
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 12/5004/03. The contractual start date was in July 2013. The final report began editorial review in July 2014 and was accepted for publication in November 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Sanderson et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Objectives and context of the review
Objectives
The main objective of the literature review reported here is to draw out lessons from procurement and supply chain management (P&SCM) theories and from empirical evidence from a range of other sectors and countries, to assist NHS managers and clinicians in developing more effective approaches to commissioning and procurement. The review meets an expressed need in the NHS management community flowing from two primary sources.
First, the NHS is under pressure to save money through a combination of cost cutting, productivity improvements and innovation in service delivery. As we discuss in the next section of this chapter, there have been various organisational and process reforms in NHS commissioning and procurement since 1991 intended to improve cost-efficiency and cost-effectiveness (e.g. the development of national framework contracts by the NHS Purchasing and Supply Agency, creation of regional procurement hubs). Despite these reforms, a recent report from the National Audit Office1 shows that there are still significant variations and inefficiencies in current NHS procurement practice. At the same time, the NHS is under massive pressure to make its contribution to the government’s ongoing deficit reduction plans. A more efficient and effective approach to procurement, which accounts for around 30% of hospital operating costs, will play a key role in delivering these savings. 2 Procurement has also been identified as a key part of the Quality, Innovation, Productivity and Prevention initiative. 3
Second, the review is needed to assist NHS managers and clinicians in meeting the challenges thrown up by the new commissioning structures and policies introduced by the Health and Social Care Act 20124 in which general practitioners (GPs), other clinicians and managers in Clinical Commissioning Groups and in NHS England are required to exercise commercial skills and make contract award decisions in the context of wider health-care markets of which many have very limited experience and knowledge.
It is useful here to reflect briefly on the differences in NHS parlance between the terms ‘commissioning’ and ‘procurement’. ‘Commissioning’ is used to refer to the planning, acquisition, and monitoring and evaluation of health-care services. 5 As of April 2013 this is the remit of Clinical Commissioning Groups for local services and of NHS England and its area teams for specialist and GP services. One NHS usage of the term ‘procurement’ is to refer to the ‘acquisition’ aspect of this commissioning cycle, whereby NHS commissioners identify, select and contract with providers and monitor their performance in delivering these health-care services. 6 Procurement is also used in the NHS to refer to the acquisition of other goods and services [e.g. dressings, medical equipment, information technology (IT) equipment, temporary staff] needed to support health-care delivery. 2 Procurement defined in this way is undertaken both by NHS commissioning organisations and by NHS health-care providers.
Thus, the common feature of procurement as it is commonly understood in the NHS is a focus on the ‘acquisition’ of goods and services. Service planning, or assessing needs and specifying how and when those needs might be met, is not typically seen as an aspect of the procurement process, particularly as it relates to the commissioning cycle. The suggestion that underpins this review, however, is that the NHS definition of procurement is perhaps too narrow. It is our intention to show that it is unhelpful to see needs assessment and the specification of priorities and requirements as separate, non-procurement activities in the commissioning cycle, because effective procurement practice should begin with a clear statement of what an organisation needs or wants to buy. 7 We do acknowledge that even if one accepts our broader definition of procurement it is not entirely synonymous with NHS commissioning, but suggest nonetheless that there is a more significant overlap than is typically understood in the NHS, which allows us to draw out lessons for the commissioning cycle from the P&SCM literature. The review will, therefore, provide a vital source of knowledge and guidance to GPs, other clinicians and NHS managers responsible for commissioning as the reforms are implemented over the coming years.
The four objectives of this literature review and synthesis are as follows:
Objective 1: To explore the main strands of the literature about P&SCM (e.g. in institutional and production economics, operations management, organisation theory, the resource-based view of strategy, business-to-business marketing, public management) and to identify the main theoretical and conceptual frameworks which relate to decisions about, and the effective management of, providers or suppliers of goods and services.
Objective 2: To understand to what extent existing evidence on the experiences of NHS managers and clinicians involved in commissioning and procurement matches these theories and to provide an explanatory framework for understanding the characteristics of effective policy and practice in the NHS.
Objective 3: To assess the empirical evidence about how different P&SCM practices and techniques can contribute to better procurement processes and outcomes.
Objective 4: To map and evaluate different approaches to improving P&SCM practice, including modelling, diagnostic and facilitation tools, and identify how these approaches relate to theories about effective P&SCM.
Context of the review
In order to set the scene for the rest of the review, the remainder of this first chapter presents a summary of the main policy changes that have shaped commissioning and procurement in the English NHS since 1991. The broad policy context of NHS commissioning and procurement has been defined by the European Union (EU) public procurement rules, which were first introduced in 1993 as part of the Single European Market programme. Since then these rules have been subject to successive waves of reform, broadly intended to achieve simplification and a lightening of the regulatory burden. 8 The detail of how the rules are applied differs for the commissioning of health-care services, where the requirements are less onerous, as compared with the procurement of clinical and non-clinical goods and services. Nevertheless, all NHS commissioning and procurement decisions are expected to conform to the fundamental principles of the rules, namely transparency and non-discrimination in dealings with providers or suppliers.
The organisational and structural context of English NHS commissioning and procurement at the time of writing is a result of periodic restructuring and reform over more than 20 years, since the purchaser–provider split was first created in April 1991. 9 This restructuring and reform is characterised to some extent by continuity, in the sense that each successive wave of reform has retained and built on aspects of what went before. This has led to the coexistence of several different, sometimes competing, forms of organisation and governance, what Exworthy et al. 10 call quasi-hierarchy, quasi-market and quasi-network. Each wave of reform has also, however, made some important changes to the organisational ecology and to the distribution of authority over and accountability for the non-pay expenditure of the NHS. This blend of change and continuity can be illustrated if we consider snapshots of the organisational settlement at four points in time, which show the outcomes of significant policy reforms. Each successive snapshot also reveals an increasingly complex set of organisational arrangements. The first, in Figure 1, shows the results of reforms made between 1991 and 1997.
FIGURE 1.
Structure and organisation of NHS commissioning and procurement circa 1997. TPP, Total Purchasing Pilot.
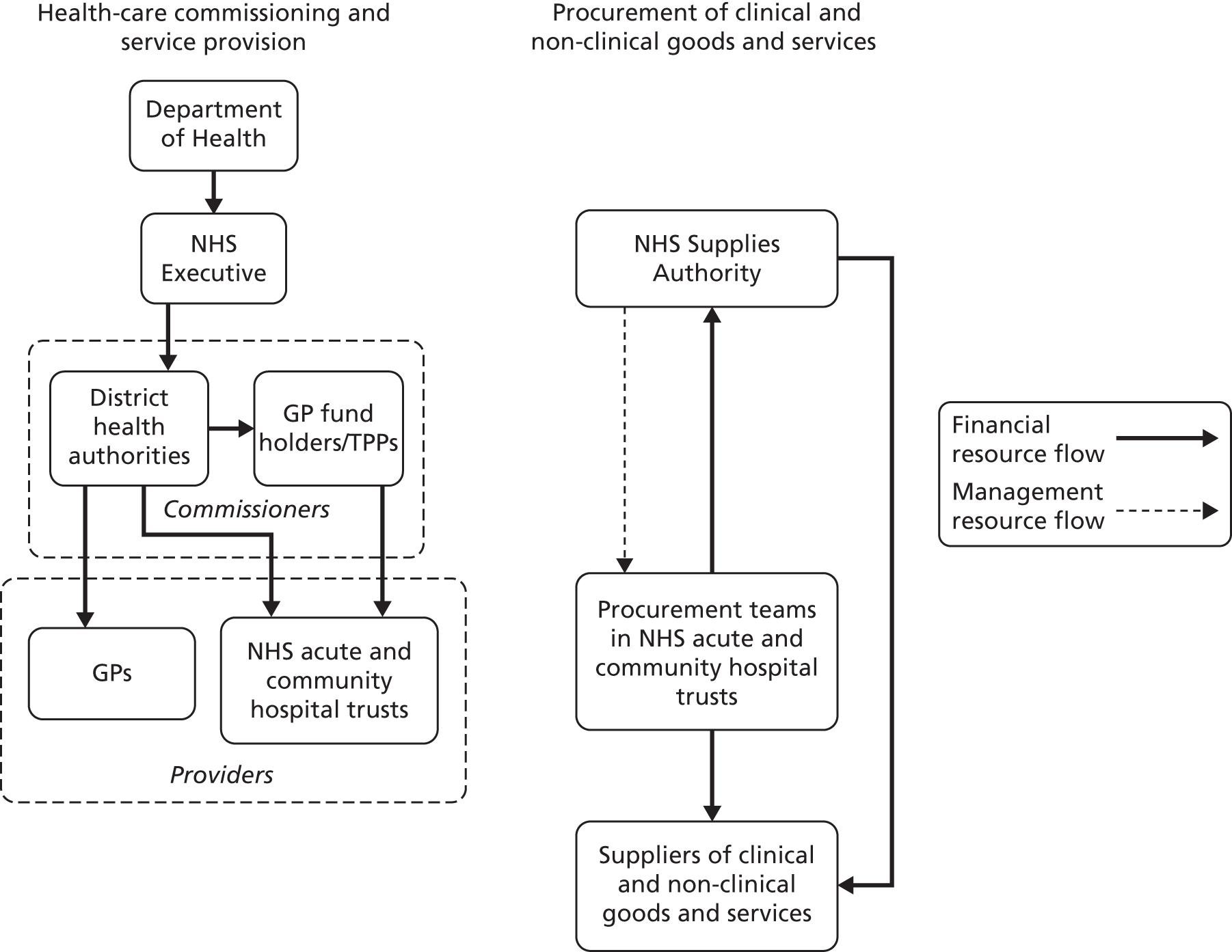
In 1997 two main sets of actors were responsible for NHS health-care commissioning: the district health authorities and GPs acting as fund-holders. This plurality in NHS commissioning arrangements had been established as a key component of the purchaser–provider split in April 1991, with GP fund-holding seen as a way of encouraging service providers to be more responsive to the needs of particular groups of patients. While district health authorities were deemed to have sufficient purchasing power, at least in theory, to extract performance improvements from service providers, they were seen as relatively unresponsive to differing local needs. 11 District health authorities commissioned primary (GP) and secondary (NHS hospital trust) health-care services for a geographically defined population. They negotiated annual block or cost and volume contracts with NHS hospital trusts, based on historical data, for the provision of specified numbers and types of clinical interventions. In principle, hospital trusts in different areas were supposed to compete with one another for these district health authority contracts,12 but in reality most trusts maintained the long-standing relationships with their local health authority that had been in place under the unitary, pre-1991, system.
Commissioning through the GP fund-holding route operated either on the basis of single practices or through co-operative arrangements known as Total Purchasing Pilots. These Total Purchasing Pilots, which had evolved from less formal networks known as multifunds, were designed to give GPs greater purchasing power in their dealings with the financially much larger NHS hospital trusts. They also helped address the lack of co-ordination and higher agency or transaction costs (costs of negotiating, drafting and monitoring contracts) associated with individual GP fund-holding practices. 13 Each Total Purchasing Pilot commissioned on behalf of a population of about 300,000 people, similar to that served by a typical district health authority. By 1997, commissioning through the variants of GP fund-holding accounted for around 10% of the secondary health-care services budget. 14
Turning to the procurement of clinical and non-clinical goods and services, in 1997 this was organised and managed by a combination of the NHS Supplies Authority (NHS Supplies), operating at the national level, and procurement teams based in each NHS trust. NHS Supplies was set up in 1991 to address inefficiencies arising from fragmented procurement and unco-ordinated supply routes that had been identified by the National Audit Office. It initially had a regional structure, with six divisions buying on behalf of trusts in their respective geographical areas and providing a logistics service. In 1995, this regional structure was replaced by a national one. NHS Supplies continued to provide a logistics service, but its remit was extended to provide a national contracting function, which operated through a combination of procurement consultancy advice and framework agreements for use by trusts. A direct customer service function, which managed trust-based procurement teams, was also introduced. A major challenge to the efficacy of NHS Supplies, however, was that NHS trusts were not required to use its services. NHS Supplies competed with other logistics providers and buying agencies to sell its services to trusts; it received no central funding from the Department of Health. Trusts were also free to directly employ and manage their own procurement team, who could select and contract with suppliers without any reference to practice elsewhere in the NHS. 15 It is unsurprising then that, 5 years after the creation of NHS Supplies, the Audit Commission produced a report showing that there were still huge variations in the prices and service levels of suppliers selling the same items to different trusts. 16
Following the election of the New Labour government in 1997 there were a number of further reforms in the structure and organisation of NHS commissioning and procurement, which meant that by 2001 the picture was markedly different (Figure 2).
FIGURE 2.
Structure and organisation of NHS commissioning and procurement circa 2001.

On the health-care commissioning side, Labour replaced the market-style relations of the GP fund-holding model with what was intended to be a more collaborative system of longer-term service delivery agreements. Under GP fund-holding, practices had real budgets, which they could spend without consulting other practices in their area; this was replaced with a system of indicative budgets. While GP fund-holding arrangements had been voluntary, all GPs were now expected to work in a more co-ordinated way by being required to join a primary care group in their area. Each primary care group was also required to include nurse and local authority representatives to further enhance the scope for collaborative working. 17 By 2001, 481 primary care groups had evolved into 303 primary care trusts, which replaced district health authorities as the lead NHS organisations responsible for health-care commissioning. 18 Primary care trusts also replaced NHS community hospital trusts as providers of community health services such as district nursing and some mental health services. Most mental health services continued, though, to be provided by mental health trusts. Positioned above the primary care trusts, at a regional level, were 28 Strategic Health Authorities. These were responsible for performance management, ensuring that national NHS priorities were integrated into local plans, and the commissioning of some specialist services from NHS acute trusts.
By 2001 there had also been some significant changes in the organisations responsible for procurement of clinical and non-clinical goods and services. Most significant was the replacement of NHS Supplies in 2000 by two separate organisations, the NHS Purchasing and Supply Agency and the NHS Logistics Authority (NHS Logistics), each of which took on some of the functions of NHS Supplies. The Purchasing and Supply Agency was responsible for the national contracting function (consultancy advice to trusts and framework agreements), but it also had a much wider remit to act as the NHS’s centre of excellence on procurement and supply management and to improve procurement performance across all levels of the NHS in England. 19 Unlike NHS Supplies, the Purchasing and Supply Agency was a part of the Department of Health and received central funding, which gave it a much more stable platform from which to carry out its wider policy and practice development remit. NHS Logistics retained the procurement and distribution functions of NHS Supplies, and like its predecessor it was a special health authority funded by charging NHS trusts to use its services. The direct customer service function of NHS Supplies had disappeared, however. All trust-based procurement practitioners were now directly employed and managed by their trust. In addition to this restructuring at the national level, the Purchasing and Supply Agency formally recognised the need for a mechanism to co-ordinate procurement at a regional level by introducing NHS supply management confederations. These were voluntary, virtual organisations without a prescribed structure or dedicated funding. 15 Each confederation was intended to bring together all NHS hospital trusts and primary care trusts within the boundaries of a Strategic Health Authority so that they could procure commonly used goods and services in a more co-ordinated manner. As before, however, NHS hospital trusts remained free if they chose to procure their goods and services directly from suppliers without reference to contracts being agreed by other NHS organisations.
A number of further changes in the structure and organisation of NHS commissioning and procurement over the next 5 or 6 years brings us to the situation in 2007 (Figure 3).
FIGURE 3.
Structure and organisation of NHS commissioning and procurement circa 2007.
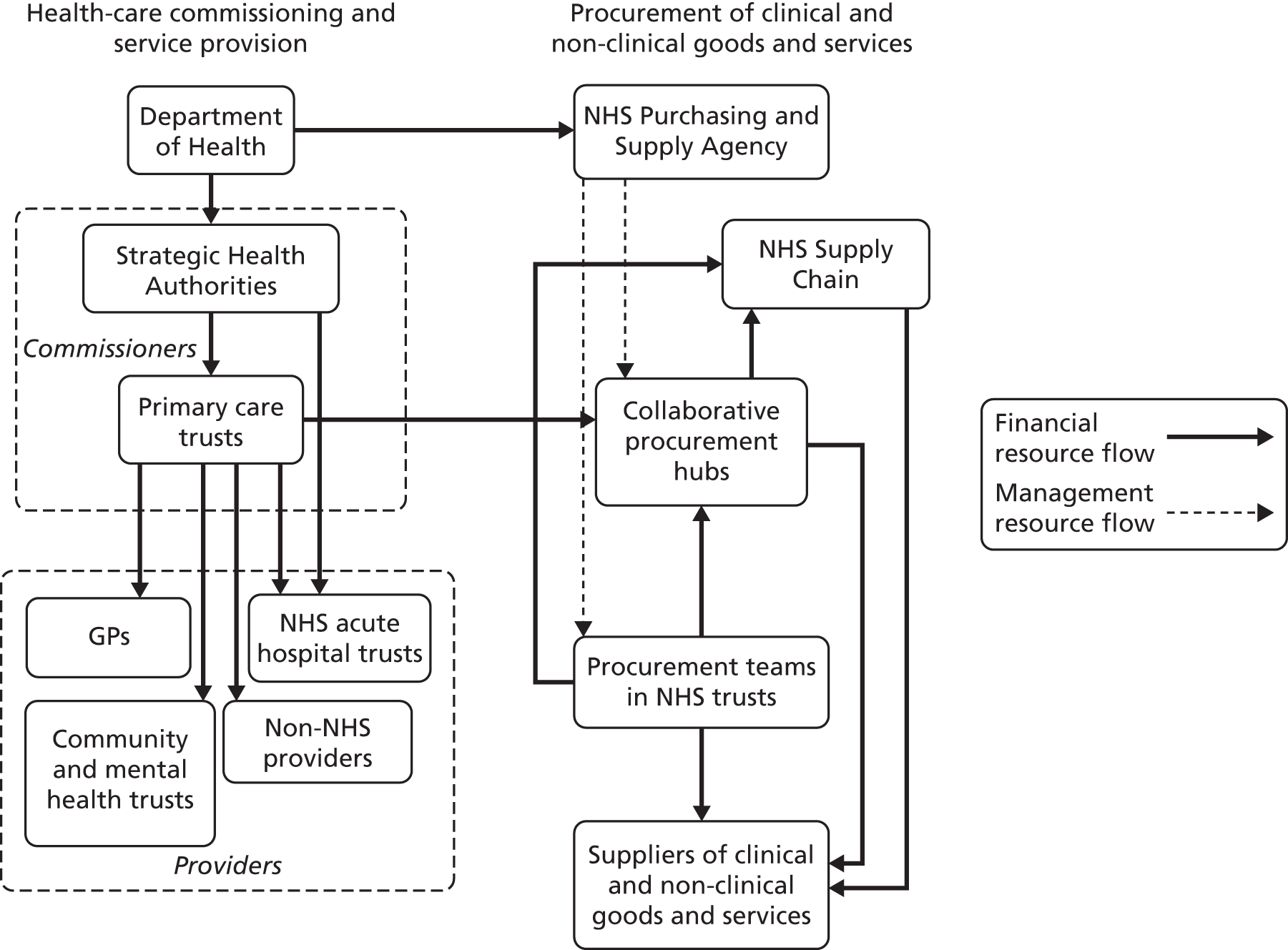
On the commissioning side, a policy of practice-based commissioning designed to encourage greater GP involvement and collaborative working between practices was introduced in 2005. This was to some extent a return to the principles of GP fund-holding and Total Purchasing Pilots, but the important difference was that primary care trusts gave GPs only virtual ‘indicative’ budgets to commission health-care services. Accountability for and authority over the actual spending was retained by the primary care trusts. 20 In 2006 the number of Strategic Health Authorities was reduced through amalgamation from 28 to 10, but they retained the same role of performance-managing the primary care trusts and ensuring that national priorities were embedded in local strategies. The number of primary care trusts was also reduced through a process of amalgamation from 303 to 152. This was a response to the argument that they had not been powerful enough in financial and management resource terms to commission effectively, to ‘insist on quality and challenge the inefficiencies of providers’ (p. 3). 21 Finally, under the Transforming Community Services programme primary care trusts were required to formally separate their community health service provider functions from their commissioning function. 22 Community health services were taken on by a range of different providers in the NHS and in the third and private sectors.
Alongside this restructuring of primary care trusts, there were a number of other initiatives designed to improve the quality and cost-effectiveness of commissioning. These included the World Class Commissioning initiative introduced in 2007, which involved the evaluation of primary care trust commissioning performance against a set of 10 competencies to identify areas for improvement. 23 One possible solution to weaknesses in any of these competencies was proposed in the Framework for Procuring External Support for Commissioners, which showed primary care trusts how to buy in private sector commissioning support. 24 Commissioners were also given a number of new mechanisms designed to influence the behaviour and performance of providers, under the broad umbrella of the payment-by-results policy. Payment by results replaced the traditional block or cost and volume contracts used in the NHS with a system under which providers were paid a fixed tariff for each episode of a particular type of care. This was intended to encourage providers to reduce their costs to below the tariff level and to increase patient throughput, thereby reducing waiting times. Payment-by-results tariffs were introduced for all elective secondary care from 2005 (representing about 30% of activity); outpatient, non-elective and accident and emergency services were covered by tariffs from 2006; and by 2008 the payment-by-results system covered ‘90% of significant inpatient, day-case and outpatient activity’ (p. 12). 25 An associated reform introduced from 2004 meant that better-performing NHS trusts were given foundation trust status. Foundation trusts had greater autonomy from and less accountability to the central NHS, which crucially allowed them to act in a more business-like way in pursuit of lower costs. 26
Aligned with this was the Commissioning for Quality and Innovation scheme, under which up to 2.5% of the value of provider contracts was linked to compliance with stipulated quality standards. 27 There was also an effort to put providers under some competitive pressure to perform through the ‘Patient Choice’ policy. 22 This gave patients the right, with the support of their GP, to choose their provider for elective secondary care. A similar policy agenda was being developed at this time in social care through the vehicle of personal health budgets. These enabled individuals to commission their own social care services rather than being reliant on their local authority. The ‘personalisation’ agenda is beyond the scope of this review, as we focus on health-care commissioning and procurement, but for a useful discussion see Needham. 28 Patients making these choices were expected to have access to a range of performance data, and consequently commissioning decisions were intended to be a driver for greater responsiveness and cost-effectiveness from providers. 29 The choices available to commissioners were also extended through a policy of ‘Any Willing Provider’, which allowed private sector providers to offer elective secondary care at NHS tariff prices as long as they were able to meet NHS quality standards. Efforts to stimulate a growth in the private provider market came from the Commercial Directorate of the Department of Health, which offered contracts for the setting up of independent sector treatment centres to carry out this elective treatment. One estimate suggested that by 2008 around 15% of NHS elective procedures would be delivered by the private sector,30 but in practice contestability on the provider side was tempered by a policy announced in 2009 that NHS organisations would be ‘preferred providers’ assuming they were delivering satisfactory services (p. 10). 21
On the procurement side, the structure in 2007 was broadly similar to that in 2001. Two important changes had taken place in the intervening years, however. First, the functions of the NHS Logistics Authority and parts of the Purchasing and Supply Agency were outsourced in 2006 to a private sector supplier. A 10-year contract was awarded to DHL, which made a commitment to deliver innovation through significant IT investments and cost savings in excess of £1B. Following this outsourcing, NHS Logistics changed its name to NHS Supply Chain. Second, under the auspices of the Supply Chain Excellence Programme launched in 2003 by the Commercial Directorate of the Department of Health, the Purchasing and Supply Agency established a number of collaborative procurement hubs at regional level. These took the place of the virtual and variously configured NHS supply management confederations. The hubs were relatively homogeneous organisational structures, with their own management and financial resources, designed to undertake co-ordinated procurement on behalf of their member trusts. As before, however, NHS trusts also retained the freedom to procure their goods and services directly from suppliers.
Finally, we turn to the situation in 2014 (Figure 4). On the commissioning side the picture looks significantly different from that in 2007, although there are echoes of previous organisational arrangements designed to get GPs more involved, in particular GP fund-holding and Total Purchasing Pilots. Following the passage of the coalition government’s Health and Social Care Act,4 the 152 primary care trusts and 10 Strategic Health Authorities were replaced in April 2013 by 211 Clinical Commissioning Groups and by NHS England, which comprises 27 area teams. Clinical Commissioning Groups are mandatory membership organisations of all the GPs serving a geographically defined resident population. They must also involve clinicians other than GPs in their governing body, but the legal requirements here are minimal (one nurse and one secondary care clinician in each Clinical Commissioning Group). The division of commissioning responsibilities between the Clinical Commissioning Groups and NHS England has been redistributed to recognise that the former are essentially led by GPs. So, the area teams of NHS England are responsible for commissioning GP as well as specialist services in their regions. They also hold the Clinical Commissioning Groups to account and provide them with developmental support, an echo of the role played by the Strategic Health Authorities. The Clinical Commissioning Groups are responsible for commissioning secondary care, community health and mental health services from NHS and non-NHS providers under the ‘Any Qualified Provider’ policy. To further add to the organisational complexity, the task of public health commissioning previously managed by the primary care trusts has been transferred to the 152 English local authorities. These, in turn, have established health and well-being boards as a forum for strategic co-ordination and to enhance the accountability of Clinical Commissioning Groups to their local population. 31
FIGURE 4.
Structure and organisation of NHS commissioning and procurement circa 2014.
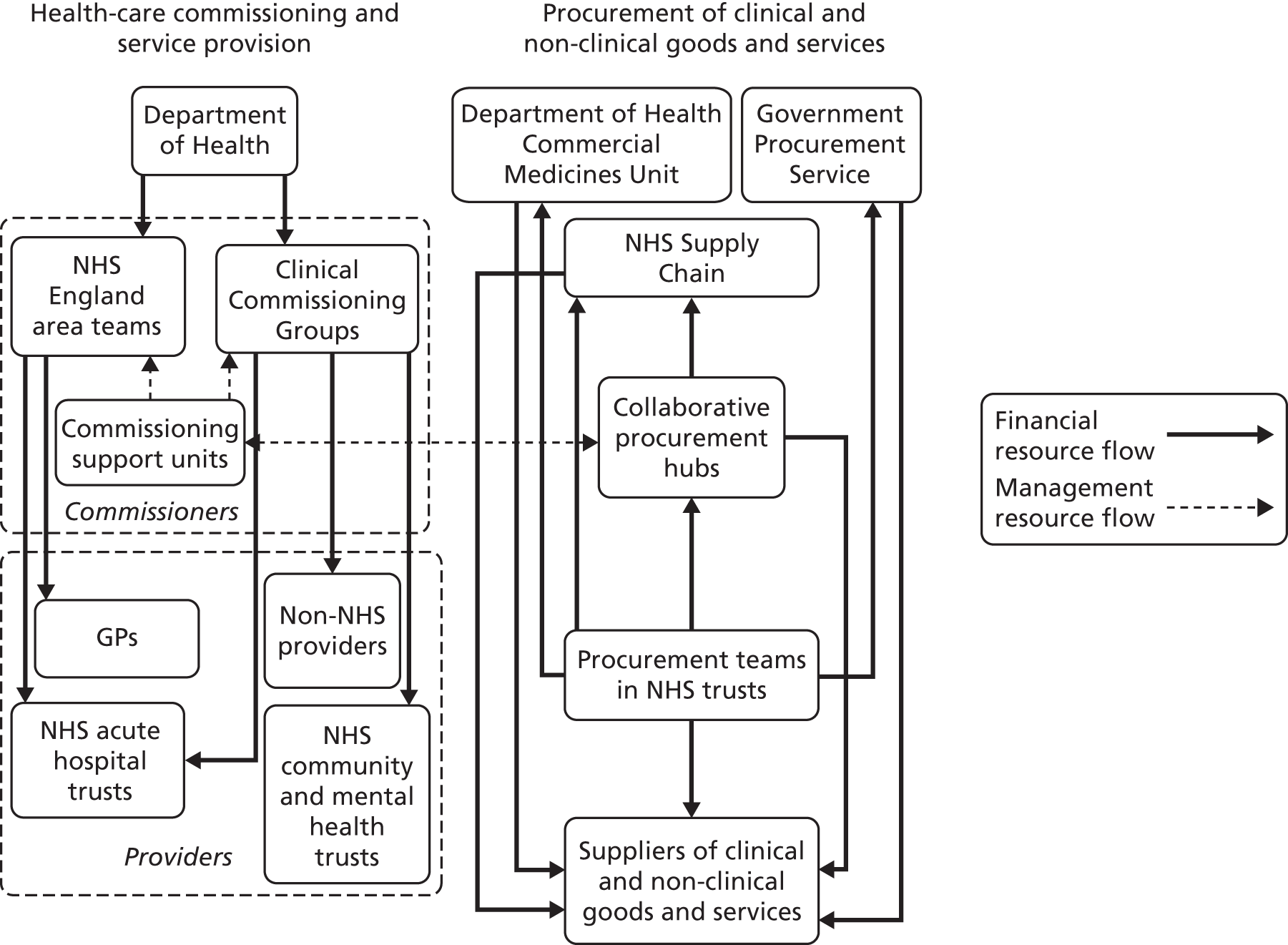
The relationship between clinicians and non-clinical managers looks very different under the new model of commissioning from that under previous commissioning arrangements. The previous relationship, based on a managerial hierarchy, has been replaced by one with a more commercial and contractual edge. A separate group of 19 commissioning support units, staffed by non-clinical managers, has been created to give procurement and contract management support to the Clinical Commissioning Groups. The commissioning support units do not have managerial authority over, or legal accountability for, the commissioning decisions made by the Clinical Commissioning Groups. The Clinical Commissioning Groups are ‘autonomous organisations exposed to full financial risk’ (p. 9)31 and are free to contract with the commissioning support units or to make other arrangements for commissioning support, for instance with private sector service providers. Under previous arrangements, ultimate managerial authority and ‘legal accountability remained with a managerially-led structure sitting above the clinical group’ (p. 9). 31 These were the district health authorities in the case of GP fund-holders and Total Purchasing Pilots or the primary care trusts in the case of practice-based commissioning.
There have also been some significant changes since 2007 on the procurement side of the picture. Perhaps the most significant change was the abolition of the Purchasing and Supply Agency in 2010, which means there is currently no organisation fulfilling its policy role as a national centre of excellence dedicated to improving procurement and supply management practice across the NHS. There has recently been recognition that this was an important and necessary role, and there are plans to create a new Centre of Procurement Development in the Department of Health which will mirror much of what the Purchasing and Supply Agency was previously doing. 32 On the operational procurement side, the Purchasing and Supply Agency’s responsibility for national drugs contracts has been transferred to the Department of Health Commercial Medicines Unit, and its responsibility for negotiating national framework agreements for categories such as energy, telecoms and IT services has been transferred to the Government Procurement Service, which works across all central government departments.
In some areas, though, the picture remains relatively unchanged. NHS Supply Chain is still operating on an outsourced basis under the terms of the 10-year contract agreed with DHL in 2006. Nine collaborative procurement hubs are still operating at a regional level. In some cases these hubs have merged with coterminous commissioning support units, which is a potentially very significant development because those working in the hubs will bring their commercially honed procurement and contract management skills to bear on the commissioning of health care. Finally, NHS hospital trusts remain absolutely free to procure their own goods and services directly from suppliers without reference to contracts being agreed by other organisations such as NHS Supply Chain and the collaborative procurement hubs. Consequently, as was recognised in the recently published Procurement Development Programme for the NHS,32 there are still significant variations in the products being used, the prices being paid and the service levels being received by different trusts.
Round-up
Having established the broad policy context of commissioning and procurement in the English NHS, we turn in the next chapter to a discussion of the approach, focus and method that we have adopted in our review of the P&SCM literature.
Chapter 2 Approach, focus and method
Approach
The approach that we have taken in this study is a theory-based realist review. We chose this route on the basis of our judgement that what constitutes an effective approach to P&SCM is likely to be highly context dependent. We begin by scoping the range of theories and conceptual frameworks used to describe and explain various aspects of P&SCM practice, including a discussion of underlying assumptions about units of analysis, actor behaviour and intended outcomes. We then examine the literature about NHS commissioning/procurement policy and practice to see to what extent the various P&SCM theories provide an insight into what is intended and what happens in this specific context. Next, we examine and assess the empirical evidence about the effect of different P&SCM practices and techniques on procurement processes and outcomes in different sectors and organisational contexts. We end by mapping and evaluating approaches to improving P&SCM practice, drawing on the logic of portfolio analysis to examine the importance of context. Our conclusions offer the basis of an explanatory framework for understanding the characteristics of effective P&SCM practice in the different contexts and types of NHS organisations.
The study is an evidence synthesis of a diverse theoretical and empirical literature on P&SCM. We draw on material from a variety of different disciplines, sectors and countries to identify lessons for more cost-effective policy and practice in the NHS. The research terrain is characterised by considerable complexity in terms of the multiple sources of evidence across different disciplinary traditions, by weakness and ambiguity in terms of association and causation, and by the influence of contextual factors on the appropriateness, effectiveness and outcomes of different P&SCM practices and techniques. Given these characteristics, a conventional systematic review, with its emphasis on a hierarchy of evidence and randomised controlled trials as the chosen research design to address questions of effectiveness, would not be appropriate. Indeed, a traditional literature review would almost certainly be unable to take account of the multiple and interconnected variables that have an impact on the effectiveness of P&SCM practices and techniques.
A realist review approach, on the other hand, emphasises the contingent nature of the evidence and addresses questions about what works in which settings, for whom, in what circumstances and why. Realist review has a ‘generative model of causality’, which argues that ‘to infer a causal outcome (O) between two events, one needs to understand the underlying mechanism (M) that connects them and the context (C) in which the relationship occurs’ (pp. 21–2). 33 A realist review can also be used to generate a theory map exposing the differences between programme theories and theories in use. The purpose is to ‘articulate programme theories and then interrogate existing evidence to find out whether and where these theories are pertinent and productive’ (p. 74). 34 This is appropriate given that a key aim of this study is to illuminate differences between how P&SCM might be carried out and current NHS policy and practice. The value of realist review and evaluation is exemplified by a number of studies of commissioning strategies in the NHS. 35–37 We therefore chose to use this as our overarching research design. Denyer et al. 38 and Jagosh et al. 39 provide a useful discussion of the key terms used in realist review. Box 1 contains a summary.
An implicit or explicit explanatory theory that can be used to evaluate programmes of action or specific interventions. A theory is middle-range if it can be tested with empirical evidence and does not deal with more abstract social, economic or cultural forces (as does a grand theory such as Marxism).
Context–mechanism–outcome (CMO) configurationsCMO configurations are used to generate causal explanations associated with the empirical evidence. The process draws out and reflects on the relationship between context, mechanism and outcome either in a whole programme of action or in specific aspects/interventions. Drawing out CMO configurations is a basis for generating and/or refining the middle-range theory that represents the final product of a realist review.
ContextThe surrounding factors, the external and internal environment and the characteristics of actors, which influence behavioural change. Programmes of action or interventions are always embedded in a particular context. Factors include the experience and competency of individual actors, the cultural norms or history of a community in which a programme or intervention is implemented, the nature and scope of existing social networks, and the geographical location. Context can be understood as any factor that shapes the behaviour of a mechanism triggered by an intervention.
MechanismThe generative force that leads to outcomes. It typically represents the reasoning of one or more actors in response to the programme of action or the intervention with which they are faced. Mechanisms are about how actors interpret, make sense of and respond to the incentives or resources associated with a programme or intervention. Identifying mechanisms allows realist review to go beyond describing ‘what happened’ (the outcome) to explaining ‘why it happened, for whom and under what circumstances’.
OutcomeThe results of a programme of action or an intervention, which can be intended or unintended, proximal, intermediate or final. Examples of outcomes resulting from P&SCM interventions are supplier/provider cost reduction and improved quality and responsiveness.
Realist synthesis belongs to the family of theory-driven review. It begins with knowledge and theory and ends with more refined knowledge and theory, in the process ‘stalking and sifting’ ideas and empirical evidence. 33 In this research, the synthesis addresses questions in particular about how P&SCM practices (interventions) are carried out, how and why these practices are influenced by context and circumstances, the impact of these practices on procurement outcomes, and the appropriateness and effectiveness of approaches to improving P&SCM. The focus is, therefore, very much on the mechanisms within these practices rather than on the practices per se. Realist review learns from, rather than controls for, real-world phenomena. Our study thereby acknowledges that no two procurement processes are exactly the same in terms of the context or the actors involved.
The limitation of realist synthesis is that it is a relatively new method, still in development and with a relatively small number of exemplar studies. 33 Nevertheless, in 2011–13 there was an effort to propose and codify a set of quality and publication standards for realist synthesis through the Realist And Meta-narrative Evidence Syntheses: Evolving Standards (RAMESES) study. 40,41 These standards represent an important development in establishing realist synthesis as a coherent, consistent and robust review methodology. Moreover, based on the reviews and literature published to date, it is an approach that seems to address the limitations of traditional systematic review methods when dealing with complex social interventions across different circumstances, using a range of mechanisms, and with varying underlying beliefs and assumptions. 38,42,43 Realist synthesis is focused on offering explanations (what is) rather than making normative judgements (what should be), and on developing principles and guidance rather than making rules. Pawson et al. (p. 24)33 comment that ‘realist review delivers illumination rather than generalisable truths and contextual fine-tuning rather than standardisation.’
Gough et al. 44 support this message in their comparison of different types of systematic review. They note that realist synthesis is both configurative, in that it begins by clarifying the nature of the theory or theories that might explain a specific programme of action or a particular intervention, and aggregative, in that it gathers a body of evidence to test those theories. In addition, unlike standard systematic reviews, realist synthesis considers empirical evidence from a broad range of sources and ‘will assess its value in terms of its contribution rather than according to some pre-set criteria’ (p. 6). 44 For the purpose of this evidence synthesis, we believe that this is the most appropriate approach to take. It will offer insights for managers and clinicians to take note of and make use of in enhancing their P&SCM practice. This judgement is further reinforced by Popay’s45 analysis of alternative approaches to systematic review, summarised in Table 1, which underlines that only realist synthesis focuses on mechanisms rather than whole programmes. In our case, this allowed us to focus on particular discrete aspects of the procurement process (specification of requirement, provider selection and evaluation, contract drafting and negotiation, contract and relationship management and so on) rather than having to consider P&SCM practice as the overall unit of analysis.
| Approach | Unit of analysis | Focus of observation | End product | Application |
|---|---|---|---|---|
| Meta-analysis | Programme | Effect sizes | Relative power of like programmes | Whole programme application |
| Narrative review | Programme | Holistic comparison | Recipes for successful programmes | Whole or majority replication |
| Realist synthesis | Mechanisms | Mixed fortunes of programmes in different settings | Theory to determine best application | Mindful employment of appropriate mechanisms |
One of the principles of realist synthesis is the importance of sense-making. The metanarrative mapping approach to synthesising evidence is attractive, because it acknowledges different disciplinary traditions and changes to dominant narratives over time. This approach has been used, for example, to reveal changing paradigms across different disciplines in relation to studies about the diffusion of innovations. 46 P&SCM is also a good example of an area of practice where the dominant narrative has shifted over time, from the highly technical and rational discourse of production economics to a more hybridised one in which, among others, issues of power, politics and bounded rationality from various branches of organisation theory are now playing a much greater role. We therefore use a metanarrative mapping exercise within the realist framework specifically to address our first research question (RQ), which is to identify and explain the emergence of different theories about P&SCM practice.
It is important to emphasise here that in recognition of the very diverse theoretical and empirical literature about P&SCM we consciously draw on evidence from a broad range of peer-reviewed journals, books and policy documents. This does not mean, however, that our search strategy is comprehensive or exhaustive. Rather we use purposive sampling to focus on literature that helps us to address the context–mechanism–outcome (CMO) configurations that drive the review. In realist review, the relevance and rigour of the literature is primarily judged not by its academic provenance but by the light it sheds on the particular CMO configuration under consideration. 33,44
A key test for studies funded by the National Institute for Health Research’s (NIHR’s) Health Services and Delivery Research (HSDR) programme is that the RQs and subsequent research findings are relevant to and useful for the target audience, those responsible for the organisation and delivery of health-care services. Similarly, realist review emphasises the need for theorising to be highly practical, with practitioners helping to shape the investigation of what works, in which circumstances, how and why. 47 In accordance with the principles of realist review, therefore, we saw our RQs as provisional and we discussed, refined and amplified these with an expert advisory and stakeholder group composed of 16 people. This had four representatives of the target audience of NHS managers and clinicians, including a senior manager from a commissioning support unit, the Head of Contracting and Procurement from a Clinical Commissioning Group, a GP and chairperson of the NHS Alliance, and a commissioner of social care services for a local authority. To provide a broader perspective the advisory group also had eight academic researchers and consultants with an active interest in P&SCM, two non-NHS procurement practitioners, the chief executive of a third sector provider of NHS services representing service users/patients, and a representative of the UK Chartered Institute of Procurement and Supply (the professional body for procurement managers).
We convened this group on a face-to-face basis in Birmingham in month 3 of the study, and ran a facilitated workshop to elicit and discuss programme theories about different approaches to P&SCM and to explore and amplify the RQs. One outcome of the workshop was a list of additional questions of interest to the advisory group, which are listed in the next section. We held one further face-to-face meeting of the group in month 6 of the study to seek their feedback on some of the early findings. Further provisional findings and a draft of the final report were shared electronically with the group, and feedback comments were received. This embeds the linkage between practitioner and researcher communities, which is advocated as a key feature of realist synthesis and helps to translate findings from research into practice. 48
Focus of the review
According to Pawson et al. 33 there are five key steps in a realist review. These are, first, clarifying the scope, second, searching for evidence, third, appraising the literature and extracting the data, fourth, synthesising the evidence and drawing conclusions and, fifth, disseminating the conclusions and implementing recommendations with practitioners and policy-makers. The quality and publication standards developed by the RAMESES study40,41 have added further depth and detail to each of these steps. Our study adheres broadly to this guidance on the realist synthesis approach rather than following it to the letter. So, while we identify a range of alternative theories relevant to the P&SCM process and test their explanatory value in terms of CMO configurations at various stages of the process, we stop short of generating new theory on the basis of this testing. Our broad approach to realist synthesis is justified by complexity and breadth of the research topic. We are looking at aspects of the broad P&SCM process rather than at a specific policy programme or interventions within a programme.
This chapter begins to clarify the scope of our study by identifying the RQs and discussing the purpose of the review. Chapter 3 completes the scoping by articulating the main P&SCM theories to be explored and by using them to create a realist synthesis framework for evaluating the evidence. Chapters 4, 5, 6 and 7 focus on the appraisal and synthesis of the evidence, and Chapter 8 draws conclusions.
We used the four research objectives described in Chapter 1 to generate four concomitant RQs. These are presented below. Guided by the realist approach to clarifying the scope of the study, these questions were treated as provisional and they were refined and amplified through discussion with the advisory and stakeholder group. This discussion generated a number of additional questions of interest, also presented below. The study did not explicitly seek to address these additional questions, but rather used them as points of reference during the review.
RQ1: What are the main disciplinary sources of ideas about P&SCM and what are the principal theories, conceptual frameworks and main paradigms?
RQ2: How can theories about P&SCM in general help NHS managers and clinicians in their commissioning and procurement activities, in particular in the light of recent and planned changes to commissioning structures, incentives and processes in the NHS?
Additional questions of interest to members of the advisory group:
-
How does/can the NHS use incentives in commissioning and procurement?
-
How does/can the NHS deliver on contractual obligations? How can NHS managers and clinicians ensure that third party contractual obligations are delivered?
-
How do different sets or layers of rules or guidelines in the NHS affect commissioning activities? What are the differences from private sector practice?
-
How should NHS managers and clinicians commission services for different client groups?
-
How does commissioning differ across different services within the health sector? What is the significance and impact of commissioning from different types of providers (private, third sector)?
-
What is the impact on NHS commissioning of variations in demand between/within health localities?
-
How does commissioning for health vary in different institutional contexts within the UK?
RQ3: What is the empirical evidence about the impact of different P&SCM practices and techniques on outcomes at different stages of the procurement process and in different settings and organisational contexts?
Additional questions of interest to members of the advisory group:
-
Who is responsible for the various P&SCM activities and at which stages of the process? How and where is responsibility handed over, and who is responsible for co-ordinating this?
-
Who is responsible for the overall design of the supply chain? Where is the P&SCM design/management function located within an organisation and what are the implications of this?
-
How can a market be developed and managed? To what extent can alternative suppliers shape the market environment?
-
When and where within a supply chain does competition work? When and where is collaboration better? How can these two approaches be co-ordinated?
-
When, or for which categories of spend, can P&SCM activities be outsourced?
-
For which categories of spend can P&SCM activities benefit from economies of scale? Which categories of spend require local design/implementation of P&SCM activities?
RQ4: What are the different approaches to improving P&SCM practice and which are likely to work best in the different contexts and types of NHS organisations?
Additional questions of interest to members of the advisory group:
-
Is there evidence of ‘best practice’ from the private sector? If so, how useful is this in the NHS context?
-
What constitutes ‘evidence’ in ‘evidence-based commissioning’?
-
What are the particularities of commissioning in health that could lessen the importing and implementation of models and practice from other sectors?
-
What constitutes ‘a success’ in P&SCM activities and what constitutes ‘a failure’?
Research methodology
A detailed description of the research methodology is presented in Table 2. It is worth noting here that the four main objectives outlined in Chapter 1, and their associated RQs, are closely inter-related. For example, the mapping and evaluation of different approaches to improving P&SCM practice (objective 4) is founded on literature presenting and discussing theories about P&SCM, the application of those theories in NHS and other contexts, and evidence about how various practices affect procurement outcomes. Equally, although Table 2 suggests a sequential set of phases, in realist review there is iteration between the phases. So, for example, theories about P&SCM and explanations about effective procurement practices in NHS contexts were shaped and reshaped throughout the course of the study.
| Phase | Actions |
|---|---|
| Define the scope of the review |
|
| Search for, extract and appraise the evidence (see Table 3 for more detail) |
|
| Synthesise findings |
|
| Draw conclusions and make recommendations in relation to the original objectives of the study |
|
Further specific details about the search, appraisal and extraction strategy used in the study are provided in Table 3. With respect to managing a large volume of papers, from diverse sources, a purposive sampling strategy was used to set strict boundaries in relation to relevance, allowing for iteration. Relevance was judged against each of our four research objectives and their associated RQs. Data selection, leading to decisions about inclusion or exclusion, was less linear and predetermined than in traditional systematic reviews. Decisions here were based on pre-existing knowledge of the subject area and the use of expert judgement on what to include in or exclude from the review, drawing upon advice from the research team and from the advisory group as required.
| Phase | Actions |
|---|---|
| Decide purposive sampling strategy |
|
| Define search sources, terms and methods |
|
| Develop data extraction forms |
|
| Test for rigour and relevance |
|
| Set thresholds for saturation |
|
The appraisal process focused on the rigour and relevance of the selected data. Rigour was assessed by looking at the credibility and robustness of the methodology used in a piece of research. Literature reporting anecdotal qualitative evidence and quantitative research drawing on a small data set were judged to be insufficiently rigorous. Relevance was assessed by considering whether or not a particular paper or piece of evidence within a paper was addressing the theories being tested, and by asking whether or not it might add valuable insights for NHS managers and clinicians. Data extraction was done using forms that were specifically tailored to each of our RQs, but in each case we focused on gathering data that revealed the nature of context, mechanisms and outcomes. For RQ1, for example, we extracted data about the contextual assumptions, proposed explanatory mechanisms and intended outcomes embedded in different P&SCM theories. For RQ2, by contrast, we extracted data about the empirical context studied within the NHS, the commissioning or procurement interventions taking place within that context, the mechanisms thought to be triggered by those interventions, and the observed outcomes. Examples of completed data extraction forms are provided in Appendix 1.
Analysis and synthesis of the extracted data were done iteratively and sequentially. First, a body of evidence related to each RQ and expressed in terms of context, mechanism and outcome was built up. This was followed by a process of comparing and contrasting evidence from different studies to identify recurrent patterns of CMO configurations in respect of each RQ. Finally, we undertook synthesis by seeing how far one or more P&SCM theories might be useful in interpreting and explaining these recurrent patterns in our evidence. This sequence of steps was then iterated by analysing further evidence in relation to each RQ through the lens of context, mechanism and outcome. Provisional findings and conclusions from this process were shared periodically with the advisory and stakeholder group to sense-check their relevance and value for NHS managers and clinicians. We also used the expertise and experience of the advisory group to help us frame our final conclusions and recommendations.
Literature search
An initial literature search was conducted in early October 2013 across the electronic resources listed below. The results of this search were then iteratively updated and refined during the remainder of October and early November. The resources used included the leading bibliographic databases in their respective disciplinary fields to ensure both quality and breadth of coverage and to minimise duplication. They were also selected for their relevance to each of our RQs.
-
ABI/INFORM® Global (ProQuest): This is a large business journal database providing the full text of articles from over 2300 business and management journals and abstracts from a further 1000. Coverage includes business, management, marketing and strategy.
-
Applied Social Sciences Index and Abstracts (ASSIA) (ProQuest): ASSIA is an indexing and abstracting tool covering health, social services, economics, politics and education.
-
Business Source Premier (EBSCOhost): This complements ABI/INFORM® Global by providing full-text access to more than 2000 business and management journals (mostly different journals from those on ABI/INFORM® Global) as well as trade journals.
-
Health Management Information Consortium (HMIC) (Ovid): This database brings together information from two key institutions: the Library and Information Services of the Department of Health and The King’s Fund Information and Library Service.
-
International Bibliography of the Social Sciences (IBSS) (ProQuest): This includes over 2.6 million references to journal articles, books, reviews and selected chapters.
-
Scopus (Elsevier): This is a large abstract and citation database, which provides access to 19,000 titles from a wide range of international publishers.
-
Social Science Citation Index (SSCI) (via the Web of Knowledge): This index covers almost 2500 journals across more than 50 social science disciplines and is one of the databases that make up the Web of Science, which is accessible via the Web of Knowledge.
Specific titles
The journals listed below were considered to be particularly relevant by the research team. They were covered by the chosen bibliographic databases as indicated.
-
Academy of Management Journal (1963 + ABI, BSP, IBSS, Scopus, SSCI)
-
American Economic Review (1911 + ABI, BSP, IBSS, Scopus, SSCI)
-
British Journal of Management (1990 + ABI, BSP, IBSS, Scopus, SSCI)
-
Environment and Planning C: Government and Policy (1983 + IBSS, Scopus, SSCI)
-
Harvard Business Review (1922 + ABI, BSP, Scopus, SSCI)
-
Health Services Management Research (1998 + ABI, ASSIA, BSP, Scopus, HMIC)
-
Industrial Marketing Management (1971 + ABI, BSP, Scopus, SSCI)
-
International Journal of Operations and Production Management (1980 + ABI, BSP, Scopus, SSCI)
-
Journal of Business and Industrial Marketing (1994 + BSP, Scopus, SSCI)
-
Journal of Business-to-Business Marketing (1993 + ABI, BSP, Scopus, SSCI)
-
Journal of Economic Behaviour and Organisation (1984 + ABI, ASSIA, BSP, IBSS, Scopus, SSCI)
-
Journal of Economic Literature (1969 + ABI, BSP, IBSS, SSCI)
-
Journal of Health Economics (1982 + ABI, ASSIA, HMIC, IBSS, Scopus, SSCI)
-
Journal of Health, Organisation and Management (1992 + ABI, ASSIA, HMIC, Scopus)
-
Journal of Health Services Research and Policy (1995 + ASSIA, Scopus, SSCI)
-
Journal of Law, Economics and Organisation (1985 + ABI, BSP, IBSS, Scopus, SSCI)
-
Journal of Marketing Management (1992 + ABI, BSP, IBSS, Scopus)
-
Journal of Purchasing and Supply Management (2003 + ABI, BSP, Scopus, SSCI)
-
Nonprofit and Voluntary Sector Quarterly (1996 + ABI, ASSIA, Scopus, SSCI)
-
Policy and Politics (1979 + IBSS, Scopus, SSCI)
-
Production and Operations Management (1996 + ABI, BSP, Scopus)
-
Production Planning and Control (1990 + ABI, BSP, Scopus)
-
Public Administration (1965 + ABI, BSP, IBSS, Scopus, SSCI)
-
Public Administration Review (1965 + ABI, BSP, IBSS, Scopus, SSCI)
-
Supply Chain Management (1996 + ABI, BSP, Scopus, SSCI).
The following titles were also searched individually:
-
Harvard Business Review
-
California Management Review.
The literature search was conducted using keywords relating to the specific focus of each of our RQs as set out in Appendix 2. The keywords were combined with the Boolean operators ‘AND’ and ‘OR’, which narrowed and widened the search respectively. Combinations with Boolean operators were not used if search terms were found to be infrequently employed, to maximise the capture of material. In addition, the terms were variously input into the search function at the level of title, abstract or subject heading in order to ensure adequate breadth and depth of the search as relevant to the RQ. Search terms were truncated (i.e. the root of a word is used with an asterisk) to capture various relevant suffixes of a term for maximum coverage. Speech marks were used if it was necessary to keep multiple words together as a single search term, further ensuring relevance.
The search was limited to retrieve material in English only. It was deemed unnecessary to limit the search by any date of publication, as the purpose of the research involved reviewing the P&SCM and related terms since their earliest usage. The vast majority of the search was limited to peer-reviewed literature, which was taken as an indication of quality, though this was relaxed where appropriate (e.g. for RQ2, to collect relevant grey literature).
The results of the literature search were exported into EndNote X5 (Thomson Reuters, CA, USA), an electronic reference management tool. Four EndNote libraries were created, one for each of the RQs. The functions of EndNote enable the references in each library to be sorted into separate subfolders to allow greater focus in the review process, and to be searched and ordered in various ways, for example by keywords, by publication date or by type (article, book chapter, report, etc.). The software also allows electronic versions of the texts to be attached and stored as part of the reference.
In the first phase of the literature review, each of the libraries was examined by the principal investigator (JS) and the researcher (TM) together to ensure that the imported references were relevant to the corresponding RQs, and references were reallocated as necessary. In phase 2, abstracts and summaries were reviewed by the principal investigator and the researcher to remove duplicate references and any material not related to our RQs, for example studies dealing with purchasing power parity and with legal commissions. In the final phase, full articles and texts were scanned and a judgement was made to select for detailed review or to discard based on the exclusion criteria described below. Further hand searching, snowballing and Rich Site Summary updates were also used to add to the literature under scrutiny.
Literature excluded from the review
The following study topics and types were excluded from the review, as they were judged not relevant to our RQs, nor were they of interest to members of the advisory group:
-
studies based exclusively on theoretical/mathematical modelling or simulation, as the realist review approach focuses on experiences of practice
-
studies relating to individual consumer buying/purchasing or related behaviour, rather than business or industrial buying/purchasing
-
empirical studies exhibiting inadequate methodological rigour, for example quantitative research based on a small sample or qualitative research reporting anecdotal evidence.
Literature included in the review
The initial literature search identified 3562 results. Based on the first phase of the review, these were distributed across the RQs as follows:
-
RQ1: 1048 texts
-
RQ2: 720 texts
-
RQ3 and RQ4: 1794 texts.
Following the second phase of the review, with the removal of duplicate references and any texts dealing with unrelated subjects, 1800 texts remained. These were distributed across the RQs as follows:
-
RQ1: 472 texts
-
RQ2: 412 texts
-
RQ3 and RQ4: 916 texts.
In the final phase, after the application of criteria for exclusion and the inclusion of additional material from hand searching, snowballing and updating, 879 texts were selected for full review as follows:
-
RQ1: 191 texts (all of which were journal articles)
-
RQ2: 194 texts (138 journal articles, 25 research reports, 16 book chapters and 15 NHS policy documents)
-
RQ3 and RQ4: 494 texts (all of which were journal articles).
Round-up
Having described and justified the approach, focus and detailed methodology of our literature review, we turn in the next chapter to a discussion of the various theories that have been used to interpret and explain the P&SCM process.
Chapter 3 Theories about procurement and supply chain management
Introduction
The primary aim of this chapter is to address RQ1, which asks: what are the main disciplinary sources of ideas about P&SCM and what are the principal theories, conceptual frameworks and main paradigms? We begin in the next section by identifying what are the main disciplinary sources of ideas about P&SCM. We then discuss the principal theories and conceptual models used to understand, explain and guide P&SCM practice. We also categorise these various theories into a number of broad literatures focused upon particular aspects of the P&SCM process.
In addition, this chapter builds on work by authors such as Giannakis and Croom,49 Halldorsson et al.,50 and Möller51 who have developed metatheoretical analyses to suggest how different theories can inform thinking about and practice in different aspects of P&SCM. The underlying aim of this type of analysis can be either to develop a contingency perspective on middle-range P&SCM theories (Halldorsson et al.,50 Möller51) or to go in search of a unified general theory to support the development of a cognate P&SCM discipline (Giannakis and Croom49). Our aim is to make a contribution to the development of a contingency perspective by adopting a realist review method, focusing on which P&SCM theory works, for whom and under what circumstances. We recognise, as does Möller,51 that the search for a unified general theory is likely to be fruitless given the ontological differences between several of the component theories, and that theory, like practice, ought to be sensitive to context. To this end, the chapter also develops and discusses a realist interpretation framework of P&SCM theories. This framework is then used in the rest of the report as a basis for examining what lessons can be learned from the general literature on P&SCM for practice in the NHS.
Definitions of procurement and supply chain management
Before turning to the primary task of this chapter we need to define our main terms, ‘procurement’ and ‘supply chain management’, and the relationship between them for the purposes of this report. Larson and Halldorsson52 provide a useful basis for this discussion in a paper which considers the scope and meaning of supply chain management (SCM). They note, as many others have done (e.g. see Svensson,53 Giannakis and Croom,49 Giunipero et al. 54), that the literature offers a multiplicity of definitions of SCM. Some of these definitions share references to the co-ordinated management of both an organisation’s upstream (supplier) and downstream (customer) relationships to achieve superior value for end-customers. Other definitions are solely focused on the integrated management of an organisation’s upstream, supply-side relationships. The interesting question raised by Larson and Halldorsson52 is: how should we define and think about procurement in relation to SCM defined in these two different ways? They identify four perspectives on this question, which they call ‘traditionalist’, ‘relabeling’, ‘unionist’ and ‘intersectionist’. These are illustrated in Figure 5.
FIGURE 5.
Four perspectives on procurement and supply chain management (adapted from Larson and Halldorsson52).
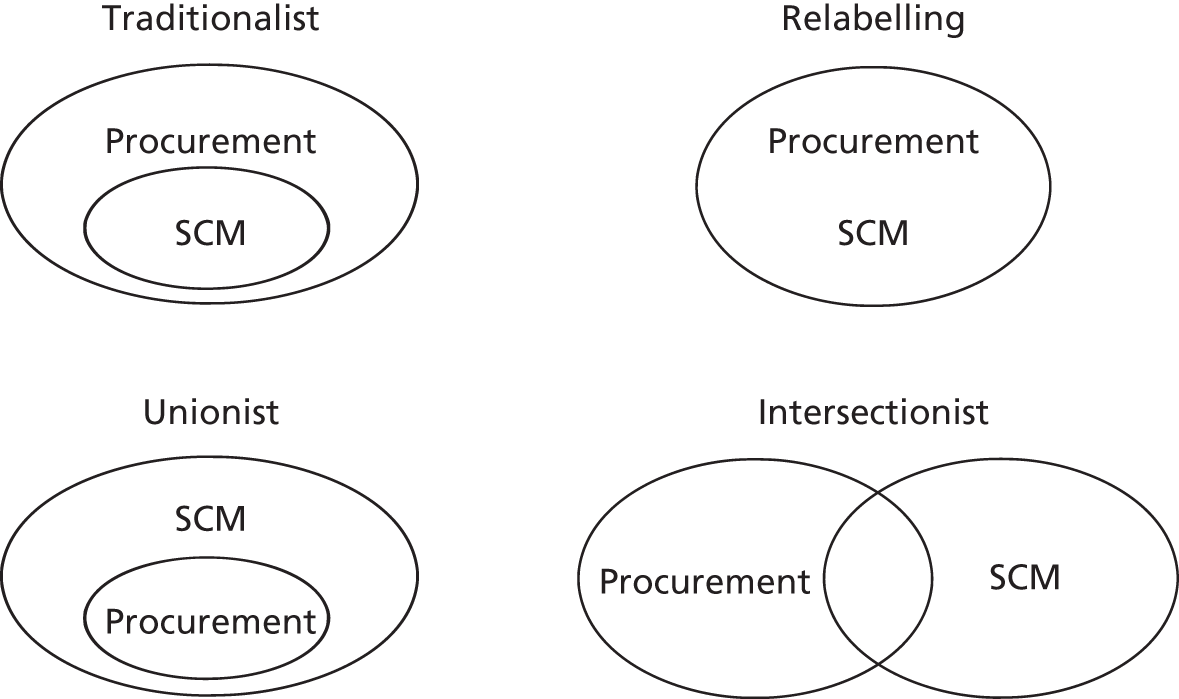
The first two perspectives are associated with the notion of SCM as integrated management of an organisation’s supply-side relationships. The traditionalist perspective sees SCM as a strategic aspect or subset of procurement, concerned particularly with supplier development and building collaborative supply relationships. Procurement in this perspective is broader than SCM and is defined as all activities associated with acquiring and managing the organisation’s supply inputs. The relabelling perspective suggests that in many organisations procurement is ‘evolving’ into SCM. This appears to mean that SCM is seen as a more modern and enlightened version of procurement, involving a generally less aggressive and more collaborative approach to supplier management.
The unionist and intersectionist perspectives are both associated with the idea that SCM involves the co-ordinated management of an organisation’s upstream and downstream relationships. Consequently, these perspectives cast SCM in very broad terms and suggest that it encompasses a wide range of activities and functions including procurement, logistics, operations and marketing. The unionist perspective is perhaps the more radical of the two in that it subsumes and attempts to integrate what have traditionally been seen as separate organisational functions. The intersectionist perspective, on the other hand, retains procurement, operations, marketing, etc. as separate functions and sees SCM as the co-ordination of cross-functional efforts across multiple organisations.
The definitions of ‘procurement’ and ‘supply chain management’ adopted for the purposes of our review are presented in Box 2.
Procurement is the process encompassing all activities associated with acquiring and managing the organisation’s supply inputs. Supply chain management is the subset of procurement activities concerned particularly with the monitoring, management and development of ongoing supplier relationships and the associated flows of supply inputs.
These definitions are perhaps closest to Larson and Halldorsson’s52 traditionalist perspective. We have adopted these supply-side-focused definitions to delimit the scope of our literature review in a way that focuses attention on particular aspects of the NHS and the interactions between its constituent organisations. This review is not concerned with literature that might cast light on an organisation’s management of its relationships with customers or, more appropriately for the NHS, patients or service users. The focus is instead firmly on the literature that addresses an organisation’s interactions with its external suppliers or, in NHS parlance, providers.
Disciplinary sources of ideas about procurement and supply chain management
Reflecting on the findings of a number of extant literature reviews, it is clear that the P&SCM literature is theoretically diverse and fragmented and draws on a very wide range of underpinning disciplines. Burgess et al. (p. 710)55 define a discipline as ‘a body of practice that is well supported by occupational groupings that identify with a defined territory of activity’ and that has an infrastructure (e.g. professional associations, publications) ‘designed to transfer and create knowledge’. They review 100 randomly selected journal articles and identify eight main disciplines, including marketing, logistics, strategy, sociology, economics and operations management, that underpin the P&SCM literature. This disciplinary diversity is further underlined by the fact that these 100 articles are published in 31 different journals covering many disciplinary areas.
Harland et al. 56 review only 41 papers, but with a specific focus on work that considers disciplinary issues and the nature of theory and conceptual development in the area of P&SCM. They find that P&SCM is characterised by ‘borrowing theories from other disciplines’ (p. 745), particularly economics (e.g. game theory and transaction cost analysis) and sociology (e.g. social capital theory). They also identify that their relatively small sample of papers are published in 20 different journals, both specialist and general management, representing disciplines as diverse as production economics, operations management and marketing.
Chen and Paulraj57 review over 400 papers and identify a similar diversity of disciplines contributing to P&SCM thinking, including logistics, marketing, information management and operations management. Giunipero et al. 54 also review just over 400 papers published in nine different journals heavily associated with P&SCM research. They comment that ‘SCM [supply chain management] has been a melting pot of various disciplines, with influences from logistics and transportation, operations management and materials and distribution management, marketing, as well as purchasing and information technology’ (p. 66). Finally, the paper by Chicksand et al. 58 takes a different approach and reviews a much larger sample of 1113 papers, but drawn from three specialist journals only. Despite this narrower search strategy, the paper once again notes the highly multidisciplinary nature of P&SCM research. It identifies economics, strategy and sociology as key sources of theory in topic areas of interest to P&SCM researchers.
Principal theories and procurement and supply chain management literatures
As this brief discussion indicates, P&SCM research is underpinned by a very diverse disciplinary base. Consequently, this area of research is also marked by the use of many different theories and associated models and conceptual frameworks. In an extensive review of organisational buying behaviour research, Johnston and Lewin59 identify the use of several sociologically grounded decision-making process models and frameworks. Buvik60 identifies the use of theoretical perspectives drawing on sociology (organisational decision-making theory, resource dependency theory) and economics (agency theory, transaction cost analysis, game theory). Burgess et al. 55 similarly identify the use of theories from sociology (interorganisational networks and organisational learning) and economics (transaction cost and agency theory), and they add theory drawn from strategic management (resource-based view of firm).
Halldorsson et al. 50 argue that practices in the domain of P&SCM are best understood by applying multiple theoretical perspectives drawn from economics (agency theory and transaction cost analysis), sociology (social exchange theory, resource dependency theory) and strategic management (resource-based view). Shook et al. 61 make the same case for the use of a number of well-established theoretical perspectives as a basis for better understanding and explaining activities such as outsourcing, supplier selection and buyer–supplier relationship management. They make use of 10 different theories, again drawn from sociology (institutional, resource dependency, network, organisational decision, critical), economics (agency and transaction cost analysis), and strategy (resource-based view and strategic choice). They also identify the value of systems theory for thinking about the need for, and the value of, co-ordinated and collaborative relationships in supply networks. This theory was drawn originally from the natural sciences (biology and physics), but has been developed for use in management and organisations.
Finally, Chicksand et al. 58 use their extensive review of articles from three specialist P&SCM journals to identify what they see as the dominant theoretical perspectives. Again, they mention agency theory and transaction cost analysis drawn from economics; network and resource dependency theory drawn from sociology; and dynamic capabilities and the resource-based view drawn from the strategy literature. They also identify a version of systems theory that they call the integrated SCM perspective.
When engaging with the P&SCM literature, then, we are faced with a diverse and fragmented use of theory. Reflecting on the discussion here, though, we can start to discern a picture of those theories that are employed most often. A representative list of the most prevalent theoretical perspectives and models would include various models of organisational decision-making, agency theory, transaction cost theory, social exchange theory, resource dependency theory, dynamic capabilities and the resource-based view, systems theory and game theory. This purely descriptive listing of the dominant theories is only of limited use, however, given our realist review objective of understanding how theory might guide practice in different contexts, for different actors and in different aspects of P&SCM. We therefore need a basis on which to categorise these theories that connects with our realist review objective.
To categorise these theories it is useful to consider Möller’s51 notion of a research domain such as P&SCM as having several inter-related or nested layers (single actor, group, organisation, interorganisational, network, industry). We can also make use of Giannakis and Croom’s49 idea of different P&SCM decision domains (synthesis, synergy and synchronisation) in accordance with the diversity of activities and processes involved. Our approach draws on these notions of nested layers and decision domains by categorising the programme theories in terms of their primary explanatory focus on a particular broad phase in the P&SCM process. As can be seen in Box 3, which illustrates a typical P&SCM process, we can crudely identify four broad phases each associated with one or more steps or activities in the process.
Phase 1: precontract (demand management)
-
Identification of need and development of a specification of the physical and performance characteristics of the required goods or services.
-
Identification of potential sources of supply (market search).
-
Qualification of potential suppliers and their goods or services.
-
Design of the request for proposal/quotation and the solicitation of bids.
Phase 2: selection and contracting
-
Bid evaluation and supplier selection.
-
Negotiation of contractual terms and conditions with selected suppliers.
Phase 3: post contract, relationship management (soft management tasks)
-
Monitoring of supplier performance and the management of ongoing supplier relationships.
Phase 4: post contract, operational delivery (hard management tasks)
-
Establishment of SCM strategies, control systems and performance measurement systems.
-
Management of inventories of purchased parts, materials and supplies.
-
Recycling or disposal of unused materials and obsolete finished products (reverse logistics).
Source: adapted from Corey. 62
By identifying these four broad phases we are able to propose a fourfold categorisation of broad literatures, each associated with particular theories, as shown in Table 4. These are (1) the organisational buying behaviour literature grounded in various theories and models of organisational decision-making; (2) the economics of contracting literature grounded in agency theory and transaction cost economics (TCE); (3) the networks and interorganisational relationships literature grounded in social exchange theory, resource dependency theory and aspects of industrial economics; and (4) the integrated SCM literature grounded in systems theory and behavioural economics, in particular game theory.
| Literature and cognate theories/models | Primary focus in procurement process |
|---|---|
Organisational buying behaviour
|
Phase 1, steps 1–4 (but also concerned with aspects of step 5 and step 7) |
Economics of contracting
|
Phase 2, steps 5 and 6 (but also concerned with aspects of step 7) |
Networks and interorganisational relationships
|
Phase 3, step 7 (but also concerned with aspects of step 6 and step 8) |
Integrated SCM
|
Phase 4, steps 8–10 (but also concerned with aspects of step 7) |
It should be noted that, while each broad literature is primarily focused on one of the four phases, there are inevitably overlaps, as the process steps are not discrete, nor do they occur in a strictly sequential manner. While phases 1 and 2 do occur in sequence, phases 3 and 4 are typically concurrent. Moreover, aspects of phase 3, for example the history of managing a supplier relationship, can affect activities in phase 2 if an existing supplier is being considered for a new or renewed contract.
We now discuss each broad literature in turn, presenting the basic assumptions and the implications for P&SCM practice of the associated theories. We also discuss the major criticisms of each theory.
Organisational buying behaviour
The organisational buying behaviour literature focuses primarily on what might be called the precontract or the demand management phase of the procurement process. Box 4 provides a summary of the implications of this literature for P&SCM practice.
-
Procurement decisions differ in terms of the level of risk that they pose for the organisation.
-
Organisational buying behaviour is a multiactor, multiagenda process, and consequently procurement decisions are a potential locus of intraorganisational power and politics.
-
Higher-risk procurement decisions (more important, more complex, more uncertain and more urgent) tend to be characterised by greater intraorganisational conflict and hence power and politics are more important in reaching a decision outcome.
The main disciplinary underpinning of this literature is in organisational sociology, with a focus on political models of decision-making. The basic assumptions underpinning such models are that actors have bounded rationality and differing motivations and preferences, and that intraorganisational conflict is inevitable in situations of joint decision-making. 63 By viewing organisational buying behaviour as a multiactor, multiagenda process, this literature conceptualises buying decisions as being a potential locus of intraorganisational politics. This, in turn, highlights the possibility for power to be used to resolve conflicts of interest. 64–68 Deciding what to buy, drawing up a specification, choosing a shortlist of potential suppliers, assessing the bids submitted and selecting a supplier are seen as intensely political rather than purely technical decisions. The literature also acknowledges, though, that decision-making conflicts can be resolved without the use of power, through problem-solving and persuasion. 69
This literature has its roots in the seminal texts on industrial buying and marketing by Robinson et al. ,70 Webster and Wind71 and Sheth. 69 A core idea common to these early models is that organisational buying behaviour should be treated as a process, in which there are a number of phases or stages representing a sequence of activities. 72 Robinson et al. 70 encapsulated this in their ‘buy-grid framework’, which presents a number of what they termed ‘buy-phases’. In broad terms, the key activities identified by these authors are akin to those shown as steps 1–4 in Box 4, although there is also some interest in step 7 in the form of supplier performance evaluation and feedback.
All of these early models also suggest that there are contextual factors at three levels influencing the nature of buying decisions. 59 At the first level there are environmental or situational factors, for example suppliers, competitors, technology, regulation, politics and culture. Second, there are organisational factors such as the buying organisation’s size, structure, orientation, technology, reward systems and goals. Third, there are factors associated with the characteristics of different types of purchase or what Robinson et al. 70 call ‘buy-classes’, such as product type, purchase novelty, purchase complexity and time pressure.
Finally, all three models posit a number of variables or dimensions that are used to characterise the actors involved in organisational buying decisions, the ways in which they are expected to behave and the decision-making criteria they are expected to use. Tanner72 suggests that these early researchers are thus exploring three different questions: who participates, what happens and what causes or influences a specific decision?
The core concept drawing all of these strands together to explain variation in organisational buying behaviour is the level of risk associated with a given procurement situation. 59 Risk is seen as a function of purchase importance, complexity, uncertainty and time pressure,73 and the key antecedents of these variables are primarily found in the contextual factors discussed above: environmental, organisational and purchase characteristics. So, for example, purchase uncertainty might be related to uncertainty in the buying organisation’s environment or to characteristics of the buying firm such as technical competence. Purchase importance might be a function of the buying organisation’s size and the type of product or service being bought (e.g. capital equipment or supplies). Purchase complexity might also be related to the type of product or service and to the nature of the buying task (new spend or renewal of an existing contract). Finally, time pressure might be a function of the nature of the buying task. The relationship suggested by the literature between different levels of procurement risk and various aspects of organisational buying behaviour intended to mitigate that risk is illustrated in Figure 6.
FIGURE 6.
The relationship between procurement risk and organisational buying behaviour.
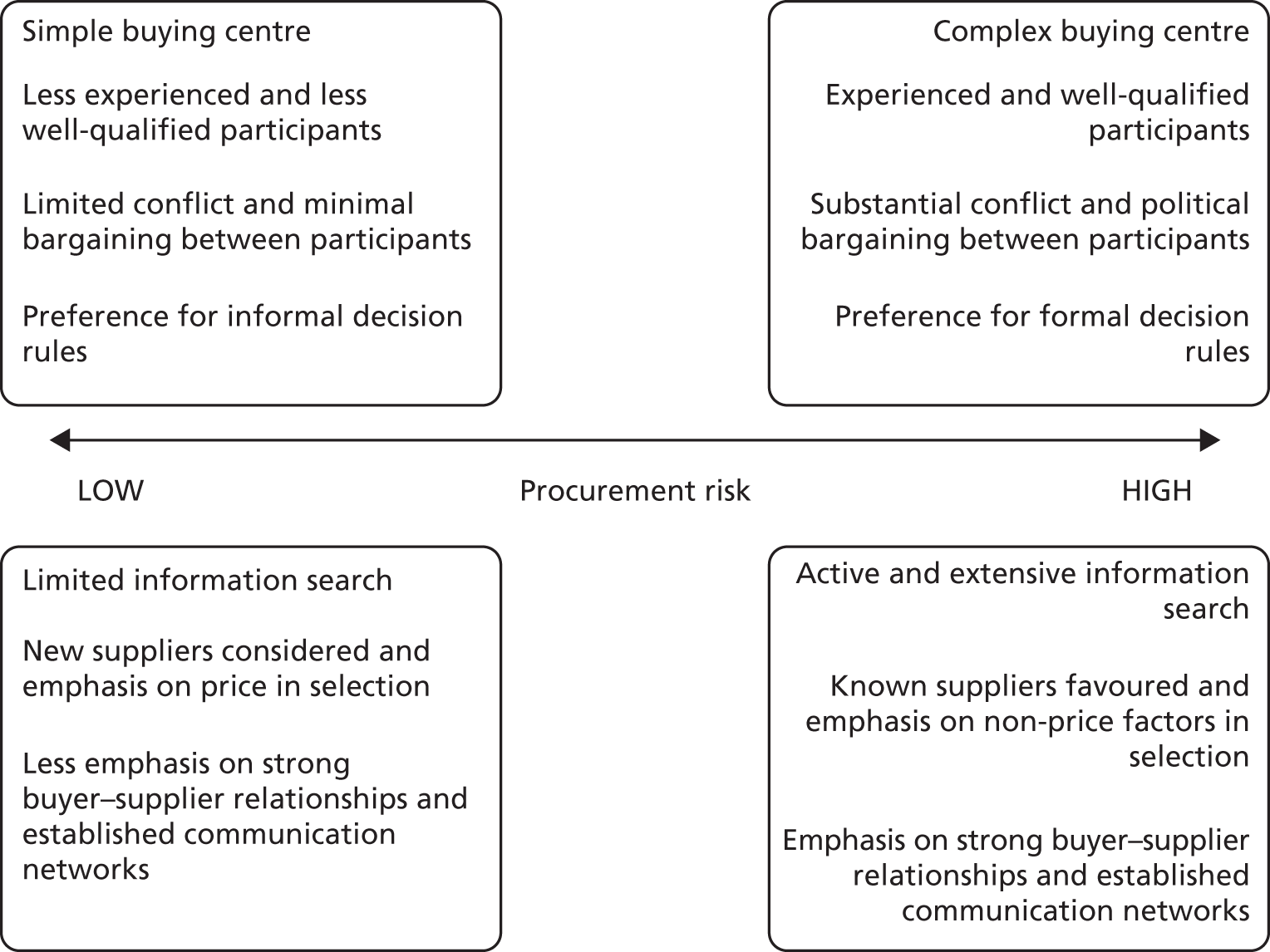
It is argued that, as the risk associated with a buying decision increases, the group of actors involved in making the decision, known in this literature as the buying centre, will become larger and more complex. In other words, more people will be involved in high-risk buying decisions and they will be drawn from a wider range of departments or organisational subunits with different preferences and agendas. The participants involved in a high-risk buying decision will also typically be more highly qualified and experienced, and will be motivated to commit greater attention throughout each stage of the procurement process. Role theory has been used by a number of authors to examine which organisational functions participate in buying decisions and what specific roles they play. 74,75
The literature associates high-risk buying decisions with greater conflict between participants and with greater use of aggressive bargaining strategies to resolve such conflicts. 69 The likelihood of intraorganisational conflict is increased as a result of the greater diversity in departmental perspectives and motivations. The use of power and politics rather than a collaborative or problem-solving approach to conflict resolution is a result of the high stakes associated with important purchasing decisions, particularly where certain departments represented in the buying centre might be negatively affected by the purchase outcome. In these circumstances, participants will be reluctant to make concessions without some type of compensation. In a complementary vein, other authors have discussed actor behaviour through the lens of behaviour choice theory. 76,77 This theory focuses on the choices made by buyers about how they will undertake the buying process. As Tanner72 argues, the actors involved in a buying decision may be more focused on using the process to demonstrate and develop their management and decision-making skills than on the outcome of acquiring a particular good or service.
As Johnston and Lewin59 note, the particular decision rules used in any given procurement situation are fundamentally firm-specific, but the literature does still suggest that, in general, there will be a preference for more formal control mechanisms and decision guidelines as procurement risk increases. The logic here is that, as the buying centre for a high-risk decision will be larger and more complex, the governance mechanisms need to be much more explicit and detailed to ensure that they are clearly understood by all involved. By contrast, because lower-risk procurement decisions are expected to involve a smaller and less diverse group of decision-makers, the decision-making process can be governed more informally and tacitly.
In terms of searching for information about supplier options, the literature suggests that this will become more active and extensive as procurement risk increases. For a high-stakes buying decision, buying centre participants will be strongly motivated to access a wide variety of formal (trade journals and sales literature) and informal (personal industry contacts) information sources. This can be seen as an effort to mitigate the uncertainty and complexity that characterise high-risk procurement decisions. Moreover, it is argued that known suppliers offering well-proven products and services will be favoured in high-risk situations, and there will be an emphasis on non-price selection criteria (i.e. quality, delivery performance, service levels). Price will play a decisive role in selection only if there are two or more suppliers that appear equally capable of satisfying the buying centre’s non-price requirements. For less important, less complex, less uncertain and therefore lower-risk procurement decisions, by contrast, buying centre participants will use price as the dominant selection criterion and seek to stimulate competition from as wide a range of suppliers as possible.
Building on the points above, the literature also suggests that, in situations of high risk, buying centre participants will favour suppliers with which their organisation has strong prior relationships and well-established networks of communication. These features are seen as an important means of mitigating purchase uncertainty, complexity and time pressure by facilitating buyer–supplier co-operation and information exchange.
Turning now to criticisms of the organisational buying behaviour literature, these are primarily made by contributors to the literature offering a competing vision of how it should develop. Two main strands can be identified in such critiques. First, it is argued that the literature has traditionally been too focused on discrete transactions from the buying organisation perspective and has given little, if any, insight into ongoing buyer–supplier relationships. 78 Second, it is suggested that the literature has been too narrow in its conception of what should be the focus of the procurement process. As we have discussed, the organisational buying behaviour literature traditionally places emphasis on the mitigation of risk in procurement decisions. The possibility that the procurement process might deliver cost and innovation benefits from suppliers receives very little attention.
Wilson79 brings these two strands together by suggesting that fundamental changes in the business environment facing many organisations (intensified and globalised competition, more rapid technological innovation) have forced them to adopt a ‘total quality management’ perspective emphasising higher quality at lower cost and with increased flexibility. The need to deliver these objectives has, in turn, led them to adopt longer-term and more co-operative relationships with many of their suppliers. Wilson’s78 argument is that the traditional organisational buying behaviour literature cannot provide an adequate explanation of these changes and that it needs to be replaced by theory focusing on buyer–supplier relationships. Tanner72 counters this argument, however, by suggesting that the organisational buying behaviour literature may still have insights to offer to an understanding of buyer–supplier relationships, particularly in terms of thinking about what happens inside the buying organisation that has an impact on relationships with particular suppliers.
Economics of contracting
Steps 5–6 in the typical P&SCM process are the focus of the economics of contracting literature, grounded in institutional economics. Box 5 provides a summary of the implications of this literature for P&SCM practice.
-
Suppliers can and do exhibit various forms of opportunistic behaviour, which can damage the value for money received by the buyer.
-
Supplier opportunism is a problem, because buyers either face information asymmetry (agency theory) or suffer from bounded rationality (TCE).
-
These hazards of opportunism should be addressed either through a complete contract (agency theory) or through the appropriate alignment of governance mechanisms with transactions (TCE)
-
Transaction cost economics suggests a simple, low-cost governance mechanism (spot market) for transactions with a low potential for opportunism, while more complex and higher-cost bilateral or unified governance mechanisms are suggested for more hazardous transactions.
Key strands of this literature draw on agency theory and TCE. Agency theory applies broadly to circumstances in which one actor (the principal) delegates responsibility for the execution of valued activities to another (the agent), and the principal needs to ensure that these activities are undertaken in a way that serves his or her interests rather than those of the agent. 80 It is perhaps best known as a basis for understanding issues of ownership and control within business organisations, where managers are expected to act as agents on behalf of owners. 81,82 This principal–agent relationship can also be seen, though, when a buyer (principal) engages a supplier (agent) to deliver a good or service. 83–85 TCE is perhaps more obviously concerned with issues of buyer–supplier interaction, focusing on the question of how to organise business transactions most efficiently. 86
Dealing first with underlying assumptions, we can observe that these theories share a basic assumption that suppliers can and do exhibit various forms of opportunistic behaviour, which can damage the value for money received by the buyer. Opportunism is defined as self-interest seeking with guile,86 which extends the notion that actors simply aim to maximise their self-interest in an open and honest way to include blatant and subtle strategic behaviour. These theories, therefore, focus attention on the various behavioural hazards that can arise when a buyer engages an external supplier to deliver a good or service. They are underpinned by an assumption that both buyer and supplier are individual utility maximisers, and that consequently the latter is not likely to always act in the interests of the former.
These theories diverge on the issue of actor rationality, however. Agency theory assumes, like classical economics, that actors are rational and are, therefore, unencumbered in their capacity to make decisions based on all of the information available to them. It does acknowledge, however, that information relevant to an interaction between a principal and an agent is not necessarily perfectly or costlessly available to both parties. Rather, one party might be less well informed than the other and, therefore, be faced with a situation of information asymmetry. TCE, by contrast, assumes that actors have inherent bounded rationality. This means that they make rational decisions, but within the limits imposed by a restricted cognitive capacity.
These different assumptions about actor rationality have important implications for the suggestions made by these theories about how best to manage the hazards of supplier opportunism. The theories discuss the mechanisms, contractual or otherwise, that are available to mitigate such hazards and identify the agency or transaction costs that are incurred in using these mechanisms. The focus for agency theory is on the use of contractual mechanisms. With an assumption of full rationality, agency theory argues that it is possible ex ante to design complete contracts covering every conceivable contingency that might impact on a buyer–supplier transaction. The agency costs incurred in mitigating supplier opportunism are thus primarily associated with contract drafting, to design incentive structures and monitoring regimes, and with contract enforcement or supplier bonding. 80
By contrast, the focus for TCE is more broadly on the use of what are called governance mechanisms. These range from arm’s length spot market interactions, through closer and more involved forms of bilateral governance, to the use of internal hierarchy where a transaction takes place within the boundaries of a single organisation. TCE assumes bounded rationality. This means that contracts designed ex ante tend to be incomplete and, therefore, cannot solely be relied upon to mitigate supplier opportunism. 87,88 Thus, in order to prevent a supplier from exploiting the gaps in a contract, the buyer needs to use extracontractual mechanisms to incentivise appropriate behaviour. This can be the threat of simple spot market contestation, which has very low transaction costs, or the use of more complex bilateral or unified management mechanisms (monitoring, negotiation and adjudication) that have higher transaction costs. TCE is concerned with mitigating the hazards of opportunism in the most cost-efficient way for each transaction. The basic argument, then, is about the appropriate alignment of governance alternatives with transactions. A simple, low-cost governance mechanism (spot market) is suggested for transactions with a low potential for opportunism, while more complex and higher-cost bilateral or unified governance mechanisms are suggested for more hazardous transactions. 86
Among the opportunistic behaviours discussed by the literature are adverse selection, strategic misrepresentation and moral hazard. All of these behaviours involve a supplier exploiting an information asymmetry advantage over a buyer to win and execute a contract on an unfair or misleading basis. The information economics literature draws attention to the notion of search, experience and credence goods. 89,90 Using this categorisation, we can think about the types of goods or services most likely to be characterised by such an information asymmetry between buyer and seller.
Search goods (e.g. office furniture) are the least likely to pose a problem of information asymmetry, because they are simple enough for the buyer to be able to have a detailed understanding of how they are made and delivered. Consequently, the quality of a supplier’s offering and the veracity of its pricing can be accurately assessed before the purchase occurs. In this case, it is possible ex ante to design a simple complete contract as proposed by agency theory or to use spot market governance as proposed by TCE.
Experience goods (e.g. IT services) pose an increased problem of information asymmetry, because the value for money of a supplier’s offering can be assessed only after the good has been delivered for an extended period of time. Here, agency theory would suggest that one could still design ex ante a complete contract using standard terms and conditions to specify desired performance outcomes, but that this should probably be offered on a short-term trial basis in the first instance to incentivise supplier adherence. TCE would suggest a bilateral governance mechanism, which might include financial performance bonds (bonuses), to complement an incomplete contract.
The problem of information asymmetry is most acute, however, in the case of credence goods. Here the buyer cannot acquire the necessary information, even after consumption, to assess whether or not he has received good value for money. Professional services, including legal services and management consultancy, are all classic examples of credence goods which are particularly prone to adverse selection and moral hazard problems. 91 Literature on the hazards associated with buying professional services (see e.g. Ellram et al. ,92 Homburg and Stebel,93 Mitchell et al. ,94 Schiele and McCue95) argues that the buyer’s requirements will typically be complex and, to some extent, unique and therefore very difficult to specify in detail in a contract. The supplier will therefore be in a position to deliver, or underdeliver, the service in a way that increases its returns, but which the buyer will find it difficult to detect. In this case, agency theory still suggests that the solution is to design a contract ex ante, but that this should be a hybrid partly specifying desired performance outcomes and partly creating incentives for non-opportunistic behaviour during contract delivery. This draws on arguments made by the behavioural variant of agency theory,82 which moves closer to the tenets and recommendations of TCE by acknowledging that complete ex-ante contracting is sometimes impossible.
Hold-up is another opportunistic behaviour, discussed using a TCE lens in particular. 86,96 This refers to a situation where a supplier is able to cease (hold up) delivery of a good or service until the buyer agrees to a deal more favourable to the supplier. The buyer is forced to agree to the supplier’s demands, because it is locked in to the contract by significant and asymmetric sunk cost investments in assets such as land, buildings, machinery or management systems/knowledge. 97 Hold-up is often seen as a particularly acute hazard in long-term contracts, associated with large and complex capital investments. The complexity and long time scales associated with such contracts tend to result in contractual incompleteness, which creates the scope for renegotiation and therefore hold-up. Projects funded under the UK’s Private Finance Initiative (PFI) have many of these characteristics. 98 TCE reasoning would suggest that hold-up in this kind of situation is best addressed through a form of bilateral governance, which creates incentives for renegotiation to be handled in an efficient and joint maximising manner. 99
The criticisms levelled at the economics of contracting literature fall into two main categories. First, the validity and robustness of its behavioural assumptions is challenged. Critics argue that the assumption of pervasive actor opportunism, founded on an individualistic and maximising view of human nature, is simplistic and ignores the complexity of individual motivation and behaviour in an organisational context. 100,101 Some emphasise that satisficing is perhaps more realistic as a way of conceptualising decision-making, and that adhering to group norms to achieve social legitimacy is perhaps more important than maximising personal (economic) utility. 102,103 Agency theory’s assumption of the possibility of complete ex-ante contracting, based on actor rationality, is also seen as dubious given widespread evidence of contractual incompleteness. Second, this literature is criticised for what is seen as an overly narrow focus on the costs associated with discrete transactions. These theories are solely interested in understanding how to achieve efficient outcomes at the level of individual transactions, and ignore the fact that these transactions often occur in the context of, and are influenced by, ongoing buyer–supplier relationships. 104,105 It is to this issue of buyer–supplier relationships that we turn in the next section.
Networks and interorganisational relationships
A third broad category of literature, addressing networks and interorganisational relationships,106 focuses our attention particularly on the ongoing management of supplier relationships (phase 3), but also touches on supply innovation and performance improvement (phase 4, step 8). Box 6 provides a summary of the implications of this literature for P&SCM practice.
-
It is important to see individual buyer–supplier relationships as part of and interacting with a wider network of relationships.
-
Firms and other organisations rely on each other’s resources (i.e. access to raw materials, goods, services, finance, knowledge) for their survival and success.
-
A proper understanding of buyer–supplier relationships requires attention to both economic (investment and adaptation) and behavioural (conflict and mutuality) aspects.
-
Some argue that relationships and networks are essentially emergent and unmanageable, while others argue that specific networks can be intentionally designed, created and managed as partially closed systems to deliver enhanced value either through innovation or cost reduction or through a combination.
This literature, like that addressing organisational buying behaviour, has its roots in organisational and economic sociology, but here the focus is outwards, on the ongoing interactions between firms in the context of their wider environment. Given the breadth of this literature, it is useful to discuss it in terms of a number of different subsets, which have overlapping theoretical roots but differ in some of their basic assumptions, particularly about the scope for planned management action in a network context.
The first major subset is commonly referred to as the industrial network approach and is associated with the work of authors in the Industrial Marketing and Purchasing Group. 107–109 These authors draw primarily on resource dependency theory110 and social exchange theory. 111,112 Key themes common to this strand of research are the dynamic nature of interactions between buyers and sellers over time, the gradual emergence of close, high-trust relationships in some cases, and the importance of seeing individual buyer–supplier relationships as part of and interacting with a wider network of relationships. The unit of analysis here is both the buyer–supplier relationship and the network within which it is embedded. The focus of discussion is on both the structure and the dynamics of relationships and networks. This literature has thus made a major contribution to the development of the concept of the supply network, and has shown how a proper understanding of buyer–supplier relationships requires attention to both economic (investment and adaptation) and behavioural (conflict and mutuality) aspects.
The Actors–Resources–Activities framework108 has been a particularly influential model in this approach. This draws on resource dependency theory to show how firms and other organisations rely on each other’s resources (i.e. access to raw materials, goods, services, finance, knowledge) for their survival and success. 110,113 It is assumed, then, that buyers and suppliers are linked in a network through resource dependency and that these linkages or relationships are characterised by the exchange of existing resources and the cocreation of new resources. 114 The model also draws on social exchange theory to examine how buyer–supplier relationships operate and evolve over time, using concepts such as expectations, co-operation, trust, commitment, communication and conflict behaviour. 115 Actors are assumed to be self-interested rather than opportunistic, and to recognise that serving their self-interest requires them to interact with others in a network context. One of the key insights offered is that a single buyer–supplier relationship can be characterised by both competitive and co-operative behaviour, either simultaneously on different levels within each organisation or at different times in the relationship. Another is that change in buyer–supplier relationships is best seen in emergent, unplanned terms rather than as a result of conscious planning. In this way, firms are seen as organic and adaptive rather than mechanistic and rational.
Two other key assumptions of the industrial network approach should be emphasised. The first is that the specific context and history of a buyer–supplier relationship are crucial for understanding how and why the actors in that relationship behave as they do. As Möller51 puts it, ‘actor behaviour is highly embedded in a layered manner’ (p. 330), which suggests that it is difficult to draw general lessons from particular relationship and network cases. Second, actors are assumed to have bounded rationality and as a consequence have only a limited understanding of their network environment. Moreover, the content of this limited understanding is assumed to be highly specific at an individual or group level, with different actors even within the same organisation enacting different interpretations or worldviews of the same network. 116 The industrial network approach therefore provides richly detailed, context- and time-specific representations of the complexity of relationship and network interactions. As a consequence, though, it is short on specific managerial implications, and ‘can provide only relatively broad guidelines regarding how to manage in a network environment’ (p. 330). 51 Specific guidance must be accompanied by an in-depth historical understanding of a particular network situation and must always remain context dependent.
An associated subset of the literature, focusing in particular on the role of trust in interorganisational relationships, is relational contract theory. This is associated most prominently with the work of Macneil, who argues that exchange transactions necessarily occur in a ‘social matrix’ and follow characteristic ‘relational patterns’ (pp. 344–5). 117 He suggests, therefore, that a purely economic analysis of buyer–supplier relationships, based on rational calculations of advantage in single, discrete exchanges, is likely to be of limited utility in explaining real-world behaviour. Moreover, a buyer–supplier relationship cannot be understood solely in terms of the contract that creates its legal basis, because there are also important ‘relational norms’ such as flexibility, solidarity and reciprocity that derive from the social context of an exchange. 104
There are other subsets of the networks and interorganisational relationships literature, however, with more normative managerial implications. One is that dealing with notions of focal networks118 and strategic nets. 119–121 Like the industrial network approach, this draws on resource dependency theory and social exchange theory, but it presents a more proactive managerial vision by including insights on actor cognition and organisational learning. 122,123
The term focal network refers to the idea that, although business networks are borderless or open in a descriptive sense, resource-constrained firms and their boundedly rational decision-makers deal primarily with those network actors they are able to see and regard as relevant to their objectives. The key issues for this perspective are to understand the roles and network positions that an actor can try to achieve in its perceived focal network, and to understand the process by which an actor forms its picture or theory of the network. It is argued that an actor’s learning capacity is a key influence on this process of building a network theory,124 which in turn influences the actor’s network perceptions, interpretations and actions. 125
The idea of a strategic net is used to complement this concept of a focal network by suggesting that specific networks can be intentionally designed, created and managed as partially closed systems to deliver enhanced value either through innovation or cost reduction or through a combination. Each one of the members of a specific network, in turn, has jointly agreed-upon roles and responsibilities aimed at achieving the chosen value creating goals. 120,126,127 There is an underlying contingency principle, here, in that the particular value-creating goals of a network are assumed to influence how it is structured and governed and the managerial capabilities that are required. The members of a strategic net are assumed to be self-interested, but to recognise that their individual self-interest is best served by working collectively. This is, in effect, a networked version of the dynamic capabilities perspective from the strategic management literature. 128,129 It is in sharp contrast to the notion of business networks as emergent and non-manageable entities that is put forward by the industrial network approach. 114
Another managerially relevant subset of this literature is that addressing the concept of power relationships in supply chains. 130–133 This work again draws on resource dependency theory,134 but brings in additional strands from industrial economics. 135 The underlying behavioural assumptions here are the same as those adopted by the other network approaches discussed above: actors are self-interested and have bounded rationality. On the issue of how manageable business relationships and networks are, the power approach takes up a similar position to that espoused by the strategic nets perspective. It agrees that firms are, descriptively speaking, in an open system, but that they have a focal network that is visible and of particular relevance to their objectives. It differs, however, in its strong emphasis on the role of buyer–supplier power in shaping how this relationship and network management is expressed. While the strategic nets perspective focuses solely on the notion of firms acting collectively, through jointly agreed-upon roles and responsibilities, the power approach argues that the management of a network might sometimes take this mutual, collective form, but on other occasions take the form of a dominant firm directing the behaviour of others in its sphere of influence.
The power approach provides a conceptual framework identifying four basic power structures (buyer dominance, supplier dominance, interdependence and independence) and proposes that the nature of the power structures underpinning buyer–supplier relationships have an impact on the scope for collaborative interactions to improve supply network performance. This is because such interactions represent a substantial investment, which firms will undertake only if they have a strong incentive to do so. It is argued that this incentive to collaborate is strong either where one firm is dependent on another or where firms are interdependent. It is further argued that the incentive to collaborate is much weaker in circumstances of buyer–supplier independence. 136 The power approach uses these arguments to propose the notion of power regimes within supply networks comprising one or more buyer–supplier relationships. 137 These are identifiable subsets of a network, each of which is characterised by a particular combination of power structures and each of which is, therefore, more or less likely to support collaborative interactions. To date, these ideas have been developed and empirically tested primarily in private sector supply chains,131 although Sanderson131,133 has focused extensively on the public–private interface in UK defence industry supply chains.
Integrated supply chain management
Finally, we turn to the literature that focuses on what might be called the operational delivery steps (phase 4) in the typical procurement process, but also engages with questions about the monitoring and management of supplier relationships (step 7). Box 7 provides a summary of the implications of this literature for P&SCM practice. The integrated SCM literature encompasses work from logistics,138,139 materials management140 and operations management. 141,142 Its underlying theoretical bases are behavioural economics, in particular game theory, and systems theory.
-
A supply network as a whole can and should be seen as an entirely closed and therefore manageable system.
-
Integrated SCM requires co-operative buyer–supplier behaviour on an extended basis across the network.
-
Co-operation becomes more likely if buyer and supplier interact with one another on a repeated basis; repeated interactions enable them to get to know each other, to build trust and to overcome the lack of information available in a one-off interaction.
-
Integrated SCM can be focused on supply chain efficiency (cost reduction) or effectiveness (innovation and flexibility).
Game theory, originally developed by von Neumann and Morgenstern,143 argues that many economic decisions involving more than one actor (e.g. a buyer and a supplier) take the form of a sequential, strategic game involving anticipation by one player of the other player’s actions. Games such as the Prisoner’s Dilemma have been used to show how co-operative behaviour becomes more likely if two actors interact with one another on a repeated basis. This is because repeated interactions enable them to get to know each other, to build trust and to overcome the lack of information available in a one-off interaction about the other party’s likely behaviour. In a one-off interaction, where the other party’s intentions are unknown, the model suggests that both actors will behave competitively to try to maximise their individual utility. Based on this theoretical provenance, the underlying assumptions of the integrated SCM approach are that actors are rational, but may face information problems; and that actors are self-interested utility maximisers, but will co-operate through repeated interactions where greater net gains can be had from doing so. The integrated SCM literature has applied this reasoning to develop an understanding of how buyers and suppliers can be encouraged to co-operate on a long-term basis and innovate to create a larger pool of value rather than competing over a static pool of value. 144 A crucial aspect of this approach is the idea that buyers and suppliers should be trusting and transparent with one another, sharing information through mechanisms such as open book costing to signal their commitment and future intentions. 145
Systems theory was initially developed within the natural sciences (biology and physics),146 but has subsequently become widespread in organisation and management theory as a means of explaining processes within and between firms. This theory brings with it an assumption that no system, in this case a supply network, should be thought of in terms of its component parts. Rather, it is argued that the processes and outputs of a system can be understood only by considering it in its totality. Reflecting on our earlier discussion of business networks as either open (unmanageable) or closed (manageable) systems, we can suggest that the integrated SCM approach goes even further than the focal network or the power perspective in arguing that a supply network as a whole can and should be seen as an entirely closed and therefore manageable system.
Some of the earliest work to use systems thinking to suggest that supply networks should be seen and managed as an integrated whole comes from Jones and Riley,147 Houlihan148 and Novack and Simco. 149 These authors recognise that there is a continuous chain of functional areas in firms through which materials flow and that extends from raw material suppliers to final distributors interacting with end-customers. The focus here is on material flow, with the associated flow of information between supply chain actors being largely ignored. Similar work has been produced in what might be called the traditional logistics perspective, with authors such as Scott and Westbrook150 discussing how to better manage fluctuations in material flows at the interfaces between supply chain actors. The main focus in this perspective is on improving supply chain efficiency by reducing inventory levels. Recognising the limitations of these early works, authors such as Lee and Billington151,152 and Christopher138 move the debate on by emphasising the importance of system-wide co-ordination of both materials and information flows. It is argued, as we noted above, that the sharing of information is an essential means of signalling commitment to drive ongoing collaborative behaviour. These authors also introduce the idea that supply chains should be managed to improve both their cost efficiency and their service and quality effectiveness.
One particularly influential application of systems thinking is the work by Forrester153 on the dynamic behaviour of firms and their supply chains. Forrester identifies the so-called bullwhip effect, which suggests that the demand information passing from buyer to supplier along a supply chain can be distorted, leading to overproduction and excess inventory. This has led some authors to go beyond arguments about how to improve pre-existing supply chains and to consider how an entire supply system might be redesigned in order to improve its efficiency and effectiveness. 154–158 Such authors have favoured the use of mathematical modelling techniques to simulate the dynamic behaviour of supply chain actors and their performance consequences using a range of possible supply chain designs. Popular variants of this thinking in recent years have been lean,159,160 agile161,162 and build-to-order supply. 163
Perhaps the most significant criticism that is levelled at the integrated SCM literature comes from authors in the networks and interorganisational relationships literature, which is unsurprising given their interest in broadly the same empirical domain. The former literature is seen by authors in the latter as being far too technicist and rationalist in its conception of the scope for management control in supply networks. 107–109,111,114,115 The integrated SCM literature assumes that actors are rational and that they will respond in a predictable way to purely economic incentives. It is assumed that the actors in a supply chain will be able to recognise the additional value that can be generated by working together as a tightly co-ordinated whole, and will simply behave accordingly. Critics argue that this is not realistic,107–109,111,114,115 because it ignores the messy complexities and constraints of buyer–supplier relationships and networks, with their social as well as their economic dimensions. Failing to acknowledge these complexities and constraints gives one a very narrow understanding of what influences behaviour and outcomes in relationships and networks.
Developing a realist interpretation framework of procurement and supply chain management theories
As we have discussed, the P&SCM research domain draws on a very diverse range of disciplinary bases, theories and models. Consequently, it is difficult to identify a single, coherent and dominant body of thought relating to P&SCM such that it might start to take on a disciplinary status. 50 This is not necessarily a negative situation, however. As Anderson164 has argued, a subject’s scientific status is enhanced if the knowledge base is widely distributed and there are multiple ideas, concepts and perspectives on its constituent parts. P&SCM encompasses a wide range of organisational processes, activities and actors, in many different contexts and types of organisations. It therefore makes sense to adopt a multidisciplinary perspective when seeking to explore and understand this complex and multifaceted aspect of organisational and business life.
This chimes with the fundamental tenets of realist review, which proposes that the focus should be on explaining what works, for whom, in what circumstances and why, rather than making normative judgements about what should be. The logic of realist review, therefore, is to explore theory and evidence to see what light is shed on the relationship between context, intervention (practice), mechanism (theoretical explanation) and outcome in a particular programme or initiative. Given its emphasis on context, realist review is about reflecting on the explanatory scope of different theories to develop contingent principles and guidance rather than to make universal rules. 33 With this in mind, we need to develop an interpretation framework, or a theory map, that surfaces the contextual assumptions, key explanatory mechanisms and intended outcomes embedded in each of the P&SCM theories discussed above. This is presented in Table 5.
| Literature and cognate theories/models | Contextual assumptions | Key explanatory mechanisms | Intended outcomes |
|---|---|---|---|
| Organisational buying behaviour | |||
|
|
|
|
| Economics of contracting | |||
|
|
|
|
| Networks and interorganisational relationships | |||
|
|
|
|
| Integrated SCM | |||
|
|
|
|
This framework illuminates two important points. First, it reinforces the idea that there is no single, universal theory of P&SCM, nor is there ever likely to be one given the diversity of contextual assumptions, mechanisms and intended outcomes which might be relevant to this broad and multifaceted research domain. As we discussed earlier, P&SCM has a number of interrelated or nested layers, each of which can be seen as a legitimate unit of analysis. As Table 2 shows, each broad literature focuses our attention on one of these layers or units of analysis, whether it is the intraorganisational (buying) group, the buyer–supplier transaction, interorganisational relationships or the wider supply network. This suggests, as others have argued,50,61 that these different literatures should be seen as complementary. Second, the framework suggests that practitioners engaged in P&SCM activities face choices about which theory might work best as a basis for interpreting their situation and for guiding their actions.
Conclusions
Having delineated the wide range of literatures, theories and models of relevance to P&SCM practice, we can begin to draw some conclusions using the CMO logic of realist review.
One important conclusion suggested by the realist interpretation framework in Table 5 is that it may be more appropriate to focus on some mechanisms than on others depending on what an organisation’s interest is in terms of intended outcome. If, for example, the intended outcome is to mitigate the technical or competence risks associated with a particular procurement decision (e.g. the reliability of a supplier’s offering or its compatibility with the buyer’s systems), then the mechanisms of interest should be the characteristics of the buying centre, the handling of intraorganisational conflict, and the nature of decision rules, information search and purchase history, predicated on the organisational buying behaviour literature. Alternatively, if the intended outcome is more about mitigating the behavioural risks of a procurement decision (various manifestations of supplier opportunism), then the mechanisms of interest should be the contractual or governance safeguards supporting the transaction, predicated on agency theory or TCE respectively.
Procurement decisions are often about much more than risk mitigation, however. Where there is an interest in the benefits that can flow from P&SCM practice (value appropriation, value-creating innovation, or improved efficiency and responsiveness), then the mechanisms associated with the interorganisational relationships literature or the integrated SCM literature are the appropriate focus. The former literature focuses attention on the mechanism of the buyer–supplier relationship and its position in a wider network of relationships and suggests that value appropriation, and potentially value creation, is a function of understanding and cultivating these interactions. The integrated SCM literature has a similar interest in buyer–supplier relationships, but sees these in mechanism terms as an integrated extended supply chain operating on the basis of close co-ordination and collaborative effort to deliver a more efficient or responsive outcome.
These insights are at a generic level, however. Thus, a second important conclusion that we can draw from our discussion is that the precise characteristics of the mechanism–outcome configurations outlined above are likely to vary depending on the context. For example, the organisational buying behaviour literature informs us that the various characteristics of a procurement decision (e.g. size and complexity of buying centre, formality of decision rules, extent and intensity of information search) vary depending on the level of risk associated with that decision, which in turn depends on the characteristics of the purchase. 59 Similarly, the integrated SCM literature tells us that choosing the appropriate techniques to integrate and co-ordinate a supply network, and the outcomes that those techniques are likely to have, depend on the nature of the product or service delivered by the network. 165 The interorganisational power literature also suggests that management choices, in this case concerning the extent to which a buyer and a supplier collaborate with one another, are shaped by the power context. 166
These observations draw our attention to the work of writers such as Kraljic167 and Fisher168 who offer so-called portfolio models of P&SCM practices. Kraljic’s landmark paper167 suggests that buying organisations should categorise their purchases along two dimensions: the level of supply market complexity and the importance of the purchase. Using these dimensions Kraljic identifies four types of purchase (strategic, leverage, bottleneck and non-critical), and he suggests how each should be managed in terms of the characteristics of the procurement process (i.e. specification, supplier selection criteria, negotiation style, contract design, relationship style). Fisher168 offers a similar contingency argument, but categorises whole supply chains in terms of the nature of the end product or service, identifying them as either functional or innovative. He suggests that supply chains delivering functional products have a predictable demand pattern and should therefore be integrated and co-ordinated using lean supply techniques. Conversely, he suggests that supply chains delivering innovative products have an unpredictable demand pattern and should be managed using agile or responsive supply techniques. In summary, this discussion suggests that the general mechanisms in each P&SCM theory proposed as explaining different outcomes might best be understood as an expression of specific practices or interventions used in particular contexts.
We take forward these issues raised by questions of context, mechanism and outcome in the next two chapters. In Chapter 4 we discuss the particular context of NHS commissioning and procurement by considering what the P&SCM theories discussed in this chapter might reveal about the underlying mechanisms and the intended outcomes embedded in NHS commissioning and procurement policy. In Chapter 5 we review evidence on the nature of NHS commissioning and procurement practice and consider how far the theories discussed here are relevant and useful to understanding that practice.
Chapter 4 Procurement and supply chain management theories in NHS policy
Introduction
This chapter and the next together address RQ2, which asks: how can theories about P&SCM in general help NHS managers and clinicians in their commissioning and procurement activities, in particular in the light of recent and planned changes to commissioning structures, incentives and processes in the NHS? We are interested, then, in the relevance and utility of the theories discussed in Chapter 3 for helping us to make sense of English NHS commissioning and procurement, and for understanding what effective policy and practice might look like. This chapter deals with policy and the next with practice.
We begin in the next section by examining a number of the key themes – mechanisms and intended outcomes, in realist review parlance – underpinning the changing NHS policy landscape and discuss how these might be understood in terms of the P&SCM theories that we have identified. Then in Chapter 5 we review evidence on the nature of NHS commissioning and procurement practice, and consider the relevance and utility of the P&SCM theories for understanding the CMO configurations of these practices. Our discussion of the evidence is presented using the four broad procurement process phases identified in Chapter 3 (demand management, selection and contracting, relationship management and operational delivery) to enable us to focus on the CMO configurations in these discrete aspects.
Key themes in NHS commissioning and procurement policy
By tracing the changing policy landscape in NHS commissioning and procurement since 1991, and its manifestation in a shifting organisational settlement, we can discern an overarching market-orientated and modernising discourse of innovation, choice and competition intended to deliver greater efficiency and responsiveness to patient needs. A number of key features of this discourse are illustrated in Table 6, showing how changes since 1991 have moved the NHS away from the model established at its inception in 1948.
| Key dimension | 1948 model | New model |
|---|---|---|
| National standards | None | National Institute for Health and Care Excellence sets national policies on access to different health technologies Treatment standards embedded in national service frameworks and monitored/regulated by Care Quality Commission |
| Service providers | Local monopoly: NHS only | Any qualified provider: NHS, private or third sector Monitor (regulator) to ensure fair competition through adherence to competition law |
| Working practices | Rigid professional demarcations | Modernised flexible professionals |
| Patient–clinician relation | Clinician as decider, patient as passive recipient of predetermined treatment plan | Clinician as advisor, facilitating patient voice (freedom to choose where and when to receive treatment) |
| Resource allocation | Managerially led, centralised and hierarchical | Clinically led and decentralised; devolved to primary care |
Some tensions have arisen within this overarching discourse as a result of contradictory practices and structural continuities persisting from the pre-1991, unitary system. Competing forms of governance – hierarchy, market and collaborative network – continue to coexist. 10 Policy rhetoric about introducing market-style competition into the NHS has often been undermined by hierarchical management interventions, such as underwriting the deficits of individual NHS trusts at the end of the financial year to avoid service disruption and damaging political fallout. 169 Commissioners have preferred to spend their budget on familiar local providers, what Exworthy and Peckham170 call ‘localism’, which suggests a reliance on well-established network-style relationships. Nonetheless, successive reforms to the structures and processes of NHS commissioning and procurement do broadly reflect these notions of innovation, choice and competition. In what follows, we examine three main policy themes – mechanisms and intended outcomes, in realist review parlance – which draw upon this overarching discourse. In particular, we discuss how these themes (summarised in Box 8) might be understood in terms of the P&SCM theories that we identified in Chapter 3.
-
Clinically led commissioning and evidence-based procurement.
-
Co-ordination or consolidation of spending through collaborative commissioning and procurement structures.
-
Market-based reforms to separate purchaser and provider, introduce patient choice and stimulate competition on the provider side.
Clinically led commissioning and evidence-based procurement
As we have noted, there have been various policy initiatives since the purchaser–provider split in 1991 designed to introduce clinically led commissioning by devolving budgets to GP practices. These are GP fund-holding, the Total Purchasing Pilots, practice-based commissioning and most recently the creation of Clinical Commissioning Groups. Although various distinctions can be drawn between these initiatives (i.e. indicative or real budgets, voluntary or mandatory participation by GPs), all are based on the same underlying theoretical assumptions and therefore posit the same relationship between mechanisms and intended outcomes. First, all of these initiatives assume that GPs are in a better position than non-clinical managers to make appropriate and effective commissioning decisions, because they have the clinical expertise necessary to properly understand the treatment options available from providers. Second, these initiatives assume that GPs know the specific local needs of their patients better than a remote administrative body such as a district health authority or a primary care trust and can therefore make more responsive and tailored commissioning decisions. Third, GPs will make better and more efficient commissioning decisions if they are accountable for the money that is spent and are able to reinvest in their practice a share of any budgetary surplus. Finally, as GPs are the actors providing continuity of care for patients in their area, they have a strong incentive to refer their patients to the best-performing providers of secondary care, those with the shortest waiting times and the best quality of care. It is assumed that this will in turn put pressure on other providers to improve. 11,171,172
By identifying these underlying mechanism–outcome configurations we can see the relevance of two of the P&SCM literatures to this policy theme. The organisational buying behaviour literature draws our attention to the central issue of risk management in buying decisions. 59 One of the arguments made is that the participants involved in higher-risk buying decisions will typically be highly qualified and experienced, and will be motivated to commit greater attention throughout each stage of the buying process. 75 Clinically led commissioning draws on this argument by suggesting that greater involvement by GPs, with their clinical expertise and experience, will lead to more appropriate and effective decisions that better mitigate clinical risk. Moreover, it is assumed that GPs will be motivated to give greater attention to specific, local needs in the commissioning process, because they have a closer, ongoing relationship with their patients. The economics of contracting literature, in particular agency theory,80 is also relevant here even though the GP–patient relationship is not based on a formal contract. As Greener and Mannion36 note, clinically led commissioning is intended to better align the interests of patients (principals) and GPs (agents) by creating ‘incentives for GPs to refer patients to the best-performing providers, increasing their responsiveness, and encouraging GPs to save money by prescribing or referring only when necessary’ (p. 60).
Alongside these clinically led commissioning initiatives, there has been an intention to ensure that procurement decisions are better informed and more consistent across the NHS. Historically in the NHS there was no systematic comparative evaluation of the efficacy of health technologies (drugs, clinical techniques and medical devices). Consequently, the procurement of different technologies was largely determined by the subjective judgements of clinicians and the marketing efforts of suppliers. Different decisions in different areas led to so-called postcode prescribing. A policy intention to address such inequalities through evidence-based procurement led to the setting up in 1999 of what is now called the National Institute for Health and Care Excellence (NICE). This body undertakes evaluations of health technologies and sets national policies for their use in the NHS. Given its limited resources, however, NICE focuses its attention on those technologies which are particularly complex and where the potential benefits are uncertain or on those which may have a major clinical impact. 15 In other words, it evaluates the highest-risk treatments.
Again, the organisational buying behaviour literature can help us make sense of the role played by NICE as a mechanism for systematic information search and as a source of decision rules for buying. The literature suggests that searching for information about supplier options will become more active and extensive as procurement risk, linked to uncertainty and complexity, increases. The literature also suggests that there will be a preference for more formal decision rules as procurement risk increases. Such decision rules act as a governance mechanism to bring clarity and co-ordination where there are a diverse range of conflicting preferences. 59 NICE can thus be seen as a response to the need to mitigate and manage the high risks associated with particular health technology procurement decisions.
Co-ordination or consolidation of spending
Our discussion of the changing policy landscape has identified a number of initiatives involving the co-ordination or consolidation of spending, at local, regional or national level, through joint commissioning and procurement structures. On the health-care-commissioning side these are the Total Purchasing Pilots which operated from 1995 to 1999,172 the primary care groups introduced in 1999 as a forerunner to primary care trusts,173 the area teams of NHS England established in April 2013 to commission specialist services at a regional level, and the Clinical Commissioning Groups established at the same time to replace primary care trusts. 31 Primary care trusts were also encouraged from the early stages of their development to commission jointly. 174 In 2006 this joint commissioning was enforced and formalised by merging adjoining primary care trusts, reducing their number from 303 to 152.
As discussed above, each of these initiatives (with the exception of regional commissioning by NHS England) has GP-led commissioning as a core principle, but each has also focused attention on the benefits that are available if commissioning is done jointly or collaboratively by bringing together a number of GP practices. The primary benefit identified, and therefore the main theoretical assumption behind collaborative commissioning, is that GP practices acting jointly will achieve greater purchasing power in their dealings with NHS hospital trusts and with other providers. 175–177 This should enable them, in turn, to hold providers to account for their performance more effectively and to engage with providers on performance improvement. Collaborative commissioning by groups of GP practices has also been identified as a means of addressing the lack of co-ordination and higher agency or transaction costs associated with commissioning by individual fund-holding practices. 20 These initiatives are thus seen as a way of increasing purchasing power and of economising on agency or transaction costs, the costs of negotiating, drafting and monitoring contracts.
On the procurement side, the co-ordination or consolidation of spending by NHS trusts has been facilitated at the national level by NHS Supplies, later NHS Logistics and now NHS Supply Chain. The NHS Purchasing and Supply Agency also played a role here through its national contracting function. At the regional level, co-ordination has been through the virtual NHS Supply Management confederations, and later the formally constituted collaborative procurement hubs. These organisational initiatives are, like those in collaborative commissioning, intended to increase the procurement leverage available to NHS trusts and help them economise on agency or transaction costs by buying goods and services on their behalf where they have common requirements.
A key aspect of these initiatives has been efforts to develop and implement e-procurement systems in the NHS. 15 The Purchasing and Supply Agency played a significant role here as part of the Supply Chain Excellence Programme launched in 2003. E-procurement systems are a crucial source of basic information about the demand requirements of NHS trusts (volume and usage patterns), which suppliers are being used and how they are performing on price, quality and delivery times. This information is essential to understanding the scope for co-ordination or consolidation of spending at regional or national level. In addition, e-procurement is a key enabler for organisations such as NHS Supply Chain to work in a more integrated way with suppliers in an effort to create leaner supply chains with faster lead times and lower inventory levels. Using IT to improve information sharing with suppliers has been integral to NHS Supply Chain’s efforts to meet a target of cost savings in excess of £1B over the life of its 10-year contract.
Identifying these underlying mechanism–outcome configurations draws our attention to contributions from three of the P&SCM literatures. First, and most prominently, we can see the relevance of the networks and interorganisational relationships literature, specifically that dealing with resource dependency theory134 and interorganisational power. 133,178 This literature proposes that the power structure underpinning a buyer–supplier relationship shapes the supplier’s willingness to perform well and the buyer’s ability to hold the supplier to account for poor performance. It is argued that either a dominant or an interdependent position for the buyer will provide the necessary performance incentive. The literature also suggests that the power structure impacts on a supplier’s willingness to work collaboratively with the buyer to improve its performance. Again, it is argued that the supplier’s incentive to work with the buyer to improve its performance will be strongest where the buyer is dominant or buyer and supplier are interdependent. Seen in the context of this argument, policy initiatives to achieve joint commissioning or collaborative procurement can be understood as an attempt to give commissioners or NHS trusts greater power resources in their interactions with providers or suppliers, to achieve if not dominance then at least interdependence.
A second relevant literature is an extension of agency theory discussing collaboration between principals. In this case the principals are either the commissioners or the NHS trusts acting as buyers. This extended agency theory suggests that, where there are multiple principals asking a single agent (provider or supplier) to act on their behalf, the principals should collaborate and offer a joint contract if they share a common set of information and can make a commitment to shared outcomes or common requirements. 179 By offering a joint contract in these circumstances, the principals would serve their self-interests by setting shared rather than competing incentives, thereby economising on agency costs. 174 Finally, aspects of the integrated SCM literature are relevant to understanding the role of e-procurement in helping to co-ordinate NHS trust demand and match it with supply more efficiently. This literature focuses our attention on the sharing of information with suppliers as a means of signalling commitment to drive ongoing performance improvement.
Market-based reforms
The introduction of various market-based reforms into the NHS has been a prominent and much discussed policy theme over the past two decades. 180–184 This theme concerns changes in the nature of only health-care commissioning, with the progressive development of market-style structures and processes intended to engender enhanced patient choice and greater provider competition and thereby stimulate improved performance. The procurement of clinical and non-clinical goods and services has not been the target of these reforms.
The initial manifestation of these reforms was the creation, in 1991, of the internal market based on the purchaser–provider split. Before this, the NHS had been managed on a hierarchical basis, without a clear distinction between who was planning and paying for health care and who was providing it. After 1991, there was an intention to create the essential components of a market, a plurality of commissioners (district health authorities and GP fund-holders) and a significant number of independent self-governing community and acute trusts on the provider side. These provider trusts were supposed to compete with one another to offer the services needed by the commissioning organisations. 9 This initial Conservative government attempt to introduce market forces into the NHS was tempered by the New Labour government elected in 1997 with talk of more collaboration in the form of longer-term service delivery agreements. The fundamental structural characteristic of the internal market, separation between commissioners and providers, remained in place, however.
Then, after a period of quiescence, New Labour moved during its second and third terms to re-establish the momentum by introducing its own set of market-based reforms. These had four main strands. First, a policy of fixed-price reimbursement, payment by results, was progressively introduced, beginning with elective secondary care in 2005 and then covering outpatient, non-elective and accident and emergency services over the next 3 years. Payment by results replaced the traditional block or cost and volume contracts used in the NHS with a system under which providers were paid a fixed tariff for each episode of a particular type of care. It was intended to encourage providers to be more efficient by reducing their costs to below the tariff level and by increasing patient throughput, thereby reducing waiting times. 185 Second, there was an effort to put providers under some competitive pressure to perform through the ‘Patient Choice’ policy. 22 This gave patients the right, with the support of their GP, to choose their provider for elective secondary care. 29 Third, the choices available to commissioners were extended through a policy of ‘Any Willing Provider’, which allowed private sector providers to offer elective secondary care at payment-by-results tariff prices as long as they were able to meet NHS quality standards. The ‘Right to Request Scheme’ launched in 2008 was intended to stimulate a similar extension of provider choice in community health care by enabling NHS staff to ‘spin out’ their services into social enterprises. 186 Finally, from 2004 better-performing NHS trusts were given foundation trust status, which meant they had greater autonomy from and less accountability to the central NHS. This earned autonomy included the freedom to act in a more business-like way, for example raising capital to invest in new services as a means of generating additional revenue. 26 The intention was to give foundation trusts the same autonomy enjoyed by non-NHS providers.
Since 2010, the coalition government has extended patient choice and the payment-by-results tariff system into mental and community health services, and it has reaffirmed a commitment to diversity and competition on the provider side through its ‘Any Qualified Provider’ policy. This extends the previous government’s market access policy by further opening up primary care and community health services to non-NHS providers. Significantly, the coalition has also removed the previous government’s preference for NHS providers where they were delivering satisfactory performance by establishing a market regulator, Monitor, tasked with ensuring fair and open competition between all potential providers. The government has also made clear that it intends all NHS trusts to take on foundation trust status to give them the autonomy needed to compete effectively. 187
Having identified the key mechanism–outcome configurations underpinning this policy theme, we suggest that two of the P&SCM literatures can provide relevant insights. The first, and perhaps most obvious, is the economics of contracting literature, encompassing agency theory and TCE. This literature is relevant, because, as one reading of the reforms would have it:
Contracts were the fulcrum of the internal market. The separation of purchasers and providers could work only if there was agreement over what health care should be provided and at what price.
pp. 255–6188
At first glance, agency theory, with its argument about complete contracts as the best way of aligning the divergent interests of purchaser (principal) and provider (agent), seems the most relevant lens. 189 The notion of complete contracting was fairly explicit in early guidance from the Department of Health,12 which proposed that purchasers should operationalise their requirements, including those relating to quality standards, through contractual specifications. Contracts were thus seen as an effective way of controlling provider behaviour and enhancing their accountability by making the performance required of them explicit. 188
This view on the role and nature of contracts in the NHS has been widely criticised as too simplistic, however, and TCE has been suggested as a more relevant and useful theoretical lens. 171,188,190 It is argued that the commissioning and provision of many health-care services is characterised by the features identified by Williamson86 as leading to incomplete contracting. Williamson argues that, in conditions of bounded rationality, uncertainty and complexity, the transaction costs of trying to negotiate, draft and enforce a detailed and comprehensive contract will be too high and will lead either to hierarchical management of a transaction or to a form of co-operative bilateral governance akin to Macneil’s104,191 relational contracting.
Not all transactions have these characteristics, of course, and a complete contract as specified by agency theory may sometimes be possible and desirable. For example, the introduction of the payment-by-results tariff system can be interpreted as an attempt to adopt the principles of complete contracting. 192 Payment-by-results tariffs are set on the basis of a predetermined national average cost, or on occasion ‘best practice’ cost, for particular procedures and are intended to incentivise providers to behave more efficiently at the level of individual episodes of care. 27 Williamson’s argument suggests, however, that complete contracting cannot be a ubiquitous solution and that the three forms of transaction governance he identifies, market, bilateral and hierarchical, are likely to coexist in the NHS. This is indeed what has been observed in a number of studies. 10,171,192,193
These observations about the continuing coexistence of different forms of governance in the NHS suggest that the interorganisational relationships literature might also enhance our understanding of this policy theme. A major criticism of the economics of contracting literature is that these theories are solely interested in efficient contracting or governance at the level of discrete transactions, and largely ignore the wider context of ongoing buyer–supplier relationships and their position in a network of other relationships. 105 Work by a number of authors (cf. Allen,188 Ferlie and McGivern,194 Gray and Higgins,184 Guven-Uslu192) addresses this criticism by drawing on the networks and interorganisational relationships literature, particularly that dealing with trust, commitment and collaboration,114,115,195,196 to understand how market-based reforms in the NHS have been enacted in practice. It has been observed, for example, that, even after the introduction of the internal market:
the purchaser–provider relationship within the NHS worked largely through inter-organisational cooperation, heavily reliant on goodwill trust and a willingness to commit to relationships with partner organisations over the medium to long term.
p. 45184
The same authors also recognise that continuing market-based reforms in the NHS (‘Any Qualified Provider’, payment by results, awarding hospitals foundation trust status) are likely to suppress or undermine elements of this interorganisational co-operation, but they do not conclude that it will simply be washed away. The networks and interorganisational relationships literature will remain a relevant lens for helping us to interpret the impact of the reform process in NHS commissioning.
Round-up
Having examined the relevance of the various P&SCM theories to the changing NHS policy context, we turn in the next chapter to a review of evidence about NHS commissioning and procurement practices. We consider the relevance and utility of the P&SCM theories for understanding the CMO configurations of these practices. Our discussion of the evidence is presented using the four broad procurement process phases identified in Chapter 3 (demand management, selection and contracting, relationship management and operational delivery) to enable us to focus on the CMO configurations in these discrete aspects.
Chapter 5 Procurement and supply chain management theories in NHS practice
Evidence on demand management in the NHS
Demand management refers to decisions about what needs to be commissioned or procured, who might be the potential providers or suppliers, and what criteria are to be used to select the provider or supplier. We argued in Chapter 3 that demand management is typically discussed in terms of the arguments made in the organisational buying behaviour literature. The evidence on demand management in the NHS is also discussed in terms of these kinds of arguments, but there are few direct and explicit references to the organisational buying behaviour literature. Papers look at commissioning and procurement decisions in terms of the role, expertise and experience of decision-makers; the size and composition of decision-making units; the nature of the decision-making process; and the criteria that influence specific decisions. There is evidence of the political nature of some commissioning and procurement decisions and the impact of power on the resolution of conflicts between the preferences of different actors. 197,198 There is also evidence of the use of sense-making behaviours, persuasion rather than power, to influence commissioning decisions. 199
Looking at evidence on the expertise of decision-makers, the size and composition of decision-making units and the criteria that influence their decisions, a number of themes suggested by the organisational buying behaviour literature emerge. Lian and Laing200 examine the role of health professionals in the purchasing of occupational health services by private sector firms. Their data show that, given the complexity and intangibility of health services, purchasing managers are heavily reliant on the expertise of their health service providers to help them make effective purchasing decisions. Although these data are not drawn from the NHS, Lian and Laing conclude that the lessons learned in their research can and should be applied to the NHS in what amounts to clinically informed, if not quite clinically led, commissioning.
Continuing this theme, there have been a number of studies into the efficacy of smaller-scale GP-led commissioning as opposed to larger-scale managerially led commissioning. 13,20,171,172,201,202 These studies are equivocal in their conclusions. On one hand they conclude that locally based initiatives such as GP fund-holding and total purchasing pilots were more responsive in securing improvements in primary care to meet the needs of particular groups of patients. On the other they observe that, despite the clinical expertise of GPs, there is no firm evidence that they have been able to make better commissioning decisions on secondary or specialist care than non-clinical managers. As Wyke et al. (p. 256)172 put it, GP-led commissioning is likely to be more effective:
in circumstances where the main purchasing task is to alter the balance and location of care between hospital and extramural settings . . . Other forms of purchasing or management may be more appropriate when the principal challenge facing the system is to improve the mix or quality specifications of specialist services.
Dopson and Locock171 suggest that this may be partly about an asymmetry between the generalist clinical knowledge of GPs and increasing specialisation at the secondary care level. It could also be argued that GPs might find it difficult to translate their clinical experience of working with individual or relatively small groups of patients to commissioning services on behalf of much bigger populations.
Laing and Cotton203 observe that GP fund-holders tended to respond to this knowledge asymmetry by using provider reputation and their past experiences of a working with a provider as bases of commissioning decisions rather than using formal measures of previous service outcomes. The setting up of NICE in 1999 was an attempted response to the perceived inequities caused by such informal decision criteria. Work by Hughes and Doheny204 on the procurement of a high-cost cancer treatment concludes, however, that such decisions are only partially influenced by NICE guidance and are still subject to significant local professional judgement. They argue that this is a function of the staged, conditional and complex nature of NICE guidance.
Using research in the context of practice-based commissioning, Checkland et al. 205 provide some valuable insights into the nature of a good commissioning manager. As an exemplar of success they identify what they call ‘the manager as animateur’, that is a primary care trust manager who works in a particularly ‘active, yet non-hierarchical’ way with disparate groups of GPs to align their objectives (p. 14). 205 Drawing out the implications of their findings for the Clinical Commissioning Groups, they conclude that it may be unhelpful to engage in an either/or debate about whether GPs or non-clinical managers should lead. Rather, the focus should be upon the role of managers as facilitators of the desired behaviours by GPs.
Evidence of the political character of decision-making processes in NHS commissioning and procurement has been provided by a number of authors. Horrocks et al. 206 and Martin207 look at the involvement of patient groups and members of the public in commissioning decisions. They conclude that the power of these actors to have a meaningful influence on decisions is highly contingent on factors such as decision scope and the coherence of a group’s ‘voice’ on the matter under consideration. In many instances they find that such groups play a largely symbolic role, merely legitimising decisions made by the NHS professionals. Allen et al. (p. 508)208 note that, despite the rise of managed professional business archetypes in the NHS, health-care professionals continue to dominate procurement decisions ‘through the referrals they make, the tests they order, and the drugs they prescribe.’ Lonsdale and Watson198 apply a political model of procurement decision-making to the buying of pathology equipment and consumables in a NHS acute hospital trust, and identify the key role of powerful actors, most notably senior clinicians, in pursuing their own preferences as a major driver of fragmented expenditure leading to extracting poor value for money from suppliers. Cox et al.,197 similarly, discuss the ways in which the clinician-dominated character of many NHS trust procurement decisions leads to fragmented patterns of expenditure and thereby damages value for money and the scope to improve supplier performance.
Checkland et al. 199 discuss sense-making by middle-level managers in primary care trusts and show how this might impart some influence in a highly political decision-making process, but through the use of persuasion rather than power. They identify two important sense-making behaviours: selective attendance at meetings, with priority being given to those where the agenda is not tightly predefined; and the production of artefacts (meeting minutes or presentation slides) to shape the parameters and terms of the decision-making process. They conclude that these sense-making behaviours may now be more difficult to enact for managers working in the commissioning support units. Their contractual relationship with the Clinical Commissioning Groups may limit free discussion in scheduled meetings and reduce the scope to develop shared understandings of any artefacts that are produced.
Evidence on selection and contracting in the NHS
‘Selection and contracting’ refers to the decision to award a contract to a provider or supplier, to the process of agreeing contractual terms and conditions, and to efforts to ensure that those terms and conditions are honoured either through monitoring and enforcement or, where necessary, dispute resolution. We argued in Chapter 3 that selection and contracting is typically discussed in terms of the arguments made in the economics of contracting literature, encompassing agency theory and TCE. This literature focuses our attention on the potential for provider or supplier opportunism and on the mechanisms that might be used to mitigate such behaviour. Agency theory proposes the use of complete contracts written ex ante. TCE suggests a range of governance mechanisms from spot market, through co-operative bilateral governance, to administrative hierarchy depending on the characteristics of a transaction.
Research on selection and contracting in the NHS also explicitly acknowledges the relevance of these theories. TCE is, though, typically regarded as a more appropriate and useful lens given the difficulties of writing complete contracts ex ante for the delivery of health-care services characterised by uncertainty, complexity and acute information asymmetry. 171,188,190,209 Health-care services share these credence good characteristics89 with professional services such as management consultancy and legal services. 92,95 Some writers181,188,210 also draw on what they see as complementary ideas from relational contract theory,104,191 demonstrating that this phase of the procurement process overlaps and interacts with the postcontract relationship management phase.
We turn first to evidence on provider selection and contracting by NHS commissioners. Allen’s188 study of contracting for district nursing services by a health authority and GP fund-holders shows that the conditions needed for writing complete contracts did not pertain. She observed information asymmetry greatly favouring providers and notes that it was not possible to specify the nature of the services fully or to monitor them fully, because district nursing is complex, consisting of a wide range of continuing activities. She also observed that where efforts had been made to negotiate and draw up contractual documents these ‘were far from complete and were poorly drafted’ (p. 261). 188 Her primary conclusion is that some aspects of these contracts mirrored the co-operative relational mechanisms that would be predicted in these circumstances by TCE or relational contract theory, but that the picture was complicated by the wider institutional context of the NHS. This imposed a number of hierarchical, administrative controls on the award and operation of these contracts, and meant that, although they were clearly not complete, they could not be characterised as entirely relational either.
Other studies reach similar conclusions about the limitations in a NHS commissioning context of complete or classical contracting based on agency theory. Bennett and Ferlie181 study contracting for complex, multiagency human immunodeficiency virus/acquired immunodeficiency syndrome services within the NHS. They observe that the model of classical contracting is only ‘patchily evident’ in the four health authorities covered by their research. They find more evidence, in line with TCE and relational contract theory, of purchasers encouraging co-operative relationships with providers ‘to preserve stability’ (p. 49). 181 They also find that the wider institutional or regulatory context of the NHS constrains the ability of purchasers to develop classical contracts with an unrestricted choice of providers. Hughes et al. 210 study contracting for secondary care services in the NHS, comparing the situations in England and Wales in the period 2008–10. They find that despite policy differences, with commissioners in England being encouraged to use more classical and harder-edged service contracts while those in Wales were emphasising co-operation and flexibility in the contracting process, practices on the ground were still remarkably similar. In particular they find, in tune with relational contract theory, that ‘long-term relationships and trust between purchasers and providers had an important role in both systems when the financial viability of organisations was at risk’ (p. 1). 210 This recourse to relational contracting is explained partly by the exigencies of local geography, history and patient expectations and partly, once again, by administrative pressures in the wider NHS context.
By way of contrast, Coleman et al. 211 provide evidence that classical, complete contracting does sometimes occur in a more fully developed form in the NHS, but not without problems. Their research, done in 2009–10 with two case study primary care trusts, shows that contracting for Alternative Providers of Primary Care was clearly of a transactional nature, defined as ‘sticking more rigidly to specified timescales and targets and having the ability to penalise poor performance and ultimately terminate contracts’ (p. 8). 211 They argue that there was a strong incentive to use this transactional approach, because the primary care trusts were contracting with new and often untried providers with which they had no prior relationships. There was a concern, therefore, to specify as clearly and as completely as possible the performance expected of providers and the penalties available to commissioners in the event of poor performance. The paper also identifies obvious problems with complete contracting, however, in particular very high transaction costs associated with contract negotiation and drafting and with the monitoring of performance against detailed targets.
Allen et al. (p. 29)180 provide complementary evidence of the high transaction costs incurred by health-care service commissioners and providers in tendering processes and suggest that these may ‘vitiate the efficiency gains of competition.’ Mannion, Marini and Street212 suggest there may also be transaction cost problems with efforts to introduce complete contracting in the form of payment by results, flowing in particular from the monitoring of provider behaviour to mitigate the potential for opportunistic gaming of the system through activities such as up-coding.
Turning to research evidence on supplier selection and contracting by NHS trusts, we also see an acknowledgement of the relevance and utility of agency theory and TCE as theoretical frames of reference. Lonsdale and Watson98 provide evidence from the management of PFI contracts by six NHS trusts, covering both the construction of hospital buildings and the delivery of facilities management services. Accounts from the trusts’ procurement and contract management teams suggest the existence of two main types of supplier opportunism: moral hazard (quality shading) and hold-up (precontractual drift and postcontractual variations). The scope for this opportunism is explained in terms of the complexity, ambiguity and uncertainty of the trusts’ requirements, which can in turn generate contractual incompleteness. Interestingly though, and in contrast with much of the evidence on the use of contracts in NHS service commissioning, the procurement teams in these cases had a preference for mitigating supplier opportunism through contracts written ex ante and associated mechanisms for competitive pressure and monitoring rather than using co-operative bilateral governance. Most of those interviewed ‘believed that buyers could, not always, but on many occasions, manage opportunism through the contractual process’ (p. 691). 98 Thus, while TCE is a relevant source here of explanations for the problems of supplier opportunism, hold-up in particular, agency theory is a more appropriate reference point for managers’ efforts to mitigate these problems. One possible explanation for this preference for classical contracting is that ‘none of the trusts had any history with their PFI suppliers; they had all established new relationships’ (p. 695). 98 As discussed above, however, classical contracting is not a panacea when dealing with complex, ambiguous and uncertain requirements, and most of the trusts in Lonsdale and Watson’s study were still struggling to control the opportunism of their suppliers.
Lonsdale et al. 209 provide a very similar analysis of supplier opportunism in their study of NHS trusts’ procurement of agency nursing services in the period 1997–2007. They identify various types of opportunism related to information asymmetry (adverse selection and moral hazard) between trusts and nursing agencies. They observe that trusts working individually and in concert with the NHS Purchasing and Supply Agency tackled this opportunism in the first instance through a combination of contractual and monitoring mechanisms, in particular detailed framework agreements and quality audits. They also observe, however, that over time the trusts’ procurement management response went beyond the purely contractual mechanisms recommended by agency theory to draw on the kind of co-operative bilateral governance mechanisms suggested by TCE. Recognising continuing problems of contractual incompleteness, linked to difficulties in specifying service requirements precisely and matching nurses appropriately with those requirements, trusts sought to develop preferred supplier and master vendor agreements ‘to ensure reliability and commitment and assist with the development of closer relationships’ (p. 814). 209
Evidence on relationship management in the NHS
As discussed in Chapter 3, analysis of the ongoing management of buyer–supplier relationships is typically framed in terms of arguments made by the networks and interorganisational relationships literature. This literature has a number of different subsets, but these share overlapping theoretical roots grounded in social exchange theory, resource dependency theory and relational contract theory. Key explanatory mechanisms of common interest to these various subsets are the dynamic nature of interactions between buyers and suppliers over time; the gradual emergence of close, high-trust relationships in some cases; recognition of and a need to cope with dependency on others; and the embedded nature of individual relationships in a wider network. The common interest in terms of outcomes is in how value is distributed between the members of a network and how value might be created through innovation.
The networks and interorganisational relationships literature is of clear relevance and utility in a NHS context, because, as Allen et al. 208 have argued, the NHS can be understood as ‘a network of multiple, extended supply chains, with purchaser and provider relationships operating as critical coordinating mechanisms at every level’ (pp. 506–7). Moreover, the reform process supporting greater patient choice in NHS service provision through the introduction of wider supply-side competition has made this network view of the NHS even more salient. 184 Unsurprisingly, then, a good deal of the research evidence on relationship management in the NHS is discussed in terms of concepts drawn from this literature. For ease of discussion, we can usefully divide relevant papers into those placing more emphasis on mechanisms such as trust and collaboration drawn from social exchange and relational contract theories, and those emphasising mechanisms such as power drawn from resource dependency theory. It should be remembered, of course, that these mechanisms are not discrete and that much of the research evidence is interpreted through a combination of conceptual lenses.
In the former category, Connel and Mannion213 and Goddard and Mannion214 look at the continuing importance of trust and co-operation in facilitating relationships between commissioners and providers in health and social care markets despite efforts to increase competitive tension. Their findings are mirrored by those of Bennett and Ferlie,181 Allen188 and Hughes et al. 210 discussed in the previous section. Frosini et al. 183 discuss how competition is characterised and experienced by NHS and non-NHS acute care providers. They find that the forces of structural (market) competition are muted, that there are many examples of collaboration between NHS and non-NHS providers, and that patients and GPs are loyal to local providers with whom they have historical relationships. This evidence for the embeddedness of relationships leads them to conclude that collaboration might be a better lever than competition for improvements in service quality. Chambers et al. 35 provide evidence of the effectiveness of a close, high-trust relationship between GPs and a private sector co-commissioner and provider in a case of whole system redesign in primary care. Their research suggests that commissioning based on a public–private partnership-type model is appropriate where innovation in a complex service is required, in this case aimed at service redesign for people with long-term conditions.
Porter et al. 215 provide complementary evidence in their study of how services are commissioned by three English primary care trusts for people with diabetes, stroke and dementia. They find that the quasi-market reforms implemented in the NHS have had little effect in these services and that commissioning is still largely relational, based on trust and collaboration with incumbent providers. They suggest that ‘the adaptive persistence of relational commissioning’ is unsurprising given the absence of ‘conditions for a well-functioning quasi-market’, such as clear demand information, clear specification of service requirements and an effective choice of providers (p. 1). 215 Sheaff et al. 216 further reinforce this theme of relational resilience in their research into how the NHS quasi-market reforms have affected four English health networks. They find that the reforms have had only a relatively limited impact on these networks. The biggest changes were evidenced in the formalised, managerial artefacts (e.g. reports, bids, guidelines) produced by the networks. There were also changes in some of the networks’ espoused values, those which both guided and legitimised changes in artefact production, but their underlying behavioural assumptions, essentially about the legitimacy and value of collaborative working, were largely unaffected.
Some research suggests, however, that the quasi-market reforms have had a more significant disruptive effect on trust and collaborative relationships between NHS commissioners and providers. This disruption brings mechanisms such as power more to the fore. Writing just after the implementation of the purchaser–provider split, Freemantle et al. 217 report on the development of relationships between district health authorities and their local hospital trusts. They observe a range of relationship types from ‘a rather cosy and comfortable co-existence to political chaos and absence of communication’ (p. 538). 217 In both cases, they conclude that the providers were considerably more powerful than the district health authorities. North218 examines a district health authority’s efforts to implement a purchasing strategy for stroke care services. She observes that the district health authority attempted to stick closely to the ideals of the internal market by dealing with the local hospital trusts on a formal arm’s length basis, even though there was no real competition for the providers in the area of acute stroke care. The health authority overcompensated for this lack of effective competition in acute care, by maintaining a threat of market testing for non-acute services. The result, North concludes, was a breakdown in reciprocity and, because the health authority’s assumption of market power was false, intransigence by the trusts. Guven-Uslu192 observes a similar lack of reciprocity and relationships in which two primary care trusts are dependent on a foundation trust hospital in her study of the use of management accounting information in commissioning under the payment-by-results system.
The work of Gray and Higgins184 provides evidence of the complex interplay between collaborative, trust-based relationships and competitive, power-based relationships in the NHS commissioner–provider interface. Evidence about the implementation of the payment-by-results tariff system by a primary care trust and two hospital trust providers in the Midlands region shows on one hand that their relationships move to being more arm’s length and focused on the threat of contractual sanctions. On the other hand, there is also evidence of a continuing legacy of more collaborative ways of working drawing on notions of goodwill trust to resolve disputes. Gray and Higgins184 suggest, however, that this legacy of collaboration is likely to come under a more sustained threat as hospitals are awarded foundation trust status and begin to seek out new income streams in services not covered by the payment-by-results system. Cast in the language of resource dependency theory, this implies a move by foundation trust hospitals to reduce their dependency on relationships facing increased competitive disruption from non-NHS providers.
Allen et al. 26 also investigate the impact of being granted foundation trust status on the relationships of NHS hospitals with commissioners and other providers in the local health economy. They find some evidence of efforts by foundation trust hospitals to reduce their interdependency with other NHS organisations and to achieve greater control over their own destiny. On the foundation trusts’ relationships with commissioners they find that ‘their clearer financial objectives, coupled with autonomy in decision-making, had meant that FTs [foundation trusts] were not always acting co-operatively with their local PCTs [primary care trusts] about service developments’ (p. 98). 26 On the foundation trusts’ relationships with other providers they find that ‘the hospitals in the study had developed a stronger sense of their own identity and of the need to protect their services and future income streams in the face of competition for funds’ (p. 98). 26
In one of the few papers that go beyond this focus purely on dyadic interorganisational power, Addicott and Ferlie219 examine the nature of power relations in wider network contexts. They look at how power was exercised and by whom in five managed clinical networks for cancer services in London. Rather than being emergent or based on long-standing relationships between health-care professionals, the creation of managed clinical networks was mandated by the Department of Health. The networks brought together multiple teaching and local district hospitals with service commissioners and health authorities within relatively small geographical areas. The policy objectives of these networks were to streamline patient care and to foster collaborative knowledge sharing to drive service innovation. There is an echo here of the idea of a strategic net,120 which is an intentionally designed network intended to deliver enhanced value.
The difficulty with the idea of managed clinical networks, and with strategic nets for that matter, is that they will deliver innovation only if there is a balance of power and a willingness to work towards common goals. As Addicott and Ferlie219 show, this was not the case in the networks examined by their research. Instead, they found a set of power relations that they characterise as ‘bounded pluralism’, wherein ‘a dominant coalition of medical professionals from the cancer centres battled to enact organisational change in their favour’ and ‘the interests of smaller district hospitals were seemingly ignored’ (p. 402). 219 Using the language of resource dependency theory, the power of these dominant medical professionals came from their possession of scarce and valuable (in the context of these networks) specialist knowledge about cancer. Crucially, this research suggests that collaborative interorganisational relationships and networks cannot be centrally imposed on the NHS given the power of certain elite subgroups of medical professionals. Collaboration can and does take place in NHS networks, but the nature of power relations is an important factor in when and where it occurs.
Evidence on operational delivery in the NHS
Finally, we turn to research evidence dealing with the operational delivery phase of the procurement process. This phase overlaps with the ongoing relationship management phase discussed above, but focuses more on the physical delivery tasks, inventory or capacity management, performance measurement and management, and process redesign to achieve improvements in efficiency and effectiveness. As we suggested in Chapter 3, discussions about operational delivery are typically framed in terms of the integrated SCM literature. This encompasses work from logistics, materials management and operations management, and is underpinned by behavioural economics in the form of game theory and systems theory. The key explanatory mechanism in this literature is collaboration between actors across an extended supply chain or network to build trust, facilitate shared understanding of problems and achieve co-ordinated effort to improve performance. It is seen as possible and desirable for the supply chain to be managed as an integrated and co-ordinated whole.
The integrated SCM literature is of relevance and utility in a NHS context, because it has an explicit and heavy emphasis on technical problem identification and continuous performance improvement. Ideas such as lean, agile and total quality management are relevant and useful in a context where resources are constrained, but high standards of quality (related to patient safety and dignity) and speed and responsiveness (related to patient satisfaction) have to be maintained. As a number of authors have observed,208,220,221 this literature has been highly influential in the work of the NHS Institute for Innovation and Improvement and its predecessor the NHS Modernisation Agency. Unsurprisingly, then, the research evidence on operational delivery in the NHS is typically discussed in terms of concepts drawn from this literature. This research can be broadly divided into papers which discuss the mapping and improvement of patient care pathways and associated processes (e.g. pathology, radiology, patient records), and papers looking at the management of interorganisational supply chains delivering clinical and non-clinical goods and services to health-care providers.
Turning to the first category of papers, we find work that explores the scope to introduce lean or agile principles into health-care organisations and that models patient flow through the phases of a treatment episode, seeing it as analogous to product flow in an industrial process. These papers therefore typically focus on what might be called the internal supply chain, which links the activities of various departments within a single NHS organisation. The extant literature suggests that lean and associated Six Sigma improvement techniques have been used and studied in the NHS more than agile techniques.
Grove et al. 222 present findings from a value stream mapping exercise in NHS primary care health visiting services. Value stream mapping is used to identify wasteful activity as a necessary precursor to the implementation of lean process improvement. Waste is defined as activities that are of no value to the customer or in this case the service user. Grove et al. 222 find that 65% of the 67 processes undertaken as part of the health visiting service are waste and could be removed in a redesigned process. They also find that the vast majority of these waste processes are administrative, which emphasises that waste is defined from the service user perspective. Proudlove et al. 221 report on the implementation of Six Sigma techniques in the NHS and draw out lessons for the potential implementation of lean thinking. They find that there are significant challenges in using Six Sigma techniques in the ‘messy, complex environment of the NHS’ (p. 33). 221 These are associated with ‘difficulties in identifying customers and processes’, ‘the use of clear and appropriate terminology’, and ‘tensions experienced between speed and rigour’ in the analysis undertaken (p. 33). 221 Issues of resistance to change and the need for team coaching are also surfaced. They also find, though, that those involved in using the techniques did gain value from the structured mapping of processes and detailed guidance on the use of improvement tools.
Lodge and Bamford223 provide evidence on the application of lean principles to patient referral and booking processes in a NHS trust radiology department. They find that the introduction of a single intranet-based system to replace three different and less functional information systems used by different parts of the department led to a reduction in waiting times of up to 30% in some cases. They too point to initial resistance to the use of lean techniques, and the need for persistent stakeholder management, consistent communication about the change process, and the provision of detailed practical training as key elements in overcoming that resistance. de Souza and Pidd224 discuss three case studies of lean process improvement in NHS trusts, one covering the management of medical records, one addressing lengths of stay in elderly care and one looking at waiting times for an audiology service. Like other authors they identify a wide range of behavioural and organisational barriers to implementing lean process improvement in the NHS. They also make some valuable observations about problems of perception and terminology linked to lean’s origins in Japanese manufacturing industry. Based on their case evidence, they conclude that lean can be implemented successfully in a health-care context, but that the barriers ‘have considerably delayed its adoption compared to manufacturing’ (p. 65). 224
Despite the popularity of lean thinking in the NHS, some authors have provided evidence that agile management techniques may be more appropriate given the level of uncertainty characterising some patient care pathways. Bourlakis et al. 225 provide what they claim to be an original and holistic mapping of actors and activities in hospital supply chains for elective care, based on interviews with senior operations managers in three NHS trusts. They map the supply chains in each of the main phases (preoperative, admission and procedure, and postoperative) and ask what impact the Patient Choice policy, which implies increased uncertainty, will have on the management of these chains. Their key finding is that the historical configurations of these supply chains (i.e. named consultant beds, division of wards by speciality, inflexible clinician employment contracts) are likely to be too inflexible to meet the growing demands of Patient Choice. This suggests a need for greater agility and responsiveness, and indeed they find that hospital managers are beginning to recognise the need to work more collaboratively with other hospitals, sharing skills and supplies ‘in order to enhance the flexibility of their supply chains’ (p. 419). 225
We turn next to research looking at the management of interorganisational supply chains delivering goods and services to NHS health-care providers. Some authors220,225 note that relatively little work has been done to examine the impact of integrated SCM thinking and techniques on the procurement activities of NHS trusts and other relevant organisations such as NHS Supply Chain and the collaborative hubs. Rather than a lack of interest from scholars, however, this suggests that integrated SCM thinking and practice have simply not been taken up in a big way by those in NHS procurement. 226 Evidence supporting this observation came in a 2011 report, which suggested that these kinds of improvement tools and techniques are being underutilised in supply chains delivering physical goods to the NHS. 1 It is perhaps unsurprising, then, that what little NHS research evidence does exist tends to be very narrowly focused, either on the implementation problems in particular supply chains or on the limited range of integrated SCM practices or technologies that have been tried, particularly e-procurement.
Browne et al. 227 provide a mapping of the wound-dressing supply chain in the English NHS. Their aim is to understand the nature and effectiveness of information transfer across the supply chain to see if it facilitates the manufacture of dressings to meet the needs of users. This picks up the lean idea of designing supply chains so that they deliver only what the customer or end-user values. They find that, although information transfer in the supply chain has been streamlined by the implementation of an e-procurement system, the communication of end-user needs to wound dressing suppliers is not facilitated. The end-to-end flow of information required for a properly integrated and effective supply chain is prevented by the lack of mechanisms for generating user information and integrating it into the procurement process. One suggestion is for nurses, end-users by proxy, to be better represented in the procurement process. Campling et al. 228 provide corroborating evidence from a complementary study of the same supply chain. They find that ‘the lack of user focus is preventing the transfer of valid user information; those stakeholders who need feedback on the functioning of products such as manufacturers and suppliers are not gaining quality information’, which results in ‘haphazard supply’ and ‘unmet user needs’ (p. 213). 228
Breen and Crawford229 and Cullen and Taylor230 provide evidence on the use of e-procurement in NHS pharmaceutical supply chains. In both papers e-procurement is regarded as an important component in the more integrated, co-ordinated and efficient management of the supply chain. Both papers also reflect on the policy drivers for e-procurement adoption coming from the Department of Health and being channelled through the NHS Purchasing and Supply Agency. Breen and Crawford229 report a survey on the extent of implementation of a very simple e-procurement technology, electronic data interchange, in hospital pharmacies in the north-west of England. They find that 58% of the pharmacies surveyed are using electronic data interchange to communicate with suppliers (place orders, receive invoices, etc.) and that these pharmacies typically see significant net benefits in using this technology, in terms of both cost savings and operational improvements. They also explore the reasons why such a significant minority of the pharmacies in their survey are not using electronic data interchange, and find a mixture of barriers including lack of funding, lack of senior management support and problems in IT development. Cullen and Taylor’s230 work considers the factors, as perceived by users, that influence the successful implementation of e-procurement systems in NHS pharmaceutical supply chains. The survey in this case is much more extensive, however, with coverage of both the NHS (buyer side) and the pharmaceutical manufacturers and wholesalers (supplier side). The study finds that information quality, system quality and trust are the most important factors influencing the use of e-procurement in this particular supply chain context. This suggests therefore that decisions about system design and whether or not e-procurement is implemented ‘on the back of existing trading relationships and using processes that are familiar to the user’ are likely to be crucial management choices (p. 1180). 230
Finally, Bakker et al. 231 also focus on the factors influencing the adoption of e-procurement in the NHS. They present interview findings from five NHS trusts, nine suppliers, the NHS Purchasing and Supply Agency and NHS Logistics. Their study is empirically much broader than either of those discussed above, because they examine practice in supply chains delivering four different types of products (cardiac stents, orthopaedic footwear, intravenous fluid bags and blood sample bottles). In addition, unlike other studies, which typically look at internal and external drivers for e-procurement use in isolation, they consider the interaction between internal context (organisational, IT and buying need characteristics) and external context (supply chain, demand and industry characteristics). Perhaps unsurprisingly they find that decisions about the adoption of e-procurement are likely to be subject to tensions between these internal and external factors. Such decisions are, therefore, best framed in terms of a trade-off between internal and external pressures, with the stronger pressures influencing the nature of the system adopted or a compromise solution being sought where the pressures are in balance.
Conclusions
The discussion here and in the previous chapter has shown that all of the P&SCM literatures discussed in Chapter 3 are of some relevance and use in helping us to make sense of policy and practice in NHS commissioning and procurement. This suggests, in turn, that the CMO configurations embedded in these theories can offer some guidance to NHS practitioners about how to proceed when seeking to achieve certain intended outcomes in particular circumstances.
That said, our review of the NHS literature also reveals that some of these P&SCM theories are seen by researchers as more relevant than others in the particular contextual circumstances of the NHS. These theories have therefore been used much more heavily and explicitly as frames of reference. TCE, agency theory and aspects of the networks and interorganisational relationships literature dealing with trust and collaboration, in particular relational contract theory, are the most frequently used. Some aspects of the integrated SCM literature, in particular such concepts as lean, also feature heavily, but typically in an intraorganisational context. By contrast, our review suggests that the organisational buying behaviour literature, the resource dependency models of power relationships in supply chains and the interorganisational integrated SCM literature have been applied less explicitly or in a heavily circumscribed way in the NHS context.
This suggests that there are a number of knowledge gaps in the NHS research literature where the relevance and utility of some P&SCM theories have not yet been properly articulated and explored. We suggest three main gaps, summarised in Box 9.
-
Knowledge about the decision-making roles, processes and criteria at work in the Clinical Commissioning Groups and the commissioning support units, and about how these commissioning organisations should operate to be effective. The organisational buying behaviour literature is likely to be of particular utility.
-
Knowledge about how interorganisational buyer–supplier relationships develop over time in the context of a wider network of organisational interactions, and about how trust and collaborative efforts can be engendered to deliver supply improvement and innovation in the NHS. The work on power relationships in supply chains is likely to be of particular significance, as it draws attention to the resources that Clinical Commissioning Groups need to have at their disposal to balance the influence of potentially powerful supply-side actors and bring about desired innovations and improvements.
-
Knowledge about the scope to apply integrated SCM thinking and techniques (lean, agile, Six Sigma, build-to-order supply) to supply chains delivering physical goods to the NHS. The use of such ideas is currently heavily focused on improving patient care pathways.
Having established these knowledge gaps, we turn in the next chapter to a review of empirical evidence about the impact of different P&SCM practices and techniques on outcomes at different stages of the procurement process and in different settings and organisational contexts. Our aim is to begin to address these gaps by drawing lessons for the NHS from this wider body of empirical evidence about what works in which settings, for whom, in what circumstances and why.
Chapter 6 Evidence on the impact of procurement and supply chain management practices and techniques
Introduction
This chapter addresses RQ3, which asks: what is the empirical evidence about the impact of different P&SCM practices and techniques on outcomes at different stages of the procurement process in different settings and organisational contexts? We are interested, then, in ascertaining the extent of the evidence base that supports the various practices and techniques that have been advanced within the academic literature and, in many cases, have become a familiar part of the P&SCM landscape.
The chapter is structured in line with the four-phase model of the P&SCM process (see Figure 6) and is guided by the realist review approach of assessing the efficacy of particular practices in particular contexts, that is the investigation of CMO configurations. It is divided into six main parts. In the next five parts, evidence concerning practices and techniques in the four phases of the P&SCM process is presented. Conclusions are then drawn on the strength of the evidence base underpinning the practices and techniques advanced in the literature.
As established earlier, there are various strands to the literature relevant to P&SCM that have developed within very different areas of business management and economics. The consequence of this is that the testing of the efficacy of practices and techniques in one stage of the procurement process, while in many cases systematic and co-ordinated, has largely been undertaken in isolation from the testing in the others. This fact is one of the key conclusions of the chapter.
Evidence on practices and techniques associated with demand management
As discussed in Chapter 3, a critical part of the task of obtaining best value for money from suppliers actually takes place within the buying organisation, away from any contact with the supplier. This section will look at six aspects of demand management: the structure of procurement, collaborative buying, internal resource allocation, specification development, e-procurement systems and internal behaviours.
Organisational structure of the procurement function
Right at the outset, a fundamental issue for buying organisations is the way in which the procurement function is structured. The options include centralised structures, localised structures and hybrid structures. It is important to be clear what the adoption of a particular procurement structure does and does not mean. A procurement structure dictates the reporting lines of procurement staff and their location within the organisation. It does not necessarily dictate the nature of the actual procurement. For example, decentralised procurement structures do not necessarily preclude organisation-level procurement.
The potential benefits of a centralised structure have been reported as the maximisation of purchasing power, process standardisation, enhanced data collection/analysis, capacity for commodity/service specialists and the ability to attract high-quality procurement staff. Suggested drawbacks are detachment from business need, excessive bureaucracy, causing delays to internal customer requests, and reduced early involvement in the procurement process. The benefits and drawbacks of decentralised procurement structures are largely the opposite of those of centralisation, with the key advantage being close and early contact with internal customers. Hybrid structures, such as the Centre-led Action Network system,232 however, are a third option and have been advanced as a way of getting the best of both worlds. In a Centre-led Action Network system, there is a small central team that undertakes certain organisation-level procurements (e.g. energy), sets standards, seeks to encourage best practice and, crucially, promotes joint procurement initiatives between different business units’ procurement teams where there are obvious synergies.
Arguments have been made that no structure represents ‘best practice’, as any structure must be tailored to the nature of the organisation. For example, centralised procurement is unlikely to suit a geographically dispersed conglomerate. It also needs to be recognised that no management structure will ever be successful in achieving its objectives without effective leadership and management actions. Nevertheless, the choice of procurement structure is still an important one. Consequently, the lack of high-quality academic research on this issue is striking. What evidence exists mainly concerns centralised structures and the findings are broadly in line with the advantages and disadvantages outlined above. Reduced prices and transaction costs resulting from centralisation are reported by Karjalainen233 in the Finnish public sector, Kastanioti et al. 234 in European health-care systems, Sorenson and Kanavos235 also in European health-care systems and Sorte236 in the Brazilian public sector. However, Kastanioti et al. 234 express concerns about the long-term effects of centralised procurement on the health-care sectors under study, Sorenson and Kanavos235 find evidence of an excessive focus on cost in centralised public procurement and McCue and Pitzer237 find no clear evidence in their study of the US public sector of benefits from either centralisation or decentralisation but do find evidence for adopted structures simply being the outcome of broader organisational preferences. Thatcher and Sharp,238 meanwhile, report on the benefits to local economies of decentralised NHS procurement.
Purchasing category management
An argument against centralised procurement is that organisations can obtain many of the potential benefits of centralisation without adopting it. Even where organisations have adopted decentralised or Centre-led Action Network procurement structures, it is still possible, it is said, to have expenditure aggregation and common standards. This is through the adoption of purchasing category management. 239 Here, rather than buying certain categories of expenditure separately, different business units come together and agree certain specifications and approved suppliers, and a governance arrangement for supplier management. Purchasing category management has been one of the most prominent developments in procurement over the past 20 years. However, it has not been an area of academic interest. The closest issue that has attracted academic attention is collaborative buying, to which our attention now turns.
Collaborative buying
Related to both the structure of procurement and purchasing category management is the practice of collaborative buying, sometimes referred to as ‘consortia buying’, ‘group purchasing’ or ‘joint buying’. This is where different organisations join forces to buy collectively in the hope of benefiting from greater purchasing power, more comprehensive information and reduced transaction costs. While, on the face of it, collaborative buying appears an obvious and straightforward practice, there are in fact many complicating factors, including the development of common specifications, the timing of group purchases and the governance of collaborative buying entities.
Despite these challenges, most of the empirical papers on collaborative buying are at least cautiously positive. In the US health-care context, where collaborative buying is customary, Burns and Lee240 report cost savings and Nollet and Beaulieu241 report lower transaction costs, while Camillus and Rosenthal242 report a by-product of better information, including investments in pooling regional health-care data, the promotion of public reporting of quality and cost information and the co-ordination of pay-for-performance initiatives. In the different context of European manufacturing, Tella and Virolainen243 also report cost savings and benefits from synergies.
The empirical literature also provides advice on the development of collaborative buying arrangements. Walker et al.,244 assessing efforts within the UK’s NHS and local authorities, found that organisational and party politics, a lack of common coding, and supplier resistance were issues that needed to be overcome. Nollet and Beaulieu,245 also looking at health purchasing, this time in the USA and Europe, emphasised the need for the group structure to evolve and for attention to be given to supplier management, while Schotanus et al. ,246 studying purchasing groups in the Netherlands, highlighted the need for voluntary participation, effective communication within the groups and perceived fairness over savings distribution.
In general, the message of the empirical literature here would appear to be that, although there is no veto on collaborative buying arrangements caused by context, such arrangements, while containing the potential to provide varied benefits, are not a panacea and have to be effectively managed in terms of structure, the accommodation of member needs, and benefits allocation. In this sense, there are parallels to the literature on marketing co-operatives.
Assignment of internal resource and indicative procurement and supply strategies
A further preliminary internal step is the segmentation of purchases, something that needs to be undertaken whatever the decisions made regarding the issues discussed above. A key development here was the first article on procurement to appear in the influential Harvard Business Review, by Kraljic. 167 Up to the early 1980s, the classification of purchases had usually been based upon expenditure levels. In a wide-ranging article, Kraljic167 offered a segmentation matrix that recognised that purchases differed in more respects than just expenditure. Purchases, he argued, should be classified by internally focused factors, such as the importance of the purchase to the organisation’s objectives, and externally focused factors, such as the competitiveness of the supply market. Combining these factors led to four purchase profiles and it was argued that different high-level procurement and supply management strategies and skill levels were required for each profile. Non-critical items were said to require an approach focused upon minimising transaction costs and could be delivered by junior staff – or even outsourced. Leverage items would require the use of buying power and warranted middle-ranking skills. The requirements of bottleneck items related to the need to avoid supply interruptions and demanded specialist attention. Finally, strategic items required a long-term approach and senior management attention.
This matrix has been very widely used by procurement departments within both the public and private sectors over the past 30 years. 247 Despite this, there has been a relative lack of empirical research assessing its efficacy. Much of what exists is largely positive, though, not least because the matrix is an effective facilitator of cross-functional discussion about expenditure profiles, procurement and supply management strategies and staff allocation. 248–250 Having said this, researchers have stressed the need to tailor the segmentation matrix to the specific needs of the organisation, through being very precise about the specific criteria on each axis, and by then carefully designing the measurement system along those axes. 251–254 Gelderman251 also reminds managers that the segmentation matrix was only the first part of Kraljic’s methodology; there is a further matrix for strategic items that considers buyer–supplier power, a concept discussed later in the chapter.
Developing appropriate specifications
In recent years, there has been a growing appreciation that buying organisations can stifle the performance of suppliers through restrictive, input-based specifications. A key aspect of context here is the type of buying situation. Clearly, where requirements are very basic, this issue does not apply. However, in more complex areas of expenditure, buying organisations are increasingly being encouraged to develop output-based, performance-based or even outcome-based specifications. Accordingly, Javed et al. 255 in Australian facilities management, Karlsson et al. 256 in European manufacturing, Kashiwagi et al. 257 in UK power generation and Patil and Molenaar258 in US construction, all explored the link between this more ‘progressive’ type of specification and value-for-money outcomes, particularly in terms of improved supplier innovation. In all studies, there were shown to be benefits to this approach, although the Kashiwagi et al. 257 and Patil and Molenaar258 studies showed that there were risks as well as opportunities and a need for new organisational capabilities.
E-procurement
A key development, of course, since the early 1990s is the use of e-procurement technology within buying organisations. The scope of e-procurement simply maps on to the procurement process itself; each stage of the process can now be undertaken online. E-procurement set-ups include spend data software, market analysis software, e-tendering, e-auctions (and the more recent ‘advanced sourcing’ technology), online contracts and purchase-to-pay systems.
There have been many studies looking at the factors that affect the success of e-procurement implementation. First, engagement with internal end-users has been seen as key, as end-user resistance to using the technology has been identified as a key implementation impediment. 259–263 Second, linked to this, was the need for top management support. 260,264,265 Third, and again linked, the quality and suitability of the e-procurement system, its usability and the quality of information provided to end-users were also seen as key. 259,266–270 Fourth, it is reported that there is a need to engage with suppliers over their involvement with the e-procurement system259,260,266,271,272 and to be aware of the capacity of e-procurement to exclude certain types of companies that are not capable of developing the necessary technology to participate, for example small and medium-sized enterprises. 273 Finally, in research findings concerning reverse e-auctions, Mithas and Jones274 outlined a series of parameters for successful buyer outcomes, including competition levels, reserve prices and information sharing.
In terms of outcomes, Soares-Aguiar and Oalma-dos-Reis272 noted that a key motivation for e-procurement implementation was the fear of falling behind competitors that had already become adopters and had started to enjoy the benefits. The main benefit revealed by the literature, not surprisingly, is cost reduction, from lower purchase prices and/or lower transaction costs, for example via increased standardisation of specifications, supply base reduction and greater contract compliance. 269,275–279 These studies revealed that cost reductions took place within a range of different contexts. A further benefit has been shown to be improved buyer–supplier relationships,280,281 although research by Tassabehji282 suggested that relationship improvements might be elusive in some cases, as, while buying organisations were enjoying short-term cost reductions from reverse e-auctions, suppliers were obtaining little or no benefits. Finally, Cox et al. 166 and Croom and Brandon-Jones,283 both of whose studies were in the UK public sector, highlighted the potential of e-procurement systems to exclude certain types of problem buyer behaviour, for example maverick buying.
Technical and organisational enablers of successful demand management
A final issue concerns the enablers of successful demand management. Demand management activities, for example, developing specifications or entering into collaborative buying arrangements, involve cross-functional or even interorganisational decision-making. There is disagreement about the implications of this. Certain contributors to the literature believe the challenges of cross-functional/interorganisational decision-making require technical management solutions. Empirical studies to this effect include those by Hult,284 Kocabasoglu and Suresh,285 Rhyne286 and Trent and Monczka,287 all studying US companies, and McIvor and McHugh’s288 study of a multinational telecommunications company. All of these studies stress the importance of effective senior management leadership and cross-functional team working that brings together interested parties and allows them to work through the various organisational buying issues.
Other contributors, however, while accepting the need for such technical solutions, have stressed that political skills and strategies are also required. The key difference with these latter contributions is that there is recognition of fundamental conflicts of interest, arising from, for example, attachments to certain specifications and suppliers. Cox et al. 197 and Lonsdale and Watson198 provide evidence on the difficulties of resolving conflicts of interest over such matters in the UK’s NHS and the implications it can have for value for money. Karjalainen et al. 289 note similar issues in the Finnish public sector in relation to off-contract or maverick buying. In response to such conflicts within the buying process, Lonsdale and Watson198 suggest that procurement managers seek to build alliances with co-operative end-users within the buying organisation in order to prevail in decision-making. Cox et al. 197 and Croom and Brandon-Jones283 highlight the potential of e-procurement systems to exclude certain types of problem behaviour. However, it is also conceded by Lonsdale and Watson198 that a more ‘political’ view of organisations implies an acceptance that not all internal conflicts are easily solved.
Summary
As can be seen, the evidence base on practices and techniques associated with demand management is stronger in some areas than others. In terms of an evaluation, with regard to alternative structures for the procurement function, collaborative buying initiatives and e-procurement systems there does not appear to be any evidence that there are restrictions of context, but there are clear warnings regarding implementation. An exception to the absence of contextual restrictions is in relation to e-auctions. Such a practice appears to play a lesser role in highly complex procurements. The studies looking at progressive approaches to specification do not suggest any restrictions of context either, although clearly output and performance-based specifications will make more sense in the case of more complex areas of third party expenditure (Box 10).
-
There is no evidence of context restricting decisions regarding procurement structures, collaborative buying and e-procurement, but there are ‘rules’ regarding implementation.
-
The Kraljic segmentation matrix, however, embodies the CMO logic.
-
A key issue concerns management views on the degree to which their organisations are ‘political’. Demand management decision-making more difficult in ‘political’ organisations.
The segmentation matrix pioneered by Kraljic,167 and developed by many others, is a very different matter, as the matrix has been specifically developed on the basis of a CMO logic. Different high-level strategies and internal resource allocations are deemed necessary for different purchases that are segmented on the basis of internal importance and external supply conditions. This matrix has much wider implications for this literature review and will be discussed more in Chapter 7.
Finally, if certain empirical studies are to be believed, sitting on top of all these practices and techniques is another factor: the degree to which an organisation’s decision-making is political. Whether or not this is an issue of context is open to question. In any case, political decision-making does not affect mechanism selection for optimal outcomes. Rather, its effect will be to make any mechanism selection or implementation decision more difficult, as managers may face internal opposition.
Evidence on practices and techniques associated with supplier selection
This section looks at three levels of analysis relating to supplier selection decisions and processes: competition, criteria and data analysis.
Preface to the empirical literature on supplier selection
Following the demand management phase, the buying organisation will approach the market, ultimately putting out a request for quotation or proposal (also known as invitation to tender). Having received bids, the buying organisation will need to select one or more suppliers. The academic literature has generated a range of empirical studies investigating how buying organisations might best go about this, with the evidence, not surprisingly, emphasising the benefits of adopting practices and techniques that are both systematic and objective; see, for example, Carter et al. ,290 Choi and Hartley,291 Hsu et al. ,292 Kaufmann et al. 293 and Talluri and Narasimhan. 294 The practices and techniques recommended are on three levels: the running of a competitive tendering process; the use within the process of objective selection criteria to evaluate the relative merits of the shortlisted suppliers; and the use of a structured process for analysis of supplier data.
Running a competitive tendering process
Studies on the use of competitive tendering processes in private sector markets are almost without limit, and, of course, neoclassical economists claim support for the perfect competition model, so instead the focus here will be on public sector studies. There has been much attention given to public sector competitive tendering over recent decades. In the UK, this was initially because of the policy interventions of the Conservative administrations of the 1980s, which started a movement towards a ‘contracting state’ that has continued to the present day. A good deal of this attention has been via public auditing, so the literature terrain is extended here to include such studies and prominent government-commissioned policy reviews.
An early study into compulsory competitive tendering in UK local government was carried out by the Institute for Local Government Studies (for the former Department of Environment) and reported savings from such tendering to be about 7%, although there was significant variation across different services. 295 Further into the 1990s, Domberger and Rimmer296 looked at competitive tendering across European public sectors and reported substantial cost savings, whereas Szymanski297 reviewed the results of compulsory competitive tendering in UK local government-provided refuse services and also found that cost reductions had been achieved.
More recently, three major studies have reviewed the effects of competition in the public sector. Davies et al. 298 conducted a literature review and reported that there was some evidence of performance and efficiency improvements attributable to competition in the UK health and education sectors, although there were also arguably other managerial factors at play in the improvements. Julius299 reviewed the literature on the use by the UK public sector of private and third sector organisations and reported that most studies found the cost savings from competitive tendering to be between 10% and 30% without having an adverse impact upon service quality. The European Commission300 study into the impact and effectiveness of the EU procurement directives reported lower purchase costs of between 2% and 10%, evidence (albeit limited) of the savings being made without the social and environmental aspects of the procurement exercises being diminished and a ratio of 4 : 1 in terms of the benefits of the directives versus the costs of them.
The evidence suggests, therefore, that consistent cost reductions are achieved from competitive tendering in different contexts. However, service quality, not thought to have been affected by cost reductions according to Julius,299 has remained a concern to others. For example, Domberger and Rimmer296 admitted that their data were unable to discern whether or not the cost savings had been at the expense of quality and, while Szymanski297 argued that the cost reductions reported in his study could not be attributed to lower service specifications, he was not (because of data limitations) able to rule out the possibility that suppliers, during contract execution, were not meeting the service levels required by the specifications. Furthermore, a study by Guccio et al. 301 into Italian public works contracts found that 25% of contracts were subject to renegotiation costs of about 10%. These last two scenarios, possibly due to moral hazard and hold-up respectively, are examined later in the chapter.
The above studies were aimed at assessing the effects of competition on buyer value for money. Related to this, although different, is empirical research on the effect of buyer–supplier power on value for money, that is the effect of running a selection process under different demand-side and supply-side structures. Research by Cox et al. 130,136,302 provides case studies showing both value for money and buyer–supplier relationships affected by the buyer–supplier power relation. In these studies, organisations that had selected powerful suppliers were seen to find difficulty in persuading those suppliers to partake in cost reduction or product/service enhancement activities requiring collaboration. Similar findings have been presented by Alderman and Ivory303 and Mortensen and Arlbjorn. 304 It is argued therefore that buyer–supplier power should be one of the selection criteria. 305
A final relevant issue here concerns the literature on the choice between sourcing a good or service using a single supplier and sourcing using multiple suppliers. Much of this literature is based on hypothetical quantitative simulations, for example Burke et al. 306 There have also been empirical studies, though, although there is no agreement on the issue and, in any case, the decision is highly situation-specific. Two studies reflect this. Aláez-Aller and Longás-García,307 looking at the Spanish automotive industry, found that a firm’s choice over this sourcing decision tended to change over time as needs and priorities changed, while Krause and Scannell,308 reporting on a study involving 312 firms, stated that service firms tended more towards using competitive sourcing strategies, whereas product firms tended more towards using approaches based upon assessment and direct involvement.
In the IT and services area, a group of academics led by Lacity and Willcocks have undertaken many empirical studies leading them to the conclusion that ‘multi-sourcing’ (defined here as the use of multiple suppliers, as the situation requires, in combination with selective in-house provision) is the most successful sourcing strategy and increasingly being adopted by organisations that had previously been sold single-source solutions; see, for example, Lacity and Willcocks. 309,310 Some of this was attributed to the fact that multisourcing allowed buying organisations to avoid problems associated with hold-up in the presence of uncertainty, supplier complacency and loss of access to innovation from the wider supply market.
The development of selection criteria
With respect to selection criteria, the most relevant issue of context here is purchase type. The evidence stresses the need for supplier evaluation scorecards to contain criteria that are relevant to the purchase in question. Given that the empirical studies have, not surprisingly, focused upon purchase types that are significant to the organisations in question (as against ‘non-critical’ items, in Kraljic’s language167), the evidence has focused upon the benefits of organisations including selection criteria beyond basic cost considerations. First, selection criteria focused upon quality are shown to assist in optimal supplier selection. 292,311,312 A link between an appropriate focus upon quality and the buying organisation’s own customers’ satisfaction is reported and the selection of suppliers offering high quality is said to be critical to organisations’ ability to compete effectively in highly competitive markets.
Second, there is also evidence to support the inclusion of relational attributes in the selection criteria, particularly when organisations are purchasing complex and innovative products or services. 313–316 Heywood and Lonsdale317 reported, in a public sector context, that buying organisations could get suppliers to provide evidence of such attributes by requiring them to demonstrate that their solution will deliver a good cultural fit, continuous improvements, sustainability, effective change management, inclusiveness, long-term benefits and benefit sharing. The benefits of including relational attributes in the selection criteria (often using qualitative data) for complex and innovative products and services are said to include reduced transaction costs, reduced production costs and improved buyer organisation performance. 315,318–320
The experimental study of Huang et al. 321 also suggested that buying organisations wishing to develop trust with a supplier, as part of relational buyer–supplier exchange, should ensure that the supplier selection process, as well as the criteria, contributes to its development rather than hinders it. The authors were particularly referring to the need for the selection process to maintain face-to-face contact throughout, rather than moving to computer-mediated contact after the initial stages.
Third, as some have argued that buyer–supplier power has an impact on the value for money achieved by buying organisations, it has naturally been argued that power should be one of the selection criteria used by buying organisations. References regarding this were reported in the previous subsection.
Analysis of supplier data
The third level concerns a structured process for the analysis of supplier data. A number of studies have claimed evidence for the benefits of using the analytical hierarchy process, a structured framework for evaluating alternatives. The method allows the prioritising of different decision criteria and has obvious application to the supplier selection process, as well as the subsequent supplier performance management task. 322 Constantino et al. 323 report the benefits of using the analytical hierarchy process in the context of the Italian public sector, while Kahraman et al. 324 and Sevkli et al. 325 report benefits from the use of analytical hierarchy process-based methods in a Turkish manufacturing context. Similar methods are reported as beneficial to supplier selection outcomes by Yigin et al. 326 and Towers and Song. 327 Clearly, structured analysis of supplier data is possible using less mathematical processes and, of course, is frequently undertaken that way in practice. Not surprisingly, however, such informal decision-making has not been deemed worthy of academic study.
Summary
The main contextual factor in relation to the different aspects of supplier selection would appear to be the nature of the purchase. The highlighted studies showed that competitive processes are able to deliver beneficial outcomes in a range of different contexts, but there is also a suggestion in some studies that competition is less effective when purchases start to provide the potential for moral hazard and hold-up (something explored on pp. 66–7). Selection criteria, meanwhile, are also shown to be affected by the nature of the purchase, with criteria designed in line with the complexity and importance of the purchase being an important factor in successful procurement outcomes. Finally, in terms of supplier data analysis, while studies highlight the benefits of using analytical hierarchy process-based methods, analysis may well be less formal in the case of minor purchases (Box 11).
-
The key aspect of context in relation to supplier selection is purchase type.
-
There is evidence that the introduction of competition into the public sector has delivered benefits, but a suggestion also that complex procurements encounter difficulties and additional challenges.
-
Selection criteria need to align with purchase type.
-
There is evidence of benefits from using robust data analysis techniques for assessing supplier bid data.
Evidence on practices and techniques associated with contracting
This section looks at various aspects of contracting, although, like the contracting literature, it focuses upon the challenges of uncertainty and incomplete contracting.
Preface to the empirical literature on contracting
Having selected a supplier or suppliers, the buying organisation needs to develop some form of contract. The phrase ‘some form of contract’ is used advisedly, as in many situations the contract developed will be, to differing degrees, incomplete. Indeed, most of the key literature on business-to-business contracting is concerned with contractual incompleteness and its management. Despite the dominance of this concern, however, it is necessary to cover all aspects of contracting here, starting with the most standard of situations.
When buying standard goods and services, buying organisations, if they wish to (some major retailers, for example, choose not to) will be able to develop a complete contract. That is, all necessary details about the product or service – specification, required amount, price and delivery – will be known prior to purchase and can be included in a legally binding document. 86 This situation is by no means the norm in business to business markets, though, and while ‘contract law might not have evolved very much away from these assumptions . . . contract scholarship has’ (p. 304). 328
Demand risk and framework agreements
A more complex, if not the most complex, situation is where the buying organisation has clarity over the specification of its requirement, but is unclear about its demand for it. For example, an organisation may be aware of the types of agency staff or medical consumables it needs, but is not fully clear about its demand over a period of, say, a year. Using historical data, the organisation will be able to estimate the parameters of demand, but the parameters may differ by a significant percentage. Here, organisations have frequently opted to develop framework agreements with preferred suppliers that specify the type or types of goods or services required and the price of those goods or services, but do not commit the buying organisation to any level of demand – although there will usually be certain supplier expectations, which affects prices. 329 Framework agreements are aimed at helping the buying organisation manage demand risk, reduce transaction costs, control the supplier base and, as a side-benefit, reduce maverick buying. Such agreements are not a panacea, though. Procurement managers often provide inadequate choice for end-users, suppliers are often dissatisfied with actual demand and such agreements can end up being used where commitment contracts are a better option.
The academic evidence on the use of framework agreements in business to business markets is scarce. Balcik and Ak330 report on their usage by disaster relief agencies and how suitability is affected by disaster scale; Karjalainen233 finds evidence for price and process cost savings in the Finnish public sector; Lacoste331 found framework agreements of assistance in balancing co-operation and competition in a manufacturing context; and Lam and Gale332 looked at UK public sector construction and found no significant benefits in terms of price, but significantly reduced transaction costs. Away from academic sources, the National Audit Office333 reported that the potential for the framework agreements used by the UK government to deliver lower prices was affected by a lack of co-ordination between central ministries.
Uncertainty and contractual incompleteness
The most complex contracting situations are those characterised by uncertainty, and the most significant strand of management literature on contracting concerns the implications of the contractual incompleteness that arises from uncertainty. In the context of a chapter about practices and techniques, a key issue concerns the use of trust as a self-enforcement mechanism in the context of contractual incompleteness. A self-enforcement mechanism is a tangible or intangible mechanism that causes contractual obligations to be fulfilled without the need for protracted negotiations or conflict. For example, a contract might be self-enforcing because there is an incentive for the supplier to fulfil its obligations. Alternatively, a contract might be self-enforcing because there is a desire on the part of the supplier to fulfil its obligations.
Trust as a self-enforcement mechanism
Trust, in this context, has been defined as the expectation of one party that the other party will not renege on its obligations, while recognising that reneging is a possibility, even if opportunities arise for profitable reneging. 334 While it is accepted that trust is not easy or costless to develop, something that we were reminded of by Spekman et al. ’s335 cross-sector and multinational study, it has been argued that it leads to lower search, negotiation, contracting and monitoring costs. In addition, trust is believed to increase the chances of buyers and suppliers developing a value adding relationship via the increased willingness it creates on both parts to share information and make joint investments. 336
Many studies have been undertaken into the efficacy of trust as a self-enforcement mechanism, with many showing a positive association between trust and the performance of buyer–supplier relationships. Dyer337 argued that evidence from the Japanese automotive industry supported the use of trust as a self-enforcement mechanism, and a study by Dyer and Chu338 covering over 300 buyer–supplier relationships in the Japanese, US and Korean automotive industries suggested that perceived trustworthiness led to both reduced transaction costs and greater information sharing, and that greater information sharing and trust were mutually reinforcing. More recently, Keast et al. 339 reported that the cost reductions achieved in a section of the US health-care sector were attributable to the ‘spirit of partnership’, while Krishnan et al. ’s340 study of US electronics manufacturing reported improved buyer–supplier relationship performance to be a consequence of collaborative contracts.
In order to cast more light on both the processes involved in the creation of trust and the impact of trust upon buyer–supplier relationship performance, Malhotra and Murnighan341 conducted a study under laboratory conditions in the USA. A key finding was that, because under informal, non-binding contracts any co-operation in the buyer–supplier relationship can be viewed by the other party as a function of a manager’s personal inclination, the absence of a formal contract, in which co-operation might simply be mandated, provides the optimal basis for the development of trust.
Of relevance to the CMO philosophy of this realist review, a number of studies have a particular focus on the impact of national culture on the development of trusting relationships between buyers and suppliers. These studies often use models such as that of Hofstede342 in an attempt to highlight the impact of particular aspects of national culture. A number of studies have found a relationship between national culture and the successful development of trust relations between buyers and suppliers. That is, certain national cultural attributes are found to support the development of trust. 343–347
Trust and contract
Malhotra and Murnighan’s study341 highlights a critical divide in the literature regarding the role of trust in helping organisations to cope with the contractual incompleteness that arises out of uncertainty. They argued, as we have seen, that formal, binding contracts have a deleterious effect on trust. In other words, trust is an alternative to contract. Others differ on this and argue that trust and formal contracting actually complement each other. An important study providing evidence supporting this point of view was that by Poppo and Zenger,348 who surveyed information systems managers in the USA and reported: ‘Managers appear to couple their increasingly customized contracts with high levels of relational governance (and vice versa). Moreover, this interdependence underlies their ability to generate improvements in exchange performance’ (p. 707).
Many others report similar findings. Caniels et al. 349 found in their study of the Norwegian oil and gas sector that trust was effective as a self-enforcement mechanism, enabling the successful delivery of project outcomes, only when it was accompanied by contractual incentives and control systems. Blomqvist et al. 350 reporting on cross-country research and development alliances and Kadefors351 reporting on the Swedish facilities management sector agree and focus on how the actual process of developing a formal contract and monitoring performance thereafter can facilitate the development of trust. It was found that the negotiations can lead to increased mutual understanding and shared learning. Bovaird and Halachmi,352 meanwhile, argue that formal contracts can complement intentional trust but only if they are not too restrictive. Finally, Olander et al. 353 report the findings of qualitative research concerning research and development contracts and conclude that trust and contracts are complements, but that their roles differ at different stages of the procurement and contract management process. Trust is reported as the prime mechanism at the early exploration stages; trust and contract are said to support each other in the development stages; and the emphasis is then believed to be more on the contract during the later stages.
Contracts, opportunism and protection
A different position is taken by Williamson. 86 There are, he said, sufficient managers and/or organisations that are prepared to act opportunistically in order for opportunism to be a default assumption entering the contracting process, not least because opportunistic actors are often hard to identify a priori and selection decisions in business to business markets are often time-consuming and expensive to reverse. Accordingly, the contracting process needs to have a strong focus on the safeguarding role. This perspective is clearly in conflict with trust theories, but only partially in conflict with theories promoting the idea of trust and contract as complementary.
Depending on the purchase type in question, in particular the level of uncertainty present, the safeguarding role could include the following: detailing a tight legal contract, making credible commitments, assigning property or control rights and/or developing incentives and monitoring rights. All of these measures are designed, and recommended to managers, on the basis that they allow the two parties to structure a contractual agreement that makes it in the economic interests of both parties to refrain from opportunistic behaviour. Such behaviour could, for example, include various forms of hold-up from a TCE perspective and adverse selection and moral hazard from an agency theory perspective.
The TCE model has been the subject of many empirical studies. Macher and Richman354 reported that, at the time of their publication, there had been over 900 papers testing the model. There have also been a number of reviews of the empirical literature. Our attention will be restricted to a selection of these reviews. Macher and Richman’s354 own review concluded that there is considerable support for many of the central propositions within the transaction cost model. This is a view supported by Schepker et al. (p. 197),355 who comment that:
the empirical literature strongly supports TCE. As transactional attributes increase, so too does the risk that exchange hazards will undermine exchange performance.
Not all of the empirical literature reviews have been as unequivocal, however. David and Han (p. 39)356 concluded that the results of the many empirical studies were mixed, commenting that:
While we found support in some areas (e.g., with regard to asset specificity), we also found considerable disagreement on how to operationalize some of TCE’s central constructs and propositions, and relatively low levels of empirical support in other core areas (e.g., surrounding uncertainty and performance).
Carter and Hodgson357 offered a similar view on the model’s empirical support and added that the outcomes in the empirical studies could just as easily be explained by theories from within the strategic management field. Lacity and Willcock’s358 review of IT outsourcing studies that used the TCE lens, likewise, produced mixed results, particularly with respect to the impact of asset specificity on governance decisions. Interestingly, this review also revealed that studies testing the idea that a key driver of IT outsourcing was simply a desire to copy peer organisations found significant support. Finally, Lonsdale99 offered case studies that supported the contention that the omission of the concept of power from the model was a shortcoming.
Turning our attention to agency theory, it is noticeable that, perhaps because of the very wide application of the theory, the number of procurement and supply management-related empirical studies that are based specifically upon agency theory, as against contractual incentives or monitoring in general, is limited. 359 However, there are some. Lonsdale et al. ,360 using cross-sector evidence from 180 procurement managers, found that transactions characterised by asset specificity and uncertainty were susceptible to adverse selection and moral hazard and that these problems of opportunism could be addressed to a degree by buying organisations if they adopted defensive procurement and supply management actions. Steinle et al. 359 looked at 87 buyer–supplier relationships in their study and reported that moral hazard was common when the relationship was characterised by information asymmetry. Zsidisin and Ellram,361 surveying procurement managers in the USA, found that managerial efforts to manage supply risk were substantially in line with the central premises of agency theory. Finally, in a reminder that academic study separates management issues and mechanisms in a manner alien to the real business world, Lonsdale99 looked at the procurement and contract management strategy of a UK central government agency and found that efforts to avoid adverse selection and moral hazard sat alongside efforts to avoid hold-up as part of an overall approach.
There is also research, however, that shows the importance of care when setting incentives, contractual or otherwise. Gibbons,362 in his review article of the literature on incentives, highlights empirical research that has borne out the comment of Kerr363 that, in a very literal sense, ‘you get what you reward.’ This has been shown to be the case in the health-care sector, with various types of incentives promoting gaming and other distortions. 212
Reflections on the empirical literature on uncertainty and contractual incompleteness
The empirical findings reported in this section, while revealing vast disagreements, have enormous implications for procurement and supply management. First, whatever view is taken on the role of trust, the findings emphasise the fact that a reliance on market forces is unlikely to be an adequate basis for policy in the area of public sector contracting. A sharp in, sharp out approach to contracting out and outsourcing is feasible where the product or service is relatively basic, but, as uncertainty and asset specificity increase, the ability to develop complete contracts and retain a credible threat of returning to the market should supplier performance be unsatisfactory decreases significantly and other actions and mechanisms are necessary.
Second, the findings confirm the view that highly experienced and knowledgeable procurement and contract managers – those with feasible foresight86 – are needed if procurement practice is to remain effective as uncertainty and asset specificity increase. This places a question mark over any policy to outsource public services rapidly to the private or non-profit sectors, as highly knowledgeable procurement and contract managers with considerable experience of procuring complex services are arguably neither cheap nor in plentiful supply. Indeed, this fact has arguably affected the outcomes achieved from the purchaser–provider split in the NHS over the past 20 years or so.
Third, the TCE model argues that, when uncertainty and asset specificity increase beyond a certain point, in-house provision will be the most efficient governance mechanism. The make/buy decision is beyond the scope of this literature review, but this contention of TCE is very relevant to the NHS. Indeed, this issue was raised by contributors to the recent Health Select Committee report on commissioning, particularly in the context of the purchaser–provider split and the possibility that the NHS had incurred the costs of competition without enjoying the benefits. 21
Summary
There are deep disagreements, therefore, regarding the development of the contract. However, certain summary points can be made. First, there is insufficient evidence to make judgements about framework agreements as a procurement technique. Second, while there is disagreement in the contract economics literature over the role that trust plays as a self-enforcement mechanism (as either an alternative to contract or a complement), there is consensus that, as levels of asset specificity increase, the ability to threaten incumbent suppliers with a return to the market decreases; that is, competitive pressure becomes an increasingly ineffective self-enforcement mechanism. Third, the disagreements regarding the role of trust highlight that the behavioural disposition of supplier managers is a critical contextual factor in terms of the contractual mechanism adopted. Misalignment between supplier behaviour and contract choice can lead to very adverse outcomes. Fourth, there is the suggestion in the empirical literature that managerial behaviour is itself a function of a contextual factor: nation and national culture. There is evidence to suggest that opportunistic behaviour is more likely in some national contexts than others. Finally, an issue is raised in the public sector literature regarding the impact of buyer–supplier power on the ability of buying organisations (and suppliers) to negotiate contracts effectively, not least in terms of establishing the necessary self-enforcement mechanisms (Box 12).
-
Purchase type affects contracts and contracting, with uncertainty frequently causing contractual incompleteness in business-to-business markets.
-
Contracting is affected by supplier behaviour; an alignment is required.
-
A debate exists over the nature of supplier behaviour, in particular the relevance of the concept of trust.
-
There is evidence that supplier behaviour, in turn, can be affected by nation.
-
The ability to implement the contractual mechanisms suggested by the literature is, according to some, affected by the relative power of the negotiating parties.
Evidence on practices and techniques associated with relationship management
Contract development and supplier relationship management are linked activities; the contract will often seek to facilitate certain supplier management activities during the contract period. As a result, it is not surprising that, while two distinct literatures exist, there are overlaps between them. The main emphases within the two literatures, however, are very different, with a prominent concern of the literature on supplier relationship management being the possibility of buyer–supplier collaboration and performance improvement. It is recognised within this literature, of course, that buyers and suppliers will not always have an interest in collaborative relationships. The interest will depend, in part, on the financial value and strategic importance of the contract and, as a result, in the case of contracts of relatively low value and importance, the management activity might be restricted to simply ensuring that the supplier is fulfilling its obligations under the contract, that is supplier performance management (see Cox et al. 136 for case evidence on decision processes leading to such relationships). The interest in collaboration may also be affected by whether one or both parties wish to create new knowledge and assets or exploit existing knowledge and assets, an issue raised by Parmigiani and Rivera-Santos364 in their recent, highly regarded review of the wider interorganisational relationships literatures. Whatever the case, complex and high-value collaborative buyer–supplier relationships undoubtedly have the greatest potential for academic study and have consequently received the greatest attention.
One other dimension needs a brief note here. In the case of collaborative relationships, a distinction can be made between collaboration that is discretionary and that which is non-discretionary (although some collaboration combines both). Some close working between buyers and suppliers is simply the result of it not being possible for the buying organisation to buy a product or service ‘off the shelf’; that is, it is non-discretionary. Other close working is discretionary and the result of a wish to create additional value, through either cost reduction or product/service enhancement. In the context of all of the above, in what follows, empirical evidence on the nature, behaviours, antecedents and effect of the collaborative form of buyer–supplier relationships is reported.
The nature of collaborative buyer–supplier relationships
Right from the beginnings of this literature in the 1980s, there have been a number of key activity types that have been argued to be integral to a collaborative buyer–supplier relationship. These activity types have been the focus of much empirical testing. One is buyer–supplier information exchange and communication, particularly regarding the product or service, demand forecasts, feedback on the actions of the other party and suggestions for how the production process might be improved. Many studies have sought to assess the importance of effective information exchange and communication for successful collaboration, with the evidence suggesting that it is of high importance. Studies by Bastl et al. 365 on manufacturing companies, Chang and Lin366 on Taiwanese manufacturing, Hsu et al. 367 on practice in the USA and Europe, Kawai et al. 368 on Japanese manufacturing, Krause and Ellram369 and Paulraj et al. 370 on US practice and Lacity and Willcocks358 on IT outsourcing all found that information exchange was a key element of successful collaboration. Oosterhuis et al. 371 and van de Vijver,372 both looking at relationships within Dutch manufacturing sectors, concurred, but made the qualification that information exchange and communication are factors in successful collaboration only when uncertainty exists and leads to the two parties believing there is a need for this type of collaborative activity.
Joint decision-making and input has also long been considered a key aspect of successful buyer–supplier collaboration. Studies by Biehl et al. 373 into Canadian manufacturing, Lindblom et al. 374,375 into category management and Perez-Arostegui et al. 376 into supplier involvement in product design all report positive effects of joint decision-making and input on collaboration. Similarly, joint investment, often to facilitate necessary adaptations, has also been a key element in the literature on collaborative buyer–supplier relationships, and, of course, in the aforementioned transaction cost literature too. Inemek and Matthyssens377 researching manufacturing sectors in Turkey, Jap378 researching US manufacturing and Rahman et al. 379 researching manufacturing sectors in Malaysia all report the role of transaction-specific investments in collaboration.
Managerial behaviours in collaborative relationships
In addition to tangible management activities, models of buyer–supplier collaboration have also stressed the importance of sympathetic managerial behaviours to successful collaboration. Again showing the overlaps between this literature and the contracting literature, the type of behaviour that has been deemed most important is trustworthy behaviour. Many studies have been undertaken, with most reporting its positive effect on buyer–supplier collaboration. For example, Chung and Jin380 looking at Korean retail sectors found evidence that trust was effective in minimising opportunism within relationships. Similarly positive findings have been reported in various contexts by Hansen,381 Jiang et al. ,382 Johnston et al. ,383 Lane and Bachmann,345 Sengün and Wasti,384 Squire et al. ,385 Tangpong et al. 386 and Lacity and Willcocks. 358 Wood and Ellis387 concur over the importance of trust, but stress the difficulties in maintaining it. Similar management behaviours shown to be important to successful collaboration in research studies include fairness,388 ethical behaviour,389 reciprocation390 and commitment. 391
The impact of collaborative relationships on business performance
Thus far, studies looking at the actions and behaviours that contribute to successful buyer–supplier collaboration have been reported. However, such collaboration is not an end in itself and many studies have sought to ascertain the extent to which collaboration improves business performance. The literature on this takes its cue from the pioneering empirical studies undertaken into the Japanese automotive industry in the late 1980s and early 1990s, studies that led to best-selling books such as The Machine that Changed the World,392 Lean Thinking160 and Beyond Partnership. 159 These studies charted the manner in which, and the extent to which, collaborative buyer–supplier relationships had improved the performance of Japanese automotive supply chains and allowed Japanese manufacturers to take market share from Western automotive firms, especially those in the USA.
Many other subsequent studies have also found significant business improvements arising from such collaboration. Bensaou,393 also researching the automotive sectors of Japan and the USA, charted improved business performance and ascribed it to the way collaboration between buyers and suppliers allowed both parties to deal better with uncertainty. In similar studies, Biehl et al. 373 on Canadian manufacturing ascribed performance improvements to joint decision-making; Cai and Yang394 on Chinese practice ascribed it to co-operative norms; Carter389,395 on US practice ascribed it to ethical behaviour; Forker et al. 396 on US manufacturing ascribed it to perceptions alignment; Hsu et al. 367 ascribed it to information sharing; Humphreys et al. 397 on Chinese manufacturing ascribed it to supplier development; Jap378 on US manufacturing ascribed it to co-ordination and joint investments; Paulraj et al. 370 on US practice ascribed it to communication; and Rajagopal and Rajagopal398 ascribed it to relationship quality.
There is, therefore, a large body of knowledge that has established the actions and behaviours that can promote collaboration between buyers and suppliers, and the performance improvements that such collaboration can deliver. However, the literature also delivers a number of warnings about buyer–supplier collaboration. First, Day et al. 399 highlight the danger of relationships becoming too embedded. Trust was shown in their study to be a potential constraint on relationship performance as well as an enabler. This view is supported by Villena et al. 400 Second, collaboration can be affected by changing commercial pressures,387 something that needs to be taken into account when entering a partnering arrangement that involves significant costs. Commercial pressures can cause partnering to be abandoned by one party. 303 Third, Lane and Bachmann345 highlight the importance of supportive social and political institutions to collaboration, something not present in all nations. Li et al. 401 also focus on nation and report that it can affect the balance required between formal controls (including contract) and the social controls of collaborative relationships. For example, their study found that formal and social controls were complements in relationships between Chinese and non-Chinese companies, but substitutes in relationships between two Chinese companies.
Fourth, there is much discussion on the impact of power on collaborative buyer–supplier relationships. It has been found in some studies that the benefits of collaboration are not always shared equally. 402 Many have ascribed this to the existence and exploitation of power within collaborative relationships. Managers are warned not to assume that a desire to ‘partner’ is synonymous with a desire to treat the other party as an equal and share benefits equally. Various studies have provided evidence of asymmetrical power relations affecting collaborative buyer–supplier relationships. 99,133,136,302,403–406
The above studies on power focus mainly on distributional issues. There have been further studies about the impact of power on business performance. McHugh et al. 407 found that the use of power could have a negative effect on relationship performance. Henke et al. ,408 however, found that the use of power to obtain price reductions can coexist with trusting relationships if power is used in a responsible manner, while Tangpong et al. 409 found that buyers using their dominance increased operational efficiency, but reduced product innovation. Overall, therefore, while there is no single message emerging from studies concerning power, there is considerable evidence to suggest that managers should include considerations of power in their relationship decision-making.
Summary
Given that the contract will often look to set the scene for the subsequent buyer–supplier relationship, it is not surprising that the same contextual variables affect the mechanisms that need to be adopted in order to achieve successful outcomes. These are the nature of the purchase (asset specificity, uncertainty and complexity are drivers of non-discretionary as well as discretionary collaborative activity), supplier behaviour (opportunism can affect the outcome of a collaborative relationship and, crucially, affect decisions over whether or not a collaborative relationship is the right mechanism to adopt in a particular situation), nation and national culture (as mentioned on p. 66, empirical studies have established a link between national culture and business behaviour) and buyer–supplier power (again, power can affect the outcome of a collaborative relationship and, crucially, affect decisions over whether or not a collaborative relationship is the right mechanism to adopt in a particular situation) (Box 13).
-
The same contextual variables that affect contracting choices and outcomes are seen to affect relationship management choices and outcomes.
-
Purchase type affects the extent of relationship activities, with the focus on relatively minor purchases being ‘supplier performance management’.
-
There is evidence of collaboration delivering significant benefits, but there are also warnings regarding supplier selection for collaboration and the implementation of collaborative relationships.
-
One such warning concerns buyer–supplier power relations.
Evidence on practices and techniques associated with operational delivery
In the previous section, we discussed evidence showing that buyer–supplier collaboration has the potential to deliver successful outcomes to buying organisations, particularly in some purchase contexts. However, many writers have questioned the logic of restricting collaboration to single dyads within the supply chain or network. It is believed that the whole system needs to be improved; otherwise all that will be achieved are islands of excellence. Accordingly, over the past 25 years, despite the confusion noted by Giunipero et al. 54 in their recent review about what should be the scope of SCM research, and again inspired by the aforementioned studies of the Japanese automotive industry, a rich research stream has developed looking at efforts made to implement practices and techniques to improve the whole supply chain or network. The two most famous parts of this research stream have been the lean and agile approaches to SCM, although, as is shown, there are complications beneath that neat divide.
Lean supply chain practices and techniques
The lean philosophy, which concentrates on the elimination of waste in supply chains, has been adopted in a diverse range of sectors, from original equipment manufacturing410 to food production and distribution. 411 Case studies of its application have been conducted in developing country contexts,412 as well as in the developed nations, where the majority of studies are set. Even where actions associated with it, such as supply base reduction, cannot be confirmed as a direct application of lean philosophy, there is widespread awareness of it. See, for example, Loader’s413 survey of English local authorities. Studies of lean SCM have been prevalent in health-care settings too. de Souza220 reviewed over 90 studies, Mazzocato et al. 414 present a realist review of 33 studies, and Guimaraes and de Carvalho415 present multiple case studies of strategic outsourcing as a lean technique across 15 different countries.
The principal lean technique assessed is just-in-time, the practice of keeping low stock levels and pulling products from suppliers when required. A number of empirical studies of just-in-time implementation demonstrate improved firm performance. 416,417 Explanations include speed and synchronization,418 improved information flows,419 and increased management focus. 420,421 González-Benito’s421 study is, however, a rare example of any contingent element in this area of research. Indeed, Bayo-Moriones et al. 422 argue that organisational context, for example the size and age of the firm, matters less than infrastructural features such as advanced technologies and quality management. The majority of studies, while they provide rich contextual detail, such as the country and sector, to support their methodological rigour, contain little reflection on how this may affect implementation. Instead, there is an assumption that just-in-time practices can be mimicked and implemented in a wide range of contexts,423–425 and variables regarding successful implementation are considered managerial, for example top management commitment and leadership. 426–428
A significant proportion of research into just-in-time also highlights the importance of improved buyer–supplier relationships,429–432 which are said to contribute towards the continued successful employment of just-in-time practices. Stamm and Golhar431 find genuine commitment in improving relationships, while Yasin et al. 432 find that operator and management training contribute towards improved linkages and firm success. Meanwhile, O’Neal429 charts a move from adversarial to co-operative exchange attitudes through the use of just-in-time, and Nassimbeni430 highlights greater buyer–supplier interaction on both quality and design in development activities. However, again reflecting the theme of power disparities, Karlsson and Norr433 question if just-in-time is really anything more than an exercise in risk displacement, a transfer of the more powerful buyer’s stock-holding problems on to the weaker parties in the network. Though they confirm this hypothesis, they also find that this is not necessarily a problem for dependent suppliers, and total economic effectiveness is still achieved.
Much of this body of work focuses specifically on just-in-time supply, but a number of studies discuss distinct practices of just-in-time production,434 just-in-time purchasing and just-in-time selling435 and just-in-time inventory management. 427 However, their findings emphasise the complementarity of these practices and suggest a total system just-in-time approach for better performance, be that in terms of organisational improvements, cost savings, improved quality, improved site management or a combination. Within the health-care context, Persona et al. 436 chart how just-in-time automatic supply of ward materials through the use of intelligent trolleys in Italian hospitals resulted in smaller quantities of stored products, out-of-date medicines and order errors.
While these just-in-time practices are based on storing less stock for leaner operations, another lean technique goes further by delegating the management of inventory to the vendor. Vendor-managed inventory has been tested in a number of contexts, though most frequently for various types of manufacturing437,438 and in health care. 436,439 Within health care, Stanger440 studied vendor-managed inventory for blood supplies in German hospitals, although this was hesitantly implemented for fear of losing control of this resource. The key to the successful implementation of this technique is reported to include the availability and usability of good-quality data438,441 and, again, the development of collaborative relationships between buyers and suppliers. 439 Kauremaa et al. ,442 however, notice the commercial aspect to vendor-managed inventory, arguing that, while buyers have an interest in more efficient supply, suppliers are attracted to vendor-managed inventory because the practice has lock-in potential. Here we see a sign of the empirical research reporting motivations beyond just multilateral attempts to develop the supply chain. In addition to transactional efficiency gains, the benefits of vendor-managed inventory noted in the empirical research include improved learning spillovers,443 closer buyer–supplier relationships444 and, in a European health-care context, clinician time release. 445
A further lean technique that has been the subject of empirical research, albeit on a lesser scale, is value stream mapping. This technique involves a detailed assessment of supply chain operations in order to identify and eliminate waste, facilitate cost reductions and increase productivity. Empirical research on the application of value stream mapping is mainly associated with assembly lines in manufacturing, such as in the automotive industry. 446,447 Finally, a combined lean Six Sigma approach has gained academic attention as a method for continuous quality improvement and innovation in a wide range of contexts. This has been found to be effective in generating improvements, although these are dependent on adequate support from higher management levels. 448,449
Agile and leagile supply chain practices and techniques
An alternative to lean SCM is agile, which concentrates on responsiveness as the primary goal, as against the elimination of waste. Agile SCM is most suited to environments where demand is uncertain or fluctuates, such as in direct selling or retail,450 particularly fashion. 162 In comparison with lean, agile practices and techniques have had fairly limited academic attention. Power et al. 451 found that customer focus, differentiated application of both hard and soft methodologies to meet customer requirements, and supplier involvement in these processes are critical success factors in the creation of more agile supply chains. K et al. 452 support this point, highlighting collaborative distribution and order commitment as practices associated with successful agility. Flexibility of production and distribution for improved responsiveness to customers has also been reported as critical. 450–452 One technique that is not exclusively associated with agility, but certainly assists with supply chain flexibility, is build-to-order, and there have been a number of positive studies of this. 453,454
A key reason for the relative lack of evidence on agile SCM is related to its presence in the compound approach of ‘leagile’. This approach involves breaking down the production process into modules. These generic modules are developed using a lean approach and then customised under an agile approach. The moment when production moves from lean to agile is called the decoupling point. 455 There have been a number of studies of this compound practice. 455–460 Again, though, research has not been as extensive as with lean and a significant proportion of it is illustrative in nature rather than a test of application. However, good-quality evidence from the literature on build-to-order environments demonstrates well the positioning and shifting of the decoupling point461 and the trade-off between volume and mix flexibilities. 462
Summary
In terms of a CMO configuration, the demand profile of a product or service is deemed a key contextual variable in the choice between lean, agile and leagile supply chain approaches. This relates to Fisher’s model,168 although that does not contain the leagile option. Other possible contextual variables, such as nation or sector, are downplayed, however, by those specifically working in the agile and leagile areas.
Further contextual variables that might affect the outcomes produced by lean, agile and leagile mechanisms are suggested by other procurement and supply chain academics. Here, we again see the appearance of both power and business behaviour, with some arguing that certain power structures and behaviours within supply chains can make the successful implementation of lean, agile and leagile supply chain practices and techniques problematic463 (Box 14).
-
There is evidence that lean and agile methods can deliver significant benefits.
-
There has been a relative lack of investigation into the contextual variables that might affect choices and outcomes, apart, that is, from the demand profile.
-
Academics from outside the lean and agile literatures, however, offer the familiar contextual variables of buyer–supplier power and supplier behaviour.
Conclusion
This chapter has provided a selective overview of the empirical research undertaken on P&SCM practices and techniques. The chapter is divided in line with the four main phases of the P&SCM process and informed by the CMO realist literature review approach. Box 15 summarises the main findings.
-
Evidence relevant to the procurement and SCM process is located in disparate literatures. While certain elements of the process have been systematically studied, very little research exists that has covered all stages in the process.
-
In general, the evidence base is weaker on practices and techniques associated with organisational buying behaviour than it is on the other process stages.
-
Management matters. There is significant evidence that organisations that adhere to key economic and management principles achieve superior value-for-money outcomes.
-
The most important consideration for the selection of management mechanisms is the nature of the purchase.
-
Other highly influential contextual variables are supplier managerial behaviour, national culture and buyer–supplier power relations.
-
Not all research has incorporated these contextual variables into its research design. This needs to be recognised when considering the findings of this chapter.
-
There is a need for research covering all of the stages in the procurement and SCM process (and the connections between them) that has key contextual variables accounted for in research design.
As mentioned previously, the literature relevant to P&SCM is located in disparate literatures. Consequently, while certain elements of the P&SCM process have been systematically studied, there is very little research that has covered all phases and made the connections between them. In P&SCM, the initial demand management phase affects the supplier selection phase, this in turn affects contract development and so on. Nevertheless, great strides have been made in understanding this complex process over the past 30 years and some concluding comments can be made about where matters currently stand.
First, there is a smaller evidence base for practices and techniques associated with demand management, e-procurement apart, than for the other process phases. This is largely because the main literature that has focused upon this phase has not had the testing of specific practices and techniques as a high priority. The other phases in the P&SCM process have a better-developed evidence base, although there is relatively little evidence on supplier selection criteria and framework agreements, at least in relation to their importance. The evidence bases on public sector competition, contracting, buyer–supplier relationship management and lean SCM practices and techniques, in particular, are stronger.
Second, there is significant evidence that management matters. A number of economic and management principles, embodied in myriad practices and techniques, have frequently been shown to assist buying organisations in getting superior value-for-money outcomes. There is, therefore, a clear argument to adopt the realist CMO logic in understanding the P&SCM process, and both the literature and management practice have made advances over the past 30 years.
Third, a number of economic and management principles emerge from the empirical literature as key contextual variables. The most important consideration for the selection of management mechanisms is the nature of the purchase. The appropriateness of mechanisms throughout the P&SCM process is dependent upon many purchase characteristics, including financial value, complexity, asset specificity, uncertainty and demand characteristics. Other highly influential contextual variables are buyer–supplier power relations and supplier managerial behaviour in terms of levels of trust and opportunism, which is, in turn, influenced by national culture.
In terms of this second group of contextual variables, there is an important point to make regarding this empirical review. While the bulk of the empirical literature was produced with an understanding of the relevance of the nature of the purchase to mechanisms and outcomes, a feature of the literature is that significant parts of it, particularly studies related to buyer–supplier relationships and supply chain practices and techniques, have not recognised the contextual variables of behaviour, nation and power. While this does not invalidate an analysis of the empirical literature, it does mean that some studies do not necessarily constitute a totally fair test. For example, some have concluded that certain mechanisms have not led, or have not consistently led, to successful outcomes. However, it is possible that such studies have not picked up that it is not the mechanisms themselves that are responsible for the unsuccessful outcomes, but their deployment in inappropriate contexts where failure was predictable. The same is true in reverse, when conclusions are drawn from sympathetic empirical contexts and are then suggested to have universal validity.
Ultimately, what is required is a structured research programme that addresses both the fragmented nature of the P&SCM literature, so that the interdependencies of all of the process phases are better understood, and the absence of key contextual variables in certain parts of the existing literature, so that all mechanisms are subjected to a fair test. No such research programme has been undertaken, although the incomplete contracting literature comes closest and Lonsdale99 provides an end-to-end template from within that literature.
Chapter 7 Portfolio approaches to improving procurement and supply chain management practice
Introduction
This chapter addresses RQ4, which asks: what are the different approaches to improving P&SCM practice and which are likely to work best in the different contexts and types of NHS organisations? As we have seen in previous chapters, the P&SCM process is complex and involves multiple contexts, phases and actors. As we have also seen, there are a very wide variety of practices or management interventions that can be used in each phase of the P&SCM process. With this in mind, we suggest that arriving at an answer to RQ4 requires an approach that enables us to simplify the complex interplay of contexts, phases, actors and practices in the P&SCM process. In order to do this we need to be able to categorise different P&SCM contexts and relate them to particular types of management practices aimed at achieving particular intended outcomes. Our review of the literature suggests that the most appropriate way of tackling this question is to use a portfolio approach.
The notion of a portfolio approach to management is rooted in the finance literature, in particular the work by Markowitz464 (see also discussion by Turnbull465) on the management of risk in equity investments. The basic premise of this work is that rational investors will categorise investment opportunities according to their particular risk–return ratios and then choose a balanced portfolio of investments that maximise the overall expected return for a given level of risk. There are two broader insights from this argument, which have subsequently been applied to various areas of management thinking and practice including P&SCM. 465 The first is that decision-makers will typically face a range of different contexts, each requiring particular management practices to deliver intended outcomes. The logic of portfolio models is thus in tune with the CMO logic of realist review. The second insight is that the decisions made and the practices deployed in these different contexts should be seen as interdependent, because organisations are resource constrained. The portfolio approach emphasises the need for managers to make trade-offs in their decision-making to achieve an appropriate balance of outcomes across the different contexts which they face.
Turnbull465 points out that references to portfolio approaches to management first started to appear in the P&SCM literature in the early 1980s. The paper by Kraljic167 has been particularly influential, spawning the development and testing of a number of similar procurement portfolio models by other authors. The limited empirical evidence that exists suggests that portfolio models are popular with procurement practitioners252,466 and their use is associated with greater sophistication in the procurement function. 467 Broadly speaking, we can categorise these various models into one of three types based on their main focus or unit of analysis. These are purchase category-focused analysis,167,248,252 relationship-focused analysis249,405,468,469 and supply chain-focused analysis. 168
In the remainder of this chapter we discuss these three types of portfolio analysis. We show in particular how each type of analysis focuses our attention on a different phase of the overall P&SCM process and a different underpinning literature. We suggest that each might therefore help us to address one of the three knowledge gaps in the NHS research literature that we identified in Chapter 5.
Purchase category-focused portfolio analysis
Kraljic167 is generally recognised to have made a seminal contribution to the development of portfolio analysis in the P&SCM literature. His ideas appear in some form in the portfolio models developed and discussed by many other authors. 248,249,252,403,466,468,469 The basic aims of Kraljic’s work are to provide a framework for categorising an organisation’s purchases according to the level of risk associated with each and to give advice about how best to manage these different types of purchase in the form of general procurement strategies and related practices.
Kraljic suggests that organisations should categorise their purchases based on two broad dimensions, the complexity of the supply market and the importance or profit impact of the good or service. He argues that supply market complexity should be assessed in terms of criteria such as the number and availability of potential suppliers, the level of competitive pressure, the pace of technological change, entry barriers, substitution possibilities, and logistics or storage costs. The importance or profit impact of a good or service is defined by criteria such as the volume purchased, the cost as a percentage of the organisation’s total purchasing expenditure, and the impact on the quality or reliability of the organisation’s end product. Using these criteria, assessed on a simple ‘high’ or ‘low’ basis, organisations can allocate their various purchases into one of the four categories shown in Figure 7.
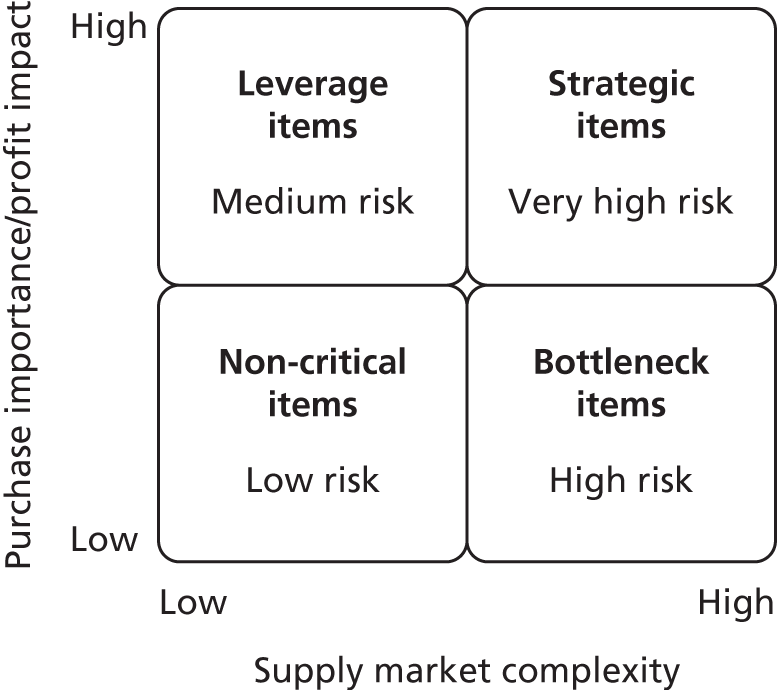
As Figure 7 shows, Kraljic’s argument suggests that organisations are faced with four broad levels of purchase risk. These different levels of risk are based on a combination of the likelihood of the buying organisation facing problems in the supply market and the impact that any problems might have on the buying organisation’s ability to successfully and, if relevant, profitably deliver its good or service. So, for example, strategic items are very high risk because the buying organisation is highly likely to face supply market problems, and those problems, should they occur, will have a significant impact. Leverage items, by contrast, pose a lower risk because, although they are important to the buying organisation’s success and any supply market problems would have a big impact, the likelihood of such problems is minimal.
The other key elements of Kraljic’s work are the general procurement strategies recommended in each category and his advice on how the buying process should be organised and managed. His work therefore clearly focuses our attention on the demand management phase of the P&SCM process. His core argument is that ‘each of these four categories requires a distinctive purchasing approach, whose complexity is in proportion to the strategic implications’ (p. 112). 167 Kraljic illustrates his argument with the experiences of four case study companies. His different purchasing approaches are summarised in Table 7.
| Purchase category | Strategy and associated practices | Required information | Decision level |
|---|---|---|---|
| Strategic items | Strategy: develop long-term supply relationships Practices: accurate demand forecasting; detailed market research; contract staggering; risk analysis; contingency planning; logistics, inventory and supplier control |
Highly detailed market data Long-term supply and demand trend information Good competitive intelligence Industry cost curves |
Top level (e.g. director of procurement) |
| Bottleneck items | Strategy: ensure supply volume or capacity, if necessary at cost premium Practices: control of suppliers; security of inventories; back-up plans |
Medium-term demand and supply forecasts Very good market data Inventory costs Maintenance plans |
Higher level (e.g. head of procurement) |
| Leverage items | Strategy: exploit purchasing power Practices: seek out new suppliers; product substitution; targeted price negotiations; contract/spot purchasing mix; consolidate/optimise order volume |
Good market data Short- to medium-term demand planning Accurate supplier performance data Price forecasts |
Medium level (e.g. chief buyer) |
| Non-critical items | Strategy: streamline purchasing process Practices: standardise requirements; monitor/consolidate order volume; optimise inventory |
Good market overview Short-term demand forecast Economic order quantity inventory levels |
Lower level (e.g. junior buyer) |
The guidance in Table 7 clearly picks up on the idea expressed in the organisational buying behaviour literature that the buying process is expected to be undertaken differently depending on the level of risk associated with a purchase. For example, Kraljic’s recommended strategies and associated practices have clear echoes of the organisational buying behaviour literature’s discussion of expected behaviour in different purchase situations. As we discussed in Chapter 3, the organisational buying behaviour literature suggests that known suppliers offering well-proven products and services will be favoured in high-risk situations, and there will be an emphasis on non-price selection criteria (i.e. quality, delivery performance, service levels). The organisational buying behaviour literature also suggests that, in situations of high risk, buying centre participants will favour suppliers with which their organisation has strong prior relationships and well-established networks of communication. These insights are strongly mirrored by Kraljic’s recommended strategies and practices in the highest-risk purchase categories, strategic and bottleneck items, where he suggests a need for closely controlled and long-term relationships. By contrast, the organisational buying behaviour literature suggests that, for lower-risk procurement decisions, buying centre participants will use price as the dominant selection criterion and seek to stimulate competition from as wide a range of suppliers as possible. Again, these insights are reflected in Kraljic’s recommendations for the lower-risk purchase categories, leverage and non-critical items, where he suggests that buying organisations should standardise and consolidate their requirements and seek to exploit supply market competition for a better price.
We can make the same observation of a mirroring of the organisational buying behaviour literature in Kraljic’s suggestions about the required information and the appropriate decision level in his different purchasing approaches. In terms of searching for information about supplier options, the organisational buying behaviour literature suggests that this will become more active and extensive as procurement risk increases. Kraljic similarly suggests that information search should be more detailed and extensive in the higher-risk purchase categories. As regards decision level, the organisational buying behaviour literature suggests that the participants involved in a high-risk buying decision will typically be more highly qualified and experienced. Kraljic suggests that decisions about the higher-risk purchase categories should be handled by the more senior members of the procurement function, who by extension should be the most highly qualified and experienced. Despite this narrow functional focus, Kraljic does also recognise the organisational buying behaviour literature’s suggestion that more people will be involved in high-risk buying decisions and that they will be drawn from a wider range of departments or organisational subunits. He notes that ‘greater integration, stronger cross-functional relations, and more top-management involvement are all necessary’ in higher-risk purchase categories (p. 116). 167
Given this resonance with the organisational buying behaviour literature, we propose that Kraljic’s work might be useful in addressing the first knowledge gap identified in Chapter 5 about the decision-making roles, processes and criteria at work in the Clinical Commissioning Groups and the commissioning support units, and about how these commissioning organisations should operate to be effective. In particular, Kraljic’s work provides a simple, clear and systematic framework that might be of use when shaping commissioning strategies and allocating scarce management resources to acquire different types of health-care services. For the same reasons we also suggest that Kraljic’s model might be of value to NHS trusts undertaking procurement of different types of health-care-related goods and services.
There are, however, criticisms of Kraljic’s work, which suggest that there might be some challenges in drawing simple lessons from it for commissioning and procurement in the NHS. These criticisms are of three main types. First, Kraljic’s framework is thought to be too simplistic in its analysis of purchasing context and its recommended procurement strategies to deal with the complexity of organisational decision-making. As Dubois and Pedersen470 suggest, it seems problematic to deduce strategies from an analysis based on just two dimensions and where the potential for interaction between those dimensions is not acknowledged. Second, and in a related vein, Kraljic’s recommended strategies are seen as too generic and too static or reactive. Some authors argue that the framework fails to acknowledge the possibility of different, more nuanced strategies within each category and does not provide guidance for buying organisations to move their purchases proactively from one category to another more favourable position. 248,252,467,471 Third, there are what have been called ‘measurement issues’ (p. 21). 467 Authors point to difficulties in deciding the operational meaning of purchase importance and supply complexity,472 difficulties in knowing if all of the appropriate variables are being used to measure these dimensions466 and difficulties in deciding how to weight these variables to produce a combined value on each dimension. 249
Despite this range of criticisms, the available evidence suggests that Kraljic’s thinking is popular with management practitioners,252,466 which indicates that they find it of value in their decision-making. Work by Gelderman and van Weele248,252 examines why this might the case by looking at how managers handle these proposed weaknesses in practice. In case study research with three Dutch industrial companies, two large international businesses and one smaller nationally focused company, they found that the Kraljic framework was used in a customised way that suited the particular context and needs of each company. They comment that ‘the generic nature of the Kraljic approach allows for customisation, implying that users have to make all kinds of decisions, implementing the portfolio analysis’ (p. 210). 252 This customisation applied to the nature of the dimensions used, the variables used to measure each dimension and the methods used to measure the individual variables and to arrive at an overall value against each dimension. This suggests that these companies regarded Kraljic’s work as a broad orientating device which could be used as a basis for analysing their purchased goods and services rather than as something given and immutable.
Moreover, the companies did not move from positioning their goods and services to pursuing procurement strategies in an unthinking and deterministic way. Rather, in each of the cases ‘the positioning of items was followed by a process of reviewing the positions in the matrix and a process of reflection on the consequences’ (p. 210). 252 The companies saw the Kraljic framework as indicative, as a means to stimulate and focus discussion about procurement activities and as a vehicle for exploring and resolving conflicting preferences between stakeholders. Finally, Gelderman and van Weele found that rather than simply following Kraljic’s generic strategic recommendations the companies pursued a range of nuanced strategies either to hold a position within a purchase category or to move to another category. The companies saw the framework as a useful means of identifying ways to reorganise and respecify their purchase requirements to better mitigate risk or achieve greater value for money.
Based on these findings, then, it seems that Kraljic’s portfolio approach is of value to practitioners so long as it is used in a customised, indicative and reflective way, as an aid to intelligent decision-making. It might therefore provide a basis on which NHS commissioning and procurement organisations could organise their demand management processes to be effective in acquiring different types of goods and services.
Relationship-focused portfolio analysis
Another criticism made of Kraljic’s portfolio approach is that it does not take into account the supplier’s perspective. 466,471 It addresses issues of complexity on the supply side, but this is done at a generic market level and from the perspective of the buying organisation only. Kraljic’s work is, therefore, seen to lack a proper engagement with buyer–supplier relationships. It could be argued that this criticism is somewhat unfounded in that Kraljic’s framework is clearly not intended to address buyer–supplier relationships. It is a means of thinking in a more structured and systematic way about how buying organisations should behave when purchasing different types of goods and services. Nonetheless, the different procurement approaches suggested by Kraljic inevitably have implications for suppliers, will provoke a response from suppliers and will be delivered through interactions with suppliers, so a complementary set of portfolio thinking is required.
Responding to the observation that Kraljic does not try to deal with these issues, another strand of the portfolio literature has developed with an explicit focus on the development and management of appropriate forms of buyer–supplier relationship in different contexts. This relationship focused portfolio analysis therefore clearly draws our attention to the relationship management phase of the P&SCM process. Consequently, the theoretical underpinnings of these frameworks lie principally in the interorganisational relationships literature, although use is also made of ideas from the economics of contracting literature. In particular there are frameworks drawing on resource dependency theory to address issues of power in buyer–supplier relationships,403,469 and frameworks using resource dependency theory, social exchange theory and TCE to focus on the social and economic factors shaping buyer–supplier relationships. 249,468 We discuss each of these broad types in turn below.
Given the basis of these various frameworks in the interorganisational relationships literature, we suggest that they might be useful in addressing the second knowledge gap in the NHS research literature identified in Chapter 5. This gap is about how buyer–supplier relationships develop over time and about how, in particular, collaborative efforts can be facilitated and maintained to deliver supply improvement and innovation in the NHS.
The basic premise of portfolio frameworks emphasising the role of power in buyer–supplier relationships is that the nature of the power structure between a buyer and a supplier has a strong influence on the kind of relationship that each party is willing and able to develop. Work by Cox et al. 473 is based on a model for understanding the nature of buyer–supplier power structures that uses ideas from resource dependency theory134 and from industrial economics. 135 This model suggests that buyers and suppliers will interact on the basis of one of four power structures: buyer dominance, supplier dominance, interdependence and independence. The nature of the power structure is seen as a function of the relative dependence of each party on the other. So, buyer dominance implies supplier dependence, supplier dominance implies buyer dependence and the other two structures imply a balance of dependence, either high (interdependence) or low (independence). Dependence is, in turn, seen as a function of two main underlying factors: how important each party is to the objectives of the other and how much choice each party has beyond a particular exchange partner. There are echoes here of the two dimensions used in Kraljic’s framework, but this is more explicitly concerned with importance and choice for both parties rather than just for the buyer.
Cox et al. 136,473 link this power model to the relationship portfolio framework shown in Figure 8. They suggest that buyers and suppliers can potentially form one of six main types of relationship, and that power is a key influence on which is possible. They illustrate their argument with a series of short case studies involving both public and private sector organisations.
FIGURE 8.
A portfolio of buyer–supplier relationships. Reproduced with the permission of Wiley from Cox A, Lonsdale C, Watson G, Qiao H. Supplier relationship management: a framework for understanding managerial capacity and constraints. Eur Bus J 2003;15:135–45. 473 Copyright Robertson Cox Ltd, 1998, reproduced with permission.
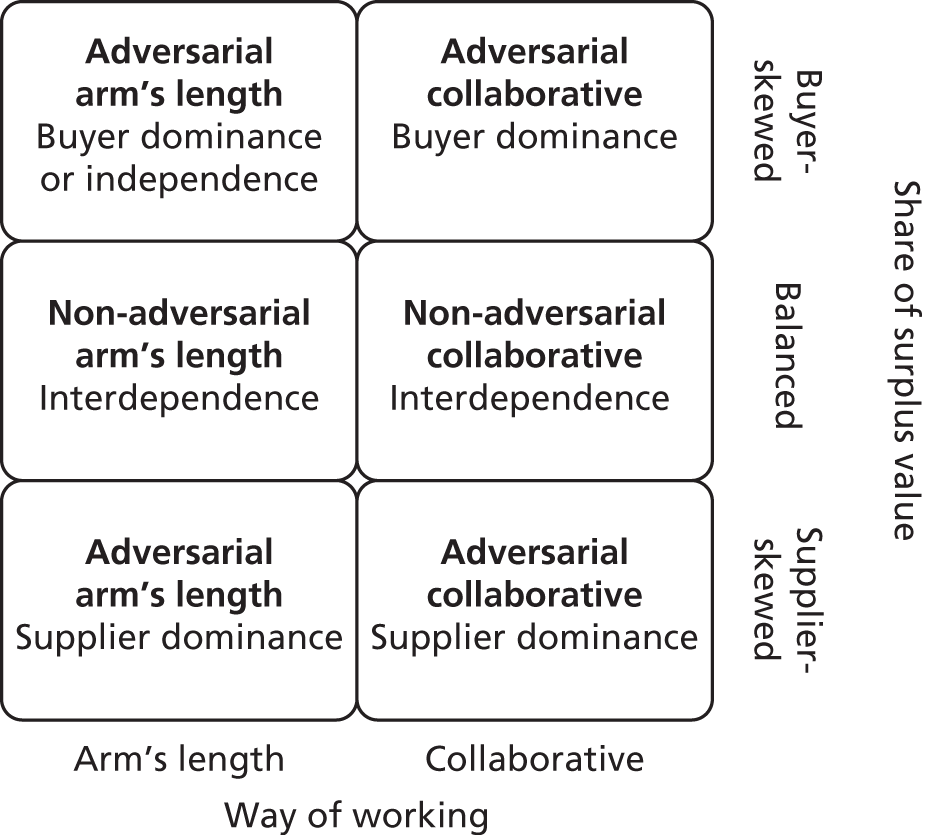
As Figure 8 shows, Cox et al. argue that buyer–supplier relationships differ along two dimensions. ‘Way of working’ is about how closely buyer and supplier interact with another in terms of such things as information sharing, operational linkages and relationship-specific investments. A collaborative relationship is closer on all of these dimensions than an arm’s length one. The ‘share of surplus value’ dimension relates to the commercial balance of a relationship in terms of who bears the costs and who receives the benefits. In a buyer-skewed relationship, for example, the supplier bears the bulk of the costs and the buyer receives most of the benefits. This framework has two key implications. First, collaboration is possible only where either one party dominates the other or where both parties are highly dependent on one another. This is because such interactions represent a substantial investment, which organisations will undertake only if they have a strong incentive to do so. Dependency is deemed to create such an investment incentive whereas independence does not. Second, the framework suggests that collaboration is not necessarily about an equal sharing of costs and benefits. Collaboration can be successfully undertaken even where one party is dominant and therefore receives a greater share of the relationship benefits and bears a smaller share of the costs. This is what Cox et al. call adversarial collaboration.
Work by Caniëls and Gelderman403,469 explores similar issues around the link between power and buyer–supplier relationships, and uses the same underlying concepts drawn from resource dependency theory. In this case, though, the discussion of power is used to extend Kraljic’s framework and to draw out its implications for buyer–supplier relationships. Data from a survey of 248 Dutch purchasing managers are used to test if proposed associations between power structure and relationship style in each quadrant of the Kraljic matrix are borne out in practice. The associations proposed by Caniëls and Gelderman are shown in Figure 9. Their findings support the expected link between power structure and relationship style in all of the quadrants except that for strategic items. Here they find that long-term collaborative relationships are the norm, but that supplier dominance tends to be a more common power structure than interdependence.
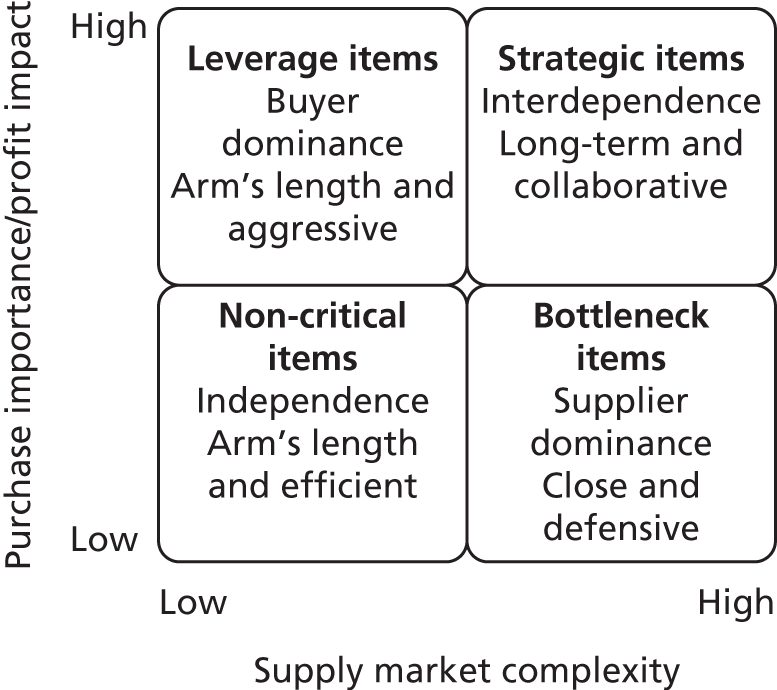
Caniëls and Gelderman conclude that these findings suggest two things. First, the nature of the power structure between a buyer and a supplier does have an important influence on the type of relationship that they are able to develop with one another. Second, collaborative relationships underpinned by a power structure in which one party is dominant will not necessarily be ineffective, as a number of authors have argued. 474–476 These findings appear to support the notion of adversarial collaboration suggested by Cox et al. 136,473 This suggests that a dominant power position can be an effective basis for managing a close exchange relationship if the weaker party sees its dependency as legitimate and the stronger party does not abuse its position.
Other relationship-focused portfolio frameworks are less explicitly concerned with the role of power. They draw on resource dependency theory, social exchange theory and TCE to examine the broader social and economic factors which influence the development and management of different kinds of buyer–supplier relationships.
Olsen and Ellram249 propose a three-step portfolio model to assist in managing buyer–supplier relationships. The first step, analysis of the organisation’s purchases, builds consciously on Kraljic’s framework. The suggested dimensions along which purchases should be categorised are, like those in Kraljic’s model, the strategic importance of a purchase and the difficulty of managing the purchase situation. A number of factors are suggested that might be used in measuring these dimensions. These are again very similar to those in Kraljic’s model, but, as suggested by Gelderman and van Weele,252 it is recognised that the precise factors used may vary with each organisation.
It is in the second and third steps of their model that Olsen and Ellram show how Kraljic’s framework might be extended with a more conscious focus on buyer–supplier relationships. They argue that the procurement strategies and implicit relationship styles proposed by Kraljic’s matrix are ideal types and that they ignore the nature of the actual relationships that an organisation has with its suppliers in each purchase category. The second step of their model, then, is to analyse these actual relationships to see how effectively they are delivering what Kraljic recommends as ideal. Olsen and Ellram suggest that relationships are analysed against two dimensions, the relative attractiveness of the supplier and the strength of the relationship. They propose that supplier attractiveness, which is analogous to supplier competence or capability, should be measured by a range of economic and technological factors inspired by resource dependency theory, and by organisational and cultural factors inspired by social exchange theory. The factors proposed to assess the strength of the relationship are about how effectively the buyer and supplier interact with one another. These are consciously derived from social exchange theory, dealing with the level of commitment, co-operation and longevity in a relationship.
Having compared actual with ideal, step 3 of the Olsen and Ellram model is about the development of action plans to ensure that the relationships in each purchase category are as effective as possible in delivering Kraljic’s ideal type procurement strategies. Three broad types of action plan are suggested. First, for those relationships where supplier attractiveness is high or moderate and relationship strength is low or moderate, the suggested plan is to strengthen the relationship by allocating more resources. Second, where a supplier’s attractiveness is low the suggested plan is either to commit resources to developing that supplier if the relationship strength is high or moderate, or to switch to a more attractive supplier if the relationship strength is low. Third, Olsen and Ellram recognise that relationship management is about making trade-offs between different relationships in an organisation’s portfolio, given resource constraints. Accordingly, they suggest that organisations should examine all of their relationships to see where allocated resources can be reduced in order to reuse them in implementing type 1 and type 2 action plans.
Bensaou468 provides a very similar step-wise model to analyse and propose different styles of buyer–supplier relationship to match particular contextual circumstances. His model draws on TCE to describe the key contextual factors influencing the development of different types of relationship. Based on a survey of 447 managers from three US and 11 Japanese car manufacturers he finds that the level and balance of relationship-specific investments, akin to the TCE notion of asset specificity, are crucial factors influencing what is the most appropriate style of relationship for a buyer and a supplier to develop. Specific investments are those ‘that are difficult or expensive to transfer to another relationship or that may lose their value when redeployed to another supplier or customer’ (p. 36). 468 This association between specific investment and relationships is summarised in Figure 10.
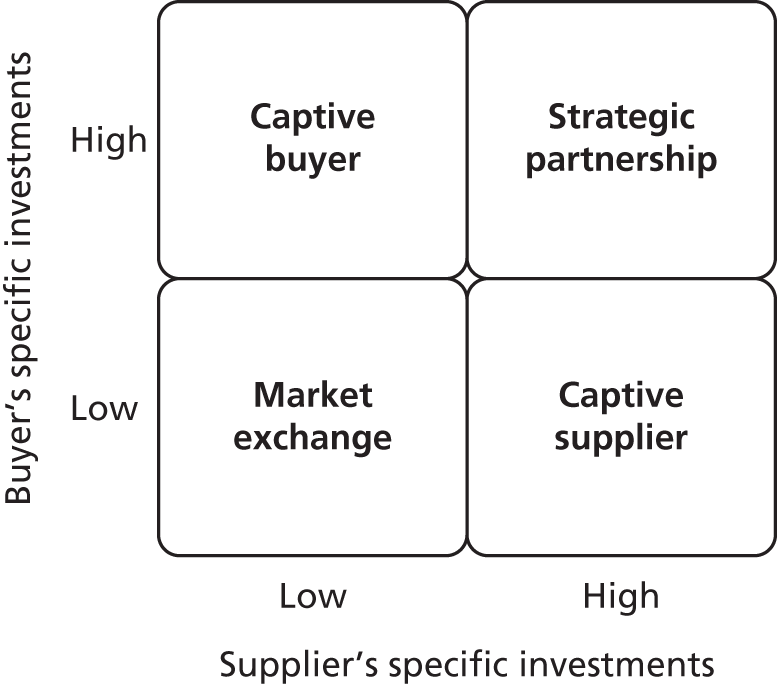
As well as identifying which type of relationship is most appropriate in the context of different levels and distributions of specific investments, Bensaou also provides guidance on the characteristics of an effective management approach for each type of relationship. As shown in Table 8, he describes each management approach in terms of three generic dimensions: information-sharing practices, boundary spanners’ task characteristics and the social climate.
| Relationship type | Information-sharing practices | Boundary spanners’ task characteristics | Social climate |
|---|---|---|---|
| Strategic partnership | Frequent and rich media exchange Regular mutual visits |
Highly ill defined and unstructured Non-routine, frequent, unplanned events Significant time spent with other party on co-ordination issues Early supplier involvement in design |
High mutual trust and commitment Extensive joint action and co-operation Emphasis on fairness and excellent reputation |
| Captive buyer | Exchange of detailed information on a continuous basis Frequent mutual visits |
Structured and highly predictable Significant time spent with supplier |
Mutual trust not well developed Strong effort by buyer to develop co-operation Supplier not concerned with its reputation |
| Captive supplier | Little information exchange Few mutual visits, typically initiated by supplier |
Limited time spent with supplier Some focus on complex, co-ordinating tasks |
High mutual trust, but narrowly focused Limited direct joint action and co-operation Greater burden put on supplier |
| Market exchange | Limited information exchange, focused at time of contract negotiation Structured routines for operational co-ordination and monitoring |
Limited time spent with supplier Highly routine and structured tasks, little interdependence with other party |
Positive social climate No systematic joint effort and co-operation Some emphasis on fairness and good reputation |
To sum up, our discussion shows that there are various relationship portfolio frameworks that might help to address the knowledge gap in the NHS research literature about how buyer–supplier relationships develop over time. In particular, these frameworks show that collaboration is not always appropriate or possible and that contextual factors such as power, supplier attractiveness, relationship strength and relationship-specific investments are likely to have an important influence on the development of collaboration.
It is important to recognise, however, that these frameworks can provide only a partial understanding of the scope for improvement in buyer–supplier relationships, because they focus at the dyadic level. As Dubois and Pedersen470 suggest, we need also to see relationships in their wider network context, because this may have an important influence on how they are best managed. With this in mind, we turn in the final section of this chapter to portfolio analysis that focuses at the level of the supply chain.
Supply chain-focused portfolio analysis
Unlike the relationship portfolio models discussed above, this literature focuses solely on approaches to using collaborative relationships between buyers and suppliers across an extended chain to deliver improved performance. These models draw directly on arguments made in the integrated SCM literature and focus our attention on the operational delivery phase of the P&SCM process. As discussed in Chapter 6, the integrated SCM literature can broadly be divided into work addressing the concept of lean and the elimination of waste through practices such as just-in-time delivery and value stream mapping, and work dealing with supply chain agility and responsiveness through practices such as flexible production and build-to-order supply. We also noted work that suggests using a combination of these approaches to create so-called leagile supply chains. The key aim of supply chain-focused portfolio analysis is to identify the contextual factors that influence when it is appropriate to adopt these different SCM approaches. We suggest therefore that this kind of analysis might be useful in addressing the third knowledge gap in the NHS research literature that we identified in Chapter 5. This gap is about the scope to apply different integrated SCM thinking and techniques to supply chains delivering physical goods to the NHS.
Although we can identify a number of supply chain-focused portfolio models,457,477–480 each of these is fundamentally derived from the framework developed by Fisher. 168 Fisher’s core argument is that the decision on which SCM approach, lean or agile, is most appropriate is determined by the nature of the product delivered by a supply chain to the end-customer. He provides a number of case examples to support his argument. Fisher identifies two types of product, functional and innovative, which he distinguishes on the basis of the predictability of end-customer demand and, by extension, the degree of uncertainty in the wider supply chain. He argues that functional products are ‘the staples’ that satisfy the buyer’s ‘basic needs’, and that, because such needs change very little over time, these products have ‘stable, predictable demand and long life cycles’ (p. 106). 168 He also notes that, because there is little variety and customisation in functional product offerings, firms compete primarily on price, and typical profit margins are low. Conversely, in the case of innovative products Fisher168 argues that, while innovation might enable firms to limit direct competition and earn higher profit margins through first mover advantage, their ‘very newness . . . makes demand for them unpredictable’ (p. 106). He also argues that innovative products will typically exhibit a short life cycle and a greater number of variants as suppliers offer buyers a range of different options in order to test the market. These characteristics are assumed to further increase the unpredictability of demand.
Fisher then suggests that, in order to link these product types appropriately to one of the two broad approaches to SCM, we need to understand which objective, supply chain efficiency or responsiveness, is most important for a firm seeking to successfully and profitably deliver each type of product. His answer in the case of a functional product is to keep physical supply chain costs, the costs of producing, storing and distributing the product, as low as possible, because of the price sensitivity of buyers. The practices necessary to create such a lean supply chain are summarised in Table 9. In the case of an innovative product, Fisher suggests that firms should place greater emphasis on supply chain flexibility and responsiveness, because of the significant impact on profitability of having either too little or too much of a product when first mover advantage is crucial and the life cycle is short. The key objective in this case is to have the right product, available in the right quantities, at the right time. 457 The practices necessary to create such an agile supply chain are also summarised in Table 9.
| Dimension of SCM approach | Lean supply with functional product | Agile supply with innovative product |
|---|---|---|
| Asset/resource utilisation | Maintain high average utilisation rates | Deploy excess buffer capacity |
| Inventory management | Generate high turns and minimise inventory | Deploy significant buffer stocks of generic or modular inventory |
| Lead-time focus | Reduce lead time as long as cost is not increased | Invest aggressively in ways to reduce lead time |
| Key supplier selection criteria | Cost and quality | Speed, flexibility and quality |
| Product design | Simplify design to use fewer parts and reduce errors/need for rework | Use modular design to postpone final product assembly for as long as possible |
| Information exchange and enrichment | Highly desirable | Obligatory |
| Forecasting mechanism | Algorithmic | Intelligent consultation |
This discussion suggests that Fisher’s portfolio framework and others derived from it might be a relatively simple and potentially useful source of guidance for those in NHS procurement organisations seeking to improve the performance of supply chains delivering clinical and non-clinical goods and services. There are, however, a number of possible limitations to the utility of these frameworks that should be borne in mind. These limitations are a function of the particular contextual circumstances on which these models are typically focused.
First, and most obvious, they are designed to be applied to supply chains delivering physical products rather than services to end-customers. Consequently, some of the analytical categories (e.g. product life cycle, product variety, lead time and inventory management) may not be easily transferable to a service setting. That said, as we discussed in Chapter 5, lean concepts have been used to identify waste in health-care service delivery and to generate ideas for improvement, which suggests that these challenges of terminology can be overcome. Second, these models are typically focused on the context of relatively high-volume manufacturing supply chains where there is a repeated production process. There has been relatively little discussion of the models’ usefulness in generating management advice for supply chains in a low-volume or one-off project context, which may characterise some of the more specialist areas of health care. Third, these frameworks are typically focused upon supply chains serving private consumer demand rather than the organisational buyer demand that one would see in NHS procurement. Consequently, there is little discussion of the possibility that the end-customer might well play an extensive and active role in design and specification decisions, which might in turn have an impact on the predictability of demand.
Work by Sanderson and Cox132 deals directly with these last two limitations. They argue that, although the logic of Fisher’s model is challenged by applying it in the context of a shipbuilding supply chain, with one-off project characteristics and an active organisational buyer, it can still provide a useful frame of reference for thinking about how best to manage supply chains. Their case study evidence suggests that functional products such as electrical cable might not necessarily have a predictable demand profile when they are supplied into a complex project context in which ‘the design and build schedule . . . are incomplete and subject to on-going change’ (p. 21). 132 If one follows Fisher’s advice unreflectively this generates a paradox, with a more costly agile supply approach being recommended for a functional product where cost efficiency should be paramount. Sanderson and Cox suggest that one way out of this paradox is to use a leagile approach, which is recommended for supply chains where ultimate customer demand is highly volatile and unpredictable, but end-users are also price sensitive. 457,477
Conclusion
To sum up, then, this chapter has discussed three different types of portfolio analysis and has shown how they might help us to address three key knowledge gaps in the NHS research literature. In broad terms, we suggest that these various portfolio approaches might be a useful means of improving P&SCM practice in the NHS, because they identify key contextual factors in the demand management, relationship management and operational delivery phases of the process and suggest appropriate forms of management intervention to deliver intended outcomes. It is important to emphasise, however, that these portfolio models should not be used in a rigid, deterministic or unreflective manner. Our discussion has also shown that these models can and often should be used in a customised way to take account of the particularities of specific organisational contexts.
Chapter 8 Conclusions
Introduction
The approach taken in this report is a theory-based realist review and synthesis. This route was chosen on the basis of a judgement that what constitutes effective practice in P&SCM is likely to be highly context dependent. A realist review approach emphasises the contingent nature of the evidence and addresses questions about what works in which settings, for whom, in what circumstances and why. In this chapter we summarise the main findings from our synthesis of the P&SCM literature and highlight some of the principal literature sources. We also discuss a number of areas for further research.
This study aimed to assist NHS managers and clinicians in developing more effective commissioning and procurement practice by:
-
exploring the main strands of the literature about P&SCM and identifying the main theoretical and conceptual frameworks
-
assessing how far these P&SCM theories are relevant and useful in helping us to make sense of policy and practice in NHS commissioning and procurement
-
assessing the empirical evidence about how different P&SCM practices and techniques, informed by different theories, might contribute to better procurement processes and outcomes
-
evaluating various context-sensitive portfolio approaches to improving P&SCM practice, and showing how these relate to theories about effective P&SCM.
Our review shows that the P&SCM literature draws on a very diverse range of disciplinary bases, theories and models. This is not surprising given that P&SCM encompasses a wide range of organisational processes, activities and actors, in many different contexts and types of organisations. It makes sense to adopt a multidisciplinary perspective. That said, some of these P&SCM theories have been used more than others to explore the particular contextual circumstances of the NHS. This suggests that there are a number of knowledge gaps in the NHS research literature where the relevance and utility of some P&SCM theories have not yet been properly articulated and explored.
The empirical evidence on the efficacy of different P&SCM practices and techniques, suggested by different theories, is also highly fragmented and at times contradictory. It does suggest, though, that matching management practice appropriately with context is crucial. Key contextual factors include the level of purchase risk, the potential for opportunism rather than trustworthy behaviour, and the structure of power underpinning a buyer–supplier interaction. We suggest that various portfolio approaches to P&SCM are likely to assist in the appropriate matching of management practice with context in order to deliver particular intended outcomes.
Theories about procurement and supply chain management
The P&SCM research domain draws on a very diverse range of disciplinary bases, theories and models. It is not possible to identify a single, coherent and dominant body of thought relating to P&SCM. 22 We have, though, identified four broad literatures, each associated with particular theories. This fourfold categorisation is based on a clustering of theories by their primary explanatory focus on a particular broad phase in the P&SCM process. These are:
-
the organisational buying behaviour literature, grounded in various theories and models of organisational decision-making,59,69–72 which focuses on the demand management phase
-
the economics of contracting literature, grounded in agency theory and TCE,83–86 which focuses on the selection and contracting phase
-
the networks and interorganisational relationships literature, grounded in social exchange, resource dependency, relational contract and dynamic capabilities theories,106,108,117,120,473 which focuses on the relationship management phase
-
the integrated SCM literature, grounded in systems theory and behavioural economics,138–142 which focuses on the operational delivery phase.
We addressed this theoretical diversity by developing a realist interpretation framework that surfaces the contextual assumptions, key explanatory mechanisms and intended outcomes of these various P&SCM theories. This framework suggests that practitioners engaged in P&SCM activities face choices about which theory might work best as a basis for interpreting their situation and for guiding their actions. It may be more appropriate to focus on some mechanisms than on others, depending on what an organisation’s interest is in terms of intended outcome. Where, for example, there is an interest in the benefits that can flow from P&SCM practices (value appropriation, value-creating innovation or improved efficiency and responsiveness), then mechanisms encouraging collaboration (power or trust) are the appropriate focus. These mechanisms are associated with the interorganisational relationships literature or the integrated SCM literature. Alternatively, where there is an interest in managing the risks associated with a procurement decision (competence or behavioural), then there should be a focus on decision-making in the buying process predicated on the organisational buying behaviour literature, and on contractual or governance safeguards based on the economics of contracting literature.
These insights are at a generic level, however. We found that the precise characteristics of the mechanism–outcome configurations outlined above are likely to vary depending on the context. For example, the organisational buying behaviour literature informs us that the various characteristics of a procurement decision (e.g. size and complexity of buying centre, formality of decision rules, extent and intensity of information search) should vary depending on the level of risk associated with that decision, which in turn depends on the characteristics of the purchase. 59 In a NHS context, we can contrast situations within hospital trusts, where they are purchasing generic medical supplies or aspects of facilities management (e.g. waste management), with situations involving Clinical Commissioning Groups and local councils, where various stakeholders are putting together tenders for integrated health and social care for elderly people (e.g. the collaboration between Kingston Clinical Commissioning Group and The Royal Borough of Kingston upon Thames).
Similarly, the integrated SCM literature tells us that choosing the appropriate techniques to integrate and co-ordinate a supply network, the generic alternatives being so-called ‘lean’, ‘agile’ and ‘leagile’ techniques, and the outcomes that those techniques are likely to have, depend on the nature of the product or service delivered by the network. 165 The interorganisational power literature also suggests that management choices, in this case concerning the extent to which a buyer and a supplier collaborate with one another, are shaped by the power context. 136
Mapping this on to the NHS, we can see places within the service where the main emphasis on improvement will involve using ‘lean’ techniques to improve process flow (e.g. the layout within hospitals of wards, stores, etc.) and others where the need is for the rapid formation and dissolution of informal multidisciplinary NHS and social care worker teams to address locally specific health needs – a process more in line with ‘agile’ techniques. However, as mentioned, enthusiasm for these integrated SCM techniques needs to be tempered with an appreciation of how operational ambitions can be constrained by contextual factors, such as power. In the examples above, this could mean plans for hospital reorganisation might be constrained by the costs imposed by a powerful PFI contractor, and flexible health and social care delivery might be obstructed by power and politics within the different public sector organisations.
These observations draw our attention to the work of writers such as Kraljic,167 Fisher168 and Bensaou,468 who offer so-called portfolio models of P&SCM practices. These models suggest that the general mechanisms in each P&SCM theory used to explain different outcomes should be understood as an expression of specific practices or management interventions used in particular contexts. The use of such models can be particularly useful in organisations where procuring entities have recently been created and/or where people with limited commercial experience are involved in commercial decisions. The models can frame debates over procurement decisions and provide a short cut to a certain level of understanding for those with a non-commercial background. Such models are often used by procurement managers in their dealings with internal customers for this reason. With Clinical Commissioning Groups still being in their infancy, the models could have a similar role to play in the NHS.
Evidence on the impact of procurement and supply chain management practices and techniques
Chapter 6 supplemented the identification of P&SCM practices and techniques by summarising the evidence about their impact that has been collected over the past 30 years. We found that empirical evidence on the efficacy of different P&SCM practices and techniques, informed by different theories, is highly fragmented and at times contradictory. Research to test the efficacy of practices and techniques in one phase of the P&SCM process, while in many cases systematic and co-ordinated, has largely been undertaken in isolation from testing in the other phases. There is very little empirical research that has considered all of the phases in the process and examined the connections between them.
The evidence does, however, provide support for many of the practices and techniques and also, crucially for the approach taken within this literature review, suggests that matching management practice appropriately with context is crucial in all phases. Key contextual variables identified by the literature are the characteristics of a purchase (including financial value, complexity, asset specificity, uncertainty and demand profile), the behavioural orientation of suppliers (trustworthiness or opportunism), national culture and buyer–supplier power.
Specific findings from each phase of the P&SCM process:
-
The evidence base on practices and techniques associated with demand management is stronger in some areas than in others. The evidence on alternative structures for the procurement function,233–238 collaborative buying initiatives239,242–246 and e-procurement systems259–261,263,264,267,272 does not suggest any clear-cut contextual influences on management choice, but there are warnings regarding implementation. Studies looking at output- and performance-based specifications also suggest that context does not have a significant impact on the appropriateness of these practices, although they are regarded as more useful in the case of complex purchase requirements. 255–258,481 Evidence shows, though, that an e-auction tends to be less appropriate in highly complex procurements. 274 The literature also contains evidence supporting both technical284–288 and political management approaches197,198,289 to dealing with the challenges of multiactor decision-making.
-
Evidence on supplier selection emphasises the benefits of adopting practices and techniques that are both systematic and objective. 290–292,294,482 There is evidence that competitive tendering processes are able to deliver beneficial outcomes in a range of different contexts,296,299 but there is also a suggestion in some studies that competition is less effective when purchases start to provide the potential for moral hazard and hold-up. 297,301 Selection criteria are also shown to be affected by the nature of the purchase, with criteria designed in line with the complexity and importance of the purchase being a key factor in successful procurement outcomes. 313–316 Finally, a number of studies highlight the benefits of using structured, computational methods, such as the analytical hierarchy process method, to evaluate and compare supplier bids. 323–325,327
-
Evidence on the negotiation and drafting of contracts is characterised by a number of areas of disagreement, particularly over whether contracts and trust are complements or substitutes,341,348–351,353 and over the extent to which the arguments of agency theory and TCE are robust in explaining management practice. 354–357,361 There is substantial evidence, however, that, as the purchase requirement becomes more complex, innovative or bespoke, and levels of asset specificity and uncertainty increase commensurately, the buyer’s scope to develop a complete contract and to retain a credible threat of returning to the market decreases significantly. As we found in the NHS research literature, the evidence shows that this kind of purchase requirement is often associated with the use of extracontractual governance mechanisms as proposed by TCE. 355
-
The bulk of the evidence on relationship management tends to focus on buyer–supplier collaboration and to ignore less complex and more arm’s length forms of interaction. Researchers have looked extensively at the practices underpinning successful collaboration and have identified information exchange,365,366,368,370–372 joint decision-making373,374,376 and joint investment377–379 as critical. Trust is seen as a key mechanism crucial to building and sustaining collaboration. 380–386 Similar mechanisms identified in the literature are fairness,388 ethical behaviour,389 reciprocation390 and commitment. 391 Many studies have found that significant performance improvements in dimensions such as cost, quality and flexibility flow from buyer–supplier collaboration. 367,373,389,393,398 There is also evidence, however, of the dangers and challenges that collaboration can bring. Trust can be a constraint on performance,399,400 and collaboration can be undermined by changing commercial pressures,303,387 by social and cultural factors345,401 and by the irresponsible exploitation of a power advantage. 407,409
-
Evidence on the practices and techniques associated with operational delivery focuses primarily on those that support the creation of a lean supply chain. The main lean technique reported on is just-in-time, and a number of studies demonstrate improved firm performance. 416,418–421 Other important lean practices include vendor-managed inventory436–439 and value stream mapping. 446,447 Evidence on the benefits of vendor-managed inventory in a European health-care setting points to clinician release time. 445 Research on the key drivers for successful implementation of lean practices tends to focus on factors such as top management commitment and leadership,426–428 good buyer–supplier relationships430,432 and the quality and availability of information. 441 Evidence on agile supply chain practices and techniques is much less substantial, but a number of writers do show how these practices have enhanced firm performance measured in terms of flexibility and responsiveness to changing customer demand. 450,451,453 There is also some evidence, however, of potentially negative aspects of lean and agile practices, including risk displacement from a powerful buyer onto a weaker supplier433 and buyer lock-in as a result of dedicated investments. 442
It was known prior to the start of the research that there had been very little empirical testing across all of the four P&SCM phases and that there had been substantial testing of both supplier relationships and integrated SCM practices and techniques. What was, perhaps, a little surprising was that the evidence base for many aspects of demand management and certain aspects of supplier selection was quite limited. Both these areas are critical to the securing of good value for money, and inter-related with other phases of the P&SCM process, and thus worthy of greater investigation. Overall, though, NHS managers responsible for commissioning and procurement are able to draw upon an area of academic study that has been subject to considerable empirical investigation.
Relevance and utility of procurement and supply chain management theories for NHS policy and practice
As was suggested by the brief examples that appeared in Theories about procurement and supply chain management, we found that all four of the P&SCM literatures identified by our review are of some relevance and use in making sense of policy and practice in NHS commissioning and procurement. This suggests that the CMO configurations embedded in these theories can offer some guidance to NHS practitioners about how to proceed when seeking to achieve certain intended outcomes in particular circumstances.
This is not surprising because, while all sectors of an economy and public sector have unique features, there is little to support the claims often heard within the service of NHS exceptionalism. The multiple stakeholder involvement, political sensitivities, path dependencies, technical complexities, policy and legal/regulatory constraints, and unbalanced commissioning–provider relationships (i.e. the relationship between Clinical Commissioning Group and hospital trust in many parts of the NHS) are features that, to a lesser or even greater extent, are seen elsewhere. Indeed, commissioning and procurement within the NHS has many echoes of procurement within the defence and aerospace sectors (for relevant discussion see Cox et al. ,130 Sanderson and Cox132 and Sanderson133). This is not to say that the NHS does not face complex challenges; it clearly does. It is just to say that they are similar to the challenges faced by managers within other sectors.
Accordingly, in Chapter 4 we discussed three key themes in NHS commissioning and procurement policy. We found that:
-
The organisational buying behaviour literature provides a relevant lens for understanding clinically led commissioning and evidence-based procurement. In particular it draws our attention to the importance of decision-maker experience and expertise, decision-maker attentiveness, systematic and extensive information search, and formal decision rules in higher-risk commissioning or procurement decisions. 15,59,75
-
The economics of contracting literature, particularly agency theory, provides a relevant lens for understanding clinically led commissioning, which is intended to better align the interests of patients (principals) and GPs (agents);36 agency theory, in the form of models addressing collaboration between principals174,179 is also relevant to policies driving the co-ordination or consolidation of NHS spending; agency theory and TCE are relevant to the various market-based reforms introduced into the NHS since the purchaser–provider split in 1991, the former focusing on the role of contracts189 and the latter drawing our attention to the likelihood of incomplete contracting in the case of many health-care services. 171,188,190
-
The networks and interorganisational relationships literature, particularly that addressing power133,473 is relevant to joint commissioning or collaborative procurement initiatives, which can be seen as an attempt to give commissioners or NHS trusts greater power resources in their interactions with providers or suppliers; this literature, particularly that dealing with trust, commitment and collaboration, is also relevant to understanding why interorganisational co-operation has persisted alongside competition and market-based reforms in the NHS. 90,184,192,194
-
Aspects of the integrated SCM literature are relevant to understanding the implementation of collaborative procurement initiatives, in particular the role of e-procurement in helping to co-ordinate NHS trust demand and match it with supply more efficiently.
The relevance of the P&SCM literature to the NHS was reflected in the evidence on NHS commissioning and procurement practice that was discussed in Chapter 5. Dividing the evidence in terms of the four broad phases of the P&SCM process, we found that:
-
Evidence on demand management in the NHS is discussed in terms of arguments and concepts associated with the organisational buying behaviour literature, although there are few direct and explicit references to that literature. Papers look at commissioning and procurement decisions in terms of the role, expertise and experience of decision-makers;205,320 the size and composition of decision-making units;20,171,172,201,202,483 and the criteria that influence specific decisions. 203,204 There is evidence of the political nature of some commissioning and procurement decisions and the impact of power on the resolution of conflicts between the preferences of different actors. 198,206–208,484 There is also evidence of the use of sense-making behaviours, persuasion rather than power, to influence commissioning decisions. 199
-
Evidence on selection and contracting in the NHS explicitly acknowledges the relevance of the economics of contracting literature. Some authors discuss the use of classical, complete contracting, inspired by agency theory, particularly where commissioners or procurement teams are dealing with new and often untried providers with which they have had no prior relationships. 98,180,211 This work also identifies problems with complete contracting, however, in particular very high transaction costs incurred by commissioners and providers in contract negotiation and drafting and in the monitoring of performance against detailed targets. TCE is typically regarded as a more appropriate and useful lens given the difficulties of writing complete contracts ex ante for the delivery of health-care services characterised by uncertainty, complexity and acute information asymmetry. 171,188,190,209 Some writers181,188,210 also draw on what they see as complementary ideas from relational contract theory, demonstrating that this phase of the procurement process overlaps and interacts with the postcontract relationship management phase.
-
The research evidence on relationship management in the NHS is typically discussed in terms of concepts drawn from the networks and interorganisational relationships literature. Papers are broadly divided into those placing more emphasis on mechanisms such as trust and collaboration drawn from social exchange and relational contract theories, and those emphasising mechanisms such as power drawn from resource dependency theory. In the former category, evidence shows the continuing importance of trust and co-operation in facilitating effective relationships between NHS commissioners and providers, particularly in the case of complex services and long-term care, despite efforts to increase competitive tension through the quasi-market reform process. 35,183,213–216 Some research suggests, however, that the quasi-market reforms have had a more significant disruptive effect on trust and collaborative relationships between NHS commissioners and providers. This work brings mechanisms such as power more to the fore and suggests that, while collaboration can and does take place in NHS networks, the nature of power relations is an important factor in when and where it occurs. 180,184,192,217–219
-
Evidence on operational delivery in the NHS is often discussed in terms of concepts drawn from the integrated SCM literature. Ideas such as lean, agile and total quality management are seen as relevant and useful in a context where resources are constrained, but high standards of quality (related to patient safety and dignity) and speed and responsiveness (related to patient satisfaction) have to be maintained. This research can be broadly divided into papers which discuss the mapping and improvement of patient care pathways and associated processes,221–225 and papers looking at the management of interorganisational supply chains delivering clinical and non-clinical goods and services to health-care providers. 227–231 Papers in the former category, dealing with intraorganisational health-care processes, are predominant in the literature. 220
In overall terms we found that some of these P&SCM theories have been used much more heavily and explicitly than others as frames of reference in the particular contextual circumstances of the NHS. TCE, agency theory and aspects of the networks and interorganisational relationships literature dealing with trust and collaboration, in particular relational contract theory, are the most frequently used. Some aspects of the integrated SCM literature, in particular concepts such as lean, also feature heavily, but typically in an intraorganisational context focused on improving patient care pathways. By contrast, our review found that the organisational buying behaviour literature, the resource dependency models of power relationships in supply chains, and the interorganisational integrated SCM literature have been applied less explicitly or in a heavily circumscribed way in the NHS context. This suggests a number of research gaps that are outlined later in the chapter.
Portfolio approaches to improving procurement and supply chain management practice in the NHS
It has been established that the P&SCM process is complex and involves multiple contexts, phases and actors. There is also a very wide variety of practices or management interventions that can be used in each phase of the P&SCM process. In order to think about how we might improve P&SCM practice, we need an approach that enables us to simplify the complex interplay of contexts, phases, actors and practices in the P&SCM process. We need to be able to categorise different P&SCM contexts and relate them to particular types of management practices aimed at achieving particular intended outcomes. Our review of the literature suggested that a portfolio approach would be the most effective way of achieving such a categorisation.
In Chapter 7 we identified three types of portfolio analysis based on their main focus or unit of analysis:
We found that these various portfolio approaches might be a useful means of improving commissioning and procurement practice in the NHS, because they identify key contextual factors in the demand management, relationship management and operational delivery phases of the P&SCM process respectively, and suggest appropriate forms of management intervention to deliver intended outcomes. We emphasised, however, that these portfolio models should not be used in a rigid, deterministic or unreflective manner. Our review has also shown that these models can and often should be used in a customised way to take account of the particularities of specific organisational contexts.
It is beyond the scope of this project to undertake primary research in order to provide detailed empirical analysis on how portfolio models could be used in the NHS and with what results. However, a few illustrations can point the way. In some respects, the Kraljic167 purchase category portfolio model is already being used in the NHS. For example, on the hospital trust procurement side, ‘non-critical’ items have long been organised in order to minimise transaction costs, most recently via the NHS Supply Chain online catalogue. Equipment purchases, by contrast, are seen as ‘strategic’ items and given greater attention by the more senior members of a hospital trust’s procurement function. A number of non-clinical services, such as those related to the estates function (cleaning, catering, waste management, security and estate maintenance) have been treated as ‘leverage’ items, not always with satisfactory outcomes (e.g. poor cleaning outcomes). Hospital trusts have also, on occasions, taken Kraljic’s advice regarding the need to investigate the potential for spend aggregation; that is aggregating demand across the trust or even buying jointly with other trusts. As the National Audit Office1 has pointed out, though, practice in this respect is patchy.
On the commissioning side, relationships with acute trusts will always be in the ‘strategic’ quadrant in Kraljic’s model. The long-term nature of such relationships then brings into play relationship portfolio models. The model of Cox et al. 136,473 is useful here. Many commissioning managers complain that their relationships with hospital trusts are in the supplier-dominated adversarial collaboration category. The Cox et al. model offers suggestions here for moving the relationship into the non-adversarial collaborative category (e.g. the removal of certain clinical services from what is often a monopoly provider in order to promote an element of competitive threat and increasing the attractiveness of the commissioning organisation as a ‘customer’, through efforts to promote efficiencies that can benefit both parties). However, perhaps more to the point, the model also points managers towards the type of negotiation and attention to detail that is required when operating in the supplier-dominated adversarial collaboration category. The relationship portfolio model of Cox et al. is also useful for the other clinical services that Clinical Commissioning Groups are responsible for (e.g. smoking cessation and sexual health services), where commissioners will have greater room for manoeuvre.
Areas for further research
As mentioned, our review and synthesis has revealed a number of important knowledge gaps in the NHS research literature where the relevance and utility of some P&SCM theories have not yet been properly articulated and explored. We suggest three main areas for further research to help fill these gaps. For each area, we also show how this further research might help to address some of the questions raised at the outset by members of our advisory group (see Chapter 2) and that this study has not answered:
-
We have identified a relatively limited number of studies looking at NHS commissioning and procurement, which make use of the arguments and concepts offered by the organisational buying behaviour literature. In most cases this literature is not explicitly acknowledged and most of the studies consider only certain discrete factors such as decision-maker characteristics, the size and composition of decision-making units, and the criteria that influence decisions, rather than looking at the interaction between these factors and their impact on specific decision-making processes. The issues arising out of conflicting preferences and the role of power and politics in resolving such conflicts are also not well understood, particularly in the context of NHS commissioning organisations. We recommend empirical research to examine in detail the processes through which those working in Clinical Commissioning Groups and commissioning support units are making different kinds of commissioning decisions and to see if the various factors proposed by the organisational buying behaviour literature can help us to make sense of these processes. This would provide an evidence base on which to consider how Clinical Commissioning Groups and commissioning support units might improve their decision-making effectiveness. This research might also provide answers to a number of questions identified by the advisory group, for example ‘How should NHS managers and clinicians commission services for different client groups?’ and ‘How does commissioning differ across different services within the health sector?’
-
We have identified a number of studies that consider the role, impact and persistence of collaborative relationships between commissioners and providers in the NHS. The bulk of this work draws on concepts such as trust and reciprocity from social exchange theory and relational contract theory in particular. We identified only a limited number of studies that use resource dependency theory to think about the role of power as an influence on the scope for and the nature of collaboration between organisations in the NHS context. Moreover, those NHS studies that do consider the role of power tend in most cases to look at dyadic relationships and to ignore the wider network in which those relationships are embedded. We recommend a study to examine the role of power in NHS health-care networks, looking in particular at the resources that Clinical Commissioning Groups might have at their disposal to encourage collaborative relationships with potentially powerful providers to bring about desired innovations and improvements. Some related questions identified by the advisory group that this research might also address are ‘Who is responsible for the overall design of the supply chain?’ and ‘When and where within a supply chain is collaboration better than competition?’
-
Our review identified that relatively little work has been done to examine the impact of integrated SCM thinking and techniques on the procurement activities of NHS trusts, NHS Supply Chain and the collaborative hubs. Rather than a lack of interest from scholars, this suggests that integrated SCM thinking and practice have not been taken up in a big way by those in NHS procurement as a means of improving the management of their supply chain relationships with suppliers of health-care-related products. The few relevant studies that do exist tend to be very narrowly focused, either on implementation problems in particular supply chains or on specific integrated SCM practices or technologies such as e-procurement. We recommend empirical research to explore how much awareness and understanding of integrated SCM thinking and techniques exists in NHS procurement organisations, to see which, if any, practices are currently being used and what scope there might to be implement such practices in a more comprehensive way. In addressing this last question, the proposed research would consider the nature of power relations between NHS procurement organisations and their various suppliers, drawing on the argument that power might be a key influence on the willingness of suppliers to co-operate with such practices. A related question raised by the advisory group that this research might also be expected to address is: ‘What are the particularities of commissioning in health that could hinder the importing and implementation of models and practices from other sectors?’
Concluding remarks
We acknowledge that our study has limitations, particularly associated with the relative newness of the realist synthesis method and the diverse nature of the sources of evidence on which the review is based. There are still relatively few exemplar studies using a realist review approach and, as a consequence, detailed guidance on data extraction, appraisal and synthesis is limited. That said, suggested standards of good practice have recently started to emerge. 40,41 Recognising the complexity and breadth of the topic addressed, however, this study adheres broadly to those standards rather than following them closely. Given the very diverse theoretical and empirical literature about P&SCM, we have intentionally used evidence from a broad range of peer-reviewed journals, books and policy documents. This does not mean, however, that our search strategy is comprehensive. Rather, we have used purposive sampling to focus on literature that helps us to address the CMO configurations that drive the review. Our conclusions and our recommendations for further research need to be seen in this context.
A further potential limitation relates to the fact that we were able to include only a minor element of patient and public involvement in the study. Although we took the view that patient and public involvement was perhaps not as central to our review as it would be for an empirical research study focusing directly on the delivery of health care, we still recognised, in line with the principles of realist review, the need for linkage with health service users as well as medical and procurement practitioners and academic experts. Our intention therefore was to include a number of individuals from the NHS user community in our expert advisory and stakeholder group. Ultimately, though, we were able to recruit only the chief executive of a third sector provider of NHS services to represent the voice of service users. This suggests that our study may well have missed some patient insights in framing the review and interpreting the findings. Despite these limitations, we suggest that our study still offers theoretically informed and contextually sensitive guidance to assist NHS managers and clinicians in enhancing their commissioning and procurement practice in the dynamic and challenging circumstances that they face.
This study shows that those engaged in P&SCM activities face choices about how to proceed. The theories and evidence reviewed show that there is no one best way for NHS managers and clinicians to undertake their commissioning and procurement responsibilities. Instead, we have endeavoured to provide some insights about which mechanisms might be triggered by particular management practices used at particular stages of the P&SCM process and in particular contexts, resulting in particular outcomes. We understand, of course, that these insights must be presented in a more easily digestible form if our research is to have a meaningful impact on NHS commissioning and procurement practice in the years ahead. A practitioner guide will therefore be developed based on our findings with the help of our advisory group. This will offer a steer about the choices that practitioners face around demand management, selection and contracting, relationship management and operational delivery, and the likely outcomes of those choices in different contextual circumstances.
Acknowledgements
This study was funded by the NIHR HSDR programme, under grant 12/5004/03. We are grateful to the members of our advisory group for their valuable insights and feedback comments, which assisted with the writing and refining of this report, and also to the Health Services Management Centre Library at the University of Birmingham for assistance with searching the NHS-specific literature.
Contributions of authors
Dr Joe Sanderson (Senior Lecturer in Procurement and Supply Management) As principal investigator designed the study and led the literature review, report writing and editorial process.
Dr Chris Lonsdale (Reader in Procurement and Supply Management) Contributed to the literature review and synthesis for specific RQs and wrote sections for the final report.
Professor Russell Mannion (Professor of Health Systems) Advised on the overall design and execution of the study and contributed to the report writing.
Dr Tatum Matharu (Research Fellow) Carried out the literature search, contributed reviews for specific RQs and compiled sections for the final report.
Publications
Sanderson J, Lonsdale C, Mannion R, Matharu T. Lessons for the NHS from a realist review of the literature on procurement and supply chain management. Poster presented at the Health Services Research Network Conference, Nottingham, June 2014.
Sanderson J, Lonsdale C, Mannion R, Matharu T. Lessons for the NHS from the literature on procurement and supply chain management. Paper presented at the European Health Management Association Conference, Birmingham, June 2014.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- The Procurement of Consumables by NHS Acute and Foundation Trusts. London: National Audit Office; 2011.
- Securing Best Value for NHS Patients: Requirements for Commissioners to Adhere to Good Procurement Practice and Protect Patient Choice. London: DH; 2013.
- Equity and Excellence: Managing the Transition. London: DH; 2011.
- Health and Social Care Act 2012. London: The Stationery Office; 2012.
- Commissioning Framework for Health and Well-Being. London: DH; 2007.
- Procurement Guide for Commissioners of NHS-Funded Services. London: DH; 2010.
- Lonsdale C, Glasby J. Commissioning for Health and Well-Being. Bristol: Policy Press; 2012.
- Reforming Public Procurement: EU Proposals for a New Public Procurement Directive. Brussels: NHS European Office; 2012.
- Working for Patients: The Health Service in the 1990s. London: DH; 1989.
- Exworthy M, Powell M, Mohan J. Markets, bureaucracy and public management: the NHS: quasi-market, quasi-hierarchy and quasi-network?. Public Money Manag 1999;19:15-22. http://dx.doi.org/10.1111/1467-9302.00184.
- Exworthy M. A review of recent structural changes to District Health Authorities as purchasing organisations. Environ Plann C Gov Policy 1993;11:279-89. http://dx.doi.org/10.1068/c110279.
- Contracts for Health Services: Operational Principles. London: DH; 1989.
- Mays N, Goodwin N, Bevan G, Wyke S. What is total purchasing?. BMJ 1997;315:652-5. http://dx.doi.org/10.1136/bmj.315.7109.652.
- Le Grand J, Mays N, Mulligan JA. Learning from the NHS Internal Market: A Review of the Evidence. London: The King’s Fund; 1998.
- Harland C, Rudd A, Knight L, Forrest S, Bakker E, Knight L, et al. Public Procurement: International Cases and Commentary. London: Routledge; 2007.
- Goods for Your Health. London: Audit Commission; 1996.
- Callaghan ME. Prospects for collaboration in primary care: relationships between social services and the new PCGs. J Interprof Care 2000;14:19-26. http://dx.doi.org/10.1080/713678538.
- Shifting the Balance of Power. London: DH; 2001.
- Eaton D. The NHS Purchasing and Supply Agency. Br J Healthcare Manag 2000;6:519-21. http://dx.doi.org/10.12968/bjhc.2000.6.11.19333.
- Curry N, Goodwin N, Naylor C, Robertson R. Practice Based Commissioning: Reinvigorate, Replace or Abandon?. London: The King’s Fund; 2008.
- Commissioning. London: The Stationery Office; 2010.
- Our Health, Our Care, Our Say. London: DH; 2006.
- World Class Commissioning. London: DH; 2007.
- World Class Commissioning: An Introduction. London: DH; 2009.
- Changes to Primary Care Trusts. London: The Stationery Office; 2005.
- Allen P, Keen J, Wright J, Dempster P, Townsend J, Hutchings A, et al. Investigating the governance of autonomous public hospitals in England: multi-site case study of NHS foundation trusts. J Health Serv Res Policy 2012;17:94-100. http://dx.doi.org/10.1258/jhsrp.2011.011046.
- Commissioning. London: The Stationery Office; 2011.
- Needham C. Personalised commissioning, public spaces: the limits of the market in English social care services. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S5.
- Fotaki M, Roland M, Boyd A, McDonald R, Sheaff R, Smith L. What benefits will choice bring to patients? Literature review and assessment of implications. J Health Serv Res Policy 2008;13:178-84. http://dx.doi.org/10.1258/jhsrp.2008.007163.
- Health Reform in England. London: DH; 2005.
- Naylor C, Ross S, Curry N, Holder H, Marshall L, Tait E. Clinical Commissioning Groups: Supporting Improvement in General Practice?. London: The King’s Fund; 2013.
- Better Procurement, Better Value, Better Care: A Procurement Development Programme for the NHS. London: DH; 2013.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review: a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10:21-34. http://dx.doi.org/10.1258/1355819054308530.
- Pawson R. Evidence-Based Policy: A Realist Perspective. London: Sage Publications; 2006.
- Chambers N, Sheaff R, Mahon A, Byng R, Mannion R, Charles N, et al. The practice of commissioning healthcare from a private provider: learning from an in-depth case study. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S4.
- Greener I, Mannion R. A realistic evaluation of practice-based commissioning. Policy Polit 2009;37:57-73. http://dx.doi.org/10.1332/030557309X395614.
- Sheaff R, Chambers N, Charles N, Exworthy M, Mahon A, Byng R, et al. How managed a market? Modes of commissioning in England and Germany. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S8.
- Denyer D, Tranfield D, Van Aken JE. Developing design propositions through research synthesis. Organ Stud 2008;29:393-41. http://dx.doi.org/10.1177/0170840607088020.
- Jagosh J, Macaulay AC, Pluye P, Salsberg J, Bush PL, Henderson J, et al. Uncovering the benefits of participatory research: implications of a realist review for health research and practice. Milbank Q 2012;90:311-46. http://dx.doi.org/10.1111/j.1468-0009.2012.00665.x.
- Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med 2013;11:1-14.
- Wong G, Greenhalgh T, Westhorp G, Pawson R. The Quality Standards for Realist Syntheses and Meta-Narrative Reviews. RAMESES Project n.d. www.ramesesproject.org/media/Quality_standards_for_RS_and_MNR_v4final.pdf (accessed 15 September 2014).
- Greenhalgh T, Kristjansson E, Robinson V. Realist review to understand the efficacy of school feeding programmes. BMJ 2007;335:858-61. http://dx.doi.org/10.1136/bmj.39359.525174.AD.
- Pilbeam C, Alvarez G, Wilson H. The governance of supply networks: a systematic literature review. Supply Chain Manag 2012;17:358-76. http://dx.doi.org/10.1108/13598541211246512.
- Gough D, Thomas J, Oliver S. Clarifying differences between review designs and methods. Systematic Rev 2012;1. http://dx.doi.org/10.1186/2046-4053-1-28.
- Popay J. Moving beyond Effectiveness in Evidence Synthesis: Methodological Issues in the Synthesis of Diverse Sources of Evidence. London: NICE; 2006.
- Greenhalgh T, Hurwitz B, Greenhalgh T, Skultans V. Narrative Research in Health and Illness. Oxford: Blackwell Publishing; 2004.
- Pawson R, Manzano-Santaella A. A realist diagnostic workshop. Evaluation 2012;18:176-91. http://dx.doi.org/10.1177/1356389012440912.
- Lomas J. Using linkage and exchange to move research into policy at a Canadian foundation. Health Affair 2000;19:236-40. http://dx.doi.org/10.1377/hlthaff.19.3.236.
- Giannakis M, Croom SR. Toward the development of a supply chain management paradigm: a conceptual framework. J Supply Chain Manag 2004;40:27-3. http://dx.doi.org/10.1111/j.1745-493X.2004.tb00167.x.
- Halldorsson A, Kotzab H, Mikkola JH, Skjøtt-Larsen T. Complementary theories to supply chain management. Supply Chain Manag 2007;12:284-96. http://dx.doi.org/10.1108/13598540710759808.
- Möller K. Theory map of business marketing: relationships and networks perspectives. Ind Market Manag 2013;42:324-35. http://dx.doi.org/10.1016/j.indmarman.2013.02.009.
- Larson PD, Halldorsson A. What is SCM? And where is it?. J Supply Chain Manag 2002;38:36-44. http://dx.doi.org/10.1111/j.1745-493X.2002.tb00141.x.
- Svensson G. Holistic and cross-disciplinary deficiencies in the theory generation of supply chain management. Supply Chain Manag 2003;8:303-16. http://dx.doi.org/10.1108/13598540310490062.
- Giunipero LC, Hooker RE, Joseph-Matthews S, Yoon TE, Brudvig S. A decade of SCM literature: past, present and future implications. J Supply Chain Manag 2008;44:66-8. http://dx.doi.org/10.1111/j.1745-493X.2008.00073.x.
- Burgess K, Singh PJ, Koroglu R. Supply chain management: a structured literature review and implications for future research. Int J Oper Prod Manag 2006;26:703-29. http://dx.doi.org/10.1108/01443570610672202.
- Harland CM, Lamming RC, Walker H, Philips WG, Caldwell ND, Johnsen TE, et al. Supply management: is it a discipline?. Int J Oper Prod Manag 2006;26:730-53. http://dx.doi.org/10.1108/01443570610672211.
- Chen IJ, Paulraj A. Towards a theory of supply chain management: the constucts and measurements. J Oper Manag 2004;22:119-50. http://dx.doi.org/10.1016/j.jom.2003.12.007.
- Chicksand D, Watson G, Walker H, Radnor Z, Johnston R. Theoretical perspectives in purchasing and supply chain management: an analysis of the literature. Supply Chain Manag 2012;17:454-72. http://dx.doi.org/10.1108/13598541211246611.
- Johnston WJ, Lewin JE. Organizational buying behavior: toward an integrative framework. J Bus Res 1996;35:1-15. http://dx.doi.org/10.1016/0148-2963(94)00077-8.
- Buvik A. The industrial purchasing research framework: a comparison of theoretical perspectives from micro economics, marketing and organization science. J Bus Ind Mark 2001;16:439-50. http://dx.doi.org/10.1108/EUM0000000006019.
- Shook CL, Adams GL, Ketchen DJ, Craighead CW. Towards a ‘theoretical toolbox’ for strategic sourcing. Supply Chain Manag 2009;14:3-10. http://dx.doi.org/10.1108/13598540910927250.
- Corey R. Procurement Management: Strategy, Organisation and Decision-Making. Boston, MA: CBI Publishing Co.; 1978.
- March JG, Simon HA. Organizations. New York, NY: Wiley; 1958.
- Kohli A. Determinants of influence in organizational buying: a contingency approach. J Mark 1989;53:50-65. http://dx.doi.org/10.2307/1251342.
- Pettigrew A. The Politics of Organizational Decision-Making. London: Tavistock Press; 1973.
- Ronchetto JR, Hutt MD, Reingen PH. Embedded influence patterns in organizational buying systems. J Mark 1989;53:51-62. http://dx.doi.org/10.2307/1251379.
- Ryan MJ, Holbrook MB. Decision-specific conflict in organizational buyer behaviour. J Mark 1982;46:62-8. http://dx.doi.org/10.2307/1251703.
- Smeltzer L, Goel S. Sources of purchasing managers’ influence within the organization. Int J Purchasing Mater Manag 1995;31:2-11.
- Sheth JN. A model of industrial buyer behavior. J Mark 1973;37:50-6. http://dx.doi.org/10.2307/1250358.
- Robinson PJ, Faris CW, Wind Y. Industrial Buying and Creative Marketing. Boston, MA: Allyn and Bacon; 1967.
- Webster FE, Wind Y. A general model for understanding organizational buying behavior. J Mark 1972;36:12-9. http://dx.doi.org/10.2307/1250972.
- Tanner JF Jr. Organizational buying theories: a bridge to relationships theory. Ind Mark Manag 1999;28:245-55. http://dx.doi.org/10.1016/S0019-8501(98)00052-2.
- McQuiston DH. Novelty, complexity, and importance as causal determinants of industrial buyer behavior. J Mark 1989;53:66-79. http://dx.doi.org/10.2307/1251414.
- Johnston WJ, Bonoma TV. The buying center: structure and interaction patterns. J Mark 1981;45:143-56. http://dx.doi.org/10.2307/1251549.
- Tanner JF, Castleberry SB. The participation model: factors related to buying decision participation. J Business-to-Business Mark 1993;1:35-61. http://dx.doi.org/10.1300/J033v01n03_03.
- Henthorne TL, LaTour MS, Williams AJ. How organizational buyers reduce risk. Ind Mark Manag 1993;22:41-8. http://dx.doi.org/10.1016/0019-8501(93)90019-4.
- Puto CP, Patton WE, King RH. Risk handling strategies in industrial vendor selection decisions. J Mark 1985;49:89-98. http://dx.doi.org/10.2307/1251179.
- Wilson EJ. Theory transitions in organizational buying behaviour research. J Bus Ind Mark 1996;11:7-19. http://dx.doi.org/10.1108/08858629610151271.
- Wilson EJ. Organizational Buying in the Quality Revolution. Bingley: Emerald; 1994.
- Jensen MC, Meckling WH. Theory of the firm: managerial behavior, agency costs and ownership structure. J Financ Econ 1976;3:305-60. http://dx.doi.org/10.1016/0304-405X(76)90026-X.
- Fama EF, Jensen MC. Separation of ownership and control. J Law Econ 1983;26:301-25. http://dx.doi.org/10.1086/467037.
- Eisenhardt KM. Agency theory: an assessment and review. Acad Manag Rev 1989;14:57-74.
- Klein B. Why hold-ups occur: the self-enforcing range of contractual relationships. Econ Inquiry 1996;34:444-63. http://dx.doi.org/10.1111/j.1465-7295.1996.tb01388.x.
- Klein B, Crawford RG, Alchian AA. Vertical integration, appropriable rents, and the competitive contracting process. J Law Econ 1978;21:297-326. http://dx.doi.org/10.1086/466922.
- Hart O. Incomplete contracts and public ownership: remarks, and an application to public–private partnerships. Econ J 2003;113:C69-C76. http://dx.doi.org/10.1111/1468-0297.00119.
- Williamson OE. The Economic Institutions of Capitalism. New York, NY: Free Press; 1985.
- Segal I. Complexity and renegotiation: a foundation for incomplete contracts. Rev Econ Stud 1999;66:57-82. http://dx.doi.org/10.1111/1467-937X.00078.
- Tirole J. Incomplete contracts: where do we stand?. Econometrica 1999;67:741-81. http://dx.doi.org/10.1111/1468-0262.00052.
- Akerlof GA. The market for ‘lemons’: quality uncertainty and the market mechanism. Q J Econ 1970;84:488-500. http://dx.doi.org/10.2307/1879431.
- Eisingerich AB, Bell SJ. Maintaining customer relationships in high credence services. J Serv Mark 2007;21:253-62. http://dx.doi.org/10.1108/08876040710758559.
- Arrow KJ. The Limits of Organization. New York, NY: WW Norton; 1974.
- Ellram LM, Tate WL, Billington C. Offshore outsourcing of professional services: a transaction cost economics perspective. J Oper Manag 2008;26:148-63. http://dx.doi.org/10.1016/j.jom.2007.02.008.
- Homburg C, Stebel P. Determinants of contract terms for professional services. Manag Accounting Res 2009;20:129-45. http://dx.doi.org/10.1016/j.mar.2008.10.001.
- Mitchell V-W, Moutinho L, Lewis BR. Risk reduction in purchasing organisational professional services. Serv Ind J 2003;23:1-19. http://dx.doi.org/10.1080/02642060308565621.
- Schiele JJ, McCue CP. Professional service acquisition in public sector procurement: a conceptual model of meaningful involvement. Int J Oper Prod Manag 2006;26:300-25. http://dx.doi.org/10.1108/01443570610646210.
- Joskow PL. Contract duration and relationship-specific investments: empirical evidence from coal markets. Am Econ Rev 1987;77:168-85.
- Lonsdale C. Locked-in to supplier dominance: on the dangers of asset specificity for the outsourcing decision. J Supply Chain Manag 2001;37:22-7. http://dx.doi.org/10.1111/j.1745-493X.2001.tb00096.x.
- Lonsdale C, Watson G. Managing contracts under the UK’s Private Finance Initiative: evidence from the National Health Service. Policy Polit 2007;35:683-700. http://dx.doi.org/10.1332/030557307782453010.
- Lonsdale C. Post-contractual lock-in and the UK Private Finance Initiative (PFI): the cases of National Savings and Investments and the Lord Chancellor’s Department. Public Adm 2005;83:67-88. http://dx.doi.org/10.1111/j.0033-3298.2005.00438.x.
- Osterloh M, Frey BS. Motivation, knowledge transfer, and organizational forms. Organ Sci 2000;11:538-50. http://dx.doi.org/10.1287/orsc.11.5.538.15204.
- Ghoshal S, Moran P. Bad for practice: a critique of the transaction cost theory. Acad Manag Rev 1996;21:13-47.
- Gibbons R. Transaction-cost economics: past, present, and future?. Scand J Econ 2010;112:263-88. http://dx.doi.org/10.1111/j.1467-9442.2010.01609.x.
- Perrow C. Complex Organizations: A Critical Essay. New York, NY: McGraw Hill; 1986.
- Macneil IR. Relational contract theory: challenges and queries. Northwestern Univ Law Rev 2000;94:877-1547.
- Mouzas S, Blois K. Contract research today: where do we stand?. Ind Mark Manag 2013;42:1057-62. http://dx.doi.org/10.1016/j.indmarman.2013.07.025.
- Oliver C. Determinants of inter-organisational relationships: integration and future directions. Acad Manag Rev 1990;15:241-65.
- Ford D, Gadde LE, Håkansson H, Snehota I. Managing Business Relationships. Chichester: Wiley; 2003.
- Hakansson H, Snehota I. Developing Relationships in Business Networks. Andover: Cengage Learning; 1995.
- Turnbull P, Ford D, Cunningham M. Interaction, relationships and networks in business markets: an evolving perspective. J Bus Ind Mark 1996;11:44-62. http://dx.doi.org/10.1108/08858629610125469.
- Pfeffer J, Salancik GR. The External Control of Organizations: A Resource Dependence Perspective. New York, NY: Harper & Row; 1978.
- Cropanzano R, Mitchell MS. Social exchange theory: an interdisciplinary review. J Manag 2005;31:874-900. http://dx.doi.org/10.1177/0149206305279602.
- Emerson RM. Social exchange theory. Annu Rev Sociol 1976;2:335-62. http://dx.doi.org/10.1146/annurev.so.02.080176.002003.
- Aldrich H. Organizations and Environments. Upper Saddle River, NJ: Prentice-Hall; 1979.
- Håkansson H, Ford D. How should companies interact in business networks?. J Bus Res 2002;55:133-9. http://dx.doi.org/10.1016/S0148-2963(00)00148-X.
- Dwyer FR, Schurr PH, Oh S. Developing buyer–seller relationships. J Mark 1987;51:11-27. http://dx.doi.org/10.2307/1251126.
- Weick KE. Sensemaking in Organizations. London: Sage Publications; 1995.
- Macneil IR. Values in contract: internal and external. Northwestern Univ Law Rev 1983;78:340-418.
- Alajoutsijärvi K, Möller K, Rosenbröijer C-J. Relevance of focal nets in understanding the dynamics of business relationships. J Business-to-Business Mark 1999;6:3-35. http://dx.doi.org/10.1300/J033v06n03_02.
- Jarillo JC. Strategic Networks: Creating the Borderless Organization. Oxford: Butterworth-Heinemann; 1993.
- Möller K, Rajala A. Rise of strategic nets: new modes of value creation. Ind Mark Manag 2007;36:895-908. http://dx.doi.org/10.1016/j.indmarman.2007.05.016.
- Parolini C. The Value Net: A Tool for Competitive Strategy. New York, NY: Wiley; 1999.
- Knight L. Network learning: exploring learning by interorganizational networks. Human Relations 2002;55:427-54. http://dx.doi.org/10.1177/0018726702554003.
- Peters LD, Johnston WJ, Pressey AD, Kendrick T. Collaboration and collective learning: networks as learning organisations. J Bus Ind Mark 2010;25:478-84. http://dx.doi.org/10.1108/08858621011066062.
- Möller K. Sense-making and agenda construction in emerging business networks: how to direct radical innovation. Ind Mark Manag 2010;39:361-71. http://dx.doi.org/10.1016/j.indmarman.2009.03.014.
- Ramos C, Ford ID. Network pictures as a research device: developing a tool to capture actors’ perceptions in organizational networks. Ind Mark Manag 2011;40:447-64. http://dx.doi.org/10.1016/j.indmarman.2010.07.001.
- Möller K, Svahn S. Managing strategic nets: a capability perspective. Mark Theory 2003;3:209-34. http://dx.doi.org/10.1177/14705931030032002.
- Möller K, Rajala A, Svahn S. Strategic business nets: their type and management. J Bus Res 2005;58:1274-84. http://dx.doi.org/10.1016/j.jbusres.2003.05.002.
- Teece DJ, Pisano G, Shuen A. Dynamic capabilities and strategic management. Strateg Manag J 1997;18:509-33. http://dx.doi.org/10.1002/(SICI)1097-0266(199708)18:7<509::AID-SMJ882>3.0.CO;2-Z.
- Teece DJ. Explicating dynamic capabilities: the nature and microfoundations of (sustainable) enterprise performance. Strategic Manag J 2007;28:1319-50. http://dx.doi.org/10.1002/smj.640.
- Cox A, Ireland P, Lonsdale C, Sanderson J, Watson G. Supply Chains, Markets and Power: Mapping Buyer and Supplier Power Regimes. London: Routledge; 2002.
- Sanderson J. Opportunity and constraint in business-to-business relationships: insights from strategic choice and zones of manoeuvre. Supply Chain Manag 2004;9:392-401. http://dx.doi.org/10.1108/13598540410560775.
- Sanderson J, Cox A. The challenges of supply strategy selection in a project environment: evidence from UK naval shipbuilding. Supply Chain Manag 2008;13:16-25. http://dx.doi.org/10.1108/13598540810850283.
- Sanderson J. Buyer–supplier partnering in UK defence procurement: looking beyond the policy rhetoric. Public Adm 2009;87:327-50. http://dx.doi.org/10.1111/j.1467-9299.2008.01734.x.
- Emerson RM. Power-dependence relations. Am Sociol Rev 1962;27:31-4. http://dx.doi.org/10.2307/2089716.
- Porter M. Competitive Strategy. New York, NY: Free Press; 1980.
- Cox A, Lonsdale C, Watson G, Wu Y. Supplier relationship management as an investment: evidence from a UK study. J Gen Manag 2005;30:27-42.
- Cox AW, Watson G, Sanderson J. Power Regimes: Mapping the DNA of Business and Supply Chain Relationships. Stratford-upon-Avon: Earlsgate Press; 2000.
- Christopher M. Logistics and Supply Chain Management: Strategies for Reducing Risks and Improving Services. London: Pearson Education; 2010.
- Cooper MC, Lambert DM, Pagh JD. Supply chain management: more than a new name for logistics. Int J Logistics Manag 1997;8:1-14. http://dx.doi.org/10.1108/09574099710805556.
- Van Weele AJ. Purchasing Management: Analysis, Planning and Practice. London: Chapman and Hall; 1994.
- Slack N, Chambers S, Johnston R. Operations Management. London: FT Pitman; 2010.
- Waller DL. Operations Management: A Supply Chain Approach. London: Thomson; 2003.
- von Neumann J, Morgenstern O. Theory of Games and Economic Behaviour. New York, NY: John Wiley and Sons; 1944.
- Macbeth D, Ferguson N. Partnership Sourcing: An Integrated Supply Chain Approach. London: Pitman; 1994.
- Lamming RC, Caldwell ND, Harrison DA, Phillips W. Transparency in supply relationships: concept and practice. J Supply Chain Manag 2001;37:4-10. http://dx.doi.org/10.1111/j.1745-493X.2001.tb00107.x.
- Von Bertalanffy L. Theory of open systems in physics and biology. Science 1950;111:23-9. http://dx.doi.org/10.1126/science.111.2872.23.
- Jones TC, Riley DW. Using inventory for competitive advantage through supply chain management. Int J Phys Distr Logistics 1985;15:16-2.
- Houlihan JB. International supply chain management. Int J Phys Distr Logistics 1985;15:22-38.
- Novack RA, Simco SW. The industrial procurement process: a supply chain perspective. J Bus Logistics 1991;12:145-67.
- Scott C, Westbrook R. New strategic tools for supply chain management. Int J Phys Distr Logistics 1991;21:23-3. http://dx.doi.org/10.1108/09600039110002225.
- Lee HL, Billington C. Managing supply chain inventory: pitfalls and opportunities. Sloan Manag Rev 1992;33:65-73.
- Lee HL, Billington C. Material management in decentralized supply chains. Oper Res 1993;41:835-47. http://dx.doi.org/10.1287/opre.41.5.835.
- Forrester JW. Industrial Dynamics. Cambridge, MA: MIT Press; 1961.
- Disney SM, Naim MM, Towill DR. Dynamic simulation modelling for lean logistics. Int J Phys Distr Logistics 1997;27:174-96. http://dx.doi.org/10.1108/09600039710170566.
- Mason-Jones R, Naim MM, Towill DR. The impact of pipeline control on supply chain dynamics. Int J Logistics Manag 1997;8:47-62. http://dx.doi.org/10.1108/09574099710805664.
- Towill DR, Evans GN, Cheema P. Analysis and design of an adaptive minimum reasonable inventory control system. Prod Plann Control 1997;8:545-57. http://dx.doi.org/10.1080/095372897234885.
- Towill DR, Naim MM, Wikner J. Industrial dynamics simulation models in the design of supply chains. Int J Phys Distr Logistics 1992;22:3-13. http://dx.doi.org/10.1108/09600039210016995.
- Wikner J, Towill DR, Naim M. Smoothing supply chain dynamics. Int J Prod Econ 1991;22:231-48. http://dx.doi.org/10.1016/0925-5273(91)90099-F.
- Lamming R. Beyond Partnership: Strategies for Innovation and Lean Supply. New York, NY: Prentice Hall; 1993.
- Womack J, Jones D. Lean Thinking: Banish Waste and Create Wealth in Your Corporation. New York, NY: Simon and Schuster; 1996.
- Christopher M. The agile supply chain: competing in volatile markets. Ind Mark Manag 2000;29:37-44. http://dx.doi.org/10.1016/S0019-8501(99)00110-8.
- Mason-Jones R, Towill DR. Total cycle time compression and the agile supply chain. Int J Prod Econ 1999;62:61-73. http://dx.doi.org/10.1016/S0925-5273(98)00221-7.
- Gunasekaran A, Ngai EWT. Build-to-order supply chain management: a literature review and framework for development. J Oper Manag 2005;23:423-51. http://dx.doi.org/10.1016/j.jom.2004.10.005.
- Anderson P. Marketing, scientific progress and scientific method. J Mark 1983;47:18-31. http://dx.doi.org/10.2307/1251395.
- Cigolini R, Cozzi M, Perona M. A new framework for supply chain management: conceptual model and empirical test. Int J Oper Prod Manag 2004;24:7-41. http://dx.doi.org/10.1108/01443570410510979.
- Cox A, Chicksand D, Ireland P, Davies T. Sourcing indirect spend: a survey of current internal and external strategies for non-revenue-generating goods and services. J Supply Chain Manag 2005;41:39-51. http://dx.doi.org/10.1111/j.1055-6001.2005.04102004.x.
- Kraljic P. Purchasing must become supply management. Harvard Bus Rev 1983;61:109-17.
- Fisher ML. What is the right supply chain for your product?. Harvard Bus Rev 1997;75:105-17.
- Klein R. The troubled transformation of Britain’s National Health Service. New Engl J Med 2006;355:409-15. http://dx.doi.org/10.1056/NEJMhpr062747.
- Exworthy M, Peckham S. The contribution of coterminosity to joint purchasing in health and social care. Health Place 1998;4:233-43. http://dx.doi.org/10.1016/S1353-8292(98)00018-5.
- Dopson S, Locock L. The commissioning process in the NHS: the theory and application. Public Manag Rev 2002;4:209-29. http://dx.doi.org/10.1080/14616670210130552.
- Wyke S, Mays N, Street A, Bevan G, McLeod H, Goodwin N. Should general practitioners purchase health care for their patients? The total purchasing experiment in Britain. Health Policy 2003;65:243-59. http://dx.doi.org/10.1016/S0168-8510(03)00040-X.
- Baxter K, Bachmann M, Bevan G. Primary care groups: trade-offs in managing budgets and risk. Public Money Manag 2000;20:53-62. http://dx.doi.org/10.1111/1467-9302.00202.
- Baxter K, Weiss M, Le Grand J. Collaborative commissioning of secondary care services by primary care trusts. Public Money Manag 2007;27:207-14. http://dx.doi.org/10.1111/j.1467-9302.2007.00581.x.
- Practical Guidance on Joint Commissioning for Project Leaders. London: DH; 1995.
- Creating a Patient-Led NHS: Delivering the NHS Improvement Plan. London: DH; 2005.
- Millar R, Powell M, Dixon A. What was the programme theory of New Labour’s health system reforms?. J Health Serv Res Policy 2012;17:7-15. http://dx.doi.org/10.1258/jhsrp.2011.010189.
- Cox AW, Ireland P, Lonsdale C, Sanderson J, Watson G. Supply Chain Management: A Guide to Best Practice. London: FT Prentice Hall; 2003.
- Dixit A. Incentives and organizations in the public sector. J Human Resources 2002;37:696-727. http://dx.doi.org/10.2307/3069614.
- Allen P, Turner S, Bertlett W, Perotin V, Matchaya G, Zamora B. Provider diversity in the English NHS: a study of recent developments in four local health economies. J Health Serv Res Policy 2012;17:23-30. http://dx.doi.org/10.1258/jhsrp.2011.011015.
- Bennett C, Ferlie E. Contracting in theory and practice: some evidence from the NHS. Public Adm 1996;74:49-66. http://dx.doi.org/10.1111/j.1467-9299.1996.tb00857.x.
- Dickinson H, Shaw S, Glasby J, Smith J. The limits of market-based reforms. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-I1.
- Frosini F, Dixon A, Robertson R. Competition in the NHS: a provider perspective. J Health Serv Res Policy 2012;17:16-22. http://dx.doi.org/10.1258/jhsrp.2011.010194.
- Gray K, Higgins M. Legacy, trust, and turbulence in the NHS healthcare commissioning process: an exploratory study. Int J Healthcare Manag 2012;5:40-7. http://dx.doi.org/10.1179/2047971912Y.0000000002.
- Reforming NHS Financial Flows: Introducing Payment by Results. London: DH; 2002.
- Miller R, Millar R, Hall K. New development: spin-outs and social enterprise – the ‘right to request’ programme for health and social care services. Public Money Manag 2012;32:233-6. http://dx.doi.org/10.1080/09540962.2012.676283.
- Equity and Excellence: Liberating the NHS. London: DH; 2010.
- Allen P. A socio-legal and economic analysis of contracting in the NHS internal market using a case study of contracting for district nursing. Soc Sci Med 2002;54:255-66. http://dx.doi.org/10.1016/S0277-9536(01)00025-9.
- Propper C. Agency and incentives in the NHS internal market. Soc Sci Med 1995;40:1683-90. http://dx.doi.org/10.1016/0277-9536(94)00285-2.
- Bartlett W. Quasi-markets and contracts: a markets and hierarchies perspective on NHS reforms. Public Money Manag 1991;11:53-61. http://dx.doi.org/10.1080/09540969109387669.
- Macneil IR. Contracts: adjustment of long-term economic relations under classical, neoclassical, and relational contract law. Northwestern Univ Law Rev 1978;72:854-905.
- Guven-Uslu P. Uncertainty and commitment in commissioning of health services. Public Money Manag 2012;32:349-56. http://dx.doi.org/10.1080/09540962.2012.703419.
- Bate A, Donaldson C, Murtagh MJ. Managing to manage healthcare resources in the English NHS? What can health economics teach? What can health economics learn?. Health Policy 2007;84:249-61. http://dx.doi.org/10.1016/j.healthpol.2007.04.001.
- Ferlie E, McGivern G. Relationships between Health Care Organisations: A Critical Overview of the Literature and Research Agenda. London: National Co-ordinating Centre for NHS Service Delivery and Organisation programme; 2003.
- Cousins PD. A conceptual model for managing long-term inter-organisational relationships. Eur J Purchasing Supply Manag 2002;8:71-82. http://dx.doi.org/10.1016/S0969-7012(01)00006-5.
- Granovetter M. Economic action and social structure: the problem of embeddedness. Am J Sociol 1985:481-510. http://dx.doi.org/10.1086/228311.
- Cox A, Chicksand D, Ireland P. Sub-optimality in NHS sourcing in the UK: demand-side constraints on supply-side improvement. Public Adm 2005;83:367-92. http://dx.doi.org/10.1111/j.0033-3298.2005.00454.x.
- Lonsdale C, Watson G. The internal client relationship, demand management and value for money: evidence from the UK National Health Service. J Purchasing Supply Manag 2005;11:159-72. http://dx.doi.org/10.1016/j.pursup.2005.11.001.
- Checkland K, Harrison S, Snow S, Coleman A, McDermott I. Understanding the work done by NHS commissioning managers. J Health Organ Manag 2013;27:149-70. http://dx.doi.org/10.1108/14777261311321752.
- Lian PCS, Laing AW. The role of professional expertise in the purchasing of health services. Health Serv Manag Res 2004;17:110-20. http://dx.doi.org/10.1258/095148404323043136.
- Gridley K, Spiers G, Aspinal F, Bernard S, Atkin K, Parker G. Can general practitioner commissioning deliver equity and excellence? Evidence from two studies of service improvement in the English NHS. J Health Serv Res Policy 2012;17:87-93. http://dx.doi.org/10.1258/jhsrp.2011.010176.
- Mannion R. General practitioner-led commissioning in the NHS: progress, prospects and pitfalls. Br Med Bull 2011;97:7-15. http://dx.doi.org/10.1093/bmb/ldq042.
- Laing AW, Cotton S. Purchasing health care services: information sources and decisional criteria. J Mark Manag 1996;12:719-34. http://dx.doi.org/10.1080/0267257X.1996.9964449.
- Hughes D, Doheny S. Deliberating Tarceva: a case study of how British NHS managers decide whether to purchase a high-cost drug in the shadow of NICE guidance. Soc Sci Med 2011;73:1460-8. http://dx.doi.org/10.1016/j.socscimed.2011.08.023.
- Checkland K, Snow S, McDermott I, Harrison S, Coleman A. ‘Animateurs’ and animation: what makes a good commissioning manager?. J Health Serv Res Policy 2012;17:11-7. http://dx.doi.org/10.1258/jhsrp.2011.011010.
- Horrocks J, Lyons C, Hopley P. Does strategic involvement of mental health service users and carers in the planning, design and commissioning of mental health services lead to better outcomes?. Int J Consumer Stud 2010;34:562-9. http://dx.doi.org/10.1111/j.1470-6431.2010.00912.x.
- Martin GP. Whose health, whose care, whose say? Some comments on public involvement in new NHS commissioning arrangements. Critical Public Health 2009;19:123-32. http://dx.doi.org/10.1080/09581590802385672.
- Allen B, Wade E, Dickinson H. Bridging the divide: commercial procurement and supply chain management – are there lessons for healthcare commissioning in England?. J Public Procurement 2009;9:504-34.
- Lonsdale C, Kirkpatrick I, Hoque K, De Ruyter A. Supplier behaviour and public contracting in the English National Health Service. Public Adm 2010;88:800-18. http://dx.doi.org/10.1111/j.1467-9299.2010.01846.x.
- Hughes D, Allen P, Doheny S, Petsoulas C, Vincent-Jones P. Co-operation and conflict under hard and soft contracting regimes: case studies from England and Wales. BMC Health Serv Res 2012;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S7.
- Coleman A, Checkland K, McDermott I, Harrison S. The limits of market-based reforms in the NHS: the case of alternative providers in primary care. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S3.
- Mannion R, Marini G, Street A. Implementing payment by results in the English NHS: changing incentives and the role of information. J Health Organ Manag 2008;22:79-88. http://dx.doi.org/10.1108/14777260810862425.
- Connell N, Mannion R. Conceptualisations of trust in the organisational literature: some indicators from a complementary perspective. J Health Organ Manag 2006;20:417-33. http://dx.doi.org/10.1108/14777260610701795.
- Goddard M, Mannion R. From competition to co-operation: new economic relationships in the National Health Service. Health Econ 1998;7:105-19. http://dx.doi.org/10.1002/(SICI)1099-1050(199803)7:2<105::AID-HEC333>3.0.CO;2-K.
- Porter A, Mays N, Shaw SE, Rosen R, Smith J. Commissioning healthcare for people with long term conditions: the persistence of relational contracting in England’s NHS quasi-market. BMC Health Serv Res 2013;13. http://dx.doi.org/10.1186/1472-6963-13-S1-S2.
- Sheaff R, Benson L, Farbus L, Schofield J, Mannion R, Reeves D. Network resilience in the face of health system reform. Soc Sci Med 2010;70:779-86. http://dx.doi.org/10.1016/j.socscimed.2009.11.011.
- Freemantle N, Watt I, Mason J. Developments in the purchasing process in the NHS: towards an explicit politics of rationing. Public Adm 1993;71:535-48. http://dx.doi.org/10.1111/j.1467-9299.1993.tb00990.x.
- North N. Implementing strategy: the politics of healthcare commissioning. Policy Polit 1998;26:5-14. http://dx.doi.org/10.1332/030557398782018301.
- Addicott R, Ferlie E. Understanding power relationships in health care networks. J Health Organ Manag 2007;21:393-405. http://dx.doi.org/10.1108/14777260710778925.
- de Souza LB. Trends and approaches in lean healthcare. Leadership in Health Services 2009;22:121-39. http://dx.doi.org/10.1108/17511870910953788.
- Proudlove N, Moxham C, Boaden R. Lessons for lean in health care from using Six Sigma in the NHS. Public Money Manag 2008;28:27-34.
- Grove AL, Meredith JO, Macintyre M, Angelis J, Neailey K. Lean implementation in primary care health visiting services in National Health Service UK. Qual Saf Health Care 2010;19. http://dx.doi.org/10.1136/qshc.2009.039719.
- Lodge A, Bamford D. New development: using lean techniques to reduce radiology waiting times. Public Money Manag 2008;28:49-52.
- de Souza LB, Pidd M. Exploring the barriers to lean health care implementation. Public Money Manag 2011;31:59-66. http://dx.doi.org/10.1080/09540962.2011.545548.
- Bourlakis M, Clear F, Patten L. Understanding the UK hospital supply chain in an era of patient choice. J Mark Manag 2011;27:401-23. http://dx.doi.org/10.1080/0267257X.2011.547084.
- Towill D, Christopher M. An evolutionary approach to the architecture of effective healthcare delivery systems. J Health Organ Manag 2005;19:130-47. http://dx.doi.org/10.1108/14777260510600059.
- Browne N, Cowley S, Grocott P. The wound dressing supply chain within England’s National Health Service: untravelling the context for users. J Nurs Manag 2004;12:51-6. http://dx.doi.org/10.1046/j.1365-2834.2003.00436.x.
- Campling N, Grocott P, Cowley S. Disconnection: the user voice within the wound dressing supply chain. J Nurs Manag 2008;16:204-13. http://dx.doi.org/10.1111/j.1365-2834.2007.00818.x.
- Breen L, Crawford H. Improving the pharmaceutical supply chain: assessing the reality of e-quality through e-commerce application in hospital pharmacy. Int J Qual Reliability Manag 2005;22:572-90. http://dx.doi.org/10.1108/02656710510604890.
- Cullen AJ, Taylor M. Critical success factors for B2B e-commerce use within the UK NHS pharmaceutical supply chain. Int J Oper Prod Manag 2009;29:1156-85. http://dx.doi.org/10.1108/01443570911000177.
- Bakker E, Zheng J, Knight L, Harland C. Putting e-commerce adoption in a supply chain context. Int J Oper Prod Manag 2008;28:313-30. http://dx.doi.org/10.1108/01443570810861543.
- Russill R. Purchasing Power. London: McGraw Hill; 1997.
- Karjalainen K. Estimating the cost effects of purchasing centralisation: empirical evidence from framework agreements in the public sector. J Purchasing Supply Manag 2011;17:87-9. http://dx.doi.org/10.1016/j.pursup.2010.09.001.
- Kastanioti C, Kontodimopoulos N, Stasinopoulos D, Kapetaneas N, Polyzos N. Public procurement of health technologies in Greece in an era of economic crisis. Health Policy 2013;109:7-13. http://dx.doi.org/10.1016/j.healthpol.2012.03.015.
- Sorenson C, Kanavos P. Medical technology procurement in Europe: a cross-country comparison of current practice and policy. Health Policy 2011;100:43-50. http://dx.doi.org/10.1016/j.healthpol.2010.08.001.
- Sorte WF. Assessing the efficiency of centralised public procurement in the Brazilian ICT sector. Int J Procurement Manag 2013;6:58-75. http://dx.doi.org/10.1504/IJPM.2013.050610.
- McCue CP, Pitzer JT. Centralised vs. decentralised purchasing: current trends in governmental procurement practices. J Public Budgeting Accounting Financ Manag 2000;12:400-20.
- Thatcher J, Sharp L. Measuring the local economic impact of National Health Service procurement in the UK: an evaluation of the Cornwall Food Programme and LM3. Local Environ 2008;13:253-70. http://dx.doi.org/10.1080/13549830701669005.
- O’Brien J. Category Management in Purchasing: A Strategic Approach to Maximize Business Profitability. London: Kogan Page; 2009.
- Burns LR, Lee JA. Hospital purchasing alliances: utilisation, services, and performance. Health Care Manag Rev 2008;33:203-15. http://dx.doi.org/10.1097/01.HMR.0000324906.04025.33.
- Nollet J, Beaulieu M. Should an organisation join a purchasing group?. Supply Chain Manag 2005;10:11-7. http://dx.doi.org/10.1108/13598540510578333.
- Camillus JA, Rosenthal MB. Health care coalitions: from joint purchasing to local health reform. Inquiry – Excellus Health Plan 2008;45:142-52.
- Tella E, Virolainen V-M. Motives behind purchasing consortia. Int J Prod Econ 2005;93,94:161-8. http://dx.doi.org/10.1016/j.ijpe.2004.06.014.
- Walker H, Schotanus F, Bakker E, Harland C. Collaborative procurement: a relational view of buyer–buyer relationships. Public Adm Rev 2013;73:588-98. http://dx.doi.org/10.1111/puar.12048.
- Nollet J, Beaulieu M. The development of group purchasing: an empirical study in the healthcare sector. J Purchasing Supply Manag 2003;9:3-10. http://dx.doi.org/10.1016/S0969-7012(02)00034-5.
- Schotanus F, Telgen J, de Boer L. Critical success factors for managing purchasing groups. J Purchasing Supply Manag 2010;16:51-60. http://dx.doi.org/10.1016/j.pursup.2009.10.002.
- Syson R. Improve Purchase Performance. London: Pitman; 1992.
- Gelderman CJ, van Weele AJ. Strategic direction through purchasing portfolio management: a case study. J Supply Chain Manag 2002;38:30-7. http://dx.doi.org/10.1111/j.1745-493X.2002.tb00127.x.
- Olsen RF, Ellram LM. A portfolio approach to supplier relationships. Ind Mark Manag 1997;26:101-13. http://dx.doi.org/10.1016/S0019-8501(96)00089-2.
- Steele P, Court B. Profitable Purchasing Strategies. London: McGraw Hill; 1996.
- Gelderman CJ. Rethinking Kraljic: towards a purchasing portfolio model, based on mutual buyer–supplier dependence. Danish Purchasing &Amp; Logistics Forum 2000;37:9-15.
- Gelderman CJ, van Weele AJ. Handling measurement issues and strategic directions in Kraljic’s purchasing portfolio model. J Purchasing Supply Manag 2003;9:207-16. http://dx.doi.org/10.1016/j.pursup.2003.07.001.
- Lee DM, Drake PR. A portfolio model for component purchasing strategy and the case study of two South Korean elevator manufacturers. Int J Prod Res 2010;48:6651-82. http://dx.doi.org/10.1080/00207540902897780.
- Padhi SS, Wagner SM, Aggarwal V. Positioning of commodities using the Kraljic Portfolio Matrix. J Purchasing Supply Manag 2012;18:1-8. http://dx.doi.org/10.1016/j.pursup.2011.10.001.
- Javed AA, Lam PTI, Zou PXW. Output-based specifications for PPP projects: lessons for facilities management from Australia. J Facil Manag 2013;11:5-30. http://dx.doi.org/10.1108/14725961311301448.
- Karlsson C, Nellore R, Soderquist K. Black box engineering: redefining the role of product specifications. J Product Innovation Manag 1998;15:534-49. http://dx.doi.org/10.1016/S0737-6782(98)00029-0.
- Kashiwagi D, Parmar D, Savicky J. The impact of minimising specifications and management at the University of Hawaii. J Facil Manag 2003;2:131-41. http://dx.doi.org/10.1108/14725960410808168.
- Patil SS, Molenaar KR. Risks associated with performance specifications in highway infrastructure procurement. J Public Procurement 2011;11:482-509.
- Angeles R, Nath R. Business-to-business e-procurement: success factors and challenges to implementation. Supply Chain Manag 2007;12:104-15. http://dx.doi.org/10.1108/13598540710737299.
- Arbin K. E-procurement maturity in industry. Int J Electron Bus 2003;1:396-407. http://dx.doi.org/10.1504/IJEB.2003.004112.
- Hartley JL, Lane MD, Duplaga EA. Exploring the barriers to the adoption of e-auctions for sourcing. Int J Oper Prod Manag 2006;26:202-21. http://dx.doi.org/10.1108/01443570610641675.
- Kulp SL, Taylor R, Brandyberry G, Potts K. Using organizational control mechanisms to enhance procurement efficiency: how GlaxoSmithKline improved the effectiveness of e-procurement. Interfaces 2006;36:209-19. http://dx.doi.org/10.1287/inte.1060.0209.
- Massa S, Testa S. ICTs adoption and knowledge management: the case of an e-procurement system. Knowledge Process Manag 2007;14:26-3. http://dx.doi.org/10.1002/kpm.267.
- Gunasekaran A, Ngai EWT. Adoption of e-procurement in Hong Kong: an empirical research. Int J Prod Econ 2008;113:159-75. http://dx.doi.org/10.1016/j.ijpe.2007.04.012.
- Rotchanakitumnuai S. Assessment of e-procurement auction with a balanced scorecard. Int J Phys Distr Logistics 2013;43:39-53. http://dx.doi.org/10.1108/09600031311293246.
- Bhakoo V, Chan C. Collaborative implementation of e-business processes within the health-care supply chain: the Monash Pharmacy Project. Supply Chain Manag 2011;16:184-93. http://dx.doi.org/10.1108/13598541111127173.
- Brandon-Jones A, Carey S. The impact of user-perceived e-procurement quality on system and contract compliance. Int J Oper Prod Manag 2011;31:274-96. http://dx.doi.org/10.1108/01443571111111928.
- Chang H-L, Wang K, Chiu I. Business–IT fit in e-procurement systems: evidence from high-technology firms in China. Info Syst J 2008;18:381-404. http://dx.doi.org/10.1111/j.1365-2575.2008.00300.x.
- Devaraj S, Vaidyanathan G, Mishra AN. Effect of purchase volume flexibility and purchase mix flexibility on e-procurement performance: an analysis of two perspectives. J Oper Manag 2012;30:509-20. http://dx.doi.org/10.1016/j.jom.2012.08.001.
- Vaidyanathan G, Devaraj S. The role of quality in e-procurement performance: an empirical analysis. J Oper Manag 2008;26:407-25. http://dx.doi.org/10.1016/j.jom.2007.08.004.
- Ketikidis PH, Kontogeorgis A, Stalidis G, Kaggelides K. Applying e-procurement system in the healthcare: the EPOS paradigm. Int J Syst Sci 2010;41:281-99. http://dx.doi.org/10.1080/00207720903326878.
- Soares-Aguiar A, Palma-dos-Reis A. Why do firms adopt e-procurement systems? Using logistic regression to empirically test a conceptual model. IEEE Transactions on Engineering Management 2008;55:120-33. http://dx.doi.org/10.1109/TEM.2007.912806.
- Walker H, Brammer S. The relationship between sustainable procurement and e-procurement in the public sector. Int J Prod Econ 2012;140:256-68. http://dx.doi.org/10.1016/j.ijpe.2012.01.008.
- Mithas S, Jones JL. Do auction parameters affect buyer surplus in e-auctions for procurement?. Prod Oper Manag 2007;16:455-70. http://dx.doi.org/10.1111/j.1937-5956.2007.tb00272.x.
- Croom SR, Brandon-Jones A. Key issues in e-procurement: procurement implementation and operation in the public sector. J Public Procurement 2005;5:367-87.
- Croom S, Johnston R. E-service: enhancing internal customer service through e-procurement. Int J Serv Ind Manag 2003;14:539-55. http://dx.doi.org/10.1108/09564230310500219.
- Davila A, Gupta M, Palmer R. Moving procurement systems to the internet: the adoption and use of e-procurement technology models. Eur Manag J 2003;21:11-23. http://dx.doi.org/10.1016/S0263-2373(02)00155-X.
- Henriksen HZ, Mahnke V. E-procurement adoption in the Danish public sector: the influence of economic and political rationality. Scand J Info Syst 2005;17:85-106.
- Subramaniam C, Shaw MJ. A study of the value and impact of B2B e-commerce: the case of web-based procurement. Int J Electron Commerce 2002;6:19-40.
- Tai Y-M, Ho C-F, Wu W-H. The performance impact of implementing Web-based e-procurement systems. Int J Prod Res 2010;48. http://dx.doi.org/10.1080/00207540903117915.
- Tassabehji R, Taylor WA, Beach R, Wood A. Reverse e-auctions and supplier–buyer relationships: an exploratory study. Int J Oper Prod Manag 2006;26:166-84. http://dx.doi.org/10.1108/01443570610641657.
- Tassabehji R. Understanding e-auction use by procurement professionals: motivation, attitudes and perceptions. Supply Chain Manag 2010;15:425-37. http://dx.doi.org/10.1108/13598541011080419.
- Croom S, Brandon-Jones A. Impact of e-procurement: experiences from implementation in the UK public sector. J Purchasing Supply Manag 2007;13:294-303. http://dx.doi.org/10.1016/j.pursup.2007.09.015.
- Hult GTM. Managing the international strategic sourcing process as a market-driven organizational learning system. Decision Sci 1998;29:193-216. http://dx.doi.org/10.1111/j.1540-5915.1998.tb01349.x.
- Kocabasoglu C, Suresh NC. Strategic sourcing: an empirical investigation of the concept and its practices in U.S. manufacturing firms. J Supply Chain Manag 2006;42:4-16. http://dx.doi.org/10.1111/j.1745-493X.2006.00008.x.
- Rhyne DM. The impact of demand management on service system performance. Serv Ind J 1988;8:446-58. http://dx.doi.org/10.1080/02642068800000064.
- Trent RJ, Monczka RM. Effective cross-functional sourcing teams: critical success factors. Int J Purchasing Mater Manag 1994;30:2-11.
- McIvor R, McHugh M. Partnership sourcing: an organization change management perspective. J Supply Chain Manag 2000;36:12-20. http://dx.doi.org/10.1111/j.1745-493X.2000.tb00247.x.
- Karjalainen K, Kemppainen K, van Raaij E. Non-compliant work behaviour in purchasing: an exploration of reasons behind maverick buying. J Bus Ethics 2009;85:245-61. http://dx.doi.org/10.1007/s10551-008-9768-2.
- Carter JR, Maltz A, Maltz E, Goh M, Yan T. Impact of culture on supplier selection decision making. Int J Logistics Manag 2010;21:353-74. http://dx.doi.org/10.1108/09574091011089790.
- Choi TY, Hartley JL. An exploration of supplier selection practices across the supply chain. J Oper Manag 1996;14:333-43. http://dx.doi.org/10.1016/S0272-6963(96)00091-5.
- Hsu C-C, Kannan VR, Leong GK, Tan K-C. Supplier selection construct: instrument development and validation. Int J Logist Manag 2006;17:213-39. http://dx.doi.org/10.1108/09574090610689961.
- Kaufmann L, Carter CR, Buhrmann C. The impact of individual debiasing efforts on financial decision effectiveness in the supplier selection process. Int J Phys Distr Logistics 2012;42:411-33. http://dx.doi.org/10.1108/09600031211246492.
- Talluri S, Narasimhan R. A methodology for strategic sourcing. Eur J Oper Res 2004;154:236-50. http://dx.doi.org/10.1016/S0377-2217(02)00649-5.
- Walsh K. Competitive Tendering for Local Authority Services: Initial Experiences. London: The Stationery Office; 1991.
- Domberger S, Rimmer S. Competitive tendering and contracting in the public sector: a survey. Int J Econ Bus 1994;1:439-53. http://dx.doi.org/10.1080/758536232.
- Szymanski S. The impact of compulsory competitive tendering on refuse collection services. Fiscal Stud 1996;17:1-19. http://dx.doi.org/10.1111/j.1475-5890.1996.tb00491.x.
- Davies C, Anand P, Artigas L, Holloway J, McConway K, Newman J, et al. Links between Governance, Incentives and Outcomes: A Review of the Literature. London: National Co-ordinating Centre for NHS Service Delivery and Organisation programme; 2005.
- Julius D. Public Service Industry Review: Understanding the Public Services Industry – How Big, How Good, Where Next?. London: Department for Business, Enterprise and Regulatory Reform; 2008.
- Evaluation Report: Impact and Effectiveness of EU Public Procurement Legislation. Brussels: European Commission; 2011.
- Guccio C, Pignataro G, Rizzo I. Determinants of adaptation costs in procurement: an empirical estimation on Italian public works contracts. Applied Econ 2011;44:1891-909. http://dx.doi.org/10.1080/00036846.2011.556589.
- Cox A, Watson G, Lonsdale C, Sanderson J. Managing appropriately in power regimes: relationship and performance management in 12 supply chain cases. Supply Chain Manag 2004;9:357-71. http://dx.doi.org/10.1108/13598540410560748.
- Alderman N, Ivory C. Partnering in major contracts: paradox and metaphor. Int J Proj Manag 2007;25:386-93. http://dx.doi.org/10.1016/j.ijproman.2007.01.002.
- Mortensen M, Arlbjørn J. Inter-organisational supplier development: the case of customer attractiveness and strategic fit. Supply Chain Manag 2012;17:152-71. http://dx.doi.org/10.1108/13598541211212898.
- Cox A. Power, value and supply chain management. Supply Chain Manag 1999;4:167-75. http://dx.doi.org/10.1108/13598549910284480.
- Burke GJ, Carrillo JE, Vakharia AJ. Single versus multiple supplier sourcing strategies. Eur J Oper Res 2007;182:95-112. http://dx.doi.org/10.1016/j.ejor.2006.07.007.
- Aláez-Aller R, Longás-García JC. Dynamic supplier management in the automotive industry. Int J Oper Prod Manag 2010;30:312-35. http://dx.doi.org/10.1108/01443571011024647.
- Krause DR, Scannell TV. Supplier development practices: product- and service-based industry comparisons. J Supply Chain Manag 2002;38:13-21. http://dx.doi.org/10.1111/j.1745-493X.2002.tb00125.x.
- Lacity MC, Willcocks LP. Global Information Technology Outsourcing: In Search of Business Advantage. Chichester: Wiley; 2001.
- Lacity MC, Willcocks LP. Information Systems and Outsourcing: Studies in Theory and Practice. Basingstoke: Palgrave Macmillan; 2008.
- Tracey M, Tan CL. Empirical analysis of supplier selection and involvement, customer satisfaction, and firm performance. Supply Chain Manag 2001;6:174-88. http://dx.doi.org/10.1108/EUM0000000005709.
- Wilson EJ. The relative importance of supplier selection criteria: a review and update. Int J Purchasing Mater Manag 1994;30:35-41.
- Ellram LM. The supplier selection decision in strategic partnerships. Int J Purchasing Mater Manag 1990;26:8-14.
- Humphreys PK, Shiu WK, Chan FTS. Collaborative buyer–supplier relationships in Hong Kong manufacturing firms. Supply Chain Manag 2001;6:152-62. http://dx.doi.org/10.1108/EUM0000000005708.
- Sieweke J, Birkner S, Mohe M. Preferred supplier programs for consulting services: an exploratory study of German client companies. J Purchasing Supply Manag 2012;18:123-36. http://dx.doi.org/10.1016/j.pursup.2012.03.001.
- Swift CO. Preferences for single sourcing and supplier selection criteria. J Bus Res 1995;32:105-11. http://dx.doi.org/10.1016/0148-2963(94)00043-E.
- Heywood T, Lonsdale C. Power in procurement. PPP Journal 2012;76:1-2.
- Kannan VR, Tan KC. Supplier selection and assessment: their impact on business performance. J Supply Chain Manag 2002;38:11-2. http://dx.doi.org/10.1111/j.1745-493X.2002.tb00139.x.
- Kannan VR, Tan KC. Buyer–supplier relationships. Int J Phys Distr Logistics 2006;36:755-75. http://dx.doi.org/10.1108/09600030610714580.
- Lian PCS, Laing AW. Public sector purchasing of health services: a comparison with private sector purchasing. J Purchasing Supply Manag 2004;10:247-56. http://dx.doi.org/10.1016/j.pursup.2004.11.005.
- Huang X, Gattiker TF, Schwarz JL. Interpersonal trust formation during the supplier selection process: the role of the communication channel. J Supply Chain Manag 2008;44:53-75. http://dx.doi.org/10.1111/j.1745-493X.2008.00066.x.
- Kaplan RS, Norton DP. The balanced scorecard: measures that drive performance. Harvard Bus Rev 1992:71-9.
- Costantino N, Dotoli M, Falagario M, Fanti MP. Using fuzzy decision making for supplier selection in public procurement. J Public Procurement 2011;11:403-27.
- Kahraman C, Cebeci U, Ulukan Z. Multi-criteria supplier selection using fuzzy AHP. Logistics Info Manag 2003;16:382-94. http://dx.doi.org/10.1108/09576050310503367.
- Sevkli M, Koh SCL, Zaim S, Demirbag M, Tatoglu E. An application of data envelopment analytic hierarchy process for supplier selection: a case study of BEKO in Turkey. Int J Prod Res 2007;45:1973-200. http://dx.doi.org/10.1080/00207540600957399.
- Yigin IH, Taskin H, Cedlmoglu IH, Topal B. Supplier selection: an expert system approach. Prod Plann Control 2007;18:16-24. http://dx.doi.org/10.1080/09537280600940655.
- Towers N, Song Y. Assessing the future challenges in strategic sourcing commodity from China: a case-study analysis. Asia Pacific Bus Rev 2010;16:527-44. http://dx.doi.org/10.1080/13602380903068071.
- Eigen ZJ. Empirical studies of contract. Annu Rev Law Soc Sci 2012;8:291-306. http://dx.doi.org/10.1146/annurev-lawsocsci-011912-083704.
- Smith J, Woodin J, Walsh K, Smith J. Healthcare Management. Maidenhead: Open University Press; 2011.
- Balcik B, Ak D. Supplier selection for framework agreements in humanitarian relief. Prod Oper Manag 2013;22:1-14.
- Lacoste SM. Coopetition and framework contracts in industrial customer–supplier relationships. Qualitative Market Res 2014;17:43-57. http://dx.doi.org/10.1108/QMR-01-2012-0006.
- Lam T, Gale K. Highway maintenance: impact of framework agreements upon project financial performance. Construction Manag Econ 2014;32:460-72. http://dx.doi.org/10.1080/01446193.2014.892628.
- The Performance and Management of Hospital PFI Contracts. London: National Audit Office; 2010.
- Nooteboom B. Trust: Forms, Foundations, Functions, Failures and Figures. Cheltenham: Edward Elgar; 2002.
- Spekman RE, Kamauff JW, Myhr N. An empirical investigation into supply chain management: a perspective on partnerships. Supply Chain Manag 1998;3:53-67. http://dx.doi.org/10.1108/13598549810215379.
- Chiles TH, McMackin JF. Integrating variable risk preferences, trust, and transaction cost economics. Acad Manag Rev 1996;21:73-99.
- Dyer JH. Does governance matter? Keiretsu alliances and asset specificity as sources of Japanese competitive advantage. Organ Sci 1996;7:649-66. http://dx.doi.org/10.1287/orsc.7.6.649.
- Dyer JH, Chu W. The role of trustworthiness in reducing transaction costs and improving performance: empirical evidence from the United States, Japan, and Korea. Organ Sci 2003;14:57-68. http://dx.doi.org/10.1287/orsc.14.1.57.12806.
- Keast RK, Maxwell S, Barkman S, Chetcuti S, Oral H, Eagle KA. Cardiovascular supply cost negotiations partnering for the future. Health Care Manag (Frederik) 2010;29:68-75. http://dx.doi.org/10.1097/HCM.0b013e3181cca421.
- Krishnan R, Miller F, Sedatole K. The use of collaborative interfirm contracts in the presence of task and demand uncertainty: a discussion. Contemporary Accounting Res 2011;28:1397-422. http://dx.doi.org/10.1111/j.1911-3846.2011.01124.x.
- Malhotra D, Murnighan JK. The effects of contracts on interpersonal trust. Administrative Sci Q 2002;47:534-59. http://dx.doi.org/10.2307/3094850.
- Hofstede G. Culture’s Consequences: International Differences in Work-Related Values. Beverly Hills, CA: Sage Publications; 1980.
- Cannon JP, Doney PM, Mullen MR, Petersen KJ. Building long-term orientation in buyer–supplier relationships: the moderating role of culture. J Oper Manag 2010;28:506-21. http://dx.doi.org/10.1016/j.jom.2010.02.002.
- Dash S, Bruning E, Guin KK. Antecedents of long-term buyer–seller relationships: a cross cultural integration. Acad Mark Sci Rev 2007;11:1-28.
- Lane C, Bachmann R. The social constitution of trust: supplier relations in Britain and Germany. Organ Stud 1996;17:365-95. http://dx.doi.org/10.1177/017084069601700302.
- Kibbeling MIG, Gelderman CJ, Ulijn JM, van Weele AJ, Calvi R. A Dutch–French comparison of dependence, trust and commitment in buyer–supplier relationships: a purchasing portfolio approach. Int J Bus Globalisation 2009;3:353-73. http://dx.doi.org/10.1504/IJBG.2009.024609.
- Steward MD, Morgan FN, Crosby LA, Kumar A. Exploring cross-national differences in organizational buyers’ normative expectations of supplier performance. J Int Mark 2010;18:23-40. http://dx.doi.org/10.1509/jimk.18.1.23.
- Poppo L, Zenger T. Do formal contracts and relational governance function as substitutes or complements?. Strategic Manag J 2002;23:707-25. http://dx.doi.org/10.1002/smj.249.
- Caniels MCJ, Gelderman CJ, Vermeulen NP. The interplay of governance mechanisms in complex procurement projects. J Purchasing Supply Manag 2012;18:113-21. http://dx.doi.org/10.1016/j.pursup.2012.04.007.
- Blomqvist K, Hurmelinna P, Seppanen R. Playing the collaboration game right: balancing trust and contracting. Technovation 2005;25:497-504. http://dx.doi.org/10.1016/j.technovation.2004.09.001.
- Kadefors A. Contracting in FM: collaboration, coordination and control. J Facil Manag 2008;6:178-88. http://dx.doi.org/10.1108/14725960810885943.
- Bovaird T, Halachmi A. Learning from international approaches to Best Value. Policy Polit 2001;29:451-63. http://dx.doi.org/10.1332/0305573012501468.
- Olander H, Hurmelinna-Laukkanen P, Blomqvist K, Ritala P. The dynamics of relational and contractual governance mechanisms in knowledge sharing of collaborative R&D projects. Knowledge Process Manag 2010;17:188-204. http://dx.doi.org/10.1002/kpm.356.
- Macher JT, Richman BD. Transaction cost economics: an assessment of empirical research in the social sciences. Bus Polit 2008;10.
- Schepker DJ, Oh W-Y, Martynov A, Poppo L. The many futures of contracts: moving beyond structure and safeguarding to coordination and adaptation. J Manag 2013;40:193-225. http://dx.doi.org/10.1177/0149206313491289.
- David RJ, Han S-K. A systematic assessment of the empirical support for transaction cost economics. Strategic Manag J 2004;25:39-58. http://dx.doi.org/10.1002/smj.359.
- Carter R, Hodgson GM. The impact of empirical tests of transaction cost economics on the debate on the nature of the firm. Strategic Manag J 2006;27:461-76. http://dx.doi.org/10.1002/smj.531.
- Lacity MC, Willcocks LP. The practice of outsourcing business and IT services: evidence of success, robust practices and contractual challenges. Legal Info Manag 2012;12:2-8. http://dx.doi.org/10.1017/S1472669612000060.
- Steinle C, Schiele H, Ernst T. Information asymmetries as antecedents of opportunism in buyer–supplier relationships: testing principal–agent theory. J Business-to-Business Mark 2014;21:123-40. http://dx.doi.org/10.1080/1051712X.2014.903457.
- Lonsdale C, Sanderson J, Watson G, Peng F. Beyond intentional trust: supplier opportunism and management control mechanisms in public sector procurement and contracting [published online ahead of print 7 February 2014]. Policy Polit 2014.
- Zsidisin GA, Ellram LM. An agency theory investigation of supply risk management. J Supply Chain Manag 2003;39:15-27. http://dx.doi.org/10.1111/j.1745-493X.2003.tb00156.x.
- Gibbons R. Incentives in organizations. J Econ Perspect 1998;12:115-32. http://dx.doi.org/10.1257/jep.12.4.115.
- Kerr S. On the folly of rewarding A, while hoping for B. Acad Manag J 1975;18:769-83. http://dx.doi.org/10.2307/255378.
- Parmigiani AA, Rivera-Santos M. Clearing a path through the forest: a meta-review of inter-organisational relationships. J Manag 2011;37:1108-36. http://dx.doi.org/10.1177/0149206311407507.
- Bastl M, Johnson M, Lightfoot H, Evans S. Buyer–supplier relationships in a servitized environment. Int J Oper Prod Manag 2012;32:650-75. http://dx.doi.org/10.1108/01443571211230916.
- Chang H-C, Lin C-H. Interfirm influence strategies and their impact on developing buyer–supplier relationships. Int J Commerce Manag 2008;18:10-3. http://dx.doi.org/10.1108/10569210810871461.
- Hsu C-C, Kannan VR, Tan K-C, Leong GK. Information sharing, buyer–supplier relationships, and firm performance. Int J Phys Distr Logistics 2008;38:296-310. http://dx.doi.org/10.1108/09600030810875391.
- Kawai T, Sakaguchi J, Shimizu N. Transition of buyer–supplier relationships in Japan. J Accounting Organ Change 2013;9:427-47. http://dx.doi.org/10.1108/JAOC-07-2011-0033.
- Krause DR, Ellram LM. Success factors in supplier development. Int J Phys Distr Logistics 1997;27:39-52. http://dx.doi.org/10.1108/09600039710162277.
- Paulraj A, Lado AA, Chen IJ. Inter-organisational communication as a relational competency: antecedents and performance outcomes in collaborative buyer–supplier relationships. J Oper Manag 2008;26:45-64. http://dx.doi.org/10.1016/j.jom.2007.04.001.
- Oosterhuis M, van der Vaart T, Molleman E. Perceptions of technology uncertainty and the consequences for performance in buyer–supplier relationships. Int J Prod Res 2011;49:6155-73. http://dx.doi.org/10.1080/00207543.2010.527386.
- van de Vijver M, Vos B, Akkermans H. A tale of two partnerships: socialization in the development of buyer–supplier relationships. J Supply Chain Manag 2011;47:23-41. http://dx.doi.org/10.1111/j.1745-493X.2011.03244.x.
- Biehl M, Cook W, Johnston DA. The efficiency of joint decision making in buyer–supplier relationships. Ann Operations Res 2006;145:15-34. http://dx.doi.org/10.1007/s10479-006-0023-x.
- Lindblom A, Olkkonen R, Ollila P, Hyvönen S. Suppliers’ roles in category management: a study of supplier–retailer relationships in Finland and Sweden. Ind Mark Manag 2009;38:1006-13. http://dx.doi.org/10.1016/j.indmarman.2008.05.004.
- Lindblom A, Olkkonen R, Ollila P, Hyvönen S. Suppliers’ control over category management in Finnish and Swedish supplier–retailer relationships. Int J Integrated Supply Manag 2009;5:1-18. http://dx.doi.org/10.1504/IJISM.2009.026202.
- Perez-Arostegui MN, Benitez-Amado J, Huertas-Perez J-F. In search of loyalty: an analysis of the determinants of buyer–supplier relationship stability under a quality management approach. Total Qual Manag Bus Excellence 2012;23:703-17. http://dx.doi.org/10.1080/14783363.2012.669999.
- Inemek A, Matthyssens P. The impact of buyer–supplier relationships on supplier innovativeness: an empirical study in cross-border supply networks. Ind Mark Manag 2013;42:580-94. http://dx.doi.org/10.1016/j.indmarman.2012.10.011.
- Jap SD. Pie-expansion efforts: collaboration processes in buyer–supplier relationships. JMR 1999;36:461-75.
- Rahman AA, Bennett D, Sohal A. Transaction attributes and buyer–supplier relationships in AMT acquisition and implementation: the case of Malaysia. Int J Prod Res 2009;47:2257-78. http://dx.doi.org/10.1080/00207540802471298.
- Chung J-E, Jin B. In-group preference as opportunism governance in a collectivist culture: evidence from Korean retail buyer–supplier relationships. J Bus Ind Mark 2011;26:237-49. http://dx.doi.org/10.1108/08858621111126983.
- Hansen JM. The evolution of buyer–supplier relationships: an historical industry approach. J Bus Ind Mark 2009;24:227-36. http://dx.doi.org/10.1108/08858620910939778.
- Jiang Z, Henneberg SC, Naudé P. Supplier relationship management in the construction industry: the effects of trust and dependence. J Bus Ind Mark 2012;27:3-15. http://dx.doi.org/10.1108/08858621211188920.
- Johnston DA, McCutcheon DM, Stuart FI, Kerwood H. Effects of supplier trust on performance of cooperative supplier relationships. J Oper Manag 2004;22:23-38. http://dx.doi.org/10.1016/j.jom.2003.12.001.
- Sengün AE, Wasti SN. Trust, control, and risk: a test of Das and Teng’s conceptual framework for pharmaceutical buyer–supplier relationships. Group Organ Manag 2007;32:430-64. http://dx.doi.org/10.1177/1059601106293959.
- Squire B, Cousins PD, Brown S. Cooperation and knowledge transfer within buyer–supplier relationships: the moderating properties of trust, relationship duration and supplier performance. Br J Manag 2009;20:461-77. http://dx.doi.org/10.1111/j.1467-8551.2008.00595.x.
- Tangpong C, Hung K-T, Ro YK. The interaction effect of relational norms and agent cooperativeness on opportunism in buyer–supplier relationships. J Oper Manag 2010;28:398-414. http://dx.doi.org/10.1016/j.jom.2009.12.001.
- Wood GD, Ellis RCT. Main contractor experiences of partnering relationships on UK construction projects. Construction Manag Econ 2005;23:317-25. http://dx.doi.org/10.1080/0144619042000287714.
- Blancero D, Ellram L. Strategic supplier partnering: a psychological contract perspective. Int J Phys Distr Logistics 1997;27:616-29. http://dx.doi.org/10.1108/09600039710188684.
- Carter CR. Ethical issues in international buyer–supplier relationships: a dyadic examination. J Oper Manag 2000;18:191-208. http://dx.doi.org/10.1016/S0272-6963(99)00016-9.
- Lee C-J, Johnsen RE. Asymmetric customer–supplier relationship development in Taiwanese electronics firms. Ind Mark Manag 2012;41:692-705. http://dx.doi.org/10.1016/j.indmarman.2011.09.017.
- Frödell M. Criteria for achieving efficient contractor–supplier relations. Engineering, Construction Architectural Manag 2011;18:381-93. http://dx.doi.org/10.1108/09699981111145826.
- Womack J, Jones DT, Roos D. The Machine that Changed The World. New York, NY: Rawson Associates; 1990.
- Bensaou M. Interorganizational cooperation: the role of information technology an empirical comparison of US and Japanese supplier relations. Info Syst Res 1997;8:107-24. http://dx.doi.org/10.1287/isre.8.2.107.
- Cai S, Yang Z. Development of cooperative norms in the buyer–supplier relationship: the Chinese experience. J Supply Chain Manag 2008;44:55-70. http://dx.doi.org/10.1111/j.1745-493X.2008.00045.x.
- Carter CR. Precursors of unethical behavior in global supplier management. J Supply Chain Manag 2000;36:45-56. http://dx.doi.org/10.1111/j.1745-493X.2000.tb00069.x.
- Forker LB, Ruch WA, Hershauer JC. Examining supplier improvement efforts from both sides. J Supply Chain Manag 1999;35:40-5. http://dx.doi.org/10.1111/j.1745-493X.1999.tb00061.x.
- Humphreys PK, Li WL, Chan LY. The impact of supplier development on buyer–supplier performance. Omega 2004;32:131-43. http://dx.doi.org/10.1016/j.omega.2003.09.016.
- Rajagopal, Rajagopal A . Buyer–supplier relationship and operational dynamics. J Oper Res Soc 2009;60:313-20. http://dx.doi.org/10.1057/palgrave.jors.2602560.
- Day M, Fawcett SE, Fawcett AM, Magnan GM. Trust and relational embeddedness: exploring a paradox of trust pattern development in key supplier relationships. Ind Mark Manag 2013;42:152-65. http://dx.doi.org/10.1016/j.indmarman.2012.12.004.
- Villena VH, Revilla E, Choi TY. The dark side of buyer–supplier relationships: a social capital perspective. J Oper Manag 2011;29:561-76. http://dx.doi.org/10.1016/j.jom.2010.09.001.
- Li Y, Xie E, Teo H-H, Peng MW. Formal control and social control in domestic and international buyer–supplier relationships. J Oper Manag 2010;28:333-44. http://dx.doi.org/10.1016/j.jom.2009.11.008.
- New S, Burnes B. Developing effective customer–supplier relationships: more than one way to skin a cat. Int J Qual Reliability Manag 1998;15:377-88. http://dx.doi.org/10.1108/02656719810196342.
- Caniëls MCJ, Gelderman CJ. Power and interdependence in buyer supplier relationships: a purchasing portfolio approach. Ind Mark Manag 2007;36:219-29. http://dx.doi.org/10.1016/j.indmarman.2005.08.012.
- Doran D, Thomas P, Caldwell N. Examining buyer–supplier relationships within a service sector context. Supply Chain Manag 2005;10:272-7. http://dx.doi.org/10.1108/13598540510612749.
- Kähkönen A-K, Virolainen VM. Sources of structural power in the context of value nets. J Purchasing Supply Manag 2011;17:109-20. http://dx.doi.org/10.1016/j.pursup.2011.01.001.
- Meehan J, Wright GH. Power priorities: a buyer–seller comparison of areas of influence. J Purchasing Supply Manag 2011;17:32-41. http://dx.doi.org/10.1016/j.pursup.2010.05.002.
- McHugh M, Humphreys P, McIvor R. Buyer–supplier relationships and organizational health. J Supply Chain Manag 2003;39:15-2. http://dx.doi.org/10.1111/j.1745-493X.2003.tb00151.x.
- Henke JW, Jr, Parameswaran R, Pisharodi RM. Manufacturer price reduction pressure and supplier relations. J Bus Ind Mark 2008;23:287-300. http://dx.doi.org/10.1108/08858620810881566.
- Tangpong C, Michalisin MD, Melcher AJ. Toward a typology of buyer–supplier relationships: a study of the computer industry. Decision Sci 2008;39:571-93. http://dx.doi.org/10.1111/j.1540-5915.2008.00203.x.
- Adamides ED, Karacapilidis N, Pylarinou H, Koumanakos D. Supporting collaboration in the development and management of lean supply networks. Prod Plann Control 2008;19:35-52. http://dx.doi.org/10.1080/09537280701773955.
- Perez C, de Castro R, Simons D, Gimenez G. Development of lean supply chains: a case study of the Catalan pork sector. Supply Chain Manag 2010;15:55-68. http://dx.doi.org/10.1108/13598541011018120.
- Arkader R. The perspective of suppliers on lean supply in a developing country context. Integrated Manufacturing Systems 2001;12:87-93. http://dx.doi.org/10.1108/09576060110384280.
- Loader K. Is local authority procurement ‘lean’? An exploration to determine if ‘lean’ can provide a useful explanation of practice. J Purchasing Supply Manag 2010;16:41-50. http://dx.doi.org/10.1016/j.pursup.2009.10.001.
- Mazzocato P, Savage C, Brommels M, Aronsson H, Thor J. Lean thinking in healthcare: a realist review of the literature. Qual Saf Health Care 2010;19:376-82. http://dx.doi.org/10.1136/qshc.2009.037986.
- Guimarães CM, de Carvalho JC. Strategic outsourcing: a lean tool of healthcare supply chain management. Strategic Outsourcing: An International Journal 2013;6:138-66. http://dx.doi.org/10.1108/SO-11-2011-0035.
- Green KW, Inman RA. Using a just-in-time selling strategy to strengthen supply chain linkages. Int J Prod Res 2005;43:3437-53. http://dx.doi.org/10.1080/00207540500118035.
- Green KW, Inman RA. The impact of JIT-II-selling on organizational performance. Ind Manag Data Syst 2007;107:1018-35. http://dx.doi.org/10.1108/02635570710816720.
- Bartezzaghi E, Turco F, Spina G. The impact of the just-in-time approach on production system performance: a survey of Italian industry. Int J Oper Prod Manag 1992;12:5-17. http://dx.doi.org/10.1108/EUM0000000001292.
- Germain R, Dröge C. Effect of just-in-time purchasing relationships on organizational design, purchasing department configuration, and firm performance. Ind Mark Manag 1997;26:115-25. http://dx.doi.org/10.1016/S0019-8501(96)00113-7.
- Dion PA, Banting PM, Picard S, Blenkhorn DL. JIT implementation: a growth opportunity for purchasing. Int J Oper Prod Manag 1992;28:32-8.
- González-Benito J. Effect of the characteristics of the purchased products in JIT purchasing implementation. Int J Oper Prod Manag 2002;22:868-86. http://dx.doi.org/10.1108/01443570210436181.
- Bayo-Moriones A, Bello-Pintado A, Merino-Díaz-de-Cerio J. The role of organizational context and infrastructure practices in JIT implementation. Int J Oper Prod Manag 2008;28:1042-66. http://dx.doi.org/10.1108/01443570810910188.
- Fawcett SE, Birou LM. Exploring the logistics interface between global and JIT sourcing. Int J Phys Distr Logistics 1992;22:3-14. http://dx.doi.org/10.1108/09600039210010324.
- Vickery SK. International sourcing: implications for just-in-time manufacturing. Prod Inventory Manag J 1989;30:66-72.
- Wafa MA, Yasin MM, Swinehart K. The impact of supplier proximity on JIT success: an informational perspective. Int J Phys Distr Logistics 1996;26:23-34. http://dx.doi.org/10.1108/09600039610116495.
- Ansari A. Strategies for the implementation of JIT purchasing. Int J Phys Distr Mater Manag 1986;16:5-12. http://dx.doi.org/10.1108/eb014640.
- Heinbuch SE. A case of successful technology transfer to health care: total quality materials management and just-in-time. J Manag Med 1995;9:48-56. http://dx.doi.org/10.1108/02689239510086524.
- Kannan VR, Keah Choon T. Just in time, total quality management, and supply chain management: understanding their linkages and impact on business performance. Omega 2005;33:153-62. http://dx.doi.org/10.1016/j.omega.2004.03.012.
- O’Neal CR. JIT procurement and relationship marketing. Ind Mark Manag 1989;18:55-63. http://dx.doi.org/10.1016/0019-8501(89)90021-7.
- Nassimbeni G. Factors underlying operational JIT purchasing practices: results of an empirical research. Int J Prod Econ 1996;42:275-88. http://dx.doi.org/10.1016/0925-5273(95)00190-5.
- Stamm CL, Golhar DY. Customer and supplier linkages for small JIT manufacturing firms. J Small Bus Manag 1991;29:43-9.
- Yasin MM, Small MH, Wafa MA. Organizational modifications to support JIT implementation in manufacturing and service operations. Omega 2003;31:213-26. http://dx.doi.org/10.1016/S0305-0483(03)00024-0.
- Karlsson C, Norr C. Total effectiveness in a just-in-time system. Int J Oper Prod Manag 1994;14:46-65. http://dx.doi.org/10.1108/01443579410058522.
- Danese P, Romano P, Bortolotti T. JIT production, JIT supply and performance: investigating the moderating effects. Ind Manag Data Syst 2012;112:441-65. http://dx.doi.org/10.1108/02635571211210068.
- Claycomb C, Germain R, Dröge C. Total system JIT outcomes: inventory, organization and financial effects. Int J Phys Distr Logistics 1999;29:612-30. http://dx.doi.org/10.1108/09600039910299940.
- Persona A, Battini D, Rafele C. Hospital efficiency management: the just-in-time and Kanban technique. Int J Healthc Technol Manag 2008;9:373-92. http://dx.doi.org/10.1504/IJHTM.2008.019674.
- Tanskanen K, Jan H, Elfving J, Talvitie U. Vendor-managed-inventory (VMI) in construction. Int J Productivity Perform Manag 2009;58:29-40.
- Vigtil A. Information exchange in vendor managed inventory. Int J Phys Distr Logistics 2007;37:131-47. http://dx.doi.org/10.1108/09600030710734848.
- Shih SC, Rivers PA, Hsu HYS. Strategic information technology alliances for effective health-care supply chain management. Health Serv Manag Res 2009;22:140-50. http://dx.doi.org/10.1258/hsmr.2009.009003.
- Stanger SHW. Vendor managed inventory in the blood supply chain in Germany. SOIJ 2013;6:25-47. http://dx.doi.org/10.1108/17538291311316054.
- Claassen MJT, van Weele AJ, van Raaij EM. Performance outcomes and success factors of vendor managed inventory (VMI). Supply Chain Manag 2008;13:406-14. http://dx.doi.org/10.1108/13598540810905660.
- Kauremaa J, Småros J, Holmström J. Patterns of vendor-managed inventory: findings from a multiple-case study. Int J Oper Prod Manag 2009;29:1109-39. http://dx.doi.org/10.1108/01443570911000159.
- Yao YO, Dong Y, Dresner M. Supply chain learning and spillovers in vendor managed inventory. Decision Sci 2012;43:979-1001. http://dx.doi.org/10.1111/j.1540-5915.2012.00379.x.
- Beier FJ. The management of the supply chain for hospital pharmacies: a focus on inventory management practices. J Bus Logistics 1995;16:153-73.
- Guimarães CM, de Carvalho JC, Maia A. Vendor managed inventory (VMI): evidences from lean deployment in healthcare. SOIJ 2013;6:8-24. http://dx.doi.org/10.1108/17538291311316045.
- Seth D, Gupta V. Application of value stream mapping for lean operations and cycle time reduction: an Indian case study. Prod Plann Control 2005;16:44-59. http://dx.doi.org/10.1080/09537280512331325281.
- Wee HM, Wu S. Lean supply chain and its effect on product cost and quality: a case study on Ford Motor Company. Supply Chain Manag 2009;14:335-41. http://dx.doi.org/10.1108/13598540910980242.
- Byrne G, Lubowe D, Blitz A. Using a Lean Six Sigma approach to drive innovation. Strat Leadership 2007;35:5-10. http://dx.doi.org/10.1108/10878570710734480.
- Timans W, Antony J, Ahaus K, van Solingen R. Implementation of Lean Six Sigma in small- and medium-sized manufacturing enterprises in the Netherlands. J Oper Res Soc 2012;63:339-53. http://dx.doi.org/10.1057/jors.2011.47.
- Baker P. The design and operation of distribution centres within agile supply chains. Int J Prod Econ 2008;111:27-41. http://dx.doi.org/10.1016/j.ijpe.2006.09.019.
- Power DJ, Sohal AS, Rahman S-U. Critical success factors in agile supply chain management: an empirical study. Int J Phys Distr Logistics 2001;31:247-65. http://dx.doi.org/10.1108/09600030110394923.
- K AK, Bakkappa B, Metri BA, Sahay BS. Impact of agile supply chains’ delivery practices on firms’ performance: cluster analysis and validation. Supply Chain Manag 2009;14:41-8. http://dx.doi.org/10.1108/13598540910927296.
- Coronado MAE, Lyons AC. Evaluating operations flexibility in industrial supply chains to support build-to-order initiatives. Bus Process Manag J 2007;13:572-87. http://dx.doi.org/10.1108/14637150710763586.
- Engelhardt-Nowitzki C. Improving value chain flexibility and adaptability in build-to-order environments. Int J Phys Distr Logistics 2012;42:318-37. http://dx.doi.org/10.1108/09600031211231317.
- Ben Naylor J, Naim MM, Berry D. Leagility: integrating the lean and agile manufacturing paradigms in the total supply chain. Int J Prod Econ 1999;62:107-18. http://dx.doi.org/10.1016/S0925-5273(98)00223-0.
- Aronsson H, Abrahamsson M, Spens K. Developing lean and agile health care supply chains. Supply Chain Manag 2011;16:176-83. http://dx.doi.org/10.1108/13598541111127164.
- Mason-Jones R, Naylor B, Towill DR. Engineering the leagile supply chain. Int J Agile Manag Syst 2000;2:54-61. http://dx.doi.org/10.1108/14654650010312606.
- Qrunfleh S, Tarafdar M. Lean and agile supply chain strategies and supply chain responsiveness: the role of strategic supplier partnership and postponement. Supply Chain Manag 2013;18:571-82. http://dx.doi.org/10.1108/SCM-01-2013-0015.
- Rahimnia F, Moghadasian M. Supply chain leagility in professional services: how to apply decoupling point concept in healthcare delivery system. Supply Chain Manag 2010;15:80-91. http://dx.doi.org/10.1108/13598541011018148.
- Stratton R, Warburton RDH. The strategic integration of agile and lean supply. Int J Prod Econ 2003;85:183-98. http://dx.doi.org/10.1016/S0925-5273(03)00109-9.
- Lyons A, Coronado A, Michaelides Z. The relationship between proximate supply and build-to-order capability. Ind Manag Data Syst 2006;106:1095-111. http://dx.doi.org/10.1108/02635570610710773.
- Salvador F, Rungtusanatham M, Forza C, Trentin A. Mix flexibility and volume flexibility in a build-to-order environment. Int J Oper Prod Manag 2007;27:1173-91. http://dx.doi.org/10.1108/01443570710830584.
- Cox A, Sanderson J, Watson G. Supply chains and power regimes: toward an analytic framework for managing extended networks of buyer and supplier relationships. J Supply Chain Manag 2001;37:28-35. http://dx.doi.org/10.1111/j.1745-493X.2001.tb00097.x.
- Markowitz H. Portfolio selection. J Finance 1952;7:77-91.
- Turnbull PW. A review of portfolio planning models for industrial marketing and purchasing management. Eur J Mark 1990;24:7-22.
- Nellore R, Söderquist K. Portfolio approaches to procurement: analysing the missing link to specifications. Long Range Plann 2000;33:245-67. http://dx.doi.org/10.1016/S0024-6301(00)00027-3.
- Gelderman CJ, van Weele AJ. Purchasing portfolio models: a critique and update. J Supply Chain Manag 2005;41:19-28. http://dx.doi.org/10.1111/j.1055-6001.2005.04103003.x.
- Bensaou M. Portfolios of buyer–supplier relationships. Sloan Manag Rev 1999;40:35-44.
- Caniëls MCJ, Gelderman CJ. Purchasing strategies in the Kraljic matrix: a power and dependence perspective. J Purchasing Supply Manag 2005;11:141-55. http://dx.doi.org/10.1016/j.pursup.2005.10.004.
- Dubois A, Pedersen A-C. Why relationships do not fit into purchasing portfolio models: a comparison between the portfolio and industrial network approaches. Eur J Purchasing Supply Manag 2002;8:35-42. http://dx.doi.org/10.1016/S0969-7012(01)00014-4.
- Cox A. Understanding buyer and supplier power: a framework for procurement and supply competence. J Supply Chain Manag 2001;37:8-15. http://dx.doi.org/10.1111/j.1745-493X.2001.tb00094.x.
- Ramsay J. Power measurement. Eur J Purchasing Supply Manag 1996;2:129-43. http://dx.doi.org/10.1016/0969-7012(96)00002-0.
- Cox A, Lonsdale C, Watson G, Qiao H. Supplier relationship management: a framework for understanding managerial capacity and constraints. Eur Bus J 2003;15:135-45.
- Anderson J, Wilson B. Determinants of continuity in conventional industrial channel dyads. Mark Sci 1989;8:42-58. http://dx.doi.org/10.1287/mksc.8.4.310.
- Frazier GL, Rody RC. The use of influence strategies in interfirm relationships in industrial product channels. J Mark 1991;55:52-69. http://dx.doi.org/10.2307/1252203.
- McDonald F. The importance of power in partnership relationships. J Gen Manag 1999;25:43-59.
- Ben Naylor J, Naim MM, Berry D. Leagility: interfacing the lean and agile manufacturing paradigm in the total supply chain. Int J Prod Econ 1999;62:107-18. http://dx.doi.org/10.1016/S0925-5273(98)00223-0.
- Christopher M, Towill DR. Supply chain migration from lean and functional to agile and customised. Supply Chain Manag 2000;5:206-13. http://dx.doi.org/10.1108/13598540010347334.
- Aitken J, Christopher M, Towill D. Understanding, implementing and exploiting agility and leanness. Int J Logistics 2002;5:59-74. http://dx.doi.org/10.1080/13675560110084139.
- Lee HL. Aligning supply chain strategies with product uncertainties. Calif Manag Rev 2002;44:105-19. http://dx.doi.org/10.2307/41166135.
- McGovern T, Hicks C. Specifications and supplier development in the UK electrical transmission and distribution equipment industry. Int J Prod Econ 2006;104:164-78. http://dx.doi.org/10.1016/j.ijpe.2004.08.005.
- Kaufmann L, Kreft S, Ehrgott M, Reimann F. Rationality in supplier selection decisions: the effect of the buyer’s national task environment. J Purchasing Supply Manag 2012;18:76-91. http://dx.doi.org/10.1016/j.pursup.2012.04.004.
- Hearts and Minds: Commissioning from the Voluntary Sector. London: Audit Commission; 2007.
- Cox A, Chicksand D, Ireland P. Overcoming demand management problems: the scope for improving reactive and proactive supply management in the UK health service. J Public Procurement 2005;5:1-22.
Appendix 1 Sample extraction forms
| Title of paper | Johnston and Lewin (1996), Organizational Buying Behaviour: Toward an Integrative Framework, Journal of Business Research, 35 |
| Name of reviewer | JS |
| Type of paper: single theoretical perspective or comparative overview | Single – reviews and synthesizes 25 years of OBB research following the classic work by RFW, WW and S in late 1960s and early 1970s |
| Contextual assumptions: underlying worldview and behavioural assumptions | Units of analysis are the buying centre (multiactor) and the process steps/stages Actors have differing motivations and preferences Actors have bounded rationality Inevitable conflicts in decision-making are resolved either thru persuasion or power and politics |
| Mechanisms: core concepts used to explain why outcomes happen, e.g. power, trust, collaboration, contract, governance, innovation, transparency, etc. | Characteristics of the buying centre (size and complexity, experience and expertise of members) Handling of conflict in buying centre Nature of decision rules and information search Purchase history (nature of buyer–supplier relations) |
| Intended outcomes: e.g. waste minimisation, improved quality, quicker response to change, value for money, risk minimisation etc. | Minimisation of purchase risk |
| Overall relevance to RQ1: core or peripheral | Core – an excellent review and synthesis of the major contributions to the OBB perspective, revealing the core context, mechanism and outcome dimensions |
| Title of paper | An economic analysis of the limits of market based reforms in the English NHS Allen, Pauline BMC Health Services Research 2013;13(s1): S1 |
| Name of reviewer | TM |
| Type of paper: theoretical lens, research design | Theory: neoclassical economics, new institutional economics and socio-legal theory Application of market concepts to research evidence of the operation of the quasi market in the NHS |
| Context: features of the environment and of actors identified in study | NHS in England – past three decades of reforms |
| Interventions: describe nature of what is happening | (Secondary) analysis of application of market principles/’third way’ to NHS. Evidence used from previous studies conducted by researchers based in the UK using economic and socio-legal logic |
| Mechanisms: why are the interventions used expected to generate the intended outcomes? | Markets are not perfect and therefore need regulation. Markets are not concerned with equity Hierarchies are not efficient, but they involve authority and accountability for resource allocation Quasi markets combine advantages of both competition and fairness |
| Outcomes: intended and/or actual | Theoretical imitations of quasi markets, supported by evidence: Demand side: patients reliant on parts of the state (GPs) to make decisions for them – no real agency Supply side: little competition between suppliers Pricing: where pricing is fixed, competition may have improved quality, though this is difficult to confirm Contracting: contracts have proved difficult to complete, so remain relational Regulation: little evidence of use or need, due to central rules about ensuring both competition and co-operation |
| Relevant findings | Quasi market mechanisms are ineffective as they operate under the national polity, which continues to be hierarchical Author argues that healthcare goals such as fairness of access cannot be delivered by a market structure, and warns against the extension of market principles evident in the Coalition Government’s policies |
| Methodological strength of paper in its domain | Theoretical analysis with secondary evidence. Methodological approaches of the studies used were not discussed (due to constraints of space) |
| Overall rigour and relevance (i.e. an original and scholarly contribution? does it address our RQ?) | Of peripheral relevance – as not an empirical study – but relevant to capture commentary from experts relating to post-HSC Act 2012 for RQ2, RQ4 and for overall report |
| Title of paper | Buyer–supplier relationships in a servitized environment Bastl, Marko Johnson, Mark Lightfoot, Howard Evans, Steve 2012, International Journal of Operations & Production Management |
| Name of reviewer | TM |
| Type of paper: | Case study research, using Cannon and Perreault’s relationship connectors framework |
| Context: features of the environment and of actors identified in study | A manufacturing company and two of its two suppliers – 16 employees on multiple organisational levels, and evidence from both sides of a relationship |
| Interventions: what is happening | Adoption of servitization |
| Mechanisms: why – generative force | Structural – relationship connectors – more open exchange of information (situated agency), strengthened operational linkages, structural changes in relationship and support for integrated solutions More agency-based mechanisms: relational norms in contracting and reduction of win–lose mentality |
| Outcomes: intended and/or actual | Servitization strategy impacts upon buyer–supplier relationships |
| Relevant findings | The authors use the case study approach to examine the tripartite relationship between a manufacturing company and two of its two suppliers as the buyer adopts a servitization strategy. The authors use Cannon and Perreault’s relationship connectors framework to analyse the data and find that the implications are notable in all five relationship connectors (information exchange, operational linkages, legal bonds, co-operative norms and buyer and supplier adaptation). This advances the understanding of the implications that the adoption of servitization has on the manner in which two parties interrelate and conduct commercial exchange |
| Methodological strength of paper in its domain | Good, solid |
| Overall rigour and relevance | Good rigour and relevance, depending on how much products and services can be bundled in the new competitive environment (perhaps via commissioning support units?) RQ3 – Phase 3 – buyer–supplier relationships |
Appendix 2 Keywords used for literature search
Research question 1: theories about procurement and supply chain management
In ABI/INFORM®, Applied Social Sciences Index and Abstracts, Business Source Premier, International Bibliography of the Social Sciences, Scopus and Social Sciences Citation Index
Title: procur*; purchas*; buy*; ‘supply chain manag*’; SCM; logistics
AND
Title: framework OR literature OR model*OR review OR theor*
Research question 2: evidence about procurement and supply chain management in the NHS
In health specialist database, Health Management Information Consortium
Title: procur* OR purchas* OR buy* OR ‘supply chain’ OR logistics OR commission*
In ABI/INFORM®, Applied Social Sciences Index and Abstracts, Business Source Premier, International Bibliography of the Social Sciences, Scopus and Social Sciences Citation Index
Title: procur*; purchas*; buy*; ‘supply chain’; logistics; commission*
AND
Subject heading: health* OR NHS OR ‘National Health Service’
Research questions 3 and 4: evidence about procurement and supply chain management practices and approaches to improvement
In ABI/INFORM®, Business Source Premier and Scopus
Title: ‘needs assessment’; specification*; demand management; ‘activity based costing’ OR ABC; ‘vendor assessment’ OR ‘supplier assessment’; ‘vendor rating’ OR ‘supplier rating’; ‘vendor evaluation’ OR ‘supplier evaluation’; ‘strategic sourcing’; network sourcing’; ‘partnership sourcing’; ‘balanced sourcing’; ‘category management’; ‘e-procurement’; ‘e-auction*’; ‘e-business’; ‘collaborative procurement’; ‘purchasing consorti*’ OR ‘procurement consorti*’; contract* AND collaborat*; contract* AND network*; contract* AND partner*; negotiat* AND collaborat*; negotiat* AND network*; negotiat* AND partner*; ‘contract management’; ‘just in time’ OR JIT; ‘supplier managed inventory’ OR ‘vendor managed inventory’; ‘electronic data interchange’; ‘economic order quantity’ OR EOQ; ‘build to order’ OR ‘made to order’; ‘life cycle cost’ OR ‘whole life cost’; ‘total cost of ownership’ OR TCO; ‘target costing’; ‘lean supply’; ‘value stream ma*’ OR VSM; ‘value analysis’; ‘agile supply’; ‘leagile supply’; ‘six sigma’
AND
Abstract: buy* OR purchas* OR procur* OR suppl*
Title: ‘approved supplier*’ OR ‘preferred supplier*’; ‘supplier selection’; ‘supplier management’; ‘supplier development’; ‘supplier relation*’
AND
Abstract: buy* OR purchas* OR procur* OR supply
Abstract: ‘vendor appraisal’ OR ‘supplier appraisal’
AND
Abstract: buy* OR purchas* OR procur* OR suppl*
Abstract: ‘purchasing portfolio matrix’; ‘purchasing hub’ OR ‘procurement hub’; ‘service level agreement’ OR SLA; ‘framework agreement’; ‘supplier improv*’; ‘supplier compliance’; ‘supplier rationali*’ OR ‘supplier based rationali*’; ‘contract compliance’; ‘purchasing cards’ OR ‘procurement cards’
Glossary
- Agile supply chain management
- Collaborative management of buyer–supplier relationships in an extended chain or network, designed to achieve flexibility and responsiveness to uncertain changes in demand.
- Category management
- Aggregation of expenditure within specified categories (e.g. information technology, facilities), with different organisational subunits working together to agree common specifications and approved suppliers.
- Contractual incompleteness
- As a result of uncertainty, a contract is drawn up which does not take account of all possible future contingencies or eventualities and therefore is said to contain gaps.
- Demand management
- Precontractual steps in the procurement process, including identification of need, development of specification, identification and approval of potential sources of supply, and design of request for proposal.
- E-procurement
- Managing the procurement process in an online or electronic environment, including software to analyse expenditure and supply markets, and to manage tendering, contracts and payment of invoices.
- Framework agreement
- Agreement with a preferred supplier that specifies the nature of the goods or services to be procured and the prices to be paid, but does not commit the buying organisation to a specified level of demand, most useful where demand is uncertain.
- Industrial marketing and purchasing
- Broad term used to describe the study of organisational or business-to-business marketing and purchasing activity and to distinguish it from consumer marketing and purchasing, associated with a group of academics primarily based in the UK and Scandinavia.
- Integrated supply chain management
- Theoretical perspective which assumes that supply networks can and should be seen as entirely closed and therefore manageable systems, and that buyers and suppliers should be encouraged to interact co-operatively across an extended network to optimise their collective performance.
- Just-in-time
- Practice of keeping minimal levels of stock in a supply chain and pulling products from suppliers as and when they are required.
- Lean supply chain management
- Collaborative management of buyer–supplier relationships in an extended chain or network, designed to minimise waste and inefficiency.
- Organisational buying behaviour
- Literature which focuses on the precontract or demand management phase of the procurement process, seeing it as a multiactor, multiagenda process and, therefore, as a locus of intraorganisational power and politics.
- Portfolio approach
- Approach to procurement decision-making and management which suggests that there are choices about how goods and services might be procured and that these should be made appropriately in line with the nature of what is being procured and with circumstances.
- Procurement
- Process encompassing all activities associated with identifying the need for, specifying, acquiring and managing an organisation’s supply inputs.
- Supply chain management
- Subset of procurement activities concerned particularly with the monitoring, management and development of ongoing supplier relationships and the associated flows of supply inputs.
- Transaction cost economics
- Theoretical perspective which focuses on how to manage buyer–supplier transactions most efficiently while minimising the potential for supplier opportunism.
- Value stream mapping
- Technique involving a detailed assessment of operational activities and processes, both within an organisation and between organisations, to identify and eliminate waste, facilitate cost reductions and increase productivity.
- Vendor-managed inventory
- Technique whereby a buyer delegates the management of its inventory to a supplier so that stock is replenished efficiently and only when it falls below a certain specified level.
List of abbreviations
- ASSIA
- Applied Social Sciences Index and Abstracts
- CMO
- context–mechanism–outcome
- EU
- European Union
- GP
- general practitioner
- HMIC
- Health Management Information Consortium
- HSDR
- Health Services and Delivery Research
- IBSS
- International Bibliography of the Social Sciences
- IT
- information technology
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- P&SCM
- procurement and supply chain management
- PFI
- Private Finance Initiative
- RAMESES
- Realist And Meta-narrative Evidence Syntheses: Evolving Standards
- RQ
- research question
- SCM
- supply chain management
- SSCI
- Social Science Citation Index
- TCE
- transaction cost economics