which CLAHRCs were mobilised and, in particular, it influenced actors’ work to embed CLAHRCs. Although few actors diagnosed the need for an organisational/system-level approach themselves, the development of knowledge broker roles did diffuse through many CLAHRCs, as actors worked to embed their models (as discussed in Chapter 8, Findings of longitudinal data analyses). However, we suggest that the diffusion of the knowledge broker role was driven by mimetic isomorphism, rather than the initial diagnosis of the problem of CLAHRCs as being organisational/systems level in nature.
Prognostic framing
Prognostic framing involves the articulation of a proposed solution to the problem and the strategies for carrying out the plan152,153 Research suggests that there tends to be a correlation between an issue’s diagnostic and prognostic framings, which means that the identification of specific problems and causes tends to constrain the range of possible ‘reasonable’ solutions and strategies advocated. 152,153 In this way we suggest that there is a generative rather than deterministic relationship between diagnostic and prognostic framing.
Marrying research to local needs
All of the CLAHRC senior-level actors were aware of the importance of tailoring their activity to the needs of local NHS organisations and their staff, users and carers. A general position from CLAHRC directors and senior staff was that, in order to close the T2 and determine a research agenda, different actors had to work together. This included clinicians delivering health services, and patients and carers receiving the health services.
The research the academics carry out in collaboration with their partners is seen as more relevant, and clinicians and patients have more ownership of the research findings and so are more likely to engage with them at the end of the process. It’s greater engagement throughout, leading to greater uptake and engagement at the end.
Clinical science academic 2, HEI-facing, case G
In a number of the CLAHRCs, the local need was defined not only by local NHS organisations, but also by the end user/carer who was the recipient of the service.
We have a very strong ethos, our principles are around capacity development and they are around public patient engagement, so we have a strategy that crosses over, so they are very cross cutting.
Clinical science academic, HEI-facing, case F
However, the manner in which this came through their prognostic frames was shaped, to a greater or lesser degree, by the local context and actors’ social positions. In many of the CLAHRCs, the focus of activity was more determined by the current research strengths (including engagement and implementation) of the HEI partner.
I must say though that implementation has been absolutely central to what we have done before and a few years ago we were sitting around tables saying ‘well we know it works in the NHS, but we can’t continue it in the NHS because there is no means of doing that’, so that was actually our experience, we had done all of this before, but with no means of implementation.
Clinical science academic 2, HEI-facing, case C
We suggest that this was particularly the case where the local context was one that resulted in a more collective bid-writing process. In such instances, work was undertaken to align existing research activity to local NHS needs.
Each of those themes were reasonably clear about where they wanted their research to go. They’ve remained pretty fixed. Certainly in conceptual terms, the details have evolved. Conceptually what we want to do is to understand how services are currently defined or designed, defined and developed and improved [ . . .] To understand that current practice and then to look at ways that new practices that are sympathetic to the skills and knowledge of the people within that organisation could be introduced.
Clinical science academic 4, HEI-facing, case B
There were a number of reasons why many of the CLAHRCs worked from areas of existing research strengths and then mapped them on to the needs of the local NHS providers. First was the idea that research would translate into practice best where there was a mass of high-calibre researchers, i.e. focus activity where the HEI was strongest. Second, in order to gain legitimacy with the NIHR, there was the perception that, for the purposes of getting past the commissioners of the CLAHRCs, there would be a need to ‘go in with the research superstars’. Where this was the case many actors worked hard, under a constrained time period, to align existing and potential programmes of research with local NHS needs.
In many ways we arrived at a marriage of convenience, through which we coproduced a research agenda for the CLAHRC in around 3 months, from start to finish. Other CLAHRCs were far more fortunate in that they were less time constrained and so could spend longer in aligning the interests of research and practice. Although we were working to a very tight time schedule, at least we could ‘hit the ground running’.
Social science academic 2, case E
As outlined in Chapter 3, two CLAHRCs were particularly independent as a result of the director being very NHS-facing and/or being able to secure large amounts of funding in a single body that enabled them to specify the research themes/programmes in detail beforehand, rather than designing activity around a portfolio of existing research projects:
From that perspective it actually gave us a lot of freedom to separate from the pull of ‘oh we need more research money or we need to make up for the loss of the clear funding’, which was a big challenge at the time. So we were completely free from that from some extent to be creative and to really focus on what we saw as the main call for the programme around how do you implement research into everyday practice. Rather than thinking we’ve got lots of research teams that we need to bring more funding in for, we can start with practice defined problems.
CLAHRC management 1, case D
Research the ‘doing’
Similar to marrying research to local needs, some actors prognostically framed CLAHRCs as vehicles that should research the ‘doing’ of practice. Here they focused on tailoring their efforts on examining attempts at improving services in their local NHS organisations. There were two main methods of doing so.
First, in one CLAHRC that was more of a greenfield site, the decision was taken to prognostically frame the CLAHRC in terms of aligning CLAHRC activity with practice through the use of a quality improvement methodology. The idea here was to operate on the basis of improving the quality of service first and foremost, and to look at how research could be employed in the process of doing so.
Well I suppose the guiding philosophy for the whole CLAHRC is that we actually want to make a difference, this isn’t just research, so in terms of what we are about it should be about making it better for patients and then making it better for staff. I know that sounds a tad grandiose, but the reality is that is kind of the premise, so we always try and bring it back to what are we trying to do and we are actually trying to make it better for patients. If we know we don’t do something terribly well, how do we learn from that and change it into something we do do terribly well.
Clinical science academic, NHS-facing, case D
The prognostic frame was based on the assumption that the ‘research’ should not be divorced from the ‘doing’.
An implementation project which is using the evidence, but recognising that what we don’t know is the best way of implementing it in a specific setting . . . which is the whole point is second translational gap… Therefore, we aim to generate new evidence on how you implement things and how you do things in the real world. We’re not generating pure new evidence for this translational gap.
CLAHRC management 3, case D
The idea was to generate new evidence about the how of implementation. In doing so, the model required that a number of different forms of evidence needed to be generated.
For evidence-based implementation we have a concept that there are three types of evidence that you need to be looking at. First, there’s evidence of what to implement, which often comes from previous controlled trials. Second, there’s evidence of how to implement, which we know a lot about and leadership once it’s working, ownership, measurement for improvement and those types of things. Third, there’s evidence of what happens when you implement things. We start essentially using the three steps of the model for improvement; what is it that you’re trying to achieve? How will you know that a change is an improvement? And, what changes can you make or test to see if they make you a desired improvement? And so it’s recognising it’s not about solutions, it’s about ideas.
CLAHRC management 1, case D
The management of this approach involved asking NHS actors in the locality to engage with the CLAHRC to help the support innovation initiatives and to research the process on an ongoing basis. As we will outline in Chapter 6, this shaped the way in which the CLAHRC engaged with different stakeholders in rolling out its activities.
The second approach differed in that it did not employ a strict quality improvement methodology and, rather than seeking new service innovation projects, it sought to engage with existing initiatives. Therefore, researching practice worked through a process of establishing what the important service innovation projects were in the local region, with a specific eye on selecting the larger, more organisationally focused projects and then building into the project performance and ongoing evaluation systems, both formative and summative.
It took me a long time to understand what was going on in the XXX CLAHRC, and the other day the penny finally dropped. He’s a genius. Rather than scrabbling around for bits of matched funding here and there, he’s taken a bigger picture perspective. He’s said to the local NHS organisations, ‘what are the big service innovation projects that you have at the moment? I’ll get the CLAHRC to work into them to provide a real-time evaluation’. You can’t get any more embedded than that can you? And it deals with the issue of matched funding all in one. Genius!
Social science academic 2, case E
The added advantage of this approach, which was different from the ‘marrying approach’, was that it enabled researchers to be embedded into the local NHS organisations’ activities from day one. In this way it was more than a ‘marrying activity’, it was more about a ‘working into’ process. The model was also one that aligned well with established ways of working for the NHS organisation and one in which management were able to retain control over resources and the way projects were run over the course of a CLAHRC.
Balancing research and practice
Interesting issues that were raised in prognostic framing were concerned with decisions around the allocation of funding between research and implementation activities, and the relationship between the two elements. The initial guidelines, which set out what CLAHRCs were to achieve, were interpreted by some as being very flexible, to the point of being unclear.
I think it was partly challenging because the CLAHRC bidding process set out a framework but there was huge room for manoeuvre within it, there was huge scope for flexibility and thinking about where the research sits and where the innovation sits and where is the balance between those two things, also in looking at what the areas of public health need were . . .
Clinical science academic 1, NHS-facing, case H
The bid formation process differed across CLAHRCs and, although the NIHR allocated 80% of the funding to research and 20% to implementation, CLAHRC directors took different approaches in how they allocated funding, and to which projects. Many emphasised research more than implementation because of the need for scientific credibility in the eyes of the NIHR, that would ultimately make the funding decision. As outlined in the previous chapter, this was driven by the founding conditions for a number of the CLAHRCs, which meant that much of the funding was already allocated to clinical science academics to attract them to engage with CLAHRCs. In addition to the founding conditions, a number of more NHS-facing actors identified that the actual form had a bias towards research.
It was very interesting completing the application form, we found a tension between the research part and the implementation part. In the implementation sections, there was nowhere to include references, whereas the research section there was. The implicit assumption was that we know how to do implementation.
CLAHRC management 1, case D
The actor above interpreted the lack of a space for references as a clear indication of the NIHR’s view that implementation was not the priority. The actor found the emphasis more on the research position surprising. Instead, the CLAHRC should have been about learning about the practice of implementation. In addition to the balance of funding, there was a real issue about the relationship between the CLAHRCs’ research and implementation activities. For some actors the solution was to integrate the research and implementation into the different research themes, and for others the solution was to run the two activities in parallel:
I think coming back to what the CLAHRCs stand for which is this idea of knowledge mobilisation and implementation and behaviour change, as well as applied research, that run parallel to each other.
Clinical science academic, HEI-facing, case F
Where CLAHRCs were prognostically framed to have research and implementation running in parallel, real tensions arose in terms of time horizons. Conversely, where the implementation was to be organised in a separate theme, implementation was prioritised over research.
So my understanding is what they did, which is actually entirely what you want them to do, which is to look for evidence-based guidance which is not being implemented locally and to do that. So in a sense, while they’re [the implementation theme] waiting for the researchers to get their act together and come up with a product, they deal with all the things that we know need dealing with.
Clinical science academic 3, HEI-facing, case C
A number of such actors followed the diagnosis that the problem centred on the T2, but over time they became increasingly aware that the problem was much more complex than they first envisaged:
I think there was probably a bit of a misunderstanding about what applied clinical research is and what the translational gap is and I suppose, we didn’t struggle, but it took quite a long time for us to be physically clear about how we were going to link in to implementation and what that meant about how you transfer knowledge and how you change culture in terms of how people look at research in terms of how it changes practice. [ . . ] a lot of my clinical science academic colleagues who probably aren’t particularly clear about what this sort of research is and possibly in the past they have seen it as soft and perhaps not as important research.
Clinical science academic 2, HEI-facing, case I
In terms of prognostic frames there was also confusion over the remit of CLAHRCs:
What the CLAHRC did was to give us a narrative, or a conversation. To begin with I think it completely puzzled people. All the agencies that had signed up to the creation of this thing then looked at their baby and thought: ‘What the heck is that?’ We have found over the first couple of years that as the narrative has been rehearsed in different audiences, they have come back and explained to us what that story actually has to be about. I would say that now going out and explaining to people what a CLAHRC is has become possible. At the beginning it was impossible.
Clinical science academic 3, NHS-facing, case G
A lack of clarity was played out differently within a number of the CLAHRCs. For example, an implementation lead for one of the CLAHRCs commented in relation to their own CLAHRC that:
I feel that at a strategic level there is a lot of ambiguity. I really don’t believe that we have been given a vision of what the CLAHRC is trying to do and what that means in practical terms, so how it feels in my individual role is that there are lots of autonomous teams doing their own work, that there is almost a culture of competition between teams to outdo each other, that we are not functioning as a collaborative at a CLAHRC level [. . .].
Implementation lead, case C
Even when the principles of the prognostic frame were clear, actors faced the added complexity of the NHS being in a continuous state of flux. This was reflected in several interviews:
However, this [NHS flux] is problematic because the NHS is continually shifting and you are never quite sure whether you have got the right person, so it is quite complicated in organisations [. . .].
Clinical science academic 2, HEI-facing, case I
Building capacity across the institutions
All of the CLAHRC directors and senior teams understood the importance of capacity building, which they focused on in a number of different ways.
First, actors highlighted the importance of establishing collaborative methods of working across organisational and professional boundaries. In doing so, CLAHRCs were framed as building bridges between research and practice whereby academics could be engaged in practice and work with practitioners to overcome local health challenges.
Well if we’re successful I think the kind of collaborative working between academics and health professionals, . . . would in some ways become embedded so that it would be kind of a natural relationship. A collaborative relationship that would have come to be seen as the normal way of doing things.
Clinical science academic 2, HEI-facing, case G
Second, it was felt to be important that the legacy of CLAHRCs spans and encompasses the health system more broadly. This aligns with a more systems-level view of thinking, in that CLAHRCs should be thinking not only about specific projects, but also about the integrative whole of what they can achieve.
It is really important that the benefits of our engagement with the NHS go beyond just a single PCT, or a couple of PCTs; they have to spread out to other providers and to other academics and other CLAHRCs and networks and for that to happen. The science has to be spot on so that we can write this up in a way that people listen and take it seriously and that we can come up with creative ways of disseminating our findings working directly with clinicians and managers that we can trust.
Social science academic, case H
Third, actors believed that capacity can be developed through the education of NHS staff to become more receptive to KT.
Whatever happens to CLAHRC in 3 years’ time, if there are 500 people that have been through this programme [. . .] you’ll have a bunch of people who’ll be able to implement any project or service improvement initiative using the same language, which are both clinicians and managers. So whatever happens to CLAHRC, which will be one of our long-term legacies.
CLAHRC management 3, case D
Through a range of secondments, fellowships, education programmes, knowledge brokers, training activities and collaborations between the HEI and NHS partners, the directors sought to use CLAHRCs as a vehicle to equip researchers and practitioners with the skills and education to drive research into practice. In addition, PPI educational initiatives were also set up across CLAHRCs to varying degrees. However, such programmes were generally fragmented and not prioritised because of the difficulties in terms of the time and cost of setting up and running user groups.
We’ve set up a service user advisory group for people with significant problems, to support the PPI part of the research [. . .] because of the knowledge and experience of the practitioner researchers, all of us, and the knowledge of services, we have been able to set that up, had we not had this type of structure.
Practitioner researcher, case B
The CLAHRC directors evidenced their understandings of the implementation gap by developing programmes to support health-care practitioners, which created stronger links between researchers and practice, and by the better application of research into clinical work. Capacity building through career trajectories was envisaged through collaborative work between researchers and practice, secondments, and research contracts. Success, however, varied across CLAHRCs, as we explain in Chapter 9. Through capacity building, CLAHRC directors sought to increase the absorptive capacity of the NHS partners and how they engaged, disseminated and applied clinical knowledge into practice. The vision of CLAHRC directors was one in which the creation of such linkages between the HEI and NHS partners and between researchers and practitioners would create a legacy that would continue after CLAHRCs had ended.
Conclusion
In this chapter we have examined the initial diagnostic and prognostic frames employed by actors in envisaging the CLAHRCs. Envisaging is important as it the first stage of any organisational/strategic change project whereby actors form a vision of the change they want to enact, based on the interplay between themselves and the context in which they are situated. 26 In the chapters that follow we will examine how the envisaging process shaped the later stages of engaging, embedding and reflecting as CLAHRCs were mobilised.
In terms of diagnostic framing,152 we witnessed variation across actors located in different social positions as to their view of the problem that CLAHRCs had been established to solve. As outlined in Chapter 4, an actor’s social position is important because it may influence his or her perception of the field. 105 However, it is important to note that not all actors had a clear idea about what they diagnosed the problem to be. In general, we found that HEI-facing clinical science academics were more likely to diagnostically frame the problem as translational in nature, i.e. the problem was one of how to make research more accessible. In contrast, a number of more NHS-facing clinical academics framed the problem away from translation, by focusing on who actually defined the problem.
Finally, actors located in social positions which we defined as ‘other’ were more likely to view the T2 as an organisational- or systems-level problem. The idea of KT has tended to focus on engendering individual-level behaviour change and, as outlined in our review of the KT literature, has often played down the role of context. The more organisational- or system-level view focuses on how individuals’ actions are shaped by their context. Therefore, in order to engender meaningful change, context needs to be reshaped accordingly.
Overall, we view the relationship between diagnostic framing and prognostic framing as generative rather than deterministic in nature. All of the CLAHRC main actors understood the importance of marrying research to local NHS needs; however, important differences emerged in relation to their desire to research practice, the balance and interaction between research and practice, and capacity building. In terms of researching the ‘doing’, a small number of CLAHRCs started with front-line service issues and worked backwards, shaped by the diagnostic frame which identified the importance of who defined the problem. The balance and interaction between research and implementation was a common issue for many CLAHRCs, which played out in different ways according to how the two elements were initially structured in relation to one another. We will discuss this later in the report. Finally, in terms of capacity building, all the main actors in CLAHRCs prognostically framed their understanding around the promotion of capacity building.
Chapter 6 Engaging Collaboration for Leadership in Applied Health Research and Care stakeholders
In this chapter we examine the work undertaken to engage the key stakeholders of CLAHRCs. Engaging stakeholders is an important element of IW, in which IEs mobilise support for their cause27,28 and cultivate co-operation. 29–31 As we outline below, lead CLAHRC actors drew on existing networks, from within their institutions as well as mobilising outsiders, in engaging key stakeholders to become involved in CLAHRCs.
Through engaging key stakeholders, actors sought to develop normative networks, which are the interorganisational connections through which practices become normatively sanctioned and which form the relevant peer group with respect to normative compliance, monitoring and evaluation. 22
In the following sections we describe the engaging processes in which those central to CLAHRC worked to draw support from key stakeholders during the bid process and in the mobilisation of CLAHRCs. In doing so, we draw a distinction between the work that was undertaken in ‘winning the minds’ of key stakeholders, in terms of getting actors to sign up to CLAHRC, and the work that was undertaken to ‘win the hearts’ of key stakeholders, in getting actors to embrace the key principles of CLAHRC. We suggest that this is a key distinction that has largely been neglected in research on institutional entrepreneurship. The distinction highlights that actors signing up to a CLAHRC is only a necessary, but not sufficient, condition for acting in a manner that is consistent with the ideals of CLAHRCs.
Winning the minds and hearts of Collaboration for Leadership in Applied Health Research and Care stakeholders
In engaging key stakeholders, actors drew on their social capital with other actors across the HEI and NHS landscape and across different levels of seniority to secure support for their CLAHRCs, but also to access research ideas during the initial bid formation. By leveraging their social capital to influence others, actors were able to champion the support of close allies and orchestrate collective action from those supporting the CLAHRC initiative. 24 We term this work ‘winning the minds of key CLAHRC stakeholders’. This comprised three mains forms of work: (1) ‘drawing on the support of key stakeholders’, (2) ‘doing the rounds’ and (3) ‘spreading the word’. In addition, we highlight work that was undertaken to ‘win the hearts’ of key stakeholders through alignment and consensus building.
Drawing on the support of key stakeholders
A starting point for many of the key actors was to draw on their existing relationships with key NHS actors in their regions. It was easier for CLAHRC senior actors to communicate the idea of a CLAHRC to stakeholders with whom they had good existing relationships.
Because I have worked very closely with the NHS, I knew the CEO [chief executive officer] of the PCT and I knew the chief exec [executive] because I have always worked in the NHS, they were on my side straight away.
Clinical science academic, HEI-facing, case F
One CLAHRC director commented on the ease with which he was able to elicit support from key NHS figures, which he attributed to his existing relationship with senior NHS managers and an ability to articulate what CLAHRCs could do for their organisations.
You have to be somebody who can see the scientific world in the context of the service world you know, you have to be able to first of all articulate a vision for how the world of chief execs [executives] relates to the world of research firstly. And secondly, you have to be able [. . .] to go like a militant and say ‘Come on everybody, will you stump up for this lot?’ And of course to do that, you’re completely cold-calling and that’s not good either.
Clinical science academic, HEI-facing, case A
The director had the status in the clinical domain, but, importantly, also understood how chief executives think and was able to key into their agendas. The framing of engagement around senior management’s priorities was an approach taken by other CLAHRCs:
It was easy to do a pitch to a CEO because I could say to them: ‘What are your strategic objectives? What are the problems you have got in your organisation? We can help you address these problems [. . .]’. So they signed up very quickly.
Clinical science academic, HEI-facing, case F
An advantage of securing the support of leading NHS figures was that CLAHRC directors could then exert some ‘mild pressure’ on other NHS actors to agree to sign up to the CLAHRC. A number of CLAHRC actors used the leading NHS actors’ social capital to help achieve buy-in at a senior level. Much of this work was done behind closed doors, through telephone calls and by having ‘a quick word’ with senior NHS staff who had discretion over funding allocation.
The structure of the CLAHRC bid itself required cofunding from the local health community and he was critical. [A NHS senior manager the NHS partner] is quite well known and respected by the acute trust and it is very unusual as well that there is a XXXXXX NHS senior manager who was able to marshal support from the other trusts around this patch to put in their money . . . He had to get them to put their hands in their pockets. If he wasn’t there it would have been much more difficult to mobilise. He just rang up a few people and they said ‘sure, fine, we will sign that over and sort that out later’. It was done in about two and a half months.
Social science academic 1, case E
Where actors were able to draw on the support of key NHS actors, they were able to encourage them to sell the concept of the CLAHRC to those who held the purse strings. In such cases, the agreement of NHS organisations to sign up ‘in principle’ was achieved. However, there was a considerable difference between signing up ‘in principle’ and how this was to be operationalised when it came to the details of rolling out the CLAHRCs.
Doing the rounds
‘Doing the rounds’ became a core part of many CLAHRC directors’ activities as the CLAHRCs were being established. Often this activity was a core part of ensuring that NHS organisations signed up to CLAHRCs. ‘Doing the rounds’ was particularly evident in NHS regions where there was an absence of key stakeholders who could help to mobilise other NHS organisations to support the CLAHRC initiative.
It’s a bit one-way street in the sense of CLAHRC coming to the trust as opposed to the trust going to CLAHRC. I think the senior directors of the trust acknowledge CLAHRC, it’s all linked in to sort of the world science situation, but I think the devil is in the detail, and they’re not particularly interested in the detail. I don’t think that’s a conscious decision, I just think they just simply don’t see it on their radar.
CLAHRC management, case C
However, even when key NHS stakeholders were engaged to help mobilise support there was still a considerable amount of work that needed to be done in order to get the NHS organisations fully on board, and signed up to specific projects. As one CLAHRC senior academic commented:
It’s one thing getting people to ‘agree in principle’, but then someone still has to go into each of the NHS organisations and work out how this is going to work in practice. At the moment I feel a bit like a tawdry salesperson. I think I’ve done the same pitch about 30 odd times.
Social science academic 2, case E
‘Doing the rounds’ was a very time intensive activity. The work focused on translating what the ‘in principle’ funding was to be used for in practice. This required a great deal of groundwork to ensure that NHS organisations followed through with their initial promise of support, and that the activity of the CLAHRCs and the needs of the NHS partner organisations were aligned. As described in the previous chapters, both existing and new projects were used in the CLAHRC bid to present projects that would be rolled out over the CLAHRC period. CLAHRC directors looked for projects and ideas that were already ‘on the shelf’, but which also fitted the project brief.
We did a lot of groundwork by going out to see various chief executives and various other medical directors on the patch in both primary and secondary care [. . .] we got 80 to 90 per cent of coverage just by getting out there and talking to people. What we also did is conduct a series of informal interviews with a whole variety of people, clinicians and researchers around the patch.
Clinical science academic, NHS-facing, case D
Across both the ‘high-level pitch’ and ‘doing the rounds’ actors had to demonstrate the value of CLAHRCs to the NHS organisations. In the previous chapter on envisaging we examined how actors ‘married research to local needs’ and/or ‘researched the doing’ of practice, both of which were ways of demonstrating value to NHS organisations. In addition to demonstrating value, a key issue of selling centred on what constituted ‘matched funding’.
We had to really use the term ‘matched funding’, as people in trusts became aware of this [resource] requirement, there has to be conversations about this. It doesn’t necessarily mean that we’re going to be asking you for £100,000 every year or whatever. What we’re really looking for is equivalent resources of that level.
CLAHRC management 4, case I
A number of CLAHRC actors interpreted matched funding as a requirement to mean cash. Others interpreted matched funding more broadly to include ‘resourcing in kind’, including physical resources, staff and workspaces or even the adoption of existing NHS research programmes. For the majority of CLAHRCs, matched funding was in the form of staff seconded from the NHS partners and HEIs, who then worked across projects on the different themes.
It became clear to me early on that people agreeing to provide matched funding was one thing, actually getting the cash was a completely different issue. Trying to get actual money was difficult as people think bottom line: What do I get for this? Given the design of our CLAHRC, what I wanted more than money was the time of NHS staff. I soon realised that asking for ‘people time’ rather than actual cash made the sales pitch much easier. In asking for people time, we were ensuring that the CLAHRC was working to their agenda.
Social science academic 2, case E
The high-level pitch for capital which was carried out by CLAHRC senior actors was much harder sell. One CLAHRC director lamented this issue and was surprised to find out how each CLAHRC had interpreted ‘matched funding’ in significantly different ways.
All of our match funding is actual money from XXXX . . . In fact, I found out from going to the programme managers meeting there was . . . ‘complex accounting’ that went to show that they had matched funding, but actually it is not funding at all, it is not money you can do anything with.
Social science academic 3, case C
However, for some, the resourcing-in-kind model was greatly beneficial as it meant that the resources were fully embedded into the host NHS organisation. As one CLAHRC director commented:
I’d rather have people than money, as you’ll only spend the money on people anyway. The big advantage is that they are embedded in the NHS. Also, if money gets tight it has the additional advantage of being a ‘hidden’ resource, it is not bottom line cash that the partner can take back if they get short.
Social science academic 2, case C
Spreading the word
The work around ‘spreading the word’ involved engaging actors lower down NHS and HEI organisational hierarchies. Furthermore, in contrast to the ‘higher-level selling’ that was undertaken by the CLAHRC senior-level actors, ‘spreading the word’ was undertaken by a broader group of actors. In particular, research leads and CLAHRC management worked to ‘spread the word’ of CLAHRCs at a more grass-roots level, and in doing so raised awareness of what CLAHRCs could do in local NHS organisations. The objective of ‘spreading the word’ was to engage people on the front line who were making the decisions about services.
The managers are the decision makers, they make decisions about what gets done, so it’s about getting the decision makers rather than any one particular group. They are in a position to decide whether this particular bit of research is useful to them and they make a decision based on it. In many ways it is down to the grass-roots level, and the clinician who is involved in the day-to-day practice.
Clinical science academic 2, HEI-facing, case I
In order to ‘spread the word’, CLAHRC staff had to attend numerous meetings in which they explained the role of CLAHRCs, what the concept was about and how it may work to the benefit of the NHS organisations. These processes helped to bridge divides between research and practice and encouraged the creation of new networks across different institutions.
We tried to get meetings in the diaries with those people and we explained the CLAHRC, explained our role, because we realised in the beginning that they didn’t know what the CLAHRC is, they didn’t know what the concept is about [. . .] So it was very much a discussion of explaining what we are here for, that we are funded partly by the XXX and we have agreed to do some work with them [. . .].
Knowledge broker 1, case C
In addition, a number of CLAHRCs employed direct incentives to attract interest from NHS organisations. Specifically, CLAHRCs that held back funding at the initial stage by not committing it to specific projects were able to offer financial incentives to actors to encourage engagement with them.
We do offer some financial incentive, we do give money you know. If you come and play with us, there is real cash available, which means quite a lot.
Clinical science academic, NHS-facing, case D
In using a financial incentive to secure engagement, however, there was a risk that actors engaged with CLAHRCs for the purpose of gaining resources. CLAHRCs may have engaged stakeholders’ minds, but this did not mean that they had signed up to the ideals of CLAHRC. A common theme from many CLAHRC senior staff was the difficulty in ensuring that actors, once engaged, really understood that CLAHRCs were there to do a different type of research, one that was not akin to a traditional research project.
It’s almost inevitable, people [academics] see that we’ve got funding and so we do get quite a lot of research applications (laughs). We put the message out to say no, we’re not necessarily looking for that, . . . and we wouldn’t discount an application on that basis. We say, ‘we’re not funding original research but your idea is interesting’. This is about implementation and we try to get them to think differently about it. But I think that’s one of the major challenges for CLAHRCs.
CLAHRC management 2, case D
The work around spreading the word was captured by a statement from a social science academic who complained about the work expended in engaging stakeholders:
One of the most important activities that I engaged in was talking the CLAHRC into existence. It’s the classic stuff discourse theorists write about, and it was no different. The CLAHRC exists in one form, virtue of naming it, it was my job then to make sure that people knew what it was and that it was going to happen.
Social science academic 3, case C
Across all of the CLAHRCs we found evidence of the focal actors working to ‘win the minds’ of key CLAHRC stakeholders. In doing so, all CLAHRCs were able to mobilise and build networks; however, such activities were a necessary, but not sufficient, condition for closing the T2. In the next section we examine the issue of winning the hearts as well as minds of key CLAHRC stakeholders.
Aligning and consensus building
Although the high-level pitch to ‘draw on the support of key stakeholders’ and ‘doing the rounds’ espoused a rhetoric of closing the T2, significant institutional tensions remained between the worlds of research and practice, which were played out at the grass-roots level.
This particular research led said to me: ‘I have absolutely no desire to do that whatsoever. The only reason I got involved in CLAHRC was because I work in the office next to XXXX and it seemed a good way of keeping my research going for the next 5 years.’ At which point I thought: ‘doesn’t the C in CLAHRC stand for collaboration?’.
Clinical science academic 6, NHS-facing, case C
This conflict was common across the majority of CLAHRCs, to greater or lesser degree, and manifested itself as a tension between the ideals of research and implementation across the different institutions.
Many of us have had conversations with NHS decision-makers over individual projects and they are a bit like ‘no you can’t do that’ or ‘that is not the right way to do it’ or whatever; and that is an important lesson that we are trying to learn jointly with the NHS, to collectively share the idea and do something different.
Clinical science academic 2, HEI-facing, case I
The HEI-facing clinical academics as well as other academics, including social science academics, felt that those in practice were critical to research. These differences of common goals and visions caused tensions between research and practice at times, hindering alignment and consensus building between the institutions and, consequently, the translation of research into practice.
The average person in the NHS will often have seen research in the past as a damn nuisance, more work for no more time and there will be no answer, or it will be something that requires us to spend more money, so they will come reluctant. But to try and find, for them to start thinking ‘ah yes, this could actually be useful to us’, that is a step they are in the process of taking as well and they are making that step at different speeds and different steps and so on.
Clinical science academic 2, HEI-facing, case I
Even when key stakeholders were signed up to CLAHRCs, significant tensions remained. Many actors were oriented towards their dominant institutions, which meant that, although their minds had been engaged in terms of their involvement with CLAHRCs, their hearts still had to be won over. A number of CLAHRC actors highlighted the importance of IW as they worked to align interests of the different institutions to build consensus as to nature of CLAHRC activities.
Some people were signed up at the beginning and some were not . . . and some people just do not get it. Part of our job, and we know it’s an ongoing battle I guess, is to try and get them to align with our set of goals and try and build a consensus around that.
CLAHRC management 2, case D
However, the issue of aligning and consensus building was acknowledged as being difficult work to engage in. Institutional forces worked, in many actors’ view, to drive continued differences in actors’ institutional orientation.
Our currency is research publications, grant income, all of the kind of traditional fodder that keeps an academic in a job and develops kudos, and marrying those two up in a proper way in the NHS context, which the CLAHRCs are in, is really challenging. It is not a small undertaking and I think we probably underestimated it in the early days, or we didn’t give enough thought to how we might do that once we got rolling.
Social science academic, case H
Consequently, ensuring alignment and building consensus was not something that could be achieved in a short time frame. Rather, it was largely through repeated interaction between clinical science academics and practitioners that the potential synergies between research and practice became evident to many CLAHRC actors. Over time, clinical science academics developed a general awareness of the local health-care landscape. Furthermore, all parties increasingly recognised the potential synergies between research and implementation. This encouraged academics and practitioners to work together in carrying out, disseminating and implementing research.
I do think it has brought about some modifications in behaviour and that’s developed some links and perhaps a little bit better understanding of the two different organisations and their cultures. I see that probably as being, maybe a bit more on the university side in terms of other ways of going about getting research done.
CLAHRC management 2, case I
However, the timescales in which alignment and consensus could be achieved were challenging within the time frame of CLAHRCs. This was as a result of the need to bring together the different cultures of the HEI and NHS that rewarded different behaviours.
If CLAHRC’s going to act as a bridge between those two and try to bring about some cultural change so the interaction is better and evidence is produced in a way that the NHS can use more readily, then I think a 5-year programme is a start but it’s not enough to change people’s views, to see it as a potential career. And I think therefore they need to be more permanent organisations.
CLAHRC management 2, case I
The influence of envisaging and founding conditions on engaging
In attempting to engage the minds and hearts of CLAHRC stakeholders, a number of challenges were identified early on in the process. The challenges were grounded in the institutional differences between the fields of research and practice, but also reflected decisions relating to the envisaged CLAHRC structures and the different hierarchical status and roles of the different actors involved. Consequently, some actors found working across the boundary of research and practice more challenging than others.
The influence of envisaging on engaging
Achieving alignment and consensus between the different partners was more difficult and took longer than originally planned for the vast majority of CLAHRC actors. One important influence on the ability of CLAHRC actors to achieve alignment and consensus across researchers and practitioners was the envisaged CLAHRC structure, which was determined by the presence of large research projects, the gravity point between research and practice, and the structural relationship between research and practice. The phrase that was coined by one actor to capture this balance was the gravity point between research and implementation. Interestingly, the term gravity point suggests that CLAHRCs were being pulled in competing directions by opposing institutional forces.
For example, CLAHRCs were envisaged to encompass large research projects but, in practice, were less likely to account for the lead time necessary to network with practice and align the research projects with the needs of practice.
I think that probably people who funded CLAHRC didn’t really take into account the lead time that you need. And that was very challenging because you have a CLAHRC starting from day one or whatever it was, really very soon after the decisions were made [. . .] there were people we needed to recruit in order to actually the projects going.
Clinical manager, case I
The result was that during the process of trying to align the interests of research and practice, and build a consensus between the two, a number of NHS partners were left frustrated. In contrast, where CLAHRCs were led by more NHS-facing directors and had an emphasis on the implementation of existing research rather than carrying out new research, there was a clearer alignment between the interests of research and practice. This point was neatly summarised by a CLAHRC manager when commenting on the variation in engagement of NHS partner organisations both across and within CLAHRCs.
I think there is something about some of the trusts feeling that they are owed something by CLAHRC, that they are entitled to something and some of them are, the ones that have that sort of view sometimes feel they are not getting their entitlement. For others, there is much more of a partnership being developed where they realise it is sort of up to them to engage as well and partly what they get out of it depends on how much they choose to engage. Others have tended to sit back and say ‘come on then, come and do stuff’.
CLAHRC management 2, case I
Similarly, the way in which the relationships between research and practice were envisaged were reflected in different structural relationships between research and implementation across CLAHRCs. Where there was a clear separation between the research and implementation themes and there was a tendency for the two groups to work in relative isolation. Consequently, the alignment of goals and consensus across the two groups was less likely. Although these tensions were evident to some degree or another in all of the CLAHRCs, they were more apparent in those CLAHRCs that envisaged and set up research and implementation as two separate entities.
There’s been an absence of coherent, joined-up thinking between those two [research and implementation] strands in the CLAHRC. I think a lot of the [NHS-facing] clinical science academics very much work in a much more pragmatic way and in a much more applied way and perhaps that didn’t gel with the more theoretical thinking that even the health psychologists as well as the social scientists brought to the table.
Social science academic 4, case C
It is important to note, however, that over time both parties became increasingly aware of how each other worked, but this process took time to establish and with varying degrees of success within and across CLAHRCs. The result was that, across the four CLAHRCs we studied in detail, there was significant learning by both parties as to how they could maximise the return from forming CLAHRC relationships and working in a CLAHRC-type way. We build on this point in Chapter 9.
The commissioners are now beginning to understand what they are party to and how they might be able to exploit it better and the researchers are beginning to understand what this huge thing called the NHS actually is and how it works and what they need to do to change and how that is slightly different to publishing another paper on whatever.
Clinical science academic 1, NHS-facing, case H
The influence of professional status and role on engaging
In addition to the influence of envisaging, issues of status and role shaped how actors engaged with CLAHRCs. During these initial networking stages there were challenges in how researchers engaged with practice and vice versa. This made the problem of translation more complex than originally envisaged. Researchers, and especially junior researchers, found that it was difficult to engage with clinicians and practice.
I’ve certainly found the clinicians generally very difficult to work with. I mean not all of them, some of them are wonderful. The clinicians, even though they know theoretically they should be on board, they’re not really always that helpful.
Researcher, case I
From the data it was evident that it was easier for senior actors to engage with practice because they were seen as legitimate in their institutions and also because, as a result of their status and role, they were able to bridge divides and form new networks. This finding is consistent with our SNA findings in Chapter 8, which show that CLAHRC actors of higher professional status were more likely to form connections than their lower-status counterparts.
Senior academics are more willing to cross boundaries, I think that there’s perhaps a sense of ability to do it [. . .] there may be a sense of their reputation or their legitimacy in that area, that might help them. Hence, I think that senior people are very motivated or much more motivated to make this work.
Social science academic 1, case B
More junior-level researchers, in many cases, found developing a network of relationships with practitioners more challenging, despite being central to a number of research projects. In some cases this was because junior researchers were on different career paths to well-established senior clinical academics and practitioners, and were often temporary. However, some junior researchers deemed the rewards of engaging with practice to be less than those accruing from their next journal publication, which they believed to be key if they were to develop a successful academic career in higher education. Therefore, a lack of status worked against junior actors in trying to develop new relationships across the research–practice divide, but this was buttressed by institutional incentives to focus on their core research publications.
In terms of actors’ roles, we found evidence that practitioners were more willing to bridge the divide to research than their research counterparts were to do the opposite, a finding that is corroborated through our SNA work in Chapter 8. One respondent talked of the ease with which a number of senior practitioners could bring their insights into academia, but that the reverse situation whereby an academic researcher going into a practice situation commonly provided more problematic.
Each of the practitioners has worked in health-care and worked in supporting service users and their families over many years. They’re quite senior in the context of their career but more so their experience and expertise. So they’re bringing that to academia, they’re bringing that to the CLAHRC [. . .]. Some of the other studies whereby an academic researcher alone going into a clinical situation or a care situation probably wouldn’t have got the same sort of results as quickly as a clinician going in there really.
CLAHRC management 1, case B
We suggest that the ability of practitioners, particularly senior-level practitioners, to network across the research–practice divide may be facilitated by their day-to-day practice. As one CLAHRC manager commented:
Obviously a researcher on a study is going to have a bit more tunnel vision, because they’re doing research, that’s what they’re supposed to do. Whereas a co-ordinator sitting in the NHS trust will be seeing various people from different backgrounds, and will be asking them for help. You know, they expect CLAHRC to go and find evidence for them or to do evaluations for them. Whereas many of the researchers are not interested in doing an evaluation because it’s just not academically interesting enough for them. So there’s a real sort of disjoin there [between academics and clinicians].
CLAHRC management 3, case I
Conclusion
In this chapter we have examined work undertaken by CLAHRC actors in engaging CLAHRC stakeholders, both during the bid formation and once CLAHRCs had been funded. The first form of work related to winning the minds of CLAHRC stakeholders about the CLAHRC initiative. Across all of our research sites we found evidence of actors leveraging their existing networks and social capital to bring together collectives of people to support the CLAHRC concept. In particular, senior CLAHRC actors worked to sign up people through (1) ‘drawing on the support of key stakeholders’, (2) ‘doing the rounds’ and (3) ‘spreading the word’. In all cases, work began by signing up the ‘big names’ in a locality, from both HEIs and the NHS. Work was then undertaken to deepen engagement and, thereby, mobilise the social movement with those lower down organisational hierarchies. Interestingly, there was a need to engage more powerful actors, with ‘strong arm’ political skills, to act on the CLAHRCs’ behalf in each locality. 109,156
As we outlined above, all CLAHRC directors and senior players were able to engage key stakeholders and those lower down organisational hierarchies. Engagement, however, was a necessary, but not sufficient, condition for closing the T2. The other form of work related to ‘winning the hearts’, which centred on alignment and consensus building. Actors, in engaging with the CLAHRC initiative, may have done so for a number of reasons as shaped by institutional forces and, in doing so, some may have fully aligned with the espoused ideals CLAHRC. An important role for actors was the work that they did to frame discourse in a manner that resonated with the interests and values of the different stakeholder groups. 27,28,152,157 Actors who worked to align stakeholders’ interests with CLAHRC ideals and build consensus across different stakeholder groups highlighted the inherent difficulties in doing so and the importance of repeated interactions across group boundaries.
The key difficulties associated with ‘winning the minds and hearts’ of CLAHRC actors, to embrace the ideals of CLAHRCs, were influenced by the way in which the CLAHRCs were envisaged and the professional status and roles of the individuals involved. Where CLAHRCs were structured around large existing research projects, the centre of gravity of the CLAHRC was more towards HEIs than the NHS, and a clear separation of research and implementation was more likely to result. In these cases, alignment and consensus building was much more difficult to achieve. We found that the bridging of the research–practice divide was more problematic for junior staff than for senior staff, demonstrating the importance of role and status to the process. Overall, there was a disparity between engaging management to enact CLAHRC ideals with actors on the ground. This may well highlight the distinction between getting the management in CLAHRCs to enact CLAHRC ideals and then getting those on the ground to do so as well. We will discuss these issues further through the SNA in Chapter 8.
Chapter 7 Embedding the Collaborations for Leadership in Applied Health Research and Care
In this chapter we describe the work carried out by actors to embed the CLAHRCs across four in-depth cases. By ‘embedding’ we refer to the process through which actors sought to shape existing institutional practices to align them with the ideals of CLAHRC. In doing so we adopt a broader definition of embedding than Townley32 and Zilber,33 based on Currie et al. ’s97 argument that Lawrence and Suddaby’s22 classification of the different types of IW for entrepreneurship and maintenance may be overly restrictive (see Chapter 2). Arguably, if embedded into existing institutions, such as the NHS and HEIs, the ideals of CLAHRC could be sustained over a longer period. We identified four main processes of embedding: (1) the education of actors in the skills and knowledge necessary to support the new institution,82 (2) the creation of new roles,22 (3) the creation of tools and routines through the infusion of the normative foundations of an institution into participants’ day-to-day routines and organisational practices32 and (4) the construction of a CLAHRC identity, which was especially important as identities describe the relationship between an actor and the field in which that actor operates. 104
The IW for embedding CLAHRCs developed over the 5-year funding period. Of particular note was the degree of mimetic isomorphism78 across the different CLAHRCs, particularly after the first few years of operation. Here we draw particular attention to the ‘knowledge broker’ role, which was first developed by one CLAHRC and then imitated through diffusion across many other CLAHRCs.
Education
All the CLAHRC senior actors understood that, in order for research to be translated into practice, those working in practice needed to be able to access education to promote the ideals of CLAHRC and to provide people with relevant skills. In response to this need, actors developed a number of different educational interventions to try and embed CLAHRCs.
CLAHRCs ran a number of courses and workshops to bridge the research–practice divide. These provided practitioners with knowledge and skills on change management, project management and research methodology. By providing education, those in practice were able to build up a level of competence in order to improve and change services and patient care based on research findings. The development of research-related courses was intended to enable professionals in NHS organisations to better understand and utilise research, and to implement findings in practice. In bridging the divides between the two institutions, the intention was that academics would work with practitioners and educated them on how better to use and implement evidence, and further provided them with the skills to generate new evidence.
You’d tend to get clinicians that are interested in changing some aspect of service delivery and they want to try to pilot a new approach and they want to evaluate that to see whether it works or not, whether the evidence can be found to demonstrate that that is a worthwhile change and something that perhaps the trust should consider rolling out more widely.
CLAHRC management 2, case I
Meetings and workshops were developed by CLAHRCs to educate health professionals on strategies to implement research into practice. As part of this, CLAHRCs contacted NHS partners offering courses on research evidence and service evaluation to suit NHS trusts’ needs.
We gave them a menu and they chose from that the ones that they thought would be suitable for the staff in their trust. It would be things like how to find evidence, how to critically appraise it, specific skills in terms of relating to descriptive statistics or interview and questionnaire design.
CLAHRC management 2, case I
In a number of cases the educational interventions were designed to break down organisational and professional cultures and barriers associated with the T2. In one CLAHRC, for example, there were a series of workshops and events that encouraged collaboration across different professional groups and brought together people from within the CLAHRC as well as those from the local health landscape.
We start with organisational culture, we look at change management, we look at team climates, communities of practice, professions, knowledge exchange. We sort of start at the organisational macro change because of course they have different levels of change that they want to achieve in their projects.
Implementation lead, case B
In addition to raising awareness about the importance of research and understanding of how to interpret research findings, educational interventions were also employed to communicate important tools to translate research into practice.
It’s about rebuilding capacity of clinicians . . . giving them advice tools and approaches for implementing change in their practice.
Social science academic 1, case B
In part, actors’ attempts at capacity building in the CLAHRCs focused on the development of educational programmes, which included postgraduate courses at HEIs and educational courses for mid-level career professionals from clinical practice.
We focus on the person and they do a little project which enables them to learn and grow and develop. We’ve had about 40 of these and these people have gone on and done various things. These people who are mid-levels in their careers, so we’ve got a number who’ve gone off because of being involved with CLAHRC, have gone off and done PhDs, they’ve gone to improved, more senior positions.
CLAHRC management 2, case D
As we discussed in Chapter 5, some of the actors central to CLAHRCs diagnostically framed CLAHRCs as an individual-level problem rather than an organisational- and systems-level problem. Accordingly, attempts to develop internal capabilities were commonly focused on the individual, and centred on changing individual-level behaviour, through specific educational interventions. The primary focus of much of the educational work was to inform and develop the skills of front-line staff who worked on CLAHRC projects; the primary focus of much of the educational work was to inform and develop the skills of the front-line staff who worked on CLAHRC, with the intention of helping the projects function more effectively.
Creating new roles
A number of CLAHRC actors developed new roles to build capabilities and enable clinicians and management in practice to gain a deeper understanding of research and its role in implementation, service design, innovation and improvement. Of particular note was the creation of the ‘knowledge broker’, a role which was operationalised under a number of different titles by different CLAHRC actors [e.g. ‘knowledge transfer associate’ (KTA), ‘boundary spanner’, ‘co-ordinator’ and ‘diffusion fellow’].
The knowledge broker roles are those that span and link different organisations and/or organisational fields. In the case of CLAHRCs, the knowledge broker roles were developed to provide a link between HEIs and NHS organisations to encourage collaborative work. The concept of the knowledge broker was first employed by one CLAHRC, led by a social scientist, who wanted to embed CLAHRC ways of working through the diffusion of knowledge in a situated manner. Here, the actor had diagnostically framed the problem facing CLAHRCs as an organisational/systems-level problem. The knowledge broker role was designed to address this need to engender organisational/systems-level change. The role was designed so that knowledge brokers would be able to act beyond the scope of any specific project, be located in the NHS partner organisation, but be co-opted into the CLAHRC on a part-time basis, thereby diffusing CLAHRC practice to NHS partner organisations and, in doing so, help to build capacity.
Through a process of mimetic isomorphism, the knowledge broker roles diffused to other CLAHRCs in a number of different incarnations. The roles included fellowships and secondments of nurses and clinicians to engage in research. CLAHRCs employed knowledge brokers to act as translators across epistemic boundaries and help bridge divides between professional groups. The process of knowledge brokerage had the potential to engender understanding and appreciation of the value of others’ perspectives of the translational problem. Such knowledge brokering had to extend beyond the research–practice boundary to encompass epistemic boundaries within the academic research domain.
We work with secondees who come in from their own organisations to work with CLAHRC on particular projects and then lead those projects. We are talking about doing, they are more interactive than training, but we are doing workshop sessions with groups and they are with us doing things like the evaluations of these projects so that it is not us doing it to them.
Social science academic 2, case C
The creation of such roles built capacity across HEIs and NHS organisations, which drew the two institutions closer together while providing actors from the NHS with research skills which they were then able to apply in their clinical work.
I think there is capacity building in the research group as well, but I think what we are not doing enough of is trying to work out whether there is capacity building that could be done and used in the service by bringing these sides together more closely.
Social science academic 2, case C
In addition, knowledge brokers were used as boundary spanners who crossed the divide between research and practice and established links between partners. They built capacity through the development of new relationships.
Their job is to know what the CLAHRC is doing in their trust and help identify the key priorities and set up a team, what we might call a translation team, which is where we try to get trusts engaging with a really important topic for their trust to try to bring about this thinking of ‘oh right, research is actually quite a useful thing then and it can help us [. . .].’ It was absolutely fundamental I think in trying to bring the researchers and the NHS together.
Clinical science academic 2, HEI-facing, case I
Knowledge brokers who worked between practice and academia benefited from the skills and knowledge gained through the role. In one CLAHRC the knowledge broker role was designed to second health professionals from practice into the CLAHRC to better understand challenges around research methods, implementation and KT.
I think what we decided to do is we try to second people into the CLAHRC much more so they work 1 or 2 days a week with us and are much more involved with running the projects and learning very much from working with the knowledge transfer associates [KTAs] how you do knowledge transfer.
Knowledge broker 1, case C
Knowledge brokers were then able to apply their new skills and knowledge to embed new ways of working back into their own work. The knowledge brokers from clinical settings benefited from the acquisition of research skills that were valued in clinical work.
[. . .] it is a little bit of career progression because they move a little bit away from just being clinically focused, but also develop a career through quality improvement and work within the health economy [. . .].
Knowledge broker 1, case C
The model of employing knowledge brokers also helped to mediate potential problems that arose within CLAHRCs which had structured research and implementation to operate as separate themes. In such cases the role of the knowledge broker was to work closely with practice to develop educational programmes and tools for the local NHS organisations. These were later embedded into practice.
Linked to the SNA results in Chapter 8, we highlight the importance of knowledge brokers in CLAHRCs and their role in fostering relationships between the HEI and NHS, and the translation and implementation of research into clinical practice.
Embedding tools and routines in practice
The third form of IW around embedding related to tools and routines in practice. A number of CLAHRCs either employed existing, well-developed tools and routines or sought to develop new ones that could be embedded into HEI and NHS organisations.
In terms of the use of the existing tools and routines, one CLAHRC developed a distinctive model that employed well-tested service improvement methodologies. The director, a NHS-facing clinical academic, organised his CLAHRC around a portfolio of ‘bid and deliver’ projects. Actors were required to apply for funding from the CLAHRC based on proposals for improving services and/or propose new implementation processes using evidence from existing research. As part of this model, the CLAHRC central team provided a range of tools to practice-facing teams to help manage the service improvement process to enhance patient outcomes, and then to monitor the efficacy of the process.
We apply a standardised method or suite of tools to enable all of those projects to implement evidence into practice. So the precondition is that they apply to us for funding and say ‘we’ve got a piece of evidence, we‘ve got an intervention, which evidence shows to be effective, and what we need to be able to roll that out in our local context’. And the point of the model for improvement, and the point of this suite of tools, is to enable them to apply that within their own context.
CLAHRC management 3, case D
From the start of the projects, tools were embedded into the host NHS organisation. The aim was then to diffuse the tools across the local landscape. Afterwards CLAHRC management monitored these projects and the use of tools to ensure that they were being integrated into daily practice, and that the use of tools translated through into improved patient outcomes. The CLAHRC provided the toolkit and framework to close the T2.
You’re not telling people how to do it, you’re saying this is the idea, you implement it the most effective way for your community hospital and we will support you using our methods. So for the COPD [chronic obstructive pulmonary disease] bundle, that started here XXX and now every single acute trust in our sector use that [. . .] So for the [local hospitals] they are doing that and that is completely embedded and they are still monitoring now, 18 months after the project’s finished [. . .].
CLAHRC management 3, case D
To ensure that there was a cycle of continuous improvement, and that the tools implemented in practice were used effectively, the clinicians were required to update the data from the projects using a web-based reporting tool. CLAHRC management was then able to monitor any issues arising in clinical practice and work with the NHS organisations to ensure that issues, including leadership, research methods and how best to implement research, were addressed.
We’ve set up a web reporting tool, and teams would use that, the suite of improving methods and planning doing study-out cycles and process and outcome measures. But the sustainability tool is one of those. So the individual departments have got a login, they’ll put their score in, the scores for the project are put together and then a composite score is produced and then the charts are produced. And the idea is that the team will look at what their risks are and come up with a strategy to address them.
CLAHRC management 3, Case D
The model of employing standardised service improvement methodologies and tools was directly related to the manner in which the director, who was a NHS-facing clinical academic, had envisaged the CLAHRC. Here, the director viewed CLAHRCs as a vehicle to improve patient care through the implementation of existing research and through addressing the needs of practice and how to support them. The role of CLAHRCs was to close the implementation gap through system/organisation-level change rather than focusing on individuals and the different institutions as separate entities.
In contrast, many other CLAHRCs conducted research first and then developed tools, or found appropriate existing tools, which they then could implement. Here, the emphasis was that research needed to be developed before it could be implemented. Or, in cases where the implementation theme was run in parallel, the implementation team often waited for the research to be conducted first. In a number of cases, implementation teams merely generated their own projects independent of the research themes.
Where the research had to generate new insights, tools and routines before they could be implemented, a slower process of transferring the new tools and routines into practice occurred. However, a number of CLAHRC actors did successfully develop useful tools through formal research-based collaborations, which were then adopted by local NHS organisations. For example, the researcher documented below collaborated with practice in the initial stages of the research project to identify how patient care could be improved with the development of educational tools. Collaborations with the local university enabled the translation of research into new systems and interventions that were then adopted and made routine even after projects had ended.
A policy simulator which lets you answer ‘what if’ questions about where you put resources into the health service. And it will tell you what happens, well it would predict what happens to the population over time. So you can change the interventions you apply, the resources you apply, it will simulate that population. Some of that work goes on in existing collaborations that we already have with the University XXX and epidemiologists there, who have basically delivered for us the sets of requirements that ultimately got translated into systems.
Researcher, case C
A number of other educational tools were developed by CLAHRCs, which later became embedded in practice and enabled evidence to be collated to identify the impact the new care pathway analysis tool had on patient outcomes over time.
What the purpose of this work is to do is to develop a software tool whereby you can define what a standardised care pathway is, you can go into a database containing historical medical data for patients and then you can compare what actually happened to those patients and the trajectory of their disease with what should have happened [. . .] Then you can then use the care pathway analysis tool to see what impact this had on their care and in fact you can then use that as evidence that you feed back into the policy simulator to refine them all.
Researcher, case C
In addition to developing new tools, and in response to the NHS needs, CLAHRC actors also identified existing tools that were documented in research but which had not been translated into practice.
There is research that says that you should be looking after these patients in these particular ways but unless they actually know who these patients are, we can’t actually do that. So the actual finding of people and actually making sure that right ones are on the register has been one aspect of enabling the sort of research about medications to actually be taken forward.
Social science academic 1, case C
An example of the development of a tool in response to NHS needs was:
[. . .] [W]e have actually brought in a tool that XXX [another CLAHRC] developed for running searches on registers to identify patients with chronic kidney disease. Actually it is interesting because in the first project we didn’t give them like a toolkit of how do you increase the number of people on your register, but the PDSA [plan, do, study, act] cycles virtually every practice that was one of the first PDSA cycles they had to do, run searches on their register, find where they were missing identification of patients.
Implementation lead, case C
The development of new evidence-based tools by CLAHRCs in collaboration with practice and the local HEI were embedded in practice and gained interest from the local health community.
And then as a result of going into these practices and learning more about the practice of the practitioners, we’ve then run education which has been very specific to the practices and as a result of that GPs [general practitioners] have said to us ‘Oh this has been so helpful, I feel far more confident now about managing patients’.
Social science academic 1, case C
This approach was also evident in other CLAHRCs that engaged with practitioners to equip them with the skills to be able to manage patient care. Clinical academics and knowledge brokers sought to bring research to practitioners and provided training for them to make services more patient focused.
Training is about patient-centred assessments, negotiation skills with patients, some of it is about actually delivering a new treatment, so a psychological therapy. Some of it’s about cultural competence, delivering care to people from ethnic groups and working together, part of our intervention is training people in primary care to work more closely together in a collaborative sense, so that care is integrated.
Social science academic 4, case C
Other CLAHRCs provided change management advice and new ways of working to practitioners. These were then embedded into the local health landscape to ensure that the tools and methods were used after CLAHRC had ended.
I mean we have very much taken an improvement collaborative approach and we’ve tweaked it and we’re in phase 3 now. I think we have managed to leave something behind in very practical skills, ways of working that they will keep using.
Implementation lead, case C
The institutionalisation of new ways of working and values to improve patient outcomes through the education of those in practice was central to CLAHRCs.
We are providing education to GPs and practice nurses around care, how to treat heart failure care, how to conduct systematic reviews, how to do data searches these kinds of things.
Researcher, case I
However, how successful actors were at embedding differed across the four CLAHRCs we studied. The IW around the creation of roles, tools and routines in practice helped to reinforce change across the NHS organisations and create linkages between the different institutions. In doing so, CLAHRC actors sought to embed the CLAHRC way of working into their partner organisations to build capacity.
Constructing a Collaboration for Leadership in Applied Health Research and Care identity
Identity construction as a form of IW has traditionally been associated with the development of new, and the transformation of existing, professional identities. 158,159 In highlighting the work that was undertaken to promote the development of a CLAHRC identity, we acknowledge the importance of IW around embedding – education, creating new roles, tools and routines – which helped develop a receptive context for such work. As such, identity work was not evident at the inception of CLAHRCs, rather it gathered momentum over time. We suggest that the development of a CLAHRC identity is important as it provided legitimacy for the roles and work that spanned the fields of research and practice.
A lot of the tools we use, whilst they have specific aims, such as process mapping, model for improvement or whatever, they have specific aims in relation to helping the project deliver, but the major side effects or benefits . . . are that first of all they allowed people to start communicating together and secondly they act as team-building tools.
CLAHRC management 1, case D
The construction of a CLAHRC identity was central to the promotion of CLAHRC ideals and in enabling greater stakeholder engagement with the CLAHRC initiative. To help develop a CLAHRC identity, one CLAHRC ran collaborative events to bring together practice and research, which stimulated a culture of ideas sharing and teamwork.
We have a mixture of people coming to events; it’s academics, patients, clinicians, health professionals and NHS managers. And that has helped to develop the ethos of bringing NHS management, clinicians, patients and academia together for the common purpose of closing the second translational gap. I think that has had the desired effect of creating that CLAHRC identity but also bringing people together to understand by working together they’re more likely to actually deliver the outcomes that they’ll want, which is essentially improve services for patients. So that’s worked quite well.
CLAHRC management 3, case D
Identity-building work was also centrally enabled by the NIHR and through numerous SDO learning events. CLAHRC directors, as a unit, saw the need for this higher-level branding as a way to develop and build a CLAHRC identity and secure the call for CLAHRC II funding.
There are learning events across all the CLAHRCs, we have a very strong learning culture. We have a very strong ethos, our principles are around capacity development and they are around public patient engagement, so we have a strategy that crosses over, so they are very cross cutting.
Clinical science academic, HEI-facing, case F
Alongside the encouragement of engagement with the ideals of CLAHRC, the development of a CLAHRC identity provided researchers and those working in the CLAHRCs with enhanced legitimacy within practice, which fostered better engagement and collaboration. The CLAHRC identity acted as a form of ‘brand’, which signalled that the researcher was more likely to be open to engaging fully with practice, which, in turn, meant that NHS staff were more willing to collaborate with them.
Clearly having a 5-year programme that’s dedicated to a specific aim, does give you an identity which then I think probably does help when you reach out to collaborate because you can say ‘Hi, I’m from the XXX CLAHRC, this is what we do’. And they might go ‘Oh yeah, okay, I get CLAHRCs’. So they carry some weight and there is some salience in using the CLAHRC name as a means to collaborate.
Social science academic 4, case C
We found, however, that the development of a strong CLAHRC identity was not prevalent in all CLAHRCs we examined. Where identity work was not as prevalent, we suggest that the cause was a number of more senior actors maintaining their pre-existing professional identities as their dominant identity. In CLAHRCs where there was a clear separation between research and implementation, actors commonly reverted back to their normal ways of working, which reinforced existing professional identities. This was particularly evident from senior academics and clinicians who were already highly embedded in their institutions, and so were less receptive to adopting the emerging CLAHRC identity.
I don’t know how much people will identify themselves with CLAHRC or its aims, I think very loosely. They see themselves as doing research in diabetes; the fact that that study is funded by CLAHRC, they might have been funded by Diabetes UK you know, it’s just a different funder. I personally think that it hasn’t been possible to get people focused on all of the aims of CLAHRC and to work towards them. I think people have used the money that have in their themes to do largely what they wanted to do and that largely meets one of the aims of CLAHRC.
CLAHRC management 2, Case I
Although CLAHRC identity was seen as important, a number of actors stressed that this was merely a means to an end, and that it was more important to focus on the development of a CLAHRC ‘way of thinking and doing’ through the creation of institutional norms and values to support CLAHRC activities. This then would enable the continuation of CLAHRC ways of working even after CLAHRCs ended.
When they’re no longer CLAHRC they can still take those ideas and use them for other things. So the next time they develop a project, even if it’s not CLAHRC funded, well a lot of them will know next time there’s no more money but in the past if they’ve done one successful project they’ve applied for the next round. So that’s how it’s worked. [. . .] Does it really matter if they’re saying ‘We’re CLAHRC, we’re CLAHRC’, what it’s about is it’s about the ethos and the values. If they are using our techniques and applying that, that’s what they want. Whether they call themselves CLAHRC is irrelevant; they are CLAHRC because they’re following the ethos which wasn’t there before.
CLAHRC management 3, Case D
Conclusion
The embedding of CLAHRCs centred on four inter-related areas of work: education, the creation of new roles, embedding tools and routines, and the construction of a CLAHRC identity. Across the four CLAHRCs we witnessed significant differences in how CLAHRC actors sought to embed the CLAHRC. We also noted a significant degree of isomorphism over time, whereby CLAHRCs looked to learn lessons from other CLAHRCs. Here, we draw attention to the archetypes of models for organising knowledge transfer and highlight that no one CLAHRC conformed to any specific archetype because of the process of isomorphism.
In terms of the IW, we saw evidence of education across all our in-depth cases, but educational programmes were conducted in different ways. In line with the study of Hargadon and Douglas,82 we found that the institutionalisation of the CLAHRC was supported by education. However, much of the educational work focused on enhancing the efficiency of existing CLAHRC projects, as opposed to capacity building in general.
The creation of new roles was most evident in the creation of the knowledge broker role, which emerged in one CLAHRC and then diffused to other CLAHRCs. An important reason for the diffusion of knowledge brokers was that NHS staff who had been seconded into such roles for only a fraction of their working week could then be counted as matched funding. The knowledge broker role is a form a hybrid role, which is based around the ideals of situated learning and the diffusion of practice, both of which influence capacity building for organisational- and systems-level change. 160
The two remaining forms of IW for embedding were more varied across the four CLAHRCs. In terms of tools and routines,32 while we witnessed evidence that CLAHRCs had been able to gain some traction in shaping NHS decision-making on a local scale, the reciprocal influence back into HEIs was more inconsistent. In addition, where tools and routines had been embedded in NHS partner organisations, this was largely done on a project basis. Similarly, the work to develop a strong CLAHRC identity varied, and was influenced by the extent to which senior CLAHRC actors had been willing to take on a CLAHRC identity. Where senior actors were unwilling to take on a CLAHRC identity, then this provides an interesting insight into how such actors view themselves, and their relationship to the field, which will orient their thoughts and actions accordingly. 104
Finally, in examining the different work undertaken to embed CLAHRCs, it is interesting to note the extent to which the different forms of work are inter-related and mutually reinforcing. We suggest that the CLAHRCs that have been the most successful in embedding their activity have sought to engage in multiple forms of embedding work. When asked about whether or not CLAHRCs had been able to engender institutional change, one senior-level actor replied:
Give us a chance. We’re now at the position where the local NHS organisations fully trust us, and that’s taken 5 years. We’ve made some changes at a local level, but an institutional level? All I can say is give us another 5 years and hopefully we’ll have scratched the surface.
Social science academic 3, case C
The issue of embedding is important as it relates to how the CLAHRCs were able to reshape existing institutions to close the T2. At present, the CLAHRCs have made significant progress in embedding the principles of CLAHRCs at a very local level, but arguably the macro-level institutions remain untouched.
Chapter 8 The Evolution of Collaboration for Leadership in Applied Health Research and Care Networks
In this chapter we complement our in-depth qualitative research with a SNA of the development of CLAHRC actors’ ego networks of interaction over two points in time. As outlined in Chapter 3, the analyses are based on the data collected from the four in-depth CLAHRCs in two survey waves. The first wave of data collection, in 2011 (wave I), produced 81 complete responses, and the second wave, in 2013 (wave II), produced 86 responses. Our approach to the SNA was based on regression and bivariate analyses of individuals’ ego networks. These allowed us to assess the effect of certain predictors on criterion variables.
Actors’ ego networks were examined by measuring a number of dependent variables (DVs), described in the subsequent sections of this chapter. Across all of our analyses we employed the 12 independent variables outlined below, which allowed us to use descriptive statistics to assess how actors’ social positions shaped their ego networks. Table 2 shows the coding and descriptive statistics for these variables. Please note that the different independent variables employed to capture the different dimensions of an actor’s social position are consistent with our qualitative work in Chapter 4. However, rather than being able to code actors’ positions from their interview transcripts, we asked actors to classify themselves along the following dimensions/variables.
| Variable definition | Variable coding | Descriptive statistics: wave I (wave II) | |||
|---|---|---|---|---|---|
| Min. | Max. | Mean | SD | ||
| Dominant orientation | Academia 1; practice 0 | 0 (0) | 1 (1) | 0.63 (0.65) | 0.49 (0.48) |
| Focus of interest | Clinical 1; non-clinical 0 | 0 (0) | 1 (1) | 0.89 (0.77) | 0.32 (0.42) |
| CLAHRC theme affiliation | Research 1; implementation 0 | 0 (0) | 1 (1) | 0.76 (0.59) | 0.43 (0.49) |
| Professional status | Scale of 4 highest status through to 1 lowest status | 1 (1) | 4 (4) | 2.49 (2.31) | 0.95 (0.84) |
| Network members’ professional status | Higher score, higher status | 1 (1) | 4 (4) | 2.90 (2.73) | 0.72 (0.64) |
| Number of knowledge brokers in an actor’s network | Count data | 0 (0) | 5 (5) | 0.46 (1.41) | 1.03 (2.26) |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | Count data | 0 (0) | 20 (14) | 3.97 (4.23) | 3.72 (3.37) |
| Number of an actor’s network connections in the same professional category (based on dominant role) | Count data | 0 (0) | 28 (11) | 4.70 (3.93) | 3.95 (2.33) |
Dominant orientation This variable concerned the distinction between those actors who were primarily academics (i.e. HEI-facing) and those who were health-care practitioners (i.e. NHS-facing). Actors were asked to assign themselves to one category.
Focus of interest This relates to whether or not an actor was clinical or non-clinical. The distinction was made between those who were focused on clinical issues, in terms of both practice and academia (including academics in health services departments), and those who were not clinically focused, including social scientists and engineers.
CLAHRC theme affiliation This relates to whether or not an actor was affiliated to a research theme or an implementation theme. Actors were asked to indicate which theme they were most closely affiliated to.
Professional status A four-point scale was used, with ascending seniority. The highest rank of 4 was given to actors in the most senior positions (e.g. directors of CLAHRCs, principal theme leads, directors of trusts, professors, etc.). The rank of 3 was given to actors with relatively senior roles including co-theme leads, readers and senior lecturers, and senior practitioners below the level of director. The rank of 2 was assigned to lecturers, research associates and health-care practitioners. Finally, the rank of 1 was assigned to actors in roles such as research assistants, PhD students, junior nurses, etc.
Network members’ professional status This is the mean score of all of the professional status rankings for the members of an actor’s network.
The remaining three independent variables of interest were the number of knowledge brokers in a network; the number of professionals in an actor’s network with whom the respondent had not worked with before joining the CLAHRC; and the number of an actor’s network connections in the category with the same dominant orientation. Each of these was measured as a count variable.
In addition to the variables presented above, we included control variables as follows: a dummy variable for gender and for three of our four CLAHRCs. In the analysis, we comment on the significance of the CLAHRC dummy variables.
Findings of cross-sectional data analyses
In this first part of this chapter we report the results of cross-sectional analyses of data from both survey waves.
Networks across academics and practitioners
The first analysis examined networks across academics and practitioners. These networks were characterised by measuring the proportion of the representatives of the other category in the network of a given actor (i.e. for academics, the proportion of practitioners in the network; and, for practitioners, the proportion of academics in the network). The proportions ranged from 0 to 1 (i.e. 100%), with mean values of 0.29 (wave I) and 0.34 (wave II), and standard deviations (SDs) of 0.28 and 0.27 respectively. The results of order of least squares (OLS) regression analysis show that the independent variables account for significant variation in the formation of connections across academics and clinicians in both survey waves (Table 3; R2 = 0.68 and R2 = 0.66 in waves I and II respectively). Thus, in the survey waves I and II regression predictors explained 68% and 66% of variance in the criterion.
| Predictor | Criterion | |
|---|---|---|
| Wave I | Wave II | |
| Dominant orientation (academic 1; practitioner 0) | –0.28a | –0.48b |
| Focus of interest (clinical 1; non-clinical 0) | 0.31c | –0.06 |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.18d | 0.08 |
| Professional status (highest status 4 – lowest status 1) | 0.25c | 0.22c |
| Network members’ professional status (average professional status score) | 0.09 | –0.15 |
| Number of knowledge brokers in network | 0.05 | 0.36c |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.54a | 0.01 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | –0.58a | –0.37a |
| Gender (female 1; male 0) | 0.01 | –0.18b |
| CLAHRC dummies | Not significant | Not significant |
| R 2 | 0.68 | 0.66 |
In the presence of regression controls, the dominant orientation variable exerted a negative, moderately weak, effect in wave I (β = –0.28; p < 0.05) and a negative, moderately strong, effect in wave II (β = –0.48; p < 0.001). Hence, practitioners in both survey waves were found to be more likely to form connections with academics than vice versa. This finding suggests that academics’ professional ego networks are generally limited to colleagues who are directly useful in the reproduction of their professional expertise. In contrast, for practitioners, the involvement of academics in their network appears to be more relevant for their professional work, namely the development, evaluation and implementation of health-care interventions.
Actors’ professional status was found to exert a statistically significant positive influence on academic–practitioner networking in both wave I (β = 0.25; p < 0.01) and wave II (β = 0.22; p < 0.01). Actors of higher professional status, in both academic and practice domains, were more likely to establish connections with the representatives of the other professional category. In contrast, since lower-status professionals are less secure in their work, they may have more to lose by becoming involved in practices that are not effectively aligned with the prevailing professional standards of promotion, and the institutions that surround them. For example, in academic organisations junior researchers may be less inclined to invest time in forming professional networks that are not likely to be directly relevant to their career mobility in accordance with existing institutional structures (they would rather focus on, for example, generating research publications that are valued highly under the REF). An alternative, but consistent, explanation is that lower-status professionals may have been actively ‘managed’ and directed away from such networking by their superiors (higher-status professionals), who may benefit from this dissuasion through the maintenance of a ‘workforce’ which services their need for academic publications and research completions.
An actor’s social position based on the established network of professional connections was found to a have a restrictive effect on actors’ networking across the academic–practitioner divide. The number of connections with members of the same professional category (for academics, those with other academics, and for practitioners, those with other practitioners) exerted a significant, moderate to strong, negative effect on the formation of networks across academics and clinicians involved in CLAHRCs in wave I (β = –0.58; p < 0.001) and II (β = –0.37; p < 0.001) respectively. Thus, formation of new connections across academics and practitioners was less pronounced among those respondents who had more connections with members of their professional category prior to joining the CLAHRC.
The formation of new connections, measured as the number of people with whom a given respondent had not worked with prior to joining a CLAHRC, was found to exert a significant, strong, positive effect on academic–practitioner networking (β = 0.54; p < 0.001) in wave I. Thus, the formation of connections between academics and practitioners in the initial survey wave was higher among those participants who had a higher a number of new professional contacts in their network.
Based on the above, we suggest that CLAHRC actors who are less embedded in existing professional networks are more likely to form connections across academic–practitioner boundaries. Involvement in previous professional networks, in part, generated a closure to the formation of new networks across distinct domains of activity. Since network expansion may alter the power balance or institutional standards of existing networks, members with higher degrees of embeddedness in existing networks may be less inclined to form new ones.
We note, however, that the potentially constraining effects of embeddedness were stronger in wave l than in wave II. In particular, the effect of the number of people with whom a given respondent had not worked with prior to joining a CLAHRC was insignificant in wave II (p > 0.05). In terms of the bridging of the academic–practitioner networking gap, these findings may suggest that, in the later phase of the operation of CLAHRCs, their members become more open to reconcile their commitment to their prior professional network with the formation of new expert networks established during their involvement in CLAHRCs.
Bridging the academic–practitioner divide: decision-making in Collaboration for Leadership in Applied Health Research and Care-related projects or research objectives and/or research questions
Next we examined how our independent variables influenced the bridging of the academic–practitioner divide in decision-making. We focused first on the influence exerted on decisions concerning CLAHRC related project or research objectives and/or research questions (RORQs) by the representatives of the opposite professional category (i.e. for academics it is the influence exerted by practitioners, and for practitioners it is the influence exerted by academics). The DV was measured as the mean score for the relevant members, based on a five-point Likert-type scale, with 5 indicating the highest influence and 1 the lowest influence. Values ranged from 1 to 5, with means of 2.63 and 2.47, and SDs of 1.88 and 1.78, for wave I and wave II respectively. In survey waves I and II, regression predictors explained 41% and 51% of variance in the DV respectively. Regression coefficients are shown in Table 4.
| Predictor | Criterion | |
|---|---|---|
| Wave I | Wave II | |
| Dominant orientation (academic 1; practitioner 0) | –0.23 | –0.42a |
| Focus of interest (clinical 1; non-clinical 0) | 0.07 | 0.07 |
| CLAHRC theme affiliation (research 1; implementation 0) | 0.01 | 0.21b |
| Professional status (highest status 4 – lowest status 1) | 0.32a | 0.29a |
| Network members’ professional status (average professional status score) | –0.15 | –0.14 |
| Number of knowledge brokers in network | 0.13 | 0.09 |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.36c | 0.08 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | –0.09 | –0.21b |
| Gender (female 1; male 0) | 0.06 | –0.08 |
| CLAHRC dummies | Not significant | Significant |
| R 2 | 0.41 | 0.51 |
Consistent with the findings for the formation of networks across academics and practitioners, professional status was found to exert a significant, moderately weak, positive effect in both wave I (β = 0.32; p < 0.01) and wave II (β = 0.29; p < 0.01). Thus, higher-status academics and practitioners were more likely than those of a lower status to incorporate the input of CLAHRC actors of the opposite professional domain (irrespective of their status) in decision-making concerning CLAHRC related RORQs. It is important to note, however, that the ability to make decisions about RORQs may be concentrated in the hands of higher-status professionals. Therefore, high-status professionals may be able to incorporate or encourage the input of actors from the opposite domain, which lower-status professionals cannot do.
Similarly, the formation of new professional connections was found to exert a significant, moderately weak, positive effect on decision-making in wave I (β = 0.36; p < 0.05). Above and beyond the influences of individual and organisational controls, professionals who had a higher number of participants in their network with whom they had not worked before joining CLAHRC were more likely to bridge the academic–practitioner decision-making gap with regard to the formation of CLAHRC RORQs. This finding was not replicated in wave II.
Consistent with the findings for academic–practitioner networking, dominant orientation was found to exert a significant, moderate, negative effect on the criterion variable in the wave II (β = –0.42; p < 0.01). In survey wave I, dominant orientation was found to be correlated (bivariate analysis) with bridging the academic–practitioner decision-making gap (r = –0.38; p < 0.001), but not as a predictor in multivariate regression. These results suggest that, at least in the later phase of the CLAHRCs operations, academics were somewhat less likely to be influenced in their professional decisions by practitioners than vice versa. We suggest that this result may, in part, reflect academics’ current preoccupation with the REF and their concern with the professional work necessary to reproduce their position in the academic status hierarchy. These displace the desire to increase involvement with clinicians in CLAHRC related decision-making, which has a noticeably lower pay-off in academic domain.
Bridging the academic–practitioner divide: decision-making in Collaboration for Leadership in Applied Health Research and Care-related research process, design and methodology
We then examined how the SNA independent variables affected the bridging of the academic–practitioner divide with regard to the influence representatives of the opposite professional category had on decisions concerning CLAHRC related research process, design and methodology (PDM). The DV was measured as the mean score for the relevant members based on a five-point Likert-type scale with 5 indicating the highest influence and 1 the lowest influence. Values range from 1 to 5, with means of 2.51 (wave I) and 2.34 (wave II), and with SDs of 1.83 and 1.77 respectively. In wave I and II, regression predictors explained 40% and 49% of variance respectively, as shown in Table 5.
| Predictor | Criterion | |
|---|---|---|
| Wave I | Wave II | |
| Dominant orientation (academic 1; practitioner 0) | –0.30a | –0.45b |
| Focus of interest (clinical 1; non-clinical 0) | 0.13 | –0.04 |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.10 | 0.24c |
| Professional status (highest status 4 – lowest status 1) | 0.22c | 0.27d |
| Network members’ professional status (average professional status score) | –0.08 | –0.16 |
| Number of knowledge brokers in network | 0.18 | 0.09 |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.06 | 0.01 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | 0.04 | –0.20c |
| Gender (female 1; male 0) | 0.05 | –0.08 |
| CLAHRC dummies | Not significant | Significant |
| R 2 | 0.40 | 0.49 |
Consistent with the results for academic–practitioner networking and bridging of the academic clinical decision-making gap in the development of CLAHRC RORQs, dominant orientation was found to exert a negative, moderately weak (β = –0.30; p < 0.05) and moderately strong (β = –0.45; p < 0.001) effects in waves I and II. These results suggest that practitioners are more likely to be influenced by academics in making decisions concerning the CLAHRC related research PDM than vice versa. One explanation of this results is that academics may be viewed as the ‘experts’ in research PDM and may even promote themselves on that basis.
Similarly, for the predictor of professional status there was a significant, moderately weak positive effect in wave II (β = 0.27; p < 0.01) and a significant weak positive trend for the effect on criterion in the wave I (β = 0.21; p < 0.1). The bridging of the academic–practitioner decision-making gap with regard to the CLAHRC related research PDM is also more likely to be exercised by the higher-status professionals in CLAHRCs. As above, this finding may reflect perceived expertise with decision-making authority over research PDM.
Finally, our analysis also revealed a significant positive trend for the effect of CLAHRC theme affiliation in the wave II (β = 0.24; p = 0.07). Thus, in the later stages of CLAHRCs, academics and practitioners involved in research themes are more likely to be influenced by the representatives of the opposite professional category in making the decisions concerning CLAHRC related PDM than implementation theme members. This was consistent with the pattern observed for the bridging of academic–practitioner decision-making gap in the formation of CLAHRC related RORQs.
Networks across research and implementation themes
The networks across research and implementation themes were then examined, with a focus on the proportion of the representatives of the opposite theme in the network (for the representatives of research themes, the proportion of implementation theme members in the network was used; for implementation theme members, the proportion of research theme representatives in the network was used). Here values ranged from 0 to 1 (i.e. 100%), with mean values of 0.21 and 0.24, and SDs of 0.23 and 0.26, for waves I and II respectively. Compared with the notable explanatory power of regression equations estimating the bridging of academic–practitioner networking and decision-making gaps, regression predictors explained significantly less variance in the formation of connections across members of research and implementation themes (Table 6; 37% and 7% in waves I and II respectively).
| Predictor | Criterion | |
|---|---|---|
| Wave I | Wave II | |
| Dominant orientation (academic 1; practitioner 0) | –0.08 | –0.05 |
| Focus of interest (clinical 1; non-clinical 0) | –0.13 | 0.11 |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.27a | –0.02 |
| Professional status (highest status 4 – lowest status 1) | 0.14 | –0.09 |
| Network members’ professional status (average professional status score) | 0.14 | 0.24 |
| Number of knowledge brokers in network | –0.05 | 0.14 |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.09 | 0.01 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | –0.02 | –0.04 |
| Gender (female 1; male 0) | –0.04 | –0.12 |
| CLAHRC dummies | Not significant | Not significant |
| R 2 | 0.37 | 0.07 |
In wave I, we identified a significant weak negative trend (β = –0.27; p < 0.1) for the effect of CLAHRC theme affiliation on the formation of networks across research and implementation themes. In wave II, CLAHRC theme affiliation was found to exert no effect on the criterion. Thus, at least in the initial phase of the operation of CLAHRCs, members of implementation themes were somewhat more likely to form connections with their counterparts from research themes than vice versa. While recognising a relatively weak effect of theme affiliation on criterion in the wave I, the observed discrepancy in results across the survey waves could be perhaps attributed to the marginal relative increase in the formation of research-implementation theme bridging networks among members of research themes in the later phase of the operation of CLAHRCs. This assumption is tentatively supported by the positive standardised regression coefficient (β = 0.24) for the effect (although statistically insignificant) of the CLAHRC theme affiliation on the change in the criterion over time (see Chapter 9, We committed too much resource upfront, for longitudinal analyses).
Networks across actors’ foci of interest
The final DV for our cross-sectional analysis relates to networks across actors’ foci of interest, as measured by the proportion of the professionals who had a different focus of interest in an actor’s network (e.g. for clinically focused actors it is non-clinically focused actors and vice versa). Values ranged from 0 to 0.83 (i.e. 83%), with mean values of 0.10 and 0.25, and SDs of 0.21 and 0.24, for waves I and II respectively.
The regression analysis explained a rather notable proportion of variance in the formation of networks across actors with a clinical and non-clinical focus of interest for both waves. Table 7 shows that 74% and 37% of the variation in the criterion variable was explained for waves I and II respectively. The results of regression analyses for the first and second surveys respectively, identified, a significant negative, moderately positive, strong effect (β = –0.54; p < 0.001) and a significant negative trend (β = –0.25; p = 0.06) for the effect of an actor’s focus of interest on networking across foci of interest. In both survey waves respondents with a non-clinical focus of interest (for example, from business schools, social science departments, etc.) were more likely to form network connections with their counterparts with a clinical focus of interest than vice versa.
| Predictor | Criterion | |
|---|---|---|
| Wave I | Wave II | |
| Dominant orientation (academic 1; practitioner 0) | 0.01 | 0.33a |
| Focus of interest (clinical 1; non-clinical 0) | –0.54b | –0.25c |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.30d | 0.10 |
| Professional status (highest status 4 – lowest status 1) | 0.16a | –0.03 |
| Network members’ professional status (average professional status score) | –0.05 | 0.12 |
| Number of knowledge brokers in network | 0.01 | 0.56b |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.06 | –0.12 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | 0.03 | –0.23c |
| Gender (female 1; male 0) | 0.16a | 0.06 |
| CLAHRC dummies | Not significant | Not significant |
| R 2 | 0.74 | 0.37 |
In the second wave, the regression analysis also identified a significant, moderately strong, positive effect of involvement with knowledge brokers on the criterion variable (β = 0.56; p < 0.001). Thus, at least in the later phase of the operation of CLAHRCs, participants with a higher number of knowledge brokers in the CLAHRC network (variously identified as KTAs, CLAHRC co-ordinators, improvement managers, etc.) tended to be more inclined to form network ties with actors with different foci of interest.
Consistent with the pattern identified for the formation of connections across members of research and implication themes, the data analysis identified a significant, moderately weak, negative effect of CLAHRC theme affiliation on the criterion variable in wave I (β = –0.30; p < 0.01). Thus, in the presence of regression controls, CLAHRC participants who were clustered in implementation themes were more likely than their colleagues from research themes to form network ties with actors with the different (opposite) foci of interest.
In the second wave, actors’ dominant orientation was found to exert a significant, moderately weak, positive effect (β = 0.33; p < 0.05). Thus, in contrast to the pattern observed for the bridging of the academic–clinical gap, academics were more likely than health-care practitioners involved in CLAHRCs to bridge the clinical–non-clinical focus of interest gap.
Finally, there was a significant, weak, positive effect of members’ professional status in wave I on the criterion variable (β = 0.16; p < 0.05). Thus, consistent with the pattern of results identified for the bridging of the academic–practitioner gap, CLAHRC actors of higher professional status were more likely than their lower-status counterparts to form connections across the clinical–non-clinical focus of interest gap.
Findings of longitudinal data analyses
In this section we report the results of the longitudinal analyses for the change actors’ networking behaviour between wave I and wave II. As above, we employ the same independent variables, but developed measures of change in the DVs across wave I and wave II, given by DVchange = DVwave II – DVwave I.
Although every attempt was made to secure the involvement of the same participants in the network survey over time, high staff turnover in one of our in-depth case sites resulted in a very low overlap between the samples of participants obtained in the waves I and II. As a result, during the second survey wave we managed to obtain longitudinal data for only three participants out of 15 surveyed in the first wave in one CLAHRC. As a result of the very low response rate, the decision was made to exclude the three respondents from longitudinal analyses. Therefore, the longitudinal analyses reported in this section are based on data from 42 of the 66 participants initially surveyed from three CLAHRCs.
Longitudinal networks across academics and practitioners
We measured change in networks across academics and practitioners by calculating the proportion of the representatives of the opposite professional category in the networks of academics and practitioners at wave II minus the same proportion at wave I (Pchange = Pwave II – Pwave I). Potential values ranged from –1 to 1, with actual values ranging from –0.85 to 0.63, with a mean of –0.03 and SD of 0.27. The independent variables accounted for 46% of variation in the change over time in the formation of networks across academics and clinicians (Table 8; R2 = 0.46). In contrast to the pattern observed in the cross-sectional analyses, the results of the longitudinal data analyses identified a positive, very strong, significant effect of dominant orientation (β = 0.79; p < 0.01). This finding provides a strong indication that the proportion of health-care practitioners in the network of CLAHRC academics has increased noticeably over the 2-year period of the operation of CLAHRCs.
| Predictors | Criterion |
|---|---|
| Dominant orientation (academic 1; practitioner 0) | 0.79a |
| Focus of interest (clinical 1; non-clinical 0) | 0.49b |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.50b |
| Professional status (highest status 4 – lowest status 1) | 0.26 |
| Network members’ professional status (average professional status score) | –0.35c |
| Number of knowledge brokers in network | 0.38c |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | –0.40b |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | 0.01 |
| Gender (female 1; male 0) | 0.04 |
| CLAHRC dummies | Not significant |
| R 2 | 0.46 |
Data analyses also identified a significant, moderately strong, positive effect of actors’ focus of interest (β = 0.49; p < 0.05) and a significant, moderately strong, negative effect of CLAHRC theme affiliation (β = –0.50; p < 0.05) on the change in academic–practitioner networking over time. Thus, actors whose focus of interest was clinical (as opposed to non-clinical) and who were members of implementation themes (as opposed to research themes) were likely to experience an increase in the formation of networks across academics and practitioners over time.
In contrast to the pattern identified in the cross-sectional analysis of wave I data, the results of longitudinal analyses revealed a negative, moderately strong, significant effect of the embeddedness in the prior professional network on the change in academic–practitioner networking over time (β = –0.40; p < 0.05). This result suggests that respondents with fewer professionals with whom they did not work before joining CLAHRC in their network (measured by the score obtained in the survey wave I) were more likely to bridge the academic–practitioner networking gap over time.
Thus, participants who were more embedded in the existing network of connections between both academics and practitioners at the time of the establishment of CLAHRCs were more likely to form new connections that crossed the gap over the 2-year period of CLAHRC operation.
It should also be noted that the regression analyses identified a significant positive trend for the effect of knowledge brokers (β = 0.38; p < 0.1) and a significant negative trend for the effect of network members’ professional status (β = –0.35; p < 0.1). Thus, members with a higher number of knowledge brokers in their CLAHRC network and members embedded in a lower professional status network were more likely to bridge the academic–practitioner networking gap over time.
Bridging the academic–practitioner divide in decision-making
Table 9 presents the results of OLS regression analysis for change in the bridging of the academic–practitioner decision-making gap between waves I and II. The DVs measure a change in the influence on decisions concerning CLAHRC related RORQs and decisions concerning CLAHRC related PDM by actors from opposing dominant orientations (for academics, it is the influence exerted by practitioners; and, for practitioners, it is the influence exerted by academics). For both DVs potential values could range from –5 to 5, with actual minimum values of –5 and maximum values of 5 for both RORQs and PDM. Mean values of –0.70 and –0.55, and SDs of 2.09 and 2.12 were found for RORQs and PDM respectively. Regression equations in both cases explained a notable proportion of variance in the change in the bridging of the academic–practitioner decision-making gap concerning CLAHRC-related RORQs (64%) and CLAHRC-related research PDM (54%) over time.
| Predictors | Criterion | |
|---|---|---|
| RORQs | PDM | |
| Dominant orientation (academic 1; practitioner 0) | 0.84a | 0.90a |
| Focus of interest (clinical 1; non-clinical 0) | 0.59b | 0.64b |
| CLAHRC theme affiliation (research 1; implementation 0) | –0.37c | –0.36c |
| Professional status (highest status 4 – lowest status 1) | 0.04 | 0.18 |
| Network members’ professional status (average professional status score) | –0.04 | –0.17 |
| Number of knowledge brokers in network | 0.58b | 0.55c |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | –0.29 | –0.08 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | –0.73a | –0.78a |
| Gender (female 1; male 0) | –0.02 | 0.04 |
| CLAHRC dummies | Not significant | Not significant |
| R 2 | 0.64 | 0.54 |
As with the pattern observed for the bridging of the academic–practitioner networking gap, dominant orientation was consistently found to exert a very strong, positive, significant effect on change in both RORQs (β = 0.84; p < 0.001) and PDM (β = 0.90; p < 0.001). This finding provides a strong indication that, over the 2-year period of involvement in CLAHRCs, academics became increasingly influenced by practitioners in making the decisions concerning CLAHRC-related project and research objectives, and PDM.
Similarly, the professional connections variable was found to exert a very strong, negative, significant effect on change in both DVs, RORQs (β = –0.73; p < 0.001) and PDM (β = –0.78; p < 0.001). Thus, CLAHRC academics and practitioners with fewer connections with members of the same professional category were likely to become more concerned with bridging the academic–practitioner decision-making gap over time. Consistent with the pattern observed for the bridging of the academic–practitioner networking gap in cross-sectional data analysis, this finding highlights the restrictive influence of the embeddedness in an existing network of connections in one’s own professional domain (either academic or practitioner). Considering this finding in the context of the results presented in Table 7, we suggest that it is not embeddedness in networks per se that has a restrictive influence on the involvement in collaborative knowledge generation and work among academics and practitioners. Rather, the restrictive influence is related to actors’ embeddedness in networks that are largely constituted by actors from their own dominant orientation.
The number of knowledge brokers in the CLAHRC network was found to exert a significant, moderately strong, positive effect on change in both DVs, RORQs (β = 0.58; p < 0.01) and PDM (β = 0.55; p < 0.05). This finding underscores the importance of knowledge brokers in fostering the involvement of academics and practitioners in CLAHRC related decision-making.
Our analysis also identified a significant, moderately strong, positive effect of actors’ focus of interest on change in both DVs, RORQs (β = 0.59; p < 0.01) and PDM (β = 0.64; p < 0.01). Similarly, CLAHRC theme affiliation was found to exert a significant, moderately weak, negative effect on both criterion measures, RORQs (β = –0.37; p < 0.05) and PDM (β = –0.36; p < 0.05). Thus, CLAHRC members whose focus of interest was on clinical issues, and those who were members of implementation themes, were more likely to bridge the academic–practitioner decision-making gap from wave I to wave II than their counterparts whose focus on interests was on non-clinical issues and who were involved in research themes. These findings were consistent with the pattern of results observed for the change in the bridging of the academic–practitioner clinical networking gap.
Networks across research and implementation themes
We examined change in actors’ networks across research and implementation themes by examining the change in the proportion of the representatives of the opposite theme in the network over time. Potential values could range from –1 to 1, with an actual minimum value of –0.8 and maximum value of 0.78, a mean of –0.02 and a SD of 0.28.
When CLAHRC participants’ characteristics were regressed on change in the formation of networks among members of research and implementation themes over time, the model explained only approximately one-quarter of variance in the criterion (Table 10; R2 = 0.24). The results of data analyses revealed a significant positive trend for the effect of knowledge brokers on criterion (β = 0.45, p < 0.1). Thus, the number of knowledge brokers in the CLAHRC network was found to be positively associated with the tendency of the members of research and implementation themes to become more integrated in the formation of mutually overlapping networks. None of the other predictors were found to exert a significant effect on the criterion in either the multivariate or bivariate analyses.
| Predictors | Criterion |
|---|---|
| Dominant orientation (academic 1; practitioner 0) | –0.16 |
| Focus of interest (clinical 1; non-clinical 0) | –0.28 |
| CLAHRC theme affiliation (research 1; implementation 0) | 0.24 |
| Professional status (highest status 4 – lowest status 1) | –0.10 |
| Network members’ professional status (average professional status score) | –0.07 |
| Number of knowledge brokers in network | 0.45a |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | –0.23 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | –0.28 |
| Gender (female 1; male 0) | 0.06 |
| CLAHRC dummies | Significant |
| R 2 | 0.24 |
Changes in networks across clinical and non-clinical foci of interest
The final DV examined the changes in actors’ networks across foci of interest, as measured by the change in the proportion of the professionals in a given actor’s network who had a different focus of interest to the actor between wave I and wave II. Potential values could range from –1 to 1, with an actual minimum value of –0.75 and maximum value of 0.33, a mean of –0.05, and a SD of 0.23.
Our regression model explained half of the variance in the change in the formation of networks spanning actors with clinical and non-clinical foci of interest (Table 11; R2 = 0.51). CLAHRC theme affiliation was found to exert a significant, moderately strong, positive effect (β = 0.44; p < 0.05), suggesting that members of CLAHRC research themes were more likely to experience an increase in the formation of networks across clinical and non-clinical actors than their colleagues from implementation themes. None of the other predictors entered in OLS regression were found to be statistically significant.
| Predictors | Criterion |
|---|---|
| Dominant orientation (academic 1; practitioner 0) | –0.05 |
| Focus of interest (clinical 1; non-clinical 0) | 0.16 |
| CLAHRC theme affiliation (research 1; implementation 0) | 0.44a |
| Professional status (highest status 4 – lowest status 1) | –0.23 |
| Network members’ professional status (average professional status score) | 0.31 |
| Number of knowledge brokers in network | 0.06 |
| Number of professionals in an actor’s network with whom respondent had not worked before joining CLAHRC | 0.12 |
| Number of an actor’s network connections in the same professional category (based on dominant orientation) | 0.10 |
| Gender (female 1; male 0) | –0.11 |
| CLAHRC dummies | Not significant |
| R 2 | 0.51 |
Conclusion
The results of our SNA highlight the enabling role of individuals’ social position in promoting institutional entrepreneurship associated with the development of network ties across actors’ different dominant orientations (academic vs. practitioner) and foci of interest (clinical vs. non-clinical). 106,114 Specifically, our SNA highlighted that there were systematic variations in actors’ ability to bridge the research–practice boundary. First, practitioners were more likely to develop networks that bridged the divide than academics. Second, actors with many existing connections in their own professional field (i.e. are more embedded) were less likely to bridge the divide than those with fewer connections (i.e. were less embedded). Third, junior actors found it more difficult than their more senior counterparts to bridge the divide. However, on a positive note, our longitudinal analysis suggests that the CLAHRC initiative has led to the development of more relationships that span the research–practice divide.
From wave I to wave II practitioners networked more with, and were influenced more by, academics than vice versa. However, our results suggest that between our two waves of analysis, academics experience a notable increase both in the proportion of practitioners in their CLAHRC network and in the extent to which they are influenced by practitioners in CLAHRC related decision-making. The involvement of academics in CLAHRCs appears to have a positive impact on the institutionalisation of their new collaborative working patterns with practitioners.
Underscoring the role of individuals’ social status in the institutionalisation of new work patterns,24,161,162 the bridging of the academic–practitioner networking and decision-making gaps is found to be more pronounced among the CLAHRC actors of higher professional status. There was no significant change in the effect of participants’ professional status over time. Since higher-status CLAHRC members are more secure in their professional roles, they may be more empowered to exhibit work patterns that deviate from the established jurisdictional standards of their profession. 163 In turn, for lower-status professionals, investing time in work that is not effectively aligned with the reproduction of existing professional standards may compromise their career mobility. Alternatively, but with the same effect, lower-status professionals may have been actively ‘managed’ and directed away from such networking by their superiors (higher-status professionals), who may benefit from this dissuasion through the maintenance of a ‘workforce’ which services their need for academic publications and research completions.
In terms of the enabling role of individuals’ social position, based on the availability and mobilisation of social connections, the findings underscore the role of knowledge brokers in the institutionalisation of KT practices. 164,165 Across our two waves of analyses, CLAHRC members with a higher number of knowledge brokers in their network were more likely to be influenced by the members of the opposition professional domain in CLAHRC-related decision-making. In wave II, the number of knowledge brokers in the network was also found to be positively associated with the formation of networks across academics and practitioners, and members of research and implementation themes. These results suggest that knowledge brokers served to facilitate communication and integration of professional networks among academics and practitioners.
In contrast to the enabling role of individuals’ social position based on professional status and involvement with knowledge brokers, the embeddedness of participants in the network of the same dominant orientation (for example, academics networked with academics) had a restrictive effect on the bridging of the academic–practitioner networking and decision-making gaps. Embeddedness in a network that did not span professional divides appears to have inhibited the involvement of CLAHRC members in the process of institutionalising new collaborative patterns of work. This may be because such patterns undermined the power and autonomy of their professional domain. 166,167
The role of the embeddedness in the prior network of professional connections (irrespective of contacts’ dominant orientations) is more ambivalent. In the initial phase, participants with higher embeddedness in the network of connections formed before joining a CLAHRC are less likely to form networks across academics and practitioners. However, during the 2-year period of involvement in CLAHRCs these members became increasingly involved in the formation of mutually overlapping networks. One interpretation of this finding is that in the initial phase members who were more embedded in their prior network of connections sought to preserve the established power and work standards by resisting the inclusion of new members from the opposite professional domain. However, as these academics and practitioners become more familiar and/or secure with the goals and means of CLAHRCs, they become increasingly open to the formation of networks with the representatives of the opposite professional domain. In doing so, they became involved in the bridging of the academic–practitioner network gap.
Chapter 9 Reflecting on Collaborations for Leadership in Applied Health Research and Care
As outlined in the previous chapters, the initial founding conditions of CLAHRCs shaped the way in which the dominant actors in each region envisaged, through diagnostic and prognostic framing, their CLAHRCs. As the CLAHRCs were mobilised and enacted, through the processes of engaging and embedding, important information on the efficacy of specific decisions that were taken at the envisaging stage and beyond were revealed. Increasingly over time, those managing and leading the projects reflected on the way CLAHRCs were set up and run.
Interestingly, there was significant variation between different actors’ ability to reflect on initial decisions and to learn from mistakes in order to improve CLAHRCs. A small number of senior CLAHRC actors appeared to be less able, or perhaps less willing, to reflect on their mistakes and to learn from them. In contrast, many other CLAHRC actors openly discussed their mistakes and saw them as important learning lessons. We suggest that the reflective ability of CLAHRC actors was key to organisational learning, especially in new ventures. 168
CLAHRC actors identified multiple issues when they reflected on the problems they had faced in mobilising the CLAHRCs. Key issues were (i) the difficulties of getting the CLAHRC up and running, (ii) commitment to large-scale projects upfront, (iii) difficulties in achieving a balance between research and implementation, (iv) issues surrounding the need for different actors to learn to work together and to establish a common understanding of what implementation and, finally, (v) an increasing awareness of the need to develop career structures that reward CLAHRC behaviour.
We did not hit the ground running
The CLAHRCs were designed around a 5-year programme of activity, and the expectation was that the CLAHRCs would be able to ‘hit the ground running’. However, it soon became apparent to many CLAHRC senior staff that they, and the NIHR, had significantly underestimated the problems of enacting the CLAHRCs.
As outlined in Chapter 6, matched funding had been ‘agreed in principle’, and, although it later proved useful as it was seen to increase the engagement from practice and the partners’ commitment to the projects, there were tensions around what matched funding actually meant and then initially securing and allocating it.
I mean one of the original challenges for CLAHRC is when we used the term ‘matched funding’, that as people in trusts became aware of this requirement, there has to be conversations about well this doesn’t necessarily mean that we’re going to be asking you for £100,000 every year or whatever. What we’re really looking for is equivalent resources of that level.
CLAHRC management 4, case I
Many of the CLAHRC directors and project leaders felt that the NIHR had assumed that there would be no lead time during the CLAHRC set-up and that projects would run from the start of CLAHRCs. However, the initial set-up process was a time-consuming element of enacting the CLAHRCs. Since matched funding included staff, many of the necessary positions were unfilled during the first year of the CLAHRC, which delayed projects.
Well we had the funding, I think we heard about the funding in about the September of 2008 and I think some funding started sort of like in the October. Well there was nobody in place. You can’t spend the money if you haven’t got staff actually in post. And we couldn’t start recruiting until we knew we’d got the money.
Clinical science academic 3, HEI-facing, case I
When you’re putting in grants for something like CLAHRC, you’re forced into a position of assuming that you can hit the ground running, but in fact that doesn’t happen.
Clinical science academic, NHS-facing, case E
The short time between the submission of bids and the beginning of the CLAHRC initiative led to differences between project proposals and their initiation. For example, a number of projects were unable to start because the projects had not been finalised with the partner organisations or had to go through a long ethics process. Other projects had been allocated funding upfront and left with none towards the end of the projects during the stages when implementation of the research in practice was due to take place. These factors led to delays in the use of funding and a lack of planning in the allocation of the funding over the course of CLAHRC – a concern to senior members of the CLAHRC.
I think the money all came in initially in quite a big lump. The way that the funding was done, I don’t think we’d do it the same way again. We had a lot of funding in the first 2 years, there was a lot of pressure to get people employed and get the studies going as soon as possible because otherwise we’d have lost the money. So our last 2 years, the money is much, much smaller.
Clinical science academic 3, HEI-facing, case I
In addition to ensuring the release of resources from partner organisations, a series of additional issues arose related to the practicalities of trying work across the HEI–NHS interface. There was a need to learn how to manage the expectations of both organisations, and to understand how both parties operated.
I think from my point of view there maybe should be at the beginning more emphasis put on the infrastructure set up and because everybody was grappling around because there’s two organisations plus all the others grappling around, they‘ve never been so collaborative before.
CLAHRC management 1, case B
In particular, enabling the release and spending of resources was problematic, especially with regards to recruitment. In many CLAHRCs there were difficulties with getting job specifications and posts approved, and harmonising grades across organisations. These all took a great deal of time to solve. One CLAHRC director commented that:
It’s like walking in treacle. I’ve got all of this money now but I can’t spend it. University HR [human resources] keeps dragging its heels as it informs me that it has not had these types of appointments. It’s a real case of ‘the computer says no’, and then it’s just left on someone’s desk gathering dust because it’s not an easy case. The worst thing is, if I’m not careful I’m going to get it in the neck from the NIHR, but it is out of my hands.
Social science academic 2, case E
On reflection, I would say you need to put in at least 6 months where you’re assuming that people are not doing the projects, they’re actually recruiting now and thinking about recruiting and they’re thinking about some of the things they didn’t have time to do before they started.
Clinical science academic, NHS-facing, case E
The race to get the CLAHRCs up and running meant that tensions between CLAHRC partners caused divides among clinicians, academics and managers. For example, conflict occurred between those in clinical practice who sought to improve services and academics who needed to pursue their research agendas with minimal contact with practice.
I’m not sure there was enough clarity around the original brief. I think the turnaround time for establishing a CLAHRC was far too small and if they were really serious about collaboration and partnership working, working with projects of local importance, they would have allowed time to establish those relationships and to put together work packages that could be longer-term aims of a wider range of organisations.
CLAHRC management 4, case I
Overall, there was a general feeling that at the beginning of the CLAHRCs, rather than hitting the ground running, many projects experienced significant delays.
We committed too much resource upfront
As outlined in Chapter 5, during the envisaging process in which the CLAHRC bids were developed, senior actors looked to draw together existing projects that they thought would be attractive to the NIHR on research grounds. Often these existing projects were already running, or were based around failed research grant applications. A number of CLAHRC directors committed significant amounts of funding upfront to specific programmes of activity, which occasionally resulted in HEI-facing clinical academics viewing the funding as being akin to a ‘normal research grant’. This resulted in many clinical academics aligning with dominant institutions, and privileging research publications above implementation.
As director I feel a bit like a teacher who is trying to keep one chapter ahead of the students. I can see where they want to go. Sometimes I really feel like shaking them. They come to me and say ‘I need more money to do this research’ as if it is just another research grant. But this can be a liability as we are being evaluated on how well we can translate the research into practice; we need to focus more energy and money on the transfer to practice.
Clinical science academic 1, HEI-facing, case C
A number of CLAHRC directors and senior staff committed resources early in the process to convince the NIHR of the quality of their CLAHRC’s research base, and used this commitment of resources to encourage academics to sign up to the CLAHRC. Where the founding conditions led to a more collective process, many clinical academics actively negotiated for ‘their own share’ of the potential CLAHRC resources. However, the commitment of resources upfront to specific programmes of research removed an important performance management lever. On reflection, a number of directors felt that they had no choice but to hand over the control of resources too early.
That was an interesting lesson. We committed much of the money upfront on project in good faith. I wish, with hindsight, that we had drip-fed the resource on a more bid and deliver basis to ensure that some of the usual suspects to not merely revert back to type. The irritating thing is that some of these people looked me in the eye and signed up to the ideals of CLAHRC, but once they got the money it was business as usual.
Social science academic 3, case C
Most CLAHRCs followed a similar pattern of allocating the funding at the start of the project. However, one CLAHRC, directed by a NHS-facing clinical academic, released the funding in stages to different projects and over several project rounds. In doing so, this particular CLAHRC was able to monitor the progress of projects to ensure that they were completed with demonstrable and measurable outputs. The particular founding conditions of this CLAHRC, with its relatively autonomous envisaging process, meant that the director and his team were able to pursue a different internal management model.
Well you could do staged release of funds but again, as I said, the problem is more in the perception of what a good bid looks like. I’m sure everybody thought that’s probably a good idea but we don’t want to jeopardise this money by saying if you’re going to suggest that you’re going to hold money back, then you’re not telling people what you’re going to do with that money and you’re implying that it might not be needed at all.
CLAHRC management 4, case I
Interestingly, a number of other CLAHRC directors viewed the model of ‘bid and deliver’ as a possible alternative approach if CLAHRCs were refinanced.
We would be more responsive, so we’d set aside resource for including funds for as yet unknown projects or priorities. And we would probably rather than just give all our resources to people internal to CLAHRC, we’d set aside some resources that people could bid to as well. And getting a wider set of people involved in the CLAHRC and getting buy-in from a wider community. We would probably encourage a wider variety of project types within the CLAHRC, we would encourage people to not just to do research projects but all sorts of projects, projects on service development and implementation of the existing evidence would be fine for things for us to be funding.
CLAHRC management 4, case I
The loss of control over resources was a significant issue that a number of CLAHRC directors had sought to address during the 5 years of the initiative. In two CLAHRCs, we saw significant work to regain control over resources through reallocating funding from projects that were underperforming, driving work focused on implementation and enforcing stricter performance measures to monitor project outputs.
I think it’s very difficult when you’ve given large sums of money upfront, distributed all of the budget upfront to people, you’ve got no levers. They are independent people, they have got other work they are doing, they are not entirely CLAHRC employees, so there are other things that they’re doing. You have no control. The only control you would have had would have been to retain significant sections of the budget and pass it out for work that met CLAHRC aims. So I think that’s been the biggest mistake really was allocating all the money upfront.
CLAHRC management 2, case I
We had to search for the right balance between research and implementation
The need to rebalance research and implementation activities was caused by the lack of clear envisaging around what CLAHRCs were set up to achieve. As part of this, lack of clarity was the problem that actors were unclear about the emerging agenda and its impact. However, in a number of cases, the lack of clear envisaging around diagnostic framing meant that the resulting prognostic framing led to the promotion of research at the expense of implementation.
I think that overall people had very little understanding of what impact actually meant in the beginning. I think in the beginning there wasn’t any clear picture at all, so people generally worked with their initial understanding of impact which was how well setup is the research trial, is the methodology accurate and are the findings publishable? Ideally in a top tier journal, so that kind of assessment of impact. I think was kind of pervasive in the CLAHRC as a whole.
Social science academic 2, case B
Consequently, an ongoing debate within many CLAHRCs focused on understanding the appropriate balance between research and implementation activities. Across CLAHRCs we saw significant variation in gravity points, and within many CLAHRCs there were debates to decide where their own gravity point should be. Over time, a clear pattern emerged where a number of CLAHRC directors actively worked to rebalance their CLAHRCs to shift the gravity point towards implementation.
There are the ongoing negotiations about where the gravity of the CLAHRC lies, is it primarily about research with a bit of implementation, is it primarily about implementation with the research on the side, and I think there are a number of parallel things going on with this CLAHRC to try and balance that out, so rather than having one centre of gravity you have lots of little points of interest.
Social science academic, case I
Research and implementation were often carried out in parallel, along different timelines and with different outputs. The possibility of future CLAHRC refinancing drove the reallocation of research and implementation activities. External advisory reviews, which emphasised implementation, also influenced some CLAHRCs’ attempts to address the gravity point. In others rebalancing was seen as a response to the needs of local services and partner NHS organisations, who had provided matched funding to CLAHRCs and wanted evidence of translational work and improvements in health services.
The issue for our CLAHRC is we are still 80% core funded for applied research and 20% for implementation, but actually that is not the right balance if you want to achieve the kind of change that we are actually looking for, so we have got to use every little bit of extra resource that we can to beef up the knowledge translation activities which include education about how they do that in trusts, or education about this, that and the other in trusts.
Clinical science academic 2, HEI-facing, case I
Shifting the gravity point was easier in CLAHRCs that were set up with a large number of research projects led by clinical academics and where research for practice was carried out in collaboration with NHS organisations, in comparison with CLAHRCs which had structured research and implementation as separate themes.
We started by being very science driven because academic researchers, they know how to do academic research and it’s changed to the focus being much more on listening to services, responding to services, making services change and to me as a clinician, of course, that’s been a very welcome, kind of, development.
Clinical science academic 5, HEI-facing, case B
A complete change in the design of research projects would have been required to enable the rebalancing of the gravity point in CLAHRCs that had separated research and implementation.
Everyone I think you would speak to would say that the structural split, and I quite understand why it occurred, was there in the beginning . . . Although we have talked endlessly about how we need to draw those [themes] together, we have done very little about that because it’s very difficult to do so.
Social science academic 2, case C
In such cases, the implementation leads and knowledge brokers working in the research themes were left frustrated, as they felt that the partner NHS organisations were expecting results from the research much earlier than the projects were able to deliver.
[. . .] because there are these separate research themes they are still driven by conventional academic goals, which is publication, getting their papers out . . . I think our researcher colleagues just couldn’t get their heads around what we meant by implementation.
Implementation lead, case C
Conversely, in one CLAHRC that had a greater initial emphasis on implementation, senior actors were increasingly active in promoting the importance of research and publication about service improvement projects. Overall, the structural separation of research and implementation hindered interaction between the two themes, and exacerbated the dominant orientation towards HEI or NHS institutions. These problems became increasingly apparent over time.
We needed to learn to work together (what is implementation?)
Linked to the process of envisaging the CLAHRC, there was ambiguity surrounding the definition of ‘implementation’ from implementation leads, knowledge brokers and NHS-facing clinical academics.
We didn’t create a strong enough vision of what we meant by implementation. I had in my head what I thought it was and other people had their own versions in their own heads, but I think collectively we didn’t sit down and say ‘what are the absolute things’. So the things I am saying to you that it has to be non-linear, it has to be multifaceted, they were maybe there implicitly, but I think it would have really helped if we had made those much more transparent early on.
Implementation lead, case C
There was the assumption from those who set up the CLAHRCs that the HEIs and NHS partners would come together at the start and work immediately in collaboration. However, tensions between the academic and clinical work exacerbated divides between research and implementation activities and prevented collaboration.
I think more traditional health-care academics find it really alien and are quite resistant to engaging whereas frontline staff or people who have been involved with quality improvement before really get it and they really appreciate it a lot more, but even then the frontline staff often get it but struggle with the measures, whereas the more academic staff have got their outcome measures sorted before the project has even started [. . .].
CLAHRC management 1, case D
Differences in expectations caused tensions between the outputs of NHS and HEI organisations. While policy-makers called for interdisciplinary research, on the ground this was often inconsistent with performance management frameworks, such as REF, which were seen to drive out interdisciplinary research.
There’s a tension here between what the service delivery units want which is normally a slightly faster horse and the researchers who want to reinvent the horse. We can either take the approach that we can try and deliver a slightly faster horse or try and work out mechanisms for making sure that innovation can take place and can be spread and can be adopted.
Clinical science academic 4, HEI-facing, case B
The disparities across academic and clinical fields about translational research often led to differences in targets and improving health care. As a result, academics set targets that did not reflect what was required in clinical practice. These misaligned goals, a lack of mutual understanding, cultural tensions and a perceived lack of commitment are institutional in nature as individuals from different settings were pulling in different directions. Rebalancing research and implementation was particularly difficult where clinical academics were employed by the HEI and their success was measured by their academic output.
The NIHR hasn’t got its act together properly, and all CLAHRCs would acknowledge that, on CLAHRC impact. So we have to look at publications and grant income and blah-blah-blah, none of which are anything to do with putting stuff into practice. And then they ask us to do what they call added value examples on the end of the annual report [. . .] now if I’m having to go to our local commissioners and say what’s the value of CLAHRC, I tell a very different story. They’re not interested in how many papers are published or how many research grants we’ve got, they are interested in what’s the impact on our local population and how much has it cost us?
Social science academic 3, case C
Simultaneously, the same clinical academics had committed funding and resources from the NHS partner organisations and were expected to deliver outputs to the services. As a result of these different performance measures, and because of the epistemological divides between the research community and practitioners, research and implementation were often seen to be working separately and in different directions.
I think that the academic has a role and a responsibility in the process to do research in a different way perhaps, so that impact can be held. And I guess also in a business school you’re used to needing to relate to the world of practice. But I think what’s become more difficult is that it seems to me that since the beginning of our CLAHRC, there is less integration across the whole in many ways [. . .].
Social science academic 2, case B
In addition to the tensions across research and practice, an epistemological tension also occurred within the academic community between clinical and social science academics.
I really don’t feel understood by the medical community as to what kind of value we can offer because what we want to do is to conceptualise and generate theory. The problem is that they just want us to tell them how to do it.
Social science academic 2, case B
Social science academics were generally seen to be preoccupied with generating theory around KT and organisational theory rather than research that was practical and relevant to the concerns of CLAHRCs. Furthermore, a number of actors from clinical backgrounds were often hostile to what they viewed as social scientists’ ‘soft’ research skills. Social scientists were viewed as generating unscientific research that fell below the clinical gold standard of RCTs.
It does annoy me how social sciences come along and criticise randomised control trials, which is something they don’t know a lot about. So they come along and say blah, blah, blah about randomised control trials and I just know they are talking rubbish. They don’t understand what randomised control trials do. I feel that the current sway of those [social] sciences is undervaluing clinical science and is likely, if we continue to do that it is likely to drive away and offend an awful lot of clinical researchers.
Clinical science academic 2, HEI-facing, case I
Despite emerging tensions between clinical and social science academics, there was an underlying feeling that CLAHRCs needed to harness the expertise of both sides of the divide. NHS clinical academics were more likely to recognise the value of social scientists, specifically of organisational scientists, in helping them bridge the T2.
There’s a double boundary and people talk about the knowledge boundary and the second translation gap, research into practice, but it’s much more complicated than that. And you really see it when you’re in social science because you’re really in a sense trying to work with both of these sides, clinical academic and clinical practitioner, and both of them have a knowledge gap, as far as you’re concerned.
Social science academic 2, case B
We need to do more to develop Collaboration for Leadership in Applied Health Research and Care career structures
Collaborations for Leadership in Applied Health Research and Care enabled more senior HEI-facing clinical academics to attract resources to fund research projects and, thus, enable them to further their academic careers. In addition to CLAHRCs being attractive to actors leading different research projects, the collaborative work involved was beneficial to knowledge brokers, secondees from practice, and boundary spanners who were able to learn new skills from the local HEIs and NHS partners. Skills and knowledge gained on implementation, service change and improvement enhanced the careers of those working in practice or between the two organisations.
It’s been good for me but I think the clinical areas here have benefited as well, just by me getting out there and selling their story and telling their story from their side to the senior managers and the theme leads and the deputy leads who sometimes can forget what it’s like out there.
Implementation manager, case I
However, many felt that the CLAHRC did not progress their career. In particular, junior and mid-career academics found it more challenging to progress with their academic careers and publication rate through CLAHRC.
So I’m stuck at the top of Grade seven, so from my point of view of my career, it’s not done me any good at all, in terms of moving up the university scale. It’s been interesting in terms of moving from a position where I was conducting research, either as a researcher or as a principal investigator, to the position of managing a range of research related activities, including service evaluation projects and doing some teaching and developing you know, online learning resources and those sorts of things. So it’s provided quite a lot of variety and interest. But from a career point of view, as things stand now, I think it’s probably been detrimental to my career.
CLAHRC management 2, case I
Some actors believed that working in CLAHRCs was a disadvantage to academic careers, particularly for those who carried out implementation or management roles. For those from health management or clinical practice, CLAHRCs provided them with an opportunity to become more familiar with research projects and academic work. This benefited their careers in health organisations where this form of experience and expertise was valued.
Well people who want to go into academic careers, starting in service-based research it [CLAHRC] does not seem to me a good thing. It’s fine for people like me who are clinical science academics, very good in fact, very good, it’s fine for people who are clinicians who want to move into academic work but actually for those people who come from academia, I think it’s a wasteland.
Clinical academic 5, HEI-facing, case B
The difficulty facing HEI academics was that the CLAHRC did not enable them to focus on developing a strong publication record. For example, one CLAHRC that was set up with research and implementation themes running in parallel adopted a problem-based approach in which knowledge brokers fed into practice and identified gaps in translation. They then worked with practice to improve health services through the translation of research and implementation of new tools and practice. CLAHRC actors working in the implementation theme, but located in the HEIs, generally felt that, although there were clear improvements in practice, the processes of implementation to create new institutions were focused more on practice-based solutions and less on the generation of new research and publications. This was seen as detrimental to their academic careers.
[. . .] within our CLAHRC here, there wasn’t a great focus on research in the implementation process and that’s really where you would be able to get some sort of academic payback from it, from being able to study it and write it up. I do not think in terms of the things you’re judged on, it’s not been hugely beneficial to me to being in the CLAHRC. [. . .] Our knowledge [brokers] I actually think that it’s been a great opportunity for them, they’ve developed some really good transferable skills around how you facilitate change, how you work with stakeholders.
Implementation lead, case C
There were concerns that junior academics on work-based contracts or those who worked across academic disciplines were unable to produce outputs recognised by the performance measures of the HEIs.
Is this person, is this new role going to be a bit of business school or a bit of social science or a bit of clinical research, or is it really going to be a hybrid? And if it’s going to be a hybrid, what on earth is it? Because it’s a risk and actually I think if you look at the people who’ve fulfilled those roles it has by and large damaged their careers because they haven’t been able to focus on the academic research that they probably should have done to secure tenure or to develop their career.
Social science academic 3, case E
Although junior actors in CLAHRCs were seen as central to CLAHRC success, they were often left without a clear career structure.
And equally, there’s nowhere for them to go because the university career structure doesn’t recognise it. So it’s almost like for the people in the roles, I think actually unless you can get in, use it and get out, it’s dangerous. And I think the people who have gone in, taken something from it and then moved on, have probably done better.
Social science academic 3, case E
Career progression and incentives for junior academics were poor across the CLAHRCs often because of the nature of the job contracts. Although fellowships, PhDs, and Master’s courses were integrated into the CLAHRCs, these were seen as another stream of funding for postgraduate studies rather than the development of an academic career pathway.
What they should have done in this CLAHRC, is devised the career model that would have gone through and said to people ‘Right, you can’t do it for 5 years, we’re only going to let you do it for 2 years and then at the end of that you should move on’. I don’t know? But I think that is the single biggest worry and I’m on the record in books for saying I think contract research is really exploitative and I’m really anti-contract research.
Social science academic 3, case E
In general, CLAHRCs were more beneficial to those working in practice who were able to built research skills that were seen as an asset in clinical practice. For academics, however, and especially junior academics, CLAHRCs were generally seen as a temporary contract and organisation that was unable to provide them with a sustainable academic career. Senior academics, however, were able to benefit from CLAHRC funding as it provided them with another funding stream for their research projects and publications.
I don’t think having the name and the identity of the CLAHRC or being part of this wider group has made it for me, as a non-clinical, as a researcher who works in health services research, I still rely on the contacts that I’ve always had and I’ve started to develop through independent research. You work with academic clinicians and they open up doors and it’s a slow, slow process as you develop your career.
Social science academic 4, case C
Conclusion
CLAHRCs were an experiment and the intention, from the first round of funding, was for CLAHRCs to be thought of as ‘learning organisations’. In the beginning, CLAHRCs were ‘new’ organisations and, although existing relationships and research activity were utilised in many, they still had to build infrastructure, which included creating new physical workspaces, filling new posts and building relationships between HEIs and practice.
I think the problem with the first CLAHRC was it was totally new, people were trying to imagine something that had not been there before and make it exciting, interesting and doable enough to get the money and actually be able to go out and do this work. I think what a second CLAHRC might look like, even if the goalposts change, if we were given different direction from NIHR, I think provided we were given sufficient time, would be a slightly different experience and hopefully a better one. But I think obviously there’s been a lot of learning that we can then use.
Clinical manager, case I
With CLAHRCs nearing an end and the potential of CLAHRC refinancing, CLAHRC actors described that, although there had been challenges across all of the CLAHRCs, there were important positive outputs, such as service improvements, the creation of new roles, new research, collaborations between research and practice and an overall increased awareness of the need to translate research into practice more effectively to improve patient care.
I think one of the successes is the attitude and behaviour change of the research community. I think they are a lot more mindful because of the CLAHRC of the challenges that the NHS has in implementing evidence and engaging with research. They’re much more likely to be running research projects that would have a reasonable chance of continued use in the NHS, whereas before, to be honest, they might not have cared, and what they were really working for is a grant and associated publications.
CLAHRC management 4, case I
While there were clear challenges and lessons learnt across all of the CLAHRCs in terms of envisaging, engaging and embedding, all the CLAHRCs demonstrated efforts to shape and create new institutions to foster knowledge exchange and learning and to build capacity across the different institutions in various ways.
Chapter 10 Models of organising for knowledge translation
Overall, our study uncovered different ways of organising KT activities to accommodate the institutional pressures and tensions entailed between HEI and NHS organisations. Drawing on data across the nine CLAHRCs, we provide insights into the critical IW and leadership challenges associated with the different CLAHRC models. 169 The culmination of our analyses of the models organising for KT is the development of five schematic archetypes. These archetypes are not representative of all the characteristics of one particular CLAHRC, but rather a synthesis of the distinctive strategies used by CLAHRCs.
Academics have previously highlighted that real organisations seldom, if ever, reflect all the features of an ideal archetype, instead they encompass varying features of different archetypes. 170 In acknowledgement, we highlight that the nine CLAHRCs generally organised their KT approach predominantly around one of the archetypes, but simultaneously drew on features from several archetypes through the process of isomorphism. Thus, while our descriptions are based on the empirical cases, our purpose is not to delineate the relationship of particular CLAHRCs to specific models, but rather to reveal the breadth of KT approaches that developed in this ‘natural experiment’ where there was a unified context, goal, and where organisational approaches emerged independently.
Archetype A: enabling a multidisciplinary research process
One way of organising KT activity entails the purposeful integration of multiple stakeholder groups into the research process. This could include researchers from multiple backgrounds and practitioners from diverse organisations participating in designing the research question, collecting data and receiving ongoing feedback about research progress and findings. An important emphasis in this approach is to alter the culture of research from a single disciplinary silo activity to accommodate more diversity in order to improve research relevance. Archetype A is presented in Figure 2.
FIGURE 2.
Archetype A.
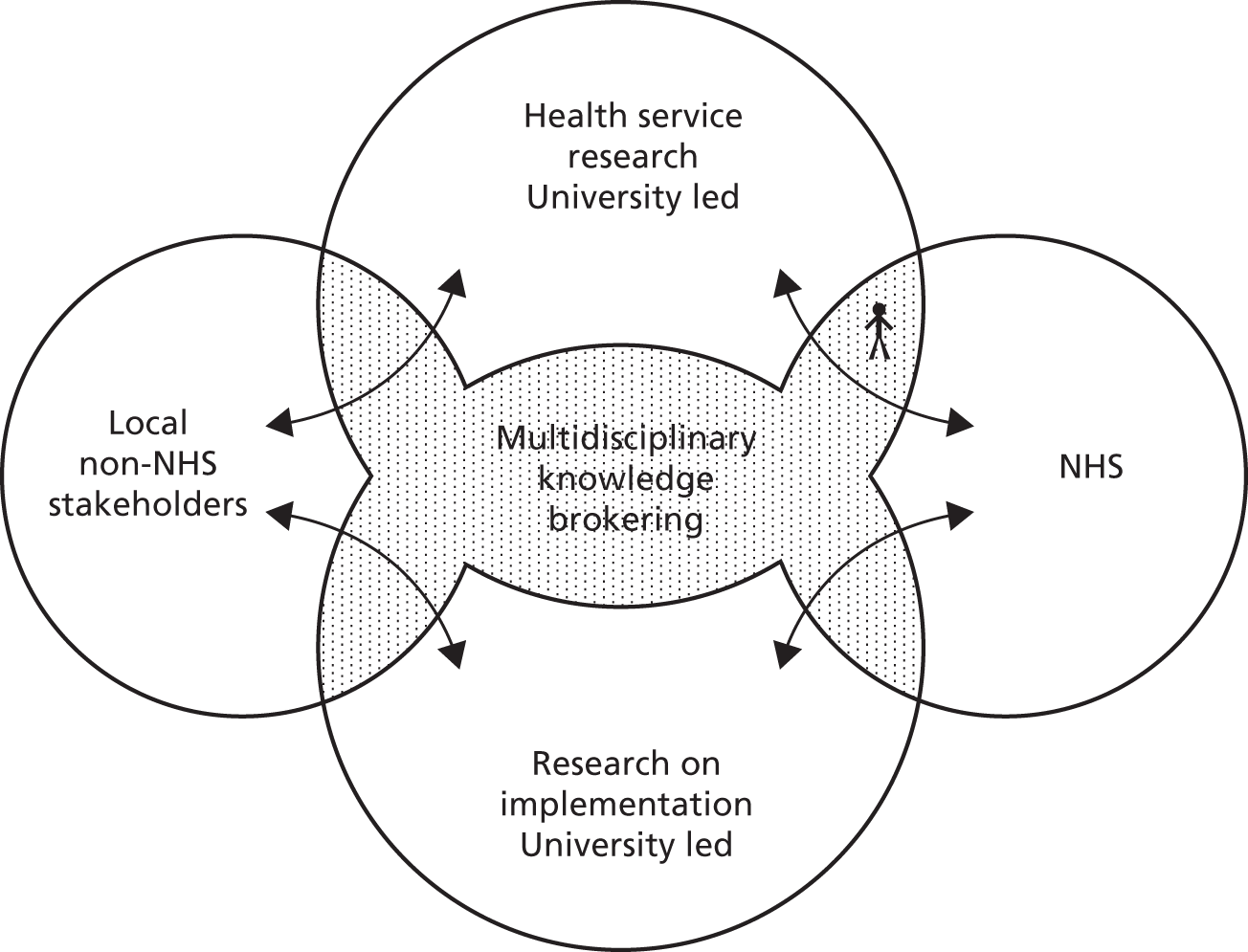
The salient knowledge boundaries that are bridged in the model are between researchers and practitioners, and between academic disciplines. This archetype emphasises rigour in the research process, seeks to adapt the potential relevance of the research output, as well as develop stakeholder ownership among potential users of the research output. This model can readily incorporate PPI either by widening the group engaged in the research process, developing involvement as a research concern in its own right. From the perspective of the researchers this model of KT radically alters the research process itself.
In the context of the CLAHRCs, this model can also emphasise research on KT as a process and science of implementation. Rather than focusing explicitly on local implementation of research outputs, implementation groups can draw on a multiple stakeholder perspective to examine the dynamics of implementation itself. Thus, a core output of this model is to generate conceptual and systematic knowledge regarding implementation and KT as a social process.
The strength of this KT model, in which researchers retain high levels of autonomy, is its lack of compromise on the rigour of research as well as its ability to address complex problems in a systematic manner. Allowing high levels of researcher autonomy can enable research teams to adjust and renegotiate research projects to fit with the needs and emergent context of stakeholders involved. However, this level of coproduction is dependent on adequate flexibility in the research design as well as the researchers’ mind set.
A challenge of delivering KT activity is its high dependence on collaboration. The breakdown of stakeholder boundaries is difficult to manage and risks the retreat of existing groups back to their silos and patterns of historical relationships. A continued challenge for IEs in engaging stakeholders with this organisational archetype is generating and sustaining broad engagement across organisational and disciplinary boundaries. Leaders, therefore, need to maintain loose couplings across the diverse agendas, and must not be seen to favour one stakeholder group above another in order to avoid alienation and the return to compartmentalisation.
The institutional challenge in embedding this model of collaboration is the need to fundamentally sustain change to enable the research process to become more inclusive and leverage multiple perspectives. While researchers retain autonomy and rigour over the research process, here they are required to broaden their perspective by engaging with user stakeholder groups. The research breadth is further challenged by the need to accommodate multiple research paradigms, such as between social science and medical world views.
Archetype B: loosely autonomous research streams with designated knowledge brokers
Knowledge transfer activity can also be organised around loosely structured collaborative research projects, which have a number of designated boundary spanners and knowledge brokers attached to each project. In this way, research is envisaged as being efficiently organised and controlled by HEI researchers. The research questions can, however, be negotiated with the designated knowledge brokers who have critical knowledge of provider issues and established relationships with the research team.
One way to implement this model would be to have knowledge brokers with varying levels of time commitment and seniority within NHS organisations to broker relationships with relevant target audiences and, thus, enable IEs to have broader levels of engagement across the stakeholder groups and status levels. Given that each NHS organisation has a unique context, and each research theme has their own particular dynamics, after designated individuals are charged with spanning the boundary across these domains, they can develop locally suitable ways of facilitating KT between the groups. Individuals can work to their strengths and nest activities into their own practices, ensuring that the new boundary dynamics become sustainable through long-term relationships and the promotion of the embedding of KT process to sustain institutional change. Archetype B is presented in Figure 3.
FIGURE 3.
Archetype B.
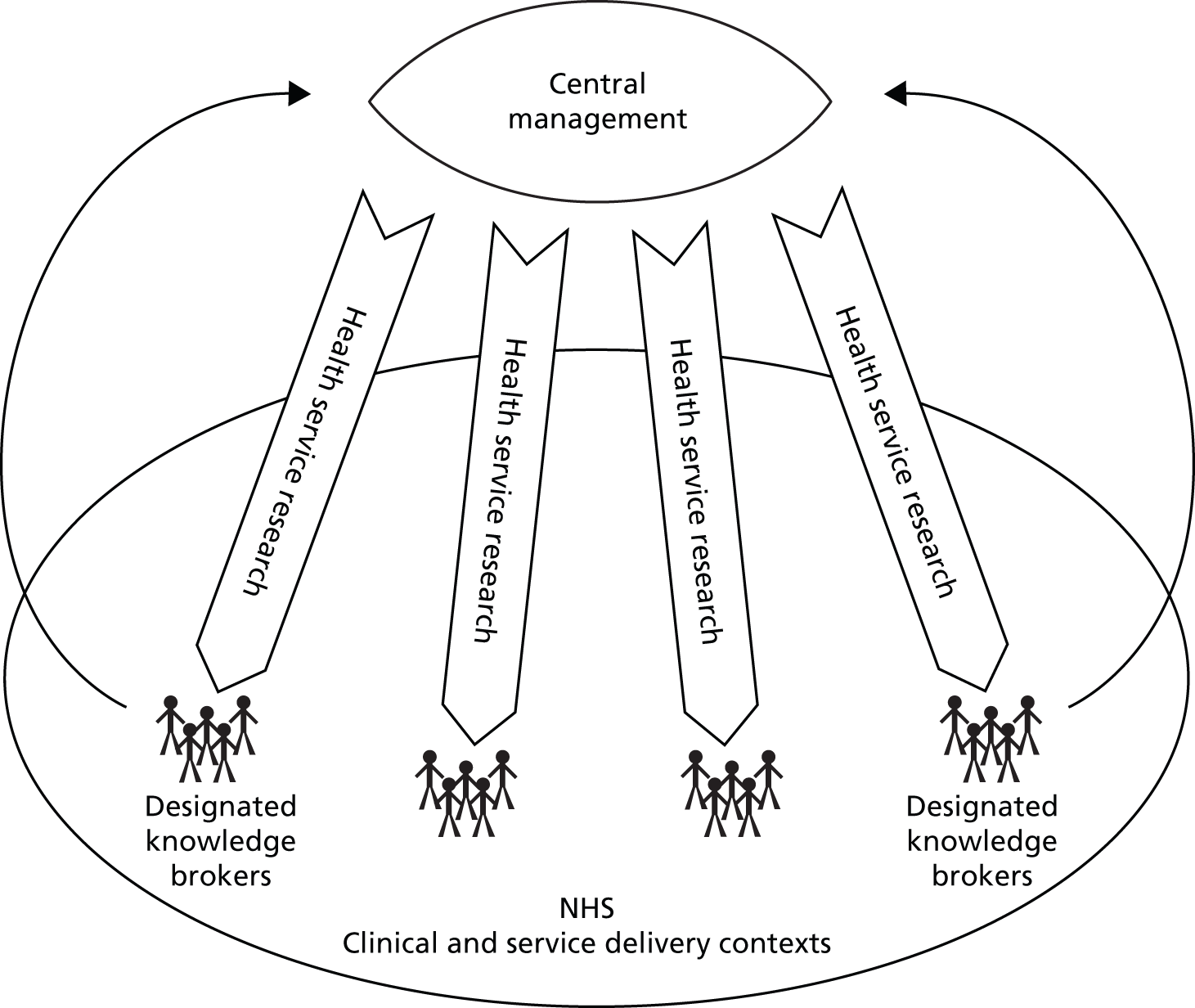
A key strength of this archetype is the development of a focused and skilled team of knowledge brokers who have the primary responsibility to manage the KT process between researchers and health providers, and who function as a primary means for engaging the work of KT. The knowledge brokers span the boundaries across two distinct stakeholder groups that consist of a number of managers who are familiar with frontline care delivery and, thus, implementation issues. They would be seconded to work within the CLAHRC for a designated portion of their week to enable dialogue between researchers and providers. Training programmes designed to integrate across diverse stakeholder world views could be tailored to suit the profile of provider organisations involved as well as the level and experience of the participants and would support the embedding of institutional change in working towards KT.
An ongoing challenge for leaders of this institutional change process is the tension between sustaining a strong traditional research focus and motivating engagement processes with stakeholders. Current institutional forces within HEIs promote a research process that focuses on the novelty and rigour of knowledge production, which has escalated in the UK context by emphasis on the REF and high impact publications. Consequently, there is pressure to orientate researchers away from an interest in knowledge dissemination and engagement with providers, towards the production of interesting and publishable findings.
The effects can be significant, as performance management systems and careers structures in HEIs tend to privilege academic publication and prevent the embedding of institutional change. Similarly, in the current fiscal climate of health care, it remains a challenge for NHS organisations to continue to release the designated knowledge brokers from their normal roles so that they can engage with researchers and CLAHRC activities. NHS staff face pressing day-to-day matters, which frequently draw them back into their former routines as the urgency of research can pale in the face of a current crisis.
Archetype C: independent (modular) research and implementation activities
Archetype C envisages organising activity through the separation of research and implementation activities, and their maintenance in a parallel modular fashion. Given the distinct temporal dynamics of research and implementation activities, separation enables focus on research activities that will yield clear outputs in the short term by highly trained academic researchers working on topics they know can be delivered and published. The research themes may broaden their concerns to consider the practical relevance of their work, but this is not their key focus. PPI can be incorporated within the research process, but is likely to be more problematic to incorporate this within the implementation themes, as fewer standard mechanisms exist to guide their involvement. Archetype C is presented in Figure 4.
FIGURE 4.
Archetype C.
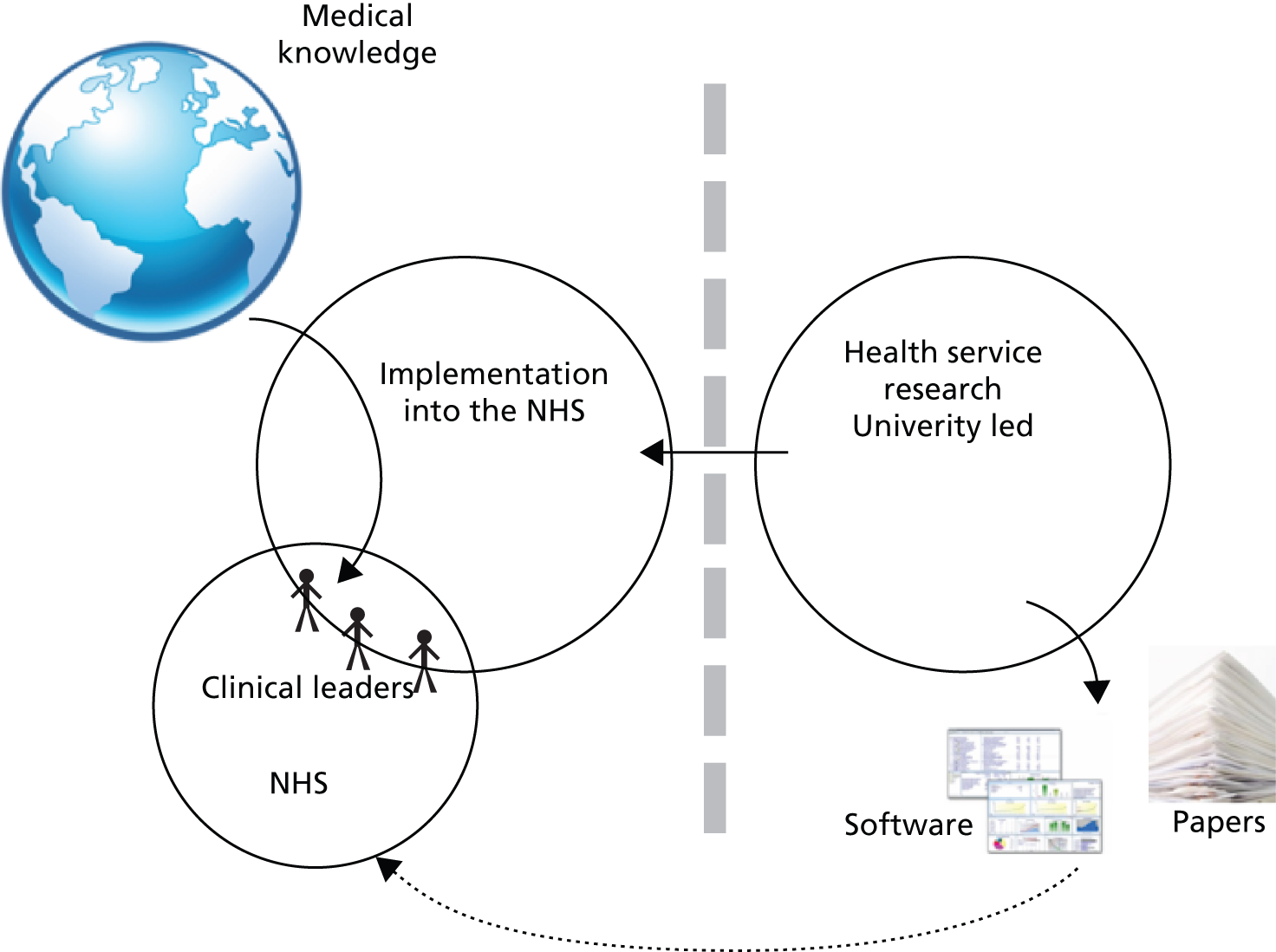
Focusing on the existing health research available, the implementation themes are explicitly kept separate to engage with appropriate stakeholders regarding their current evidence concerns to influence health service provision to incorporate existing research findings. Given the wealth of well-established research and rigorous best practice protocols, this model of implementation is efficient. The knowledge boundary that challenges leaders and institutional change is the one between the research and implementation themes within the KT organisation, as the two groups have clearly delineated and differentiated practices and goals. Thus, while changes may embed within implementation themes, who now are using more extant research and practice guidelines to inform their practice, there is little need to engage regularly with researchers and influence their research agenda per se.
An important vehicle for engaging clinicians in this organisational archetype is the speed by which implementation activities can be improved, and the benefits noted by clinicians or service providers. Rather than waiting for the end of a lengthy research study, implementation actors can develop local capacity and influence practice more quickly using existing knowledge outputs. The slow temporal rhythm of research, as compared with clinical and management environment, was a consistent cause of strain across all CLAHRCs. While research production and knowledge creation was a slow and meticulous process, NHS clinicians and managers were confronted daily with making decisions in contexts where there was insufficient information.
Though NHS workers were prepared to engage in the coproduction of research questions and content, by the time the outcomes and findings were clear, the questions often lost relevance. Instead there were new issues that needed to be addressed. Consequently, the potential risk of archetype C is that the research and implementation themes run in parallel – by the time the research themes have developed research to be implemented, the implementation theme has already developed a full portfolio of activity.
Archetype D: collaborating through loose networks
Archetype D takes advantage of existing informal structures and builds organically onto existing relationships. While recognising that KT activity occurs in a context of existing relationships and collaborations, this model seeks first and foremost to develop and extend what is already in place. This model might be particularly relevant in a context in which multiple ties between researchers and health providers are strong, which was an important element of the founding conditions of CLAHRCs. Existing relationships of trust and goodwill can provide a basis for building and embedding the new partnership projects and a means for mediating between competing organisational priorities and goals. In this way governance structures can be more informal and can be guided by mutual goodwill. Networked project groups can also incorporate public and patient participation in line with the locally perceived importance or relevance of lay involvement. Similarly, other stakeholders, such as social services, charities or private businesses can also be accommodated within specific project groups, as enabled by project goals and local relationships. Archetype D is presented in Figure 5.
FIGURE 5.
Archetype D.
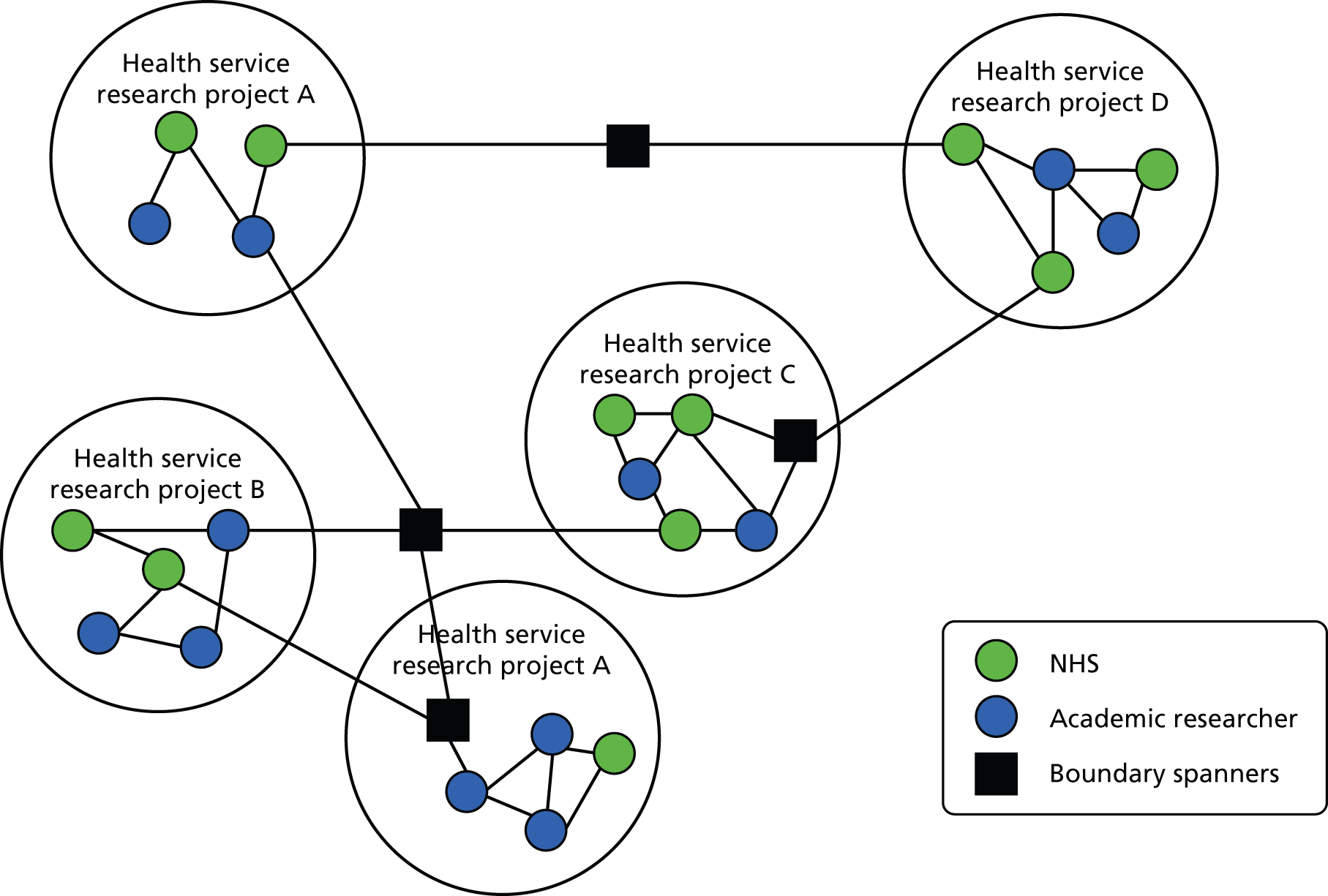
As such, IEs use a strategy of engaging a broad array of stakeholders in a more informal manner, and draw on areas with least resistance to embedding change. An advantage of this archetype is that genuine engagement is possible between providers and academic researchers, as neither is able to carry out the networked activity without the adequate coparticipation and engagement with the other.
The leaders’ challenge in embedding this model is maintaining an adequate group of knowledge brokers who can span between project groups and build scale beyond the smaller collaboration level. In particular, there is a need to bring in new members from provider organisations to influence practice as widely as possible. Given the less formalised nature of this model, designating and governing the knowledge brokers is challenged by the competing institutional pressures they face. In addition, brokers need to be strategically located in order to maximise their network impact and broker across unconnected groups or network entities.
Archetype E: centrally controlled service improvement projects
The final envisaged archetype is managerially focused and enables the retention of high levels of control over both research and implementation activities through ongoing accountability mechanisms and monitoring of project teams. The key mechanism for exercising control is centralised budget management and formal accountability in accordance with central management priorities. Thus, while the CLAHRCs’ decision-making powers typically addressed the research end in other archetypes, this archetype for organising KT places a higher emphasis on service effectiveness and the efficiency of research uptake through clearly defined projects. Research activity is aligned with service improvement goals of provider organisations rather than theoretic interests of academic departments. The embedding of the institutional change is driven by the responsiveness of projects to current provider needs, with service implementation and improvement initiatives written in to project deliverables. Archetype E is presented in Figure 6.
FIGURE 6.
Archetype E.
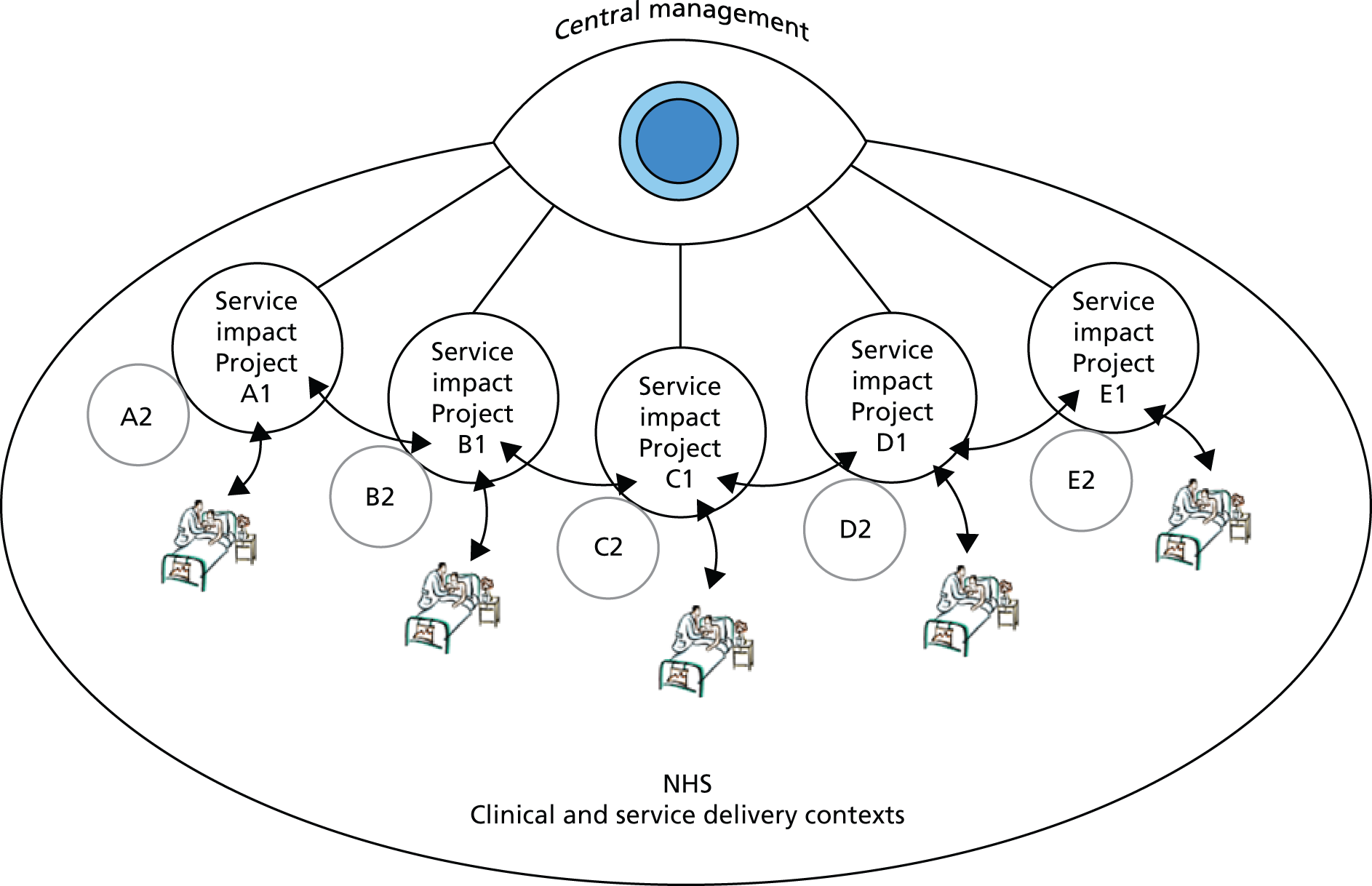
A key strength of this archetype is the horizontal and symmetrical approach to KT, such as collaborative research design, evaluation and implementation at the project level, which serves to embed the institutional change. Centralised managerial control structures project findings and enables accountability for levels of service impact. Frequent updates on the status and outcomes can be requested. As these projects necessarily involve highly integrated provider and researcher relationships, learning, knowledge transfer and social relationships among project teams are enabled and may lead to broader engagement. Central management take responsibility for organising events, workshops, and regular cross-boundary activities in order to promote learning and further KT objectives.
Importantly, a high proportion of the CLAHRC project members who envisaged and initially supported this organisational form were not full-time university researchers, but individuals involved in service provision or part-time consultants hired to implement change. As many of those participating in KT activities are from NHS providers, they will be accustomed to the more rigid control and hierarchy culture common in provider organisations and project management teams.
The low extent of researcher autonomy may mean that engaging and embedding top-level researchers is more of a challenge and could compromise rigorous research, leading to less theoretical innovation and lower levels of publication impact. While concern for service improvement is of interest to local providers of that specific service, its highly contextual nature limits the broad applicability of findings and the international interest in the research outputs.
Summary
In this chapter we have presented five different archetypes for organising KT to communicate the breadth of different approaches that have been tried and tested by the different CLAHRCs. Over time there has been significant isomorphism across the CLAHRCs as senior members of CLAHRCs have imported best practice and learning from other CLAHRCs. Of particular note has been the diffusion of the knowledge broker role, devised by a social science academic in one CLAHRC. This has been subsequently imitated by many other CLAHRCs.
We note, however, that while we have presented archetypes, these models are more or less likely to occur under different founding conditions. The founding conditions of CLAHRCs shaped actors’ envisaging of the models of CLAHRCs they implemented. Therefore, the founding conditions will influence which archetypes the different CLAHRC actors drew on. We suggest that both archetypes A and C, or elements of them, are more likely to be promoted by HEI-facing clinical academics. In contrast, archetype B, or elements of archetype B, will be championed more heavily by actors from a social sciences background. Archetype D, or elements of archetype D, is more likely to be enacted in brownfield sites with good existing relationships across research and practice in the local region. Finally, archetype E, or elements of archetype E, are more likely to be enacted under the founding conditions of a CLAHRC being led by a NHS-facing clinical academic, and where there are lower levels of existing activity, such as greenfield sites. Table 12 details the institutional features, strengths, weaknesses and leadership challenges of each proposed archetype model of organising for KT.
| Institutional features | Strengths | Weakness | Leadership challenge |
|---|---|---|---|
| Archetype A: multidisciplinary knowledge brokering | |||
| Research governance maintained by academics yet they are accountable to a wider group of stakeholders; this can increase researcher absorptive capacity of service provider values and concerns Wider research agenda promotes research into implementation processes from multiple perspectives |
Increased stakeholder involvement enables integration of perspectives, thus suited to researching complex multidimensional problems Research includes the KT process, which may be done from multiple perspectives New culture of inclusive and multidisciplinary research can generate wider genre of research, beyond medical paradigm |
Risk of alienation and retreat to institutionalised silos of activity if boundaries are not actively managed, rather than sustaining new culture of multistakeholder research | Complexity of research and integration of (shifting) stakeholder agendas can increase the time needed to generate research outputs Brokering and negotiation needed across multiple stakeholder groups Engaging practitioners and health service providers in research increases their level of ownership, supporting the implementation of research findings; yet implementation process not formally controlled |
| Archetype B: designated KBs | |||
| Research governance maintained by academics, including process and questions; yet select KBs are invited to interact with research teams KBs are aware of research agenda and nature of likely findings, and thus able to develop implementation goals early in research process |
Research capacity within service providers is developed through KBs Researchers can develop sustained dialogue with provider representatives to facilitate ongoing relationship following project completion Designated KBs have ownership for supporting KT into specific service contexts |
Difficulty appointing KBs at the right level of seniority to effect and resource service change There is a risk that researchers can focus on exploration and disregard concerns of service orientated KBs and knowledge exploitation, given no formal accountability between academics and service providers |
Central management organise and support KBs KBs receive formal training in brokering techniques and skills, increasing individual and system-level absorptive capacity to draw on research knowledge to influence service delivery |
| Archetype C: modular independence | |||
| Functional separation of research and implementation processes, which run in parallel fashion Research governance maintained by academics who determine research questions and process |
Quick start to implementation process as not waiting for new research findings to be produced Autonomous research process attractive to highly qualified academics who are not needing to change their research practice; this increases likelihood of high-impact generalisable findings Existing external knowledge used, such as systematic reviews and other published accounts of research outputs |
Boundary between implementation and research themes, stymying integration between their efforts Low coproduction of research topic risks knowledge outputs having low relevance to local stakeholders |
Central management responsible for developing implementation skills No explicit link with in-house research process Highly autonomous research process with no explicit need to accommodate new significant stakeholder groups |
| Archetype D: building on existing networks | |||
| Governance of research process shared between academics and service providers Academics and service providers involved in research process; existing relationships and high levels of trust form the basis for the collaboration Research questions heavily influenced by local provider concerns |
Low levels of inertia to overcome at early stages, as individuals already have connections and goodwill ties High levels of possible integration and tailoring of research projects with local provider needs Strengthening existing ties enables solid basis for legacy to remain once funding for overall initiative ceases |
Cliques and silos can arise from unconnected groups within network as no designated brokers are accountable or assigned High levels of informal and horizontal networking can make the overall coherence and vision difficult to integrate |
Informal governance is difficult to hold to account Difficult to extend the network beyond a certain size when working more informally as this is not centrally managed and more ad hoc; ICTs can help facilitate this |
| Archetype E: central management control | |||
| Research explicitly managed by central controls, who hold governance oversight Research directly influenced or determined by local provider concerns Central management systematically collects and collates research findings |
Project-level control by central management enables high levels of accountability Sustained investment in local service improvement Integrates into culture and goals of a hierarchical health service system |
Incremental nature of service orientated research and alienation of academics decreases likelihood of high-impact publications Supports a bureaucratic culture and orientation which works against innovation |
Research supported by systematic approaches to quality management, ensuring consistency Low levels of research autonomy risks alienation of high-calibre academics |
Chapter 11 Conclusions
The aims of this work, as detailed in the introduction of this report, were:
-
to provide a formative evaluation of CLAHRCs in relation to the generation of applied research, and the impact on practice and capacity building, across CLAHRCs
-
to apply institutional theory to identify and examine the challenges facing CLAHRCs
-
to apply the concept of institutional entrepreneurship to make a theoretically informed analysis of how to engender and sustain the translation and exchange of research knowledge into service facing innovation in CLAHRCs.
By drawing on institutional theory,78,79 and the emerging literature on institutional entrepreneurship,20,39 we argue that the T2 in health care is institutional in nature. Importantly, for the CLAHRC initiative to enable sustainable change and in order to begin to close the T2, actors need to reshape existing institutions in a manner that supports behavioural change.
Through our research we have developed a process-based model of institutional entrepreneurship (see Chapter 3, Figure 1) to render visible the IW undertaken by actors. In addition, we conducted SNA at two time points to examine how institutional change was reflected in the dynamic patterns of actors’ interactions across the research–practice divide. Our key findings are presented in Chapters 4–10. Here, we will highlight some of the main conclusions from our work.
Although our work is based on CLAHRCs, which are just one form of translational initiative, we suggest that the lessons emerging are germane to other forms of translational initiatives such as the AHSCs, BRCs, BRUs, the health innovation and education clusters (HIECs) and the NHS Innovation Hubs. The issues surrounding the different stages of our model of institutional entrepreneurship are likely to resonate with other initiatives, particularly in relation to how the founding conditions shape the subsequent development of any initiative. In addition, the KT archetypes presented in Chapter 10 are not necessarily specific to CLAHRCs and are generalisable to other forms of translational initiatives.
Main findings
A central idea that emanates from our work is that the founding conditions of CLAHRCs, in terms of the social positions of the key actors and the local-level field conditions, played a central role in shaping how CLAHRCs were envisaged, how stakeholders were engaged, how CLAHRCs were embedded and the nature of reflection that actors carried out. We note, however, that the effects were particularly pronounced during the actors’ envisaging stage of CLAHRCs, which then subsequently shaped the issues arising from engaging, embedding and reflecting. Overall, our work suggests that actors’ social positions will shape their propensity to engage in institutional entrepreneurship, or conversely institutional maintenance, to promote institutional change or stability respectively.
The interplay between the founding conditions and the social positions of IEs shaped conceptions of, and activities encompassed within, CLAHRCs, and especially within HEIs. In some cases, the CLAHRC initiative was seen as a vehicle for progressing research bids that had failed to be funded. In others, CLAHRCs were seen as a way of ‘wrapping up’ existing research activity akin to a large-scale programme grant. In such cases, CLAHRC activity was more academically oriented than NHS defined. This model, in part, aligned with a view of those leading the CLAHRC bid development: that the NIHR privileged research excellence in its commissioning objectives. CLAHRC funding therefore ran the risk of reinforcing pre-existing research agendas and modes of research. Some CLAHRC bids could be viewed as offering little more than pre-existing activity. Although CLAHRC funding here enabled pre-existing activity to be accelerated, leveraged and potentially institutionalised for a greater gain than previously possible in the absence of support for large-scale activity. Furthermore, the CLAHRC initiative led to a translational focus that was more service oriented.
Although most of the CLAHRC bids were derived from pre-existing research activity, this proved to be advantageous in the mobilisation of CLAHRCs even if their value-added was reduced. Conversely, two of the CLAHRCs characterised their bid as more greenfield than brownfield activity and, therefore, claimed greater innovation around service-user involvement and focus on service problems. Such CLAHRC bids might sidestep translational ‘lock-in’ to established ways of doing things, but may prove more difficult to mobilise in the face of the greenfield context.
Where CLAHRCs were more oriented towards service improvement in the bidding process there was a difference in whether individual-level behavioural change or wide-scale organisational and system change was required. Here antecedent conditions and position of lead actors played a large part in determining this. Where a CLAHRC was more clinical science oriented, the focus was on the need to change individual-level behaviour. In comparison, social scientists, and at least one senior NHS manager, privileged the need for wider-scale organisational- and system-level change. However, a number of actors became increasingly focused on the importance of capacity building, which was in part fuelled by, and reinforced interest in, the diffusion of the knowledge broker role. Overall, the recognition of the type of change needed was dependent on the configuration of social actors within each CLAHRC. The process of envisaging, as shaped by local-level field conditions and key actors’ social positions, influenced the way in which CLAHRCs were designed and enacted. We suggest that the effectiveness of the initiative was fundamentally shaped by the envisaging process which ‘locked in’ CLAHRCs to a path of action.
During the engagement process, we found that senior CLAHRC actors had to work hard to ‘win the minds’ of key stakeholders and that this was a process that was much harder than many people anticipated. In particular, there was a disparity between the need to obtain resources from NHS partner organisations and then engagement of on-the-ground actors. The ‘winning of minds’ was a necessary but not sufficient condition for encouraging stakeholders to sign up to the ideals of CLAHRC. Additional work was undertaken in the form of aligning and consensus building, which helped to develop the normative component of the CLAHRC networks.
Work to embed CLAHRCs was undertaken across all four of our cases through education and the creation of new roles. Education worked to enhance NHS organisations’ capacity to absorb research. However, the focus of much of the educational work was on enhancing the efficacy of existing CLAHRC projects as opposed to capacity building. In terms of the creation of new roles, the dominant approach was the creation of the knowledge broker role, which emerged in one CLAHRC and then diffused through mimetic isomorphism to other CLAHRCs. The two remaining forms of embedding work – the embedding of tools and routines, and the creation of a CLAHRC identity – were more variable across the case studies. Overall, the difficulties associated with enacting institutional change required long time horizons. In terms of engaging and embedding, we highlight that the work has been more difficult than many CLAHRC actors imagined, highlighting the importance of continuity in resource deployment to such initiatives.
The activity of reflection was the final form of work and was particularly prevalent in the run up to CLAHRC refinancing. There were multiple lessons learned by many senior CLAHRC actors as they mobilised their CLAHRCs: (1) CLAHRCs were more difficult to get up and running than the envisaged form at the outset, which led to delays; (2) the commitment of resource to large-scale projects upfront ran the risk of handing over managerial control; (3) the balance (or gravity point) between research and implementation was difficult and required changes in the emphasis of CLAHRC activity over time; (4) actors across organisational and epistemological boundaries needed to learn how to understand one another and work towards a common understanding of what implementation actually was; and, finally, (5) career structures needed to be better developed to promote and reward CLAHRC behaviour. From the case studies, it could be argued that formalised learning events drawing people from outside CLAHRC and the wider health-care landscape, and other translational initiatives, to share learning in establishing and mobilising new initiatives, with those from all of the CLAHRCs.
Our SNA complemented our qualitative case studies, and provided evidence that the systematic variations in actors’ ability to bridge the research–practice divide related to actors’ social positions in terms of dominant orientations, professional status and existing relationships. For example, practitioners were more likely than academics and actors with many existing connections in their own professional field to develop networks that bridged the divide. Furthermore, junior actors found it more difficult than their senior counterparts to bridge the divide. Our longitudinal analysis, however, suggests that the CLAHRC initiative led to the development of more relationships that spanned the research–practice divide and provides evidence that CLAHRCs have enabled actors to more effectively bridge the research–practice divide.
Finally, given the different founding conditions, and the malleability of the CLAHRC mission presented in the original tender document, there was variation in how the CLAHRCs were organised and structured. 171 Based on our analysis we suggest that a number of different archetype models have emerged which CLAHRCs have drawn on. These models, as outlined in Chapter 10, are more or less likely to occur under different founding conditions. We present a detailed summary of the strengths and weaknesses of the different models in Table 12, in the previous chapter which includes institutional features, strengths, weaknesses and leadership challenges.
Implications for practice
Based on the main findings of our study, we contend that there are important lessons for those involved with, and those attempting to promote, institutional change that can support sustainable KT practices.
First, we encourage policy-makers to consider whether they need to set out a more defined template for translational initiatives in the initial calls for such initiatives or if variation is encouraged. We suggest that the less defined the template, the greater the variation will be in what actors envisage. Second, policy-makers need to understand the importance of both antecedent conditions to the development of any funding bids and the social position of the main actors leading bid development. Although established and known clinical academics are likely to be trusted to lead the development of a funding bid around translational research activity, and the presence of pre-existing organisational relationships are important for mobilisation, privileging such dimensions of any bid may constrain more radical change. Our study highlighted that strategic change and outcomes of innovation may be ‘locked-in’ in a way reflecting traditional clinical research at an early stage of bid development. We suggest that this conclusion is germane to all forms of translational initiative, which will fundamentally shape how any initiative plays out over time. To emphasise, strategies for change are not built independently from the structural context in which they are embedded, inclusive of consideration of the social position of the IEs leading translational innovation and antecedent conditions to bid development.
Second, regarding prescriptions for the development of implementation of KT networks, we tentatively suggest the following points. First, thought is given to selection of their leadership. More emphasis might be placed on those who exhibit recognition of system-level issues, and capability to work across organisational and professional boundaries, rather than remain within their academic research silos. At the same time, we need to recognise that leaders of KT networks require legitimacy from powerful individuals (such as clinical academics) to drive change in research and clinical practice. IEs need to be embedded in existing power structures, but willing to change such structures, if evidence-based innovation is to ensue on the ground. Second, any lock-in at early stages of development of KT networks might be mediated through relaxing any requirement to develop a detailed programme of activity in order to drawdown funding. The coproduction of a research agenda, which balances a service- and research-centred model for translation, might be engendered by more ‘open’ funding.
Third, our work pertaining to the different archetypes of the models of organising KT demonstrates that there are a range of different models that IEs may draw on in leading translational initiatives. We suggest, however, that IEs will seldom have a free choice as to the type of model they should pursue. Rather, we suggest that the founding conditions (local context and the social positions of the focal actors) will influence which archetypes the different actors draw on.
Fourth, practitioners need to be aware of how professional role, hierarchical status and embeddedness may shape actors’ willingness and ability to span the research–practice divide. We suggest that in addition to the social position of IEs influencing their orientation towards institutional change, social position can influence the extent to which others help enact that change (by actually bridging the research–practice divide). In essence, policy-makers need to understand that actors’ behaviours are shaped by institutional forces, and that sustainable change necessitates institutional change.
Study limitations
Our study, as with all studies, has a number of limitations. First, the qualitative work initially focused on nine CLAHRCs and then four CLAHRCs were examined in depth. Examining only four CLAHRCs in depth may have influenced the development of our process-based model of institutional entrepreneurship. However, given potential conflicts of interest with other projects and the practicality of being able to examine all nine CLAHRCs in depth, we feel that the four CLAHRCs we focused on provided us with nuanced insights of institutional entrepreneurship in translational initiatives and lessons for future initiatives.
Second, as outlined in Chapter 3, because of the nature of the CLAHRC initiative, our research protocol following ethics approvals, and a need for particular sensitivity given ongoing CLAHRC refinancing, meant that we were not able to present the data in as fine-grained a manner as we would ordinarily have liked to. Furthermore, we do not draw explicitly on our observational data because of the sensitive nature of much of the information. Consequently, we are slightly constrained in terms of ability to communicate the specific nuances of the different CLAHRCs on a case-by-case, and individual IE, basis.
Third, the high churn of staff in a number of the CLAHRCs we studied in depth meant that it was difficult to develop a large sample of common respondents across the two waves of our analysis. As detailed in Chapter 8, in one CLAHRC we were able to obtain longitudinal data for only three participants out of 15 surveyed in the first wave in one CLAHRC. As a result of a very low response rate, the decision was made to exclude the three respondents from longitudinal analyses. Therefore, the longitudinal analyses reported in this section are based on data from 42 of the 66 participants initially surveyed from three CLAHRCs.
Finally, we recognise that our study examines one form of translational initiative, in a particular national context. Research that investigates transferability to other translational initiatives internationally, moving beyond Anglo-(North) American contexts, seems particularly important given how the NHS context, notably system-level incentives, impacts the way that translational initiatives are received. 172 However, we have sought to mediate the influence of the specific empirical context by developing a theoretically informed process-based model of institutional entrepreneurship, and also the archetype models of KT, so as to maximise the generalisable lessons that may be drawn from our research.
Future research
In this report we have examined the CLAHRC initiative as a whole, as an interesting case of a translational research initiative, and have commented on only the broad social position of the key actors. We did so because an internal case analysis with a fine-grained interrogation of each actor’s unique social position would have undermined their anonymity. It would be interesting, however, for future research to explore the issue of actors’ social positions at a micro level. For example, recent work about health care by Lockett et al. 173 has employed the work of Bourdieu,105 to examine the relationship between each individual actor’s unique social position and the way in which the opportunities and problems of change were conceptualised. Evidence of which, in a focused manner, is provided by our SNA work (see Chapter 8) which indicates that an actor’s social position, based on role, hierarchy and existing networks, may have an important influence on their willingness and ability to bridge the worlds of research and practice. In addition, there might be closer consideration of the influence of brownfield compared with greenfield in shaping actors’ behaviour.
Although we have documented important learning by CLAHRCs in Chapter 9, we suggest that the process through which translational initiatives are refinanced may be an important opportunity for the promotion of further learning via the promotion of reflective thinking. The very process of having to critically examine past performance, identify the key lessons learned, and to translate the lessons into the renewed strategy may help the leaders of translational research initiatives to break away from being ‘locked in’ to existing ways of working that were established through the envisaging of the initiative in its formative years.
Associated with learning, we suggest that there is a need to examine how actors are led to reflect on the emerging lessons from their endeavours. We suggest that, consistent with the work of Lockett et al. ,173 research could examine whether or not actors in different social positions are more or less likely to develop reflective skills. Indeed, the work of Lockett et al. 173 suggests that the diversity of an actor’s social capital may be important in this regard. Hence, we argue that it may be revealing to link actors’ ego networks, and particularly the diversity of their networks, to their capacity to reflect.
Given that institutional change commonly requires the sustained efforts of IEs engaged in IW, we suggest that the first round of CLAHRC funding is only the start of the process of institutional change to close the T2. Therefore, there is a real need to undertake more longitudinal work to examine how translational research initiatives continue to promote institutional change and identify the outputs, both in terms of research and in practice.
Furthermore, our work is based on the study of CLAHRCs, which are just one form of translational initiative. We suggest that important lessons may also be gleaned from comparative work across other forms of translational initiatives such as the AHSCs, BRCs, BRUs, HIECs and the NHS Innovation Hubs. For example, the recent launch of AHSNs has raised the issue of how different translational initiatives could work together. According to a DH report,174 Innovation, Health and Wealth, the role of AHSNs will be to work with stakeholders from across the NHS and the scientific community, academia, the third sector, and local authorities to link up regional innovation systems and drive the diffusion of innovation. In doing so, the goal of AHSNs will be to improve patient and population health outcomes through the translation of research into practice and the development and implementation of integrated health-care systems. Rather than treating each translational initiative as a stand-alone entity, we suggest that research could examine the synergies across the initiatives and analyse how institutional change may be brought about in a more collective fashion.
Acknowledgements
We are grateful to the NIHR-HSDR for funding this project. In addition, we would like to thanks all of our research participants, especially those involved in our four in-depth case sites, who have given up over the course of this study numerous hours of their time. Finally, we would like to thank the members of SSAP, and service users, who provided us with invaluable guidance and insight in developing the research and honing our analysis. We thank Alice MacNeil and Bassel Namih for their assistance in producing this report.
Contributions of authors
Andy Lockett (Professor, strategy and entrepreneurship, University of Warwick) led the study and the writing of the report, conducted some of the fieldwork and data analysis.
Nellie El Enany [Assistant Professor, organisational behaviour, University of Warwick (was a research fellow for a period on the project)] contributed to the writing of the report, fieldwork and analyses of the data.
Graeme Currie (Professor, public management, University of Warwick) contributed to the writing of the report and analyses of the data.
Eivor Oborn (Professor, health care management, University of Warwick) contributed to the writing of the report, conducted the literature review into knowledge transfer, fieldwork and analyses of the data, particularly the KT models.
Michael Barrett (Professor of Information Systems and Innovation Studies, University of Cambridge) led the study from the University of Cambridge, helped with the writing of the report, conducted the literature review into knowledge transfer, fieldwork and analyses of the data, particularly the KT models.
Girts Racko [Assistant Professor, organisational behaviour, University of Warwick [was a research fellow for a period on the project)] helped with the writing of the report, conducted the literature review into knowledge transfer, fieldwork and analyses of the SNA data.
Simon Bishop [Lecturer, organisational behaviour, University of Nottingham [was a research fellow for a period on the project)] conducted the literature review on institutional entrepreneurship and fieldwork.
Justin Waring (Professor, public management, University of Nottingham) conducted fieldwork.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- The Theory and Practice of Knowledge brokering in Canada’s Health System. Ottawa, ON: Canadian Health Services Research Foundation; 2003.
- Lomas J. The in-between world of knowledge brokering. BMJ 2007;334:129-32. http://dx.doi.org/10.1136/bmj.39038.593380.AE.
- Woolf SH. The meaning of translational research and why it matters. JAMA 2008;299:211-13. http://dx.doi.org/10.1001/jama.2007.26.
- Dzau VJ, Ackerly DC, Sutton-Wallace P, Merson MH, Williams RS, Krishnan KR, et al. The role of academic health science systems in the transformation of medicine. Lancet 2010;375:949-53. http://dx.doi.org/10.1016/S0140-6736(09)61082-5.
- Butler D. Translational research: Crossing the valley of death. Nature 2008;453:840-2. http://dx.doi.org/10.1038/453840a.
- Fontanarosa PB, DeAngelis CD. Basic science and translational research in JAMA. JAMA 2002;287. http://dx.doi.org/10.1001/jama.287.13.1728.
- Cooksey D. A Review of UK Health Research Funding. London: The Stationery Office; 2006.
- Rycroft-Malone J, Kitson A, Harvey G, McCormack B, Seers K, Tichen A, et al. Ingredients for change: revisiting a conceptual framework. Qual Saf Health Care 2002;11:174-80. http://dx.doi.org/10.1136/qhc.11.2.174.
- Kitson A, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A. Evaluating the successful implementation of evidence into practice using the PARIHS framework: theoretical and practical challenges. Implement Sci 2008;3. http://dx.doi.org/10.1186/1748-5908-3-1.
- Graham I, Tetroe J. Learning from the U.S. department of veterans affairs quality enhancement research initiative: QUERI Series. Implement Sci 2009;4:1-6. http://dx.doi.org/10.1186/1748-5908-4-13.
- Dussault G, Davis J, Gruman J, Thorton W. CHSRF at the Crossroads: Capitalizing on Success – Report of the International Review Panel to the Board of Trustees of the Canadian Health Services Research Foundation. Ottawa, ON: Canadian Institutes of Health Research; 2007.
- Wehrens R, Bekker M, Bal R. Within The Netherlands, Dutch Academic Collaborative Centres for Public Health: Development through time – Issues, dilemmas and coping strategies. Evidence Policy 2012;8:149-70. http://dx.doi.org/10.1332/174426412X640063.
- Nutley SM, Walter I, Davies HTO. Using Evidence: How Research can Inform Public Services. Bristol: Policy Press; 2007.
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Q 2004;82:581-629. http://dx.doi.org/10.1111/j.0887-378X.2004.00325.x.
- Currie G, Suhomlinova O. The impact of institutional forces upon knowledge sharing in the UKNHS: The triumph of professional power and the inconsistency of policy. Public Adm 2006;84:1-30. http://dx.doi.org/10.1111/j.0033-3298.2006.00491.x.
- Martin G, Currie G, Lockett A. Prospects for knowledge exchange in health policy and management: institutional and epistemic boundaries. J Health Serv Res Policy 2011;16:211-17. http://dx.doi.org/10.1258/jhsrp.2011.010132.
- Martin G, Currie G, Finn R. Bringing genetics into primary care: findings from a national evaluation of pilots in England. J Health Serv Res Policy 2009;14:204-11. http://dx.doi.org/10.1258/jhsrp.2009.008158.
- Albert M, Laberge S, Hodges BD, Regehr G, Lingard L. Biomedical scientists’ perception of the social sciences in health research. Soc Sci Med 2008;66:2520-31. http://dx.doi.org/10.1016/j.socscimed.2008.01.052.
- Morgan M, Barry C, Donovan J, Sandall J, Wolfe C, Boaz A. Implementing ‘translational’ biomedical research: convergence and divergence among clinical and basic scientists. Soc Sci Med 2011;73:945-52. http://dx.doi.org/10.1016/j.socscimed.2011.06.060.
- Lockett A, Currie G, Waring J, Finn R, Martin G. The role of institutional entrepreneurs in reforming healthcare. Soc Sci Med 2012;74:356-63. http://dx.doi.org/10.1016/j.socscimed.2011.02.031.
- Currie G, Finn R, Martin G. Accounting for the ‘dark side’ of new organizational forms: the case of healthcare professionals. Hum Relat 2008;61:539-64. http://dx.doi.org/10.1177/0018726708091018.
- Lawrence TB, Suddaby R, Clegg SR, Hardy C, Lawrence TB, Nord WR. Handbook of Organization Studies. London: Sage Publications; 2006.
- Lounsbury M, Crumley ET. New practice creation: an institutional perspective on innovation. Organ Stud 2007;28:993-1012. http://dx.doi.org/10.1177/0170840607078111.
- Maguire S, Hardy C, Lawrence TB. Institutional entrepreneurship in emerging fields: HIV/AIDS treatment advocacy in Canada. Acad Manag J 2004;47:657-79. http://dx.doi.org/10.2307/20159610.
- Pettigrew AM, Ferlie EB, McKee L. Shaping Strategic Change. London: Sage Publications; 1992.
- Gioia DA, Chittipeddi K. Sensemaking and sensegiving in strategic change initiation. Strat Manag J 1991;12:433-48. http://dx.doi.org/10.1002/smj.4250120604.
- Fligstein N. Social skill and institutional theory. Am Behav Sci 1997;40:397-405. http://dx.doi.org/10.1177/0002764297040004003.
- Greenwood R, Suddaby R, Hinings CR. Theorizing change: the role of professional associations in the transformation of institutionalized fields. Acad Manag J 2002;45:58-80. http://dx.doi.org/10.2307/3069285.
- Fligstein N. Social skill and the theory of fields. Sociol Theory 2001;19:105-25. http://dx.doi.org/10.1111/0735-2751.00132.
- Lawrence TB, Hardy C, Phillips N. Institutional effects of interorganizational collaboration: the emergence of proto-institutions. Acad Manag J 2002;45:281-90. http://dx.doi.org/10.2307/3069297.
- Rao H. Caveat emptor: The construction of nonprofit consumer watchdog organizations. Am J Sociol 1998;103:912-61. http://dx.doi.org/10.1086/231293.
- Townley B. The institutional logic of performance appraisal. Organ Stud 1997;18:261-85. http://dx.doi.org/10.1177/017084069701800204.
- Zilber T. Institutionalization as an interplay between actions and actors: the case of a rape crisis center in Israel. Acad Manag J 2002;45:234-54. http://dx.doi.org/10.2307/3069294.
- Dopson S, Fitzgerald L. Knowledge to Action?: Evidence-Based Health Care in Context. Oxford: Oxford University Press; 2005.
- Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, et al. Lost in knowledge translation: time for a map?. J Contin Educ Health Prof 2006;26:13-24. http://dx.doi.org/10.1002/chp.47.
- Mitton C, Adair C, McKenzie E, Patten S, Perry B. Knowledge transfer and exchange: review and synthesis of the literature. Milbank Q 2007;85:729-68. http://dx.doi.org/10.1111/j.1468-0009.2007.00506.x.
- Weiss C. Many meanings of research utilization. Public Adm Rev 1979;39:426-31. http://dx.doi.org/10.2307/3109916.
- Oborn E, Barrett M, Racko G. Knowledge Translation in Healthcare: Incorporating Theories of Learning and Knowledge from the Management Literature. J Health Organ Managt 2013;27.
- Battilana J, Leca B, Boxenbaum E. How Actors Change Institutions: towards a Theory of Institutional Entrepreneurship. Acad Manag Ann 2009;3:65-107. http://dx.doi.org/10.1080/19416520903053598.
- Bridging the “Know-Do” Gap: Meeting on Knowledge Translation in Global Health. Meeting report. Geneva: WHO; 2005.
- Eccles MP, Mittman BS. Welcome to implementation science. Implement Sci 2006;1. http://dx.doi.org/10.1186/1748-5908-1-1.
- Nicolini D, Powell J, Conville P, Martinez-Solano L. Managing knowledge in the healthcare sector. A review. Int J Manag Rev 2008;10:245-63. http://dx.doi.org/10.1111/j.1468-2370.2007.00219.x.
- Rycroft-Malone J, Wilkinson JE, Burton CR, Andrews G, Ariss S, Baker R, et al. Implementing health research through academic and clinical partnerships: a realistic evaluation of the Collaborations for Leadership in Applied Health Research and Care (CLAHRC). Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-74.
- Eccles MP, Armstrong D, Baker R, Cleary K, Davies H, Davies S, et al. An implementation research agenda. Implement Sci 2009;4. http://dx.doi.org/10.1186/1748-5908-4-18.
- Oborn E. Facilitating implementation of the translational research pipeline in neurological rehabilitation. Curr Opin Neurol 2012;25:676-81. http://dx.doi.org/10.1097/WCO.0b013e32835a35f2.
- McKibbon KA, Lokker C, Wilczynski NL, Ciliska D, Dobbins M, Davis DA, et al. A cross-sectional study of the number and frequency of terms used to refer to knowledge translation in a body of health literature in 2006: a tower of babel?. Implement Sci 2010;5. http://dx.doi.org/10.1186/1748-5908-5-16.
- Mosteller F. Innovation and evaluation. Science 1981;211:881-6. http://dx.doi.org/10.1126/science.6781066.
- Caplan N. The two-communities theory and knowledge utilization. Am Behav Sci 1979;22:459-70. http://dx.doi.org/10.1177/000276427902200308.
- Jacobson N, Butterill D, Goering P. Development of a framework for knowledge translation: understanding user context. J Health Serv Res Policy 2003;8:94-9. http://dx.doi.org/10.1258/135581903321466067.
- Sackett DL, Rosenberg WMC. The need for evidence-based medicine. J R Soc Med 1995;88:620-4.
- Gabbay J, Le May A. Practice-Based Evidence for Healthcare: Clinical Mindlines. Abingdon: Routledge; 2011.
- Swan J, Bresnen M, Newell S, Robertson M. The object of knowledge: the role of objects in biomedical innovation. Hum Relat 2007;60:1809-37. http://dx.doi.org/10.1177/0018726707084915.
- Graham ID, Tetroe J, Group KTTR. Some theoretical underpinnings of knowledge translation. Acad Emerg Med 2007;14:936-41. http://dx.doi.org/10.1111/j.1553-2712.2007.tb02369.x.
- Freeman AC, Sweeney K. Why general practitioners do not implement evidence: qualitative study. Br Med J 2001;323:1100-02A. http://dx.doi.org/10.1136/bmj.323.7321.1100.
- Mitton C, Adair CE, McKenzie E, Patten S, Waye-Perry B, Smith N. Designing a knowledge transfer and exchange strategy for the Alberta Depression Initiative: contributions of qualitative research with key stakeholders. Int J Mental Health Syst 2009;3. http://dx.doi.org/10.1186/1752-4458-3-11.
- Harvey G, Fitzgerald L, Fielden S, McBride A, Waterman H, Bamford D, et al. The NIHR collaboration for leadership in applied health research and care (CLAHRC) for greater manchester: combining empirical, theoretical and experiential evidence to design and evaluate a large-scale implementation strategy. Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-96.
- Baumbusch JL, Kirkham SR, Khan KB, McDonald H, Semeniuk P, Tan E, et al. Pursuing common agendas: a collaborative model for knowledge translation between research and practice in clinical settings. Res Nurs Health 2008;31:130-40. http://dx.doi.org/10.1002/nur.20242.
- Lomas J. Using ‘linkage and exchange’ to move research into policy at a Canadian foundation. Health Aff (Millwood) 2000;19:236-40. http://dx.doi.org/10.1377/hlthaff.19.3.236.
- Bowen S, Martens P. Demystifying knowledge translation: learning from the community. J Health Serv Res Policy 2005;10:203-11. http://dx.doi.org/10.1258/135581905774414213.
- Trostle J, Bronfman M, Langer A. How do researchers influence decision-makers? Case studies of Mexican policies. Health Policy Plan 1999;14:103-14. http://dx.doi.org/10.1093/heapol/14.2.103.
- Knowledge Translation Strategy 2004–2009: Innovation in Action. Ottawa, ON: Canadian Institute of Health Research; 2004.
- Sudsawad P. The National Center for the Dissemination of Research; 2007.
- National Institute on Disability and Rehabilitation Research . Department of Education: National Institute on Disability and Rehabilitation Research – Notice of Final Long-Range Plan for Fiscal Years 2005-2009. Fed Regist 2006;71:8166-200.
- Keith RE, Hopp FP, Subramanian U, Wiitala W, Lowery JC. Fidelity of implementation: development and testing of a measure. Implement Sci 2010;5. http://dx.doi.org/10.1186/1748-5908-5-99.
- Kontos PC, Poland BD. Mapping new theoretical and methodological terrain for knowledge translation: contributions from critical realism and the arts. Implement Sci 2009;4. http://dx.doi.org/10.1186/1748-5908-4-1.
- Logan J, Graham ID. Toward a comprehensive interdisciplinary model of health care research use. Sci Commun 1998;20:227-46. http://dx.doi.org/10.1177/1075547098020002004.
- Dobrow MJ, Goel V, Upshur REG. Evidence-based health policy: context and utilisation. Soc Sci Med 2004;58:207-17. http://dx.doi.org/10.1016/S0277-9536(03)00166-7.
- Estabrooks CA, Squires JE, Cummings GG, Birdsell JM, Norton PG. Development and assessment of the Alberta Context Tool. BMC Health Serv Res 2009;9. http://dx.doi.org/10.1186/1472-6963-9-234.
- Eccles M, Grimshaw J, Walker A, Johnston M, Pitts N. Changing the behavior of healthcare professionals: the use of theory in promoting the uptake of research findings. J Clin Epidemiol 2005;58:107-12. http://dx.doi.org/10.1016/j.jclinepi.2004.09.002.
- Wensing M, Oxman A, Baker R, Godycki-Cwirko M, Flottorp S, Szecsenyi J, et al. Tailored implementation for chronic diseases (TICD): a project protocol. Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-103.
- Oxman AD, Fretheim A, Flottorp S. The OFF theory of research utilization. J Clin Epidemiol 2005;58:113-16. http://dx.doi.org/10.1016/j.jclinepi.2004.10.002.
- Chamberlain P, Brown CH, Saldana L. Observational measure of implementation progress in community based settings: the stages of implementation completion (SIC). Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-116.
- Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf 2008;34:228-43.
- Stetler CB, Damschroder LJ, Helfrich CD, Hagedorn HJ. A Guide for applying a revised version of the PARIHS framework for implementation. Implement Sci 2011;6. http://dx.doi.org/10.1186/1748-5908-6-99.
- Rycroft-Malone J. The PARIHS framework – a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual 2004;19:297-304. http://dx.doi.org/10.1097/00001786-200410000-00002.
- Greenhalgh T. What is this knowledge that we seek to “exchange”?. Milbank Q 2010;88:492-9. http://dx.doi.org/10.1111/j.1468-0009.2010.00610.x.
- Ward V, Smith S, House A, Hamer S. Exploring knowledge exchange: a useful framework for practice and policy. Soc Sci Med 2012;74:297-304. http://dx.doi.org/10.1016/j.socscimed.2011.09.021.
- DiMaggio PJ, Powell WW. The iron cage revisted – institutional isomorpohism and collective rationality in organizational fields. Am Sociol Rev 1983;48:147-60. http://dx.doi.org/10.2307/2095101.
- Meyer JW, Rowan B. Institutionalized organizations – formal-structure as myth and ceremony. Am J Sociol 1977;83:340-63. http://dx.doi.org/10.1086/226550.
- Scott WR. Institutions and Organizations. Thousand Oaks, CA: Sage Publications; 2001.
- Dobbin F, Dowd TJ. How policy shapes competition: early railroad foundings in Massachusetts. Adm Sci Q 1997;42:501-29. http://dx.doi.org/10.2307/2393736.
- Hargadon AB, Douglas Y. When innovations meet institutions: Edison and the design of the electric light. Adm Sci Q 2001;46:476-501. http://dx.doi.org/10.2307/3094872.
- Leblebici H, Salancik GR, Copay A, King T. Institutional change and the transformation of interorganizational fields – an organizational history of the united-states radio broadcasting industry. Adm Sci Q 1991;36:333-63. http://dx.doi.org/10.2307/2393200.
- Friedland R, Alford RR, Powell WW, DiMaggio PJ. The New Institutionalism in Organizational Analysis. Chicago, IL: The University of Chicago Press; 1991.
- Scott WR, Scott WR, Meyer JW. Institutional Environments and Organizations: Structural Complexity and Individualism. Thousand Oaks, CA: Sage Publications; 1994.
- Rao H, Morrill C, Zald MN, Staw BM, Sutton RI. Research in Organizational Behavior (Vol. 22): An Annual Series of Analytical Essays and Critical Reviews. San Diego, CA: JAI Press; 2000.
- D’Aunno T, Succi M, Alexander JA. The role of institutional and market forces in divergent organizational change. Adm Sci Q 2000;45:679-703. http://dx.doi.org/10.2307/2667016.
- Lounsbury M. A tale of two cities: Competing logics and practice variation in the professionalizing of mutual funds. Acad Manage J 2007;50:289-307. http://dx.doi.org/10.5465/AMJ.2007.24634436.
- Scott WR. Institutions and Organizations. Thousand Oaks, CA: Sage Publications; 1995.
- Hoffman AJ. Institutional evolution and change: Environmentalism and the US chemical industry. Acad Manage J 1999;42:351-71. http://dx.doi.org/10.2307/257008.
- Oliver C. The antecedents of deinstitutionalization. Organ Stud 1992;13:563-88. http://dx.doi.org/10.1177/017084069201300403.
- Greenwood R, Diaz AM, Li SX, Lorente JC. The Multiplicity of Institutional Logics and the Heterogeneity of Organizational Responses. Organ Sci 2010;21:521-39. http://dx.doi.org/10.1287/orsc.1090.0453.
- Health and Social Care Act 2012: Elizabeth II. London: The Stationery Office; 2012.
- Liberating the NHS: No Decision About Me, Without Me – Government Response to the Consulation. London: DH; 2012.
- University Clinical Partnership: Harnessing Clinical and Academic Resources. London: The Nuffield Trust; 2000.
- Becher T, Trowler P. Academic Tribes and Territories: Intellectual Enquiry and the Cultures of Disciplines. Buckingham: The Society for Research into Higher Education; 2001.
- Currie G, Lockett A, Finn R, Martin G, Waring J. Institutional work to maintain professional power: recreating the model of medical professionalism. Organ Stud 2012;33:937-62. http://dx.doi.org/10.1177/0170840612445116.
- Bourdieu P. The Logic of Practice. Cambridge: Polity; 1990.
- Beckert J. Agency, entrepreneurs, and institutional change. The role of strategic choice and institutionalized practices in organizations. Organ Stud 1999;20:777-99. http://dx.doi.org/10.1177/0170840699205004.
- DiMaggio PJ, Powell WW, DiMaggio PJ. The New Institutionalism in Organizational Analysis. Chicago, IL: The University of Chicago Press; 1991.
- Lawrence TB. Institutional strategy. J Manag 1999;25:161-87. http://dx.doi.org/10.1016/S0149-2063(99)80008-7.
- DiMaggio PJ, Zucker L. Institutional Patterns and Organizations: Culture and Environment. Cambridge, MA: Ballinger; 1988.
- Oakes LS, Townley B, Cooper DJ. Business planning as pedagogy: Language and control in a changing institutional field. Adm Sci Q 1998;43:257-92. http://dx.doi.org/10.2307/2393853.
- Bourdieu P, Wacquant LJD. An Invitation to Reflexive Sociology. Chicago, IL: University of Chicago Press; 1992.
- Bourdieu P. Outline of a Theory of Practice. Cambridge, UK: Cambridge University Press; 1977.
- Battilana J. Agency and institutions: The enabling role of individuals’ social position. Organization 2006;13:653-76. http://dx.doi.org/10.1177/1350508406067008.
- Dacin MT, Ventresca MJ, Beal BD. The embeddedness of organizations: dialogue & directions. J Manag 1999;25:317-56. http://dx.doi.org/10.1177/014920639902500304.
- Greenwood R, Suddaby R. Institutional entrepreneurship in mature fields: the big five accounting firms. Acad Manage J 2006;49:27-48. http://dx.doi.org/10.5465/AMJ.2006.20785498.
- Garud R, Jain S, Kumaraswamy A. Institutional entrepreneurship in the sponsorship of common technological standards: The case of Sun Microsystems and Java. Acad Manag J 2002;45:196-214. http://dx.doi.org/10.2307/3069292.
- Hillman AJ, Hitt MA. Corporate political strategy formulation: a model of approach, participation, and strategy decisions. Acad Manag Rev 1999;24:825-42.
- Hinings CR, Greenwood R, Zucker L. Institutional Patterns and Organizations: Culture and Environment. Cambridge, MA: Ballinger; 1988.
- Jain S, George G. Technology transfer offices as institutional entrepreneurs: the case of Wisconsin Alumni Research Foundation and human embryonic stem cells. Industrial Corporate Change 2007;16:535-67. http://dx.doi.org/10.1093/icc/dtm017.
- Slack T, Hinings B. Institutional pressures and isomorphic change – an empirical-test. Organ Stud 1994;15:803-27. http://dx.doi.org/10.1177/017084069401500602.
- Haveman HA, Rao H. Structuring a theory of moral sentiments: institutional and organizational coevolution in the early thrift industry. Am J Sociol 1997;102:1606-51. http://dx.doi.org/10.1086/231128.
- Hirsch PM. From ambushes to golden parachutes: corporate takeovers as an instance of cultural framing and institutional integration. Am J Sociol 1986;91:800-37. http://dx.doi.org/10.1086/228351.
- Seo MG, Creed WED. Institutional contradictions, praxis, and institutional change: A dialectical perspective. Acad Manag Rev 2002;27:222-47.
- Hardy C, Maguire S, Greenwood R, Oliver C, Suddaby R, Sahlin-Andersen K. Handbook of Organizational Institutionalism. London: Sage Publications; 2008.
- Nasra R, Dacin MT. Institutional arrangements and international entrepreneurship: the state as institutional entrepreneur. Entrepreneurship Theory Pract 2009;34:583-609. http://dx.doi.org/10.1111/j.1540-6520.2009.00354.x.
- Sherer PD, Lee K. Institutional change in large law firms: a resource dependency and institutional perspective. Acad Manag J 2002;45:102-19. http://dx.doi.org/10.2307/3069287.
- Townley B. The role of competing rationalities in institutional change. Acad Manag J 2002;45:163-79. http://dx.doi.org/10.2307/3069290.
- Rao H, Monin P, Durand R. Institutional change in Toque Ville: nouvelle cuisine as an identity movement in French gastronomy. Am J Sociol 2003;108:795-843. http://dx.doi.org/10.1086/367917.
- Lawrence T, Suddaby R, Leca B. Institutional work: refocusing institutional studies of organization. J Manag Inquiry 2011;20:52-8. http://dx.doi.org/10.1177/1056492610387222.
- Jarzabkowski P, Matthiesen J, Van de Ven AH, Lawrence TB, Suddaby R, Leca B. Institutional Work: Actors and Agency in Institutional Studies of Organizations. Cambridge, UK: Cambridge University Press; 2009.
- Lee TW. Using Qualitative Methods in Organizational Research. Newbury Park, CA: Sage Publications; 1999.
- Locke K. Grounded Theory in Management Research. London: Sage Publications; 2001.
- Yin RK. Case Study Research: Design and Methods. Thousand Oaks, CA: Sage Publications; 2003.
- Eisenhardt KM, Graebner ME. Theory building from cases: opportunities and challenges. Acad Manag J 2007;50:25-32. http://dx.doi.org/10.5465/AMJ.2007.24160888.
- Jick TD. Mixing qualitative and quantitative methods – triangulation in action. Adm Sci Q 1979;24:602-11. http://dx.doi.org/10.2307/2392366.
- Gephart RP. The textual approach – risk and blame in disaster sensemaking. Acad Manag J 1993;36:1465-514. http://dx.doi.org/10.2307/256819.
- Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago, IL: Aldine; 1967.
- Bernard HR. Research Methods in Anthropology: Qualitative and Quantitative Approaches. Walnut Creek, CA: Altamira Press; 2002.
- Miles BM, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. 2nd edn. Thousand Oaks, CA: Sage Publications; 1994.
- Pope C, Ziebland S, Mays N. Qualitative research in health care – analysing qualitative data (reprinted from Qualitative Research in Health Care). BMJ 2000;320:114-16. http://dx.doi.org/10.1136/bmj.320.7227.114.
- Abbott A, Ragin C, Becker H. What is a case? Exploring Foundations of Social Inquiry. New York, NY: Cambridge University Press; 1992.
- Strauss A, Corbin J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park, CA: Sage Publications; 1990.
- Corley KG, DA G. Identity ambiguity and change in the wake of a corporate spin-off. Adm Sci Q 2004;49:173-208.
- Van Maanen J. Tales of the Field: On Writing Ethnography. Chicago, IL: University of Chicago Press; 1988.
- Wodak R, Seale C, Gubrium JF, Silverman D. Qualitative Research Practice. Thousand Oaks, CA: Sage Publications; 2004.
- Mantere S, Schildt HA, Sillince JAA. Reversal of strategic change. Acad Manag J 2012;55:172-96. http://dx.doi.org/10.5465/amj.2008.0045.
- Van de Ven AH. Engaged Scholarship: A Guide for Organizational and Social Research. Oxford: Oxford University Press; 2007.
- Eisenhardt KM. Building theories from case study research. Acad Manag Rev 1989;14:532-50.
- Requirements for Social Work Training. London: DH; 2002.
- Best Research for Best Health. London: DH; 2006.
- McLaughlin H. Keeping service user involvement in research honest. Br J Soc Work 2010;40:1591-608. http://dx.doi.org/10.1093/bjsw/bcp064.
- Callard F, Rose D, Wykes T. Close to the bench as well as at the bedside: involving service users in all phases of translational research. Health Expect 2012;15:389-400. http://dx.doi.org/10.1111/j.1369-7625.2011.00681.x.
- Hansen WB, Reese EL. Network Genie. Greensboro, NC: Tanglewood Research; 2008.
- Burt RS. Network items and the general social survey. Soc Netw 1984;6:293-339. http://dx.doi.org/10.1016/0378-8733(84)90007-8.
- Nigam A, Ocasio W. Event attention, environmental sensemaking, and change in institutional logics: an inductive analysis of the effects of public attention to Clinton’s health care reform initiative. Organ Sci 2010;21:823-41. http://dx.doi.org/10.1287/orsc.1090.0490.
- Emirbayer M. Manifesto for a relational sociology. Am J Sociol 1997;103:281-317. http://dx.doi.org/10.1086/231209.
- Emirbayer M, Mische A. What is agency?. Am J Sociol 1998;103:962-1023. http://dx.doi.org/10.1086/231294.
- Nigam A, Golden B. Professional Roles, Frames, Politics, and the Selection and Change of Organizational Routines. Working Paper 2010.
- Suddaby R, Greenwood R. Rhetorical strategies of legitimacy. Adm Sci Q 2005;50:35-67.
- Creed WED, Scully MA, Austin JR. Clothes make the person? The tailoring of legitimating accounts and the social construction of identity. Organ Sci 2002;13:475-96. http://dx.doi.org/10.1287/orsc.13.5.475.7814.
- Déjean F, Gond JP, Leca B. Measuring the unmeasured: an institutional entrepreneur strategy in an emerging industry. Hum Relat 2004;57:741-64. http://dx.doi.org/10.1177/0018726704044954.
- Demil B, Bensédrine J. Process of legitimation and pressure toward regulation. Int Stud Manag Organ 2005;35:58-79.
- Perkmann M, Spicer A. ‘Healing the scars of history’: Projects, skills and field strategies in institutional entrepreneurship. Organ Stud 2007;28:1101-22. http://dx.doi.org/10.1177/0170840607078116.
- Hsu CL. Market ventures, moral logics, and ambiguity: Crafting a new organizational form in post-socialist china. Sociol Qu 2006;47:69-92. http://dx.doi.org/10.1111/j.1533-8525.2006.00038.x.
- Brock DM, Powell MJ, Hinings CR. Restructuring the Professional Organization: Accounting, Healthcare and Law. London: Routledge; 1999.
- Covaleski MA, Dirsmith MW, Heian JB, Samuel S. The calculated and the avowed: techniques of discipline and struggles over identity in Big Six public accounting firms. Adm Sci Q 1998;43:293-327. http://dx.doi.org/10.2307/2393854.
- Rowley E, Morriss R, Currie G, Schneider J. Research into practice: collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Nottinghamshire, Derbyshire, Lincolnshire (NDL). Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-40.
- Battilana J. The enabling role of social position in diverging from the institutional status quo: evidence from the UK National Health Service. Organ Sci 2011;22:817-34. http://dx.doi.org/10.1287/orsc.1100.0574.
- Washington M, Zajac EJ. Status evolution and competition: theory and evidence. Acad Manage J 2005;48:282-96. http://dx.doi.org/10.5465/AMJ.2005.16928408.
- Phillips DJ, Zuckerman EW. Middle-status conformity: theoretical restatement and empirical demonstration in two markets. Am J Sociol 2001;107:379-42. http://dx.doi.org/10.1086/324072.
- Dorado S. Institutional entrepreneurship, partaking, and convening. Organ Stud 2005;26:385-414. http://dx.doi.org/10.1177/0170840605050873.
- Kleinman DL, Vallas SP. Science, capitalism, and the rise of the ‘knowledge worker’: the changing structure of knowledge production in the United States. Theory Soc 2001;30:451-92. http://dx.doi.org/10.1023/A:1011815518959.
- Ferlie E, Fitzgerald L, Wood M, Hawkins C. The nonspread of innovations: the mediating role of professionals. Acad Manag J 2005;48:117-34. http://dx.doi.org/10.5465/AMJ.2005.15993150.
- Freidson E. Professionalism, the Third Logic: On the Practice of Knowledge. Chicago, IL: University of Chicago Press; 2001.
- Ucbasaran D, Shepherd DA, Lockett A, Lyon SJ. Life after business failure: the process and consequences of business failure for entrepreneurs. J Manag 2013;39:163-202. http://dx.doi.org/10.1177/0149206312457823.
- Oborn E, Barrett M, Prince K, Racko G. Balancing exploration and exploitation in transferring research into practice: a comparison of five knowledge translation entity archetypes. Implement Sci 2013;8.
- Greenwood R, Hinings CR. Organizational design types, tracks and the dynamics of strategic change. Organ Stud 1988;9:293-316. http://dx.doi.org/10.1177/017084068800900301.
- Currie G, Lockett A, El Enany N. From what we know to what we do: lessons learned from the translational CLAHRC initiative in England. J Health Serv Res Policy 2014;18:27-39.
- Atun R. Health systems, systems thinking and innovation. Health Policy Plan 2012;27:iv4-8. http://dx.doi.org/10.1093/heapol/czs088.
- Lockett A, Currie G, Finn R, Martin G, Waring J. The influence of social position sensemaking about organizational change. Acad Manag J 2014.
- Innovation, Health and Wealth. London: DH; 2011.
Appendix 1 Interview schedules, observation guide and social network analysis questionnaire
Phase 1 interview schedule: indicative questions
Please could you tell me about your background, and about how you became involved with this CLAHRC.
What is your role in relation to this CLAHRC?
How is your CLAHRC going about addressing the divide between clinical research and the application of research in practice?
What challenges has it encountered in this process?
How has it got around these challenges?
What individuals and groups are most closely involved in the work of the CLAHRC?
What are the roles of these individuals and groups? Who is most important in the process?
Are there any individuals or groups who are not so closely involved, but should be?
Is there anything else you think might be of interest to me, but which I haven’t mentioned?
Phase 2 interview schedule: indicative questions
(If not involved in phase 1.) Please could you tell me about your background, and about how you became involved with this CLAHRC?
(If not involved in phase 1.) What is your role in relation to this CLAHRC?
(If not involved in phase 1.) Please could you tell me about how things have progressed since I last spoke to you? Please could you tell me if there have been any changes to your role or to the CLAHRC as a whole?
Please could you describe to me in detail what your work in making this CLAHRC happen has involved? What have been the challenges? How has it differed from what your role involved before you linked up with the CLAHRC?
What organisations do you work with most closely in this work? Have there been any particular challenges in engaging them? How have you got round these challenges?
What individuals do you work with most closely in this work? Have there been any particular challenges in engaging them? How have you got round these challenges?
Are there any particular aspects of the environment in which your CLAHRC works that are especially challenging to the objectives of the CLAHRC? For example, policy structures, gaps between organisations, expectations of different professional groups? In an ideal world, how would these be different? In the real world, how can you work around these?
Is there anything else you think might be of interest to me, but which I haven’t mentioned?
Observation guide: indicative issues to look for
Who is in the room? What are their roles (differences in terms of status, professional function, age, gender, etc.)?
How do different actors express their views/concerns etc. in different ways?
What is the role of local context, both in terms of history and politics in the locality, play into emerging relationships and CLAHRC activities?
Who are the most powerful actors in the region and how do they interact with one another? And what are people’s views of those actors and how does that vary by actors’ social positions?
How does the CLAHRC director, and his/her senior management team, relate to other CLAHRC members?
How do the different actors interact with one another, in terms of their use of language and their body language? Are certain groups more vocal/dominant?
What is the focus of attention of different actors, and how does it vary by their social positions?
What is the culture and climate within the CLAHRC?
What important debates appear to be stifled, and why?
Social network analysis questionnaire
-
Please enter your first and last name (this will be made anonymous following data collection)
-
[……………….]
-
Please enter your professional/occupational role
-
[……………….]
-
The questions below relate to the people who have influenced your decision-making about the CLAHRC theme or project(s) which you help to manage or lead. Please think about the last 6 months of work on your theme/project(s) (or since you joined if shorter). We would like you to nominate all of the people who have influenced your decision-making about the theme/project(s) during this period. We define ‘influence’ as the capacity to shape ideas, select between different courses of action or in some way substantially affect decisions about one or more aspects of the theme/project(s). Influence may relate to any aspect of the theme/project including the objectives, questions, design, process, methodology, implementation or dissemination activities.
-
In the text boxes below, please enter the names of the people who have influenced your decision-making about the theme/project(s) during this period. When you have added all of the people you wish to add, scroll to the bottom of the page and go to the next question.
-
Please enter the professional/occupational role of the people you have identified. If they hold more than one role, please enter all that apply.
-
Again thinking about the last 6 months of your project(s) or theme (or your first 6 months in post), please indicate the extent to which the people you listed influenced your decisions on your theme/project(s) OBJECTIVES AND/OR RESEARCH QUESTIONS (1 = no influence at all, 5 = the highest level of influence).
-
Again thinking about the last 6 months of your project(s) or theme (or your first 6 months in post), please indicate the extent to which the people you listed influenced your decisions on your theme/project(s) PROCESS, DESIGN AND/OR METHODOLOGY (1 = no influence at all, 5 = the highest level of influence).
-
Again thinking about the last 6 months of your project(s) or theme (or your first 6 months in post), please indicate the extent to which the people you listed influenced your decisions on how your theme/project(s) RESEARCH OR IMPLEMENTATION ACTIVITIES SHOULD BE USED TO CHANGE PRACTICE (1 = no influence at all, 5 = the highest level of influence).
-
For each person you have identified, please indicate whether you had worked with that person prior to your involvement in the CLAHRC.
-
Again thinking about the last 6 months of your project(s) or theme (or your first 6 months in post), please identify UP TO FOUR people who have most strongly influenced your decisions about your project(s) OVERALL.
-
Involvement in CLAHRC has provided me with additional funding or other resources.
-
Involvement in CLAHRC has allowed me to acquire new knowledge or skills.
-
Involvement in CLAHRC has led to a loss of control/autonomy over the decisions I make about my project compared with other projects I have been involved with.
-
Involvement in CLAHRC has led to more efficient or more effective use of resources in the organisation(s) that I work for.
-
Involvement in CLAHRC has allowed me to build new relationships which improve the work I do.
-
Involvement in CLAHRC is very time consuming because the CLAHRC involves collaboration with a range of different stakeholders.
-
Involvement in CLAHRC has led to a heightened public profile for my organisation(s).
-
Involvement in CLAHRC has led to a heightened public profile for my own work.
Thank you for taking our survey. Your response is very important to us.
List of abbreviations
- AHSC
- academic health science centre
- AHSN
- academic health science network
- BRC
- biomedical research centre
- BRU
- biomedical research unit
- CEO
- chief executive officer
- CIHR
- Canadian Institute for Health Research
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- DH
- Department of Health
- DV
- dependent variable
- EBM
- evidence-based medicine
- GP
- general practitioner
- HEI
- higher education institution
- HIEC
- health innovation and education cluster
- HSDR
- Health Services and Delivery Research
- IE
- institutional entrepreneur
- IW
- institutional work
- KT
- knowledge translation
- KTA
- knowledge transfer associate
- NIHR
- National Institute for Health Research
- OLS
- order of least squares
- PARIHS
- Promoting Action on Research Implementation in Health Services
- PCT
- primary care trust
- PDM
- process, design and methodology
- PDSA
- plan, do, study, act
- PPI
- patient and public involvement
- RCT
- randomised control trial
- REF
- Research Excellence Framework
- RORQ
- research objective and/or research question
- SD
- standard deviation
- SDO
- Service Delivery and Organisation
- SHA
- strategic health authority
- SIC
- stages of implementation completion
- SNA
- social network analysis
- SSAP
- scientific and stakeholders’ advisory panel
- T2
- second translational gap