

Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project number 14/70/153. The contractual start date was in January 2016. The final report began editorial review in July 2019 and was accepted for publication in January 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Murray et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Background and rationale
This project considered children and young people who have little or no intelligible speech and need to use symbol communication aids to communicate. The children who benefit from such aids constitute a heterogeneous group, and they often have several co-occurring impairments that may include motor deficits (ranging from no control over any limb to minor impairment of one or more limbs), sensory and perceptual deficits (specifically hearing and vision) and, in some instances, cognitive deficits. When successfully prescribed, communication aids can have significant positive impacts on health and quality of life, reducing the risk of social isolation and mental health issues. 1–3
In an earlier study,4 0.5% of the population were estimated to require augmentative and alternative communication (AAC). This equates to 529 people per 100,000 population. Since 2014, NHS England has commissioned communication aid services as specialised services, delivering services to 1 in 2000 people, including, potentially, 8627 children and young people aged under 25 years. 5 Services were previously fragmented, and so this relatively new care pathway has limited decision-making resources to support the delivery or to assist in the monitoring of quality of provision.
The need for the current research was reflected in the second priority selected by the James Lind Alliance Childhood Disability Research Priority Setting Partnership, which asked ‘what is the best way to select the most appropriate communication strategies?’6,7 The proposed work reflected the need identified by the National Institute for Health Research’s (NIHR’s) call for research into the evaluation of health services to enhance the management of long-term conditions in children and young people.
Why focus on decision-making?
We know that communication aids, when successfully provided, can have a positive impact on the health and quality of life of children through to adulthood. 4 Unfortunately, symbol communication aids for children are reportedly prescribed without reference to evidence or best practice. 8,9 This may contribute to levels of aid abandonment, which in turn have an impact on the educational, employment and quality-of-life outcomes for aid users, and potentially result in higher costs to the NHS. 10,11 The process of communication aid decision-making has not been comprehensively documented or evaluated, and research evidence remains limited. 12–15 Currently, there are inadequate decision-making tools available to support the robust and effective identification and provision of communication aids. 16–19
In a 3-year government initiative, the financial cost to the NHS of inappropriate or non-provision of a communication aid was estimated to be £500,000 per individual over their lifetime. 10 The social and economic consequences of an inappropriate aid are reinforced by research that suggests that communication aid abandonment figures are between 30% and 50%. 3,11,20,21
Symbol communication aid decision-making is multifaceted, involving consideration of the child, the aid and the context of use. Symbol communication aids comprise three interconnected components: (1) the mode of communication (the aid), (2) the means of access and (3) the language representation system (e.g. the symbol).
The mode is the method by which the message is transmitted to the communication partner. This may range from noting the direction of the child’s gaze to indicate a choice, to the use of a computer-based speech output device. This project focused on computer-based devices because of the changes in specialised service provision in the UK. Service changes affected the resources that were available to pay for electronic symbol communication systems. However, the research focus does not imply that paper-based symbol communication systems have less merit in the development of communication skills. Indeed, as will become apparent in later chapters, they figured in many discussions during the current research.
Children with severe physical involvement cannot access the communication mode directly. In such instances, they need to be taught to use an indirect approach, for example using a scanning system involving switch operation. Means of access was not an intended focus of the proposed research, as we were interested in the language assessment and language representation considerations during the recommendation process. As will become apparent, it was a considerable focus for many participants and so was given greater consideration than originally anticipated.
The language representation system on a symbol communication aid may include different types of symbol set to substitute for spoken words, for example photographs, line drawings or a formalised set of symbols such as Picture Communication Symbols® (Tobbii Dynavox LLC, Pittsburgh, PA, USA). 22 The clinical decision-making debate concerning choice of language representation system was a particular focus of this research.
What do we already know about augmentative and alternative communication decision-making?
The challenge of making appropriate clinical decisions about communication aids for children with significant communication disability has long been debated in the field of practice, and the existing research highlights multiple issues.
Communication aids are a key intervention for children who cannot speak. The positive effects of using these systems include well-being, sense of belonging and educational attainment. 16,17,23–25
Expert professionals make variable decisions about appropriate technologies based on their knowledge of available systems, the medical and physical characteristics of the child, and the immediate rather than long-term use of communication aids. 14,26,27
Limited research evidence is available to determine the characteristics and features of communication aids and how these relate to successful use by a child. 2,12,28–30
Patient and family involvement in the decision-making process is often minimal, although it is recognised as key to the effective adoption of communication aids. 19,20,31–33
Little is known about the impact of acquiring language through aided communication on the educational and social experiences of these children. 18,34
Although there is literature on typical language and communication development, there is little research on symbolic-aided language learning trajectories or on how clinical decision-making tools may support recommendations. 28,34–45
Why decision-making episodes as the contexts for studying augmentative and alternative communication recommendation processes?
Currently there is a lack of understanding about the most valuable aspects of clinical expertise and a poor understanding about patient values in the clinical decision process. 45 Without research evidence to reinforce clinical expertise there is no means of determining the actual quality of provision. 26,27 Professionals make decisions between different communication aids based on clinical judgement, without the benefit of guidelines based on research evidence or patient values. 14,19,31,46,47
Aims and objectives
The overall aim was to contribute to improved long-term outcomes for children and young people with little or no intelligible speech who need symbol communication aids to communicate.
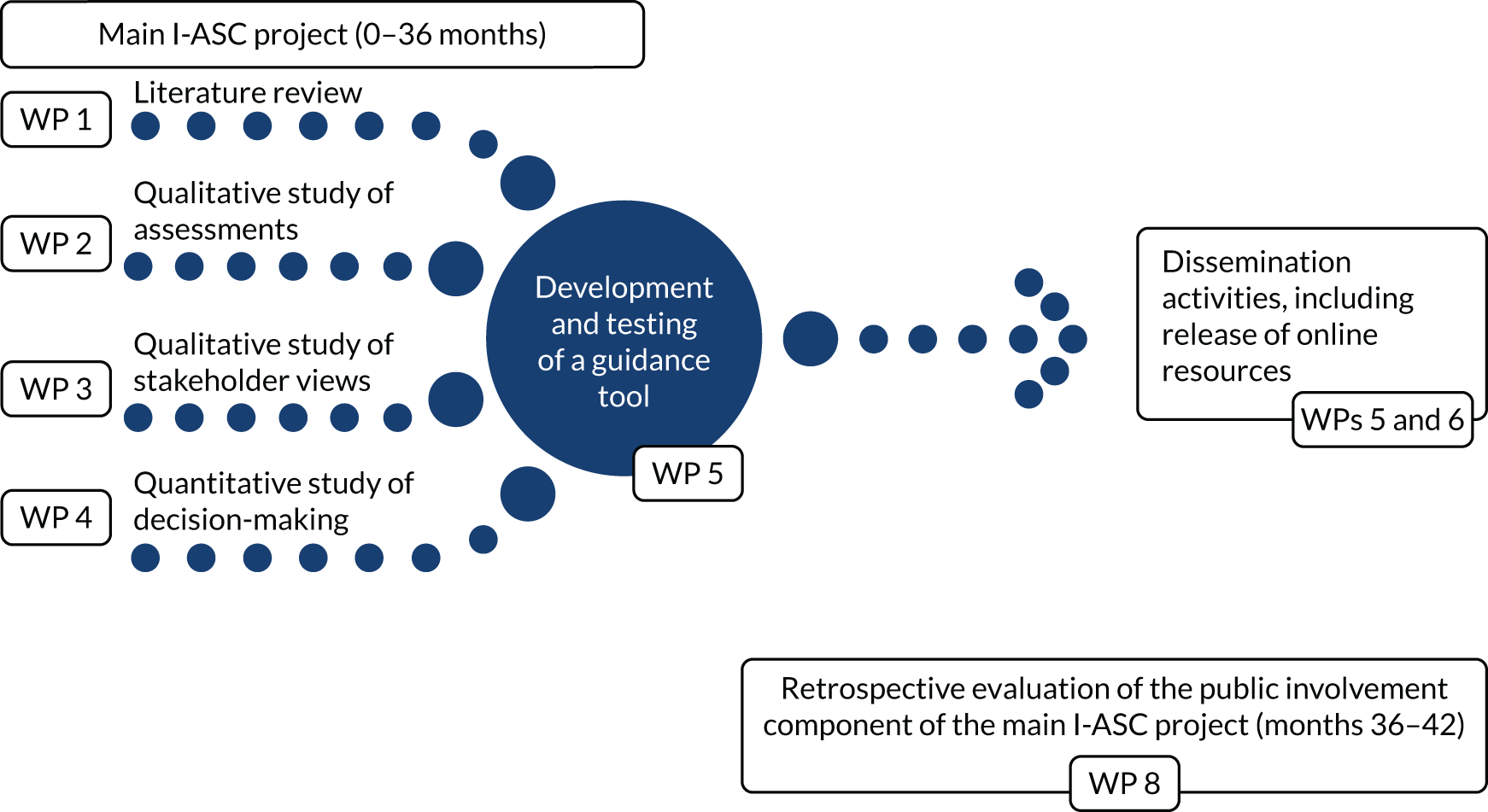
The specific aim was to influence current practice and enhance the consistency and quality of clinical decision-making in the provision of symbol communication aids. The research was delivered through specific work packages (WPs). WP 1 comprised three systematic literature reviews; WPs 2 and 3 were qualitative and included focus groups and individual interviews with different stakeholder groups; WP 4 was quantitative and delivered two surveys to professionals involved in communication aid recommendations; WP 5 focused on the development of resources to inform decision-making; WP 6 focused on disseminating the research findings; and WP 7 concerned project management. In 2018, a further work package was agreed (WP 8) and this sat separately from the preceding WPs, focusing on a retrospective evaluation of the public involvement aspects of the research. This WP is addressed separately throughout this report (Figure 1).
FIGURE 1.
Schematic representation of the main I-ASC project WPs and retrospective public involvement work package.
Research objectives
-
To understand what is perceived as important in terms of symbol communication aid provision; how decisions are made; and what barriers and facilitators have an impact on these decisions (WPs 1–4).
-
To understand and agree the range of attributes that should be considered when making these decisions, related to the child, the family and the communication aid (WPs 1–4).
-
To establish how professionals currently make decisions (by exploring their stated preferences) and how they consider attributes (WPs 2–4). (Throughout, the term ‘professional’ is taken to mean any health professional or educationalist with a specific remit to determine the best symbol communication system for a child with little or no intelligible speech. The majority of these professionals are based in the NHS, but some were in independent practice.)
-
To explore how this process takes account of the perspectives of all involved, specifically how children and adults reflect on their experiences and how parents and professionals perceive the effectiveness of existing or historic recommendations (WPs 2–5).
Then, on the basis of the information gathered from WPs 1–4:
-
to develop decision guidance for professionals and all others involved to support their decision-making in matching symbol communication aids to children (WP 5)
-
to disseminate this guidance and the results of the project to influence practice and improve the quality and consistency of decisions (WPs 5 and 6).
Research questions
The study investigated four key research questions in order to meet the aims and objectives of the project:
-
What attributes related to the child and of generic communication aids do professionals consider important in making decisions about communication aid provision? (WPs 1–4)
-
What other factors influence or inform the final decision? (WPs 1–4)
-
What attributes are considered important by other participants (e.g. the child and family) and what impact do these have in the short, medium and long term? (WPs 1 and 3)
-
What decision support guidance and resources would enhance the quality, accountability and comparability of decision-making? (WPs 1–5)
Public involvement evaluation
In December 2018 a contract variation was awarded for a retrospective evaluation of public involvement activity in the I-ASC project to be completed. This is referred to elsewhere in the report as work package 8 (WP 8). As this WP was not an aspect of the original funding award, it was designed as a post hoc methodology to evaluate the public involvement contribution to the I-ASC project. Consequently, there were additional research objectives and questions.
Research objectives
-
To describe processes that support public involvement across all aspects of co-production in the research process.
-
To describe protocols that facilitate marginalised and vulnerable public involvement groups to make meaningful contributions to the research process.
-
To appraise the costs and benefits of extensive public involvement in research.
-
To develop guidance and practical tools to facilitate the co-production of research with public involvement co-researchers from hard-to-reach cohorts.
-
To disseminate this guidance in order to improve the quantity and quality of public involvement in the co-production of research.
Research questions
-
How and what can we learn from an evaluation of public involvement in a nationally funded project focusing on vulnerable and hard-to-reach patients?
-
How can public involvement research, implementing current guidance with vulnerable and hard-to-reach groups, be structured to avoid pitfalls and improve impact?
Work package 8 is described in the final chapter of this report (see Chapter 10), as it offers insights that transcend the research questions (1–4) related to decision-making.
Chapter 2 Methodology overview
Introduction
Design
The overarching research paradigm used was pragmatism. 48,49 Pragmatism accepts the existence of singular and multiple realities and focuses on finding solutions to practical problems. Within this paradigm, a mixed-methods approach is commonplace, and specifically supports an ethnographic frame of reference. This perspective was adopted specifically for WPs 2–4, with an exploratory approach to data modelling that would typically include focus groups, interviews and surveys. An ethnographic lens also supports mixed methods that take qualitative perspectives (WPs 2 and 3: observed and lived experiences) and apply them to quantitative interrogation (WP 4). This approach also defines the WP dedicated to an evaluation of public involvement (WP 8).
Method
In summary, for the main I-ASC research (WPs 1–4), our methodological investigation adopted a three-tier approach: first, three linked systematic reviews (WP 1); second, qualitative exploration of stakeholder perspectives through focus groups and interviews (WPs 2 and 3); and, third, quantitative investigation of professional perspectives using two surveys (WP 4). Chapters 4–7 provide the detailed methods used in these WPs.
The public involvement evaluation (WP 8) detailed in Chapter 10 adopted a mixed-methods approach.
Ethics approvals
Ethics approval was obtained from Manchester Metropolitan University (reference 1316, approved 18 November 2015) and the North West – Lancashire NHS Research Ethics Committee (REC reference 16/NW/0165, approved 13 April 2016). Ethics amendment 1 (public involvement contract variation) was approved by the North West – Preston NHS Research Ethics Committee (REC reference 16/NW/0165, approved 18 December 2018). The project’s Integrated Research Application System (IRAS) ID is 186234: ‘Symbol Communication Aids for Children who are Non-speaking: CDM’.
Data collection techniques
Primary data collection activities
Primary data collection activities were focus groups, individual semistructured interviews and surveys. All data collection was UK-wide.
Data management
Data were managed in accordance with the General Data Protection Regulation and Manchester Metropolitan University’s data protection policy.
Three linked systematic literature reviews: contextualising the evidence
The aim of the systematic literature reviews (WP 1) was to identify the current state of knowledge about AAC relevant to the overall project aims. The usual use of systematic reviews is to identify robust research in a focused area, either to inform interventions or to identify gaps that require further research. Owing to the dispersed nature of AAC research,50 a multifaceted search strategy was developed to navigate the literature. The review process followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 51 Systematic reviews were completed exploring the following questions:
-
What are the language and communication characteristics of children and adults acquiring language through aided AAC systems?
-
What are the language and communication characteristics of communication aids considered in decision-making for AAC prescription?
-
What does the literature tell us about how professionals make decisions about communication aid recommendations for children?
The outputs from these systematic reviews supported the survey developments (WP 4) and informed the heuristic resources (WP 5).
Analysis procedures: qualitative and quantitative processes
With the exception of the systematic review process, this project adopted a sequential mixed-methods approach to data modelling. Two WPs had a qualitative focus (WPs 2 and 3), one WP was quantitative (WP 4) and one WP used mixed methods (WP 8). Justifications for the WP approaches are provided in the relevant chapters.
Qualitative data analysis: in summary
Coding scheme design
Two methods of data coding were adopted to support the analysis of focus group and interview data: thematic analysis52 and framework approach. 53 The former supported the inductive development of a network from open coding, and the latter enabled the deductive and inductive development of themes. With both approaches, analysis followed the stages of data interpretation, that is familiarisation with the data through to mapping and interpretation.
Intercoder reliability testing
Intercoder reliability testing was set up for all qualitative activity. This included lead researchers for the relevant WPs reading the transcripts to gain a sense of the data. Two researchers independently re-read and assigned initial codes to meaningful segments of the data, which was followed by discussion and some preliminary consensus on coding and then core research group members sharing and discussing coding. The key researchers led an iterative process of code refinement to develop the thematic network or map to the existing framework. Finally, the network and frameworks were illustrated using quotations from the data and presented to the wider research group for sense checking, credibility and transferability. Two researchers external to the core research group (critical friend group or additional co-investigator staff involved in the public involvement WP) provided independent coding reliability reviews to reduce the impact of researcher bias.
Quantitative data analysis
Two stated preference surveys investigated the decision-making of AAC practitioners. The first method, termed best–worst scaling (BWS) case 1, allowed the relative importance of factors in decision-making to be assessed. It quantified what AAC professionals regarded as the most important factors related to both children and their AAC systems. The second method, a discrete choice experiment (DCE), built on the findings from the BWS. Professionals completed this survey by making choices related to which of three hypothetical AAC systems they would choose for a stated hypothetical child.
Analysis was grounded in random utility theory and for BWS included estimates of the β parameters obtained from random parameters logit models. Analysis in the DCE included a one-sample Kolmogorov–Smirnov test.
Public involvement (formerly patient and public involvement)
Two public involvement co-researchers, an adult who used a symbol communication aid and a parent of a communication aid user, were integral to the project development and the delivery of each WP. The public involvement co-researchers led the dissemination WP (WP 6). Their involvement throughout drew on their expertise in the areas of using a symbol communication aids, working for a company assessing and supplying communication aids, mentoring, personal knowledge of the impact of technology changes, project management, financial management, leading a UK charity, and marketing and publicity management, as well as first-hand experience of the current clinical decision-making process.
The project delivery also benefited from a critical friend group that comprised a young person who used AAC, support staff, parents of AAC users, professionals and researchers.
The public involvement in the I-ASC project resulted in an additional award to the project (contract variation) in December 2018 to evaluate the impact of public involvement across the project. As previously stated, this evaluation is detailed in Chapter 10.
Chapter 3 Overview of the data set
Introduction
The aim of the I-ASC project was to involve all stakeholder groups in contributing data to at least two WPs. This was achieved and is reflected in the numbers in Table 1. In this chapter, summary details of participant demographics are provided, with detailed participant characteristics included in the relevant WP chapters. The public involvement evaluation is not detailed here (see Chapter 10).
| Geographical location of event | WP (n) | Total (n) | |||||
|---|---|---|---|---|---|---|---|
| 2 (focus groups) | 3 (interviews) | 4 (BWS) | 4 (DCE) | 5 (heuristic testing) | 6 (heuristic feedback an dissemination) | ||
| North West England | 4 | 14 | 16 | 7 | 5 | 131 | 177 |
| South East England | 13 | 14 | 7 | 34 | |||
| Yorkshire and The Humber | 17 | 9 | 12 | 22 | 3 | 185 | 248 |
| Wales | 9 | 8 | 17 | ||||
| West Midlands | 5 | 4 | 9 | 11 | 4 | 28 | 61 |
| Northern Ireland | 7 | 5 | 1 | 13 | |||
| East Midlands | 7 | 7 | 11 | 25 | |||
| South West England | 3 | 5 | 7 | 1 | 16 | ||
| East of England | 13 | 4 | 13 | 30 | |||
| London | 3 | 4 | 17 | 3 | 80 | 107 | |
| Scotland | 2 | 12 | 3 | 23 | 3 | 53 | 96 |
| North East England | 2 | 21 | 23 | ||||
| Non-UK | 1 | 3 | 5 | 70 | 79 | ||
| Total | 31 | 75 | 93 | 155 | 25 | 547 | 926 |
Data collection sites
Data collection sites were UK-wide and encompassed NHS and non-NHS (e.g. educational and charitable provisions) locations. Table 1 summarises the data collection locations by geographical area and contributors to each WP. Research participant numbers are provided for WPs 1–4. Contributions to heuristic development received during feedback trials and at dissemination events (WPs 5 and 6) are also provided. Please note that we have excluded the numbers of participants in the public involvement evaluation (WP 8) from this table as these are not relevant to the decision-making objectives of the main I-ASC study but are detailed in Chapter 10.
Participant demographics
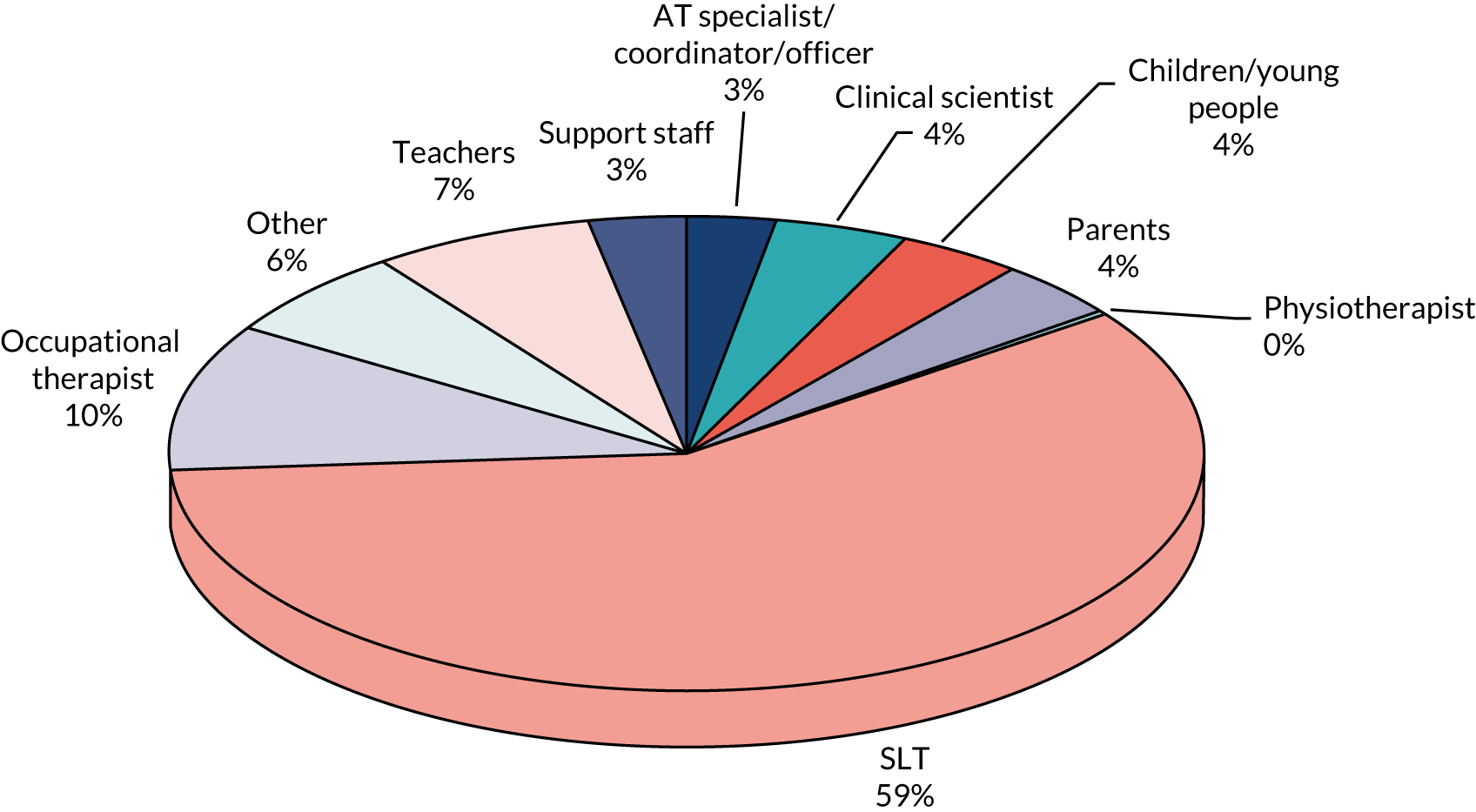
Work packages 2—4 allow for participants to be described by perspective (e.g. parent, professional). These are given in Table 2. There is a predominance of speech and language therapists (SLTs) across the whole data set and this is presented visually in Figure 2. This is not surprising as SLTs are traditionally recognised as the key professionals involved in AAC decision-making.
| Participant type | WP (n) | Total (n) | |||
|---|---|---|---|---|---|
| 2 (focus groups) | 3 (interviews) | 4 (BWS) | 4 (DCE) | ||
| Child/young person/adult | 15 | 15 | |||
| Parent | 16 | 16 | |||
| Teacher | 7 | 4 | 11 | 22 | |
| Teaching assistant | 2 | 5 | 7 | ||
| Key worker | 1 | 1 | |||
| Support worker | 2 | 2 | |||
| Therapy assistant | 1 | 1 | |||
| Personal assistant | 1 | 1 | |||
| SLT | 15 | 20 | 66 | 117 | 218 |
| Assistive technology co-ordinator | 2 | 2 | |||
| AAC officer | 1 | 1 | |||
| Physiotherapist | 1 | 1 | |||
| Occupational therapist | 7 | 4 | 7 | 9 | 27 |
| Assistive technology specialist | 5 | 5 | 10 | ||
| Other | 7 | 8 | 15 | ||
| Clinical scientist | 5 | 1 | 4 | 5 | 15 |
| Total | 31 | 75 | 93 | 155 | 354 |
FIGURE 2.
Participant backgrounds across WPs 2–4. AT, assistive technology; PT, physiotherapist.
Recruitment figures across sites
It was not feasible to define accurately the recruitment figures related to specific sites owing to the anonymous survey completion component of our data set (WP 4). However, it is possible to indicate that we recruited the following across different components of the research programme:
-
six focus groups with specialised and local professionals (n = 31)
-
interviews with children, young people and adults with lived experience, their families and the professional teams who support them (n = 75)
-
two surveys of professionals (n = 248).
This indicates that a total of 354 participants contributed to the data collection components of the research project. This figure includes NHS and non-NHS participants.
An additional 25 volunteers supported heuristic resource development and a further 547 people attended dissemination events and provided feedback.
Conclusion
In the original project submission, we had anticipated such recruitment numbers for focus groups and interviews. We had hoped for enhanced survey completion figures and suspect that the actual numbers reflect an artefact of survey methodologies and, anecdotally, the content of the surveys and the time constraints on NHS employees.
Chapter 4 Setting the scene for the complexities of decision-making in augmentative and alternative communication: systematic literature reviews (work package 1)
Systematic reviews
Introduction
The broad aim of WP 1 was to identify the current state of knowledge about AAC relevant to the overall project aims. Systematic reviews are usually used to identify robust research in a focused area, either to inform interventions or to identify gaps that require further research. As Arksey and O’Malley54 identify, there are many forms of ‘review’, with many published reviews not meeting the robust standards and replicability required of a full systematic review. To ensure the highest standards of rigour and accountability, the study followed widely accepted, published protocols to guide the process, starting with the fundamental definition: ‘Systematic reviews aim to identify, evaluate, and summarize the findings of all relevant individual studies over a health-related issue, thereby making the available evidence more accessible to decision makers.’55
Rather than seeking to inform intervention or to identify the next steps in research, the aim of WP 1 was to identify the current state of knowledge in three areas needed to inform subsequent WPs. In particular, the quantitative component, WP 4 (BWS/DCE), required data on the characteristics of children who use AAC and the features of symbol communication aids to build the surveys and vignettes. Accordingly, reviews are framed as research questions, the answers to which would inform the BWS and DCE. The third area, which informed all subsequent aspects of the research project, was the current state of knowledge concerning decision-making regarding the provision or prescription of AAC. Because the reviews were not concerned with interventions, neither the usual PICO (patient problem, intervention, component and outcome) approach56 nor the AAC adaptation of PESICO (person, environments, stakeholders, intervention, comparison and outcome)57 was appropriate for structuring the research questions.
Generic point
Guidance sought from the NHS NW Research Design Service on the extent of double screening required indicated (Sarah A Rhodes, NIHR Research Design Service – North West, and University of Manchester, 8 October 2019, personal communication) that 100% double reviewing was not necessary as the reviews did not seek evidence of the effectiveness of interventions. The reviewers for systematic reviews 1 and 3 were very experienced and had several published systematic reviews, including Cochrane reviews. One of the reviewers for systematic review 2 had no previous experience of systematic reviewing; accordingly, it was decided that, for systematic review 2, 100% of the records would be double reviewed.
Systematic review 1: the language and communication characteristics of children and adults who use augmentative and alternative communication while language acquisition is under way
The research question was ‘What are the language and communication characteristics of children and adults acquiring language through aided AAC systems?’
Method
The review process followed PRISMA,51 was registered with PROSPERO (www.crd.york.ac.uk/prospero/display_record.php?RecordID=36785) and commenced on 22 March 2016.
Search procedure
A multifaceted search strategy was developed to navigate the literature. Five electronic databases were selected, namely EMBASE™ (Elsevier, Amsterdam, the Netherlands), ProQuest® (ProQuest LLC, Ann Arbor, MI, USA), EBSCOhost (EBSCO Information Services, Ipswich, MA, USA), Scopus® (Elsevier) and Web of Science™ (Clarivate Analytics, Philadelphia, PA, USA). A hand-search of the Augmentative and Alternative Communication journal was completed and reference lists from a range of sources were also examined (Box 1 provides the search strategy).
(Symbol* OR (aided AND (communicat* OR language)) OR (Graphic AND Representation) OR ((Augmentative OR Alternative) AND Communication) OR Bliss OR Rebus OR Minspeak OR AAC OR (Assistive AND Technolog*) OR (Complex Communication Need*))
AND
Speech OR Language OR Communicat*
AND
Learn* OR Develop* OR Acqui*
Inclusion criteria
Participants
Studies were included if the participants were children, young people or adults whose speech was insufficient to meet everyday needs. Studies were excluded if the participants were typically developing or had an acquired condition. Where a study included both eligible and ineligible data, it was included only if the reported data could be disaggregated. As the focus of the review was language and communication, outcomes needed to include some indication of language or communication measures. Studies of people at pre-symbolic levels of communication were excluded.
Study types
Any primary, non-intervention research study of any design conducted from 1970 to 2018 was included. Searches were conducted in English, but records returned in any language were considered for the review.
Screening process
The search process yielded 53,158 records, which were imported into EndNote™ [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA] for screening. One researcher conducted the title and abstract review and full-text review. An independent researcher completed inter-rater reliability checks. This researcher independently applied the inclusion and exclusion criteria to a sample of search records. The sample combined half of the included papers with a sample of the excluded papers as a reliability measure and the agreement rate was 100%.
Quality appraisal
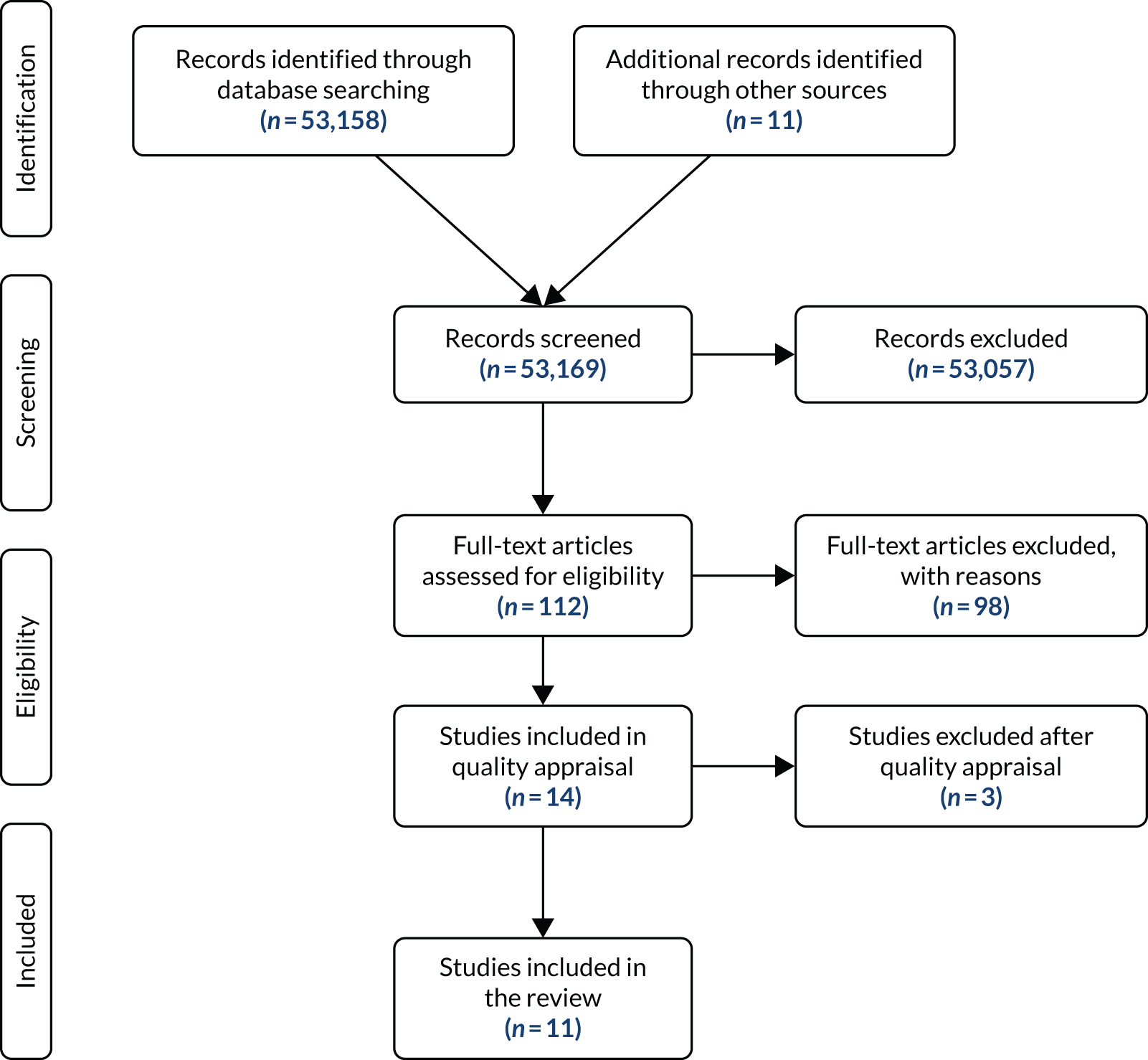
The inclusion/exclusion criteria were used to screen all returned records, resulting in 112 studies being included in the full-text review. Following the full-text review, 14 papers were identified for quality appraisal (Figure 3). Two quality appraisal tools appropriate to the study designs were used: the Critical Appraisal Skills Programme (CASP) Qualitative Checklist58 and the Evidence-Based Management Survey Checklist. 59 The 14 papers were appraised using relevant quality indicators and weight of evidence and relevance to the research question. 60 Two researchers independently completed this process before comparing the results. Eleven studies were agreed to meet the quality threshold. Three studies were excluded as they did not meet the agreed quality threshold: one from the USA,61 one from Ireland62 and one from Canada. 1
FIGURE 3.
Systematic review 1 PRISMA flow chart of language and communication characteristics of children.
Data extraction
Two researchers extracted relevant data from the studies. Information on study characteristics was extracted.
Results
The review comprised 11 research papers (Table 3), which represented 14 separate studies. Across all papers, 143 children and adult participants had used aided AAC. Most participants in the review papers had severe speech and physical impairments with no learning difficulties. The results, therefore, reflect children and adults with this profile, who are only one group of people who use AAC.
| Study (authors, country) | Description of study participants | AAC system(s) used | Aspect of language/communication studied | Outcomes |
|---|---|---|---|---|
| Blockberger and Johnston,30 USA and Canada |
20 children aged 5.8–17.1 years who could speak no more than 10 words and had no known hearing loss or second language issues Diagnoses: cerebral palsy, developmental delay, syndromes or no diagnosis Attained age-equivalent scores on the PPVT (receptive vocabulary assessment) of between 4 and 8:11 years. The children were compared with 20 children with typical development and 15 children with language delay |
Each of the children had their own individualised communication system, often combining unaided modes and light and high tech. Symbols used ranged from PCS, Minspeak® (Semantic Compaction Systems, Pittsburgh, PA, USA) and Dynasims to traditional orthography |
Understanding and expression of three grammatical morphemes: Possessive ‘s’ (e.g. Jack’s cars) Past tense ‘ed’ (e.g. ‘I walked to school’) Third person regular ‘s’ (e.g. ‘she walks’) |
The children using AAC had greater difficulty learning and using grammatical morphemes (both comprehension and expression) than children of the same age with typical development or younger children with language delays who had the same language learning level |
| Sutton,63 Canada |
Four adults with SSPI Two male and two female ranging in age from 18 to 29 years Receptive vocabulary (PPVT) age-equivalent abilities 8:4–11:10 years |
All had used Blissymbols for > 9 years with displays of 461–900 symbols One produced some intelligible spoken words Three produced vocalisations Participants were estimated to interact with 15–40 communication partners per week |
Social verbal competence |
Varying pattern of social verbal competence was observed across participants. Achievement scores did not reflect age, number of years using Blissymbols, number of symbols available or receptive vocabulary. However, number of communication partners per week and scores on the measure of social verbal competence seemed to correspond Participants had the most success with the informing function (three out of four scoring at a level of 13–14 years). Difficulty noted with the authority context (expressing in a formal register). Three out of four had most difficulty with the feelings function and one had most difficulty with the ritualising function Participants had the most success with speech acts that can be fulfilled with one word |
| Geytenbeek et al.,64 the Netherlands |
68 children out of 87 (19 did not pass screening) with severe cerebral palsy (GMFCSa levels 4 and 5). Anarthria (productive spoken vocabulary of fewer than five words). Able to match spoken words to objects. Children with severe hearing loss were excluded. Children without Dutch-speaking parents were excluded Also included 806 children with typical development |
Not specified | Language comprehension |
The children followed a typical developmental pathway but at a slower rate. The children using AAC were more delayed in learning ‘who’ questions and complex sentence types (significant difference in all sentence types) Children with dyskinetic cerebral palsy had better outcomes on complex syntactic analysis than children with spastic cerebral palsy |
| Lund and Light,16 USA | Seven young men with SSPI3 related to cerebral palsy. They ranged in age from 19 to 23 years and had a range of cognitive skills |
All had used AAC for at least 15 years. Systems used were communication boards (n = 2), computers (n = 3), Lightwriter (n = 1) and DynaVox (Tobii Technology, Pittsburgh, PA, USA) (n = 1) Five used indirect selection and two used direct selection |
Language comprehension | All participants scored below average on language comprehension |
| Redmond and Johnston,65 USA |
Four children with SSPI related to cerebral palsy or another neuromuscular condition Aged 11–15 years; had fewer than five spoken words and used AAC as their primary communication system; had normal hearing and normal corrected visual acuity; and were school-aged. Monolingual English; had no issues with an auditory detection probe Comparison groups: 11 children aged 4–6 years with typical development; 13 children aged 7–10 years with typical development; 21 adults |
Indirect access to black-and-white line drawings (no symbols) (n = 1) Direct access to a Liberator (PRC-Saltillo, Wooster, OH, USA) device with Minspeak (n = 1) Direct access to a DynaVox device with dynasyms (n = 1) Direct Lightwriter with traditional orthography (n = 1) The length of time the children had been using AAC was not specified |
Morphological competence: ability to recognise grammatical errors | Despite the wide variation in profile of the children with SSPI, a similar pattern of performance was observed across all four children. The children were able to identify when the past tense ending was missing from an irregular verb but they missed more errors than their peers who were typically developing but were matched as having the same vocabulary skills. Three out of four did better than vocabulary-matched peers in identifying when a regular past tense ending had been used where an irregular past tense ending should have been. The children with SSPI were more likely than vocabulary-matched peers to accept errors when a regular verb was missing the ending. Bare stem regular verbs were particularly challenging for children with SSPI and past tense irregular verbs were an area of strength |
| Soto and Hartmann66 and Soto et al.67 (two papers – results presented together), USA |
Four children aged 5–11 years with SSPI, average cognitive abilities and no hearing or vision difficulties Three girls and one boy Medical diagnoses: arthrogryposis and cleft palate (repaired) (n = 1), cerebral palsy (n = 2), muscular atrophy (n = 1) |
|
Narrative skills through five elicitation tasks |
Among the four children, narrative contribution ranged from very limited detail to appropriate levels of detail. Topic maintenance was a clear strength. Heavy reliance on co-construction with communication partner but could direct the conversation back to a previous point. However, lack of use of conversational control strategies, overuse of one-word utterance and the limitations of the AAC device often results in all children having to yield conversational control Appropriate event sequencing was observed in book-based activities but not in other activities. For the two youngest children, language production lacked structure and inclusion of basic story grammar elements There was a lack of action verbs and concrete supporting details in the narratives. Referencing was absent except for eye gaze use (could be considered ‘proto-referencing’) and occasional use of pronouns by some children Conjunctive cohesion: use of one-word utterances and short phrases meant that there were limited opportunities to use linking devices (such as ‘and’ or ‘because’). Pragmatic use of conjunctions was not evident and there was a lack of narrative coherence and fluency in narrative-telling |
| Soto and Toro-Zambrana,68 USA |
Three adults with SSPI related to cerebral palsy aged 25–32 years Two male and one female |
Blissymbol communication boards with 120 to 500 symbols | Morphosyntactic complexity of language output | The participants were able to convey a wide range of meanings with different language structures using their restricted vocabularies. They demonstrated use of a range of compensatory strategies to aid communication in the absence of the desired vocabulary being available |
| Sutton and Gallagher,69 Canada |
Two adults with SSPI related to cerebral palsy One male aged 25 years and one female aged 26 years |
Communication displays with 450 Blissymbols and alphabet access via numerical codes and yes/no responses | Ability to learn how to use encoding to mark regular and irregular past-tense endings | Suggests that individuals using AAC may have a reduced repertoire of language skills that may be related to modality restrictions (i.e. communicating through symbols has an impact on language learning) |
| Trudeau,70 Canada |
27 children with severe speech impairment aged 7:5–17:5 years whose first language was French Using AAC system for at least 3 months with at least 30 symbols Excluded if using an alphabet system or semantic compaction or if speech problem occurred after primary language development (2 years) |
15 had VOCAs with graphic symbols (range over 30–1000 with number of symbols unknown for four participants) Seven had symbol boards (with 60–700 symbols); 16 used direct selection; two used mixed methods; and two used scanning AAC experience ranged from 6 months to 41 years (unknown for six participants) |
Ability to construct and interpret symbol sequences |
The majority of participants showed consistent patterns in how they interpreted and constructed graphic symbol sequences, with a small number showing differences across interpretation and construction of sequences. As most were consistent, this suggests that learning to understand and learning to use graphic symbol sequences develop at the same time (rather than comprehension preceding expression) The majority used the spoken word order in the construction task unless they needed to change it to avoid ambiguity in the meaning Performance was not related to age or severity of the motor impairment or receptive vocabulary; however, performance was related to syntactic skills and cognitive abilities |
| van Balkom et al.,71 the Netherlands | Four adolescents with cerebral palsy |
All four participants used multimodal communication with communication boards; described as experienced graphic symbol users The participants’ communication boards had between 215 and 400 symbols One participant used single words; one used single words and PCS; two used rebus and single words |
Ability to describe pictures in children’s books |
Word order deviations from spoken language were observed Participants used an average of two graphic signs per message The majority of the graphic symbol messages were a succession of nouns with the use of nouns or noun combinations observed in the place of action verbs in some cases The participants demonstrated overt metalinguistic skills, such as the use of self-corrections, repetitions and other strategies, to overcome the restrictions of limited vocabularies to convey meanings |
Studies examined the language abilities of children and adults who were experienced aided communicators; the review results are detailed below.
Language understanding
Two studies16,64 reported on language understanding. In one study,16 68 children demonstrated their spoken sentence understanding. The results indicated that, although children followed a typical pattern of development, spoken sentence understanding was more typical of a child younger than their (chronological) age. In the second study,64 of seven young men who had been using AAC for ≥ 15 years, all participants scored below average (i.e. younger than their age) on language understanding. Participants did not have identified learning difficulties, so the results suggested that factors affecting language development included language learning opportunities and the influence of communicating with graphic symbols. Currently, we know too little; further research is needed to identify how AAC systems and language learning opportunities best support children to achieve their potential.
Expressive use of symbols
Three studies68,70,71 considered how participants generated graphic symbol output. There was variation across participants, with many using limited vocabularies successfully to communicate a range of messages and language structures. In one study, 72 adolescents used an average of two symbols per message to tell stories. It was clear that they used extra skills to communicate with fewer words, for example using strategies such as ‘it sounds like’. Some participants used different word orders from the spoken language in their environment. These word-order variations were used to make the intended message clearer. Word-order patterns did not appear to be related to age or motor impairment severity but did correspond to the child’s language-understanding abilities. In summary, there was wide variation in the language abilities of and graphic symbols used by children using aided AAC, and some children had developed highly creative skills to overcome the restriction of small expressive vocabularies. The limited data suggest that research is needed to understand how children develop these strategies and how to support the effective use of these.
Narrative skills
Two papers from one research project looked at the storytelling abilities of children who use AAC,66,67 which varied widely across participants. One study66 found that some children could give many details in their story, while others were unable to do this. All participants had some difficulty with independently telling stories and using different story elements. The results indicated that maintaining the topic of the story was an area of strength. Children overly relied on one-word messages and because of the limitations of their communication aids they often depended on their communication partner and allowed the partner to take control of the story. Specifically, children did not use many action words (e.g. ‘run’ or ‘jump’) or pronouns (e.g. ‘he’ and ‘she’) in their stories. Nor did they use joining words (e.g. ‘and’ or ‘because’). As a result, it was harder to follow their storylines. These findings suggested that children may need more opportunities to tell stories and may need AAC vocabularies that support storytelling.
Grammatical morphemes
Grammatical morphemes are small words or word parts of a language that can be used to change meaning. For example, adding the past-tense ending ‘–ed’ turns ‘I look’ into ‘I looked’ to show that the action happened in the past. Some studies looked at how children who use AAC understand and use grammatical morphemes. 30,65,69 The results suggest that children who use AAC find it harder to understand and use grammatical morphemes than children who are speaking. Children may leave out grammatical morphemes because they have limited opportunities to use them or because communicating with symbols may make it harder to learn grammatical morphemes. These results indicate that children may need more opportunities to learn grammar morphemes even if they are not expected to use them in everyday communication (e.g. drill and practice activities). It can be proposed that more thought needs to be given to AAC system design to support children learning to use grammatical morphemes.
Social competence
Using a test of social competence, one study63 looked at the ability of four young adults to adjust their communication abilities based on different social situations. Participants had most success with communicating messages that could be fulfilled with one word (e.g. ‘yes’) and with providing information (e.g. ‘That’s my coat’). Participants had difficulty expressing messages more formally (e.g. ‘Could I look at that?’) and expressing feelings (e.g. ‘I love it!’). The participants’ performance scores did not reflect their age, the number of symbols available on their AAC system or their language understanding. A further result was that participants who interacted with more people on a weekly basis achieved higher scores on the social competence test. This suggests that having more communication opportunities is important in supporting ongoing communication skill development.
Systematic review 2: the language and communication attributes of communication aids
The research question was ‘What are the language and communication characteristics of communication aids considered in decision-making for AAC prescription?’.
Method
Search procedure
A review protocol was drawn up using the PRISMA-P51 template and a search strategy was developed based on the research question. The search strategy is detailed in Box 2. The review commenced in March 2016.
(Symbol* OR (aided AND (communicat* OR language)) OR (Graphic AND Representation*) OR “Alternative Communication” OR “Augmentative Communication” OR “Augmentative and Alternative” OR “Alternative and Augmentative” OR AAC OR (Assistive AND Technolog*) OR (Complex Communication Need*))
AND
(attribute* OR feature* OR quality OR qualities OR characteristic* OR design* OR specification* OR (vocabulary AND (organisation OR organization))
This box has been reproduced from Judge et al. 72 with permission from Taylor & Francis Group (https://www.tandfonline.com/). The box includes minor additions and formatting changes to the original box.
Searches were carried out on the EBSCOhost, EMBASE, ProQuest, Scopus, Web of Science, the Cochrane Library and Augmentative and Alternative Communication journal electronic databases. When possible, searches were refined by excluding categories that could not be related to AAC (e.g. animal studies).
Inclusion and exclusion criteria
Studies were included if their focus was the implementation of a graphic symbol AAC system. Papers were excluded if the focus was entirely on literacy. Any primary research study of any design conducted from 1970 to 2018 was included. Searches were conducted in English, but records returned in any language were considered for the review. Unfortunately, a translation of one paper from Korean could not be sourced within the available timeframe.
Screening process
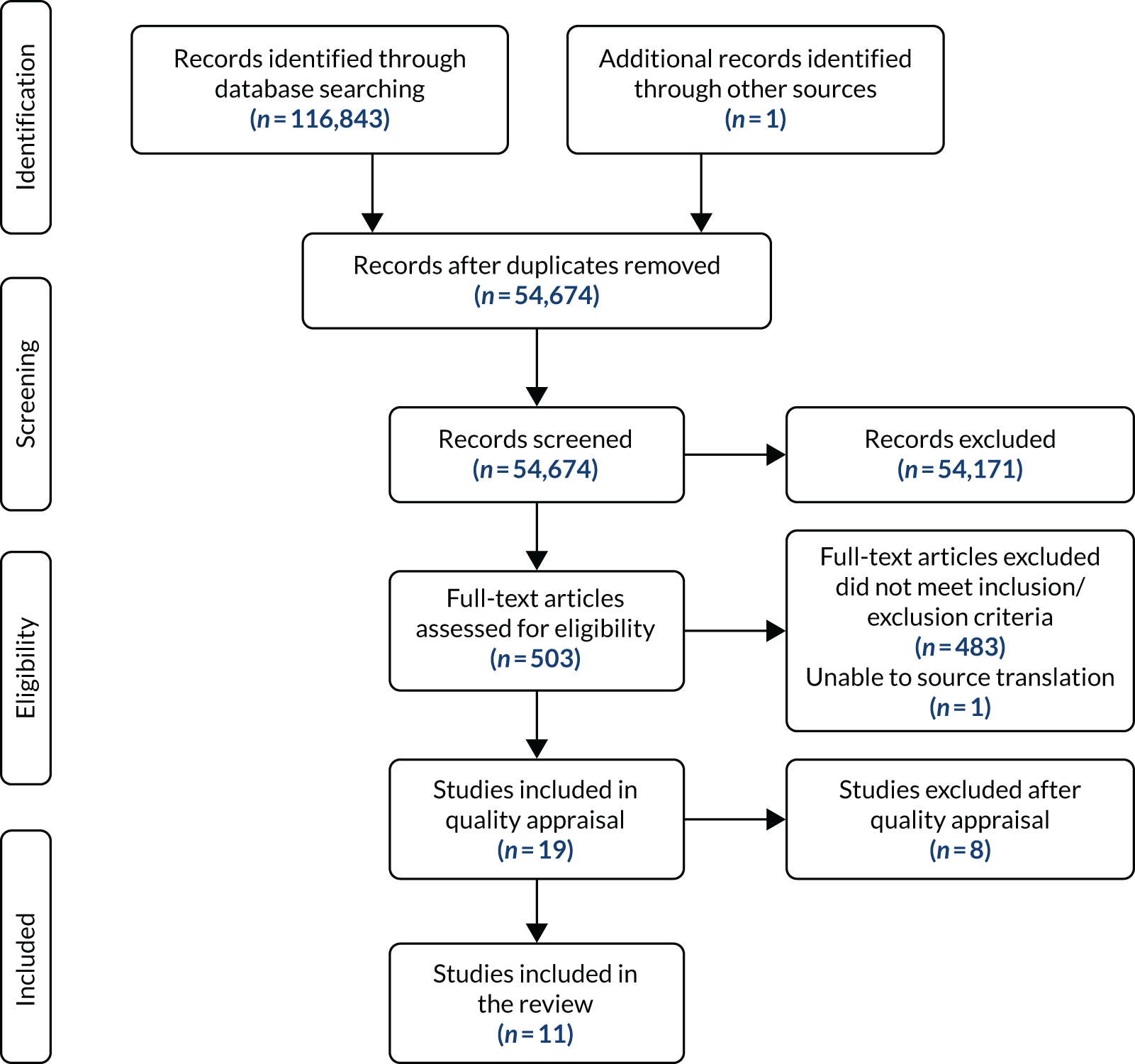
The citations were downloaded to a local database and managed using the JabRef software tool (www.jabref.org). Owing to the number of papers, the initial review process was carried out in two stages. An initial title and abstract review stage excluded articles not related to AAC. Two researchers independently carried out a title and abstract review of the remaining literature to screen for relevance to the research question. Any paper marked by either researcher as meeting the inclusion criteria was retained for full-paper review. Both researchers reviewed the full text of the remaining papers independently. Papers included by both researchers were included in the review. Papers included by only one researcher were discussed until consensus was achieved, with a third researcher available if needed. Figure 4 details the review screening process.
FIGURE 4.
Systematic review 2 PRISMA flow chart of language and communication characteristics of communication aids. This figure has been reproduced from Judge et al. 72 with permission from Taylor & Francis Group (https://www.tandfonline.com/). The figure includes minor additions and formatting changes to the original figure.
Quality appraisal
The Crowe Critical Appraisal Tool73 was used as the basis for quality appraisal as it supports the inclusion of a variety of study designs. It was chosen also because it allowed the outcome of the appraisal to be used as a criterion for acceptability. A score of < 40% on the tool was agreed to indicate that the paper was rated as weak. Quality appraisal was carried out by the two researchers independently. Papers rated as weak by both researchers were excluded from the review. 74–80
Data extraction
Two researchers worked jointly to extract relevant data from the studies. The following study characteristics were extracted: study design, participant sample size and characteristics, existing graphic symbol system(s) used by participants, language or communication attribute studied, intervention, measures and results.
Results
Data extraction was completed on 11 papers (Table 4). The included studies reported data from 66 relevant participants; 88% were reported as having cerebral palsy, 58% were reported to be children or young people and 58% were reported to be male. Eight of the studies, involving 73% of participants, took place in North America (USA, n = 6;81–86 Canada, n = 288,89) and the remaining three studies were carried out in the UK, Australia and South Africa. Five of the papers were published before 2000 and nine were published before 2005. Seven of the papers could be described as single-case (within-subject) experimental or quasi-experimental design, using the typology proposed by Tate;92 the remaining papers consisted of two surveys and two case studies.
| Study (authors, country) | Design | Sample size and characteristics | Existing graphic symbol system(s) used | Language or communication attribute studied |
|---|---|---|---|---|
| Hochstein et al.,81 USA (theme 1) |
Quasi-experimental 2 × 2 × 2 mixed factorial Only 2 × 2 relevant to this review |
Eight participants diagnosed with CP:
|
Not specifically detailedAll participants selected had to have a lack of familiarity with both of the two presentation systemsThe speech impaired children who had familiarity with AAC systems were only allowed to have familiarity with non-computerised systems or level static systems in which the levels had to be manually placed | Display levels and vocabulary abstractness
|
| Hochstein et al.,82 USA (theme 1) |
Quasi-experimental 2 × 2 × 2 mixed factorial Only 2 × 2 relevant to our review |
Two groups of eight (16 in total): CCN and speech skills (not relevant to review) CCN group: |
CCN group:
|
Presentation scheme: static or dynamic
|
| Reichle et al.,83 USA (theme 1) | Within subject, alternating treatment, repeated measures |
‘Sarah’: 16 years old, severe ‘mental retardation’, receptive language score in first percentile on formal assessment Approximately equal exposure to each display strategy prior to the study |
Macintosh PowerBook 540c (Apple, Inc., Cupertino, CA, USA) with Speaking Dynamically™ (Tobii Dynavox Llc, Pittsburgh, PA, USA) v1.2 software
|
Arrangement/layout of symbols:
|
| Hurlbut et al.,84 USA (theme 2) |
Quasi-experimental Authors describe as ‘within subject: multi-element baseline’ |
Three males with quadriplegic CP (range of type and severity)
|
|
|
| Light et al.,85 USA (theme 2) | Within subjects, repeated measures | Six physically disabled adults with functional literacy
|
Used communication aid for at least 1 year prior to study
|
|
| Light and Lindsay,86 USA (theme 2) | Within subjects, repeated measures | 12 adult participants with congenital disabilities
|
|
|
| Bornman and Bryden,87 South Africa (theme 3) | Descriptive survey | 12 South African adults with CCN who use AAC
|
|
|
| Yorkson et al.,88 Canada (theme 3) | Descriptive statistics |
Nine non-speaking adult users of AAC systems: two female, six male. Aged 20–36 years Eight CP, one CVA (not applicable to this review); moderate to severe physical handicap; range of spelling skills (< 2nd grade to 6th grade); intellectual ability broadly WNL |
Of participants with CP:
|
|
| Yorkson et al.,89 Canada (theme 3) | Case description including analysis of vocabulary list produced: percentage of structure words; and comparison with standard vocabulary lists | One participant, GT: 36 years, female; CP and spastic quadriparesis; not able to produce intelligible words; no formal education; recognised 5–10 sight words, no functional spelling; approximate age equivalence of 11 years 7 months in receptive language level skills; and motor limitations appeared to be greater obstacle to communication than language skills |
|
|
| Black et al.,90 UK (theme 4) | User-centred design and formative evaluation |
Three children with quadriplegic CP:1 and 3 – little functional speech 2 – functional speech, but sequencing/memory difficulties 1 – uses graphic symbols, ‘emerging literacy’, some whole-word reading 2 – literacy not clear ‘can copy type’ 3 – knows about 400 PCSs; can type simple sentences using on-screen keyboard |
|
|
| Stewart and Wilcock,91 Australia |
Single-case experimental design ABACA design across three cases: A, no prediction; B, regular prediction; and C, internal prediction |
Three participants:
|
|
|
Themes
Thematic analysis of the included papers resulted in three main themes of vocabulary organisation and design, symbol system and encoding, and vocabulary selection.
Vocabulary organisation and design
Three papers reported data from studies related to vocabulary organisation and design. These studies involved participants trialling communication aids with different combinations of static and dynamic organisational schemas. The primary aim of the first study81 was to investigate the nomothetic approach; however, the study had the secondary aim of examining the effect of display levels and vocabulary concreteness on the use of a communication aid. The study compared organisation schemas described as single level or dual level with a small number of symbols in a task where the participant was asked to match a symbol to a word spoken to them. The single-level display produced fewer errors, and concrete items were found to be easier to recall by participants than abstract ones. The second study82 was of similar design. In this study the static organisation promoted higher rates of vocabulary recognition during initial learning with the dynamic organisation scheme achieving higher rates after training (the seventh and eighth trials in the study). One study83 alternated organisational schemas between schemas they termed fixed, dynamic passive and dynamic active. The study involved a symbol-to-photograph matching task using a 30-symbol set with a single participant described as having ‘severe mental retardation’. For this participant there was no significant difference between dynamic active and fixed organisations tested in terms of speed or accuracy of symbol selection. The quality appraisal process identified two potential challenges to the validity of this result when considering it in the context of communicative use. First, it is not clear that the symbol-to-photograph matching task would transfer to unprompted use in communicative environments. Second, the method does not adequately explain the results for the ‘dynamic active’ condition. The method states that page changing occurred every time a symbol was pressed, with each screen displaying only half of the available symbols; this would suggest that for a randomly presented photograph the matched symbol would not be present on the communication screen for around half of all responses. The reported accuracy results are all > 60% (rising to > 90%) and so it appears that the experimenter chose the photograph to correspond to the current screen or that the method or condition was not fully described.
Symbol system and encoding
Three papers reported data from studies related to either the symbol system or the encoding methods used in symbol communication aids. One study84 had the aim of establishing which of two symbol systems was more easily acquired and maintained when an individual is trained in their use. Blissymbolics, a predominantly ideographic symbol system,93 was compared with line-drawn iconic pictures illustrated with the intention of showing a high degree of similarity to the object they represent. Twenty of each of the symbols were placed on a single-page communication board and provided to three males with cerebral palsy as part of a within-subjects study. Stimulus generalisation was evident in both symbol systems, but higher scores were reported with iconic pictures. Although students made spontaneous responses using both symbol types during daily activities, iconic pictures were used more frequently. A number of factors were identified in quality appraisal as limiting the interpretation of these results. Participants were all described as having ‘severe retardation’; however, the inclusion/exclusion criteria were not listed and it was reported that teachers felt that participants’ receptive language was above that reported in the test results. The test used to assess receptive and expressive language is not validated for this level of physical disability and it is not made clear if the assessment was carried out by the researchers or taken from records. The choice of items for the intervention was based on items that were readily visible in the environment, which limited the symbol vocabulary to nouns. Furthermore, in the spontaneous use task, both types of symbol were included on the communication board, which is unlikely to be representative of use in a naturalistic communication task. No description of the analysis or statistical methods is provided.
Two studies85,86 investigated the process of using short codes to create longer messages, termed ‘message encoding’. Both studies compared letter codes based on the first letters of salient words in the message (e.g. CE would expand to ‘can I have something to eat’), letter category codes based on the first letters of a category plus a specifier (e.g. RE would mean a ‘Requests to do with Eating’) and iconic codes derived from the icons and semantic associations proposed by Baker,94 that is, Minspeak® (e.g. the icon of an apple followed by a question mark would stand for food and requests). The first study found that the salient letter technique was associated with higher recall than the letter code or iconic technique. In both studies, concrete messages were also found to have significantly higher recall than abstract ones. There was no interaction effect between these two factors. The accuracy of code recall increased for all learning and testing sessions in both studies. The quality appraisal identified that the participant cohort in the first study was biased towards functionally literate individuals and those with cerebral palsy. The authors noted this and attempted to address it in the second study; however, in this study, all of the participants included were above the age of 6–7 years in reading ability and all but one had cerebral palsy.
Vocabulary selection
Three papers investigated the process of selecting the symbol vocabulary to use on a communication aid. One study87 aimed to investigate the social validity of a specific vocabulary set by determining the importance of identified vocabulary items to 12 adults who used AAC. The results suggested that participants concurred with most (80%) of the vocabulary selected by a variety of knowledgeable informants. The authors identified that the study had a low response rate, and participants were recruited as a purposive sample, which may have provided skewed data. There were also no test–retest or internal consistency reliability measures of the data collection tool. Two studies looked at vocabulary selection. The first study89 involved nine participants who contributed their vocabulary lists, which were compared with each other and then against standard vocabulary lists. The second study89 presented a case description of the process of vocabulary selection and a comparison of the selected vocabulary against standard vocabulary lists. Inspection of participants’ vocabulary lists highlighted that these were small vocabularies compared with estimates of common English words or standard vocabulary lists. Comparing against the standard lists showed that the larger vocabulary lists contained a greater proportion of users’ vocabularies, but no standard vocabulary list contained all words included in even relatively small user vocabularies.
Systematic review 3
The research question was ‘What does the literature tell us about how professionals make decisions in communication aid recommendations for children?’
Method
The review process followed the PRISMA guidelines. 51 The review was registered with PROSPERO (www.crd.york.ac.uk/prospero/; accessed 11 September 2018) and commenced on 14 July 2016.
Search procedure
Owing to the dispersed nature of AAC research,50 a multifaceted search strategy was developed to navigate the literature. Five electronic databases were selected, namely EMBASE, ProQuest, EBSCOhost, Scopus and Web of Science. A hand-search of the Augmentative and Alternative Communication journal was completed and reference lists from a range of sources were also examined. Box 3 summarises the search strategy.
(Symbol* OR (aided AND (communicat* OR language)) OR (Graphic AND Representation) OR “Augmentative Communication” OR “Alternative Communication” OR “Augmentative and Alternative” OR “Alternative and Augmentative” OR AAC OR (Assistive AND Technolog*) OR (Complex Communication Need*))
AND “Decision-making” OR “Decision-making” OR “Prescrib*” OR “Prescription” OR “Recommend*” OR Heuristic OR Framework
Inclusion criteria
Participants
Studies were included if the participants were professionals involved in decision-making about communication aid recommendations for children aged 0–18 years with developmental disabilities. Studies of professional decision-making about communication aid recommendation for adults with developmental disabilities were also included, as studies of adults who have grown up with communication aids have the potential to shed light on the outcomes of recommendations made in childhood. Studies of communication aid recommendation for adults with acquired disabilities, and for individuals at a pre-symbolic level of functioning, were excluded.
Communication aids
Studies of decision-making related to both light-tech aids and high-tech aids were included, as were studies in which the communication aids recommended used graphic symbol or traditional orthography representation. Studies related to manual sign or tangible symbols were excluded.
Study types
Any primary research study of any design conducted from 1970 to 2018 was included. Searches were conducted in English but records returned in any language were considered for the review.
Screening process
The search process yielded 29,591 records, which were imported into EndNote for screening. The lead researcher conducted the title and abstract review and full-text review. An independent researcher completed inter-rater reliability checks. This researcher independently applied the inclusion and exclusion criteria to a sample of search records. The independent researcher reviewed a sample of 403 records of included and excluded papers using agreed evaluation criteria. The agreement rate was 100%.
Quality appraisal
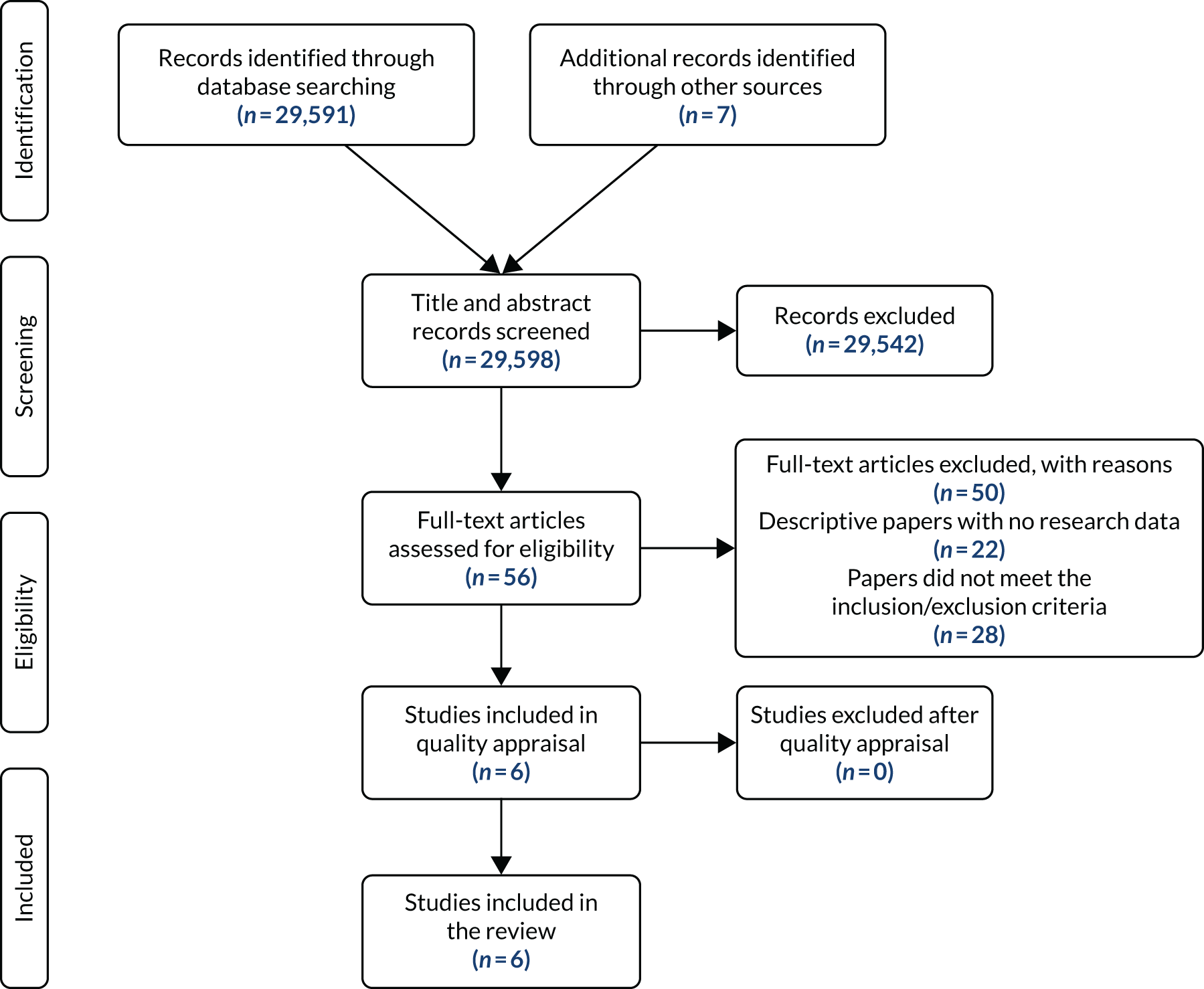
The inclusion/exclusion criteria were used to screen all returned records, resulting in 56 studies being included in the full-text review. Following the full-text review, six papers were identified for quality appraisal (Figure 5). Quality indicators were derived from two quality appraisal tools appropriate to study designs: the Critical Appraisal Skills Programme (CASP) Qualitative Checklist58 and the Evidence-Based Management Survey Checklist. 59 The six papers were appraised using relevant quality indicators and weight of evidence and relevance to the research question. 60 Two researchers independently completed this process before comparing the results. Five studies were agreed to meet quality thresholds. One study was deemed acceptable following consensus discussion.
FIGURE 5.
Systematic review 3 PRISMA flow chart of clinical decision-making by professionals.
Data extraction
Two researchers worked jointly to extract relevant data from the studies. The following study characteristics were extracted: sample size and characteristics, data collection and analysis, team composition and service delivery model, experience level of team members, decision-making processes, child and parent involvement in decision-making, language representation and organisation considerations.
Terminology
Across the included studies, different terminology was used to describe the professionals involved. For ease of reading, the term speech and language therapist (SLT) has been applied to both speech and language therapists and speech–language pathologists (SLPs). The term specialist speech and language therapist describes a SLT with reported expertise in communication aid recommendation. The term generalist SLT describes a SLT who is involved in aid recommendation but is reported to have broad experience across clinical areas. The term professional describes any person involved in the aid recommendation processes in a paid capacity, including health and education professionals.
Results
Of the six included studies, three were from the USA27,95,96 two were from Canada9,26 and one was from South Africa;97 all were published in peer-reviewed journals from 1992 to 2017. In total, there were 405 participants (Table 5). The studies employed qualitative designs9,27,96 or survey designs. 26,95,97 Analysis generated either descriptive statistics and correlations or themes.
| Study (authors, country) | Sample size and characteristic | Data collection | Data analysis | Team composition and service delivery model | Professional experience level | Decision-making processes | Child and parent involvement | Language representation and organisation |
|---|---|---|---|---|---|---|---|---|
| Batorowicz and Shepherd,26 Canada | 92 professionals | Surveys | Descriptive statistics and estimation of degree of association among variables |
Size: professionals worked in teams of 5–33 people Composition: occupational therapists,a SLTs,b technology specialists, communication disorder assistants, educators and an audiologist Model: transdisciplinary prescription review |
6 months–25 years | A small team completes an assessment and provides a case presentation to a wider team. Discussion is used to share perspectives, innovation and creativity. The wider team is involved in the decision-making process | Parents were involved but not in the final decision | n/s |
| Dada et al.,97 South Africa | 77 SLTs with a minimum of 1 year’s AAC experience | Survey |
Descriptive statistics and estimation of degree of association among variables Thematic analysis |
85% of participants worked in a team Composition: teams included occupational therapists, teachers, physiotherapists, nurses, doctors, social workers, caregivers and psychologists |
9% had ≤ 2 years’ experience 45% had 3–5 years’ experience 9% had 6–10 years’ experience 36% had > 10 years’ experience 55% worked with children and 21% worked with children and adults (results for SLTs working with adults only and results pertaining to intervention only have been disaggregated) |
74% used a combination of standardised tests and functional and authentic assessments 21% used only functional assessments 5% used observation in natural settings Areas rated as important were communication of basic needs, choice-making and child preferences. Feature-matching was also used |
Child’s aid preference was rated important and respondents considered the child and family to be team members (89%). Participants rated having active family involvement higher than having families observe assessments |
Symbol iconicity and the system’s ability to support language developed were both rated as important 54% focused on a core vocabulary for the initial vocabulary selection and 45% indicated use of core and fringe for initial vocabularies 86% used category-based organisation, 7% based on parts of speech and 8% used a combination of both Language representation decisions were influenced by resource availability, ease of learning, previous clinical experience, child’s skills, family’s views, peer recommendation, published research, and access to social media |
| Dietz et al.,27 USA | 25 SLTs | Semistructured interviews | Thematic analysis |
Size: most worked in isolation or consulted other professionals as needed Team composition and model: not specified |
Three levels of experience Generalist SLTs: SLTs who provided a range of clinical services including AAC but did not specialise in AAC Specialist SLTs: SLTs who provided AAC services for at least 50% of their caseload and had skills in AAC assessment including supporting others Research/policy SLTs: SLTs who prepared future SLTs and who carried out AAC research |
Generalist SLTs: decisions based on standardised assessments, broader information-gathering and deficit focused Specialist SLTs: used functional communication tasks, focus on multimodality and the need for personalisation, multiple appointments to facilitate aid trialling |
Generalist SLTs: n/s Specialist SLTs: parents consulted to provide information and discuss results. Provided with feedback/reassurance – believe assessment should include an education role |
Generalist SLTs: gathered information on object and picture recognition skills but did not integrate this into decision-making Specialist SLTs: gathered information about language representation/organisation and vocabulary personalisation |
| Lindsay,9 Canada | 7 SLTs; 4 occupational therapists | Semistructured interviews | Thematic analysis |
Size: teams involving different professionals (including assistive technology consultants and communication disorder assistants) Model: transdisciplinary prescription review |
At least 1 year’s experience of AAC funding authorisation |
A small team assesses the child and makes a case presentation to a larger team. Discussion is used to make the recommendation decision Participants felt that device trials would support decision-making, but were precluded from trialling by the service model Child had to demonstrate proficiency with the aid to access funding |
Child’s level of prerequisite skill was more important than parental wishes. Parental preferences did influence recommendation | n/s |
| Locke and Mirenda,95 USA | 210 special education teachers | Survey | Descriptive and correlational measures |
Size: variable Composition: 16 types of professionals listed as team members (including hearing specialists and rehabilitation engineers) Model: multidisciplinary, 24%; interdisciplinary, 39%; and transdisciplinary, 32% |
78% had > 3 years’ experience teaching children with communication disorders | n/s | Parents were considered team members | n/s |
| Lund et al.,96 USA | 8 SLTs | Semistructured case study interviews | Thematic analysis | Composition: participants indicated they would work with different team members depending on the child’s diagnosis (e.g. occupational therapist for a child with cerebral palsy, psychologist for a child with autism) |
SLTs with expertise in AAC (participants and expertise definitions drawn from Dietz et al. 27) Specialist SLTs, n = 4 Research SLTs, n = 4 |
Major themes: Areas of assessment (what was assessed) Evaluation preparation Methods of assessment (how) Parent education The child’s medical diagnosis influenced the decision-making process |
Considering parental preference, information-sharing, parental education and managing expectations were discussed | Child’s receptive language and medical diagnosis influenced vocabulary size and organisation decisions |
Team composition and service delivery model
A range of professionals was identified as contributing to communication aid recommendation; both single professional and multiprofessional models were utilised in practice. Three types of team structure emerged:
-
Individual SLTs working in isolation with families. 27,97 Both generalist and specialist SLTs reported working alone without team support. 27
-
Team models used included multidisciplinary, interdisciplinary and transdisciplinary models. 95,97 Team composition varied, with up to 16 professional backgrounds contributing to individual teams, for example hearing specialists, occupational therapists and rehabilitation engineers. 95,97
-
The two Canadian studies9,26 reported the use of a prescription review model. In this structure, specialist team representatives conduct an assessment and then refer back to the whole specialist team for a case presentation and discussion. The case presentation is a critical feature in decision-making, with the larger team taking shared responsibility for the final recommendation. Team size in one of the studies ranged from 5 to 33 members. 26
Across the studies there were different perspectives on how team composition and structure influenced decision-making. Working in a team was reported in one study to be a moderate support for decision-making. 26 While the potential advantages of team working were recognised by SLTs working in isolation, some service structures were cited as preventing team working. 27 Other studies reported that teams formed on an ‘as needed basis’95 or professionals were consulted as needed,27 suggesting that teams were transient and not working together over a period of time to develop shared knowledge and skills. One study9 identified that the lack of time to work together as a team was a challenge to providing appropriate aid recommendations for children and another study97 reported that collaborating with other team members was challenging, with reasons unspecified.
Experience level of team members and decision-making processes
Three studies26,27,96 reported that the professionals’ experience level influenced the decision-making processes. Experience level was reported to influence both the timeframes and the tasks undertaken in the recommendation process. 27 Specialist SLTs reported using longer time periods to make a recommendation. Specialist SLTs incorporated up to 8 weeks of therapy to identify an appropriate communication aid. 27 Although all specialist SLT participants in the review reported a need for more extended timeframes to make appropriate recommendations, some were constrained by service structures. Specialist SLTs in the study by Lindsay9 concluded that a consultative model limited the time available to make recommendations. Specifically, they identified a lack of device trialling as a barrier to effective decision-making. In another study,27 generalist SLTs reportedly engaged in shorter assessment processes but spent more time preparing in advance than specialist SLTs.
Child and family involvement in decision-making
An absence of active child or family involvement in decision-making was evident in most studies in the review. Two studies95,97 described family members as core team members and respondents in one of those studies rated active family involvement as more important than family observation. 97 The remaining studies9,26,27,96 described professional-led models in which parents were consulted for their views rather than being partners in the decision-making process. In one study,26 professional decision-making processes specifically excluded full parental involvement and professionals indicated that clients should not be involved in the meeting at which the final communication recommendation decision was made (the reasons for this were not explored). In another study,9 professionals reported that obtaining attitudinal and practical support for communication aids from parents and teachers was a key challenge.
Although limited evidence of families having active involvement in decision-making was identified, most studies reported that professionals considered child and family preferences during the process. In one study,27 child preferences were ascertained through parents and teachers to inform decision-making. However, no study reported professionals directly obtaining child views on aid selection. One study9 reported that strong parental opinions about technology were likely to influence the final decision made. Another96 reported that specialist SLTs valued parental preferences. These specialist SLTs described recommendation processes that included sharing information with parents and managing parents’ expectations. 96
Consideration of language representation and organisation in decision-making
Consideration of how language is represented and organised within communication aids appeared to have variable importance across the included studies. In one study,9 it was not a key consideration, whereas hardware features, such as reliability and performance, were. Another study27 reported that some generalist SLTs mentioned symbol representation in their description of their assessment process but these SLTs primarily focused on object and picture recognition tasks and did not elaborate on how they used the information to inform system selection. By contrast, the specialist SLTs in the same study reported that they focused on vocabulary personalisation and assessment of language representation and organisation. They also reported using tasks to compare communicative efficiency in message generation across different systems to inform their recommendation. SLTs favoured systems that supported less effortful and more efficient generation of utterances. 27 However, they were likely to choose a more abstract representation system if the child demonstrated the ability to learn it, even if it was not the easiest system for the child to use. 27 This rationale suggests that SLTs focus on maximising linguistic and communicative potential and consider developmental trajectories in their decision-making.
In the two most recent studies,96,97 language representation and organisation decision-making were explored in more detail. The first study96 explored the decision-making processes of eight specialist SLTs in making aid recommendations. Each SLT was asked to talk aloud the process they would undertake to recommend an aid for two children described to them in case studies. In this study, child characteristics appeared to have a strong influence on decisions made about vocabulary size and organisation. SLTs reported that information about receptive language abilities would inform their decisions for both of the children described. However, the child’s current expressive language ability was not reported as a key consideration. The study indicated that specialist SLTs considered a child’s medical diagnosis when selecting a vocabulary. For example, SLTs said that they would consider how the motor skills of a child with cerebral palsy might influence the selection of array size. By contrast, the SLTs said that cognitive loading would be the priority area they would consider when choosing the array size for a child with autism.
The second study97 surveyed South African SLTs about their communication aid recommendation practices. Respondents indicated that symbol iconicity was an important consideration, as was the software package’s ability to support language development. The majority of respondents indicated that vocabulary selection was informed by ecological or environmental inventories. Wordlists and family preferences were considered by some respondents to inform vocabulary selection. 97 Slightly more than half of respondents focused on core vocabulary (a small set of words frequently used across contexts) for initial vocabulary selections. Slightly fewer than half also included fringe vocabulary (a larger set of words used less frequently) alongside core words in their initial selections. 97 In terms of vocabulary organisation, the majority of respondents (86%) indicated that category-based was their preferred choice, with a small number (7%) using organisations based on parts of speech or parts of speech combined with category-based organisation (8%). 97
Summary and conclusions from the three systematic reviews
Three systematic reviews of the literature were undertaken examining the existing evidence base related to:
-
the language and communication characteristics of children and adults who use AAC while the process of language acquisition is under way
-
the language and communication attributes of communication aids used by children
-
clinical decision-making in communication aid recommendation processes.
Collectively, it is evident that, although the evidence base in the field of AAC is growing, gaps remain in a number of areas related to the specific focus of the current study. There is a paucity of UK and European research to inform clinical practice in this context.
The language and communication characteristics of children who use augmentative and alternative communication
The first review indicated that the evidence base on the language profile of children who grow up using aided AAC is emerging, but knowledge gaps remain. The available literature indicates a wide variation in language abilities in children and adults with severe speech and physical impairment who use aided AAC. In some studies, this variation did not appear to be related to language understanding, access to symbols or age, but did appear to be linked to opportunities to use symbols in communication contexts, and to the number of regular communication partners. This finding suggests that it may be necessary to have a greater focus on language development alongside communication skills in AAC interventions. For example, the opportunity to learn how to use grammatical markers in structured tasks may be important, even if a child will not be expected to use them communicatively (i.e. for efficiency purposes). The review indicates that access to more communication opportunities with more partners is likely to promote language development. Providing access to communication aids with the vocabulary to support the use of grammatical morphemes, storytelling and different social functions would be welcome. Communicating with symbols did affect how children developed skills; despite restricted vocabularies, in many cases children developed specific strategies to support communication, demonstrating creative and innovative ways to express themselves.
The language and communication attributes of communication aids
The second review demonstrates that there is little research evidence on which practitioners can base their decision-making about which specific symbol communication aid to choose. Readers looking for information to directly inform their clinical practice are unlikely to be able to draw significant conclusions from the available literature. Considerable inconsistencies in the terminology used were identified. Currently, the few attributes that have been studied are inconsistently defined. If clinical practice reflects the literature, it is possible that the concept of communication aids having language and communication attributes is not strongly ingrained. It may be that communication aids are not viewed as a conglomeration of attributes from which to choose but rather as a complete product. This review identifies a need for further work to better describe and understand the impact of the attributes that make up graphic symbol communication aids.
Clinical decision-making in communication aid recommendations
The available research related to decision-making in AAC is primarily qualitative. It is not possible to infer optimal approaches to decision-making from this literature review. The prevailing expert opinion indicates that having extended assessment periods involving functional communication opportunities and communication aid trialling is considered best practice; some service models may constrain the process and preclude the use of longer timeframes. Citations suggest that many children who use communication aids do not have access to experienced SLTs. These studies indicate that specialist support for generalist SLTs may be important for enhancing the quality of communication aid recommendation processes for children. Maintaining clinical expertise has been linked to having ongoing experience in an area connected with appropriate learning opportunities and mentoring support. 98 For generalist SLTs, whose role may limit their development and maintenance of expertise, providing decision guidance supports may help them to make high-quality recommendations.
Although it is recognised that children and their families should be central to communication aid recommendation processes, with consensus-building critical to future success,99 this third systematic review implies that, in many instances, families were excluded from the decision-making process. 26 Identifying how families may be supported and empowered to have a central role in decision-making in communication aid selection is merited.
This third systematic review also indicated that we have limited understanding of how decisions are made about language representation and organisation within aid recommendations. These factors are likely to be particularly important for children, as they are using communication aids during the language acquisition process. The limited reporting on language organisation decision-making may indicate that professionals prioritise hardware considerations9 or may not relate information gathered on symbolic understanding to language representation and organisation decisions. 27 When language representation and organisation decisions were discussed, the child’s characteristics such as their medical diagnosis, their ability to learn more abstract symbols and their receptive language abilities were reported as influencing factors. 96 Across studies, there was minimal evidence to suggest that information about children’s expressive communication abilities is gathered and used to inform aid recommendation. Systematic review 3 suggests that consideration of language representation and organisation may not be sufficiently prioritised and decisions may not always be underpinned by adequate clinical information and evidence.
Outputs for work package 4
In addition to serving as the literature reviews for the I-ASC study, systematic reviews 1 and 2 were used to derive the child characteristics and communication aid attributes to be used in the quantitative surveys in WP 4 (see Chapter 7).
Chapter 5 Specialised provision and decision-making factors (work package 2)
Introduction, background and rationale
Parts of this chapter have been reproduced from Lynch et al. 100 [© 2019 Lynch et al. 100 Published by Informa UK Limited, trading as Taylor & Francis Group. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon in any way] and Murray et al. 101 [© 2019 Murray et al. 101 Published by Informa UK Limited, trading as Taylor & Francis Group. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon in any way].
This WP was designed to explore the decision-making processes of professionals who specialise in AAC assessment and recommendation during a real-time assessment episode. AAC practice has evolved over time, with a wider range of children and young people with varying abilities and challenges accessing specialist services. 102 Hereafter, for ease of reading, children is the term used throughout this report to describe children and young people. In addition, the range of dedicated and non-dedicated technology available has increased considerably. 102 Professionals need to stay abreast of the latest technology to identify the most appropriate communication aids for children. 103 An additional challenge in making communication aid recommendations for children is that the system chosen must not only support expressive and receptive communication, but also facilitate the process of ongoing language acquisition. 104
Typically, communication aid recommendations are based on an assessment of the child’s capabilities, motivators and progress to date, and an evaluation of their environment and the communication partner resources, to contextualise the current and predicted needs. 105 The success of communication aid recommendation processes relies, in part, on the professional team’s competencies to make clinical decisions. Yet little is known and understood about decision-making processes AAC professionals use when recommending communication aids, especially in the UK. 12,101
As identified in Chapter 4, three recent studies in the international literature shed light on decision-making processes in communication aid recommendation. Dietz et al. 27 conducted semistructured interviews with 25 SLPs (in three groups: generalist, specialist and research SLPs). The authors found differences in approach and work practices between generalist SLPs and specialist/research SLPs. Generalist SLPs focused on speech and language deficits, whereas specialist SLPs focused on functional communication. Specialist SLPs recognised the value of working in teams but typically worked independently. In a follow-up study,96 eight specialist and research SLPs were given case reports of two children with different medical and communication presentations. Participants explained the clinical decisions they would make for these children. Results showed that the specialist SLPs approached the AAC assessment differently for each of the children; they focused on facilitating language development for the child with cerebral palsy, and on the motivation to communicate for the child with autism spectrum condition. In the third study,97 SLPs’ AAC prescribing practices were evaluated. In contrast to the two previous studies considered, Dada et al. 97 reported that most respondents indicated that they worked in teams and used a combination of standardised assessment and functional communication tasks to inform their decisions. Research evidence had limited influence on their choices, whereas available resources and the clinical expertise of colleagues had a strong influence.
The UK perspective informing work package 2
Across the literature included in our reviews, no UK study relating to clinical decision-making in communication aid recommendation was found. As the specific service contexts in the UK are likely to influence research findings, UK-focused research is required. In England and Wales, AAC services are provided through a hub-and-spoke model commissioned by NHS England. Specialised ‘hub’ services deliver electronic-AAC services to 10% of children and adults who need AAC, with the majority of people accessing AAC services through local ‘spoke’ services. Criteria for referral to specialised services include demonstrating the a receptive–expressive language gap, the ability to combine concepts, the need for graphic symbols to communicate through an electronic system, or the need for a complex access solution. In other parts of the UK, AAC specialised services have referral criteria that enable local professionals to refer any child with any type of AAC need. At the time the report was developed, to our knowledge, there were no published studies of how teams in the UK arrive at decisions about communication aid recommendation. International studies have primarily focused on single-discipline professionals (e.g. SLTs) and their role in communication aid recommendation, with limited consideration of team-based decision-making. Previous studies have examined professionals’ reports of decision-making processes through case studies, but have not looked at real-time decision-making in communication aid assessments. 96 For these reasons, this WP was intended to explore decision-making practices during a specialised multidisciplinary assessment appointment conducted in real time.
Research questions considered in work package 2
-
What attributes related to the child, and generic communication aids, do professionals consider important in making decisions about communication aid provision?
-
What other factors influence or inform the final decision?
Methods
A qualitative approach utilising a focus group procedure was adopted for understanding decision-making processes and exploring professional practices. 106
Participant sampling strategy
Professionals
The managers of specialised communication aid services from across the UK were contacted in writing and invited to participate. Purposive sampling ensured that the specialised services from which the managers were recruited had different funding structures (e.g. government-funded public services, charitable organisations) and were from across the UK. The inclusion criteria were being a professional team member (e.g. SLT, occupational therapist) involved in making a communication aid recommendation for a child aged 0–18 years referred to a specialised service. All professional team members involved in the clinical decision-making for a particular child were invited to participate, so this included the local service staff who completed the specialist referral.
Children and families
Each participating team of professionals identified families who had been referred to the specialised service for an assessment. These families were contacted and provided with study information. They were asked to give written consent to their consultation being discussed, so, although not participants in the traditional sense, they were facilitators of the process. This was to ensure that the research agenda had no impact on their assessment. The researchers provided the specialised teams with a list of broad demographic child characteristics to encourage diversity among those invited to take part.
Procedure
One appointment during a naturally occurring communication aid assessment acted as the starting point for each focus group discussion. A further rationale for a focus group approach was that AAC assessments are typically carried out by teams and a focus group method allowed the collective decision-making of the team to be explored.
The focus group took place immediately after the appointment. The two researchers conducting the focus group did not attend the appointment to reduce the likelihood that the discussions would be influenced by their assumptions. The focus groups were audio recorded and lasted 45–75 minutes. The researchers moderated the discussion, using a topic guide to facilitate a semistructured format (see the focus group discussion guide on the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 20 April 2020). Follow-up questions were used for clarification and to encourage more in-depth discussion. The focus groups were transcribed orthographically, and all identifying information was removed. Participants were offered a copy of their transcript to check both at the time of the focus group and in a follow-up e-mail. None of the participants asked to see their transcript.
Materials
A topic guide was created with semistructured content based on the evidence from the literature considered in the systematic review process (see the focus group discussion guide on the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 20 April 2020).
Analysis
Focus group transcripts were imported into NVivo 10TM software (QSR International, Warrington, UK) for data management. An inductive thematic analysis52 approach to coding was used, encompassing the stages of data interpretation from initial familiarisation, identification of potential themes, indexing and charting through to mapping and interpretation.
Rigour
Two researchers independently read the transcripts and suggested initial coding and potential thematic networks. Discussion between researchers enabled coding comparison, debate and agreement. Initial coding networks were shared and debated with core research team members. Reviews were amended and incorporated into the draft network. Networks and suggested coding were also shared with two independent reviewers. Consensus coding was agreed, with the two lead researchers agreeing and amending all transcriptions and coding protocols to reflect this.
Results
Six teams of professionals were recruited to the study and gave written consent. Seven young people and their families gave written consent to be the focus of discussion. A total of six focus groups were completed and ranged in size from 2 to 13 participants, with a mean of 5 participants. While a typical focus group ranges from 5 to 10 participants,106 focus group size in the present study was determined by service structure and delivery processes (Table 6). The focus groups included one specialised team operating a prescription review model of decision-making,9 where two children were discussed. In this service model, representatives from the specialised service conducted a communication aid assessment with the local professional team and the family. At a future date, the specialised team representatives met with their wider specialised team to discuss their provisional decisions for that child. In this way, the whole specialised team contributed to decision-making. This focus group captured the specialised services consensus in decision-making for two children.
| Focus group | Number of participants | Professional background |
|---|---|---|
| 1 | 4 |
|
| 2 | 13a |
|
| 3 | 3 |
|
| 4 | 5 |
|
| 5 | 4 |
|
| 6 | 2 |
|
The purposive sampling of children included a range of profiles that made them eligible for referral to specialised services in the UK (Table 7).
| Identifier and gender | Age (years) | Diagnosis | Type of assessment episode (for high-tech aid) |
|---|---|---|---|
| C1 Female | 5 | Cerebral palsy, ambulant, direct access | Assessment for first communication aid |
| C2 Female | 5 | Physical disability and medical condition, wheelchair user, direct access | Assessment for first communication aid |
| C3 Female | 18 | Learning disability, autism features, wheelchair user, direct access | Assessment for new communication aid following experience with a number of communication aids |
| C4 Male | 7 | Cerebral palsy, wheelchair user, indirect access | Assessment for a second communication aid |
| C5 Male | 9 | Medical condition, wheelchair user, direct access | Assessment for a new communication aid following experience with a number of communication aids |
| C6 Male | 4 | Cerebral palsy, wheelchair user, autism features, partner-assisted scanning and eye gaze access | Assessment for first communication aid |
| C7 Male | 5 | Cerebral palsy, hearing impairment, wheelchair user, partner-assisted scanning and eye gaze access | Assessment for first communication aid |
A thematic network emerged with two global themes, six organising themes and 38 basic codes (Table 8). The global themes were competing considerations and cultural and contextual influencers. The range of elements presented in the network is indicative of the myriad of interactive factors considered when recommending communication aids. The first global theme demonstrated competing considerations contained in the three organising themes: child characteristics, access features, and communication aid attributes. The second global theme included cultural and contextual factors outside the child and aid that influenced decision-making and captured the influences of work processes and team structures, resources and the wider social context. The second global theme comprised three organising themes: ways of working, transitions, and available resources. See Murray et al. 100 and Lynch et al. 101 for a detailed review of these findings. In the sections that follow, we provide summative insights into the rich data set; themes are presented alphabetically, but this ordering does not reflect a hierarchy of importance.
| Global theme 1: Competing considerations | Global theme 2: cultural and contextual influencers |
|---|---|
| Organising theme: Child characteristics | Organising theme: Ways of working |
| Age | Balancing decisions |
| Assumed abilities | Basis for referral |
| Child preference | Extraneous factors |
| Communication ability | How decisions are made |
| Cognitive skills | Information brokering |
| Diagnosis | Inheriting decisions |
| Expectations and aspirations | Policy |
| Linguistic level | Roles and responsibilities |
| Motor abilities and operational competence | Service delivery model |
| Personality and temperament | Team theory |
| Progress and communication opportunities | |
| Organising theme: Access features | Organising theme: Transitions |
| Access method | Future planning |
| Positioning and mounting | Technology change |
| Organising theme: Communication aid attributes | Organising theme: Available resources |
| Hardware aesthetics | Attitude |
| Hardware reliability | Cost |
| Hardware data storage and processing | Intervention |
| Software consistency and intuitiveness of design | Support |
| Software ease of editing | Team knowledge and skill |
| Software graphic representation | Training |
| Software vocabulary | |
Competing considerations
This global theme summarised the perspectives of feature-matching that related to the child, to the communication aid and to effective access.
Child characteristics
In summary, participants considered many child characteristics in their decision-making. They took into account physical characteristics such as motor abilities and operational competence, age and medical diagnosis. These characteristics were often at the forefront of the decision-making process, particularly motor abilities, as it was suggested that children could not demonstrate their abilities unless a reliable access method was identified. Participants considered linguistic level, cognitive abilities and communication ability, as well as personality traits and temperament. Information about the level of functioning informed decisions; however, when assessments had not been completed prior to referral, teams relied on observational assumptions during an appointment. Linguistic level, specifically receptive language and cognitive ability, was a factor perceived to influence the selection of a vocabulary package. However, at times, participants relied on partial information to infer a child’s linguistic ability during an assessment episode.
A child’s history with AAC also influenced the recommendation. Participants evaluated a child’s progress in the light of the communication opportunities the child had experienced and how their skills had developed. Participants used this information to predict the expected rate of the child’s progress. Future expectations and aspirations for the child appeared to influence recommendation choices concerning language organisation and graphic representation.
Access features
Teams identified access as one of the most time-consuming considerations, indicating that addressing access was often where the process of recommendation began. Participants considered a hierarchy of access options and sought to minimise operational demands on the child. The importance of low-tech systems for supporting communication as access skills developed was noted. Considerable focus was given to positioning the child and the communication aid to ensure that systems were available throughout the day and across settings. It should be noted that access was not the intended focus of the research, but it recurred across the data set and hence has been included.
Communication aid attributes
Participants considered trade-offs across many communication aid attributes. For particular children, specific hardware attributes were prioritised, some of which were considered in relation to the child’s physical characteristics. For example, size and weight were important for very small children. Children’s preferences influenced which communication aid attributes were considered, for example appearance and voice quality. Reliability and ruggedness became more salient for those teams with previous experience of communication aid breakdown. Professionals recognised the negative influence on learning and buy-in when communication aids were not available for long periods because of protracted repair processes. There was limited discussion of other hardware attributes (e.g. battery life and additional assistive technology features). The software attributes prioritised reflected the needs of the child and of those providing support. Prioritised components included consistent layouts, intuitive design, and vocabulary packages to support current and future needs. Vocabulary package selection was influenced by predicted progress and literacy development. Limited consideration was given to the type of vocabulary or graphic representation. For some professionals, ease of editing for those supporting the child was a key consideration.
Clinical implications
A collective evaluation of these competing considerations suggests that those charged with the responsibility of proposing specific communication aids face a complex task that includes identifying particular child characteristics, access features, and communication aid attributes in their recommendations. These elements are not separate or fixed components of the decision-making process, but are constantly moving in relation to each other, suggesting that trade-offs are a component of decision-making.
Cultural and contextual influencers
This global theme summarised the context within which decisions are enacted. This includes people, places, learning resources and situations.
Ways of working
Some factors identified were related to the team and their working practices. Participants described using discussion and technology trialling to support decision-making. Trade-offs when choosing an aid for each child emerged as a recurring feature across focus groups. For example, participants said that preserving existing learning was a consideration in decisions about a second or subsequent aid, so they might choose a system from the same ‘family’ as a previous recommendation. A further team-related factor was the use of implicit theoretical frameworks as a mechanism for supporting decisions; however, these were insufficiently explicit to other members of the team, impacting on the transparency of the decision-making process. Other influencers included service structures; for example, the process of referral, service delivery restrictions and perceived roles of team members influenced how teams prepared for or carried out assessment processes. Variation in practice was reported. Extraneous factors such as luck and local policies influenced decisions; for example, local policies could determine which graphic symbol system would be used in school(s). Finally, challenges with accessing client-specific information meant that some recommendations were made without this key information available.
Transitions
Participants reported that expected changes in a child’s life created urgency in the recommendation process. The rapid change in technology also had potential to influence the timing of recommendations.
Available resources
Attitudinal and practical support were key influences in decision-making. When full attitudinal or practical support was not achievable, a recommendation was still made, but the expected outcomes might change. Consideration of the aid cost was not salient in the data set, although the relative cost was considered. Participants indicated that pre-existing knowledge of the child’s environment influenced their choices. Broader changes in technology and AAC awareness also influenced recommendations. Participants recognised that children needed a high level of input post recommendation but that they did not have jurisdiction over intervention support. When resources were more limited, training was perceived to maximise the available input. Although interventions were deemed the remit of those referring to specialised services, training was seen as part of the recommendation set-up.
Clinical implications
Taking cultural and contextual influencers collectively, the process of making a communication aid recommendation is shaped by many factors. The specific cultural and contextual influencers varied across children and services, suggesting that each decision involved balancing a range of influencers.
The perceived complexity of communication aid decision-making resulted in the development of an I-ASC explanatory model of AAC decision-making. Figure 6 provides a schematic representation of the process. ‘Competing considerations’ was identified as the first global theme as it denotes the interaction between child characteristics, access features and communication aid attributes. The ‘competing’ label describes the process of choosing the best fit based on a series of trade-offs rather than necessarily arriving at the perfect option. In the explanatory model, these competing considerations are illustrated by the cog wheels. The interaction of the elements of the child, access and communication aid is shown by the potential of the cog wheels to rotate in either direction as the team debates and considers issues within the decision and, ultimately, moves towards consensus. The cog–wheel interplay indicates an intensity in the trade-off between one decision made related to a characteristic, feature or attribute and how that instantly has an impact on the interlinked cogs that depict the remaining two organising themes. Once a decision is made about these factors, it can be influenced by issues external to the child or the aid. In the second global theme, ‘contextual and cultural influencers’, we found that environmental factors related to both the child’s culture and context and the professional’s work setting influenced decision-making. These cultural and contextual influencers, as illustrated by the funnel and its contents, denote factors that further influence clinical decision-making outside the feature matching process. The model denotes the two global themes and the arrows are indicative of the fluid and iterative process of decision-making.
FIGURE 6.
The I-ASC explanatory model of AAC decision-making.
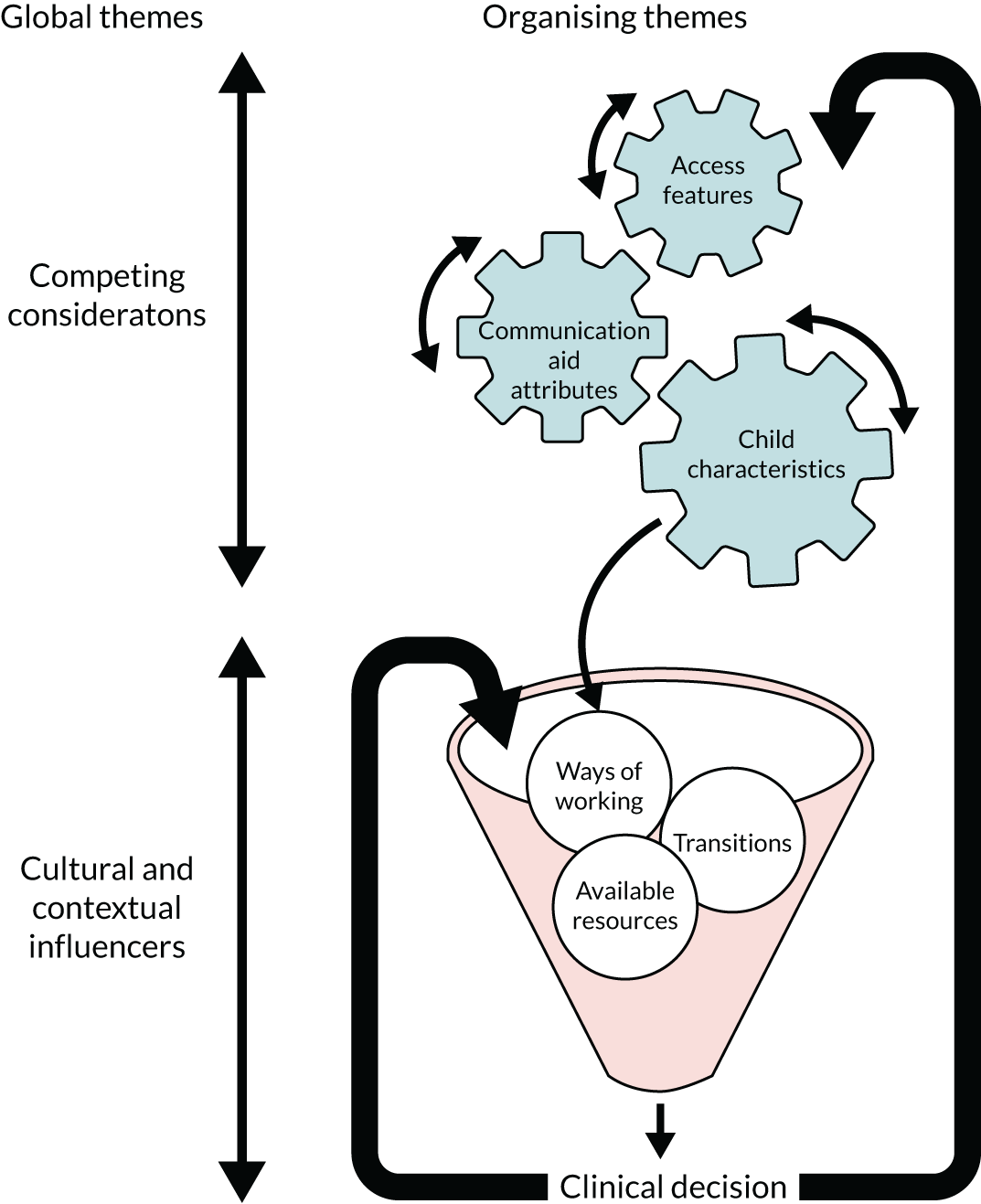
Discussion
This WP, the first in the UK to our knowledge to focus on interdisciplinary decision-making during real-time recommendation processes, highlights the fundamental complexities of those decisions. 102 To reach the point of recommendation, teams work through multiple layers of consideration to identify the best-fitting symbol communication aid. 103–105 To our knowledge, studies have not explored the decisions made when a multiprofessional team deliberates AAC options for a child immediately following an actual AAC assessment. These findings offer insight into interprofessional dialogue during the AAC decision-making process.
Symbol communication aid recommendations are a product of the process whereby child characteristics, access features and aid attributes are permutated to allow the most appropriate aid for each child to be identified. However, this study confirms that these decisions are distilled through the cultural and contextual influencers of the child’s environment. The current findings suggest that cultural and contextual influences have a considerable impact on the decisions made for children. For example, participants reported that a lack of attitudinal support from those in a child’s environment would limit their expectations for the extent of the child’s aid use. This reinforces the findings of previous studies of aid abandonment, which also identified attitude and support as critical factors of successful outcomes. 11 Future research could focus on addressing external influencing factors during the recommendation process.
There was consensus among participants that children who are recommended symbol communication aids should have high levels of intervention input following recommendation. The availability of intervention and training support remains ill defined at a local service level. Future research could focus on investigating intervention support following aid recommendation.
Decisions made about a child’s first communication aid have ramifications for future aid recommendations. Participants indicated a desire to build on existing knowledge and skills, indicating that particular care is needed when making decisions about first communication aids. Further research may also be needed to explore whether or not decision-making processes for second and subsequent communication aids have different qualities from those after an initial assessment. Further research is needed to explore the long-term impact of clinical decisions related to communication aid use (see Chapter 6).
A further contextual influence that was entirely external to the child was the service providing the aid recommendation. This had considerable influence on the nature of the decisions made: from the time available to who was involved and what was done. This finding reflects those of previous studies in which professionals recognised the influence of particular service delivery models on aid recommendation processes. 9,26 Delivering aid recommendations in the real world will inevitably be influenced by service-related factors. Further research considering service design initiatives is warranted to enhance service delivery within real-world constraints, for example enhancing information-gathering procedures in time-constrained models (see Chapter 8).
The decision-making processes used by specialised participants were multifaceted and not always explicit. Implicit processes may preclude children, families, and professions with less AAC experience from participating in decisions. Previous research has indicated that families may be excluded from or marginalised during decision-making26 and may not be empowered to undertake a decision-making role. 107 The I-ASC findings reinforce the need for decision-making tools and supports to enhance transparent and inclusive processes (see Chapters 6 and 8).
Clinical and research implications
The children in this WP represented a small section of the broader AAC community (as determined by the referral criteria for specialised services), and yet each child discussed had a unique set of abilities, attributes and resources. This highlights the individualised nature and the complexity of the decision-making process involved in recommending a communication aid. Related studies have indicated that non-specialist practitioners face challenges in making effective AAC recommendations;27 the present study suggests that, even for experienced professionals, the breadth of factors is likely to be challenging.
This study identified different priority considerations for AAC team members from those that have been reported in previous research. In the present study, professionals prioritised children’s unique physical characteristics and the access features of specific devices in their decision-making. Access was often viewed as the starting point and the most complicated aspect of the recommendation process. These considerations appeared more prominently in the present study, in contrast to previous studies,27,96 which described access features as a lesser consideration. There was relatively little focus on the individual’s language and communication abilities as a factor for consideration. In particular, there was little evidence of a requirement for formal assessment of these abilities, and, instead, there was a tendency to rely on informal observations or assumptions about a child’s intrinsic abilities in these domains. These differences in emphasis may reflect the responsibility that all UK specialised services have to support children with highly complex access issues. Alternatively, it may reflect the broader range of participants’ professional backgrounds, in that this study incorporated a range of professionals involved in AAC services, not just SLTs. It may also indicate that, in real time, the factors considered may be different from those reported in hypothetical situations or in retrospective reports, where professionals have more opportunity to reflect on their decision-making. Different specialised service referral criteria exist across the countries of the UK; for example, the specialised service referral criteria in England and Wales require that children be able to demonstrate an ability with AAC. Therefore, it is important that children who show slower progress in the stages of their AAC journey, and who do not meet referral criteria, have access to appropriate pathways so that they can achieve their potential. A perceived difficulty in developing access skills can be a significant barrier to language and communication experiences. During the process of developing consistent access, consideration of how to support language and communicative development may merit greater research and intervention prioritisation. 104
The communication aid attributes considered by participants in this study resonate with previous research. For example, reliability and ease of editing were important considerations for both the current UK participants and their Canadian counterparts. 9 By contrast, consideration of graphic representational forms seems to differ from that in a South African study. 97 Participants in this UK study favoured more abstract symbols for children with higher cognitive abilities, whereas South African SLTs favoured more iconic symbols. Across both studies, professionals prioritised the selection of core vocabulary. However, the South African SLTs indicated a preference for category-based vocabulary organisation, whereas there was limited discussion of layout organisation in the present study. Future research could usefully explore the merits of different graphic representations systems and their organisation.
Limitations and future directions
Although the focus groups provided a snapshot of clinical processes in real time, which allowed a concentrated examination of specific decision-making episodes, the method may have precluded reflection on how decisions could change over time. In addition, the families at the centre of the discussions were excluded to avoid any undue influence on the services they received. All but one focus group contained members of more than one profession, and the number and ratio of professional perspectives varied across the focus groups. The thematic network and explanatory model cannot be considered exhaustive, as the themes pertained to particular children with specific characteristics and diagnoses. Each child appeared to have an individualised assessment process, and children with other profiles may have additional characteristics, features and attributes. Further research is warranted to examine the impact of the decision-making process over time, to take account of child and family priorities, and to explore decision-making for children with different profiles (see Chapter 6).
Conclusion
The recommendation of communication aids is multifaceted, requiring effective interaction between local and specialised services. The identification of all characteristics, features and attributes relevant to individual children is complex and results in a unique set of considerations for each child. Cultural and contextual influencers have a considerable impact on decision-making, suggesting that greater consideration is needed to mitigate outside influences negatively shaping decisions for children. Suggested clinical implications from these findings, and I-ASC developed resources to support enhanced decision-making, are available at https://iasc.mmu.ac.uk/; an example screenshot is given in Figure 7.
FIGURE 7.
Excerpt from the heuristic illustrating ways of working: balancing decisions – practical guidance and I-ASC resource links. Reproduced with permission from Nick Holland, Manchester Metropolitan University, Manchester, UK.

Chapter 6 A case series from a service user’s perspective of decision-making (work package 3)
Introduction
The aim of this WP was to describe symbol communication aid decisions and their impact over time from a service user perspective, including the person using AAC, their family members and their team network. WP 3 was constructed to provide a retrospective view of the impact of symbol communication aid recommendations. Hence, the service users in this work strand include children, young people and adults who can reflect on their assessment experiences, as well as their family members. As contributors to these data included adults who use AAC, for ease of reading, children, young people and adults will be referred to as AAC users throughout this chapter.
Although AAC users are the central stakeholders in a communication aid assessment, their opinions are often limited in AAC research and practice. Yet eliciting their views is recognised as essential to designing services that are responsive and targeted to their needs. 108,109 Evidence-based practice suggests that practice is best informed by the application of three perspectives: currently available research, clinical expertise and the patient voice. 110 This WP captured service users’ views and values, as well as clinical expertise, to contribute to an evidence-based practice triad. 110
Research objective
The objective was to explore how this process takes account of the perspectives of all involved, specifically how children and adults (reflecting on their experiences), parents and professionals perceive the effectiveness of historical recommendations.
Research questions
-
What attributes related to the child, and to generic communication aids, do professionals consider important in making decisions about communication aid provision?
-
What other factors influence or inform the final decision?
-
What attributes are considered important by other participants (e.g. the child and their family) and what impact do these have in the short, medium and long term?
Methods
Design
A qualitative approach was adopted, using semistructured interviews.
Participants
Augmentative and alternative communication users, family members and professionals historically involved were invited to participate in interviews about their experiences of communication aid assessments. Interviews were conducted in clusters (Table 9). Participants were identified through professional networks and two national AAC charities (Communication Matters and 1Voice). Purposive sampling was used to obtain a spread of interview clusters across the UK. AAC users differed in age and abilities, and were representative of families accessing different service types and structures. For each interview cluster, a potential AAC user was identified and invited to take part. In addition, their parent and the team involved in their AAC assessment were invited to participate (see Tables 9 and 10).
| Interview cluster | Participants by type in each cluster | Total number | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | AAC user | Parent (mother) | Specialist SLT and local SLT | Key worker | 5 | |||
| 2 | AAC user | Parent (mother) | Teacher | Teaching assistant | SLTs (n = 2) | 6 | ||
| 3 | AAC user | Parent (mother) | Teacher | Teaching assistant | Specialist SLT and local SLT | 6 | ||
| 4 | AAC user | Parent (mother) | Teacher | Teaching assistant | Specialist SLT and local SLT | Local occupational therapist | 7 | |
| 5 | AAC user | Parent (mother) | Teacher | Teaching assistant | Local SLT | Local occupational therapist | 6 | |
| 6 | AAC user | Parent (mother) | Teacher | Teaching assistant | Assistive technology co-ordinator | 5 | ||
| 7 | AAC user | Parent (mother) | Specialist SLT | Specialist occupational therapist | 4 | |||
| 8 | AAC user | Parent (mother) | Specialist SLT and local SLT | 4 | ||||
| 9 | AAC user | Parent (mother) | Specialist SLT and local SLT | 4 | ||||
| 10 | AAC user | Parent (mother) | Teacher | Local SLT | AAC officer | 5 | ||
| 11 | AAC user | Parent (mother) | Teacher | Local SLT | Assistive technology co-ordinator | 5 | ||
| 12 | AAC user | Parent (mother) | Personal assistant | 3 | ||||
| 13 | AAC user | Parent (mother) | Local SLT | Support workers (n = 2) | 5 | |||
| 14 | AAC user | Parent (father) | Specialist SLT and local SLT | Local occupational therapist | Local clinical scientist | 6 | ||
| 15 | AAC user | Parent (mother); parent (father) | Local SLT | 4 | ||||
Augmentative and alternative communication users
Augmentative and alternative communication users were recruited to discuss their experiences of communication aid assessments. Using purposive sampling, 15 AAC users were recruited. This process aimed to identify people with a range of profiles (Table 10).
| Identifier/sex | Age (years) | Diagnosis | AAC set-up |
|---|---|---|---|
| C8 (female) | 9 |
Global developmental delay Moderate learning disability |
PODD book Direct access |
| C9 (male) | 4 |
Cerebral palsy Cognitively able |
PODD 70 Tobii I12 with Picture WordPower B Using partner-assisted scanning and high-tech eye gaze |
| C10 (male) | 7 |
Cerebral palsy Mild learning disability |
Communication book Accent 800 (Liberator Ltd) with easyChat 16 (Liberator Ltd) Direct access |
| C11 (female) | 11 |
Cerebral palsy Mild learning disability |
Accent 1400 (Liberator Ltd) Access via two head switches |
| C12 (male) | 10 |
Cerebellar atrophy Moderate learning disability |
Accent 1000 (Liberator Ltd) with easyChat 60 (Liberator Ltd) |
| C13 (male) | 4 | Global developmental delay | Grid Pad (Smartbox Assistive Technology, Malvern, UK) rigged with Symbol Talker A (Smartbox Assistive Technology) |
| C14 (female) | 12 |
Acquired brain injury Learning disability |
Accent (Liberator Ltd) with Grid 3 (Smartbox Assistive Technology) |
| C15 (male) | 15 |
Cerebral palsy Cognitively able |
NOVA chat 8 (Liberator Ltd) Direct access |
| C16 (male) | 7 |
Cerebral palsy Learning disability |
Grid Pad with Grid 3 Eye gaze |
| C17 (male) | 11 |
Autism spectrum condition Severe learning disability |
iPad (Apple Inc., Cupertino, CA, USA) with Clicker Communicator Core 2 (Crick Software Ltd, Northampton, UK) Direct access |
| C18 (female) | 19 |
Autism spectrum condition Severe learning disability |
iPad with Grid Player Smartbox Assistive Technology on Symbol Talker A Direct access |
| C19 (male) | 36 |
Cerebral palsy Cognitively able |
Accent 1400 with NuEye™ (Prentke Romich Company, Wooster, OH, USA) Eye gaze |
| C20 (female) | 7 |
Cerebral palsy Mild learning disability |
Communication book Grid Pad with the Grid and an iPad with Grid Player; both on Symbol Talker A Direct access |
| C21 (male) | 18 |
Cerebral palsy Moderate learning disability |
PODD book iPad with Clicker Communicator Direct access |
| C22 (female) | 21 |
Cerebral palsy Moderate learning disability |
Alphabet board iPad with Grid Player ECO™2 (Liberator Ltd) with LLL 128 Direct access |
Parents
Parents were invited to participate, and 16 agreed (Table 11). The participants comprised 14 mothers and two fathers.
| Parent identifier | Relationship | Age group (years) | Ethnicity |
|---|---|---|---|
| P1 | Mother | 25–34 | White British |
| P2 | Mother | 35–44 | White British |
| P3 | Mother | 25–34 | White British |
| P4 | Mother | 35–44 | White British |
| P5 | Mother | 45–54 | White British |
| P6 | Mother | 35–44 | White Irish |
| P7 | Mother | 45–54 | White British |
| P8 | Mother | ≥ 65 | White British |
| P9 | Mother | 45–54 | White British |
| P10 | Father | 35–44 | White British |
| P11 | Mother | 35–44 | White British |
| P12 | Father | 35–44 | White British |
| P13 | Mother | 35–44 | White British |
| P14 | Mother | 45–54 | White British |
| P15 | Mother | 45–54 | White British |
| P16 | Mother | 45–54 | White British |
Professional and support teams
Team members involved in any aspect of a communication aid assessment process were invited to participate. Forty-four participants from a range of backgrounds contributed (see Table 9).
Procedure
Data collection was conducted by researchers who either had lived experience of AAC or were experienced in speech and language therapy.
Augmentative and alternative communication users
Recruitment and consent processes included a range of formats to support access to study information, including a YouTube (YouTube, LLC, San Bruno, CA, USA) participant information video (https://youtu.be/GWL1pFVVIlE; accessed 10 September 2020) and symbolised information leaflets and consent forms (Figure 8; for participant information leaflets and consent forms, see the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 20 April 2020).
FIGURE 8.
Screenshots from the YouTube participant information video (https://youtu.be/GWL1pFVVIlE; accessed 10 September 2020). Reproduced with permission from Gareth Preston, Manchester Metropolitan University, Manchester, UK, 2020, personal communication.

Once informed consent was obtained, the research team worked with each AAC user, their family and the team to identify how best to support user participation in the study. For those AAC users for whom it was appropriate, a topic guide of interview questions was provided in advance to allow them to prepare responses using their communication aids (for the AAC user interview topic guide, see the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 20 April 2020). These interviews were video-recorded and transcribed.
For AAC users who required more support, materials were used to support them in sharing their views. Storybooks were developed detailing fictional (but plausible) experiences of AAC users participating in communication aid assessments. The storybooks were used to contextualise the interview content, prime them to recall their own communication aid assessment and introduce related vocabulary that could be used during the interview to express views about communication aid attributes and aspects of the assessment process (Figure 9; see also https://iasc.mmu.ac.uk/wp-content/uploads/2019/05/I-ASC-Katie-Gets-a-Communication-Aid-Book.pdf; accessed 10 September 2020).
FIGURE 9.
Sample pages from the storybooks developed to support data collection.
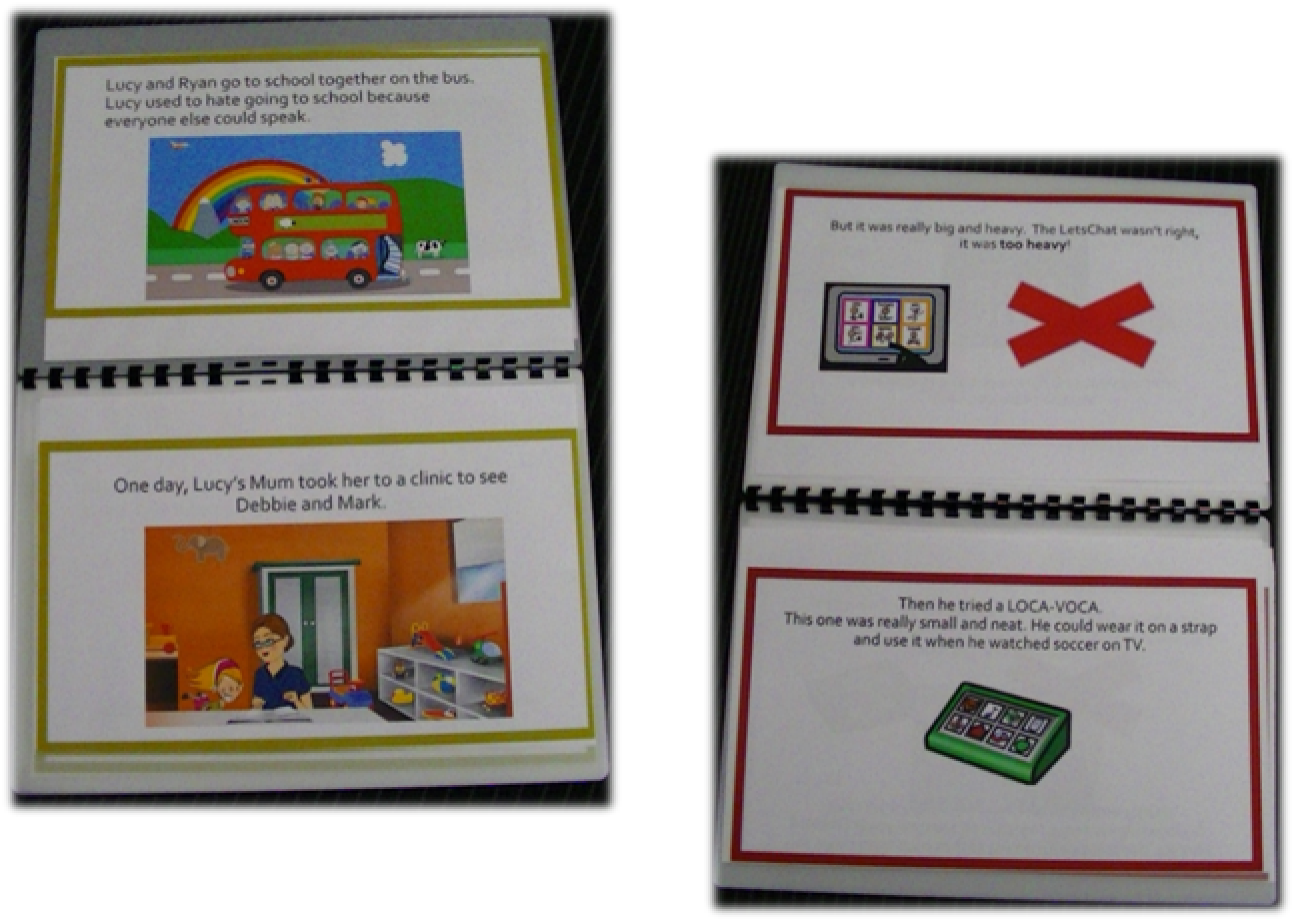
For AAC users who were unable to respond to the questions in the interview with their own communication aid (because of vocabulary limitations of their current communication system), a Talking Mats™111 (Talking Mats Ltd, Stirling, UK) approach was used to support them to express their opinions. Talking Mats is an evidence-based dynamic communication framework that can be used to support individuals with communication difficulties to understand, and express views. 112 The framework is based on three sets of graphic symbols that are presented to the individual with communication difficulties:
-
graphic symbols to introduce a topic
-
graphic symbols related to options within each topic
-
a visual scale that allows individuals to indicate their general feelings about each option (i.e. like, don’t like, don’t mind).
Graphic symbols support the particular topic being discussed. Integral to the approach is placing the graphic symbols on a topic board (or mat) along the visual rating scale. This allows topic options to be considered collectively and changed in relation to each other. It can be photographed to serve as a visual record of an individual’s opinions on a particular topic (Figure 10).
FIGURE 10.
Sample visual record of one young person’s views of their communication aid.
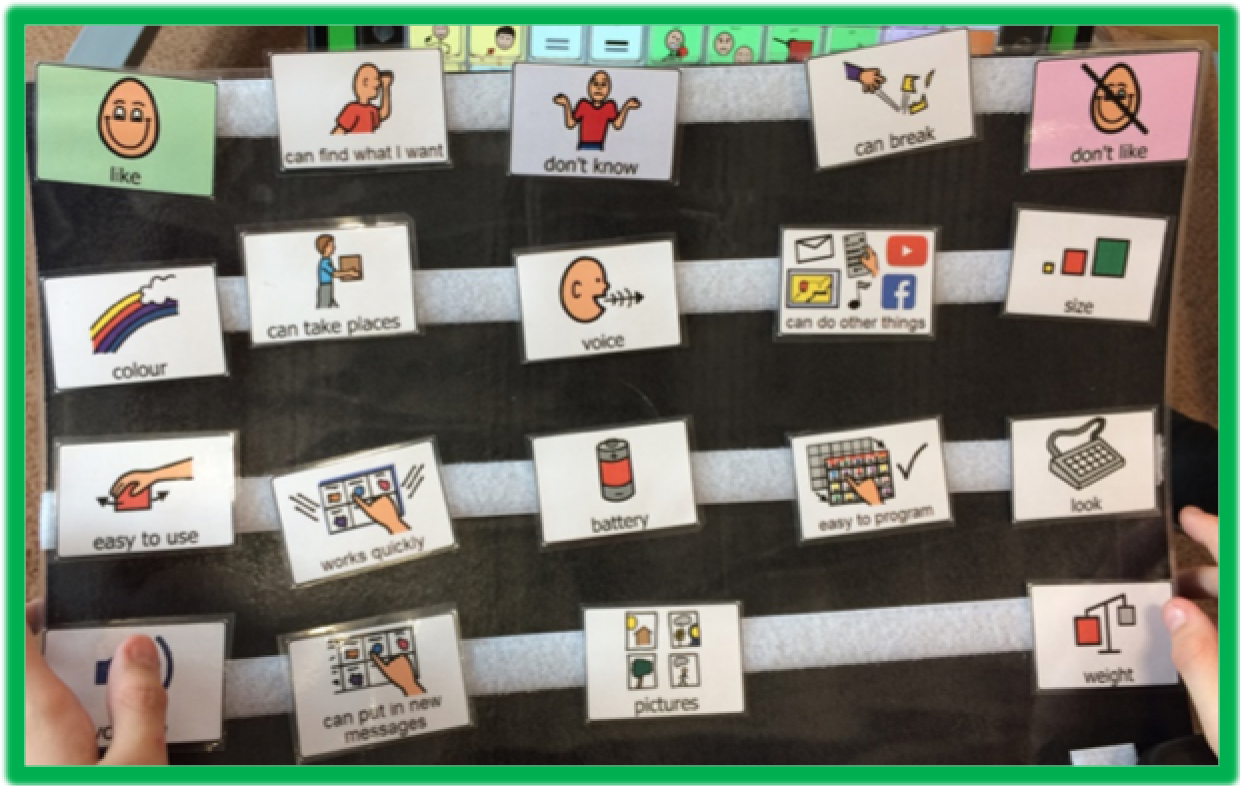
In this study, a Talking Mats approach was used with a number of AAC users to support understanding and expression of views in relation to communication aid assessment. Prior to the interview, telephone discussions were held with the family and/or team members to support the development of appropriate topic-based graphic symbols. In the interview, unrelated topics of interest to the AAC user were introduced first, such as food or television programmes. Using unrelated topics facilitated the introduction of the Talking Mats framework and ensured conceptual understanding of the approach prior to using it to obtain views on their communication aid and assessment process.
Once procedural understanding had been established, a hierarchy of topics was introduced, starting with concrete topics and progressing to more abstract concepts. Later topics discussed with each AAC user were tailored based on their response to the initial topics. Responses were augmented by additional information provided through yes/no responses, communication aid output and co-constructed messages. Each Talking Mat record was photographed and the full interview was video-recorded to capture all communication information for later analysis. Interview field notes were written up after each interview to aid interpretation of the photographs. The videos were reviewed by research team members, and all data expressing views, irrespective of the communication modes used, were transcribed.
Parents and professional support teams
Interviews were carried out in clusters, with the AAC user, parents and team members all interviewed on the same day (or on consecutive days for the AAC user). Interviews were conducted in a setting convenient to the participants, which included home, school and clinic.
Interviews were conducted in a semistructured way with a topic guide used to support data collection (for the interview topic guides, see the project web page: www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 20 April 2020). The topic guides were informed by the systematic literature review and the findings from WP 2 focus groups. Interviews lasted from 20 to 60 minutes and were audio-recorded and transcribed verbatim.
Analysis
To support the prominence of the AAC user voice in the analysis, it was agreed that the parental and professional team content would be analysed separately from the AAC user data. The processes of analysis are described in the following sections.
Augmentative and alternative communication users
The interview transcriptions of those AAC users who completed interviews in a traditional format (i.e. gave spoken responses) were imported into NVivo. For AAC users who completed interviews using supported formats, the Talking Mats photographs, researcher interviewer field notes and video transcription notes were imported into NVivo. These data were held in a separate NVivo record from the parent and team member data for analysis purposes; however, the same framework analysis approach was used. 113 Using this approach, two researchers read and reread the interview records and viewed the images to obtain an overall sense of the data and to develop their initial impressions. An initial coding process identified how meaningful data segments related to framework codes. The two researchers discussed initial coding, recognising commonalities and discrepancies, and arrived at consensus that informed coding development. Other research team members undertook a data review process. The purpose of this review was to support robustness of the qualitative process. These researchers reviewed portions of coding against the operational coding definitions and asked questions about the overall procedure, meanings and interpretations. Coding consensus was agreed. The NVivo software provided an audit trail and supported credibility.
Parent and professional teams
Interview transcripts were imported into NVivo for data management purposes. Following the inductive development of a thematic network in WP 2, a framework analysis approach was used in this WP to support the coherent development of themes. 113 Two researchers who were specialist AAC SLTs read and reread the transcripts to obtain an overall sense of the data and to develop their initial impressions. An initial coding process explored how meaningful data segments related to framework codes. The two researchers discussed initial coding, recognising commonalities and discrepancies that informed the coding development. Further independent coding reviews were conducted by two external researchers to ensure credibility and transferability. 52 In addition, a peer review process was undertaken by other research team members, as described in the preceding section, Augmentative and alternative communication users.
Results
Introduction
In summary, a decision-making framework converged with the inductive thematic network developed in WP 2. Consequently, the framework resonated with the I-ASC explanatory model of AAC decision-making detailed in WP 2 (see Chapter 5) capturing the complexity inherent in AAC decision-making for AAC users. The participants in WP 3 contributed insights and observations right across the explanatory model (the model presented in WP 2 is not repeated here). There were many commonalities with the themes arising in WP 2, for example a reduced focus on language assessment with identified information gaps present in the decision-making process. These data shed light on the longitudinal impact of decisions made in communication aid recommendation processes. Owing to the breadth and depth of the data, a cross-section of findings is detailed in this chapter. These findings have been selected to contrast with and complement the findings provided in WP 2 (see Chapter 5). Detailed findings are synthesised in Chapter 8 with links provided to online I-ASC resources.
Overview of augmentative and alternative communication users’ perspectives
I love my communication aid, because I can pretty much say anything.
The majority of AAC users were able to express opinions about their communication aids and their communication aid assessments. Some could provide views on specific aspects of the communication aid (e.g. the colour, battery life reliability or aid size) (Figures 11 and 12).
FIGURE 11.
A visual record of a young person’s view on their communication aid. This young person indicated that they liked the size, colour, voice and look of their communication aid. They also like the (speaking) volume. They did not like the battery life, how difficult it was to program and the time it took them to communicate. They did not have an opinion on what the communication aid was like for playing games.
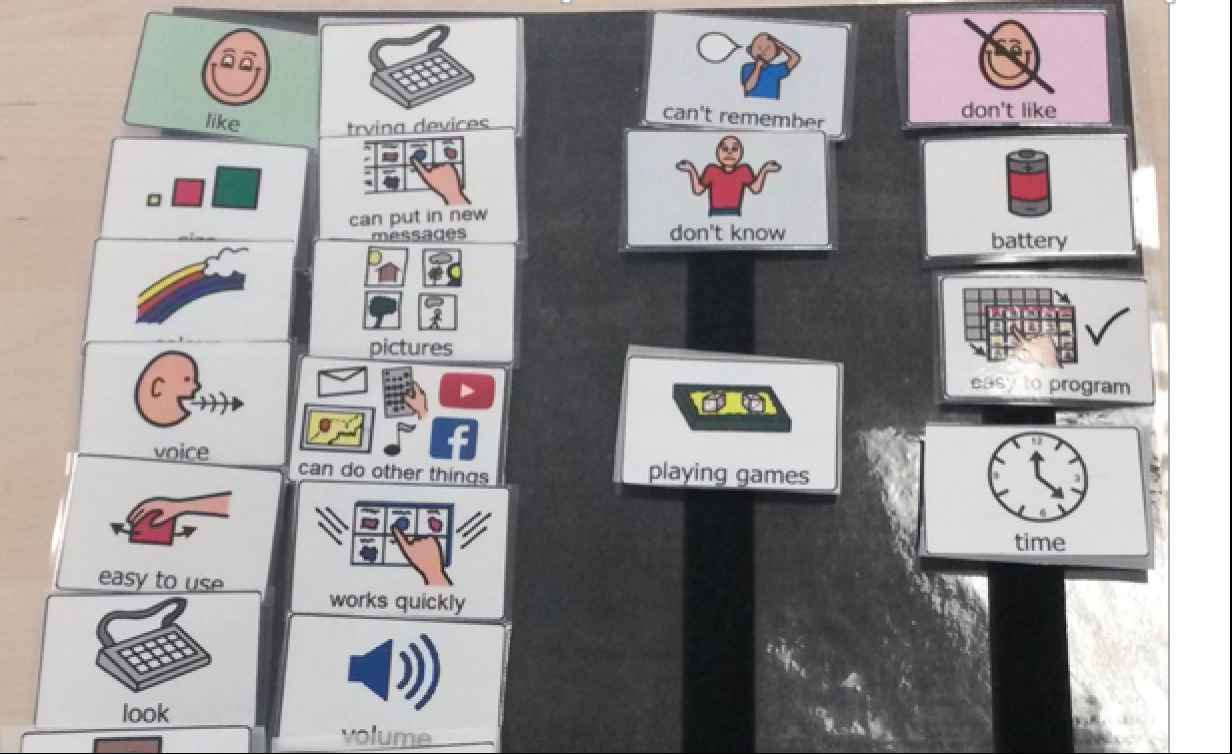
FIGURE 12.
A visual record of a child’s view of their communication aid. In this example from a very young child, they demonstrate that they can express that they liked the size, colour and voice of the communication aid. They liked that it worked quickly and was easy to use. They did not like how to put in new messages and that it was hard to take around places.
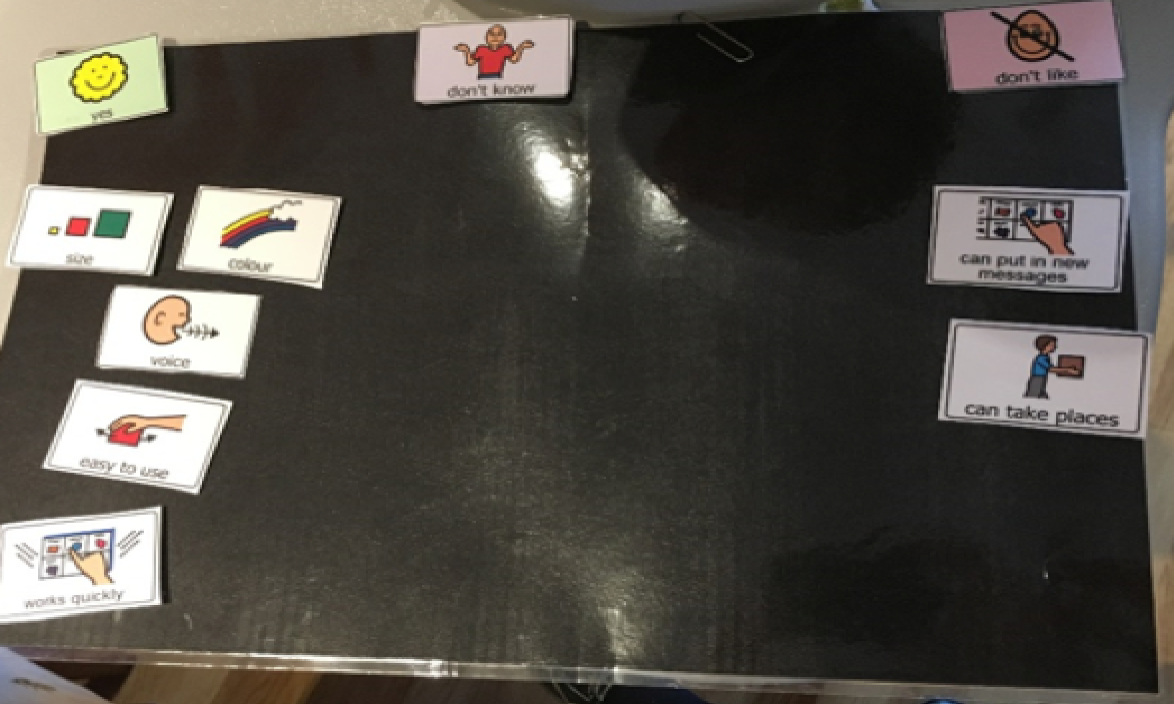
They could also express their preferences about how they liked to use their communication aids [e.g. talking to grandparents on Skype™ (Microsoft Corporation, Redmond, WA, USA), talking to friends, talking about places they like to use their communication aids, being able to go to the shops independently]. Young children (as young as 4 years) and those with multiple challenges were able to express their views with support (see Figures 11 and 12).
Augmentative and alternative communication users have the ability to take an active role in decision-making related to communication aid assessment and recommendation. Building opportunities for AAC users to express their views during assessment processes may support the selection of communication aids that are more closely aligned with their views and preferences.
Augmentative and alternative communication user analysis
Older children, young people and adults were able to provide insights into the impact of clinical decision-making processes for them as AAC users. These views were coded across the following organising themes within the analysis framework described in Chapter 5 (WP 2):
-
communication aid attributes – hardware aesthetics and hardware reliability
-
ways of working – inheriting decisions and service delivery model
-
transitions – technology change
-
available resources – intervention.
Communication aid attributes
Hardware attributes were identified and discussed as priorities by many participants.
Communication aid attributes: hardware aesthetics
Hardware aesthetics were expressed as preferences for smaller and lighter communication aids: ‘As small, I can use it on my knees’. For one participant, size was the most important decision-making factor:
My previous communication aid was really heavy and difficult to carry around and I was just about to go to secondary school so we were looking for a communication device that was lighter, smaller and easier to carry around.
Another participant indicated they would prefer a larger screen than they currently had, highlighting the individual nature of each decision-making process and the need to seek individual views.
Some participants highlighted challenges of not having access to their communication aid during the whole day, for example if they were not able to use it in a swimming pool or when travelling in a car, limiting their communication options (Box 4).
One participant expressed that he would like to use his eye gaze communication aid in the car (which is not possible as it requires a floor mount that cannot be used in a car).
Expressed using the Talking Mat: Don’t like + can take places
Participant was asked is it hard to take the eye gaze places? Indicated Yes through eye movement
Participant indicated symbol for CAR
Would you like to use your eye gaze in the car? Indicated yes through eye movement
In addition to weight and size, some participants expressed preferences for more modern and mainstream-looking devices:
My parents have suggested going back to a typewriter because people are able to see what you are typing on both sides of the device but I prefer a tablet-styled device because it is modern and blends better with other devices.
This supports views expressed in other aspects of the study that devices having a mainstream look was important, particularly for adolescents. One participant highlighted the importance of a good voice that can be understood as a priority communication aid attribute: ‘I think good voice and you understand it’.
Communication aid attributes: hardware reliability
A key consideration was the operational reliability of the aid and how long the battery lasted. Both were priorities for individuals who had experienced insufficiently reliable systems: ‘It is bad because every week they break’.
Given the impact that these attributes have on the AAC users in this study and the relatively low importance ratings these received in the BWS (see Chapter 7), these findings reinforce the notion that obtaining users’ views and preferences and incorporating them into decision-making needs to be considered in assessment processes.
Ways of working: inheriting decisions
A factor some AAC users raised was the impact of decisions made in previous communication aid recommendations and the implications that such decisions had for the future. Graphic symbol sets and systems are used in AAC to represent language. Learning to use these symbols to communicate takes considerable time, learning effort and support, similar to learning how to read. The graphic symbol sets used are proprietary and, as a result, some graphic symbols and language organisation packages are available only on specific communication aids. As one participant noted, once the time and learning has been invested in one language representation system, there are significant opportunity costs in switching to another form of language representation:
I wanted same language because if I move away from my language system, I guess I will be not happy because I don’t know nothing.
This limitation of being able to use a language representation system on only one retailer’s communication aids essentially means that individuals are precluded from choosing another type of aid. This restriction implies that, when a communication aid needs to be replaced, individuals do not receive a full assessment but move to the newest aid that can run a similar language representation system. New developments in other aids that may enhance communication are not easily available to them. This highlights the long-term ramifications of the choices about communication aids made when a child is very young. It is important to recognise that these early decisions may be taken forward into multiple future communication aid options. The clinical implication of this finding suggests a need for extra care to be taken over early communication aid recommendations with a mind to the long-term impact of the choice made; alternatively, communication aid manufacturers need to recognise how to support all graphic symbol communication platforms.
Ways of working: service delivery model
Data on service delivery models mirror findings from other aspects of the I-ASC study. AAC users reported varied levels of support and service delivery models, which had an impact on their experience of communication aid assessment and the subsequent intervention. Some participants were able to access good services in a timely way – ‘They [the AAC service] were fantastic, very quick’ – whereas others waited long periods for services or reported the need to fight for the services they needed: ‘I had a very long fight with people about paying [for the communication aid]’. Service availability appeared to be affected by geographical location (across the UK) and by the age of person. Young adults experienced being discharged from services and struggling to access support to enable them to continue to communicate independently. Further research and service appraisal could determine equity of access to services, especially at the time when young people who use AAC transition into adulthood.
Transitions: technology change
In contrast to inheriting decisions that may impede choice, technology change was identified as an important and positive factor for some participants; technology change opens up new ways of communicating, interacting with other technology such as computers, and enhances access speed and efficiency: ‘I started using my eye equipment last August which is fantastic and easier and quicker’. Some of the young adults reflected on the changes in technology during their lifetimes and welcomed what systems can do now: ‘When I was at school, no equipment like this was around but then they started coming’.
Available resources: intervention and team knowledge and skill
The AAC users valued having access to the intervention support and resources needed to fulfil communication aid recommendations. For example, one participant described being fortunate to have access to these resources in a timely manner: ‘I was very lucky, because 2 years I had speech therapy every day for an hour or two’. This reinforces the belief that detailing appropriate support for an aided communication intervention at the time of recommendation may enable appropriate provision.
Summary
The majority of AAC users, irrespective of age and individual abilities and challenges, were able to express their views about their communication aids and their communication aid recommendation processes. Many are able to take on an active role in decision-making about communication aid recommendations. Their participation may help shape recommendations to align more closely with their preferences. Strong views were reported about communication aid aesthetics and reliability, in contrast to views expressed elsewhere in the study (see Chapter 7).
The AAC user data also highlight the significance of decisions about first communication aid recommendations. Because learning and time are invested in one language representation system, the choices available in future communication aid assessments can be reduced. Particular care is needed when making early decisions, and the long-term implications of these should be considered.
The variability of service delivery models and access to resources that support children in getting communication aids and learning to use them is reflected in the data. Further research could review the availability of and access to services following a recommendation.
Parental and professional team analysis
Essentially in our case a decision was made when he was born to keep him alive and to my mind that is essentially a contract being signed by society. That’s the same with so many children now who through lots of new technology and developments are now able to continue to be with us and be part of our families and communities, and you have to embrace it.
Parent
Overview
Sixty parents and professional team members shared their experiences of decision-making in communication aid assessments and their views on how those decisions affected the lives of AAC users.
Owing to available reporting space, salient key findings from three themes detailed below are presented both to illustrate what is working well and to illuminate areas in which improvements could be made:
-
child characteristics – communication opportunities and progress
-
communication aid attributes – software graphic representation
-
ways of working – roles and responsibilities.
The remainder of the analysis from this work package has been synthesised and translated into clinical guidance, with I-ASC resources to support decision-making (e.g. https://iasc.mmu.ac.uk/i-asc-explanatory-model-of-aac-decision-making/ways-of-working/) (Figure 13).
FIGURE 13.
Heuristic excerpt: ways of working: roles and responsibilities. Reproduced with permission from Nick Holland, Manchester Metropolitan University, Manchester, UK.

Child characteristics
Communication opportunities and progress
Positive aspirations for the young person were a main factor when considering how to build communication opportunities:
He is going to go on and have a career so we are thinking long term. He is going to have to build friendships, relationships, so we need something that’s going to help him to achieve his full potential really, making sure that communication isn’t the barrier to any of these things happening.
SLT
When appropriately recommended and implemented, communication aids were recognised as supporting AAC users to communicate independently and reach their potential:
The high-tech device really has opened up her world to being able to communicate what she wants to say independently.
SLT
Participants described how the use of communication aids had the power to shift perceptions of what was possible. These ‘little eureka moments’ showcased the young person’s potential and raised expectations about their future:
She told her she had a headache and she wanted a tablet, she had a pain which was a very big first for mum. She had never told her mum that she had a pain in her head before. So there were those little eureka moments that we talk about that were really lovely.
Assistive technology professional
The young person communicating something they had never expressed before or independently communicating for the first time were important watersheds in people’s perception of their young person’s communication development:
In a café, he asked for a hot chocolate and a cookie, which was pretty mind-blowing really for him. The bit that got [child name] mother what she was so excited about was, it was that spur of the moment. They just went off and did it. It was a case of, we are going to the pub as a family, and what do you fancy for dinner? There’s the menu, and they read him out the things and then he found it on the [device name] and ordered what he wanted, and it was lovely, it was really lovely.
Teaching assistant
By demonstrating what they could do with their communication aids, AAC users changed others’ perceptions of them. This highlights the need for having the right communication supports in place so that children and young people can show their potential:
She threw a complete 2-year-old tantrum and was taken out into the kitchen. She told her dad she didn’t want to watch that on the telly through the [device name]. But she still continued having this big, big strop. So, we gave her 20 minutes to calm down and then we said, ‘Hello [child name] how do you feel now?’ ‘I feel sorry.’ Up until then, we didn’t know that she had any empathy, that she felt those feelings. Nobody knew whether she was just playing up because she was playing up or whether it was a disability-linked issue.
Parent
The communication opportunities experienced by AAC users, coupled with their ability to demonstrate communication skills, influenced the perceptions and expectations of those around them. Such abilities also affected their access to services. For example, in some areas, being assessed for a specialised communication aid was predicated on being able to demonstrate existing abilities with AAC that met the referral criteria. One SLT observed that being able to demonstrate these abilities often required particular communication opportunities:
It is often about what low-tech AAC supports they’ve had in place and how the children are [used] to communicating in any way but particularly [by] combining symbols (to suggest linguistic competence).
SLT
This particular commentary highlights that children with limited or no access to appropriate AAC support at a local level may not be able to demonstrate the level of ability required to access specialised services and therefore may miss support at both levels. Research needs to address how children access appropriate support at a local level to ensure that they experience the best possible communication opportunities to develop skills that may later enable them to meet specialised referral criteria. For example, young children may need highly motivating and lower-effort opportunities to build their experience of being successful and active communicators:
We just gave him access to communication from the start. The very first thing we did is we made a human jack-in-the-box, we put his teaching assistant in the box and every time [child name] hit a switch for a different message, he actually jumped out of the box.
Teaching assistant
There was a recognition that these opportunities did not just happen but required skilled individuals in the child’s environment to structure opportunities to afford the child control and the experience of active communication; in typically ‘speaking’ children, this is taken for granted:
Everybody’s communication opportunities have to grow. What concerns me the most is, yes, we have given him this aid, but for it to grow with him, that’s reliant on us understanding how it grows. We have been fortunate here because we’ve got a specialist teaching assistant, who’s had lots of training and is very motivated and enthusiastic, so he can oversee those elements.
Teaching assistant
This example highlights how critical the right support is for an AAC user to benefit from the communication aid recommended. Experienced and knowledgeable staff members are needed to help children learn the power of communication through technology.
It was notable in the I-ASC data that those who progressed quickly and demonstrated greater proficiency were offered more communication opportunities than those who made slower progress. Where rapid progress was observed, there was a greater focus on making a communication aid available for more of the day, for example by providing appropriate mounting systems:
Mounting it to her wheelchair would probably be our long-term plan, but at the moment we just want her to be a bit more proficient and use it in the classroom.
Assistive technology professional
Some AAC users had their opportunities with their communication aids limited for different reasons. For example, sometimes communication aids could be used only in school or for certain activities:
I’m not sure if it always goes out onto the playground with him but I’ve had conversations with his teaching assistant before that it really should go out with him because it’s one of his social times of the day.
Teaching staff member
The demands of keeping up with vocabulary needs and customisation was another reason why opportunities to use a communication aid could be limited:
He brings it home on weekends because the school keep it in the week to add things on it. So he brings it home at weekends but he hasn’t been using it until lately at home.
Parent
Communication aid attributes
Software graphic symbol representation and organisation
Graphic symbol systems are used to represent language. There are many types of graphic symbol that can be chosen for children at different stages of language skill. Different symbol sets are available on different communication aids and symbols can be organised in many different ways. Many participants indicated that, despite being core to how children learn how to communicate through aided means, consideration of the type of graphic representation or how it was organised did not feature strongly in the decision-making debate:
It is not particularly the software because we customise most of it anyway. It’s really about the people around the child that are the key. To be able to programme it yourself, to be able to use it, to encourage [child name] by modelling, I think all of those skills are actually more important than the software itself.
Teacher
Data suggest that the choice of graphic representation may be influenced by the acceptability of different systems to those in the environment, rather than by the child’s learning needs and learning style preferences:
Don’t get me wrong, there is a place for [named software 1]. But we have quite a few new members of staff and I think sometimes they got a bit flustered by it. Whereas with [named software 2], the response we got from the staff and their ability to support him was quite different. It wasn’t as daunting for them as well and the same with his parents.
SLT
Participants reported that the type of graphic representation used by children often changed. Changes occurred as children changed communication aids or contexts, for example when they started school. Participants reported that they often aimed to retain previous learning in terms of vocabulary layout, but it was not seen as important to retain the same graphic representation system, particularly with children who had a good understanding of their current symbol set:
He had gone down the route of [symbol set 1]. I don’t have too much of a problem with changing to something like [symbol set 2] because for some children that isn’t really an issue but his mum was very, very keen that he stick with the [symbol set 1].
SLT
It is unclear from this finding if decisions related to the choice of graphic representation and organisation are driven by the preferences of those supporting the child or by the resources in the child’s environment, rather than by the system preferences of the child.
The need for customised child-specific vocabulary layouts was considered for individuals starting out with AAC to build early motivation to communicate:
We fostered the choice-making, but did it in a way that he would find fun and interesting. And those boards just grew arms and legs. There was more and more and more of them. So she put all that into a book but it got so big with so much vocabulary that it became unmanageable and it became far too big.
Teaching staff member
Choosing how the vocabulary was organised was made in one of two ways. The first way was the use of ‘try it and see’. Participants reported giving a child a few different layouts to try and they then gauged the child’s response to these layouts, choosing the one that they felt worked best. The second way was by selecting the vocabulary layout that was already being used in the child’s school or other setting. This lends further support to the notion that contextual factors often have a greater prominence in decision-making than child characteristics do. This implies a need for more structured assessment of children’s symbolic understanding and potential for communicating with graphic symbols, so that this information can inform the choice of graphic symbols and vocabulary organisation.
Ways of working
Roles and responsibilities
There was considerable comment about who took responsibility for different aspects of the decision-making and implementing processes. Across the interview clusters, there was variation in team size, team perspectives and the way decisions were made. There were examples of good practice and outcomes. Good practice appeared to be related to either having a comprehensive team with the required expertise involved in the appraisal or having a few people assuming multiple roles to ensure that all aspects of the process were completed:
Because we had that team approach, I think we did cover everything. It would have been different if we hadn’t had the expertise of everybody involved. I think having that team approach really worked. If we had taken any particular member of the team away, it would have fallen down then. I am hopeful that he feels the same way but I think we covered it quite comprehensively.
SLT
There were less positive examples of information gaps or an absence of collaborative working. For example, one professional discussed how an aid had been provided to a child and their family without any instructions or training:
We feel responsible for the communication aid, but because it is another organisation’s kit. You know, you presume. You can presume that it has come with a set of instructions. Actually, they have just provided it [the communication aid].
SLT
Although there were several examples of different service structures and processes, there was a sense that, as long as roles were clearly defined and mutually understood, team responsibilities could work well for the AAC user. One example of good practice was having someone in the role of champion or driver of the process:
The class teacher was highly involved and was always really supportive, and there was a very supportive learning support assistant as well. They always attended all the assessments and when he moved class, both teachers attended one of the assessments so the school were very supportive and I personally think that was part of the success.
SLT
Sometimes a professional took on this role but often a parent fulfilled this role and created the drive for success:
His mum’s involvement and her being so proactive in taking the lead in putting all that stuff in there, for me was the crux of it being so successful and in such a short period of time. It could be quite laboured and it could take a very long time if you didn’t get the support of parents.
Teaching staff member
This view was echoed by a parent who had taken on this role for her child:
It’s all about advocating and you’ve got to play a significant role in pushing things forward, and if you’re not able to do that then you’re stuffed basically because the system cannot cope with a parent who isn’t heavily involved in all the processes.
Parent
Another suggestion of good practice was having a case holder for each child who uses a communication aid. A case holder could be described as an individual who takes responsibility, follows up, checks in and makes sure that the aid is still meeting the child’s needs and that any roadblocks are addressed:
I didn’t get to go in myself to do the pick-up and the feedback to classroom staff. But then I probably wouldn’t have felt so anxious about that if there’d been a case-holding SLT involved.
SLT
Discussion and conclusions
This WP illustrates the value that communication aids can have for children and young people when appropriately chosen and adequately implemented. Children can experience the power of everyday communication, participate in their communities and demonstrate their potential.
Decision-making in communication aid recommendations is complex and multifactorial; three key factors were considered here. It is important to provide the child with communication opportunities sufficient in quantity and quality to show their abilities. Children who cannot meet the referral criteria for specialist AAC assessment service need to have alternative routes to access communication opportunities to enable them to develop their communication skills. Choices of graphic representation and organisation are, in many cases, driven more by contextual factors, such as what is already being used or what those in the environment feel comfortable using, than by child preferences and learning style. This implies that there is a need for more comprehensive information-gathering related to children’s symbolic understanding, learning preferences and potential with graphic symbols. Greater consideration is needed of changing graphic representation systems and the potential loss of existing learning. Children and young people across the UK receive varied AAC services delivered through different service structures and by professionals with different backgrounds. Examples of good practice were evident in different working structures. Services that worked well for children had strong communication links across professionals and clearly defined roles and responsibilities across team members, with all aspects of assessment and implementation accounted for and held by an individual. Children who experienced success often had AAC champions or case holders. This was a person who advocated for the child and their communication needs, as well as taking on responsibility for considerable levels of support.
Chapter 7 Investigating augmentative and alternative communication professionals’ priorities and decision-making using stated preference methods (work package 4)
Introduction
This chapter reports research that aimed to measure the factors that are most important to AAC professionals and to provide quantitative evidence about their decision-making in the complex environment, considered in preceding chapters of this report. This research does not consider in detail environmental factors, which are considered elsewhere in the extended research project and other literature,103,114,115 but focuses on factors related to children and AAC devices.
We used stated preference surveys to investigate the decision-making of AAC practitioners. Several existing studies highlight important factors in decision-making,4,64,115,117 but the present study was the first, to our knowledge, to address the topic using quantitative stated preference methods. These methods are used widely in health research and broadly consist of survey respondents being presented with a series of hypothetical decision-making situations and being asked to state their preferences in some way. The hypothetical nature of the situations presented means that it is possible to study decision-making situations for which it would otherwise be difficult or impossible to gather data (e.g. patient preferences for treatments that are still in development). As a methodology, it can also make it easier to disentangle the effect of factors that are confounded in real-life decision situations (e.g. treatment efficacy being highly correlated with the severity of side effects).
This chapter presents two stated preference studies. The first investigated AAC professionals’ stated priorities when making decisions using a method termed BWS case 1, which allows the relative importance of several factors in decision-making to be assessed. This study quantified what AAC professionals regarded as the most important factors to consider about children and their potential AAC systems. The second was a DCE that built on the BWS findings. Participants were shown a vignette describing a hypothetical child with a range of believable characteristics, who would benefit from AAC. Professionals then made several choices about which of three hypothetical AAC systems they would choose for the hypothetical child. Analysing the choices revealed the trade-offs that professionals made between different attributes of AAC systems and showed how those trade-offs changed and interacted with the characteristics of the children considered.
To our knowledge, no previous stated preference work had been carried out in the field. Therefore, a BWS case 1 study was chosen as a starting point, as it quantified which of several child- and AAC-system-related factors (37 in total) AAC professionals considered most important in decision-making. This method was preferred over alternatives such as ranking as it imposes a lower cognitive burden,118 thereby increasing the chances of gathering high-quality research data.
Decision-making in health is more often studied using DCEs, and a DCE was carried out following the BWS. Owing to the cognitive demand of DCE tasks, they typically include only a small number of attributes, usually around five or six. However, they have the advantage of giving more information about the attributes, and, because participants make choices between alternatives, DCE tasks resemble real-world decision-making more closely than does stating priorities, as in BWS.
Carrying out a BWS followed by a DCE meant that the two studies complemented each other, with the BWS giving information about many factors in decision-making and the DCE examining fewer factors in more detail. The BWS also improved the relevance of the subsequent DCE by providing quantitative evidence about which factors were most suitable for including as attributes.
Study 1: best–worst scaling case 1 survey
Methods
Participant recruitment
The target population was any UK-based professional involved in AAC decision-making and who worked, either wholly or partly, with children. To make statistical modelling as robust as possible, the aim was to obtain as large a sample as feasible and to reach a geographically widespread UK audience. Recruitment e-mails were sent to a mailing list developed by the research team of attendees at previous project events. The e-mails were also sent to the mailing list of Communication Matters, a UK-wide AAC charity (www.communicationmatters.org), and to the administrators of various service providers with a request to forward it to their members. In addition, personalised invitations were sent to the research team’s professional contacts with a request to circulate these. Responses were collected between 24 March 2017 and 15 May 2017.
Procedures
Characteristic and attribute development
In the study described here, the term ‘AAC attribute’ refers to hardware features (voice, portability, etc.) and software features (vocabulary, navigation, etc.), whereas the term ‘characteristic’ refers to a child’s diagnosis, physical and cognitive features, motivation, personality traits and so on.
Two systematic literature reviews were conducted to provide material for the candidate characteristics and communication aid attributes to be included in the survey (see Chapter 4). 72,101,119
It is considered good practice to construct attributes for stated preference studies using qualitative methods. 120 An aspect of the wider research project was being able to provide material for characteristics and attributes from a number of sources (see Chapters 5 and 6).
Project team members with expertise in AAC, speech and language therapy and qualitative research extracted qualitative findings from the above sources. Through consensus discussions, the findings were condensed into an initial list of 31 potential characteristics related to children and 29 attributes related to AAC devices.
As fewer characteristics/attributes mean greater statistical power and more precise results, the goal was to reduce their number as far as possible. Thus, using an iterative process, the research team held further consensus discussions to clarify characteristic/attribute definitions, combine similar ones, and discard those whose influence was captured largely by another characteristic/attribute (e.g. age and educational stage). This process continued until no further reductions could be made without excluding key factors. The result was a list of 19 child-related characteristics and 18 communication aid attributes, shown in Appendices 1 and 2.
Survey design and implementation
Owing to the large number of characteristics and attributes, they were separated into two parts, administered as a single survey. In each question, participants were shown a list of six characteristics/attributes and asked to select which was the most and which was the least important factor in their decision about provision of an AAC device.
For each BWS component, participants answered 10 questions (i.e. 20 BWS questions for the whole survey). Two survey designs were constructed using Sawtooth Software (Sawtooth Software, Inc., Provo, UT, USA), each of which had five versions. Sawtooth uses an algorithm to generate designs that balances, as far as possible, (a) the number of times each attribute/characteristic is presented, (b) the number of times each combination of two attributes/characteristics appears and (c) the number of times each attribute/characteristic is shown in a given position, in order of priority. Each of the five BWS child component versions (denoted A, B, C, D and E) was then paired with a BWS AAC device component (denoted 1, 2, 3, 4 and 5), making five questionnaire versions: A1, B2, C3, D4 and E5. Five more versions were created by reversing the order of the child and AAC device components (1A, 2B, 3C, 4D and 5E), making 10 questionnaire versions in total. After completing both BWS components, participants answered questions about themselves and their work. The survey was tested with five AAC professionals who were not part of the research team. Based on feedback, alterations were made to the visual presentation and to the wording of instructions and characteristics/attributes.
Analysis
Analysis was grounded in random utility theory. 121 This means that individuals are assumed to choose whichever option gives the greatest utility. The utility of an option is modelled as having a deterministic component, determined by the option’s attributes, and a random component, which represents aspects of the decision-making environment not observable by the researcher. All analysis was carried out using R version 3.3.1 (The R Foundation for Statistical Computing, Vienna, Austria).
The utility individual i receives from choosing option k ∈ {1,2, . . ., 6} in choice situation j is modelled as:
where xjkl is a dummy variable indicating whether or not option k includes attribute/characteristic l, βil is a parameter representing an individual i’s preference for attribute/characteristic l, εijk is an independently and identically distributed extreme value error term, and NA is the total number of attributes/characteristics.
Estimates of the β parameters were obtained from random parameters logit (also commonly known as mixed logit) models. For a given attribute, l, individuals’ parameters were assumed to be normally distributed with mean β¯il and variance σl2. The distribution mean was allowed to depend on respondent characteristics according to:
where βl0 is a constant, the Zim are M variables representing characteristics of individual i, the δlm are parameters giving the dependence of preference on characteristics, and ηil is a normally distributed error term.
Results are presented using relative importance scores (RISs), which give the importance of characteristics/attributes on a ratio scale. Thus, a characteristic/attribute with a RIS of 10 is twice as important as one with a RIS of 5, and a characteristic/attribute with a RIS of 2 is only half as important as one with a RIS of 4. The RIS of all characteristics/attributes is transformed to sum to 100, implying that a characteristic/attribute with a RIS of 100/19 ≈ 5.26 for children and 100/18 ≈ 5.55 for AAC devices was of average importance. The RIS of attribute/characteristic l for individual i was calculated using:
where β^il is the estimated individual-level coefficient on attribute/characteristic l for respondent i. 122 The mean RIS for each attribute was then calculated across participants.
We performed t-tests of the null hypotheses that each attribute/characteristic was of average relative importance, and also for each pair of attributes/characteristics of the null that they were of equal relative importance. Whether or not the RIS differed according to each of the demographic variables in Appendix 3 was examined using t-tests. Based on test results, characteristics and attributes were divided into three groups: (1) those with a RIS significantly higher than average, (2) those with a RIS not significantly different from average, and (3) those with a RIS significantly lower than average. We tested whether or not all characteristics and attributes differed in importance, and each RIS was tested to determine if there were differences according to respondent demographics (Table 12).
| Characteristic/attribute | Mean score | 95% CI | p-value |
|---|---|---|---|
| Child characteristics | |||
| Child’s receptive and expressive language abilities | 11.4 | 10.6 to 12.3 | < 0.001a |
| Support for AAC from communication partners | 11 | 10.2 to 11.8 | < 0.001a |
| Communication ability with aided AAC | 10.4 | 9.73 to 11.1 | < 0.001a |
| Child’s determination and persistence | 9.93 | 9.13 to 10.7 | < 0.001a |
| Physical abilities for access | 8.94 | 8.11 to 9.75 | < 0.001a |
| Predicted future needs and abilities | 7.04 | 6.15 to 8.03 | 0.002a |
| Level of learning ability | 6.86 | 5.77 to 7.84 | 0.012 |
| Insight into own communicative skills | 5.67 | 4.78 to 6.53 | 0.438 |
| Attention level | 5.08 | 3.88 to 6.42 | 0.811 |
| Access to professional AAC support | 4.88 | 3.9 to 5.93 | 0.538 |
| Speech skills and intelligibility | 4.38 | 3.54 to 5.3 | 0.101 |
| Functional visual skills | 3.64 | 2.7 to 4.65 | 0.007a |
| History of aided AAC use | 2.55 | 1.66 to 3.34 | < 0.001a |
| Presence of additional diagnoses | 2.21 | 1.53 to 2.93 | < 0.001a |
| Level of fatigue | 1.96 | 1.45 to 2.51 | < 0.001a |
| Literacy ability | 1.65 | 1.02 to 2.32 | < 0.001a |
| Educational stage | 1.14 | 0.53 to 1.72 | < 0.001a |
| Primary diagnosis | 1.09 | 0.53 to 1.72 | < 0.001a |
| Mobility | 0.19 | 0.02 to 0.59 | < 0.001a |
| AAC device attributes | |||
| Vocabulary or language package(s) | 11 | 9.9 to 12 | < 0.001a |
| Consistency of layout and navigation | 10.6 | 9.64 to 11.5 | < 0.001a |
| Ease of customisation | 9.92 | 9.02 to 10.9 | < 0.001a |
| Durability and reliability | 9.62 | 8.65 to 10.6 | < 0.001a |
| Type of vocabulary organisation | 9.36 | 8.44 to 10.3 | < 0.001a |
| Number of key presses required to generate symbol or text output | 7.98 | 7.04 to 8.92 | < 0.001a |
| Size of output vocabulary | 6.62 | 5.69 to 7.56 | 0.062 |
| Range of access methods | 5.9 | 5.08 to 6.77 | 0.500 |
| Number of cells per page | 5.28 | 4.2 to 6.34 | 0.673 |
| Portability | 5.1 | 4.09 to 6.11 | 0.458 |
| Graphic representation | 4.82 | 3.87 to 5.8 | 0.211 |
| Battery life | 4.3 | 3.34 to 5.3 | 0.038 |
| Supplier support | 3.22 | 2.44 to 4.01 | < 0.001a |
| Ease of mounting on a range of equipment | 2.65 | 1.92 to 3.45 | < 0.001a |
| Cost | 1.44 | 0.83 to 2.15 | < 0.001a |
| Additional assistive technology functions | 1 | 0.51 to 1.57 | < 0.001a |
| Voice | 0.97 | 0.42 to 1.59 | < 0.001a |
| Appearance | 0.31 | 0.05 to 0.75 | < 0.001a |
Response quality was assessed as follows. Kolmogorov–Smirnov tests were used to check whether or not individuals were biased towards selecting an attribute/characteristic in a given position (e.g. at the top of the list). We calculated the proportion of times participants made either contradictory choices (e.g. stating that attribute A is more important than attribute B in one question, and then stating the opposite in another question) or choices that violated transitivity (the principle that if attribute A is more important than attribute B, and if attribute B is more important than attribute C, then attribute A is more important than attribute C). As individuals who make logical choices should be consistent and transitive, and should make an even spread of choices in each position, poor performance may indicate a lack of understanding or inattentiveness.
No responses were excluded from the main analysis based on these measures. Respondents were split according to whether their choices displayed above or below the median proportion of consistency and transitivity and we examined whether or not the relative importance score differed significantly between the two groups. Models were re-estimated including only participants making consistent and transitive choices at least 80% of the time (this removed participants with the greatest number of inconsistent and intransitive choices while retaining sufficient data to estimate models).
Statistical significance was judged at the 5% level, with adjustment for multiple testing using Holm’s sequential Bonferroni correction. 123
Results
A total of 113 participants answered at least one question, and 93 completed the survey. However, the latter figure includes some non-completers who might have returned the survey later. Non-completers answered a median of four questions. No data are available for those who did not respond to invitations, so it is not possible to compare them with responders. Recruitment involved requests for e-mails to be forwarded, making it impossible to know how many people received information about the survey; thus, a response rate cannot be assessed.
Participant demographics
Table 13 summarises the participants’ characteristics. A large majority of the participants were female (n = 84, 90%) and of white British ethnicity (n = 80, 86%), which we believe to be reasonably representative of AAC professionals in the UK. For example, data from the Health and Care Professionals Council showed that 96% of SLTs in the UK are female, and the Higher Education Statistics Agency found in 2017/18 that 79% of speech and language therapy students were white (Tom Griffin, Royal College of Speech and Language Therapists, 2019, personal communication). Almost half reported that they had > 10 years’ experience of working with AAC (n = 42, 45%). Most had a professional background as a SLT (n = 66, 71%). Almost half reported that at least 80% of their role was related to AAC (n = 41, 44%), with relatively few (n = 9, 10%) reporting this to be < 20%. Around three-quarters of participants reported that they spent some of their time working in an educational establishment (n = 71, 76%), with a majority working in health-care settings (n = 58, 62%). Just under half visited people’s own homes (n = 43, 46%). (Note that participants could report multiple settings and thus percentages do not sum to 100%.) It is difficult to determine how representative this is, although it includes SLTs, occupational therapists, teachers and assistive technology specialists, in line with UK guidelines for the composition of AAC services.
| Characteristic | Number of participants | % |
|---|---|---|
| Age (years) | ||
| 18–24 | 2 | 2.15 |
| 25–34 | 29 | 31.18 |
| 35–44 | 34 | 36.56 |
| 45–54 | 19 | 20.43 |
| 55–64 | 9 | 9.68 |
| Sex | ||
| Female | 84 | 90.32 |
| Male | 7 | 7.53 |
| Prefer not to say | 2 | 2.15 |
| Ethnicity | ||
| White: English/Welsh/Scottish/Northern Irish/British | 80 | 86.02 |
| White: any other white background | 7 | 7.53 |
| White: Irish | 4 | 4.3 |
| Asian/Asian British: Chinese | 1 | 1.08 |
| Mixed/multiple ethnic group: white and Asian | 1 | 1.08 |
| Experience (years) | ||
| < 1 | 2 | 2.15 |
| 1–4 | 27 | 29.03 |
| 5–10 | 22 | 23.66 |
| > 10 | 42 | 45.16 |
| Professional background | ||
| SLT | 66 | 70.97 |
| Other | 9 | 9.68 |
| Occupational therapist | 7 | 7.53 |
| Assistive technology specialist | 5 | 5.38 |
| Teacher | 4 | 4.3 |
| Clinical scientist | 4 | 4.3 |
| Per cent of role relating to AAC | ||
| 1–20 | 9 | 9.68 |
| 20–40 | 15 | 16.13 |
| 40–60 | 19 | 20.43 |
| 60–80 | 9 | 9.68 |
| 80–100 | 41 | 44.09 |
| Workplace | ||
| Education establishments | 71 | 76.34 |
| Health-care setting | 58 | 62.37 |
| Person’s own home | 43 | 46.24 |
| Residential care | 22 | 23.66 |
| Day-care settings | 18 | 19.35 |
| Other | 3 | 3.23 |
Response quality
The median number of contradictory/intransitive choices was six (4.88%) for child characteristics and eight (5.93%) for AAC device attributes (percentages relative to the number of opportunities participants had to make contradictory or intransitive choices).
Child characteristics
Table 12 shows the relative importance score for child characteristics, which were split into three groups: those of greater than average importance, those of average importance and those of less than average importance. Six out of 19 child characteristics (31.6%) were considered to be of greater than average importance, while five (26.3%) were considered to be of average importance and eight (42.1%) were considered to be of less than average importance. Characteristics considered to be of greater than average importance were child’s receptive and expressive language abilities, support for AAC from communication partners, child’s communication ability with aided AAC, child’s determination and persistence, physical abilities for access, and predicted future needs and abilities. Characteristics considered to be of lower than average importance were functional visual skills, history of AAC use, presence of additional diagnoses, level of fatigue, literacy ability, educational stage, primary diagnosis, and mobility.
The results of tests for statistically significant differences in the RIS of every pair of characteristics (i.e. those that did not arise by chance) are provided in Appendix 4. It is impossible to distinguish the importance of any characteristic from that of any adjacently ranked characteristic. Nevertheless, out of 171 pairwise comparisons, 115 (67.3%) were significantly different. Characteristics with above-average RIS were more similar in importance than those with below-average RIS. For example, child’s receptive and expressive language abilities, ranked first, was only 1.6 times as important as predicted future needs and abilities, ranked sixth, whereas functional visual skills, ranked 12th, was almost 19 times as important as mobility, ranked 19th. The survey was able to detect only six significant differences in RIS according to respondent demographics, all in characteristics that were of less than average importance.
Augmentative and alternative communication device attributes
Table 12 shows the RIS for AAC device-related attributes. Splitting AAC device-related attributes into three groups reveals that six (33.3%) attributes each were considered to be of greater than average importance, average importance and less than average importance. Those of greater than average importance were vocabulary or language package(s), consistency of layout and navigation, ease of customisation, durability and reliability, type of vocabulary organisation, and number of key presses required to generate symbol or text. Those of less than average importance were supplier support, ease of mounting on a range of equipment, cost, additional assistive technology features, voice and appearance.
The results show that it is impossible to distinguish the importance of any attribute from any adjacently ranked attribute (see Appendix 5). However, out of 153 pairwise combinations, 102 (66.7%) were significantly different. Again, attributes with above-average RIS were more tightly grouped in terms of importance than those with below-average RIS. The top-ranked attribute, vocabulary or language package(s), was only 1.4 times more important than the sixth-ranked attribute, number of key presses required to generate symbol or text output, and yet supplier support, ranked 13th, was over 10 times more important than appearance, which was ranked 18th.
Robustness checks
Respondents did not exhibit a tendency to choose attributes/characteristics in one position in the list over any other (p-value > 0.999 for children, p-value = 0.939 for AAC devices). No significant differences were observed in the RIS of participants who made above and those who made below the median proportion of consistent and transitive choices. The results of estimating models with only the 75 participants whose choices were consistent and transitive at least 80% of the time were qualitatively similar to those from the full sample. Details of the results are available on request to Dr Edward Webb, University of Leeds, Leeds, UK.
Discussion
Participants obeyed the axioms of consistency and transitivity around 95% of the time, evidence that they understood the tasks and found them meaningful. This compares favourably with response quality observed in other stated preference studies. 124 In addition, participants showed no tendency to be biased towards choosing attributes/characteristics that appeared at the top of the list.
For child characteristics, a trend emerges that physical abilities were considered less important than cognitive and learning, language and communication abilities, and personality traits. Only one physical characteristic, physical abilities for access, was ranked as having greater than average importance. Receptive and expressive language, communication ability with aided AAC, and level of learning ability were ranked as having greater than average importance, whereas literacy ability and educational stage were both considered to be of less than average importance. Child’s determination and persistence and insight into own communicative skills were ranked as having greater than average importance, with attention level just below average importance.
The prioritisation of child’s determination and persistence suggests recognition of the high demands that aided communication may place on children and their need to continue trying to communicate. It suggests that interventions focused on reducing the demands of aided communication (e.g. incorporating low-tech AAC to reduce operational demands when linguistic demands are higher125) and incorporating strategies that help children develop greater resilience and a willingness to continue trying may have positive long-term outcomes.
Support for AAC by communication partners was the second most important child characteristic, significantly more important than 14 other child characteristics. This suggests that there is a critical reliance on support in the child’s environment for AAC device recommendations, and reinforces findings elsewhere in this report that an exploration of environmental influences would be useful.
The future trajectory of a child, represented by predicted future needs and abilities, is of above-average importance, while past experiences, represented by history of AAC use, is of below-average importance. This is an interesting finding, given reported concerns regarding the abandonment or non-use of AAC devices. 11,126
Primary and secondary diagnoses were among the least important characteristics. This may be because key features of diagnoses are intentionally captured by other characteristics.
In terms of AAC device attributes, greater importance tended to be ascribed to language and communication interface aspects than to hardware aspects. Only a single hardware-related attribute, durability and reliability, was more important than average, with all the other above-average importance attributes relating to the vocabulary organisation aspects interfacing with the AAC device. Vocabulary and language package(s) and consistency of layout and navigation were the highest-ranked attributes. Ease of customisation was ranked third, but not significantly differently from the two language and communication attributes. Range of access methods was rated just above average importance.
Four out of the six of the highest-ranked AAC device attributes pertain to the vocabulary in the software of the device and how it is organised. Furthermore, physical features such as ease of mounting on a range of equipment, voice and appearance were ranked as below-average importance. Previous studies suggest that attributes such as aesthetics and ease of mounting are valued by people who use AAC. 13 In addition, consideration of the results by the project team’s public involvement co-researchers indicated that there were potentially differing views on some of the attributes ranked least important by professionals (voice, appearance, ease of mounting, and additional assistive technology features).
Comparing the results with other available evidence suggests that professionals have a greater focus on features that specifically influence the communicative use of the AAC device and that they may give less priority to attributes that may be less relevant in a clinic setting than in everyday life. These priorities may be different from those of children who use AAC and their families, suggesting a need for tools to support consensus-building and agreement of priorities to inform AAC device recommendation across all stakeholders.
Cost was one of the least important AAC device attributes, suggesting a positive impact of the recent policy change in the UK that introduced dedicated funding for AAC devices.
Graphic representation stands out as the only language attribute ranked as having less than average relative importance. Recent studies suggest ambivalence towards challenges or levels of cognitive difficulty associated with perceived levels of graphic representation. 23
Limitations
A disadvantage of BWS case 1 is that, although it is possible to show the relative importance of characteristics and attributes, it is not possible to demonstrate which are of absolute importance. However, the characteristics and attributes were developed using existing literature and the views of practitioners, indicating that all included characteristics and attributes were important to a certain extent. Another disadvantage is that the stated importance of characteristics/attributes may not reflect the variability that participants see in practice. The sample size of 93 was relatively small, approximately half of the average sample size of BWS case 1 studies in health. A larger sample size would have been desirable; however, recruiting even the achieved number of participants proved challenging.
Study 2: discrete choice experiment
Methods
Survey development
Attributes for the DCE were selected from the attributes used in study 1 (BWS) during consensus discussions between the research team with lived AAC experience and expertise in AAC service delivery and research and health economics. The criteria for selecting the attribute sets were that they should (1) form coherent and realistic descriptions of children and systems, (2) address the research aims of the wider research project, (3) include mainly attributes with high relative importance scores in the BWS study and (4) contain a small enough number of attributes that the choice tasks would not overburden respondents. This resulted in four child attributes and five system attributes.
A set of levels was generated for each attribute during further consensus discussions, with the criteria that levels should (1) reflect the characteristics of children and systems usually encountered by AAC professionals, (2) cover a wide range of characteristics of a given attribute and (3) be few in number to aid model estimation. The language used for attributes was refined from that used in the BWS to reflect a different type of choice task.
The final list of four child attributes with associated levels and descriptions is given in Table 14 and the list of AAC system attributes with associated levels and descriptions is given in Table 15.
| Child attributes (levels) | Description |
|---|---|
| Receptive and expressive language | Child’s ability to understand communication from and communicate with others without AAC |
| Delayeda | Both receptive and expressive abilities below expectation given child’s age |
| Receptive language exceeding expressive language | Ability to understand communication from others greater than ability to communicate with others |
| Communication ability with AAC | How well a child can communicate when using AAC |
| No previous AAC experiencea | Has never communicated using AAC before |
| Able to use AAC for a few communicative functions | Can use AAC for some basic functions (e.g. simple requests) |
| Able to use AAC for a range of communicative functions | Can use AAC for more complex tasks (e.g. constructing sentences) |
| Child’s determination and persistence | Attitude of child towards communication and using AAC |
| Does not appear motivated to communicate through any methods and meansa | Child is not inclined to develop communication skills |
| Motivated to communicate through symbol communication systems | Child has demonstrated motivation and willingness to use AAC |
| Only motivated to communicate through methods other than symbol communication | Child may be motivated to communicate, but is not inclined to use AAC |
| Predicted future skills and abilities | Professional assessment of how child’s communication abilities will develop |
| Regressiona | Abilities projected to become worse in future (e.g. owing to a degenerative condition such as Rett syndrome) |
| Plateau | Abilities will not change significantly in future (e.g. a child aged 16–17 years) |
| Progression | Communication abilities will develop in future |
| AAC system attributes (levels) | Description |
|---|---|
| Vocabulary sets (1) | Words and/or symbols pre-provided on system, usually as part of a software package |
| No vocabulary seta | AAC practitioners/child’s support network provides all vocabulary content |
| Fixed vocabulary set | A single, largely uncustomised, fixed set of vocabulary |
| Vocabulary set with staged progression | A series of largely uncustomised vocabulary sets with predetermined progression through them that simulates language development (e.g. an initial set including just basic words, with subsequent sets introducing more grammatical structure) |
| Size of vocabulary (7) | How many words/symbols system can output |
| Up to 50 vocabulary itemsa | Implies only simple communication functions possible |
| 50–1000 vocabulary items | Implies combining words/symbols to create grammatical structures |
| More than 1000 vocabulary items | Does not imply more complex communication than 50–1000 items, but means a greater load on child’s memory |
| Type of vocabulary organisation (5) | How words/symbols are organised within the system |
| Visual scenea | Interface shows photographs, most likely of scenes familiar to the child, with areas of it highlighted to represent words |
| Taxonomic | Words/symbols organised according to subject, analogous to non-fiction books in a library |
| Semantic–syntactic | Words/symbols organised according to sentence structure (e.g. verbs, nouns, adjectives) |
| Pragmatic | Words/symbols organised around function in language rather than grammar (e.g. request, mood) |
| Graphic representation (12) | Type of symbols used by system |
| Photographsa | Photographs, possibly of items personal to the child |
| Pictographic symbol set | Non-photorealist pictures with specific meanings attached. May be accompanied by text |
| Ideographic symbol system (with rules or encoding) | Stylised symbols combined with fixed rules and grammar analogous to Chinese/Japanese characters (e.g. Blissymbols) |
| Text | Text unaccompanied by other symbols |
| Consistency of layout (2) | How consistent positions of words/symbols are in system interface, and how consistent navigation to find different symbols is |
| Consistency of some aspects of layouta | Words/symbols in multiple categories appear in different positions across categories, but always in the same place in a given category |
| Consistency of all aspects of layout | All/nearly all words/symbols always appear in same position in interface |
| Idiosyncratic layout | Layout that has been personalised for an individual child |
A decision situation in this DCE had two components: a child vignette and a set of systems to allocate to that child. For the first component, there were 54 possible vignettes. Research colleagues with expertise in AAC and speech and language therapy identified and removed 18 vignettes that represented unrealistic combinations, leaving a total of 36. Each participant was asked to answer questions about three vignettes randomly selected from these 36.
Experience with the BWS study led to the belief that it would be difficult to recruit a large sample to this study. To maximise the number of data, we chose a relatively heavy response burden of 12 choices among three systems. From the 432 possible AAC systems, researchers removed 158 unrealistic combinations. From the remaining 274 combinations, a D-efficient survey design was generated using NGene (© ChoiceMetrics; www.choice-metrics.com) with five blocks, meaning that there were 60 choice tasks in total. Participants were randomly allocated to a block independently of the child vignettes.
At the start of the survey, participants were asked whether or not they contributed to decision-making about AAC systems. Those who answered ‘no’ were not shown the DCE tasks and answered only demographic questions. For the first four DCE questions, participants were asked to imagine choosing a system for the first randomly selected child vignette, for the second four questions they chose for the second child vignette, and for the final four questions they chose for the third vignette. The children in the first, second and third vignettes were referred to as child A, child B and child C, respectively. The order of system attributes was randomised between participants but consistent within the choices seen by a given participant. Finally, participants answered some questions about themselves and their experiences with AAC (Table 16).
| Characteristic | Mean | SE |
|---|---|---|
| Age (years) | 40.8 | 11 |
| Experience (years) | 11.4 | 9.2 |
| % of role relating to AAC | 53.7 | 34.3 |
| Sex, n | ||
| Female | 155 | 90.1 |
| Male | 10 | 5.81 |
| Prefer not to say | 7 | 4.07 |
| Ethnicity, n | ||
| White – English/Welsh/Scottish/Northern Irish/British | 149 | 86.6 |
| White – other | 12 | 6.98 |
| Other | 6 | 3.49 |
| White – Irish | 5 | 2.91 |
| Professional background, n | ||
| SLT | 125 | 72.7 |
| Occupational therapist | 16 | 9.3 |
| Teacher | 14 | 8.14 |
| Other | 12 | 6.98 |
| Assistive technology specialist | 5 | 2.91 |
| Clinical scientist | 5 | 2.91 |
| Age groups worked with, n | ||
| Primary school age | 99 | 57.6 |
| Secondary school age | 94 | 54.7 |
| Preschool age | 85 | 49.4 |
| All age groups | 56 | 32.6 |
| Higher education | 30 | 17.4 |
| Further education | 21 | 12.2 |
| Other | 12 | 6.98 |
| Adults | 10 | 5.81 |
| Among most common three diagnoses seen in practice, n | ||
| Physical disability (e.g. neuromuscular, cerebral palsy) | 140 | 81.4 |
| Intellectual disability/developmental delay | 118 | 68.6 |
| Autism spectrum disorder | 113 | 65.7 |
| Syndromes | 61 | 35.5 |
| Neurological | 45 | 26.2 |
| Specific speech/language impairment | 22 | 12.8 |
| Dyspraxia | 14 | 8.14 |
The DCE was administered online for ease of recruitment. It was tested by five AAC professionals, after which the wording of some attributes and levels was altered.
Recruitment was completed using e-mail lists gathered at previous project events, as well as the mailing list of Communication Matters and authors’ professional contacts. Owing to the small pool of potential respondents, we had to allow those who may have completed the BWS survey to complete the DCE. Responses were collected between 20 October 2017 and 4 March 2018.
Analysis
Responses were again analysed using a random utility framework. The utility to participant ε of allocating AAC system s to child c is modelled as:
where αs is an alternative specific constant, xs is a vector of dummy variables indicating the level of each attribute for system s, βic is a vector of coefficients describing i’s assessment of the appropriateness of each level of each system attribute for child c and εi is an independently and identically distributed extreme value error term.
The coefficient on level l of system attribute a, βialc, depends on the characteristics of the child according to:
where γial0 is a constant, zc is a vector of dummy variables indicating the level of each attribute for child c, and γial is a vector of coefficients indicating how i’s valuation of level l of system attribute α depends on child attributes.
For each child and system attribute, one level was selected as a baseline (indicated by asterisks in Tables 14 and 15).
A full model with all interaction terms and two alternative specific constants implies 98 parameters, too many to reliably estimate given the number of data collected. A strategy was required to allow the identification of a suitable model with fewer parameters. The first stage was a series of stepwise multinomial logit regressions, beginning with a model with all 98 parameters. The parameter with the lowest p-value, excluding the γ0 constant terms, was eliminated, and a model with 97 parameters was estimated. Then the parameter with the lowest p-value was excluded and a new model was run. This continued an iterative process until only the 12 γ0 constant terms remained (one for each non-baseline system level).
The Bayesian information criterion was used to select the preferred multinomial logit model. This model was then re-estimated as a mixed logit model to accommodate heterogeneity of participants’ preferences. The β-coefficients on system attribute levels were assumed to be drawn from a normal distribution with both mean and variance depending on child attributes. If p is the number of parameters of the preferred multinomial logit model, then models with between p – 2 and p + 2 parameters were re-estimated as mixed logit models. The mixed logit model minimising the Bayesian information criterion was chosen as the final preferred model.
Multinomial logit models were estimated using maximum likelihood and mixed logit models were estimated using simulated maximum likelihood, both implemented using the Choice Modelling Centre’s code for R version 1.1 (University of Leeds, Leeds, UK). Analysis was carried out using R version 3.3.1.
The statistical significance of parameters was assessed at the 5% level after adjusting for multiple testing using Holm’s sequential Bonferroni correction. 123
It is possible to gain an insight into the size of impact child attributes have on AAC professionals’ decision-making. A measure is introduced termed relative interaction attribute importance, similar to relative attribute importance, which is often used to present DCE results. Relative interaction attribute importance measures the amount that preferences for attributes of choice objects are impacted by a given interaction attribute associated with a choice situation relative to other interaction attributes. In this study it measures how much preferences for AAC systems are influenced by child characteristics.
Relative interaction attribute importance is calculated with respect to a single choice object attribute by taking the difference between the greatest increase an interaction attribute causes to a choice object attribute’s part worth utility and the greatest decrease, expressed as a percentage of the differences for all interaction attributes. Formally, the relative interaction attribute importance for interaction attribute i with respect to choice attribute c is:
where γicmax and γicmin are, respectively, the maximum and minimum coefficients for interaction attribute i with respect to choice attribute c, and NI is the number of interaction attributes. The overall relative interaction attribute importance for i is similarly calculated as:
where now γimax and γimin are, respectively, the maximum and the minimum coefficients for interaction attribute i across all choice attributes.
Results
In total, 172 participants completed the survey, of whom 155 indicated that they contributed to decision-making about AAC systems and answered DCE questions. Participants’ characteristics are summarised in Table 5 and are similar to those of BWS participants. The sample reported working with children of a wide range of ages. Approximately 30% specifically reported working with all age groups, while 50–60% reported working with children from one of the following age groups: preschool, primary school and secondary school. The sample also reported working with children with a wide range of diagnoses, for example physical disability (≈ 80%), intellectual disability/developmental delay (≈ 70%) and autism spectrum disorder (≈ 65%).
Table 17 shows the results of the final preferred model, with 24 coefficients, 12 of which were interaction terms, and no alternative specific constants. The ‘constant’ terms give participants’ priorities in AAC system allocation when shown a vignette with all attributes at baseline levels:
Child A/B/C has delayed receptive and expressive language and no previous AAC experience. Child A/B/C does not appear motivated to communicate through any means. Child A/B/C is predicted to regress in future in terms of skills and abilities (regression).
| AAC system attribute | Child attribute | Estimate | 95% CI | p-value |
|---|---|---|---|---|
| Vocabulary sets (baseline none) | ||||
| Fixed | Constant | 0.283 | 0.0937 to 0.472 | 0.003a |
| Staged progression | Constant | 0.364 | 0.0882 to 0.64 | 0.010a |
| Predicted to progress | 1.36 | 0.922 to 1.79 | 0.000a | |
| Size of vocabulary (baseline 50 items) | ||||
| 50–1000 items | Constant | 0.131 | –0.149 to 0.41 | 0.360 |
| Motivated to communicate through symbol communication systems | 1.01 | 0.552 to 1.46 | 0.000a | |
| More than 1000 items | Constant | –0.929 | –1.35 to –0.511 | 0.000a |
| Receptive language exceeding expressive language | 0.692 | 0.328 to 1.06 | 0.000a | |
| Able to use AAC for a range of communicative functions | 1.14 | 0.515 to 1.77 | 0.000a | |
| Motivated to communicate through symbol communication systems | 1.31 | 0.781 to 1.85 | 0.000a | |
| Predicted to progress | 0.902 | 0.445 to 1.36 | 0.000a | |
| Type of vocabulary organisation (baseline visual scene) | ||||
| Taxonomic | Constant | 0.0629 | –0.261 to 0.387 | 0.703 |
| Motivated to communicate through symbol communication systems | 0.707 | 0.303 to 1.11 | 0.001a | |
| Semantic–syntactic | Constant | –0.178 | –0.503 to 0.146 | 0.282 |
| Motivated to communicate through symbol communication systems | 0.826 | 0.441 to 1.21 | 0.000a | |
| Pragmatic | Constant | 0.443 | 0.201 to 0.685 | 0.000a |
| Graphic representation (baseline photos) | ||||
| Pictographic symbol set | Constant | –0.41 | –0.769 to –0.0513 | 0.025 |
| Motivated to communicate through symbol communication systems | 1.36 | 0.886 to 1.83 | 0.000a | |
| Predicted to progress | –0.814 | –1.24 to –0.387 | 0.000a | |
| Ideographic symbol system | Constant | –1.25 | –1.66 to –0.85 | 0.000a |
| Motivated to communicate through symbol communication systems | 1.67 | 1.14 to 2.2 | 0.000a | |
| Text | Constant | –0.709 | –1.02 to –0.398 | 0.000a |
| Motivated to communicate through symbol communication systems | 1.39 | 0.933 to 1.84 | 0.000a | |
| Consistency of layout (baseline some aspects) | ||||
| Consistency of all aspects | Constant | 0.892 | 0.655 to 1.13 | 0.000a |
| Idiosyncratic layout | Constant | 1.46 | 1.18 to 1.73 | 0.000a |
For such a vignette, vocabulary sets with fixed and staged progression were preferred to no pre-provided vocabulary. There were no significant differences in preferences between up to 50 and 50–1000 vocabulary items, but over 1000 items was considered significantly worse. There was no significant preference among having vocabulary organised using visual scene, taxonomic or semantic-syntactic schemes, but pragmatic organisation was preferred. There was no preference of graphic representation between using photographs and using pictographs. However, text was preferred less than either of those two modes of graphic representation, and ideographic symbols were considered even less favourably. Finally, having only some consistent aspects of system layout was preferred less than having consistency across all aspects or an idiosyncratic layout.
Compared with this ‘baseline’ vignette, a practitioner is much more likely [odds ratio (OR) 3.88] to choose a system with vocabulary sets with staged progression than one with no preinstalled set if the child is predicted to progress in skills and ability. An intermediate number of vocabulary items (50–1000) becomes more preferable than a small number of items (≤ 50) for a child who is motivated to communicate using AAC. Having > 1000 items becomes significantly more preferable for children who have certain characteristics: receptive language exceeding expressive language, an ability to use a range of AAC functions, being motivated to communicate using AAC and predicted to progress in skills and abilities.
There are two significant interactions between type of vocabulary organisation and motivation. A child who is motivated to communicate through symbol communication systems becomes more likely to be allocated a system with taxonomic (OR 2.03) or semantic–syntactic (OR 2.29) organisation than one with visual scene organisation.
Motivation to communicate using AAC also has a large influence on the type of graphic representation preferred. It increases the probability of the child being allocated a system with pictographic symbols (OR 3.88), ideographic symbols (OR 5.31) or text (OR 4.00) rather than photographs. However, being predicted to progress in skills and abilities makes a system with pictographic symbols less preferable.
Figure 14 illustrates the relative interaction attribute importance of child attributes and system attributes. Consistency of layout is omitted as preferences for this attribute are not affected by which vignette is shown. Predicted future skills and abilities is the only child attribute to influence preferences for type of vocabulary set. It is one of only two child attributes to influence preferences for graphic representation, although determination and persistence is more impactful (67% vs. 33%). Determination and persistence is the only child attribute to impact preferences for type of vocabulary organisation. All child attributes influence preferences for vocab size; communication ability with AAC (32%) and determination and persistence (28%) have a relatively more important impact than future skills and abilities (22%) and receptive and expressive language (17%). Overall, future skills and abilities has the greatest relative importance (38%), followed by determination and persistence (19%), communication ability with AAC (20%) and, finally, receptive and expressive language (12%).
FIGURE 14.
Relative interaction attribute importance for each DCE AAC system attribute and averaged over all attributes. Error bars show 95% confidence intervals.

Discussion
This DCE has revealed AAC professionals’ priorities when they allocate AAC systems to children. It has also shown that these priorities interact with the characteristics of the children they encounter. This is in line with previous research showing that AAC professionals recognise the importance of matching an AAC system to an individual’s needs. 127,128 However, this study reveals the magnitude of preference changes. For example, for a child with delayed receptive and expressive language, no previous AAC experience and no motivation to communicate, and who is predicted to regress, a system with more than 1000 vocabulary items is less likely to be chosen than one with fewer than 50 items (OR 0.395). However, if a child has a receptive–expressive language gap, can use AAC for a range of functions, is motivated to use AAC and is predicted to progress, a system with more than 1000 vocabulary items is much more likely to be chosen (OR 22.5).
A child’s motivation to communicate using AAC has the greatest number of interactions with AAC system attributes. This motivation tends to drive AAC professionals towards what can be regarded as more ‘ambitious’ choices, for example more vocabulary items. Visual scene as a method of vocabulary organisation and photographs as a method of graphic representation are relatively simple methods, both involving items/scenes from an individual’s own life. Both become less preferred for a child motivated to communicate via AAC, in favour of more abstract methods of organisation (taxonomic and semantic–syntactic) and modes of graphical representation that require more grammar (pictographs, ideographs and text). This may be interpreted as AAC professionals believing that motivated children will be better able to use more complex AAC systems, in line with previous findings that attitude towards AAC, and valuing an AAC system are important factors in successful adoption of AAC. 11,128
No significant differences were found in allocation preferences between children predicted to regress in and those predicted to maintain skills and abilities. However, if a child is predicted to progress in skills and abilities, this has a large impact on AAC professionals’ decision-making, and future skills and abilities is the highest-ranked attribute in terms of relative interaction attribute importance. As with motivation, it tends to lead to more ambitious choices, with more vocabulary items being preferred and pictographs becoming depreciated as a mode of graphic representation compared with the more complex ideographs and text. However, it is important to note that, unless the child is also motivated to communicate via AAC, photographs are still the most preferred mode. This is a possible indication that they remain a good starting point for a child who is not engaged, regardless of prognosis.
Even in the context of high rates of abandonment, AAC professionals have high expectations of motivated children who are expected to progress, even if their receptive and expressive language are both delayed and they have no previous AAC experience. One interpretation is that participants wished to minimise asymmetries by choosing text as the expressive output for children who they believed could cope with it. These ambitious choices are also encouraging given the greatly increased aspirations for effective societal participation of AAC users. 129–131 Choosing ambitiously is also in line with official guidance,132 and is one of Williams et al. ’s133 five principles for AAC: ‘AAC must support full participation in all aspects of 21st century life’.
There were non-linear preferences for vocabulary size for many child vignettes, which may be interpreted as professionals not wishing to restrict children to only 50 items, and wanting to avoid the additional memory load of > 1000 items. Between 20 and 1000 items was considered better than only 50 items for all children, although the difference was not always significant.
It is important to note that for a given child vignette it is possible to determine only relative preferences for system attributes, not absolute preferences. Although it is possible to compare how relative priorities change between vignettes, it is not possible to compare how suitable in absolute terms a given system is for two children.
General discussion
Comparing the results of studies 1 and 2, some similarities are apparent. For example, graphic representation was the lowest-ranked attribute in terms of importance in the BWS to be included in the DCE, and, if the relative importance of AAC system attributes is calculated for each child vignette in the DCE, it is never the most important. However, many differences can be seen. Language abilities was the most important child attribute in the BWS, yet its relative interaction attribute importance in the DCE was below predicted future abilities, ranked sixth in the BWS. However, caution should be used in interpreting these results as divergent or contradictory. First, some changes to the language of attributes were made to better suit the DCE format, and thus they may not be directly comparable. In addition, the different methodologies did not measure the same things. For example, BWS measured the importance of AAC system attributes over the case mix that AAC professionals encounter in practice, whereas the respondents to the DCE were presented with a specific vignette. Likewise, relative interaction attribute importance is a measure of the largest impact that a child attribute can possibly have on preferences given the levels chosen in a DCE, whereas the BWS measured how important an attribute was (relative to other attributes) over the case mix seen in practice. Thus, the BWS and DCE results may be viewed as complementary, revealing their own insights into different aspects of a decision.
The current study is the first to use stated preference methods to investigate what AAC practitioners working with children prioritise during decision-making. As such, it is a strength that attributes/characteristics were selected using qualitative methods involving both an evidence synthesis and focus groups with people who use AAC/families and AAC professionals with a variety of backgrounds. This process means that we can be relatively confident that important features of decision-making have not been omitted.
The differing methodologies of studies 1 and 2 complement each other. Using BWS case 1 in study 1 allowed information to be gathered about a large number of attributes. Using DCE in study 2 allowed more detailed information to be collected about the trade-offs and interactions between a smaller number of the most important attributes.
General conclusion
This WP represents a first step in quantifying the priorities and identifying the most crucial characteristics of children and features of AAC devices that professionals consider when making their choices and recommendations.
Important insight has been gained, showing that children’s physical characteristics are perceived to be relatively less important in AAC professionals’ decision-making than their language and communication, cognitive and learning abilities and personality traits. The communication, language and interface features of AAC devices are considered to be relatively more important by professionals than hardware and physical features.
This work package has revealed which characteristics of a child most influence an AAC professional’s decision-making. In particular, whether a child is motivated to communicate using AAC or is predicted to progress in skills and abilities has a large impact on their priorities.
There is much scope for future quantitative research in this field. We studied only AAC professionals. It would be beneficial to directly compare results from AAC professionals with those from other stakeholders in the decision-making process, particularly people who use AAC and their families.
Chapter 8 Practical outcomes: heuristic development and dissemination (work packages 5 and 6)
Introduction
The results from the I-ASC project highlight that the process of making AAC decisions related to children and symbol communication aids can be improved. It is clear that these decisions involve a range of individuals with different skills and knowledge and that the voice of the child or young person and their family is probably often under-represented in these decisions.
One aim of the project was to develop initial decision guidance for all stakeholders, the intention being that this guidance would support the best possible decisions made in matching symbol communication aids to children.
Approaches to producing such guidance and improving decisions within health care may centre on developing clinical protocols aimed at professionals or decision aids promoting patient involvement in decision-making. Such approaches often adopt an algorithmic structure (i.e. if you see ‘a’ you do ‘b’). The working hypothesis of the I-ASC project was that development of such algorithmic clinical protocols would not be an appropriate outcome of the project. Decision aids are tools designed to help people participate in decision-making about personal health-care options (URL: http://ipdas.ohri.ca/what.html; accessed 10 September 2020). This stance on participation is reinforced by Coulter et al. ,134 who have described the challenges of developing a systematic decision aid.
The literature reviews completed in the I-ASC project highlighted a lack of high-quality empirical research that could inform decision supports. The qualitative and choice experiment work further highlighted the heterogeneity and complexity of the decision-making context that needs to be considered before a recommendation is made. Consequently, the concept of a heuristic was used to guide the development of the I-ASC approach.
A heuristic ‘supports a person to ‘discover or learn’. 135 The I-ASC heuristic resource was conceptualised as supporting the decision-making process concerning symbol communication aids for children and young people by providing all involved with a structured way of thinking about their decisions. The heuristic resource was intended to meet the original project aim of improving decision-making while acknowledging that the context of the evidence base and the challenges of creating formal protocols relating to AAC recommendations remain underspecified.
The relevant project objective was that the combined outputs from WPs 1–4 result in the development of an evidence-based prototype decision resource and decision-making heuristic.
The heuristic developments targeted four areas of practice:
-
specialised and local specialist service provision
-
user and family involvement in the decision-making process
-
undergraduate and postgraduate education
-
a national clinical audit to determine which data should be collected routinely.
The protocol led us to complete a mapping exercise in which the results from WPs 1–4 were compared and mapped across the themes resulting from the inductive analysis that emerged from WP 2. The I-ASC research identified a comprehensive range of attributes, characteristics and features that participants considered when making their decisions. These formed the basis for the production of the heuristic resource. The I-ASC resource can thus be considered a heuristic developed from the project data, which we propose may be used to aid future AAC decision-making.
The development of the components of the heuristic aimed to ensure that the resource was accessible to a range of groups of individuals, including children, young people, families and non-specialists, with different levels of knowledge and experience.
Heuristic conceptualisation
The I-ASC heuristic was conceptualised as having a number of content layers (Figure 15) representing varying abstractions of the data collected as part of the I-ASC project. Any layer has the potential to support an individual in considering their clinical decisions. Figure 15 provides a visual summary of the I-ASC heuristic and its relation to the underlying data. The heuristic shows the methods of representing the findings, including the I-ASC explanatory model and the methods of utilising these components through resources, and offers a way of understanding and accessing it through key questions.
FIGURE 15.
The I-ASC heuristic structure.
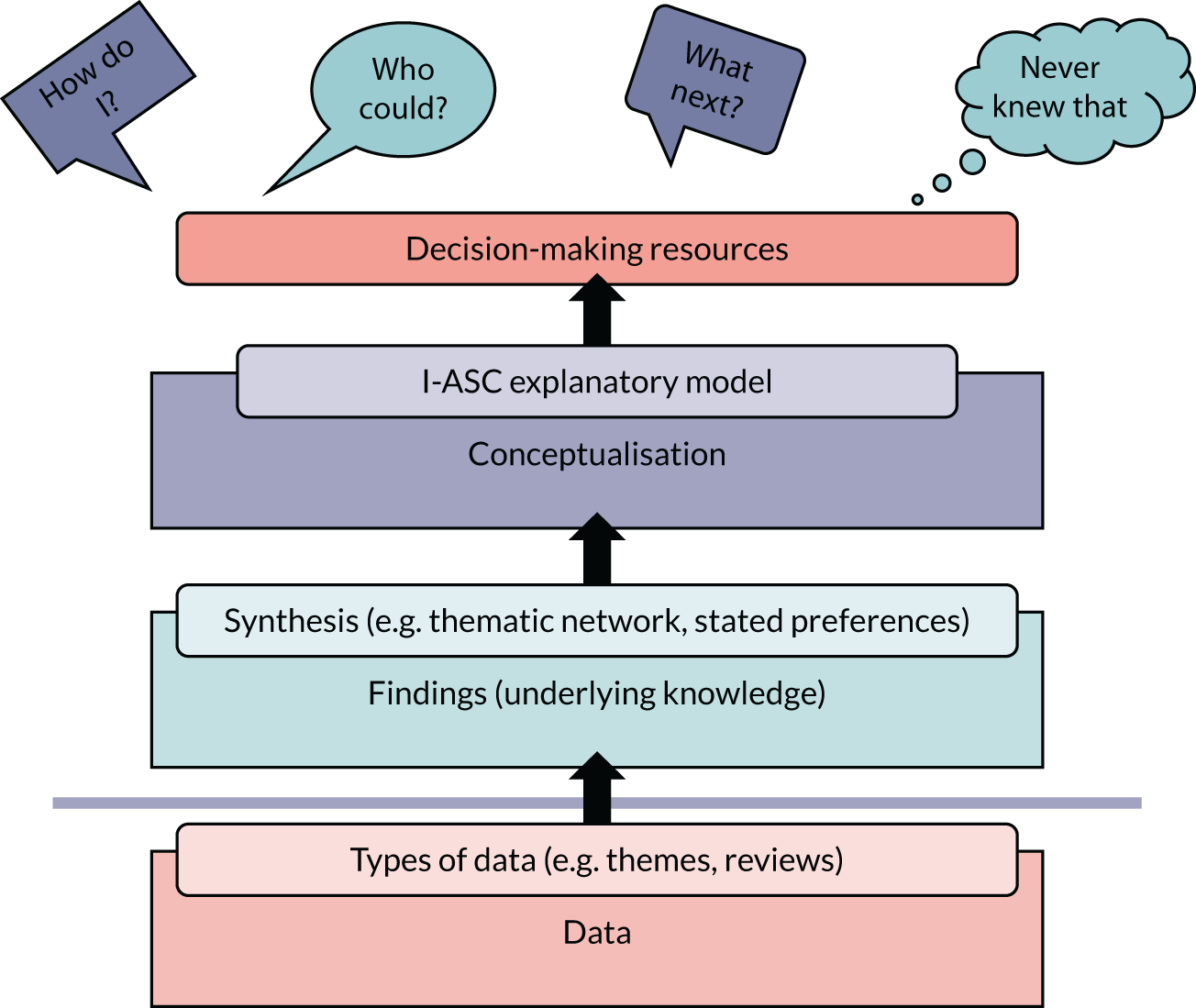
The foundation layer contains the underlying data and findings produced from the I-ASC project, composed of a synthesis of the raw data produced from the systematic reviews, qualitative and quantitative investigations, and existing theory.
These findings are conceptualised in the heuristic using an explanatory model. The I-ASC explanatory model originally emerged from the qualitative and quantitative data analysis, and the synthesis highlights the competing considerations in and contextual and cultural influences on communication aid decisions. Each consideration and influencer is subdivided into characteristics, attributes, features, resources, transitions and ways of working. Further synthesis enabled the evidence from the systematic review process to be included.
The final layer of the heuristic is the provision of resources. This layer, along with the underlying explanatory model, is assumed to be the main interface with individuals involved in symbol communication aid decisions. Resources were produced to support consideration of the characteristics, attributes, features, available resources, transitions and ways of working that are defined in the model.
The remainder of this chapter details the process of the heuristic construction.
Underlying data
The heuristic represents the findings from the raw data collected in the I-ASC project and analyses of these data. Raw data are not included in the heuristic except as illustrative quotations. Analysis of the raw data has produced a wide range of decision-related descriptors (quantitative data), themes (qualitative data) and literature considerations (existing theory). These data remain stored with MMU/Leeds partners, as per data management procedures. Information will largely be publicly available via the I-ASC website resource (https://iasc.mmu.ac.uk), existing research and practice outputs72,100,101 under review and in preparation.
Synthesis of findings
Each WP in the project produced a series of findings that addressed specific research questions (see Chapters 4–7). Synthesising these findings required cross-referencing to outputs from the project, namely analysis iterations, published papers and papers in preparation. Consequently, this established a network of findings from multiple data sources related to a range of considerations and influencers of decisions associated with symbol communication aids for children. The synthesis of the findings created an ontology, helping us to capture knowledge by identifying decision-making concepts and the relationships between these concepts. The ontology cannot predict in what way these considerations and influencers should be deliberated within each decision, but it can provide a structure from which to problem-solve the components that could be relevant to each child or young person.
Method of synthesis
The project team reviewed each data source, that is, an internal analysis was carried out of the WP data sources. Different members of the team had led different aspects of data analysis, so this synthesis enabled all members to review the entire I-ASC data set. This was completed via documentary review (Table 18), team discussion and debate. This consensus approach allowed us to identify findings that could inform decision-making in some way by starting with those identified by the lead researchers from their WPs.
| Subtheme(s) | Service delivery model |
|---|---|
| Organising theme(s) | Ways of working |
| Global theme | Cultural and contextual influencers |
| Source(s) | WP 1: systematic review 3 (Lynch et al.119) |
| WP 2: focus group (Lynch et al.100) | |
| WP 3: individual interviews (Westminster presentation136) | |
| Illustrative quotation or data point | While the potential advantages of team working were recognised by SLTs working in isolation, some service structures were cited as preventing team workingSR3 |
| We have worked with [local therapist name] a lot, you know if it was a different therapist, you might have been explaining more, but we’ve known [local therapist name] for yearsWP 2, focus group | |
| It is quite tricky because it’s your child, and as a parent you generally have a casting vote on your child’s decisions. But I don’t think it entirely works like that in a world of disabilityWP 3, parent interview | |
| Synthesis of the data | A range of professionals were identified as contributing to communication aid recommendation, and both single professional and multiprofessional models are utilised in practice |
| Four types of team structure emerged: multidisciplinary, interdisciplinary, transdisciplinary and prescription review | |
| Family representation and voice is variable across recommendation processes | |
| Link to I-ASC resources | Implications of findings (clinical implications), and decision resources |
| Team roles and responsibilities | |
| AAC log resources | |
| Communication aid attribute list and spidergram resource | |
| Links to other themes | Roles and responsibilities |
| Team knowledge and skill | |
| Team theory |
In this way, we determined if each finding was a consideration related to the child or the communication aid, or an influencer driven by context, following the principles of documentary analysis.
Representation: the I-ASC explanatory model
An explanatory model emerged from the qualitative analysis of data in WP 2 (see Chapter 5) and, through the process of synthesising findings, it was expanded to represent the whole scope of the I-ASC project’s contribution to decision-making for children who are non-speaking.
The use of the explanatory model within the heuristic resource was designed to provide a way of accessing the findings and support critical thinking about decisions related to symbol communication aids. The explanatory model, illustrated in Figure 6, is a schematic representation of the complexity of the decision-making process of the team around the child.
The label ‘competing considerations’ was identified as the first of two global themes as it denotes the interaction between child characteristics, access features and communication aid attributes. 101 The label indicates the need to choose the best fit based on a series of trade-offs rather than perfect options. In the explanatory model, these competing considerations are illustrated by the cogs. The interaction of the child, access and communication aid is shown by the potential of the cogs to rotate in either direction as the team debates and considers issues while making the decision and, ultimately, moves towards consensus. The interplay between the cogs indicates an intensity in the trade-off between one decision made relating to a characteristic, feature or attribute and the impact that instantly has on the interlinked cogs. Once a decision is made about these factors, the decision can be influenced by issues external to the child or the aid. 100
In the second global theme, ‘contextual and cultural influencers’, we found that environmental factors related to both the child’s culture and context and the professional’s work setting influenced decision-making. These cultural and contextual influencers, as visualised using the funnel and its contents, denote factors that further influence clinical decision-making outside the feature-matching process.
While the cog and funnel components denote the two global themes, the arrows are indicative of the fluid and iterative process of decision-making. The model is a visual artefact that can prompt discussion and structured thinking about the topic. It is not intended to replace the underlying findings and has been carefully constructed and explained in the online resource (https://iasc.mmu.ac.uk/) to avoid any overextrapolation of the findings.
Together, the model and the associated explanations of findings have been linked to downloadable resources (https://iasc.mmu.ac.uk/resources/). These resources are tools to support evidence-informed decision-making and are described in the following section.
Resource conceptualisation
Resources to accompany the heuristic were designed to support decisions about symbol communication aids. These resources (https://iasc.mmu.ac.uk/resources/) provide access to the underlying findings of the heuristic and are aimed at specific groups (e.g. children, families, professionals) or target specific stages of the observed decision-making process (e.g. first AAC appointment, review appointment).
The resources provided in the heuristic at the phase-1 launch were not designed to cover every aspect of the explanatory model or all findings. The resources provided in the phase-1 release were mapped to ensure coverage across the basic themes of the model, and different stages of the decision-making process. These resources were designed to act as sample resources and also to exemplify the process of linking a resource to the explanatory model.
The creation of resources emerged from aspects of the research including (1) resources developed and used as part of the data collection processes, (2) analysis of the data, (3) synthesis of existing research and (4) researchers’ and participants’ experience/expertise.
To disseminate the initial I-ASC heuristic resource, an online resource was developed (https://iasc.mmu.ac.uk/). An extensive range of resources were produced and they are also differentiated in terms of targeting different audience groups, different stages of the decision-making process and AAC development, and are offered in different formats.
Heuristic resource development (and testing phase)
During production of the heuristic and resources a number of approaches to testing and involvement in content creation were part of the work package (WP 5) and dissemination activities (WP 6).
In WP 5 we targeted a reference group of testers who represented all stakeholder groups (n = 25) and provided them with a number of I-ASC resources to test, comment on and offer suggested edits. Feedback enhanced the clarity of the content. Nothing suggested compromised the influence of the I-ASC findings within the resources.
Dissemination activities were also used as a means of informal testing and feedback [see Dissemination (work package 6)].
I-ASC heuristic resource publication
As already indicated, the main heuristic publication is available through an online resource (https://iasc.mmu.ac.uk/) consisting of website content and downloadable and linked resources.
The heuristic platform was developed as a subdomain of the Manchester Metropolitan University website. The website provides information about the I-ASC project and represents the heuristic through the I-ASC explanatory model. The website is structured as follows:
-
The main web page contains a header/footer with logos and key information links (Figure 16).
-
The main content area has six blocks (Figure 17) linking to content pages [i.e. about the project (and acknowledgements), the I-ASC explanatory model, resources, policy, public involvement, frequently asked questions].
-
The key content pages are structured around the main research aims.
-
The explanatory model (Figure 18) section makes the findings, ontology and resources accessible to all site users.
FIGURE 16.
I-ASC website navigation header. Reproduced with permission from Nick Holland, Manchester Metropolitan University, Manchester, UK.

FIGURE 17.
Main heuristic resource website navigation blocks. Reproduced with permission from Nick Holland, Manchester Metropolitan University, Manchester, UK.

FIGURE 18.
Heuristic explanatory model navigation page. Reproduced with permission from Nick Holland, Manchester Metropolitan University, Manchester, UK.

The resource was created in standard desktop publishing software to ensure futureproofing in terms of revisions and maintenance. The I-ASC site remains hosted by Manchester Metropolitan University and has been approved by its information technology and digital team. Visual identity and branding associates the heuristic with Manchester Metropolitan University and the I-ASC project. This has included agreement of colour palette, use of NIHR and research partner logos, use of the I-ASC logo and consistent use of the short title of the project as ‘I-ASC: Identifying Appropriate Symbol Communication Aids’. We received NIHR advice on how to ensure that all downloadable materials acknowledge NIHR as the funding body. This information is included on all resource pages and is provided in detail in the Acknowledgements.
Heuristic audience
As stipulated in the research award and in the original project protocol, the online heuristic is aimed at a range of individuals, including those directly involved in supporting the best match between the child and the communication device, as well as those with indirect input into this process. The I-ASC findings have clarified who such individuals are and where they may be located. During the life of the project, we have also tested reaction from all potential stakeholder groups. Appendix 6 offers a summary of key groups who may benefit from the online I-ASC heuristic, and its associated resources.
Future heuristic resource development
The initial release of the I-ASC heuristic contains a significant but initial amount of content. Future phases of development (outside the funded project) will add further findings and associated resources. This will ensure that the resource remains current and relevant.
The heuristic resource has also been set up in such a way that it promotes contributions from stakeholder groups, for example a request to inform the I-ASC team of any existing resources that would be good to highlight. The heuristic demonstrates how existing resources can be mapped to the I-ASC explanatory model and it is hoped that this will be used in the future as a way for authors to describe and categorise their resources and to indicate how they can be used to support consistent symbol communication decision-making.
It is anticipated that the careful construction of I-ASC resources will support users to collect data that could be useful for informing future research activities.
The online resource seeks feedback from site visitors. Over time, this will add to our understanding of the usefulness of the heuristic. Editorial revisions will be supported by Manchester Metropolitan University. All original project team members will be given an opportunity to contribute to updates, but the majority of maintenance responsibility will fall to Professor Janice Murray.
Conclusion
The I-ASC heuristic resource has been developed through an interdisciplinary effort and is the first resource of its kind to be constructed from a research evidence base. As enshrined in the original project aim, we anticipate that this resource will contribute to more equitable and informed practice, particularly the recommendation process for symbol communication aids.
As the heuristic resource is informed by the personal experiences of children, young people and their families, we anticipate that the I-ASC resources will promote the inclusion of the voices of these service users as being central to the recommendation process.
The findings from the I-ASC research are extensive, enabling the online resource to be an evolving entity, as more of the evidence summarised throughout this report is uploaded for general use by those who have an interest in AAC decision-making. It is anticipated that the heuristic resource and explanatory model will be utilised by other researchers and those developing resources in the future as a way of mapping research and resources on to aspects of the decision-making process.
Dissemination (work package 6)
The public involvement co-researchers led this work package. As individuals with personal experience of the implications of AAC recommendations, their plans were ambitious for the project team and meaningful for all stakeholder groups. From the commencement of the project, we began our dissemination activities. Initially, dissemination focused on raising awareness to support engagement from those in the AAC practice field and the family support community to aid recruitment to the various data collection WPs. As this group is small and well connected, this approach was key throughout the project and enabled us to recruit effectively to each WP. Dissemination activities included presentations at the Royal College of Speech and Language Therapists 2019 conference, Clinical Excellence Networks (AAC), national and international AAC conferences (e.g. International Society for Augmentative and Alternative Communication 2016, Communication Matters 2017 and 2018, AGOSCI 2019), family advocacy organisations, to undergraduate and postgraduate students. Three final dissemination events were delivered in October 2018 at the Scottish Parliament, Edinburgh, the Museum of Science and Industry, Manchester, and in Westminster, London. These events involved contributions from parliamentarians, CEOs, commissioners and representatives of organisations with an interest in AAC users with communication disabilities. Debate was robust, with several contributors commending the I-ASC research team for their application of research findings to real-world experiences. Members of the research team were invited to present at study days and international conferences over this following year, for example the International Society for Augmentative and Alternative Communication pre-conference workshop 2020 in Mexico. This has been rescheduled to 2021. In addition, a 1-day workshop is planned for January 2021 that will be delivered, virtually, in collaboration with the AAC charity Communication Matters.
Other dissemination achievements include publications in peer-reviewed and practice journals. We also have an online presence that has enabled us to immediately disseminate soundbites from the research findings. All dissemination activities have been recorded on Researchfish.
Chapter 9 Discussion and conclusions
Introduction
Perceptions of augmentative and alternative communication decision-making and satisfaction
The I-ASC research set out to better understand the process of symbol communication aid recommendation from all stakeholder perspectives. This aim was set in the context of children and young people with special needs having a statutory right to an Education, Health and Care Plan. The principles enshrined in the Special Educational Needs and Disability Code of Practice132 incorporate the need for early identification and intervention, inclusion, removing learning barriers and successful preparation for adulthood. Specific reference is made in the code to NHS England’s responsibility for supporting the identification and provision of AAC. Previous research suggests that an estimated 0.5% of the population require AAC. This equates to 529 people per 100,000 population. The financial costs to the NHS of the inappropriate provision or non-provision of a communication aid have been estimated at £500,000 per individual. 10 The potential social and economic consequences of an inappropriate aid is evidenced in research showing communication aid abandonment figures of between 30% and 50%. 11 By concentrating on enhancing the decision-making process for prescribing symbol communication aids, this project has the potential to have an impact on the long-term quality-of-life outcomes of children and young people who rely on these aids, and also to be of wider social and economic benefit. For a more extensive consideration of factors described in this chapter see Lynch et al. ,100 Murray et al. 101 and Webb et al. 116
The research context
The I-ASC research focused on the interplay between the symbol communication aid, the young person benefiting from it, and the contexts of use and interaction.
In the documentary space available, key points are developed in this chapter, with cross-references given to our online resource. The online resource provides a comprehensive synthesis of findings that have been translated into guidance to inform research and clinical decision-making (https://iasc.mmu.ac.uk/).
Symbol communication aid: decision-making
Four research questions guided our exploration of decision-making:
-
What attributes related to the child, and generic communication aids, do professionals consider important when making decisions about communication aid provision? ‘Professional’ was the generic term agreed by the research team to denote any professional who might contribute to the decision-making process. This included health and education employees.
-
What other factors influence or inform the final decision?
-
What attributes are considered important by other participants (e.g. the child and family) and how do these impact in the short, medium and long term?
-
What decision support guidance and resources would enhance the quality, accountability and comparability of decision-making?
The key findings related to each question are summarised below, with particular reference to the clinical implications and areas for further research.
Attributes and characteristics identified as important to professionals
Research question 1: what attributes related to the child, and generic communication aids, do professionals consider important in making decisions about communication aid provision?
The I-ASC research, through its mixed-methods approach to investigation, offers new knowledge to support future decision-making in symbol communication aid recommendation. Prior to the I-ASC project, the research related to clinical decision-making in AAC was primarily qualitative and not related to real-time decision-making processes. 27 This current state of knowledge is likely to be a consequence of two things: AAC research being a relatively young field of inquiry, and the heterogeneity of the individuals who benefit from AAC prescription, which makes it challenging to complete large-scale cohort studies. 95–97
As the I-ASC explanatory model emerged it superseded terminology chosen for the original research questions; hence, the following discussion related to the child or young person now adopts the I-ASC terminology of child characteristics, and reference to communication aid attributes and access features will be used throughout this chapter.
Influence from the I-ASC literature synthesis
Child and young person
Consideration of the existing evidence in terms of child or young person characteristics reveals a confusing literature that appears focused on the experiences the child or young person needs to access support for language development, rather than describing the inherent characteristics and abilities that might inform decision-making (e.g. current language profile, sensory impairments).
In a small number of studies, child characteristics, such as their medical diagnosis, their ability to learn more abstract symbols and their receptive language abilities, were reported as factors in the decision-making process. 96 An ability to demonstrate skills was also reported as a factor, resonating with other aspects of I-ASC research (e.g. referral criteria to specialised services requiring the demonstration of AAC-related communication skill). Existing research suggests that, if such skill was evident, a more abstract representation system would be chosen, even if this was not the easiest system for the child to use. 14 This suggests that SLTs focus on maximising linguistic and communicative potential and consider developmental trajectories in their decision-making. It also suggests evidence of a gap in provision of support for young people who do not yet meet specialised referral criteria.
Children and young people having access to high-quality communication opportunities with more conversational partners was viewed as likely to promote their language development, but only if they were afforded access to sufficient vocabulary on their communication aid. Although not explicitly stated, the characteristics of resilience and motivation were implied in the recognition that the child/young person persevered in trying to convey a message with often limited vocabulary options.
Communication aid
The literature review demonstrated that little research exists to help us understand what evidence professionals use to appraise the attributes of specific symbol communication systems. This was reinforced by the considerable inconsistencies in the terminology used across the research cited; where attributes have been studied, they have been inconsistently defined.
Influence from I-ASC specialised assessment episodes
I-ASC findings from a specialised assessment context (WP 2) suggest that the recommendation process is a product of trade-offs between child characteristics, access features, communication aid attributes and contextual ways of working, resources and transitions. This WP, to our knowledge the first to include real-time AAC decision-making processes in the UK, indicates that recommendations may differ from the hypothetical decision-making processes reported in the literature, or in other WPs of the I-ASC study. The findings introduce the notion that professionals make real-time decisions with insufficient information about the current language skills of a child or young person. This appears to be an artefact of assumed responsibility and information brokering, whereby specialised professionals regard language-level insights as the domain of the local SLT (the typical referral pathway), and the local SLT may not be able to gather this information or may not have shared the information by the time a specialised assessment takes place. This requires better understanding of the contextualised ways of working, as well as the available resources to support informed decision-making.
A further finding is that decision-making at the time of a child’s first communication aid assessment may have potential ramifications for future aid recommendations and their communication development. This was evidenced during review recommendations by participants’ desire to build on existing knowledge and skills by choosing later aids and graphic representation systems from the same family as the first aid. This was reinforced by some findings in WP 3, where commentary highlighted the impact of decisions made about the first communication aid and the long-term implications of these early decisions. For example, the learning time invested in using one language representation system influences and reduces the choices of future communication aid assessments. These collective findings indicate that particular care is needed when making decisions about a child’s first communication aid.
A final finding of note in this section is access features being prioritised ahead of all other considerations. This may be an artefact of current specialised referral criteria in the UK. Rightly or wrongly, more time was given to debating (independent) access features than to discussing current or future language skills and communication potential. This finding suggests that a review of specialised assessment focus may be welcome.
Influence from I-ASC survey methodologies
To our knowledge, our quantitative work (WP 4) was the first in the field of AAC research to use stated preference methods to investigate what professionals identify as important child characteristics or communication aid attributes during decision-making. The two survey methodologies brought different but complementary knowledge to our understanding of decision-making. Using BWS allowed information to be gathered about a large number of attributes, while using a DCE allowed more detailed information to be collected about the trade-offs and interactions between a smaller number of the more important communication aid attributes and how these related to the child characteristics available.
For example, graphic representation is an attribute that never reached an average level of importance in either survey. This suggests that decisions are made about communication systems with insufficient regard given to the way in which the language (and therefore the communication) system is made available. Perhaps contradictorily (but mentioned with caution as the different methodologies did not measure the same things), current language ability was the most important child attribute in the BWS, but the child’s predicted future (language) abilities had most prominence in the DCE. Again, rather contradictorily, in WPs 2 and 3 there was evidence of decisions being made when detailed knowledge of the child’s current language skills was unavailable. This suggests that greater heed needs to be paid to current, rather than future, language abilities during the decision-making process.
Summary
Overall, important insight has been gained through this research process showing that, when an offline interrogation is used, children’s physical characteristics are perceived to be relatively less important in AAC professionals’ decision-making than their language, communication, cognitive and learning abilities. However, in real-time decision-making contexts, the opposite appears to be true, with access needs and personality traits featuring above all other considerations.
How the current and potential skill development of the child or young person is measured during the decision-making process remains poorly defined. The impact of external forces, such as cultural and contextual influencers, is reported relatively rarely in final decisions, although it is recognised as influential by those completing the recommendation process. This reinforces the apparent complexity of symbol communication aid recommendations. Of note, and perhaps the most influencing factors in decision-making resonating with other aspects of the I-ASC work, AAC professionals’ decision-making can be influenced strongly by two particular child characteristics: whether or not a child is perceived as motivated to communicate using AAC and if they are predicted to progress in terms of their skills and abilities. If these two child characteristics truly influence professionals' decision-making, the way in which such characteristics are appraised by professionals remains unclear and is worthy of further research.
Factors influencing or informing final decisions
Research question 2: what other factors influence or inform the final decision?
Influence from the I-ASC literature synthesis
The literature suggests that best practice informed by expert opinion constitutes an extended assessment period that includes trialling communication aids. Realistically, the available service delivery models have an impact on decision-making time frames, with current research evidence suggesting a variable perspective of aid trialling opportunities.
We also found that, although children and their families should be central to communication aid recommendations, with consensus-building critical to future success,99,103 in many instances families were excluded from the decision-making process. 26
Influence from I-ASC specialised assessment episodes
Many children and young people who may benefit from communication aids do not have access to experienced (local) SLTs (WP 2). Yet current decisions appear strongly influenced by cultural and contextual elements in the child’s immediate environment, or by their service provider, rather than determined by the child’s communication profile or need. Additionally, our findings offer insight into interprofessional dialogue during the decision-making process. For example, an identified lack of attitudinal support from those in the child’s environment would limit expectations of their aid use and inform the recommendation. This reinforces findings from previous studies of aid abandonment, in which attitude and support were identified as critical factors in (un)successful outcomes. 11
Professionals acknowledged that, owing to their knowledge and skill, they applied specific theoretical frames of reference that were often implicit in recommendations (i.e. profession specific), and that this may preclude the understanding of, and participation in, decisions by children, families and other professionals. One clinical outcome from this research would be a means for professionals to share theoretical frames of reference and be more explicit in decision-making processes.
Influence from I-ASC case series
Participants of different ages and with a range of abilities were able to express their views about their communication aids and their recommendation processes. This achievement was not without the time and sensitive co-creation of resources and techniques to enable many contributions. Given the time and resources, children/young people could take an active role in decision-making. The longer-term consequence may be that their participation shapes recommendations so that these align more closely with their preferences and motivators.
The service providing the aid recommendation had considerable influence on the nature of the decision, affecting the time available to conduct a recommendation, as well as who was involved and the funding support. This reflects previous studies in which professionals recognised the influence of particular service delivery models. 9,26 Delivering aid recommendations in the real world will inevitably be influenced by service-related factors, but our key finding is that considerable variation in service experience still exists across the UK.
A cautionary comment arising from the I-ASC findings is that choices in graphic representation and organisation are, in many cases, driven more by contextual factors, for example by what is familiar to support personnel in the environment, than by sensitivity to the child’s preferences or linguistics needs. One clinical implication is that there is a need for more comprehensive information-gathering related to children’s symbolic understanding and preferences to inform decisions about their potential to use communication.
Influence from I-ASC survey methodologies
The surveys completed in WP 4 suggest that professionals make particular decisions when given the time to consider them. These may differ from those made in real-time (i.e. during appointments; see WPs 2 and 3). In the BWS survey, professionals identified a number of important aid attributes, prioritising consistency of (vocabulary) layout and navigation, along with choice of vocabulary package, while least important was voice and communication aid appearance. In the DCE choices were influenced by the perceived motivation of the child/young person and their anticipated capacity to develop or gain skills.
Summary
Decision-making is influenced by several factors, some of which are not within the control of decision-makers (e.g. service structure and provision). This results in variable experiences for children/young people and their families, and at times may even result in their exclusion from the final decision-making process.
Knowledge, skill and attitude influences recommendations; if people are known to have less desirable insights, decisions may be affected by these external influencers rather than determined by what may best meet the child/young person’s actual need. This was reinforced by the recognition that decisions were often made with inadequate appraisal of existing language skills.
Real-time decisions (those influenced by several cultural and contextual factors) differed from simulated decisions (vignettes and choices), suggesting that caution is required when interpreting simulated decision-making scenarios, and that there is greater need to explore the demands of decision-making within typical service delivery constraints. This exploration of factors offers insight into several areas for further research.
Important short-, medium- and long-term factors informing decision-making
Research question 3: what attributes are considered important by other participants (e.g. the child and family) and how do these impact in the short, medium and long term?
Influence from the I-ASC literature synthesis
The literature suggests that, although children and young people and their families are key to the success of any recommendation, using our applied inclusion and exclusion criteria we could find no studies that specifically sought the views of children about the most appropriate communication system for them.
Influence from I-ASC case series
Augmentative and alternative communication users in the I-ASC data set had specific preferences related to communication aid attributes. In particular, they had strong views about aesthetics, reliability and battery life. These attributes have particular salience in everyday use. Given the lower rating of importance these attributes were given in other WPs in the I-ASC research (i.e. by professionals), this suggests that it would be beneficial to place users’ views at the forefront of the clinical decision-making process. I-ASC’s contribution to meaningful decision-making suggests that if this is to be achieved sensitively and meaningfully, then an inclusive attitude, recognising all stakeholder perspectives, is required.
An emphasis on providing sufficient quantity and quality of communication opportunities recurs in the data (WP 3) in relation to adult-held positive aspirations for the child/young person's ability to learn their aided language system. Unnecessarily changing the child/young person's graphic (language) representation system based on ill-defined decisions will have an impact on the child/young person's language learning trajectories.
Summary
Children and young people need to be central to decisions.
In contrast with professionals, users and family members value different aesthetic and user-centred attributes for their preferred communication aid. This reinforces the need for decision-making teams to be mindful of all parties’ perspectives.
Communication and learning opportunities, and how these are maintained over time, require further investigation. Dosage of learning practice and translation into conversation success remains poorly understood.
Guidance and resources
Research question 4: what decision support guidance and resources would enhance the quality, accountability and comparability of decision-making?
Influence from the I-ASC literature synthesis
Our literature synthesis suggests that the evidence base in the field of AAC is growing, but gaps remain in terms of clearly defining child characteristics as part of a decision-making process. The terminology to describe the attributes of communication aids appears to be poorly defined and interchangeable. Unhelpfully, there is a paucity of UK and European research to enhance definitions by providing contextual and cultural relevance.
The literature synthesis of service delivery models identified varying practices, often informed by geographically specific funding mechanisms. It seems likely that variation in delivery models will continue; what have not been adequately defined are the gains and losses to the service user across the range of delivery constraints. The I-ASC heuristic resource supports thinking to clarify the benefits and constraints of differing service delivery models (e.g. identifying roles in the decision-making process: https://iasc.mmu.ac.uk/wp-content/uploads/2019/04/I-ASC-Choosing-roles-in-AAC-decision-making-and-implementation.pdf; accessed 11 September 2020).
Influence from I-ASC specialised assessment episodes
UK-specialised AAC assessment reaches a small proportion of children/young people who benefit from AAC. 4 The majority of AAC beneficiaries never access specialised services; this is particularly true in England and Wales. I-ASC data suggest that it is critical to support local AAC service providers, who are charged with supporting the majority of children, many of whom do not meet the referral criteria for specialised AAC assessment services. One of this research project’s contributions to increasing the knowledge and skill of the local workforce is the I-ASC heuristic resource. This includes research-informed guidance, references to published research and the development of bespoke decision-making resources (e.g. https://iasc.mmu.ac.uk/wp-content/uploads/2019/04/I-ASC-Communication-system-recommendation-reflective-practice-checklist.pdf; accessed 11 September 2020). Throughout, the heuristic resource was developed with consideration given to multiple audiences with varying levels of AAC knowledge and skill.
Influence from I-ASC case series
Across the UK, examples of good practice were evident in different working structures and models. In services that worked well, professionals had strong communication links and team members had clearly defined roles and responsibilities. Young people who experienced success often had an AAC champion, who took on responsibility for considerable levels of support. The likelihood is that different service delivery models will remain, but guidance materials and decision-making resources could improve equity across services and enhance the child’s/young person’s experience [e.g. ways of working – system trial evaluations (completed example); https://iasc.mmu.ac.uk/wp-content/uploads/2019/05/I-ASC-Communication-system-trial-evaluation-example.pdf; accessed 11 September 2020].
Influence from I-ASC survey methodologies
The two surveys reviewed different aspects of decision-making and identified slightly different decision priorities. This reinforces the suggestion from other aspects of the research that the AAC decision-making terrain is complicated. Certain child characteristics appeared to be noted above all others, for example motivation and anticipated progress; by contrast, the communication aid attributes valued varied across surveys and ranged from organisational/navigational components, to the amount of vocabulary available, to the language representation system. The picture remains confusing, and it must be remembered that these were simulated decision-making episodes, which may vary from real-time decision-making (WP 2). Real-time decision-making requires people to engage with trade-offs and contextual realities. The I-ASC heuristic resource was based on some of these conflicts and trade-offs, offering people a way to be more explicit in those trade-offs [e.g. competing considerations – communication aid attributes and the spidergram resource to support debate; https://iasc.mmu.ac.uk/wp-content/uploads/2019/05/I-ASC-Competing-considerations-descriptors.pdf (accessed 11 September 2020); https://iasc.mmu.ac.uk/wp-content/uploads/2019/05/I-ASC-How-to-use-the-spidergram-resource.pdf (accessed 11 September 2020)].
Summary
The I-ASC research has informed and directed the development of guidance tools and resources. Originally, this output was conceptualised as a heuristic to inform and support critical thinking during the symbol communication aid decision-making process. The contents appraised here offer a snapshot of the range of materials developed thus far to support the application of a research-informed explanatory model. The materials available have been designed for all stakeholders to support enhanced and consistent AAC decision-making.
Methodological innovations: translational research
The I-ASC research offers a number of methodological innovations. Its qualitative approach to enquiry enabled us to undertake an in-depth exploration of real-time symbol communication aid decision-making with multidisciplinary teams. To our knowledge, the combination of real-time and multidisciplinary informed decision-making has not been reported previously in the AAC research literature. The I-ASC project also offers a unique quantitative approach as a first step in quantifying professionals’ priorities and identifying the most crucial characteristics of children and young people and the agreed attributes of communication aids. These two data collection processes have gone some way to supporting research-informed discussion and challenging terminological confusions in the AAC field; they highlight the need for caution about assumptions related to child ability and potential progress.
The I-ASC approach to including children and young people and adults in the data set was innovative, albeit not groundbreaking, in AAC research. It included people with lived experience of AAC as data collectors, as well as developers of data collection protocols and procedures, and those deemed hard to include in data sets. Although some of the data collection techniques used are familiar to those in the field of AAC research, our approach ventured beyond techniques to include an ethos of equal contribution through supported inclusion. To enable public involvement co-researchers to take up an active role in data collection, as well as ensuring we gathered the views of children/young people who have often been regarded as hard to include in research, we undertook considerable preparation and planning activity to ensure that these individuals were included and successfully facilitated during data collection activities. I-ASC offers a template for supporting and streamlining the inclusion of children and young people in future research projects, and in associated data collection and analysis.
The aim of synthesising all findings has enabled us through the I-ASC work to propose new theory and ways of conceptualising the decision-making process. Making this theory accessible to all stakeholder groups via the online heuristic supports the achievement of one of the original aims of the study, namely to promote consistent, informed symbol communication aid recommendations (https://iasc.mmu.ac.uk).
Benefits of I-ASC approach to public involvement
As detailed from the outset of this report, one cornerstone of the I-ASC research was the inclusion of public involvement researchers as core team members. The influence of this approach on the outcomes of the project are detailed and appraised in Chapter 10.
Limitations
There are a number of limitations to this work, with many components already identified in the relevant WPs presented across this report. In summary, the key limitation remains that, although we attempted to include a wide range of personal and clinical perspectives in the data, the heterogeneity of the broader client group, in combination with the different experience levels of the professionals who support them, would suggest that we cannot guarantee that we have captured all of the key influences on symbol communication aid decision-making. Although this study represents a significant data set within the field of AAC research, the sample size remains relatively small. The generalisability of the findings from across this mixed-methods approach to data sampling is significant in the field of AAC research, but our findings would benefit from further testing and ongoing evaluation.
Further research
This report has already raised several points of note for further research. The following is a prioritised list related to I-ASC findings. Key areas for future work should include how to:
-
Appraise the existing language abilities of children/young people prior to a decision-making episode. This requires skilled professionals and appropriately standardised language and communication assessment tools. Currently, such tools remain unavailable for use with the children/young people considered in this research. This requires studies exploring existing standardised language assessment tools and how they might be modified for this group of children/young people.
-
Explore whether or not decision-making processes for second and subsequent communication aids have different qualities from those during an initial assessment. Currently, re-referrals lack research-informed knowledge to support follow-up recommendations or service delivery demands. This requires further investigation of referral and re-referral pathways.
-
Identify AAC systems and language learning opportunities that best support children to achieve their potential. Currently, we have limited knowledge about how to determine the number of language learning (teaching) opportunities required to enable an AAC user to become proficient or independent in their use of an AAC system. To better understand aided-language learning demands, longitudinal intervention studies are required.
-
Better describe attributes of graphic symbol communication aids. This requires quantitative and qualitative investigations of graphic symbol components and their usefulness to learning language through non-spoken media.
-
Explore external influencing factors during the recommendation process. This suggests that research that looks at the local context is welcome. These contexts describe who and what may make aided communication more effective. As stated earlier, local professionals are responsible for 90% of the needs of those who might benefit from AAC. As yet, insufficient understanding of local delivery means that we have little understanding of what that looks like. Future investigation would be well served by considering what local provision looks like and who is responsible for the elements that it should include.
-
Use quantitative methods to compare the results from AAC professionals with those from other stakeholders in the decision-making process, particularly people who use AAC and their families. For example, the I-ASC findings suggest that the perspectives of professionals and AAC users and their families about priorities differ. The research presented here suggests that there is value in revisiting stakeholder perspectives through survey designs derived from the I-ASC research methodologies.
Final conclusions
This research project describes symbol communication recommendation processes that offer further understanding of what is perceived as important in making decisions. The study has gone some way to defining the barriers to and facilitators of research-informed decision-making. However, as intimated throughout, this work has raised as many questions as it has offered answers, suggesting that ongoing research is needed to better support this complex field of intervention.
Chapter 10 Evaluation of public involvement across the I-ASC project
Introduction to work package
Background and rationale
The beneficiary focus of the I-ASC project was children with severe communication impairment and physical disability; consequently, public involvement across the life of the project involved those with such disability or family members. This participant group is considered as one of the most hard to reach or include as public involvement representatives. 137–139 Figure 1 shows where public involvement activity occurred throughout the I-ASC project. This WP was not an aspect of the original funding award. Funding was awarded to the team in a contract variation in December 2018 as a result of recognition of the public involvement activity across the life of the I-ASC project and its potential contribution to enhancing future public involvement activity in research. This WP was designed as a post hoc methodology to evaluate the public involvement contribution to the I-ASC project to identify processes that supported public involvement in research and made involvement accessible to marginalised and vulnerable groups. The evaluation aimed to investigate the costs and benefits of extensive public involvement in research to inform guidance materials and resources about how to include vulnerable groups in research and the benefits of their inclusion.
The recent NIHR National Standards for Public Involvement in Research140 provide clear benchmarks to improve the planning for and involvement of the public in research roles. However, a review of the literature by Moulam et al. 141 identified five key areas of challenge for public involvement in research that make it difficult for researchers to achieve these practice standards:
-
A current lack of specific guidance on how to overcome policy barriers (e.g. relating to ethics approval, occupational health and employment) to successfully involve the public in research, and a disparity of interpretation locally, regionally and nationally. 139,142
-
A tokenistic approach through the use of the same small pool of participants, with an emphasis on consultation rather than participation, often using ‘consumer surveys’ to tick the box of inclusive research. 138
-
Power imbalances between the perceived expert professional view and the expert individual’s lived experience, leading to a lack of parity in the research process between co-researchers (public involvement) and researchers. 143,144
-
A perception among researchers and funders that including the public both as research participants and as co-researchers is time-consuming and too costly, owing to the mistaken beliefs that members of the public can be ‘too hard’ to involve, have nothing to add and are frequently ‘too difficult to reach’, and that a proxy is good enough. 137–139
-
Existing guidance and toolkits are aimed at mainstream adults, not at children or vulnerable groups, and fail to support best practice in delivery, expectations and outcomes; they also lack guidance about making adjustments for vulnerable groups to take part in research. 137–139
This WP aimed to demonstrate how it is possible to address these challenges with a cohort (people with severe communication disability) regarded conceptually as the most difficult to involve in the research process. Although the National Standards for Public Involvement in Research140 and other guidance documents145 provide considerable information about what to do in terms of public involvement, they provide less information about to how to do it in the context of I-ASC research. The I-ASC project can offer insight that supports multidisciplinary researchers and practitioners working in health care and education in how to achieve public involvement when working with those with significant speech, communication and physical disabilities. Similarly, this project can offer insight that supports those with significant disability to fully understand their role and commitment as public involvement co-researchers. (For clarity, in this document ‘researcher’ is used to define those with the traditional researcher characteristics, e.g. professional/academic, and the term ‘co-researcher’ is used to define those with a public involvement perspective. Collectively, all are actually ‘co-researchers’.)
Research objectives
-
To qualify and quantify processes that support public involvement across all aspects of co-production in the research process.
-
To quantify the protocols that facilitate marginalised and vulnerable public involvement groups to make meaningful contributions to the research process.
-
To appraise the costs and benefits of extensive public involvement in research.
-
To develop guidance and practical tools to facilitate the co-production of research with public involvement co-researchers from diverse, hard-to-reach cohorts.
-
To disseminate this guidance and the results of the project to improve the quantity and quality of public involvement meaningfully in the co-production of research.
Research questions
-
How and what can we learn from an evaluation of public involvement in a nationally funded project focusing on vulnerable and hard-to-reach people?
-
How can public involvement research, implementing current guidance with vulnerable and hard-to-reach groups, be structured to avoid pitfalls and improve impact?
Methods
Summary of study design
A mixed-methods design was adopted. Individual and focus group semistructured interviews were used to explore participants’ preconceptions and the phenomena that have an impact on how public involvement is conceptualised and delivered in research projects that explore a clinical need. 146 All of these participants had been involved in the I-ASC project in some capacity. The economic evaluation adopted a mixed-methods cost–consequences analysis in an attempt to quantify and qualify the impact of the implementation together with the benefits of public involvement co-production of research. 147 A resource utilisation questionnaire (see the project web page at www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 6 July 2020) was designed so that qualitative and quantitative data on resource use could be collected.
Staffing of this work package
Although the project chief investigator retained overall responsibility for delivery, as the participants in this WP were researchers and contributors to the main I-ASC project, it was important to employ a research team who were independent of that experience. Consequently, this included two professors from Manchester Metropolitan University acting as co-investigators, and a research fellow lead researcher responsible for data collection, analysis and reporting, as well as one original public involvement co-researcher leading on the quantitative economic evaluation component.
Sampling strategy
Participants were recruited from four broad groups using purposive sampling. These participant groups included public involvement representatives, academics, policy implementers, administrators and practitioners:
-
individuals who were involved with the construction, delivery and dissemination content of the I-ASC project, that is the interdisciplinary project team (n = 7)
-
members of the I-ASC team who were engaged in discrete sections of the project (e.g. WP 4 delivery) (n = 3)
-
those in the wider I-ASC team who supported the project from an organisational and operational perspective, (e.g. human resources staff) (n = 5)
-
NIHR Advisory Board and the I-ASC critical friend group who supported the project and represented all stakeholder groups in the research (n = 7).
Materials
Topic guides were created for the individual and focus group interviews. The content of these guides was informed by a review of the published literature and guidance relating to public involvement. Participants in groups 1, 2 and 3 were asked to complete individual interviews. Interview topic guides (see the project web page at www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 6 July 2020) were designed to elicit responses from each individual about their experience of the project implementation; they included questions relating to participants’ role in any public involvement activity, their perceptions of how co-researchers were integrated into the project, the co-researcher role, how the team were supported to work alongside co-researchers and any perceived benefits or learning they gained from this experience of public involvement.
Members of the interdisciplinary project team (group 1) also took part in a focus group. The topic guide (see the project web page at www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 6 July 2020) reflected the collective implementation and process and procedures undertaken. It included questions about the perceived benefits to the project overall from the co-production of research with the co-researchers, if and how public involvement activity affected research timelines and resource use, how the public involvement aspects might be improved, and in what ways the public involvement approach adopted for I-ASC could be implemented or adapted for use in different research contexts.
Participants from the NIHR Advisory Board and the I-ASC critical friend group (group 4) were originally to be interviewed in a focus group. A topic guide was created, which included similar questions to those used in the focus group topic guide for the interdisciplinary project team (group 1) but reflected the fact that these participants were advisors on the project (see the interview topic guides on the project web page at www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 6 July 2020). For logistical reasons, most participants in group 4 were actually interviewed individually. The interview and focus group topic guides were also designed to provide data for a narrative evaluation of the public involvement input to the I-ASC project as part of the economic analysis.
The full research team and the wider support team (groups 1, 2 and 3) were asked to complete a resource utilisation questionnaire (see the project web page at www.journalslibrary.nihr.ac.uk/programmes/hsdr/1470153/#/; accessed 6 July 2020). This paper questionnaire was designed using current guidance on public involvement in research with the specific aim of examining resource use associated with the public involvement aspects of the project. 148–151 Owing to the limited number of participants to be included, the questionnaire was developed with a qualitative focus, offering participants comment boxes to provide their responses. It included questions relating to resources, including the time commitment of project staff and additional staff who had not been initially anticipated to contribute to the project, facilities, equipment and consumables. The resource utilisation questionnaire was designed so that data could be collected anonymously, with a participant identification code used to identify each respondent. To complement these data, a cost–consequences evaluation was planned to appraise the awarded and actual budgetary expenditure across the life of the project related to public involvement. However, owing to the post hoc nature of this evaluation we found that we were unable to disaggregate all of the associated costs related to the evolution of public involvement roles across the life of the project.
Procedure
Participant recruitment
Participants in all groups had been identified already as they had all been involved previously in the I-ASC project, as researchers/co-researchers/support staff/Advisory Group and critical friend. The chief investigator provided the contact details of these individuals, with their consent, to the WP lead. An electronic participant information sheet and the topic guide were sent to all potential participants. Those who wanted to take part were invited to attend an interview and provided written informed consent on a consent form at the beginning of the interview.
Data collection
Across the participant groups, three possible data collection activities were completed: (1) individual interviews, (2) one focus group and (3) a resource utilisation questionnaire. Individual semistructured interviews were conducted face to face in accessible, confidential rooms on university premises or over Skype. Interviews lasted between 25 and 100 minutes depending on each participant’s responses. The focus group for group 1 took place on university premises and lasted approximately 90 minutes. For group 1, individual interviews took place before the focus group to ensure that group thinking did not influence individual viewpoints. Two participants who used AAC were invited to prepare their responses in advance and pre-programme their AAC devices if they wanted to do this. One participant prepared written responses to questions and e-mailed these to the WP lead before the interview. This participant’s responses were read aloud to them during the interview and they were asked if they wanted to revise these or add any information. This participant received communication support during their individual interview from their support assistant, who was also a participant. The second participant who used AAC and their support assistant, also a participant, requested to be interviewed together, so that personal and communication support could be provided where needed. This AAC user did not pre-programme their responses using their AAC device. All interviews were recorded digitally and field notes were completed. After they had completed their interviews, participants in groups 1, 2 and 3 were asked to complete and return the resource utilisation questionnaire.
Analysis
A mixed-methods approach was adopted. Interview and focus group data were analysed thematically using the framework analysis approach. 53 This approach was selected because it enables organising themes and basic themes to be generated both deductively from the research objectives and the findings of the literature review (see above) and inductively from open data coding. The digital recordings from the interviews and focus group were transcribed verbatim into a Microsoft Word (Microsoft Corporation, Redmond, WA, USA) file. Each Microsoft Word file was imported into NVivo to facilitate data analysis.
Analysis followed the five-stage framework analysis process53 of familiarisation with the data through to mapping and interpretation of the data. This enabled the overall thematic framework to be modified (see Appendix 7).
The resource utilisation questionnaires were analysed thematically using the framework analysis approach. 53 The questionnaire responses were collected, scanned and stored electronically in accordance with agreed project protocols for data management. As above, each Microsoft Word file was imported into NVivo to facilitate data analysis, and a similar five-stage framework analysis approach was completed. A financial analysis of proposed and actual budgetary spend was completed so that quantitative data relating to resource use could be considered.
Rigour
Different approaches were used to ensure methodological rigour. 152 An experienced qualitative researcher reviewed the initial thematic framework and was able to suggest slight changes to it. Another researcher used the thematic framework to code a sample of four transcriptions (one per participant group). Coding consensus was achieved through discussion and slight amendments were made to the thematic framework in response to differences in coding identified.
Results
Participants
Sixteen participants were recruited to take part in this WP (Table 19). Not all participants completed all data collection activities (as previously outlined). Sixteen participants agreed to be interviewed.
| Group | Number of participants/project role |
|---|---|
| 1: interdisciplinary project team | Researchers (n = 4) |
| Co-researchers (n = 2) | |
| 2: I-ASC team members engaged on discrete sections of project | Researchers (n = 3) |
| 3: wider I-ASC team who supported project from an organisational and operational perspective | University technical officer (n = 1) |
| University manager (n = 1) | |
| 4: NIHR Advisory Board and I-ASC critical friend group | Critical friend group members (n = 2) |
| Advisory Board members (n = 2) | |
| Personal assistant of participant who uses AAC (n = 1) |
Findings from individual and focus group interviews
Five themes were generated from the deductive and inductive coding of individual interview and focus group data: (1) the nature of public involvement in the I-ASC project; (2) the resources used to enable public involvement; (3) the benefits provided by public involvement; (4) the challenges associated with public involvement; and (5) the facilitators of successful public involvement. Organising themes and basic themes were also identified in the data; these are discussed below.
The nature of public involvement in the I-ASC project
This theme was generated from data relating to how public involvement was planned and implemented in the I-ASC project (Table 20).
| Organising themes | Basic themes |
|---|---|
| Purpose of PI | Clarity of aims at start |
| Lack of mutual understanding | |
| Use of guidance/standards | |
| The co-researcher role is multifaceted and can evolve | Initial definition evolved in response to project need |
| Researchers’ expectations of co-researcher input and the reality | |
| Co-researcher understanding of own role | |
| Being representative and being a researcher | |
| Giving a different perspective | |
| Providing healthy challenge | |
| Input at different stages | |
| Team composition | Recruitment processes and challenges |
| Co-researchers bring different skills, needs and experience | |
| Representativeness/number of co-researchers | |
| General diversity of team | |
| Collaboration/partnership working | Genuine integration in team |
| Different levels of integration and involvement | |
| Potential barriers to integration and involvement | |
| Tokenism/box-ticking | Lack of tokenism in the I-ASC project |
| Degree of co-researcher integration | |
| Public recognition of PI approach | |
| Other people’s views of co-researchers |
Participants’ responses indicated that purposeful public involvement was integral to and achievable during all stages of the I-ASC project:
[The chief investigator] had a very clear view as to what she wanted and that she wanted PI [public involvement] involvement right from the start to the finish of the project.
Co-researcher, group 1
So I’ve been working on the I-ASC project as a co-researcher and I’ve been working on interviewing people, doing presentations regarding the project, and I have done some work on the website and social media.
Co-researcher, group 1
Having them there, very evident and very involved, not just people who we were reporting to. I think that worked well . . . It made us reflect on what . . . we were saying and what we were planning all the way through the project . . .
Researcher, group 1
Participants described how the roles of the co-researchers evolved from early conceptualisations in response to the needs of the project with the skills and experience that the co-researchers were able to provide. Notably, one co-researcher brought many professional skills that were utilised in the project and contributed more time to the project than had been initially anticipated. Researchers in the team emphasised that this set of circumstances should be neither perceived as commonplace in public involvement research nor expected in future projects:
[The co-researcher] has been involved over and above what might be well what we previously expected or what might be reasonable for any other projects . . .
Researcher, group 1
Participants perceived different aspects of the co-researcher role: (1) to provide the perspective of a representative of a particular population (in this case, a user of AAC or personal assistant/family member); (2) to challenge established and accepted norms in the research process (e.g. the way in which research outcomes were described and reported); and (3) to contribute actively to research activities (e.g. data collection, analysis and dissemination). Researchers valued all contributions and were able to provide examples of the benefits associated with each aspect to the conduct and outcomes of the project.
This theme provided information about how researchers and co-researchers worked in partnership to deliver the project. Participants perceived the co-researchers to be well integrated in the research team and actively involved in the project; they rejected the notion that public involvement in the project could be viewed as tokenistic:
. . . you know the last thing this research has been . . . is tokenistic. It has taken full account of the views of [the co-researchers] in making certain that people who use AAC and families are accounted for.
Co-researcher, group 1
I think the project has gained from its genuine, rather than tokenistic inclusion . . .
Researcher, group 2
. . . I do believe that they have been actively involved in it, and not just token box-ticking, which is what I frequently see when you include any stakeholder . . .
Critical friend, group 4
Participants suggested that there were differences in individual levels of integration and involvement between the co-researchers and proposed a number of potential reasons for this:
I think I would say that [one co-researcher] was a very integrated member of the research team. [They are] familiar with being involved on research projects and [are] an assertive communicator in a very positive way . . . I think for [a different co-researcher], the experience of being involved in a research project was newer and more challenging . . . And there are sort of practical logistical reasons which probably made some of that challenging.
Researcher, group 2
Participants’ responses enable us to identify potential barriers to co-researchers’ integration within research teams and to their involvement in research activity: (1) lack of experience of public involvement (on the part of researchers and co-researchers), (2) perceived power imbalances resulting from different professional status and experience, (3) structural barriers that exclude people with disabilities from inhabiting traditional research roles and (4) differences in researchers’ and co-researchers’ communicative abilities, skills and methods.
Resources used to enable public involvement during the I-ASC project
This theme was generated from data relating to the resources used to plan and implement public involvement in the I-ASC project (Table 21).
| Organising themes | Basic themes |
|---|---|
| Time | Time setting up PI (before funding was secured) |
| Time spent enabling co-researchers to work in building | |
| Additional time spent on project management by chief investigator | |
| General comments about additional time required | |
| Training and support within team to enable PI | Training and support to engage in team work |
| Training and support for researchers to support a co-researcher | |
| Training co-researchers in research methods | |
| Training personal assistants to support co-researchers | |
| Shared social time to aid team-building | |
| Miscellaneous support | |
| Making the environment accessible | Accessible facilities and equipment |
| Making communication accessible | |
| Support for a co-researcher with a physical or communication disability | |
| Paid personal support for co-researchers | |
| Hidden costs | Additional time provided by co-researchers |
| Professional skills provided by co-researchers | |
| Co-researcher motivation, flexibility |
Participants indicated that resources were utilised to ensure that meaningful public involvement was integrated into the project. They suggested that research projects that involve public involvement take more time and cost more money than traditional research projects:
I’d be really keen to be involved again in this kind of project but recognise that it needs a lot of time and money to support that to happen properly.
Researcher, group 1
Various members of employed staff inside and outside the core research team needed to devote time to facilitate the involvement of the co-researchers. Initially, the chief investigator and the co-researchers used unfunded resource in terms of time to incorporate public involvement within the original project funding application. Participants reported that an important amount of researcher time was required to overcome structural barriers to the co-researchers gaining access to their role on the project. This included time spent ensuring that the building was physically accessible to a co-researcher who uses a wheelchair (in addition to the purchase of specialist equipment) and time spent attempting to obtain employment contracts and research passports for both co-researchers.
Considerable resources were used to provide training and support for researchers and co-researchers to work together effectively. This included supporting co-researchers to be able to understand and participate in the research environment (e.g. research methods training); supporting researchers to engage in teamwork successfully with co-researchers; and specific training for personal assistants and researchers to deliver effective, personalised care and communication support for one of the co-researchers. This last type of support can be resource intensive, resulting in significant cost.
Participants identified several ‘hidden costs’ of public involvement that were not anticipated when the original project funding application was submitted. At the project planning stage, public involvement contributions were unfunded, apart from out-of-pocket expenses. Additionally, the project funding projections required to support the delivery of the public involvement elements of the project were underestimated; subsequently, the chief investigator needed to use unfunded time to manage some aspects of the project and secure additional non-NIHR funding to support enhanced co-researcher involvement. Participants emphasised that the co-researchers also used unpaid time to work on the project during the project conceptualisation and funding application stages. At times, the financial reward received by co-researchers may not have been commensurate with the level of professional skill and experience informing their contributions to the project.
Benefits provided by public involvement during the I-ASC project
This theme was generated from data relating to the ways in which participants perceived the I-ASC project to benefit from public involvement (Table 22).
| Organising themes | Basic themes |
|---|---|
| Benefits to services | Direct changes to service delivery/organisation |
| Greater awareness among professionals and researchers of lived experience of clinical population and carers | |
| Benefits to service users and society | PI provides role models, challenges stereotypes and empowers clinical population |
| PI enables co-researchers to learn new skills | |
| PI is rewarding for co-researchers | |
| PI enables co-researchers to engage in meaningful activity/inhabit the worker role | |
| PI enables co-researchers to engage in paid work | |
| Benefits to knowledge about how to do research | Co-researcher perspective provides methodological insights |
| Co-researcher direct input to research process is associated with more successful research | |
| New learning about how to make research outputs accessible and engaging to the public | |
| New learning about how to do PI | |
| Demonstrates positive value of PI in research and clinical service delivery | |
| Benefits to knowledge about the clinical topic | PI is associated with superior research outputs (increased face validity) |
| Research that includes PI is valued more externally (aids research conduct and implementation of findings) | |
| Benefits to team working | PI is inherently rewarding |
| PI is associated with improved communication within the team | |
| Co-researchers help the team feel grounded and focused on the research | |
| Co-researchers bring additional skills to the team | |
| Co-researchers help the team feel more ambitious about their work | |
| Ambivalence and uncertainty about benefits | The benefits are hard to identify/quantify |
| The benefits will take time to see |
Some participants reported that they found it difficult to identify or quantify concrete benefits that they could attribute to the public involvement contribution to the project; there was also a perception that benefits may become more apparent in the long term. However, the majority of participants were able to identify a range of important benefits to the project that they associated with its public involvement elements.
Researchers, particularly those in clinical service delivery, suggested that their experience of working with the co-researchers had made them more aware of the lived experience of people who use AAC and their families; one participant stated that their involvement with the co-researchers had inspired them to make changes to the way in which clinical service delivery was organised locally to ensure that service users’ voices were represented:
. . . it’s probably inspired me to do more of that within our service outside of research, which we are doing. So we got a member of staff that’s now an honorary member of staff. He’s someone that uses AAC.
Researcher, group 1
Participants indicated that the public contributions made by the co-researchers during the data collection and dissemination phases have challenged public perceptions about the ability of people with disabilities to be involved in research. Furthermore, the co-researchers have proved empowering role models to other AAC users, their families and the people who work with them:
Having co-researchers involved in the interviews, again, really had an impact on participants . . . So I think the message that sends to families of young AAC users is very powerful and very important.
Researcher, group 1
. . . people listening to [the co-researchers] have really been fascinated, interested in their role and viewed them as very competent people who are doing the presentation . . .
Researcher, group 1
The data suggest that the opportunities provided by being involved in the project empowered the co-researchers; their involvement enabled them to learn new skills, engage in meaningful and financially rewarding work activity, gain confidence and feel valued for their contributions:
Being on this project as a co-researcher has been a huge learning curve for me in plenty of aspects . . .
Co-researcher, group 1
. . . it’s been good to get the opportunity to work within the field again.
Co-researcher, group 1
. . . it has helped me to feel valued for skills that I haven’t used for a good number of years.
Co-researcher, group 1
The data suggest that the I-ASC project research process benefited in different ways from public involvement. Researchers were able to identify methodological insights into data collection and analysis that originated from the co-researchers’ unique perspectives. Actively involving co-researchers in data collection was associated with improvements in the quantity and quality of data sourced:
I think engaging the co-researchers in actual data collection, as I said, allowed data to be accessed.
NIHR Advisory Board member, group 4
Researchers commented that as a result of the direct contributions by the co-researchers they had learned new approaches to making research dissemination more accessible and engaging to the public:
. . . [the co-researcher] might say, ‘I don’t understand that,’ . . . that would make us go away and think, ‘Well . . . yeah, actually it doesn’t make sense logically what we’ve just said’ or ‘it’s just not clear enough’ . . . So it’s definitely helped frame how we’ve reported the results, which is really important.
Researcher, group 3
Researchers reported benefiting from witnessing the positive value of public involvement and from new learning about how to involve the public in research (e.g. in terms of how to recruit and support co-researchers with specific needs):
. . . it has made me think twice about how I go about recruiting PPI, PI involvement [patient and public involvement/public involvement] . . . paying much more heed to what I suspect are the skill and experience sets required for a particular activity.
Researcher, group 1
Participants associated public involvement during the project with superior research outputs. They reported that they believed that clinical resources originating in the project would be more useful and useable and that any publications would be stronger. Participants described the project outputs as having increased face validity and thereby greater credibility with research consumers as a result of the co-researchers’ involvement. This was associated with the potential for enhanced research impact:
And its impact will be greater because it was a co-produced project.
Researcher, group 2
Researchers reported that working alongside co-researchers was rewarding. They associated public involvement with improvements in team communication processes and identified ways in which the co-researchers’ contributions helped the team to feel grounded. One participant suggested that comments from co-researchers during discussions about research dissemination had helped the team to feel more ambitious about the way they conceptualised and communicated their research findings:
. . . it gave the project team a bit more braveness in being able to do it I think.
Researcher, group 1
Challenges associated with public involvement during the I-ASC project
This theme was generated from data relating to the challenges that participants associated with incorporating public involvement into the I-ASC project (Table 23).
| Organising themes | Basic themes |
|---|---|
| Challenges for researchers | Identifying co-researchers |
| Representativeness of co-researchers | |
| Making research roles and activities accessible | |
| Gaining support for co-research from carers | |
| Providing equitable reward | |
| Having enough time and money to involve co-researchers fully | |
| Competing demands: research and supporting co-research | |
| Dealing with challenging views | |
| Involving people with disabilities in research is challenging, takes more time | |
| Challenges for people who use AAC and their personal assistants | Accessing research roles |
| People may not have the time or ability to be involved | |
| Securing personalised support to be a co-researcher | |
| Being able to challenge or ask for help | |
| Being able to communicate effectively in the research environment | |
| Other people’s responses to co-researchers |
Different types of challenge were identified in the data that could have an impact on researchers and co-researchers involved in other projects. Participants suggested that identifying individuals who want to be co-researchers and are representative of a specific clinical population could be difficult. Researchers expressed concerns that the co-researchers working on the I-ASC project might not be representative of the wider population of people who use AAC and their families:
. . . I think that was a challenge in that [the co-researchers] might say things or interpret bits of data or interpret things that had happened in one way, whereas I think we might know from our practice in going to see the very wide variety of people in lots of different socioeconomic circumstances, that there is a wider reflection, there is a wider spread of opinions, perspectives, realities in terms of how people live than they had.
Researcher, group 1
Participants identified that the co-researchers were not representative of younger people or children who use AAC, the project’s targeted clinical population. Researchers suggested that the research outputs might have been strengthened by including a wider group of co-researchers. Although the critical friend group was intended to go some way to addressing this concern, it was clear that the group demographic did not deliver a child-oriented perspective.
As reported above, the team needed to overcome structural barriers to enable co-researchers to take part in research activities. It was not possible to obtain an NHS research passport for one co-researcher because of their employment status; they could not be employed by the university as this would have jeopardised their entitlement to state disability benefits, and this excluded them from certain data collection activities. Researchers indicated that involving people with communication and physical disabilities in research is inherently challenging and takes more time than research that does not involve these groups. For example, practical adjustments needed to be made to the research environment to make it more accessible to co-researchers who use wheelchairs. The project team experienced considerable difficulty in recruiting consistent support from the personal assistants of one of the co-researchers to enable this individual to participate fully during the early stages of the project. Participants also acknowledged challenges in making research activities accessible to people with different types of educational background and life experience.
Participants emphasised that the team encountered challenges when attempting to pay the co-researchers equitably for their time. Structural barriers related to employment contractual arrangements and the welfare benefits system prevented the co-researchers from being paid on an equal basis to the researchers. Researchers associated this with a lack of parity within the team:
So that actually made the relationship different. Even though we wanted you [the co-researchers] as equal partners, actually, we weren’t able to have you as equal partners in terms of reimbursement at that point.
Researcher, group 1
Perceived power relationships between researchers and co-researchers also presented a source of challenge to communication within the project team. Researchers suggested that they felt challenged by some of the co-researchers’ views or responses during team discussions but did not always feel empowered to challenge those views themselves:
I think there was sense that everyone was equal but then I think some of the researchers felt maybe we couldn’t always challenge [the co-researchers] . . . so then it’s not fully equal, in a way.
Researcher, group 1
Individuals may not have sufficient time or resources to be involved in research activities, or they may not be able to secure sufficient personalised support to be involved. Individuals may not feel empowered to challenge researchers’ views or to ask for support to understand research concepts. This is especially important for people who use AAC, whose communication in group discussions is likely to need to be supported by the whole group:
. . . I think if [the co-researcher] wasn’t understanding something, I don’t necessarily think [they] challenged it back said, ‘I don’t understand that’.
Researcher, group 1
Individuals who use AAC may find other people’s reactions to their involvement challenging and potentially disempowering. For example, one research participant appeared surprised that a person who used AAC was actively involved in the project:
. . . there was one person we were interviewing, he was then surprised that [the co-researcher] was asking questions. And I was like, I couldn’t, I cannot believe this has happened to [the co-researcher].
Researcher, group 1
Facilitators of successful public involvement on the I-ASC project
This theme relates to potential methods to facilitate public involvement in research and was constructed from participants’ responses relating to their experience of and reflections about the I-ASC project (Table 24).
| Organising themes | Basic themes |
|---|---|
| Establishing the co-researcher role | Having a clear vision of the co-researcher role |
| Securing equitable employment status | |
| Ensuring that PI enablement is part of local/national policy | |
| Acknowledging that representativeness is not realistic | |
| Forward planning | Understanding local processes |
| Being realistic about time and resource requirements | |
| Communicating openly about expectations and options with individuals, their personal assistants and their families | |
| Enabling shared understanding of each other’s roles | |
| Involving co-researchers from start to finish | |
| Providing timely, individualised training and support for co-researchers | |
| Considering group size and mix | |
| Team ethos | Ensuring an assets-based, inclusive approach |
| Understanding each other, being open to challenge | |
| Communicating well | |
| Spending time together as a team |
Participants indicated that they felt it was important that the co-researcher role was clearly defined and firmly established within the research infrastructure to facilitate public involvement in future studies. Their responses suggest that research teams need to have a clear vision of what the co-researcher role involves while acknowledging that this will depend on the aims and objectives of individual projects. For example, it would be beneficial for researchers to understand and acknowledge that co-researchers bring unique perspectives to each project and cannot represent the views of an entire clinical population. Members of the public need to be motivated to engage in public involvement roles and supported to participate in ways that correspond to their abilities and preferences.
Participants indicated that public involvement could be facilitated if members of the public were able to access employed research roles on an equitable basis:
. . . I think one of the things that would have improved that was if there had been a budget to actually reimburse [the co-researchers] at that preparatory stage, because [they] were completely volunteering [their] input there.
Researcher, group 1
To achieve this, various mechanisms for enabling public involvement at local and national levels were proposed: funders need to explicitly encourage full costing for public involvement roles in their award application processes; support needs to include recruitment to public involvement roles, in terms of how to cost salaries, define the role (e.g. proposing a template job description) and identify potential candidates; policy could be enhanced and practical support and research training made available to enable people to access co-researcher roles; research teams should publish real-world exemplars of public involvement research to share learning and good practice with others.
Participants identified several ways of improving the planning of individual projects to facilitate public involvement. They emphasised the importance of understanding local processes (e.g. human resources) for identifying and recruiting co-researchers:
. . . know your university processes, has it been done before? . . . and actually try and pre-empt those challenges and barriers and start those initial conversations earlier . . .
University manager, group 3
Participants recognised a need for researchers to be realistic about the time, funding and other resources (e.g. accessible environments) required to facilitate co-researchers’ participation. In addition, participants highlighted the importance of enabling clear and open reciprocal communication between researchers and members of the public about each group’s expectations of the co-researcher role, available participation options and individual preferences. The co-researchers suggested that it was important to plan for co-researchers to be involved throughout the lifetime of a project, rather than at discrete stages, to help them to fully understand and contribute to the research activity:
It’s having that broad base of knowledge from the start of the project right through has actually helped to add the value, hopefully, rather than being a bit of a butterfly and coming in on a particular element.
Co-researcher, group 1
Participants emphasised the value of securing consistent, personalised, flexible and high-quality support for co-researchers with disabilities during research projects. It is also important that other members of the research team feel supported to work confidently with co-researchers with disabilities:
. . . if they’ve got cognitive impairment or mobility issues or communication, dealing with those kinds of issues, I guess it would be easy for most clinicians if they’re familiar with this. I suppose I’m in a different [position] because I’m a methodologist . . . so getting help on that front would be important.
Researcher, group 2
Additionally, co-researchers should be offered training in research methodology and flexible working options (e.g. the opportunity to work from home) to support their participation.
Another theme identified in the data related to the need for leaders to create a team ethos that facilitates public involvement. Participants’ responses indicate that an asset-based, inclusive approach to project management can facilitate participation by members of the public:
It’s about the value, the recognition as equals. The fact we’ve looked at [the co-researchers’] individual needs and built it in, not made it a problem. You know, it’s that attitude of . . . it’s asset-based rather than a sort of negative-based approach.
University manager, group 3
Co-researchers need to feel confident in expressing their needs and strengths when making decisions about how they might contribute to projects. All members of the research team need to take time to get to know one another so that they can understand each other’s roles, backgrounds and expectations. Participants suggested that spending some social time together, especially in the early stages of a project, could facilitate such team-building. This may support team members to appreciate their colleagues’ viewpoints and better value their contributions to group discussions:
Try to get to know your colleagues and value and understand what they’re bringing to the project.
Co-researcher, group 1
Participants highlighted the importance of open, inclusive and respectful communication within the team; they identified that some team members may need support to manage challenging conversations between researchers and members of the public, which might arise when individual perspectives appear to conflict. Importantly, they were able to identify practical approaches to making communication during research activities more accessible to people with communication disability who use AAC.
Findings from resource utilisation questionnaires
During the qualitative analysis of the resource utilisation questionnaire, five themes emerged from this analysis; these differed slightly from those that emerged from the interview and focus group data analysis. They included (1) the nature of public involvement in the I-ASC project, (2) communication, (3) power relations, (4) time, and (5) the challenges associated with public involvement. The organising themes and basic themes generated from the qualitative data are shown in Table 25. This analysis revealed that data relating to the nature of public involvement in the project and the time and challenges associated with public involvement activity were broadly consistent with the findings generated from the interviews and focus groups.
| Organising themes | Basic themes |
|---|---|
| Nature of PI on the I-ASC project | Including PI researchers across all aspects of a project is possible |
| The PI co-researchers made a valuable contribution | |
| Communication | Communication in meetings can take longer, although this was not perceived to make meetings longer |
| There was a need for more one-to-one meetings (face to face or over Skype) rather than online communications | |
| Power relations | There was a wish for more one-to-one mentoring and support |
| Considerable research time was put into recruiting support for and mentoring and empowering the PI co-researchers | |
| PI co-researchers are individuals and can be very different; what can be expected of them and from them will vary by person | |
| Time | Working on whole-team tasks (team meetings) with PI co-researchers made little or no difference overall to the delivery of the project on time |
| The PI co-researchers made a valuable contribution, delivering work they were responsible for on time | |
| Team members found some aspects of including PI co-researchers on the team more time-consuming than anticipated | |
| Sorting out NHS ethics and R&D approval took twice as long as expected | |
| Recruiting and training support assistants who provided support to a PI co-researcher | |
| Role playing prior to data collection interviews | |
| Challenges associated with PI | Unexpected time commitment of ethics, R&D, NHS Passports |
| Unexpected time recruiting and training personal support staff | |
| Budgeting for inclusion of PI co-researchers had an impact on some project activities | |
| Balancing additional workload with other academic/personal commitments |
Quantitative analysis
The original investigative intention had been to carry out a financial analysis of the proposed and actual budgets. However, owing to the retrospective nature of this analysis, the process of data extrapolation and exploration had the potential to be misleading. For example, both of the public involvement co-researchers had taken on additional tasks as a result of the illness and absence of core research collaborators (e.g. they made a greater contribution to data analysis, data evaluation and preparations for dissemination). This project was fortunate to (1) have the skills in the public involvement co-research team, (2) have their time and willingness to take on additional duties, and (3) have the capacity to move budgets around to accommodate their reimbursement for such activities. The anxiety that merely looking at pounds, pence and time would be misleading was reinforced by the project risk analysis documentation highlighting how we managed staff illness and absence. Nonetheless, data indicate that resource use in the project was high in terms of staff time, training time and personalised support/care costs. An awareness of the financial implications, and an attempt to offer informed suggestions for future bid construction, leads us to suggest the following considerations for any future submission attempting the level of public involvement we have delivered (i.e. in addition to the I-ASC staffing approved during the project delivery phases):
-
additional time from the chief investigator to support methodological rigour, training and support (half a day per week)
-
a project manager role to support all administrative necessities, such as research passports, occupational health processes, human resources processes (half a day per week)
-
additional time from research fellow staff to support logistical, theoretical, analytical and delivery and dissemination processes (1 day per week)
-
appropriate budget to support the reimbursement of public involvement contributors/researchers (e.g. vouchers for those who cannot be paid directly without jeopardising state benefit provision)
-
appropriate budget to identify a research assistant role to support anyone who needs it (e.g. someone with a severe communication disability can be effectively supported to deliver research objectives when given adequate support by a well-informed research assistant).
Although we found it difficult to quantify the actual resource use associated with public involvement contributions, these suggested additions to any research team could inform the future appraisal of public involvement contributions.
In conclusion, even with a post hoc analysis, a key conclusion would be to recommend mindfulness of how to collate public involvement contributions during a project and that this should be a part of any ongoing framework to support inclusive public involvement opportunities.
Discussion
This was a post hoc investigation of the public involvement component of the I-ASC project, the resources used to achieve it and the perceived impact of public involvement. A retrospective, mixed-methods design was used to collect data from individuals directly involved in the project. This investigation was planned in response to an identified need to improve the evidence base relating to (1) how public involvement can be successfully integrated into research projects139 and (2) how public involvement can be evaluated to demonstrate its effectiveness. 153
The qualitative data describing the implementation of public involvement in the I-ASC project provide an exemplar that other researchers could use to identify ways of making involvement more accessible to vulnerable public involvement groups. These data show that the co-researchers’ participation was enabled at all stages of the research process and suggest that these individuals were integrated into the research team as equal partners. Co-researchers contributed actively to diverse research activities and were not consulted merely on specific aspects, as in other studies, suggesting that their participation was not tokenistic. 138
The data provide indicators to help further refine the co-researcher role. In this project, the role was observed to serve different functions in response to project need and individual availability, preferences, skills and experience. Participants were eager to stress that they felt that one co-researcher’s contribution to the project was exceptionally extensive in terms of the skills and experience they brought to their role and the amount of time they could devote to public involvement. Participants felt that this type of involvement should not be expected in all studies. However, it could also be argued that this individual’s level of involvement was enabled by facilitative aspects of the project’s management processes and team ethos. Future research could explore how researchers and members of the public conceptualise the co-researcher role.
This WP identified a number of potential barriers to and facilitators of successful public involvement that could be used to inform policy development and identify improvements to research infrastructure. The findings complement existing evidence relating to various structural and cultural barriers that still prevent the public from accessing research roles, participating equitably in research activity and receiving fair financial rewards for their contributions. 139,154,155 The findings suggest that the co-researcher role needs greater clarification, recognition and status at national level in order to increase access for diverse groups of people. The data emphasise the potential benefits of improved planning for public involvement and an asset-based team ethos that promotes inclusivity, mutual respect and open communication; these findings complement existing evidence. 154–156
This investigation has extended the evidence base by providing new evidence about the challenges associated with involving individuals with severe communication disability, a vulnerable public involvement group that is at risk of being excluded from public involvement research. The challenges of involving the individual who uses AAC and has physical disabilities were clearly greater than those associated with involving the other co-researcher without these disabilities. This study has identified practical ways that communication and physical access can be facilitated for individuals with disabilities. These findings will be used to inform guidance and practical resources to develop future public involvement practice.
The output from this WP is an online toolkit, including guidance for funders, policy-makers and researchers to develop research protocols, and guidance for public involvement co-researchers and potential participants to explain prospective roles and input. The toolkit includes videos and guidance materials to facilitate increased and meaningful public involvement in research for those with significant speech, communication and physical disability of all ages (see https://iasc.mmu.ac.uk/publicinvolvement). Guidance informs all other public involvement informed research (e.g. critical care research, public health research). The resources will enable researchers to understand the place of public involvement in co-production in research.
The interview and focus group data indicate that incorporating significant public involvement in a research study significantly increases resource use in terms of staff time, training and support activities. Resource costs are likely to be higher when members of the public have disabilities. There may be additional costs if researcher and co-researcher time is not fully costed during the research funding application process.
The qualitative data identify a number of potential benefits that active public involvement can bring to research projects. These include refinements to participant recruitment and data collection and analysis methods and improvements to the validity, credibility and accessibility of the research outputs. These findings complement similar observations made in other studies. 153,156 This evaluation suggests that actively involving individuals with communication disabilities and their families is likely to bring additional benefits, including improving the accessibility of research outputs to the target audience.
The data indicate that the concept of public involvement in research affords important benefits to members of the public who choose to be involved. The active involvement in research projects of service users and family members can provide positive role models for others, both internally to other members of the research team and externally to the general public. This confirms observations made in other studies139,155 but provides novel evidence relating to this particular population.
The post hoc nature of this evaluation means that the current data do not enable us to quantify the increase in resource use or the value of benefits associated with public involvement activity during the project. Even considering the main methodological limitation of this investigation, namely its retrospective design, the data do provide indicators of parameters that could be included in a conceptual framework for evaluating the cost–benefit of public involvement in future research studies. Future studies evaluating the cost–benefit of public involvement may quantify the actual costs and benefits associated with such activity. This information could be useful for both funders and researchers in planning efficient resource allocation to enhance the impact of such activity.
This evaluation, applied for in 2018, was motivated in part by an identified need to develop protocols to evaluate the impacts of public involvement qualitatively and quantitatively. 153 Recently, authors have suggested that an economic evaluation of and justification for public involvement is unnecessary and irrelevant. 154–156 These authors highlight the accepted ethical and epistemological justifications for public involvement. They conceptualise public involvement as an emergent, context-dependent activity providing multiple levels of impact that can develop over the long term, and argue that public involvement should not be considered an intervention to be defined, controlled and measured using traditional evaluation methodologies. However, it must be recognised that cost parameters informed by systematic public involvement evaluations are welcome to support effective inclusion of public involvement co-researchers, and to ensure that funding requests are adequate. Future studies should attempt to identify the optimum methods to evaluate public involvement costs and benefits (including impact) and to explore ways to describe the contributions that public involvement co-researchers can make to research studies. In the meantime, this post hoc evaluation of the impact of the integrated involvement of those described as hard to reach and vulnerable offers some useful insights into how to plan, budget and support meaningful contributions. This perspective is reinforced by Staley and Barron,155 who suggest that researchers’ descriptions of the impact of public involvement should be considered valid measures.
Conclusions
This WP was designed to evaluate public involvement in the I-ASC project to identify the costs and benefits of co-produced research and to develop practical guidance and tools to facilitate meaningful public involvement in future projects that focus on vulnerable and hard-to-reach patients. The WP generated rich qualitative data that describe how public involvement, including of those with significant disabilities, can be enabled at all stages of a research project. These qualitative data have been used to develop specific guidance (e.g. how to obtain a research passport for co-researchers, how to provide personalised support) included in a public involvement toolkit that is hosted on the I-ASC website (https://iasc.mmu.ac.uk/publicinvolvement). This knowledge has already been disseminated through initial training events for researchers and prospective co-researchers, in peer-reviewed journals and practice publications141 and at scientific and service-user conferences. 157,158
We were unable to evaluate the costs and benefits of public involvement quantitatively in this study owing to methodological limitations. Our findings do provide indicators that could be used to inform future, prospective quantitative investigations of the resources required for and benefits associated with public involvement. Consistent data generated from both the interviews and the elements of an economic evaluation suggest that successful public involvement, especially of individuals with disabilities, requires significant resources in terms of staff time, training and personal support. These data highlight the need for mechanisms to enable researchers to pay public involvement co-researchers for their contributions to research funding bid preparations, which remains, at present, a ‘hidden’ cost of public involvement research.
Acknowledgements
Funders
The I-ASC project was funded by the NIHR Health Services and Delivery Research programme. Throughout the project we were supported by two NIHR advisors, Samantha Low and Jennifer Cook.
Participants
This research was possible only because of the responsiveness and support of the many participants involved in different aspects of the I-ASC research project.
Advisory Board and Critical Friend Group
Thank you to the members of these two groups. They offered wise counsel, critical appraisal and genuine guidance, resulting in a far more robust outcome to the project. Advisory Board: Professor Catherine Mackenzie, Jenny Herd, Sally Townend and Professor Luke Vale. Critical Friend Group: Professor Martine Smith, Professor Pamela Enderby, Dr Arne RiseHole, Gregor Gilmour, Angie McCormack, Liz Pryde and Nat Mills.
Contributions of others
Thanks to Professor Shakila Dada and Associate Professor Beata Batorowicz for their constructive contributions to work strand delivery.
Thanks to Dr Joan Murphy, Talking Mats, for her kind support of our data collection techniques.
Thanks to the Speech and Language Therapy Department at the Central Remedial Clinic, Dublin, and specifically Murieann McCleary (Speech and Language Therapy Manager), who supported pilot testing and evaluation during data collection preparations and provided resource production feedback.
Thanks to Chris Sherlock, Janet Scott, Professor Jois Stansfield, Gregor Gilmour, Ruth McMorran, Jenny Herd, colleagues from ATTherapy, Gavin Drysdale, Margaret Drysdale, Linda Page and Judith Chapman for their time in testing and helping us refine resources.
Thanks to Sarah Hannis, Natalie Rowland, Nazifa Khatun and Gemma Sleman for their artistic support in developing story books to support children and young people to engage in the assessment process.
Thanks to Jon Moulam for his support as photographer at the Scottish Parliament dissemination event.
Thanks to Douglas Millar, Heather Palmer and Jean Alexander, who supported organisational aspects of the dissemination event at the Scottish Parliament (Edinburgh). Particular thanks to Fulton MacGregor, MSP, for sponsoring the event, and to Gavin Drysdale, who gave the opening address.
Thanks to Sam Gray for supporting organisational aspects of our dissemination event at MOSI (Manchester), and especial thanks to Carolyn Young, Anna Reeves (Deputy Lieutenant) and Gregor Gilmour, for their contributions to the event.
Thanks to Robert McLaren, Policy Connect, for his support in aiding delivery of our Westminster (London) dissemination event and in securing sponsors and contributors: the Rt Hon John Bercow, MP; Seema Malhotra, MP; Lord Ramsbotham; Kamini Gadhok; Professor Brian Lamb; Anne Longfield; Marie Gascoigne; Sara Bainbridge; Dr Michael Clarke; Carolyn Young; Liz Hewson; and Kim Bates.
www.1voice.info/ for their support in the recruitment of participants for different aspects of the project.
Thanks to Professor Bronwyn Helmsley for her support of public involvement co-created research.
Contributions of authors
The research was conducted by three collaborative partners, Manchester Metropolitan University (lead), Barnsley Assistive Technology Service and the University of Leeds.
Manchester Metropolitan University
Research team: Professor Janice Murray, Professor Juliet Goldbart, Dr Yvonne Lynch, Liz Moulam, Stuart Meredith and Helen Whittle.
Professor Janice Murray (https://orcid.org/0000-0001-8809-4256) managed the entire project, led the delivery of WPs 2 and 3, co-led data collection in WP 2, led and contributed to data analysis in WPs 1–4, co-led WP 5 developments, supported WP 6 construction and delivery, and oversaw WP 8 delivery. She has also led on the development and delivery of several outputs, for example journal publications (WPs 2, 3 and 8), professional publications, conference and workshop presentations and represented the project team at public and policy-driven events. Another key role has been supporting public involvement co-researcher involvement and less experienced research staff (e.g. Barnsley). Janice was lead author for Chapters 1, 2, 5, 8 and 9, and was overall editorial lead.
Dr Yvonne Lynch (https://orcid.org/0000-0003-3209-3099) was the lead researcher for WPs 1–3. She also facilitated the development of attribute descriptors to support the delivery of WP 4. She led preparations for data collection and delivered data collection, data analysis and writing for publication. She was a key lead on the development of WP 5 (heuristic). She was also a key researcher related to aspects of project management/delivery, such as ethics approval preparations across the UK and data management protocols. Within WP 6 (dissemination) she led several dissemination events (e.g. CENs, international conference workshops). She was the lead author of Chapters 3 and 6 and had significant input to Chapters 1, 2, 4, 5, 7 and 9. She also led the report formatting.
Professor Juliet Goldbart (https://orcid.org/0000-0003-1290-7833) led WP 1 and contributed to a number of WP 6 (dissemination) events both nationally and internationally. She was lead author of Chapter 4 and contributed to Chapters 7 and 8.
Liz Moulam (https://orcid.org/0000-0003-3810-1037) was a key contributor to the data collection in WP 3 and the data analysis in WPs 1–3. She contributed to preparations for data collection in WP 4. She also made a significant contribution to the developments in WP 5. She co-led WP 6 and the delivery of WP 8. Liz also made significant contribution to local, national and international presentation events (e.g. the Communication Matters International Conference), as well as supporting academic and practice-based outputs from WPs 2–5. Liz made significant author contributions to Chapters 5, 6, 8 and 10.
Mark Jayes was the lead researcher for the qualitative components of WP 8 and the lead author of Chapter 10.
Stuart Meredith was a key contributor to the data collection in WP 3 and the data analysis in WPs 2 and 3. He also contributed to preparations for WP 4 data collection. He co-led the delivery of WP 6 and contributed to the outputs from WPs 1–5 and 8. He made significant author contributions to Chapters 6, 8 and 10.
Helen Whittle (https://orcid.org/0000-0003-4969-0826) contributed to data collection and analysis in WP 3; in addition, she supported the analysis of data in WPs 1 and 4 and contributed to the delivery of events associated with WP 6. A further key role was acting as support for Stuart Meredith during project meetings and data collection activities. Helen made significant author contributions to Chapters 6, 8 and 10.
Public involvement (work package 8) research team
Liz Moulam, Professor Sue Powell, Professor Francis Fatoye and Dr Mark Jayes. Francis Fatoye led the development and delivery of the cost–consequence analysis component of the WP. Liz Moulam was the lead delivery researcher for this component. Sue Powell offered project management support to Liz Moulam and Mark Jayes.
Support team
Kelly Lavender-Smith, Zoe Lingard, Zoe Johnston, Christopher Wills, Helen Bell, Gareth Preston, Dr Sue Caton, Dr Christina Sotiropoulou-Drosopoulou, Dr Sam Wright, Radek Loucka, Monwara Begum, Marie Basting, Charlotte Saunders, Chloe Levett-Smith, Sarah Brown, Wanausha Khafaf, Kerry Wilkins and Natasha Robinson.
Barnsley Assistive Technology Service, Barnsley Hospital Foundation Trust
Research team: Simon Judge and Nicola Randall.
Simon Judge (https://orcid.org/0000-0001-5119-8094) was the researcher lead for one systematic review in WP 1 and its associated journal publication, and contributed to the attribute debate that informed WP 4. He co-led developments in WP 5 (heuristic) and has presented I-ASC findings at national events. Simon made author contributions to Chapters 4, 7 and 8.
Nicola Randall (https://orcid.org/0000-0002-8353-3325) substantially contributed to one systematic review in WP 1 and its associated journal publication, and contributed to the attribute debate that informed WP 4. She contributed to the data collection and analysis in WP 3 and to dissemination events (WP 6) both nationally and internationally (e.g. International Society for Augmentative and Alternative Communication conference 2018 in Australia). She supported content development within WP 5 (heuristic). Nicola made author contributions to Chapters 6 and 7.
Support team
Andrea Lee, Gemma Sleman and Beccy Masters.
University of Leeds
Research team: Professor Stephane Hess, Dr David Meads and Dr Edward Webb.
Dr Edward Webb (https://orcid.org/0000-0001-7918-839X) led and delivered WP 4 and its associated journal publications. He also contributed to national and international conference presentations. He was the lead author of Chapter 7.
Dr David Meads (https://orcid.org/0000-0003-1369-2483) and Professor Stephane Hess (https://orcid.org/0000-0002-3650-2518) acted in an advisory capacity for the delivery of WP 4 and its associated outputs. Both made significant contributions to the authorship of Chapter 7.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Patient data
This work uses data provided by patients and collected by the NHS as part of their care and support. Using patient data is vital to improve health and care for everyone. There is huge potential to make better use of information from people’s patient records, to understand more about disease, develop new treatments, monitor safety, and plan NHS services. Patient data should be kept safe and secure, to protect everyone’s privacy, and it’s important that there are safeguards to make sure that it is stored and used responsibly. Everyone should be able to find out about how patient data are used. #datasaveslives You can find out more about the background to this citation here: https://understandingpatientdata.org.uk/data-citation.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care.
References
- Hamm B, Mirenda P. Post-school quality of life for individuals with developmental disabilities who use AAC. Augment Altern Commun 2006;22:134-47. https://doi.org/10.1080/07434610500395493.
- McDonald R, Harris E, Price K, Jolleff N. Elation or frustration? Outcomes following the provision of equipment during the Communication Aids Project: data from one CAP partner centre. Child Care Health Dev 2008;34:223-9. https://doi.org/10.1111/j.1365-2214.2007.00787.x.
- Smith MM, Murray J. Parachute without a ripcord: the skydive of communication interaction. Augment Altern Commun 2011;27:292-303. https://doi.org/10.3109/07434618.2011.630022.
- Enderby P, Judge S, Creer S. Examining the need for and provision of AAC methods in the UK. Advances in clinical neuroscience & rehabilitation. White Rose 2013;13:20-3.
- Office for National Statistics . Population Estimates 2014. www.ons.gov.uk/ons/taxonomy/index.html?nscl=Population+Estimates+by+Age+and+Sex#tab-data-tables (accessed 11 September 2020).
- James Lind Alliance . Childhood Disability Research Priority Setting Partnership. 2014. www.lindalliance.org/ChildhoodDisabilityPSP.asp (accessed 13 July 2020).
- Morris C, Simkiss D, Busk M, Morris M, Allard A, Denness J, et al. Setting research priorities to improve the health of children and young people with neurodisability: a British Academy of Childhood Disability-James Lind Alliance Research Priority Setting Partnership. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2014-006233.
- van der Meer L, Sigafoos J, O’Reilly MF, Lancioni GE. Assessing preferences for AAC options in communication interventions for individuals with developmental disabilities: a review of the literature. Res Dev Disabil 2011;32:1422-31. https://doi.org/10.1016/j.ridd.2011.02.003.
- Lindsay S. Perceptions of health care workers prescribing augmentative and alternative communication devices to children. Disabil Rehabilitation: Assistive Technology 2010;5:209-22. https://doi.org/10.3109/17483101003718195.
- Gross J. Two Years On: Final Report of the Communication Champion for Children 2011.
- Johnson JM, Inglebret E, Jones C, Ray J. Perspectives of speech language pathologists regarding success versus abandonment of AAC. Augment Altern Commun 2006;22:85-99. https://doi.org/10.1080/07434610500483588.
- Baxter S, Enderby P, Evans P, Judge S. Barriers and facilitators to the use of high-technology augmentative and alternative communication devices: a systematic review and qualitative synthesis. Int J Lang Commun Disord 2012;47:115-29. https://doi.org/10.1111/j.1460-6984.2011.00090.x.
- Judge S, Townend J. Choosing Voice Output Communication Aids: A Proposed Decision-making Tool. Barcelona: International Society for Augmentative and Alternative Communication; 2010.
- McFadd E, Wilkinson K. Qualitative analysis of decision making by speech-language pathologists in the design of aided visual displays. Augment Altern Commun 2010;26:136-47. https://doi.org/10.3109/07434618.2010.481089.
- World Health Organization . International Classification of Functioning, Disability and Health (ICF) 2001.
- Lund SK, Light J. Long-term outcomes for individuals who use augmentative and alternative communication: part I – what is a ‘good’ outcome?. Augment Altern Commun 2006;22:284-99. https://doi.org/10.1080/07434610600718693.
- Lund SK, Light J. Long-term outcomes for individuals who use augmentative and alternative communication: part II – communicative interaction. Augment Altern Commun 2007;23:1-15. https://doi.org/10.1080/07434610600720442.
- Parkes J, McCullough N, Madden A. To what extent do children with cerebral palsy participate in everyday life situations?. Health Social Care Community 2010;18:304-15. https://doi.org/10.1111/j.1365-2524.2009.00908.x.
- Bryen D, Chung Y, Lever S. What you might not find in a typical transition plan! Some important lessons from adults who rely on augmentative and alternative communication. Perspectives Augment Altern Commun 2010:5-8. https://doi.org/10.1044/aac19.2.32.
- Bailey RL, Parette HP, Stoner JB, Angell ME, Carroll K. Family members’ perceptions of augmentative and alternative communication device use. Lang Speech Hear Serv Sch 2006;37:50-6. https://doi.org/10.1044/0161-1461(2006/006).
- Smith MM, Connolly I. Roles of aided communication: perspectives of adults who use AAC. Disabil Rehabil Assist Technol 2008;3:260-73. https://doi.org/10.1080/17483100802338499.
- Murray J, Goldbart J. Augmentative and alternative communication: a review of current issues. Paediatr Child Health 2009;19:464-8. https://doi.org/10.1016/j.paed.2009.05.003.
- Dada S, Alant E. The effect of aided language stimulation on vocabulary acquisition in children with little or no functional speech. Am J Speech Lang Pathol 2009;18:50-64. https://doi.org/10.1044/1058-0360(2008/07-0018).
- Lund SK, Light J. Long-term outcomes for individuals who use augmentative and alternative communication: part III – contributing factors. Augment Altern Commun 2007;23:323-35. https://doi.org/10.1080/02656730701189123.
- Schlosser R, Lee D. Promoting generalization and maintenance in augmentative and alternative communication: a meta-analysis of 20 years of effectiveness research. Augment Altern Commun 2000;16:208-27. https://doi.org/10.1080/07434610012331279074.
- Batorowicz B, Shepherd TA. Teamwork in AAC: examining clinical perceptions. Augment Altern Commun 2011;27:16-25. https://doi.org/10.3109/07434618.2010.546809.
- Dietz A, Quach W, Lund SK, McKelvey M. AAC assessment and clinical-decision making: the impact of experience. Augment Altern Commun 2012;28:148-59. https://doi.org/10.3109/07434618.2012.704521.
- Binger C, Light J. The effect of aided AAC modelling on the expression of multi-symbol messages by preschoolers who use AAC. Augment Altern Commun 2007;23:30-43. https://doi.org/10.1080/07434610600807470.
- Binger C, Kent-Walsh J, Berens J, Del Campo S, Rivera D. Teaching Latino parents to support the multi-symbol message productions of their children who require AAC. Augment Altern Commun 2008;24:323-38. https://doi.org/10.1080/07434610802130978.
- Blockberger S, Johnston JR. Grammatical morphology acquisition by children with complex communication needs. Augment Altern Commun 2003;19:207-21. https://doi.org/10.1080/07434610310001598233.
- Goldbart J, Marshall J. ‘Pushes and pulls’ on parents of children who use AAC. Augment Altern Commun 2004;20:194-200. https://doi.org/10.1080/07434610400010960.
- King G, Batorowicz B, Shepherd TA. Expertise in research-informed clinical decision making: working effectively with families of children with little or no functional speech. Evid Based Commun Assess Intervention 2008;2:106-16. https://doi.org/10.1080/17489530802296897.
- Milner P, Kelly B. Community participation and inclusion: people with disabilities defining their place. Disabil Soc 2009;24:47-62. https://doi.org/10.1080/09687590802535410.
- Murray J, Goldbart J. Emergence of working memory in children using aided communication. J Assistive Technologies 2011;5:214-32. https://doi.org/10.1108/17549451111190623.
- von Tetzchner S. Introduction to the special issue on aided language processes, development, and use: an international perspective. Augment Altern Commun 2018;34:1-15. https://doi.org/10.1080/07434618.2017.1422020.
- Smith MM, Batorowicz B, Sandberg AD, Murray J, Stadskleiv K, van Balkom H, et al. Constructing narratives to describe video events using aided communication. Augment Altern Commun 2018;34:40-53. https://doi.org/10.1080/07434618.2017.1422018.
- Stadskleiv K, Batorowicz B, Massaro M, van Balkom H, von Tetzchner S. Visual-spatial cognition in children using aided communication. Augment Altern Commun 2018;34:68-7. https://doi.org/10.1080/07434618.2017.1422017.
- Deliberato D, Jennische M, Oxley J, Nunes LRDP, Walter CCF, Massaro M, et al. Vocabulary comprehension and strategies in name construction among children using aided communication. Augment Altern Commun 2018;34:16-29. https://doi.org/10.1080/07434618.2017.1420691.
- Batorowicz B, Stadskleiv K, Renner G, Sandberg AD, von Tetzchner S. Assessment of aided language comprehension and use in children and adolescents with severe speech and motor impairments. Augment Altern Commun 2018;34:54-67. https://doi.org/10.1080/07434618.2017.1420689.
- Murray J, Sandberg AD, Smith MM, Deliberato D, Stadskleiv K, von Tetzchner S. Communicating the unknown: descriptions of pictured scenes and events presented on video by children and adolescents using aided communication and their peers using natural speech. Augment Altern Commun 2018;34:30-9. https://doi.org/10.1080/07434618.2017.1420690.
- Binger C, Light J. The morphology and syntax of individuals who use AAC: research review and implications for effective practice. Augment Altern Commun 2008;24:123-38. https://doi.org/10.1080/07434610701830587.
- Choi BC, Pak AW. Multidisciplinarity, interdisciplinarity and transdisciplinarity in health research, services, education and policy: 1. Definitions, objectives, and evidence of effectiveness. Clin Invest Med 2006;29:351-64.
- Fallon K, Light J, Achenbach A. The semantic organisation patterns of young children: implications for augmentative and alternative communication. Augment Altern Commun 2003;19:74-85. https://doi.org/10.1080/0743461031000112061.
- Goetghebeur MM, Wagner M, Khoury H, Rindress D, Gregoire JP, Deal C. Combining multicriteria decision analysis, ethics and health technology assessment: applying the EVIDEM decision making framework to growth hormone for Turner syndrome patients. Cost Eff Resour Alloc 2010;8:4-14. https://doi.org/10.1186/1478-7547-8-4.
- Scherer M, Jutai J, Fuhrer M, Demers L, Deruyter F. A framework for modelling the selection of assistive technology devices (ATDs). Disabil Rehabil Assist Technol 2007;2:1-8. https://doi.org/10.1080/17483100600845414.
- Murray J, Martin A, Pennington L, Marshall J, Enderby P, Goldbart J. A case study template to support experimental design in augmentative and alternative communication and assistive technology. Disabil Rehabil Assist Technol 2014;9:60-9. https://doi.org/10.3109/17483107.2013.851744.
- Schlosser RW. Evidence-based practice for AAC practitioners. Perspect Augment Altern Commun 2006;15:8-9. https://doi.org/10.1044/aac15.3.8.
- Creswell J, Plano Clark V. Designing and Conducting Mixed Methods Research. Thousand Oaks, CA: SAGE Publications Ltd; 2007.
- Feilzer MY. Doing mixed methods research pragmatically: implications for the rediscovery of pragmatism as a research paradigm. J Mixed Methods Res 2010;4:6-16. https://doi.org/10.1177/1558689809349691.
- Schlosser R, Wendt O, Angermeier KL, Shetty M. Searching for evidence in augmentative and alternative communication: navigating a scattered literature. Augment Altern Commun 2005;21:233-55. https://doi.org/10.1080/07434610500194813.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000097.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Ritchie J, Spencer L, Bryman, Burgess. Qualitative Data Analysis for Applied Policy Research. London: Routledge; 1994.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19-32. https://doi.org/10.1080/1364557032000119616.
- Gopalakrishnan S, Ganeshkumar P. Systematic reviews and meta-analysis: understanding the best evidence in primary healthcare. J Family Med Prim Care 2013;2:9-14. https://doi.org/10.4103/2249-4863.109934.
- Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak 2007;7. https://doi.org/10.1186/1472-6947-7-16.
- Schlosser RW, Koul R, Costello J. Asking well-built questions for evidence-based practice in augmentative and alternative communication. J Commun Disord 2007;40:225-38. https://doi.org/10.1016/j.jcomdis.2006.06.008.
- Critical Appraisal Skills Programme C . Critical Appraisal Skills Programme Qualitative Checklist n.d. https://casp-uk.net/casp-tools-checklists/ (accessed 11 September 2020).
- Center for Evidence-Based Management . Critical Appraisal of a Survey Tool n.d. www.cebma.org/wp-content/uploads/Critical-Appraisal-Questions-for-a-Survey.pdf (accessed 3 March 2017).
- Gough D. Weight of evidence: a framework for the appraisal of the quality and relevance of evidence. Res Papers Educ 2007;22:213-28. https://doi.org/10.1080/02671520701296189.
- Kliewer C. Young children’s communication and literacy: a qualitative study of language in the inclusive preschool. Ment Retard 1995;33:143-52.
- Smith M. Reading ability of nonspeaking students. Augment Altern Commun 1992;8:57-66. https://doi.org/10.1080/07434619212331276043.
- Sutton AC. The social-verbal competence of AAC users. Augment Altern Commun 1989;5:150-64. https://doi.org/10.1080/07434618912331275156.
- Geytenbeek JJ, Heim MJ, Knol DL, Vermeulen RJ, Oostrom KJ. Spoken language comprehension of phrases, simple and compound-active sentences in non-speaking children with severe cerebral palsy. Int J Lang Commun Disord 2015;50:499-515. https://doi.org/10.1111/1460-6984.12151.
- Redmond SM, Johnston SS. Evaluating the morphological competence of children with severe speech and physical impairments. J Speech Lang Hear Res 2001;44:1362-75. https://doi.org/10.1044/1092-4388(2001/106).
- Soto G, Hartmann E. Analysis of narratives produced by four children who use augmentative and alternative communication. J Commun Disord 2006;39:456-80. https://doi.org/10.1016/j.jcomdis.2006.04.005.
- Soto G, Hartmann E, Wilkins DP. Exploring the elements of narrative that emerge in the interactions between an 8-year-old child who uses an AAC device and her teacher. Augment Altern Commun 2006;22:231-41. https://doi.org/10.1080/07434610500431777.
- Soto G, Toro-Zambrana W. Investigation of Blissymbol use from a language research paradigm. Augment Altern Commun 1995;11:118-30. https://doi.org/10.1080/07434619512331277219.
- Sutton AE, Gallagher TM. Verb class distinctions and AAC language-encoding limitations. J Speech Hear Res 1993;36:1216-26. https://doi.org/10.1044/jshr.3606.1216.
- Trudeau N, Sutton A, Morford JP, Côté-Giroux P, Pauzé AM, Vallée V. Strategies in construction and interpretation of graphic-symbol sequences by individuals who use AAC systems. Augment Altern Commun 2010;26:299-312. https://doi.org/10.3109/07434618.2010.529619.
- van Balkom H, Donker-Gimbere W, von Tetzchner S, Jensen MH. Augmentative and Alternative Communication: European Perspectives. London: Whurr; 1996.
- Judge S, Randall N, Goldbart J, Lynch Y, Moulam L, Meredith S, et al. The language and communication attributes of graphic symbol communication aids – a systematic review and narrative synthesis [published online ahead of print April 23 2019]. Disabil Rehabil Assist Technol 2019. https://doi.org/10.1080/17483107.2019.1604828.
- Crowe M. Crowe Critical Appraisal Tool n.d. https://conchra.com.au/wp-content/uploads/2015/12/CCAT-form-v1.4.pdf (accessed 20 September 2017).
- Bhattacharya S. Design of an iconic communication aid for individuals in India with speech and motor impairments. Assist Tech 2009;21:173-87. https://doi.org/10.1080/10400430903246035.
- Bruno J. Customizing a Minspeak1 system for a preliterate child: a case example. Augment Altern Commun 1989;5:89-100. https://doi.org/10.1080/07434618912331275066.
- Judge S, Townend G. Perceptions of the design of voice output communication aids. Int J Lang Commun Disord 2013;48:366-81. https://doi.org/10.1111/1460-6984.12012.
- Mirenda P. Designing pictorial communication systems for physically able-bodied students with severe handicaps. Augment Altern Commun 1985;1:58-64. https://doi.org/10.1080/07434618512331273541.
- O’Keefe B, Brown L, Schuller R. Identification and rankings of communication aid features by five groups. Augment Altern Commun 1998;14:37-50. https://doi.org/10.1080/07434619812331278186.
- Sigafoos J, Iacono T. Selecting augmentative communication devices for persons with severe disabilities: some factors for educational teams to consider. A N Z J Dev Disabil 1993;18:133-46. https://doi.org/10.1080/07263869300034901.
- Smith-Lewis M. Discontinuity in the development of aided augmentative and alternative communication systems. Augment Altern Commun 1994;10:14-26. https://doi.org/10.1080/07434619412331276730.
- Hochstein D, McDaniel M, Nettleton S, Neufeld KH. The fruitfulness of a nomothetic approach to investigating AAC. Am J Speech-Language Pathol 2003;12:110-20. https://doi.org/10.1044/1058-0360(2003/057).
- Hochstein DD, McDaniel MA, Nettleton S. Recognition of vocabulary in children and adolescents with cerebral palsy: a comparison of two speech coding schemes. Augment Altern Commun 2004;20:45-62. https://doi.org/10.1080/07434610410001699708.
- Reichle J, Dettling E, Drager K, Leiter A. Comparison of correct responses and response latency for fixed and dynamic displays: performance of a learner with severe developmental disabilities. Augment Altern Commun 2000;16:154-63. https://doi.org/10.1080/07434610012331279014.
- Hurlbut BI, Iwata BA, Green JD. Nonvocal language acquisition in adolescents with severe physical disabilities: Bliss symbol versus iconic stimulus formats. J Appl Behav Anal 1982;15:241-58. https://doi.org/10.1901/jaba.1982.15-241.
- Light J, Lindsay P, Siegel L, Parnes P. The effects of message encoding techniques on recall by literate adults using AAC systems. Augment Altern Commun 1990;6:184-201. https://doi.org/10.1080/07434619012331275454.
- Light J, Lindsay P. Message-encoding techniques for augmentative communication systems. J Speech Hear Res 1992;35:853-64. https://doi.org/10.1044/jshr.3504.853.
- Bornman J, Bryen DN. Social validation of vocabulary selection: ensuring stakeholder relevance. Augment Altern Commun 2013;29:174-81. https://doi.org/10.3109/07434618.2013.784805.
- Yorkston K, Dowden P, Honsinger M, Marriner N, Smith K. A comparison of standard and user vocabulary lists. Augment Altern Commun 1988;4:189-210. https://doi.org/10.1080/07434618812331274807.
- Yorkston K, Honsinger M, Dowden P, Marriner N. Vocabulary selection: a case report. Augment Altern Commun 1989;5:101-8. https://doi.org/10.1080/07434618912331275076.
- Black R, Waller A, Turner R, Reiter E. Supporting personal narrative for children with complex communication needs. ACM Trans Comput Hum Int 2012;19. https://doi.org/10.1145/2240156.2240163.
- Stewart H, Wilcock A. Improving the communication rate for symbol-based, scanning voice output device users. Technol Disabi 2001;13:141-50. https://doi.org/10.3233/TAD-2000-13301.
- Tate RL, Perdices M, Rosenkoetter U, Wakim D, Godbee K, Togher L, et al. Revision of a method quality rating scale for single-case experimental designs and n-of-1 trials: the 15-item Risk of Bias in N-of-1 Trials (RoBiNT) Scale. Neuropsychol Rehabil 2013;23:619-38. https://doi.org/10.1080/09602011.2013.824383.
- Blissymbolics Communication International . Blissymbolics 2018. www.blissymbolics.org/.
- Baker B. Minspeak. Byte 1982;7.
- Locke PA, Mirenda P. Roles and responsibilities of special education teachers serving on teams delivering AAC services. Augment Altern Commun 1992;8:200-14. https://doi.org/10.1080/07434619212331276193.
- Lund SK, Quach W, Weissling K, McKelvey M, Dietz A. Assessment with children who need augmentative and alternative communication (AAC): clinical decisions of AAC specialists. Lang Speech Hear Serv Sch 2017;48:56-68. https://doi.org/10.1044/2016_LSHSS-15-0086.
- Dada S, Murphy Y, Tonsing K. Augmentative and alternative communication practices: a descriptive study of the perception of South African speech-language therapists. Augment Altern Commun 2017;33:189-200. https://doi.org/10.1080/07434618.2017.1375979.
- Hill K, Romich B. AAC evidence-based clinical practice: a model for success. AAC Inst Press 2002;2:1-6.
- Parette P, VanBiervliet A, Hourcade JJ. Family-centered decision making in assistive technology. J Special Education Technol 2000;15:45-5. https://doi.org/10.1177/016264340001500104.
- Lynch Y, Murray J, Moulam L, Meredith S, Goldbart J, Smith M, et al. Decision-making in communication aid recommendations in the UK: cultural and contextual influencers. Augment Altern Commun 2019;35:180-92. https://doi.org/10.1080/07434618.2019.1599066.
- Murray J, Lynch Y, Meredith S, Moulam L, Goldbart J, Smith M, et al. Professionals’ decision-making in recommending communication aids in the UK: competing considerations. Augment Altern Commun 2019;35:167-79. https://doi.org/10.1080/07434618.2019.1597384.
- Light J, McNaughton D. Supporting the communication, language, and literacy development of children with complex communication needs: state of the science and future research priorities. Assist Technol 2011;24:34-4. https://doi.org/10.1080/10400435.2011.648717.
- Van Niekerk K, Dada S, Tönsing K. Influences on selection of assistive technology for young children in South Africa: perspectives from rehabilitation professionals. Disabil Rehabil 2019;41:912-25. https://doi.org/10.1080/09638288.2017.1416500.
- Smith MM. Language development of individuals who require aided communication: reflections on state of the science and future research directions. Augment Altern Commun 2015;31:215-33. https://doi.org/10.3109/07434618.2015.1062553.
- Beukelman D, Mirenda P. Augmentative and Alternative Communication Supporting Children and Adults with Complex Communication Needs. Baltimore, MD: Paul H Brookes Publishing Co.; 2013.
- Barbour R. Doing Focus Groups. London: SAGE Publications Ltd; 2008.
- Serpentine EC, Tarnai B, Drager KDR, Finke EH. Decision making of parents of children with autism spectrum disorder concerning augmentative and alternative communication in Hungary. Communication Disord Q 2011;32:221-31. https://doi.org/10.1177/1525740109353938.
- Blackstone SW, Williams MB, Wilkins DP. Key principles underlying research and practice in AAC. Augment Altern Commun 2007;23:191-203. https://doi.org/10.1080/07434610701553684.
- O’Keefe BM, Kozak NB, Schuller R. Research priorities in augmentative and alternative communication as identified by people who use AAC and their facilitators. Augment Altern Commun 2007;23:89-96. https://doi.org/10.1080/07434610601116517.
- Sackett D, Straus SE, Richardson WS, Rosenberg W, Haynes BR. Evidence Based Medicine: How to Practice and Teach EBM. New York, NY: Churchill Livingstone; 1997.
- Murphy J. Talking Mats: speech and language research in practice. Speech Lang Ther Pract 1998.
- Murphy J, Cameron L. The effectiveness of Talking Mats® for people with intellectual disability. Br J Learning Disabil 2008;36:232-41. https://doi.org/10.1111/j.1468-3156.2008.00490.x.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Chung YC, Stoner JB. A meta-synthesis of team members’ voices: what we need and what we do to support students who use AAC. Augment Altern Commun 2016;32:175-86. https://doi.org/10.1080/07434618.2016.1213766.
- Thistle JJ, Wilkinson KM. Building evidence-based practice in AAC display design for young children: current practices and future directions. Augment Altern Commun 2015;31:124-36. https://doi.org/10.3109/07434618.2015.1035798.
- Webb EJD, Meads D, Lynch Y, Randall N, Judge S, Goldbart J, et al. What’s important in AAC decision making for children? Evidence from a best-worst scaling survey. Augment Altern Commun 2019;35:80-94. https://doi.org/10.1080/07434618.2018.1561750.
- Cheung KL, Wijnen BF, Hollin IL, Janssen EM, Bridges JF, Evers SM, et al. Using best-worst scaling to investigate preferences in health care. PharmacoEconomics 2016;34:1195-209. https://doi.org/10.1007/s40273-016-0429-5.
- Louviere JJ, Street D, Burgess L, Wasi N, Islam T, Marley AA. Modeling the choices of individual decision-makers by combining efficient choice experiment designs with extra preference information. J Choice Model 2008;1:128-64. https://doi.org/10.1016/S1755-5345(13)70025-3.
- Lynch Y, Goldbart J, Dada S, Moulam S, Murray J. A literature review on the language abilities of children and young adults who use aided AAC during language development. Commun Matters J 2018;32:16-20.
- Coast J, Al-Janabi H, Sutton EJ, Horrocks SA, Vosper AJ, Swancutt DR, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ 2012;21:730-41. https://doi.org/10.1002/hec.1739.
- Louviere JJ, Hensher DA, Swait JD. Stated Choice Methods: Analysis and Applications. Cambridge: Cambridge University Press; 2000.
- Orme B. MaxDiff System Technical Paper. Sawtooth Software Research Paper Series. Orem, UT: Sawtooth Software, Inc.; 2005.
- Holm S. A simple sequentially rejective multiple test procedure. Scan J Stat 1979:65-70.
- Rezaei A, Patterson Z. Detecting, Non-Transitive, Inconsistent Responses in Discrete Choice Experiments. Montréal, QC: CIRRELT; 2015.
- Beukelman D. Magic and cost of communicative competence. Augment Altern Commun 1991;7:2-10. https://doi.org/10.1080/07434619112331275633.
- Moorcroft A, Scarinci N, Meyer C. A systematic review of the barriers and facilitators to the provision and use of low-tech and unaided AAC systems for people with complex communication needs and their families. Disabil Rehabil Assist Technol 2019;14:710-31. https://doi.org/10.1080/17483107.2018.1499135.
- Munton T. Augmentative and Alternative Communication (AAC) Support in Scotland: A Review of the Research Literature and Cost Benefit Analyses. Edinburgh: NHS Education for Scotland; 2013.
- Light J, McNaughton D. Communicative competence for individuals who require augmentative and alternative communication: a new definition for a new era of communication?. Augment Altern Commun 2014;30:1-18. https://doi.org/10.3109/07434618.2014.885080.
- Light J, McNaughton D, Beukelman D, Fager SK, Fried-Oken M, Jakobs T, et al. Challenges and opportunities in augmentative and alternative communication: research and technology development to enhance communication and participation for individuals with complex communication needs. Augment Altern Commun 2019;35:1-12. https://doi.org/10.1080/07434618.2018.1556732.
- Calculator SN. Augmentative and alternative communication (AAC) and inclusive education for students with the most severe disabilities. Int J Inclusive Educ 2009;13:93-113. https://doi.org/10.1080/13603110701284656.
- Isakson CL, Burghstahler S, Ajato A. AAC, employment and independent living. Assist Technol Outcomes Benefits 2006;3:67-79.
- Department for Education and Department of Health and Social Care . SEND Code of Practice: 0 to 25 Years 2014.
- Williams MB, Krezman C, McNaughton D. ‘Reach for the stars’: five principles for the next 25 years of AAC. Augment Altern Commun 2008;24:194-206. https://doi.org/10.1080/08990220802387851.
- Coulter A, Stilwell D, Kryworuchko J, Mullen PD, Ng CJ, van der Weijden T. A systematic development process for patient decision aids. BMC Med Inform Decis Mak 2013;13. https://doi.org/10.1186/1472-6947-13-S2-S2.
- Collins Concise English Dictionary of the English Language 1978.
- Murray J, Lynch Y, Whittle H, Moulam L, Randall N. Westminster presentation: dissemination event supported by Policy Connect. Chaired by Lord Ramsbottom. Identifying appropriate symbol communication aids for children who are non speaking: enhancing clinical decision making. London: Portcullis House; 2018.
- Frankena TK, Naaldenberg J, Cardol M, Meijering JV, Leusink G, van Schrojenstein Lantman-de Valk HM. Exploring academics’ views on designs, methods, characteristics and outcomes of inclusive health research with people with intellectual disabilities: a modified Delphi study. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2016-011861.
- Ocloo J, Matthews R. From tokenism to empowerment: progressing patient and public involvement in healthcare improvement. BMJ Qual Saf 2016;25:626-32. https://doi.org/10.1136/bmjqs-2015-004839.
- Staniszewska S, Denegri S, Matthews R, Minogue V. Reviewing progress in public involvement in NIHR research: developing and implementing a new vision for the future. BMJ Open 2018;8. https://doi.org/10.1136/bmjopen-2017-017124.
- National Institute for Health Research (NIHR) . National Standards for Public Involvement in Research 2018.
- Moulam L, Meredith S, Whittle H, Lynch Y, Murray J, Mclaughlin H, et al. The Routledge International Handbook on Service User Involvement in Human Services Education and Research. London: Routledge; 2020.
- Gibson A, Britten N, Lynch J. Theoretical directions for an emancipatory concept of patient and public involvement. Health 2012;16:531-47. https://doi.org/10.1177/1363459312438563.
- Green G. Power to the people: to what extent has public involvement in applied health research achieved this?. Res Involve Engage 2016;2. https://doi.org/10.1186/s40900-016-0042-y.
- Snow R. What makes a real patient?. The BMJ Opinion 2016. https://blogs.bmj.com/bmj/2016/07/19/rosamund-snow-what-makes-a-real-patient/ (accessed 11 September 2020).
- Hickey G, Brearley S, Coldham T. Guidance on Co-producing a Research Project. Southampton: INVOLVE; 2018.
- Hammersley M, Atkinson P. Ethnography: Principles in Practice. London: Routledge; 2007.
- Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford: Oxford University Press; 2015.
- Burau V, Carstensen K, Fredens M, Kousgaard MB. Exploring drivers and challenges in implementation of health promotion in community mental health services: a qualitative multi-site case study using normalization process theory. BMC Health Serv Res 2018;18. https://doi.org/10.1186/s12913-018-2850-2.
- Pfadenhauer LM, Gerhardus A, Mozygemba K, Lysdahl KB, Booth A, Hofmann B, et al. Making sense of complexity in context and implementation: the Context and Implementation of Complex Interventions (CICI) framework. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0552-5.
- May CR, Mair F, Finch T, MacFarlane A, Dowrick C, Treweek S, et al. Development of a theory of implementation and integration: normalization process theory. Implement Sci 2009;4. https://doi.org/10.1186/1748-5908-4-29.
- May CR, Johnson M, Finch T. Implementation, context and complexity. Implement Sci 2016;11. https://doi.org/10.1186/s13012-016-0506-3.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: SAGE Publications Ltd; 1985.
- Brett J, Staniszewska S, Mockford C, Herron-Marx S, Hughes J, Tysall C, et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect 2014;17:637-50. https://doi.org/10.1111/j.1369-7625.2012.00795.x.
- Beckett K, Farr M, Kothari A, Wye L, le May A. Embracing complexity and uncertainty to create impact: exploring the processes and transformative potential of co-produced research through development of a social impact model. Health Res Policy Syst 2018;16. https://doi.org/10.1186/s12961-018-0375-0.
- Staley K, Barron D. Learning as an outcome of involvement in research: what are the implications for practice, reporting and evaluation?. Res 2019;5. https://doi.org/10.1186/s40900-019-0147-1.
- Dovey-Pearce G, Walker S, Fairgrieve S, Parker M, Rapley T. The burden of proof: the process of involving young people in research. Health Expect 2019;22:465-74. https://doi.org/10.1111/hex.12870.
- L Moulam, M Jayes. The Rhetoric and Reality of Co-Producing Research With Those Who Use AAC n.d.
- L Moulam, M Jayes, J Murray, S Judge, S Meredith, H Whittle. Public Involvement in Research: The I-ASC Project As a Context for Exploring Public Involvement Possibilities 2019.
Appendix 1 Best–worst scaling child characteristics and descriptions
| Child-related characteristic | Description |
|---|---|
| Access to professional AAC support | Access to professional support such as teacher, speech-language therapist or others with knowledge and skills in AAC |
| Attention level | Ability to attend to tasks and sustain attention |
| Child’s determination and persistence | Motivation and persistence to communicate (or not) |
| Child’s receptive and expressive language abilities | Ability to understand and produce language (through aided or unaided means) |
| Communication ability with aided AAC | The communication functions and roles a child can carry out using aided AAC system |
| Educational stage | The child’s current education setting and stage |
| Functional visual skills | Ability to use gaze to eye point for communication |
| History of aided AAC use | What is the child’s experience to date with aided AAC systems |
| Insight into own communicative skills | The child’s awareness and understanding of their own communicative skills |
| Level of fatigue | Whether fatigue impacts on aided AAC |
| Level of learning ability | Ability to learn and retain information and problem solve (includes the child’s developmental level) |
| Literacy ability | Ability to read and write (aided or unaided) |
| Mobility | Ability to move independently or with assistance, with or without powered or partner propelled wheelchairs |
| Physical abilities for access | Ability to use direct or indirect access methods to control AAC system |
| Predicted future needs and abilities | Based on all the information available what are the predicted or expected future needs and abilities of the child that could impact on AAC |
| Presence of additional diagnoses | Whether the child has another diagnosis in addition to the condition associated with the need for AAC, for example hearing, vision, epilepsy, behavioural issues |
| Primary diagnosis | The main medical diagnosis the child associated with the need for AAC |
| Speech skills and intelligibility | Ability to use speech to communicate |
| Support for AAC from communication partners | Includes the attitudes, skills and knowledge of people close to the child that will impact on use and learning of AAC |
Appendix 2 Best–worst scaling augmentative and alternative communication device attributes and descriptions
| AAC device attribute | Description |
|---|---|
| Additional assistive technology functions | Whether the aided AAC system supports other assistive technology functions, such as offering computer features |
| Appearance | Appearance and feel including the hardware and the interface |
| Battery life | How long the battery lasts between charges |
| Consistency of layout and navigation | Consistency of layout of symbols or text on pages |
| Cost | Cost of purchase including warranty or repair |
| Durability and reliability | How robust the aided AAC system is, how frequently or easily it stops working |
| Ease of customisation | How intuitive and easy is it to add and change vocabulary and customise other features such as changing the volume |
| Ease of mounting on a range of equipment | The compatibility of the aided AAC system with different mounting systems and to be used with different equipment (e.g. power chair) |
| Graphic representation | Type of symbol or text used |
| Number of cells per page | The number of cells or locations for symbols or text on each page in an aided AAC system |
| Number of key presses required to generate symbol or text output | Number of selections required to generate symbol or text output |
| Portability | Ease of carrying or moving the aided AAC system |
| Range of access methods | Range of access methods offered to allow control of the aided AAC system |
| Size of output vocabulary | The size of the output vocabulary available within the aided AAC system |
| Supplier support | Technical and training support provided by AAC device company |
| Type of vocabulary organisation | Format used to organise the vocabulary within the aided AAC system for example |
| Vocabulary or language package(s) | Preprogrammed vocabulary set(s) |
| Voice | The type and quality of voice output provided by the aided AAC system |
Appendix 3 Demographic variables included in regression models
| Demographic group | Number (%) in group |
|---|---|
| Participants aged ≥ 35 years | 62 (67.4) |
| Participants with ≥ 5 years of AAC experience | 64 (69.6) |
| Participants with a professional background as a SLT | 66 (71.7) |
| Participants whose role is at least 60% AAC related | 50 (54.3) |
| Participants who work in an educational setting | 71 (77.1) |
| Participants who work in a health-care setting | 58 (63.0) |
| Participants who work in a person’s own home | 43 (46.7) |
| Participants who reported neuromuscular conditions as one of the three most common diagnoses they see | 71 (77.2) |
| Participants who report intellectual/developmental delay as one of the three most common diagnoses they see | 66 (71.7) |
| Participants who report autism as one of the three most common diagnoses they see | 59 (64.1) |
Appendix 4 Pairwise comparison of relative importance scores for best–worst scaling child characteristics
| Characteristic | Support for AAC from communication partners | Communication ability with aided AAC | Child’s determination and persistence | Physical abilities for access | Predicted future needs and abilities | Level of learning ability | Insight into own communicative skills | Attention level | Access to professional AAC support | Speech skills and intelligibility | Functional visual skills | History of aided AAC use | Presence of additional diagnoses | Level of fatigue | Literacy ability | Educational stage | Primary diagnosis | Mobility |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Child’s receptive and expressive language abilities | – | – | – | a | a | a | a | a | a | a | a | a | a | a | a | a | a | a |
| Support for AAC from communication partners | – | – | – | a | a | a | a | a | a | a | a | a | a | a | a | a | a | |
| Communication ability with aided AAC | – | – | a | a | a | a | a | a | a | a | a | a | a | a | a | a | ||
| Child’s determination and persistence | – | a | a | a | a | a | a | a | a | a | a | a | a | a | a | |||
| Physical abilities for access | – | – | a | a | a | a | a | a | a | a | a | a | a | a | ||||
| Predicted future needs and abilities | – | – | – | – | a | a | a | a | a | a | a | a | a | |||||
| Level of learning ability | – | – | – | – | a | a | a | a | a | a | a | a | ||||||
| Insight into own communicative skills | – | – | – | – | a | a | a | a | a | a | a | |||||||
| Attention level | – | – | – | – | – | a | a | a | a | a | ||||||||
| Access to professional AAC support | – | – | – | a | a | a | a | a | a | |||||||||
| Speech skills and intelligibility | – | – | – | a | a | a | a | a | ||||||||||
| Functional visual skills | – | – | – | – | a | a | a | |||||||||||
| History of aided AAC use | – | – | – | – | – | a | ||||||||||||
| Presence of additional diagnoses | – | – | – | – | a | |||||||||||||
| Level of fatigue | – | – | – | a | ||||||||||||||
| Literacy ability | – | – | – | |||||||||||||||
| Educational stage | – | – | ||||||||||||||||
| Primary diagnosis | – |
Appendix 5 Pairwise comparison of relative importance scores for best–worst scaling augmentative and alternative communication device attributes
| Attribute | Consistency of layout and navigation | Ease of customisation | Durability and reliability | Type of vocabulary organisation | Number of key presses required | Size of output vocabulary | Range of access methods | Number of cells per page | Portability | Graphic representation | Battery life | Supplier support | Ease of mounting on a range of equipment | Cost | Additional assistive technology functions | Voice | Appearance |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vocabulary or language package(s) | – | – | – | – | a | a | a | a | a | a | a | a | a | a | a | a | a |
| Consistency of layout and navigation | – | – | – | – | a | a | a | a | a | a | a | a | a | a | a | a | |
| Ease of customisation | – | – | – | a | a | a | a | a | a | a | a | a | a | a | a | ||
| Durability and reliability | – | – | a | a | a | a | a | a | a | a | a | a | a | a | |||
| Type of vocabulary organisation | – | a | a | a | a | a | a | a | a | a | a | a | a | ||||
| Number of key presses required to generate symbol or text output | – | – | – | a | a | a | a | a | a | a | a | a | |||||
| Size of output vocabulary | – | – | – | – | – | a | a | a | a | a | a | ||||||
| Range of access methods | – | – | – | – | a | a | a | a | a | a | |||||||
| Number of cells per page | – | – | – | – | – | a | a | a | a | ||||||||
| Portability | – | – | – | – | a | a | a | a | |||||||||
| Graphic representation | – | – | – | a | a | a | a | ||||||||||
| Battery life | – | – | a | a | a | a | |||||||||||
| Supplier support | – | – | a | a | a | ||||||||||||
| Ease of mounting on a range of equipment | – | – | – | a | |||||||||||||
| Cost | – | – | – | ||||||||||||||
| Additional assistive technology functions | – | – | |||||||||||||||
| Voice | – |
Appendix 6 Beneficiaries of the I-ASC heuristic
| Group | Subgroups (service sectors) | What they gain from the I-ASC heuristic |
|---|---|---|
| Direct beneficiaries | ||
| Children and young adults (individuals who use, or could use, AAC) |
|
Resources to support:
|
| Families and support network (those around the individual) |
|
Resources to support:
|
| Professionals (professionals who are or should be available to children and young people with AAC needs) |
|
Resources to support considering decisions:
|
| Indirect beneficiaries | ||
| Others |
|
|
|
Further education Higher education |
|
|
| Communication aid developers and suppliers |
|
|
| Researchers and HE |
|
|
Appendix 7 Revised thematic framework: public involvement
| Global themes | Organising themes | Basic themes |
|---|---|---|
| Nature of PI in I-ASC | Purpose of PI |
|
| What was the co-researcher role? |
|
|
| Team composition: recruitment, diversity and experience |
|
|
| Collaboration/partnership working: facilitators/barriers, team relationships, inclusion, individualised support, flexibility |
|
|
| Tokenism/box-ticking |
|
|
| Resources used to enable PI | Time |
|
| Training and support within team to enable PI |
|
|
| External support |
|
|
| Consumables |
|
|
| Equipment |
|
|
| Hidden costs |
|
|
| Benefits of PI | Benefits to services |
|
| Benefits to service users and society |
|
|
| Benefits to knowledge about how to do research |
|
|
| Benefits to knowledge about the clinical topic |
|
|
| Benefits to team working |
|
|
| Ambivalence and uncertainty about benefits |
|
|
| Challenges of PI | Challenges for researchers |
|
| Challenges for people who use AAC and their carers |
|
|
| Facilitators of successful PI | Establishing the co-researcher role |
|
| Planning |
|
|
| Team ethos |
|
Glossary
- Assistive technology co-ordinator
- A role commonplace in school settings that supports a generic review and implementation of all aspects of technology, including augmentative and alternative communication technologies.
- Augmentative and alternative communication
- The international term for various methods of communication that can support speech intelligibility and are used to get around problems with ordinary speech. Augmentative and alternative communication includes simple systems, such as pictures, gestures and pointing, as well as more complex techniques involving powerful computer technology.
- Augmentative and alternative communication device
- Typically, an electronic communication aid with a voice output option.
- Augmentative and alternative communication system
- A system can be an unaided (e.g. sign system), an aided non-electronic (e.g. communication chart) or an aided electronic (e.g. computer-based) communication arrangement.
- Communication aid
- Generically, any type of aided augmentative and alternative communication system.
- Graphic symbol
- A visual representation of a concept or a written word. Each symbol may be iconic or ideographic. There are several graphic symbol communication systems in use, for example the Picture Communication System.
- Symbol communication
- This type of communication uses symbols, rather than written words, within the communication aid.
- Symbolic-aided language
- A graphic representational system with a symbol-based rather than written word-based focus.
List of abbreviations
- AAC
- augmentative and alternative communication
- BWS
- best–worst scaling
- DCE
- discrete choice experiment
- I-ASC
- Identifying Appropriate Symbol Communication
- NIHR
- National Institute for Health Research
- OR
- odds ratio
- PRISMA
- Preferred Reporting Items for Systematic reviews and Meta-Analyses
- REC
- Research Ethics Committee
- RIS
- relative importance score
- SLP
- speech–language pathologist
- SLT
- speech and language therapist
- WP
- work package