
Notes
Article history
The research reported here is the product of an HS&DR Evidence Synthesis Centre, contracted to provide rapid evidence syntheses on issues of relevance to the health service, and to inform future HS&DR calls for new research around identified gaps in evidence. Other reviews by the Evidence Synthesis Centres are also available in the HS&DR journal.
The research reported in this issue of the journal was funded by the HS&DR programme as project number 13/05/11. The contractual start date was in March 2014. The final report began editorial review in September 2014 and was accepted for publication in December 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Jane Dalton is a publicly elected governor at York Teaching Hospital NHS Foundation Trust.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Dalton et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
The need to fully engage staff, patients and the public in discussions and decisions about changes to the way health services are delivered has been recognised for many years. In England, local authority health overview and scrutiny committees must be consulted by local NHS bodies about proposals for substantial changes to services. Committees can refer proposals to the Secretary of State for Health if they are not satisfied with the consultation process or consider that the proposals are not in the interests of the health service in their area. The Independent Reconfiguration Panel (IRP) provides independent advice to the Secretary of State in such cases. 1 More recently, the Health and Social Care Act 20122 established a new mechanism (Healthwatch) to drive patient involvement locally and nationally across the NHS. Best-practice guidance is available from several sources, such as NHS England’s Planning and Delivering Service Changes for Patients3 and Transforming Participation in Health and Care. 4 Proposals for service changes by commissioners and other bodies are required to pass four tests, the first of which is to be able to demonstrate evidence of strong public and patient engagement. The remaining tests seek to demonstrate consistency with current and prospective need for patient choice; a clear clinical evidence base; and support for proposals from clinical commissioners.
While much of the guidance reflects common sense, there is a need to establish the strength of the evidence base around different approaches to public engagement and involvement and in terms of impact. Proposed changes to health service delivery are often controversial locally and sometimes nationally. Effective public engagement may help resolve controversy and result in a broad consensus on the way forward. Successful implementation of this process may, in turn, bring about greater satisfaction that services adequately reflect public preferences; and may ultimately improve clinical outcomes or better access to services. In contrast, inadequate consultation may result in lack of agreement, leading to proposals being delayed or referred to the IRP or ultimately the courts. Any evidence that can clarify factors associated with positive public engagement will be of value both to NHS decision-makers and to society as a whole.
A wide variety of approaches to public engagement and involvement are available. Examples include surveys, face-to-face and telephone interviews, public meetings, focus groups, online consultations (including use of social media), local referenda and citizens’ juries (also known as citizen panels or stakeholder dialogues). The available literature describing and evaluating how these approaches have operated in practice appears to be disparate and widely scattered. Recent systematic reviews have looked at the impact of patient and public involvement (PPI) on UK health care in general5 and at strategies for interactive public engagement in development of health-care policies and programmes. 6 In the primary literature, examples include an academic study of a ‘decision conference’ including patients and caregivers, to consider eating disorders services;7 a general discussion of the issues in a journal aimed at health service managers;8 and a number of case studies published by the NHS Confederation. 9–13
The objective of this project was to bring together evidence from published and grey literature sources, to assess what is known about effective patient and public engagement in reconfiguration processes and to identify implications for further health-care practice and research.
Chapter 2 Methods
General approach
The project was resourced as a rapid evidence synthesis. There is no generally accepted definition of this term and a number of other terms have been used to describe rapid reviews incorporating systematic review methodology modified to various degrees. Our intention was to carry out a review using systematic and transparent methods to identify and appraise relevant evidence and produce a synthesis that goes beyond identifying the main areas of research and listing their findings. However, we foresaw that the process would be less exhaustive and the outputs somewhat less detailed than might be expected from a full systematic review. Added to this, we expected to find limited evidence on the subject in the peer-reviewed primary literature.
Research questions
We sought to address the following five questions:
-
How have patients and the public been engaged in decisions about health service reconfiguration in the past?
-
How has PPI affected decisions about health service reconfiguration?
-
Which types of PPI have had the greatest impact on these decisions?
-
Which methods of PPI are likely to be sustainable/repeatable?
-
How have differing opinions about reconfiguration between patients, the public, clinical experts and other senior decision-makers been negotiated and resolved?
Scope and definitions
The focus of the review is reconfiguration of health service provision in the NHS. We also considered evidence on health services delivered by non-NHS providers (e.g. voluntary sector/private sector) and the joint provision of health and social care where this impacts directly on NHS provision. Where relevant, we considered international evidence from other health systems which are comparable and relevant to the NHS. In addition to England/the UK, the included systematic reviews covered studies conducted worldwide; other research and case studies additionally covered Scotland and Canada.
Reconfiguration includes large-scale system change, such as relocation of hospitals, (re)location of specialist care and changes in provision of urgent/emergency/out-of-hours care. We did not consider small-scale change, for example at hospital ward level or within a general practitioner (GP) practice. Reconfiguration has been defined in the literature as a deliberately induced change of some significance in the distribution of medical, surgical, diagnostic and ancillary specialties that are available in each hospital or other secondary or tertiary acute care unit in locality, region or health-care administrative area. 14
In the literature, the terms ‘engagement’ and ‘involvement’ are often used interchangeably. For the purposes of public involvement in research, INVOLVE (www.invo.org.uk) distinguishes between active involvement of patients or members of the public in research projects and engagement, which provides information and knowledge about research in an accessible way (e.g. through science festivals or open days). This distinction is difficult to sustain in the context of proposals for service reconfiguration where provision of information may (or may not) lead to active involvement. Events such as public meetings or citizens’ juries have elements of both information provision and active contribution of patients or members of the public to developing or modifying (or rejecting) proposals for change. In this review we define patient/public engagement or democratic involvement as including any means of seeking and responding to the views of patients and the wider public at any stage of the process of reconfiguration (including identifying possible options for change). We have not attempted to standardise the various terminology used to indicate service user engagement across the included studies. In our search strategy, other terms included ‘user’ and ‘carer’ engagement and involvement (see Appendix 1). The scope included existing patients, carers and their representative groups; and the general public and their representatives [e.g. local councillors and Members of Parliament (MPs)].
Inclusion and exclusion criteria
We looked for relevant evidence in three main areas:
-
Systematic reviews of methods of/approaches to patient/public engagement. We included only reviews that were relevant to PPI in decisions about health service reconfiguration. Reviews of PPI in research were excluded.
-
Empirical studies of any design evaluating methods of/approaches to patient/public engagement. Studies that focused on involvement in research were excluded.
-
Case studies examining how PPI worked in specific examples of system change in the recent past. We expected that these were more likely to be found in the grey literature than in peer-reviewed publications. Case studies of this kind were likely to provide a biased sample of ‘successful’ rather than typical PPI but were more likely to provide useful data to inform future practice. We also searched for case studies where public involvement failed to produce an agreed way forward or resulted in unintended consequences, using the website of the IRP as a starting point.
The following were excluded:
-
‘emergency’ reconfigurations triggered by failure of a service provider, such as a NHS trust
-
consultation/involvement of NHS staff, except as part of a broader consultation where staff and PPI could not be separated
-
patient/public representation on bodies where reconfiguration was part of the remit but was not the main focus
-
patient/public engagement methods where complaints management was the focus (e.g. patient advice and liaison service and the Healthwatch independent advocacy arm).
Literature search
Search strategy for reviews
A search strategy was developed on the Cochrane Database of Systematic Reviews (Wiley) to identify any systematic reviews or overviews of systematic reviews of user engagement. As user engagement is described in a variety of ways in the literature, a wide range of text words, synonyms and subject headings were included in the search strategy. Key terms for user engagement were identified by scanning key papers, discussion with the review team and use of database thesauri. Searches were restricted to reviews published from 2000 onwards. No language restrictions were applied to the searches. The search strategy was adapted for use in each of the review databases searched. Text word searches were limited to searching in only the title field for databases where this was possible. The following databases were searched in March/April 2014: the Cochrane Database of Systematic Reviews, the Campbell Library, Database of Abstracts of Reviews of Effects (DARE), Database of Promoting Health Effectiveness Reviews, the Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI-Centre), Evidence Library and Health Systems Evidence (www.mcmasterhealthforum.org/hse/).
Search strategy for primary studies
A search strategy for primary studies was developed using MEDLINE (OvidSP). The existing strategy for reviews described above (containing terms for user engagement) was combined using the Boolean operator ‘AND’ with a second set of terms for reconfiguration. As this was a rapid review, a number of limits were used to focus the strategy: focusing of subject headings, a date limit of 2000 onwards and restriction to English-language studies. The range of databases searched was more limited than would be usual for a full systematic review. In particular, no specific databases of conference proceedings, theses or foreign-language studies were searched. Relevant databases covering literature from health, health management and social science were searched in March/April 2014: MEDLINE and MEDLINE In-Process & Other Non-Indexed Citations, Applied Social Sciences Index and Abstracts, Health Management Information Consortium, PsycINFO, Social Care Online and the Social Science Citation Index. The MEDLINE strategy was adapted for use in each database.
Search strategy to locate grey literature
In addition to the database searches, a wide range of websites relevant to UK health policy, health service delivery and organisation, and user engagement were searched to identify any policy documents, reports, case studies or grey literature. Websites were selected on the basis of expert knowledge and judgement. A list of relevant websites was drawn up by the review team and further additions to the list were suggested by our collaborators and external contacts. Each website was browsed manually and/or searched using the website search function where available, depending on the size of literature contained on the website. Searches were carried out in April/May 2014. Relevant documents hosted on the websites relating to user engagement in the reconfiguration of services published since 2000 in English were retrieved and downloaded. Further links within each website to documents on other websites were not explored. To supplement the website searches, a focused search of Google was carried out to locate UK reports on service reconfiguration. Using the Google advanced search facility, the search was limited to UK portable document format files (PDFs) published in English from 2000 onwards with the term ‘reconfiguration’ in the title of the web page. The first 100 results were scanned for relevance. Further case studies were identified through contact with local hospitals and other experts and researchers working in the field of user engagement.
Records were managed within an EndNote library (EndNote version X6, Thomson Reuters, CA, USA). After deduplication, 2322 records in total were identified.
Further details of the search strategies and results can be found in Appendix 1.
Study selection, data extraction and quality assessment
Search results were initially screened by a single reviewer to eliminate obviously irrelevant items. Full-text copies were ordered or downloaded for potentially relevant records. Final study selection was carried out by two reviewers independently, with disagreements resolved by discussion or involvement of a third reviewer if necessary.
We used EPPI-Reviewer 4 (Evidence for Policy and Practice Information and Co-ordinating Centre, University of London, London, UK) to record decisions about study selection and for data extraction and quality assessment. We developed separate data extraction forms to record key information for different evidence sources (systematic reviews, case studies and other research). For case studies, data extraction was done in two stages: basic details were extracted for all included case studies; then a number of ‘exemplars’ were selected for more detailed data extraction and analysis. Exemplars were those case studies that provided most detailed and current information about the methods used for patient/public engagement and involvement and/or assessed the impact of engagement/involvement in reconfiguration decisions. Data extraction was performed by one reviewer and checked by a second.
We assessed systematic reviews for methodological quality and reliability using the approach of DARE. We planned to assess published primary research studies using appropriate design-specific tools described in the guidance of the Centre for Reviews and Dissemination for undertaking systematic reviews in health care (2009). 15 Unpublished case studies and non-peer-reviewed reports were not formally assessed for quality (risk of bias) but we sought to identify any instances of more rigorously conducted and fully reported case studies. Issues considered were:
-
the extent to which an appropriate diversity of perspectives (e.g. across service user and NHS) was considered in assessing the impact of patient/public engagement
-
the extent to which the case study was conducted and reported with transparency
-
reflexivity on any specifically adopted perspective, together with adequacy and clarity of reporting on intervention context, methods and impact.
Synthesis
We carried out a narrative synthesis using multiple frameworks to guide our analysis. In addition to the five research questions specified in the study protocol, we considered chronological aspects of reconfiguration decisions in terms of the seven stages specified in the NHS England guidance on planning and delivering service changes (Box 1). 3 Levels of engagement/involvement were assessed where possible, using the version of Arnstein’s ‘ladder of engagement and participation’ presented in the NHS England guidance on transforming participation in health and care (Table 1). 4 We used the available literature to determine the extent to which evidence supported or disagreed with the recent guidance and to highlight areas where the evidence was conflicting or insufficient.
-
Setting the strategic context.
-
Proposal.
-
Discussion.
-
Assurance.
-
Consultation.
-
Decision.
-
Implementation.
Source: Planning and Delivering Service Changes for Patients (pp. 14–15). 3
| Devolving | Placing decision-making in the hands of the community and individuals, for example Personal Health Budgets or a community development approach |
| Collaborating | Working in partnership with communities and patients in each aspect of the decision, including the development of alternatives and the identification of the preferred solution |
| Involving | Working directly with communities and patients to ensure that concerns and aspirations are consistently understood and considered, for example partnership boards, reference groups and service users participating in policy groups |
| Consulting | Obtaining community and individual feedback on analysis, alternatives and/or decisions, for example surveys, door knocking, citizens’ panels and focus groups |
| Informing | Providing communities and individuals with balanced and objective information to assist them in understanding problems, alternatives, opportunities and solutions, for example websites, newsletters and press releases |
In synthesising the case studies, we focused on those case studies identified as exemplars (those case studies that provided more detail, see Study selection, data extraction and quality assessment). We were particularly interested in identifying case studies with an element of independent evaluation by an organisation not involved in the reconfiguration being examined.
Given the resources available for the project, we planned to focus on only a small number of exemplars. For other case studies, we extracted basic details only and used these studies to supplement the analysis of themes emerging from the exemplar case studies.
Chapter 3 Nature of the evidence
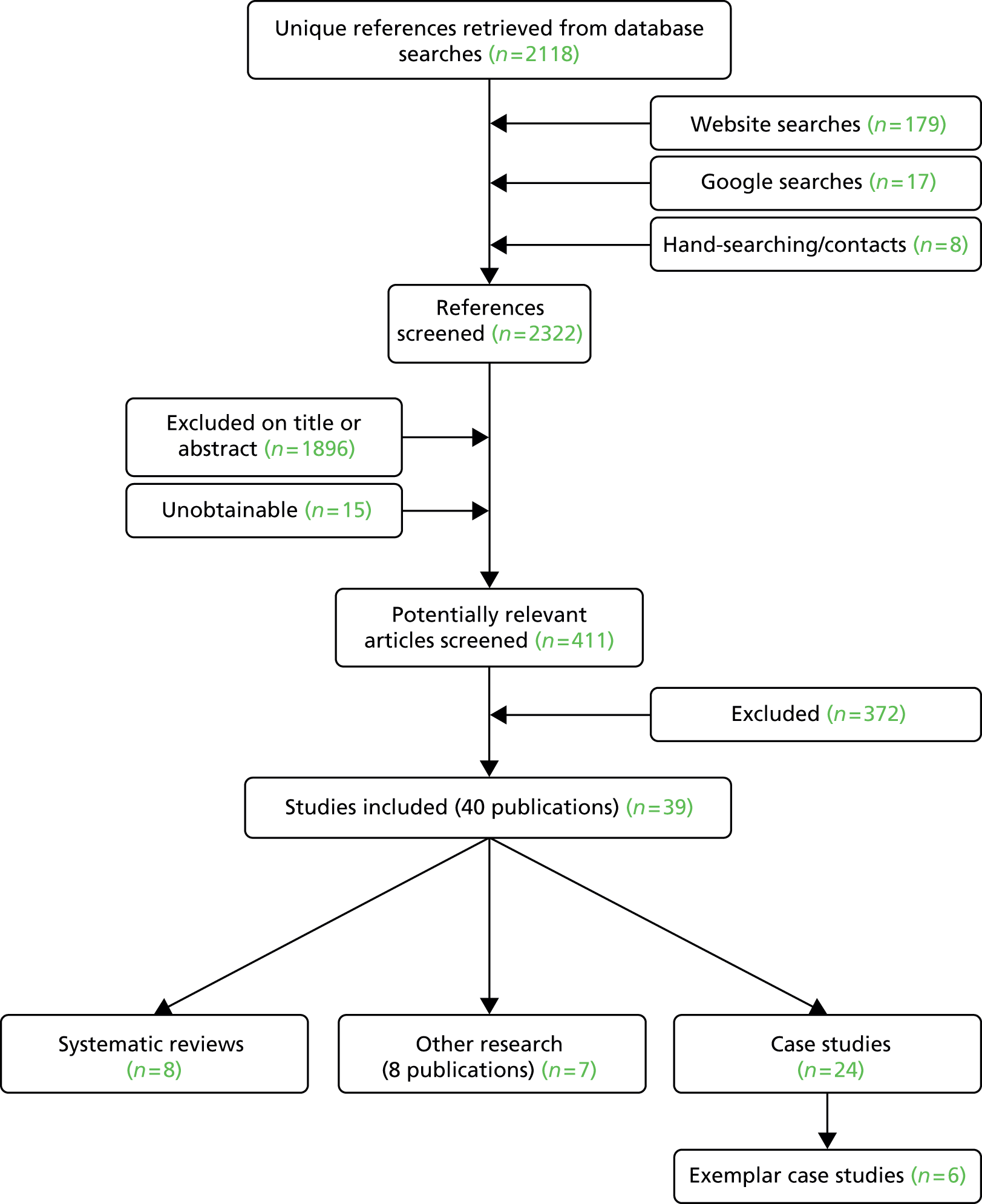
We included eight systematic reviews,5,6,16–21 eight papers (describing seven distinct pieces of work) that were classified as other health-care-related research1,22–28 and 24 case studies. 7–13,29–45 See Figure 1 for details.
FIGURE 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Full data extraction tables for the systematic reviews, other research, case studies and case study exemplars are available in the appendices, along with details of the systematic reviews quality assessments (see Appendices 2–6).
Overview
We identified eight systematic reviews conducted between 2002 and 2012 (see Appendix 2). The number of included studies in these reviews ranged from 8 to 344. Study locations included various European countries, the USA, Canada, Australia, New Zealand, Israel and Japan. All reviews included some proportion of UK studies. Four reviews contained a majority of studies located in the UK16–18,21 and two reviews5,19 had a complete focus on the UK setting (Table 2 and Appendix 2). Reading across the reviews, there was some overlap of studies. Owing to resource limitations, further examination of the nature and extent of this overlap was not carried out.
| Study reference | Type(s) of reconfiguration | Who was engaged/involved? | Method(s) of engagement/involvement |
|---|---|---|---|
| Conklin et al. (2012)16 | Relevant studies (where reconfiguration was the goal). Examples: resource allocation relating to local health integration networks; shaping policies and decisions about primary care provision and delivery; health-care priority setting; health policy decisions about the delivery of women’s health services; decision-making about local health services | Special interest groups; the public; patients; staff; NHS lay board members. More specific definitions of ‘the public’ varied and were generally unclear across the studies. Terms used by the study authors: representatives of patient organisations; ordinary citizens; individuals with no particular axe to grind; those whose voices might not otherwise be heard | Surveys; conference and website; community health councils; public meetings; local patient groups; citizen panels/juries; group simulation using roulette wheel; collaboration between agencies/groups/individuals |
| Crawford et al. (2002)17 | Various services, including primary care, mental health, learning and physical disability, general health care, community services, inpatient and outpatient, social care, maternity, neurology and human immunodeficiency virus. Most studies looked at smaller-scale change. Approximately one-quarter of studies focused on larger-scale change, including changes to organisation of care and/or services. Of these studies, two involved a plan for hospital closure | Most studies described participants as patients. Others reported involvement of carers, service users, staff, Health and Welfare Council, Community Health Council, citizens, lay board of directors or mixed populations | Patient groups; consultation meetings; committees and forums; interviews; citizen’s juries; survey; focus groups; representation on planning boards and panels; mixed methods |
| Crawford et al. (2003)18 | Specific reconfiguration not described. Reconfiguration contexts described as various within health, social and community care; non-health public sector (including postal services, social security, education, housing); private sector (including consumer goods, travel, entertainment); and voluntary sector (disability/neurological services) | Current, past and potential service users and their representatives; providers | Various, covering time-limited methods (to elicit user perceptions/preferences) and long-term approaches (building relationships with service users). Some initiated by provider; others initiated by service users. Public sector tended to use more deliberative approaches. Examples: surveys; focus groups; deliberative approaches (such as citizen’s juries, public conferences); user/community groups; formal bodies (such as Community Health Councils, patient groups, advocates and link workers) |
| Daykin et al. (2007)19 | General/strategic development; cancer services; mental health; older people’s services | Staff; members of the public; patients | Employment of an individual to work with community groups; interprofessional cancer education programme; user groups; forums for service users and officials; community-based exercise facility for people with mental health problems; citizen’s juries; community initiative to elicit and respond to the views of older people; regional-level action research programme with staff |
| Mockford et al. (2012)5 | General | Patients/carers; public | Lay membership of boards, panels and working groups; user groups |
| Rose et al. (2003)21 | Promoting democracy and representation and/or cultural change (over 50% of included studies). Strategic planning, restructuring of services (very few studies), and policy initiatives. New service provision and the employment of service users in organisations | Most studies focused on service users and professional staff. A quarter of studies involved carers. Others involved: user groups, carer groups, public, Community Health Councils | Most studies focused on collective consumerism, involving consultation, representation, partnership, evaluation, involvement in staff recruitment. Methods not explicitly stated |
Quality of the reviews
The quality of the eight systematic reviews varied. Seven reported an adequate search and provided study details, and all presented implications for research and/or practice. However, the extent to which review conclusions were reliably supported by the evidence presented (in the traditional sense of critically appraising systematic reviews) was limited by the fact that only two reviews formally assessed the quality of included studies. Seven of the reviews involved mixed evidence sources such as reviews, qualitative and quantitative (largely observational) studies, grey literature and discussion papers.
Types of reconfiguration
Although all eight reviews were related to service reconfiguration, not all framed their objective in these terms. Where reconfiguration was described beyond general terms, review authors referred to priority setting, local planning and policy development, and decisions about health service resource allocation. Service user engagement was explored across a range of specialist services and generic service or policy development. Examples of specific clinical service changes included those which were related to cancer,6,19 mental health,17 women’s health and maternity,16,17 and older peoples’ services. 19 Reviews also examined system-wide change, such as the shaping of primary care and community services;17,18 one review included two studies concentrating on plans for hospital closure. 17 Some reviews adopted a wider remit, capturing more than merely health implications. These particular reviews focused (in addition to health-care services) on proposals for change in areas such as environmental planning, education and housing. 18,20
Engagement methods and who was involved
There was no consistent definition of service user engagement or involvement. Where this was reported, engagement was specified in the review authors’ terms and did not appear substantially linked to any wider conceptual or theoretical framework.
A range of methods was employed in the engagement process. The extent to which methods were explicitly specified varied. Those that were primarily informative in nature included, for example, communication via traditional publicity and the provision of website materials. 16,20 Other methods indicated more active involvement of service users in eliciting feedback by opinion polls and surveys. 17,18,20 Consultation and deliberative methods featured in all reviews, being largely operationalised as collaborative partnerships, citizens’ juries, working groups, consensus conferences and other mechanisms. Where public meetings and community forums were described, without further detail it was often difficult to determine their positioning on the ladder of engagement and participation (see Table 1). Across many reviews, a mixture of methods was used to capture the service user voice. Four reviews discussed the potential sustainability of methods. 6,16,18,20
Across the reviews, service users were frequently described as ‘the public’, although this term tended to be defined loosely and variably. Others engaged in the process were patients, carers, staff, local residents, councillors, MPs and stakeholders (invariably not defined). The engagement of multiple audiences was referred to in many cases.
Impact
Most reviews were broadly agreed on the paucity of evidence of impact in relation to service user engagement and reconfiguration. More robust evaluative research was generally recommended. Many review authors cited the critical influence of contextual variables on successful engagement; one referred in particular to geographic variability. 16 The absence of measurable outcomes was a problem;5,16,21 the lack of independent research was reported to be a considerable limiting factor. 18
Successful engagement was defined variably across the included studies, with many describing impact on processes rather than service reconfiguration per se; for example, changes in service user views about services, organisational culture change with regard to commitment to user engagement, and shifts in learning about future processes represented outcomes in two reviews. 16,17
There was some evidence of impact on service delivery outcomes in terms of changes to service provision5,17 and, in particular for location and access issues,5 priorities integrated into a regional programme and new resources found for services resulting from the activities of citizens’ juries and other community collaborations. 16 One review included two studies that reported a successful challenge to hospital closure, resulting in the proposal being modified or abandoned. 17
Negative consequences of engagement were rarely reported. However, two reviews referred to service users interpreting the engagement process as tokenism,17 and community stakeholders were reported to experience unintended consequences (feeling ostracised) when challenging statutory sector partners. 16
While there was little evidence to support the isolated success of any particular engagement method,19,20 there were positive indications for those characterised as more deliberative in nature and involving face-to-face interactions,6,16,19,20 and for engagement efforts comprising multiple methods. 19 There was mixed support for partnership working, which was seen as central to success in one review6 and as having no systematic relationship with any form of organisational change in another. 21
Tentative success factors in service user engagement appeared to be organisational support for the process; a willingness of users to engage; clarity surrounding the aims of engagement; and adequate resourcing of evaluations. 6,18,19,21
There was little discussion about the potential sustainability of methods. In one review, the institutionalisation of partnerships was seen as a key driver,6 while regional meetings were seen as potentially repeatable in another. 16
Systematic reviews in summary
Reviews were conducted with a reasonable level of attention to methodological rigour. Because of the diversity and nature of the study designs, the quality of the studies included in the reviews was difficult to determine. A variety of health services were studied, and a range of engagement methods (described by various terminologies) adopted. Not all systematic reviews focused completely on health service reconfiguration. Where this was the case, review objectives seemed closely aligned to reconfiguration (e.g. the focus was on priority setting or decisions about resource allocation for future services).
The isolated impact of service user engagement (as distinct from the engagement of staff and other stakeholders) was sometimes difficult to distinguish. Reviews focused largely on the impact of service user engagement on outcomes related to process (e.g. shifts in organisational views about engagement) rather than those related to the impact of engagement on reconfiguration success.
Positive indications were noted from engagement methods that were more deliberative, those involving face-to-face interactions and those comprising multiple methods. Tentative factors leading to successful service user engagement were organisational support, willingness of users to engage, clarity about the aims of engagement and adequate resourcing of evaluations.
Other research
Overview
We identified eight publications that described seven other research projects in the area (see Figure 1). All were located in the UK (four in England, two in Scotland and one UK-wide). The papers were selected based on relevance to this review. They were not evaluated for methodological quality. Although they were diverse in methodology, it was possible to identify three broad categories of discussion papers about service user engagement and reconfiguration.
Influencing factors, trade-offs and options appraisal
Three papers focused in part on engagement in proposed changes in accident and emergency services. 22–24 Changes to community hospital provision were additionally explored in the Scottish-based paper; in this paper, discussion of services involving day-long deliberative panels, surveys and interviews with the public and NHS stakeholders resulted in the identification of several key drivers underpinning successful service user engagement. 24 These were reported primarily as the need for common understanding on the case for change, careful selection of methods of public engagement, focus on location and access, and a strong clinical case for change.
In-depth interviews and flash cards were used to elicit information about preferences and trade-offs among patients and members of the public in two English localities. 22,23 Discussion revealed that most participants were unwilling to accept trade-offs (particularly longer journey times to access higher-quality care). A key message for commissioners and policy-makers was to avoid assuming that presenting the clinical case for change, together with very visible clinical leadership of the proposals, would result in associated community support. While this could be viewed as a negative or unexpected consequence of engagement, hostility to the proposal identified in this research demonstrated an important step in the process of arriving at a democratically derived solution.
Mechanisms for independent scrutiny and lessons from failures
A review of IRP reviews sought to highlight common themes arising from various cases of service reconfiguration referred to the organisation between 2003 and 2010. 1 The report illustrated the following precursors to referral: inadequate community and stakeholder engagement in the early stages of planning and change; inadequate promotion of the clinical case for change; overlooking the broad vision of integration; underplaying benefits of change; limited content and methods of conveying information; lack of preparedness to respond on key issues such as money, transport and emergency care; and inadequate attention to responses throughout and beyond the consultation.
The issue of independent scrutiny was further discussed in an expert opinion paper exploring the robustness of local and national scrutiny mechanisms (local overview and scrutiny committees, judicial scrutiny and the role of the IRP) relating to a range of NHS service reconfigurations. 25 The report concluded that local overview and scrutiny committees were assertive in questioning and challenging proposals. Uncertainties were uncovered relating to decisions about exactly when consultation was required and the definition of ‘substantial’ change. Costs and benefits of local authority scrutiny were also discussed.
Recommendations for local leaders of service reconfiguration from a further expert opinion paper placed strong emphasis on involving patients in the coproduction of services (where patients and organisations were engaged from the start as equals in shaping the case for redesigning services to meet their needs and preferences) and having less reliance on formal consultation. 28
The nature of communication and role of the media
The first of two papers focused on how primary care trusts (PCTs) could most effectively communicate proposals for service reconfiguration to the general public. 26 Using focus groups and case studies, the authors discussed the use of language. Results showed that certain words and phrases (such as ‘budget’, ‘value for money’ and ‘competitive tendering’) were not fully understood and sometimes misunderstood by service users. Consequently, the potential tension between organisational transparency and communicating in a way that successfully engaged people was exposed. In Scotland, media coverage of changes to rural maternity services was observed in another report. 27 This report documented variations in reporting across a number of newspapers and British Broadcasting Corporation (BBC) coverage, with positive and negative accounts of the service change.
Other health-care-related research in summary
Other health-care-related research comprised discussion papers and debates, with some examination of public views about engagement and/or service reconfiguration. The research highlighted the existence of key steps in the reconfiguration process that could result in referral to the IRP if not followed correctly (see Mechanisms for independent scrutiny and lessons from failures). 1 The research also indicated where service user engagement could be construed negatively; the importance of effective use of language in communicating with multiple audiences; variations in media opinion about service change; and consequent potential to influence service users in their decision-making.
Case studies
Overview of case studies not examined in depth
We identified 24 case studies, but detailed data extraction was not carried out for 18 of these because of variability in the consistency and depth of reporting. The basic details of these case studies are summarised as follows.
Most case studies highlighted potential indicators of success but failed to provide enough detail about methods of engagement and/or report the association of these methods with specific impact. 8,10,11,13,29–38 Most studies were located in England and in the NHS setting. Specific types of reconfiguration included hospital mergers, integration of health and social care, and changes linked to primary care, maternity, emergency, acute care and pain services. Other types of reconfiguration were less well specified, such as the centralisation of services or unspecified large-scale reconfiguration. A wide range of participants was involved in the engagement process, including patients and the public, NHS staff, foundation trust members and governors, voluntary sector organisations, MPs and others.
Two reports focused on the history and development of specific models of patient and public engagement. These included a detailed account of activities from the Somerset Health Panels39 and a description of how a Public Involvement Network model was developed in Dorset, England. 40 Another report which looked at the planning of regional supportive cancer services in Ontario, Canada, focused generally on barriers to effective patient involvement. 41
The final case study reference was a web link to 24 reports produced between 2005 and 2012 by the Scottish Health Council on behalf of the Scottish Government. 42 As with the English NHS, Scottish Health Boards are required to involve patients and local communities adequately in relation to significant NHS service change. Across these reports, types of reconfiguration varied. Details centred on aspects of the consultation process and on learning points to improve future public consultations.
Case study exemplars
Six case studies were identified as being exemplars of good practice on the basis of one or more of the following: completeness and quality of reporting (particularly on methods and impact); diversity of perspectives employed; reflexivity in reporting; and demonstrable impact resulting from a specified engagement process. 7,9,12,43–45 See Tables 3 and 4, and Appendix 6.
| Study reference | Setting | Type(s) of reconfiguration | Who was engaged/involved? | Methods |
|---|---|---|---|---|
| Airoldi (2013)7 | PCT eating disorder service | Priority-setting in eating disorder services, with emphasis on improving services in a climate of decreasing resources | Patients, caregivers, clinicians, health-care managers. There were five patients/carers out of 24 in the group. Follow-up was conducted with a wider set of stakeholders (not specified) in the local health economy | Decision conferences: working meetings attended by key stakeholders, led by an impartial facilitator. Participants assessed the value of services based on (1) cost and (2) population health benefit. Additionally: semistructured and unstructured interviews; e-mail correspondence; direct observation of workshops; use of flipchart notes and minutes of board meetings; follow-up events and interviews at 1 and 2 years after consultation. A steering group and an independent evaluator oversaw the process, in addition to input from the case study author |
| Gamble and Sloss (2011)43 | Urgent care/ED | Redesign of minors care within the ED. To include integration of a walk-in centre (separately located at the time; engagement work on the walk-in centre does not form part of the present study); improved integration with the out-of-hours GP service; and consideration of a potential GP triage service | Patients, carers, staff, hospital governors | Observation sessions in ED; focus group; real-time feedback (patient experience questionnaire via standpoint machine); inpatient national survey results specific to York ED. Other engagement work was proposed (no details in this report) as part of the trust’s wider communications strategy on proposals to create an urgent care centre. The proposed work included attendance at local events, presentations to specialist interest groups and information-giving at the hospital open day |
| NHS Confederation (2013)12 | Acute and emergency care | ‘Better Healthcare in Bucks’: centralisation of emergency care. Providing care closer to home for most patients. Establishment of clinical centres of excellence | Patients, public, primary care and hospital-based clinicians, other health service staff, MPs, local health overview and scrutiny committee, voluntary organisations | Public meetings, clinical summits, online surveys, website, video showing interviews with lead clinicians, printed materials, local media campaign, presentations and site visits. A wide-reaching communications programme (internal and external) was implemented to support the service change |
| NHS Confederation (2013)9 | Acute hospital (maternity services) | Redesign of maternity services | Patients and their representatives: women and their families, GPs, local councillors and MPs, including the Joint Health Overview Scrutiny Group. Parent groups, Sure Start. Others engaged in the process: community midwives, hospital-based clinicians | Online responses, public meetings, face-to-face meetings with key stakeholders, letters, articles in relevant local and national media, website updates, ‘ground-breaking events’, posters and postcards, employment of a redesign lead at the trust. Public engagement ran alongside a comprehensive staff-training programme |
| Sainsbury Centre for Mental Health (2010)44 | Mental health day and vocational services | Service redesign as part of a wider review of modernising day and vocational services for people with mental health problems | Service users, commissioners, external consultants | A working group (comprising eight service users) was established to take part in the review of services, in response to invitation leaflets and posters distributed to local day centres. Three members of the working group joined a separate project steering group, which also included representatives from commissioners and external consultants. The group’s remit included design of the review of services; research with service users to gather views about services; contributing to decisions about service redesign; contributing to the development of service specifications and tender documents; and helping to select future providers in the tendering process |
| NHS Scarborough and Ryedale CCG (2014)45 | Primary care | Urgent care services | Patients, public, clinicians, partner organisations (representatives from primary care, secondary care, local authority, voluntary sector), local and regional scrutiny committees, local media | Distribution of consultation document and video; interactive workshop for clinicians and partner organisations; presentations to local and regional health scrutiny committees; surveys; public meetings; focus groups; Facebook (Facebook Inc. CA, USA) posts |
| Key factors of successful engagement/reconfiguration from case study exemplars | |
|---|---|
| Study and reference | Key themes |
| NHS Scarborough and Ryedale CCG (2014)45 |
|
| York Teaching Hospital NHS Foundation Trust (Gamble and Sloss 201143) |
|
| Buckinghamshire and Oxfordshire PCT/Buckinghamshire Healthcare NHS Trust (NHS Confederation 201312) |
|
| Sandwell and West Birmingham NHS Trust (NHS Confederation 20139) |
|
| Sainsbury Centre for Mental Health (201044) |
|
| NHS Sheffield PCT (Airoldi et al. 20137) |
|
Overview
Consultations took place between 2007 and 2014. All were conducted in the UK. Four case studies were commissioned by NHS organisations [foundation or acute care trusts, PCT, Clinical Commissioning Group (CCG)], one was carried out by the Sainsbury Centre for Mental Health and the other was commissioned by The Health Foundation.
Quality of the case studies
Based on our three assessment criteria, the overall quality of these case studies was good (defined as adequate and clear reporting; evidence of reflexivity; and diverse perspectives considered). Report authors had generally considered diverse perspectives in the conduct of their case studies. There was evidence of reflexivity in the reporting (authors had reflected on findings and discussed the implications for practice in many cases), and reporting depth and clarity was considered largely good to excellent.
Types of reconfiguration
Proposed changes to services covered urgent and emergency care;43,45 centralisation of emergency care, providing services closer to home and developing clinical centres of excellence;12 acute hospital maternity services;9 mental health services;44 and priority-setting for eating disorder services. 7
Populations engaged
Multiple audiences were involved in all except one case study where the consultation focused more narrowly on patients and members of the public (although this piece of work was part of a wider engagement and communication strategy). 43 Across the case studies, other people engaged in the process included patient representatives, NHS staff and clinicians, overview and scrutiny committees, carers, local councillors and MPs, partner organisations (including the voluntary sector), specific statutory bodies (e.g. Sure Start), media, commissioners and external consultants.
Case study exemplars in focus: engagement methods and impact
NHS Scarborough and Ryedale Clinical Commissioning Group
A 3-month consultation was commissioned by Scarborough and Ryedale CCG in relation to urgent care services. 45 The consultation was intense and wide-reaching (an estimated 200,000 people were contacted), and this involved gathering the views of service users and the general public about their experiences of current provision, together with their thoughts about a proposed new model of urgent care. Clinicians, partner organisations (representatives from primary care, secondary care, local authority and voluntary sector organisations) and local media were also consulted.
Multiple engagement methods were employed, including the distribution of a consultation document and accompanying video; an interactive workshop for clinicians and partner organisations; presentations to local and regional health scrutiny committees; questionnaires (paper and online); a series of public meetings and focus groups; and use of social media.
The demonstrable impact of this consultation was a number of key considerations being taken forward to inform a service tender specification for urgent care services. Important issues identified by service users were the need for appropriate location of services with attention to parking, transport, and security (a significant finding was that people would not be willing to travel further for an improved service, echoing findings from other research). 22–24 Service users also called for the appropriate design of services for a range of potential users; appropriate access to medical records and liaison with NHS 111 (where necessary); and adequate information to aid decision-making about how and when to access urgent care. It was strongly felt that patient experience should form part of ongoing performance and quality measures for urgent care services. In November 2014, the successful provider of these services was announced with effect from April 2015. From the CCG’s press release, it was evident that issues raised in the public consultation (such as access and car parking) had been taken on board in the reconfigured service.
This case study highlights the potential effectiveness of wide-reaching stakeholder consultation including those opposing change. Use of an extensive range of engagement methods (including those to access hard-to-reach populations and others most likely to access urgent care services) and intensive reflection on local context appeared to be significant drivers. The direct impact of this engagement on successful service reconfiguration will require further evaluation.
York Teaching Hospital NHS Foundation Trust
The trust conducted a 3-month consultation focusing on public and patients/patient representatives in relation to redesigning the minors care pathway with a view to developing an integrated urgent care service within its emergency department. 43 This piece of work formed part of a wider consultation on urgent care services including the integration of a walk-in centre (separately located at the time), improved integration with the out-of hours GP service and consideration of a potential GP triage service. The project was set in the broader strategic context of helping to maximise effective future streaming of patients across minor and major care within the emergency department.
Uniquely in this series of exemplars, the methodology underpinning the particular engagement exercise was experience-based design. 46 This methodology focuses on capturing and understanding patient, carer and staff experience of services, with a view to using them to inform actions for the physical redesign of systems and processes.
Three key engagement methods were used: observation sessions in the emergency department by hospital governors and members of the local involvement network; focus groups with service users who had attended the emergency department in the preceding year; and real-time feedback (a questionnaire on a standpoint machine located in the emergency department waiting area).
A number of key issues arising from this engagement exercise were fed into an action plan for the emergency department redesign at micro and macro levels. Various aspects relating to physical redesign were linked directly to the trust’s capital works programme (e.g. major alterations to the reception area and the provision of a designated quiet area for people with particular clinical needs such as those suffering from dementia). Indeed, in identifying the needs of patients with dementia as a priority, the emergency department consultation proposed a review of wider activity around the referral and service access for these patients.
This case study highlighted the potential effectiveness of consultations that were more narrowly focused, time-limited and based on a specific methodological framework.
Buckinghamshire and Oxfordshire Primary Care Trust Cluster/Buckinghamshire Healthcare NHS Trust
The redesign of emergency care featured again in the next case study reported by the NHS Confederation and carried out across NHS hospital sites in Buckinghamshire. 12 This study focused on the proposed centralisation of emergency care, alongside other objectives to provide care closer to home and to establish a number of clinical centres of excellence. Similar to York (previous subsection), this was a short-term consultation but with wider reach involving patients, public, primary care and hospital-based clinicians and other NHS staff, MPs, local overview and scrutiny committees and voluntary sector organisations.
A range of engagement methods was used, including public meetings, clinical summits, online surveys, website access, video recordings showing interviews with lead clinicians, printed materials, a local media campaign, presentations and site visits. Public meetings were seen as opportunities to provide assurance on fears about service closure.
Results of the engagement programme led to direct action in response to patient concerns about transport and access to services. Concerns were considered in more depth by a multidisciplinary task group comprising council members, hospital representatives and ambulance service representatives. A direct outcome of this partnership work was the subsequent provision of free travel on local bus networks and the establishment of a county-wide community transport hub.
For service redesign, implementation began 6 months after the consultation had ended. An emergency medical centre at one site was replaced with a new minor injuries unit, together with the transfer of some inpatient medical wards, a new day unit and a step-down ward. The engagement process was reported to continue beyond the implementation stage.
Key messages from this case study were the importance of reaching a shared understanding of the case for change at local level (involving partnerships with primary and secondary care) and possibly by focusing on one aspect of care to encourage wider debate about services; starting public engagement early and listen to/accommodate the views of all interest groups where possible; encouraging clinicians to make the case for change, focusing on the potential to improve services rather than cost savings; and engaging face-to-face with local politicians and stakeholders. This case study also demonstrated the direct impact of engagement in bringing together a multidisciplinary team to address a specific issue of patient and public concern (transport and service access), and how positive action could result from collaboration with agencies outside the health-care system.
Sandwell and West Birmingham NHS Trust
Maternity service redesign was the focus of an engagement exercise spanning 4 years at Sandwell and West Birmingham NHS Trust, reported by the NHS Confederation. 9 The proposed redesign arose from a pre-consultation exercise that resulted in three options for the delivery of maternity care across the region. On these three options a range of participants were consulted over a 3-month period. Participants included patients and their representatives, GPs, local councillors and MPs, community midwives and hospital-based clinicians.
Methods of engagement include online activities, public meetings, face-to-face meetings with key stakeholders, use of local and national media, ‘ground-breaking events’, posters and postcards, and the employment of a redesign lead at the hospital trust.
Response to the consultation was reported to be overwhelmingly in favour of the option to establish a community birth centre, with specialist care taking place at an inner-city hospital location. It was proposed that women and their families would contribute to the design of the new facilities. The option was approved and its implementation ran in parallel with an intensive communications and engagement programme and a staff training programme.
The nexus between engagement, service reconfiguration and health outcomes was tentatively demonstrated in this case study. The maternity services at Sandwell and West Birmingham NHS Trust resulted in the highest normal birth rate in the country in 2011/12, a national award from the Royal College of Midwives for promoting natural birth was received in 2013, and in the same year the trust’s maternity services were upgraded to level 2 of the Clinical Negligence Scheme in recognition of safety standards. The unforeseen consequence of this reconfiguration (and one which will reportedly be taken forward as a lesson for future consultations) was that some women preferred to give birth in the Black Country, rather than in the specialist unit in Birmingham. It was unclear from the report whether this was potentially related to socioeconomic status or to broader cultural influences.
Many of the key messages for future service user engagement mentioned earlier were illustrated in this case study. Additionally, this study provided novel insight to cultural factors that can exert a strong influence on patient choice of service location and thus potentially affect the success of reconfiguration.
Sainsbury Centre for Mental Health
A case study carried out over 2 years by the Sainsbury Centre for Mental Health focused on engagement as part of a wider review of modernising day and vocational services for people with mental health problems. 44 Participants included in the process comprised service users, commissioners and external consultants.
A working group (consisting of eight service users) was established to take part in the review of services. Three members of the group joined a separate project steering group, which also included representatives from commissioners and external consultants. The group’s remit was to design the review of services, gather service user views and contribute to decisions about service redesign (e.g. the development of service specifications and tender documents, and helping to select future service providers).
This case study focused heavily on a process evaluation of the consultation, and several key considerations were highlighted relating to the need for clarity of purpose; attention to detail (e.g. the provision of background contextual information to aid the process of service redesign); openness between commissioners and staff about the implications of service change; and effective management and resolution of conflict and hostility. A list of specific issues was presented in terms of what worked well and what worked less well. Key indicators of successful engagement were reported to be suitable practical arrangements (inclusivity, minimal use of jargon and an agreed working agreement); decision-making based on genuine and valued partnerships with service users; consideration of service user well-being (in terms of whether or not they felt their input was worthwhile); and commitment to ongoing development of the engagement process.
Outcomes directly relating to service redesign were less well documented. Many service users were reported to feel positively about their involvement in the process, in terms of personal lives and services offered. Three new models were proposed in relation to the provision of future day and vocational services.
NHS Sheffield Primary Care Trust
The final case study in this section focused on a 6-month engagement programme relating to the redesign of eating disorder services in Sheffield (delivered by the PCT at that time), reported by The Health Foundation. 7 Participants in the process included patients, caregivers, clinicians and health-care managers. Follow-up was conducted with a wider set of stakeholders (unspecified) in the local health economy.
Methods of engagement included decision conferences attended by key stakeholders and led by an impartial facilitator; interviews; e-mail correspondence; direct observation of workshops; use of flipchart notes and minutes of board meetings; and post-consultation follow-up events.
Results of the decision conferences had a direct impact on the development of a business case. The objective of the business case was to reallocate resources by expanding capacity in primary care and increasing community or outpatient services, with a view to reducing the number of referrals of patients to residential care. The case was approved, spending for the eating disorder service was reduced by more than 15% and reductions were sustained in subsequent years.
Key messages for overcoming resistance to service change were the collective character of deliberations and encouraging ownership of the model and its results; analysis of the whole pathway and helping to identify opportunity costs of alternative budgetary choices; strong patient presence; development of a model based on cost-effectiveness analysis principles; and strong managerial leadership.
Exemplars in summary
The series of case studies chosen as exemplars of good practice were conducted across a range of health-care services and implementation contexts, with diverse audiences and using multiple engagement methods. Key messages focused mainly on the potential mechanisms for successful engagement, and less so on possible negative outcomes. In two case studies attempts were clearly made to link engagement efforts with impact on service reconfiguration and further on health9 and financial outcomes. 7
Chapter 4 Synthesis
This chapter focuses on evidence emerging from the review (but particularly the case study exemplars). We first summarise the evidence in relation to the ‘ladder of engagement and participation’,4 second we consider the NHS England guidance3 and finally we draw together the material to answer our five research questions.
Ladder of engagement and participation
The NHS England guidance on transforming participation in health and care uses a ‘ladder of engagement and participation’4 (based on the work of Sherry Arnstein47) to classify different ways in which patients and the public can participate in health (see Table 1). The ladder has five levels: informing, consulting, involving, collaborating and devolving. It is argued that participation becomes more meaningful towards the top of the ladder (devolving). Although there is academic debate about the limitations of this model, in terms of its narrow focus on transfer of power between providers and services,48 it has been widely used in studies of engagement and participation in health.
For the included case studies, we assessed only the levels of engagement reported in those selected as exemplars. Among the six exemplars, the highest level was devolving in one case,7 collaborating in four12,43–45 and involving in one. 9 Thus, these generally well-reported case studies were characterised by relatively high levels of engagement, which would be expected to allow meaningful interaction between participants and NHS decision-makers. This sample of case studies was too small to allow any assessment of whether or not levels of engagement had increased over time.
The levels of engagement in the studies reported in the included systematic reviews were also high. The highest level reported was collaborating (which involved working in partnership with communities and patients on all aspects of a decision) for all except one review. The broad review of user involvement in change management by Crawford et al. was judged to include examples of devolving (placing decision-making in the hands of the community or individuals). 18 The high levels of engagement may partly reflect the broad coverage of the included systematic reviews.
The levels of engagement reported or discussed in studies in the ‘other research’ category were generally lower than in the case studies or reviews. Two reports related to the collaborating level. 15,28 The Scottish Health Council report sought input from public panels and NHS stakeholders on how to enhance public involvement in NHS service change. 42 The other report was an expert opinion report on how NHS managers should seek to frame debates around reconfiguration. 28 As with the systematic reviews, both reports were broad in scope, although much more specifically focused on service change.
Overall, the ‘ladder of engagement’ was of some help in differentiating among studies but its use was based on the assumption that the methods reported provide genuine opportunities for engagement and were not just offered to meet legal or bureaucratic requirements. The extent to which this was true may depend on contextual factors that were difficult to assess from paper reports.
NHS England stages of reconfiguration
The NHS England guidance covers seven stages (Table 5), ranging from ‘setting the strategic context’ through to ‘implementation’, although the boundaries between these are not always clear-cut. Some themes and issues arose at multiple stages of the process. It should be noted at the outset that most of the evidence appeared to adopt the perspective of health system decision-makers responsible for the process of service change, and comments about ‘successful’ engagement or service change should be seen in those terms.
| NHS England stage | Guidance/recommendations | Relevant exemplars | Findings/comments |
|---|---|---|---|
| 1: setting the strategic context | Continuous dialogue with communities on local health priorities and needs | Airoldi et al. (2013);7 Sainsbury Centre for Mental Health (2010);44 NHS Scarborough and Ryedale CCG (2014)45 | Limited evidence of this from reports |
| 2: proposal | Identify range of possible service changes. Statutory duty to involve service users. Good practice to involve patients, the public and wider stakeholders in the early stages of building a case for change | Airoldi et al. (2013);7 Sainsbury Centre for Mental Health (2010);44 NHS Scarborough and Ryedale CCG (2014)45 | Difficult to identify as a discrete stage; often mixed with wider public consultation |
| 3: discussion | Formal discussion with local stakeholders, including relevant health and well-being boards and local authority health scrutiny bodies | Airoldi et al. (2013);7 Gamble and Sloss (2011);43 NHS Confederation (2013);12 NHS Confederation (2013);9 Sainsbury Centre for Mental Health (2010);44 NHS Scarborough and Ryedale CCG (2014)45 | Also difficult to identify as a discrete stage. Limited research |
| 4: assurance | Demonstrate clinical case for change, the robustness of the reconfiguration programme, workforce and financial plans, and the alignment between the proposal and commissioning plans (where relevant) | Airoldi et al. (2013);7 Gamble and Sloss (2011);43 NHS Confederation (2013);12 NHS Confederation (2013);9 NHS Scarborough and Ryedale CCG (2014)45 | Limited evidence to demonstrate explicit attention to the assurance stage of the guidance, other than three exemplar case studies reporting that clinical case for change was proposed |
| 5: consultation | Continuous engagement with service users throughout the period of reconfiguration, with options to focus on specific reconfiguration and allow for a range of approaches for appropriate tailoring | Airoldi et al. (2013);7 Gamble and Sloss (2011);43 NHS Confederation (2013);12 NHS Confederation (2013);9 Sainsbury Centre for Mental Health (2010);44 NHS Scarborough and Ryedale CCG (2014)45 | Continuous engagement with service users throughout the period of consultation featured heavily across the evidence base. Many engagement activities were designed with specific populations in mind |
| 6: decision | The need for commissioners to determine which (if any) of the configuration options are to be pursued; at the same time notifying all relevant stakeholders | Airoldi et al. (2013);7 NHS Confederation (2013);12 NHS Confederation (2013)9 | Some evidence that decisions had been made and communicated to service users and stakeholders in respect of reconfiguration. The particular influence of overview and scrutiny committees in this process was highlighted |
| 7: implementation | The need for clarity about implementation plans, and maintenance of an ongoing dialogue with service users in relation to the bedding down of service reconfiguration | Airoldi et al. (2013);7 NHS Confederation (2013);12 NHS Confederation (2013)9 | Some attention to the implementation stage was evident in a limited number of articles, mainly in the exemplar case studies in terms of follow-up with service users or communication at this stage |
We did not systematically attempt to assess the extent to which stages of the NHS guidance were addressed in the case studies not selected as exemplars. When considering the stages of the NHS guidance addressed in the other research studies, the extent to which attention to specific stages influenced the overall success of the engagement process and other outcomes was unclear.
Table 5 summarises which of the stages were covered by the literature, with a focus on the relevant exemplar case studies.
Stage 1: setting the strategic context
Exemplar case studies
Three of our exemplar case studies covered this phase of reconfiguration. 7,44,45 The extensive literature on public involvement in commissioning and other decision-making bodies was excluded, as we looked only at examples that were explicitly focusing on service change and reconfiguration. The main issue emphasised by the guidance was continuous dialogue with local communities and representative bodies on local health priorities and needs.
Of the three case studies, only the NHS Scarborough and Ryedale CCG urgent care redesign involved a broad public consultation. 45 The other case studies involved setting the strategic context with small groups of service users/carers. 7,44 The Scarborough and Ryedale report noted the involvement of CCG governing body members, local clinicians, voluntary/third sector organisations and local authority scrutiny committees prior to the wider public consultation. However, the extent to which the urgent care consultation was influenced by a process of continuous dialogue with local communities and stakeholders was unclear from the report of the consultation. 45
We did not systematically attempt to assess the stage(s) of engagement covered by case studies not selected as exemplars. However, a number of case studies reported attempts by UK health authorities to engage the public and patients in discussion of broad strategic issues prior to developing proposals for service change. An example is the ‘Big Health Debate’ organised by Liverpool PCT in 2006 and involving structured discussion and voting on different options to inform redesign of primary care and community services. 34 Another case study, referring to work done in Cornwall and the Isles of Scilly, stressed the importance of engaging with the public to gain information and establish trust in a situation where there had been a history of conflict over proposals for service change. 35 In a case study in Surrey and Sussex, where some hospitals faced a potential loss of acute services, extensive ‘pre-consultation’ in the absence of firm proposals was reported to have increased public concern. 37 These examples reinforced the importance of local contextual factors in influencing how proposals for service change are received and discussed; the Surrey and Sussex example, in particular, may reflect a lack of success in engaging with the public to discuss the strategic context and drivers of change before introducing potentially unpopular proposals.
Systematic reviews
Among the included systematic reviews, a 2009 scoping review by Mitton et al. looked at public participation in health-care priority-setting. 20 The review included a wide variety of empirical studies, mainly focusing on macro-level priority-setting. Despite a lack of rigorous evaluations, two-thirds of included studies reported that participation processes were successful (as defined by the original study authors). Use of deliberative methods (often as part of an ongoing process rather than one-off events) and face-to-face contact were associated with higher levels of perceived successful participation. In studies where affecting an actual decision was the intention of the engagement process, this was reported to be achieved in 60% of cases, not achieved in 10%, and unclear or not reported in 30% (actual numbers of studies unclear). Other systematic reviews provided limited information about this stage of the service change process.
Other research
Three pieces of ‘other research’ were judged to address this stage of the service change process. 1,27,28 The IRP report on lessons from reviews identified inadequate community and stakeholder engagement in the early stages of planning change as a key factor in proposals referred to the panel for formal review. 1 In Scotland, the study of media coverage of reconfiguration of maternity services at Caithness General Hospital reported that the issue was framed as a conflict between Highland Health Board management and local people, with a lack of information about issues underpinning the proposed changes. 27 Issues around how proposals for service change were framed were also central to an expert opinion report published by the NHS Confederation. 28 This report stressed the need to focus on drivers of change and potential benefits of new models of service without overusing the term ‘reconfiguration’.
Summary
Overall, the limited available evidence suggested that early strategic engagement with patients and the public along with other stakeholders could contribute to the process of developing and implementing proposals for service change. Although there was a lack of rigorous evaluations, opportunities for ongoing face-to-face interaction appeared to be viewed positively. 20 One-off deliberative approaches allowing groups of patient or public representatives to express views on possible service changes in a structured way have also been reported as successful. 7,34 This early stage of discussing service change is important because it can influence how the issue is framed and perceived by the patients and public with whom decision-makers are trying to engage. Case studies emphasised the importance of local contextual factors which those responsible for service change may or may not be able to influence. The Surrey and Sussex case study cited in Exemplar case studies37 involved a phased roll-out of engagement to different groups, which could have had a negative impact on those who entered the process later.
Stage 2: proposal
Exemplar case studies
At the proposal stage, the NHS England guidance stresses the importance of identifying a range of potentially viable options for change and involving patients, the public and other stakeholders at an early stage in building a case for change. Three of our exemplar case studies assessed methods and impact of public and patient involvement at this stage;7,44,45 these were the same three exemplars as for the previous stage, emphasising the difficulty of separating the two stages. In addition, a further case study from the NHS Confederation reported in some detail the methods of public engagement at the proposal stage in Greater Manchester but without evidence of impact. 11
As with the previous stage, the NHS Sheffield PCT eating disorders7 and Sainsbury Centre for Mental Health44 case studies involved small groups of service users/carers rather than the general public. Key themes of the eating disorder case study included collective deliberation encouraging ownership of the process and its results; analysis of the pathway as a whole; and framing the problem in terms of patient benefit, seen as a result of the presence of patients as part of the group developing the proposal. In this case study, the group was able to identify the opportunity cost of alternative budget allocations and develop a model based on theoretical principles which provided a credible rationale for difficult decisions. 7 Some similar themes of service users and commissioners working together to identify potential new models of service emerged from the Sainsbury Centre for Mental Health case study, although this did not involve a cost-effectiveness analysis. 44
The NHS Scarborough and Ryedale CCG case study45 reported on a broad public consultation that primarily included elements of stages 2, 3 and 5 of the NHS England guidance (proposal, discussion and consultation). It appeared that patients and the public were involved from an early stage, although the exact details of how the CCG had developed its ‘vision’ for urgent care services were not clear. The CCG did use a wide variety of methods to involve patients and the public in the process. The consultation had an impact in identifying issues that needed to be considered in the specification and tendering process for a new urgent care service. Overall, this case study did not fit closely to the NHS England model, as a broad public consultation appeared to have begun at an earlier stage than envisaged in the NHS England guidance. This may reflect the context of reconfiguring the service by means of a service specification and tendering process. However, although not included as an ‘exemplar’ case study, the ‘Healthier Together’ consultation in Greater Manchester also involved early engagement of wider groups of patients and the public in discussing the need for change and broad principles involved rather than commenting on specific proposals for service change. 11
Systematic reviews
Of the eight systematic reviews considered, the only review to address this stage of service change was the broad overview of interactive methods of public engagement by Abelson et al. 6 Two other systematic reviews contained potentially relevant evidence but their broad scope made it difficult to fit them with the stages mentioned in the NHS England guidance. 5,18
Findings from the empirical literature synthesis by Abelson et al. indicated that interactive public engagement can be implemented successfully in various situations. 6 Success appeared to depend on contextual factors, including organisational commitment and the topic under discussion. The authors noted that participant satisfaction and topic-specific learning appeared higher when the engagement process was well designed, but process satisfaction was not necessarily linked to perceived impact on policy decision-making. Group debate was identified as an important contributor to participant satisfaction. This finding fitted with the reports of case studies involving small groups of service users contributing to service change proposals in eating disorders and mental health services. 7,44
A systematic review of the impact of PPI on the UK NHS did not report any examples that could be specifically linked to this stage of service change. 5 The same was true of a broad (but written from a UK perspective) systematic review of user involvement in change management. 17
Other research
Other research studies considered relevant to this stage were the same as those for the previous stage,1,27,28 plus a report from the Scottish Health Council. 24 The IRP review identified specific issues resulting in referrals that imply insufficient attention to involving patients and the public at the proposal stage, specifically ‘important content missing from reconfiguration plans and limited methods of conveying information’. 1 The NHS Confederation report emphasises the possibility of ‘co-production’ of improved services by patients/the public and NHS managers and warns against over-reliance on formal consultation. 28 This picks up on a theme also mentioned by Abelson et al. 6 and the NHS Sheffield PCT and Sainsbury Centre for Mental Health case studies. 7,44 Finally, although Thomson et al. ’s27 study focused primarily on media coverage, their background explanation implied that proposals for reconfiguration of maternity services in Caithness were developed with little or no patient or public input, and this could have been a contributory factor to the subsequent controversy.
The Scottish Health Council research involved public participants recruited via a citizens’ panel in day-long deliberative events to obtain their views on how to improve public involvement in NHS major service change. NHS stakeholders were involved through interviews and a national online survey. In the proposal stage, both the public panels and NHS stakeholders offered views on factors that should be taken into account when developing options for change. While both groups felt that improving the quality of current services was the most important factor, the report author identified a major difference between the public and NHS stakeholder views, summed up as ‘the public felt strongly that local accessibility was more important than access to specialist capacity even when the services were of a lesser quality’. 24 This finding agreed with research in England (see Stage 4: assurance) in relation to evidence for change not persuading communities to accept change. 22,23 The report also noted the importance of trying to reach a resolution of conflicting views before applying a scoring system to different options, ‘otherwise many or some of those taking part could weight options to support particular points of view’. 24
Summary
Studies of PPI at this stage divided into those that involved relatively small groups of service users/public members and those that involved broader public engagement to inform the development of more specific proposals for service change. The latter type of engagement was used in the NHS Scarborough and Ryedale CCG,45 but it was unclear how this fitted in with the NHS England guidance, which appeared to reserve widespread public engagement to later stages.
Case studies7,44 and one systematic review6 suggested that positive results (for both participant satisfaction and potential influence on decisions) could be achieved when patient/public members and commissioners worked together and were able to form a common view of how service change could bring benefits to patients. However, evidence from public opinion surveys suggested that the public and NHS commissioners may have different priorities, which, if not resolved, could cause problems for the later stages of the service change process. 24
Stage 3: discussion
The discussion stage of the NHS England guidance involves discussion with local representative bodies such as health and well-being boards and local authority health scrutiny committees. 3
Exemplar case studies
Most of the exemplar case studies included some reference to engagement with health scrutiny committees, councillors, MPs or other public representatives. 7,9,12,43–45 However, this was not the main focus in any of the exemplars, and meetings, discussions or ‘engagement’ were generally referred to without any further details. The role of scrutiny committees in particular was addressed in more detail in studies included in the ‘other research’ category as discussed below.
One case study, not suitable for use as an exemplar, referred to the situation in Wyre Forest, where local opposition to loss of services at Kidderminster Hospital was expressed through the political process. 36 Opponents of the proposed reconfiguration formed a political group and elected representatives to Parliament and the local district council. However, while this was a famous case in the history of NHS reconfiguration, the outcome also appeared to reflect local contextual factors that had not been replicated elsewhere.
Systematic reviews
Three systematic reviews included some evidence on the discussion phase of service change;6,16,17 the relevance of three others was unclear. 5,18,19 Overall, the information presented in these reviews was too general to be helpful in analysing public involvement through discussion with representatives or representative bodies in the context of service change in the UK NHS. Two UK-specific systematic reviews did not contain any relevant evidence. 5,19
Other research
Five studies in this category were judged relevant to the discussion phase. 1,24,25,27,28 The most important was the 2007 Nuffield Trust report on the ‘politics of reconfiguration’, which included a discussion and case studies of the operation of local authority scrutiny committees. 25 The case studies illustrated how scrutiny committees worked with patient groups, clinicians and other stakeholders. The role of scrutiny committees in referring reconfiguration proposals to the IRP was also discussed, a theme also raised in the IRP overview of lessons learned from reviews. 1 The authors of the Nuffield Trust report considered scrutiny committees to be assertive in questioning and challenging proposals but basing their challenge on evidence rather than being opposed in principle to any change. 25 This conclusion was supported by the case studies (although as with all case studies their representativeness/generalisabilty was uncertain) and to some extent by the report’s status as an independent academic evaluation.
The NHS Confederation report on reframing the debate around reconfiguration also considered the role of public representatives. Taking a broadly NHS managerial perspective, the report advocated the need for local and national leaders to work with patient groups and clinicians to support service changes where these are supported by evidence of improved clinical outcomes. 28
In the Scottish context, the Scottish Health Council report on enhancing public involvement in major NHS service change reported the views of a small sample of the public on proposals for independent scrutiny of reconfiguration plans prior to public consultation. 24 Public panels expressed some support for independent review but were less clear about the stage in the process at which this should take place. In Thomson et al. ’s study of media coverage of reconfiguration of maternity services at Caithness General Hospital, the role of councillors and Members of the Scottish Parliament was mentioned. 27 In this case study, the representatives appeared as supporting a public campaign against the reconfiguration proposals rather than being involved in a formal consultation process.
Summary
Discussion of service change proposals with public representative bodies is an important statutory part of the process. Although this was treated as a separate stage from wider public consultation in the NHS England guidance, case studies suggested that the two stages often took place simultaneously or overlap with one another. 9,12,45 Local authority scrutiny committees were important because of their role in referring contested proposals to the IRP. An independent academic review in 2007 gave a generally positive assessment of how these committees were operating, based on a small number of case studies. 25
Stage 4: assurance
The main issues emphasised by this stage of the guidance are to demonstrate the clinical case for change, the robustness of the reconfiguration programme, workforce and financial plans, and the alignment between the proposal and commissioning plans (where relevant).
Exemplar case studies
Five of our exemplar case studies indicated some attention to this phase of reconfiguration,7,9,12,43,45 although explicit detail was lacking and it was not possible to conclude definitively. Three studies referred to the need to set out the case for clinical change prior to service redesign. 9,12,45 One case study reported the discussion of costs and alternative budget allocations, and the framing of intent for patient benefit. 7 In a further study, coverage of this stage was implied but lacking in detail. 43
Systematic reviews
Some of the included systematic reviews loosely referred to a form of assurance being part of the engagement process, for example those focusing on priority-setting, resource allocation, health service and policy planning, local goal-setting and (among the engagement methods) the provision of information about options for change. 6,16,17,19 Firm demonstration of assurance was not evident in any of the reviews.
Other research
In pieces of work classed as ‘other research’, only the review of referrals to the IRP demonstrated clearly that the assurance stage of reconfiguration had been addressed, along with consideration of all other stages. 1 In the remainder of papers it was implied, with reference in the text to evidence for change not persuading communities to accept change,22,23 high levels of financial disclosure being given to participants,26 the need for clinically driven case for change and making the case for value,28 and a hindering factor to successful engagement being lack of issues underpinning change. 27
Summary
There was limited reporting to demonstrate attention paid to the assurance stage of the guidance. Explicit attempts were reported in three exemplar case studies in demonstrating the clinical case for change prior to service redesign. 9,12,45 Firm demonstration of attention to assurance was not evident in any of the systematic reviews, although indirectly it may have been present where reference was made to priority-setting, resource allocation, health service and policy planning, and local goal-setting.
Stage 5: consultation
The main issues emphasised by this stage of the guidance is continuous engagement with service users throughout the period of reconfiguration, with emphasis on methods that focus on specific reconfiguration options and allow for a range of approaches for appropriate tailoring.
Exemplar case studies
All of our exemplar case studies demonstrated efforts to achieve adequate consultation at various stages of service reconfiguration according to the guidance. 7,9,12,43–45 All studies employed multiple engagement methods. Many justified the choice of a specific method in terms of intent to target a specific population, for example using social media to capture the voice of younger people45 and focus groups to gather the views of mental health patients attending the emergency department. 43
Systematic reviews
Five systematic reviews were selected here to demonstrate compliance with the guidance on consultation. 6,16,17,19,21 Multiple engagement methods featured heavily, with a notable frequency of community-based initiatives such as citizens’ juries,6,16,17,19 emphasis on partnerships and collaborations,16 and collective consumerism. 19 Targeting attempts were illustrated across the reviews, for example in a specific community initiative to elicit and respond to the views of older people. 19
Other research
All pieces of other health-care-related research reported some attention to the consultation stage, and this was illustrated by use of multiple methods. 1,22–28 An attempt to tailor future consultations for specific populations was demonstrated in an exercise to test public understanding of frequently used NHS terminology. 26 The paper focusing on a Scottish Health Board debate had prime focus on different messages emanating from media coverage of proposed changes to maternity services. 27 The paper demonstrated that media coverage (as a method of consultation) could be manipulative, in contrast to other reported consultation attempts in this review that have sought to demonstrate transparency and rigour.
Summary
Continuous engagement with service users throughout the period of consultation featured heavily across the case study exemplars, systematic reviews and other research. Multiple engagement methods were reported, many of which aimed to target specific populations. 19,26,27,43,45 The nature of the evidence made it difficult to identify any specific methods as better or worse than others, but emphasised the need to use methods appropriate to the local setting and the population groups most affected by proposed service changes. Consultation methods involving direct interaction with small groups of service users were often considered successful but raised issues around the representativeness of those involved.
Stage 6: decision
The main issue emphasised by this stage of the guidance is the need for commissioners to determine which (if any) of the configuration options are to be pursued, at the same time notifying all relevant stakeholders.
Exemplar case studies
Three exemplar case studies7,9,12 provided evidence that decisions had been reached on issues concerning service redesign following engagement programmes. The implication was, additionally, that stakeholders had been notified of such decisions, but methods of communication were not explicit. In particular, there was evidence that decision conferences had played an important part leading to the approval of a business case to reallocate resources for services. 7 Multiple engagement methods were followed by a decision to replace an emergency medical centre with a new minor injury unit and other wards. 12 The creation of new maternity services appeared to result from another successful multimethod engagement programme. 9
Systematic reviews
Two systematic reviews showed that engagement using multiple methods (and particularly the use of citizens’ juries) was successful in influencing decisions about the commissioning of new services. 16,17 Proposals for hospital closures were modified or abandoned, as reported by Crawford et al. ,17 demonstrating further the impact of potential for engagement to influence the process of decision-making.
Other research
Decisions about service reconfiguration were referred to in other health-care-related research. 1,24–27 The particular influence of overview and scrutiny committees was highlighted in relation to details on various proposals accepted and rejected. 25 Decision uncertainty was reflected in the paper focusing on media portrayal of maternity services in Scotland. 27
Stage 7: implementation
The main issues emphasised by this stage in the guidance are the need for clarity about implementation plans and for maintenance of an ongoing dialogue with service users on the bedding down of service reconfiguration.
Exemplar case studies
Three exemplar case studies referred to some measure of follow-up with service users or communications strategies to support the implementation process. 7,9,12
Systematic reviews and other research
Efforts to maintain dialogue with service users was implied in the results of a systematic review in repeatability of regional meetings. 16 The implementation stage was covered, along with other stages, in the IRP review of referrals. 1
Summary
Some attention to the implementation stage was evident in a limited number of articles, mainly in the exemplar case studies in terms of follow-up with service users or communication at this stage. None of the included systematic reviews or other research addressed the implementation stage.
Research questions addressed
We did not attempt to assess systematically the extent to which our research questions were addressed in the case studies not selected as exemplars. Engagement methods were often not described in sufficient detail to provide meaningful reporting. Where reported, the range of methods did not appear materially different from those identified in the other types of research above. Similarly, the lack of details about methods precluded meaningful analysis with respect to demonstrable impact on service reconfiguration. The measure of impact on decisions about health service reconfiguration, sustainability of engagement methods, and resolving and negotiating differing opinions about reconfiguration were also not sufficiently reported in these studies.
Tables 6–8 summarise the evidence (by type of research) on the extent to which the five research questions were addressed.
| Research question | Systematic reviews | |||||||
|---|---|---|---|---|---|---|---|---|
| Abelson et al. (2010)6 | Conklin et al. (2012)16 | Crawford et al. (2002)17 | Crawford et al. (2003)18 | Daykin et al. (2007)19 | Mitton et al. (2009)20 | Mockford et al. (2012)5 | Rose et al. (2003)21 | |
| 1: How have patients and the public been engaged in decisions about health service reconfiguration in the past? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| 2: How has PPI affected decisions about health service reconfiguration? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ||
| 3: Which types of PPI have had the greatest impact on these decisions? | ✗ | ✗ | ✗ | |||||
| 4: Which methods of PPI are likely to be sustainable/repeatable? | ✗ | ✗ | ✗ | ✗ | ✗ | |||
| 5: How have differing opinions about reconfiguration between patients, public and clinical experts and other senior decision-makers been negotiated and resolved? | ||||||||
| Research question | Other research | ||||||
|---|---|---|---|---|---|---|---|
| Barratt et al. (2014)22,23 | Boyes (2008)24 | Day and Klein (2007)25 | IRP (2010)1 | NHS Confederation (2010)26 | NHS Confederation (2013)28 | Thomson et al. (2008)27 | |
| 1: How have patients and the public been engaged in decisions about health service reconfiguration in the past? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | |
| 2: How has PPI affected decisions about health service reconfiguration? | ✗ | ✗ | ✗ | ||||
| 3: Which types of PPI have had the greatest impact on these decisions? | ✗ | ✗ | |||||
| 4: Which methods of PPI are likely to be sustainable/repeatable? | ✗ | ✗ | ✗ | ✗ | |||
| 5: How have differing opinions about reconfiguration between patients, public and clinical experts and other senior decision-makers been negotiated and resolved? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | |
| Research question | Exemplar case studies | |||||
|---|---|---|---|---|---|---|
| Airoldi et al. (2013)7 | Gamble and Sloss (2011)43 | NHS Confederation (2013)12 | NHS Confederation (2013)9 | Sainsbury Centre for Mental Health (2010)44 | NHS Scarborough and Ryedale CCG (2014)45 | |
| 1: How have patients and the public been engaged in decisions about health service reconfiguration in the past? | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| 2: How has PPI affected decisions about health service reconfiguration? | ✗ | ✗ | ✗ | ✗ | ✗ | |
| 3: Which types of PPI have had the greatest impact on these decisions? | ✗ | ✗ | ||||
| 4: Which methods of PPI are likely to be sustainable/repeatable? | ✗ | ✗ | ||||
| 5: How have differing opinions about reconfiguration between patients, public and clinical experts and other senior decision-makers been negotiated and resolved? | ✗ | ✗ | ✗ | |||
Question 1: How have patients and the public been engaged in decisions about health service reconfiguration in the past?
All of our exemplar case studies,7,9,12,43–45 the systematic reviews5,6,16–21 and all except one piece of work classed as other health-care-related research22–28 adequately answered this question.
Methods of engagement varied in nature and intensity (from informative to deliberative), and use of mixed methods to capture service user voice seemed to be the general approach. The engagement process ranged from being a one-off event, to deliberations spanning several months or years. Details on the sustainability of methods were lacking.
Question 2: How has patient and public involvement affected decisions about health service reconfiguration?
Five exemplar case studies,7,9,12,43,45 all six systematic reviews5,16–20 and three pieces of other health-care-related research25,27,28 contributed to answering this question, demonstrating some element of impact from service user engagement. As mentioned earlier in this review, impact was variably defined across the included papers, and more frequently in terms of process measures rather than outcomes related to the success or failure of service reconfiguration.
Of particular note was the impact reported in one exemplar. 9 In this case study, multiple engagement methods resulted in service user preference for a particular maternity service configuration in Sandwell and West Birmingham. 9 Not only did the consultation appear to achieve broad consensus about future service provision, the resulting reconfiguration was associated with improvements in wider outcomes relating to patient health and safety, for example percentage of ‘normal’ births. Various other levels of impact were demonstrated in our exemplars, for example from wide-reaching consultations that added robustness to a service tender specification for urgent care services (with specific issues raised by the public, in terms of access and car parking, subsequently helping to inform the agreed service model),45 to the direct impact of engagement on securing initiatives to improve transport and access to health-care services. 12
Systematic reviews focused largely on process outcomes, with key factors to successful engagement (with potential to influence successful reconfiguration) being organisational readiness and commitment to service user engagement; clarity about the aims of engagement; and adequate resources of the process and evaluation of engagement. 18,19 In examining discussion papers and debates about service user engagement and/or service reconfiguration, other health-care-related research was helpful in identifying some of the negative outcomes on service reconfiguration, such as the variable impact of media coverage. 27
Question 3: Which types of patient and public involvement have had the greatest impact on these decisions?
Two exemplar case studies,9,12 three systematic reviews16,18,20 and two pieces of other health-care-related research25,27 contributed to answering this question.
Information was sparse in general, but exemplars indicated differential success in regular face-to-face meetings, discussions with politicians and local stakeholders, and initiatives to ensure that all interested parties were listened to. 12 Social media was highlighted as a particularly effective method for engaging young people in decisions about reconfiguration. 9
Systematic reviews highlighted the influential effect of a range of methods, including small group meetings and plenary sessions, surveys, citizens’ juries16 and deliberative methods. 20 One systematic review concluded that there was no best method for involving users in the NHS. 18
Other health-care-related research focused on the particular influence of overview and scrutiny committees,25 and the potential to encourage polarised views in the decision-making process through different angles of media coverage. 27
Question 4: Which methods of patient and public involvement are likely to be sustainable/repeatable?
Two exemplar case studies,7,12 five systematic reviews6,16–18,20 and five pieces of other health-care-related research22–24,26,28 provided insight to answering this question, although details on the sustainability of methods were lacking.
Sustainability of multiple methods was implied in one exemplar case study, which reported continuous dialogue with service users at the end of the implementation period. 12 Two systematic reviews emphasised the sustainability of methods that encouraged partnership working and collaboration;6,16 and a further review cited the ongoing application of multiple engagement methods over a mean duration of 4 years. 20 In other health-care-related research, the repeatability of focus groups was implied, as these were continued after consultation. 26
Question 5: How have differing opinions about reconfiguration between patients, public and clinical experts and other senior decision-makers been negotiated and resolved?
Three exemplar case studies7,12,45 and seven pieces of other health-care-related research1,22–25,27,28 contributed some evidence to answering this question. There was no evidence from systematic reviews.
The exemplars highlighted potential mechanisms for negotiating and resolving differing opinions between various stakeholders. These included decision conferences, public meetings and the overview and scrutiny committee function. Other health-care-related research implied the possible success of in-depth interview techniques to elicit trade-offs between service alternatives. 22,23 Public deliberative panels,24 coproduction of services48 and public campaigns27 were other possible mechanisms, as was referral to the IRP. 1
Chapter 5 Discussion
The objective of this rapid evidence synthesis was to bring together evidence from published and grey literature sources, to assess what is known about effective patient and public engagement in reconfiguration processes and to identify implications for further research. The review was guided by five research questions, existing NHS guidance on seven stages of reconfiguration3 and a theoretical framework outlining five incremental intensities of service user involvement. 4
Evidence was gathered from three main areas: systematic reviews of methods of/approaches to patient/public engagement; empirical studies of any design evaluating methods of/approaches to patient/public engagement; and case studies where public/patient engagement appears to have worked or not worked well. The review successfully identified a number of case study exemplars of good practice.
Summary of the evidence
Methods of engagement identified in this rapid evidence synthesis were varied in nature and intensity, and generally involved a mixed methods approach. Engagement programmes were conducted across a range of health services with diverse audiences. There was no evidence on the isolated impact of any particular engagement method or collection of methods, and there was little detail about their sustainability.
The impact of engagement was variably measured and demonstrated. Impact was more frequently defined in terms of process measures rather than success or failure of reconfiguration. Key process factors identified were organisation readiness and commitment to service user engagement, clarity of aims and adequate resources. Little was reported on the potential negative impact of service user engagement, but the variable effect of media coverage (which may encourage polarised views) was highlighted, and lessons from past referrals to the IRP may be helpful.
Early engagement can help to contextualise and influence the perceptions of service users. Ongoing face-to-face interaction may be beneficial, and deliberative methods may provide further help to ensure a wide representation of service user voice. Social media may be useful, particularly to engage with young people. It is helpful to form common views between the public and commissioners, but different priorities may present difficulties.
This was a difficult area to research, the evidence was limited and rigorous evaluations were lacking. Much of the evidence was from single case studies, which may have limited generalisability in other settings. The evidence to support methods of service user engagement in health service reconfiguration was inconclusive; we were unable to recommend a particular method to effect a specific outcome. The lack of independent research was noted (case studies identified were likely to be biased towards successful reconfiguration from the perspective of NHS managers), as was the absence of measurable outcomes and clear definitions of successful reconfiguration.
Reflections on the evidence
Much of the evidence presented in this review related to the UK NHS setting. For those embarking on future service user engagement programmes, the exemplars identified may indeed represent what good evidence looks like. Clearly reported objectives, methods and contextual detail, and reflective reporting are key elements to achieve this.
The review uncovered a broad range of engagement methods, from those simple and informative in nature, to more deliberative methods involving the development of shared understanding with service users and identifying solutions through partnership and collaborative working. No single specific method of engagement appeared to be more effective than another; the use of mixed methods of engagement was frequently reported. While there may be an argument for evaluating the collective effect of multiple methods (on the basis that this is reflective of practice), the relative effects of different engagement methods from a cost-effectiveness viewpoint may be a topic warranting further research.
Service user engagement was rarely evaluated in terms of its direct impact on the success or failure of service reconfiguration. Interim and process outcomes were frequently reported (such as changes in service user views about services, organisational culture change with regard to commitment to user engagement, or shifts in learning about future processes). This poses a question for future research about what is really meant by impact in evaluations of service user engagement and health service reconfiguration. Until more clarity is reached about objectives and outcomes, the evidence is likely to remain inconclusive. Future evaluation of interventions is vital.
Although it was not explicitly stated, impact appeared to be context-specific; the relative success of this was set against a backdrop of local dynamics, historical issues and baseline service user expectations. Furthermore, the impact of interventions to involve patients and the public in reconfiguration decisions was likely to be mediated by contextual factors which could vary widely across settings as well as over time. Some of these factors were at least in part predictable and could be used to select appropriate engagement methods. Examples are the nature of the area (such as urban or rural), age structure and socioeconomic characteristics of the local population and the types of services affected by reconfiguration proposals.
Additionally, local responses to configuration proposals can be inherently unpredictable, making it difficult or impossible to discuss alternatives and seek ways to resolve different opinions. Many community groups have opposed loss or downgrading of services in their local hospital; only in one setting (Wyre Forest) did they succeed in getting a representative elected to Parliament and gain control of the local council. 36 This example dates from the early 2000s and the fact that it has not been repeated since suggests the existence of some highly unusual local factors. In another example, a campaign against changes to hospital services in Surrey and Sussex was strengthened by the support of well-known local residents, a factor unlikely to be reproduced in less affluent areas. 37
The exemplars and other case studies included in our review cover a range of different services and geographical settings. An obvious distinction is that between services for the general population (e.g. primary and urgent care), for specific sections of the population (e.g. maternity services) and for people with specific conditions (e.g. specialist mental health services). The balance between engaging with the general public and with patients, patient groups and carers, and hence the methods used, tend to reflect the type of service. The type of setting (e.g. urban, suburban or rural) may also influence the process of engaging with patients and the public, although it is likely that the increasing use of online and social media-based methods will reduce the importance of geographical factors over time. It is also likely that other, more subtle factors influence the appropriateness of using different methods of engagement in different circumstances. A fuller analysis of this type of issue would require a larger sample of well-reported exemplars than we were able to obtain for this review, but this could be a topic for future primary research. A robust conceptual model of the rationale and goals of PPI in reconfiguration decisions would be helpful for this type of research.
In the synthesis, a pragmatic decision was taken to map the evidence against existing policy and guidance. We turned to potential triangulation between the evidence, the NHS stages of reconfiguration and levels of engagement; the extent to which the different sources correlate with each other and offer a consolidated framework to those considering service user engagement in health service reconfiguration. Generally, convergence of concepts from the different sources was difficult to determine, as it was not possible to distinguish with confidence the seven stages and the five levels of engagement in the included evidence. It was clear, however, that the ‘ladder of engagement and participation’ (based on the work of Sherry Arnstein47) provided less theoretical contribution than the NHS England stages. In respect of the ladder, examples of devolved decisions to the community were not well represented in our evidence. One might propose that devolvement might more appropriately apply to smaller-scale service change than to the various larger-scale reconfigurations considered in this review.
Given the nature of the review questions, it was clear that evidence was unlikely to be generalisable in the traditional sense of identifying elements which frame the research questions (populations, interventions, comparators and outcomes). We suggest that generalisability of the evidence to future service reconfigurations may lie in the approach (e.g. using the seven NHS England Stages) to guide the engagement process, rather than attempting to generalise based on the mechanics or the context underpinning that approach.
We focused our search for evidence on studies of direct relevance to PPI in service reconfiguration. Resource constraints meant that we have not systematically reviewed the theoretical and empirical literature on PPI in health care generally (although this was covered to some extent in the systematic reviews we have included). For theoretical frameworks we concentrated on those that have informed current NHS guidance (NHS England’s stages of service change3 and the ‘ladder of engagement and participation’). Arnstein’s ladder dates back to the 1960s and other theoretical frameworks have been developed more recently. For example, Gibson et al. 50 suggested that earlier models of PPI were unable to respond effectively to the current context of declining faith in traditional political structures and processes and the diversity of values, ideologies and social groups trying to make their voices heard. They proposed a four-dimensional framework for analysing the nature of PPI. This framework encourages knowledge accumulation from multiple sources, with emphasis on the development of reasoned, interactive and equitable discussions between lay and professional people. The framework, they argued, could assist the development of new structures and processes that may allow professionals and lay people to work together more productively than most current structures permit. 50
Another critique of current practice in PPI generally related to the issue of power imbalance between patients and members of the public and NHS managers and clinicians. This was the original purpose of Arnstein’s ‘ladder of involvement and participation’, to suggest that most involvement activity was more tokenistic than genuine participation. 47 Harrison and Mort coined the phrase ‘technology of legitimation’, arguing that PPI ‘can be seen as a means by which managerial legitimacy is maintained in the context of an increasingly pluralistic policy arena’. 51 Similar issues were raised by Martin in a study of service user involvement in the establishment of cancer genetics services in England. 52
In view of resource constraints and the service-focused nature of this review, we were unable to address these issues in any depth, but we recognise that it is important for NHS decision-makers to be aware of and reflect on these critiques. However, these issues relate to all types of PPI in health care (and in policy- and decision-making generally) and are not specific to service reconfiguration, which was the main focus of this review.
Reflections on the review process
The topic area had parallels with the evaluation of complex interventions and public health research; engagement was often part of a multicomponent intervention from which it was difficult to isolate individual effects, and the long-term impact was difficult to measure.
Reconfiguration was defined for this review as large-scale system change [e.g. relocation of hospitals, (re)location of specialist care, changes in provision of urgent/emergency/out-of-hours care] as opposed to small-scale change (e.g. at hospital ward level, within a GP practice). It became evident during the study selection process that the distinction between large-scale and small-scale change was not always straightforward, and this was not helped by variable use of terminology to describe service change. Judgements had to be made, and discussions took place between reviewers to reach agreement on inclusion, particularly where articles reported on a mixture of different levels of change, and often as part of an overarching strategy.
Given the rapid nature and limited resources available, limitations were placed on the review process. For example, strict criteria were applied on the reporting aspects of articles to tighten the focus to those most likely to provide useful information. Studies contained within reviews were not extensively followed up, and the overlap of studies across reviews was not examined. For case studies, a number of websites provided external links to other case studies, for example the Scottish Health Council;42 external links were not followed, but instead a signpost was provided, together with a summary of characteristics of those studies.
Of interest for future search strategies in service-facing reviews, two of the exemplar case studies were retrieved through contacts and not by the review search strategy. Contact with experts routinely forms part of traditional searching and this aspect represented a particularly important contribution to the present review.
The variable quality of evidence across the included systematic reviews may be a consequence of the composite nature of that evidence. Mixed methods evidence appeared to be a defining feature of the topic area selected for this review. Assessing the quality of a review based on mixed methods and/or multiple sources presented difficulties in applying traditional assessment criteria based on individual study design. Currently, there is no robust reliability assessment tool for mixed methods reviews.
Early specification of criteria for evaluating the quality of case studies in this review (based on clarity and transparency of reporting) enabled the successful identification of evaluations that might serve as exemplars of good practice. This was a relatively straightforward aspect of the review. Based on our three assessment criteria, the overall quality of these case studies was good (defined as adequate and clear reporting; evidence of reflexivity; and diverse perspectives considered). However, given that good reporting was an inclusion criterion for case studies, selection bias was a possibility in this review.
Chapter 6 Conclusions
Key conclusions from the project
The overall quality of evidence in our review is mixed. The included systematic reviews comprised multiple types of evidence and study designs, and most reviews did not report any quality assessment of included studies. A number of potentially helpful case studies were found, but the quality of reporting was generally poor. Six case studies were selected as exemplars on the basis of clearly reported evaluations, and these provided focus for our analysis. One of the key findings from this review is that meaningful engagement is hard to achieve, and research to evaluate its impact is difficult to conduct.
Nevertheless, our review demonstrated that it was possible to address these difficulties. Great advances have been made to set out frameworks for engaging users in discussions and decisions about service reconfigurations. We have found a number of exemplar case studies which show that meaningful engagement can be achieved. Moreover, although the evidence base was not large, we have found studies that were able to provide insight into the value of user engagement and its impact on shaping service reconfiguration. In particular, this review succeeded in clarifying some of the factors associated with positive service user engagement.
Patients and the public can be engaged through a wide variety of methods ranging from public meetings and distribution of information to the use of social media. People can be engaged as individuals, in small groups and in larger groups. In selecting which methods to employ locally, decision-makers will need to take into account the nature of the local population and of the proposed service changes. In general, engagement was most likely to be successful when the process started at an early stage of planning service change, offered opportunities for genuine interaction and was led and supported by clinicians involved in delivering the relevant services. Interactive methods involving small groups, such as citizens’ juries, could be very successful, although there may be difficulties in recruiting genuinely representative samples.
Our review also highlighted the importance of engaging with public representatives, in England primarily in the form of local authority scrutiny committees. The committees are important because of their power to refer disputed reconfiguration proposals to the IRP, an outcome that NHS decision-makers should seek to avoid. The IRP’s summary of lessons from its reviews1 was an important resource, as was the availability of informal advice from the IRP.
The IRP report noted that problems often arose because NHS decision-makers paid insufficient attention to issues considered important to the public. There was evidence from case studies45 and public opinion research22–25 that many people were unwilling to accept longer journey times in return for the promise of better-quality care at specialised centres. Since reconfiguration often involved centralisation of services, tackling such issues may warrant consideration by the leadership of the NHS at the national and local levels. There were potentially divergent issues to consider across other challenges to the NHS, such as decentralisation of services across several locations or moving services from one location to another.
Drawing on the included systematic reviews and exemplar case studies, our review broadly addressed the first two research questions, seeking to identify methods and impact of service user engagement in health service reconfiguration. Evidence on differential impact of methods, the sustainability of methods and outcomes, and methods of resolving differences between interested parties was less well documented. We noted some difficulty in distinguishing the stages of reconfiguration presently recommended by NHS England, but we uncovered some congruence between this guidance and what appears to be happening in practice, particularly in relation to the concentration of activity noted at stages 3 (discussion) and 5 (consultation). There is also some accordance between these specific NHS England stages and the theoretical basis provided by Arnstein’s ladder of participation. Across all evidence types, engagement activity appeared to move beyond basic information-giving towards the consultation and collaboration steps in the Arnstein’s ladder. It appears that future activity might usefully engage more readily with earlier and later stages in the process.
Given that service reconfiguration dominates the health policy agenda in almost all countries, it is essential to build upon the practical and research foundations that have already been laid.
Strengths of this review
The rapid nature of this review provides a timely, service-facing response to identify methods and impact of service user engagement in health service reconfiguration. This will be particularly valuable as the UK NHS navigates a way through arguably the biggest financial and operational challenge since its inception in 1948. The needs of service users are positioned at the heart of all service reconfigurations.
While providing a rapid response, the review also maintained the highest quality standards through the adoption of a systematic and explicit review process, featuring:
-
a thorough and comprehensive search to identify both published and unpublished studies
-
a strong pragmatic focus, with less emphasis on academic deliberation, and more on knowledge translation to a service-based audience
-
input of external advisors to corroborate the findings.
Weaknesses of this review
Despite its strengths, there were potential weaknesses in this review. These related to the fact that inconsistent terminology featured frequently, and inadequate descriptions of reconfiguration were encountered, which made it difficult on occasion to decide on the eligibility of studies for inclusion. To mitigate this, such cases were discussed fully to ensure consistent judgements were made. If there was doubt about the value of a study, it was not included. The rapid time frame for the review also meant that the detail of some studies was not followed up (e.g. studies contained within web links), although appropriate summaries and signposts were provided. All of this meant that relevant studies may have been overlooked.
The nature of the evidence also presented potential problems. Most of the recommendations emanated from a small sample of case studies. These were potentially biased, as they documented successful engagement in reconfiguration, largely from a NHS commissioner or provider perspective. While many practical examples of engagement are available, they are generally poorly reported in terms of methods, context, impact and sustainability over time.
Implications for health care
The NHS England stages of reconfiguration3 may provide a helpful framework on which to base plans for future service user engagement programmes. However, this framework should not necessarily be considered as a linear process or a set of distinct elements. Arnstein’s ‘ladder of engagement and participation’ (based on the work of Sherry Arnstein47) contained in NHS England guidance4 seems to offer less practical value. The four-dimensional framework developed by Gibson et al. 50 may be worth further evaluation.
Within the NHS England framework, some key factors contributing to successful engagement and/or service reconfiguration appear to be:
-
ensuring a clear understanding of the local context
-
early engagement; consulting widely
-
demonstrating clinical-led case for change, with focus on service improvement rather than cost savings
-
demonstrating openness and developing shared understanding of change through local partnership working
-
promoting ownership of the change model and feedback results of engagement
-
implementing strong managerial leadership
-
using mixed approaches, particularly deliberative methods of engagement, targeted where necessary for different population groups
-
considering access and transport issues as part of service change
-
evaluation; follow-up
-
expecting the unexpected.
Of these key factors, one aspect that seemed the most pressing was the striking need for robust evaluation and follow-up in user engagement programmes. Where evaluation has taken place – particularly in some potentially valuable case studies – it was largely poorly reported and difficult to appraise from a research viewpoint. Potential limiting factors are time constraints in health-care practice and naturally less concern for academic rigour. However, present reporting made it difficult to learn and move forward. Evaluation of user engagement in future health service reconfiguration is vital if we are to avoid reinventing the wheel each time public interaction is required. Ideally, evaluation should be conducted independently of those directing the engagement programme and should be embedded throughout the entire process from planning to implementation. The reporting system in Scotland may provide some helpful pointers. 42 Specific attention should be paid to explicitly and consistently describing the contextual characteristics of the situation; the methods of engagement, outcomes measured and overall impact (including positive and negative impact, and differential effects of engagement methods); the sustainability of efforts (through appropriate follow-up); and the lessons to be learned. The need to publish evidence on methods and impact of patient and public voice activity is touched upon in NHS England’s Transforming Participation in Health and Care. 4
Implications for research
One of the difficulties of the review was that much of the research was context-specific, which made generalisation difficult. Reconfiguration of services might be considered for the general population (such as primary care); for people with diagnosed conditions (such as mental health problems); for people seeking specific services (such as maternity services); or across geographical areas. Although the contexts are diverse, many challenges will be common.
The NHS England guidance on stages of reconfiguration may be of value in providing a generalisable approach and basis for user engagement in practice. The guidance may also provide a foundation for the design of future research on the evaluation of user engagement in service reconfiguration. These aspects are recommended areas of future research, together with an exploration of how the guidance might apply beyond the NHS setting.
In addition, further longer-term evaluations are needed to test the sustainability of methods of engagement and their impact over time. Prospective evaluations with contemporaneous data collection, including use of observational methods, may be the most suitable methods to achieve this. More research may also be warranted on the specific impact of interventions in negotiating and resolving differing opinions between patients, the public and clinical experts. Cost-effectiveness evaluation of engagement methods would be beneficial.
Acknowledgements
The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Health Service and Delivery Research editors have tried to ensure the accuracy of the authors’ work and would like to thank the reviewers for their constructive comments; however, they do not accept liability for damages or losses arising from material published in this web report.
Contributions of authors
Jane Dalton, Duncan Chambers and Alison Eastwood carried out the study selection, data extraction and critical appraisal, and wrote up the report.
Melissa Harden conducted all searching.
Andrew Street and Gillian Parker provided expertise and advice, contributed to the development of the protocol and commented on drafts of the report.
External advice
The review authors are grateful to the following individuals for their valuable comments on the review protocol and/or the draft report:
Dr Helen Barratt, Hon. Clinical Lecturer (National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care North Thames). Dr Barratt was particularly helpful in providing information on further study sources and in relation to interpretation of the review findings.
Dr David Evans, Professor in Health Services Research (Public Involvement), University of the West of England.
Lucy Brown, Head of Communications, York Teaching Hospital NHS Foundation Trust.
Kay Gamble, Lead for Patient Experience, York Teaching Hospital NHS Foundation Trust.
Representatives of York Teaching Hospital NHS Foundation Trust were engaged with this review via Dr Jane Dalton (in her role as a publicly elected governor at the trust). This process was helpful in providing local context to the research and to enable discussion on potential exemplars for the review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Learning from Reviews: An Overview. London: Independent Reconfiguration Panel; 2010.
- Health and Social Care Act 2012. London: The Stationery Office; 2012.
- Planning and Delivering Service Changes for Patients. Leeds: NHS England; 2013.
- Transforming Participation in Health and Care: ‘The NHS Belongs to Us All’. Leeds: NHS England; 2013.
- Mockford C, Staniszewska S, Griffiths F, Herron-Marx S. The impact of patient and public involvement on UK NHS health care: a systematic review. Int J Qual Health Care 2012;24:28-3. http://dx.doi.org/10.1093/intqhc/mzr066.
- Abelson J, Montesanti S, Li K, Gauvin F, Martin E. Effective Strategies for Interactive Public Engagement in the Development of Healthcare Policies and Programs. Ottawa, ON: Canadian Health Services Research Foundation; 2010.
- Airoldi M. Disinvestments in practice: overcoming resistance to change through a sociotechnical approach with local stakeholders. J Health Polit Policy Law 2013;38:1149-71. http://dx.doi.org/10.1215/03616878-2373175.
- Clarke R, Rozansky D. The battle for hearts and minds. Health Serv J 2013;123:24-5.
- Service Redesign Case Study: Redesigning Maternity Services in Sandwell and West Birmingham. London: NHS Confederation; 2013.
- Service Redesign Case Study: The Southern Health Acquisition of Ridgeway. London: NHS Confederation; 2013.
- Service Redesign Case Study: Healthier Together – the Greater Manchester Experience. London: NHS Confederation; 2013.
- Service Reconfiguration Case Study: Better Healthcare in Bucks. London: NHS Confederation; 2013.
- Service Redesign Case Study: Providing Specialist Emergency Care in Northumbria. London: NHS Confederation; 2013.
- Spurgeon P, Cooke M, Fulop N, Walters R, West P, . Evaluating Models of Service Delivery: Reconfiguration Principles. London: National Coordinating Centre for the Service Delivery and Organisation (NCCSDO) Research Programme; 2010.
- Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. York: CRD, University of York; 2009.
- Conklin A, Morris Z, Nolte E. What is the evidence base for public involvement in health-care policy? Results of a systematic scoping review. Health Expect 2015;18:153-65. http://dx.doi.org/10.1111/hex.12038.
- Crawford MJ, Rutter D, Manley C, Weaver T, Bhui K, Fulop N, et al. Systematic review of involving patients in the planning and development of health care. BMJ 2002;325:1263-5. http://dx.doi.org/10.1136/bmj.325.7375.1263.
- Crawford M, Rutter D, Thelwall S. User Involvement in Change Management: a Review of the Literature. London: National Co-ordinating Centre for NHS Service Delivery and Organisation R&D; 2003.
- Daykin N, Evans D, Petsoulas C, Sayers A. Evaluating the impact of patient and public involvement initiatives on UK health services: a systematic review. Evid Policy 2007;3:47-65. http://dx.doi.org/10.1332/174426407779702201.
- Mitton C, Smith N, Peacock S, Evoy B, Abelson J. Public participation in health care priority setting: a scoping review. Health Policy 2009;91:219-28. http://dx.doi.org/10.1016/j.healthpol.2009.01.005.
- Rose D, Fleischmann P, Tonkiss F, Campbell P, Wykes T. User and Carer Involvement in Change Management in a Mental Health Context: Review of the Literature. London: National Co-ordinating Centre for NHS Service Delivery and Organisation R&D; 2003.
- Barratt H, Fulop N, Raine R. Factors That Influence Public Willingness to Accept Proposals for Major Service Change: Evidence from the English NHS n.d.
- Barratt H. Factors That Influence Patient and Public Views about Proposals for Major Service Change: Evidence from the English NHS n.d.
- Boyes L. Enhancing Public Involvement in Major NHS Service Change. Glasgow: Scottish Health Council; 2008.
- Day P, Klein R. The Politics of Scrutiny: Reconfiguration in NHS England. London: The Nuffield Trust; 2007.
- Talking It Through: the Importance of Communications when Discussing Local Service Change. London: NHS Confederation; 2010.
- Thomson E, Farmer J, Tucker J, Bryers H. Informing debate or fuelling dispute? Media communication of reconfiguration in Scotland’s rural maternity care. Soc Policy Adm 2008;42:789-812. http://dx.doi.org/10.1111/j.1467-9515.2008.00638.x.
- Changing Care, Improving Quality: Reframing the Debate on Reconfiguration. London: NHS Confederation; 2013.
- Brown L. Report to Monitor on the Communications and Engagement Activity Carried Out to Date to Meet Consultation Requirements. York: York Teaching Hospital NHS Foundation Trust; 2012.
- Bruce G, Wistow G, Kramer R. Connected care re-visited: Hartlepool and beyond. J Integr Care 2011;19:13-21. http://dx.doi.org/10.5042/jic.2011.0156.
- Carver N, Halpin J, Lloyd B, Brierley S. Reconfiguration: talking services into shape. Health Serv J 2011;121:21-3.
- Caseley C. Lend an ear to your service users. Health Serv J 2010;120:24-5.
- Cohen A, Fairclough L, Jass J. Optimising community and stakeholder engagement in a merger of community health centres. Healthcare Manag Forum 2011;24:192-5. http://dx.doi.org/10.1016/j.hcmf.2011.08.002.
- Davies J. When Norma, Dot and Beckie had their say about NHS care. Health Serv J 2006;116:14-5.
- Greenwood L. Building bridges. Health Serv J 2007;117:20-2.
- Mason P. Power to the people. Nurs Times 2002;98:26-7.
- Moore A. Where managers fear to tread, myths and legends may rush in. Health Serv J 2006;116:16-7.
- Public Participation Case Study: Dorset Patients Involved in Redesign of Pain Services. Leeds: NHS England; 2013.
- Coe NL. Health panels: the development of a meaningful method of public involvement. Policy Studies 2012;33:263-81. http://dx.doi.org/10.1080/01442872.2012.694267.
- Nicholson-Banks K. Involving local people to improve services. Br J Healthcare Manag 2010;16:10-7. http://dx.doi.org/10.12968/bjhc.2010.16.1.45894.
- Gold SK, Abelson J, Charles CA. From rhetoric to reality: including patient voices in supportive cancer care planning. Health Expect 2005;8:195-209. http://dx.doi.org/10.1111/j.1369-7625.2005.00334.x.
- Scottish Health Council . Major Service Change Reports n.d. www.scottishhealthcouncil.org/publications/major_service_change_reports.aspx (accessed 1 May 2014).
- Gamble K, Sloss P. Report on the Findings from the Patient & Public Engagement in the Emergency Department Project. York: York Teaching Hospital NHS Foundation Trust; 2011.
- An Evaluation of Mental Health Service User Involvement in the Re-Commissioning of Day and Vocational Services. London: Sainsbury Centre for Mental Health; 2010.
- Right Care, First Time: Urgent Care Public Consultation Report. Scarborough: Scarborough and Ryedale Clinical Commissioning Group; 2014.
- NHS Institute for Innovation and Improvement . The EBD Approach (Experience Based Design): Using Patient and Staff Experience to Design Better Healthcare Services 2009. www.institute.nhs.uk/quality_and_value/experienced_based_design/the_ebd_approach_%28experience_based_design%29.html (accessed 19 August 2014).
- Arnstein SR. A ladder of citizen participation. J Am Inst Plan 1969;35:216-24. http://dx.doi.org/10.1080/01944366908977225.
- Tritter JQ, McCallum A. The snakes and ladders of user involvement: moving beyond Arnstein. Health Policy 2006;76:156-68. http://dx.doi.org/10.1016/j.healthpol.2005.05.008.
- Williams J, Cheung WY, Cohen D, Hutchings H, Jerzembek G, Rapport F, et al. Evaluating Innovations in the Delivery and Organisation of Gastroenterology Services Initiated Directly or Indirectly by the Modernising Endoscopy Service of the NHS Modernisation Agency (ENIGMA). London: National Co-ordinating Centre for NHS Service Delivery and Organisation R&D; 2008.
- Gibson A, Britten N, Lynch J. Theoretical directions for an emancipatory concept of patient and public involvement. Health (London) 2012;16:531-47. http://dx.doi.org/10.1177/1363459312438563.
- Harrison S, Mort M. Which champions, which people? Public and user involvement in health care as a technology of legitimation. Soc Policy Adm 1998;32:60-7. http://dx.doi.org/10.1111/1467-9515.00086.
- Martin GP. Representativeness, legitimacy and power in public involvement in health-service management. Soc Sci Med 2008;67:1757-65. http://dx.doi.org/10.1016/j.socscimed.2008.09.024.
- Dixon-Woods M, Cavers D, Agerwal S, Annandale E, Arthur A, Harvey J. Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med Res Methodol 2006;6. http://dx.doi.org/10.1186/1471-2288-6-35.
- Lomas J. Reluctant rationers: public input to health care priorities. J Health Serv Res Policy 1997;2:103-11. http://dx.doi.org/10.1186/1471-2288-6-35.
- Rowe G, Frewer LJ. A typology of public engagement mechanisms. Sci Technol Hum Value 2005;30:251-90.
Appendix 1 Search strategies
Search strategies for reviews
The Cochrane Database of Systematic Reviews via The Cochrane Library, Wiley
URL: http://onlinelibrary.wiley.com/
Date range searched: inception to March 2014.
Date of search: 27 March 2014.
Records retrieved: 30.
#1 MeSH descriptor: [Consumer Participation] explode all trees (993)
#2 MeSH descriptor: [Public Opinion] this term only (54)
#3 MeSH descriptor: [Consumer Organizations] this term only (9)
#4 MeSH descriptor: [Consumer Advocacy] this term only (10)
#5 MeSH descriptor: [Patient Advocacy] this term only (59)
#6 ((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver*) near/2 (particip* or engage* or involve* or consult* or opinion* or voice* or dialogue or view* or input* or partner* or represent* or collaborat* or advoc*)):ti (777)
#7 ((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver*) near/2 (jury* or juries or panel* or forum*)):ti (10)
#8 community next health next council*:ti (0)
#9 local next involvement next network*:ti (0)
#10 healthwatch:ti (0)
#11 national next voices:ti (0)
#12 foundation next trust next governor*:ti (0)
#13 FT next governor*:ti (0)
#14 co-produc* or coproduc*:ti (13)
#15 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 in Cochrane Reviews (Reviews and Protocols) (30)
Key: MeSH descriptor = indexing term (MeSH heading); * = truncation; :ti = terms in title field; near/2 = terms within two words of each other (any order); next = terms are next to each other.
The Campbell Library
URL: www.campbellcollaboration.org/lib/
Date range searched: 2003–2014.
Date of search: 25 March 2014.
Records retrieved: 32.
1 title is particip* or title is engage* or title is involve* or title is consult* or title is opinion* or title is voice* or title is dialogue or title is view* or title is input* or title is partner* or title is represent* or title is collaborat* or title is advoc* (15)
2 title is ‘citizen jury’ or title is ‘citizen juries’ or title is forum* or title is panel* (0)
3 keywords is ‘citizen jury’ or keywords is ‘citizen juries’ or keywords is forum* or keywords is panel* (0)
5 keywords is particip* or keywords is engage* or keywords is involve* or keywords is consult* or keywords is opinion* or keywords is voice* or keywords is dialogue or keywords is view* or keywords is input* or keywords is partner* or keywords is represent* or keywords is collaborat* or keywords is advoc* (17)
8 title is ‘community health council’ or title is ‘community health council*’ or title is ‘local involvement network’ or title is ‘local involvement networks’ or title is Healthwatch or title is ‘national voices’ or title is co-produc* or title is coproduc* or title is ‘foundation trust governor’ or title is ‘foundation trust governors’ or title is ‘FT governor’ or title is ‘FT governors’ (0)
9 keywords is ‘community health council’ or keywords is ‘community health council*’ or keywords is ‘local involvement network’ or keywords is ‘local involvement networks’ or keywords is healthwatch or keywords is ‘national voices’ or keywords is co-produc* or keywords is coproduc* or keywords is ‘foundation trust governor’ or keywords is ‘foundation trust governors’ or keywords is ‘ft governor’ or keywords is ‘ft governors’ (0)
Key: * = truncation; ‘ ‘ = phrase search
Database of Abstracts of Reviews of Effects (DARE)
Centre for Reviews and Dissemination Internal Content Management System (includes those records published in DARE on the Centre for Reviews and Dissemination website and records retrieved for possible inclusion in DARE but rejected).
Date range searched: inception to 25 March 2014.
Search date: 25 March 2014.
Records retrieved: 356.
-
MeSH DESCRIPTOR consumer participation
-
MeSH DESCRIPTOR patient participation
-
MeSH DESCRIPTOR public opinion
-
MeSH DESCRIPTOR patient advocacy
-
MeSH DESCRIPTOR consumer advocacy
-
MeSH DESCRIPTOR consumer organisations
-
#1 OR #2 OR #3 OR #4 OR #5 OR #6
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 particip*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 engage*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 involve*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 consult*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 opinion*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 voice*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 dialogue):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 view*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 input*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 partner*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 represent*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 collaborat*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 advoc*):ti
-
((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver* or care giver or care givers) adj2 (jury* or juries or panel* or forum*)):ti
-
(‘community health council’ or ‘community health councils’):ti
-
(‘local involvement network’ or ‘local involvement networks’):ti
-
healthwatch:ti
-
‘national voices’:ti
-
(‘foundation trust governor’ or ‘foundation trust governors’ or ‘FT governor’ or ‘FT governors’):ti
-
(co-produc* or coproduc*):ti
-
#8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27
-
#7 OR #28
-
FROM 2000 TO 2014
-
#29 AND #30
Key: MeSH descriptor = indexing term (MeSH heading); * = truncation; :ti = terms in title field; adj/2 = terms within two words of each other (any order); ‘ ‘ = phrase search.
Database of Promoting Health Effectiveness Reviews (DoPHER)
URL: http://eppi.ioe.ac.uk/webdatabases/Search.aspx
Date range searched: inception to 27 March 2014.
Date of search: 27 March 2014.
Records retrieved: 40.
121 Freetext: ‘Patient* engage*’ (0)
123 Freetext: ‘user* engage*’ (1)
125 Freetext: ‘client* engage*’ (0)
127 Freetext: ‘consumer* engage*’ (0)
129 Freetext: ‘citizen* engage*’ (0)
131 Freetext: ‘citizen* engage*’ (0)
133 Freetext: ‘public engage*’ (0)
135 Freetext: ‘communit* engage*’ (7)
137 Freetext: ‘stakeholder* engage*’ (0)
139 Freetext: ‘Patient* particip*’ (4)
141 Freetext: ‘user* particip*’ (1)
143 Freetext: ‘client* particip*’ (0)
145 Freetext: ‘consumer* particip*’ (1)
147 Freetext: ‘citizen* particip*’ (0)
149 Freetext: ‘public particip*’ (0)
151 Freetext: ‘communit* particip*’ (6)
153 Freetext: ‘stakeholder* particip*’ (1)
155 Freetext: ‘Patient* involve*’ (5)
157 Freetext: ‘user* involve*’ (0)
159 Freetext: ‘client* involve*’ (0)
161 Freetext: ‘consumer* involve*’ (0)
163 Freetext: ‘citizen* involve*’ (0)
165 Freetext: ‘public involve*’ (0)
167 Freetext: ‘communit* involve*’ (16)
169 Freetext: ‘stakeholder* involve*’ (0)
171 121 OR 123 OR 125 OR 127 OR 129 OR 131 OR 133 OR 135 OR 137 OR 139 OR 141 OR 143 OR 145 OR 147 OR 149 OR 151 OR 153 OR 155 OR 157 OR 159 OR 161 OR 163 OR 165 OR 167 OR 169 (40)
Key: * = truncation; ‘ ‘ = phrase search.
EPPI-Centre Evidence Library
URL: http://eppi.ioe.ac.uk/cms/Default.aspx?tabid=62
Date range searched: inception to 27 March 2014.
Date of search: 27 March 2014.
Records retrieved: 1.
The list of EPPI-Centre reviews was browsed for relevance. One relevant record was retrieved.
Health Systems Evidence
URL: www.mcmasterhealthforum.org/healthsystemsevidence-en
Date range searched: inception to 1 April 2014.
Date of search: 1 April 2014.
Records retrieved: 95.
The search was carried out using the predefined database topic search of consumer and stakeholder involvement. In total, 95 records were retrieved.
Search strategies for primary studies
MEDLINE In-Process & Other Non-Indexed Citations and MEDLINE via OvidSP
Date range searched: 1946 to 20 March 2014.
Date of search: 24 March 2014.
Records retrieved: 467.
-
exp *Consumer Participation/ (16,670)
-
*Public Opinion/ (7243)
-
*Patient Advocacy/ (11,992)
-
*Consumer Advocacy/ (1551)
-
*Consumer Organisations/ (661)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 particip$).ti,ab. (31,113)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 engage$).ti,ab. (4448)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 involve$).ti,ab. (22,446)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 consult$).ti,ab. (6340)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 opinion$).ti,ab. (4103)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 voice$).ti,ab. (1435)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 dialogue).ti,ab. (515)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 view$).ti,ab. (7186)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 input$).ti,ab. (1662)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 partner$).ti,ab. (5922)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 represent$).ti,ab. (11,498)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 collaborat$).ti,ab. (2831)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 advoc$).ti,ab. (3722)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 (jury$or juries or panel$or forum$)).ti,ab. (1668)
-
community health council$.ti,ab. (95)
-
local involvement network$.ti,ab. (8)
-
healthwatch.ti,ab. (32)
-
national voices.ti,ab. (0)
-
(foundation trust governor$or FT governor$).ti,ab. (3)
-
(co-produc$or coproduc$).ti,ab. (2003)
-
or/1–25 (131,571)
-
(reconfigur$or re-configur$).ti. (686)
-
((reconfigur$or re-configur$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ab. (327)
-
((redesign$or re-design$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (1609)
-
((reorganis$or re-organis$or reorganiz$or re-organiz$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (2498)
-
(brain or cortical or cortex).ti,ab. (887,140)
-
30 not 31 (2202)
-
((restructur$or re-structur$) adj5 (service$or system$or care or healthcare or NHS or hospital$)).ti,ab. (1848)
-
((major or large-scale or substantial$or extensive$) adj5 (chang$or reform$or modif$or transform$or shap$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (1727)
-
27 or 28 or 29 or 32 or 33 or 34 (8160)
-
26 and 35 (388)
-
Health Facility Merger/ (4446)
-
Health Facility Moving/ (250)
-
Health Facility Closure/ (2151)
-
Hospital Restructuring/ (4532)
-
((hospital$or service$or care or healthcare or NHS) adj3 (closure$or closing or close$or merg$or relocat$or re-locat$or transfer$or decommission$or de-commission$or disinvest$or dis-invest$)).ti,ab. (9594)
-
or/37–41 (19,523)
-
26 and 42 (447)
-
36 or 43 (810)
-
exp animals/not humans/ (3,903,063)
-
44 not 45 (810)
-
letter.pt. (830,574)
-
editorial.pt. (349,409)
-
47 or 48 (1,179,918)
-
46 not 49 (797)
-
limit 50 to yr = ‘2000 -Current’ (492)
-
limit 51 to english language (467)
Key: / = indexing term (MeSH heading); exp = exploded MeSH heading; * = focussed MeSH heading; $ = truncation; .ti,ab. = terms in either title or abstract fields; adj2 = terms within two words of each other (any order).
Applied Social Sciences Index and Abstracts via ProQuest
URL: www.proquest.com/
Date range searched: inception to 26 March 2014.
Date of search: 26 March 2014.
Records retrieved: 234.
((((SU.EXACT(‘Participation’) OR SU.EXACT(‘Community participation’) OR SU.EXACT(‘Citizen participation’) OR SU.EXACT(‘Patient participation’) OR SU.EXACT(‘Consumer participation’) OR SU.EXACT(‘Client participation’)) OR SU.EXACT(‘Engagement’) OR SU.EXACT(‘User involvement’) OR SU.EXACT(‘Consumer representation’) OR SU.EXACT(‘Advocacy’) OR SU.EXACT(‘Citizens’ juries’) OR SU.EXACT(‘Community health councils’) OR SU.EXACT(‘Public opinion’)) AND la.exact(‘English’) AND pd(2000–2014)) OR (TI,AB((Patient* OR user* OR client* OR consumer* OR citizen* OR public OR communit* OR stakeholder* OR carer* OR caregiver* OR care-giver* OR ‘care giver’ OR ‘care givers’) NEAR/2 (particip* OR engage* OR involve* OR consult* OR opinion* OR voice* OR dialogue OR view* OR input* OR partner* OR represent* OR collaborat* OR advoc*)) AND la.exact(‘English’) AND pd(2000–2014)) OR (TI,AB((Patient* OR user* OR client* OR consumer* OR citizen* OR public OR communit* OR stakeholder* OR carer* OR caregiver* OR care-giver* OR ‘care giver’ OR ‘care givers’) NEAR/2 (jury* OR juries OR panel* OR forum*)) AND la.exact(‘English’) AND pd(2000–2014)) OR (TI,AB(‘community health council’ OR ‘community health councils’ OR ‘local involvement network’ OR ‘local involvement networks’ OR Healthwatch OR ‘national voices’ OR co-produc* OR coproduc* OR ‘foundation trust governor’ OR ‘foundation trust governors’ OR ‘FT governor’ OR ‘FT governors’) AND la.exact(‘English’) AND pd(2000–2014))) AND ((((TI(reconfigur* OR re-configur*) OR AB((reconfigur* OR re-configur*) NEAR/5 (service* OR system* OR care OR healthcare OR hospital* OR NHS)) OR TI,AB((redesign* OR re-design*) NEAR/5 (service* OR system* OR care OR healthcare OR hospital* OR NHS)) OR TI,AB((reorganis* OR re-organis* OR reorganiz* OR re-organiz*) NEAR/5 (service* OR system* OR care OR healthcare OR hospital* OR NHS)) OR TI,AB((restructur* OR re-structur*) NEAR/5 (service* OR system* OR care OR healthcare OR NHS OR hospital*)) OR TI,AB((major OR large-scale OR substantial* OR extensive*) NEAR/5 (chang* OR reform* OR modif* OR transform* OR shap*) NEAR/5 (service* OR system* OR care OR healthcare OR hospital* OR NHS))) OR (SU.EXACT(‘Organisational change’) OR SU.EXACT(‘Reorganisation’) OR SU.EXACT(‘Structural change’) OR SU.EXACT(‘Restructuring’))) AND la.exact(‘English’) AND pd(2000–2014)) OR ((SU.EXACT(‘Closure’) OR SU.EXACT(‘Mergers’) OR SU.EXACT(‘Relocation’) OR TI,AB((hospital* OR service* OR care OR healthcare OR NHS) NEAR/3 (closure* OR closing OR close* OR merg* OR relocat* OR re-locat* OR transfer* OR decommission* OR de-commission* OR disinvest* OR dis-invest*))) AND la.exact(‘English’) AND pd(2000–2014)))
Key: SU.EXACT = subject heading; TI,AB = terms in the title or abstract fields; NEAR/2 = terms within two words of each other (any order); * = truncation; ‘ ‘ = phrase search; la.exact = language limit; pd = publication date limit.
Health Management Information Consortium via OvidSP
Date range searched: 1979 to January 2014.
Date of search: 25 March 2014.
Records retrieved: 574.
-
exp Participation/ (7731)
-
exp opinions/ (10,525)
-
exp consumer representation/ (829)
-
exp advocates/ (96)
-
exp patient & public involvement services/ (126)
-
commission for patient & public involvement in health/ (4)
-
local representative committees/ (11)
-
citizens juries/ (84)
-
patient partnership strategy/ (16)
-
community health councils/ (366)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 particip$).ti,ab. (2004)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 engage$).ti,ab. (595)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 involve$).ti,ab. (3277)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 consult$).ti,ab. (1437)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 opinion$).ti,ab. (645)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 voice$).ti,ab. (196)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 dialogue).ti,ab. (43)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 view$).ti,ab. (2158)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 input$).ti,ab. (164)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 partner$).ti,ab. (868)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 represent$).ti,ab. (645)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 collaborat$).ti,ab. (300)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 advoc$).ti,ab. (469)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 (jury$or juries or panel$or forum$)).ti,ab. (357)
-
community health council$.ti,ab. (554)
-
local involvement network$.ti,ab. (78)
-
healthwatch.ti,ab. (53)
-
national voices.ti,ab. (8)
-
(foundation trust governor$or FT governor$).ti,ab. (18)
-
(co-produc$or coproduc$).ti,ab. (87)
-
or/1-30 (26,280)
-
exp organisational change/ (3458)
-
Structural change/ (140)
-
change management/ (1926)
-
(reconfigur$or re-configur$).ti. (106)
-
((reconfigur$or re-configur$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ab. (199)
-
((redesign$or re-design$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (483)
-
((reorganis$or re-organis$or reorganiz$or re-organiz$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (670)
-
((restructur$or re-structur$) adj5 (service$or system$or care or healthcare or NHS or hospital$)).ti,ab. (463)
-
((major or large-scale or substantial$or extensive$) adj5 (chang$or reform$or modif$or transform$or shap$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (412)
-
32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 (6932)
-
31 and 41 (671)
-
exp ‘contraction of services’/ (668)
-
exp service relocation/ (208)
-
site relocation/ (57)
-
((hospital$or service$or care or healthcare or NHS) adj3 (closure$or closing or close$or merg$or relocat$or re-locat$or transfer$or decommission$or de-commission$or disinvest$or dis-invest$)).ti,ab. (1910)
-
43 or 44 or 45 or 46 (2586)
-
31 and 47 (249)
-
42 or 48 (879)
-
limit 49 to yr = ‘2000 -Current’ (574)
-
limit 50 to english (574)
Key: / = indexing term (MeSH heading); exp = exploded MeSH heading; $ = truncation; .ti,ab. = terms in either title or abstract fields; adj2 = terms within two words of each other (any order).
PsycINFO via OvidSP
Date range searched: 1806 to March week 4, 2014.
Date of search: 28 March 2014.
Records retrieved: 390.
-
*Participation/ (4167)
-
client participation/ (1323)
-
*Public Opinion/ (5012)
-
advocacy/ (3187)
-
*Involvement/ (3321)
-
community involvement/ (2575)
-
collaboration/ (5449)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 particip$).ti,ab. (14,125)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 engage$).ti,ab. (4401)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 involve$).ti,ab. (7873)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 consult$).ti,ab. (2157)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 opinion$).ti,ab. (4010)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 voice$).ti,ab. (775)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 dialogue).ti,ab. (455)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 view$).ti,ab. (4369)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 input$).ti,ab. (664)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 partner$).ti,ab. (3358)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 represent$).ti,ab. (3527)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 collaborat$).ti,ab. (2313)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 advoc$).ti,ab. (1823)
-
((Patient$or user$or client$or consumer$or citizen$or public or communit$or stakeholder$or carer$or caregiver$or care-giver$) adj2 (jury$or juries or panel$or forum$)).ti,ab. (850)
-
community health council$.ti,ab. (12)
-
local involvement network$.ti,ab. (6)
-
healthwatch.ti,ab. (6)
-
national voices.ti,ab. (0)
-
(foundation trust governor$or FT governor$).ti,ab. (0)
-
(co-produc$or coproduc$).ti,ab. (438)
-
or/1-27 (66,071)
-
exp organisational change/ (8947)
-
((reconfigur$or re-configur$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (146)
-
((redesign$or re-design$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (438)
-
((reorganis$or re-organis$or reorganiz$or re-organiz$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (733)
-
((restructur$or re-structur$) adj5 (service$or system$or care or healthcare or NHS or hospital$)).ti,ab. (659)
-
((major or large-scale or substantial$or extensive$) adj5 (chang$or reform$or modif$or transform$or shap$) adj5 (service$or system$or care or healthcare or hospital$or NHS)).ti,ab. (526)
-
((hospital$or service$or care or healthcare or NHS) adj3 (closure$or closing or close$or merg$or relocat$or re-locat$or transfer$or decommission$or de-commission$or disinvest$or dis-invest$)).ti,ab. (1858)
-
or/29-35 (13,057)
-
28 and 36 (509)
-
limit 37 to yr = ‘2000 – 2014’ (400)
-
limit 38 to english language (390)
Key: / = indexing term (MeSH heading); exp = exploded MeSH heading; * = focussed MeSH heading; $ = truncation; .ti,ab. = terms in either title or abstract fields; adj2 = terms within two words of each other (any order).
Social Care Online
URL: www.scie-socialcareonline.org.uk/
Date range searched: inception to 7 April 2014.
Search date: 7 April 2014.
Records retrieved: 171.
-
[- PublicationYear:’2000 2014’]
AND
-
[- SubjectTerms:’’participation’’ including narrower terms – OR SubjectTerms:’’public opinion’’ including this term only – OR SubjectTerms:’’advocacy’’ including this term only – OR SubjectTerms:’’interest groups’’ including this term only – OR SubjectTerms:’’consultation’’ including this term only – OR SubjectTerms:’’user views’’ including this term only – OR SubjectTerms:’’collaboration’’ including this term only – OR SubjectTerms:’’co-production’’ including this term only]
AND
-
[- SubjectTerms:’’change management’’ including this term only – OR SubjectTerms:’’service closure’’ including this term only]
OR
-
[- AllFields:’reconfigur*’ – OR AllFields:’’re-configur*’’ – OR AllFields:’redesign*’ – OR AllFields:’’re-design*’’ – OR AllFields:’reorganis*’ – OR AllFields:’’re-organis*’’ – OR AllFields:’reorganiz*’ – OR AllFields:’’re-organiz*’’ – OR AllFields:’restructur*’ – OR AllFields:’’re-structur*’’]
Key: SubjectTerms = subject heading search; AllFields = terms in any field; * = truncation; ’ ’ = phrase search.
Social Science Citation Index via Web of Science, Thomson Reuters
URL: http://thomsonreuters.com/thomson-reuters-web-of-science/
Date range searched: 1956–26 March 2014.
The Social Science Citation Index was searched using a date limit of 2000–14.
Date of search: 28 March 2014.
Records retrieved: 437.
# 17 (#16 AND #9) AND LANGUAGE: (English) (437)
# 16 #15 OR #14 OR #13 OR #12 OR #11 OR #10 (5505)
# 15 (TS = ((hospital* or service* or care or healthcare or NHS) NEAR/3 (closure* or closing or close* or merg* or relocat* or re-locat* or transfer* or decommission* or de-commission* or disinvest* or dis-invest*))) AND LANGUAGE: (English) (2633)
# 14 (TS = ((major or large-scale or substantial* or extensive*) NEAR/5 (chang* or reform* or modif* or transform* or shap*) NEAR/5 (service* or system* or care or healthcare or hospital* or NHS))) AND LANGUAGE: (English) (701)
# 13 (TS = ((restructur* or re-structur*) NEAR/5 (service* or system* or care or healthcare or NHS or hospital*))) AND LANGUAGE: (English) (855)
# 12 (TS = ((reorganis* or re-organis* or reorganiz* or re-organiz*) NEAR/5 (service* or system* or care or healthcare or hospital* or NHS))) AND LANGUAGE: (English) (516)
# 11 (TS = ((redesign* or re-design*) NEAR/5 (service* or system* or care or healthcare or hospital* or NHS))) AND LANGUAGE: (English) (727)
# 10 (TS = ((reconfigur* or re-configur*) NEAR/5 (service* or system* or care or healthcare or hospital* or NHS))) AND LANGUAGE: (English) (220)
# 9 #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 (61,671)
# 8 (TS = (co-produc* or coproduc*)) AND LANGUAGE: (English) (909)
# 7 (TS = (‘foundation trust governor*’ or ‘FT governor*’)) AND LANGUAGE: (English) (2)
# 6 (TS = ‘national voices’) AND LANGUAGE: (English) (0)
# 5 (TS = healthwatch) AND LANGUAGE: (English) (6)
# 4 (TS = ‘local involvement network*’) AND LANGUAGE: (English) (6)
# 3 (TS = ‘community health council*’) AND LANGUAGE: (English) (12)
# 2 (TS = ((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver*) NEAR/2 (jury* or juries or panel* or forum*))) AND LANGUAGE: (English) (1509)
# 1 (TS = ((Patient* or user* or client* or consumer* or citizen* or public or communit* or stakeholder* or carer* or caregiver* or care-giver*) NEAR/2 (particip* or engage* or involve* or consult* or opinion* or voice* or dialogue or view* or input* or partner* or represent* or collaborat* or advoc*))) AND LANGUAGE: (English) (59,787)
Key: TS = topic tag (searches terms in title, abstract, author keywords and keywords plus fields); * = truncation; ‘ ‘ = phrase search; NEAR/2 = terms within two words of each other (any order).
Search strategies to locate grey literature
The following websites were browsed manually and/or searched using the website search function where available, depending on the size of literature contained on the website. The searches were carried out during the period 11 April 2014 to 2 May 2014. The search was limited to documents published in English from 2000 onwards. A total of 187 relevant documents were identified.
| Website | Results |
|---|---|
| Center for Studying Health System Change www.hschange.org/ |
0 |
| Department of Health www.gov.uk/government/publications |
15 |
| Foundation Trust Governors Association www.ftga.org.uk/ |
0 |
| Health Services and Delivery Research (HSDR) programme www.nets.nihr.ac.uk/programmes/hsdr |
11 |
| Health Services Management Centre, University of Birmingham www.birmingham.ac.uk/schools/social-policy/departments/health-services-management-centre/index.aspx |
8 |
| Healthcare Improvement Scotland www.healthcareimprovementscotland.org/ |
0 |
| Healthwatch England www.healthwatch.co.uk/ |
0 |
| Independent Reconfiguration Panel www.irpanel.org.uk/view.asp?id = 0 |
52 |
| Joseph Rowntree Foundation www.jrf.org.uk/ |
5 |
| National Voices www.nationalvoices.org.uk/ |
2 |
| NHS Confederation www.nhsconfed.org/Pages/home.aspx |
20 |
| NHS England www.england.nhs.uk/ |
4 |
| NHS Improving Quality www.nhsiq.nhs.uk/ |
3 |
| NHS Institute for Innovation and Improvement www.institute.nhs.uk/ |
5 |
| NHS Scotland www.show.scot.nhs.uk/ |
7 |
| NHS Wales www.wales.nhs.uk/ |
2 |
| National Institute for Health and Care Excellence www.nice.org.uk/ |
3 |
| RAND Corporation www.rand.org/ |
0 |
| Scottish Health Council www.scottishhealthcouncil.org/patient__public_participation/patient__public_participation.aspx |
16 |
| Social Care Institute for Excellence (SCIE) www.scie.org.uk/ |
12 |
| The Health Foundation www.health.org.uk/publications/ |
6 |
| The King’s Fund www.kingsfund.org.uk/ |
9 |
| The Nuffield Trust www.nuffieldtrust.org.uk/ |
4 |
| The Picker Institute Europe www.pickereurope.org/ |
3 |
| Total | 187 |
A focused search of Google, using the advanced search, was carried out to locate reports on service reconfiguration. The search was limited to UK PDFs published in English from 2000 onwards with the term ‘reconfiguration’ in the title of the web page. The first 100 results were scanned for relevance. The search was carried out on 2 May 2014 and identified 18 reports.
Appendix 2 Systematic reviews data extraction
Study: Abelson et al. (2010)6
Authors’ objectives: To evaluate the effectiveness of interactive strategies for engaging the public in the development of health-care policies and programmes at provincial/regional level. Particular attention is given to public engagement of rural populations (and to the New Brunswick context in Canada), in both official languages (English and French) and regarding the determinants of health.
Inclusion criteria: Original and review articles of empirical studies of public engagement methods, practices and evaluations in the development of health-care policy and programmes. Theoretical and conceptual work that helps inform the evaluation of public engagement. Key background papers of methodological and theoretical issues relating to public engagement. Languages restricted to English and French.
Exclusion criteria: Not stated.
Search dates: 2000–9.
Number of included studies: 34.
Included study designs: Cochrane review (1); systematic review (1); scoping review (1); narrative reviews (2); empirical studies evaluating a public engagement intervention in health care (12) (including three comparative evaluations; where reported, comparisons were different intensities, not different interventions); non-empirical papers of evaluation approaches and methods (8); Canadian grey literature documents containing empirical and non-empirical studies (9).
Countries of included studies: 12 published empirical studies include Canada (7); the UK (3); the USA (1); and Australia (1).
Types of reconfiguration: Published empirical studies: priority-setting, planning and policy development in a number of areas including local health goal-setting; health promotion and healthy public policy; cancer-specific and general health service planning and delivery; and policy development related to new health technologies.
Definitions of engagement/involvement: Review authors’ definition: a category of methods for involving citizens in health-care decision-making that incorporates at least three elements, (1) the provision of information to participants about the topic/issue being discussed; (2) the opportunity for interactive discussion among participants and potentially between participants which the public engagement sponsors; (3) an explicit process for collecting individual or collective input. Definitions are also provided for included reviews.
Who was engaged/involved: Urban/rural/Francophone/Aboriginal populations. Participants recruited from community-based organisations; local residents/citizens/stakeholders/hard-to-reach groups.
Methods of engagement/involvement: Ad hoc deliberative meetings (e.g. citizens’ panels/juries) held over 1–3 days; long-term collaborative partnerships over several months or years. Three studies looked at partnerships as models of, or inputs to, effective and sustainable public engagement.
Method of synthesis: Critical interpretive synthesis (Dixon-Woods et al. 200653): conceptual translation of quantitative/qualitative/non-empirical studies.
Conceptual/theoretical framework or logic model used: There is a contextual framework mentioned (figure 1, p. 6) but it is not explicitly stated that this was used. Many of the included studies employed a conceptual framework in their evaluation.
Research questions addressed: 1, 4.
Stages of involvement: 1, 2, 3, 4?, 5.
Levels of involvement: Informing; consulting; involving; collaborating.
Results: Results from the review of reviews indicated that greater conceptual clarity is needed about the meaning of effective public engagement and common evaluative criteria, as is more rigorous evaluation of the effects of public engagement on a range of outcomes of interest. Key messages from the 12 published empirical studies: interactive public engagement can be implemented successfully in various situations, and success is dependent on contextual variables. Organisational commitment and topic-related characteristics appear to be key contextual variables. Public engagement mechanisms need to be adapted to the wider context of policy development around the issue, including topic, the group(s) to be engaged, the history of the issue and the perceived power dynamics. Skills required to conduct interactive processes can be learned in a supportive organisational environment. Participant satisfaction and increased topic-specific learning is higher when the engagement process is well designed, although process satisfaction does not necessarily lead to perceived impact of participation on policy decision-making. Group debate features as an important contributor to satisfaction. Partnerships are central to the effectiveness of community-based public engagement strategies. Institutionalisation of partnerships beyond the active phase can enable sustainable change. Interactive public engagement can influence participant views, but is less likely to change more dominant views. Results from the Canadian grey literature highlighted the need for open processes of engagement, with the involvement of policy-makers and participants in setting indicators, benchmarks and goals in evaluating public engagement activity. Further results are reported in the paper from the published non-empirical literature (focusing on theoretical and conceptual work in public engagement evaluation). Further results are also reported on engaging the public about the determinants of health; engaging rural populations; public engagement in different languages; and combining theory and practice.
Authors’ conclusions: Current interest in public engagement among Canadian health system managers and policy-makers needs to be matched by clear thinking from all interested parties (researchers, managers and policy-makers) about the terminology, goals, theoretical properties and benefits of public engagement.
Comments: Not all focused on reconfiguration. Related to this review are those focusing on priority-setting and resource allocation. Not clear if any study overlap with Mitton et al. (2009),20 as Mitton did not present study details. Crawford et al. (2002)19 also included in the Abelson review.
Study: Conklin et al. (2012)16
Authors’ objectives: To evaluate the outcomes of public involvement in health-care decision-making, priority-setting, resource allocation and health service planning at the macro and meso levels.
Inclusion criteria: Focus on evaluation studies. For this review, involvement was conceptualised as taking a broader societal perspective on public involvement where the public were (1) lay citizens/community members, (2) representatives of organised social interest groups, such as coalitions, partnerships, (3) organisations of staff members and/or patients/customers/clients, and input was from a broad group (not individual) perspective. Any outcome or impact was eligible, as defined by the study authors.
Exclusion criteria: Surveys of beliefs/attitudes about participation. Studies that examined involvement in service development, shared decision-making of individual treatment, clinical decisions, participatory action research, therapeutic and service delivery decisions, and clinical guidelines. Studies of preferences for participation among health-care professionals or users. Reviews, editorials, commentaries. Studies in languages other than English, German or French.
Search dates: Published articles from November 2000 to April 2010 were sought.
Number of included studies: 19.
Included study designs: Nine descriptive case studies; 10 empirical studies (cross-sectional; comparative pre–post design; qualitative; mixed methods). Follow-up (where reported) ranged from 1 year to 7 years.
Countries of included studies: Majority in England, Canada, the USA and Northern Ireland. Others included France, the Netherlands, Italy and Israel.
Types of reconfiguration: Relevant studies (where reconfiguration was the goal). Examples: resource allocation relating to local health integration networks; shaping policies and decisions about primary care provision and delivery; health-care priority setting; health policy decisions about the delivery of women’s health services; decision-making about local health services.
Definitions of engagement/involvement: The review authors defined six levels of involvement (consultation, participation, engagement, partnership, community development, representation), but stated that these were often used interchangeably, even within included studies.
Who was engaged/involved: Special interest groups; the public; patients; staff; NHS lay board members. More specific definitions of ‘the public’ varied and were generally unclear across the studies. Terms used: representatives of patient organisations; ordinary citizens; individuals with no particular axe to grind; those whose voices might not otherwise be heard.
Methods of engagement/involvement: Surveys; conference and website; community health councils; public meetings; local patient groups; citizen panels/juries; group simulation using roulette wheel; collaboration between agencies/groups/individuals.
Method of synthesis: Narrative.
Conceptual/theoretical framework or logic model used: Not stated.
Research questions addressed: 1, 2, 3, 4.
Stages of involvement: 3, 4, 5, 6, 7.
Levels of involvement: Informing; consulting; involving; collaborating.
Results: Where reported, details of specific and measurable data on outcomes were generally lacking. Studies demonstrated how public involvement had influenced decision-making and led to acceptance and implementation (one study involving small group meetings/plenary sessions); practical changes/improvement were achieved (three studies involving surveys and group meetings); priorities (identified through the involvement activity) were integrated to a regional programme (one study); and resources had been found for new services (three studies involving citizen’s juries, community group representations/collaborations). One study demonstrated repeatability of regional meetings (a deliberative consultation activity) in two other organisations. Other studies suggested that the impact or influence of public involvement on shaping strategic decisions was found to be minimal (three studies), geographically variable (two studies) or mixed (one study). Common outcome measures were participant views or ‘change’ as a measure of influence of public engagement on decisions, policy and practice. Some studies reported improved learning or knowledge of processes involved in consultation and priority-setting, and benefits for deliberative procedures. Negative consequences of public involvement were reported as costs and unintended outcomes for participating stakeholders when challenged by members of the public.
Authors’ conclusions: Evidence of impact on public involvement in health-care policy remains scarce, despite the growing body of work. Firm conclusions about effective and appropriate involvement activities are difficult to draw. Focus on outcomes risks missing the normative argument that involving the public in the health-care policy process may be seen to be of intrinsic value.
Comments: This review was designed as a scoping review.
Study: Crawford et al. (2002)17
Authors’ objectives: To examine the effects of involving patients in the planning and development of health care.
Inclusion criteria: Studies of patient involvement (defined as the active participation in the planning, monitoring and development of health services of patients, patient representatives and the wider public as potential patients) in the planning and development of health care.
Exclusion criteria: Studies of patient involvement in research, community development, health promotion, self-management and self-help, and the role of doctors and patients in determining individual treatment choices. Studies measuring patient satisfaction or patient preferences without describing how information was used to help develop a service.
Search dates: 1966 to 2000.
Number of included studies: 42.
Included study designs: Case reports (31); surveys (5); review of minutes of meetings (3); action research (3). Four of the included studies used qualitative research methods.
Countries of included studies: The UK (28); Sweden; the USA; Australia; and Canada.
Types of reconfiguration: Various services, including primary care, mental health, learning and physical disability, general health care, community services, inpatient and outpatient, social care, maternity, neurology, human immunodeficiency virus. Most studies looked at smaller-scale change. Approximately one-quarter of studies focused on larger-scale change, including changes to organisation of care and/or services. Of these studies, two involved a plan for hospital closure.
Definitions of engagement/involvement: Review author’s definition: active patient participation in the planning, monitoring and development of health services of patients, patient representatives and the wider public as potential patients.
Who was engaged/involved: Most studies described participants as patients. Others reported involvement of carers, service users, staff, health and welfare council, community health council, citizens, lay board of directors or mixed populations.
Methods of engagement/involvement: Patient groups, consultation meetings, committees and forums; interviews; citizen’s juries; survey; focus groups; representation on planning boards and panels; mixed methods.
Method of synthesis: Narrative.
Conceptual/theoretical framework or logic model used: No.
Research questions addressed: 1, 2, 4.
Stages of involvement: 3?, 4?, 5, 6.
Levels of involvement: Informing; consulting; involving; collaborating.
Results: Most frequently cited effects of patient involvement were the production of new or improved sources of information for patients and making services more accessible (smaller-scale changes). Seven reports described new services being commissioned, and two reports described hospital closure proposals being modified or abandoned as a result of patient involvement. There was a mixed response from patients in terms of satisfaction with the process of involvement. Organisational attitudes to involving patients became more favourable (four reports), resulted in culture change to being more open to involving patients (two reports) and resulted in further involvement projects (two reports). Other reports (6) discussed less favourable consequences, such as involvement being used to legitimise decisions already made, or a slower decision-making process.
Authors’ conclusions: Involving patients has contributed to changes in the provision of services across a range of different settings. The evidence base for the effects on use of services, quality of care, satisfaction or health of patients does not exist.
Comments: This review appears to be a subset (based on health-care context only) of that in Crawford et al. (2003)18 (which contains a wider scope of sectors). The wider review has a different objective: to look at transferability of user involvement from other sectors to health care. Therefore, it appears appropriate to treat these as two separate reviews.
Study: Crawford et al. (2003)18
Authors’ objectives: To evaluate user involvement in change management across a range of sectors (health, other public services, voluntary and private sectors). To identify factors that promote successful user engagement, and identify relevance to the NHS.
Inclusion criteria: Any study design focusing on the aims, processes and outcomes of service user involvement in change management at local organisational level.
Exclusion criteria: Studies not directly related to change management (such as campaigns for change in policy at national level).
Search dates: Databases: published after 1980, to 2002. Other searches (where reported) to 2002.
Number of included studies: 344 (of those reporting outcomes, 55 related to public sector health, social care and community care; 19 related to public sector non-health; and 23 related to the private sector). See Appendix 3.
Included study designs: Most were qualitative process evaluations or discussion papers on case studies.
Countries of included studies: Largely the UK. Others: Australia, Sweden, Denmark, the USA, Canada, Austria, Japan. See Appendix 3.
Types of reconfiguration: Specific reconfiguration not described. Reconfiguration contexts described as various within health, social and community care; non-health public sector (including postal services, social security, education, housing); private sector (including consumer goods, travel, entertainment); and voluntary sector (disability/neurological services).
Definitions of engagement/involvement: Review authors’ definition: taking an active part in change management at the organisational level.
Who was engaged/involved: Current, ex- and potential service users and their representatives. Providers.
Methods of engagement/involvement: Various, covering time-limited methods (to elicit user perceptions/preferences) and long-term approaches (building relationships with service users). Some initiated by provider; others initiated by service users. Public sector tended to use more deliberative approaches. Examples: surveys, focus groups; deliberative approaches (such as citizen’s juries, public conferences); user/community groups; formal bodies (such as community health councils, patient groups, advocates and link workers).
Method of synthesis: Thematic (using qualitative methods).
Conceptual/theoretical framework or logic model used: Not stated.
Research questions addressed: 1, 2, 3, 4.
Stages of involvement: Not clear. Difficult to apply to such a general review.
Levels of involvement: Informing; consulting; involving; collaborating; devolving.
Results: User involvement in health care (represents the majority of evidence in this review): small numbers of reports attributed changes in services to user involvement. The impact of changes on service quality has not been evaluated. User involvement in other public sector services: similar issues to health care, but greater emphasis on involving local residents who are not service users. Emphasis on complaints procedure in social services. User involvement in the voluntary sector: very limited number of reports. Emphasis on user-led services. User involvement in the private sector: user engagement more frequently applied to shaping products and services (not structural or organisational policy change). Less emphasis on methods of involvement than other sectors. Quality of evidence reported to be poor (reported for private sector only). See Crawford et al. (2003)18 pp. 10–11.
Authors’ conclusions: There is little evidence of independent research in any of the sectors examined. No best method for involving users within the NHS. Methods need to be selected on the basis of aims of involvement, capacity of local users and providers, and financial/other constraints. Facilitators of successful user involvement appear to be increase clarity of aims of involvement to service users; increase willingness of users to engage; reduce organisational resistance to user involvement; and increase appropriately resourced evaluation on where user involvement has made a difference.
Comments: In the first 55 studies (on public sector health, social care and community care) this review overlaps with Crawford et al. (2002)17 (their review of 42 studies focusing on health care).
Study: Daykin et al. (2007)19
Authors’ objectives: To evaluate the impact of strategies, including the Patient Advice and Liaison Service, for PPI in health care.
Inclusion criteria: Initial inclusion criteria: quantitative studies (with measurable outcomes) or qualitative research focusing on defined PPI/user involvement interventions in an identified health-care population. English language and published between 2000 and 2005. Second stage inclusion criteria: randomised controlled trial/experimental studies. Quantitative studies measuring outcomes against an identified baseline. Qualitative and mixed methods studies focusing on successful or unsuccessful elements of the strategy under investigation.
Exclusion criteria: Second stage exclusion criteria: studies focusing on individual treatment and care. Anecdotal reporting only, no recognisable research process.
Search dates: 2000 to 2005.
Number of included studies: Eight evaluations.
Included study designs: Four case studies; two independent evaluations using qualitative methods; one project evaluation using mixed methods; one action research study.
Countries of included studies: The UK.
Types of reconfiguration: General/strategic development; cancer services; mental health services; older people’s services.
Definitions of engagement/involvement: Definition not stated.
Who was engaged/involved: Staff, members of the public, patients.
Methods of engagement/involvement: Employment of an individual to work with community groups; interprofessional cancer education programme; user groups; forums for service users and officials; community-based exercise facility for people with mental health problems; citizen’s juries; community initiative to elicit and respond to the views of older people; regional-level action research programme with staff.
Method of synthesis: Narrative.
Conceptual/theoretical framework or logic model used: Realist framework: identifying contexts and mechanisms that lead to favourable or unfavourable outcomes.
Research questions addressed: 1, 2.
Stages of involvement: Not clear. Possibly 3, 4?, 5.
Levels of involvement: Informing; consulting; collaborating.
Results: Difficulties were reported in documenting impacts from PPI. Problems were a result of time lag between intervention and outcomes, and difficulty isolating the direct impact of PPI from other potential contributory factors. Social benefits (two studies): engagement with community groups and activists can assist in shifting service provision towards a social model of care. New services provided as a result of PPI intervention. PPI can help to destigmatise mental illness and offer a means of reintegration to the community. Other outcomes were reported, but they did not correspond with the review inclusion criteria (e.g. focused on improvements to individual care and in relation to community health improvement). Prerequisites for effective PPI identified as follows. Structure and resources: organisational structures that support partnership working; community capacity for change; programme-level structures to support staff and safeguard users’ well-being; and mechanisms to identify impact of user involvement on decisions. Politics and discourse: commitment to deliberative process involving discursive democracy and community development. Attitudes and culture: adaptations and change by staff needed to enable successful participation of users in service development. Specific results in relation to Patient Advice and Liaison Service are reported in the paper.
Authors’ conclusions: Authors’ conclusion appeared to focus on limitations of the evidence, in terms of relevance to the evaluation of PPI and quality criteria.
Comments: The review authors excluded a number of reviews on the basis that they did not meet the review criteria.
Study: Mitton et al. (2009)20
Authors’ objectives: To examine methods and impact of public engagement in health-care priority-setting decision-making.
Inclusion criteria: Study design: English-language studies in peer-reviewed journals. Population: ordinary or lay citizens/community members; representatives of organised social interest groups (including coalitions, partnerships); organisation staff members/employees and/or patients/customers/clients. Intervention: public engagement or involvement in decision-making. Setting/context: decisions at macro (high-level funding) and meso (specific services and programmes) levels; decisions about treatment eligibility at group or typical patient level; monitoring and evaluation relating to priority-setting or resource allocation. Perspective: societal.
Exclusion criteria: Study design: news items, letters, editorials, book reviews, non-peer-reviewed journal articles. Population: exclusively professionals or experts. Context/setting: studies of wider policy frameworks and choices, (such as clinical rationing) unless they focused directly on how public engagement was used to develop such frameworks. Perspective: individual.
Search dates: 1981 to 2006.
Number of included studies: 175 articles (190 distinct cases of public engagement).
Included study designs: Observational.
Countries of included studies: The USA (40%), the UK (26%), the rest of Europe (8%), Canada (9%), Australia/New Zealand (7%) and elsewhere (10%).
Types of reconfiguration: Largely macro-level decision-making. General assessments of public priorities for government spending or development of broad vision statements in health care (97 cases). Non-health care (largely environmental science; urban planning) (77 cases). Most health care reconfiguration focused on public health and health promotion. Others on general policy and spending, regional health authorities and integrated systems, mental health, acute care, pharmaceuticals or health technology assessment, and long-term care. Sixteen cases included health and non-health care sectors.
Definitions of engagement/involvement: Three levels: communication; consultation; participation.
Who was engaged/involved: Where defined (167 of 190 cases): public as individuals (speaking on their own behalf) (42). Public as organised interest groups (speaking on behalf of a membership) (20). Public as patients or consumers of services (speaking on issues outside their personal experience) (14). Most of the 190 cases reported engagement with multiple public audiences. Thirty-eight per cent of cases reported particular attention to disadvantaged populations or groups with special needs.
Methods of engagement/involvement: Communication: traditional publicity; public meeting/hearing; drop-in centre; internet information; telephone hotline. Consultation: opinion poll/survey; referendum; consultation document with select population; electronic consultation/interactive website; focus group; study circle or open space; standing citizens’ advisory panel. Participation: citizens’ jury or consensus conference; negotiated rule-making or task force; deliberative poll or planning cell; town meeting with voting. Most cases (93 of 183 codable) used multiple methods. In total, 405 techniques were employed. Fifty-eight per cent consultation; 24% communication; 18% participation. From the codable data, 49% one-off events; 45% ongoing over a period of time (mean duration approximately 4 years). Forty per cent of cases involved face-to-face interaction, and this was more likely to occur within deliberative engagement processes.
Method of synthesis: Narrative.
Conceptual/theoretical framework or logic model used: Lomas (1997):54 three-level scale to assess the scope of public engagement (with added fourth category of monitoring and evaluation). Rowe and Frewer (2005):55 coding framework for intensity and methods of public engagement.
Research questions addressed: 1, 2, 3, 4.
Stages of involvement: 1 (largely macro-level priority-setting).
Levels of involvement: Informing; consulting; involving; collaborating.
Results: Evaluation of effectiveness carried out in only 32% of included cases, and most of this was process evaluation. No direct experimental comparison of different methods. Despite the lack of evaluation, two-thirds of included articles concluded that participation processes were successful (as defined by the study authors). Six per cent of cases were deemed to be unsuccessful and 14% inconclusive. Cases using deliberative methods were more successful than those employing lower levels of engagement (e.g. communication or consultation). Cases with face-to-face contact were perceived to be more successful than those without direct interaction. In studies where the intention of engagement was making a difference (or leading to a decision other than what would have been arrived at in the absence of engagement), 60% of cases stated an impact; 10% stated this had not been achieved; and in 30% of cases the impact was unclear or unspecified.
Authors’ conclusions: Some practices for public engagement in priority-setting are promising; for example, use of multiple methods and balancing broad consultations with in-depth engagement using new deliberative techniques. Lack of evaluation limits the ability to suggest supportive evidence for any particular approach to public engagement in priority-setting.
Study: Mockford et al. (2012)5
Authors’ objectives: To identify the impact of PPI on UK NHS health-care services and to identify the economic cost of PPI. Secondary objectives were to examine how PPI has been defined, theorised and conceptualised, and how the impact of PPI is captured or measured.
Inclusion criteria: Studies of user/patient activity which involved patients, carers or the public working (1) in a collaborative way with health professionals or management or (2) in a user-led way. All types of study designs were eligible except those specifically excluded.
Exclusion criteria: Studies of children’s services; health research; NHS research and development; voluntary sector; independent health-care services; and educational services. Studies of involvement as part of an individual’s health care. Discussion papers, ‘think pieces’ and editorials.
Search dates: 1997 to 2009.
Number of included studies: 28 (42 publications).
Included study designs: Case studies (20); ‘evaluations’ (5); secondary data analyses (2); survey (1).
Countries of included studies: The UK.
Types of reconfiguration: General.
Definitions of engagement/involvement: Not reported. Authors stated that included studies rarely provided an explicit definition of PPI, engagement or similar terms.
Who was engaged/involved: Patients/carers; the public.
Methods of engagement/involvement: Lay membership of boards, panels and working groups; user groups.
Method of synthesis: Narrative.
Conceptual/theoretical framework or logic model used: No.
Research questions addressed: 1, 2.
Stages of involvement: Unclear.
Levels of involvement: Consulting; involving; collaborating.
Results: Results indicated that PPI took many forms and had a range of impacts on health-care services, including design, location of and access to services; provision of additional services; reorganisation of existing services; and changes in organisation of acute trusts. Reporting quality was poor and there was little evidence on costs.
Authors’ conclusions: There is a need for significant strengthening of the evidence base around the impact of PPI on NHS health-care services. Development of clear concepts and robust forms of measurement is required.
Comments: Focused on small-scale (such as ward-level) change as well as larger-scale change.
Study: Rose et al. (2003)21
Authors’ objectives: To evaluate user and carer involvement in organisational change management in a mental health context.
Inclusion criteria: English-language articles published between 1987 and 2002. Studies of user and carer involvement in organisational change in a mental health context.
Exclusion criteria: Participants aged under 18 years and over 65 years. User/carer involvement in auditing and evaluation of services, where changes resulting from involvement are not described.
Search dates: 1987 to 2002.
Number of included studies: At least 112.
Included study designs: Most included studies were discussion papers (61 discussing practice; 43 discussing concept; some discussed both). There were 34 qualitative papers, 16 quantitative papers (including four trials), seven organisational reports and two unpublished dissertations.
Countries of included studies: The UK (71); the USA (42); Europe (1); Australia/New Zealand (3); and more than one country (9).
Types of reconfiguration: Promoting democracy and representation and/or cultural change (over 50% of included studies). Strategic planning, restructuring of services (very few studies) and policy initiatives. New service provision and the employment of service users in organisations.
Definitions of engagement/involvement: Review authors’ definition: consumerism (individual), including day-to-day personal care planning; consumerism (collective), group involvement in the planning, delivery, implementation and monitoring of services; citizenship.
Who was engaged/involved: Majority of studies focused on service users and professional staff. One-quarter of studies involved carers. Others involved: user groups, carer groups, the public, community health councils.
Methods of engagement/involvement: Majority of studies focused on collective consumerism, involving consultation, representation, partnership, evaluation, involvement in staff recruitment. Methods not explicitly stated.
Method of synthesis: Narrative. Use of coding frame to elicit most frequently occurring aspects of user involvement activity.
Conceptual/theoretical framework or logic model used: Review authors’ definition could also be classed as a conceptual framework for the review: consumerism (individual), including day-to-day personal care planning; consumerism (collective), group involvement in the planning, delivery, implementation and monitoring of services; citizenship. Adapted version of Arnstein’s ladder of participation was also used.
Research questions addressed: 1.
Stages of involvement: 5.
Levels of involvement: Consulting; involving; collaborating.
Results: Outcomes were rarely measurable (and based on subjective judgement of the study author). Fifty-eight papers reported unknown or unclear outcomes; 52 papers reported positive outcomes; 14 reported negative outcomes of user involvement. The included trials did not focus on reconfiguration. Among the other studies, various relationships were proposed between the type of user involvement and type of change. For example, collective consumerism was associated with restructuring and strategic planning but could equally be conceptualised as tokenism. Partnership working showed no systematic relationship with any form of organisational change (small number of reports). Citizenship and campaigning were associated with change of mission. User control was associated with new service provision. Drivers for successful user involvement included a facilitating organisational culture, information provision, funding and service user training.
Authors’ conclusions: The review shows a complex picture of user and carer involvement in change management. The evidence is diverse and of variable quality.
Appendix 3 Systematic reviews quality assessment
| Study reference | Adequate search? | Quality assessed? | Quality assessment used in analysis? | Study details reported? | Research/practice implications identified? | Conclusions supported by evidence? |
|---|---|---|---|---|---|---|
| Abelson et al. (2010)6 | Yes | No | N/A | Yes | Yes | Reliability unclear. No quality assessment of empirical studies, including comparative studies |
| Conklin et al. (2012)16 | No. Limited to two databases. Published studies only. Three languages | No | N/A | Yes | Yes | Not clear. Restrictions in search, and absence of quality assessment |
| Crawford et al. (2002)17 | Yes | No (authors justified on the basis of no available criteria for case reports) | N/A | Yes | Yes | Yes |
| Crawford et al. (2003)18 | Yes | No formal quality assessment. Assessment based on relevance to review question | N/A | Yes (for studies reporting outcomes) | Yes | Yes |
| Daykin et al. (2007)19 | Yes | Yes – CASP | Yes, although not explicitly used. Full results not reported | Yes | Yes | Yes |
| Mitton et al. (2009)20 | Yes | No | N/A | No | Yes | Unclear. No study details to verify the authors’ conclusions about methods and impact. No quality assessment of included studies (although all observational) |
| Mockford et al. (2012)5 | Yes | Yes | Yes | Yes | Yes | Yes |
| Rose et al. (2003)21 | Yes | No | N/A | No | Yes | Unclear. No study details to verify results, which are essentially based on vote counting. Not possible to verify authors’ conclusion in relation to variable quality |
Appendix 4 Other research data extraction
| Author(s); Country | Focus/design; Setting; Date | Type(s) of reconfiguration; Who was engaged/involved | Stages;a Levels of involvement; Method(s) of engagement/involvement | Results of engagement/involvement | Key themes and comments |
|---|---|---|---|---|---|
| Barratt et al. (2014)22,23 England |
Interview study to examine factors that influence patient and public response to proposals for major service change, including willingness to accept the trade-offs inherent in decisions about reorganising care. Analysis ‘combined inductive and deductive approaches, drawing on sociocultural perspectives of risk as an analytic focus’23 Two urban areas, one where service changes were being considered (‘Greenville’) and one where no changes were proposed (‘Hilltown’) Not reported |
Proposed reconfiguration involving closure of local emergency department Participants (n = 28) were classified as Greenville parents (5); Greenville older people (6); Greenville activists/patient reps (9); and Hilltown NHS patients (8). It was not reported how participants were recruited |
Stages: 4?, 5 Levels: informing; consulting In-depth interviews: Participants were invited to use flash cards to select their priorities for emergency care, including aspects they might be prepared to have less of (e.g. rapid access) in return for more of another (e.g. consultant-delivered care) |
Main findings of the study were most participants were unwilling to accept the trade-offs involved in consolidating services. There was a widespread belief that timely access is associated with better outcomes. As a result, participants were not prepared to accept a longer journey to hospital. Participants did not consider expected improvements in care as a result of centralising services to be gains worth having. They believed care quality would be negatively affected because greater patient numbers would mean more pressure on staff. Participants in both areas held similar views. The authors also stated that, in the area where service changes were being considered, presentation of evidence by clinicians was not effective but instead fuelled hostility to the proposals | Timely access to services; emergency care; clinical leadership insufficient; clinical evidence not accepted; public perceptions; centralisation of services; quality of care; safety concerns. Implications as stated by authors: commissioners and policy-makers should not assume that evidence will persuade communities to accept service change. Commissioners should instead make explicit plans for changes in patient flows and should clarify the roles of key staff groups. No quantitative data were reported |
| Boyes (2008)24 Scotland |
To identify potentially effective methods for involving the public in the option generation and appraisal and decision-making stages of NHS major service change. Methods included a literature review; deliberative panels; interviews with NHS stakeholders; an online survey; and a ‘Service Change Dialogue’ NHS services in Scotland 2007 (public panels and other events) |
Focus was any type of major service change. Public panels considered an actual case from their area (accident and emergency service change in Monklands and closure of community hospitals in Coldstream and Jedburgh) and a vignette setting out a hypothetical option Public participants recruited from Scottish Council Foundations Citizens’ Panel; none had actively taken part in public involvement relating to major NHS service change in their local area (Borders or Lanarkshire). NHS stakeholders were involved through interviews and a national online survey |
Stages: 2, 3, 5, 6 Levels: informing; consulting; involving; collaborating Public engagement/involvement in this research was through participation in day-long deliberative panels |
The public panels made a number of recommendations under the broad headings: reach a common understanding on the need for change; carefully select methods and tools for engaging the public; location matters most to the public; consult on a range of feasible options; the public need compelling evidence that proposed changes will lead to better health outcomes; strengthen accountability; improve quality of feedback; independent review; and learn, adapt and improve. Full details in the report | Demonstrate need for change; different types/methods of involvement; access to services; provide range of options; demonstrate benefits of reconfiguration; feedback; external scrutiny. Report commissioned by the Scottish Health Council |
| Day and Klein (2007)25 England |
Expert opinion review of the ‘machinery for independent scrutiny of organisational and service change in the NHS’ (p. 7). Main focus is local authority scrutiny, covering OSCs; judicial scrutiny; the role of the Secretary of State; and the IRP NHS services affected by reconfiguration proposals 2003–7 (examples of reconfigurations are discussed in text) |
Closure of small local hospital (Keynsham); major reconfiguration involving redistribution of services among three acute hospitals (Tees) Keynsham: joint OSC involving Bath and North East Somerset Council, Bristol City Council and South Gloucestershire Council; also local organisations, patient groups and GPs. Tees: joint OSC involving six local authorities; also the public and ‘stakeholders’ |
Stages: 3, 5, 6 Levels: informing; consulting; involving Keynsham: five OSC meetings; consultation with local organisations, patient groups and GPs; visit to facilities that would provide care once Keynsham Hospital closed; advice from IRP on consultative process and reconfiguration plans. Tees: consultation on external review by Professor Ara Darzi, including 150 public meetings, 350 meetings with stakeholders and distribution of a consultation document to 377,000 properties |
Keynsham: joint OSC accepted proposal to close Keynsham Hospital subject to 21 recommendations in line with IRP advice. The NHS trusts involved accepted most of the joint OSC recommendations. Tees: joint OSC was satisfied with consultation although public response rate was only 10%. OSC report drew heavily on evidence from local clinicians. Five proposals were accepted and four rejected. Proposals for reconfiguration of maternity and paediatric services were referred to the IRP, which in January 2007 recommended accepting them in a modified form | Different types/methods of involvement; external scrutiny; clinician opposition to reconfiguration; political influence. Report also highlighted the importance in the Tees’ example of opposition from clinicians likely to be affected by change. Overall, the authors considered OSCs to be assertive in questioning and challenging proposals but basing their challenge on evidence rather than being opposed in principle to any change. The report also discussed uncertainty over when consultation is required and the definition of ‘substantial’ change; and the possibility of judicial review when disagreements cannot be resolved locally. The authors suggested that reconfiguration proposals should include a risk assessment of what might go wrong in the process of implementation. Elements required to assess costs and benefits of local authority scrutiny were also discussed |
| IRP (2010)1 UK |
Review of 17 reviews carried out by the IRP since 2003. Common themes arising Includes maternity services; children’s services; accident and emergency; impatient emergency trauma; surgery; medical care; general care for older people; services for older people with mental health problems; microbiology services; oesophago-gastric cancer surgery services Reviews took place from 2003 to 2010 |
Various (details provided) NHS leaders, local councillors, community representatives |
Stages: 1–7 (as necessary) Levels: informing; consulting; involving The role of the IRP is to advise the Secretary of State for Health on contested NHS reconfigurations in England, and specifically to give advice about proposals formally referred to the Secretary of State for decision |
N/A | Clinical, managerial, procedural issues deemed to be significant in referrals that have been subject to formal review: inadequate community and stakeholder engagement in the early stages of planning change. The clinical case has not been convincingly described or promoted. Clinical integration across sites and a broader vision of integration into the whole health community has been weak. Proposals that emphasise what cannot be done and underplay the benefits of change and plans for additional services. Important content missing from reconfiguration plans and limited methods of conveying information. Health agencies caught on the back foot about three issues most likely to excite local opinion: money, transport and emergency care. Inadequate attention to responses during and after the consultation |
| NHS Confederation (2010)26 England |
Report focuses on how PCTs can best communicate with the public about decisions on local service change. Based on two pieces of research carried out by Ipsos MORI on behalf of the PCT Network: focus group research with the general public (testing common words and phrases used by the NHS in describing service change) and case studies of local PCT service changes (interviews with senior leaders at NHS South Gloucestershire, NHS West Sussex, South East London PCTs and NHS East and North Hertfordshire) NHS services affected by reconfiguration proposals. Report takes a commissioner’s (PCT) perspective Dates of focus groups and case studies were not reported |
Any: report focuses on general principles of communication and language use General public via focus groups (no further details reported). In the only case study discussed separately (South Gloucestershire), members of campaign groups were engaged |
Stages: 4?, 5, 6 Levels: informing; consulting; involving Focus groups to assess public reaction to various statements on the roles of PCTs as well as phrases used to explain policy issues such as commissioning and local decision-making. In the South Gloucestershire case study, engagement methods included personal involvement of the chief executive; revisiting evidence for the proposed solution; membership for campaign groups in the PCT’s reference group; and high levels of disclosure of financial and other information to reference group members |
Based on the PCT case studies and the IRP report on lessons from reviews, the following themes were identified: consult early; target the right stakeholders; develop proposals in partnership with health-care professionals; communicate a strong narrative; be open to the evidence; demonstrate genuine involvement; make personal leadership a priority; be prepared for further dialogue with a hostile audience; and continue discussions after consultation. Findings from focus groups suggested that words/phrases that created confusion for the public included ‘budget’, ‘clinicians’, ‘competitive tendering’, ‘engagement’, ‘postcode lottery’, ‘safety’ and ‘value for money’. The public disliked phrases that suggested the PCT was abdicating responsibility; unrealistic or exaggerated examples; and comparisons between different services. The authors suggested that the findings show there is sometimes a tension between being transparent about the need for change and communicating in a way the public can relate to | Communication; language use; public perceptions; focus groups; clinical leadership; managerial leadership. Also includes ‘Key points for communicators’ |
| NHS Confederation (2013)28 (Authors state relevant to UK as a whole) |
Expert opinion report examining why reconfiguration proposals have failed in the past and how clinicians, managers and patients can work together to reframe the debate by stressing the benefits of developing new models of care. Report based on over 50 structured interviews and a series of workshops and meetings, with input from the Academy of Medical Royal Colleges, the NHS Confederation and National Voices (coalition of health and social care charities in England) NHS services affected by reconfiguration proposals Dates of interviews and workshops not reported. Report published 2013 |
Report addresses issues around reconfiguration in general, illustrated by a range of case studies providing brief details of successful and unsuccessful approaches from practice. Three types of reconfiguration featured prominently: moving care out of hospitals; centralising specialist services; and reacting to hospital trusts that are unsustainable People involved in contributing to the report included members of patient groups and charities and public representatives (MPs). Case studies give examples of involving patients/patient groups, clinicians, managers and NHS staff generally |
Stages: 1, 2, 3, 4?, 5 Levels: informing; consulting; involving; collaborating Methods in case studies include a dedicated transport group to consider access; Patient and Client Council (Northern Ireland); Marie Curie programme to redesign services for palliative care patients. Other methods and examples discussed in the text |
The authors identified six key principles to serve as a foundation for most reconfiguration plans: health care is constantly changing; there are significant benefits to delivering new models of care; reconfiguration is a catch-all term and drivers of change need to be understood to consider potential benefits; patients can coproduce better services; a ‘whole-system’ approach is essential; and change requires consistency of leadership. Recommendations for local leaders were coproduce any change with patients – do not rely on formal consultation; create a clinically driven case for change; make the case for value; provide a forum to consider access; and develop plans openly with staff. Recommendations for national leaders were also presented. The report also identified primary concerns in the following areas and suggested possible ways of addressing them: access; resources; ‘the system’; leadership; communication; and collaboration | Demonstrate need for change; clinical leadership; managerial leadership; political leadership; access to services; different types/methods of involvement; patient groups; coproduction; communication; language use |
| Thomson et al. (2008)27 Scotland |
Content and qualitative analysis of media coverage of reconfiguration of maternity services in Caithness (Scotland) and its impact on public participation in policy decision-making Rural maternity unit (Caithness General Hospital, Wick) September 2003 to December 2004 |
Change from consultant-led to midwife-led obstetric unit The public, including campaign groups; public representatives (Members of the Scottish Parliament, councillors and church leaders). Limited details in paper, as focus was on media coverage |
Stages: 1; 2; 3; 4?; 5, 6 Levels: informing; consulting Debate between proponents (Highland Health Board) and opponents of reconfiguration as portrayed by local and national media |
The authors’ thematic analysis (‘qualitative document analysis’ based on ‘ethnographic content analysis’) covered four newspapers and the BBC Scotland website. There were 145 articles covering issues around the Caithness reconfiguration, containing 173 positive and 435 negative (antichange) comments. Only the BBC news website had more positive than negative quotes (27 vs. 19). There was a general framing of the issue in terms of polarised opposition between Highland Health Board management (based in Inverness) and local people. There was a lack of information about issues underpinning change. In response to the public campaign, Highland Health Board offered several service options to the public, but they continued to demand a consultant-led service. Eventually, three consultant posts were advertised and filled but uncertainty about the future of the service remained at the end of the study | Media coverage; polarisation; public perception; conflict; maternity services; rural health services |
Appendix 5 Case studies data extraction
| Author(s) and country | Setting, date and organisation commissioning report | Type(s) of reconfiguration and who was engaged/involved | Comments |
|---|---|---|---|
| Airoldi et al. (2013)7 England (used as an exemplar) |
Sheffield PCT eating disorders service June to December 2009 N/A. The Health Foundation provided financial support to the author |
Priority-setting in eating disorder services, with emphasis on improving services in a climate of decreasing resources Patients, caregivers, clinicians, health-care managers. There were five patients/carers out of 24 in the group. Follow-up was conducted with a wider set of stakeholders (not specified) in the local health economy |
|
| Brown (2012)29 England |
NHS Foundation Trust October 2010 to February 2012 York Teaching Hospital NHS Foundation Trust (report to Monitor) |
Merger of York and Scarborough Hospital Trusts Foundation trust members and governors; general public; PCTs/CCGs; neighbouring NHS trusts; local involvement networks; MPs; overview and scrutiny committees; media; community groups/forums; hospital Leagues of Friends |
Focus on methods of communication with stakeholders, no information on impact. Links engagement with communications strategy |
| Bruce et al. (2011)30 England |
Health and social care services in Hartlepool; Bolton; Warrington (two sites); Basildon; Brandon (Suffolk); Hammersmith and Fulham; Burnley; and Clacton and Jaywick (Essex) 2004 to 2010 N/A (authors were members of Turning Point which developed the Connected Care model for integrated care) |
Redesign of services to promote integration of health and social care General public (including community researchers) and community groups |
Article focuses on barriers to implementing integrated care and partnership working, with limited details of methods/impact of community engagement |
| Carver et al. (2011)31 England |
NHS services across Hertfordshire 2007 to 2008 N/A (article written by NHS managers involved in reconfiguration and other stakeholders) |
Centralisation of inpatient and emergency services; commissioning of two local general hospitals; establishment of a county-wide network of urgent care centres Patients; the general public; community groups and other stakeholders; the NHS staff; MPs, council leaders and other local politicians; local media; health overview and scrutiny committee |
Focus on methods and indicators of successful engagement. Highlights links between engagement and communication strategies |
| Caseley (2010)32 England |
London boroughs of Bexley, Bromley, Greenwich and Lewisham Not reported N/A |
Large-scale reconfiguration involving four hospital sites and community services for more than 1 million people Stakeholder groups (including organisations working with under-represented groups); the general public (via meetings and consultation documents distributed to households, businesses, NHS and community organisations); NHS staff; other NHS organisations (neighbouring PCTs and London Ambulance Service); local authority scrutiny committees; stakeholder reference group |
Focus on methods and indicators of successful engagement. Highlights link between engagement and communication strategy |
| Clarke and Rozansky (2013)8 England |
NHS services in south-west and north-west London Not reported N/A (authors worked for OPM, an independent research organisation and consultancy involved in the reconfigurations discussed) |
Major reconfiguration proposals covering five hospitals in south-west London (Better Services, Better Value); limited details of plans in north-west London (Shaping a Healthier Future) The general public; community groups; others (not specified) |
Article mentions how plans for surgery and palliative care were modified as a result of public feedback. In north-west London additional travel analysis was undertaken to address public concerns. Authors stated that reconfiguration depends on people being prepared to travel further for better quality and safer care. People believe their own experience rather than published data, especially when complicated formulae have been used to calculate average travel times |
| Coe (2012)39 England |
NHS services in Somerset 1994 to 2003 N/A (author was research lead for Somerset health panels between 1999 and 2003) |
Panels discussed various issues related to reconfiguration, for example provision of 24-hour GP cover; confidential drug services for young people; services for elderly people; local outpatient services vs. centralised General public: members were recruited for three rounds only, by independent recruiters trained by the core research team. Recruiters visited homes at different times of the day/week to reach a wider range of potential participants |
Not a case study of specific reconfiguration but includes background on history of PPI in the NHS and compares health panels with other similar methods |
| Cohen et al. (2011)33 Canada |
Community health services in Ontario, Canada Summer 2009 to July 2010 N/A (authors were from organisations involved in the reconfiguration) |
Merger of two organisations providing community health services Clients and community members of the two organisations; corporate members; funders; Provincial Association of Ontario Health Centres and Community Health Centre network; management team and staff team; union representing staff; partner organisations; local politicians |
Limited information on methods used (surveys and focus groups), emphasis on need for ongoing engagement |
| Davies (2006)34 England |
NHS services in Liverpool November 2006 N/A |
Redesign of primary care and community-based services The public, health professionals and representatives of voluntary organisations and other stakeholders |
Article focuses mainly on an event (the Big Health Debate) organised by Liverpool PCT and involving structured discussion and voting on different options |
| Gamble and Sloss (2011)43 England (used as an exemplar) |
Urgent care/emergency department Consultation took place between September and November 2011 York Teaching Hospital NHS Foundation Trust/NHS North Yorkshire and York |
Redesign of minors care within the emergency department. To include integration of a walk-in centre (separately located at the time; engagement work on the walk-in centre does not form part of the present study); improved integration with the out-of-hours GP service; and consideration of a potential GP triage service Patients, carers, staff, hospital governors |
The approach to patient and public engagement was based on the methodology of EBD. EBD focuses on capturing and understanding experiences of services as part of service redesign. The report formed part of a paper to be presented to the local health overview and scrutiny committee |
| Gold et al. (2005)41 Canada |
Cancer services in Ontario 1999 to 2003 N/A |
Planning of regional supportive cancer care networks Patients, defined as people currently receiving cancer care or cancer survivors; representatives of patient support groups |
Main focus is barriers that hindered effective patient involvement |
| Greenwood (2007)35 England |
NHS services in Cornwall and Isles of Scilly; Calderdale and Huddersfield; and Sandwell and Birmingham Not reported N/A |
Cornwall: pre-consultation to gain information and establish trust with local communities; Calderdale: reconfiguration of maternity services; Sandwell: large-scale reconfiguration involving new acute hospital supported by five community hospitals and 95% of GP practices to be new or refurbished The public; NHS staff (including primary care managers in Calderdale and Huddersfield); local authority scrutiny committee; stakeholder and community groups (including hospital League of Friends) |
Focus on methods and indicators of successful engagement. Highlights link between engagement and communication strategies |
| Scottish Health Council (no date)42 Scotland |
NHS services affected by proposals for major service change 2005 to 2012 Reports produced by the Scottish Health Council on behalf of the Scottish Government |
Any reconfiguration deemed by the Scottish Government to involve a major service change. Latest reports (2012) involve maternity services in Grampian and service changes at Dumfries and Galloway Royal Infirmary Scottish NHS Boards are required to involve patients and local communities. Details vary among reports on the website |
Reports outline proposed service changes, details of the consultation process, whether or not it was considered adequate and any learning points to improve future public consultations |
| Mason (2002)36 England |
Acute hospital (Kidderminster Hospital) June 2002 (refers to elections in May 2002) N/A |
Restoration of emergency and acute surgery services The general public; local MP and councillors elected to represent campaign group (Health Concern) |
Emphasis on role of campaigning groups and use of electoral process to challenge or reverse decisions to downgrade local hospital services |
| Moore (2006)37 England |
NHS services in Surrey and Sussex 2006 to 2007 N/A |
Potential loss of acute services at two major district general hospitals and downgrading of three others The public (through extensive pre-consultation); clinicians and other NHS staff; local authority scrutiny committees |
Focuses on methods, including possible negative consequences of a lengthy pre-consultation in the absence of firm proposals and a staged approach to engaging different groups |
| NHS Confederation (2013)11 England |
Health services across Greater Manchester area February 2012 to March 2013 NHS Confederation/NHS Greater Manchester |
Area-wide service review to inform future reconfiguration focusing on integrated care; emergency surgery; acute emergency and urgent medicine; and women’s and children’s services The public; local media; voluntary organisations; patients/patient groups; MPs; local government; staff |
Consultation Institute engaged to provide advice and produce a report into recent reconfiguration consultations (not publicly available) |
| NHS Confederation (2013)12 England (used as an exemplar) |
Acute and emergency care Consultation started in January 2012 for 3 months, building on earlier work done in the recent past. Final proposals published in May 2012. NHS Confederation report published March 2013 NHS Confederation/Buckinghamshire and Oxfordshire PCT Cluster/Buckinghamshire Healthcare NHS Trust |
‘Better Healthcare in Bucks’: centralisation of emergency care. Providing care closer to home for most patients. Establishment of clinical centres of excellence Patients, the public, primary care and hospital-based clinicians, other health service staff, MPs, local health overview and scrutiny committee, voluntary organisations |
The engagement process was carried out by the programme team attached to those commissioning the piece of work. However, independent companies were employed to facilitate engagement workshops, collate and analyse the data, and to produce an independent report leading to preparation of a business case. ‘Better Health in Bucks’ was given an Association of Healthcare Communications and Marketing award for its consultation and engagement programme |
| NHS Confederation (2013)13 England |
Emergency services provided by Northumbria NHS Foundation Trust Unclear: report states that the process involved 3 months of engagement followed by 3 months of consultation but other statements refer to a much longer time scale. Building of the new hospital started in November 2012 NHS Confederation/Northumbria NHS Foundation Trust |
Centralisation of emergency services and construction of a new specialist emergency care hospital The public (including specifically residents close to proposed new hospital site); local GPs; MPs; overview and scrutiny committees; clinical teams |
Limited information on methods. Distinction between engagement and consultation unclear. Staged approach to engaging different groups appeared to work well (contrast with Moore 2006)37 |
| NHS England (2013)38 England |
Community pain services in Dorset Not reported; new service commenced June 2013 NHS England |
Redesign of community pain service Patients recruited via a local patient group and the Dorset Pain Society; GPs and secondary care, public health and allied health professionals also involved |
Very limited details reported |
| NHS Confederation (2013)9 England (used as an exemplar) |
Acute hospital (maternity services) 2009 to 2013 NHS Confederation/Sandwell and West Birmingham NHS Trust |
Redesign of maternity services Patients and their representatives: women and their families, GPs, local councillors and MPs, including the Joint Health Overview Scrutiny Group. Parent groups, Sure Start. Others engaged in the process: community midwives, hospital-based clinicians |
|
| NHS Confederation (2013)10 England |
NHS Foundation Trust Summer 2011 to November 2012 NHS Confederation/Southern Health NHS Foundation Trust |
Merger of Ridgeway Partnership (Oxfordshire Learning Disabilities NHS Trust) into Southern Health Service users and carers; staff; board members; clinicians; media. Ridgeway Partnership membership engagement group became a primary focus for engagement |
Case study mainly focuses on methods. Highlights issues around people with learning disabilities and around ‘takeover’ of a small NHS Trust by a larger one |
| Nicholson-Banks (2010)40 England |
NHS services in Dorset (NHS Bournemouth and Poole) May to August 2009 (launch of network) N/A (author is Patient and Public Engagement Manager for NHS Bournemouth and Poole) |
N/A (paper describes public involvement network model and process of setting up the network) The public: members were recruited through PCT Health Information Shop; Healthpoint (based in a large local library); distributing information at local events; online registration through PCT website; and a mailing campaign to 3000 local households |
Not a case study of reconfiguration. Paper describes model, including choice of five different levels of involvement. Authors report that over 100 people signed up to join the network between May and July 2009 |
| Sainsbury Centre for Mental Health (2010)44 England (used as an exemplar) |
Mental health day and vocational services 2007 to 2009 Sainsbury Centre for Mental Health |
Service redesign as part of a wider review of modernising day and vocational services for people with mental health problems Service users, commissioners, external consultants |
This report is essentially a process evaluation of service user engagement. There was no direct evaluation of impact of service user engagement on service provision |
| NHS Scarborough and Ryedale CCG (2014)45 England (used as an exemplar) |
Primary care Consultation took place from 6 January to 30 March 2014 NHS Scarborough and Ryedale CCG |
Urgent care services Patients, the public, clinicians, partner organisations (representatives from primary care, secondary care, local authority, voluntary sector), local and regional scrutiny committees, local media |
Appendix 6 Exemplar case studies data extraction
| Author(s); Stages;a Levels of involvement;Critical appraisal (perspectives, reflexivity and reporting)b | Methods | Results | Key themes |
|---|---|---|---|
| Airoldi et al. (2013)7 Stages: 1, 2, 3, 4, 5, 6, 7. Mainly 2 Levels: informing; consulting; involving; collaborating; devolving Perspectives: yes Reflexivity: yes (see discussion in paper, pp. 1164–8) Reporting: very good |
Decision conferences: working meetings attended by key stakeholders, led by an impartial facilitator. Participants assessed the value of services based on (1) cost and (2) population health benefit. Additionally: semistructured and unstructured interviews; e-mail correspondence; direct observation of workshops; use of flipchart notes and minutes of board meetings; follow-up events and interviews at 1 and 2 years after consultation. A steering group and an independent evaluator oversaw the process, in addition to input from the case study author | A business case was developed to reallocate resources based on the results of the decision conferences. The objective of the business case was to reduce the number of referrals to residential care by expanding capacity in primary care and increasing community services or outpatient services at the local hospital. The business case was approved, and authority was given to expand local and community services to provide capability to treat borderline cases without referral to residential care. The financial net effect of this change was a reduction in spending for the eating disorder service by more than 15%. Two years later, the new care model had been implemented and savings were achieved. The authors cite several success factors in overcoming resistance to change (see also key themes) | Key factors to successfully overcoming resistance to service change: (1) the collective character of deliberations, encouraging ownership of the model and its results; (2) the analysis of the whole pathway, helping to identify the opportunity cost of alternative budget allocations; (3) the presence of patients, reinforcing the need to frame the problem in terms of patient benefit; (4) the development of a model based on a theoretical framework (i.e. cost-effectiveness analysis principles), which provided a credible rationale for difficult decisions; (5) managerial leadership |
| Gamble and Sloss (2011)43 Stages: 3, 4?, 5 Levels: informing; consulting; involving; collaborating Perspectives: main focus of this report is on the patient/service user perspective Reflexivity: no Reporting: good |
Observation sessions in ED; focus group; real-time feedback (patient experience questionnaire via standpoint machine); inpatient national survey results specific to York ED. Other engagement work was proposed (no details in this report) as part of the trust’s wider communications strategy on proposals to create an urgent care centre. The proposed work included attendance at local events, presentations to specialist interest groups, and information-giving at the hospital open day | Based on the results of the engagement work, an action plan was compiled for specific low-level changes to be made in a number of areas (including car park, reception and waiting area, information and communication aspects, treatment areas, and toilets). Higher-level change was indicated (where appropriate) in the action plan between the engagement work and the wider ED redesign programme | Use of EBD as a framework to facilitate public and patient engagement. Action points and linkages to micro- and macro-level change. Link between engagement work and trust’s wider communications strategy |
| NHS Confederation (2013)12 Stages: 3, 4, 5, 6, 7 Levels: informing; consulting; involving; collaborating Perspectives: yes Reflexivity: yes Reporting: very good |
Public meetings, clinical summits, online surveys, website, video showing interviews with lead clinicians, printed materials, local media campaign, presentations and site visits. A wide-reaching communications programme (internal and external) was implemented to support the service change | Patient concerns about transport and access to services were addressed by a group (comprising council, hospital and ambulance service representatives) set up to consider issues in more depth and conduct further engagement work. Free travel on local bus networks became available, and a county-wide community transport hub was established. A core element of the engagement work was to address confusion about where patients would access treatment for particular conditions. Public meetings provided the forum for response from the programme team to help allay fears about service closure. Implementation commenced in November 2012, with the replacement of an emergency medical centre at one site with a new minor injuries unit, followed by the transfer of some inpatient medical wards, and provision of a new day unit and step-down ward. Continued dialogue with stakeholders was ongoing at the completion of the implementation stage | (1) Reach a shared understanding of the case for change across the local health economy (involving partnership between primary and secondary care); (2) start public engagement as early as possible; (3) encourage clinicians to make the case for change, focusing on improvement of services rather than cost savings; (4) hold regular face-to-face discussions with politicians and local stakeholders; (5) listen to all interest groups and accommodate their views where possible; (6) discussions about one aspect of care can provide a useful forum for a wider debate about the shape of services; (7) access to services is important, including transport issues. NB: report claims public understanding of increased travel times, but content does not appear to support this |
| NHS Confederation (2013)9 Stages: 3, 4, 5, 6, 7 Levels: informing; consulting; involving Perspectives: yes Reflexivity: yes regarding negative consequence, cultural preference for place of birth. Will be taken into account for future public consultations Reporting: good |
Online responses, public meetings, face-to-face meetings with key stakeholders, letters, articles in relevant local and national media, website updates, ‘ground-breaking events’, posters and postcards, employment of a redesign lead at the trust. Public engagement ran alongside a comprehensive staff training programme | Agreement achieved on one of three options offered, that is creation of a new midwife-led unit in Oldbury, to work alongside the newly opened colocated (with specialist care) midwifery-led unit at City Hospital. Positive impact on maternity care. Trust since achieved highest normal birth rate in the country; awards for safety and promotion of natural birth. Negative impact: unforeseen consequence of reconfiguration was that some patients preferred to give birth in the Black Country, rather than in the area where the new facilities were located | Before developing options for service redesign, set out clearly the clinical case for change. Support clinicians in leading change and in leading discussions with the public. Be open about what you intend to do, why you intend to do it and what will happen in the interim. Do not include options you will not consider. To keep people informed, ensure that that the consultation results are fed back. Expect the unexpected – alongside high-quality care and facilities, cultural factors can also exert a strong influence on choice of service location. Use new and social media to engage with younger audiences |
| Sainsbury Centre for Mental Health (2010)44 Stages: 1, 2, 3, 5 Levels: informing; consulting; involving; collaborating Perspectives: yes Reflexivity: yes. What worked well, what worked less well, future suggestions Reporting: largely good. However, it was unclear whether the three new service models were the result of the engagement/reconfiguration process or they represented the initial proposals under consideration |
A working group (comprising eight service users) was established to take part in the review of services, in response to invitation leaflets and posters distributed to local day centres. Three members of the working group joined a separate project steering group, which also included representatives from commissioners and external consultants. The group’s remit included design of the review of services; research with service users to gather views about services; contributing to decisions about service redesign; contributing to the development of service specifications and tender documents; and helping to select future providers in the tendering process | The process evaluation (involving interviews and focus groups with service user members of the working group) identified key factors for successful user involvement in future service re-commissioning. (1) Clarity of purpose: including roles and skills needed from service users; potential conflicts; expectations about support, supervision and training; arrangements for reimbursements and rewards. (2) Attention to detail: provision of background contextual information (e.g. government policy guidance) to help service users and staff in the process of service transformation. (3) Openness: between commissioners and staff about the potential implications of change and their future roles. (4) Conflict management and resolution: commissioners need to consider the impact on service users involved in the process, so that conflicts do not become a focus for hostility. The authors provided a list of specific issues leading to what worked well and what worked less well. Many service users felt positively about their involvement, in terms of impact on their personal lives and services offered. Three new service models were proposed as the basis of future day and vocational services provision, with service points available across the locality | Mental health; service user involvement |
| NHS Scarborough and Ryedale CCG (2014)45 Stages: 1, 2, 3, 4, 5 Levels: informing; consulting; involving; collaborating Perspectives: yes. Wide consultation; multistakeholder. Recognition of public concerns, for example petitions Reflexivity: yes. Several references/cross-references to contextual reflections, for example rural vs. urban differences in response; contextual sensitivities regarding Castle Health Centre Reporting: excellent. NB: not independent. This is a CCG report |
Distribution of consultation document and video; interactive workshop for clinicians and partner organisations; presentations to local and regional health scrutiny committees; surveys; public meetings; focus groups; Facebook posts | Estimated consultation reach of 200,000 people. 724 primary contacts made. Based directly on the findings of the public consultation, a number of key considerations (below) were to be taken forward to inform a service tender specification for urgent care services (to be awarded at the end of August 2014). (1) Appropriate location of services; parking and transport considerations; security; and appropriate design for a range of potential service users. (2) Inclusion of particular services; access to patient medical records, liaison with NHS 111. (3) Education: appropriate publication of information to enable decision-making about accessing urgent care. (4) Quality: patient experience to form part of urgent care service performance and quality measures; new service should maintain or build upon current quality. (5) Interim walk-in service: needed to bridge the end of the current contract to the start of the new one. Results also found that people would not be prepared to travel further for an improved service (supports Barratt et al.’s work22,23) | Wide stakeholder consultation (including consideration of methods to reach hard-to-reach populations and/or those most likely to access urgent care services, for example young people; parents of younger children; and the elderly); ability to achieve wide reach; use of extensive range of methods; importance of reflections on local context; precursor to service tender; access to services; engagement with opponents of reconfiguration |
List of abbreviations
- BBC
- British Broadcasting Corporation
- CCG
- Clinical Commissioning Group
- DARE
- Database of Abstracts of Reviews of Effects
- EPPI-Centre
- Evidence for Policy and Practice Information and Co-ordinating Centre
- GP
- general practitioner
- IRP
- Independent Reconfiguration Panel
- MP
- Member of Parliament
- PCT
- primary care trust
- PPI
- patient and public involvement