
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 12/129/32. The contractual start date was in November 2013. The final report began editorial review in June 2015 and was accepted for publication in November 2015. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
At the time of receiving funding for this project Jo Rycroft-Malone was a member of the National Institute for Health Research Health Services and Delivery Research (HSDR) programme’s Commissioning Board and is now its Programme Director. She is editor-in-chief of the HSDR programme.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2016. This work was produced by Rycroft-Malone et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Older people’s care context
The UK’s population is getting older: it is estimated that by 2031 one in five people will be over 65 years old. 1 In the UK older people (aged ≥ 65 years) account for approximately 16% of the population throughout England and Wales, with 14.7% of over-65s residing in Northern Ireland and 20% living in Scotland. 2 Research suggests that older people require care that encompasses both health and social care functions. 3,4 These needs require access to a wide range of generalist and specialist services including from statutory, independent and voluntary services. 5 Older people are the main recipients of care in the NHS, and thus care costs are relatively higher than those for working-age people. 6 The provision of health and social care for older people may be more complex because of existing conditions. For example, it is estimated that 40% of people in hospital care over the age of 65 years have dementia. 7
A series of recent investigations and high-profile cases have questioned current practices in services provided to older people. Both Francis Inquiries were focused on older people’s care. 8 The Care Quality Commission9 identified concerns over the skills, training and availability of the care workforce within hospital settings to deliver dignified and appropriate care and followed on from several other critical reports of the standards of care offered to older patients within the NHS. In particular, the Parliamentary and Health Service Ombudsman10 called for standards of NHS care for older people to be improved. Health Service Journal/Serco8 reference a range of recent publications in which concerns about older people’s inpatient care have been highlighted, including those from the Joint Committee on Human Rights,11 Age UK/NHS Confederation12 and the Office for National Statistics. 13 Furthermore, the preferences and experiences of older people may not always be reflected in care policies, structures and practices. 14,15
The rapid increase in the older-person population is driving current pressures to develop new service models, processes, roles and expertise for delivering effective and efficient care, especially when people have distinctive and often individualised care needs. Monetary investment in joint funding between the NHS and social care can support preventative care in older people’s services, for example falls prevention and reduced social isolation, and improve discharge pathways. 16 The NHS is increasingly moving to multisectorial services which are integrated around the patient,17 which should promote models of care for the future which prioritise social and medical needs and should be relationship based. 18 However, integration has been in danger of being reduced to political rhetoric19 owing to a lack of joined-up integration across services,20 and fragmented commissioning structures. 21 The personalisation agenda, whereby people fund their own care, direct payments and personal budgets, will lead to changes in the workforce in the future, with more emphasis on personal assistants and social enterprises. 22
As part of these changes, greater use and development of the support workforce in health and social care is likely to remain a long-term priority for NHS managers and other sector organisations. High-quality care provision for older people is a strategic priority. Public policy interest in the support workforce has heightened recently as policy-makers have faced a litany of care delivery failures. 23
Faced with an ageing population, escalating levels of complexity and need in NHS and social care services, and changes in workforce design (which include reduced working hours for doctors, nurse training and advancing roles), the demands on the support workforce will most likely increase in the future. 24
The support workforce
The health and social care support workforce is defined as providers of ‘face to face care or support of a personal or confidential nature to service users in a clinical or therapeutic settings, community facilities or domiciliary settings, but who do not hold qualifications accredited by a professional association and is not formally regulated by a statutory body’25 (quote contains public sector information licensed under the Open Government Licence v3.0). The support workforce delivers care alongside the regulated, professional workforce in their day-to-day duties under supervision. 24
Establishing a clear role definition for the support workforce is challenging. Role labels vary across health and social care services, from health-care assistants (HCAs) and support workers26 to health-care support workforce27 to care assistants or therapy assistants. 28
In acute NHS care, terms used to describe the support workforce include HCAs, nursing assistants, nursing auxiliaries, assistant practitioners and personal/clinical or health-care support workers. 23,29 The role is ill-defined in social care, with terms being used interchangeably to generally describe the support workforce, for example support worker, community support worker and social work assistant. 30 There is a lack of a common definition of the support worker role, largely due to the variety of duties that they perform. 31 This diversity and lack of clarity means that often support workers are ‘figuring it out in the moment’. 32
Across health and social care, the support workforce is large; an estimated 1.3 million people are working on the frontline of care,26 which can be categorised into the different types of roles they perform, including direct care, indirect care, administration and facilitation. In the UK, health-care support workers account for 47% of the total NHS workforce;33 thus, they constitute the largest group of staff. 28 Care assistants and health-care support workers account for 60% of estimated contact time with patients. 19,33 In England alone, support workers account for over 300,000 of the people employed in the NHS. 24 UK statistics are similar to those found across the globe. For example, assistant and support workers account for 50% of the health and social care workforce in Australia;34 in Canadian nursing homes, the unregulated support workforce provides 75–80% of direct care35 and health-care aides provide up to 80% of care for older adults in long-term care settings. 36,37 In the UK, most health-care support workers are female. 26,38 The health-care support workforce has been described as tending to comprise ‘mature women with partners and children’39 and to be more embedded within the local community than professional nurses. 40
In general, there is evidence to suggest that support workers are not deployed as effectively as possible and are often undervalued. 29,39 Research concerning this workforce has generally focused on their role and contribution in the acute care sector. 41 In this context, support workers have been described a providing the fundamentals of care by the bedside. 23 Research evidence addresses the development of staff (including support workers) to promote patient-centred care in particular situations, such as dementia services,29,42 and there is evidence about role boundaries for support workers in the context of different professional groups. 39,43 However, we could find only one study that has specifically explored the role of support workers in older people’s services. 44 Moreover, there are evidence gaps in understanding roles across different care settings,24 for example the community, independent sector, home care, third sector and social enterprise. This is despite an escalation in numbers of support worker roles; for example, an unprecedented rise in the numbers of community nursing assistants has occurred over the past 20 years. 45 In the face of policy developments such as personalisation and integrated care, a better understanding of support worker roles within community-based settings will become even more important.
Policy context for support workforce development
The use and role development of the support workforce has been somewhat ad hoc43 and largely dependent on the various activities they perform. 31 In the NHS policy context, the importance of HCA roles has not been underestimated, but the discourse about them has, at times, been ambiguous. 46 The literature reflects a general lack of clarity about the role of support workers,47 with roles developing organically rather than systematically, and, consequently, their preparation and continuing development has tended to be haphazard. 40
Probably the most significant review to emerge in the UK recent years relating to the support workforce is the Cavendish Review. 26 In response to the Francis Inquiry, Cavendish undertook an independent inquiry of the support workforce to ensure that all patients would be treated with care and compassion. 48 Based on the recommendations of the Cavendish report, a new certificate (the Care Certificate) is now under development, which will need to be completed in order to allow new HCAs and support workers to work unsupervised in care settings. 48 The Care Certificate is equally applied to the support workforce across health and social care, replacing the National Minimum Training Standards and Common Induction Standards, and reflecting the ‘6 Cs’ (care, compassion, competence, communication, courage and commitment). 49
In addition, in the UK, a group of recent publications4,26,50–53 have made recommendations for training for nursing assistants and HCAs. These reports have steered the commissioning of the Shape of Caring review. 49 In NHS care, Talent for Care has seen the development of a national strategy for all support roles in the Agenda for Change pay bands 1–4. The Talent for Care consultation in 2014 found universal support across the UK for a national strategic framework to develop the support workforce,27,50 underpinned by the Department of Health,50 which directed Health Education England to improve the training and development for the support workforce. However, although a number of publications point to the need to improve the skills and training approaches currently used to develop support workers,9 education, training and development for the support workforce remain challenging. 33 Further, there are other challenges for the support workforce, including career pathways, role substitution, regulation and retention, described as follows.
Career pathways
One of the recommendations from Cavendish26 was to strengthen the care career trajectory for the support workforce, and there is evidence that a number of health-care support workers aspire to develop their careers. 40 In social care, there is acknowledgement of the benefits of career pathways for support workers, but the picture is mixed. 30 It seems that, currently, the degree of synergy between workforce development and opportunities for job and role development is not always clear. Leadership, supervision and support should be developed in order to get the best out of people. 26,48
Role substitution
Support workers have been traditionally represented as low-cost labour source. 23 In recent times, the division of labour in hospital care has led to delegation of nursing tasks to care assistant roles. 54 Traditional workforce boundaries have altered drastically, with the support workforce taking on tasks previously undertaken by registered staff. 31,38 Although the growth in the support workforce has sometimes been driven by initiatives to reduce costs, involving role substitution for registered staff, there is a degree of evidence to show that support workers can act as an additional resource to enhance older people’s experiences by improving the contact with care practitioners. 35,44 In social care, there is role overlap between support worker and professional roles. 30 When the support worker role is perceived as a substitute for professional nurse tasks,46 this can potentially compromise morale.
Regulation
Regulation for health-care support workers has been debated at length in recent years but as yet remains unresolved. 46 In the UK, a major review of health support workers commissioned in 1999 examined health support workers’ roles and regulation. 55 Core competencies in Scotland were introduced in 2001, which informed further work about regulation for health-care support workers. 56 The current ambiguity about regulation means that there is little control over employment, responsibilities, education, competence, title and pay. 38 In social care, registration of home-care support workers has been recommended,57 with codes of conduct developed for health and social care workers58,59 in addition to governance frameworks. 60
Retention
Consistent employment patterns for clinical health-care support workers have been reported. 40 However, in social care, retention in home care is problematic, with one of the highest staff turnover rates at around 21%, twice the national average. 61 Securing new support staff and retaining those who are already employed in home care should be key priorities. 59 For joint working, staff retention is important, as it has been reported that frequent staff turnover can have consequences for the numbers of staff who champion integration. 16 Recommendations have been made for employers to be supported to test care values at recruitment stage. 26 However, in home care, high turnover demand and low pay can compromise values-based recruitment. 61
Workforce development interventions
For this review, workforce development interventions are defined as the support required to equip those providing care to older people with the right skills, knowledge and behaviours to deliver safe and high-quality services. 22 Evidence about interventions to develop the health and social care support workforce in older people’s care and services is limited, and there have been calls for evidence to inform services about how to improve standards for the future. 40 This is especially timely in the light of the introduction of new service models, for example training for staff in integrated services whereby the workforce is expected to work in different organisations and across traditional boundaries. 16 However, there is scant evidence to show how approaches to training and education can link with impacts for the people who are the users of services. 16 In social care, evaluations have already concluded that National Vocational Qualifications (NVQs) are inadequate and that there is a lack of clarity regarding training. 30
For the design and delivery of workforce development, current provision is inconsistent. 27 Access to good developmental opportunities (e.g. recent reporting of comprehensive and innovative training programmes62) sits alongside variation in mandatory training and induction. 26 NHS trusts and other services have adopted different approaches to workforce design and development models, which confounds attempts to show a universal picture across health and social care. Recommendations included the need to shift to more work-based approaches to learning and development for all staff including the support workforce. 63 In social care, lack of attention to developing skills for support workers to implement person-centred care planning has been noted. 30 In Scotland, recommendations about consultation with stakeholders in the design of workforce training, study skills and support systems were made to improve support workers’ education and training. 40
Previous work on the development of professionals has focused on advancing workers from novices to experts. 64 However, such models of education have focused on individuals who are already highly educated and with additional years of experience to build on, which is often not the case for the support workforce. The general lack of clarity and diversity in models, roles and care settings has resulted in a gap in knowledge about what makes for effective interventions. Moreover, much previous work has focused on how professionals learn, including the different processes for adopting new practices, rather than on considering contextual and structural barriers such as the role of organisational strategy and professional regulation. Further, workforce development interventions are characteristic of complex social programmes with inter-related components, the impacts of which are likely to be contingent on multiple personal, work-related and organisational factors.
Summary
Calls for change across recruitment, training and education for support workforce have been made. 26 The evidence presented in this chapter has shown where gaps exist in knowledge about how to develop staff across health and social care services. The issues highlighted show how it is timely for a review of workforce development for the support workforce, to understand what works and to develop the skills and knowledge of staff.
Review question and aims
This review was designed to identify interventions at individual, team and organisational levels that have the potential to enhance skills and care standards in the support workforce for older people. In addition, the review was designed to uncover how and why workforce development interventions may impact, and on whom, in order to guide future workforce development policy and practice.
Our research question asked ‘how can workforce development interventions improve skills and care standards of support workers within older people’s health and social care services?’.
The main aims of the study were to:
-
identify support worker development interventions from different public services and to synthesise evidence of impact
-
identify the mechanisms through which these interventions deliver support workforce and organisational improvements that are likely to benefit older people
-
investigate the contextual characteristics that will mediate the potential impact of these mechanisms on clinical care standards for older people
-
develop an explanatory framework that synthesises review findings of relevance to services delivering care to older people
-
recommend improvements for the design and implementation of workforce development interventions for support workers.
Chapter 2 Methods
Introduction
Following recognised realist principles and published guidance,65–67 and drawing on the previous experience of the team in undertaking realist review,68,69 we followed a number of stages in completing this project. However, unlike the stages of a traditional systematic review, which tend to follow a linear path, the process of a realist review is more iterative. This is because the review is theory and stakeholder driven, and it is the process of theory development and refinement that guides the search for evidence, the review of evidence (which evolves through the process) and, ultimately, the synthesis process. This process goes back and forth, and although we have presented the methods in stages below we have attempted to reflect an iterative process in the narrative. In this chapter, we provide a detailed description of each of the areas of evidence (stakeholder views, published literature and interview data) which informed programme theory development, refining and testing. In this report we have used the RAMESES (Realist and Meta-review Evidence Synthesis: Evolving Standards) publication standards (i.e. specific publication guidelines for realist syntheses). 67
Stakeholder engagement, including patient and public involvement
Stakeholders are key drivers in realist work. The realist synthesis focus is driven by ‘negotiation between stakeholders and reviewers and therefore the extent of stakeholder involvement throughout the process is high’. 67 Stakeholder contributions for realist synthesis can include clarification, checking meaning and developing theory. 70,71 For this review, stakeholder engagement was designed to help the research team elaborate on the review context, refine the review questions, contribute to programme theory development and interpret the evidence. Stakeholders were involved in a process of (a) prioritising and (b) refining the theory areas and making additions.
The research team adopted a systematic approach to stakeholder identification based on an impact and influence matrix72 to ensure that the most appropriate people were contributing to the review. Lists of potential stakeholders were drawn up to show who they were and to consider their potential input for the review. Stakeholder categories included users of services (i.e. older people, their care partners and families, and the public/media); providers of services (i.e. unregulated practitioners, professional practitioners and service providers/service managers, and education providers); service commissioners/funders and other relevant bodies (e.g. inspectorate bodies, advocacy, and professional bodies and government/policy-makers). Stakeholder engagement also incorporated the interactions with the Project Advisory Group members.
We identified 13 categories of people/groups who could bring different perspectives to the study (see Appendix 1 for information about stakeholder engagement). To help to identify levels of involvement with the project, the categories were then analysed further to consider the interests of the stakeholders and how, hypothetically, they could affect/be affected by the study’s aims and objectives. Consideration was given to the stakeholders’ interest, their particular influence (that would inform the study), potential impact level, expected concerns and stakeholder management throughout the study’s duration. The results of the stakeholder analysis were mapped onto a matrix to give consideration to the levels of influence and impact, expecting that levels of engagement for different stakeholders would change during the study’s duration. In addition, we searched for people active in representing older people at community level to secure patient and public involvement (PPI) in the project team and steering group. Three individuals were nominated and accepted the team’s invitation to participate. They became project team members and are coauthors of this report (for profiles see http://opswise.bangor.ac.uk/meet-team.php.en).
Stakeholder engagement in the review was as follows:
-
participating in workshops to explore the nature of, and identify key issues in, workforce development for the older persons’ support workforce
-
advising on priority issues within the review theory areas
-
commenting on iterations of the plausible hypotheses and context–mechanism–outcome (CMO) configurations
-
advising on specific stakeholders to participate in interviews
-
advising on knowledge mobilisation – including through a ‘WeNurses’ Twitter chat (Twitter, Inc., San Francisco, CA, USA) (see Appendix 2 for a summary).
In addition, PPI representatives attended all monthly meetings of the project team, and were consulted on specific issues in between. Representatives also attended initial exploratory workshops along with other stakeholders and this led the construction of some review artefacts, including a plain English glossary of review terms (see Appendix 3).
Changes to the review process
No changes to the review process were made subsequent to the publication of the review protocol. 73
Rationale for using realist synthesis
Realist synthesis is theory driven. In this way, realist synthesis works under the principle that it is the unseen elements of a programme (the mechanisms) that lead to its success or failure. Contingent relationships are expressed as CMOs, to show how particular contexts or conditions trigger mechanisms to generate outcomes. Mechanisms are ‘the pathway from resource to reasoning and response’,74 and resources can be described as those that are ‘material, cognitive, social or emotional’. 75 The reasoning and response may stem from the perspectives of the receivers, the organisers or those involved in the delivery of programmes/interventions.
As Pawson and Tilley remind us, social programmes (i.e. workforce development interventions/programmes) are ‘theories incarnate’. 76 Programme theory ‘describes the theory built into every programme’77 and is expressed in this way: ‘if we provide these people with these resources it may change their behaviour’. 75 Different sources of evidence are used to construct programme theories but they emerge from a systematic process that includes stakeholder engagement, an overview of relevant extant theory77 and scrutiny of primary research. 78 In this review, theory development work was undertaken in phases 1 and 2, to articulate theories about ‘what works’ in workforce development for the support workforce in health and social care and the conditions that might make them successful.
Workforce development interventions for the support workforce for older people are complex social programmes, involving people, structures and organisations. In this review, workforce development interventions were defined as the support required to equip those providing care to older people with the right skills, knowledge and behaviours to deliver safe and high-quality services. 22 As such, the way in which they might work will be contingent on a variety of factors and, therefore, synthesising evidence to explain this required an approach that could accommodate both complexity and contingency. We consequently undertook a theory-driven approach to evidence synthesis, which was underpinned by the realist philosophy of science and causality. 67,73
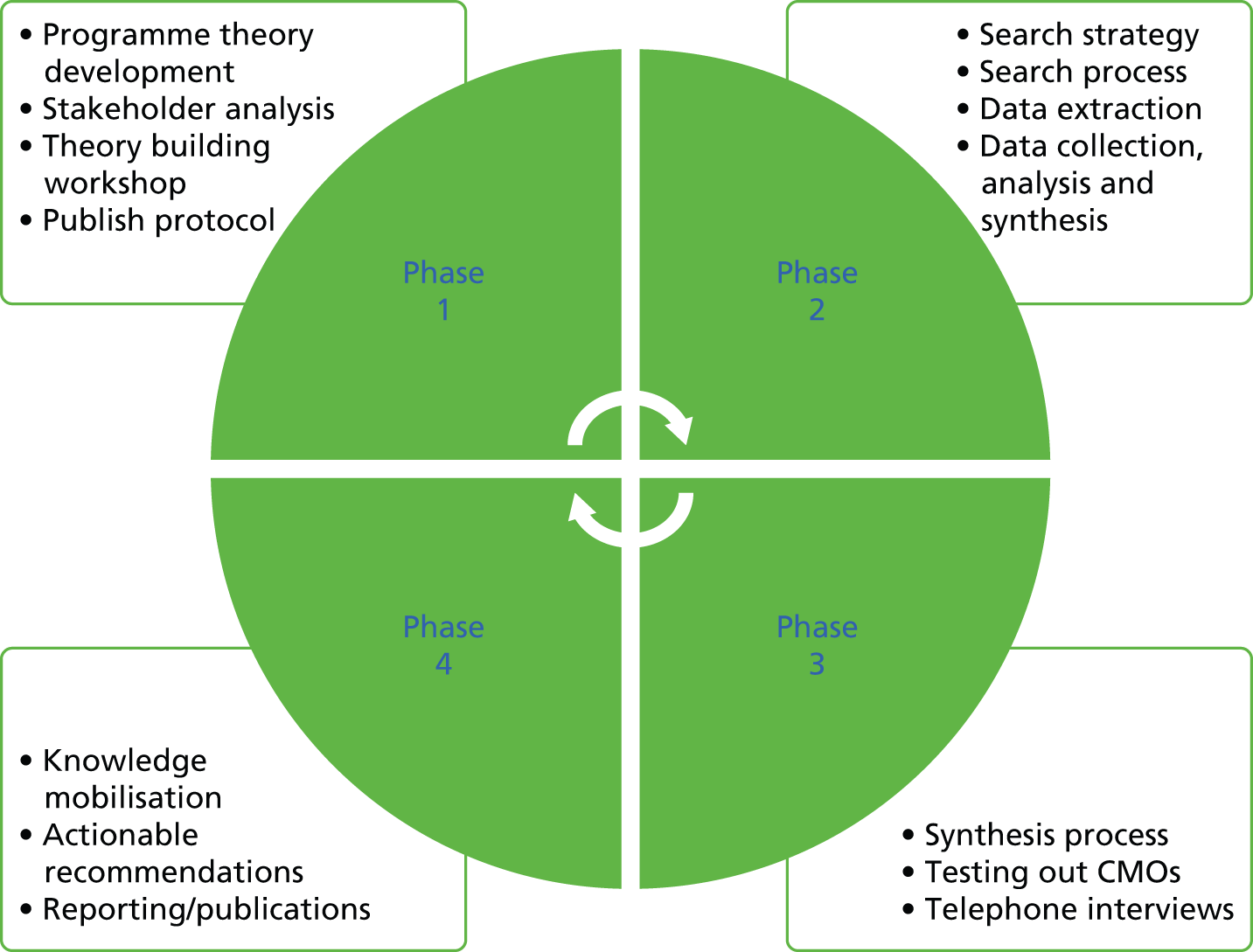
Programme theory development and refinement involved in a number of interconnected processes (Figure 1), including:
-
scoping the literature
-
concept mining
-
conceptualising workforce development – stakeholder workshop, which was guided by soft systems
-
identification of theory areas
-
-
searching processes
-
selection and appraisal of documents
-
data extraction, analysis and synthesis processes.
FIGURE 1.
Phases of the study.
The process and outputs of each of these activities are described in more detail in the following text.
Scoping the literature
Concept mining
Concept mining was undertaken to map evidence about the support workforce, workforce development interventions, older people’s services, how interventions might operate and any reported enablers or barriers to the successful implementation of interventions. Concept mining in realist synthesis describes a process of searching through different bodies of evidence for information that could help build theories. In this review, concept mining involved searching through different bodies of evidence (including the commissioning brief, policy/guidance and grey literature) for information that could build theories about workforce development.
The starting point for the review was the commissioning brief, which was subsequently reflected in the funded proposal. 79 Particular points worth reiterating here relate to the nature of the work of the support worker; how training and support interventions should reflect variety in need across different organisations/settings; the focus of training (task/core competencies vs. values-based approaches); effectiveness and cost-effectiveness; ‘best’ interventions; teaching methods, organisational development and performance management; and impacts of workforce development interventions (for individual support workers, teams and older people).
In a background search of some policy documents,41,60,63 we found literature about the perceptions of support worker roles, gaps identified in skills training, how training and development should be structured for the support worker, approaches to workforce development, professionalism and the working environment. Key concepts identified from this background search included:
-
how support workers who feel valued and empowered are more likely to promote dignified care
-
how management support in the workplace can enhance autonomy and decision-making
-
the challenges of over-reliance on personal experience without specific guidance
-
continuing professionalisation of care work so that support worker roles can be promoted
-
how personal development can build knowledge and skills
-
dimensions of quality, including dignity, communication and understanding of the older person as an individual
-
use of multiple, flexible learning and teaching strategies to promote confidence
-
increase of the attractiveness of care work through the provision of development opportunities.
To guide our development of the programme theories, we conducted an initial exploration of theory which might help to show how workforce development should work and identify what factors can supposedly support or hinder its success, for example learning from theories of professional learning, which included the role played by informal learning80 and role progression, and the development of expertise in developing learning. 81 We drew on the work of authors64 to consider how the mental activity required for skill acquisition varies from novice to expert (i.e. workforce development interventions should meld with the support worker’s developmental stage). Theories of adult and transformational learning were also relevant to be considered in the context of how interventions may be underpinned by holistic education, taking into account cognitive, affective and psychomotor domains. 82 We also examined how workforce development is defined in other disciplines, for example education83,84 and employment. 85 We considered variation in workforce development implementation for the support workforce,26 issues of workforce changes and substitution31 and how to link different development interventions and workforce functions. 33 Theories of behaviour change were also considered, as they focus attention on how to develop individual skills and knowledge. 86 From an implementation perspective (i.e. literature that might help to explain how interventions/programmes get implemented in practice), we considered how knowledge use may be influenced by factors related to the work environment and facilitation,87 and, from education, how the choice of intervention should suit the context. 88 We also mined the practice development literature to be cognisant of how workplace cultures can be improved. 89 We also felt it important to take into account the role of organisational and other contextual influences that might influence workforce development intervention design, delivery and evaluation, including individual, team and organisational foundations for learning organisations90,91 and other factors which enhance or act as barriers to learning. 92
Conceptualising workforce development
At the beginning of the project we held a workshop in which stakeholders contributed to the development of the scope and issues that are relevant to the workforce development of support workers with older people’s health and social care services (see Appendix 4 for workshop participants). The workshop was facilitated by two members of the research team (CB and LW). Stakeholders were purposively sampled to ensure representation from relevant constituencies (i.e. health, social care, education, third sector, patients and the public).
The structure of the workshop was guided by soft systems thinking, a learning approach which offers an interpretive perspective of the complex and adaptive nature of human systems, such as workforce development, within the ‘real world’. 93,94 Soft systems methodology complements the realist approach used in this review, as it takes into account how complex systems within which programmes or interventions are situated may be underpinned by different perspectives. 95 We found that applying the principles of soft systems methodology helped the team to operationalise the workshop in a structured way. In addition, soft systems methodology helped us to guide stakeholders’ thinking, so that they could shed light on some of the complexities behind workforce development for support workers. We chose this approach as we assumed workforce development to be transformative of both individuals and contexts, with the potential for both complementary and conflicting structures, processes, impacts and perspectives. We applied the principles of soft systems in two ways:
-
the use of the CATWOE mnemonic (see below) to structure data collection, discussion and analysis
-
the generation of rich pictures describing how workforce development works.
The CATWOE mnemonic provided a structured way of thinking about the complexity of workforce development programmes by focusing on the beneficiaries of workforce development (customers), the roles and functions of people within workforce development (actors), the changes that workforce development makes (transformations), the beliefs about what is important in workforce development (world views), issues of leadership (ownership) and physical and other constraints on the system (environment). 95
The first phase of the workshop included table discussions around the CATWOE issues (Table 1).
| CATWOE elements | Trigger questions |
|---|---|
| Beneficiaries (customers) and roles and functions (actors) | What are the roles of older people and others in workforce development? |
| Who should be involved in designing workforce development programmes and strategies? In what ways? | |
| Transformations | What changes are required? |
| Where are interventions likely to work/fail? | |
| World views | What are the current problems/challenges facing the staff now? |
| How should these issues be picked up in workforce programmes and strategies? | |
| What are the political/professional and other influences on the support workforce that we need to consider? | |
| Ownership | Who/what can influence success in developing workforce interventions? |
| Constraints (environment) | Can you foresee any constraints/barriers? |
The output from these discussions was used to develop rich pictures to illustrate the complexity of a workforce development ‘system’ by linking the CATWOE elements, for example:
The rich pictures provided the basis on which to develop a stakeholder-driven textual summary of how workforce development for the support workforce for older people should operate:
-
The effectiveness of workforce development interventions/programmes for the older people’s support workforce can span outcomes for the workforce (e.g. knowledge, skills and attitudes, career progression and personal/professional development); for the delivery of services; for older people and their carers (e.g. service effectiveness and experience); and for organisations (e.g. service quality). Interventions/programmes are most effective when positive impacts from workforce development can be identified in all of these areas. For example, changes in the knowledge and skills of the support workforce will often require changes in organisational systems or processes for benefits to be accrued by older people, and vice versa. When these impacts do not meet the expectations of older people or health organisations, then positive, individual changes from workforce development programmes/interventions might be evident but might not be sustained.
-
Workforce development will be effective when it is aligned with organisational and other career development frameworks and opportunities. When these frameworks are used to design and evaluate workforce development, benefits for individual members of the workforce may have greater visibility and meaning.
-
Effective workforce development is designed, implemented and evaluated with the older people’s support workforce and practice. Programmes or interventions that are neither grounded in the reality of daily work completed by the older people’s support workforce, nor delivered within in the workplace, are less likely to be effective.
-
Effectiveness can be mediated by the personal characteristics of members of the older people’s support workforce (e.g. motivation, self-esteem, confidence and learning styles); aspects of human and social geography; characteristics of the organisations in which the support workforce is operating; workforce and service policy; and public experiences and expectations.
Identification of theory areas
This initial conceptualisation was used to generate a longlist of issues in four theory areas for focusing the review (see Appendix 5). These were reviewed and prioritised by stakeholder workshop participants and then by the Project Advisory Group members in a face-to-face meeting. They were broadly grouped into theory areas: career development and strategy, design and delivery, and mediating factors and impacts.
Searching processes
As theory development work was under way, the process of developing the search strategy continued, led by the project’s information scientist (BH) and involving the research team and feedback from the steering group. The process involved searching for evidence relevant to the theory areas.
Reflecting the realist approach, the search strategy was broad and eclectic96 and combined a primary search and purposive searches in order to capture the most relevant evidence to support or refute the ideas within the initial programme theories. For the primary search, a list of search terms was created from the theory development work (concept mining and conceptualising workforce development). Search terms used for the support worker captured data to inform the mediating factors theory area (e.g. personal characteristics, gender, cultural issues). In addition, further searches found other data relevant to mediating factors (e.g. leadership or policy).
Test searches were set up in MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Social Services Abstracts (SSA) and titles/abstracts were inspected for search terms. Longlists of terms were drawn up for support workers, workforce interventions, and outcomes for support workers, older people/carers/families and organisations. The search term list for the support workforce was adjusted to include terms that emerged from scrutinising the literature, for example care attendants, health-care aides, personal support workers, hybrid workers and care providers (see Appendix 6). Search term lists were rationalised and checked against MeSH (medical subject headings) when available, and checked alongside the developing set of programme theories. Search terms for support workers in education and policing were also retrieved, for example para educator, special education assistant, aide, instructional assistant, paraprofessional, police community support officer, special constable, and operational support grade. The logic for deliberately looking beyond health was to refine the emerging findings from the health and social care literature, and to ascertain whether or not there is any cross-sector learning given that support roles exist in other public services.
Primary search of databases
The major health, social and welfare databases were searched using keywords identified through the search development and database specific ‘keywords’ adapted for each information source (see Appendix 7 for an example of search strategy). The primary search was limited to material from 1986 (the date of the conception of NVQs) to 2013. Methodological filters were not used to avoid excluding any potentially relevant papers. Systematic searches were conducted in 10 electronic databases subscribed to by Bangor University: PsycINFO; SSA; Sociological Abstracts; MEDLINE; NHS Economic Evaluation Database; Web of Science; CINAHL; The Cochrane Library; Applied Social Sciences Index and Abstracts; and Database of Abstracts and Reviews of Effects.
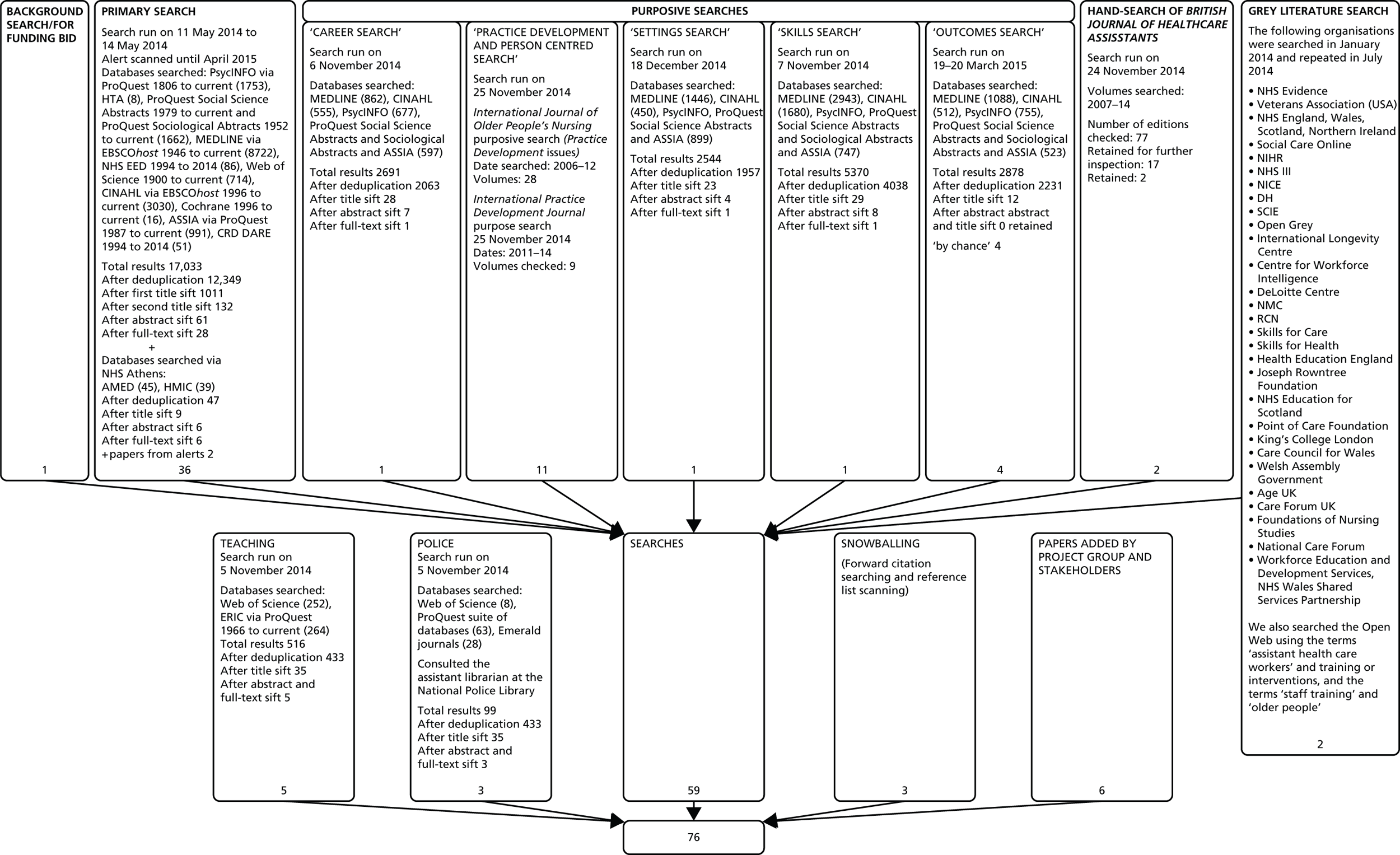
The searches took place in April and May 2014. References were stored in RefWorks database software (ProQuest, Ann Arbor, MI, USA: www.proquest.com/products-services/research-tools/). The systematic databases search yielded 17,033 references; 4684 of these were duplicates, leaving 12,349 hits included for title screening. Hits for each database are shown in Figure 2. Alerts were set up for the database searches and alerts were scanned up to April 2015.
FIGURE 2.
Results of search and retrieval. AMED, Allied and Complementary Medicine Database; ASSIA, Applied Social Sciences Index and Abstracts; CRD, Centre for Reviews and Dissemination; DARE, Database of Abstracts of Reviews of Effects; DH, Department of Health; ERIC, Education Resources Information Center; HMIC, Health Management Information Consortium; NHS EED, NHS Economic Evaluation Database; NICE, National Institute for Health and Care Excellence; NIHR, National Institute for Health Research; NMC, Nursing and Midwifery Council; RCN, Royal College of Nursing; SCIE, Social Care Institute for Excellence.
Purposive searches
In realist synthesis, a Cochrane-type systematic search strategy is unlikely to yield all sources to inform the testing and refinement of the programme theories. 97
In a review related to complex evidence, only 30% of sources were obtained from the database and hand-searches, while 51% were identified by snowballing and 24% were obtained through personal knowledge/contacts. 98
In the current review, purposive searches of the evidence were conducted to provide specific focus on the programme theories. The primary search for references was augmented by other searches for support worker role evaluations or intervention research which made specific reference to embedded implementation or impact (e.g. around careers, location, settings, skills or outcomes). Purposive searches were also conducted in Allied and Complementary Medicine Database, Health Management Information Consortium, education, policing and the practice development literature. In addition, a hand-search was conducted in the British Journal of Healthcare Assistants. Other papers were added through snowballing, from database alerts and from project group and stakeholders (see Figure 2). Internet-based searches for grey literature were conducted for workforce development project reports, national inspection and regulation quality reports, and evaluative information about these initiatives.
Selection and appraisal of documents
Evidence was excluded only if did not relate to the theory areas. The test for inclusion was if the evidence provided was ‘good and relevant enough’ to be included96 (see below for further information about how this criteria was operationalised). Drawing on the previous experiences of the research team,66,69 data were extracted if they were ‘good and relevant enough’. 96
The test of ‘good and relevant’ enough is potentially vague and could lead to a lack of transparency about decision-making. Therefore, through critical discussion within the core team, we developed an additional subset of constructs which were added to the data extraction form in the form of a flow chart (see Appendix 8). The flow chart provided a set of additional questions which affirmed the judgement made of the extracted data, and reported its potential to contribute to the review. ‘Good enough’ was deconstructed as the quality of evidence expressed through fidelity, trustworthiness and value. ‘Relevance’ related to the contribution of the evidence to the theories. Member checking with reviewing took place within the research team. Title-sifting was cross-checked across three team members (JRM, CB and LW). Levels of agreement across reviewers were scored for 6% of the total titles. The title-sifting example was also checked with JRM, CB, LW and BH.
Data extraction, analysis and synthesis processes
In realist synthesis, theory development, refinement and testing is an iterative process of review and refinement and is made visible through bespoke data extraction forms. 66,96 As such, data extraction was undertaken in an iterative way across the review. 99 Initially, a bespoke data extraction form was developed from the four theory areas (see Appendix 9) to provide a template to extract evidence (if it met the test of relevance; see above). Member checking with extraction took place within the core research team. A sample of evidence was cross-checked across three team members (JRM, CB and LW).
Data were organised into evidence tables representing the four theory areas (see Appendix 10 for an example). In addition, data were organised into evidence tables representing a continuum ranging from conceptual (awareness, knowledge and understanding) to instrumental (attitudes and perceptions) to direct impact (practice change). 100 As we were extracting data we also began the process of synthesis.
The realist synthesis is theory-driven and uses abduction to understand CMO configurations. 101 Synthesis is a process of triangulation102 that melds different sources of evidence in a process of theory development, testing and refining. Through the previous experiences of the research team66,69 and building on the suggestions of Pawson96 and the principles of realist enquiry, we undertook an abductive and retroductive analysis of evidence across the tables to look for emerging demiregularities (patterns). Reflecting the interpretive nature of the review, the quality and relevance of the evidence was assessed during the synthesis process103 through weighing up the contribution of each piece of information to the development of the explanatory account and to the review question and aims. 74,104
This contrasts with traditional Cochrane-type reviews, which support the use of more quantitative statements of ‘how much’ evidence (and of what type) to underpin the findings.
This process was facilitated by the development of a set of plausible hypotheses – ‘if . . . then’ statements about what might work, for whom, how, why and in what circumstances – about workforce development interventions for the support care workforce:
-
If workforce development is closely related to practice (cognitive and/or physical), then the intervention is more relevant and more likely to be applied.
-
Taking staff away from practice for workforce development results in them feeling as if there has been an investment made in them and gives them more headspace, and they are more likely to feel valued by employer/organisation.
-
Depending on the nature/issue/purpose of the workforce development intervention, a multiprofessional approach to learning/delivery is more likely to be effective and engender cohesion.
-
When design and delivery of workforce development is seen to be credible, support workers will engage more/it will have more relevance.
-
When workforce development integrates personal perspective and professional perspective so that the support worker knows what is expected of them, it may have more relevance.
-
When/if workforce development fits with the organisational strategy/philosophy, then the support worker will feel more valued.
-
If the focus of workforce development is on where people are coming from/starting from, and design and deliver interventions around this, then the interventions are going to be more effective.
-
If workforce development is operating at more than one level (individual, team, organisation, system), then the impact is likely to be greater.
-
If workforce development is appropriately targeted at individual, team, organisation, system, then it is more likely to be effective.
-
When workforce development reinforces behaviour and learning, it is more likely to be effective.
-
When workforce development is aligned with incentives, it is more likely to be effective.
-
If there is a clearly articulated predefined theory/postulated mechanism of action about workforce development, then it is more likely to be effective.
-
When implementation features are embedded in the design and delivery of workforce development, it is more likely to be effective.
Reflecting the iterative refinement of the theory development process, these plausible hypotheses led to a revision in the data extraction form (see Appendix 11). We did a further ‘dive’ into the evidence with this revised data extraction form.
Following data extraction of the whole pool of evidence, tables were developed that summarised the evidence we extracted relevant to each plausible hypothesis. These evidence tables were then used as the basis for further deliberations about the emerging contingencies we could see within and across the extracted data. The extraction and synthesis process was managed on a day-to-day basis by the local research team (LW, CB and JRM) with regular input (face to face and via e-mail) from the wider project team, including our patient and public representatives.
This deliberative and iterative process enabled iteration from plausible hypotheses to the uncovering of CMO configurations (see Appendix 12 for summary of tracking of plausible hypotheses to CMO configurations). The result was eight configurations, which are summarised in Table 2.
| Context | Mechanism | Outcomes |
|---|---|---|
| ‘Making it real’ [to the work of the (individual) support worker] | ||
| When intervention design and delivery is proximal to the work of the HCA/support worker in that it is close to and pays attention to practice . . . | . . . this prompts resonance, in that the workforce development intervention is relevant because it resonates with individuals participating in it, makes it understandable, is congruent to their experience, has work-related meaning and significance Achieved through activities – vignettes, stories, reflection, reflective conversations . . . building on the oral tradition of the support workforce Situating in the workplace However, taking away from practice can also provide legitimate space, stops disruption, providing opportunities for access to different sorts of expertise . . . |
. . . which results in cognitive and practice changes for individuals including cognitive changes (e.g. seeing things differently, changing mental models, deepening knowledge, self-esteem, confidence, focusing attention on the right things, being able to see what is important, seeing the person as a person) AND practice changes/impacts: appropriate caring behaviours |
| Where the support worker is ‘coming from’ | ||
| If workforce design and delivery pays attention to the support worker’s personal and role starting points and expectations . . . | . . . this prompts increased engagement with the development opportunity, which leads to . . . | . . . personal cognitive impacts (e.g. personal efficacy), instrumental impacts (e.g. skills development) and potentially, organisational impacts (e.g. staff commitment) |
| Tapping into motivations | ||
| If workforce development is incentivised (to turn up to the workforce development intervention and in ongoing engagement), and in some professional and service contexts . . . | . . . then the HCA/support worker will feel rewarded and recognised . . . | . . . and so feel that they have a stake in the workforce development . . . increased participation and engagement |
| Joining things up | ||
| If workforce development interventions are developed in the context of the presence of an organisation’s strategy . . . | . . . this prompts alignment . . . | . . . and leads to more sustained, lasting impact of the workforce development intervention, reducing turnover/supporting retention strategy |
| Co-design | ||
| If the right mix of people (including service users) are engaged in design of workforce development programmes/interventions . . . | . . . this prompts co-design because the workforce development accommodates a collective view about what needs to be done . . . | . . . and leads to workforce development that is more credible, meaningful and impactful for the HCA/support worker |
| ‘Journeying together’ | ||
| If the right mix of people (including service users) are engaged in delivery of workforce development programmes/interventions . . . | . . . this prompts learning together (‘journeying together’) . . . | . . . and leads to engendering cohesion, greater understanding of each other’s roles, impacts on residents’ perceptions of care |
| Taking a planned approach | ||
| If there is use of theory and a planned approach in design, delivery and evaluation of workforce development . . . | . . . this prompts a more systematic process in planning, and delivering workforce development . . . | . . . and leads to greater potential to demonstrate impact, and learn about workforce development effectiveness |
| Spreading impact | ||
| If the workforce development programme/intervention is comprehensive in that it is multilayered (micro, meso, macro) and multifaceted . . . | . . . this prompts paying attention to the way components reinforce each other . . . | . . . which leads to increasing the potential for impacts to embed and spread across organisations |
An evidence-based narrative was developed under each CMO configuration by drawing on evidence in and across the data tables.
Programme theory testing
To enhance the trustworthiness of the resulting CMO configurations and to facilitate the development of a final review narrative, we conducted 10 semistructured, audio-recorded interviews with stakeholders. We used a mixture of purposive and snowballing sampling to obtain the perspectives of people who would reflect those who would have a stake in the findings. The interviews were structured for the purposes of testing out the CMO configurations, with data confirming or disputing each mapped directly onto the CMOs. The interviews facilitated the development of the final CMO narrative. Our sample comprised managers, directors for training/development and support workers. An interview schedule was developed based on the CMO configurations to elicit stakeholders’ views on whether or not they resonated with their experience, and whether or not and how they might operate in practice (see Appendix 13). All the interviews were conducted by telephone and lasted between 45 and 60 minutes. All interviews were audio-recorded and concurrent detailed notes were made.
The audio-recordings were fully transcribed. As the interviews were structured for the purposes of ‘testing’ out the CMO configurations, data confirming or disputing each were mapped directly onto the CMOs. In fact, the interviews provided mainly confirmatory evidence of the CMOs and provided some additional contextual evidence to each. Evidence from the interviews is combined in the narrative for each of the CMO configurations reported in the next chapter.
Ethics
The study fell outside the scope of NHS and social care requirements for ethics review; however, we sought ethics approval from Bangor University’s research ethics committee to conduct the interviews. Approval was granted on 27 August 2014 (number 2014-06-03) (see Appendix 14).
Chapter 3 Findings
Introduction
As Chapter 2 outlined, the theory development, refinement and testing process led to the distillation of eight CMO configurations. These are explanations that, cumulatively, constitute a programme theory about ‘what works’ in workforce development for the older persons’ support workforce. These CMO configurations emerged from the evidence and were verified with stakeholders. They are not mutually exclusive and we hypothesise that, in order for workforce development interventions to have maximum impact, paying attention to elements of each will be important.
In realist review the analytical task is to draw across the evidence base to provide explanations expressed in the form of CMOs; in other words, it is rare that one CMO is reflected in its entirety in a single piece of evidence. Therefore, we describe each CMO configuration in terms of the underpinning evidence, drawing on the included studies (see Appendix 15), interviews and stakeholder perspectives which have been embedded in the conduct of the review. Illustrative excerpts from the literature and quotations from interviews are embedded in these explanations to highlight meaning and salient points. We also include some practical examples of the ways in which the components of each CMO were visible in the interventions included in the review.
The review process, including findings from stakeholder interviews, resulted in eight CMO configurations. These are explanations that, cumulatively, constitute a programme theory about ‘what works’ in workforce development for the older persons’ support workforce. These are:
-
making it real to the work of the support worker
-
where the support worker is coming from
-
tapping into support workers’ motivations
-
joining things up around workforce development
-
co-design
-
‘journeying together’
-
taking a planned approach in workforce development
-
spreading the impacts of workforce development across organisations.
Context–mechanism–outcome 1: making it real to the work of the support worker
If intervention design and delivery is close to the work of the support worker (context), then this prompts resonance with individuals participating in it (mechanism), which can result in cognitive and practice changes in them (outcome) (Box 1).
Tools and techniques: videos, role play, ‘homework’, simulation, debriefing, care planning, visual tools.
Supervision of practice: group, follow-up, one-to-one supervision.
Working together: debriefing, sharing experiences, case conferences.
Focusing on the individual: case studies, biographies, vignettes, goal planning.
Context and mechanism
A strong relationship was evident between the proximity of the workforce development intervention and real-life work of the support worker, and specifically whether their work was immersed or disconnected from the intervention. Proximity was a feature of development initiatives that were closely aligned to the work of the support worker, delivered in practice or closely related to practice. 105–127
Proximity prompted feelings of resonance, when the intervention focused on what the support worker might experience in their work and what was familiar and relevant to them. There were two different forms of proximity in the evidence:
-
cognitive proximity,106–110,112,113,115,117–119,121–125,128 which was evident in intervention specifics or content, and judged by the extent to which the applicability of the intervention to the support worker’s own work practice could be observed, and/or
-
physical proximity,105,107,111,114–116,120,126,127 reflected in intervention delivery, was physically located in the support worker’s workplace.
Cognitive proximity
When the design of interventions was intentionally focused on the role and work of the support worker, this was more likely to prompt resonance. This was exemplified by learning tools and techniques that drew on real-life work, supervision of practice, working together and focusing on the individual, including the use of films. 108,109 To teach person-centred caregiving skills to support workers from an older persons’ service, one intervention included the viewing of Putting Person Before Task, a 7-minute film showing support workers modelling person-centred care, as the basis for participation in further role-playing activities. Visual depictions of the reality of older persons’ services and experiences were also used to make the intervention more engaging:121
Visual tools such as photographs of various situations and story-telling became the bases for discussion. The emphasis was on doing, experiencing, discussing, and team problem-solving-rather than didactic teaching.
p. 3121
Cognitive proximity also featured in interventions that paid attention to the personal backgrounds of older people. Case studies of care home residents were used in one intervention to enable support workers to link the needs of care home residents with their knowledge of the person. 121 Resonance with the work of the support worker was also evident in interventions which focused on individual older people within workers’ services [in this case, certified nursing assistants (CNAs)] through, for example, the creation of care home residents’ biographies:108
. . . an innovative way of making personal information about residents available to CNAs. Creating videotapes of CNA/resident caregiving interactions and using them, in conjunction with behavioral observation instruments, is an innovative way to promote CNAs’ self-awareness of the person centeredness of their caregiving behaviors.
p. 697108
Interventions similarly driven by biography invited support workers to share their feelings about caring with people with dementia128 and helped staff to get to know the person they were caring for:118
. . . collecting biographical material about people’s lives helped them to gain a more dynamic and complete picture of those for whom they were caring, and that knowledge of people’s life stories enabled them to find out more about residents’ needs and behavior.
p. 701118
Role play, with a facilitator playing the role of an older person in a residential care setting, was used to teach communication skills so that the support worker could learn how to individualise their approach. 117 Support workers learned the significance of information in the individual biographies of the older person in shaping communication. In addition, homework sessions were included to promote self-reflection about actual practice, in which participants were asked to design a short- and a long-term care plan to address the specific needs of an individual resident,117 and ‘overcome a care-related problem that they identified within their own clinical settings’. 110 This was reviewed at sessions with their peers and mentors. The use of care planning strategies that drew on real-world challenges, such as how to deal with challenging families, also ensured that the intervention had work-related meaning and significance for the support worker. 110
In training for care staff to recognise depression in residential care settings,127 a bespoke care planning intervention was implemented over an 8-week period, with support workers working together with residents to plan their care, and supported through weekly one-to-one supervision sessions over the 8 weeks. Interview data reinforced the utility of developing, sharing and reviewing care plans to bring learning to life; for example:
I think one of the things that we did that was really . . . beneficial, was writing our own care plans together, and looking at how intricate we were as people, and how bizarre some of the things were that were important to us, as people, and I think for me it was quite a learning curve as a manager.
Telephone interview, participant 1
In a series of seminars provided by a multidisciplinary team, a similar attempt was made to ensure that the intervention was congruent with the support worker’s own experiences of work:
The main aim of goal planning was to encourage care staff to formulate a specific and detailed care plan with a view to positively changing problematic areas of a resident’s behavior.
p. 234125
Other aspects of workforce development interventions that enabled proximity to the work of the support worker included experiential learning approaches,121 which ‘enabled the [support worker] to experience (in some degree), the difficulties that frail residents faced, and to identify the care practices that could be used to ameliorate those difficulties. . .’ (p. 3). 121 In a different report, proximity to the work of the support worker was supported by a clinical component to the education course which consisted of ’24 hours of “hands-on” patient care in a long-term facility under the direction of the course instructor’. 106 Fortnightly group supervision was complemented by individual training sessions for support workers in care home settings,107 whereby trainers observed support workers at their work and provided feedback. When there were opportunities for support workers to share experiences through group debriefing,115 groups were established ‘to use the experience of caring for a resident who has died as a basis for learning about end-of-life care’ (p. 120). 115 In this case, the groups were led by a nurse specialist in palliative care, and open dialogue approaches were used to encourage engagement. In addition, it was reported that debriefing promoted ‘reflection in action’ and made the intervention realistic for participants. 119
Cognitive proximity also featured in other examples, including case conference style approaches in which registered professionals chose the topics and led the case presentation and discussion. 124 This helped to capture support workers’ imagination and challenge their own thinking. The benefits of more interactive approaches that included the discussion of cases were reinforced in interviews; for example:
We’re also using supervision and appraisal very much as a training tool, so I think we’ve missed a trick there with those, it’s been a little bit ‘are you OK’ ‘yes you are that’s fine off you go’, actually using that to really encourage discussion looking at particular case studies, so it’s more like a clinical supervision . . .
Telephone interview, participant 1
In addition to the use of vignettes, practice tools and biography to bring work with older people ‘to life’ for participants, desirable aspects of the support worker’s work were made evident in other parts of workforce development interventions. This included an application process, which used a questionnaire, a written essay and an interview, for participants to access the intervention. In this example, applicants were expected to model professional conduct,106 and contracting was included at the start of the intervention to promote the modelling of professional behaviours106 and to specify prerequisites related to the support worker role. 129,130
There was also evidence to illustrate the advantages of drawing on the experience of older people themselves in the delivery of workforce development in making learning real. For example, in a paper that reported a feasibility study of an education programme, we found that the delivery included people with aphasia as educators,131 which was designed to improve nursing assistant students’ knowledge of aphasia, and supported examining the experiences of participants with aphasia.
Physical proximity
Proximity to the work of the support worker also featured in a physical/geographical sense, when interventions were deliberately based in the workplace. 106,107,114,127 These included interventions that facilitated competency-based assessments,126 focused on behaviour strategies to support the work of the support worker,112 for example learning how to give instruction in small steps or improving the level of stimulation in a service setting.
Alternatively, some workforce development interventions were designed to enable support workers to make, and understand, the close link between the intervention and the context of work. When an intervention was situated in the workplace and designed to fit with the working pattern of the staff, being held during shift changes, this maintained a ‘theoretical and practical link with the daily routine of the institution. Each topic to be taken up in the training program would be closely linked to life in the institution, with the aim of fulfilling the special needs of the residents of the particular institution’ (p. 591). 112
There was consistency with literature about teaching assistants in schools, in which evidence also supported the importance of physical proximity. Where workforce development for teaching assistants was held in the workplace,123 there were increases in the congruence of the intervention with teaching assistants’ experiences, which encouraged co-learning with other colleagues, thereby encouraging teachers and support workers to learn from each other in partnership. 123
Taking support workers out of the workplace for workforce development
We found a different perspective or contradictory evidence around physical proximity, specifically about the positive impacts of removing support workers from their work area, and that learning could be better enabled through the provision of separate space with less disruption. 105,123,131–133
For example, facilitating workforce development on weekend days away from support workers’ jobs was linked with positive impacts about participants’ knowledge and attitudes. 105 An intervention to improve participants’ awareness and knowledge about aphasia, delivered in a college setting, demonstrated improved learning about aphasia. In addition, in this study, participants demonstrated greater incorporation of new learning into their work. Interview data affirmed the feasibility and positive impacts of taking staff out of their work context to participate in workforce development, but noted caution in ensuring no negative consequences for the organisation:
. . . variety and change of scenery does make a difference to people’s learning habits and what they learn and how they learn without a doubt, and I agree with that completely. We also have to do what works well for our organisation, within our care delivery demands as well. So it’s finding that balance.
Telephone interview, participant 3
In two other interviews, reference was also made to the benefits of providing opportunities for support workers to gain understanding of other organisations settings, in which it was ‘interesting to see how different some of the homes operate’ (telephone interview, participant 8) and useful for ‘. . .cross-fertilisation’ (telephone interview, participant 1). Further, from the education literature, we noted reports of interventions which encouraged taking teaching assistants out of the classroom to visit other schools and view different practices. 123
Regardless of the pros and cons of the physical proximity of workforce development, the interviews highlighted the need to think systematically about the delivery location by focusing on its combination of practical or theoretical content:
I think a lot of it depends on the type of training. If you’re going to have an academic session that’s looking at the impact of immobility on tissue for instance, you want to have a session on pressure area care. That can be beneficial in the care home setting, so in [xxxx] there would be some quite logical sense in doing that because you can then say, OK we’re going to go along and see so and so after we’ve done this and we’ll look at our tissue areas and their pressure areas and we’ll look at the colour of them, we’ll look at the state of her skin, we’ll look at the state of her hydration and nutrition, and you can then make the training wheel. That kind of training I consider to be essentially practical. If you’re looking at something that’s perhaps more theoretical, going to talk about say, let’s say it’s going to be the impact of certain drugs on someone who’s got vascular dementia, the effect they’re going to have . . . that works quite well in more of a classroom setting because you can focus, you won’t have the distractions of being in your workplace, you won’t have call bells going off, you and your students will be able to concentrate on the academic side, the technical and the academic rather than the practical.
Telephone interview, participant 9
This interviewee went on to describe the positive personal impacts for support workers that taking them out of the workplace might bring, when ‘taking someone away from their workplace and sending them to somewhere, as a novelty value, creates a break. And that in itself is quite a positive thing’ (telephone interview, participant 9).
Taking participants out of the context of practice may also have implications for continuity of learning, in that learning that has happened away from the setting may have to be reinforced when back in practice to ‘make it real’.
Outcomes
Proximity in workforce development, in either a cognitive or a physical sense, prompted resonance with the individuals participating in it and/or was more likely to lead to cognitive and/or practice changes. Cognitive impacts for support workers included empowerment114,127 and improvements in self-esteem,114 together with increased knowledge and understanding of the behaviours of older people in their care. 108 When interventions were proximal through the use of person-centred training, role play and homework, this led to changes in support workers’ mental models of their role and work. 117,124 For example, coaching in the workplace led to an ‘ah-ha’ moment for one care assistant and a positive difference in a care home resident’s behaviour as a result of the changes in behaviour of the support worker. 117
Practice changes included better cohesion and paying more attention to older people in efforts to meld theory and practice,111 and improved relationships with family members. 113 The use of real-life case studies of older people in residential care settings, as well as visual tools and storytelling, also prompted resonance with the support worker’s practice. Improvements in the appropriateness and adequacy of care, including for those older people with the greatest needs, were affected after intervention. 121
In situating interventions in the workplace, practice changes as a result of making learning more real for the support worker included more attention being paid to older people111 and relationships with family members improving,113 as well as more general aspects of service quality; for example:
Following completion of the educational programme, there was significant increase in the proportion of care that was judged appropriate and adequate provided by healthcare assistants to residents than before.
p. 8121
Summary
In this CMO configuration, we found that a relationship between the cognitive or physical proximity of the support worker and the workforce development prompted resonance with participating individuals which was important in terms of potentially influencing positive cognitive and/or practice changes. The relationship between proximity and resonance was made visible through the use of tools and techniques to draw on real life, supervision of practice, working together, and evidence to prompt understanding and appreciation of older people themselves.
Context–mechanism–outcome 2: where the support worker is coming from
If workforce design and delivery pays attention to the individual support worker’s personal starting points and expectations of the role (context), then this prompts better engagement with the intervention (mechanism). Paying attention to the individual within workforce development can promote positive personal cognitive (e.g. personal efficacy) and instrumental impacts (e.g. skill development) and, potentially, impacts for the organisation (e.g. staff commitment) (outcome) (Box 2).
Personal attributes (e.g. paying attention to personal resources, personal issues/backgrounds, experiences/age, challenges, existing strengths, how one perceives others, values).
Abilities (e.g. assessment of communication skills, technology, literacy, language).
Personal feelings and expectations (e.g. reflection, exploring individual development needs and expectations).
Context and mechanism
There were numerous examples of workforce development interventions paying attention to support workers’ personal and professional perspectives, previous career, age and experiences, values and perceptions of older people’s services, abilities, expectations and life skills. 106,107,109,113,121,122,129,130,134–140 We were able to trace an evidence thread between tailoring to these factors and engagement with the intervention, as the support worker is able to appreciate what is expected of them in the context of ‘where they are at’. This finding was also reflected in interview data. For example:
. . . a lot of what we’re trying to do is get people to see that the skills and talents that they have outside of the service . . . things that can be brought to work. Maybe other residents are interested in these things, maybe they can support all different parts of life of the home and not necessarily just doing their set job, and in that way you can sort of, contributing to the sense of it being a whole home approach, having a thriving community and having a lots of different kinds of varying activities going on in the service.
Telephone interview, participant 6
Starting points included experience of work within older people’s services, as exemplified in this excerpt from a report of a gerontological training intervention,132 in which ‘sessions were experiential as well as didactic, drawing upon trainees’ experiences and challenges; this set the tone for interactive skills which “role modeled” communication skills for interaction with clients and families’. 132
A broad range of individual attributes was evident, on which successful interventions were constructed including emotional resources. The value of harnessing existing support workers’ emotional strengths and personal resources to enhance the effectiveness of workforce development activities was evidenced in examples of interactive training processes and interventions. In one example, in the context of ‘. . . often a lack of training in emotional issues, and especially in working with residents’ families’113 a workshop-style training intervention for staff in long-term residential care based in Australia113 included affirming participants’ existing strengths and skills. Analysis of the participants’ feedback demonstrated how life experiences were valued and used to explore how they managed the emotional aspects of their work.
In a short programme aimed at sensitising nursing assistants in a long-term care setting to ageing and the experiences of older people,129 the intervention focused on the self and reflection, including linking this to individuals’ existing values:
During the introduction, an exercise entitled ‘As We Grow’ was used to elicit an atmosphere conducive to self-examination. This exercise required participants to write down seven of the most important things in their lives (i.e., people, animals, careers, possessions, etc.). 129
Extending beyond self-awareness, workforce interventions to teach person-centred care-giving skills to support workers also indicated benefits in the workers’ emotional engagement with older people. 109 Person-centred caregiving was associated with interpersonal complexity, or support workers’ abilities to view older people in ways that are not stereotypical. The intervention included discussion about the importance of identifying how individuals perceive others and found that ‘cognitive complexity is associated with motivational factors, such as the goal of forming personal relationships with residents. Being able to select talented caregivers would be of direct benefit to facilities and could reduce the need for training’. 109
Other attributes accounted for in workforce development included individuals’ earlier life or work-related experiences of learning. An evaluation of a simulation-based intervention demonstrated that both previous experiences of formal education and a reliance on experiential learning about the support worker role were instrumental in influencing support workers’ learning experience. 122 This was highlighted by a ward manager reflecting on the programme that ‘in the past most [support workers] have learned with time, and through experience, working alongside trained nurses, knowing the expectations of the trained staff. That’s probably time served . . . experience’. 122 Interviews with service managers confirmed the importance of experience and age in tailoring workforce development to the individual:
So we actually look at what the individual has achieved already, and then we match that up with things that they could also do . . . that they’ve not done for whatever reason . . . we do take a lot of interest in each individual.
Telephone interview, participant 5
In addition to acknowledging the role of emotional attributes and prior experiences of learning, some evidence targeted the mental models that support workers held about the nature of care settings, services and older people. 124 In a case study set in a residential care in the USA, two mental models (described as the ‘golden rule’ and ‘mother wit’) were identified as guiding certified nurse assistants in their work and their interactions with older people. Understanding individuals’ mental models, because they ‘might not be a good basis for appropriate care actions’,124 can be a starting point for reframing them.
Although not linked specifically to workforce development, an acknowledgement of the importance of personal resources was reflected in the non-health evidence. In a report of a research study about the police community support officer (PCSO) role in England, we found a similar pattern between the age and life experiences of the support officers and their effectiveness within the role, which appeared to be easier for ‘the older PCSOs – those who had a wider range of life experiences from which to draw. This is not to say that the younger PCSOs were not effective in the role – they were, and they often seemed to be more at ease behind a computer screen than their older colleagues’. 140
Abilities
Our second interview participant raised the importance of paying attention to individual ability: ‘there’s something about acknowledging the stage that learner is at in their career or their learning pathway’ (telephone interview, participant 2). There was also evidence of drawing on individuals’ own abilities in the design and evaluation of workforce development. Individuals’ communication skills were the focus of a training package for care home staff to enhance their interactions with older people,139 and in a critical analysis of a communication skills training programme for nurse aides set in the USA. 138 The effectiveness of communication skills was assessed prior to the intervention during 5-minute care interactions with residents, using a communication skills checklist. This was also important in establishing that ‘an increase in the use of effective skills and instructions, and a decrease in ineffective instructions by [support workers] during care interactions and maintenance of these changes for 3 months’138 had occurred.
Evaluation of a computerised educational programme for nursing assistants in end-of life care134 included exploration of ‘the following characteristics: 1) ease of use; 2) clarity of presentation; 3) appropriateness of reading level and content; and 4) relevance to nursing assistant practice’. 134 In this example, the use of learning approaches that paid attention to the existing abilities of the nursing assistants in literacy and language were explanatory:134
. . . needs of users with low literacy skills and diverse learning styles are addressed by incorporating slides, art (line drawings or illustrations), video clips and audio clips. Other features to increase ease of use for those with diverse learning needs include a glossary, indices, a simple search engine, and self-grading quizzes.
p. 504134
Similarly, in a work-based learning programme for support workers in assisted living based in Oregon, USA,135 paying attention to literacy and language needs enabled the intervention planners to factor in additional time to maximise the effectiveness of the programme for staff.
Role expectations
We also found that the design of some workforce development interventions supported the sharing of individual expectations about the support worker role. Participation in a simulation-based educational programme required support workers to express their own expectations about their role development. 122 Interventions promoted the career development of support workers, including the use of job analysis to understand existing and required competencies for the role. 135 Other interventions focused on career progression, incorporating principles such as professionalism, self-efficacy, self-worth and maximising intrinsic motivation,132 so that the design was ‘grounded in an intention to encourage a more career-focused orientation’. 132
Outcomes
Situating and tailoring workforce development in the context of the personal and role starting points and expectations of support workers was more likely to prompt commitment, leading to increased levels of engagement with the intervention and potentially with the older people’s service. This was achieved through improvements in team working, clinical knowledge and skills, and relationships with residents. 141 For employers, impacts were in terms of better management of challenges,105 including support workers being ‘more creative in handling challenges that come up for them’. 105 Through a cycle of reinforcement, these impacts appeared to extend to a better appreciation of staff by family members:113
The results may also suggest that when staff members feel more appreciated by family members, they feel more able to have cooperative conversations and feel more empathy. The above can lead to staff forming better and more cooperative relationships with family members, which may improve their working life.
p. 319113
In an intervention which featured self-assessment and lifestyle change for the support worker, caring for themselves could help support workers to better care for older people, expressed through increased feelings of worth and belonging. 107 In another intervention designed to promote a career-focused view and enhance professionalism, self-efficacy and self-worth, a deeper commitment to care work was found. 132
Personal outcomes related to more confidence, pride and feeling rewarded141 and valued. 142 These outcomes also emerged in interviews, but were linked to service improvement, for which one manager felt that it ‘is as much about the worker, as it is about the resident, and it works because they feel valued. It’s reciprocation, I mean look at, it is, if you treat somebody as a human being and you listen to them and you really, really support them to do their best, they start to totally reciprocate with residents’ (telephone interview, participant 1).
Summary
If workforce development pays attention to the individual support worker’s personal and role starting points, for example personal resources, abilities and personal feelings and expectations, then this leads to increased levels of engagement with the intervention. Workforce development interventions can examine support workers’ personal resources, build on, recognise and value different abilities, and harness existing resources in development activity. In addition to engagement with the intervention, this may enhance support workers’ engagement in their service. It also leads to personal outcomes such as confidence, empathy, self-esteem and satisfaction, which may be linked to other outcomes for older people, families and services.
Context–mechanism–outcome 3: tapping into support workers’ motivations
If workforce development opportunities include elements of incentivisation (context), then it is likely that participants will feel recognised and rewarded (mechanism). The relationship between incentivisation and having a stake in workforce development can lead to greater emotional and practical participation and engagement with the intervention (outcomes) (Box 3).
Certification (e.g. manuals, certificate of completion).
Prizes and perks (e.g. public postings, lottery).
Financial/monetary investment (e.g. salary bonus or increase, stipend, course fee).
Context and mechanism
Incentivisation was noted to be a strong thread within the analysis, interpreted as efforts within the design and delivery of interventions to motivate individuals and to ensure attendance at, and completion of, the intervention. These efforts included certification to recognise engagement in interventions105,120,127,140 and the use of prizes112,138,143 and financial incentives. 106,127,133,141,144
In its simplest form, we found evidence that the use of ‘certificates of attendance’ triggered a sense of reward105,120,127 through the branding, badging and accreditation of the intervention that support workers were taking part in. This excerpt of interview data reinforces the link between acknowledging participation in workforce development and individuals feeling rewarded and motivated:
And I remember one person saying to me, do you know what, I’ve never had a certificate for any work I’ve ever done before. Never at school, never got anything, now I’ve got two certificates in one day I can’t believe it. You know, it motivates some people. Even if it’s only for a couple of days or a couple of weeks or whatever, because before they know it they’re on the next course, and remember how well you did on that one, let’s see how you can do on this one.
Telephone interview, participant 5
In a communication skills programme120 and an intervention to recognise depression in care home settings,127 certificates were also used to recognise completion of the intervention. Successful completion of a short curriculum for direct care workers (described as nurse aides, personal assistants and adult day-care assistants working in older people’s care), set in the USA, resulted in completion certificates for the participants being provided, but these were designed to be relevant for employers in the local area. 105
From the policing literature, we found supporting evidence that certification should be offered to recognise support officers’ development of skills and abilities:140
. . . when a PCSO contemplates leaving the organisation to move on to other work, many are left with the impression that they ‘have nothing to show for it’ when it comes to their experiences as a PCSO. Many of the abilities they have gained are of course transferable to other organisations.
p. 23140
Theoretically, certificates of engagement and achievement in workforce development should increase prospects for those support workers who wish to progress within or move between organisations. However, we found little evidence that examined the consequences of this type of incentive mechanism, other than in the above aspirational excerpt from the policing literature.
Other than rewarding attendance and participation by certification, other incentives were used to motivate support workers to complete and engage in ongoing workforce development programmes. Practical approaches included public posting of progression reports for support workers and using prizes as rewards for specific performance targets. 138,143 In an intervention in which support workers were taught to use communication skills with residents with cognitive impairments, a comprehensive staff motivational system was used to encourage individuals to sustain their new performance and skills. 143 Some incentives were designed to include an element of choice, so that the prize was more relevant for the individual choosing it. However, in the example below, the personalisation of incentives within a lottery-style draw was constructed in addition to a public recognition of performance:
For each shift, the individual winning the lottery was provided with his or her choice of incentives from a list of choices determined by each nursing home . . . Across nursing homes, the most frequently chosen incentives were the opportunity to leave work earlier than scheduled, extra pay, and goodie bags.
p. 453143
Lottery-style approaches to incentivisation featured in other evidence, including a development to incorporate ‘Informed Teams’ (a specific programme of staff development in care home settings which integrates skills in routine practice with staff development to meet staff’s needs) as a vehicle for staff development in care homes. 112 Weekly draws and prizes were used to encourage staff participation in daily meetings and skill sessions, as well as other incentives used to encourage engagement by the participants. Lottery reward systems were also associated with intervention tasks in the case of the completion of self-monitoring documentation. 138 The impact on staff engagement was evident by the fact that when the reward system was withdrawn, compliance with the self-monitoring task decreased significantly. In this context, lottery-based reward systems may be successful only in raising awareness of expectations of workforce development, rather than in affecting more fundamental and sustained cognitive and behavioural changes. From interview data, we also found that there was an impact in terms of staff feeling recognised and rewarded if incentives were offered:
. . . it may seem insignificant to others unless you’ve ever been to one, we do a presentation every year for the learners and the staff who achieved, we have something called the smile award. And it’s a little initiative that I find that . . . makes the difference. And we’re not giving them £50 bunch of flowers, we’re giving them a nice pen, certificate and a badge and they love it.
Telephone interview, participant 7
A range of different organisations used monetary investment to engage the support workforce with development. The evidence to support the use of financial incentives was limited to some North American and European settings,106,133,141 and so may reflect particular professional and service contexts. A financial contribution from the support worker, such as a small course fee to attend a clinical module,106 could also lead to a sense of personal stake in the workforce development/intervention. Financial incentives or remuneration from workforce development budgets were generally noted to be directed towards support workers’ turning up. 106,127,144
Financial incentives or remuneration from workforce development budgets were also noted to be directed towards support workers’ completing interventions. The ‘Win A Step Up’, a programme of continuing education by on-site trainers for nursing assistants in care homes in North Carolina, was designed to decrease turnover and improve quality of care. 141 The programme reported using financial incentives in the form of staff bonuses to ensure successful completion of the intervention.
An intervention that included peer mentorship for care assistants in a care home setting used the financial incentive of a 10–20% increase in peer mentors’ salary, or overtime or a reduction in workload, in recognition of the additional work that the mentors took on. 133 We also found reference to financial incentives being used to reward enhanced skills in stakeholder interviews: ’. . . we reward, once staff attain a certain level of skills and experiences, we reward that through pay’ (telephone interview, participant 3).
Outcomes
Monetary incentives were reported as generating positive impacts for the individual support worker. For example, managers reported support workers’ enhanced confidence and pride and feeling more rewarded,141 and self-esteem. 144 Outcomes from lottery-style incentives were related to personal engagement with the intervention (‘generate excitement’ about the project intervention strategies112), their work and the organisation in the development of a culture in which ‘. . . the work environment supports skill use with constructive feedback and recognition’112 (p. 254).
There were also reports of positive impacts on the quality of support workers’ interactions with patients’ relatives from interventions which included evidence of incentivisation. 144
When communication skills training used a motivational system which included prizes and perks, the outcomes included increases in positive staff behaviours that were also sustained over time. 143
Summary
We uncovered a number of ways in which engagement in workforce development was incentivised for support workers, including the use of certificates, prizes and perks or financial/monetary investment. Incentivisation may make it more likely that participants will feel that they have a stake in the intervention and feel more valued and motivated to participate, which can lead to better engagement with the intervention. Lottery-based incentives on their own may not trigger sustained changes in desired workforce development outcomes and the use of financial incentives may be effective in only some service and professional contexts. There may also be a case for tailoring incentives to make them relevant to the support worker.
Context–mechanism–outcome 4: joining things up around workforce development
If interventions are developed in the context of an organisation’s goals, including their human resource and quality improvement strategies (context), then this prompts alignment between the aims of the intervention and the goals of the organisation, such that they mutually reinforce each other (mechanism). This leads to more sustained and lasting impact of the intervention, reducing turnover and supporting the organisations’ retention strategy (outcome) (Box 4).
Care management (e.g. quality of care, integration).
Staff development (e.g. leadership, coaching, supervision, appraisal, mentoring).
Organisational strategy (e.g. recruitment, retention, policy, quality improvement).
Context and mechanism
When the organisation’s strategic direction was made explicit in the reporting of how workforce development interventions were developed, this generally showed alignment with the intervention’s aims. There was evidence of joining up the organisation’s human resource strategy with support workers’ development needs. 142 This included the development of leadership roles for senior support workers and preceptorship for new staff,110 coaching roles to ensure that support workers can benefit from coaching,117,124 supervision,109 appraisal systems140,145,146 and mentoring. 127,147,148
Other ways in which organisations prioritised development for the support workforce included reference to policies such as a mandatory attendance policy,112 allocating time for workforce development112 and general efforts to develop support worker roles through bespoke workforce development strategies. 117,126 Examples were organisational direction/goals to describe care management priorities that were important to the organisation, for example quality of care. 108
However, we noted how the success of workforce development interventions was often contingent on how the organisation prioritised quality improvement. 112 For example, in a report describing the development and pilot testing of a 6-week intervention for certified nursing assistants,108 the authors explained how the intervention aimed to ‘identify and operationalise person-centred caregiving behaviours’. 108 In this way, the intervention was set in the context of organisational efforts to improve the quality of long-term care more broadly, through focusing on relationships and promoting culture change within care settings.
Some interventions, including an advanced education programme for nursing assistants in care home settings110 and the development of a curriculum for paraprofessionals,142 were based on the needs of the service providers. We also found studies that assessed the feasibility of interventions for support workers to recognise depression among residents in care homes for older people. Here, support for staff to receive the intervention echoed the organisation’s direction following concern from managers. 127 In another example,110 the aims of the intervention were aligned with the interests of external stakeholders (in this case, colleges of health-care education) in improving services.
Aligning support worker development with the strategic aims of the organisation was also evident in the context of paying attention to the integration of health and social care. For example, a report of an in-reach team project described the aims to develop a group of carers and support them in their role in integrated care for the older person. 149 The benefit of developing the intervention to meld with the organisation’s strategic direction in this case supported previous research findings about the benefits of up-skilling support workers in integrated care. We also found, in a paper describing the implementation of a support worker role in general practice, evidence to support linking support workforce development to the organisation’s ethos about interprofessional working. 147
Outcomes
Alignment between the organisational goals and workforce development interventions had the potential for greater sustainability because the type of impacts realised could lead to longer-lasting effects, for example enhancing support workers’ commitment to their work,108 promoting better understanding of their work,145,149 helping to develop positive attitudes,142 promoting more tolerance and more interest in residents’ behaviours,127 enhancing self-reflection117 and leading to improvements in knowledge. 110,152
Alignment of organisational human resource strategies and intervention design appeared to lead to better outcomes in terms of staff turnover and retention. In this extract, the choice of competency-based programmes which enhanced the competence and confidence of the support worker was perceived to be effective in increasing job satisfaction, retention and career progression:
. . . develop work-based learning programs that move low-wage frontline workers up health career ladders by improving skills and knowledge. The initiative focused on developing competency-based training programs that would increase job satisfaction, staff retention, and career advancement and improve quality of care . . .
p. 283135
Summary
Aligning workforce development with the organisation’s strategy has the potential to be reinforcing, in that the context and content of development are relevant to the goals of the organisation. This reinforcement has the potential to lead to longer-lasting types of impacts for the individual and the organisation, thus enhancing the sustainability of the investment made in the support worker’s development. However, there was little evidence in this context of a ‘joined-up’ approach to a workforce development which linked learning with opportunities for career development, personal growth and monetary and other rewards for skill and role development.
Context–mechanism–outcome 5: co-design
If the right mix of people are engaged in the design of workforce development programmes/interventions reflecting the complexity of workforce needs and desired development (context), then this prompts co-design and a collective view about what needs to be done (mechanism), which can lead to workforce development that is (perceived to be) more credible, meaningful and relevant for the support worker with greater potential for positive outcomes for practice (outcomes) (Box 5).
In partnership: multiagency working, academic, community.
With individuals: specialists, support workers, national experts, credible people.
Context and mechanism
We found that a key factor in intervention design was the make-up of the people involved in it. The significance of getting the right mix of people involved in the design of intervention/development programmes was made visible through reports of:
-
design involving partnership and involvement of charitable trust funding141 and partnerships with specialists,115,142 multiagency collaboration in the design of programmes/interventions (e.g. joint project work132), collaboration with academic staff150 and communities (e.g. continuous care retirement site109)
-
use of expertise128,151 in design (e.g. expert panel,152 professional teachers,128 core curriculum designed with national experts134 and involving people with experience106,150)
-
involvement of relevant staff in design,111,113,153 including the support workforce (e.g. intervention design based on interviews with nursing assistants132).
Partnership between organisations
When there was partnership working between different agencies in the design of workforce development programmes/interventions, a co-design approach was reflected in the reporting. A workforce development programme for nursing assistants in care homes set in the USA was described as an established partnership with established goals:141
The program is a partnership between the North Carolina Department of Health and Human Services and the University of North Carolina Institute on Aging.
p. 72141
Similarly, in a report of a skills development programme for direct service workers,132 the authors describe the extent of the multiagency collaboration involved, and how taking a co-design approach informed the development of the intervention because it brought ‘together the strengths and interests of multiple parties in academia, provider agencies, and professional associations garnered statewide support for the effort and ensured that concerns were addressed’. 132 This was discussed in the context of the development of a state-funded training curriculum (which focused on improving problem-solving, communication and stress management skills, in order to increase professionalism and self-efficacy) for care staff. 132
We found examples to show how partnerships were formed with academic and community partners in a collective approach. For example, a 6-week college-based course, which constituted part of the preparation for support workers in the care home sector to achieve the NVQ award, was developed, designed and delivered within a higher education institution in London. 150
In a report of a pilot study that described the development and evaluation of a 2-hour programme for trainee nursing assistants to promote person-centred caregiving skills with older people, collaboration with community partners was instrumental in developing ‘an operational definition of person centred caregiving’109 for trainee nursing assistants.
Partnerships with the right individuals
Paying attention to the intention of the intervention related to who was involved in the design process. We found that the intent behind collaborative intervention design was often twofold. For example, planning an intervention for support workers to develop their skills to deliver the right care was also aimed at supporting their personal development. 151
Similarly, ‘Recognition, Respect, and Responsibility: Enhanced Care Assistant Training’ was developed as a curriculum for nursing/home care aides to improve problem-solving and communication, in addition to developing stress management skills in order to increase professionalism and self-efficacy:132
Underlying the curriculum development was an emphasis on four self-efficacy-enhancing methods: mastery experience, modeling, social persuasion, and altering emotional states . . . The ultimate goal was to empower the direct care worker not just in terms of skills enhancement but to increase their overall perception of self-worth.
p. 116132
In a community-academic project to deliver a gerontological intervention training for paraprofessional service providers,142 the design of the curriculum involved the trainees themselves selecting the topics, and social workers with training in older people’s care were involved in the development and delivery of the intervention. A policy of drawing on people’s experience and expertise was reflected in the report of developing curricula, including trainers holding a Master of Social Work degree related to gerontology and experience of working in a gerontological practice setting. 142 This approach enhanced a collective view about what needed to be done.
Similarly, in an action research study that explored and developed quality end-of-life care in two nursing homes using reflective debriefing groups ‘. . . to encourage open dialogue using the oral tradition of healthcare assistants’,115 groups were led by a researcher who was a nurse specialist in palliative care. 115 We also found evidence of curriculum content in which design was supported by national experts in the topic136 or topic experts in gerontology. 128 In one example, a factor of significance for the programme’s success alluded to by the authors, was the credibility of the contributors to the curriculum design because they were ‘national experts in palliative care and staff education’. 128
Other evidence pointed to the significance of involving the most appropriate staff in the design of interventions, including the support workforce themselves. For example, certified nursing assistants were included on a multidisciplinary expert panel to develop an educational programme for one faculty. 151 Elsewhere, the evidence supported the principle of consulting with staff. 113 In a report of an educational programme for nursing assistants working in long-term care nursing assistants, the programme was designed by an expert panel including a physician, a nurse practitioner, a nursing assistant, a palliative care nurse, a hospice director and an administrator. The authors suggested that the addition of the support workers enhanced the quality of the programme because ‘Participants suggested improvements to the content and format of the workshops, especially the provision of more concrete and practical strategies for working with families’. 113
Support worker engagement was also evident in the co-design of a framework for career progression for health-care support workers incorporating three phases of continuing professional development. 151 The programme was organised and co-ordinated by a dedicated support worker training team comprising four registered nurses plus senior support workers in the role of peripatetic NVQ care assessors.
Complementing the attention on involving support workers, interviewees also highlighted the significance of involving family members in the design of workforce development; for example:
. . . very often they (relatives) will have, sometimes even more of an influence we find because very often older people themselves will not like to cause trouble, will just want somebody who’s kind to them, whereas actually the relatives will often come in with a slightly dispassionate view and have different expectations and standards. And so their input I think is really important. In terms of design I would say, again where I’ve worked in the past these things are often designed by a learning and development team of experts, but actually involving staff, managers and residents and relatives gives it a far richer input.
Telephone interview, participant 2
Outcomes
Having the right mix of people engaged in the design of workforce development programmes/interventions prompted co-design and a collective view about aims and objectives. For example, a programme funded by a charitable trust enabled the team to work together to assess the support workforce and develop a workforce intervention to improve their job satisfaction and retention. 141 When intervention design and development engaged with the right people, such as one example that drew on a dedicated support worker development team including registered nurses and support workers in the role of assessor,151 this implied a more collective approach and streamlined pathways, including linking theory and practice.
When the evidence led to our conclusions that getting the right mix of people involved in the design of interventions can prompt co-design and a collective view, workforce development was more likely to be credible, meaningful and relevant for the support worker, and promoted the potential for positive practice change, as reflected in reports of individual and practice changes.
Individual change
A collaborative approach to the design of one programme (which was developed in order to assist candidates to achieve the NVQ care award) found that, following the programme, the support workers became more orientated towards deep and strategic approaches to learning. 150 A group of papers in which the authors reported involving experts in the design of programmes/interventions134,144,150,152 noted positive outcomes relating to individual knowledge, ways of learning and enhanced self-esteem. 144 One report of a curriculum whereby topics were prioritised by the paraprofessionals and trainers held a Master of Social Work degree related to gerontology, and worked (or had experience of working) in a gerontological practice setting,142 concluded that it was more relevant ‘to the hands-on staff and the connection to the University made them feel special’. 142
Practice change
There was also evidence of practice change; for example, in a report of an intervention design based on partnership (‘Win A Step Up’), nursing assistants who undertook the event were found to be showing slightly, but not significantly, more person-centred behaviours than students in the control condition. 141 The same study reported that residents in the intervention condition had higher levels of satisfaction in their interactions with nursing assistants than did those in the control condition, and managers described improvements in job satisfaction and retention of participating nursing assistants. 141
In a report that described the extent of multiagency collaboration in the development of the curriculum for care staff, and for which the curriculum was developed in conjunction with support workers, a statistically significant change was found in the outcome measurements, suggesting the likelihood that the intervention changed the way participants performed their jobs. 132 In another example in which staff were contacted to get their views on the programme in the development stages111 it was reported that their work was more cohesive and that they devoted more attention to residents. The benefits of consulting with staff about course content pre intervention were noted in a study report of a programme based on the ongoing relationships between nursing staff and residents’ families. 113 In this study, significant increases in scores for staff feeling appreciated by families and feeling pleased with conversations with families, and in family members being pleased with conversations with staff members, were reported.
Summary
In this configuration, we found that the right mix of people engaging in the design of workforce development can be instrumental to the impact of the intervention on the individual support worker and his or her practice. When a collective approach to design is visible, workforce development is more likely to be meaningful, credible and relevant for the individual, and adds potential benefits for practice.
Context–mechanism–outcome 6: ‘journeying together’
If the right mix of people are engaged in delivering workforce development programmes/interventions (context), then this can prompt learning together (mechanism), which leads to stronger cohesion across groups and greater understanding of others’ roles and less duplication, and impacts on residents’ perceptions of care (outcomes) (Box 6).
Internal facilitators; trainers, coworkers, supervisors, administrative staff, registered staff.
Credible people; patients, experts.
Bringing people together; multidisciplinary approach, working together, mutual learning.
Context and mechanism
Evidence related to engaging with the right mix of people in the delivery of workforce development was noted to provide opportunities for learning together and promote cohesiveness. Having the right people in intervention delivery could be interpreted in terms of who they are and approaches for learning or ‘journeying together’. There was also evidence about the different benefits of bringing different groups of staff together to participate in workforce development alongside support workers.
Involving different groups in enabling workforce development
Several papers referred to internal facilitators drawn from across a service who had distinct responsibility for supporting the delivery of workforce development. In a report of a work-based learning programme for direct care workers in assisted living,135 support workers’ coworkers, supervisors and administrative staff took on a training role. This was highlighted as a critical component of the workforce development, using ‘train the trainers’ as facilitators had completed a comprehensive programme of education. This involvement meant that they were learning as well, and ‘each organization’s training team begins to develop implementation plans specific to its organization’,135 which also links to CMO 4, ‘joining things up around workforce development’.
A programme for HCAs working in dementia care, which focused on person-centred care, used group sessions and reflection to promote learning together. 154 The group sessions were facilitated by registered nurses, and the pilot study enabled reciprocal learning to take place through facilitator training and also ‘meant that the workbooks presented up-to-date knowledge, evidence-based practice and real life situations that take place in the wards for patients and staff’,154 which links back to CMO 1, ‘making it real to the work of the support worker’. There is a suggestion that adopting this approach to programme delivery can result in positive outcomes for support workers including personal recognition of the role they play:
I thought that just being a healthcare assistant I was just a small cog in the machine. Now I feel I have an important role in the team as HCAs spend more time with patients than anyone else. 154
In the policing literature, we also found evidence to support the beneficial effects of coworkers learning together, specifically the potential to increase the relevance and resonance of development opportunities:
PCSOs preferred to shadow other PCSOs in their initial training periods and might also benefit from being trained by PCSOs, rather than police officers who may not fully appreciate the realities of the job for these workers.
p. 4140
We also found that evidence from the education literature supported the finding that undertaking workforce development together prompted learning together,123 as explained in a research report that focused on the management, role and training of learning support assistants. The opportunities provided for teachers’ own learning and mentorship promoted staff development and collaborative practice. 123
Involving different staff groups in supporting the delivery of workforce development was dependent on the degree to which individuals possessed expertise and were able to bring it to bear on the learning. 106,128,131,139,143,150 For example, an evaluation of a Nursing Assistant Communication Skills Programme120 identified that the commitment and expertise of the social worker were crucial in prompting learning together. In addition, undertaking workforce development interventions for both support workers and their supervisors prompted learning together. In a report of a research study which set out to examine the effects of a relationship-enhancing programme of care on resident/care provider outcomes, a three-session educational programme about the dynamics of providing support for care providers was provided for supervisors/managers. 136
Learning together was also supported in interviews in which reference was made to the benefits of undertaking workforce development for both novice and more experienced support workers together because it can prompt sharing and the reinforcement of existing policies and practice:
. . . because it’s our policy that when people have a training session the course itself will be populated by experienced carer workers. We would not just put a course together or a classroom together of people who are all brand new to care, we like to have senior care workers who are updating or refreshing certain topics, also a mix of the two, because we feel that again it’s, you have the skills and experiences being shared there, and also the people who have been working for this organisation can quickly or earlier reinforce that yes, the company’s policy to do this, it’s policy to do that, etc., etc., and they’ll be flagged and highlighted during the training sessions as well so a mixture of experience and new carers is always how we package care training, definitely.
Telephone interview, participant 3
Outcomes
In the evidence that we found linked engaging with the right mix of people to deliver workforce development and learning together, outcomes related to stronger cohesion across groups105 and sharing of experience. Data from interviews also showed that ‘having a good cross-section of people who’ve got an interest is key to the whole success of the training’ (telephone interview, participant 4). In a report of a 24-hour curriculum for non-clinical direct care workers caring for older people,105 in which different groups of direct care workers undertook the intervention together, the findings found that participants:
. . . expressed increased feelings of worth and belonging (e.g., ‘I liked meeting others like me to share stories, and I feel more understood’)
p. 122105
There was also evidence to link learning together to less duplication of effort and a greater understanding of others’ roles, impacts on residents’ perceptions of care, and improvements in skills and communication during interactions with residents. 128,138
Summary
There is evidence to suggest that if different groups of people are engaged in delivering workforce development interventions then learning together can lead to greater understanding of others’ roles, and potential impacts on residents’ perceptions of care. The ways in which ‘journeying together’ was made visible included through the use of internal facilitators and credible people and by bringing people together through joint sessions.
Context–mechanism–outcome 7: taking a planned approach in workforce development
If workforce development draws on theory (both explicit and implicit), or there is evidence of a planned approach (context), then this prompts the adoption of a systematic process in its design and delivery (mechanism), which leads to greater potential to demonstrate impact and learn about workforce development effectiveness (outcome) (Box 7).
Models (e.g. stress reduction, team functioning).
Theories (e.g. self-efficacy, stress theory, planned behaviour, feminist, empowerment, competence and environmental press, family therapy, systems theory).
Frameworks (e.g. person-centred practice framework, emancipatory practice, group reflection).
Methods (e.g. biographical approach, behavioural approach to care planning).
Context and mechanism
In this configuration, we were able to trace an evidence thread around the impacts of a clearly articulated predefined theory/planned approach and a more systematic approach in the design and delivery of workforce development. We found explicit references to the use of models,112,128,132,133,155 theories112,113,132,136,144 and frameworks,115,136,155–157 linked to the methods then used132,153,156 in three key areas:
-
the development of the support workforce contribution to services
-
the individual support worker him- or herself
-
the delivery of workforce development itself.
Improving services
There was a wide range of evidence referring to the use of systematic approaches to workforce development for service quality. 112,115,136,155,157 For example, we found a report of using ‘Informed Teams’ (a specific programme of staff development) in care home settings. 112 ‘Informed Teams’ is described in the paper as a staff development programme which integrates skills in routine practice with staff development to meet staff’s needs. In this paper, Lawton and Nahemow’s158 1973 theory of competence and environmental press (stimuli associated with a behaviour) was applied to staff development activities that address staff/patient needs in an attempt to understand the characteristics in nursing home context, recognising that behaviour and affective responses are functions of people’s personal resources:
Although the theory describes older adults’ adaptive behaviour, it is also applicable to nursing home staff members’ in the context of the nursing home work environment.
p. 246112
The explicit use of theory was also important in the translation of learning within workforce development programmes into changes in support workers’ practice. For example, in a skills enhancement training curriculum for support workers to improve their problem-solving, communication and stress management skills, the theory of planned behaviour was linked to understanding how competency development could be transferred from an intervention to their work,132 as it assumes that ‘performance of a behaviour is determined by the individual’s evaluation that the behaviour will produce positive consequences’. 132
There was also evidence of how theories can be applied to illustrate the impact of the work setting on the success of the intervention, for example feminist theories and theories of empowerment showing how work issues can be understood in care settings114 as a precursor to workforce development. For example, ‘. . . it is important to teach women about the social structures that affect them. It is also important to help them understand these structures as well as how they can get involved in and influence their own work situation and work environment’. 114
Development of the support worker
Evaluation of a training programme aimed at strengthening self-esteem and empowering staff by enhancing their understanding of factors that influence them demonstrated that support workers could influence and improve their work situation. The authors indicate an implicit theory underpinning the workforce development in a nursing home setting:114
Our presumption was that one way of improving the situation for staff would be to help them develop their self-esteem and feel empowered though a training programme. This programme focused on helping participants to understand factors in the work situation that influence them and on empowering them.
p. 835114
To understand how the support workers could potentially influence their working situation and become more empowered, explicit theories from Kanter159 and Spreitzer160 were used and made visible through ‘the homework lesson . . . a way to see problems in a larger context and not to blame oneself, thus to strengthen self-determination and through participants being encouraged to attend to structures in the organization’. 114
The stress reduction model was used to frame the exploration of communication and interpersonal caring skills and bereavement in a gerontological training curriculum for care assistants (which included content to improve problem-solving, communication and stress management skills) in order to increase professionalism and self-efficacy. 138 Embedding distinct theoretical approaches ‘Need-Driven Dementia Compromised Behavior (Algase et al., 1996; Kolanowski and Whall, 2000) and the Progressively Lowered Stress Threshold Model (Hall and Buckwalter, 1987)’132 in the design of the curriculum made more visible the desired achievement of the programme goal ‘. . . to design a curriculum that helped participants understand, in a more comprehensive manner, the cognitive changes and physiological changes of their clients’ (p. 115). 132 Potentially melding theories with the goals of the programme would increase understanding about the effectiveness of the workforce development.
Workforce development design
There was reference to theoretically-driven learning strategies, considered to be instrumental to intervention design and delivery, promoting greater learning about effectiveness of different approaches, for example the use of a biographical approach which encourages people to talk about their life and their experiences while enabling the building and strengthening relationships with older people and their relatives. 118
Outcomes
The design of a workforce development intervention to enhance the communication skills of paraprofessional caregivers in dementia care was underpinned by Brooker’s VIPS model of person-centredness. 128 This model incorporated four elements about person-centredness in dementia care: valuing people with dementia, recognising people with dementia as individuals, acknowledging people’s perspectives and promoting a conducive environment to optimise well-being for people with dementia [V (value), I (individualised), P (perspective) and S (social environment)]. 128 In this example, the model was used as a heuristic to help participants thread together the themes of the programme and their learning. Utilising the person-centred and hope themes within the model to measure specific outcomes highlighted the impact of the intervention and provided an opportunity for learning about workforce development effectiveness. 128
Explicit reference to theory was also visible in evaluation reports of interventions that focused on personal development for support workers. 144 For example, in a report of an evaluation study of an intervention designed for auxiliary and assistant nurses, stress theory illuminated the potential of reducing work-related stress for the support workers through enhancing their control over their work:
. . . strengthening staff resources of job control, work support, and learning (Karasek and Theorell, 1990), as well as attaining new coping skills, is health promoting
p. 354144
Furthermore, the use of stress theory in a planned approach led to greater potential to demonstrate impact as it illuminated learning about factors that can affect support workers and how they can be empowered.
Summary
There was evidence of both implicit and explicit use of theory and planned approaches in workforce development, in relation to the development of the support worker contribution to services, their personal development and the use of specific learning methodologies. The use of theory could be associated with taking a more systematic approach to workforce development, which meant that the achievement of learning outcomes was made more obvious within programmes. We expect that this is a key requirement for wider programme evaluation and process learning about workforce development.
Context–mechanism–outcome 8: spreading the impacts of workforce development across organisations
If workforce development interventions are comprehensive, in that they are multilayered (focus on individuals, groups and organisations) and reflect broader developments relevant to the support workforce (context), then this prompts attention to the way in which components of interventions reinforce one another (mechanism), increasing the potential for impacts to embed and spread across organisations (outcome) (Box 8).
Team functioning: leadership, mentoring, supervision.
Organisational factors: workplace structure, environment, culture.
Context and mechanism
There were some examples (but these were limited) of workforce development interventions which demonstrated a more comprehensive approach, for example by not only incorporating the individual support worker perspective, but addressing their role within groups, teams or the organisation as a whole. In these cases it appeared more likely that attention was focused on how interventions can reinforce one another. This finding was prominent in papers which featured, alongside the reporting of the intervention, evidence about innovation leadership, mentoring, supervision and team functioning. 112,117,132,133,141,144,154
Working through teams
Some support worker development was nestled within the development of others and organisations, as well as themselves, with the implication that development at one level is inherently linked to development at other levels. This finding was also supported in interview data; for example:
. . . it’s about being part of the team. If you want to be part of this team, you have to be able to work to a very good level, and um, because you know, we’re all, we’re a team here. Everybody’s in the team, and I can’t work without them, they can’t work without me . . . that’s the same for everybody . . . carers can’t work without the kitchen, because the kitchen provide all the food for the residents . . . so everybody has to, we’re all as important as one another, so we’re a team.
Telephone interview, participant 5
Findings in this CMO configuration resonate with ‘journeying together’ in that bringing the right people together for workforce development was shown to be important to prompt learning together in a number of sources that we uncovered in the review. 105,136,140,148,157,161,162 In this CMO the evidence indicates the importance of bringing together people at different levels and from different places in the organisation in and of itself. For example, in an evaluation of an acute care programme of practice development (which focuses on development within the context of the organisation as a whole), the authors explained their rationale for bringing people at different levels together for the intervention:161
The overall metaphor for the sessions was of a ‘journey’ together over a period of time. Each session had a particular focus which contributed to different stages of this ‘journey’, and enabled participants to move from being strangers to each other to getting to know each other, to working collaboratively.
p. 9161
Working through organisations
In a report of a 1-year practice development project set in the context of older people’s care to improve quality of care,163 a sustained and collective approach to supporting the workforce was adopted in the project design to generate a better chances of success for the desired improvements in team functioning. Focusing attention on the multilayered nature of the system led to an appreciation of how interventions could reinforce one another:
On-going work was aimed at implementing cultural and structural changes agreed by the multidisciplinary team, supported by research evidence, in order to establish new norms of clinical practice and leadership.
p. 340163
Workforce development drawing on principles of culture change was also evident in an example of a peer-mentoring programme for support workers in care home settings, reflecting the commitment and values of the entire facility. 133
The concept of coaching supervision was used to extend the impact of an intervention to improve team working between support workers and registered nurses. 141 The project implementation plan introduced the concept of coaching supervision to educate supervisors about how to support staff to solve their issues. This approach to the design and development of the intervention meant that in addition to improvements in team functioning reported by managers, the impacts extended beyond the participants of the programme to include improvements in nursing care and supportive leadership.
Efforts to demonstrate a comprehensive approach to workforce development were evident in linking elements to the wider context of the organisation. This was reinforced in interview data in which we found reference to longer-lasting impacts of workforce development if this was focused across the organisation:
. . . we find that anything to really have a lasting impact it’s got to be something that’s a whole home approach, so if we’re doing something with the support workers we also need to be working separately with the managers, with the activity leads, and we need to be doing that over a long period of time, because otherwise it’s a limit to how much it becomes an everyday way of working . . . they need to see that other people want to do it, that their manager is talking about it in staff meetings, celebrating it when they’re doing something that’s been a learning from the course. And it that only happens if . . . joined up.
Telephone interview, participant 6
And:
So we’ll be making a programme on infection control and we’ll be talking about everything from the kitchen through to the front-line care workers, the handy person and the reception staff. And getting them all to think about this as how it impacts everybody in the care home. Equally the condition related programmes, again we encourage all the staff from the kitchens and the laundry to come in and watch so that they understand more of the condition that somebody’s living with. And we find that’s very, very powerful in terms of spreading understanding, spreading tolerance and acceptance, also spreading, thinking about how best to support people.
Telephone interview, participant 6
In the broader context of the organisation in which the support workforce is situated, we found evidence supporting linking systemic change management and multidisciplinary approaches in efforts to drive innovation in workforce development,164 particularly in settings in which implementing change is challenging. There were also examples of workforce development interventions having a comprehensive focus on workplace structure, environmental and cultural factors. 113,114,135,157 For example, a training programme tailored to one long-term residential care facility was based on the ongoing relationship between nursing staff and residents’ families. 113 A series of workshops for staff were designed for the participants, who included personal care assistants, senior nurses and their supervisors. The role play employed in the workshops enabled participants to experience a range of different situations and to empathise not only with family members, but also with other staff members. The authors suggest that the development of the intervention highlights the need to consider the range of organisational and systematic factors which can influence the success of similar interventions.
Outcomes
The evidence shows how factors related to team functioning and organisational factors can enhance the potential for impacts to spread across organisations. In the papers in which we uncovered evidence about team functioning, examples of impacts that could be embedded included better management of challenges by staff,105 changes in job performance132 and improved ability to demonstrate empathic and reliable behaviours and relational care. 136 From the evidence in papers which highlighted organisational factors, we found that outcomes related to supporting staff and improving retention,133 supporting leadership141 and improving quality of care. 163 There is also evidence to suggest that particular interventions, such as ongoing supervision, mentorship and coaching, can promote longer-lasting impacts. 109,117
We found limited examples of whole-system approaches to development; the exception to this would be practice development-type programmes. 163 This intervention works at multiple levels (individual, team and organisation) and in doing so has the potential to lead to impacts at an organisational level, which could last longer than one-off interventions aimed at the individual support worker.
Summary
Workforce development programmes/interventions that are comprehensive (i.e. multilevelled/multicomponent) have the potential to prompt attention to be paid to the way in which interventions/activities reinforce one another. This approach could lead to the potential for embedding workforce development and scaling up, so that the impact is felt across organisations. Scaling up is made visible through evidence that shows team functioning features, and when attention is paid to organisational factors.
Chapter summary
The CMOs presented in this chapter highlight evidence-based statements of what works in the development of the older persons’ support workforce. These have been presented individually to enable understanding. In practice, these are integrated and interactive, highlighting the idea of workforce development as a complex intervention or programme. We include a figurative representation of this complexity in Chapter 4.
Chapter 4 Conclusions, implications and recommendations
Our review has resulted in an explanatory account of how the design and delivery of workforce development interventions work to improve the skills and care standards of support workers within older people’s health and social care services. In developing this account we have drawn on a range of evidence, including from different public service contexts, namely policing and teaching. We have generated eight CMO configurations that are explanatory statements reflecting the complexity of workforce development in this setting. An embedded stakeholder engagement strategy was used to ensure the interpretive depth and the policy and practice relevance of the emerging findings.
In this chapter we reflect on the review in relation to our stated aims, including:
-
a typology of the workforce development interventions we identified in the literature
-
a summary of the mechanisms through which interventions work and the contexts that might mediate through an explanatory framework that synthesises the CMO configurations
-
implications for practice (design and delivery of interventions) and recommendations for future research.
Typology of workforce development interventions
We distilled four types of workforce development from the evidence included in this review, which are reported in Table 3. This typology is driven by the focus of the workforce development, and describes groups of interventions that precipitate changes around different aspects of the support worker role, their work environment and the support worker as an individual. Consequently, this typology refers principally to impacts, rather than to different approaches to delivering workforce development (such as face to face, work-based, blended or e-learning) or the types of changes associated with learning (such as cognitive, affective or psychomotor).
| Focus of workforce development | Characteristics |
|---|---|
| Competence | Workforce development that focuses on the support workers’ competence in a specific aspect of their work such as monitoring (pulse, blood pressure, temperature), pain assessment and moving and handling116,126,135,142,144,149,152,165 |
| Aspects of caring | Workforce development that targets general caring issues issue of significance to the older person [e.g. dignity, health ageing, relationships, communication (including aphasia), end-of-life care, infection control, managing family relationships, care planning, managing challenging behaviour]. This may or may not be accompanied by competence-based training105,108,111,113,115,120,122,126,128,129,132,134–139,141,143,152,157,161,165–170 |
| Improving team and/or service context | Workforce development that seeks to improve organisational context and/or culture and the role of the support worker within it (e.g. values, culture change, teamwork, awareness of each other’s roles, improving the learning environment, working across sectors/boundaries, quality and safety, leadership, conflict resolution)106,107,112,115,122,128,130,133,141,151,152,156,163,171,172 |
| Personal development | Workforce development that seeks to enhance the personal growth of the support worker and which may not be directly related to their day-to-day work (e.g. self-efficacy, confidence, self-esteem, motivation, career development, employability, stress management)114,132,134,135,143,144,151,166,173 |
However, while presenting this in a typology, we draw attention to the fact that there is a considerable degree of overlap in the evidence underpinning the classification. The evaluations of workforce development included in this review often describe the evaluation of a suite of activities/interventions and, therefore, these types should not be considered mutually exclusive.
Programme theory
Cumulatively, our eight CMO configurations provide a programme theory or contingent explanation, which is grounded in evidence from the literature and in stakeholder perspectives, about how workforce development works in improving outcomes for support workers, organisations and older people. Although the theory is specific to workforce development for support workers in the context of older people’s services, we believe that the CMO explanations are sufficiently abstract to be transferable across other workforce development approaches and service contexts:
-
Making it real to the work of the support worker. If intervention design and delivery is close to the work of the support worker (context), then this prompts resonance with individuals participating in it (mechanism), which can result in cognitive and practice changes in them (outcome).
-
Where the support worker is coming from. If workforce design and delivery pays attention to the individual support worker’s personal and role starting points and expectations (context), then this prompts better engagement with the intervention (mechanism). Paying attention to the individual can promote positive personal cognitive (e.g. personal efficacy) and instrumental impacts (e.g. skill development) and, potentially, impacts for the organisation (e.g. staff commitment) (outcome).
-
Tapping into support workers’ motivations. If workforce development opportunities include elements of incentivisation (context), then it is likely that participants will feel recognised and rewarded (mechanism). The relationship between incentivisation and having a stake in workforce development can lead to greater emotional and practical participation and engagement with the intervention (outcomes).
-
Joining things up around workforce development. If interventions are developed in the context of an organisation’s goals including their human resource and quality improvement strategies (context), then this prompts alignment between the aims of the intervention and the goals of the organisation, such that they mutually reinforce each other (mechanism). This leads to a more sustained, lasting impact of the intervention, reducing turnover and supporting the organisations’ retention strategy (outcome).
-
Co-design. If the right mix of people are engaged in the design of workforce development programmes/interventions (reflecting the complexity of workforce needs and desired development) (context), then this prompts co-design and a collective view about what needs to be done (mechanism), which can lead to workforce development that is (perceived to be) more credible, meaningful and relevant for the support worker with greater potential for positive outcomes for practice (outcomes).
-
Journeying together. If the right mix of people are engaged in delivering workforce development programmes/interventions (context), then this can prompt learning together (mechanism), which leads to greater understanding of others’ roles and less duplication and impacts on residents’ perceptions of care (outcomes).
-
Taking a planned approach. If there is use of theory (both explicit and implicit), or evidence of a planned approach, in workforce development (context), then this prompts the adoption of a systematic process in its design and delivery (mechanism), which leads to greater potential to demonstrate impact and learn about workforce development effectiveness (outcome).
-
Spreading the impacts. If workforce development interventions are comprehensive, in that they are multilayered (focus on individuals, groups and organisations) and reflect broader developments relevant to the support workforce (context), then this prompts attention on the way in which components of interventions reinforce one another (mechanism), increasing the potential for impacts to embed and spread across organisations (outcome).
Each of these CMO configurations is grounded in evidence generated from the review and stakeholder perspectives. Our starting point in the review, for example through the application of soft systems, represented workforce development interventions as complex programmes, in that they are transformative of people and organisations, involve multiple components which affect different types of change at different levels and are mediated by a wide range of political, social, environmental and other factors. We posit that the complexity of workforce development is also encapsulated in the cumulative nature of the CMO configurations; that, when describing ‘what works’ in workforce development, the whole is greater than the individual contributions of each CMO configuration: that is, for maximum impact it would be important to pay attention to the features of them all.
As each CMO configuration includes a different type of contingent change in individual or organisational behaviour or understanding, it is inevitable that workforce development programmes draw on a range of theoretical traditions and perspectives, some of which come through in the analysis more strongly than others. The mid-range theories which relate to the CMO configurations identified in this synthesis are summarised in Table 4.
| CMO | Illustrative theories | Implications |
|---|---|---|
| Making it real | Theories of adult learning | These theories pay attention to the different roles and balance of ‘teacher-led’ and ‘student-led’ approaches to learning for adults. The theoretical debate highlights the importance of previous life experiences as a foundation for learning, and experiential learning that helps individuals make sense of their learning in terms of application to the realities of work (e.g. Knowles174) |
| Paying attention to the individual | Expertise | In addition to theories of adult learning which emphasise the importance of a participant’s biography in shaping learning, models of skill acquisition also highlight a series of phases which characterise the development of expertise.175–178 These phases provide an indication of the different understandings of the learning requirements, decision-making processes and commitment which need to be accommodated in workforce development programmes |
| Incentives | Self-determination (intrinsic and extrinsic factors) | Self-determination theory examines the motivations for human behaviour and, specifically, the roles of both intrinsic and external factors in influencing motivation. Although there has been some debate about the potential for extrinsic factors, such as the reward-based incentives uncovered in this synthesis, a recent meta-analysis indicates that both are important.179 While incentives may be effective in influencing the quantity of appropriate behaviours, such as participation in workforce development, intrinsic factors may be crucial in ensuring the quality of participation |
| Strategy | Organisational change | Workforce development programmes operate in a given context, in which context or the conditions represent a mix of social, cultural and material factors.180 Differentiation can be made between the contextual conditions within organisations (e.g. structural characteristics, networks and communications, culture, climate and readiness for change) and external to the setting (e.g. the economic, political and cultural factors)181 Other conceptualisations of context focus on the interplay between layers of context,182 combinations of experiential aspects of culture, leadership and learning climate183 and in the development of person-centred cultures184 An implication of theorising about context is the important role that context can play in mediating workforce development programme effects, and the need to account for context in programme design and implementation184,185 Components of context may be considered as driving or restraining workforce development impacts,186 and so provide a focus for planning and tailoring implementation activity187 |
| Co-design | Coproduction | Although coproduction is commonly used to describe the process of engaging stakeholders in designing services, it is also linked to stakeholder engagement in the processes of knowledge creation and mobilisation188 As with theories of adult learning, there is a recognition of the importance of acknowledging the different forms of tacit and formal, codified knowledge that are important, which may be brought to bear on a topic (e.g. Rycroft-Malone et al.189). In addition, different stakeholders bring different priorities and expectations to the design process in workforce development, and may draw on and contribute different knowledge bases which, cumulatively, enrich the learning process and environment184 |
| Learning together | Interprofessional learning PPI |
Theories of interprofessional learning include the concept of ‘contact’ in which exposure to others to enable positive attitudes to grow between different groups within the older person’s service190 Building on aspects of coproduction, the involvement of patient and public stakeholders in aspects of workforce development, including in supporting its delivery, points to a range of different theoretical perspectives. These may involve different explanations of the impacts of involving lay stakeholders in workforce development191 The evidence in this synthesis relates principally to the ethical dimensions of including service user insights on workforce development challenges |
| Using theory | Programme theory | A wide range of approaches to evaluation have a common focus on the use of different forms of theory (e.g. logic), although these will reflect different ontological and epistemological perspectives. Regardless of perspective, theory plays a key role in articulating the change within a workforce development programme and directing evaluation activity192 |
| Spreading the impacts | Complexity theory | Complexity theory (e.g. Anderson193) focuses on the non-linear nature of transformative change within workforce development programmes. Elements of complexity theory include aspects of feedback (between programme components), connectedness (between programme and contexts) and the emergence of new programme elements. Within this synthesis, complexity theory points to the challenges of directing and delivering changes through workforce development in the context of changing organisational and other landscapes, and the potential for unplanned change. Key features of complexity theory that are relevant to the implementation of workforce development interventions include understanding behaviour of the whole (system) rather than its constituent parts, that components of interventions and systems interact with each other, continually emerge and evolve, and that history cannot easily be dismantled and, therefore, will impact on intervention implementation |
The breadth of more abstract theoretical perspectives pointed to in this review presents a further resource that people designing and delivering workforce development programmes can draw on. Rarely will workforce development be underpinned by just one of these theoretical perspectives, and so different insights from different perspectives are likely to be integrated in workforce development practice. In addition, they provide an added layer of explanation about why the CMO configurations may operate in the way they do.
Explanatory framework
The resulting explanatory framework (Figure 3) draws together the key features of the CMO configurations and the relationships between them into a theoretical, and potentially practical, heuristic. To enhance the transferability of the programme theory, the explanatory framework has been designed to illustrate the interconnectedness between and across the CMO configurations.
FIGURE 3.
Explanatory framework for workforce development in the support workforce.

This was an interpretive task, which involved creative processes borrowed from codesign methods and critical creativity. 184,194
This involved the identification of linking components (from the CMO configurations) and representing them (and their connections) in figurative form. In this process, some mechanisms are now more embedded in the final iteration of the programme theory as represented in this framework. The framework represents the starting point or local context, mechanisms and potential impacts of workforce development for support workers in its wider implementation context. We would argue that the findings of this review have resonance beyond the context of the older persons’ care setting, as they highlight issues relevant to workforce development more generally.
Specifically, we suggest that the design and delivery of workforce development needs to take into account the starting points for change; these issues form a local or specific context and include:
-
the broader organisational strategy and goals – incorporating what the strategy and goals are, and how the development need or gap aligns with the needs and strategy of the older people’s service, such as workforce development plans, and the adaptation of health and social care policies/procedures for local needs and ways of working
-
personal factors about the support worker – including their personal background, career aspirations, their existing strengths including life skills, development needs, values and experience, etc.
-
the specific requirements of the workforce development challenge in the context of improving the service for older people – including where the focus for change comes from (e.g. older person, family, carers, support workers) and the development needs, which may be clinical, technical, behavioural, cultural, individual, team organisational, etc.
In combination, these factors provide an initial context in that they determine ‘where they (individuals and organisations) are coming from’, and, therefore, if these issues are not attended to in design and delivery they may reduce the impact of the intervention/programme. The comprehensiveness of a workforce development intervention or programme will be determined by systematically considering the starting point of the local context.
Pawson77 argues for the development of conceptual platforms that represent the basic structure for programmes, which can be considered as necessary ingredients of a particular programme or intervention. We have found that the design and delivery of workforce development has a greater chance of ‘working’, or will be enhanced, by paying attention to a number of mechanisms. The mechanisms include:
-
Resonance – making the interventions/programmes’ components and activities cognitively and emotionally relevant and meaningful to the support workers’ themselves (personally, i.e. their starting point, aspirations, skills, experience) and to the reality of their day-to-day work as carers. The evidence would suggest that where these personal cognitively and emotional connections exist there is more personal interest in the development opportunity and greater motivation to engage.
-
Alignment – aligning the different pieces of workforce development– such as individual (support worker, patient/resident/person) with team and organisation needs/requirements through the use of a planned approach and/or theory. The evidence would suggest that alignment makes it easier for people to access opportunities, there is an obvious fit with their personal/role/career ambitions (as appropriate) and they can more easily apply any learning because it is directed at changes desired by the organisation and recognised appropriately for any achievements.
-
Proximity – embedding development opportunities and activities with examples/experiences from the reality of practice, including (when appropriate) learning being delivered within the workplace. There is evidence to suggest that closely aligning learning to the day-to-day work may be more effective in shifting from cognitive (the thinking) to instrumental (the doing) impacts for support workers, older people and the organisation.
-
Learning together – learning alongside peers or others that are part of the system (depending and as relevant to the development need and focus of intervention) to reflect the realities of service delivery. Learning and development opportunities that provide space for sharing, communicating and working on challenges together appear to be successful in building a better understanding of roles and in fostering productive and positive relationships between support workers, colleagues and older people.
-
Incentives – offering meaningful intrinsic (e.g. feeling like you are doing a good job) and extrinsic (e.g. pay awards) incentives for engaging with development opportunities, and for achieving and recognising/rewarding the attainment of specific goals. In this way individual motivation for taking advantage of and continuing involvement in development opportunities can be enhanced.
-
Coproduction – co-designing and co-delivering development opportunities with relevant stakeholders and participants, including residents/patients/carers and support workers themselves. Taking this approach recognises the different perspectives and, therefore, contributions different stakeholders will have about the issue. Incorporating these perspectives provides an opportunity to build a platform for shared learning in addition to increasing the chances of its success because of a sense of involvement and ownership in the process and product.
Systematically attending to the starting point of local context and mechanisms, including through the use of theory, could increase the potential of the workforce development interventions/programmes to result in sustained impacts for the individual (support worker and resident/patient/care receiver) and the organisation, including personal development, changes in and development of knowledge, attitudes, skills and care processes, and, if aligned appropriately, potential impact on the wider organisational context.
Within the framework these impacts revolve around the local context and mechanisms rather than being specifically aligned to one or more of them. This dynamic reflects our underlying argument that for workforce development to have the greatest potential for impact, there needs to be some alignment between local context and mechanisms, which will be determined by, for example, where the support worker is starting from and what the organisation and client group needs are. Alignment necessitates approaching the design and delivery of workforce development in a planned manner, including through the articulation and use of a theory for the development programme itself. This should link workforce development inputs and activities through to expected changes, paying attention to context, and may draw on explicit mid-range theory.
Workforce development as conceptualised here operates within a broader service, political, regulatory and social context. As such, features of this implementation context will mediate the successful implementation of workforce development interventions/programmes. Representation of implementation context should be considered not as some form of multilayered ‘backdrop’ to a workforce development programme. Rather, it could be more helpful to think of it as clusters of factors or issues which give the impacts of workforce development programmes meaning and purpose. For example, the development of support worker skills makes sense only if set within the context of role developments within services and settings; changing attitudes about older people makes sense only if situated within a wider context of social and cultural values. The interface between these aspects of implementation context and the design and delivery of workforce development programmes provides the conditions in which the identified mechanisms of action are triggered.
Review strengths and limitations
Strengths
We consider that the methodological approach used in this review was a key strength. As is the intention in a realist review, we have developed a theory-driven explanation of how workforce development for support workers might work, in the form of eight CMO configurations that make up a programme theory. Realist review is not concerned with developing statements or recommendations that have statistical certainty about questions of effectiveness or cost-effectiveness. Traditional approaches to evidence synthesis generally rely on a statistical analysis of the findings, for example the confidence interval around effect size. The philosophical underpinnings of realist reviews necessitate a focus on theoretical depth, breadth and transferability. It would be inappropriate, therefore, to produce a quantitative account of the contribution of each CMO configuration within the programme theory. However, we have paid attention to the weight of the threads of evidence (stakeholder views, published literature and interview data) across the programme theory. This was an accumulative and deliberative analytical process across phases of the review, which we have attempted to document in a transparent way in Chapter 2. The programme theory framework we have developed can be used to guide support worker workforce development initiatives/programmes in the future, pointing to what should be paid attention to and what might work: that is, it provides a plausible and credible account of what works, how, why and in what circumstances.
Realist review takes a particular position on how research quality is judged. 78,195 Rejecting the hierarchy of evidence in favour of an approach that facilitated a search for ‘nuggets’ to help us build up an explanation of how and why a workforce development programme or intervention may or may not work, we did not reject evidence based ‘simply’ on quality. In our extraction process we included trigger questions relating to ‘fidelity’ (did the evidence link to the theory areas?), ‘nuggets’ (did the evidence provide valuable information?), ‘trustworthiness’ (can the evidence be relied on?) and ‘relevance’ (does the evidence contribute to the review?). These trigger questions formalised our approach to coming to a decision about evaluating the usefulness of the evidence to the review.
Another strength of this review was the embedded approach to stakeholder engagement, including with PPI representatives and in novel ways through, for example, the use of Twitter and a Twitter chat. Adjunct to the study website and blog, we operated a Twitter account as suggested in a project advisory group meeting, which provided a communication channel about the study’s topic and fostered additional networking with relevant stakeholders. As part of the networking, we were invited to lead on a @WeNurses Twitter chat about workforce development for support workers. A member of the project advisory group hosted the chat, which was useful to elicit the views of the nursing community and inform ongoing discussions. The chat also led to networking with practitioners with a vested interest in the topic area. A summary of the main points from the Twitter chat is provided in Appendix 2. This facilitated the development of a credible account, while helping us to mobilise knowledge about the work throughout the lifetime of the project.
Limitations
In realist terms, findings are contingent on there and then conditions from stakeholders’ perspectives and as reported in the evidence base. We acknowledge that decision-making at key stages in the review process in this review rests with this unique team and group of stakeholders. However, we have paid attention to providing a transparent account of our approach in this review including a clear audit trail. Although we have identified the junctures at which key decisions were made, it would be impossible within the confines of this report to provide an exhaustive account of the day-to-day decisions we have had to make as part of undertaking the review. Readers should have some confidence in the fact that the review has been conducted by a team experienced in realist review using an approach to decision-making that has been team based (LW, CB and JRM), as well as a decision log/reflective diary. We sought additional support for decision-making from the wider team in our regular monthly meetings.
We suggest that a limitation of this review is the extent and detail of the evidence that we were able to access. As described in our funded protocol, we drew on a wide range of evidence to inform the development of this explanatory account, including from literature outside of health. We had expected, given the prevalence of support work roles in other public services (in the case of this review, policing and teaching), that the available evidence base would be larger. We used relevant networks and key contacts to ensure that we were not missing any key pieces of evidence, and this led to the discovery of some reports. These reports and other sources of evidence from these public services tended to be descriptive rather than empirical.
Reflecting on the nature of the evidence base that was included in the review, overall we found that reports of studies evaluating workforce development interventions tended to lack detail. Specifically, these reports tended to lack detail about the interventions that were being evaluated; for example, authors would state that ‘care planning’ or ‘vignettes’ were used, but did not provide details about these approaches/tools. In addition, we found a lack of specificity in reports about what were the perceived and actual intended impacts from the workforce development initiatives being implemented and/or evaluated.
Implications and recommendations
Implications for practice
The following implications for the practice of designing and delivering older persons’ support workforce development interventions are directly related to the eight CMO configuration of the programme theory:
-
Workforce development programmes should be organised to reflect the realities of the support worker role and work in a number of ways; for example:
-
Inclusion of material and examples drawn from the reality of practice, for example vignettes, care planning, role playing, stories, theatre and drawing on the experiences of older people, in addition to building on the ‘oral tradition’ of support workers.
-
Integrating learning within the expectations and boundaries of the role that support workers have, such as designing learning opportunities through, for example, (self-)assessments of where the support worker ‘is at’ in relation to their career/work ambitions, including the ambition of coming to work to do ‘the best that you can today’.
-
Bringing learning into the workplace on a sessional or integrated basis. This may be more or less relevant depending on the need to access expertise to support learning, the availability of a conducive learning environment and whether or not taking the workforce out of the service context may be desirable or necessary to address specific development needs and/or to work together with people in different contexts (e.g. cross-fertilisation of ideas and knowledge, disrupting the daily routine to foster new perspectives).
-
-
Workforce development should be constructed to build on the life skills and experiences that individuals bring to the support worker role, and enable role development and career progression (as appropriate) for the individual and their organisation. This implication is consistent with some of the recommendations from the Shape of Caring review that development should be appropriately aligned with an individual’s skills, experience and ambitions. Some care workers will not have ambitions to progress beyond their current role; others will have different career ambitions. Furthermore, individual care workers contribute to their role based on very different life experiences and skills. Therefore, an individual (and regular) assessment of a person’s skills, experiences and ambitions will enable workforce development to be designed around an individuals’ perspective on these issues.
-
Workforce development should incorporate strategies and techniques that might incentivise and motivate individual engagement in workforce development. These strategies and techniques should be designed to address both extrinsic and intrinsic motivators when possible. It may also be appropriate to make the incentives as relevant as possible to the support worker(s). To sustain motivation, extrinsic motivators should address explicit criteria for attainment, for example rewarding the achievement of specific goals such as attendance at learning events, and changing behaviours and performance.
-
There should be a systematic approach to the design of workforce development which ensures that it is aligned with organisational strategy around, for example, priorities such as quality and integration across health and social care. When this alignment is evident, for example by making explicit transparent links in course content and evaluation with the workforce development initiative and other strategies, such as quality improvement, it should be possible to realise more sustained improvements in workforce knowledge and skills because it should have a cumulative effect.
-
Designing workforce development interventions should include the involvement of the right stakeholders from the beginning of the development process. Stakeholders will probably include relevant agencies, for example organisations/institutions that can provide specialist input and/or educational accreditation/credibility, and individuals, for example support care workers, patients, residents and carers. Co-design processes, including interactive workshops and value clarification activities, will recognise and incorporate the views, expertise and values of each stakeholder constituency.
-
The delivery of workforce development interventions should include opportunities to involve others beyond the support worker him- or herself, for example in shared learning events. There will be learning and development issues, for example improving teamwork, supporting individuals’ transfer of care, what is healthy ageing, dignity in dementia, relationships between staff and families, where it would be relevant and promote resonance and to learn among peers. Involving older people in learning opportunities may be a particularly powerful way to effect changes in value and behaviour, for example regarding antidiscriminatory practice and challenging behaviours. This also links back to the first implication about making learning meaningful and close to the reality of practice.
-
Workforce development design and delivery should be approached in a theory-driven and systematic way. Programme specifications and curriculum plans, for example, should include reference to and inclusion of relevant theory/theories, frameworks and the learning methods/approaches/tools used linked to those underpinning heuristics. In addition, theoretically driven and systematic approaches should be used to evaluate learning and development interventions.
-
Workforce development should be considered a complex programme that is transformative of people and organisations. Therefore, workforce development should not be ad hoc and fragmented. Paying attention to workforce development in the context of the whole system, which includes individuals, teams and the organisation in its wider context, is more likely to result in wider, and potentially more systemic, impacts. This will require joining up and aligning various organisational strategies and associated goals such as human resource management (recruitment, retention, development, exit), organisational development, quality and safety, and resource management.
There are more general implications about support worker development, which were consistently mentioned by professional and lay stakeholders throughout the conduct of the project. These provide a broader context to the delivery of workforce development for this group of care workers:
-
Support workers make up approximately 60% of the health and social care workforce in the UK. 26
-
Professional and lay stakeholders consistently highlighted the importance of investing in the support workforce as a firm foundation on which to improve the quality of health and social care. While recognising the importance of being clinically competent, they also stressed the importance of some fundamental aspects of service delivery, including dignity, compassion and communication. Therefore, workforce development opportunities need to balance the technical with the professional and emotional aspects of caring work with older people.
Related to implication 2, investment in the development of the older persons’ support workforce provides a visible and clear recognition of the value attached to the contribution of support workers. Our evidence identified the use of some incentives to encourage participation with, and engagement in, workforce development. However, there was little evidence of a ‘joined-up’ approach to a workforce development in this context which linked learning with opportunities for career development, personal growth and monetary and other rewards for skill and role development.
Recommendations for future research
Our recommendations for future research relate both to aspects of research methods and to the further evaluation and explication of our programme theory.
With respect to research methods, the synthesis demonstrated generally poor reporting of workforce development interventions. In future research, we recommend that:
-
The typology proposed in this synthesis could be used to describe the focus of the intended workforce development.
-
Authors provide clear and detailed description of the component(s) of the intervention, including the theory of change for the workforce development intervention being clearly reported. This will make the ongoing synthesis of evidence around workforce development easier to manage and provide opportunities for learning and improvement.
-
The complexity of workforce development was highlighted in stakeholder workshops that drew on soft systems thinking, and in the CMO configuration around sustaining the impacts of workforce development across organisations. We recommend that drawing on complexity theory may provide new insights into ‘what works’ in relation to implementing workforce development interventions, and encourage researchers to explore alternative evaluation approaches which reflect different ontological perspectives in the evaluation of workforce development.
The eight CMO configurations resulting from this review provide a programme theory or contingent explanation, grounded in evidence from literature and stakeholder perspectives, about how workforce development works in improving outcomes for support workers, organisations and older people. Research questions relating to the development of the programme theory are as follows:
-
What is the right mix of workforce and organisational related policy to deliver a sustainable support workforce for older people’s services? What are the components of a fully integrated workforce planning and development strategy?
-
How can the sustainability of workforce development be addressed in the challenging context of the older persons’ support workforce?
-
What are the features of a whole-system approach to workforce development operating within a specific geographical context, and which pays attention to social (e.g. characteristics of the service user and workforce populations) and other (e.g. environmental) characteristics?
-
What is the appropriate mix of opportunities for personal and work-related development that balances individual support workers’ engagement in learning with the need to sustain a workforce with the capacity to deliver an effective service?
-
What approaches to the design and delivery of workforce development might be more effective in engaging hard-to-reach groups within the older persons’ support workforce?
-
What are the most effective ways to engage and integrate different stakeholder perspectives, including patient and public representatives, in the design and delivery of workforce development that enables support workers to address the needs older people?
-
What interventions can accelerate support workers’ implementation of gains in knowledge and skill into routine service delivery?
-
What are the best ways of including incentives in workforce development programmes that build on the motivations and aspirations of individual support workers?
Methodological recommendations
We have reflected on the processes we used to apply the principles of the particular methodological approach for this review, and suggest some recommendations for future use of realist synthesis as an emerging approach for research inquiry. In particular, we recommend that:
-
Realist synthesis should be considered for future work to explain the intricacies of programme such as workforce development. The focus on theory development at mid-range level provides practicable guidance for providers, commissioners and users of workforce development.
-
We have suggested that the design and delivery of workforce development has a greater chance of being successful if attention is paid to the mechanisms which represent the basic structure for such programmes. In this review, we found that the combination of desk work and active stakeholder engagement was a good framework for identifying key mechanisms and recommend that future realist studies build on the specific approach that we undertook.
-
Future application of realist methodology can draw on the account that we have provided of the approach and work conducted throughout this review, using the tools and processes used and/or developed. Our tools include a living document to log decisions and reflections, and a set of constructs within the data extraction form to guide decision-making. Soft systems methodology guided our understanding of factors which we found can influence the success or otherwise of workforce development at a system level. Our engagement processes included additional support for decision-making from the wider team in our regular monthly meetings, and active engagement and communication with stakeholders and PPI representatives through, for example, workshop, group work, glossary, website, blog and use of social media.
-
Although Pawson offers principles to guide the analysis process in realist synthesis, it is not suggested that these be used prescriptively. We chose the abductive analysis of evidence in this review as it reflects the realist quest to elicit generative mechanisms that explain the contingent nature of phenomena. We considered that retroduction was appropriate for this review, as we could draw from a wide range of experience and expertise. We suggest that future research develop and build on these and other approaches for analysis to ensure that realist researchers can access resources and guidance that reflects their particular research aims and objectives.
Conclusion
This evidence synthesis has constructed a realist, contingent programme theory which explains ‘what works’ and ‘how’ in the development of the older persons’ support workforce. Our programme theory captures the complexity of workforce development through its transformative potential, pointing to the need for approaches to design and delivery which are themselves underpinned by robust theory. The scope of workforce development should be comprehensive, attending to the interface between local context, mechanisms and implementation contexts, which shape engagement in, and the impacts of, workforce development. Our explanatory framework may provide a useful heuristic for designers and developers to use in the development and implementation of workforce development strategies for the older persons’ support workforce.
Acknowledgements
We would like to acknowledge the contribution and support of stakeholders and participants who engaged in a variety of different meetings and activities across the life of the project.
Professor Anthony Arthur; Marie Batey; Lynne Bedson; Sharon Blackburn; Tanis Hand; Mandy Hughes; Kirk Lawler; Charlette Middlemiss; Jerome Rampersad; Dr Theresa Shaw; Dr Louise Stewart; Karen Wakelin; Christopher Watts; Ian Thomas; Ulla Webber-Jones; Lowri Welnitschuk; Dr Sion Williams; Clare Woodcock; and Dr Gill Windle.
We are also very grateful to Nyree Hulme for her help with research administration and for her work on compiling and formatting this report, to Heledd Owen-Griffiths for being a note-taker during the telephone interviews and to Heledd and Alys Elen Williams for transcribing the interviews.
Contributions of authors
Professor Jo Rycroft-Malone was the co-principal investigator, co-led the study design, was involved in all aspects of the review process and is co-lead author of this report.
Professor Christopher R Burton was the co-principal investigator, co-led the study design, chaired the monthly research team meetings, facilitated the advisory group and stakeholder group meetings, was involved in all aspects of the review process and is co-lead author of this report.
Dr Lynne Williams took day-to-day responsibility for project management and for the review process, co-facilitated stakeholder and advisory group meetings, was involved in all aspects of the review process and co-led the preparation of this report.
Mr Stephen Edwards was a lay research team member. He participated in monthly meetings, provided feedback and input in between meetings, prepared a glossary of terms and participated in the preparation of the final report.
Mrs Denise Fisher was a lay research team member. She participated in monthly meetings, provided feedback and input in between meetings, prepared a glossary of terms and participated in the preparation of the final report.
Dr Beth Hall was a coapplicant on the grant, was involved in study design, was involved in monthly research team meetings, led the information searching, retrieval and organisation, gave feedback in between meetings and participated in the preparation of this report.
Professor Brendan McCormack was a coapplicant on the grant, was involved in study design, involved in monthly research team meetings, gave feedback in between meetings and participated in the synthesis process and in the preparation of this report.
Professor Sandra Nutley was a coapplicant on the grant, was involved in study design and monthly research team and stakeholder meetings, gave feedback in between meetings, helped to sift evidence within the context of education, and participated in the synthesis process and in the preparation of this report.
Dr Diane Seddon was a coapplicant on the grant, was involved in study design and monthly research team and advisory group meetings, gave feedback in between meetings and participated in the synthesis process and in the preparation of this report.
Mr Roger Williams was a lay research team member. He participated in monthly meetings, provided feedback and input in between meetings, prepared a glossary of terms and participated in the preparation of the final report.
Data sharing statement
All available data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Wise J. Number of ‘oldest old’ has doubled in the past 25 years. BMJ 2010;340. http://dx.doi.org/10.1136/bmj.c3057.
- Ageing, Longevity and Demographic Change: A Fact Pack of Statistics from the International Longevity Centre. London: International Longevity Centre; 2013.
- Shield F, Enderby P, Nancarrow S. Stakeholder views of the training needs of an interprofessional practitioner who works with older people. Nurse Educ Today 2006;26:367-76. http://dx.doi.org/10.1016/j.nedt.2005.11.006.
- Independent Inquiry into Care Provided by Mid Staffordshire NHS Foundation Trust. January 2005–March 2009. London: The Stationery Office; 2010.
- Reed J, Cook G, Childs S, McCormack B. A literature review to explore integrated care for older people. Int J Integr Care 2005;5:1-8.
- NHS and Social Care Funding: The Outlook to 2021/22. London: The Nuffield Trust; 2012.
- Cracks in the Pathway Summary. People’s Experiences of Dementia Care as They Move between Care Homes and Hospitals. London: Care Quality Commission; 2014.
- Commission on Hospital Care for Frail Older People. London; 2014.
- Dignity and Nutrition Inspection Programme: National Overview. London: Care Quality Commission; 2011.
- Care and Compassion? Report of the Health Service Ombudsman on Ten Investigations into NHS Care of Older People. London: The Stationery Office; 2011.
- The Human Rights of Older People in Healthcare. Eighteenth Report of Session 2006–7. London: The Stationery Office; 2007.
- Delivering Dignity. Securing Dignity in Care for Older People in Hospitals and Care Homes. London: Age UK/NHS Confederation; 2012.
- National Bereavement Survey (VOICES). London: Office for National Statistics; 2012.
- Rudd AG, Hoffman A, Down C, Pearson M, Lowe D. Access to stroke care in England, Wales and Northern Ireland: the effect of age, gender and weekend admission. Age Ageing 2007;36:247-55. http://dx.doi.org/10.1093/ageing/afm007.
- Gott M, Small N, Barnes S, Payne S, Seamark D. Older people’s views of a good death in heart failure: implications for palliative care provision. Soc Sci Med 2008;67:1113-21. http://dx.doi.org/10.1016/j.socscimed.2008.05.024.
- Evidence Review – Integrated Health and Social Care. Oxford: Institute of Public Care, Oxford Brookes University; 2013.
- Five Year Forward Review. London: NHS; 2014.
- Gage C. Vibrant communities: the care homes of the future. J Dement Care 2014;22:22-5.
- Shaping the Future: Education and Training for Nurses and Care Assistants. London: Council of Deans of Health; 2014.
- Better Care for Frail Older People. Working Differently to Improve Care. London: Deloitte Centre for Health Studies; 2014.
- Public Expenditure on Health and Social Care. London: Health Select Committee; 2014.
- Capable, Confident, Skilled – A Workforce Development Strategy for People Working, Supporting and Caring in Adult Social Care. Leeds: Skills for Care; 2011.
- Kessler I, Spilsbury K, Heron P. Developing a high-performance support workforce in acute care: innovation, evaluation and engagement. Health Serv Deliv Res 2014;2.
- The NHS. Confederation. The support workforce in the NHS. SDO Network Research Digest 2011;1.
- Saks M, Allsop J, Chevannes M, Clark M, Fagan R, Genders NEA. Review of Health Support Workers: Report to the UK Departments of Health. Leicester: De Montfort University; 2000.
- Cavendish C. The Cavendish Review: An Independent Review into Healthcare Assistants and Support Workers in the NHS and Social Care Settings. London: Department of Health; 2013.
- The Talent for Care – Feedback From Consultation on the Development of the Healthcare Support Workforce. London: Health Education England; 2014.
- Moran A, Nancarrow SA, Enderby P. Mechanisms to enhance the effectiveness of allied health and social care assistants in community-based rehabilitation services: a qualitative study. Health Soc Care Community 2015;23:389-98. http://dx.doi.org/10.1111/hsc.12158.
- Schneider J, Scales K, Bailey S, Lloyd J. Challenging Care: The Role and Experience of Health Care Assistants in Dementia Wards. London: National Institute for Health Research; 2010.
- Manthorpe J, Martineau S. Support Workers: Their Role and Tasks. London: Social Care Workforce Research Unit, King’s College London; 2008.
- Nancarrow SA, Borthwick AM. Dynamic professional boundaries in the healthcare workforce. Sociol Health Illn 2005;27:897-919. http://dx.doi.org/10.1111/j.1467-9566.2005.00463.x.
- Janes N, Sidani S, Cott C, Rappolt S. Figuring it out in the moment: a theory of unregulated care providers’ knowledge utilization in dementia care settings. Worldviews Evid Based Nurs 2008;5:13-24. http://dx.doi.org/10.1111/j.1741-6787.2008.00114.x.
- Healthcare Support Workers in England: Five Proposals for Investing in Education and Development to Deliver High Quality, Effective and Compassionate Care. London: Council of Deans of Health; 2013.
- Assistant and Support Workers: Workforce Flexibility to Boost Productivity – Full Report. Canberra, ACT: Department of Health Australia; 2014.
- Estabrooks CA, Squires JE, Carleton HL, Cummings GG, Norton PG. Who is looking after mom and dad? Unregulated workers in Canadian long-term care homes. Can J Aging 2015;34:47-59. http://dx.doi.org/10.1017/S0714980814000506.
- Berta W, Laporte A, Deber R, Baumann A, Gamble B. The evolving role of health care aides in the long-term care and home and community care sectors in Canada. Hum Resour Health 2013;11. http://dx.doi.org/10.1186/1478-4491-11-25.
- Cummings GG, Spiwek T, Hewko S, Cooper S, Lynch S, Huynh H. Shining a Light on the Unregulated Healthcare Aide Workforce. Edmonton, AB: University of Alberta; 2013.
- Griffiths P, Robinson S. Moving Forward With Healthcare Support Workforce Regulation. A Scoping Review: Evidence, Questions, Risks and Options. London: National Nursing Research Unit, King’s College London; 2010.
- Kessler I, Heron P, Dopson S, Magee H, Swain D, Askham J. The Nature and Consequences of Support Workers in a Hospital Setting. London: National Institute for Health Research Service Delivery and Organisation programme; 2010.
- Healthcare Support Workers. The Development of the Clinical Support Worker Role: A Review of the Evidence. Edinburgh: NHS Education for Scotland; 2010.
- Tadd W, Hillman A, Calnan S, Calnan M, Bayer T, Read S. Dignity in Practice: An Exploration of the Care of Older Adults in Acute NHS Trusts. London: National Institute for Health Research Service Delivery and Organisation programme; 2011.
- Bond J, Bamford C, Arksey H, Poole M, Kirkley C, Hughes J, et al. Person- and Carer-Centred Respite Care for People with Dementia: Developing Methods of Evaluating the Effectiveness of Different Models. Final Report. National Institute for Health Research Service Delivery and Organisation programme; 2009.
- Spilsbury K, Adamson J, Atkin K, Bartlett C, Bloor K, Borglin GEA. Evaluation of the Development and Impact of Assistant Practitioners Supporting the Work of Ward-Based Registered Nurses in Acute NHS (Hospital) Trusts in England. London: National Institute for Health Research Service Delivery and Organisation programme; 2010.
- Nancarrow S, Enderby PM, Moran A, Dixon S, Parker S. The Relationship between Workforce Flexibility and the Costs and Outcomes of Older Peoples’ Services. London: National Institute for Health Research Service Delivery and Organisation programme; 2010.
- Spilsbury K, Pender S, Bloor K, Borthwick R, Atkin K, McCaughan DEA. Support matters: a mixed methods scoping study on the use of assistant staff in the delivery of community nursing services in England. Health Serv Deliv Res 2013;1.
- Kessler I, Heron P, Dopson S. The Modernization of the Nursing Workforce: Valuing the Healthcare Assistant. Oxford: Oxford University Press; 2012.
- Manthorpe J, Martineau S, Moriarty J, Hussein S, Stevens M. Support workers in social care in England: a scoping study. Health Soc Care Community 2010;18:316-24. http://dx.doi.org/10.1111/j.1365-2524.2010.00910.x.
- Glasper A. Making caring a career: the role of the healthcare assistant. Br J Nurs 2013;22:1028-9. http://dx.doi.org/10.12968/bjon.2013.22.17.1028.
- Raising the Bar. Shape of Caring: A Review of the Future Education and Training of Registered Nurses and Care Assistants. London: Health Education England; 2015.
- Frontline Care. London: The Prime Minister’s Commission on the Future of Nursing and Midwifery in England; 2010.
- Berwick Review into Patient Safety. London: Department of Health; 2013.
- Keogh B. Review into the Quality of Care and Treatment Provided by 14 Hospital Trusts in England: Overview Report. NHS England; 2013.
- Quality with Compassion: The Future of Nursing Education. Royal College of Nursing; 2012.
- Arborio AM. Climbing invisible ladders: how nurse’s aides craft lateral careers. Ethnography 2004;5:75-105. http://dx.doi.org/10.1177/1466138104041589.
- Saks M, Allsop J. Social policy, professional regulation and health support work in the United Kingdom. Soc Policy Society 2007;6:165-77. http://dx.doi.org/10.1017/S1474746406003435.
- Balancing Risk and Safety for Our Community – Unlicenced Health Workers in the Health and Aged Care Systems. Canberra, ACT: Australian Nursing Federation; 2009.
- Llewellyn M, Longley M, Fisk M, Boutall T, Wallace C, Roberts M. Care at Home. Challenges, Possibilities and Implications for the Workforce in Wales. Cardiff: Care Council for Wales; 2010.
- Skills for Care/Skills for Health . Code of Conduct for Healthcare Support Workers and Adult Social Care Workers in England 2013.
- Code of Practice for Social Care Workers. Cardiff: Care Council for Wales; 2010.
- Governance Framework for Development of the Health and Social Care Support Worker Role in Adult Services. Cardiff: Care Council for Wales; 2012.
- Key to Care: Report of the Burstow Commission on the Future of the Home Care Workforce. London: Local Government Information Unit; 2014.
- Care Quality Commission . The Partnership in Care Limited Prince of Wales House Inspection Report 2015. www.cqc.org.uk/sites/default/files/new_reports/AAAA2076.pdf (accessed 7 January 2015).
- Delivering Dignity: Securing Dignity in Care for Older People in Hospitals and Care Homes. Independent Commission on Dignity in Care; 2012.
- Dreyfus SE, Dreyfus HL. A Five Stage Model of the Mental Activities Involved in Directed Skill Acquisition. Berkley, CA: University of California; 1980.
- Pawson R, Tilley N. Realistic Evaluation. London: Sage Publications; 1997.
- Rycroft-Malone J, McCormack B, Hutchinson AM, DeCorby K, Bucknall TK, Kent B, et al. Realist synthesis: illustrating the method for implementation research. Implement Sci 2012;7. http://dx.doi.org/10.1186/1748-5908-7-33.
- Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med 2013;11. http://dx.doi.org/10.1186/1741-7015-11-21.
- McCormack B, Wright J, Dewar B, Harvey G, Ballantine K. A realist synthesis of evidence relating to practice development: findings from the literature analysis. Pract Dev Health Care 2007;6. http://dx.doi.org/10.1002/pdh.211.
- McCormack B, Rycroft-Malone J, DeCorby K, Hutchinson AM, Bucknall T, Kent B, et al. A realist review of interventions and strategies to promote evidence-informed healthcare: a focus on change agency. Implement Sci 2013;8. http://dx.doi.org/10.1186/1748-5908-8-107.
- Hardwick R, Pearson M, Byng R, Anderson R. The effectiveness and cost-effectiveness of shared care: protocol for a realist review. Syst Rev 2013;2. http://dx.doi.org/10.1186/2046-4053-2-12.
- McConnell T, O’Halloran P, Porter S, Donnelly M. Systematic realist review of key factors affecting the successful implementation and sustainability of the Liverpool care pathway for the dying patient. Worldviews Evid Based Nurs 2013;10:218-37. http://dx.doi.org/10.1111/wvn.12003.
- Post J, Preston L, Sachs S. Managing the extended enterprise: the new stakeholder view. California Manage Rev 2002;45:6-28. http://dx.doi.org/10.2307/41166151.
- Rycroft-Malone J, Burton C, Hall B, McCormack B, Nutley S, Seddon D, et al. Improving skills and care standards in the support workforce for older people: a realist review. BMJ Open 2014;4. http://dx.doi.org/10.1136/bmjopen-2014-005356.
- Hewitt G, Sims S, Harris R. The realist approach to evaluation research: an introduction. Int J Therapy Rehabil 2012;19:250-9. http://dx.doi.org/10.12968/ijtr.2012.19.5.250.
- Pawson R. Nothing as practical as a good theory. Evaluation 2003;9:471-90. http://dx.doi.org/10.1177/1356389003094007.
- Westhorp G, Prins E, Kusters C, Hultink M, Guijt I, Brouwers J. Realist Evaluation: An Overview. Wageningen: Centre for Development Innovation; 2011.
- Pawson R. The Science of Evaluation: A Realist Manifesto. Thousand Oaks, CA: Sage; 2013.
- Pawson R. Evidence-Based Policy: A Realist Perspective. London: Sage Publications; 2006.
- Interventions to Improve Skills and Care Standards in the Clinical Support Workforce for Older People (Proposal) n.d. www.nets.nihr.ac.uk/__data/assets/pdf_file/0018/81801/CB-12–129–32.pdf (accessed 19 October 2015).
- Eraut M. Informal learning in the workplace. Stud Continuing Educ 2004;26:247-73. http://dx.doi.org/10.1080/158037042000225245.
- Daley BJ. Novice to expert: an exploration of how professionals learn. Adult Educ Q 1999;49:133-47. http://dx.doi.org/10.1177/074171369904900401.
- Bloom BS. Taxonomy of Educational Objectives: The Classification Of Education Goals. Cognitive Domain. Handbook 1. New York, NY: Longman; 1956.
- Grubb WN. From Isolation to Integration: Occupational Education and the Emerging Systems of Workforce Development. Centerpoint; 1999.
- Jacobs RL. Understanding Workforce Development: Definition, Conceptual Boundaries, and Future Perspectives. Winnipeg, MB: University of Manitoba; 2002.
- Hughes D, Bimrose J, Barnes S, Bowes L, Orton M. A Systematic Literature Review of Research into Career Development Interventions for Workforce Development. Derby: Centre for Guidance Studies, University of Derby; 2005.
- Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. ‘Psychological Theory’ Group . Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care 2005;14:26-33. http://dx.doi.org/10.1136/qshc.2004.011155.
- Rycroft-Malone J, Kitson A, Harvey G, McCormack B, Seers K, Titchen A, et al. Ingredients for change: revisiting a conceptual framework. Qual Saf Health Care 2002;11:174-80. http://dx.doi.org/10.1136/qhc.11.2.174.
- Nutley S, Davies H, Davies HTO, Nutley S, Smith PC. What Works? Evidence-Based Policy and Practice in Public Services. Bristol: The Policy Press; 2009.
- McCormack B, Dewar B, Wright J, Garbett R, Harvey G, Ballantine K. A Realist Synthesis of Evidence Relating to Practice Development. NHS Quality Improvement Scotland; 2006.
- Easterby-Smith M. Disciplines of organizational learning: contributions and critiques. Hum Relations 1997;50:1085-113. http://dx.doi.org/10.1177/001872679705000903.
- Berta W, Teare GF, Gilbart E, Ginsburg LS, Lemieux-Charles L, Davis D, et al. The contingencies of organizational learning in long-term care: factors that affect innovation adoption. Health Care Manage Rev 2005;30:282-92. http://dx.doi.org/10.1097/00004010-200510000-00002.
- Ellinger AD, Cseh M. Contextual factors influencing the facilitation of others’ learning through everyday work experiences. J Workplace Learn 2007;19:435-52. http://dx.doi.org/10.1108/13665620710819384.
- Lane DC, Oliva R. The greater whole: towards a synthesis of system dynamics and soft systems methodology. Eur J Oper Res 1998;107:214-35. http://dx.doi.org/10.1016/S0377-2217(97)00205-1.
- Williams B. Soft Systems Methodology. The Kellogg Foundation; 2005.
- Checkland P. Systems Thinking, Systems Practice. Chichester: John Wiley and Sons; 1999.
- Pawson R. Digging for nuggets: How ‘bad’ research can yield ‘good’ evidence. Int J Soc Res Methodol 2006;9:127-42. http://dx.doi.org/10.1080/13645570600595314.
- Westhorp G, Walker B, Rogers P, Overbeeke N, Ball D, Brice G. Enhancing Community Accountability, Empowerment and Education Outcomes in Low and Middle-Income Countries: A Realist Review. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2014.
- Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ 2005;331:1064-5. http://dx.doi.org/10.1136/bmj.38636.593461.68.
- Brennan N, Bryce M, Pearson M, Wong G, Cooper C, Archer J. Understanding how appraisal of doctors produces its effects: a realist review protocol. BMJ Open 2014;4. http://dx.doi.org/10.1136/bmjopen-2014-005466.
- Nutley SM, Walter I, Davies HTO. Using Evidence: How Research Can Inform Public Services. Bristol: Policy Press; 2007.
- Jagosh J, Macaulay AC, Pluye P, Salsberg J, Bush PL, Henderson J, et al. Uncovering the benefits of participatory research: implications of a realist review for health research and practice. Milbank Q 2012;90:311-46. http://dx.doi.org/10.1111/j.1468-0009.2012.00665.x.
- Greenhalgh J, Pawson R, Wright J, Black N, Valderas JM, Meads D, et al. Functionality and feedback: a protocol for a realist synthesis of the collation, interpretation and utilisation of PROMs data to improve patient care. BMJ Open 2014;4. http://dx.doi.org/10.1136/bmjopen-2014-005601.
- Gough D. Weight of evidence: a framework for the appraisal of the quality and relevance of evidence. Res Pap Educ 2007;22:213-28. http://dx.doi.org/10.1080/02671520701296189.
- Leeman J, Chang, YK, Lee EJ, Voils CI, Sandelowski M. Implementation of antiretroviral therapy adherence interventions: a realist synthesis of evidence. J Adv Nurs 2010;66:1915-30. http://dx.doi.org/10.1111/j.1365-2648.2010.05360.x.
- Braun KL, Cheang M, Shigeta D. Increasing knowledge, skills, and empathy among direct care workers in elder care: a preliminary study of an active-learning model. Gerontologist 2005;45:118-24. http://dx.doi.org/10.1093/geront/45.1.118.
- Cherry B, Marshall-Gray P, Laurence A, Green A, Valadez A, Scott-Tilley D, et al. The geriatric training academy: innovative education for certified nurse aides and charge nurses. J Gerontol Nurs 2007;33:37-44.
- Clare L, Whitaker R, Woods RT, Quinn C, Jelley H, Hoare Z, et al. AwareCare: a pilot randomized controlled trial of an awareness-based staff training intervention to improve quality of life for residents with severe dementia in long-term care settings. Int Psychogeriatr 2013;25:128-39. http://dx.doi.org/10.1017/S1041610212001226.
- Coleman CK, Medvene LJ. A person-centered care intervention for geriatric certified nursing assistants. Gerontologist 2013;53:687-98. http://dx.doi.org/10.1093/geront/gns135.
- Grosch K, Medvene L, Wolcott H. Person-centered caregiving instruction for geriatric nursing assistant students: development and evaluation. J Gerontol Nurs 2008;34:23-3. http://dx.doi.org/10.3928/00989134-20080801-07.
- Lerner NB, Resnick B, Galik E, Russ KG. Advanced nursing assistant education program. J Contin Educ Nurs 2010;41:356-62. http://dx.doi.org/10.3928/00220124-20100401-10.
- Ron P, Lowenstein A. In-service training of professional and para-professional staff in institutions for the aged. Educ Gerontol 2002;28:587-97. http://dx.doi.org/10.1080/03601270290099787.
- Stevens AB, Hochhalter AK, Hyer L, Intrieri RC, Hyer L, Intrieri R. Geropsychological Interventions in Long-Term Care. New York, NY: Springer Publishing Co; 2006.
- Tisher TB, Dean S, Tisher M. Aged care residential facility and family interface: a training program for staff. Clin Gerontol 2009;32:309-23. http://dx.doi.org/10.1080/07317110902895952.
- Wadensten B, Engström M, Häggström E. Public nursing home staff’s experience of participating in an intervention aimed at enhancing their self-esteem. J Nurs Manag 2009;17:833-42. http://dx.doi.org/10.1111/j.1365-2834.2009.00968.x.
- Hockley J. Learning, support and communication for staff in care homes: outcomes of reflective debriefing groups in two care homes to enhance end-of-life care. Int J Older People Nurs 2014;9:118-30. http://dx.doi.org/10.1111/opn.12048.
- Nilsson A, Andrén M, Engström M. E-assessment of prior learning: a pilot study of interactive assessment of staff with no formal education who are working in Swedish elderly care. BMC Geriatr 2014;14. http://dx.doi.org/10.1186/1471-2318-14-52.
- Boettcher IF, Kemeny B, DeShon RP, Stevens AB. A system to develop staff behaviors for person-centered care. Alzheimers Care Q 2004;5:188-96.
- Clarke A, Hanson EJ, Ross H. Seeing the person behind the patient: enhancing the care of older people using a biographical approach. J Clin Nurs 2003;12:697-706. http://dx.doi.org/10.1046/j.1365-2702.2003.00784.x.
- McKenzie Smith M, Turkhud K. Simulation-based education in support of HCA development. Br J Healthc Assist 2013;7:392-7. http://dx.doi.org/10.12968/bjha.2013.7.8.392.
- McCallion P, Toseland RW, Lacey D, Banks S. Educating nursing assistants to communicate more effectively with nursing home residents with dementia. Gerontologist 1999;39:546-58. http://dx.doi.org/10.1093/geront/39.5.546.
- Smith B, Kerse N, Parsons M. Quality of residential care for older people: does education for healthcare assistants make a difference?. N Z Med J 2005;118.
- Lewis R, Kelly S, Whitfield M, McKenzie-Smith MM, Strachan A. An Evaluation of a Simulation-Based Educational Programme to Equip HCAs with the Necessary Non-Technical Skills to Undertake Their Role Safely and Effectively, Specifically in Relation to the Measurement of Vital Signs. Sheffield Hallam University; 2013.
- Farrell P, Balshaw MH, Polat F. The Management, Role and Training of Learning Support Assistants. London: Department for Education and Employment; 1999.
- Anderson RA, Ammarell N, Bailey D, Colón-Emeric C, Corazzini KN, Lillie M, et al. Nurse assistant mental models, sensemaking, care actions, and consequences for nursing home residents. Qual Health Res 2005;15:1006-21. http://dx.doi.org/10.1177/1049732305280773.
- Proctor R, Stratton Powell H, Burns A, Tarrier N, Reeves D, Emerson E, et al. An observational study to evaluate the impact of a specialist outreach team on the quality of care in nursing and residential homes. Aging Ment Health 1998;2:232-8. http://dx.doi.org/10.1080/13607869856713.
- Hancock H, Campbell S, Ramprogus V, Kilgour J. Role development in health care assistants: the impact of education on practice. J Eval Clin Pract 2005;11:489-98. http://dx.doi.org/10.1111/j.1365-2753.2005.00569.x.
- Moxon S, Lyne K, Sinclair I, Young P, Kirk C. Mental health in residential homes: a role for care staff. Ageing Soc 2001;21:71-93. http://dx.doi.org/10.1017/S0144686X01008054.
- Passalacqua SA, Harwood J. VIPS communication skills training for paraprofessional dementia caregivers: an intervention to increase person-centered dementia care. Clin Gerontol 2012;35:425-45. http://dx.doi.org/10.1080/07317115.2012.702655.
- Thomson M, Burke K. A nursing assistant training program in a long term care setting. Gerontol Geriatr Educ 1998;19:23-35. http://dx.doi.org/10.1300/J021v19n01_03.
- McCormack B, Dewing J, Breslin L, Coyne-Nevin A, Kennedy K, Manning M, et al. Developing person-centred practice: nursing outcomes arising from changes to the care environment in residential settings for older people. Int J Older People Nurs 2010;5:93-107. http://dx.doi.org/10.1111/j.1748-3743.2010.00216.x.
- Welsh JD, Szabo GB. Teaching nursing assistant students about aphasia and communication. Semin Speech Lang 2011;32:243-55. http://dx.doi.org/10.1055/s-0031-1286178.
- Coogle CL, Parham IA, Jablonski R, Rachel JA. The value of geriatric care enhancement training for direct service workers. Gerontol Geriatr Educ 2007;28:109-31. http://dx.doi.org/10.1300/J021v28n02_08.
- Hegeman CR. Peer mentoring of nursing home CNAs: a way to create a culture of caring. J Soc Work Long-Term Care 2003;2:183-96. http://dx.doi.org/10.1300/J181v02n01_13.
- Ersek M, Wood BB. Development and evaluation of a nursing assistant computerized education programme. Int J Palliat Nurs 2008;14:502-9. http://dx.doi.org/10.12968/ijpn.2008.14.10.31495.
- White DL, Cadiz DM. Efficacy of work-based training for direct care workers in assisted living. J Aging Soc Policy 2013;25:281-300. http://dx.doi.org/10.1080/08959420.2013.816124.
- McGilton KS, O’Brien-Pallas LL, Darlington G, Evans M, Wynn F, Pringle DM. Effects of a relationship-enhancing program of care on outcomes. J Nurs Scholarsh 2003;35:151-6. http://dx.doi.org/10.1111/j.1547-5069.2003.00151.x.
- Graber DR, Mitcham MD, Coker-Bolt P, Wise HH, Jacques P, Edlund B, et al. The caring professionals program: educational approaches that integrate caring attitudes and empathic behaviors into health professions education. J Allied Health 2012;41:90-6.
- Bourgeois MS, Dijkstra K, Burgio LD, Allen RS. Communication skills training for nursing aides of residents with dementia: the impact of measuring performance. Clin Gerontol 2004;27:119-38. http://dx.doi.org/10.1300/J018v27n01_10.
- Bryan K, Axelrod L, Maxim J, Bell L, Jordan L. Working with older people with communication difficulties: an evaluation of care worker training. Aging Ment Health 2002;6:248-54. http://dx.doi.org/10.1080/13607860220142495.
- O’Neill M. PCSOs as the Paraprofessionals of Policing: Findings and Recommendations from a Research Project. Dundee: University of Dundee; 2014.
- Morgan JC, Konrad TR. A mixed-method evaluation of a workforce development intervention for nursing assistants in nursing homes: the case of WIN A STEP UP. Gerontologist 2008;48:71-9. http://dx.doi.org/10.1093/geront/48.Supplement_1.71.
- Stevens-Roseman ES, Leung P. Enhancing attitudes, knowledge and skills of paraprofessional service providers in elder care settings. Gerontol Geriatr Educ 2004;25:73-88. http://dx.doi.org/10.1300/J021v25n01_05.
- Burgio LD, Allen-Burge R, Roth DL, Bourgeois MS, Dijkstra K, Gerstle J, et al. Come talk with me: improving communication between nursing assistants and nursing home residents during care routines. Gerontologist 2001;41:449-60. http://dx.doi.org/10.1093/geront/41.4.449.
- Petterson IL, Donnersvard HA, Lagerstram M, Toomingas A. Evaluation of an intervention programme based on empowerment for eldercare nursing staff. Work Stress 2006;20:353-69. http://dx.doi.org/10.1080/02678370601070489.
- McLellan H, Bateman H, Bailey P. The place of 360 degree appraisal within a team approach to professional development. J Interprof Care 2005;19:137-48. http://dx.doi.org/10.1080/13561820400024290.
- Gethin-Jones S. Focus on the micro-relationship in the delivery of care. Br J Healthc Assist 2013;7:452-5. http://dx.doi.org/10.12968/bjha.2013.7.9.452.
- Vail L, Bosley S, Petrova M, Dale J. Healthcare assistants in general practice: a qualitative study of their experiences. Prim Health Care Res Dev 2011;12:29-41. http://dx.doi.org/10.1017/S1463423610000204.
- Cooper C, Anscombe J, Avenell J, McLean F, Morris J. A National Evaluation of Community Support Officers 2006.
- Nelson S, Wild D, Szczepura A. The forgotten sector: workforce development in residential care for older people. Nurs Residential Care 2009;11:200-3. http://dx.doi.org/10.12968/nrec.2009.11.4.41063.
- Cowan DT, Roberts JD, Fitzpatrick JM, While AE, Baldwin J. The approaches to learning of support workers employed in the care home sector: an evaluation study. Nurse Educ Today 2004;24:98-104. http://dx.doi.org/10.1016/j.nedt.2003.10.002.
- Arblaster G, Streather C, Hugill L, McKenzie M, Missenden J. A training programme for healthcare support workers. Nurs Stand 2004;18:33-7. http://dx.doi.org/10.7748/ns2004.07.18.43.33.c3640.
- Parks SM, Haines C, Foreman D, McKinstry E, Maxwell TL. Evaluation of an educational program for long-term care nursing assistants. J Am Med Dir Assoc 2005;6:61-5. http://dx.doi.org/10.1016/j.jamda.2004.12.001.
- Kuske B, Luck T, Hanns S, Matschinger H, Angermeyer MC, Behrens J, et al. Training in dementia care: a cluster-randomized controlled trial of a training program for nursing home staff in Germany. Int Psychogeriatr 2009;21:295-308. http://dx.doi.org/10.1017/S1041610208008387.
- Chapman A, Law S. Bridging the gap: an innovative dementia learning program for healthcare assistants in hospital wards using facilitator-led discussions. Int Psychogeriatr 2009;21:S58-63. http://dx.doi.org/10.1017/S1041610209008680.
- McCormack B. A conceptual framework for person-centred practice with older people. Int J Nurs Pract 2003;9:202-9. http://dx.doi.org/10.1046/j.1440-172X.2003.00423.x.
- Yalden J, McCormack B, O’Connor M, Hardy S. Transforming end of life care using practice development: an arts-informed approach in residential aged care. Int Pract Dev J 2013;3:1-18.
- McCormack B, Dewing J, Breslin L, Tobin C, Manning M, Coyne-Nevin A, et al. The Implementation of a Model of Person-Centred Practice in Older Person Settings. Final Report. Dublin: National Council for the Continuing Professional Development of Nursing and Midwifery and Health Service Executive; 2010.
- Lawton MP, Nahemow L, Eisdorfer C, Lawton MP. The Psychology of Adult Development and Aging. American Psychological Association; 1973.
- Kanter RM. Men and Women of the Corporation. New York, NY: Basic Books; 1993.
- Spreitzer GM. Encyclopedia of Industrial and Organizational Psychology. Thousand Oaks, CA: Sage Publications; 2006.
- Webster J, Coats E, Noble G. Enabling dignity in care through practice development with older people. Pract Dev Health Care 2009;8:5-17. http://dx.doi.org/10.1002/pdh.272.
- Noelker LS, Ejaz FK. Training direct care workers for person-centered care. Public Policy Aging Report 2005;15:17-9. http://dx.doi.org/10.1093/ppar/15.4.17.
- McCormack B, Wright J. Achieving dignified care for older people through practice development: a systematic approach. Nursing Times Research 1999;4:340-52. http://dx.doi.org/10.1177/136140969900400504.
- Aubry F, Etheridge F, Couturier Y. Facilitating change among nursing assistants in long term care. Online J Issues Nurs 2012;18. http://dx.doi.org/10.3912/OJIN.Vol18No01PPT01.
- Latta LE, Ross J. Exploring the impact of palliative care education for care assistants employed in residential aged care facilities in Otago, New Zealand. Sites 2011;7:30-52. http://dx.doi.org/10.11157/sites-vol7iss2id155.
- Goodridge D, Johnston P, Thomson M. Impact of a nursing assistant training program on job performance, attitudes, and relationships with residents. Educ Gerontol 1997;23:37-51. http://dx.doi.org/10.1080/0360127970230104.
- Ruckdeschel K, Van Haitsma K. A workshop for nursing home staff: recognizing and responding to their own and residents’ emotions. Gerontol Geriatr Educ 2004;24:39-51. http://dx.doi.org/10.1300/J021v24n03_04.
- Howatson-Jones L, Thurgate C, Graber M, Harnett CM, Thompson JS, Jordan DA. Biographical learning: a process for promoting person-centredness in nursing. Int Pract Dev J 2013;3.
- Medvene LJ, Lann-Wolcott H. An exploratory study of nurse aides communication behaviours: giving positive regard as a strategy. Int J Older People Nurs 2010;5:41-50. http://dx.doi.org/10.1111/j.1748-3743.2009.00183.x.
- Brown J, Nolan M, Davies S, Nolan J, Keady J. Transforming students’ views of gerontological nursing: realising the potential of ‘enriched’ environments of learning and care: a multi-method longitudinal study. Int J Nurs Stud 2008;45:1214-32. http://dx.doi.org/10.1016/j.ijnurstu.2007.07.002.
- Manley K, Sanders K, Cardiff S, Webster J. Effective workplace culture: the attributes, enabling factors and consequences of a new concept. Int Pract Dev J 2011;1:1-29.
- Noelker L, Ejaz F, Menne H, Jones J. The impact of stress and support on nursing assistant satisfaction with supervision. J Appl Gerontol 2006;25:307-23. http://dx.doi.org/10.1177/0733464806290935.
- Bailey S, Scales K, Lloyd J, Schneider J, Jones R. The emotional labour of health-care assistants in inpatient dementia care. Ageing Soc 2015;35:246-69. http://dx.doi.org/10.1017/S0144686X13000573.
- Knowles MS. Andragogy in Action. San Francisco, CA: Jossey-Bass; 1984.
- Benner P. From Novice to Expert, Excellence and Power in Clinical Nursing Practice. Menlo Park, CA: Addison-Wesley Publishing Company; 1984.
- Dreyfus SE. The five-stage model of adult skill acquisition. Bull Sci Technol Soc 2004;24:177-81. http://dx.doi.org/10.1177/0270467604264992.
- Manley K, Hardy S, Titchen A, Garbett R, McCormack B. Changing Patients’ Worlds through Nursing Practice Expertise. A Royal College of Nursing Research Report, 1998–2004. London: Royal College of Nursing; 2005.
- Hardy S, Titchen A, McCormack B, Manley K. Revealing Nursing Expertise through Practitioner Enquiry. Chichester: Wiley-Blackwell; 2009.
- Cerasoli CP, Nicklin JM, Ford MT. Intrinsic motivation and extrinsic incentives jointly predict performance: a 40-year meta-analysis. Psychol Bull 2014;140. http://dx.doi.org/10.1037/a0035661.
- Kontos PC, Poland BD. Mapping new theoretical and methodological terrain for knowledge translation: contributions from critical realism and the arts. Implement Sci 2009;4. http://dx.doi.org/10.1186/1748-5908-4-1.
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 2004;82:581-629. http://dx.doi.org/10.1111/j.0887-378X.2004.00325.x.
- Iles V, Sutherland K. Organisational Change: A Review for Health Care Managers, Professionals and Researchers. London: National Co-ordinating Centre for NHS Service Delivery and Organisation; 2001.
- McCormack B, Kitson A, Harvey G, Rycroft-Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of context. J Adv Nurs 2002;38:94-104. http://dx.doi.org/10.1046/j.1365-2648.2002.02150.x.
- McCormack B, McCance T. Person-Centred Nursing: Theory and Practice. Oxford: Wiley-Blackwell; 2010.
- Baker R, Camosso-Stefinovic J, Gillies G, Shaw EJ, Cheater F, Flottorp S, et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev 2015;4. http://dx.doi.org/10.1002/14651858.cd005470.pub3.
- Lewin K. Defining the ‘field at a given time’. Psychol Rev 1943;50. http://dx.doi.org/10.1037/h0062738.
- Straus S, Tetroe J, Graham ID. Knowledge Translation in Health Care: Moving from Evidence to Practice. Wiley-Blackwell and BMJ Books; 2009.
- Van de Ven AH. Engaged Scholarship: A Guide for Organizational and Social Research. Oxford University Press; 2007.
- Rycroft-Malone J, Seers K, Titchen A, Harvey G, Kitson A, McCormack B. What counts as evidence in evidence-based practice?. J Adv Nurs 2004;47. http://dx.doi.org/10.1111/j.1365-2648.2004.03068.x.
- Carpenter J, Dickinson H. Interprofessional Education and Training. Bristol: Policy Press; 2008.
- Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Health Care 2006;15:307-10. http://dx.doi.org/10.1136/qshc.2005.016527.
- Stame N. Theory-based evaluation and types of complexity. Evaluation 2004;10:58-76. http://dx.doi.org/10.1177/1356389004043135.
- Anderson P. Perspective: complexity theory and organization science. Organ Sci 1999;10:216-32. http://dx.doi.org/10.1287/orsc.10.3.216.
- McCormack B TA. Critical creativity: melding, exploding, blending. Educ Action Res 2006;14:239-66. http://dx.doi.org/10.1080/09650790600718118.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist review – a new method of systematic review designed for complex policy interventions. J Health Serv Res Policy 2005;10:21-34. http://dx.doi.org/10.1258/1355819054308530.
- Noelker L, Ejaz F, Menne H, Bagaka J. Factors affecting frontline workers’ satisfaction with supervision. J Aging Health 2009;21:85-101. http://dx.doi.org/10.1177/0898264308328641.
- Parry R, Vass C. Training and assessment of physiotherapy assistants. Physiotherapy 1997;83:33-40. http://dx.doi.org/10.1016/S0031-9406(05)66108-1.
- Ryan T, Nolan M, Enderby P, Reid D. Part of the family: sources of job satisfaction amongst a group of community-based dementia care workers. Health Soc Care Community 2004;12:111-18. http://dx.doi.org/10.1111/j.0966-0410.2004.00471.x.
- Godfrey A. What impact does training have on the care received by older people in residential homes?. Soc Work Educ 2000;19:55-6. http://dx.doi.org/10.1080/026154700114658.
- Sutherland J. The PCSO Review – An Evaluation of the Role, Value and Establishment of Police Community Support Officers ithin Cambridgeshire Constabulary. Cambridgeshire Constabulary; 2014.
- Jolly A, Evans S. Teacher assistants move to the front of the class: job-embedded learning pays off in student achievement. J Staff Develop 2005;26:8-13.
- Groom B. Building relationships for learning: the developing role of the teaching assistant. Support Learn 2006;21:199-203. http://dx.doi.org/10.1111/j.1467-9604.2006.00432.x.
- Collins J, Simco N. Teaching assistants reflect: the way forward?. Reflect Pract 2006;7:197-214.
- Righter B. Training for teaching assistants. Eng Educ 1987;78:135-6.
- Santo Pietro M. Training nursing assistants to communicate effectively with persons with Alzheimer’s Disease: a call for action. Alzheimers Care Q 2002;3:157-64.
Appendix 1 Stakeholder information
Stakeholder categories
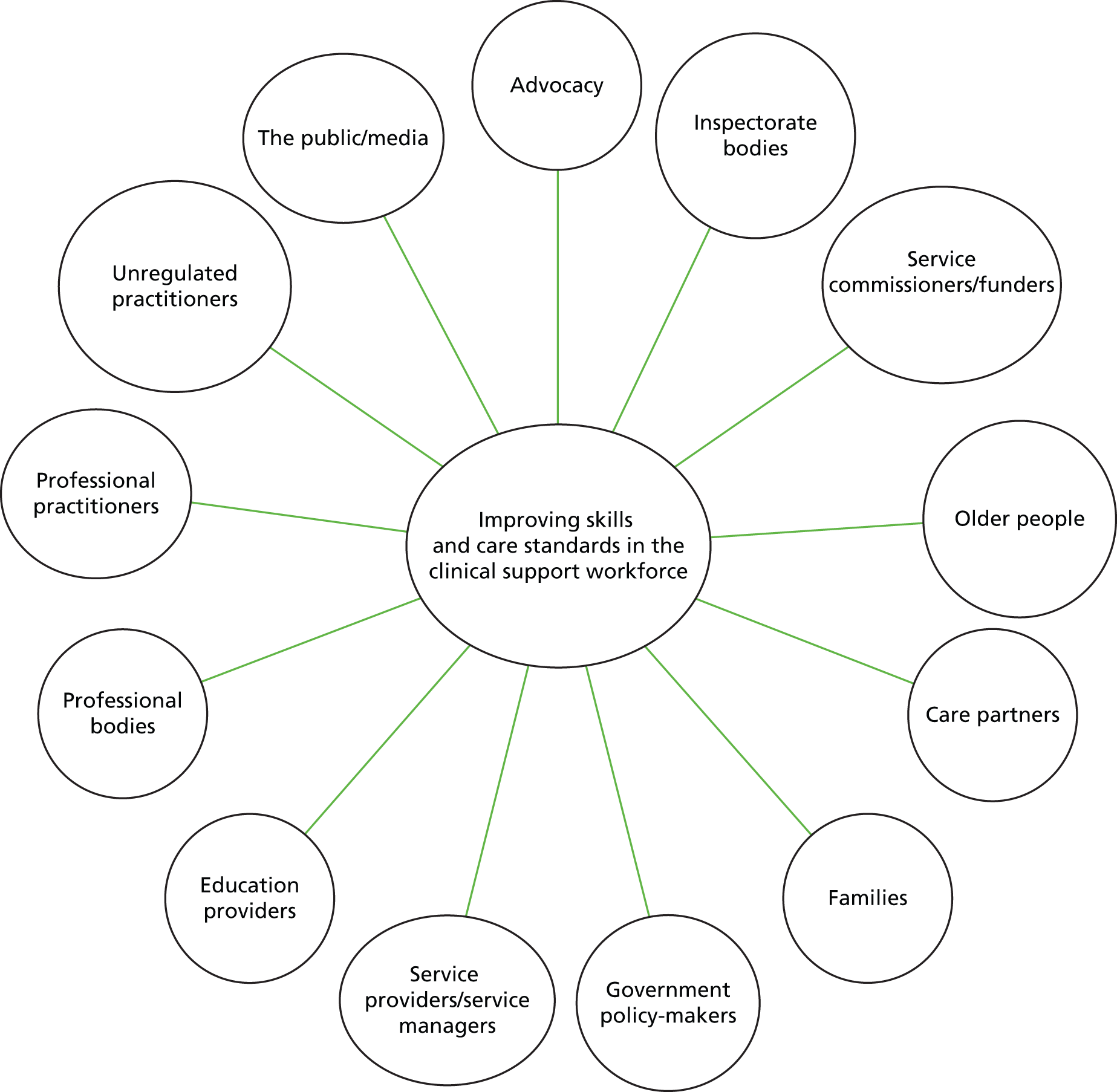
Hypothetical stakeholder matrix (start of project)
| ↑ | High influence | Government/policy-makers The public/media |
Service commissioners/funders | Older people Care partners Families |
| Moderate influence | Education providers | Inspectorate bodies | Professional practitioners Service providers/service managers Advocacy Professional bodies |
|
| Little or no influence | Unregulated practitioners | |||
| Little or no impact | Moderate impact | High impact |
Hypothetical stakeholder matrix (end of project)
| ↑ | High influence | Government/policy-makers The public/media |
Older people Care partners Families Service commissioners/funders Professional bodies |
|
| Moderate influence | Inspectorate bodies Advocacy bodies |
Service providers/service managers Education providers Unregulated practitioners |
||
| Little or no influence | ||||
| Little or no impact | Moderate impact | High impact |
Appendix 2 WeNurses Twitter chat summary, 23 October 2014
The chat host used her personal experiences with a care assistant colleague who had influenced her own practice to kickstart the discussion, which led to many personal recollections among the Twitter audience about their own experiences of working alongside care assistants. Individuals who made lasting impressions were those care assistants who demonstrated qualities such as kindness, humility and respect, promoting compassionate care and commitment. Examples of care assistants showing good organisational skills were shared, and other commendable attributes were considered to be care assistants’ abilities to teach others about essential care, supporting the nursing team in different ways, including increasing registered nurses’ confidence levels. One comment highlighted how care assistants are perceived to have a pivotal role in the patient’s journey, and others see the care assistant as the ‘glue’ for team working and ‘the eyes and ears’ for wards – in this way, the roles are described as ‘good barometers’ for care. Audience members agreed that although care assistants are vital members of the team, they can also be underestimated.
Moving to the questions relating to role development, the Twitter audience had clear views on making training relevant to practice, and one comment suggested that, for care assistants, delivering training should be ‘through their eyes’. The principles of training and development should be the same as for other staff groups, so understanding individual learning styles was considered to be important, so that training can accommodate different needs. The quality of training was discussed, and views on content included teaching listening skills to promote empathy with patients, and delivering training in different ways (e.g. scenario based, project work, short modules, patient stories). The main focus should be on developing relationships. Audience members had experiences of care assistants wanting more training than that offered; however, for others, there was recognition that additional training and development beyond refreshers may not be desired. Sometimes, care assistants may not want additional training, but still want to be respected for doing their job well. Practical teaching and supervision, peer support, supervision and valuing their role as teachers for other (new) care assistants were discussed as important ways to develop individuals.
Career pathways for care assistants was a hot topic, perceived by some as important so that individuals can flourish, promoting their talent and skills, and possibly linked to nursing registration and retention. However, it may not be the approach for all. Whatever the route care assistants choose to take in their career, equal opportunity is important. The importance of celebrating care assistants’ achievements was discussed vigorously, linked to awards and recognition events.
Care assistants should be able to be involved in decision-making, to voice their opinions and influence change and to access leadership training if they wish. In terms of care assistant development, there is a need to recognise the impact of changes and developing skills on efficiency and patient care experiences. Team working to promote quality of care is key.
Appendix 3 Plain English glossary of review terms
Appendix 4 OPSWISE theory-building workshop attendance, 30 January 2014
| Name | Role and organisation |
|---|---|
| Lynne Bedson | Higher education/further education lecturer in health, programme leader of assistant practitioner course, Llandrillo College, Rhos-on-Sea, UK |
| Christopher R Burton | Noreen Edwards Chair of Rehabilitation and Nursing Research, Health Foundation Improvement Science Fellow, Bangor University, Bangor, UK |
| Mandy Hughes | Workforce Modernisation Manager – Skills Development, Betsi Cadwaladr University Health Board, Wrexham, UK |
| Sandra Nutley | Professor of Public Policy and Management, School of Management, University of St Andrews, St Andrews, UK |
| Jo Rycroft-Malone | Professor of Implementation and Health Services Research, Head of School of Healthcare Sciences, Bangor University, Bangor, UK |
| Diane Seddon | Senior research fellow, School of Social Sciences, Bangor University, Bangor, UK |
| Ulla Webber-Jones | Workforce development–training officer (older people’s care), Gwynedd Council, Porthmadog, UK |
| Lowri Welnitschuk | Nursing, Primary, Community and Specialist Medicine group, Betsi Cadwaladr University Health Board, Wrexham, UK |
| Lynne Williams | Lecturer in adult nursing, research fellow, Bangor University, Bangor, UK |
| Roger Williams | PPI member, Community Health Council representative |
| Sion Williams | RCBC Wales Senior Health Career Research Fellow/Senior Lecturer in Nursing, Bangor University, Bangor, UK |
| Gill Windle | Senior research fellow, Dementia Services Development Centre, Bangor University, Bangor, UK |
| Clare Woodcock | Experienced support worker, student nurse, Bangor University, Bangor, UK |
Appendix 5 Longlist of issues in theory areas
-
Workforce development will be most effective when it is aligned with organisational and other career development frameworks, and opportunities and benefits for individuals, teams and organisations may have greater visibility and meaning.
Theory-area questions:
-
What impact does career development have on outcomes for the workforce?
-
How do the ways in which support worker roles and personal development are met through workforce development impact on outcomes?
-
How do organisational and work factors mediate on the outcomes for workforce development, services and older people and their care providers?
-
How do the means in which workforce development interventions are streamlined/connected impact on outcomes for the workforce, service and older people and their care providers?
-
What is the impact of support worker roles being promoted as a positive career option?
-
-
Effective workforce development is designed using flexible, interactive, experiential approaches, and implemented and evaluated in close proximity to the work of the older people’s support workforce and practice. Programmes or interventions that are neither grounded in the reality of daily work completed by the older people’s support workforce, nor delivered within in the workplace, are less likely to be effective.
Theory-area questions:
-
How does the location of workforce development impact on outcomes for the workforce, delivery of services, and older people and their care providers?
-
How does the flexibility in delivery of workforce development interventions/programmes impact on outcomes?
-
How do educational models and styles impact on the outcomes for workforce development?
-
How do the ways in which support workers are involved in setting the workforce development agenda impact on the development of support worker roles?
-
-
Effectiveness can be mediated by the personal characteristics of members of the older people’s support workforce, practice development aspects of human and social geography; characteristics of the organisations in which the support workforce are operating workforce and service policy; and public experiences and expectations.
Theory-area questions:
-
What impact do the people involved in the design and delivery of workforce development have on the outcomes for the workforce, service and older people and their care providers?
-
How does workforce development enhance the public perception of support workers’ roles?
-
How does the role of personal and other characteristics of the workforce influence workforce development outcomes?
-
How do leadership styles impact on the outcomes for workforce development?
-
What is the impact of policy (e.g. health and social care) on the outcomes of workforce development for the workforce, services, older people and their care providers?
-
How do strategies for commissioning, validating, accrediting and quality assurance impact on outcomes for workforce development, services, older people and their care providers?
-
What is the impact of multicultural issues on the outcomes for workforce development in this context?
-
What is the impact of gender issues on the outcomes for workforce development in this context?
-
-
The effectiveness of workforce development interventions and programmes for the support workforce for older people’s services can span outcomes for the workforce, the delivery and quality of services through organisations and for older people and their families/ care providers. Interventions/programmes are most effective when positive impacts from workforce development can be identified in all the above areas. When these impacts do not meet the expectations of older people or health and social care organisations, then positive, individual changes from workforce development programmes/interventions might be evident and/or achieved, but not sustained.
Theory-area questions:
-
How do workforce development interventions balance core and specific skills for the support workforce for older people’s services?
-
How do programmes instil and encourage confidence in the support workforce to contribute to quality improvement?
-
How do workforce development interventions for support staff develop the concept of relationships in older people’s services?
-
How do workforce development interventions impact on outcomes for the workforce (i.e. motivation, job satisfaction, self-esteem and confidence)?
-
How does workforce development meet the current and expected knowledge, skills and attitudes required of the support workforce?
-
Appendix 6 Search terms
-
Aide.
-
Allied health assistant.
-
Assistant.
-
Assistant care worker.
-
Assistant care workforce.
-
Assistant nurse.
-
Assistant practitioner.
-
Care assistant.
-
Care attendant.
-
Care practitioner.
-
Care provider.
-
Care worker.
-
Carer.
-
Clinical support worker.
-
Community health worker.
-
Community nursing assistant.
-
Community rehabilitation team therapist.
-
Community support worker.
-
Direct care worker.
-
Generic worker.
-
Health advisor.
-
Health aide.
-
Health care aide.
-
Health care assistant.
-
Health care support worker.
-
Health care worker.
-
Health trainer.
-
Health worker.
-
Healthcare aide.
-
Healthcare assistant (HCA).
-
Healthcare support staff.
-
Healthcare Support Worker (HCSW).
-
Healthcare worker.
-
Helper.
-
Home care support worker.
-
Hybrid worker.
-
In-home aide.
-
Intermediate Care.
-
Medical assistant.
-
Mentor.
-
Multidisciplinary healthcare support worker.
-
Nurse aide.
-
Nursing Assistant.
-
Nursing support worker.
-
Officer.
-
Outreach worker.
-
Paraprofessional.
-
Peer support.
-
Peer worker.
-
Personal assistant.
-
Personal care aide.
-
Personal care assistant.
-
Personal support worker.
-
Physical therapy assistant.
-
Physiotherapy assistant.
-
Rehabilitation assistant.
-
Rehabilitation assistant.
-
Rehabilitation support worker.
-
Rehabilitation worker.
-
Support Staff.
-
Support worker.
-
Support workforce.
-
Technician.
-
Therapy aide.
-
Therapy assistant.
-
Therapy support worker.
-
Unlicensed worker.
-
Unregulated worker.
Appendix 7 Example search strategy
MEDLINE 1946: current via EBSCOhost
Date range searched: 1 January 1986 to 11 May 2014.
Date of search: 11 May 2014.
Search strategy
S1 TI (advisor* or aide* or assistant* or attendant* or carer* or helper* or mentor* or officer* or paraprofessional* or “peer support*” or practitioner* or staff or technician* or trainer* or worker* or workforce or “care provider”)
S2 TI (“older person” or “older people” or “older adult*” or elder* or “nursing home*” or “residential home*” or “senior citizen*” or gerontology or geriatric* or “aged people” or “aged person*” or aging or senior* or “old person” or “old people” or “old age” or pensioner* or later-life or “later life” or “third age” or retiree* or “long term care” or dementia or stroke)
S3 (MH “Aged+”) OR (MH “Aged, 80 and over”) OR (MH “Health Services for the Aged”)
S4 S2 or S3
S5 S1 AND S4
S6 TI or AB(“accelerated development program*” or “nursing assistant champion*” or “staff support” or accountabilit* or ambassador* or appraisal* or apprenticeship* or barrier* or “behaviour change*” or “behavior change*” or boundar* or “care ambassador scheme*” or career or certification or “change in practice*” or “clinical education program*” or communication or coaching or credit* or “decision support” or delegation or develop* or education or e-learning or “emotional support” or “expectation* of staff” or framework* or governance or incentive* or induction* or information or “job specification*” or knowledge or leadership or learning or “learning technolog*” or network* or nurse-led or “organi?ational change*” or “organi?ational context*” or “organi?ational culture*” or “organi?ational improvement*” or “organi?ational value*” or “orientation program*” or “performance management” or “person centred” or “person centered” or planning or polic* or practice* or “practice change*” or “practice centred approach*” or “professional development” or “protected time” or qualification* or registration or regulation* or relationship* or responsibilit* or reward* or role* or service or simulation or skill* or “staff development” or storytelling or strateg* or supervision or team* or training or well-being or wellbeing or “well being” or “workforce development”)
S7 (MH “Communication+”) or (MH “Delegation, Professional”) or (MH “Clinical Governance”) or (MH “Access to Information+”) or (MH “Knowledge”) or (MH “Leadership”) or (MH “Organizational Objectives”) or (MH “Organizational Innovation”) or (MH “Organizational Culture”) or (MH “Policy Making+”) or (MH “Peer Review+”) or (MH “Professional-Patient Relations+”) or (MH “Interprofessional Relations+”) or (MH “Personnel Management+”) or (MH “Patient Care Team+”) or (MH “Credentialing+”) or (MH “Professional Role+”) or (MH “Clinical Competence”) or (MH “Staff Development”)
S8 S6 or S7
S9 S5 and S8
S10 restricted 1986-to date
Appendix 8 ‘Relevant and good enough’ flow chart
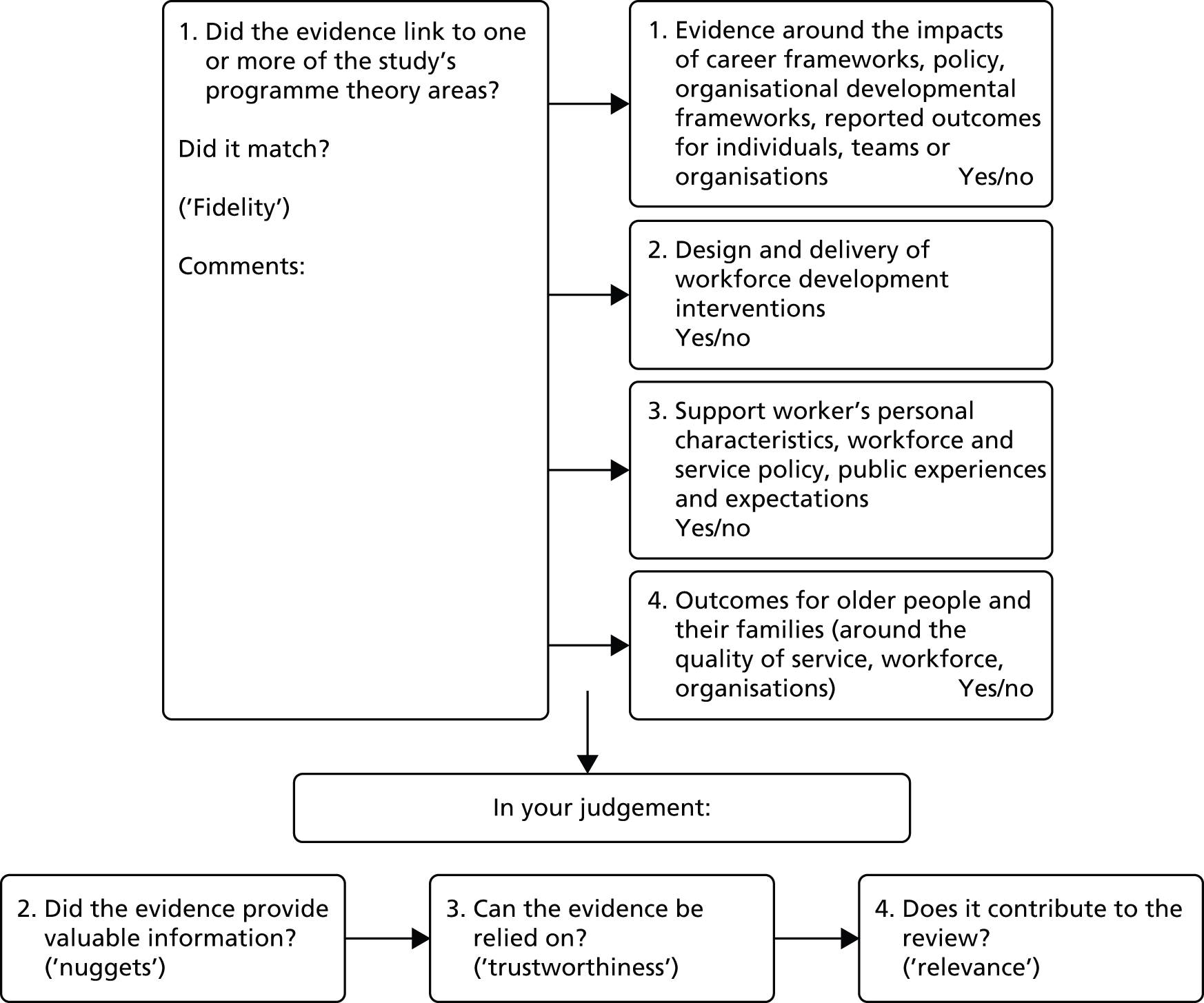
Appendix 9 Data extraction form final
| Q1 Document ID/title | |
| Q2 Authors/year published | |
| Q3 Document type (e.g. research study/policy/local evidence/opinion?) | |
| Q4 What is the study’s aim/purpose? | |
| Q5 What is the intervention (if applicable)? | |
| Q6 What information is there about the design/method used and was it appropriate for the aims/purpose of the study? | |
| Q7 Sample – type/size? What information is there about population and setting? |
|
| Q8 What data collection method was used? | Questionnaires and interviews |
| Q9 Theory areas | Is there evidence about |
| Theory area 1: fit with career development, policy and strategy | Career development Personal development Organisation and work factors Role promotion |
| Theory area 2: design, delivery and evaluation | Approaches to workforce development interventions Location Flexibility Educational models/styles Core/specific skills Support workers’ level of involvement in workforce development planning |
| Theory area 3: mediating factors regarding effectiveness | Personal characteristics of support workers Public perception Leadership Policy Commissioning, validating, accrediting, quality assurance Multiculturalism Gender |
| Theory area 4: impacts – what, for whom, how and where? | Older people and their families/carers Support workforce Delivery and quality of services Organisations |
Appendix 10 Evidence table example
| Evidence source | Theory area 1: Fit with career, development, policy, strategy and structures |
|---|---|
| 1. Arblaster et al. (2004)151 | Suggestion that career development for HCAs is best promoted through using a phased approach to CPD and progression, and linking national strategy to frame design (Essence of Care, in this case):the training and development pathway incorporates three phases of continuing professional development: the Essence of Care programme, and NVQ Care levels 2 and 3. These enable HCSWs to develop skills and achieve recognition of these skills, with the opportunity to progress to nurse trainingp. 34Suggestion that the academic gap is addressed through linking with a study skills module as integral part of developmental pathway for HCAs, based on collaboration with HEIs, and discussions with student nurses who had completed the NVQ route. The benefits of a structured approach to progression in an NHS Trust (UK context) discussed, and use of manager nomination model for progression to the next level:. . . implementing a structured approach to the training and development of HCSWs ensures gradual development in both theory and practice. It also enables HCSWs to plan their professional development and identify a career pathwayp. 37Owing to the organisation’s policy of employing large numbers of HCAs, consistency issues (NVQ vs. ‘on the job’). Emphasis made on linking with partners to deliver training programmes (using practice facilitators, specialist nurses, external agencies) and highlighting the importance of organisational commitment to develop competency for health-care support workers Support for HCAs is often reliant on the support they receive from their peers in practice. Few qualified nurses in place as assessors because of work demands led to health-care support workers becoming the assessors:It was apparent from discussion with HCSWs that much of their support in practice came from successful NVQ Care candidates who had experienced the process first hand. This suggested that there was the potential for HCSWs to train as NVQ Care assessorsp. 35Managerial support important to reduce ‘the potential risks associated with devolving responsibility for assessment of competency in the skills required to deliver fundamental care from registered nurses to unqualified staff’ (p. 35) |
| 2. Aubry et al. (2012)164 | There were challenges for developing support workers entering long-term care services, where a focus on innovation is driven by policy and academia. So, a mismatch between training and reality was found:It’s impossible; trainers don’t see the reality of things in long term care facilities . . . We were told that we had 45 minutes per resident but we actually have no more than 15 minutesp. 6A gap was noted between valuing care, which takes time, and the value of work efficiencyEarly stages of the recruits’ integration into the ward behaviors were spent on the orientation or training phase. This was a short period of time (two to five days) during which the new recruit worked under the watchful eye of the referent, experienced nursing assistantp. 7This quote shared by staff member in charge of new recruit activity:We look at recruits working; we see how they are when they start; we see what happens. It takes a certain pace, it’s Go! A toileting, go! Another . . . And we help them to keep the pace because they don’t learn that during their trainingp. 7The link between systemic change management and multidisciplinary approaches was considered essential to drive innovation in long-term care settings:implementing change in LTCOs remains a complex task that is often based on intuition and anecdotes and characterized by very uncertain outcomesp. 2A strategic analysis approach was employed to understand the relationship between the development of nursing assistants in long-term care services and the organisational context, and how this relationship impacted on developing change management strategies:Crozier’s framework makes it possible to define the means of understanding the collective structure of the nursing assistants’ work during the many change endeavors facing LTCOs, as described below in the study findingsp. 3Challenges and constraints can lead to homogeneity among nursing assistants, that they develop (informal) strategies, and discussed how these are shared with new staff. The paper’s findings suggest that using informal practices and team working can facilitate change:overlooking the potential input of nursing assistants in the development of an innovative care program or else soliciting the input of an individual nursing assistant, rather than that of the ‘team,’ can foster resistance to changep. 9 |
| 3. Braun et al. (2005)105 | Based around home/community health-care/direct-care workers with older people in the USA in non-Medicare ageing network. Suggested identified gap in non-clinical training/education:our goals were to provide a foundation for nonclinical direct care workers by imparting a basic knowledge of aging, improving assessment and reporting skills, increasing empathy for older adults, teaching strategies to manage stress, and validating the importance of direct care workersp. 119Disjointed approaches can lead to lack of meaning for direct-care workers:direct care workers in this study had relatively few years of education and little knowledge of basic aging processes, differential effects of aging and disease, and good self-care principles. Many conceptualized their jobs as custodial, rather than therapeutic, and did not see the value of their workp. 122Caring for themselves can impact on the care that direct-care workers provide for older people (p. 119) The degree of control direct-care workers had on their development and practice influenced the success of the intervention:another probable reason for success is that we focused on improving basic knowledge and attitudes that were under the control of the direct care worker, rather than on teaching clinical behaviours that may require concurrent organisational or systems changep. 123 |
| 7. Coogle et al. (2007)132 | Significant linkage through multiagency collaboration to the development of the curriculum for care staff:This initial collaboration of pertinent stakeholders was crucial to the development of the training program . . . Bringing together the strengths and interests of multiple parties in academia, provider agencies, and professional associations garnered statewide support for the effort and ensured that concerns were addressedp. 112Likely that the application of training content resulted in a deepened commitment to care work as well which was ‘grounded in an intention to encourage a more career-focused orientation’ And:enhance professionalism by enabling support workers to better handle challenging situations, aggressive behaviour, and work-related stresspp. 115–16 |
| 8. Cowan et al. (2004)150 | Linked the development of effective learning strategies with nurse registration, practice and post-registration continuing education, to facilitate access to lifelong learning for support workers employed in care homes for older people in the UK (linked to European Commission directive on lifelong learning) |
| 12. Hegeman (2003)133 | Reported how a not-for-profit organization was supportive of the project in one long-term care setting in the USA. The author linked peer-mentoring programme to improving culture change, as it had the potential to improve the retention of staff when turnover staff was high, which also ultimately reduced costs for the organisation:peer mentoring is also-in itself-a way to create a culture of caring among aides within a long-term care facility. When carefully-selected, experienced CNAs who embody the caring values of their facility become successful peer mentors, there are clear potential organisational changesp. 186CNAs who demonstrated a culture of caring were recognized for this, thereby increasing their own satisfaction (and this supported retention):the behaviours and attitudes the new CNA is exposed to, making it more likely they will be the traits which are learned and emulatedp. 187 |
| 29. Hockley (2014)115 | Report of action research about how to develop strategies to develop quality care in nursing homes. Time constraints, low morale and need to develop a culture of learning were identified as work factors Experience-based learning was considered to be a way to draw out the ways in which people learn – didactic, experiential, critical thinking (p. 125) Highlighted the importance of the provision of support and learning for care assistants:Care assistants play an important part in end of life care because they have often cared for the resident(s) for many months, even years. They can feel excluded when nurses “take over the care” when a resident is dying . . .p. 126 |
| 14. Morgan and Konrad (2008)141 | The ratings of perceived career rewards improved for participants who completed a specific programme in North Carolina nursing homes Programme strengthened view of care work as career opportunity, not ‘just a job’ |
| 15. Nelson et al. (2009)149 | Union membership and conditions of employment were perceived as being important by care staff participants (in this UK-based paper). Participants identified with a lack of status, regulation and accountability:Should be able to be part of RCN (Royal College of Nursing)—we are a missed and forgotten groupFeels like a back door profession—that anyone can enter. Should be regulated like nurses and be able to be struck offp. 202Issues around care staff development, accountability and scope of practice:Some new role care staff showed awareness of the links between responsibility, accountability and liability, e.g. ‘More questioning now, more assertive and aware, more realisation that it is our head that rolls’, but this was not universal: ‘Don’t think people realise the responsibility.’; ‘Think improvements should be made re insurancep. 202Issues were identified in the paper around relationships and ways of working and implication was made that care assistant development roles require time ‘to establish the carers’ new roles but also for the in-reach team to overcome various issues with community nurses, including ways of working to avoid duplication of activities’ |
| 30. Nilsson et al. (2014)116 | E-assessment of prior learning, a pilot study of interactive assessment of staff with no formal education who are working in older people’s care. One-third of all staff working in Swedish older people’s care lacked formal competence for their jobs (p. 2). Staff were often considered to be working temporarily, suggesting that this was putting extra demands on organisations. All staff working in older people’s care have to show basic professional skills for the tasks involved (p. 2) Upper secondary school care programme curriculum was seen as benchmark for national standards. Assessing informal/non-formal learning was seen as way of improving lifelong learning (p. 2) |
| 16. Noelker et al. (2006)172 | In a study of nursing assistants in care settings in Ohio, USA, a link was made between supervision and turnover, with reference to previous authors:associated high turnover with poor supervision by licensed nurses who typically receive little or no training in management skills such as leadership, motivation, and team building . . .p. 308Significance of respect being shown by managers towards care assistants Information was provided to suggest the influence of the characteristics of the workplace:it is expected that personal and job-related stressors will be more widely reported by NAs working in for-profit facilities compared to nonprofit facilities based on research indicating that staffing practices and working conditions in for-profit facilities place greater demands on nursing staff . . .p. 309There was reference to the general lack of training that was available for nursing assistants:the required minimum 75 hours of entry-level training is widely regarded as inadequate to train workers properly . . .p. 310 |
| 17. Noelker et al. (2009)196 | Lack of training for supervisors in care settings, in Ohio, USA, and also continuing education:More than half the supervisors said their continuing education either did not cover or was not helpful in improving their abilities to do the following: demonstrate good leadership, handle racial issues in the workplace, motivate staff, manage insubordination, and deal with difficult workersp. 94Other factors were considered to be important for targeting to improve workplace support:the positive effects of peer mentoring at hire and having job orientation and continuing education programs that workers view as adequate for their needs suggest these programs should be given more careful attention in efforts to improve satisfaction with supervisionp. 98 |
| 20. Petterson et al. (2006)144 | Study set in nursing homes in Sweden and the report referred to the use of stress theory to plan interventions in order to support:strengthening staff resources of job control, work support, and learning . . ., as well as attaining new coping skills, is health promotingp. 354The intervention was introduced as an empowerment project for care assistants:Job control is defined as learning authority (access to competence and new learning) and authority over decisions (work influence and participation). By increased job control and support, the self-confidence of employees is enhanced, stimulating their engagement and activityp. 356The project has inspired new efforts on professional authority and career development for auxiliary and assistant nurse. Advancement opportunities have been created for these nurses by a recently permanent stepwise career ladder, which serves as a model for (older)care organizations in other municipalities in Sweden and has attained international attentionp. 367 |
| 23. Stevens et al. (2006)112 | Context of care homes in the USA. Suggested that staff development programmes should:recognize the complex interplay between the personal competencies of residents and staff and their environmentsp. 249Staff training programmes that can change: ‘residents’ environments to better match residents’ competencies’ (p. 249) The Informed Teams model was introduced and suggestion made that ‘active organisational support is a prerequisite’ (p. 253) |
| 24. Stevens-Roseman and Leung (2004)142 | Paraprofessional training for staff working with older people in the US context. The paper includes reference to the significance of the organisational/manager role of reinforcement:By reinforcing paraprofessionals’ strengths and worth, trainers convey the impact and the process of building on strengths. This skill can then be applied by trainees in recognizing the worth of (older people) during the course of their workp. 86 |
| 26. Tisher et al. (2009)113 | Based in an older people’s care setting in Australia, showed evidence to suggest that organisations need to support training with shift in culture, supporting staff to manage workloads, emotional burden, and allowing time for staff to share experiences. In particular, organisational role to support staff to develop more co-operative relationships with families |
| 28. White and Cadiz (2013)135 | Direct care workers in assisted living in Oregon found that a focus on the environment is significant to success – e.g. investment in supervisors, organisational policy changes made to support trainees (e.g. tuition advancement)In addition to the content targeting AL workers, the results of this study offer additional support for a work-based learning design for frontline workers. The emphasis on one-on-one and small group learning provides a structure for engaging and supporting all levels of staff, both as trainers and learnersp. 296 |
| 42. Clarke et al. (2003)118 | Describes the findings of a developmental study undertaken over a 6-month period to investigate the introduction of a biographical approach to care on a unit in one NHS hospital in the UK:the focus of the study was on the experiences and views of older people (and, wherever possible, their families) and practitioners working in the field. Practitioners were central to the research process and were involved throughout the planning, delivery and dissemination of the studyp. 700 |
| 45. McLellan et al. (2005)145 | Describes how a new interprofessional primary care practice team was defined and how it implemented a new appraisal system drawing on the principles of 360-degree appraisal, in order to:support and reinforce positive and responsible inter-professional team workingtake into account the concerns and requirements of both the team members and the service organizationembrace the appraisal requirements of different professional groups and partner organizationsp. 140It was suggested that the appraisal system could complement existing organisational systems:These included short monthly one-to-one meetings between the service development manager and each team member to discuss workload, performance and development, and also team discussions about roles, responsibilities, values, team policies and service developmentsp. 140 |
| 46. Parry and Vass (1997)197 | Discussion about some of the issues relevant to the role and training of physiotherapy assistants. Process of role definition, assessment and training of an individual, developed in the context of a larger research study. Points about assuming capabilities, and importance of supervision, are reflected in interviews with physiotherapists. Expectations and knowing staff were mentioned as important by several participants, as was the need to give assistants responsibility and a role within the teamLevel of supervision depends on competence and experience . . . It’s a professional judgement (that’s true of supervising juniors too!)They need to have a feeling of positive contribution – involvement in decision makingp. 36 |
| 48. Vail et al. (2011)147 | HCA role in general practice. Progression, acknowledgement of the role, and how personal characteristics sometimes influence development. The report emphasised the importance of recognition and the environment for role development, and showed some negative attitudes about the role:Although the three youngest HCAs were positive about their role and claimed to enjoy it, they spoke more often about negative aspects of the job, such as low pay and the lack of opportunities to progressp. 34These quotes below indicate negative attitude towards pay and progression:I think we should be on more money we’re at risk from needle stick injuries and infections and all the rest of it. And we’re on fourteen and a half thousand [pounds]. I don’t understand how they got to that figure. I think we’re undervalued for the skills that we’ve gotp. 34I do get frustrated because there’s only a certain amount I can do without my general nursing qualification. I’m actually hoping to go to University. I’d like to learn more and do more (HCA14)p. 34Concerns were expressed by some participants about the limitations of the HCA role:[I]t’s being not able to go further and get that extra knowledge that you want, you know, when you get so far and you’re just … you’re hungry for it and you can’t get it (HCA3)p. 35There was reference to lack of awareness and understanding within the GP team about the HCA roleHere was a little bit frustrating for me when I first started because they were … they were unaware of what I was and what I could do . . . because they’d never had a Health care assistant before (HCA11)p. 35Shed some light on the perceived status of HCA role as illustrated by these quotes:Over half of the HCAs commented on their role being of minor importance within the GP team. The interviewees often referred to their tasks as ‘menial’, ‘silly’, and ‘mundane’, and implicitly or explicitly compared them to the ‘more important’ responsibilities of the nursesp. 35I think I take the pressure off the nurses because I can do little jobs for them, which means that they can move on and do other things that are more important (HCA2)p. 36Obviously, I’m not allowed to give injections and do smears and that, but just silly little things like doing a leg dressing or stitch removal (HCA1)p. 36Practices, therefore, need to ensure that their wider workforce is fully prepared when taking on an HCA for the first time. HCAs in this study appreciated their colleagues’ support and encouragement on both a day-to-day basis and also in relation to role developmentp. 39 |
| 52. Ryan et al. (2004)198 | Interview data gathered from a group of community-based dementia care workers, and the aim of the study was to identify the sources of job satisfaction and reward. Ideas around the organisation which were considered to promote job satisfaction for support workers. These ideas could be considered as important for individual and team development. Factors which supported support workers through promoting job satisfaction were illustrated in the following quotes:open channels of communication between the support workers and more senior colleagues, which facilitated exchange of information, advice and ideas. Support workers particularly valued opportunities to explore ‘difficult’ situations with other team membersp. 113weekly team meetings were seen as essential in helping to engender cohesion and provided the forum for much of the above discussion. However, one support worker noted that things could be improved if attendance at team meetings was made mandatoryp. 114support workers stressed that the ready availability of more senior colleagues was pivotal to them feeling well supported, especially at difficult times. This fostered a feeling of security amongst the staff team as well as contributing to a thorough assessment of risk (for both staff and users of the service)p. 114It was not just immediate managers who valued the contribution of the support workers since senior personnel within the National Health Service trust were also perceived to value the service and support the workers’ contribution to itp. 114These data exemplify the significance of being valued by fellow colleagues and senior managers, of feeling protected from potential overwork and emotional harm. This was essential because the support workers were relatively autonomous in their day-to-day work, which was another major factor contributing to their feelings of job satisfactionp. 114 |
| 49. Bailey et al. (2015)173 | Insight into the emotional labour of the HCA role, with the concept of detachment being viewed as positive for engagement as opposed to being perceived negatively. Ideas for teaching/supervision. The concept of detachment is perceived in a positive light, offering case studies to illustrate points:This presents detachment as an active emotional choice; a putting aside of certain feelings in the interests of completing one’s job, as we also observed. This does not mean that detachment may not, in some cases, indicate a disinterested or uncaring attitude on the part of HCAsp. 18Insight into organisational responsibility for the development of support workers:To negotiate the complexities of their patients’ needs, dispositions and communication abilities, while also delivering the practical aspects of good care, demands a high level of emotional output and superior skills in self-regulation, which are little-recognised characteristics of the role of HCAsp. 20Ideas about training and supervision:. . . HCAs must be given the space to reflect on the relationship between thought and action in their everyday encounters with patients. Therefore, we suggest that developing a model of supervision along the lines of qualified nurses’ clinical supervision, which is delivered by someone outside the ward, could greatly benefit HCAsp. 21 |
| 50. Noelker and Ejaz (2005)162 | Challenges faced by support workers working in long-term care. Calls are made for ensuring a person-centred care approach to improve conditions and quality of care. Training and education support workers wish to have, and how can they best be supported to advance and be empowered. It is suggested that retention of support workers can be improved by career-advancing ladders and tuition reimbursement, as well as provision of education in collaboration with nursing courses. It is suggested that, where workplaces demonstrate worker empowerment and person-centred care, retention and quality of care may be improved |
Appendix 11 Focused data extraction form
Appendix 12 Tracking final context–mechanism–outcomes
The final CMOs are as follows:
-
making it real to the work of the support worker
-
paying attention to the individual support worker
-
tapping into support workers’ motivations
-
joining things up around workforce development
-
getting the right people round the table in designing workforce development
-
‘journeying together’
-
taking a planned approach to workforce development design, delivery and evaluation
-
spreading impact.
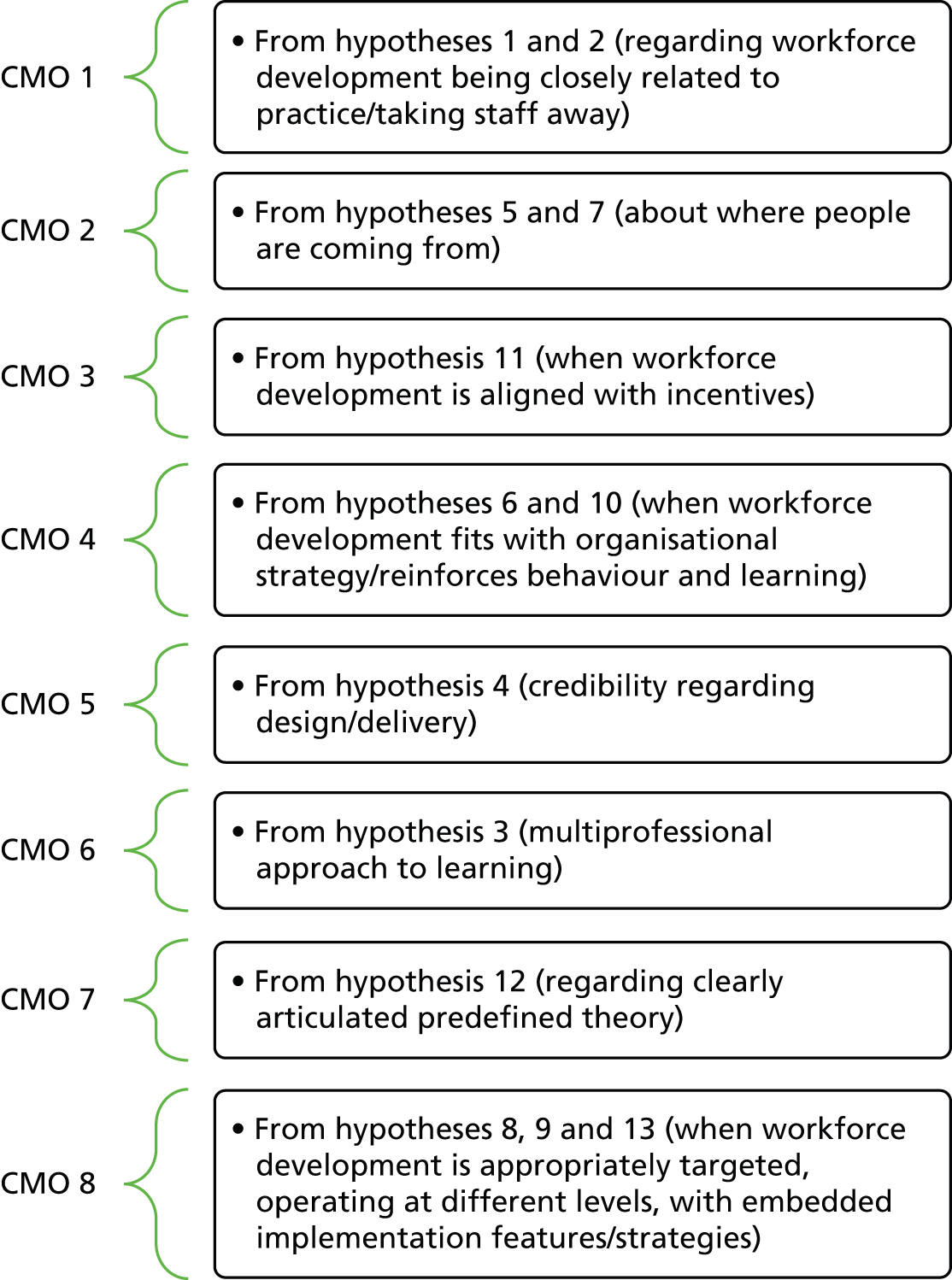
Appendix 13 Interview spine
In preamble to set the scene: as managers/trainers, what do you want to see for the support workforce? What are your current programmes?
-
We are interested in why some workforce development programmes resonate more with [SUPPORT WORKERS] than others. From your experience, what are the workforce development programmes that best reflect the reality of the daily work that [SUPPORT WORKERS] engage in? What is it that makes them ‘real’ for participants? Work-based?
Prompt around characteristics: work-related; in the workplace; theory-skill mix; complex versus simple developments; short-term versus programme – seeking examples.
-
If you wanted to design a workforce development programme that really resonated with [SUPPORT WORKERS], how should this be done? Who should be involved in their design?
Prompt around people and design processes – seeking examples.
-
What teaching and learning strategies (too professional) are most helpful in making workforce development ‘real’ for participants? What effective strategies have you come across? What else needs to be done?
Prompt around strategies and techniques (including patient stories, reflection, etc., ask for examples from own experiences) – seeking examples.
-
Are there situations where the delivery of workforce development for [SUPPORT WORKERS] should include other members of the older persons’ services in health and social care?
Prompt around the relevant issues (e.g. simple vs. complex workforce development) and impact (e.g. role appreciation and team-building) – seeking examples.
-
Are there good examples of where older people themselves (or carers/families/support workers) have been involved in the design and/or delivery of workforce development? Did it work? Why did this work?
-
What are the benefits and disadvantages of delivering workforce development for [SUPPORT WORKERS] in the workplace?
Prompt around benefits (e.g. real/getting experts in/translates into practice – who delivers) how this is facilitated/and disadvantages (e.g. noise and space/difficult for time out).
-
How can we effectively build on the values and experiences (caution: may not always be positive) that [SUPPORT WORKERS] bring to their work and role?
Prompt around previous life and work experiences; recruitment issues, e.g. values; revisiting and challenging existing ways of working for those longer in the role – seeking examples.
-
What are the best ways of incentivizing [SUPPORT WORKERS] to engage in workforce development programmes? What’s the tipping point? Managers’ incentivisation?
Prompts around certification, accreditation, fit with career development frameworks; and financial incentives from and to the [SUPPORT WORKER] – seek examples and explanations of why incentives worked for different groups/types of [SUPPORT WORKERS].
-
What is needed at organisational level to make workforce development successful?
Prompts around organisational strategy; culture/leadership/senior buy-in; clarity and consistency of expectations across the organisation; programmatic approaches versus one-off programmes – seeking examples of good organisational practice.
-
What would be the most important changes to make to workforce development programmes (yours/and in general) that would increase their impact for [SUPPORT WORKERS]? What about for health and social care organisations?
Appendix 14 Ethics approval
Appendix 15 Table of included papers
| Reference number | Authors and date | Title | Source |
|---|---|---|---|
| 151 | Arblaster G, Streather C, Hugill L, McKenzie M, Missenden J (2004) | A training programme for healthcare support workers | Nursing Standard |
| 164 | Aubry F, Etheridge F, Couturier Y (2012) | Facilitating change among nursing assistants in long term care | Online Journal of Issues in Nursing |
| 105 | Braun KL, Cheang M, Shigeta D (2005) | Increasing knowledge, skills, and empathy among direct care workers in elder care: a preliminary study of an active-learning model | The Gerontologist |
| 106 | Cherry B, Marshall-Gray P, Laurence A, Green A, Valadez A, Scott-Tilley D, Merritt P (2007) | The geriatric training academy: innovative education for certified nurse aides and charge nurses | Journal of Gerontological Nursing |
| 107 | Clare L, Whitaker R, Woods RT, Quinn C, Jelley H, Hoare Z, et al. (2013) | AwareCare: a pilot randomized controlled trial of an awareness-based staff training intervention to improve quality of life for residents with severe dementia in long-term care settings | International Psychogeriatrics |
| 108 | Coleman C, Medvene L (2013) | A person-centered care intervention for geriatric certified nursing assistants | The Gerontologist |
| 132 | Coogle C, Parham I, Jablonski R, Rachel J (2007) | The value of geriatric care enhancement training for direct service workers | Gerontology and Geriatrics Education |
| 150 | Cowan D, Roberts J, Fitzpatrick J, While A, Baldwin J (2004) | The approaches to learning of support workers employed in the care home sector: an evaluation study | Nurse Education Today |
| 134 | Ersek M, Wood B (2008) | Development and evaluation of a nursing assistant computerised education programme | International Journal of Palliative Nursing |
| 166 | Goodridge D, Johnston P, Thomson M (1997) | Impact of a nursing training program on job performance, attitudes, and relationships with residents | Educational Gerontology |
| 109 | Grosch K, Medvene L, Wolcott H (2008) | Person-centred care-giving instruction for geriatric nursing assistant students: development and evaluation | Journal of Gerontological Nursing |
| 133 | Hegeman C (2003) | Peer mentoring of nursing home CNAs: a way to create a culture of caring | Journal of Social Work in Long-Term Care |
| 110 | Lerner N, Resnick B, Galik E, Gunther Russ K (2010) | Advanced nursing assistant education program | The Journal of Continuing Education in Nursing |
| 141 | Morgan J, Konrad T (2008) | A mixed-method evaluation of a workforce development intervention for nursing assistants in nursing homes: the case of WIN A STEP UP | The Gerontologist |
| 149 | Nelson S, Wild D, Szczepura (2009) | The forgotten sector: workforce development in residential care for older people | Nursing and Residential Care |
| 172 | Noelker L, Ejaz F, Menne H, Jones J (2006) | The Impact of Stress and Support on Nursing Assistant Satisfaction With Supervision | Journal of Applied Gerontology |
| 196 | Noelker L, Ejaz F, Menne H, Bagaka J (2009) | Factors affecting frontline workers’ satisfaction with supervision | Journal of Aging and Health |
| 152 | Parks SM, Haines C, Foreman D, McKinstry E, Maxwell TL (2005) | Evaluation of an educational program for long-term care nursing assistants | Journal of the American Medical Directors Association |
| 128 | Passalacqua S, Harwood J (2012) | VIPS communication skills training for paraprofessional dementia caregivers: an intervention to increase person-centered dementia care | Clinical Gerontologist |
| 144 | Petterson IL, Donnersvard HA, Lagerstrom M, Toomingas A (2006) | Evaluation of an intervention programme based on empowerment for eldercare nursing staff | Work and Stress |
| 111 | Ron P, Lowenstein A (2002) | In-service training of professional and para-professional staff in institutions for the aged | Educational Gerontology |
| 167 | Ruckdeschel K, Van Haitsma K (2004) | A workshop for nursing home staff: recognizing and responding to their own and residents’ emotions | Gerontology and Geriatrics Education |
| 112 | Stevens AB, Hochhalter AK, Hyer L, Intieri RC (2006) | Meeting the needs of nursing home residents and staff | Geropsychological Interventions in Long Term Care |
| 142 | Stevens-Roseman ES, Leung P (2004) | Enhancing attitudes, knowledge, and skills of paraprofessional service providers in elder care settings | Gerontology and Geriatrics Education |
| 129 | Thomson M, Burke K (1998) | A nursing assistant training program in a long term care setting | Gerontology and Geriatrics Education |
| 113 | Tisher T, Dean S, Tisher M (2009) | Aged care residential facility and family interface: a training program for staff | Clinical Gerontologist |
| 114 | Wadensten B, Engström M, Häggström E (2009) | Public nursing home staffs experience of participating in an intervention aimed at enhancing their self-esteem | Journal of Nursing Management |
| 135 | White DL, Cadiz DM (2013) | Efficacy of work-based training for direct care workers in assisted living | Journal of Aging and Social Policy |
| 115 | Hockley J (2014) | Learning, support and communication for staff in care homes: outcomes of reflective debriefing groups in two care homes to enhance end-of-life care | International Journal of Older People’s Nursing |
| 116 | Nilsson A, Andrén M, Engström M (2014) | E-assessment of prior learning: a pilot study of interactive assessment of staff with no formal education who are working in Swedish elderly care | BMC Geriatrics |
| 124 | Anderson RA, Ammarell N, Bailey D Jr, Colón-Emeric C, Corazzini KN, Lillie M, et al. (2005) | Nurse assistant mental models, sensemaking, care actions, and consequences for nursing home residents | Qualitative Health Research |
| 117 | Boettcher IF, Kemeny B, DeShon R, Stevens AB (2004) | A system to develop staff behaviours for person-centered care | Alzheimer’s Care Quarterly |
| 136 | McGilton K, O’Brien-Pallas L, Darlington G, Evans M, Wynn F, Pringle DM (2003) | Effects of a relationship-enhancing program of care on outcomes | Journal of Nursing Scholarship |
| 130 | McCormack B, Dewing, L, Breslin L, Coyne-Nevin, Kennedy K, Manning M, et al. (2010) | Developing person-centred practice: nursing outcomes arising from changes to the care environment in residential settings for older people | International Journal of Older People’s Nursing |
| 163 | McCormack B, Wright J (1999) | Achieving dignified care for older people through practice development: a systematic approach | Nursing Times Research |
| 156 | Yalden J, McCormack B, O’Connor M, Hardy S (2013) | Transforming end of life care using practice development: an arts-informed approach in residential aged care | International Practice Development Journal |
| 161 | Webster J, Coats, E, Noble G (2009) | Enabling dignity in care through practice development with older people | Practice Development in Health Care |
| 168 | Howatson-Jones L, Thurgate C, Graber M, Harnett C, Thompson JS, Jordan DA (2013) | Biographical learning: a process for promoting person-centredness in nursing | International Practice Development Journal |
| 171 | Manley K, Sanders K, Cardiff S, Webster J (2011) | Effective workplace culture: the attributes, enabling factors and consequences of a new concept | International Practice Development Journal |
| 157 | McCormack B, Dewing J, Breslin L, Tobin C, Manning M, Coyne-Nevin A, et al. (2010) | The Implementation of a Model of Person-centred practice in older persons setting | Health Service Executive |
| 155 | McCormack B (2003) | A conceptual framework for person-centred practice with older people | International Journal of Nursing Practice |
| 118 | Clarke A, Hanson, EJ, Ross H (2003) | Seeing the person behind the patient: enhancing the care of older people using a biographical approach | Journal of Clinical Nursing |
| 169 | Medvene L, Lann-Wolcott H (2009) | An exploratory study of nurse aides’ communication behaviours: giving ‘positive regard’ as a strategy | International Journal of Older People Nursing |
| 170 | Brown J, Nolan M, Davies S, Nolan J, Keady J (2008) | Transforming students’ views of gerontological nursing: realising the potential of ‘enriched’ environments of learning and care: a multi-method longitudinal study | International Journal of Nursing Studies |
| 145 | McLellan H, Bateman H, Bailey P (2005) | The place of 360 degree appraisal within a team approach to professional development | Journal of Interprofessional Care |
| 197 | Parry R, Vass C (1997) | Training and assessment of physiotherapy assistants | Physiotherapy |
| 137 | Graber DR, Mitcham MD, Coker-Bolt P, Wise HH, Jacques P, Edlund B, et al. (2012) | The caring professionals program: educational approaches that integrate caring attitudes and empathic behaviours into health professions education | Journal of Allied Health |
| 147 | Vail L, Bosley S, Petrova M, Dale J (2011) | Healthcare assistants in general practice: a qualitative study of their experiences | Primary Health Care Research |
| 173 | Bailey S, Scales K, Lloyd J, Schneider J, Jones R (2015) | The emotional labour of healthcare assistants in inpatient dementia care | Ageing and Society |
| 162 | Noelker LS, Ejaz FK (2005) | Training direct-care workers for person-centered care | Public Policy and Aging Report |
| 131 | Welsh JD, Szabo GB (2011) | Teaching nursing assistant students about aphasia and communication | Seminars in Speech and Language |
| 198 | Ryan T, Nolan M, Enderby P, Reid D (2004) | Part of the family: sources of job satisfaction amongst a group of community –based dementia care workers | Health and Social Care in the Community |
| 146 | Gethin-Jones S (2013) | Focus on the micro-relationship of care | British Journal of Healthcare Assistants |
| 119 | McKenzie Smith M, Turkhod K (2013) | Simulation-based education in support of HCA development | British Journal of Healthcare Assistants |
| 199 | Godfrey A (2000) | What impact does training have on the care received by older people in residential homes? | Social Work Education |
| 120 | McCallion P, Toseland RW, Lacey D, Banks S (1999) | Educating nursing assistants to communicate more effectively with nursing home residents with dementia | The Gerontologist |
| 121 | Smith B, Kerse N, Parsons M (2005) | Quality of residential care for older people: does education for healthcare assistants make a difference? | The New Zealand Medical Journal |
| 122 | Lewis R, Kelly S, Whitfield M, Mckenzie-Smith M, Strachan A (2013) | An evaluation of a simulation-based educational programme to equip HCAs with the necessary non-technical skills to undertake their role safely and effectively, specifically in relation to the measurement of vital signs | Yorkshire and Humber Strategic Health Authority |
| 125 | Proctor R, Stratton Powell H, Burns A, Tarrier N, Reeves D, Emerson E, et al. (1998) | An observational study to evaluate the impact of a specialist outreach team on the quality of care in nursing and residential homes | Aging and Mental Health |
| 143 | Burgio LD, Allen-Burge R, Roth DL, Bourgeois MS, Dijkstra K, Gerstle J, et al. (2001) | Come talk with me: improving communication between nursing assistants and nursing home residents during care routines | The Gerontologist |
| 138 | Bourgeois MS, Dijkstra K, Burgio LD, Allen RS (2004) | Communication skills training for nursing aides of residents with dementia | Clinical Gerontologist |
| 165 | Latta LE, Ross J (2010) | Exploring the impact of palliative care education for care assistants employed in residential aged care facilities in Otago, New Zealand | Sites |
| 126 | Hancock H, Campbell S, Ramprogus V, Kilgour J (2005) | Role development in healthcare assistants: the impact of education on practice | Journal of Evaluation in Clinical Practice |
| 154 | Chapman A, Law S (2009) | Bridging the gap: an innovative dementia learning program for healthcare assistants in hospital wards using facilitator-led discussions | International Psychogeriatrics |
| 127 | Moxon S, Lyne K, Sinclair I, Young P, Kirk C (2001) | Mental health in residential homes: a role for care staff | Ageing and Society |
| 153 | Kuske B, Luck T, Hanns S, Matschinger H, Angermyer M, Behrens J, et al. (2009) | Training in dementia care: a cluster-randomised controlled trial of a training program for nursing home staff in Germany | International Psychogeriatrics |
| 139 | Bryan K, Axelrod L, Maxim J, Bell L, Jordan L (2002) | Working with older people with communication difficulties: an evaluation of care worker training | Aging and Mental Health |
| 200 from policing | Sutherland J (2014) | The PCSO review- an evaluation of the role, value and establishment of police community support officers within Cambridgeshire Constabulary | Cambridgeshire Constabulary |
| 140 from policing | O’Neill M (2014) | PCSOS as the Paraprofessionals of Policing | Leverhulme Trust |
| 148 from policing | Cooper C, Anscombe J, Avenell J, McLean F, Morris J (2006) | A National Evaluation of Community Support Officers | Home Office Research Study 297 |
| 123 from education | Farrell P, Balshaw MH, Polat F (1999) | The Management, Role and Training of Learning Support Assistants | Department for Education and Employment |
| 201 from education | Jolly A, Evans S (2005) | Teacher assistants move to the front of the class: job-embedded learning pays off in student achievement | The Journal of Staff Development |
| 202 from education | Groom B (2006) | Building relationships for learning: the developing role of the teaching assistant | Support for Learning |
| 203 from education | Collins J, Simco N (2006) | Teaching assistants reflect: the way forward? | Reflective Practice: International and Multidisciplinary Perspectives |
| 204 from education | Righter B (1987) | Training for Teaching Assistants | Engineering Education |
| 205 | Santo Pietro M (2002) | Training nursing assistants to communicate effectively with persons with Alzheimer’s Disease: a call for action | Alzheimer’s Care Quarterly |
Glossary
- Abductive analysis
- An approach to see something new in evidence or observation and inference is made to the best explanation about the cause.
- Agenda for Change
- In the NHS, the current system for grading and pay for staff.
- Care Certificate
- Standards for the work of non-regulated health and social care workers.
- CATWOE
- A mnemonic to describe the main elements included in soft systems methodology (customers, actors, transformations, world views, owner and environment).
- Concept mining
- In realist synthesis, describes a process of searching through different bodies of evidence for information that could build theories.
- Context
- The conditions which influence the success or failure of different interventions or programmes.
- Knowledge mobilisation
- A process of ensuring that the study findings reach the right audience using the right channels.
- Mechanism
- What is the change; what influences the reasoning and behaviour of people.
- Outcome
- Patterns resulting from the interplay between context and mechanism.
- Plausible hypotheses
- ‘If . . . then’ statements about what might work, for whom, how, why and in what circumstances.
- Programme theory
- The theory behind a given programme.
- RAMESES
- Specific publication standards for realist syntheses.
- Realist review
- The process of evidence review which follows the realist approach (also known as the Realist synthesis).
- Realist synthesis
- The process of evidence review which follows the realist approach (also known as the Realist review).
- Retroductive analysis
- In realist approaches, an analytical approach to understanding the cause of an event.
- Soft systems methodology
- A systematic approach to addressing a real-world situation.
- WeNurses
- Regular Twitter chat (Twitter, Inc., San Francisco, CA, USA) for the nursing profession.
- Workforce development
- In this study, interventions to improve skills and care standards of support workers in older people’s health and social care services.
List of abbreviations
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CMO
- context–mechanism–outcome
- CNA
- certified nursing assistant
- HCA
- health-care assistant
- NVQ
- National Vocational Qualification
- PCSO
- police community support officer
- PPI
- patient and public involvement
- SSA
- Social Services Abstracts