
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 13/182/07. The contractual start date was in December 2015. The final report began editorial review in July 2016 and was accepted for publication in November 2016. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Gillian Parker has in the past received, and is currently in receipt of, a number of other research grants from the National Institute for Health Research, all won in open competition.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2017. This work was produced by Thomas et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Policy and research interest in carers – those who provide support, on an unpaid basis, to ill, disabled or older people to enable them to live in their own homes – has grown in importance over the past 30 years. Since the first UK review of evidence on carers,1 the national and international body of research literature has grown substantially. It now covers data on, inter alia, the prevalence of caregiving, the impact and outcomes of caring on people with caregiving responsibilities, issues related to combining paid work and care, and the effectiveness of support and services for carers. Although some studies cover carers in general, others examine issues from the perspective of specific subgroups of carers, for example older carers, children and young people who provide care, and carers of people with specific conditions. Likewise, studies adopt different designs, ranging from randomised controlled trials (RCTs) to small-scale qualitative pieces of work.
Since 1995, the UK government has introduced legislation and policy measures aimed specifically at carers, as well as setting up the cross-departmental Standing Commission on Carers. The revised 2008 national strategy for carers2 contained the then-government’s 10-year vision for carers. The ‘next steps’ document,3 published 2 years later, outlined a cross-departmental approach to carers policy from identification to support; this also highlighted the need to develop the evidence base on supporting carers. The document pointed out that, although much is now known about the challenges that carers face and the impact that caring can have, much less is known about how to improve outcomes for carers. In May 2016, NHS England launched a toolkit4,5 to assist with identifying and assessing carer health and well-being as part of its ongoing commitment to carers. 6,7 The toolkit includes a template ‘Memorandum of Understanding’ to help local partners work collaboratively to support carers.
In 2009, the Department of Health commissioned a meta-review for the Standing Commission on Carers from the Social Policy Research Unit at the University of York to inform their thinking about how best to improve outcome for carers, as well as identifying future research areas. 8
The overall aim of that review was to provide the Department of Health with an overview of the evidence base relating to the outcomes and cost-effectiveness of support for unpaid carers of ill, disabled or older people. The specific objectives of the proposed study were:
-
to undertake a scoping review of existing literature reviews, including systematic reviews, on support and interventions for carers
-
to map out the extent, range and nature of the identified reviews on support and interventions for carers
-
to summarise the main findings of the identified reviews
-
to identify gaps and weaknesses in the evidence base.
The review encompassed carers of all ages (including children and young adults) supporting adults, including those making the transition from children’s to adults’ services, but did not cover people supporting adults with mental health problems except in the scoping work.
The review followed a protocol with inclusion and exclusion criteria, search terms, search strategy, quality control tools and approach to data extraction and synthesis.
The following parameters for the review were used:
-
include literature reviews published since 2000 to date and written in English only
-
no geographical restriction, that is, include reviews covering both national and international research
-
include published reviews only, that is, exclude research in progress and grey literature.
The overall conclusion of the meta-review was that the strongest evidence of effectiveness of any sort was in relation to education, training and information for carers. These types of interventions – particularly when active and targeted rather than passive and generic – appeared to increase carers’ knowledge and abilities as carers. There was some suggestion that this might also improve carers’ mental health or their coping; however, the review concluded that this possibility remained to be tested rigorously in research specifically designed to do so and that explored both effectiveness and costs.
Beyond this, there was little convincing evidence about any of the interventions included in the reviews. This was not the same as saying that these interventions had no positive impact. Rather, what the review revealed was poor-quality primary research, often based on small numbers, testing interventions that had no theoretical underpinning, with outcome measures that might have little relevance to the recipients of the interventions.
The National Institute for Health Research (NIHR) is keen to update the evidence in this area. Given the increase in published evidence since the original meta-review,8 and the introduction of the latest Care Act in 2014,9 an updated meta-review was considered helpful to inform both the NHS and possible future research commissioning in relation to the needs of different types of carers and information on types of support interventions.
For the update, we set out to assess what is known about effective interventions to support carers of all ages supporting adults who are ill, disabled or older. We adopted a pragmatic approach given the limited time and resources available.
Chapter 2 Methods
Introduction
We adapted, as necessary, the methods adopted in the original meta-review. 8
Search strategy
The database search strategies from the original meta-review were checked and updated. Updates were necessary for some of the strategies to account for changes to the search interface or provider, or where new indexing terms had been introduced or changed since the searches were last run in August 2009.
The searches were rerun in January 2016 on all of the databases searched in the original meta-review: Applied Social Sciences Index and Abstracts (ASSIA), Cochrane Database of Systematic Reviews, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Database of Abstracts of Reviews of Effects (DARE), EMBASE, Health Management Information Consortium (HMIC), Health Technology Assessment database, MEDLINE, MEDLINE In Process & Other Non-Indexed Citations, NHS Economic Evaluations Database, PsycINFO, Social Care Online, Social Sciences Citation Index (SSCI) and Social Services Abstracts. In addition, PROSPERO was searched to identify any recently completed systematic reviews.
As with the original meta-review, a study design search filter was used to limit the search to reviews only, if an appropriate filter was available. When possible, searches were restricted to records added to the database during the period 2009–16. All searches were restricted to English-language papers only.
Owing to the higher than anticipated volume of hits from the database searches and the time constraints of the project, we did not undertake any supplementary searches.
The records retrieved from each database were downloaded and imported into EndNote X7.4 (Thomson Reuters, CA, USA) for deduplication. The records were then further deduplicated against the EndNote library containing the original results from the 2009 searches. The total number of results after the deduplication process was 10,094. A further 72 results of potentially relevant systematic reviews were found from PROSPERO.
The search strategies and results for each database can be found in Appendix 1.
Study selection and quality assessment
The search results were downloaded in EndNote X7.4 and split equally between two reviewers, who screened the titles and abstracts to eliminate obviously irrelevant items. A 20% sample was split equally between two additional reviewers to double screen. In addition, one reviewer used text-mining software in EPPI-Reviewer 4 (Evidence for Policy and Practice Information and Co-ordinating Centre, Social Science Research Unit, Institute of Education, University of London, UK) to assess all of the records excluded at titles and abstracts stage to ensure that no relevant records had been missed during the single reviewer initial screening stage. Full-text copies were subsequently ordered or downloaded for potentially relevant records. We applied a cut-off date of 31 March 2016 for the receipt of full papers that had been ordered. We used a Microsoft Excel® 2013 (Microsoft Corporation, Redmond, WA, USA) spreadsheet to record full-paper screening decisions simultaneously for study selection and quality assessment, using the inclusion/exclusion criteria in Table 1 and the quality assessment criteria in Box 1 (taken largely from the original meta-review). 8 The screening of full papers was carried out by two reviewers independently, with disagreements resolved by discussion or the involvement of a third reviewer if necessary.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Population of interest | |
|
|
| Types of interventions | |
|
|
| Geographical coverage | |
|
|
| Language | |
|
|
| Period of interest | |
|
|
| Type of literature review | |
|
|
The set of criteria applied to relevant reviews embodies seven questions:
-
Is there a well-defined question?
-
Is there a defined search strategy?
-
Are inclusion/exclusion criteria stated?
-
Are study designs and number of studies clearly stated?
-
Have the primary studies been quality assessed?
-
Have the studies been appropriately synthesised?
-
Has more than one person been involved at each stage of the review process?
The criteria are scored as follows: yes = 1; in part = 0.5; and no or not stated = 0. High-scoring reviews (i.e. those reviews that scored ≥ 4) will go forward for full data extraction for the meta-review. Only brief summary information will be extracted from reviews of lower quality (i.e. those scoring < 4).
Reproduced from Parker et al. ,8 with permission from the Social Policy Research Unit, University of York.
As well as selecting reviews based on the inclusion and exclusion criteria, we assessed the quality of the reviews to inform which were subject to full review.
The quality assessment criteria that we used (see Box 1) are adapted from those developed by Egan et al. 10 in their systematic meta-review of psychosocial risk factors in home and community settings. These criteria had themselves been adapted for epidemiological reviews from two critical appraisal guides: the University of York’s Centre for Reviews and Dissemination’s (CRD) DARE criteria for quality assessment of reviews11 and a systematic review tool created by Oxman and Guyatt. 12
The first review, as commissioned by the Department of Health, did not include the carers of adults with mental health problems, except in the scoping work. 8 The main reason for this was the very different nature of the literature in this area. The concept of ‘carers’ for adults with mental health problems, even when these problems are severe and enduring, is more difficult to define than in other areas, and in some parts of the literature it remains contested. This difficulty is reflected in the nature of interventions evaluated; although these may be targeted at family members, their intended outcome is usually improved mental health for the adult being supported. The literature can also encompass interventions for people with drug and alcohol dependencies, which raises the same issue: that although interventions may have an impact on family members (or ‘carers’), this is not usually their primary purpose. We have discussed these challenges and complexities in reviewing this area elsewhere. 13,14 However, the search strategies for the first review did not exclude interventions for carers of adults with mental health problems, so that the likely size of the evidence base could be estimated. No reviews focused on carers in this area were actually identified in the first review. 8
We took the same approach to searching in the updated review, to allow us to see whether or not the evidence base had grown. This time we did find reviews in this area, which we included in the updated work reported here. However, the issues relating to the definitions of ‘carers’ in this field, and the nature of intervention, remain.
Post-protocol decisions prior to data extraction
From the initial searches and selection, it was clear that there had been substantial development in the volume, content and complexity of the literature since the original meta-review was carried out in 2010. Consequently, > 100 reviews were selected for potential inclusion in the update. It appeared that the average quality of reviews identified had improved since the first review, which potentially offered the opportunity for a ‘best evidence’ approach. Given the time and resource available, we needed to find a way to focus attention on those reviews that would provide the most robust information. Therefore, we revisited a number of decisions from the original protocol to focus our work.
The following post-protocol issues were discussed and agreed.
-
Review protocols were excluded on the basis that:
-
in their current form they were not a published systematic review and, therefore, they failed to meet our inclusion criteria
-
CRD’s PROSPERO database had been searched to locate publications from relevant protocols (we contacted the authors of such protocols but there were no available publications)
-
for older protocols we would expect our search strategy to have picked up relevant publications (given that not everything is registered on PROSPERO).
-
-
Conference abstracts were excluded on the basis that:
-
in their current form they were not a full systematic review publication and, therefore, they failed to meet our inclusion criteria
-
they did not provide sufficient detail to allow them to be assessed for inclusion
-
we were confident that our robust search strategy would have identified any relevant reviews underpinning these conference abstracts.
-
-
We found one review15 of interventions for carers of people with delirium. After discussion, we excluded this on the basis that delirium is an acute condition that would be expected to resolve. ‘Carers’ of people with delirium might thus be so for a very short period of time, whereas the focus of our work, and of NIHR’s interest, was on people who carry caring responsibility over an extended period.
-
We also found three reviews16–18 of case or care management. Although these examined outcomes for carers, they were excluded for two reasons:
-
Case or care management, as currently understood in the UK context, is less an intervention and more a framework within which needs are identified and assessed, care is planned, interventions and services are delivered and ongoing needs are monitored. Any type or number of specific interventions or services (or none), both for the ill or disabled person and (less frequently) the carer, might thus be delivered as a result of receiving case/care management.
-
The focus of case/care management is the ill or disabled person, albeit that the carer’s needs might also be considered during assessment and care planning.
-
The growth in the literature since the first review posed other challenges; for example, there were reviews that dealt with dyad interventions, interventions directed at the ill or disabled person and/or carers, and multiple-component interventions. There was also the issue of geographic coverage, whereby it was not clear if interventions or delivery contexts were fully transferable to UK health and social care systems. We also encountered the issue, evident in the original meta-review, of reviews in which the main focus was not on outcomes for the carer, but such outcomes were reported. We discussed these issues prior to data extraction and agreed a consistent way forward on whether to include or exclude. We included reviews of interventions aimed at patient–carer dyads only when carer outcomes were reported separately. When carer outcomes were reported but were not the main focus, a judgement was made as to the usefulness of this contribution to our meta-review. In relation to geographic applicability, we focused on reviews of interventions from developed countries with similar health-care systems, regardless of any differences in payment arrangements. We included multicomponent interventions on the basis that identifying the differential effectiveness of component parts may be limited to what was reported by the review authors.
Applying the adapted quality assessment criteria and scoring system by Egan et al. 10 used in the original meta-review revealed 61 high-quality systematic reviews. This was a larger proportion than expected. However, we noted that a review could achieve high-quality status using this system on the basis of adequate reporting of research question, search strategy, inclusion criteria and study designs/numbers but with insufficient attention to quality assessment, synthesis and transparency in the review process. Reviews with such shortcomings would be scrutinised closely for overall reliability, or may fail altogether the criteria for inclusion in DARE. DARE is a database of quality-assessed systematic reviews meeting specific criteria that was produced by the CRD, University of York; included are reviews that evaluate the effects of health and social care interventions, including delivery and organisation of services. Full details of the DARE process are available. 11 Therefore, we decided to refine the scoring system in the original meta-review and introduce a second tier of criteria (using the quality threshold for DARE) to further differentiate the ‘high’-quality reviews by splitting them into ‘high’ and ‘medium’ quality.
To be classed as ‘high’ quality, reviews had to reach a minimum score of 4 points, comprising (as mandatory) 1 point each for inclusion criteria, search strategy and synthesis and, additionally, 1 point for either quality assessment or number/design of included studies.
Most of the reviews identified at this stage were about ill or disabled people with specific conditions or impairment, for example dementia, stroke or cancer. Therefore, prior to data extraction of the included high-quality reviews, we grouped them according to impairment or condition to establish any discernible patterns and weightings in the evidence base. After this, we examined the distribution of reviews, by quality and by condition/impairment. This allowed us to adopt a ‘best evidence available’ approach to each of the condition/impairment areas identified.
Twenty-seven reviews were reclassified as high quality and progressed to detailed data extraction. The remaining 25 reviews (i.e. those that were high quality using the adapted Egan et al. 10 criteria but failed to meet the threshold for inclusion on DARE) were classed as medium quality, and we proceeded to basic data extraction. Bibliographic details were provided for nine reviews of low quality (using the adapted Egan et al. 10 criteria).
Data extraction
We followed the approach to data extraction used in the original meta-review. 8 For data extraction of high- and medium-quality reviews, we developed and piloted data collection forms for the first 11 reviews. For high-quality reviews, we summarised the review characteristics by target carer group, sociodemographic information, intervention (and comparator, when reported), outcomes, cost-effectiveness, number/study design and location of included studies, and findings. We then recorded key information according to the seven outcomes measured in the original meta-review, as follows: physical health, mental health, burden and stress, coping, satisfaction, well-being or quality of life, ability and knowledge. When it was unclear where best to place the review authors’ description of the outcome in our list of seven categories, this was discussed and agreed between two reviewers. For basic data extraction of medium-quality reviews, we summarised target carer groups, sociodemographic information, interventions (and comparators, when reported), a brief summary of outcomes measured, cost-effectiveness, number/study design and location of included studies. All data extraction forms were constructed as Microsoft Word® 2013 (Microsoft Corporation, Redmond, WA, USA) tables. For low-quality reviews, we recorded bibliographic detail only. Data extraction was carried out by one reviewer and checked by a second. Appendix 2 provides a summary of review characteristics for the high-quality reviews. All other data extraction tables are available on request.
Synthesis
Given the substantial growth in volume and complexity of the literature since the original meta-review,8 we adopted a pragmatic approach to the synthesis. We focused our synthesis primarily on the included high-quality reviews, aiming to identify any intervention effect (positive or negative, derived from narrative or quantitative synthesis), size of effect or heterogeneity, together with details of the population, intervention/comparator and outcome. We followed with a discussion of review quality, (when possible) highlighting the better-quality primary studies relating to any findings of interest. We then summarised information from the medium- and low-quality reviews to establish any material differences from the high-quality reviews in terms of review coverage.
Public and patient engagement
We engaged early with a group of carers who were known to us and were willing to give their views on the overall findings of our review. We had originally intended to involve the carers at an earlier stage of the work. However, discussion with the carers suggested that it was a better use of their time to ask them to comment on the draft findings, rather than to ask them to come to meetings in which they would be involved in a process that, because we were updating a previous meta-review, had relatively little scope for change and was largely technical.
A draft version of the report was sent to four individuals who had agreed to help, all of whom were female relatives (spouses and daughters) of people with different types of dementia. All were aged < 70 years. We provided them with a short brief on the purpose of the project and how we thought they might be able to help put the results into context, and asked them to share their views within 4 weeks. We offered the carers various options for feeding back their views: meeting the research team over a cup of coffee, talking to a researcher over the telephone or providing written comments. All chose to provide written comments via e-mail. In the end, however, only two of the carers were able to return comments in the time available.
Chapter 3 Results
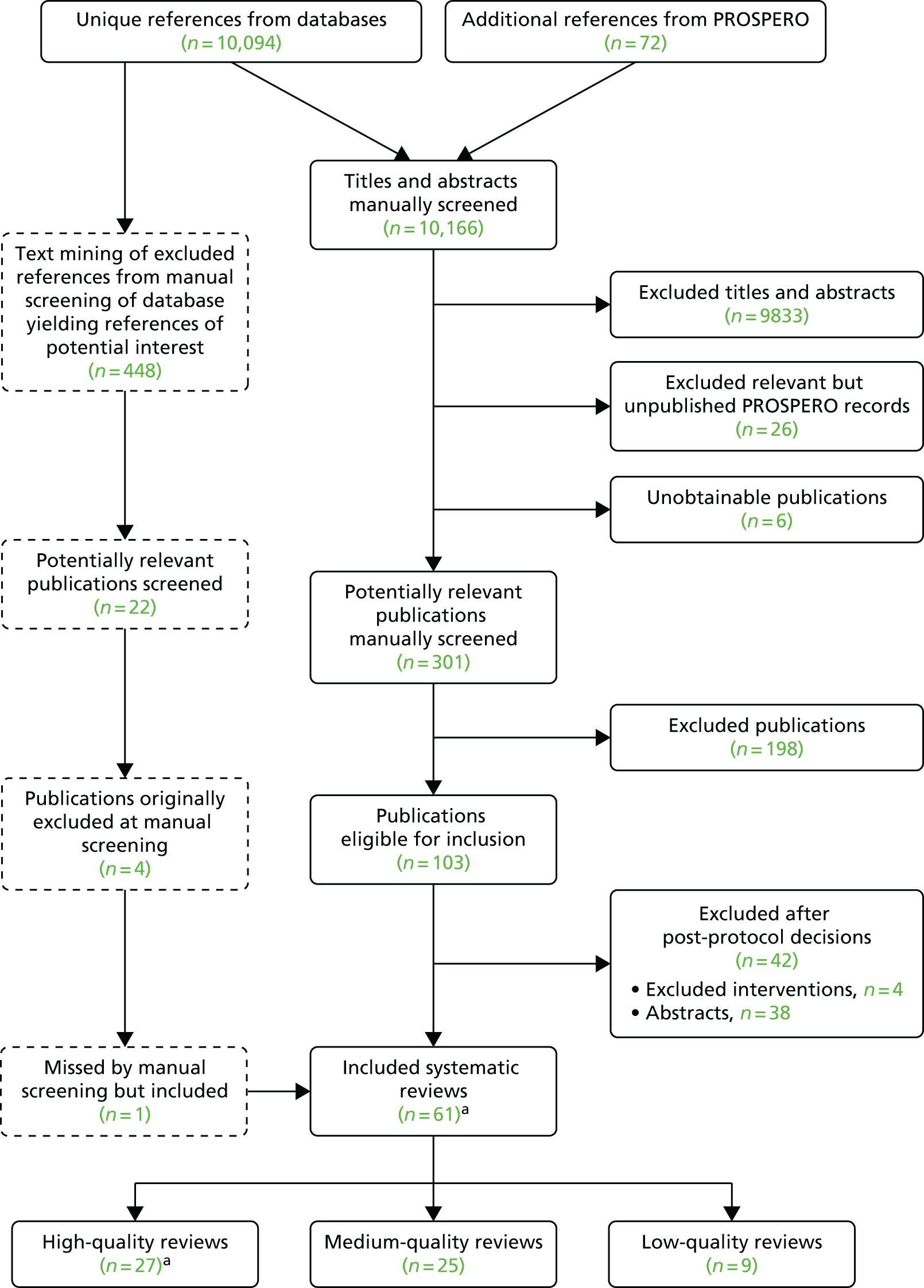
We initially identified 103 systematic reviews. Applying our post-protocol decision on a higher threshold for quality assessment (based on DARE), we finally included 61 reviews (27 of high quality, 25 of medium quality and nine of low quality). One of the 25 medium-quality reviews was identified through the text-mining exercise. We excluded 38 reviews only published in abstract form and four reviews with excluded interventions (delirium and case management). Figure 1 provides details.
FIGURE 1.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart. a, One review had two publications.
In this chapter, we start by presenting the results from reviews we defined as high quality. We have grouped the findings from different reviews in relation to impact on carers’ physical health, mental health, burden and stress, coping, satisfaction (with the intervention), well-being or quality of life, and ability and knowledge. We further subgroup according to the condition of the person the carer was helping. We conclude with a summary on the cost-effectiveness of interventions to support carers, followed by a summary of conclusions drawn by the reviews. The full details of all of the included high-quality reviews are given in Tables 2–9 and Appendix 2. To complete the evidence picture, we then outline the other reviews classed as medium quality (see Table 10) and low quality (see Table 11), highlighting any substantive differences from the high-quality reviews in terms of types of carers, interventions and outcomes. The full bibliographic details are included in the References.
Overview of the high-quality reviews
Twenty-seven high-quality reviews (28 papers) (including eight Cochrane reviews) were included in this meta-review. 19–46 The details of the quality scoring of these reviews are given in Table 2.
| First author, year of publication | 1. Is there a well-defined question? | 2. Is there a defined search strategy? | 3. Are inclusion/exclusion criteria stated? | 4. Are study design and number of studies clearly stated? | 5. Have the primary studies been quality assessed? | 6. Have the studies been appropriately synthesised? | 7. Has more than one person been involved at each stage of the review process? | Total score |
|---|---|---|---|---|---|---|---|---|
| Carers of people with dementia | ||||||||
| Boots, 201419 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Chien, 201120 | 1 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 6 |
| Eggenberger, 201321 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 6.5 |
| Godwin, 201322 | 1 | 1 | 1 | 1 | 0 | 1 | 0.5 | 5.5 |
| Hurley, 201423 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Jensen, 201524 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Lins, 201425 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Marim, 201326 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Maayan, 201427 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| McKechnie, 201428 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Orgeta, 201429 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Schoenmakers, 201030 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 5.5 |
| Smith, 201432 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Vernooij-Dassen, 201131 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Carers of people with cancer | ||||||||
| Lang, 201433 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Northouse, 201034 | 0.5 | 1 | 1 | 1 | 0 | 1 | 0.5 | 5 |
| Regan, 201235 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Waldron, 201336 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Carers of people with stroke | ||||||||
| aCheng, 201237 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| aCheng, 201438 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Ellis, 201039 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 6.5 |
| Forster, 201240 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Legg, 201141 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Carers of people with various conditions at the end of life | ||||||||
| Candy, 201142 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Gomes, 201343 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Nevis, 201444 | 1 | 1 | 1 | 1 | 0.5 | 1 | 0 | 5.5 |
| Carers of people with mental health problems | ||||||||
| Macleod, 201145 | 1 | 1 | 1 | 1 | 0.5 | 1 | 0 | 5.5 |
| Yesufu-Udechuku, 201546 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
Of the reviews, 1419–32 focused on interventions for carers of people with dementia, four33–36 focused on carers of people with cancer, four37–41 focused on carers of people with stroke, three42–44 focused on carers of people with various conditions at the end of life and two45,46 focused on carers of people with mental health problems. Not all reviews reported the geographic location of the included primary studies. When this was reported, coverage was worldwide. Many studies originated in the USA and Europe (including several in the UK). When sociodemographic data were reported, carers in general were white, female and spouses or adult children, with the age at which they started their caregiving roles ranging from their early forties up to at least 70 years.
In general, the review characteristics were highly variable. When data were extracted on statistical heterogeneity, this is reported (focusing on where intervention effects are indicated) in the results that follow.
A wide range of interventions was included (see Appendix 2 and Tables 3–9). Multicomponent interventions were the focus in many reviews; those with psychosocial or psychoeducational content featured prominently,28,34–38,46 as did those containing education and/or communication skills training. 21,24,26,40,44,45 Other (more specific) interventions included stroke liaison workers,39 volunteer mentoring,32 meditation-based activity,23 art-making classes33 and home-based exercise. 29 Control or comparator groups (when reported) were usual care, no control, other active intervention, wait list or placebo. The details of what was delivered to control groups were sparse or were not reported. Many different outcome measures were reported (see Appendix 2 and Tables 3–9).
Quality of the primary studies
A quality assessment of primary studies was carried out in 2519–21,23–33,35–46 of the 27 included reviews. In most cases, it was possible to determine at least the overall quality of the included studies. However, Shoenmakers et al. 30 applied quality assessment only as an inclusion criterion and did not report further on the quality of the primary studies. In Ellis et al. ,39 only selective coding was carried out, making it impossible to gauge the overall quality. In Eggenberger et al. ,21 quality assessment criteria were presented in the paper, but detailed results were not. Similarly, in Macleod et al. ,45 risk of bias was reported to have been assessed, but the results of this were not presented. Two reviews22,34 did not perform any quality assessment of primary studies.
When it was possible to determine from results reported in the reviews, the methodological quality of primary studies was variable. In reviews targeting carers of people with dementia, only one26 specifically reported that all of the included studies had a low risk of bias. 26 A majority of studies in another review20 was reported as being of high or moderate quality, and a further review presented an average quality score of 75 out of 100. 32 In other reviews, the quality of primary studies appeared to be moderate,23,25,29 variable19,21,28 or very low. 27 One review described overall quality as satisfactory;31 another reported separately on the quality of primary studies for different outcomes (overall low to moderate). 24 In reviews targeting carers of people with cancer, one33 suggested that studies were of moderate quality,33 one35 reported moderate to strong evidence35 and one36 reported fair to good-quality evidence. 36 Limitations and variable study quality were also reported in reviews of interventions for carers of people with stroke. 37,38,40,41 Reviews addressing carers of people with various conditions at the end of life indicated studies of unclear quality,42 mixed-quality studies43 or studies at serious risk of bias, particularly in those focusing on carer outcomes. 44 Low- to moderate-quality primary studies were reported in one review46 focusing on carers of people with mental health problems. 46
Approach to synthesis
In most reviews, the analysis was grouped by intervention or outcome. The multicomponent nature of many interventions meant that it was difficult to identify causal relationships. Eleven reviews undertook narrative synthesis19,21–23,28,32,35,36,43–45 and six undertook quantitative synthesis. 20,26,27,29,30,34 Ten reviews24,25,31,33,37–42,46 contributed both narrative and quantitative syntheses. Two references37,38 relate to the same review.
Overlap of primary studies
From the outset, it was clear that there was some overlap of primary studies in the reviews we included. The effect of this overlap is difficult to judge without substantial additional analysis, but it could run the risk of exaggerating effects from the undue influence of individual studies, and present difficulties arising from contradictory assessments of the same study.
Carer outcomes
Physical health
Evidence about carers’ physical health was reported in seven reviews (in eight papers). 28,34,35,37–39,42,43 Physical health (when defined) included physical distress, physical functioning, somatic complaints, perceived or subjective health status and sleep improvement. Some formal outcome measures were reported. All results are presented in Table 3.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| McKechnie, 201428 | Computer-mediated psychosocial (complex multifaceted) interventions with/without professional support | Physical health | 2/14 | HSQ-12; Caregiver Health and Health Behaviours scale | Narrative | No intervention effects | Unclear | ||
| Carers of people with cancer | |||||||||
| Northouse, 201034 | Psychoeducation, skills training, therapeutic counselling | Physical functioning | 7/29 | NR | Meta-analysis (Hedges’ g) | 0.11 | –0.05 to 0.27 | NS | Post intervention: 0–3 months |
| Psychoeducation, skills training, therapeutic counselling | Physical functioning | 6/29 | NR | Meta-analysis (Hedges’ g) | 0.22 | 0.04 to 0.41 | < 0.05 | Post intervention: 3–6 months | |
| Psychoeducation, skills training, therapeutic counselling | Physical functioning | 2/29 | NR | Meta-analysis (Hedges’ g) | 0.26 | 0.02 to 0.49 | < 0.05 | Post intervention: ≥ 6 months | |
| Regan, 201235 | Couples-based psychosocial interventions | Physical distress | 2/23 | SRHS; PAL-C; BCTRI; FACT-G; EPIC; SF-36 | Narrative | Significant reductions following disease management, psychoeducation/telephone counselling intervention (one study) and a multicomponent ‘FOCUS’ intervention (one study). Results were not reported for one study | Unclear | ||
| Carers of people with stroke | |||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual interventions; many were multifaceted Counselling and psychoeducation |
Physical functioning | 2/18 | SF-36 | Narrative | No significant differences for counselling, social problem solving or physical exercise training | Unclear | ||
| Counselling and psychoeducation | Somatic complaints | 1/18 | SF-36 | Narrative | No significant differences for social problem-solving interventions | Unclear | |||
| Counselling and psychoeducation | Perceived health status | 4/18 | SF-36 | Narrative | No significant differences for social problem-solving, counselling, psychoeducation or social support interventions | Unclear | |||
| Counselling and psychoeducation | Physical functioning (for all interventions) | 4/18 | Various, including SF-36 or global family assessments | Meta-analysis (SMD) | –0.14 | –0.37 to 0.09 | 0.23 | Immediately post intervention | |
| Counselling and psychoeducation | Physical functioning (for all interventions) | 4/18 | NS differences for subgroup analysis by intervention | Unclear | |||||
| Counselling and psychoeducation | Somatic complaints | 2/18 | Various, including SF-36 or global family assessments | Meta-analysis (SMD) | –0.10 | –0.37 to 0.16 | 0.45 | Immediately post intervention | |
| Counselling and psychoeducation | Somatic complaints | 2/18 | NS differences for subgroup analysis by intervention | ||||||
| Ellis, 201039 | Stroke liaison workers for patients and carers: proactive and structured approach; reactive and flexible approach; proactive and focused approach | Caregiver subjective health status (includes carer strain but unable to separate) | 15/16 | Majority used a measure of Carer Strain Index | Meta-analysis (SMD) | 0.04 | –0.05 to 0.14 | 0.37 | Unclear |
| Carers of people with various conditions at the end of life | |||||||||
| Candy, 201142 | Usual care plus direct interventions for carers | Sleep improvement | 1/11 | Pittsburgh Sleep Quality Index; Actigraph Sleep Watch | Narrative | No difference in sleep improvement for brief behavioural intervention | End of intervention | ||
| Gomes, 201343 | Home palliative care vs. usual care | Pre-bereavement physical function, general health, pain | 2/23 | SF-36 subscales | Narrative | Moderate evidence of no statistically significant differences apart from physical functioning (p < 0.05) | Unclear | ||
| Post-bereavement physical function, general health, pain | 3/23 | SF-36 subscales | Narrative | Conflicting results | Unclear | ||||
| Reinforced vs. standard home palliative care | General health | 2/23 | GHQ-12 and GHQ-28 | Narrative | Moderate evidence of no statistically significant differences | Unclear | |||
| Carers of people with mental health problems | |||||||||
| No reviews | |||||||||
Carers of people with dementia
A narrative synthesis in McKechnie et al. ,28 focusing on computer-mediated psychosocial interventions (with or without professional support), reported no intervention effects on the physical health outcome for carers (two studies, both of medium quality). Physical health was not defined in this review, but outcome measures were reported, such as the Health Status Questionnaire-12 and the Caregiver Health and Health Behaviours Scale.
Carers of people with cancer
Two reviews34,35 reported improved physical health outcomes for carers of people with cancer. 34,35 In Regan et al. ,35 a narrative synthesis showed reductions in physical distress following couples-based psychosocial support involving disease management, psychoeducation, telephone counselling and the development of family coping skills (two studies, one of strong and one of moderate quality). In Northouse et al. ,34 a meta-analysis revealed a small statistically significant intervention effect for physical functioning (a range of self-care behaviours and sleep quality) beyond 3 months from the delivery of multicomponent psychoeducation activities (six studies, quality not reported).
Carers of people with stroke
Two reviews37–39 provided narrative and quantitative syntheses, neither of which revealed any significant group differences or intervention effects on the physical health of carers of people with stroke. Across the reviews, physical health was defined as physical functioning, somatic complaints and carer subjective health status. Interventions in these reviews were dissimilar (the first review focused on multicomponent psychosocial activities; the second review focused on stroke liaison workers). In Ellis et al. ,39 a large proportion (15 out of 16) of included studies was used in the meta-analysis (quality scores were not reported).
Carers of people with various conditions at the end of life
Two reviews42,43 provided narrative syntheses for physical health outcomes. When defined beyond general health, physical health included sleep quality; outcome measures included Short-Form questionnaire-36 items (SF-36) subscales, General Health Questionnaire (GHQ)-12 and GHQ-28, and specific sleep quality measures. The results generally showed no improvements or showed conflicting results. However, in Gomes et al. 43 there was a statistically significant effect for physical functioning following home palliative care (not defined further) in two studies (at unclear or high risk of bias).
Carers of people with mental health problems
No reviews were identified that addressed physical health for carers of people with mental health problems.
Mental health
Carers’ mental health was a frequently reported outcome in the 24 included reviews. 19–25,27–35,37–43,45,46
Mental health was variably defined (when reported). The terms depression, anxiety, psychological distress and self-efficacy were commonly used. Some reviews defined the outcome more broadly as psychological well-being or carer mental health. The outcome measures were generally well reported and diverse. Frequently used measures were the Centre for Epidemiologic Studies Depression Scale (CES-D), Brief Symptom Inventory, Beck Depression Inventory, Hospital Anxiety and Depression Scale (HADS) and the GHQ-12 and GHQ-28. The following results focus primarily on the detail for positive intervention effects. Providing further detail on reviews showing no significant effects for mental health outcomes was not considered to be informative, but a brief summary of results from these reviews is provided below. All results are reported in Table 4.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| Boots, 201419 | Internet-based interventions including information, caregiving strategies and support | Depression | 2/12 | Unclear | Narrative | Small significant improvement | Unclear | ||
| Self-efficacy | 4/12 | Unclear | Narrative | Small significant improvement | Unclear | ||||
| Chien, 201120 | Support groups led by professionals or other trained group members | Overall mental health | 19/30 | NR | Meta-analysis (Hedges’ g) | –0.44 | –0.73 to 0.15 | End of intervention | |
| Overall mental health | 6/30 | NR | Meta-analysis (Hedges’ g) | –0.53 | –1.07 to 0.01 | NR | Follow-up of 1–3 months | ||
| Depression | 17/30 | NR | Meta-analysis (Hedges’ g) | –0.40 | –0.72 to –0.08 | NR | End of intervention | ||
| Depression | 6/30 | NR | Meta-analysis (Hedges’ g) | –0.57 | –1.09 to –0.05 | NR | Follow-up of 1–3 months | ||
| Eggenberger, 201321 | Face-to-face communications skills training (small groups or individually) | Depression | 1/4 | HDRS | Narrative | One study reported a mean decline of depression levels from 6.9 (SD 4.1) to 6.3 (SD 4.5); p < 0.041 | Unclear | ||
| Godwin, 201322 | Technology-driven multicomponent support including information and social support: Caregiver’s Friend | Depression | 1/8 | CES-D | Narrative | Significant decrease in depression compared with control | Unclear | ||
| REACH | Depression | 1/8 | CES-D | Narrative | Significant reductions in depression | 6 and 18 months’ follow-up | |||
| Caregiver’s Friend or REACH | Anxiety | 2?/8 | STAI | Narrative | Both reported significantly decreased anxiety compared with control | Unclear | |||
| Hurley, 201423 | Meditation-based intervention | Depression | 7/8 | CES-D; HDRS; SCL-90; POMS | Narrative | Five studies (including two RCTs) found statistically significant reductions in depression score pre–post intervention; two studies (including one RCT) found non-statistically significant trends for reduced scores. There were mixed results at follow-up | End of intervention or follow-up (4 weeks to 4 months) | ||
| Jensen, 201524 | Educational interventions aimed at teaching skills relevant to dementia caring | Depression | 2/7 RCTs | CES-D; Montgomery–Åsberg Depression Rating Scale | Meta-analysis (SMD) | –0.37 | –0.65 to –0.09 | 0.010 | 5 to 6 months’ follow-up |
| Depression | 1/7 | CES-D; Montgomery–Åsberg Depression Rating Scale | Meta-analysis (SMD) | 0.12 | –0.15 to 0.38 | NR | 15 months’ follow-up | ||
| Lins, 201425 | Telephone counselling with or without additional intervention | Self-efficacy | 4//9 RCTs | Caregiving Self-efficacy by Steffen; Self-Efficacy Scale by Fortinsky | Narrative | Mixed results from two RCTs of telephone counselling without additional intervention. Positive effects were reported in the control groups. Mixed results reported following telephone counselling with video sessions and workbook; positive effects were noted in both intervention and control groups (two studies) | Unclear | ||
| Depressive symptoms | 4/9 RCTs | CES-D; BSI | Narrative | Mixed results over time after telephone counselling with (one RCT) or without (two RCTs) video sessions. A statistically significant group difference was reported favouring telephone counselling combined with video sessions and a workbook (one RCT) | Unclear | ||||
| Telephone counselling without other intervention | Depressive symptoms | 3/9 RCTs | CES-D; GDS; BSI; BDI; | Meta-analysis (SMD) | 0.32 | 0.01 to 0.63 | 0.0444 | Unclear | |
| Telephone counselling combined with video sessions | Anxiety | 1/9 RCTs | BSI | Narrative | Anxiety significantly reduced over time in both interventions and control groups | Unclear | |||
| Maayan, 201427 | Interventions providing respite care vs. no respite | Depression | 1/4 RCTs | HDRS | Meta-analysis (MD) | 0.18 | –3.82 to 3.46 | NR | Unclear |
| Respite vs. polarity therapy | Depression | 1/4 RCTs | CES-D | Meta-analysis (MD) | 6.0 | 0.31 to 11.69 | NRa | Unclear | |
| Respite vs. no respite | Anxiety | 1/4 RCTs | Hamilton Anxiety Scale | Meta-analysis (MD) | 0.05 | –3.76 to 3.86 | NR | Unclear | |
| Psychological distress | 1/4 RCTs | BSI | Meta-analysis (MD) | 0.04 | –0.29 to 0.37 | NR | Unclear | ||
| McKechnie, 201428 | Computer-mediated psychosocial interventions (complex and multifaceted) with and without professional support | Depression | 7/14 | CES-D; Composite measure (detail NR) | Narrative | Four studies found improvements in CES-D; three medium-quality studies found no effect (when reported) | Unclear | ||
| Anxiety | 2/14 | STAI | Narrative | Reduction in STAI | Unclear | ||||
| General Mental Health | 3/14 | GHQ; HSQ-12; HSQ-20; subscales from Revised Ways of Coping | Narrative | Three studies generally did not find any intervention effect | Unclear | ||||
| Self-efficacy | 3/14 | Caregiving self-efficacy scale | Narrative | There were inconsistent findings across one high-quality study and two medium-quality studies | Unclear | ||||
| Orgeta, 201429 | Home-based supervised endurance or aerobic exercise; telephone-based exercise; 12-week exercise programme | Depression | 3/4 RCTs | BDI; 11-item Iowa short form for CES-D | Meta-analysis (SMD) | –0.35 | –0.73 to 0.03 | 0.07 | Unclear |
| Depression | 2/4 RCTs | BDI only | Meta-analysis (SMD) | –0.35 | –0.73 to 0.03 | NR | Unclear | ||
| Anxiety | 2/4 | Taylor Manifest Anxiety Scale (short form) | Meta-analysis (SMD) | –0.22 | –0.60 to 0.16 | 0.26 | Unclear | ||
| Schoenmakers, 201030 | Active intervention in a dementia care home Using psychological interventions |
Depression | 15/26 | GHQ-12 or -28; CES-D, Zung Depression Scale, BDI, PST-BSI | Meta-analysis (MD) | 0.03 | –0.42 to 0.35 | 0.86 | Unclear |
| Depression | 15/26 | GHQ-12 or GHQ-28; CES-D, Zung Depression Scale, BDI, PST-BSI | Meta-analysis (MD) | Authors report no significant change to results following sensitivity analysis | Unclear | ||||
| Using communication technologies | Depression | 2/26 | Unclear | Meta-analysis (MD) | 0.07 | –2.62 to 2.75 | 0.96 | Unclear | |
| Using case management | Depression | 3/26 | Unclear | Meta-analysis (MD) | –0.32 | –0.73 to 0.091 | 0.13 | Unclear | |
| Smith, 201432 | Volunteer mentoring – peer support | Anxiety and depression | 2/4 | HADS | Narrative | Peer support: one study found no positive improvements in depression, but ‘after secondary analysis, peer support was found to have a modest buffering effect on depressive symptoms for carers experiencing the most stressful situations’ | Unclear | ||
| Volunteer mentoring – telephone befriending | Anxiety and depression | 1/4 | HADS | Narrative | Telephone befriending: no improvement was found for carers in the intention-to-treat population but carers receiving the befriending intervention for at least 6 months reported a statistically significant improvement in depression scores (p = 0.04) | Final follow-up at 15 months | |||
| Vernooij-Dassen, 201131 | Cognitive reframing (one element of CBT) | Anxiety | 4/11 RCTs | STAI; HAM-A; BSI anxiety subscale | Meta-analysis (SMD) | –0.21 | –0.39 to –0.04 | NR | Unclear |
| Depression | 6/11 RCTs | CES-D, BDI, BSI depression subscale; MAACL depression subscale | Meta-analysis (SMD) | –0.66 | –1.27 to –0.05 | NR | Unclear | ||
| 5/11 RCTs (removal of one RCT owing to heterogeneity) | CES-D, BDI, BSI depression subscale; MAACL depression subscale | Meta-analysis (SMD) | –0.24 | –0.42 to –0.07 | NR | Unclear | |||
| Carers of people with cancer | |||||||||
| Lang, 201433 | Art-making class/creative arts interventions: art therapy | Anxiety | 2/2 | BAI | Meta-analysis (WMD) | 4.83 | 3.12 to 6.55 | < 0.001 | Unclear |
| Northouse, 201034 | Psychoeducation, skills training, therapeutic counselling | Self-efficacy | 8/29 | NR | Meta-analysis (Hedges’ g) | 0.25 | 0.03 to 0.47 | < 0.05 | During first 3 months of intervention |
| 4/29 | NR | Meta-analysis (Hedges’ g) | 0.20 | 0.03 to 0.37 | < 0.05 | 3–6 months post intervention | |||
| 1/29 | NR | Meta-analysis (Hedges’ g) | 0.29 | 0.03 to 0.56 | < 0.05 | 6 months post intervention | |||
| Distress and anxiety | 16/29 | NR | Meta-analysis (Hedges’ g) | 0.20 | 0.08 to 0.32 | < 0.05 | During first 3 months of intervention | ||
| 11/29 | NR | Meta-analysis (Hedges’ g) | 0.16 | 0.03 to 0.29 | < 0.05 | 3–6 months post intervention | |||
| 6/29 | NR | Meta-analysis (Hedge’s g) | 0.29 | 0.06 to 0.51 | < 0.05 | 6 months post intervention | |||
| Depression | 16/29 | NR | Meta-analysis (Hedges’ g) | 0.06 | NR | NR | During first 3 months of intervention | ||
| 11/29 | NR | Meta-analysis (Hedges’ g) | 0.06 | NR | NR | 3–6 months post intervention | |||
| 3/29 | NR | Meta-analysis (Hedges’ g) | –0.03 | NR | NR | 6 months post intervention | |||
| Regan, 201235 | Couples-based psychosocial interventions | Psychological distress | 7/23 | Various | Narrative | Significant improvements for intervention partners vs. control (two studies); within-group improvements from baseline (three studies); improvements for intervention partners compared with control group partners (four studies); within-group improvements at the final follow-up compared with baseline (one study) | Unclear | ||
| Carers of people with stroke | |||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual interventions Psychoeducation, behaviour and cognitive–behavioural interventions |
Anxiety | 3/18 | NR | Narrative | Inconsistent findings between studies of psychoeducation, behaviour and cognitive–behavioural interventions | Unclear | ||
| Psychoeducation or social problem-solving | Depression | 3/18 | NR | Narrative | Inconsistent findings for psychoeducation and social problem-solving | Unclear | |||
| Individual or group counselling, social support or social problem-solving | Psychological health | 3/18 | NR | Narrative | Inconsistent findings for individual or group counselling, social support or social problem-solving | Unclear | |||
| Psychoeducation or social support | Depression | 5/18 | NR | Meta-analysis (SMD) | 0.14 | –0.19 to 0.46 | 0.41 | Post intervention | |
| Psychological or counselling | Psychological health | 5/18 | NR | Meta-analysis (SMD) | 0.12 | –0.07 to 0.31 | 0.22 | Post intervention | |
| Ellis, 201039 | Stroke liaison workers for patients and carers | Caregiver mental health | 13/16 RCTs | NR | Meta-analysis (SMD) | –0.02 | –0.12 to 0.08 | 0.67 | Unclear |
| Caregiver subjective health status (includes measure of carer strain but cannot separate) | 15/16 RCTs | NR | Meta-analysis (SMD) | 0.04 | –0.05 to 0.14 | 0.37 | Unclear | ||
| Forster, 201240 | Passive education interventions | Depression | 2/21 RCTs | HADS | Narrative | No significant differences were reported for passive information studies | Unclear | ||
| Active education interventions | Depression | 1/21 RCTs | HADS | Narrative | Carers in the active intervention group were significantly less depressed than those in control groups (p < 0.0001, no figures reported) | Unclear | |||
| Passive or active education interventions | Psychological distress | 4/21 RCTs | NR | Meta-analysis (OR) | 1.13 | 0.65 to 1.97 | 0.65 | Unclear | |
| Legg, 201141 | Non-pharmacological interventions | Anxiety | 1/8 RCTs | NR | Narrative | No significant differences reported | Unclear | ||
| Teaching ‘procedural knowledge’ | Depression | 5/8 RCTs | HADS; GHQ-28; CES-D | Narrative | One RCT reported significant effects on depression for ‘teaching procedural knowledge’ (MD –0.61, 95% CI –0.85 to –0.37; p < 0.001) | Unclear | |||
| Information and support | Depression | 2/8 | HADS; GHQ-28; CES-D | Meta-analysis (SMD) | –0.06 | –0.31 to 0.18 | 0.62 | Unclear | |
| Psychoeducational interventions | Depression | 2/8 | HADS; GHQ-28; CES-D | Meta-analysis (SMD) | 0.20 | –0.17 to 0.57 | 0.28 | Unclear | |
| Carers of people with various conditions at the end of life | |||||||||
| Candy, 201142 | Usual care plus direct interventions for carers | Psychological distress | 8/11 RCTs | HADS; CES-D | Meta-analysis (SMD) | –0.15 | –0.28 to –0.02 | 0.020 | End of interventions |
| Gomes, 201343 | Home palliative care vs. usual care | Pre-bereavement outcomes: psychosocial well-being | 6/23 | SF-36 subscales | Narrative | Conflicting results for home palliative care vs. usual care | Unclear | ||
| Post-bereavement outcomes: grief | 4/23 | Various measures | Narrative | Strong evidence of no statistically significant differences between groups | Unclear | ||||
| Post-bereavement outcomes: psychological well-being | 5/23 | SF-36 subscales | Narrative | Conflicting results | Unclear | ||||
| Reinforced vs. standard home palliative care | Psychological well-being | 2/23 | HADS; STAI | Narrative | Moderate evidence of no statistically significant difference | Unclear | |||
| Intensity of grief | 1/23 | NR | Narrative | Limited evidence of no statistically significant difference | 4 months after patient death | ||||
| Caregiver distress | 1/23 | CBrI | Narrative | Limited evidence of positive effect in favour of added component | Unclear | ||||
| Carers of people with mental health problems | |||||||||
| Macleod, 201145 | Support from community mental health nurses – education | Somatic symptoms, anxiety, insomnia, social dysfunction, severe depression | 1/68 | NR | Narrative | No effects on somatic symptoms, anxiety, insomnia, social dysfunction or severe depression | Unclear | ||
| Support from community mental health nurses – family education | Anxiety and distress | 2/68 | NR | Narrative | A decrease in depression | Unclear | |||
| Support from community mental health nurses – family interventions | Depression | 6/68 | NR | Narrative | One study out of six reported a decrease | Unclear | |||
| Support from community mental health nurses – mutual support | Mood | 1/68 | NR | Narrative | Improved mood | Unclear | |||
| Yesufu-Udechuku, 201546 | Interventions delivered by health and social care services Psychoeducation compared with control |
Psychological distress | 2/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.30 | –0.84 to 0.24 | NR | End of intervention |
| 2/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.34 | –0.76 to 0.08 | NR | 6-months’ follow-up | |||
| 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –1.79 | –3.01 to –0.56 | NR | Over 6-months’ follow-up | |||
| Support group | Psychological distress | 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.99 | –1.48 to –0.49 | NR | End of intervention | |
| 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.99 | –1.48 to –0.49 | NR | Up to 6-months’ follow-up | |||
| Psychoeducation plus support | Psychological distress | 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.28 | –0.84 to 0.29 | NR | Over 6 months post intervention | |
| Problem-solving bibliotherapy | Psychological distress | 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –1.57 | –1.79 to –1.35 | NR | End of intervention | |
| 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –1.54 | –1.95 to –1.13 | NR | Up to 6-months’ follow-up | |||
| Self-management | Psychological distress | 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.32 | –0.73 to 0.09 | NR | End of intervention | |
| Practitioner-delivered vs. postal psychoeducation | Psychological distress | 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | –0.38 | –1.0 to 0.25 | NR | End of intervention | |
| 1/21 RCTs | GHQ-12 and GHQ-28; BDI; K10; CIS-Rb | Meta-analysis (SMD) | 0 | –0.62 to 0.61 | NR | Up to 6-months’ follow-up | |||
Carers of people with dementia
The reviews of interventions for carers of people with dementia focused mainly on depression, anxiety and self-efficacy. These outcomes are highlighted in the following sections. Other outcomes analysed were psychological distress, psychological well-being, carer mental health and general mental health.
Depression
Narrative syntheses revealed positive intervention effects on depression in Eggenberger et al. 21 following a home-care education intervention with professional support (one good-quality study); Boots et al. ,19 relating to web-based carer support interventions (two studies, one of higher quality and one of lower quality); Godwin et al. ,22 focusing on the Caregiver’s Friend: Dealing with Dementia (involving the delivery of positive caregiving strategies via text and video) or Resources for Enhancing Alzheimer’s Caregiver Health (REACH) interventions (two studies, quality not reported); Hurley et al. ,23 relating to meditation-based interventions (five studies, although the results were mixed at follow-up; all of moderate quality); Lins et al. ,25 for combined telephone counselling, video sessions and workbook (one moderate-quality study); McKechnie et al. ,28 for computer-mediated interventions (four studies, all of high quality); and Smith and Greenwood,32 for anxiety and depression after a befriending intervention (one study after 15 months, of high quality). Quantitative syntheses showed statistically significant positive intervention effects on depression in Jensen et al. ,24 following educational interventions (two studies, one of high quality and one of low quality; no evidence of statistical heterogeneity at I2 = 0%); Vernooij-Dassen et al. ,31 in relation to cognitive reframing (six studies, all of which had some methodological limitations); Chien et al. ,20 for carer support groups (17 studies with high statistical heterogeneity at I2 = 86.03%; six studies maintained the effect at 1–3 months’ follow–up; the studies were of moderate to high quality); and Lins et al. ,25 for depressive symptoms after telephone counselling (three studies of moderate quality; no evidence of statistical heterogeneity at I2 = 0%).
Anxiety
Narrative syntheses showed positive intervention effects for anxiety in Godwin et al. 22 focusing on the Caregiver’s Friend and REACH interventions (number of studies unclear, no quality reported); and McKechnie et al. 28 after computer-mediated interventions (two studies of high quality). Quantitative syntheses showed statistically significant positive intervention effects for anxiety in Vernooij-Dassen et al. 31 following cognitive reframing interventions (four studies, all of which had some methodological limitations).
Self-efficacy
Narrative syntheses showed a small positive intervention effect for self-efficacy in Boots et al. 19 after internet-based support interventions (four studies, one of high quality and three of low quality). In Lins et al. ,25 there were generally mixed effects, but positive effects were noted in the control group (four studies of telephone counselling with or without additional intervention, all of mixed quality).
Other reviews27,29,30 reported mixed, inconclusive or non-significant results for mental health outcomes. No negative intervention effects were reported.
Carers of people with cancer
Improvement in psychological distress was reported in Regan et al. 35 after couples-based psychosocial help (seven studies; intervention vs. control or within groups from baseline; moderate to strong quality). Statistically significant pooled effects were reported for reductions in anxiety following art therapy in Lang and Lim33 (two studies of moderate quality) and in Northouse et al. 34 for distress and anxiety in the first 6 months after psychoeducation interventions, which then increased from small to moderate at beyond 6 months (16 studies, quality not reported). In the same review, a similar positive and statistically significant intervention effect was reported for improved self-efficacy (eight studies, quality not reported) and small, non-statistically significant intervention effects were recorded for depression (18 studies, quality not reported).
Carers of people with stroke
Interventions aiming to improve mental health for carers of people with stroke mainly included psychoeducation and/or counselling, social support and problem-solving, and information provision. There were generally no significant findings and/or the findings were inconsistent. 37–41 When reported, the overall quality of primary studies in these reviews was variable or fair. Legg et al. 41 reported a statistically significant reduction in depression following an intervention focusing on ‘teaching procedural knowledge’ (formal multidisciplinary training of caregiver in the prevention and management of common problems related to stroke) (one study of higher quality). In Forster et al. 40 there was a statistically significant reduction in depression in the active information provision intervention group (one study at some risk of bias).
Carers of people with various conditions at the end of life
Home palliative care and other multicomponent interventions were used to target mental health in carers of people with various conditions at the end of life. Gomes et al. 43 suggested that a reinforced version of home palliative care (comprising added brief psychoeducation delivered by care advisors) had a positive effect on carer distress (one study of lower quality). A meta-analysis in Candy et al. 42 showed reductions in psychological distress at the end of interventions comprising multiple components (eight studies; no evidence of statistical heterogeneity at I2 = 0%; low-quality evidence).
Carers of people with mental health problems
In Macleod et al. ,45 improvements were reported for depression following family interventions (one study, quality not reported), for mood following a mutual support intervention (one study, quality not reported), and for anxiety and distress following supportive family education (two studies, quality not reported); all interventions actively involved carers (e.g. through family education and mutual support assisted by mental health nurses). In addition, statistically significant effects were reported in Yesufu-Udechuku et al. 46 for psychological distress after 6 months’ follow-up of psychoeducation (one study of high quality) and up to 6 months’ follow-up after a support group intervention (one study of low quality). In the same review, problem-solving bibliotherapy [not defined by the review, but a definition can be found in Wikipedia47 (see Glossary)] was found to be effective in reducing psychological distress up to 6 months’ follow-up (one study of moderate quality).
There were no effects on somatic symptoms, anxiety, insomnia, social dysfunction or severe depression following an education intervention in Macleod et al. 45 (one study, quality not reported). Similarly, absence of intervention effect was reported in Yesufu-Udechuku et al. 46 for psychoeducation up to 6 months with or without support (three studies of low quality), and following a self-management intervention (one study of moderate quality) for psychological distress.
Burden and stress
Carer burden and stress was reported in 21 reviews (22 papers). 19–31,33,34,37,38,40,41,43,45,46
Burden and stress were not well-defined outcomes in most reviews, but various outcome measures were reported: the Zarit Burden Scale, the Caregiver Appraisal Inventory, the Caregiver Strain Index (CSI) and others. The measurement tools used in respect of burden were fairly consistent across the reviews. All results are reported in Table 5.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at | |
|---|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | ||||||||||
| Carers of people with dementia | ||||||||||
| Boots, 201419 | Internet-based interventions | Burden | 4/12 | Unclear | Narrative | Mixed results | Unclear | |||
| Stress and strain | 1/12 | Unclear | Narrative | Small significant reduction | Unclear | |||||
| Chien, 201120 | Support groups led by professionals or other trained group members | Burden | 24/30 | Unclear | Meta-analysis (Hedges’ g) | –0.23 | –0.33 to –0.13 | NR | Unclear | |
| 24/30 | Unclear | Meta-analysis (Hedges’ g) | In sensitivity analysis authors reported that effects persisted over time | Unclear | ||||||
| Eggenberger, 201321 | Communication skills | Burden | Unclear | Unclear | Narrative | No significant improvement of family caregiver burden, albeit one study reported a positive effect on burden | Unclear | |||
| Godwin, 201322 | Technology-driven multicomponent support: Caregiver’s Friend | Stress and strain | 1/8 | CSI | Narrative | Significantly reduced stress and strain | Unclear | |||
| ComputerLink | Stress and strain | 1/8 | CSI | Narrative | No overall reduction in strain but reductions were reported for relationship and emotional strain | Unclear | ||||
| Hurley, 201423 | Meditation-based interventions | Burden | 5/8 | Zarit Burden Interview (various versions); RMBC | Narrative | Three studies (including one RCT) found statistically significant reductions in levels of burden pre–post intervention; one study found a non-significant trend and one study found no difference in pre–post intervention levels. There were mixed results at follow-up | Unclear | |||
| Jensen, 201524 | Educational interventions aimed at teaching skills | Burden | 5/7 RCTs | Zarit Burden Scale | Meta-analysis (SMD) | –0.52 | –0.79 to –0.26 | < 0.0001 | Unclear | |
| Shorter intervention length | Burden | ?/7 | Zarit Burden Scale | Meta-analysis (SMD) | –0.86 | –1.24 to –0.47 | NR | Unclear | ||
| Longer intervention length | Burden | ?/7 | Zarit Burden Scale | Meta-analysis (SMD) | –0.36 | –0.60 to –0.13 | Unclear | Unclear | ||
| Lins, 201425 | Telephone counselling with or without additional intervention | Distress | 2/9 RCTs | Scale B of SCB; TCIAT | Narrative | Mixed results for telephone counselling without additional intervention (one RCT). No significant difference between groups following telephone counselling with video sessions and workbook (one RCT) | Unclear | |||
| Burden | 2/9 RCTs | CAI; subunits Upset and Annoyance from RMBC | Narrative | Results of telephone counselling combined with video sessions were not reported (one RCT). No difference between groups following telephone counselling combined with video sessions and workbook (one RCT); and telephone counselling without additional interventions (one RCT) showed reductions in both intervention and control groups (statistical significance not reported) | Unclear | |||||
| Telephone counselling without additional intervention | Burden | 4/9 RCTs (moderate quality) | Zarit Burden Interview; CAI; SCB; RMBC including subunits | Meta-analysis (SMD) | 0.45 | –0.01 to 0.90 | 0.005 | Unclear | ||
| Marim, 201326 | Interdisciplinary education and support programmes | Burden | 7/7 RCTs | Zarit Burden Interview | Meta-analysis (MD) | –1.79 | –4.27 to 0.69 | 0.16 | Unclear | |
| Sensitivity analysis – removal of heterogeneous RCTs | Burden | 4/7 | Zarit Burden Interview | Meta-analysis (MD) | –1.62 | –2.16 to –1.08 | < 0.00001 | Unclear | ||
| Maayan, 201427 | Respite care | Burden | 1/4 RCTs | Zarit Burden Scale | Meta-analysis (MD) | –5.51 | –12.38 to 1.36 | 0.12 | Unclear | |
| Respite care vs. polarity therapy | Stress | 1/4 RCTs | PSS | Meta-analysis (MD) | 5.80 | 1.43 to 10.17 | 0.0093 | Unclear | ||
| McKechnie, 201428 | Computer-mediated psychosocial interventions (complex multifaceted) | Stress and burden | 9/14 | RMBC | Narrative | Five medium-/high-quality studies found positive intervention effects. There were inconsistent findings across the remaining studies | Unclear | |||
| Orgeta, 201429 | Home-based supervised endurance or aerobic exercise; telephone-based exercise promotion; 12-week exercise programme | Perceived stress | 3/4 RCTs Involving two analyses of two RCTs |
PSS | Meta-analysis (SMD) | –0.18 –0.19 |
–0.45 to 0.08 –0.57 to 0.19 |
0.17 0.33 |
Unclear Unclear |
|
| Burden | 2/4 RCTs | SCB | Meta-analysis (SMD) | –0.43 | –0.81 to –0.04 | 0.03 | Unclear | |||
| Burden | 2/4 RCTs | SCB | Narrative | Two other meta-analyses using the same two RCTs for same outcome but using different tools (unclearly reported) found NS differences | Unclear | |||||
| Schoenmakers, 201030 | Active intervention in home care – psychosocial intervention | Burden | 6/26 | Zarit Burden Interview; Lawton Subjective Burden Instrument | Meta-analysis (MD) | –2.94 | –6.28 to 0.40 | 0.08 | Unclear | |
| Respite | Burden | 2/26 | Zarit Burden Interview; Lawton Subjective Burden Instrument | Meta-analysis (MD) | 0.30 | 0.12 to 0.48 | 0.001 | Unclear | ||
| Vernooij-Dassen, 201131 | Cognitive reframing (one element of CBT) | Burden | 3/11 RCTs | Zarit Burden Interview; Caregiver Strain instrument | Meta-analysis (SMD) | –0.14 | –0.32 to 0.03 | 0.12 | Unclear | |
| Stress or distress | 4/11 RCTs | Revised Burden Interview; PSS; investigator developed scales | Meta-analysis (SMD) | –0.24 | –0.40 to –0.07 | 0.0059 | Unclear | |||
| Stress | 3/11 RCTs | Revised memory and behaviour checklist | Meta-analysis (SMD) | –0.21 | –0.45 to 0.03 | 0.09 | Unclear | |||
| Carers of people with cancer | ||||||||||
| Lang, 201433 | Art-making class | Stress | 1/2 | Salivary cortisol | Narrative | Clinically effective in reducing stress among family caregivers. There was no statistically significant reduction in mean cortisol level; 0.089 (SD 0.05) to 0.087 (SD 0.06) | Unclear | |||
| Creative arts intervention | Stress | 1/2 | DABS | Narrative | A statistically significant reduction in stress in family caregivers from baseline 13.27 (SD 6.00) to post intervention 9.85 (SD 5.84; p = 0.001) | Unclear | ||||
| Northouse, 201034 | Psychoeducation; skills training; therapeutic counselling | Burden | 11/29 RCTs | NR | Meta-analysis (Hedges’ g) | 0.22 | 0.08 to 0.35 | < 0.001 | During 3 months post intervention | |
| Psychoeducation; skills training; therapeutic counselling | Burden | 5/29 | NR | Meta-analysis (Hedges’ g) | 0.10 | NR | NR | 3–6 months post intervention | ||
| Carers of people with stroke | ||||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual interventions Psychoeducation and counselling |
Burden | 6/18 | CBS; CSI | Narrative | Inconsistent findings were reported | Unclear | |||
| 6/18 | CBS; CSI | Narrative | Authors report similar results for subgroup analysis by intervention | Unclear | ||||||
| Psychosocial interventions (counselling and psychoeducation) | Burden | 5/18 | Various | Meta-analysis (SMD) | –0.04 | –0.25 to 0.17 | 0.70 | Immediately post intervention | ||
| 5/18 | Various | Meta-analysis (SMD) | Authors report similar results were found for subgroup analysis by intervention | Unclear | ||||||
| Forster, 201240 | Passive or active education | Burden | 3/21 RCTs | Various | Narrative | No evidence of effect for passive information compared with control (one UK RCT). Conflicting results were reported for active information interventions (two RCTs, one UK) | Unclear | |||
| Legg, 201141 | Non-pharmacological interventions including support and information; teaching procedural knowledge/vocational education, psychoeducation | Stress or strain | 1/8 RCTs | CSI | Narrative (SMD) | –8.67 | –11.39 to –6.04 | 0.001 | Unclear | |
| Global measures of stress or distress | 2/8 RCTs | GHQ-28 | Narrative | No significant differences | Unclear | |||||
| Support and information interventions | Global measures of stress or distress | 2/8 RCTs | CSI, author defined | Meta-analysis (SMD) | –0.29 | –0.86 to 0.27 | 0.11 | Unclear | ||
| Psychoeducational interventions | Stress or strain | 2/8 RCTs | Zarit Burden Inventory; Relatives’ Stress Index | Meta-analysis (SMD) | 0.01 | –0.34 to 0.36 | 0.94 | Unclear | ||
| Carers of people with various conditions at the end of life | ||||||||||
| Gomes, 201343 | Home palliative care vs. usual care | Pre-bereavement: burden | 3/23 | Montgomery–Borgatta Caregiver Burden Scale; Zarit Burden Inventory | Narrative | Conflicting results | Unclear | |||
| Reinforced vs. standard home palliative care | Caregiver burden | 3/23 | Caregiver Demand Scale; CSI; Zarit Burden Inventory | Narrative | Conflicting results | Unclear | ||||
| Carers of people with mental health problems | ||||||||||
| Macleod, 201145 | Support from community mental health nurses Education |
Burden | 5/68 | NR | Narrative | Mixed findings from studies evaluating education intervention | Unclear | |||
| Supportive family education | Burden | 6/68 | NR | Narrative | Mixed findings for supportive family education with five (four RCTs) studies reporting a decrease in burden and one RCT reporting no significant changes between groups | Unclear | ||||
| Behavioural family therapy | Burden | 6/68 | NR | Narrative | Reductions in carer burden was reported in six studies (three RCTs) for behavioural family therapy | Unclear | ||||
| Cognitive–behavioural family therapy | Burden | 6/68 | NR | Narrative | Mixed results were reported for cognitive–behavioural family therapy with five studies reporting no change in carer burden; one study reported a reduction in carer burden but low number of participants | Unclear | ||||
| Other family interventions | Burden | 8/68 | NR | Narrative | For other intervention approaches only one study out of eight reported improvements for carer burden | Unclear | ||||
| Community support services | Burden | 7/68 | NR | Narrative | Five of seven studies reported reduced burden as a result of assertive community treatment (two studies), clinical case management (one study), home counselling (one study) and multidisciplinary support (one study) | Unclear | ||||
| Mutual support groups | Burden | 2/68 | NR | Narrative | Improvements in burden were reported | Unclear | ||||
| Day-care services | Burden | 3/68 | NR | Narrative | Inconsistent findings | Unclear | ||||
| Supportive family educations | Stress | 1/68 | NR | Narrative | One RCT reported reduced stress for supportive family education | Unclear | ||||
| Yesufu-Udechuku, 201546 | Delivered by health and social care services: psychoeducation vs. postal psychoeducation | Family burden | 1/21 RCT (low quality) | NR | Meta-analysis (SMD) | –0.41 | –1.04 to 0.21 | NR | End of intervention | |
| 1/21 RCT (low quality) | NR | Meta-analysis (SMD) | –0.41 | –1.03 to 0.22 | NR | Up to 6-months’ follow-up | ||||
Carers of people with dementia
For carer burden, narrative syntheses showed statistically significant pre–post intervention reductions (although mixed results at follow-up) for meditation-based interventions in Hurley et al. 23 (three studies of seemingly low to moderate quality). Reductions in burden were found for both intervention and control groups in Lins et al. 25 following telephone counselling without additional intervention (one study at low to unclear risk of bias). Stress and burden were reduced following computer-mediated interventions in McKechnie et al. 28 (five medium- to high-quality studies out of nine in total; the remaining studies had inconsistent findings).
Quantitative syntheses similarly revealed positive intervention effects on carer burden. In Jensen et al. ,24 a moderate reduction was observed following education interventions (five studies; moderate statistical heterogeneity at I2 = 40%; moderate quality), with shorter interventions showing greater effect than longer interventions (no statistical heterogeneity at I2 = 0%). Physical activity was favoured over usual care in Orgeta and Miranda-Castillo29 (two studies; no statistical heterogeneity at I2 = 0%; unclear/low risk of bias). In Marim et al. ,26 education and support interventions were favoured over usual care, and the effect was statistically significant when four homogenous studies remained in the meta-analysis (low risk of bias). Mixed or inconsistent effects were reported for communication skills training interventions in Eggenberger et al. ,21 and for internet-based support interventions in Boots et al. 19 No intervention effects were reported for respite care in Maayan et al. ,27 for cognitive reframing interventions in Vernooij-Dassen et al. 31 or for psychosocial interventions in Schoenmakers et al. 30 An adverse intervention effect was noted for respite care with a statistically significant increase in carer burden in Schoenmakers et al. 30 (two studies; no statistical heterogeneity at I2 = 0%; quality not reported).
Other outcomes and results were reported. Decreases in carer stress were reported as a result of the control condition (polarity therapy) in Maayan et al. 27 (one study at largely unclear risk of bias), and stress or distress was reduced in Vernooij-Dassen et al. ,31 favouring multiple types of cognitive reframing interventions (four studies, all with some methodological limitations), although the analysis was driven by one large study. In Godwin et al. 22 (quality not reported), carer strain was significantly reduced following the Caregiver’s Friend intervention; a small significant decrease in stress and strain was also observed as a result of internet-based support in Boots et al. 19 (one study of moderate quality). In Chien et al. ,20 a statistically significant effect (outcome not explicitly defined) was reported as a result of carer support groups (24 studies; low statistical heterogeneity at I2 = 12.59%; moderate to high quality), and this appeared to be sustained over time (six studies). The remaining results for other outcomes were mixed or inconsistent.
Carers of people with cancer
In Lang and Lim,33 two types of art-based therapy resulted in clinically significant (one study) or statistically significant (one study) reductions in family carers’ stress from baseline (both studies were reported to be of moderate quality). Furthermore, in Northouse et al. ,34 a meta-analysis showed an overall small but significant decrease in carer burden following interventions comprising information or skills building, relationship management or self-care (11 studies, quality not reported), and this effect was sustained up to 6 months post intervention (five studies).
Carers of people with stroke
An intervention focusing on vocational training (teaching procedural knowledge) resulted in statistically significant reductions in stress or strain, compared with a control group, in Legg et al. 41 (one study, largely at low risk of bias). In the same review, no significant differences in global measures of stress, strain or distress were reported following interventions containing support and information or psychoeducational activities. Further absence of effect or inconsistent findings were noted for carer burden in Cheng et al. 37,38 in relation to psychoeducation and counselling or psychosocial interventions, or from information giving (passive or active) in Forster et al. 40
Carers of people with various conditions at the end of life
Conflicting results for carer burden were observed in Gomes et al. 43 comparing home palliative care with usual care (three studies) or reinforced home palliative care (comprising added brief psychoeducation delivered by care advisors) versus standard home palliative care (three studies).
Carers of people with mental health problems
In Macleod et al. ,45 carer burden was reduced following behavioural family therapy (six studies), community support services comprising assertive community treatment (two studies), clinical case management (one study), home counselling (one study), multidisciplinary support (one study) and mutual support groups (two studies). In the same review, mixed or inconsistent findings for carer burden were reported following cognitive–behavioural family therapy (five studies), education interventions (five studies), day-care services (three studies) and supportive family education (six studies); however, supportive family education was associated with reduced carer stress (one study). The quality of primary studies appeared to have been assessed, but the results of this were not reported in this review. There were no statistically significant differences between practitioner-delivered and postal psychoeducation from one study in Yesufu-Udechuku et al. 46
Coping
Coping outcomes for carers were reported in nine reviews. 19,27,31,32,34,35,42,43,45 Definitions of coping (when reported) varied. These included coping skills; strategies (including problem-solving and reduction of ineffective coping such as avoidance and denial); caregiving competence; perceived affective and confidant support; ability to achieve previously set objectives; confidence in caregiving skills; and control of worry, loneliness and reliance on support systems. Some outcome measures were reported, including the Caregiver Burden Index, the CSI and the subscale of the Duke UC Functional Support Questionnaire. All results are reported in Table 6.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| Boots, 201419 | Internet-based interventions | Ability to achieve previously set objectives | 1/12 | Unclear | Narrative | Small significant improvement | Unclear | ||
| Coping skills | 1/12 | Unclear | Narrative | No intervention effect | Unclear | ||||
| Coping skills | 2/12 | Interviews and focus groups | Narrative (qualitative) | Positive effects | |||||
| Confidence in caregiving skills | 3/12 | Interviews and focus groups | Narrative (qualitative) | Positive effects | Unclear | ||||
| Maayan, 201427 | Interventions providing respite care Respite vs. no respite |
Perceived affective support | 1/4 | Subscale of Duke UC Functional Support Questionnaire | Meta-analysis (MD) | –0.44 | –2.85 to 1.97 | 0.72 | Unclear |
| Perceived confidant support | 1/4 | Subscale of Duke UC Functional Support Questionnaire | Met-analysis (MD) | 1.30 | –1.04 to 3.64 | 0.28 | Unclear | ||
| Smith, 201432 | Volunteer mentoring (befriending, mentoring and peer support): telephone peer support | Coping | 1/4 | NR | Narrative (using qualitative data) | An ‘increase in coping skills and caregiving competence and a decrease in loneliness and reliance on other forms of social support’. Unclear whether this applies to all carers (study included stroke carers as well as dementia) or just to dementia. Carers also reported as receiving emotional support for peer supporters | Unclear | ||
| Vernooij-Dassen, 201131 | Cognitive reframing (one element of CBT) | Coping/self-efficacy | 4/11 RCTs | Ways of Coping Checklist-Revised; Ways of Coping; Caregiving Competence (Pearlin) | Meta-analysis (SMD) | 0.64 | –0.17 to 1.45 | 0.12 | Unclear |
| Carers of people with cancer | |||||||||
| Northouse, 201034 | Psychoeducational interventions | Coping strategies | 10/29 | NR | Meta-analysis (Hedges’ g) | 0.47 | 0.16 to 0.78 | 0.001 | First 3 months post intervention |
| Coping strategies | 4/29 | NR | Meta-analysis (Hedges’ g) | 0.20 | 0.02 to 0.38 | < 0.05 | Between 3 and 6 months | ||
| Coping strategies | 2/29 | NR | Meta-analysis (Hedges’ g) | 0.35 | 0.10 to 0.58 | < 0.05 | Beyond 6 months | ||
| Regan, 201235 | Couples-based psychosocial interventions | Couple communication | 2/23 | Qualitative interviews and SSQ (undefined) | Narrative | Both reported greater improvements for intervention patients and partners than control patients and partners | Immediately following intervention | ||
| Couple communication | 1/23 | SSQ (undefined) | Narrative | Sustained improvements for intervention partners compared with control partners | Final follow-up (undefined) | ||||
| Carers of people with stroke | |||||||||
| No reviews | |||||||||
| Carers of people with various conditions at the end of life | |||||||||
| Candy, 201142 | Usual care plus direct interventions for carers | Coping with the caring role | 7/11 | CBI; CSI | Meta-analysis (SMD) | –0.05 | –0.24 to 0.14 | 0.59 | End of intervention |
| Gomes, 201343 | Home palliative care: reinforced vs. standard home palliative care | Coping | 2/23 | NR | Narrative | No statistically significant differences | Unclear | ||
| Carers of people with mental health problems | |||||||||
| Macleod, 201145 | Support from community mental health nurses Family interventions |
Coping | 7/68 | NR | Narrative | Conflicting findings | Unclear | ||
| Mutual support groups | Coping | 2/68 | NR | Narrative | Improvements reported | Unclear | |||
| Community support services | Coping | 1/68 | Reported as ‘non-validated outcome measure’ | Narrative | Improvements reported | Unclear | |||
Carers of people with dementia
In Boots et al. ,19 a small improvement in the ability to achieve previously set objectives was reported (one study of low quality), together with positive effects in coping skills (two studies of low quality) and confidence in caregiving skills (three studies of low quality). Smith and Greenwood32 reported that one qualitative study (seemingly of moderate quality) of telephone peer support showed an increase in coping skills and caregiving competence, together with reduced loneliness and reliance on other forms of social support. It was unclear if the latter results applied only to carers of people with dementia.
Reviews conducted by Maayan et al. 27 on respite care and by Vernooij-Dassen et al. 31 on cognitive reframing reported no significant intervention effects on coping outcomes.
Carers of people with cancer
Moderate and statistically significant intervention effects on coping strategies were reported up to and beyond 6 months after psychoeducation in Northouse et al. 34 (10 studies, quality not reported). Greater improvements in communication between couples were reported following couples-based psychosocial interventions in Regan et al. 35 (two studies of moderate to strong quality).
Carers of people with stroke
No reviews were identified that focused on coping outcomes for carers of people with stroke.
Carers of people with various conditions at the end of life
Two studies in Gomes et al. ,43 focusing on reinforced versus standard home palliative care, and seven studies in Candy et al. ,42 looking at multicomponent education and support, failed to show statistically significant intervention effects on carer coping.
Carers of people with mental health problems
Conflicting results for carer coping were reported in Macleod et al. 45 in respect of family interventions, with improvements following behavioural family therapy (two studies) and an intervention based on Atkinson and Coia’s framework (comprising 20 hours of education, communication, problem-solving and stress coping) (one study) and four studies showing no change. Improvements in coping were reported for mutual support groups (two studies) and receipt of community support services (one study). The quality of primary studies was not reported in this review.
Satisfaction
Satisfaction with the intervention was reported in eight reviews (nine papers). 21,25,37–41,43,46 The outcome was rarely defined further. Several outcome measures were reported; some of them related to carer satisfaction in general. All results are reported in Table 7.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| Eggenberger, 201321 | Communication skills training | Satisfaction | 1/12 | Unclear | Narrative | Almost 100% caregiver satisfaction with the intervention, the most pertinent feedback being that caregivers wished that they had received the intervention at a far earlier stage of their relatives’ illness trajectory | Unclear | ||
| Lins, 201425 | Telephone counselling with or without additional intervention | Satisfaction | 2/9 RCTs | Unclear | Narrative | Results of telephone counselling without additional intervention not reported by one primary study. A significant decrease in carer satisfaction reported over time in both groups following telephone counselling combined with video sessions (one study) | Unclear | ||
| Evaluation of experience | 2/2 | Qualitative data | Narrative | Telephone counselling meets the important needs of carers (16 descriptive themes) | Unclear | ||||
| Carers of people with cancer | |||||||||
| No reviews | |||||||||
| Carers of people with stroke | |||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual interventions: psychoeducation, counselling or support compared with usual care | Intervention satisfaction | 3/18 | Various | Narrative | Caregivers were generally more satisfied than those in usual care group | Unclear | ||
| Ellis, 201039 | Stroke liaison workers | Carer satisfaction | Various/16 | Questionnaire | Narrative | Conflicting findings with 15 questions resulting in four analyses reporting significant effects in favour of intervention (1–3 RCTs). Most of the results were based on a varying number of RCTs from 2 to 15 for each outcome | Unclear | ||
| Forster, 201240 | Passive or active education: active intervention of information about recovery and rehabilitations | Carer satisfaction | 2/21 RCTs | Various stroke scales and questionnaires (unspecified) | Meta-analysis (OR) | 1.78 | 0.88 to 3.60 | 0.11 | Unclear |
| Information about allowances and services (passive and active) | Carer satisfaction | 3/21 RCTs | Various, including Pound Scale | Meta-analysis (OR) | 1.30 | 0.71 to 2.37 | 0.39 | Unclear | |
| Passive education about allowances and services | Carer satisfaction | 1/21 RCTs | Unvalidated questionnaire | Meta-analysis (OR) | 0.61 | 0.16 to 2.23 | 0.46 | Unclear | |
| Active education about allowances and services | Carer satisfaction | 2/21 | Stroke scales (unspecified) | Meta-analysis (OR) | 1.59 | 0.81 to 3.13 | 0.18 | Unclear | |
| Legg, 201141 | Non-pharmacological interventions | Intervention satisfaction | 1/8 RCTs | Caregiver Satisfaction Questionnaire | Narrative | Attempts made to assess satisfaction with characteristics of the intervention but no comparison was made between study groups | Unclear | ||
| Carers of people with various conditions at the end of life | |||||||||
| Gomes, 201343 | Home palliative care vs. usual care | Pre bereavement: satisfaction with interventions – caregiver view on place of death | 2/23 | NR | Narrative | Conflicting results | Unclear | ||
| Home palliative care vs. usual care | Post bereavement: satisfaction with care | 6/23 | Various including FAMCARE | Narrative | Conflicting results | Unclear | |||
| Reinforced vs. standard home palliative care | Satisfaction with care | 1/23 | NR | Narrative | Limited evidence of no statistically significant difference | Unclear | |||
| Carers of people with mental health problems | |||||||||
| Yesufu-Udechuku, 201546 | Psychoeducation interventions delivered by health and social care services vs. control | Satisfaction with services | 1/21 | Consumer Satisfaction Questionnaire | Meta-analysis (SMD) | –0.42 | –1.06 to 0.22 | NR | End of intervention |
| Psychoeducation interventions delivered by health and social care services vs. control | Satisfaction with services | 1/21 | Consumer Satisfaction Questionnaire | Meta-analysis (SMD) | –0.41 | –1.04 to 0.23 | NR | Up to 6 months’ follow-up | |
Carers of people with dementia
In Eggenberger et al. 21 there was almost complete satisfaction among carers receiving communication skills training (one study at some risk of bias). There were conflicting results using different measures in Lins et al. ;25 decreases in carer satisfaction were reported in both intervention and comparator groups following telephone counselling with or without additional intervention (one study at some risk of bias). In the same review, descriptive themes derived from qualitative data (largely based on one study of moderate quality) suggested that telephone counselling adequately met the important needs of carers.
Carers of people with cancer
No reviews were identified that examined satisfaction with the intervention in carers of people with cancer.
Carers of people with stroke
In their study of carers of people with stroke, Cheng et al. 37,38 found that carers receiving psychoeducation, counselling or support were generally more satisfied with the interventions than those receiving usual care (three studies; two appeared to be of moderate quality and the quality of the other was unclear). No statistically significant differences were found in Forster et al. 40 for carer satisfaction with information about recovery and rehabilitation (two studies), or for information about allowances and services (three studies). Conflicting findings about satisfaction with stroke liaison workers were reported in Ellis et al. ,39 and there were no comparative results on satisfaction with multicomponent non-pharmacological interventions in Legg et al. 41
Carers of people with various conditions at the end of life
Conflicting results about satisfaction with home palliative care versus usual care were reported in Gomes et al. 43 at the pre- or post-bereavement stages (2–6 studies). In the same review, no statistically significant difference in carer satisfaction was reported in one study when home palliative care was compared with the reinforced version (comprising added brief psychoeducation delivered by care advisors).
Carers of people with mental health problems
In Yesufu-Udechuku et al. ,46 no statistically significant differences were reported for carer satisfaction with psychoeducation versus control at any time up to 6 months’ follow-up (one study of low quality).
Well-being and quality of life
Twenty reviews (21 papers)19,22,24,25,27,28,31,33–46 reported on aspects related to carer well-being and quality of life. In addition to the general terms of well-being and quality of life, various others were used to describe this outcome. These included social isolation, social support needs, caregiving experience, sleep quality, marital–family relationships, social functioning and ability to perform activities of daily living. Many different outcome measures were reported. All results are reported in Table 8.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| Boots, 201419 | Internet-based interventions | QoL | 1/12 | Unclear | Narrative | No intervention effect | Unclear | ||
| Social isolation | 1/12 | Unclear | Narrative | No intervention effect | Unclear | ||||
| Social isolation | 1/12 | Qualitative interviews and focus groups | Narrative | Positive intervention effect | Unclear | ||||
| Godwin, 201322 | Technology-driven support – multicomponent (using computer or web-based applications) Caregiver’s Friend |
Social support | 1/8 | Revised ways of coping social subscale | Narrative | Improvement in intention to get social support | Unclear | ||
| ComputerLink | Social support | 2/8 | IEFSS (social isolation) | Narrative | No significant changes in social isolation | Unclear | |||
| REACH | Social support | 2/8 | RSS | Narrative | Mixed results | Unclear | |||
| Jensen, 201524 | Educational interventions aimed at teaching skills relevant to dementia caring | QoL | 4/7 RCTs | SF-36 and WHO-QOL-BREF subdomains | Narrative | Significant effect on ‘emotional role’ subdomain (two RCTs); two RCTs did not measure this. Significant effects on physical role and functioning, general health, vitality and bodily pain subdomains (one RCT). No effect on physical subdomain (two RCTs); one RCT did not report on this. Non-significant trends towards effect on social subdomain (two RCTs). No effect for any study on psychological or environmental subdomains. No overall effect of QoL possible | Unclear | ||
| Lins, 201425 | Telephone counselling with or without additional intervention | QoL | 1/9 | SF-36 general health | Narrative | Authors reported a non-significant reduction in QoL in both intervention (telephone counselling without additional intervention) and control groups | After 12 months | ||
| Social support | 2/9 | Caregiver Social Support scale; ISSB; MSPSS | Meta-analysis (SMD) | 0.25 | –0.24 to 0.73 | 0.32 | One study at 6 months; one at 12 months | ||
| Maayan, 201427 | Respite care vs. polarity therapy | Mental component of QoL | 1/4 RCTs | SF-36 Mental component summary score | Meta-analysis (MD) | –0.90 | –6.35 to 4.55 | 0.75 | Unclear |
| Physical component of QoL | 1/4 RCTs | SF-36 Physical component summary score | Meta-analysis (MD) | –4.50 | –9.96 to 0.69 | 0.089 | Unclear | ||
| QoL | 1/4 RCTs | QoL-AD | Meta-analysis (MD) | –1.80 | –5.74 to 2.14 | 0.37 | 8 weeks’ follow-up | ||
| Quality of sleep | 1/4 RCTs | Pittsburgh Sleep Quality Index | Meta-analysis (MD) | 1.70 | –0.55 to 3.95 | 0.14 | Unclear | ||
| McKechnie, 201428 | Computer-mediated psychosocial (complex and multifaceted) | Social support | 3/14 | ISSB; MSPSS; Revised UCLA Loneliness Scale; Family and Friendship Contacts Scale | Narrative | Inconsistent findings | Unclear | ||
| Computer-mediated psychosocial (complex and multifaceted) | Positive aspects of caring | 2/14 | Positive aspects of Caregiving; Stress-related Growth Scale | Narrative | Inconsistent findings | Unclear | |||
| Vernooij-Dassen, 201131 | Cognitive reframing (one element of CBT) | QoL | – | – | Narrative | Although several instruments have been developed to assess quality of life, these measures were not used in the included studies | – | ||
| Carers of people with cancer | |||||||||
| Lang, 201433 | Art-making class; creative arts | Emotional level | 1/2 | DABS | Narrative | A statistically significant increase (p < 0.01) in the post evaluation family caregiver emotional mean score of 151.42 (SD 24.05) over the pre-evaluation score of 139.55 (SD 19.09) | Unclear | ||
| Northouse, 201034 | Psychoeducation; skills training; therapeutic counselling | Caregiving benefit | 5/29 | NR | Meta-analysis (Hedges’ g) | 0.17 | NR | NS | Up to 3 months post intervention |
| 2/29 | NR | Meta-analysis (Hedges’ g) | 0.31 | 0.02 to 0.61 | < 0.05 | 3–6 months post intervention | |||
| 1/29 | Meta-analysis (Hedges’ g) | 0.48 | NS | Over 6 months | |||||
| Marital–family relationships | 10/29 | NR | Meta-analysis (Hedges’ g) | 0.20 | 0.02 to 0.38 | < 0.05 | Up to 3 months post intervention | ||
| 8/29 | NR | Meta-analysis (Hedges’ g) | 0.13 | NR | NS | 3–6 months post intervention | |||
| 5/29 | NR | Meta-analysis (Hedges’ g) | –0.04 | NR | NS | Over 6 months | |||
| Social functioning | 4/29 | NR | Meta-analysis (Hedges’ g) | –0.14 | NR | NS | Up to 3 months post intervention | ||
| 6/29 | NR | Meta-analysis (Hedges’ g) | 0.12 | NR | NS | 3–6 months post intervention | |||
| 2/29 | NR | Meta-analysis (Hedges’ g) | 0.39 | 0.03 to 0.74 | Reported as significant | Over 6 months | |||
| Regan, 201235 | Couples-based psychosocial interventions: FOCUS (involving families in coping skills and uncertainty reduction) | QoL impact on physical and emotional functioning | 4/23 | Partner QoL using FACT-G; FACT-B; SF-36; QoL SP; IIRS | Narrative | Weak to moderate improvement | Immediately after intervention | ||
| 2/23 | Partner QoL using FACT-G; FACT-B; SF-36; QoL SP; IIRS | Narrative | Weak to moderate improvement | 6 and 12 months’ follow-up | |||||
| Interventions aimed at couples focusing on counselling therapy | Relationship functioning | 4/23 | CARES, QMI, RDAS, 0–10 scale (undefined) | Narrative | Greater improvements for intervention partners than for control partners | Immediately following intervention | |||
| 4/23 | CARES, QMI, RDAS, 0–10 scale (undefined) | Narrative | Greater improvements for intervention partners than for control partners at the final follow-up point | Final follow-up (undefined) | |||||
| Waldron, 201336 | Psychosocial interventions based on cognitive–behavioural approach | QoL | 4/6 RCTs | Quality of life: CQoLI; FACT scale (version 3); SF-36 Combined POMS-SF and CSI |
Narrative | Conflicting findings: effect sizes ranged from nil to small (0.048 to 0.271). Two studies showed no effects of the intervention and two showed a small effect. Studies with larger effect sizes resulted from interventions focused on problem-solving and communication skills | Unclear | ||
| Carers of people with stroke | |||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual interventions Social problem-solving |
QoL (physical domain) | 1/18 | SF-36 | Narrative | There ‘appears’ to be no significant differences | Unclear | ||
| Social problem-solving | QoL (social domain) | 1/18 | SF-36 | Narrative | No significant differences | Unclear | |||
| Counselling, psychoeducation, social support | Social functioning | 4/18 | Various | Narrative | Conflicting results | Unclear | |||
| Psychoeducation and counselling | QoL (physical domain) | 4/18 | Various | Meta-analysis (SMD) | –0.14 | –0.36 to 0.08 | 0.21 | Immediately post intervention | |
| 2/18 | Various | Meta-analysis (SMD) | –0.10 | –3.35 to 0.16 | 0.46 | 6–11 months post intervention | |||
| QoL (psychological domain) | 4/18 | Various | Meta-analysis (SMD) | –0.17 | –0.39 to 0.05 | 0.12 | Immediately post intervention | ||
| 2/18 | Various | Meta-analysis (SMD) | –0.07 | –0.32 to 0.18 | 0.60 | 6–11 months post intervention | |||
| QoL (social domain) | 3/18 | Various | Meta-analysis (SMD) | 0.02 | –0.22 to 0.27 | 0.85 | Immediately post intervention | ||
| 2/18 | Various | Meta-analysis (SMD) | 0.07 | –0.58 to 0.71 | 0.84 | 6–11 months post intervention | |||
| Counselling | Family functioning | 2/18 | Various | Meta-analysis (SMD) | –0.12 | –0.23 to –0.01 | 0.03 | Immediately post intervention (but differences in dose and duration noted) | |
| Psychoeducation and counselling | Social functioning | 3/18 | SF-36 | Meta-analysis (SMD) | 0.02 | –0.22 to 0.27 | 0.85 | Immediately post intervention | |
| Ellis, 201039 | Stroke liaison workers | Carer extended activities of daily living | 5/16 RCTs | Various | Meta-analysis (SMD) | –0.13 | –0.28 to 0.01 | 0.07 | Unclear |
| Forster, 201240 | Passive or active education | Social activities | 2/21 RCTs | Various | Narrative | No significant differences for active interventions compared with controls. No data reported | Unclear | ||
| Passive interventions | Perceived health status | 1/21 RCTs | Various | Narrative | No significant differences were reported. No data reported | Unclear | |||
| Active interventions | Perceived health status | 3/21 RCTs | Various | Narrative | Conflicting results. Data not reported | Unclear | |||
| Legg, 201141 | Non-pharmacological interventions: teaching procedural knowledge | Health-related QoL | 1/8 RCT | EuroQol; SF-36 | Narrative (MD) | –11.97 | –15.59 to –8.35 | < 0.001 | Unclear |
| Support and information | Health-related QoL | 2/8 RCTs | EuroQol; SF-36 | Narrative | Inconsistent findings | Unclear | |||
| Carers of people with various conditions at the end of life | |||||||||
| Candy, 201142 | Usual care plus direct interventions | QoL | 6/11 RCTs | CQoLI – Cancer; one unidentified questionnaire to assess well-being | Meta-analysis (SMD) | 0.08 | –0.11 to 0.26 | 0.42 | End of intervention |
| Gomes, 201343 | Home palliative care vs. usual care | Pre bereavement: social well-being | 3/23 | SF-36 subscales; CES-D subscales; PGC Morale Scale | Narrative | Inconclusive evidence | Unclear | ||
| Reinforced vs. standard home palliative care | QoL | 2/23 | CQoLI – Cancer | Narrative | Conflicting results | Unclear | |||
| Nevis, 201444 | Educational interventions Patient and caregiver education/communication vs. usual palliative care |
QoL | 1/6 RCTs | City of Hope QoL; CQoLI – Cancer | Narrative (MD) | –0.16 | –0.30 to –0.02 | 0.02 | Unclear |
| Education intervention: problem-solving training and therapy (coping skills) vs. usual hospice care | QoL | 1/6 RCTs | City of Hope QoL; CQoLI – Cancer | Narrative (MD) | –0.87 | –1.24 to –0.50 | 0.03 | Unclear | |
| Carers of people with mental health problems | |||||||||
| Macleod, 201145 | Support from community mental health nurses | Well-being | 1/68 | NR | Narrative | Improvements in well-being following an individual family intervention | Unclear | ||
| Yesufu-Udechuku 201546 | Interventions delivered by health and social care services: psychoeducation | Experience of caregiving | 8/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –1.03 | –1.69 to –0.36 | Reported as significant | End of intervention |
| 4/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.92 | –1.51 to –0.32 | Reported as significant | Up to 6-months’ follow-up | |||
| 3/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –1.29 | –2.4 to –0.18 | NR | Over 6 months | |||
| Support groups | Experience of caregiving | 3/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –1.16 | –1.96 to –0.36 | NR | End of intervention | |
| 3/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.67 | –0.99 to –0.35 | Reported as significant | Up to 6-months’ follow-up | |||
| 2/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –1.95 | –4.22 to 0.31 | NR | Over 6-months’ follow-up | |||
| Psychoeducation and support | Experience of caregiving | 1/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.5 | –0.61 to 0.51 | NR | Over 6-months’ follow-up | |
| Problem-solving bibliotherapy | Experience of caregiving | 1/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.17 | –2.45 to 2.11 | NR | End of intervention | |
| 1/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –1.09 | –2.52 to 0.34 | NR | Up to 6-months’ follow-up | |||
| Self-management | Experience of caregiving | 1/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.19 | –0.58 to 0.2 | NR | End of intervention | |
| Enhanced psychoeducation vs. standard psychoeducation | Experience of caregiving | 1/21 RCTs | ECI; FBIS; SBAS; Family Burden Questionnaire; Zarit Caregiver Burden Scale | Meta-analysis (SMD) | –0.64 | –1.25 to –0.03 | NR | End of intervention | |
| Enhanced psychoeducation vs. standard psychoeducation | QoL | 1/21 RCTs | SF-36 | Meta-analysis (SMD) | –0.31 | –0.93 to 0.31 | NR | End of intervention | |
| Problem-solving bibliotherapy | QoL | 1/21 RCTs | SF-36 | Meta-analysis (SMD) | –0.14 | –0.5 to 0.23 | NR | End of intervention | |
| 1/21 RCTs | SF-36 | Meta-analysis (SMD) | –0.5 | –0.87 to –0.12 | NR | Up to 6-months’ follow-up | |||
Carers of people with dementia
For quality of life, reviews (narrative and quantitative syntheses) generally reported conflicting or non-significant intervention effects. The interventions contained within these reviews included internet-based support in Boots et al. 19 and respite care in Maayan et al. 27 In Lins et al. 25 there were non-significant reductions in quality of life for both intervention (telephone counselling with or without additional intervention) and control groups after 12 months (one study at some risk of bias). In Jensen et al. 24 it was not possible to estimate the overall effect on quality of life and in Vernooij-Dassen et al. 31 the results were not reported (despite intentions to measure this outcome).
Mixed effects on social isolation were reported following the receipt of internet-based support interventions in Boots et al. 19 (two studies). In Godwin et al. ,22 there were no significant changes in social isolation following the ComputerLink intervention (a computer network involving information, communication and decision support) (two studies). In the same review, intention to seek social support was increased as a result of the Caregiver’s Friend intervention (one study, quality not reported); and there were mixed results for the REACH intervention (two studies). A non-statistically significant increase in social support reported by the carer was observed following telephone counselling without additional intervention in Lins et al. 25 (two studies; no statistical heterogeneity at I2 = 0%; low quality), whereas inconsistent findings for this outcome were found following computer-mediated psychosocial interventions (three studies) in McKechnie et al. 28 In this review, there were also mixed effects for caregiving experience (two studies). Respite care interventions did not show any statistically significant effect on sleep quality in one study from Maayan et al. 27
Carers of people with cancer
Some small improvements in carer quality of life were reported in Waldron et al. 36 following psychosocial interventions based on problem-solving and communication skills (two studies of good quality), and mixed effects were reported in Regan et al. 35 up to 12 months after receipt of the FOCUS intervention (four studies). However, in Regan et al. 35 greater improvements in relationship functioning were reported for couples after couples-based counselling therapy (five studies of moderate to strong quality). A statistically significant increase in carers’ ‘emotional level’ (mean score measured by the Derogatis Affects Balance Scale) was reported as a result of art-based therapy in Lang and Lim33 (one study of moderate quality). In Northouse et al. ,34 psychoeducation interventions resulted in small statistically significant effects for caregiving benefit (defined as personal growth, rewarding experience, investment and self-esteem) during the first 3–6 months (two studies), and for marital–family relationships during the first 3 months post intervention (10 studies). Statistical significance was not sustained in the longer term for either of these outcomes. In the same review, social functioning was improved beyond 6 months post intervention (two studies), despite non-statistically significant improvements recorded at earlier time points. The quality of primary studies was not reported in this review.
Carers of people with stroke
Significant positive effects were recorded for health-related quality of life following an intervention based on teaching procedural knowledge in Legg et al. 41 (one study at low risk of bias), and for family functioning after counselling versus no treatment in Cheng et al. 37,38 (two studies seemingly of moderate quality).
Most other results indicated no significant differences or inconsistent findings for outcomes in relation to well-being and quality of life in carers of people with stroke. In Cheng et al. ,37,38 the results from narrative and quantitative syntheses showed largely non-significant differences in relation to the effects of social problem-solving, counselling, psychoeducation and social support groups on the physical, social and psychological domains of quality of life (number of studies in each analysis ranged from one to four across narrative and quantitative syntheses), and for social functioning (three studies in quantitative synthesis; four studies in narrative synthesis). In Forster et al. ,40 active and passive education interventions showed no significant differences or mixed effects on carers’ engagement in social activities (two studies) and carers’ perceived health status (four studies). In Ellis et al. ,39 there were no significant differences between interventions involving stroke liaison workers and control in relation to carers’ participation in extended activities of daily living (five studies).
Carers of people with various conditions at the end of life
There were statistically significant positive effects on quality of life from education interventions (one study with serious risk of bias) and from problem-solving training and therapy versus usual care (one study with serious risk of bias) in Nevis. 44 Gomes et al. 43 reported inconclusive evidence for social well-being after home palliative care versus usual care (three studies); and conflicting findings for quality of life after reinforced versus standard home palliative care (two studies). Marginal, non-statistically significant intervention effects on quality of life were reported in Candy et al. 42 as a result of multicomponent support interventions (six studies).
Carers of people with mental health problems
Individualised family interventions were associated with improved carer well-being in Macleod et al. 45 (one study, no quality reported). In Yesufu-Udechuku et al. ,46 experience of caregiving was significantly improved following psychoeducation, in different patient groups (schizophrenia and psychosis), and up to and beyond 6 months’ follow-up (between one and eight studies were included in the analyses; high statistical heterogeneity at I2 = 89%; very low quality). In the same review, the effects were also statistically significant for the positive effect of support groups on caregiving experience at the end of the intervention (three studies; high statistical heterogeneity at I2 = 85%; very low quality) and at up to 6 months’ follow-up (three studies; no statistical heterogeneity at I2 = 0%; low quality), and for enhanced psychoeducation versus standard psychoeducation in carers of patients with bipolar disorder (one study of moderate quality). There were no statistically significant differences for caregiving experience following psychoeducation plus support (one study), problem-solving bibliotherapy (one study) or a self-management intervention (one study). Yesufu-Udechuku et al. 46 also reported no significant effects on quality of life following psychoeducation (one study) or problem-solving bibliotherapy (one study).
Ability and knowledge
Carers’ ability and knowledge was reported in nine reviews (10 papers). 19,21,28,34,37,38,40,43,45,46 When reported, more detailed author definitions of this outcome included the carers’ sense of competence or mastery, decision-making confidence, knowledge of the disease and caring, information needs and learning new skills. Various outcome measures were reported, including the Caregiver Demand Scale, Lawton Positivity Questionnaire and Preparedness for Caregiving Scale. All results are reported in Table 9.
| First author, year of publication | Type of interventions | Outcome | n/N | Measures used | Synthesis approach (summary statistic) | Meta-analysis results | 95% CI | p-value | Outcome calculated at |
|---|---|---|---|---|---|---|---|---|---|
| Or summary of narrative synthesis | |||||||||
| Carers of people with dementia | |||||||||
| Boots, 201419 | Internet-based interventions | Sense of competence | 1/12 | Unclear | Narrative | Small significant improvement | Unclear | ||
| Decision-making confidence | 1/12 | Unclear | Narrative | Small significant improvement. | Unclear | ||||
| Knowledge of disease and caring | 3/12 | Interviews and focus groups | Narrative | Positive effects | Unclear | ||||
| Eggenberger, 201321 | Communication skills training | Knowledge and competencies | 3/12 | Unclear | Narrative | Significant effects on family caregivers’ knowledge and competencies, especially concerning awareness of communication problems and communication strategies Unclear from text if this finding is separate from studies reported below |
Unclear | ||
| Ability to deal with challenging behaviours | 1/12 | Unclear | Narrative | The RCT explicitly focused on training consultants to train family caregivers and showed a ‘significant decrease in frequency (57%), severity of (52%), and reactivity to challenging behaviour (62%; p < 0.001)’ | Unclear | ||||
| Reports of communication problems and problem behaviours | 1/12 | Unclear | Narrative | Family caregivers’ reports of communication problems significantly decreased, whereas the reports of problem behaviours remained stable [F(1.39) = 10.2; p < 0.003] | Unclear | ||||
| McKechnie, 201428 | Computer-mediated psychosocial (complex multifaceted) | Programme impact | 6/14 | Various non-standardised measures | Narrative | Five of six studies reported positive intervention effects | Unclear | ||
| Carers of people with cancer | |||||||||
| Northouse, 201034 | Psychoeducation; skills training; therapeutic counselling | Information needs | 3/29 RCTs | NR | Meta-analysis (Hedges’ g) | 1.36 | 0.92 to 1.77 | < 0.001 | First 3 months post intervention |
| Carers of people with stroke | |||||||||
| Cheng, 2012,37 201438 | Psychosocial, group and individual: psychoeducation | Caregiver competency | 3/18 | Various | Narrative | Interventions had a significant effect on caregiver competency, but dose of interventions was unclear | Unclear | ||
| 3/18 | Various | Meta-analysis (SMD) | 0.10 | –0.32 to 0.52 | 0.65 | Unclear | |||
| Forster, 201240 | Passive or active education | Knowledge | 2/21 RCTs | Various | Narrative | No significant differences between groups | Unclear | ||
| 4/21 RCTs | Various | Meta-analysis (SMD) | 0.74 | 0.06 to 1.43 | 0.03 | Unclear | |||
| NS differences in meta-analysis for passive or active interventions | Unclear | ||||||||
| Carers of people with various conditions at the end of life | |||||||||
| Gomes, 201343 | Home palliative care vs. usual care | Pre-bereavement outcomes: learning new caregiving skills | 1/23 | Lawton Positivity Questionnaire | Narrative | Moderate evidence of no statistically significant difference | Unclear | ||
| Reinforced vs. standard home palliative care | Sense of mastery | 2/23 | General Caregiver; CDS; Preparedness for Caregiving scale | Narrative | Moderate evidence showed no statistically significant difference | Unclear | |||
| Carers of people with mental health problems | |||||||||
| Macleod, 201145 | Support from community mental health nurses: education | Knowledge | 10/68 | NR | Narrative | Mixed findings for an education intervention with one study reporting no knowledge gain and nine studies reporting improved knowledge | Unclear | ||
| Supportive family education | Knowledge | 6/68 | NR | Narrative | Mixed findings with five studies reporting an improvement in knowledge and one study reporting no significant differences | Unclear | |||
| Family interventions | Knowledge | 8/68 | NR | Narrative | Knowledge gains that were maintained for behavioural family therapy (four studies), cognitive–behavioural family therapy (one study); group psychoeducation (one study), psychosocial intervention (one study) and a culturally modified family intervention (one study) | Up to 1 year | |||
| Community support services (integrated community treatment programme) compared with standard care | Knowledge | 1/68 | NR | Narrative | No effect on knowledge for an integrated community treatment programme compared with standard care | Unclear | |||
| Mutual support groups | Knowledge | 1/68 | NR | Narrative | Gains in knowledge | Unclear | |||
| Yesufu-Udechuku, 201546 | Interventions delivered by health and social care services: individual psychoeducation vs. group psychoeducation | Knowledge (medication) | 1/21 RCTs | NR | Narrative | Carers found individual psychoeducation less helpful than group psychoeducation for understanding of medication (p < 0.004) | Unclear | ||
| Individual psychoeducation vs. group psychoeducation | Knowledge (community resources) | 1/21 RCTs | NR | Narrative | In the same study, carers receiving the group psychoeducation intervention found the sessions less useful than did carers in the individual psychoeducation group (p < 0.004) | Unclear | |||
Carers of people with dementia
Positive intervention effects of internet-based interventions were reported in Boots et al. 19 in relation to carers’ sense of competence (one study of lower quality), confidence in decision-making (one study of good quality) and knowledge of the disease and caring (three studies of lower quality). In McKechnie et al. ,28 ability and knowledge were included in the measurement of programme impact following computer-mediated psychosocial interventions. In this review, five studies out of six (poorer quality) reported positive effects. It appears that there were positive intervention effects following communication skills training in Eggenberger et al. ;21 however, the lack of clarity in reporting in this review makes it difficult to draw meaningful results.
Carers of people with cancer
A large statistically significant effect on carers’ appraisal of information needs during the first 3 months post intervention was reported as a result of interventions involving psychoeducation, skills training and counselling in Northouse et al. 34 (three studies, no quality reported).
Carers of people with stroke
There were mixed findings across narrative and quantitative syntheses in two reviews that measured carers’ ability and knowledge. In Cheng et al. ,37,38 psychosocial interventions had a significant effect on carer competency (three studies), but in a pooled analysis the effect was not statistically significant (three studies). It was difficult to determine the quality of these primary studies individually, but the review authors reported overall moderate quality. In Forster et al. ,40 narrative synthesis showed no significant group differences following education interventions (two small studies). In the same review, however, a pooled analysis of other studies showed statistically significant differences in carer knowledge between education (particularly active education; e.g. involving participatory sessions or meetings) and control groups (four studies; high statistical heterogeneity at I2 = 88%; some risk of bias in all studies).
Carers of people with various conditions at the end of life
In Gomes et al. ,43 there were no statistically significant effects on learning new caregiving skills or sense of mastery following home palliative care versus usual care (one study of moderate-quality evidence) or for standard home palliative care versus a reinforced version (two studies of moderate-quality evidence).
Carers of people with mental health problems
In Macleod et al. ,45 carers’ knowledge appeared to be improved as a result of family interventions that were (variously) behavioural family therapy (four studies); cognitive–behavioural therapy (one study); group psychoeducation (one study); psychosocial intervention (one study); a culturally modified family intervention (one study); and mutual support groups (one study). In the same review, findings were mixed for education interventions (10 studies) and supportive family education (six studies), and there was no effect on knowledge from an integrated community treatment programme (one study). The quality of primary studies was not reported in this review. In Yesufu-Udechuku et al. ,46 group psychoeducation was associated with an improved understanding about medications (one study) compared with individual interventions; and individual psychoeducation was more helpful than when delivered in group format for learning about available community resources (one study). These results were statistically significant, but were based on low-quality evidence.
Cost-effectiveness of interventions to support carers
Three reviews32,40,43 reported on cost-effectiveness. In Forster et al. ,40 the total annual health and social care costs were significantly lower for carers of stroke patients who received an education and training intervention (one study at some risk of bias). The cost reduction was probably due to differences in length of hospital stay. In Smith and Greenwood,32 there was no evidence of cost-effectiveness from a volunteer befriending intervention for carers of people with dementia (one study of high quality). There was inconclusive evidence of cost-effectiveness from six high-quality studies looking at the total costs of home palliative care versus usual care for carers of people with various conditions at the end of life in Gomes et al. 43
Overall conclusions drawn by the high-quality reviews
In this section, we summarise the conclusions reported by the authors of the 27 high-quality reviews, grouping them by the condition of the person who was being cared for. We proceed to highlight the best evidence of effectiveness considering the reliability of the authors’ conclusions based on the evidence presented, together with overall quality of the review.
Carers of people with dementia (14 reviews)
In a review of 12 studies, Boots et al. 19 concluded that internet-based support interventions may improve carer well-being and that multicomponent activities allowing carer interaction (e.g. carer discussion forums) are more effective than those offering primarily information. This tentative conclusion is based on results of mixed-quality primary studies that generally reported conflicting or non-significant effects. However, some positive effects were reported. The best evidence of effectiveness was in relation to small positive intervention effects on depression (one higher-quality study), self-efficacy (one higher-quality study) and on carer stress and strain (one moderate-quality study). Positive intervention effects were also found for carer confidence in decision-making (one good-quality study). Although there were some limitations in reporting, this was a largely well-conducted review.
Chien et al. 20 concluded that carers of people with dementia benefit from support groups and that the use of theoretical models to aid intervention design had a significant impact on the effect size for psychological well-being and depression. The overall quality of 30 primary studies included in this review was reported to be high or moderate. For depression, the effect size was small to moderate but with high statistical variation in the analysis of 17 studies. A small reduction in carer burden and stress was indicated in a further analysis of 24 studies with low statistical heterogeneity; the effect appeared to persist over time. Although the quality of primary studies was generally good, the lack of control group data, the high statistical heterogeneity for mental health outcomes and the reporting limitations in this review meant that it was difficult to be totally confident about the review authors’ conclusions.
In Eggenberger et al. ,21 the authors concluded that communication skills training had a significant impact on family carers’ communication skills, competencies and knowledge. This review of 12 studies had substantial reporting limitations and generally contained studies of variable quality. This makes it difficult to assess the reliability of the authors’ conclusions. The best evidence of effectiveness arose from one good-quality study that found reduced depression in carers after a home-care education intervention with professional support, and another good-quality study of communication skills training resulting in total carer satisfaction.
Godwin et al. 22 concluded that each of the included technology-driven multicomponent support interventions (including Caregiver’s Friend: Dealing with Dementia, ComputerLink and REACH) had some positive findings, but there was insufficient evidence to support or refute the effects. Evidence from the primary studies supports this conclusion on positive effects for all outcomes except social isolation. Although overall the review was reasonably well conducted, it comprised only eight studies with no quality assessment; control group and follow-up data were lacking.
In a review of seven studies looking at carer education focused on skills training, Jensen et al. 24 concluded that educational programmes have a moderate effect in reducing carer burden and a small effect in reducing depression; the effects were unclear for quality of life and transition to long-term care. The analysis of depression included two studies (one of high quality). The result for carer burden was based on five moderate-quality studies with some statistical heterogeneity, and that favoured interventions of shorter duration. This review appeared largely well conducted and provided additional analysis of outcomes separated by low- and high-income countries.
In a well-conducted and well-reported review by Hurley et al. 23 (containing eight studies), the authors reported tentative evidence for the effectiveness of meditation-based interventions for improving scores of depression and carer burden. This conclusion was supported by primary study evidence at the end of the intervention in five moderate-quality studies for depression, and in three low- to moderate-quality studies for carer burden. The results for both outcomes were mixed at follow-up.
A well-conducted Cochrane review by Lins et al. 25 (containing 11 studies) concluded that telephone counselling without any additional intervention can reduce depressive symptoms and also meets the important needs of carers. The conclusion on depressive symptoms was supported in the analysis of three moderate-quality studies with no evidence of statistical heterogeneity. A positive effect on depression was also found in a moderate-quality study focusing on an enhanced version of the intervention comprising telephone counselling with additional video sessions and workbook. Two moderate-quality, qualitative studies substantiated the review authors’ conclusion on carer satisfaction with the intervention. Positive control group effects for self-efficacy and satisfaction were also reported, but the quality of studies in these analyses was mixed. This was a well-conducted review, and theoretical underpinnings of the included studies were reported.
The authors in Maayan et al. 27 concluded that current evidence does not demonstrate any benefits or adverse effects from respite care in carers of people with dementia, but the results should be interpreted cautiously. The authors’ conclusion was supported by this largely well-conducted Cochrane review containing four primary studies of very low quality.
Marim et al. 26 concluded that interdisciplinary education and support programmes have a positive impact on carer burden when compared with standard care. The conclusion was supported by this well-conducted and well-reported review of seven studies containing high-quality primary studies.
In their review of 14 studies, McKechnie et al. 28 concluded that computer-mediated psychosocial interventions can benefit carers of people with dementia. The best evidence of effectiveness related to improvements in scores for depression in the analyses of four high-quality studies, for anxiety from two high-quality studies and for reductions in stress and burden from five (out of nine) medium- to high-quality studies, with remaining studies in the last analysis showing inconsistent results. Not all of the included studies had control groups, and there were potential limitations regarding the transparency of the review process.
The review by Orgeta and Miranda-Castillo29 suggested that home-based physical activity interventions were effective in reducing subjective carer burden, compared with usual care. The analysis showed a moderate intervention effect based on two studies with unclear or low risk of bias and no evidence of statistical heterogeneity. This review was well reported in terms of methods, interventions and results. However, the overall review findings are based on four clinically heterogeneous studies with largely unknown risk of bias and limited follow-up data.
The conclusion from Schoenmakers et al. 30 suggested weak evidence for interventions to support family carers of people with dementia. Although this conclusion was generally supported by the primary study evidence, it was not possible to confirm the quality of the 19 included studies, as quality assessment was used only to select studies for the review. A small to moderate statistically significant adverse effect was reported in respect of increased carer burden resulting from respite care. The review authors speculated that this effect may be a result of carers’ uneasiness with respite nursing quality and the sudden release of free time for themselves.
In the generally well-conducted review by Smith and Greenwood32 (containing three studies), the authors concluded that there is limited quantitative evidence to support volunteer mentoring for carers of people with dementia. This contrasted with qualitative evidence that carers value the opportunity to talk with others about their experiences. The best evidence of effectiveness arose from one high-quality study of a telephone befriending intervention and consequent statistically significant improvement in scores for carer anxiety and depression after 15 months. Cost-effectiveness was reported for this study but no positive impact was found. Other benefits were apparent, but it was unclear whether they applied only to carers of people with dementia or also to carers of those with stroke. Such benefits were demonstrated in one moderate-quality qualitative study in terms of coping skills and caregiving competence, reduced loneliness and reliance on social support.
The authors of the well-conducted Cochrane review by Vernooij-Dassen et al. 31 (containing 11 studies) suggested that cognitive reframing for family carers shows promise as part of an individualised, multicomponent intervention. The inclusion of cognitive reframing appeared to reduce psychological morbidity and subjective stress, but without any effects on appraisals of coping or burden. In support of this conclusion, moderate to large effects were reported for reduced depression in the analysis of six studies; small-sized effects for anxiety from the analysis of four studies; and similarly small effects for stress and distress from four studies. All primary studies had some methodological limitations, but the overall quality was considered by the review authors to be satisfactory.
Carers of people with cancer (four reviews)
The authors in Lang and Lim33 concluded that art therapy is effective in reducing anxiety, stress and negative emotions in family carers of patients with cancer. This conclusion reflects a statistically significant pooled effect in two studies for anxiety; effects for reduced stress from baseline in each of two studies; and an improvement in carer emotional balance in one study. This was a well-reported review of moderate-quality primary studies. However, the findings may be limited by the reliance on two small-sized studies, each with the same lead author.
In their well-reported review of 29 studies, Northouse et al. 34 concluded that multicomponent interventions, including psychoeducation, skills training and counselling, can have a positive effect on many important carer outcomes, including small to medium effects on burden, ability to cope, self-efficacy and quality of life. These positive effects were all substantiated in the primary studies. Additionally, small statistically significant positive effects were reported for self-care behaviours and sleep quality in six studies when measured beyond 3 months from intervention delivery; small effects were noted for distress and anxiety, and moderate effects were sustained beyond 6 months following psychoeducation in 16 studies. In an analysis of three studies, a large statistically significant effect was reported for carers’ appraisal of information needs during the first 3 months post intervention. The review reported on theoretical frameworks underpinning the intervention. Despite the large number of positive intervention effects reported, the reliability of the review findings is limited by the absence of primary study quality assessment. Additionally, although most interventions were delivered jointly to patients and carers, the authors stated that many were designed primarily to address patient care.
Regan et al. 35 included six moderate- to strong-quality primary studies out of 23 studies overall. The authors concluded that couples-based psychosocial interventions showed promise, particularly in respect of improving couple communication and relationship functioning, and reducing psychological distress. These conclusions were supported by the evidence presented. In addition, there were reductions in physical distress in one study of disease management, psychoeducation and telephone counselling; and in another study evaluating the FOCUS intervention (family coping skills and uncertainty reduction). Improvements were also noted following the FOCUS intervention for quality of life [physical and emotional functioning (two studies)].
In their review of six studies, Waldron et al. 36 concluded that psychosocial/psychoeducation interventions focusing on problem-solving and communication skills may improve quality of life in carers of people with cancer. The evidence was provided by a small effect size in the analysis of two good-quality studies. The review was well conducted and well reported.
Carers of people with stroke (four reviews)
The review authors in Cheng et al. 37,38 suggested that there was limited evidence of effect for psychosocial interventions on family functioning of carers for people with stroke. This conclusion is based on a small effect size favouring counselling over no treatment from the analysis of two moderate-quality studies. In addition, satisfaction with psychoeducation, counselling or support was higher than for usual care in two moderate-quality studies. This was a well-conducted review with small numbers of studies included in each analysis across multiple outcomes. Theoretical frameworks underpinning the interventions were reported.
In the Cochrane review of individual patient data (involving 4759 patients and carers) by Ellis et al. ,39 the authors concluded that there was no evidence of effectiveness for the introduction of stroke liaison workers to help carers and patients, although some studies found improved user satisfaction with service provision. The conclusions were supported by the evidence presented in this largely well-conducted review. However, the reliability of the findings is limited by the inability to judge the overall quality of the primary studies.
Another Cochrane review by Forster et al. 40 (containing 21 studies) concluded that education-based interventions can improve carer knowledge of stroke. The conclusion is supported by evidence for active education programmes, but only in a pooled analysis of four studies containing substantial heterogeneity and at some risks of bias. The interventions in this review showed evidence of cost-effectiveness, possibly linked to benefits in length of hospital stay. The review was well conducted, but the overall findings are limited by the fact that only a small subset of the included studies related to carer outcomes.
Finally, a well-conducted Cochrane review by Legg et al. 41 (containing eight studies) concluded that interventions based on ‘teaching procedural knowledge’ (formal multidisciplinary training of caregivers in the prevention and management of common problems related to stroke), delivered to carers prior to the hospital discharge of stroke patients, appear to be the most promising. The authors’ tentative conclusion is justified on the basis of one small higher-quality study of ‘teaching procedural knowledge’. This intervention showed a small statistically significant reduction in carer depression, together with a statistically significant more substantial reduction in stress and improved quality of life.
Carers of people with various conditions at the end of life (three reviews)
The well-reported Cochrane review by Candy et al. 42 (containing 11 studies) proposed that multicomponent support interventions can help to reduce carers’ psychological distress. However, the evidence is derived from a pooled analysis of eight low-quality studies showing only a small effect size at the end of the intervention.
In the Gomes et al. 43 review of 23 studies, the authors stated that there was clear and reliable evidence that carer grief was not affected detrimentally after the receipt of home palliative care. This arises from a positive effect on carer distress favouring a reinforced version of the intervention, but it was based on one low-quality study and so the conclusion should be considered as tentative. A cost-effectiveness analysis involving six high-quality studies was inconclusive. This was a well-conducted review.
Nevis44 concluded that educational and problem-solving interventions were effective in improving carer quality of life but with no decrease in resource use. This conclusion was based on two (out of six included) studies containing serious risk of bias. No costs were reported.
Carers of people with mental health problems (two reviews)
In a large review of 68 studies focusing on multicomponent support interventions involving mental health nurses, Macleod et al. 45 concluded that, although findings were mixed, there was some evidence of effectiveness for a range of approaches. The primary evidence confirmed positive effects on carer mental health outcomes, burden and stress, coping, well-being and knowledge. The quality of primary studies (although claimed by the authors to be assessed) was not reported, so it is not possible to judge the reliability of these findings. Aside from this and some reporting discrepancies, the review was largely well conducted.
A well-conducted review by Yesufu-Udechuku et al. 46 (containing 21 studies) concluded that carer-focused interventions, including psychoeducation, support groups, problem-solving and self-management, appear to improve quality of life and reduce psychological distress, but no single specific intervention could be recommended. The best evidence of effectiveness for psychological distress is derived from statistically significant effects in one small high-quality study of psychoeducation, and from one moderate-quality study of problem-solving bibliotherapy measured up to 6 months post intervention. Quality of life (caregiving experiences, not further defined) was also improved, but the evidence was based largely on very low-quality studies with substantial heterogeneity.
Overview of the medium-quality reviews
Twenty-five reviews were classed as medium quality (Table 10). 48–72 Most reviews failed to meet the high quality standard owing to inadequate synthesis of the primary studies.
| First author, year of publication | Target carer group(s) | Sociodemographic informationa | Intervention(s) (and comparator, when reported) | Outcomes | Costs/cost-effectivenessb | Total number of studies/study designs/locations | Commentaryc |
|---|---|---|---|---|---|---|---|
| Carers of people with dementia | |||||||
| Brodaty, 201249 | Family caregivers of patients with dementia | Limited detail on ethnicity and/or sex for approximately half of the included studies | Categories of interventions and components were given six groupings: skills training, education, activity planning and environmental redesign, enhancing support, self-care techniques and miscellaneous (including exercise and collaboration with professional). Comparators (when reported) were active intervention, wait list, no treatment or usual care | Caregiver reactions to patient behavioural and psychological symptoms | NR | A total of 23 studies were included with 16 RCTs and seven pseudo-RCTs Study locations: USA, n = 15; UK, n = 2; and n = 1 for each of Russia, the Netherlands, Ireland, Canada, Italy and Norway |
(a) Multiple studies by the same author are included in the two main meta-analyses (b) Study details/quality assessment |
| Elvish, 201248 | Carers of patients with dementia including spouses and family | NR | Interventions were grouped into four categories: psychoeducational skill building, psychotherapy counselling, multicomponent and technology-based interventions. Comparators included treatment as usual, information provision and alternative treatments | Psychosocial outcomes were the focus of the review with the majority of studies measuring depression, burden and social support | NR | Twenty studies featured in the review, with 17 quantitative and three qualitative, from the following regions: USA, n = 12; USA/UK/Australia, n = 2; UK, n = 1; Taiwan, n = 1; Switzerland, n = 1; Mexico, n = 1; Denmark, n = 1; and not reported, n = 1 | (b) Synthesis/study details |
| Elvish, 201357 | Carers of patients with dementia | NR | A range of psychological interventions were included and categorised into psychoeducational-skill building, psychotherapy/counselling, multicomponent studies and technology based. Comparator included no attention, waiting list, alternative intervention or usual treatment (unspecified) | A range of outcomes were measured including depression, burden and social support and well-being | NR | Twenty studies were included in the review, featuring 17 quantitative and three qualitative Locations of data collection were the USA, n = 12; the UK/USA/Australia, n = 2; UK, n = 1; Taiwan, n = 1; Switzerland, n = 1; Mexico, n = 1; Denmark; and unreported, n = 1 |
Authors state in inclusion criteria that studies had to include random assignment. However, no mention of RCT is made anywhere else in the paper (b) Study details/synthesis |
| Greenwood, 201654 | Carers of people with Alzheimer’s disease and related dementias; dementia; chronic diseases | Carers were mostly female and aged between 61 and 72 years | Interventions in general practice were included, typically featuring educational and behavioural components | A variety of measured outcomes included depression, burden, knowledge and health | NR | The review included four studies comprising two RCTs, one quasi-experimental trial and one uncontrolled before-and-after study Study locations: USA, n = 3; and Spain, n = 1 |
(b) Study details/synthesis |
| Jones, 201252 | Carers of dementia patients | NR | Psychosocial and service delivery interventions targeting carers or family, comparators (when reported) were usual care | A range of outcomes included quality of life, burden and stress, depression and coping | All studies reported cost-effectiveness data. Types of data reported included mean cost, incremental cost-effectiveness ratio, cost per quality-adjusted life-year and loss of employment hours | Included eight studies focusing on interventions for carers: psychosocial or service delivery interventions. Of these there were four RCTs, three cohort studies and one based on the Monte Carlo Markov model Study locations: UK, n = 2; Canada, n = 2; USA, n = 2; the Netherlands, n = 1; and Finland, n = 1 |
(a) Grouped into pharmacological, psychosocial and service delivery, but in the discussion it is unclear which they are referring to – much more general (b) Study details/synthesis |
| Lord, 201555 | Carers (defined as family or friend) of patients with dementia | NR | Interventions featured decision-making aids and advanced care planning. Comparators (when reported) were no support or usual care | Outcome measures included burden, decision-making and knowledge | NR | Included three studies relevant to carer interventions (total of 30 studies in review that focused on barriers and facilitators). There were two RCTs (one in the UK) and a before-and-after study | (b) Synthesis |
| Martín-Carrasco, 201456 | Carers of patients with dementia | NR | Interventions were classified into categories of non-professional support or support groups, counselling and psychoeducation. Comparators included waiting lists and usual treatment (unspecified). Some RCTs used an alternative intervention as the comparator | Measured outcomes included depression, burden and anxiety | NR | A total of 35 RCTs were included in the review | (a) Lack of quality assessment (b) Study details/synthesis |
| Moon, 201351 | Caregivers of patients with dementia including family | Predominantly white, female spouse participants | Support group, counselling, cognitive simulation, skills training and multidyad memory notebook interventions featured in included studies. Those with comparators mainly used wait lists | Outcomes covered a range of measures, including those for depression, coping and knowledge | NR | Twelve studies were included in the review, with five RCTs, five single-group designs and two qualitative studies. Study locations were not reported | (b) Study details/synthesis |
| Olazoran, 201053 | Carers of patients with Alzheimer’s disease and related disorders | NR | Variety of interventions categorised as non-pharmacological including caregiver education, support, case management respite care and multicomponent. Control groups varied (including usual care, attention control) | A range of outcome measures included quality of life, burden, psychological well-being and mood | NR | A total of 179 studies were in the review, of which 53 RCTs were included with interventions directed solely at the caregiver. Study locations were not reported | (a) No table of characteristics naming the studies. Only included as count data and citations; appendix lists examples (b) Synthesis/no quality assessment of primary studies |
| Zabalegui, 201450 | Carers of patients with dementia | NR | Interventions targeted the caregiver or caregiver and patient, covering three general categories: psychoeducational, supportive and multicomponent interventions. Comparators were not reported | A range of outcomes measured included knowledge, satisfaction, coping, management of anxiety and depression, and well-being | Cost-effectiveness data came from a single study of an intervention to improve patient functioning and caregiver sense of competence. It found 35% higher proportion of successful treatment than for control | 23 RCTs met inclusion criteria Study locations: USA, n = 11; UK, n = 4; other Europe, n = 7; and Hong Kong, n = 1 |
(a) Lack of sociodemographic information and detail about who is included in carers group for conclusions (b) Synthesis |
| Carers of people with cancer | |||||||
| Chambers, 201159 | Partners of men with prostate cancer | Some studies targeted minority groups, with majority for white North American males with some higher education and their partner. Mean age of partners ranged from 56 to 61 years | Psychoeducational and coping skills interventions for patient and/or partner (only one intervention aimed solely at partners). These included a telephone-based coping skills programme, home and telephone intervention, and nursing support, most frequently with usual care as comparators | Focus on female spouse quality of life | NR | Relating to the research question for partner interventions there were five included studies (part of a wider review evaluating effects on patients, 25 studies) | (a) Limited synthesis to address multiple research questions, discussion and conclusions unclear to which question they refer (b) Inclusion criteria/synthesis |
| Caress, 200960 | Family members of cancer patients | NR | Interventions reviewed fell into four categories: interventions with some focus on skills development, interventions to enhance care through managing symptoms, interventions with problem-solving focus and interventions with a learning focus. Few studies had comparison groups and, when reported, they included standard care, other intervention or waiting list | A range of outcomes measured included skills, emotional components and knowledge | NR | Total of 19 studies were included in the review from the following regions: USA, n = 14; UK, n = 2; Canada, n = 1; Australia, n = 1; and Taiwan, n = 1 Of these nine were RCTs, with three pre–post-test designs and two repeated measures as well as quasi-experimental, descriptive, feasibility and mixed methods. Longitudinal designs featured in seven studies |
Databases searched are limited and many indexed up to 2007, although inclusion ran to June 2008 Lack of participant characteristics (b) Synthesis |
| Gauthier, 201262 | Caregivers of cancer patients; spouses and partners | Mostly female spouses. Mean age ranged from 50 to 66 years | A range of bereavement interventions such as muscle relaxation and group psychotherapy, and end-of-life patient care | A number of outcomes were collected including anxiety, grief and depression | NR | There were nine studies (10 articles) including: two RCTs, one RCT with a qualitative element, two pre–post studies, one longitudinal study, one retrospective study and two descriptive studies | (b) Synthesis |
| Harding, 201258 | Carers of patients with cancer or receiving palliative care | Includes unpaid carers and family; no further details reported | Six intervention models were identified in the review: one-to-one psychological models, psychological interventions for patient–carer dyads, palliative care/hospice interventions, information and training interventions, respite interventions, group interventions and physical interventions (yoga) | A range of outcomes were measured, including quality of life, perceived competence and carer distress | NR | A total of 33 studies were included, with nine RCTs, eight qualitative designs and seven pre–post studies, as well as retrospective, prospective, observational and quasi-experimental methods. 11 studies featured a single group Data were collected in the following regions: USA, n = 11; Australia, n = 7; UK, n = 6; Canada, n = 4; Sweden, n = 2; Israel, n = 1; Japan, n = 1; and South Africa, n = 1 |
(a) Very brief synthesis; data extraction table vital to understanding study types and interventions (b) Study details/synthesis |
| Kaltenbaugh, 201563 | Caregivers of cancer patients | Majority of caregivers were partners/spouses and female, with an average age between 49 and 57 years. Many carers had some college-level attendance and many described themselves as ‘somewhat comfortable using the internet’ | Internet-based interventions that included online CBT, communication services and information services. Interventions included those that were multicomponent or single component Comparison groups included usual care, another intervention and no internet access |
Measured outcomes covered psychological, physical and social domains, as well as usability and feasibility | NR | A total of six studies met inclusion criteria with three RCTs, one secondary analysis of a RCT, one feasibility study and one quantitative focus group data | (b) Synthesis |
| Ussher, 200961 | Caregivers of cancer patients | Most carers reported as being aged > 40 years In most studies the majority of caregivers were women, although six studies included 98–100% men as carers |
Psychosocial interventions, including counselling, psychotherapy, psychoeducation, education with or without support and couple interventions. When reported, comparison groups included usual care, waiting list or another intervention | A broad range of outcomes was measured including quality of life, coping and depression | NR | Twenty-two studies were included with 13 RCTs and nine non-RCT (one pseudo-RCT; one comparative study with concurrent control; one comparative study without concurrent control; six case series). Note: text and tables differ on numbers. Detail taken from tables 1 and 2 | (a) Unclear outcomes and synthesis. Appears to be a focus on positive findings. Data in tables and text do not match relating to number of studies or study details (b) Synthesis; numbers of studies in tables and text do not tally, and distribution between RCT and non-RCT differs, as does total included |
| Carers of people with stroke | |||||||
| Bakas, 201464 | Caregivers of stroke survivors | Stated as ‘not reported’ in primary data | Caregiver and patient–caregiver dyad interventions that were categorised into three types: skill building, psychoeducational provision and support. Interventions were delivered face to face or via telephone. Studies featured comparators including waiting list controls, historical comparison and crossover | A variety of outcomes were measured, including caregiver preparedness, burden and quality of life | NR | 32 studies were included with 22 RCTs, as well as three single-group designs, six random/quasi-random studies and one time-lag design | (a) PRISMA diagram gives reasons for exclusion, but no defined inclusion and exclusion criteria are presented except as referred to in the research questions. No formal quality assessment (b) Synthesis |
| Heslin, 201665 | Carers (mainly individual other than any health, social or voluntary care provider) of stroke survivors | Predominantly white, female carers | Interventions included information provision, structured assessment and active intervention directed as caregiver or caregiver and patient. When reported, comparators were standard care or another intervention | A range of outcomes included emotional health, quality of life and satisfaction | Three out of 10 reported economic outcomes for patients. Measured outcomes include resource use, costs and QALYs | A total of 10 studies were included, consisting of eight RCTs, one cohort study and one non-randomised, controlled trial. All included an economic evaluation. Studies were conducted in the USA, n = 5; UK, n = 4; and Germany, n = 1 | (a) No formal quality assessment, although comments made on quality (b) Synthesis |
| Carers of people with various conditions at the end of life | |||||||
| Glasdam, 201068 | Caregivers of patients with cancer, stroke or cardiovascular diseases | When reported, caregivers were mainly partners, family members, friends, neighbours, other | Interventions provided focused on discussion and guidance, knowledge and support for caregivers. Comparators were typically standard care | A variety of outcomes were measured including depression, burden, coping, satisfaction and knowledge | NR | A total of 32 studies were included in the review: 29 RCTs and three controlled trials Study locations: USA, n = 1; and Western Europe, n = 10 |
(b) Inclusion criteria; synthesis; quality assessment |
| Hudson, 201069 | Family carers of palliative care patients | When reported, family members included spouses and partners | A variety of psychosocial interventions included psychoeducation, social support and sleep interventions. When reported, comparators were usual care with or without active intervention | Outcomes measured included well-being, psychological health, sleep quality, burden, coping, quality of life and preparedness | NR | 14: five RCTs, two prospective studies, five pre–post and two qualitative | (a) Brief synthesis mainly descriptive and discussion in relation to other research (b) Synthesis/quality assessment |
| Loi, 201470 | Carers of patients with a range of patient groups including dementia and stroke survivors | Caregivers were predominantly female and Caucasian with an average age of 65 years | Physical activity interventions featuring walking, strength/circuit training, t’ai chi and hatha yoga or physical activity plus education. Comparators included usual activity or a nutritional programme | Outcome measures included burden, stress, depression and anxiety | NR | Seven studies were included in the review with four RCTs, two protocol trials and one non-randomised trial Study locations: USA and Australia |
(a) Lack of clarity regarding study types in text/table. Authors mention the difficulties of dementia care and most studies focus on this group, but conclusions do not specify this as a feature (b) Synthesis |
| Pottie, 201471 | Carers of hospice care patients with conditions including cancer and dementia | Primarily female and Caucasian carers (when reported) | Interventions included problem-solving, psychosocial and support interventions | A range of outcome measures were used including depression, anxiety and stress, quality of life, burden and satisfaction with services | NR | A total of 58 studies were included, with a range of designs that featured 22 quantitative, 21 quasi-experimental, 11 qualitative and three RCT methods, with some secondary analyses. It appears that a smaller subset of studies were analysed for direct caregiver interventions The geographic focus of the study was the USA |
(a) Particularly unclear what interventions are included, as they are only discussed briefly in the text with outcomes. Tables focus on methods and outcomes (b) Inclusion criteria/study details/quality assessment/synthesis |
| Walczak, 201672 | Caregivers of patients at the end of life | NR | Interventions targeted end-of-life communication skills including guided meetings and web-based end-of-life education | A range of outcomes measured included communication, psychological morbidity and burden | NR | The review included 45 studies with three focusing on caregivers featuring: two RCTs and one pre–post study Study locations (focusing on caregivers): France, USA, Japan |
(b) Lack of clear characteristics of studies on features of intervention, outcomes and populations |
| Carers of people with mental health problems | |||||||
| Chien, 200966 | Family caregivers for patients with severe mental illness | Majority of carers were female (ranging from 52% to 96%), age range between 41 and 61 years; and parents or spouses | A range of mutual support groups for family caregivers, including family groups, professionally led programmes and education | Outcome measures included burden, knowledge and coping | NR | Twenty-five studies were included in the review with six RCTs and experimental studies, four qualitative studies and 15 quasi-experimental or non-experimental studies Locations of data collection: USA, n = 12; UK, n = 3; Hong Kong, n = 3; Australia, n = 2; and Spain, Israel, Taiwan, Ireland and Belgium, all n = 1 |
(b) Synthesis |
| Chien, 201067 | Family carers of patients with severe mental illness | Majority of caregivers were female aged between 40 and 58 years, either spouses or parents, and Chinese. Most were from a middle social class | The focus of the review was mutual support groups | Outcomes included burden, coping, anxiety and distress, depression, family functioning, quality of life and satisfaction | NR | A total of 12 studies were included in the review, with five experimental or RCTs; three quasi-experimental; and four qualitative designs Study locations: Hong Kong, n = 5; USA, n = 2; Australia, n = 2; Taiwan, n = 1; Belgium, n = 1; and UK, n = 1 |
(a) This looks like another version of the 2009 review by Chien.66 However, the search dates are slightly different The focus of the reviews are mental health67 and psychotic disorders;66 Chien 201067 includes patients with dementia The earlier review66 contains more studies than later review.67 Poorly reported review methods (b) Synthesis (not easily separated for caregivers and patients) |
Patterns in the medium-quality literature were similar to those found in the high-quality reviews. The most commonly featured carers in reviews were those looking after people with dementia,48–57 followed by those caring for people with cancer. 58–63 Reviews also featured carers of people with stroke,64,65 carers of people with mental health problems66,67 and carers of people with various conditions. 68–72 In reviews that included primary studies of carers of people with different conditions, carers of patients at the end of life were represented,69,71,72 as were carers of people with conditions including cancer, stroke, dementia and cardiovascular disease. 68,70 The types of interventions reported in the medium-quality reviews were broadly similar to those reported in the high-quality reviews. A large proportion of activities were multicomponent psychosocial or educational in nature. One review55 looked at interventions featuring decision-making aids, advanced care planning and decision-making outcomes in carers of people with dementia. Outcomes measured in the medium-quality reviews covered the whole range as specified in the high-quality reviews; similar to the high-quality reviews, the greatest focus was on mental health, burden and stress, and quality of life. Three reviews50,52,65 included a cost-effectiveness analysis. There were no substantive differences from the high-quality reviews in terms of geographical coverage of the included primary studies or the sociodemographic characteristics of carers, when these were reported. As might be expected, there was overlap of included primary studies between the medium- and high-quality reviews in similar areas.
Overview of the low-quality reviews
Nine reviews were classed as low quality (Table 11). 73–81 Six of these focused on carers of people with dementia,73–78 two focused on carers of people with mental health problems79,80 and one focused on carers of people with multiple conditions. 81 In terms of types of interventions and outcomes, the literature appeared broadly similar to that covered in medium- and high-quality reviews.
| First author, year of publication | Title of article |
|---|---|
| Carers of people with dementia | |
| Beinart, 201275 | Caregiver burden and psychoeducational interventions in Alzheimer’s disease: a review |
| Lee, 201574 | Do technology-based support groups reduce care burden among dementia caregivers? A review |
| Mason, 200977 | Telephone interventions for family caregivers of patients with dementia: what are best nursing practices? |
| Neville, 201576 | Literature review: use of respite by carers of people with dementia |
| Nunnemann, 201278 | Caregivers of patients with frontotemporal lobar degeneration: a review of burden, problems, needs, and interventions |
| Van Mierlo, 201273 | Personalised caregiver support: effectiveness of psychosocial interventions in subgroups of caregivers of people with dementia |
| Carers of people at the end of life (various conditions) | |
| Alcide, 201581 | Adult hospice social work intervention outcomes in the United States |
| Carers of people with mental health problems | |
| Bailey, 201380 | Burden and support needs of carers of persons with borderline personality disorder: a systematic review |
| Fiorillo, 201379 | Efficacy of supportive family interventions in bipolar disorder: a review of the literature |
Chapter 4 Discussion and conclusions
In this final chapter, we outline the conclusions of our meta-review, highlighting areas of promise for practice. We also summarise the strengths and limitations of the meta-review, of the reviews we drew on to carry out our work and of the underlying primary research that informed those reviews. Finally, we discuss the implications of this meta-review for health-care practice and for research.
Overall conclusions from the meta-review
As with the original work,8 reviews of interventions that might support carers of people with dementia were predominant in our updating work. Some 14 of the 27 included high-quality reviews fell into this category. This undoubtedly reflects the continued interest internationally in both policy and practice in relation to dementia care. However, this time we found also high-quality reviews of interventions to support carers of people with mental health problems, which were absent previously. We also found a number of high-quality reviews on cancer, stroke and end-of-life care for people with various conditions.
The NIHR’s original interest, as outlined in Chapter 1, was to update the evidence about how best to support carers, given the introduction of the Care Act in 2014. 9 It was felt that a review could usefully evaluate particular interventions, such as carer champions, respite care, resilience programmes and health checks, and their cost-effectiveness. However, as this report shows, of these interventions only respite care has been subject to systematic review to date.
As in the earlier work, multicomponent interventions dominated the reviews, with a particular emphasis on psychosocial or psychoeducational content. Education or training for carers and communication skills training were also evident. In terms of outcomes, the most common focus across all carer groups was on mental health, burden and stress, and well-being/quality of life. This was the case with the earlier work. Also as with the earlier work, reviews usually reported on multiple outcomes, some of which were not clearly defined. Some reviews classed outcomes in one way, whereas others classed the same outcomes in another way. This was a particular issue around mental health outcomes, for which some reviews included ‘stress’ in their synthesis of mental health outcomes, whereas others treated this as a separate outcome.
Strengths and limitations
This update of the evidence base on interventions to support carers was carried out over a relatively short time scale (7 months). It has attempted to synthesise rapidly the overall messages of the identified reviews and the strength of these, drawing on the higher-quality reviews that we identified.
The evidence base has clearly grown both in volume and complexity since the original meta-review. The growth allowed us to take a rigorous approach to the quality of included reviews, but even this left us with some question marks about the methodological aspects of some reviews (see The included reviews and primary studies).
However, despite the speed of the process, this rapid review is built on strong foundations. Our systematic approach, with clear search strategies, fully documented inclusion and exclusion criteria, decision-making by more than one member of the team, and clearly documented data extraction and quality assessment, provides confidence that we have not missed any major sources of evidence and that our conclusions are firmly rooted in the best evidence available.
The very nature of a meta-review means that it is difficult to uncover definitively what interventions work, for whom and why. Other limitations may include the restriction to reviews published in English; the short time scale, which prevented a systematic investigation of primary study overlap across the included reviews; and a number of post-protocol decisions that were dictated by the growth in literature since the original meta-review.
Views of carers
As described in Chapter 2 (see Public and patient engagement), we asked carers to give us their views on the overall findings of our work. We were particularly interested in whether or not they felt that the interventions for which the reviews seemed to have found evidence were ones that carers might find helpful.
As outlined earlier, in the end only two carers were able to provide comments, which is a limitation, but the comments they did provide were detailed and pertinent. Both were carers of people with dementia, although in different circumstances. Carers of people with dementia both are more heavily involved and experience the impact of caring to a greater extent than most other carers, so one might take the view that if we can get support ‘right’ for them, then we can also get it ‘right’ for many other types of carer.
These advisers highlighted for us that carers of people with different conditions experience different caring experiences and trajectories. Thus, what might be useful and effective for one sort of carer might not be useful or effective for another. Similarly, what might be useful and effective at one stage in the trajectory might not be useful or effective at another stage. This underlined the difficulty, as they saw it, of knowing what a true ‘control’ carer or condition might be in a controlled research design.
The advisers also felt that variations in caring situations and across carers made it difficult to see that a single intervention could be the ‘answer’ in supporting carers. Rather, as one put it, ‘because of the complexities of the situations there is unlikely to be a one size fits all that will be right at any one time’. As a result, she felt that any opportunity to engage with carers and the cared-for person might ‘just press the right supportive button at that moment’, and hence a ‘pick and mix’ approach, whereby various support options were on offer, would be the ideal.
All of the interventions that the high-quality reviews had suggested might have a positive effect on carers were seen as acceptable, but the advisers pointed out that what was actually available to carers was limited and incomplete, and that although education and training for the carer might have a part to play, this was no substitute for ‘direct intervention on the carer’s own behalf’. They also raised the issue of the value to carers of standard services, including respite, that were provided to the person they cared for.
The included reviews and primary studies
The overall impression of the reviews is one of higher quality since the earlier work; they were generally well conducted and well reported (reflecting also the use, this time, of a higher quality threshold), although there were also some methodological limitations. Even the reviews that we defined as high quality did not always assess – or, if assessed, report – the quality of the primary studies that they included. This was particularly disappointing in relation to some of the reviews of carers of people with mental health problems, as in our previous work we did not find any reviews in this area.
Although the authors’ conclusions generally reflected the evidence they presented, in some places, whether a result of the quality of the primary research available (see below) or of the limitations of the reviews themselves (i.e. small-sized reviews), many relied on the analysis of small numbers of studies, and in some cases single studies, to underpin their conclusions. In some reviews, too, it was difficult to interpret effect sizes, for example when synthesis relied on standardised mean differences without reported confidence intervals and when there was unclear reporting on what was being measured and how.
As with any review of reviews, there was evidence of overlap of primary studies; that is, different reviews of similar topics drew on the same primary studies. It was also the case that some reviews included interventions with elements that in other reviews were defined differently. An example of this is Chien et al. ,20 whose review of ‘caregiver support groups’ included groups that had psychoeducational or educational components. These overlaps increase the risk of exaggerated effects. A formal investigation of primary study overlap was beyond the resources available for this project.
Another weakness of the reviews, which may reflect the quality of the primary studies, was the lack of information about what support, if any, carers in control groups were receiving. There is little consistency in the messages about the type of interventions that have been argued to have positive effects for carers, particularly for carers of people with dementia. This raises the question of if ‘anything is better than nothing’. With little understanding of the experiences of control groups, we have no way of addressing this question.
There was a lack of clarity of reporting in some reviews relating to the analysis of comparators. It was unclear whether some analyses were using data from primary studies collected before and after the intervention or whether the findings were related to differences between intervention and comparator groups. In some analyses it appeared that there may have been a combination of both.
The primary studies from the included reviews had worldwide coverage, but our focus on health systems in developed countries means that the results can largely be seen as relevant to the UK context.
Despite the passage of time since the original work, and the greater emphasis in that time on quality standards for evaluation research, many reviews pointed to the poor quality of primary research. This seemed particularly the case with the evidence on support for carers of people with mental health problems. The few reviews that used a high cut-off point for quality thus rarely included more than a handful of studies.
The inclusion of multiple interventions in a single review, and the use of multicomponent interventions in the primary research, as well as the overlap referred to above, made it difficult, in many parts of our work, to interpret cause and effect (in the few places where effect was evident).
The original meta-review highlighted the problem of intervention research, whereby no theory of change or intervention logic has been developed that could sensibly inform the choice of appropriate outcome domains. This remains an issue but, in the updated work, some review authors also acknowledged this problem and, in one case, focused exclusively on interventions for which such theory was evident. 31 The lack of an underpinning theory means that primary research often includes multiple outcome measures, none of which is identified as primary, adding further to the difficulties of ascribing cause and effect.
Finally, as with the original work, we found very little information about the cost-effectiveness of any of the interventions reviewed.
Reviews showing promise for carers
In Table 12 we draw together findings from across the meta-review to show, overall, what evidence there may be for interventions that may have an effect on carers. We have defined such evidence as analysis based on more than one study, when the quality of the primary studies was appraised and reported to be moderate or above for at least two studies, when the intervention type was clearly defined and when the results of the synthesis were not mixed or inconsistent.
| Type of carer | Outcome improved | Type of intervention |
|---|---|---|
| Dementia | Anxiety | Cognitive reframing31 |
| Anxiety | Psychosocial interventions (computer mediated)28 | |
| Burden | Educational interventions aimed at teaching skills24 | |
| Burden | Interdisciplinary education and support26 | |
| Burden (although outcome not explicitly defined) | Support groups20 | |
| Burden and stress | Cognitive reframing31 | |
| Burden and stress | Psychosocial interventions (computer mediated)28 | |
| Depression | Cognitive reframing31 | |
| Depression | Meditation-based interventions23 | |
| Depression | Psychosocial interventions (computer mediated)28 | |
| Depression | Support groups20 | |
| Depression | Telephone counselling25 | |
| Cancer | Mental health | Art therapy33 |
| Physical distress | Couples-based psychosocial interventions35 | |
| Psychological distress | Couples-based psychosocial interventions35 | |
| Quality of life | Psychosocial intervention based on problem solving and communication skills36 | |
| Quality of life: relationship functioning | Counselling therapy35 | |
| Stroke | Family functioning | Counselling37,38 |
In addition to the effects summarised in the table, the review of respite care for carers of people with dementia identified a negative impact on carer burden (which was similar to a finding in the original meta-review), although this was based on unclear primary study quality. 30
We can see from Table 12 that there is some evidence that an intervention that involves contact between carers of people with dementia and other people who know about dementia may improve some aspects of carers’ mental health and of their perceptions of burden and stress. The very different types of intervention that appear to produce this effect, when we have no clear understanding of what control groups were experiencing as ‘usual care’, inevitably raises again the ‘something better than nothing’ question. Thus, this evidence could reflect a type of Hawthorne effect: when people feel better simply because they are in the active arm of a research project and are therefore having greater contact with people outside their normal context. Given the restricted lives some carers lead, any contact may have beneficial effects. Alternatively, the evidence could reflect the real value of being able to share experiences with and learn from others, whether carers or professionals; but this benefit does appear to be regardless of how the sharing and learning is achieved.
In relation to those caring for a person with cancer, the message seems a little clearer. Here, interventions with a psychosocial element may improve carers’ physical and mental health, quality of life and relationship functioning. Art therapy (which perhaps could also be characterised as providing some psychosocial support) may also affect mental health positively.
The only other group of carers for which there are any clear messages is those helping someone who has had a stroke. Here, counselling was able to improve family functioning.
Implications for practice and research
Practice
This meta-review, like the earlier one, was established to explore the evidence on interventions specifically designed and intended to support carers, not to explore the ways in which generic services might also help carers. It is important to remember this, because we know from other types of research that services intended for the person being supported are often crucial to the carers’ own health and well-being. For example, if people with dementia attend day activities and are offered things to do that engage their interest and give them an opportunity to meet other people, carers may benefit both from the short break it gives them and from any positive effect the activity may have on the mood of the person with dementia. Similarly, if people who are nearing the end of their life receive good-quality palliative care, both they and their close family members may benefit.
In the original meta-review, the strongest evidence of effectiveness of any sort was in relation to education, training and information for carers. When active and targeted, such interventions increased carers’ knowledge and abilities as carers, with some indication that they might also thereby improve carers’ mental health or coping. This updated meta-review suggests that interventions with this sort of content, for carers of people with dementia, may also have a positive impact on subjective burden.
However, the updated meta-review suggests other possibilities for effective support for carers. These are as follows.
-
For carers of people with dementia:
-
Opportunities to share with and learn from others (whether carers or professionals) may have a positive impact on depression and anxiety, and on subjective burden.
-
Opportunities to reframe the way they think about dementia may have a positive impact on mental health and on subjective burden and stress.
-
Learning meditation techniques may have a positive impact on depression.
-
Psychosocial interventions delivered via a computer may have a positive impact on depression and anxiety and on subjective burden and stress.
-
-
For carers of people with cancer:
-
Psychosocial interventions may have a positive impact on carers’ physical and psychological ‘distress’ and quality of life.
-
Art therapy may have a positive impact on carers’ mental health.
-
Counselling may have a positive impact on relationship functioning.
-
-
For carers of people with stroke:
-
Counselling may have positive impact on family functioning.
-
None of the above suggests that a ‘one intervention fits all’ approach would meet the needs of all carers; neither do we know which elements of multicomponent interventions have the most effect.
Research
The implications for research are much as they were previously:
-
There remains a dearth of good-quality primary research about the effectiveness of most support interventions for carers. In large part, we suspect that this is driven by the lack of underpinning theories of change or intervention logic that would allow the right questions about the right outcomes to be asked. This applies as much to recent initiatives in Britain, such as carers’ champions and health checks for carers (for which we were unable to identify any review evidence), as it does to more established interventions.
-
The issue of respite care and its effectiveness, or not, in supporting carers of people with dementia remains a paradox, given the apparent conflict between the empirical evidence and the views of carers. On the one hand, the earlier meta-review and this one found reviews suggesting that respite care might have negative effects for carers of people with dementia. On the other hand, our carer advisers and the qualitative literature suggest that respite care is essential to carers feeling that they can continue to care. A major issue with the reviews of respite care, however, is the assessment of the quality of the respite being evaluated and, in some cases, careful distinction between the different types of respite on offer. Furthermore, there have been recent developments that may provide a different sort of respite from traditional models. Examples of such new models include memory cafés and the use of volunteers to provide people with dementia with meaningful daytime occupation; however, these have not yet been fully evaluated. Primary research that explores what type of respite is better or worse, for whom, and in relation to outcomes that carers themselves think are valuable is urgently needed. This should be research that articulates clear intervention logic driven by carers’ views about outcomes, and that carefully triangulates both quantitative and qualitative findings.
-
Reviews that separate out different parts of multicomponent interventions and then model their unique impact are beginning to emerge, but much more of this type of sophisticated systematic reviewing is needed. A review that attempted to separate out and assess the effects of different elements of formal ‘psychosocial’ support, and to set this alongside evidence of the effect of informal support delivered via different modes, would be a start.
-
Such reviews would also need to model differential impact for different types of carers. By definition, carers are a very diverse group; as our carer advisers pointed out, expecting a single type of intervention to meet the needs of all carers and at all stages of caring is unrealistic. There appears to be a particular gap in the review evidence relating to young carers and carers from minority groups.
-
Heavily involved carers, by definition, have very little, if any, time to spare from their daily routines, yet these are the people most likely to need support. Finding ways of engaging meaningfully with them in research processes, without imposing additional burdens, is a challenge for all empirical and review work in this field. The use of ‘virtual’ advisory groups for evaluation research, whereby user organisations act as a conduit through which carers can engage in research projects via face-to-face meetings, telephone or e-mail, as and when they have time, is proving very useful in other NIHR-funded projects at York. 82 However, this model has inevitable resource implications, as it takes time to set up and needs to be moderated independently of the research team.
Acknowledgements
We would like to offer our appreciation to Andrew Street, of the Centre for Health Economics, University of York, for comments on drafts of the report; to James Thomas, of the University College London Institute of Education for expertise, advice and assistance with text mining; and to Hollie Melton for her contribution to data extraction and text mining. Thanks are also due to the group of carer advisers for their invaluable comments on the final draft of the report.
Contributions of authors
Study selection, data extraction, critical appraisal and write-up of the report were carried out by Sian Thomas (Research Fellow, Evidence Synthesis) and Jane Dalton (Research Fellow, Evidence Synthesis), as was commenting on the protocol.
All searching was conducted by Melissa Harden (Information Specialist), who also wrote the search sections of the report and commented on the draft report.
Alison Eastwood (Professor, Evidence Synthesis) oversaw the project, contributed advice and expertise, and commented on all drafts of the report and protocol.
Gillan Parker (Professor of Social Policy Research, Applied Health and Social Care Research) developed the protocol, carried out some of the data extraction and wrote the discussion and conclusion sections of the report, as well providing expertise and advice and commenting on all drafts.
External advice
We engaged with a group of carers who were known to us, and who were willing to give their views on the overall findings of our review. A finished version of the report was sent to four individuals, together with a short brief on the purpose of the project and how we thought they might be able to help.
Data sharing statement
All available data can be obtained from the corresponding author. All data will be shared in a way that safeguards the confidentiality and anonymity of carers in our advisory group.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Parker G. With Due Care and Attention: A Review of Research on Informal Care. London: Family Policy Studies Centre; 1985.
- Carers at the Heart of 21st-century Families and Communities. London: Department of Health; 2008.
- Recognised, Valued and Supported: Next Steps for the Carers Strategy. London: Department of Health; 2010.
- Dementia and Elderly Care News . Improving Integration of Carer Support: Toolkit to Assist Identification and Assessment of Carer Health and Wellbeing (NHS England). 2016. https://dementianews.wordpress.com/2016/05/19/integration-of-carer-support-toolkit-for-identification-and-assessment-carer-health-and-wellbeing-nhs-england/ (accessed 3 June 2016).
- Carers Toolkit. Leeds: NHS England; 2016.
- NHS England’s Commitment to Carers. Leeds: NHS England; 2014.
- Commitment to Carers – Improving Carer Health and Wellbeing. Leeds: NHS England; 2016.
- Parker G, Arksey H, Harden M. Meta-review of International Evidence on Interventions to Support Carers. York: Social Policy Research Unit, University of York; 2010.
- Care Act 2014. Chapter 23. London: The Stationery Office; 2014.
- Egan M, Tannahill C, Petticrew M, Thomas S. Psychosocial risk factors in home and community settings and their associations with population health and health inequalities: a systematic meta-review. BMC Public Health 2008;8. http://dx.doi.org/10.1186/1471-2458-8-239.
- Chambers D, Wade R, Wilson P. Training Manual for Selecting Reviews and Writing Abstracts for the Database of Abstracts of Reviews of Effects (DARE). York: CRD, University of York; 2012.
- Oxman AD, Guyatt GH. Validation of an index of the quality of review articles. J Clin Epidemiol 1991;44:1271-8. https://doi.org/10.1016/0895-4356(91)90160-B.
- Parker G, Beresford B, Clarke S, Gridley K, Pitman R, Spiers G, et al. Technical Report for SCIE Research Review on the Prevalence and Incidence of Parental Mental Health Problems and the Detection, Screening and Reporting of Parental Mental Health Problems. York: Social Policy Research Unit, University of York; 2008.
- Beresford B, Clarke S, Gridley K, Parker G, Pitmam R, Spiers G, et al. Technical Report for SCIE Research Review on Access, Acceptability and Outcomes of Services/Interventions to Support Parents with Mental Health Problems and their Families. York: Social Policy Research Unit, University of York; 2008.
- Carbone MK, Gugliucci MR. Delirium and the family caregiver: the need for evidence-based education interventions. Gerontologist 2015;55:345-52. http://dx.doi.org/10.1093/geront/gnu035.
- Berthelsen CB, Kristensson J. The content, dissemination and effects of case management interventions for informal caregivers of older adults: a systematic review. Int J Nurs Stud 2015;52:988-1002. http://dx.doi.org/10.1016/j.ijnurstu.2015.01.006.
- You EC, Dunt D, Doyle C, Hsueh A. Effects of case management in community aged care on client and carer outcomes: a systematic review of randomized trials and comparative observational studies. BMC Health Serv Res 2012;12. http://dx.doi.org/10.1186/1472-6963-12-395.
- Reilly S, Miranda-Castillo C, Malouf R, Hoe J, Toot S, Challis D, et al. Case management approaches to home support for people with dementia. Cochrane Database Syst Rev 2015;1. http://dx.doi.org/10.1002/14651858.CD008345.pub2.
- Boots LM, de Vugt ME, van Knippenberg RJ, Kempen GI, Verhey FR. A systematic review of internet-based supportive interventions for caregivers of patients with dementia. Int J Geriatr Psychiatry 2014;29:331-44. http://dx.doi.org/10.1002/gps.4016.
- Chien LY, Chu H, Guo JL, Liao YM, Chang LI, Chen CH, et al. Caregiver support groups in patients with dementia: a meta-analysis. Int J Geriatr Psychiatry 2011;26:1089-98. http://dx.doi.org/10.1002/gps.2660.
- Eggenberger E, Heimerl K, Bennett MI. Communication skills training in dementia care: a systematic review of effectiveness, training content, and didactic methods in different care settings. Int Psychogeriatr 2013;25:345-58. http://dx.doi.org/10.1017/S1041610212001664.
- Godwin KM, Mills WL, Anderson JA, Kunik ME. Technology-driven interventions for caregivers of persons with dementia: a systematic review. Am J Alzheimers Dis Other Demen 2013;28:216-22. http://dx.doi.org/10.1177/1533317513481091.
- Hurley RV, Patterson TG, Cooley SJ. Meditation-based interventions for family caregivers of people with dementia: a review of the empirical literature. Aging Ment Health 2014;18:281-8. http://dx.doi.org/10.1080/13607863.2013.837145.
- Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: systematic review and meta-analysis of randomised controlled trials. Int J Geriatr Psychiatry 2015;30:130-43. http://dx.doi.org/10.1002/gps.4208.
- Lins S, Hayder-Beichel D, Rücker G, Motschall E, Antes G, Meyer G, et al. Efficacy and experiences of telephone counselling for informal carers of people with dementia. Cochrane Database Syst Rev 2014;9. http://dx.doi.org/10.1002/14651858.CD009126.pub2.
- Marim CM, Silva V, Taminato M, Barbosa DA. Effectiveness of educational programs on reducing the burden of caregivers of elderly individuals with dementia: a systematic review. Rev Lat Am Enfermagem 2013;21:267-75. https://doi.org/10.1590/S0104-11692013000700033.
- Maayan N, Soares-Weiser K, Lee H. Respite care for people with dementia and their carers. Cochrane Database Syst Rev 2014;1. http://dx.doi.org/10.1002/14651858.CD004396.pub3.
- McKechnie V, Barker C, Stott J. Effectiveness of computer-mediated interventions for informal carers of people with dementia – a systematic review. Int Psychogeriatr 2014;26:1619-37. http://dx.doi.org/10.1017/S1041610214001045.
- Orgeta V, Miranda-Castillo C. Does physical activity reduce burden in carers of people with dementia? A literature review. Int J Geriatr Psychiatry 2014;29:771-83. https://doi.org/10.1002/gps.4060.
- Schoenmakers B, Buntinx F, DeLepeleire J. Supporting the dementia family caregiver: the effect of home care intervention on general well-being. Aging Ment Health 2010;14:44-56. http://dx.doi.org/10.1080/13607860902845533.
- Vernooij-Dassen M, Draskovic I, McCleery J, Downs M. Cognitive reframing for carers of people with dementia. Cochrane Database Syst Rev 2011;11. http://dx.doi.org/10.1002/14651858.CD005318.pub2.
- Smith R, Greenwood N. The impact of volunteer mentoring schemes on carers of people with dementia and volunteer mentors: a systematic review. Am J Alzheimers Dis Other Demen 2014;29:8-17. http://dx.doi.org/10.1177/1533317513505135.
- Lang D, Lim LC. Effects of art therapy for family caregivers of cancer patients: a systematic review. JBI Database System Rev Implement Rep 2014;12:374-94. https://doi.org/10.11124/jbisrir-2014-1096.
- Northouse LL, Katapodi MC, Song L, Zhang L, Mood DW. Interventions with family caregivers of cancer patients: meta-analysis of randomized trials. CA Cancer J Clin 2010;60:317-39. http://dx.doi.org/10.3322/caac.20081.
- Regan TW, Lambert SD, Girgis A, Kelly B, Kayser K, Turner J. Do couple-based interventions make a difference for couples affected by cancer? A systematic review. BMC Cancer 2012;12. http://dx.doi.org/10.1186/1471-2407-12-279.
- Waldron EA, Janke EA, Bechtel CF, Ramirez M, Cohen A. A systematic review of psychosocial interventions to improve cancer caregiver quality of life. Psycho-Oncology 2013;22:1200-7. http://dx.doi.org/10.1002/pon.3118.
- Cheng HY, Chair SY, Chau JP. The effectiveness of caregiver psychosocial interventions on the psychosocial wellbeing, physical health and quality of life of stroke family caregivers and their stroke survivors: a systematic review. JBI Database System Rev Implement Rep 2012;10:679-797. https://doi.org/10.11124/jbisrir-2012-66.
- Cheng HY, Chair SY, Chau JP. The effectiveness of psychosocial interventions for stroke family caregivers and stroke survivors: a systematic review and meta-analysis. Patient Educ Couns 2014;95:30-44. http://dx.doi.org/10.1016/j.pec.2014.01.005.
- Ellis G, Mant J, Langhorne P, Dennis M, Winner S. Stroke liaison workers for stroke patients and carers: an individual patient data meta-analysis. Cochrane Database Syst Rev 2010;5. http://dx.doi.org/10.1002/14651858.CD005066.pub2.
- Forster A, Brown L, Smith J, House A, Knapp P, Wright JJ, et al. Information provision for stroke patients and their caregivers. Cochrane Database Syst Rev 2012;11. http://dx.doi.org/10.1002/14651858.CD001919.pub3.
- Legg LA, Quinn TJ, Mahmood F, Weir CJ, Tierney J, Stott DJ, et al. Non-pharmacological interventions for caregivers of stroke survivors. Cochrane Database Syst Rev 2011;10. http://dx.doi.org/10.1002/14651858.CD008179.pub2.
- Candy B, Jones L, Drake R, Leurent B, King M. Interventions for supporting informal caregivers of patients in the terminal phase of a disease. Cochrane Database Syst Rev 2011;6. http://dx.doi.org/10.1002/14651858.CD007617.pub2.
- Gomes B, Calanzani N, Curiale V, McCrone P, Higginson IJ. Effectiveness and cost-effectiveness of home palliative care services for adults with advanced illness and their caregivers. Cochrane Database Syst Rev 2013;6. http://dx.doi.org/10.1002/14651858.CD007760.pub2.
- Nevis I. Educational intervention in end-of-life care: an evidence-based analysis. Ont Health Technol Assess Ser 2014;14:1-30.
- Macleod SH, Elliott L, Brown R. What support can community mental health nurses deliver to carers of people diagnosed with schizophrenia? Findings from a review of the literature. Int J Nurs Stud 2011;48:100-20. http://dx.doi.org/10.1016/j.ijnurstu.2010.09.005.
- Yesufu-Udechuku A, Harrison B, Mayo-Wilson E, Young N, Woodhams P, Shiers D, et al. Interventions to improve the experience of caring for people with severe mental illness: systematic review and meta-analysis. Br J Psychiatry 2015;206:268-74. http://dx.doi.org/10.1192/bjp.bp.114.147561.
- Wikipedia . Bibliotherapy n.d. https://en.wikipedia.org/wiki/Bibliotherapy (accessed 21 June 2016).
- Elvish R, Lever SJ, Johnstone J, Cawley R, Keady J. Psychological Interventions for Carers of People with Dementia: A Systematic Review of Quantitative and Qualitative Evidence. Lutterworth: British Association for Counselling & Psychotherapy; 2012.
- Brodaty H, Arasaratnam C. Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia. Am J Psychiatry 2012;169:946-53. http://dx.doi.org/10.1176/appi.ajp.2012.11101529.
- Zabalegui A, Hamers JP, Karlsson S, Leino-Kilpi H, Renom-Guiteras A, Saks K, et al. Best practices interventions to improve quality of care of people with dementia living at home. Patient Educ Couns 2014;95:175-84. http://dx.doi.org/10.1016/j.pec.2014.01.009.
- Moon H, Adams KB. The effectiveness of dyadic interventions for people with dementia and their caregivers. Dementia 2013;12:821-39. http://dx.doi.org/10.1177/1471301212447026.
- Jones C, Edwards RT, Hounsome B. A systematic review of the cost-effectiveness of interventions for supporting informal caregivers of people with dementia residing in the community. Int Psychogeriatr 2012;24:6-18. http://dx.doi.org/10.1017/S1041610211001207.
- Olazaran J, Reisberg B, Clare L, Cruz I, Pena-Casanova J, del Ser T, et al. Nonpharmacological therapies in Alzheimer’s disease: a systematic review of efficacy. Dement Geriatr Cogn Disord 2010;30:161-78. http://dx.doi.org/10.1159/000316119.
- Greenwood N, Pelone F, Hassenkamp AM. General practice based psychosocial interventions for supporting carers of people with dementia or stroke: a systematic review. BMC Fam Pract 2016;17. http://dx.doi.org/10.1186/s12875-015-0399-2.
- Lord K, Livingston G, Cooper C. A systematic review of barriers and facilitators to and interventions for proxy decision-making by family carers of people with dementia. Int Psychogeriatr 2015;27:1301-12. http://dx.doi.org/10.1017/S1041610215000411.
- Martín-Carrasco M, Ballesteros-Rodríguez J, Domínguez-Panchón AI, Muñoz-Hermoso P, González-Fraile E. Interventions for caregivers of patients with dementia. Actas Esp Psiquiatr 2014;42:300-14.
- Elvish R, Lever SJ, Johnstone J, Cawley R, Keady J. Psychological interventions for carers of people with dementia: a systematic review of quantitative and qualitative evidence. Couns Psychother Res 2013;13:106-25. https://doi.org/10.1080/14733145.2012.739632.
- Harding R, List S, Epiphaniou E, Jones H. How can informal caregivers in cancer and palliative care be supported? An updated systematic literature review of interventions and their effectiveness. Palliat Med 2012;26:7-22. http://dx.doi.org/10.1177/0269216311409613.
- Chambers SK, Pinnock C, Lepore SJ, Hughes S, O’Connell DL. A systematic review of psychosocial interventions for men with prostate cancer and their partners. Patient Educ Couns 2011;85:e75-88. http://dx.doi.org/10.1016/j.pec.2011.01.027.
- Caress AL, Chalmers K, Luker K. A narrative review of interventions to support family carers who provide physical care to family members with cancer. Int J Nurs Stud 2009;46:1516-27. http://dx.doi.org/10.1016/j.ijnurstu.2009.03.008.
- Ussher JM, Perz J, Hawkins Y, Brack M. Evaluating the efficacy of psycho-social interventions for informal carers of cancer patients: a systematic review of the research literature. Health Psychol Rev 2009;3:85-107. http://dx.doi.org/10.1080/17437190903033401.
- Gauthier LR, Gagliese L. Bereavement interventions, end-of-life cancer care and spousal well-being: a systematic review. Clin Psychol Sci Pract 2012;19:72-9. https://doi.org/10.1111/j.1468-2850.2012.01275.x.
- Kaltenbaugh DJ, Klem ML, Hu L, Turi E, Haines AJ, Hagerty Lingler J. Using web-based interventions to support caregivers of patients with cancer: a systematic review. Oncol Nurs Forum 2015;42:156-64. http://dx.doi.org/10.1188/15.ONF.156-164.
- Bakas T, Clark PC, Kelly-Hayes M, King RB, Lutz BJ, Miller EL. American Heart Association Council on Cardiovascular and Stroke Nursing and the Stroke Council. Evidence for stroke family caregiver and dyad interventions: a statement for healthcare professionals from the American Heart Association and American Stroke Association. Stroke 2014;45:2836-52. http://dx.doi.org/10.1161/STR.0000000000000033.
- Heslin M, Forster A, Healey A, Patel A. A systematic review of the economic evidence for interventions for family carers of stroke patients. Clin Rehabil 2016;30:119-33. http://dx.doi.org/10.1177/0269215515575334.
- Chien WT, Norman I. The effectiveness and active ingredients of mutual support groups for family caregivers of people with psychotic disorders: a literature review. Int J Nurs Stud 2009;46:1604-23. http://dx.doi.org/10.1016/j.ijnurstu.2009.04.003.
- Chien WT, Brown LD, Wituk S. Mental Health Self-help: Consumer and Family Initiatives. New York, NY: Springer; 2010.
- Glasdam S, Timm H, Vittrup R. Support efforts for caregivers of chronically ill persons. Clin Nurs Res 2010;19:233-65. http://dx.doi.org/10.1177/1054773810369683.
- Hudson PL, Remedios C, Thomas K. A systematic review of psychosocial interventions for family carers of palliative care patients. BMC Palliat Care 2010;9. http://dx.doi.org/10.1186/1472-684X-9-17.
- Loi SM, Dow B, Ames D, Moore K, Hill K, Russell M, et al. Physical activity in caregivers: what are the psychological benefits?. Arch Gerontol Geriatr 2014;59:204-10. http://dx.doi.org/10.1016/j.archger.2014.04.001.
- Pottie CG, Burch KA, Thomas LP, Irwin SA. Informal caregiving of hospice patients. J Palliat Med 2014;17:845-56. http://dx.doi.org/10.1089/jpm.2013.0196.
- Walczak A, Butow PN, Bu S, Clayton JM. A systematic review of evidence for end-of-life communication interventions: who do they target, how are they structured and do they work?. Patient Educ Couns 2016;99:3-16. http://dx.doi.org/10.1016/j.pec.2015.08.017.
- Van Mierlo LD, Meiland FJ, Van der Roest HG, Dröes RM. Personalised caregiver support: effectiveness of psychosocial interventions in subgroups of caregivers of people with dementia. Int J Geriatr Psychiatry 2012;27:1-14. http://dx.doi.org/10.1002/gps.2694.
- Lee E. Do technology-based support groups reduce care burden among dementia caregivers? A review. J Evid Inf Soc Work 2015;12:474-87. http://dx.doi.org/10.1080/15433714.2014.930362.
- Beinart N, Weinman J, Wade D, Brady R. Caregiver burden and psychoeducational interventions in Alzheimer’s disease: a review. Dement Geriatr Cogn Dis Extra 2012;2:638-48. http://dx.doi.org/10.1159/000345777.
- Neville C, Beattie E, Fielding E, MacAndrew M. Literature review: use of respite by carers of people with dementia. Health Soc Care Community 2015;23:51-3. http://dx.doi.org/10.1111/hsc.12095.
- Mason BJ, Harrison BE. Telephone interventions for family caregivers of patients with dementia: what are best nursing practices?. Alzheimers Care Today 2009;10:172-8.
- Nunnemann S, Kurz A, Leucht S, Diehl-Schmid J. Caregivers of patients with frontotemporal lobar degeneration: a review of burden, problems, needs, and interventions. Int Psychogeriatr 2012;24:1368-86. http://dx.doi.org/10.1017/S104161021200035X.
- Fiorillo A, Sampogna G, Del Gaudio L, Luciano M, Del Vecchio V. Efficacy of supportive family interventions in bipolar disorder: a review of the literature. J Psychopathol 2013;19:134-42.
- Bailey RC, Grenyer BF. Burden and support needs of carers of persons with borderline personality disorder: a systematic review. Harv Rev Psychiatry 2013;21:248-58. http://dx.doi.org/10.1097/HRP.0b013e3182a75c2c.
- Alcide A, Potocky M. Adult hospice social work intervention outcomes in the United States. J Soc Work End Life Palliat Care 2015;11:367-85. http://dx.doi.org/10.1080/15524256.2015.1107806.
- Gridley K, Brooks J, Birks Y, Baxter K, Parker G. Improving care for people with dementia: development and initial feasibility study for evaluation of life story work in dementia care. Health Serv Deliv Res 2016;4. http://dx.doi.org/10.3310/hsdr04230.
- Centre for Reviews and Dissemination . Search Strategies for DARE 2015. www.crd.york.ac.uk/crdweb/searchstrategies.asp (accessed 21 March 2016).
- Wilczynski NL, Haynes RB. Hedges Team. EMBASE search strategies achieved high sensitivity and specificity for retrieving methodologically sound systematic reviews. J Clin Epidemiol 2007;60:29-33. https://doi.org/10.1016/j.jclinepi.2006.04.001.
- Montori VM, Wilczynski NL, Morgan D, Haynes RB. Hedges Team. Optimal search strategies for retrieving systematic reviews from MEDLINE: analytical survey. BMJ 2005;330. https://doi.org/10.1136/bmj.38336.804167.47.
Appendix 1 Database search strategies
The search strategies for each individual database are presented below. Please note that the strategies were taken directly from the database search interfaces at the time that the searches were run. This detailed recording of each individual database search strategy preserves the necessary details to allow the searches to be reproduced and increases transparency of the search methods.
Applied Social Sciences Index and Abstracts
Searched via ProQuest (www.proquest.com/).
Date range searched: inception to 21 January 2016.
Searched on 21 January 2016.
Records retrieved: 1371.
Search strategy
The search strategy below incorporates a section to restrict the search to reviews only. This part of the strategy was based on the CRD search strategy for retrieving reviews from ASSIA.
((SU.EXACT(“Informal care”) OR SU.EXACT(“Carers”) OR SU.EXACT(“Respite care”) OR TI,AB(caregiv* OR care-giv* OR carer* OR ”informal care” OR befriending OR caretak* OR “care taker” OR “care takers” OR “care taking” OR “children caring” OR “families caring” OR respite) OR TI,AB(families NEAR/2 support)) AND ((TI,AB(metaanaly* OR meta-analy*) OR SU.EXACT(“Literature reviews”) OR SU.EXACT(“Systematic reviews”) OR TI,AB,IF(“meta study” OR meta-synthes* OR meta-evaluat*) OR TI,AB,IF(synthes* NEAR/3 literature*) OR TI,AB,IF(synthes* NEAR/3 research*) OR TI,AB,IF(synthes* NEAR/3 studies) OR TI,AB,IF(synthes* NEAR/3 data) OR TI,AB,IF(synthes* NEAR/3 trials) OR TI,AB,IF(synthes* NEAR/3 findings) OR TI,AB,IF(synthes* NEAR/3 evidence) OR TI,AB,IF(quantitative-synthes*) OR TI,AB,IF(pooled-analys*) OR TI,AB,IF((data NEAR/3 pool*) AND studies)) OR (TI,AB,IF(pooling NEAR/1 studies) OR TI,AB,IF(medline OR medlars OR embase OR cinahl OR cochrane OR scisearch OR psychinfo OR psycinfo OR psychlit OR psyclit) OR TI,AB,IF((hand OR manual* OR database* OR computer* OR electronic*) NEAR/3 search*) OR TI,AB,IF((electronic* OR bibliographic*) NEAR/3 database*) OR TI,AB,IF(overview*) OR TI,AB,IF(“evaluation review*”) OR TI,AB,IF(“what works”) OR TI,AB,IF(“evaluation synthes*”) OR TI,AB,IF(review*)))) AND la.exact(“English”)
Additional limits: date – from 1 January 2000 to 21 January 2016.
Key
SU.EXACT = subject heading.
TI,AB = terms in the title or abstract fields.
NEAR/2 = terms within two words of each other (any order).
* = truncation.
“ ” = phrase search.
la.exact = language limit.
Cochrane Database of Systematic Reviews
Searched via Wiley (http://onlinelibrary.wiley.com/).
Issue 1 of 12, January 2016.
Searched on 21 January 2016.
Records retrieved: 408.
Search strategy
#1 MeSH descriptor: [Caregivers] this term only (1313)
#2 MeSH descriptor: [Respite Care] this term only (33)
#3 caregiv*:ti,ab,kw (4322)
#4 care next giv*:ti,ab,kw (351)
#5 carer*:ti,ab,kw (1060)
#6 "informal care":ti,ab,kw (72)
#7 befriending:ti,ab,kw (41)
#8 caretak*:ti,ab,kw (147)
#9 care next taker*:ti,ab,kw (10)
#10 care next taking:ti,ab,kw (10)
#11 children next caring:ti,ab,kw (2)
#12 families next caring:ti,ab,kw (10)
#13 families near/2 support:ti,ab,kw (48)
#14 respite:ti,ab,kw (74)
#15 (parent or parents or mother or mothers or father or fathers) near/2 care:ti,ab,kw (460)
#16 (parent or parents or mother or mothers or father or fathers) near/2 caring:ti,ab,kw (18)
#17 (parent or parents or mother or mothers or father or fathers) near/2 support:ti,ab,kw (252)
#18 (parent or parents or mother or mothers or father or fathers) near/2 supporting:ti,ab,kw (35)
#19 (sons or daughters or friends) near/2 care:ti,ab,kw (5)
#20 (sons or daughters or friends) near/2 caring:ti,ab,kw (0)
#21 (sons or daughters or friends) near/2 support:ti,ab,kw (43)
#22 (sons or daughters or friends) near/2 supporting:ti,ab,kw (0)
#23 (husband* or wives or wife or spouse* or grandparent* or grandchild* or neighbour* or neighbor* or relatives) near/2 care:ti,ab,kw (42)
#24 (husband* or wives or wife or spouse* or grandparent* or grandchild* or neighbour* or neighbor* or relatives) near/2 caring:ti,ab,kw (11)
#25 (husband* or wives or wife or spouse* or grandparent* or grandchild* or neighbour* or neighbor* or relatives) near/2 support:ti,ab,kw (125)
#26 (husband* or wives or wife or spouse* or grandparent* or grandchild* or neighbour* or neighbor* or relatives) near/2 supporting:ti,ab,kw (3)
#27 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #23 or #24 or #25 or #26 (6318)
Note that the result at line #27 is the total for all of the databases within The Cochrane Library.
Key
MeSH descriptor = indexing term [medical subject heading (MeSH)].
* = truncation.
ti,ab,kw = terms in either title or abstract or keyword fields.
near/2 = terms within two words of each other (any order).
next = terms are next to each other.
“ “ = phrase search.
Cumulative Index to Nursing and Allied Health Literature (CINAHL Plus)
Searched via EBSCOhost (www.ebscohost.com/).
Date range searched: inception to 20 January 2016.
Searched on 21 January 2016.
Records retrieved: 2262.
Search strategy
The search strategy below incorporates a section to restrict the search to reviews only. This part of the strategy was based on the CRD search strategy for retrieving reviews from CINAHL. 83
| # | Query | Results |
|---|---|---|
| S45 | S42 OR S44 | 2262 |
| S44 | S40 AND S43 | 64 |
| S43 | (ZD “in process”) | 106,037 |
| S42 | S40 AND S41 | 2198 |
| S41 | EM 2009- | 2,529,422 |
| S40 | S15 AND S38 Limiters - Publication Year: 2000-2016; English Language | 3785 |
| S39 | S15 AND S38 | 4458 |
| S38 | S36 not S37 | 272,014 |
| S37 | PT book review | 35,119 |
| S36 | S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S33 OR S34 OR S35 | 283,972 |
| S35 | AB systematic* N10 overview* or AB methodologic* N10 overview* or AB quantitative* N10 overview* or AB research* N10 overview* or AB literature* N10 overview* or AB studies N10 overview* or AB trial* N10 overview* or AB effective* N10 overview* | 3802 |
| S34 | AB systematic* N10 review* or AB methodologic* N10 review* or AB quantitative* N10 review* or AB research* N10 review* or AB literature* N10 review* or AB studies N10 review* or AB trial* N10 review* or AB effective* N10 review* | 90,517 |
| S33 | S31 AND S32 | 54,536 |
| S32 | AB systematic* or AB methodologic* or AB quantitative* or AB research* or AB literature* or AB studies or AB trial* or AB effective* | 960,291 |
| S31 | PT review | 133,870 |
| S30 | TX electronic* N2 database* or TX electronic* N2 data base* or TX bibliographic* N2 database* or TX bibliographic* N2 data base* | 5971 |
| S29 | (MH “Reference Databases+”) or (MH “Reference Databases, Health+”) | 46,371 |
| S28 | TX hand N2 search* or TX manual N2 search* or TX database* N2 search* or TX computer* N2 search* | 16,812 |
| S27 | TX pooled analy* or TX data N2 pool* | 4964 |
| S26 | TX medline or medlars or embase or scisearch or psycinfo or psychinfo or psychlit or psyclit | 49,214 |
| S25 | TX synthes* N3 literature* or TX synthes* N3 research or TX synthes* N3 studies or TX synthes* N3 data | 6052 |
| S24 | (MH “Literature Searching+”) or (MH “Computerized Literature Searching+”) | 7088 |
| S23 | MH “Literature Review+” | 39,465 |
| S22 | TI review* or TI overview* | 134,359 |
| S21 | PT systematic review | 52,406 |
| S20 | PT nursing interventions | 1487 |
| S19 | AB cochrane or TI Cochrane | 15,534 |
| S18 | TI meta-analy* or AB meta-analy* | 26,870 |
| S17 | TI metaanaly* or AB metaanaly* | 534 |
| S16 | (MH “Meta Analysis”) | 23,952 |
| S15 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 | 52,385 |
| S14 | TI respite or AB respite | 1075 |
| S13 | TI families N2 support OR AB families N2 support | 5650 |
| S12 | TI “families caring” or AB “families caring” | 200 |
| S11 | TI “children caring” or AB “children caring” | 27 |
| S10 | TI “care taking” or AB “care taking” | 131 |
| S9 | TI "care taker*" or AB "care taker*" | 54 |
| S8 | TI caretak* or AB caretak* | 1106 |
| S7 | TI befriending or AB befriending | 92 |
| S6 | TI “informal care” or AB “informal care” | 606 |
| S5 | TI carer* or AB carer* | 8500 |
| S4 | TI “care giv*” or AB “care giv*” | 2470 |
| S3 | TI caregiv* or AB caregiv* | 27,550 |
| S2 | MH “Respite Care” | 1153 |
| S1 | MH “Caregivers” | 22,274 |
Key
MH = indexing term (CINAHL heading).
* = truncation.
TI = terms in the title.
AB = terms in the abstract.
“ “ = phrase search.
N2 = terms within two words of each other (any order).
PT = publication type.
TX = all text – search of all the database's searchable fields.
EM 2009- = limits search to records entered into the database from 2009 to present.
ZD in process = searches for any records that are in process and do not yet have an entry date.
Database of Abstracts of Reviews of Effects
Searched via Wiley (http://onlinelibrary.wiley.com/).
Issue 2 of 4, April 2015.
Searched on 21 January 2016.
Records retrieved: 153.
See above under Cochrane Database of Systematic Reviews for search strategy used.
EMBASE
Searched via Ovid (http://ovidsp.ovid.com/).
Date range searched: 1974 to 20 January 2016.
Searched on 21 January 2016.
Records retrieved: 4869.
Search strategy
The search strategy for EMBASE below incorporated the Hedges best optimisation of sensitivity and specificity filter for retrieval of systematic reviews in EMBASE. 84
-
Caregivers/ (28,457)
-
Caregiver support/ (1813)
-
Respite Care/ (874)
-
caregiv$.ti,ab. (54,102)
-
care giv$.ti,ab. (6712)
-
carer$.ti,ab. (13,826)
-
informal care.ti,ab. (1329)
-
befriending.ti,ab. (136)
-
caretak$.ti,ab. (4320)
-
care taker$.ti,ab. (245)
-
care taking.ti,ab. (322)
-
children caring.ti,ab. (42)
-
families caring.ti,ab. (257)
-
(families adj2 support).ti,ab. (1603)
-
respite.ti,ab. (1705)
-
or/1-15 (87,059)
-
meta-analys$.mp. (160,679)
-
search$.tw. (356,113)
-
review.pt. (2,121,136)
-
17 or 18 or 19 (2,456,581)
-
16 and 20 (12,459)
-
limit 21 to yr = “2000 – Current” (10,497)
-
limit 22 to english language (9443)
-
exp Animal/ (21,018,527)
-
exp animal-experiment/ (1,902,970)
-
nonhuman/ (4,667,343)
-
(rat or rats or mouse or mice or hamster or hamsters or animal or animals or dog or dogs or cat or cats or bovine or sheep).ti,ab,sh. (5,214,665)
-
24 or 25 or 26 or 27 (22,616,514)
-
exp human/ (16,646,006)
-
exp human-experiment/ (346,372)
-
29 or 30 (16,647,452)
-
28 and 31 (16,646,482)
-
28 not 32 (5,970,032)
-
23 not 33 (9397)
-
(2009$ or 2010$ or 2011$ or 2012$ or 2013$ or 2014$ or 2015$ or 2016$).em. (9,456,931)
-
34 and 35 (4869)
Key
/ = indexing term (Emtree heading).
exp = exploded indexing term (Emtree heading).
$ = truncation.
ti,ab = terms in either title or abstract fields.
pt = publication type.
sh = subject heading field.
em = entry week.
mp = multi-purpose – searches in title, original title, abstract, subject heading, name of substance and registry word fields.
tw = text word search in title or abstract fields.
adj2 = terms within two words of each other (any order).
Health Management Information Consortium
Searched via Ovid (http://ovidsp.ovid.com/).
Date range searched: 1979 to November 2015.
Searched on 21 January 2016.
Records retrieved: 909.
Search strategy
The search strategy for HMIC incorporated a strategy for finding reviews that was translated from the CRD search strategy for retrieving reviews from ASSIA.
-
Carers/ (4005)
-
Informal Care/ (393)
-
exp Respite Care/ (448)
-
caregiv$.ti,ab. (1161)
-
care giv$.ti,ab. (743)
-
carer$.ti,ab. (6824)
-
informal care.ti,ab. (424)
-
befriending.ti,ab. (82)
-
caretak$.ti,ab. (66)
-
care taker$.ti,ab. (1)
-
care taking.ti,ab. (28)
-
children caring.ti,ab. (14)
-
families caring.ti,ab. (60)
-
(families adj2 support).ti,ab. (220)
-
respite.ti,ab. (611)
-
or/1-15 (10,299)
-
exp LITERATURE REVIEWS/ (5537)
-
meta analysis/ (726)
-
(metaanaly$ or meta-analy$).ti,ab. (1605)
-
(meta study or meta synthes$ or meta evaluat$).ti,ab. (40)
-
(synthes$ adj3 (literature$ or research$ or studies or data or trials or findings or evidence)).ti. (104)
-
quantitative synthes$.ti,ab. (22)
-
pooled analys$.ti,ab. (98)
-
((data adj3 pool$) and studies).ti,ab. (93)
-
(pooling adj2 studies).ti,ab. (3)
-
(medline or medlars or embase or cinahl or cochrane or scisearch or psychinfo or psycinfo or psychlit or psyclit).ti,ab. (2342)
-
((hand or manual$ or database$ or computer$ or electronic$) adj3 search$).ti,ab. (1424)
-
((electronic$ or bibliographic$) adj3 database$).ti,ab. (972)
-
review$.ti,ab. (35,957)
-
overview$.ti,ab. (4451)
-
evaluation synthes$.ti,ab. (0)
-
evaluation review$.ti,ab. (6)
-
what works.ti,ab. (274)
-
or/17-33 (41,527)
-
16 and 34 (1523)
-
limit 35 to yr=”2000 –Current” (909)
Key
/ = indexing term.
exp = exploded indexing term.
$ = truncation.
ti,ab. = terms in either title or abstract fields.
adj2 = terms within two words of each other (any order).
Health Technology Assessment database
Searched via Wiley (http://onlinelibrary.wiley.com/).
Issue 2 of 4, April 2015.
Searched on 21 January 2016.
Records retrieved: 37.
See above under Cochrane Database of Systematic Reviews for search strategy used.
MEDLINE
Searched via Ovid (http://ovidsp.ovid.com/).
Date range searched: 1946 to January week 2 2016.
Searched on 21 January 2016.
Records retrieved: 3109.
Search strategy
The search strategy for MEDLINE below incorporated the Hedges optimised sensitivity and specificity balanced search filter for retrieval of systematic reviews in MEDLINE. 85
-
Caregivers/ (24,035)
-
Respite Care/ (914)
-
caregiv$.ti,ab. (35,082)
-
care giv$.ti,ab. (4089)
-
carer$.ti,ab. (8206)
-
informal care.ti,ab. (930)
-
befriending.ti,ab. (93)
-
caretak$.ti,ab. (3226)
-
care taker$.ti,ab. (132)
-
care taking.ti,ab. (215)
-
children caring.ti,ab. (31)
-
families caring.ti,ab. (211)
-
(families adj2 support).ti,ab. (1061)
-
respite.ti,ab. (1196)
-
or/1-14 (57,920)
-
meta-analysis.mp,pt. (86,024)
-
review.pt. (1,996,933)
-
search$.tw. (244,702)
-
16 or 17 or 18 (2,177,630)
-
15 and 19 (8440)
-
exp animals/ not humans/ (4,173,052)
-
20 not 21 (8396)
-
(2009$ or 2010$ or 2011$ or 2012$ or 2013$ or 2014$ or 2015$ or 2016$).ed. (5,415,956)
-
22 and 23 (3442)
-
limit 24 to english language (3109)
Key
/ = indexing term (MeSH heading).
exp = exploded indexing term (MeSH heading).
$ = truncation.
ti,ab = terms in either title or abstract fields.
pt = publication type.
ed = entry date.
mp = multi-purpose – searches in title, original title, abstract, subject heading, name of substance and registry word fields.
tw = text word search in title or abstract fields.
adj2 = terms within two words of each other (any order).
MEDLINE In-Process & Other Non-Indexed Citations
Searched via Ovid (http://ovidsp.ovid.com/).
Database last updated on 20 January 2016.
Searched on 21 January 2016.
Records retrieved: 401.
Search strategy
The search strategy below incorporated a strategy for finding reviews that was translated from the CRD search strategy for retrieving reviews from MEDLINE. 83
-
caregiv$.ti,ab. (4875)
-
care giv$.ti,ab. (439)
-
carer$.ti,ab. (1055)
-
informal care.ti,ab. (137)
-
befriending.ti,ab. (22)
-
caretak$.ti,ab. (283)
-
care taker$.ti,ab. (26)
-
care taking.ti,ab. (32)
-
children caring.ti,ab. (5)
-
families caring.ti,ab. (15)
-
(families adj2 support).ti,ab. (141)
-
respite.ti,ab. (95)
-
or/1-12 (6675)
-
systematic$ review$.ti,ab. (14,947)
-
meta-analytic$.ti,ab. (564)
-
meta-analysis.ti,ab. (12,106)
-
metanalysis.ti,ab. (13)
-
metaanalysis.ti,ab. (101)
-
meta analysis.ti,ab. (12,106)
-
meta-synthesis.ti,ab. (90)
-
metasynthesis.ti,ab. (31)
-
meta synthesis.ti,ab. (90)
-
meta-regression.ti,ab. (562)
-
metaregression.ti,ab. (44)
-
meta regression.ti,ab. (562)
-
(synthes$ adj3 literature).ti,ab. (287)
-
(synthes$ adj3 evidence).ti,ab. (736)
-
integrative review.ti,ab. (244)
-
data synthesis.ti,ab. (628)
-
(research synthesis or narrative synthesis).ti,ab. (252)
-
(systematic study or systematic studies).ti,ab. (1782)
-
(systematic comparison$ or systematic overview$).ti,ab. (384)
-
evidence based review.ti,ab. (243)
-
comprehensive review.ti,ab. (1391)
-
critical review.ti,ab. (1391)
-
quantitative review.ti,ab. (48)
-
structured review.ti,ab. (64)
-
realist review.ti,ab. (43)
-
realist synthesis.ti,ab. (34)
-
or/14-39 (28,503)
-
medline.ab. (9796)
-
pubmed.ab. (11,032)
-
cochrane.ab. (7101)
-
embase.ab. (7697)
-
cinahl.ab. (2226)
-
psyc?lit.ab. (27)
-
psyc?info.ab. (2869)
-
(literature adj3 search$).ab. (5471)
-
(database$ adj3 search$).ab. (5031)
-
(bibliographic adj3 search$).ab. (196)
-
(electronic adj3 search$).ab. (2097)
-
(electronic adj3 database$).ab. (2731)
-
(computeri?ed adj3 search$).ab. (232)
-
(internet adj3 search$).ab. (310)
-
included studies.ab. (1997)
-
(inclusion adj3 studies).ab. (1444)
-
inclusion criteria.ab. (7790)
-
selection criteria.ab. (1962)
-
predefined criteria.ab. (146)
-
predetermined criteria.ab. (55)
-
(assess$ adj3 (quality or validity)).ab. (6110)
-
(select$ adj3 (study or studies)).ab. (5529)
-
(data adj3 extract$).ab. (5037)
-
extracted data.ab. (965)
-
(data adj2 abstracted).ab. (311)
-
(data adj3 abstraction).ab. (161)
-
published intervention$.ab. (13)
-
((study or studies) adj2 evaluat$).ab. (13,837)
-
(intervention$ adj2 evaluat$).ab. (901)
-
confidence interval$.ab. (25,616)
-
heterogeneity.ab. (11,555)
-
pooled.ab. (6160)
-
pooling.ab. (835)
-
odds ratio$.ab. (17,406)
-
(Jadad or coding).ab. (12,700)
-
or/41-75 (104,006)
-
review.ti. (40,392)
-
77 and 76 (12,082)
-
(review$ adj4 (papers or trials or studies or evidence or intervention$ or evaluation$)).ti,ab. (16,644)
-
40 or 78 or 79 (41,167)
-
13 and 80 (413)
-
limit 81 to yr = “2000 –Current” (410)
-
limit 82 to english language (401)
Key
$ = truncation.
? = optional wildcard – stands for zero or one character.
ti,ab = terms in either title or abstract fields.
adj2 = terms within two words of each other (any order).
NHS Economic Evaluations Database
Searched via Wiley Online Library (http://onlinelibrary.wiley.com/).
Issue 2 of 4, April 2015.
Searched on 21 January 2016.
Records retrieved: 67.
See above under Cochrane Database of Systematic Reviews for search strategy used.
PsycINFO
Searched via Ovid (http://ovidsp.ovid.com/).
Date range searched: 1806 to January week 2 2016.
Searched on 21 January 2016.
Records retrieved: 2783.
Search strategy
The search strategy below incorporated an adapted version of the CRD search strategy for retrieving reviews from PsycINFO. 83
-
Caregivers/ (21,578)
-
Respite Care/ (405)
-
caregiv$.ti,ab. (38,420)
-
care giv$.ti,ab. (2332)
-
carer$.ti,ab. (7251)
-
informal care.ti,ab. (734)
-
befriending.ti,ab. (192)
-
caretak$.ti,ab. (4009)
-
care taker$.ti,ab. (46)
-
care taking.ti,ab. (161)
-
children caring.ti,ab. (52)
-
families caring.ti,ab. (230)
-
(families adj2 support).ti,ab. (1351)
-
respite.ti,ab. (1288)
-
or/1-14 (54,825)
-
metaanaly*.ti,sh. (68)
-
meta-analy*.ti,sh. (13,305)
-
cochrane*.ti. (155)
-
(review* or overview*).ti,ab. (481,630)
-
meta analysis/ (3771)
-
meta analysis.md. (14,073)
-
(review adj2 literature).ti. (3525)
-
“literature review”.md. (116,490)
-
“systematic review”.md. (13,184)
-
(synthes* adj3 (literature* or research or studies or data)).ti. (653)
-
pooled analys*.ti,ab. (532)
-
((data adj2 pool*) and studies).ti,ab. (747)
-
((hand or manual* or database* or computer* or electronic*) adj2 search*).ti,ab. (6637)
-
((electronic* or bibliographic*) adj2 (database* or data base*)).ti,ab. (3073)
-
or/16-29 (514,573)
-
(“review software other” or “review media” or editorial or letter or “review book”).dt. (169,661)
-
(electronic collection or dissertation abstract or encyclopedia).pt. (450,365)
-
(rat or rats or mouse or mice or hamster or hamsters or animal or animals or dog or dogs or cat or cats or bovine or sheep).ti,ab,sh. (282,974)
-
31 or 32 or 33 (844,164)
-
30 not 34 (350,835)
-
15 and 35 (5976)
-
limit 36 to (english language and yr=”2000 –Current”) (4431)
-
(2009$ or 2010$ or 2011$ or 2012$ or 2013$ or 2014$ or 2015$ or 2016$).up. (1,393,644)
-
37 and 38 (2783)
Key
/ = subject heading.
$ = truncation.
* = truncation.
ti,ab = terms in either title or abstract fields.
adj2 = terms within two words of each other (any order).
sh = subject heading field.
md = methodology field.
dt = document type.
pt = publication type.
up = update code – date the record was released into the database.
PROSPERO
Searched via www.crd.york.ac.uk/PROSPERO/.
Searched on 16 February 2016.
Records retrieved: 72.
Searched in review title field for the following terms:
Carer or carers or caregiver or caregivers or caregiving – 72 results
Care-giver or care-givers or care-giving – 0
Caretaker or caretakers or caretaking – 0
Care-taker or care-takers or care-taking – 0
Informal care or befriending or respite or family support – 0
Social Care Online
Searched via www.scie-socialcareonline.org.uk/.
Searched on 22 January 2016.
Records retrieved: 1706.
Seven searches in total were carried out to enable download of results (currently limited to 500 only).
Search 1
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
ContentTypes: ‘systematic review’
140 results.
Search 2
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
ContentTypes: ‘research review’
418 results.
Search 3
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
SubjectTerms: “systematic reviews” including this term only
OR SubjectTerms: “ ‘literature reviews’ ” including this term only
270 results.
Search 4
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
PublicationTitle: ‘review’
466 results.
Search 5
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
PublicationTitle: ‘overview’
47 results.
Search 6
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
AllFields: ‘metaanalysis’
OR AllFields: ‘meta-analysis’
OR AllFields: “ ‘meta study’ ”
OR AllFields: ‘meta-synthesis’
OR AllFields: ‘synthesis’
OR AllFields: “ ‘pooled analysis’ ”
OR AllFields:” ‘pooling studies’ ”
OR AllFields: “ ‘what works’ ”
149 results.
Search 7
SubjectTerms: “ ‘carers’ ” including this term only
OR SubjectTerms: “ ‘young carers’ ” including this term only
OR SubjectTerms: “ ‘informal care’ ” including this term only
OR SubjectTerms: “ ‘befriending schemes’ ” including this term only
OR AllFields: ‘caregiver’
OR AllFields: ‘care-giver’
OR AllFields: ‘carer’
OR AllFields: “ ‘informal care’ ”
OR AllFields: ‘befriending’
OR AllFields: ‘caretaker’
OR AllFields: ‘care-taker’
OR AllFields: “ ‘care taking’ ”
OR AllFields: “ ‘children caring’ ”
OR AllFields: “ ‘families caring’ ”
OR AllFields: ‘respite’
AND
AllFields: ‘medline’
OR AllFields: ‘medlars’
OR AllFields: ‘embase’
OR AllFields: ‘cinahl’
OR PublicationTitle: ‘cochrane’
OR AbstractOmitNorms: ‘cochrane’
OR AllFields: ‘scisearch’
OR AllFields: ‘psychinfo’
OR AllFields: ‘psycinfo’
OR AllFields: ‘psychlit’
OR AllFields: ‘psyclit’
OR PublicationTitle: ‘search’
OR AbstractOmitNorms: ‘search’
216 results.
Social Sciences Citation Index
Searched via Web of Science – ISI Web of Knowledge (www.isinet.com/).
Date range searched: 1900 to 20 January 2016.
Searched on 22 January 2016.
Records retrieved: 4970.
Search strategy
The search strategy below incorporates a section to restrict the search to reviews only. This part of the strategy was based on the CRD search strategy for retrieving reviews from the Social Science Citation Index.
| # 28 | 4970 | (#27) AND LANGUAGE: (English) Indexes = SSCI Timespan = 2000–2016 |
| # 27 | 5555 | (#26) AND LANGUAGE: (English) Indexes = SSCI Timespan = 1900–2016 |
| # 26 | 5762 | #25 AND #13 Indexes = SSCI Timespan = 1900–2016 |
| # 25 | 46,020 | #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18 OR #17 OR #16 OR #15 OR #14 Indexes = SSCI Timespan = 1900–2016 |
| # 24 | 1116 | TS=(“respite”) Indexes = SSCI Timespan = 1900–2016 |
| # 23 | 1795 | TS=(“families” NEAR/2 “support”) Indexes = SSCI Timespan = 1900–2016 |
| # 22 | 176 | TS=(“families caring”) Indexes = SSCI Timespan = 1900–2016 |
| # 21 | 48 | TS=(“children caring”) Indexes = SSCI Timespan = 1900–2016 |
| # 20 | 48 | TS=(“care-taker*”) Indexes = SSCI Timespan = 1900–2016 |
| # 19 | 1946 | TS=(caretak*) Indexes = SSCI Timespan = 1900–2016 |
| # 18 | 137 | TS=(“befriending”) Indexes = SSCI Timespan = 1900–2016 |
| # 17 | 1410 | TS=(“informal care”) Indexes = SSCI Timespan = 1900–2016 |
| # 16 | 7344 | TS=(carer*) Indexes = SSCI Timespan = 1900–2016 |
| # 15 | 2261 | TS=(care-giv*) Indexes = SSCI Timespan = 1900–2016 |
| # 14 | 34,552 | TS=(caregiv*) Indexes = SSCI Timespan = 1900–2016 |
| # 13 | 328,533 | #12 OR #11 OR #10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 Indexes = SSCI Timespan = 1900–2016 |
| # 12 | 1458 | TS=(“evaluation synthes*”) OR TS=(“evaluation review*”) OR TS=(“what works”) Indexes = SSCI Timespan = 1900–2016 |
| # 11 | 33,260 | TS=(overview*) Indexes = SSCI Timespan = 1900–2016 |
| # 10 | 240,643 | TS=(review*) Indexes = SSCI Timespan = 1900–2016 |
| # 9 | 7436 | TS=(electronic* SAME database*) OR TS=(bibliographic* SAME database*) Indexes = SSCI Timespan = 1900–2016 |
| # 8 | 22,111 | TS=(“hand” SAME search*) OR TS=(manual* SAME search*) OR TS=(database* SAME search*) OR TS=(computer* SAME search*) OR TS=(electronic* SAME search*) Indexes = SSCI Timespan = 1900–2016 |
| # 7 | 16,945 | TS=(“medline” OR “medlars” OR “embase” OR “cinahl” OR “cochrane” OR “scisearch” OR “psychinfo” OR “psycinfo” OR “psychlit” OR “psyclit”) Indexes = SSCI Timespan = 1900–2016 |
| # 6 | 2629 | TS=(“data” SAME pool*) AND TS=”studies” Indexes = SSCI Timespan = 1900–2016 |
| # 5 | 991 | TS=(“quantitative synthes*” OR “pooled analys*” OR “pooling studies”) Indexes = SSCI Timespan = 1900–2016 |
| # 4 | 18,329 | TS=(synthes* SAME (literature* OR research* OR “studies” OR “data” OR “trials” OR “findings” OR “evidence”)) Indexes = SSCI Timespan = 1900–2016 |
| # 3 | 16,867 | TS=(“literature review*”) Indexes = SSCI Timespan = 1900–2016 |
| # 2 | 597 | TS=(meta-study OR meta-synthes* OR meta-evaluat*) Indexes = SSCI Timespan = 1900–2016 |
| # 1 | 52,989 | TS=(metaanaly* OR meta-analy*) Indexes=SSCI Timespan=1900-2016 |
Key
TS = topic tag; searches terms in title, abstract, author keywords and keywords plus fields.
* = truncation.
“ ” = phrase search.
SAME = terms within same sentence.
Social Services Abstracts
Searched via ProQuest (www.proquest.com/).
Date range searched: inception to 22 January 2016.
Searched on 22 January 2016.
Records retrieved: 673.
Search strategy
The search strategy below incorporates a section to restrict the search to reviews only. This part of the strategy was based on the CRD search strategy for retrieving reviews from ASSIA.
(SU.EXACT(“Caregivers”) OR SU.EXACT(“Respite Care”) OR TI,AB(caregiv* OR care-giv* OR carer* OR “informal care” OR befriending OR caretak* OR “care taker” OR “care takers” OR “care taking” OR “children caring” OR “families caring” OR respite) OR TI,AB(families NEAR/2 support)) AND (TI,AB(metaanaly* OR meta-analy*) OR SU.EXACT(“Literature Reviews”) OR TI,AB,IF(“meta study” OR meta-synthes* OR meta-evaluat*) OR TI,AB,IF(synthes* NEAR/3 literature*) OR TI,AB,IF(synthes* NEAR/3 research*) OR TI,AB,IF(synthes* NEAR/3 studies) OR TI,AB,IF(synthes* NEAR/3 data) OR TI,AB,IF(synthes* NEAR/3 trials) OR TI,AB,IF(synthes* NEAR/3 findings) OR TI,AB,IF(synthes* NEAR/3 evidence) OR TI,AB,IF(quantitative-synthes*) OR TI,AB,IF(pooled-analys*) OR TI,AB,IF((data NEAR/3 pool*) AND studies) OR TI,AB,IF(pooling NEAR/1 studies) OR TI,AB,IF(medline OR medlars OR embase OR cinahl OR cochrane OR scisearch OR psychinfo OR psycinfo OR psychlit OR psyclit) OR TI,AB,IF((hand OR manual* OR database* OR computer* OR electronic*) NEAR/3 search*) OR TI,AB,IF((electronic* OR bibliographic*) NEAR/3 database*) OR TI,AB,IF(overview*) OR TI,AB,IF("evaluation review*") OR TI,AB,IF("what works") OR TI,AB,IF("evaluation synthes*") OR TI,AB,IF(review*))
Additional limits: date – from 1 January 2000 to 22 January 2016; language – English.
Key
SU.EXACT = subject heading.
TI,AB,IF = terms in the title or abstract or keyword fields.
NEAR/2 = terms within two words of each other (any order).
* = truncation.
“ ” = phrase search.
Appendix 2 Review characteristics tables
| First author, year | Target carer group(s) | Intervention(s) (and comparators, when reported). Include whether or not part of multicomponent intervention/targeted at group/individual | List all outcomes reported in the review | Sociodemographic informationa | Costs/cost-effectivenessb | Total number of included studies: study designs/dates/sample size/location | Brief summary of review findings (reported by authors) | Our commentary |
|---|---|---|---|---|---|---|---|---|
| Boots, 201419 | Carers of people with dementia or mild cognitive impairment | Internet-based interventions, including information, caregiving strategies, telephone or e-mail support, and carer discussion forums. Some were tailored to carer needs. Control group conditions are reported in the paper (5/12 studies) | Self-efficacy; stress/burden; depressive symptoms; coping; quality of life; experience of intervention; sense of competence; decision-making confidence; and ability to achieve pre-set objectives Other (single study) outcomes are reported in the paper |
Spouses; children. Mostly female; mean age range (when reported) 47–73 years | NR | 12 studies (three RCTs; four mixed methods; one single-group pre–post-test design; one quasi-experimental design; two pre-test post-test multiple group designs; one formative evaluation) Study dates: 1995–2013 Sample size range: 11–700 Location: NR |
Internet interventions for informal carers of people with dementia may improve carer well-being. Multicomponent, tailored interventions allowing carer interaction are likely to be more effective than those that primarily provide information. Authors report variable quality of included studies | Variable quality of included studies (overall low). Well conducted, but reporting of outcomes was difficult to follow. There was a positive control group intervention effect in one study. When reported, follow-up was 30 days to 12 months (not clear what time points are used in results) |
| Chien, 201120 | Non-professional carers of people with dementia | Support groups for carers led by professionals or other group members who had received professional training. Support groups included mutual support groups, educational psychology groups and training groups. Groups organised on the internet, by telephone ‘or in the community’ (not further defined) were excluded Control groups were general care, waiting list or minimal support including information, personal consultation, traditional support groups and short-break services |
Well-being, depression, burden and social outcome variables Overall mental health meta-analysis is described variously as ‘psychological wellbeing’ and ‘caregivers’ mental health’. Separate analysis for depression |
The majority of carers were women (average 72.5%); the average age of carers ranged from 43.6 to 71.8 years; spouse carers ranged from 27% to 100%. Eight studies referred to mild dementia and 14 referred to moderate dementia (no further details on remaining studies) | NR | Experimental or quasi-experimental studies. Total of 30 studies with various numbers for each outcome. 20 were described as using random sampling; others non-random sampling January 1998 to December 2009 English language only Quality assessment scale developed (reported in the paper). Sample sizes for individual studies and location were not reported |
Support groups benefit carers. All outcomes studied demonstrated significant positive effects. Moderate effect sizes were found for psychological well-being, depression and ‘social outcomes’; a small effect size was found for burden. The review states that the use of theoretical models underpinning the group design and length and intensity of group sessions had a significant impact on effect size for psychological well-being and depression. There is no discussion of limitations of the review | It was not clear if the target population included volunteers. It is difficult to validate the findings, as no study tables were included in the paper and no references were given to online availability. Details on outcome measures and what was used in each analysis was limited. There were very high levels of heterogeneity in the mental health and depression outcomes, but no indication that the meta-analyses were rerun to deal with this. There were many subgroup analyses related to type of group, type of participants and study characteristics. Subgroup analysis regarding the control condition (crucial in this topic area) would have been helpful. Overall, it is difficult to be confident about the conclusions drawn by the review |
| Eggenberger, 201321 | Both professional and family carers. Some results presented separately. People with dementia aged > 65 years living in residential or community settings or in acute care. Diagnosis of dementia following DSM-IV | Communication skills training by means of face-to-face interaction in small groups or individually with aim of improving basic communicative skills with people with dementia Communication defined as ‘a reciprocal process of sharing and receiving verbal information by means of language’. Interaction was defined ‘as a reciprocal communicative action by means of non-verbal information‘. Excluded were expressive and creative interventions intended to improve memory or physical function; and interventions underpinned by specific theoretical approaches already systematically reviewed Six studies compared the intervention with usual care/no intervention; three compared it with a placebo. The remaining studies were before-and-after designs. Placebos were booklet, relaxation group, or a group given instructions on behavioural aspects of dementia (recipients of placebo were unclear) Three carer studies: all included discussion, two included videos, two included role play; one included ‘input’ (not further defined) and one ‘reflection’. Interventions varied from 2 to 15 hours of training |
For carers: observed communication skills and attitudes, burden, stress. Self-reported data on knowledge, skills and attitudes | NR | NR | RCTs, CCTs, before-and-after studies English and German Searching from inception of databases to January 2010 12 papers included: seven RCTs, two CCTs and three before-and-after studies. Eight studies conducted in the USA; three conducted in Germany; and one conducted in the UK. Only four studies (two RCTs, one CCT and one before-and-after study) focused on family carers. Total of 162 family carers were included, ranging from 22 to 95 in different studies |
Review concludes that communication skills training can have a significant impact on family carers’ ‘communication skills, competencies, and knowledge’ (abstract) The authors refer to the practical difficulties of research in this area, especially in residential settings, and the high attrition rates due to turnover |
Inadequate reporting of findings from the included studies. The reliability of the authors’ conclusion on impact for carers is unclear |
| Godwin, 201322 | Carers of people with Alzheimer’s disease or related dementia. One of the included interventions specifically targeted carers who were employed | Technology-driven multicomponent support (using computer or web-based applications). Three interventions were reported: Caregiver’s Friend: Dealing with Dementia, ComputerLink and REACH. All included an information and social support element | Social support; strain; depression; anxiety | White women; average age range 46.9 to > 60 years | NR | Eight studies (representing three ‘parent’ studies of four unique RCTs) Study dates: 1995–2007 Sample size: 772 Location: NR |
Each of the interventions had some positive findings. Intervention content and delivery were variable, as were outcome measures. There is insufficient evidence to support or refute technology-driven interventions for carers of people with dementia | Reasonably well-conducted review. Results are synthesised by intervention. No quality assessment/small number of included studies. No information on control groups or follow-up data |
| Hurley, 201423 | Family carers of people with dementia | Meditation-based interventions (including mindfulness and concentration techniques) were generally compared with no control. Two studies had active controls: passive relaxation (listening to music); education or respite | Depression; carer burden | Mean age 61 years; 87.25% female | NR | Eight studies (five case series; three RCTs) Study dates: 2004–12 Sample size: total 181; range: 6–45 Location: NR |
There is tentative evidence that meditation-based interventions improve levels of depression and carer burden | Well-conducted and well-reported review. The quality of RCTs appeared to be moderate; the quality of case series appeared to be good. Follow-up in four studies ranged from 4 weeks to 4 months |
| Jensen, 201524 | Carers of people with dementia living in the community, providing day-to-day care | Educational interventions aimed at teaching skills relevant to dementia caring. Not educational material or information. Provided as part of routine clinical interaction. Excluded were interventions that focused on one or two domains only (e.g. communication skills or anger management). Also excluded were multicomponent interventions where education was combined with other things. Three trials were of one-to-one and four of group-based interventions. All delivered by health professionals. Varied from 2.5 to 24 hours in total. Controls were usual care and/or waiting list control | Carer burden, carer quality of life (primary outcomes); depression (secondary outcome) | Not summarised. Average age of carers reported for individual studies | NR | Seven RCTs Study dates: 2001–11 No restriction on geography or ‘socioeconomic’ setting Sample sizes ranged from 50 to 292, with a total of 764 |
Abstract says that educational programmes have a moderate effect on carer burden and a small effect on depression. Evidence of effect on quality of life and long-term care transitions remain unclear. Discussion says that: . . . quality of evidence for education of caregivers [was] moderate for caregiver burden and low for quality of life, depression . . . Refers to limitations of primary research in terms of sample size and likely power. Further rigorous trials with cost-effectiveness analysis are recommended |
Studies are from different countries; one each from France, Russia, Peru, USA, Germany, Austria, Switzerland, Spain and Iran. Analysis of carer burden separates low- from high-income countries, defining low income as Russia and Peru In four out of the seven studies, subdomain results only and not always the same subdomains, making meta-analysis impossible |
| Lins, 201425 | Carers of people with dementia | Telephone counselling with or without additional intervention (educational video and/or workbook). Most interventions were conducted on an individual basis. Control groups included usual care with or without brief telephone contact at intervals; and friendly calls | Depressive symptoms (primary outcome) Burden; distress; anxiety; quality of life; self-efficacy; satisfaction; social support; adverse effects/harm |
Mixture of male and female spouses; children; other family members Mean age in most RCTs: 60–66 years |
NR | 11 studies (nine RCTs and two qualitative studies) Study dates: 1999–2008 Sample size range: 32–229 Locations: USA (eight RCTs) and Germany (one RCT) |
There is moderate-quality evidence that telephone counselling without any additional intervention can reduce depressive symptoms. Important needs of carers are met and there were no adverse effects. All RCTs had some high risk of bias. The quality of qualitative studies was moderate. Results should be interpreted with caution | Well-conducted and well-reported Cochrane review. Theoretical background of the included studies is reported (table 4). Positive control group effects were reported. Limited post-intervention follow-up |
| Maayan, 201427 | People with dementia and their carers (including those living in the community with a full-time carer) | Interventions providing respite care, defined as any service or groups of services designed to provide temporary periods of relief or rest (or both) for carers. Controls included those receiving otherwise comparable services without respite, but who were eligible and willing to participate in such care, or a comparison with an alternative intervention. Respite had to amount to < 50% of total care and could be at home or in an institution. Respite models varied. Studies had to use standardised approaches to the diagnosis of dementia | Secondary outcomes for carers included burden, psychological stress and health, physical health, economic impact and quality of life. Outcomes actually reported in studies were carer attitude, physical health, psychological well-being (depression, affect), burden, support received, and health and social service use | Varied reporting of sex, age and ethnicity of carers. One study was of two different Native American groups. No subgroup analysis planned | NR | Four RCTs with a total of 753 participants Study dates: 1989–2003 Locations: USA (three studies) and Canada (one study) |
Current evidence does not demonstrate any benefits or adverse effects from the use of respite care for people with dementia or their carers. Results may reflect the lack of high-quality research rather than lack of actual benefit. Well-designed trials are needed in this area. Short duration of follow-up is highlighted as a weakness in studies of a long-term condition. Review authors stated that the quality of evidence was very low | Cochrane review Three studies compared outcomes of the respite intervention group with those of the control group. One compared respite with polarity therapy. There were few similarities between studies. However, only three studies were actually used in analysis because one was said to have reported results in an ‘unusable’ form Two of the outcomes (not one as reported) showed positive impact of polarity therapy vs. respite |
| Marim, 201326 | Carers of elderly people with dementia and Alzheimer’s disease | Interdisciplinary education and support programmes compared with standard care delivery. Most were multicentre interventions delivered weekly over 3–12 months | Carer burden | NR | NR | Seven RCTs Study dates: 1994–2011 Carer sample size: intervention, n = 317; control, n = 276 Locations: France, Canada, Peru, Russia, USA and Spain |
Education and support programmes have a positive impact in reducing carer burden when compared with standard care. All included RCTs had low risk of bias | Well-conducted and well-reported review. Further intervention details are given in Portuguese (figure 3). No follow-up data |
| McKechnie, 201428 | Carers of people with dementia | Computer-mediated psychosocial (complex multifaceted) interventions with and without professional support | Carer burden/stress, depression, anxiety, self-efficacy, social support, physical aspects of caring, programme impact (including acceptability of the intervention, perceived changes in abilities and knowledge) | Chinese (two studies) and Cuban American (one study) | NR | 14 studies, several with mixed methods (only quantitative components addressed), including six RCTs, one controlled trial, four single-group pre–post-test design, two single-group post-test design, one two-group pre–post-test design Carer sample size 1165; range 18–329 Study dates: 2003–11 Locations (when reported): USA, Canada, Scandinavia and the Netherlands |
Intervention effectiveness is mixed, but generally positive. Findings support the provision of computer-mediated interventions for carers of people with dementia | Transparency of review process unclear. Variable quality of included studies. Not all studies had control groups. Limited follow-up data. Most studies used multiple outcome measures |
| Orgeta, 201429 | Carers of people with dementia | Home-based supervised endurance or aerobic exercise; telephone-based exercise promotion; 12 weeks’ exercise programme. Other durations of intervention are reported in the paper. Comparator: usual care (no specific physical activity intervention) | Depression; perceived stress; carer burden; anxiety | Sedentary older women (average age 62 years); spouses (white Caucasian); carers in good health | NR | Four RCTs (plus three ongoing studies) Study dates: 1997–2011 Sample size: 346; range 23–173 Location: NR |
There is moderate-quality evidence that physical activity reduced subjective carer burden (SMD –0.43, 95% CI –0.81 to –0.04), compared with usual care. Authors report moderate quality of included studies. Further high-quality trials are needed | Good reporting of review methods, interventions and results. Small number of clinically heterogeneous studies containing some unknown risk of bias. Limited follow-up (ranged from end of intervention to 6 months post intervention) |
| Schoenmakers, 201030 | Family carer of a person with dementia | Active intervention in dementia home care vs. usual care, waiting list or placebo. Six types of intervention classified as cognitive–behavioural family or group training (psychosocial interventions); respite care; telephone or internet-based support; case management, physical exercise; and communication skills | Carer depression and burden | Sociodemographics are not summarised or reported in the study details table | NR | RCTs and controlled studies with at least a 6-month follow-up reported Study dates: 1980–2007 26 included studies. 15 used for depression outcome and six used for burden |
Psychosocial intervention in dementia home care was found to beneficial on carers’ burden in a non-significant way. An almost negligible decrease in depression was found in the psychosocial intervention arm, whereas multidisciplinary case management contributed to a large albeit insignificant decrease of depression in carers. Respite care was responsible for an increase in burden Review demonstrated weak evidence that supporting family carers could beneficial in terms of outcomes explored |
Very different results found from reviews covering similar types of interventions (and same primary studies in some cases). This is perhaps because of the tight focus on type of study and only those reporting longer-run outcomes (at least 6 months) and reporting results that could be subject to meta-analysis. That said, some included studies appeared to have shorter follow-up periods |
| Smith, 201432 | Carers of people with dementia (Studies that included other conditions than carers of people with dementia could be included if at least 50% were carers of people with dementia. One study also included carers of people who had a stroke) |
Volunteer mentoring (defined as befriending, mentoring and peer support). Specifically not professional support. Included studies focused on peer support and befriending only. Review reports that ‘typically’ interventions lasted for 1 hour, once per week, although telephone support offered potentially more flexibility. Table 1 indicates that one study compared the intervention with ‘usual care’ | Not reported in the text | Not summarised. Mean age in primary studies ranged from 58% to 68%; female carers ranged from 64% to 75% Ethnicity reported in one (UK) study only (99% ‘white’) Low uptake of intervention and high rates of dropout (between 19% and 30%) |
Results of economic evaluation from one high-quality RCT reported no evidence of cost-effectiveness | Quantitative, qualitative and mixed-methods primary studies. Searching from database inception to January 2013 English language only Four papers from three studies were included: one from the USA, one from Canada and one from the UK. Two were RCTs (one with an accompanying observational study paper) and one was a qualitative study |
Quantitative findings highlighted a weak but statistically significant reduction in depression after 6 months of befriending. The review demonstrates the lack of demonstrated efficacy of volunteer mentoring for carers of people with dementia. The review highlights the contrast between the quantitative studies (that show little impact) and the qualitative studies that suggest ‘carers value the support the schemes can give’. The review also points out that the outcomes measured in the quantitative studies ‘may not be focusing on the aspects of volunteer mentoring which are most important to carers’ | Abstract perhaps draws too much attention to the single (and small) significant finding. But paper does highlight several important issues related to this type of intervention research with carers |
| Vernooij-Dassen, 201131 | Family carers of people living in the community with any type of dementia | Cognitive reframing (one element of cognitive–behavioural therapy). In dementia care this focuses on: . . . family carers’ maladaptive, self-defeating or distressing cognition so about their relatives’ behaviours and about their own performance in the caring role This is hypothesised to improve coping, reduce burden and psychological morbidity, improve quality of life and reduce health-care costs Intervention delivery could be group or individual setting. There were no restrictions on type of control, which could be usual control or placebo. It appears that studies included other elements, in addition to cognitive reframing |
Psychological morbidity and distress, including depression and anxiety; quality of life of carers; carers’ appraisal of role performance, including burden, coping and self-efficacy; appraisal of problem behaviours; use of health care by people with dementia. Actually reported were anxiety, depression, stress, carer burden, coping or self-efficacy, reactions to memory or behaviour problems, quality of life and service use | Carers ages ranged from 19 to 84 years, average 59 years Relationship to people with dementia: spouse (40.2%); adult child (28.1%); and other (6.7%). In 25% of cases, no relationship was specified |
NR | RCTs. Eleven were included | Cognitive reframing for family carers of people with dementia seems to reduce psychological morbidity and subjective stress but without altering appraisals of coping or burden. Results suggest that it may be an effective component of individualised, multicomponent interventions | Studies of cognitive reframing were compared with usual care or placebo. To demonstrate the effectiveness of cognitive reframing, it may have been more helpful to compare with interventions that specifically do not include this element. Multicomponent interventions were excluded, but some of the included interventions appeared diverse in their content beyond cognitive reframing. Follow-up data were not reported; this may have been helpful when considering the clinical relevance of variable follow-up in relation to mental health outcomes |
| First author, year of publication | Target carer group(s) | Intervention(s) (and comparators, when reported). Include whether or not part of multicomponent intervention/targeted at group/individual | List all outcomes reported in the review | Sociodemographic informationa | Costs/cost-effectivenessb | Total number of included studies: study designs/dates/sample size/location | Brief summary of review findings (reported by authors) | Our commentary |
|---|---|---|---|---|---|---|---|---|
| Lang, 201433 | Adult (aged > 18 years) family carers of patients with cancer receiving active (potentially life-saving) treatment | Art-making class/creative arts intervention (including painting, decorating jewellery boxes, monoprints, silk scarves, wall hangings, Mandela creations, mosaic tile trays and ribbon gems) | Stress; anxiety | Two-thirds of participants were female aged between 18 and 81 years (one study); mean age 51.43 years (one study). Some had high school education; Catholic religion; and Hispanic origin | NR | Two quasi-experimental (pre–post-test) studies; 2004 and 2007 Total sample size: 109 Location: South Florida; south-eastern USA |
Art therapy is effective in reducing anxiety, stress and negative emotions in family carers of patients with cancer. Further research is needed to establish the impact of art therapy on coping | Well-reported Joanna Briggs Institute review. Meta-analysis is based on two primary studies with same lead author and small sample size (n = 109). Other results from the individual studies are also reported |
| Northouse, 201034 | Carers of people in various stages of cancer | Psychoeducation (including information on symptom management); skills training (including coping and communication); therapeutic counselling (encouraging therapeutic leadership). Most interventions were delivered jointly to patient and carer (63%); nine studies focused on carers alone. Interventions were delivered largely face to face (69%); others by telephone and group delivery | Carer burden (strain or demanding activity, overinvestment, negative reaction to activities relating to caring for the patient) Caregiving benefit (personal growth, rewarding experience, investment, self-esteem) Information needs Coping strategies (active coping, problem solving, reduction of ineffective coping such as avoidance and denial) Self-efficacy (perceived confidence, preparation, and/or mastery to provide care and manage patients’ symptoms) Physical functioning (self-care behaviours such as exercise, recreational activities, improvements in sleep quality) Distress and anxiety (emotional distress, worry, negative affect or mood) Depression Marital–family relationships (marital or sexual satisfaction, family support, couple communication) Social functioning (ability to carry out domestic and family roles; increased interactions with family members, friends and peers) |
Spouses (84%); others were adult children, siblings, family members and friends; most were female (64%) and Caucasian (84%); age range 18–92 (mean 55) years | NR | 29 RCTs Study dates: 1983–2009 Sample size range: 14–329 Location: NR |
Interventions targeted to family carers of cancer patients can have a positive effect on many important carer outcomes. Small to medium intervention effects were found for improved carer burden, ability to cope, self-efficacy and quality of life | Well-reported review. Authors organised the data collection (incorporating multiple outcome measures) in the following conceptual framework: stress and coping theory; cognitive–behavioural theory; quality-of-life frameworks. Authors state that many of the interventions were designed primary to address patient care |
| Regan, 201235 | Partners of people with cancer | Couples-based psychosocial interventions (involving spousal partner). Most were ‘dyadic’ (where both patient and partner engage simultaneously with similar roles). Others comprised coaching (whereby the partner adopts a ‘proxy’ therapist role); individual (whereby patient and partner receive the same or similar intervention separately). Intervention focus: communication; coping skills, including relaxation, stress management and information; education in symptom management, side effects of treatment. Intervention delivery included face to face, telephone and video | Quality of life Physical and psychological distress (emotional distress, anxiety, depression, worry, negative thoughts and/or negative mood) Social adjustment Sexuality Relationship functioning (defined as quality of the relationship between patients and partners and their satisfaction with the relationship) Appraisal variables Coping Self-efficacy Couple communication (defined as how couples communicate and discuss thoughts, feelings and practical issues surrounding the cancer between each other) Problem-solving |
Mean age 53.37 years (SD 4.34 years); over half female; 85% Caucasian. Most were highly educated spouses of patients | NR | 23 studies (six RCTs; 13 CCTs; and four cohort studies) Sample size range: 6–484 Published 2000 to 2011 Location: NR |
Couples-based interventions improved outcomes for intervention couples compared with control couples (small to medium effect sizes; Cohen’s d 0.35 to 0.45). Interventions were most efficacious in improving communication, psychological distress and relationship functioning. There was limited impact on physical distress and social adjustment | Well-conducted and well-reported review. Quality of included studies was moderate to strong. The review authors state that various theoretical frameworks underpinned the interventions (frameworks not reported). Regarding the authors’ findings on communication, this was not a primary outcome. The section on couple communication reports two studies with positive outcomes (one from qualitative interview, no results). Very limited evidence. Large amount of heterogeneity: multiple intervention content, multiple outcome measures, multiple results. We have extracted only the primary outcomes. Others are available in the paper |
| Waldron, 201336 | Adult carers of patients with cancer at various stages of the illness trajectory | Psychosocial interventions based on a cognitive–behavioural approach and including psychoeducation. Most were delivered by nurses face to face. Half of the included trials offered interventions jointly to cancer patients and carers. Interventions included coping skills training; problem-solving; improving sleep habits; and improving communication between carer and patient. Comparisons included usual care or attention control | Quality of life (covering coping, depression, self-efficacy, strain, negative appraisal) | Spouse or significant other; family members; friends. Mean age 56.5 years; 82% female | NR | Six RCTs Study dates: 2005–7 Sample size: 1115 carers (range 30–329) Location: NR |
The quality of included studies was fair to good. Interventions focusing on problem-solving and communication skills may improve carer quality of life. Further research is needed to investigate the efficacy of interventions across all stages of the cancer caregiving experience | Well-conducted and well-reported review. Other results for psychosocial factors (single studies) are reported in the paper |
| First author, year of publication | Target carer group(s) | Intervention(s) (when reported, include whether or not part of multicomponent intervention/targeted at group/individual) | List all outcomes reported in the review | Sociodemographic informationa | Costs/cost-effectivenessb | Total number of included studies: study designs/dates/sample size/location | Brief summary of review findings (reported by authors) | Our commentary |
|---|---|---|---|---|---|---|---|---|
| Cheng, 2012,37 201438 | Family carers of stroke survivors | Psychosocial, group and individual; many were multifaceted including counselling, psychoeducation, peer group/social support group. 12 studies were aimed at carers only; six studies were aimed at carers and stroke survivors. Control groups (when reported) received no treatment, matched historic cohort, usual care, attention/wait-list control or active control | Multiple including physical function, somatic complaints, perceived health status, carer competency, satisfaction of services, quality of life, physical, psychological and family functioning. Several other (single study) outcomes were reported | Mean age ranged from 47.9 to 71.3 years; most were female and spouse of stroke survivor; in seven studies carers had at least high school education; one study included more sons than daughters as carers | NR | 18 (13 RCTs; two pseudo-RCTs; three observational) Study dates: 1988–2010 Sample size: 1723 (range 17–257) carers Locations: USA, Australia, Europe (including one in the UK) and Taiwan (Province of China) |
The review demonstrated limited evidence of positive effect of psychosocial interventions on family functioning of carers. Methodological quality of included studies was fair (p. 725). There is a need for more well-designed RCTs to determine optimal dose and format of psychosocial interventions owing to the diversity of interventions | (Joanna Briggs Institute review) This was a well-conducted review. Authors’ conclusions are based on 2 out of 18 studies. Only a small number of studies were reported for each outcome. Theoretical frameworks underpinning the primary studies were reported |
| Ellis, 201039 | Carers of patients with stroke or TIA | Stroke liaison workers for patients and carers: proactive and structured approach (four RCTs); reactive and flexible (eight RCTs); proactive and focused approach (six RCTs) Control groups generally received usual care/minimal active control or no treatment |
Carer subjective health status (1775 carers) (primary outcome) Carer extended activities of daily living (752 carers) Carer mental health (1629 carers) Carer satisfaction |
There is no reported synthesis in the text | NR | 16 RCTs Study dates: 1984 to 2009 Sample size: 4759 patients and carers overall (unclear how split overall, but separated for individual outcomes) Locations: Australia, the Netherlands, the UK and the USA |
There is no evidence for the effectiveness of this multifaceted intervention in improving outcomes for all groups of patients or carers. Both patients and carers do report improved satisfaction with some aspects of service provision | Cochrane review (individual patient data) Carer subjective mental health status includes measure of carer strain. There is a separate outcome for mental health Some control group effects were reported Well-conducted review |
| Forster, 201240 | Carers of people who have experienced stroke or TIA | Education. Passive (nine RCTs): including written information (generic or individualised), delivered by written methods or multimedia computer program. Active (12 RCTs): interventions included lectures, specialist nurses or multicomponent interventions | Included patient and carer outcomes. Only carer outcomes reported here Knowledge (six RCTs) Carer knowledge (four RCTs) Psychological distress (four RCTs) Depression (three RCTs) Burden (three RCTs) Social activities (two RCTs) Perceived health status and quality of life (four RCTs) Satisfaction (five RCTs) |
Patients were at least 60 years old in most (n = 19) studies Carers were younger than patients |
Costs to health and social services (one UK RCT with some risks of bias) Total health and social care costs over 1 year for patients whose carers received intervention were significantly lower [MD –£4043 (US$7249; €6072), 95% CI to –£1595 to £6544]. The cost differences were largely due to differences in length of hospital stay |
21 RCTs Study dates: 1987 to 2010 2289 patients; 1290 carers. Sample size range: 36–300 The USA (three studies), the UK (11 studies), Australia (three studies), Sweden (one study), the Netherlands (one study), Taiwan (one study) and Thailand (one study) |
There is evidence that information improves patient and carer knowledge of stroke, aspects of patient satisfaction and reduces patient depression scores. The reduction in depression score was small and may not be clinically significant Authors’ report RCTs are of variable quality |
Cochrane review update This is a well-conducted review Only a small subset of the included RCTs related to carer outcomes were included |
| Legg, 201141 | Carers of stroke survivors or patients with aphasia (one study) | Non-pharmacological interventions including support and information, teaching procedural knowledge/vocational education, psychoeducational interventions. Intervention delivery included internet; individual or group using face to face, telephone or combination. Control groups included (when reported) waiting list control, no treatment, sham or usual care | Carer stress and strain (primary outcome), Global measures of stress or distress, anxiety, depression, health-related quality of life | Approximately half of the included RCTs reported information. When reported, mean age ranged from 58 to 64.4 years; per cent male, 9–32.6% | NR | Eight RCTs Study dates: 2000–7 Sample size: 1007 carers Locations: USA, Australia, Sweden, the UK (two studies) and Korea |
Authors refer to a lack of description of important characteristics relating to population However, ‘vocational educational’ type interventions delivered to carers prior to the stroke survivor’s discharge from hospital appear the most promising intervention. But this is based on one small study. There were limitations in design and conduct of all studies |
(Cochrane review) This was a well-conducted review. As the authors note, the conclusion is based on one small study |
| First author, year of publication | Target carer group(s) | Intervention(s) (and comparators, when reported). Include whether or not part of multicomponent intervention/targeted at group/individual | List all outcomes reported in the review | Sociodemographic informationa | Costs/cost-effectivenessb | Total number of included studies: study designs/dates/sample size/location | Brief summary of review findings (reported by authors) | Our commentary |
|---|---|---|---|---|---|---|---|---|
| Candy, 201142 | Adult (aged > 18 years) carers of adults in the terminal phase of a disease (10 of 11 included trials focused on cancer patients; one trial on life-limiting conditions such as general disability, chronic illness, heart disease or cancer) | Usual care plus direct interventions for carers (9 of 11 RCTs) Five of these RCTs included interventions also directed at the patient. Interventions included involvement of a nurse or social worker (seven RCTs); grief therapy (one RCT); advice and support, including problem-solving, emotional support, financial advice, future planning and patient care education (five RCTs); extra support during hospice care (one RCT); FOCUS programme (strategies to improve communication and coping) (two RCTs); family life review (one RCT); family grief therapy (one RCT); brief behavioural intervention to improve sleep quality (one RCT); and pain management education (one RCT) Indirect interventions for carers (focused on patients) (two RCTs) Reported separately in the paper |
Psychological health (including distress, coping and quality of life) Physical health (sleep quality) Other (secondary outcomes) are reported in the paper |
Middle-aged spouses or an adult child of the patient In 10 of 11 RCTs the mean age of carers was between 50 and 65 years |
NR | 11 RCTs Study dates: 1984–2008 Total sample size: 1836 carers Locations: USA, Australia and the UK |
There is evidence that interventions directly supporting carers can reduce psychological distress. Further research is needed to establish the effects on physical health, and potential harms | Well-reported Cochrane review Multiple interventions are included in the meta-analyses, and therefore individual exposures and effects are not clear (although the review authors appear to acknowledge this and take steps to address it in their meta-analytic framework on p. 8) |
| Gomes, 201343 | 14 out of 23 studies involved carers of people with multiple conditions (mostly cancer; others had congestive heart failure, COPD, HIV/AIDS, MS) | Home palliative care (19 different models of specialist and intermediate home palliative care; mostly multidisciplinary involving 2–13 professionals; intervention components, format and duration varied; four models were theoretically grounded); reinforced home palliative care plus carer support (four models). Added components were brief psychoeducation interventions delivered by care advisors (one model was theoretically based). Home palliative care was compared with reinforced version. Other controls were usual care (which varied across studies) | Place of death (primary outcome) plus various other patient outcomes Carer outcomes: pre-bereavement well-being and quality of life (psychological, social, physical, pain and general health); caregiving-related outcomes (burden, mastery, positive aspects of caregiving, unmet needs, coping and distress with patients symptoms); post-bereavement outcomes (grief, well-being and quality of life) |
Mainly female spouses; median/mean age 56–63 years | 16 studies measured resource, including emergency department visits, intensive care stays, admission, days and proportion of time spend in nursing homes and hospitals, length of hospital admissions, including last one before death, overall institutional days, outpatient clinic visits, use of community services, medication and other resources, carer post-bereavement health-care use and absenteeism from work Overall evidence of cost-effectiveness (six high-quality studies measuring total costs) inconclusive |
23 studies (16 RCTs, of which six were high quality; four CCTs; two CBAs; and one ITS with a nested CBA) Study dates: 1978–2010 Total sample: 41,603 (comprising 4042 carers and 37,561 patients) Locations: USA (11 studies), Europe (10 studies, including five in the UK), Canada (one study) and Australia (one study) |
There is clear and reliable evidence that home palliative care increases the chance of dying at home and reduces symptom burden for patients, but has no impact on carer grief (three RCTs, of which two were high quality, and one CBA; 2113 carers). Evidence on cost-effectiveness is inconclusive (high-quality evidence; figure 3) | Well-conducted review. Various other subgroup analyses reported in the paper. Two RCTs found positive effects on rewards from caregiving in favour of reinforced over standard home palliative care (p. 28), but this appears to be satisfaction with caregiving not satisfaction with the intervention. Overall quality of primary (effectiveness) studies is mixed (figure 2) and authors state that body of evidence has methodological limitations (p. 35) Authors’ conclusion: focus is on primary outcome but unclear why grief is the only carer outcome singled out. There were several others, although none suggested any notable intervention effect |
| Nevis, 201444 | Carers of people nearing the end of life (4/6 included studies were patients with advanced cancer; two of these studies targeted carers; other studies focused on patients with advanced chronic disease) | Educational interventions for health-care providers (three studies); patients nearing the end of life and informal carers (one study); patients only (one study); and informal carers alone (one study). Comparators: usual care or usual education | Quality of life | Mean age of carers: 71 years (one study); NR in second study targeting carers. Higher proportion of males than females in one study; NR in second study | Resource use reported (no significant decrease) but not costs | Six RCTs, of which two targeted and involved informal carers Study dates: 2006 and 2011 Both studies of carers conducted in USA. Sample size 661 |
Moderate-quality evidence that educational interventions improved patient symptom control and informal carer quality of life. No decrease in resource use. Serious risk of bias limitations were reported in studies reporting for carer outcomes (table A1) | Very limited evidence and small effect sizes for carer outcomes. Our data extraction focuses on the two RCTs targeting and reporting on carers |
| First author, year of publication | Target carer group(s) | Intervention(s) (and comparators, when reported). Include whether or not part of multicomponent intervention/targeted at group/individual | List all outcomes reported in the review | Sociodemographic informationa | Costs/cost-effectivenessb | Total number of included studies: study designs/dates/sample size/location | Brief summary of review findings (reported by authors) | Our commentary |
|---|---|---|---|---|---|---|---|---|
| Macleod, 201145 | Carers of people diagnosed with schizophrenia | Support from community mental health nurses (delivering intervention either directly or as part of a multidisciplinary team) Interventions broadly categorised as education (10 studies), supportive family education (13 studies), family interventions (29 studies), community support services (nine studies), mutual support groups (four studies); and day-care services (three studies) Delivery varied and included individual and group Comparisons included standard care, waiting list or other intervention (details reported in paper) |
Burden, carer knowledge, somatic symptoms, anxiety, insomnia, social dysfunction, problem-solving, severe depression | None reported except one study reported including Latino carers | NR | 68 studies (37 RCTs, six non-RCTs, three non-randomised matched controls, seven quasi-experimental, 11 single sample, one longitudinal and one pilot). Note two studies not reported in tables Study dates: 1982–2008 Sample sizes: 4–1048 (when reported) Locations: Europe (including the UK), the USA, Canada, Chile, China, Japan, Malaysia, India and Australia |
Findings were mixed. There was some evidence supporting a range of approaches that mental health nurses could offer to carers. But there is a need for further pragmatic studies to determine the extent that the interventions can be delivered within nursing practice | Discrepancies noted in number of studies in tables, and in reporting of results in text and tables Authors report some limited data on theoretical framework used in individual studies. Review authors also report results on ‘health’ or ‘general health’ but do not define what this encompasses, and some of it appears to be mental health. Therefore, these studies have not been included in the data extraction. This was a well-conducted review but has some limitations and discrepancies in the reporting of the results |
| Yesufu-Udechuku, 201546 | Carers of people with severe mental illness (most patients had a diagnosis of psychosis and schizophrenia) | Delivered by health and social care services and included psychoeducation and/or support group, problem-solving bibliotherapy and self-management Studies with comparators listed these as treatment as usual |
Experience of caregiving (authors do not clearly define what this means; for our review purposes recorded in quality-of-life and well-being outcome sheets); quality of life; satisfaction with services; psychological distress; knowledge | Median of mean age of carers was 49 years. Median study included 76% women. Studies of support group interventions were conducted only in East Asian populations | NR | 21 RCTs. Note one trial had three arms and will have been counted multiple times. 1589 carers, median sample size 63, range 40–225 Published between 1987 and 2013 Locations: China, UK, USA, Australia, Iran, Canada, Spain, Chile and Ireland |
Carer-focused interventions appear to improve the experience of caring and quality of life, and reduce psychological distress of those caring for people with severe mental illness, but not one specific intervention can be recommended. Interventions for carers should be considered as part of integrated services for people with severe mental health problems Authors state several limitations with the evidence base, including quality of RCTs being low to moderate. Analyses may be underpowered |
This was a well-conducted and well-reported review The primary outcome was ‘carer experience’, which is not explicitly defined |
Glossary
- Bibliotherapy
- Defined by Wikipedia as ‘an expressive therapy that involves the reading of specific texts with the purpose of healing. It uses an individual’s relationship to the content of the books and poetry and other written words as therapy’ (see https://en.wikipedia.org/wiki/Bibliotherapy) (reproduced under the terms of the Creative Commons Attribution-ShareAlike 3.0 Unported License).
- Caregiver’s Friend: Dealing with Dementia
- An intervention involving the delivery of positive caregiving strategies via text and video.
List of abbreviations
- ASSIA
- Applied Social Sciences Index and Abstracts
- CES-D
- Centre for Epidemiologic Studies Depression Scale
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CRD
- Centre for Reviews and Dissemination
- CSI
- Caregiver Strain Index
- DARE
- Database of Abstracts of Reviews of Effects
- GHQ
- General Health Questionnaire
- HADS
- Hospital Anxiety and Depression Scale
- HMIC
- Health Management Information Consortium
- NIHR
- National Institute for Health Research
- RCT
- randomised controlled trial
- REACH
- Resources for Enhancing Alzheimer’s Caregiver Health
- SF-36
- Short-Form questionnaire-36 items
- SSCI
- Social Sciences Citation Index