

Notes
Article history
This issue of the Health Services and Delivery Research journal series contains a project commissioned/managed by the Methodology research programme (MRP). The Medical Research Council (MRC) is working with NIHR to deliver the single joint health strategy and the MRP was launched in 2008 as part of the delivery model. MRC is lead funding partner for MRP and part of this programme is the joint MRC–NIHR funding panel ‘The Methodology Research Programme Panel’.
To strengthen the evidence base for health research, the MRP oversees and implements the evolving strategy for high-quality methodological research. In addition to the MRC and NIHR funding partners, the MRP takes into account the needs of other stakeholders including the devolved administrations, industry R&D, and regulatory/advisory agencies and other public bodies. The MRP funds investigator-led and needs-led research proposals from across the UK. In addition to the standard MRC and RCUK terms and conditions, projects commissioned/managed by the MRP are expected to provide a detailed report on the research findings and may publish the findings in the HS&DR journal, if supported by NIHR funds.
The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2021. This work was produced by Michie et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2021 Queen’s Printer and Controller of HMSO
Chapter 1 General introduction
Improving health by changing behaviour
Addressing many of the huge challenges facing the world today will require changes in behaviour at all levels, from governments to individual citizens. Whether it be climate change and environmental degradation, war and other conflicts, epidemic and pandemic diseases, or poverty and inequalities, the solution often lies in changing deeply ingrained patterns of behaviour. Many of the world’s leading causes of mortality result from diseases, such as cardiovascular disease, lung cancer, stroke and human immunodeficiency virus (HIV), where behaviour contributes significantly to exposure to risk – smoking, poor diet, excessive alcohol consumption, physical inactivity and unprotected sex being cases in point. 1,2 In Western societies, such behaviour-related diseases contribute to approximately half of premature deaths. 3–6 Population health can also suffer significantly from a lack of certain behaviours (e.g. people not accessing health care when needed, not engaging with screening or vaccination programmes and not adhering to medication or other treatments and advice). The behaviour of health-care providers is also critical to population health, which can be significantly impaired if health professionals do not implement evidence-based practice, such as ensuring that the prescription and use of antibiotics is necessary and appropriate,6–9 or fail to follow infection prevention and control guidelines. 10
As well as reducing premature mortality and disability, behaviour change interventions have the potential to reduce health-care expenditure. 11,12 The latest analysis of the global burden of disease concluded that investing in preventing and controlling these diseases offers a high return for countries at all income levels and contributes to economic growth. 13 Interventions that target health-related patterns of behaviours have the potential to transform the health of populations, often at low cost,12–14 and there is good evidence that interventions have a positive impact on both health and equity across a number of areas. 15,16 Despite this, the effects of these interventions tend to be small, there is wide variation in effectiveness across contexts and the effects are often not maintained long term. 17,18 The effects are also usually not at the scale required to bring about a population-level impact (see Cochrane database for examples19–21).
Changing health-related patterns of behaviour across diverse populations and settings is not easy; it requires complex interventions (i.e. interventions that contain several interacting componets22) that target multiple levels within systems (e.g. communities or organisations) and can sustain their impact over time. 16 This in turn requires sophisticated methods for developing and evaluating interventions, including how to draw on theory and how to report interventions to maximise replicability and potential for faithful implementation. At present, authors do not reliably provide explicit reporting on the theoretical propositions underpinning interventions, their development and their evaluation. 15,22,23 Where theory-based interventions are reported, there is often little detail about how the theory was applied in the development or evaluation phase. 24–26 This is partly due to the paucity of methods to support this process. Methods are needed to support intervention reporting to move beyond describing them simply as being theory informed27 towards reporting how and why theoretical principles are tested. 28–31 One of the areas in which progress could be made is in the methods for intervention development and for accumulating knowledge across intervention evaluations. Progress has been made in improving, harmonising and standardising the reporting of interventions aimed at changing behaviour32–36 and their theoretical underpinnings. 37–40 This includes specifying interventions in enough detail to allow replication and to do this using consistent and shared terminology. 15,17,41,42
Behaviour change techniques: essential components of behaviour change interventions
Behavioural interventions are often delivered as part of complex systems that include a number of behaviour change techniques (BCTs). BCTs are conceptualised as fine-grained intervention components that on their own have the potential, in the right circumstances, to bring about behaviour change. 17,32,43,44 The Behaviour Change Technique Taxonomy version 1 (BCTTv1) is a formal, standardised system used to characterise behaviour change interventions, developed with input from 400 experts across 12 countries. 17,42 It consists of 93 BCTs organised into 16 groupings and provides labels and definitions of intervention techniques. This extensive shared vocabulary enables researchers and others to specify and describe the components of behavioural interventions, allowing better reporting and facilitating accurate replication and implementation of interventions. The BCTTv1 incorporates a number of cross-behaviour BCT taxonomies33,34 and some behaviour-specific taxonomies for physical activity,36 alcohol use,35 smoking45 and condom use. 39 The BCTTv1 has been used to specify the potentially ‘active ingredients’ in many types of intervention, for example those aiming to change physical activity and dietary behaviours,40,46 oral hygiene behaviours,47 hazardous and harmful drinking,48 sexual health behaviours,49–51 blood pressure control/management behaviours,52 antibiotic prescribing53,54 and type 2 diabetes preventative behaviours. 55
As well as being widely used for intervention reporting, the BCTTv1 is used to support intervention design and development and to synthesise information across intervention evaluations. Systematic reviewers have used it to identify BCTs in published reports of intervention evaluations and to generate evidence of the effectiveness of not only the intervention as a whole, but also the component techniques, either individually or as theoretical combinations that work synergistically. 25,26,56–59 This approach is recommended by the National Institute for Health and Care Excellence (NICE) in its guidance that research should investigate which BCTs are effective in promoting the initiation and maintenance of behaviour change. 15 Studies of published interventions have found that interventions using BCT combinations were more effective than those that used only one BCT. 60–62 For example, interventions that combine self-monitoring with BCTs that support self-regulation of behaviour, such as goal-setting or action-planning, have been found to be associated with improved effectiveness. 60 More than 350 articles reporting interventions coded by BCTTv1 are available for researchers and others to use in a searchable database, which is updated as researchers add to it (see www.bct-taxonomy.com/interventions; accessed 1 March 2020).
Specifying intervention content by BCTs has transformed methods for reporting the content of behaviour change interventions, which facilitates greater precision and consistency in research. 42,63 However, identifying which specific BCTs or BCT combinations are likely to be effective for a particular behaviour in its context is challenging. A review of 135 studies examined methods used to do this and found that, although a range of methods existed, they all have limitations. 64 The methods were (1) experimental manipulation of BCTs (where it is important to specify BCTs in the interventions, both in the experimental and in the control groups22,37,65–67), (2) observational studies comparing outcomes in the presence or absence of BCTs, (3) meta-analyses of BCT comparisons, (4) meta-regressions evaluating effect sizes with and without specific BCTs, (5) reviews of BCTs found in effective interventions and (6) meta-classification and regression trees (CART).
From the review findings, Michie et al. 68,69 concluded that there are limitations to all of these methods for drawing conclusions about BCT efficacy and that research in this area would be strengthened by triangulation of methods. Similarly, policy-makers and practitioners, when making decisions about what combination of BCTs to use in an intervention, should draw on findings across different methods. Another approach that would provide a fuller understanding of the impact that an intervention has on behaviour and health, and strengthen work in this area, is to link BCTs to other intervention features in an ontology of behaviour change interventions. 68,69 Research is currently under way to develop a Behaviour Change Intervention Ontology to support this approach (see www.humanbehaviourchange.org; accessed 1 March 2020).
An important aim of this work is to increase our knowledge of the mechanisms of action (MoAs) through which the BCTs have their effect. The need for this has been recognised beyond behavioural science, for example, by the Cochrane Collaboration’s Effective Practice and Organisation of Care (EPOC) Group70 and by NICE. 71,72 By linking BCTs to their hypothesised MoAs as described in behavioural theory, researchers and intervention designers may target MoAs more deliberatively, leading to interventions that are more likely to be effective. In addition, knowledge of these links makes it easier for investigators to design studies that can evaluate the processes underlying effective interventions and thus test and advance theory. Furthermore, it enables a theoretical understanding of interventions that have not been, or at least have not been reported as being, based on theory.
Behaviour change theory: specifying the mechanisms of action of behaviour change
Theories of behaviour change summarise accumulated knowledge about how behaviour change occurs, as well as explaining variation across behaviours, settings and populations. They have the potential to be useful tools in designing interventions to change behaviour, if applied systematically and appropriately. 28,29,37,73,74 This is reflected, for example, in the UK Medical Research Council’s framework for designing and evaluating complex interventions22 and the Intervention Mapping framework75 for planning health promotion programmes.
Theories of behaviour change attempt to explain and predict when, why and how behaviours do or do not occur and change. This involves proposing MoAs, defined as ‘the processes through which a behaviour change technique affects behaviour’, and moderators of change along various causal pathways. MoAs are theoretical constructs from theories of behaviour and behaviour change, such as ‘self-efficacy’ or ‘knowledge’, that mediate the effect of a BCT on a behaviour. By contrast, moderators are variables such as the population or the setting that may modify the effect of a BCT on a behaviour. As part of a multidisciplinary consensus exercise, theory was defined as:
A set of concepts and/or statements with specification of how phenomena relate to each other [providing] an organising description of a system that accounts for what is known, and explains and predicts phenomena.
There are numerous formal theories, which are more or less generalisable across behaviours, settings and populations. They vary in complexity and range of application, and many overlap. A multidisciplinary literature review led by psychologists, sociologists, anthropologists and economists identified 83 theories of behaviour and behaviour change, containing > 1700 theoretical constructs. 30,76 Because the review had strict inclusion criteria, there are likely to be many other relevant theories not included. Despite the abundance of theories, there is a paucity of guidance for researchers and intervention designers as to how they should decide about which theory or theories to draw on and how they should apply them to intervention design or evaluation. The result is that a relatively small number of theories dominate the field, and often they are poorly applied or their application is poorly reported. 26,77
Efforts to help in this process include the theoretical domains framework (TDF), which is an integrative framework of theoretical constructs relevant to understanding and changing behaviour. The framework was developed to make theories more usable and accessible to an interdisciplinary audience. 38,78,79 The TDF specifies 14 theoretical domains, each of which includes several theoretical constructs that are similar in definition but derive from different theories. The TDF has been used in intervention development and design,31,80,81 as well as in systematic reviews. 82–84 Although there are integrative frameworks, such as the TDF, and general intervention development frameworks, such as intervention mapping,22,75,85,86 a consensus is needed about how the individual MoAs specified in these theories can be linked with particular BCTs. 30,37 This would allow interventions to be developed in a way that was more precisely informed by theory than is generally current practice and would enable the theoretical understanding of interventions that were found to be effective but were not explicitly developed based on theory. However, we do not yet have an agreed method for systematically linking BCTs to individual hypothesised MoAs.
Linking behaviour change techniques with theoretical mechanisms of action
Although the BCTTv1 provides a shared language with which to describe intervention content, it does not directly specify which MoAs these BCTs target in the intervention. For interventions to have a good chance of being effective, their active components (i.e. BCTs) should target relevant MoAs.
There are a large number of BCTs and theories and models of behaviour and behaviour change. However, research investigating links between BCTs and MoAs has been sparse, despite a range of frameworks for developing behaviour change interventions [e.g. intervention mapping,87 precede–proceed model,88 the behaviour change wheel (BCW)89]. The importance of understanding the processes through which behaviour change may occur (a theory of change) has been recognised internationally, for example by the Cochrane Collaboration’s EPOC Group,70 NICE’s Public Health guidelines in the UK71,72 and the Science of Behavior Change programme of research in the USA. The Science of Behavior Change programme of research is building evidence about a discrete set of interventions by experimentally testing methods for changing specified MoAs (see https://commonfund.nih.gov/behaviorchange/index; accessed 1 June 2019). There is a need for many programmes of research to accumulate evidence about the processes by which the full range of BCTs have their effects; this will maximise our potential to develop effective interventions.
Preliminary work identifying links between BCTs and MoAs has been conducted in both primary research and evidence syntheses. 15,34,68,75,88,90 For example, a set of 35 BCTs has been mapped to theoretically derived domains in the TDF. 34 This approach has been used in developing behaviour change interventions31,34 and to identify theoretical mediators of change within process evaluations. 91–93 Associations between BCTs and theory have also been investigated in evidence syntheses such as systematic literature reviews and meta-analyses,26,94 and in primary research in relation to changing particular mechanisms of action, such as self-efficacy95–98 and behavioural intention. 99 Guidance about selecting BCTs to target processes of change have been developed in the form of intervention development frameworks (e.g. the BCW,85 Intervention Mapping75 and the TDF78,79). However, these are at a general level and do not include guidance or evidence about links between specific BCTs and MoAs.
This work shows the interest in and need for developing links between BCTs and their MoAs. However, there is no transparent, agreed method for identifying these links. This is needed to provide the tools for those (1) developing ‘theory-based’ interventions and (2) attempting to make theoretical sense of interventions that specify the BCTs used in interventions but without referring to theory and/or that specify MoAs but without identifying specific BCTs in interventions. Achieving this would enable evidence accumulation to continue to advance more systematically and efficiently.
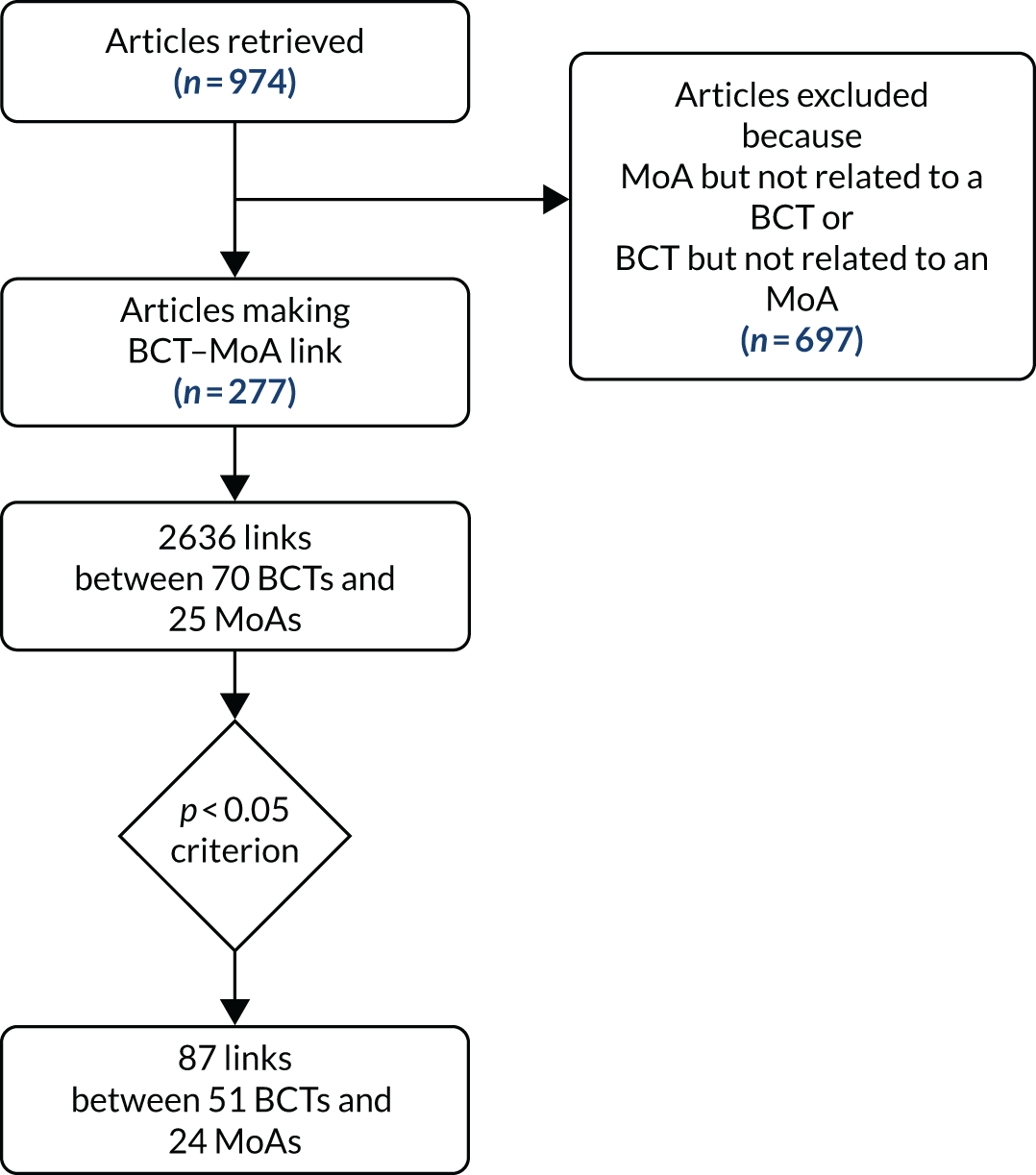
In this report, we present a programme of research using a range of methods to identify and operationalise links between behaviour change techniques and (1) specific mechanisms of action and (2) behavioural theories. 100 These are links as reported by behaviour change researchers in developing and/or evaluating behaviour change interventions, and as judged by experts in a consensus exercise. These links are therefore hypothesised rather than necessarily tested and shown to be robustly supported by evidence. It thus provides a valuable resource for researchers as to which links are most and least likely to be effective in changing behaviour through changing a particular MoA. The links are presented in the form of matrices and interactive heatmaps that allow data from three studies to be easily extracted for each link and additional data or comments to be added by users (https://theoryandtechniquetool.humanbehaviourchange.org/tool). The data come from two complementary sources. In study 1, the data are derived from a synthesis of published literature, which encapsulates thinking in past peer-reviewed work. Study 2 is of expert consensus, which encapsulates current thinking. Study 3 triangulates the data from the previous two studies, providing a reconciliation of findings about the hypothesised links between behaviour change techniques and their MoAs. Study 4 examines links between groups of BCTs and theories as a whole. The sequence of studies in this research programme is shown in the flow diagram in Figure 1. The matrices of links resulting from these studies will provide a methodological online resource available to behaviour change scientists and intervention designers, providing a more efficient and systematic way to identify and evaluate the theoretical processes hypothesised to underlie BCTs.
FIGURE 1.
Flow diagram outlining the sequence of studies.

Aims
-
To identify and integrate hypothesised links between (1) BCTs and MoAs and (2) BCTs and behavioural theories.
-
To generate a freely available, searchable online resource to support theory-based intervention development and evaluation.
Objectives
-
Intervention development and evaluation:
-
To triangulate literature analysis and expert consensus to identify links between BCTs and both MoAs and behaviour change theories.
-
To graphically represent the strength of BCT and MoA links through searchable matrices of the findings from literature synthesis, expert consensus and triangulation.
-
-
Efficient evidence accumulation:
-
To create an accessible and freely available online resource that allows researchers to share data, publications and conference reports relevant to individual links.
-
To seek engagement and collaborations with international scientific and intervention development communities.
-
The objectives of each study are listed below.
Study 1: identifying the links between behaviour change techniques and mechanisms of action described by authors of published intervention articles101
Objectives
-
Determine the number of times BCT–MoA links are described in studies.
-
Determine which specific BCTs are most frequently described as targeting specific MoAs.
-
Determine which specific MoAs are most frequently described as being affected by specific BCTs.
-
Determine whether or not specific BCT–MoA links demonstrate greater frequency than anticipated based on the average number of times the BCT–MoA link is described.
Study 2: an expert consensus approach to linking behaviour change techniques and mechanisms of action102
Objectives
-
Develop consensus on the MoAs through which BCTs may affect behaviour (i.e. links).
-
Develop consensus on the MoAs through which BCTs may not affect behaviour (i.e. non-links).
-
Develop consensus on the specificity of BCT–MoA links, specifically whether BCTs affect behaviour through one specific, or multiple, MoAs.
The study additionally sought to:
-
Determine for which BCT–MoA links experts did not reach consensus.
-
Determine whether or not all BCTs may be linked with at least one MoA.
-
Determine whether or not all MoAs may be linked with at least one BCT.
Study 3: triangulating evidence of links between behaviour change techniques and mechanisms of action from literature synthesis and expert consensus103
Objectives
-
Investigate the agreement between the studies in study 1101 and study 2102 by developing BCT–MoA link matrices to:
-
Determine the extent of agreement between the two studies for individual and overall MoAs.
-
Determine BCT–MoA links that for both studies were greater than the pre-set criteria as being either linked (i.e. met criteria for a link in both expert consensus and literature synthesis) or not linked (i.e. met criteria for a non-link in the expert consensus and the literature synthesis).
-
Determine BCT–MoA links for which agreement was not reached.
-
Utilise ‘reconciliation experts’ to resolve BCT–MoA links for which agreement was not reached.
-
Study 4: do combinations of behaviour change techniques that occur frequently in interventions reflect underlying theory?104
Objectives
-
Determine the extent to which BCTs are frequently used together.
-
Determine how experts link groups of BCTs to specific theories.
-
Determine whether or not the theories that experts most frequently linked to specific BCT groups found across interventions are comparable to the theories that authors explicitly reported within interventions using similar groups of BCTs.
Chapter 2 Identifying the links between behaviour change techniques and mechanisms of action described by authors of published intervention articles
Abstract
Objective
To identify the links between BCTs and MoAs, as described in published intervention articles.
Methods
Two coders extracted links between BCTs and MoAs from 277 behaviour change intervention articles. The relative frequency of these was examined through a series of one-tailed binomial tests.
Results
Seventy-seven BCTs were coded. Seventy BCTs were linked to at least one MoA, with links present for 25 of 26 possible MoAs. In total, 2636 BCT–MoA links were extracted from the intervention articles, with up to five MoAs linked to each BCT (mean = 1.71, range 1–5) and up to eight BCTs linked to each MoA (mean = 3.63, range 1–8).
Conclusions
The database of BCT–MoA links identified in this study provides a resource that can be used for intervention development (e.g. to identify BCTs that can be used to target relevant MoAs) and evaluation (e.g. to advance our understanding of theory by elucidating the processes of change underlying effective interventions).
Introduction
Cumulative progress in behavioural science could be improved by advancing our understanding of the processes through which behaviour change interventions have their effects. As outlined in Chapter 1, behaviour change interventions consist of BCTs that are the smallest, irreducible components, or the potentially ‘active ingredients’ that can bring about change in behaviour. The theoretical constructs that represent the processes by which these BCTs change behaviour are termed MoAs. Identifying links between individual BCTs and MoAs could aid intervention design (e.g. by enabling us to identify relevant intervention strategies that influence a particular MoA) and evaluation (e.g. by allowing us to better understand the processes of change in successful interventions).
A number of sources of evidence can inform our understanding of these links. One valuable source of evidence is the published intervention literature. By examining this literature, we can examine links described or hypothesised by intervention authors and/or links that have been empirically tested (e.g. through experimental studies and meta-analyses). Although the available evidence for the latter (i.e. that resulting from empirical tests of individual links) appears to be limited,26 extracting and examining researchers’ descriptions of links may provide a useful data set. For example, where published interventions describe the rationale behind BCT selection, including the MoA(s) a specific BCT is believed to target (e.g. based on a theoretical model, previous research, clinical guidelines), this can shed light on researchers’ thinking and inform our understanding of BCT–MoA links.
Any one intervention may include a number of BCT–MoA links, as behavioural interventions tend to be delivered as part of a complex system, and can involve a number of co-occurring BCTs. BCTs can enable behaviour change by augmenting factors that facilitate change, or by mitigating factors that inhibit change. For example, in a smoking cessation intervention, researchers may hypothesise that providing an individual with emotional social support will change behaviour by increasing motivation. Similarly, persuading someone about their capabilities may be hypothesised to change behaviour by decreasing negative emotions such as shame or worry.
In the above example, motivation and negative emotions can be conceptualised as MoAs. In this context, MoAs are constructs from theories of behaviour and behaviour change that can be viewed as ‘mediating’ the effects of interventions. They may be constructs that relate to the individual (i.e. psychological processes, e.g. self or identity) or to the social or physical environment (e.g. social influences from peers).
The rationale underlying the selection of BCTs is not clearly described in every intervention article and there is also not always a clear, linear pathway for how BCT X changes behaviour by changing MoA Y. However, given the increasingly available array of tools for intervention development and reporting,17,18,41 many of which offer some form of guidance regarding which BCTs can target which MoAs, it is reasonable to assume that there is a corpus of literature from which BCT–MoA links can be identified.
This study aimed to identify the hypothesised links between BCTs and MoAs to inform (1) how researchers can target MoAs of interest (i.e. informing an understanding about which BCTs to select) and (2) explanations of intervention effects (i.e. informing an understanding of the MoAs through which BCTs are having their effects). We also aimed to understand whether or not any BCT–MoA links were described with a relatively high level of frequency in the included corpus of intervention articles. Therefore, based on the published intervention literature, this study sought to determine:
-
the number of times BCT–MoA links are described by authors within studies
-
which specific BCTs are most frequently described as targeting specific MoAs
-
which specific MoAs are most frequently described as being influenced by specific BCTs
-
whether or not specific BCT–MoA links are seen with greater frequency than anticipated based on the average number of times the BCT–MoA link is described.
Method
Overview of search methods
We set out to collate published behaviour change intervention articles that reported the development and/or evaluation of an intervention, where there was at least one explicit link between a BCT and a MoA.
To do this efficiently (given time and resource constraints), our search strategy prioritised intervention articles where (1) intervention authors described BCTs using a taxonomy within the article, or systematic reviewers had retrospectively identified BCTs and (2) researchers had used a theoretical framework to identify/describe MoAs. Although we did not set out to conduct a systematic review, we developed a search strategy that we considered broad enough to capture a range of articles, covering a variety of behavioural domains, years and countries. A systematic review was not conducted as the main aim of the study was to locate a corpus of literature in which BCT–MoA links were most likely to be identifiable, and not to address a research question (e.g. to test how frequently or infrequently such links can be found in a representative body of literature), which would require a systematic review methodology. Additionally, it was considered infeasible given time and resource constraints. Our search strategy thus included (1) electronic (database) searches, (2) e-mails to behavioural science experts and (3) reviews of the reference lists of relevant systematic reviews. More detail on each of these is provided below. Note that the search was not explicitly restricted to health behaviour change interventions. However, because of the nature of our search strategy, all of the included papers were health related.
Searching electronic databases
We searched for intervention articles that had cited any of five published BCT taxonomies,17,33,35,36,45 the Theory Coding Scheme77 or the TDF. 38,78 This was done to identify articles that were likely to have explicitly described BCTs and/or MoAs. These ‘forward-searches’ were conducted in Web of Science and Google Scholar.
E-mailing behavioural science experts
The project’s International Advisory Board (IAB) (see Appendix 1), which included 42 members from 10 countries, was contacted and asked to send relevant intervention articles. We also e-mailed several national and international professional and scientific societies including the US Society for Behavioral Medicine, the European Health Psychology Society, UK Society for Behavioural Medicine and the British Psychological Society’s Division of Health Psychology. Researchers who received the request were also asked to relay the e-mail to relevant colleagues in their networks.
Reviewing interventions included in systematic reviews
Where the above search methods led to the identification of a relevant systematic review (i.e. one in which BCTs and/or theory had been coded), we reviewed the associated reference lists of included intervention articles. This included the review by NICE published as part of its guidance on behaviour change. 15 We downloaded and screened all relevant intervention articles identified through these reviews.
Inclusion criteria
Articles were included if they described a behaviour change intervention and if they included at least one identifiable link between a BCT and a MoA. Such links could be described in the text or in a table or figure provided that the MoA was clearly described as the process through which the authors hypothesised that the BCT would change behaviour. For example, an article would be included in which the intervention asked participants to reflect on their identity as a ‘smoker’ and hypothesised that this technique would change behaviour by changing participants’ self-image. We did not have any criteria relating to year of publication, target behaviour, journal, study quality or article type.
Intervention articles were excluded if descriptions were not detailed enough to allow us to identify a link. In some cases, the intervention was described in detail and a number of theoretical constructs were discussed. However, it was not clear whether or not the authors were proposing that the constructs were MoAs through which specific BCTs would change behaviour. In other cases, authors included lists of BCTs described as linked to a list of MoAs. It was not always clear, however, whether the authors were hypothesising that all of the listed BCTs were linked to all of the listed MoAs, or that there were more specific links. Thus, these articles were also excluded, because of uncertainty about specific individual links. We also excluded unpublished theses, articles and reports that were not peer-reviewed, and articles that did not report a behavioural outcome.
Screening procedure
The full texts of all intervention articles retrieved through the search methods above were reviewed by two researchers. Guidelines for screening were developed and updated iteratively, and discrepancies were resolved through discussion. All articles were first screened by the two researchers independently, until inter-rater reliability was at an acceptable level (κ = 0.9). Articles were subsequently screened by one reviewer; a summary of inter-rater reliability across all stages of screening and coding is shown in Appendix 2.
Overview of data extraction
Data were extracted in several stages. General data about the study were extracted into a ‘source’ table that was connected to another ‘links’ table using a unique identifying number. General data included author(s), year, study type (e.g. randomised controlled trial), target behaviour and whether or not the authors identified a theoretical model as underpinning the development of the intervention. BCTs were identified and extracted, irrespective of whether or not they were linked to a MoA. MoAs (if any) were then identified for each BCT. More detail on the coding of BCTs – and BCT–MoA links – is provided in Identifying links between behaviour change techniques and mechanisms of action.
Identifying behaviour change techniques
Behaviour change techniques were identified using the BCTTv117,33 by two researchers who were trained in BCT coding. Each article was initially coded by the two researchers independently, until inter-rater reliability was acceptable [prevalence and bias adjusted kappa (PABAK) = 0.9; see Appendix 2]. Subsequently, articles were coded by one researcher and checked by another researcher. PABAK105 was used to calculate inter-rater reliability because of its ability to account for high prevalence of negative agreement. 105 Coding guidelines were developed (see Report Supplementary Material 1 for BCT coding guidelines) based on those used for the BCTTv1 online training (www.bct-taxonomy.com). Examples of guidelines were that (1) BCTs should be coded only if they targeted one or more of the target behaviours or key preparatory behaviours of the intervention (2) the whole intervention description should be read before beginning to code BCTs, (3) where BCTs were previously coded in the intervention articles using BCTTv1, the authors’ original coding was maintained and (4) where an earlier taxonomy had been used (e.g. that used by Abraham and Michie33), coding was updated in line with BCTTv1 guidelines.
Identifying links between behaviour change techniques and mechanisms of action
For each of the BCTs identified, researchers examined whether the authors had described a link to one or more MoAs. MoAs were identified when they were described as a theoretical construct through which behaviour change was hypothesised to occur, and were clearly linked to one or more BCTs. Data regarding each link between a BCT and a MoA were extracted by two researchers independently. Percentage agreement was used to calculate reliability between coders. This was because coding was not conducted using a ‘finite’ list of MoAs during data extraction.
Coding guidelines were developed and updated iteratively where necessary and discrepancies were resolved through discussion. Examples of coding guidelines were that (1) each BCT–MoA link should be extracted only once in any intervention article, regardless of how many times it was described in the article and (2) the most specific links possible should be coded. For example, if BCT X was linked to the MoA ‘perceived efficacy’ and perceived efficacy was said to be made up of self-efficacy and response-efficacy, BCT X was linked to self-efficacy and response-efficacy.
The following data were extracted for each link:
-
BCT label and number (from the BCTTv1 taxonomy)
-
MoA label and definition [as specified by the author(s)]
-
explicitness of the link (some inference needed vs. no inference needed)
-
whether or not the links included groups of BCTs or MoAs (one BCT linked to one MoA vs. one or more BCTs linked to one MoA/one or more MoAs linked to one BCT)
-
whether or not the link was tested empirically in the article (MoA not measured and BCT–MoA link not tested vs. MoA measured but BCT–MoA link not tested vs. BCT–MoA link tested).
Categorising mechanisms of action
Following data extraction, to allow for more efficient data synthesis, we categorised all extracted MoAs into a set of 26 general MoAs (see Appendix 3). These were the 14 domains from the TDF38 and the 12 additional most frequent MoA constructs from a set of 83 theories of behaviour change identified by a multidisciplinary literature review led by psychologists, sociologists, anthropologists and economists. 30 Two coders categorised MoAs until intercoder reliability was > 90% (see Appendix 4 for guidelines). Discrepancies were resolved through discussion and MoAs that could not be categorised into any of the 26 were categorised as ‘other’.
Data analysis
Research questions 1–3
Descriptive analyses were used to examine the frequency of links between BCTs and MoAs, reflecting the number of articles in which a particular link was described. This was used to address the first three research questions:
-
How frequently is each possible BCT–MoA link described?
-
Which BCTs are frequently described as targeting a specific MoA?
-
Which MoAs are frequently described as influenced by a specific BCT?
Research question 4
The fourth research question concerned the relative frequency of each link. To address this, the observed frequency of occurrence was compared with the expected frequency of occurrence for each link using a series of one-tailed exact binomial tests using R (The R Foundation for Statistical Computing, Vienna, Austria). 106 A one-tailed test was used because the objective was to identify the ‘presence’ of links rather than their absence. These analyses were performed on the links for which MoAs could be categorised only (i.e. excluding the MoAs categorised as ‘other’).
As we did not have an a priori expected frequency of links that could be used for comparison, we calculated an expected frequency that represented an approximation of the frequency one may observe if the links between BCTs and MoAs are random. This value was calculated as the probability that a specific BCT was coded (calculated by dividing the frequency with which the BCT was linked with any MoA by the total number of BCT–MoA links) multiplied by the probability that a specific MoA was coded (calculated by dividing the frequency with which the MoA was linked with any BCT by the total number of BCT–MoA links).
The p-values from the binomial tests provide an indication of the likelihood of a particular link being identified. These values enable us to examine the frequency of a specific link (e.g. BCT X linked to MoA Y), by comparing this with the frequency with which BCT X and MoA Y were identified in any intervention. The binomial tests therefore provide indications of relative frequency such as links that are high in frequency relative to other links identified in the intervention articles. It is worth noting that this means that if a specific BCT or MoA was not identified often across the intervention articles, a link containing that BCT or MoA may emerge as relatively frequent – regardless of the absolute frequency of that link. By contrast, if a specific BCT or MoA was identified very frequently and linked to a range of BCTs or MoAs across the articles, links containing this BCT or MoA would be lower in relative frequency.
The links that we list as ‘relatively frequent’, based on these analyses, are those that emerged with a p-value of < 0.05. This was selected as an arbitrary minimum criterion for a particular link, and we present these data to serve as one indication of relative frequency only. No statistical inferences about the links that fall above or below this value are made. We welcome others applying more or less stringent criteria as they see appropriate.
We present the data resulting from these analyses (i.e. including those links that did not reach this threshold) in ‘heat maps’, generated using R. In these heat maps, individual values (in this case, the p-values) are given a colour that represents their relative frequency. We present the data in this way to provide the full data set ‘at a glance’ to aid readers in interpreting the findings.
Results
Characteristics of intervention articles
A total of 974 intervention articles were identified through our search methods. Of those, 697 (72%) were excluded after screening the full text based on our coding guidelines (e.g. the paper was not reporting on an intervention, the intervention description was not detailed/clear enough to code BCTs, or there was an underpinning theory described but individual links between specific BCTs and MoAs were not clear). The most common reasons for exclusion were that papers did not provide a ‘codable’ description of a link between at least one BCT and a MoA and/or they did not clearly identify MoAs.
In total, 277 intervention articles described at least one BCT–MoA link, covering > 10 target behaviours. These included physical activity (40%), dietary behaviours (18%), alcohol intake (10%) and smoking (cessation) (6%). The years of publication ranged from 1982 to 2016, with almost half (49%) published in or after 2010. Over three-quarters (78%) of articles reported on the outcome(s) of a behavioural intervention, rather than describing their design or development. No theoretical basis was specified for the intervention in 14% of the articles. In addition, 13% mentioned theory but did not specify how theory was applied to developing or evaluating interventions. The analyses and discussions described in this chapter are based on the 277 included articles. A full summary of study characteristics are in the study information and materials on Open Science Framework (https://osf.io/7qjvn/; (accessed 1 January 2020). Figure 2 is a flow diagram of the search strategy and the selection process of the articles.
FIGURE 2.
Flow diagram of search strategy.
Characteristics of extracted links
From the 277 articles, we extracted 2636 BCT–MoA links. Some inference was required to identify 33% of these links. In some cases, for example, a theoretical construct was identified as a MoA in the introduction of the paper (e.g. where authors were describing the underpinning theory of the intervention) and the intervention description then described an intervention component as aiming to target this construct. Because we needed the additional statement in the introduction identifying this construct as a MoA to code the link, we would code this as a link needing some inference. This is in contrast with where authors provided an explicit hypothesis [e.g. ‘we are including this intervention component (BCT X) as we hypothesise that it will change this mechanism (MoA Y), which in turn will change behaviour’].
Across the included articles, we identified 77 BCTs, of which 70 had at least one link to a MoA. The BCTs that were most frequently linked to a MoA were ‘4.1 instruction on how to perform the behaviour’ (182 times) and ‘1.2 problem-solving’ (177 times). The MoA that was most frequently linked to a BCT was ‘beliefs about capabilities’ (733 times), followed by ‘intention’ (318 times). From our set of 26 MoAs, ‘norms’ was the only MoA not identified. There was an empirical test of only 9% of the links within the intervention articles.
Frequency of extracted links (research questions 1–3)
We extracted approximately 10 links per study [mean = 9.56, standard deviation (SD) = 13.80]. Of the extracted links, 12% involved a single BCT and a single MoA, whereas 88% involved more than one BCT or MoA (e.g. one BCT linked to a list of three MoAs). The maximum number of BCTs identified as linked to a single MoA was eight (mean = 3.63, range 1–8). The maximum number of MoAs linked to a single BCT was five (mean = 1.71, range 1–5). A full list of the 2636 BCT–MoA links is available on the Open Science Framework study site (https://osf.io/7qjvn/).
Do any specific behaviour change technique—mechanism of action links occur more frequently than might be expected given the average frequency of behaviour change technique—mechanism of action links? (Research question 4)
There were 87 links that occurred with a relatively high level of frequency, based on the p < 0.05 criterion. This included 51 out of 93 (55%) BCTs and 24 out of 26 (92%) MoAs. Of the MoAs that were linked to a BCT at least once (i.e. all except ‘norms’), only ‘optimism’ was not linked to any BCT at the p < 0.05 threshold. This MoA was derived from the TDF. 38 Several BCTs were coded frequently but did not meet the p < 0.05 threshold for being linked to a MoA. For example, the BCT ‘1.5 review behaviour goals’ was coded 36 times and ‘3.3 social support (emotional)’ was coded 14 times. However, the relative frequency with which these were linked to a MoA did not meet the threshold.
A heat map that displays a visual representation of link frequency, where darker colours represent p-values closer to zero, can be seen in Figure 3 and are also available online as part of an interactive online tool (https://theoryandtechniquetool.humanbehaviourchange.org/tool; see Discussion for more details).
FIGURE 3.
Heat map representing the relative frequency of BCT–MoA links.
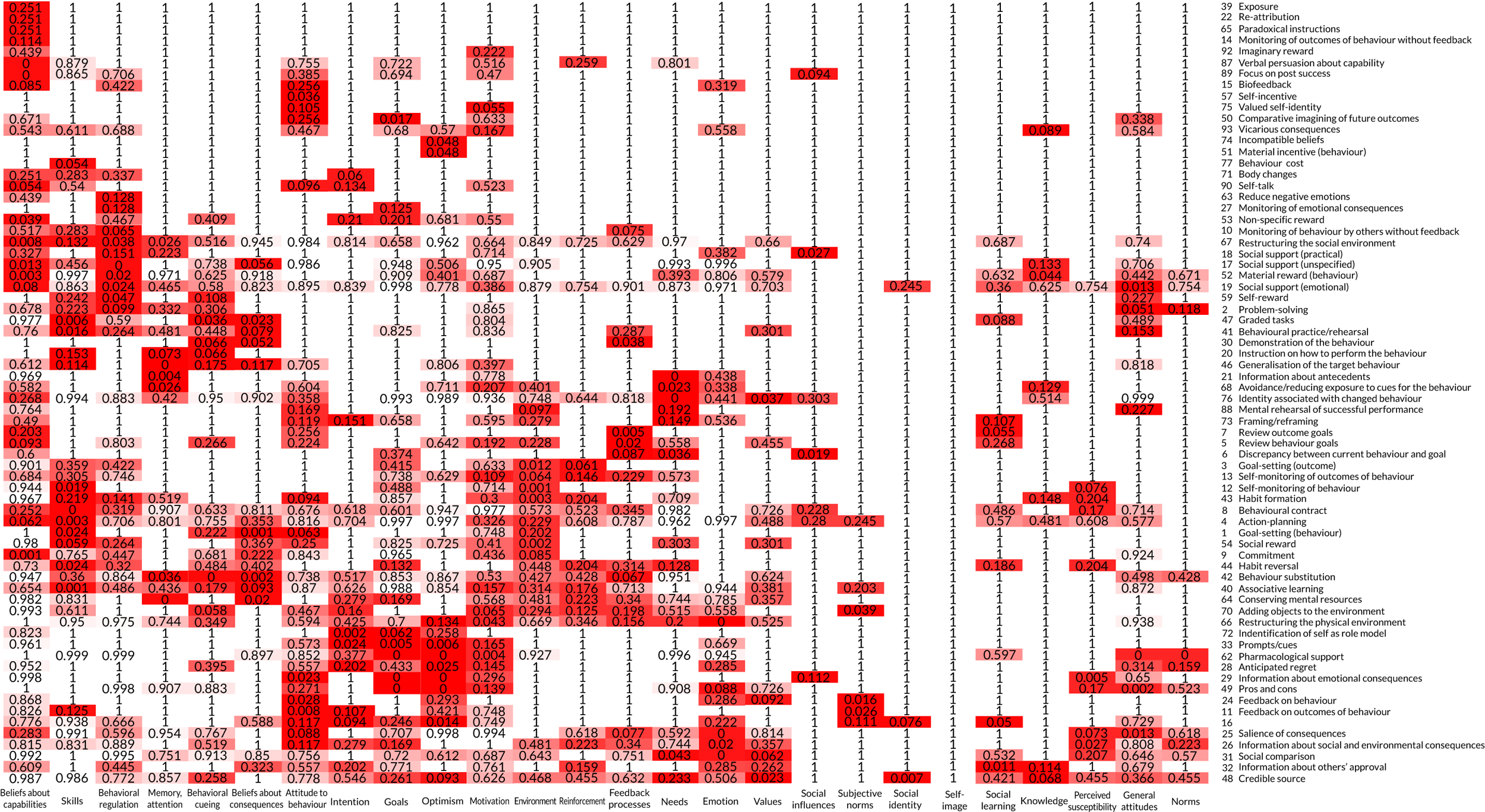
Each cell contains a numerical value (i.e. p-value) and is coloured to reflect the relative ‘heat’ of that value (in this case, the relative frequency of a particular link). Rows and columns (i.e. BCTs and MoAs, respectively) are clustered by similarity, such that BCTs linked to similar MoAs are clustered together and MoAs linked to similar numbers of BCTs are clustered together.
The 51 BCTs and the MoAs that were most frequently linked are shown in Table 1. These summarise the descriptions provided by authors of this set of interventions regarding how these 51 BCTs change behaviour. For some BCTs, there is one MoA for which there appears to be agreement. For example, the BCT ‘8.7 graded tasks’ that was frequently coded across interventions, was linked to only one MoA (‘beliefs about capabilities’) with a relatively high level of frequency (p = < 0.001). For other BCTs, there are links to multiple MoAs. In some of these cases, there is one seemingly ‘dominant’ MoA. For example, although the BCT ‘1.2 problem-solving’ was frequently linked to three MoAs, the link to ‘beliefs about capabilities’ (p = 0.008; occurring 65 times) occurred substantially more frequently than the next highest two: ‘environmental context and resources’ (p = 0.026; occurring nine times) and ‘skills’ (p = 0.038; occurring 18 times).
| BCT | MoA | Frequency | p-value |
|---|---|---|---|
| Instruction on how to perform the behaviour (4.1) | Knowledge | 17 | 0.013 |
| Skills | 20 | 0.024 | |
| Goal-setting (behaviour) (1.1) | Behavioural regulation | 15 | 0.003 |
| Problem-solving (1.2) | Beliefs about capabilities | 65 | 0.008 |
| Environmental context and resources | 9 | 0.026 | |
| Skills | 18 | 0.038 | |
| Social support (unspecified) (3.1) | Social influences | 34 | < 0.001 |
| Social/professional role and identity | 5 | 0.037 | |
| Demonstration of the behaviour (6.1) | Beliefs about capabilities | 60 | 0.003 |
| Skills | 17 | 0.020 | |
| Social learning/imitation | 3 | 0.044 | |
| Action-planning (1.4) | Behavioural regulation | 14 | 0.001 |
| Feedback on behaviour (2.2) | Subjective norms | 19 | < 0.001 |
| Knowledge | 13 | 0.013 | |
| Information about health consequences (5.1) | Knowledge | 18 | < 0.001 |
| Beliefs about consequences | 26 | < 0.001 | |
| Attitude towards the behaviour | 19 | < 0.001 | |
| Perceived susceptibility/vulnerability | 10 | < 0.001 | |
| Intention | 28 | 0.004 | |
| Behavioural practice/rehearsal (8.1) | Skills | 24 | < 0.001 |
| Beliefs about capabilities | 47 | 0.013 | |
| Social comparison (6.2) | Subjective norms | 31 | < 0.001 |
| Social influences | 9 | 0.043 | |
| Information about social and environmental consequences (5.3) | Beliefs about consequences | 20 | < 0.001 |
| Attitude towards the behaviour | 16 | < 0.001 | |
| Knowledge | 13 | 0.002 | |
| Self-monitoring of behaviour (2.3) | Behavioural regulation | 18 | < 0.001 |
| Credible source (9.1) | General attitudes/beliefs | 2 | 0.007 |
| Social/professional role and identity | 4 | 0.023 | |
| Adding objects to the environment (12.5) | Environmental context/resources | 8 | < 0.001 |
| Prompts/cues (7.1) | Memory, attention and decision processes | 8 | < 0.001 |
| Behavioural cueing | 6 | 0.002 | |
| Environmental context/resources | 5 | 0.036 | |
| Graded tasks (8.7) | Beliefs about capabilities | 28 | < 0.001 |
| Pros and cons (9.2) | Beliefs about consequences | 12 | < 0.001 |
| Attitude towards the behaviour | 9 | < 0.001 | |
| Feedback processes | 3 | 0.005 | |
| Motivation | 5 | 0.023 | |
| Framing/reframing (13.2) | Self-image | 2 | < 0.050 |
| Attitude towards the behaviour | 7 | 0.014 | |
| Behaviour substitution (8.2) | Behavioural regulation | 5 | 0.016 |
| Social reward (10.4) | Reinforcement | 3 | 0.020 |
| Focus on past success (15.3) | Beliefs about capabilities | 23 | < 0.001 |
| Restructuring the physical environment (12.1) | Environmental context/resources | 9 | < 0.001 |
| Behavioural cueing | 3 | 0.020 | |
| Behavioural contract (1.8) | Goals | 4 | 0.002 |
| Information about others’ approval (6.3) | Subjective norms | 13 | < 0.001 |
| Intention | 12 | 0.043 | |
| Verbal persuasion about capability (15.1) | Beliefs about capabilities | 27 | < 0.001 |
| Feedback on outcomes of behaviour (2.7) | Subjective norms | 5 | 0.020 |
| Feedback processes | 2 | 0.027 | |
| Reduce negative emotions (11.2) | Beliefs about capabilities | 12 | 0.039 |
| Salience of consequences (5.2) | Attitude towards the behaviour | 4 | 0.025 |
| Commitment (1.9) | Values | 1 | 0.039 |
| Self-monitoring of outcomes of behaviour (2.4) | Behavioural regulation | 5 | 0.024 |
| Information about emotional consequences (5.6) | Beliefs about consequences | 6 | 0.005 |
| Attitude towards the behaviour | 5 | 0.006 | |
| Emotion | 2 | 0.024 | |
| Goal-setting (outcome) (1.3) | Goals | 4 | 0.003 |
| Social support (practical) (3.2) | Social influences | 4 | 0.023 |
| Environmental context and resources | 3 | 0.026 | |
| Discrepancy between current behaviour and goal (1.6) | Goals | 3 | 0.001 |
| Behavioural regulation | 3 | 0.019 | |
| Avoidance/reducing exposure to cues for the behaviour (12.3) | Needs | 1 | 0.027 |
| Identification of self as role model (13.1) | Self-image | 2 | 0.011 |
| Restructuring the social environment (12.2) | Environmental context/resources | 3 | 0.004 |
| Social influences | 6 | < 0.001 | |
| Non-specific reward (10.3) | Reinforcement | 2 | 0.005 |
| Habit formation (8.3) | Behavioural cueing | 3 | 0.001 |
| Behavioural regulation | 3 | 0.024 | |
| Review outcome goals (1.7) | Goals | 2 | 0.012 |
| Mental rehearsal of successful performance (15.2) | Motivation | 3 | 0.008 |
| Values | 1 | 0.026 | |
| Material incentive (behaviour) (10.1) | Attitude towards the behaviour | 1 | 0.048 |
| Monitoring of behaviour by others without feedback (2.1) | Needs | 1 | 0.019 |
| Social influences | 2 | 0.036 | |
| Generalisation of target behaviour (8.6) | Skills | 2 | 0.047 |
| Comparative imagining of future outcomes (9.3) | Beliefs about consequences | 3 | 0.017 |
| Identity associated with changed behaviour (13.5) | Values | 1 | 0.016 |
| Motivation | 2 | 0.028 | |
| Anticipated regret (5.5) | Emotion | 2 | 0.002 |
| Habit reversal (8.4) | Behavioural regulation | 4 | 0.006 |
| Behavioural cueing | 2 | 0.023 | |
| Memory, attention and decision processes | 2 | 0.036 | |
| Associative learning (7.8) | Reinforcement | 1 | 0.038 |
| Self-incentive (10.7) | Motivation | 1 | 0.036 |
| Incompatible beliefs (13.3) | Attitude towards the behaviour | 1 | 0.048 |
For those BCTs for which there are multiple MoAs linked, the data suggest that the authors may be hypothesising specific causal pathways (e.g. attitude → intention → behaviour). For instance, the BCT ‘5.1 information about health consequences’ was linked to the MoAs ‘beliefs about consequences’ (p < 0.001), ‘knowledge’ (p < 0.001), ‘perceived susceptibility/vulnerability’ (p < 0.001), ‘attitude towards the behaviour’ (p < 0.001) and ‘intention’ (p = 0.004).
Table 2 shows the 24 MoAs and the BCTs that were most frequently linked. It can be interpreted as a summary of the BCTs that the authors believe are suitable to target these 24 MoAs. In some cases, there is one clear BCT for a given MoA. For example, the MoA ‘perceived susceptibility/vulnerability’ was linked only to the BCT ‘5.1 information about health consequences’ (p < 0.001) and the MoA ‘social learning/imitation’ was linked only to the BCT ‘6.1 demonstration of the behaviour’ (p = 0.044).
| MoA | BCT | Frequency | p-value |
|---|---|---|---|
| Attitude towards the behaviour | Information about health consequences (5.1) | 19 | < 0.001 |
| Information about social and environmental consequences (5.3) | 16 | < 0.001 | |
| Pros and cons (9.2) | 9 | < 0.001 | |
| Information about emotional consequences (5.6) | 5 | 0.006 | |
| Framing/reframing (13.2) | 7 | 0.014 | |
| Salience of consequences (5.2) | 4 | 0.025 | |
| Material incentive (behaviour) (10.1) | 1 | 0.048 | |
| Incompatible beliefs (13.3) | 1 | 0.048 | |
| Behavioural cueing | Habit formation (8.3) | 3 | 0.001 |
| Prompts/cues (7.1) | 6 | 0.002 | |
| Restructuring the physical environment (12.1) | 3 | 0.020 | |
| Habit reversal (8.4) | 2 | 0.023 | |
| Behavioural regulation | Self-monitoring of behaviour (2.3) | 18 | < 0.001 |
| Action-planning (1.4) | 14 | 0.001 | |
| Goal-setting (behaviour) (1.1) | 15 | 0.003 | |
| Habit reversal (8.4) | 4 | 0.006 | |
| Behaviour substitution (8.2) | 5 | 0.016 | |
| Discrepancy between current behaviour and goal (1.6) | 3 | 0.019 | |
| Self-monitoring of outcomes of behaviour (2.4) | 5 | 0.024 | |
| Habit formation (8.3) | 3 | 0.024 | |
| Beliefs about capabilities | Graded tasks (8.7) | 28 | < 0.001 |
| Verbal persuasion about capability (15.1) | 27 | < 0.001 | |
| Focus on past success (15.3) | 23 | < 0.001 | |
| Demonstration of the behaviour (6.1) | 60 | 0.003 | |
| Problem-solving (1.2) | 65 | 0.008 | |
| Behavioural practice/rehearsal (8.1) | 47 | 0.013 | |
| Reduce negative emotions (11.2) | 12 | 0.039 | |
| Beliefs about consequences | Information about health consequences (5.1) | 26 | < 0.001 |
| Information about social and environmental consequences (5.3) | 20 | < 0.001 | |
| Pros and cons (9.2) | 12 | < 0.001 | |
| Information about emotional consequences (5.6) | 6 | 0.005 | |
| Comparative imagining of future outcomes (9.3) | 3 | 0.017 | |
| Environmental context and resources | Restructuring the physical environment (12.1) | 9 | < 0.001 |
| Adding objects to the environment (12.5) | 8 | < 0.001 | |
| Restructuring the social environment (12.2) | 3 | 0.004 | |
| Problem-solving (1.2) | 9 | 0.026 | |
| Social support (practical) (3.2) | 3 | 0.026 | |
| Prompts and cues (7.1) | 5 | 0.036 | |
| Emotion | Anticipated regret (5.5) | 2 | 0.002 |
| Information about emotional consequences (5.6) | 2 | 0.024 | |
| Feedback processes | Pros and cons (9.2) | 3 | 0.005 |
| Feedback on outcomes of behaviour (2.7) | 2 | 0.027 | |
| General attitudes/beliefs | Credible source (9.1) | 2 | 0.007 |
| Goals | Discrepancy between current behaviour and goal (1.6) | 3 | 0.001 |
| Behavioural contract (1.8) | 4 | 0.002 | |
| Goal-setting (outcome) (1.3) | 4 | 0.003 | |
| Review outcome goals (1.7) | 2 | 0.012 | |
| Intention | Information about health consequences (5.1) | 28 | 0.004 |
| Information about others’ approval (6.3) | 12 | 0.043 | |
| Knowledge | Information about health consequences (5.1) | 18 | < 0.001 |
| Information about social and environmental consequences (5.3) | 13 | 0.002 | |
| Instruction on how to perform the behaviour (4.1) | 17 | 0.013 | |
| Feedback on behaviour (2.2) | 13 | 0.013 | |
| Memory, attention and decision processes | Prompts/cues (7.1) | 8 | < 0.001 |
| Habit reversal (8.4) | 2 | 0.036 | |
| Motivation | Mental rehearsal of successful performance (15.2) | 3 | 0.008 |
| Pros and cons (9.2) | 5 | 0.023 | |
| Identity associated with changed behaviour (13.5) | 2 | 0.028 | |
| Self-incentive (10.7) | 1 | 0.036 | |
| Perceived susceptibility/vulnerability | Information about health consequences (5.1) | 10 | < 0.001 |
| Needs | Monitoring of behaviour by others without feedback (2.1) | 1 | 0.019 |
| Avoidance/reducing exposure to cues for the behaviour (12.3) | 1 | 0.027 | |
| Reinforcement | Non-specific reward (10.3) | 2 | 0.005 |
| Social reward (10.4) | 3 | 0.020 | |
| Associative learning (7.8) | 1 | 0.038 | |
| Self-image | Framing/reframing (13.2) | 2 | < 0.050 |
| Identification of self as role model (13.1) | 2 | 0.011 | |
| Skills | Behavioural practice/rehearsal (8.1) | 24 | < 0.001 |
| Demonstration of the behaviour (6.1) | 17 | 0.020 | |
| Instruction on how to perform the behaviour (4.1) | 20 | 0.024 | |
| Problem-solving (1.2) | 18 | 0.038 | |
| Generalisation of target behaviour (8.6) | 2 | 0.047 | |
| Social influences | Social support (unspecified) (3.1) | 34 | < 0.001 |
| Restructuring the social environment (12.2) | 6 | < 0.001 | |
| Social support (practical) (3.2) | 4 | 0.023 | |
| Monitoring of behaviour by others without feedback (2.1) | 2 | 0.036 | |
| Social comparison (6.2) | 9 | 0.043 | |
| Subjective norms | Feedback on behaviour (2.2) | 19 | < 0.001 |
| Social comparison (6.2) | 31 | < 0.001 | |
| Information about others’ approval (6.3) | 13 | < 0.001 | |
| Feedback on outcomes of behaviour (2.7) | 5 | 0.020 | |
| Social learning/imitation | Demonstration of the behaviour (6.1) | 3 | 0.044 |
| Social/professional role and identity | Credible source (9.1) | 4 | 0.023 |
| Social support (unspecified) (3.1) | 5 | 0.037 | |
| Values | Identity associated with changed behaviour (13.5) | 1 | 0.016 |
| Mental rehearsal of successful performance (15.2) | 1 | 0.026 | |
| Commitment (1.9) | 1 | 0.039 |
In other cases, clusters of theoretically linked BCTs were linked to one MoA. An example is the MoA ‘emotion’ being linked to the BCT ‘5.5 anticipated regret’ (p = 0.002) and ‘5.3 information about emotional consequences’ (p = 0.024).
Discussion
This study provides the first data set summarising links between BCTs and MoAs, as described by authors of published intervention articles. There were 2636 links identified in this study, including 70 BCTs and 25 MoAs. Eighty-seven links were identified with a relatively high level of frequency (i.e. meeting the criterion of p-value of < 0.05). The findings of this study provide a summary of links that are described frequently (e.g. providing information about the health consequences of a behaviour is frequently hypothesised to increase knowledge), as well as those links that appear to be absent. Advancing the science of behaviour change at a theoretical and methodological level, through this and similar initiatives (see www.scienceofbehaviourchange.org), helps to provide a grounding from which researchers and practitioners can build innovative new interventions by combining BCTs, knowing where important gaps are and providing a basis for new hypotheses.
The findings indicate that, in some cases, there is one clear BCT for a given MoA and one clear MoA for a given BCT. In other cases, there are BCTs linked to more than one MoA and MoAs linked to more than one BCT. Some of the links that can be seen in our data set map closely to the theoretical literature. For example, in Bandura’s theory of self-efficacy,107 a number of intervention strategies that can be used to increase self-efficacy are described, including mastery experience, vicarious experience and verbal persuasion. These intervention strategies are comparable to the BCTs ‘8.1 behavioural practice/rehearsal’, ‘6.1 demonstration of the behaviour’ and ‘15.1 verbal persuasion about capability’, respectively, all of which were linked to the MoA ‘beliefs about capabilities’, a construct that is conceptually identical to self-efficacy in this study.
Although we identified at least one link for 91% of the coded BCTs and 92% of the MoAs, in a number of cases no clear links were identified. Two of the MoAs in our set of 26 were not linked to BCTs enough to meet the criterion of a p-value of < 0.05. These were ‘optimism’ and ‘norms’, both of which are found to be frequently occurring in behavioural theories. 30 This may reflect a lack of clarity or agreement in the behavioural intervention literature regarding the types of BCTs that should be employed to target these MoAs.
How can the findings be used?
The heat map (see Figure 3 and Tables 1 and 2), can be used both to identify BCTs that have the potential to target relevant MoAs (e.g. for intervention design and development) as well as to understand the MoA(s) through which BCTs are having their effects (e.g. for intervention evaluation and/or to advance our theoretical knowledge). For example, to include BCTs that will most likely have an effect on relevant MoAs (i.e. an ‘optimal’ BCT–MoA link), one can refer to Tables 1 and 2, which list the links that met the criterion of a p-value of < 0.05. By drawing on these findings, researchers may identify creative ways to target MoAs of interest (e.g. by including less commonly used BCTs).
Given the scope of this work, we cannot draw inferences about the extent to which these BCT–MoA links have been empirically tested. However, our data set can be used to develop a framework for designing and conducting empirical tests. This would help to inform the cumulative development of evidence that can provide clarity and reduce ambiguity about these links. This would also help researchers to examine those BCT–MoA links that currently appear to be underused. Thus, the database of BCT–MoA links resulting from this study can be used to identify links that have been (1) frequently described in the literature and that require empirical study and (2) infrequently reported and appear to be understudied.
There are several additional points to note. It is clear that, despite the importance of a rigorously applied theoretical basis15,22 to optimise effectiveness and enhance our understanding of intervention effects,23 a large number of intervention articles lack clarity in their description of the theoretical underpinning of the study. In this study, 72% of the articles identified through the search methods did not explicitly describe links between BCTs and MoAs. These findings are consistent with previous meta-analytic findings, which indicated that, although 50% of the interventions reviewed reported a theoretical basis, 90% did not report links between all BCTs and individual theoretical constructs. 26 Without clear descriptions of the hypothesised links between BCTs and MoAs, it can be difficult to draw generalisable theoretical conclusions.
Furthermore, it seems clear from this study that conceptualisations of what authors may refer to as a ‘theory-based’ intervention are highly variable. A large number of interventions that are reported to be based on theory in fact draw on implicit or partially applied theories. 24–26 Intervention descriptions often lack clarity about exactly how theory has been applied. This is particularly the case in the selection of BCTs and the links to, and measurement of, relevant theoretical constructs. We can only systematically advance our theoretical understanding of how interventions work if authors explicitly report how and why theoretical principles were tested28–31 rather than simply describing the intervention as being informed by theory. 27 A reliance on the latter, and a tendency to rely on implicit theoretical assumptions, has hampered intervention research.
It is worth noting that most of the links between BCTs and MoAs were not extracted as individual links, but as groups. This may indicate that authors considered there to be synergistic relationships among BCTs and/or MoAs (e.g. BCTs A, B and C and/or MoAs X, Y and Z work together in the behaviour change process). Another explanation is a lack of specificity in the selection of BCTs, targeting of MoAs and/or lack of detail in reporting interventions.
Limitations
There are a number of limitations to the current work. We did not undertake a full systematic review; the intervention articles were purposively selected to maximise the likelihood of being able to identify BCT–MoA links. This was because the aim of the study was to identify the links that were described in intervention articles, rather than to set out to examine the clarity with which they tended to be described. Although we attempted to collate articles from the international research community (e.g. by contacting the Society of Behavioral Medicine in the USA and the European Health Psychology Society), there is a wide range of published intervention evaluations that our data set of articles may not represent.
The extracted BCT–MoA links were based on authors’ descriptions and hypotheses. Very few had been tested empirically in the articles. Therefore, we were unable to synthesise the results of empirical tests of these links. This indicates that there is a need for empirical research that systematically tests the links that have been frequently described. With this aim in mind, work is ongoing in the USA to identify, measure and manipulate MoAs using experimental methods (see www.scienceofbehaviourchange.org).
We cannot use the findings of this study to draw conclusions about the links that did not appear in the included intervention articles. The links that appeared to be absent may reflect a belief among authors that they do not exist, or that they may be links that do not tend to be considered by intervention designers (despite being potentially useful). These links may also include MoAs that authors find difficult to operationalise, or those that authors tend to use implicitly and are therefore less likely to explicitly describe in detail.
Next steps
This was the first of three related studies that aim to examine the links between BCTs and (1) MoAs and (2) behavioural theories. 100 In the next stage, links between BCTs and MoAs were identified through an expert consensus study.
Chapter 3 An expert consensus approach to linking behaviour change techniques and mechanisms of action
Abstract
Objective
To build a shared knowledge of the links between BCTs and MoAs through expert consensus.
Methods
International behaviour change experts (n = 105) participated in a modified nominal group technique to examine links between 61 frequently used BCTs and 26 MoAs. Experts participated in three rounds to rate, discuss and re-rate links between BCTs and MoAs. Consensus was reached if at least 80% of experts agreed about a link.
Results
Of 1586 possible BCT–MoA link combinations (61 BCTs × 26 MoAs), 83.6% (51/61) of BCTs were definitely linked to at least one MoA [mean (SD) 1.44 (0.96), range 1–4], 76.9%. Twenty out of 26 MoAs were definitely linked to at least one BCT [mean (SD) 3.27 (2.91), range 9]. A total of 90 links were considered ‘definite’ (5.7%) and 464 (29.2%) were considered ‘definitely not’ links. Finally, 1032 (65.1%) were considered ‘possible’ or ‘unsure’ links. There were 10 BCTs (e.g. ‘action-planning’ and ‘behavioural substitution’) and six MoAs (e.g. ‘needs’ and ‘optimism’) with no identified links.
Conclusions
The identified agreed links between BCTs and MoAs provide a framework for specifying empirical tests of links in future studies and for researchers interested in developing and/or synthesising behavioural interventions.
Introduction
Identifying specific links between BCTs and MoAs is important for both developing interventions and understanding the processes through which interventions affect behaviour change. One method for generating evidence on the links between BCTs and MoAs would be to conduct experimental studies of BCT–MoA links by manipulating BCTs and measuring MoAs and subsequently conducting meta-analyses of their findings. 108 However, the sheer number of potential BCTs and MoAs and, consequently, BCT–MoA links render these methods relatively infeasible.
Indirect approaches, such as the examination of hypothesised links between BCTs and MoAs in published intervention literature (see Chapter 2), provide a valuable alternative source of evidence. However, the published intervention literature is limited by various publication biases. These include the selection of research projects (at least in part) being driven by funding requirements, reporting of projects by researchers and the selection of which findings to present for publication. Examining the current thinking of international experts in behaviour change provides a complementary source of evidence, capable of generating useful information on a large set of BCT–MoA links. Using an expert consensus approach permits a synthesis of the current hypotheses of experts in the field, limits the impact that publication or funding-related biases have and is informed by existing theory and evidence.
Expert consensus methods can be used to facilitate the development of research questions, solutions to existing problems and priorities for action. 109 Through expert consensus methodologies, differing ideas can be discussed, reported and organised to establish areas of consensus and priorities for further investigation. Furthermore, these methods cultivate the experts’ ownership of the resulting research, thereby increasing the likelihood that future research and practice will be influenced by the outcomes of the study. 110
This chapter reports the second in a series of four studies to develop and test a methodology for generating links between BCTs and MoAs. This study aimed to build consensus around the mechanisms through which BCTs may alter behaviour. The primary research questions were:
-
Which BCTs do experts agree influence behaviour through specific MoAs?
-
Which BCTs do experts agree do not influence behaviour through specific MoAs?
-
Do experts agree that BCTs influence behaviour through one or multiple MoAs?
The secondary research questions were:
-
Which links between BCTs and MoAs do experts disagree on?
-
Do experts agree on at least one link with a MoA for all BCTs?
-
Do experts agree on at least one link with a BCT for all MoAs?
Methods
Design
A formal consensus method drawing on nominal group technique (NGT)111 was used to examine the links between BCTs and MoAs across three rounds: (1) initial rating, (2) discussion and (3) final rating.
Participants
Experts with experience in behaviour change intervention design, evaluation and/or evidence synthesis were selected to represent a range of academic disciplines, professional backgrounds and geographical regions.
Recruitment
Participants were recruited via e-mail. E-mails were sent to (1) experts who had participated in in-person BCT training, online BCT training (www.bct-taxonomy.com/) and/or the BCTTv1 project42 (see www.ucl.ac.uk/health-psychology/bcttaxonomy), (2) members of the IAB for the research programme and (3) contact lists from professional societies and centres (University College London’s Centre for Behaviour Change, the Special Interest Group of the US Society of Behavioral Medicine, European Health Psychology Society, UK Society for Behavioural Medicine and Division of Health Psychology of the British Psychological Society). Recruited participants were also asked to recommend other participants, creating a ‘snowballing’ recruitment process.
Participants interested in becoming an expert judge (n = 227) completed a self-reported survey (see Appendix 5) to evaluate their experience and expertise in behaviour change interventions. Eligibility criteria included (1) above-average self-rated expertise in BCTs, behaviour change theories and behaviour change interventions, (≥ 4 using a 7-point scale ranging from ‘0 – no expertise’ to ‘7 – profound expertise’) and (2) some experience with behaviour change intervention(s) that ‘used specific BCTs’ and ‘was specifically grounded in behaviour change theory/theories’. Just over half (54.2%) of interested participants were eligible. Eligible experts were sent a second questionnaire to collect demographic information to ensure that the selected panel contained experts reflecting a range of countries, professional backgrounds and academic disciplines (see Appendix 5).
Reviews of previous expert consensus studies found that panels with approximately 20 participants demonstrate stability of consensus. 112 Therefore, the final sample of experts (n = 105) was sufficient to establish consensus. Furthermore, dividing the experts into subgroups of 20 or more experts would also be sufficient. Approximately half of the experts were from the UK, 20% were from other European countries, 20% were from North America and 10% were from Africa, Australia or New Zealand. The majority of experts worked in an academic setting (75%) and in the field of psychology (60%).
Procedure
The expert ratings in rounds 1 and 3 were administered via the web-based survey software Qualtrics (Provo, UT, USA; www.qualtrics.com). The expert discussion in round 2 was managed via the online forum ‘Loomio’ (version 1.0, Loomio, Wellington, New Zealand). In rounds 1 and 3, experts rated links between a discrete set of BCTs and MoAs. To reduce participant burden, we limited the number of BCTs and MoAs included in the study. A subset of the 93 BCTs was identified by establishing those that were commonly used in the literature. In this instance, BCTs identified more than twice (n = 61) across a set of 40 systematically identified and coded intervention descriptions covering a range of different behaviours were used to determine the subset of BCTs. 42 We also restricted the set of MoAs included to the 14 theoretical domains described in the TDF38 and the 12 most frequently occurring MoAs (that did not overlap with the TDF domains) identified in a systematic review of 83 behaviour change theories. 30 A total of 61 BCTs and 26 MoAs were included in the final study; a full list of MoAs and their definitions provided in Table 3.
| Mechanism label | Mechanism definition |
|---|---|
| Knowledge | An awareness of the existence of something |
| Skills | An ability or proficiency acquired through practice |
| Social/professional role and identity | A coherent set of behaviours and displayed personal qualities of an individual in a social or work setting |
| Beliefs about capabilities | Beliefs about one’s ability to successfully carry out a behaviour |
| Optimism | Confidence that things will happen for the best or that desired goals will be attained |
| Beliefs about consequences | Beliefs about the consequences of a behaviour (i.e. perceptions about what will be achieved and/or lost by undertaking a behaviour, as well as the probability that a behaviour will lead to a specific outcome) |
| Reinforcement | Processes by which the frequency or probability of a response is increased through a dependent relationship or contingency with a stimulus or circumstance |
| Intentions | A conscious decision to perform a behaviour or a resolve to act in a certain way |
| Goals | Mental representations of outcomes or end states that an individual wants to achieve |
| Memory, attention and decision processes | Ability to retain information, focus on aspects of the environment and choose between two or more alternatives |
| Environmental context and resources | Aspects of a person’s situation or environment that discourage or encourage the behaviour |
| Social influences | Those interpersonal processes that can cause oneself to change one’s thoughts, feelings or behaviours |
| Emotion | A complex reaction pattern involving experiential, behavioural and physiological elements |
| Behavioural regulation | Behavioural, cognitive and/or emotional skills for managing or changing behaviour |
| Norms | The attitudes held and behaviours exhibited by other people within a social group |
| Subjective norms | One’s perceptions of what most other people within a social group believe and do |
| Attitude towards the behaviour | The general evaluations of the behaviour on a scale ranging from negative to positive |
| Motivation | Processes relating to the impetus that gives purpose or direction to behaviour and operates at a conscious or unconscious level |
| Self-image | One’s conception and evaluation of oneself, including psychological and physical characteristics, qualities and skills |
| Needs | Deficit of something required for survival, well-being or personal fulfilment |
| Values | Moral, social or aesthetic principles accepted by an individual or society as a guide to what is good, desirable or important |
| Feedback processes | Processes through which current behaviour is compared against a particular standard |
| Social learning/imitation | A process by which thoughts, feelings and motivational states observed in others are internalised and replicated without the need for conscious awareness |
| Behavioural cueing | Processes by which behaviour is triggered from either the external environment, the performance of another behaviour, or from ideas appearing in consciousness |
| General attitudes/beliefs | Evaluations of an object, person, group, issue or concept on a scale ranging from negative to positive |
| Perceived susceptibility/vulnerability | Perceptions of the likelihood that one is vulnerable to a threat |
To increase the feasibility of the task for experts, BCTs were divided across the five participant groups. To reduce the possibility of bias in ratings due to familiarity with BCTs, BCTs were allocated to the five groups through stratified random allocation by ordering BCTs according to the frequency with which they were used in a comprehensive review of behaviour change interventions. 42 The 105 experts were block-randomised to one of five groups. Block randomisation was used to distribute experts from different countries, professional backgrounds and academic disciplines across the five groups. Each group of 21 experts rated links between either 13 or 14 BCTs and 26 MoAs, encompassing either 338 or 364 possible links. Details of the links rated by each expert group are in Appendix 5.
Conduct of the consensus exercise
Round 1: initial ratings of behaviour change technique–mechanism of action links
Round 1 established an initial level of consensus for each BCT–MoA link. Experts responded to the question ‘Does the BCT [e.g. self-monitoring (behaviour)] change behaviour through the MoA [e.g. beliefs about one’s ability to successfully carry out a behaviour (beliefs about capabilities)]?’. Answers were provided on a 5-point scale (ranging from ‘1 – definitely no’ to ‘5 – definitely yes’). The 26 MoAs were randomised to appear in a different order for each BCT to reduce potential bias due to ordering effects.
Round 2: discussion of uncertain and disagreed links
During round 2, experts discussed the BCT–MoA links from round 1 for which were there was most uncertainty or disagreement. The discussion on Loomio was anonymous and asynchronous. Experts discussed (1) the 10 links rated ‘don’t know/uncertain’ by the largest proportion of experts (within-group) and (2) the 10 most disagreed links (i.e. links with a nearly equivalent proportion of experts rating ‘definitely no’ and ‘definitely yes’). Experts were prompted to discuss these ‘uncertain’ and ‘disagreed’ links to enhance the utility of the exercise. Experts also had the opportunity to suggest and discuss other links, as well as their views on the expert consensus exercise more generally.
To ensure anonymity, experts were assigned a user identification code to use as a pseudonym. Experts were not required to participate in live discussions. To facilitate participation across geographical regions, experts had a defined 2-week period to comment on the discussion. The research team served as anonymous discussion moderators to answer questions raised by experts, periodically prompt discussion by summarising key points from the experts’ comments, and conduct informal polls of experts’ opinions. Round 2 occurred 1 week after experts received their statistical summaries from round 1.
Round 3: final ratings of all behaviour change technique–mechanism of action links
During round 3, experts determined agreement on the BCT–MoA links by re-rating the same links from round 1. Feedback from experts during the discussion round indicated minor modifications needed to be made to the wording and response options of the question answered in round 3 (see Appendix 5). For round 3, experts answered the question, ‘When [BCT] works, does it work through changing [MoA definition (MoA label)]?’. Experts were able to respond using the options ‘definitely yes’, ‘definitely no’, ‘uncertain’ or ‘possibly’.
Materials
Round 1
Experts were e-mailed the definitions of their assigned 13 or 14 BCTs and 26 MoAs, along with the guidelines for the task (see Appendix 5). For each question, BCT and MoA definitions were provided alongside a diagram depicting the causal behaviour change flow from each BCT to MoA link as shown in Figure 4.
FIGURE 4.
Diagram depicting the causal behaviour change flow from each BCT to MoA link.
As shown in Figure 4, experts were provided with this diagram during round 1 of the consensus exercise, for each question, which depicts that a BCT influences a MoA, which in turn influences behaviour change.
Round 2
Experts were e-mailed a personalised statistical summary of round 1 results. Summaries included frequency distributions of both their own and their group’s responses for each BCT–MoA link (see Appendix 5). To enhance interpretation and understanding of the summaries, ‘definitely yes’ and ‘probably yes’ response options were combined into ‘yes’, and ‘definitely no’ and ‘probably no’ were combined into ‘no’. ‘Uncertain’ (don’t know/uncertain) remained unchanged.
Round 3
Experts were provided with transcripts of their group’s discussion from round 2, in addition to the personalised statistical summaries previously circulated. The statistical summaries and discussion transcripts from the previous rounds enabled experts to reconsider and provide final ratings for each link. Experts were instructed to provide their final ratings taking into consideration both their own thoughts from the previous rounds, as well as the thoughts and ratings of the other experts in their group.
Procedures to evaluate effects of group membership
A total of 52 BCT–MoA links were rated across all five groups and 105 experts. To detect whether or not the results were influenced by group membership, two BCTs were rated by all experts during both round 1 and round 3. These BCTs were the two BCTs most frequently identified in studies evaluating the BCTTv1:17 ‘4.1 instruction on how to perform behaviour’ and ‘3.1 social support (unspecified)’. Similarly, to ensure valid comparisons between the discussions across the five groups, all five expert groups discussed two of the 52 BCT–MoA links shared across all groups. These links were between (1) the most disagreed link between the BCT ‘4.1 instruction on how to perform the behaviour’ and MoA ‘intention’ and (2) the most uncertain link between the BCT ‘3.1 social support (unspecified)’ and MoA ‘attitude towards the behaviour’.
Data analysis
Data from round 3 were analysed to answer the three primary and three secondary research questions (see Background). To answer all research questions, the proportion of experts who rated the same response option (i.e. ‘definitely yes’, or ‘definitely no’) was calculated using Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA) to identify which links reached consensus. For a link to reach consensus, > 80% of experts needed to agree a BCT was either ‘definitely linked’ or ‘definitely not linked’ to a MoA. In addition, to answer secondary research question 1, the distribution of proportions for each of the response options were examined (i.e. the proportion of experts rating ‘definitely yes’ vs. ‘definitely no’).
To facilitate a visual analysis of the descriptive data, four heat maps were produced in R for the final round 3 ratings. A heat map is a visual depiction of a data matrix where the values in the cells are represented by colours shaded to indicate the strength or ‘heat’ of a particular value. In the heat map, BCTs represent rows that are linked to MoA columns. In each of the heat maps, the cell values presented are the proportion of experts who agree that a BCT and MoA are (1) ‘definitely’ linked (Figure 5), (2) ‘definitely not’ linked (Figure 6), (3) ‘possibly’ linked (see Appendix 5) and (4) ‘uncertain’ whether or not they are linked (see Appendix 5).
FIGURE 5.
A heat map of the percentage of experts rating a BCT as ‘definitely’ linked to a MoA. ATB, attitude towards the behaviour; BCap., beliefs about capabilities; BCon., beliefs about consequences; BR, behavioural regulation; GAB, general attitudes and beliefs; MADP, memory, attention, and decision processes; PSV, perceived susceptibility and vulnerability; SPRI, social/professional role and identity.

FIGURE 6.
A heat map of the percentage of experts rating a BCT as ‘definitely not’ linked to a MoA. ATB, attitude towards the behaviour; BCap., beliefs about capabilities; BCon., beliefs about consequences; BR, behavioural regulation; GAB, general attitudes and beliefs; MADP, memory, attention, and decision processes; PSV, perceived susceptibility and vulnerability; SPRI, social/professional role and identity.
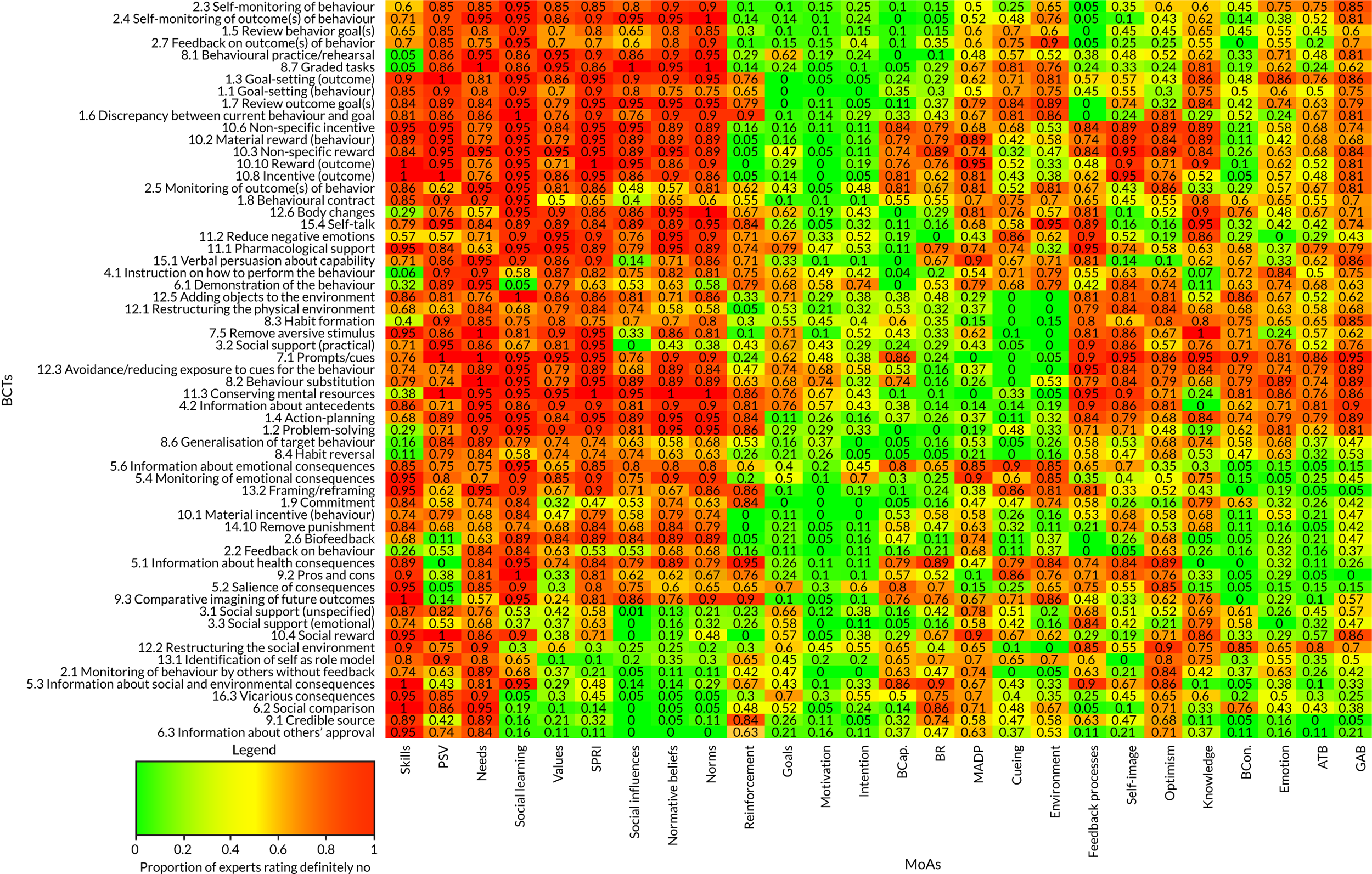
To facilitate this visual analysis, the heat map clusters rows (BCTs) and columns (MoAs) by similarity. For example, in the ‘definitely’ linked case, BCTs linked to similar MoAs (such as BCT X and Y both being linked to MoAs 1, 5 and 7) are clustered closer together vertically. In addition, MoAs linked to similar numbers of BCTs are clustered together horizontally (e.g. MoA 1 and 2 are both linked to five BCTs). This clustering presents patterns in the data but does not imply any statistical inference.
To examine any possible effects of group membership on experts’ ratings, intraclass correlation coefficients (ICCs) were calculated. The ICCs were calculated using the ratings data from the 52 BCT–MoA links rated by all experts. The round 1 ICCs indicate whether or not group allocation had any influence on the ratings. Round 3 ICCs indicate the extent to which the within-group discussion (round 2) influenced the ratings. To understand the extent to which variance in the experts’ ratings can be attributed to group membership, the ICC value can be translated into a percentage. For example, if the ICC value is 0.03, this means that 3% of the variance in ratings can be attributed to group membership properties. Without standard criteria to assess ICC values for group ratings, the results describe, rather than evaluate, the influence of group membership on experts’ ratings. We predicted small ICCs for round 1 due to the block randomisation procedures and larger round 3 ICCs because of the likely influence of group-specific discussion about the links.
Results
Round 1
All experts (n = 105) participated in round 1. More than 80% of experts rated 13 (0.81%) BCT–MoA links as ‘definite’ and 3 (0.19%) as ‘definitely not’ links. At least 50% of experts agreed on 83 ‘definite’ (5%), 147 (9%) ‘possibly’, 53 (3%) ‘possibly not’ and 296 (19%) ‘definitely not’ BCT–MoA links. No BCT–MoA links were rated by > 50% of experts as ‘uncertain’.
Round 2
During round 2, experts collectively discussed 102 links: (1) the 10 most uncertain links in their group; (2) the 10 most disagreed links in their group; and (3) the two links discussed by all five groups. Expert participation in round 2 decreased slightly, with 88% (92/105) of experts actively participating. On average, experts provided 14 comments (mean 13.96, SD 7.103, range 1–40 comments). A maximum of four experts per group did not participate in the discussion, with some groups commenting more than others (range 213–353 comments). However, there were no significant differences in the mean number of comments per expert across groups [F (4, 95) = 1.684; p = 0.161]. The results suggest that experts were highly involved in the task, and comments suggest that experts found the task helpful. Example of comments are:
I put uncertain, as I too could not see how [instruction on how to perform the behaviour] would necessarily facilitate intention to act as [expert] points out . . . I think the example about smoking from [another expert] illustrates when this would not apply very effectively. I would change my rating to ‘no’ now.
I have found this one of the most challenging to call and therefore waited to see the arguments of others as I was unable to decide a camp. I too do not feel that intention is the primary MoA [for BCT social comparison], but I see the argument put forward by [expert]. [. . .] However, my hunch is still that this is not a key MoA therefore I will rate it as ‘no’.
Ratings from round 1 and feedback from round 2 indicated that experts experienced difficulty with the initial rating task. In particular, experts had difficulty discerning between ‘possibly yes’ and ‘possibly no’ options, and suggested that including only one ‘possibly’ option would improve the task. For example, one expert provided feedback that: ‘The two [‘probably’] options created a lot of grey area, which experts interpreted differently’. Experts also expressed difficulty linking any BCTs with specific MoAs. For example, experts had difficulty rating BCTs linked with intentions. One expert noted, ‘In general, I struggled with INTENTION as a key MoA for most BCTs. I see Intention as so proximal to behaviour (and analogous to overall motivation) that it is almost always a result of other (more critical) MoAs, no matter which theoretical perspective one adopts’. An expert in a different group made a similar comment: ‘While I believe “intention” is not a key MoA in this case, and am thus happy to keep my no vote, I also struggled with ‘intention’ as MoA in general - I thought it would be involved but not necessarily key to achieving change for almost all BCTs’. Experts also expressed challenges in singular thinking about the BCTs linked with MoAs: ‘It is very difficult to think about the individual BCTs in isolation. My brain is forced to think about models of behaviour change, directions of causality and other BCTs before making a decision “yes”, “no” or “unsure”. Although I might say “yes” to a specific BCT, it’s likely that what I’m really saying is that the BCT in question is part of a cluster, but probably plays the biggest part in that cluster’.
Round 3
Nearly all experts (n = 100, 95%) participated in round 3, rating 1586 links between 61 BCTs and 26 MoAs. Consensus was reached for 90 ‘definite’ (research question 1) and 464 ‘definitely not’ (research question 2; see Appendix 5) BCT–MoA links. Of the 102 links discussed in round 2 with either high disagreement and/or uncertainty, agreement was reached for eight links.
Out of the 61 BCTs rated, 51 were ‘definitely’ linked to at least one MoA. Of the 26 MoAs, 21 were ‘definitely’ linked to at least one BCT (research questions 5 and 6). The specificity with which BCTs linked to MoAs is illustrated in Figure 7, the frequency with which BCTs were definitely linked to MoAs by > 80% of experts is depicted in the dark blue bars, and the frequency with which MoAs were linked to BCTs by > 80% of experts is depicted in the light blue bars.
FIGURE 7.
The frequency of BCT–MoA links as rated by experts.
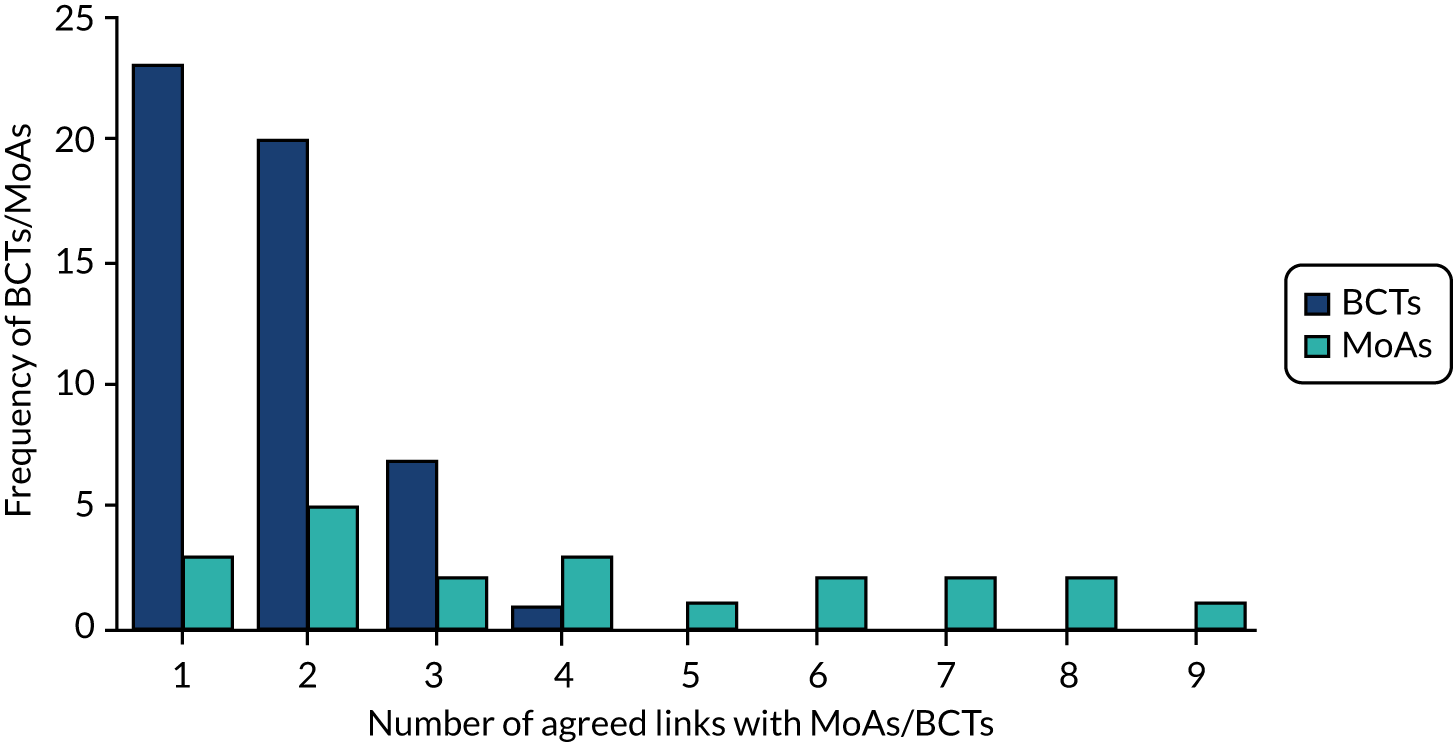
Twenty-three BCTs were linked to only one MoA, and 20 BCTs were linked to only two MoAs (research question 3). MoAs were linked to between one and nine BCTs. The MoA ‘motivation’ was linked to nine different BCTs. The 10 BCTs with no ‘definite’ links to MoAs included:
-
1.4 action-planning
-
2.1 monitoring of behaviour by others without feedback
-
2.5 monitoring of outcomes of behaviour without feedback
-
8.2 behavioural substitution
-
8.6 generalisation of the target behaviour
-
9.1 credible source
-
10.6 non-specific incentive
-
11.1 pharmacological support
-
12.6 body changes
-
15.4 self-talk.
The five MoAs with no definite links to BCTs included (1) general attitudes and beliefs, (2) needs, (3) optimism, (4) social professional role and identity, and (5) values.
The visual representations of the expert consensus on BCT–MoA links are presented in two heat maps (see Figures 5 and 6). The BCTs that experts agreed were linked to similar MoAs are vertically closer together in the heat map, and MoAs that are linked to a similar frequency of BCTs are closer horizontally.
A larger number of links did not meet the consensus criterion (n = 1032, 65%). This was due to strong disagreement among the experts for 163 links. ‘Strong disagreement’ was recorded when at least one-third of experts responded ‘definitely yes’, one-third responded ‘definitely no’ and one-third responded either ‘possibly’ or ‘don’t know/uncertain’ (research question 4). For 340 links, between 50% and 80% of experts agreed on 255 and 85 links as ‘definitely not’ and ‘definitely’ links (respectively). The remaining experts provided ratings of ‘possibly’ and ‘don’t know/uncertain’. No meaningful trends emerged among the remaining 529 links.
Analysis of between-group differences in rating patterns (intraclass correlation coefficients)
To assess whether or not there were differences in expert ratings because of group membership, we examined the ICCs for the BCTs shared across groups [i.e. instruction about how to perform the behaviour and social support (unspecified)]. The ICCs for round 1 were small for all BCT–MoA links (range 0.00–0.10), suggesting that group allocation did not affect ratings (Table 4).
| MoA | Social support (unspecified) | Instruction on how to perform a behaviour | ||||
|---|---|---|---|---|---|---|
| Round 1 | Round 3 | Δ | Round 1 | Round 3 | Δ | |
| Knowledge | 0.05 | –0.01 | –0.06 | –0.03 | –0.04 | –0.01 |
| Skills | 0.05 | 0.07 | 0.02 | 0.00 | 0.02 | 0.02 |
| Behavioural regulation | 0.07 | 0.12 | 0.05 | 0.09 | 0.11 | 0.02 |
| Social influences | 0.00 | –0.01 | –0.01 | –0.01 | 0.01 | 0.02 |
| Memory, attention, decision processes | 0.01 | 0.02 | 0.01 | 0.04 | 0.02 | –0.02 |
| Social professional role/identity | 0.02 | 0.10 | 0.08 | 0.01 | 0.02 | 0.01 |
| Beliefs about capabilities | 0.09 | 0.18 | 0.09 | 0.02 | 0.01 | –0.01 |
| Beliefs about consequences | 0.03 | 0.05 | 0.02 | –0.03 | 0.01 | 0.04 |
| Optimism | –0.04 | 0.01 | 0.05 | –0.02 | 0.01 | 0.03 |
| Intention | 0.00 | 0.10 | 0.1 | –0.02 | 0.08 | 0.1 |
| Goals | 0.04 | 0.07 | 0.03 | 0.07 | 0.06 | –0.01 |
| Reinforcement | 0.10 | 0.13 | 0.03 | 0.03 | 0.04 | 0.01 |
| Emotion | 0.03 | 0.08 | 0.05 | 0.00 | 0.03 | 0.03 |
| Environment | 0.01 | 0.01 | 0 | 0.03 | 0.00 | –0.03 |
| Norms | –0.01 | –0.02 | –0.01 | 0.00 | 0.01 | 0.01 |
| Subjective norms | 0.00 | –0.03 | –0.03 | –0.02 | 0.03 | 0.05 |
| Attitude towards the behaviour | 0.01 | 0.24 | 0.23 | –0.01 | 0.23 | 0.24 |
| Motivation | 0.03 | 0.07 | 0.04 | 0.00 | 0.00 | 0 |
| Self-image | –0.03 | 0.00 | 0.03 | 0.04 | 0.07 | 0.03 |
| Needs | –0.02 | 0.09 | 0.11 | –0.03 | 0.05 | 0.08 |
| Values | –0.02 | 0.17 | 0.19 | 0.00 | 0.06 | 0.06 |
| Feedback processes | –0.01 | 0.02 | 0.03 | 0.00 | 0.02 | 0.02 |
| General attitudes and beliefs | 0.08 | 0.26 | 0.18 | 0.03 | 0.10 | 0.07 |
| Social learning | 0.04 | 0.21 | 0.17 | 0.07 | 0.05 | –0.02 |
| Cueing | 0.07 | 0.06 | –0.01 | –0.02 | 0.05 | 0.07 |
| Perceived susceptibility/vulnerability | 0.03 | 0.03 | 0 | 0.05 | 0.05 | 0 |
As predicted, ICCs increased from round 1 to round 3 for 37 BCT–MoA links, reflecting an increase in within-group agreement after the discussion round. In round 3, 1 out of 52 (1.9%) ICCs was large [for the MoA ‘general attitudes and beliefs’ with the BCT ‘3.1 social support (unspecified)’], and 13 out of 52 (25%) were moderately-sized. Ten of the moderately sized ICCs were for the BCT ‘3.1 social support (unspecified)’, suggesting that round 2 discussions engendered more agreement on the meaning of this BCT in some groups than others.
Discussion
In the current expert consensus study, 90 BCT–MoA links between 51 (of 61 commonly used) BCTs and 20 (of 26 frequently used) MoAs were identified, which may provide promise for intervention development and evidence synthesis. Experts agreed that 464 links definitely did not exist and, as such, should not be targeted by interventions, whereas no consensus was reached for 1032 links; therefore, further research is required. No links were identified in either direction for 10 frequently used BCTs and six MoAs, which may be of particular interest for future research on behaviour change.
The pattern of results indicates that, for most of the BCTs evaluated in this task, the key MoAs for behaviour change are ‘motivation’ and ‘intention’. A large number of BCTs were also hypothesised to operate through the MoAs: (1) ‘beliefs about capabilities’, (2) ‘beliefs about consequences’ and (3) ‘behavioural regulation’. Nearly all experts agreed on which BCTs are linked to ‘reinforcement’, ‘cueing’ and ‘environmental context and resources’. The extent of agreement for these links could possibly be explained by the specificity with which the theoretical literature describes techniques for changing these MoAs. In addition, several of the groupings that occur in BCTTv1 (which is structured hierarchically and groups BCTs that are similar in function within 16 clusters)17 also appear within the heat map (in terms of vertical proximity). This could indicate shared hypotheses across different consensus studies about how BCTs change behaviour.
There was no consensus for some of the most frequently used BCTs (e.g. ‘1.4 action-planning’, ‘9.1 credible source’, ‘8.2 behavioural substitution’) on the MoAs they target. Experts actively participated in this consensus exercise, so it is possible that through additional rating rounds, a greater number of participants, and/or an additional consensus exercise with different experts, the number of agreed BCT–MoA links could increase. An alternative explanation is that in several different theories these BCTs are linked to different MoAs and possibly only work in combination with other BCTs. This alternative explanation supports feedback from the experts that it was often difficult to make BCT–MoA judgements in isolation. For example, several MoAs that occur frequently within theories of behaviour change (e.g. ‘needs’, ‘values’, ‘optimism’) were not linked to any BCTs. It is possible that these MoAs do not occur in isolation and rather need to be targeted by multiple BCTs, as noted by experts during the discussion round.
The BCT–MoA-behaviour change effect depends on both the path from BCT to MoA and the path from MoA to behaviour change. The extent to which experts agreed on a link could have been influenced by experts’ beliefs about either of these effects. For example, if the experts had confidence in the BCT’s ability to alter the MoA, but limited confidence in the link between the MoA and behaviour change, experts may have rated that the BCT was not linked to the MoA. Experts echoed this concern during the discussion round. The present study cannot ascertain whether experts’ ratings were influenced more by their hypotheses about the effect of the BCT on the MoA, or the effect of the MoA on behaviour change. The modified question wording in round 3, which was altered in response to comments from experts, may have limited this to a degree by asking experts to consider their judgements in round 3 in response to the hypothetical, ‘When this BCT works . . .’. Further research is needed to explore the rationale behind experts’ ratings. For example, 95% of experts agreed that ‘1.1 goal-setting (behaviour)’ changes behaviour by eliciting changes in intentions; despite comments during the discussion round on experts’ difficulty linking BCTs to intention. This finding may be a result of experts’ knowledge of previous research findings that changes in intentions are associated with small to medium changes in behaviour.
In this study, we chose a stringent criterion to evaluate expert consensus. In a systematic review of expert consensus studies, the percentage of experts in agreement was the most frequently used method to determine consensus. Studies using percentage of experts in agreement applied a range of criteria to establish consensus (50–97%), with the median threshold value at 75%. 113 The relatively small number of experts rating each link compared with the number of links rated by each expert was a major factor in the decision to use such a stringent criterion. Future research should generate empirical evidence for the links where more than two-thirds of the experts agreed (i.e. the more moderately shaded links in Figure 5).
At present, when selecting BCTs for use in an intervention, intervention developers tend to consult theory, published literature and their own hypotheses to determine what may be most effective for modifying the relevant MoAs and consequently changing the behaviour of interest. The current data provide evidence about the shared judgements of experts and an additional resource for both the development of interventions and the generation of data-driven hypotheses. Similarly, these data can also be used for evaluation of how an intervention has its effect. Furthermore, the data indicating which BCTs are not linked to specific MoAs, and which MoAs are not linked to specific BCTs, may also be useful for understanding what mechanisms do not provide promise. Therefore, these results generate hypotheses about effective links, which can foster empirical research to test the most promising BCT–MoA links and increase our understanding of how intervention components have their effects.
Limitations
The range of links identified in this study was restricted to the subset of BCTs and MoAs evaluated (i.e. 61 of 93 BCTs in the BCTTv1). We also chose a specific set of experts based on our inclusion/exclusion criteria. A different recruitment strategy or panel of experts may have led to different results. However, several measures were taken in this study to limit this possibility, including the large sample size and variety of recruitment procedures used. Some of the expert groups were able to agree on certain BCT–MoA links more than other groups; however, most of the links with better agreement in some groups were for the BCT ‘3.1 social support (unspecified)’. In previous studies this BCT has demonstrated lower than average reliability. 17,32 We changed the question prompt and the rating scale used from round 1 to round 3, which could have limited the consensus among experts. The difficulty experts had with the original question and rating scale may have limited the total number of links agreed on at the end of the consensus exercise. Lastly, we restricted the set of MoAs in the study based on the frequency with which they appear in behaviour change theories. Therefore, it is possible that there are other important MoAs that were not considered in this study.
Future directions
This study focused on theoretically based MoAs that have not necessarily been explicitly linked in theories or theoretical frameworks. A given theory may propose how MoAs interact to change behaviour. Thus, there is reason to explore whether the BCT–MoA links have additive (independent), synergistic, or antagonistic effects, as such effects have been explored in previous research. 60–62 Therefore, the next study (see Chapter 4) presents triangulated data on the two previous studies (see Chapters 2 and 3) to increase confidence in the links identified through both the literature synthesis and the present expert consensus study. Future analyses of the collected data could also include a qualitative analysis of the expert discussions conducted throughout the project.
Conclusions
This study provides a systematically derived summary of experts’ judgements about how BCTs change behaviour. The results can be used to inform intervention development, evaluation and synthesis of effectiveness evidence. The majority of BCT–MoA links for which there was uncertainty among the experts could be of particular interest for future studies. These results offer a first level of evidence-based hypotheses, which can be confirmed or refuted through further empirical research to delineate how BCTs have their effects on behaviour.
Chapter 4 Triangulating evidence of links between behaviour change techniques and mechanisms of action from literature synthesis and expert consensus
Abstract
Background
A methodology is required to link BCTs and their MoAs to enhance the understanding of intervention effects and theory development. Links were previously examined through literature synthesis (see Chapter 2) and expert consensus (see Chapter 3). However, concordance between these sources of evidence is unknown.
Purpose
To examine concordance between evidence from literature synthesis and expert consensus studies for hypothesised BCT–MoA links, reconcile discrepancies, and develop a readily accessible, online resource.
Methods
(1) ‘Links’ and ‘non-links’ were identified from 1456 possible links (between the 56 BCTs and 26 MoAs) identified by previous studies (see Chapters 2 and 3). (2) Agreement between the two sets of data was investigated statistically. (3) Uncertainties and differences were reconciled by 16 behaviour change experts who engaged in a consensus process.
Results
Thirty-seven ‘links’ and 460 ‘non-links’ (of the possible 1456 links) were identified. Results were concordant between the two studies for 25 MoAs, with literature synthesis explaining over 35% of variance for each MoA in multilevel models. Following reconciliation, a total of 465 ‘non-links’ and 92 ‘links’ (covering 51/56 BCTs and 22/26 MoAs) were identified
Conclusions
Triangulation established the level of concordance between hypothesised BCT–MoA ‘links’ and ‘non-links’ identified through (1) literature synthesis and (2) expert consensus. Researchers and intervention designers seeking guidance on the mechanisms by which BCTs may change behaviour can use results through the Theory and Technique Tool (TaTT) (https://theoryandtechniquetool.humanbehaviourchange.org/).
Introduction
Interventions to change behaviour are necessary to address many current global challenges, including health, climate and environmental issues. 1,2 Interventions depend on having a sound theoretical and evidence base for optimal development. Considerable progress has been made in specifying BCTs, which are the ‘active ingredients’ of an intervention aimed at changing behaviour. The BCTTv1 specifies 93 BCTs with labels and definitions. 17,42,114 However, it is still unclear how BCTs should be selected for inclusion in an intervention. For example, how would a physiotherapist aiming to increase physical activity in a patient following stroke choose among BCTs as diverse as ‘demonstration of the behaviour’ and ‘giving rewards if and only if the activity is performed’? In addition, finding that an intervention successfully changed behaviour, one might wish to understand the process by which BCTs were enacted. However, this process is understudied and underspecified and lacks evidence.
A scientist or practitioner developing an intervention typically has an idea or theory of how their intervention might change behaviour, which guides their selection of techniques to incorporate in the intervention. For example, a physiotherapist may consider that the intervention may need to increase the patient’s motivation or skills. These ideas about intervention development can benefit from progress in behavioural science regarding influences on behaviour, which mediate the effect of behaviour change interventions (i.e. the MoAs of the interventions). Deciding which BCTs may affect change in these MoAs is a key part of intervention development, but one where there has been little evidence-based guidance. For example, if a physiotherapist believed that motivation was the MoA, it is unclear what evidence could guide their BCT choice.
To implement a successful intervention or interpret the findings from evidence synthesis, it is also important to learn how and why the intervention worked. Understanding the MoA through which the BCTs worked may provide insight into further relevant BCTs, or methods of enhancing the effectiveness of the included BCTs. Thus, gaining evidence about the links between BCTs and MoAs may facilitate both the selection of BCTs to target an MoA in designing an intervention, and the interpretation of the MoA of BCTs delivered in an effective intervention.
There is a clear scientific need to identify links between BCTs and MoAs. In the USA, the Science of Behavior Change programme of the National Institutes of Health is testing the effect of experimentally changing MoAs. 115–117 Furthermore, the experimental medicine approaches to behaviour change advocate testing mediation of intervention effects via MoAs to identify routes to behaviour change. 118 In the intervention mapping framework, linking the hypothesised determinants of behaviour to behaviour change methods is a key step in their systematic approach to intervention design. 119 Given the enormous number of possible combinations of MoAs and BCTs, it would be unrealistic and potentially a waste of resources to test the mediating effect of each possible link empirically. Therefore, guidance on those BCT–MoA combinations that are most likely to be effective (‘links’) and ineffective (‘non-links’) would be a useful and practical scientific advance.
The previous chapters provided preliminary evidence on BCT–MoA links, with Chapter 2101 involving a synthesis of literature reporting behaviour change interventions and Chapter 3102 involving an expert consensus study. The findings have similarities but are not identical. What we need now is a triangulation study to establish the degree of agreement between these two sources of evidence, to identify points of disagreement and to reconcile any discrepancies. Otherwise, intervention designers or those interpreting and evaluating interventions may be faced with conflicting, diverging or confusing evidence.
Triangulation of evidence using different methods to answer the same question is good scientific practice. Compared with simple replication of the same methods, one can have more confidence in the validity of the findings if biases in the design, techniques and analytic methods are not repeated. 120 The literature synthesis study101 (see Chapter 2) provides findings that reflect the previous thinking and methods of intervention designers addressing a variety of different behaviour change targets across disciplines and countries. However, findings are limited by reporting methods and publication constraints. Conversely, the experts involved in the consensus study102 (see Chapter 3) used their knowledge of current evidence and theory in reaching their decisions. However, for practical reasons they could consider only a restricted set of BCTs and MoAs. Therefore, triangulating findings derived from these two methods would strengthen confidence in the results.
Both previous studies produced a matrix of links between BCTs and MoAs. Although some concordance is expected between matrices, there are important differences between the two sets of data that limit the extent of possible concordance. First, experts in the consensus study could agree that a possible ‘link’ was improbable and therefore probably a ‘non-link’, whereas in the literature study it was only possible to find that a link had not occurred and there was no way of separating improbable links from those that simply had not been used in the 277 interventions examined. Second, the literature study could examine any and every BCT and MoA that authors had investigated. However, for practical reasons the consensus study included a set restricted to 61 BCTs and 26 MoAs. Thus, concordance could only be examined for the possible links included in both studies.
It is important first to examine concordance to identify points of agreement between Chapters 2 and 3, and then to examine whether or not the two methods achieve agreement that goes beyond chance coincidence. Otherwise any guidance to researchers, policy-makers and practitioners would be built on misleading evidence. Therefore, this chapter aims to:
-
investigate the degree of agreement between the findings of the two studies reported in Chapters 2 and 3 using statistical methods to evaluate concordance between them
-
reconcile remaining uncertainties and discrepancies between the literature synthesis and expert consensus studies (Chapters 2 and 3) using a new group of experts.
Based on these findings, we aimed to make the results more accessible to potential users by developing an online resource that provides researchers and intervention designers with information on the ‘links’ and ‘non-links’ between BCTs and MoAs.
Methods
Study design
The study comprised two parts: (1) concordance and (2) reconciliation. First, the BCT–MoA links found in the literature synthesis of 277 published reports of behaviour change interventions (see Chapter 2), and in the consensus reached by > 100 experts (see Chapter 3), were triangulated. This involved examining concordance between the two sets of results for 56 BCTs and 26 MoAs (i.e. 1456 possible links). The relationship between the study findings was then examined statistically, first for all MoAs and then for each MoA separately. Comparison of the results from the two previous studies identified potential links where both studies agreed (i.e. ‘links’ and ‘non-links’), as well as potential links where the evidence was marginal or the findings of the two studies disagreed. Second, the latter ‘inconclusive’ findings were brought into a reconciliation study where 16 new behaviour change experts engaged in a consensus process to establish whether or not they could be resolved.
Part 1: concordance study – comparing the findings of the literature synthesis and expert consensus studies
The data
The literature study identified 70 BCTs, and MoAs were categorised to 26 MoAs resulting in 2636 potential BCT–MoA links from the 277 interventions included. The expert consensus investigated 61 BCTs over the same 26 MoAs. The two studies shared 56 BCTs and all 26 MoAs, making a total of 1456 BCT–MoA combinations occurring in both studies. In the literature study, the measure of the frequency of a link was the p-value from the binomial test examining whether or not the link occurred more frequently than would be expected by chance, with lower p-values indicating a more frequent link. For the expert consensus study, the measure was the proportion of experts rating the link ‘definitely yes’ (for a link) or ‘definitely no’ (for a non-link). These two measures derived for each of the 1456 BCT–MoA combinations were the data used in the multilevel statistical models.
The BCT–MoA combinations showing concordance were identified by examining the potential links exceeding the criteria set in advance for each study. For the literature study, the criterion was set at a p-value of ≤ 0.05 and for the expert consensus study at ≥ 80% experts’ agreement. Although these criteria are somewhat arbitrary, the p-value criterion is similar to the criterion for statistical significance, and the consensus criterion is similar to that used as criteria in sensitivity/specificity analyses and in Delphi studies. 121 The matrices of links and non-links for each study were compared to establish agreed links and non-links, but also to identify marginal results and potential links that met criterion in one, but not the other, study.
Analyses to identify concordant behaviour change technique—mechanism of action combinations
The results of the previous literature synthesis and expert consensus studies were summarised in two independent matrices of 56 BCTs × 26 MoAs. Cells were compared to identify potential BCT–MoA links as:
-
a ‘link’ (i.e. meets the criterion for a link in both studies)
-
a ‘non-link’ (i.e. meets the criterion for a non-link in both studies)
-
‘inconclusive’ which could be either –
-
‘marginal’ [i.e. near criterion level of evidence in the literature (0.05 ≤ p ≤ 0.10) and/or expert consensus, e.g. link agreed by 70–80% of experts], or
-
‘discrepancy’ [i.e. no link in literature synthesis (p > 0.05), but meets criterion for a link in expert consensus or link in literature synthesis but no evidence of link in expert consensus].
-
-
‘evidence lacking’ [i.e. absence of link in literature synthesis, no evidence meeting criterion for link or non-link in expert consensus (< 80% agreed link or non-link)].
The inconclusive category of marginal and discrepant links needed to be reconciled and so were brought forward to the reconciliation study. The other three categories show agreement between the two studies that there was a link, a non-link or a lack of evidence and are therefore classed as ‘concordant’.
Analysis to test concordance statistically
Although the simple comparison of matrices allows classification of each potential BCT–MoA link, it is also important to quantify the degree of agreement between the data sets from the two studies. Multilevel modelling was used to investigate the prediction of expert consensus results from the p-values from the literature synthesis. Using the expert consensus rather than the literature synthesis as the dependent variable allowed the analyses to be conducted separately for prediction of the proportion of experts asserting each BCT–MoA combination a link (i.e. rating ‘definitely yes’) and the proportion asserting a non-link (i.e. rating ‘definitely no’). In addition, the consensus data had a better distribution than the literature synthesis data as there were fewer ties.
Data were analysed using MLwiN 3.01, in a two-level model with BCTs nested within MoAs. The intercept was allowed to vary randomly at both levels. By allowing the probability of a link from the literature synthesis to vary at the MoA level, it was possible to examine the relationship between the data sets from the two studies and to investigate whether or not the relationship varied across MoAs. Estimates of the variance explained were calculated using procedures reported by Nakagawa and Schielzeth122 and Johnson. 123
The data from the literature study included BCTs that showed a link to at least one MoA but not to other MoAs, and these latter BCT–MoA combinations had a resulting p-value of 1. However, they differed from other p-values of 1 that were positively established and, therefore, are probably more reliable than p-values depending on the absence of evidence. Therefore, the data were analysed both with and without BCT–MoA combinations where p = 1.
Part 2: reconciliation study – resolving discrepancies and marginal links identified in the concordance study
Participants: reconciliation experts
Behaviour change experts who work on the design, evaluation and/or synthesis of behaviour change interventions based on theory and who had not participated in the earlier study were recruited from a database created in the earlier expert consensus study. This database was supplemented by experts recommended by the IAB of the research programme. Sixteen experts were invited from the large number of experts on the database, based on objective evidence of their experience in conducting systematic reviews and publishing research articles. They completed the self-assessment of expertise and breadth of background used previously. 102 They were based in the UK (n = 11), the USA (n = 1), Canada (n = 2), Australia (n = 1) and Russia (n = 1).
Procedure
Three rounds of consensus methods were used to reconcile the 179 discrepancies and marginal BCT–MoA links found in the concordance study.
First, detailed guidelines for the study, including the sources of the data to be presented, were e-mailed to the 16 experts. Then, they were sent the following 179 inconclusive BCT–MoA links:
-
‘literature +ve, experts –ve’ – 48 BCT–MoA combinations with evidence of a link in literature synthesis but, in expert consensus, ‘definitely no’ link, disagreement about link or link not included in expert consensus (see Appendix 6)
-
‘experts +ve, literature –ve’ – 53 BCT–MoA combinations with ‘definitely’ evidence of a link in expert consensus but no evidence of a link in literature synthesis (see Appendix 6)
-
‘marginal evidence’ in either the literature synthesis (0.05 ≤ p ≤ 0.1) or the expert consensus study [70–79% of experts answered ‘definitely yes’ (n = 78)] (see Appendix 6).
Experts were sent the 179 BCT–MoA combinations in a random order along with the information from the literature and previous expert consensus studies and access to definitions of all BCTs and MoAs. Experts were asked to take account of this evidence and make a judgement rating each potential link ‘definitely yes’, ‘definitely no’ or ‘uncertain/don’t know’. Owing to error, 11 links were omitted from the reconciliation study and six were incorrectly included in the reconciliation study and therefore removed from analyses. Following completion, the experts were each sent a personalised summary with their own ratings alongside the frequency distributions for each BCT–MoA combination for all the experts.
Experts engaged in online, asynchronous, anonymous discussions (via Loomio) of the 25 BCT–MoA combinations about which there continued to be considerable uncertainty or disagreement. They were encouraged to focus on links for which they were uncertain or where their ratings were different from those of other experts. The discussion was moderated by a member of the research team who summarised and raised issues from time to time.
In addition to their personalised ratings from round 1, experts had access to the two sources of evidence from the earlier studies and were e-mailed transcripts of the round 2 discussions. Thus, the experts had detailed information to allow them to reconsider their previous ratings, taking into account both the evidence from the two studies and the ratings and opinions of other experts. As before, they rated each BCT–MoA combination in a random order, rating each potential link ‘definitely yes’, ‘definitely no’ or ‘uncertain/don’t know’. The criterion for a resolved ‘link’ was ≥ 80% of the reconciliation experts rating it ‘definitely yes’ and a ‘non-link’ occurring when ≥ 80% experts rated the link as ‘definitely no’.
Results
The flow chart in Figure 8 summarises the stages of the research and the data at each stage.
FIGURE 8.
Flow chart showing stages in the research and the links between BCTs and MoAs.
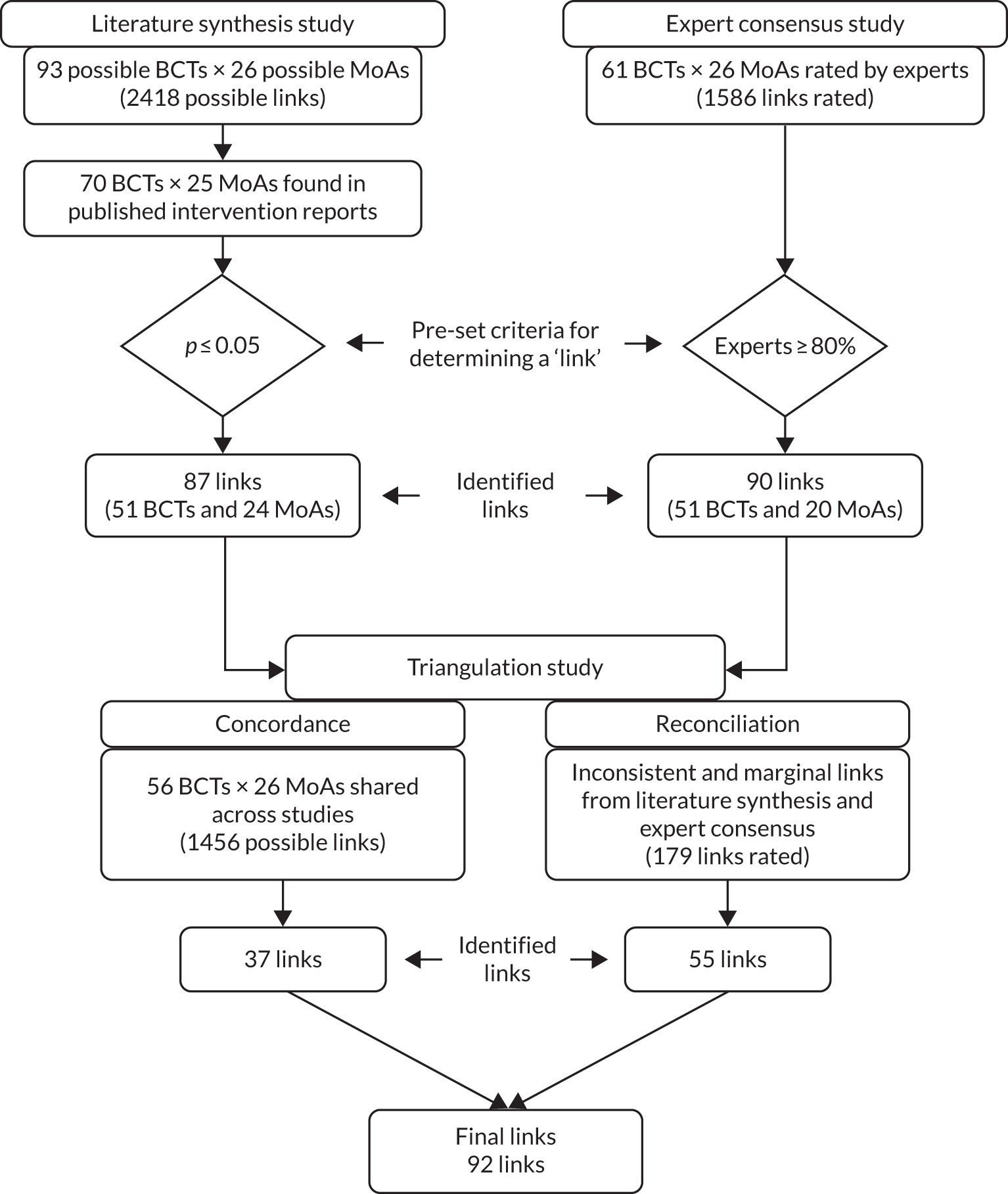
Results of concordance study: identifying concordant links
There was concordant evidence for links and non-links for 497 potential BCT–MoA links. A total of 37 links were identified (i.e. they met the pre-set criterion for a link in both the literature synthesis and the expert consensus studies). These links covered 28 BCTs and 18 of the 26 MoAs (Table 5). In addition, 460 non-links (i.e. experts agreed that the BCTs did not act through these MoAs and there was no evidence of a link in the literature) were found, involving 61 BCTs and 22 MoAs (see Appendix 6).
| BCT | MoA | Literature synthesis study | Expert consensus study: proportion of experts (definitely yes) | |
|---|---|---|---|---|
| Frequency (number of papers) | p-value | |||
| 1.2 Problem-solving | Beliefs about capabilities | 65 | 0.008 | 0.95 |
| 1.3 Goal-setting (outcome) | Goals | 4 | 0.003 | 1.00 |
| 1.6 Discrepancy between current behaviour and goal | Goals | 3 | 0.001 | 0.81 |
| 1.7 Review outcome goals | Goals | 2 | 0.012 | 0.89 |
| 2.7 Feedback on outcomes of behaviour | Feedback processes | 2 | 0.027 | 0.80 |
| 3.1 Social support (unspecified) | Social influences | 34 | < 0.001 | 0.87 |
| 3.2 Social support (practical) | Environmental context and resources | 3 | 0.026 | 0.90 |
| Social influences | 4 | 0.023 | 0.81 | |
| 4.1 Instruction on how to perform the behaviour | Skills | 20 | 0.024 | 0.86 |
| 5.1 Information about health consequences | Knowledge | 18 | < 0.001 | 0.89 |
| Beliefs about consequences | 26 | < 0.001 | 0.95 | |
| Perceived susceptibility/vulnerability | 10 | < 0.001 | 0.84 | |
| 5.3 Information about social and environmental consequences | Beliefs about consequences | 20 | < 0.001 | 0.95 |
| 5.6 Information about emotional consequences | Beliefs about consequences | 6 | 0.005 | 0.90 |
| 6.1 Demonstration of the behaviour | Social learning/imitation | 3 | 0.044 | 0.84 |
| 6.2 Social comparison | Social influences | 9 | 0.043 | 1.00 |
| Subjective norms | 31 | < 0.001 | 0.81 | |
| 6.3 Information about others’ approval | Subjective norms | 13 | < 0.001 | 0.89 |
| 7.1 Prompts/cues | Behavioural cueing | 6 | 0.002 | 1.00 |
| Environmental context and resources | 5 | 0.036 | 0.90 | |
| 8.1 Behavioural practice/rehearsal | Skills | 24 | < 0.001 | 0.95 |
| Beliefs about capabilities | 47 | 0.013 | 0.86 | |
| 8.3 Habit formation | Behavioural cueing | 3 | 0.001 | 0.85 |
| 8.7 Graded tasks | Beliefs about capabilities | 28 | < 0.001 | 0.90 |
| 9.2 Pros and cons | Beliefs about consequences | 12 | < 0.001 | 0.90 |
| Attitude towards the behaviour | 9 | < 0.001 | 0.81 | |
| Motivation | 5 | 0.023 | 0.86 | |
| 9.3 Comparative imagining of future outcomes | Beliefs about consequences | 3 | 0.017 | 1.00 |
| 10.3 Non-specific reward | Reinforcement | 2 | 0.005 | 0.95 |
| 10.4 Social reward | Reinforcement | 3 | 0.020 | 1.00 |
| 12.1 Restructuring the physical environment | Environmental context/resources | 9 | < 0.001 | 0.95 |
| Behavioural cueing | 3 | 0.020 | 0.89 | |
| 12.2 Restructuring the social environment | Environmental context/resources | 3 | 0.004 | 0.95 |
| 12.5 Adding objects to the environment | Environmental context/resources | 8 | < 0.001 | 0.95 |
| 13.1 Identification of self as role model | Self-image | 2 | 0.011 | 0.90 |
| 13.2 Framing/reframing | Attitude towards the behaviour | 7 | 0.014 | 0.81 |
| 15.1 Verbal persuasion about capability | Beliefs about capabilities | 27 | < 0.001 | 1.00 |
Thus, there was concordance between the studies for a total of 497 (31.3%) of the total 1586 possible links at this stage. There were 179 BCT–MoA combinations (11.5%) where evidence was inconclusive as either it was marginal or there was a discrepancy between the results of the two studies; these inconclusive links were brought forward to be rated and discussed by experts in the reconciliation study.
For the remaining BCT–MoA combinations, there was not enough evidence to classify them as links or non-links but neither was there potential for resolution as there was neither disagreement between the studies nor evidence approaching the thresholds for links or non-links. These 904 BCT–MoA combinations where < 80% of experts agreed a link was definitely present or definitely absent and a p-value of > 0.05 in the literature study constituted the 56.9% of links where there was a ‘lack of evidence’.
Results of multilevel modelling to quantify agreement between the results of the literature synthesis and expert consensus studies
The overall evidence of agreement is first presented visually, as scatterplots with regression lines, in Figure 9 for expert consensus on a ‘link’. The p-values from the literature study are plotted against the proportion of ‘definitely yes’ and ‘definitely no’ responses in the expert consensus study, with each line representing one MoA for all MoAs except ‘norms’, which was not found. In each case, lower p-values indicate higher frequency of links. The negative slope of the regression lines indicates that lower p-values were associated with a higher frequency of ‘yes’ responses by experts. Thus, the slopes indicate agreement between the two sources of evidence and this pattern is apparent for each MoA. Each line represents the prediction from the multilevel model. The thick line is the overall regression line. Other lines represent each MoA. The dots indicate the predicted values for actual data points. The occasions when no link was proposed in the literature synthesis study (coded as p = 1) have been omitted.
FIGURE 9.
Relationship between findings from the literature synthesis and expert consensus studies when links between BCTs and MoAs have been proposed (i.e. ‘yes’, BCT and MoA linked). Note that each dot represents one BCT (with BCTTv1 label). The line represents the prediction from the multilevel model omitting BCTs for which p = 1 in the literature study (but the expert consensus values for such BCTs are shown).
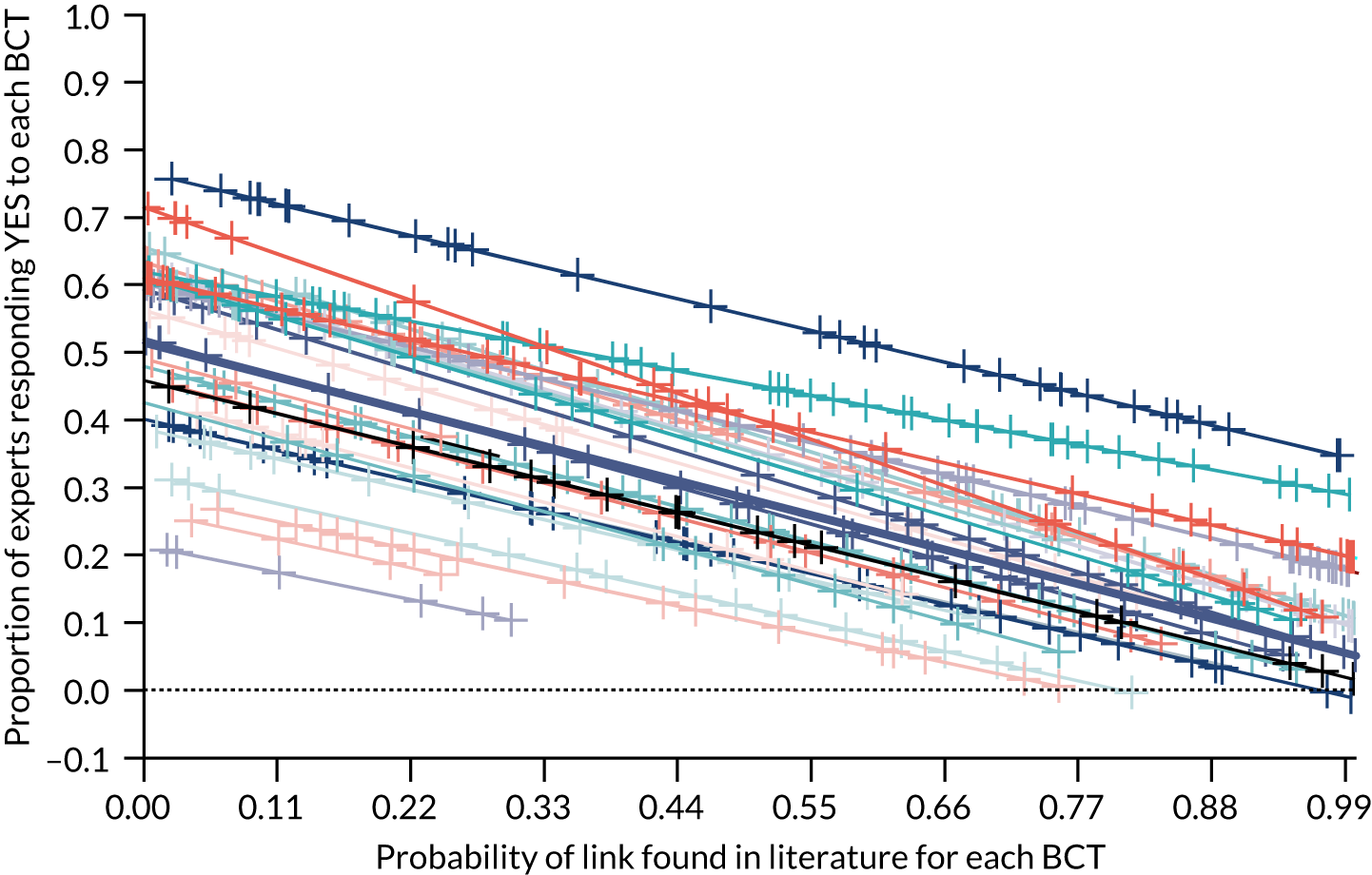
Figure 10 illustrates the findings for a single MoA with the p-values from the literature study plotted against the proportion of experts responding ‘yes’ (or ‘no’) showing the regression line and with each data point being one BCT labelled as in BCTTv1. 17 The MoA ‘behavioural cueing’ is strongly associated in both studies with the BCT ‘7.1 prompts and cues’ and BCT ‘12.5 adding objects to the environment’ for ‘yes’ responses by experts, indicating agreement that these BCTs may act via this MoA in changing behaviour.
FIGURE 10.
Relationship between literature and expert consensus when links between BCTs and MoA ‘behavioural cueing’ have been proposed. Note that each dot represents one BCT (with BCTTv1 label). The line represents the prediction from the multilevel model omitting BCTs for which p = 1 in the literature study (but the expert consensus values for such BCTs are shown).
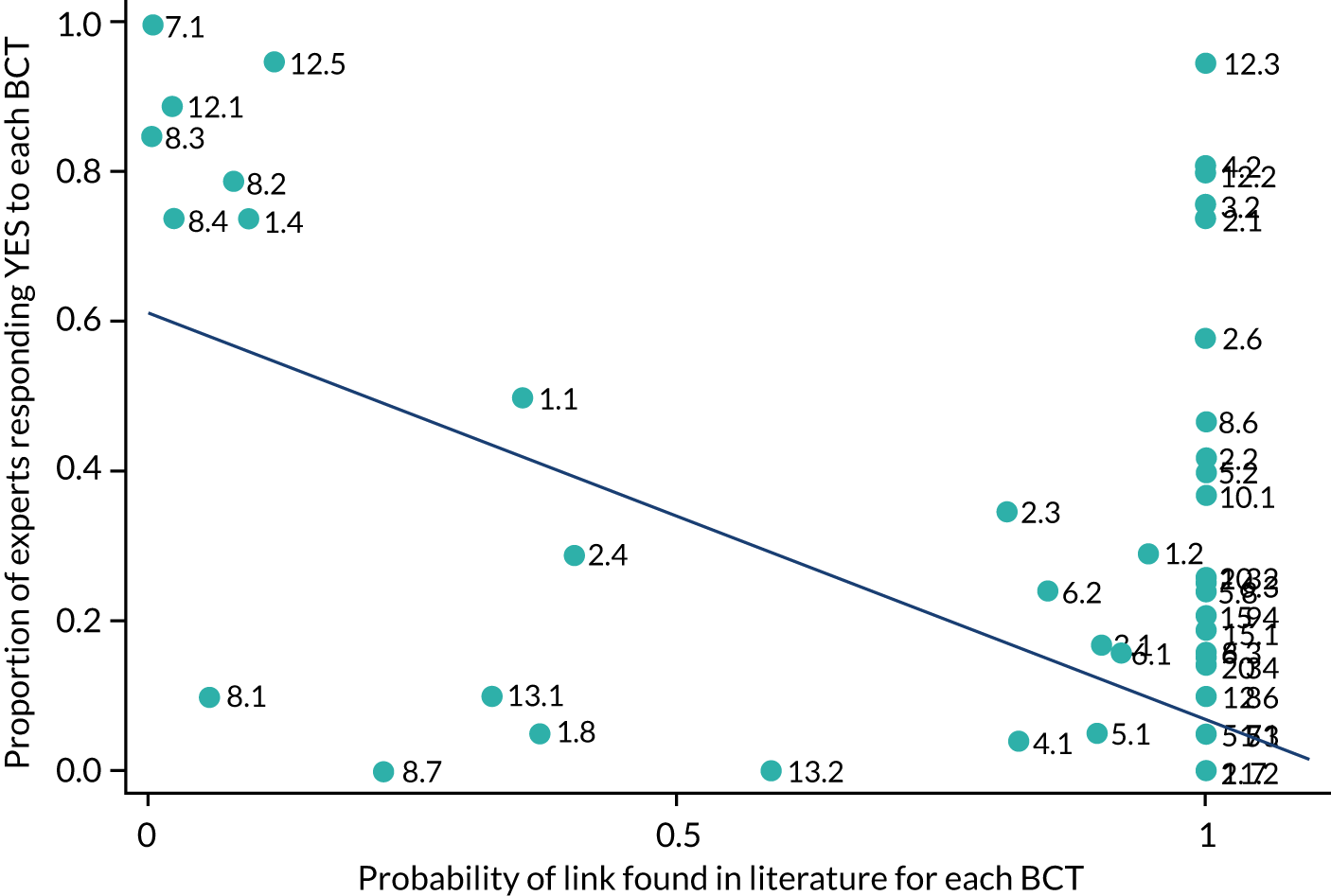
Detailed scatterplots for each of the 25 MoAs (not for ‘norms’ as this was not found in the literature study), showing which BCTs are linked to which MoAs in the two studies along with the labels for each BCT, can be accessed in Report Supplementary Material 2.
The multilevel models are reported in Table 6 and details of unstandardised regression intercepts and slopes for each MoA are shown in Table 7. Because the results are broadly similar whether p-values of 1 (which occur when a BCT is not linked to the target MoA) are included or removed, the latter are reported here, but both are presented in Tables 6 and 7. The total variance explained by the ‘yes’ model was 42.8%. The comparable value for the ‘no’ responses was 45.0%. As there was little difference in slopes between MoAs, larger intercepts for ‘yes’ responses indicate greater agreement across studies that a link exists: the slopes indicate the relationship between the studies for each MoA. Apart from the MoA ‘norms’, which was not found in the literature synthesis study, each MoA shows negative slopes for ‘yes’ responses and positive slopes for ‘no’ responses, indicating moderate concordance between the results of the two studies for virtually all MoAs.
| ‘Yes’ expert consensus | ‘No’ expert consensus | |||
|---|---|---|---|---|
| All data | p = 1 omitted | All data | p = 1 omitted | |
| Fixed effects, estimated beta weights (standard error) | ||||
| Intercept | 0.474 (0.037)*** | 0.510 (0.036)*** | 0.295 (0.030)*** | 0.270 (0.029)*** |
| Literature | –0.325 (0.031)*** | –0.464 (0.042)*** | 0.327 (0.240)*** | 0.439 (0.035)*** |
| Random effects, variances (standard error) | ||||
| Level 2: MoA | ||||
| Intercept | 0.029 (0.01)*** | 0.025(0.009)* | 0.017 (0.007)* | 0.014 (0.006) |
| Literature | 0.016 (0.007)* | 0.014 (0.011) | 0.006 (0.004) | 0.005 (0.007) |
| Level 1: BCT | ||||
| Intercept | 0.045 (0.002)*** | 0.059 (0.004)*** | 0.056 (0.002)*** | 0.058 (0.003)*** |
| MoA | ‘Yes’ all | ‘Yes’, p = 1 BCTs removed | ‘No’ all | ‘No’, p = 1 BCTs removed | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Int | Slp | n | Int | Slp | n | Int | Slp | n | Int | Slp | |
| Knowledge | 56 | 0.48 | –0.37 | 29 | 0.52 | –0.50 | 56 | 0.30 | 0.36 | 29 | 0.26 | 0.43 |
| Skills | 56 | 0.35 | –0.29 | 36 | 0.40 | –0.41 | 56 | 0.47 | 0.35 | 36 | 0.39 | 0.54 |
| Social/professional role and identity | 56 | 0.24 | –0.19 | 19 | 0.32 | –0.40 | 56 | 0.46 | 0.35 | 19 | 0.39 | 0.52 |
| Beliefs about capabilities | 56 | 0.58 | –0.36 | 51 | 0.60 | –0.43 | 56 | 0.18 | 0.29 | 51 | 0.14 | 0.38 |
| Optimism | 56 | 0.22 | –0.15 | 19 | 0.29 | –0.38 | 56 | 0.38 | 0.29 | 19 | 0.36 | 0.49 |
| Beliefs about consequences | 56 | 0.63 | –0.44 | 37 | 0.66 | –0.55 | 56 | 0.19 | 0.35 | 37 | 0.20 | 0.37 |
| Reinforcement | 56 | 0.54 | –0.33 | 20 | 0.56 | –0.51 | 56 | 0.26 | 0.31 | 20 | 0.26 | 0.44 |
| Intentions | 56 | 0.59 | –0.25 | 42 | 0.62 | –0.33 | 56 | 0.14 | 0.22 | 42 | 0.08 | 0.34 |
| Goals | 56 | 0.61 | –0.38 | 28 | 0.63 | –0.53 | 56 | 0.19 | 0.29 | 28 | 0.18 | 0.37 |
| Memory, attention and decision processes | 56 | 0.43 | –0.33 | 28 | 0.48 | –0.47 | 56 | 0.29 | 0.36 | 28 | 0.27 | 0.43 |
| Environmental context and resources | 56 | 0.71 | –0.54 | 22 | 0.71 | –0.62 | 56 | 0.20 | 0.40 | 22 | 0.22 | 0.37 |
| Social influences | 56 | 0.60 | –0.50 | 28 | 0.62 | –0.53 | 56 | 0.27 | 0.43 | 28 | 0.26 | 0.40 |
| Emotion | 56 | 0.42 | –0.29 | 20 | 0.46 | –0.47 | 56 | 0.27 | 0.30 | 20 | 0.29 | 0.43 |
| Behavioural regulation | 56 | 0.59 | –0.36 | 36 | 0.61 | –0.41 | 56 | 0.20 | 0.32 | 33 | 0.15 | 0.38 |
| Norms | – | – | – | – | – | – | – | – | – | – | – | – |
| Subjective norms | 56 | 0.41 | –0.34 | 25 | 0.46 | –0.44 | 56 | 0.36 | 0.40 | 25 | 0.30 | 0.46 |
| Attitude towards the behaviour | 56 | –0.57 | –0.43 | 27 | 0.59 | –0.54 | 56 | 0.20 | 0.35 | 27 | 0.21 | 0.37 |
| Motivation | 56 | 0.76 | –0.40 | 36 | 0.77 | –0.43 | 56 | 0.04 | 0.27 | 36 | 0.03 | 0.29 |
| Self-image | 56 | 0.34 | –0.17 | 15 | 0.39 | –0.41 | 56 | 0.30 | 0.27 | 15 | 0.30 | 0.47 |
| Needs | 56 | 0.15 | –0.12 | 6 | 0.21 | –0.36 | 56 | 0.57 | 0.21 | 6 | 0.55 | 0.66 |
| Values | 56 | 0.24 | –0.13 | 4 | 0.27 | –0.38 | 56 | 0.39 | 0.29 | 4 | 0.42 | 0.55 |
| Feedback processes | 56 | 0.60 | –0.42 | 12 | 0.61 | –0.52 | 56 | 0.28 | 0.36 | 12 | 0.24 | 0.42 |
| Social learning/imitation | 56 | 0.38 | –0.33 | 10 | 0.43 | –0.46 | 56 | 0.47 | 0.36 | 10 | 0.41 | 0.54 |
| Behavioural cueing | 56 | 0.60 | –0.37 | 21 | 0.61 | –0.54 | 56 | 0.23 | 0.29 | 21 | 0.26 | 0.42 |
| General attitudes/beliefs | 56 | 0.46 | –0.34 | 3 | 0.49 | –0.47 | 56 | 0.28 | 0.34 | 3 | 0.27 | 0.43 |
| Perceived susceptibility/vulnerability | 56 | 0.37 | –0.31 | 11 | 0.43 | –0.49 | 56 | 0.41 | 0.36 | 11 | 0.38 | 0.50 |
Results of reconciliation study
The 179 links for which there was inconclusive evidence across the literature synthesis and expert consensus studies were brought forward to be discussed and rated by the reconciliation experts. They reached the criterion for agreement that there was a link, that is ≥ 80% rated it ‘definitely yes’, for 55 possible links shown in Table 8. The criterion for agreement on a ‘non-link’, that is ≥ 80% rated it ‘definitely no’ link, was reached for five links (see Appendix 6).
| BCT | MoA | Literature synthesis study | Expert consensus study | Reconciliation study | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Yes (%) | Possibly (%) | Don’t know (%) | No (%) | Yes (%) | Don’t know (%) | No (%) | ||
| 8.2 Behaviour substitution | Behavioural regulation | 5 | 0.016 | 79 | 5 | 0 | 16 | 93.75 | 6.25 | 0 |
| 5.1 Information about health consequences | Attitude towards the behaviour | 19 | < 0.001 | 68 | 21 | 0 | 11 | 81.25 | 18.75 | 0 |
| 5.3 Information about social and environmental consequences | Attitude towards the behaviour | 16 | < 0.001 | 76 | 5 | 9.5 | 9.5 | 93.75 | 6.25 | 0 |
| 5.3 Information about social and environmental consequences | Knowledge | 13 | 0.002 | 67 | 24 | 0 | 9 | 81.25 | 18.75 | 0 |
| 2.3 Self-monitoring of behaviour | Behavioural regulation | 18 | < 0.001 | 70 | 15 | 0 | 15 | 93.75 | 6.25 | 0 |
| 9.1 Credible source | General attitudes/beliefs | 2 | 0.007 | 68 | 26 | 0 | 6 | 87.5 | 12.5 | 0 |
| 15.4 Self-talk | Beliefs about capabilities | 8 | 0.054 | 42 | 47 | 0 | 11 | 81.25 | 18.75 | 0 |
| 15.3 Focus on past success | Beliefs about capabilities | 23 | < 0.001 | N/A | N/A | N/A | N/A | 100 | 0 | 0 |
| 1.2 Problem-solving | Behavioural regulation | 13 | 0.13 | 100 | 0 | 0 | 0 | 100 | 0 | 0 |
| 1.6 Discrepancy between current behaviour and goal | Feedback processes | 1 | 0.08 | 100 | 0 | 0 | 0 | 100 | 0 | 0 |
| 10.8 Incentive (outcome) | Motivation | N/A | N/A | 100 | 0 | 0 | 0 | 87.5 | 12.5 | 0 |
| 1.1 Goal-setting (behaviour) | Intention | 17 | 0.33 | 95 | 5 | 0 | 0 | 87.5 | 12.5 | 0 |
| 1.1 Goal-setting (behaviour) | Goals | 4 | 0.23 | 95 | 0 | 5 | 0 | 87.5 | 12.5 | 0 |
| 5.1 Information about health consequences | Intention | 28 | 0.004 | 63 | 26 | 0 | 11 | 81.25 | 18.75 | 0 |
| 2.2 Feedback on behaviour | Feedback processes | 3 | 0.07 | 95 | 5 | 0 | 0 | 100 | 0 | 0 |
| 7.1 Prompts/cues | Memory, attention and decision processes | 8 | < 0.001 | 76 | 24 | 0 | 0 | 93.75 | 6.25 | 0 |
| 11.3 Conserving mental resources | Memory, attention and decision processes | 1 | 0.07 | 100 | 0 | 0 | 0 | 81.25 | 18.75 | 0 |
| 10.1 Material incentive (behaviour) | Reinforcement | 0 | 1 | 95 | 5 | 0 | 0 | 93.75 | 6.25 | 0 |
| 10.4 Social reward | Social influences | 2 | 0.56 | 95 | 5 | 0 | 0 | 81.25 | 18.75 | 0 |
| 11.2 Reduce negative emotions | Emotion | 1 | 0.21 | 95 | 0 | 5 | 0 | 87.5 | 12.5 | 0 |
| 12.3 Avoidance/reducing exposure to cues | Environmental context and resources | 1 | 0.22 | 95 | 5 | 0 | 0 | 93.75 | 6.25 | 0 |
| 12.3 Avoidance/reducing exposure to cues | Behavioural cueing | 0 | 1 | 95 | 5 | 0 | 0 | 100 | 0 | 0 |
| 12.5 Adding objects to the environment | Behavioural cueing | 2 | 0.12 | 95 | 5 | 0 | 0 | 93.75 | 6.25 | 0 |
| 14.10 Remove punishment | Reinforcement | N/A | N/A | 95 | 5 | 0 | 0 | 93.75 | 6.25 | 0 |
| 1.5 Review behaviour goals | Goals | 2 | 0.064 | 90 | 0 | 0 | 10 | 87.5 | 12.5 | 0 |
| 6.2 Social comparison | Norms | 0 | 1 | 90 | 5 | 0 | 5 | 81.25 | 18.75 | 0 |
| 6.2 Social comparison | Feedback processes | 2 | 0.21 | 90 | 5 | 0 | 5 | 100 | 0 | 0 |
| 11.2 Reduce negative emotions | Behavioural regulation | 0 | 1 | 90 | 5 | 5 | 0 | 81.25 | 18.75 | 0 |
| 7.5 Remove aversive stimulus | Environmental context and resources | N/A | N/A | 90 | 5 | 5 | 0 | 87.5 | 12.5 | 0 |
| 10.8 Incentive (outcome) | Reinforcement | N/A | N/A | 90 | 0 | 5 | 5 | 87.5 | 12.5 | 0 |
| 10.10 Reward (outcome) | Reinforcement | N/A | N/A | 90 | 5 | 5 | 0 | 100 | 0 | 0 |
| 10.10 Reward (outcome) | Motivation | N/A | N/A | 90 | 10 | 0 | 0 | 81.25 | 18.75 | 0 |
| 6.3 Information about others’ approval | Norms | 0 | 1 | 90 | 5 | 5 | 0 | 93.75 | 6.25 | 0 |
| 10.2 Material reward (behaviour) | Reinforcement | 0 | 1 | 90 | 0 | 5 | 5 | 87.5 | 12.5 | 0 |
| 4.2 Information about antecedents | Knowledge | 3 | 0.051 | 86 | 14 | 0 | 0 | 93.75 | 6.25 | 0 |
| 4.1 Instruction on how to perform the behaviour | Knowledge | 17 | 0.013 | 74 | 18 | 1 | 7 | 81.25 | 0 | |
| 5.2 Salience of consequences | Beliefs about consequences | 2 | 0.43 | 85 | 10 | 0 | 5 | 81.25 | 18.75 | 0 |
| 6.3 Information about others’ approval | Social influences | 4 | 0.20 | 84 | 16 | 0 | 0 | 87.5 | 12.5 | 0 |
| 8.7 Graded tasks | Skills | 4 | 0.45 | 81 | 14 | 0 | 5 | 81.25 | 18.75 | 0 |
| 2.3 Self-monitoring of behaviour | Feedback processes | 2 | 0.17 | 80 | 15 | 0 | 5 | 81.25 | 18.75 | 0 |
| 2.6 Biofeedback | Knowledge | 0 | 1 | 79 | 16 | 0 | 5 | 81.25 | 12.5 | 6.25 |
| 6.1 Demonstration of the behaviour | Beliefs about capabilities | 60 | 0.003 | 58 | 37 | 5 | 0 | 87.5 | 0 | |
| 4.1 Instruction on how to perform the behaviour | Beliefs about capabilities | 62 | 0.08 | 79 | 17 | 0 | 4 | 87.5 | 12.5 | 0 |
| 9.1 Credible source | Attitude towards the behaviour | 7 | 0.09 | 79 | 21 | 0 | 0 | 100 | 0 | 0 |
| 10.1 Material incentive (behaviour) | Beliefs about consequences | 0 | 1 | 79 | 10.5 | 0 | 10.5 | 87.5 | 12.5 | 0 |
| 10.6 Non-specific incentive | Reinforcement | N/A | N/A | 79 | 5 | 0 | 16 | 93.75 | 6.25 | 0 |
| 15.4 Self-talk | Motivation | 2 | 0.1 | 79 | 16 | 0 | 5 | 87.5 | 12.5 | 0 |
| 1.3 Goal-setting (outcome) | Motivation | 3 | 0.09 | 76 | 19 | 0 | 5 | 87.5 | 12.5 | 0 |
| 4.2 Information about antecedents | Behavioural regulation | 2 | 0.22 | 76 | 10 | 0 | 14 | 81.25 | 18.75 | 0 |
| 9.2 Pros and cons | General attitudes and beliefs | 0 | 1 | 76 | 24 | 0 | 0 | 87.5 | 12.5 | 0 |
| 11.3 Conserving mental resources | Behavioural regulation | 1 | 0.15 | 76 | 14 | 0 | 10 | 81.25 | 18.75 | 0 |
| 1.4 Action-planning | Behavioural cueing | 4 | 0.09 | 74 | 16 | 0 | 10 | 81.25 | 18.75 | 0 |
| 5.2 Salience of consequences | Perceived susceptibility/vulnerability | 1 | 0.16 | 70 | 25 | 0 | 5 | 81.25 | 18.75 | 0 |
| 2.2 Feedback on behaviour | Motivation | 8 | 0.09 | 68 | 32 | 0 | 0 | 81.25 | 18.75 | 0 |
| 5.5 Anticipated regret | Beliefs about consequences | 2 | 0.06 | N/A | N/A | N/A | N/A | 87.5 | 12.5 | 0 |
Overall agreement was reached for 60 (33.52%) of the 179 BCT–MoA links. For the remaining 119 possible links there was insufficient evident to indicate either a ‘link’ or a ‘non-link’ and so they remain inconclusive. Fourteen of the 60 resolved links confirmed the literature synthesis finding, 42 confirmed the previous expert consensus finding and four links confirmed the marginal evidence provided by both studies (i.e. where 0.05 ≤ p ≤ 0.1 in literature synthesis and 70–79% of experts answered ‘definitely yes’).
Thus, finally, a total of 92 BCT–MoA links were identified, of which 37 and 55 were identified during the concordance and reconciliation stages, respectively. Links covered 51 out of 61 BCTs and 22 out of 26 MoAs. There were seven links for which the BCT had not been identified in the literature study and three that were found in the literature synthesis but not in the expert consensus study.
In summary, the results provide evidence for 92 hypothesised links as well as evidence that 465 links do not exist, and that more evidence is needed for the remaining links investigated.
Development of an online tool to make results accessible to users: the Theory and Technique Tool
An online interactive tool was developed to include each of the 1456 BCT–MoA links in an interactive format incorporating the data from all studies. Each BCT–MoA combination was classified as a ‘link’, a ‘non-link’, ‘inconclusive’ or ‘no evidence’ and presented in a colour-coded matrix of BCTs by MoAs. Clicking on any BCT–MoA cell of the matrix reveals the evidence for that combination from the three studies. Figure 11 shows a section of the matrix in a screenshot of the homepage of the tool, which can be accessed at https://theoryandtechniquetool.humanbehaviourchange.org/ (accessed 1 January 2020). Figures 12 and 13 show the screenshot following clicking on a ‘link’ and a ‘non-link’ and Figures 14 and 15 show the Resources and Collaboration portals, respectively.
FIGURE 11.
Theory and Technique Tool (TaTT) illustration showing home page.
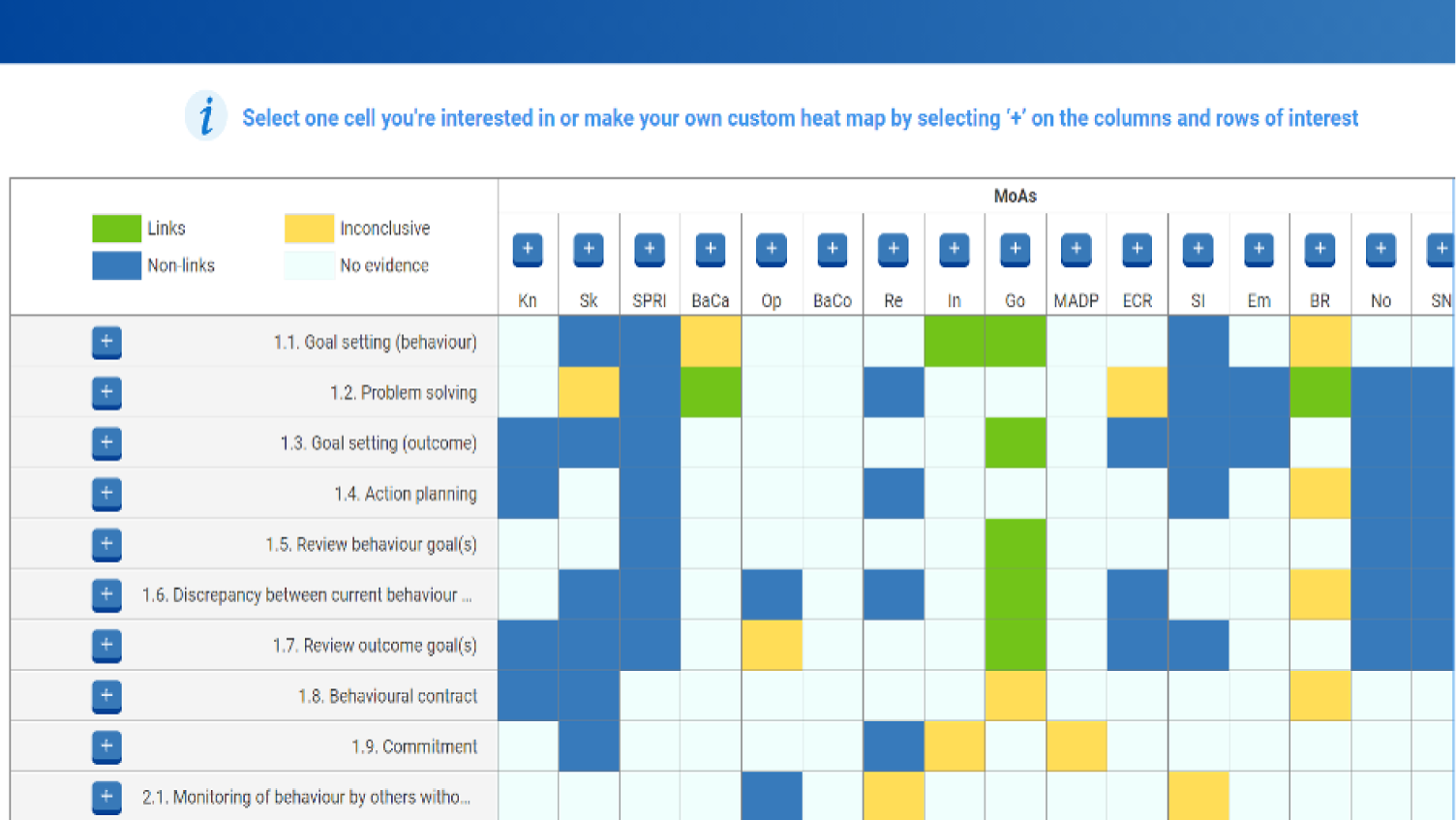
FIGURE 12.
Theory and Technique Tool (TaTT) illustration of results of clicking on a cell for a ‘link’.
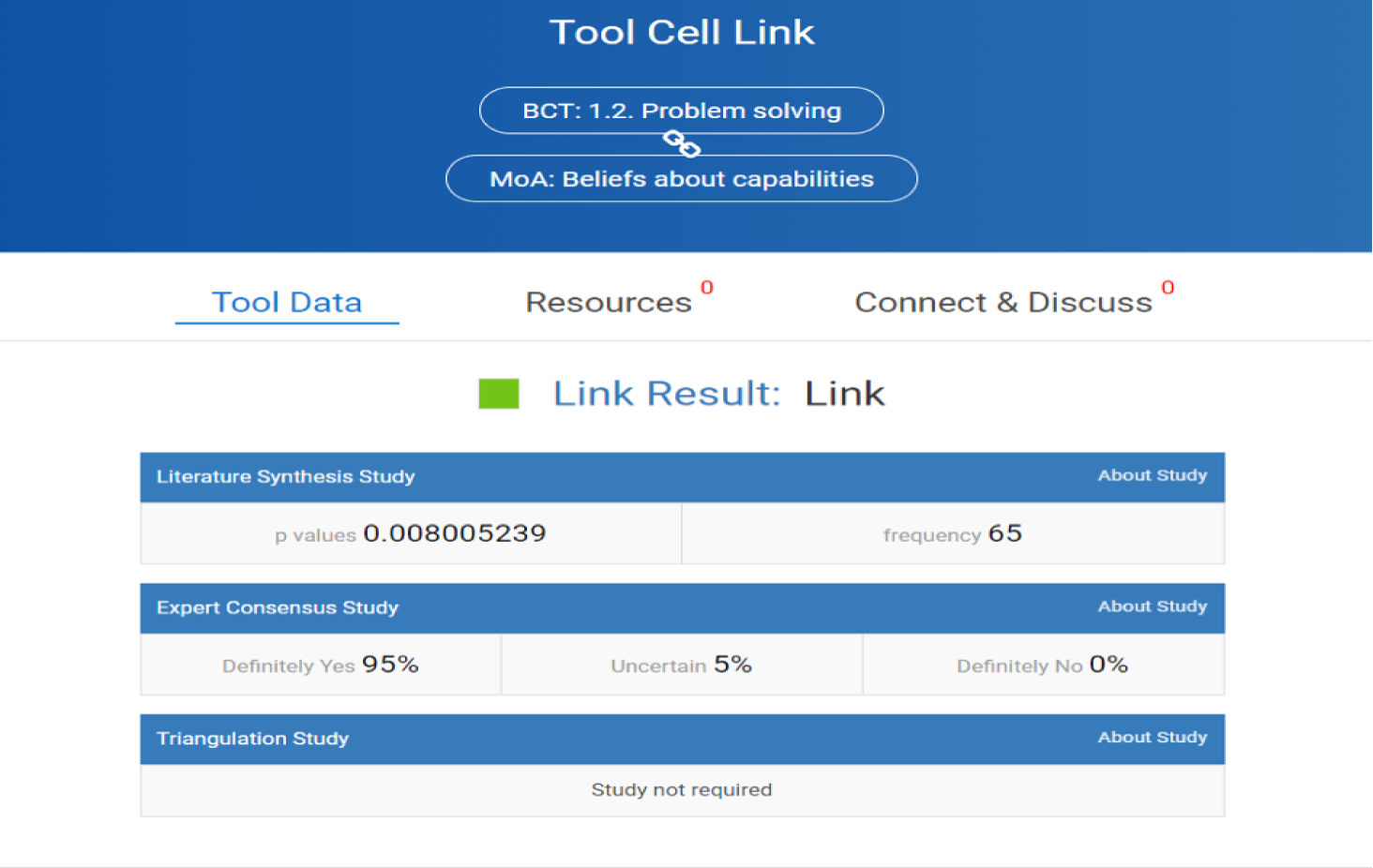
FIGURE 13.
Theory and Technique Tool (TaTT) illustration of results of clicking on a ‘non-link’.
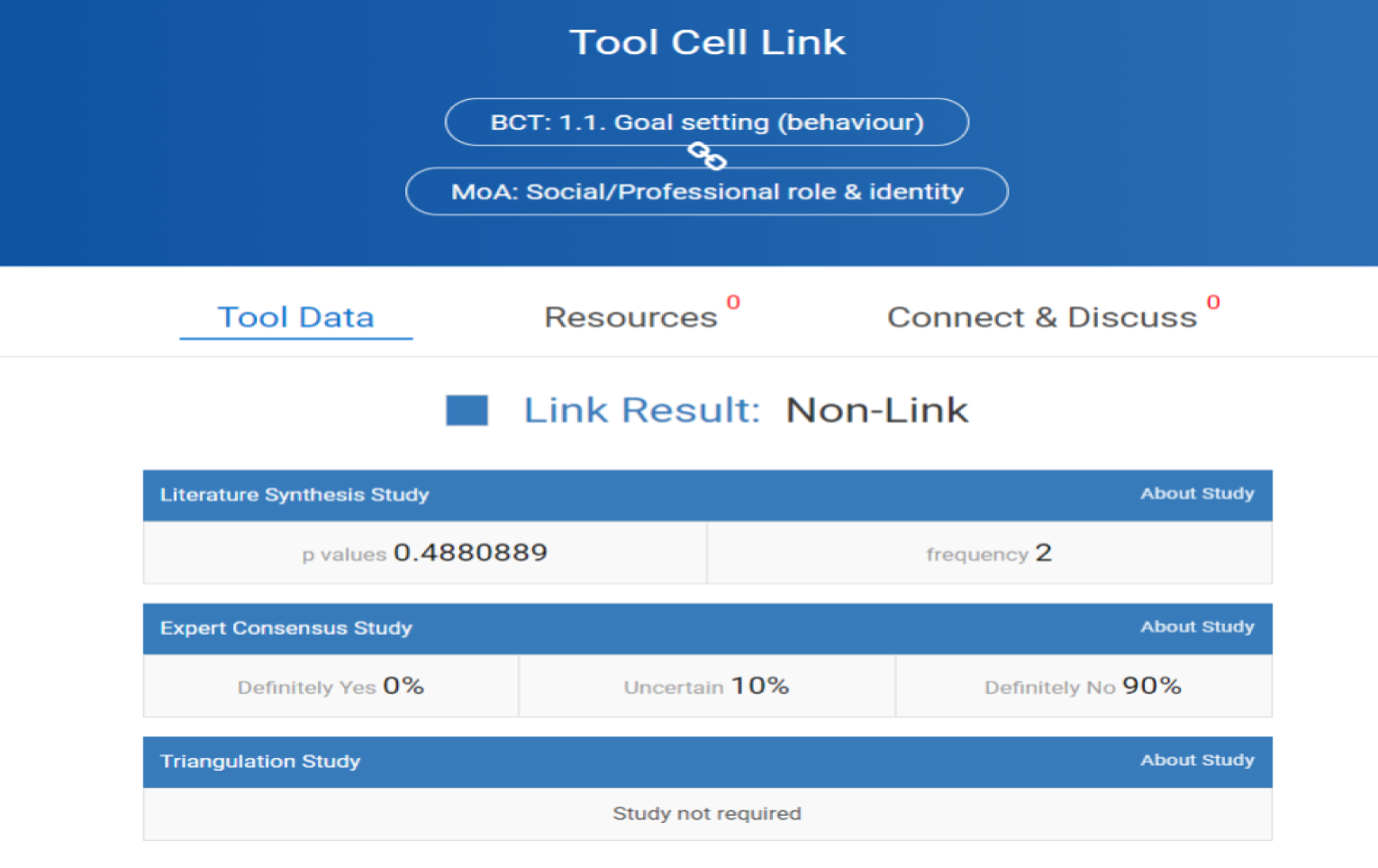
FIGURE 14.
Theory and Technique Tool (TaTT) illustration of screens for Resources.
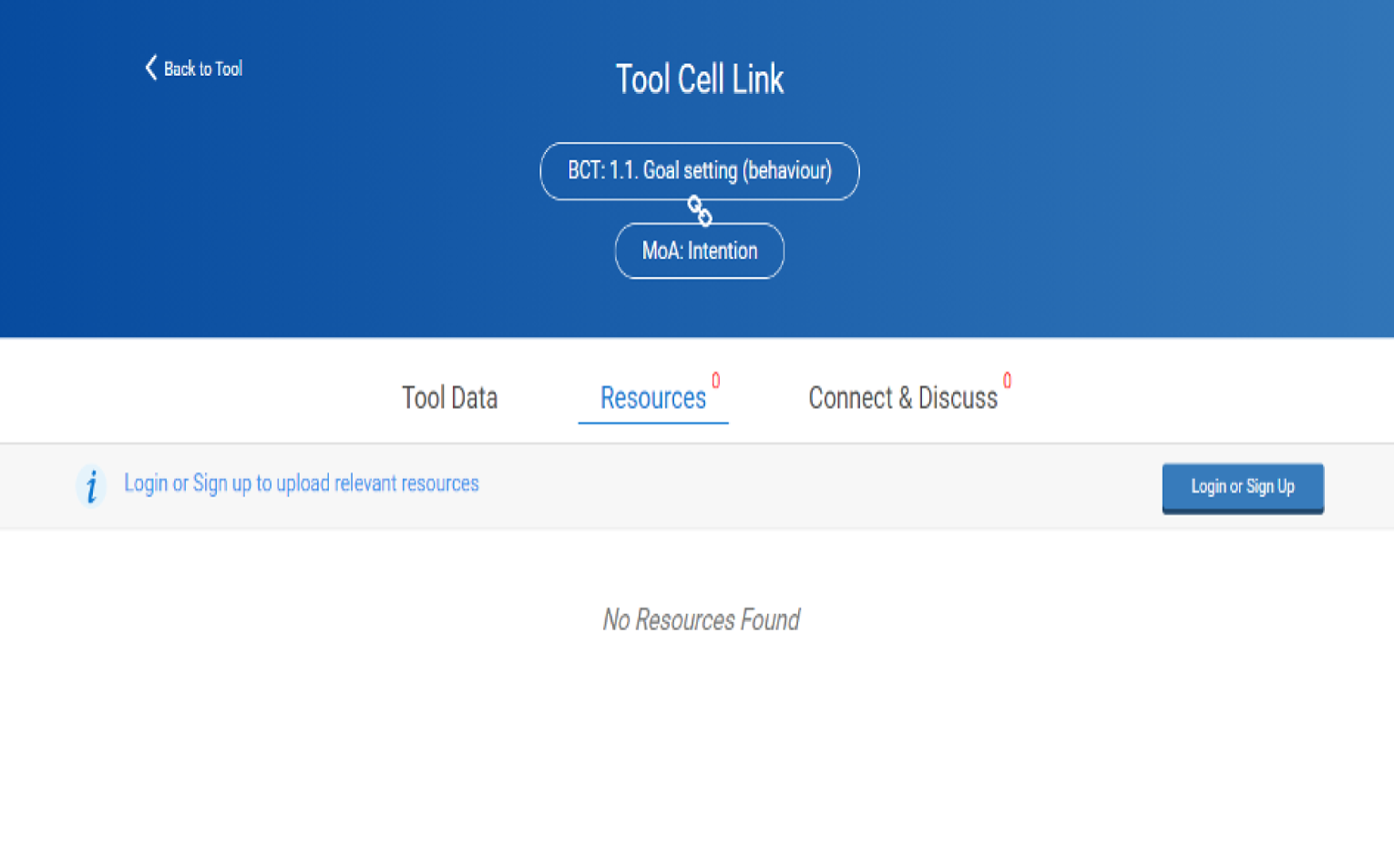
FIGURE 15.
Theory and Technique Tool (TaTT) illustration of screens for Connect & Discuss.
Discussion
This study aimed to triangulate evidence between a literature synthesis study of 277 intervention reports and a consensus study of 100 experts. Both studies provided evidence of potential links between BCTs and their MoA. However, by examining the degree of agreement between findings based on two quite different methods, the results provide more reliable evidence of hypothesised links. As a consequence, results could be used to provide a useful resource for evidence synthesis, the design and evaluation of interventions, and for identifying priorities for empirical research on BCT–MoA relationships.
Overall, there was evidence of agreement between the results of the two previous studies for 25 of the 26 MoAs investigated (as ‘norms’ was not found in the literature). There was also agreement for both links (where experts responded ‘definitely yes’) and non-links (where experts responded ‘definitely no’). Comparison of the matrices of BCT–MoA combinations reaching the threshold for a ‘link’ or a ‘non-link’ identified 37 links and 460 non-links. Following resolution by a further 16 ‘reconciliation’ experts, this increased to 92 hypothesised links that could be used to guide the design of interventions. In addition, 465 ‘non-links’ were agreed on, indicating the specific BCTs in BCT–MoA combinations that are unlikely to be effective in changing specific MoAs. The results also identified BCT–MoA combinations where there is insufficient evidence to hypothesise that specific BCTs would or would not effect change via specific MoAs.
Triangulation of the data obtained by two different methods resulted in evidence of substantial agreement. This provides evidence of replicability and thus greater confidence in the shared findings and a more secure basis for both interpreting intervention results theoretically and designing interventions. Although the methods used are quite different, they are not completely independent. On the one hand, experts’ judgements are likely to have been influenced by their knowledge of the published literature and, on the other hand, experts are likely to have designed and published some of the studies reviewed in the literature synthesis. Nevertheless, the results go beyond simple confirmation by replication of quantitative findings by identical methods, and instead used a reconciliation study to clarify discrepant and marginal findings.
The reconciliation experts resolved 60 of the 179 inconclusive BCT–MoA combinations, most often by agreeing with the previous expert consensus rather than the literature synthesis. This is likely to have occurred because of experts in both the previous expert consensus and the reconciliation studies being likely to have an awareness of current literature, whereas the literature synthesis may have provided more of a historical record of studies of behaviour change interventions. In addition, the experts in both studies could consider possible combinations, whereas the literature survey was restricted to what had actually been done and reported. Furthermore, reconciliation experts had much greater information than the original experts and comments in the discussion round of the reconciliation study indicated that they took into account all the previous evidence as well as their own opinions. However, the majority of reconciliation experts were European, perhaps due to the origin of BCT research being in the UK. Therefore, it is possible that different results may be obtained with experts from other continents but, given the spread of BCT research, this seems unlikely.
The links are relevant to a wide range of theoretical frameworks as they address the main current theoretical domains and commonly investigated theoretical constructs. The results provide a resource that may guide the selection of BCTs when an intervention designer has a hypothesis about the theoretical construct that influences the target behaviour. For example, a physiotherapist aiming to increase the activity of the stroke patient who was motivated but forgetful may find, from Figure 10, that the inclusion of the BCT ‘7.1 prompts and cues’ may be helpful.
Findings may also be used to support future research. For example, a researcher conducting a theory-based literature synthesis may use the hypothesised BCT–MoA links to suggest alternative theoretical explanations to those proposed or illustrated as being implicit within the original studies. A similar method was used in Gardner et al. ’s124 theoretical synthesis of audit and feedback interventions. The authors started by identifying techniques used in interventions and then mapped them to ‘. . . the most relevant behaviour change theories . . .’. 124 For example, from the BCTs ‘2.3 self-monitoring of behaviour’ and ‘1.4 action-planning’ they worked via the MoAs in control theory to reach a more coherent interpretation of the intervention trial results. 62 Therefore, the links identified in the current study may be helpful in clarifying other diverse intervention results. Nevertheless, it is important to remember that the current data do not provide empirical evidence of links but only indicate hypothesised links. More work is required to test whether or not the BCTs actually work by the hypothesised MoAs. The online TaTT may assist in selecting BCT–MoA combinations for further investigation and in integrating the resulting evidence.
The expert consensus and literature synthesis methods may have produced similar results as both may be informed by dominant theories of behaviour change. 125 For example, if experts had social cognitive theory126 in mind, it is plausible that a link between MoA ‘beliefs about capabilities’ might be linked to BCTs designed to enhance self-efficacy. Interventions reported in the literature are more likely to have been driven by theories involving rational, reflective, deliberative behaviour change MoAs than more recent studies involving more impulsive, associative, automatic processes, which have gained greater prominence in more recent times with the increasing emphasis on dual-processing theories. 127 For example, a greater emphasis on non-deliberative processes may lead to more intervention studies changing the physical environment. 127 In either case, identifying concordant links may enable intervention designers to make stronger connections between their theoretical framework, and resulting interventions may be more likely to overcome the criticism that interventions are more often theory-inspired than theory-based. 26,77 Even so, because of the complexity of behaviour change, the strength of BCT–MoA links may differ in different populations, settings and behavioural domains. Therefore, it would be valuable to investigate the moderating effects of context and behaviour in assessing the effects of interventions. 69
Although hypothesised links and non-links have been identified, results were inconclusive for a large number of BCT–MoA combinations. This may simply be reflective of the recency of the field. However, it may also reflect the lack of a shared terminology to enable aggregation of evidence as is a current focus of the Human Behaviour Change Project. 69 Furthermore, the current study did not investigate the co-occurrence of BCTs and it is possible that some BCTs may have a synergistic or antagonistic effect on the action of another BCT on the specified MoA. In most theories of behaviour change, theoretical constructs work together to change behaviour, and intervention mapping87 identifies parameters that add to the effectiveness of behaviour change methods. If interventions were designed with theoretical clusters in mind, then one would expect to see recurring clusters as similar theories are used and, consequently, this is investigated in Chapter 5. However, it was clear in the literature synthesis study that a single BCT could be used to target several MoAs, and that MoAs were frequently targeted by more than one BCT. BCTs working via several MoAs may be particularly useful in practical situations but less informative in clarifying theoretical questions.
The online tool provides detailed evidence for each BCT–MoA combination, giving users easy access to the information that they need without having to base an intervention plan on common sense or implicit theorising. It provides users with the results of the current, and two previous, studies and additionally allows them to interact with the tool by adding information, posting comments and collaborating with other users.
Conclusion
The concordance and reconciliation studies have triangulated two distinct sources of evidence: literature synthesis and expert consensus. The resulting set of hypothesised links between BCTs and MoAs provide a resource for researchers and practitioners (see Appendices 5 and 6 and in the interactive online TaTT). Evidence of the ‘links’ and ‘non-links’ could be used to guide intervention development and the theoretical interpretation of results of behaviour change interventions. Moreover, this study has revealed key areas where we lack evidence on potential BCT–MoA links, offering many opportunities for further research to strengthen the TaTT. Thus, the work reported could provide the basis for more systematic, co-ordinated research studies to examine and strengthen the evidence base underlying behaviour change interventions.
Chapter 5 Do combinations of behaviour change techniques that occur frequently in interventions reflect underlying theory?
Abstract
Background
Behaviour change interventions typically include several BCTs combined in accordance with the theory underlying the intervention. The theory may be stated explicitly, or unreported or implicit. However, the combination of BCTs used may provide insight into the theory underlying the intervention.
Purpose
This study aimed to identify groups of BCTs occurring together in behaviour change interventions and investigate whether or not these can be considered to be underpinned by specific theories.
Methods
In the first phase, groups of co-occurring BCTs were identified from 277 behaviour change intervention reports using factor analysis. In a subsequent consensus exercise, 25 experts were provided with these BCT groups and asked to identify theories consistent with these BCT groups and engage in discussion and ratings of links. The theories associated with each BCT group by the expert consensus were compared with those theories specified in the original reports where interventions used comparable groups of BCTs.
Results
The factor analysis identified five groups of co-occurring BCTs (range 3–13 BCTs per group). The experts reached ≥ 80% agreement on five links between three BCT groups and five behaviour change theories. Four of these theories have also been explicitly stated by several authors in the analysed intervention reports when interventions used a comparable set of BCTs.
Conclusions
The analyses found groups of BCTs that occurred together in interventions and experts could reach consensus on linking these groups to behaviour change theories. Thus, it may be possible to identify behaviour change theories underpinning groups of BCTs even when these have not been explicitly stated. Authors of published studies that made an explicit link between BCTs and theory also mentioned these theories, increasing confidence in this conclusion.
Introduction
There has been increasing emphasis on the desirability of drawing on theory when developing interventions to change behaviour or when interpreting the findings of evaluations of interventions. 15,41,71,72,128,129 Theories help to make sense of the complexity of behaviour change processes by summarising, in concise form, what is known about key entities and the relationships between these entities. Systematic application of theory can guide action by identifying MoAs to target with an intervention. Having an explicit, theory-based rationale for an intervention also enables that theory to be tested and refined on the basis of evaluation results. Because theory provides an organising framework, it can also be very helpful in synthesising evidence across studies about processes of change, thus building our knowledge about not only what interventions are effective in specific circumstances, but also how interventions have their effects. However, applying theory to interventions is not just a question of selecting a theory. The process also requires one to understand which combinations of BCTs are most likely to be effective in changing the MoAs specified by the theory, and hence the behaviour(s) of interest.
Despite the increasingly recognised importance of applying theory to developing interventions,15,41,71,72,128,129 the reporting of the use of theory is variable, often incomplete and the underpinning theory may not be explicitly stated. Rather, it may have to be inferred from the intervention report. 28,101 In these cases, it may be possible to identify clusters of BCTs associated with specific theories, thus giving an indication of the likely theoretical basis of the intervention.
In many cases, theories do not directly point to which BCTs, or BCT combinations, link to their component MoAs and thus they do not provide direct guidance to intervention developers. This is illustrated in relation to a frequently cited theory of behaviour change, the theory of planned behaviour. According to one of its authors, ‘Once it has been decided which beliefs the intervention will attempt to change, an effective intervention method must be developed. This is where the investigator’s experience and creativity come into play. The theory of planned behaviour can provide general guidelines, described below, but it does not tell us what kind of intervention will be most effective’. 130 Other theories provide more guidance about principles to draw on in developing interventions. For example, Bandura’s107 social-cognitive theory proposes four methods of intervention to increase self-efficacy: graded mastery, social modelling, social persuasion and re-interpretation of physiological states. Theories of risk perception posit that interventions will be more effective if they use techniques that increase perceived self- and response-efficacy alongside increasing fear arousal, as increasing fear arousal without increasing people’s beliefs that they can do something to reduce the threat is likely to be ineffective or even counter-productive. 131
When an intervention’s theoretical underpinning is not explicitly stated, it may be inferred from the BCTs included in the intervention. For example, the intervention ‘audit and feedback’ has considerable evidence of its effectiveness in changing clinician behaviour but there is less knowledge about how the intervention brings about its effects. 132 The combination of BCTs included in audit and feedback was analysed to investigate possible theoretical underpinnings. Three key BCTs were identified: ‘1.1 goal-setting’, ‘1.4 action-planning’ and ‘2.2 feedback on behaviour. 124 These were all linked to a self-regulation theory of behaviour change: control theory. 133 The theory posits that these BCTs work synergistically rather than additively, increasing the power of using them together. The authors of the updated Cochrane review62 were able to use this knowledge in a theory-based analysis of audit and feedback, which found that interventions including all three BCTs were more effective than those using feedback alone. 62 This is a good example of ‘retro-fitting’ a theoretical base from frequently co-occurring groups of BCTs that makes explicit what may have been an implicit theoretical understanding of those who developed the intervention. When implicit theories are made explicit, they become more useable and useful to others and therefore help to advance understanding and practice. 26,134,135
This chapter reports the final study in the programme of research, which investigated whether or not frequently occurring combinations of BCTs used in behaviour change interventions could be linked to behaviour change theories. We addressed this question with three main aims:
-
To what extent do BCTs co-occur across published reports of behaviour change interventions?
-
To what extent do behaviour change experts identify links between identified groups of BCTs and behaviour change theories?
-
For explicitly theory-based interventions, to what extent do the experts’ identification of theories linked to groups of BCTs match the theories stated by authors of interventions using similar groups of BCTs?
Methods
Study design
The study had three phases. The first was an analysis of 277 peer-reviewed reports of behaviour change intervention generated in a previous literature synthesis study101 in which interventions were coded according to their component BCTs as defined by the BCTTv1. The second phase was an expert consensus exercise, and the third was a comparison of the output of the literature analysis and expert consensus. 101–103
First, a factor analysis of the BCTs identified in interventions in the literature synthesis study (see Chapter 2)101 examined which BCTs tend to co-occur across interventions. Second, an expert consensus exercise established links between each of these BCT groups and theories of behaviour change (see Chapter 3). 102 Third, the data set of intervention reports was re-examined to identify interventions that used one of the BCT groups and were explicitly guided by a theory of behaviour change. Using this information, the similarity of the BCT group–theory links identified through expert consensus was compared with those specified in the literature by the intervention authors. 103
Phase 1: identify groups of behaviour change techniques that frequently co-occur in published intervention reports
Procedure
To identify groups of BCTs frequently co-occurring in the 277 intervention reports (see Chapter 2), exploratory factor analysis was used. This took account of the fact that BCTs are correlated across interventions and avoided imposing structure on the observed variables that cluster analysis, for example, does. 136
Analyses
There were no missing data because of the nature of the data. Exploratory factor analyses were conducted in Mplus v8 (Muthén & Muthén, Los Angeles, CA, USA), which allows for factor analysis of categorical and/or binary variables using the maximum likelihood estimator136 and an oblique rotation (geomin rotation). Exploratory factor analysis was conducted to identify groups of two or more BCTs that co-occurred across interventions. Given that a total of 77 BCTs were identified across the 277 intervention reports, those occurring in < 5% of interventions were excluded, thus improving the power of the analysis. Twenty-nine BCTs were excluded, leaving 48 in the analysis, coded in binary form: BCT presence versus absence.
Determining the number of factors retained
The number of factors retained was informed first by retaining factors with eigenvalues of > 1136 and then by examining scree plots (see Appendix 7), before examining multiple indices to give a conservative assessment of model fit. 136,137 The indices were comparative fit index (CFI) > 0.90, root-mean-square-error approximation (RMSEA) < 0.05 and the p-value for χ2 > 0.05. Finally, a solution in which BCTs did not load on more than one factor was preferred.
Identifying behaviour change technique factor group membership
The factor loadings in the factor solution with the fewest number of cross-loading BCTs were used to identify BCT co-occurrence. To give a conservative estimate for factor membership, given the large number of BCTs analysed across a relatively small number of interventions,137,138 only those BCTs with a factor loading ≥ 0.45 were retained. If a BCT had a loading > 0.45 on more than one factor, the BCT was retained on the factor for which it had the highest loading.
Phase 2: expert consensus exercise to identify links between behaviour change technique groups and theories
Participants
Twenty-five international experts with experience in designing, evaluating and/or synthesising evidence about theory-based behaviour change interventions and advanced knowledge of behavioural theories and BCTs were recruited from a pool of previous participants in our consensus exercises. 100,102,103 The number was chosen as expert panels of at least 20 members have been found to show stability in previous consensus studies. 112 In total, 56% were from the UK, 24% were from other European countries, 16% were from North America and 4% were from Australia. Two-thirds had a background in psychology.
Materials
For each round of the consensus exercise, experts were provided with the BCT groups identified in phase 1, along with the factor loading for each BCT and its definition, based on the BCTTv142 (see Appendix 8). To enable experts to identify theories that could be linked to each BCT group, they were given access to 83 theories of behaviour change as described in an e-edition of the ABC of Behaviour Change Theories. 30 Experts were asked to base their answers on the BCT definitions rather than making judgements based on the labels only. For each BCT group, they could identify none, one or more than one theory from the 83 provided or from their own knowledge or other sources. Full details of the procedure are provided in Appendices 8 and 9.
Procedure
The expert consensus exercise followed a modified consensus development method, based on the NGT. 109,111 The online exercise had four rounds: (1) an open response task round to generate links between BCT groups and theories, (2) initial rating of BCT–theory links to assess consensus, (3) discussion about links lacking consensus and (4) final rating of BCT–theory links. Responses were recorded using Qualtrics survey software and the discussion was hosted on the online forum Loomio.
Round 1
In an open response task, experts were asked to list all possible theories underpinning each of the five BCT groups identified in phase 1 by drawing on their own knowledge and theories from the ABC of Behaviour Change Theories book. 30
Round 2
Experts were presented with the five BCT groups along with the theories identified by more than one expert as linked to one of the BCT groups. The order of presenting the BCT groups and theories was randomised. Experts were asked to rate how confident they were (on a three-point scale: very confident, uncertain/don’t know or not at all confident) that the BCT group was linked to a given theory. Those BCT group–theory links that met the criterion of ≥ 80% experts being ‘very confident’ or ‘not at all confident’ responses were not presented for subsequent discussion and rating.
Round 3
Experts were provided with their own responses from round 2 and a summary of the responses of the other experts’ responses. They were then invited to exchange views about the BCT group–theory links for which there was not consensus in round 2 in an anonymous, asynchronous online forum over a period of 2 weeks. There were two types of links not achieving consensus: (1) those with high uncertainty (i.e. high percentage of ‘uncertain/don’t know’ responses) and (2) links with high disagreement (i.e. those where there were similar proportions of experts rating ‘very confident’ and ‘not at all confident’). For each BCT group–theory link, there were separate discussion threads; experts were invited to focus on the links that they were uncertain about or on which they disagreed with others. The discussion was summarised every now and again by a moderator who also raised issues for the experts to consider as they arose.
Round 4
Experts were provided with their round 2 certainty ratings for links between the five BCT groups and theories that did not reach consensus and were also given a link to the online discussion forum. Experts were asked to give their final ratings of their confidence in the BCT group–theory links on a three-point scale (very confident, uncertain/don’t know or not at all confident).
Experts were also asked to choose up to three theories that they were most confident were linked to a group of BCTs and were given the opportunity to change the BCTs in the groups by adding or removing BCTs. In doing this, they were encouraged to consider both the frequency and the strength of links between BCTs within a group (i.e. the factor loadings) and between BCTs and the theory’s component constructs.
Data analysis
-
Round 1: the number of unique theories listed by experts, the number of theories linked to each BCT group, and the number of theories linked to more than one BCT group were documented.
-
Round 3: the number of comments per online discussion thread and the number of comments per expert were documented.
-
Round 2 and round 4: using the consensus criterion of ≥ 80% of experts being ‘very confident’ or ‘not at all confident’ about a BCT group–theory link, data were used to identify which BCT groups were most frequently linked with confidence to theories.
-
Round 4: the frequency with which experts added or removed BCTs from a BCT group was documented.
Phase 3: comparison of behaviour change technique groups-theory links as generated by literature analysis and by expert consensus
Procedure
From the 277 published intervention reports,101 with interventions coded for component BCTs according to BCTTv1,42 those that contained more than half of the BCTs from a particular BCT group were included in further analysis. The data set was further refined by selecting those interventions for which there was an explicit statement that the intervention had been developed on the basis of one or more theories (0 = no theory mentioned, 1 = theory mentioned but not specified as underlying interventions, and 2 = theory-guided intervention). A second researcher checked a random 20% of the intervention reports for accurate selection of intervention reports and discrepancies were resolved through discussion (see Table 11).
Results
Phase 1: identify groups of frequently co-occurring behaviour change techniques from published intervention reports
The factor solution A factor solution between one and eight factors resulted from an exploratory factor analysis examining eigenvalues and scree plots. Although 16 factors had an eigenvalue of > 1, after eight factors the change in eigenvalues became increasingly consistent and small. Factor solutions between five and eight factors had satisfactory model fit across multiple fit indices (Table 9).
| Number of factors | RMSEA | CFI | χ2 (df); p-value |
|---|---|---|---|
| Target values for acceptable model fit | < 0.05 | > 0.90 | p > 0.05 |
| 1 | 0.034 | 0.746 | 1219.28 (1080); 0.001 |
| 2 | 0.030 | 0.802 | 1141.23 (1033); 0.01 |
| 3 | 0.027 | 0.845 | 1072.09 (987); 0.03 |
| 4 | 0.024 | 0.891 | 1001.81 (942); 0.09 |
| 5 | 0.019 | 0.932 | 935.27 (898); 0.19 |
| 6 | 0.015 | 0.960 | 876.23 (855); 0.30 |
| 7 | 0.013 | 0.973 | 827.62 (813); 0.35 |
| 8 | 0.005 | 0.996 | 774.32 (772); 0.47 |
The five-factor solution was judged to have the most acceptable model fit, with the most parsimonious solution and all pre-specified criteria for fit met. In the five-factor solution, only one BCT (‘12.3 avoidance/reducing exposure to cues for the behaviour’) loaded on more than one factor; a much larger number of BCTs cross-loaded in the eight-factor solution. The BCT groups were found not to be very highly correlated, although BCT group 2 had a significant interfactor correlation with two other BCT groups (Table 10).
| BCT group | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1 | 1.00 | |||
| 2 | 0.191* | 1.00 | ||
| 3 | 0.076 | 0.141 | 1.00 | |
| 4 | 0.122 | 0.192 | 0.020 | 1.00 |
| 5 | 0.206 | 0.274* | 0.062 | 0.112 |
Co-occurring behaviour change techniques by factor
Twenty-nine of the 48 BCTs were assigned to the five factors, based on the criterion of factor loadings of > 0.45. These are presented in rank-order in Table 4. BCTs with the highest factor loadings are the most descriptive of the group. The only BCT to have a factor loading of > 0.5 for more than one factor (‘12.3 avoidance/reducing exposure to cues for the behaviour’) was selected to load on BCT group 3, as it had a higher factor loading for this group than for group 5.
The BCT groups contained between three and 13 BCTs, and several of the BCTs within groups belonged to the same BCTTv1 clusters. For example, seven of the 13 BCTs in BCT group 1 belong to the BCTTv1 cluster ‘1.0 goals and planning’, and two of three BCTs in BCT group 2 belong to BCTTv1 cluster ‘2.0 feedback and monitoring’. Three of the seven BCTs in BCT group 3 belong to the BCTTv1 grouping ‘5.0 natural consequences’ and two BCTs belong to the BCTTv1 grouping ’12.0 antecedents’. There were no BCTs in BCT groups 4 or 5 that belonged to the same BCTTv1 cluster.
Phase 2: expert consensus exercise to identify links between behaviour change technique groups and theories
Round 1
All 25 invited experts participated and between them listed 81 theories across the five BCT groups. Five did not come from the ABC of Behaviour Change Theories book30 provided for the task. Of these, 75 theories were linked to a BCT group by more than one expert and were, therefore, carried forward to round 2. Thirty-six theories were identified as potentially underpinning BCT group 1; 45 for BCT group 2; 68 for BCT group 3; 25 for BCT group 4; and 20 for BCT group 5. Eight theories were identified as potentially underpinning all five BCT groups: the COM-B model (capability, opportunity, motivation model of behaviour), social cognitive theory, self-efficacy theory, self-determination theory, Health Action Process Approach (HAPA), theory of planned behaviour, integrated theory of health behaviour change and the relapse prevention model. Ten theories were identified as potentially linked to four BCT groups. These results are summarised in Appendix 10.
Round 2
All experts participated in round 2 and between them rated their confidence in 194 BCT group–theory links. There was consensus for eight BCT group–theory links: for four pairings, ≥ 80% of experts were ‘very confident’ that the BCT group and the theory were linked. BCT group 1 linked with both ‘HAPA’, and ‘self-regulation theory.’ BCT group 4 linked with ‘self-efficacy theory’ and social cognitive theory’. For the four other pairings that reached consensus in round 2, ≥ 80% of experts were ‘not at all confident’ that they were linked. At least 50% of experts were ‘very confident’ in a further 31 links, ‘uncertain/don’t know’ about 10 links and ‘not at all confident’ about 57 links. For 23 BCT group–theory links there was high disagreement (n = 11) and/or uncertainty (n = 12) among experts, defined as nearly equal numbers of experts rating ‘very confident’ and ‘not at all confident’; and > 50% of experts indicating that they were ‘uncertain/don’t know’.
Round 3
All experts participated, discussing the 23 BCT group–theory links about which there was uncertainty or high disagreement in round 2. The total number of comments per expert ranged from 1 to 25 (mean 11.6, SD 7.08) and per discussion thread ranged from 7 to 22 (mean 12.29, SD 4.06). Although experts found the discussion helpful, they also found some of it difficult, as illustrated by the following quotations.
Helpful:
The discussion on this one has been very persuasive. I originally put uncertain for many of the reasons other[s] have highlighted above. From reading the justifications given above, I am happy to change to ‘not confident’.
Uncertain about how many BCTs in the BCT group needed to link to the theory:
. . . a little confused about the task, particularly in terms of whether all the different techniques had to relate to the theory in question, or whether just one of them might. Because in practice, when developing an intervention, people often draw on several different theories.
Lack of familiarity with some theories:
I was not aware of the Action theory model of consumption and I am not familiar with consumer behaviour. Mostly these aspects made me mark ‘not at all confident’.
I’m not very familiar with PRIME theory so not sure I could ever be ‘very confident’ about making a judgement about it!
Experts reported a tendency to be influenced by familiarity more than by the BCTs in rating confidence:
When I saw the percentages of agreement by other experts in the final round I got the feeling that those theories that are well known to health psychologists received higher confidence ratings than rather unknown theories – no matter whether the BCT groups really fitted.
Overwhelmed by the large number of theories to think about:
As there were so many theories involved I guess that none of the invited experts were experts for each of those theories . . . I had to look up most of the theories, because the exercise made me more and more confused about what I thought I knew about the theories I work most with as there was just too much information to process.
Round 4
All but one of the 25 experts participated in round 4, providing final confidence ratings about the 186 BCT group–theory links for which there was not consensus in round 2. Consensus was reached that > 80% of experts were ‘very confident’ about one link (0.54%), between BCT group 3 and the theory of planned behaviour, and ‘not at all confident’ about 13 links (7%). Expert consensus did not emerge for any of the 23 links for which there was high disagreement and/or uncertainty following round 2.
For the 81 theories generated in round 1, 10 experts reported the theory of planned behaviour was the theory that they were most confident about being linked to BCT group 3. Despite 42% of experts linking BCT group 3 to the theory of planned behaviour, six of the 10 experts who reported they were ‘most confident’ in the link indicated that they would not maintain all seven BCTs in the group, given a link to the theory. Three experts (12.5%) chose to remove BCT ’13.2 framing/reframing’ from the BCT group, and three removed BCT ’12.3 avoidance/reducing exposure to cues for the behaviour’.
Although consensus was not reached for any theory with BCT groups 2 and 5, 13 experts (54%) rated control theory, 12 experts (50%) rated feedback intervention theory, and 10 experts (42%) rated self-regulation theory in their top three most confident theories to be linked to BCT group 2. Similarly, 12 experts (50%) rated operant learning theory and 8 (33%) rated self-efficacy theory in their top three most confident theories for BCT group 5.
Consensus exercise outcome
There was consensus about five BCT group–theory links, with three BCT groups linked to more than one theory, but no theory linked to more than one BCT group. A full list of the BCT–theory links that experts did not agree on can be found in Appendix 11.
Phase 3: comparison of behaviour change technique groups–theory links as generated by literature analysis and by expert consensus
Of the 277 intervention reports, 177 contained at least half of the BCTs from a BCT group. Of the 177 intervention reports reflecting the BCT groups, 168 (61% of the total) included explicit mentioning of theory as underpinning the development of the intervention. The number of intervention reports for each of the five BCT groups and the number of BCTs in each group are shown in Table 11.
| BCT group | BCTs in BCT group (n) | Intervention reports (n) | Theory-guided interventions (n) | BCTs from BCT group used in intervention (n) | Intervention reports with [n] BCTs from BCT group (n) |
|---|---|---|---|---|---|
| 1 | 13 | 19 | 14 | 7 | 6 |
| 8 | 9 | ||||
| 9 | 2 | ||||
| 10 | 2 | ||||
| 2 | 3 | 73 | 40 | 2 | 54 |
| 3 | 19 | ||||
| 3 | 7 | 12 | 9 | 4 | 7 |
| 5 | 3 | ||||
| 7 | 2 | ||||
| 4 | 3 | 122 | 94 | 2 | 66 |
| 3 | 56 | ||||
| 5 | 3 | 13 | 11 | 2 | 11 |
| 3 | 2 |
To identify BCT group–theory links that were supported by both sources of evidence, theories that achieved consensus among the experts were compared with evidence from the literature regarding the number of intervention reports in which a theory was explicitly identified as underlying an intervention (Table 12).
| BCTs in BCT group | Factor loading | Theories identified by expert consensus | Experts ‘very confident’ in the link (%) | Theories identified in published intervention reports | Intervention reports with link (n) |
|---|---|---|---|---|---|
| BCT group 1 | |||||
| 1.5 Review behaviour goals | 0.823 | HAPA | 84 | Social cognitive theory | 5 |
| 1.4 Action-planning | 0.783 | Self-regulation theory | 80 | Self-determination theory | 4 |
| 15.3 Focus on past success | 0.729 | Theory of planned behaviour | 3 | ||
| 1.3 Goal-setting (behaviour) | 0.717 | HAPA | 3 | ||
| 15.4 Self-talk | 0.712 | TTM | 1 | ||
| 3.3 Social support (emotional) | 0.705 | IMB skills model | 1 | ||
| 1.2 Problem-solving | 0.624 | Control theory | 1 | ||
| 2.3 Self-monitoring of behaviour | 0.613 | Chronic disease self-management model | 1 | ||
| 8.7 Graded tasks | 0.570 | I-Change | 1 | ||
| 1.3 Goal-setting (outcome) | 0.560 | Motivational interviewing | 1 | ||
| 1.6 Discrepancy between current behaviour and goal | 0.523 | Relative deprivation | 1 | ||
| 2.4 Self-monitoring of outcomes of behaviour | 0.503 | Limited resources | 1 | ||
| 1.8 Behavioural contract | 0.489 | Narrative transportation theories | 1 | ||
| Implementation intentions | 1 | ||||
| BCT group 2 | |||||
| 2.7 Feedback on outcomes of behaviour | 0.807 | Social cognitive theory | 17 | ||
| 2.2 Feedback on behaviour | 0.740 | TPB | 9 | ||
| 6.2 Social comparison | 0.626 | Self-efficacy theory | 5 | ||
| Self-determination | 4 | ||||
| TTM | 3 | ||||
| IMB skills model | 3 | ||||
| Operant learning theory | 3 | ||||
| Precaution adaptation process model | 3 | ||||
| I-Change | 3 | ||||
| HAPA | 2 | ||||
| Health belief model | 2 | ||||
| Control theory | 2 | ||||
| Social comparison | 2 | ||||
| TRA | 2 | ||||
| Social impact theory | 2 | ||||
| Self-regulation theory | 2 | ||||
| TDF | 2 | ||||
| Protection motivation theory | 1 | ||||
| Social–ecological model | 1 | ||||
| Social support principles (Heaney and Israel139) | 1 | ||||
| Social support theories | 1 | ||||
| Social norms theory | 1 | ||||
| Behavioural self-regulation model | 1 | ||||
| Health education model | 1 | ||||
| EnRG framework | 1 | ||||
| Motivational interviewing | 1 | ||||
| Social identity theory | 1 | ||||
| Habit strength theory | 1 | ||||
| Dual process theory | 1 | ||||
| ANGELO model | 1 | ||||
| Perspectives on change model | 1 | ||||
| Knowledge-attitude-behaviour model | 1 | ||||
| CBT | 1 | ||||
| BCT group 3 | |||||
| 5.2 Salience of consequences | 0.665 | Theory of planned behaviour | 80 | Theory of planned behaviour | 3 |
| 12.3 Avoidance/reducing exposure to cues for the behavioura | 0.651 | Social cognitive theory | 1 | ||
| 6.3 Information about others’ approval | 0.599 | TTM | 1 | ||
| 12.2 Restructuring the social environment | 0.498 | HAPA | 1 | ||
| 5.3 Information about social and environmental consequences | 0.475 | PRIME | 1 | ||
| 5.1 Information about health consequences | 0.460 | TRA | 1 | ||
| 13.2 Framing/reframing | 0.453 | I-Change | 1 | ||
| TDF | 1 | ||||
| Implementation process theories | 1 | ||||
| BCT group 4 | |||||
| 8.1 Behavioural practice/rehearsal | 0.726 | Self-efficacy theory | 92 | Social cognitive theory | 40 |
| 6.1 Demonstration of the behaviour | 0.621 | Social cognitive theory | 84 | TPB | 20 |
| 4.1 Instruction on how to perform the behaviour | 0.563 | TTM | 11 | ||
| TRA | 6 | ||||
| Self-efficacy theory | 6 | ||||
| Health belief model | 5 | ||||
| TDF | 5 | ||||
| IMB skills model | 4 | ||||
| Social learning theory | 4 | ||||
| Self-determination | 4 | ||||
| CBT | 4 | ||||
| Self-regulation theory | 3 | ||||
| HAPA | 2 | ||||
| Control theory | 2 | ||||
| COM-B | 2 | ||||
| Operant learning theory | 2 | ||||
| I-Change | 2 | ||||
| Health promotion model | 2 | ||||
| PRIME | 1 | ||||
| Protection motivation theory | 1 | ||||
| Health proportion model | 1 | ||||
| Social–ecological model | 1 | ||||
| Family based theoretical framework | 1 | ||||
| Social inoculation theory | 1 | ||||
| Precaution adaptation process model | 1 | ||||
| Precaution adoption | 1 | ||||
| Organisational theory | 1 | ||||
| Self-management model | 1 | ||||
| Chronic disease self-management model | 1 | ||||
| Adapted physical activity model | 1 | ||||
| EnRG framework | 1 | ||||
| Motivational interviewing | 1 | ||||
| Planning | 1 | ||||
| Habit strength theory | 1 | ||||
| Dual process theory | 1 | ||||
| ANGELO model | 1 | ||||
| Knowledge–attitude–behaviour model | 1 | ||||
| Elaboration likelihood model | 1 | ||||
| Frames model | 1 | ||||
| Adult learning theory | 1 | ||||
| Implementation process theories | 1 | ||||
| Habit theory | 1 | ||||
| Implementation intentions | 1 | ||||
| Implementation model | 1 | ||||
| Self-control theory | 1 | ||||
| Empowerment theory | 1 | ||||
| BCT group 5 | |||||
| 12.6 Body changes | Social cognitive theory | 4 | |||
| 10.9 Self-reward | Self-efficacy theory | 3 | |||
| 11.2 Reduce negative emotions | Self-determination | 2 | |||
| TTM | 1 | ||||
| PRIME | 1 | ||||
| Self-management model | 1 | ||||
| I-Change | 1 | ||||
| Motivational interviewing | 1 | ||||
| CBT | 1 | ||||
For both BCT groups 1 and 3, one theory was linked to the BCT group by the experts, and these two theories were supported by both sources of evidence: the ‘HAPA’ was linked to group 1 and the ‘theory of planned behaviour’ to group 3. For group 4, two theories were supported by both sources of evidence: ‘social cognitive theory’ and ‘self-efficacy theory’. These were mentioned in the literature 48 (40 and 8, respectively) of the 152 times theories were mentioned (32%). The ‘theory of planned behaviour’ was not agreed on by experts for this BCT group. However, the ‘theory of planned behaviour’ was mentioned in the literature 20 times for group 4 intervention reports.
Experts did not identify any theory for groups 2 and 5. Intervention reports using group 2 BCTs mentioned ‘social cognitive theory’ 17 of the 82 times that theories were mentioned. For group 5, authors most commonly referred to ‘social cognitive theory’ and ‘self-efficacy theory’ 7 out of 15 times that theories were mentioned.
In the intervention reports, a number of the same theories were linked to multiple BCT groups. Table 13 lists the six theories that were linked to multiple BCT groups, and which of the five BCT groups each theory was linked to.
| BCT group | SCT | TTM | HAPA | TPB | SDT | SET |
|---|---|---|---|---|---|---|
| 1 | ✗ | ✗ | ✗ | ✗ | ✗ | |
| 2 | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| 3 | ✗ | ✗ | ✗ | ✗ | ✗ | |
| 4 | ✗ | ✗ | ✗ | ✗ | ✗ | |
| 5 | ✗ | ✗ | ✗ | ✗ |
Social cognitive theory and the transtheoretical model were linked to all five BCT groups, HAPA was linked to BCT groups 1–4, theory of planned behaviour to BCT groups 1–4, self-determination theory was linked to BCT groups 1, 2, 4 and 5, and self-efficacy theory was linked to BCT groups 2, 3 and 5.
Discussion
This study identified five distinct co-occurring groups of BCTs in an analysis of 277 published reports of behaviour change interventions, with few BCTs statistically loading on more than one factor (BCT group). The results suggest that there is a shared explanatory model among authors concerning which BCTs are likely to have a synergistic effect when combined. This assumption may have been implicit rather than explicitly stated. There was consensus among experts on three of these groups of co-occurring BCTs linking to one or more of five theories. Although several theories were mentioned below criterion level, experts did not reach the criterion for a link of the same theory to multiple BCT groups, suggesting that experts were able to implicitly identify a theory based on sets of frequently co-occurring BCTs.
Examination of the component BCTs suggested that group 1 focused on intention, goals and planning; group 3 focused on changing beliefs about norms and behaviour, and antecedents and consequences of behaviour; and group 4 focused on instruction, demonstration, practice and modelling. The links with theory were coherent, with group 1 being linked to the HAPA and self-regulation theory, group 3 being linked to the theory of planned behaviour, and group 4 being linked to social cognitive theory and self-efficacy theory.
These results demonstrate that it is possible to infer theories underpinning behaviour change interventions by examining groups of BCTs used together in interventions. This enables the theoretical understanding of interventions that have not been explicitly developed on the basis of theory. However, two groups of BCTs found to co-occur in intervention reports were not consistently linked to a theory, despite experts being provided with descriptions of 83 theories and having knowledge of others. It may be that intervention developers were not basing their interventions on likely MoAs, or that they were and the absence of a linked theory reflected a gap in theoretical knowledge in the field.
Expert discussion in the consensus study suggested that there was confusion about how to apply theories to intervention development resulting from the large number of theories and lack of guidance about their application. This is likely to explain the substantial number of interventions that were not reported as theory-based, as shown in Table 11. There appears to be much greater clarity about links between individual BCTs and individual MoAs than about links between BCT groups and theories (groups of mechanisms), as evidenced by the triangulation study reported in Chapter 4. 103 This study found 92 links identified in both the literature analysis and the expert consensus. 101,102 Further research comparing these links with the BCT group–theory links would provide another layer of validation of both sets of links.
In the comparison of the literature analysis and the expert consensus exercise, four out of the five links were also made by study authors, demonstrating consistency between explicit theorising in published reports and implicit theorising by working in reverse order, starting with co-occurring BCT groups. In considering the likelihood of a match between the theory associated with a group of BCTs as agreed by the experts and the theory reported by the study authors, it is important to bear in mind that in each case a choice is made from a very large number of possible theories. The experts were offered a source with 83 theories but were free to name any additional theories. The authors had no restrictions and one can assume that they could have chosen from at least 83 theories. However, there may be other constraints on the number of possible theories that experts or authors were choosing from. Nevertheless, given the current level of understanding in theory and intervention development, this methodology seems unlikely to enable readers to pinpoint a precise theoretical underpinning for a published intervention based on the combination of BCTs used. The strongest match was for group 4 and social cognitive theory (and self-efficacy theory), where 40 (+ 8) of 152 experts’ responses matched the authors’ theory. This may have been more successful as Bandura107 gives clear guidance on the methods that can be used to enhance a key construct in the theory, namely self-efficacy, whereas for other popular theories, such as the theory of planned behaviour, no such guidance is offered. If so, then developing a shared approach to working from theory to MoAs to the choice of BCTs could advance this field. The evidence and the TaTT described here may contribute to clearer delineation of the steps between theory and intervention.
Limitations
The results of the current study should be interpreted in the light of the size of the database: 277 interventions of evaluations with a health focus. Further investigation with more, or more diverse, interventions may produce different findings. Another further limitation is that factor analysis requires judgement when, as in this case, there are several possible numbers of factors with an acceptable model fit. We selected the factor solution with the fewest number of cross-loading BCTs; however, a different solution may have yielded different results. Another word of caution is that the 25 experts were mainly from health and psychology backgrounds. A larger and more diverse group may have provided different judgements. However, the congruence between the expert consensus and the literature analysis (see Chapters 2–4) provides a degree of confidence in the results.
A drawback of intervention designers and researchers not using theory routinely in their work is that it precludes the use of organising summary frameworks that enable the accumulation of knowledge over studies and domains about processes of change. 128 However, parallel programmes of research are addressing this problem. The first is the application of an ontology-based modelling system to represent 77 theories both diagrammatically and in computer-readable format in a searchable database. 140 The second is the development of a behaviour change intervention ontology, an organising knowledge framework, produced as part of the Human Behaviour-Change Project69 [www.humanbehaviourchange.org (accessed 1 January 2020)].
Conclusions
The five BCT group–theory links identified across literature analysis and expert consensus can inform intervention development, evaluation and evidence synthesis. This supports clear and systematic thinking about how theories may be applied by identifying appropriate groups of BCTs. It also enables evaluation of the processes of change of interventions that have not been explicitly developed on the basis of theory. The comparison between the expert consensus and (where available) the authors’ explicit theories suggests that it may also be possible to retro-fit theory to interventions when authors have not made an explicit theory link, but this is likely to be most successful when theories are specific about intervention methods. The evidence from this and related work can lead to advances in intervention design, theoretical thinking about behaviour change and creating effective interventions.
Chapter 6 Discussion and recommendations
Summary of purpose, methods and results
Many of the health challenges worldwide may be addressed by changing people’s behaviour. Behaviours such as physical inactivity, alcohol misuse, smoking and some dietary behaviours contribute to deaths and disability from cancers, cardiovascular diseases, type 2 diabetes, and so on, and interventions have been designed to change behaviours with a view to reducing exposures to these health risks. However, although there have been many interventions, the effects of these are variable and further information is needed to enhance their success. More information is needed about how interventions work to generate more useful theories of behaviour change, to guide research and to achieve more successful implementable interventions. Recent research has developed a taxonomy of 93 well-defined BCTs but we need more information on their MoAs (i.e. how these techniques might work to change behaviour). We therefore aimed to examine links between BCTs and MoAs and to make the results available in a format that is usable by researchers, practitioners and policy-makers.
First, we conducted a literature synthesis study in which the links made by authors of 277 behaviour change intervention studies were extracted and links occurring with significant frequency were identified. Second, behaviour change experts were engaged in a three-round consensus study in which they discussed and rated their confidence that each of 61 BCTs worked through each of 26 MoAs: 90 links and 460 ‘non-links’ reached the pre-set threshold of 80% agreement. The third study aimed to triangulate the findings of the first two and to reconcile differences. We viewed triangulation as important both as good scientific practice, and to be able to discuss discrepancies and identify new agreed links. We found agreement between the frequency of links in the first study and links or non-links in the second. Discrepant or uncertain BCT–MoA combinations were brought to a reconciliation consensus study with a new group of experts. Following their discussions and ratings, the final total was 92 links and 465 non-links. In the fourth study, we explored whether or not it was possible to deduce any shared thinking about how BCTs work together from the combinations of BCTs that authors frequently use together in interventions, particularly as the theories underlying published behaviour change interventions are often implicit or under-reported. We examined whether or not groups of BCTs identified through factor analysis revealed shared theoretical underpinnings. We found that experts agreed on underlying theory for three groups of BCTs and that the theories were also identified by authors using similar sets of BCTs.
Our results provide a framework that policy-makers and practitioners can use to guide the selection of BCTs to include in interventions. Table 14 suggests how the TaTT might be used as a guide to intervention by a policy-maker faced with a problem of spreading infection or by a general practitioner managing a diabetic patient who is having difficulty with weight loss.
| Person | Problem | Possible MoA | Potentially useful BCTs | BCTs that are unlikely to be useful |
|---|---|---|---|---|
| Policy-maker | Spread of infection | Lack of knowledge | Information about health consequences | Reward |
| Lack of skills (e.g. hand-washing) | Instruction on how to perform the behaviour | Goal-setting | ||
| General practitioner | Patient with diabetes struggling to lose weight | Lack of motivation | Pros and cons | – |
| Inability to regulate behaviour | Behaviour substitution | Information about health consequences |
Given the state of the field, the findings from our programme of research cannot be used to infer that the BCTs are effective in targeting the MoA, only that the links identified are ‘best bets’ for interventions to be effective in changing behaviour by changing the MoA, and that non-links are unlikely to be effective. However, as researchers become more mindful of the hypothesised links between BCTs and MoAs, they will be in a better position to generate the evidence needed to test the effectiveness of the proposed linkages. The creation of the TaTT based on the findings of studies 1, 2 and 3 provides easy identification of links for which effectiveness needs to be tested [https://theoryandtechniquetool.humanbehaviourchange.org/ (accessed 1 January 2020)]. The tool makes our results usable by researchers, practitioners and policy-makers. We believe that by enabling the pooling of resources and facilitating online interactive discussion and collaboration, the TaTT will be a key tool for generating the empirical work that is needed to move the field forward.
Strengths and limitations
We have identified several strengths of this programme of work:
-
Need and relevance – this project is a response to the needs of the field of behavioural science and intervention development more generally. The development of the BCTTv1 was an advance in providing behavioural science with a method for specifying intervention components using a common language. Over the last decade or so, there has been increasing recognition within behavioural medicine and population health research of the desirability of informing intervention development and evaluation with theory; however, there is a lack of guidance for doing this.
-
Triangulation – the methodology for generating final results was based on an analysis that triangulated two sources of evidence. The first was an analysis of published literature (see Chapter 2) reporting how authors conceptualise links between BCTs and MoAs over 10 behavioural domains and ranging from 1982 to 2016. The second was a consensus exercise of 100 experts spanning Europe, North America, Australasia and Africa. The study demonstrated agreement about both the presence of links and also the absence of links (i.e. agreement that BCTs were not linked to MoAs).
-
Multidisciplinary – we received advice from a scientific advisory board representing a deliberately broad range of countries, disciplines and topics of study.
-
Online tool – we made the findings maximally accessible and therefore useable by developing an open access online TaTT resource (https://theoryandtechniquetool.humanbehaviourchange.org/) that enables users to quickly find whether links are present, absent, uncertain or unknown along with the data that these categories are based on.
-
BCT and MoA combinations – in recognition of the fact that BCTs are often used in combination and theories usually involve more than one MoA, we investigated combinations of BCTs and theories as a whole in addition to single BCT–MoA links.
-
Dissemination and engagement – we disseminated widely using social media [e.g. blogs, Twitter (www.twitter.com; Twitter, Inc., San Francisco, CA, USA)] as well as via scientific conferences and journal articles. 101–104 We also engaged the research and intervention designer communities via workshops that gave participants experience of using the TaTT as well as learning about the work and considering future research possibilities and applications of the TaTT.
-
Collaboration enablement – in recognition of the desirability of making research as efficient and productive as possible, we included facilities for collaborating and sharing resources within the TaTT (https://theoryandtechniquetool.humanbehaviourchange.org/). This is a facility for researchers to upload information, evidence and research about specific links and/or seek collaborators for joint research.
A limitation of the work is that a project of this scale could not investigate all possible BCTs and MoAs, given the size and complexity of this kind of data set. The BCTTv1 provides labels, definitions and evidence from previous studies, which allowed identification of frequently cited BCTs for inclusion. However, there was no similar taxonomy of MoAs and, therefore, no reliable set of labels and definitions. As a result, the MoAs investigated represent the broad theoretical domains of the theoretical domains framework38 supplemented by MoAs occurring frequently in behaviour change theories. Furthermore, BCT–MoA combinations that are not covered here could be investigated as links or non-links. In addition, we were not able to include all behavioural domains in our analyses nor behavioural experts from all continents. The literature search identified more studies addressing lifestyle behaviours and fewer dealing with health service utilisation or the behaviour of health-care professionals. The behavioural experts were selected based on self-definition by those responding to our calls and were predominantly working in the field of psychology (60%) and in academic settings (75%). However, we made efforts to cover a range of domains and the MoAs were largely generated via a review of theories guided by anthropologists, sociologists, economists and psychologists. For future work, we would recommend checking expertise by web searches and using a multidisciplinary advisory board to generate experts from wider disciplinary backgrounds.
Another important issue to bear in mind is that this work is based on expert opinion, reporting and judgement; it is not based on empirical evidence about the range of effectiveness of links in published evaluations. This work did not set out to do this, but it lays the basis for others to systematically review the evidence for the links and to empirically test the links.
Sustainability of resources developed for use by the research community is a challenge, given that there is no model for the long-term sustainability of such resources outside the commercial one. The Cochrane Collaboration and the Equator set of guidelines including Consolidated Standards of Reporting Trials (CONSORT) have transformed the quality of scientific research and evidence synthesis. However, they are maintained with difficulty on the basis of piecemeal grants. For the BCTTv1 and the TaTT, we are exploring the model of a not-for-profit company to sustain and develop the resources as the need and opportunities arise.
Recommendations for researchers and intervention designers
TaTT can be used by researchers and intervention designers in the following ways.
Existing interventions:
-
Intervention reporting – enables reporting of intervention techniques and theoretical mechanisms in a standardised fashion, using a shared language. It enables the explicit reporting of theoretical processes underpinning interventions.
-
Intervention improvement – enables an analysis of current interventions in terms of the number of BCT–MoA links that are consistent with the evidence summarised in the TaTT and those that are inconsistent. This information can be used to inform potential improvements.
-
Intervention tailoring – offers suggestions for intervention designers regarding potential BCTs to use given the need to engage groups of individuals who differ in MoAs (e.g. knowledge, attitudes towards the behaviour).
Intervention development:
-
Provides information about which BCTs could be used to target MoAs that the intervention is designed to target (e.g. increasing intention, changing emotions), and which BCTs not to use.
-
Suggests theoretically coherent combinations of BCTs.
Understanding how interventions work:
-
Process evaluation –selecting BCT–MoA combinations that are links in TaTT provides a systematic method for identifying the MoAs to evaluate (or not evaluate) for component BCTs.
-
Intervention effects – suggests likely MoAs for interventions that have been developed without being explicitly based on theory, based on the BCTs included, providing a basis for intervention testing.
-
Ineffective interventions – supports the generation of hypotheses about why ineffective interventions did not have predicted effects by identifying ‘non-links’ between BCTs and MoAs.
Theory development:
-
Facilitates the specification of propositions within theories about links between interventions and theoretical mechanisms, enhancing the ability to develop studies that can test these propositions and, in turn, generate an evidence base that can inform the refinement of theories.
Future research
Evidence for the links identified
The links identified need to be tested empirically to examine if, for each of the 92 identified BCT–MoA links:
-
delivering the BCT affects the MoA
-
the effects of the BCT on behaviour change are mediated by changes in the MoA.
Examining intervention effectiveness in evidence synthesis
Currently the research literature is typically too heterogeneous to find an adequate number of studies examining the effectiveness of interventions based on a single BCT, MoA or BCT–MoA link. The findings reported here can inform strategies for synthesising evidence about intervention effects by suggesting groupings of interventions and/or component BCTs that are likely to be theoretically coherent either because they share MoAs or because they are linked to MoAs that are likely to act synergistically with each other. This would enable the answering of the following questions:
-
Are interventions that include the BCTs that target the same MoA effective?
-
Are interventions that include BCTs that target MoAs that act synergistically effective?
Generating new evidence about effective behaviour change technique–mechanism of action links
To date there has been no systematic way of selecting BCT–MoA links to investigate. The research findings reported here have identified BCT–MoA links that experts consider promising but have not been investigated in published studies. More studies should investigate these links, as in the following research question:
-
Are interventions based on BCT–MoA links made by experts but that currently lack published evidence (1) feasible and (2) effective?
Selecting intervention components
It is impossible to test the effectiveness of all possible combinations of BCTs to include in interventions. Fractional factorial designs are a method of testing ‘likely’ combinations but depend on evidence of which combinations may be most promising. The current findings provide an evidence base for selecting ‘best bets’, and the following research question:
-
In fractional factorial designs, are combinations of BCTs targeted at complementary MoAs more effective than combinations lacking the evidence provided by the current research?
Research collaboration and productivity
The TaTT provides a research portal for online collaboration as a means of gaining information about previous and current research on links and identifying potential collaborators, hence increasing efficiency and reducing waste in research investment. Questions for future investigation include:
-
How is the TaTT collaborative portal used?
-
Is information exchanged?
-
Are new collaborations forged?
-
Does collaboration generate efficient research?
Acknowledgements
This research was funded by the Medical Research Council via its Methodology Panel: ‘Developing methodology for designing and evaluating theory-based complex interventions: an ontology for linking behaviour change techniques to theory’ (reference MR/L011115/1). We thank the 42 members of our IAB (see Appendix 1) who gave invaluable advice at strategic points during the project and the 105 experts from across the world who took part in the two consensus studies in this programme of research. Finally, our thanks go to our many colleagues who have given invaluable feedback when the work has been presented at different stages at UK and international conferences and workshops.
Contributions of authors
Susan Michie (https://orcid.org/0000-0003-0063-6378) (Professor of Health Psychology and Principal Investigator) and Marie Johnston (https://orcid.org/0000-0003-0124-4827) (Professor of Health Psychology, co-investigator) led the development of the research proposal, study design and protocol. Together with co-investigators Alexander J Rothman (https://orcid.org/0000-0003-3163-1895) (Professor of Psychology), Marijn de Bruin (https://orcid.org/0000-0003-3100-6803) (Professor of Health Psychology) and Michael P Kelly (https://orcid.org/0000-0002-2029-5841) (Professor and Senior Visiting Fellow), they provided the scientific leadership for the project.
Rachel N Carey (https://orcid.org/0000-0002-3299-9723) (Research Associate) and Lauren EC Bohlen (https://orcid.org/0000-0003-4207-9872) (Research Associate) contributed to the design of the four studies and led the conduct of the research.
Hilary NK Groarke (https://orcid.org/0000-0001-6282-3254) (Research Assistant) led the conduct of study 4.
Niall C Anderson (https://orcid.org/0000-0003-1834-9086) (Senior Research Associate) contributed to and revised the final draft of this manuscript.
Silje Zink (https://orcid.org/0000-0003-4077-8629) (Research Assistant) prepared, contributed to and revised the final draft of this manuscript.
All the authors contributed to the development of the protocol and the writing of the manuscript, including its final version.
Publications
Carey RN, Connell LE, Johnston M, Rothman AJ, de Bruin M, Kelly MP, Michie S. Behaviour change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med 2018;53:693–707.
Connell LE, Carey RN, de Bruin M, Rothman AJ, Johnston M, Kelly MP, Michie S. Links between behaviour change techniques and mechanisms of action: an expert consensus study. Ann Behav Med 2018;53:708–20.
Johnston M, Carey RN, Connell LB, Johnston DW, Rothman AJ, de Bruin M, et al. Linking behaviour change techniques and mechanisms of action: triangulation of findings from literature synthesis and expert consensus [published online ahead of print August 4 2020]. Transl Behav Med 2020.
Bohlen LC, Michie S, de Bruin M, Rothman AJ, Kelly MP, Groarke HN, et al. Do combinations of behaviour change techniques that occur frequently in interventions reflect underlying theory? Ann Behav Med 2020;54:1–16.
Data-sharing statement
We have published our data set online through Open Science Framework (https://osf.io/7qjvn/) and through our interactive online tool (https://theoryandtechniquetool.humanbehaviourchange.org/tool), with the aim of the data being transparent and usable by the research community. We provide the full database of links and not just those links that met the p < 0.05 criterion, such that researchers can draw on all of the data as needed (e.g. using criteria of their choosing). We welcome further data extraction and/or additional analyses by researchers who are interested in examining these characteristics.
Data in the form of BCT coding of the 277 interventions identified through this study have been added to an open access online database that collates intervention articles in which BCTs have been identified (www.bct-taxonomy.com/interventions). Researchers can search this database using a number of criteria, including author, year, BCT and target behaviour. It also includes an option for researchers to upload their or others’ articles where BCTs have been coded using BCTTv1. The study findings have been incorporated into the interactive, online BCT–MoA tool, which allows users to select a particular BCT–MoA link and view the associated data. There is also a facility for researchers to add data and other information (e.g. ongoing research projects) relating to a particular link. We hope that this resource will facilitate collaborative research efforts to accumulate empirical evidence about each of the links in the matrix. Any other queries should be addressed to the corresponding author for consideration.
Disclaimers
This report presents independent research funded under a MRC–NIHR partnership. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the MRC, NETSCC, the HS&DR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the MRC, NETSCC, the HS&DR programme or the Department of Health and Social Care.
References
- Ezzati M, Riboli E. Behavioral and dietary risk factors for noncommunicable diseases. N Engl J Med 2013;369:954-64. https://doi.org/10.1056/NEJMra1203528.
- Kontis V, Mathers CD, Rehm J, Stevens GA, Shield KD, Bonita R, et al. Contribution of six risk factors to achieving the 25×25 non-communicable disease mortality reduction target: a modelling study. Lancet 2014;384:427-37. https://doi.org/10.1016/S0140-6736(14)60616-4.
- García MC, Bastian B, Rossen LM, Anderson R, Miniño A, Yoon PW, et al. Potentially preventable deaths among the five leading causes of death – United States, 2010 and 2014. MMWR Morb Mortal Wkly Rep 2016;65:1245-55. https://doi.org/10.15585/mmwr.mm6545a1.
- Bauer UE, Briss PA, Goodman RA, Bowman BA. Prevention of chronic disease in the 21st century: elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014;384:45-52. https://doi.org/10.1016/S0140-6736(14)60648-6.
- Garcia MC, Faul M, Massetti G, Thomas CC, Hong Y, Bauer UE, et al. Reducing potentially excess deaths from the five leading causes of death in the rural United States. MMWR Surveill Summ 2017;66:1-7. https://doi.org/10.15585/mmwr.ss6602a1.
- Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A, et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst Rev 2013;4. https://doi.org/10.1002/14651858.CD003543.pub3.
- Lorencatto F, Charani E, Sevdalis N, Tarrant C, Davey P. Driving sustainable change in antimicrobial prescribing practice: how can social and behavioural sciences help?. J Antimicrob Chemother 2018;73:2613-24. https://doi.org/10.1093/jac/dky222.
- Pinder R, Sallis A, Berry D, Chadborn T. Behaviour Change and Antibiotic Prescribing in Healthcare Settings – Literature Review and Behavioural Analysis. London: Public Health England; 2015.
- Rzewuska M, Charani E, Clarkson JE, Davey PG, Duncan EM, Francis JJ, et al. Prioritizing research areas for antibiotic stewardship programmes in hospitals: a behavioural perspective consensus paper. Clin Microbiol Infect 2019;25:163-8. https://doi.org/10.1016/j.cmi.2018.08.020.
- Burke JP. Infection control – a problem for patient safety. N Engl J Med 2003;348:651-6. https://doi.org/10.1056/NEJMhpr020557.
- Soler R, Orenstein D, Honeycutt A, Bradley C, Trogdon J, Kent CK, et al. Community-based interventions to decrease obesity and tobacco exposure and reduce health care costs: outcome estimates from communities putting prevention to work for 2010–2020. Prev Chronic Dis 2016;13. https://doi.org/10.5888/pcd13.150272.
- Cecchini M, Sassi F, Lauer JA, Lee YY, Guajardo-Barron V, Chisholm D. Tackling of unhealthy diets, physical inactivity, and obesity: health effects and cost-effectiveness. Lancet 2010;376:1775-84. https://doi.org/10.1016/S0140-6736(10)61514-0.
- Nugent R, Bertram MY, Jan S, Niessen LW, Sassi F, Jamison DT, et al. Investing in non-communicable disease prevention and management to advance the Sustainable Development Goals. Lancet 2018;391:2029-35. https://doi.org/10.1016/S0140-6736(18)30667-6.
- Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. IMAGE Study Group . Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-119.
- National Institute for Health and Care Excellence (NICE) . Behaviour Change: Individual Approaches 2014.
- National Institute for Health and Care Excellence (NICE) . Behaviour Change: General Approaches 2007.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:81-95. https://doi.org/10.1007/s12160-013-9486-6.
- Webster R, Michie S, Estcourt C, Gerressu M, Bailey J. the MenSS Trial Group . Increasing condom use in heterosexual men: development of a theory-based interactive digital intervention. Transl Behav Med 2016;6:418-27. https://doi.org/10.1007/s13142-015-0338-8.
- Ussher MH, Taylor A, Faulkner G. Exercise interventions for smoking cessation. Cochrane Database Syst Rev 2012;1. https://doi.org/10.1002/14651858.CD002295.pub4.
- Cahill K, Perera R. Competitions and incentives for smoking cessation. Cochrane Database Syst Rev 2008;3. https://doi.org/10.1002/14651858.CD004307.pub3.
- Marteau T, Hollands GJ, Kelly M, Kaplan RM, Spittel M, David DH. Emerging Behavioral and Social Science Perspectives on Population Health. Rockville, MD: Agency for Healthcare Research and Quality and Office of Behavioral and Social Sciences Research, National Institutes of Health; 2015.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance . Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Sniehotta FF, Presseau J, Araújo-Soares V. On the development, evaluation and evolution of health behaviour theory. Health Psychol Rev 2015;9:176-89. https://doi.org/10.1080/17437199.2015.1022902.
- Bernard P, Carayol M, Gourlan M, Boiché J, Romain AJ, Bortolon C, et al. Moderators of theory-based interventions to promote physical activity in 77 randomized controlled trials. Health Educ Behav 2017;44:227-35. https://doi.org/10.1177/1090198116648667.
- Arnott B, Rehackova L, Errington L, Sniehotta FF, Roberts J, Araujo-Soares V. Efficacy of behavioural interventions for transport behaviour change: systematic review, meta-analysis and intervention coding. Int J Behav Nutr Phys Act 2014;11. https://doi.org/10.1186/s12966-014-0133-9.
- Prestwich A, Sniehotta FF, Whittington C, Dombrowski SU, Rogers L, Michie S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol 2014;33:465-74. https://doi.org/10.1037/a0032853.
- Moore GF, Evans RE. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM Popul Health 2017;3:132-5. https://doi.org/10.1016/j.ssmph.2016.12.005.
- Prestwich A, Webb TL, Conner M. Using theory to develop and test interventions to promote changes in health behaviour: evidence, issues, and recommendations. Curr Opin Psychol 2015;5:1-5. https://doi.org/10.1016/j.copsyc.2015.02.011.
- Rothman AJ, Klein WM, Cameron LD. Advancing innovations in social/personality psychology and health: opportunities and challenges. Health Psychol 2013;32:602-8. https://doi.org/10.1037/a0032116.
- Michie S, West R, Campbell R, Brown J, Gainforth H. ABC of Behaviour Change Theories. London: Silverback Publishing; 2014.
- French SD, Green SE, O’Connor DA, McKenzie JE, Francis JJ, Michie S, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the Theoretical Domains Framework. Implement Sci 2012;7. https://doi.org/10.1186/1748-5908-7-38.
- Abraham C, Wood CE, Johnston M, Francis J, Hardeman W, Richardson M, et al. Reliability of identification of behavior change techniques in intervention descriptions. Ann Behav Med 2015;49:885-900. https://doi.org/10.1007/s12160-015-9727-y.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27:379-87. https://doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. App Psychol 2008;57:660-80. https://doi.org/10.1111/j.1464-0597.2008.00341.x.
- Michie S, Whittington C, Hamoudi Z, Zarnani F, Tober G, West R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012;107:1431-40. https://doi.org/10.1111/j.1360-0443.2012.03845.x.
- Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479-98. https://doi.org/10.1080/08870446.2010.540664.
- Michie S, Johnston M. Theories and techniques of behaviour change: developing a cumulative science of behaviour change. Health Psychol Rev 2012;6:1-6. https://doi.org/10.1080/17437199.2012.654964.
- Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci 2012;7. https://doi.org/10.1186/1748-5908-7-37.
- Abraham C, Good A, Huedo-Medina T, Warren M, Johnson B. Reliability and utility of the SHARP taxonomy of behaviour change techniques. Psychol Health 2012;27:1-2.
- Young MD, Collins CE, Callister R, Plotnikoff RC, Doran CM, Morgan PJ. The SHED-IT weight loss maintenance trial protocol: A randomised controlled trial of a weight loss maintenance program for overweight and obese men. Contemp Clin Trials 2014;37:84-97. https://doi.org/10.1016/j.cct.2013.11.004.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Michie S, Wood C, Johnston M, Abraham C, Francis J, Hardeman W. Behaviour change techniques: the devlelopment and evaluation of a taxonomic method for reporting and describing behaviour change interventions. Health Technol Assess 2015;19. https://doi.org/10.3310/hta19990.
- Cane J, Richardson M, Johnston M, Ladha R, Michie S. From lists of behaviour change techniques (BCTs) to structured hierarchies: comparison of two methods of developing a hierarchy of BCTs. Br J Health Psychol 2015;20:130-50. https://doi.org/10.1111/bjhp.12102.
- Wood CE, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. Applying the behaviour change technique (BCT) taxonomy v1: a study of coder training. Transl Behav Med 2015;5:134-48. https://doi.org/10.1007/s13142-014-0290-z.
- Michie S, Hyder N, Walia A, West R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict Behav 2011;36:315-19. https://doi.org/10.1016/j.addbeh.2010.11.016.
- Po’e EK, Heerman WJ, Mistry RS, Barkin SL. Growing Right Onto Wellness (GROW): a family-centered, community-based obesity prevention randomized controlled trial for preschool child–parent pairs. Contemp Clin Trials 2013;36:436-49. https://doi.org/10.1016/j.cct.2013.08.013.
- Schwarzer R, Antoniuk A, Gholami M. A brief intervention changing oral self-care, self-efficacy, and self-monitoring. Br J Health Psychol 2015;20:56-67. https://doi.org/10.1111/bjhp.12091.
- Newbury-Birch D, Coulton S, Bland M, Cassidy P, Dale V, Deluca P, et al. Alcohol screening and brief interventions for offenders in the probation setting (SIPS Trial): a pragmatic multicentre cluster randomized controlled trial. Alcohol Alcohol 2014;49:540-8. https://doi.org/10.1093/alcalc/agu046.
- Newby KV, French DP, Brown KE, Lecky DM. Increasing young adults’ condom use intentions and behaviour through changing chlamydia risk and coping appraisals: study protocol for a cluster randomised controlled trial of efficacy. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-528.
- Booth AR, Norman P, Goyder E, Harris PR, Campbell MJ. Pilot study of a brief intervention based on the theory of planned behaviour and self-identity to increase chlamydia testing among young people living in deprived areas. Br J Health Psychol 2014;19:636-51. https://doi.org/10.1111/bjhp.12065.
- Dale H, Raftery B, Locke H. Behaviour change and sexual health: SHARE programme evaluation. Health Educ 2014;114. https://doi.org/10.1108/HE-12-2012-0056.
- Bobrow K, Brennan T, Springer D, Levitt NS, Rayner B, Namane M, et al. Efficacy of a text messaging (SMS) based intervention for adults with hypertension: protocol for the StAR (SMS Text-message Adherence suppoRt trial) randomised controlled trial. BMC Public Health 2014;14. https://doi.org/10.1186/1471-2458-14-28.
- Treweek S, Bonetti D, Maclennan G, Barnett K, Eccles MP, Jones C, et al. Paper-based and web-based intervention modeling experiments identified the same predictors of general practitioners’ antibiotic-prescribing behavior. J Clin Epidemiol 2014;67:296-304. https://doi.org/10.1016/j.jclinepi.2013.09.015.
- Prior M, Elouafkaoui P, Elders A, Young L, Duncan EM, Newlands R, et al. Evaluating an audit and feedback intervention for reducing antibiotic prescribing behaviour in general dental practice (the RAPiD trial): a partial factorial cluster randomised trial protocol. Implement Sci 2014;9. https://doi.org/10.1186/1748-5908-9-50.
- Kaholokula JK, Wilson RE, Townsend CK, Zhang GX, Chen J, Yoshimura SR, et al. Translating the Diabetes Prevention Program in Native Hawaiian and Pacific Islander communities: the PILI ‘Ohana Project. Transl Behav Med 2014;4:149-59. https://doi.org/10.1007/s13142-013-0244-x.
- Jones CJ, Smith H, Llewellyn C. Evaluating the effectiveness of health belief model interventions in improving adherence: a systematic review. Health Psychol Rev 2014;8:253-69. https://doi.org/10.1080/17437199.2013.802623.
- Morton K, Beauchamp M, Prothero A, Joyce L, Saunders L, Spencer-Bowdage S, et al. The effectiveness of motivational interviewing for health behaviour change in primary care settings: a systematic review. Health Psychol Rev 2015;9:205-23. https://doi.org/10.1080/17437199.2014.882006.
- Shahab L, Beard E, Gardner B. BCT Analysis of Existing, Cost-Effective Interventions 2012. https://discovery.ucl.ac.uk/id/eprint/1450790/ (accessed 1 January 2020).
- Shahab L, Lorencatto F, Beard E. BCT Analysis of Behaviour Change Interventions Reported in Studies of Cost Effectiveness 2013. https://discovery.ucl.ac.uk/id/eprint/1450790/ (accessed 1 January 2020).
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol 2009;28:690-701. https://doi.org/10.1037/a0016136.
- Dombrowski SU, Sniehotta FF, Johnston M, Broom I, Kulkarni U, Brown J, et al. Optimizing acceptability and feasibility of an evidence-based behavioral intervention for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: an open-pilot intervention study in secondary care. Patient Educ Couns 2012;87:108-19. https://doi.org/10.1016/j.pec.2011.08.003.
- Ivers N, Jamtvedt G, Flottorp S, Young JM, Odgaard-Jensen J, French SD, et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev 2012;6. https://doi.org/10.1002/14651858.CD000259.pub3.
- Johnson BT, Michie S, Snyder LB. Effects of behavioral intervention content on HIV prevention outcomes: a meta-review of meta-analyses. J Acquir Immune Defic Syndr 2014;66:259-70. https://doi.org/10.1097/QAI.0000000000000235.
- Michie S, West R, Sheals K, Godinho CA. Evaluating the effectiveness of behavior change techniques in health-related behavior: a scoping review of methods used. Transl Behav Med 2018;8:212-24. https://doi.org/10.1093/tbm/ibx019.
- Michie S, Abraham C, Eccles MP, Francis JJ, Hardeman W, Johnston M. Strengthening evaluation and implementation by specifying components of behaviour change interventions: a study protocol. Implement Sci 2011;6. https://doi.org/10.1186/1748-5908-6-10.
- de Bruin M, Viechtbauer W, Hospers HJ, Schaalma HP, Kok G. Standard care quality determines treatment outcomes in control groups of HAART-adherence intervention studies: implications for the interpretation and comparison of intervention effects. Health Psychol 2009;28:668-74. https://doi.org/10.1037/a0015989.
- de Bruin M, Viechtbauer W, Schaalma HP, Kok G, Abraham C, Hospers HJ. Standard care impact on effects of highly active antiretroviral therapy adherence interventions: a meta-analysis of randomized controlled trials. Arch Intern Med 2010;170:240-50. https://doi.org/10.1001/archinternmed.2009.536.
- Michie S, Johnston M. Optimising the value of the evidence generated in implementation science: the use of ontologies to address the challenges. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0660-2.
- Michie S, Thomas J, Johnston M, Aonghusa PM, Shawe-Taylor J, Kelly MP, et al. The Human Behaviour-Change Project: harnessing the power of artificial intelligence and machine learning for evidence synthesis and interpretation. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0641-5.
- Patterson SM, Hughes C, Kerse N, Cardwell CR, Bradley MC. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst Rev 2012;5. https://doi.org/10.1002/14651858.CD008165.pub2.
- Kelly M, Morgan A, Ellis S, Younger T, Huntley J, Swann C. Evidence based public health: A review of the experience of the National Institute of Health and Clinical Excellence (NICE) of developing public health guidance in England. Soc Sci Med 2010;71:1056-62. https://doi.org/10.1016/j.socscimed.2010.06.032.
- Kelly MP, Moore TA. Methodological, theoretical, infrastructural, and design issues in conducting good outcome studies. Res Social Work Prac 2011;21:644-53. https://doi.org/10.1177/1049731511405070.
- Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health 2010;31:399-418. https://doi.org/10.1146/annurev.publhealth.012809.103604.
- Rothman AJ. Capitalizing on opportunities to refine health behavior theories. Health Educ Behav 2009;36:150-5. https://doi.org/10.1177/1090198109340514.
- Bartholomew LK, Parcel GS, Kok G, Gottlieb NH, Fernández ME. Planning Health Promotion Programs: An Intervention Mapping Approach. San Francisco, CA: Jossey-Bass; 2011.
- Davis R, Campbell R, Hildon Z, Michie S. Theories of behaviour and behaviour change across disciplines: a scoping review. Health Psychol Rev 2015;9:323-44. https://doi.org/10.1080/17437199.2014.941722.
- Michie S, Prestwich A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol 2010;29:1-8. https://doi.org/10.1037/a0016939.
- Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. ‘Psychological Theory’ Group. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care 2005;14:26-33. https://doi.org/10.1136/qshc.2004.011155.
- Atkins L, Francis J, Islam R, O’Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci 2017;12. https://doi.org/10.1186/s13012-017-0605-9.
- Thomas S, Mackintosh S. Use of the theoretical domains framework to develop an intervention to improve physical therapist management of the risk of falls after discharge. Phys Ther 2014;94:1660-75. https://doi.org/10.2522/ptj.20130412.
- McKenzie JE, French SD, O’Connor DA, Mortimer DS, Browning CJ, Russell GM, et al. Evidence-based care of older people with suspected cognitive impairment in general practice: protocol for the IRIS cluster randomised trial. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-91.
- Godin G, Bélanger-Gravel A, Eccles M, Grimshaw J. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implement Sci 2008;3. https://doi.org/10.1186/1748-5908-3-36.
- Guillaumie L, Godin G, Vézina-Im LA. Psychosocial determinants of fruit and vegetable intake in adult population: a systematic review. Int J Behav Nutr Phys Act 2010;7. https://doi.org/10.1186/1479-5868-7-12.
- Zhu D, Norman IJ, While AE. The relationship between health professionals’ weight status and attitudes towards weight management: a systematic review. Obes Rev 2011;12:e324-37. https://doi.org/10.1111/j.1467-789X.2010.00841.x.
- Michie S, Atkins L, West R. The Behaviour Change Wheel: A Guide to Designing Interventions. London: Silverback Publishing; 2014.
- Green LW, Kreuter MW. Health Promotion Planning: An Educational and Environmental Approach. Mountain View, CA: Mayfield Publishing; 1991.
- Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, Ruiter RA, et al. A taxonomy of behaviour change methods: an intervention mapping approach. Health Psychol Rev 2016;10:297-312. https://doi.org/10.1080/17437199.2015.1077155.
- Gielen AC, McDonald EM, Gary TL, Bone LR, Glanz K, Rimer BK, et al. Health Behavior and Health Education: Theory, Research, and Practice. Hoboken, NJ: John Wiley & Sons; 2008.
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 2011;6. https://doi.org/10.1186/1748-5908-6-42.
- Lenert L, Norman GJ, Mailhot M, Patrick K. A framework for modeling health behavior protocols and their linkage to behavioral theory. J Biomed Inform 2005;38:270-80. https://doi.org/10.1016/j.jbi.2004.12.001.
- Araújo-Soares V, McIntyre T, MacLennan G, Sniehotta FF. Development and exploratory cluster-randomised opportunistic trial of a theory-based intervention to enhance physical activity among adolescents. Psychol Health 2009;24:805-22. https://doi.org/10.1080/08870440802040707.
- Fletcher A, Wolfenden L, Wyse R, Bowman J, McElduff P, Duncan S. A randomised controlled trial and mediation analysis of the ‘Healthy Habits’, telephone-based dietary intervention for preschool children. Int J Behav Nutr Phys Act 2013;10. https://doi.org/10.1186/1479-5868-10-43.
- Foy R, Francis JJ, Johnston M, Eccles M, Lecouturier J, Bamford C, et al. The development of a theory-based intervention to promote appropriate disclosure of a diagnosis of dementia. BMC Health Serv Res 2007;7. https://doi.org/10.1186/1472-6963-7-207.
- Dalgetty R, Miller CB, Dombrowski SU. Examining the theory-effectiveness hypothesis: a systematic review of systematic reviews. Br J Health Psychol 2019;24:334-56. https://doi.org/10.1111/bjhp.12356.
- Ashford S, Edmunds J, French DP. What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br J Health Psychol 2010;15:265-88. https://doi.org/10.1348/135910709X461752.
- Williams SL, French DP. What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behaviour – and are they the same?. Health Educ Res 2011;26:308-22. https://doi.org/10.1093/her/cyr005.
- Golley R, Hendrie G, Slater A, Corsini N. Interventions that involve parents to improve children’s weight-related nutrition intake and activity patterns–what nutrition and activity targets and behaviour change techniques are associated with intervention effectiveness?. Obes Rev 2011;12:114-30. https://doi.org/10.1111/j.1467-789X.2010.00745.x.
- Olander EK, Fletcher H, Williams S, Atkinson L, Turner A, French DP. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 2013;10. https://doi.org/10.1186/1479-5868-10-29.
- Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol Bull 2006;132:249-68. https://doi.org/10.1037/0033-2909.132.2.249.
- Michie S, Carey RN, Johnston M, Rothman AJ, de Bruin M, Kelly MP, et al. From theory-inspired to theory-based interventions: a protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Ann Behav Med 2018;52:501-12. https://doi.org/10.1007/s12160-016-9816-6.
- Carey RN, Connell LE, Johnston M, Rothman AJ, de Bruin M, Kelly MP, et al. Behavior change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med 2019;53:693-707. https://doi.org/10.1093/abm/kay078.
- Connell LE, Carey RN, de Bruin M, Rothman AJ, Johnston M, Kelly MP, et al. Links between behavior change techniques and mechanisms of action: an expert consensus study. Ann Behav Med 2019;53:708-20. https://doi.org/10.1093/abm/kay082.
- Johnston M, Carey R, Bohlen LC, Johnston DW, Rothman A, de Bruin M, et al. Linking behavior change techniques and mechanisms of action: triangulation of findings from literature synthesis and expert consensus. Ann Behav Med 2018. https://doi.org/10.31234/osf.io/ur6kz.
- Bohlen LC, Michie S, de Bruin M, Rothman AJ, Kelly MP, Groarke HN, et al. Do combinations of behaviour change techniques that occur frequently in interventions reflect underlying theory?. Ann Behav Med 2020;54:1-16. https://doi.org/10.1093/abm/kaaa078.
- Byrt T, Bishop J, Carlin JB. Bias, prevalence and kappa. J Clin Epidemiol 1993;46:423-9. https://doi.org/10.1016/0895-4356(93)90018-V.
- R-Package . A Language and Environment for Statistical Computing. R Foundation for Statistical Computing 2013.
- Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977;84:191-215. https://doi.org/10.1037//0033-295x.84.2.191.
- Harkin B, Webb TL, Chang BP, Prestwich A, Conner M, Kellar I, et al. Does monitoring goal progress promote goal attainment? A meta-analysis of the experimental evidence. Psychol Bull 2016;142:198-229. https://doi.org/10.1037/bul0000025.
- Harvey N, Holmes CA. Nominal group technique: an effective method for obtaining group consensus. Int J Nurs Pract 2012;18:188-94. https://doi.org/10.1111/j.1440-172X.2012.02017.x.
- Vella K, Goldfrad C, Rowan K, Bion J, Black N. Use of consensus development to establish national research priorities in critical care. BMJ 2000;320:976-80. https://doi.org/10.1136/bmj.320.7240.976.
- Van de Ven AH, Delbecq AL. The nominal group as a research instrument for exploratory health studies. Am J Public Health 1972;62:337-42. https://doi.org/10.2105/AJPH.62.3.337.
- Jorm AF. Using the Delphi expert consensus method in mental health research. Aust N Z J Psychiatry 2015;49:887-97. https://doi.org/10.1177/0004867415600891.
- Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 2014;67:401-9. https://doi.org/10.1016/j.jclinepi.2013.12.002.
- Michie S, Johnston M, Carey R, Gellman M, Turner JR. Encyclopedia of Behavioral Medicine. New York, NY: Springer; 2016.
- Riddle M, Ferrer R. The science of behavior change. APS Observer 2015;28.
- Nielsen L, Riddle M, King JW, Aklin WM, Chen W, Clark D, et al. The NIH Science of Behavior Change Program: transforming the science through a focus on mechanisms of change. Behav Res Ther 2018;101:3-11. https://doi.org/10.1016/j.brat.2017.07.002.
- Sumner JA, Beauchaine TP, Nielsen L. A mechanism-focused approach to the science of behavior change: an introduction to the special issue. Behav Res Ther 2018;101:1-2. https://doi.org/10.1016/j.brat.2017.12.005.
- Sheeran P, Klein WM, Rothman AJ. Health behavior change: moving from observation to intervention. Annu Rev Psychol 2017;68:573-600. https://doi.org/10.1146/annurev-psych-010416-044007.
- Eldredge LKB, Markham CM, Ruiter RA, Kok G, Fernandez ME, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. Hoboken, NJ: John Wiley & Sons; 2016.
- Munafo MR, Smith GD. Repeating experiments is not enough. Nature 2018;553:399-401. https://doi.org/10.1038/d41586-018-01023-3.
- Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res 2010;19:539-49. https://doi.org/10.1007/s11136-010-9606-8.
- Nakagawa S, Schielzeth H. A general and simple method for obtaining R2 from generalized linear mixed-effects models. Methods Ecol Evol 2013;4:133-42. https://doi.org/10.1111/j.2041-210x.2012.00261.x.
- Johnson PC. Extension of Nakagawa. Schielzeth’s R2GLMM to random slopes models. Methods Ecol Evol 2014;5:944-6. https://doi.org/10.1111/2041-210X.12225.
- Gardner B, Whittington C, McAteer J, Eccles MP, Michie S. Using theory to synthesise evidence from behaviour change interventions: the example of audit and feedback. Soc Sci Med 2010;70:1618-25. https://doi.org/10.1016/j.socscimed.2010.01.039.
- Revenson TA, Gurung RA. Handbook of Health Psychology. New York, NY: Routledge; 2018.
- Bandura A. Human agency in social cognitive theory. Am Psychol 1989;44:1175-84. https://doi.org/10.1037/0003-066x.44.9.1175.
- Hollands GJ, Bignardi G, Johnston M, Kelly MP, Ogilvie D, Petticrew M, et al. The TIPPME intervention typology for changing environments to change behaviour. Nat Hum Behav 2017;1. https://doi.org/10.1038/s41562-017-0140.
- Muthukrishna M, Henrich J. A problem in theory. Nat Hum Behav 2019;3:221-9. https://doi.org/10.1038/s41562-018-0522-1.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Ajzen I. Behavioral Interventions Based on the Theory of Planned Behavior 2006. https://people.umass.edu/aizen/pdf/tpb.intervention.pdf (accessed 21 November 2019).
- Peters G-JY, Ruiter RA, Kok G. Threatening communication: a critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psychol Rev 2013;7:8-31. https://doi.org/10.1080/17437199.2012.703527.
- Jamtvedt G, Young JM, Kristoffersen DT, O’Brien MA, Oxman AD. Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev 2006;2. https://doi.org/10.1002/14651858.CD000259.pub2.
- Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull 1982;92:111-35. https://doi.org/10.1037/0033-2909.92.1.111.
- Dombrowski SU, Sniehotta FF, Avenell A, Johnston M, MacLennan G, Araújo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev 2012;6:7-32. https://doi.org/10.1080/17437199.2010.513298.
- Prestwich A, Conner M, Hurling R, Ayres K, Morris B. An experimental test of control theory-based interventions for physical activity. Br J Health Psychol 2016;21:812-26. https://doi.org/10.1111/bjhp.12198.
- Muthén LK, Muthén B. Exploratory Factor Analysis, Confirmatory Factor Analysis, and Structural Equation Modeling For Continuous Outcomes 2008. https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.367.3079&rep=rep1&type=pdf (accessed 1 January 2020).
- Stevens JP, Stevens JP, Pituch KA. Applied Multivariate Statistics for the Social Sciences. New York, NY: Routledge; 2012.
- Guadagnoli E, Velicer WF. Relation of sample size to the stability of component patterns. Psychol Bull 1988;103:265-75. https://doi.org/10.1037/0033-2909.103.2.265.
- Heaney CA, Israel BA, Glanz K, Rimer BK, Viswanath K. Behavior and Health Education: Theory, Research, and Practice. San Francisco, CA: Jossey-Bass; 2008.
- West R, Godinho CA, Bohlen LC, Carey RN, Hastings J, Lefevre CE, et al. Development of a formal system for representing behaviour-change theories. Nat Hum Behav 2019;3:526-36. https://doi.org/10.1038/s41562-019-0561-2.
- Flay BR, Petraitis J. A new theory of health behavior with implications for preventive interventions. Adv Med Sociol 1994;4:19-44.
- Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Specialist 2009;23:161-72. https://doi.org/10.1097/NUR.0b013e3181a42373.
- Ewart CK. Social action theory for a public health psychology. Am Psychol 1991;46.
Appendix 1 International Advisory Board
-
Henk Aarts, Utrecht University, the Netherlands
-
Larry An, University of Michigan, MI, USA
-
Ron Borland, Cancer Council Victoria, VIC, Australia
-
Jos Bosch, University of Amsterdam, the Netherlands
-
Noel Brewer, University of North Carolina, NC, USA
-
Angela Bryan, University of Colorado, CO, USA
-
Simon Christmas, Simon Christmas Ltd/King’s College London, UK
-
Linda Collins, Penn State University, PA, USA
-
Mark Conner, University of Leeds, Leeds, UK
-
Susan Curry, University of Iowa, IW, USA
-
Karina Davidson, Columbia University, NY, USA
-
Heather Gainforth, University of British Columbia, BC, Canada
-
Karen Glanz, University of Pennsylvania, PA, USA
-
Jeremy Grimshaw, University of Ottawa, ON, Canada
-
Wendy Hardeman, University of East Anglia, Norwich, UK
-
Tessa Hart, Moss Rehabilitation Research Institute, PA, USA
-
Eric Hekler, Arizona State University, AZ, USA
-
Kate Hunt, University of Glasgow, Glasgow, UK
-
Blair Johnson, University of Connecticut, CT, USA
-
Robert Kaplan, National Institutes of Health, MD, USA
-
Abby King, Stanford University, CA, USA
-
William Klein, National Cancer Institute (NIH), MD, USA
-
Kai Larsen, University of Colorado, CO, USA
-
Aleksandra Luszczynska, SWPS University of Social Sciences and Humanities, Wrocław, Poland
-
Kevin Masters, University of Colorado Denver, CO, USA
-
Kevin McCaul, North Dakota State University, ND, USA
-
Robin Mermelstein, University of Illinois at Chicago, IL, USA
-
Gerry Molloy, NUI Galway, Republic of Ireland
-
Miquel Porta, Universitat Autònoma de Barcelona, Spain
-
William Riley, National Cancer Institute (NIH), MD, USA
-
Robert Ruiter, Maastricht University, the Netherlands
-
Ralf Schwarzer, Freie Universität Berlin, Germany
-
Bonnie Spring, Northwestern University, IL, USA
-
Annette Stanton, University of California (LA), CA, USA
-
Pedro Teixeira, University of Lisbon, Portugal
-
Bas van den Putte, University of Amsterdam, the Netherlands
-
Robert West, University College London, UK
-
Reinout Wiers, University of Amsterdam, the Netherlands
-
Danny Wight, University of Glasgow, UK
-
David Williams, Brown University, RI, USA
-
Sally Wyke, University of Glasgow, UK
-
Marco Yzer, University of Minnesota, MN, USA.
Appendix 2 Intercoder reliability for intervention report coding
| Stage of coding | Index | Reliability | Number of papers coded before reliability achieved |
|---|---|---|---|
| Screening | Kappa | 0.9 | 22 |
| BCT coding | PABAK | 0.9 | 93 |
| Link coding | Percentage agreement | 90% | 183 |
Appendix 3 The 26 mechanisms of action
Mechanisms of action are defined as ‘the processes through which a BCT affects behaviour’. These 26 MoAs are taken from the 14 theoretical domains as described in the theoretical domains framework38 and the 12 most frequently occurring mechanisms derived from a set of 83 behaviour change theories. 30
| Number | Mechanism definition | Mechanism label |
|---|---|---|
| 1 | An awareness of the existence of something | Knowledge |
| 2 | An ability or proficiency acquired through practice | Skills |
| 3 | A coherent set of behaviours and displayed personal qualities of an individual in a social or work setting | Social/professional role and identity |
| 4 | Beliefs about one’s ability to successfully carry out a behaviour | Beliefs about capabilities |
| 5 | Confidence that things will happen for the best or that desired goals will be attained | Optimism |
| 6 | Beliefs about the consequences of a behaviour (i.e. perceptions about what will be achieved and/or lost by undertaking a behaviour, as well as the probability that a behaviour will lead to a specific outcome) | Beliefs about consequences |
| 7 | Processes by which the frequency or probability of a response is increased through a dependent relationship or contingency with a stimulus or circumstance | Reinforcement |
| 8 | A conscious decision to perform a behaviour or a resolve to act in a certain way | Intention |
| 9 | Mental representations of outcomes or end states that an individual wants to achieve | Goals |
| 10 | Ability to retain information, focus on aspects of the environment and choose between two or more alternatives | Memory, attention and decision processes |
| 11 | Aspects of a person’s situation or environment that discourage or encourage the behaviour | Environmental context and resources |
| 12 | Those interpersonal processes that can cause oneself to change one’s thoughts, feelings or behaviours | Social influences |
| 13 | A complex reaction pattern involving experiential, behavioural and physiological elements | Emotion |
| 14 | Behavioural, cognitive and/or emotional skills for managing or changing behaviour | Behavioural regulation |
| 15 | The attitudes held and behaviours exhibited by other people within a social group | Norms |
| 16 | One’s perceptions of what most other people within a social group believe and do | Subjective norms |
| 17 | The general evaluations of the behaviour on a scale ranging from negative to positive | Attitude towards the behaviour |
| 18 | Processes relating to the impetus that gives purpose or direction to behaviour and operates at a conscious or unconscious level | Motivation |
| 19 | One’s conception and evaluation of oneself, including psychological and physical characteristics, qualities and skills | Self-image |
| 20 | Deficit of something required for survival, well-being or personal fulfilment | Needs |
| 21 | Moral, social or aesthetic principles accepted by an individual or society as a guide to what is good, desirable or important | Values |
| 22 | Processes through which current behaviour is compared against a particular standard | Feedback processes |
| 23 | A process by which thoughts, feelings and motivational states observed in others are internalised and replicated without the need for conscious awareness | Social learning/imitation |
| 24 | Processes by which behaviour is triggered from either the external environment, the performance of another behaviour, or from ideas appearing in consciousness | Behavioural cueing |
| 25 | Evaluations of an object, person, group, issue or concept on a scale ranging from negative to positive | General attitudes/beliefs |
| 26 | Perceptions of the likelihood that one is vulnerable to a threat | Perceived susceptibility/vulnerability |
Appendix 4 Guidelines for categorisation of mechanisms
-
Read and re-read the 26 MoA labels and definitions (in BCT–MoA Link Coding Guidelines).
-
Ensure that all decisions are based on definitions, not labels.
-
If a definition is given and it clearly fits one of the 26 MoA definitions, add the label and number of the MoA in the spreadsheet.
-
If a definition is given and it fits into more than one of the 26 MoA definitions (e.g. a definition encompasses both attitude towards behaviour AND beliefs about consequences), highlight in yellow for review.
-
If a definition is given and you are unsure which of the 26 MoA definitions it fits into, highlight in yellow for review.
-
If no definition is given:
-
Double-check the PDF (portable document format) and add any relevant information where possible (e.g. how the MoA was measured or what theory it came from)
-
If no additional information found and/or still unclear, highlight in yellow for review
-
-
If the definition says ‘as per [theory]’ – check the theory definition, if unclear, highlight in yellow for review.
-
-
Where categorisation of MoAs within one paper means that there are multiple identical links, highlight these in yellow. For example, where intrinsic motivation is linked to BCT X and Y, and extrinsic motivation is linked to BCT X and Y, and these are both categorised into ‘motivation’ (i.e. meaning motivation is linked to BCT X and Y twice), highlight these BCT numbers in yellow in the links spreadsheet.
-
Where no definition given but the label is exactly label of one of the 26 MoAs, it is OK to categorise as such (this includes self-efficacy → beliefs about capabilities, outcome expectancies → beliefs about consequences and social support → social influences).
-
For uncertain MoAs:
-
Check whether construct is similar/identical to one of the component constructs of the TDF domain or frequently occurring MoA
-
If no definition or information is given about construct in the paper, and the label is not similar to any MoA, code as ‘other’.
-
| Construct label | Construct definition (from theory) | MoA categorisation |
|---|---|---|
| Intention | TPB: the cognitive representation of one’s readiness to perform the behaviour; considered to be the immediate antecedent of behaviour | Intention (8) |
| Attitude | TPB: favourable or unfavourable evaluation or appraisal of the behaviour | Attitude towards the behaviour (17) |
| Perceived susceptibility | HBM: the extent to which one believes that one is at risk of contracting a particular disease or developing a particular health problem | Perceived susceptibility/vulnerability (26) |
| Perceived threat | HBM: perceptions of the threat posed by a disease or health problem, based on one’s perceived susceptibility to, and the perceived severity of, a disease or health problem | Perceived susceptibility/vulnerability (26) |
| Perceived behavioural control | TPB: the perceived ability to perform the behaviour | Beliefs about capabilities (4) |
| Self-efficacy | SCT: perceived judgements of one’s ability to cope effectively in different circumstances | Beliefs about capabilities (4) |
| Self-efficacy | SET: belief that one is capable of carrying out a specific behaviour that will lead to desired outcomes | Beliefs about capabilities (4) |
| Behavioural intention | HAPA: a conscious decision to perform a behaviour | Intention (8) |
| Self-regulation | HAPA: actual or perceived environmental factors that prevent performance of an intended behaviour | Behavioural regulation (14) |
| Motivation | I-change: one’s intention to carry out a particular type of behaviour; determined by attitudes, social influences and self-efficacy | Intention (8) |
| Index | Reliability (of MoAs not highlighted in yellow) | Number of MoAs categorised before reliability achieved |
|---|---|---|
| Percentage agreement | 90% | 20 |
Appendix 5 Expert consensus
FIGURE 16.
Self-rated expertise in designing or helping design behaviour change interventions using specific BCTs and/or theory. Values indicate the number of experts who rated the extent to which they had designed or helped design a behaviour change intervention using specific BCTs, or behaviour change theory (see also Appendix A; questions 1a and 1c).
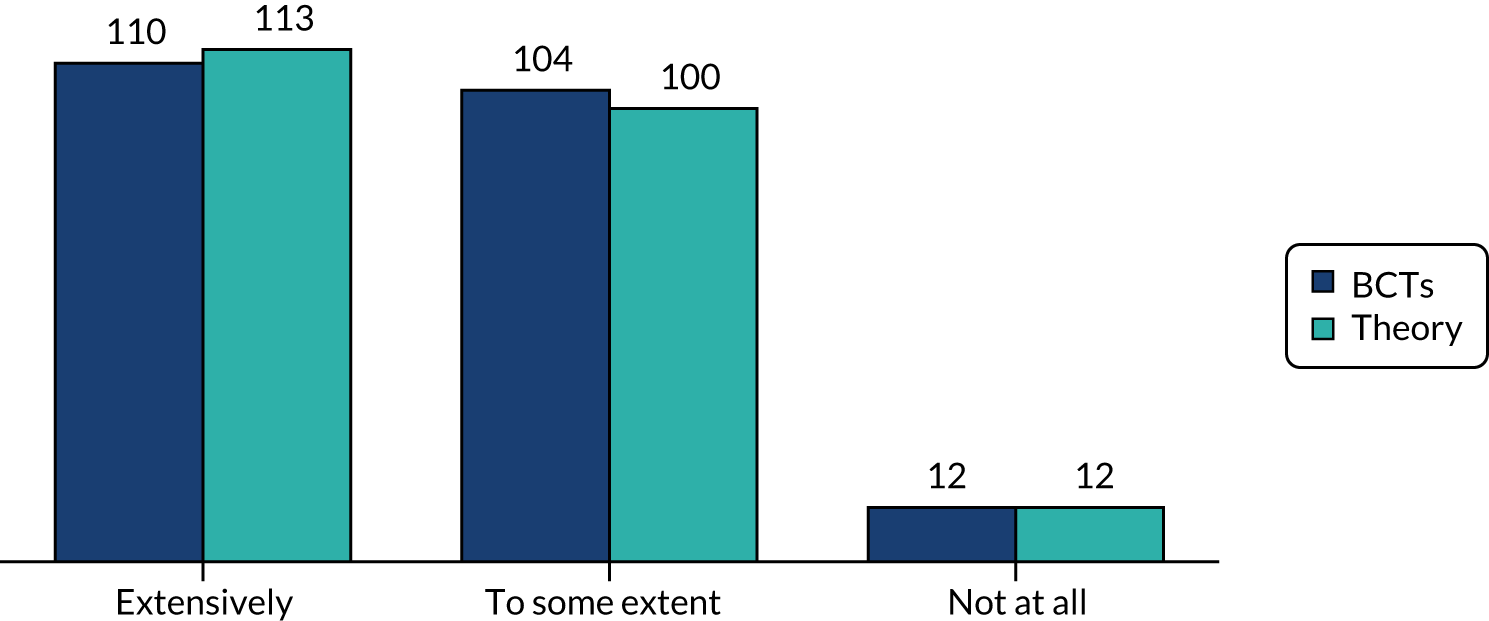
FIGURE 17.
Self-rated expertise in behaviour change theories, BCTs, and behaviour change interventions. Values indicate the number of experts who rated the extent of their expertise in behaviour change theories, BCTs, and behaviour change interventions.
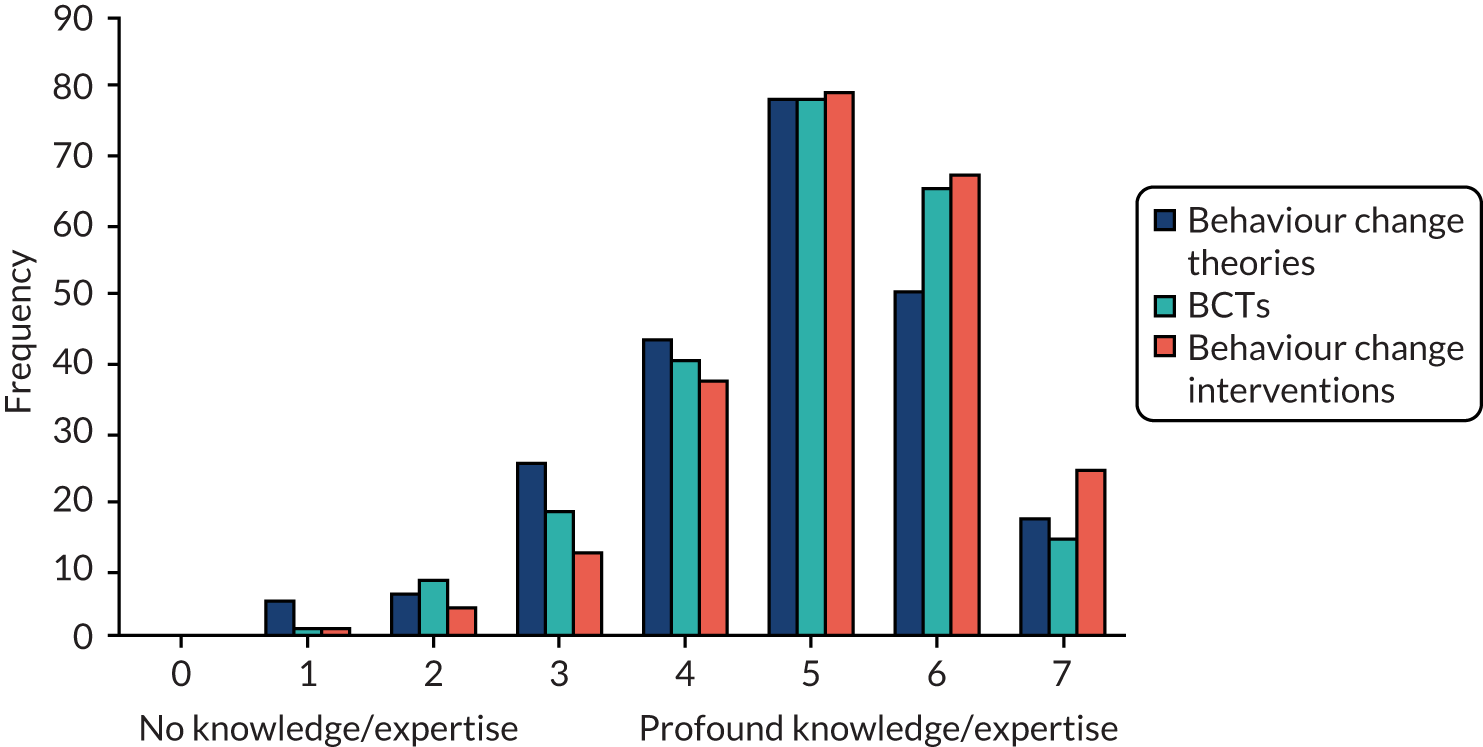
| Group A | Group B | Group C | Group D | Group E |
|---|---|---|---|---|
| 1.1 Goal-setting (behaviour) | 5.1 Information about the health consequences | 3.2 Social support (practical) | 9.1 Credible source | 5.3 Information about social and environmental consequences |
| 2.7 Feedback on outcome(s) of behaviour | 1.4 Action-planning | 12.5 Adding objects to the environment | 2.2 Feedback on behaviour | 1.2 Problem-solving |
| 2.3 Self-monitoring of behaviour | 6.1 Demonstration of the behaviour | 7.1 Prompts/cues | 2.1 Monitoring of behaviour by others without feedback | 1.3 Goal-setting (outcome) |
| 1.5 Review behaviour goal(s) | 1.6 Review outcome goal(s) | 8.1 Behavioural practice/rehearsal | 12.1 Restructuring the physical environment | 2.5 Monitoring of outcome of behaviour without feedback |
| 8.3 Habit formation | 11.1 Pharmacological support | 2.4 Self-monitoring of outcome(s) of behaviour | 3.3 Social support (emotional) | 4.2 Information about antecedents |
| 5.2 Salience of consequences | 10.2 Material reward (behaviour) | 6.1 Social comparison | 2.6 Biofeedback | 1.6 Discrepancy between current behaviour and goal |
| 12.2 Restructuring the social environment | 10.3 Non-specific reward | 13.2 Framing/reframing | 10.1 Material incentive (behaviour) | 15.1 Verbal persuasion about capability |
| 1.8 Behavioural contract | 10.6 Non-specific incentive | 11.2 Reduce negative emotions | 1.9 Commitment | 10.4 Social reward |
| 5.6 Information about emotional consequences | 8.2 Behaviour substitution | 9.2 Pros and cons | 6.3 Information about others’ approval | 11.3 Conserving mental resources |
| 5.4 Monitoring of emotional consequences | 15.4 Self-talk | 7.5 Remove aversive stimulus | 8.6 Generalisation of target behaviour | 10.8 Incentive (outcome) |
| 13.1 Identification of self as role model | 12.3 Avoidance/reducing exposure to cues for the behaviour | 8.7 Graded tasks | 8.4 Habit reversal | 10.10 Reward (outcome) |
| 16.3 Vicarious consequences | 12.6 Body changes | 14.10 Remove punishment | 9.3 Comparative imagining of future outcomes |
Content of the guidelines for round 1 of the consensus exercise
Aims of study
This study aims to develop a shared understanding of behaviour change techniques (BCTs) and the mechanisms of action through which they influence behaviour. A summary of the project is appended to this document (Appendix A).
Who are the participants?
You are one of 105 experts from 18 countries, selected because you have a high level of expertise in theories and techniques of behaviour change.
What are we asking you to do?
The consensus exercise is a modified Nominal Group Technique (NGT),109 involving 3 rounds. In round 1, you will be directed to an online questionnaire. You will be presented with 13 BCTs, one at a time, and asked to consider whether each BCT changes behaviour through any of a given set of 26 mechanisms. Thus, you will be asked to respond to 13 sets of 26 questions, where each set relates to 1 BCT × 26 mechanisms. You will be prompted to take a break after completing each set – you may complete round 1 in one sitting or several.
What is a behaviour change technique (BCT)?
BCTs are the potentially active ingredients of behaviour change interventions. For this study, BCTs will be taken from the 93-item BCT Taxonomy Version 1 (BCTTv1; www.ncbi.nlm.nih.gov/pubmed/23512568).
What is a mechanism of action?
These are defined as ‘the processes through which a BCT affects behaviour’. The following diagram may be helpful in conceptualising the processes through which a particular BCT might affect behaviour.
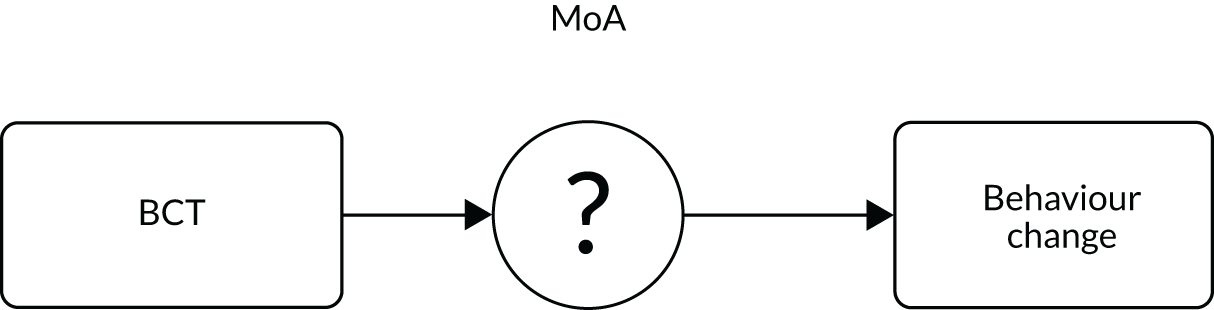
Notes
-
We are not evaluating the effectiveness of BCTs in this study (i.e. how likely it is that a particular BCT changes behaviour). When rating BCT–mechanism links (see example below), please focus on the mechanisms you believe a BCT might change, in order to change behaviour.
-
There are many mechanisms of action through which a BCT might affect behaviour. When considering whether a given BCT affects behaviour through a particular mechanism, you may draw on evidence, theory and/or experience.
-
In order to ensure consistency across experts, and with the aim of developing a shared understanding of BCT–mechanism links, it is very important that you base your answers on the definitions, rather than labels, of the BCTs and mechanisms. Definitions for all BCTs and mechanisms will appear on screen during the consensus exercise, and these can also be found in Appendices B and C. Please read and re-read these definitions before beginning the task.
Sample question
Does the behaviour change technique goal-setting (behaviour) change behaviour through the mechanism: an awareness of the existence of something (knowledge)?
□ Definitely no
□ Probably no
□ Uncertain/don’t know
□ Probably yes
□ Definitely yes
Note: Additional information provided in the guidelines document was excluded from this paper, this information included a project summary, BCT definitions and MoA definitions. For more information about the project see the project protocol, published in Annals of Behavioral Medicine,100 for BCT definitions see the BCT taxonomy app or website: www.bcts.23.co.uk, (accessed 1 January 2020), and for more information about the MoAs included in this study, see Table 19.
FIGURE 18.
Sample statistical summary sent to experts after the completion of round 1 for the BCT goal-setting (behaviour). Note, the above distribution depicts the frequency with which experts thought that the BCT ‘goal-setting (behaviour) was linked to any of the 26 MoAs. For round 1, yes = definitely yes and probably yes, no = definitely no and probably no.
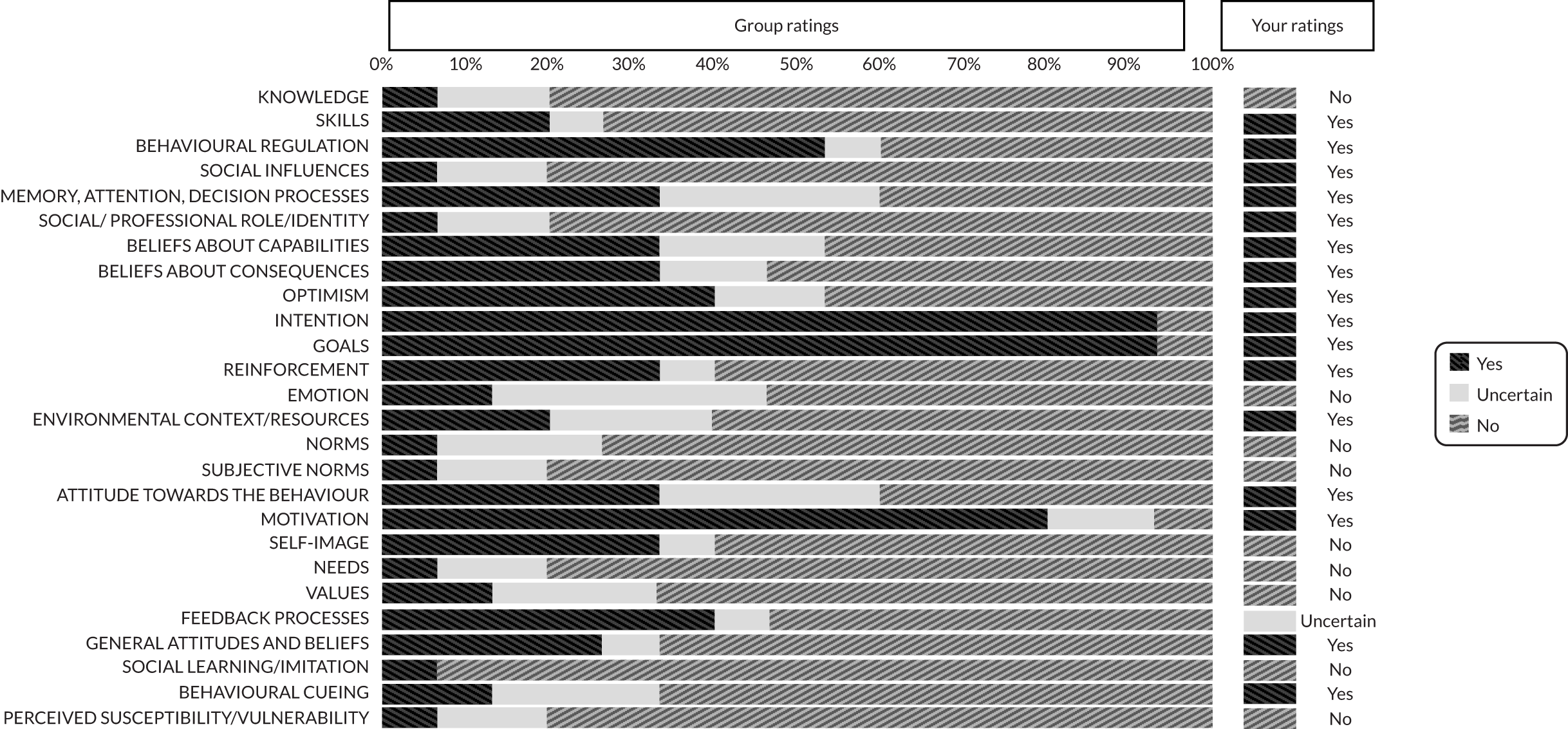
FIGURE 19.
Proportion of experts rating ‘possibly’.
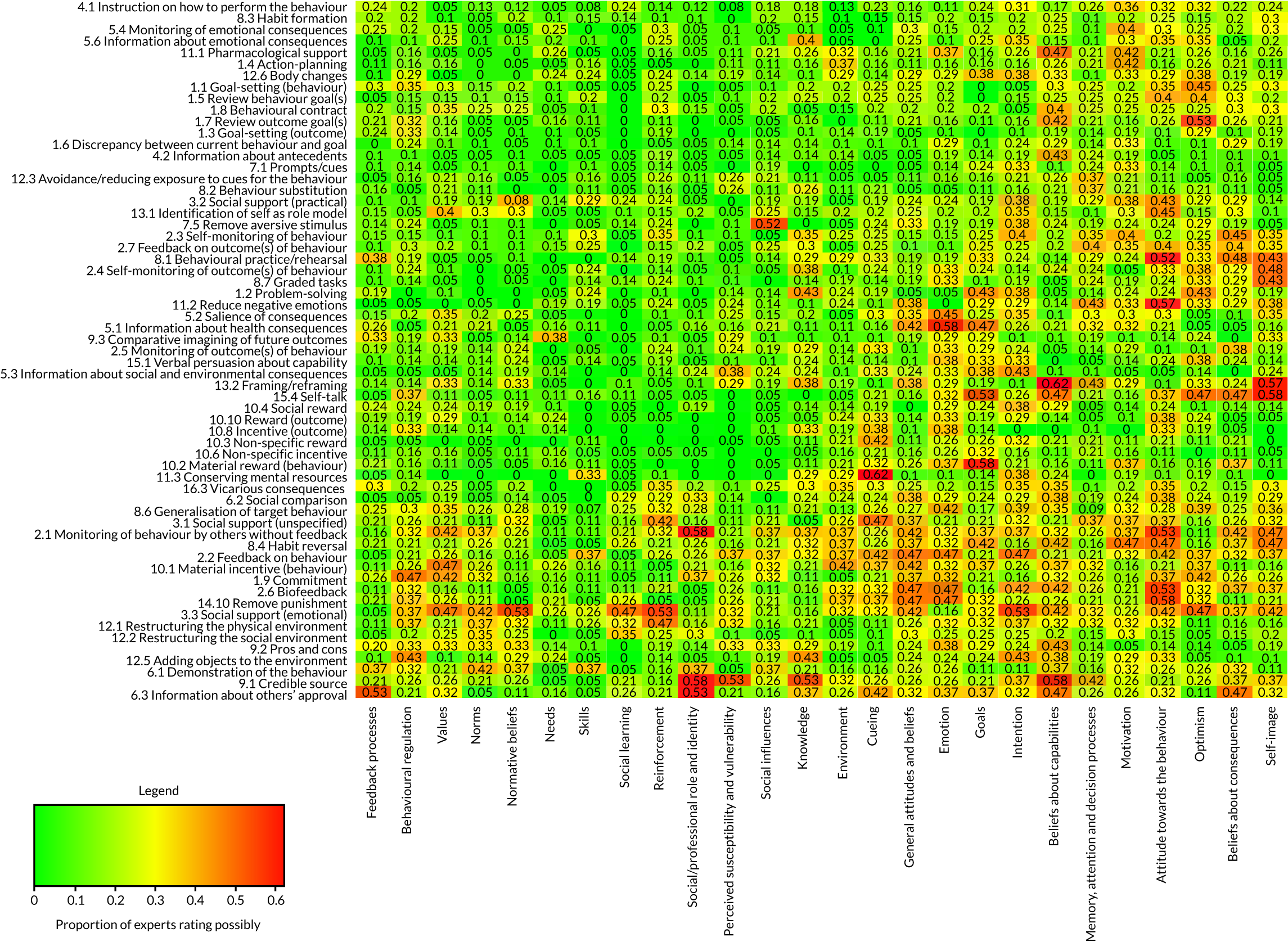
FIGURE 20.
Proportion of experts rating ‘uncertain/don’t know’.
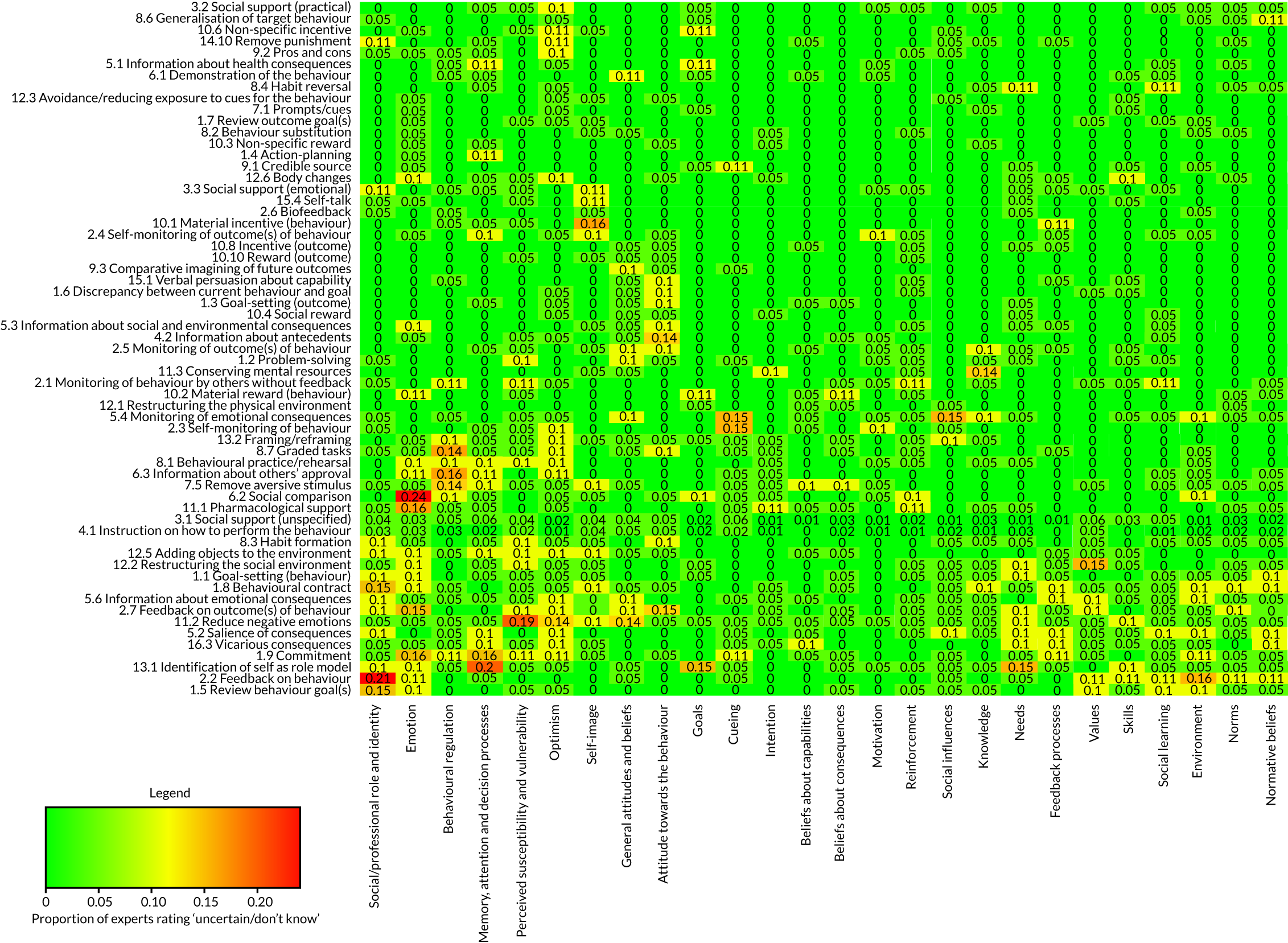
| BCT | MoA | |||
|---|---|---|---|---|
| ‘Definitely yes’ linked | Proportion of experts | ‘Definitely no’ not linked | Proportion of experts | |
| 1.1 Goal-setting (behaviour) | Goals | 0.95 | Social learning | 0.90 |
| Intention | 0.95 | Social/professional role and identity | 0.90 | |
| Motivation | 0.80 | Perceived susceptibility and vulnerability | 0.90 | |
| Skills | 0.85 | |||
| Social influences | 0.80 | |||
| Needs | 0.80 | |||
| 1.2 Problem-solving | Behavioural regulation | 1 | Normative beliefs | 0.95 |
| Beliefs about capabilities | 0.95 | Norms | 0.95 | |
| Social learning | 0.95 | |||
| Social/professional role and identity | 0.90 | |||
| Values | 0.90 | |||
| Needs | 0.90 | |||
| Reinforcement | 0.86 | |||
| Social influences | 0.81 | |||
| General attitudes and beliefs | 0.81 | |||
| Emotion | 0.81 | |||
| 1.3 Goal-setting (outcome) | Goals | 1 | Perceived susceptibility/vulnerability | 1.00 |
| Intention | 0.86 | Social/professional role and identity | 0.95 | |
| Norms | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Skills | 0.90 | |||
| Social influences | 0.90 | |||
| Subjective norms | 0.90 | |||
| Knowledge | 0.86 | |||
| Emotion | 0.86 | |||
| Values | 0.86 | |||
| General attitudes and beliefs | 0.86 | |||
| Environmental context and resources | 0.81 | |||
| Needs | 0.81 | |||
| 1.4 Action-planning | Social/professional role and identity | 0.95 | ||
| Norms | 0.95 | |||
| Subjective norms | 0.95 | |||
| Needs | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Social influences | 0.89 | |||
| General attitudes and beliefs | 0.89 | |||
| Perceived susceptibility/vulnerability | 0.89 | |||
| Knowledge | 0.84 | |||
| Reinforcement | 0.84 | |||
| Values | 0.84 | |||
| Feedback processes | 0.84 | |||
| 1.5 Review behaviour goal(s) | Feedback processes | 0.95 | Social learning/imitation | 0.90 |
| Goals | 0.90 | Norms | 0.85 | |
| Perceived susceptibility/vulnerability | 0.85 | |||
| Social/professional role and identity | 0.80 | |||
| Subjective norms | 0.80 | |||
| Needs | 0.80 | |||
| 1.6 Discrepancy between current behaviour and goal | Feedback processes | 1 | Social learning/imitation | 1.00 |
| Goals | 0.81 | Social/professional role and identity | 0.90 | |
| Reinforcement | 0.90 | |||
| Norms | 0.90 | |||
| Subjective norms | 0.90 | |||
| Environmental context and resources | 0.86 | |||
| Needs | 0.86 | |||
| Perceived susceptibility/vulnerability | 0.86 | |||
| Skills | 0.81 | |||
| Optimism | 0.81 | |||
| Behavioural cueing | 0.81 | |||
| General attitudes and beliefs | 0.81 | |||
| 1.7 Review outcome goal(s) | Goals | 0.89 | Social/professional role and identity | 0.95 |
| Social influences | 0.95 | |||
| Norms | 0.95 | |||
| Subjective norms | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Environmental context and resources | 0.89 | |||
| Perceived susceptibility/vulnerability | 0.89 | |||
| Knowledge | 0.84 | |||
| Skills | 0.84 | |||
| Needs | 0.84 | |||
| Behavioural cueing | 0.84 | |||
| 1.8 Behavioural contract | Intention | 0.80 | Social learning/imitation | 0.95 |
| Needs | 0.90 | |||
| Perceived susceptibility/vulnerability | 0.90 | |||
| Skills | 0.85 | |||
| Knowledge | 0.80 | |||
| 1.9 Commitment | Intention | 0.84 | Skills | 0.84 |
| Motivation | 0.84 | Reinforcement | 0.84 | |
| Social learning/imitation | 0.84 | |||
| 2.1 Monitoring of behaviour by others without feedback | Needs | 0.89 | ||
| Optimism | 0.84 | |||
| 2.2 Feedback on behaviour | Feedback processes | 0.95 | Needs | 0.84 |
| Social learning/imitation | 0.84 | |||
| 2.3 Self-monitoring of behaviour | Feedback processes | 0.80 | Social learning/imitation | 0.95 |
| Norms | 0.90 | |||
| Subjective norms | 0.90 | |||
| Social/professional role and identity | 0.85 | |||
| Needs | 0.85 | |||
| Values | 0.85 | |||
| General attitudes and beliefs | 0.85 | |||
| Perceived susceptibility/vulnerability | 0.85 | |||
| Social influences | 0.80 | |||
| 2.4 Self-monitoring of outcome(s) of behaviour | Feedback processes | 0.81 | Norms | 1 |
| Social influences | 0.95 | |||
| Subjective norms | 0.95 | |||
| Needs | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Social/professional role and identity | 0.90 | |||
| Perceived susceptibility/vulnerability | 0.90 | |||
| Values | 0.86 | |||
| General attitudes and beliefs | 0.81 | |||
| 2.5 Monitoring of outcomes of behaviour without feedback | Needs | 0.95 | ||
| Social learning/imitation | 0.95 | |||
| Skills | 0.86 | |||
| Social/professional role and identity | 0.86 | |||
| Optimism | 0.86 | |||
| Beliefs about capabilities | 0.81 | |||
| Memory, attention, and decision processes | 0.81 | |||
| Environmental context and resources | 0.81 | |||
| Norms | 0.81 | |||
| Values | 0.81 | |||
| General attitudes and beliefs | 0.81 | |||
| 2.6 Biofeedback | Feedback processes | 0.89 | Social/professional role and identity | 0.89 |
| Norms | 0.89 | |||
| Subjective norms | 0.89 | |||
| Social learning/imitation | 0.89 | |||
| Social influences | 0.84 | |||
| Values | 0.84 | |||
| 2.7 Feedback on outcome(s) of behaviour | Feedback processes | 0.80 | Subjective norms | 0.80 |
| Social learning/imitation | 0.95 | |||
| Environmental context and resources | 0.90 | |||
| Norms | 0.90 | |||
| Perceived susceptibility/vulnerability | 0.85 | |||
| 3.1 Social support (unspecified) | Social influences | 0.87 | Skills | 0.87 |
| Perceived susceptibility/vulnerability | 0.82 | |||
| 3.2 Social support (practical) |
Environmental context and resources Social Influences |
0.90 0.81 |
Perceived susceptibility/vulnerability | 0.95 |
| Feedback processes | 0.90 | |||
| Self-image | 0.86 | |||
| Needs | 0.86 | |||
| Values | 0.81 | |||
| 3.3 Social support (emotional) | Emotion | 0.84 | Feedback processes | 0.84 |
| 4.1 Instruction on how to perform the behaviour | Skills | 0.86 | Needs | 0.90 |
| Perceived susceptibility/vulnerability | 0.90 | |||
| Values | 0.87 | |||
| Emotion | 0.84 | |||
| Social/professional role and identity | 0.82 | |||
| Subjective norms | 0.82 | |||
| Norms | 0.81 | |||
| 4.2 Information about antecedents | Knowledge | 0.86 | Needs | 0.95 |
| Behavioural cueing | 0.81 | Social/professional role and identity | 0.90 | |
| Norms | 0.90 | |||
| Subjective norms | 0.90 | |||
| Values | 0.90 | |||
| Feedback processes | 0.90 | |||
| General attitudes and beliefs | 0.90 | |||
| Skills | 0.86 | |||
| Self-image | 0.86 | |||
| Social learning/imitation | 0.86 | |||
| Optimism | 0.81 | |||
| Reinforcement | 0.81 | |||
| Social influences | 0.81 | |||
| Attitude towards the behaviour | 0.81 | |||
| 5.1 Information about health consequences | Beliefs about consequences | 0.95 | Reinforcement | 0.95 |
| Knowledge | 0.89 | Social learning/imitation | 0.95 | |
| Perceived susceptibility and vulnerability | 0.84 | Skills | 0.89 | |
| Optimism | 0.89 | |||
| Behavioural regulation | 0.89 | |||
| Subjective norms | 0.89 | |||
| Social/professional role and identity | 0.84 | |||
| Environmental context and resources | 0.84 | |||
| Self-image | 0.84 | |||
| Needs | 0.84 | |||
| 5.2 Salience of consequences | Beliefs about consequences | 0.85 | Skills | 0.95 |
| Social learning/imitation | 0.90 | |||
| Optimism | 0.85 | |||
| Needs | 0.85 | |||
| Social/professional role and identity | 0.80 | |||
| Beliefs about capabilities | 0.80 | |||
| 5.3 Information about social and environmental consequences | Beliefs about consequences | 0.95 | Skills | 1 |
| Motivation | 0.86 | Social learning/imitation | 0.95 | |
| Behavioural regulation | 0.90 | |||
| Feedback processes | 0.90 | |||
| Beliefs about capabilities | 0.86 | |||
| Optimism | 0.86 | |||
| Needs | 0.81 | |||
| 5.4 Monitoring of emotional consequences | Emotion | 0.80 | Skills | 0.95 |
| Social/professional role and identity | 0.90 | |||
| Memory, attention and decision processes | 0.90 | |||
| Norms | 0.90 | |||
| Subjective norms | 0.90 | |||
| Social learning/imitation | 0.90 | |||
| Environmental context and resources | 0.85 | |||
| Values | 0.85 | |||
| Perceived susceptibility/vulnerability | 0.80 | |||
| 5.6 Information about emotional consequences | Beliefs about consequences | 0.90 | Social influences | 0.80 |
| Social learning/imitation | 0.95 | |||
| Behavioural cueing | 0.90 | |||
| Skills | 0.85 | |||
| Social/professional role and identity | 0.85 | |||
| Memory, attention and decision processes | 0.85 | |||
| Environmental context and resources | 0.85 | |||
| Beliefs about capabilities | 0.80 | |||
| Social influences | 0.80 | |||
| Norms | 0.80 | |||
| Subjective norms | 0.80 | |||
| 6.1 Demonstration of behaviour | Social learning/imitation | 0.84 | Needs | 0.95 |
| Perceived susceptibility/vulnerability | 0.89 | |||
| Self-image | 0.84 | |||
| 6.2 Social comparison | Social influences | 1 | Skills | 1 |
| Normative beliefs | 0.81 | Needs | 0.95 | |
| Feedback processes | 0.90 | Behavioural regulation | 0.86 | |
| Norms | 0.90 | Perceived susceptibility/vulnerability | 0.86 | |
| 6.3 Information about others’ approval | Normative beliefs | 0.89 | Skills | 0.95 |
| Norms | 0.89 | Needs | 0.84 | |
| Social influences | 0.84 | |||
| 7.1 Prompts/cues | Behavioural cueing | 1 | Needs | 1 |
| Environmental context and resources | 0.90 | Perceived susceptibility/vulnerability | 1 | |
| Knowledge | 0.95 | |||
| Social/professional role and identity | 0.95 | |||
| Self-image | 0.95 | |||
| Values | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| General attitudes and beliefs | 0.95 | |||
| Beliefs about consequences | 0.90 | |||
| Norms | 0.90 | |||
| Subjective norms | 0.90 | |||
| Feedback processes | 0.90 | |||
| Beliefs about capabilities | 0.86 | |||
| Optimism | 0.86 | |||
| Attitude towards the behaviour | 0.86 | |||
| Emotion | 0.81 | |||
| 7.5 Remove aversive stimulus | Environmental context and resources | 0.90 | Knowledge | 1 |
| Needs | 1 | |||
| Skills | 0.95 | |||
| Social/professional role and identity | 0.95 | |||
| Values | 0.90 | |||
| Subjective norms | 0.86 | |||
| Self-image | 0.86 | |||
| Perceived susceptibility/vulnerability | 0.86 | |||
| Norms | 0.81 | |||
| Feedback processes | 0.81 | |||
| Social learning/imitation | 0.81 | |||
| 8.1 Behavioural practice/rehearsal | Skills | 0.95 | Norms | 0.95 |
| Beliefs about capabilities | 0.86 | Needs | 0.95 | |
| Values | 0.95 | |||
| Social/professional role and identity | 0.90 | |||
| Subjective norms | 0.90 | |||
| Social influences | 0.86 | |||
| Social learning/imitation | 0.86 | |||
| Perceived susceptibility/vulnerability | 0.86 | |||
| General attitudes and beliefs | 0.81 | |||
| 8.2 Behaviour substitution | Needs | 1 | ||
| Social/professional role and identity | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Social influences | 0.89 | |||
| Emotion | 0.89 | |||
| Norms | 0.89 | |||
| Subjective norms | 0.89 | |||
| General attitudes and beliefs | 0.89 | |||
| Self-image | 0.84 | |||
| 8.3 Habit formation | Behavioural cueing | 0.85 | Perceived susceptibility/vulnerability | 0.90 |
| Needs | 0.85 | |||
| General attitudes and beliefs | 0.85 | |||
| Knowledge | 0.80 | |||
| Optimism | 0.80 | |||
| Norms | 0.80 | |||
| Values | 0.80 | |||
| Feedback processes | 0.80 | |||
| 8.4 Habit reversal | Skills | 0.84 | Needs | 0.84 |
| 8.6 Generalisation of the target behaviour | Needs | 0.89 | ||
| Perceived susceptibility/vulnerability | 0.84 | |||
| 8.7 Graded tasks | Beliefs about capabilities | 0.90 | Social influences | 1 |
| Skills | 0.81 | Norms | 1 | |
| Needs | 1 | |||
| Subjective norms | 0.95 | |||
| Values | 0.95 | |||
| Social/professional role and identity | 0.86 | |||
| Social learning/imitation | 0.86 | |||
| Perceived susceptibility/vulnerability | 0.86 | |||
| Knowledge | 0.81 | |||
| Behavioural cueing | 0.81 | |||
| 9.1 Credible source | Skills | 0.89 | ||
| Needs | 0.89 | |||
| Reinforcement | 0.84 | |||
| 9.2 Pros and cons | Beliefs about consequences | 0.90 | Social learning/imitation | 1 |
| Motivation | 0.86 | Skills | 0.90 | |
| Attitude towards the behaviour | 0.81 | Behavioural cueing | 0.86 | |
| Social/professional role and identity | 0.81 | |||
| Self-image | 0.81 | |||
| Needs | 0.81 | |||
| 9.3 Comparative imagining of future outcomes | Beliefs about consequences | 1 | Skills | 1 |
| Intention | 0.81 | Social learning/imitation | 0.95 | |
| Motivation | 0.86 | Reinforcement | 0.90 | |
| Norms | 0.90 | |||
| Environment | 0.86 | |||
| Social influences | 0.86 | |||
| Social/professional role and identity | 0.81 | |||
| 10.1 Material incentive (behaviour) | Reinforcement | 0.95 | Social learning/imitation | 0.84 |
| Motivation | 0.84 | |||
| 10.2 Material reward (behaviour) | Reinforcement | 0.89 | Social/professional role and identity | 0.95 |
| Social learning/imitation | 0.95 | |||
| Perceived susceptibility/vulnerability | 0.95 | |||
| Knowledge | 0.89 | |||
| Skills | 0.89 | |||
| Memory, attention and decision processes | 0.89 | |||
| Social influences | 0.89 | |||
| Norms | 0.89 | |||
| Subjective norms | 0.89 | |||
| Self-image | 0.89 | |||
| Optimism | 0.84 | |||
| 10.3 Non-specific reward | Reinforcement | 0.95 | Social/professional role and identity | 0.95 |
| Motivation | 0.84 | Subjective norms | 0.95 | |
| Self-image | 0.95 | |||
| Needs | 0.95 | |||
| Values | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Perceived susceptibility/vulnerability | 0.95 | |||
| Optimism | 0.89 | |||
| Social influences | 0.89 | |||
| Behavioural regulation | 0.89 | |||
| Norms | 0.89 | |||
| Knowledge | 0.84 | |||
| Skills | 0.84 | |||
| Feedback processes | 0.84 | |||
| General attitudes and beliefs | 0.84 | |||
| 10.4 Social reward | Social comparison | 0.95 | Perceived susceptibility/vulnerability | 1 |
| Motivation | 0.81 | Skills | 0.95 | |
| Memory, attention and decision processes | 0.90 | |||
| Social learning/imitation | 0.90 | |||
| Knowledge | 0.86 | |||
| Needs | 0.86 | |||
| General attitudes and beliefs | 0.86 | |||
| 10.6 Non-specific incentive | Skills | 0.95 | ||
| Social/professional role and identity | 0.95 | |||
| Social influences | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Perceived susceptibility/vulnerability | 0.95 | |||
| Knowledge | 0.89 | |||
| Optimism | 0.89 | |||
| Norms | 0.89 | |||
| Subjective norms | 0.89 | |||
| Self-image | 0.89 | |||
| Beliefs about capabilities | 0.84 | |||
| Values | 0.84 | |||
| Feedback processes | 0.84 | |||
| 10.8 Incentive (outcome) | Intention | 0.95 | Skills | 1 |
| Beliefs about consequences | 0.90 | Perceived susceptibility/vulnerability | 1 | |
| Reinforcement | 0.90 | Social/professional role and identity | 0.95 | |
| Self-image | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Subjective norms | 0.90 | |||
| Social influences | 0.86 | |||
| Norms | 0.86 | |||
| Values | 0.86 | |||
| Beliefs about capabilities | 0.81 | |||
| Memory, attention and decision processes | 0.81 | |||
| General attitudes and beliefs | 0.81 | |||
| 10.10 Reward (outcome) | Reinforcement | 0.90 | Skills | 1 |
| Motivation | 0.90 | Perceived susceptibility/vulnerability | 1 | |
| Beliefs about consequences | 0.86 | Social/professional role and identity | 0.95 | |
| Self-image | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Subjective norms | 0.90 | |||
| Social influences | 0.86 | |||
| Norms | 0.86 | |||
| Values | 0.86 | |||
| Beliefs about capabilities | 0.81 | |||
| Memory, attention and decision processes | 0.81 | |||
| General attitudes and beliefs | 0.81 | |||
| 11.1 Pharmacological support | Skills | 0.95 | ||
| Subjective norms | 0.95 | |||
| Values | 0.95 | |||
| Feedback processes | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Social/professional role and identity | 0.89 | |||
| Norms | 0.89 | |||
| Perceived susceptibility/vulnerability | 0.84 | |||
| 11.2 Reduce negative emotions | Emotion | 0.95 | Subjective norms | 0.95 |
| Behavioural regulation | 0.90 | Values | 0.95 | |
| Social/professional role and identity | 0.90 | |||
| Norms | 0.90 | |||
| Feedback processes | 0.90 | |||
| Social learning/imitation | 0.90 | |||
| Knowledge | 0.86 | |||
| Behavioural cueing | 0.86 | |||
| 11.3 Conserving mental resources | Memory, attention and decision processes | 1 | Social/professional role and identity | 1 |
| Norms | 1 | |||
| Subjective norms | 1 | |||
| Perceived susceptibility/vulnerability | 1 | |||
| Social influences | 0.95 | |||
| Needs | 0.95 | |||
| Values | 0.95 | |||
| Feedback processes | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Self-image | 0.90 | |||
| Reinforcement | 0.86 | |||
| Emotion | 0.86 | |||
| General attitudes and beliefs | 0.86 | |||
| Beliefs about consequences | 0.81 | |||
| 12.1 Restructuring the physical environment | Environmental context and resources | 0.95 | Social/professional role and identity | 0.84 |
| Behavioural cueing | 0.89 | Optimism | 0.84 | |
| Self-image | 0.84 | |||
| Needs | 0.84 | |||
| 12.2 Restructuring the social environment | Environmental context and resources | 0.95 | Skills | 0.90 |
| Behavioural cueing | 0.80 | Optimism | 0.90 | |
| Needs | 0.90 | |||
| Beliefs about consequences | 0.85 | |||
| Feedback processes | 0.85 | |||
| Attitude towards the behaviour | 0.80 | |||
| 12.3 Avoidance/reducing exposure to cues for the behaviour | Environmental context and resources | 0.95 | Needs | 0.89 |
| Behavioural cueing | 0.95 | Feedback processes | 0.95 | |
| Social learning/imitation | 0.95 | |||
| Social/professional role and identity | 0.89 | |||
| Subjective norms | 0.89 | |||
| Needs | 0.89 | |||
| General attitudes and beliefs | 0.89 | |||
| Knowledge | 0.84 | |||
| Norms | 0.84 | |||
| Self-image | 0.84 | |||
| 12.5 Adding objects to the environment | Environmental context and resources | 0.95 | Social learning/imitation | 1 |
| Behavioural cueing | 0.95 | Skills | 0.86 | |
| Social/professional role and identity | 0.86 | |||
| Beliefs about consequences | 0.86 | |||
| Norms | 0.86 | |||
| Values | 0.86 | |||
| Optimism | 0.81 | |||
| Social influences | 0.81 | |||
| Self-image | 0.81 | |||
| Feedback processes | 0.81 | |||
| Perceived susceptibility/vulnerability | 0.81 | |||
| 12.6 Body changes | Norms | 1 | ||
| Subjective norms | 0.95 | |||
| Social learning/imitation | 0.95 | |||
| Knowledge | 0.90 | |||
| Values | 0.90 | |||
| Social/professional role and identity | 0.86 | |||
| Social influences | 0.86 | |||
| Memory, attention and decision processes | 0.81 | |||
| Feedback processes | 0.81 | |||
| 13.1 Identification of self as role model | Self-image | 0.90 | Perceived susceptibility/vulnerability | 0.90 |
| Skills | 0.80 | |||
| Optimism | 0.80 | |||
| Needs | 0.80 | |||
| 13.2 Framing/reframing | Attitude towards the behaviour | 0.81 | Skills | 0.95 |
| Needs | 0.95 | |||
| Social/professional role and identity | 0.90 | |||
| Social learning/imitation | 0.90 | |||
| Reinforcement | 0.86 | |||
| Norms | 0.86 | |||
| Behavioural cueing | 0.86 | |||
| Environmental context and resources | 0.81 | |||
| Feedback processes | 0.81 | |||
| 14.1 Behaviour cost | Reinforcement | 0.95 | Skills | 0.84 |
| Social/professional role and identity | 0.84 | |||
| Subjective norms | 0.84 | |||
| 15.1 Verbal persuasion about capability | Beliefs about capabilities | 1 | Needs | 0.95 |
| Social/professional role and identity | 0.90 | |||
| Memory, attention and decision processes | 0.90 | |||
| Social learning/imitation | 0.90 | |||
| Norms | 0.86 | |||
| Values | 0.86 | |||
| General attitudes and beliefs | 0.86 | |||
| Perceived susceptibility/vulnerability | 0.86 | |||
| Feedback processes | 0.81 | |||
| 15.4 Self-talk | Knowledge | 0.95 | ||
| Environment | 0.95 | |||
| Norms | 0.95 | |||
| Perceived susceptibility/vulnerability | 0.95 | |||
| Social influences | 0.89 | |||
| Subjective norms | 0.89 | |||
| Values | 0.89 | |||
| Feedback processes | 0.89 | |||
| Social learning/imitation | 0.89 | |||
| Social/professional role and identity | 0.84 | |||
| Reinforcement | 0.84 | |||
| Needs | 0.84 | |||
| 16.3 Vicarious consequences | Social learning/imitation | 0.85 | Skills | 0.95 |
| Norms | 0.80 | Needs | 0.90 | |
| Perceived susceptibility/vulnerability | 0.85 | |||
| MoA | BCT | |||
|---|---|---|---|---|
| ‘Definitely yes’ linked | Proportion of experts | ‘Definitely no’ not linked | Proportion of experts | |
| Knowledge | 4.2 Information about antecedents | 0.86 | ||
| 5.1 Information about health consequences | 0.89 | |||
| Skills | 4.1 Instruction on how to perform the behaviour | 0.86 | ||
| 8.1 Behavioural practice/rehearsal | 0.95 | |||
| 8.4 Habit reversal | 0.84 | |||
| 8.7 Graded tasks | 0.81 | |||
| Social/professional role and identity | 1.1 Goal-setting (behaviour) | 0.90 | ||
| 1.2 Problem-solving | 0.90 | |||
| Beliefs about capabilities | 15.1 Verbal persuasion about capability | 1 | 2.1 Monitoring of outcomes of behaviour without feedback | 0.81 |
| 1.2 Problem-solving | 0.95 | 5.2 Salience of consequences | 0.80 | |
| 8.7 Graded tasks | 0.90 | 5.3 Information about social and environmental consequences | 0.86 | |
| 8.1 Behavioural practice/rehearsal | 0.86 | 5.6 Information about emotional consequences | 0.80 | |
| 7.1 Prompts/cues | 0.86 | |||
| 10.6 Non-specific incentive | 0.84 | |||
| 10.8 Incentive (outcome) | 0.81 | |||
| Optimism | ||||
| Beliefs about consequences | 5.1 Information about health consequences | 0.95 | ||
| 5.2 Salience of consequences | 0.85 | |||
| 5.3 Information about social and environmental consequences | 0.95 | |||
| 5.6 Information about emotional consequences | 0.90 | |||
| 9.2 Pros and cons | 0.90 | |||
| 9.3 Comparative imagining of future outcomes | 1 | |||
| 10.8 Incentive (outcome) | 0.90 | |||
| 10.10 Reward (outcome) | 0.86 | |||
| Reinforcement | 10.1 Material incentive (behaviour) | 0.95 | 1.2 Problem-solving | 0.86 |
| 10.2 Material reward (behaviour) | 0.89 | |||
| 10.3 Non-specific reward | 0.95 | |||
| 10.8 Incentive (outcome) | 0.90 | |||
| 10.10 Reward (outcome) | 0.90 | |||
| 14.1 Behaviour cost | 0.95 | |||
| Intention | 1.1 Goal-setting (behaviour) | 0.95 | ||
| 1.3 Goal-setting (outcome) | 0.86 | |||
| 1.8 Behavioural contract | 0.80 | |||
| 1.9 Commitment | 0.84 | |||
| 9.3 Comparative imagining of future outcomes | 0.81 | |||
| 10.8 Incentive (outcome) | 0.95 | |||
| Goals | 1.1 Goal-setting (behaviour) | 0.95 | ||
| 1.3 Goal-setting (outcome) | 1 | |||
| 1.5 Review behaviour goal(s) | 0.90 | |||
| 1.6 Discrepancy between current behaviour and goal | 0.81 | |||
| 1.7 Review outcome goal(s) | 0.89 | |||
| Memory, attention and decision processes | 11.3 Conserving mental resources | 1 | ||
| Environmental context and resources | 3.2 Social support (practical) | 0.90 | ||
| 7.1 Prompts/cues | 0.90 | |||
| 7.5 Remove aversive stimulus | 0.90 | |||
| 12.1 Restructuring the physical environment | 0.95 | |||
| 12.2 Restructuring the social environment | 0.95 | |||
| 12.3 Avoidance/reducing exposure to cues for the behaviour | 0.95 | |||
| 12.5 Adding objects to the environment | 0.95 | |||
| Social influences | 3.1 Social support (unspecified) | 0.87 | 1.1 Goal-setting (behaviour) | 0.80 |
| 3.2 Social support (practical) | 0.90 | 1.2 Problem-solving | 0.81 | |
| 6.2 Social comparison | 1 | 5.6 Information about emotional consequences | 0.80 | |
| 6.3 Information about others’ approval | 0.84 | |||
| Emotion | 3.3 Social support (emotional) | 0.84 | 1.2 Problem-solving | 0.81 |
| 5.4 Monitoring of emotional consequences | 0.80 | |||
| 11.2 Reduce negative emotions | 0.95 | |||
| Behavioural regulation | 1.3 Problem-solving | 1 | ||
| 11.2 Reduce negative emotions | 0.90 | |||
| Norms | 6.2 Social comparison | 0.90 | 1.2 Problem-solving | 0.95 |
| 6.3 Information about others’ approval | 0.89 | |||
| 16.3 Vicarious consequences | 0.80 | |||
| Subjective norms | 2.7 Feedback on outcomes of behaviour | 0.80 | ||
| Attitude towards the behaviour | 13.2 Framing/reframing | 0.81 | 4.2 Information about antecedents | 0.81 |
| 9.2 Pros and cons | 0.81 | 7.1 Prompts/cues | 0.86 | |
| 12.2 Restructuring the social environment | 0.80 | |||
| Motivation | 1.1 Goal-setting (behaviour) | 0.80 | ||
| 1.9 Commitment | 0.84 | |||
| 5.3 Information about social and environmental consequences | 0.86 | |||
| 9.2 Pros and cons | 0.86 | |||
| 9.3 Comparative imagining of future outcomes | 0.86 | |||
| 10.1 Material incentive (behaviour) | 0.84 | |||
| 10.3 Non-specific reward | 0.84 | |||
| 10.4 Social reward | 0.81 | |||
| 10.10 Reward (outcome) | 0.90 | |||
| Self-image | 13.1 Identification of self as role model | 0.90 | ||
| Needs | 1.1 Goal-setting (behaviour) | 0.80 | ||
| 1.2 Problem-solving | 0.90 | |||
| 2.1 Monitoring of behaviour by others without feedback | 0.89 | |||
| 12.3 Avoidance/reducing exposure to cues for the behaviour | 0.89 | |||
| Values | 1.2 Problem-solving | 0.90 | ||
| Feedback processes | 1.5 Review behaviour goal(s) | 0.95 | ||
| 1.6 Discrepancy between current behaviour and goal | 1 | |||
| 2.2 Feedback on behaviour | 0.95 | |||
| 2.3 Self-monitoring of behaviour | 0.80 | |||
| 2.4 Self-monitoring of outcome(s) of behaviour | 0.81 | |||
| 2.6 Biofeedback | 0.89 | |||
| 2.7 Feedback on outcome(s) of behaviour | 0.80 | |||
| 6.2 Social comparison | 0.80 | |||
| Social learning/imitation | 6.1 Demonstration of behaviour | 0.84 | ||
| 16.3 Vicarious consequences | 0.85 | |||
| Behavioural cueing | 4.2 Information about antecedents | 0.81 | ||
| 7.1 Prompts/cues | 1 | |||
| 8.3 Habit formation | 0.85 | |||
| 12.1 Restructuring the physical environment | 0.85 | |||
| 12.1 Restructuring the social environment | 0.80 | |||
| 12.3 Avoidance/reducing exposure to cues for the behaviour | 0.95 | |||
| 12.5 Adding objects to the environment | 0.95 | |||
| General attitude and beliefs | 1.2 Problem-solving | 0.81 | ||
| Perceived susceptibility/vulnerability | 5.1 Information about health consequences | 0.84 | 1.1 Goal-setting (behaviour) | 0.90 |
Appendix 6 Evidence from triangulation
| BCT | MoA | Literature synthesis study | Expert consensus study | ||||
|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Experts definitely yes (%) | Experts possibly (%) | Experts don’t know (%) | Experts definitely no (%) | ||
| 2.1 Monitoring of behaviour by others without feedback | Needs | 1 | 0.018 | 0 | 11 | 0 | 89 |
| 2.7 Feedback on outcomes of behaviour | Subjective norms | 5 | 0.018 | 0 | 10 | 10 | 80 |
| 5.6 Information about emotional consequences | Social influences | 2 | 0.022 | 5 | 10 | 5 | 80 |
| 12.3 Avoidance/reducing exposure to cues for the behaviour | Needs | 1 | 0.026 | 5 | 5 | 0 | 90 |
| BCT | MoA | Literature synthesis study | Expert consensus study | ||||
|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Experts definitely yes (%) | Experts possibly (%) | Experts don’t know (%) | Experts definitely no (%) | ||
| 8.2 Behaviour substitution | Behavioural regulation | 5 | 0.016 | 79 | 5 | 0 | 16 |
| 5.3 Information about social and environmental consequences | Attitude towards the behaviour | 16 | < 0.001 | 76 | 5 | 9.5 | 9.5 |
| 7.1 Prompts/cues | Memory, attention and decision processes | 8 | < 0.001 | 76 | 24 | 0 | 0 |
| 4.1 Instruction on how to perform the behaviour | Knowledge | 17 | 0.011 | 74 | 18 | 1 | 7 |
| 8.4 Habit reversal | Behavioural regulation | 4 | 0.006 | 74 | 21 | 0 | 5 |
| 8.4 Habit reversal | Behavioural cueing | 2 | 0.034 | 74 | 26 | 0 | 0 |
| 8.6 Generalisation of the target behaviour | Skills | 2 | 0.044 | 74 | 10 | 0 | 16 |
| 2.4 Self-monitoring of outcomes of behaviour | Behavioural regulation | 5 | 0.024 | 71 | 24 | 0 | 5 |
| 1.8 Behavioural contract | Goals | 4 | 0.002 | 70 | 0 | 20 | 10 |
| 2.3 Self-monitoring of behaviour | Behavioural regulation | 18 | < 0.001 | 70 | 15 | 0 | 15 |
| 5.6 Information about emotional consequences | Emotion | 2 | 0.02 | 70 | 10 | 5 | 15 |
| 5.1 Information about health consequences | Attitude towards the behaviour | 19 | < 0.001 | 68 | 32 | 5 | 11 |
| 9.1 Credible source | General attitudes and beliefs | 2 | 0.006 | 68 | 26 | 0 | 6 |
| 5.3 Information about social and environmental consequences | Knowledge | 13 | 0.001 | 67 | 24 | 0 | 9 |
| 12.2 Restructuring the social environment | Social influences | 6 | < 0.001 | 65 | 5 | 5 | 25 |
| 5.1 Information about health consequences | Intention | 28 | 0.005 | 63 | 26 | 0 | 11 |
| 11.2 Reduce negative emotions | Beliefs about capabilities | 12 | 0.039 | 62 | 14 | 5 | 19 |
| 5.6 Information about emotional consequences | Attitude towards the behaviour | 5 | 0.005 | 60 | 35 | 0 | 5 |
| 1.4 Action-planning | Behavioural regulation | 14 | 0.002 | 58 | 16 | 0 | 26 |
| 2.1 Monitoring of behaviour by others without feedback | Social influences | 2 | 0.034 | 58 | 37 | 0 | 5 |
| 6.1 Demonstration of the behaviour | Beliefs about capabilities | 60 | 0.001 | 58 | 37 | 5 | 0 |
| 8.4 Habit reversal | Memory, attention and decision processes | 2 | 0.034 | 58 | 16 | 5 | 21 |
| 10.1 Material incentive (behaviour) | Attitude towards the behaviour | 1 | 0.047 | 58 | 21 | 0 | 21 |
| 5.2 Salience of consequences | Attitude towards the behaviour | 4 | 0.029 | 55 | 30 | 0 | 15 |
| 6.3 Information about others’ approval | Intention | 12 | 0.038 | 53 | 32 | 5 | 10 |
| 8.3 Habit formation | Behavioural regulation | 3 | 0.022 | 45 | 20 | 0 | 35 |
| 2.2 Feedback on behaviour | Knowledge | 13 | 0.010 | 42 | 32 | 0 | 26 |
| 15.4 Self-talk | Beliefs about capabilities | 8 | 0.045 | 42 | 47 | 0 | 11 |
| 1.6 Discrepancy between current behaviour and goal | Behavioural regulation | 3 | 0.017 | 33 | 24 | 0 | 43 |
| 1.1 Goal-setting (behaviour) | Behavioural regulation | 15 | 0.004 | 35 | 35 | 0 | 30 |
| 6.1 Demonstration of the behaviour | Skills | 17 | 0.015 | 26 | 37 | 5 | 32 |
| 1.9 Commitment | Values | 1 | 0.049 | 21 | 42 | 5 | 32 |
| 9.1 Credible source | Social/professional role and identity | 4 | 0.021 | 11 | 58 | 0 | 31 |
| 3.1 Social support (unspecified) | Social/professional role and identity | 5 | 0.035 | 10 | 28 | 4 | 58 |
| 2.2 Feedback on behaviour | Subjective norms | 19 | < 0.001 | 5 | 16 | 11 | 68 |
| 9.2 Pros and cons | Feedback processes | 3 | 0.005 | 0 | 29 | 0 | 71 |
| 5.5 Anticipated regret | Social influences | 2 | 0.002 | N/A | N/A | N/A | N/A |
| 7.8 Associative learning | Reinforcement | 1 | 0.049 | N/A | N/A | N/A | N/A |
| 10.7 Self-incentive | Motivation | 1 | 0.034 | N/A | N/A | N/A | N/A |
| 13.5 Identity associated with changed behaviour | Values | 1 | 0.016 | N/A | N/A | N/A | N/A |
| 15.2 Mental rehearsal of successful performance | Environmental context/resources | 3 | 0.001 | N/A | N/A | N/A | N/A |
| 15.2 Mental rehearsal of successful performance | Values | 1 | 0.034 | N/A | N/A | N/A | N/A |
| 15.3 Focus on past success | Beliefs about capabilities | 23 | < 0.001 | N/A | N/A | N/A | N/A |
| BCT | MoA | Literature synthesis study | Expert consensus study | ||||
|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Experts definitely yes (%) | Experts possibly (%) | Experts don’t know (%) | Experts definitely no (%) | ||
| 1.2 Problem-solving | Behavioural regulation | 13 | 0.16 | 100 | 0 | 0 | 0 |
| 1.6 Discrepancy between current behaviour and goal | Feedback processes | 1 | 0.07 | 100 | 0 | 0 | 0 |
| 11.3 Conserving mental resources | Memory, attention and decision processes | 1 | 0.06 | 100 | 0 | 0 | 0 |
| 10.8 Incentive (outcome) | Motivation | N/A | N/A | 100 | 0 | 0 | 0 |
| 1.1 Goal-setting (behaviour) | Intention | 17 | 0.34 | 95 | 5 | 0 | 0 |
| 1.1 Goal-setting (behaviour) | Goals | 4 | 0.23 | 95 | 0 | 5 | 0 |
| 1.5 Review behaviour goals | Feedback processes | 0 | 1 | 95 | 5 | 0 | 0 |
| 2.2 Feedback on behaviour | Feedback processes | 3 | 0.07 | 95 | 5 | 0 | 0 |
| 10.1 Material incentive (behaviour) | Reinforcement | 0 | 1 | 95 | 5 | 0 | 0 |
| 10.4 Social reward | Social influences | 2 | 0.55 | 95 | 5 | 0 | 0 |
| 11.2 Reduce negative emotions | Emotion | 1 | 0.21 | 95 | 0 | 5 | 0 |
| 12.3 Avoidance/reducing exposure to cues | Environmental context and resources | 1 | 0.24 | 95 | 5 | 0 | 0 |
| 12.3 Avoidance/reducing exposure to cues | Behavioural cueing | 0 | 1 | 95 | 5 | 0 | 0 |
| 12.5 Adding objects to the environment | Behavioural cueing | 2 | 0.11 | 95 | 5 | 0 | 0 |
| 14.10 Remove punishment | Reinforcement | 0 | 1 | 95 | 5 | 0 | 0 |
| 10.8 Incentive (outcome) | Intention | N/A | N/A | 95 | 0 | 0 | 5 |
| 1.5 Review behaviour goals | Goals | 2 | 0.07 | 90 | 0 | 0 | 10 |
| 6.2 Social comparison | Norms | 0 | 1 | 90 | 5 | 0 | 5 |
| 6.2 Social comparison | Feedback processes | 2 | 0.20 | 90 | 5 | 0 | 5 |
| 7.1 Prompts/cues | Environmental context and resources | 5 | 0.05 | 90 | 5 | 0 | 5 |
| 11.2 Reduce negative emotions | Behavioural regulation | 0 | 1 | 90 | 5 | 5 | 0 |
| 7.5 Remove aversive stimulus | Environmental context and resources | N/A | N/A | 90 | 5 | 5 | 0 |
| 10.8 Incentive (outcome) | Beliefs about consequences | N/A | N/A | 90 | 5 | 0 | 5 |
| 10.8 Incentive (outcome) | Reinforcement | N/A | N/A | 90 | 0 | 5 | 5 |
| 10.10 Reward (outcome) | Reinforcement | N/A | N/A | 90 | 5 | 5 | 0 |
| 10.10 Reward (outcome) | Motivation | N/A | N/A | 90 | 10 | 0 | 0 |
| 6.3 Information about others’ approval | Norms | 0 | 1 | 90 | 5 | 5 | 0 |
| 10.2 Material reward (behaviour) | Reinforcement | 0 | 1 | 90 | 0 | 5 | 5 |
| 2.6 Biofeedback | Feedback processes | 0 | 1 | 89 | 11 | 0 | 0 |
| 1.3 Goal-setting (outcome) | Intention | 5 | 0.27 | 86 | 9 | 0 | 5 |
| 4.2 Information about antecedents | Knowledge | 3 | 0.05 | 86 | 14 | 0 | 0 |
| 5.3 Information about social and environmental consequences | Motivation | 5 | 0.24 | 86 | 5 | 0 | 9 |
| 9.3 Comparative imagining of future outcomes | Motivation | 1 | 0.26 | 86 | 9 | 0 | 5 |
| 10.10 Reward (outcome) | Beliefs about consequences | N/A | N/A | 85 | 5 | 0 | 10 |
| 5.2 Salience of consequences | Beliefs about consequences | 2 | 0.46 | 85 | 10 | 0 | 5 |
| 16.3 Vicarious consequences | Social learning/imitation | 1 | 0.10 | 85 | 5 | 5 | 5 |
| 1.9 Commitment | Intention | 5 | 0.13 | 84 | 16 | 0 | 0 |
| 1.9 Commitment | Motivation | 1 | 0.53 | 84 | 16 | 0 | 0 |
| 3.3 Social support (emotional) | Emotion | 1 | 0.16 | 84 | 16 | 0 | 0 |
| 6.3 Information about others’ approval | Social influences | 4 | 0.19 | 84 | 16 | 0 | 0 |
| 8.4 Habit reversal | Skills | 1 | 0.58 | 84 | 5 | 0 | 11 |
| 10.1 Material incentive (behaviour) | Motivation | 0 | 1 | 84 | 16 | 0 | 0 |
| 10.3 Non-specific reward | Motivation | 1 | 0.29 | 84 | 11 | 0 | 5 |
| 4.2 Information about antecedents | Behavioural cueing | 0 | 1 | 81 | 5 | 0 | 14 |
| 8.7 Graded tasks | Skills | 4 | 0.42 | 81 | 14 | 0 | 5 |
| 9.3 Comparative imagining of future outcomes | Intention | 1 | 0.66 | 81 | 10 | 0 | 9 |
| 2.4 Self-monitoring of outcomes of behaviour | Feedback processes | 1 | 0.20 | 81 | 9 | 5 | 5 |
| 10.4 Social reward | Motivation | 3 | 0.20 | 81 | 14 | 0 | 5 |
| 1.1 Goal-setting (behaviour) | Motivation | 3 | 0.80 | 80 | 20 | 0 | 0 |
| 1.8 Behavioural contract | Intention | 4 | 0.44 | 80 | 5 | 5 | 10 |
| 2.3 Self-monitoring of behaviour | Feedback processes | 2 | 0.16 | 80 | 15 | 0 | 5 |
| 5.4 Monitoring of emotional consequences | Emotion | 0 | 1 | 80 | 15 | 0 | 5 |
| 12.2 Restructuring the social environment | Behavioural cueing | 0 | 1 | 80 | 10 | 0 | 10 |
| 16.3 Vicarious consequences | Norms | 0 | 1 | 80 | 5 | 10 | 5 |
| BCT | MoA | Literature synthesis study | Expert consensus study | ||||
|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Experts definitely yes (%) | Experts possibly (%) | Experts don’t know (%) | Experts definitely no (%) | ||
| 1.7 Review outcome goals | Intention | 1 | 0.62 | 79 | 16 | 0 | 5 |
| 1.7 Review outcome goals | Feedback processes | 0 | 1 | 79 | 21 | 0 | 0 |
| 1.9 Commitment | Goals | 1 | 0.35 | 79 | 21 | 0 | 0 |
| 2.6 Biofeedback | Knowledge | 0 | 1 | 79 | 16 | 0 | 5 |
| 3.3 Social support (emotional) | Social influences | 2 | 0.17 | 79 | 21 | 0 | 0 |
| 4.1 Instruction on how to perform the behaviour | Beliefs about capabilities | 62 | 0.06 | 79 | 17 | 0 | 4 |
| 8.4 Habit reversal | Intention | 1 | 0.79 | 79 | 16 | 0 | 5 |
| 8.2 Behaviour substitution | Behavioural cueing | 2 | 0.0784 | 79 | 21 | 0 | 0 |
| 9.1 Credible source | Attitude towards the behaviour | 7 | 0.08 | 79 | 21 | 0 | 0 |
| 10.1 Material incentive (behaviour) | Beliefs about consequences | 0 | 1 | 79 | 11 | 0 | 11 |
| 10.6 Non-specific incentive | Reinforcement | N/A | N/A | 79 | 5 | 0 | 16 |
| 14.10 Remove punishment | Beliefs about consequences | 0 | 1 | 79 | 10.5 | 0 | 10.5 |
| 15.4 Self-talk | Motivation | 2 | 0.08 | 79 | 16 | 0 | 5 |
| 1.3 Goal-setting (outcome) | Motivation | 3 | 0.08 | 76 | 19 | 0 | 5 |
| 2.4 Self-monitoring of outcomes of behaviour | Beliefs about capabilities | 7 | 0.73 | 76 | 24 | 0 | 0 |
| 2.4 Self-monitoring of outcomes of behaviour | Motivation | 0 | 1 | 76 | 5 | 9.5 | 9.5 |
| 3.2 Social support (practical) | Behavioural cueing | 0 | 1 | 76 | 19 | 0 | 5 |
| 4.2 Information about antecedents | Behavioural regulation | 2 | 0.23 | 76 | 10 | 0 | 14 |
| 8.7 Graded tasks | Motivation | 1 | 0.82 | 76 | 19 | 0 | 5 |
| 9.2 Pros and cons | General attitudes and beliefs | 0 | 1 | 76 | 24 | 0 | 0 |
| 11.3 Conserving mental resources | Behavioural regulation | 1 | 0.15 | 76 | 14 | 0 | 10 |
| 15.1 Verbal persuasion about capability | Social influences | 1 | 0.79 | 76 | 10 | 0 | 14 |
| 15.1 Verbal persuasion about capability | Motivation | 1 | 0.73 | 76 | 14 | 0 | 10 |
| 16.3 Vicarious consequences | Subjective norms | 1 | 0.58 | 75 | 20 | 0 | 5 |
| 1.4 Action-planning | Goals | 3 | 0.32 | 74 | 16 | 0 | 10 |
| 1.4 Action-planning | Behavioural cueing | 4 | 0.10 | 74 | 16 | 0 | 10 |
| 1.7 Review outcome goals | Motivation | 0 | 1 | 74 | 16 | 0 | 10 |
| 2.1 Monitoring of behaviour by others without feedback | Behavioural cueing | 0 | 1 | 74 | 26 | 0 | 0 |
| 2.6 Biofeedback | Reinforcement | 0 | 1 | 74 | 21 | 0 | 5 |
| 2.6 Biofeedback | Motivation | 1 | 0.24 | 74 | 21 | 0 | 5 |
| 8.6 Generalisation of the target behaviour | Beliefs about capabilities | 0 | 1 | 74 | 21 | 0 | 5 |
| 9.1 Credible source | Social influences | 5 | 0.22 | 74 | 26 | 0 | 0 |
| 10.1 Material incentive (behaviour) | Intention | 0 | 1 | 74 | 26 | 0 | 0 |
| 10.6 Non-specific incentive | Intention | N/A | N/A | 74 | 16 | 0 | 10 |
| 10.6 Non-specific incentive | Motivation | N/A | N/A | 74 | 16 | 0 | 10 |
| 14.10 Remove punishment | Motivation | 0 | 1 | 74 | 21 | 0 | 5 |
| 6.2 Social comparison | Values | 0 | 1 | 71 | 19 | 0 | 10 |
| 9.2 Pros and cons | Memory, attention and decision processes | 0 | 1 | 71 | 14 | 5 | 10 |
| 9.3 Comparative imagining of future outcomes | Attitude towards the behaviour | 0 | 1 | 71 | 14 | 5 | 10 |
| 10.8 Incentive (outcome) | Goals | N/A | N/A | 71 | 14.5 | 0 | 14.5 |
| 12.6 Body changes | Self-image | 0 | 1 | 71 | 19 | 0 | 10 |
| 13.2 Framing/reframing | Beliefs about consequences | 5 | 0.28 | 71 | 24 | 5 | 0 |
| 13.2 Framing/reframing | Motivation | 3 | 0.29 | 71 | 29 | 0 | 0 |
| 15.1 Verbal persuasion about capability | Self-image | 0 | 1 | 71 | 14.5 | 0 | 14.5 |
| 1.5 Review behaviour goals | Intention | 5 | 0.11 | 70 | 15 | 0 | 15 |
| 1.5 Review behaviour goals | Behavioural regulation | 2 | 0.30 | 70 | 15 | 0 | 15 |
| 2.7 Feedback on outcomes of behaviour | Beliefs about capabilities | 7 | 0.78 | 70 | 20 | 0 | 10 |
| 2.7 Feedback on outcomes of behaviour | Reinforcement | 1 | 0.33 | 70 | 15 | 5 | 10 |
| 5.2 Salience of consequences | Perceived susceptibility/vulnerability | 1 | 0.17 | 70 | 25 | 0 | 5 |
| 8.3 Habit formation | Memory, attention and decision processes | 1 | 0.21 | 70 | 10 | 5 | 15 |
| 8.3 Habit formation | Environmental context and resources | 0 | 1 | 70 | 10 | 5 | 15 |
| 16.3 Vicarious consequences | Social influences | 0 | 1 | 70 | 25 | 0 | 5 |
| 2.2 Feedback on behaviour | Motivation | 8 | 0.06 | 68 | 32 | 0 | 0 |
| 11.3 Conserving mental resources | Environment | 1 | 0.08 | 67 | 28 | 0 | 5 |
| 9.1 Credible source | Social learning/imitation | 2 | 0.07 | 63 | 21 | 0 | 16 |
| 2.2 Feedback on behaviour | Reinforcement | 4 | 0.07 | 58 | 26 | 0 | 16 |
| 13.2 Framing/reframing | General attitude and beliefs | 1 | 0.08 | 52 | 38 | 5 | 5 |
| 2.7 Feedback on outcomes of behaviour | Motivation | 3 | 0.10 | 50 | 35 | 0 | 15 |
| 1.2 Problem-solving | Skills | 18 | 0.05 | 43 | 24 | 5 | 28 |
| 1.2 Problem-solving | Environment | 9 | 0.05 | 43 | 24 | 0 | 33 |
| 10.4 Social reward | Beliefs about capabilities | 18 | 0.08 | 43 | 29 | 0 | 28 |
| 1.1 Goal-setting (behaviour) | Beliefs about capabilities | 44 | 0.07 | 35 | 30 | 0 | 35 |
| 8.3 Habit formation | Motivation | 2 | 0.06 | 35 | 20 | 0 | 45 |
| 1.8 Behavioural contract | Behavioural regulation | 3 | 0.07 | 25 | 15 | 5 | 55 |
| 2.1 Monitoring of behaviour by others without feedback | Reinforcement | 1 | 0.08 | 16 | 31.5 | 10.5 | 42 |
| 10.2 Material reward (behaviour) | Goals | 1 | 0.09 | 16 | 58 | 10 | 16 |
| 12.6 Body changes | Emotion | 1 | 0.07 | 14 | 29 | 9 | 48 |
| 1.7 Review outcome goals | Optimism | 1 | 0.06 | 11 | 53 | 5 | 31 |
| 1.9 Commitment | Memory, attention and decision processes | 2 | 0.09 | 11 | 26 | 16 | 47 |
| 2.6 Biofeedback | Beliefs about capabilities | 5 | 0.07 | 11 | 42 | 0 | 47 |
| 5.2 Salience of consequences | Subjective norms | 8 | 0.09 | 10 | 25 | 5 | 60 |
| 8.1 Behavioural practice/rehearsal | Behavioural cueing | 5 | 0.05 | 10 | 33 | 0 | 57 |
| 4.2 Information about antecedents | Skills | 3 | 0.10 | 9 | 5 | 0 | 86 |
| 10.3 Non-specific reward | Self-image | 1 | 0.07 | 5 | 0 | 0 | 95 |
| 13.2 Framing/reframing | Self-image | 2 | 0.06 | 5 | 57 | 5 | 33 |
| 5.5 Anticipated regret | Beliefs about consequences | 2 | 0.06 | N/A | N/A | N/A | N/A |
| 7.8 Associative learning | Behavioural cueing | 1 | 0.07 | N/A | N/A | N/A | N/A |
| 7.8 Associative learning | Memory, attention and decision processes | 1 | 0.08 | N/A | N/A | N/A | N/A |
| 13.3 Incompatible beliefs | Attitude towards the behaviour | 1 | 0.09 | N/A | N/A | N/A | N/A |
| 13.4 Valued self-identity | Intention | 2 | 0.05 | N/A | N/A | N/A | N/A |
| 13.4 Valued self-identity | Motivation | 1 | 0.10 | N/A | N/A | N/A | N/A |
| 13.5 Identity associated with changed behaviour | Social/professional role and identity | 1 | 0.09 | N/A | N/A | N/A | N/A |
| 14.1 Behaviour cost | Behavioural regulation | 1 | 0.05 | N/A | N/A | N/A | N/A |
| 15.2 Mental rehearsal of successful performance | Motivation | 2 | 0.09 | N/A | N/A | N/A | N/A |
| BCT | MoA | Literature synthesis study | Expert consensus study | |
|---|---|---|---|---|
| Frequency (number of papers) | p-value | Proportion of experts (‘definitely no’) | ||
| 1.1 Goal-setting (behaviour) | Social/professional role and identity | 2 | 0.49 | 0.90 |
| Social learning/imitation | 1 | 0.48 | 0.90 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.90 | |
| Skills | 7 | 0.71 | 0.85 | |
| Social influences | 2 | 0.96 | 0.80 | |
| Needs | 1 | 0.28 | 0.80 | |
| 1.2 Problem-solving | Norms | 0 | 1 | 0.95 |
| Subjective norms | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social/professional role and identity | 2 | 0.66 | 0.90 | |
| Needs | 0 | 1 | 0.90 | |
| Values | 0 | 1 | 0.90 | |
| Reinforcement | 2 | 0.63 | 0.86 | |
| Social influences | 3 | 0.97 | 0.81 | |
| Emotion | 1 | 0.81 | 0.81 | |
| General attitudes and beliefs | 0 | 1 | 0.81 | |
| 1.3 Goal-setting (outcome) | Perceived susceptibility/vulnerability | 0 | 1 | 1.00 |
| Social/professional role and identity | 0 | 1 | 0.95 | |
| Norms | 0 | 1 | 0.95 | |
| Social learning/imitation | 1 | 0.15 | 0.95 | |
| Skills | 4 | 0.1405 | 0.90 | |
| Social influences | 1 | 0.71 | 0.90 | |
| Subjective norms | 0 | 1 | 0.90 | |
| Knowledge | 0 | 1 | 0.86 | |
| Emotion | 0 | 1 | 0.86 | |
| Values | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.86 | |
| Environmental context and resources | 1 | 0.518 | 0.81 | |
| Needs | 0 | 1 | 0.81 | |
| 1.4 Action-planning | Social/professional role and identity | 2 | 0.39179 | 0.95 |
| Norms | 0 | 1 | 0.95 | |
| Subjective norms | 2 | 0.94 | 0.95 | |
| Needs | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social influences | 0 | 1 | 0.89 | |
| General attitudes and beliefs | 0 | 1 | 0.89 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.89 | |
| Knowledge | 3 | 0.8715 | 0.84 | |
| Reinforcement | 1 | 0.71 | 0.84 | |
| Values | 1 | 0.20 | 0.84 | |
| Feedback processes | 0 | 1 | 0.84 | |
| 1.5 Review behaviour goals | Social learning/imitation | 0 | 1 | 0.90 |
| Norms | 0 | 1 | 0.85 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.85 | |
| Social/professional role and identity | 0 | 1 | 0.80 | |
| Subjective norms | 0 | 1 | 0.80 | |
| Needs | 0 | 1 | 0.80 | |
| 1.6 Discrepancy between current behaviour and goal | Social learning/imitation | 0 | 1 | 1.00 |
| Social/professional role and identity | 0 | 1 | 0.90 | |
| Reinforcement | 0 | 1 | 0.90 | |
| Norms | 0 | 1 | 0.90 | |
| Subjective norms | 0 | 1 | 0.90 | |
| Environmental context and resources | 0 | 1 | 0.86 | |
| Needs | 0 | 1 | 0.86 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.86 | |
| Skills | 0 | 1 | 0.81 | |
| Optimism | 0 | 1 | 0.81 | |
| Behavioural cueing | 0 | 1 | 0.81 | |
| General attitudes and beliefs | 0 | 1 | 0.81 | |
| 1.7 Review outcome goals | Social/professional role and identity | 0 | 1 | 0.95 |
| Social influences | 0 | 1 | 0.95 | |
| Norms | 0 | 1 | 0.95 | |
| Subjective norms | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Environmental context and resources | 0 | 1 | 0.89 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.89 | |
| Knowledge | 0 | 1 | 0.84 | |
| Skills | 1 | 0.422 | 0.84 | |
| Needs | 0 | 1 | 0.84 | |
| Behavioural cueing | 0 | 1 | 0.84 | |
| 1.8 Behavioural contract | Social learning/imitation | 0 | 1 | 0.95 |
| Needs | 0 | 1 | 0.90 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.90 | |
| Skills | 3 | 0.26 | 0.85 | |
| Knowledge | 0 | 1 | 0.80 | |
| 1.9 Commitment | Skills | 0 | 1 | 0.84 |
| Reinforcement | 1 | 0.198 | 0.84 | |
| Social learning/imitation | 0 | 1 | 0.84 | |
| 2.1 Monitoring of behaviour by others without feedback | Optimism | 0 | 1 | 0.84 |
| 2.2 Feedback on behaviour | Needs | 0 | 1 | 0.84 |
| Social learning/imitation | 0 | 1 | 0.84 | |
| 2.3 Self-monitoring of behaviour | Social learning/imitation | 0 | 1 | 0.95 |
| Norms | 0 | 1 | 0.90 | |
| Subjective norms | 0 | 1 | 0.90 | |
| Social/professional role and identity | 1 | 0.72 | 0.85 | |
| Needs | 1 | 0.23 | 0.85 | |
| Values | 0 | 1 | 0.85 | |
| General attitudes and beliefs | 0 | 1 | 0.85 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.85 | |
| Social influences | 1 | 0.98 | 0.80 | |
| 2.4 Self-monitoring of outcomes of behaviour | Norms | 0 | 1 | 1 |
| Social influences | 3 | 0.13 | 0.95 | |
| Subjective norms | 0 | 1 | 0.95 | |
| Needs | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.9 | |
| Values | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.81 | |
| 2.5 Monitoring of outcomes of behaviour without feedback | Needs | 0 | 1 | 0.95 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Skills | 0 | 1 | 0.86 | |
| Social/professional role and identity | 0 | 1 | 0.86 | |
| Optimism | 0 | 1 | 0.86 | |
| Beliefs about capabilities | 2 | 0.11 | 0.81 | |
| Memory, attention and decision processes | 0 | 1 | 0.81 | |
| Environmental context and resources | 0 | 1 | 0.81 | |
| Norms | 0 | 1 | 0.81 | |
| Values | 0 | 1 | 0.81 | |
| General attitudes and beliefs | 0 | 1 | 0.81 | |
| 2.6 Biofeedback | Social/professional role and identity | 0 | 1 | 0.89 |
| Norms | 0 | 1 | 0.89 | |
| Subjective Norms | 1 | 0.32 | 0.89 | |
| Social learning/imitation | 0 | 1 | 0.89 | |
| Social influences | 0 | 1 | 0.84 | |
| Values | 0 | 1 | 0.84 | |
| 2.7 Feedback on outcomes of behaviour | Social learning/imitation | 0 | 1 | 0.95 |
| Environmental context and resources | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Perceived susceptibility/vulnerability | 1 | 0.22 | 0.85 | |
| 3.1 Social support (unspecified) | Skills | 6 | 0.88 | 0.87 |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.82 | |
| 3.2 Social support (practical) | Perceived susceptibility/vulnerability | 0 | 1 | 0.95 |
| Feedback processes | 0 | 1 | 0.9 | |
| Self-image | 0 | 1 | 0.86 | |
| Needs | 0 | 1 | 0.86 | |
| Values | 0 | 1 | 0.81 | |
| 3.3 Social support (emotional) | Feedback processes | 0 | 1 | 0.84 |
| 4.1 Instruction on how to perform the behaviour | Needs | 0 | 1 | 0.9 |
| Perceived susceptibility/vulnerability | 1 | 0.754 | 0.9 | |
| Values | 0 | 1 | 0.87 | |
| Emotion | 1 | 0.84 | 0.84 | |
| Social/professional role and identity | 2 | 0.70 | 0.82 | |
| Subjective norms | 4 | 0.97 | 0.82 | |
| Norms | 0 | 1 | 0.81 | |
| 4.2 Information about antecedents | Needs | 0 | 1 | 0.95 |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Subjective norms | 0 | 1 | 0.9 | |
| Values | 0 | 1 | 0.9 | |
| Feedback processes | 0 | 1 | 0.9 | |
| General attitudes and beliefs | 0 | 1 | 0.9 | |
| Skills | 3 | 0.098 | 0.86 | |
| Self-image | 0 | 1 | 0.86 | |
| Social learning/imitation | 0 | 1 | 0.86 | |
| Optimism | 0 | 1 | 0.81 | |
| Reinforcement | 0 | 1 | 0.81 | |
| Social influences | 0 | 1 | 0.81 | |
| Attitude towards the behaviour | 0 | 1 | 0.81 | |
| 5.1 Information about health consequences | Reinforcement | 0 | 1 | 0.95 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Skills | 2 | 0.99 | 0.89 | |
| Optimism | 0 | 1 | 0.89 | |
| Behavioural regulation | 1 | 0.999 | 0.89 | |
| Subjective norms | 3 | 0.95 | 0.89 | |
| Social/professional role and identity | 0 | 1 | 0.84 | |
| Environmental context and resources | 0 | 1 | 0.84 | |
| Self-image | 1 | 0.60 | 0.84 | |
| Needs | 0 | 1 | 0.84 | |
| 5.2 Salience of consequences | Skills | 0 | 1 | 0.95 |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Optimism | 0 | 1 | 0.85 | |
| Needs | 0 | 1 | 0.85 | |
| Social/professional role and identity | 0 | 1 | 0.8 | |
| Beliefs about capabilities | 3 | 0.95 | 0.8 | |
| 5.3 Information about social and environmental consequences | Skills | 1 | 0.99 | 1 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Behavioural regulation | 0 | 1 | 0.9 | |
| Feedback processes | 2 | 0.17 | 0.9 | |
| Beliefs about capabilities | 7 | 0.999 | 0.86 | |
| Optimism | 0 | 1 | 0.86 | |
| Needs | 0 | 1 | 0.81 | |
| 5.4 Monitoring of emotional consequences | Skills | 1 | 0.13 | 0.95 |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Memory, attention and decision processes | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Subjective norms | 0 | 1 | 0.9 | |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Environmental context and resources | 0 | 1 | 0.85 | |
| Values | 0 | 1 | 0.85 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.8 | |
| 5.6 Information about emotional consequences | Social learning/imitation | 0 | 1 | 0.95 |
| Behavioural cueing | 0 | 1 | 0.9 | |
| Skills | 0 | 1 | 0.85 | |
| Social/professional role and identity | 0 | 1 | 0.85 | |
| Memory, attention and decision processes | 0 | 1 | 0.85 | |
| Environmental context and resources | 0 | 1 | 0.85 | |
| Beliefs about capabilities | 3 | 0.96 | 0.8 | |
| Social influences | 0 | 1 | 0.8 | |
| Norms | 0 | 1 | 0.8 | |
| Subjective norms | 1 | 0.69 | 0.8 | |
| 6.1 Demonstration of the behaviour | Needs | 0 | 1 | 0.95 |
| Perceived susceptibility/vulnerability | 1 | 0.67 | 0.89 | |
| Self-image | 1 | 0.63 | 0.84 | |
| 6.2 Social comparison | Skills | 2 | 0.99 | 1.00 |
| Needs | 0 | 1 | 0.95 | |
| Behavioural regulation | 0 | 1 | 0.86 | |
| Perceived susceptibility/vulnerability | 1 | 0.56 | 0.86 | |
| 6.3 Information about others’ approval | Skills | 1 | 0.98 | 0.95 |
| Needs | 0 | 1 | 0.84 | |
| 7.1 Prompts/cues | Needs | 0 | 1 | 1 |
| Perceived susceptibility/vulnerability | 1 | 0.43 | 1 | |
| Knowledge | 4 | 0.50 | 0.95 | |
| Social/professional role and identity | 1 | 0.62 | 0.95 | |
| Self-image | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| General attitudes and beliefs | 0 | 1 | 0.95 | |
| Beliefs about consequences | 3 | 0.85 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Subjective norms | 0 | 1 | 0.9 | |
| Feedback processes | 0 | 1 | 0.9 | |
| Beliefs about capabilities | 14 | 0.95 | 0.86 | |
| Optimism | 1 | 0.43 | 0.86 | |
| Attitude towards the behaviour | 2 | 0.86 | 0.86 | |
| Emotion | 1 | 0.516 | 0.81 | |
| 7.5 Remove aversive stimulus | Knowledge | N/A | N/A | 1 |
| Needs | N/A | N/A | 1 | |
| Skills | N/A | N/A | 0.95 | |
| Social/professional role and identity | N/A | N/A | 0.95 | |
| Values | N/A | N/A | 0.9 | |
| Subjective norms | N/A | N/A | 0.86 | |
| Self-image | N/A | N/A | 0.86 | |
| Perceived susceptibility/vulnerability | N/A | N/A | 0.86 | |
| Norms | N/A | N/A | 0.81 | |
| Feedback processes | N/A | N/A | 0.81 | |
| Social learning/imitation | N/A | N/A | 0.81 | |
| 8.1 Behavioural practice/rehearsal | Norms | 0 | 1 | 0.95 |
| Needs | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Subjective norms | 1 | 0.996 | 0.9 | |
| Social influences | 1 | 0.99 | 0.86 | |
| Social learning/imitation | 2 | 0.13 | 0.86 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.81 | |
| 8.2 Behaviour substitution | Needs | 0 | 1 | 1 |
| Social/professional role and identity | 1 | 0.30 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social influences | 0 | 1 | 0.89 | |
| Emotion | 0 | 1 | 0.89 | |
| Norms | 0 | 1 | 0.89 | |
| Subjective norms | 0 | 1 | 0.89 | |
| General attitudes and beliefs | 0 | 1 | 0.89 | |
| Self-image | 0 | 1 | 0.84 | |
| 8.3 Habit formation | Perceived susceptibility/vulnerability | 0 | 1 | 0.9 |
| Needs | 0 | 1 | 0.85 | |
| General attitudes and beliefs | 0 | 1 | 0.85 | |
| Knowledge | 0 | 1 | 0.8 | |
| Optimism | 0 | 1 | 0.8 | |
| Norms | 0 | 1 | 0.8 | |
| Values | 0 | 1 | 0.8 | |
| Feedback processes | 0 | 1 | 0.8 | |
| 8.4 Habit reversal | Needs | 0 | 1 | 0.84 |
| 8.6 Generalisation of the target behaviour | Needs | 0 | 1 | 0.89 |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.84 | |
| 8.7 Graded tasks | Social influences | 0 | 1 | 1 |
| Norms | 0 | 1 | 1 | |
| Needs | 0 | 1 | 1 | |
| Subjective norms | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.86 | |
| Social learning/imitation | 0 | 1 | 0.86 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.86 | |
| Knowledge | 1 | 0.92 | 0.81 | |
| Behavioural cueing | 2 | 0.22 | 0.81 | |
| 9.1 Credible source | Skills | 4 | 0.77 | 0.89 |
| Needs | 0 | 1 | 0.89 | |
| Reinforcement | 1 | 0.63 | 0.84 | |
| 9.2 Pros and cons | Social learning/imitation | 0 | 1 | 1 |
| Skills | 0 | 1 | 0.9 | |
| Behavioural cueing | 0 | 1 | 0.86 | |
| Social/professional role and identity | 0 | 1 | 0.81 | |
| Self-image | 0 | 1 | 0.81 | |
| Needs | 1 | 0.11 | 0.81 | |
| 9.3 Comparative imagining of future outcomes | Skills | 0 | 1 | 1 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Reinforcement | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Environment | 0 | 1 | 0.86 | |
| Social influences | 0 | 1 | 0.86 | |
| Social/professional role and identity | 0 | 1 | 0.81 | |
| 10.1 Material incentive (behaviour) | Social learning/imitation | 0 | 1 | 0.84 |
| 10.2 Material reward (behaviour) | Social/professional role and identity | 0 | 1 | 0.95 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.95 | |
| Knowledge | 1 | 0.23 | 0.89 | |
| Skills | 0 | 1 | 0.89 | |
| Memory, attention and decision processes | 0 | 1 | 0.89 | |
| Social influences | 1 | 0.19 | 0.89 | |
| Norms | 0 | 1 | 0.89 | |
| Subjective norms | 0 | 1 | 0.89 | |
| Self-image | 0 | 1 | 0.89 | |
| Optimism | 0 | 1 | 0.84 | |
| 10.3 Non-specific reward | Social/professional role and identity | 0 | 1 | 0.95 |
| Subjective norms | 0 | 1 | 0.95 | |
| Self-image | 1 | 0.055 | 0.95 | |
| Needs | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.95 | |
| Optimism | 0 | 1 | 0.89 | |
| Social influences | 0 | 1 | 0.89 | |
| Behavioural regulation | 0 | 1 | 0.89 | |
| Norms | 0 | 1 | 0.89 | |
| Knowledge | 0 | 1 | 0.84 | |
| Skills | 0 | 1 | 0.84 | |
| Feedback processes | 0 | 1 | 0.84 | |
| General attitudes and beliefs | 0 | 1 | 0.84 | |
| 10.4 Social reward | Perceived susceptibility/vulnerability | 0 | 1 | 1 |
| Skills | 2 | 0.80 | 0.95 | |
| Memory, attention and decision processes | 2 | 0.27 | 0.9 | |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Knowledge | 0 | 1 | 0.86 | |
| Needs | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.86 | |
| 10.6 Non-specific incentive | Skills | N/A | N/A | 0.95 |
| Social/professional role and identity | N/A | N/A | 0.95 | |
| Social influences | N/A | N/A | 0.95 | |
| Social learning/imitation | N/A | N/A | 0.95 | |
| Perceived susceptibility/vulnerability | N/A | N/A | 0.95 | |
| Knowledge | N/A | N/A | 0.89 | |
| Optimism | N/A | N/A | 0.89 | |
| Norms | N/A | N/A | 0.89 | |
| Subjective norms | N/A | N/A | 0.89 | |
| Self-image | N/A | N/A | 0.89 | |
| Beliefs about capabilities | N/A | N/A | 0.84 | |
| Values | N/A | N/A | 0.84 | |
| Feedback processes | N/A | N/A | 0.84 | |
| 10.8 Incentive (outcome) | Skills | N/A | N/A | 1 |
| Perceived susceptibility/vulnerability | N/A | N/A | 1 | |
| Social/professional role and identity | N/A | N/A | 0.95 | |
| Self-image | N/A | N/A | 0.95 | |
| Social learning/imitation | N/A | N/A | 0.95 | |
| Subjective norms | N/A | N/A | 0.9 | |
| Social influences | N/A | N/A | 0.86 | |
| Norms | N/A | N/A | 0.86 | |
| Values | N/A | N/A | 0.86 | |
| Beliefs about capabilities | N/A | N/A | 0.81 | |
| Memory, attention and decision processes | N/A | N/A | 0.81 | |
| General attitudes and beliefs | N/A | N/A | 0.81 | |
| 10.10 Reward (outcome) | Skills | N/A | N/A | 1 |
| Social/professional role and identity | N/A | N/A | 1 | |
| Memory, attention and decision processes | N/A | N/A | 0.95 | |
| Social influences | N/A | N/A | 0.95 | |
| Social learning/imitation | N/A | N/A | 0.95 | |
| Perceived susceptibility/vulnerability | N/A | N/A | 0.95 | |
| Knowledge | N/A | N/A | 0.9 | |
| Norms | N/A | N/A | 0.9 | |
| Self-image | N/A | N/A | 0.9 | |
| Subjective norms | N/A | N/A | 0.86 | |
| General attitudes and beliefs | N/A | N/A | 0.81 | |
| 11.1 Pharmacological support | Skills | 1 | 0.13 | 0.95 |
| Subjective norms | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Feedback processes | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.89 | |
| Norms | 0 | 1 | 0.89 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.84 | |
| 11.2 Reduce negative emotions | Subjective norms | 0 | 1 | 0.95 |
| Values | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.9 | |
| Feedback processes | 0 | 1 | 0.9 | |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Knowledge | 0 | 1 | 0.86 | |
| Behavioural cueing | 0 | 1 | 0.86 | |
| 11.3 Conserving mental resources | Social/professional role and identity | 0 | 1 | 1 |
| Norms | 0 | 1 | 1 | |
| Subjective norms | 0 | 1 | 1 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 1 | |
| Social influences | 0 | 1 | 0.95 | |
| Needs | 0 | 1 | 0.95 | |
| Values | 0 | 1 | 0.95 | |
| Feedback processes | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Self-image | 0 | 1 | 0.9 | |
| Reinforcement | 0 | 1 | 0.86 | |
| Emotion | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.86 | |
| Beliefs about consequences | 0 | 1 | 0.81 | |
| 12.1 Restructuring the physical environment | Social/professional role and identity | 1 | 0.36 | 0.84 |
| Optimism | 1 | 0.22 | 0.84 | |
| Self-image | 0 | 1 | 0.84 | |
| Needs | 0 | 1 | 0.84 | |
| 12.2 Restructuring the social environment | Skills | 0 | 1 | 0.9 |
| Optimism | 0 | 1 | 0.9 | |
| Needs | 0 | 1 | 0.9 | |
| Beliefs about consequences | 0 | 1 | 0.85 | |
| Feedback processes | 0 | 1 | 0.85 | |
| Attitude towards the behaviour | 0 | 1 | 0.8 | |
| 12.3 Avoidance/reducing exposure to cues for the behaviour | Feedback processes | 0 | 1 | 0.95 |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.89 | |
| Subjective norms | 1 | 0.38 | 0.89 | |
| General attitudes and beliefs | 0 | 1 | 0.89 | |
| Knowledge | 0 | 1 | 0.84 | |
| Norms | 0 | 1 | 0.84 | |
| Self-image | 0 | 1 | 0.84 | |
| 12.5 Adding objects to the environment | Social learning/imitation | 0 | 1 | 1 |
| Skills | 0 | 1 | 0.86 | |
| Social/professional role and identity | 0 | 1 | 0.86 | |
| Beliefs about consequences | 0 | 1 | 0.86 | |
| Norms | 0 | 1 | 0.86 | |
| Values | 0 | 1 | 0.86 | |
| Optimism | 0 | 1 | 0.81 | |
| Social influences | 0 | 1 | 0.81 | |
| Self-image | 0 | 1 | 0.81 | |
| Feedback processes | 0 | 1 | 0.81 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.81 | |
| 12.6 Body changes | Norms | 0 | 1 | 1 |
| Subjective norms | 0 | 1 | 0.95 | |
| Social learning/imitation | 0 | 1 | 0.95 | |
| Knowledge | 0 | 1 | 0.9 | |
| Values | 0 | 1 | 0.9 | |
| Social/professional role and identity | 0 | 1 | 0.86 | |
| Social influences | 0 | 1 | 0.86 | |
| Memory, attention and decision processes | 0 | 1 | 0.81 | |
| Feedback processes | 0 | 1 | 0.81 | |
| 13.1 Identification of self as role model | Perceived susceptibility/vulnerability | 0 | 1 | 0.9 |
| Skills | 2 | 0.44 | 0.8 | |
| Optimism | 1 | 0.16 | 0.8 | |
| Needs | 0 | 1 | 0.8 | |
| 13.2 Framing/reframing | Skills | 3 | 0.67 | 0.95 |
| Needs | 0 | 1 | 0.95 | |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Reinforcement | 0 | 1 | 0.86 | |
| Norms | 0 | 1 | 0.86 | |
| Behavioural cueing | 1 | 0.587 | 0.86 | |
| Environmental context and resources | 0 | 1 | 0.81 | |
| Feedback processes | 0 | 1 | 0.81 | |
| 14.1 Behaviour cost | Skills | N/A | N/A | 0.84 |
| Social/professional role and identity | N/A | N/A | 0.84 | |
| Subjective norms | 0 | 1 | 0.84 | |
| 15.1 Verbal persuasion about capability | Needs | 0 | 1 | 0.95 |
| Social/professional role and identity | 0 | 1 | 0.9 | |
| Memory, attention and decision processes | 0 | 1 | 0.9 | |
| Social learning/imitation | 0 | 1 | 0.9 | |
| Norms | 0 | 1 | 0.86 | |
| Values | 0 | 1 | 0.86 | |
| General attitudes and beliefs | 0 | 1 | 0.86 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.86 | |
| Feedback processes | 0 | 1 | 0.81 | |
| 15.4 Self-talk | Knowledge | 0 | 1 | 0.95 |
| Environment | 0 | 1 | 0.95 | |
| Norms | 0 | 1 | 0.95 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.95 | |
| Social influences | 0 | 1 | 0.89 | |
| Subjective norms | 0 | 1 | 0.89 | |
| Values | 0 | 1 | 0.89 | |
| Feedback processes | 0 | 1 | 0.89 | |
| Social learning/imitation | 0 | 1 | 0.89 | |
| Social/professional role and identity | 0 | 1 | 0.84 | |
| Reinforcement | 0 | 1 | 0.84 | |
| Needs | 0 | 1 | 0.84 | |
| 16.3 Vicarious consequences | Skills | 1 | 0.69 | 0.95 |
| Needs | 0 | 1 | 0.9 | |
| Perceived susceptibility/vulnerability | 0 | 1 | 0.85 | |
| BCT | MoA | Literature synthesis study | Expert consensus study | Reconciliation study | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frequency (number of papers) | p-value | Experts definitely yes (%) | Experts possibly (%) | Experts don’t know (%) | Experts definitely no (%) | Experts definitely yes) (%) | Experts don’t know (%) | Experts definitely no (%) | ||
| 2.1 Monitoring of behaviour by others without feedback | Needs | 1 | 0.019 | 0 | 11 | 0 | 89 | 6.25 | 12.5 | 81.25 |
| 12.3 Avoidance/reducing exposure to cues for the behaviour | Needs | 1 | 0.027 | 5 | 5 | 0 | 90 | 0 | 0 | 100 |
| 2.2 Feedback on behaviour | Subjective norms | 19 | < 0.001 | 5 | 16 | 11 | 68 | 6.25 | 12.5 | 81.25 |
| 4.2 Information about antecedents | Skills | 3 | 0.10 | 9 | 5 | 0 | 86 | 0 | 0 | 100 |
| 10.3 Non-specific reward | Self-image | 1 | 0.06 | 5 | 0 | 0 | 95 | 0 | 12.5 | 87.5 |
Appendix 7 Scree plot of eigenvalues from exploratory factor analysis
FIGURE 21.
Scree plot of eigenvalues from exploratory factor analysis.
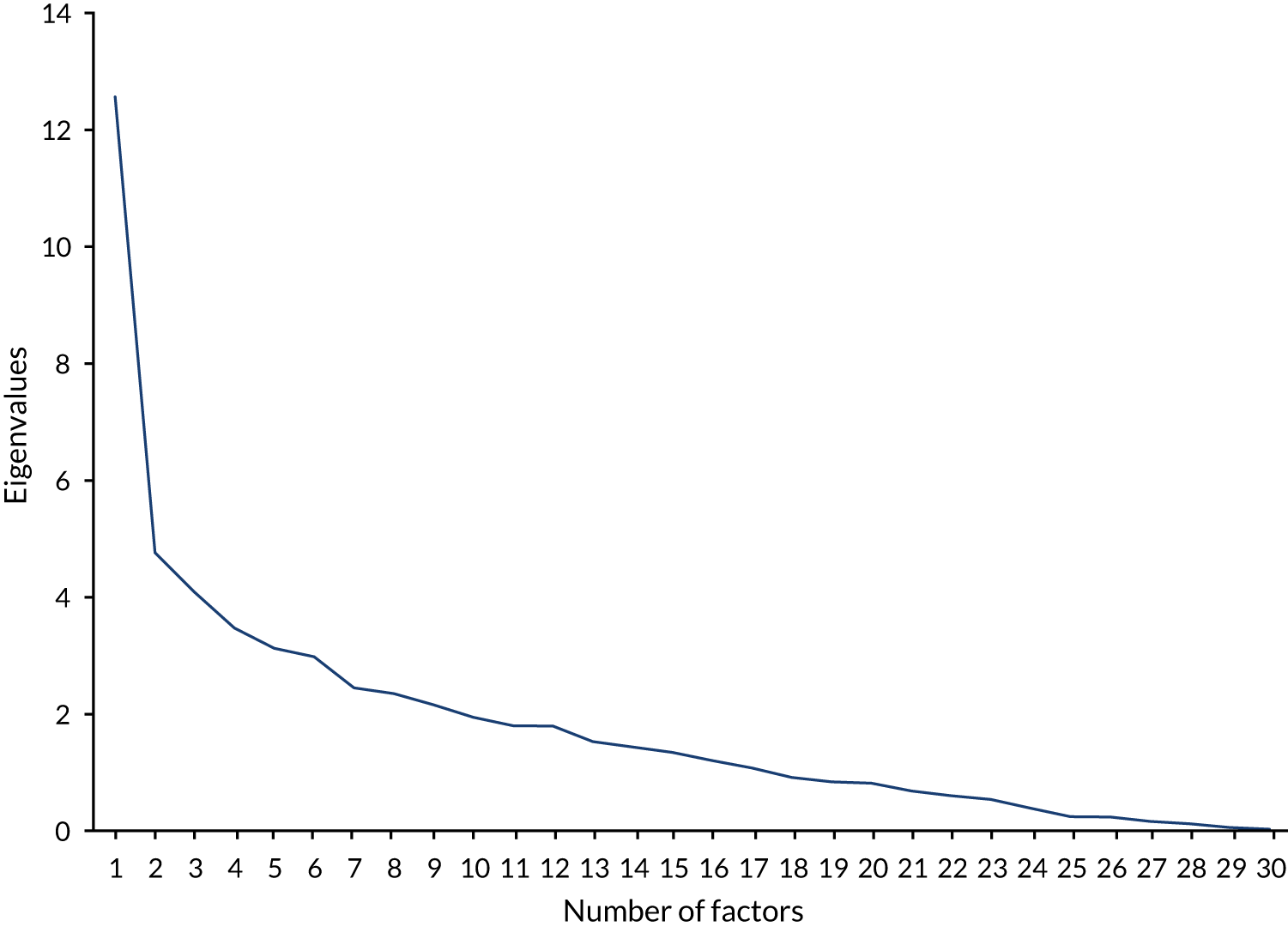
Appendix 8 Behaviour change technique labels and definitions presented by behaviour change technique group
| BCT group | Factor loading | BCTTv1 number and label | BCT definition |
|---|---|---|---|
| 1 | 0.823 | 1.5 Review behaviour goals | Review behaviour goal(s) jointly with the person and consider modifying goal(s) or behaviour change strategy in light of achievement. This may lead to resetting the same goal, a small change in that goal or setting a new goal instead of (or in addition to) the first, or no change |
| 0.783 | 1.4 Action-planning | Prompt detailed planning of performance of the behaviour (must include at least one of context, frequency, duration and intensity). Context may be environmental (physical or social) or internal (physical, emotional or cognitive) | |
| 0.729 | 15.3 Focus on past success | Advise to think about or list previous successes in performing the behaviour (or parts of it) | |
| 0.717 | 1.1 Goal-setting (behaviour) | Set or agree a goal defined in terms of the behaviour to be achieved | |
| 0.712 | 15.4 Self-talk | Prompt positive self-talk (aloud or silently) before and during the behaviour | |
| 0.705 | 3.3 Social support (emotional) | Advise on, arrange or provide emotional–social support (e.g. from friends, relatives, colleagues, ‘buddies’ or staff) for performance of the behaviour | |
| 0.624 | 1.2 Problem-solving | Analyse, or prompt the person to analyse factors influencing the behaviour and generate or select strategies that include overcoming barriers and/or increasing facilitators | |
| 0.613 | 2.3 Self-monitoring of behaviour | Establish a method for the person to monitor and record their behaviour(s) as part of a behaviour change strategy | |
| 0.570 | 8.7 Graded tasks | Set easy-to-perform tasks, making them increasingly difficult, but achievable, until behaviour is performed | |
| 0.560 | 1.3 Goal-setting (outcome) | Set or agree a goal defined in terms of a positive outcome of wanted behaviour | |
| 0.523 | 1.6 Discrepancy between current behaviour and goal | Draw attention to discrepancies between a person’s current behaviour (in terms of the form, frequency, duration or intensity of that behaviour) and the person’s previously set outcome goals, behavioural goals or action plans (goes beyond self-monitoring of behaviour) | |
| 0.503 | 2.4 Self-monitoring of outcomes of behaviour | Establish a method for the person to monitor and record the outcome(s) of their behaviour as part of a behaviour change strategy | |
| 0.489 | 1.8 Behavioural contract | Create a written specification of the behaviour to be performed, agreed by the person and witnessed by another | |
| 2 | 0.807 | 2.7 Feedback on outcomes of behaviour | Monitor and provide feedback on the outcome of performance of the behaviour |
| 0.740 | 2.2 Feedback on behaviour | Monitor and provide informative or evaluative feedback on performance of the behaviour (e.g. form, frequency, duration, intensity) | |
| 0.626 | 6.2 Social comparison | Draw attention to others’ performance to allow comparison with the person’s own performance | |
| 3 | 0.665 | 5.2 Salience of consequences | Use methods specifically designed to emphasise the consequences of performing the behaviour with the aim of making them more memorable (goes beyond informing about consequences |
| 0.651 | 12.3 Avoidance/reducing exposure to cues for the behaviour | Advise on how to avoid exposure to specific social and contextual/physical cues for the behaviour, including changing daily or weekly routines | |
| 0.599 | 6.3 Information about others’ approval | Provide information about what other people think about the behaviour. The information clarifies whether others will like, approve or disapprove of what the person is doing or will do | |
| 0.498 | 12.2 Restructuring the social environment | Change, or advise to change the social environment to facilitate performance of the wanted behaviour or create barriers to the unwanted behaviour (other than prompts/cues, rewards and punishments) | |
| 0.475 | 5.3 Information about social and environmental consequences | Provide information (e.g. written, verbal, visual) about social and environmental consequences of performing the behaviour | |
| 0.460 | 5.1 Information about health consequences | Provide information (e.g. written, verbal, visual) about health consequences of performing the behaviour | |
| 0.453 | 13.2 Framing/reframing | Suggest the deliberate adoption of a perspective or new perspective on behaviour (e.g. its purpose) to change cognitions or emotions about performing the behaviour (includes ‘cognitive structuring’) | |
| 4 | 0.726 | 8.1 Behavioural practice/rehearsal | Prompt practice or rehearsal of the performance of the behaviour one or more times in a context or at a time when the performance may not be necessary, to increase habit and skill |
| 0.621 | 6.1 Demonstration of the behaviour | Provide an observable sample of the performance of the behaviour, directly in person or indirectly (e.g. via film, pictures, for the person to aspire to or imitate), includes ‘modelling’ | |
| 0.563 | 4.1 Instruction on how to perform the behaviour | Advise or agree on how to perform the behaviour (includes ‘skills training’) | |
| 5 | 0.834 | 12.6 Body changes | Alter body structure, functioning or support directly to facilitate behaviour change |
| 0.736 | 10.9 Self-reward | Prompt self-praise or self-reward if and only if there has been effort and/or progress in performing the behaviour | |
| 0.509 | 11.2 Reduce negative emotions | Advise on ways of reducing negative emotions to facilitate performance of the behaviour (includes ‘stress management’) |
Appendix 9 Content of the guidelines for rounds 1–4 of the consensus exercise
Overview
Background and aim
The Theories and Techniques of Behaviour Change Project (www.ucl.ac.uk/behaviour-change-techniques; accessed 1 January 2020) aims to identify hypothesised links between BCTs and (1) the MoAs through which they influence behaviour and (2) behavioural theories. The final phase of this research aims to examine whether groups of co-occurring BCTs can be linked to specific theories.
Participants
You are one of 25 experts from 10 countries, selected because you have a high level of expertise in theories and BCTs and provided valuable input in our previous consensus exercise.
Overview of study
The consensus exercise is a modified nominal group technique, involving 4 rounds. In round 1, you will be directed to an online questionnaire and asked to list all possible theories that might underlie a particular BCT group. You will be asked to do this for 5 BCT groups (see Appendix A). In round 2, you will be presented with the same 5 BCT groups, and asked to consider the extent to which each BCT group is linked to a particular theory; the theories you are asked to consider will be those identified by experts in round 1. In round 3, you will be invited to participate in an online, asynchronous (i.e. each member can participate at a time of their choosing), anonymous discussion, in which you will be encouraged to exchange views with other experts. Finally, in round 4, you will be asked to provide final ratings on links between BCT groups and theories (which may or may not be the same as your round 2 ratings). At this point, you will also have the opportunity to add and/or remove BCTs from each BCT group for each theory.
More detail on rounds 1 and 2 can be found below; guidelines for rounds 3 and 4 will be sent out separately.
Round 1 guidelines
Information provided
In Appendix A, you will find 5 groups of co-occurring BCTs (i.e. BCTs that were found to appear together frequently in interventions, identified through an exploratory factor analysis). These BCT groups will be presented to you on screen during the consensus exercise. In addition, you will receive a complementary online book containing a description of 83 theories (ABC of Behaviour Change Theories), which you may draw on during the task. Log-in details to access this online book will be sent to you by e-mail.
Question
You will be presented with 5 BCT groups, one at a time, and asked to list all theories that you consider to be associated with each group, in the following question:
An intervention was developed that includes the BCTs listed above. Which behavioural theory or theories do you think could have guided the development of this intervention?
Response options
To respond, you will be provided with an open text box in which you can list one or more theories, drawing on the ABC of Behaviour Change Theories and/or your own knowledge and expertise (see Appendix B for a preview of the round 1 questionnaire).
Round 2 guidelines
Information provided
You will have access to the same information as above (i.e. the 5 BCT groups and the online book, ABC of Behaviour Change Theories).
Question
You will be presented with 5 BCT groups, one at a time, and asked to respond to the following question for all theories listed by experts in round 1:
An intervention was developed that includes the BCTs listed above. How confident are you that this group of BCTs is linked to [Theory X]?
Response options
-
‘Very confident’: Very confident that this group of BCTs is linked to [Theory X].
-
‘Uncertain/don’t know’: Uncertain about whether or not this group of BCTs is linked to [Theory X].
-
‘Not at all confident’: Not at all confident about whether or not this group of BCTs is linked to [Theory X].
When providing your ratings, please remember:
-
In order to ensure consistency across experts, and with the aim of developing a shared understanding of BCT mechanism of action links, it is very important that you base your answers on the definitions, rather than labels, of the BCTs.
-
Definitions for all BCTs will appear on the screen during the consensus exercise, and these can also be found in Appendix A. Please read and re-read these definitions before beginning the task. Definitions can also be accessed via www.bcts.23.co.uk, or through the BCTTv1 smartphone app, which can be downloaded for free via the Apple App and Google Play stores.
-
In answering the questions, you may draw on your own knowledge and expertise and/or the theories in the ABC of Behaviour Change Theories.
-
Round 3 guidelines
Overview
Thank you for completing the first two rounds of this study. In round 3, we are asking for your input on links between groups of co-occurring BCTs and theories where there remains uncertainty and/or disagreement. The purpose of this round is to discuss these uncertainties and disagreements to help guide your final round ratings. By providing your input in this round, you will add to our shared understanding of the links between BCT groups and theories, and help to build consensus. This is your opportunity to share your thoughts with other behaviour change experts about the task.
Information provided
In Appendix A, you will find confidential data from round 2 of this consensus exercise, including a summary of all experts’ responses, and a reminder of your own responses. You will be able to see the group data on screen as part of the round 3 discussion. However, we recommend that you read through Appendix A in full before round 3 begins, in order to give you a chance to reflect on the data to inform your contribution to the discussion.
In Appendix B, you will find step-by-step instructions for how to use ‘Loomio’, the online discussion forum on which round 3 will be hosted.
What the task involves
-
We are asking experts to contribute to an online discussion forum, in which you will have the opportunity to share your views about BCT group–theory links rated in round 2, and to comment on other experts’ views.
-
The online discussion will involve the group of 25 experts who are participating in this study. Your contributions will be anonymous (i.e. you will use an assigned expert ID and not your name).
-
We estimate that your participation in round 3 should take approximately 1.5 hours in all. While you may log in and participate at any time(s) of your choosing, we would recommend that you log in at least three times over the round 3 period. This is to ensure that you have had a chance to contribute fully to the discussion.
-
A moderator from the research team will periodically summarise the discussion and raise issues for further consideration.
How to participate
Step-by-step instructions for participating in the online discussion can be found in Appendix B. In summary:
-
You will be sent a link to the discussion via an e-mail from the research team. When you click on this link, a website called ‘Loomio’ will open and you will be prompted to register an account or log in. You can log in using the details you previously registered (i.e. during the last expert consensus study). If, for any reason, you need to register a new account (e.g. if you no longer have a Loomio account), it is very important that you do this using your expert ID and not your name.
-
There will be a number of discussion groups on which you can comment, each specific to a BCT group–theory link for which there was high uncertainty or disagreement in round 2 (see Appendix A). There will be other discussion groups in which you can contribute thoughts about the task more generally and/or about other BCT group–theory links.
-
It may be helpful to focus on the ratings of BCT group–theory links for which (1) you remain very uncertain, and/or (2) your responses differed from those of the other experts. However, we would also value your thinking on other aspects of the task.
Round 4 guidelines
Overview
Thank you for completing the first three rounds of this study. In round 4, we are asking you to provide your final ratings for links between groups of BCTs and behavioural theories. You will be directed to an online questionnaire and asked to consider whether a group of BCTs is linked to a particular theory. In addition, for each BCT group, you will be asked to indicate the theory or theories (up to three) you are most confident are linked. For these theories, you will also have the opportunity to consider whether there are BCTs that should be added to and/or removed from the BCT group.
Information provided
During the final round, you will see data on screen from round 2 (i.e. ‘In round 2, X% of experts were very confident that this BCT group is linked to this theory’). For the links that were discussed in round 3, there will be hyperlinks to the relevant discussion page on Loomio (note that you will need to be signed in to view this content). You will not be asked to discuss links for which there was consensus in round 2.
Definitions for the BCTs in each BCT group will be presented on screen during the consensus exercise (these are also available in Appendix A). BCT definitions can also be accessed via www.bcts.23.co.uk, and through the BCTTv1 smartphone app, which can be downloaded for free via the Apple App and Google Play stores.
To view theory descriptions, you may draw on the ABC of Behaviour Change Theories book, as in the previous rounds.
What the task involves:
-
You will be presented with 5 BCT groups, one at a time, and asked to respond to the following question (for all theories where consensus was not reached in round 2):
An intervention was developed that includes the BCTs listed above. How confident are you that this group of BCTs is linked to [Theory X]?
Response format
-
In this round, the response options for this question will be:
-
‘Confident that they are linked’: Confident that this group of BCTs is linked to [Theory X].
-
Note: You may use this option if you believe most (i.e. not necessarily all) of the BCTs in a group are linked to this theory.
-
-
‘Uncertain/don’t know’: Uncertain about whether or not this group of BCTs is linked to [Theory X].
-
‘Confident that they are not linked’: Confident that this group of BCTs is not linked to [Theory X].
-
-
Following completion of the above, you will be asked to identify the theory or theories that you are most confident are linked to each BCT group.
-
For each BCT group, you will be presented with the theories you rated as ‘confident that there is a link’ and asked to select those you are most confident about.
-
You may base your judgements on the frequency and/or strength of links between the BCTs within a group and the constructs of the theory.
-
Response format
-
The response format for this question will be a click-and-drag format. You will be asked to select a theory and ‘drag’ it into the ‘most confident’ box. You will be able to do this for up to three theories. If you select more than one theory, you will be able to reorder theories within the box.
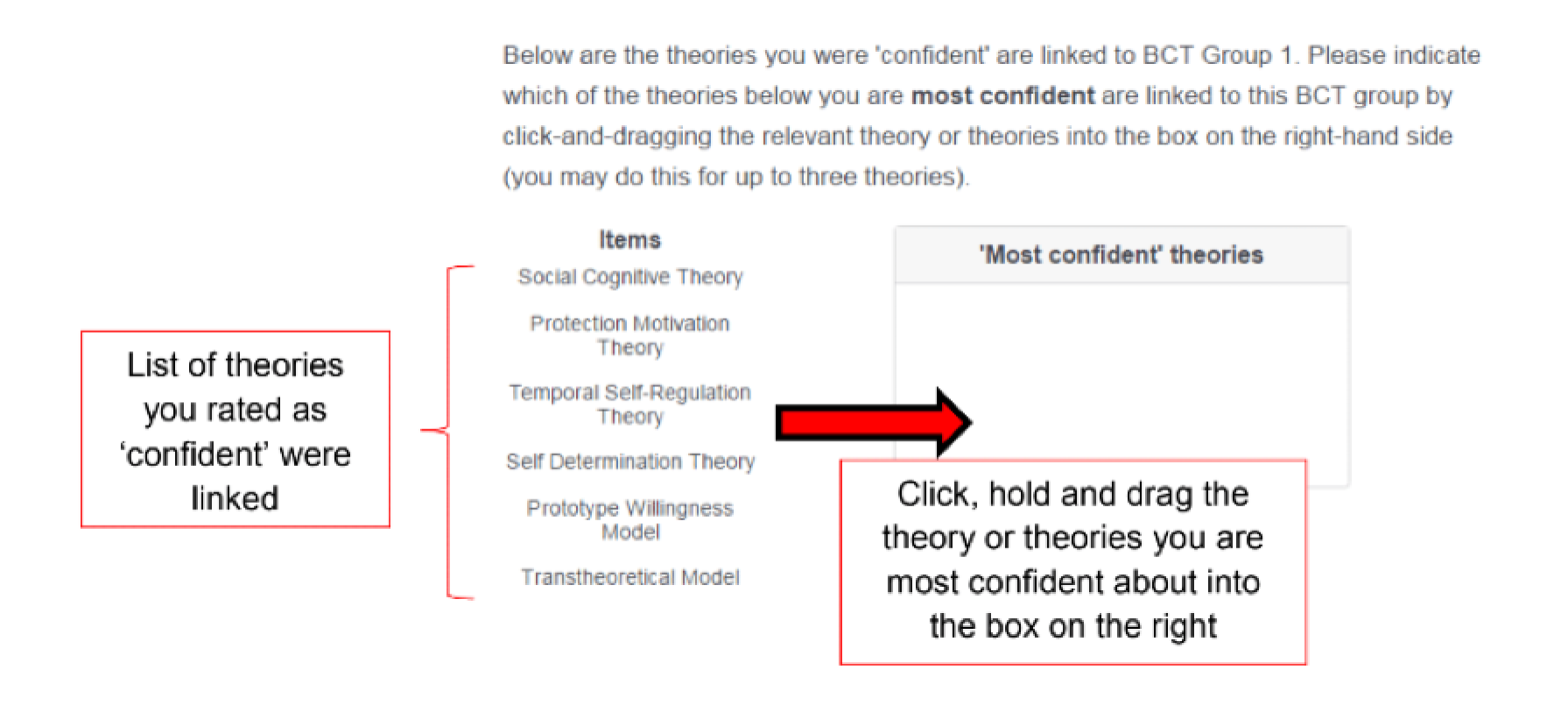
-
Finally, for each of the theories you identified in the previous step, you will be asked to indicate whether or not there are BCTs you think should be added to, or removed from, the BCT group. You will be provided with an open text box to indicate which (if any) BCTs you would add and/or remove.
Appendix 10 Names of theories linked to behaviour change technique groups by more than two experts in the expert consensus exercise
| BCT group 1 | BCT group 2 | BCT group 3 | BCT group 4 | BCT group 5 | |
|---|---|---|---|---|---|
| Theories linked (n) | 36 | 45 | 68 | 25 | 20 |
| Action theory model of consumption | Action theory model of consumption | Action theory model of consumption | |||
| Affective events theory | |||||
| AIDS risk reduction model | |||||
| Behavioural ecological model of adolescent AIDS prevention | |||||
| CEOS theory | CEOS theory | CEOS theory | CEOS theory | ||
| Change theory | Change theory | ||||
| Classical conditioning theory | Classical conditioning theory | Classical conditioning theory | |||
| COM-B model | COM-B model | COM-B model | COM-B model | COM-B model | |
| Consumption and social practice theory | |||||
| Containment theory | |||||
| Control theory | Control theory | Control theory | |||
| Differential Association Theory | |||||
| Diffusion of innovations theory | Diffusion of innovations theory | Diffusion of innovations theory | Diffusion of innovations theory | ||
| Ecological model for preventing type 2 diabetes in minority youth | |||||
| Extended information processing model | |||||
| Extended parallel process model | Extended parallel process model | Extended parallel process model | |||
| Feedback intervention theory | Feedback intervention theory | ||||
| Focus theory of normative conduct | Focus theory of normative conduct | Focus theory of normative conduct | |||
| General theory of crime | General theory of crime | ||||
| General theory of deviant behaviour | General theory of deviant behaviour | ||||
| Goal-directed theory | Goal-directed theory | ||||
| Goal-framing theory | |||||
| Goal-setting theory | Goal-setting theory | Goal-setting theory | Goal-setting theory | ||
| HAPA | HAPA | HAPA | HAPA | HAPA | |
| Health behaviour goal model | Health behaviour goal model | Health behaviour goal model | |||
| Health behaviour internalisation model | |||||
| Health belief model | Health belief model | Health belief model | Health belief model | ||
| Health promotion model | Health promotion model | Health promotion model | Health promotion model | ||
| I-Change model | I-Change model | I-Change model | I-Change model | ||
| Information–motivation–behavioural skills model | Information–motivation–behavioural skills model | Information–motivation–behavioural skills model | |||
| Information–motivation–behavioural skills model of adherence | |||||
| Integrated model of behavioural prediction | Integrated model of behavioural prediction | Integrated model of behavioural prediction | |||
| Integrated theoretical model for alcohol and other drug abuse prevention | Integrated theoretical model for alcohol and other drug abuse prevention | ||||
| Integrated theory of drinking behaviour | |||||
| Integrated theory of health behaviour change (Ryan141) | Integrated theory of health behaviour change (Ryan141) | Integrated theory of health behaviour change (Ryan141) | Integrated theory of health behaviour change (Ryan141) | Integrated theory of health behaviour change (Ryan141) | |
| Integrative model of factors influencing smoking and attitude and health behaviour change | Integrative model of factors influencing smoking and attitude and health behaviour change | ||||
| Integrative model of factors influencing smoking behaviours | Integrative model of factors influencing smoking behaviours | Integrative model of factors influencing smoking behaviours | |||
| Integrative model of health attitude and behaviour change (Flay and Petraitis142) | Integrative model of health attitude and behaviour change (Flay and Petraitis142) | Integrative model of health attitude and behaviour change (Flay and Petraitis142) | |||
| Model of pro-environmental behaviour | |||||
| Motivation–opportunities–abilities model | Motivation–opportunities–abilities model | Motivation–opportunities–abilities model | |||
| Norm activation theory | |||||
| Operant learning theory | Operant learning theory | Operant learning theory | Operant learning theory | ||
| Precaution adoption process model | |||||
| PRIME theory | PRIME theory | PRIME theory | PRIME theory | ||
| Problem behaviour theory | Problem behaviour theory | Problem behaviour theory | |||
| Prospect theory | |||||
| Protection motivation theory | Protection motivation theory | Protection motivation theory | Protection motivation theory | ||
| Prototype willingness model | Prototype willingness model | Prototype willingness model | |||
| Reflective impulsive model | Reflective impulsive model | ||||
| Regulatory fit theory | |||||
| Relapse prevention model | Relapse prevention model | Relapse prevention model | Relapse prevention model | Relapse prevention model | |
| Risk as feelings theory | |||||
| Self-determination theory | Self-determination theory | Self-determination theory | Self-determination theory | Self-determination theory | |
| Self-efficacy theory | Self-efficacy theory | Self-efficacy theory | Self-efficacy theory | Self-efficacy theory | |
| Self-regulation theory | Self-regulation theory | Self-regulation theory | |||
| Six-staged model of communication effects | Six-staged model of communication effects | ||||
| Social action theory (Ewart143) | Social action theory (Ewart143) | ||||
| Social action theory (Weber) | Social action theory (Weber) | ||||
| Social change theory | Social change theory | ||||
| Social cognitive theory | Social cognitive theory | Social cognitive theory | Social cognitive theory | Social cognitive theory | |
| Social consensus model of health education | |||||
| Social development model | |||||
| Social ecological model of behaviour change | Social ecological model of behaviour change | ||||
| Social identity theory | Social identity theory | ||||
| Social influence model of consumer participation | Social influence model of consumer participation | ||||
| Social learning theory | Social learning theory | Social learning theory | |||
| Social norms theory | Social norms theory | ||||
| Systems model of health behaviour change | Systems model of health behaviour change | Systems model of health behaviour change | Systems model of health behaviour change | ||
| Temporal self-regulation theory | Temporal self-regulation theory | ||||
| Theory of interpersonal behaviour | Theory of interpersonal behaviour | Theory of interpersonal behaviour | Theory of interpersonal behaviour | ||
| Theory of normative social behaviour | Theory of normative social behaviour | ||||
| Theory of planned behaviour | Theory of planned behaviour | Theory of planned behaviour | Theory of planned behaviour | Theory of planned behaviour | |
| Theory of reasoned action | |||||
| Theory of triadic influence | Theory of triadic influence | ||||
| Transcontextual model of motivation | Transcontextual model of motivation | ||||
| Transtheoretical model of behaviour change | Transtheoretical model of behaviour change | Transtheoretical model of behaviour change | Transtheoretical model of behaviour change |
Appendix 11 Links between theories and behaviour change technique groups agreed not to be present by ≥ 80% experts
| BCT group | BCT | Experts ‘not at all confident’ in the link (%) |
|---|---|---|
| 1 | Health belief model | 80 |
| Focus theory of normative feedback | 88 | |
| Diffusion of innovations theory | 87.5 | |
| Prototype willingness model | 83.33 | |
| 2 | Protection motivation theory | 83.33 |
| 3 | Control theory | 87.5 |
| Diffusion of innovations theory | 83.33 | |
| Operant learning theory | 83.33 | |
| Self-efficacy theory | 83.33 | |
| Social identity theory | 87.5 | |
| Temporal self-regulation theory | 83.33 | |
| 4 | Classical conditioning theory | 83.33 |
| Diffusion of innovations theory | 80 | |
| Health belief model | 80 | |
| 5 | Self-determination theory | 87.5 |
| Goal-setting theory | 83.33 | |
| Theory of planned behaviour | 83.33 |
Glossary
- Eigenvalues
- A special set of scales associated with a linear system of equations (e.g. matrix equation).
- Maximum likelihood estimator
- A method of estimating the parameters of a probability distribution by maximising a likelihood function so that under the assumed statistical model the observed data are most probable.
- Multilevel modelling
- Statistical models of parameters that vary at more than one level.
- Oblique rotation
- A transformational system used in factor analysis when two or more factors (latent variables) are correlated.
- One-tailed binomial test
- An exact test of statistical significance.
List of abbreviations
- BCT
- behaviour change technique
- BCTTv1
- Behaviour Change Technique Taxonomy version 1
- BCW
- behaviour change wheel
- CFI
- comparative fit index
- EPOC
- Effective Practice and Organisation of Care
- HAPA
- Health Action Process Approach
- IAB
- International Advisory Board
- ICC
- intraclass correlation coefficient
- MoA
- mechanism of action
- NGT
- nominal group technique
- NICE
- National Institute for Health and Care Excellence
- PABAK
- prevalence and bias adjusted kappa
- RMSEA
- root-mean-square-error approximation
- SD
- standard deviation
- TaTT
- Theory and Technique Tool
- TDF
- Theoretical Domains Framework
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/hsdr09010).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.