
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 12/5001/14. The contractual start date was in June 2013. The final report began editorial review in June 2014 and was accepted for publication in December 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Disclaimer
This report contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Galdas et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Long-term conditions
Improving the treatment and management of long-term conditions (LTCs) is currently one of the most significant challenges facing the NHS. 1 Around 15 million people in the UK suffer from a LTC such as hypertension, asthma, diabetes, coronary heart disease, chronic kidney disease or other health problems that cannot currently be cured but can be managed through medication, therapy and/or lifestyle modification. 2 The figure is set to grow dramatically over the next 10 years, particularly those individuals living with three or more LTCs at once.
The increasing burden of LTCs coupled with the financial pressures facing the NHS in the coming years is leading to a shift in health-care delivery. Offering existing LTC care and services as currently configured – that is ‘doing more of the same’ – will not be adequate if NHS and social care services are to be sustainable in the future and are to appropriately target need while being resource efficient. 3 The current NHS therefore requires a ‘paradigm shift’ in the provision of health care to meet the needs of a population in which most of the disease burden is attributable to LTCs. 4
Empowering and supporting the increasing number of people living with LTCs to develop their knowledge, skills and confidence to manage their own health has become a key strategic objective of the NHS. 5 So-called ‘supported self-management’ is seen as a core platform for optimising quality, effectiveness and efficiency of LTC care because of the potential to improve health outcomes, help patients make better use of available health-care support, and avoid interventions that are burdensome for patients, inappropriate to their needs and inefficient for the NHS. 3,6 Delivered on a large scale, self-management support interventions have the potential to help reduce the overall costs of care in the NHS without compromising patient outcomes. 7
Self-management
There is currently no universally accepted definition of self-management, and the terms ‘self-care’ and ‘self-management’ are often used interchangeably in the literature. In this report, ‘self-management’ is considered as distinct from ‘self-care’. ‘Self-care’ refers to a set of behaviours which individuals perform to prevent the onset of illness or disability and maintain quality of life. 8 ‘Self-management’ refers to an individual’s ability to effectively manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with a LTC. 9 Thus, in this review we have adopted the definition of a ‘self-management support intervention’ used in the recent Health Services and Delivery Research Reducing Care Utilisation through Self-management Interventions (RECURSIVE) review:7
An intervention primarily designed to develop the abilities of patients to undertake management of health conditions through education, training and support to develop patient knowledge, skills or psychological and social resources.
Knowledge of the most effective ways to support patient self-management of LTCs is growing. Significant investment has been made by a number of research funders in studies to explore the role of various forms of self-management support, including studies of the Expert Patient Programme10 and assistive technologies through the Whole System Demonstrator. 11 A number of systematic reviews have also been carried out on different aspects of self-management support. These have focused on interventions targeting specific conditions (e.g. diabetes or mental health),12,13 types of intervention (e.g. lay-led programmes)14 or particular outcomes (e.g. medicines adherence). 15 Despite a developing evidence base, there remains a lack of clarity concerning the effectiveness of self-management interventions, and major ‘knowledge gaps’ remain, especially around ‘what works, for whom, and why?’
Men and self-management support
Despite growing evidence for their effectiveness, self-management support interventions are considerably limited in their ‘reach’, that is the numbers of patients able or willing to access and engage with the intervention. 16–18 Existing self-management support services have tended to engage only a minority of the eligible population. Evidence suggests that, despite men being more likely than women to develop the most common and disabling LTCs such as chronic pulmonary disease, diabetes and cardiovascular diseases,19,20 fewer than one-third of participants engaging with existing support services are male. 13,21–23 This pattern of attendance is consistent with a growing body of research into male identity and the management of illness that is revealing preventable risk factors, poor engagement in self-management and reluctance to access existing health services may account for a high proportion of mortality and morbidity in men. 20,24–29
Increasing recognition of the evidence pointing towards men’s gender-specific needs has led to calls for tailored and targeted health-care interventions to be delivered to men,19,29 including the recent European Commission report on the State of Men’s Health in Europe. 20 Delivering gender-sensitive health services to meet the statutory requirements of the Public Sector Equality Duty30 is also a matter of great concern to the NHS at present. The duty, which forms part of the Equality Act 2010, places statutory responsibility on all NHS organisations to take account of any evidence that men and women have different needs, experiences, concerns or priorities when developing policies and services. This means fully integrating an awareness of male and female health needs strategically and operationally throughout an organisation. 31,32
Compliance with the Public Sector Equality Duty30 is currently being implemented by the vast majority of NHS organisations through the refreshed Equality Delivery System. 32 Considering the different needs of men and women in the commissioning, design and delivery of NHS services to meet the legal requirements of the Public Sector Equality Duty30 will remain a crucial factor in service planning in the future, and the area of self-management support is an example of where gender-related differences are likely to exist.
However, existing data on self-management support are not available in a form suitable for assessing whether or not gender has an impact on the effects of these types of interventions; therefore, the data cannot be used as a basis for supporting evidence-based decisions about commissioning and designing services to meet the specific needs of men with LTCs and the legal requirements laid out in the Public Sector Equality Duty. 30 The relative effectiveness, cost-effectiveness, accessibility and acceptability of self-management interventions for men with LTCs have yet to be established. 14
The aim of this review was to address this ‘knowledge gap’ by conducting a comprehensive assessment of the current evidence to judge if self-management support interventions are effective and cost-effective in men. In addition, the review aimed to identify men’s experiences of, and perceptions of, self-management support to identify whether or not interventions and activities aimed at supporting self-management are acceptable and accessible to men.
Our synthesis was designed to make a conceptual and empirical contribution to the evidence base on both self-management support and men’s health. A key goal of this project was to provide clear guidance on whether or not self-management support interventions need to be adapted so that they are more effective in, accessible to and acceptable for men; this would help commissioners and practitioners meet the legal requirements of the Public Sector Equality Duty30 and allow men to gain appropriate support to limit any adverse consequences of living with a LTC.
The results of the SELF-MAN review should be considered alongside the recent Practical systematic Review of Self-Management Support for long-term conditions (PRISMS)33 and RECURSIVE7 reviews, which offer broader assessments of the role and effectiveness of self-management support in LTCs, and the degree to which current models of support reduce health service utilisation, respectively.
Research questions
-
How effective, cost-effective, accessible and acceptable are self-management support interventions for men with LTCs?
-
What are the key recommendations for service commissioners and research funding bodies on delivery of self-management support for men with LTCs and the research priorities of the future?
Review objectives
-
To assess the effectiveness, cost-effectiveness, accessibility and acceptability of self-management support interventions in men with LTCs.
-
To identify experiences of, and perceptions of, interventions and activities aimed at supporting self-management of LTCs among men of differing age, ethnicity and socioeconomic background.
-
To identify gaps in the available evidence and identify critical areas for future research.
Chapter 2 Quantitative review methods
A systematic review and meta-analysis was conducted based upon a protocol published on the PROSPERO database (registration number CRD42013005394, URL: www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013005394).
Deviations from the original protocol are presented in Box 1.
The target population are male adults (aged 18 years or over) living with one or more long-term conditions.
The 1-year time frame of this project made consideration of all possible LTCs impracticable. We therefore focused on a range of ‘exemplar conditions’ informed by the strategy adopted by the recent PRISMS review:33 asthma, type 1 diabetes, type 2 diabetes, depression, hypertension, heart failure, chronic obstructive pulmonary disease, arthritis, chronic kidney disease, chronic pain (including back pain) and human immunodeficiency virus. In addition, we also considered the literature on generic non-disease-specific interventions (such as the Expert Patients Programme) as well as self-management interventions for men-only conditions (i.e. disorders of the prostate and testicles).
Identifying and locating studies of relevance from existing high quality systematic reviews via the Cochrane Database of Systematic Reviews (CDSR), Database of Abstracts of Reviews of Effects (DARE) and PROSPERO.
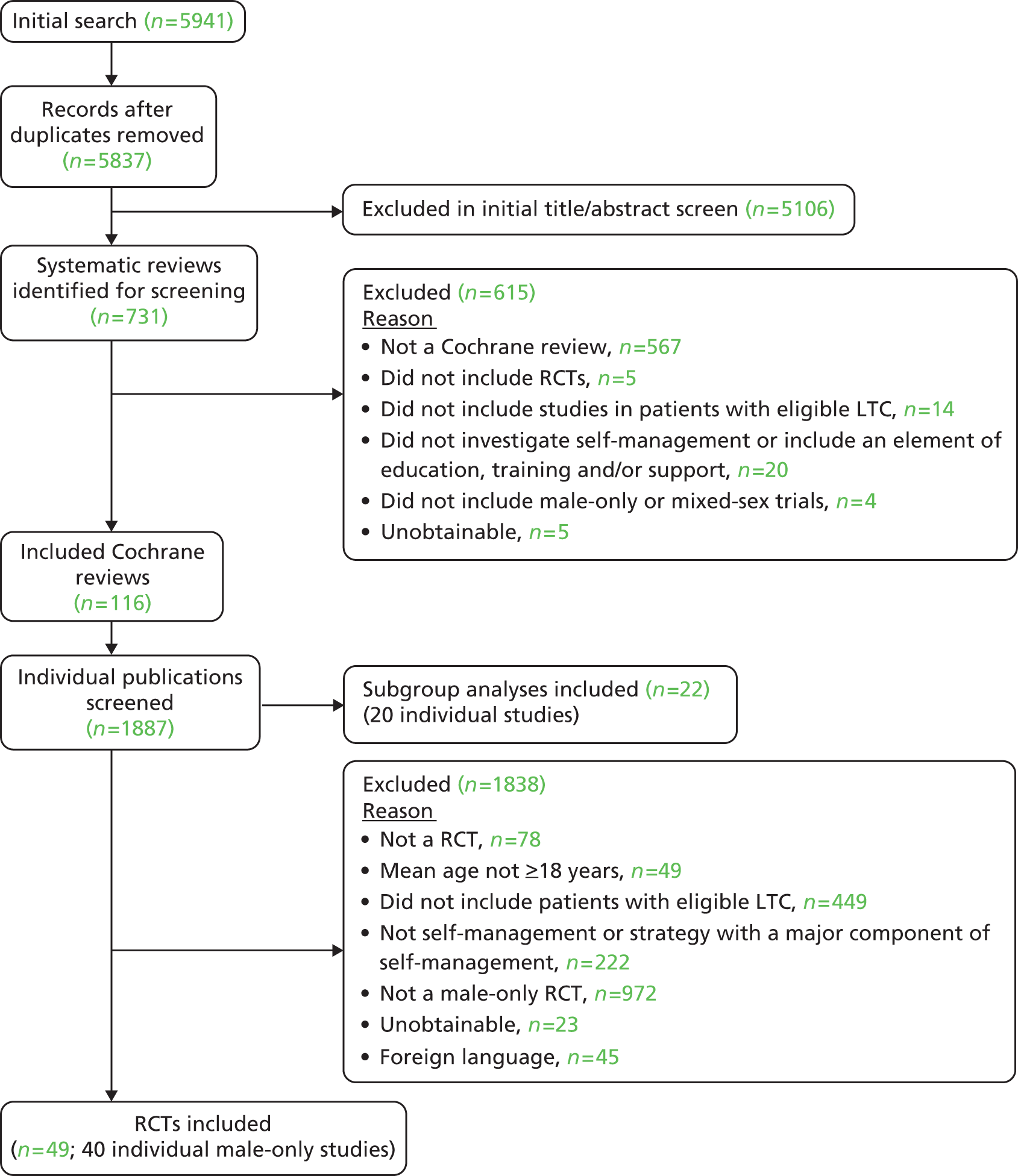
Dual screening of the systematic review literature on self-management support interventions led to the identification of 706 potentially eligible reviews that met our study inclusion criteria via the CDSR, DARE and PROSPERO. The team considered the screening, extraction and synthesis of all randomised controlled trials (RCTs) included in these 706 reviews to be unmanageable within the project time frame and an inefficient use of research resources to answer our research questions. We therefore limited the review to relevant RCTs identified through Cochrane systematic reviews (n = 116). We considered the incremental benefit of including studies identified through non-Cochrane systematic reviews to be low, as the majority of relevant high-quality RCTs are likely to be included in Cochrane systematic reviews.
A data extraction tool will be created to extract data on patient populations (e.g. gender, age, other demographic factors, long-term conditions and other clinical characteristics), self-management interventions (including details on components using the BCT [behavioural change techniques] taxonomy as a guide).
We found that coding and synthesising interventions using the BCT taxonomy and methodology developed by Michie et al. 34 was not feasible because a shared language was not used to describe ‘active ingredients’ of interventions; there was a lack of precision and detail reported in studies to enable coding at a granular level; and reporting was inconsistent on whether or not an intervention was intended to target a specific behaviour change. We therefore extracted data on intervention components and structured aspects of our analysis using the categories of self-management support informed by the PRISMS and RECURSIVE projects.
Search strategy
We searched the following databases using a search strategy developed in conjunction with an information specialist from the Centre for Reviews and Dissemination, University of York (see Appendix 1): Cochrane Database of Systematic Reviews (CDSR); Database of Abstracts of Reviews of Effects (DARE) (up to July 2013); PROSPERO (International Prospective Register of Systematic Reviews) (up to July 2013); and Medical Literature Analysis and Retrieval System Online (MEDLINE) (January 2012 to July 2013). The breadth of the literature identified meant we took a pragmatic approach and limited our search to CDSR; see Box 1.
Inclusion/exclusion criteria
Randomised controlled trials (RCTs) investigating self-management support interventions in men with LTCs (identified via Cochrane systematic reviews of self-management support interventions) were included. Studies which analysed the effects of self-management support interventions in sex groups within a RCT were also identified and synthesised separately.
The following population, intervention, comparison and outcome criteria were used:
-
Population and setting: adults, 18 years of age or older, diagnosed with a LTC.
We limited the review to studies of patients with 14 ‘exemplar’ LTCs (informed by disease areas prioritised in the PRISMS study and team discussions): asthma, diabetes, depression, hypertension, heart failure, chronic obstructive pulmonary disease (COPD), arthritis, chronic kidney disease, chronic pain, human immunodeficiency virus (HIV), testicular cancer, prostate cancer, prostate hyperplasia and chronic skin conditions in any setting. Studies including inpatients with depression were excluded. Studies including patients with multimorbidity involving at least one ‘exemplar’ condition were considered.
-
Intervention: a self-management support intervention.
We adopted the broad definition of a self-management support intervention used in the recent Health Services and Delivery Research RECURSIVE review:7
An intervention primarily designed to develop the abilities of patients to undertake management of health conditions through education, training and support to develop patient knowledge, skills or psychological and social resources.
There is no single agreed definition of what a self-management support intervention encompasses; interventions are highly variable. We therefore developed further standardised criteria which more clearly defined what we considered to be a self-management support intervention of relevance to this review. They are outlined in Box 2.
In line with the recent RECURSIVE7 and PRISMS33 reviews, we excluded any self-management that did not involve some level of professional or peer-led input, guidance or facilitation. For example, we included physical activity-based interventions if they involved an element of education, training or service support, but we excluded studies which involved exercise only. Although we recognise that self-management can be undertaken without any support from health services, we took this stance because it is seldom the subject of intervention studies. 7
We excluded studies involving only self-monitoring of blood pressure in hypertension and glucose monitoring in diabetes, as we considered these to be well-established practices with a well-developed evidence base. The substantial nature of this literature also meant that reviewing these studies was not feasible within the project time frame.
-
Comparison: any comparison group.
We considered studies using ‘care as usual’ or any other intervention.
-
Outcomes: effectiveness, cost-effectiveness.
We extracted data on the effect of interventions on health status, clinical measures, health behaviour, health-care use, self-efficacy, knowledge and understanding, communication with health-care professionals (HCPs) and effects on members/carers.
-
Study design: RCTs identified via eligible Cochrane systematic reviews.
Only papers published in the English language were included, as translation was not feasible in the time frame of the project. In instances where records were unobtainable, attempts were made to contact authors to request the information.
The intervention should, through some means of education, training or support, help people with a LTC by:
-
developing knowledge, skills, psychological or social resources relating to the management of their condition
-
adopting healthy life habits
-
helping individuals recognise the signs of deteriorating health status
-
planning actions to take at signs of relapse or exacerbation
-
knowing what resources are available and how to access them
-
developing skills for helping individuals adhere to a treatment plan
-
communicating effectively with health professionals and/or a support network
-
solving problems
-
identifying objectives and goals and developing action plans.
Identification of studies
We piloted the screening criteria on a sample of papers before undertaking the main screening, in order to identify and resolve any inconsistencies. Screening was conducted in two phases:
-
identification of relevant Cochrane systematic reviews
-
identification of relevant RCTs within included Cochrane systematic reviews.
For phase 1, an initial screen by title and abstract was conducted by one researcher. Two researchers then screened each article independently according to the screening criteria to identify relevant systematic reviews. Disagreements were resolved by a third researcher (principal investigator) as required.
For phase 2, each Cochrane review was screened independently for eligible RCTs by two researchers. The eligibility of each RCT was checked using the study information presented within Cochrane reviews before full papers were sourced. Full texts of each RCT were independently screened by two researchers and disagreements were resolved by a third researcher (principal investigator) as required.
For this review we focused on identifying male-only RCTs and trials which analysed the effects of interventions by sex groups. Agreement on Cochrane review eligibility was 89% and agreement on male-only RCT inclusion/exclusion and identification of RCTs containing sex group analyses was > 90%.
Data extraction
We designed a data extraction sheet and piloted this on a sample of papers prior to the main data extraction. Relevant data from each included article were extracted by a member of the review team and checked for completeness and accuracy by a second member of the team. Disagreements were discussed and resolved by a third person (principal investigator) as required. In instances where key information for meta-analysis was missing, efforts were made to contact authors. We extracted data on study and population characteristics, intervention details (setting, duration, frequency, individual/group, delivered by), outcome measures of health status, clinical measures, health behaviour, health-care use, self-efficacy, knowledge and understanding, communication with HCPs and items for quality assessment (Cochrane risk of bias tool35). Items for economic evaluations [hospital admission, service use, health-related quality of life (HRQoL), incremental cost-effectiveness ratios] were also extracted.
Where studies were reported in multiple publications, each publication was included and relevant data were extracted.
Quality assessment strategy
We extracted data on the methodological quality of all included male-only RCTs and appraised this using the Cochrane risk of bias tool. Quality appraisal was undertaken by two researchers independently and disagreements were resolved through discussion. Sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting and other sources of bias were assessed, assigning low, high or unclear risk of bias, as appropriate. The purpose of the quality appraisal was to describe the quality of the evidence base, not to give an inclusion/exclusion criterion.
Randomised controlled trials containing sex group analyses were assessed for quality using assessment criteria adapted from Pincus et al. 36 and Sun et al. 37 ‘Yes’, ‘No’ and ‘Unclear’ were recorded as responses to the following quality appraisal questions:
-
Was the group hypothesis considered a priori?
-
Was gender included as a stratification factor at randomisation?
-
Was gender one of a small number of planned group hypotheses tested (≤ 5)?
-
Was the study free of other bias (randomisation, allocation concealment, outcome reporting)?
Data analysis
Meta-analysis was conducted using Review Manager version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark).
Data were extracted, analysed and presented as standardised mean difference (SMD) to account for the different instruments used, unless otherwise stated. As a guide to the magnitude of effect, we categorised an effect size of 0.2 as representing a ‘small’ effect, 0.5 a ‘moderate’ effect and 0.8 a ‘large’ effect. 38
A random-effects model was used to combine study data. Statistical heterogeneity was assessed with the I2 value, with ‘low’ heterogeneity set at ≤ 25%, ‘moderate’ 50% and ‘high’ 75%.
In instances where studies contained multiple intervention groups, each group was extracted and analysed independently, dividing the control group sample size to avoid double counting in the analysis.
The following outcome measures were used in the analysis where possible: HRQoL, depression, anxiety, fatigue, stress, distress, pain and self-efficacy. Where a study contained more than one measure of a particular outcome (e.g. depression measured by the Centre for Epidemiologic Studies Depression Scale39 and Beck Depression Inventory40), the tool most established in the wider literature was chosen for meta-analysis. If the tool had multiple subscales, a judgement was made about the most relevant subscale. Where studies reported at multiple time periods, outcome measures reported at or closest to 6 months were used, as measures around this time were by far the most frequently reported.
Unless otherwise specified in the results section, positive effect sizes indicate beneficial outcomes for HRQoL and self-efficacy outcomes, while negative effect sizes indicate beneficial outcomes for depression, anxiety, fatigue, stress, distress and pain outcomes.
We conducted four types of analysis, described below.
Analysis 1: ‘within-Cochrane review analysis’
Analysis 1 sought to determine whether studies in males show larger, similar or smaller effects than studies in females and mixed-sex groups within interventions included within the ‘parent’ Cochrane review. We screened all included Cochrane reviews of self-management support interventions to identify those that contained analysis on outcomes of interest and at least two relevant male-only RCTs. Where an eligible review was identified that met these criteria, the studies were categorised as male only, mixed sex and female only (Figure 1).
FIGURE 1.
Analysis 1: ‘within-Cochrane review analysis’.
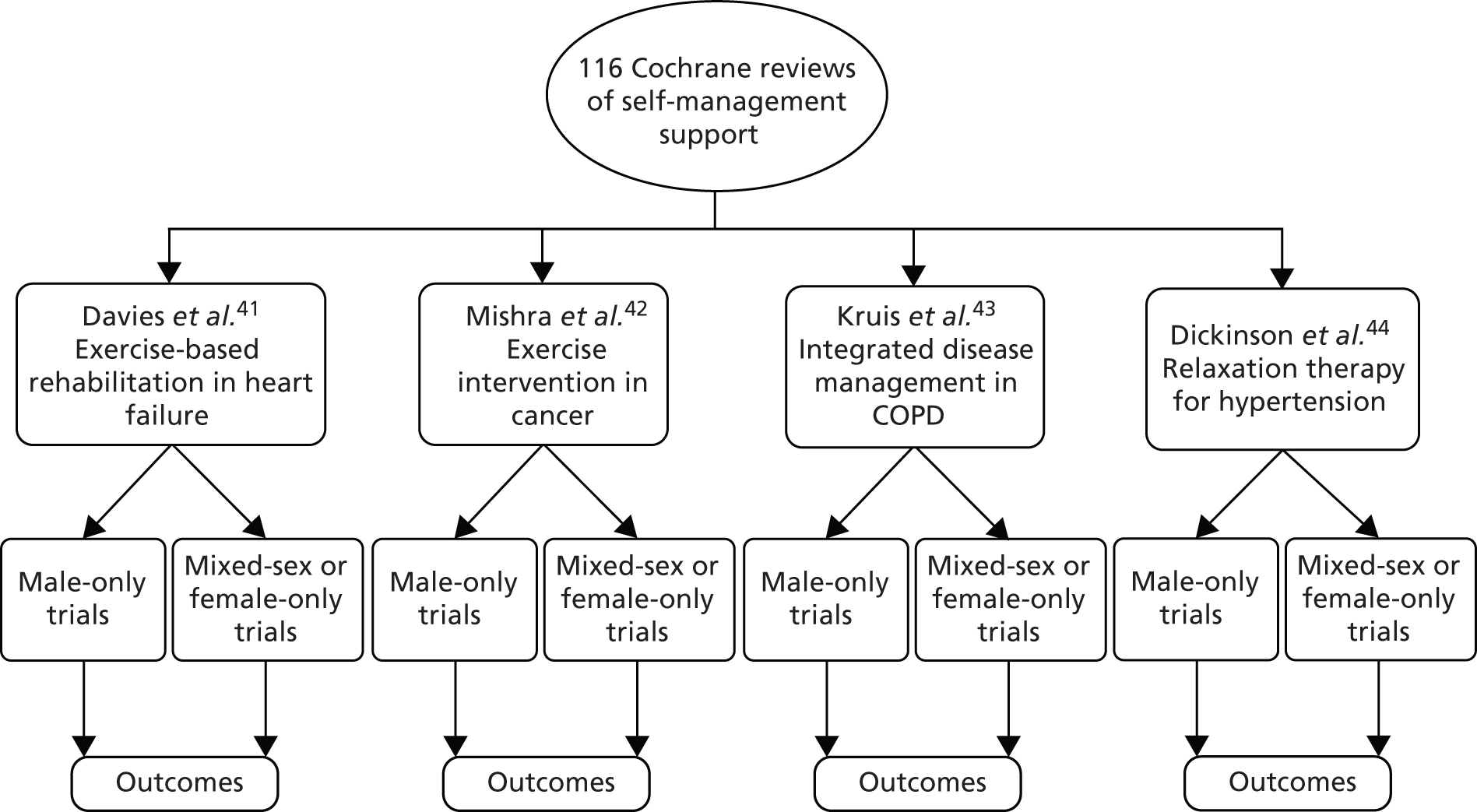
Such comparisons across trials do not have the protection of randomisation, and there may be differences between the studies included in each sex group which account for differences in effects between groups. We presented data on the comparability of these trials within these three categories, including the age of the included patient populations, and on the quality of the studies (using allocation concealment as an indicator of quality).
We report the effect size [together with significance and 95% confidence interval (CI)] of self-management support in each sex group (male only, mixed sex, female only). We conducted analyses to test whether or not interventions showed significantly different effects in sex groups. It should be noted that the power to detect significant differences in such analyses can be limited.
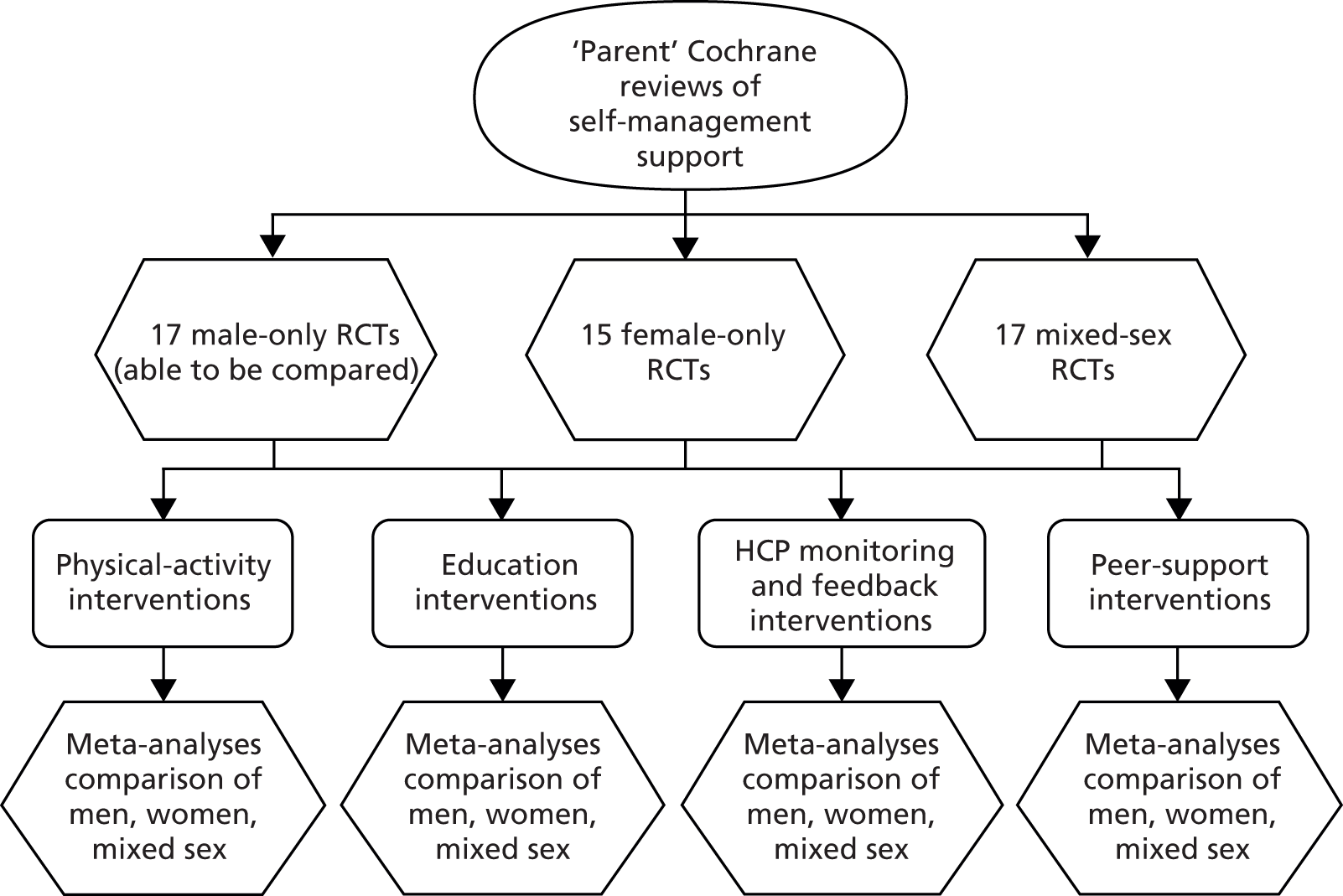
Analysis 2: ‘across-Cochrane review analysis’
Analysis 2 sought to determine whether studies in males show larger, similar or smaller effects than studies in females and mixed-sex groups within types of self-management support pooled across reviews.
In analysis 2, data were pooled according to broad intervention type across reviews, rather than within individual reviews as in analysis 1 (Figure 2). This allowed us to determine whether broad types/components of self-management support interventions show larger, similar or smaller effects in males than in females and mixed populations. Limitations in the data meant that we were able to conduct analyses on only physical activity, education, peer support, and HCP monitoring and feedback interventions.
FIGURE 2.
Analysis 2: ‘across-Cochrane review analysis’.
Such comparisons across trials do not have the protection of randomisation, and there may be differences between the studies included in each sex group which account for differences in effects between groups. We presented data on the comparability of these trials within these three categories, including the age of the included patient populations, and on the quality of the studies (using allocation concealment as an indicator of quality).
We report the effect size (together with significance and 95% CI) of self-management support in each sex group (male only, mixed sex, female only). We conducted analyses to test whether or not interventions showed significantly different effects in sex groups. It should be noted that the power to detect significant differences in such analyses can be limited.
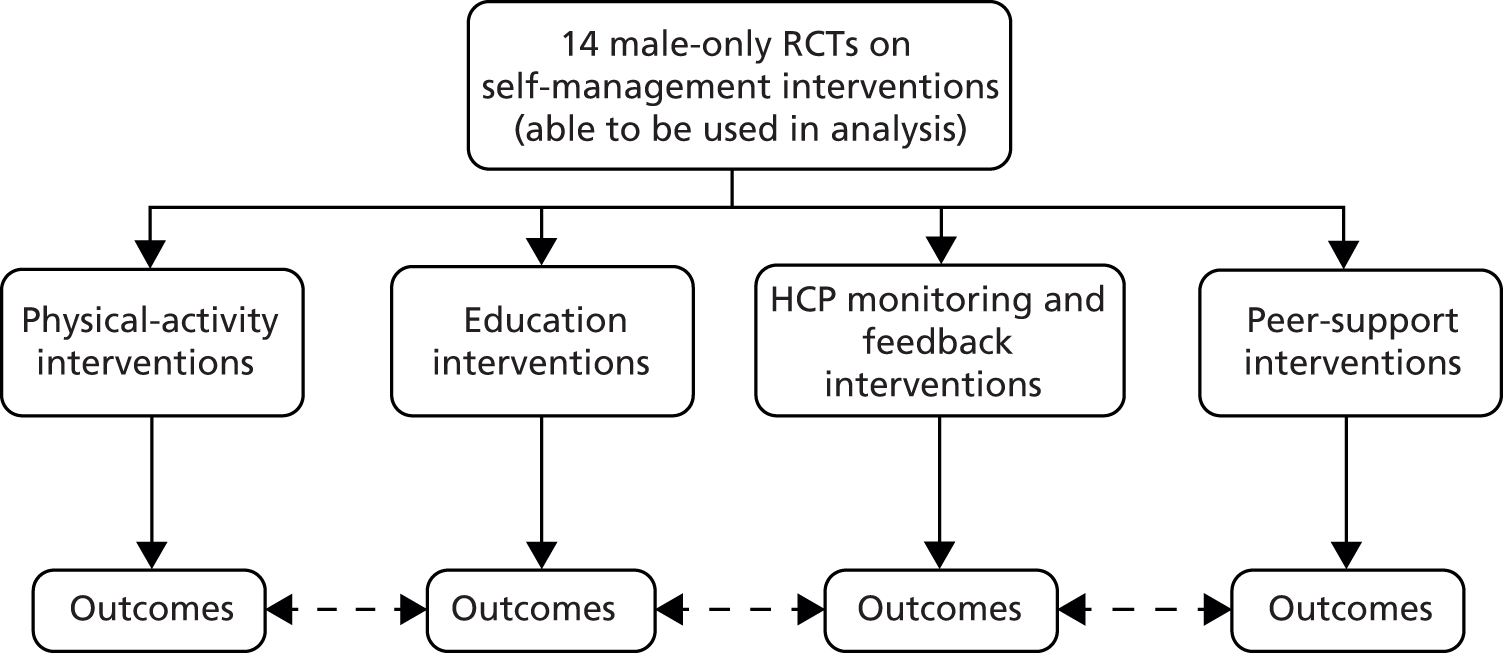
Analysis 3: ‘male-only intervention type analyses’
We conducted a meta-analysis on trials including males only, according to broad intervention type – physical activity, education, peer support, and HCP monitoring and feedback – and compared effects between intervention types (Figure 3). This allowed us to determine whether or not certain broad categories of self-management support intervention were effective in men.
FIGURE 3.
Analysis 3: ‘male-only intervention type analyses’.
Analysis 4: ‘within-trial sex group analysis’
We identified RCTs which analysed the effects of self-management support interventions in sex groups. We sought to extract relevant data on the direction and size of moderating effects in secondary analysis (i.e. whether males show larger, similar or smaller effects than females), and assess these effects in the context of relevant design data, such as sample size, and the quality of the secondary analysis (Figure 4).
FIGURE 4.
Analysis 4: ‘within-trial sex group analysis’.
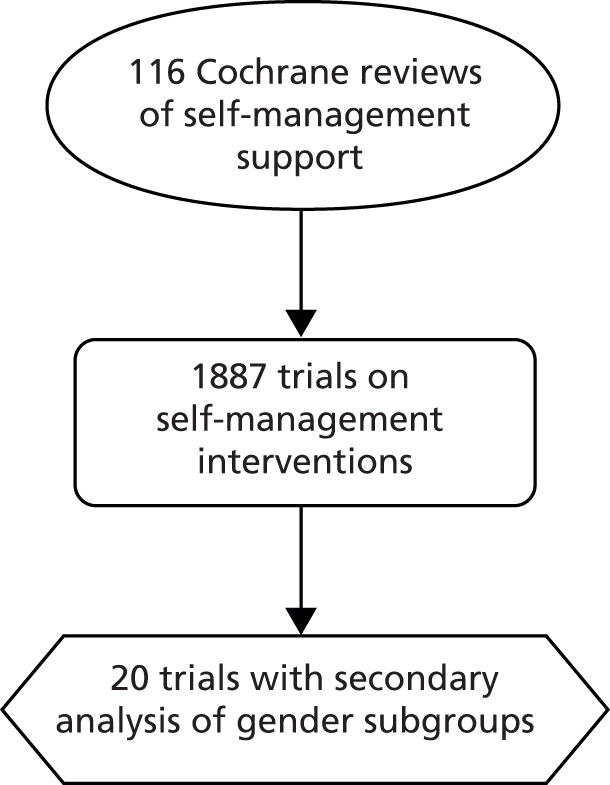
Sex group analyses within trials do in theory provide greater comparability in terms of patient and intervention characteristics than analyses 1–3.
A mixture of LTCs was included within each analysis, constituting the main analysis. Although this was not in the original protocol, we attempted to conduct an analysis by each disease area. We found there were sufficient data to conduct a sex-comparative analysis in only cancer studies; the results are presented in Appendix 2.
Coding interventions for analysis
The plan to use the behavioural change techniques (BCT) taxonomy was dropped (see Box 1 on protocol deviations). Post hoc, we took a pragmatic approach to coding interventions. Development of the intervention categories was informed by the published literature identified in this project and previous work conducted by the PRISMS and RECURSIVE project teams. 7,33 Table 1 provides a list of the categories and their associated description. Categories were designed to be broadly representative of the interventions identified and facilitate comparison of intervention types in the analysis. Two members of the review team independently assessed the ‘type’ of self-management support intervention in each study in order to categorise it, and disagreements were identified and resolved by discussion with a team member.
| Self-management support intervention category | Description |
|---|---|
| Physical activity | Includes any study where physical activity occurs, that is a class or self-directed home-based work. Those containing purely advice or promotion should be captured under education |
| Education | Includes any study where education is taught or educational materials are provided to patients. This may include skills training and dietary or physical activity guidance |
| Peer support | Peer support provided by ‘peers’, that is other patients. This may be in the form of a ‘buddy’ system or through interaction at support groups. HCP support may be captured under HCP monitoring and feedback |
| Psychological interventions | Includes professional counselling or therapy |
| HCP monitoring and feedback | Support in the form of health monitoring and/or feedback on a regimen/promoted lifestyle change. Excludes support provided by peers, which should be captured under peer support |
| Action plans | A plan of actions or responses agreed with and used by the patient in response to particular situations; for example, if symptoms exacerbated, dose adjustment according to symptoms |
| Financial incentives | Includes any intervention where financial barriers are removed or incentives are used to motivate patients to follow a particular intervention or lifestyle change |
Economic evaluation
The review of cost-effectiveness studies was initially planned as a two-stage review. First, we would review economic evaluations of self-management interventions on males only. Subsequently, we would review all economic evaluations with group analyses in which the costs and effects for males and females could be separated.
Study quality was assessed using a modified version of the Drummond checklist where appropriate. 45
Study characteristics
Setting and sample
We identified a total of 40 RCTs on self-management support interventions conducted in male-only samples (some trials have more than one reference) (Figure 5). The majority of the studies were conducted in the USA (n = 23),46–70 with the remainder conducted in the UK (n = 6),71–78 Canada (n = 5),79–83 Spain (n = 3),84–88 Sweden (n = 1),89 Poland (n = 1)90 and Greece (n = 1). 91 Males with prostate cancer were the most frequently studied male-only population (n = 15) included in this review. 48,49,52,58,59,61,64–66,68,69,72,78,80,89 Other disease areas included hypertension (n = 6),47,71,79,82,83,85,86 COPD (n = 6),54,55,73–76,81,84,87,88 heart failure (n = 4),62,67,90,91 type 2 diabetes (n = 3),46,50,51,70 diabetes of unspecified type (n = 1),56 arthritis (n = 1)63 and testicular cancer (n = 1). 77 One multimorbidity study recruited obese men with type 2 diabetes and chronic kidney disease. 57 The age of participants ranged from 25 to 89 years and, where reported, ethnicity was predominantly white. Only one study reported socioeconomic status using a validated tool;63 the majority of other publications included a description of education or annual income.
FIGURE 5.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for the quantitative review.
Self-management support interventions
A total of 51 distinct self-management support interventions were reported across the 40 included male-only studies. Physical activity (n = 16),49,57,62,72–76,78,80,81,84,87–91 education (n = 36),46–55,58–61,63–67,70–72,77,79–81,83–88 peer support (n = 17)47,49,53,56,68–72,80 and HCP monitoring and feedback (n = 25)46,47,50–52,56,57,60,61,66–68,70,71,75,76,78–80,82–89 were the most frequently reported components of these interventions. Three interventions with a psychological component,64,77 two interventions containing a financial incentive component82,83 and one study containing an action plan component19 were also identified.
Twenty-three of the interventions were aimed at individuals,46,48,50–52,54,55,60,61,64,65,67–69,75–78,82–86 20 were aimed at groups47,53,58,59,62,66,70,71,79,89–91 and the remainder used a mixed individual and group approach (n = 6). 49,56,72–74,80,81,87,88 It was unclear what approach was used in two studies. 57,63 Over half of the interventions lasted 0–5 months (n = 28),47,53,58–64,67–69,71–80,85,86 12 interventions ranged between 6 and 11 months,46,52,54–57,66,70,84,90,91 six interventions were 12 months or longer49,65,81,82,84,87,88 and in five cases the total programme duration was unclear. 48,83,89
The mode of administration of the interventions varied. They included telephone-based support (n = 6),60,61,65,67 face-to-face delivery (n = 21),47,53–55,58,59,62–64,66,68–70,77,83,89–91 remote unsupervised activities (n = 2),75,76,78 a combination of face-to-face delivery and remote unsupervised activities (n = 20),46–51,57,71–74,79–82,84–89 and a combination of face-to-face delivery and telephone support (n = 2). 52,56
In terms of setting, interventions were reported to be home-based (n = 11),46,52,60,61,65,67,75,76,78 at a non-home location such as a dedicated gym, pharmacy, hospital clinic, work, university laboratory, coffee shop or other community-based venue (n = 12),53–55,62–64,68–70,77,85,86,90 a combination of home and non-home-based venue (n = 14)48–51,56,57,72–74,79–84,87,88 or not clearly reported in the publication (n = 14). 47,58,59,66,71,89,91
Half of the studies79–82,46,48–51,53,56,58,59,66,70,72,78,84,87,88 reported on some aspect of compliance with the self-management intervention and most participants were followed up for 6 months or less (n = 24) following participation in the intervention.
Table 2 provides an overview of study details and Table 3 includes detailed descriptions of the self-management support intervention.
| Author, year, country | Study aim | Participants: intervention | Participants: control | LTC | Self-management support strategy: intervention group | Self-management support strategy: control group | Follow-up from baseline | Attrition |
|---|---|---|---|---|---|---|---|---|
| Adsett et al. 1989,79 Canada | To compare compliance and efficacy of relaxation therapy with medication, alone or in combination, in reducing the effects of physical and psychological stressors, anxiety and anger | n = 11. Mean age 42.45 years (± 8.24 years). Age range N/R. Ethnicity N/R. SES N/R | n = 12. Mean age 47.50 years (± 9.35 years). Age range N/R. Ethnicity N/R. SES N/R | Hypertension | Relaxation therapy with placebo drug | Relaxation therapy with beta blocker | 1 month, 3 months | n = 15. No further detail |
| n = 12. Mean age 46.58 years (± 7.77 years). Age range N/R. Ethnicity N/R. SES N/R | n = 12. Mean age 49.42 years (± 6.84 years). Age range N/R. Ethnicity N/R. SES N/R | Education with placebo drug | Education with beta blocker | |||||
| Allen et al. 1990,46 USA | To compare the effectiveness of self-monitoring with blood glucose testing and routine urine testing and their respective costs | n = 27. Mean age 58.2 years (± 9.7 years). Age range N/R. Ethnicity 59% white. Mean education 11.1 years (± 4.0 years) | n = 27. Mean age 57.9 years (± 10.7 years). Age range N/R. Ethnicity 67% white. Mean education 10.9 years (± 3.1 years) | Type 2 diabetes | Blood testing and dietary guidance | Urine testing and dietary guidance | 6 months | Five removed because of inappropriate randomisation. I, 1; C, 1 |
| Bennett et al. 1991,71 UK | To investigate the effectiveness of minimal stress management or stress management, through TAM, on cardiovascular reactivity and behaviour | n = 15. Across-group mean age 46 years. Age range N/R. Ethnicity N/R. SES N/R | n = 14. Across-group mean age 46 years. Age range N/R. Ethnicity N/R. SES N/R | Hypertension | Minimal SMT | Waiting list | 2, 6 months | SMT I, 2; TAM I, 0; C, 0 |
| n = 15 (TAM). Across-group mean age 46 years. Age range N/R. Ethnicity N/R. SES N/R | SM including behaviour modification (TAM) | |||||||
| Berglund et al. 2007,89 Sweden | To assess the effect of a psychosocial rehabilitation programme on anxiety and depression and HRQoL | n = 53. Across-group mean age 69 years. Across-group age range 43–86 years. Ethnicity N/R. Elementary school education 52% | n = 51. Across-group mean age 69 years. Across-group age range 43–86 years. Ethnicity N/R. University graduate 28% | Anxiety and depression | Physical training | Standard care | 6, 12 months | 23 dropouts at baseline. Missing data at 6 months n = 23, 12 months n = 19 |
| n = 55. Across-group mean age 69 years. Across-group age range 43–86 years. Ethnicity N/R. Elementary school education 30% | Information | |||||||
| n = 52. Across-group mean age 69 years. Across-group age range 43–86 years. Ethnicity N/R. Elementary school education 39% | Physical training and information | |||||||
| Bosley and Allen 1989,47 USA | To evaluate training procedures to alter psychological responses to stress, to reduce blood pressure | n = 41. Across-group mean age 57 years. Across-group age range 42–68 years. Ethnicity 100% black. Majority skilled/unskilled labour | n = 41. Across-group mean age 57 years. Across-group age range 42–68 years. Ethnicity 100% black. Majority skilled/unskilled labour As above |
Hypertension | Cognitive self-management | Standard care | 2 months | N/R |
| n = 41. Across-group mean age 57 years. Across-group age range 42–68 years. Ethnicity 100% black. Majority skilled/unskilled labour | Attention placebo | 2 months | N/R | |||||
| Bourke et al. 2011,72 UK | To assess the feasibility of a tapered exercise programme in combination with dietary advice in men with prostate cancer | n = 25. Mean age 71.3 years (SD 6.4 years). Across-group age range 60–87 years. Ethnicity N/R. SES N/R | n = 25. Mean age 72.2 years (SD 7.7 years). Across-group age range 60–87 years. Ethnicity N/R. SES N/R | Prostate cancer | Exercise and dietary advice | Standard care | 3, 6 months | I, 10; C, 12 |
| Burgio et al. 2006,48 USA | To test the effects of preoperative pelvic floor muscle training vs. usual care on continence | n = 57. Mean age 60.7 years (SD 6.6 years). Across-group age range 53–68 years. Ethnicity 22.8% black. 83.3% high school graduates. 50% employed outside home | n = 55. Mean age 61.1 years (SD 7.2 years). Across-group age range 53–68 years. Ethnicity 32.7% black. 85.7% high school graduates. 54.7% employed outside home | Prostate cancer | Exercise | Standard care | 1.5, 3, 6 months | I, 6; C, 4. |
| Carmack Taylor et al. 2006,66 USA | To evaluate the efficacy of a 6-month group-based lifestyle physical activity programme on QoL for prostate cancer patients | n = 46. Across-group mean age 69.2 years. Across-group age range 44.8–89.0 years. Across-group ethnicity 73.1% white. Across-group employment status 54.5% retired. Across-group education status 48.9% college or advanced degree | n = 37. Across-group mean age 69.2 years. Across-group age range 44.8–89.0 years. Across-group ethnicity 73.1% white. Across-group employment status 54.5% retired. Across-group education status 48.9% college or advanced degree | Prostate cancer | LP | Standard care and information leaflets | 6, 12 months | LP I, 11; EP I, 7; C, 3 |
| n = 51. Across-group mean age 69.2 years. Across-group age range 44.8–89.0 years. Across-group ethnicity 73.1% white. Across-group employment status 54.5% retired. Across-group education status 48.9% college or advanced degree | EP | |||||||
| Cockcroft et al. 198174 and 1982,73 UK | To examine the effects of exercise on chronic respiratory disability | n = 18. Mean age 61.2 years (± 5.02 years). Age range N/R. Ethnicity N/R. SES N/R | n = 16. Mean age 60.2 years (± 4.72 years). Age range N/R. Ethnicity N/R. SES N/R | COPD | Exercise | Waiting list | 2, 4, 8–9 months | I, 1; C, 4 |
| Culos-Reed et al. 2010,80 Canada | To investigate the effects of physical activity, for men receiving androgen deprivation therapy for prostate cancer treatment, on activity behaviour, QoL and fitness | n = 53. Mean age 67.2 years (SD 8.8 years). Age range 46–82 years. Ethnicity N/R. Completed university/college 32.7%. Annual income > CA$80,000 31.3% | n = 47. Mean age 68 years (SD 8.4 years). Age range 49–86 years. Ethnicity N/R. Partially completed university/college 25.5%. Annual income CA$20,000–CA$39,999 31.8% | Prostate cancer | Exercise, education and peer support | Waiting list | 4, 6, 12 months | I, 11; C, 23 |
| Daubenmier et al. 2006,49 USA | To assess the impact of a lifestyle intervention on HRQoL, perceived stress and self-reported sexual function in those electing for active surveillance | n = 44. Mean age 64.8 years (SD 7.1 years). Age range N/R. Ethnicity 84.1% white. Graduate degree 46%. Full-/part-time work 54% | n = 49. Mean age 66.5 (SD 7.6 years). Age range N/R. Ethnicity 96% white. Graduate degree 35%. Retired/disabled 51% | Prostate cancer | LP | Standard care | 12 months | I, 4; C, 7 |
| Fernandez et al. 2009,84 Spain | To determine if a simple home-based pulmonary rehabilitation programme for patients with severe COPD is safe and effective | n = 30. Mean age 66 years (± 8 years). Age range N/R. Ethnicity N/R. SES N/R | n = 20. Mean age 70 years (± 5 years). Age range N/R. Ethnicity N/R. SES N/R | COPD | Exercise and education | Standard care including education | 12 months | One removed from analysis. I, 3; C, 5 |
| Gallagher et al. 198451 and 1987,50 USA | To evaluate the effect of an unmeasured diet on control of blood sugar, insulin dosage, serum lipids and weight as compared with traditional calorie-defined diet | n = 28. Mean age 47.8 years (SD 16.2 years). Age range N/R. Ethnicity N/R. SES N/R | n = 23. Mean age 44.5 years (SD 12.7 years). Age range N/R. Ethnicity N/R. SES N/R | Type 2 diabetes | Unmeasured diet and dietary education | Calorie-defined diet and dietary education | 48 months | I, 1; C, 3 |
| Garcia-Vera et al. 199785 and 2004,86 Spain | To evaluate whether or not SMT reduces blood pressure and blood pressure variability | n = 22. Mean age 45.6 years (± 9.9 years). Age range N/R. Ethnicity N/R. SES N/R | n = 21. Mean age 45.1 years (± 7.8 years). Age range N/R. Ethnicity N/R. SES N/R | Hypertension | SMT | Waiting list | 4 months | I, 1; C, 3 |
| Giesler et al. 2005,52 USA | To assess the efficacy of a cancer-care intervention on QoL | n = 48. Mean age 66.7 years (± 8 years). Age range N/R. Ethnicity 92% Caucasian. High school diploma 29% | n = 51. Mean age 61.1 years (± 8 years). Age range N/R. Ethnicity 88% Caucasian. College degree 35% | Prostate cancer | Psychoeducational strategy | Standard care | 12 months | 14 dropouts, nearly equal between groups |
| Gifford et al. 1998,53 USA | To evaluate the acceptability, practicality and short-term efficacy of a health education programme to improve disease self-management with symptomatic HIV/AIDS | n = 25. Mean age 45.2 years (SD 9.4 years). Age range N/R. Ethnicity 68% white. Some graduate school education 36%. Unemployed 56%. Annual income < US$20,000 55% | n = 33. Mean age 45.3 years (SD 8.1 years). Age range N/R. Ethnicity 82% white. Completed college 33%. Unemployed 70%. Annual income US$20,000–40,000 40% | HIV/AIDS | Education | Standard care | 3 months | I, 9; C, 4 |
| Gourley et al. 199854 and Solomon et al. 1998,55 USA | To determine patient satisfaction with pharmacist-led care | n = 43. Mean age 69.3 years (SD 5.9 years). Age range N/R. Ethnicity 90.7% Caucasian (sic). Some college or technical school education 37.2%. Mean annual family income US$20,908 | n = 55. Mean age 69.3 years (SD 9.2 years). Age range N/R. Ethnicity 83.6% Caucasian (sic). Some college or technical school education 40.0%. Mean annual family income US$21,022 | COPD | Education and support | Standard care | 6 months | N/R |
| Guell et al. 2000,81 Canada | To examine the short- and long-term effects of an outpatient pulmonary rehabilitation programme | n = 30. Mean age 64 years (± 7 years). Across-group age range 46–74 years. Ethnicity N/R. SES N/R | n = 30. Mean age 66 years (± 6 years). Across-group age range 46–74 years. Ethnicity N/R. SES N/R | COPD | Education, breathing exercise and general exercise | Standard care | 6, 9, 12, 24 months | I, 6; C, 7 |
| Haynes et al. 1976,82 Canada | To assess the application of behavioural-oriented strategies on compliance and blood pressure control | n = 20. Mean age N/R. Age range N/R. Ethnicity N/R. SES N/R | n = 18. Mean age N/R. Age range N/R. Ethnicity N/R. SES N/R | Hypertension | Behavioural strategies | Standard care | 12 months | I, 0; C, 1 |
| Heisler et al. 2010,56 USA | To compare reciprocal peer-support with nurse care management | n = 125. Mean age 61.8 years (SD 6.1 years). Age range N/R. Ethnicity 80% Caucasian (sic). Some college or technical or vocational training 73%. Annual income ≤ US$30,000 63% | n = 119. Mean age 62.3 years (SD 6.6 years). Age range N/R. Ethnicity 84% Caucasian (sic). Some college or technical or vocational training 70%. Annual income ≤ US$30,000 63% | Diabetes (type not specified) | Peer support | Nurse care management | 6 months | I, 9; C, 5 |
| Klocek et al. 2005,90 Poland | To examine changes in QoL and oxygen consumption compared in two exercise programmes | n = 14. Mean age 54 years (± 7 years). Age range N/R. Ethnicity N/R. Years of education 12 | n = 14. Mean age 55 years (± 9 years). Age range N/R. Ethnicity N/R. Years of education 13 | Heart failure | Rehabilitation programme with constant level of workload | Standard care | 6 months | N/R |
| n = 14. Mean age 57 years (± 8 years). Age range N/R. Ethnicity N/R. Years of education 14 | Rehabilitation programme with progressive level of workload | |||||||
| Koukouvou et al. 2004,91 Greece | To investigate whether or not exercise-based rehabilitation affects psychological profile and QoL and examine correlations between changes in cardiorespiratory capacity and psychological status | n = 16. Mean age 52.3 years (SD 9.2 years). Across-group age range 36–66 years. Ethnicity N/R. SES N/R | n = 10. Mean age 52.8 years (SD 10.6 years). Across-group age range 36–66 years. Ethnicity N/R. SES N/R | Heart failure | Supervised exercise rehabilitation programme | Standard care | 6 months | I, 2; C, 1 |
| Leehey et al. 2009,57 USA | To measure if exercise improves cardiovascular health and weight loss, decreases proteinuria, improves glucose and lipid control and decreases inflammation | n = 7. Across-group mean age 66 years. Across-group age range 55–81 years. Ethnicity N/R. SES N/R | n = 6. Across-group mean age 66 years. Across-group age range 55–81 years. Ethnicity N/R. SES N/R | Kidney disease and type 2 diabetes | Exercise | Standard care including disease education | 1.5, 6 months | I, 0; C, 2 |
| Lepore 1999,58 USA | To investigate if psychoeducational support groups enhance QoL | n = 12. Age N/R. Age range N/R. Ethnicity 100% Caucasian (sic). Median annual income US$50,000–75,000 | n = 12. Age N/R. Age range N/R. Ethnicity 100% Caucasian (sic). Median annual income US$50,000–75,000 | Prostate cancer | Psychoeducational support group | Standard care | 2 months | N/R |
| Lepore et al. 2003,59 USA | To compare QoL outcomes of patients randomised to standard care, education alone or education and peer discussion | n = 84. Mean age 64.8 years (SD 7.7 years). Age range N/R. Ethnicity 76% Caucasian (sic). High school graduate 26%. Retired 43%. Latest occupation professional/technical 34% | n = 80. Mean age 65.6 years (SD 6.6 years). Age range N/R. Ethnicity 72% Caucasian (sic). College graduate 21%. Retired 38%. Latest occupation professional/technical 33% | Prostate cancer | Education | Standard care | 0.5, 6, 12 months | 29 lost to follow-up |
| n = 86. Mean age 64.8 years (SD 8.0 years). Age range N/R. Ethnicity 78% Caucasian (sic). College graduate 29%. Retired 42%. Latest occupation professional/technical 30% | Education and peer discussion | |||||||
| Lucy 1994,60 USA | To measure the impact of a psychosocial intervention on psychological distress | n = 9. Mean age 38 years (± 8.1 years). Across-group age range 25–68 years. Ethnicity n = 7 Caucasian (sic). Full-time employment n = 6. Annual income US$20,000–29,000 | n = 8. Mean age 38.75 years (± 12.7 years). Across-group age range 25–68 years. Ethnicity n = 5 Caucasian (sic). Full-time employment n = 4. Annual income US$30,000–39,000 | HIV | Telecare support | Waiting list | 4 months | N/R |
| McGavin et al. 197776 and 1976,75 UK | To evaluate a home-based exercise scheme | n = 12. Mean age 61.4 years (± 5.6 years). Age range 53–69 years. Ethnicity N/R. SES N/R | n = 12. Mean age 57.2 years (± 7.9 years). Age range 40–69 years. Ethnicity N/R. SES N/R | COPD | Exercise | No intervention | ≈ 3 months | I, 4; C, 0 |
| Mishel et al. 2002,61 USA | To test the efficacy of an individualised uncertainty management intervention | Overall n = 239. Group n N/R. Across-group mean age 64.0 years (SD 6.9 years). Age range N/R. Across-group ethnicity 56% Caucasian. Across-group income > US$3000 per month 45%. > 12 years education 57% | Overall n = 239. Group n N/R. Across-group mean age 64.0 years (SD 6.9 years). Age range N/R. Across-group ethnicity 56% Caucasian. Across-group income > US$3000 per month 45%. > 12 years education 57% | Prostate cancer | Patient uncertainty management | Standard care and general health information | 7 months | 5% dropout across groups |
| Overall n = 239. Group n N/R. Across-group mean age 64.0 years (SD 6.9 years). Age range N/R. Across-group ethnicity 56% Caucasian. Across-group income > US$3000 per month 45%. > 12 years education 57% | Patient and close family member uncertainty management | |||||||
| Moynihan et al. 1998,77 UK | To determine the efficacy of adjuvant psychological therapy in patients with testicular cancer | n = 36. Across-group mean age 62 years. Age range N/R. Ethnicity N/R. Across-group social class III n = 25 | n = 37. Across-group mean age 62 years (± 85 years). Age range N/R. Ethnicity N/R. Across-group social class III n = 25 | Testicular cancer | Psychological therapy | Standard care | 12 months | I, 3; C, 2 |
| Mueller et al. 2007,62 USA | To assess exercise capacity, mortality, cardiac events and physical activity patterns in chronic heart failure patients undergoing a rehabilitation programme | n = 25. Across-group mean age 55 years (± 10 years). Age range N/R. Ethnicity N/R. SES N/R | n = 25. Across-group mean age 55 years (± 10 years). Age range N/R. Ethnicity N/R. SES N/R | Heart failure | Residential rehabilitation programme | Standard care | 1 month, 6.2 years | I, 11; C, 12 |
| Parker et al. 1984,63 USA | To compare patients receiving a comprehensive arthritis education programme with a standard-care control group | Overall n = 18. Group n N/R. Mean age 55.3 years (± 10.8 years). Age range N/R. Ethnicity N/R. Hollingshead index 56.9 (± 7.5) | Overall n = 18. Group n N/R. Mean age 55.8 years (± 10.2 years). Age range N/R. Ethnicity N/R. Hollingshead index 56.9 (± 16.7) | Arthritis | Education | Standard care | 3 months | n = 22 selected; n = 18 with complete data. No further detail |
| Parker et al. 2009,64 USA | To assess the short- and long-term effects of a SM or SA intervention | SM: n = 53. Mean age 59.8 years (SD 6.9 years). Age range N/R. Ethnicity 71% white. College graduate 39% | n = 52. Mean age 60.9 years (SD 5.9 years). Age range N/R. Ethnicity 92% white. College graduate 35% | Prostate cancer | SM | Standard care | 12 months | SM I, 21; SA I, 17; C, 20 |
| SA: n = 54. Mean age 60.7 years (SD 7.2 years). Age range N/R. Ethnicity 70% white. College graduate 39% | SA | |||||||
| Puente-Maestu et al. 200088 and 2003,87 Spain | To compare two exercise training programmes and evaluate any long-term effects | n = 20. Mean age 65.6 years (SD 43.7 years). Age range N/R. Ethnicity N/R. SES N/R | n = 21. Mean age 63.3 years (SD 4.3 years). Age range N/R. Ethnicity N/R. SES N/R | COPD | Unsupervised exercise | Supervised exercise | 2, 15 months | I, 10; C, 8 |
| Sackett et al. 1975,83 Canada | To evaluate strategies for increasing medication compliance. Factorial design | Overall n = 230. Group n N/R. Age N/R. Age range N/R. Ethnicity N/R. SES N/R | Augmented convenience n = 114, normal convenience n = 116, mastery learning n = 115, no mastery learning n = 115 | Hypertension | Augmented convenience and mastery learning | Normal convenience and no mastery learning | 6 months | Augmented convenience, 6; normal convenience, 4; mastery learning, 8; no mastery learning, 2 |
| Scura et al. 2004,65 USA | To evaluate the feasibility of a telephone social support intervention to increase physical, emotional, functional and interpersonal adaption of men to prostate cancer | n = 7. Across-group mean age 66 years (SD 8.3 years). Across-group age range 51–78 years. Across-group ethnicity 59% Caucasian (sic). Across-group mean annual income ≤ US$40,000 | n = 10. Across-group mean age 66 years (SD 8.3 years). Across-group age range 51–78 years. Across-group ethnicity 59% Caucasian (sic). Across-group mean annual income ≤ US$40,000 | Prostate cancer | Telephone support and education | Education | 2.5, 7.5, 12 months | N/R |
| Wakefield et al. 2008,67 USA | To compare a telephone intervention and a videophone intervention on changes in communication, nurse perception and patient satisfaction | n = 14. Mean age 72 years (± 9.2 years). Age range N/R. Ethnicity 86% Caucasian (sic). High school education 29% | N/R | Heart failure | Telephone support | Standard care | 3 months | Telephone I, 39; video I, 18; C, N/R |
| n = 14. Mean age 68.1 years (± 8.3 years). Age range N/R. Ethnicity 100% Caucasian (sic). High school education 57% | Video call support | |||||||
| Weber et al. 2004,68 USA | To investigate the effects of a peer support programme between men recently treated with radical prostatectomy and long-term survivors | n = 15. Mean age 57.5 years (SD 6.7 years). Across-group age range 48–67 years. Ethnicity 87% white. High school education 40%. Mean annual income US$50,000–74,000 33%. Full-time employment 80% | n = 15. Mean age 59.7 years (SD 6.6 years). Across-group age range 48–67 years. Ethnicity 80% white. High school education 40%. Mean annual income > US$75,000 33%. Full-time employment 47% | Prostate cancer | Peer support | Standard care | 2 months | I, 2; C, 0 |
| Weber et al. 2007,69 USA | To enhance self-efficacy through dyadic support in men who have undergone radical prostatectomy for prostate cancer | n = 37. Mean age 59.5 years. Across-group age range 47–74 years. Ethnicity 86.5% white. Four-year degree education 29.7%. Mean annual income > US$75,000 37.8% | n = 35. Mean age 60 years. Across-group age range 47–74 years. Ethnicity 80% white. Some college education 28.6%. Mean annual income > US$75,000 29.4% | Prostate cancer | Peer support | Standard care | 2 months | Two patients relocated/lost to follow-up, unclear which group. I, 2; C, 5 |
| White et al. 1986,70 USA | To compare the effectiveness of advice and education vs. group management with peer support | n = 16. Mean age 62.4 years (± 5.5 years). Age range N/R. Ethnicity N/R. Employment 25%. More than high school education 31.3% | n = 16. Mean age 60.7 years (± 6.4 years). Age range N/R. Ethnicity N/R. Employment 31.3%. More than high school education 37.5% | Type 2 diabetes | Group management and peer support | Education and advice | 6 months | I, 4; C, 5 |
| Windsor et al. 2004,78 UK | To determine if aerobic activity reduces fatigue incidence and prevents deterioration of physical functioning during radiotherapy | n = 33. Mean age 68.3 years (± 0.9 years). Across-group age range 52–82 years. Ethnicity N/R. SES N/R | n = 33. Mean age 69.3 years (± 1.3 years). Across-group age range 52–82 years. Ethnicity N/R. SES N/R | Prostate cancer | Exercise and HCP support | Standard care | 1 month | I, 1; C, 0 |
| Author, year, country | Self-management intervention description and intervention coding | Method of recruitment | Setting of intervention | Duration of intervention session and frequency | Total duration | Individual or group | Mode of administration | Delivered by/intervention training |
|---|---|---|---|---|---|---|---|---|
| Adsett et al. 1989,79 Canada | Training in progressive muscle relaxation, monitoring practice and strategies for stressful situations. Education on hypertension, lifestyle and stress. Patients were given a take-home tape of first relaxation session for home practice and kept daily logs. Compliance was assessed weekly (Edu, M&F) | Recruitment from work place (Dominion Foundries) | Work and home based | 1 hour, weekly | 8 weeks | Group | Face to face and remote unsupervised | Therapists trained on intervention |
| Education (same as relaxation group) on hypertension, lifestyle and stress. Weekly logs of activities, food intake and exercise were kept and reviewed weekly (Edu, M&F) | Work and home based | 1 hour, weekly | 8 weeks | Group | Face to face and remote unsupervised | Therapists trained on intervention | ||
| Allen et al. 1990,46 USA | Patients were trained to perform blood glucose tests at least 36 times per month. Proficiency was checked prior to the start of study and throughout. Each patient was also instructed on a diet, which largely focused on increasing fibre intake. Booklets on diet and weight loss were provided and compliance was checked at 3 and 6 months (Edu, M&F) | Medical centres | Home based | N/A. Follow-up at 3 and 6 months | 24 weeks | Individual | Face to face and remote unsupervised | Dietitian, diabetes teaching nurse, physician or physician associate. Intervention training N/R |
| Bennett et al. 1991,71 UK | Stress management training: small groups were educated on BP, stress and relaxation techniques, self-instruction techniques, cognitive restructuring and meditation. Sessions involved role-play and group problem-solving. Participants were set behavioural assignments and kept a diary (Edu, Peer, M&F) | Medical centres | N/R | 2 hours, weekly | 8 weeks | Group | Face to face and remote unsupervised | Therapist. Intervention training N/R |
| Type A behaviour management: same content as stress management training. Additionally, specific attention was paid to the identification and modification of type A behaviours including time urgency management and anger control (Edu, Peer, M&F) | N/R | 2 hours, weekly | 8 weeks | Group | Face to face and remote unsupervised | Therapist. Intervention training N/R | ||
| Berglund et al. 2007,89 Sweden | The training programme involved light physical fitness training, relaxation, breathing exercises and pelvic floor exercises. A booster session was held after 2 months (Phy, M&F) | Consecutive hospital patients within 6 months of diagnosis | N/R | 1.25 hours, 7 sessions | N/R | Group | Face to face and remote unsupervised | Physiotherapist. Intervention training N/R |
| Information was provided on prostate cancer, treatment and potential side effects in the form of lectures. Opportunities for group discussion and demonstration of products for incontinence and sexual aid formed part of the sessions (Edu, Peer) | N/R | 1.25 hours, 7 sessions | N/R | Group | Face to face | Nurse. Intervention training N/R | ||
| This programme combined the physical and information programmes (Phy, Edu, Peer) | N/R | 2.25 hours, 7 sessions | N/R | Group | Face to face and remote unsupervised | Physiotherapist and nurse. Intervention training N/R | ||
| Bosley and Allen 1989,47 USA | Education on stress, emotional arousal and hypertension. Participants were trained to monitor own behaviour and physiological responses in stressful situations. Group practice, identification of faulty appraisal, recognition of inaccurate labelling of situations and home practice formed part of the intervention (Edu, Peer, M&F) | Community recruitment | N/R | 45 minutes, weekly | 8 weeks | Group | Face to face and remote unsupervised | Psychologist with matched ethnicity. Intervention training N/R |
| Presentation on the dynamics of stress and hypertension, followed by group discussion sessions on how to handle stressful situations (Edu, Peer) | N/R | 45 minutes, weekly | 8 weeks | Group | Face to face | Psychologist with matched ethnicity. Intervention training N/R | ||
| Bourke et al. 2011,72 UK | Supervised aerobic and resistance exercise training and self-directed exercise. Incorporating exercise into daily activities and available support structures were explored for each patient. All participants received a nutrition advice pack, which recommended reductions in saturated fat and refined carbohydrates, increased fibre and moderate alcohol consumption. Small group healthy eating seminars were also held (Phy, Edu, Peer) | Sedentary patients from outpatient clinics | Dedicated exercise suite and home based. Healthy eating seminar location N/R | ≥ 0.5 hours, three times per week. Healthy eating seminar fortnightly, duration N/R | 12 weeks | Group and individual | Face to face and remote unsupervised | Exercise physiologist. Intervention training N/R |
| Burgio et al. 2006,48 USA | A single session of biofeedback to learn pelvic floor control, reinforced with verbal instructions. Patients were provided with written instructions for 45 pelvic floor exercises and encouraged to continue at home in various positions and to integrate into daily activities (Edu) | Pre-surgery patients at urology clinics | Hospital and home based | One session, duration N/R. Frequency of home practice N/R | N/R | Individual | Face to face and remote unsupervised | N/R |
| Carmack Taylor et al. 2006,66 USA | Cognitive behavioural skills training including self-monitoring, goal-setting, problem-solving to overcome barriers, cognitive restructuring and self-rewards to integrate physical activity into daily life. Patients self-monitored and were followed up to solve issues and set new goals (Edu, M&F) | Cancer centres. Recruitment in five cohorts | N/R | 1.5 hours per session; one orientation session, 16 weekly sessions and four sessions twice a week | 24 weeks | Group | Face to face | Expert speakers, physical and lifestyle co-ordinator. Intervention training N/R |
| Facilitated group discussion on various topics: diet and prostate cancer, side effects of treatment and sexuality. Expert speakers presented at some sessions (Edu, Peer) | N/R | 1.5 hours per session; one orientation session, 16 weekly sessions and four sessions twice a week | 24 weeks | Group | Face to face | Expert speakers | ||
| Cockcroft et al. 198174 and 1982,73 UK | Rehabilitation centre-based exercise including stationary cycle pedalling, rowing machines, swimming and daily walks. Recommended home exercises included stair climbing and level walking (Phy) | N/R | Rehabilitation centre and home based | Twice-daily walks, duration unknown | 16 weeks | Group and individual | Face to face and remote unsupervised | N/R |
| Culos-Reed et al. 2010,80 Canada | Group exercise tailored to ability consisting of walking, stretching and light resistance work. Exercise equipment was provided to facilitate home-based exercise. Peer support was encouraged and education/discussion sessions were held on goal-setting, monitoring behaviour, overcoming barriers, role of positive attitude, social support, relapse support and nutrition (Phy, Edu, Peer, M&F) | Prostate cancer survivors on long-term therapy | Home based and fitness centre | Home-based exercise 3–5 times per week, duration N/R. Fitness centre exercise weekly for 1.5 hours, then monthly during maintenance phase | 16 weeks | Individual and group | Face to face and remote unsupervised | Fitness professional. Intervention training N/R |
| Daubenmier et al. 2006,49 USA | A plant-based vegan diet with 10% of calories from fat, 3 hours of moderate exercise per week and 1 hour of stress management practice per day. Participants attended a 1-week retreat to familiarise themselves with the intervention. Subsequently, weekly support group meetings were held to enhance programme adherence (Phy, Edu, Peer) | N/R | Residential retreat and home based. Support group meeting location N/R | Recommended 3 hours of exercise per week and 1 hour of stress management per day. Support group meetings weekly, duration N/R | 48 weeks including 1-week residential retreat | Individual and group | Face to face and remote unsupervised | N/R |
| Fernandez et al. 2009,84 Spain | Respiratory education combined with inspiratory, upper and lower limb muscular training. Training logs were kept and patients were followed up by a physiotherapist. Educational materials were also provided on exercises (Phy, Edu, M&F) | Patients receiving long-term oxygen therapy | Hospital and home based | Two education sessions for 1 hour each. 1 hour of exercise, five times per week | 44 weeks | Individual | Face to face and remote unsupervised | Physiotherapist and nurse. Intervention training N/R |
| Gallagher et al. 198451 and 1987,50 USA | Diet with an unspecified calorie intake consisting of three meals per day and a snack avoiding refined sugars and saturated fats. Education on the diet and dietary consultations occurred every 3 months (Edu, M&F) | Hospital diabetic outpatient unit | Home based | N/A. Consult every 3 months | 4 years | Individual | Face to face and remote unsupervised | Dietitian |
| Garcia-Vera et al. 199785 and 2004,86 Spain | Education and training on hypertension, relaxation and problem-solving. Patients received a self-help book, problem-solving sheets, relaxation tapes and recording sheets to track medication use and stressful events. Homework assignments were set and reviewed by a therapist (Edu, M&F) | Referrals from medical centres | Health centre and university laboratory | Five sessions over 1 week and then two sessions every 2 weeks | 8 weeks | Individual | Face to face and remote unsupervised | Therapist. Intervention training N/R |
| Giesler et al. 2005,52 USA | A programme of symptom management and psychoeducational strategies. The intervention focused primarily on sexual and urinary problems, bowel dysfunction, cancer worry, dyadic adjustment and depression (Edu, M&F) | Medical centres and hospital cancer units | Home based | Monthly, duration unknown | 24 weeks | Individual | Face to face and telephone | Nurse. Intervention training N/R |
| Gifford et al. 1998,53 USA | Self-care education sessions covering evaluating symptoms, seeking care for new symptoms, medication use and problems, communication skills with caregiver/health professionals, coping with symptoms using cognitive–behavioural therapy, and relaxation. Additionally exercise, fitness programmes, nutrition plans and goal-setting. Interaction was encouraged through role-playing, information sharing and other forms of participation (Edu, Peer) | Community recruitment and medical centres | Community settings | Weekly, duration unknown | 7 weeks | Group | Face to face | Lay leaders from community trained on intervention |
| Gourley et al. 199854 and Solomon et al. 1998,55 USA | A pharmacist provided regular assessment and educational interventions to optimise disease management. Patients’ questions and concerns were also managed (Edu) | Hospital and medical centres | Pharmacy clinic | Monthly, duration unknown | 24 weeks | Individual | Face to face | Pharmacist. Intervention training N/R |
| Guell et al. 2000,81 Canada | Breathing retraining and relaxation techniques, low-level stair walking, flat surface exercise, stationary cycle pedalling and walking with arm and leg co-ordination. Education sessions covered anatomy, basic respiratory physiology, nature of the disease and interventions. Physiotherapy for effective cough and postural drainage was offered (Phy, Edu) | Consecutive eligible patients at an outpatient clinic | Hospital gym and home based. Unclear where educational classes held | Phased exercise programme: 30 minutes of supervised classes and 30–60 minutes of home-directed exercise up to 5 times per week. Education component details N/R | 48 weeks | Group and individual | Face to face and remote unsupervised | N/R |
| Haynes et al. 1976,82 Canada | Each patient was interviewed to identify habits and tailor medication taking. Loaned BP devices were provided and BP and medication taking were tracked. During fortnightly follow-ups, if BP had lowered, financial credit was given towards owning the BP device. Patients were also praised and encouraged on progress (M&F, Finance) | N/R | Work and home based | 30 minutes, every 2 weeks | 48 weeks | Individual | Face to face and remote unsupervised | Female programme co-ordinator |
| Heisler et al. 2010,56 USA | Action plans were generated based on individual laboratory and BP results. Each patient was then paired with a peer and encouraged to make regular contact with automated reminders. Each pair received training on communication skills and topic guides for phone calls. In addition three optional group sessions to raise queries, discuss concerns and review action plan progress were held (Peer, M&F, Action) | Patients from two medical centres with poor glycaemic control | Home based. Group session location N/R | One 3-hour training session. Weekly peer calls encouraged. Three optional group sessions lasting 1.5 hours each | 24 weeks | Individual and group | Face to face and telephone | Care manager trained on motivational interviewing and empowerment. Patient peer supporters trained on peer communication |
| Klocek et al. 2005,90 Poland | Exercise consisting of warm-up, then consistent workload training on a cycle ergometer (60% maximal heart rate for age) and post-training relaxation (Phy) | Consecutive patients from hospital cardiac unit | Cardiac rehabilitation outpatient unit | 1 hour, three times per week | 24 weeks | Group | Face to face | Physician and rehabilitation specialist |
| Exercise consisting of warm-up, interval training with gradually increasing workload on a cycle ergometer and post-training relaxation (Phy) | Cardiac rehabilitation outpatient unit | 1 hour, three times per week | 24 weeks | Group | Face to face | Physician and rehabilitation specialist | ||
| Koukouvou et al. 2004,91 Greece | A gradually modified physical training programme incorporating stationary cycling, walking or jogging, calisthenics, stair climbing and step aerobic exercises. Resistance exercises were added in after the first 3 months (Phy) | Referrals from hospital cardiac clinic | N/R | 1 hour, 3–4 times per week | 24 weeks | Group | Face to face | N/R |
| Leehey et al. 2009,57 USA | Education and instruction on walking, shoe selection and developing a walking programme. Gradually increasing treadmill walking and unsupervised home-based walking programme. Patients were followed up and monitored by staff (Phy, M&F) | Individuals from an outpatient clinic | Laboratory gym setting and home based | Gradually increasing from 30 minutes, thrice weekly | 24 weeks | N/R | Face to face and remote unsupervised | N/R |
| Lepore 1999,58 USA | Patients and partners were invited to expert lecture and question sessions followed by separate peer discussions for men and wives. Topics were prostate cancer overview, nutrition and exercise, side effects, stress management, communication and intimacy, and follow-up care. Those missing meetings received a tape recording of the lecture and any handouts (Edu, Peer) | Patients after treatment for prostate cancer | N/R | 1.75 hours, weekly | 6 weeks | Group | Face to face | Clinical psychologist and oncology nurse. Intervention training N/R |
| Lepore et al. 2003,59 USA | Expert-delivered lectures on prostate cancer biology and epidemiology, control of physical side effects, nutrition, stress and coping, relationships and sexuality, follow-up care, and future health concerns. Printed materials were provided in each lecture and 10 minutes of questions were permitted, minimising group discussion (Edu) | Urology and radiology clinics | N/R | 1 hour, weekly | 6 weeks | Group | Face to face | Expert speakers. No further detail |
| Expert lectures as above as well as facilitated group discussion with a male psychologist for men and separate discussion for partners with a female oncology nurse (Edu, Peer) | N/R | 1.75 hours, weekly | 6 weeks | Group | Face to face | Expert speakers, male psychologist and female oncology nurse. Intervention training N/R | ||
| Lucy 1994,60 USA | Psychosocial support, monitoring of health, stress, mood and interpersonal satisfaction. Monitored weekly over the phone. Information and education on HIV/AIDS. Referrals to other services when appropriate (Edu, M&F) | Press release | Home based | 0.4–0.75 hours, weekly | 16 weeks | Individual | Telephone | N/R |
| McGavin et al. 197776 and 1976,75 UK | Home stair-climbing exercises starting from a minimum of two steps up and down for 2 minutes building to 10 steps for 10 minutes. Participants recorded their progress and the programme was reviewed after 2 weeks and monthly thereafter (Phy, M&F) | N/R | Home based | 2–10 minutes ≥ once a day, ≥ 5 times per week | 12 weeks | Individual | Remote unsupervised | N/R |
| Mishel et al. 2002,61 USA | Patients’ concerns directed the skills training. Strategies included information, cognitive reframing, directing to local resources, problem-solving techniques, encouragement and patient–doctor communication skills to enhance participation in care (Edu, M&F) | Medical centres and community | Home based | Weekly, duration unknown | 8 weeks | Individual | Telephone | Nurse trained in the intervention |
| Patients’ concerns directed the skills training. Strategies included information, cognitive reframing, directing to local resources, problem-solving techniques, encouragement and patient–doctor communication skills to enhance participation in care. In addition, the spouse or family support member also received weekly telephone calls (Edu, M&F) | Medical centres and community recruitment | Home based | Weekly, duration unknown | 9 weeks | Individual | Telephone | Nurse trained in the intervention | |
| Moynihan et al. 1998,77 UK | A cognitive and behavioural treatment programme, designed for cancer patients, covering current problems, coping strategies, muscle relaxation, raising self-esteem, overcoming feelings of helplessness and promoting a ‘fighting spirit’ (Edu, Psy) | Newly diagnosed hospital patients | Hospital based | 1 hour. Six sessions offered although exact number tailored per patient | ≥ 8 weeks | Individual | Face to face | Experienced cancer/mental health nurse trained in therapy techniques |
| Mueller et al. 2007,62 USA | Patients resided at a rehabilitation centre for 1 month, undertaking cycling and walking. Exercise levels were adjusted accordingly (Phy) | Consecutive referrals to rehabilitation centre | Residential rehabilitation centre | 1.5–2 hours, seven times per week | 4 weeks | Group | Face to face | N/R |
| Parker et al. 1984,63 USA | Intensive education programme covering disease process, therapies and medication, joint protection and conservation, coping with psychological stresses, and unproven treatment methods (Edu) | Hospitalised patients | Hospital based | One session for 7 hours | 7 hours | N/R | Face to face | Rheumatology patient educators |
| Parker et al. 2009,64 USA | Individual clinical psychologist sessions and stress management guides covering relaxation skills (60% of the time), problem-focused coping strategies, having realistic recovery expectations and an imagined exposure of day of surgery. Further information on cancer and the adverse effects of treatment were also provided (Edu, Psy) | Patients before prostate surgery | Hospital based | 1–1.5 hours, four sessions around surgery | < 3 weeks | Individual | Face to face | Clinical psychologist |
| Individual clinical psychologist sessions providing support to patients (Psy) | Patients before prostate surgery | Hospital based | 1–1.5 hours, four sessions around surgery | < 3 weeks | Individual | Face to face | Clinical psychologist | |
| Puente-Maestu et al. 200088 and 2003,87 Spain | Each participant was supplied with a pedometer and asked to walk 3–4 km in 1 hour, 4 days per week. Subjects were followed up and encouraged to continue with training during a maintenance phase. During this period, patients were interviewed every 3 months to reinforce compliance. Education sessions were also held on medication use and nutrition (Phy, Edu, M&F) | Respiratory physician referrals | Home based. Location of education sessions N/R | Exercise 1 hour, four times per week. Education session 0.75–4 hours, frequency N/R. Maintenance phase N/R | 56 weeks | Individual. Education sessions N/R | Face to face and remote unsupervised | Nurse and dietitian. Intervention training N/R |
| Sackett et al. 1975,83 Canada | Enhanced access to physicians through free appointments during work hours and reimbursement for 90% of prescription drug costs. Education audiotapes and booklet on hypertension, effect on organs, health, life expectancy, therapy benefits and compliance skills. Education reinforcement occurred periodically (Edu, M&F, Finance) | Recruitment from work place (Dominion Foundries) | Work and home based | N/R | N/R | Individual | Face to face | Audiotape plus ‘patient educator’ |
| Scura et al. 2004,65 USA | The programme consisted of telephone-based HCP support with structured educational components (Edu, M&F) | N/R | Home based | Weekly decreasing to monthly, duration N/R | 48 weeks | Individual | Telephone | Oncology research assistant |
| Wakefield et al. 2008,67 USA | Nurse telephone support covering patient activation and partnerships, health information, monitoring of symptoms and compliance strategies in regard to heart failure (Edu, M&F) | Recruited from larger RCT | Home based | N/R | 12 weeks | Individual | Telephone | Nurse. Intervention training N/R |
| Nurse video-telephone support covering patient activation and partnerships, health information, monitoring of symptoms and compliance strategies with regard to heart failure (Edu, M&F) | Home based | N/R | 12 weeks | Individual | Telephone | Nurse. Intervention training N/R | ||
| Weber et al. 2004,68 USA | Patients were matched with a peer (long-term survivor of prostate cancer) to provide social support following surgery for prostate cancer. Dyads were matched on race (Peer) | Post-surgery hospital patients | Coffee shop | Weekly, duration unknown | 8 weeks | Individual | Face to face | Support partner trained on discussion topics and skills |
| Weber et al. 2007,69 USA | Men were paired with support partners (survivors of prostate cancer who had undergone radical prostatectomy) and encouraged to discuss thoughts and feelings on diagnosis and sexual/urinary side effects. Discussions were held away from loved ones at a location which was suitable for private conversations (Peer) | Post-surgery patients from urology clinics | N/R | Weekly, duration unknown | 8 weeks | Individual | Face to face | Support partner trained to recognise clinical depression, communicate with active listening and record progress |
| White et al. 1986,70 USA | The programme facilitated peer interaction and support through idea sharing and advice to manage disease. Weekly serum glucose levels were posted and discussed. Education on the adverse effects of hyperglycaemic and hypoglycaemic reactions, importance of weight control and exercise was provided (Peer, Edu, M&F) | Hospital diabetic outpatient unit | Hospital based | 1 hour, weekly in first month, twice a week for second month and monthly thereafter | 24 weeks | Group | Face to face | Peers and clinical psychologist with brief training on obese diabetic patient management |
| Windsor et al. 2004,78 UK | A home-based programme of moderate intensity involving continuous walking for at least 30 minutes. All patients kept a log of activity and the exercise group was contacted to encourage adherence (Phy, M&F) | Consecutive outpatients waiting for radiotherapy | Home based | 30 minutes, ≥ 3 times per week | 4 weeks | Individual | Remote unsupervised | N/R |
Quality assessment: risk of bias
Study quality was assessed using the Cochrane risk of bias tool,92 which covers six key domains: sequence generation, allocation concealment, blinding performance, incomplete outcome data, selective outcome reporting and other sources of bias.
Studies were often poorly reported, making judgements of quality difficult. With the exception of selective outcome reporting, the most frequent rating for all domains was an unclear risk of bias. For the selective outcome-reporting domain, a low risk of bias was most frequently reported assignment. Table 4 describes the risk of bias allocation for each study by each domain. Figure 6 presents a summary of the male-only study quality assessment findings.
| Author, year, country | Sequence generation | Allocation concealment | Blinding performance | Incomplete outcome data | Selective outcome reporting | Other sources of bias |
|---|---|---|---|---|---|---|
| Adsett et al. 1989,79 Canada | Low | Low | Low | Low | High | Unclear |
| Allen et al. 1990,46 USA | Low | Unclear | High | High | High | Low |
| Bennett et al. 1991,71 UK | Unclear | Unclear | Low | Unclear | Unclear | Unclear |
| Berglund et al. 2007,89 Sweden | Low | Unclear | Unclear | Unclear | High | Unclear |
| Bosley and Allen 1989,47 USA | Unclear | Low | Unclear | High | Unclear | High |
| Bourke et al. 2011,72 UK | Unclear | Low | Low | Unclear | Low | Unclear |
| Burgio et al. 2006,48 USA | Low | Low | Unclear | Unclear | High | Unclear |
| Carmack Taylor et al. 2006,66 USA | Low | Unclear | Low | Unclear | Low | Unclear |
| Cockcroft et al. 198174 and 1982,73 UK | Low | Unclear | High | Unclear | High | Unclear |
| Culos-Reed et al. 2010,80 Canada | Unclear | Unclear | Unclear | High | High | Unclear |
| Daubenmier et al. 2006,49 USA | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Fernandez et al. 2009,84 Spain | Low | Unclear | Unclear | High | Low | Unclear |
| Gallagher et al. 1984,51 and 1987,50 USA | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Garcia-Vera et al. 199785 and 2004,86 Spain | Unclear | Unclear | Low | Low | Low | Unclear |
| Giesler et al. 2005,52 USA | Low | Unclear | Low | Unclear | Low | Unclear |
| Gifford et al. 1998,53 USA | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Gourley et al. 199854 and Solomon et al. 1998,55 USA | Low | Unclear | High | Unclear | Low | Unclear |
| Guell et al. 2000,81 Canada | Unclear | High | Low | Low | High | Unclear |
| Haynes et al. 1976,82 Canada | Low | Unclear | Low | Unclear | Unclear | Unclear |
| Heisler et al. 2010,56 USA | Unclear | Low | Low | Unclear | Low | Unclear |
| Klocek et al. 2005,90 Poland | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Koukouvou et al. 2004,91 Greece | Unclear | Unclear | Unclear | Unclear | Low | High |
| Leehey et al. 2009,57 USA | Low | Unclear | Unclear | High | Low | Unclear |
| Lepore 1999,58 USA | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Lepore et al. 2003,59 USA | Low | Low | Low | Unclear | Low | Low |
| Lucy 1994,60 USA | Unclear | Unclear | Unclear | Low | Low | High |
| McGavin et al. 197776 and 1976,75 UK | Unclear | Unclear | Unclear | High | High | Unclear |
| Mishel et al. 2002,61 USA | Low | Unclear | Unclear | Unclear | Low | High |
| Moynihan et al. 1998,77 UK | Unclear | Low | Unclear | Low | Unclear | Unclear |
| Mueller et al. 2007,62 USA | Low | Unclear | Unclear | Unclear | Low | Unclear |
| Parker et al. 1984,63 USA | Low | Unclear | Unclear | High | Unclear | Unclear |
| Parker et al. 2009,64 USA | Low | Unclear | Low | Unclear | Unclear | Unclear |
| Puente-Maestu et al. 200088 and 2003,87 Spain | Low | Unclear | Low | Unclear | Low | Unclear |
| Sackett et al. 1975,83 Canada | Low | Unclear | Low | Unclear | High | High |
| Scura et al. 2004,65 USA | Unclear | Unclear | Unclear | Unclear | High | High |
| Wakefield et al. 2008,67 USA | Unclear | Unclear | Unclear | Unclear | Unclear | High |
| Weber et al. 2004,68 USA | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Weber et al. 2007,69 USA | Unclear | Unclear | Unclear | Unclear | High | Unclear |
| White et al. 1986,70 USA | Low | Unclear | Unclear | Unclear | Low | Unclear |
| Windsor et al. 2004,78 UK | Unclear | Low | Unclear | Low | Low | Low |
FIGURE 6.
Summary of male-only study Cochrane risk of bias findings.
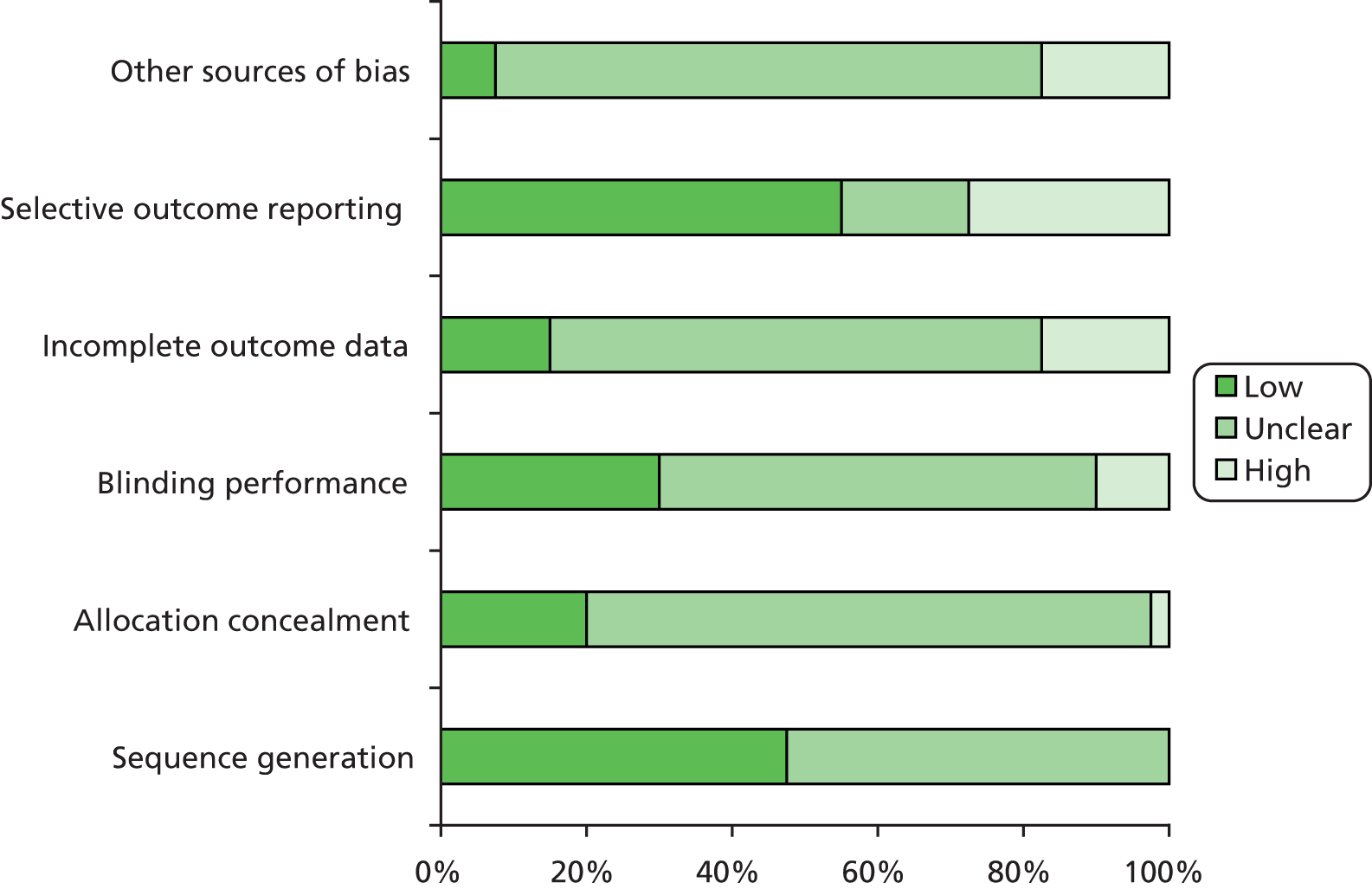
Chapter 3 Qualitative review methods
The objective of the qualitative metaethnography was to systematically identify experiences of, and perceptions of, interventions or specific activities aimed at supporting or promoting self-management of LTCs among men of differing age, ethnicity and socioeconomic background.
A summary of the methods used in the metaethnography is provided in Appendix 3, using the enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) reporting standards for qualitative evidence synthesis, developed by Tong et al. 93
The evidence synthesis was conducted using a metaethnography approach originally described by Noblit and Hare. 94 This approach was chosen because of its emphasis on conceptual development and generating new insights (i.e. being interpretive rather than integrative94) and because it is compatible with synthesising all types of qualitative research. 95
Metaethnography involves seven stages: getting started, deciding what is relevant, reading the studies, determining how studies are related to each other, translating studies into each other, synthesising translations and expressing the synthesis;94 these seven, often overlapping, stages are depicted in Figure 7.
FIGURE 7.
Seven steps of metaethnography.
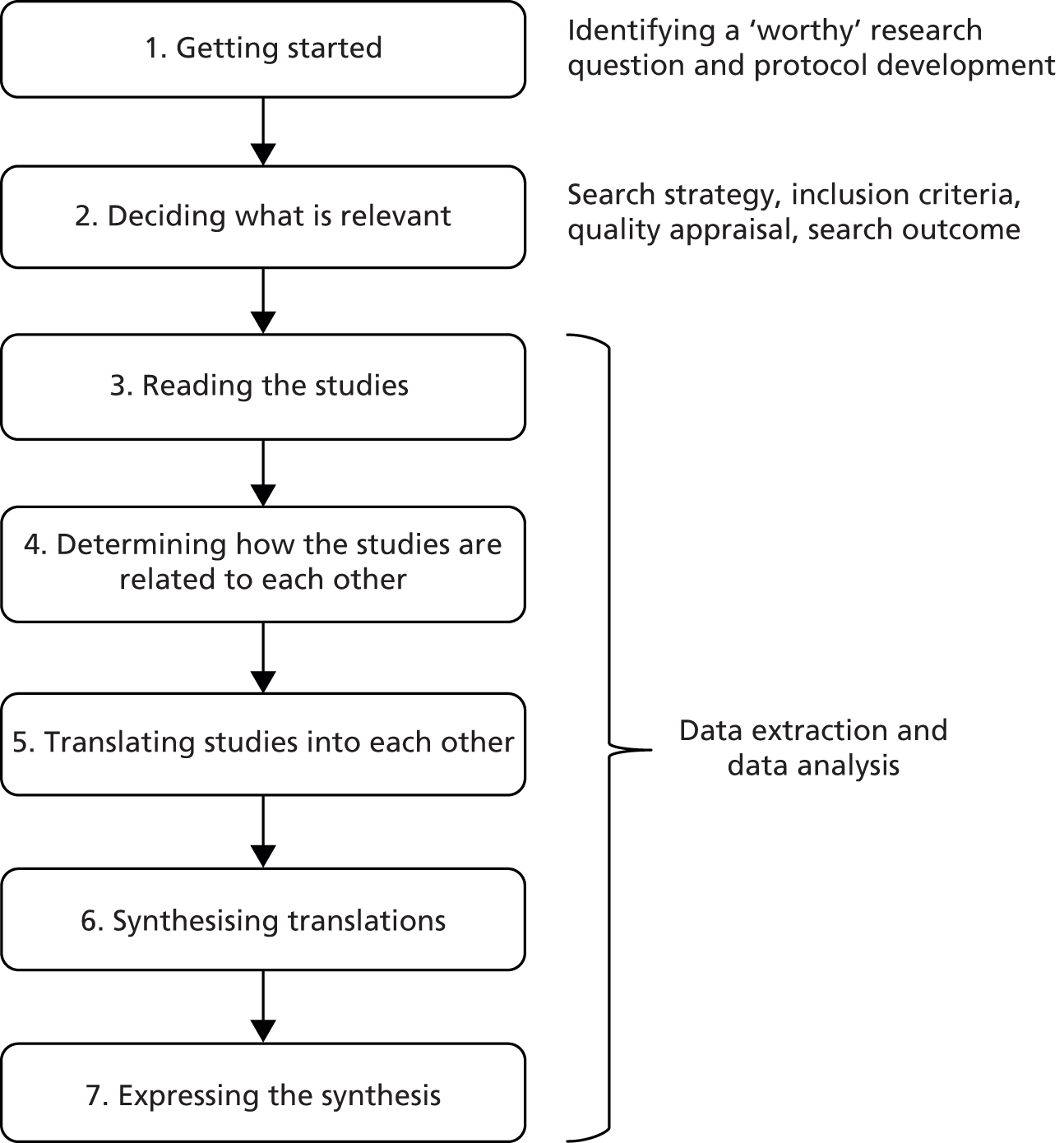
Step 1: getting started
The first stage involved identifying a ‘worthy’ research question and one that could be addressed through qualitative evidence synthesis. 94 This stage took place in developing the original funding application for the current review and its justification is presented in Chapter 1.
Step 2: deciding what is relevant
The second stage, ‘deciding what is relevant’, was viewed as comprising the search strategy, inclusion criteria and quality appraisal, consistent with the experiences of Atkins et al. 96 These are presented next, before steps 3–7 are described in the section Data extraction strategy and data analysis.
Search methods
Search strategy
A comprehensive electronic search strategy (Appendix 4) was developed in liaison with information specialists. It sought to identify all available studies, rather than using purposive sampling to identify all available concepts. Five electronic databases were searched in July 2013 [Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, MEDLINE, PsycINFO and Social Science Citation Index].
Because of challenges with methodological indexing of qualitative research,97 the electronic search was complemented by checking reference lists, and using an adapted strategy published elsewhere98 that includes ‘thesaurus terms’ (keywords indexed in electronic databases, e.g. ‘Qualitative Research’), ‘free text terms’ (commonly used research methodology terms searched for in the titles, abstracts and keywords) and ‘broad-based terms’ (i.e. the broad free-text terms ‘qualitative’, ‘findings’ and ‘interview$’ and the thesaurus term ‘Interviews’). Terms relating to gender were combined with other terms to narrow the search and increase the precision of the strategy (e.g. ‘men’, ‘male’, ‘masculine$’, ‘gender’, ‘sex difference$’, ‘sex factors’).
Study selection: study screening methods and inclusion criteria
Records were initially screened by one reviewer (ZD) on the basis of the title and abstract. Decisions were recorded in EndNote X7.0.2 (Thomson Reuters, CA, USA), a reference management database. All articles identified as potentially eligible for inclusion were obtained in full. Attempts were made to identify and obtain published findings for unpublished literature that was otherwise eligible, for example doctoral theses or conference proceedings.
The full-text literature was screened independently by two reviewers (ZD and PG) using the inclusion criteria listed in Table 5. Studies that explored the experiences of men alone, or included a clear and explicit comparison between men and women, were included. Studies which focused on self-management experiences of people with LTCs more generally (i.e. did not consider experiences of, or perceptions of, a self-management support intervention or activity) were excluded. The approach to screening was inclusive; for example, studies where the qualitative findings were limited (e.g. Iredale et al. ,99 Ramachandra et al. ,100 Smith et al. 101) and mixed-sex studies with limited findings on gender comparisons (e.g. Barlow et al. 102,103) were retained in case they contributed to the synthesis.
| Question | Answer |
|---|---|
| Does the study present qualitative data?a | Yes/no |
| Are the participants identified as having long-term conditions (LTCs)?b | Yes/no |
| Were data collected in relation to self-management support activities and interventions rather than, for example, the lived experience of a LTC?c | Yes/no |
| Is the sample either male only or mixed (with explicit comparison by gender)? | Yes/no |
| Is the sample composed of adults (or predominantly adult)? | Yes/no |
| Is the paper dated 1970 or later?d | Yes/no |
| Is the paper published and peer-reviewed in an academic journal? | Yes/no |
| Is the paper written in English? | Yes/no |
Classification of self-management interventions and support activities in the qualitative evidence synthesis
The original study protocol sought to code self-management interventions and support activities using the most up-to-date version of the taxonomy of BCT. 104–106 As in the quantitative review (see Chapter 2, Coding interventions for analysis), we found that the level of detail reported on self-management interventions or activities in the qualitative literature was limited in detail, precision and consistency, making coding with the BCT taxonomy unfeasible.
Most of the qualitative literature did not focus on behaviour change per se or seek to address men’s views and experiences of behaviour change techniques; for example, some papers were concerned with the dynamics of social support groups, or the use of other self-management support and information. The BCT taxonomy is applicable to only studies that are judged as targeting behaviour change; we were therefore limited to ‘lifestyle’ and ‘psychological’ studies. Only a minority of the studies (n = 13) provided sufficient information on interventions to allow even rudimentary coding with the BCT taxonomy, and these are presented in Appendix 5. Issues around application of the BCT taxonomy are returned to in the discussion chapter (see Chapter 6).
The lack of detail reported in the qualitative literature also made it unfeasible to classify interventions using the system developed for the quantitative review. Whereas the quantitative review concerned trials of specific interventions, approximately half of the studies in the qualitative review99,101,107–130 included more than one intervention or activity (e.g. ‘any cancer support group’).
We therefore developed a broad system for classifying interventions and support activities that offered a pragmatic way to group studies and make the analysis process more manageable. The categories are shown in Table 6.
| Self-management category | Description |
|---|---|
| Face-to-face support group | Any face-to-face support group. This could include peer- or professional-led groups and groups that were time-limited or rolling in nature. These groups usually involved sharing of personal information and experiences, sometimes including lectures and question-and-answer sessions. Groups classified here did not include activities such as physical activity or practising stress management techniques |
| Internet information and/or support | Any internet-based support activity, involving support through forums and discussion boards and/or information, through either boards or searching websites |
| Information (including online) | Any use of information, regardless of source |
| Psychological | Any intervention or activity with a clear psychological component (e.g. professional counselling) and/or described by the authors as psychological |
| Lifestyle | Any intervention or activity that includes components of training and/or education which seeks to address behaviour change (e.g. physical activity, diet, medication taking) |
| Various | Any combination of activities (e.g. any self-management services; counselling and peer support) |
Quality assessment strategy
The purpose of quality appraisal in the review was to provide descriptive information on the quality of the included studies rather than as a basis for inclusion. We considered that studies of weaker quality either would not contribute or would contribute only minimally to the final synthesis. 94,131 We therefore chose not to use design-specific appraisal tools (which the original protocol stated we would) because we placed emphasis on conceptual contribution, which did not require a detailed design-specific appraisal of methodological quality. With that in mind, we used the Critical Appraisal Skills Programme (CASP) tool. 132
The CASP tool comprises 10 checklist-style questions (see Appendix 6) for assessing the quality of various domains (including aims, design, methods, data analysis, interpretation, findings and value of the research). Because of the checklist nature of the CASP tool, we developed some additional questions informed by other metaethnography studies96,131 that enabled us to extract and record more detailed narrative summaries of the main strengths, limitations and concerns of each study (see Appendix 7).
The CASP tool was used in the light of the experiences reported by other researchers who recommended that, despite rather low inter-rater agreement, such an approach ‘encourag[es] the reviewers to read the papers carefully and systematically, and serves as a reminder to treat the papers as data for the synthesis’ (p. 44). 131
Its focus is on procedural aspects of the conduct of the research rather than the insights offered. 133 The quality appraisal (which focused on methodological quality) did not form part of the inclusion criteria because, as recognised by Campbell et al. ,131 it is conceptual quality that is most important for evidence synthesis and it is the process of synthesis that judges the ‘worth’ of studies, with conceptually limited studies making a limited contribution. 94 Additionally, it is acknowledged that agreement is often slight, with low reproducibility. 131,133 Appraisal was conducted by two reviewers independently (ZD and PG), with discrepancies resolved through discussion.
Search outcome
The electronic search strategy identified 6330 unique references. Screening based on title and abstract identified 149 papers for full-text screening. Dual screening of these full-text articles identified 34 studies (reported in 38 papers) to be included in the review. Reasons for excluding the remaining 111 articles are shown in Table 7.
| Reason | n | ||||
|---|---|---|---|---|---|
| Not LTC | Not self-management intervention/support activity | Not male only/explicit gender comparison | Not qualitative data collection and analysis | ||
| ✗ | ✗ | 1 | |||
| ✗ | 53 | ||||
| ✗ | ✗ | 30 | |||
| ✗ | ✗ | 3 | |||
| ✗ | ✗ | ✗ | 2 | ||
| ✗ | 9 | ||||
| ✗ | ✗ | 4 | |||
| ✗ | 9 | ||||
| Totals | 1 | 89 | 45 | 18 | 111 |
Inter-rater agreement on the decision to include was 88.6%. The majority of disagreements (n = 17) concerned the definition of self-management intervention or activity. Having discussed the 17 disagreements, we agreed that five studies on which there was disagreement would be included. 100,103,110,116,134
An additional four studies were identified through reference checks and efforts to locate published literature linked to unpublished work identified through the electronic search. 111,112,135,136 An additional two papers (women only), although individually ineligible, were located as ‘linked papers’ for two of the original 34 studies,114,120 giving a total of 38 studies (reported in 44 papers), as shown in Figure 8.
FIGURE 8.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for the qualitative review.
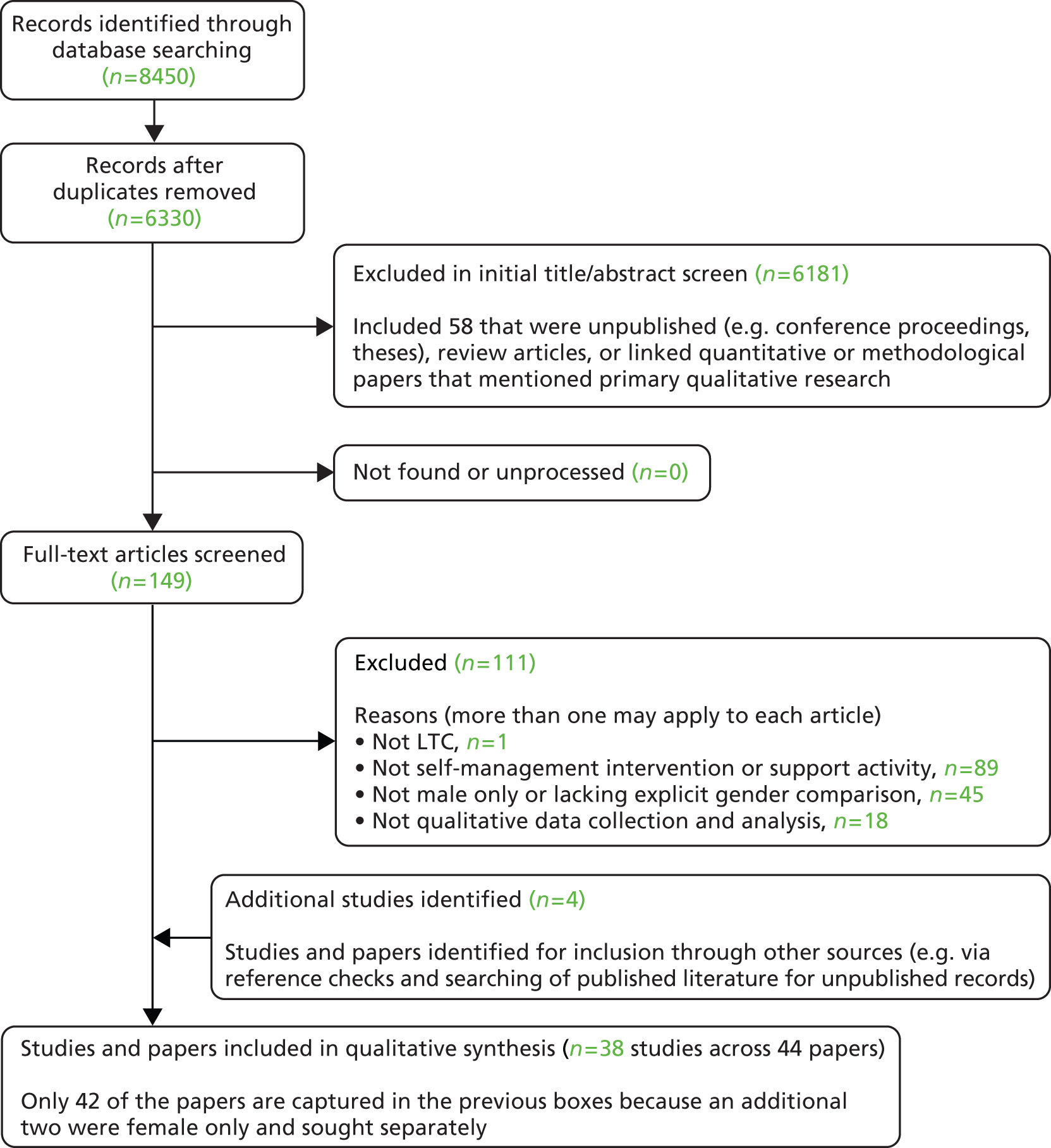
Data extraction strategy and data analysis
The lead reviewer (ZD) extracted all papers using data extraction forms previously tested and refined through a pilot study of four papers. All study details (including aim, participant details, methodology, method of data collection and analysis) were extracted into Microsoft Excel® version 14 (Microsoft Corporation, Redmond, WA, USA) and checked by a second reviewer (PG). Extraction and analysis of study findings was undertaken by a group of coreviewers within the research team (ZD, PG, LK, CB, KM, KH) and followed steps 3–7 of the metaethnography process described by Noblit and Hare. 94 Despite being numbered sequentially, these phases do not occur in a linear process. 94
Step 3: reading the studies
The metaethnography process involved three levels of constructs, as described by Schutz137 and operationalised by Atkins et al. :96
-
first-order: participant quotes and participant observations, while recognising that in secondary analysis these represent the participants’ views as selected by the study authors in evidencing their second-order constructs
-
second-order: study authors’ themes/concepts and interpretations, also described by Noblit and Hare94 as ‘metaphors’
-
third-order: our ‘interpretations of interpretations of interpretations’ (p. 35),94 based on our analysis of the first-order and second-order constructs extracted from the studies.
Each paper was read in full and copied verbatim into NVivo version 10 (QSR International, Warrington, UK) for line-by-line coding by the lead reviewer. Coding involved repeated reading and line-by-line categorising of first-order and second-order constructs, using participants’ and authors’ words wherever possible, and reading for possible third-order constructs.
Third-order constructs were developed by building second-order constructs into broader categories and themes in a framework which was revised iteratively using the hierarchical functions of the NVivo software (i.e. using ‘parent’ and ‘child’ nodes).
Rather than simply being a synthesis of the second-order constructs, third-order-constructs were derived inductively from the extracted data; this was an interpretive process that was not limited to interpretations offered by the original authors of included studies.
Coding by coreviewers (i.e. other members of the research team) was idiosyncratic but commonly involved working with printed papers, noting key ‘metaphors’ (themes, concepts and ideas) in the margins and highlighting first-order and second-order evidence that supported the coreviewers’ interpretations. The lead reviewer, ZD, met with each coreviewer to discuss/debrief coding decisions and ensure the credibility (i.e. the congruence of coding decisions with the original author interpretations) of the overall analytical process.
Step 4: determining how the studies are related
To offer a ‘way in’ to the synthesis, we adopted a similar approach to that of Campbell et al. :131 initially grouping studies by the broad categories of self-management intervention and support activity shown in Table 6. Each coreviewer was allocated one or more category of studies to analyse. The lead reviewer then read each category of studies in the following order: face-to-face group support, online support, online information, information, psychological, lifestyle and ‘various’; within this, she read the studies in alphabetical order of first author rather than nominating ‘key’ papers. All included papers were analysed, rather than reading until saturation of concepts.
The lead reviewer and coreviewer independently completed matrices to report the second-order constructs and emerging third-order constructs for each paper (which for the lead reviewer were based on a more comprehensive line-by-line coding using NVivo). This facilitated the juxtaposing of metaphors and/or constructs alongside each other, leading to initial assumptions about relationships between studies.
Step 5: translating studies into one another
A defining element of metaethnography is the ‘translation’ of studies into each other, whereby metaphors, together with their inter-relationships, are compared across studies. Facilitated by discussions using the matrices of second- and third-order constructs, we translated studies firstly within types of support activity and then, secondly, across types.
The lead reviewer initially developed the constructs in relation to face-to-face support (the largest category of studies) and read other categories of studies with reference to this, using a constant comparison approach to identify and refine concepts. The ‘models’ function in NVivo was used to depict relationships between third-order constructs; this helped to develop the line-of-argument synthesis, which is discussed next.
Step 6: synthesising translations
Studies can be synthesised in three ways:94
-
reciprocal translation, where the findings are directly comparable
-
refutational translation, where the findings are in opposition
-
a line-of-argument synthesis, where both similarities and contradictions are found and translations are encompassed in one overarching interpretation that aims to discover a whole among the set of parts, uncovering aspects that may be hidden in individual studies.
Because we found similarities and contradictions, we developed a line-of-argument synthesis (rather than reciprocal or refutational translation) that encompassed four key concepts, each of which was based around a set of third-order constructs.
Step 7: expressing the synthesis
The output of the synthesis, that is communicating our third-order concepts and overarching line-of-argument synthesis, is described by Noblit and Hare94 as ‘expressing the synthesis’ (p. 29). They state that ‘the worth of any synthesis is in its comprehensibility to some audience’ (p. 82),94 emphasising the importance of communicating the synthesis effectively, being mindful of the intended audience and using concepts and language that are meaningful (and understandable). We worked to make the synthesis comprehensible by discussion with coreviewers and, critically, through involvement of the patient and public involvement (PPI) group. The synthesis is presented in Chapter 5 and will also be expressed through other dissemination activities, for example the SELF-MAN symposium (www.self-man.com), mini-manuals and journal publications.
Rigour
We undertook several steps to enhance the rigour of our analysis. Authors’ themes and interpretations (second-order constructs) were independently extracted by two reviewers, each of whom additionally suggested their own interpretations of the study findings (third-order constructs).
We were influenced by a recent Health Technology Assessment metaethnography which found multiple reviewers offered ‘broad similarities in interpretation, but differences of detail’ (p. x). 131 We therefore treated the lead reviewer’s analyses as the ‘master copy’ and compared these with the coreviewers’ extractions and interpretations. Peer debriefing meetings were held between the lead reviewer and each coreviewer to discuss matrices of second-order and third-order constructs which facilitated the consideration of alternative interpretations.
The third-order constructs and line-of-argument synthesis were further refined at a full-day meeting (January 2014) attended by the lead qualitative reviewer and wider team of five coreviewers involved in coding, extraction, analysis and interpretation (PG, KH, LK, KM, CB).
We identified the need to be reflexive about our interpretations and recognised potential sources of influence on our interpretations; for example, two reviewers (PG, KH) identified having a ‘constructions of masculinity’ lens, and we agreed to focus the line-of-argument synthesis on interpretations offered by authors of studies being synthesised, rather than framing our interpretations around constructions of masculinity. We considered it a strength that the six reviewers involved reflected a wide range of backgrounds and perspectives. Although PPI colleagues were not involved in the coding process, the line-of-argument synthesis and four key concepts were discussed with the PPI group to ensure credibility.
Public and patient involvement
The SELF-MAN research team worked with a specially constituted public and patient advisory group comprising men living with one or more LTCs who were involved in either running or attending a LTC support group in the north of England. Members were recruited via the research team’s existing networks. Stakeholders’ support groups were all condition-specific – arthritis (n = 1), diabetes (n = 1), heart failure (n = 2) and Parkinson’s disease (n = 1) – although some men lived with multiple LTCs. All stakeholders attended a welcome meeting prior to the commencement of the study to prepare them for the involvement in the research, and were provided with ongoing support and guidance by the chief investigator throughout the research process. Members were reimbursed for travel, expenses and time throughout the duration of the project (in line with current INVOLVE recommendations138).
The overarching aims of PPI in the project were, first, to help ensure that the review findings spoke to the self-management needs and priorities of men with LTCs, and, second, to ensure the development of appropriate outputs that would have benefit and relevance for service users. A recognised limitation of our group was that stakeholder representation was drawn from face-to-face group-based support interventions.
The stakeholder group met on three half-days over the course of the 12-month project. On each occasion, the group provided positive affirmation that the project was being conducted in accordance with its stated objectives. In the first two meetings, the group offered feedback and advice to the investigative team on preliminary and emerging analysis of the qualitative data throughout the research process: specifically, the development of third-order constructs and the line-of-argument synthesis. Responding to their input, we made revisions to some of our interpretations, particularly in relation to the importance of physical aspects of environments in which interventions took place. The group’s input also highlighted the need for future research to address depression as a common and often overlooked comorbidity in men (see Chapter 7, Recommendations for future research), and that they welcomed recommendations for sustainability of support groups and improving communication within groups. When considering the key outcomes to be assessed in the quantitative review, stakeholders also recommended that emphasis should be placed on quality-of-life outcome measures when considering whether or not a self-management support intervention is effective.
In the final meeting, the stakeholder group provided detailed recommendations for the content of the Self-Manual: Man’s Guide to Better Self-Management of Long Term Conditions (not yet available). It advised that the guide should be rephrased from ‘how to’ self-manage to ‘how to better’ self-manage because men may view themselves as already self-managing and therefore not identify with the former.
Six or seven stakeholders attended each meeting. The female partner of one of the men attended and contributed to discussions at each meeting. Members of the group each received reimbursement of travel expenses and a £150 honorarium for each meeting they attended. In the final meeting, the stakeholders provided feedback on their involvement in the research process overall, focusing on what was done well and what could be improved. Feedback indicated that most stakeholders had a positive experience, particularly valuing the opportunity to have their ‘voices heard’ and make a potential impact on future service delivery. Recommendations for improvements mostly centred on ensuring prompt reimbursement of expenses incurred in attending the meetings.
Chapter 4 Results from quantitative review
Summary of analytical approach
We used four analytical strategies to evaluate the effectiveness of self-management support interventions in men, described in detail in Chapter 2 (see Data analysis). Included male-only studies which did not contribute to the meta-analysis (i.e. non-extractable data, no comparative outcomes, etc.) are presented in Appendix 8.
Summaries of each of the four analytical strategies are provided below.
Analysis 1: ‘within-Cochrane review analysis’
We screened all included Cochrane reviews of self-management support interventions (n = 116) to identify those that contained analysis on outcomes of interest and at least two relevant male-only RCTs. Where an eligible review was identified that met this criterion (n = 4),41–44 the data were pooled into male-only, mixed-sex and female-only groups. This allowed us to determine whether males show larger, similar or smaller effects than females and mixed-sex groups within interventions included in the ‘parent’ Cochrane review (all other things being equal). The forest plot in Figure 9 presents an example of analysis showing the effect of exercise-based interventions in HRQoL outcomes in male-only trials compared with mixed-sex trials, taken from the analysis of the Cochrane review by Davies et al. 146
FIGURE 9.
Example forest plot of ‘within-Cochrane review analysis’. Different intervention groups within the Klocek 2005 study are referred to by ‘a’ and ‘b’. df, degrees of freedom; IV, inverse variance.
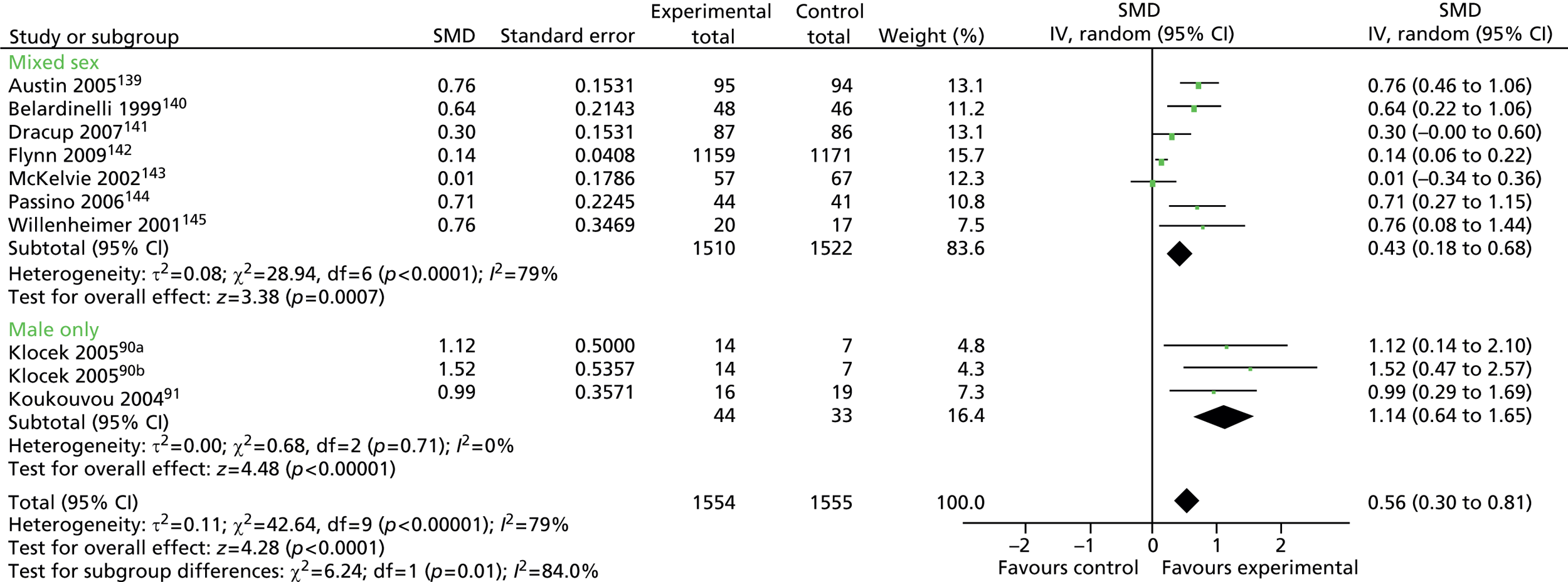
Analysis 2: ‘across-Cochrane review analysis’
To expand on analysis 1, studies with mixed-sex samples (n = 17)147–162 and female-only samples (n = 14)163–177 were identified from ‘parent’ Cochrane reviews that contained the male-only studies. Data were pooled according to broad intervention type rather than using the ‘by review’ approach taken in analysis 1.
This allowed us to determine whether broad types/components of self-management support interventions show larger, similar or smaller effects in men than in women and mixed populations. Limitations in the data meant we were able to conduct analyses on only physical activity, education, peer support, and HCP monitoring and feedback interventions. The forest plot in Figure 10 is an example of analysis showing the effect of physical activity interventions on HRQoL outcomes in male-only, mixed-sex and female-only groups.
FIGURE 10.
Example forest plot ‘by intervention-type analysis in men, women and mixed-sex groups’. df, degrees of freedom; IV, inverse variance; SD, standard deviation.

Analysis 3: ‘male only by intervention-type analysis’
We conducted a meta-analysis on trials with males only, according to broad intervention type – physical activity, education, peer support, and HCP monitoring and feedback – and compared effects between intervention types. This allowed us to determine whether or not certain broad categories of self-management support intervention were more effective in men. The forest plot in Figure 11 is an example of analysis showing the effect on HRQoL outcomes of interventions with a physical activity component compared with interventions without a physical activity component in male-only trials.
FIGURE 11.
Example forest plot of ‘male only by intervention-type analysis’. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
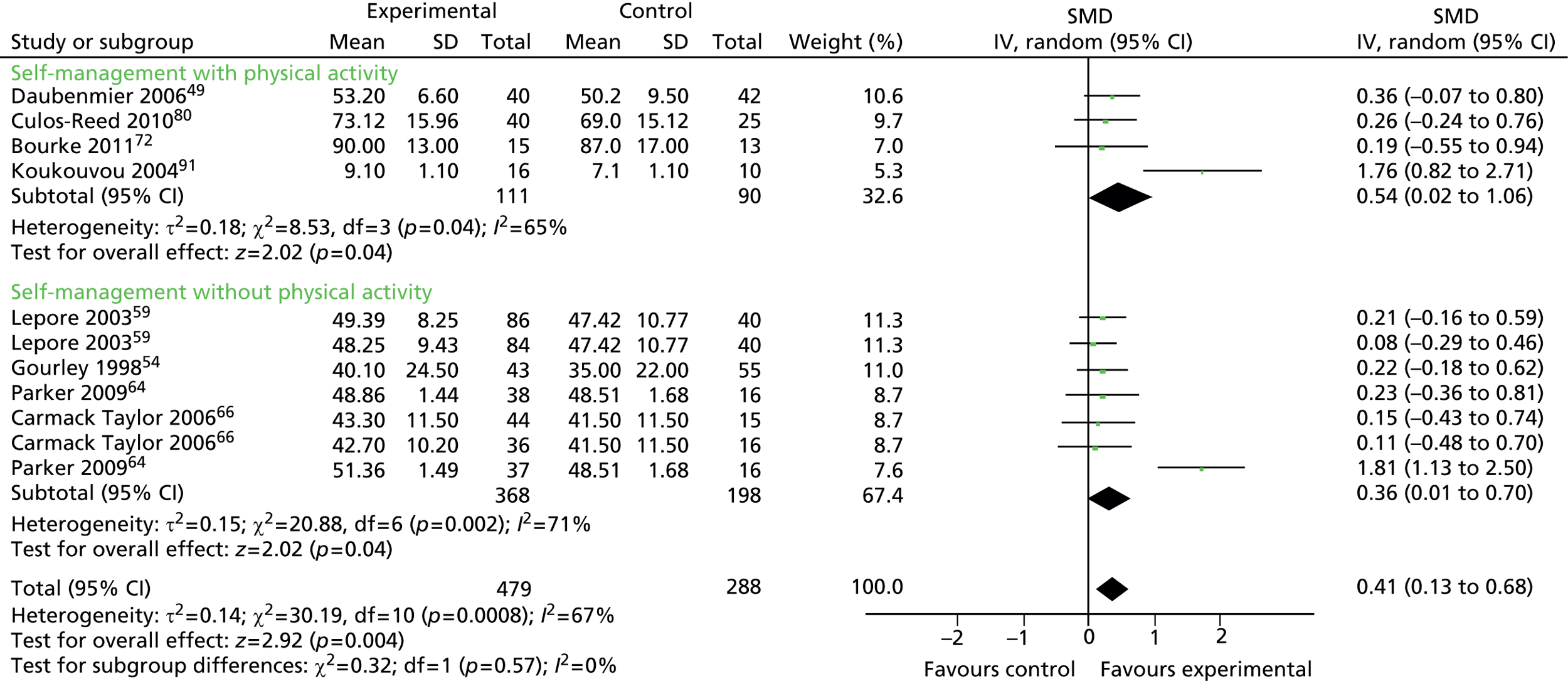
Analysis 4: ‘within-trial gender group analysis’
We identified RCTs which analysed the effects of self-management support interventions in gender groups. We sought to extract relevant data on the direction and size of moderating effects in secondary analysis (i.e. whether males show larger, similar or smaller effects than females), and assess these effects in the context of relevant design data, such as sample size, and the quality of the secondary analysis.
Results from analysis 1: ‘within-Cochrane review analysis’
We identified four Cochrane reviews of self-management support interventions41–44 that met criteria for analysis (i.e. that contained analysis on outcomes of interest and at least two relevant male-only RCTs within an analysis). These reviews were used to determine if, within a group of interventions included in a single Cochrane review, RCTs in male-only samples demonstrate different effect sizes from RCTs in mixed-sex and female-only samples.
Exercise based rehabilitation for heart failure: Davies et al. (2010)146
Selection criteria
Randomised controlled trials of exercise-based interventions with six months follow up or longer compared to usual medical care or placebo. The study population comprised adults of all ages (> 18 years) with evidence of chronic systolic heart failure.
Davies et al. 146
Analysis conducted
Given the limited number of male-only studies, we were able to conduct an analysis for only HRQoL (all scales).
Health-related quality of life (all scales)
The original Cochrane review analysis on HRQoL (all scales) contained nine studies: two male-only trials (considering three different exercise interventions) and seven mixed-sex studies (including seven different exercise interventions).
In terms of the comparability of trials across samples, allocation concealment was predominantly unclear in both groups. The mean age across male-only studies (54.3 years) was slightly younger than in the mixed-sex studies (61.5 years), and heart failure severity varied across studies [New York Heart Association (NYHA) I–IV], which may have introduced some clinical heterogeneity.
Table 8 reports the effect sizes for RCTs with different gender composition. Across all samples, significant positive effects on HRQoL were identified for exercise-based rehabilitation interventions [SMD 0.56 (95% CI 0.30 to 0.81), p < 0.001, I2 = 79%]. Significant effects were identified in both male-only and mixed-sex groups, with ‘large’ effects in the male-only group (SMD 1.14, 95% CI 0.64 to 1.65; p = 0.71; I2 = 0%) in comparison with the overall and mixed-sex groups, which achieved ‘moderate’ effect sizes. A test for group differences identified statistically significant differences between groups (p = 0.01), indicating that the intervention effect appears to be greater in RCTs in male participants.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | 1.14 (0.64 to 1.65) | Low |
| Mixed sex (n = 7) | 0.43 (0.18 to 0.68) | High |
Exercise interventions on health-related quality of life for people with cancer during active treatment: Mishra et al. (2012)42
Selection criteria
We included all randomized controlled trials (RCTs) and quasi-randomized controlled clinical trials (CCTs) comparing exercise interventions with usual care or other type of non-exercise comparison intervention to maintain or enhance, or both, overall HRQoL or at least one distinct domain of HRQoL. Included trials tested exercise interventions that were initiated when adults with cancer were undergoing active cancer treatment or were scheduled to initiate treatment.
Mishra et al. 42
Analysis conducted
Given the limited number of male-only studies, we were able to conduct an analysis for only HRQoL (all scales) and fatigue.
Health-related quality of life (all scales, follow-up closest to 6 months) and fatigue
The original Cochrane review analysis on HRQoL contained 27 studies: five male only, seven mixed sex and 14 female only. Three male-only studies were removed from the analysis because they did not meet our inclusion criteria, leaving a total of 24 studies in the analysis.
In terms of the comparability of trials across samples, allocation concealment was predominantly unclear in all groups. The mean age across male-only studies (69.2 years) was much greater than mixed-sex (50.8 years) and female-only studies (46.2 years). Additionally, type and severity of cancer varied greatly across studies, which may account for some clinical heterogeneity.
Table 9 reports the effect sizes for each group. Overall, significant positive effects on HRQoL were identified for exercise-based interventions (SMD 0.26, 95% CI 0.06 to 0.45; p < 0.001; I2 = 68%). The magnitude of effect was very similar in male-only, mixed-sex and female-only samples, although none of these analyses reached statistical significance.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | 0.25 (–0.10 to 0.60) | Low |
| Mixed sex (n = 7) | 0.23 (–0.00 to 0.46) | Low |
| Female only (n = 14) | 0.25 (–0.04 to 0.54) | High |
Fatigue
The original Cochrane review analysis on fatigue contained 28 studies: seven male-only, eight mixed-sex and 13 female-only studies reporting on fatigue outcomes. Four male-only studies were removed from the analysis because they did not meet our inclusion criteria, leaving a total of 24 studies in the analysis.
In terms of the comparability of trials across samples, allocation concealment was predominantly unclear in the mixed-sex and female-only groups and low in the male-only group. One study in the mixed-sex group had a high risk of allocation bias. 161 The mean age across male-only studies (68.9 years) was much greater than across mixed-sex (47.5 years) and female-only studies (50.9 years). Additionally, type and severity of cancer varied greatly across studies, which may account for some clinical heterogeneity.
Table 10 reports the effect sizes for each group. Overall, significant positive effects on fatigue outcomes were found in favour of exercise-based interventions (SMD –0.22, 95% CI –0.35 to –0.08; p = 0.02; I2 = 42%). The magnitude of effect was very similar in male-only, mixed-sex and female-only samples, although in only the female-only group did it reach statistical significance.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 3) | –0.18 (–0.45 to 0.09) | Low |
| Mixed sex (n = 8) | –0.21 (–0.45 to 0.02) | Low |
| Female only (n = 13) | –0.23 (–0.44 to –0.02) | Moderate |
Relaxation therapies for the management of primary hypertension in adults: Dickinson et al. (2008)44
Selection criteria
RCTs of a parallel design comparing relaxation therapies with no active treatment, or sham therapy; follow-up 8 weeks; participants over 18 years, with raised systolic blood pressure (SBP) 140 mmHg or diastolic blood pressure (DBP) 85 mmHg; SBP and DBP reported at end of follow-up. 44
Analysis conducted
Given the limited number of male-only studies, we were able to conduct an analysis comparing only gender groups for systolic and diastolic blood pressure (SBP and DBP; < 6 months’ follow-up) outcomes.
Systolic and diastolic blood pressure (< 6 months’ follow-up)
The original Cochrane review analysis on SBP and DBP contained 13 studies: three male-only and 10 mixed-sex studies. One of the male-only studies (Carson 1998, as cited by Dickinson et al. 200844) was removed because it did not meet our inclusion criteria, leaving a total of 12 studies in the analysis.
In terms of the comparability of trials across samples, allocation concealment bias, age and diagnosis did not appear to vary across studies, so they do not appear to account for the high degree of heterogeneity. Male only: allocation concealment all unclear, mean age 46.0 years, majority diagnosis essential hypertension. Mixed sex: allocation concealment all unclear, mean age 47.1 years, majority diagnosis essential hypertension.
Table 11 reports the effect sizes for each group. Overall, SBP and DBP were statistically significantly reduced by relaxation therapies: SMD –0.48 (95% CI –0.79 to –0.16; p < 0.001; I2 = 65%); and SMD –0.52 (95% CI –0.87 to –0.17; p < 0.001; I2 = 72%), respectively. Analysis by male-only and mixed-sex groups found a similar magnitude of effects on SBP but larger effects in male-only studies in DBP (SMD –0.69, 95% CI –0.89 to –0.09; p < 0.001; I2 = 73%), although statistically significant effects were evident in only the mixed-sex group.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | ||
| SBP | –0.45 (–1.20 to 0.30) | Moderate |
| DBP | –0.69 (–1.66 to 0.27) | High |
| Mixed sex (n = 10) | ||
| SBP | –0.49 (–0.85 to –0.12) | Moderate |
| DBP | –0.49 (–0.89 to –0.09) | High |
Integrated disease management interventions for patients with chronic obstructive pulmonary disease: Kruis et al. (2013)43
Selection criteria
Randomized controlled trials evaluating IDM [integrated disease management] programs for COPD compared with controls were included. Included interventions consisted of multidisciplinary (two or more health care providers) and multi-treatment (two or more components) IDM programs with a duration of at least 3 months.
Analysis conducted
Given the limited number of male-only studies, we were able to conduct an analysis comparing only gender groups for 6-minute walking distance (6MWD) and forced expiratory volume (FEV; % predicted) outcomes.
Six-minute walking distance (short-term)
The original Cochrane review analysis on 6MWD contained 14 studies: two male-only and 12 mixed-sex studies.
In terms of the comparability of trials across samples, allocation concealment was predominantly low across studies, but one study in the male-only group (Guell et al. 2000,81 as cited by Kruis et al. 201343) and three studies in the mixed-sex group (Engstrom 1999,178 Guell et al. 2006,179 Mendes 2010,180 as cited by Kruis et al. 201343) were allocated a high risk of bias, which may have distorted findings. The mean age across male-only studies (66.0 years) was similar to the mixed-sex group (67.1 years). Disease severity was inconsistently reported and could not be summarised.
Table 12 reports the effect sizes for each group. 6MWD is presented as mean difference (MD). Overall, significant positive effects on 6MWD were identified for integrated disease management interventions, with an improvement of 43 m (MD 43.86, 95% CI 21.83 to 65.89; p < 0.001; I2 = 79%). Group analysis found that statistically significant effects on 6MWD were evident in both groups: male only and mixed sex. The effects were more substantive in the male-only group (MD 69.06, 95% CI 43.69 to 94.43; p = 0.90; I2 = 0%) than the overall effect and mixed-sex group, although the test for group differences identified no significant differences between groups (p = 0.10).
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | 69.06 (43.69 to 94.43) | Low |
| Mixed sex (n = 12) | 39.7 (15.50 to 64.08) | High |
Forced expiratory volume in 1 second (% predicted) short-term
The original Cochrane review analysis on FEV in 1 second (FEV1) contained four studies: two male-only and two mixed-sex studies reporting.
In terms of the comparability of trials across samples, allocation concealment was predominantly low, but one study in the male-only group (Guell et al. 2000,81 as cited by Kruis et al. 201343) was allocated a high risk of bias. The mean age across male-only studies (66.0 years) was similar to the mixed-sex group (69.0 years).
Table 13 reports the effect sizes for each group. Overall, no significant effects on FEV1 were identified for integrated disease management interventions (SMD –0.05, 95% CI –0.30 to 0.20; p = 0.35; I2 = 9%), or in either sex group. A trend in favour of the control group was observed for the male-only group, while the mixed-sex group showed a marginal effect in favour of the intervention.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | –0.34 (–0.74 to 0.06) | Low |
| Mixed sex (n = 2) | 0.11 (–0.18 to 0.41) | Low |
Analysis 1: summary of key findings
Table 14 presents a summary of the main findings of analysis 1.
| Review | Outcome | Significant effecta | Gender group differences |
|---|---|---|---|
| Davies et al.: exercise rehab | Overall HRQoL | ✓ | |
| Male HRQoL | ✓ | Significant difference between groups: greater effect in males | |
| Mixed-sex HRQoL | ✓ | ||
| Mishra et al.: exercise interventions | Overall HRQoL | ✓ | N/A |
| Male HRQoL | ✗ | N/A | |
| Mixed-sex HRQoL | ✗ | ||
| Women HRQoL | ✗ | ||
| Overall fatigue | ✓ | ||
| Male fatigue | ✗ | N/A | |
| Mixed-sex fatigue | ✗ | ||
| Women fatigue | ✓ | ||
| Dickinson et al.: relaxation therapy | Overall SBP and DBP | ✓ | |
| Male SBP and DBP | ✗ | No significant difference between groups | |
| Mixed-sex SBP and DBP | ✓ | ||
| Kruis et al.: integrated disease management | Overall 6MWD | ✓ | |
| Male 6MWD | ✓ | No significant difference between groups | |
| Mixed-sex 6MWD | ✓ | ||
| Overall FEV1 (% predicted) | ✗ | ||
| Male FEV1 (% predicted) | ✗ | N/A | |
| Mixed-sex FEV1 (% predicted) | ✗ |
Overall, our analyses showed that physical activity (exercise-based interventions) had a positive impact on HRQoL, and that this may be particularly beneficial to men. Further clinical outcomes – SBP, DBP, FEV1, 6MWD and fatigue – were inconclusive in terms of gender differences.
Results from analysis 2: ‘across-Cochrane review analysis’
We identified studies with mixed-sex samples and female-only samples from the ‘parent’ Cochrane reviews that contained the male-only studies identified in analysis 1. Data were pooled according to broad intervention type rather than using the ‘by review’ approach taken in analysis 1.
This allowed us to determine whether broad types/components of self-management support interventions show larger, similar or smaller effects in men than in women and mixed populations. Limitations in the data meant we were able to conduct analyses on only physical activity, education, peer support, and HCP monitoring and feedback interventions.
Physical activity self-management support interventions: male-only studies versus mixed-sex and female-only studies
Health-related quality-of-life scales: positive scores indicate better status
Across all Cochrane reviews, four male-only studies,49,72,80,91 four mixed-sex studies147,148,150,157 and six female-only studies164,167,168,172,176,177 reported HRQoL outcomes which could be used for meta-analysis. Table 15 reports the effect sizes for each group.
| Group | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 4) | 0.54 (0.02 to 1.03) | Moderate |
| Mixed sex (n = 3) | 0.24 (–0.03 to 0.51) | Low |
| Female only (n = 6) | 0.36 (–0.02 to 0.75) | High |
Allocation concealment was predominantly unclear except in the female-only studies, which had a mostly low risk of bias. The mean age across male-only studies (63.9 years) was slightly older than in the mixed-sex (52.0 years) and female-only (52.2 years) groups, which may account for some clinical heterogeneity.
Overall, significant positive effects on HRQoL were identified for self-management support interventions containing a physical activity component (SMD 0.38, 95% CI 0.16 to 0.60; p = 0.005; I2 = 56%).
A moderate effect size, which reached statistical significance, was evident in the male-only group and was larger than the overall effect size (SMD 0.54, 95% CI 0.02 to 1.06; p = 0.04; I2 = 65%). Small and similar effect sizes were observed in the mixed-sex and female-only group but neither reached statistical significance. Testing for group differences found no statistically significant differences between groups (p = 0.58), indicating that the intervention effect did not vary significantly between men, women and mixed-sex groups.
Depression scales: negative scores indicate better status
Three male-only studies (including four interventions),80,89,91 five mixed-sex studies147,151,152,157 and eight female-only studies163,165,175 reported on depression scales which could be used for meta-analysis. Table 16 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 3) | –0.42 (–1.07 to 0.23) | High |
| Mixed sex (n = 5) | 0.00 (–0.50 to 0.50) | High |
| Female only (n = 8) | –1.07 (–1.80 to –0.33) | High |
| Female only excluding outlier (n = 7) | –0.43 (–0.72 to –0.14) | Moderate |
Allocation concealment was predominantly unclear except in the female-only studies, which had a mostly low risk of bias. The mean age across male-only studies (62.8 years) was older than in the mixed-sex (46.7 years) and female-only (51.9 years) groups, which may account for some clinical heterogeneity.
Overall, self-management support interventions containing a physical activity component significantly improved depression scores (SMD –0.55, 95% CI –0.93 to –0.17; p < 0.001; I2 = 88%). Only the female-only group reached statistical significance on depression scales, and the effect size was large and greater than the overall effect size (SMD –1.07, 95% CI –0.80 to –0.33; p < 0.001; I2 = 93%). Small effects were observed in male-only RCTs and mixed-sex RCTs, but neither reached statistical significance. A test for group differences found no statistically significant differences between groups (p = 0.16), indicating that the intervention effect did not vary significantly between men, women and mixed-sex groups.
Heterogeneity in the female-only group is exceedingly high. Visual examination of the forest plot (see Figure 23) identifies the presence of an outlier: the Banerjee 2007 study. 163 A post-hoc analysis was conducted to determine if removal of this study from the female-only group maintained the significant treatment effect but reduced heterogeneity (see Table 16).
Anxiety scales: negative scores indicate better status
Two male-only studies (including three interventions),89,91 four mixed-sex studies147,151,152,157 and three female-only studies163,165,175 reported on anxiety scales which could be used for meta-analysis. Table 17 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | –0.35 (–1.36 to 0.66) | High |
| Mixed sex (n = 4) | –0.12 (–0.33 to 0.09) | Low |
| Female only (n = 3) | –1.76 (–3.80 to 0.29) | High |
| Female only excluding outlier (n = 2) | –0.41 (–0.96 to 0.14) | Moderate |
Allocation concealment was predominantly unclear except in the female-only studies, which had a mostly low risk of bias. The mean age across male-only studies (60.6 years) was older than in the mixed-sex (47.6 years) and female-only (49.1 years) groups, which may account for some clinical heterogeneity.
Overall, significant positive effects on anxiety were identified for self-management support interventions containing a physical activity component (SMD –0.66, 95% CI –1.21 to –0.10; p < 0.001; I2 = 90%); however, heterogeneity was substantially high. This appears to be partially attributable to an outlier in the female-only group: the Banerjee 2007 study. 163 A post-hoc analysis, removing this study, reduced heterogeneity to moderate levels in the female-only group.
The effect size was largest in the female-only group, although none of the groups reached statistically significant effects on anxiety outcomes.
Fatigue scales: negative effect size indicates better status
Four male-only studies,72,80,81,88 six mixed-sex studies147,151–153,157,161 and six female-only studies166,170–173,176 reported on fatigue scales which could be used for meta-analysis. Table 18 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 4) | –0.41 (–0.70 to –0.12) | Low |
| Mixed sex (n = 6) | –0.01 (–0.28 to 0.26) | Moderate |
| Female only (n = 6) | –0.23 (–0.46 to 0.00) | Low |
Allocation concealment was predominantly unclear, with one study in the male-only group (Guell et al. 200081) allocated a high risk of bias. The mean age across male-only studies (67.0 years) was higher than in the mixed-sex (48.2 years) and female-only (53.3 years) groups, which may account for some clinical heterogeneity.
Overall, marginally significant positive effects on fatigue outcomes were identified for self-management support interventions containing a physical activity component (SMD –0.17, 95% CI –0.33 to –0.02; p = 0.03; I2 = 43%).
Only the male-only group reached statistical significance on fatigue scales, and the effect was greater than the overall effect size (SMD –0.41, 95% CI –0.70 to –0.12; p < 0.71; I2 = 0%). Small effect sizes were observed in mixed-sex and female-only groups, but neither reached statistical significance. Testing for group differences found no statistically significant differences (p = 0.13), indicating that the intervention effect did not vary significantly between men, women and mixed-sex groups.
Education self-management support interventions: male-only studies versus mixed-sex and female-only studies
Health-related quality of life: positive effect size indicates better status
Seven male-only studies (including nine interventions),49,54,59,64,66,72,80 seven mixed-sex studies (including eight interventions)148,150,154,155,157,158,181 and one female-only study168 reported HRQoL outcomes which could be used for meta-analysis. Table 19 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 7) | 0.36 (0.06 to 0.67) | High |
| Mixed sex (n = 7) | 0.07 (–0.08 to 0.21) | Low |
| Female only (n = 1) | 0.21 (–0.21 to 0.63) | Not available |
| Male only excluding outlier (n = 6) | 0.20 (0.04 to 0.36) | Low |
Allocation concealment was predominantly unclear, except in the female-only group, which had a low risk of bias. The mean age across male-only studies (66.7 years) was similar to the mixed-sex group (61.1 years) but higher than the female-only group (52.5 years).
Overall, small but significant positive effects on HRQoL were identified for self-management support interventions containing an education component (SMD 0.23, 95% CI 0.07 to 0.40; p = 0.001; I2 = 58%).
When each gender group was examined, statistically significant effects on HRQoL were evident only in the male-only group and were greater than the overall effect size (SMD 0.36, 95% CI 0.06 to 0.67; p < 0.001; I2 = 73%). No effect was observed in the mixed-sex group and small, non-significant effects were found in the female-only group. Testing for group differences found no significant difference between groups (p = 0.22).
The high heterogeneity in the male-only group may be attributable to an outlier. A post-hoc analysis, removing the outlying study,64 reduced heterogeneity to 0%, while maintaining a significant, albeit reduced, effect size in the male-only group (SMD 0.20, 95% CI 0.04 to 0.36; p = 0.99; I2 = 0%).
Depression scales: negative scores indicate better status
Five male-only studies (including eight interventions),53,59,66,80,89 five mixed-sex studies147,156–158,160 and two female-only studies169,174 reported depression outcomes which could be used for meta-analysis. Table 20 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 5) | –0.10 (–0.27 to 0.07) | Low |
| Mixed sex (n = 5) | –0.16 (–0.35 to 0.03) | Moderate |
| Female only (n = 2) | 0.26 (–0.78 to 1.30) | High |
Allocation concealment was predominantly unclear in all gender groups. The mean age across male-only studies (63.0 years) was slightly older than in the mixed-sex (47.14 years) and female-only (51.4 years) groups, which may account for some clinical heterogeneity.
Overall, self-management support interventions containing an education component did not have a statistically significant effect on depression outcomes, although a slight trend in favour of education was observed (SMD –0.11, 95% CI –0.23 to 0.01; p = 0.18; I2 = 25%).
None of the individual gender groups reached statistically significant effects on depression outcomes, and all effect sizes were small or marginal. Unlike the male-only and mixed-sex groups, the female-only group showed indications of worsening depression outcomes following interventions with education components.
Anxiety scales: negative scores indicate better status
Two male-only studies (including four interventions)66,89 and three mixed-sex studies147,157,158 reported anxiety outcomes which could be used for meta-analysis. Table 21 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | –0.01 (–0.29 to 0.27) | Low |
| Mixed sex (n = 3) | –0.12 (–0.38 to 0.14) | Moderate |
Allocation concealment was predominantly unclear in all groups. The mean age across male-only studies (66.7 years) was older than in the mixed-sex group (50.7 years).
Overall, self-management support interventions containing an education component did not have a statistically significant effect on anxiety outcomes (SMD –0.06, 95% CI –0.21 to 0.09; p = 0.60; I2 = 0%). Effect sizes in the groups were marginal and none reached statistical significance. The number of studies and sample size were small in this analysis, which may account for the lack of effect shown.
Fatigue scales: negative scores indicate better status
Five male-only studies53,72,80,81,87,88 and one mixed-sex study157 reported fatigue outcomes which could be used for meta-analysis. Table 22 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 5) | –0.36 (–0.61 to –0.10) | Low |
| Mixed sex (n = 1) | –0.57 (–1.32 to 0.18) | Not available |
Allocation concealment was predominantly unclear across studies, with one study in the male-only group reported as having a high risk of bias for allocation concealment (Guell et al. 2000). 81 The mean age across male-only studies (62.6 years) was substantially older than for mixed-sex studies (40.9 years).
Overall, significant positive effects on fatigue were identified for self-management support interventions containing an education component (SMD –0.38, 95% CI –0.62 to –0.14; p = 0.82; I2 = 0%). The effect size in the male-only group was similar (SMD –0.36, 95% CI –0.61 to –0.10; p = 0.74; I2 = 0%). A moderate effect size was observed in the mixed-sex group, although the effect was non-significant.
Conclusions cannot be drawn on the mixed-sex group, as only one study was included.
Peer support self-management support interventions: male-only studies versus mixed-sex and female-only studies
Health-related quality of life: positive scores indicate better status
Five male-only studies,49,59,66,72,80 one mixed-sex study150 and three female-only studies147,173,177 reported HRQoL outcomes which could be used for meta-analysis. Table 23 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 5) | 0.23 (0.04 to 0.43) | Low |
| Mixed sex (n = 1) | 0.16 (–0.24 to 0.56) | Not available |
| Female only (n = 2) | 0.61 (–0.08 to 1.30) | High |
Allocation concealment was predominantly unclear in all groups. The mean age across male-only studies (67.4 years) was slightly higher than in the mixed-sex group (59.7 years) and substantially higher than in the female-only group (50.9 years), which may account for some clinical heterogeneity.
Overall, small but significant positive effects for HRQoL were identified for self-management support interventions containing a peer support component (SMD 0.35, 95% CI 0.13 to 0.57; p = 0.02; I2 = 56%).
When each group was examined, statistically significant effects on HRQoL were evident in only the male-only group, although the effect was smaller than the overall effect size (SMD 0.23, 95% CI 0.04 to 0.43; p = 0.97; I2 = 0%). A moderate effect was found in the female-only group, although this effect was non-significant. Testing for group differences found no statistically significant differences between groups (p = 0.54), indicating that the intervention effect did not vary significantly between men, women and mixed-sex groups; however, the mixed-sex and female-only groups were small and this may account for the lack of effect.
Depression: negative scores indicate better status
Seven male-only studies (including eight interventions),53,59,66,68,69,80,89 two mixed-sex studies,156,159 and one female-only study172 reported depression outcomes which could be used for meta-analysis. Table 24 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 7) | –0.23 (–0.42 to –0.05) | Low |
| Mixed sex (n = 2) | 0.28 (–0.34 to 0.90) | Moderate |
| Female only (n = 1) | –0.32 (–0.62 to –0.03) | Not available |
Allocation concealment was predominantly unclear in all groups. The mean age across male-only studies (61.7 years) was substantially higher than in the mixed-sex (46.3 years) and female-only (51.3 years) groups, which may account for some clinical heterogeneity.
Overall, no significant effects on depression were identified for self-management support interventions containing a peer support component (SMD –0.17, 95% CI –0.35 to 0.01; p = 0.07; I2 = 42%).
When each group was examined, small but statistically significant effects on depression were evident in the male-only group (SMD –0.23, 95% CI –0.42 to –0.05; p = 0.29; I2 = 18%). A slightly larger significant effect size was determined in the female-only group. However, only one female-only study was included, so definitive conclusions cannot be drawn. Testing for group differences found no statistically significant differences between groups (p = 0.22), indicating that the intervention effect did not vary significantly between men, women and mixed-sex groups.
Fatigue: negative scores indicate better status
Three male-only studies53,72,80 and two female-only studies172,176 reported fatigue outcomes which could be used for meta-analysis. Table 25 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 3) | –0.24 (–0.56 to 0.09) | Low |
| Female only (n = 2) | –0.29 (–0.56 to –0.01) | Low |
Allocation concealment was predominantly unclear and the mean age was higher for male-only studies (61.2 years) than for female-only studies (52.15 years).
Overall, small significant effects on fatigue were identified for self-management support interventions containing a peer support component (SMD –0.27, 95% CI –0.48 to –0.06; p = 0.91; I2 = 0%).
Although effect size was similar in the male-only and female-only groups, only the female-only group reached statistical significance, benefiting fatigue outcomes. Testing for group differences confirmed that the effect did not vary between male and female groups (p = 0.82).
Self-efficacy: positive scores indicate better status
Three male-only studies53,68,69 and one mixed-sex study156 reported self-efficacy outcomes which could be used for meta-analysis. Table 26 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 3) | 0.57 (0.25 to 0.88) | Low |
| Mixed sex (n = 1) | 2.54 (2.15 to 2.92) | Not available |
Allocation concealment was unclear for all studies and the mean age across male-only studies (54.0 years) was greater than in the mixed-sex study (43.1 years), which may account for some clinical heterogeneity.
Overall, no significant effects on self-efficacy were identified for self-management support interventions containing a peer support component, and substantial heterogeneity was apparent (SMD 1.02, 95% CI –0.12 to 2.17; p < 0.001; I2 = 95%]. Significant effects were identified in both groups, although only one study was included within the mixed-sex group so definitive conclusions cannot be drawn.
Health-care professional monitoring and feedback self-management support interventions: male-only studies versus mixed-sex and female-only studies
Health-related quality of life: positive scores indicate better status
Two male-only studies66,80 and four female-only studies164,167,168,177 reported HRQoL outcomes which could be used for meta-analysis. Table 27 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 2) | 0.18 (–0.17 to 0.53) | Low |
| Female only (n = 4) | 0.42 (–0.22 to 1.05) | High |
Allocation concealment was predominantly unclear in the male-only group and low in the female-only group. The mean age across male-only studies (68.2 years) was substantially older than in the female-only group (52.2 years), which may account for some clinical heterogeneity.
Overall, no significant effects on HRQoL were identified for self-management support interventions containing a HCP follow-up and monitoring component (SMD 0.34, 95% CI –0.07 to 0.75; p = 0.003; I2 = 72%), although a small effect in favour of HCP follow-up and monitoring was observable in both groups and was greater in the female-only group.
Depression: negative scores indicate better status
Three male-only studies,66,80,89 one mixed-sex study149 and two female-only studies164,167 reported depression outcomes which could be used for meta-analysis. Table 28 reports the effect sizes for each group.
| Group | Effect size SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| Male only (n = 3) | –0.17 (–0.45 to 0.11) | Low |
| Mixed sex (n = 1) | –0.26 (–1.12 to 0.60) | Not available |
| Female only (n = 2) | –0.26 (–0.70 to 0.19) | Low |
Allocation concealment was predominantly unclear except in the female-only group, in which all studies had a low risk of bias for allocation concealment. The mean age across male-only studies (68.2 years) was substantially older than in the mixed-sex (44.0 years) and female-only (54.0 years) groups.
Overall, no significant effects on depression were identified for self-management support interventions containing a HCP follow-up and monitoring component (SMD –0.20, 95% CI –0.43 to 0.03; p = 0.89; I2 = 0%), although a trend in favour of HCP follow-up and monitoring was observable in all groups and was greatest in mixed-sex and female-only groups.
Analysis 2: summary of key findings
A summary of the main findings is presented in Table 29.
| Outcome | Overall effect | Male only | Mixed sex | Female only | Group differences |
|---|---|---|---|---|---|
| Physical activity | |||||
| HRQoL | ✓ | ✓ | ✗ | ✗ | None |
| Depression | ✓ | ✗ | ✗ | ✓ | None |
| Anxiety | ✓ | ✗ | ✗ | ✗ | N/A |
| Fatigue | ✗ | ✓ | ✗ | ✗ | None |
| Education | |||||
| HRQoL | ✓ | ✓ | ✗ | ✗ | None |
| Depression | ✗ | ✗ | ✗ | ✗ | N/A |
| Anxiety | ✗ | ✗ | ✗ | No studies | N/A |
| Fatigue | ✓ | ✓ | ✗ | No studies | N/A |
| Stress scales | ✗ | ✗ | No studies | No studies | N/A |
| Pain scales | ✗ | ✗ | No studies | No studies | N/A |
| Peer support | |||||
| HRQoL | ✓ | ✓ | ✗ | ✗ | None |
| Depression | ✗ | ✓ | ✗ | ✓ | None |
| Anxiety | ✗ | ✗ | No studies | No studies | N/A |
| Fatigue | ✓ | ✗ | No studies | ✓ | None |
| Stress scales | ✗ | ✗ | No studies | No studies | N/A |
| Pain scales | ✗ | ✗ | No studies | No studies | N/A |
| Self-efficacy | ✗ | ✓ | ✓ | No studies | N/A |
| HCP monitoring and feedback | |||||
| HRQoL | ✗ | ✗ | No studies | ✗ | N/A |
| Depression | ✗ | ✗ | ✗ | ✗ | N/A |
| Distress | ✗ | ✗ | No studies | No studies | N/A |
Our analyses showed that self-management support interventions containing physical activity, education or peer support components may be particularly beneficial for HRQoL outcomes in men.
Depression outcomes were improved in only men receiving a self-management support intervention with a peer support component. Education and physical activity support intervention components were beneficial to fatigue outcomes, and findings indicate that there may be greater benefit to men.
Results from analysis 3: ‘male only by intervention-type analysis’
To investigate whether particular broad types of self-management support intervention were more or less effective in men, we conducted a meta-analysis on trials in men alone and compared effects between intervention types. Limitations in the data meant that we were able to conduct analyses on only physical activity, education, peer support, and HCP monitoring and feedback interventions.
Physical activity component versus no physical activity component interventions in male-only trials
Table 30 reports the effect sizes for interventions with physical activity and those without, on HRQoL, depression, anxiety and fatigue outcomes.
| Outcome | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| With physical activity component | ||
| HRQoL (n = 4) | 0.54 (0.02 to 1.06) | Moderate |
| Depression (n = 3) | –0.44 (–1.14 to 0.25) | High |
| Anxiety (n = 2) | –0.37 (–1.46 to 0.72) | High |
| Fatigue (n = 4) | –0.41 (–0.70 to –0.12) | Low |
| Without physical activity component | ||
| HRQoL (n = 4) | 0.36 (0.01 to 0.70) | High |
| Depression (n = 6) | –0.26 (–0.46 to –0.05) | Low |
| Anxiety (n = 2) | –0.09 (–0.43 to 0.26) | Low |
| Fatigue (n = 1) | –0.18 (–0.70 to 0.34) | Not available |
Interventions with a physical activity component were found to have greater effects than those without. However, no statistically significant group differences between interventions with physical activity and those without were found, indicating that the effects observed did not significantly vary by the presence or absence of a physical activity intervention component.
Small significant effects were observed for depression outcomes in interventions without a physical activity component; the effect was larger with a physical activity component but non-significant. Significant effects were found for HRQoL outcomes in interventions with and without a physical activity component. Those interventions with a physical activity component achieved a greater magnitude of effect (moderate effect size) than those interventions without this component (small effect size). Anxiety and fatigue outcomes both reported small effect sizes in favour of physical activity, although only fatigue outcomes were significant. Several of the groups in this analysis had small sample sizes and high levels of heterogeneity. Because data were insufficient, reasons for heterogeneity could not be explored.
Education component versus no education component interventions in male-only trials
Table 31 reports the effect sizes for each group on HRQoL, depression and anxiety outcomes.
| Outcome | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| With education component | ||
| HRQoL (n = 7) | 0.34 (0.07 to 0.60) | Moderate |
| Depression (n = 5) | –0.10 (–0.27 to 0.08) | Low |
| Anxiety (n = 2) | –0.02 (–0.32 to 0.28) | Low |
| Fatigue | Analysis not possible | |
| Without education component | ||
| HRQoL (n = 2) | 0.95 (–0.55 to 2.45) | High |
| Depression (n = 4) | –0.83 (–1.43 to –0.23) | Moderate |
| Anxiety (n = 2) | –0.71 (–2.66 to 1.24) | High |
| Fatigue | Analysis not possible | |
Only interventions containing an education component were found to benefit HRQoL outcomes significantly. Although a large effect size for HRQoL was observed for interventions without education, the effect was non-significant and heterogeneity was high. Improvements in depression outcomes significantly favoured interventions without an education component. This effect size was large and significantly distinct from the group of interventions with an education component, indicating that the effect is associated with the characteristics of those interventions without an education component. Anxiety outcomes were not significantly benefited with or without an education component, and analysis of fatigue outcomes was not possible. Limited data and the magnitude of heterogeneity in some groups mean that the results should be interpreted with caution.
Peer support component versus no peer support component interventions in male-only trials
Table 32 reports the effect sizes for each group on HRQoL, depression, anxiety and fatigue outcomes.
| Outcome | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| With peer support component | ||
| HRQoL (n = 5) | 0.25 (0.03 to 0.47) | Low |
| Depression (n = 7) | –0.24 (–0.45 to –0.04) | Low |
| Anxiety (n = 2) | 0.01 (–0.34 to 0.36) | Low |
| Fatigue (n = 3) | –0.24 (–0.56 to 0.09) | Low |
| Without peer support component | ||
| HRQoL (n = 5) | 0.62 (0.08 to 1.16) | High |
| Depression (n = 4) | –0.50 (–1.17 to 0.16) | High |
| Anxiety (n = 3) | –0.46 (–1.47 to 0.55) | High |
| Fatigue (n = 2) | –0.53 (–0.93 to –0.14) | Low |
Self-management support interventions with or without a peer support component statistically significantly benefited HRQoL outcomes. The effect was greater in those studies without a peer support component, although heterogeneity was high and group differences were non-significant (p = 0.21).
A small but significant effect was found for depression outcomes in interventions containing a peer support component. A moderate effect was observed for interventions without this component, but the effect was non-significant and heterogeneity was high. Fatigue outcomes favoured interventions without a peer support component, demonstrating a moderate effect. Analysis of anxiety outcomes was not possible. Limited data and the magnitude of heterogeneity in some groups mean that results should be interpreted with caution.
Health-care professional monitoring and feedback component versus no health-care professional monitoring and feedback component interventions in male-only trials
Table 33 reports the effect sizes for each group for HRQoL and depression outcomes.
| Outcome | Effect size: SMD (95% CI) | I2 heterogeneity |
|---|---|---|
| With HCP monitoring and feedback component | ||
| HRQoL (n = 2) | 0.20 (–0.19 to 0.59) | Low |
| Depression (n = 3) | –0.14 (–0.48 to 0.19) | Low |
| Anxiety | Analysis not possible | |
| Fatigue | Analysis not possible | |
| Without HCP monitoring and feedback component | ||
| HRQoL (n = 7) | 0.47 (0.14 to 0.81) | High |
| Depression (n = 7) | –0.36 (–0.65 to –0.07) | Moderate |
| Anxiety | Analysis not possible | |
| Fatigue | Analysis not possible | |
Only self-management support interventions without a HCP monitoring and feedback component significantly benefited HRQoL and depression outcomes; small effect sizes were observed in both cases. No further outcomes could be analysed because data were insufficient.
Analysis 3: summary of key findings
Table 34 presents a summary of the main findings.
| Component | Outcome | With component | Without component | Group differences |
|---|---|---|---|---|
| Physical activity | HRQoL | ✓ | ✓ | No significant differences between groups for each outcome |
| Depression | ✗ | ✓ | ||
| Anxiety | ✗ | ✗ | ||
| Fatigue | ✓ | ✗ | ||
| Education | HRQoL | ✓ | ✗ | For depression outcomes, significant difference between groups. No other significant outcome group difference found |
| Depression | ✗ | ✓ | ||
| Anxiety | ✗ | ✗ | ||
| Peer support | HRQoL | ✓ | ✓ | No significant differences between groups for each outcome |
| Depression | ✓ | ✗ | ||
| Anxiety | ✗ | ✗ | ||
| Fatigue | ✗ | ✓ | ||
| HCP monitoring and feedback | HRQoL | ✗ | ✓ | No significant differences between groups for each outcome |
| Depression | ✗ | ✓ |
Our analyses showed no significant differences in interventions with or without a physical activity component or peer support component on HRQoL, depression, anxiety and fatigue outcomes. No significant differences in HRQoL and depression outcomes were identified in interventions with or without a HCP monitoring and feedback component.
A significant group difference was observed for depression outcomes: interventions without an education component benefited depression outcomes.
Interventions with peer support were also identified as the only intervention component able to demonstrate a significant benefit to depression outcomes.
Results from analysis 4: ‘within-trial, gender group analysis’
We identified individual RCTs which analysed the effects of self-management support interventions in gender groups, with the aim of comparing these results with our meta-analysis findings: analyses 1–3.
In the original protocol we sought to extract relevant data on the direction and size of moderating effects in secondary analysis (i.e. whether males show larger, similar or smaller effects than females), and assess these effects in the context of relevant design data, such as sample size, and the quality of the secondary analysis. However, we found that data on the effect of gender in self-management support interventions are inconsistently, and often poorly, reported in trials. Moreover, we found that data were frequently not reported in a way that could allow comparison between effect sizes in males and females.
We extracted data from trials (n = 20) where an effect of gender had been reported for intervention and control groups,182–204 and those data are presented in Appendix 9. However, interpretation of those data is difficult because the outcomes reported are variable.
The data showed some indication that gender can influence the effect of self-management support interventions. However, the key implication arising from this analysis is that improvements in reporting gender differences in trials of self-management support interventions are urgently needed (see Chapter 7, Recommendations for future research).
Results from cost-effectiveness analysis
Economic evaluation is defined as a study where costs are estimated and presented alongside the consequences of intervention versus one or more comparator. 205 We did not find any economic evaluations of self-management interventions in male-only studies.
In addition, no studies reported outcome measures and/or resource-use measures that could be used to reliably inform UK-based decision-making. Most studies were dated before 2000, were from outside the UK and used a non-generic outcome measure.
In secondary studies, we reviewed economic evaluations where a male group could be identified. Only one study (Hagen et al. 2003206) fitted the criteria for review. The results of the quality assessment checklist are presented in Table 35. In brief, this intervention aimed to encourage individuals with low back pain to undertake moderate physical activity. The economic evaluation was a cost–benefit analysis based on a RCT. While the study showed that both males and females benefit from the intervention (in terms of return to and time spent at work), the omission of out-of pocket expenses, as well as other health-related resource-use items and health-related outcome measures, renders the study of limited use for UK decision-makers.
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7a | Q7b | Q8a | Q8b | Q9 | Q10a | Q10b | Q11 | Q12 | Q13 | Q14 | Q15a | Q15b | Q16a | Q16a | Q16b | Q16c | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hagen et al. 2003206 | ✓ | ✓ | 4 | 5 | 12 | ✗ | ✗ | ✗ | ✓ | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ | ✗ | ✗ | N/A | ✓ | 12 | ✗ | ✗ |
| Q1 Study clarity | Q5 Economic study design | Q11 Discounting | |||||||||||||||||||||
| Q2 Comprehensive description of competing alternatives | 9 = Cost-effectiveness analysis (CEA) | Q12 Incremental analysis | |||||||||||||||||||||
| Q3 Perspective | 10 = Cost–consequence analysis (CCA) | Q13 Allowance for uncertainty | |||||||||||||||||||||
| 1 = Societal (30%) | 11 = Cost–utility analysis (CUA) | Q14 Missing data handled appropriately | |||||||||||||||||||||
| 2 = Health care system and patient (6%) | 12 = Cost–benefit analysis (CBA) | Q15a Economic model | |||||||||||||||||||||
| 3 = Health care system (54%) | Q6 Design adequacy given study type | Q15b Appropriateness of economic model | |||||||||||||||||||||
| 4 = Not clear (11%) | Q7a Relevant costs identified | Q16a Type of funder | |||||||||||||||||||||
| Q4 Study design | Q7b Relevant consequences identified | 12 = Public/voluntary sector (73%) | |||||||||||||||||||||
| 5 = Randomised control trial (RCT) (62%) | Q8a Costs measured accurately | 13 = Private sector (13%) | |||||||||||||||||||||
| 6 = Case control trial (CCT) (11%) | Q8b Consequences measured adequately | 14 = Do not state (13%) | |||||||||||||||||||||
| 7 = Before and after (21%) | Q9 Statistical analysis appropriateness given the design | Q16b Generalisability | |||||||||||||||||||||
| 8 = Decision model (6%) | Q10a Subgroup analysis | Q16c Presentation and discussion of key results | |||||||||||||||||||||
| Q10b Subgroups pre-specified |
Summary of key messages from quantitative review
We used a number of analytic techniques and assessed a number of different outcomes, and there was no consistent finding of differential effects in self-management interventions. Although there were some differences of note (summarised below), overall there is insufficient evidence to make strong statements about whether men show larger, similar or smaller effects in self-management support interventions than women and mixed-sex groups.
Interventions containing a physical activity component
We did not identify consistent statistical differences in the effect of physical activity interventions between men, women and mixed-sex groups. Interventions with a physical activity component were found to improve HRQoL and fatigue outcomes and there is some indication that this may be particularly beneficial for men.
Depression outcomes did not appear to improve in studies with a physical activity component, but did significantly improve in those without this component. Analysis of physical activity intervention studies by gender found no effect in men for depression, but significant improvements were found in women. No demonstrable effects for anxiety outcomes were found in any analysis, and data were too limited to explore further outcomes.
Interventions containing an education component
We did not find consistent statistical differences in the effect of education interventions on HRQoL and fatigue outcomes between men, women and mixed-sex groups. Interventions with an education component were found to improve HRQoL and fatigue outcomes and there is some indication that this may be particularly beneficial for men, although data were limited.
Notably, depression outcomes were significantly improved in studies without an education component, and this effect was statistically different from the group of interventions with this component. No demonstrable effect for anxiety outcomes was found in any analysis, and data were too limited to explore further outcomes.
Interventions containing a peer support component
We did not find consistent statistical differences in the effect of peer support interventions between men, women and mixed-sex groups. Interventions with or without a peer support component both significantly improved HRQoL outcomes, although a by-gender analysis of interventions with peer support found this effect was significant in only male-only studies. Fatigue outcomes were significantly improved in only interventions without peer support.
Interventions with peer support were identified as the only interventions to demonstrate a significant beneficial effect on depression outcomes in men, whereas significant benefits on depression were found in women for both physical activity and peer support interventions. No demonstrable effects for anxiety outcomes were found in any analysis, and data were too limited to explore further outcomes through gender comparison.
Interventions containing a HCP monitoring and feedback component
We did not identify consistent statistical differences in the effect of interventions with a HCP monitoring and feedback component between men, women and mixed-sex groups. Limited data were available to conduct a robust analysis on interventions with a HCP monitoring and feedback component. HRQoL and depression outcomes appeared significantly improved by only interventions without this component. The data were too limited to explore further outcomes by gender comparison.
Chapter 5 Results from qualitative review
General study characteristics
A total of 38 studies, reported in 44 papers, were included in the review. 99–103,107–129,134–136,207–218 Three studies were reported across multiple papers that were individually eligible for inclusion. 118–121,124–126 An additional two papers that did not meet the eligibility criteria as they had female-only samples are included in the synthesis because they presented data about women that formed the basis of gender comparisons made by the authors of included studies reporting findings from male participants. 114,122 The details of all included studies are presented in Table 36 and provide the context for the interpretations of each study.
| Study (first author, year, country) | Aim | Classification of support activity used in qualitative synthesis | Condition | Data collection (IV, FG, OP, PO) and sample size | Methodological approach | Sample (size, sex, condition details, age, ethnicity, locality/settlement, socioeconomic status, employment, sexuality, relationship) |
|---|---|---|---|---|---|---|
| Adamsen 2001,207 Denmark | Men’s experiences of a tailored intervention involving physical activity and information relay for men with cancer | Lifestyle | Cancer: any | FG 10 men, PO 17 men, total 17 men | Descriptive/interpretive | Range of cancers and varying stages; mean age 56.5 years (range 21–71 years); ethnicity N/R; ‘broad range’ of education, employment, relationship status |
| Arrington 2005,208 USA | Communication practices of man-to-man prostate cancer support groups | Support group (face to face) | Cancer: prostate | PO N/R (20 groups of men) | Discourse analysis | All ‘senior citizens’; ‘almost exclusively retired, elderly’; no further details reported |
| Baird 2001,134 USA | Self-care factors influencing adherence to a cardiac rehabilitation programme | Lifestyle | Cardiac: coronary artery disease | IV five men | Phenomenology | Majority myocardial infarction (four myocardial infarction, one sudden cardiac arrest; one following cerebrovascular accident, two following percutaneous transluminal coronary angioplasty and one following coronary artery bypass graft surgery); aged 60–70 years; 80% Caucasian (four Caucasian, one African American); 100% retired; mix of previous ‘blue-collar’ and ‘white-collar’ occupations; 100% married |
| Barlow 2009,103 UK | Experiences of patients with multiple sclerosis of the Chronic Disease Self-Management Course | Lifestyle | Multiple sclerosis | IV three men, seven women | Descriptive/interpretive (part of mixed-methods study) | Disease duration 4–19 years; aged 35–60 years |
| Barlow 2009,102 UK | Experiences of patients with myocardial infarction of the Chronic Disease Self-Management Course and cardiac rehabilitation | Lifestyle | Cardiac: myocardial infarction | IV 10 men, nine women | Descriptive/interpretive (part of mixed-methods study) | 14 with comorbidity; median age 68 years (range 59–74 years); 1 employed; majority (16) married/residing with partner; all had attended at least five of the six intervention sessions |
| Bedell 2000,108 USA | Daily life experiences of gay men with HIV/AIDS living alone in New York, NY, USA | Support group (face to face) | HIV/AIDS | IV 8 men | Descriptive/interpretive | Varying severity (six diagnosed with AIDS for ≥ 2 years, two not yet developed); all had prior/current difficulty with daily activities; aged 25–50 years; majority white (six white, two African American); all urban; majority ‘middle-class’; education ranged from 1 year’s college to doctorate; four employed, three on public assistance, one neither; all gay; all lived alone |
| Bell 2010,107 Canada | Composition, processes and patients’ views of differently designed and structured cancer support groups | Support group (face to face) | Cancer: (1) women with metastatic cancer; (2) colorectal cancer patients; and (3) Chinese patients with cancer | IV three men, 17 women. PO: metastatic group no men, 25 women; colorectal group 14 men, 16 women; Chinese group 35 men, 61 women (including 48 caregivers) | Descriptive/interpretive | Interview sample: time since diagnosis 3 months to 3 years, 13 in treatment, seven after treatment; time in group 1 month to 4 years; median age fifties (range forties to seventies); ethnicity N/R. Metastatic observation sample: no men, 25 women; 25 in treatment; median age fifties (range thirties to sixties); majority white. Colorectal observation sample: 14 men, 16 women; one before treatment, eight in treatment, 12 after treatment; median age fifties (range thirties to seventies); majority white. Chinese observation sample: 35 men, 61 women; five before treatment, 30 in treatment, 15 after treatment; median age fifties (range twenties to eighties); all Chinese |
| Bourke 2012,209 UK | Men’s experiences of a lifestyle intervention for men with prostate cancer undergoing androgen suppression therapy | Lifestyle | Cancer: prostate | FG 12 men (three groups) | Descriptive/interpretive | All T3–T4 prostate cancer receiving androgen suppression therapy ≥ 6 months; details N/R but linked trial reports for intervention group of 25: mean treatment 30 months (SD 31 months); mean age 71.3 years (SD 6.4 years) |
| Broom 2005,109 Australia | Impact of internet use on disease experience of prostate cancer and the doctor–patient relationship | Internet (information and/or support) | Cancer: prostate | IV 33 men | Descriptive/interpretive | ‘Range’ of prognoses and treatments; ‘varying ages’ |
| Chambers 2012,210 Australia | Men’s experiences of a mindfulness-based cognitive therapy group intervention in men with advanced prostate cancer | Psychological | Cancer: prostate | IV 12 men | Descriptive/interpretive | N/R for interview sample, therefore based on 19 men taking part in intervention. Mean time since diagnosis 68.9 months (SD 51.2 months, range 1–167 months); majority had hormone treatment; range of surgery and radiotherapy (16 received hormone therapy including nine ongoing; 11 external beam radiation therapy; three brachytherapy; three radical prostatectomy surgery; one orchidectomy); mean age 67.0 years (SD 6.5 years, range 58–83 years); 79% completed university, college or vocational training; 37% employed, 63% retired; 84% married or in a relationship, 16% widowed, divorced or separated |
| Chenard 2007,110 USA | Impact of stigma on self-care behaviours of HIV-positive gay men | Support group (face to face) | HIV/AIDS | IV 15 men, FG 5 men (one group), total 20 men | Grounded theory | All HIV-positive ≥ 1 year, 85% ≥ 5 years; median age 44 years (range 26–62 years; 70% over 30 years); all gay |
| Corboy 2011,111 Australia | Perceived barriers to using psychosocial support services in men with cancer living in rural Australia | Various | Cancer: prostate | IV nine men (82 surveyed and subsample interviewed) | Descriptive/interpretive | Men with ‘any’ cancer eligible but all participants had prostate cancer; mean age 69 years (SD 9.3 years); all rural (five accessible, four moderately, based on Accessibility/Remoteness Index of Australia classification); all married; two employed, one sick leave, six retired |
| Cramer 2013,112 UK | Men’s experiences of depression and anxiety groups and the role of health professionals in accessing support | Support group (face to face) | Depression/anxiety | IV 17 men, PO 30 (four groups, unclear if this includes some women), total 38 (may include women) | Descriptive/interpretive | Details N/R; sampling described as aiming to increase ethnic diversity and diversity in type of help sought |
| Dickerson 2006,114 USA (linked study to Dickerson 2011113) | Experiences of patients with cancer using the internet for information and support to manage self-care, including symptom management | Internet (information and/or support) | Cancer: any | IV 20 women (intended as mixed but only managed to recruit women) – compared with Dickerson 2011113 | Phenomenology | Various cancer types (11 breast, three gynaecological, one gastrointestinal, three lymphomas, two haematological); seven new diagnosis, seven in treatment, six survivors (> 5 years); mean age 52.3 years (SD 8.7 years, range 34–65 years); mean education 15 years (SD 2 years, range 12–18 years); mean 14 hours weekly internet use (SD 12 hours, range 2–40 hours); mean 6 years using internet (range 2–10 years) |
| Dickerson 2011,113 USA | Experiences of men with cancer using the internet | Internet (information and/or support) | Cancer: any | IV 15 men (comparison made with 20 women in above study) | Phenomenology | Majority prostate cancer (14 prostate, one leukaemia); one new diagnosis, four in treatment, 10 survivors (> 5 years); mean age 63 years (SD 10 years, range 47–78 years); mean education 17 years (SD 3 years, range 12–20 years); mean 11 hours weekly internet use (SD 10 hours, range 1–35 hours); mean 7 years using internet (range 1–10 years); 10 attend ‘Us, Too’ face-to-face support group |
| Eldh 2006,135 Sweden | Phenomena of participation and non-participation in nurse-led clinic for chronic heart failure, as observed in visits and experienced by patients and nurses | Lifestyle | Cardiac: heart failure | IV three men, PO three men (11 visits), total three men | Phenomenology | Classed as II/III using NYHA classes of heart failure; aged 53, 77 and 79 years |
| Emslie 2007,115 UK | Experiences of men and women with depression in articulating emotional distress and engaging with health professionals | Various | Depression | IV 16 men, 22 women | Descriptive/interpretive | Majority (34 of 38) experienced multiple/prolonged depressive episodes; 18 of 38 hospitalised; 10 of 38 bipolar depression; wide age range (from < 30 to ≥ 66 years; 3 aged < 30 years, 14 aged 30–40 years, 11 aged 41–55 years, six aged 56–65 years, four aged ≥ 66 years); majority white British (33 of 38), others one each of black, Asian, south European, north European, American) |
| Evans 2007,116 UK | Acquisition and evaluation of CAM information in men with cancer | Information | Cancer: any | IV 34 men (total sample is 43 but paper focus is on 34 who did use CAM) | Descriptive/interpretive | Various cancer types (10 colorectal, 10 prostate, three lung, 11 other: thymic, tonsillar, pancreatic, bone, lymphoma, bladder, renal, oesophageal, leukaemia); varying stages (10 localised, 10 remission, eight metastatic, six palliative care); mean age 57 years (range 31–83 years); all white; ‘range’ of manual, non-manual and professional occupational backgrounds (over half professional); 22 used CAM before diagnosis |
| Ferrand 2008,218 France | Motives for regular physical activity in men and women with type 2 diabetes using the French patients’ association Move for Health | Lifestyle | Diabetes: type 2 | IV nine men, 14 women | Descriptive/interpretive | Men: six diagnosed ≥ 5 years; six medicated including two insulin; mean age 67.0 years (SD 6.1 years); 6 post-secondary education; one employed, eight retired; seven married, one widowed and one never married. Women: mean 56.3 years (SD 9.5 years), total range 35–78 years; 13 diagnosed ≥ 5 years; 10 medicated including four insulin; mean age 56.3 years (SD 9.5 years); four post-secondary education; three employed, seven retired, four homemakers; seven married, one widowed, five separated/divorced and one never married |
| Galdas 2012,211 Canada | Canadian Punjabi Sikh men’s experiences of adopting lifestyle changes following myocardial infarction | Lifestyle | Cardiac: myocardial infarction | IV 27 men | Descriptive/interpretive | Majority reported comorbidity (10 diabetes, eight high blood pressure, seven high cholesterol, three depression); mean age 65.7 years (range 41–86 years); all Canadian Punjabi Sikh; lived in Canada mean 20 years (range 2–42 years); majority retired, seven employed, 13 receiving pension or disability income; 24 married, three widowed; 15 attended cardiac rehabilitation |
| Gibbs 2005,119 Australia | Factors influencing utilisation of self-management services in men with arthritis | Various | Arthritis | IV 17 men | Grounded theory (and participatory research) | Time since diagnosis 4 months to 25 years; varied health status (self-reported three poor, eight fair, six good); median age 41–60 years (two aged 18–25 years, three aged 26–40 years, seven aged 41–60 years, three aged 61–75 years, two aged ≥ 75 years); majority Anglo/Celtic (sic) (12 Anglo/Celtic including one also Aboriginal; one UK/European; one Greek; one Chilean; one Italian; one Filipino/Asian); varied education (one primary school only, five completed secondary, one passed secondary, seven vocational, three university, three N/R); nine employed, six retired, one student, one unemployed; range of employment roles (health services, research, managerial, information technology, motor mechanics, farming); sexuality not asked but one homosexual, one bisexual, others referred to female partners although acknowledge may not identify as heterosexual; varied involvement in self-management programmes (0–4 different programmes) |
| Gibbs 2007,118 Australia | Work as a barrier to accessing self-management services in men with a chronic illness (arthritis) | Various | Arthritis | IV 17 men | Grounded theory (and participatory research) | See 2005 paper119 (pooled) |
| Gooden 2007,212 Australia | Comparison of ways in which men with prostate cancer and women with breast cancer share issues online | Internet (information and/or support) | Cancer: prostate (men) and breast (women) | OP 77 men (591 postings), 69 women (272 postings) | Descriptive/interpretive (part of mixed methods) | No sample characteristics because of methods; however, quality of writing in postings suggested ‘reasonably well educated and articulate’ |
| Gray 1996,122 Canada | Comparison of men’s experiences of prostate cancer self-help groups and women’s experiences of breast cancer self-help groups | Support group (face to face) | Cancer: prostate (men) and breast (women) | IV 12 men, IV/FG 27 women | Descriptive/interpretive | Men: ‘representation from among long-term survivors and men with advanced disease’; aged 45–80 years. Women: range of time since diagnosis (four < 1 year, 11 < 3 years, 10 longer term); range of severity including six with recurrence; aged 33–73 years (15 aged < 50 years). All white, reflecting groups; ‘predominantly middle class and well educated’ (three had less than high school) |
| Gray 1997,121 Canada (linked study to Gray 1997120) | Men’s experiences of prostate cancer self-help groups | Support group (face to face) | Cancer: prostate | IV 12 men | Descriptive/interpretive | See above |
| Gray 1997,120 Canada (linked study to Gray 1996122) | Women’s experiences of breast cancer self-help groups | Support group (face to face) | Cancer: breast (women) | IV/FG 27 women, linked study | Descriptive/interpretive | See above |
| Harris 2007,117 Canada | Experiences of counselling and peer support services in gay men with HIV/AIDS | Various | HIV/AIDS | IV 12 men | Phenomenology | Mean 9.75 years since diagnosis (range 4–15 years); mean age 43 years (range 27–56 years); range of education (four some high school credits, five completed high school, three ‘completed some’ university/college education); seven employed, two retired, three not working; varied income (five < $20,000, three $30,000–49,999, one > $50,000, three N/R); all gay (five previously married to women); all involved in local community-based agencies; most reported following their antiretroviral medications; 6 men had used peer support 1–2 times per week for eight years on average; seven men had received counselling 1–2 times per fortnight for 4 years on average |
| Iredale 2007,99 UK | Perceptions of information needs in men with breast cancer | Information | Cancer: breast (male) | IV 30 men (subsample of 161 men surveyed in full study) | Descriptive only (supplement to quantitative study) | Details for interview sample N/R. Details for full sample surveyed (n = 161): mean 35 months since diagnosis (range 2–120 months); 55% current breast cancer; mean age 67.3 years (range 27–88 years); 64% secondary education or above; 78% married/residing with partner, 8% single, 6% divorced/separated, 8% widowed |
| Kendall 1992,123 USA | Experiences of community support groups in gay men with HIV/AIDS | Support group (face to face) | HIV/AIDS | IV 29 men | Descriptive/interpretive | Mean 3 years and 2 months since HIV diagnosis (range 3 months to 9 years); range of disease severity (eight asymptomatic; eight mild, transient symptoms; eight ‘full-blown AIDS, not terminal’; five ‘full-blown AIDS in terminal stage’); mean age 37 years (range 25–58 years); majority Caucasian (27 Caucasian, two African American); majority highly educated (mean 16 years’ education; only one without college education); 53% employed, 46% disability allowance; all gay; 11 in a relationship (length ranging 1 month to 14 years); 31% strong family support, 46% strong friend support but ‘in general . . . did not feel well-supported’; mean three HIV support groups attended (range 1–8) |
| Kronenwetter 2005,210 USA | Men’s experiences of a prostate cancer lifestyle trial for men with early prostate cancer | Lifestyle | Cancer: prostate | IV 26 men | Descriptive/interpretive | Mean age 67 years (range 50–85 years); majority Caucasian (> 90%); majority college education, university education or ‘specialised training’ (> 90%); ‘over half’ retired; 21 (81%) had ‘partners/spouses’ |
| Martin 2013,211 UK | Men’s experiences of a nurse-led workshop for men with testicular cancer | Lifestyle | Cancer: testicular | IV 6 men | Descriptive/interpretive | Mean age 35 years (range 29–45 years) |
| Mfecane 2011,212 South Africa | Phenomenon of therapeutic citizenship in HIV/AIDS support groups, as observed in visits and experienced by men in rural South Africa | Lifestyle | HIV/AIDS | IV 25 men; PO n N/R (14 months, presumably includes some women) | Ethnography | Interview sample: aged 28–50 years; all South African; all rural; all ‘poor, working-class community’; majority unemployed; approximately half single (six married, four cohabitating, three partners living apart, 12 single); all had ≥ 1 child but minority lived with their children |
| Oliffe 2008,125 Canada | Factors influencing sustainability of prostate cancer support groups | Support group (face to face) | Cancer: prostate | PO 333 men (15 groups of men and partners) | Ethnography | Details of group members N/R |
| Oliffe 2010,126 Canada | How prostate cancer support groups simultaneously facilitate health promotion and illness demotion | Support group (face to face) | Cancer: prostate | PO 333 men (15 groups of men and partners), IV 52 men, total 333 men | Ethnography | Interview sample: mean 6.8 years since diagnosis; majority received treatment (49); mean age 70 years (range 53–87 years); 25 Anglo-Canadian, 25 northern European; majority retired (42); all attended ≥ 2 meetings in past year (inclusion criteria); mean 5.3 years accessed support groups; 16 were long-term members (had been attending for > 12 months), 16 were short-term members (had been attending for < 12 months); 20 held leadership roles (e.g. facilitator, secretary) |
| Oliffe 2011,124 Canada | How men who attend prostate cancer support groups engage with health literacy and consumerism | Support group (face to face) | Cancer: prostate | PO n N/R (16 groups of men and partners), IV 54 men, total n N/R | Ethnography | Interview sample: majority received treatment (50); mean age 71 years (range 53–87 years); all Canadian, ‘many’ northern European ancestry; majority retired (44); all attended ≥ 2 meetings in past year (inclusion criterion); 16 were long-term members (had been attending for > 12 months), 16 were short-term members (had been attending for < 12 months); 22 held leadership roles (e.g. facilitator, secretary) |
| Ramachandra 2009,100 UK | Acceptability of a brief self-led psychological intervention in patients with cancer | Psychological | Cancer: metastatic prostate (men) and metastatic breast (women) | IV unclear whether four men and three women or three men and two women (46 in total trial: 24 men, 22 women; unclear whether feedback at 6 weeks or 12 weeks) | Descriptive only (supplement to quantitative study) | Interview sample details N/R. Full trial details: men mean age 72.4 years; women mean age 60.8 years |
| Sandstrom 1996,127 USA | Utilisation of peer support groups by gay men with HIV/AIDS | Support group (face to face) | HIV infection/AIDS | IV 25 men | Grounded theory | All advanced diagnoses; 10 symptomatic HIV (including three with severe complications), 15 diagnosed with AIDS; age ranged 20–56 years (seven twenties, 11 thirties, six forties and one fifties); majority white (two African American); 12 ‘attended college or completed college degrees’; 20 urban; all gay; 16 had used support groups at some time, including nine briefly (‘usually 1–4 months’) and seven for ≥ 1 year |
| Seale 2006,128 UK | Compare the language of men and women with cancer in research interviews and online support groups | Internet (information and/or support) | Cancer: prostate (men) and breast (women) | IV 52 men, 47 women; OP 900 men, 153 women; total 952 men, 200 women | Descriptive/interpretive | Interview sample details N/R; online postings sample details N/R; Ziebland 2004219 (cited by authors) reports interview sample details for 49 men and 37 women as respective mean ages 62 years (range 51–83 years) and 44 years (range 19–75 years) |
| Seymour-Smith 2008, 213 UK | How men and women negotiate their identities as members of cancer self-help groups | Support group (face to face) | Cancer: testicular (men) and breast (women) | IV 4 men, 7 women | Discourse analysis | Men aged 26–31 years, women aged 33–64 years; all white UK; men’s sample includes 1 group leader |
| Smith 2002,101 USA | Views of African American men with prostate cancer who do not use the Man to Man support group | Support group (face to face) | Cancer: prostate | FG 4 men | Descriptive only (supplement to quantitative study) | All African American; all members of ‘100 Black Men’ organisation |
| Sullivan 2003,136 USA | Comparison of communication practices of men with prostate cancer and women with ovarian cancer supporting each other online | Internet (information and/or support) | Cancer: prostate (men) and ovarian (women) | OP 176 men (616 postings), 134 women (1256 postings). Messages from patients and HCPs were analysed in this study | Descriptive/interpretive | Sample details not known (because of methods) |
| Trapp 2013,214 USA | Men’s preferences for cancer support groups | Support group (face to face) | Cancer: any | IV five men | Descriptive/interpretive | Various cancer types (two melanoma, brain cancer, lymphoma, leukaemia); various stages (two metastatic, one stage III); four had previous cancer diagnosis; aged 30–69 years (30, 62, 62, 64, 69 years); all Caucasian and from USA; urban; majority highly educated (one high school, two graduate, two postgraduate); all had been employed (some retired/unable to work); two married, two single and one widowed |
| Vanable 2012,129 USA | Views of men with HIV who have sex with men, about sexual risk reduction programmes, to develop a tailored intervention | Various | HIV/AIDS | IV 21 men, FG 31 men, total 52 men | Descriptive/interpretive | Mean 8 years since diagnosis; 50% reported undetectable viral load; mean age 41.4 years (SD 8.1 years, range 24–63 years, ‘mostly middle-aged’); majority Caucasian (61% Caucasian, 33% African American, 6% other); 48% employed, 48% unemployed; mean monthly income $1023 (SD 699); all men who have sex with men; 33% cohabiting, 19% in relationship but living apart, 48% ‘did not have a primary partner’; mean 4.8 sexual partners in past year (SD 10.9) |
| Wallace 2007,130 USA | Psychosocial needs of men with prostate cancer | Various | Cancer: prostate | FG 16 men (2 groups) | Descriptive/interpretive | Mean 4.3 years since diagnosis (range 6 months to 12 years); mean age 66.8 years (range 49–81 years); majority Caucasian (one African American, one other); range of education (eight high school, five college and three graduate school); annual income range $20,000–100,000; majority married (15 married and one divorced) |
Country
The majority of the studies were conducted in the USA (n = 13 studies)101,110,113,114,123,128–130,136,208,213,217 and the UK (n = 11),99,100,102,108,112,115,116,128,209,214,216 with the remainder in Australia (n = 5),109,111,118,210,212 Canada (n = 5)107,117,120,125,211 and the following: Denmark,207 France,218 South Africa215 and Sweden135 (n = 1 each).
Condition
The most common disease area was cancer (n = 22),99–101,107,109,111,116,122,125,128,130,136,207–210,212–214,216,217 followed by HIV/acquired immunodeficiency syndrome (AIDS) (n = 7),108,110,117,123,127,129,215 cardiac (n = 4: coronary artery disease n = 1,134 heart failure n = 1,135 myocardial infarction n = 2102,211), mental health (n = 2: depression n = 1,115 depression/anxiety n = 1112), arthritis (n = 1),118 type 2 diabetes (n = 1)218 and multiple sclerosis (n = 1). 103 The majority of cancer studies focused on male sex-specific cancers (prostate n = 14,100,101,109,111,121,125,128,136,208–210,212,213 testicular n = 2214,216), sometimes including comparisons with female cancers (prostate vs. breast n = 4;100,122,128,212 prostate vs. ovarian n = 1;136 testicular vs. breast n = 1). 216 The remaining six cancer papers concerned a mixture of cancer types (‘any’, n = 4),113,116,207,217 male breast cancer (n = 1)99 and a comparison across colorectal cancer in men and women, cancer in male and female Chinese patients, and metastatic cancer in women (n = 1). 107
Sex
The majority of the 38 included studies had male-only samples (n = 26),99,101,108–111,113,116,117,119,121,123,125,127,130,134,135,207–211,213–215,217 but 12 studies included mixed-sex samples. 100,102,103,107,113,115,122,128,136,212,216,218 Two of the mixed-sex studies reported separate male-only and female-only data. 113,114,120–122 Two of the 26 male-only studies involved participant observation of mixed-sex groups, but did not report the number of female participants because the focus of the study was men. 112,215 The number of males and females in the sample was reported for all of the mixed-sex sample studies except one. 100
Methodology
As shown in Table 36, the majority of studies (n = 35)99–103,107–113,115–117,119,122–124,127–130,134,135,207,209–211,213–218 gathered participants’ views using interviews or focus groups. Data were collected solely through interviews in 22 studies,99,100,102,108,109,111,113,115–117,119,121,123,127,134,210,211,213,214,216–218 solely through focus groups in three studies101,130,209 and through a combination of interviews and focus groups in three studies. 110,120–122,129 A further five studies used a combination of interviews and participant observation107,112,124–126,135,215 and one study combined focus groups and participant observation. 207 Only one study used participant observation without another form of data collection. 208 Three studies analysed internet message board postings;128,136,212 one of them also used interviews in combination with internet postings. 128
Studies varied in terms of their philosophical and methodological traditions. The majority (n = 25)102,107–109,111,112,115,116,120–123,128–130,136,207,209–214,217,218 were considered to be interpretive/descriptive studies, either because they did not specify a distinct methodological approach or philosophical orientation or because they used analytical methods associated with certain traditions (e.g. grounded theory method of constant comparative analysis), or were in some way informed by these perspectives, but were judged to have adopted the approach inconsistently throughout the study. For the purposes of this report, such studies were classified by the review team as interpretive/descriptive despite the authors’ acknowledging other approaches, for example ethnography,107 phenomenology136,210 and grounded theory. 109,115,127,129,130,211,212
Three studies were descriptive only, and all three of these were reported alongside quantitative research. 99–101 Four studies reported taking a phenomenological approach,113,114,117,134,135 two used ethnography,124–126,215 two used discourse analysis208,218 and two used grounded theory,115,118,119 including one that used participatory research. 118,119
Sample size
Studies varied greatly in sample size, which partly reflected type of data collection. Studies utilising internet message board postings had relatively large sample sizes (range n = 146–1053), with postings across studies being made by a total of 1053 men and 356 women with LTCs. Studies employing participant observation varied in sample size, between three135 and 333,124–126 while in some it was not possible to determine the sample size of men with LTCs. 107,112,124,208,215 Samples for studies involving interviews and focus groups ranged between three135 and 99. 128 One of the interview studies did not report the number of participants interviewed;100 in the remainder, a total of 583 men and 114 women took part in interviews or focus groups.
Sample characteristics
Reporting of sample characteristics was often limited. This was found across study designs, not just those studies where collection of demographic information was potentially constrained by the type of data collection (i.e. participant observation and analysis of online postings) or by the intervention’s being accessed independently of the research study itself (e.g. participation in a support group).
Age was the most frequently reported characteristic, being reported in 26 studies. In a further five studies, age was reported for a wider sample from which a smaller qualitative subsample was drawn, but was not reported for the smaller qualitative sample. 99,100,128,206,207 Participant age ranges varied greatly, reflecting different LTCs, with younger samples restricted to studies concerning testicular cancer (range 29–45 years211) and HIV/AIDS (range 25–50 years;108 26–62 years;110 27–56 years;117 25–58 years;123 20–56 years127).
Ethnicity was reported in 18 studies. Of these, four studies reported that the full sample comprised only white/Caucasian participants116,120–122,216,217 and a further 10 studies reported the majority of the sample as white/Caucasian. 108,115,118,119,123–127,129,130,134,210 Three studies recruited samples that were entirely non-white: Canadian Punjabi Sikh,211 black South African215 and African American. 101 One study, a focus of which was ethnicity, included two predominantly white samples and one exclusively Chinese sample. 107
Relationship status (e.g. single, cohabiting) was reported in 14 studies. Sexuality was reported in one study focusing on arthritis119 and six of the seven studies concerning HIV/AIDS; the exception was a South African study of men with HIV/AIDS. 215
Measures/descriptions of socioeconomic status varied. Where these were reported, most commonly the measures used included employment status (n = 15), educational attainment (n = 14), occupation status (n = 4) and annual income (n = 3).
Details of the LTCs (e.g. time since diagnosis, treatment history, stage of condition, prognosis) were reported in 23 studies.
Reporting of participant characteristics alongside data extracts
Participant characteristics were often not presented alongside excerpts/data in the individual studies. Three studies reported group-level data, without presenting individual-level data. 100,101,208 Of the remaining 35 studies, participant identifiers were presented in 23 studies. A participant identification number or pseudonym was given in 18 studies, although this did not always link to any characteristics.
In this review, one of the inclusion criteria for mixed-sex studies was that the authors explicitly reported at least some comparison by gender. Gender could be determined for all data cited in the majority of the mixed-sex studies; however, two studies by Barlow et al. 102,103 reported gender only in brief sections concerning ‘gender differences’, and not in the remainder of the findings.
Age was reported alongside data extracts for eight studies. 107,112,116–119,124,126,215,217 Individual reporting of ethnicity and relationship status was confined to one study each. 217 Employment status was reported in only two studies. 118,119,217 Individual treatment information was presented in six studies107,109,112,124,126,213,217 and information about individuals’ conditions (e.g. stage) in four studies. 107,109,116,217 Some of the details concerning ethnicity, treatment information and condition did not need to be reported with individual data because samples were homogeneous.
Types of self-management support
The details of the self-management support are presented in Table 37. As described in Chapter 3, Public and patient involvement, studies in the qualitative reviews were grouped using the broad categories listed in Table 6. The most common type of self-management support described in the studies was face-to-face support groups (12 studies),101,107,108,110,112,120,123,124,127,208,216,217 followed by ‘lifestyle’ interventions (11 studies). 102,103,134,135,207,209,211,213–215,218 Five studies involved internet information and/or support;109,113,114,128,136,212 two of these studies were focused on analyses of postings on online forums and discussion boards. 136,212 Two studies concerned information more broadly, not limited to online access. 99,116 Two studies described the interventions as ‘psychological’. 100,210 The remaining six studies were grouped as ‘various’, which included studies that concerned ‘any’ experiences of self-management or psychosocial support services,111,115,118,119 experiences of both one-to-one support and peer support117,130 and views on potential interventions. 129
| Study (first author, year) | Description | Classification of support activity used in qualitative synthesis |
|---|---|---|
| Adamsen 2001207 | Group programme involving physical activity and keynote speakers; structured as 13 2-hour sessions over 16 weeks; led by health professionals (oncology and physiotherapy) at a hospital facility; developed for men with cancer | Lifestyle |
| Arrington 2005208 | One prostate cancer face-to-face support group (‘Man to Man’) involving keynote speakers, question and answer session and ‘breakout’ groups; structured as monthly 2-hour sessions; led by health professional (physician); open to family members | Support group (face to face) |
| Baird 2001134 | Cardiac rehabilitation programme involving supervised exercise (including cardiac monitoring), assistance with medication, education on stress management, diet and other health behaviours; led by professional. Phase II lasts 4 weeks, Phase III lasts 4 months, Phase IV involves exercise prescription and open-ended use of cardiac therapy facility | Lifestyle |
| Barlow 2009103 | Group programme involving education, group discussion, skills training, goal-setting, problem-solving, role-play and reporting back on progress; structured as six weekly 2-hour sessions; led by trained lay tutors who have LTC, held in community settings; developed for any LTC | Lifestyle |
| Barlow 2009102 | Group programme involving education, group discussion, skills training, goal-setting, problem-solving, role-play and reporting back on progress; structured as six weekly 2-hour sessions; led by trained lay tutors who have LTC, held in community settings; developed for any LTC | Lifestyle |
| Bedell 2000108 | Any face-to-face support group | Support group (face to face) |
| Bell 2010107 | Three professionally facilitated face-to-face cancer support groups, all with ‘drop-in’ format: (1) women’s metastatic group, involving meditation and group sharing, held bimonthly (sic); (2) mixed-sex colorectal group, involving group sharing and occasional speakers, held monthly, open to caregivers too; and (3) mixed-sex Chinese group, involving lecture, group sharing and discussion, held monthly, open to family members too | Support group (face to face) |
| Bourke 2012209 | Group programme involving supervised physical activity, self-directed physical activity, healthy eating group seminars and nutrition advice pack; structured as twice-weekly supervised exercise for the first 6 weeks and weekly for the next 6 weeks, with 15- to 20-minute seminars every fortnight; supervised by ‘exercise specialists’ at a university rehabilitation suite; developed for men with prostate cancer | Lifestyle |
| Broom 2005109 | Any Internet use to access information and support | Internet (information and/or support) |
| Chambers 2012210 | Group programme involving mindfulness-based cognitive therapy, including education, skills training, handbook, audio CD and self-led home-based practice; structured as eight weekly 2-hour sessions and optional extended practice session; led by psychologist; developed for cancer patients | Psychological |
| Chenard 2007110 | Any face-to-face support group for patients with HIV/AIDS | Support group (face to face) |
| Corboy 2011111 | Any cancer psychosocial support services | Various |
| Cramer 2013112 | Various peer-led and professional-led face-to-face support groups for men with depression or anxiety; mixture of ‘drop-in’ format (usually weekly or monthly) and more structured psychoeducational with set number of sessions; majority mixed-sex groups; some funded by voluntary sector, some by statutory sector; some self-referral, others via general practitioner | Support group (face to face) |
| Dickerson 2011113 (linked: Dickerson 2006114) | Any internet use to access information and support; and any experiences of interactions with HCP relating to this | Internet (information and/or support) |
| Eldh 2006135 | Nurse-led clinic involving medication management and education about the condition, its management and health behaviours; held at a hospital outpatient clinic | Lifestyle |
| Emslie 2007115 | Experiences of any self-management support interventions for depression (e.g. cognitive–behavioural therapy/talking therapies) | Various |
| Evans 2007116 | Any information accessed relating to complementary and alternative medicine | Information |
| Ferrand 2008218 | Group physical activity including exercise classes, groups and events; organised by a patients’ association (‘Move for Health’); activities available throughout the week on an ongoing basis; led by patients and sometimes cosupervised by ‘medico-sporting educators’ | Lifestyle |
| Galdas 2012211 | Cardiac rehabilitation programme involving education on the condition and health behaviours, using classes, workshops and individual counselling sessions; held weekly at a hospital facility | Lifestyle |
| Gibbs 2005119 (linked: Gibbs 2007118) | Any arthritis self-management services | Various |
| Gooden 2007212 | One prostate cancer and one breast cancer online support group (‘discussion board’) | Internet (information and/or support) |
| Gray 1996122 (linked: Gray 1997120,121) | Various face-to-face prostate cancer and breast cancer support groups; held in the community and described as ‘self-help’; the three prostate cancer groups described as affiliated with ‘Us, Too’, ‘Man to Man’ and ‘a local hospital but later took on a more independent status’; affiliations for the breast cancer groups are not presented | Support group (face to face) |
| Harris 2007117 | Any individual counselling and individual/group peer support; counselling involving trained professional counsellor or therapist, who may or may not be living with HIV/AIDS; peer support is facilitated by trained peers living with HIV/AIDS | Various |
| Iredale 200799 | Any information accessed relating to the condition (male breast cancer) | Information |
| Kendall 1992123 | Any face-to-face community support group for patients with HIV/AIDS | Support group (face to face) |
| Kronenwetter 2005213 | Group programme involving physical activity, skills training (stress management), peer support and dietary advice; structured as weekly 4-hour sessions, case management and home visits; held in community settings; developed for men with prostate cancer | Lifestyle |
| Martin 2013214 | Group workshop involving education, survivor stories, group discussion and goal-setting; structured as one-off 4-hour session; led by nurse and self-management tutor; developed for men with testicular cancer | Lifestyle |
| Mfecane 2011215 | Group (mixed-sex) programme involving education and group discussion about the condition, its management and health behaviours ‘challeng[ing] traditional health and gender beliefs’ and encouraging to ‘convert’ to a ‘responsible’ lifestyle; facilitator trained by non-government and government organisations; some facilitators also had HIV; medication conditional on group attendance; held at public health clinic; developed for HIV/AIDS | Lifestyle |
| Oliffe 2008125 (linked: Oliffe 2010,126 2011124) | Various face-to-face prostate cancer support groups; varied format but usually involving education and group sharing; two-thirds involved formal sharing and half had a formal presentation by a speaker, typically involving refreshment breaks where one-to-one and small group discussion happened; all peer-led; majority 2-hour sessions (range 35–120 minutes) | Support group (face to face) |
| Ramachandra 2009100 | Self-administered psychological intervention involving well-being diary, mindfulness CD and planning activities, following briefing on the theory and practical aspects of the intervention; telephone contact happened in weeks 1, 2, 4 to answer queries and encourage practice; developed for cancer patients | Psychological |
| Sandstrom 1996127 | Any face-to-face support group for patients with HIV/AIDS | Support group (face to face) |
| Seale 2006128 | Any internet use to access information and support; includes online postings from one prostate cancer and one breast cancer online support group (‘forum/discussion board’) | Internet (information and/or support) |
| Seymour-Smith 2008216 | One lay-led testicular cancer and one lay-led breast cancer face-to-face support group | Support group (face to face) |
| Smith 2002101 | One prostate cancer face-to-face support group (‘Man to Man’) involving keynote speakers, led by health professional (physician); open to family members | Support group (face to face) |
| Sullivan 2003136 | One prostate cancer and one ovarian cancer online support group (‘mailing list’) | Internet (information and/or support) |
| Trapp 2013217 | One mixed-sex face-to-face cancer support group | Support group (face to face) |
| Vanable 2012129 | Possible self-management support interventions for men with HIV who have sex with men | Various |
| Wallace 2007130 | Any psychosocial support, including one-to-one and face-to-face support groups | Various |
Study design did not form part of the inclusion criteria and, therefore, study designs varied considerably. In eight studies, participants accessed self-management interventions or support activities as part of research participation; three of these were non-controlled studies207,210,214 and five involved random allocation to the intervention of a trial. 100,102,103,209,213 All of these studies concerned lifestyle or psychological interventions, as shown in Table 38.
| Intervention type | Allocation to intervention | Total number of studies | |||
|---|---|---|---|---|---|
| Participants all received same intervention given as part of research study | Participants all received same intervention (e.g. specific support group) but not given as part of research study | Participants received a range of different interventions of the same type (e.g. any support group) but not given as part of research study | Participants received various interventions and different types of interventions (e.g. counselling and peer support) but not given as part of research study | ||
| Lifestyle | Adamsen 2001207 Barlow 2009103 Barlow 2009102 Bourke 2012209 Kronenwetter 2005213 Martin 2013214 |
Baird 2001134 Eldh 2006135 Ferrand 2008218 aGaldas 2012211 Mfecane 2011215 |
11 | ||
| Psychological | Chambers 2012210 Ramachandra 2009100 |
2 | |||
| Face-to-face support groups | Arrington 2005208 Seymour-Smith 2008216 Trapp 2013217 |
Bell 2010107 Gray 1996,122 1997120,121 Kendall 1992123 Oliffe 2008,125 2010,126 2011124 aBedell 2000108 aChenard 2007110 aCramer 2013112 aSandstrom 1996127 aSmith 2002101 |
12 | ||
| Internet information and/or support | Gooden 2007212 Sullivan 2003136 |
Dickerson 2006,114 2011113 Seale 2006128 aBroom 2005109 |
5 | ||
| Information (including online) | Iredale 200799 Evans 2007116 |
2 | |||
| Various | Harris 2007117 aCorboy 2011111 aEmslie 2007115 aGibbs 2005,119 2007118 aVanable 2012129 aWallace 2007130 |
6 | |||
Self-management support that happened independently of research participation did not usually focus on one single intervention or support activity; the exceptions were five lifestyle interventions,134,135,211,215,218 three face-to-face support groups208,216,217 and two sets of online forums. 136,212
As shown in Table 38, in 12 studies, not all participants had engaged in self-management support as part of the research study per se: lifestyle (n = 1);211 face-to-face support groups (n = 5);101,108,110,112,127 online information and/or support (n = 1);109 various (n = 5). 111,115,118,119,129,130 Rather, these studies provided an evaluation of participants’ experiences of current or previous involvement with these activities.
Summary of study quality
As discussed in Chapter 3, Quality assessment strategy, we used the CASP tool (see Appendix 6) to provide descriptive information on the quality of the included studies to inform interpretation of the evidence, rather than as a basis for inclusion/exclusion.
We found the CASP tool was of limited value in providing an overall comparison between the ‘quality’ of the included studies (see Table 39), and total scores were not considered to be a meaningful reflection of the quality of the research. The tool was, however, useful for enabling the review team to identify and document specific methodological concerns and limitations relating to individual studies (see Appendix 7).
| Study (first author, year) | 1: clear statement of aims | 2: qualitative methodology appropriate | 3: research design appropriate | 4: recruitment strategy appropriate | 5: data collected in way that addressed research issue | 6: researcher–participants relationship considered | 7: ethical issues | 8: data analysis rigorous | 9: clear statement of findings | 10: research valuable |
|---|---|---|---|---|---|---|---|---|---|---|
| Adamsen 2001207 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes |
| Arrington 2005208 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Unclear | Yes | Yes |
| Baird 2001134 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Limited |
| Barlow 2009103 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Limited |
| Barlow 2009102 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Limited |
| Bedell 2000108 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Bell 2010107 | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes |
| Bourke 2012209 | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes |
| Broom 2005109 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Chambers 2012210 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Chenard 2007110 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Corboy 2011111 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Cramer 2013112 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Dickerson 2006114 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Dickerson 2011113 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Eldh 2006135 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Emslie 2007115 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Evans 2007116 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Ferrand 2008218 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Galdas 2012211 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Gibbs 2005119 | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes |
| Gibbs 2007118 | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes |
| Gooden 2007212 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Gray 1996122 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Gray 1997121 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Gray 1997120 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Harris 2007117 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Iredale 200799 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Limited |
| Kendall 1992123 | Yes | Yes | Yes | Unclear | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Kronenwetter 2005213 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Martin 2013214 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Limited |
| Mfecane 2011215 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes |
| Oliffe 2008125 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Oliffe 2010126 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Oliffe 2011124 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ramachandra 2009100 | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Unclear | Yes | Limited |
| Sandstrom 1996127 | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Unclear | Yes | Yes |
| Seale 2006128 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Seymour-Smith 2008217 | Yes | Yes | Yes | Unclear | Yes | Unclear | Yes | Yes | Yes | Yes |
| Smith 2002101 | Yes | Yes | Unclear | Unclear | Yes | Unclear | Yes | Unclear | Yes | Limited |
| Sullivan 2003136 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Trapp 2013217 | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes | Yes | Yes |
| Vanable 2012129 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
| Wallace 2007130 | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes | Yes |
All studies were judged to have provided an adequately clear statement of aims (CASP item 1) and findings (item 9). Qualitative methodology (item 2) was considered appropriate for all studies and the research design (item 3) was judged appropriate for all studies except one101 which could not be determined from the information provided. Inadequate detail was provided in seven studies to judge the appropriateness of the recruitment strategy (item 4);101,107,118,119,123,209,216,217 the remainder were judged appropriate. Sufficient details were presented to enable a judgement that data were collected in a way that addressed the research issue (item 5) in all but one study. 100 Only five studies provided sufficient information that demonstrated consideration of self-reflexivity and the relationship between the researcher and participant (or data; item 6). 115,117,124–126,136,217 None of the studies raised any significant ethical concerns; however, seven did not report the appropriate ethical permissions (item 7);110,113,114,120–123,127,208,214 this may partly reflect the age of the studies and changing reporting requirements regarding ethical approval over time. The two quality appraisal items that were most difficult to determine were whether or not the data analysis was rigorous (item 8) and the value of the research (item 10). Eight studies were judged to present insufficient detail to evaluate the rigour;99–102,127,207,208,215 the remainder were judged adequate. Although all studies were assumed to offer some potential value through ‘novel findings or perspectives’ in their individual research area, seven studies were judged to be of limited value for the current review,99–103,134,214 for example, because they reported minimal qualitative data or had a different focus from the current research questions (perceptions and experiences of self-management interventions or support activities).
Although not reflected by the CASP ratings (Table 39), the qualitative reviewer comments highlighted concern across the literature with the (in)adequacy of descriptions of the samples and, as described earlier, lack of participant identifiers accompanying data excerpts, which hampered assessment of the extent to which authors had taken into consideration all available data.
Line-of-argument synthesis
As described in Chapter 3, Data extraction strategy and data analysis, we developed a line-of-argument synthesis that encompassed both similarities and contradictions that were evident in the literature. The second-order findings extracted from the studies are presented in Appendix 10, alongside the third-order constructs that we developed through our analysis and which formed the basis of our key concepts and line-of-argument synthesis.
Our analysis identified four key, interconnected concepts associated with men’s experience of, and perceptions of, self-management support. Our line-of-argument synthesis using these concepts provides an interpretation of men’s perceptions of the acceptability of self-management support and what may act as facilitators and barriers to access to and use of interventions and activities. The synthesis also offers an understanding of how masculine identities play a central and enduring role in men’s experience of self-management support. The four key concepts and their constituent third-order constructs are shown in Figure 12, and the inter-relationship between the concepts are depicted in Figure 13. The four key concepts that constitute our line-of-argument synthesis are summarised below:
FIGURE 12.
Four key concepts and constituent third-order constructs.
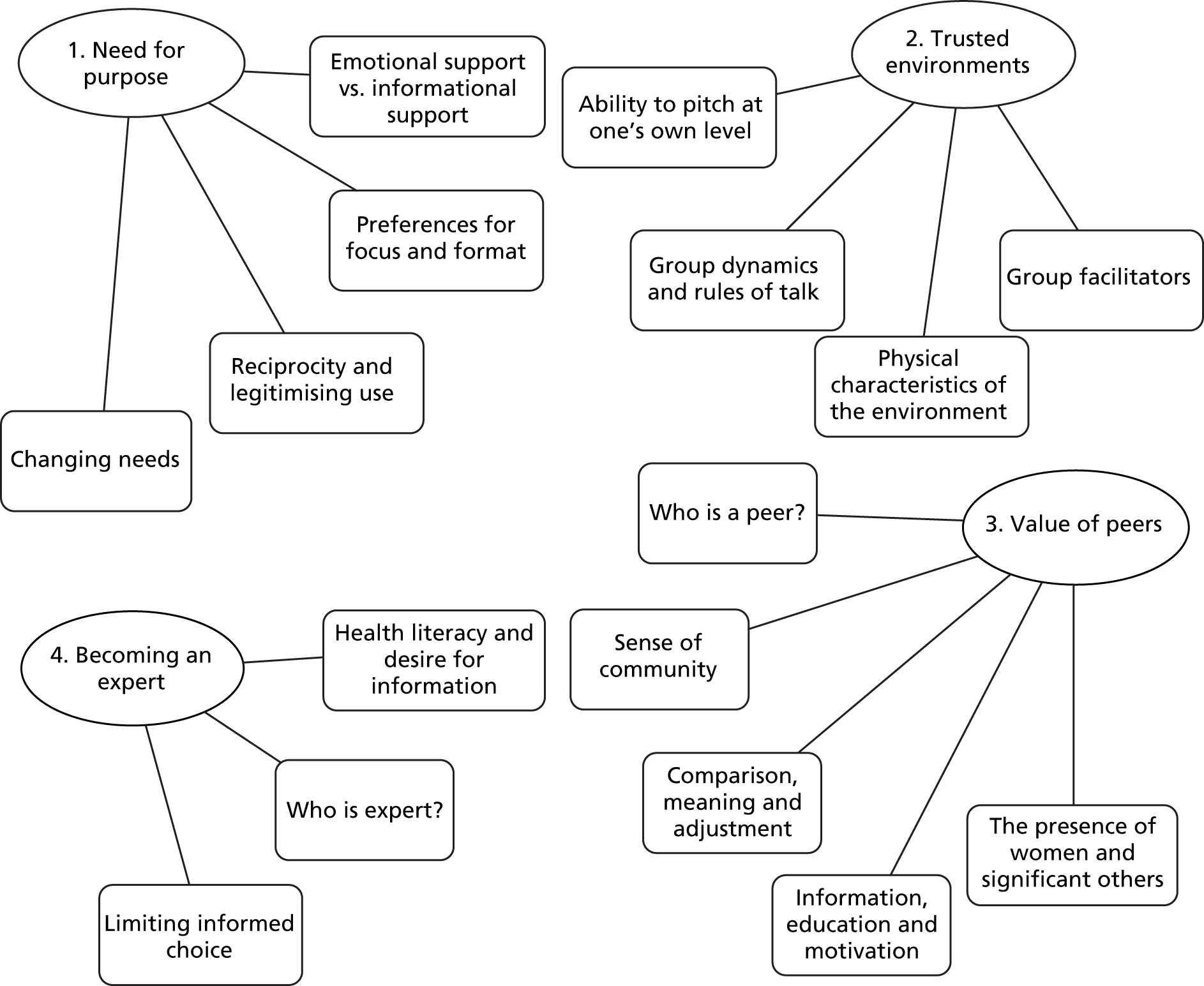
FIGURE 13.
Four key concepts and their inter-relationship.
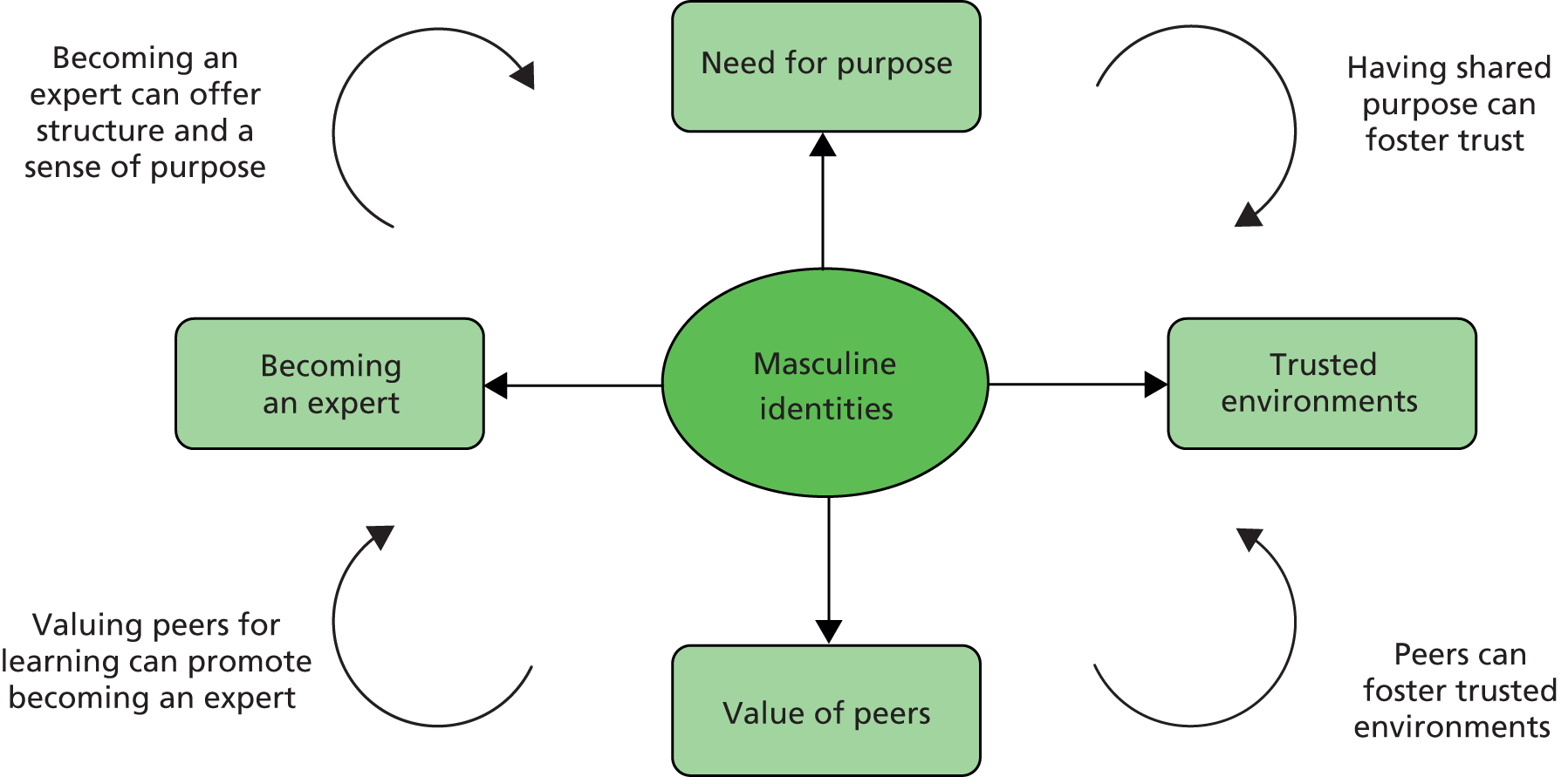
-
Need for purpose
Men commonly expressed the need to feel that there was a clear purpose when accessing and continuing to use self-management support that was perceived to address an unmet need. Evident across study findings were tensions between men’s perceived need to fulfil roles and obligations linked to their identity as a man, and acceptance of living with and needing help to manage a health condition that could potentially threaten that identity. Family or friends were often instrumental in legitimising a need and encouraging men’s involvement in support interventions.
There was a clear preference for structured, action-orientated support that was consistent with a male predilection for problem-focused coping. Support that did not transgress culturally valued masculine ideals of independence, strength and control were often considered to be more accessible and acceptable. Men valued both information and emotional types of support, but appeared more comfortable with the latter occurring as a ‘by-product’ of other shared activities, or tackled ‘sideways on’, in order to avoid challenges to masculine norms associated with emotional self-sufficiency. Receiving and sharing information could provide men with both reassurance and emotional support, and was commonly seen as more acceptable than ‘just talking’.
-
Trusted environments
The need for men to access interventions in a safe, private, trusted space/environment was apparent across the literature. Building a ‘trusted environment’ was critical for accessibility and acceptability, especially where men may have felt vulnerable or lacking in confidence; this included interventions involving physical activity and group-based activities such as emotional sharing that might be seen as incongruous with masculine ideals and behavioural norms. The trustworthy nature of an environment could be fostered or evaluated in different ways: for some men, it meant a male-only environment where they felt able to speak freely, or an online environment that maintained anonymity; for others, feeling able to set the pace and activity at a level where they felt comfortable, or being permitted different types of involvement or contribution at different times, was considered an important factor.
The setting of an intervention, group size and structure, processes for dealing with emotional or taboo topics, and the characteristics of the facilitator or health professional were all shown to have a bearing on whether or not an intervention was perceived to be ‘trustworthy’ by men and, therefore, accessible and acceptable.
-
Value of peers
Interaction with peers who had a shared illness experience was valued across self-management support activities (either face to face or online) and they offered a sense of belonging, connectedness and normality for many men. Shared experience and understanding frequently helped to foster a ‘trusted environment’ and could offer men living with LTCs opportunities for social comparison and learning, and lead to implications (which men often did not foresee) for sense of community, issues of belonging, meaning and adjustment, as well as peer education and mutual motivation.
Comparison and learning from peers were common and not limited to information about the condition or its management. Examples in the literature showed possibilities for learning about well-being more generally, gaining a sense of community and developing social skills that fostered the development of relationships. Group lifestyle interventions noted the importance of peers and group identity for encouraging adoption of physical activity through motivating each other, a sense of camaraderie and social commitment that were congruous with masculine identities. Private ‘male-only’ spaces away from ‘significant others’ were valued by some, but the presence of friends and family in face-to-face interventions was also reported to encourage talking and emotional sharing.
-
Becoming an expert
Study findings illustrated that men involved in self-management support interventions often evolved into ‘experts’ and providers of information in their own right: a role that could complement a ‘need for purpose’ and offer a way to regain control and reclaim a sense of identity fractured through chronic illness. Contrary to prevailing commentaries on gender differences, the literature showed that men valued health education, with the use of medical terminology and evidence often helping to foster group identity in face-to-face support groups. Acceptable support required the provision of practical information and strategies that could be integrated into daily life, rather than simply providing general health messages.
Evidence of the use of multiple types of support intervention was apparent, particularly information provision/education and online or face-to-face support groups, with some men becoming informed consumers of services and treatments. Findings also highlighted the potential of information and education to provoke anxiety and overwhelm; boundaries were sometimes set around the amount of information that was needed or should be sought, to maintain an ability to cope. Evident were preferences for men to be able to devolve decision-making and management to HCPs and retain the ability to adopt a passive rather than proactive role when this was desired.
The full synthesis is described below with reference to these four key concepts and the third-order constructs that constitute them. First-order constructs (participant quotes or observations) as well as secondary constructs (the original author’s or authors’ interpretations) extracted from the included studies are incorporated to illustrate and add depth to the concepts.
Although the term ‘men’ is used throughout the description of the synthesis, it is important to note that we found that a number of the constructs pertain to both men and women living with LTCs. Where we identified variation between men and women in the ways in which concepts are enacted, experienced or expressed, we have provided examples accordingly.
Need for purpose
We didn’t come just to discuss things.
First-order; p. 532207
Our analyses suggested that, for men to access and continue to use self-management support, many felt that they had to identify that an intervention had a clear purpose and addressed an unmet need. Related to this were tensions between men’s perceived need to fulfil roles and obligations linked to their identity as a man, and acceptance of living with and needing help to manage a condition that could potentially threaten that identity.
The concept is discussed below with reference to four third-order constructs that constitute the overall concept:
-
emotional support versus informational support
-
preferences for focus and format
-
reciprocity and legitimising use
-
changing needs.
Emotional support versus informational support
In describing the functions of self-management support activities, studies commonly presented emotional support as distinct from informational support and considered the relative importance of each, particularly when drawing gender comparisons. Several studies with mixed-gender samples stated that men living with LTCs had a preference for informational support, while women preferred emotional support. 102,103,107,113,122,128,136,216,218
However, a number of investigations with male-only samples, spanning different types of LTCs, self-management support activities and methods of data collection, reported that men valued both information and emotional support. 108,117,207,209,213 In one study, support groups were seen as offering both important informational support and an outlet to share feelings and fears. 108
Some authors recognised that, while many men value emotional support, they may feel less comfortable than women with reporting this as a motivation for using interventions, as this may transgress the enactment of dominant (hegemonic) masculine ideals of stoicism118,124–126,216 and ‘emotional self-sufficiency’. 112 Notably, some men did identify company and intimacy as the primary motivation for joining peer support groups,123,217 including a preference of ‘connection over information’ (p. 626),217 contrary to a supposedly common perception of men as ‘solitary and emotionally restricted’ (p. 619). 217
However, there was an indication that men and women valued informational and emotional types of support equally, but received (and offered) this in different (gendered) ways. For some men, receiving ‘factual’ information could offer reassurance, which also served to provide emotional support109,113 and ‘reduce uncertainty and unpredictability of disease and to increase feelings of control’ (p. 87). 208
Although emotional support in online postings in discussion board/internet support groups was not as immediately evident among men as in women, having ‘well-informed and balanced information’ could itself provide emotional support212 and the act of sharing information was associated with feeling ‘esteemed, valued and accepted’ (p. 100). 136 It could, therefore, be considered ‘intimate’ communication; this provides further confirmation that emotional support and informational support are inter-related for some men, possibly more so than in women. Emotional support may, however, be less visible and under-recognised in men’s interactions because of a disinclination to use overtly emotional or nurturing language:
Researchers need to be alert to instances of talk that represent strong emotional content, but which do not employ emotion words.
Second-order; p. 111212
Other examples of men’s preferred forms of emotional support included encouragement that focused on strength, perseverance, and camaraderie,212 and support conveyed covertly through humour207,209 or supportive silence. 207,208 Participant observation studies107,124–126,208,215 illustrated that separation of emotional and information support may be increased through group processes, rather than necessarily reflecting men’s true preferences (discussed further in Trusted environments). Some authors tended to persist with traditional perspectives about male preference for information and action in their analyses, rather than considering inter-relatedness or group processes. 103,107,122
Types of support and types of coping
Gender differences in the way support was provided and received were reported to be closely tied to gender differences in preferences for types of coping. Men were found to express preference for ‘action-oriented’, ‘activity-based’ support consistent with a male predilection for problem-focused coping. 126,207,216 This was often contrasted with a female preference for sharing personal experiences,103,107,122 consistent with emotion-focused coping.
Some studies reported that men were keen to emphasise structure and activity as important and thus distance their participation in self-management support activities that were considered ‘feminine’,119 for example ‘touchy-feely’ discussions. 216 ‘Doing’ was seen as a way to regain control and reclaim a sense of identity, which had been disrupted through chronic illness. 115,203 This was commonly contrasted with ‘just talking’. 111,112,115,117,209
[D]oing the exercises we thought we were getting something out of it. Just having these talks [referring to group discussions], is not doing a lot of good.
First-order209
A sense of ‘doing’ could be particularly valued where the management of a condition was not viewed as ‘active’; for example, ‘watchful waiting’ in prostate cancer may be viewed as ‘nothing is being done’. 213
Sometimes the phrase ‘just talking’ distinguished talk that was considered ‘unproductive’ or ‘emotional masturbation’115 from talk that was perceived as constructive and purposeful, for example, through providing information, being problem-focused or ‘unburdening’ via emotional sharing.
In the two studies that focused on mental health112,115 this distinction contrasted talking therapies (such as cognitive–behavioural therapy) that offer practical results with other forms of talking therapy. Emslie et al. 115 found that men placed importance on getting practical results from talking therapies; this was in comparison with other forms of therapy, which were conceptualised as ‘just talking’. Similarly, several men in Cramer’s study112 disliked the idea of counselling because they did not see the point of ‘talking about things that happened in the past and could not be changed’.
Preferences for focus and format
Across all types of support, men were commonly reported to have expressed preferences for structure and activity, which links with expressed preferences for problem-solving. Physical activity was consistently valued as offering a purpose and focus, sometimes linked to self-reported physical improvement207,209,218 and feeling ‘healthier’ or energised. 213 Three studies reported that structuring meetings around talks by invited speakers, or embracing activities such as activism and lobbying by the group, could also provide a useful focus for the group. 120–122,124–127
Several studies reported that having structure and/or activities could offer opportunities for ‘opening up’ emotionally,207,218 ‘regardless of [men’s] intentions’122 through approaching emotional issues or mental health ‘sideways on’. 112
Men may be more comfortable, and environments considered more ‘trusted’, when self-management activities do not have emotional support as an explicit component, with emotional support instead arising as a ‘by-product’ of other shared activities. Aligned with this is the need to avoid transgressing culturally valued masculine ideals of independence, strength and control, which confirms the notion, expressed by some study authors, that support services can be made more acceptable to men if they ‘focus less on emotional expressiveness and more on instrumental changes and control’115 and are thereby reframed as a way of demonstrating these traditional masculine ‘traits’. 111
There was evidence that the need for using structure and activity to tackle emotional sharing ‘sideways on’ may vary between different groups of men. For example, differences were observed in the HIV/AIDS literature, in which all of the support groups for gay men with HIV/AIDS focused on emotional sharing, in contrast to some of the other male-only support groups. 122,124–126,208 A focus on structure and activities did not seem necessary for these men to ‘open up’,108,110,123,127 although there was some suggestion that sharing certain types of feelings (e.g. fear and shame) may take longer for some men. 123
In contrast, it was deemed necessary for an intervention in South Africa for men with HIV to be strongly structured and to include educational components. This was reflective of culturally dominant notions of masculine identities and how men were not comfortable with emotional expression. 215 Similar intersections between culture and gender arose in the cancer literature, with Bell et al. 107 noting that a ‘tangible product’ such as education or coping skills may increase acceptability of support groups to men for whom ‘sharing’ is an ‘unfamiliar concept’.
Reciprocity and legitimising use
Seeking and accepting support could pose greater threats to identity for men who adhere to the masculine ideals of stoicism and self-sufficiency. In these cases, men may feel the need to ‘justify or legitimize their involvement’ as part of their performance of masculinity in the face of presumed hegemonic ideals. 216 This may be particularly true of group-based interventions or those with an active element of social support or self-revelation.
One example of men legitimising their involvement in such interventions was the way in which men ‘denied any agency’ in seeking support, instead portraying themselves as having ‘stumbled’ across support groups. 216 This is consistent with several other studies which reported an instrumental role for family or friends in men’s help seeking (rather than the man himself), for example in identifying a need for support, accompanying men when attending activities, or helping to access and navigate information. 111,113,116,122,128,130,134,208
Therefore, feelings of reciprocity and mutuality could be important for men when accessing interventions as a way to legitimise their involvement and lessen perceptions of need or vulnerability, as noted by Seymour-Smith:
Perhaps once men establish that their primary concern is to offer help to others it may became less problematic to admit to benefiting from the group themselves.
Second-order; p. 794216
Similarly, participants in one study found it critical to both receive and exchange information;127 this phenomenon was viewed in another study as a ‘transaction’217 that involved ‘give and take’, not just receiving. Although this was not a male-only phenomenon,107,120 there was some suggestion in the literature that men placed greater importance on reciprocity. Seymour-Smith216 argued that the tendency to emphasise the benefit of others through one’s involvement was gendered, with women describing receiving help and men portraying themselves as offering help.
Authors’ analyses of online postings also reported that, although reciprocity is important for both genders, men may be more likely to engage in information sharing and women may be more likely to engage in personal or emotional sharing. 136
The role of reciprocity could vary at different stages in an individual’s use of self-management support. A number of support group studies (spanning various conditions) reported that information seeking was commonly given as a main reason for initial attendance whereas, later on, men said that they continued to attend to ‘give back’, both to other individuals (especially newcomers) and to the group as a whole, thereby strengthening a group’s sustainability. 107,125,216
This sense of ‘giving back’ could also extend beyond group members, to wider society, for example through lobbying involvement, through raising awareness or, in the case of patients accessing interventions as part of a research study, as a way of expressing ‘gratitude’ to care providers,100,209 or being able to contribute to research to benefit future patients. 209
Contributing to the group and to the experiences of others could be important for identity and self-esteem, and was reported to be of particular importance to men. 216 Contributions could occur informally through relationships within groups and could also occur through taking on leadership and committee membership roles. 112,122,125 Such business-like approaches were argued to be particularly valued by some men,122 perhaps reflecting the ways in which LTCs can challenge men’s identities as men, for example through loss of identity through loss of work. 118,119
However, the process of ‘giving back’ was not always positive. Some studies reported that men who had acquired leadership roles as lay volunteers felt that they were burdensome, and that such men risked ‘burnout’ particularly when faced with worsening health. 125,127
Changing needs
The purpose of interventions could change with evolving individual circumstances and ensuing changes in men’s needs and requirements for support.
The need for support and motivations for attending and continuing to use interventions was reported to vary according to men’s existing informal support and availability of significant others (e.g. partner, family, friends). Such observations were a stronger feature of the male-only literature than the gender comparison literature. Some men attributed choosing not to access support groups to their strong informal support network. 101,127
There was some evidence that emotional support might be particularly sought and valued where social isolation commonly accompanied LTCs, for example among men with mental health problems112 and HIV/AIDS. 117,123,127 Sandstrom127 provide a key illustration of this third-order construct, identifying that men with greater existing support still accessed groups but sought different support; that is, they primarily sought informational support and did not remain involved with the support groups for as long. Sandstrom127 also found that existing support did not solely relate to people; it could also concern knowledge of the condition, how it is viewed in society and ease of access to information through other means, such as literature.
Other studies reported that attending a support group could allow men to seek emotional support outside their informal network for different reasons: not because of a lack of informal support but because, for example, they wished to ‘protect’ their significant others from being burdened or otherwise negatively affected by their concerns. We return to this later in relation to the concept ‘value of peers’ (see Value of peers).
Existing commitments were reported to act as potential barriers to accessing interventions and activities, for example being busy with other activities101 and work. 118 Sometimes commitments intersected with men’s identities; for example, Gibbs’s analysis118 reported that, in the case of work, men identified themselves as providers and prioritised work over health; the type of employment (e.g. self-employment, farming) or, indeed, culture did not necessarily act as a barrier. Prioritising work over health was most relevant in the middle years, when men carry greatest obligations, compared with younger men (who may view accessing self-management support as a temporary disruption to work) and older men (who may not have the competing demands of work as they approach retirement, or are retired, or see declining health as an expected part of ageing). 118
Similarly, Corboy et al. 111 concluded that, contrary to the perception that men in rural areas may struggle to access self-management support because of ‘logistical barriers’ (e.g. travel and availability of services), an issue of greater concern may be that coming from rural communities may influence their beliefs about engaging in specific types of activities, especially those involving emotional support. Consistent with this, Chambers et al. 210 reported anecdotally that men from rural regions were harder to recruit to their mindfulness-based intervention, which they thought could be linked to relatively ‘conservative views’ about meditation compared with their ‘urban counterparts’. Another potential issue faced by men from small communities (e.g. rural communities and gay communities) was increased concerns about privacy, anonymity and confidentiality that may pose particular barriers to emotional sharing in these circumstances. 111,117
Men’s needs frequently varied with changing health status or stage of condition, most often with worsening health or prognosis. 111,112,116,117,127 Denial of a condition, or a reluctance to be labelled as someone with a disease, was a barrier to accessing interventions or support activities for some men,101 as expressed by one participant in Gibbs’s study:
I do not want to accept myself as a person with arthritis, and going along there would be taking a step down that road.
First-order; p. 296119
Once again, evident here were tensions between men’s perceived need to fulfil roles and obligations linked to their identity as a man, and acceptance of living with, and needing help to manage, a condition that may threaten that identity. Although this could initially be a barrier to accessing support, Gibbs119 reported that changing needs due to worsening health could over-ride this in the context of rheumatoid arthritis, when severe pain and restrictions made it impossible to sustain valued social identities and roles. Gibbs119 also argued that men may have multiple LTCs, each with individual needs and carrying implications for identity.
Across all LTCs it was acknowledged that, whereas initially someone may view a condition as controllable and seek information to ‘take on’ or ‘fight’ their condition, the same person may later want to focus on managing adjustment and seeking emotional support instead. In the context of peer-support groups, authors observed that it was, therefore, important to ensure that groups catered to the needs of longer-term members, as well as newcomers:123,125,208
Participants saw the success of this group being due to the structure provided by the leader in arranging more experiences for older members than those that can be provided in open and unstructured crisis groups.
Second-order; p. 33123
[I]n addition to meeting the information needs of newly diagnosed men, the group meetings needed to offer ‘new’ information to maintain the interest of long-term members, because their commitment to the group was often premised on continuing to learn, as well as ‘giving back’ to newly diagnosed men.
Second-order; p. 149125
Key messages: need for purpose
-
Men can experience tensions between a perceived need to fulfil valued social roles and obligations linked to their identity (especially those related to masculinities), and acceptance of living with and needing support to manage a condition that could potentially threaten that identity.
-
Family or friends can be instrumental in legitimising a need and encouraging men’s involvement in self-management support.
-
Structured, action-orientated support that leads to tangible results and does not transgress culturally valued masculine ideals of independence, strength and control may improve the acceptability of support interventions for men.
-
Men value both informational support and emotional support, but may perceive, engage in and access these in gender-specific ways.
-
Receiving and sharing information can provide men with both reassurance and emotional support, and may be viewed as more acceptable than ‘just talking’.
-
Men’s needs and preferences for different types and functions of self-management support may vary with their changing health, although not necessarily in a linear fashion.
Trusted environments
I finally screwed up the courage to say something . . . I looked around expecting people to look shocked or disapproving. . . . People just nodded . . . and reacted like it was no big deal. After that, I was able to talk more openly.
First-order; pp. 57–8127
We found that men (and women) needed to access support in a safe, private, trusted space/environment. Building a ‘trusted environment’ appeared critical for accessibility and acceptability, especially in any circumstances where individuals may feel particularly vulnerable or lack confidence. For men, it seemed that this was most relevant to emotional sharing and physical activity, where a support activity or men’s capabilities might be seen as incongruous with masculine ideals and behavioural norms. The trustworthy nature of an environment could be fostered in different ways, reflected in the four third-order constructs that constitute the overall concept:
-
ability to pitch at one’s own level
-
group dynamics and rules of talk
-
physical characteristics of the environment
-
facilitators.
Ability to pitch at one’s own level
For some men, a trusted environment meant being able to set the pace and activity at a level where they felt comfortable, and allowed different types and amounts of involvement or contribution at different times. In studies where the intervention/support was focused around physical activity, authors highlighted the importance of matching the pace or intensity of exercise to individuals’ current physical health and limitations. 100,207
The option for varied involvement was also important for face-to-face group support and online forums, but for different reasons. One study of prostate cancer support groups noted the value men placed on the ability to listen without feeling an expectation to talk; members were ‘allowed’ to just listen:
Men who did not want to talk could listen without worrying about being put on the spot to say something, whereas others could comfortably share questions and comments from within the group.
Second-order; p. 564126
Varying levels of contribution were also observed in analyses of online forums, where some men were noted to have ‘lurked’ rather than (or prior to) posting. 109,136,212 ‘Lurking’ may have been a necessary step for some men in the ‘opening up’ process, affording an opportunity to ‘participate without feeling the pressure to share their specific experience’ and allowing men who may not feel able to ask questions to gain some benefit from the interactions of those who are more active. 109 Authors also contended that ‘lurking’ may reflect men’s desire to learn the rules of talk before actively participating136,209 in order to become ‘comfortable in knowing “how to” participate’;136 this is discussed further in the ‘becoming an expert’ concept (see Becoming an expert).
Group dynamics and rules of talk
Some authors reported that, given its potential to transgress culturally dominant expectations that men should behave in a strong and stoical manner, any topic that was particularly emotive and/or required emotional expression could be considered ‘taboo’ by men. 126,208,215 This could be overcome by the anonymity afforded by online communities, which allowed some men to ‘open up’ to emotional expression and intimacy that would otherwise be considered (prohibitively) difficult in face-to-face interactions. 109
In face-to-face support groups, authors reported that group dynamics could work to either promote the discussion of taboo topics or stifle them. In prostate cancer support groups, for example, ‘rational and objective’ discussions on functionality rather than feelings legitimised a supportive and collective problem-solving group dynamic that encouraged men to ‘open up’ about potentially taboo topics, such as erectile dysfunction. 126 This way of talking also allowed men to ‘open up’ to different ways of thinking about activities not usually considered to fit with stereotypical masculine roles, such as cooking or abstaining from alcohol consumption. 126,215
Groups where participants perceived a shared experience and shared understanding with others (both face to face and online) offered permission for men to discuss taboos such as sexual functioning:
being chauvinistic males we tend to keep it to ourselves . . . But when I’m amongst people like this I feel safe and confident.
First-order; p. 4209
Such dynamics also provided permission to show emotions freely,207 facilitating circumstances in which men could ‘say anything you want’217 and ‘feel free to rant’. 136 However, some studies reported that men felt that there should be limits to this and that the talk should remain ‘constructive’ and ‘productive’, offering practical strategies rather than being dominated by members who want to ‘moan’. 111,127
Group dynamics could also work to stifle emotional expression, highlighted in Corboy’s suggestion that individual men’s lack of emotional sharing may in fact reflect ‘limited opportunity rather than unwillingness on the men’s behalf’ (p. 179). 111 Studies indicated that men’s inhibitions around emotional talk in peer support groups may reflect group dynamics rather than the wishes of all of the male attendees. Practices that were noted to discourage or ‘squelch’208 emotional talk and sharing included topic turning by facilitators208 or group members, with ‘conversation quickly mov[ing] towards “safer” topics’. 107 Thus, although a focus on problem-solving and the practical aspects of potentially emotive topics could represent a positive way to facilitate the discussion of potentially taboo topics among men,126 it was also interpreted as a practice employed to avoid emotional talk and listening to underlying concerns and experiences:208,215
Jim was visibly disturbed by the effect of the hormone on his body, but rather than address that concern, the group moved into a discussion of financial matters, an instrumental issue.
First-order; p. 93208
Avoidance of emotional topics was reported in some studies as consistent with men’s individual preferences. 103 Elsewhere, it appeared that such group processes may not meet all men’s needs208 and that some men needed to be ‘allowed’ to vent, particularly as part of psychological adjustment to their diagnosis. 108,117,127
Evident in a minority of study findings was the use of humour as a way to foster trust and allow greater ‘opening up’ among men, both as a way to address emotion (compared with ‘incidental’ use by women212) and as a way to encourage camaraderie and a ‘male-trust culture’ in relation to physical activity. 207 Conversely, however, three mixed-sex sample studies reported use of humour in women but not men. 114,120,136
Our analysis found that peers were a key factor in establishing safety and trust, which we describe in further detail in the ‘value of peers’ concept later in this chapter (see Value of peers). Regardless of the nature of relationships between those accessing face-to-face group interventions, it was evident that those attending a group needed to demonstrate certain core values, such as respect and a willingness to listen, that were critical for ensuring a ‘trusted environment’:
even though I didn’t feel a great affinity toward a lot of people we showed respect for each other, we listened.
First-order; p. 1190207
Sharing core values could be particularly important where men were facing health issues which they perceived to be stigmatised or stigmatising. For example, in the HIV/AIDS literature, men were seen to place a high value on other group members sharing in common both diagnosis and sexuality. 123
For some men, trusted environments were quite clearly about male-only spaces,207,209 but for others they were not. Some men taking part in physical activity did not want (female) partners to be present207,209 whereas, in the context of cardiac rehabilitation services, some men found that female partner involvement could influence both access of support and implementation of lifestyle changes. 134,211 Thus, for some men, environments were made more trusted and accessible through inclusion of female ‘significant others’. For other men, the exclusion of female family and friends from self-management groups promoted greater trust, enabling men, for example, to speak without worrying about ‘negative consequences’ in their existing social networks. 127
Physical characteristics of the environment
There was some indication in the literature that men and women differed in their preferred size of support group, reflecting gender differences in preferred purpose and focus of self-management support activity. For example, Gray et al. 122 found that women preferred smaller support groups, consistent with an emphasis on ‘intimacy and peer knowledge’, in contrast with a male emphasis on ‘information and advocacy’, better served by larger support groups. Kendall123 reported men’s need for HIV/AIDS support groups to be small enough for all to talk and be heard. Additionally, emotional sharing and intimacy was noted to require familiarity,208 which was seen to be facilitated by small, closed groups, given the ‘lack of structure and consistency of group membership’ in large, open groups. 123
Some men reported not feeling comfortable in group situations; this was occasionally linked to dynamics within the group such as concerns over the ‘trustworthiness’ of group members, whereas for others it was about preferring one-to-one interactions and feeling listened to. 127
Contrasting views were reported among men on the extent to which security and trust were offered by face-to-face support compared with online support. Among the men in Broom’s109 study, some favoured online support because it offered ‘anonymity’ and was ‘potentially liberating’ and ‘disembodying’, whereas others felt distrust in such situations and were wary of the ‘potential for deception and misinformation’ in anonymous online settings,109 feeling people’s information and experiences would be ‘hard to verify’. 114 Others felt potential mistrust of information about their condition and its management; this was true regardless of setting, which may reflect a distrust of information provided by non-professionals (discussed in Becoming an expert) rather than characteristics of the setting per se.
Issues of anonymity were also raised in relation to health professionals, with some men (and women) with mental health needs preferring to ‘preserv[e] a degree of anonymity’ rather than receive support from, for example, their general practitioner. 115 Despite online forums usually being ‘publicly visible’, men (and women) viewed them as ‘relatively private places for the discussion of intimate personal information’. 128 As discussed earlier in this chapter, online support groups can sometimes offer fewer barriers for group members to discuss taboo subjects about expressing their experiences than face-to-face groups136 by freeing men from the constraints of adhering to culturally dominant ideals and norms of masculine behaviour, such as expectations to be ‘strong, well, tough, inexpressive’. 119
There was limited evidence on the importance of the characteristics of the physical environment in contributing to building a trusted environment for self-management support; evidence was largely confined to studies reporting influences on men’s engagement in physical activity. In Bourke et al. ’s209 study, men who participated in a lifestyle intervention valued doing physical activity in a university rehabilitation suite, and the location of the intervention within this setting helped to motivate the men to ‘get stuck in’. Their discussion of the use of this setting also highlighted their lack of confidence in community exercise facilities and the ability for these facilities to accommodate their specific needs. Similarly, Galdas et al. 211 found that men attending cardiac rehabilitation valued being supervised and monitored by health-care specialists when exercising; this ensured they ‘felt safe’, whereas self-led exercise was accompanied by ‘fragility and uncertainty’. With the exception of Kronenwetter et al. ,213 who questioned if the ‘community itself (vs traditional health care setting)’ (which was not described in further detail) ‘allows the staff to connect to participants in a more meaningful way’ (p. 106), authors did not disentangle the role of supervision from other aspects of the setting.
Both peer and professional facilitators and supervisors of support activities were seen to play a crucial role in nurturing a ‘trusted environment’. Dissatisfaction with health-care providers was widely reported among both men and women. Some studies highlighted the key role of HCPs as enablers of or barriers to interventions – often regarded as ‘gatekeepers’ – and the need for interventions to be more considerate of points of access. The role of health-care providers could vary with condition and was particularly important in relation to mental health. 112,115 In particular, some men found it critical to establish a one-to-one relationship with the facilitator before attending depression and/or anxiety support groups, and there was a clear sense that it was important for health-care providers to consider carefully how they approached men: for example, not placing the onus on men to make changes. 112
Several ‘lifestyle’ interventions highlighted the importance of facilitators for motivating patients, supervising activities where men lacked confidence (especially physical activity) and maintaining behaviour change. 134,207,213,218 These all emphasised the need for both professional facilitators and peer support:
[professional staff] had an important role . . . in maintaining and changing physical activity . . . However, . . . getting together with people who share similar circumstances seems vital.
Second-order; p. 518218
The staff was overwhelmingly mentioned as positive, helpful, and extremely supportive. . . . the peer community was the most highly valued part.
Second-order; p. 106213
Professional staff ensured security and they motivated the men.
Second-order; p. 533207
Facilitators of groups were key in fostering group dynamics and, as discussed earlier, this could lead to the promotion or stifling of emotional expressiveness. In relation to their ‘lifestyle’ intervention, Adamsen et al. reported the importance of a sympathetic and skilled facilitator to create the potential for establishing trusting relationships between group members and to provide a secure environment; they noted that the presence of a professional ‘allowed’ the men to speak about their personal situation. 207
The extent to which facilitators promoted emotional sharing partly depended on their credentials and whether they were a peer or a professional. Observation of prostate cancer support groups, for example, reported that professional facilitators (particularly those who were health professionals) may be a barrier to emotional sharing and voicing of certain views between men. 208 Similarly, in the context of online discussion boards, a ‘professional presence’ may inhibit members from ‘sharing their own expertise’. 212 The extent to which facilitators were viewed as impartial and having no agenda of their own is discussed further in Becoming an expert.
In some of the studies, men expressed views on the attributes they valued in facilitators or HCPs. Some men valued warm, supportive facilitators123 whereas others expressed the need for organised leaders who would bring in new members. 125 The capacity of the facilitator to meet the needs of all members was often seen to be important, whether through provision of new information to maintain client interest125 or through ensuring that the group was not monopolised by particular individuals. 123,127 In comparing experiences of general practitioner support for mental health, Emslie et al. 115 noted that, whereas women valued ‘listening skills’ in health professionals, men valued ‘skills which helped them to talk’.
There was little evidence regarding men’s preferences for the sociodemographic characteristics (i.e. age, gender or ethnicity) of facilitators and care providers, although one study focusing on mental health reported that some men may find it easier to talk to male care providers. 112 Some men were said to favour facilitators who were themselves peers;112,125 however, this could place high demands on lay volunteers, as discussed earlier, in Need for purpose.
Key messages: trusted environments
-
Support interventions can be made more accessible and acceptable to men if they are offered in a safe, private, trusted space/environment.
-
Sociocultural expectations of men to behave in a strong and stoical manner can inhibit emotional expression and stifle the discussion of ‘taboo’ topics that might be challenging to masculine identities.
-
Allowing participants the ability to set the pace, activity and level of involvement/contribution may be necessary to allow some men to participate in interventions without feeling inadequate about their bodies or their physical capabilities or feeling pressure to share their specific experience.
-
Group dynamics in face-to-face support groups can work to either support or stifle emotional expression. Facilitators of support groups are key to fostering group dynamics.
-
Environments can be made more trusted and accessible for some men through inclusion of female partners; for others, a male-only environment may promote trust by enabling men to speak without ‘negative consequences’.
-
The ‘trusted environments’ afforded by online communities, and face-to-face groups where participants perceive a shared experience and understanding, can help men to transcend cultural expectations of masculinity and ‘open up’ emotionally.
Value of peers
[Y]ou can’t separate support from understanding. . . . there’s nothing more supportive to me than when someone says, ‘Yeah, I know’ or ‘I understand’ or ‘it’s happened to me’ . . . that commonality.
First-order; pp. 623–4217
Interactions with ‘peers’ were widely reported as being important for accessibility and acceptability across the range of self-management support activities. Shared understanding through commonalities in defining aspects of the men’s experiences (e.g. of the health condition or treatment, and their combined effects on roles and identities) offered men living with LTCs opportunities for social comparison and learning. This carried implications for a sense of belonging, community and meaning, and for adjustment, as men were helped to come to terms with their health problems. Peers also contributed to education, evaluating information, and motivation for initiating and maintaining behaviour change.
The concept is discussed below with reference to five third-order constructs that constitute the overall concept:
-
Who is a peer?
-
Sense of community.
-
Comparison, meaning and adjustment.
-
Information, education and motivation.
-
The presence of women and significant others.
Who is a peer?
The ways in which men were able to identify with ‘peers’ with similar health conditions whom they encountered in self-management support activities were complex. Within face-to-face groups there appeared to be a delicate balance between other participants appearing sufficiently heterogeneous so that all would feel welcome, ‘eligible’ and included, but also sufficiently homogeneous (i.e. ‘similar enough’) that men felt at least some shared sense of identify with other group members.
Through analysis of the data presented in the studies, it appeared that differences in some social characteristics (such as age, ethnicity, class/economic background) were often transcended by ‘trumping’ commonalities, in particular the shared experience of a particular health issue and gender. 113,207 In these cases, perceptions of shared experiences and understandings offered ‘connection’217 and could help to foster a ‘trusted environment’ that allowed men to ‘open up’ and engage in emotional sharing. An assumed empathy based on experiences that were sufficiently similar, or ‘roughly in the same boat’,210 appeared to allow men a ‘break’ from their illness (and disrupted identities) as they felt able to fall back on a degree of ‘intuition’ thanks to ‘truly understanding’117 how others felt. This meant that, for some men, less needed to be explicitly voiced,110,207 as one participant in Adamsen et al. ’s study explained:
We don’t need to convolute things by asking how someone feels today because we can see it . . . We understand just when to laugh and sometimes when we should be quiet.
First-order; p. 531207
For some men, however, the range in the severity of condition among people in the group meant that they did not identify with each other or, indeed, did not wish to identify with each other, as discussed at the beginning of this section. In contrast, other men reported welcoming a range of diagnoses and severity in a group setting:103,210,217
their problems were more common than they had realised and this helped to reduce feelings of isolation, uniqueness and the belief that people who did not have multiple sclerosis would not be able to understand their condition.
Second-order; p. 1173103
Some studies suggested that men valued attending support interventions with those who were peers across ‘several layers’. In this way, seeing others as ‘sufficiently like me’ might require having multiple things in common, something beyond simply a shared health issue. This was particularly evident in the HIV/AIDS literature on support groups focused on emotional sharing, in which several studies reported that gay men valued the fact that group members had both diagnosis and sexuality in common. 110 An analysis of this issue across other health conditions and issues is somewhat limited, however, as sexuality was rarely considered outside the HIV/AIDS literature, although Gooden and Winefield212 did report that online postings (in relation to prostate and breast cancer) were ‘limited to heterosexual references’, potentially discouraging the involvement of others.
There was some evidence of a lack of identification with ‘peers’ among both men and women. For example, one study reported that men found it frustrating and disappointing to be surrounded by individuals who had the same health condition as them yet whom they did not view to be positive role models, either because of other differences in broader social values or because of their outlook concerning the condition. 127 This study also reported that men who had already undergone some process of adjustment to their illness found that interacting with those in ‘crisis’, who had not (yet) ‘come to terms’ with their diagnosis, could lead to negative interactions. This was voiced explicitly by one participant in Sandstrom’s127 study, who described feeling as though he was ‘walking into a wake’ and not wanting to feel worse for having attended the group.
Men attending a testicular cancer workshop211 also reported needing more in common than simply the same condition; in this case, men identified preferences for survivor stories that involved others of similar ages and socioeconomic/employment/cultural backgrounds (‘typical lad or bloke’ rather than ‘professionals’; not ‘too American’).
In contrast to the majority of the literature, which automatically positioned other men with LTCs as peers, there were two examples where men preferred to draw on support from those more closely known to them, describing others with the same condition as ‘strangers’. 101,211 As argued by Galdas et al. , such findings highlight the need to consider other influences, such as ‘the demands of cultural customs and societal bonds’ that may limit accessibility of self-management interventions ‘premised on individualist or spousal-centred models’ (p. 262). 211
Sense of community
For many men, the ‘peers’ they encountered through self-management support (either face to face or online) offered a welcome opportunity to experience a sense of belonging and of normality. 112,113,126,136,212 Such validation that, as men with a chronic health condition, they could regain a male ‘insider’ rather than ‘outsider’ status appeared to be important across several different health conditions studied (e.g. cardiac conditions,134 prostate cancer130), although there is some suggestion from the literature reviewed that this may be particularly important for men living with more ‘stigmatised’ conditions, such as mental health problems and HIV/AIDS:110,112,123,129
[the diagnosis was] such an emotional thing that I needed to be with people who had gone through this.
First-order; p. 185130
Seeing other people are here with the same problems makes me feel a little better, not so strange.
First-order; p. 236134
The online friendships . . . where the patients shared their symptom stories, served to validate a patient’s experience and lead them to the realization that they were not alone, which fostered a positive attitude toward treatment completion and hope for the future.
Second-order; p. 392113
Other authors described self-management groups as ‘communities’. Kendall123 suggested HIV/AIDS support groups were ‘spiritually bound’ communities where men shared not only common language but also ideals and values. Elsewhere, the distinction between ‘group’ and ‘community’ appeared more linked to whether contact between peers was limited to planned activities or extended beyond these. Gooden and Winefield’s212 analysis of online postings suggested that both men and women wanted to extend their contact with other contributors beyond the online forums, whereas Sullivan136 reported that this phenomenon was more common among female participants. Consistent with this, studies on face-to-face support groups reported that some men ‘were quick to distance themselves’ from others accessing interventions and preferred to focus on information exchange rather than ‘friendship or camaraderie’126 and that women more commonly wanted ‘buddies’ outside the formal group. 107 Other studies suggested that men valued ‘connections’ and ‘intimacy’ with others123 and ‘true friendships’ which men saw as extending beyond scheduled support group meetings (p. 625). 217 There was also evidence of some men feeling rejected when contact did not occur outside such meetings, or dissatisfaction when relationships felt superficial. Gray et al. ,121 for example, noted that ‘much of the felt intimacy was left unsaid’ and there was ‘little deliberate attention paid to facilitating men making personal connections’.
For some men, the involvement of family and friends could nurture a community that extended beyond meetings. 213 In contrast, observations of prostate cancer support groups208 found that contact did not continue beyond prescribed meetings, because of the presence of partners at these groups or the older age of group members, who may have had less flexibility around transport. Opportunities to develop relationships beyond group meetings may therefore be affected by material barriers or existing informal support.
Comparison, meaning and adjustment
Many men’s accounts indicated that much of the value they derived through being with peers occurred as a result of self-comparison. Some men were seen as ‘living examples’126 of hope, optimism and inspiration. This helped some men achieve a sense of perspective:
The experience of simply being able to speak to others who were in a similar situation was useful to participants. Social comparisons were engaged in and seen as helpful.
Second-order; p. E7214
However, exposure to others’ (ill) health was not always seen as a positive opportunity. For instance, being around other ‘sick people’ could challenge men’s established ways of coping (such as denial) or potentially reinforce an unwanted identity. 101,127 Sandstrom,127 for example, found that some men with HIV feared the prospect of seeing other men at a more advanced stage of their illness and the accompanying insights into their own potential future.
One study210 on acceptance-based mindfulness therapy offered a contrasting insight. Men with less advanced prostate cancer were reported to view others with more advanced disease, including those who died during the study period, as providing inspiration, reassurance and encouragement, and this ‘seemed to enhance acceptance’. 210 This may reflect the nature of the condition or the nature of the intervention, which involved reflection with others, a focus on acceptance and the role of the intervention facilitators.
Information, education and motivation
The value men placed on opportunities to learn from their peers was evident across the qualitative literature. Often, men (and women) viewed peers as experts and ‘credible sources’ from which to garner information and learn about self-management. There was evidence that some men considered learning from peers to be more acceptable than learning from health professionals because they perceived ‘power’ to be more equal in their relationships with their peers. 117 One participant in Vanable et al. ’s study described being taught by health professionals as sometimes feeling like being ‘preached at’. 129
Learning from peers could occur through explicit exchange of information (e.g. ‘tips’ and strategies218) via face-to-face or online interaction, but also through reading accounts of ‘survivor stories’. 116,214 The majority of group ‘lifestyle’ interventions noted the importance of peers and group identity for encouraging the adoption of increased physical activity, which men and study authors attributed to mutual motivation that developed through a sense of team spirit, camaraderie, social commitment and obligation;134,207,209,218 such processes may be seen as congruous with masculine identities.
Similar views were expressed by some men in relation to group-based psychological interventions:
I felt part of a . . . team, and really wanted to be there for other people no matter what condition I was in.
First-order; p. 1190210
A role-modelling approach to learning was adopted in one self-management intervention in rural South Africa, which aimed to encourage men with HIV to adopt health behaviours that were widely seen to challenge sociocultural notions of masculinity, such as using condoms, eating healthy food, having one sexual partner and abstaining from alcohol. 215 However, learning from peers was not limited to conditions or their management. Examples in the literature showed possibilities for learning about well-being more generally (e.g. ‘mixing health and illness messages’126), gaining a sense of community123,213 and developing ‘social skills’ that ‘foster the development of relationships’117 through processes such as becoming more ‘self-aware’ by having one’s views challenged by other group members. 123
The presence of women and significant others
Findings varied in relation to the involvement in interventions of men’s ‘significant others’, and whether or not they were considered peers. Some studies reported on self-management support activities which actively involved men’s partners. There was some suggestion that wanting family and friends involved in support activities may vary with condition and with activity/intervention type. For example, prostate cancer was often described as a ‘couple’s disease’ and studies of face-to-face support groups and online discussion forums described widespread participation of female partners. 109,122,136 Internet forums used by men with prostate cancer also had a presence of family members136,212 and some prostate cancer support groups were attended by family members. 208 In contrast, involvement of partners was not reported in any of the HIV/AIDS support groups. 108,110,123,127
Men in one study spoke of the value they placed on opportunities to hear the views and experiences of other patients’ friends and family at support groups. 217 Significant others were said to be welcomed by men at some ‘lifestyle’ interventions134,213 but not others. 207,209 Valuing separation from friends and family for engaging in interventions to promote physical activity was also found in Ferrand et al. ’s study of men and women with type 2 diabetes:
Participants described their personal histories with familial difficulties and their depression related to the disease, and indicated that it was important to them to exercise in a supportive context. They reported developing competence, autonomy and a relatedness in the patient association.
Second-order; p. 514218
Some men (and women) distinguished the value of the support provided through taking part in an intervention or group interaction with ‘peers’ encountering the same health issues, as distinct from the support they valued from friends and family. 108,121,126,127,217 As mentioned earlier, one underlying reason cited for preferring this separation was the opportunity to be able to ‘say anything’217 without fear of ramifications and the related desire to protect friends and family from the ‘burden’ of their own condition and associated needs:
you have also created an enormous burden on others . . . I belong to the support group, because . . . we all understand each other. There are a few people there who are very important to me. They’re not friends. . . . there’s that distance. We just get together to unburden.
First-order; p. 200108
Space away from friends and family appeared to be particularly important where participants experienced worsening health or were struggling with emotional impact. Importantly, such separation of support meant that men did not need to ‘rely’ on friends and family for emotional support, which helped to ‘diminish feelings of dependency’ within these relationships. 127
The importance of being with other men for physical activity-based interventions was evident in some studies207,209 but not others. 218 The apparent need for ‘men’s spaces’207,209 was sometimes conflated with a need for creating spaces away from partners and other family, rather than away from female patients per se. Indeed, one study which reported on women’s expressed preferences for groups attended by only other women clarified that this meant ‘women with the same condition’; that is, groups which excluded HCPs, friends and family, to avoid ‘compromis[ing] the special quality of women’s intimacy with women’ or ‘divert[ing]’ attention to family. 122
In studies that reported questioning men directly about their preferences for male-only versus mixed-sex interventions, a preference for mixed-sex groups was sometimes expressed. For example, some men with mental health problems suggested that mixed-sex groups would encourage more talking, and more emotional talking in particular. 112 Similarly, men with a range of different cancers felt that mixed-sex groups might increase more ‘free flowing’ and ‘higher quality’ discussion. 217 These comments from men directly contrasted with the views of some facilitators of mental health support groups, who felt that mixed groups could lead to avoidance of certain topics (e.g. those related to sexual functioning) and to different dynamics. 112 Bell et al. , having observed mixed-sex cancer support groups, also noted the possibility that mixed-sex groups may not meet the gender-specific needs of both men and women:
[mixed-sex groups] may flatten the ‘gendered’ dimensions of typical support groups . . . there was less emotional sharing than might appeal to women, and less formal provision of information than might appeal to men.
Second-order; p. 443107
Key messages: value of peers
-
Interaction, either face-to-face or online, with peers who have a shared illness experience can offer a sense of belonging, connectedness and normality for men living with a LTC; but it can also have potentially negative implications for self-identity.
-
In some cases, especially among men living with LTCs perceived to be ‘stigmatised’, identifying others as peers might require having multiple things in common.
-
Men can view peers as ‘credible sources’ from which to learn about self-management through interaction, information exchange or social comparison.
-
Peers and group identity can encourage and motivate behaviour through a sense of camaraderie and social commitment.
-
Attendance of women and significant others at self-management support can have both positive and negative impacts on men’s perception of acceptability and accessibility; this may vary with condition and with activity/intervention type.
Becoming an expert
People [men] are hungry for information, what is the latest in research . . . People are just dying to get their hands on the latest information.
First-order; p. 17121
Men involved in self-management support often evolved into ‘experts’ and providers of information. Our synthesis aligned such roles with a ‘need for purpose’ and a way to regain control and reclaim or reframe a sense of identity fractured through the experience of chronic illness. Across a range of self-management support activities, men’s actions and expressed experiences illustrated that many valued health information highly. Some authors reported frequent use of medical research and terminology by men, which they interpreted as helping to foster group identity in face-to-face support groups.
The concept ‘becoming an expert’ is discussed below with reference to three third-order constructs that constitute the overall concept:
-
Health literacy and the desire for information.
-
Who is expert?
-
Limited informed choice.
Health literacy and the desire for information
Studies of face-to-face and online support groups, and studies of men’s use of information, consistently illustrated that, contrary to prevailing assumptions about gender differences in health behaviour, men placed great value on health information and education. 102,103,107,109,113,116,122,124,126,128,136,208,212,214
On the basis of observations of prostate cancer support groups, some authors commented on the frequent use of medical terminology and numerical information in health education. 124,208 This was interpreted by Oliffe et al. 124 as a way to foster group identity, whereas Sullivan136 argued that such language was used by men to demonstrate knowledge and a hierarchy/superiority, consistent with the construction of dominant (hegemonic) masculinities. Similarly, analyses of online postings identified expectations placed on men to have high levels of health literacy, read key articles, use medical terminology and abbreviations, and provide personal history information in a digest format. 113,136,212 By contrast, women’s cancer forums did not contain detailed reports, instead using brief summaries of medical information. 128,136,212
Study authors proposed that the prevalent use of medical terminology in men’s online support forums may reflect the demographics of those men who chose to access this type of support, as well as the presence of health professionals in the forums studied. 46,136 Although the characteristics of the persons putting up online posts were not available for researchers analysing postings, Gooden and Winefield reported that the ‘quality of writing’ of men and women indicated ‘reasonably well educated and articulate’ users (p. 112)212 and Sullivan reported that online discussions may be likely to be of most benefit to ‘well-educated, analytically minded’ men (p. 98). 136
While it was evident throughout the literature that men had a desire for information and knowledge, overly complex or technical information could also act as a barrier to learning. Oliffe et al. ’s study of prostate cancer support groups noted the importance of men being able to learn from their peers ‘in their own way’ and without feeling the threat of being derided for their lack of knowledge about specific health and illness issues, and observed instances where information was not fully accessible to men as a result of ‘complex content or the style and language’. 124 In the context of online discussion groups, Broom109 suggested that individual ability to access and comprehend information could limit empowerment.
Studies of ‘lifestyle’ interventions also found that some men did not express preferences for technical information, but instead emphasised the need for accessible information, presented in ‘everyday language’. 214 Accessibility required that the information be tailored and contextualised, which the authors reported may be particularly important for younger men. 99,214 Other studies indicated that ‘contextualising’ information meant considering not only demographic characteristics that men could relate to, but also guidance on how to translate information into knowledge that could be integrated with daily life. For example, through analysing men’s comments, study authors noted the importance of strategies or ‘usable information’ on ‘the why’s and how you do it’214 rather than standardised or general health messages that could be seen as lacking ‘respect for the individual and his context’. 135
An unfavourable aspect of knowledge and information that was notable in some study findings was the potential to provoke anxiety in men (and women) and overwhelm them. 128 As a result, some men described setting boundaries around what they wanted to know in order to maintain their coping strategies. 116 Evans et al. distinguished between ‘proactive seekers’ and ‘passive recipients’ of information and argued that this might reflect different stages and experiences of illness, rather than an underlying personality style. 116 Significant others were also described as playing a key role for some men in obtaining information, and may have helped to protect them from feeling overwhelmed by information; for example, some studies reported that men used ‘lay referral networks’ or ‘Internet-savvy’ friends and family, often their wife or daughter, to navigate and ‘filter’ information resources. 113,116,128 It is of note that, among the studies that paid attention to gender and the use of internet-based resources, gender differences were not observed regarding the use of family and friends to overcome technological barriers. 113,116,128
Who is expert?
Men living with a LTC varied in whom they considered to be an ‘expert’. As described earlier, peers were identified in several studies as trusted sources of information that could provide highly valued advice thanks to shared understanding. 112,117,129,218 However, caution was evident about the reliability of information from lay patients, rather than ‘qualified’ professionals,111 with the suggestion that ‘qualified’ professionals may be more appropriate to provide factual information, whereas support could be better offered by peers, as Wallace and Storms129 concluded:
Participants clearly indicated that although educational needs may be filled by enhanced education within urology practices, support needs must be filled by prostate cancer patients and survivors, not health care professionals.
Second-order; p. 186130
Preferences for information sources were sometimes interpreted by study authors as being linked to gender differences in preferences for particular types of information, with a suggestion in one study for a male preference for medical information and education and a female preference for personal experience,107 although this was contradicted in other studies, which found that both types of information were valued highly by men and women. 124,216
The findings of a number of studies reported that men often evolved into experts and providers of information. Linked to the ‘need for purpose’ concept, the opportunity for ‘reciprocity’, ‘mutuality’ and ‘giving back’107,126,127,209,217 through providing information was frequently positioned as a key motivator for (ongoing) use of group support and ‘lifestyle’ interventions, with associated benefits for self-identity and self-esteem.
Similarly, the literature on information and online support illustrated how men sought information from peers in order to become experts themselves;109,113,136 using peer counsellors was said to offer similar benefits. 117 Authors argued that becoming equipped with information could also be about processing and accepting past treatment decisions (including those made by others), rather than necessarily influencing future ability for shared decision-making. 109,113 Alongside face-to-face information sharing, some men sought other patients’ stories of their personal experiences through media and books as well as via internet resources, to navigate, for example, complementary and alternative medicine information. 116
Studies of online and information provision interventions reported that men were often ‘selective’ about the sources of evidence they used,113 considering and weighing up the utility of varying ‘forms of evidence’, including personal stories and more factual/medical information. 116 Information was sometimes validated by comparing sources, either by doing so themselves or by seeking from care providers the ‘stamp of approval’ of information or information providers. 116 Evident in this literature was consideration of the potential agendas of information sources, for example not having ‘wholesale acceptance’ of commercial sites116 and being cautious about information and online support, treating it with a ‘pinch of salt . . . grain of truth’. 113 Similarly, men were described in some studies as being cautious about health professionals, who may have conflicting agendas or vested interests. 124,130
Our synthesis indicated that becoming an ‘expert’ could extend beyond information gathering, to developing skills in navigating health services, facilitating patient–HCP interactions and attaining partnership in decision-making. 113,124 Men were described as gaining ‘currency’ and ‘power’ through having knowledge,113 ultimately becoming informed consumers who ‘shopped around’ for health-care providers and treatments, as described by Oliffe et al. :
Consumer discourses and strategies to contest power relations with health care professionals underpinned many men’s search for prostate cancer information and their commitment to assisting other men.
Second-order, p. 555124
The opportunity to build confidence and expertise in communicating with care providers also occurred as part of an intervention, for example through face-to-face question-and-answer sessions or online interactions. 124,136,208,209 Such involvement with care providers was described as being particularly valued where men felt dissatisfied with clinical interactions, for example owing to lack of time with health professionals and lack of power and partnership. 111,209
Importantly, however, the literature showed that not all men wanted to develop an in-depth understanding of what treatments might be available. This was reflected in varied findings on the extent to which men welcomed the opportunity to act in the role of ‘consumer’ of health services. Some men described not wishing to be active patients/consumers, instead preferring to devolve decision-making to health professionals as experts who ‘know [their] stuff’. 109
Although contemporary health policy may promote a move away from the traditional paternalistic model to shared decision-making, coproduction and a consumerist approach involving the ‘expert patient’, suggestions that the balance may have gone too far were evident, as illustrated by one man in Evans et al. ’s study:
Imagine being in a fast flowing river and the guy on the bank has got half a dozen different aids to help you, and he’s shouting to you ‘which one do you want?’
First-order116
Limited informed choice
Self-management support activities (particularly information-based interventions, online and face-to-face support groups) were often positioned by activity providers as promoting informed choice and empowering men as consumers of health care, rather than advising or prescribing. 109,113,124,136,212 However, although providers (and often men) positioned activities in such ways, some study authors argued that apparent ‘choice’ was sometimes limited to certain options that were endorsed by the group, for example ‘conventional’ treatments rather than ‘alternative approaches’. This was most evident where views varied about the appropriate management of a condition, for example prostate cancer,124 and in relation to complementary and alternative medicine. 212
Arrington et al. ’s208 observations of prostate cancer support groups identified a prevailing attitude that prostate cancer was controllable and should therefore be ‘fought’, favouring ‘active’ forms of treatment. Similarly, Oliffe et al. ’s124 analysis of observations of such groups proposed that informed choice was limited for those men with prostate cancer who opted for conservative management (watchful waiting or active surveillance) given groups’ favouring of ‘proactive’ options.
Similar themes were identified in a study of men with heart failure, where the authors suggested that, despite apparently promoting informed choice, a nurse-led clinic was positioned as helping men make the ‘correct’ choices rather than true free choices that take into account individual preferences and circumstances. 135
Alongside informed choice, several interventions and activities across condition types were described as encouraging involvement in wider lobbying and activism activities. In the HIV/AIDS literature, this included expectations about public disclosure of patients’ LTC215 and influencing public attitudes about the condition, which could vary with changing public awareness. 127
[I]t’s about saving lives . . . that’s why you talk about it.
First-order; p. 793216
Gray et al. 120–122 reported that men with prostate cancer were more pro-lobbying than women with breast cancer, although the authors recognised that this may partly reflect different histories of the conditions in relation to public awareness. Seymour-Smith216 (in reporting experiences of men with testicular cancer and women with breast cancer) also reported a male preference for a group agenda, including education and raising awareness, which may have reflected a male tendency to ‘legitimise’ attendance by demonstrating that their attendance is of benefit to others (as discussed previously in Need for purpose).
Some men expressed the view that activism/lobbying was futile and should not be the focus of a support group. 127 Elsewhere, Oliffe et al. 125 observed variation in men’s views around activism and proposed that this may reflect resources available for lobbying when the group’s sustainability was the more pressing concern, and whether the focus was the local support group or the wider (prostate cancer) community.
Key messages: becoming an expert
-
Men may value opportunities to learn from peers and health professionals in order to develop their capacity to be informed consumers of health care.
-
Acceptability of health information may be improved through the use of medical information/evidence and terminology, which may also help to foster group identity in face-to-face support groups.
-
Education may be made more accessible and acceptable for some men by contextualising and individualising information in the form of strategies or ‘usable information’ that can be incorporated into daily life.
-
Developing expert knowledge on management and treatment options can be a way for some men to regain a sense of control and identity fractured through chronic illness.
-
Although some men may place a high value on technical information and knowledge, overly complex information can also act as a barrier to learning and may also provoke anxiety or feelings of being overwhelmed.
-
Men can become empowered to better navigate health services, facilitate patient–HCP interactions and attain partnership in decision-making; however, some men may wish to retain the ability to adopt a passive rather than proactive role in health-care decision-making.
-
Some support interventions can be positioned as helping men make the ‘correct’ choices rather than true free choices that take into account their individual preferences and circumstances.
Chapter 6 Discussion
In this chapter we briefly summarise the principal findings before discussing the findings from both quantitative and qualitative reviews in further detail in the context of the existing evidence base. One of the objectives of this review was to integrate the findings of the meta-analysis with those of the metaethnography. This type of integration is still a relatively new approach with a lack of consensus about methods for doing so, or standards for reporting. In the second section of this chapter we have chosen to present and juxtapose the findings of the two reviews alongside one another in parallel synthesis. 220
Summary of principal findings
This review aimed to assess the effectiveness, cost-effectiveness, accessibility and acceptability of self-management support interventions in men with LTCs.
In terms of effectiveness, the evidence is limited, and there was no consistent finding of differential effects to make a definitive statement about whether males show larger, similar or smaller effects in self-management support interventions than females.
There is some evidence to suggest that multicomponent interventions that include a physical activity, education or peer support component have a positive impact on quality of life in men. Self-management support interventions with a peer support component, and those without an education component, appear to have a positive impact on depression outcomes in men.
In terms of comparative impact in men, there is some evidence to suggest that interventions with a physical activity, education or peer support component may be particularly beneficial for improving quality of life in men in comparison with women or mixed-sex groups, although there is currently insufficient robust evidence to draw definitive conclusions in this regard.
In terms of cost-effectiveness, there is a lack of evidence available to make an assessment about whether or not self-management interventions are cost-effective for males, or whether or not gender has an impact on cost-effectiveness.
In terms of acceptability and accessibility, men may feel less comfortable participating in interventions if they are perceived to be incongruous with their identity, particularly when support is perceived to transgress culturally dominant masculine ideals associated with independence, strength and control. Men may find self-management support more attractive when it is perceived as action-oriented, having a clear purpose and offering personally meaningful information and practical strategies that can be integrated into daily life.
In order to overcome barriers to access and fully engage with interventions, some men may need support to be delivered in an environment that offers a sense of shared understanding, connectedness and normality, and involves and/or is facilitated by those considered to be ‘peers’.
Parallel synthesis of review findings
Recognition of gender-specific health concerns has led to growing calls for tailored and targeted health interventions to be delivered to men. 22,23 However, the current evidence base does not provide a strong steer on how to design and deliver services to address men’s distinct health concerns. 221
Bringing together the main findings from our two reviews in parallel synthesis points towards some key ‘ingredients’ of the content and process of self-management support that may be important in helping to optimise interventions to be more effective, accessible and acceptable to men.
Physical activity
Self-management support interventions involving a physical activity component appear to have a positive impact on quality-of-life and fatigue outcomes in men, and may be particularly beneficial and appealing to men in comparison with women. The metaethnography suggested that providing opportunities for physical activity can improve the acceptability of self-management support for some men (and perhaps particularly in the early stages of engagement with an intervention) by offering a sense of structure, purpose and practical/tangible results that may be consistent with an expressed male preference for problem-focused coping.
The physical activity interventions that were included in our analyses varied in format, duration and intensity, and it was not possible to establish a type of activity that might be most effective in men, particularly in men with such a wide range of conditions. However, in terms of acceptability and accessibility, the metaethnography suggests that enabling men to take part at a pace and intensity that matches their current physical health, and in an environment in which they feel safe, supported and among peers who share similar circumstances, may be of equal importance to the type of physical activity offered.
Studies of physical activity interventions that have been delivered in venues associated with male identities, such as football and rugby clubs, have shown these to be particularly acceptable and ‘trusted’ environments for men engaging in weight management programmes. 222,223 The findings from our metaethnography suggest that delivering self-management support interventions in similar environments might also improve accessibility and acceptability for men with LTCs.
Peer support
Contrary to conventional commentaries that position men as solitary, stoic and emotionally restricted,221 the quantitative review indicated that interventions involving peer support appear to have a positive impact on quality-of-life and depression outcomes in men. This may be explained in part by findings in the metaethnography illustrating that many men value the sense of belonging and community offered by peer interaction, which was widely reported to help men adjust and come to terms with their health problems. This chimes with the results of the evaluation of the UK Expert Patients Programme – a lay-led self-management education programme – which showed that (male and female) participants placed a high value on the social support and social networks gained through contact with new people. 224 The metaethnography suggests that peer support may be particularly important for men when they have a chronic problem which makes them feel that they ‘stand out from the herd’;225 that they are distinct from other men and perhaps unable to ‘perform’ their masculinity in different contexts in ways which they have been accustomed to at other times in their adult life.
It was not possible to identify a particular format for peer support that was most effective in men. However, the metaethnography emphasised that interventions involving constructive and purposeful discussion (e.g. providing and sharing information and being problem-focused), perhaps particularly in the context of other group-based activities, may generally be seen as more appealing and acceptable to men than peer support that offers ‘just talking’ or emoting, especially where peer support lacks an effective facilitator.
Many authors did not consider that men may provide and receive emotional support in different ways from women, or use different language to express emotion. There was evidence in the review findings that emotional support which occurs as an apparent ‘by-product’ of other shared activities, rather than being tackled ‘head on’ or positioned as the main purpose of an intervention, may improve the acceptability of interventions for some men. Indeed, using the word ‘support’ in the advertising of interventions may discourage some men because it can be associated with indebtedness or weakness. 126,226
Despite many male ‘gender-sensitised’ health interventions being predicated on the provision of a male-only environment,221,227–229 it was not possible to determine whether or not male-only peer support groups were more effective than mixed-sex groups.
Although analyses of peer support interventions in male-only groups were included in the quantitative review, none of these interventions had been designed specifically for men alone. There was also evidence of mixed views in the metaethnography about whether or not interventions (and those involving peer support in particular) were seen as more acceptable to men if they were restricted to males alone.
The metaethnography showed that some men wished to attend male-only groups, but others did not consider this to be essential. There was evidence that being able to ‘identify’ with the illness experience of others appeared to be of greatest importance for some men with LTCs. These findings are in line with a recent review of weight-management programmes in men with obesity. 222 However, also evident were indications that having multiple things in common with peers (including gender) may improve accessibility and acceptability. Similar findings were reported in the recent Football Fans in Training (FFIT) study, which attracted ‘like-minded’ and ‘like-bodied’ men, who shared an interest in football and had similar physiques and levels of fitness (‘people like them’). 230
To improve acceptability, consideration may need to be given to the benefits and disadvantages of providing group-based support or interventions to men with the same LTC or a range of conditions, and of including only those at a similar stage of illness or a range of severity. The PRISMS review33 highlighted the importance of delivering self-management appropriate to the individual patient at a particular time point in relation to the level of functional disruption and flare-ups. The analyses in this review highlighted the potential for the commonalities that bind a heterogeneous group of men together to spill over into unhelpful interactions. It may be that some groups become too reliant on an apparent homogeneity (based, for example, on illness type and/or sexuality) and that this element of identity then becomes fractured by other inherent elements (e.g. political views).
Education and information
Men appear to benefit from multicomponent interventions involving education, and may do particularly well in terms of quality-of-life and fatigue outcomes compared with women. Acceptable and accessible self-management education for men may require the provision of practical, ‘useable’ health information and strategies that can be integrated into daily life rather than providing ‘general’ health messages alone. These findings resonate with distinctions identified in other studies230,231 between information that is based on ‘personal experiences’ and ‘general facts’, and adds weight to suggestions that providing information about other people’s experiences – such as the lay-led narrative/‘story-telling’ methods embodied by the Expert Patients Programme224 – may help to inspire confidence and develop individuals’ capabilities to make health-related decisions autonomously. 232
Consistent with existing evidence,233 the metaethnography also identified that men may place particular value on technical information and scientific evidence relating to their condition(s). Being able to ‘give back’, by providing information and becoming an ‘expert’ on management and treatment options, might be a particular motivator for some men to access and continue to use support interventions, by offering a way to regain control and reclaim or reframe a sense of identity and ‘masculine capital’223,234 that may have been lost through the experience of chronic illness.
Importantly, overly complex information could act as a barrier to learning and may also provoke anxiety or feelings of being overwhelmed in some men. It is interesting to juxtapose these findings with results from the effectiveness review that showed that improvements in depression outcomes in men significantly favoured interventions without an education component. The FFIT study235 similarly found that men valued practical ‘tips’ and technical but not overly scientific information (‘science but not rocket science’), and the review findings reinforce the need to make information accessible for men. Affording men opportunities to learn at their own pace without any threat of being derided for their lack of knowledge may be one strategy that can help improve accessibility.
Masculine identities
Recent evidence has shown that the accessibility and acceptability of behaviour change interventions can be improved when the context, content and delivery style of interventions are tailored to be in alignment with valued aspects of men’s identities. 222,223,230,235 A theme evident throughout the metaethnography was the tensions that men experienced between a perceived need to fulfil roles and obligations linked to their identities as men, and acceptance of living with, and needing help to manage, a LTC that could potentially threaten those identities. It was clear from the metaethnography that the physical and mental impacts of living with a LTC could pose significant challenges to men’s masculinity; this theme has been recognised elsewhere as a ‘loss of self’236 as men try to renegotiate and recapture aspects of masculine identity they feel have been lost through illness. 225
These findings echo a thread that ran through the qualitative findings in the PRISMS review. 33 The authors contextualised the disruption LTCs can have on ‘normal’ life with Bury’s theory of biographical disruption and the need to reconstruct one’s identity by adjusting to the physical, emotional and societal implications of illness. 237,238
The findings from this review place this ‘disruption’ in the context of men’s gender identity, furthering the recommendation from PRISMS that support needs to be tailored to patients’ existing health beliefs, preferred lifestyle and cultural background. Specifically, the findings of the metaethnography suggest that self-management support is most likely to be successful in engaging men when working with, not against, cultural ideals of masculinity. In other words, as Hunt et al. have stated, support interventions need to engage men without being anathema to valued aspects of their identities. 223
Here, the findings from this review highlight the potential importance of positioning and marketing self-management support interventions in ways that pre-empt or overcome potential threats to masculine identities; for instance, demonstrating for potential users a clear purpose, and the opportunity for exchange/reciprocity among users, as well as recognising that such marketing should address changing needs and recognise different purpose in initial and ongoing use. This links to the need for some men to tackle emotional issues ‘sideways on’, as a ‘by-product’ of other shared activities. Intimacy and emotional sharing may become hampered if it is made too explicit a goal for support interventions. Crucially, it was suggested that ‘trusted environments’ afforded by online communities and face-to-face groups can help men to overcome cultural expectations of masculinity and enable them to ‘open up’ emotionally.
Men may also feel the need to ‘legitimise’ their involvement in self-management support as part of performance of, or alignment with, hegemonic masculinity. 216 The findings from the metaethnography suggest that family or friends may be crucial in helping men to identify a need for support and in encouraging access and engagement with available interventions. However, it was not feasible to explore this within the quantitative data.
It is important to note that, while culturally dominant (hegemonic) masculine ideals were a prominent feature of our metaethnography, the findings need to be interpreted with caution. A body of recent work has begun to question the simplistic link between constructions of hegemonic masculinity and men’s health-care practices. 239 Evidence of the fluid and contextually dependent nature of gender in the wider body of men’s health literature240,241 suggests that the studies included in our review may not adequately capture the complexity of how masculinities intersect with men’s health behaviour.
Thus, there is unlikely to be a ‘one-size-fits-all’ approach to gender-sensitising self-management support for men. Indeed, the metaethnography suggested that men and women may both benefit from particular intervention components/types (e.g. peer support, information sharing) if they have similar personal preferences and/or a shared illness experience. Although the review findings point towards some key considerations that may be important in helping to optimise interventions to be more effective, accessible and acceptable to men, clearly gender is not a ‘stand-alone’ variable that determines access and engagement. The factors discussed here in relation to the content and processes of designing and delivering self-management support may help to improve acceptability and accessibility in certain groups of men (e.g. those who adhere to hegemonic masculine constructions) but not others.
Strengths and limitations of our methods
Quantitative review
Although the analyses suggest that certain components/broad types of self-management support intervention may be more effective in men, the findings from this review need to be interpreted with caution. In several analyses, the number of studies and/or sample size was small, which means that they may have limited power to detect important differences.
Clinical and high statistical heterogeneity were also evident in some cases, and caution must be used in interpreting results in these instances. Reasons for heterogeneity were explored where possible, although limitations in reporting and small numbers of included studies made detailed exploration difficult. As other recent reviews in this area have identified, few studies in the extant self-management literature provide ‘cost’ data. Economic evaluations where a male group could be identified were reviewed. Only one study met the criteria for review and hence we were unable to assess whether or not self-management interventions are cost-effective for males, or whether or not gender has an impact on cost-effectiveness.
The size of the self-management literature and the 1-year time frame of this project meant that some deviations from the protocol became necessary. This involved limiting the search to studies of relevance identified from Cochrane systematic reviews. The search was efficient and broad, generating a substantial sample frame of 1887 potentially relevant studies (identified from 116 Cochrane reviews) that were screened for eligibility against our inclusion criteria. However, the pragmatic nature of the search strategy has obvious limitations. It is highly likely that other relevant studies might have been identified had we conducted a separate search of the primary research literature, or included literature identified from DARE and PROSPERO databases as per the original protocol. Translation of foreign-language papers was also unfeasible, and relevant data may have been missed for this reason. However, it seems unlikely that these additional sources would have provided significant numbers of new studies that would have had a profound impact on the results of the syntheses.
The short time frame of the project also made consideration of all possible LTCs impracticable. It is difficult to determine whether or not the results would have been significantly moderated had other disease categories been included, but, like other recent reviews,7,33 we included a range of ‘exemplar conditions’ that had a diversity of core characteristics which affect on the design and delivery of self-management interventions in terms of models and mode of delivery of care.
Two types of analyses of effectiveness were planned: first, comparing the impact of self-management interventions in males alone with the relevant results from systematic reviews of self-management when delivered to mixed populations (in order to assess the direction and magnitude of any differences); and, second, comparing data on the direction and size of moderating effects in secondary analysis in individual trials (i.e. whether males show larger, similar or smaller effects than females). The extent to which it was feasible to answer the review questions using this two-pronged approach was significantly limited by the availability and relevance of studies and extractable data. As a result, the analytical strategy was expanded to incorporate two additional levels of abstraction.
The innovative approach to analysis used in this review is an obvious strength. The review questions were examined using multiple methods and levels of abstraction to see if there were any key trends across the multiple analyses. Combining the findings from the meta-analyses and metaethnography in parallel synthesis also helped generate insights into why certain types of self-management support might be more successful, appealing and accessible to men. Despite this, however, the analytical approach has some intrinsic limitations.
Analyses 1 and 2 were based upon comparisons of primary trials within and across reviews, where trials differed in the gender composition of their samples. This approach is limited, as such comparisons do not have the protection of randomisation, and represent rigorous comparisons only to the degree that other differences between the studies do not account for these differences. Analysis 1, ‘within-review analyses’, should, however, provide a measure of comparability in terms of the included interventions and populations. We presented data on the comparability of these trials (in terms of the included patient populations) and the quality of the studies (using allocation concealment as an indicator of quality) to help in the interpretation of the results. Similarly, analysis 3, ‘male only by intervention type analyses’, did not compare studies according to gender composition, which may increase the comparability, but the same types of issues apply.
The fourth approach to analysis, ‘secondary analysis within trials’, maximises comparability among participants and removes variation associated with intervention type and study quality. However, these data were considerably limited in scope and so contributed little to the main review findings.
In relation to outcomes, it was originally intended to extract data on a wide range of measures. However, it became evident that extractable, relevant and comparable data were predominantly available only in quality-of-life domains, thus limiting much of the findings to this outcome measure. Limitations in the reporting of outcome data also meant it was possible to conduct analyses on only four broad types of intervention, and limitations in the way that interventions were reported in the literature also meant we were unable to code these comprehensively according to the BCT taxonomy.
Metaethnography
The difficulty in systematically identifying qualitative studies in research databases is well recognised. 97 A strength of this review was the thoroughness of our search, which involved the title/abstract screening of 6330 unique records and offers a comprehensive picture of the available qualitative research. The approach adopted in the metaethnography did not preclude synthesis across studies of different types of intervention or support activities, but the limited amount of data and analysis reported in studies meant it was not possible to unpick the accessibility and acceptability of particular types compared with others. In addition, the synthesis is likely to have been heavily influenced by the literature on face-to-face group-based support interventions. There are three possible reasons for this: firstly, this was the most common type of intervention/activity represented in the qualitative literature; secondly, the analysis began with this category of studies, potentially influencing subsequent interpretations; and, thirdly, the stakeholder representation in the PPI group recruited for the purpose of this review was drawn from face-to-face group-based support interventions. A key strength of this review, however, was the involvement of six researchers from multidisciplinary backgrounds with diverse theoretical perspectives and a wealth of expertise in the areas of men’s health and gender studies, self-management, health psychology and LTCs. Involvement of the PPI group at key stages of the analytical process also allowed the consideration of service-user perspectives that appreciably strengthened the rigour of the analysis and the potential applicability and impact of the findings.
It was appropriate to synthesise qualitative data from studies that used different theoretical traditions; that is a strength for gaining conceptual insights. In the analyses, we questioned if certain concepts (e.g. group dynamics, legitimising use) were limited to studies adopting certain methodologies that did not seek participants’ views directly (e.g. discourse analysis); however, there was evidence of such concepts across methodologies. A recognised challenge in metaethnography is the ability to identify and separate first-, second- and third-order constructs. The ability to access first-order constructs was largely determined by the authors’ selection of data in presenting their second-order constructs. Similarly, distinguishing between second- and third-order concepts was somewhat artificial because selection and extraction of second-order constructs could not be separated from the reviewers’ subjective interpretive processes.
Descriptions of interventions were significantly limited in the qualitative literature, which precluded the possibility of coding according to the BCT taxonomy. For example, studies on face-to-face group support rarely described key characteristics such as whether groups were peer-led or professionally facilitated; whether groups were open (‘drop-in’) or closed; whether groups were rolling or finite; the setting (e.g. community); and whether or not referral by health professional was required. Furthermore, the qualitative studies often concerned one or more broad type of activity (e.g. support group) rather than the evaluation of a specific intervention with stated characteristics. The majority of studies in the metaethnography concerned experiences of self-management support where access happened independently of research participation. Although this could be considered a strength in terms of ecological validity, it is likely that negative experiences and barriers to accessibility and acceptability were under-represented because studies were largely concerned with the experiences of those currently accessing interventions, rather than those who either do not engage initially or do not continue to engage. As Emslie et al. have noted, studies are likely to have missed the truly ‘strong and silent’ men. 242
Chapter 7 Conclusions and recommendations
Implications for health-care practice and service delivery
Self-management support is likely to be more accessible and acceptable to men when it takes account of valued aspects of masculine identities.
Findings from this review echo recommendations for self-management support to be tailored to individual preferences and lifestyles;33,243 for men with LTCs, this is likely to involve consideration of their identity as a man. Health professionals and service commissioners might usefully consult with male service users about how to make existing support interventions more appealing to men and congruent with their identities.
It may yield benefits if self-management support is gender-sensitised in context (e.g. delivered in a trusted environment among peers), content (e.g. action-orientated), delivery style (e.g. a problem-solving/practical approach) and marketing (e.g. emphasis on purpose/tangible results). However, health professionals need to recognise that men are not a homogeneous group and that there is unlikely to be a ‘one-size-fits-all’ approach that meets the requirements of all male service users. Men and women may both benefit from particular intervention components/types (e.g. peer support, information sharing) if they have similar personal preferences and/or a shared illness experience, and men may also be willing to accept different types of interventions or activities once they feel they are in a trusted environment with peers, including interventions or activities which at the outset may have appeared to present some challenge to aspects of male identity.
Gender appears to have an impact on the effectiveness of self-management support.
Limitations in the data meant we were not able to provide a definitive answer to the review questions relating to effectiveness, and any recommendations in this regard therefore need to be tentative. As there is currently insufficient evidence to make strong statements about differential effectiveness in men, the focus for services should be on ensuring the accessibility and acceptability of self-management support interventions to ensure equitable uptake and engagement among men.
However, health professionals and those involved in designing interventions may wish to consider whether or not certain components and intervention types are particularly effective in men. In the current data that are amenable to analysis, evidence of effects on quality of life point towards men benefiting the most from interventions with a physical activity, education or peer support component, although more research is needed to fully determine and explore this.
Recommendations for future research
-
Clear and consistent reporting of components of self-management support interventions.
Support interventions need to be clearly and consistently described by researchers using a shared language. It is suggested that researchers clearly report on whether or not an intervention was intended to target a specific behaviour change and report adequate detail to allow for coding with the BCT taxonomy, where applicable.
-
Understanding what interventions work in men and why.
Clearly, further primary research is needed to examine which models of service delivery are most effective and cost-effective in providing self-management support to men. Any intervention developed should be theory-led, and our review findings point towards some broad BCT which could act as a starting point for testing the ‘active ingredients’ successful at promoting self-management in men. Parallel primary qualitative research is also needed to test theory and develop our understanding of what makes interventions, and their ‘active ingredients’, accessible and acceptable for men with LTCs. The complex and contextually dependent nature of men’s engagement with self-management support interventions highlighted in this review suggests that a study drawing on realist principles244 might be one method of analysis which might have utility.
-
Including gender in the analysis of effectiveness of self-management support.
The ability to conduct the analyses was limited by a lack of consideration and/or poor reporting of gender as a moderator of outcome data in primary studies. Few studies provided outcome data separately for men and women. There is a need for researchers to consider gender consistently in their analyses and provide consistent and comprehensive reporting of outcomes by gender. Access to primary databases through archives or the supplementary material functions of online publications may be one way of facilitating such analyses, and concerns about power and precision may be managed through adoption of appropriate meta-analysis techniques. 157
-
Consideration of the cost-effectiveness of self-management interventions for men.
There is a dearth of evidence on the cost-effectiveness of self-management interventions for men. Without an evidence base it is not possible to assess whether or not self-management interventions are cost-effective for males and females or whether or not gender affects cost-effectiveness. While the lack of evidence is surprising, it is conceivable that existing studies of self-management interventions in the UK could be accessed and retrospective analyses performed. All trials will collect data on gender and many cost-effectiveness analyses could be conducted by simply running a group analysis by gender. This would generate estimates of whether or not the intervention is likely to be cost-effective in men. Similarly, where funding is granted for evaluation of self-management interventions, it is suggested that researchers should consider the inclusion of gender as a pre-specified group analysis for the economic evaluation.
-
Consideration of men of differing age, ethnicity and socioeconomic background.
The self-management experiences and perceptions of men of differing age, ethnicity and socioeconomic background need to be explored. Men are a heterogeneous group, yet consideration of how these factors intersect with men’s gender identities is rarely a focus of empirical research.
-
Understanding depression in men with LTCs.
Depression is a prevalent comorbidity among those living with a chronic physical condition and is recognised in current National Institute for Health and Care Excellence guidelines. 176 Although several quantitative studies examined depression outcome measures, depression as a comorbidity was recognised in only one study included in our qualitative review. Studies tended to discuss addressing men’s ‘fears’ (e.g. of treatments or worsening health) and psychological processes (e.g. ‘coming to terms’ with a diagnosis or prognosis) rather than depression symptomatology or psychological morbidity per se. Further primary research is indicated to explore this under-recognised comorbidity in men.
Acknowledgements
We would like to thank Cori Dressler and Adejoke Oluyase for contributing to assessing studies for inclusion and extracting data on the quantitative review. We thank Kath Wright and the staff at Centre for Reviews and Dissemination, University of York, for their assistance with the searches and Dr Rosaleen O’Brien, Glasgow Caledonian University, for her contributions to the study design. We would also like to sincerely thank Ali Finlayson, David Houghton, Stan Williams, Barry Cassidy, and Richard and Fiona Benson for their involvement and contributions in the PPI/stakeholder group.
Contributions of authors
Paul Galdas (senior lecturer, health sciences) managed the project and had primary responsibility for writing the study protocol and final report.
Zoe Darwin (research fellow, health sciences) assessed studies for inclusion, extracted data on all qualitative studies, conducted qualitative analyses and wrote the report.
Jennifer Fell (research fellow, health sciences) assessed quantitative studies for inclusion, extracted data on all quantitative studies, conducted meta-analyses and wrote the report.
Lisa Kidd (research fellow, public health) made contributions to the design and conduct of the study, conducted qualitative analyses and contributed to the writing of the report.
Peter Bower (professor, primary care) made contributions to the design and conduct of the study, conducted and advised on meta-analyses, and contributed to the writing of the report.
Christian Blickem (research fellow, primary care) made contributions to the design and conduct of the study, conducted qualitative analyses and contributed to the writing of the report.
Kerri McPherson (senior lecturer, health psychology) made contributions to the design and conduct of the study, conducted qualitative analyses and contributed to the writing of the report.
Kate Hunt (professor, gender and health) made contributions to the design and conduct of the study, conducted qualitative analyses and contributed to the writing of the report.
Simon Gilbody (professor, health sciences) made contributions to the design and conduct of the study, conducted and advised on meta-analyses, and contributed to the writing of the report.
Gerry Richardson (senior research fellow, health economics) made contributions to the design and conduct of the study, extracted data on economic evaluations, advised on economic methodology and contributed to the writing of the report.
Data sharing statement
Data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Coutler A, Roberts S, Dixon A. Delivering Better Services for People with Long-Term Conditions: Building the House of Care. London: The King’s Fund; 2013.
- Improving Chronic Disease Management. London: DH; 2004.
- Long Term Conditions Compendium of Information. London: DH; 2012.
- NHS Networks . About Us n.d. www.networks.nhs.uk/nhs-networks/commissioning-for-long-term-conditions/about-us (accessed 7 February 2014).
- Department of Health (DH) . The Mandate: A Mandate from the Government to the NHS Commissioning Board: April 2013 to March 2015 2013. www.gov.uk/government/uploads/system/uploads/attachment_data/file/256497/13-15_mandate.pdf (accessed 7 February 2014).
- Self-Care: A Real Choice. London: DH; 2005.
- Panagioti M, Richardson G, Murray E, Rogers A, Kennedy A, Newman S, et al. Reducing Care Utilisation through Self-management Interventions (RECURSIVE): a systematic review and meta-analysis. Health Serv Deliv Res 2014;2.
- Parsons S, Bury M, Carter S, Hurst P, Magee H, Taylor D. Self Management Support Amongst Older Adults: The Availability, Impact and Potential of Locally Based Services and Resources 2010.
- Supporting People with Long Term Conditions: An NHS and Social Care Model to Support Local Innovation and Integration. London: DH; 2005.
- Rogers A, Kennedy A, Bower P, Gardner C, Gately C, Lee V, et al. The United Kingdom Expert Patients Programme: results and implications from a national evaluation. Med J Aust 2008;189:21-4.
- Steventon A, Bardsley M, Billings J, Dixon J, Doll H, Hirani S, et al. Whole System Demonstrator Evaluation Team. Effect of telehealth on use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial. BMJ 2012;344.
- Deakin T, McShane C, Cade J, Williams R. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev 2005;2. http://dx.doi.org/10.1002/14651858.cd003417.pub2.
- Duncan E, Best C, Hagen S. Shared decision making interventions for people with mental health conditions. Cochrane Database Syst Rev 2010;1. http://dx.doi.org/10.1002/14651858.cd007297.pub2.
- Foster G, Taylor S, Eldridge S, Ramsay J, Griffiths C. Self-management education programmes by lay leaders for people with chronic conditions. Cochrane Database Syst Rev 2007;4. http://dx.doi.org/10.1002/14651858.cd005108.pub2.
- Nieuwlaat R, Wilczynski N, Navarro T, Hobson N, Jeffery R, Keepanasseril A, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev 2014;11. http://dx.doi.org/10.1002/14651858.cd000011.pub4.
- Furler J, Harris M, Rogers A. Equity and long-term condition self-management. Chronic Illn 2011;7:3-5. http://dx.doi.org/10.1177/1742395310386978.
- Kennedy A, Bower P, Reeves D, Blakeman T, Bowen R, Chew-Graham C, et al. Implementation of self management support for long term conditions in routine primary care settings: cluster randomised controlled trial. BMJ 2013;346. http://dx.doi.org/10.1136/bmj.f2882.
- Chodosh J, Morton SC, Mojica W, Maglione M, Suttorp MJ, Hilton L, et al. Meta-analysis: chronic disease self-management programs for older adults. Ann Intern Med 2005;143:427-38. http://dx.doi.org/10.7326/0003-4819-143-6-200509200-00007.
- White A, McKee M, Richardson N, Visser R, Madsen SA, Sousa BC, et al. Europe’s men need their own health strategy. BMJ 2011;343. http://dx.doi.org/10.1136/bmj.d7397.
- The State of Men’s Health in Europe Report. Brussels: European Commission; 2011.
- Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown W, Bandura A, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care 2001;39:1217-23. http://dx.doi.org/10.1097/00005650-200111000-00008.
- Kennedy A, Reeves D, Bower P, Lee V, Middleton E, Richardson G, et al. The effectiveness and cost-effectiveness of a national lay-led self care support programme for patients with long-term conditions: a pragmatic randomised controlled trial. J Epidemiol Community Health 2007;61:254-61. http://dx.doi.org/10.1136/jech.2006.053538.
- Bury M, Newbould J, Taylor D. A Rapid Review of the Current State of Knowledge Regarding Lay Led Self Management of Chronic Illness: Evidence Review. London: National Institute for Health and Care Excellence; 2005.
- Banks I. No man’s land: men, illness and the NHS. BMJ 2001;323:1058-60. http://dx.doi.org/10.1136/bmj.323.7320.1058.
- Galdas PM, Cheater F, Marshall P. Men and health help-seeking behaviour: literature review. J Adv Nurs 2005;49:616-23. http://dx.doi.org/10.1111/j.1365-2648.2004.03331.x.
- Courtenay WH. Key determinants of the health and well-being of men and boys. Int J Mens Health 2003;2:1-30. http://dx.doi.org/10.3149/jmh.0201.1.
- O’Brien R, Hunt K, Hart G. ‘It’s caveman stuff, but that is to a certain extent how guys still operate’: men’s accounts of masculinity and help-seeking. Soc Sci Med 2005;61:503-16. http://dx.doi.org/10.1016/j.socscimed.2004.12.008.
- McCartney G, Mahmood L, Leyland AH, Batty GD, Hunt K. Contribution of smoking-related and alcohol-related deaths to the gender gap in mortality: evidence from 30 European countries. Tob Control 2011;20:166-8. http://dx.doi.org/10.1136/tc.2010.037929.
- Wilkins D, Payne S, Granville G, Branney P. The Gender and Access to Health Services Study: Final Report. London: Department of Health; 2008.
- Equality Act 2010: Public Sector Equality Duty: What Do I Need to Know? A Quick Start Guide for Public Sector Organisations. London: The Stationery Office; 2011.
- Branney P. What is the UK Gender Duty and why is it linked to men’s health?. Crit Public Health 2012;22:121-6. http://dx.doi.org/10.1080/09581596.2011.646955.
- NHS Constitution . A Refreshed Equality Delivery System for the NHS: EDS2 Making Sure That Everyone Counts 2013. www.england.nhs.uk/wp-content/uploads/2013/11/eds-nov131.pdf (accessed 2 November 2014).
- Taylor S, Pinnock H, Epiphanou E, Pearce G, Parke H, Schwappach A, et al. A rapid synthesis of the evidence on interventions supporting self-management for people with long-term conditions: PRISMS – Practical systematic Review of Self-Management Support for long-term conditions. Health Serv Deliv Res 2014;2.
- Michie S, Johnston M, Abraham C, Francis J, Hardeman W, Eccles M. BCT Taxonomy Training Manual: Self-Directed 2013. www.ucl.ac.uk/health-psychology/bcttaxonomy (accessed 23 November 2014).
- The Cochrane Collaboration . The Cochrane Collaboration'S Tool for Assessing Risk of Bias n.d. http://ohg.cochrane.org/sites/ohg.cochrane.org/files/uploads/Risk%20of%20bias%20assessment%20tool.pdf (accessed 3 July 2013).
- Pincus T, Miles C, Froud R, Underwood M, Carnes D, Taylor SJ. Methodological criteria for the assessment of moderators in systematic reviews of randomised controlled trials: a consensus study. BMC Med Res Methodol 2011;11. http://dx.doi.org/10.1186/1471-2288-11-14.
- Sun X, Briel M, Busse JW, You JJ, Akl EA, Mejza F, et al. Credibility of claims of subgroup effects in randomised controlled trials: systematic review. BMJ 2012;344. http://dx.doi.org/10.1136/bmj.e1553.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Erlbaum; 1988.
- Devins GM, Orme CM. Center for epidemiologic studies depression scale. Test Critiques 1985;2:144-60.
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996.
- Davies EM, Moxham T, Rees K, Singh S, Coats A, Ebrahim S, et al. Exercise based rehabilitation for heart failure. Cochrane Database Syst Rev 2014;4.
- Mishra SS, Scherer RW, Snyder C, Geigle PM, Berlanstein DR, Topaloglu O. Exercise interventions on health-related quality of life for people with cancer during active treatment. Cochrane Database Syst Rev 2012;8.
- Kruis A, Smidt N, Assendelft W, Gussekloo J, Boland M, Rutten-van Mölken M, et al. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2013;10. http://dx.doi.org/10.1002/14651858.cd009437.pub2.
- Dickinson HO, Campbell F, Beyer FR, Nicolson DJ, Cook JV, Ford GA, et al. Relaxation therapies for the management of primary hypertension in adults. Cochrane Database Syst Rev 2008;1.
- Drummond MF, Schulpher MJ, Torrance BJ, O’Brien BJ, Stoddart GL. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 1997.
- Allen BT, DeLong ER, Feussner JR. Impact of glucose self-monitoring on non-insulin-treated patients with type II diabetes mellitus: randomized controlled trial comparing blood and urine testing. Diabetes Care 1990;13:1044-50. http://dx.doi.org/10.2337/diacare.13.10.1044.
- Bosley F, Allen TW. Stress management training for hypertensives: cognitive and physiological effects. J Behav Med 1989;12:77-89. http://dx.doi.org/10.1007/BF00844750.
- Burgio KL, Goode PS, Urban DA, Umlauf MG, Locher JL, Bueschen A, et al. Preoperative biofeedback assisted behavioral training to decrease post-prostatectomy incontinence: a randomized, controlled trial. J Urol 2006;175:196-201. http://dx.doi.org/10.1016/S0022-5347(05)00047-9.
- Daubenmier JJ, Weidner G, Marlin R, Crutchfield L, Dunn-Emke S, Chi C, et al. Lifestyle and health-related quality of life of men with prostate cancer managed with active surveillance. Urology 2006;67:125-30. http://dx.doi.org/10.1016/j.urology.2005.07.056.
- Gallagher A, Henderson W, Abraira C. Dietary patterns and metabolic control in diabetic diets: a prospective study of 51 outpatient men on unmeasured and exchange diets. J Am Coll Nutr 1987;6:525-32. http://dx.doi.org/10.1080/07315724.1987.10720212.
- Gallagher AM, Abraira C, Henderson WG. A four-year prospective trial of unmeasured diet in lean diabetic adults. Diabetes Care 1984;7:557-65. http://dx.doi.org/10.2337/diacare.7.6.557.
- Giesler RB, Given B, Given CW, Rawl S, Monahan P, Burns D, et al. Improving the quality of life of patients with prostate carcinoma: a randomized trial testing the efficacy of a nurse-driven intervention. Cancer 2005;104:752-62. http://dx.doi.org/10.1002/cncr.21231.
- Gifford AL, Laurent DD, Gonzales VM, Chesney MA, Lorig KR. Pilot randomized trial of education to improve self-management skills of men with symptomatic HIV/AIDS. J Acquir Immune Defic Syndr Hum Retrovirol 1998;18:136-44. http://dx.doi.org/10.1097/00042560-199806010-00005.
- Gourley GA, Portner TS, Gourley DR, Rigolosi EL, Holt JM, Solomon DK, et al. Humanistic outcomes in the hypertension and COPD arms of a multicenter outcomes study. J Am Pharm Assoc 1998;38:586-97.
- Solomon DK, Portner TS, Bass GE, Gourley DR, Gourley GA, Holt JM, et al. Clinical and economic outcomes in the hypertension and COPD arms of a multicenter outcomes study. J Am Pharm Assoc 1998;38:574-85.
- Heisler M, Vijan S, Makki F, Piette JD. Diabetes control with reciprocal peer support versus nurse care management: a randomized trial. Ann Intern Med 2010;153:507-15. http://dx.doi.org/10.7326/0003-4819-153-8-201010190-00007.
- Leehey DJ, Moinuddin I, Bast JP, Qureshi S, Jelinek CS, Cooper C, et al. Aerobic exercise in obese diabetic patients with chronic kidney disease: a randomized and controlled pilot study. Cardiovasc Diabetol 2009;8. http://dx.doi.org/10.1186/1475-2840-8-62.
- Lepore S. Psychoeducational support group enhances quality of life after prostate cancer. Harwood Academic 1999;8:81-92.
- Lepore SJ, Helgeson VS, Eton DT, Schulz R. Improving quality of life in men with prostate cancer: a randomized controlled trial of group education interventions. Health Psychol 2003;22:443-52. http://dx.doi.org/10.1037/0278-6133.22.5.443.
- Lucy J. The Effects of TELECARE on Psychosocial Symptoms in HIV-Seropositive Individuals. Pasadena, CA: Fuller Theological Seminary; 1994.
- Mishel MH, Belyea M, Germino BB, Stewart JL, Bailey DE, Robertson C, et al. Helping patients with localized prostate carcinoma manage uncertainty and treatment side effects: nurse-delivered psychoeducational intervention over the telephone. Cancer 2002;94:1854-66. http://dx.doi.org/10.1002/cncr.10390.
- Mueller L, Myers J, Kottman W, Oswald U, Boesch C, Arbrol N, et al. Exercise capacity, physical activity patterns and outcomes six years after cardiac rehabilitation in patients with heart failure. Clin Rehabil 2007;21:923-31. http://dx.doi.org/10.1177/0269215507079097.
- Parker JC, Singsen BH, Hewett JE, Walker SE, Hazelwood SE, Hall PJ, et al. Educating patients with rheumatoid arthritis: a prospective analysis. Arch Phys Med Rehabil 1984;65:771-4.
- Parker PA, Pettaway CA, Babaian RJ, Pisters LL, Miles B, Fortier A, et al. The effects of a presurgical stress management intervention for men with prostate cancer undergoing radical prostatectomy. J Clin Oncol 2009;27:3169-76. http://dx.doi.org/10.1200/JCO.2007.16.0036.
- Scura KW, Budin W, Garfing E. Telephone social support and education for adaptation to prostate cancer: a pilot study. Oncol Nurs Forum 2004;31:335-8. http://dx.doi.org/10.1188/04.ONF.335-338.
- Carmack Taylor CL, Demoor C, Smith MA, Dunn AL, Basen-Engquist K, Nielsen I, et al. Active for Life After Cancer: a randomized trial examining a lifestyle physical activity program for prostate cancer patients. Psycho-Oncology 2006;15:847-62. http://dx.doi.org/10.1002/pon.1023.
- Wakefield BJ, Bylund CL, Holman JE, Ray A, Scherubel M, Kienzle MG, et al. Nurse and patient communication profiles in a home-based telehealth intervention for heart failure management. Patient Educ Couns 2008;71:285-92. http://dx.doi.org/10.1016/j.pec.2008.01.006.
- Weber BA, Roberts BL, Resnick M, Deimling G, Zauszniewski JA, Musil C, et al. The effect of dyadic intervention on self-efficacy, social support, and depression for men with prostate cancer. Psycho-Oncology 2004;13:47-60. http://dx.doi.org/10.1002/pon.718.
- Weber BA, Roberts BL, Yarandi H, Mills TL, Chumbler NR, Wajsman Z. The impact of dyadic social support on self-efficacy and depression after radical prostatectomy. J Aging Health 2007;19:630-45. http://dx.doi.org/10.1177/0898264307300979.
- White N, Carnahan J, Nugent CA, Iwaoka T, Dodson MA. Management of obese patients with diabetes mellitus: comparison of advice education with group management. Diabetes Care 1986;9:490-6. http://dx.doi.org/10.2337/diacare.9.5.490.
- Bennett P, Wallace L, Carroll D, Smith N. Treating type A behaviours and mild hypertension in middle-aged men. J Psychosom Res 1991;35:209-23. http://dx.doi.org/10.1016/0022-3999(91)90075-Y.
- Bourke L, Doll H, Crank H, Daley A, Rosario D, Saxton JM. Lifestyle intervention in men with advanced prostate cancer receiving androgen suppression therapy: a feasibility study. Cancer Epidemiol Biomarkers Prev 2011;20:647-57. http://dx.doi.org/10.1158/1055-9965.EPI-10-1143.
- Cockcroft A, Berry G, Brown EB, Exall C. Psychological changes during a controlled trial of rehabilitation in chronic respiratory disability. Thorax 1982;37:413-16. http://dx.doi.org/10.1136/thx.37.6.413.
- Cockcroft AE, Saunders MJ, Berry G. Randomised controlled trial of rehabilitation in chronic respiratory disability. Thorax 1981;36:200-3. http://dx.doi.org/10.1136/thx.36.3.200.
- McGavin C, Gupta S, Lloyd E, McHardy G. A controlled trial of self-regulated physical training in chronic bronchitis. Br J Dis Chest 1976;1.
- McGavin CR, Gupta SP, Lloyd EL, McHardy GJ. Physical rehabilitation for the chronic bronchitic: results of a controlled trial of exercises in the home. Thorax 1977;32:307-11. http://dx.doi.org/10.1136/thx.32.3.307.
- Moynihan C, Bliss JM, Davidson J, Burchell L, Horwich A. Evaluation of adjuvant psychological therapy in patients with testicular cancer: randomised controlled trial. BMJ 1998;316:429-35. http://dx.doi.org/10.1136/bmj.316.7129.429.
- Windsor PM, Nicol KF, Potter J. A randomized, controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localized prostate carcinoma. Cancer 2004;101:550-7. http://dx.doi.org/10.1002/cncr.20378.
- Adsett CA, Bellissimo A, Mitchell A, Wilczynski N, Haynes RB. Behavioral and physiological effects of a beta blocker and relaxation therapy on mild hypertensives. Psychosom Med 1989;51:523-36. http://dx.doi.org/10.1097/00006842-198909000-00004.
- Culos-Reed SN, Robinson JW, Lau H, Stephenson L, Keats M, Norris S, et al. Physical activity for men receiving androgen deprivation therapy for prostate cancer: benefits from a 16-week intervention. Support Care Cancer 2010;18:591-9. http://dx.doi.org/10.1007/s00520-009-0694-3.
- Guell R, Casan P, Belda J, Sangenis M, Morante F, Guyatt GH, et al. Long-term effects of outpatient rehabilitation of COPD: a randomized trial. Chest 2000;117:976-83. http://dx.doi.org/10.1378/chest.117.4.976.
- Haynes RB, Sackett DL, Gibson ES, Taylor DW, Hackett BC, Roberts RS, et al. Improvement of medication compliance in uncontrolled hypertension. Lancet 1976;1:1265-8. http://dx.doi.org/10.1016/S0140-6736(76)91737-2.
- Sackett DL, Haynes RB, Gibson ES, Hackett BC, Taylor DW, Roberts RS, et al. Randomised clinical trial of strategies for improving medication compliance in primary hypertension. Lancet 1975;1:1205-7. http://dx.doi.org/10.1016/S0140-6736(75)92192-3.
- Fernandez AM, Pascual J, Ferrando C, Arnal A, Vergara I, Sevila V. Home-based pulmonary rehabilitation in very severe COPD: is it safe and useful?. J Cardiopulm Rehabil Prev 2009;29:325-31. http://dx.doi.org/10.1097/HCR.0b013e3181ac7b9d.
- Garcia-Vera MP, Labrador FJ, Sanz J. Stress-management training for essential hypertension: a controlled study. Appl Psychophysiol Biofeedback 1997;22:261-83. http://dx.doi.org/10.1007/BF02438980.
- Garcia-Vera MP, Sanz J, Labrador FJ. Blood pressure variability and stress management training for essential hypertension. Behav Med 2004;30:53-62. http://dx.doi.org/10.3200/BMED.30.2.53-64.
- Puente-Maestu L, Luisa Sanz M, Sanz P, de Ona RJ, Arnedillo A, Casaburi R. Long-term effects of a maintenance program after supervised or self-monitored training programs in patients with COPD. Lung 2003;181:67-78. http://dx.doi.org/10.1007/s00408-003-1007-0.
- Puente-Maestu L, Sanz ML, Sanz P, Cubillo JM, Mayol J, Casaburi R. Comparison of effects of supervised versus self-monitored training programmes in patients with chronic obstructive pulmonary disease. Eur Resp J 2000;15:517-25. http://dx.doi.org/10.1034/j.1399-3003.2000.15.15.x.
- Berglund G, Petersson LM, Eriksson KC, Wallenius I, Roshanai A, Nordin KM, et al. ‘Between Men’: a psychosocial rehabilitation programme for men with prostate cancer. Acta Oncol 2007;46:83-9. http://dx.doi.org/10.1080/02841860600857326.
- Klocek M, Kubinyi A, Bacior B, Kawecka-Jaszcz K. Effect of physical training on quality of life and oxygen consumption in patients with congestive heart failure. Int J Cardiol 2005;103:323-9. http://dx.doi.org/10.1016/j.ijcard.2004.10.021.
- Koukouvou G, Kouidi E, Iacovides A, Konstantinidou E, Kaprinis G, Deligiannis A. Quality of life, psychological and physiological changes following exercise training in patients with chronic heart failure. J Rehabil Med 2004;36:36-41. http://dx.doi.org/10.1080/11026480310015549.
- Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 2011. www.cochrane-handbook.org (accessed 2 November 2014).
- Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol 2012;12. http://dx.doi.org/10.1186/1471-2288-12-181.
- Noblit GW, Hare RD. Meta-ethnography: Synthesizing Qualitative Studies. Newbury Park, CA: Sage Publications; 1988.
- Flemming K, Graham H, Heirs M, Fox D, Sowden A. Smoking in pregnancy: a systematic review of qualitative research of women who commence pregnancy as smokers. J Adv Nurs 2012;69:1023-36. http://dx.doi.org/10.1111/jan.12066.
- Atkins S, Lewin S, Smith H, Engel M, Fretheim A, Volmink J. Conducting a meta-ethnography of qualitative literature: lessons learnt. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-21.
- Flemming K, Briggs M. Electronic searching to locate qualitative research: evaluation of three strategies. J Adv Nurs 2007;57:95-100. http://dx.doi.org/10.1111/j.1365-2648.2006.04083.x.
- Shaw RL, Booth A, Sutton AJ, Miller T, Smith JA, Young B, et al. Finding qualitative research: an evaluation of search strategies. BMC Med Res Methodol 2004;4. http://dx.doi.org/10.1186/1471-2288-4-5.
- Iredale R, Williams B, Brain K, France E, Gray J. The information needs of men with breast cancer. Br J Nurs 2007;16:540-4. http://dx.doi.org/10.12968/bjon.2007.16.9.23432.
- Ramachandra P, Booth S, Pieters T, Vrotsou K, Huppert FA. A brief self-administered psychological intervention to improve well-being in patients with cancer: results from a feasibility study. Psycho-Oncology 2009;18:1323-6. http://dx.doi.org/10.1002/pon.1516.
- Smith RL, Crane LA, Byers T, Nelson-Marten P. An evaluation of the Man to Man self-help group in Colorado and Utah. Cancer Pract 2002;10:234-9. http://dx.doi.org/10.1046/j.1523-5394.2002.105002.x.
- Barlow JH, Turner AP, Gilchrist M. A randomised controlled trial of lay-led self-management for myocardial infarction patients who have completed cardiac rehabilitation. Eur J Cardiovasc Nurs 2009;8:293-301. http://dx.doi.org/10.1016/j.ejcnurse.2009.02.002.
- Barlow J, Edwards R, Turner A. The experience of attending a lay-led, chronic disease self-management programme from the perspective of participants with multiple sclerosis. Psychol Health 2009;24:1167-80. http://dx.doi.org/10.1080/08870440802040277.
- Abraham C, Michie S. A taxonomy of behaviour change techniques used in interventions. Health Psychol 2008;27:379-87. http://dx.doi.org/10.1037/0278-6133.27.3.379.
- Michie S, West R. Behaviour change theory and evidence: a presentation to Government. Health Psychol Rev 2013;7:1-22. http://dx.doi.org/10.1080/17437199.2011.649445.
- Michie S, Hyder N, Walia A, West R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict Behav 2011;36:315-19. http://dx.doi.org/10.1016/j.addbeh.2010.11.016.
- Bell K, Lee J, Foran S, Kwong S, Christopherson J. Is there an ‘ideal cancer’ support group? Key findings from a qualitative study of three groups. J Psychosoc Oncol 2010;28:432-49. http://dx.doi.org/10.1080/07347332.2010.488140.
- Bedell G. Daily life for eight urban gay men with HIV/AIDS. Am J Occupat Ther 2000;54:197-206. http://dx.doi.org/10.5014/ajot.54.2.197.
- Broom A. Virtually he@lthy: the impact of internet use on disease experience and the doctor–patient relationship. Qual Health Res 2005;15:325-45. http://dx.doi.org/10.1177/1049732304272916.
- Chenard C. The impact of stigma on the self-care behaviors of HIV-positive gay men striving for normalcy. J Assoc Nurs Aid Care 2007;18:23-32. http://dx.doi.org/10.1016/j.jana.2007.03.005.
- Corboy D, McDonald J, McLaren S. Barriers to accessing psychosocial support services among men with cancer living in rural Australia: perceptions of men and health professionals. Int J Mens Health 2011;10:163-83. http://dx.doi.org/10.3149/jmh.1002.163.
- Cramer H, Horwood J, Payne S, Araya R, Lester H, Salisbury C. Do depressed and anxious men do groups? What works and what are the barriers to help seeking?. Prim Health Care Res Devel 2013;5:287-301. http://dx.doi.org/10.1017/S1463423613000297.
- Dickerson SS, Reinhart A, Boemhke M, Akhu-Zaheya L. Cancer as a problem to be solved: internet use and provider communication by men with cancer. Comput Inform Nurs 2011;29:388-95. http://dx.doi.org/10.1097/NCN.0b013e3181f9ddb1.
- Dickerson SS, Boehmke M, Ogle C, Brown JK. Seeking and managing hope: patients’ experiences using the internet for cancer care. Oncol Nurs Forum 2006;33:E1-E10. http://dx.doi.org/10.1188/06.ONF.E8-E17.
- Emslie C, Ridge D, Ziebland S, Hunt K. Exploring men’s and women’s experiences of depression and engagement with health professionals: more similarities than differences? A qualitative interview study. BMC Fam Pract 2007;8. http://dx.doi.org/10.1186/1471-2296-8-43.
- Evans M, Shaw A, Thompson EA, Falk S, Turton P, Thompson T, et al. Decisions to use complementary and alternative medicine (CAM) by male cancer patients: information-seeking roles and types of evidence used. BMC Complement Altern Med 2007;7. http://dx.doi.org/10.1186/1472-6882-7-25.
- Harris GE, Alderson K. An investigation of gay men’s experiences with HIV counselling and peer support services. Can J Community Ment Health 2007;26:129-42. http://dx.doi.org/10.7870/cjcmh-2007-0017.
- Gibbs L. Identifying work as a barrier to men’s access to chronic illness (arthritis) self-management programs. Int J Mens Health 2007;6:143-55. http://dx.doi.org/10.3149/jmh.0602.143.
- Gibbs L. Applications of masculinity theories in a chronic illness context. Int J Mens Health 2005;4:287-300. http://dx.doi.org/10.3149/jmh.0403.287.
- Gray R, Fitch M, Davis C, Phillips C. A qualitative study of breast cancer self-help groups. Psycho-Oncology 1997;6:279-89. http://dx.doi.org/10.1002/(SICI)1099-1611(199712)6:4<279::AID-PON280>3.0.CO;2-0.
- Gray RE, Fitch M, Davis C, Phillips C. Interviews with men with prostate cancer about their self-help group experience. J Palliat Care 1997;13:15-21.
- Gray R, Fitch M, Davis C, Phillips C. Breast cancer and prostate cancer self-help groups: reflections on differences. Psycho-Oncology 1996;5:137-42. http://dx.doi.org/10.1002/(SICI)1099-1611(199606)5:2<137::AID-PON222>3.0.CO;2-E.
- Kendall J. Promoting wellness in HIV-support groups. J Association Nurs AIDS Care 1992;3:28-3.
- Oliffe JL, Bottorff JL, McKenzie MM, Hislop TG, Gerbrandt JS, Oglov V. Prostate cancer support groups, health literacy and consumerism: are community-based volunteers re-defining older men’s health?. Health 2011;15:555-70. http://dx.doi.org/10.1177/1363459310364156.
- Oliffe JL, Halpin M, Bottorff JL, Hislop TG, McKenzie M, Mroz L. How prostate cancer support groups do and do not survive: British Columbian perspectives. Am J Mens Health 2008;2:143-55. http://dx.doi.org/10.1177/1557988307304147.
- Oliffe JL, Gerbrandt JS, Bottorff JL, Hislop TG. Health promotion and illness demotion at prostate cancer support groups. Health Promot Pract 2010;11:562-71. http://dx.doi.org/10.1177/1524839908328990.
- Sandstrom KL. Searching for information, understanding, and self-value: the utilization of peer support groups by gay men with HIV/AIDS. Soc Work Health Care 1996;23:51-74. http://dx.doi.org/10.1300/J010v23n04_05.
- Seale C, Ziebland S, Charteris-Black J. Gender, cancer experience and internet use: a comparative keyword analysis of interviews and online cancer support groups. Soc Sci Med 2006;62:2577-90. http://dx.doi.org/10.1016/j.socscimed.2005.11.016.
- Vanable PA, Carey MP, Brown JL, Littlewood RA, Bostwick R, Blair D. What HIV-positive MSM want from sexual risk reduction interventions: findings from a qualitative study. AIDS Behav 2012;16:554-63. http://dx.doi.org/10.1007/s10461-011-0047-3.
- Wallace M, Storms S. The needs of men with prostate cancer: results of a focus group study. Appl Nurs Res 2007;20:181-7. http://dx.doi.org/10.1016/j.apnr.2006.08.008.
- Campbell R, Pound P, Morgan M, Daker-White G, Britten N, Pill R, et al. Evaluating meta ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess 2011;15. http://dx.doi.org/10.3310/hta15430.
- Critical Appraisal Skills Programme . Critical Appraisal Skills Programme (CASP) Qualitative Research Checklist 31.05.13: 10 Questions to Help You Make Sense of Qualitative Research 2013. www.casp-uk.net/wp-content/uploads/2011/11/CASP-Qualitative-Research-Checklist-31.05.13.pdf (accessed 15 July 2013).
- Dixon-Woods M, Sutton A, Shaw RL, Miller T, Smith JA, Young B, et al. Appraising qualitative research for inclusion in systematic reviews: a quantitative and qualitative comparison of three methods. J Health Serv Res Policy 2007;12:42-56. http://dx.doi.org/10.1258/135581907779497486.
- Baird KK, Pierce LL. Adherence to cardiac therapy for men with coronary artery disease. Rehabil Nurs J 2001;26:233-7. http://dx.doi.org/10.1002/j.2048-7940.2001.tb01962.x.
- Eldh AC, Ehnfors M, Ekman I. The meaning of patient participation for patients and nurses at a nurse-led clinic for chronic heart failure. Eur J Cardiovasc Nurs 2006;5:45-53. http://dx.doi.org/10.1016/j.ejcnurse.2005.06.002.
- Sullivan CF. Gendered cybersupport: a thematic analysis of two online cancer support groups. J Health Psychol 2003;8:83-103. http://dx.doi.org/10.1177/1359105303008001446.
- Schutz A. Collected Papers. The Hague: Martinus Nijhoff; 1971.
- INVOLVE . Payment for Involvement: A Guide for Making Payments to Members of the Public Actively Involved in NHS, Public Health and Social Care Research 2010.
- Austin J, Williams R, Ross L, Moseley L, Hutchison S. Randomised controlled trial of cardiac rehabilitation in elderly patients with heart failure. Eur J Heart Fail 2005;7:411-17. http://dx.doi.org/10.1016/j.ejheart.2004.10.004.
- Belardinelli R, Georgiou D, Cianci G, Purcaro A. Randomized, controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation 1999;99:1173-82. http://dx.doi.org/10.1161/01.CIR.99.9.1173.
- Dracup K, Evangelista LS, Hamilton MA, Erickson V, Hage A, Moriguchi J, et al. Effects of a home-based exercise program on clinical outcomes in heart failure. Am Heart J 2007;154:877-83. http://dx.doi.org/10.1016/j.ahj.2007.07.019.
- Flynn KE, Pina IL, Whellan DJ, Lin L, Blumenthal JA, Ellis SJ, et al. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009;301:1451-9. http://dx.doi.org/10.1001/jama.2009.457.
- McKelvie RS, Teo KK, Roberts R, McCartney N, Humen D, Montague T, et al. Effects of exercise training in patients with heart failure: the Exercise Rehabilitation Trial (EXERT). Am Heart J 2002;144:23-30. http://dx.doi.org/10.1067/mhj.2002.123310.
- Passino C, Severino S, Poletti R, Piepoli MF, Mammini C, Clerico A, et al. Aerobic training decreases B-type natriuretic peptide expression and adrenergic activation in patients with heart failure. J Am Coll Cardiol 2006;47:1835-9. http://dx.doi.org/10.1016/j.jacc.2005.12.050.
- Willenheimer R, Rydberg E, Cline C, Broms K, Hillberger B, Oberg L, et al. Effects on quality of life, symptoms and daily activity 6 months after termination of an exercise training programme in heart failure patients. Int J Cardiol 2001;77:25-31. http://dx.doi.org/10.1016/S0167-5273(00)00383-1.
- Davies P, Taylor F, Beswick A, Wise F, Moxham T, Rees K, et al. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev 2010;7. http://dx.doi.org/10.1002/14651858.cd007131.pub2.
- Mutrie N, Campbell AM, Whyte F, McConnachie A, Emslie C, Lee L, et al. Benefits of supervised group exercise programme for women being treated for early stage breast cancer: pragmatic randomised controlled trial. BMJ 2007;334. http://dx.doi.org/10.1136/bmj.39094.648553.AE.
- Johansson B, Brandberg Y, Hellbom M, Persson C, Petersson LM, Berglund G, et al. Health-related quality of life and distress in cancer patients: results from a large randomised study. Br J Cancer 2008;99:1975-83. http://dx.doi.org/10.1038/sj.bjc.6604789.
- Cheville AL, Girardi J, Clark MM, Rummans TA, Pittelkow T, Brown P, et al. Therapeutic exercise during outpatient radiation therapy for advanced cancer: feasibility and impact on physical well-being. Am J Phys Med Rehabil 2010;89:611-9. http://dx.doi.org/10.1097/PHM.0b013e3181d3e782.
- Demark-Wahnefried W, Clipp EC, Morey MC, Pieper CF, Sloane R, Snyder DC, et al. Lifestyle intervention development study to improve physical function in older adults with cancer: outcomes from Project LEAD. J Clin Oncol 2006;24:3465-73. http://dx.doi.org/10.1200/JCO.2006.05.7224.
- van Vilsteren MC, de Greef MH, Huisman RM. The effects of a low-to-moderate intensity pre-conditioning exercise programme linked with exercise counselling for sedentary haemodialysis patients in The Netherlands: results of a randomized clinical trial. Nephrol Dial Transplant 2005;20:141-6. http://dx.doi.org/10.1093/ndt/gfh560.
- Puig AL, Goodwin SM, Sherrard L. The efficacy of creative arts therapies to enhance emotional expression, spirituality, and psychological well-being of newly diagnosed Stage I and Stage II breast cancer patients: a preliminary study. Arts Psychother 2006;33:218-28. http://dx.doi.org/10.1016/j.aip.2006.02.004.
- Cohen L, Warneke C, Fouladi RT, Rodriguez MA, Chaoul-Reich A. Psychological adjustment and sleep quality in a randomized trial of the effects of a Tibetan yoga intervention in patients with lymphoma. Cancer 2004;100:2253-60. http://dx.doi.org/10.1002/cncr.20236.
- Bennett JA, Lyons KS, Winters-Stone K, Nail LM, Scherer J. Motivational interviewing to increase physical activity in long-term cancer survivors: a randomized controlled trial. Nurs Res 2007;56:18-27. http://dx.doi.org/10.1097/00006199-200701000-00003.
- Coultas D, Frederick J, Barnett B, Singh G, Wludyka P. A randomized trial of two types of nurse-assisted home care for patients with COPD. Chest 2005;128:2017-24. http://dx.doi.org/10.1378/chest.128.4.2017.
- Dominique LG, Annelie D, Madan A, Pierre B, Ginette D. Impact of the yoga Bali method on quality of life and depressive symptoms among women diagnosed with breast cancer undergoing chemotherapy. Psycho-Oncology 2010;19:136-40.
- Bower P, Kontopantelis E, Sutton A, Kendrick T, Richards DA, Gilbody S, et al. Influence of initial severity of depression on effectiveness of low intensity interventions: meta-analysis of individual patient data. BMJ 2012;346. http://dx.doi.org/10.1136/bmj.f540.
- Cadmus LA, Salovey P, Yu H, Chung G, Kasl S, Irwin ML. Exercise and quality of life during and after treatment for breast cancer: results of two randomized controlled trials. Psycho-Oncology 2009;18:343-52. http://dx.doi.org/10.1002/pon.1525.
- Chandwani KD, Thornton B, Perkins GH, Arun B, Raghuram NV, Nagendra HR, et al. Yoga improves quality of life and benefit finding in women undergoing radiotherapy for breast cancer. J Soc Integr Oncol 2010;8:43-55.
- Raghavendra RM, Nagarathna R, Nagendra HR, Gopinath KS, Srinath BS, Ravi BD, et al. Effects of an integrated yoga programme on chemotherapy-induced nausea and emesis in breast cancer patients. Eur J Cancer Care 2007;16:462-74. http://dx.doi.org/10.1111/j.1365-2354.2006.00739.x.
- Courneya KS, Friedenreich CM, Quinney HA, Fields AL, Jones LW, Fairey AS. A randomized trial of exercise and quality of life in colorectal cancer survivors. Eur J Cancer Care 2003;12:347-57. http://dx.doi.org/10.1046/j.1365-2354.2003.00437.x.
- Heckman TG, Carlson B. A randomized clinical trial of two telephone-delivered, mental health interventions for HIV-infected persons in rural areas of the United States. AIDS Behav 2007;11:5-14. http://dx.doi.org/10.1007/s10461-006-9111-9.
- Banerjee B, Vadiraj HS, Ram A, Rao R, Jayapal M, Gopinath KS, et al. Effects of an integrated yoga program in modulating psychological stress and radiation-induced genotoxic stress in breast cancer patients undergoing radiotherapy. Integr Cancer Ther 2007;6:242-50. http://dx.doi.org/10.1177/1534735407306214.
- Donnelly CM, Blaney JM, Lowe-Strong A, Rankin JP, Campbell A, McCrum-Gardner E, et al. A randomised controlled trial testing the feasibility and efficacy of a physical activity behavioural change intervention in managing fatigue with gynaecological cancer survivors. Gynecol Oncol 2011;122:618-24. http://dx.doi.org/10.1016/j.ygyno.2011.05.029.
- Emery CF, Schein RL, Hauck ER, MacIntyre NR. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol 1998;17:232-40. http://dx.doi.org/10.1037/0278-6133.17.3.232.
- Carmack CL, Amaral-Melendez M, Boudreaux E, Brantley PJ, Jones GN, Franks BD, et al. Exercise as a component in the physical and psychological rehabilitation of hemodialysis patients. Int J Rehabil Health 1995;1:13-2. http://dx.doi.org/10.1007/BF02214958.
- Jarden M, Baadsgaard MT, Hovgaard DJ, Boesen E, Adamsen L. A randomized trial on the effect of a multimodal intervention on physical capacity, functional performance and quality of life in adult patients undergoing allogeneic SCT. Bone Marrow Transplant 2009;43:725-37. http://dx.doi.org/10.1038/bmt.2009.27.
- Adamsen L, Quist M, Andersen C, Moller T, Herrstedt J, Kronborg D, et al. Effect of a multimodal high intensity exercise intervention in cancer patients undergoing chemotherapy: randomised controlled trial. BMJ 2009;339. http://dx.doi.org/10.1136/bmj.b3410.
- Danhauer SC, Mihalko SL, Russell GB, Campbell CR, Felder L, Daley K, et al. Restorative yoga for women with breast cancer: findings from a randomized pilot study. Psycho-Oncology 2009;18:360-8. http://dx.doi.org/10.1002/pon.1503.
- Thorsen L, Skovlund E, Stromme SB, Hornslien K, Dahl AA, Fossa SD. Effectiveness of physical activity on cardiorespiratory fitness and health-related quality of life in young and middle-aged cancer patients shortly after chemotherapy. J Clin Oncol 2005;23:2378-88. http://dx.doi.org/10.1200/JCO.2005.04.106.
- Courneya KS, Friedenreich CM, Sela RA, Quinney HA, Rhodes RE, Handman M. The group psychotherapy and home-based physical exercise (group-hope) trial in cancer survivors: physical fitness and quality of life outcomes. Psycho-Oncology 2003;12:357-74. http://dx.doi.org/10.1002/pon.658.
- Wang YJ, Boehmke M, Wu YW, Dickerson SS, Fisher N. Effects of a 6-week walking program on Taiwanese women newly diagnosed with early-stage breast cancer. Cancer Nurs 2011;34:E1-13. http://dx.doi.org/10.1097/NCC.0b013e3181e4588d.
- Mock V, Frangakis C, Davidson NE, Ropka ME, Pickett M, Poniatowski B, et al. Exercise manages fatigue during breast cancer treatment: a randomized controlled trial. Psycho-Oncology 2005;14:464-77. http://dx.doi.org/10.1002/pon.863.
- Stein MD, Herman DS, Bishop D, Anderson BJ, Trisvan E, Lopez R, et al. A telephone-based intervention for depression in HIV patients: negative results from a randomized clinical trial. AIDS Behav 2007;11:15-23. http://dx.doi.org/10.1007/s10461-006-9131-5.
- Kouidi E, Iacovides A, Iordanidis P, Vassiliou S, Deligiannis A, Ierodiakonou C, et al. Exercise renal rehabilitation program: psychosocial effects. Nephron 1997;77:152-8. http://dx.doi.org/10.1159/000190266.
- CG91 Depression in Adults with a Chronic Physical Health Problem: Treatment and Management. Manchester: NICE; 2009.
- Rogers LQ, Hopkins-Price P, Vicari S, Pamenter R, Courneya KS, Markwell S, et al. A randomized trial to increase physical activity in breast cancer survivors. Med Sci Sports Exerc 2009;41:935-46. http://dx.doi.org/10.1249/MSS.0b013e31818e0e1b.
- Engstrom CP, Persson LO, Larsson S, Sullivan M. Longterm effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease: a randomized controlled study. Scand J Rehabil Med 1999;31:207-13. http://dx.doi.org/10.1080/003655099444371.
- Guell R, Resqueti V, Sangenis M, Morante F, Martorell B, Casan P, et al. Impact of pulmonary rehabilitation on psychosocial morbidity in patients with severe COPD. Chest 2006;129:899-904. http://dx.doi.org/10.1378/chest.129.4.899.
- Mendes JC, Studart Leitao Filho FS, Malosa Sampaio LM, Negrinho de Oliveira AC, Hirata RP, Costa D, et al. Outpatient vs. home-based pulmonary rehabilitation in COPD: a randomized controlled trial. Multidiscip Respir Med 2010;5:401-8. http://dx.doi.org/10.1186/2049-6958-5-6-401.
- Fillion L, Gagnon P, Leblond F, Gelinas C, Savard J, Dupuis R, et al. A brief intervention for fatigue management in breast cancer survivors. Cancer Nurs 2008;31:145-59. http://dx.doi.org/10.1097/01.NCC.0000305698.97625.95.
- Blanchard EB, Eisele G, Vollmer A, Payne A, Gordon M, Cornish P, et al. Controlled evaluation of thermal biofeedback in treatment of elevated blood pressure in unmedicated mild hypertension. Biofeedback Self-Regul 1996;21:167-90. http://dx.doi.org/10.1007/BF02284694.
- GESICA Investigators . Randomised trial of telephone intervention in chronic heart failure: DIAL trial. BMJ 2005;331. http://dx.doi.org/10.1136/bmj.38516.398067.E0.
- Hagen EM, Eriksen HR, Ursin H. Does early intervention with a light mobilization program reduce long-term sick leave for low back pain?. Spine 2000;25:1973-6. http://dx.doi.org/10.1097/00007632-200008010-00017.
- Molde Hagen E, Grasdal A, Eriksen HR. Does early intervention with a light mobilization program reduce long-term sick leave for low back pain: a 3-year follow-up study. Spine 2003;28:2309-15. http://dx.doi.org/10.1097/01.BRS.0000085817.33211.3F.
- Hämäläinen H, Rönnemaa T, Toikka T, Liukkonen I. Long-term effects of one year of intensified podiatric activities on foot-care knowledge and self-care habits in patients with diabetes. Diabetes Educ 1998;24:734-40. http://dx.doi.org/10.1177/014572179802400609.
- Hanefeld M, Fischer S, Schmechel H, Rothe G, Schulze J, Dude H, et al. Diabetes Intervention Study: multi-intervention trial in newly diagnosed NIDDM. Diabetes Care 1991;14:308-17. http://dx.doi.org/10.2337/diacare.14.4.308.
- Julius U, Gross P, Hanefeld M. Work absenteeism in type 2 diabetes mellitus: results of the prospective Diabetes Intervention Study. Diabetes Metab 1993;19:202-6.
- Härkäpää K, Järvikoski A, Mellin G, Hurri H. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part I: pain, disability, compliance, and reported treatment benefits three months after treatment. Scand J Rehabil Med 1989;21:81-9.
- Heitzmann CA, Kaplan RM, Wilson DK, Sandler J. Sex differences in weight loss among adults with type II diabetes mellitus. J Behav Med 1987;10:197-211. http://dx.doi.org/10.1007/BF00846426.
- Jensen IB, Bergstrom G, Ljungquist T, Bodin L, Nygren AL. A randomized controlled component analysis of a behavioral medicine rehabilitation program for chronic spinal pain: are the effects dependent on gender?. Pain 2001;91:65-78. http://dx.doi.org/10.1016/S0304-3959(00)00420-6.
- Kankaanpää M, Taimela S, Airaksinen O, Hänninen O. The efficacy of active rehabilitation in chronic low back pain: effect on pain intensity, self-experienced disability, and lumbar fatigability. Spine 1999;24:1034-42. http://dx.doi.org/10.1097/00007632-199905150-00019.
- Katon W, Russo J, Frank E, Barrett J, Williams JW, Oxman T, et al. Predictors of nonresponse to treatment in primary care patients with dysthymia. Gen Hosp Psychiatry 2002;24:20-7. http://dx.doi.org/10.1016/S0163-8343(01)00171-2.
- Williams JW, Barrett J, Oxman T, Frank E, Katon W, Sullivan M, et al. Treatment of dysthymia and minor depression in primary care: a randomized controlled trial in older adults. JAMA 2000;284:1519-26. http://dx.doi.org/10.1001/jama.284.12.1519.
- Kendall PA, Jansen CM, Sjogren DD, Jansen GR. A comparison of nutrient-based and exchange-group methods of diet instruction for patients with noninsulin-dependent diabetes. Am J Clin Nutr 1987;45:625-37.
- Kovar PA, Allegrante JP, MacKenzie CR, Peterson MG, Gutin B, Charlson ME. Supervised fitness walking in patients with osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med 1992;116:529-34. http://dx.doi.org/10.7326/0003-4819-116-7-529.
- Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet 2010;376:1838-45. http://dx.doi.org/10.1016/S0140-6736(10)61997-6.
- Mellin G, Hurri H, Härkäpää K, Järvikoski A. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part II: effects on physical measurements three months after treatment. Scand J Rehabil Med 1989;21:91-5.
- O’Connor CM, Whellan DJ, Lee KL, Keteyian SJ, Cooper LS, Ellis SJ. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA 2009;301:1439-50. http://dx.doi.org/10.1001/jama.2009.454.
- Penttinen J, Nevala-Puranen N, Airaksinen O, Jääskeläinen M, Sintonen H, Takala J. Randomized controlled trial of back school with and without peer support. J Occup Rehabil 2002;12:21-9. http://dx.doi.org/10.1023/A:1013594103133.
- Smith B, Forkner E, Zaslow B, Krasuski RA, Stajduhar K, Kwan M, et al. Disease management produces limited quality-of-life improvements in patients with congestive heart failure: evidence from a randomized trial in community-dwelling patients. Am J Manag Care 2005;11:701-13.
- Vanninen E, Uusitupa M, Lansimies E, Siitonen O, Laitinen J. Effect of metabolic control on autonomic function in obese patients with newly diagnosed type 2 diabetes. Diabet Med 1993;10:66-73. http://dx.doi.org/10.1111/j.1464-5491.1993.tb01999.x.
- Wing RR, Blair E, Marcus M, Harvey J. Year-long weight loss treatment for obese patients with type II diabetes: does including an intermittent very-low-calorie diet improve outcome?. Am J Med 1994;97:354-62. http://dx.doi.org/10.1016/0002-9343(94)90302-6.
- Wing RR, Marcus MD, Epstein LH, Wing RR, Jawad A. A ‘family-based’ approach to the treatment of obese type II diabetic patients. J Consult Clin Psychol 1991;59:156-62. http://dx.doi.org/10.1037/0022-006X.59.1.156.
- Drummond M, Sculpher MJ, Torrance G. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 1997.
- Hagen E, Grasdal A, Eriksen HR. Does early intervention with a light mobilization program reduce long-term sick leave for low back pain: a 3-year follow-up study. Spine 2003;28:2309-15. http://dx.doi.org/10.1097/01.BRS.0000085817.33211.3F.
- Adamsen L, Rasmussen JM, Pedersen LS. ‘Brothers in arms’: how men with cancer experience a sense of comradeship through group intervention which combines physical activity with information relay. J Clin Nurs 2001;10:528-37. http://dx.doi.org/10.1046/j.1365-2702.2001.00514.x.
- Arrington MI, Grant CH, Vanderford ML. Man to man and side by side, they cope with prostate cancer: self-help and social support. J Psychosoc Oncol 2005;23:81-102. http://dx.doi.org/10.1300/J077v23n04_05.
- Bourke L, Sohanpal R, Nanton V, Crank H, Rosario DJ, Saxton JM. A qualitative study evaluating experiences of a lifestyle intervention in men with prostate cancer undergoing androgen suppression therapy. Trials 2012;13. http://dx.doi.org/10.1186/1745-6215-13-208.
- Chambers SK, Foley E, Galt E, Ferguson M, Clutton S. Mindfulness groups for men with advanced prostate cancer: a pilot study to assess feasibility and effectiveness and the role of peer support. Support Care Cancer 2012;20:1183-92. http://dx.doi.org/10.1007/s00520-011-1195-8.
- Galdas PM, Oliffe JL, Wong ST, Ratner PA, Johnson JL, Kelly MT. Canadian Punjabi Sikh men’s experiences of lifestyle changes following myocardial infarction: cultural connections. Ethn Health 2012;17:253-66. http://dx.doi.org/10.1080/13557858.2011.610440.
- Gooden RJ, Winefield HR. Breast and prostate cancer online discussion boards: a thematic analysis of gender differences and similarities. J Health Psychol 2007;12:103-14. http://dx.doi.org/10.1177/1359105307071744.
- Kronenwetter C, Weidner G, Pettengill E, Marlin R, Crutchfield L, McCormac P, et al. A qualitative analysis of interviews of men with early stage prostate cancer: the Prostate Cancer Lifestyle Trial. Cancer Nurs 2005;28:99-107. http://dx.doi.org/10.1097/00002820-200503000-00003.
- Martin F, Turner A, Bourne C, Batehup L. Development and qualitative evaluation of a self-management workshop for testicular cancer survivor-initiated follow-up. Oncol Nurs Forum 2013;40:E1-10. http://dx.doi.org/10.1188/13.ONF.E14-E23.
- Mfecane S. Negotiating therapeutic citizenship and notions of masculinity in a South African village. Afr J AIDS Res 2011;10:129-38. http://dx.doi.org/10.2989/16085906.2011.593375.
- Seymour-Smith S. ‘Blokes don’t like that sort of thing’: men’s negotiation of a ‘troubled’ self-help group identity. J Health Psychol 2008;13:785-97. http://dx.doi.org/10.1177/1359105308093862.
- Trapp SK, Woods JD, Grove A, Stern M. Male coping processes as demonstrated in the context of a cancer-related social support group. Support Care Cancer 2013;21:619-27. http://dx.doi.org/10.1007/s00520-012-1565-x.
- Ferrand C, Perrin C, Nasarre S. Motives for regular physical activity in women and men: a qualitative study in French adults with type 2 diabetes, belonging to a patients’ association. Health Soc Care Community 2008;16:511-20. http://dx.doi.org/10.1111/j.1365-2524.2008.00773.x.
- Ziebland S, Chapple A, Dumelow C, Evans J, Prinjha S, Rozmovits L. How the internet affects patients’ experience of cancer. Br Med J 2004;328:564-7. http://dx.doi.org/10.1136/bmj.328.7439.564.
- Noyes J, Popay J, Pearson A, Hannes K, Booth A, Higgins JPT, et al. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.0.1. The Cochrane Collaboration; 2008.
- Douglas FC, Greener J, Van Teijlingen E, Ludbrook A. Services just for men? Insights from a national study of the well men services pilots. BMC Public Health 2013;13. http://dx.doi.org/10.1186/1471-2458-13-425.
- Robertson C, Archibald D, Avenell A, Douglas F, Hoddinott P, van Teijlingen E, et al. Systematic reviews and integrated report on the quantitative, qualitative and economic evidence base for the management of obesity in men. Health Technol Assess 2014;18. http://dx.doi.org/10.3310/hta18350.
- Hunt K, McCann C, Gray CM, Mutrie N, Wyke S. ‘You’ve got to walk before you run’: positive evaluations of a walking program as part of a gender-sensitized, weight-management program delivered to men through professional football clubs. Health Psychol 2013;32. http://dx.doi.org/10.1037/a0029537.
- Rogers A, Kennedy A, Bower P, Gardner C, Gately C, Lee V, et al. The United Kingdom Expert Patients Programme: results and implications from a national evaluation. Med J Aust 2008;189.
- O’Brien R, Hart GJ, Hunt K. Standing out from the herd: men renegotiating masculinity in relation to their experience of illness. Int J Mens Health 2007;6:178-200. http://dx.doi.org/10.3149/jmh.0603.178.
- Gray RE, Fitch M, Phillips C, Labrecque M, Fergus K. To tell or not to tell: patterns of disclosure among men with prostate cancer. Psycho-Oncology 2000;9:273-82. http://dx.doi.org/10.1002/1099-1611(200007/08)9:4<273::AID-PON463>3.0.CO;2-F.
- Young M, Morgan P, Plotnikoff R, Callister R, Collins C. Effectiveness of male-only weight loss and weight loss maintenance interventions: a systematic review with meta-analysis. Obes Rev 2012;13:393-408. http://dx.doi.org/10.1111/j.1467-789X.2011.00967.x.
- Witty K, White A. Tackling men’s health: implementation of a male health service in a rugby stadium setting. Community Pract 2011;84.
- Robertson L, Douglas F, Ludbrook A, Reid G, Van Teijlingen E. What works with men? A systematic review of health promoting interventions targeting men. BMC Health Serv Res 2008;8. http://dx.doi.org/10.1186/1472-6963-8-141.
- Hunt K, Gray CM, Maclean A, Smillie S, Bunn C, Wyke S. Do weight management programmes delivered at professional football clubs attract and engage high risk men? A mixed-methods study. BMC Public Health 2014;14. http://dx.doi.org/10.1186/1471-2458-14-50.
- Wyke S. Information for Choice: What People Need, Prefer and Use. Oxford: Division of Public Health & Primary Health Care, University of Oxford; 2011.
- Entwistle VA, France EF, Wyke S, Jepson R, Hunt K, Ziebland S, et al. How information about other people’s personal experiences can help with healthcare decision-making: a qualitative study. Patient Educ Couns 2011;85:e291-8. http://dx.doi.org/10.1016/j.pec.2011.05.014.
- Mallyon A, Holmes M, Coveney J, Zadoroznyj M. I’m not dieting, ’I’m doing it for science’: masculinities and the experience of dieting. Health Sociol Rev 2010;19:330-42. http://dx.doi.org/10.5172/hesr.2010.19.3.330.
- de Visser RO, McDonnell EJ. ‘Man points’: masculine capital and young men’s health. Health Psychol 2013;32:5-14. http://dx.doi.org/10.1037/a0029045.
- Hunt K, Wyke S, Gray CM, Anderson AS, Brady A, Bunn C, et al. A gender-sensitised weight loss and healthy living programme for overweight and obese men delivered by Scottish Premier League football clubs (FFIT): a pragmatic randomised controlled trial. Lancet 2014;83:1211-21. http://dx.doi.org/10.1016/S0140-6736(13)62420-4.
- Charmaz K. Loss of self: a fundamental form of suffering in the chronically ill. Sociol Health Illn 1983;5:168-95. http://dx.doi.org/10.1111/1467-9566.ep10491512.
- Bury M. Chronic illness as biographical disruption. Sociol Health Illn 1982;4:167-82. http://dx.doi.org/10.1111/1467-9566.ep11339939.
- Bury M. The sociology of chronic illness: a review of research and prospects. Sociol Health Illn 1991;13:451-68. http://dx.doi.org/10.1111/j.1467-9566.1991.tb00522.x.
- Farrimond H. Beyond the caveman: rethinking masculinity in relation to men’s help-seeking. Health 2012;16:208-25. http://dx.doi.org/10.1177/1363459311403943.
- Galdas PM, Johnson JL, Percy ME, Ratner PA. Help seeking for cardiac symptoms: beyond the masculine–feminine binary. Soc Sci Med 2010;71:18-24. http://dx.doi.org/10.1016/j.socscimed.2010.03.006.
- Galdas PM, Broom A, Tovey P. Men’s Health: Body, Identity and Social Context. London: John Wiley and Sons; 2010.
- Emslie C, Ridge D, Ziebland S, Hunt K. Men’s accounts of depression: reconstructing or resisting hegemonic masculinity?. Soc Sci Med 2006;62:2246-57. http://dx.doi.org/10.1016/j.socscimed.2005.10.017.
- Kidd LA. Consequences, control and appraisal: cues and barriers to engaging in self-management among people affected by colorectal cancer – a secondary analysis of qualitative data. Health Expect 2012;17:565-78. http://dx.doi.org/10.1111/j.1369-7625.2012.00785.x.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review: a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10:21-34. http://dx.doi.org/10.1258/1355819054308530.
- Achmon J, Granek M, Golomb M, Hart J. Behavioral treatment of essential hypertension: a comparison between cognitive therapy and biofeedback of heart rate. Psychosom Med 1989;51:152-64. http://dx.doi.org/10.1097/00006842-198903000-00005.
- Cottier C, Shapiro K, Julius S. Treatment of mild hypertension with progressive muscle relaxation: predictive value of indexes of sympathetic tone. Arch Intern Med 1984;144:1954-8. http://dx.doi.org/10.1001/archinte.1984.04400010062011.
- Frankel BL, Patel DJ, Horwitz D, Friedewald WT, Gaarder KR. Treatment of hypertension with biofeedback and relaxation techniques. Psychosom Med 1978;40:276-93. http://dx.doi.org/10.1097/00006842-197806000-00002.
- Jacob RG, Shapiro AP, O’Hara P, Portser S, Kruger A, Gatsonis C, et al. Relaxation therapy for hypertension: setting-specific effects. Psychosom Med 1992;54:87-101. http://dx.doi.org/10.1097/00006842-199201000-00011.
- McGrady AV, Yonker R, Tan SY, Fine TH, Woerner M. The effect of biofeedback-assisted relaxation training on blood pressure and selected biochemical parameters in patients with essential hypertension. Biofeedback Self Regul 1981;6:343-53. http://dx.doi.org/10.1007/BF01000659.
- McGrady A. Effects of group relaxation training and thermal biofeedback on blood pressure and related physiological and psychological variables in essential hypertension. Biofeedback Self Regul 1994;19:51-66. http://dx.doi.org/10.1007/BF01720670.
- Murugesan R, Govindarajulu N, Bera TK. Effect of selected yogic practices on the management of hypertension. Indian J Physiol Pharmacol 2000;44:207-10.
- Schein MH, Gavish B, Herz M, Rosner-Kahana D, Naveh P, Knishkowy B, et al. Treating hypertension with a device that slows and regularises breathing: a randomised, double-blind controlled study. J Hum Hypertens 2001;15:271-8. http://dx.doi.org/10.1038/sj.jhh.1001148.
- Seer P, Raeburn JM. Meditation training and essential hypertension: a methodological study. J Behav Med 1980;3:59-71. http://dx.doi.org/10.1007/BF00844914.
- Yen LL, Patrick WK, Chie WC. Comparison of relaxation techniques, routine blood pressure measurements, and self-learning packages in hypertension control. Prev Med 1996;25:339-45. http://dx.doi.org/10.1006/pmed.1996.0064.
- Bendstrup KE, Ingemann Jensen J, Holm S, Bengtsson B. Out-patient rehabilitation improves activities of daily living, quality of life and exercise tolerance in chronic obstructive pulmonary disease. Eur Respir J 1997;10:2801-6. http://dx.doi.org/10.1183/09031936.97.10122801.
- Boxall AM, Barclay L, Sayers A, Caplan GA. Managing chronic obstructive pulmonary disease in the community: a randomized controlled trial of home-based pulmonary rehabilitation for elderly housebound patients. J Cardiopulm Rehabil 2005;25:378-85. http://dx.doi.org/10.1097/00008483-200511000-00012.
- Cambach W, Chadwick-Straver RV, Wagenaar RC, van Keimpema AR, Kemper HC. The effects of a community-based pulmonary rehabilitation programme on exercise tolerance and quality of life: a randomized controlled trial. Eur Respir J 1997;10:104-13. http://dx.doi.org/10.1183/09031936.97.10010104.
- Gottlieb V, Lyngso AM, Nybo B, Frolich A, Backer V. Pulmonary rehabilitation for moderate COPD. COPD 2011;8:380-6. http://dx.doi.org/10.3109/15412555.2011.610393.
- Littlejohns P, Baveystock CM, Parnell H, Jones PW. Randomised controlled trial of the effectiveness of a respiratory health worker in reducing impairment, disability, and handicap due to chronic airflow limitation. Thorax 1991;46:559-64. http://dx.doi.org/10.1136/thx.46.8.559.
- Theander K, Jakobsson P, Jorgensen N, Unosson M. Effects of pulmonary rehabilitation on fatigue, functional status and health perceptions in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Clin Rehabil 2009;23:125-36. http://dx.doi.org/10.1177/0269215508096174.
- van Wetering CR, Hoogendoorn M, Mol SJ, Rutten-van Molken MP, Schols AM. Short- and long-term efficacy of a community-based COPD management programme in less advanced COPD: a randomised controlled trial. Thorax 2010;65:7-13. http://dx.doi.org/10.1136/thx.2009.118620.
- Wakabayashi R, Motegi T, Yamada K, Ishii T, Jones RC, Hyland ME, et al. Efficient integrated education for older patients with chronic obstructive pulmonary disease using the Lung Information Needs Questionnaire. Geriatr Gerontol Int 2011;11:422-30. http://dx.doi.org/10.1111/j.1447-0594.2011.00696.x.
- Wijkstra PJ, Van Altena R, Kraan J, Otten V, Postma DS, Koeter GH. Quality of life in patients with chronic obstructive pulmonary disease improves after rehabilitation at home. Eur Respir J 1994;7:269-73. http://dx.doi.org/10.1183/09031936.94.07020269.
- Farrero E, Escarrabill J, Prats E, Maderal M, Manresa F. Impact of a hospital-based home-care program on the management of COPD patients receiving long-term oxygen therapy. Chest 2001;119:364-9. http://dx.doi.org/10.1378/chest.119.2.364.
- Courneya KS, Jones LW, Peddle CJ, Sellar CM, Reiman T, Joy AA, et al. Effects of aerobic exercise training in anemic cancer patients receiving darbepoetin alfa: a randomized controlled trial. Oncologist 2008;13:1012-20. http://dx.doi.org/10.1634/theoncologist.2008-0017.
- Hacker ED, Larson J, Kujath A, Peace D, Rondelli D, Gaston L. Strength training following hematopoietic stem cell transplantation. Cancer Nurs 2011;34:238-49. http://dx.doi.org/10.1097/NCC.0b013e3181fb3686.
- Mustian KM, Peppone L, Darling TV, Palesh O, Heckler CE, Morrow GR. A 4-week home-based aerobic and resistance exercise program during radiation therapy: a pilot randomized clinical trial. J Support Oncol 2009;7:158-67.
- Wiskemann J, Dreger P, Schwerdtfeger R, Bondong A, Huber G, Kleindienst N, et al. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011;117:2604-13. http://dx.doi.org/10.1182/blood-2010-09-306308.
- Courneya KS, Segal RJ, Mackey JR, Gelmon K, Reid RD, Friedenreich CM, et al. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: a multicenter randomized controlled trial. J Clin Oncol 2007;25:4396-404. http://dx.doi.org/10.1200/JCO.2006.08.2024.
- Oliveira MM, Souza GA, Miranda Mde S, Okubo MA, Amaral MT, Silva MP, et al. Upper limbs exercises during radiotherapy for breast cancer and quality of life. Rev Bras Ginecol Obstet 2010;32:133-8. http://dx.doi.org/10.1590/S0100-72032010000300006.
- Hwang JH, Chang HJ, Shim YH, Park WH, Park W, Huh SJ, et al. Effects of supervised exercise therapy in patients receiving radiotherapy for breast cancer. Yonsei Med J 2008;49:443-50. http://dx.doi.org/10.3349/ymj.2008.49.3.443.
- Moros MT, Ruidiaz M, Caballero A, Serrano E, Martinez V, Tres A. Effects of an exercise training program on the quality of life of women with breast cancer on chemotherapy. Rev Med Chil 2010;138:715-22. http://dx.doi.org/10.4067/S0034-98872010000600008.
- Segal R, Evans W, Johnson D, Smith J, Colletta S, Gayton J, et al. Structured exercise improves physical functioning in women with stages I and II breast cancer: results of a randomized controlled trial. J Clin Oncol 2001;19:657-65.
- Yang CY, Tsai JC, Huang YC, Lin CC. Effects of a home-based walking program on perceived symptom and mood status in postoperative breast cancer women receiving adjuvant chemotherapy. J Adv Nurs 2011;67:158-68. http://dx.doi.org/10.1111/j.1365-2648.2010.05492.x.
- Chang PH, Lai YH, Shun SC, Lin LY, Chen ML, Yang Y, et al. Effects of a walking intervention on fatigue-related experiences of hospitalized acute myelogenous leukemia patients undergoing chemotherapy: a randomized controlled trial. J Pain Symptom Manage 2008;35:524-34. http://dx.doi.org/10.1016/j.jpainsymman.2007.06.013.
- Dimeo FC, Stieglitz RD, Novelli-Fischer U, Fetscher S, Keul J. Effects of physical activity on the fatigue and psychologic status of cancer patients during chemotherapy. Cancer 1999;85:2273-7. http://dx.doi.org/10.1002/(SICI)1097-0142(19990515)85:10<2273::AID-CNCR24>3.0.CO;2-B.
- Caldwell MG. The Effects of an Endurance Exercise Regimen on Cancer-Related Fatigue and Physical Performance in Women With Breast Cancer 2009.
- Moadel AB, Shah C, Wylie-Rosett J, Harris MS, Patel SR, Hall CB, et al. Randomized controlled trial of yoga among a multiethnic sample of breast cancer patients: effects on quality of life. J Clin Oncol 2007;25:4387-95. http://dx.doi.org/10.1200/JCO.2006.06.6027.
- Pinto BM, Frierson GM, Rabin C, Trunzo JJ, Marcus BH. Home-based physical activity intervention for breast cancer patients. J Clin Oncol 2005;23:3577-87. http://dx.doi.org/10.1200/JCO.2005.03.080.
- Galdas PM, Oliffe JL, Kang HB, Kelly MT. Punjabi Sikh patients’ perceived barriers to engaging in physical exercise following myocardial infarction. Public Health Nurs 2012;29:534-41. http://dx.doi.org/10.1111/j.1525-1446.2012.01009.x.
- CASP Qualitative Checklist n.d. www.casp-uk.net/#!casp-tools-checklists/c18f8 (accessed 3 September 2013).
- Ornish D, Weidner G, Fair WR, Marlin R, Pettengill EB, Raisin CJ, et al. Intensive lifestyle changes may affect the progression of prostate cancer. J Urol 2005;174:1065-9. http://dx.doi.org/10.1097/01.ju.0000169487.49018.73.
- Mellin G, Härkäpää K, Hurri H, Järvikoski A. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part IV: long-term effects on physical measurements. Scand J Rehabil Med 1990;22:189-94.
- Wing RR, Marcus MD, Salata R, Epstein LH, Miaskiewicz S, Blair EH. Effects of a very-low-calorie diet on long-term glycemic control in obese type 2 diabetic subjects. Arch Intern Med 1991;151:1334-40. http://dx.doi.org/10.1001/archinte.1991.00400070100012.
Appendix 1 Quantitative literature search
We searched the CDSR to identify systematic reviews of self-care of LTCs. This search was supplemented with a search of the last 2 years of MEDLINE (2012–13) to identify any recent reviews that had not been added to CDSR. Details of the searches are given below.
Cochrane Database of Systematic Reviews
URL: www.thecochranelibrary.com/
Date range searched: all dates up to present.
Date of search: 18 July 2013.
Records identified: 3429.
Search strategy
#1 MeSH (medical subject heading) descriptor: [Stroke] explode all trees
#2 MeSH descriptor: [Diabetes Mellitus] explode all trees
#3 MeSH descriptor: [Asthma] explode all trees
#4 MeSH descriptor: [Hypertension] explode all trees
#5 MeSH descriptor: [Depression] explode all trees
#6 MeSH descriptor: [Depressive Disorder] explode all trees
#7 MeSH descriptor: [Dementia] explode all trees
#8 MeSH descriptor: [Pulmonary Disease, Chronic Obstructive] explode all trees
#9 MeSH descriptor: [Renal Insufficiency, Chronic] explode all trees
#10 MeSH descriptor: [Irritable Bowel Syndrome] explode all trees
#11 MeSH descriptor: [Arthritis, Rheumatoid] explode all trees
#12 MeSH descriptor: [Arthritis, Psoriatic] explode all trees
#13 MeSH descriptor: [Spondylitis, Ankylosing] explode all trees
#14 MeSH descriptor: [Lupus Erythematosus, Systemic] explode all trees
#15 MeSH descriptor: [Low Back Pain] explode all trees
#16 MeSH descriptor: [Epilepsy] explode all trees
#17 MeSH descriptor: [Multiple Sclerosis] explode all trees
#18 MeSH descriptor: [Parkinson Disease] explode all trees
#19 MeSH descriptor: [Motor Neuron Disease] explode all trees
#20 MeSH descriptor: [Motor Neuron Disease] explode all trees
#21 MeSH descriptor: [Neoplasms] explode all trees
#22 MeSH descriptor: [Inflammatory Bowel Diseases] explode all trees
#23 MeSH descriptor: [Heart Diseases] explode all trees
#24 MeSH descriptor: [Skin Diseases] explode all trees
#25 MeSH descriptor: [Chronic Pain] explode all trees
#26 MeSH descriptor: [HIV] explode all trees
#27 MeSH descriptor: [Hepatitis] explode all trees
#28 MeSH descriptor: [Anxiety] explode all trees
#29 MeSH descriptor: [Psychotic Disorders] explode all trees
#30 (long* or chronic or long-term or long-standing or persistent or ongoing) near/2 (illness* or disease* or condition*)
#31 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 or #30
#32 MeSH descriptor: [Self Administration] explode all trees
#33 MeSH descriptor: [Self Care] explode all trees
#34 “self care” or selfcare
#35 “self manag*” or selfmanag*
#36 “self monitor*” or selfmonitor*
#37 “self help” or selfhelp
#38 “self diagnos*” or selfdiagnos* or “self assess*” or selfassess*
#39 MeSH descriptor: [Self Medication] explode all trees
#40 “self medicat*” or selfmedicat* or “self remed*” or selfremed*
#41 “self treat*” or selftreat* or “self cure” or selfcure
#42 MeSH descriptor: [Self-Help Groups] explode all trees
#43 group near (support* or advice or advis* or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information)
#44 peer near (support* or advice or advis* or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information)
#45 “expert patient*”
#46 MeSH descriptor: [Telemedicine] explode all trees
#47 telemedicine or telecare or telenursing or telemonitor* or telehealth
#48 MeSH descriptor: [Remote Consultation] explode all trees
#49 (telephon* or remote or phone) near/2 (follow* or support or consult* or advice or advis* or intervention* or train* or instruction or assis* or educate or education or information or monitor*)
#50 “Action plan*”
#51 #32 or #33 or #34 or ’35 or #36 or #37 or #38 or #39 or #40 or #41 or #42 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or #50
#52 #31 and #51
#53 (man or man’s or men or men’s or male* or masculin* or gender* or sex difference* or sex factor*)
#54 #52 and #53
MEDLINE (via OvidSP)
Date range searched: 2012–2013.
Date of search: 18 July 2013.
Records identified: 282.
Search strategy
-
exp Stroke/ (82,239)
-
exp Diabetes Mellitus/ (31,2330)
-
exp Asthma/ (107,919)
-
exp Hypertension/ (208,847)
-
Depression/ (74,653)
-
Depressive Disorder/ (58,545)
-
exp Dementia/ (119,170)
-
exp Pulmonary Disease, Chronic Obstructive/ (23,545)
-
exp Renal Insufficiency, Chronic/ (81,421)
-
exp Irritable Bowel Syndrome/ (4136)
-
exp Arthritis, Rheumatoid/ (100,502)
-
exp Arthritis, Psoriatic/ (3678)
-
exp Spondylitis, Ankylosing/ (11,626)
-
exp Lupus Erythematosus, Systemic/ (49,068)
-
exp Low Back Pain/ (14,051)
-
exp Epilepsy/ (127,082)
-
exp Multiple Sclerosis/ (43,448)
-
exp Parkinson Disease/ (46,608)
-
exp Motor Neuron Disease/ (19,445)
-
exp Neoplasms/ (256,3081)
-
exp Inflammatory Bowel Diseases/ (59,128)
-
exp Heart Diseases/ (880,175)
-
exp Skin Diseases/ (811,256)
-
exp Chronic Pain/ (2312)
-
exp HIV/ (88,002)
-
exp Hepatitis/ (132,863)
-
exp Anxiety/ (54,488)
-
exp Psychotic Disorders/ (37,864)
-
((long$ or chronic or long-term or long-standing or persistent or ongoing) adj2 (illness$ or disease$ or condition$)).ti,ab. (141,407)
-
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 (5,458,249)
-
self administration/ (9551)
-
self care/ (23,254)
-
(self care or selfcare).ti,ab. (9402)
-
(self manag$ or selfmanag$).ti,ab. (7804)
-
(self monitor$ or selfmonitor$).ti,ab. (4251)
-
(self help or selfhelp).ti,ab. (4326)
-
(self diagnos$ or selfdiagnos$ or self assess$ or selfassess$).ti,ab. (9084)
-
self medication/ (3966)
-
(self medicat$ or selfmedicat$ or self remed$ or selfremed$).ti,ab. (2588)
-
(self treat$ or selftreat$ or self cure or selfcure).ti,ab. (1379)
-
self help groups/ (7760)
-
Social Support/ (50,861)
-
Social support$.ti,ab. (20,628)
-
(group adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (4297)
-
(peer adj1 (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (2566)
-
expert patient$.ti,ab. (150)
-
Telemedicine/ (10,745)
-
telemedicine.ti,ab. (5418)
-
telecare.ti,ab. (323)
-
telenursing.ti,ab. (76)
-
telemonitor$.ti,ab. (534)
-
telehealth.ti,ab. (1336)
-
Remote Consultation/ (3547)
-
((telephon$ or remote or phone) adj2 (follow$ or support or consult$ or advice or advis$ or intervention$ or train$ or instruction or assis$ or educate or education or information or monitor$)).ti,ab. (8191)
-
Action plan$.ti,ab. (3333)
-
or/31-55 (150,468)
-
systematic$ review$.ti,ab. (45,152)
-
meta-analysis as topic/ (13,800)
-
meta-analytic$.ti,ab. (3263)
-
meta-analysis.ti,ab,pt. (59,807)
-
metanalysis.ti,ab. (117)
-
metaanalysis.ti,ab. (991)
-
meta analysis.ti,ab. (43,949)
-
meta-synthesis.ti,ab. (163)
-
metasynthesis.ti,ab. (97)
-
meta synthesis.ti,ab. (163)
-
meta-regression.ti,ab. (1903)
-
metaregression.ti,ab. (236)
-
meta regression.ti,ab. (1903)
-
(synthes$ adj3 literature).ti,ab. (1201)
-
(synthes$ adj3 evidence).ti,ab. (3500)
-
integrative review.ti,ab. (665)
-
data synthesis.ti,ab. (6925)
-
(research synthesis or narrative synthesis).ti,ab. (565)
-
(systematic study or systematic studies).ti,ab. (6311)
-
(systematic comparison$ or systematic overview$).ti,ab. (1670)
-
evidence based review.ti,ab. (1077)
-
comprehensive review.ti,ab. (5770)
-
critical review.ti,ab. (9779)
-
quantitative review.ti,ab. (430)
-
structured review.ti,ab. (428)
-
realist review.ti,ab. (40)
-
realist synthesis.ti,ab. (21)
-
or/57-83 (129,596)
-
review.pt. (1,874,978)
-
medline.ab. (50,039)
-
pubmed.ab. (23,033)
-
cochrane.ab. (24,745)
-
embase.ab. (22,904)
-
cinahl.ab. (8149)
-
psyc?lit.ab. (865)
-
psyc?info.ab. (8596)
-
(literature adj3 search$).ab. (21,542)
-
(database$ adj3 search$).ab. (20,482)
-
(bibliographic adj3 search$).ab. (1089)
-
(electronic adj3 search$).ab. (6812)
-
(electronic adj3 database$).ab. (8298)
-
(computeri?ed adj3 search$).ab. (2413)
-
(internet adj3 search$).ab. (1524)
-
included studies.ab. (5132)
-
(inclusion adj3 studies).ab. (5159)
-
inclusion criteria.ab. (28,625)
-
selection criteria.ab. (17,615)
-
predefined criteria.ab. (968)
-
predetermined criteria.ab. (662)
-
(assess$ adj3 (quality or validity)).ab. (36,078)
-
(select$ adj3 (study or studies)).ab. (33,681)
-
(data adj3 extract$).ab. (24,958)
-
extracted data.ab. (5703)
-
(data adj2 abstracted).ab. (2995)
-
(data adj3 abstraction).ab. (754)
-
published intervention$.ab. (99)
-
((study or studies) adj2 evaluat$).ab. (95,592)
-
(intervention$ adj2 evaluat$).ab. (5553)
-
confidence interval$.ab. (204,605)
-
heterogeneity.ab. (85,913)
-
pooled.ab. (40,303)
-
pooling.ab. (7061)
-
odds ratio$.ab. (134,809)
-
(Jadad or coding).ab. (116,960)
-
or/86-120 (737,671)
-
85 and 121 (110,275)
-
review.ti. (228,123)
-
123 and 121 (37,651)
-
(review$ adj4 (papers or trials or studies or evidence or intervention$ or evaluation$)).ti,ab. (90,964)
-
84 or 122 or 124 or 125 (253,580)
-
letter.pt. (792,482)
-
editorial.pt. (328,780)
-
comment.pt. (522,179)
-
127 or 128 or 129 (1,220,440)
-
126 not 130 (247,307)
-
exp animals/ not humans/ (4,001,071)
-
131 not 132 (237,840)
-
30 and 56 and 133 (2068)
-
limit 134 to (english language and yr=“2012 -Current”) (282)
-
(man or man’s or men or men’s or male$ or masculin$ or gender$ or sex difference$ or sex factor$).ti,ab. (1,305,221)
-
135 and 136 (16)
PROSPERO
URL: www.crd.york.ac.uk/prospero/
Date range searched: all dates up to present.
Date of search: 18 July 2013.
Search strategy
A simple search for “self” was undertaken that identified 21 potentially relevant records.
Appendix 2 Forest plots
Analysis 1: within-Cochrane review analysis forest plots
FIGURE 14.
Health-related quality-of-life outcomes in male-only vs. mixed-sex groups. Adapted from Davies et al. 2010. 146 a and b refer to different intervention groups within the Klocek 2005 study. df, degrees of freedom; IV, inverse variance.
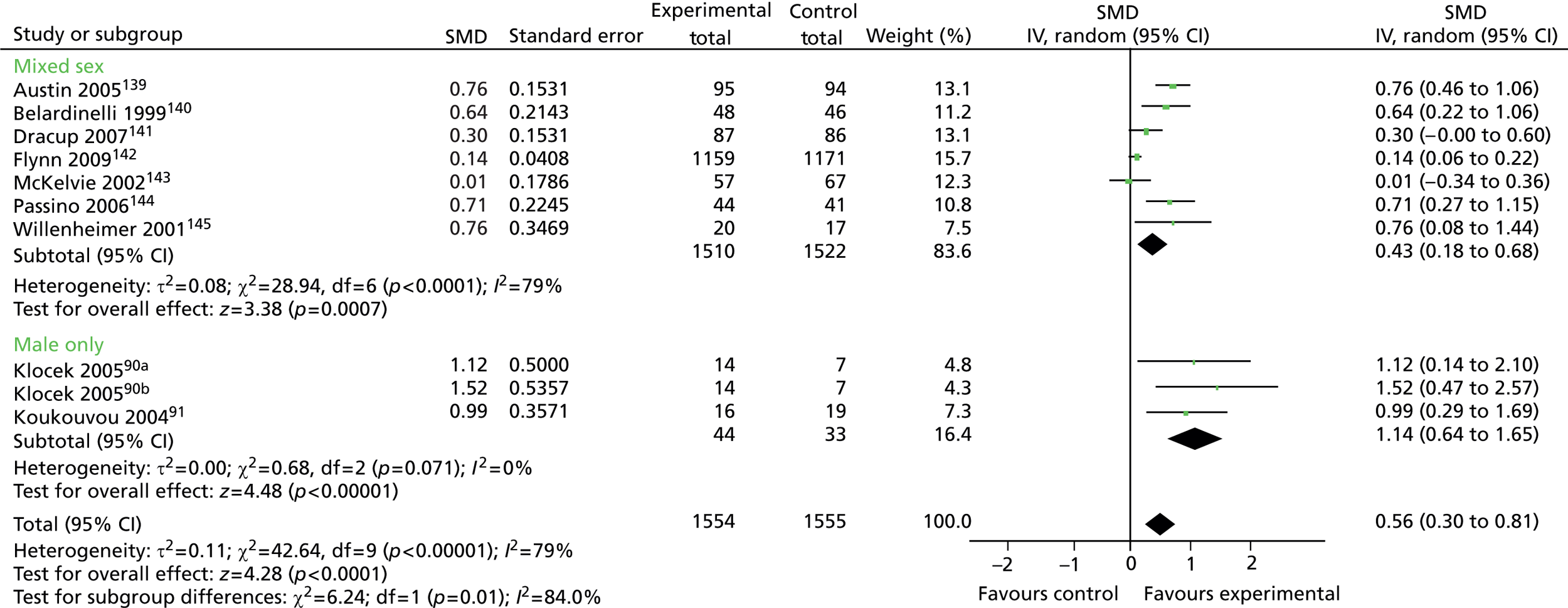
FIGURE 15.
Systolic blood pressure (< 6 months’ follow-up) in male-only vs. mixed-sex groups. Adapted from Dickinson et al. 2008. 44 df, degrees of freedom; IV, inverse variance; SD, standard deviation.
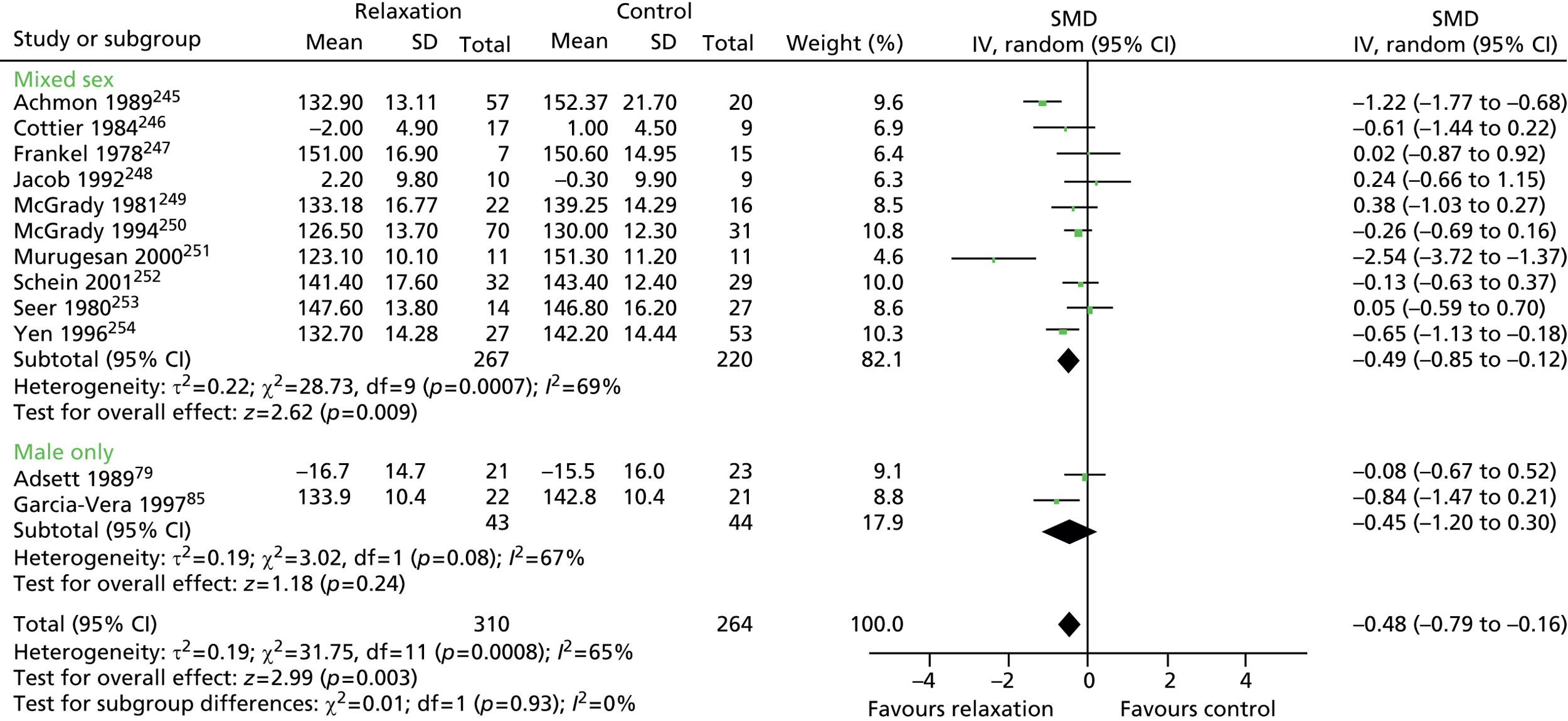
FIGURE 16.
Diastolic blood pressure (< 6 months’ follow-up) in male-only vs. mixed-sex groups. Adapted from Dickinson et al. 2008. 44 df, degrees of freedom; IV, inverse variance; SD, standard deviation.
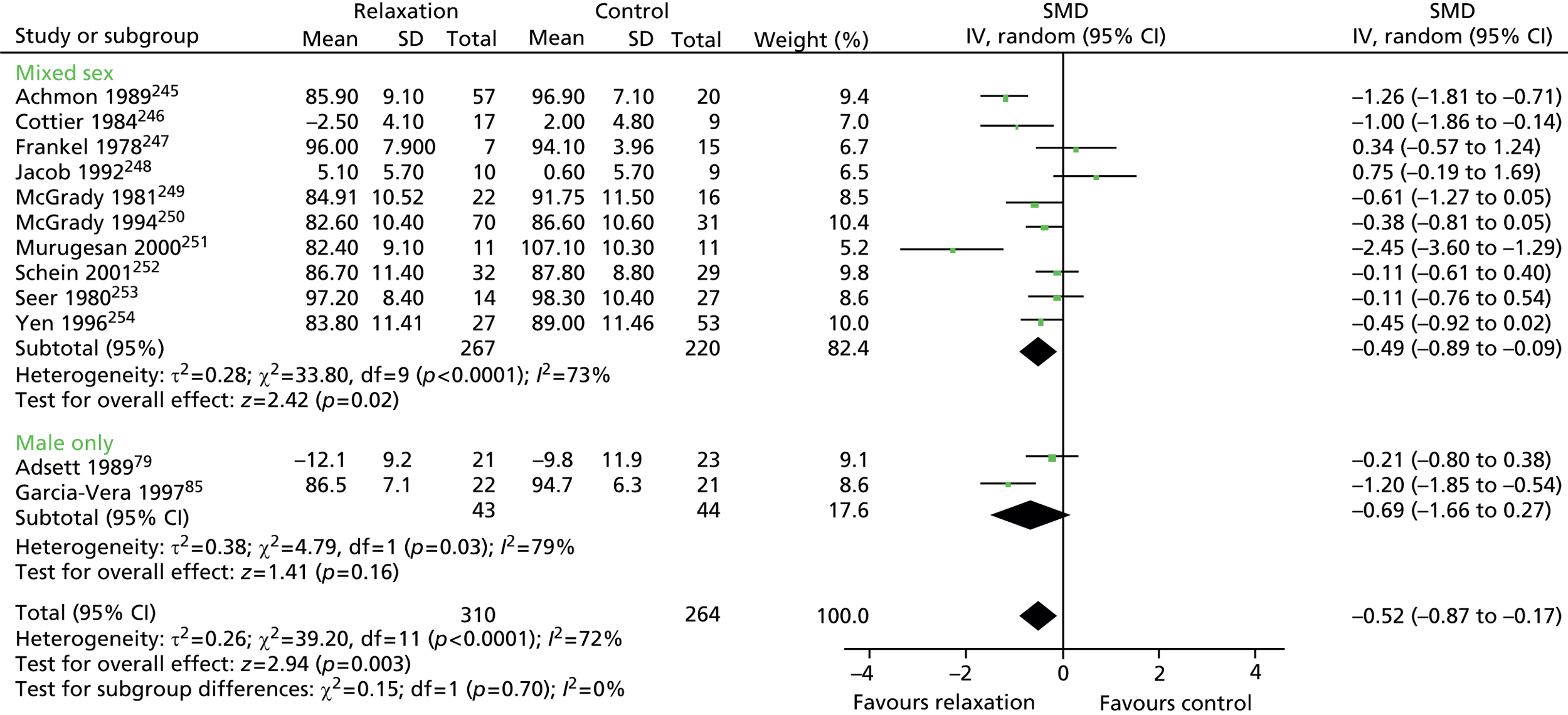
FIGURE 17.
Six-minute walking distance (≤ 12 months) in male-only vs. mixed-sex groups. Adapted from Kruis et al. 2013. 43 df, degrees of freedom; IDM, integrated disease management; IV, inverse variance; SD, standard deviation.

FIGURE 18.
Forced expiratory volume (% predicted) in male-only vs. mixed-sex groups. Adapted from Kruis et al. 2013. 43 df, degrees of freedom; IDM, integrated disease management; IV, inverse variance; SD, standard deviation.
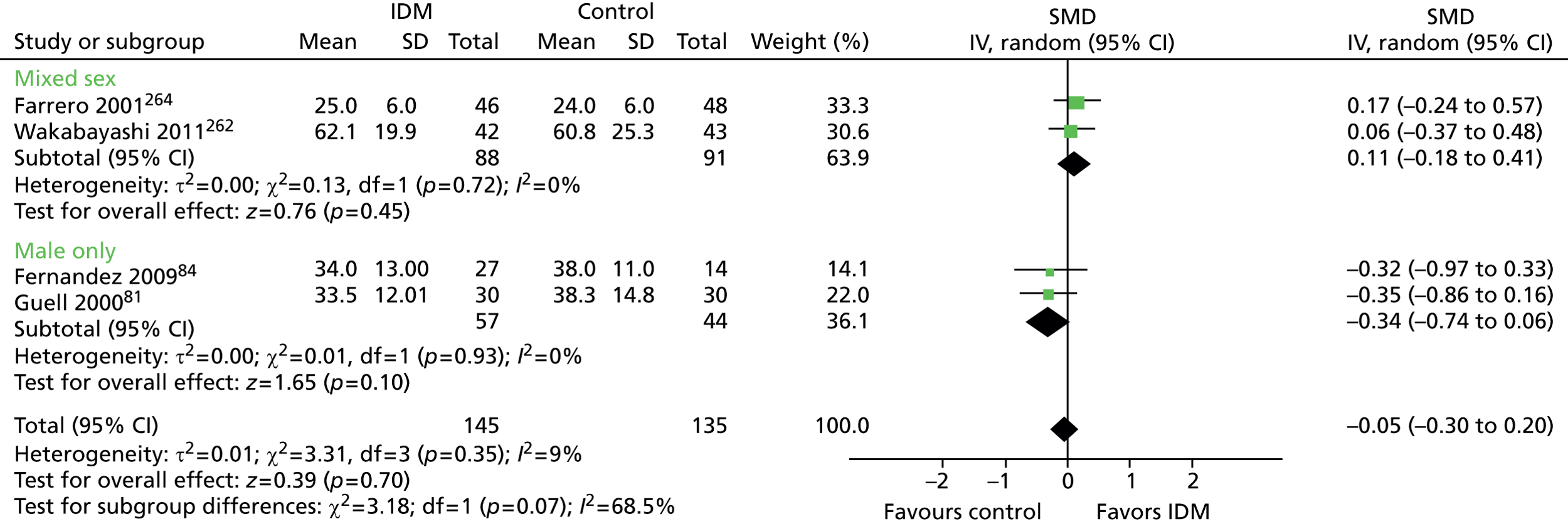
FIGURE 19.
Health-related quality-of-life (≤ 6 months) outcomes in male-only vs. mixed-sex and female-only groups. Adapted from Mishra et al. 2012. 42 df, degrees of freedom; IV, inverse variance; SD, standard deviation.

FIGURE 20.
Fatigue (≤ 6 months) outcomes in male-only vs. mixed-sex and female-only groups. Adapted from Mishra et al. 2012. 42 df, degrees of freedom; IV, inverse variance; SD, standard deviation.

Analysis 2: across-Cochrane review analysis
FIGURE 21.
Physical activity interventions: HRQoL outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
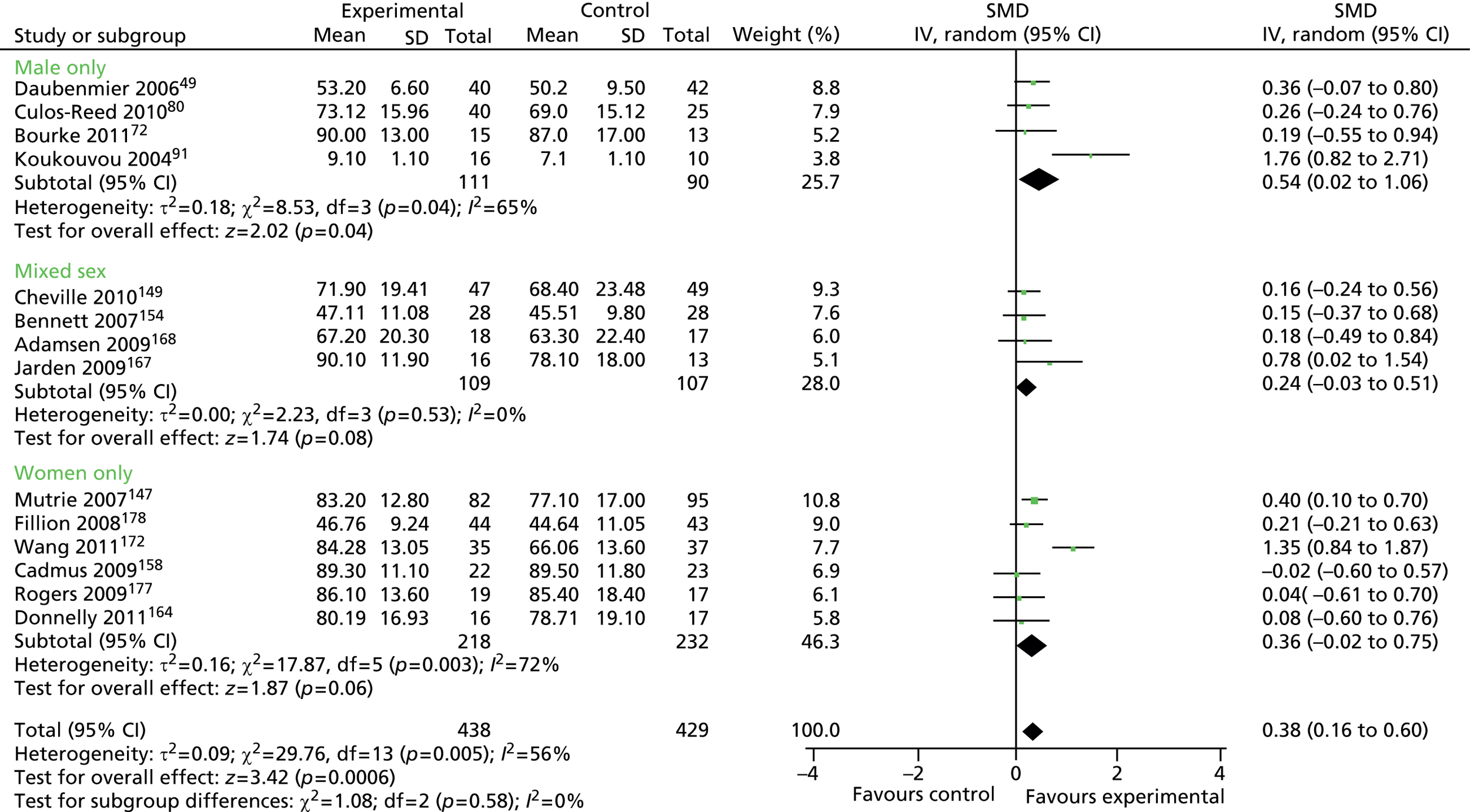
FIGURE 22.
Physical activity interventions: HRQoL outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
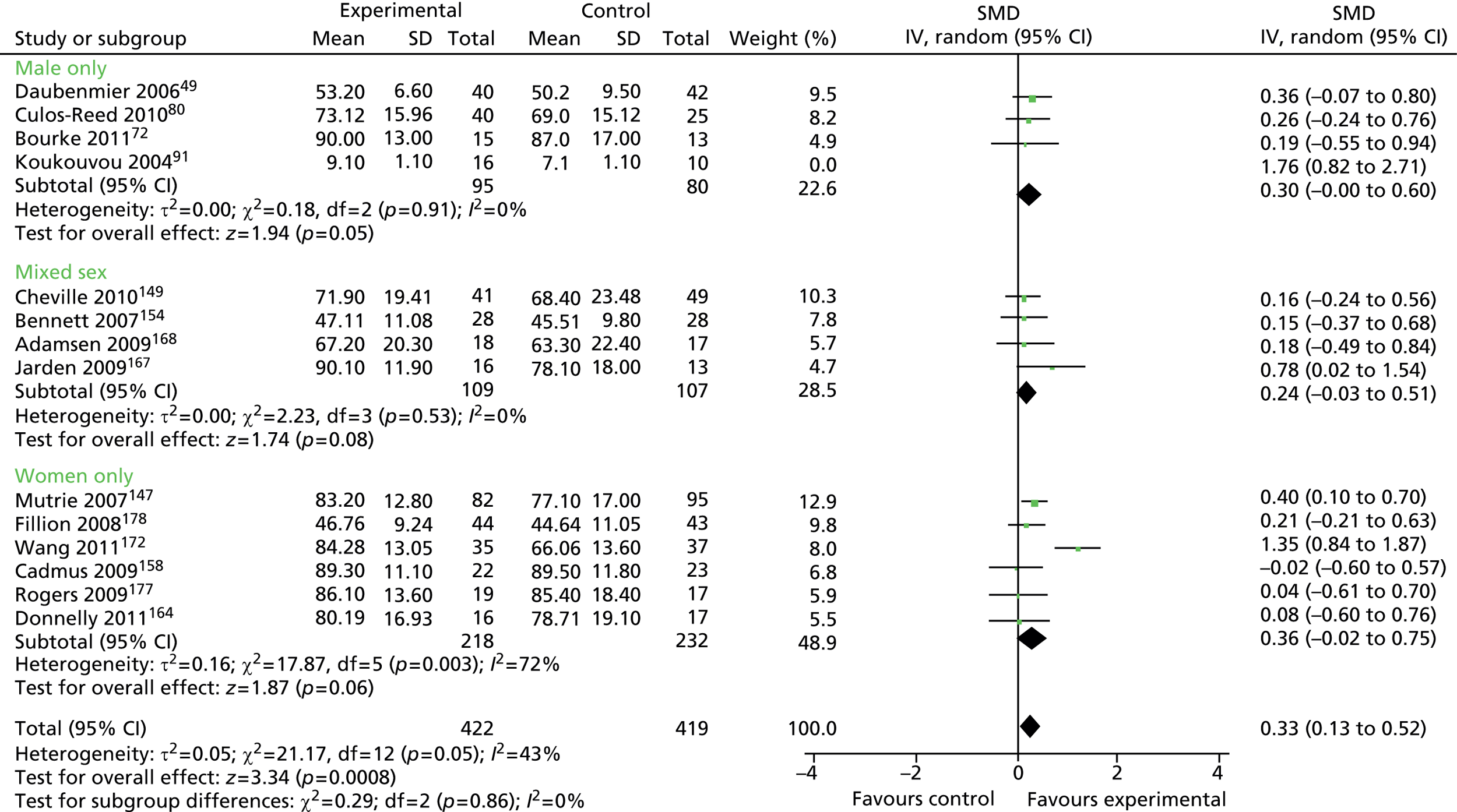
FIGURE 23.
Physical activity interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
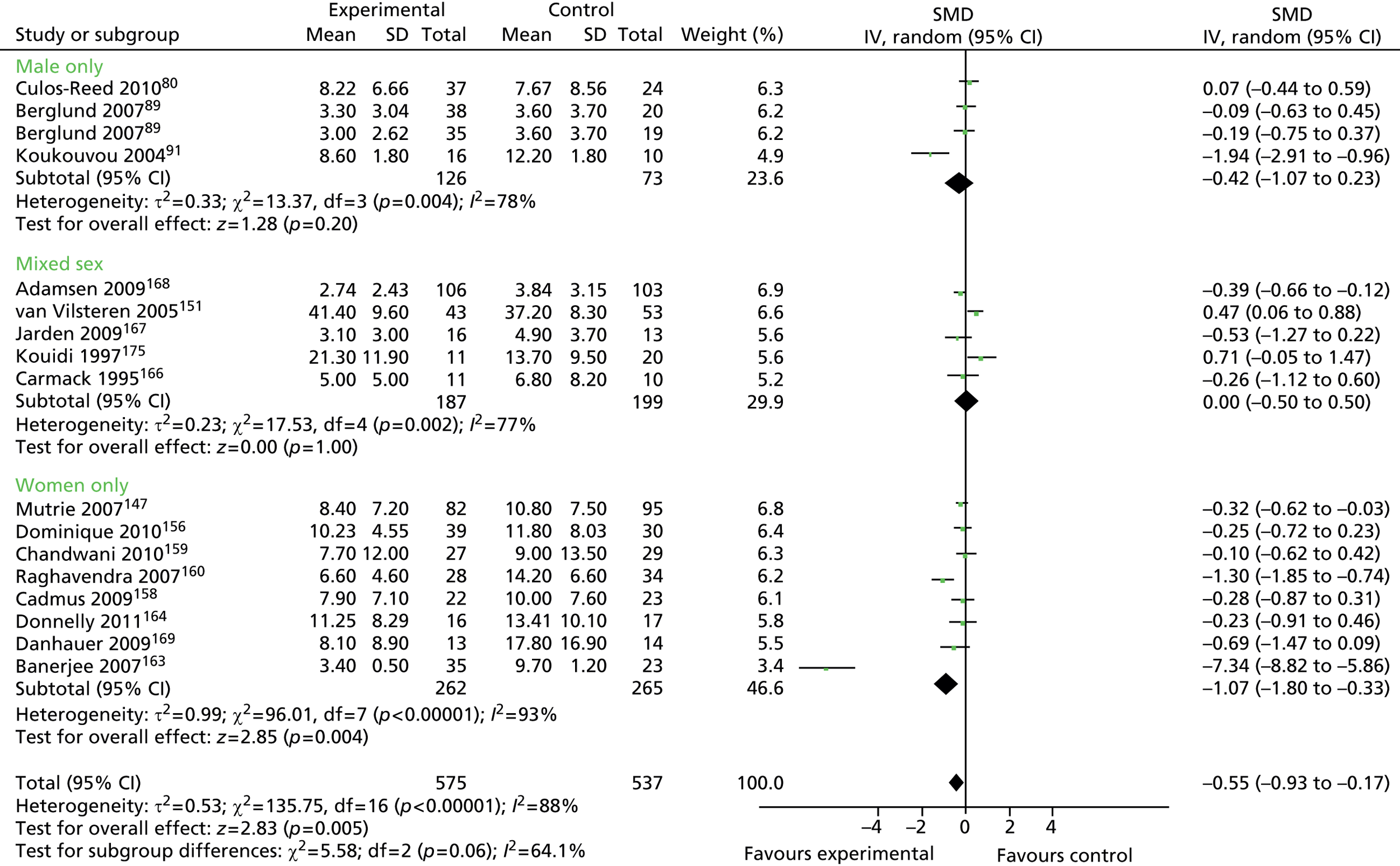
FIGURE 24.
Physical activity interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot minus outlier Banerjee 2007163). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
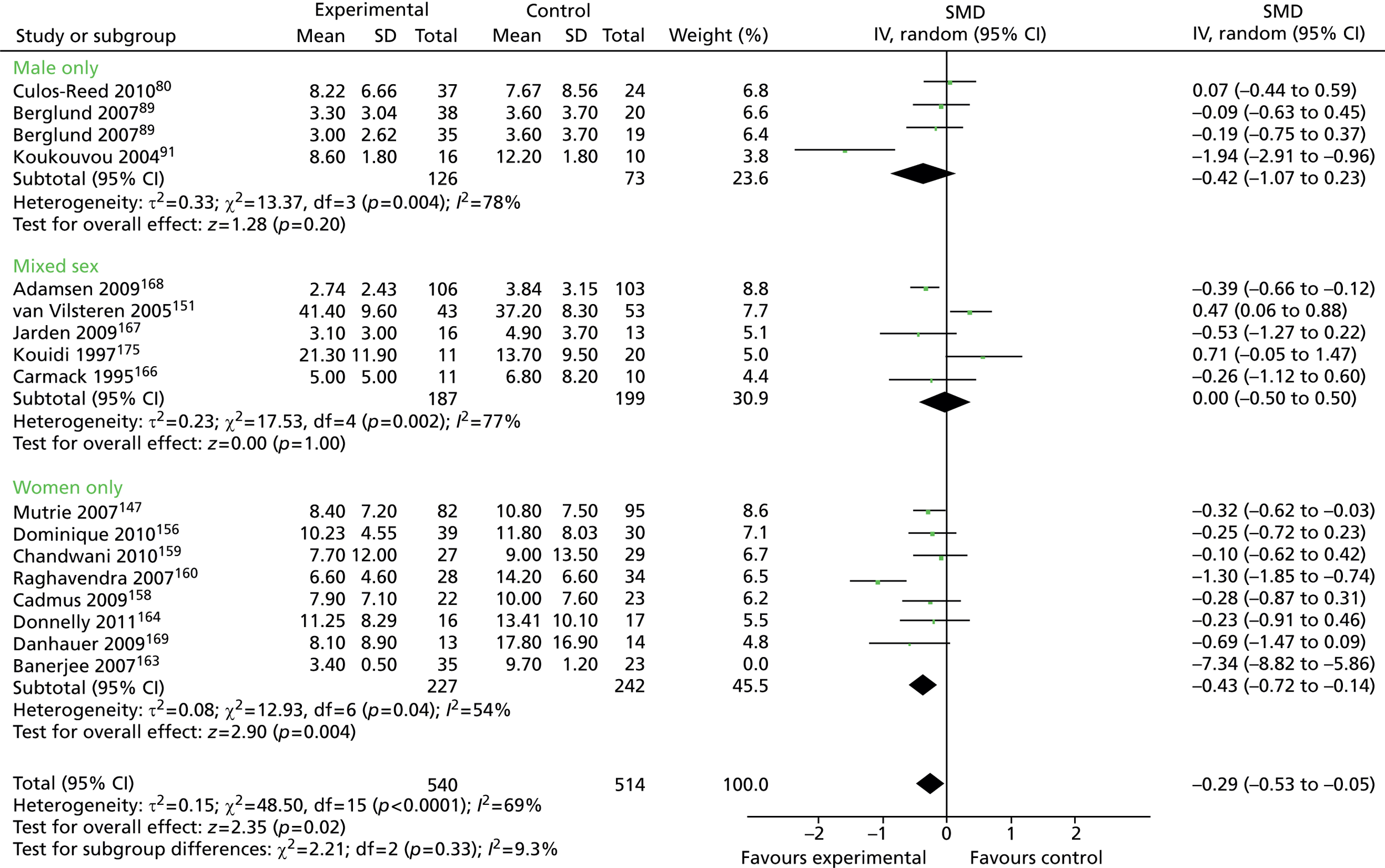
FIGURE 25.
Physical activity interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
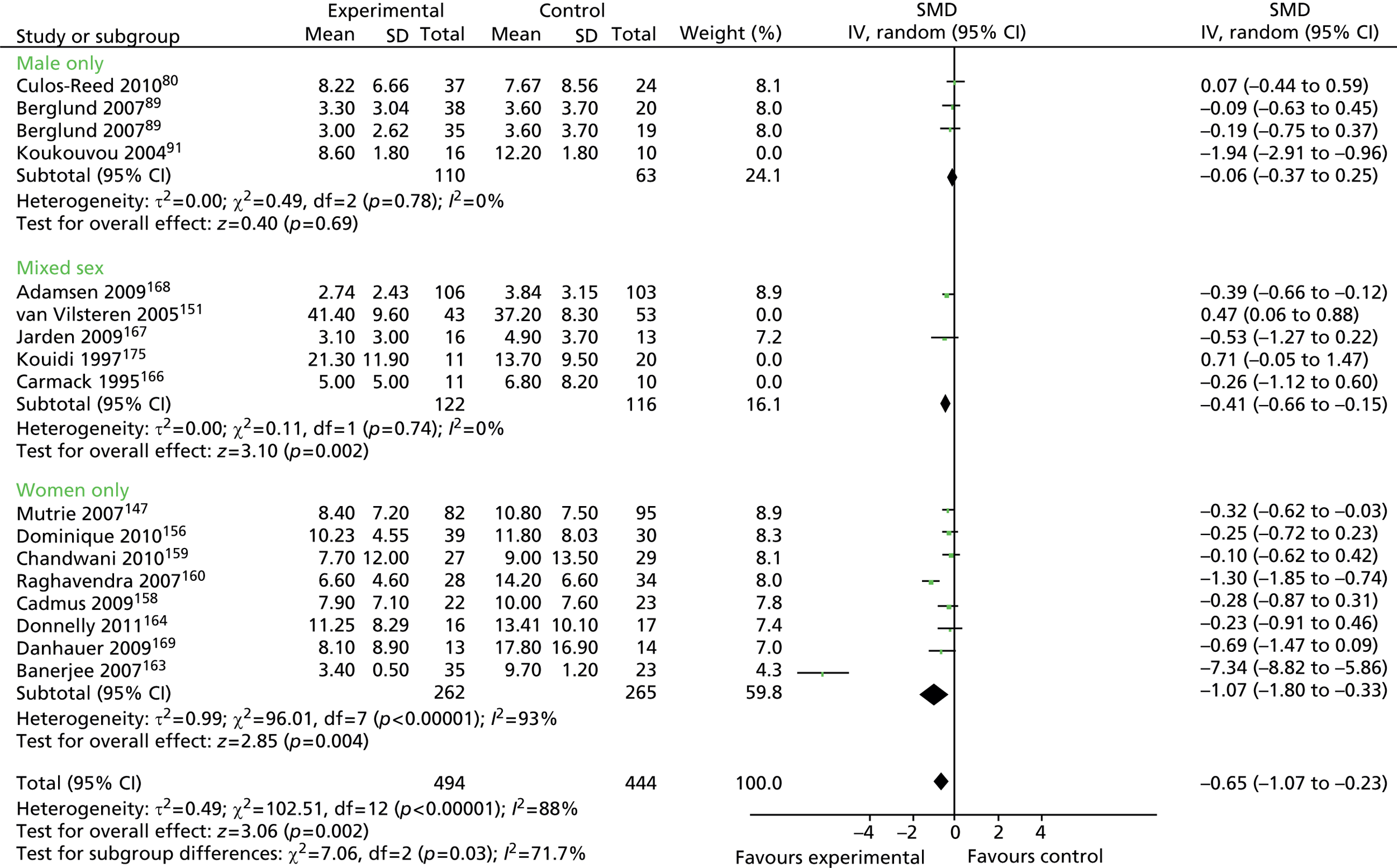
FIGURE 26.
Physical activity interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot, minus outlier Banerjee 2007163). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
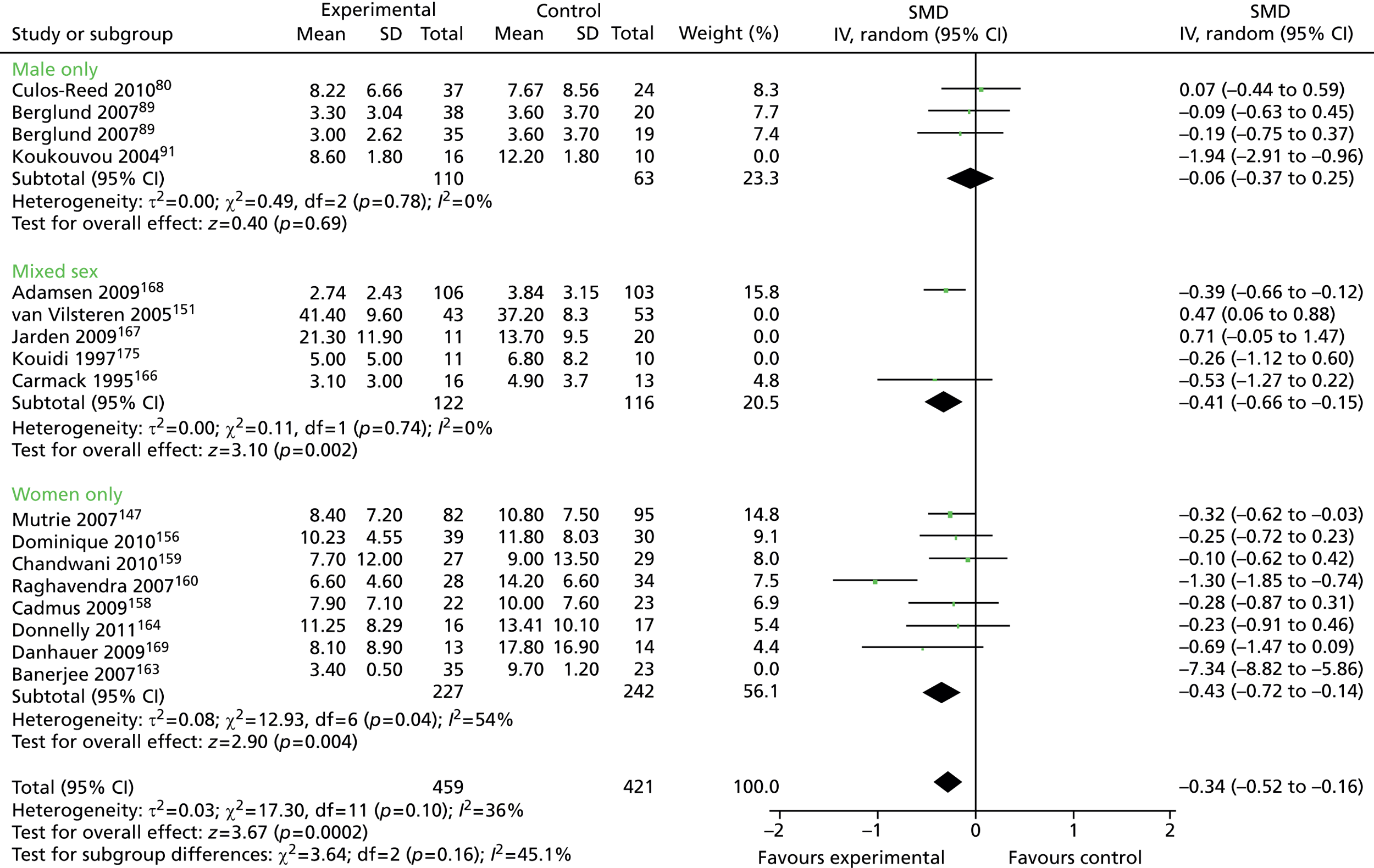
FIGURE 27.
Physical activity interventions: anxiety outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
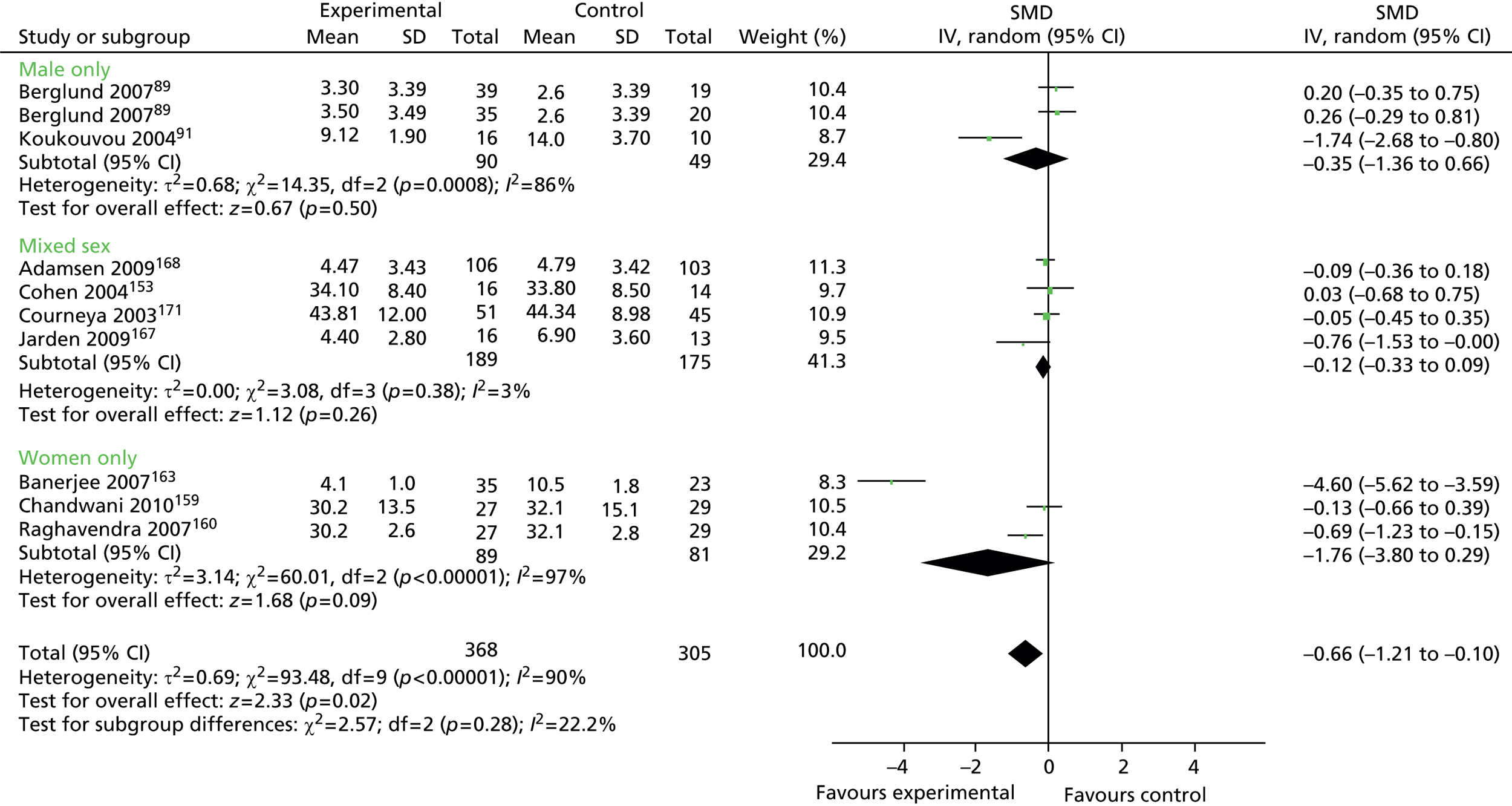
FIGURE 28.
Physical activity interventions: anxiety outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot, minus outlier Banerjee 2007163). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
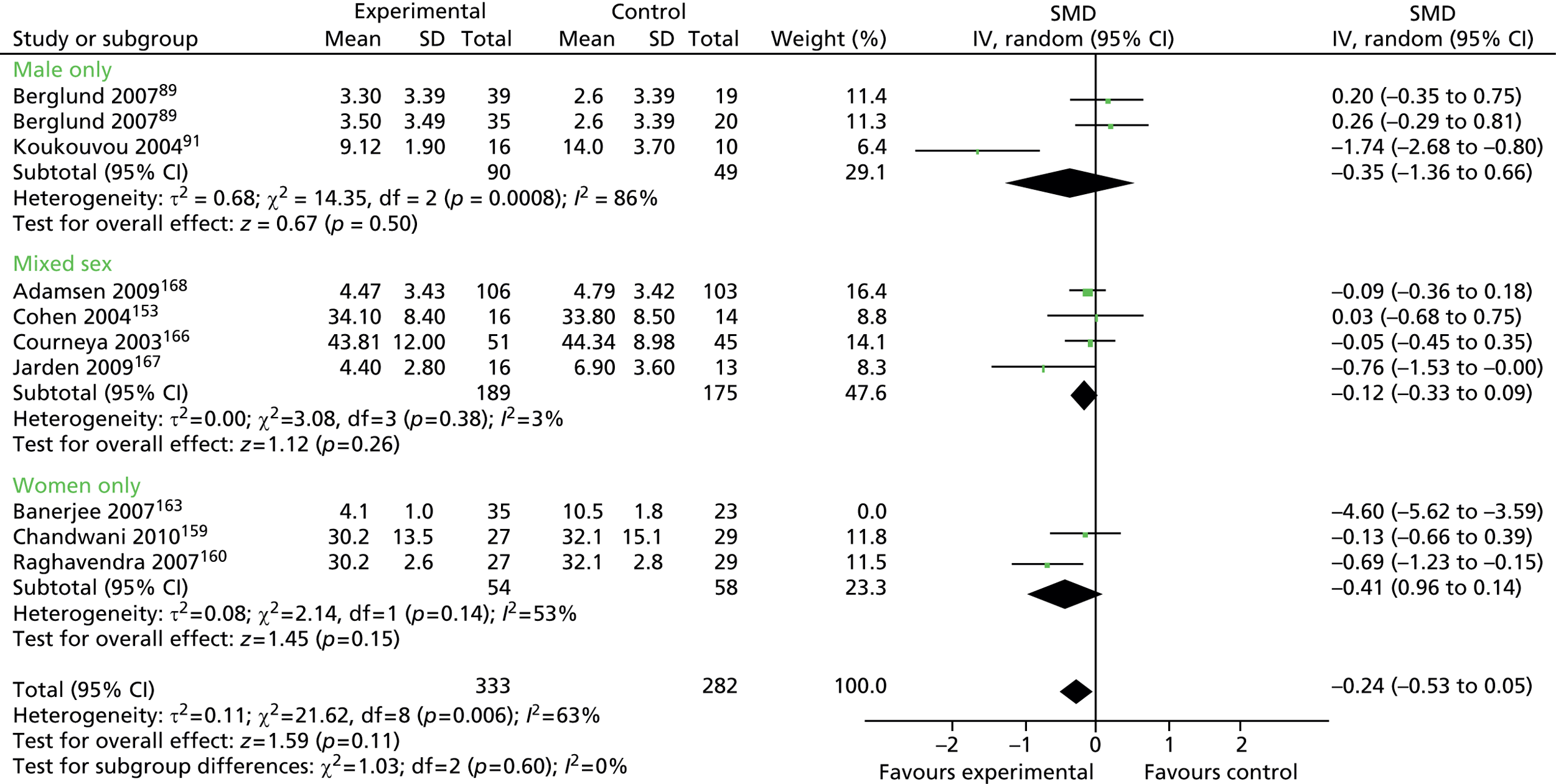
FIGURE 29.
Physical activity interventions: anxiety outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
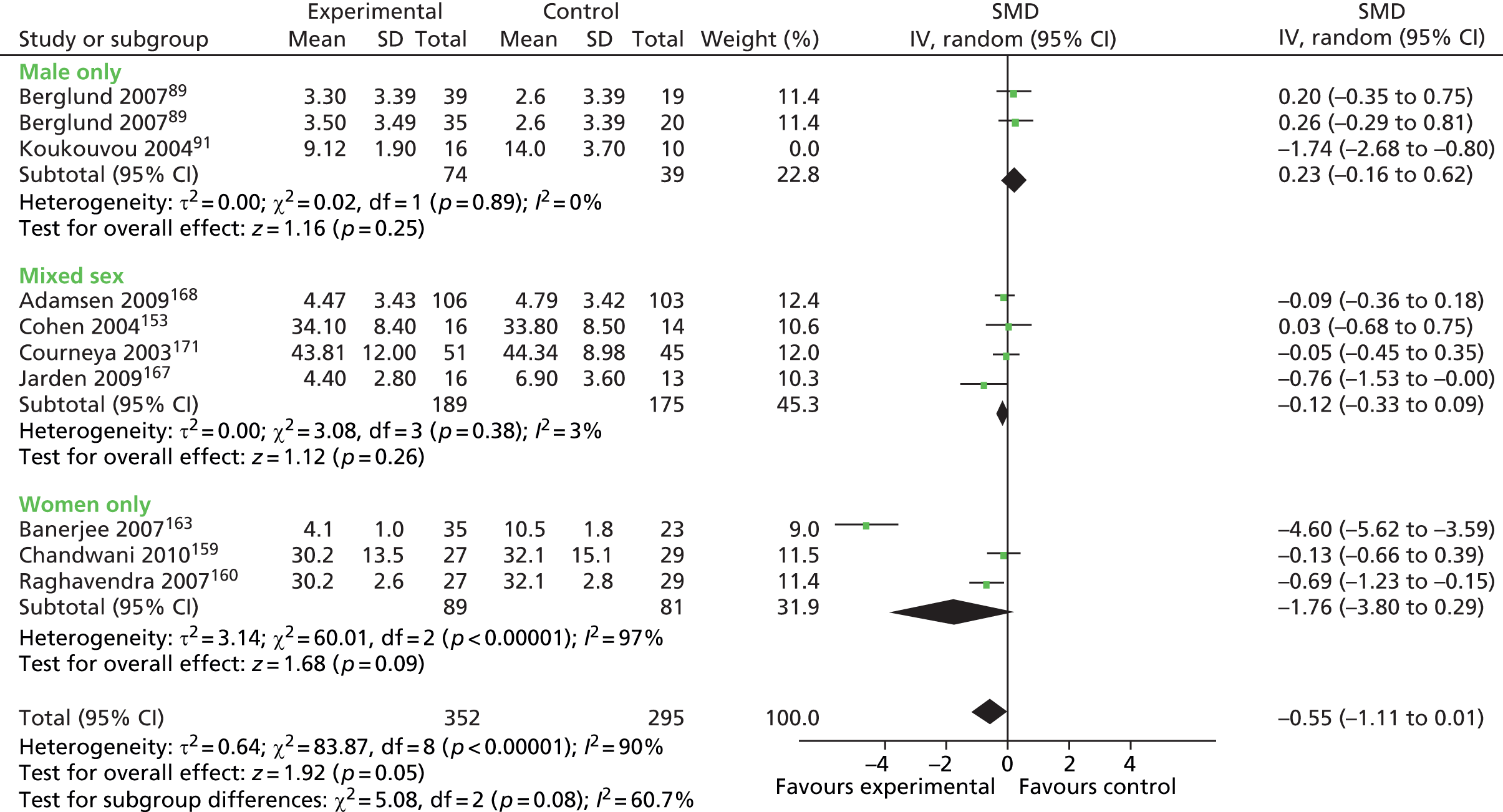
FIGURE 30.
Physical activity interventions: anxiety outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot, minus outlier Banerjee 2007163). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
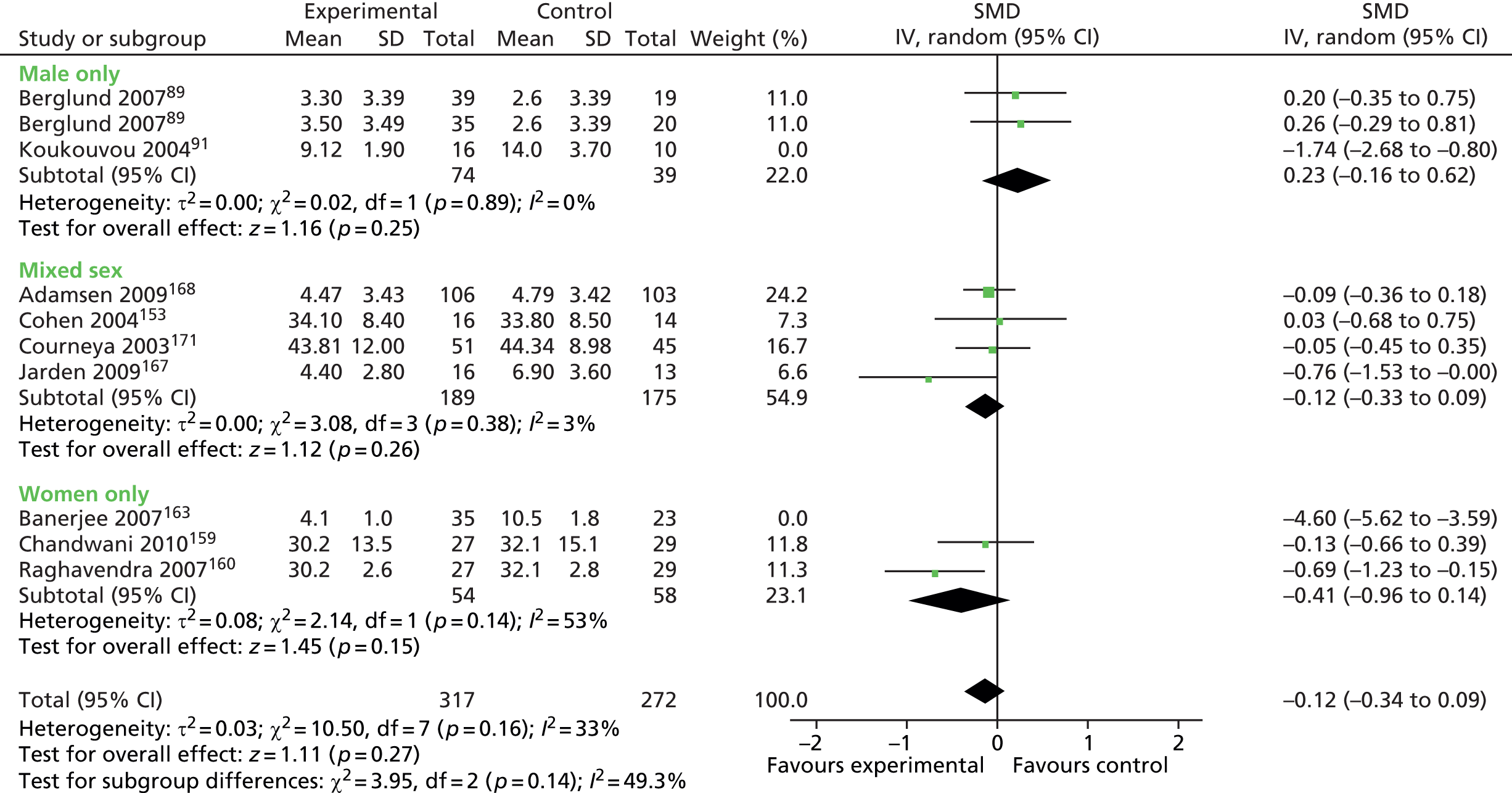
FIGURE 31.
Physical activity interventions: fatigue outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance.
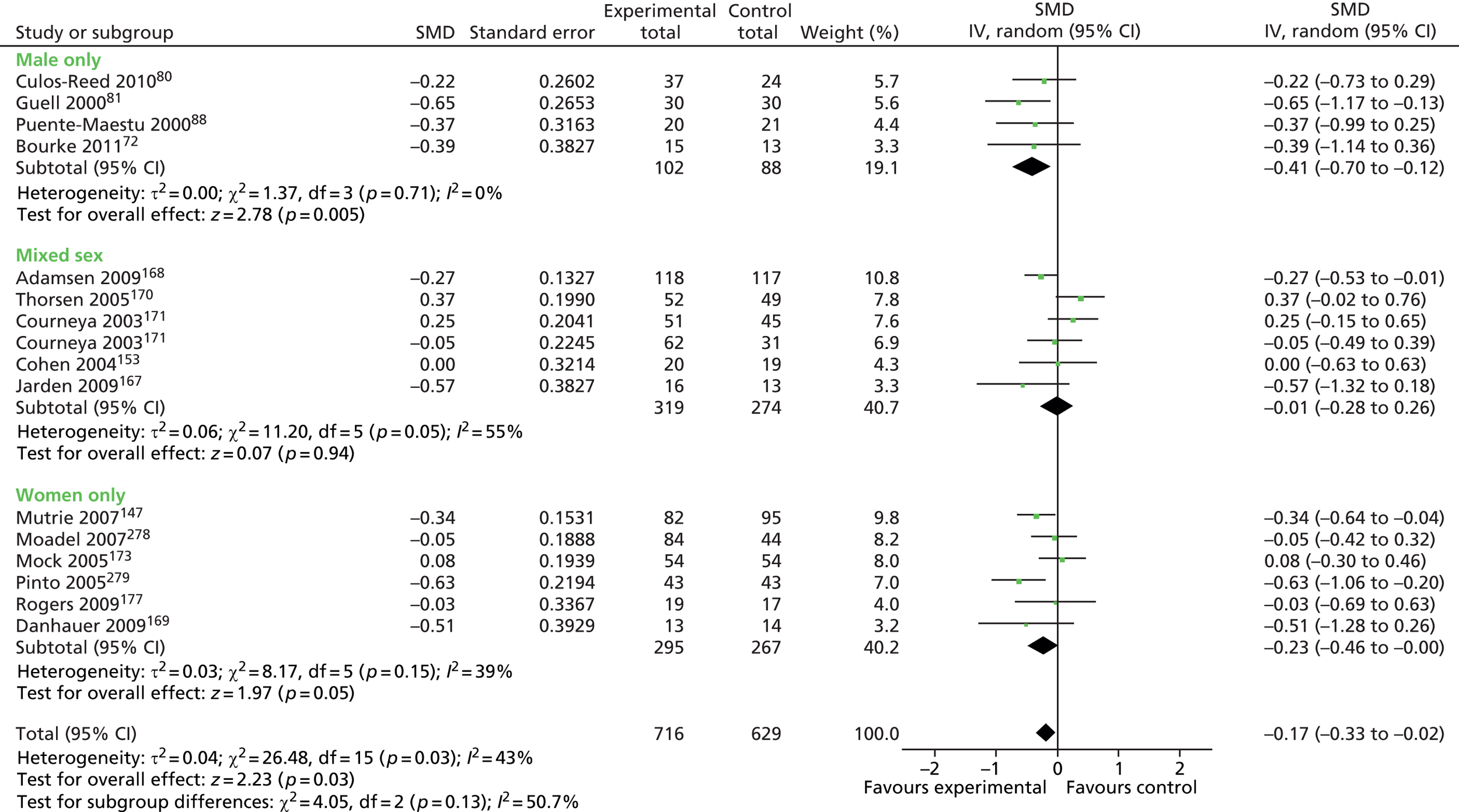
FIGURE 32.
Physical activity interventions: fatigue outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance.
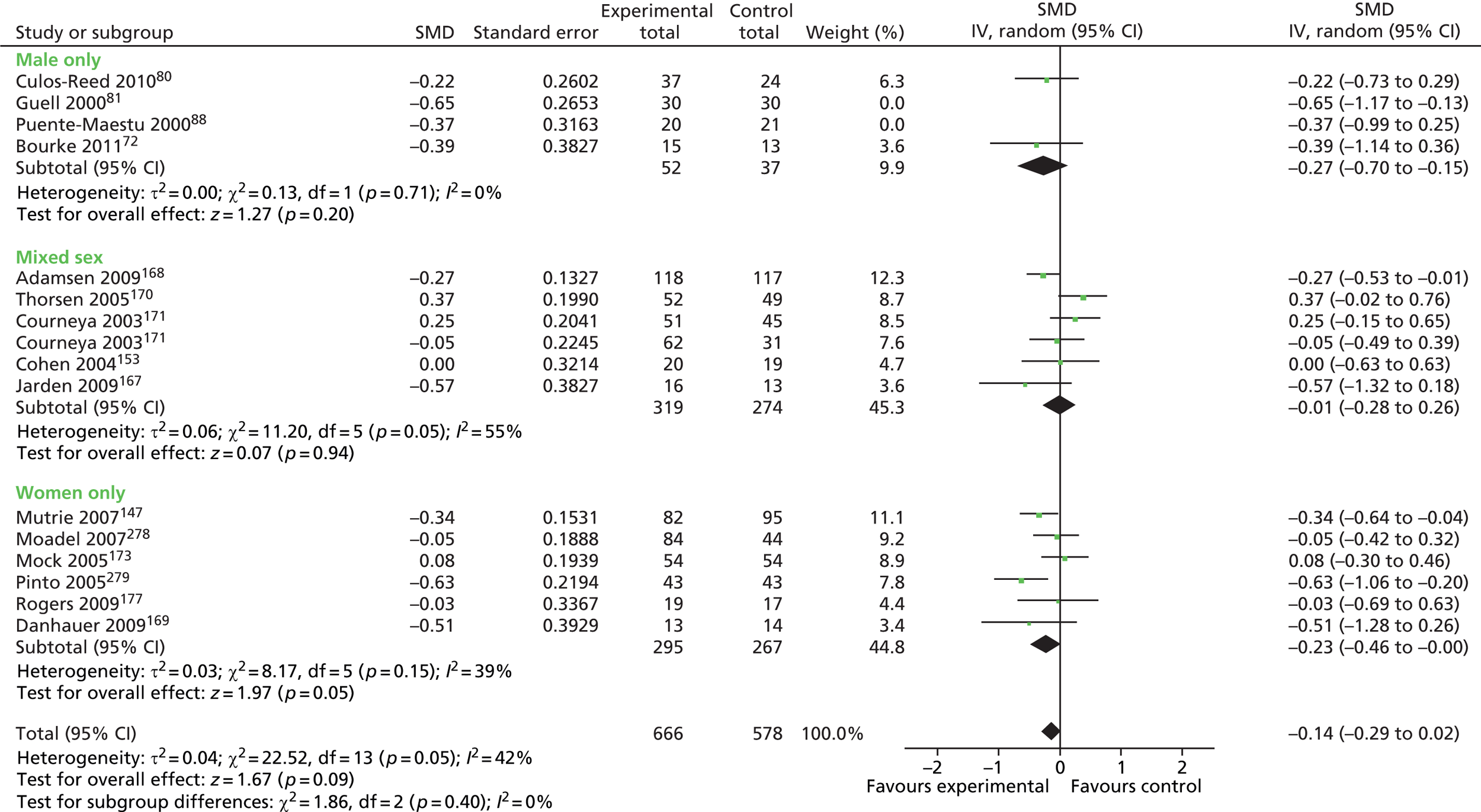
FIGURE 33.
Education interventions: HRQoL outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). a and b refer to different intervention groups within the Coultas 2005 study. 155 df, degrees of freedom; IV, inverse variance.
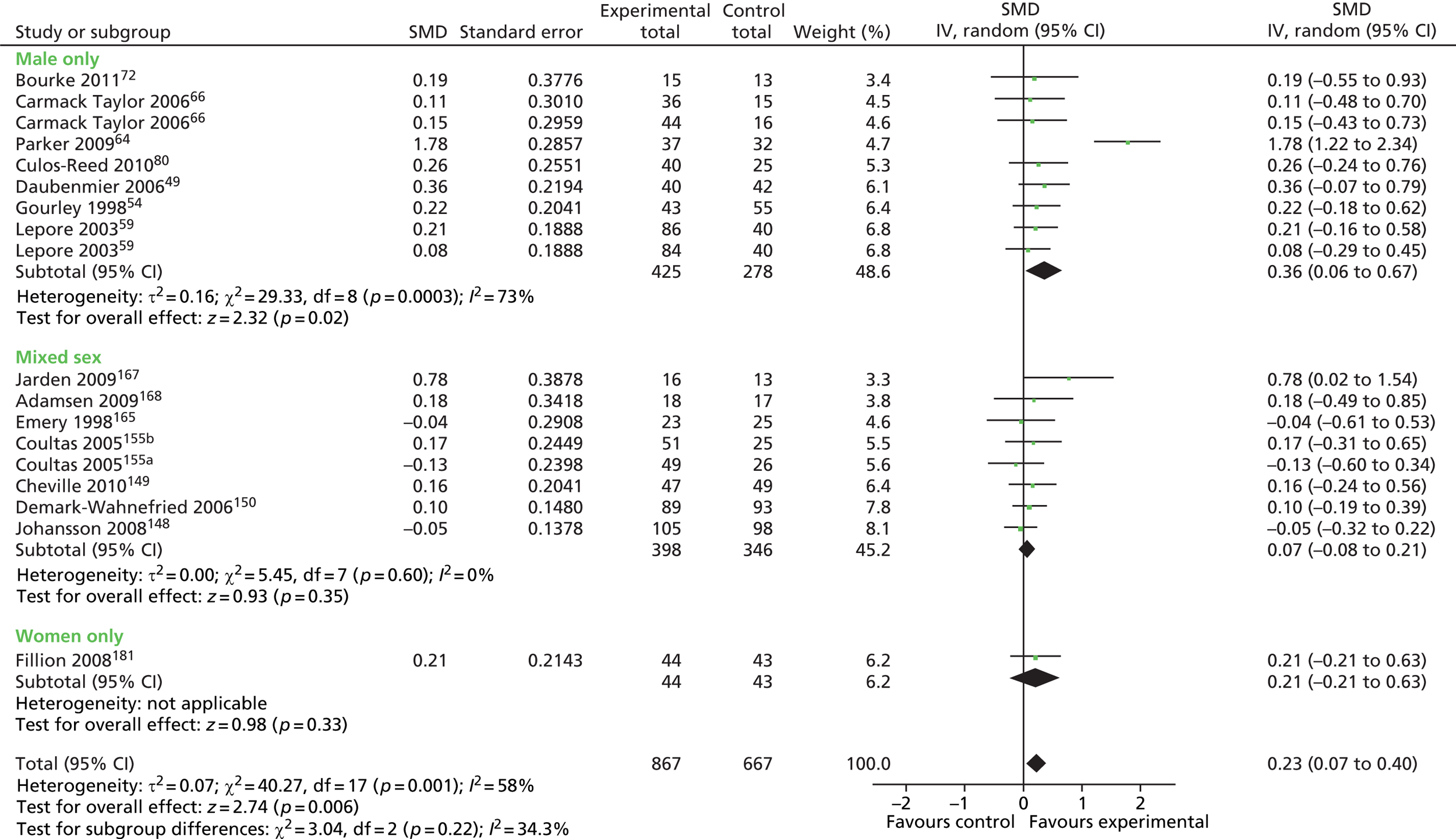
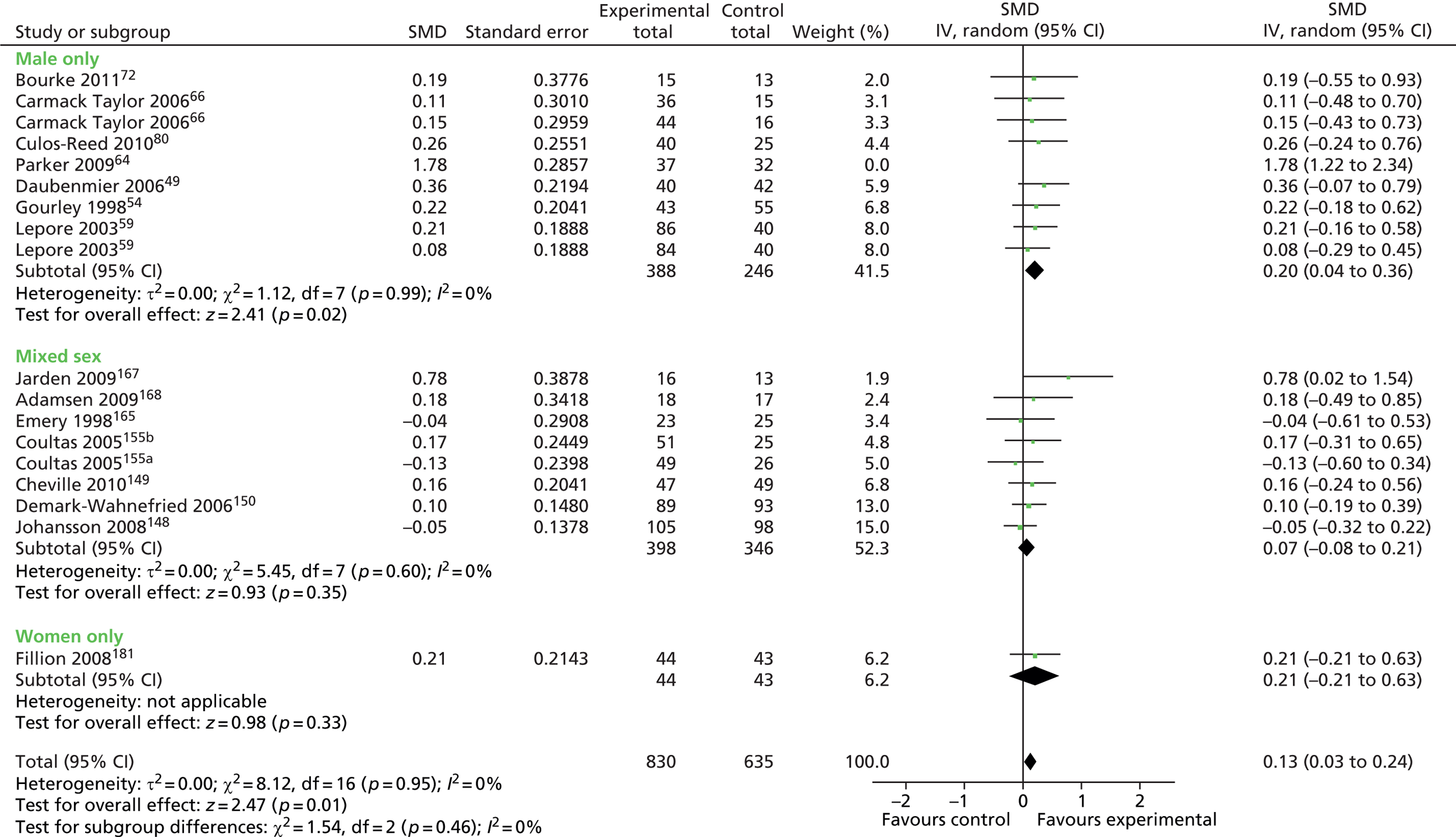
FIGURE 35.
Education interventions: HRQoL outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). a and b refer to different intervention groups within the Coultas 2005 study. 155 df, degrees of freedom; IV, inverse variance.
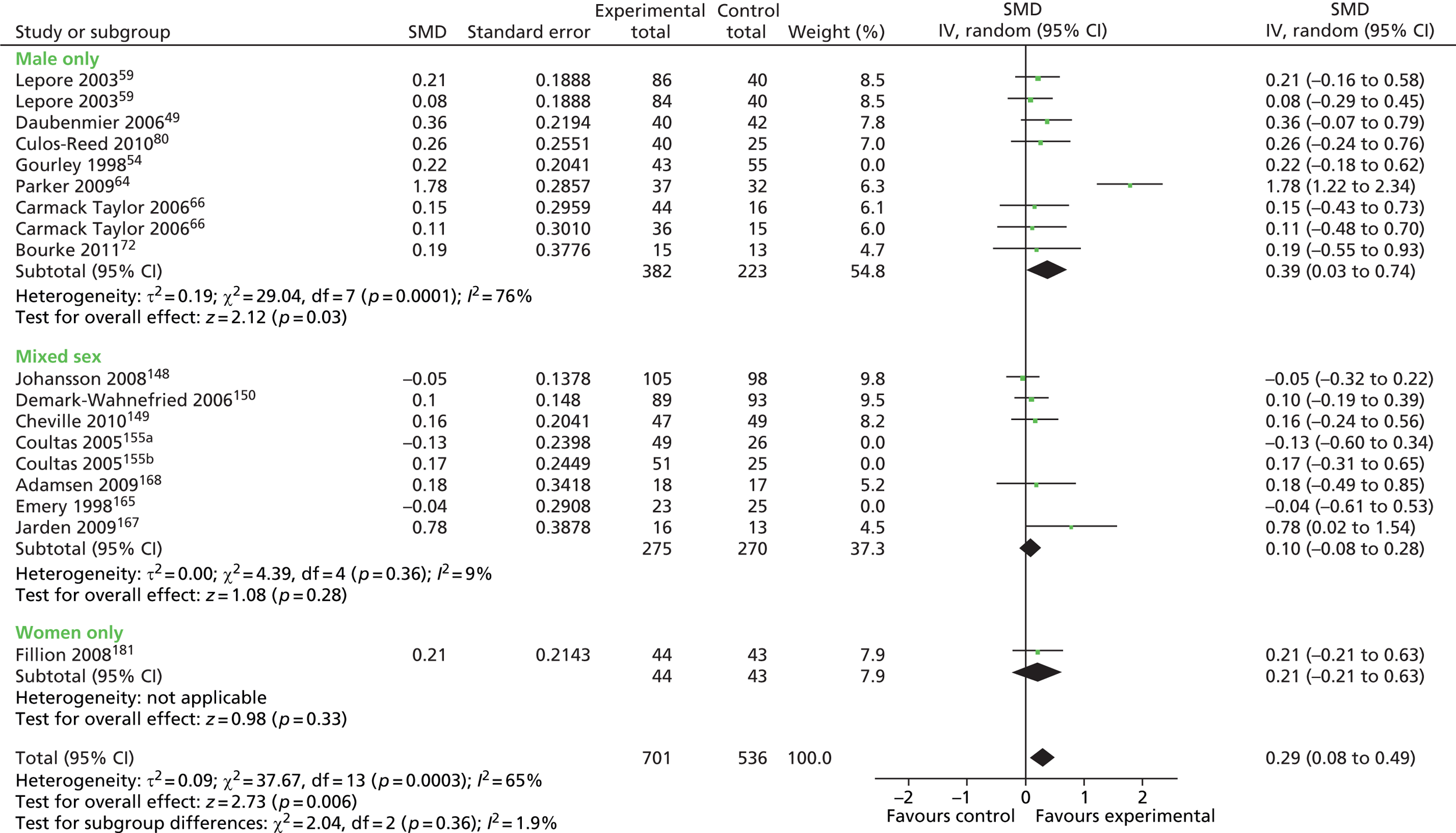
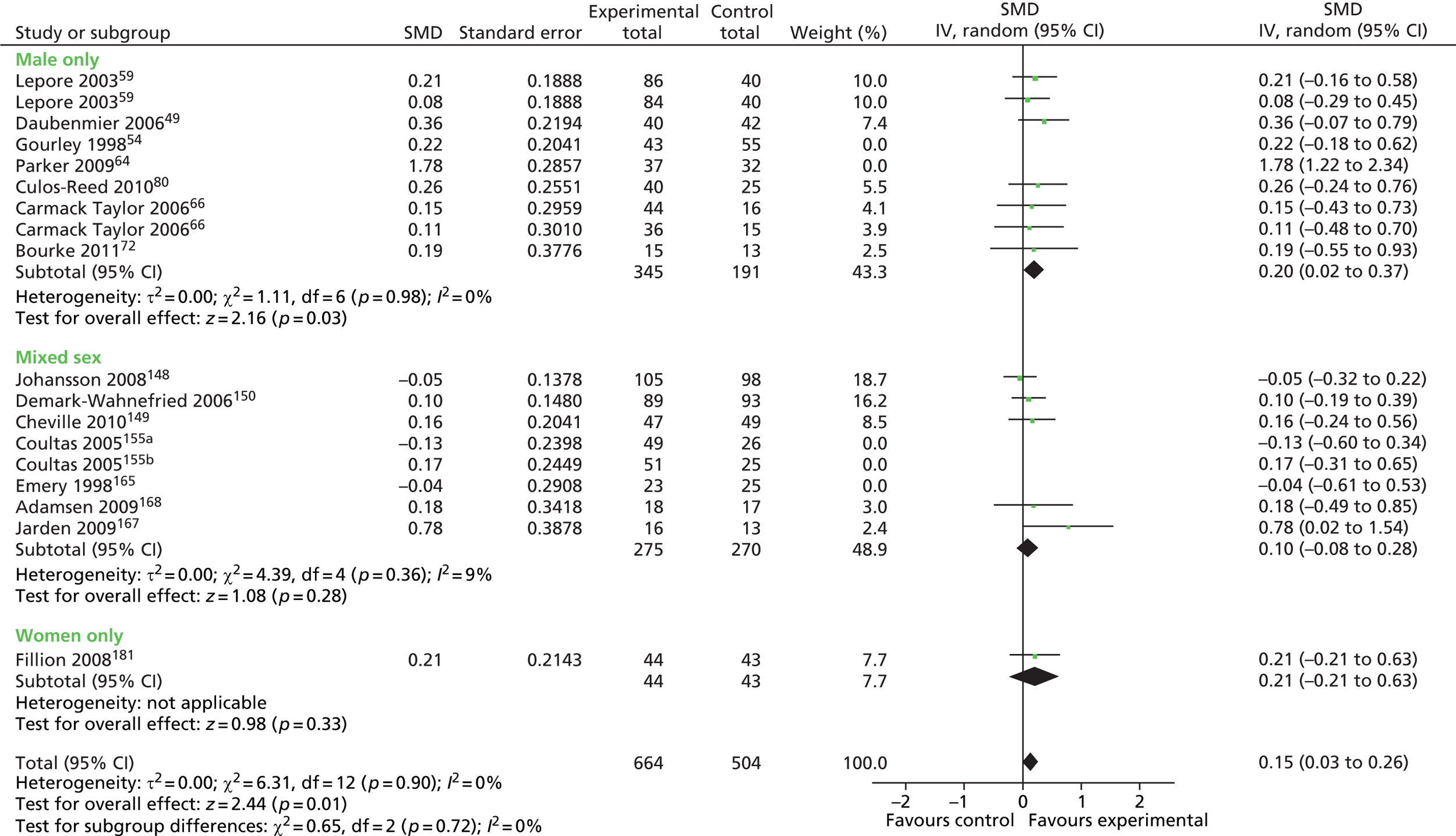
FIGURE 37.
Education interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
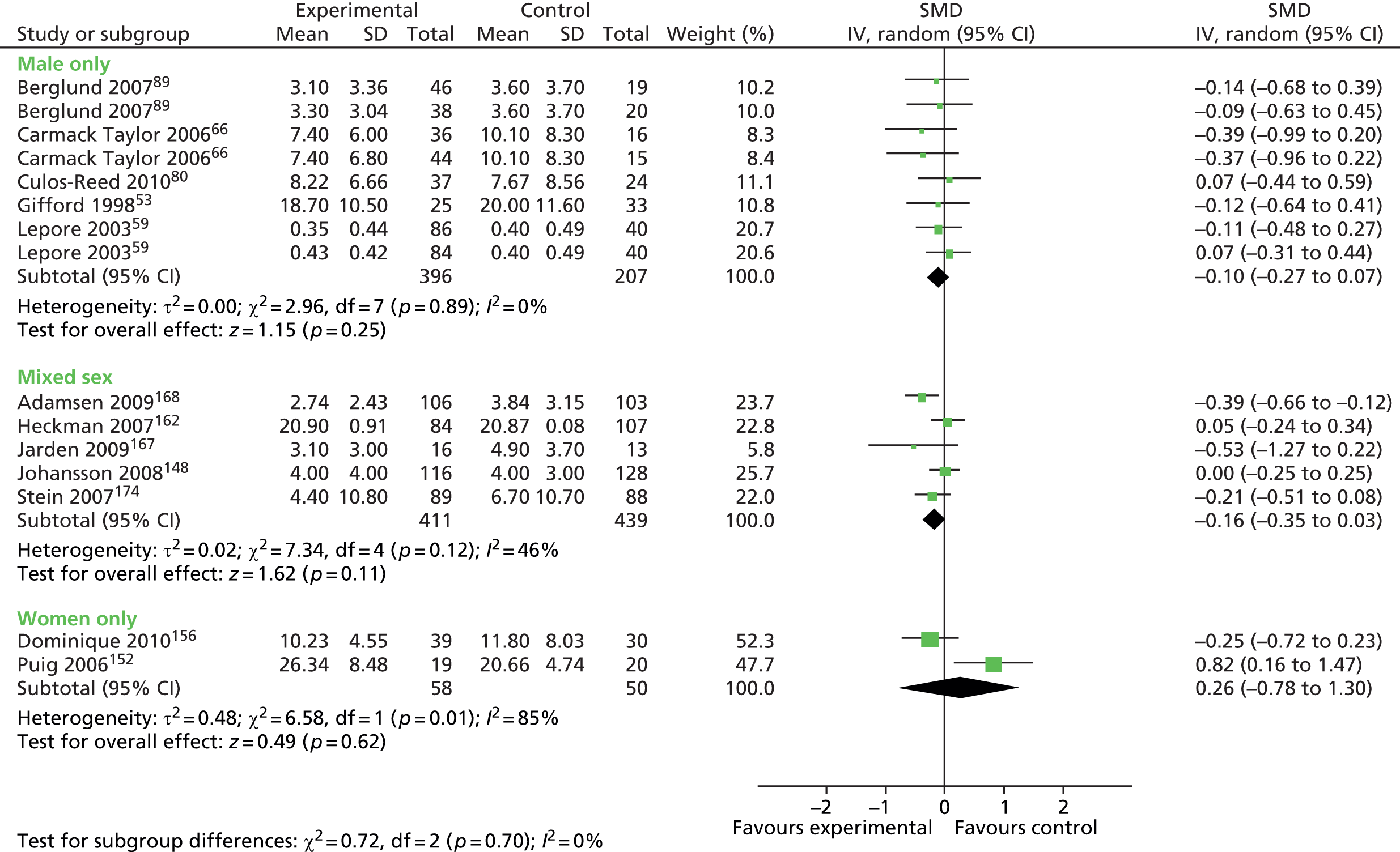
FIGURE 38.
Education interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
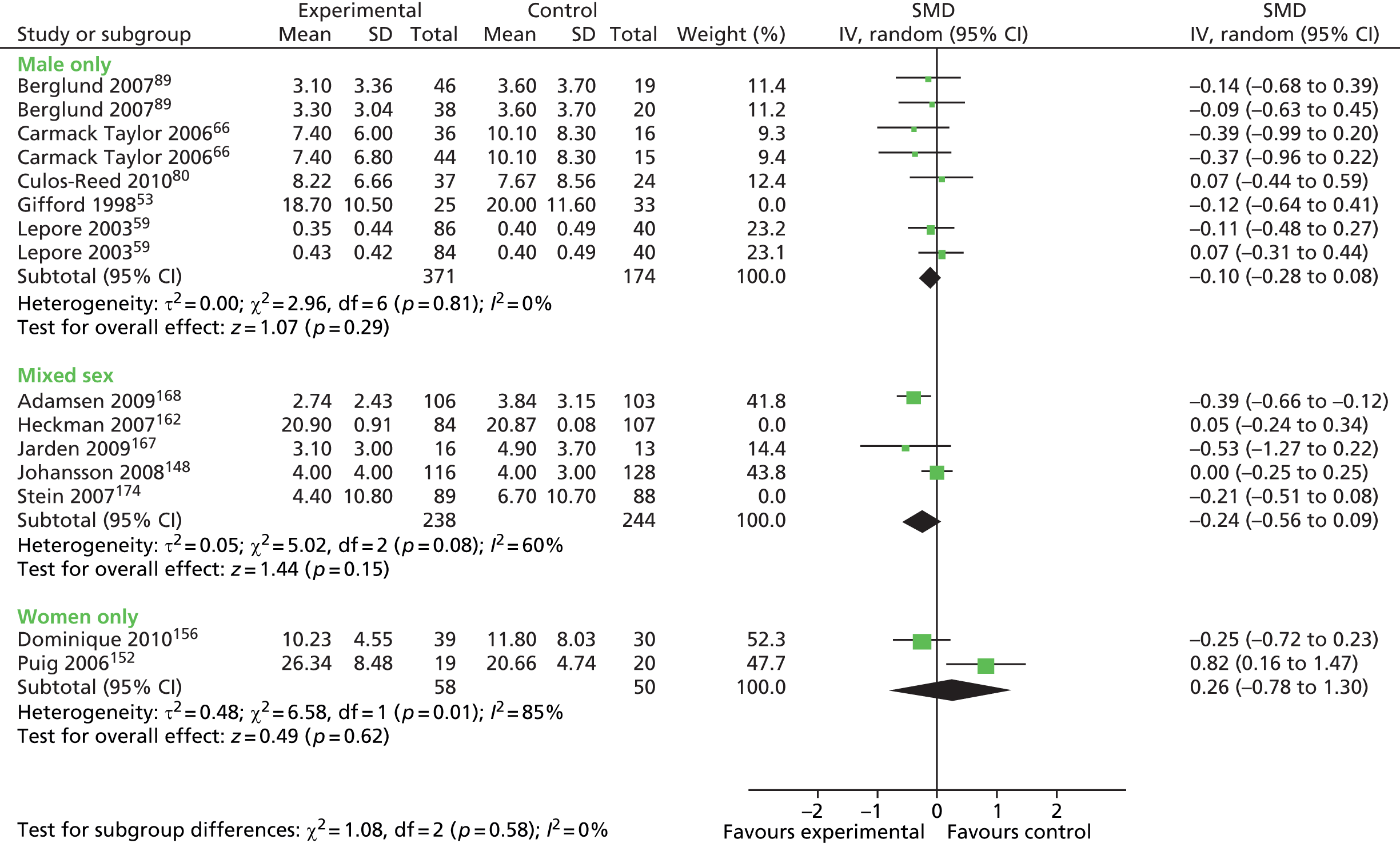
FIGURE 39.
Education interventions: anxiety outcomes in male-only vs. mixed-sex groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
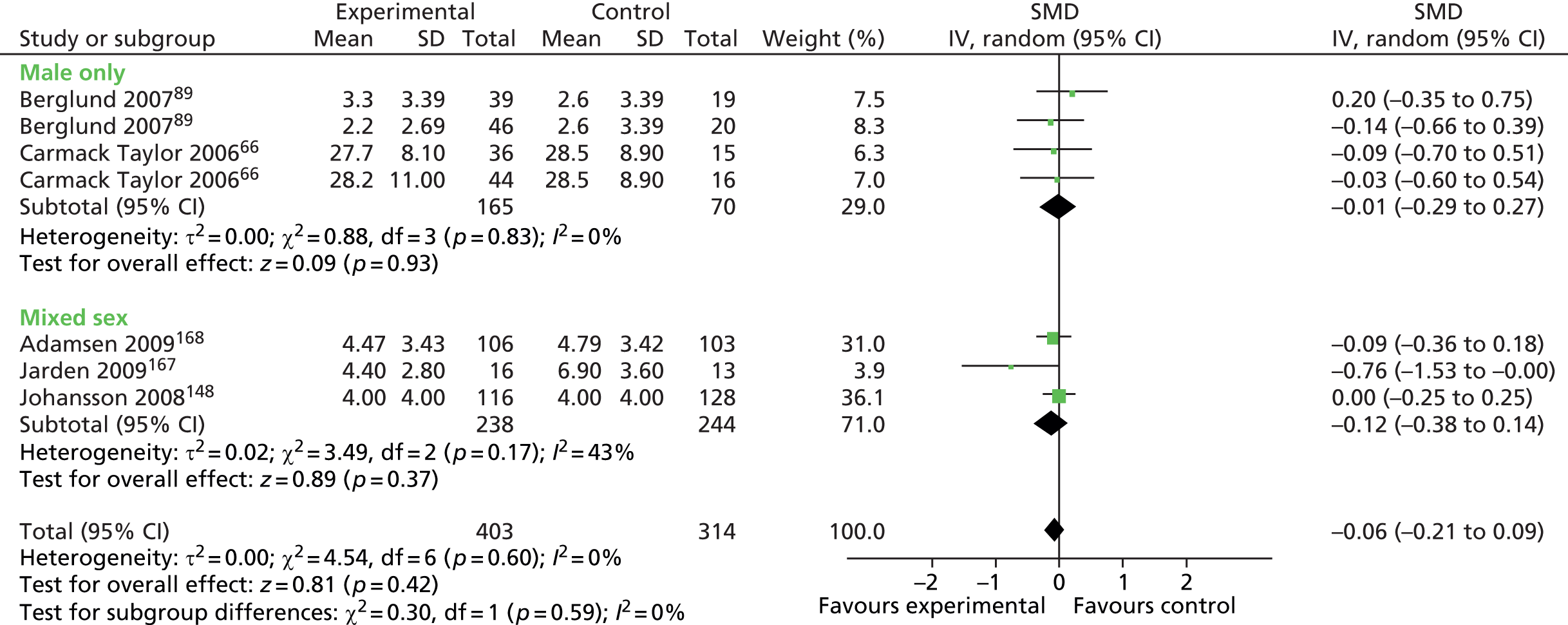
FIGURE 40.
Education interventions: fatigue outcomes in male-only vs. mixed-sex groups (mixed disease plot). df, degrees of freedom; IV, inverse variance.
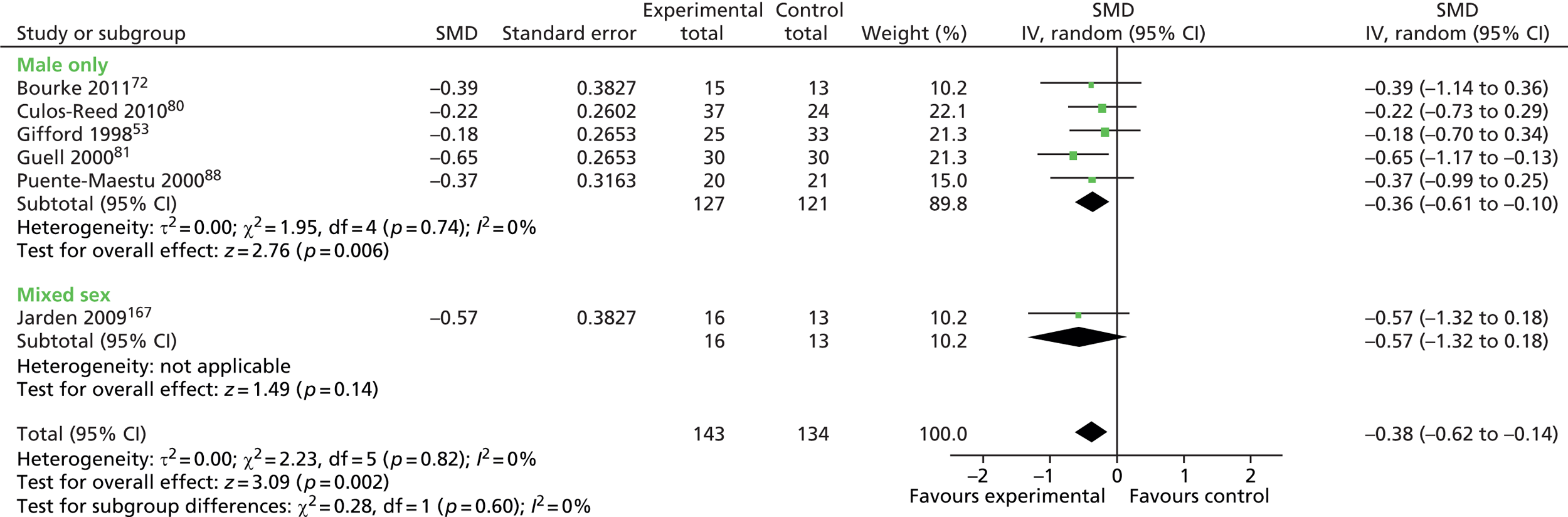
FIGURE 41.
Education interventions: fatigue outcomes in male-only vs. mixed-sex groups (cancer-only plot). df, degrees of freedom; IV, inverse variance.
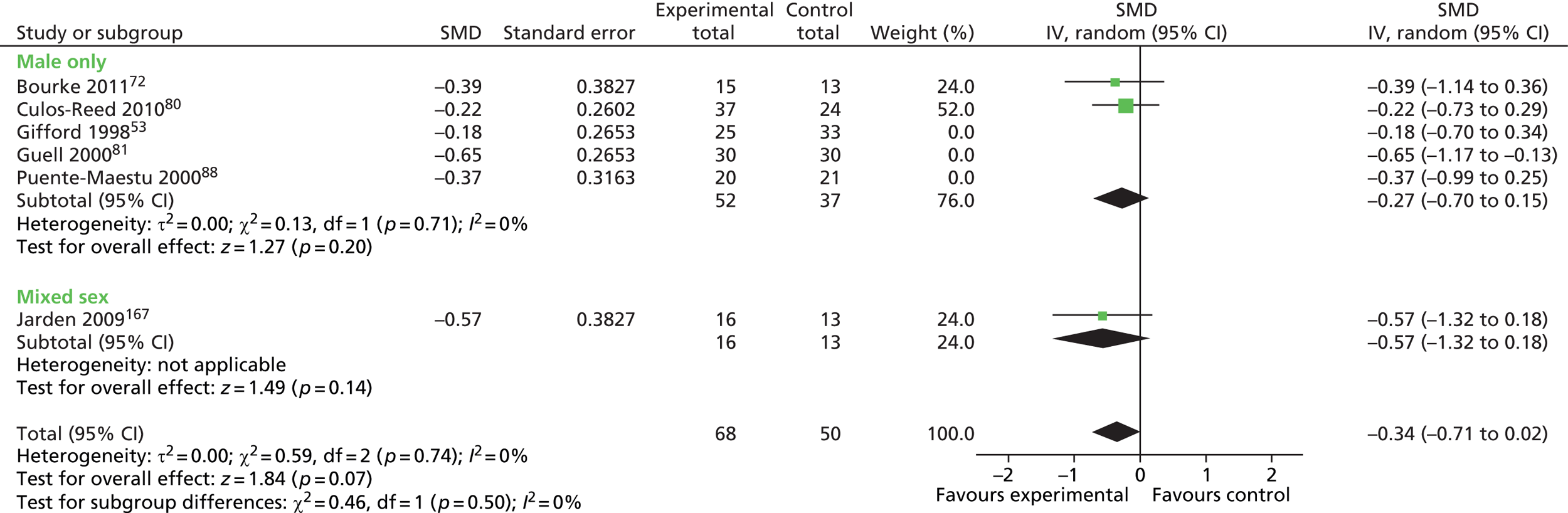
FIGURE 42.
Peer support interventions: HRQoL outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
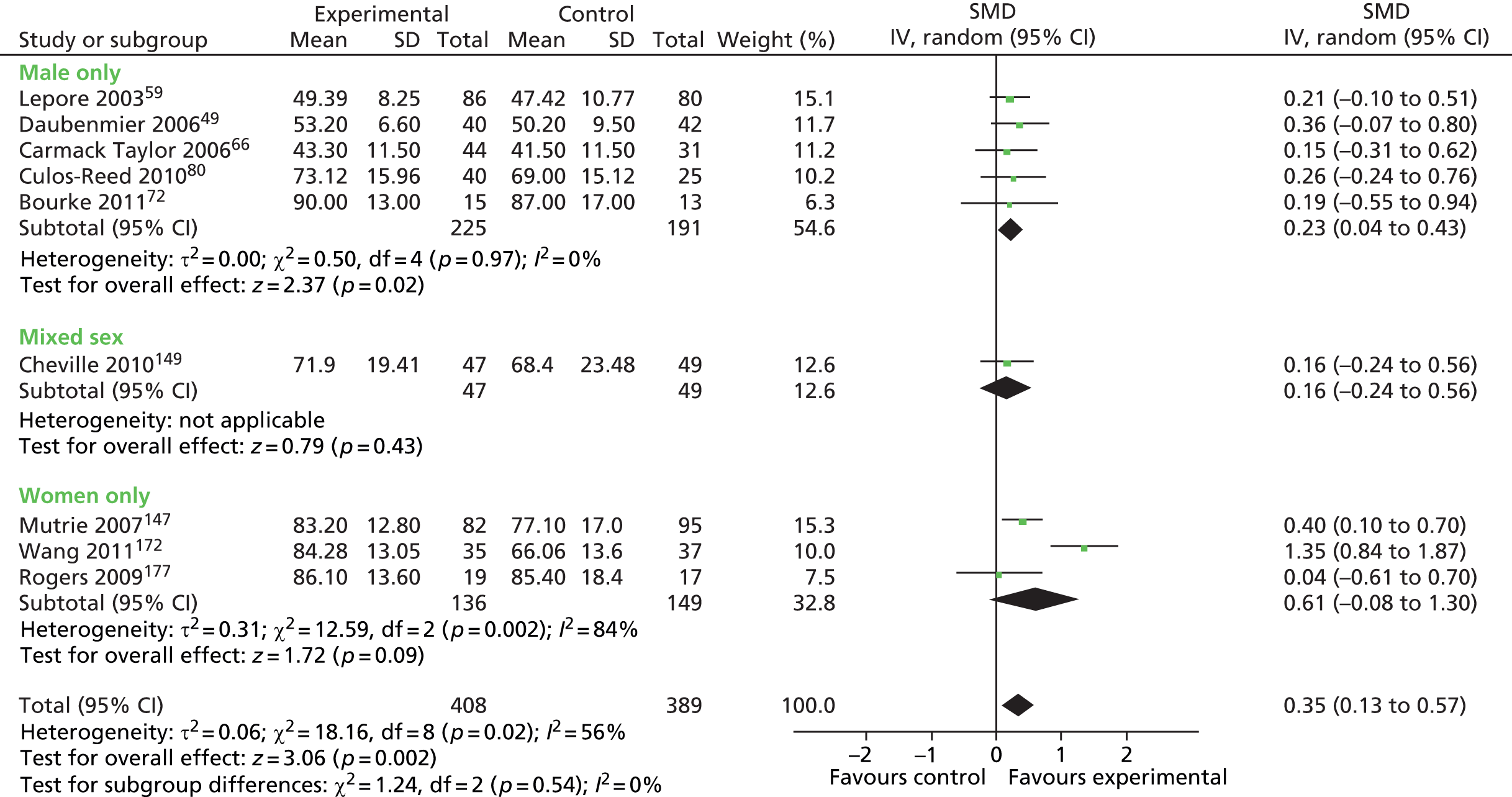
FIGURE 43.
Peer support interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
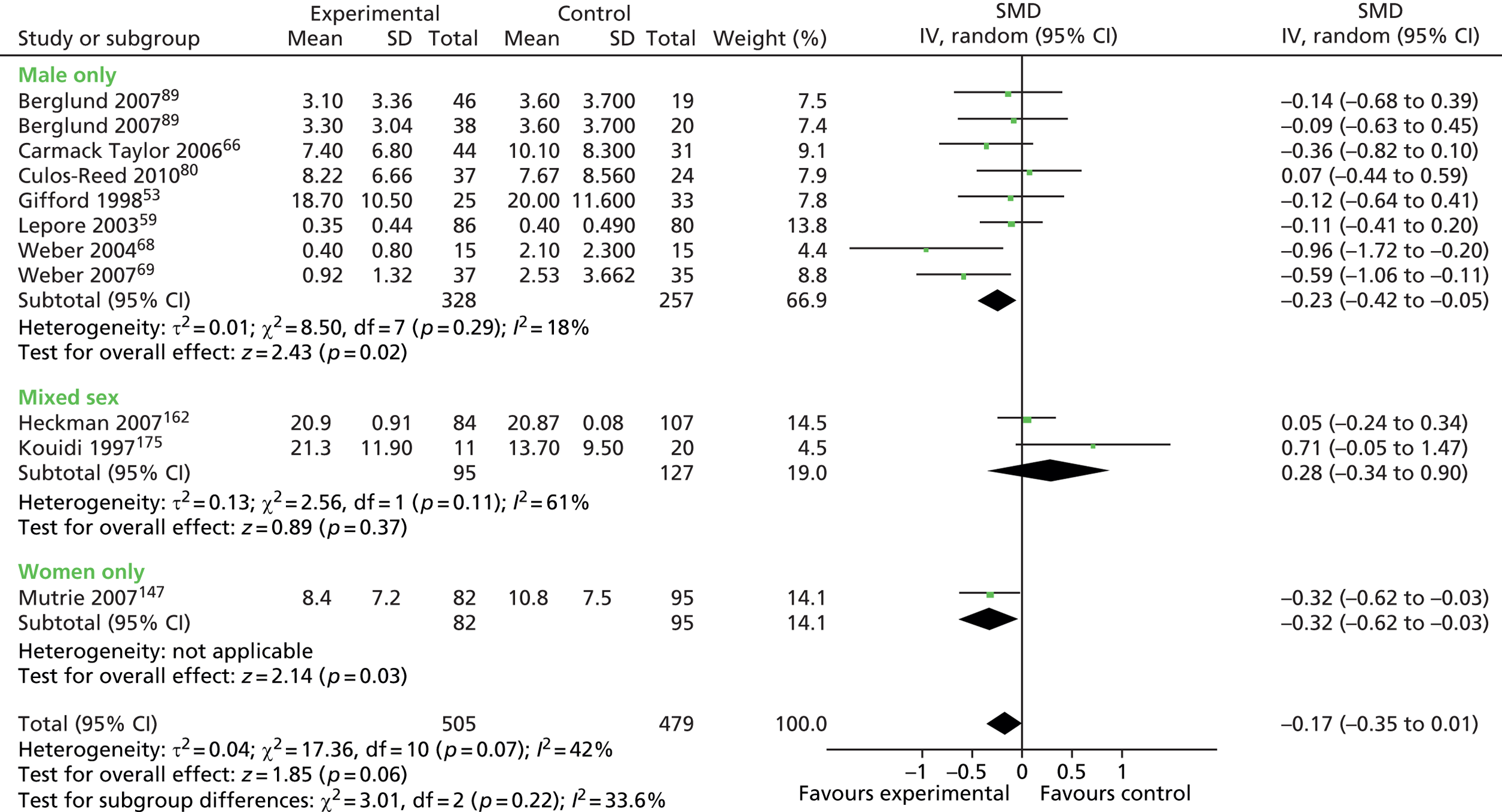
FIGURE 44.
Peer support interventions: depression outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
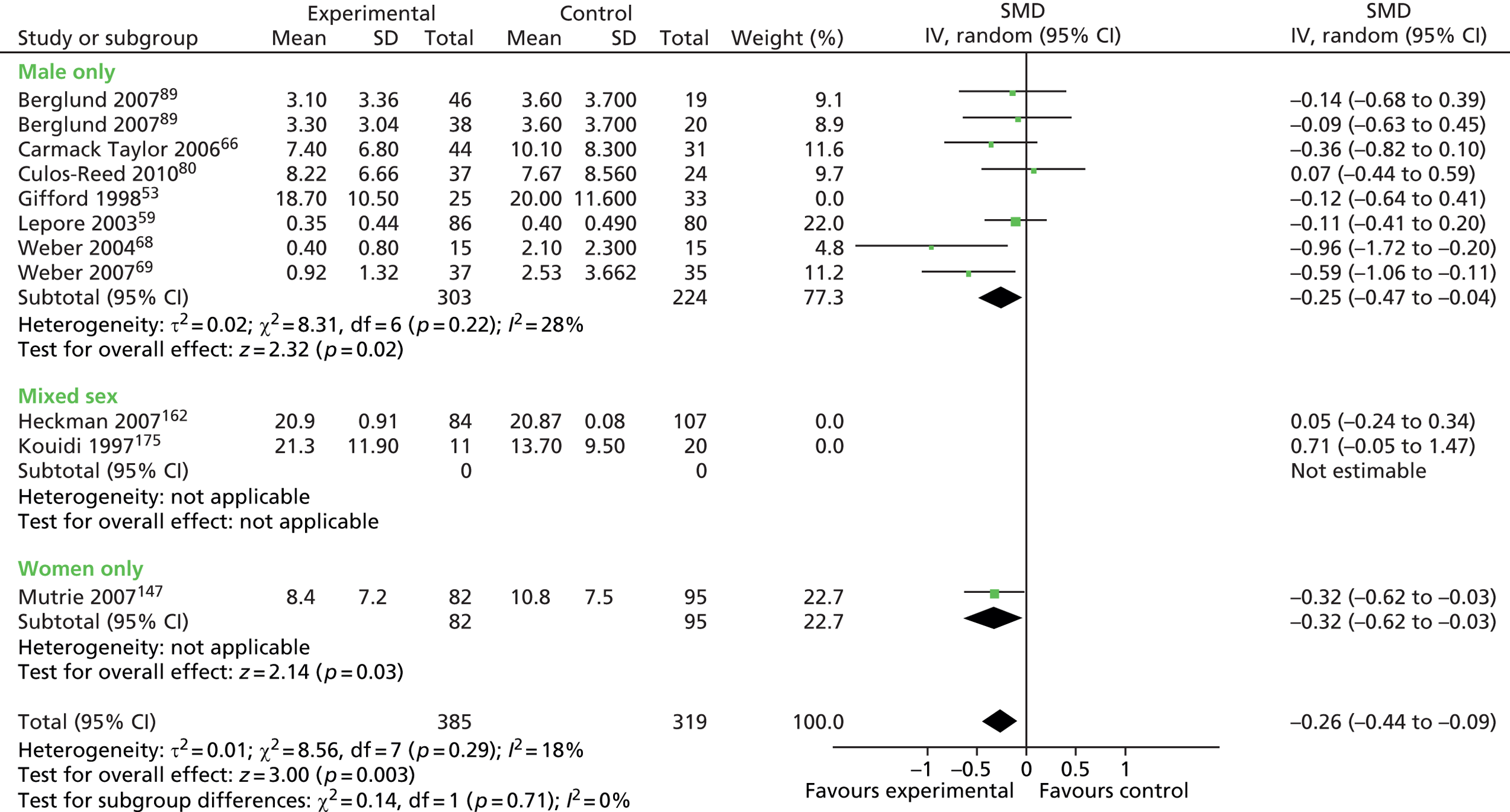
FIGURE 45.
Peer support interventions: fatigue outcomes in male-only vs. female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
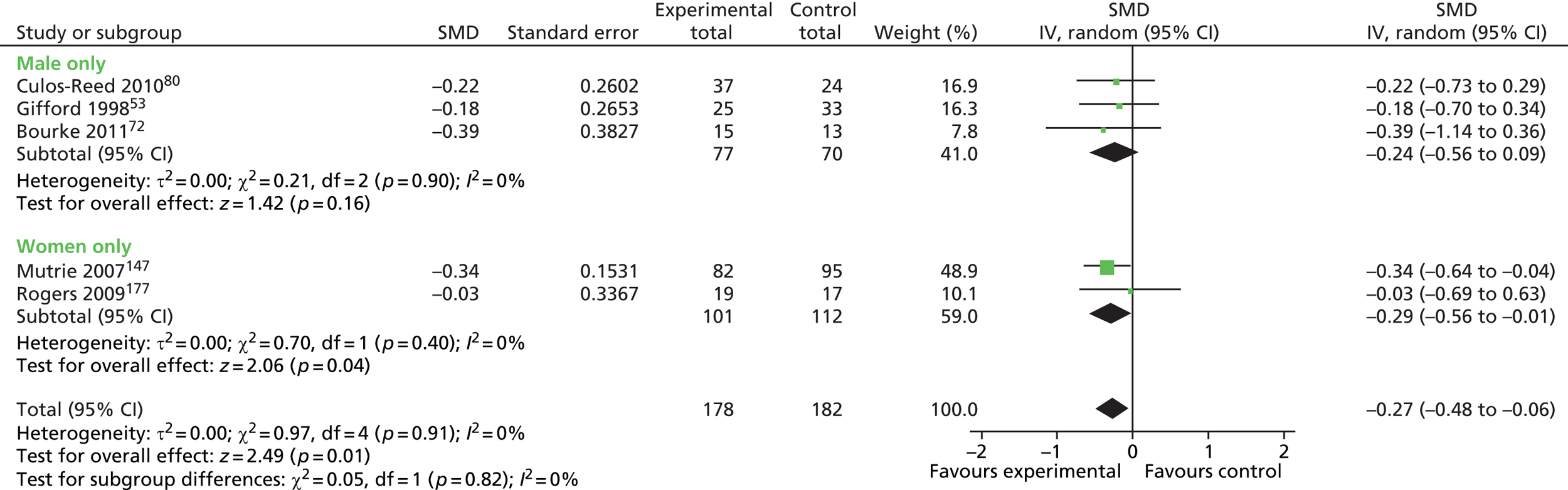
FIGURE 46.
Peer support interventions: fatigue outcomes in male-only vs. female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
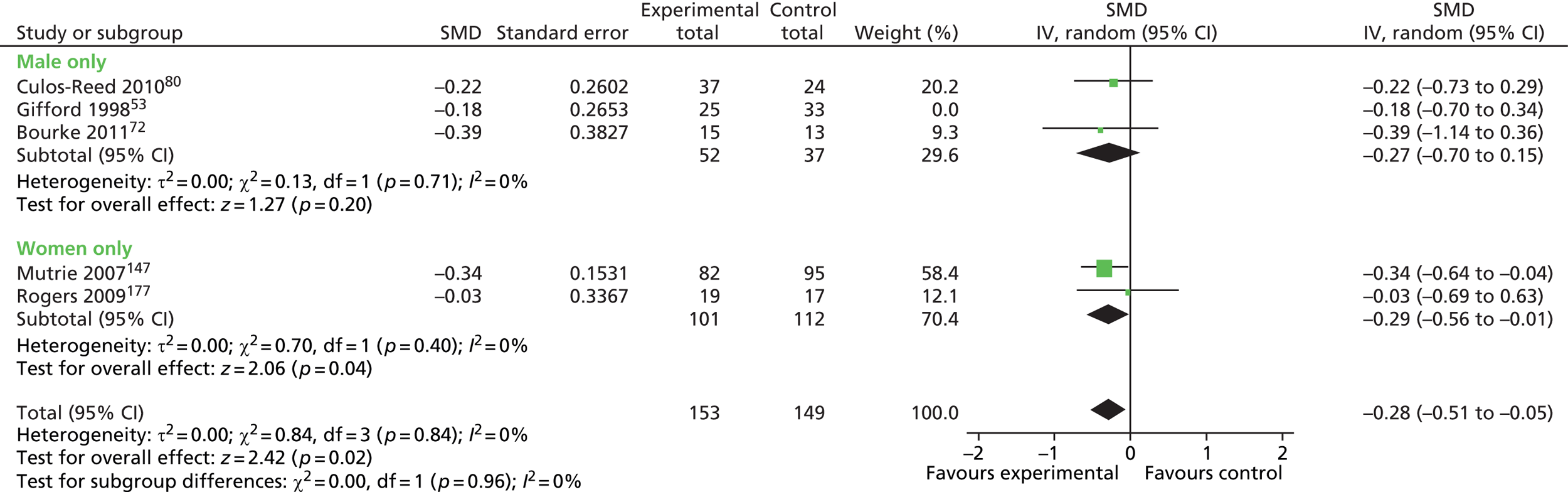
FIGURE 47.
Peer support interventions: self-efficacy outcomes in male-only vs. mixed-sex groups. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
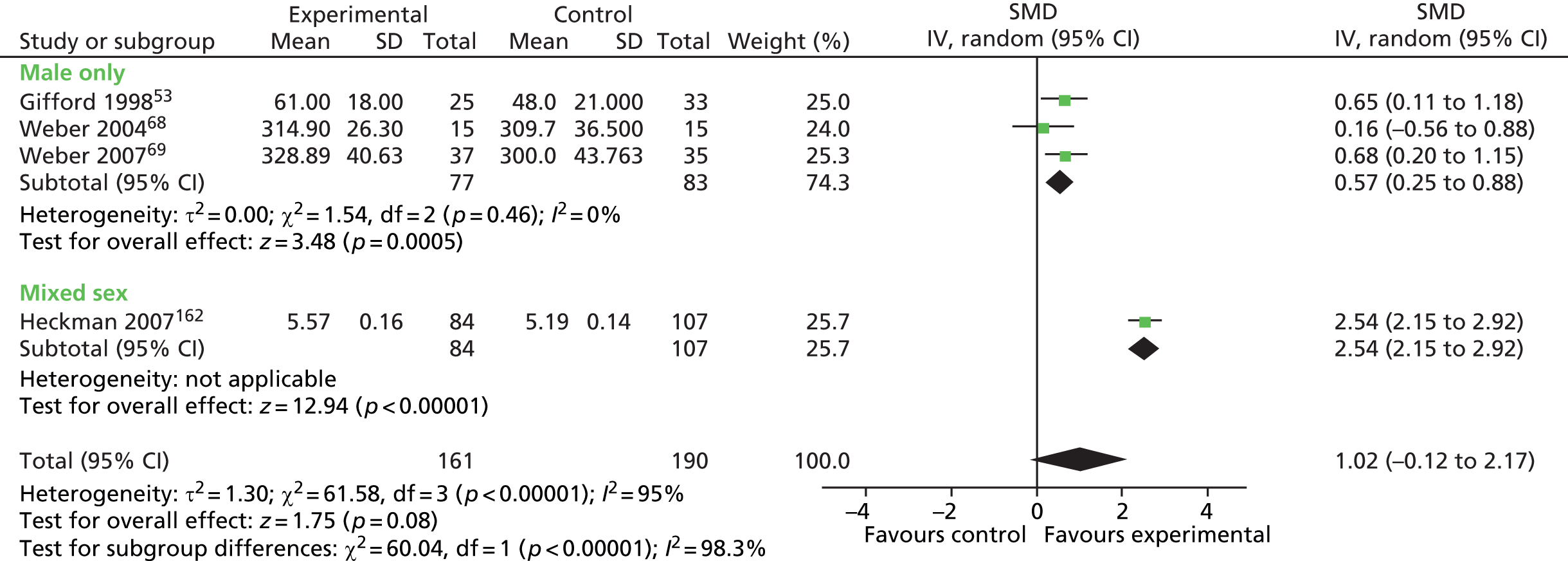
FIGURE 48.
Health-care professional monitoring and feedback: HRQoL outcomes in male-only vs. female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.

FIGURE 49.
Health-care professional monitoring and feedback: depression outcomes in male-only vs. mixed-sex and female-only groups (mixed disease plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
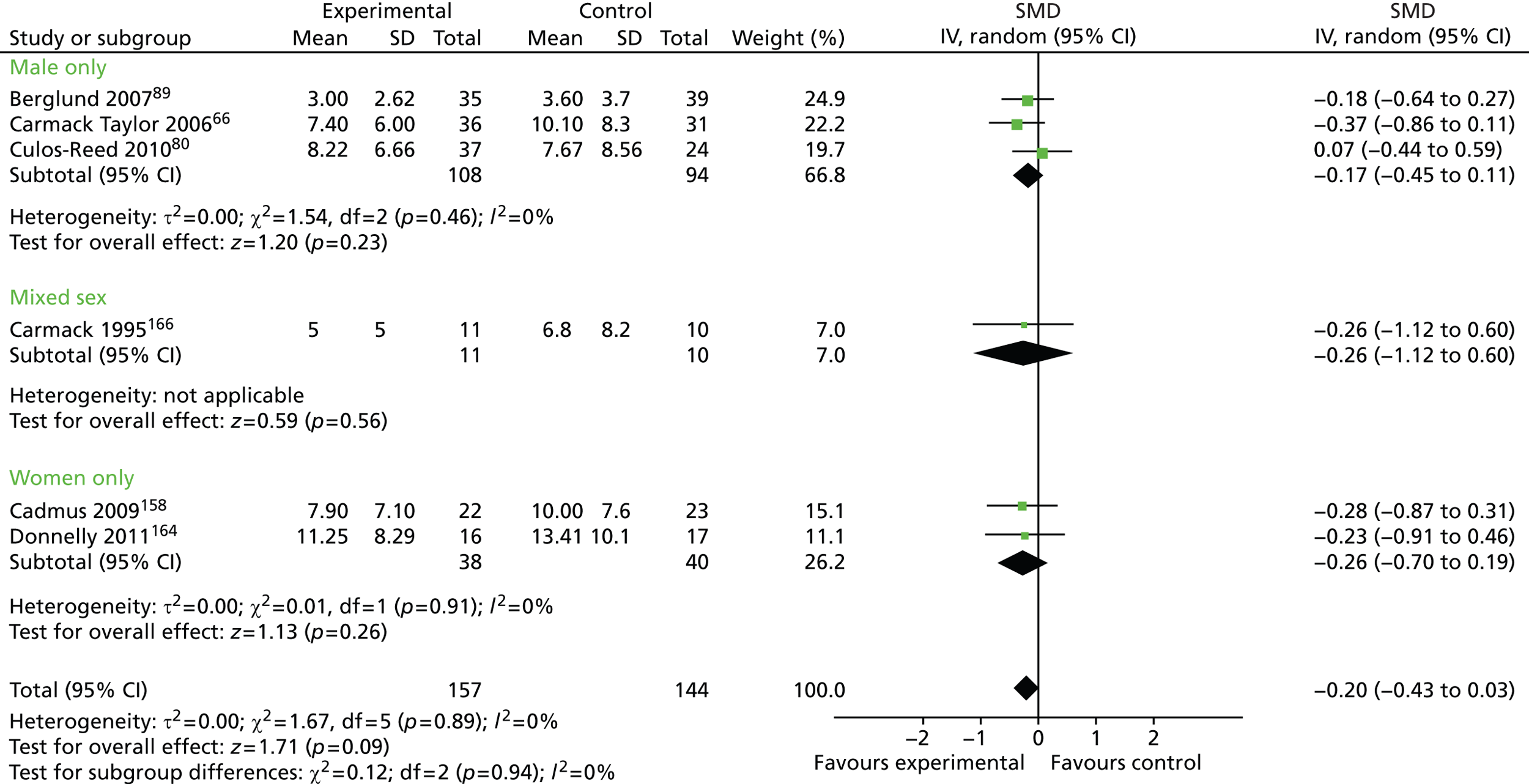
FIGURE 50.
Health-care professional monitoring and feedback: depression outcomes in male-only vs. mixed-sex and female-only groups (cancer-only plot). df, degrees of freedom; IV, inverse variance; SD, standard deviation.
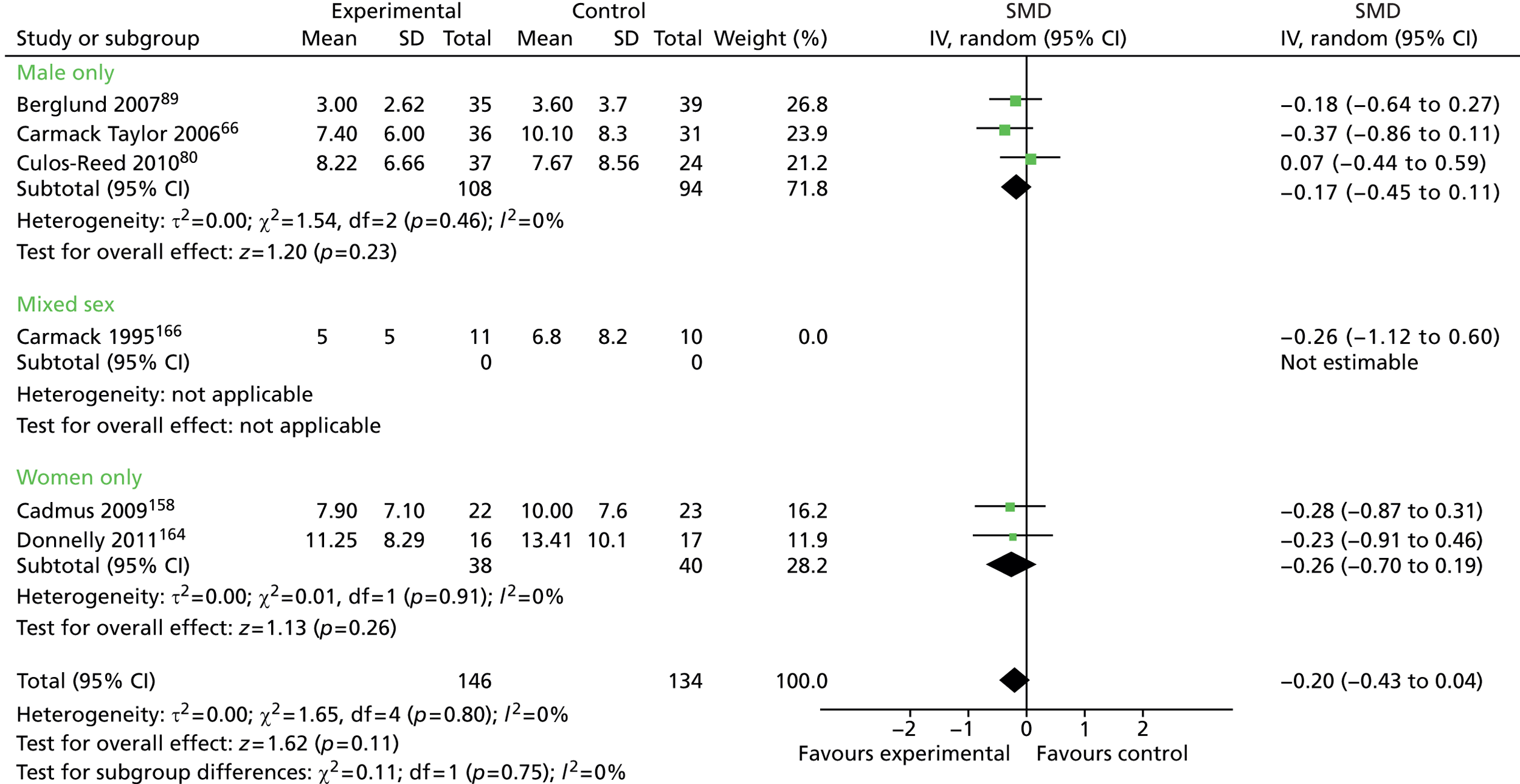
Analysis 3: male-only by intervention-type analysis
FIGURE 51.
Physical activity vs. no physical activity: HRQoL outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.

FIGURE 52.
Physical activity vs. no physical activity: depression outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
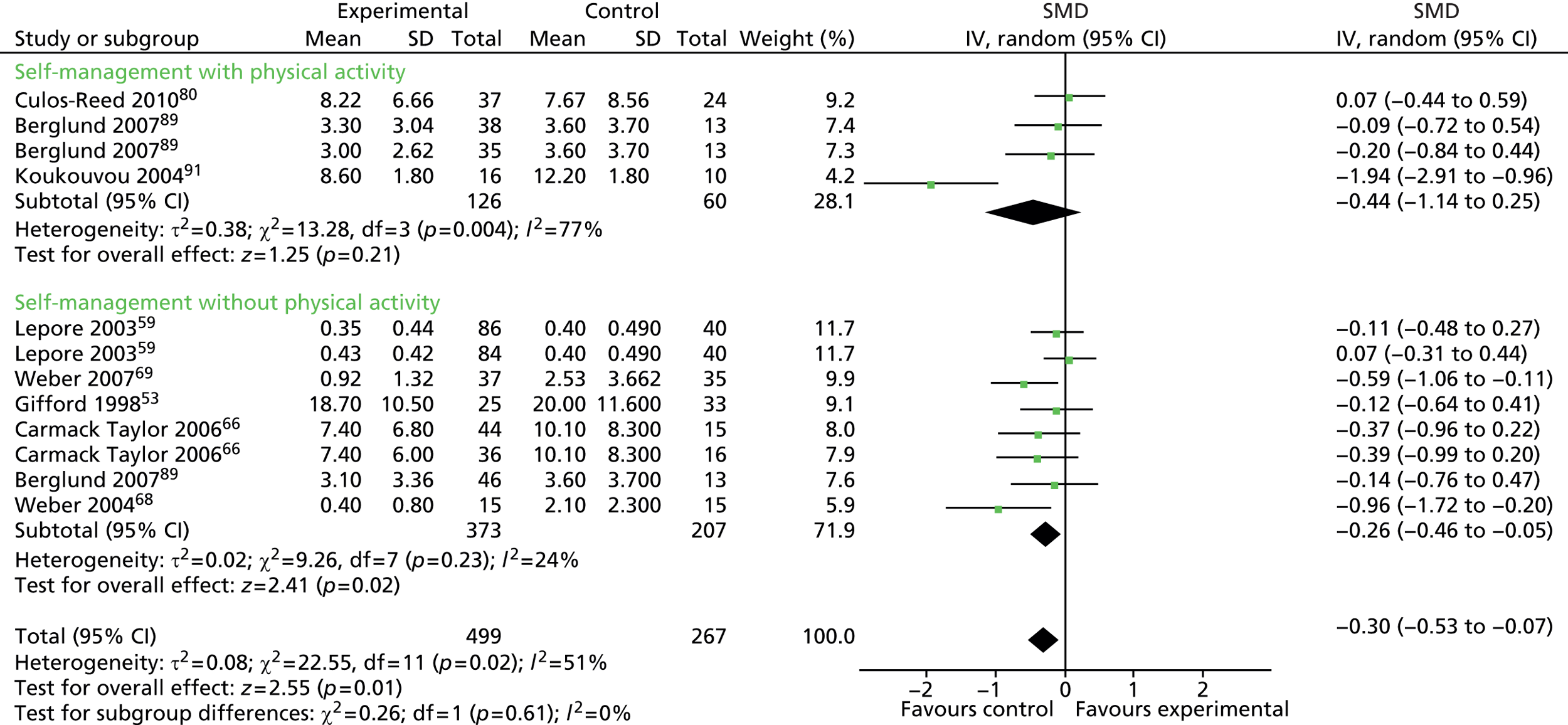
FIGURE 53.
Physical activity vs. no physical activity: anxiety outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
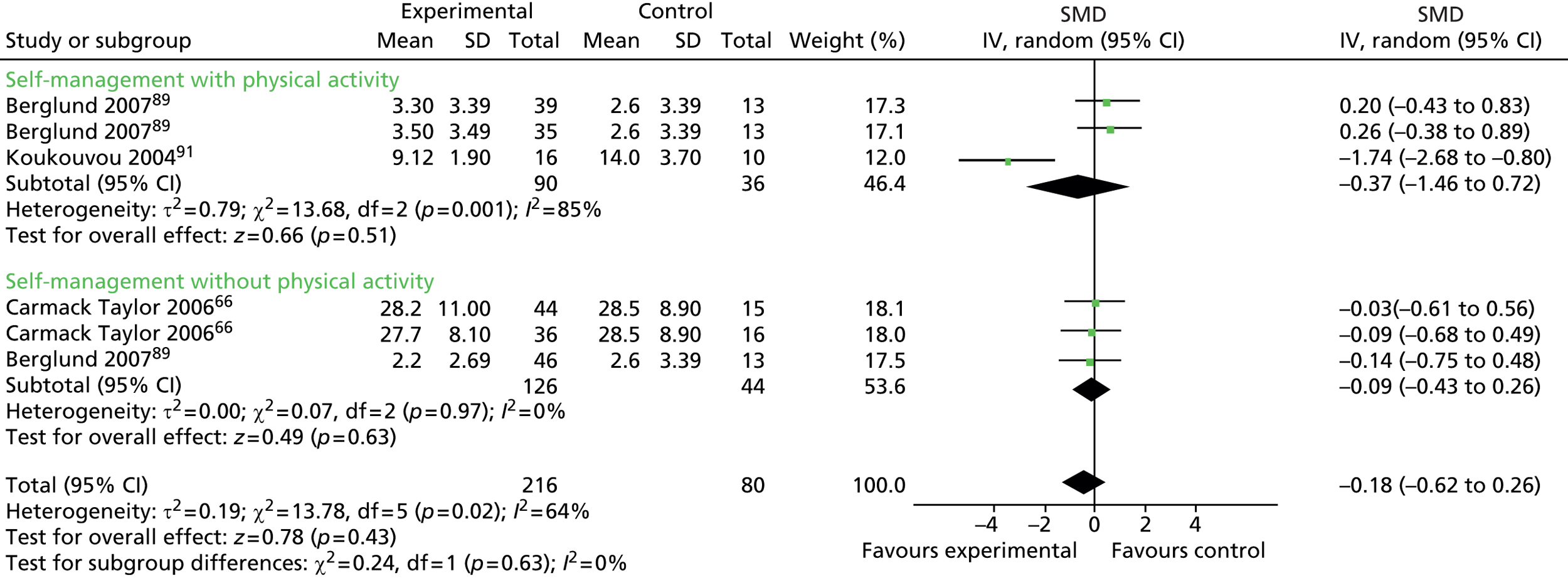
FIGURE 54.
Physical activity vs. no physical activity: fatigue outcomes. df, degrees of freedom; IV, inverse variance.
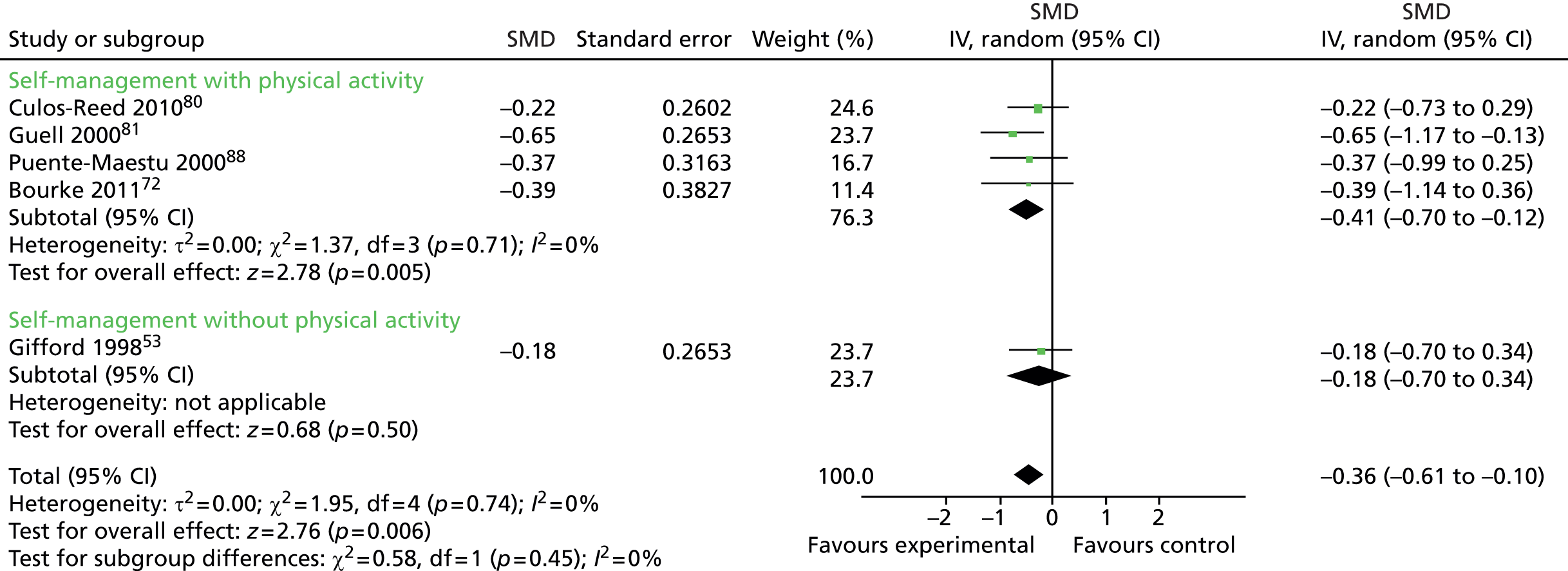
FIGURE 55.
Education vs. no education: HRQoL outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
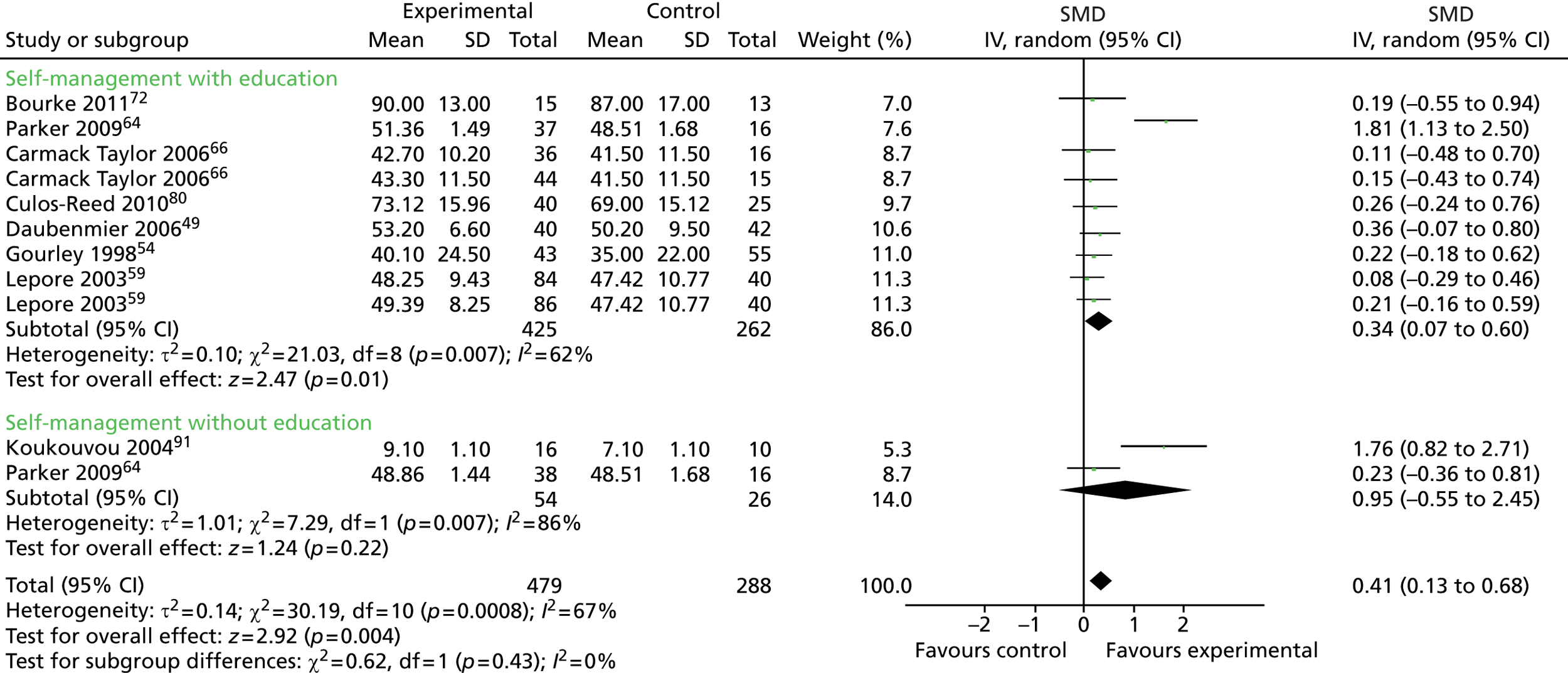
FIGURE 56.
Education vs. no education: depression outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
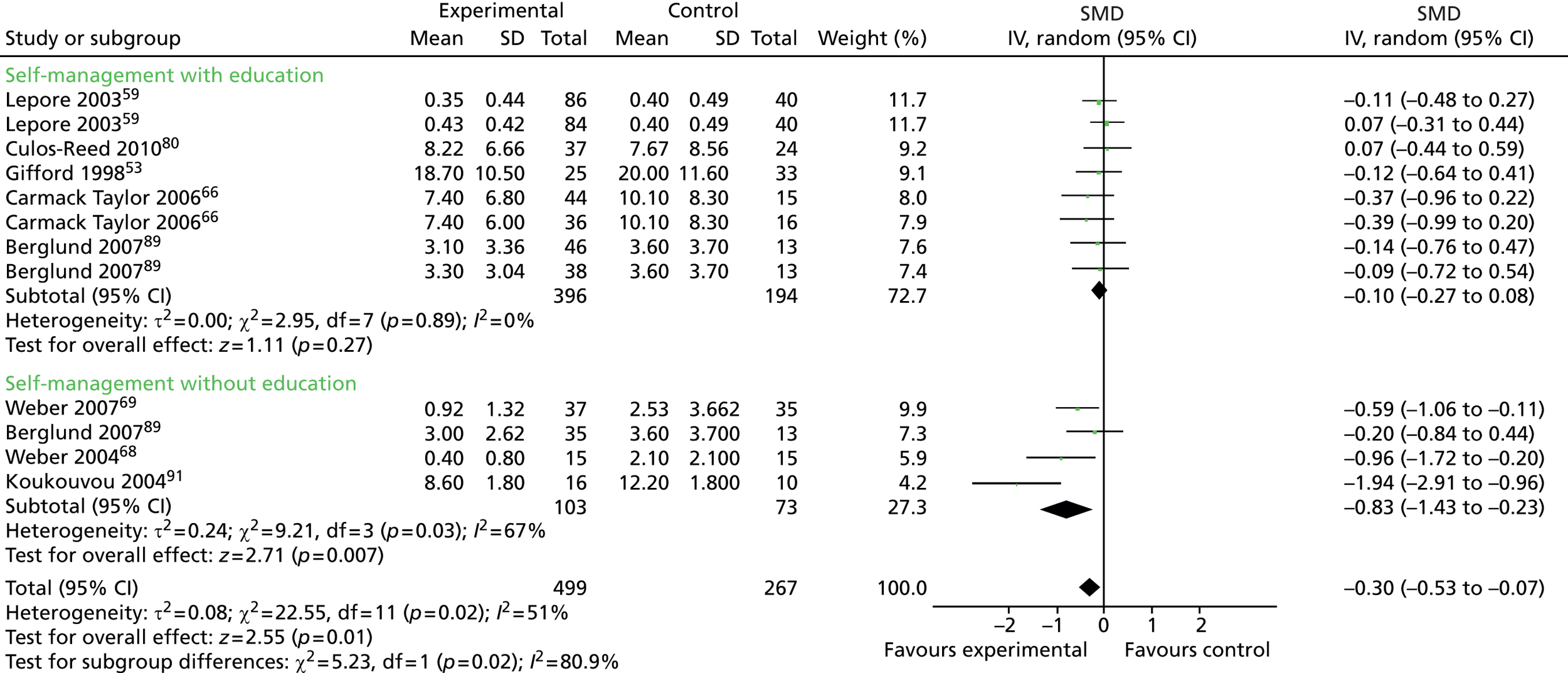
FIGURE 57.
Education vs. no education: anxiety outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
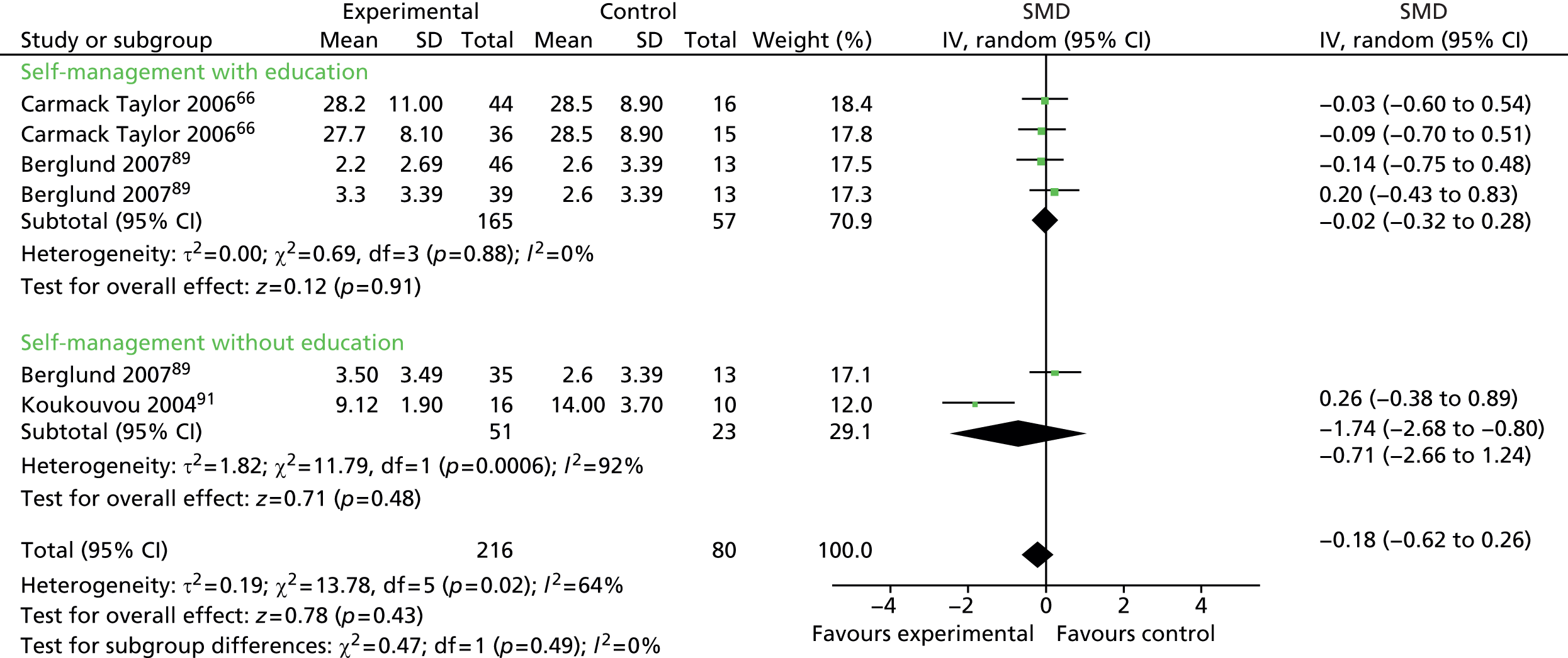
FIGURE 58.
Peer support vs. no peer support: HRQoL outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
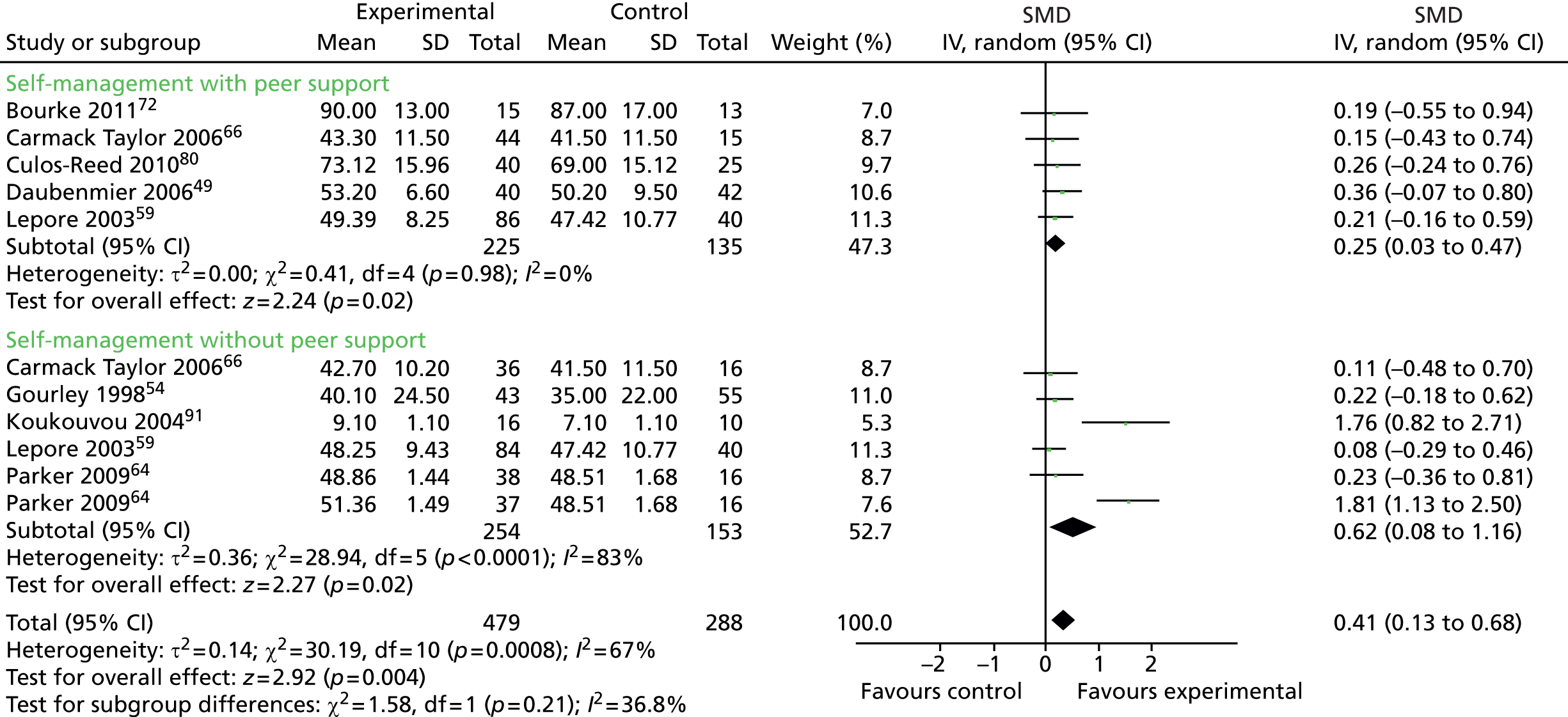
FIGURE 59.
Peer support vs. no peer support: depression outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.

FIGURE 60.
Peer support vs. no peer support: anxiety outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
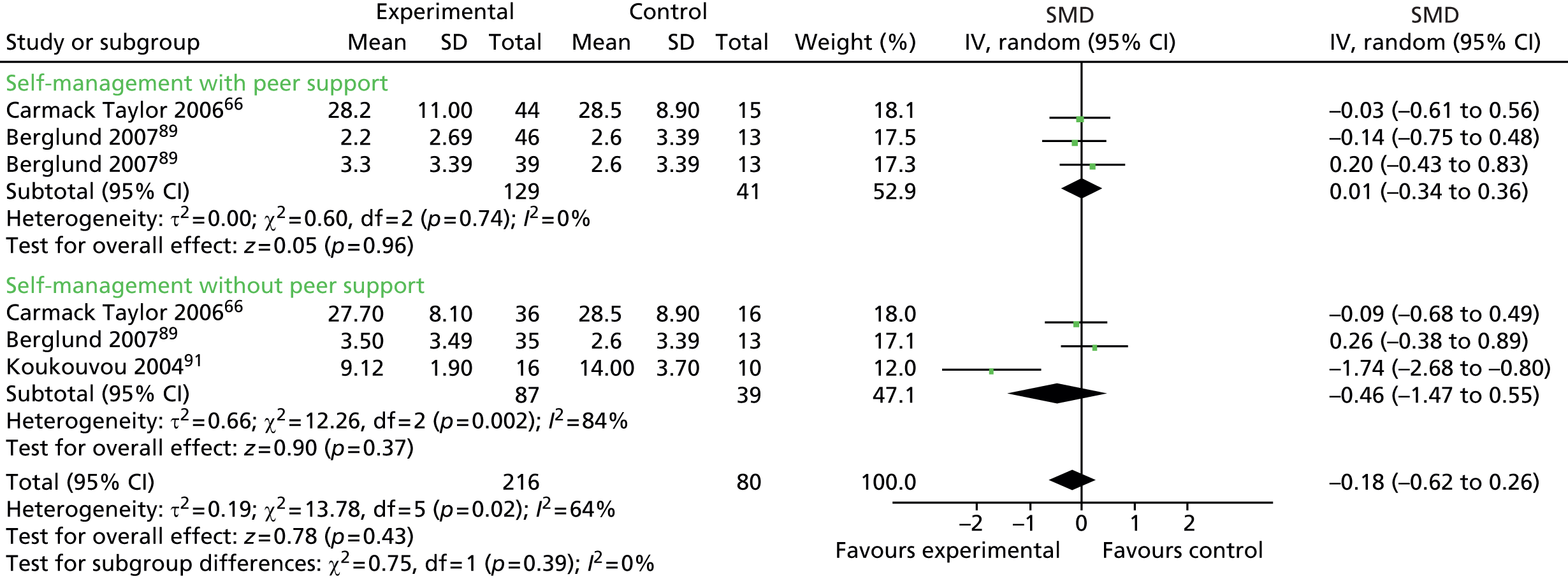
FIGURE 61.
Peer support vs. no peer support: fatigue outcomes. df, degrees of freedom; IV, inverse variance.

FIGURE 62.
Health-care professional monitoring and feedback vs. no HCP monitoring and feedback: HRQoL outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.

FIGURE 63.
Health-care professional monitoring and feedback vs. no HCP monitoring and feedback: depression outcomes. df, degrees of freedom; IV, inverse variance; SD, standard deviation.
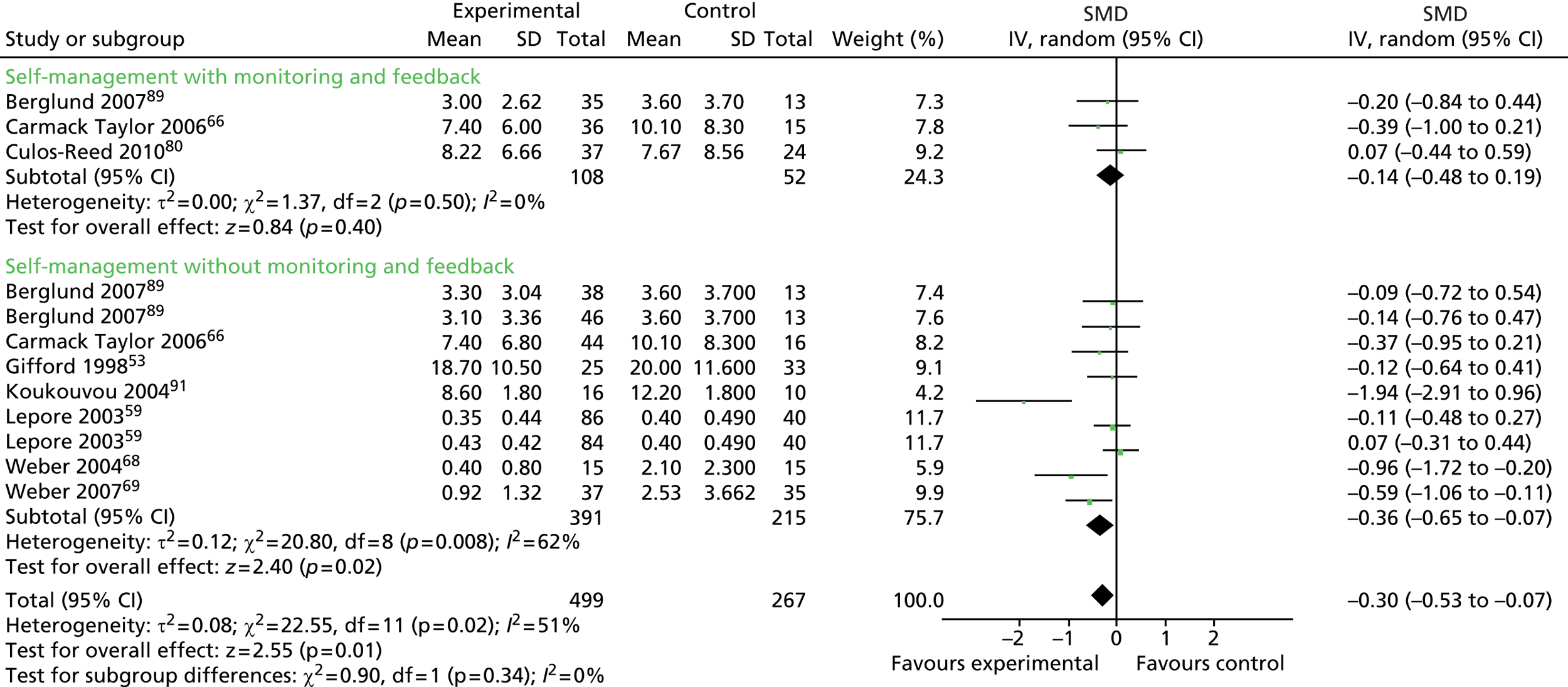
Appendix 3 Enhancing transparency in reporting the synthesis of qualitative research reporting standards
The metaethnography is summarised in Table 40, using the ENTREQ reporting standards recommended by Tong et al. 93
| No. | Item | Description |
|---|---|---|
| 1 | Aim | To identify perceptions towards, and perceived acceptability of, interventions or specific activities aimed at supporting or promoting self-management of LTCs among men of differing age, ethnicity and socioeconomic background |
| 2 | Synthesis methodology | Metaethnography was chosen because of emphasis on generating new insights and allowing synthesis across different types of qualitative research |
| 3 | Approach to searching | Pre-planned electronic search strategy complemented by checking reference lists of included studies |
| 4 | Inclusion criteria | Full details are given in Table 5. Qualitative research not restricted by study type. Adult men/mixed group with LTCs. Self-management interventions or support activities. Published 1970 onwards in English language |
| 5 | Data sources | Five electronic databases were searched in July 2013 (CINAHL, EMBASE, MEDLINE, PsycINFO and Social Science Citation Index) and reference lists were also checked |
| 6 | Electronic search strategy | The search strategy is available in Appendix 4 |
| 7 | Study-screening methods | Records initially screened on the basis of title/abstract by one reviewer (ZD). Potentially eligible studies were obtained for assessment based on full text. Full-text screening conducted by two reviewers independently (ZD, PG) |
| 8 | Study characteristics | Study characteristics are shown in Table 36 |
| 9 | Study selection results | The PRISMA flow diagram is shown in Figure 8 |
| 10 | Rationale for appraisal | Quality appraisal offered description of the literature in terms of study design, conduct and reporting, rather than forming part of the inclusion criteria |
| 11 | Appraisal items | The modified CASP132 was used to appraise quality relating to aims, design, data analysis and interpretations, and reporting |
| 12 | Appraisal process | Quality appraisal of all studies was undertaken by one reviewer (ZD). Coreviewers independently assessed quality and another reviewer (PG) resolved any disagreements |
| 13 | Appraisal results | Quality appraisal results are shown in Table 39 and Appendix 7 |
| 14 | Data extraction | Study details were extracted by one reviewer (ZD) using a pro forma and checked by a second (PG). Findings were copied verbatim into NVivo for full coding |
| 15 | Computer software | NVivo 10 |
| 16 | Number of reviewers | Reviewers comprised one lead reviewer (ZD) and five coreviewers (PG, CB, KH, LK, KM) |
| 17 | Coding | Coding was undertaken, as described by Noblit and Hare (1988)94 |
| 18 | Study comparison | Studies were grouped by broad intervention type and initially analysed in these sets, building on the analysis with each set. Both reciprocal and refutational relationships were accommodated by the approach taken |
| 19 | Derivation of themes | Third-order themes/constructs were derived inductively based on coding of all included papers. Studies were synthesised using line-of-argument synthesis to encompass similarities and contradictions between findings |
| 20 | Quotations | Quotations of participants and participant observations (first-order) and quotations of authors’ interpretations (second-order) are provided in Chapter 5 to illustrate third-order constructs |
| 21 | Synthesis output | The line of argument and its four overarching concepts are expressed in Chapter 5: need for purpose, trusted environments, value of peers, becoming an expert |
Appendix 4 Qualitative literature search
Five databases (CINAHL, EMBASE, MEDLINE, PsycINFO and Social Science Citation Index) were searched to identify qualitative studies exploring men’s perceptions of interventions aimed at the self-management of LTCs. Each of the search strategies used a combination of thesaurus and free-text terms and consisted of four sections: self-management; LTCs; men and masculinity; and a qualitative filter. The qualitative search filter was based upon the one described in the paper by Shaw et al. 98) with the addition of some further terms. A total of 8450 records were identified from the database searches. After loading into bibliographic software and deduplicating, there was a total of 6330 unique records.
Databases searched: CINAHL, EMBASE, MEDLINE, PsycINFO and Social Science Citation Index.
Cumulative Index to Nursing and Allied Health Literature
Database provider: EBSCOhost.
URL: www.ebscohost.com/biomedical-libraries/cinahl-plus-with-full-text
Date range searched: 1937 to July week 2 2013.
Search date: 16 July 2013.
Records identified: 539.
Search strategy
| Search ID# | Search terms |
|---|---|
| S25 | S22 AND S23 Published Date from: 19700101-20131231 |
| S24 | S22 AND S23 |
| S23 | LA english |
| S22 | S20 AND S21 |
| S21 | TI ( man or man’s or men or men’s or male* or masculin* or gender* or sex difference* or sex factor* ) |
| S20 | S5 AND S9 AND S19 |
| S19 | S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 |
| S18 | TX understanding* OR TX perception* OR TX perspective* OR TX meaning* OR TX belief* OR TX opinion* OR TX voice* |
| S17 | TX mixed method OR TX multi method OR TX survey OR TX ( coding or coded or codes ) OR TX framework analysis OR TX process evaluation OR TX meta synthesis OR TX meta study OR TX meta ethnograph* OR TX realist synthesis OR TX realist review OR view* |
| S16 | TX findings OR TX interview* OR MH interviews OR TX qualitative |
| S15 | TX ( (constant N1 (comparative or comparison)) ) OR TX narrative analys?s OR TX corbin* N2 strauss* OR TX glaser* N2 strauss* OR TX strauss* N2 corbin* OR TX glaser* |
| S14 | TX cluster sampl* OR TX ( theme* or thematic ) OR TX categor* OR TX observational method* OR TX field stud* OR TX focus group* OR TX questionnaire* OR TX content analysis OR TX thematic analysis OR TX constant comparative OR TX discourse analys?s OR TX ( (discourse* or discurs*) N3 analys?s ) |
| S13 | TX ( field N1 (study or studies or research) ) OR TX human science OR TX biographical method OR TX qualitative validity OR TX purposive sampl* OR TX theoretical sampl* OR TX purpos* N4 sampl* OR TX focus N1 group* OR TX ( account or accounts or unstructured or open-ended or open ended or text* or narrative* ) OR TX ( life world or life-world or conversation analys?s or personal experience* or theoretical saturation ) OR TX lived experience* OR TX life experience* |
| S12 | TX ethnonursing OR TX ethnograph* OR TX phenomenol* OR TX grounded theory OR TX ( grounded N1 (theor* or study or studies or research or analys?s) ) OR TX life stor* OR TX ( emic or etic or hermeneutic* or heuristic* or semiotic* ) OR TX data N1 saturat* OR TX participant observ* OR TX ( social construct* or postmodern* or post-structural* or post structural* or poststructural* or post modern* or post-modern* or interpret* ) OR TX ( action research or cooperative inquir* or co operative inquir* or co-operative inquir* ) OR TX ( humanistic or existential or experiential or paradigm* )TX ethnonursing OR TX ethnograph* OR TX phenomenol* OR TX grounded theory OR TX ( grounded N1 (theor* or study or studies or research or analys?s) ) OR TX life stor* OR TX ( emic or etic or hermeneutic* or heuristic* or semiotic* ) OR TX data N1 saturat* OR TX participant observ* OR TX ( social construct* or postmodern* or post-structural* or post structural* or poststructural* or post modern* or post-modern* or interpret* ) OR TX ( action research or cooperative inquir* or co operative inquir* ...Show Less |
| S11 | MH purposive sample OR MH observational methods OR MH field studies OR MH theoretical sample OR MH phenomenology OR MH phenomological research OR MH life experiences OR MH cluster sample |
| S10 | MH qualitative studies OR MH research nursing OR MH questionnaires OR MH attitudes OR MH focus groups OR MH discourse analysis OR MH content analysis OR MH ethnographic research OR MH ethnological research OR MH ethnonursing research OR MH constant comparative method OR MH qualititive validity |
| S9 | S6 OR S7 OR S8 |
| S8 | TX HIV OR TX hepatitis OR TX anxiety OR TX psychotic disorders OR TX ( (long* or chronic or long-term or long-standing or persistent or ongoing) N2 (illness* or disease* or condition*) ) |
| S7 | TX ankylosing spondylitis OR TX lupus OR TX low back pain OR TX epilepsy OR TX multiple sclerosis OR TX parkinson* disease OR TX motor neuron disease OR TX ( cancer* or neoplasm* ) OR TX inflammatory bowel disease OR TX heart disease* OR TX skin disease* OR TX chronic pain |
| S6 | TX stroke OR TX cerebrovascular accident* OR TX diabetes mellitus OR TX asthma OR TX hypertension OR TX depression OR TX dementia OR TX chronic obstructive pulmonary disease OR TX kidney disease* OR TX irritable bowel syndrome OR TX rheumatoid arthritis OR TX psoriatic arthritis |
| S5 | S1 OR S2 OR S3 OR S4 |
| S4 | TX ( (telephon* or remote or phone) N2 (follow* or support* or consult* or advice or advis* or intervention* or tain* or instruct* or assist* or educat* or inform* or monitor*) ) OR TX action plan* |
| S3 | TX self help OR TX ( group N5 (support* or advis* or advice or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information) ) OR TX ( peer N5 (support* or advis* or advice or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information) ) OR TX “expert patient*” OR TX telemedicine OR TX telecare OR TX telenurs* OR TX telemonitor* OR TX telehealth OR TX remote consultation |
| S2 | TX self assess* OR TX selfassess* OR TX self medicat* OR TX selfmedicat* OR TX self remed* OR TX selfremed* OR TX self treat* OR TX selftreat* OR TX self cure OR TX selfcure |
| S1 | TX self administration OR TX self care OR TX selfcare OR TX self manag* OR TX selfmanag* OR TX self monitor* OR TX self monitor* OR TX self help OR TX selfhelp OR TX self diagnos* OR selfdiagnos* |
EMBASE
Database provider: OvidSP.
URL: http://ovidsp.tx.ovid.com/
Date range searched: 1974 to July week 2 2013.
Search date: 16 July 2013.
Records identified: 3641.
Search strategy
-
drug self administration/ (7349)
-
self care/ (27,802)
-
(self care or selfcare).ti,ab. (12,190)
-
(self manag$ or selfmanag$).ti,ab. (10,586)
-
(self monitor$ or selfmonitor$).ti,ab. (5777)
-
(self help or selfhelp).ti,ab. (5750)
-
(self diagnos$ or selfdiagnos$ or self assess$ or selfassess$).ti,ab. (12,680)
-
self medication/ (8009)
-
(self medicat$ or selfmedicat$ or self remed$ or selfremed$).ti,ab. (3966)
-
(self treat$ or selftreat$ or self cure or selfcure).ti,ab. (1841)
-
self help/ (10,946)
-
(group adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (6528)
-
(peer adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (2905)
-
expert patient$.ti,ab. (216)
-
telemedicine/ or telehealth/ (10,429)
-
telemedicine.ti,ab. (6633)
-
telecare.ti,ab. (398)
-
telenursing.ti,ab. (79)
-
telemonitor$.ti,ab. (797)
-
telehealth.ti,ab. (1526)
-
teleconsultation/ (5403)
-
((telephon$ or remote or phone) adj2 (follow$ or support$ or consult$ or advice or advis$ or intervention$ or train$ or instruct$ or assist$ or educat$ or inform$ or monitor$)).ti,ab. (11,418)
-
Action plan$.ti,ab. (4704)
-
or/1-23 (121,561)
-
exp cerebrovascular accident/ (57,547)
-
exp Diabetes Mellitus/ (562,637)
-
exp Asthma/ (182,027)
-
exp Hypertension/ (463,753)
-
Depression/ (237,701)
-
exp Dementia/ (213,993)
-
exp lung disease/ (907,909)
-
exp kidney failure/ (220,989)
-
exp irritable colon/ (14,627)
-
exp rheumatoid arthritis/ (143,039)
-
exp psoriatic arthritis/ (9802)
-
exp ankylosing spondylitis/ (18,472)
-
exp systemic lupus erythematosus/ (63,362)
-
exp Low Back Pain/ (33,344)
-
exp Epilepsy/ (164,206)
-
exp Multiple Sclerosis/ (72,617)
-
exp Parkinson Disease/ (86,844)
-
exp Motor Neuron Disease/ (26,105)
-
exp Neoplasm/ (3,291,240)
-
exp enteritis/ (188,925)
-
exp Heart Disease/ (1,286,722)
-
exp Skin Disease/ (1,164,384)
-
exp Chronic Pain/ (29,960)
-
exp human immunodeficiency virus/ (127,466)
-
exp Hepatitis/ (207,938)
-
exp Anxiety/ (110,053)
-
exp Psychosis/ (209,438)
-
((long$ or chronic or long-term or long-standing or persistent or ongoing) adj2 (illness$ or disease$ or condition$)).ti,ab. (189,963)
-
or/25-52 (8,063,749)
-
Qualitative Research/ (20,514)
-
qualitative stud$.mp. (17,810)
-
Questionnaire/ (360,379)
-
exp Attitude/ (481,381)
-
focus group$.mp. (23,244)
-
discourse analysis.mp. (1345)
-
content analysis.mp. (12,921)
-
ethnographic research.mp. (843)
-
ethnological research.mp. (12)
-
ethnonursing research.mp. (31)
-
constant comparative method.mp. (880)
-
qualitative validity.mp. (101)
-
purposive sample.mp. (1840)
-
observational method$.mp. (1385)
-
field stud$.mp. (12,740)
-
theoretical sampl$.mp. (403)
-
phenomenology.mp. (10,872)
-
phenomenological research.mp. (282)
-
life experience$.mp. (3609)
-
cluster sampl$.mp. (4315)
-
ethnonursing.af. (90)
-
ethnograph$.mp. (6692)
-
phenomenol$.af. (19,318)
-
grounded theory.mp. (6295)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (6399)
-
life stor$.mp. (790)
-
(emic or etic or hermeneutic$ or heuristic$ or semiotic$).af. (11,669)
-
(data adj saturat$).tw. (257)
-
participant observ$.tw. (2782)
-
(social construct$ or postmodern$ or post-structural$ or post structural$ or poststructural$ or post modern$ or post-modern$ or interpret$).mp. (316,318)
-
(action research or cooperative inquir$ or co operative inquir$ or co-operative inquir$).mp. (2819)
-
(humanistic or existential or experiential or paradigm$).mp. (106,488)
-
(field adj (study or studies or research)).tw. (12,947)
-
human science.tw. (244)
-
biographical method.tw. (17)
-
qualitative validity.af. (101)
-
purposive sampl$.af. (3152)
-
theoretical sampl$.mp. (403)
-
((purpos$ adj4 sampl$) or (focus adj group$)).af. (29,569)
-
(account or accounts or unstructured or open-ended or open ended or text$ or narrative$).mp. (444,387)
-
(life world or life-world or conversation analys?s or personal experience$ or theoretical saturation).mp. (23,184)
-
lived experience$.tw. (2405)
-
life experience$.mp. (3609)
-
cluster sampl$.mp. (4315)
-
(theme$ or thematic).mp. (52,616)
-
categor$.mp. (256,510)
-
observational method$.af. (1385)
-
field stud$.mp. (12,740)
-
focus group$.af. (23,314)
-
questionnaire$.mp. (492,836)
-
content analysis.af. (12,921)
-
thematic analysis.af. (4688)
-
constant comparative.af. (1583)
-
discourse analys?s.af. (1373)
-
((discourse$ or discurs$) adj3 analys?s).tw. (1296)
-
(constant adj (comparative or comparison)).af. (2320)
-
narrative analys?s.af. (552)
-
(corbin$ adj2 strauss$).tw. (160)
-
(glaser$ adj2 strauss$).tw. (85)
-
(strauss$ adj2 corbin$).tw. (160)
-
glaser$.tw. (677)
-
or/54-114 (1,985,119)
-
findings.af. (1,487,654)
-
interview$.af. or Interviews/ (273,544)
-
qualitative.af. (155,061)
-
or/116-118 (1,820,660)
-
mixed method.mp. (1348)
-
multi method.mp. (801)
-
survey.mp. (967,244)
-
(coding or coded or codes).mp. (204,429)
-
framework analysis.mp. (515)
-
process evaluation.mp. (1563)
-
meta synthesis.mp. (182)
-
meta study.mp. (48)
-
meta ethnograph$.mp. (122)
-
realist synthesis.mp. (17)
-
realist review.mp. (40)
-
view$.mp. (401,299)
-
understanding$.mp. (510,737)
-
perception$.mp. (254,944)
-
perspective$.mp. (205,022)
-
meaning$.mp. (93,335)
-
belief$.mp. (60,452)
-
opinion$.mp. (93,410)
-
voice$.mp. (32,964)
-
or/120-138 (2,518,653)
-
115 or 119 or 139 (5,239,196)
-
24 and 53 and 140 (27,334)
-
(man or man’s or men or men’s or male$ or masculin$ or gender$ or sex difference$ or sex factor$).ti,ab. (1,749,636)
-
141 and 142 (3926)
-
limit 143 to (english language and yr=“1970 “Current”) (3641)
MEDLINE
Database provider: OvidSP.
URL: http://ovidsp.tx.ovid.com/
Date range searched: 1946 to July week 2 2013.
Search date: 16 July 2013.
Records identified: 2132.
Search strategy
-
self administration/ (9541)
-
self care/ (23,209)
-
(self care or selfcare).ti,ab. (9380)
-
(self manag$ or selfmanag$).ti,ab. (7782)
-
(self monitor$ or selfmonitor$).ti,ab. (4239)
-
(self help or selfhelp).ti,ab. (4315)
-
(self diagnos$ or selfdiagnos$ or self assess$ or selfassess$).ti,ab. (9064)
-
self medication/ (3960)
-
(self medicat$ or selfmedicat$ or self remed$ or selfremed$).ti,ab. (2585)
-
(self treat$ or selftreat$ or self cure or selfcure).ti,ab. (1376)
-
self help groups/ (7756)
-
(group adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (4288)
-
(peer adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (2289)
-
expert patient$.ti,ab. (150)
-
Telemedicine/ (10,717)
-
telemedicine.ti,ab. (5408)
-
telecare.ti,ab. (323)
-
telenursing.ti,ab. (76)
-
telemonitor$.ti,ab. (531)
-
telehealth.ti,ab. (1335)
-
Remote Consultation/ (3542)
-
((telephon$ or remote or phone) adj2 (follow$ or support$ or consult$ or advice or advis$ or intervention$ or train$ or instruct$ or assist$ or educat$ or inform$ or monitor$)).ti,ab. (8392)
-
Action plan$.ti,ab. (3326)
-
or/1-23 (97,058)
-
exp Stroke/ (82,103)
-
exp Diabetes Mellitus/ (312,012)
-
exp Asthma/ (107,810)
-
exp Hypertension/ (208,641)
-
Depression/ (74,560)
-
Depressive Disorder/ (58,515)
-
exp Dementia/ (119,030)
-
exp Pulmonary Disease, Chronic Obstructive/ (23,481)
-
exp Renal Insufficiency, Chronic/ (81,289)
-
exp Irritable Bowel Syndrome/ (4129)
-
exp Arthritis, Rheumatoid/ (100,444)
-
exp Arthritis, Psoriatic/ (3671)
-
exp Spondylitis, Ankylosing/ (11,614)
-
exp Lupus Erythematosus, Systemic/ (49,044)
-
exp Low Back Pain/ (14,032)
-
exp Epilepsy/ (127,011)
-
exp Multiple Sclerosis/ (43,404)
-
exp Parkinson Disease/ (46,577)
-
exp Motor Neuron Disease/ (19,431)
-
exp Neoplasms/ (256,0854)
-
exp Inflammatory Bowel Diseases/ (59,048)
-
exp Heart Diseases/ (879,192)
-
exp Skin Diseases/ (810,575)
-
exp Chronic Pain/ (2283)
-
exp HIV/ (87,939)
-
exp Hepatitis/ (132,754)
-
exp Anxiety/ (54,417)
-
exp Psychotic Disorders/ (37,842)
-
((long$ or chronic or long-term or long-standing or persistent or ongoing) adj2 (illness$ or disease$ or condition$)).ti,ab. (141,127)
-
25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 (5,453,163)
-
Qualitative Research/ (18,450)
-
Nursing Methodology Research/ (15,380)
-
Questionnaires/ (297,017)
-
exp Attitude/ (263,813)
-
Focus Groups/ (16,627)
-
discourse analysis.mp. (774)
-
content analysis.mp. (9908)
-
ethnographic research.mp. (470)
-
ethnological research.mp. (6)
-
ethnonursing research.mp. (27)
-
constant comparative method.mp. (787)
-
qualitative validity.mp. (6)
-
purposive sample.mp. (1504)
-
observational method$.mp. (392)
-
field stud$.mp. (9140)
-
theoretical sampl$.mp. (280)
-
phenomenology.mp. (4471)
-
phenomenological research.mp. (246)
-
life experience$.mp. (2741)
-
cluster sampl$.mp. (3430)
-
or/55-74 (540,562)
-
ethnonursing.af. (86)
-
ethnograph$.mp. (5453)
-
phenomenol$.af. (12,573)
-
grounded theory.mp. (5169)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (5241)
-
life stor$.mp. (581)
-
(emic or etic or hermeneutic$ or heuristic$ or semiotic$).af. (9134)
-
(data adj saturat$).tw. (142)
-
participant observ$.tw. (2397)
-
(social construct$ or postmodern$ or post-structural$ or post structural$ or poststructural$ or post modern$ or post-modern$ or interpret$).mp. (342,198)
-
(action research or cooperative inquir$ or co operative inquir$ or co-operative inquir$).mp. (2217)
-
(humanistic or existential or experiential or paradigm$).mp. (86,385)
-
(field adj (study or studies or research)).tw. (9888)
-
human science.tw. (208)
-
biographical method.tw. (11)
-
qualitative validity.af. (6)
-
purposive sampl$.af. (2502)
-
theoretical sampl$.mp. (280)
-
((purpos$ adj4 sampl$) or (focus adj group$)).af. (28,237)
-
(account or accounts or unstructured or open-ended or open ended or text$ or narrative$).mp. (356,979)
-
(life world or life-world or conversation analys?s or personal experience$ or theoretical saturation).mp. (10,739)
-
lived experience$.tw. (1989)
-
life experience$.mp. (2741)
-
cluster sampl$.mp. (3430)
-
(theme$ or thematic).mp. (41,510)
-
categor$.mp. (192,404)
-
observational method$.af. (392)
-
field stud$.mp. (9140)
-
focus group$.af. (23,521)
-
questionnaire$.mp. (427,353)
-
content analysis.af. (9908)
-
thematic analysis.af. (3198)
-
constant comparative.af. (1400)
-
discourse analys?s.af. (801)
-
((discourse$ or discurs$) adj3 analys?s).tw. (1040)
-
(constant adj (comparative or comparison)).af. (2007)
-
narrative analys?s.af. (439)
-
(corbin$ adj2 strauss$).tw. (121)
-
(glaser$ adj2 strauss$).tw. (74)
-
(strauss$ adj2 corbin$).tw. (121)
-
glaser$.tw. (604)
-
or/76-116 (1,392,027)
-
findings.af. (1,243,335)
-
interview$.af. or Interviews/ (232,178)
-
qualitative.af. (114,877)
-
or/118-120 (1,508,150)
-
mixed method.mp. (1071)
-
multi method.mp. (645)
-
survey.mp. (298,289)
-
(coding or coded or codes).mp. (172,882)
-
framework analysis.mp. (377)
-
process evaluation.mp. (1327)
-
meta synthesis.mp. (162)
-
meta study.mp. (32)
-
meta ethnograph$.mp. (100)
-
realist synthesis.mp. (21)
-
realist review.mp. (40)
-
view$.mp. (304,920)
-
understanding$.mp. (424,156)
-
perception$.mp. (281,912)
-
perspective$.mp. (159,128)
-
meaning$.mp. (71,143)
-
belief$.mp. (46,914)
-
opinion$.mp. (71,790)
-
voice$.mp. (28,191)
-
or/122-140 (1,641,011)
-
75 or 117 or 121 or 141 (3,834,172)
-
24 and 54 and 142 (17,068)
-
(man or man’s or men or men’s or male$ or masculin$ or gender$ or sex difference$ or sex factor$).ti,ab. (1,303,641)
-
143 and 144 (2280)
-
limit 145 to (english language and yr=“1970 “Current”) (2132)
PsycINFO
Database provider: OvidSP.
URL: http://ovidsp.tx.ovid.com/
Date range searched: 1967 to July week 2 2013.
Search date: 16 July 2013.
Records identified: 944.
Search strategy
-
drug self administration/ (1324)
-
self care skills/ (3177)
-
(self care or selfcare).ti,ab. (5161)
-
(self manag$ or selfmanag$).ti,ab. (5119)
-
(self monitor$ or selfmonitor$).ti,ab. (4407)
-
(self help or selfhelp).ti,ab. (6207)
-
(self diagnos$ or selfdiagnos$ or self assess$ or selfassess$).ti,ab. (5453)
-
self medication/ or self monitoring/ (2802)
-
(self medicat$ or selfmedicat$ or self remed$ or selfremed$).ti,ab. (1114)
-
(self treat$ or selftreat$ or self cure or selfcure).ti,ab. (319)
-
self help techniques/ (3276)
-
(group adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (5277)
-
(peer adj (support$ or advice or advis$ or monitor$ or intervention$ or train$ or instruction or consult$ or assist$ or education or educate or information)).ti,ab. (2931)
-
expert patient$.ti,ab. (69)
-
Telemedicine/ (2131)
-
telemedicine.ti,ab. (787)
-
telecare.ti,ab. (111)
-
telenursing.ti,ab. (18)
-
telemonitor$.ti,ab. (73)
-
telehealth.ti,ab. (511)
-
((telephon$ or remote or phone) adj2 (follow$ or support$ or consult$ or advice or advis$ or intervention$ or train$ or instruct$ or assist$ or educat$ or inform$ or monitor$)).ti,ab. (2739)
-
Action plan$.ti,ab. (1806)
-
or/1-22 (45,673)
-
exp cerebrovascular accidents/ (12,349)
-
exp Diabetes Mellitus/ (3472)
-
exp Asthma/ (3416)
-
exp Hypertension/ (5147)
-
exp affective disorders/ (110,959)
-
exp Dementia/ (48,408)
-
exp chronic obstructive pulmonary disease/ (673)
-
exp kidney diseases/ (1321)
-
exp Irritable Bowel Syndrome/ (738)
-
exp rheumatoid arthritis/ (1478)
-
exp Lupus/ (600)
-
exp Back Pain/ (2625)
-
exp Epilepsy/ (17,744)
-
exp Multiple Sclerosis/ (7225)
-
exp Parkinson’s Disease/ (12,717)
-
exp Motor Neurons/ (2913)
-
exp Neoplasms/ (31,677)
-
exp Heart Disorders/ (9651)
-
exp Skin Disorders/ (3112)
-
exp Chronic Pain/ (8854)
-
exp HIV/ (29,662)
-
exp Hepatitis/ (1712)
-
exp Anxiety/ (46,583)
-
exp Psychosis/ (84,763)
-
((long$ or chronic or long-term or long-standing or persistent or ongoing) adj2 (illness$ or disease$ or condition$)).ti,ab. (21,861)
-
or/24-48 (420,500)
-
Qualitative Research/ (3669)
-
qualitative study.md. (107,795)
-
Questionnaires/ (12,709)
-
exp Attitudes/ (249,245)
-
Focus Group.md. (9180)
-
discourse analysis.mp. (7586)
-
content analysis.mp. (14,282)
-
ethnographic research.mp. (1618)
-
ethnological research.mp. (5)
-
ethnonursing research.mp. (9)
-
constant comparative method.mp. (1023)
-
qualitative validity.mp. (6)
-
purposive sample.mp. (1245)
-
observational method$.mp. (673)
-
field stud$.mp. (5508)
-
theoretical sampl$.mp. (302)
-
phenomenology.mp. (13,641)
-
phenomenological research.mp. (758)
-
life experience$.mp. (21,923)
-
cluster sampl$.mp. (760)
-
or/50-69 (399,632)
-
ethnonursing.af. (94)
-
ethnograph$.mp. (16,790)
-
phenomenol$.af. (60,727)
-
grounded theory.mp. (8374)
-
(grounded adj (theor$ or study or studies or research or analys?s)).af. (28,264)
-
life stor$.mp. (2307)
-
(emic or etic or hermeneutic$ or heuristic$ or semiotic$).af. (52,465)
-
(data adj saturat$).tw. (85)
-
participant observ$.tw. (5536)
-
(social construct$ or postmodern$ or post-structural$ or post structural$ or poststructural$ or post modern$ or post-modern$ or interpret$).mp. (141,504)
-
(action research or cooperative inquir$ or co operative inquir$ or co-operative inquir$).mp. (4635)
-
(humanistic or existential or experiential or paradigm$).mp. (88,709)
-
(field adj (study or studies or research)).tw. (6759)
-
human science.tw. (483)
-
biographical method.tw. (35)
-
qualitative validity.af. (33)
-
purposive sampl$.af. (2080)
-
theoretical sampl$.mp. (302)
-
((purpos$ adj4 sampl$) or (focus adj group$)).af. (31,180)
-
(account or accounts or unstructured or open-ended or open ended or text$ or narrative$).mp. (214,353)
-
(life world or life-world or conversation analys?s or personal experience$ or theoretical saturation).mp. (9380)
-
lived experience$.tw. (5330)
-
life experience$.mp. (21,923)
-
cluster sampl$.mp. (760)
-
(theme$ or thematic).mp. (71,267)
-
categor$.mp. (109,511)
-
observational method$.af. (1149)
-
field stud$.mp. (5508)
-
focus group$.af. (30,463)
-
questionnaire$.mp. (233,969)
-
content analysis.af. (27,088)
-
thematic analysis.af. (5170)
-
constant comparative.af. (2080)
-
discourse analys?s.af. (12,824)
-
((discourse$ or discurs$) adj3 analys?s).tw. (5294)
-
(constant adj (comparative or comparison)).af. (2769)
-
narrative analys?s.af. (3473)
-
(corbin$ adj2 strauss$).tw. (380)
-
(glaser$ adj2 strauss$).tw. (281)
-
(strauss$ adj2 corbin$).tw. (380)
-
glaser$.tw. (953)
-
or/71-111 (888,147)
-
findings.af. (574,946)
-
interview$.af. or Interviews/ (348,635)
-
qualitative.af. (186,987)
-
or/113-115 (870,736)
-
mixed method.mp. (2306)
-
multi method.mp. (1283)
-
survey.mp. (148,155)
-
(coding or coded or codes).mp. (36,178)
-
framework analysis.mp. (234)
-
process evaluation.mp. (849)
-
meta synthesis.mp. (132)
-
meta study.mp. (31)
-
meta ethnograph$.mp. (80)
-
realist synthesis.mp. (9)
-
realist review.mp. (11)
-
view$.mp. (202,519)
-
understanding$.mp. (224,811)
-
perception$.mp. (314,085)
-
perspective$.mp. (182,033)
-
meaning$.mp. (104,768)
-
belief$.mp. (87,978)
-
opinion$.mp. (31,556)
-
voice$.mp. (24,191)
-
or/117-135 (1,034,662)
-
70 or 112 or 116 or 136 (1,924,978)
-
23 and 49 and 137 (6875)
-
(man or man’s or men or men’s or male$ or masculin$ or gender$ or sex difference$ or sex factor$).ti,ab. (470,427)
-
138 and 139 (1010)
-
limit 140 to (english language and yr=“1970 “Current”) (944)
Social Science Citation Index
Database provider: Web of Science.
URL: http://ip-science.thomsonreuters.com/cgi-bin/jrnlst/jloptions.cgi?PC=SS
Date range searched: 1900 to July 2013.
Search date: 16 July 2013.
Records identified: 2023.
Search strategy
TS=(self administration OR self care OR selfcare OR selfmanag* OR self manag* onitor* OR selfmonitor* OR self help OR selfhelp OR self diagnos* OR selfdiagnos* OR self assess* OR selfassess*) OR TS=(self medicat* OR selfmedicat* OR self remed* OR selfremed* OR self treat* OR selftreat*) OR TS=(self cure OR selfcure) OR TS=(group NEAR (support* or advice or advis* or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information)) OR TS=(peer NEAR (support* or advice or advis* or monitor* or intervention* or train* or instruction or consult* or assist* or education or educate or information)) OR TS=(“expert patient*” or “action plan*”) OR TS=(telemedicine OR telecare OR telenursing. OR telemonitor* OR telehealth) OR TS=((telephon* or remote or phone) NEAR (follow* or support* or consult* or advice or advis* or intervention* or train* or instruct* or assist* or educat* or inform* or monitor*))
TS=(stroke OR diabetes OR asthma OR hypertension OR depression OR dementia OR “chronic obstructive pulmonary disease”) OR TS=(“Renal Insufficiency” OR “irritable bowel syndrome” OR “rheumatoid arthritis” OR “psoriatic arthritis”) OR TS=(“ankylosing spondylitis” OR lupus OR “low back pain” OR epilepsy OR “multiple sclerosis” OR “parkinson* disease” OR “motor neuron disease”) OR TS=(neoplasms OR cancer OR “inflammatory bowel disease*” OR “heart disease*” OR “skin disease*” OR “chronic pain”) OR TS=(HIV OR hepatitis OR anxiety OR psychosis OR “psychotic disorder*”) OR TS=((long* OR chronic OR long-term OR long-standing OR persistent OR ongoing) NEAR (illness* or disease* or condition*))
TS=(“Qualitative Research” OR “qualitative stud*” OR “nursing research methodology” OR questionnaire OR attitude OR “focus groups” OR “discourse analysis”) OR TS=(content analysis” OR “ethnographic research” OR “ethnological research” OR “ethnonursing research” OR “constant comparative method” OR “qualitative validity”) OR TS=(“purposive sampl*” OR “observational research” OR “field stud*” OR “theoretical sampl*” OR phenomenology OR “phenomenological research”) OR TS=(“life experiences” OR “cluster sample*” OR ethnonursing OR ethnograph* OR phenomenol* OR “grounded theor*” OR “grounded stud*” OR “grounded research” OR “grounded analys*”) OR TS=(“life stor*” OR emic OR etic OR hermeneutic* OR heuroistic* OR semiotic* OR “data saturat*” OR “participant observ*” OR “social construct*” OR postmodern* OR “post structural*”) OR TS=(interpret* OR “action research” OR “cooperative inquir*” OR humanistic OR existential OR paradigm* OR “field stud* OR “field research” OR “human science”) OR TS=(“biographical method*” OR “qualitative validity” OR “purposive sampl*” OR “open-ended account*” OR “unstructured account*” OR narrative* OR “life world” OR “conversation analys*” OR “theoretical saturation”) OR TS=(“lived experience*” OR “life experience*” OR theme OR “thematic analys*” OR “constant comparative” OR discurs*) OR TS=((corbin* NEAR strauss*) OR (strauss* NEAR corbin*) OR (glaser* NEAR strauss*) OR strauss) OR TS=(findings OR interview* OR qualitative) OR TS=(“mixed method” OR “multi method” OR survey OR codes OR coding OR coded OR “framework analysis” OR “process evaluation” OR “meta synthesis” OR “meta study” OR “meta ethnograph*” OR “realist synthes*” OR “realist review”) OR TS=(view* OR understanding* OR perception* OR perspective* OR meaning* OR belief* OR meaning* OR voice
TI=(man or man’s or men or men’s or male* or masculin* or gender* or “sex difference*” or “sex factor*”)
#1 AND #2 AND #3 AND #4 Timespan 1970-2013
Appendix 5 Behavioural change techniques classification for qualitative studies
| Study (first author, date) | Description | Behaviour(s) being targeted | BCT classification |
|---|---|---|---|
| Adamsen 2001207 | Group programme involving physical activity and keynote speakers; structured as 13 2-hour sessions over 16 weeks; led by health professionals (oncology and physiotherapy) at a hospital facility; developed for men with cancer | Physical activity | 1.1 Goal-setting (behaviour): physical activity is expected at classes but there is no explicit reference to goal-setting 3.1 Social support: suggested by participant experiences, but not part of the intervention description 4.1 Instruction on how to perform a behaviour: exercise undertaken in class setting 6.1 Demonstration of the behaviour: exercise undertaken in class setting 6.2 Social comparison: suggested by participant experiences (‘comradeship’) 6.3 Information about others’ approval – suggested by participant experiences (‘comradeship’) 8.1 Behavioural practice/rehearsal: exercise undertaken in class setting 13.4 Valued self-identity: suggested by participant experiences 13.5 Identity associated with changed behaviour: suggested by participant experiences Note: 5.1, 5.3 and 5.6 not coded because information concerns consequences of LTC, not behaviour change |
| Baird 2001134 | Cardiac rehabilitation programme involving supervised exercise (including cardiac monitoring), assistance with medication, education on stress management, diet and other health behaviours; led by professional. Phase II lasts 4 weeks; Phase III lasts 4 months; Phase IV involves exercise prescription and open-ended use of cardiac therapy facility | Physical activity, medication taking, stress management, ‘lifestyle modification’, smoking cessation, diet modification’ | 2 Feedback and monitoring: cardiac monitoring but unclear whether or not feedback given; therefore unknown if 2.4–2.7 4.1 Instruction on how to perform a behaviour: supervised exercise 6.1 Demonstration of the behaviour: supervised exercise 8.1 Behavioural practice/rehearsal: supervised exercise (unclear how much practice) 11.2 Reduce negative emotions: stress management, although not described as being in relation to the behaviours Note: limited information on how medication is ‘assisted’ |
| Barlow 2009103 | Group programme involving education, group discussion, skills training, goal-setting, problem-solving, role play, and reporting back on progress; structured as 6 weekly 2-hour sessions; led by trained lay tutors who have LTC, held in community settings; developed for any LTC | Exercise, nutrition, pain management, relaxation techniques, psychological health, communication with family and health professionals, goal-setting | 1.1 Goal-setting (behaviour) 1.2 Problem-solving 1.3 Goal-setting (outcome) 2.2 and 2.7 Feedback on behaviour and outcome: participants report back to group on progress with goals, which presumably involves feedback 2.3 and 2.4 Self-monitoring of behaviour and outcome: participants document progress 4.1 Instruction on how to perform a behaviour: skills training 5.1 Information about health consequences (possibly 5.3, 5.6): ‘lecturettes’, although not explicit if this is about behaviour change 6.1 Demonstration of the behaviour: role play and mastery experience 6.2 Social comparison: reporting progress to group probably involves this 6.3 Information about others’ approval: reporting progress to group probably involves this 10.4 Social reward: given group feedback on progress |
| Barlow 2009102 | |||
| Bourke 2012209 | Group programme involving supervised physical activity, self-directed physical activity, healthy eating group seminars and nutrition advice pack; structured as twice-weekly supervised exercise for the first 6 weeks and weekly for the next 6 weeks, with 15- to 20-minute seminars every fortnight; supervised by ‘exercise specialists’ at a university rehabilitation suite; developed for men with prostate cancer | Exercise, nutrition/diet | 1.1 Goal-setting (behaviour): specified intensity of physical activity 1.4 Action planning: including planned duration 3.1 Social support: explored what was available 4.1 Instruction on how to perform a behaviour: skills training 5.1 Information about health consequences (possibly 5.3, 5.6): ‘small group healthy eating seminars’ 6.1 Demonstration of the behaviour: skills training 8.1 Behavioural practice/rehearsal: skills training, practice 12 Antecedents: discussed how to incorporate into daily life but detail not reported; therefore unknown which BCTs apply 12.5 Adding objects to the environment: nutrition pack |
| Chambers 2012210 | Group programme involving mindfulness-based cognitive therapy, including education, skills training, handbook, audio CD and self-led home-based practice; structured as eight weekly 2-hour sessions and optional extended practice session; led by psychologist; developed for cancer patients | Focus is 11.2, reducing negative emotions, via acceptance-based mindfulness | 1.1 Goal-setting (behaviour): pleasant activity scheduling 1.4 Action planning: pleasant activity scheduling 1.8 Behavioural contract: pleasant activity scheduling 3.1 Social support: group processes 4.1 Instruction on how to perform a behaviour: skills training 6.1 Demonstration of the behaviour: skills training in class 6.2 Social comparison: group processes 8.1 Behavioural practice/rehearsal: skills training, practice encouraged 8.3 Habit formation: repetition to build confidence 11.2 Reduce negative emotions: targeted through mindfulness 12.5 Adding objects to the environment: self-help materials including CD which provided the ‘necessary sounds’ 15 Self-belief: unclear if repetition to build confidence should be coded here |
| Eldh 2006135 | Nurse-led clinic involving medication management and education about the condition, its management and health behaviours; held at a hospital outpatient clinic | Limited detail; possibly medication taking, physical activity, diet, smoking cessation, reducing alcohol consumption | 1.1 Goal-setting (behaviour): e.g. use stairs instead of lift 2 Feedback and monitoring likely to be included but details not reported; therefore unknown which BCTs apply 5.1 Information about health consequences: assumed to include about behaviours as well as LTC and treatment side effects and dietary advice |
| Ferrand 2008218 | Group physical activity including exercise classes, groups and events; organised by a patients’ association (Move for Health); activities available throughout the week on an ongoing basis; led by patients and sometimes cosupervised by ‘medico-sporting educators’ | Physical activity | 1.1 Goal-setting (behaviour): e.g. ‘realistic goals’ (although unclear how these were set) 3.1 Social support: community group 6.2 Social comparison: participants report potential for ‘ridicule’ and that friendship is ‘additional motivation’ 6.3 Information about others’ approval: participants report potential for ‘ridicule’ and that friendship is ‘additional motivation’ 9.1 Credible source: participants describe as ‘trustworthy’ 12.5 Adding objects to the environment: classes are available |
| Galdas 2012280 | Cardiac rehabilitation programme involving education on the condition and health behaviours using classes, workshops and individual counselling sessions; held weekly at a hospital facility | ‘Lifestyle’: presumably includes physical activity and diet | 3.1 Social support: classes and workshops and counselling 5.1 Information about health consequences (possibly 5.3, 5.6): health and lifestyle education |
| Kronenwetter 2005213 | Group programme involving physical activity, skills training (stress management), peer support and dietary advice; structured as weekly 4-hour sessions, case management and home visits; held in community settings; developed for men with prostate cancer | Physical activity, diet, stress management | 1.1 Goal-setting (behaviour): specified intensity 1.4 Action planning: specified intensity 3.1 Social support: support group to encourage adherence 4.1 Instruction on how to perform a behaviour: skills training 6.1 Demonstration of the behaviour: skills training 8.1 Behavioural practice/rehearsal: skills training and practice encouraged 11.2 Reduce negative emotions: stress management |
| Martin 2013214 | Group workshop involving education, survivor stories, group discussion and goal-setting; structured as one-off 4-hour session; led by nurse and self-management tutor; developed for men with testicular cancer | Physical activity, nutrition, goal-setting, managing fatigue, self-examination | 1.1 Goal-setting (behaviour): self-examination goals 3.1 Social support: ‘opportunity to talk to someone’ outlined in modelling of intervention 5.1 Information about health consequences: education 9.1 Credible source: use of survivor stories 11.2 Reduce negative emotions: ‘finding a meaning’ outlined in modelling of intervention Notes: unclear what skills training, if any, was done in the workshop |
| Mfecane 2011215 | Group (mixed-sex) programme involving education and group discussion about the condition, its management and health behaviours ‘challeng[ing] traditional health and gender beliefs’ and encouraging to ‘convert’ to a ‘responsible’ lifestyle; facilitators trained by non-government and government organisations; some facilitators also had HIV; medication conditional on group attendance; held at public health clinic; developed for HIV/AIDS | ‘Responsible lifestyle’, including medication taking, diet, safer sex practices | 3.1 Social support: group attendance 5.1 Information about health consequences (possibly 5.6): health and lifestyle education 5.3 Information about social and environmental consequences: health and lifestyle education 9.1 Credible source: use of expert patients 12.1 Restructuring physical environment: e.g. advise to carry purse for pills 13.1 Identification of self as role model: expectation to disclose status publicly, although unclear extent to which this is considered related to ‘behaviour change’ 13.5 Identity associated with changed behaviour: ‘convert to responsible lifestyle’ and implications for identity |
| Ramachandra 2009100 | Self-administered psychological intervention involving well-being diary, mindfulness CD and planning activities, following briefing on the theory and practical aspects of the intervention; telephone contact happened in weeks 1, 2, 4 to answer queries and encourage practice; developed for cancer patients | Focus is 11.2, reducing negative emotions, via mindfulness | 1.1 Goal-setting (behaviour), pleasant activity scheduling (unclear if also 1.4 action planning and 1.8 behavioural contract) 2.3 Self-monitoring of behaviour: self-monitoring using diary 2.4 Self-monitoring of outcome(s) of behaviour: self-monitoring using diary 4.1 Instruction on how to perform a behaviour: brief introduction (i.e. skills training) and self-administered using tools provided 8.1 Behavioural practice/rehearsal: practice encouraged 11.2 Reduce negative emotions: targeted through mindfulness 12.5 Adding objects to the environment: self-help materials including diary and CD 15 Self-belief: unclear if repetition to build confidence should be coded here |
Appendix 6 Critical Appraisal Skills Programme criteria
| CASP item | Criteria used |
|---|---|
| 1. Was there a clear statement of the aims of the research? | Aim can be determined from anywhere in the paper (e.g. title, abstract, introduction, methods) |
| 2. Is a qualitative methodology appropriate? | Qualitative research is the appropriate way to address the aim or answer the research question (e.g. the research concerns experiences/views of participants, processes involved, or the nature of interactions) |
| 3. Was the research design appropriate to address the aims of the research? | Data collection, data analysis and methodological approach are appropriate to address the aim or answer the research question; the review team classified methodological approach based on whether the approach had consistently been used throughout (e.g. grounded theory required analytical methods such as constant comparison as well as the development of a core category or theory) |
| 4. Was the recruitment strategy appropriate to the aims of the research? | Authors clearly report selection of participants and this is appropriate to address the aim or answer the research question. Additional prompt:Is the sampling method clearly described?96 |
| 5. Was the data collected in a way that addressed the research issue? | Type of data collection method is clear (e.g. interview, focus group, participant observation, online postings) and has potential to address the aim or research question. Additional prompt:Is the method of data collection clearly described?96 |
| 6. Has the relationship between researcher and participants been adequately considered? | Authors demonstrate self-reflexivity in data collection and data analysis processes |
| 7. Have ethical issues been taken into consideration? | Approval from an ethics committee is reported |
| 8. Was the data analysis sufficiently rigorous? | Authors clearly describe data analysis approach and employ strategies to ensure rigour (e.g. peer debriefing, member checking, negative cases). Additional prompts:Is the method of analysis clearly described?96Are the claims made supported by sufficient evidence?96Are sufficient data presented to support the descriptive findings?131Are you confident that all of the data were taken into account?131 |
| 9. Is there a clear statement of findings? | Findings are clearly stated (e.g. in the abstract or findings) |
| 10. Is the research valuable? | Study appears valuable in own right (i.e. something has been ‘learnt’), rather than judged in relation to contribution made to the current review. Additional prompts:Does the study add to knowledge or theory in the field?131Does the study demonstrate theoretical insight, novel findings or perspectives?131 |
Appendix 7 Quality assessment comments
| Study (first author, year) | Comments (including concerns and limitations) |
|---|---|
| Adamsen 2001207 | Recruitment occurred by means of posters and leaflets but it is unclear where these were distributed. Focus group participation was limited to the 10 (out of 17) men who continued to participate, although author comments indicate the majority dropped out because of ill health. Some of the data are presented in the discussion |
| Arrington 2005208 | Authors describe the groups as ‘successful’ and comment that ‘the lack of an emotional support dimension . . . does not seem to affect participation’ (p. 99); however, there is no discussion of the extent to which participants attend multiple meetings, and participants’ views were not sought directly. Authors acknowledge sample limitations and possible ‘idiosyncrasies’ of group |
| Baird 2001134 | Unclear sampling – purposive and ‘based on . . . judgement about which men would be most representative of the population’ (p. 234). Use of phenomenology appears at odds with deductive approach to analysis, which is framed around self-care deficit theory |
| Barlow 2009103 | Men were only three of the 10 participants yet authors make claims concerning gender differences. Intention of study was not gender comparisons and it cannot be assumed that the findings consistently adopt a gender-comparative approach, so the findings are limited to the paragraph concerning gender comparisons and sex is not identified for the remainder of the data. Authors acknowledge that recruitment via community settings may have led to volunteers being ‘more committed and motivated to change, compared with patients referred by clinicians’ (p. 1178) |
| Barlow 2009102 | The claims about gender differences are not demonstrated by the data presented. Intention of study was not gender comparisons and it cannot be assumed that the findings consistently adopt a gender-comparative approach, so the findings are limited to the paragraph concerning gender comparisons and sex is not identified for the remainder of the data |
| Bedell 2000108 | Authors note that findings ‘may not be applicable to other persons with HIV/AIDS who may have inadequate resources’ (p. 202) because they use a mainly ‘educated middle-class white gay’ sample (p. 202) |
| Bell 2010107 | Unclear sampling of interviewees within groups. Men were only three of the 20 interviewees. Ethnicity, a focus of the study, was not reported for interviewees. Authors did not limit study to gender differences, but also considered ‘commonalities’ of groups. Authors acknowledge issues of generalisability beyond the groups sampled |
| Bourke 2012209 | Unclear how subsample selected for focus groups and no sample characteristics available for subsample, or comment on extent to which representative |
| Broom 2005109 | Sample mostly recruited through face-to-face support groups. Sampling until variation of certain characteristics is described; however, the description suggests convenience sampling and that no participants were turned away (p. 331). The study is reported as presenting three themes (empowerment, enhanced sense of control, and risk) but the findings are presented under five titled sections |
| Chambers 2012210 | Recruitment to the trial involved multiple routes, including face-to-face support groups. Sampling is limited to the 12 men who completed the intervention (29 expressed an interest and 19 started the intervention) |
| Chenard 2007110 | It was unclear whether data came from interviews or focus groups, because of the lack of identifiers accompanying quotes |
| Corboy 2011111 | Survey participants recruited via various routes, including support groups. Unclear how interview subsample was selected from survey pool. Unclear if interviews were simply structured around survey topics. Authors acknowledged the small sample size and that ‘men under the age of 60’ and ‘men with cancer in tumour streams other than prostate cancer’ were under-represented (p. 180) |
| Cramer 2013112 | Unclear how many of the 30 participants observed at groups were women. Authors’ argument of a relationship between socioeconomic status and preferred type of facilitator (peer/professional) does not consider that this may link to eligibility for accessing groups. Authors acknowledge that they ‘were not able to gain access to an existing black and minority ethnic group or a younger men’s group’ (p. 14) |
| Dickerson 2006114 | Linked study for Dickerson 2011, providing the women’s dataset. Study attempted to recruit both sexes but was unsuccessful |
| Dickerson 2011113 | Male sample mostly composed of men recruited via face-to-face support groups. Some of the gender comparisons appear to be inaccurately emphasised (e.g. verifying decisions, holistic nature, health-care provider interactions) |
| Eldh 2006135 | Study not intentionally male only. Small sample size (n = 3) but described as phenomenology, therefore not necessarily a problem |
| Emslie 2007115 | Participants recruited via various routes, including support groups |
| Evans 2007116 | None |
| Ferrand 2008218 | Authors recognised that the findings may not generalise to the wider diabetic population because the sample was ‘intrinsically motivated’ and composed of ‘active people . . . integrated in a patients’ association promoting physical activities for health’ (p. 519). Although there is some good evidence of rigour, there is some repetition between themes (e.g. body image) and some of the themes’ names do not reflect the overall messages |
| Galdas 2012211 | Given the focus of the study, it is not consistently possible to determine whether or not comments are from men who have accessed cardiac rehabilitation |
| Gibbs 2005119 | Unclear how or where sample recruited, despite giving good detail on maximum variation sampling. Limited information given on analysis |
| Gibbs 2007118 | Unclear how or where sample recruited, despite giving good detail on maximum variation sampling. Limited information given on analysis although some discussion of disconfirming evidence |
| Gooden 2007212 | Lack of sample characteristics; however, this is an inherent challenge with this type of research. Sampling appears appropriate |
| Gray 1996122 | No detail provided about analysis of comparing two data sets; however, the themes seem appropriate. Quotes not reported to illustrate points but available in linked studies (Gray 1997)120,121 |
| Gray 1997120 | Authors acknowledge recognised small sample size and that the findings may not generalise because of sampling of group leaders and those with ‘substantive’ involvement |
| Gray 1997121 | Linked study for Gray 1996,122 providing the women’s data set |
| Harris 2007117 | Authors note that findings may not apply to other groups because all are gay men and involved in local community-based agencies |
| Iredale 200799 | Little detail available concerning qualitative methods, reflecting the fact that this was supplemental to a quantitative survey study |
| Kendall 1992123 | Unclear recruitment, simply ‘self-referral’. Authors do not consider limitations of sample. Rich themes and comprehensive recommendations made |
| Kronenwetter 2005213 | Authors acknowledge limited generalisability due to ‘highly selected group . . . early stage disease, opting for watchful waiting, and participation in an intensive lifestyle change program’ (p. 106). No details reported about characteristics of those not interested in taking part in interviews (15 of 44 taking part in the intervention). Authors do not show self-reflexivity in relation to their theme on spirituality. Strength to have shown mix of responses and some negative comments but unfortunately did not report all of these. Original RCT (Ornish et al., 2005,282 cited by Kronenwetter et al. 2005213) shows that only half of those eligible agreed to take part in RCT because did not want to make lifestyle changes |
| Martin 2013214 | Authors note small sample size (n = 6) but justify because the first stages of intervention development. Lack of sample characteristics |
| Mfecane 2011215 | Unclear sampling for interviewees. Participant observation sample size and gender composition not reported and unable to judge extent to which interviewee subsample representative of group members. Strong thick description of context. Quotes did not always support the points being made. Authors did not acknowledge any limitations |
| Oliffe 2008125 | Authors acknowledge reliance on researcher interpretation with observational research and potential issues of recall bias |
| Oliffe 2010126 | Unclear how interviewees sampled from groups. Authors acknowledge issues of generalisability beyond the groups sampled. Authors acknowledge limited to men who attend groups and beyond study’s scope to include ‘men who chose not to participate or did not continue to participate’ (p. 569). Wide-ranging group size (4–100) not considered in observations |
| Oliffe 2011124 | Unclear how interviewees sampled from groups. Wide-ranging group size (4–100) not considered in observations |
| Ramachandra 2009100 | Unclear how interviewees sampled from intervention group. Small sample size but exact number unclear (maximum n = 7) and gender composition unclear. Little detail available concerning qualitative methods, reflecting that this was supplemental to a quantitative RCT. The claims about gender differences were not evidenced or explained (e.g. meaning of ‘psychological aspects’). Intention of study was not gender comparisons and it cannot be assumed that the findings consistently adopt a gender-comparative approach |
| Sandstrom 1996127 | Wide range of experiences of support groups reported and consideration given to how this varies with sample characteristics |
| Seale 2006128 | Study involved analysis of internet use in patients recruited from support groups, which may limit generalisability of findings. Authors note that keyword analytical method focuses on differences, and similarities may therefore be underestimated; additionally, keyword comparison missed that some women have interest in seeking and giving information |
| Seymour-Smith 2008216 | Unclear how interviewees were sampled within support groups. Author acknowledges small sample size. Several of the author’s arguments appeared open to alternative explanations concerning gendered differences around legitimising use, which were not presented |
| Smith 2002101 | Unclear how focus group members were sampled from the 100 Black Men organisation, the extent to which the men may be representative, or the nature of the organisation. Small sample size (n = 4). Little detail available concerning qualitative methods, reflecting that this was supplemental to a quantitative survey study |
| Sullivan 2003136 | Lack of sample characteristics; however, this is an inherent challenge with this type of research. Sampling appears appropriate (using postings week by week until saturation occurred); however, these numbers are not consistent with participant numbers. Analysis appears to be rigorous; however, the women’s findings include a section on humour, which feels like a different theme |
| Trapp 2013217 | Unclear how interviewees were sampled from the local group, or extent to which they were representative. Small sample size (n = 5) but this enabled rich biographical detail and thick descriptions. Authors acknowledged that findings may not apply to others and that the sample was restricted to Caucasian men. Authors reported that ‘the primary investigator maintained a limited clinical role at the site’ (p. 626), which may have influenced participants’ disclosures and/or research interpretations |
| Vanable 2012129 | Authors do not report how the sample size was determined. Authors noted that generalisability may be limited because the sample was potentially more knowledgeable about sexual risk behaviours. It was unclear whether data came from interviews or focus groups, given the lack of identifiers accompanying quotes. Authors did not consider the potential influence of data collection method, yet a participant’s comment about ‘having a blast right now’ (p. 558) in relation to a focus group suggests that this may have intersected with views expressed |
| Wallace 2007130 | Strong development of theory; however, a key point was raised in the discussion without being clear in the main finding: ‘Participants clearly indicated that although educational needs may be filled by enhanced education within urology practices, support needs must be filled by prostate cancer patients and survivors, not health care professionals’ (p. 186) |
Appendix 8 Male-only studies not used in meta-analysis: main findings
| First author, year, country, condition | Outcomes | Main findings |
|---|---|---|
| Allen 1990,46 USA, type 2 diabetes | Fasting plasma glucose, glycosylated haemoglobin, weight, total cholesterol, high-density lipoprotein cholesterol, patient preference for intervention, costs | No significant group differences were observed |
| Burgio 2006,48 USA, prostate cancer | Time to continence, proportion with severe incontinence, pad use, bladder control, return to work, return to usual activities, incontinence impact, psychological distress and quality of life | Time to continence was significantly more rapid in the intervention group (p = 0.04). At 6 months, significantly higher rates of severe or continual leakage were present in the control group (p = 0.04). Intervention subjects had a higher proportion of dry days (p = 0.04) and a lower proportion of pad use (p < 0.05). No group differences were observed for lifestyle variables, incontinence impact, psychological distress or quality of life |
| Cockcroft 198174 and 1982,73 UK, COPD | 12-minute walking distance, FEV, FVC, oxygen uptake, ventilation, cardiac frequency, maximum ventilation, maximum oxygen uptake, Lorr McNair mood questionnaire, graded response questionnaire, Eysenck personality questionnaire | The intervention group improved significantly more than control group on the 12-minute walking test and maximum oxygen intake (at 2 months only). No difference between groups was observed for treadmill exercise test, FEV1, weight, FVC or psychology scores |
| Gallagher 198451 and 1987,50 USA, type 2 diabetes | Weight, fasting blood glucose, fasting serum triglycerides, fasting cholesterol, insulin dosage, hypoglycaemic incidence and dietary recall | Fasting blood glucose, daily calorie intake, cholesterol, insulin and weight did not significantly differ between groups. Triglycerides were significantly reduced at 3 months in the intervention group but at all other time points no difference was evident. In the control group, a greater proportion of patients were 3% or more over their ideal body weight on 50% of visits (p = 0.008) |
| Giesler 2005,52 USA, prostate cancer | Prostate cancer quality of life, depression, dyadic adjustment, general quality of life (SF-36) | Prostate cancer quality of life showed significant improvements in the intervention group on the sexual function scale at 4 months (p = 0.05), sexual limitation at 7 and 12 months (p ≤ 0.05) and cancer worry at 12 months (p = 0.03). SF-36 showed no significant differences between groups at any time point |
| Haynes 1976,82 Canada, hypertension | Compliance (pill count), DBP | Compliance and DBP improved but only compliance was significantly more improved in the intervention group (p = 0.025) |
| Leehey 2009,57 USA, diabetes and kidney disease | Exercise duration, maximal oxygen consumption, oxygen consumption, heart rate, blood pressure, maximum rate pressure product, serum creatinine, serum urea nitrogen, creatinine clearance, urea clearance, glomerular filtration rate, urine albumin/creatinine, urine protein/creatinine, haemoglobin, total cholesterol, low-density cholesterol, high-density cholesterol, triglycerides, glycated haemoglobin, C-reactive protein, calorie intake, body weight, fat weight, lean weight | No significant group differences were observed |
| Lepore 1999,58 USA, prostate cancer | Quality of life, social moderators, psychosocial variables, prostate cancer knowledge | Greater improvements were seen in the intervention group in knowledge (p < 0.001), self-efficacy (p < 0.05) and distress (p < 0.05). Differences in quality of life were not evident between groups except for the mental health scale, which showed greater improvement in the intervention group (p < 0.05). Interpersonal conflict also worsened in the control group alone (p < 0.05) |
| McGavin 1977,76 and 1976,75 UK, COPD | FVC, 12-minute walking distance, bicycle exercise test with expired gas analysis | Subjective measures of breathlessness, well-being, cough and sputum significantly improved in the intervention group (p ≤ 0.02), but general activities were not significantly different between groups. No significant differences between groups were observed for FEV1 or FVC |
| Mishel 2002,61 USA, prostate cancer | Illness uncertainty, self-control, cancer knowledge, patient–provider communication, symptom distress/quality-of-life scale | Uncertainty and symptoms improved over time, but there were no differences between groups. At 4 months, cognitive reframing was significantly better in the intervention groups (p = 0.005), but not at 7 months. A similar pattern was evident for problem-solving. Patient communication and cancer knowledge showed no difference between groups. Urine flow significantly improved in the intervention groups (p = 0.03) up to 4 months, with no group differences at 7 months. Sexual function showed improvement over time for all groups (p = 0.02) and erectile function showed no group differences |
| Moynihan 1998,77 UK, prostate cancer | Anxiety, depression, mental adjustment to cancer, psychological adjustment to illness, Rotterdam symptom checklist, emotional concealment, sexual adjustment | Anxiety was more improved in the control group than in the intervention group (p = 0.03). No difference in depression scores was evident between groups |
| Parker 1984,63 USA, arthritis | Arthritis Knowledge Inventory, AIMS, BDI | No significant group differences were observed for AIMS: total score, dexterity, social role, depression or BDI. Patients gained more knowledge in the education group (p < 0.001) and showed significant improvements in AIMS physical activity, but had higher pain scores than control (p < 0.05) |
| Sackett 1975,83 Canada, hypertension | Compliance (pill count), blood pressure | Those with augmented physician access were no more compliant with medication use. Health education improved knowledge, but did not improve later medication use. Neither strategy improved the rate at which men were designated compliant/at goal blood pressures |
| Scura 2004,65 USA, prostate cancer | Functional assessment of cancer therapy scale – general, symptom experience scale – prostate, international index of erectile function scale, relationship change scale | No significant group differences were observed |
| Wakefield 2008,67 USA, heart failure | Instrumental and affective behaviour, nurses’ perceptions and patient satisfaction | A number of communication profile differences emerged between telephone and video-calls, but nurse perception and patient satisfaction were not significantly different between groups |
| White 1986,70 USA, type 2 diabetes | Serum glucose, body weight, glycohaemoglobin, diabetes knowledge, locus of control | No significant difference in weight, glycohaemoglobin levels or knowledge was observed between groups. A decline in serum glucose was observed in both groups up to 3 months. At 6 months the education alone group had significantly higher serum glucose levels (p < 0.05) |
Appendix 9 Study characteristics and main findings of trials containing gender group analysis
| First author, year, country, condition | Aim | Participants | Method of recruitment | Self-management support: intervention | Self-management support: control | Outcomes | Main findings (including gender analysis) | Attrition and compliance |
|---|---|---|---|---|---|---|---|---|
| Blanchard 1996,182 USA, hypertension | To investigate thermal biofeedback and 24-hour ambulatory blood pressure monitoring in both genders and to evaluate a maintenance programme | Main study n = 42 (28 male). Maintenance phase n = 22 (13 male). Overall mean age N/R. Age range 32–62 years. Ethnicity N/R. SES N/R | Referrals from medical centres | Thermal biofeedback practice including discussion and questions and home practice | Waiting-list control. Self-monitoring of blood pressure | Blood pressure | No significant difference in blood pressure observed between groups or by gender overall. During maintenance, no difference in blood pressure was observed between intensive and regular follow-up | Attrition in main study n = 4. Attrition in maintenance phase n = 10. Main study compliance at least five thermal biofeedback practices per week. Maintenance phase compliance 16.5 per month for first 7 months |
| GESICA 2005,183 Argentina, heart failure | To determine if a telephone intervention reduces morbidity and mortality in chronic heart failure patients | n = 1518 (1074 male). Mean age 65 years (SD 13.3 years). Age range N/R. Ethnicity N/R. SES N/R | Patients were identified from the Argentina chronic heart failure register | Heart failure nurses phoned patients for educational and monitoring purposes. An education booklet was also provided | Standard care | Mortality, hospital admission, quality of life | Usual care patients were more likely to be admitted (p = 0.026). Mortality was similar between groups. Quality of life was improved in the intervention group (p = 0.001). Admission for heart failure by gender favoured the intervention but no significant interaction was observed (p = 0.49) | Complete follow-up for 99.5% of patients. Compliance N/R |
| Molde Hagen 2003,185 Norway, chronic pain | To investigate the effects of a light mobilisation programme on sick leave and pain | n = 457 (238 male). Mean age 40.9 years (SD 10 years). Age range N/R. Ethnicity N/R. SES N/R | Sick lists from national insurance offices for lower back pain for 8–12 weeks were examined for eligibility | Encouragement to take daily walks, individualised training and stretching, and practical advice on coping with daily activities at home and work | Standard primary health care | Sick leave, pain reporting, return to work | At 3 months, 6 months and 1 year, significantly more intervention than control patients had returned to work (RR = 1.21, 95% CI 1.05 to 1.40). At 6 months, significantly more intervention men and women had returned to work, but at 12 months this was significant only for women. Significantly fewer sickness compensation days were observed in the intervention group (p < 0.001); this was significant only for men (p = 0.001). No difference between the number of men and women off sick in the intervention or control group was reported at 1, 2 or 3 years. Significantly more men than women reported off sick at 3 years (RR = 1.93, 95% CI 1.11 to 3.37) | 13 discontinued treatment and seven died during the study. Compliance N/R |
| Hämäläinen 1997,186 Finland, type 1/2 diabetes | Long-term effects of podiatrist care on knowledge, self-care and foot lesions | n = 733 (369 male). Mean age 46.9 years (SD 19.1 years), age range 10–80 years. Ethnicity N/R. SES N/R | Identified from the National Drug Reimbursement Register | Individual and tailored education, counselling and exercises for foot care. All services free of charge | Written instructions on foot care | Knowledge, self-care and podiatrist foot assessment | Intervention group knowledge scores were significantly higher than control at 1 year (p = 0.025). Self-care scores did not differ between groups, but were significantly higher in women than in men p < 0.001 and higher in the intervention group than control (p = 0.011). No difference in podiatrist assessment was observed between groups | Attrition n = 198. Compliance N/R |
| Hanefeld 1991187 and Julius 1992,188 Germany, type 2 diabetes | To evaluate the effect of IHE on diabetes and coronary incidence and risk factors | n = 1139 (635 male). Age range 30–55 years. IHE + C: mean age 45.8 years (SD 8.8 years). Ethnicity N/R. SES N/R | Identified from 16 rural and urban diabetes clinics | IHE + C included instruction on low-calorie, lipid-reduced diet, guidance on physical activity and group exercise sessions and antismoking/alcohol education. Clofibric acid prescribed | Standard care | Health behaviour (nutrition, physical activity and smoking), BMI, fasting blood glucose, medication use, cholesterol, triglycerides, blood pressure, cardiac events, mortality, work absence | Both interventions demonstrated improvements in fat consumption, physical activity, glucose control, reduced diabetic drug use, triglycerides, blood pressure (p < 0.05). Only the IHE + C significantly improved smoking. No effect on body weight, cholesterol or sick leave observed. Men appeared to have a higher incidence of myocardial infarction in all groups and women appeared to have a higher incidence of ischaemic heart disease across all groups; no statistics. Duration of sick leave was also longer in women (p < 0.01) | 88.5% completed the study. Compliance N/R |
| IHE included instruction on low-calorie, lipid-reduced diet, guidance on physical activity and group exercise sessions, and antismoking education. Placebo prescribed | ||||||||
| Härkäpää 1989,276 Finland, chronic pain | To investigate the short-term effects of two preventative/rehabilitative interventions on pain, disability and compliance with self-care | n = 459 (289 men). Intervention mean age 44.8 years. Age range 35–54 years. Ethnicity N/R. SES ‘blue collar workers’ | Invitation to those working at state railway, post, telecoms, various enterprises and farming | Inpatient: Swedish back school, back exercises, relaxation exercises, heat and electrotherapy, massage and group discussion. A programme of exercise and stretching was taught following treatment | Written and oral instructions on back exercises and ergonomics | Pain, disability index, compliance, subjective benefit | Significant decreases in pain and disability were evident in inpatient and outpatient interventions overall compared with control (p < 0.04). Decrease in pain and disability was more pronounced in women regardless of treatment group, but not significantly | n = 459 completed the programmes. Compliance in male study groups did not differ between groups. Female inpatients reported exercise more frequently than outpatients and controls |
| Outpatient: Swedish back school, back exercises, relaxation exercises, heat and electrotherapy, and group discussion. A programme of exercise and stretching was taught following treatment | ||||||||
| Heitzmann 1987,190 USA, type 2 diabetes | To assess the long-term impact of behavioural weight management strategies for men and women with type 2 diabetes | n = 46 (22 male). Mean age 52.94 years (SD 12.08 years). Age range 29–79 years. Ethnicity n = 44 white. Education n = 43 high school graduate | Referral by physician and public announcements | BMG recorded daily weight, food intake and exercise. Dietary advice and prescribed exercise regimen provided | Dietary advice and prescribed exercise regimen provided. Progressive muscle relaxation training | Relative weight (Quetelex Index), glycosylated haemoglobin, body fat | BMG subjects lost significantly more weight than CBMG and control groups (p < 0.05). Men were shown to benefit mostly from BMG in terms of weight loss (p < 0.05); no group differences were observed for women. Between-group differences in body fat and HbA1c were non-significant. Men experienced significantly greater reductions in HbA1c than women (p < 0.05) | Attrition n = 10. Compliance N/R |
| Cognitive modification group discussed role of cognition on behaviours. Dietary advice and prescribed exercise regimen provided | ||||||||
| CBMG combined cognitive modification group and BMG practices. Dietary advice and prescribed exercise regimen provided | ||||||||
| Jensen 2001,191 Sweden, chronic pain | To evaluate the long-term outcomes of a behavioural medicine rehabilitation programme | n = 214 (97 male). Mean age 43.3 years (SD 10.4 years). Age range N/R. Ethnicity 81% Swedish. Employed 80% | Recruited through insurance claims of musculoskeletal diagnosis | PT: included how to incorporate activity into daily lives, goal-setting, physical activity, relaxation and body awareness. Homework assignments were also set. All programmes included education on pain and ergonomics, rehabilitation plan and follow-up visits | Standard care | Absence from work, HRQoL (SF-36) and perceived relevance of programme | No significant difference between groups on total work absence was observed. Risk of early retirement was significantly lower for females in the PT and CBT groups than control. Behavioural medicine group: SF-36 significantly improved in three domains for women and one domain for men compared with control. PT group: one domain on SF-36 significantly improved for women compared with control. CBT group: six domains on SF-36 significantly improved for women compared with control | Attrition intervention: n = 28. Female adherence across work, domestic and lifestyle plans ranged from 41% to 60%. Male adherence across work, domestic and lifestyle plans ranged from 25% to 83% |
| CBT: aimed at improving ability to manage pain and resume normal activity level. Homework assignments were also set. All programmes included education on pain and ergonomics, rehabilitation plan and follow-up visits | ||||||||
| Behavioural medicine programme: a combination of CBT and PT. All programmes included education on pain and ergonomics, rehabilitation plan and follow-up visits | ||||||||
| Kankaanpää 1999,192 Finland, chronic pain | To investigate the efficacy of active low back rehabilitation on pain, self-experienced disability and lumbar fragility | n = 59 (37 male). Mean age at intervention men 40.7 years (SD 8.6 years), women 38.9 years (SD 8.2 years). Age range N/R. Ethnicity N/R. SES N/R | Those presenting with non-specific chronic low back pain at a health centre | Physiotherapist-led physical exercise, stretching, relaxation and ergonomic advice | Passive treatment consisting of thermal therapy and massage | Pain and disability index, isoinertial back extension endurance test, electromyography | At 12 months, pain and functional disability index scores significantly decreased in the intervention group vs. control (p < 0.05). No gender differences were observed | 90% completed the intervention and 83% were followed up at 1 year |
| Katon 2002193 and Williams 2000,194 USA and Lebanon, dysthymia | To compare the effectiveness of paroxetine and psychotherapy in patients with depression | n = 415 (150 male). Mean age 71 years. Age range 60–93 years. Paroxetine group: ethnicity 82.5% white, median annual income $15,000–$20,000, median education duration 12 years | Referrals from primary care practices | Paroxetine was titrated to effective dose. Medical therapists reviewed dose and side effects, and gave general support | Placebo drug alongside medical therapist review on dose, side effects and general support | Interview based on Primary Care Evaluation of Mental Disorders, Hamilton rating scale for depression, substance abuse and psychosis modules from structured clinical interview for diagnosis, Hopkins symptom checklist, due severity of illness index, NEO neuroticism scale | Improvement in Hamilton rating scale for depression scores was significant in the paroxetine group vs. control (p = 0.04) but not for problem-solving treatment. Gender was not a predictor of recovery. An interaction between age and gender was observed in women but not men, with younger women more likely to recover p < 0.001. Treatment status significantly interacted with recovery for men but not women, with significantly fewer men recovering in the placebo group (p = 0.008) | Compliance: 338 of 415 attended at least four treatment sessions. Paroxetine/placebo reported compliance: 96% of scheduled doses taken |
| Problem-solving treatment group: ethnicity 75.4% white, median annual income $15,000–$20,000, median education duration 12 years | Problem-solving treatment delivered by therapist | |||||||
| Kendall 1987,195 USA, type 2 diabetes | To compare the effectiveness of nutrient-based diet evaluation with a traditional diabetic diet evaluation in improving dietary adherence | n = 83 (26 male). Mean age at intervention 56.2 years (SD 16 years). Age range 21–82 years. Education 78% high school graduates | Identified from physician and hospital patient lists | Colorado State University diet guide with cassette tape teaching nutrition, diet planning and food composition | Food exchange list for menu planning with cassette tape of lists. Nutrition and diet planning was also taught | Nutrient intake, weight, skinfold, arm circumference, blood pressure, glucose, glycated haemoglobin, cholesterol, triclycerides | No significant changes between groups for total energy intake, weight, skinfold, glucose, HbA1c, blood pressure, cholesterol. Men were persistently closer to mean desired weight than women (p = 0.05). Skinfold was significantly higher in women than men (p < 0.01). DBP lower in male Colorado State University and female exchange list patients (p < 0.01). Mean serum cholesterol was significantly lower in men (p < 0.05) | n = 22 dropped out. Compliance N/R |
| Kovar 1992,179 USA, osteoarthritis | To evaluate the effects of an education and exercise programme on functional status, pain and medication use | n = 102 (17 male). Mean age 69 years. Age range 40–89 years. Intervention group ethnicity n = 50 white and education college graduate n = 20 | Patients identified from medical centres, Arthritis Foundation and various community-based sites | Indoor supervised fitness walking, patient education and discussion sessions led by physical therapist | Weekly telephone contact | 6MWD, AIMS: functional status, health status, pain, medication scales | The intervention improved walking distance, AIMS physical and AIMS pain subscales (p ≤ 0.003). No significant group difference for AIMS arthritis and medication use subscales. No between-subject or group difference in walking distance for men and women was observed (p = 0.02) | Attrition: n = 10 dropped out. Compliance: 47 of 52 completed the programme with mean attendance to sessions 21 (SD 6) out of 24 |
| Lester 2010,266 Kenya, HIV | To assess the effect of regular, structured text messages on HIV drug adherence | n = 538 (187 male). Mean age at intervention 36.7 years (SD 8.5 years). Age range 19–84 years. Ethnicity N/R. Intervention group monthly income $1–5 47%; primary school education 40% | Recruited from three HIV clinics | Weekly text from HCP enquiring on status and follow-up call as required by response | Standard care | Self-reported adherence, viral load, attrition, quality of life | Adherence was significantly improved in the intervention group (adjusted odds ratio 0.57, 95% CI 0.40 to 0.83; p = 0.002). Viral load was not significantly different between groups. No significant differences in adherence and viral load were observed between men and women | Attrition n = 114. Compliance N/A |
| Mellin 1989,283 Finland, chronic pain | The effects of back pain treatment on patients that work | n = 456 (288 male). Mean age N/R. Age range 35–54 years. Ethnicity N/R. SES N/R | Inpatients and outpatients | Combination of heat and electrotherapy, massage, back exercise, physical exercise, muscle strength training, back school and relaxation | Standard care | Lumbar spinal mobility, hip mobility, trunk strength, IPM, subjective progress | Both male and female inpatients (but not outpatients) showed significant improvements in IPM (p < 0.05) | IPM measurements could be calculated 277/287 males and 159/165 females. Compliance N/R |
| O’Connor 2009,199 USA, heart failure | To examine whether or not aerobic exercise reduces all-cause mortality or all-cause hospitalisation and improves quality of life | n = 2331 (1670 male). Median age 59 years. Age range 51–68 years. Intervention ethnicity 61.2% white. SES N/R | Medical centres within the USA, Canada and France | Structured group exercise including walking, treadmill and stationary cycling followed by home-based activity. Home exercise equipment and educational materials were provided | Standard care including educational materials and follow-up | Mortality, hospitalisation, peak oxygen consumption, 6MWD, change in NYHA class | Rates of all-cause and cardiovascular mortality or hospitalisation were not significantly different between groups; adjustment by prognostic factors led to significant benefits in exercise group. 6MWD, exercise test, peak oxygen consumption (p < 0.001) and NYHA (p = 0.03) were all significantly improved by exercise vs. control. No significant effects of intervention by gender were observed for all-cause mortality or hospitalisation | n = 736 completed training. During the supervised phase, median exercise time per week was 76 minutes, reducing to 74 minutes at 2 months and 50 minutes at 3 years |
| Penttinen 2002,200 Finland, chronic pain | To evaluate the effect of social support in the rehabilitation of non-specific back pain | n = 108 (45 males). Mean age at intervention male 41 years, female 43 years. Age range N/R. Ethnicity N/R. SES N/R | Subjects were screened at an occupational health centre unit | Swedish-type back school including physical training, ergonomic techniques and supervised group meetings including fitness training and discussion | Supervised group meetings including fitness training and discussion, but less frequent than intervention | Physical capacity, subjective disability, quality of life, analgesic use | Subjective disability significantly decreased in intervention group at 12 months (p = 0.02) but not at 6 months. Quality of life improved at 6 months (p = 0.04) but not at 12 months. At 12 months improvements were more pronounced in men but not significantly. No overall difference in mobility variables were found between groups; however, at 6 months intervention group trunk extension was significantly more improved in males and trunk flexion in females (p = 0.05). Reductions in analgesic use were observed in both intervention and control groups. At 6 months only men in the intervention group used significantly less analgesics (p = 0.005) | 15 dropped out prior to starting back school (gender N/R). Compliance N/R |
| Smith 2005,201 USA, heart failure | To assess the impact of a disease management programme on quality of life | n = 1069 (71% male). Mean age 70.9 years (SD 10.3 years). Age range N/R. Ethnicity 71.6% white. SES N/R | Patients were identified from various medical centre and health-care system databases | Disease management group received telephone education and monitoring from a nurse. Scales provided for weight monitoring | Standard care | Quality of life (SF-36) | No significant differences were observed between groups on the SF-36 domains. Males and females significantly differed on physical functioning (p = 0.009), role-emotional (p = 0.003) and role-physical (p = 0.03) SF-36 domains, with women performing worse. Subanalysis found no significant interaction between sex and intervention | 67.4% completed the protocol. Compliance N/R |
| Augmented disease management group received telephone education and monitoring from a nurse. Each patient also received a blood pressure cuff, pulse oximeter, activity monitor and scales for self-monitoring | ||||||||
| Vanninen 1993,202 Finland, type 2 diabetes | To investigate whether or not intensive diet and exercise education and continued support are more beneficial than conventional treatment | n = 83 (48 male). Mean age 53 years (SE 1 year). Age range 40–67 years. Ethnicity and SES N/R | Referrals from urban and rural health centres | Education on diet and physical activity benefits. Exercise instructions provided and activity monitored. Encouragement was given to increase activity | Basic education on diet and the benefits of physical activity | Expiration–inspiration ratio, orthostatic challenge blood pressure, fasting blood glucose, HbA1c, plasma insulin, body weight, BMI, fat-free body mass, waist–hip ratio, respiratory gas exchange during exercise test | Fasting blood glucose decreased in intervention women compared with control (p < 0.05), but not in men. HbA1c statistically decreased in intervention women compared with control at 15 months (p ≤ 0.001), but not in men. No further statistical findings | N/R |
| Wing 1991,284 USA, type 2 diabetes | To test the effectiveness of a ‘family-based approach’ for obese type 2 diabetics | n = 49 (18 male). Intervention group mean age 53.6 years (SD 7.7 years). Age range N/R. Ethnicity N/R. SES N/R | Newspaper advertisements | A weight control programme aimed at patients and spouses. Calorie and exercise goals were set and blood sugar levels checked. Support and problem-solving skills were taught and financial incentives offered for weight loss | A weight control programme aimed at patients alone. Calorie and walking goals set and blood sugar levels checked. Training on behavioural strategies was given and financial incentives offered for weight loss | Weight, BMI, HbA1c, fasting blood glucose, eating behaviour, exercise, adherence, dyadic adjustments | Significant improvements were observed over time but no between-group differences were found for weight, BMI, HbA1c and fasting blood glucose. Calories consumed were significantly lower in the alone group (p < 0.05), but no other eating behaviour differences were observed between groups. Changes in weight were better in men in the alone group and women in the together group; no statistics | 87.7% of patients and 86% of spouses completed the programme. Compliance N/R |
| Wing 1994,203 USA, type 2 diabetes | To evaluate intermittent use of a VLCD | n = 93 (33 male). Mean age at intervention 52.3 years (SD 10.7 years). Age range N/R. Ethnicity N/R. SES N/R | Newspaper advertisement | Behavioural programme consisting of exercise goals, weight review, self-monitoring review, lectures and discussion on nutrition, exercise and behaviour. Patients also adhered to an intermittent VLCD of 400–500 kcal per day | Behavioural programme consisting of exercise goals, weight review, self-monitoring review, lectures and discussion on nutrition, exercise and behaviour. Patients also adhered to a consistent LCD of 1000–1200 kcal per day | Weight, BMI, HbA1c, plasma glucose, insulin, cholesterol and triglycerides | Overall, weight loss and improved BMI were greater on VLCD (p = 0.05). Women lost significantly more weight on VLCD (p = 0.02), but no difference between groups was observed for men. Overall, no difference between groups on HbA1c, fasting glucose, insulin. Cholesterol significantly lower in LCD (p = 0.05) and DBP lower in LCD (p = 0.03) | Attrition n = 14. Attendance in first 3 months 10 of 12 meetings, last 3 months attendance at 5 of 12 meetings |
Appendix 10 Second-order findings and third-order constructs
| Study (first author, year) | Second-order findings (main themes and ideas reported by authors) | Third-order constructs and overarching concepts (our interpretations) |
|---|---|---|
| Adamsen 2001207 | (1) Why the men enrolled (motivation): ‘personal conquest’, ‘victory’, physical development, dissatisfaction with body, reputation of training facility. (2) Social obligation: professional-led, set meeting times, obligation towards group, comradeship via physical activity and humour and trust, understand ‘when to laugh/be quiet’, fight together against the ‘shit’. (3) Well-being and bodily awareness: improved well-being, new energy, self-esteem and belief in own resources, awareness of body, different levels of ability and vary with health, lectures helpful and valued psychologist speaking with them not to them and use of jokes, topics (e.g. sexuality, complementary and alternative medicine) no longer taboo | Need for purpose:
|
| Arrington 2005208 | (1) Man-to-man self-help groups are primarily used for information. (2) Emotional talk is discouraged (‘squelched’) by group processes: topics (avoided discussions of death, sex); topic turning (e.g. focusing on practical aspects instead of emotional), using comparisons, facilitators (including HCP). Other factors limiting emotional support/talk include size of groups, lack of familiarity with other members, members’ contact limited to meetings, possibly partner presence | Need for purpose:
|
| Baird 2001134 | Note: analysed with respect to self-care deficit theory. (1) Self-care agency: importance of health beliefs and ‘dispositions’ for adherence. (2) ‘Basic conditioning factors’ influence adherence to health behaviour change, e.g. age (habits may be more entrenched); health state (wanting to avoid further illness); health-care system (information, HCPs, other patients); family system (partners attend and reinforce messages outside contact time); pattern of living (habits inhibit change); environmental factors (heat at exercise facility may inhibit); resource availability and adequacy (financial barriers to resource access, e.g. lack of coverage by medical insurance) | Trusted environments:
|
| Barlow 2009103 | (1) Men were more ‘critical of the course content and delivery’. (2) Men and women reported similar benefits regarding self-management skills. (3) Men valued informational aspects whereas women valued ‘interactive processes’. (4) Some men may struggle with ‘group interaction on emotive topics’, wanting factual information from ‘tutors’ rather than ‘facilitators’ of group discussion. (5) Some patients valued range of conditions to offer different perspectives and reduce feelings of isolation | Need for purpose:
|
| Barlow 2009102 | Men valued information exchange whereas women valued ‘emotional and social interaction’ | Need for purpose:
|
| Bedell 2000108 | Central theme of ‘a reasonably stable base’; section relating to support groups: ‘people I feel I can lean on’ – informational support and an ‘outlet’ for emotional sharing; support group understand each other; want to protect family and friends from negative emotions | Need for purpose:
|
| Bell 2010107 | (1) Content of group meetings: metastatic (women’s) focuses on emotional sharing whereas colorectal (mixed sex) is emotionally ‘neutral’ and moves towards ‘safer’ topics; gender effects may be ‘flattened’ and not meet needs of men or women (some women wanted more ‘intimate atmosphere’ and ‘buddies’ outside group’); Chinese group had wide-ranging topics (including practical aspects, communication issues). (2) Commonalities between groups: similar perceived benefits (information, acceptance, understanding); motivations vary with treatment stage (initially more focused on information, later friendship and ‘give back’ and support others) | Need for purpose:
|
| Bourke 2012209 | (1) Motivations for taking part: return to physical activity, ‘give back’ to staff and future patients. (2) Supervised group design: encouraged motivation and ‘male only’ space away from partners. (3) Social interaction: felt ‘safe and confident’ around men with ‘similar’ condition, would prefer longer duration. (4) Home-based exercise: more challenging as distracted by competing priorities. (5) Diet aspect: helpful and valued information but difficult to adhere to. (6) Future participation: requires that intervention be viewed beneficial by self and feedback from exercise specialist, prefer group lifestyle programme to peer support focused on talking. (7) Exercise beyond the intervention: barriers to access including confidence and cost. (8) Disease recurrence: psychological benefits (reduced anxiety and fear). (9) Communication with HCPs: dissatisfaction with some. (10) Benefits and drawbacks of taking part: valued goal-setting, improved physical and psychological well-being but not improved urological side effects | Need for purpose:
|
| Broom 2005109 | Note: describes as three themes (empowerment, control, risk) yet presents as five sections. (1) The internet and control: information increases power and control over disease and decision-making but partly depends on HCP responses. (2) The internet and empowerment: information allows patient to ‘do something’ rather than ‘being told what to do’, but information may overwhelm and may help process past decisions even if ‘too late’ to influence decision; internet can enable other roles (e.g. helping others, taking on support group leadership roles). (3) The internet and the patient’s role: empowering effect of information may be limited by HCP strategies to ‘reclaim the consultation model’, financial ability to choose provider, individual ability to access and comprehend information, time to make a decision. (4) Trust and uncertainty: some patients are suspicious of internet and value HCP as expert, rejecting consumerism. (5) Masculinity and risk management: online setting enables some men to ‘open up’ and discuss sensitive topics by offering ‘anonymity’ and allowing different levels of involvement whereas others felt suspicious of online setting | Need for purpose:
|
| Chambers 2012210 | (1) Group identification: group identity based on shared experience of LTC (despite some variation in stage of progression), sense of ‘being there’ for others and camaraderie. (2) Acceptance of diversity: differences described in positive way, enhancing group experience, all show ‘respect’ and listen to each other. (3) Peer learning: learn coping strategies through sharing with others and considering different perspectives. (4) Acceptance of disease progression: contact with others with more advanced disease was confronting but could offer encouragement and reassurance, ‘synergistic’ with nature of intervention (acceptance-based) | Need for purpose:
|
| Chenard 2007110 | Central themes of ‘striving for normalcy’ and ‘the role of social support’. Findings relating to support groups: social support is an essential part of self-care via normalising, stigma management and ‘affirming’ social networks where disclosures are not required; limiting social support to HIV/AIDS-related environments ‘assured a level of safety’ and ‘allies’ | Trusted environments:
|
| Corboy 2011111 | Note: analysed with respect to behavioural model of health service use. (1) Predisposing characteristics: age (older men perceive symptoms as part of ageing, therefore less in need of support), social structure (varied awareness of services, some disappointment with HCPs, helps to know someone ‘in the [health-care] system’), health beliefs (some issues of stigma and embarrassment, reservations about effectiveness of support groups, including reliability of information, but male reluctance to discuss health is a myth). (2) Enabling resources: personal/family (can enable or be a barrier), community (rural can influence travel and delays in receiving appointments but greater barriers may be beliefs and fears around privacy). (3) Need for care: perceived (independence and stoicism as barrier, minimise and downplay problems), evaluated (HCPs can find it hard to judge support needs and needs can change with time) | Need for purpose:
|
| Cramer 2013112 | (1) Isolation and social benefits: men often isolated, valued support outside family or friends, valued ongoing support, may need one-to-one instead of group in periods of ‘crisis’. (2) Value of groups and strategies for attracting men: establishing trusting relationships through one-to-one work with facilitator before joining group, providing activities (e.g. food) that allow mental health to be addressed ‘sideways on’, opportunity for leadership (via roles in the group), type of facilitators (preferences may link to socioeconomic background), importance of peers (e.g. reducing stigma, learning from each other), men only may or may not inhibit sharing and talking openly about feelings. (3) Accessing support and the role of health professionals: general practitioners can act as enabler or facilitator for accessing support, counselling sometimes seen as unproductive | Need for purpose:
|
| Dickerson 2006114 (linked women’s study); Dickerson 2011113 | Sex comparisons (Dickerson 2011): men focus on problem-solving and women focus on ways of living with condition; women use family/friends more for accessing information; men want power in HCP interactions whereas women want to verify decisions; both value patient stories for symptom management and expectations but men primarily use for functional aspects (symptom management, adverse effects, treatment) whereas women use primarily for support, advice, encouragement. Men’s data set (Dickerson 2011): overall pattern – ‘cancer diagnosis as a problem to be solved’. Five themes: (1) seeking information for decision-making and treatment plan; (2) retrieving information to facilitate HCP interactions and monitor for recurrence; (3) evaluating information, including using views of HCPs; (4) patients’ (online) stories informing possible symptom management; (5) navigating the ‘healthcare system politics and power’. Women’s data set (Dickerson 2006): overall pattern – ‘Internet use as assisting in discovering ways to live with cancer as a chronic illness instead of a death sentence’. Five themes: (1) retrieving and filtering contextualised information using ‘Internet-savvy’ friends or family; (2) seeking hope while avoiding fear, using ‘manageable “bytes”’; (3) self-care regarding specific symptom management; (4) empowerment through providing ‘second opinion in decision making and validating treatment decisions’; (5) providing peer support | Need for purpose:
|
| Eldh 2006135 | (1) ‘Participation’ viewed by men as being an equal partner (shared decisions), accepting responsibility, being responsible, being seen in one’s context (treated as an individual with contextualised information). (2) ‘Non-participation’ viewed by men as being controlled (commands and instructions), lacking respect (not listened to or treated as individual), lacking information. (3) Men and HCPs had ‘conflicting values’: respective emphasis on responsibility and information, and HCPs perceived themselves as more involving and individualising than perceived by patients and participant observation | (D)evolving consumer:
|
| Emslie 2007115 | (1) Men and women may struggle to recognise and articulate mental health problems. (2) Men and women value certain aspects of HCP relationships (being listened to, taken seriously, not rushed, caring, trust, rapport) but diversity within groups regarding whether or not they prefer ‘talking to a stranger’. (3) ‘Different emphasis in communication’ with gender: men value HCP skills that help them talk whereas women value listening skills. (4) ‘Male emphasis on getting practical results from talking therapies’ using problem-solving rather than ‘just talking’ | Need for purpose:
|
| Evans 2007116 | (1) Men may be ‘proactive seekers’ or ‘passive recipients’ of CAM information: main information source is ‘lay referral’ network (family/friends, especially women, sometimes linked to proficiency with internet especially if older); approach varies with characteristics (e.g. use prior to cancer, type and stage of cancer); some did not want to seek CAM information (feeling that NHS should signpost, lacking confidence, wary, wanting NHS ‘stamp of approval’); proactive usually view as empowering (gain control, hope) whereas passive usually view as anxiety provoking or overwhelming; some individuals change from passive to proactive. (2) Patients use multiple types of evidence and from various sources (internet and ‘traditional’) and use various criteria for evaluating CAM information and therapies: often ‘discerning’ rather than ‘wholesale acceptance’; want belief and trust in therapies and providers (e.g. NHS ‘stamp of approval’) | Need for purpose:
|
| Ferrand 2008218 | (1) Social motive: ‘convivial team atmosphere’ (men and women value friendship, talk and exchange with others, being respected and valued). (2) Social motive: feeling understood and well supported (medico-sporting educators offer information exchange; women value emotional support, friendship, encouragement and group activity from peers whereas men value information, skills, strategies; few men or women mentioned family support). (3) Social motive: ‘pleasure in a group’ (women value group and doing something for self rather than family). (4) Psychological motive: well-being (valued by both but women also about bodily awareness). (5) Psychological motive: health (valued by both but women focus on flexibility, mobility, pain and men focus on stopping weight gain, increased fitness, energy, delays ageing). (6) Psychological motive: body image (found in women only, linked to confidence) | Need for purpose:
|
| Galdas 2012211 | (1) Food: diet is strongly linked to family practices and gendered division of domestic labour and a social activity at the gurdwara (Sikh temple); therefore, changes hard to maintain without family/friend support. (2) Exercise: some prefer walking and socialising with others to formal exercise regimen with ‘strangers’; education and monitoring in programme can provide self-efficacy for self-led but some still lack confidence without HCP guidance; some men who did not access intervention are already independent. (3) Faith and religion: predetermination and external locus of control shape health beliefs that could act as barrier to access, but some diversity of views | Trusted environments:
|
| Gibbs 2005119 | (1) Hegemonic masculinity influences men’s perceptions of services: perceive services as solely about support groups and emotional sharing (unaware of exercise, education, pain management); emotional sharing viewed as feminine and sign of weakness with homosexual connotations (use of sexist and sexual references in humour); however, severity of condition and its impact (including ‘emotional needs’) may ‘override hegemonic masculinity’. (2) Hegemonic masculinity influences men’s perceptions of self: condition compromises hegemonic masculinity; men may have multiple conditions each requiring identity adjustment; treating condition as a technical problem to be solved helps regain control, fitting with hegemonic masculinity | Need for purpose:
|
| Gibbs 2007118 | (1) Work as a conceptual barrier: work is an indicator of health and ability to fulfil roles, so men do not identify as needing services while still able to work. (2) Work as a structural barrier: some men lack time and energy to access services because of work commitment; however, the greater barrier is ‘placing work as a priority’ rather than employment type (e.g. rural, self-employed). (3) Work as a sociocultural barrier: men prioritise work over health rather than assigning value to health/services; however, this varies with severity of condition; priorities are similar across culture and employment types but less work priority for younger men (work is temporarily disrupted) and older men (view as part of ageing) whereas middle years face ‘greatest obligation’ (different hegemonic masculinities at different stages in life course) | Need for purpose:
|
| Gooden 2007212 | (1) Information support ‘facts about the disease’: personal experience was exchanged but professional opinion ‘took precedence’; literature was cited by both sexes but women gave short references and men provided detailed technical summaries; evidence-based practice and scientific rigour were promoted; alternative practices were considered in women’s but not men’s; informed choice and consumer perspective promoted, especially in men’s. (2) Information support ‘dealing with effects of the disease’: patients relayed own experiences but women summarised facts whereas men provided detailed medical information (including impact on bodily functions and sexual impacts); both discussed disease site and shared strategies but men focused on function and women on appearance. (3) Emotional support ‘coping philosophy’: both sexes offered ‘wisdoms’; both used humour but men’s use was lengthy and way to address emotions whereas women’s was more incidental. (4) Emotional support ‘nurturing and expressing’: women used overt emotional expression whereas men’s often implied or ‘intellectualized’; women encouraged through affection and nurturing whereas men promoted strength, perseverance and camaraderie; both challenged other members and set boundaries for communication; both expressed anger and dissatisfaction with HCPs and services; both had sense of connection and ‘the group’; both showed some telephone contact outside online group | Need for purpose:
|
| Gray 1996;122 Gray 1997121 (linked men’s study;121 linked women’s study120) | (1) Information: highly valued by both but primary for men and for women it overlaps with emotional; men value from HCPs, women value from peers. (2) Emotional support: intimacy is ‘cornerstone’ for women vs. secondary for men, developing over time. (3) Group organisation and structure: men have business-like task-centred approach whereas women’s focus is mutual support. (4) Advocacy and lobbying: men are more keen for advocacy. (5) Family participation: men are more keen for others to be involved (e.g. HCPs) whereas women want to retain intimacy with other women. (6) Community: men want to involve others whereas women want their own space. (7) Valuing laughter: women valued laughter whereas not mentioned by men. (8) Encountering death: women considered how to handle death of members whereas not mentioned by men. (9) Sexuality: men reported more sexual concerns but this may reflect conditions or emphasis on and acceptability of discussing sexuality | Need for purpose:
|
| Harris 2007117 | Individual counselling: (1) benefits – reduced isolation, especially important at key times; accept responsibility; explore and vent emotions; signpost to other support; problem-solving; information including referrals and health strategies; safe and respectful environment; discuss sensitive and private issues not appropriate for group setting; (2) counsellor qualities – various including non-judgemental, empathetic, knowledgeable conveying expertise (especially in times of crisis) while having ‘egalitarian relationship’; (3) therapeutic alliance – various including egalitarian, client involvement, accomplish goals, feel comfortable with counsellor; (4) issues addressed – several including practical, health behaviours, emotional, existential, identity. Peer support: (1) benefits – reduced isolation, camaraderie and friendship, ‘not alone’, physical resources (e.g. food), skills (e.g. social skills), vent emotions, distraction, information; (2) relationships – equal power, increased openness, ‘same boat’, ‘don’t judge’, clear communication through shared experience; (3) role models – peer support workers who ‘truly understand’ and can signpost to other resources | Need for purpose:
|
| Iredale 200799 | (1) Information received: some dissatisfaction with amount of information provided; some reported helpful HCPs who provided information and support. (2) Gender-specific information: many wanted, especially younger men (although the age observation came from quantitative data) | Becoming an expert:
|
| Kendall 1992123 | (1) Intimacy: need for connection, ‘closeness’ and ‘unity’ is primary reason for access, develops via activities (e.g. ‘sharing’). (2) Group process: ‘gay bonding’ (importance of being around other gay men, talking about gay issues, identity), ‘being realistic’ (rather than in denial), ‘confronting group members in supportive ways’ (building honesty and intimacy), ‘promoting a wellness orientation’ (intimacy as a source of wellness). (3) Group structure: closed groups are the most intimate (build trust through consistency of members); open groups can be ‘bonded’ provided enough structure and consistency; smaller groups promote well-being and time to deal with everyone’s issues; different levels of groups are needed to meet different needs (e.g. newcomers’ crisis group, intermediate group, advanced-level group dealing with ‘hard core’ issues including existential); there are valued leadership qualities (e.g. active, facilitate). (4) Meaning: gained through ‘reassessing life priorities’ (meaning of HIV in their lives) and building a caring community (spiritually bound community as ultimate goal of group) | Need for purpose:
|
| Kronenwetter 2005213 | (1) Peer community (which included involvement of family) was the most highly valued component, providing shared activities, support, socialising, ‘connection’ and ‘belonging’. (2) ‘Spirituality’ linked to the intervention was valued by some men. (3) ‘Value’ included ‘emotional reactions’ to the intervention (e.g. optimism, hope, ‘fighting spirit’, reduced anxiety and some ‘negative’ reactions), feeling ‘healthier’ and energised, becoming more emotionally available | Need for purpose:
|
| Martin 2013214 | (1) Goal-setting: some value, some struggle (e.g. if not done in work environment, if younger, if depressed, if ‘lack’ goals) and need examples. (2) Information: some want it not to be too technical, welcome ‘how to’ strategies, want tailored and ‘contextualising’. (3) Survivor stories: want examples they can relate to (e.g. not ‘too American’, not all professionals, some younger). (4) Psychological health: some expressed few emotional impacts, some valued addressing fear of recurrence, importance of survivor peers, listening and sharing, role of facilitators valued. (5) Timing: mainly wanted intervention sooner, earlier in treatment | Need for purpose:
|
| Mfecane 2011212 | (1) ‘Constructions of masculinity in Bushbuckridge’: men have ‘economic and emotional independence’, are ‘self-sufficient’, ‘stoical rather than expressive’ and the ‘dominant partners’, so not content with mixed-sex groups or sharing with women; consumption of alcohol and traditional medicines demonstrates masculinity. (2) ‘Support groups’: view facilitators as educators (experts) and patients as students; some expert patients are viewed as role models and part of health-care team; ‘top-down approach’ to effect ‘responsible behaviour’; traditional health beliefs condemned, ‘convert[ing]’ patients may involving being ‘chastised’ by staff and patients; prescribe solutions rather than listen to concerns. (3) ‘Therapeutic citizenship and masculinity’: praise support group and benefits (information, knowledge, acceptance of diagnosis, resist stigmatisation, combat hopelessness, connect with peers) but feel obliged to abandon previous identity; therefore ‘ambivalence’ (enabling for coping with condition but disabling to abandon masculine lifestyles and adopt non-masculine ones) | Need for purpose:
|
| Oliffe 2008125 | (1) ‘Micro-level influences: leadership as the lynchpin to meeting diverse individual needs’: leaders/committee organise meetings and speakers; committee preferable to avoid burden; realistic workload and leadership succession needed to ensure sustainability; leaders engage new members and establish rapport and camaraderie; leaders offer ‘new’ information to maintain interest of long-standing members who seek continued learning as well as ‘giving back’ to new members. (2) ‘Meso level influences: emancipation or affiliation’: tensions exist about whether groups should build individual identity or collective power and retain autonomy or adopt standardised format. (3) ‘Macro level influences: insufficient capacity for activism’: sustainability threatened if limited resources are redeployed from local to global activities | Need for purpose:
|
| Oliffe 2010126 | (1) ‘Living examples of healthy men’: importance of shared diagnosis for connection and normalising; some men value information exchange over camaraderie and friendship; men often value needs-driven activity-based meetings; men value living examples who offer comparison, reassurance, self-reflection, hope, optimism; roles change with time whereby men later ‘give back’ to other group members. (2) ‘Mixing health and illness messages’: discussions move ‘seamlessly’ between health and illness information; presentations and peers encourage adoption of healthy lifestyle; involvement of partners can encourage discussion of emotions. (3) ‘Tailoring trajectory and problem-specific information’: main goal of newcomers is empowerment for informed treatment choice; important to have ‘expert’ men and opportunity for discussion of specific treatment options in small groups; value sharing strategies and joint problem-solving; have permission to discuss taboo topics because discussed by other men and focus on problem-solving rather than emotional experience | Need for purpose:
|
| Oliffe 2011124 | (1) ‘Numbers and measures as the foundation of prostate cancer literacy’: across illness trajectory, men are able to exert control and partnership in decision-making through information; information focused on treatment options and side effects, conveyed using ‘group dialect’ linking biomarkers and probabilities. (2) ‘Group information processing’: information stimulated group discussion and could provide hope; access to expert speakers gave current information and opportunities to gain confidence interacting with HCPs; men had varied involvement (some listened rather than talked). (3) ‘Shopping around’: knowledge given to navigate health systems, exercise consumer rights to choose doctor and treatment, including CAM; specific strategies given for conveying ‘consumer identity’ in HCP consultations; information presented as agenda-free (although certain active options may be favoured) and not rushed, unlike clinical appointments | Need for purpose:
|
| Ramachandra 2009100 | (1) Men were less interested in ‘psychological aspects’. (2) Both sexes gave altruism and gratitude, not personal benefit, as reasons for taking part | Need for purpose:
|
| Sandstrom 1996127 | (1) ‘Becoming involved in a support group’: men became involved for different reasons (information and advice, empathy and emotional relief, camaraderie and friendship). (2) Different types of support group participation exist (long-term, brief, non-participation): long-term usually diagnosed before HIV/AIDS awareness existed, faced high stigma and lacked access to other support, therefore valued emotional sharing, information exchange, and helping others but experienced some disbenefits (grief, ‘dying out’ of group, unwanted roles); brief participants usually diagnosed since increased awareness and had greater access to more support, were more interested in instrumental support (e.g. receiving and exchanging information and coping strategies) and stopped because of ‘discomfort with emotional climate’ (dealing with emotional instability of those experiencing different stages of adjustment and feeling that facilitators should have managed these dynamics), wanting more useful information and coping strategies (e.g. constructive talk about controllable aspects), experiencing a ‘lack of exemplars of productive coping’ (not finding ‘role models’); non-participants reported sufficient support from existing networks, not wanting to be confronted by their ‘future’ (by seeing those with worse health), being in relatively good health and that they may become involved when faced with deteriorating health (both for extra support and to ‘lessen the burden’ on others) | Need for purpose:
|
| Seale 2006128 | (1) Men use internet mainly for information whereas women use mainly for social and emotional aspects, although may use for both. (2) Men more concerned with specific body areas whereas women more holistic. (3) Men more concerned with treatment information and HCPs whereas women more concerned with impact on significant others. (4) Women more concerned that information is untrustworthy and has potential to overwhelm or cause anxiety. (5) Women show greater emotional expressivity whereas men more inhibited and use ‘concerned’, ‘embarrassed’ to convey emotion. (6) Both sexes view web forums as relatively private so can discuss bodily function (and for women, privacy facilitates interactions characteristic of women’s friendship groups). (7) Family and friends are sometimes responsible for information gathering from internet (particularly in men, although this was quantitatively informed) | Need for purpose:
|
| Seymour-Smith 2008213 | (1) ‘Signalling trouble’: women ‘un-problematically’ accepted researcher’s positioning of them as members of self-help groups whereas men resisted this identity. (2) ‘Stereotypical constructions’: men talked about stereotyped versions of self-help groups (e.g. ‘touchy feely’) whereas women discussed advice and support activities in non-problematic ways. (3) ‘Four functions: a matter of identity’: men foreground gender and distance themselves from stereotypical self-help groups and how they are perceived. (4) ‘“Legitimate” involvement’: men ‘deny agency’ in seeking support group membership, instead presenting ‘stumbling across’ or attending to help others | Need for purpose:
|
| Smith 2002101 | (1) Men may report not needing support groups because they access support from existing networks (e.g. church, family). (2) Men may obtain information from other sources (e.g. friends and family with experience of LTC, HCPs, literature, internet, American Cancer Society) instead of groups. (3) Men may not access because of denial of disease. (4) Men may not access because of feeling uncomfortable discussing ‘sensitive issues such as sexuality with strangers’. (5) Men may not access because of being ‘too busy’ with other organisations and activities | Need for purpose:
|
| Sullivan 2003136 | Presents findings as consistent with ‘western society’s accepted forms of gendered communication’ whereby men value instrumental and informational support whereas women value emotional. Men’s themes: (1) ‘as we all know’ (men use technical information and medical jargon, place emphasis on medical reports and knowledge, including discussion of sexual aspects); (2) ‘I do not respond to messages without a PC digest’ (HCPs contribute and expect men to provide case histories that conform to standards; men are expected to read key articles and be well informed); (3) ‘if you want to be a partner in your own healing’ (patients should ‘arm’ selves with up-to-date medical information to become active patients and have informed decision-making). Women’s themes: (1) ‘I send my good vibes’ (women have positive optimistic interactions, expressing affection); (2) ‘at this cyber tea party’ (understanding is possible only by others with similar experiences; similar others validate and normalise experiences); (3) ‘feel free to rant’ (women vent feelings and frustrations about HCPs, treatment, side effects, bodily changes, relationships); (4) ‘put a face with a cyber name’ (women seek contact outside discussion boards and establish ‘personal relationships’ through remembering important treatment dates, etc.); (5) ‘may we all be blessed with the ability to contribute to others’ lives’ (women provide support to others as a form of coping, give each other advice to become active patients in their own health care, educate each other about condition and HCP interactions and help to ‘interpret’ information) | Need for purpose:
|
| Trapp 2013217 | (1) Predominant coping styles were ‘seeking guidance and support’ (valuing opportunity for support outside the family and the importance of shared understanding), ‘seeking information’ (focusing on learning from each other, with education happening alongside ‘connection’) and ‘acceptance’ (including dealing with uncertainty and accepting the diagnosis). (2) ‘Seeking emotional support’ was the central emotion-focused coping style (this overlapped with ‘seeking guidance and support’ but was primarily concerned with emotional needs; men valued ‘mutual give-and-take’ ‘transactions’). (3) Preferences in group qualities included an interest in connection (contrary to perception of ‘solitary and emotionally restricted’), an interest in mixed-sex groups (to increase discussion and to help understand perspectives of others, including family and friends) and interest in mixed diagnoses (to give ‘deeper understanding’ and meet practical needs of having few with shared diagnosis) | Need for purpose:
|
| Vanable 2012129 | (1) ‘Focus[ing] exclusively on safer sex may not be well received’: some men perceive negativity and blame around safer sex whereas it should be everyone’s responsibility. (2) ‘Preference for a supportive, group approach that addresses other coping challenges as well as sexual risk reduction’: appeal of informal sociable group where meet other HIV+ men, have interactive engaging group discussion, learn about each other, support each other to live ‘healthier lives’, without feeling stigmatised (by virtue of being around other HIV+ men) or ‘preached at’, instead having a facilitator but being able to ‘steer’ discussions | Need for purpose:
|
| Wallace 2007130 | (1) Some men seek support from family and friends with experience of prostate cancer. (2) HCPs are not a good source of psychosocial support; support from peers is preferred. (3) Some men lack awareness of services. (4) Support groups offer opportunity to meet peers going through same thing. (5) Support should be available immediately after diagnosis to aid decision-making. (6) Men want independent support groups because of agendas of HCPs. (7) Men want to meet peers with range of treatment experiences to inform decision-making. (8) Men want both one-to-one and peer-led group support. (9) Men want to see other men who are well years after treatment. (10) Access may be limited by viewing ‘prostate cancer as a private matter involving male potency and urinary function’ | Need for purpose:
|
Appendix 11 Behavioural change techniques classification for quantitative studies
| First author, year, country | Self-management intervention description | BCT categories |
|---|---|---|
| Adsett 1989,79 Canada | Training in progressive muscle relaxation, monitoring practice and strategies for stressful situations. Education on hypertension, lifestyle and stress. Patients were given a take-home tape of first relaxation session for home practice and kept daily logs. Compliance was assessed weekly | 2.3 Self-monitoring of behaviour 2.2 Feedback on behaviour 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Education (same as relaxation group) on hypertension, lifestyle and stress. Weekly logs of activities, food intake and exercise were kept and reviewed weekly | 2.2 Feedback on behaviour 2.3 Self-monitoring of behaviour 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
|
| Allen 1990,46 USA | Patients were trained to perform blood glucose tests at least 36 times per month. Proficiency was checked prior to the start of study and throughout. Each patient was also instructed on a diet, which largely focused on increasing fibre intake. Booklets on diet and weight loss were provided and compliance was checked at 3 and 6 months | 1.2 Problem-solving 2.4 Self-monitoring of outcome of behaviour 2.6 Biofeedback 2.7 Feedback on outcome of behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Bennett 1991,71 UK | Stress management training: small groups were educated on blood pressure, stress and relaxation techniques, self-instruction techniques, cognitive restructuring and meditation. Sessions involved role-play and group problem-solving. Participants were set behavioural assignments and kept a diary | 1.1 Goal-setting 1.2 Problem-solving 2.4 Self-monitoring of outcomes of behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 13.2 Framing/reframing |
| Type A behaviour management: same content as stress management training. Additionally, specific attention was paid to the identification and modification of type A behaviours including time urgency management and anger control | 1.1 Goal-setting 1.2 Problem-solving 2.4 Self-monitoring of outcomes of behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 13.2 Framing/reframing |
|
| Berglund 2007,89 Sweden | The training programme involved light physical fitness training, relaxation, breathing exercises and pelvic floor exercises. A booster session was held after 2 months | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Information on prostate cancer, treatment and potential side effects was provided in the form of lectures. Opportunities for group discussion and demonstration of products for incontinence and sexual aid formed part of the sessions | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences |
|
| The third intervention combined the physical and information programmes | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
|
| Bosley 1989,47 USA | Education on stress, emotional arousal and hypertension. Participants were trained to monitor own behaviour and physiological responses in stressful situations. Group practice, identification of faulty appraisal, recognition of inaccurate labelling of situations and home practice formed part of the intervention | 2.3 Self-monitoring of behaviour 2.2 Feedback on behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 9.1 Credible source 11.2 Reduce negative emotions |
| Presentation on the dynamics of stress and hypertension, followed by group discussion sessions on how to handle stressful situations | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 9.1 Credible source 11.2 Reduce negative emotions |
|
| Bourke 2011,72 UK | Supervised aerobic and resistance exercise training and self-directed exercise. Incorporating exercise into daily activities and available support structures were explored for each patient. All participants received a nutrition advice pack, which recommended reductions in saturated fat and refined carbohydrates, increased fibre and moderate alcohol consumption. Small group healthy eating seminars were also held | 1.1 Goal-setting 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Burgio 2006,48 USA | A single session of biofeedback to learn pelvic floor control, reinforced with verbal instructions. Patients were provided with written instructions of 45 pelvic floor exercise and encouraged to continue at home in various positions and to integrate into daily activities | 1.4 Action planning 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Carmack Taylor 2006,66 USA | Cognitive behavioural skills training including self-monitoring, goal-setting, problem-solving to overcome barriers, cognitive restructuring and self-rewards to integrate physical activity into daily life. Patients self-monitored and were followed up to solve issues and set new goals | 1.1 Goal-setting 2.3 Self-monitoring of behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Facilitated group discussion on various topics: diet and prostate cancer, side effects of treatment and sexuality. Expert speakers presented at some sessions | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences |
|
| Cockcroft 198174 and 1982,73 UK | Rehabilitation centre-based exercise including stationary cycle pedalling, rowing machines, swimming and daily walks. Recommended home exercises included stair climbing and level walking | 1.1 Goal-setting 2.3 Self-monitoring of behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 8.7 Graded tasks |
| Culos-Reed 2010,80 Canada | Group exercise tailored to ability consisting of walking, stretching and light resistance work. Exercise equipment was provided to facilitate home-based exercise. Peer support was encouraged and education/discussion sessions were held on goal-setting, monitoring behaviour, overcoming barriers, role of positive attitude, social support, relapse support and nutrition | 1.1 Goal-setting 1.2 Problem-solving 2.2 Feedback on behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment 11.2 Reduce negative emotions |
| Daubenmier 2006,49 USA | A plant-based vegan diet with 10% of calories from fat, 3 hours of moderate exercise per week and 1 hour of stress management practice per day. Participants attended a 1-week retreat to familiarise with the intervention. Subsequently, weekly support group meetings were held to enhance programme adherence | 1.1 Goal-setting 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 11.2 Reduce negative emotions |
| Gallagher 198451 and 1987,50 USA | Diet with an unspecified calorie intake consisting of three meals per day and a snack avoiding refined sugars and saturated fats. Education on the diet and dietary consultations occurred every 3 months | 2.2 Feedback on behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour |
| Garcia 199785 and 2004,86 Spain | Education and training on hypertension, relaxation and problem-solving. Patients received a self-help book, problem-solving sheets, relaxation tapes and recording sheets to track medication use and stressful events. Homework assignments were set and reviewed by a therapist | 1.2 Problem-solving 2.2 Feedback on behaviour 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 12.5 Adding objects to the environment |
| Giesler 2005,52 USA | A programme of symptom management and psychoeducational strategies. The intervention focused primarily on sexual and urinary problems, bowel dysfunction, cancer worry, dyadic adjustment and depression | 1.2 Problem-solving 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 9.1 Credible source 12.5 Adding objects to the environment |
| Gifford 1998,53 USA | Self-care education sessions covering evaluating symptoms, seeking care for new symptoms, medication use and problems, communication skills with caregiver/health professionals, coping with symptoms using CBT and relaxation. Additionally exercise, fitness programmes, nutrition plans and goal-setting. Interaction was encouraged through role-playing, information sharing and other forms of participation | 1.1 Goal-setting 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Gourley 1998,54 and Solomon 1998,55 USA | A pharmacist provided regular assessment and educational interventions to optimise disease management. Patients’ questions and concerns were also managed | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences |
| Guell 2000,81 Canada | Breathing retraining and relaxation techniques, low-level stair walking, flat surface exercise, stationary cycle pedalling and walking with arm and leg co-ordination. Education sessions covered anatomy, basic respiratory physiology, nature of the disease and interventions. Physiotherapy for effective cough and postural drainage was offered | 1.1 Goal-setting 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 8.7 Graded tasks |
| Fernandez 2009,84 Spain | Respiratory education combined with inspiratory, upper-limb and lower-limb muscular training. Training logs were kept and patients were followed up by a physiotherapist. Educational materials were also provided on exercises | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Haynes 1976,82 Canada | Each patient was interviewed to identify habits and tailor medication taking. Loaned blood pressure devices were provided and BP and medication taking were tracked. During fortnightly follow-ups, if BP had lowered, financial credit was given towards owning the BP device. Patients were also praised and encouraged on progress | 1.1 Goal-setting 1.4 Action planning 2.4 Self-monitoring of outcome of behaviour 2.7 Feedback on outcome of behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 10.8 Incentive (outcome) 10.10 Reward (outcome) |
| Heisler 2010,56 USA | Action plans were generated based on individual laboratory and blood pressure results. Each patient was then paired with a peer and encouraged to make regular contact, with automated reminders. Each pair received training on communication skills and topic guides for phone calls. In addition, three optional group sessions to raise queries, discuss concerns and review action plan progress were held | 1.1 Goal-setting 1.4 Action planning 2.2 Feedback on behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Klocek 2005,90 Poland | Exercise consisting of warm-up, then consistent workload training on a cycle ergometer (60% maximal heart rate for age) and post-training relaxation | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Exercise consisting of warmup, interval training with gradually increasing workload on a cycle ergometer and post-training relaxation | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
|
| Koukouvou 2004,91 Greece | A gradually modified physical training programme incorporating stationary cycling, walking or jogging, calisthenics, stair climbing and step-aerobic exercises. Resistance exercises were added in after the first 3 months | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Leehey 2009,57 USA | Education and instruction on walking, shoe selection and developing a walking programme. Gradually increasing treadmill walking and unsupervised home based walking programme. Patients were followed up and monitored by staff | 1.1 Goal-setting 1.4 Action planning 2.3 Self-monitoring of behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 8.7 Graded tasks |
| Lepore 1999,58 USA | Patients and partners were invited to expert lecture and question sessions followed by separate peer discussions for men and wives. Topics were prostate cancer overview, nutrition and exercise, side effects, stress management, communication and intimacy, and follow-up care. Those missing meetings received a tape recording of the lecture and any handouts | 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 9.1 Credible source 11.2 Reduce negative emotions |
| Lepore 2003,59 USA | Expert-delivered lectures on prostate cancer biology and epidemiology, control of physical side effects, nutrition, stress and coping, relationships and sexuality, follow-up care and future health concerns. Printed materials were provided in each lecture and 10 minutes of questions were permitted, minimising group discussion | 5.1 Information about health consequences 9.1 Credible source 12.5 Adding objects to the environment |
| Expert lectures as above as well as facilitated group discussion with a male psychologist for men and separate discussion for partners with a female oncology nurse | 3.1 Social support (unspecified) 5.1 Information about health consequences 9.1 Credible source 12.5 Adding objects to the environment |
|
| Lucy 1994,60 USA | Psychosocial support, monitoring of health, stress, mood and interpersonal satisfaction. Monitored weekly over the phone. Information and education on HIV/AIDS. Referrals to other services when appropriate | 2.5 Monitoring without feedback 3.1 Social support (unspecified) 5.1 Information about health consequences |
| McGavin 1977,76 and 1976,75 UK | Home stair-climbing exercises, starting from a minimum of two steps up and down for 2 minutes, building to 10 steps for 10 minutes. Participants recorded their progress and the programme was reviewed after 2 weeks and monthly thereafter | 1.1 Goal-setting 2.3 Self-monitoring of behaviour 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 8.7 Graded tasks |
| Mishel 2002,61 USA | Patients’ concerns directed the skills training. Strategies included information, cognitive reframing, directing to local resources, problem-solving techniques, encouragement and patient–doctor communication skills to enhance participation in care | 1.2 Problem-solving 3.1 Social support (unspecified) 13.2 Framing/reframing |
| Patients’ concerns directed the skills training. Strategies included information, cognitive reframing, directing to local resources, problem-solving techniques, encouragement and patient–doctor communication skills to enhance participation in care. In addition the spouse or family support member also received weekly phone calls | 1.2 Problem-solving 3.1 Social support (unspecified) 13.2 Framing/reframing |
|
| Moynihan 1998,77 UK | A cognitive and behavioural treatment programme, designed for cancer patients, covering current problems, coping strategies, muscle relaxation, raising self-esteem, overcoming feelings of helplessness and promoting a ‘fighting spirit’ | 1.2 Problem-solving 3.1 Social support (unspecified) 11.2 Reduce negative emotions |
| Mueller 2007,62 USA | Patients resided at a rehabilitation centre for 1 month, undertaking cycling and walking. Exercise levels were adjusted accordingly | 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal |
| Parker 1984,63 USA | Intensive education programme covering disease process, therapies and medication, joint protection and conservation, coping with psychological stresses and unproven treatment methods | 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 11.2 Reduce negative emotions |
| Parker 2009,64 USA | Individual clinical psychologist sessions and stress management guides covering relaxation skills (60% of the time), problem-focused coping strategies, having realistic recovery expectations and an imagined exposure of day of surgery. Further information on cancer and the adverse effects of treatment were also provided | 1.2 Problem-solving 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 11.2 Reduce negative emotions 12.5 Adding objects to the environment 15.2 Mental rehearsal of successful performance |
| Individual clinical psychologist sessions providing support to patients | 3.3 Social support (emotional) | |
| Puente-Maestu 200088 and 2003,87 Spain | Each participant was supplied with a pedometer and asked to walk 3–4 km in 1 hour, 4 days per week. Subjects were followed up and encouraged to continue with training during a maintenance phase. During this period, patients were interviewed every 3 months to reinforce compliance. Education sessions were also held on medication use and nutrition | 1.1 Goal-setting 1.2 Problem-solving 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 6.1 Demonstration of behaviour 8.1 Behavioural practice/rehearsal 12.5 Adding objects to the environment |
| Sackett, 1975,83 Canada | Enhanced access to physicians through free appointments during work hours and reimbursement for 90% of prescription drug costs. Education audiotapes and booklet on hypertension, effect on organs, health, life expectancy, therapy benefits and compliance skills. Education reinforcement occurred periodically | 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences 12.5 Adding objects to the environment |
| Scura 2004,65 USA | The programme consisted of telephone-based HCP support with structured educational components | 3.1 Social support (unspecified) |
| Wakefield 2008,67 USA | Nurse telephone support covering patient activation and partnerships, health information, monitoring of symptoms and compliance strategies in regard to heart failure | 2.7 Feedback on outcomes of behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences |
| Nurse video-telephone support covering patient activation and partnerships, health information, monitoring of symptoms and compliance strategies in regard to heart failure | 2.7 Feedback on outcomes of behaviour 3.1 Social support (unspecified) 4.1 Instruction on how to perform behaviour 5.1 Information about health consequences |
|
| Weber 2004,68 USA | Patients were matched with a peer (long-term survivor of prostate cancer) to provide social support following surgery for prostate cancer. Dyads were matched on race | 3.1 Social support (unspecified) |
| Weber 2007,69 USA | Men were paired with support partners (survivors of prostate cancer who had undergone radical prostatectomy) and encouraged to discuss thoughts and feelings on diagnosis and sexual/urinary side effects. Discussions were held away from loved ones at a location which was suitable for private conversations | 3.1 Social support (unspecified) |
| White 1986,70 USA | The programme facilitated peer interaction and support through idea sharing and advice to manage disease. Weekly serum glucose levels were posted and discussed. Education was provided on the adverse effects of hyperglycaemic and hypoglycaemic reactions, importance of weight control and exercise | 1.2 Problem-solving 2.2 Feedback on behaviour 2.3 Self-monitoring of behaviour 2.6 Biofeedback 2.7 Feedback on outcomes of behaviour 3.1 Social support (unspecified) 5.1 Information about health consequences 6.1 Demonstration of behaviour 9.1 Credible source 10.4 Social reward |
| Windsor 2004,78 UK | A home-based programme of moderate intensity involving continuous walking for at least 30 minutes. All patients kept a log of activity and the exercise group was contacted to encourage adherence | 1.1 Goal-setting 2.3 Self-monitoring of behaviour 3.1 Social support 4.1 Instruction on how to perform behaviour 10.5 Social incentive |
Appendix 12 Quality-of-life instruments used by quantitative studies
| Instrument name | Abbreviation | Overall domain or subscale | Direction of response | Trials using this scale |
|---|---|---|---|---|
| Functional Assessment of Cancer Therapy – General | FACT-G | HRQoL | Positive scores indicate better status | Bourke et al. 2011;72 Jarden et al. 2009;167 Rogers et al. 2009;177 Donnelly et al. 2011;164 Wang et al. 2011;172 Cadmus et al. 2009;158 Mutrie et al. 2007147 |
| European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30 | EORTC QLQ-C30 | HRQoL | Positive scores indicate better status | Culos-Reed et al. 2010;80 Johansson et al. 2008;148 Adamsen et al. 2009168 |
| Short Form health survey 36 | SF-36 P | HRQoL – physical composite | Positive scores indicate better status | Daubenmier 2006 et al.;49 Bennett et al. 2007;154 Fillion et al. 2008;181 Carmack Taylor et al. 2006;66 Lepore et al. 2003;59 Parker et al. 2009;64 Demark-Wahnefried et al. 2006;150 Coultas et al. 2005155 |
| Spitzer Quality of Life Index | Spitzer Index | HRQoL | Positive scores indicate better status | Koukouvou et al. 2004;91 Cheville et al. 2010149 |
| Health Status Questionnaire v2.0 | HSQ | HRQoL – general health subscale | Positive scores indicate better status | Gourley et al. 199854 |
| Sickness Impact Profile | SIP | HRQoL | Negative scores indicate better status | Emery et al. 1998165 |
| Centre for Epidemiologic Studies Depression Scale | CES-D | Depression | Negative scores indicate better status | Culos-Reed et al. 2010;80 Carmack Taylor et al. 2006;66 Cadmus et al. 2009;158 Carmack et al. 1995;166 Chandwani et al. 2010;159 Danhauer et al. 2009;169 Gifford et al. 1998;53 Lepore et al. 200359 |
| Beck Depression Inventory | BDI | Depression | Negative scores indicate better status | Kouidi et al. 1997;175 Donnelly et al. 2011;164 Dominique et al. 2010;156 Mutrie et al. 2007;147 Raghavendra et al. 2007;160 Heckman and Carlson 2007;162 Stein et al. 2007174 |
| Hospital Anxiety and Depression Scale | HADS | Depression subscale | Negative scores indicate better status | Koukouvou et al. 2004;91 Berglund et al. 2007;89 Adamsen et al. 2009;168 Jarden et al. 2009;167 Banerjee et al. 2007;163 Johansson et al. 2008148 |
| Self-Rating Depression Scale | – | Depression | Negative scores indicate better status | van Vilsteren et al. 2005151 |
| Profile of Mood States | POMS | Depression subscale | Negative scores indicate better status | Puig et al. 2006152 |
| Geriatric Depression Scale | GDS | Depression | Negative scores indicate better status | Weber et al. 2004;68 Weber et al. 200769 |
| Hospital Anxiety and Depression Scale | HADS | Anxiety subscale | Negative scores indicate better status | Berglund et al. 2007;89 Koukouvou et al. 2004;91 Adamsen et al. 2009;168 Jarden et al. 2009;167 Banerjee et al. 2007;163 Johansson et al. 2008148 |
| State–Trait Anxiety Index | STAI | Anxiety | Negative scores indicate better status | Cohen et al. 2004;153 Courneya et al. 2003;161 Chandwani et al. 2010;159 Raghavendra et al. 2007;160 Carmack Taylor et al. 200666 |
| Functional Assessment of Cancer Therapy – Fatigue | FACT-F | Fatigue subscale | Positive scores indicate better status | Bourke et al. 2011;72 Courneya et al. 2003;171 Courneya et al. 2003;161 Jarden et al. 2009;167 Danhauer et al. 2009;169 Mutrie et al. 2007;147 Rogers et al. 2009177 |
| Fatigue Severity Scale | FSS | Fatigue | Negative scores indicate better status | Culos-Reed et al. 201080 |
| Chronic Respiratory Questionnaire | CRQ | Fatigue subscale | Positive scores indicate better status | Guell et al. 2000;81 Puente-Maestu et al. 200088 |
| European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-C30 | EORTC QLQ-C30 | Fatigue subscale | Negative scores indicate better status | Adamsen et al. 2009;168 Thorsen et al. 2005170 |
| Brief Fatigue Inventory | BFI | Fatigue | Negative scores indicate better status | Cohen et al. 2004153 |
| Piper Fatigue Scale | PFS | Fatigue | Negative scores indicate better status | Mock et al. 2005173 |
| Functional Assessment of Chronic Illness Therapy | FACIT | Fatigue subscale | Positive scores indicate better status | Moadel et al. 2007278 |
| Fatigue Scale | – | Fatigue | Negative scores indicate better status | Gifford et al. 199853 |
| Profile of Mood States | POMS | Fatigue subscale | Negative scores indicate better status | Pinto et al. 2005279 |
| Perceived Stress Scale | PSS | Stress | Negative scores indicate better status | Daubenmier et al. 2006;49 Gifford et al. 199853 |
| Derogatis stress profile | – | Relaxation subscale | Negative scores indicate better status | Bennett et al. 199171 |
| Brief Pain Inventory | BPI | Pain | Negative scores indicate better status | Carmack Taylor et al. 200676 |
| Medical Outcomes Study | MOS | Pain severity subscale | Negative scores indicate better status | Gifford et al. 199853 |
| Symptom self-efficacy scale | – | Self-efficacy | Positive scores indicate better status | Gifford et al. 199853 |
| Standford Inventory for Cancer Patient Adjustment | SICPA | Self-efficacy | Positive scores indicate better status | Weber et al. 2004;68 Weber et al. 200769 |
| Coping self-efficacy scale | – | Self-efficacy | Positive scores indicate better status | Heckman and Carlson 2007162 |
| Diabetes emotional distress scale | – | Distress | Negative scores indicate better status | Heisler et al. 201056 |
| Brief Symptom Inventory | BSI | Psychiatric distress subscale | Negative scores indicate better status | Lucy 199460 |
Appendix 13 Study characteristics of mixed-sex and female-only studies in analysis 2
| First author, year | Disease | Mean age at intervention | Self-management intervention | Allocation concealment bias |
|---|---|---|---|---|
| Adamsen 2009168 | Cancer: breast, bowel, ovaries, testes, oesophagus, brain, cervix, pharynx, pancreas, stomach and haematological | 47.2 years | Physical activity and relaxation | Low |
| Banerjee 2007163 | Cancer: breast | N/R | Yoga | Low |
| Bennett 2007154 | Cancer: breast and other | 55.5 years | Motivational interviewing to encourage exercise plan with follow-up and feedback | Low |
| Cadmus 2009158 | Cancer: breast | 54.5 years | Physical activity with follow-up and feedback | Low |
| Carmack 1995166 | Chronic kidney disease | N/R | Physical activity with family support, and follow-up and feedback | Unclear |
| Chandwani 2010159 | Cancer: breast | 51.39 years | Yoga | Unclear |
| Cheville 2010149 | Cancer: gastrointestinal, head and neck, lung, brain, other | 59.7 years | Physical activity with education and peer support | Unclear |
| Cohen 2004153 | Cancer: lymphoma | 51 years | Yoga | Low |
| Coultas 2005155 | COPD | First intervention 68.3 years; second intervention 70.1 years | Action plan, education, and follow-up and feedback | Low |
| Courneya 2003161 | Cancer: colorectal | N/R | Physical activity with follow-up and feedback | Unclear |
| Courneya 2003171 | Cancer: various | N/R | Physical activity with psychotherapy | Unclear |
| Danhauer 2009169 | Cancer: breast | 54.3 years | Yoga | Unclear |
| Demark-Wahnefried 2006150 | Cancer: breast and prostate | 71.5 years | Telephone counselling and printed material to improve physical activity and diet | Unclear |
| Donnelly 2011164 | Cancer: gynaecological | 53.5 years | Physical activity with follow-up and feedback | Low |
| Emery 1998165 | COPD | 67 years | Education | Low |
| Fillion 2008178 | Cancer: breast | 52.5 years | Physical activity with stress management and psychoeducation | Low |
| Heckman 2007162 | HIV | N/R | Tele-support covering either information support or coping intervention | Unclear |
| Jarden 2009167 | Cancer: haematological | 40.9 years | Physical activity with education | Unclear |
| Johansson 2008148 | Cancer: breast, colorectal, gastric, prostate | N/R | Psychological support and education | Unclear |
| Kouidi 1997175 | Chronic kidney disease | 49.6 years | Physical activity with peer support | Unclear |
| Dominique 2010156 | Cancer: breast | N/R | Physical activity and relaxation | Unclear |
| Moadel 2007279 | Cancer: breast | 55.11 years | Yoga | Unclear |
| Mock 2005173 | Cancer: breast | N/R | Physical activity with follow-up and feedback | Low |
| Mutrie 2007147 | Cancer: breast | 51.3 years | Physical activity with peer support | Low |
| Pinto 2005280 | Cancer: breast | N/R | Physical activity with follow-up and feedback | Unclear |
| Puig 2006152 | Cancer: breast | N/R | Education and psychotherapy | Unclear |
| Raghavendra 2007160 | Cancer: breast | N/R | Yoga | Low |
| Rogers 2009177 | Cancer: breast | N/R | Physical activity with peer support | Unclear |
| Stein 2007174 | HIV | N/R | Tele-support psychoeducation | Unclear |
| Thorsen 2005170 | Cancer: various | N/R | Physical activity with follow-up and feedback | Unclear |
| van Vilsteren 2005151 | Chronic kidney disease | 52 years | Physical activity with psychological intervention | Unclear |
| Wang 2011172 | Cancer: breast | 48.40 years | Physical activity with peer support and follow-up and feedback | Unclear |
Appendix 14 Quality appraisal findings of trials containing a gender group analysis
| First author, year, country | Was the group hypothesis specified a priori? | Was gender included as a stratification factor at randomisation? | Was gender analysis one of a small number of planned group hypotheses tested (≤ 5)? |
|---|---|---|---|
| Blanchard 1996,182 USA | Yes | Yes | Yes |
| GESICA Investigators 2005,183 Argentina | Yes | No | No |
| Hagen 2000184 and Molde Hagen 2003,185 Norway | No | No | Unclear |
| Hämäläinen 1997,186 Finland | Unclear | Yes | Unclear |
| Hanefeld 1991187 and Julius 1992,188 Germany | No | Unclear | Unclear |
| Härkäpää 1989,189 Finland | No | Unclear | Unclear |
| Heitzmann 1987,190 USA | Yes | No | Yes |
| Jensen 2001,191 Sweden | Yes | No | Yes |
| Kankaanpää 1999,192 Finland | No | No | Unclear |
| Katon 2002193 and Williams 2007,194 USA and Lebanon | No | Unclear | Unclear |
| Kendall 1987,195 USA | Yes | Yes | Yes |
| Kovar 1992,196 USA | No | Unclear | Unclear |
| Lester 2010,197 Kenya | No | No | Unclear |
| Mellin 1989,198 Finland | Yes | Unclear | Yes |
| O’Connor 2009,199 USA | No | No | Unclear |
| Penttinen 2002,200 Finland | No | Unclear | Unclear |
| Smith 2005,201 USA | Yes | Unclear | Yes |
| Vanninen 1993,202 Finland | No | Unclear | Unclear |
| Wing 1991,203 USA | No | Unclear | Unclear |
| Wing 1994,204 USA | No | Unclear | Unclear |
List of abbreviations
- 6MWD
- 6-minute walking distance
- AIDS
- acquired immunodeficiency syndrome
- BCT
- behavioural change techniques
- CASP
- Critical Appraisal Skills Programme
- CDSR
- Cochrane Database of Systematic Reviews
- CI
- confidence interval
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- COPD
- chronic obstructive pulmonary disease
- DARE
- Database of Abstracts of Reviews of Effects
- DBP
- diastolic blood pressure
- ENTREQ
- enhancing transparency in reporting the synthesis of qualitative research
- FEV
- forced expiratory volume
- FEV1
- forced expiratory volume in 1 second
- FFIT
- Football Fans in Training
- HCP
- health-care professional
- HIV
- human immunodeficiency virus
- HRQoL
- health-related quality of life
- LTC
- long-term condition
- MD
- mean difference
- MEDLINE
- Medical Literature Analysis and Retrieval System Online
- MeSH
- medical subject heading
- NYHA
- New York Heart Association
- PPI
- patient and public involvement
- PRISMS
- Practical systematic Review of Self-Management Support for long-term conditions
- RCT
- randomised controlled trial
- RECURSIVE
- Reducing Care Utilisation through Self-managemnt Interventions
- SBP
- systolic blood pressure
- SMD
- standardised mean difference