
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 12/5004/08. The contractual start date was in September 2012. The final report began editorial review in October 2013 and was accepted for publication in February 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Hinrichs et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
Policy context
In the UK, the government has made reducing the public deficit its greatest priority, with significant implications for public sector services including health care. 1 Following a decade of growth in National Health Service (NHS) funding, this has slowed substantially from 2011–12. 2 This is set against a need to make efficiency savings of £20B by 2014–15 while improving the quality and delivery of NHS care. 3 NHS organisations are therefore under considerable pressure to contain cost while at the same time meet the growing demand for health care and ensure the quality of treatment and care. 3
There are various options by which the efficiency of the health system and of organisations operating within it may be enhanced. One way of thinking about this is to differentiate between types of inefficiencies that occur at different levels in the health-care production process, considering operational, allocative and administrative processes. 4,5 Thus, operational inefficiencies occur because of duplication of services and inefficient processes, the use of expensive inputs or errors. Allocative inefficiencies result from misalignment of resources against best possible outcomes that could be achieved. Measures to strengthen allocative efficiency would involve rebalancing services across the health system, improving care co-ordination or strengthening preventative care. 5,6 Administrative inefficiencies occur as a consequence of administrative spending which exceeds that necessary to achieve the overall goals of the organisation or system,4 also referred to as ‘back office’ functions. 4,7 Improving administrative efficiency could be achieved through, for example, (de)centralising administrative functions, simplifying administrative procedures and introducing uniform standards.
Ongoing activity in the NHS is seeking to address these different types of inefficiencies in different ways, with the potential for savings in operational and administrative functions. In particular, procurement and back office are seen as important areas to achieve efficiency gains. 2 One area that has come under scrutiny is NHS trusts’ non-pay expenditure, which, on average, accounts for around 30% of their total expenditure. 8 In 2011–12, this expenditure was estimated at £20.6B, of which over one-quarter was spent on drugs and pharmacy and just over one-fifth on clinical supplies and services (Table 1). 9
| Expenditure category | NHS expenditure | Items | |
|---|---|---|---|
| Absolute (£B) | Proportion (%) | ||
| Drugs and pharmacy | 5.5 | 27 | Generic and branded drugs, medical gases and other pharmacy-delivered supplies |
| Clinical supplies and services | 4.5 | 22 | Medical devices and consumables, dressings, X-ray machines, laboratory and occupational therapy materials |
| Premises | 3.3 | 16 | Rates, electricity, gas, oil, furnishings and fittings |
| Contract and agency staff | 2.4 | 12 | |
| Non-clinical supplies and services | 1.3 | 6 | Cleaning materials, crockery, bed linen, laundry items, uniforms, patient clothing |
| Establishment | 1.0 | 5 | Administration expenses such as printing, stationery, advertising and telephones |
| Rentals under operating lease | 0.6 | 3 | |
| Transport | 0.5 | 2 | Vehicle insurance, fuel, materials and external contracts |
| Consultancy services | 0.3 | 1 | |
| Training | 0.3 | 1 | |
| Health care provided by non-NHS bodies | 0.2 | 1 | |
| Miscellaneous | 0.6 | 3 | |
| Total expenditure | £20.6B | ||
A 2011 review of NHS spending on medical and other consumables found wide variation in purchasing across acute trusts in England, with differences in processes and product ranges procured, alongside variation in prices paid for the same items. 10 The review highlighted the scope for efficiency savings in this area of spending. It estimated the potential of savings to be £500M, which equates to 10% of the annual spend on NHS consumables. Areas identified as offering potential for even greater savings include strengthening the strategic vision for purchasing and logistics.
Procurement in the NHS
Procurement of medical supplies and other consumables by NHS trusts in England can be realised in various ways. NHS trusts can, individually or in collaboration with others, directly contract with suppliers, draw on the national supplies organisation (NHS Supply Chain) or use one of the nine regional collaborative procurement hubs. 10 These hubs are regional purchasing organisations that were introduced during the 2000s in an attempt to achieve savings for partner trusts at regional level through aggregating their procurement efforts. 11 NHS Supply Chain was formed in 2006 from the NHS Logistics Authority and parts of the NHS Purchasing and Supply Agency, which had been established in 2000 as an executive agency of the Department of Health. 12 Operated by DHL Supply Chain Limited and managed by the NHS Business Services Authority on behalf of the Department of Health, it provides, at national level, procurement and logistics customer and supplier support. 12 Purchasing decisions are otherwise controlled by individual trusts via the local route of direct contracting between individual providers and suppliers.
More recently, the 2008 Procurement Capability Review of the Department of Health and the NHS,13 conducted by the Office of Government Commerce, identified weaknesses in approaches to procurement in the NHS, for instance lack of agreed strategy and operating model. In response, and as part of its wider strategy for the NHS, the Department of Health set out a new commercial operating model for the Department of Health and the NHS. 14 Among other things, this included the introduction of regional commercial support units (CSUs), which were intended to provide commercial support to both NHS commissioning and provider organisations, and were expected to work alongside NHS Supply Chain to ensure value for money for goods and services procured (Table 2). There was also an expectation for CSUs to merge with the corresponding regional collaborative procurement hub. The new model further involved the dissolution of the NHS Purchasing and Supply Agency, and its responsibility for procurement policy and pharmaceuticals procurement was transferred to the Department of Health. 17 At the same time, and in response to Innovation Nation (2008),18 which committed each government department to include an innovation procurement plan as part of its commercial operating model, the Department of Health published the National Innovation Procurement Plan (2009). 15 It highlighted the importance of innovation procurement in safeguarding quality, productivity and sustainability in the NHS. The plan sought to provide a coherent framework for innovation procurement by organising the adoption of technology-led innovation at the regional level, supported by an innovation fund to promote faster innovation and more universal diffusion of best practice. These overall developments took place against a wider reform programme of the NHS that sought to enhance patient choice and competition between providers while emphasising the need to secure quality, innovation and productivity. 19
| Year | Policy document | Aims and core elements |
|---|---|---|
| 2009 | Necessity – Not Nicety: A New Commercial Operating Model for the NHS and Department of Health 14 | To create ‘a new commercial operating model which will address past deficiencies and which is fit to meet the opportunities and challenges of the future’a Core elements include:
|
| 2009 | National Innovation Procurement Plan 15 | To ‘bring clarity and coherence’a to innovation procurement in the NHS Core elements include:
|
| 2011 | Innovation Health and Wealth: Accelerating Adoption and Diffusion in the NHS 16 | To ‘support the adoption and diffusion of innovation across the NHS’ through setting a ‘delivery agenda that will significantly ramp up the pace of change and innovation’b Improving arrangements for procurement in the NHS identified as one of the eight themes described as core to the delivery agenda to support the NHS in achieving systematic transformation. Core activities identified under the procurement theme include:
|
| 2013 | Better Procurement, Better Value, Better Care: A Procurement Development Programme for the NHS 9 | To ‘support the modernisation of procurement across the health system and help trusts deliver the efficiencies they need’c The programme comprises four integrative elements:
|
Recognition of the importance of procurement as a means to drive up quality and value, and to stimulate innovation in the NHS more widely, was further emphasised in the 2011 Innovation Health and Wealth: Accelerating Adoption and Diffusion in the NHS report,16 which also noted how procurement would provide an important lever for economic growth. It announced the publication of a procurement strategy by the Department of Health in 2012, which would include a range of measures to help reduce waste and achieve efficiency gains in procurement as identified by the National Audit Office (2011), as described earlier. 10 This strategy was eventually published in August 2013, although referred to as a ‘procurement development programme’ rather than a strategy as such. 9 Highlighting how non-pay expenditure in NHS trusts had continued to increase over time, and at a rate higher than NHS activity and inflation during 2011–12, it set out a programme of work that seeks to stabilise non-pay spending for the period until the end of 2015–16. It proposed four core initiatives that aim to (i) deliver immediate efficiency and productivity gains; (ii) improve data, information and transparency; (iii) revisit the nature of clinical engagement in procurement; and (iv) create a national ‘enabling function’ to support leadership and build procurement capability throughout the system (see Table 2). We will return to the 2013 procurement development programme in subsequent sections of this report as it provides important context for the findings presented here.
Informing NHS learning for procurement
In its 2012 review of progress made in the NHS towards achieving efficiency savings, the National Audit Office highlighted the need for robust evidence to help the NHS make informed decisions about how to make such savings. 2 It pointed to the potential for lessons to be learned from activities and initiatives implemented elsewhere to enable the adoption of good practice.
In the field of NHS procurement, and supply chain management (SCM) more generally, there is potential to learn from other sectors, public and private, and from experiences in other countries, and to identify potential for cost containment and efficiency gains. A growing body of work has studied the applicability of SCM concepts developed in the private sector to public services to inform better use of public funds. 20 Much of the existing literature which draws on good practice in the private sector focuses on manufacturing, with the automotive sector one of the most studied industries. For example, Toyota’s ‘just in time’ supply management model, which aimed at improving return on investment and limiting inventory costs, has been explored in some depth for its transferability to other sectors. 21 The Toyota model relies on developing close links with a small number of suppliers, level production scheduling and continuous quality improvement,22 and this has also informed discourse and practice in health-care settings. 23–25
The public sector may also offer opportunities for learning. For instance, following a review of UK Ministry of Defence routine procurement items in 2007,26 the ministry introduced a number of measures intended to streamline processes and improve the cost-effectiveness of routine procurement by introducing measures such as e-procurement and reverse auctions, and changing some of the low-cost supply routes for routine items. 27 There is also potential for learning from experiences of procurement in health systems other than the English NHS. Countries that may provide useful insights into procurement and SCM in the health-care sector are Italy28 and New Zealand,29 owing to their recent reforms to strengthen efficiency in health-care procurement.
Although available evidence provides potential for models developed in other sectors to be adapted in health-care settings, there is a need to bring together the diverse literature on such approaches that may be relevant to the NHS context. Work that is available has highlighted that the NHS has a substantial potential to influence the supply chain in some of the products it purchases. 30 The 2011 review by the National Audit Office of NHS procurement of consumables argued that more efficient procurement has the potential to save costs without reducing the quality of patient care. 10 At the same time, lessons learned will have to be placed in the wider context of the quality improvement agenda31 and the need to create value in health care. 32 There is therefore a need to better understand the potential of new approaches used in other sectors to inform decision-making in the NHS, and the risks and benefits associated with these.
The work presented in this report seeks to contribute to this process by advancing our understanding of the evidence on procurement and SCM in sectors other than health care that can inform practice in the NHS. Principally drawing on a rapid evidence assessment (REA), we sought to
-
describe approaches to procurement and SCM in selected areas (including, but not limited to, manufacturing and automotive sectors, defence, information and communication technology and pharmaceutical industries)
-
identify best practices that may inform procurement and SCM in the NHS.
Defining procurement
The terminology around procurement in the health sector has proliferated in recent years, with concepts such as procurement, purchasing, commissioning or contracting frequently used interchangeably. 33 However, interpretation of these terms is likely to differ across disciplines and professions,34 and it will therefore be important to apply consistent terminology throughout this report.
At the outset, a core distinction can be made between purchasing for health care and purchasing of health-care services. 35 Purchasing for health care refers to the purchase of any physical items, and their maintenance, by health-care organisations in order to support the delivery of services. Purchasing of health-care services describes the actual process of purchasing the service itself. In the context of the English NHS, this is also referred to as NHS commissioning, although it is important to note that the term ‘commissioning’ is understood as a broader concept than purchasing. Box 1 provides an overview of definitions of a range of terms used in the context of procurement and SCM. It illustrates that boundaries of concepts are frequently not clear-cut and we will use the terms ‘procurement’ and ‘purchasing’ as equivalent while noting their conceptual differences.
Commissioning: oriented towards maximising population health and equity by purchasing health services and influencing other organisations to create conditions which enhance population health. 36 Involves a strategic approach that includes monitoring and evaluating outcomes. 33
Contracting: negotiated agreement about services that a provider will provide in return for payment; includes service specification, tendering, monitoring and reviewing contract performance. 36
Procurement: the process of managing all activities associated with the purchase of goods and services required to operate an organisation. The term ‘procurement’ is more often used within the public procurement context, whereas private organisations may refer to purchasing and/or sourcing.
Purchasing: the process of buying or funding goods and services in response to demand or usage. 33 Purchasing is often linked to resource allocation and thus regarded as a mechanism by which those who hold financial resources allocate them to those who produce health services. 37
SCM: the management of the interconnection of organisations that relate to each other through upstream and downstream linkages between the processes that produce value to the ultimate consumer in the form of products and services. 38
Effects of the changing NHS context on the study
The REA presented in this report was commissioned to commence in December 2012. Since then, the NHS has undergone a series of changes which had direct and indirect impacts on the work undertaken here. First, when submitting the research protocol for this study we had secured commitment from advisors from two hospital trusts, who had agreed to participate in the research as key informants, and to act as multipliers by enabling contacting of other staff members within their trusts for interview. Both trusts were affected by the changing NHS context; one had to withdraw its commitments because of unforeseen difficulties in securing staff time for research within current resource and financial constraints, and the second experienced changes in staff working in procurement. Given that the procurement function in hospital settings tends to work with small teams, any reduction in team size will inevitably affect availability of staff previously engaged in procurement to participate in the research. Against this background, we amended the original research protocol by extending the range of key informants to be interviewed, to include a wider range of stakeholders with expertise and/or experience in NHS procurement from other NHS trusts and related organisations.
Second, and as indicated earlier, in August 2013 the Department of Health released the new procurement development programme. 9 This has not had an impact on our approach to the REA presented in this report, although we set the discussion of findings in the light of the recommendations by the procurement development programme, in the context of insights drawn from the literature. We have, however, amended our approach to include international experiences. The original research protocol for this component of the project foresaw an assessment of general approaches to procurement and SCM strategies in a small number of health systems. However, given that the new procurement development programme for the NHS has now been released and will be implemented in due course, we believed it to be of more use to the NHS to report in detail on specific countries’ experiences that may provide useful insights into the further advancement of the procurement development programme, rather than providing general overviews of different systems as such. Following a preliminary review of the evidence, we narrowed the international component to an in-depth review of approaches in France and New Zealand. We describe the reasoning for our choices in Chapter 2, Assessing the experience of procurement and supply chain management in the health sector in selected high-income countries. It is important to note, however, that we have considered experiences in other countries by means of the REA also, and report on these throughout the evidence review.
Structure of the report
This introductory chapter has briefly set out the aims of the research and the policy context within which it was commissioned. Chapter 2 describes the methods used. Chapter 3 presents the core findings of the work, structured according to the major themes identified in the academic and grey literature, and with reference to interview findings to highlight the NHS context. Chapter 4 specifically reports on the international approaches studied. We close with Chapter 5, which discusses our overall findings, seeking to relate them to the wider health-care context, and offers recommendations for further research.
Chapter 2 Methods
The principal approach used in this study was a REA of the academic and grey literature. We complemented the assessment of evidence with interviews with a small set of stakeholders involved in procurement in the NHS, representing both the NHS and the private sector, to help place the findings of the evidence review in the NHS context. We also undertook an in-depth assessment of approaches to procurement in the health-care sector in two countries other than England to understand the potential for learning for the NHS.
Rapid evidence assessment
A REA is a comprehensive, systematic and critical assessment of the scope and quality of available evidence which follows the general principles of conducting literature reviews in health care. 39 The choice of REA was informed by the requirements for this project as set out in the commissioning brief40 and was based on the need to provide the best possible value for money within a relatively limited time frame. In contrast to formal systematic reviews, REAs tend to place more explicit limits on the scope of the review, whether by number and type of databases or other sources searched, types of research included or the language and time period in which the research was conducted. However, the REA follows the same principles as a systematic review: defining the research question; developing the review protocol, including defining inclusion and exclusion criteria, search terms and sources to be searched; undertaking the review, that is, study selection, data extraction, quality assessment and data synthesis; and reporting.
Search strategy
The literature on procurement and SCM stretches beyond peer-reviewed journals to trade publications and government reports. Given the highly theoretical nature of most of the academic publications, we included examples from smaller studies or empirical data from case studies in practice, regardless of whether this was academic or grey literature.
Our pilot testing of the search terms underwent several iterations, and the search was conducted in three stages, focusing on (1) SCM and procurement, (2) procurement in health care and (3) targeted searches of procurement and SCM in the defence and pharmaceutical industries. Here we summarise our principal approach; further details are described in Appendix 1.
-
General SCM and procurement As a first step, we undertook a systematic search for studies that described any initiatives and mechanisms in procurement and SCM across any sector. We searched MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, Academic Search Complete, Social Sciences Abstracts, Military and Government Collection, EconLit and Business Source Complete from January 2006 to November 2013.
-
Procurement in health care In a second step, we conducted a further targeted search of studies of procurement in health care, using MEDLINE only. We used medical subject headings, with the search extending from 2007 to 2013.
-
Procurement and SCM in the defence and pharmaceutical industries We conducted targeted searches of studies of procurement and SCM in the defence industry, using Google Scholar, for the period 2008–13, and procurement and SCM in the pharmaceutical industries, using Google Scholar, Web of Science and Business Source Complete, for the period 2006–13.
The first search was the most extensive with respect to databases and date range as this was the main source for evidence, whereas the two additional searches were more targeted towards the nature of studies in each particular field.
Inclusion and exclusion criteria
Table 3 summarises the inclusion and exclusion criteria which we applied when selecting studies for review.
| Type of study | Inclusion: we considered reviews and primary studies that presented empirical evidence, for example testing a hypothesis or demonstrating practice, as well as case studies of specific experiences in the sector under review Exclusion: we excluded studies that presented conceptual or theoretical work only and did not provide lessons for practice. We further excluded news articles and opinions |
| Outcomes | Inclusion: the outcomes of interest were cost savings, efficiency (e.g. time saving or general business performance) or effectiveness (improved delivery of the organisation’s aim, quality improvement). Outcomes could be reported qualitatively or quantitatively Exclusion: empirical studies that did not report outcomes were excluded |
| Time period | Searches were undertaken from 2006 onwards (in the main search), coinciding with the introduction of technologies such as RFID, which had a significant impact on approaches to SCM |
| Transferability | Inclusion: we only considered studies conducted in high-income countries. Eligible studies had to report on aspects of procurement or SCM that were potentially transferable to the NHS Exclusion: studies reporting on experiences in low- and middle-income countries were excluded unless they were incorporated as part of a multicountry comparative study |
| Type of article | We considered studies published in academic journals as well as trade and professional journals and the grey literature, as long as these provided examples of procurement and SCM applied in industries in different sectors, including health care |
Study selection
To ensure consistency in study selection, three reviewers screened the same 200 articles, each using the inclusion and exclusion criteria described in Table 3. Disagreements and discrepancies were resolved by discussion or involvement of a fourth reviewer where necessary. The full list of records (n = 13,191) was then divided between three reviewers for further screening according to the inclusion and exclusion criteria.
Data extraction
Data from studies identified as eligible for inclusion in the review were extracted into a spreadsheet template. We extracted information on context, study design and objective(s), methodological approach, reported outcomes and identified limitations. Data extraction was undertaken by three researchers. Consistency of data extraction across reviewers was checked through duplicate extraction of a random sample of studies (n = 100) by two reviewers independently. Disagreements and discrepancies were resolved by discussion or involvement of a third reviewer where necessary. Given the wide range of types of studies, to aid with the extraction and reporting of the review we have utilised the Context, Interventions, Mechanisms, Outcomes (CIMO) extraction approach, a framework used in management and organisational settings. 41 Details of all studies selected for review are included in Appendix 2.
Quality assessment of studies
Given the heterogeneity of study designs considered in this review, we did not apply a formal quality rating system, such as the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) system for evaluating the quality of evidence for reported outcomes, and typically used for health-care randomised trials. Initial scanning of identified records revealed that many studies were theoretical in nature and did not present empirical data, or that recommendations were not tested in practice. Thus, as a pragmatic approach we applied the following criteria to assess the quality of the studies:
-
The research question or aim of the study is clearly stated.
-
The approach/mechanism/intervention is clearly defined.
-
The study design is rigorous and clearly reported.
-
The results are clearly reported.
Study analysis
Data were analysed drawing on the principles of narrative synthesis, which has been recommended as the most appropriate approach for analysing diverse evidence. 42 Building on tabular presentation of findings as described above (see Data extraction), we first grouped data according to emerging themes and particular areas of learning, including, but not limited to, the following:
-
types of ‘end product’: service, product or product–service system
-
types of improvement gained: efficiency, effectiveness, other forms of optimisation and streamlining
-
types of cost savings: transaction costs, items costs, other optimisation costs
-
types of opportunities for innovation: e-procurement, collaborative agreements
-
types of outcomes achieved: purchaser experience, wider economic impacts.
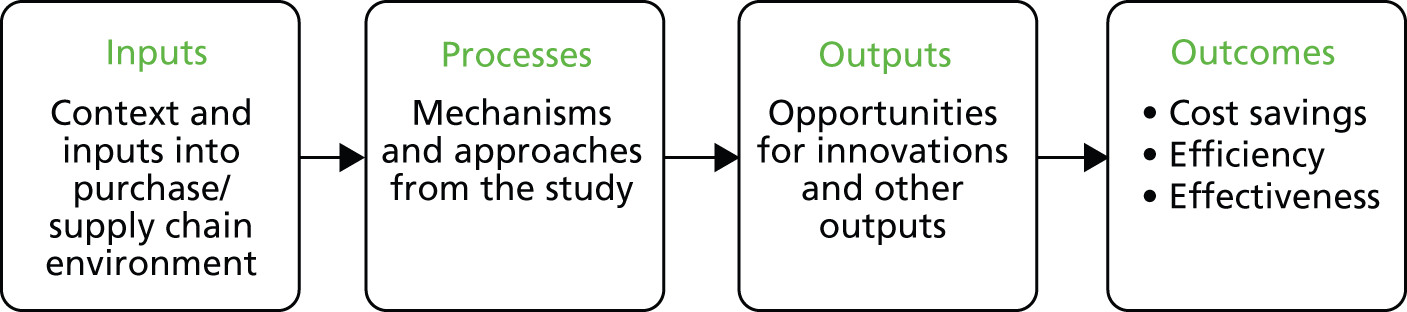
In a further step, we organised our learning from the literature into a logic model format as a means to group the emerging themes and areas of learning into a hypothetical NHS context (Figure 1). In line with the established approach to logic modelling, we distinguished inputs into an organisation (i.e. the context and environment in which purchases are made), the processes or mechanisms used for purchasing, and purchasing outputs and outcomes emerging. In line with our inclusion criteria, we sought to identify outcomes that were (or could potentially be) associated with cost savings, efficiencies and general effectiveness in achieving a given organisation’s aims. We return to a further development of this model, containing the emerging themes from the study, in the discussion (see Chapter 5, Although the evidence remains limited, it is possible to draw some general lessons).
FIGURE 1.
Framework for analysis of studies.
Key informant interviews
Purchasing practices depend on a range of industry and contextual factors which are not easily identifiable or documented in the published literature. Interviews with a small number of key informants, working with or within the health-care sector, helped to ground and validate the themes identified through the literature. They also furthered our understanding of the more practical issues facing NHS procurement in the current climate. This component of the research was designed to be exploratory only, to help place the findings of the evidence review in the NHS context and so inform how our findings might best be used to meet the needs of the NHS.
As indicated in Chapter 1, Effects of the changing NHS context on the study, the original protocol for this research foresaw the commitment of advisors from two hospital trusts who had agreed to participate in the research as key informants and to act as multipliers to identify further staff members for interview. However, the changing NHS context since commencement of the study in December 2012 has meant that one trust had to withdraw, while the second was affected by changes in staff working in procurement, so reducing the number of potential participants in the research. In consultation with the National Institute for Health Research (NIHR), we amended the original research protocol by extending the range of key informants for interview to consider a wider group of stakeholders with expertise or experience of NHS procurement, including participants from the private sector.
As a consequence of these changes to the protocol, interview participants were identified from different sources. First, we approached the trust still involved in the study in an advisory function for potential interview participants. Second, we used a combination of purposive and ‘snowball’ strategies using official websites, expert advisors’ contacts and the authors’ professional networks. These two approaches identified 21 potential interviewees, who were invited to participate by e-mail explaining the background of the study. Of those invited, five agreed to be interviewed. Table 4 provides an overview of the roles of study participants.
| Label | Sector | Role |
|---|---|---|
| Interviewee 1 | Private sector | Senior manager; provider of data management services to NHS suppliers |
| Interviewee 2 | Private sector | Senior manager; provider of procurement and business services to the NHS |
| Interviewee 3 | Private sector | Senior manager; provider of data management and joint purchasing services to the NHS |
| Interviewee 4 | Private sector | Consultant provider of procurement and improvement services to the NHS |
| Interviewee 5 | NHS | Responsible for strategic procurement in a general acute teaching hospital (foundation trust) |
| Interviewee 6 | NHS | Head of medical device procurement committee in a general acute teaching hospital (foundation trust) |
Depending on the location of the study site under consideration, interviews were undertaken face to face or by telephone, using a semistructured interview guide which was shared with the interviewee beforehand upon request. Interviews explored broad themes around issues facing procurement in the NHS today. They included questions about drivers behind buying practices, problems with NHS buying, best practices in procurement for the NHS, and challenges to and enablers of implementing best buying practice in the NHS (the full interview protocol is presented in Appendix 3).
Interviews were carried out between June and August 2013. All but one interview were undertaken by two researchers. Interviews lasted an average of 45 minutes; they were audio recorded following consent and key notes were transcribed. Transcripts were manually coded, with analyses informed by key themes guiding the interviews with respect to the interview protocol, while also seeking to identify additional emerging themes.
As indicated above, the purpose of key informant interviews in this study was exploratory only, complementing the evidence review as the main component of the study. Given the small number of interviews, data are presented only as a means to further illustrate findings from the evidence review, rather than as confirmatory evidence in their own right.
Assessing the experience of procurement and supply chain management in the health sector in selected high-income countries
The international component of this study initially sought to systematically explore the experiences in a set of countries of procurement and supply chain strategies within their health systems. However, as noted in Chapter 1, in August 2013 the Department of Health released the new procurement development programme. 9 Against this background, and given that the programme will be implemented in due course, we have amended our approach to examining countries’ experiences by focusing on specific examples that may provide useful insights into the further advancement of the procurement development programme, rather than providing general overviews of different systems as such.
Based on a preliminary review of the evidence, we considered five countries for in-depth review: France, Germany, Italy, New Zealand and the USA. Following further assessment of publicly available documentation, we have narrowed the international component to an in-depth review of approaches in France and New Zealand. These were chosen because both countries recently introduced system-level changes in the approach to procurement in the health-care sector through nationally mandated programmes, but they did so through different means. Thus, New Zealand established a national agency mandated with facilitating and leading national initiatives and managing the implementation of common administrative functions of regional health agencies [district health boards (DHBs)], while in France, a national programme seeking to advance hospital performance through sustainable procurement made systematic use of existing collaborative purchasing groups [group purchasing organisations (GPOs)] to help building and disseminating efforts at regional and local levels.
Data collection involved first a review of the published and grey literature as identified from bibliographic databases (PubMed, EBSCOhost), the World Wide Web using common search engines (Google Scholar) and relevant governmental and non-governmental agencies and organisations in the two countries under review, generally following a snowballing approach. Based on information and data extracted from publicly available documents, we drafted a report on each country. Each followed a similar structure, including (i) a summary overview of key features of the health system, (ii) a description of the policy or reform leading to system changes in procurement, (iii) an overview of the key agencies involved in delivering the changes and (iv) an assessment of achievements.
Second, the draft report was informed by one expert in each country. Experts were identified from the professional networks of the authors of this report. They were asked to review the report on their country for comment and verification of the information presented. Experts were also invited to participate in a telephone interview to further explore the nature of the system-level changes in procurement and provide additional information where appropriate, in particular on areas that are not well documented or require in-depth understanding of the country context. Interviews followed a topic guide, exploring perceived challenges around procurement in the health-care sector; the general approach to procurement and policy framework; the role of stakeholders; the role of procurement in the wider system; and the perceived effectiveness and achievements of changes in the procurement function. Interviews lasted an average of 60 minutes; they were recorded upon verbal consent by the interviewee and notes were taken. Interviews were not formally analysed as their purpose was to provide additional information only.
Ethics review
The research protocol was reviewed by the National Research Ethics Service, Research Ethics Committee East of England – Cambridge Central. It confirmed that this study would not require ethics review. However, RAND Europe is committed to following good ethical principles and practice in all research studies. In light of this, key informants were approached in their professional roles only and no sensitive personal information was collected. All references to interviewees were anonymised throughout the report. Information about the project was shared in advance and participants were given the opportunity to ask questions before consenting to take part. Verbal consent was obtained before the interview and interviewees could withdraw from the study at any point.
Patient and public involvement
Patient and public involvement (PPI) did not form a significant component of our study. However, we consulted with members of the public from INsPIRE (patIeNt & Public Involvement in REsearch), a PPI in health and social care research group for Bedfordshire and Cambridgeshire43 on the research protocol and the conceptual framework. Four individuals shared comments, especially regarding the importance of this study, the value of the international component of the study and the need to find genuine efficiency savings, if possible. We considered these in the data extraction and analysis phase. One panel member suggested that SCM professionals should be interviewed, in view of their knowledge of good practices; these individuals were included in our interviewee selection.
Chapter 3 Findings: evidence assessment
This chapter presents the findings from the REA according to the themes that emerged from the data extraction and analysis. Within this section we also report on observations from interviews with reference to the current context of working within and with the NHS.
Description of studies
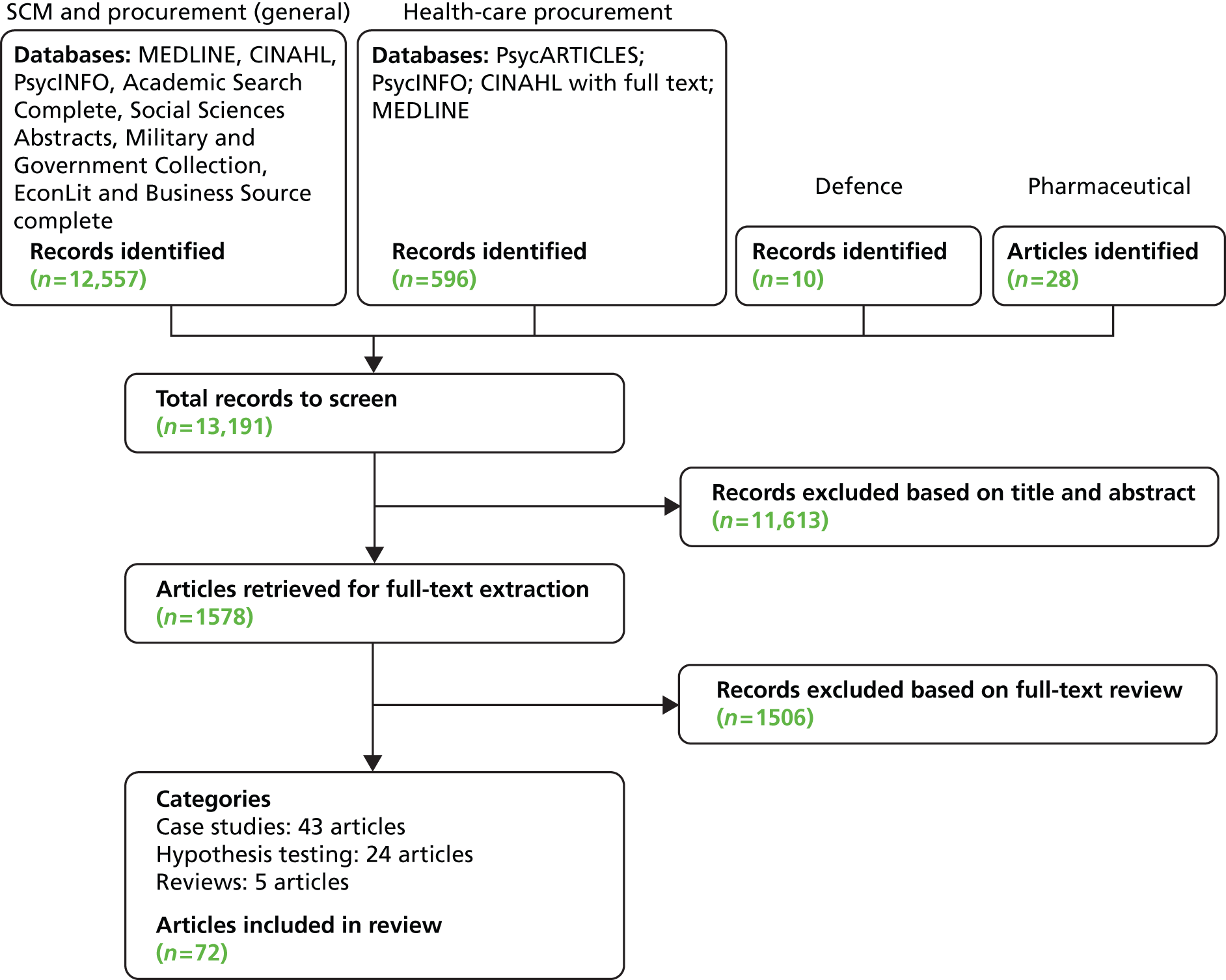
Our search identified a total of 13,191 records across the databases searched, following removal of duplicates; after initial screening of titles and abstracts, we considered 1578 references for full-text review. Of these, 72 studies were identified as eligible for inclusion in the review (Figure 2). 44–115
FIGURE 2.
Process of selection of articles for review.
It was challenging to judge the quality of studies and documents considered as eligible as these often lacked descriptions of methods and strategy of analysis. Our main aim was to capture examples of approaches in practice and, where available, evaluations of such approaches, or studies which contained at least some form of empirical evidence. Frequently, studies did not specify the precise details of the nature of the practice and reported outcomes could not be attributed to single interventions or practices. The studies included in the review were of three types:
-
Studies testing a hypothesis about practice (n = 24),47,50,51,58,63–66,68,71,74,76,77,79–82,84,85,91,93,95,102,104 validated empirically through surveys or interviews, or exploring concepts through interviews, surveys or observation; in the following we refer to these as ‘hypothesis testing’.
-
Studies describing current practice, typically in the form of case studies (n = 43). 45,46,48,49,52–57,59,60,67,69,70,72,73,78,83,86–90,92,94,96–101,103,105,106,108–115 Primary studies were set mostly in the USA (n = 20),48,52–54,57,70,87,88,90,94,96,97,99–101,105,106,108,110,113 Canada (n = 2),72,115 Australia (n = 1),92 Europe (n = 8)45,46,67,69,89,103,109,112 and the UK (n = 3);49,73,78 a few were set in multiple countries (n = 6),55,56,59,83,111,114 or their country information was not reported (n = 3)60,86,98 or unavailable. In the following we refer to these as ‘case studies’.
An overview of the studies included is shown in Table 5. Identified studies covered a range of sectors and industries, including textiles, information technology (IT),99 the automotive industry45,46,68 and manufacturing. 57,63,65,71,76,77,79,80,86,102,104,113 We further identified 21 studies addressing the health-care sector specifically. 48,49,52,54,58,62,70,72,87,88,90,94,96,97,103,105,106,108–110,115
| Theme | Case study (n) | Hypothesis testing (n) | Review (n) |
|---|---|---|---|
| Organisation and strategy | 13 | 9 | 3 |
| Collaboration and relationships | 9 | 10 | 1 |
| Materials and information management | 21 | 5 | 1 |
Analysis of studies identified three overarching themes: organisational and strategic issues; collaboration and relationships (within an organisation and with suppliers); and materials management and information flows within an organisation. Table 5 summarises the included studies according to theme, although it is important to note that studies might address more than one theme. Further detail of individual studies is presented in Appendix 2.
The following sections are organised according to the three main themes we have identified. Each section begins with a summary table of studies reporting on the theme, describing selected characteristics; further details of studies are documented in Appendix 2. We then report on a subset of studies in some more detail, to illustrate the type of evidence under each identified theme. We complement the evidence assessment presented with findings from interviews with key informants working in or with the NHS in England, where appropriate.
Organisation and strategy
A common theme identified across studies reviewed here concerned strategic and organisational issues in relation to SCM, although only a small number of studies (n = 13)45,46,48,49,52–57,59,60,67 provided examples of how this was achieved in practice. The remainder of the studies reviewed comprised those testing hypotheses (n = 9)47,50,51,58,63–66,68 and literature reviews (n = 3). 44,61,62 The studies are summarised in Table 6. Under the overarching theme, we identified further subthemes; these were green and environmental issues, group and collaborative purchasing, and supply chain integration, alignment and general quality improvement. We discuss each of these in turn.
| Reference | Country | Industry | Study type | Study aim and principal methods | Outcomes/learning |
|---|---|---|---|---|---|
| AlSagheer and Ahli (2011)44 | Multiple | Multiple | Review | To assess and analyse the impact of supply chain integration on business performance and associated challenges, using review of literature | Supply chain integration had a ‘mostly’ positive impact on business and enhances profitability, financial stability, customers’ satisfaction and accomplishing business goals |
| Azevedo et al. (2011)45 | Portugal | Automotive | Case study | To study the relationship between green practices and the supply chain performance, using interviews and secondary data | Environmental cost, quality and efficiency were the performance measures with most significant relationships with green practices (e.g. environmental packaging implies utilisation of reusable packages), but differences in opinion on other aspects |
| Azevedo et al. (2012)46 | Portugal | Automotive | Case study | To use a theoretical framework applied to a case study to determine the relationship between green and lean practices and the economic, social and environmental performance of businesses, using interviews and secondary data | Operational costs decrease with one green practice, i.e. reusable packaging, and decrease with a selection of lean practices (such as ‘just-in-sequence’, deliveries direct to point of use, geographical concentration, using electronic data interchange to share information, single sourcing) |
| Baier et al. (2008)47 | Multiple | Multiple | Hypothesis test | To look at the effect of strategic alignment and purchasing efficacy on financial performance, using survey and interviews | Results supported hypotheses which suggested that the relative fit between business strategy and purchasing strategy (labelled as strategic alignment) and between purchasing strategy and purchasing practices (referred to as purchasing efficacy) was key to achieving financial performance |
| Birk (2009)48 | USA | Health care | Case study | To report on effects of implementing a purchasing coalition | One hospital group, as members of the purchasing coalition, saved $1,105,309 on medical supplies in the year prior and $11M in capital acquisitions was saved across members. Cost saving estimated 10–25% for group buys depending on the product |
| Boniface (2012)49 | UK | Health care | Case study | To see the benefits delivered by effective purchasing, related to sustainability (e.g. switching to thinner gloves to deliver smaller carbon footprint) | Cost saving of 30% reported on gloves, due to price environmental incentives set by industry |
| Bose and Pal (2012)50 | Multiple | Multiple | Hypothesis test | To examine the effect of green SCM initiatives on stock prices of firms | Greatest impact was on manufacturing firms, and firms with high R&D to asset ratio |
| Brau et al. (2007)51 | Not reported | Multiple | Hypothesis test | To explore SCM initiative impact on the performance of small firms, using surveys | Higher integration strategy, internal integration support, external integration support, supply chain alignment, supplier integration and customer integration all positively (and significantly) associated with asset utilisation, revenue generation and competitive performance |
| Carpenter (2008)52 | USA | Health care | Case study | To report on the implementation and benefits of quality management initiatives, using surveys | 55% of respondents with quality initiatives said that the initiative reduced waste or cost, 49% said that it improved patient satisfaction, 45% that it increased communication, 44% that it reduced hospital-associated infections and 43% that it improved staff satisfaction |
| Carroll and Coker (2007)53 | USA | Military | Case study | To provide an overview of the impact of the army’s LMP | LMP benefited by streamlining processes (decreasing project time) and accessibility worldwide |
| Case (2011)54 | USA | Health care | Case study | To investigate reasons for SCM-attributable success in a health-care setting. Intervention comprised switching to a low-unit-of-measure distribution and a switch to the combined medical–surgery and pharmacy departments | Combined departments avoided the need for multiple supply chain agreements and adopted a single 7-year master agreement including medical–surgical supply, pharmacy distribution and pharmacy data analytics. Leaders estimated savings potential in tens of millions of dollars. Low-unit-of-measure distribution logistics service reduces high cost of storing, maintaining and distributing by delivering low-unit-of measure orders straight to hospital departments |
| Childerhouse and Towill (2011)55 | Multiple | Multiple | Case study | To test whether or not enhanced performance of supply chains can be attributed to the five arcs of integration – inward facing (lower quartile for suppliers and customers), periphery facing (middle range for both supplier and customer integration), supplier facing (upper quartile for suppliers, below for customers), customer facing (upper quartile for customers, below upper quartile for suppliers) and outward facing (upper quartile for suppliers and customers) – using interviews, attitudinal survey and document analysis | More integrated supply chains (i.e. more outward facing) were more productive for four out of seven productivity indicators (most relevant: customer delivery frequency; outward-facing value streams deliver average of 687 times/year compared with 77 for periphery-facing arc). Non-productivity indicators: no positive difference found between product variety and arc of integration, outward-facing arc had highest level of streamlined information flow (but it is only significant at 90% level) |
| Constantine et al. (2009)56 | Multiple (Europe and North America) | Multiple | Case study | To assess the link between supply chain performance and underlying practices driving it, using interviews | Organisations displaying strength across six broad practices (link supply chain to company strategy, segment supply chain to master most important product/service complexity, tailor the supply network to optimise service/cost/risk goals, use lean tools end to end, create integrated/robust sales and operations planning, find top talent/hold people accountable) outperformed competitors in service, inventory and logistics costs. Top companies achieved the discipline required to excel in these areas partly by improving the skills of their employees. Investments in formal IT systems did not appear to improve supply chain performance as much as some managers expected |
| Elmuti et al. (2008)57 | USA | Manufacturing | Case study | To examine the impact of a SCM system on organisational performance (ROI, productivity, expenses), using surveys and interviews | Organisational performance measures increased (between 52% and 81%) |
| Elmuti et al. (2013)58 | USA | Health care | Hypothesis test | To examine the effect of various SCM interventions (e.g. inventory control, centralising supply chain data, strategic alliances), using surveys, interviews and secondary data | Positive relationship between SCM activities and organisational performance/effectiveness, and positive correlation between outsourcing decisions and performance/effectiveness |
| Font et al. (2008)59 | UK and Europe | Tourism | Case study | Various sustainability initiatives implemented (e.g. the development of standards and assessments, environmental auditing and management, renewable energy use), using document analysis and interviews | Increased revenues and reduced costs; increased staff morale, improved relationship with suppliers and client retention |
| Fugate et al. (2006)60 | N/R | Multiple | Case study | To explore how co-ordination mechanisms in different disciplines are effective, using interviews | Price co-ordination mechanisms (i.e. discounts for the buyer) had a negative impact on firms’ and trading partners’ performance. Non-price co-ordination (e.g. allocation rules) turned out to be contrary to the literature as the interviewees saw it as detrimental to performance |
| Golicic and Smith (2013)61 | N/R | Multiple | Review | Meta-analysis to understand variables, measures, contexts or other factors that might be influencing impacts of environmental practices specific to the supply chain and their performance | The mean effect (0.294) was significant; overall environmental supply chain practices were associated with positive firm performance |
| Guimarães and de Carvalho (2011)62 | Germany, UK, Australia/New Zealand, USA, Greece | Health care | Review | To compare outsourcing activities, drivers, benefits and risks of outsourcing, using literature review | Five countries studied showed different benefits and attitudes towards outsourcing; all reported positive outcomes such as best access to technology and increased efficiency, but highlighted contextual risks such as adaptability time and some dissatisfaction with outsourced suppliers |
| Kroes and Ghosh (2010)63 | USA | Manufacturing | Hypothesis test | To evaluate the degree of congruence between a firm’s outsourcing drivers and its competitive priorities, assess the impact of this congruence on supply chain performance and investigate the relationships between the supply chain and the business performance, using surveys | Outsourcing congruence was associated with higher levels of supply chain performance, i.e. aligning outsourcing with firm strategy |
| Meehan and Muir (2008)64 | UK | Multiple | Hypothesis test | To assess SMEs’ attitudes towards benefits and barriers of SCM (defined as the degree of internal co-operation and external integration, implying end-to-end co-ordination, representing a strategic shift in a firm’s culture rather than just a business practice), using surveys | Most important benefits of SCM were a reduction in duplication of interorganisational processes, reduction in product development cycle time processes, reduction in risk, improvement in supply chain communications and improvement in customer service responsiveness |
| Merschmann and Thonemann (2011)65 | Germany | Manufacturing | Hypothesis test | To analyse the relationship between environmental uncertainty, supply chain flexibility and firm performance, using surveys and interviews | Companies that matched supply chain flexibility and environmental uncertainty performed better than those that did not (i.e. those with high environmental uncertainty should have high supply chain flexibility) |
| Paulraj and Chen (2007)66 | USA | Multiple | Hypothesis test | To illustrate that the implementation of strategic supply management initiatives can ultimately lead to a sustained competitive advantage for buyer firms and their suppliers, using surveys | There was a significant association between strategic supply management and supplier performance, and buyer performance, and a significant association between supplier performance and buyer performance |
| Rudberg and Thulin (2009)67 | Sweden | Farming | Case study | To show the implementation of advanced planning system for logistics, using case study descriptive methods | Total costs reduced by 13% annually |
| Zhu et al. (2008)68 | Multiple (UK and China) | Automotive industry | Hypothesis test | To compare pressures, practice and performance of environmental SCM (UK and China), using surveys | Performance improvement based on environmental SCM practices was only weakly supported (in the UK mainly due to fines and financial incentives for adopting environmental practices) |
‘Green’ supply chain
Our review identified seven studies45,46,49,50,59,61,68 which specifically reported on initiatives to create a more environmentally sustainable, or ‘green’ supply chain as referred to in this section (other studies also alluded to this theme but are not referenced here). For example, one meta-analysis examined the relationship between environmental SCM (environmental effort targeted towards creation, development and/or delivery of a product to end user) and the firm’s operational performance. 61 It found that, overall, environmental supply chain practices were associated with improved firm performance. An association between ‘green’ supply chain practices and organisational performance was also demonstrated by Zhu et al. (2008),68 in a study surveying automotive organisations in the UK (n = 39) and China (n = 89). It found the association to be positive, if only weakly so, with impacts of the use of environmental SCM practices on performance being due to decreased fines for environmental accidents (UK companies) and an increased volume of goods delivered on time.
Within these articles we found some examples of primary studies. One concerned the tourism sector in the UK and in Europe more widely, and sought to identify examples of good practice to promote sustainability across the whole supply chain among tour operators. 59 Drawing on interviews and document analyses across tour operators (n = 18), tour operators’ associations (n = 3) and non-governmental organisations engaged in tourism (n = 4), the authors documented changes in the supply chain such as the development of standards and assessments, environmental auditing and renewable energy use. These developments were reported to have resulted in financial gains to the organisation such as increased revenues and reduced costs, as well as non-financial gains such as improved brand reputation, staff morale and retention, long-term business relationships with suppliers, retention of clients, operational efficiency and risk management, as well as staying ahead of legislative requirements and protection of the core assets of the business. 59
Azevedo et al. (2011)45 reported one example in the automotive industry in Portugal, finding that, in one firm, operational costs and business wastage decreased following the introduction of one ‘green’ intervention (reusable packaging). Cost savings may also arise from the financial incentives for switching to green product choices; an article in a professional journal reported on various trusts switching to more sustainable practices which in some cases resulted in cost savings of around 30%. 49
In summary, evidence reviewed here suggests that a ‘green’ supply chain can increase staff morale and organisational reputation. There is also some evidence to suggest that moving to a green supply chain may be associated with cost savings. However, studies frequently failed to provide a detailed account of how such reported savings were arrived at and often relied on savings ‘implied’ as a result of incentives for purchasing more sustainable products.
Collective purchasing
We identified one study which reported empirical evidence of cost savings associated with the use of collective purchasing, by which organisations come together to aggregate purchasing. Birk (2009)48 reported on a case of 14 hospitals in the USA that formed a purchasing ‘coalition’ which secured volume purchases, committing to a specific volume as a single unit. Reported savings achieved through group purchases were in the region of 10–25%, with a reported total of US$11M of capital acquisitions saved across the hospitals participating in the coalition; one hospital was reported to have saved just over US$1M on medical supplies in a year.
The limited empirical evidence of collective purchasing as identified in the evidence review does not permit drawing general conclusions about the likely effectiveness and potential of such practices. Interviews with a small number of key informants working in or with the NHS in England highlighted that such practices formed a necessary requirement for effective procurement, mainly because of a perceived lack of specialised purchasing skills within individual NHS trusts (interviewee 3, private sector). There was recognition among interviewees that collective purchasing can help to negotiate lower product prices. This was seen to be particularly important for smaller facilities with limited ‘purchasing power’, whereas a larger hospital ‘with the international reputation gets the better deal than the small little hospital’ (interviewee 5, NHS); however, the usefulness of such collaborations would depend on the nature of products to be purchased:
Collaborative procurements hubs are probably more powerful than they’ve ever been . . . and that can only be beneficial. But that’s only for small medical devices, mainly disposables . . . Really the ones we’re talking about are the electro-medical capital equipment.
Interviewee 5, NHS
In this particular case it was suggested that direct negotiation with suppliers on larger equipment remained the preferable option for services providers.
Overall, the evidence on the effectiveness of collective purchasing identified in our study is limited and it is difficult to predict whether or not collective purchasing would be a successful strategy based solely on evidence from elsewhere. Therefore, although we note that the use of collective purchasing may have the potential to increase the purchasing ‘power’ of service providers through strengthening their position in price negotiations, further empirical evidence is needed to assess the extent to which this is effective, the specific roles of market size and volume of purchases, and the further implications for the supply chain as a whole.
Supply chain integration, alignment and quality improvement
We identified 10 studies44,47,51,55,60,63–67 which discussed the role of supply chain improvement in the context of streamlining and integration and quality improvement as a means to improve organisational performance (other studies also alluded to this theme but are not referenced here). The notion of integration was generally discussed with reference to aligning general corporate strategies and priorities among different organisations within a supply chain, and measures of success included enhanced profitability and customer satisfaction,44 as well as increased revenue. 51 The importance of strategic alignment was also discussed in the context of outsourcing of purchasing functions or other functions within an organisation. For example, one study of the manufacturing sector reported that companies whose drivers and motivations were better aligned (in this instance, the drivers for outsourcing were compared with its general competitive priorities) demonstrated better supply chain performance. 63 One study specifically focused on quality improvement measures in relation to SCM. Carpenter (2008)52 surveyed the implementation and benefits of quality management initiatives within their materials management departments across 710 health-care organisations, of which 58% were reported to have implemented a defined quality improvement programme. Initiatives included programmes such as Six Sigma, lean and rapid cycle improvement, all within their materials supplies departments. Reported outcomes included reduced waste or cost (mentioned by 55% of respondents), improved patient satisfaction (49%), increased communication (44%), reduced hospital-associated infections (44%) and improved overall staff satisfaction (43%).
Collaboration and relationships
Evidence reviewed in this study pointed to the role of the ‘softer’ features of SCM and procurement activities which may influence their effectiveness. Less than half of the studies were empirical case studies (n = 8);69,70,72,73,78,83,86,87 the remainder comprised hypotheses testing (n = 10)71,74,76,77,79–82,84,85 and one literature review. 75 The studies are summarised in Table 7. Specific areas within this category that emerged from the literature as pertinent were stakeholder engagement within an organisation; capabilities of procurement stakeholders; and relationships with suppliers. We discuss each in turn.
| Reference | Country | Industry | Study type | Study aim and principal methods | Outcomes/learning |
|---|---|---|---|---|---|
| Abrahamsson and Rehme (2010)69 | Sweden | Food retail | Case study | To find the role of logistics in retailers’ profitability, growth and market expansion by comparing the Swedish food retailing industry with modern retailers, using interviews and document analysis | Fast-growing companies (IKEA, H&M, Tesco, etc.) were ‘flow-oriented’ by managing flow of goods through constantly adapting operational resources and capacity in manufacturing and logistics to customers’ demands, partly through co-operation with suppliers |
| Barlow (2006)70 | USA | Health care | Case study | To show the impact on an organisation as a result of investing heavily in materials management via physical, mental and emotional reorganisation, a strengthened engagement of clinicians and streamlining | New contract for gloves resulted in reduced nosocomial infections translating to $1.2M in savings in one hospital and $334,000 in another. A further $750,000 in savings resulted from dealing with fewer vendors |
| Barnes and Liao (2012)71 | USA | Manufacturing | Hypothesis test | To look at the impact of strategic partnerships on firm performance (the extent to which a company can meet end-customer requirements, and operate efficiently to deliver high-quality performance), using surveys | Positive relationship between a company’s investment in strategic partnership (i.e. long-term relationships) and its overall performance |
| Bilyk (2008)72 | Canada | Health care | Case study | To examine effects in a hospital where managers, physicians and nurses take a close look at supplies they are using, streamline inventory, store information on supplies using IT inventory management databases and other best practices | A major hospital in Alberta managed a 34% reduction in direct-buy spending on operating room supplies in 1 year, and in just over 3 years decreased overall operating room supply costs by 42%, increasing on-contract spending by 52% |
| Cadden et al. (2013)73 | UK | Consumer goods | Case study | To investigate what cultural dimensions between a buyer and its supply chain partners are compatible in supporting high and poor performance outcomes, using survey and qualitative research | High-performing supply chain organisations had significantly different cultural profiles across all six dimensions. Low-performing organisations had identical profiles with significantly lower mean scores across every dimension |
| Ciliberti et al. (2011)74 | Multiple, Europe (Italy and the Netherlands) | Various | Hypothesis test | To investigate whether or not specific code of conduct is followed, using four case studies with interviews, observations and document analysis | Codes of conduct could lead to communication flows and improved supplier selection processes and solve moral hazard issues |
| Cox and Chicksand (2008)75 | UK | Food | Review | To review the demand and supply in pig and beef supply chains and provide an analysis of two red meat supply chains using power and leverage methodology; framework development for policy options | The success of collaboration practices (such as lean thinking) were context dependent |
| Danese and Romano (2011)76 | Multiple | Manufacturing | Hypothesis test | To analyse the impact of CI and SI on efficiency and the moderating role of SI, using secondary data | CI was not significantly associated with efficiency performance |
| Kannan and Tan (2010)77 | Multiple (USA and Europe) | Manufacturing | Hypothesis test | To examine whether or not performance benefits accrue to firms that involve extended supply chain partners, using surveys. The ‘extent of integration’ is the extent of the supply chain that is integrated (i.e. beyond first-tier suppliers) | Firms incorporating broad spectrum of supply chain partners in integration efforts had stronger emphasis on building interorganisational linkages; statistically significant differences between integration constructs (supplier focus, customer focus, information focus and supply chain focus). They also had a stronger relationship performance; relationships had a greater positive impact in sales improvements, new product development time and quality, but not cost reduction. Finally, they had strong customer service performance level, but not a higher market share, ROI or overall competitive position – likely because these last factors had to do with non-supply chain elements of a firm |
| Ogden and McCorriston (2007)78 | UK | Hospitality | Case study | To report the findings from a survey of UK conference and event managers, which highlights the benefits that can accrue from supplier management within this sector, using surveys | A significant proportion of venue managers reported having long-term supplier relationships, placing considerable value on the non-financial benefits that could accrue from long-term supplier relations featuring mutual trust and good working relationships |
| Pagell et al. (2007)79 | Multiple (USA and Taiwan) | Manufacturing | Hypothesis test | Implementation of two investments: greening supply chain and buyer–supplier relationships; using surveys | Buyer–supplier relationship and environmental investments were significantly associated with sustainability performance, but not with cost, quality or responsiveness performance |
| Paulraj and Chen (2007)80 | USA | Manufacturing | Hypothesis test | To explore the connection between strategic buyer–supplier relationships and logistics integration, along with the subsequent impact on a firm’s agility performance | Results show that effective external logistics integration is engendered by strategic buyer–supplier relationships and IT, and logistics integration has a positive impact on firm agility |
| Periatt et al. (2007)81 | USA | Multiple | Hypothesis test | To investigate the degree to which personality factors (neuroticism, extraversion, openness to experience, agreeableness and conscientiousness) affect customer orientation of logistics personnel, using surveys | Openness to experience, agreeableness and conscientiousness were significantly positively related to customer orientation of logistics employees (neuroticism and extraversion were not) |
| Richey et al. (2008)82 | N/R | Retail | Hypothesis test | To explore the direct impact of retailer technology utilisation behaviours on operational effectiveness, using surveys. ‘Operational effectiveness’ relates to the sales per employee. ‘Technological intensity’ refers to the variety of technologies used | Intensive technology utilisation between supplier and retailer led to better retailer operational effectiveness. Technological intensity was a particularly important determinant of retailer effectiveness for retailers who are optimistic about the use of technology |
| Roloff and Aßländer (2010)83 | Multiple | Consumer toys | Case study | To investigate a particular safety case in terms of buyer–supplier relationships and corporate autonomy; approach to data collection not reported | In this context it was found that supplier–buyer partnerships can harm corporate autonomy through mistakes made by suppliers or the company |
| Schloetzer (2012)84 | N/A | Petroleum manufacturing | Hypothesis test | To investigate the effect of process integration and information sharing in supply chains, using secondary administrative data | Process integration and information sharing could lead to productivity, sales growth and profitability |
| Thai (2012)85 | Australia | Multiple | Hypothesis test | To investigate the skills and knowledge required for logistics personnel to be successful, using surveys | The five most important skills and knowledge (in order), as currently perceived by respondents, were personal integrity, managing client relationships, problem-solving ability, cost control and the ability to plan |
| Van der Vaart and van Donk (2006)86 | Not reported | Manufacturing | Case study | To identify which business characteristics make suppliers choose buyer-focused operations as a supply chain strategy in their relationships with key buyers, using interviews as part of site visit case studies | The study found that buyer-focused operations are chosen for reasons of flexibility in mix, volume, specification and timing |
| Williams (2008)87 | USA | Health care | Case study | To provide some examples of cost containment through better SCM and increased physician engagement; approach to data collection not reported | Cost savings reported for both of the organisations examined ($4.5M and $13M respectively) |
| Kehoe (2006)88 | USA | Health | Case study | To report on the improvements in SCM due to the adoption of an electronic supply chain and engagement of stakeholders; approach to data collection not reported | One of the outcomes included an average bid savings of 21%. An average bid savings of 21% and a 70% reduction in bill completion cycle time was seen |
Stakeholder engagement
Stakeholder engagement, although alluded to as an important factor across sectors, emerged as a particular theme within the procurement literature in health care. Evidence identified for this review drew mostly on single case studies, with three studies70,72,88 reporting on four case studies located in the health-care sector in the USA and one in Canada. For example, Williams (2008)87 reported on experiences in one hospital in North Carolina which created teams of supply chain personnel, finance professionals and clinicians to inform procurement decisions. Teams reviewed data on types of products used in departments, and consulted and negotiated reduced prices with suppliers. This resulted in the standardisation of some products, which was interpreted by the authors as promoting patient safety through the use of ‘similar’ devices across the hospital. Williams (2008)87 also reported on experiences of a group of 20 hospitals in Arizona operating under the same health-care provider, where finance staff and clinicians together developed a pricing model which set a fixed price for physician preference items and was informed on a comparison of prices in the national market. This was reported to have saved the provider more than US$3M per year in cardiology, and US$13M overall. A proportion of the cost savings was invested in new equipment and technology, hypothesised to have sustained engagement of physicians. A related example of clinician engagement was reported by Kehoe (2006). 88 Inspired by SCM systems used by local groceries stores, the executive team of a financially challenged group of hospitals in Pennsylvania combined end-users, such as chief nurses, pharmacists and materials management staff, with engagement and IT investment to improve organisational performance through streamlining, standardisation and overall better materials management. The collaboration of clinicians was reported to have enabled the implementation of new processes and contributed to the success of the initiative.
An analysis of stakeholder engagement in one hospital in Canada was reported to have led to a 34% reduction in 1 year in direct spending on operating room supplies, and a reduction of overall theatre supply costs by 42% over 3 years. 72 This was achieved through involving managers, physicians and nurses in streamlining purchasing and taking a more active part in storing information on supplies and inventory to inform new purchases. Finally, Barlow (2006)70 reported on experiences of two hospitals which invested in improved materials management, while also strengthening clinician engagement in procurement decisions. This was reported to have resulted in a new contract for surgical gloves, which in turn was linked to a reduction in nosocomial infections, estimated to have equated to a total of US$1.5M in savings in the two hospitals combined.
Stakeholder engagement was also identified as an important factor in effective procurement decision-making in our exploratory interviews with key informants. In addition to the value placed upon engaging a wider range of stakeholders in itself, engaging clinicians in particular in the purchasing process was felt to lead to better information about the requirements of the purchase, as well as knowledge of other products on the market, which may lead to a more informed negotiation position for a hospital:
Clinician engagement in procurement decisions is key. They have to be involved. One of the things we’re trying to do . . . is actually set up focus groups. So we have focus groups for various types of equipment. But the focus group is involved in various types of procurement elements in their categories of equipment. And it’s bringing in expert clinicians and nursing staff in those areas to advise and to provide input into that process.
Interviewee 5, NHS
In summary, evidence reviewed here suggests that team collaboration and the engagement of practitioners such as clinicians in the health-care sector may have a core role in the procurement process. Selected examples of stakeholder engagement in health-care procurement in North America point to the notion of ‘engagement’ as good practice. However, the empirical evidence demonstrating the value of engagement with regard to overall organisational performance remains weak.
Capability
Strong professional capabilities in the purchasing function were identified as important by a small number of studies, with supportive evidence based on studies that were of a hypotheses-testing nature rather than reporting on interventions in practice. One study conducted in Australia aimed to examine the skills and knowledge required for logistics professionals to be successful in their job, and the perceived importance of these skills. 85 Using a survey of 1300 members of the Chartered Institute of Logistics and Transport in Australia, the five most important skills and knowledge (in order), as perceived by respondents, were personal integrity, managing client relationships, problem-solving ability, cost control and ability to plan. 85 The study included logistics professionals only, and the response rate was low (11%). However, the authors suggested that these skills would form an important requirement for anyone working in a more general capacity in a purchasing function. One other study in the USA investigated the degree to which personality factors affected customer orientation in logistics personnel across a range of industries. 81 It found that traits such as openness to experience, agreeableness and conscientiousness were significantly and positively related to customer orientation.
The role of capabilities and knowledge that can be linked to enhancing purchasing functions was, in part, reflected in the interviews with key informants for this study, although the nature of these capabilities was not necessarily specified:
At the moment procurement is pretty fragmented in the NHS . . . and there’s no way that most trusts can afford to employ the expertise that they need, even if it was available, which . . . it isn’t . . . There’s a lack of understanding of procurements by chief executives, even though it’s a huge element of NHS costs . . .
Interviewee 4, private sector
Respondents attributed perceived failure to adopt effective procurement models and approaches to a range of external and contextual factors, highlighting a need to ‘understand the role of procurement and what it can do’ (interviewee 2, private sector).
Capabilities required in order to undertake effective purchasing can be acquired through training and experience, although there may be options to transfer purchasing functions to other organisations in the form of outsourcing. One review synthesised the related evidence in the health-care sector. 62 It found that outsourcing purchasing functions resulted in general improvements such as improved quality services by the outsourcing companies (in Germany), some service standardisation benefits (UK) and cost reduction (Australia). However, it also highlighted the potential risks that may be involved, such as cultural change, and the need for monitoring of the outsourced suppliers.
Strengthening capability can also be interpreted more broadly in the sense of creating an ‘enabling’ environment to enhance performance. For example, Ciliberti et al. (2011)74 reported on case studies of four companies in Italy and the Netherlands, each looking at the way they had implemented a specific code of conduct and the degree to which staff adhered to the codes, using interviews, observation and document review. They found that where staff followed codes of conduct and generally accepted them, this was associated with improved communication flows, improved supplier selection processes and solving moral hazard issues.
Relationships with suppliers
A small number of studies (n = 4)71,73,78,84 were concerned with the relationships between purchasers and suppliers. We note that these studies did not link such relationships directly to outcomes. One study surveyed professionals working in conference and event management in the UK. 78 Venue managers reported having long-term supplier relationships, and highlighted the non-financial benefits that can accrue from these, such as mutual trust and good working relationships. Reported benefits included consistency, responsiveness and flexibility in service delivery. Similarly, Barnes and Liao (2012),71 reporting on a survey of around 5150 companies in the manufacturing sector in the USA (response rate 69%), pointed to a positive relationship between a company’s investment in strategic partnership, such as long-term relationships, and its overall performance, although details of how this was implemented were not described.
Conversely, key informants interviewed for this study suggested problems with engaging with suppliers, with reported challenges ranging from a perceived inability to involve small enterprises because of existing NHS framework contracts and fragmentation to ‘disincentive[s] to purchase collaboratively’ (interviewee 1, private sector). One study in the consumer goods industry also highlights the role of potential cultural conflicts, reporting that high-performing supply chain organisations had significantly different cultural profiles to those of their buyers compared with low-performing organisations. 73 The expense of equipment maintenance was highlighted by one NHS respondent, who suggested that lower maintenance cost would require long-term relationships with particular suppliers to ensure lower maintenance and serving contracts, while highlighting how this might be difficult to achieve in situations where suppliers are primarily selected on price (interviewee 5, NHS).
Overall, working relationships with suppliers appear to be important with regard to procurement by means of improved information sharing and shared values, which may support negotiation and contracting functions.
Materials and information management
A third main theme identified in this review centred on materials and stock management. Most of the evidence reviewed was based on small empirical case studies (n = 22),88–90,92,94,96–101,103,105,106,108–115 and there was variation in the quality of reported outcomes and generalisability. A smaller proportion were hypotheses-testing studies (n = 5)91,93,95,102,104 and there was one review107 (Table 8).
| Reference | Country | Industry | Study type | Study aim and principal methods | Outcomes/learning |
|---|---|---|---|---|---|
| Alfaro and Rábade (2009)89 | Spain | Food | Case study | To show the qualitative and quantitative benefits obtained from implementation of a computerised traceability system, using interviews and document analysis within longitudinal case study | Benefits included doubled production with same number of employees, 90% reduction in productive process, 20% reduction in indirect costs, 10–15% increase in warehouse capacity, 20–30% reduction in safety stock. Challenges included the need to convince senior managers of the potential for the investment |
| Belkoski (2008)90 | USA | Health care | Case study | To report on a pilot programme that demonstrates benefits of data standardisation and synchronisation and enables the system to recognise productivity gains in the supply chain | Savings reported for the two case studies but not attributed directly to the interventions |
| Bernhard et al. (2006)91 | Australia | Multiple | Hypothesis test | To test the performance of users of ERPSs and non-users, and impact on firm performance and the business process performance, using surveys | Tested performance of ERPS users and non-ERPS users and found that, on average, ERPS users scored higher but no significant difference between the samples on any measure of performance |
| Bhakoo and Chan (2011)92 | Australia | Pharmaceutical | Case study | To report on the implementation of an e-business system in health-care supply chain (manufacturer to pharmacy), using observations, document analysis, interviews | Time taken to receive goods decreased by 20%; incorrect deliveries decreased from 8% to 3.5%. Some other tasks increased in time |
| Bigné et al. (2008)93 | Spain | Tourism | Hypothesis test | To examine the impact of adoption of IT (automated systems) in travel industry, using surveys | E-communication and e-procurement positively associated with e-sales and relationship development. E-procurement positively associated with e-efficiency, i.e. cost savings |
| Callender and Grasman (2010)94 | USA | Health care | Case study | To explore the material management in the health-care sector to identify best practices, using questionnaires | Best practices identified included increased training on SCM principles; automated inventory management and ordering; information sharing and clinician involvement |
| Campo et al. (2010)95 | Spain | Retail | Hypothesis test | To analyse the direct influence of IT on retailers’ perceived performance, using surveys | No direct relationship between specific use of IT and perceived performance (standardised coefficient = 0.09 and non-significant) but positive effect was produced indirectly through information sharing and satisfaction with the relationship |
| Creedon (2006)96 | USA | Health care | Case study | To compile savings from automated procurement and buying processes, using secondary data from 200 hospitals | Manual vs. electronic requisitions (based on $20 or $30/hour), $8 vs. $2.50 for the process. Manual vs. electronic sending of purchase orders (based on $20/hour), $5 vs. $0.33. Manual vs. electronic receiving of purchase orders (based on pay of $20/hour), $1.33 vs. $0. Manual vs. electronic invoicing (based on pay of $23/hour), $345 vs. $1.15 |
| Cunningham (2006)97 | USA | Health care | Case study | To give an overview of SCM fundamentals that have resulted in cost savings; reports on interviews with hospital executives | Various savings reported from different hospitals, including price negotiations resulting in savings, improved product selection also resulting in cost savings |
| Fawcett et al. (2011)98 | Not reported | Multiple | Case study | To explore how IT investments can create differential returns when they enable the creation of specific capabilities, using surveys and interviews | Supply chain connectivity was positively and significantly related to operational performance and customer satisfaction in both time periods; however, the strength of IT’s influence on value might decrease marginally over time |
| Ghani et al. (2009)99 | USA | Computing | Case study | To test whether or not the conventional supply chain (where feedback from customer flows in the reverse direction to the distributor and then the manufacturer, who alters their products if necessary for the supplier) has no effective technology and has slow information sharing | The firm examined adopted a model whereby they sold directly to customers and different information-sharing model (suppliers can access information about sales forecast and product changes, and the information sharing goes in both directions). They reported a 15% increase in product shipments at the same time the industry volume dropped 5% (although no direct attribution can be made to their more effective SCM) |
| Gianakis and McCue (2012)100 | USA | Public sector organisations | Case study | To identify challenges, barriers and benefits of SCM processes, using reports from four case studies (approach to data collection not reported) | Savings reported for one hospital (three times expected amount) and purchasing administration time reduced |
| Jeffery et al. (2009)101 | USA | Public sector organisations | Case study | To examine the effect of RFID implementation on service performance, using interviews | Firms reported on higher profitability, reduced errors and improved overall customer satisfaction, although implementation challenges needed to be overcome at each site |
| Johnson et al. (2007)102 | Multiple (USA and Canada) | Manufacturing | Hypothesis test | To investigate whether or not the use of e-business is related to firm performance, using surveys | E-business technology dyadic co-ordination dimension was significantly associated with return on assets and return on sales, but price determination and private exchange dimensions were not |
| Krusius (2012)103 | Finland | Health care | Case study | To report on the implementation of centralised and streamlined blood collection system; approach to data collection not reported | Cost of logistics dropped by one-third over 5 years |
| Leonard and Davis (2006)104 | USA | Manufacturing | Hypothesis test | To determine whether or not electronic supply chains using electronic data interchange are more effective than non-electronic supply chains by analysing products before and after electronic data interchange implementation, using secondary product data | Electronic data interchange led to savings by enabling shorter order cycles and greater availability of component parts without affecting inventory level and supplier stockouts |
| Maggio and Perez (2006)105 | USA | Health care | Case study | To report on the implementation of an automated materials management information system; approach to data collection not reported | Time spent on administering purchasing decreased (10 hours/day to 45 minutes/day); hospital is able to consider more suppliers; errors in orders automatically verified |
| McHugh (2006)106 | USA | Health care | Case study | To investigate options to manage a clinical laboratory inventory and implement a computerised system; approach to data collection not reported | Results included 8% reduction in excess quantity; savings in operating expenses; reduction of overstock and administrative task time |
| Narayanan et al. (2009)107 | Multiple | Multiple | Review | Meta-analysis to test whether or not there is a consistent set of antecedents and realised benefits associated with electronic data interchange adoption which is supported by empirical research in multiple streams in the field | Specific benefits from electronic data interchange were inconclusive from the literature; greatest effects could be ascertained for customer-facing activities |
| Page (2011)108 | USA | Health care | Case study | To present a successful example of automated supply chains in a hospital; approach to data collection not reported | Each of the case studies led to cost savings and improved workflow efficiencies |
| Persona et al. (2008)109 | Italy | Health care | Case study | To describe effects of implementation of ‘JIT’ and ‘Kanban’ techniques in two hospitals; approach to data collection not reported | In the first hospital (JIT Kanban system) savings amounted to €21,000 in the first year of testing. In the second hospital, there was a saving of €13,100, which is equal to 24.9% of the expenses of the ward for drugs. The monthly consumption of drugs also decreased in the first month of the test |
| Raviprakash et al. (2009)110 | USA | Health care | Case study | To present the different ways of using RFID in health-care settings; approach to data collection not reported | Using RFID to locate medical equipment and mobile assets contributed to capital avoidance and utilisation efficiencies |
| Smart (2010)111 | Multiple | Multiple | Case study | To examine how users of e-procurement in buying firms have deployed these applications and how this deployment has had an impact on their use of the supply market, using case study descriptive methods | In the four cases, administrative time for purchases decreased to allow time for more strategic tasks; limited evidence |
| Tarantilis et al. (2008)112 | Greece | Construction manufacturing | Case study | To develop and test a customised web-based enterprise resource planning (ERPS to manage one enterprise process event flow, therefore increasing efficiency and control, using the design and testing of the ERPS and observing impact | Outcomes included enhanced streamlining of operations, reduced paperwork, facilitated communication (access to real-time data, documents and reports) and a reduction in project execution times from 0% to 40% |
| Walker (2010)113 | USA | Manufacturing | Case study | To describe the implementation of a new SCM system to lower inventories and improve product quality with an integration IT infrastructure, using business process analysis and mapping methods | One-time savings at $22.3M and ongoing savings at $6.83M per year; internal rate of return on the project was 29%. Inventory management improvements allowed the company to reduce its inventory by $4.2M. In addition, customers were able to reduce inventory by an average of 3.1 days in the first year, resulting in a cash savings of $19M |
| Wieland et al. (2012)114 | Multiple (Europe) | Electronics | Case study | To report on the implementation of an automated materials management information system; approach to data collection not reported | One year after implementation, total inventory levels were reduced by more than 11%; in addition, service levels of products modelled using the automated process were eight points higher than products not modelled using this process |
| Ygal et al. (2010)115 | Canada | Health care | Case study | To estimate impact of RFID tracking technology to automatically replenish medical supplies in nursing units, using interviews, observations, secondary routine data | Outcomes were estimates only and argued that the two main benefits were thought to be time saving for nurses and optimisation of inventory levels and processes, e.g. time savings would correspond to $153,883 (nurses) and $589,424 (auxiliary personnel) per year (some tasks would be transferred to store personnel, which would cost $220,130). The reduction of 67% in the walking distance due to reorganisation of storage location would save $3,097,373 (or 7.5 minutes/day/nurse/working shift). The reduction in costs associated with expired products would save $109,453 per year for stock items, and $65,367 for non-stock items |
The body of evidence identified in this theme was highly diverse, pinpointing a range of more general concepts emerging across the studies. These include automated or electronic purchasing; stock management and inventory using data management and the use of radio frequency identification (RFID) tagging; and the use of some of these processes for benchmarking and price comparisons. It is important to note that the distinction of these concepts is not clear-cut and there is considerable overlap between categories.
Electronic purchasing
By automating purchasing functions, such as through online purchases and software for internal use, organisations may benefit from more efficient inventory control, time savings and cost savings. For instance, evidence from one case study of a construction company in Greece suggested that use of a customised web-based enterprise resource planning system to manage enterprise process event flow may lead to increased efficiency and control. 112 The authors reported a substantial cost reduction in all areas affected by this new system, but they did not quantify the size of the estimated savings. The types of efficiencies achieved included avoiding paperwork; streamlining personnel-related tasks (e.g. timesheets); flexible and efficient resource planning; increased productivity; increased customer satisfaction; increased sales department efficiency through the better use of sales data; and facilitated communication such as through access to real-time data, documents and reports. The authors also reported a reduction of up to 40% in project execution times. 112 Bhakoo and Chan (2011)92 reported on a longitudinal case study of the implementation of an e-business system in a health-care supply chain (manufacturer to pharmacy) in Australia, using direct participant observation, document and archive analysis and interviews. Before project implementation, pharmacy orders were issued via telephone and fax and goods data entered manually into a central computer before being issued to other hospital areas. The electronic ordering system resulted in a reported reduction of 20% in the time taken to receive goods (from 51 minutes to 40 minutes). There was also a reported decrease in incorrect deliveries, from 8% to 3.5% per order, because of improved labelling; however, there was an increase in packing time for the supplier and time taken to label each carton.
One study reported on four examples of electronic procurement in industrial settings. 111 Reported benefits included reduced supplier numbers through better information in a large UK manufacturing business, improved productivity in a European telecommunication firm, and buyers freed up from transactional work to focus on strategic issues in both a European energy firm and a chemicals and agricultural firm. 111 The types of outcomes reported from one hospital setting in the USA which implemented automated supply chains included increased time with patients due to the release of staff time, as the automated system made more aggregated purchasing data available to help them choose from different products. 108 We further note that through automating purchases, an organisation may be able to access more suppliers. For example, the implementation of an automated supply chain information system within a hospital in the USA led to a rise in the number of suppliers the hospital engaged with, from 7 to 43. 105
These examples point to the potential for time savings and efficiencies as a result of automating processes, although the nature of the empirical evidence remains weak. The adoption of automated supply chain processes can lead to efficiencies, such as reducing time spent by buyers to verify purchase orders,100 but outcomes such as these are seldom contrasted with the investment costs required to set up these systems to allow for a full cost–benefit analysis. 105
Stock management and inventory
Stock management and inventory was an area which was most frequently studied in relation to procurement in the health-care sector in particular, and our review identified a series of small case studies based in hospitals which reported on its roles for organisational performance. Examples highlighted the design and implementation of different stock management systems which tend to rely on the adoption of new technology and the use of RFID.
Raviprakash et al. (2009)110 reported on the use of RFID technology to locate medical equipment and mobile assets within wards in health-care settings in the USA. The authors estimated that the providers may have achieved a return of $200,000 per year over the investment into the RFID system, including maintenance costs, while excluding staff productivity gains. In addition, nursing staff were estimated to have achieved a time saving of about 30 minutes per nurse shift, implying freed-up time for patient care.
In the Stakeholder engagement section we reported on one study that actively involved clinicians in inventory management in a Canadian hospital, which was supported by an automated database. 72 The analysis reported substantial savings on purchasing and supply costs, although it is difficult to attribute reported savings – for example a reduction in overall operating theatre supply costs of 42% over 3 years – to inventory management as such, because of the multiple components involved in the intervention. McHugh (2005)106 reported on the experiences of implementing a specially designed computerised system to actively manage a clinical laboratory inventory in one medical centre in California, USA. This was reported to have led to a reduction in overstock (reduced wastage, with fewer products becoming outdated before use) and reduced paperwork for clinical laboratory scientists, due to enhanced management of the supply chain. The study also reported that there were net savings in operating expenses but it did not quantify the volume of savings.
Similar findings were reported by Persona et al. (2008)109 following the implementation of ‘just-in-time’ techniques in two hospitals in Italy, designed to streamline stock management. Though it was not clear how data were collected, the reported impacts of the new approaches to stock management included savings of up to €21,000 in one hospital in the first year of testing, attributed to reductions in the quantities of stored products, out-of-date medicines and order errors. However, as in many of the examples identified in this review, the initial investment costs of implementing the new systems were not explicitly reported. One of the few examples of work that sought to take a broader cost perspective was a study by Ygal et al. (2010),115 who sought to estimate the impact of RFID tracking technology used to automatically replenish medical supplies in nursing units in a Canadian setting, using interviews, observations and secondary routine data. The authors estimated the time savings accrued to nurses and auxiliary staff to be in the region of CA$153,883 and CA$589,424 per annum, respectively, through the transfer of tasks to store personnel, and a reduction of 67% in the walking distance due to reorganisation of storage location. This equated to a saving of CA$3.1M (or 7.5 minutes per day per nurse and working shift). However, these estimates were arrived at through modelling rather than actual cost audits.
The examples of stock management and inventory reported on here reflect the wider literature on data management, as they allude to the automation of processes. This overall theme was also reflected on in our interviews with key informants, who suggested that technology solutions would play an important role in improving the usefulness of data and gathering important information that the NHS cannot currently access:
[In] the vast majority of cases, [each trust] has created its own catalogue if it’s had a catalogue at all. So master data, you’ve got to be joking. If you’re lucky, some kind of data exists in some trust. But that won’t be the same set of data as exists in another trust . . . The NHS has no idea how many items it buys of anything.
Interviewee 3, private sector
Interviewees highlighted best practices from other companies and stressed the importance of what they referred to as ‘master data’. Currently, barcodes are not routinely used in the NHS to record intake of products and this was reported to lead to problems such as cancelled operations due to unknown inventory quantities.
However, interviewees also noted that the reality of managing data about existing supplies, as well as old and new purchases, can be challenging given the existence of multiple purchasing systems for different types of supplies in each hospital, such as for pharmaceuticals, devices and equipment, and other types of non-clinical supplies: ‘Some trusts have seven different purchasing systems. Like any other organisation, they should have one purchasing system . . . So we do seven different transformations for seven different systems. But we don’t mind, it’s just difficult’ (interviewee 3, private sector).
Better data management can support the purchasing function by providing a history of purchasing information and so enabling negotiations with suppliers, as well as supporting the inventory and stock management functions. The available evidence suggests that techniques that lead to improved stock management and tracking have the potential to save costs, in part because they help to reduce waste and, in the health-care field in particular, enhance the quality and safety of patient care by ensuring stock is available when needed and on time.
Benchmarking and price comparison
A third concept emerging from the literature is related to what we have generally identified as benchmarking and price comparison, and arose mainly from studies set in the health-care sector. However, as noted earlier, the concepts identified here overlap and as we will see below, the usefulness of benchmarking and price comparison will be strongly dependent on data management systems.
Information that enables benchmarking and price comparisons may place purchasers in a better position to negotiate prices. For example, one study in the USA reported on interviews with hospital executives on their price benchmarking strategies. 97 Staff in one hospital compared supply prices with those of other hospitals, and then used this information to negotiate a 13% volume pricing discount, resulting in a reported reduction in costs of $1M. One other hospital reported having negotiated pricing on hip and knee implants, which result in reported yearly savings of $113,000.
The potential usefulness of benchmarking and price comparison was also highlighted by two NHS stakeholders interviewed in our study, who pointed to large differences in prices paid for the same devices and consumables across hospitals in the NHS. They suggested that greater transparency by suppliers providing prices to the NHS would allow hospitals to more accurately compare products that are available on the market.
Chapter 4 Experience of procurement and supply chain management in the health sector in selected high-income countries
This chapter explores experiences in a small set of high-income countries around procurement and SCM in the health sector. The international component of the work presented here sought to complement the findings of the REA reported in Chapter 3. Specifically, we report on two themes: first, a whole system change involving the centralisation of the procurement function in New Zealand; and second, the role of GPOs in Europe, focusing on recent experiences in France, where, as part of the national Hospital Performance for Responsible Procurement [Performance Hospitalière pour des Achats Responsables (PHARE)] programme launched in 2011 by the French Ministry of Health, public sector GPOs have been tasked with supporting and advancing efforts to strengthen procurement across the health system. 116
As noted in Chapter 2, the exploration of international experiences in procurement and SCM in the health sector draws, to a great extent, on the published and grey literature. This formed the basis for draft country reports, which were reviewed by one key informant in each of the countries for completeness and accuracy. Experts also provided additional information in the context of an interview, and, in the following, we refer to these additional sources of data as ‘NZ KI’ (key informant New Zealand) and ‘Fr KI’ (key informant France), respectively.
Centralisation of the procurement function in New Zealand
Main features of the New Zealand health system
Health care in New Zealand is financed largely through public sources, mainly general taxation (74.9% in 2011) and the employment-based accident compensation scheme (7.8%). 117 The remaining 17.3% is funded from private sources including private health insurance and out-of-pocket payments (10.9%); in 2011, approximately 31% of the New Zealand population (of around 4.3 million) had some private health insurance. 118 In 2011, national health expenditure was 10.3% of gross domestic product (GDP), which was higher than the Organisation for Economic Co-operation and Development (OECD) average of 9.3% (UK 9.4%), although remaining lower in terms of per capita spending, at US$3182 compared with an average spend across the OECD of US$3339 (UK US$3405). 117 Compared with 2000, health expenditure in New Zealand grew by 5.1% per year in real terms (OECD 4.1%; UK 4.5%). 117
Since 2000, with the introduction of the New Zealand Health and Disability Act, responsibility for the organisation of publicly funded health services has been devolved to 20 geographically defined DHBs. DHBs administer about 75% of public funding and they are responsible for planning, managing and purchasing publicly funded health and long-term care services for the population within their region. 119 DHBs are governed by a board whose members are elected by popular vote or appointed by the Minister of Health; they are overseen by the newly established National Health Board (see Ministerial review of New Zealand health system performance) and are required to report progress regularly against a set of performance measures and other accountability requirements set out in a nationwide service framework. 120
District health boards operate government-owned hospitals, health centres and community services, and also purchase some (mostly elective) services from private hospitals, and long-stay residential and community-based services from non-governmental organisations. 121 They purchase a significant proportion of primary care services through contracts with primary health organisations (PHOs), which were introduced as non-statutory, not-for-profit bodies following the 2001 Primary Health Care Strategy. 119 PHOs organise and manage publicly funded primary care, and subsidise low-cost access to general practitioner (GP) services, covering over 95% of the population. 122 They bring together doctors, nurses and other health professionals providing care in the community, through either employed staff or affiliated provider organisations and individual general practices; enrolment is voluntary for patients. The number of PHOs was consolidated through merger over the years, from an initial 80 to 31 by the end of 2011. 123
Health-care provision is both public and private. Specialists in public hospitals are paid a salary whereas GPs are usually independent, self-employed providers. GPs act as gatekeepers to secondary care; residents are free to choose any GP.
Ministerial review of New Zealand health system performance
In 2008, amid concerns about the future direction of health-care provision and financial sustainability, and a new commitment to create more efficient and accessible public health services, the newly elected government commissioned a Ministerial Review Group to review the performance, quality and sustainability of the New Zealand health system. 29,121 In its 2009 report Meeting the Challenge the group recommended (re)centralising some of the planning and purchasing functions. 124 The overall direction was to reduce bureaucracy, including reducing duplication of ‘back office’ functions of DHBs and PHOs and an aim to ‘reduce waste and inefficiencies within the health system’. 29 The group also advised the integration of different aspects of planning that had so far been undertaken separately and the development of a joint approach for health services, workforce, technology and capital planning across the entire public system. 124
Among the main changes introduced by the New Zealand government in response to more than 170 recommendations issued by the review125 was the establishment of the aforementioned National Health Board to oversee and guide planning at district and supradistrict levels. Appointed by the Minister of Health and supported by a business unit within the Ministry, the National Health Board is responsible for overseeing operational functions that were formerly the responsibility of the Ministry of Health. These include the funding, monitoring and planning of DHBs, as well as the planning and funding of designated national services. 126 Further significant changes included the creation of a Shared Services Establishment Board, which was to become Health Benefits Limited (HBL) (see next subsection) and a Quality and Safety Commission. 125 Furthermore, the National Health Committee, an independent statutory body, was reconfigured to provide advice to the Ministry of Health on new and existing health technologies in the health and disability sector. 127
A new central procurement agency: Health Benefits Limited
As part of its review, the Ministerial Review Group noted how New Zealand’s Pharmaceutical Management Agency (Pharmac) had contained pharmaceutical cost growth and concluded that a similar approach should be adapted to ‘other non-wage costs in back office areas that all DHBs have in common, in order to free up resources for front-line care’. 124 It thus proposed the creation of a new national procurement agency or ‘Pharmac-like national shared service agency with a mandate to manage the assessment, standardisation, management, purchasing, and/or SCM of any of the common back office functions of DHBs that are referred to it by the Minister of Health’. 124
In response, in 2010 the government established HBL as a shared services organisation for the District Health Boards. 128 It is a standalone Crown-owned company, owned by the Ministers of Health and Finance, whose purpose is to ‘help District Health Boards (DHBs) save money by reducing their administrative, support and procurement costs’129 by means of facilitating and leading national initiatives and managing the related implementation programme. 130 Overall, HBL has been tasked with delivering a total of NZ$700M (around £360M) in gross savings to the DHBs between 2010 and 2015. 131 It is anticipated that these savings will arise from cost reductions, cost avoidance, operational efficiencies achieved in administrative and support services or non-administrative areas, and sharing of good practice in administrative and support services. 130
Principles of working
Health Benefits Limited is separate from the Ministry of Health; it has its own board which reports directly to the Minister of Health. 132 A core aim of HBL’s activities is to generate savings that can be reinvested into front-line services, so supporting the wider objectives of reform activities towards patient-centred care. The responsibility for decisions about the (re)allocation of savings remains with the DHBs and other stakeholders.
As an organisation mandated to support DHBs, HBL seeks to work with DHBs ‘to help facilitate the processes required to deliver gains and savings through shared service initiatives’. 131 In its 2010–11 statement of intent (a statutory annual document), HBL highlighted that engagement and communication activities were to be targeted at different levels across the health sector and at the different needs of a range of stakeholders, including ministers, government agencies, the different administrative ties within DHBs and different suppliers. 131
In the same statement, HBL also noted that while working with DHBs to meet their needs would be of key importance in order to deliver effective shared services, there may be instances of lack of consensus on a given activity or initiative. In these instances, HBL could consider asking the Minister of Health to direct DHBs using his/her ministerial power in line with the New Zealand Public Health and Disability Act. 131 In practice, this lever has not been used so far and the Ministry of Health could draw on other, more informal methods of performance management if deemed necessary (NZ KI).
Health Benefits Limited publishes two accountability documents: a statement of intent and an annual report. 130 The statement of intent is prepared on an annual basis, reviewed and approved by the shareholding ministers. The annual report documents activity during a given year. HBL also provides the Ministry of Health with information to enable responses to parliamentary questions and process Select Committee inquiries, among other things. 131
The identification and formulation of long-term objectives and short-term outputs evolved as HBL became more established in the wider system. The 2013/14–2015/16 statement of intent describes three long-term objectives:129
-
effective and efficient provision of DHB administration and support services
-
benefits realised in DHB administration and support services
-
sustainability of benefits and implemented services and initiatives.
These objectives are to be delivered by means of defined output classes, which continued to be developed over time along with HBL’s work streams and the organisation as a whole. Thus, in its initial work programme,131 HBL identified a number of non-clinical support services as areas with the most potential for savings, which were further developed into a set of defined work streams and which, in the 2011–12 period, were identified as:133
-
collective procurement, working with Pharmac and the National Health Committee to prepare a co-ordinated strategy for procurement of medical devices (for all DHBs)
-
finance, procurement and supply chain, which includes food and laundry services
-
facilities management and support services
-
information services; and
-
human resources and workforce management.
The 2013/13–2015/16 statement of intent further refined these work streams into six distinct ‘output classes’, redefining ‘collective procurement’ as ‘Direct Services to DHBs: Shared Banking, Insurance, National Procurement’, and adding a new output class, ‘new opportunities’. 129 The following provides a brief summary of activities in the two output classes ‘collective procurement’ and ‘facilities management and support services’.
Collective (national) procurement activities
National procurement centres on identifying procurement opportunities across the health sector, including engaging with suppliers and negotiating contracts. 129 Supplier engagement involves regular (quarterly) meetings that seek to explore potential for efficiencies from the supplier perspective also (NZ KI). In 2011–12, there was an ‘emphasis on categories of goods and services or suppliers that are most likely to quickly deliver the savings needed’. 133 To this end, HBL had identified 29 categories where it led or worked with other agencies (Table 9).
| Medical goods and services | Other goods and services |
|---|---|
| Urinary catheters and bags (hospital only) Spinal and epidural packs Orthopaedic cement and togas Sutures/skin Staplers/skin adhesives Pulse oximetry Examination gloves Hypodermic needles and syringes Digital mammography Orthopaedic trauma Orthopaedic implants Rehabilitation equipment Wound care Diathermy consumables |
Ward beds and mattresses Personal protective equipment Banking and treasury Household relocation Fuel PRINCE2® training Apparel Media monitoring IT service Aggregator mobile, voice and data Recruitment services Travel management services Electricity External legal service Air travel Energy management services |
Of these, eight national procurement projects were completed during 2012–13. 129 These included medical examination gloves (Box 2) and rehabilitation equipment supply agreements, alongside hospital bed contracts and a single banking contract for all DHBs. 134
Reviewing the procurement arrangements for non-sterile gloves, HBL identified that there were 18 suppliers to the 20 DHBs, while noting that these supplied gloves from two manufacturers worldwide. The review found that prices offered by each of the suppliers varied widely and it was agreed by the sector that there was an opportunity to buy these gloves on a national basis, potentially reducing the number of suppliers and achieving lower costs.
A final national supply contract for all DHBs was signed in December 2012; this meant reducing the number of suppliers to 6 from 18. The tender process used a ‘sector-first online, real-time electronic procurement process’134 arranged by HBL which permitted preselected suppliers to bid competitively to secure orders. It is thought that this process in itself resulted in a reduction of prices by 20–25%. 135 HBL estimates that the national non-sterile gloves contract resulted in savings of NZ$700,000 across all DHBs in 2012–13, and is forecast to result in a cumulative NZ$5.9M (≈ £3M) over the 3-year term of the contract.
The collective procurement workstream also involved the establishment of HBL Clinical Council, which includes representatives of the medical and allied health professions across New Zealand. 136 The council is expected to provide advice on product groups and on opportunities to improve care quality and delivery more generally to inform HBL’s work. Equally important, perhaps, it also provides an avenue for HBL to access wider clinical networks and associations, so ensuring that ‘clinical communities remain informed of HBL’s programme’,136 which can be seen to secure ‘buy-in’ from clinicians, perceived to be a powerful lever for success (NZ KI).
Finance, procurement and supply chain programme
Health Benefits Limited has been working with DHBs on the design and implementation of a national finance, procurement and supply chain (FPSC) operating model, and by mid-2013 a single provider for warehousing and distribution services to all 20 DHBs had been agreed upon. 129,136 As part of the FPSC programme, HBL, in collaboration with DHBs, has also been working to develop a DHB National Catalogue134 and a single financial management information system for the sector. 129 The catalogue seeks to address the fragmentation of the current system in which DHBs approach purchasing of goods and services in different ways in the absence of a single register. The focus of the catalogue is on clinical and non-clinical consumables which can be reordered. 137 It is anticipated that DHBs will be able to begin purchasing from the catalogue, enabled through GS1 (global standards) net,138 progressively over 18 months, beginning from 2014, as a common computerised purchasing system is being put in place. 135
The anticipated benefits of centralising the approach to procurement through a single catalogue and the use of a single provider for supply chain services include savings through permitting bulk purchasing, consistent processes and systems, and operational cost savings, among others. 136
In this context, HBL has built a strategic partnership with healthAlliance N.Z. Limited (healthAlliance), a stand-alone company established in 2000 as a joint venture between two DHBs in the north of New Zealand to provide key non-clinical business services for both DHBs. 139 HBL became shareholder in 2011, along with two additional DHBs, each holding 20%. healthAlliance is expected to have a variety of roles as one of the FPSC shared service providers for the New Zealand health sector. 129
Assessment of the changes in procurement in New Zealand
In its first 2 years of operation, HBL was reported to have achieved cumulative savings of NZ$114.6M (≈ £60M); these were largely attributed to collective procurement initiatives. 133 Forecasts estimate further gross annual savings from around NZ$100M in 2012–13 to NZ$150M per annum in subsequent years, adding to a cumulative gross saving of NZ$795M by 2015–16 (≈ £415M). 129
The overall impacts of the establishment of HBL and the wider changes in the system towards the intended development of a sustainable health system in New Zealand have yet to be demonstrated (NZ KI). The performance of HBL as such can be assessed against the objectives it set out to achieve, that is, the extent by which HBL succeeded in contributing to gross benefits over the 5-year period after its establishment, with defined long-term outcomes providing a further benchmark for measuring success. 129 Important achievements can be seen in centralising the procurement function. Concerns among suppliers that the centralised approach might stifle innovation have been countered by the argument that the processes put in place by HBL have provided for a clear framework for suppliers to work with (NZ KI).
However, challenges remain. For example, one of the key barriers to strengthening procurement in the health sector in New Zealand, in addition to a fragmented approach to procurement activities, has been a perceived lack in procurement capacity and capability (NZ KI). There has been an interest in centralising leadership by bringing together procurement leads into one group to build capacity and optimise training, but such a move has an impact on positions locally.
When interpreting the New Zealand experience, it is important to consider that with a population of 4.3 million the New Zealand market is small. For comparison, the average population size overseen by strategic health authorities in England before the 2012 health reform was around 5 million. 140 The overall bargaining power in New Zealand is thus small compared with larger markets, which are able to leverage size vis-à-vis negotiating power (NZ KI). A key feature of the New Zealand system can be seen to lie in a perceived culture of working together for the benefit of the population (NZ KI), which may facilitate introducing system changes that may be less acceptable elsewhere.
Group purchasing organisations in the hospital sector in Europe
Background
Group purchasing organisations in the health-care sector act as ‘purchasing intermediaries’ that negotiate contracts between health-care providers and manufacturers, distributors and other suppliers of a range of medical goods and services. 141 Through pooling the purchases of these products for their customers, GPOs can negotiate lower prices from suppliers, which may result in cost savings for health-care providers. 142
Group purchasing organisations started emerging in the USA in the late 1950s. 143 According to the Healthcare Supply Chain Association, which represents 14 GPOs in the USA, about 98% of US hospitals use GPOs to purchase products, on average between two and four GPOs per facility. 144 It is estimated that GPO contracts account for just over 70% of non-labour hospital purchases. 144,145 Although a large number of GPOs operate in the USA (> 600), the market is concentrated in a small number, with six of the largest national GPOs accounting for almost 90% of all hospital purchases. 146
During the early 2000s, GPOs became subject to congressional scrutiny because of concerns about potential anticompetitive practices, including the charging of fees to manufacturers by GPOs, raising questions about conflicts of interest, among other things. 141,143 In response, in 2005 nine GPOs established the Healthcare Group Purchasing Industry Initiative to promote best practices and public accountability among its member GPOs. 146,147 Although this effectively operates as a self-regulatory body, the government has retained federal oversight. 146
Empirical evidence of the impact of GPOs on pricing for hospitals in the USA is limited. 142 Studies that are available suggest that GPOs appear to reduce health-care costs by lowering product prices,148,149 and also reduce transaction costs through commonly negotiated contracts. 148
Group purchasing in European countries
Group purchasing in the publicly funded health-care sector has become an increasingly important feature in some European health systems from the late 1990s onwards, in response to a perceived need to reduce fragmentation, inefficiencies and lack of transparency in procurement activities; examples include England, France, Germany and, more recently, Italy. 11 The nature of group purchasing differs across countries, however, with varying involvement of national or regional public agencies in the co-ordination or oversight of procurement activities in the publicly funded system. 150 For example, in Italy collaborative procurement associations or other forms of collaboration have been set up at regional level,28 and the national procurement agency is tasked with the co-ordination of a network of regional central purchasing bodies. 151 In France, public sector reforms in the mid-2000s have encouraged the formation of nationally and regionally grouped procurement consortia, including in the health-care sector,11 with GPOs playing an increasingly important role in the government’s efforts to strengthen public procurement, as we shall see in the next subsection.
In Germany, about 80% of hospitals use GPOs, and the volume of non-labour hospital spending processed through GPOs increased from an average of around 20% in 2000 to 42% in 2010. 152 The organisational structure, remit and scope of GPOs in Germany varies, ranging from hospitals jointly co-ordinating their procurement to non-binding and binding purchasing companies. 153 The main focus of hospitals joining purchasing associations or organisations has been on cost savings through custom contracting, that is, contract and price negotiations,154 although more recently GPOs have begun to offer additional services such as IT, process consulting and logistics services. 153 It has been estimated that in 2010, hospitals in Germany made cost savings in the region of €4B through the use of GPOs. 152 GPOs are also playing an increasingly important role in Austria and Switzerland;152 there are indications of an increasing consolidation and Europeanisation of GPOs, with, for example, Prospitalia, one of Germany’s leading GPOs, which has established subsidiaries in Austria and the Netherlands, also foreseeing the formation of so-called ‘super GPOs’ across the European health sector. 155
Group purchasing in European countries: the experience in France
The French health system is based on statutory health insurance (SHI) and provides all legal residents with health coverage, as per the 1999 Universal Health Coverage Act (CMU Act). 156 In 2011, SHI accounted for 73.1% of health expenditure, complemented by taxation (3.6%), out-of-pocket payments (7.5%) and private health insurance (15.7%). 117 About 95% of the population hold complementary private health insurance to cover user charges and/or excluded services (e.g. psychologists, dieticians). 157 National health expenditure in 2011 was 11.6% of GDP (UK 9.4%), with per capita spending at US$4118 compared with an average spend across the OECD of US$3339 (UK US$3405). 117 Compared with 2000, health expenditure in France grew by 2.5% per year in real terms (OECD 4.1%; UK 4.5%).
Although the Ministry of Health oversees overall health sector planning and provides guidance on health policies, regions have an increasingly important role in health-care governance through regional health agencies [agence régionale de santé (ARS)]. 156 Created in 2010 following the 2009 Hospital, Patients, Health and Territories Act, the ARS are responsible for ensuring that health-care provision meets the needs of the population by improving co-ordination between ambulatory and hospital care and health and social care services, while respecting national health expenditure objectives.
Health services are delivered by public and private providers in ambulatory care and in hospital. GPs mainly work in private practice as self-employed professionals, with around 75% working in health centres or hospitals in addition to their private practice. GPs are reimbursed on a fee-for-services basis, with fees set nationally, based on agreements between professional organisations and the SHI administration. Since 2009, GPs can also enter into individual contracts with the SHI to receive additional payment in compensation for ‘practice improvements’ (pay for performance; from 2011 this was extended to also include specialists). 158 Specialists are paid based on fee for service in both private practice and private hospital settings. Specialists employed in a public hospital receive a salary.
Patients are able to access specialists in hospitals and private practice directly. In 2004, a ‘soft’ form of gatekeeping was introduced to encourage patients to see a GP before visiting a specialist, referred to as ‘preferred doctor’ (médecin traitant). Although a voluntary scheme, there are strong financial incentives for patients to sign up, and more than 85% of the population is registered with a GP. 157
The hospital sector in France
Secondary and tertiary care is provided by a mix of public (including private not-for-profit) hospitals, covering two-thirds of hospital beds, and private for-profit hospitals. 157 There were just under 2700 hospitals in France in 2011. 117 Public hospitals are legally and financially independent but overseen by the state, whereas private not-for-profit hospitals are typically managed by associations, foundations, mutual insurance companies or others. 159 Private for-profit hospitals are civil or commercial enterprises and, increasingly, form large corporations. 157
Hospital care is financed through an activity-based funding system using diagnosis-related groups, which became fully operational in 2008. The system is used to reimburse both public/private not-for-profit and private for-profit hospitals. Private for-profit hospitals have been paid entirely through diagnosis-related groups since 2005. 160 The aforementioned 2009 Hospital, Patients, Health and Territories Act has introduced a number of changes to the governance of public and not-for-profit hospitals, increasing their autonomy and organisational flexibility. 156 This also included devolving executive responsibilities from the administrative board of the hospital (subsequently the monitoring board), which comprises representatives of the state, local authorities, hospital staff, patients and qualified personnel, to the hospital director.
In 2006, the government launched a continuum of initiatives that sought to strengthen efficiency in the French public sector, in particular the introduction of nationally and regionally grouped procurement strategies. 161 As part of this strategy, in 2011 the government introduced the PHARE programme, in an attempt to achieve further efficiency gains in the hospital sector. 162 It is estimated that procurement in the hospital sector amounts to an annual expenditure of €18B, of which around 60% is spent on medical goods and services. 163 The PHARE programme set out to realise ‘smart savings’ by means of providing hospitals with greater flexibility within a financially constrained environment while improving the quality of care provided to patients. 116 The overarching goal was to enable all the levers for effective procurement, including group purchasing or framework contracting, optimising products and services purchased and optimising procurement processes. 116
The programme identified a hospitals’ savings potential of a total of €910M over the period 2012–14. 162 This was to be achieved through the development of a purchasing function within institutions with a unique responsibility for procurement; the development of a regional procurement policy by the ARS; and the development of a national pilot project led by the Directorate General of Health Care Provision at the Ministry of Health [Direction générale de l’offre de soins (DGOS)]. 162
The programme is organised around six areas: (i) procurement performance, which seeks to mobilise all levers and build support through projects (project ARMEN; Box 3) and support for the development of regional markets; (ii) institutional support, including support for the leading 150 institutions in the development of their first shared procurement plans, and development and dissemination of dedicated tools (‘Kit ES’) and training opportunities; (iii) support for regional health agencies (ARS) as moderators and facilitators of strategic procurement at regional level, including for the development and dissemination of specific tools (‘Kit ARS’); (iv) communication including newsletters, websites and meetings of decision-makers; (v) leadership, including monitoring of progress of the programme and possible corrective action; and (vi) launch and management of high-impact cross-cutting projects such as streamlining the procurement process, procurement information systems and supply chain. 162
The ARMEN project is one of the major arms of the PHARE programme; it seeks to identify opportunities for savings in a range of purchasing domains. 164 Bringing together 10 working groups from the hospital community (purchasers, pharmacists, biologists, engineers and prescribers from health institutions), each specialises in a specific procurement area. Under the supervision of the DGOS, groups are tasked to identify good practices that have already been successfully implemented, to quantify and derive practical recommendations and directives. These ‘smart savings’ should enable institutions to improve procurement strategies and thus increase their margins to act in the interest of patients.
The first wave, conducted from March to June 2012, focused on 10 procurement areas, such as laboratory consumables, disposable medical and surgical equipment, medical equipment maintenance and repair, laundry, real estate, insurance and others. It is suggested that the resulting recommendations would allow for potential gains in the order of €1.2B in 3 years, or 13% of expenditures in the 10 sectors covered in the first wave. The second round of ARMEN was formally launched in November 2012, with a further 10 procurement areas to be explored.
By March 2013, ARMEN had quantified over 110 ‘good practices’ in procurement, with processes involving professionalisation of the dialogue between suppliers and purchasers; the development of joint activities; optimising of products and services purchased; and optimising purchasing techniques and processes. 162
Group purchasing organisations as key players within the Performance Hospitalière pour des Achats Responsables programme
One of the aims of the PHARE programme was to demonstrate ‘quick wins’ in its efforts to strengthen procurement in the health-care sector. 162 This was to be achieved, in part, through building on and bringing in the expertise of existing operators in the market, identified as the four large public, not-for-profit GPOs: UniHA, UNICANCER, Union des Groupements d’Achats Publics (UGAP) and Réseau des acheteurs hospitaliers d’Ile de France (Résah-idf). In brief, the French public sector procurement co-operative UniHA represents 56 hospitals across France, including 30 university hospitals; it represents half of all public hospital procurement in France. 165 The UNICANCER group brings together the 20 French comprehensive cancer centres and their federation and pools their strategic activities: research, purchasing, human resources, hospital strategy, quality control and information systems. 166 UGAP is the only general public procurement agency in France, which represents public sector organisations in different areas including health care. 167
We here focus in on Résah-idf, which has been tasked by the Ministry of Health, as part of the PHARE programme, to support and co-ordinate the inter-regional network of health-care group purchasers (Alliance Groupements), bringing together over 100 groups, with an annual procurement volume of €8B. 168
Réseau des acheteurs hospitaliers d’Ile de France
Réseau des acheteurs hospitaliers d’Ile de France was established in 2007 as a public, not-for-profit organisation which supports the purchasing activities of about 135 public and private not-for-profit hospitals and nursing homes in the Paris region. 169 Funded by the Paris regional health authority (L’ARS Ile de France), Résah-idf covers around 42,000 beds and an annual procurement volume of €1.5B.
As noted above, Résah-idf has been tasked to co-ordinate the inter-regional network of group purchasers in the non-university hospital sector, the Alliance Groupements. The main objective of the Alliance is to help its members achieve efficiency gains on their purchases of a total of €215M during 2013 and 2014 in the areas of pharmaceuticals, medical devices, medical goods and supplies, alongside office supplies and consumables, food, waste and estate, among other things, while seeking to continuously improve the quality of care and staff working conditions. 168 Résah-idf’s role is to support the alliance by means of sharing best practice and leading on the professionalisation of the procurement process (Fr KI). Operating in close collaboration with the regional health agencies as facilitators of strategic procurement at regional level, this has involved, for example, the organisation of two inter-regional conferences to enable networking and information exchange. 170 Support further includes the development of tools, methods and procedures to enable efficient procurement through, for example, pricing models, benchmarking activities, the provision of training, etc.
Réseau des acheteurs hospitaliers d’Ile de France also co-ordinates the European Health Public Procurement Alliance (EHPPA), established in 2012,171 and co-ordinates the procurement special interest group at the International Hospital Federation172 in an attempt to promote the exchange of good practice and advancement of procurement practices through the provision of a framework for joint procurement policies and strategies, and to enhance and professionalise the non-profit health procurement sector in Europe more broadly.
Assessment of the Performance Hospitalière pour des Achats Responsables programme
Since the inception of the PHARE programme in 2011, reported progress has included an initial pilot phase that sought to demonstrate potential savings with one region and one facility as well as encouraging key actors to engage in the programme, and a subsequent expansion of the activities to cover a larger number of regions (at least 10) and facilities (20–30). 162 Since June 2012 through 2014, the programme is being rolled out nationally, including an acceleration of exchange of best practices, support for the top 150 institutions in the implementation of their first shared procurement plans and promotion of the creation or consolidation of regional procurement policies. Given the ongoing roll-out of the programme, it is too early to assess its overall impact. Important achievements of the programme could be seen as having placed procurement as a strategic issue on the agenda, and its facilitation of the networking of actors within and across regions (Fr KI). Recent figures from the French Ministry of Health suggest that by mid-2013 savings of approximately €200M had been achieved within the PHARE programme. 163
A key feature of the French approach to public procurement in the health sector is the emphasis on the region as a hub for group purchasing activities. The regional unit, with a procurement volume in the region of €1.2–1.5B, can be seen to provide potential for the demand side to take advantage of savings achieved through collective procurement while allowing sufficient scope for suppliers to engage in the process and guarantee contracts (Fr KI). Elsewhere, there has been concern that increasing centralisation of the procurement function, whether at regional or national level, may have a negative impact on the adoption of innovation in the health-care sector, with the possible exemption of ‘breakthroughs’, because of demand standardisation and reduction of market prices. 150 Related concerns have been raised around the extent to which collective procurement may disadvantage small- and medium-sized enterprises (SMEs), for example in relation to large volumes or administrative requests under public tendering conditions. 150 Empirical evidence regarding whether GPOs promote or hinder innovation is rare and conflicting. Burns and Lee (2008),148 based on a national survey of hospital purchasing groups in the USA, did not find evidence that GPOs exclude new innovative firms from the marketplace, while Hu and Schwartz (2011),149 using modelling techniques, concluded that GPOs reduce manufacturers’ incentives to introduce innovations to existing products. These two findings are not mutually exclusive, however, and highlight the need for further research to understand the impact of GPOs and collective procurement more generally on innovation. 11
Chapter 5 Discussion, conclusions and research recommendations
In this report we have sought to assess the evidence on procurement and SCM in sectors outside and within health care that can inform practice in the NHS, drawing on a REA, interviews with a small sample of key informants in the NHS and examples from experiences in other health systems. This chapter explores how our findings contribute to advancing our understanding of the diverse evidence base on procurement and SCM and identifies key learning points, including implications for the NHS. We conclude with recommendations for further research into best practices that may inform procurement and SCM in the NHS. However, before discussing our findings it is necessary to highlight some of the limitations of the work presented here.
Limitations of the study
Search strategy
The review presented in this report sought to capture evidence in the area of procurement and SCM in a wide range of sectors to identify best practices that may inform practice in the NHS. In order to manage the potentially large number of eligible studies for review within the time frame of this study of 9 months, it was necessary to focus the search terms while keeping the search area as broad as possible. The nature of the subject area also meant that approaches to systematic searches that, in the health field, can draw on medical subject headings, were of limited applicability. This meant that we had to test the performance of free text search terms, in isolation and in combination, to assess the volume of studies of potential relevance. Given the large number of records identified by initial searches we used an iterative process to narrow the searches, working with an information scientist, to arrive at a manageable number of studies for screening and further analysis. Our final search strategy applied a fairly restricted combination of search terms, requiring presence of both ‘supply chain’ and ‘procurement or purchasing or supply chain management’ in title, abstract or subject (see Appendix 1). Although this still yielded a large number of studies (in excess of 12,000), it is possible that this approach missed studies that would have been of relevance for this review.
We further narrowed the review by including studies that reported empirical findings only. However, as empirical work in the field of procurement is limited, we broadened our definition of ‘empirical’ to also include single case studies. Given our broad approach to the search, it is perhaps not surprising that studies identified as eligible for inclusion in the review covered a very wide range of aspects in the fields of procurement and SCM, with few examples of actual interventions in practice, which may simply be a reflection of the field and the methodological approaches that are typically used. It is possible that an alternative approach which had focused on specific themes within the procurement and SCM fields might have identified studies that would have informed specific learning in particular aspects. However, the call for proposals for the present review asked for an overview of the field, and we believe such a broad approach provides a necessary starting point to guide future research that focuses in on specific questions around procurement or SCM to inform learning for health care more broadly and the NHS specifically.
We imposed a limit on the publication date of studies to be considered for review and used the year 2006 as a cut-off, excluding earlier studies. We accept that by restricting the inclusion of potentially eligible work in such a way we may have inadvertently excluded earlier studies that could have provided important lessons to be drawn. The cut-off was chosen for pragmatic reasons, noting that certain aspects such as the use of technology and sustainability have emerged as core themes only since the mid-2000s. The evidence assessment further excluded studies published in languages other than English and those set in low- and middle-income countries. Again, by imposing these exclusion criteria we may have missed potentially important developments in those settings, although we should emphasise that the health care and system infrastructure in low- and middle-income countries is very different from that of high-income settings, likely restricting the transferability of experiences to the NHS context.
Keeping these limitations in mind, we should, however, note that we feel confident that our searches and review have captured themes that we understand to be most pertinent to the field of procurement and SCM as it concerns the health-care sector. This assertion is further supported by the key themes that have emerged from interviews with a small number of stakeholders in England, which tend to mirror the themes identified from the literature.
Furthermore, we believed it to be important to also consider the health-care sector itself as a direct source for both best practice and learning, and we consider the inclusion of health-care-specific studies to be adding value to the final selection in terms of lessons learned of relevance to the NHS. These studies also added an important comparative component to our analysis, in that the concepts analysed from examples in other sectors could be compared with initiatives currently tested within health-care settings.
Finally, in our initial research protocol we proposed undertaking systematic assessments of the experience of procurement and SCM in the health-care sector in other high-income countries. However, as described earlier, following the 2013 publication of the NHS procurement development programme9 we believe that in-depth assessment of country experiences in this field more generally would have added little additional value for learning, given that the NHS procurement programme will be implemented in due course. We therefore focused on two specific examples of countries that have recently also introduced a strategic framework or reform to guide procurement in their respective health-care sectors. We accept that by following this approach we may have unduly limited the potential for learning from elsewhere, although we should note that this component of the work was aimed at complementing the REA rather than presenting a separate study in itself, which would have been outside the scope of this research.
Framework for analysis
We should note that our initial research protocol anticipated a review of the evidence on procurement and SCM in areas other than health care to inform potential lessons for the health-care sector in England by identifying models of good practice. However, on conducting an initial scan of the published evidence it became clear that distinct ‘models’ of procurement and SCM were not present in the literature and in the field overall in a way that would have allowed appraisal of models by sector. Instead, the published literature focused on different approaches to purchasing and SCM practices described for different settings. Against this background we believed it to be useful to adopt a more ‘emergent’ approach by allowing the themes to emerge from the literature itself. In addition, we note that the original protocol presented a framework for analysis which would have allowed us to categorise the learning from both the theoretical models and the individual industry sectors into specific ‘areas for improvement’ for the NHS. However, we also noted that a review of practice in other sectors would require further analyses to demonstrate transferability and applicability to the health-care sector. Firstly, transferability in identifying the types of practices, such as, for example, environmental approaches or group purchasing that could be beneficial to a health-care setting, would have to be analysed through further study. In turn, further analyses would be required to understand the mode of practice that would be applicable to specific areas within health care, for example large or small equipment and devices, consumables and stationery, where different approaches might accrue differential benefit. Such an approach was, however, beyond the scope of this study, although we acknowledge that the use of such a framework may help guide future research. We therefore chose an analytical framework that served to synthesise the themes emerging from the literature in the form of a logic model used to group the emerging themes and areas of learning to a hypothetical NHS context (presented in Chapter 2, Figure 1). However, we caveat that the model was not intended to identify causal links between identified processes and outputs specifically, and was used as a means to summarise the themes only. Its relation to the emerging themes is described further in the discussion of the findings (see Although the evidence remains limited, it is possible to draw some general lessons).
Key learning from the study
The nature and quality of the evidence of interventions in the fields of procurement and supply chain management is diverse
Thinking within and approaches to the fields of procurement and SCM have evolved considerably during the past decades, and this is reflected by wide variation in scope and domain, definitions, key trends, theories and methodologies seeking to characterise the fields. 173 SCM has been defined as a multicomponent field encompassing the four areas of logistics, marketing channels, purchasing and operations management. 173 Therefore, any review within and of this field will include studies across these areas, along with the wider range of methodologies employed across each. This broad scope is reflected in the literature identified in our initial scoping of the available evidence for this report, which can be categorised as follows:
-
hypothesis-testing studies, validated empirically through surveys or interviews
-
case studies of current practice
-
studies that test a model or theory without presenting empirical evidence
-
studies with scholarly contribution only (i.e. setting recommendations for further scholarly research only).
Of these, we only considered studies that presented some form of empirical evidence as eligible for inclusion in the full review. Evidence identified covered a range of sectors and industries, including textile, IT, the automotive industry and manufacturing, alongside the health-care sector.
Overall, the body of empirical work in the fields of procurement and SCM as identified here was limited, both in quantity and quality. At the outset it was challenging to identify examples of good practice given the very theoretical nature of much of the literature in these fields. Studies presenting practice examples tended to be rather weak in terms of methodology, lacking adequate description of methodological design, modes of data collection and strategy for analysis. This observation is not necessarily new, however. For example, Carter et al. (2003),174 in a review of studies published in the Journal of Supply Chain Management, found that nearly 90% of the articles published from 1965 to 1999 consisted of normative literature, methodology reviews and exploratory studies; only a small proportion of studies provided empirical studies involving hypothesis testing. They highlighted the need for systematic assessments of the existing literature as well as rigorously designed inductive studies that would allow for the development of frameworks and testable research propositions. Subsequent work by the same authors further highlighted a possible trend away from the use of empirical data collection (such as surveys and case studies) and corresponding methodologies towards econometric modelling, at the possible expense of empirical approaches. 175 The need for empirical work was also suggested by review work included in our report, such as the study by AlSagheer and Ahli (2011),44 who assessed the evidence base for supply chain integration in relation to business performance. This was recently also highlighted in relation to the broader field of purchasing or commissioning of health services, with Allen (2009)176 noting how lesson drawing for the NHS is challenged by weaknesses in the existing evidence base.
In addition to the relative lack of empirical evidence, our review highlights that where data are presented, studies frequently fail to assess (or describe) the robustness of their methodological approaches when linking interventions with outcomes, such as cost savings or improved performance. Typically, although not always, the review had to rely on single case studies and evaluations of an intervention were seldom presented. Where cost data were presented, analysis frequently did not consider initial investment costs associated with a given new intervention, so it is difficult to arrive at firm conclusions on return on investment and efficiency gains more broadly.
We should note that identifying evidence from the procurement and SCM fields that may be applicable to health care, or any area of the public sector, remains challenging. Thus, a recent literature review on the use of processes developed in the private sector within the public sector showed that 51% of publications focused on ‘lean’ methods (i.e. streamlining processes) and 13% on business process re-engineering, while 35% stated their use in health services. 177 That review had to draw mainly on case studies, and the authors noted that these usually failed to consider the influence of factors such as context, behavioural aspects, organisational design or policy implications. Others have argued that the majority of studies on methodologies such as lean in the public sector tend to lack a suitable comparator or generally a rigorous study design. 178
Although the evidence remains limited, it is possible to draw some general lessons
The evidence review, complemented by interviews with key stakeholders and insights from experiences in other countries, identified three general themes of potential learning: (i) organisation and strategy, (ii) collaboration and relationships, and (iii) materials and information management. We discuss the main insights below.
Organisation and strategy
Within the theme of organisation and strategy we identified three subthemes: aspects of sustainability and ‘green’ issues with respect to managing and operating an organisation; collaborative, or group, purchasing; and benchmarking and price comparisons. Available evidence suggests that opting for a ‘green’ supply chain can increase staff morale and organisational reputation. This may be due, in part, to positive associations implied by such approaches, but evidence of cost savings was primarily related to cases where financial incentives for purchasing ‘green’ products exist.
Evidence from the literature and complementary data sources both locally and internationally points to the value placed upon collaborative, or group, purchasing. Empirical evidence that is available points to the potential for cost savings that have been associated with collaborative purchasing, and the potential for purchasers to build longer-term relationships with suppliers. There was a perception among stakeholders interviewed for this study that group purchasing could provide the NHS with the financial leverage to enter into larger contracts, a perception supported from a New Zealand perspective described here, where a smaller market size can be seen to reduce bargaining power. Against this background, it is important to add that evidence from both New Zealand and France suggests that in order for group purchasing to ‘work’, conditions would have to be put in place suitable to overcome fragmented and disaggregated decision-making by individual purchasers. In New Zealand this was achieved by making group purchasing ‘mandatory’ for district health boards by virtue, while in France, the non-competitive nature of GPOs operating in the public and not-for-profit health sector may be seen to be facilitating buy-in from service providers.
Collaboration and relationships
Intrateam collaboration and the engagement of practitioners was recognised as an enabler of SCM performance in the studies considered in our review. In health care, the practitioners would be clinicians, and experience from both New Zealand and France reviewed in this report pointed to the core role of clinicians in strengthening procurement. Thus, clinician input can be seen to ensure that procurement activities meet service needs and benefit patients. Furthermore, clinicians can act as important multipliers in terms of securing buy-in in strategic procurement activities. Available evidence also noted how engaging clinicians in purchasing decisions can increase their knowledge of available products, and hence help in future supplier negotiations as the market is better informed.
One key aspect noted in relation to collaboration and relationships is that of skills and capacity. This aspect emerged as a particularly strong theme from the international case studies in New Zealand and France, where lack of procurement capacity and capability has been viewed as one of the key barriers to effective procurement in the health-care sector. In both countries, recent policy developments have placed particular emphasis on building capacity and capability for procurement, with considerations for ‘bundling’ capacity to further enhance the procurement function. The 2013 procurement development programme for the NHS also identifies procurement capabilities as a core requirement for effective procurement and sets out recommendations for strengthening leadership and capability for procurement in the NHS. 9
Maintaining a good working relationship with suppliers was also described as an important lever in strengthening the procurement function, by means of information sharing and shared values to support negotiation and contracting. Again, experiences from New Zealand and France provide useful insights in that approaches established to strengthen the procurement function seek to engage suppliers not only to facilitate information exchange, but also to gauge advice on potential efficiency reserves from the supplier perspective.
Materials and information management
By automating purchasing functions (e.g. online purchases or software for internal use) organisations may benefit from more efficient inventory control and cost savings. These outcomes were more easily measured and evaluated in the studies we reviewed, although little reference was made to these issues in the key informant interviews. This may be attributed to the large number of studies in the operations, product development and automotive sectors. Published evidence also pointed to the likely impacts of improved stock management and tracking of items within an organisation, using technologies such as RFID tagging. The most direct outcome of this is cost savings (especially with online tracking of purchases), given that costs of previous purchases and rentals could be monitored and compared over time. Studies in health-care settings noted the potential safety implications of using tracking approaches such as RFID tagging; this would allow for location of devices in hospitals and improved inventory management so that devices are readily available when needed in critical times, leading to improved efficiency in the operation of hospital functions. Benchmarking and price comparisons were noted as potentially effective tools allowing for more balanced contract negotiation with suppliers, also with the potential to generate cost savings. In the examples identified by our interviews, the potential for cost savings is explicit, but those from literature lacked rigorous empirical evidence. However, available evidence that did report on efficiency and cost savings frequently did not account for the initial investment costs and often it was not clear how reported savings were arrived at.
Overview of key learning from the studies
Building on our framework described in Chapter 2 (see Figure 1), we have organised the key learning emerging from the findings of the study presented in this report in the form of a logic model to illustrate the potential applicability of our findings to a (hypothetical) NHS context (Figure 3). Inputs refer to the knowledge of available product for purchase within an organisation, but also the professional capabilities of those working in purchasing functions, which was reflected in both the evidence review and interviews. Under processes we list the types of approaches identified in this study, such as collaboration and engagement, electronic tagging and information sharing. We further list the types of outputs that arise from these processes, which we extracted from the literature, although we caveat that most of these were reported as narratives and not evaluated after implementation. These outputs could potentially be linked to potential outcomes such as cost savings, general efficiencies (resulting, for instance, from reduced staff administration time) and more effective performance management. We note that this framework guided the analysis of the evidence, serving to illustrate the types of associations between different components as demonstrated by the evidence reviewed. However, as we have highlighted, the quality of the evidence was frequently low and did not permit drawing robust conclusions as to the direction of (implied or empirically verified) links between the processes, outputs and outcomes.
FIGURE 3.
Framework for analysis including identified lessons (themes) from the study.
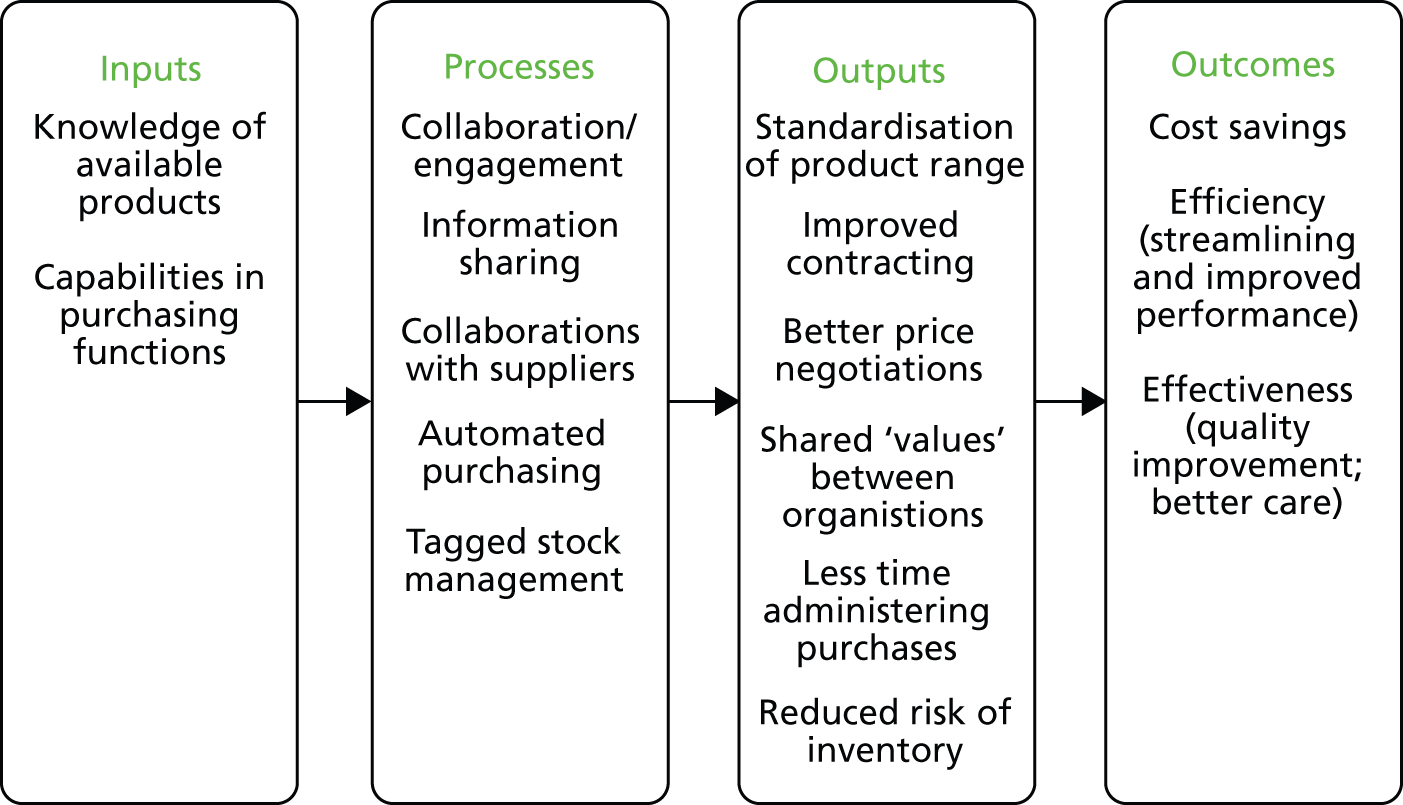
Implications for the NHS
Although we clearly caveat the challenges in taking lessons from other industries for the health-care sector, we provide some of our observations on selected aspects of the learning gained in terms of their implications for the NHS.
What type of supply chain for which device?
In Chapter 2, Rapid evidence assessment, we described the focus of lessons learned for this review to include particular items in the non-pay expenditures for the NHS: establishment, clinical supplies and services, drugs and pharmacy, and non-clinical supplies and services. This diversity of products and services that can be subsumed under the procurement function also means diversity in procurement and supply chain models. For example, according to the National Audit Office, different types of supply chains or purchasing model can be applied to different items. 179 Items essential to the achievement of the organisation’s key outputs (‘strategic items’), for instance, may require a different purchasing model to more routine, low-value items. It also implies that some of the learning from this review, such as collaborative purchasing and effective supplier relationships, may be more appropriate for either higher-value strategic items or low-value routine items. However, this current categorisation is not in line with the way supply chains are managed in the NHS (see Chapter 1, Table 1). For instance, medical devices can include anything from an X-ray machine or renal dialysis machine to an infusion pump or a simple thermometer. A thermometer may be considered a ‘routine’ purchase as it is low value, but at the same time it is critical to the achievement of the organisation’s key outputs (i.e. ‘strategic’). Categorisations of medical devices currently only exist for regulatory purposes (i.e. Food and Drug Administration and EU regulatory classifications) but not from a SCM perspective. Therefore, lessons learned from other sectors would have to be analysed according to different types of items purchased by the NHS.
What are the purchasing capabilities in the NHS?
The preceding section has highlighted the importance of professional capabilities in procurement. Capability can be built internally through experience or training, or, as indicated by international examples and interviews, can be provided externally, through professional services or outsourced purchasing support. Whatever the source of the expertise, our study highlights the importance of having appropriate skills for making appropriate purchasing decisions.
Although capabilities may be developed further in-house, there is also a consideration to be made for outsourcing purchasing functions or indeed adopting the group purchasing options suggested by the international examples included in this review.
What are the collaborative purchasing options?
In line with some of the evidence collected here, there is the potential to achieve savings by either collaborative purchasing or group purchasing. This could help in reducing variation in prices paid for routine items across trusts and so help streamline purchases further. As suggested by the evidence reviewed here, better data management and access to publicly available information on prices permitting benchmarking and transparency would be important to achieving this.
Which technologies should be employed and where?
A pattern observed in the studies reviewed is that most promising strategies likely involve substantial (up-front) investment in technology. The question for the NHS would therefore be how to use IT most effectively. This may be for better information management (i.e. to keep track of previous purchases and purchasing information) and better interorganisation information sharing (to enable a more transparent view of purchases across hospitals). However, the costs of the up-front investments for these technologies would have to be assessed in line with the overall value to the organisation. Furthermore, the (re)training of professionals and potential reassigning of procurement roles will have to be considered, if some functions are automated.
Research recommendations
The review highlights that there is an awareness among scholarly research and industry that SCM and procurement are areas for creating efficiencies and cost savings. Several dimensions within SCM and procurement for improving organisational performance and outcomes are explored: organisation and strategy (including sustainability issues), the option of collaborative purchasing, improving relationships with suppliers, building capabilities for skilful purchasing decisions and the use of technology for data and materials management. Many of these mechanisms are only described as before-and-after studies and do not include evaluations of their effects. Against this background, we have identified three recommendations for further research into this area.
-
There is a need for further research using rigorous methodology to assess the effectiveness of different types of interventions in different settings for improving purchasing and SCM. Many of the studies were essentially modelling or theoretical and tested only among stakeholders and their perceptions, rather than tried out in practice. Such studies, although rigorous within their own field, prove challenging when trying to extract lessons of good practice for other sectors and contexts.
-
Empirical research on current practices in health-care purchasing and SCM, or evaluation of new practices in health-care settings, should be implemented. A review of current practice in other industries, owing to its limitations in applicability, can only suggest general lessons and ultimately these would have to be tried out in practice. Although this review identified some empirical evidence in the form of case studies in health-care settings, these were seldom evaluated comprehensively and it has therefore proved difficult to understand how contextual factors may affect their implementation elsewhere. More in-depth case studies and evaluations of new practices, interventions and/or mechanisms used in health-care settings may provide such context-rich data. This would also allow for an analysis of different approaches to procurement according to the type of purchase made (i.e. consumables, medical devices, stationery), as these have varying requirements and supply chains.
-
An evaluation of the Department of Health’s 2013 Procurement Development Programme and its recommendations may provide an opportunity to focus evaluation efforts. In addition to local practices and approaches to procurement, the Department of Health’s Procurement Development Programme9 provides the unique opportunity to focus evaluation efforts across NHS organisations. Recommendations arising from this programme, including capacity training of procurement staff, better data management and strengthened clinician engagement, are believed to lead to efficiency savings and more streamlined SCM across the NHS. Future work could be commissioned to evaluate the effects of these individual initiatives or the programme as a whole.
-
There is a need for more interdisciplinary work across health-care management and SCM. Many of the studies found were testing a hypothesis through empirical means, and seldom was an intervention or mechanism tried out in practice. If adequate learning is to be compared across health-care management and general SCM research fields, future research is needed that acknowledges these differences but builds frameworks and approaches to adequately draw learning from each field.
Acknowledgements
We are grateful to Professor Ruth Boaden (Manchester Business School) and Dr Katri Kauppi (Aalto University School of Business) for their continuous advice and guidance in all stages of the work. We also thank Matthew Bassford, Jonathan Cave, Yun Kang and Maryse Penny (RAND) for their support in providing comparative examples in other sectors in our analyses. We would further like to thank John Warrington (Department of Health) for his guidance in helping us understand the policy context of this work. We are particularly grateful to Emma Pitchforth for her very helpful comments on an earlier draft of this report. We would like to highlight the contribution of Gail Kouril and Tomiko Envela (RAND) whose skills and expertise were essential in conducting the literature review. We should especially like to thank the interviewees and country experts for their time and interest in supporting this study. Finally, we would like to thank the NIHR Health Services and Delivery Research programme for their ongoing engagement and support.
Contributions of authors
Dr Saba Hinrichs (Analyst, Health and Healthcare) was involved in study design, data collection and analysis (literature review, interviews), and in the preparation of the report.
Deepa Jahagirdar (Associate Analyst, Health and Healthcare) was involved in data collection and analysis (literature review, interviews), and in the preparation of the report.
Céline Miani (Analyst, Health and Healthcare) was involved in data collection and analysis (literature review), and in the preparation of the report.
Benoit Guerin (Associate Analyst, Innovation and Technology Policy) was involved in data collection and analysis (literature review), and in the preparation of the report.
Dr Ellen Nolte (Research Director, Health and Healthcare) was principal investigator on the project. She was involved in study design, data collection and analysis (literature review, international case studies), and in the preparation of the report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Public Expenditure: Statistical Analyses 2013. Norwich: The Stationery Office; 2013.
- Progress in Making NHS Efficiency Savings. London: National Audit Office; 2012.
- Putting Patients First: The NHS England Business Plan for 2013/14–2015/16. London: Department of Health; 2013.
- Bentley TG, Effros RM, Palar K, Keeler EB. Waste in the US health care system: a conceptual framework. Milbank Q 2008;86:629-59. http://dx.doi.org/10.1111/j.1468-0009.2008.00537.x.
- Hurley E, McRae I, Bigg I, Stackhouse L, Boxall A-M, Broadhead P. The Australian Health Care System: The Potential for Efficiency Gains. Australian Government National Health and Hospitals Reform Commission; 2009.
- Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA 2012;307:1513-16. http://dx.doi.org/10.1001/jama.2012.362.
- Appleby J, Ham C, Imison C, Jennings M. Improving NHS Productivity: More with the Same not More of the Same. London: The King’s Fund; 2010.
- The Operating Framework for the NHS in England 2012–13. London: Department of Health; 2011.
- Better Procurement, Better Value, Better Care: A Procurement Development Programme for the NHS. London: Department of Health; 2013.
- The Procurement of Consumables by NHS Acute and Foundation Trusts. London: National Audit Office; 2011.
- Sorenson C, Kanavos P. Medical technology procurement in Europe: A cross-country comparison of current practice and policy. Health Policy 2011;100:43-50. http://dx.doi.org/10.1016/j.healthpol.2010.08.001.
- NHS Supply Chain . NHS Supply Chain: About NHS Supply Chain n.d. www.supplychain.nhs.uk/about-us/what-we-do/ (accessed September 2013).
- Procurement Capability Review. London: Office of Government Commerce; 2007.
- Necessity – Not Nicety: A New Commercial Operating Model for the NHS and Department of Health. London: Department of Health; 2009.
- National Innovation Procurement Plan. London: Department of Health; 2009.
- Innovation Health and Wealth: Accelerating Adoption and Diffusion in the NHS. London: Department of Health; 2011.
- Annual Report and Accounts for the Year Ended 31 March 2010. London: The Stationery Office; 2010.
- Innovation Nation. London: The Stationery Office; 2008.
- Equity and Excellence: Liberating the NHS. London: Department of Health; 2010.
- Cook J, DeBree K, Feroleto A. From raw materials to customers: supply chain management in the service industry. SAM Adv Manag J 2001;66:792-80.
- Yasin MM, Wafa M, Small MH. Benchmarking JIT: an analysis of JIT implementations in the manufacturing service and public sectors. Benchmarking Int J 2004;11:74-92. http://dx.doi.org/10.1108/14635770410520311.
- Kannan VR, Tan KC. Just in time, total quality management, and supply chain management: understanding their linkages and impact on business performance. Omega 2005;33:153-62. http://dx.doi.org/10.1016/j.omega.2004.03.012.
- Young T, McClean S. A critical look at Lean Thinking in healthcare. Qual Saf Health Care 2008;17:382-6. http://dx.doi.org/10.1136/qshc.2006.020131.
- Proudlove N, Moxham C, Boaden R. Lessons for lean in healthcare from using Six Sigma in the NHS. Public Money Manag 2008;28:27-34.
- Radnor ZJ, Holweg M, Waring J. Lean in healthcare: the unfilled promise?. Soc Sci Med 2012;74:364-71. http://dx.doi.org/10.1016/j.socscimed.2011.02.011.
- Improving the Efficiency of the Procurement of Routine Items. London: The Stationery Office; 1997.
- The Procurement of ‘Routine Items’: A Review of Progress. London: National Audit Office; 2008.
- Lega F, Marsilio M, Villa S. An evaluation framework for measuring supply chain performance in the public healthcare sector: evidence from the Italian NHS. Prod Plan Control 2013;24:931-47. http://dx.doi.org/10.1080/09537287.2012.666906.
- Gauld R. New Zealand’s post-2008 health system reforms: toward re-centralization of organizational arrangements. Health Policy 2012;106:110-13. http://dx.doi.org/10.1016/j.healthpol.2012.03.018.
- Phillips W, Knight L, Caldwell N, Warrington J. Policy through procurement: the introduction of digital signal process (DSP) hearing aids into the English NHS. Health Policy 2007;80:77-85. http://dx.doi.org/10.1016/j.healthpol.2006.03.008.
- Boaden R. Quality improvement: theory and practice. Br J Healthcare Manag 2009;15:12-6. http://dx.doi.org/10.12968/bjhc.2009.15.1.37892.
- Porter ME. What is value in health care?. N Engl J Med 2010;363:2477-81. http://dx.doi.org/10.1056/NEJMp1011024.
- Smith J, Woodin J, Walshe K, Smith J. Healthcare Management. Maidenhead: Open University Press; 2011.
- Murray JG. Towards a common understanding of the differences between purchasing, procurement and commissioning in the UK public sector. J Purchasing Supply Manag 2009;15:198-202. http://dx.doi.org/10.1016/j.pursup.2009.03.003.
- Raaij E, Schotanus F, Valk W. What Do We Know about Purchasing Health Care? A Systematic Literature Review and Research Agenda n.d.
- Ovretveit J. Purchasing for Health: A Multidisciplinary Introduction to the Theory and Practice of Health Purchasing. Buckingham: Open University Press; 1995.
- Figueras J. Purchasing to Improve Health Systems Performance. London: McGraw-Hill International; 2005.
- Slack N, Chambers S, Johnston R. Operations Management. Harlow: Pearson Education; 2010.
- Systematic Reviews: CRD’s Guidance for Undertaking Systematic Reviews in Health Care. York: Centre for Reviews and Dissemination, University of York; 2009.
- Call for Proposals for Rapid Evidence Syntheses for the NIHR Health Services and Delivery Research (HS&DR) Programme: Learning for the NHS on Procurement and Supply Chain Management. Southampton: NIHR; 2012.
- Denyer D, Tranfield D, van Aken JE. Developing design propositions through research synthesis. Organ Stud 2008;29:393-41. http://dx.doi.org/10.1177/0170840607088020.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Lancaster: Lancaster University; 2006.
- University of Cambridge . Patient and Public Involvement (PPI) n.d. www.medschl.cam.ac.uk/gppcru/index.php?option=com_content&view=article&id=497&Itemid=156 (accessed July 2013).
- AlSagheer A, Ahli M. Impact of supply chain integration on business performance and its challenges. Int Bus Econ Res J 2011;10:79-92.
- Azevedo SG, Carvalho H, Cruz Machado V. The influence of green practices on supply chain performance: a case study approach. Transport Res Part E: Logist Transport Rev 2011;47:850-71. http://dx.doi.org/10.1016/j.tre.2011.05.017.
- Azevedo SG, Carvalho H, Duarte S, Cruz-Machado V. Influence of green and lean upstream supply chain management practices on business sustainability. IEEE Trans Eng Manag 2012;59:753-65. http://dx.doi.org/10.1109/TEM.2012.2189108.
- Baier C, Hartmann E, Moser R. Strategic alignment and purchasing efficacy: an exploratory analysis of their impact on financial performance. J Supply Chain Manag 2008;44:36-52. http://dx.doi.org/10.1111/j.1745-493X.2008.00071.x.
- Birk S. Millions saved with purchasing coalition. Mater Manag Health Care 2009;18:26-8.
- Boniface A. Green giant. Supply Manag 2012;17:40-2.
- Bose I, Pal R. Do green supply chain management initiatives impact stock prices of firms?. Decis Support Syst 2012;52:624-34. http://dx.doi.org/10.1016/j.dss.2011.10.020.
- Brau JC, Fawcett SE, Morgan L. An empirical analysis of the financial impact of supply chain management on small firms. J Entrep Financ Bus Ventures 2007;12:55-81.
- Carpenter D. Bringing discipline to your supply chain. Hosp Health Netw 2008;82:49-52.
- Carroll K, Coker DW. Logistics modernization program: a cornerstone of army transformation. Army Logistician 2007;39:11-5.
- Case C. Gaining efficiencies through a single supply chain. Healthcare Exec 2011;26:54-5.
- Childerhouse P, Towill DR. Arcs of supply chain integration. Int J Prod Res 2011;49:7441-68. http://dx.doi.org/10.1080/00207543.2010.524259.
- Constantine B, Ruwadi B, Wine J. Management practices that drive supply chain success. McKinsey Q 2009;2:24-6.
- Elmuti D, Minnis W, Abebe M. Longitudinal assessment of an integrated industrial supply chain. Supply Chain Manag 2008;13:151-9. http://dx.doi.org/10.1108/13598540810860985.
- Elmuti D, Khoury G, Omran O, Abou-Zaid AS. Challenges and opportunities of health care supply chain management in the United States. Health Market Q 2013;30:128-43. http://dx.doi.org/10.1080/07359683.2013.787885.
- Font X, Tapper R, Schwartz K, Kornilaki M. Sustainable supply chain management in tourism. Bus Strat Environ 2008;17:260-71. http://dx.doi.org/10.1002/bse.527.
- Fugate B, Sahin F, Mentzer JT. Supply chain management coordination mechanisms. J Bus Logist 2006;27:129-61. http://dx.doi.org/10.1002/j.2158-1592.2006.tb00220.x.
- Golicic SL, Smith CD. A meta-analysis of environmentally sustainable supply chain management practices and firm performance. J Supply Chain Manag 2013;49:78-95. http://dx.doi.org/10.1111/jscm.12006.
- Guimarães CM, de Carvalho JC. Outsourcing in the healthcare sector: a state-of-the-art review. Supply Chain Forum 2011;12:140-8.
- Kroes JR, Ghosh S. Outsourcing congruence with competitive priorities: impact on supply chain and firm performance. J Oper Manag 2010;28:124-43. http://dx.doi.org/10.1016/j.jom.2009.09.004.
- Meehan J, Muir L. SCM in Merseyside SMEs: benefits and barriers. Total Qual Manag J 2008;20:223-32.
- Merschmann U, Thonemann UW. Supply chain flexibility, uncertainty and firm performance: an empirical analysis of German manufacturing firms. Int J Product Econ 2011;130:43-5. http://dx.doi.org/10.1016/j.ijpe.2010.10.013.
- Paulraj A, Chen IJ. Environmental uncertainty and strategic supply management: a resource dependence perspective and performance implications. J Supply Chain Manag 2007;43:29-42. http://dx.doi.org/10.1111/j.1745-493X.2007.00033.x.
- Rudberg M, Thulin J. Centralised supply chain master planning employing advanced planning systems. Prod Plan Control 2009;20:158-67. http://dx.doi.org/10.1080/09537280802705047.
- Zhu Q, Crotty J, Sarkis J. A cross-country empirical comparison of environmental supply chain management practices in the automotive industry. Asian Bus Manag 2008;7:467-88. http://dx.doi.org/10.1057/abm.2008.20.
- Abrahamsson M, Rehme J. The role of logistics in retailers’ corporate strategy: a driver for growth and customer value. Supply Chain Forum 2010;11:14-22.
- Barlow RD. Saving the ship during a fiscal storm. Healthc Purchas News 2006;30:10-4.
- Barnes J, Liao Y. The effect of individual, network, and collaborative competencies on the supply chain management system. Int J Prod Econ 2012;140:888-99. http://dx.doi.org/10.1016/j.ijpe.2012.07.010.
- Bilyk C. Don’t break the chain: importance of supply chain management in the operating room setting. Can Oper Room Nurs J 2008;26.
- Cadden T, Marshall D, Cao G. Opposites attract: organisational culture and supply chain performance. Supply Chain Manag 2013;18:86-103. http://dx.doi.org/10.1108/13598541311293203.
- Ciliberti F, de Haan J, de Groot G, Pontrandolfo P. CSR codes and the principal-agent problem in supply chains: four case studies. J Clean Prod 2011;19:885-94. http://dx.doi.org/10.1016/j.jclepro.2010.09.005.
- Cox A, Chicksand D. Rethinking policy options for industry: appropriateness in policies for industry and UK farming and food. Public Admin 2008;86:813-36. http://dx.doi.org/10.1111/j.1467-9299.2008.00726.x.
- Danese P, Romano P. Supply chain integration and efficiency performance: a study on the interactions between customer and supplier integration. Supply Chain Manag 2011;16:220-30. http://dx.doi.org/10.1108/13598541111139044.
- Kannan VR, Tan KC. Supply chain integration: cluster analysis of the impact of span of integration. Supply Chain Manag 2010;15:207-15. http://dx.doi.org/10.1108/13598541011039965.
- Ogden SM, McCorriston E. How do supplier relationships contribute to success in conference and events management?. Int J Contemp Hospitality Manag 2007;19:319-27. http://dx.doi.org/10.1108/09596110710747652.
- Pagell M, Krumwiede DW, Sheu C. Efficacy of environmental and supplier relationship investments: moderating effects of external environment. Int J Prod Res 2007;45:2005-28. http://dx.doi.org/10.1080/00207540600634931.
- Paulraj A, Chen IJ. Strategic buyer–supplier relationships, information technology and external logistics integration. J Supply Chain Manag 2007;43:2-14. http://dx.doi.org/10.1111/j.1745-493X.2007.00027.x.
- Periatt JA, Chakrabarty S, LeMay SA. Using personality traits to select customer-oriented logistics personnel. Transport J 2007;46:22-37.
- Richey RG, Tokman M, Skinner LR. Exploring collaborative technology utilization in retailer–supplier performance. J Bus Res 2008;61:842-9. http://dx.doi.org/10.1016/j.jbusres.2007.09.011.
- Roloff J, Aßländer M. Corporate autonomy and buyer–supplier relationships: the case of unsafe Mattel toys. J Bus Ethics 2010;97:517-34. http://dx.doi.org/10.1007/s10551-010-0522-1.
- Schloetzer JD. Process integration and information sharing in supply chains. Account Rev 2012;87:1005-32. http://dx.doi.org/10.2308/accr-10216.
- Thai VV. Competency requirements for professionals in logistics and supply chain management. Int J Logist Res Appl 2012;15:109-26. http://dx.doi.org/10.1080/13675567.2012.694859.
- Van der Vaart T, Pieter van Donk D. Buyer-focused operations as a supply chain strategy. Int J Oper Prod Manag 2006;26:8-23. http://dx.doi.org/10.1108/01443570610636996.
- Williams J. A team approach to cost containment. Healthc Financ Manag 2008;62:51-8.
- Kehoe B. Store-bought lessons. Mater Manag Health Care 2006;15:24-9.
- Alfaro JA, Rábade LA. Traceability as a strategic tool to improve inventory management: a case study in the food industry. Int J Prod Econ 2009;118:104-10. http://dx.doi.org/10.1016/j.ijpe.2008.08.030.
- Belkoski DA. Stop the supply chain insanity: retail as a model for hospitals. Healthc Financ Manag 2008;62:60-4.
- Bernhard W, Peter B, Zoltan PM, Maria-Luise O. The impact of ERP systems on firm and business process performance. J Enterprise Inform Manag 2006;19:13-29. http://dx.doi.org/10.1108/17410390610636850.
- Bhakoo V, Chan C. Collaborative implementation of e-business processes within the health-care supply chain: The Monash Pharmacy Project. Supply Chain Manag 2011;16:184-93. http://dx.doi.org/10.1108/13598541111127173.
- Bigné JE, Aldás J, Andreu L. B2B services: IT adoption in travel agency supply chains. J Serv Market 2008;22:454-64. http://dx.doi.org/10.1108/08876040810901873.
- Callender C, Grasman SE. Barriers and best practices for material management in the healthcare sector. Eng Manag J 2010;22:11-9.
- Campo S, Rubio N, Yague MJ. Information technology use and firm’s perceived performance in supply chain management. J Bus-Bus Mark 2010;17:336-64. http://dx.doi.org/10.1080/10517120903574649.
- Creedon C. Save time and money with supply chain automation. Mater Manag Health Care 2006;15:37-8.
- Cunningham J. Back to supply chain basics. Mater Manag Health Care 2006;15:32-8.
- Fawcett SE, Wallin C, Allred C, Fawcett AM, Magnan GM. Information technology as an enabler of supply chain collaboration: a dynamic-capabilities perspective. J Supply Chain Manag 2011;47:38-59. http://dx.doi.org/10.1111/j.1745-493X.2010.03213.x.
- Ghani K, Zainuddin Y, Ghani F. Integration of supply chain management with internet and enterprise resource planning (ERP) systems: case study. Global Bus Manag Res 2009;1:97-104.
- Gianakis G, McCue C. Supply management concepts in local government: four case studies. J Public Procurement 2012;12:109-41.
- Jeffery SS, Lorraine L, Mark G. The impact of RFID on service organizations: a service profit chain perspective. Manag Serv Qual 2009;19:179-94. http://dx.doi.org/10.1108/09604520910943170.
- Johnson PF, Klassen RD, Leenders MR, Awaysheh A. Utilizing e-business technologies in supply chains: the impact of firm characteristics and teams. J Oper Manag 2007;25:1255-74. http://dx.doi.org/10.1016/j.jom.2007.01.005.
- Krusius T. The national organization in a shrinking economy. ISBT Sci Ser 2012;7:99-101. http://dx.doi.org/10.1111/j.1751-2824.2012.01567.x.
- Leonard LNK, Davis CC. Supply chain replenishment: before-and-after EDI implementation. Supply Chain Manag 2006;11:225-32. http://dx.doi.org/10.1108/13598540610662121.
- Maggio MK, Perez JJ. Exceptional success. Health Manag Technol 2006;27:18-21.
- McHugh TM. Supply chain management in the clinical laboratory. Clin Leadersh Manag Rev 2006;20.
- Narayanan S, Marucheck AS, Handfield RB. Electronic data interchange: research review and future directions. Decis Sci 2009;40:121-63. http://dx.doi.org/10.1111/j.1540-5915.2008.00218.x.
- Page D. Automate your supply chain and reap the benefits. Hosp Health Netw 2011;85:41-2.
- Persona A, Battini D, Rafele C. Hospital efficiency management: the just-in-time and Kanban technique. Int J Healthc Technol Manag 2008;9:373-91. http://dx.doi.org/10.1504/IJHTM.2008.019674.
- Raviprakash AV, Prabu B, Alagumurthi N, Soundararajan V. RFID: Rx to healthcare industry. J Supply Chain Manag 2009;6:7-25.
- Smart AF. E-procurement and its impact on supply management: evidence from industrial case studies. Int J Logist Res Appl 2010;13:423-40. http://dx.doi.org/10.1080/13675567.2010.486760.
- Tarantilis CD, Kiranoudis CT, Theodorakopoulos ND. A web-based ERP system for business services and supply chain management: application to real-world process scheduling. Eur J Oper Res 2008;187:1310-26. http://dx.doi.org/10.1016/j.ejor.2006.09.015.
- Walker K. Does your supply chain management system deliver the goods? A case study. Supply Chain Forum 2010;11:86-93.
- Wieland B, Mastrantonio P, Willems S, Kempf K. Optimizing inventory levels within Intel’s Channel Supply Demand Operations. Interfaces 2012;42:517-27. http://dx.doi.org/10.1287/inte.1120.0637.
- Ygal B, Harold B, Richard P. Redesigning the replenishment process of medical supplies in hospitals with RFID. Bus Process Manag J 2010;16:991-1013. http://dx.doi.org/10.1108/14637151011093035.
- Ministère des Affaires sociales et de la Santé [Ministry of Social Affairs and Health] . The PHARE Programme n.d. www.sante.gouv.fr/achats-hospitaliers-le-programme-phare.html (accessed September 2013).
- OECD Health Data 2013. Paris: OECD; 2013.
- Gauld R, Thomson S, Osborn R, Squires D, Jun M. International Profiles of Health Care Systems, 2012. New York, NY: The Commonwealth Fund; 2012.
- Smith J. Critical Analysis of the Implementation of the Primary Health Care Strategy Implementation and Framing of Issues for the Next Phase 2009. www.health.govt.nz/system/files/documents/publications/critical-analysis-primary-health-care-strategy-sept09.doc (accessed September 2013).
- Ministry of Health . Nationwide Service Framework Library n.d. www.nsfl.health.govt.nz/apps/nsfl.nsf/menumh/General+Information (accessed September 2013).
- Fazekas M, Ettelt S, Newbould J, Nolte E. Framework for Assessing, Improving and Enhancing Healthcare Planning. Santa Monica, CA: RAND Corporation; 2010.
- World Health Organization, Ministry of Health New Zealand . Health Service Delivery Profile, New Zealand 2012 n.d. www.wpro.who.int/health_services/service_delivery_profile_new_zealand.pdf (accessed September 2013).
- Ministry of Health . Primary Health Care n.d. www.health.govt.nz/our-work/primary-health-care (accessed September 2013).
- Ministerial Review Group . Meeting the Challenge: Enhancing Sustainability and the Patient and Consumer Experience Within the Current Legislative Framework for Health and Disability Services in New Zealand n.d. www.beehive.govt.nz/sites/all/files/MRG%20Report%20Meeting%20the%20Challenge.pdf (accessed September 2013).
- Letford K, Tenbensel T. Health System Restructuring: Government Response n.d. http://hpm.org/nz/a15/2.pdf (accessed September 2013).
- National Health Board . Our Structure n.d. www.nationalhealthboard.govt.nz/about-us/our-structure (accessed September 2013).
- National Health Committee . Terms of Reference n.d. http://nhc.health.govt.nz/about-us/terms-reference (accessed September 2013).
- New Zealand House of Representatives . Briefing from Health Benefits Limited. Report of the Health Committee n.d. www.parliament.nz/resource/0000254764 (accessed September 2013).
- Statement of Intent 2013/14–2015/16. Final version 1.1. Auckland: Health Benefits Limited; 2013.
- Ministry of Justice . Health Benefits Limited n.d. www.justice.govt.nz/publications/global-publications/d/copy_of_directory-of-official-information-december-2011/alphabetical-list-of-entries-1/h/health-benefits-limited (accessed September 2013).
- Health Benefits Limited . Statement of Intent 2010 11 n.d. www.comu.govt.nz/resources/pdfs/hb/hb-sci-10.pdf (accessed September 2013).
- Belich A. Health benefits limited: don’t be fooled by the name. Specialist 2011;88:7-9.
- Annual Report 2012. Auckland: Health Benefits Limited; 2012.
- Health Benefits Limited . Pathway July 2013 n.d. http://hbl.co.nz/News/67/pathway-july (accessed September 2013).
- Health Benefits Limited . Stronger Together n.d. www.healthbenefits.co.nz/system/files/HBL%20Brand%20Book_July%202013_FINAL.pdf (accessed September 2013).
- Health Benefits Limited . Pathway September 2013 n.d. http://hbl.co.nz/News/68/pathway-september (accessed September 2013).
- Health Benefits Limited . DHB National Catalogue &Amp; GS1net – Supplier Guide n.d. www.gs1nz.org/files/3613/7947/2788/HBL_GS1net_Supplier_Guideline.pdf (accessed September 2013).
- GS1 New Zealand . DHB National Catalogue Supplier Information n.d. www.gs1nz.org/services/gs1net/gs1net-supplier-information/ (accessed September 2013).
- Statement of Intent 2012/13–2014/15. Auckland: healthAlliance; 2012.
- NHS . Strategic Health Authority Configurations n.d. www.nhs.uk/NHSEngland/aboutnhs/Documents/MapofSHAsFeb09.pdf (accessed October 2013).
- Group Purchasing Organizations: Services Provided to Customers and Initiatives Regarding Their Business Practices. Washington, DC: GAO; 2010.
- United States Government Accountability Office . Group Purchasing Organizations: Research on Their Pricing Impact on Health Care Providers n.d. www.gao.gov/products/GAO-10-323R (accessed September 2013).
- Weinstein B. The role of group purchasing organizations (GPOs) in the U.S. medical industry supply chain. Estud Econ Aplicada 2006;24:789-802.
- Healthcare Supply Chain Association . Frequently Asked Questions n.d. www.supplychainassociation.org/?page=FAQ (accessed September 2013).
- Schneller E. The Value of Group Purchasing – 2009: Meeting the Need for Strategic Savings. Scottsdale, AZ: Health Care Sector Advances, Inc.; 2009.
- Group Purchasing Organizations: Federal Oversight and Consumer Rights. Washington, DC: GAO; 2012.
- Healthcare Group Purchasing Industry Initiative . Healthcare Group Purchasing Industry Initiative n.d. www.healthcaregpoii.com/ (accessed September 2013).
- Burns L, Lee J. Hospital purchasing alliances: utilization, services, and performance. Health Care Manag Rev 2008;33:203-15. http://dx.doi.org/10.1097/01.HMR.0000324906.04025.33.
- Hu Q, Schwarz L. Controversial role of GPOs in healthcare-product supply chains. Prod Oper Manag J 2011;20:1-15. http://dx.doi.org/10.1111/j.1937-5956.2010.01121.x.
- Schnell G. Centralized Public Procurement, Decision Makers, Tenders and Innovation. Stuttgart: Simon-Kucher & Partners; 2012.
- Racca G. Collaborative procurement and contract performance in the Italian healthcare sector: illustration of a common problem in European procurement. Public Procurement Law Rev 2010;19:119-33.
- Roland Berger Strategy Consultants GmbH . Health Expenditure for Hospitals in Germany Rising. Help Purchasing Companies Save Material Costs n.d. www.management-krankenhaus.de/news/studie-gesundheitsausgaben-fuer-krankenhaeuser-deutschland-steigen (accessed September 2013).
- Purchasing in Hospitals: Strategic Purchasing in Hospitals. Purchasing Tensions Between Hospital Managers and Doctors. Frankfurt: BME e.V.; 2012.
- Schluechtermann J, Meinecke V, Nottinger A. The variety of purchasing syndicates offer something for everyone 2009;26:377-81.
- Gould B. The Present and Future Role of Group Purchasing Organizations in Europe n.d. www.smeetsadviesgroep.eu/smeetsadviesgroep/download/isv-presentaties-25-september-2012/8.-prospitalia-gpo-bradley-gould.pdf (accessed September 2013).
- Chevreul K, Durand-Zaleski I, Bahrami S, Hernández-Quevedo C, Mladovsky P. France: Health System Review. Copenhagen: The European Observatory on Health Systems and Policies; 2010.
- Durand-Zaleski I, Thomson S, Osborn R, Squires D, Jun M. International Profiles of Health Care Systems, 2012. New York, NY: The Commonwealth Fund; 2012.
- Assurance Maladie . Remuneration on Public Health Goals: Mobilizing Doctors and Health Insurance for the Quality of Care n.d. www.ameli.fr/fileadmin/user_upload/documents/DP_Bilan_ROSP_1_an_11042013_VDEF3.pdf (accessed September 2013).
- International Hospital Federation . Hospital Sector: France n.d. www.ihf-fih.org/ (accessed September 2013).
- Ettelt S, Nolte E. Funding Intensive Care – Approaches in Systems Using Diagnosis-related Groups. Santa Monica, CA/London: RAND Corporation and London School of Hygiene & Tropical Medicine; 2010.
- Oruezabala G, Rico J-C. The impact of sustainable public procurement on supplier management: the case of French public hospitals. Ind Market Manag 2012;41:573-80. http://dx.doi.org/10.1016/j.indmarman.2012.04.004.
- Ministère des Affaires sociales et de la Santé [Ministry of Social Affairs and Health] . Introduction to the PHARE Programme n.d. www.sante.gouv.fr/IMG/pdf/performance_programme_phare.pdf (accessed September 2013).
- Ministère des Affaires sociales et de la Santé [Ministry of Social Affairs and Health] . Hospital Purchases: The PHARE Programme n.d. www.sante.gouv.fr/les-achats-hospitaliers-le-programme-phare,9524.html (accessed September 2013).
- Ministère des Affaires sociales et de la Santé [Ministry of Social Affairs and Health] . The ARMEN Project n.d. www.sante.gouv.fr/le-projet-armen,12401.html (accessed September 2013).
- Healthcare Europa . UniHA Grows Despite Medtech Struggles 2013. www.healthcareeuropa.com/uniha-grows-despite-medtech-struggles/ (accessed September 2013).
- The UNICANCER Group . Organisation n.d. www.unicancer.fr/en/unicancer-group/organisation (accessed September 2013).
- UGAP . Connaître l’établissement [Knowing the Institution] n.d. www.ugap.fr/actualites/connaitre-letablissement_24046.html (accessed September 2013).
- Alliance Groupements . Who Are We? n.d. www.alliance-groupements.fr/index.php?id=fr66 (accessed September 2013).
- Resah-idf . Réseau Des Acheteurs Hospitaliers d’Ile De France n.d. www.resah-idf.com/index.php?id=fr117 (accessed September 2013).
- Resah-idf . Join Group Hospital Purchasing in Your Area n.d. www.resah-idf.com/fichiers/Plaquette_Groupement.pdf (accessed September 2013).
- European Health Public Procurement Alliance . European Health Public Procurement Alliance n.d. www.ehppa.com/ (accessed September 2013).
- International Hospital Federation . Group Purchasing Organisation (GPO) n.d. www.ihf-fih.org/Spec.-Interest-Groups/Group-Purchasing-Organisations-GPO (accessed September 2013).
- Frankel R, Bolumole YA, Eltantawy RA, Paulraj A, Gundlach GT. The domain and scope of SCM’s foundational disciplines – insights and issues to advance research. J Bus Logistics 2008;29:1-30. http://dx.doi.org/10.1002/j.2158-1592.2008.tb00066.x.
- Carter CR, Ellram LM. Thirty-five years of the Journal of Supply Chain Management: where have we been and where are we going?. J Supply Chain Manag 2003;39:27-39. http://dx.doi.org/10.1111/j.1745-493X.2003.tb00152.x.
- Carter CR, Sanders NR, Dong Y. Paradigms, revolutions, and tipping points: the need for using multiple methodologies within the field of supply chain management. J Oper Manag 2008;26:693-6. http://dx.doi.org/10.1016/j.jom.2008.07.002.
- Allen B, Wade E, Dickinson H. Bridging the divide – commercial procurement and supply chain management: are there lessons for health care commissioning in England?. J Public Procurement 2009;9:505-34.
- Radnor ZJ. Review of Business Process Improvement Methodologies in Public Services. London: AIM Research; 2010.
- Lilford R, Dobbie F, Warren R, Braunholtz D, Boaden R. Top-rated British business research: has the emperor got any clothes?. Health Serv Manag Res 2003;16:147-54. http://dx.doi.org/10.1258/095148403322167906.
- A Review of Collaborative Procurement Across the Public Sector. London: National Audit Office; 2010.
Appendix 1 Search strategy
The search strategies for the three separate searches used in the review are outlined in Figure 4 and described further below.
FIGURE 4.
Overview of main search processes (all conducted between July and August 2013).
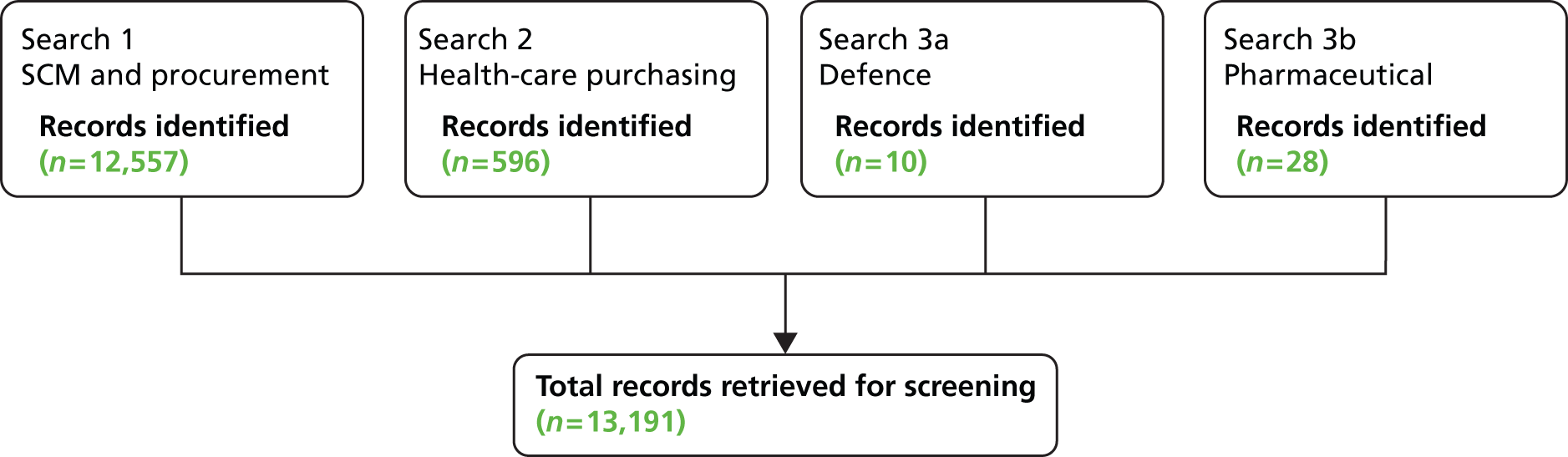
Search 1: General supply chain management and procurement
Language limitations: English.
Date limitations: 2006–present.
Type of document limitations: Exclude books, PhD/Masters theses, news items.
Country limitations: Exclude low-income countries.
Databases: MEDLINE, CINAHL, PsycINFO, Academic Search Complete, Social Sciences Abstracts, Military and Government Collection, EconLit and Business Source Complete.
Search terms
|
Procur* OR purchas* OR “supply chain management” |
|
“supply chain” |
The logic links between the different categories were: 1 AND 2.
Search terms should be found in the title, abstract or subject keyword.
Results: n = 12,577.
Search 2: Procurement in health care
Language limitations: English.
Date limitations: 2007–present.
Type of document limitations: Exclude books, PhD/master’s theses, news items.
Country limitations: Exclude low-income countries.
Databases: MEDLINE.
Search terms (Major MeSH)
|
“Group purchasing” OR “Practice valuation and purchase” OR “purchasing, hospital” OR “managed competition” |
|
“Delivery of Health care, integrated” |
The logic links between the different categories were: 1 OR 2.
Search terms should be found in the title, abstract or subject keyword.
Search 3a: Sector-specific searches (defence industry)
Language limitations: English.
Date limitations: 2008–present.
Type of document limitations: None specified.
Country limitations: None specified.
Databases: Google Scholar.
Search terms
|
“defence” AND “procurement”AND “best practice” |
|
“defence” AND “commodities” AND “best practice” |
The logic links between the different categories were: 1 OR 2.
Search terms should be found anywhere in the article.
Search 3b: Sector-specific searches (pharmaceutical industry)
Language limitations: English.
Date limitations: 2006–present.
Type of document limitations: None specified.
Country limitations: None specified.
Databases: Google Scholar, Web of Science, Business Source Complete.
Search terms
|
“pharmaceuticals” AND “procurement” |
|
“pharmaceuticals” AND “supply chain” |
|
“drug” AND “supply chain” |
The logic links between the different categories were: 1 OR 2 OR 3.
Search terms should be found anywhere in the article.
Appendix 2 Studies included in the review
| Reference | Context | Intervention/mechanism | Outcome | ||||
|---|---|---|---|---|---|---|---|
| Country | Industry | Aim of study | Design/methods | Outcomes | Source | Limitations/comments | |
| Abrahamsson and Rehme (2010)69 | Sweden | Food retail | To find the role of logistics in a retailer’s profitability and in retailers’ growth and market expansion by comparing the Swedish food retailing industry with other retailers | Examples of case studies were used because of their characteristics of profitable growth which is higher than the industry average. These cases represent one set of empirical data Data were collected through semistructured interviews with top management-level representatives with two interviewers (n = 15 interviews). The interviews complemented other data such as that from annual reports, brochures, etc. Another set of empirical data from the Swedish food sector using 15 interviews and secondary data from suppliers was collected Analysis: condensation of empirical data sets into a pattern to compare with existing theory |
International retailers’ differences from Swedish retailers include designing their supply chain with growth purpose, combining and integrating wholesaling and retailing in one company, using standardised logistics, combined IT systems and automatic replenishment, information transparency, clear division of roles in the supply chain Fast-growing companies (IKEA, H&M, Tesco, etc.) were ‘flow-oriented’ by managing flow of goods through constantly adapting operational resources and capacity in manufacturing and logistics to customers’ demands, partly through co-operation with suppliers. Matching the logistics strategy with the company’s growth strategy and value creation processes was more important than merely optimising logistics (cost and lead time reduction) vs. the traditional retail approach of logistics being primarily about cost-efficiency |
Academic | Theoretical paper analysing the retail industry, only included a few case studies, approach to data collection not reported; descriptive results rather than distinct outcomes |
| Alfaro and Rábade (2009)89 | Spain | Food | To show the qualitative and quantitative benefits obtained from implementation of a computerised traceability system | The study focused on one firm dedicated to producing canned vegetables with 326 people Longitudinal case study over 3 years (2003–6) Multiple employees interviewed with two team members. Used different informants for triangulation and accessed internal documents The firm began the implementation of the traceability system in 2002; hence information was obtained in real time. Finished products can be traced backwards and the system was used as an intranet to constantly monitor the whole production process |
Invested €18M; 50% on equipment (e.g. each forklift operator has PC with scanner), and the rest on software. Estimated payback time was 2 years, but in reality payback time was 18 months Each supplier could be audited to calculate price–quality ratio, and could analyse individual production lots. Increased trust and long-term relationships with suppliers, integration of suppliers into the firm’s strategy, 10–15% reduction in farmers’ cost and other supplier benefits (10% decrease in raw material returns, 3–5% reduction of spoilage) Other benefits included doubled production with same number of employees, 90% reduction in productive process, 20% reduction in indirect costs, 10–15% increase in warehouse capacity, 20–30% reduction in safety stock. Challenges included the need to convince senior managers of the potential for the investment |
Academic | Strong case study with data collected over length of time to gather benefits |
| AlSagheer and Ahli (2011)44 | Multiple | Multiple | To assess and analyse the impact of supply chain integration on business performance and associated challenges | An analysis of 21 research papers from 1995–2011 from 11 different journals. Comparative analyses of research papers that support and oppose the view that supply chain integration leads to better business performance. Supply chain integration involves a process of information sharing within and outside the organisation, mostly leveraging IT | Supply chain integration had a ‘mostly’ positive impact on business and enhances profitability, financial stability, customers’ satisfaction and accomplishing business goals | Academic | Paper selection and inclusion details unclear; no indication on their quality. Review highlights the need for more empirical research |
| Azevedo et al. (2011)45 | Portugal | Automotive | To study the relationship between green practices and the supply chain performance | A qualitative study considering five case studies of companies. Companies had to be verified under ISO:14001 Data were collected through semistructured interviews with different managers in the five companies about 10 green practices and six performance measures. Cross-case analysis was conducted to understand the relationships between these variables. Green practices included environmental collaboration with suppliers, environment-friendly purchasing, working with designers/suppliers to reduce product environmental impact, minimise waste and decrease consumption of hazardous and toxic materials, ISO 14001 certification, reverse logistics, environmental collaboration with customers, enviro-friendly packaging and working with customers to change specifications |
Overall, environmental cost, quality and efficiency were the performance measures with most significant relationships with green practices (e.g. environmental packaging implies utilisation of reusable packages), but differences in opinion on other aspects | Academic | Comprehensive study in terms of grounding literature and theory. It suggested opportunities to improve performance by being greener, but based on five case studies |
| Azevedo et al. (2012)46 | Portugal | Automotive | To use a theoretical framework applied to a case study to determine the relationship between green and lean practices and the economic, social and environmental performance of businesses | A case study of a single company based on informant interviews and empirical information collected from secondary data. The company already had strong environmental programme in place and complied with international standards | Operational costs decreased with only one green practice, i.e. reusable packaging, but decreased with lean practices ‘Just-in-sequence’, deliveries direct to point of use, geographical concentration, using electronic data interchange to share information, single sourcing. Further outcomes include reducing business wastage, except single sourcing. Green upstream SCM practices only contributed to reducing environmental costs Some evidence of association between green and lean practices and company’s social performance To ensure long-term success, the company continuously developed and sustained supplier relationships. Variables affecting business performance that green and lean SCM practices affected: (1) increased resource utilisation and the percentage of materials recycled, reused and remanufactured; (2) improved supplier social and environmental monitoring, business ethics and transparency, and increase in the number of local suppliers; and (3) reduced lead time, inventory levels, scrap, energy consumption and the quantity of solid and liquid waste |
Academic | Case study uses a theoretical framework developed from the literature and provides some insight into benefits of green and lean practices |
| Baier et al. (2008)47 | Multiple | Multiple | To look at the effect of strategic alignment and purchasing efficacy on financial performance | Primary data were collected from small business units in different countries with revenues > $3B in 2004. Out of 2251 eligible entities, the final sample consisted of 768 (stratified random sample); n = 141 as the response rate was 18.4% Survey interviews were developed based on the literature review and pre-tests to collect information on purchasing competitive priorities and a business strategy through a mail survey. Information on purchasing practices was collected though interview-based surveys. Information on financial performance was collected through publicly available databases The analysis involved a ‘profile-deviation analysis’ to find associations and a calculation of the overall index of financial performance considering several indicators |
Results supported hypotheses which suggested that the relative fit between business strategy and purchasing strategy (labelled as strategic alignment) and between purchasing strategy and purchasing practices (referred to as purchasing efficacy) was key to achieving financial performance | Academic | Good-quality study grounded in data. The lessons are holistic rather than numeric |
| Barlow (2006)70 | USA | Health care | To show the impact on an organisation as a result of investing heavily in materials management via physical, mental and emotional reorganisation, a strengthened engagement of clinicians and streamlining | A case study (where no methods were described) of Baptist Health System Inc., a multihospital system in Birmingham, AL. In order to address a $52M deficit, the organisation invested heavily in materials management. This included physical, mental and emotional reorganisation, a strengthened engagement of clinicians and streamlining | $9M was accounted for in actual savings in the first year and $18M in cumulative savings during the first half of a 3-year strategic plan. A new contract for gloves across the entire system helped to reduce nosocomial infections, which translated to $1.2M in savings in 6 months at one hospital and $334,000 at another. As a result, staff were dealing with fewer vendors. For instance, a team of clinicians and materials management staff succeeded in driving market share from 20% to 80% for one of their cardiovascular vendors. This generated more than $750,000 in savings | Grey | Results show substantial savings but no detail of exact data collection method nor attributable factors. News items appeared in professional magazines |
| Barnes and Liao (2012)71 | USA | Manufacturing | To look at the impact of strategic partnerships on firm performance (the extent to which a company can meet end-customer requirements, and operate efficiently to deliver high-quality performance) | An electronic survey was sent to 5147 companies in summer 2006, including purchasing/manufacturing/materials executives and chief executive officers/executives. Of these, 288 consented and 201 returned questionnaires (response rate was 69.8%) The questionnaires asked about organisational awareness (the extent to which supply chain professionals are involved in knowledge sharing), collaborative awareness (commitment to partnership), investment in strategic partnership (establishing long-term relationships) and the overall performance. Structural equation modelling was undertaken to find path coefficients to test the hypothesis of relationships between the above concepts |
The relationship was significant (beta = 0.6, p < 001), which indicated that there was positive relationship between a company’s investment in strategic partnership (i.e. long-term relationships) and its overall performance. This verified that suppliers were undoubtedly becoming increasingly important for the success of today’s companies | Academic | Strong empirical study although findings potentially restricted to manufacturing industries. Data based on the self-reporting of company executives |
| Belkoski (2008)90 | USA | Health care | To report on a pilot programme that demonstrates benefits of data standardisation and synchronisation and enables the system to recognise productivity gains in the supply chain | A small pilot intervention using a synchronised system accessible to all partners, showing accurate inventory levels. Techniques were developed based on other industry models focused on quickly and easily presenting data to medical and clinical staff, with the assumption that usable data enables more effective negotiations of product pricing and availability. Structured information systems generated management reports | Savings in excess of $900,000 associated with use of product’s services; however, not clear that this could be directly attributed to the intervention | Grey | Single case study; approach to data collection not reported |
| Bernhard et al. (2006)91 | Australia | Multiple | To test the performance between users of ERPSs and non-users, and impact on firm performance and the business process performance | The questionnaire was mailed to chief information officers of 2170 Australian companies to identify firms using or intending to use enterprise resource planning or SCM systems. The final sample size was 106 (with a response rate of 5.7%), with 102 used for analysis | Tested performance of ERPS users and non-users: on average, ERPS users scored higher but no significant difference between the samples on any measure of performance Results contradicted the claims of ERPS vendors insofar as no significant performance differences were found between ERPS adopters and non-adopters, either at the business process level or at the overall firm level. Although it could be confirmed that the longer the experience of firms with ERPS, the higher their overall performance, no evidence was found of a similar effect on business process (supply chain) performance. Only those ERPS adopters that also adopted SCM systems achieved significantly higher performance at the business process level. Results showed an indication (given that sample size was small) that ERPS users that also adopted SCM systems perform far better along the supply chain (mean 5.0) than ERPS users that did not use additional SCM systems (mean 4.24) |
Academic | Grounded in data and analyses, but contradicts other literature saying ERPSs have positive impact |
| Bhakoo and Chan (2011)92 | Australia | Pharmaceutical | To report on the implementation of an e-business system in health-care supply chain (manufacturer to pharmacy) | A longitudinal case study involving direct participant observation (40 meetings where the first author was an active participant), site visits and observations, document and archive analysis and interviews with project participants and stakeholders. Inductive data analysis was carried out Before the project, pharmacy orders were sent via telephone and fax, and goods data were entered manually into a central computer before being issued to other hospital areas |
Hospital pharmacy department benefits: time taken to receive goods reduced by 20% (from 51 minutes to 40 minutes) because purchasing staff did not need to manually check stock against invoices. Decrease in incorrect deliveries from 8% to 3.5% per order because of appropriate labelling (however, there was an increase in packing time for supplier from 1 hour 51 minutes to 2 hours 59 minutes), and time taken to label each carton went from 30 seconds to 1 minute 20 seconds, along with an additional staff member required, i.e. benefits are not always seen across the whole supply chain and one member might benefit more than the other | Academic | Strong, detailed case study, though only involves one company. Focus was on implementation of system rather than benefits; hence it is unclear benefits were fully captured. Did not report any company financial figures |
| Bigné et al. (2008)93 | Spain | Tourism | To examine the impact of adoption of IT (automated systems) in the travel industry | An e-mail survey was distributed among managers of Spanish traditional travel agencies (105/600 received; n = 105, response rate 17.5%). In-depth interviews were carried out prior to the survey to understand the context. The survey was validated using confirmatory factor analysis and psychometric testing; this generally supported reliability and the validity of constructs Analysis: using the maximum likelihood method of parameter estimation, and performance on the variance–covariance matrix |
E-communication and e-procurement were positively associated with e-sales (b = 0.18, p < 0.01 and b = 0.46, p < 0.01, respectively). E-procurement was positively associated with e-efficiency, i.e. cost savings (b = 0.51, p < 0.01) but e-communication did not have a direct relationship. E-communication and e-procurement were positively associated with relationship development (b = –0.28 and 0.27, respectively; p < 0.01 for both) | Academic | The study was cross-sectional and might not have accounted for the changes in the operational efficiency over time with IT investment. It does not consider the cost of initial IT investment. Unclear if it is applicable beyond industries with online sales |
| Bilyk (2008)72 | Canada | Health care | To examine effects in a hospital where managers, physicians and nurses take a close look at supplies they are using, streamline inventory, store information on supplies using IT inventory management databases and other best practices | Brief case report of a hospital where managers, physicians and nurses take a close look at supplies they are using, streamline inventory, store information on supplies using IT inventory management databases and other best practices | A major hospital in Alberta managed a 34% reduction in a year of direct buy spending in operating room supplies, and in just over 3 years, decreased overall operating room supply costs by 42%, increasing on-contract spending by 52% | Grey | Discusses SCM practices in a general sense, and suggests one hospital improved by implementing them, but does not discuss how they actually reduced costs specifically |
| Birk (2009)48 | USA | Health care | To report on effects of implementing a purchasing coalition | Scott & White Memorial flagship hospital teamed up with 13 other hospitals throughout the state to form Texas Purchasing Coalition. The coalition worked by securing volume purchases, committing to a specific volume as a single unit. Group buys did not require precommitment to specific versions of technologies; every option was included so that hospitals received what they needed. No other data collection method reported | One hospital group, as members of the purchasing coalition, saved $1,105,309 on medical supplies in the year prior and $11M in capital acquisitions saved across members Cost saving estimated 10–25% for group buys depending on the product |
Grey | Approach to data collection not reported. Data seem to be based only on information provided by the company and an interview |
| Boniface (2012)49 | UK | Health care | To see the benefits delivered by effective purchasing, related to sustainability (e.g. switching to thinner gloves to deliver smaller carbon footprint) | An overview article with expert interviews | Guy’s and St Thomas’ Trusts and King’s College Hospital Trust switched examination glove to thinner material to deliver smaller carbon footprint while achieving 30%-plus cost saving. Both hospitals introduced 100% recycled-content paper which is cheaper material cost than normal white | Grey | Only based on executive interviews, small article without detail |
| Bose and Pal (2012)50 | Multiple | Multiple | To examine the effect of green SCM initiatives on stock prices of firms | Event study technique: to analyse the immediate impact of announcements of events on firm value. Relevant announcements retrieved from news databases using a suitable list of keywords (included the green supply chain, closed-loop supply chain, sustainable operation, green operation, remanufacturing, green refurbishment, green disassembly, green returns management and product recovery) over a 3-day period. ‘Abnormal’ stock returns in the window around announcements were compiled using statistical analysis parametric tests. The final data set included 104 announcements (from 1997–2009) involving 48 companies in the USA, Canada, China, Germany, Japan and Taiwan | The hypothesis was only partially supported: announcements of green supply chain initiatives had an impact on CAR most significantly just as the announcement was made. Mean CAR is 0.2% but parametric test is not significant at the 10% level (though the non-parametric test is significant) Manufacturing firms observed greater positive change in stock price with such announcements (p = 0.06 for parametric, 0.08 for non-parametric) Firms with high R&D-to-asset ratio also saw positive changes (p-value < 0.1 for both tests) No support for the hypotheses that early-adopting firms or firms specifically making recycling announcements had higher CAR with the announcement. Smaller firms saw a strong positive impact (p < 0.03, p < 0.04 in non-parametric test) and firms with low growth potential also had significant findings (p < 0.05) |
Academic | Some aims and methods need clarification and context (e.g. relevance of ‘announcements’) |
| Brau et al. (2007)51 | Not reported | Multiple | To explore SCM initiative impact on the performance of small firms | A survey of 570 firms; the average response rate was 11.4% (257 large and 313 small firms with mean sales of $7.06M and $542,000, respectively). The surveys had 170 questions (on integration strategy implementation, supply chain development practices and business performance indicators). They were sent by mail and each manager was telephoned to ask to participate. Univariate and multivariate empirical tests (Tobit tests) were conducted to test SCM value to firm performance | Higher integration strategy, internal integration support, external integration support, supply chain alignment, supplier integration and customer integration all positively (and significantly) associated with asset utilisation, revenue generation and competitive performance. Higher levels of supply chain development had a negative correlation with financial performance. Customer integration was shown to be most influential Multivariate analysis: two primary SCM variables that drive competitive performance improvement were supply chain alignment and customer integration |
Academic | Strong empirical work; based on hypothesis-testing methods |
| Cadden et al. (2013)73 | UK | Consumer goods | To investigate what cultural dimensions between a buyer and its supply chain partners are compatible in supporting high and poor performance outcomes | Case study: buyer organisation plus four supplier organisations. The survey questionnaire, with 35 items to measure organisational culture, was distributed to firm staff. There was a response rate ranging from 49% to 64% within the respective partner in the best-performing supply chain, and 32% to 59% in the underperforming supply chain (the analysis was done using ANOVA). Qualitative research was undertaken after a statistical analysis involving a random selection of two personnel at strategic level and two at operational level from each participating organisation (24 in total). Open tours of the organisation were used for direct observation. Supply chain performance was measured through operational and financial metrics | High-performing supply chain organisations had significantly different cultural profiles across all six dimensions; in a supply chain scenario whereby multiple participants are involved yet each participant still has autonomy and its own organisational identity, it would appear that as long as cultures are compatible, the culture of each organisation in the supply chain could differ with successful outcomes. Low-performing organisations had identical profiles with significantly lower mean scores across every dimension. Qualitative findings found themes of blame, distrust and poor performance | Academic | Only looked at one bread and bakery supply chain system (with two high-performing and two low-performing firms) but the case study was in-depth. It is uncertain how transferable it is |
| Callender and Grasman (2010)94 | USA | Health care | To explore the material management in the health-care sector to identify best practices | Empirical data were collected from material managers, directors, distributors, manufacturers and GPO directors. The questionnaire asked about barriers for SCM implementation and best practices for material management. There were three different groups of participants (health-care providers, suppliers and GPO directors). Final sample included 35 health-care providers, 15 manufacturers and distributors and 2 GPs | Best practices in material management were identified: education (increased training in SCM principles), inventory management (using software to calculate reorder points and quantities, holding less inventory), procurement and contracting (increasing automated ordering process, standardising products), information sharing and collaboration (sharing inventory information with vendors, involving clinicians in product selection) | Academic | Response rates not reported. Study did not look for significant differences between companies that did and did not implement a best practice, data based on narrative synthesis from responses |
| Campo et al. (2010)95 | Spain | Retail | To analyse the direct influence of IT on retailers’ perceived performance | A telephone survey was distributed to store managers of retail stores selling home appliances and associated with wholesale purchase groups. Final sample: 97 in Madrid and 69 in Barcelona, with response rates of 56% and 47%, respectively; there was a sampling error of 5.10%. The questionnaire asked about IT use and relationships with providers and the perceived performance in the relationship with a provider, such as economic and marketing benefits. The technologies included software providers, own software, scanner, e-mail, provider’s web portal, own web page and telephone/fax | Firms with ‘low use of IT’ mean scores on 10-point scale: growth in sales, 6.3; increased profits, 5.6; customer loyalty, 6.2; assortment adaptation to the market environment, 6.5 Firms with ‘high use of IT’: growth in sales, 6.9; increased profits, 6.4; customer loyalty, 6.7; assortment adaptation to the market environment, 7.0 All means were significant (as an association with perceived benefits in the provider relationship as a function of IT use) No direct relationship between specific use of IT and perceived performance (standardised coefficient = 0.09 and non-significant) but positive effect is produced indirectly through information sharing and satisfaction with the relationship |
Academic | The link to performance is made through a relationship with a specific provider; therefore, the inferences about IT use and benefits seem a bit indirect, but they are about the perceived benefits associated with a specific provider |
| Carpenter (2008)52 | USA | Health care | A report on a survey of implementation and benefits of quality management initiatives | A nationwide electronic survey, involving 710 organisations, about quality management initiatives. 58% reported they have implemented a defined quality management programme. This included programmes like Six Sigma, lean and rapid cycle improvement programmes | 55% of respondents with quality initiatives reported that these initiatives reduced waste or cost, 49% that they improved patient satisfaction, 45% that they increased communication, 44% that they reduced hospital-associated infections and 43% reported that they improved staff satisfaction Gunderson Lutheran Health System went from manual to a $100,000 surgical instrument management system, increasing instrument accuracy in the operating room from 84% to 90%, and a further initiative to reduce steps required for sterilisation increased accuracy to 99.7% Wellmont Health System: a focus on standardisation and cost reduction across hospitals. Supply chain department set up equipment teams to bring items to bedside and keeping a small stock there; total inventory at flagship reduced to $600,000 from $1.8M |
Grey | Some specific case examples; approach to data collection not reported other than a national survey but this was only a secondary report on the survey |
| Carroll and Coker (2007)53 | USA | Military | To provide an overview of the impact of the army’s Logistics Modernization Program (LMP) | An overview of the LMP: enterprise resource planning solution involving vertical and horizontal integration at all levels of logistics across the army | Users benefit in three areas:
|
Grey | Approach to data collection not reported, and not much comparison of pre- and postsystem implementation |
| Case (2011)54 | USA | Health care | To investigate reasons for SCM-attributable success in a health-care setting. Intervention comprised switching to a low-unit-of-measure distribution and a switch to the combined medical–surgery and pharmacy departments | A switch to a low-unit-of-measure distribution and a switch to the combined medical–surgery and pharmacy departments; no systematic data collection | Combined departments avoided need for multiple supply chain agreements, leading to a 7-year master agreement including medical–surgical supply, pharmacy distribution and pharmacy data analytics Leaders estimated savings potential in tens of millions of dollars. Low-unit-of-measure distribution logistics service reduced high cost of storing, maintaining and distributing by delivering low-unit-of-measure orders straight to hospital departments |
Grey | Brief report on a single case study, approach to data collection not reported |
| Childerhouse and Towill (2011)55 | Multiple | Multiple | To test whether or not enhanced performance of supply chains can be attributed to the five arcs of integration: inward facing (lower quartile for suppliers and customers), periphery facing (above lower quartile for either supplier or customer, but below for the other), supplier facing (upper quartile for suppliers, below for customers), customer facing (upper quartile for customers, below upper quartile for suppliers) and outward facing (upper quartile for suppliers and customers). The quartiles are based on uncertainty | Comparative analyses of 50 value streams were conducted: 33/50 were analysed via the site-based Quick Scan audit methodology (mapping of material and information flows, key manager interviews, evaluation of company archival information, quantitative and attitudinal questionnaires); 17/50 were assessed via multiple interviews and a review of archival material provided by the companies, and open literature, quantitative questionnaires and structured interviews conducted on site. This was done over an 8-year study period Analysis: 16 indicators to examine the comparative performance (reflecting marketplace, productivity and non-productivity factors) |
Productivity indicators: more integrated supply chains (i.e. more outward facing) were more productive for four out of seven productivity indicators (most relevant: customer delivery frequency – outward-facing value streams deliver average of 687 times/year compared with 77 for periphery-facing arc) Non-productivity indicators: no positive difference found between product variety and arc of integration, outward-facing arc had highest level of streamlined information flow (but it is only significant at 90% level) More integrated supply chains had a higher structured approach to change and seamless supply chain target |
Academic | Extensive study, but complex findings as aims to rank different stages of supply chain integration. The ‘non-productivity’ factors are probably most relevant. The transferability of this is uncertain though because it focuses on 50 specific value streams, and gathered data in different ways |
| Ciliberti et al. (2011)74 | Multiple, Europe (Italy and the Netherlands) | Various | To show how SMEs can use codes of conduct to solve the principal–agent problem between chain directors and partners. A principal–agent relationship is one where one party (the principal) delegates work to another (the agent) who performs the work. This relationship can lead to adverse selection and moral hazard due to information asymmetry | Four case studies of four different companies, each looking at the way they implement a specific code of conduct (SA8000 certification), including interviews, observation and document review. The study carried out a qualitative analysis | Codes of conduct could improve the communication flows on intangible aspects of business between indirect partners within a supply chain and reduce information asymmetry between the parties Codes of conduct could contribute to solving the adverse selection problem in the process of searching for new suppliers (selected from certified firms), and to negotiating intangible issues in new contracts with current suppliers, when they accept certification Codes of conduct could contribute to solving moral hazard issues, with respect to intangible aspects of business, because monitoring improves communication on these issues, in particular in the case of third-party monitoring of all parties involved Agents could reduce moral hazard problems even more when they applied bonding practices towards their partners, including the principal, to support monitoring activities by a third party |
Academic | Codes of conduct and management systems are part of the Corporate Social Responsibility. They include health and safety codes, ethical trading initiatives, etc. |
| Constantine et al. (2009)56 | Multiple (Europe and North America) | Multiple | To assess the link between supply chain performance and underlying practices driving it | In-depth interviews were carried out with operations executives at 60 companies across Europe and North America. Interview responses were plotted on a 1–5 scale and the results were compared with supply chain performance metrics provided by the respondents on cost, inventory and service levels | Organisations displaying strength across six broad practices (link supply chain to company strategy, segment supply chain to master most important product/service complexity, tailor the supply network to optimise service/cost/risk goals, use lean tools end to end, create integrated/robust sales and operations planning, find top talent/hold people accountable) outperformed competitors in service, inventory and logistics costs Organisations scoring among the top one-third of survey participants on this dimension were 2.5 times as likely to be leaders in inventory performance and twice as likely to be leaders in service as companies in the bottom third Top companies also excelled in optimising end-to-end efficiency (the companies with the lowest supply chain costs are also more likely to entrust managers with end-to-end control over them, thus increasing the likelihood that management decisions will improve the whole business and not just certain functions) Top companies achieved the discipline required to excel in these areas partly by improving the skills of their employees. Investments in formal IT systems did not appear to improve supply chain performance as much as some managers expected (companies relying more on spreadsheets and other informal solutions were nearly twice as likely to be cost leaders – and nearly three times as likely to be inventory leaders – as companies using formal IT systems extensively) |
Grey | Rich study but it does not report details of data collection; conducted by a consulting firm, and does not comment on the quantitative impact of practices |
| Cox and Chicksand (2008)75 | UK | Food | To review the demand and supply in pig and beef supply chains and provide an analysis of two red meat supply chains using power and leverage methodology; framework development for policy options | A literature review of the demand and supply in pig and beef supply chains and an analysis of two red meat supply chains using power and leverage methodology | Government policy should not assume everyone benefits in equal measure from long-term collaborative relationships based on lean. In the pig supply chain only multiple retailers and major processors, not producers, benefitted operationally and commercially from lean. Where there was demand and supply uncertainty, it was not operationally feasible for everyone in the chain to be involved in the lean/collaboration. One policy approach, such as lean, is not likely to be appropriate in all circumstances, and so applying one policy across industries, as the UK tries to, would be even less likely. This is due to power and leverage structures, operations within pig and beef supply chains and major demand and supply differences | Academic | The study only uses two case studies but its analysis supports other studies which discuss the downside of Japanese business practices based on lean thinking |
| Creedon (2006)96 | USA | Health care | To compile savings from automated procurement and buying processes | The research based on studies at 200 hospitals compiled industry averages for times associated with various procurement processes and methodologies, comparing manual vs. automated processes. Labour costs were calculated in the average compensation: $23/hour for accounts payable clerks and $30/hour for clinicians | Manual requisitions vs. electronic requisitions (based on $20/hour or $30/hour), $8 vs. $2.50 for the process Manual vs. electronic sending purchase orders (based on $20/hour), $5 vs. $0.33 Manual vs. electronic receiving purchase orders (based on pay of $20/hour), $1.33 vs. $0 Manual versus electronic invoicing (based on pay of $23/hour), $345 vs. $1.15 |
Grey | Methods not described, takes average times for processes but no sense of the variation between hospitals |
| Cunningham (2006)97 | USA | Health care | To give an overview of SCM fundamentals that have resulted in cost savings | Interviews with hospital executives | Close examination of end-user practices to develop standards. For example, Ohio State University Medical Center looked at clinician usage and made appropriate buying changes to realise yearly savings of about $1M ($2M in the first year) Improving contract management and usage. For example, Stony Brook University Hospital optimised value of spine supplies contract by understanding its purchase prices compared with others and analysing pricing structures to evaluate different models. The result was a negotiation for a 13% volume pricing discount and lowered costs of $1M. Set priorities to achieve savings building on strengths. For example, Medical University of South Carolina altered buying practices to use tier pricing on hip and knee implants, resulting in yearly savings of $113,000. The University of California health system leveraged aggregate purchasing power of system’s five medical centres focusing on only nine high-spend products. The result was reduced costs of more than $1M Communication/effective team building. Grady Health System implemented supply chain strategy cutting expenses for examination gloves by $544,000; for a smooth transition, input was gathered from various departments, e-mail blasts, updates, etc. |
Grey | Examples report on cost savings achieved but approach to data collection not reported and appears to be based only on narratives |
| Danese and Romano (2011)76 | Multiple | Manufacturing | To analyse the impact of customer integration and supplier integration on efficiency and the moderating role of supplier integration | Data from the third round of the High Performance Manufacturing project data set were used. Twenty recipients were involved at each of the 200 sampled manufacturing plants (manager, HR manager, etc.) Analysis: controlled for industry and size. A hierarchical linear regression to derive coefficient estimates was undertaken |
Customer integration was not significantly associated with efficiency performance Supplier integration was significantly associated with efficiency (b = 0.696, p < 0.001) Interaction between customer and supplier integration was significant (b = 0.565, p < 0.01), so effect of customer integration on efficiency performance varied according to level of supplier integration Managers should not invest in customer integration alone; need both supplier and customer integration to achieve a positive effect on efficiency |
Academic | Strength of study is that it administers questionnaires to multiple people in each participating firm and a large study involving global universities. Study does not report constructs used to measure supplier and customer integration and does not report response rate |
| Elmuti et al. (2013)58 | USA | Manufacturing | To examine the effect of various SCM interventions (e.g. inventory control, centralising supply chain data, strategic alliances) | A literature review, a survey (n = 210) of organisations involved in health-care SCM and interviews (n = 30) of health-care supply professionals were conducted | There was a positive relationship between SCM activities and organisational performance/effectiveness. There was a positive correlation between outsourcing decisions and performance/effectiveness. Establishing partnerships with key suppliers was considered an enabler, whereas a lack of data standardisation, conflicting goals among supply chain partners and lack of performance measures were seen as challenges | Academic | Mostly self-reported data. There is no indication of what works and what does not in particular |
| Elmuti et al. (2008)57 | USA | Health care | To examine the impact of a SCM system on organisational performance (ROI, productivity, expenses) | The research was conducted at a single manufacturing plant for equipment and medical supplies. At time of study, the plant was in financial distress; new SCM system was implemented to improve operations and train employees. An employee perception survey was conducted prior to the new system. A second survey was distributed 36 months after the first. Information on organisational performance (efficiency, customer responsiveness, flexibility, quality, productivity and other indicators) was collected. The population sample was all 1835 employees, and the response rate was 81%. In-depth interviews with 30 managers from different departments were undertaken An analysis of the average changes in various performance indicators and a regression analysis to look at the relationship between integrated SCM and organisational performance were done |
Average percentage increase in organisational performance measures:
Interviews: respondents found integrated behavioural relationship must exist and sharing information and co-operation at all levels in a supply chain was critical |
Academic | The plant specifically asked the authors to monitor the implementation of integrated SCM Extensive study although there are uncertainties as to its transferability |
| Fawcett et al. (2011)98 | Not reported | Multiple | To explore how IT investments can create differential returns when they enable the creation of specific capabilities | A literature search going back to the 1980s was undertaken. Informal interviews were conducted with managers and advisory boards to provide feedback on research content. Three professional associations – the Council for Supply Chain Management Professionals, the Institute for Supply Management and APICS (the leading professional association for supply chain and operations management) – helped compile a mailing list consisting of their senior-level executives The survey data were collected at two different points in time, 6 years apart; n = 702, response rate of 14.69% – this was checked for non-response bias. Interactions using structural equation modelling were assessed Interview data were collected: 51 interviews in period 1 and 58 interviews in period 2. 15 companies participated in both rounds of interviews. A coding frame was developed and frequencies generated |
Supply chain connectivity was positively and significantly related to operational performance and customer satisfaction in both time periods (beta = 50.44 in period 1, p < 0.01; beta = 50.37 in period 2, p < 0.01); however, the strength of IT’s influence on value may decrease marginally over time Qualitative findings also suggested IT as key enabler of value creation in period 1, and in period 2 interviewees were saying investment in IT was essential to stay competitive though it did not deliver advantages on its own Information-sharing culture had a strong, positive influence on operational performance (beta = 0.29, p < 0.01), but no amplification of advantage exists if implemented along with supply chain connectivity Qualitative findings: proactive sharing of operational information was a leading-edge practice not implemented by a lot of companies, and willingness to share information depended on relationship trust (information = power). Four out of five managers identified lower costs as a primary benefit of their collaboration initiatives Firm’s collaboration capability primarily and most enduringly influenced operational performance, and was highly significant in both time periods (period 1: b = 0.58, p < 0.01; period 2: b = 0.72, p < 0.01). Direct effect of supply chain connectivity, information-sharing culture and supply chain collaboration positively influenced profitability and growth but fully mediated by operational performance and customer satisfaction |
Academic | Strong study with a time element to compare time period. Based on professional organisation membership, with the organisations compiling the sampling frame, but unclear how this was selected |
| Font et al. (2008)59 | UK and Europe | Tourism | To generate examples of good practice in order to promote sustainability across the whole supply chain among tour operators. Initiatives revolve around four main themes: accommodation; transport; ground handlers, representatives’ excursions and activities; and food and crafts. Examples include the development of standards and assessments, environmental auditing and management, renewable energy use | A document review and interviews (n = 25) | The benefits reported included increased revenues and reduced costs. Other reported benefits included gains from brand reputation, staff morale and retention, long-term business relationships with suppliers, retention of clients, improved operational efficiency, risk management, staying ahead of legislative requirements and protection of the core assets of the business | Academic | This article does not provide evidence of schemes that have been evaluated but ideas of what was developed and implemented and indications of what could potentially work |
| Fugate et al. (2006)60 | Not reported | Multiple | To consolidate the existing disparate research findings on co-ordination mechanisms from different disciplines and explore how practitioners perceive the use of these mechanisms. Of particular interest is identifying the mechanisms that managers use and find most effective in co-ordinating their firm’s supply chains. Co-ordination means to co-ordinate the actions of the individual supply chain members such that their decisions are aligned with global supply chain objectives | A literature review and in-depth interviews (n = 13) with senior managers of nine different firms over various sizes and sectors were conducted. The unit of analysis was the dyadic relationship between the buyer and the seller | Price co-ordination mechanisms (i.e. discounts for the buyer) had a negative impact on firms and trading partners’ performance, despite short-term benefits, because they altered demand planning. Non-price co-ordination (e.g. allocation rules) turned out to be contrary to the literature as the interviewees saw it as detrimental to performance The literature and interviews both had a positive perception of flow co-ordination mechanisms (e.g. vendor-managed inventory) and their impact on performance. There were indications that successful buyer–supplier co-ordination consisted of trust, commitment, co-operative norms, dependence, organisational compatibility and top management support |
Academic | It attained saturation after 13 interviews only |
| Ghani et al. (2009)99 | USA | Computing | To test whether or not the conventional supply chain (where feedback from customer flows in the reverse direction to the distributor and then the manufacturer, who alters their products if necessary for the supplier) has no effective technology and has slow information sharing | Case study methodology: a literature review of articles published in the past 10 years Conventional SCM: feedback from customer flows in the reverse direction to the distributor and then the manufacturer, who alters their products if necessary for the supplier. A sequential information flow is time-consuming. It is observed that there is now a sharing of SCM partners using technology to enhance effective communication. Software enables reviews of past performance, monitoring, prediction, etc. Dell case study: direct business model that eliminated retailers and sold directly to the customer. Does not have to hold much inventory or information shared with all supply chain members; suppliers can access information about sales forecast, product changes, etc., and the information sharing goes in both directions |
Dell became the number one PC maker in 2001 because of effective SCM: a 15% increase in product shipments at the same time the industry volume dropped 5% | Academic | Only one case study, approach to data collection was not reported for the case study, but a good literature review |
| Gianakis and McCue (2012)100 | USA | Public sector organisations | To identify challenges, barriers and benefits of SCM processes | Findings from the four case studies in Florida:
|
Case study 2: purchasing administrative lead time was reduced from 6.39 days on average to less than 2 days. Vendors’ satisfaction increased Case study 3: the annualised savings reached $15M, i.e. almost three times the expected savings |
Academic | |
| Golicic and Smith (2013)61 | N/R | Multiple | Meta-analysis to understand variables, measures, contexts or other factors that might be influencing impacts of environmental practices specific to the supply chain and their performance | Research on the ABI/Inform Global database using keywords such as sustainability and performance was undertaken. References from prior meta-analyses and reviews were obtained. The research included 4500 articles of published materials starting in 1990 Inclusion: a study of hypothesised and environmental supply chain practice/performance, which was tested empirically; it excluded qualitative studies or opinions and studies where performance was not the outcome or dependent variable. Only studies specifically examining the environmental supply chain practices as the independent variable were included (31 studies). Seventy-seven independent effect sizes were included (the effect size was taken to be the correlation where provided, and if not, correlations were calculated). An analysis of the fixed-effects model was conducted |
The mean effect (0.294) was significant; overall environmental supply chain practices are associated with positive firm performance. The mean effects for operational-based and accounting-based performance (0.301 and 0.256) were also significant | Academic | Unreported quality assessment for articles. Not much detail on hand-searching methods Only used published results but unpublished literature might be important in this context |
| Guimaraes and de Carvalho (2011)62 | Germany, UK, Australia/New Zealand, USA, Greece | Health care | To compare outsourcing activities, and drivers, benefits and risks of outsourcing | Synthesised evidence of outsourcing in the health-care sector using a keyword search was used. 76 articles in peer-reviewed literature, 16 articles in grey literature and 10 books were used. All of the countries outsourced non-clinical or clinical services which varied between countries | Germany: outsourcing service quality higher than internal because of IT and cost reduction. Risks: adapting problems, high hidden cost of IT outsourcing, patient claims regarding service quality UK: service standardisation benefits. Risks: results monitoring difficulty and consequent need for process monitoring Australia/New Zealand: equipment improvement, increase in patient number, staff reduction (160 to 35 in 1200-bed unit), cost reduction from AUS$200,000 to AUS$3000). Risks: supplier noncompliance and lowered quality, new monitoring costs, cultural discrepancies USA: access to best practices and top-class technology. Risks: dissatisfaction with outsourcing outcomes Greece: service quality improvement. Risks: low impact on costs, integration/co-ordination difficulties, vendor difficulty in understanding internal process, difficulty negotiating quality levels |
Academic | Little detail on search methods, reason for selecting country case studies, definitions of outsourcing or appraisal of the papers they included, although there was not much literature on the topic and was not intended as a systematic review |
| Jeffery et al. (2009)101 | USA | Public sector organisations | To examine the effect of RFID implementation on service performance | A multiple case study methodology n = 35 from city library employees and customers who were interviewed n = 15 from a road race organisation (staff, volunteers and race participants) Data collected through in-depth qualitative fieldwork. Organisations had already implemented RFID The interviews were conducted over a 2-year period and multiple researchers were used to ensure that the findings converged |
City library:
|
Academic | Strong study; analysis of two case studies, but in depth and triangulated by looking at customers, employees and managers |
| Johnson et al. (2007)102 | Multiple (USA and Canada) | Manufacturing | To assess whether or not firms’ financial performance related to the use of e-business in the supply chain | The Title 1 membership list of the Institute of Supply Management (ISM) and the CAPS Research membership directory were used to identify US respondents for firms on the Fortune 1000 manufacturing and services lists. The membership database of the PMAC was used to identify Canadian respondents for firms on the Financial Post’s 100 list The survey was sent to 640 targeted firms (n = 284; 44% response rate) Analysis: regression analysis of variables’ impact on firm performance |
E-business technology dyadic co-ordination dimension significantly associated with return on assets and return on sales (b = 1.12 and b = 1.62, respectively), but price determination and private exchange dimensions were not. Dyadic co-ordination was the e-business technology implemented to reduce co-ordination costs between buyers and suppliers such as online purchase order systems Dyadic co-ordination was also the most widely adopted e-business technology factor |
Academic | E-business technology is the digitally enabled inter- or intraorganisational internet-based information technologies used to accomplish business processes It is unclear if the effect of dyadic co-ordination over the other e-business technology dimensions may be attributable to it being the most used one as well; however, this has little implication for the significant finding of the dimension |
| Kannan and Tan (2010)77 | Multiple (USA and Europe) | Manufacturing | To examine whether or not performance benefits accrue to firms that involve extended supply chain partners. The ‘extent of integration’ is the extent of the supply chain that is integrated (i.e. beyond first-tier suppliers) | A survey of practising managers from members lists of the Institute of Supply Management and Association of Operations Management. The survey assessed supply chain integration, relationships with suppliers and firm performance relative to competitors. The survey was distributed to 2900 respondents (n = 321; response rate = 11.1%) The firms’ annual sales had a median of $100M Analysis: cluster analysis (based on firms’ SCM efforts) was used to partition respondents. Each category of supply chain participant was used as a separate variable. Sample t-tests were used to explore the difference between clusters’ integration efforts and performance |
Two clusters: one had a broad span of integration, one had a narrow span. Firms incorporating broad spectrum of supply chain partners in integration efforts had stronger emphasis on building interorganisational linkages: statistically significant differences between integration constructs (supplier focus, customer focus, information focus and supply chain focus) Firms incorporating broad spectrum of supply chain partners in integration efforts had a stronger relationship performance; relationships had a greater positive impact in sales improvements, new product development time and quality but NOT cost reduction Firms incorporating broad spectrum of supply chain partners in integration efforts had strong customer service performance level, but not a higher market share, ROI or overall competitive position – likely because these factors had to do with non-supply chain elements of a firm |
Academic | Reliance on self-reporting on firm performance and supply chain focus. Unclear about whether or not the number of entities in a supply chain would have any bearing on results, as it was not controlled for |
| Kehoe (2006)88 | USA | Health | To report on the improvements in SCM due to the adoption of an electronic supply chain (e-sourcing + e-procurement + e-materials) | Case study focusing on the West Penn Allegheny Health System (six acute care hospital campuses). The new system was inspired by an example of a grocery store. This resulted in a strategy that engaged end-users (clinicians and materials management) and received financial commitment of the organisation ($8.4M in incremental annual expenses for IT investments) | An average bid savings of 21% and a 70% reduction in bill completion cycle time was seen 96% of purchase order lines administered electronically A low-unit-of-measure distribution system was implemented for medical–surgery products and pharmaceuticals, moving the process of unpacking orders downstream. This allowed to deliver 99% fill rates (in comparison with less than 70% before) |
Grey | |
| Kroes and Ghosh (2010)63 | USA | Manufacturing | To evaluate the degree of congruence between a firm’s outsourcing drivers and its competitive priorities, to assess the impact of this congruence on supply chain performance and to investigate the relationships between the supply chain and the business performance ‘Outsourcing drivers’ refers to motivations and objectives and the goals of the outsourcing efforts are related to supply chain processes and activities. ‘Firm performance’ includes profit margin, return on assets, return on sales and sales over assets |
Internet-based survey targeted 1793 supply chain executives from professional organisation lists (n = 233, with an 18% response rate). The majority were firms with over $1B in sales volume An analysis of a structural equation modelling was conducted to test the impact of outsourcing congruence |
Outsourcing congruence was associated with higher levels of supply chain performance, i.e. aligning outsourcing with firm strategy | Academic | This may be specific to manufacturing or companies driven by product development, but some relevant messages on strategic alignment |
| Krusius (2012)103 | Finland | Health care | To report on the implementation of centralised and streamlined blood collection system | A new production model to centrally manage blood collection and production, consolidate production and testing, and synchronise production and testing with blood component demand. Hospital blood banks generate reports several times a day on blood stocks so that they are automatically filled to a pre-agreed target level. There are experienced experts in the purchasing, logistics and HR units to support blood service. Certain screening requirements for blood, based on internal data and reinvested in other screening, were changed. Collaboration with major hospitals created a database on using blood components and can gather comparative information, e.g. on diagnoses or surgeries to develop appropriate blood use and benchmark | The cost of logistics rose from about €2.75M in 2004 to €3.25M in 2007. By 2011 this cost had dropped to just over €2M. There was a focus on developing a more cost-effective service while improving customer service by redesigning processes and closing co-operation | Grey | This is an overview; approach to data collection was not reported. Not much in terms of outcome evaluation |
| Leonard and Davis (2006)104 | USA | Manufacturing | To determine whether or not electronic supply chains (using EDI) are more effective than non-electronic supply chains by analysing products before and after EDI implementation. The EDI works to exchange data/information between trading partners electronically; companies depend on EDI to streamline processes in SCM and logistics – it is an application of e-commerce ‘Supply chain effectiveness’ relates to the product of inventory level, stockouts, order cycle, fill rate, price, cost and availability |
Information was taken from one manufacturing organisation and its supplier about individual products before and after EDI implementation, and organisational impact (i.e. effectiveness) of three products was examined in one sample (using detailed transactional data over 6 months) and 55 in another (where price, cost and inventory were compared at a single point in time before and after implementation) Analysis: ANOVA equivalent test to assess differences in effectiveness in both periods and paired t-tests to investigate paired products |
Sample 1: all three products had significantly shorter order cycles after EDI was implemented, but none experienced a significant change in fill rate. Only product C had a significantly lower inventory level when EDI was used Sample 2: significant difference post EDI implementation; lowered purchase price (x = 0.767), transaction cost (x = 13.29), average transaction cost (x = 0.669) and total cost (x = 1.43) EDI led to savings by enabling shorter order cycles and greater availability of component parts without affecting inventory level and supplier stockouts |
Academic | Strong study, but single, in-depth case study. Does not provide detail on the products used for analysis and whether or not there were differences in outcomes across products |
| Maggio and Perez (2006)105 | USA | Health care | To report on the implementation of automated supply chain processes (materials management information system) in a hospital in Louisiana. In order to increase efficiency of the purchasing process, the hospital hired GHX, a company that enables hospitals and suppliers to conduct business electronically | A case study (by hospital representatives) | The hospital hoped to save more than $976,000 through contract price enforcement and an additional $290,000 in contract rebates annually The number of suppliers that the hospital could deal with increased from seven to 43. The percentage of EDI transmissions increased from 28% to 62%. Errors in orders are automatically verified (it was previously done manually) Time spent by buyers to verify purchase orders decreased from 10 hours a day to 45 minutes a day. Staff can focus on contract reviews and negotiation Clinicians spent less time sourcing and requisitioning products Charges for purchase orders that were below minimum amounts had almost been eliminated |
Grey | Some details are missing (i.e. cost of developing and implementing the new system) |
| McHugh (2006)106 | USA | Health care | To investigate options to manage a clinical laboratory inventory and implement a computerised system | An in-house design and implementation of a new inventory management system. The system was a Min-Max system: for each supply there was a calculation of a DQOH and a ROP. When the stock reached ROP, the quantity ordered (semiautomatically) is equal to the difference between ROP and DQOH. The system also tracks lot numbers and expiration dates. Software used: InvMan (COVE Laboratory Software, Sonoma, CA, USA) | There was an 8% reduction in the quantity on hand (from $550,000 to $506,000) owing to improved SCM Net savings in operating expenses were seen (although no figure was given). Additional outcomes included a reduction of overstock; reduced wastage (less products become outdated before being used); and less paperwork for clinical laboratory scientists |
Academic | |
| Meehan and Muir (2008)64 | UK | Multiple | To assess SMEs’ attitudes towards benefits and barriers of SCM. SCM is the degree of internal co-operation and external integration, implying end-to-end co-ordination, representing a strategic shift in a firm’s culture rather than just a business practice | A questionnaire asking about benefits and barriers of SCM using Likert Scale was used (n = 60, response rate 24%). A stratified sample by company size, type and industry was used to represent diversity for firms identified through NWDA database A random sampling was applied within each stratum and 250 questionnaires were distributed, addressed to the organisations’ managing director |
Most important benefits of SCM were a reduction in duplication of interorganisational processes (2.35), reduction in product development cycle time processes (2.24), reduction in risk (2.08), improvement in supply chain communications (1.93) and improvement in customer service responsiveness (1.75), where 1 is the most important Issue of lowest importance was introduction/improvement of electronic trading, maybe because SMEs place more emphasis on relational elements of SCM |
Academic | Small, geographically concentrated study, but findings largely consistent with bigger studies. SMEs could represent a range of organisations, but they did stratify the sample |
| Merschmann and Thonemann (2011)65 | Germany | Manufacturing | To analyse the relationship between environmental uncertainty, supply chain flexibility and firm performance ‘Environmental uncertainty’ relates to demand variation, product variation, complexity, sourcing complexity and order process variation ‘Supply chain flexibility’ enables a company to respond more quickly to changes in supply and demand, offers new products more quickly and is involved with processes ranging from procurement to distribution/logistics ‘Firm performance’ relates to its profitability and growth |
Face-to-face interviews (n = 32/71, response rate 45%) with executives from the consumer goods industry A web-based survey was sent out via e-mail (n = 53/364, response rate 15%) Potentially significant differences were checked between the questionnaires administered in person and via the web Analysis: a SEM and partial least squares approach to estimate coefficients |
Supply chain flexibility significantly associated with firm performance (b = 0.12), and interaction term (supply chain uncertainty × supply chain flexibility) also associated with firm performance (b = 0.59) Companies that match supply chain flexibility and environmental uncertainty performed better than those who do not (i.e. high environmental uncertainty should have high supply chain flexibility) |
Academic | Attributed significant differences between questionnaires administered in person and via web to differences in industries Results (in terms of association strength) may be highly firm- or industry-dependent |
| Narayanan et al. (2009)107 | Multiple | Multiple | To test whether or not there is a consistent set of antecedents and realised benefits associated with EDI adoption which is supported by empirical research in multiple streams in the field | A meta-analysis based on EDI literature from 1991 to 2005 was undertaken. The databases ‘included’ ABI-informs, EBSCO, keywords such as ‘electronic data interchange’ and ‘EDI’, publications lists (suggested by the contacted authors) and, in total, 182 articles. Ninety survey-based and 50 conceptual articles, 33 case studies and nine analytical studies were identified. It also examined dissertations in the UMI ProQuest Digital Database from 1986 to 2006, adding 31 dissertations. It only included 39 studies in meta-analysis | The realisation of specific individual benefits from EDI has not been conclusively established:
|
Academic | EDI: the primary enabling technology for business-to-business transactions. Studies found in the search and then synthesised to meta-analysis were largely inconsistent but the article does say that the results are generally inconclusive and low powered. The study only indicates patterns. It is also unclear whether or not biases were introduced by the fact that only a subset could be included in the meta-analysis |
| Ogden and McCorriston (2007)78 | UK | Hospitality | To report the findings from a survey of UK conference and event managers, which highlights the benefits that can accrue from supplier management within this sector | A survey of venue managers covering a cross-section of venue types was used | A significant proportion of venue managers reported having long-term supplier relationships, placing considerable value on the non-financial benefits that can accrue from long-term supplier relations featuring mutual trust and good working relationships. These included consistency, responsiveness and flexibility in service delivery. Additionally, the familiarity of regular suppliers with the venue and its procedures can lead to seamless service delivery to the customer and free up venue managers’ time | Academic | |
| Page (2011)108 | USA | Health care | To present a successful example of automated supply chains in a hospital | Examples from different hospitals were used (no methods were described) The three examples concerned New Jersey with a perpetual inventory materials management system (1), Texas with an automated materials management system (2) and New York with a just-in-time management system (3) |
Case study 2: automated materials management saved in excess of $1M, plus another $4.5M in lower pricing thanks to negotiation as a result of having better aggregated purchasing data. Increased quality of care was seen through more time dedicated to patients and more money to invest in new equipment. There were improved workflow efficiencies, higher service levels and the material management staff was cut in half Case study 3: there was an improved materials service, a reduction of inventory and a reduction of staff (25%) |
Grey | There was only a very brief description of the successful hospital system and the methods were not discussed |
| Pagell et al. (2007)79 | Multiple (USA and Taiwan) | Manufacturing | To examine the operational performance impact of two types of investments: an investment in environmental management (i.e. green initiatives) and an investment in buyer–supplier relationships | Survey data were collected as part of the GMRG’s 2002 data collection effort (n = 335) with surveys sent to manufacturing managers. The sample was augmented by sending surveys to purchasing managers in the USA and Taiwan at all included plants with a 16.4% response rate (n = 103) The manufacturing manager addressed the investments in environmental management, while the purchasing manager addressed the buyer–supplier relationships Analysis: dependent variable is operational performance, and path analysis |
Buyer–supplier relationship and environmental investments were significantly associated with sustainability performance (b = 0.20, b = 0.08; p < 0.05) but not with cost, quality or responsiveness performance. Environmental investment only linked to responsiveness performance at the 10% significance level (b = 0.40). Explanation: it is possible that, in the pursuit of improved environmental performance, organisations create processes that have fewer steps, making them faster and more predictable | Academic | Unclear whether or not it is applicable beyond manufacturing, as investment in environmental management included investments in pollution prevention, waste reduction, etc. |
| Paulraj and Chen (2007)66 | USA | Multiple | To illustrate that the implementation of strategic supply management initiatives can ultimately lead to a sustained competitive advantage for buyer firms and their suppliers. The strategic supply management relates to strategic purchasing, long-term relationship orientation, interfirm communication, cross-organisational teams and supplier integration | A cross-sectional mail survey was distributed to members of the Institute for Supply Management with the title Vice President of Purchasing, Materials Management and Supply Chain Management or Director/Manager of Purchasing, Material Management. 232/954 responses were received, 11 were discarded, resulting in n = 221 (a response rate of 23.2%). Nearly 60% of the firms had a gross income of > $100M Analysis: testing of the structural equation model and maximum likelihood estimation for parameters |
Significant association between strategic supply management and supplier performance (b = 0.23, p < 0.01), and buyer performance (b = 0.10, p < 0.05). Significant association between supplier performance and buyer performance (b = 0.51, p < 0.01) | Academic | Self-reporting and based on opinions of executives |
| Paulraj and Chen (2007)80 | USA | Manufacturing | To explore the connection between strategic buyer–supplier relationships and logistics integration, along with the subsequent impact on a firm’s agility performance | A cross-sectional mail survey was administered to members of the Institute for Supply Management with title Vice President of Purchasing, Materials Management and SCM or Director/Manager of Purchasing, Material Management. 232/954 responses were received, 11 were discarded, resulting in n = 221 (response rate 23.2%). The survey asked about numbers of suppliers, views on long-term relationship orientation, interfirm communication, buyer–supplier relationships, IT and external logistics integration. Nearly 60% of the firms had a gross income of > $100M Analysis: testing of structural equation model and maximum likelihood estimation for parameters |
Significant associations between strategic buyer–supplier relationships and external logistics integration (b = 0.39, p < 0.01), IT and external logistics integration (b = 0.27, p < 0.01) and a positive link between external logistics integration and agility performance (b = 0.18, p < 0.01) Empirical evidence that effective external logistics integration is engendered by strategic buyer–supplier relationships and IT, and logistics integration has a positive impact on firm agility IT can serve as a powerful mechanism in co-ordinating suppliers and their activities |
Academic | Targets firms based on assumption that industries are more advanced in implementation of various supply chain initiatives Unclear whether agility performance collected separately from objective data or self-reported |
| Periatt et al. (2007)81 | USA | Multiple | To explore the degree to which the ‘Big Five’ personality factors predict customer orientation of logistics employees. The ‘Big Five’ personality factors are neuroticism, extraversion, openness to experience, agreeableness and conscientiousness | Data were collected as part of a larger multiorganisational job classification study sponsored by Council of Supply Chain Management Professionals – convenience sample as organisations selected by referral and included manufacturers, 3PLs, retailers and financial institutions, with sizes from 15 to more than 100,000 staff. Responses were gathered from 354 people (with 168 different job titles), and 185 responses kept for analysis; questionnaires administered face to face to employees. Existing scales from literature to measure constructs were used. An ordinary least squares regression analysis with personality dimensions as independent variables was run | Personality explained 14% of the variance in customer orientation; openness to experience, agreeableness and conscientiousness were significantly positively related to customer orientation of logistics employees (neuroticism and extraversion were not). Concluded personality factors can be used to select customer-oriented logistics personnel | Academic | ‘Customer orientation’ may be ambiguous, as with all subjective constructs Does not control for any other factor that could influence customer orientation, for example training. Used a convenience sample, limiting generalisability |
| Persona et al. (2008)109 | Italy | Health care | To provide an empirical demonstration of efficient management results obtained by the use of the JIT and Kanban tools; also to demonstrate the implementation of better lean and SCM techniques implemented in two hospitals | The first application of the proposed procedure was implemented in the City Hospital of Padua. The second application was carried out in the Religious Hospital of Turin, where the implementation of the Kanban method has a particular development | In the first hospital (JIT Kanban system) savings amounted to €21,000 in the first year of testing. In the second hospital, there was a saving of €13,100, which is equal to 24.9% of the expenses of the ward for drugs. The monthly consumption of drugs also decreased in the first month of the test (with a reduction of about 32% in comparison with the same month in the previous year) With the introduction of small investments (modular cabinets and ‘intelligent’ trolleys), the quantities and the volumes of stored products, out-of-date medicines, order errors and unnecessary picking operations largely decreased |
Academic | The two hospitals and specific outcomes are not necessarily generalisable, but a very simple task to implement in any hospital worldwide The Kanban system in this context explained as follows Hospital 1: this technique is an application of the one move ‘card’ procedure. The containers used in this study are baskets divided into two parts. The front half of the basket contains products in use; the back half contains the stock products. These containers are kept in organiser cupboards, which are used exclusively to store hospital materials. The ward personnel are only allowed to take the products that are in the front part of the baskets. When the products in use are about to run out, the contents of the back section are moved to the front by the ward sister. By so doing, the FIFO policy is assured. The two separate parts of the basket guarantee that the products used in the wards are always up to date. Expiry problems are thus avoided Hospital 2: the necessary reorganisation of the internal logistics involves the adoption of a technique for refilling drugs and medical supplies for the wards, using the Kanban method adapted to the specific situation. The experimentation was carried out in 2005 and has been progressively extended to all the products supplied to the wards |
| Raviprakash et al. (2009)110 | USA | Health care | To present the different ways of using RFID in health-care settings | A document review. One case study is mentioned: Bon Secours Richmond Health Systems, operating three hospitals in Virginia, USA | Using RFID to locate medical equipment and mobile assets contributed to capital avoidance and utilisation efficiencies. It is estimated that the provider has gained $200,000 in benefits per year over the cost of RFID system installation and maintenance costs (excluding staff productivity gains) In the case study: nursing staff have gained about 30 minutes per nurse shift (because they do not have to hunt down equipment) |
Academic | The case study mentioned in the results section is just one part of the article, which is otherwise very generic |
| Richey et al. (2008)82 | N/R | Retail | To explore the direct impact of retailer technology utilisation behaviours on operational effectiveness. ‘Operational effectiveness’ relates to the sales per employee. ‘Technological intensity’ refers to the variety of technologies used | Methodology:
|
Intensive technology utilisation between supplier and retailer led to better retailer operational effectiveness (b = 0.48, p < 0.01). Technological intensity is a particularly important determinant of retailer effectiveness for retailers who are optimistic about the use of technology (interaction term, b = 0.39, p < 0.01) | Academic | The study does not provide information on the source of the sample. The control variables may be independently associated with operational effectiveness and not technological intensity |
| Roloff and Aßländer (2010)83 | Multiple | Consumer toys | To investigate a particular safety case in terms of buyer–supplier relationships and corporate autonomy | Narrative analysis grounded in the theory of corporate autonomy | Supplier–buyer partnerships could harm corporate autonomy through mistakes made by suppliers or the company. Mattel, Inc. allowed part of control to go to supplier, leaving its control autonomy vulnerable. Submissions of autonomy are acceptable only when all parties consent to certain rules. Relationships can become dysfunctional when corporate autonomy is violated | Academic | Only based on one case study, approach to data collection not reported |
| Rudberg and Thulin (2009)67 | Sweden | Farming | To show that advanced planning systems (APS) can act as an enabler in adapting logistics and supply chain principles and reducing costs through streamlining the supply chain. APS aims to find feasible, near-optimal plans across the supply chain as a whole, while potential bottlenecks are considered explicitly | Case study: Lantmannen (Swedish Farmers Supply and Crop Marketing Association) seed supply chain. The seed supply chain contains 30,000 farmers who act as both suppliers and customers to the four production plants and the two distribution centres. It uses data on products and material in aggregated product groups, as well as demand data and network constraints. One of the challenges is dealing with seasonal demand peaks | Total costs decreased by 13% on a yearly basis, while the quantity of sold units increased. This was equal to a total reduction in cost of 15% per tonne Other outcomes included increased communication between logistics, manufacturing, marketing and sales functions, as well as more time-efficient planning |
Academic | Strong empirical study; uncertain whether or not the outcomes are transferable |
| Schloetzer (2012)84 | N/A | Petroleum manufacturing | To investigate whether or not the potential for hold up in supply chains influences the extent of process integration and information sharing between partners | Performance scorecards and financial performance data from one manufacturer and 156 distributors were used. The study used the percentage of total revenue each partner obtains from relationship to examine partnership interdependence A quantitative analysis was undertaken and controls for the distributor size were taken into consideration |
Positive and significant paths from process integration to sales growth and sales productivity (b = 0.244, p < 0.05 and b = 0.129, p < 0.05, respectively) Positive and significant path from process integration to profitability (b = 0.349, p < 0.01) Paths from information sharing to sales growth and sales productivity were statistically significant (b = 0.201, p < 0.05 and b = 0.189, p < 0.05, respectively) Positive and significant paths from information sharing to profitability (b = 0.125, p < 0.05), i.e. favourable performance benefits could arise from more extensive process integration and information sharing between partners An asymmetry of interdependence and a negative association with information sharing (–0.257), while magnitude was positively associated with both process integration and information sharing (b = 0.195 and b = 0.391, both p < 0.05), i.e. a potential for hold up to prevent process integration and information sharing |
Academic | ‘Hold up’ is where a firm makes specific investments that are hard to redeploy if a partnership with a supplier is terminated. A proxy for ‘hold up’ was asymmetry and the magnitude of interdependence between partners (the independent variables) Confidence intervals were not reported; only standard coefficients and the statistical significance between several relationships, meaning there could be some chance of finding correlations |
| Smart (2010)111 | Multiple | Multiple | To examine how users of e-procurement in buying firms have deployed these applications and how this deployment has had an impact on their use of the supply market | Descriptive case studies |
|
Academic | Limited evidence |
| Tarantilis et al. (2008)112 | Greece | Construction manufacturing | To develop and test a customised web-based ERPS to manage one enterprise process event flow, thereby increasing efficiency and control | A literature review, system design and system implementation in one of the biggest Greek construction companies, which specialises in metallurgical constructions. The system deals with customer complaints, procurement, production planning, quality control and sales | There was a significant cost reduction in all areas affected by the system; however, there was no indication of the scale of the impact The outcomes included enhanced streamlining of company operation; an ability to manage service-related personnel (timesheets); minimal paperwork, flexible and efficient production planning, reduced project delivery times and idle times; increased productivity, increased customer satisfaction; increased sales department efficiency (better use of sales data); facilitated communication (access to real-time data, documents and reports); and a reduction in project execution times from 0% to 40% |
Academic | The benefits are summarised in the article, but detailed measures are not given |
| Thai (2012)85 | Australia | Multiple | To examine the questions of what skills and knowledge are necessary for logistics professionals to be successful in their jobs and how these skills and knowledge profiles may change in the future To investigate the perceived importance of these skills and knowledge and the implications for education and training providers in preparing students for a logistics career |
A literature review and seven interviews to guide survey design were conducted 1300 members of the Chartered Institute of Logistics and Transport in Australia were included in a survey and 147 questionnaires were returned |
All of the proposed skills and knowledge were important for logistics professionals to be successful in their jobs. The findings relating to the relative importance of business, logistics and management skill and knowledge sets were broadly consistent with earlier studies, which have found that logistics professionals should be managers first and logisticians later. In addition, the logistics-related skill and knowledge set was found to be the area which educational and training providers should particularly target to further equip the logistics workforce with substantially improved skills and knowledge to perform their jobs successfully in the future In terms of ranking, the five most important skills and knowledge (in order) as perceived by respondents were personal integrity, managing client relationships, problem-solving ability, cost control and the ability to plan |
Academic | |
| Van der Vaart and Pieter van Donk (2006)86 | Not reported | Manufacturing | To identify what business characteristics make suppliers choose buyer-focused operations as a supply chain strategy in their relationships with key buyers | A broad range of qualitative and quantitative data were collected during interviews and plant visits in a multi-case study research design. Nine units and 42 supply links with key buyers were investigated and analysed | The study confirmed that the two configurations coincided with the proposed business characteristics. On the one hand, they found that operations with shared resources fitted in with made-to-stock manufacturing, cost and speed as order-winners, and mass production. On the other hand, they found buyer–supplier links that perfectly fitted in with the configuration of buyer-focused operations: make-to-order, flexibility and quality as order-winners, and flexible manufacturing. In other words, the supply chain strategy was in line with their theoretical ideas, and buyer-focused operations were chosen for reasons of flexibility in mix, volume, specification and timing | Academic | |
| Walker (2010)113 | USA | Manufacturing | To examine the results of a project to implement a new SCM system to lower inventories and improve product quality with an integration IT infrastructure | The methods are unclear: the study provides an overview of the project post audit, motivations for the project, changes to business processes, lessons learned and outcomes of business plan realisation | Investment of $26M over 3 years. One-time savings at $22.3M and ongoing savings at $6.83M per year; internal rate of return on the project was 29% Inventory management improvements allowed the company to reduce its inventory by $4.2M. In addition, customers were able to reduce inventory by an average of 3.1 days in the first year resulting in cash savings of $19M. General and administrative costs dropped as a result of personnel reductions in billing and accounting. Other headcount reductions occurred in several support functions as a result of reduced duplication of reporting |
Academic | Approach to data collection not reported; however, study does provide a lot of details on benefits of SCM |
| Wieland et al. (2012)114 | Multiple (Europe) | Electronics | To demonstrate a MEIO project to improve efficiency and effectiveness by optimising inventory levels and locations across CSDO’s end-to-end supply chain. This paper describes the project plan, workflows and results | The MEIO system was applied in practice and tested in four steps:
|
One year after implementation, total inventory levels were reduced by more than 11%; in addition, service levels of products modelled using the MEIO process were eight points higher than products not modelled using this process The MEIO process continued to be in place at Intel Corporation and had resulted in sustained reductions in inventory levels, average service levels exceeding 90% and more than an order-of-magnitude reduction in the number of expedites |
Academic | |
| Williams (2008)87 | USA | Health care | To provide some examples of cost containment through better SCM | Case studies (the methods were not described) Moses Cone Health System, Greensboro, NC: analysis teams were created, each comprising supply chain personnel, finance professionals and clinicians. Teams reviewed data regarding types of product used in departments. They then asked physicians to ask for help in reducing supply costs, negotiating with vendors (better pricing), identifying infrequently used products and standardising supplies Babber Health (20 hospitals, Phoenix, AZ): finance professionals and clinicians developed a capped pricing model establishing a fixed price for physician preference items based on a comparison of prices in the national market |
Case study 1: the organisation saved $4.5M over a year (although no details on how this figure was calculated were given) Case study 2: the organisation saved more than $3M/year in cardiology alone, and $13M in total (the study does not state if the $13M was saved over 1 year or over several years) A portion of the cost savings is shared with physicians through investment in new equipment and technology. This sustained the engagement of physicians |
Grey | Context specific; based on two case studies |
| Ygal et al. (2010)115 | Canada | Health care | To estimate the potential impact of the use of a RFID technology system in a hospital nursing unit. The system allows medical supplies bins to be automatically replenished when they become empty | Case study including interviews, validation interviews, experiences from elsewhere and observations | Time savings would correspond to $153,883 (nurses) and $589,424 (auxiliary personnel) a year. However, some tasks would be transferred to store personnel, which would cost $220,130. The reduction of 67% in the walking distance due to reorganisation of storage location would save $3,097,373 (or 7.5 minutes/day/nurse/working shift) The reduction in costs associated with expired products would save $109,453 for stock items/year and $65,367 for non-stock items It is argued that freeing up time in the nursing shift would increase the quality of care The two main benefits were thought to be time saving for nurses and optimisation of inventory levels and processes |
Academic | This is an interesting case study. However, it is to be noted that all costs are estimates calculated from a simulation exercise Implementation costs are taken into account in the saving calculation |
| Zhu et al. (2008)68 | Multiple (UK and China) | Automotive industry | To compare pressures, practice and performance of the ESCM in China and the UK | An empirical study of 128 automotive organisations, 39 in the UK and 89 in China. Questionnaires were administered based on the literature and the industrial input (pressures to adopt ESCM practices, current ESCM practices and corresponding performance outcomes and improvements) In China a convenience sampling from workshops at a university was used. Two additional convenience sample surveys were conducted to acquire information over a 2-year period from February 2003 to April 2005 (n = 89, a 61% response rate). In the UK a postal questionnaire was sent to people in organisations (n = 39, an 18% response rate) Analysis using two-tailed independent samples t-tests |
The impact of ESCM on performance came mainly from decreased fines for environmental accidents (UK companies) and an increased amount of goods delivered on time. Both economic and operational benefits were greater for Chinese companies. The performance improvement hypothesis was only weakly supported | Academic | ESCM was used as the explicit consideration of the ecological implications for all supply chain operation activities Response set bias may be a problem in this study, as they employed scaled data gathered from two samplings in two different countries. Additionally, cultural factors may have caused differences in survey interpretations |
Appendix 3 Key informant interview protocol
Interview topic guide
-
What are the main issues facing procurement as a policy today? What should be the priorities for improving SCM?
-
How are these challenges different for:
-
consumables
-
devices (and within these, the range of purchases from capital to revenue)
-
pharmaceuticals?
-
-
How is procurement at Department of Health/government level working together with industry to overcome its challenges?
-
Where are the gaps in evidence? What don’t we know?
-
How do you feel evidence is informing policy?
-
Do we know what ‘good practice’ looks like? If not, why not? How have previous models helped? How have previous models failed?
-
What industries do you think we have the most to learn from?
-
How important are softer factors such as relationships with suppliers in NHS supply chains? Are they prioritised?
-
How do you think technology, or enhanced technology, would be accepted or perceived by people working within the NHS supply chain or policy-makers?
-
What problems do you think technology could help to solve?
-
-
How much should SCM be integrated to the rest of NHS business operations?
-
How are suppliers selected? Are decisions strategic or pragmatic?
List of abbreviations
- ARS
- agence régionale de santé [regional health agencies]
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CSU
- commercial support unit
- DGOS
- Direction générale de l’offre de soins [Directorate General of Health Care Provision]
- DHB
- district health board
- FPSC
- finance, procurement and supply chain
- GDP
- gross domestic product
- GP
- general practitioner
- GPO
- group purchasing organisation
- HBL
- Health Benefits Limited
- IT
- information technology
- NIHR
- National Institute for Health Research
- OECD
- Organisation for Economic Co-operation and Development
- PHARE
- Performance Hospitalière pour des Achats Responsables [Hospital Performance for Responsible Procurement]
- PHO
- primary health organisation
- REA
- rapid evidence assessment
- Résah-idf
- Réseau des acheteurs hospitaliers d’Ile de France
- RFID
- radio frequency identification
- SCM
- supply chain management
- SHI
- statutory health insurance
- SME
- small- and medium-sized enterprise
- UGAP
- Union des Groupements d’Achats Publics