

Notes
Article history
The research reported in this issue of the journal was funded by the HSDR programme or one of its preceding programmes as award number NIHR128616. The contractual start date was in April 2020. The draft manuscript began editorial review in February 2023 and was accepted for publication in February 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HSDR editors and production house have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Ryan et al. This work was produced by Ryan et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Ryan et al.
Chapter 1 Background
Introduction
The importance and value of the co-production of public services have been increasingly recognised since the 1980s, in terms of providing more efficient and effective services and through improving active citizenship. 1 Qualitative research into experiences of patients, social care service users and providers can provide insights into how services might be improved, but too often these insights are not followed through into changes in practice. 2 Even when improvements are achieved, practitioners may doubt whether the lessons are transferable to other settings within the same sector. The challenge of knowledge transfer is recognised in health, where there is a substantial body of work exploring how patient experience and feedback can be captured and used to improve the quality of health care. 3,4 However, it is arguably a greater challenge in social care, where the routes for incorporating evidence into practice are less well established and supported, and where the settings in which social care happens are diffuse, sometimes unknown and often unbounded. For example, social care services can be delivered in people’s homes, public places, residential homes, community centres or even schools. Cost-effective ways to integrate the perspectives and experiences of social care service users into the design of prevention, care and support initiatives led by local authorities and their partners are needed.
Experience-based co-design (EBCD)5 is a participatory action research (PAR) approach to co-designing healthcare improvements, which draws on the co-production and design science literature. PAR is a partnership approach which has its roots in community development; EBCD sought to bring these participatory principles to health care. It has been used nationally and internationally in a range of settings, including mental health, but as far as we are aware, this study is the first to apply it as a specific structured approach in social care. A distinguishing feature of EBCD has been its emphasis on rigorously collected and analysed narrative interviews with patients and staff and observations of care as the basis for subsequent co-design work. The importance of people’s experiences, knowledge and expertise is at the centre of this approach. This helps to ensure the co-design phase is solidly based on a range of real-life perspectives and builds an effective partnership between users and staff. In this project, we explored whether an ‘accelerated’ version of EBCD, evaluated positively in the NHS,6 could offer a way to design improvements in social care, and what adaptations it may require to be practical and acceptable in this setting. Loneliness was selected as the topic of focus. We first wanted to understand what the experience of loneliness is like from the perspective of people who are or have been lonely, and how it affects all aspects of their lives, relationships and well-being. We then drew on these experiences to work, in one local authority, with people who experience loneliness and use local loneliness support services, and with local authority staff, to find better ways to address people’s needs. Through this process, we evaluated the use of accelerated experience-based co-design (AEBCD) in social care and identified recommendations for adaptations.
Challenges for social care
Adult social care in England is distinct from health care and encompasses care and support arrangements for people with (generally) long-term needs and a wide range of characteristics and circumstances. Social care also has different aims of care which are much more aligned to supporting individual well-being, independence and safeguarding, with activities focusing on personal care, domestic routines and supporting people to live full lives.
Care is needs- and means-tested with the underlying core objectives of promoting independence; encouraging and enabling choice, control, and ‘personalisation’; safeguarding; and supporting people to contribute to society. Older people comprise the largest user group and account for a high proportion of social care expenditure, though important groups in terms of incidence, needs and spending include people with physical, learning or sensory disabilities and those with mental ill health. Social care is delivered by many individuals and providers. Skills for Care estimates 17,900 organisations were involved in providing or organising adult social care in England as at 2021–2. Those services were delivered in an estimated 39,0007,8 establishments providing, or involved in organising, adult social care in England, with a somewhat dynamic picture of for-profit private sector providers dominating service markets. Social care is also heavily dependent on family and other unpaid carers, with about 5.4 million in the UK. Its structure is distinct from that of health care and less familiar to the public and those working outside of local authorities or with direct responsibility for commissioned services.
Despite recent cuts, commissioning of care by the public sector remains considerable. There were almost 2 million requests for adult social care support from nearly 1.4 million new service users to local authorities in 2021–2. However, the number of people receiving long-term care has decreased slightly to 818,000. 9 Eligible people receive local council funding for their social care but typically also pay a means-tested contribution. The council funding is either paid directly by the council to the care provider or it can be paid to the person needing care as a budget called a direct payment. Direct payments can be used in a variety of approved ways to meet care needs. If people are not eligible for local council funding, they pay for their care and support themselves and are known as self-funders.
In 2021–2 around 220,000 adults, older people and carers received direct payments, and the total number of direct payment recipients employing staff remained stable (at around 70,000) between 2014–5 and 2021–2. 7,8 However, estimates of a rapidly growing self-funded care sector who are often hidden from view and under-researched are less established, although we do know that self-funders find accessing and arranging social care difficult and emotional. 10,11 The Office for National Statistics estimates that 47% of residents in care homes for older people are self-funding. 7 Copayments (user charges) are common for many public services. Monitoring care quality is possible through contracting, and regulation is the responsibility of the Care Quality Commission.
Need for social care is growing rapidly with population ageing. If today’s care and funding arrangements continue unchanged, public and private expenditure on social care for older people will rise by 162% by 2035. 8 The need to address early identification and prevention agendas to avoid escalation of need is important and urgent in both health and social care contexts. Achieving this effectively would facilitate swifter and better-managed transitions of care and better support the growing self-funder population to access care and manage their resources.
Co-production and experience-based co-design
Co-production is widely held to be an important approach to improving the design and delivery of public sector services, by making them more inclusive and responsive and increasing individual and collective well-being. It involves professionals and members of the public working together; while an evolving concept,12 one definition is: ‘the provision of services through regular, long-term relationships between professionalized service providers (in any sector) and service users or other members of the community, where all parties make substantial resource contributions.’13
Co-production requires things to be done differently to deliver the aims of efficiency, patient or service user empowerment and accountability. 14 It involves a ‘reimagining of traditional health systems and practice trajectories’15 and reflects a political agenda to address inequalities and promote democracy. 16 Co-production has a key place in the values underpinning social care and is enshrined within the statutory guidance supporting the 2014 Care Act.
Co-production can operate at individual, group and collective levels, with the latter viewed as having the most potential to lead to wider, systematic change. 1 Different layers of public value have been identified: user value; value to groups; and social, environmental and political values. 17 In exploring why professionals (in this case hospitals) support co-production, Vennik et al. 18 found a belief that increased and improved patient involvement would improve the quality of care provided, that it helped to maintain the hospital position in a competitive healthcare market and that the approach was aligned to an adherence to organisational goals and ethos.
Osborne et al. 19 argue that co-production in public services may be unintentional and may simply arise from any interaction between professionals and users that shapes the service provided. They therefore use the term co-design to signify a more intentional, active process of working together to improve services.
Experience-based co-design is a well-established co-production approach used in health care. EBCD adopts PAR methods to involve patients and healthcare professionals as equal partners in redesigning services. 20 PAR approaches are underpinned by a collective commitment to investigate and resolve social problems with the building of alliances between researchers and those with direct experience of the issue being considered. 21 EBCD also draws on user-centred design, which again involves a collaborative approach to co-designing solutions to problem areas, and uses learning theory with a focus on reflective practice and narrative-based approaches to change. 5 There are a set of six clearly defined stages to EBCD that have been described in full elsewhere. 6,22 We briefly summarise these in Table 1.
| Stage | Activity |
|---|---|
| 1 | The clarification and organisation of governance and project management arrangements. |
| 2 | Interviews with staff working in the relevant area to explore their experiences of working within the service, and observations. Staff participants are brought together in a facilitated workshop to discuss themes emerging from the data analysis and produce a list of priorities for service improvement. |
| 3 | Video- or audio-recorded in-depth interviews with patients and family carers explore their experiences of the health service. Touch points – that is, defining moments of good or poor interaction between people using the service – are identified from the data analysis. A short film is produced using interview extracts to illustrate these points and shown to patient and family carer participants in a facilitated workshop. The group identifies a set of priorities for service improvement. |
| 4 | Staff, patients and family carers come together for the first time in a third workshop and watch the film. The two priority lists are shared, and the group decides what areas they want to work on. |
| 5 | ‘Co-design working groups’ work together on these areas over the next few months. |
| 6 | The working groups reconvene in a celebration event to share progress in implementing service change ideas and decide what the next steps are. |
A review of the international spread of EBCD 10 years after its development found more than 80 projects in 6 countries (UK, Australia, New Zealand, Sweden, Canada and Netherlands). 20 The authors note that many positive evaluations have been undertaken which report not only specific changes to services or care pathway redesign but also changes in staff attitude and morale. However, they note several challenges, particularly the time involved in an average EBCD cycle (1 year) and the cost of conducting interviews and observations. These issues have led to often informal and untested adaptations to the method. Only half the studies included in the review used observations, and only just over half filmed interviews with users. These adaptations may reflect not just resource issues but also concerns about anonymity, privacy and unequal power relations. In one inpatient mental health unit, for example, filming was retained but the process of recruiting participants and interviewing was led by a user group with existing relationships within the unit. Rather than a single interview, a repeated cycle of interviewing with an art therapist was adopted, giving people time to prepare and reconstruct the story of their experiences in their own way. 23,24 Mulvale et al. 25 introduced novel elicitation methods with experience maps and co-designing visual ‘prototype’ solutions, alongside the catalyst film.
A case study synthesis of six EBCD projects in Australia covering different areas of health care found that there was a need for guidance on capability development and preparedness for all participants in the project, not only for the project leads. 26 The authors found that the variability in implementation of the approach made it difficult to identify which component parts were essential for sustained service improvement. An evaluation of EBCD in a cancer centre in two large NHS trusts in London found that the engagement in the setting and proactive involvement of key clinical leaders alongside ‘particularly skilled staff who were committed to the philosophy of the approach’ were key ingredients to its successful ‘implementation’. 27 Locock et al. further describe ‘push and pull’ factors:
[T]he ‘push’ of active support and ‘opinion’ leadership at a high level of an organisation; the ‘pull’ of active quality improvement teams on the ‘look out’ for new approaches; and the mediating effects of ‘outward-reaching’ quality improvement leaders to build potential relationships. 6
Ramos et al. 28 explored the barriers and facilitators to the approach through a literature review and small-scale qualitative interview study with EBCD project facilitators. While EBCD has commonly been focused on staff in direct care roles, the authors conclude that active management participation in the process facilitates the implementation of service improvement, and underlines the importance of the project facilitation role, full organisation support, and the relationship between the service and patients. More recently, the use of the approach has been extended in different settings including forensic services29 and domestic violence and abuse services. 30
The importance of the adaptability and flexibility of this approach to different contexts while retaining its core philosophy has been emphasised,6,27 and we now turn to a key adaptation.
Accelerated experience-based co-design
‘Accelerated’ EBCD was developed by Locock et al. ,6 who sought to examine whether efficiencies could be gained by using existing filmed interviews to create a catalyst film, rather than collecting new user interviews locally. The project drew on a secondary analysis of interview data from an existing University of Oxford archive of interviews from studies of people’s experiences of illnesses or health topics. Evaluation suggested this approach led to a similar number and type of changes compared to standard EBCD but at lower cost and time, and the same catalyst film could be used in numerous settings. This model has since been used in different settings, including a hospital-at-home service for patients with chronic obstructive pulmonary disease and for advanced care planning in later life. 4,31,32
Experience-based co-design and its accelerated form are now well-established techniques for service improvement in healthcare settings but have so far not been widely used in social care or to improve care support for people whose lives are affected by social rather than health-related issues. In this study, we produced a data set of nationally conducted interviews focusing on loneliness to explore the use of AEBCD in one local authority, Doncaster. The findings of the interview study and the catalyst film will be published on Socialcaretalk.org and available for use nationally under licence.
Thinking critically about co-production
Co-production is not without criticism, and Steen et al. 33 describe the tendency of researchers towards optimism without engaging with the ‘dark side’ of this approach. Steen et al. highlight the optimism surrounding the approach and an often-presented idealised view by scholars and others, which they argue masks a set of potential problems. Attention should be paid to the potential relinquishing of responsibility by government, local authorities and other public sector bodies. Co-production can lead to a lack of clear responsibility, with boundaries blurred between public, private and voluntary sectors. There is little evidence of sustained change, with innovations often remaining precarious and small,34 and it is important to recognise the costs associated with the approach. 35 Co-production can be dominated by people who are wealthy and well educated, leading to further exclusionary practices and a professionalisation of involvement. 36 There can also be co-destruction rather than co-production if the process is done poorly or as a tick-box exercise; it can cause conflict and lead to misunderstandings, opportunities to change services may be missed, and the approach is open to misuse and manipulation by government. This is not only a waste of resources; it can also generate mistrust. 11,35 While it is important to note that Williams et al. 37 have pointed out flaws in some of these concerns, we agree critical questions should be asked about how situated practices of co-designing, facilitating or participating in co-produced activities can reflect or disrupt power relations at a local level. 14 Tools are available to help navigate this complex terrain. Leach,38 for example, presents a normative framework to assess the efficacy of co-production which involves consideration of inclusiveness, representativeness, impartiality, transparency, deliberativeness, lawfulness and empowerment. Thinking specifically about EBCD, Donetto et al. 39 draw on Bradwell and Marr’s40 working definition of co-design process to frame how the EBCD approach is operationalised. Bradwell and Marr’s framework sets out four key dimensions of co-design process: participation (a collaborative process); development (an evolving, maturing process); ownership and power (a transforming process); and outcomes and intent (a process with practical intent in which unplanned processes and transformations are also likely). Bradwell and Marr acknowledged, as did Leach,38 that such frameworks of principles for co-production or co-design represent ideals which are difficult to achieve fully in practice but can act as a guide to key aspects deserving attention. We return to Bradwell and Marr’s40 framework when reporting on the current study in Chapter 6.
Loneliness
There is an unprecedented rise in loneliness globally, with around a third of people affected by what has been referred to as the ‘widespread disorder of our times’. 41,42 Loneliness is viewed as a serious issue associated with a range of negative health outcomes comparable to smoking and obesity. 43 In 2016, the Local Government Association, Age UK and the Campaign to End Loneliness produced a guide for local authorities on key research about, and practical steps to help tackle, loneliness. 44 This guide was updated in 2018 with additional sections on public health and preventing loneliness. 45 The report advised, among other things, that council leaders should understand local levels of loneliness and set out plans for action. In 2020, loneliness was announced as a government priority in response to the COVID-19 pandemic and government-enforced lockdown conditions. A new public campaign, #LetsTalkLoneliness, was launched alongside a £750 million charity funding package. Despite this focus, the definition of loneliness remains elusive largely because it is a subjective experience. As Fried et al. suggest: ‘We believe loneliness can be defined as a subjective negative experience that results from inadequate meaningful connections, but neither definitions nor assessments of loneliness have achieved wide-scale consensus.’46
Three main theoretical or conceptual frameworks have been offered to understand the phenomenon: existential, social and cognitive/emotional perspectives. 47 Common ground across these approaches is that loneliness is an emotionally negative experience that increases the risk of adverse effects on physical and mental health. The existential perspective conceives loneliness as a natural and necessary component of human existence,48 which involves the perception of being disconnected from others, and emotional aspects which include emptiness and feeling abandoned. 49 The social perspective focuses on the absence of needed relationships, feelings of disconnection, vulnerability, powerlessness and lack of interpersonal affirmation, with roots in attachment theory and childhood. 50 This perspective is commonly used in research, with 70% of studies in a recent review following this approach. 47 The cognitive or emotional perspective describes loneliness as a negative and involuntary experience that arises from the perceived discrepancy between desired and emotional and/or social relationships. 51 Different types of loneliness are distinguished based on chronicity. While transient loneliness may arise due to circumstances (e.g. moving house or retirement) and people tend to adjust to an unfamiliar environment or life situation, chronic loneliness alludes to feelings that last for more than 2 years and are hard to change, or to an intense feeling that is hard to endure. 52
There is controversy around the use of the term ‘chronic’, which suggests a pathologisation of loneliness and has been challenged in favour of terms like ‘persistent’ or ‘prolonged’ loneliness. 53 Research is often framed as though loneliness needs curing or management through health and social care services rather than being a relational and emotional state that can affect us all. A recent report by the Campaign to End Loneliness,54 however, underlined the importance of focusing on chronic loneliness, which affects around 2.6 million people in the UK (around the same number that experienced chronic loneliness pre COVID-19). The authors highlight how chronic loneliness is more likely to be experienced by people with poor health, disabled people, family carers and those receiving care, people living in poverty, and people from minority groups, as well as intersections of these factors. The lack of detail and focus on inequalities in research evidence about loneliness was also highlighted in the evidence synthesis by Mansfield et al. 47
A further limitation of research in this area is that it focuses on generating a quantifiable definition of the term to measure its antecedents and consequences. The prevalence of loneliness in later life, however, has not changed despite considerable attention to this area and a host of interventions across decades. 55 In a paper based on the findings of the first stage of this project (see Chapter 3), we suggest that more qualitative and conceptual/theoretical work is needed to better understand the phenomenon and develop appropriate resources. 56 Studies tend to explore deficits in interpersonal relationships, emphasising individual characteristics such as personality, social skills and physical mobility. Less research explores the role of communities and societal relationships that contribute to loneliness. 57 The word ‘loneliness’ is often used interchangeably with ‘social isolation’, which is measurable and considered an objective state. Unlike loneliness, which can be experienced in the presence of other people, it is more about the lack of ‘meaningful’ relationships than the size of a person’s social network. 58 While a lack of social contact can lead to loneliness, it is possible to live a solitary life and not feel lonely. 59 Indeed, solitude can be connected to feelings of freedom and a sense of comfort with one’s life. 47
There is recent interest in younger people and loneliness,19 in part fuelled by COVID-19, and we need to explore the concept beyond the constraints of age. Advanced age and ageing are often equated with becoming lonely, although a recent synthesis of qualitative studies exploring loneliness indicated there was a fall in the number of studies focusing on ageing to less than half the studies included in the review. 47 Victor et al. 60 found that 14% of older people who were lonely had experienced loneliness in five life stages from childhood to older age. Other qualitative studies explore loneliness in relation to groups such as disabled people or people with mental ill health and identify explicit contextual and person-related factors that contribute to feeling lonely. 61,62
Loneliness interventions
Reviews of intervention studies, for example the work of Victor et al. ,53 draw attention to insufficient separation of related concepts, such as loneliness and isolation, for underpinning the persistent difficulty in establishing ‘what works’ in tackling loneliness, for whom and in what circumstances. Fried et al. highlight how the evidence base for interventions ‘is characterised by poorly constructed trials with small samples, a lack of theoretical frameworks, undefined target groups, heterogeneous measures of loneliness, and short follow-up periods.’46
Although loneliness matters for a prevention agenda, a review of interventions among older people found that mechanisms for reducing social isolation and loneliness differed and the quality of evidence was generally weak. 63 However, local authorities continue to introduce interventions without consideration of the very little existing evidence and few robust evaluations.
Interventions often use ‘asset-based’ approaches focused on maximising personal and social network resources. 64 Asset-based approaches have gained traction in social care, where many people fund their own care and cutbacks contribute to growing unmet need, and have been enthusiastically embraced in preventative agendas around tackling loneliness and isolation within the context of the Care Act 2014, which orientates local authorities to a duty to prevent or delay the need for care.
While many reviews and evaluations have concentrated on the findings from quantitative studies of interventions, qualitative study findings have helped understand some of the nuances of complexity, pointing to why certain interventions may be experienced as more effective. For example, Gardiner et al. 63 found three characteristics common among effective interventions: attention to local context, participants doing productive activities and involving local users in design and implementation of interventions. McMullin1 compared co-production initiatives aimed at older people experiencing loneliness in England and France and identified the importance of how the social problem is framed in terms of values. The Ageing Better programme based in England explicitly linked loneliness to individual problems, while the Monalisa initiative in France was linked to wider social and political values which motivated the selection of activities which are more geared towards successful co-production. Other reviews similarly suggested factors associated with successful interventions, including adaptability, community involvement in the design and development of the intervention, and active rather than passive client engagement. 65–67 Some of the sociodemographic factors considered important when tailoring interventions included age, poverty, and being a carer, as well as aspects of the social environment such as access to transport and driving status. 68 Interventions based on social loneliness and a focus on social connections and community integration are unlikely to work. 47
Where interventions were delivered by multidisciplinary partnerships, colocation of professionals involved was shown to be beneficial, by acting as a reminder to those delivering the intervention of the availability of support from others. 69 Finally, the importance of identifying triggers or events where loneliness and/or social isolation may change – for example, life-course transitions such as retirement, and relationship and health changes – was also shown to be key. 70
The reviews reported fewer factors that hindered the effectiveness of interventions. Of those reported, most concerned digital technologies. Specifically, these were the attitudes of older people towards the required technologies and lack of interest in learning new technological skills; the cost of technology; access to technology (including digital literacy and access to devices, especially in care homes); and concerns over privacy and online safety. 67,71,72 Other non-technological factors hindering the effectiveness of interventions were the workload and lack of interest of those involved in delivery65 and difficulties that carers of people living with dementia had with relaxing at joint events due to concerns about how the person with dementia would react. 73
In general, the reviews report a lack of sufficient evidence on ‘what works’ to guide practice. Reviews note that this is not to deny that some people experience beneficial impacts from interventions intended to help address loneliness or social isolation. Rather, evidence remains weak owing to the complex nature of interventions and research quality issues, which included little theoretical exploration of how interventions can mitigate loneliness and/or social isolation and a lack of methodological rigour in their evaluation. In summary, reviews are increasingly calling for providers to move away from standard, ‘one-size-fits-all’ interventions to more tailored offers and for future research about the effectiveness of interventions to be able to discern what works for whom, how and in what context.
COVID-19 and loneliness
The impact of COVID-19 and associated government policies around social distancing have led to considerable research on loneliness in the last 2 years. This evidence is contradictory in places. Some research suggests the experience of loneliness has remained stable despite social distancing rules74 while other findings suggest the pandemic has resulted in more loneliness. 75,76 It is clear, however, that pandemic-related conditions have had an uneven impact, with some people more affected than others. A recent report from the Campaign to End Loneliness, drawing on data from the Office for National Statistics, showed an additional million people experienced loneliness during the pandemic, and this impacted more heavily on people who already experience disadvantage: ‘[T]he fallout from COVID-19 could further embed economic and health inequalities, with disadvantaged people more likely to be out of work and in ill health, increasing their risk of chronic loneliness.’77
While concerns have been raised about the impact of COVID-19-related responses on older people, with a request for more nuanced and less ageist responses,78 people over the age of 60 years had a greater resilience to loneliness and mental ill health, possibly because older people have more experience of being alone and of dealing with potentially life-threatening medical situations. 79 The pandemic has brought into focus the impact of loneliness on children, young people and people with mental ill health. 80–82 Consideration around women is raised in some studies, although again it is not clear whether this is a continuation of pre-pandemic patterns. 81,83
In summary, tackling loneliness remains a key priority for health and social care services in the UK because the health and well-being impacts of loneliness can be substantial for those experiencing it. The costs to the health and social care sectors of increased health problems can also be considerable. Mansfield et al. suggest that co-production methods would enhance research around loneliness, concluding that: ‘[w]e need to comprehend more clearly who feels lonely, when where and in what context.’47
Why Doncaster?
Doncaster has a high concentration of neighbourhoods at elevated risk of loneliness (Age UK Loneliness Map),84 including several wards (e.g. Mexborough) in the top percentile of risk nationally. Local consultations have highlighted the loss of many social spaces linked to the decline of manufacturing and mining (e.g. community centres, working men’s clubs), and concern that loneliness is worsening (Doncaster Talks). Doncaster’s local authority and public health stakeholders have determined that addressing loneliness and social isolation is a key strategic priority, recognised in the local Health and Wellbeing Board priorities for 2018–21. The Doncaster Cabinet founded a third sector-led Social Isolation and Loneliness Alliance to substantially reduce loneliness in Doncaster.
The local authority and its Alliance have been highly committed to supporting our research. Given the challenges that social care research faces in engaging practice and the time it can take to build and sustain links with local authorities, it is important to have a willing organisation that is interested in research and has a clear commitment to the topic area. Doncaster is also part of the Curiosity Partnership, a 4-year Health and Social Care Delivery Research (HSDR)-funded research capacity-building network which is further developing the use and production of research at the level of local authorities.
In addition to Doncaster Metropolitan Borough Council acting as co-applicants to the research, planning discussions were held with the Head of Strategy and Performance, Head of Programme Delivery, the Assistant Director for Communities, and the Director of Public Health as well as the co-ordinator of the council’s work with the voluntary, community and faith (VCF) sector. They remained particularly interested in engaging with the video-based presentation of qualitative research as a means for enabling evidence to feed into service development and action planning.
The rationale for this project
Research, and more generally the use of data, should play a leading role in supporting commissioning and practice in social care. However, there is a weaker research culture and a lack of quality improvement architecture in the social care sector compared to health, with implications for the involvement of decision-makers, practice and service users. At present, local authorities collect some routine outcomes data but lack (even) the data-analytic capacity of health services. Qualitative data are a more natural format for experiential information, and robustly undertaken, could be more amenable to translation into service improvement. Moreover, narrative forms of data would be more accessible to local communities seeking to engage in service improvements. There is a slight caveat here, in that loneliness as the exemplar sits in local authority prevention work and is in the orbit of public health, which is more research orientated.
Social care policy is set nationally but interpreted, shaped and implemented in 152 locally elected councils. The result is wider variation in social care practice than in health care. There are very few public sector providers, making it harder to get research messages heard or acted upon, and most of the care workforce have no research experience or training. Those who provide services are typically in highly competitive markets and operate with low profit margins.
Staff turnover is high and even those seen as ‘qualified’ social care professionals (e.g. social workers, occupational therapists) receive less research training and continuous professional development than most of their equivalents in health. They are rarely exposed to research evidence, and indeed many do not have access to online research resources during their working hours. Few social care researchers simultaneously combine academic and practice responsibilities.
In short, models of working and the organisation, funding, commissioning and delivery of social care, as well as the research landscape, are quite different from health care, and the generalisability of innovation from health to social care is unlikely to be straightforward or comfortable. This makes it vital to ensure that what seem like promising interventions that support evidence-informed practice (e.g. the work of improvement scientists in the NHS) are tested in social care contexts. We know that there is considerable room for improvement in the provision of social care support in the UK and that innovative and cost-effective approaches are needed both to help prevent the need for social care and to guide the best use of current resources.
Study aim and objectives
Aim
Our aim was to assess whether an effective and efficient co-design approach, AECBD, could be translated from health to social care, using experiences of ‘loneliness’ as an exemplar.
Objectives
-
To understand how loneliness is (1) characterised and experienced by people who are in receipt of social care in England and (2) characterised by social care staff and the voluntary sector.
-
To identify how services might be changed to help tackle the problem of loneliness experienced by users of social care.
-
To explore, with one local authority, whether an approach to service improvement, known to be effective in health care, could be adapted for use in social care.
-
To disseminate all study outputs and publish resources on a newly established Socialcaretalk.org platform for public, family carers, service users, voluntary organisations, researchers, teachers, policy-makers and providers.
Outline of this report
We have structured Chapters 2–6 of this report in line with the two chronological phases of AEBCD: discovery and co-design. We first present the methods and findings of the discovery phase. This phase comprises two elements. First, an in-depth interview study with members of the public who experience loneliness, required to create the film to use in the co-design phase to test the accelerated form of EBCD. This work is presented in Chapters 2 and 3. Second, interviews with staff working in loneliness support. Most of the staff interviewed worked in Doncaster, with themes from the findings used in the co-design phase. A small number of staff working elsewhere were also interviewed, to explore generalisability of the local findings. The methods and findings from this work are presented in Chapter 4. Figure 1 summarises the flow of reporting the discovery and co-design phases in Chapters 2–6 of the report.
FIGURE 1.
Chapters reporting the discovery and co-design phases of the study.
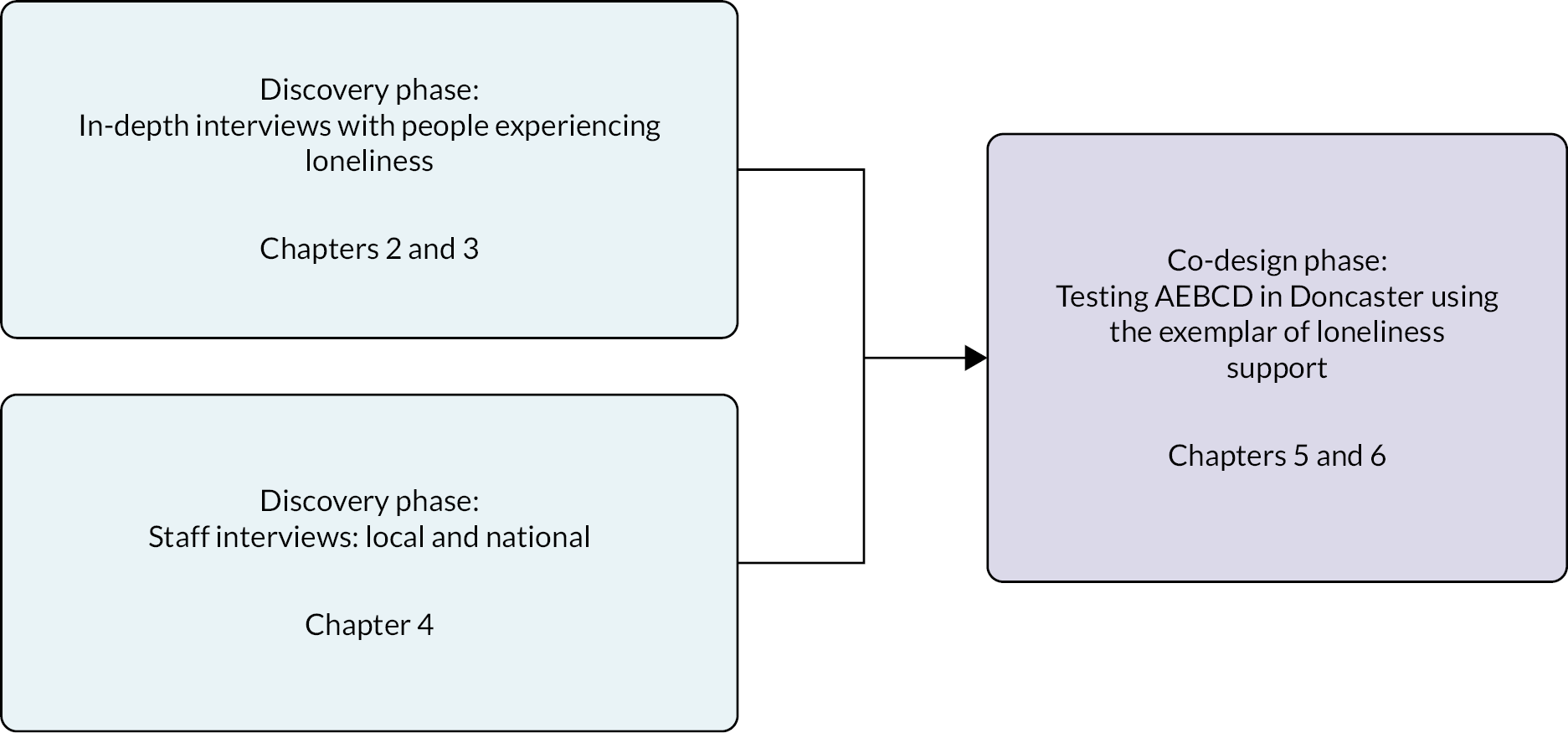
Chapters 5 and 6 present the methods and findings of the co-design phase, which was exploring whether the AEBCD intervention worked in Doncaster, along with the parallel evaluation. In Chapter 7, we outline how members of the public were involved in the project. Chapter 8 brings both stages of the project together, and we present our conclusions and recommendations for how AEBCD could be used effectively in social care settings.
Chapter 2 Discovery phase: study design, methods and public interviews
Material throughout this chapter has been reproduced from Malli et al. 56 This is an Open Access article under the terms of the Creative Commons Attribution Licence, which permits use, distribution and reproduction in any medium, provided the original work is properly cited. The text below includes minor additions and formatting changes to the original text.
Introduction
This phase of the study involved a separate, preliminary stage of qualitative research to produce a nationally generated data set based on in-depth narrative interviews with people who experience or have experienced loneliness. While we were using an accelerated EBCD approach, we had to create this initial national data set to draw on in the co-design work. By contrast, the test of AEBCD in health care used by Locock et al. 6 was able to draw on the extensive existing Oxford national archive of qualitative interviews published on Healthtalk.org (https://healthtalk.org). This archive has over 4500 interviews conducted since 2000 and covers over 120 health conditions including experiences of mental ill health, pregnancy, long-term conditions, cancers and, more recently, COVID-19. The research question underpinning these projects is ‘what are the health, information, and support needs of people with experience of the condition?’ We replicated this approach85 to create the data set from people with experience of loneliness, which has created two new resources; video, audio and text extracts from these data were used to produce a new section on loneliness and a catalyst film, both published on Socialcaretalk.org (https://socialcaretalk.org).
The Healthtalk approach
Each Healthtalk project aims to generate a diverse sample in terms of demographic characteristics and types of experiences, which means the number of participants is typically large for a qualitative study. An expert advisory panel made up of patients, third-sector representatives, health professionals and academics offers suggestions about condition-specific experiences to guide the researcher in recruitment and other aspects of the research. Participants are interviewed in depth about their experiences and asked to give permission for their interviews to be used in research, teaching, publication, broadcasting and to form part of the new online resource. They can select whether they would like data extracts to be used in text, audio, or film versions. While Healthtalk.org was originally created to provide support and information for patients and carers going through similar health issues, it has become widely used in medical and health education and the project findings are used to inform health policy, for example, in the development of National Institute for Health and Care Excellence guidelines. 86
While the aim of the current project is to assess whether AEBCD can be translated from health to social care, in this chapter, we present the methods designed to achieve the first part of objective 1, namely, to understand how loneliness is (1) characterised and experienced by people who are in receipt of social care in England and (2) characterised by social care staff and the voluntary sector.
Field review
A brief field review on the topic of experiences of loneliness was conducted to inform the interview topic guides. This review guided the selection of study participants and highlighted issues for inclusion in the interviews. It further helped the team to recognise the limitations of previous studies and find innovative ways to avoid them.
We developed the search through an iterative process, using combinations of keywords and synonyms for loneliness and social care: loneliness; social isolation; social networks; intervention; review; public health; support; lonely; alone; isolated. We searched a range of social care, health, and social science databases, including Social Care Online, Social Science Abstracts, MEDLINE, CINAHL, PsycInfo and Social Science Citation Index. We also screened reference lists of relevant papers. Literature on improvement science was included to identify individuals who write about this area and communities who could be relevant in terms of engagement and dissemination. A literature topic alert was set up for the project’s duration and on the advice of our Study Steering Committee (SSC), the literature review was updated in October 2021 to include studies focused on COVID-19 and loneliness.
The initial field review was completed during months 1–3 of the study by researchers Malli (Oxford) and Maddison (York) when the start of the fieldwork was delayed by COVID-19. From the starting point of the latest synthesis of qualitative studies across the adult life course (144 studies published up to 2018), Malli identified an additional 30 recent articles. Of these 174 studies, 98 focused on loneliness in relation to elderly people and in developed countries.
Maddison examined published research reviews of interventions designed to reduce loneliness and/or social isolation. The purpose was to explore what types of interventions are effective and why. The search was limited to English-language peer-reviewed papers published since 2000, identified via the Cochrane Library or the Social Policy and Practice database. A total of 36 papers were identified, dating from 2003 to 2022; a further 8 were identified by cross-checking the list against a key ‘grey’ report prepared for the Cabinet Office in 2018. 60 The body of research reviewing ‘what works’ in relation to interventions to reduce loneliness and/or social isolation appears recent but is growing rapidly: almost half (18/44) of the reviews identified were published in 2020 or later. The findings of the review are included in Chapter 1.
Method
An interpretative approach to knowledge production was used to understand how people make sense of their experiences, particularly loneliness. Narrative interviews were used in line with the EBCD approach. 87–90 Narrative interviews allow participants to convey stories that are meaningful to them and articulate the impact of loneliness on their lives and the lives of those around them, as well as the strategies and routes they may have used to help alleviate loneliness. 91 We were interested in understanding how participants construct and negotiate the meaning of their experiences of loneliness. 92 Our aim was to generate a deeper understanding of the experiences and meaning of loneliness through the analysis of accounts of being lonely. Blumer believed that research methods should be faithful to the empirical world under investigation, so we did not provide participants with a definition of loneliness, allowing space for subjective constructions of loneliness to emerge which could enhance our understanding of the phenomenon. Participants actively engaged in meaning-making during the process of the interviews as they were encouraged to explore and consider their experiences through careful probing and questioning.
The national, qualitative research study involved in-depth interviews with 37 people who self-identified as being lonely, conducted between October 2020 and January 2021. Participants were aged 18–71 years, with 23 identifying as female, 13 identifying as male and 1 as non-binary. A further two people were interviewed and later withdrew.
Due to COVID-19 restrictions, the interviews were conducted online (n = 30) using videoconference or by telephone (n = 7) depending upon participants’ preferences. A purposive maximum variation sampling approach was used to capture a wide range of perspectives and understand variations in people’s experiences. 93
We particularly wanted to capture the experiences of marginalised people as our review highlighted that this group could be more susceptible to experiencing loneliness. Our sample included participants with multiple intersecting identities, as outlined in detail in Table 2, which states the number of participants that identified with these marginalised identities.
| Identitiesa | Number of participants (n = 37) |
|---|---|
| Physically disabled people | 3 |
| People with mental ill health | 21 |
| People with learning disabilities | 2 |
| Autistic people | 4 |
| Bereaved people | 4 |
| LGBTQ community | 5 |
| Migrants | 6 |
| Substance users | 4 |
| People living with HIV | 4 |
| Domestic violence and abuse survivors | 4 |
| Family carers | 2 |
| People from ethnic minorities | 3 |
| People that have experienced homelessness | 3 |
Recruitment
Participants were recruited using a range of strategies including mental health charity advertisements, local authority newsletters, personal contacts through previous research and the involvement of colleagues, snowballing through existing contacts and social media platforms. More specifically, Facebook (Meta Platforms, Inc., Menlo Park, CA, USA), which has been identified as a useful tool in approaching seldom-heard populations,94, 95 was used. Flyers for the study were posted on relevant public Facebook pages and closed support groups. Due to the latter’s strict access conditions, the study was only advertised after permission was granted by the administrator through private messages providing details of the research. More than 30 closed Facebook groups were approached relating to mental illness, disabilities, drug and alcohol dependencies and lesbian, gay, bisexual, transgender and queer (LGBTQ) issues, of which 3 declined to advertise the study. Participants had to be 18 years old or over and to have experienced loneliness. Although some studies have avoided using the term ‘loneliness’ during recruitment due to negative connotations of the word,96 it was clearly stated in our flyers so as not to mislead potential participants about the topic of our study. Originally, we intended to include only people who used social care services; however, it transpired that people were often not aware of whether groups or services they had interacted with were included, and we widened our sample criteria to people who experienced loneliness.
All participants received a £30 voucher in recognition of their time and contribution to the research.
Interviews
The narrative interviews were conducted by Malli, an experienced qualitative researcher. A ‘warm-up’ discussion preceded the interview to make the participants feel at ease. This is especially pertinent to sensitive topics, such as loneliness. The interview was divided into two sections. An open question (‘Can you tell me a little bit about yourself and how loneliness came into your life?’) was used at the start of the interview to allow participants to highlight what was important to them, their values, meanings, priorities and experiences. The second part of the interview was based on the topic guide grounded in the field review and feedback from our project advisory panel. It covered loneliness and support, identity, loneliness, and the media (see Report Supplementary Material 1). To bridge the two parts of the interview, the researcher started with questions about topics raised by the participant in their primary narrative and then asked the additional questions to understand participants’ experiences of their wider lives including relationships and employment, social care services and other sources of support. We also explored how services could be improved. The interviews lasted between 45 minutes and 2 hours and were audio- and video-recorded with participants’ permission.
Transcript checking
The interviews were transcribed verbatim by professional transcribers, checked for accuracy against the recording, and deidentified. Time codes were added throughout. The transcripts were returned to participants to give them the opportunity to read and remove any sections they would not like disseminated or used in research. At that stage, they were asked to sign a form giving the copyright for their interview to the University of Oxford to enable their interview to be used in online resource production, including a resource to be published on Socialcaretalk.org and the catalyst film. The transcripts were also deposited in a University of Oxford data archive available to other bona fide research teams for secondary analysis under licence.
Data analysis
Analysis was conducted alongside the fieldwork until ‘data saturation’ was reached. We defined this as a point where new data repeated that of previous interviews without bringing new contributions to the understanding of the phenomenon. 97 A multistage inductive thematic analysis was carried out as a systematic method of generating themes and patterns within the data following the Braun and Clarke98 guidelines and using the organisational support of NVivo 12 (QSR International, Warrington, UK). A deviation from the study protocol included the use of grounded theory; this approach was felt to be more flexible, allowing us to analyse the data within the time constraints we were facing due to a delay in gaining ethics approval.
Initially, the data were read carefully by Malli in a process of familiarisation before being coded in NVivo to maintain participants’ meaning as far as possible. Malli and Ryan independently coded the first three interviews and met to discuss the different codes generated. The codes were then reordered into a more formal tree structure allowing the identification of broader categories. Malli continued to code the remaining transcripts. The descriptive codes were organised into categories and these categories were analysed conceptually in what Braun and Clarke98 describe as a process of ‘latent analysis’ to examine underlying ideas, assumptions, connections and links within the data. From this analytic stage, themes were identified, and the data were systematically reviewed to ensure that a name and clear definition for each theme were produced and that these themes worked in relation to the coded extracts. We returned to the original recordings as appropriate to aid this stage of analysis. To increase the integrity and trustworthiness of the study, the first author kept a reflective diary during the interviews, transcription and analysis phase.
Ethics
Ethics approval for the study was obtained from the Health Research Authority Research Ethics Committee (REC), after the submission was moved from Social Care REC, on 2 October 2020 (ethics reference: 20/WM/0223). COVID-19 necessitated further planning to minimise face-to-face interaction with research participants where possible. New operating procedures were introduced for the capture of data suitable for dissemination on a web platform which specifies methods to optimise video and audio quality while adhering to data security policy.
Producing a catalyst film
A core output for the co-design phase was to produce a ‘catalyst’ film using film, audio and text extracts. A ‘touch point’ coding report was produced during the analysis process detailed above. Malli selected extracts of data which highlighted key points illustrating excellent or particularly poor support. These extracts were shared with full team members and advisory panel members before meeting to discuss the content further. The planned workshop to finalise the content of the film was unable to go ahead because of COVID-19 limitations. Locock separately arranged a meeting with the Doncaster team, the evaluator, and the workshop facilitator to talk through AEBCD and the film’s use in the co-design phase of the project. The content of the catalyst film was further revised in individual discussions with public advisory panel members. Extracts included participants’ discussions of what good loneliness support looked like and what had not worked for them in terms of social care and privately provided interventions.
The DIPEx charity produced a draft version of the 20-minute film using the video and audio extracts, and the link was shared with the full team and advisory panel members by e-mail. Comments were invited and incorporated into the film. A final discussion about the film was held at an advisory panel meeting in January 2022. Feedback included concern about the quality of the sound, which led to the addition of subtitles, and the organisation of the content which has the following sections:
-
What is loneliness?
-
What does loneliness feel like?
-
What has made loneliness worse?
-
Why are people hesitant to access support in relation to loneliness?
-
What hasn’t worked for you in relation to loneliness support?
-
What does good loneliness support look like?
The film was used in the co-design workshops (see Chapters 5 and 6) and is published on Socialcaretalk.org (https://socialcaretalk.org/introduction/loneliness/).
Developing a Socialcaretalk section
The second output from this stage was the production and publication of a new section on experiences of loneliness on Socialcaretalk.org. In producing the section, the aim was to include a representation of the full data set, and this was achieved by identifying what mattered to participants and reflecting a diverse range of perspectives around loneliness in a balanced manner. From the identified categories and themes, we developed a series of lay summaries on the issues that were most important to people who self-identify as lonely (https://socialcaretalk.org/introduction/loneliness/). The summaries include contextual, evidence-based information and links to other sources of information and materials.
To ensure quality, balance and comprehensiveness, each summary was prepared by Malli, with Ryan independently mind-mapping the coding reports on which the summaries were based and adding any aspects that had been overlooked. When each summary was drafted and checked by Ryan, it was reviewed by members of the project advisory panel before final editing and publication.
Example feedback from advisory panel members included these comments:
I think they are really interesting, and the text is an excellent summary of the themes, the childhood one was so sad it brought tears to my eyes.
I think they would be brilliant to use in teaching about loneliness and really make it clear that it is much more than not having people around you but is often more of an internal state of feeling.
Chapter 3 Discovery phase: public interview findings
Material throughout this chapter has been reproduced from Malli et al. 56 This is an Open Access article under the terms of the Creative Commons Attribution Licence, which permits use, distribution and reproduction in any medium, provided the original work is properly cited. The text below includes minor additions and formatting changes to the original text.
An early finding from this research was the ambiguity relating to the relationship between participants and social care services. Unlike healthcare services, where people typically enter a healthcare setting or contact at a clearly defined contact point, there was a lack of clarity around the meaning or scope of social care and whether it is seen as an extension to community-based preventative activity such as loneliness support. Some participants used social care services such as support workers, and some used local services that may have been funded by the local authority.
Our analysis led to the identification of six key themes. Four of these – loneliness as lacking, loneliness as abandonment, lingering loneliness and the unspoken and trivialised experience of loneliness – have been published. 56 In addition to the findings reported in the paper, two additional themes were identified: the double-edged sword of social media and inevitably, though unplanned for in the initial project design, reappraising connections as an outcome of COVID-19. The section below is a summary of the published paper and the two additional themes.
Loneliness as lacking
Loneliness was linked to the loss of important close relationships and the absence of close relationships with people who could genuinely understand participants, empathise with them and affirm their value as an individual.
Loneliness as loss
Loss and bereavement strongly featured in participants’ narratives, and these deaths were often unanticipated and accompanied by additional emotional trauma. Participants were deprived of the company and affection of the person and an envisioned future together. P29, who lost her partner abruptly in her late 30s, explained:
I know this woman who lost her husband, but she was in her seventies or eighties. And I always say, ‘You lost a lot of past, but not so much future. I lost a lot of future and not so much past.’ It’s very different to be on your own when you’re, let’s say, in your seventies and maybe you are a grandparent, and you have a completely different role in life than when you are just a young person who had their whole life to go.
P29
Participants described irreplaceable bonds that could not be substituted, which worsened loneliness. P1 talked about the loss she felt after the death of her mother, whom she relied on in different ways:
I think that had a huge impact on how I interact with other people now I just, I don’t feel as connected any more. So she was always kind of like she had, she was a friend, she was a sister, she was a carer as well like, you know, she’d always sort of check up on me and she had so many roles and when that went it just left this huge hole in my life, so I think that, yeah, it sort of affected me quite badly.
P1
The unanticipated loss brought an additional layer of loneliness as participants discussed how they struggled to approach the grief of premature death. There was a lack of the comforting and supportive responses that bereaved people commonly receive. As P40 said in relation to her brother’s death:
When your 27-year-old brother dies from a heroin overdose it’s like there’s no [card company] card for that . . . people also don’t wanna talk about it because it’s a bit like ‘oh, do we bring it up?’ whereas people seem more comfortable bringing it up sort of if a parent or grandparent’s died.
P40
Loneliness as absence
For many participants, loneliness was marked by the absence of a meaningful person to turn to, a relationship that they never experienced. Many wanted a connection with someone they could talk to and confide in. The following extracts capture this absence:
I have no-one to share my life with . . . I don’t have someone to turn to, to tell my problems to, or anything like that.
P37
There’s moments when I’d like to sort of really connect with someone or when I’m feeling low, I want to sort of, because I don’t really have [um] many friends and [um] I think that’s when it does appear like [um] I feel that intense loneliness when I feel quite isolated.
P1
Even participants who perceived themselves as sociable and surrounded by casual friendships missed an intimacy and affection which was absent from their life. For P2: ‘I suppose I would really like my friendship to be like quite close, friendships should be quite close, so I want to feel like, like family’.
For P22 and many participants, the intensity of a friendship rather than the quantity of the social circle combated loneliness: ‘it no longer mattered whether I had other friends because I found another really, person who I could be really close with’.
Loneliness as abandonment
Loneliness could begin with strained family relationships and feelings of invisibility and abandonment from childhood. Others described feeling abandoned by society because of insufficient care and cuts in funding.
Being overlooked during childhood
Loneliness was discussed in relation to participants’ family and childhood experiences, including stressful environments, the emotional unavailability of close family members, and other adverse experiences such as abuse and neglect. Looking back at their childhoods, they described how loneliness was about the need to be listened to, believed, supported and protected. The impact of this abandonment could be extreme, as P32 describes, talking about her relationship with her father:
It took years for me to realise that I actually felt annihilated in his presence. I was so unacknowledged, um, that I almost felt like there was nobody reflecting me back and my grasp on my own existence was tenuous. I realised when I was very much an adult, um, that just being in his presence was enough to make me feel suicidal because I felt so unacknowledged, like somebody had rendered me invisible.
P32
The illness of his younger brother, who subsequently died, led P12 to feel neglected by his mother, while P35 felt her parents gave her brother all the attention when he was born 8 years after her:
I was an only child for eight years and then my brother came along. […] So my parents favoured him over me pretty much from the get-go, so I kind of, because everyone was always all over my brother I kind of retreated [um] and just kind of spent a lot of time in my room by myself [um] not really socialising and isolating myself I suppose.
P35
For some participants, loneliness came from keeping experiences of abuse secret. Fear of the consequences of disclosing this and perceptions of self-blame emotionally isolated participants and made them feel that they could not reach out and ask for support. P11 described how:
I was being sexually abused from the age of 9 and, and it was quite a secret thing, [um] it was something I was keeping to myself . . . think it was quite lonely because I suppose it’s a lot to deal with and at the time, I didn’t really have anyone to talk to about it.
P11
The need to keep domestic violence as a private family matter that could not be disclosed and discussed with people outside the household left P37 feeling lonelier:
I was like locked inside of the prison, you know, I couldn’t say a word I couldn’t look for help I literally felt like I’m like decaying inside, like the living dead. You know we are forbidden to talk about this to anyone and it does make you feel lonely.
P37
Being abandoned by society and those who could have helped
For many participants, loneliness was a result of being deprived of community and social care resources due to austerity cuts. Financial cuts were seen as a source of social alienation that made people feel invisible. Social clubs and support groups which for many were an important resource for active networking with ‘similar others’ were closed. P19 talked about the impact of two social clubs closing:
They lost their funding, which was hard because I was enjoying it. I was enjoying the activities they were doing. They were doing like games, cooking in one of them. All different types of stuff . . . It was hard because I was enjoying it. I enjoyed seeing people.
P19
P18 described feeling isolated and abandoned after being diagnosed with multiple sclerosis. He described getting ‘a whole bunch of pamphlets thrown at you and told you have MS, and told we’ll see you in six months for a check-up’.
Other participants discussed not being heard within the mental healthcare services. They described a process of dehumanisation and objectification from healthcare professionals that induced loneliness and social isolation. In relation to mental health care, P6 described:
If I could at least [have] told them about my experiences and what I was going through, I wouldn’t necessarily have wanted an answer, but I’d have wanted someone to listen and if someone’s listening to me, they see me, I’m not lonely any more.
P6
Finally, some participants felt that their social identity was invalidated and undervalued, which made them feel lonely. P3 reflected on her unpaid carer role:
When I’m being sort of selfish, I think maybe I made a mistake and I should have just kept my career because they certainly don’t look after carers, they’re on their own . . . Because people seem to forget that the productivity coming from unpaid carers in this country saves the state about a £132 billion every year so, you know, it’s a bit of a sore point when people say you didn’t go to work.
P3
Lingering loneliness
For many participants, loneliness was something that accompanied them throughout their life. It was perceived as an innate part of their identity that stemmed from a sense of otherness, and its presence lingered even in the company of others. Participants also described feeling trapped in a cycle of loneliness, which intensified personal isolation.
Loneliness and identity
For many participants, a sense of loneliness came from feeling ‘different’ and was inevitably ingrained in their identity. For example, P1 said ‘I think [um] being autistic [um] I feel lonely quite a lot of the time [um] so I think it’s always there, I think it’s never not a part of who I am’.
For some, being ‘different’ affected their sense of integration and belonging, and emotions were tied to loneliness. P33 said, in relation to mental illness:
I kind of always, I guess, had this like longing to belong or like be a part of other people’s lives where I wasn’t really. Um, so I spent kind of like most of my teen years extremely lonely.
P33
Being ‘different’ sometimes meant being stigmatised and fearing or experiencing rejection. In relation to her mental illness, P39 said:
It’s like damaged goods you don’t ever, nobody ever prioritises damaged goods, you look for an apple you look for a perfect one in the supermarket you don’t look for one that has got lumps and bumps.
P39
A common point was loneliness that stemmed from not being understood by people. Participants seemed to experience a profound sense of loneliness through trying to convey how they felt to people who could not relate to them. In relation to psychosis, P15 commented:
There’s a sense of loneliness that people can’t experience the same things that I’m experiencing, and people say to me, if I’m talking to somebody [um] that other people can’t see, it can be quite frustrating when people are saying, ‘But I can’t see that,’ when it’s very real to me. And that makes you feel lonely because people aren’t experiencing the same world that you’re experiencing.
P15
The absence of people with similar experiences, who could provide emotional support and validation of their identity, creates what Stein99 terms ‘experiential loneliness’:
You feel very much alone and you’re very much aware that the experiences you’re having and the feelings you’re having aren’t the same as the people around you. And as much as they try and are as supportive as they can be, I don’t think that they will ever be able to fully understand. You kind of feel like if you’re trying to communicate something to them about like, something difficult about being like gay or non-binary, they can try to understand but they won’t fully know, and I think that is a form of loneliness.
P33
Loneliness despite the presence of others
For many participants, loneliness persisted even in the presence of others. They felt the experience of emotional isolation amid a group of people, within their family or even their intimate relationship. Togetherness in some cases could make loneliness worse:
I’ve been with people and felt lonelier than when I was on my own. I don’t really know why. I guess, if you can’t relate to people, or like you don’t really feel a part of their group, then it can definitely feel lonelier to be around people.
P25
Loneliness was also experienced in absence of shared understanding, as P8 describes:
Going to the pub and being around people I still felt very isolated because of my HIV. And that people, there weren’t people who got where I was at, and understood [um] the position I was in, and what was going on in my mind. I felt very isolated. Even though I was surrounded by people.
P8
Some participants described an ‘internal’ type of loneliness, that kept them separated from the world and made them feel like an outsider. P37 describes this when referring to the relationship with her then partner:
I used different things in those times to cover over it [loneliness] and deal with it in a different way. But eventually it would come to the surface as the relationship developed [um] . . . but no, I’ve never not felt this crushing emptiness and loneliness.
P37
The vicious cycle of loneliness
Many participants reported feeling trapped in a cycle of loneliness in which the lonelier they became, the more isolated they felt from society. 100 They recognised how they should act to reduce this, while feeling that loneliness had become an integral part of their life in which they felt secure. P32 described the paradox of wanting to ease feelings of loneliness while feeling unwilling to step outside the comfort zone loneliness had become:
That might sound a bit peculiar, but I’ve begun to recognise that when I have the opportunity to socialise it’s almost as though I’ve turned in so much on myself, that [sighs] it’s becoming hard to turn outwards and meet other people again.
P32
It was apparent that loneliness can create a tendency in people to dwell in self-pity, be more sensitive to rejection, withdraw and be less trusting of the people around them. This in turn created worsening feelings of loneliness. The fear of experiencing loneliness in the future could further obstruct the enjoyment of the present.
The unspoken and trivialised experience of loneliness
Most participants discussed the difficulties of disclosing their experiences of loneliness due to the associated shame and stigma. The experience in their view was a taboo subject and silenced or associated with the public discourse of old age and failing health. On the rare occasions when loneliness was discussed, it was approached with a veneer of light-heartedness and easy-fix solutions and interventions recommended by people who did not understand their experiences.
The silencing of loneliness
A pivotal subtheme here was the notion of stigma, shame and self-blame which restricted any constructive discussion about loneliness. Many participants discussed the ‘archetype of the loner’ who is depicted as socially ‘defective’, inept and incapable of forming key relationships to combat isolation and loneliness. P39 highlighted: ‘If you’re a loner there’s something wrong with you . . . It is not a positive word to put on someone . . . there must be something, because why would someone choose to be alone?
This stereotype, which carries negative and derogatory connotations, views the person through a lens of personal and social failing and intrinsic character flaw. Subsequently loneliness is pathologised and viewed as an experience outside the boundaries of what is considered to be normal.
I think there was a lack of talking about loneliness as a thing that can happen to just normal people. It was always this person visibly has no social skills and you know is really profoundly like struggling in society, not this is another well-adjusted person who has got some confidence issues and is struggling to make friends in a new context.
P22
The ‘tyranny of positive attitude’, which is saturated with the view that we must think positive thoughts and block out negative emotions and avoid any difficult but nevertheless authentic emotions, further contributes to the silencing of the discussion of loneliness. P10 expressed ‘We’re meant to be these very successful, bubbly, happy-go-lucky people who do these great things every weekend and you know, are never stressed, are never behind at work, you know, are never struggling’.
Indeed, the stereotype and trope of the lonely elderly prevail in the collective consciousness, leaving little room for other populations to share their experiences of loneliness. By being excluded from the loneliness discourse, many participants resorted to self-blame for failing wider expectations:
They always say it’s the older people that feel lonely . . . They never talk about the younger generation. I think because society expects people at that age to be married, have children, and have their lives sorted so to speak, so they don’t think about people that might be gay, they don’t think about people that might be single, they don’t think about people that might be trans-sexual, they just think about the mainstream. And then sometimes that makes me feel guilty about being lonely or feel weird about being lonely, because I think I shouldn’t be lonely at my age, I should have lots of friends, I should have a partner. And then I think ‘what’s wrong with me? Why do I not have these things?’
P17
The stigma attached to loneliness dissuaded many participants from seeking support from services. Indeed, the intolerance towards individuals who experience loneliness acted as a barrier to help-seeking. In reference to accessing help for loneliness, P5 mentioned: ‘I would have really benefited from it at the time [support] I don’t know if I would have accepted it if anybody had said it because I also think there’s that kind of, you don’t wanna be stigmatised.'
The trivialisation of loneliness
Many participants said that the seriousness of loneliness can be diminished through a process of trivialisation. The consequences it might have for quality of life and mental health are downplayed and the reality, nuances and causes of the experience are oversimplified and even ignored. Moreover, the legitimacy and severity of loneliness are questioned and there is an implication that it may be the person’s fault. People are blamed for not being proactive, for not taking steps to make positive changes. Thus, individual agency was presented to participants as an effective approach to managing loneliness. For example:
People just go, ‘Oh, loneliness, you just need a fellow’, or ‘Loneliness, oh, get a dog’, or, it’s just people minimalise it so that it’s . . . loneliness leads to so much more than just being lonely . . . It can lead to all sorts of things that people don’t necessarily think would start from loneliness.
P13
Since the essence of loneliness is oversimplified, the interventions and advice offered by experts are unsophisticated, and, as discussed in Chapter 1, only superficially approach the problem. P5 shared her experience of being given ‘by the book’ advice from a health visitor as an early mother that was not tailored to her circumstances or needs:
You get all the health visitors come round and all that kind of stuff and I always felt like they were just saying OK, yeah but you can just fix that, you know, can you do this? Can you that? Can’t you do such things like it’s easy to, to kind of just get on with things and not feel isolated.
P5
Indicatively, participants discussed support from services that aimed to broaden people’s social networks and therefore to tackle social isolation (quantity), while they felt that they lacked a close intimate attachment to another person (quality). Thus, strategies between social isolation and emotional loneliness were used interchangeably, indicating the insufficient understanding of the differences between the two concepts. Many participants suggested that genuine attachments could not be formed in loneliness support groups since they are not based on common interests between people. For P2:
I just feel like in that [support group for loneliness] group other people will just be maybe desperate for friendships . . . like some people are lonely, they’re just happy to be friends with anyone [um] and obviously that’s not what I want. Either I want friendships to be genuine . . . you need to have a rapport, a rapport and [um] genuine fondness for each other and a likeness with [um] appreciation for each other’s company.
P2
The double-edged sword of social media
Social media has changed the way we communicate with people around us, and, for some young people and adults, it is a primary means of communication. Participants had varying views about whether social media could help people to feel less lonely. For some, online support communities allow people affected by similar issues – for example, mental health – to communicate online. This can help ease loneliness as people find ‘similar others’ and receive (and provide) emotional support. As P11 said, it could be reassuring to hear other people’s problems and know you were not the only one experiencing issues. P1 described how:
P1: I really enjoy social media and seeing there’s other autistic people which is just like amazing because it just makes me feel like I’m not alone, you know.
Interviewer: Could you tell me a little bit about that community, I’m very interested in hearing about how this community on social media has evolved and, you know, how it really helps you?
P1: Yeah, it’s just you go on there and you just realise there’s so many different kinds of people and, you know, we’re just like neurotypical people we’ve all got different personalities, but I think they understand your struggles more than neurotypical people like my mum just did with me.
Other participants were more cautious about social media and wondered if it made loneliness worse by, for example, providing glimpses into other people’s lives. Linked to this was the suggestion of a falseness inherent in social media that some participants described. People have a greater insight into the lives of their ‘friends’ than they had before platforms like Twitter and Instagram, but not all information that is shared is accurate. People may share unrealistic images and try to present only the most positive side of their lives, creating an impression of living happier, more successful, and more connected lives than they really are. People may compare themselves to their ‘more successful’ friends and feel envy. As P11 said it could also make you feel lonelier as ‘you feel like you’re looking through a window’ to the life you would like to have.
Social media could also pull people away from their physical surroundings and isolate them from people they could directly interact with. Some participants, like P33, had mixed views about social media. While it could help people feel a sense of belonging that could ease loneliness, it could also exacerbate loneliness:
Um, but on the other side of social media, um, you have like Snapchat and Instagram where people post, you know, highlight reels of their lives. Um, and I think when you’re very vulnerable to loneliness, that can be extremely, extremely dangerous and harmful because you’ll be sitting there alone in your room bombarded with constant images of people with their friends, people smiling, people at parties. Um, and because that’s all you’re seeing, but it’s not what you are doing or the life you are living, you feel like there’s something wrong with you. You’re like, why aren’t I doing that? Why is that not my life? When that’s what everyone else is doing and they look so happy doing it. And so, I think it can definitely intensify loneliness, um, to a very like severe extent.
P33
A few people questioned whether the use of social media can create loneliness and suggested that it can only worsen the existing problem. In other words, people who might experience loneliness could use social media and feel even more lonely, but loneliness is not the result of using social media.
Reappraising connections as an outcome of COVID-19
Although our study was not about the pandemic, fieldwork took place during periods of lockdown, and most people talked about experiencing loneliness due to government-imposed social distancing policies. Restricted face-to-face interaction with friends, family and social networks had mental health implications and heightened or even generated feelings of loneliness for many people. Staying at home could lead people to question how meaningful their friendships were, and how they were not able to stop them feeling lonely.
P1, for example, said that the restrictions imposed due to COVID-19 added another layer of loneliness to her life and how she felt more trapped despite not being ‘super social or anything’.
For P29, the lockdown meant she had to rely on herself in terms of the choices she made in her life:
I think that’s when you experience loneliness. It’s just like when the weight of the world is just on your shoulders. It’s like every single decision is yours. I mean, it also has to do with the fact of not being able to see people. It’s like the loneliness that I . . . during the first lockdown I literally spent two months on my own. Completely on my own. I don’t wish that to my worst enemy. It’s just like, it’s really, it can really harm your, your mind, you know? It just feels like that, it feels like ‘OK, all the decisions fall on me’.
P29
Other participants feared lockdown would worsen mental health issues, and some talked about how they tried to avoid this.
So that’s why I’m working from home I have to get up I have to do this, do this at a certain time and I work late, it’s different things each day but I have to have that, I have to have that structure because for me loneliness creates lack of control and if I don’t have control in my life then all the bad things start to happen again. See I’m a control freak I don’t ever want to control another human being but I have to control of my own life because if I lose it the loneliness comes in and it causes mental health problems again.
P6
Lockdown also created insights into the status of social relationships which, for some, turned out to be less meaningful than they had assumed.
I’ve got, I would say a good set of work friends/colleagues, people I have lunch with, but I know that since lockdown it’s been very much more evident that they are just work colleagues. They’re not people that I would see outside of that unless we’re in the office and say going, you know, for a drink after work or going to a leaving do or something. Very much they are a work set. So whilst I do have friends, it’s often, I think some of it’s transactional.
P10
During lockdown, many people realised the importance of physical contact and the impact a lack of physical contact had on loneliness. Some participants who lived alone went for days, weeks or even months without seeing people, and the lack of human touch made them feel even more alone. P21 acknowledged that a lot of loneliness during the pandemic stemmed from a lack of physical contact with other people:
. . . and while we can video chat thanks to technology and that, it just doesn’t seem to have that same personal touch like let’s say if me and my partner lived in separate houses, yes we could communicate like this like we did before we moved in together but it was never the same where I could physically hug her. I think that’s what contributes a lot to the loneliness in the pandemic because there’s that physical connection.
P21
Discussion
Our sampling approach, which focused on recruiting people who are less likely to be included in research, allowed us to explore common features of loneliness and highlighted the complexity and nuances of loneliness among adults which is not age related. Our findings underline how loneliness is more multifaceted than a discrepancy between the relationships we desire and the relationships we have, which is the basis of widely used contemporary definitions.
Experiences of loneliness were also highly subjective, often linked to the absence of a significant person and associated with participants’ societal roles and identity. Indeed, for many participants, loneliness arose from inadequate integration and feelings of alienation within society which were generated by insufficient care and community resources, stigmatisation and feelings of being abandoned by those in power. They felt dehumanised by not being heard, and unjustly treated. While research in this area has focused on micro-level characteristics that predispose people to loneliness, de Jong Gierveld101 highlighted the need to explore the wider social and economic circumstances contributing to loneliness. We found a wide range of macro-level factors that generate feelings of loneliness.
Our study provides a nuanced understanding of the reasons people may struggle to talk about loneliness as loneliness. The causes are often shrouded in shame, trivialised and ignored. Consistent with existing research (e.g. Franklin et al. 102), our participants could be reluctant to discuss the subject for fear of being stigmatised.
We recognise that the stigma attached to loneliness means that people who feel the need to shy away from the label may not have been included in our study,103 and suggest further research is needed to explore the interplay between wider structures and loneliness. Our study also highlights the need to normalise the experience of loneliness in public discourse and promote openness among those who are affected by it. As discussed in Chapter 1, existentialist theory of loneliness views loneliness as a painful and intrinsic human condition which generates personal growth,104 while a biological viewpoint is that loneliness acts as an aversive signal, like hunger or thirst. 105 Like many mental health-related issues, loneliness is discussed in the realm of private life and personal control and responsibility. Furthermore, because of the enduring stereotype of loneliness as relating to old age, younger lonely people can be left to dwell in their loneliness.
Barreto et al. ’s55 global study of loneliness found that young people feel the loneliest, with 40% of 16- to 24-year-olds reporting the experience of loneliness often or very often compared to 27% of those aged 75 years and older. We argue that loneliness should be reframed as a recurring condition of human life that transcends age, gender and geography. At the same time, it is important not to minimise its severe consequences and the need for effective support. Loneliness can be a grave issue when left unattended and when it settles long enough to create a persistent self-enforcing loop of negative thoughts, sensations, and behaviours. 106
Many participants described a form of prolonged loneliness since childhood despite not (always) living alone or lacking satisfying relationships. Their loneliness was attributed to a lingering rejection of their identity and an enduring sense of feeling different. Our research, therefore, expands existing criteria that reveal factors generating prolonged loneliness. Most participants longed for emotional togetherness, and the presence of social contact could not combat this. This could be further worsened by using social media, which was perceived by some participants as a double-edged sword.
Conclusion
Our interview study contributes to understanding how loneliness is experienced by a wide range of adults. The findings suggest that loneliness may stem from unfulfilled interpersonal social needs but also from a societal undermining and invalidation of people’s social identity. Unmet care and support needs, ignored by those with the power to help, meant participants felt unheard, in turn perpetuating feelings of abandonment and social alienation. Furthermore, the stigmatisation of loneliness left the most vulnerable to endure the phenomenon in silence. These findings should be considered when developing interventions that aim to ameliorate loneliness.
Chapter 4 Discovery phase: staff interviews, methods and findings
This chapter addresses the second part of objective 1, that is, to understand how loneliness is characterised by social care and the voluntary sector staff. The purpose of the local, Doncaster-based discovery phase staff interviews was twofold. First, to gather staff perspectives on loneliness and their views on current local support to prepare a summary to facilitate discussion in the co-design phase staff workshop; and second, to raise the profile of the co-design work and engage participants’ interest in taking part. The smaller number of national interviews was undertaken to understand whether and how the wider loneliness support context differed from that in the Doncaster area, to help with understanding the generalisability of the study findings.
Sampling and recruitment
A small study working group in Doncaster was created to support the discovery phase and co-design work. Its three members comprised a Public Health Lead from Doncaster Council (Robson), the Programme Manager of Doncaster’s local Social Isolation and Loneliness Alliance of VCF organisations offering support (the Alliance), and the evaluator (Madison) from the research team. The two Doncaster-based members facilitated sampling and recruitment by raising awareness about the study with colleagues via their respective networks. These efforts established connections with other work around loneliness, helping to build cooperation and embed the co-design phase in the wider pattern of loneliness work.
The project proposal suggested at least 8 of the 20 interviews should be with local staff; the Doncaster working group agreed on 12 local and 8 national interviews. This ratio was influenced by previous AEBCD studies which interviewed only local staff and used the interviews as a way of engaging local staff in the subsequent co-design phase, which would be seeking 10–15 local staff participants. Recruitment of local staff ensured a mix of people in managerial and front-line roles and those working for Doncaster Council and other organisations whose work included loneliness support.
National interviews were planned as a mix between staff from other local authorities in the Yorkshire and Humber region known to be working on aspects of loneliness, with the remainder involving staff from further afield. The latter group included a representative from a national loneliness charity, with the rest drawn from diverse local authority areas to explore examples of potential good practice in loneliness support. A shortlist of examples was compiled from knowledge among study working group members and evaluator discussion with the office of the Campaign to End Loneliness, which had recently published an updated report of ‘promising approaches’ to tackling loneliness. 54 From the shortlist, the study working group selected participants they felt would provide the most useful learning for Doncaster.
Data collection and analysis
Overall progress was slower than anticipated due to ongoing and severe COVID-19-related work pressures on the capacity of Doncaster Council and VCF staff working in this field. Interviews carried out by Maddison were completed between March and August 2021, conducted via videoconference or telephone and, with consent, were audio-recorded for transcription. A template interview topic guide was used (see Report Supplementary Material 2), adapted according to each participant’s work context.
A total of 19 interviews were completed with 20 participants (1 joint interview). Table 3 gives a breakdown of these participants by organisation type. Of these, 12 interviews (13 staff) were with managers and front-line staff working in a range of roles in Doncaster Council and local VCF organisations. Some participant roles focused on loneliness (e.g. befriending), while others engaged with loneliness as part of a wider brief (e.g. home care, social prescribing). The secondary aim of these interviews – to inform/engage staff about the co-design phase – was successful, with staff agreeing in principle to be recontacted.
| Organisation type | Number of participants | Total | |
|---|---|---|---|
| Local | National | ||
| Local authority | 2 | 5 | 7 |
| Private sector provider | 1 | 0 | 1 |
| VCF/third sector | 10 | 2 | 12 |
| Totals | 13 | 7 | 20 |
The seven (national) interviews involved five participants based in other local authorities and two from organisations that were able to offer a regional and national perspective on loneliness programmes.
Analysis of the Doncaster staff interviews focused on identifying and collating key points to present and discuss at the co-design phase staff workshop. Two broad headings were used: how staff understand loneliness and experiences of being lonely; and the ‘hallmarks’ of good loneliness support (a term participants preferred to ‘touch points’). Data included under the second heading included how well participants felt Doncaster was faring regarding tackling loneliness, and suggestions for improvement.
The national interviews were analysed similarly with the aim of sharing learning points for Doncaster. This included identifying additional issues around conceptualising loneliness and factors that help or hinder loneliness support interventions.
Findings from the local staff interviews
Understanding loneliness and people’s experiences of being lonely
Local staff (who were predominantly community-based or working in the VCF sector) recognised that there was more to learn from people with lived experience (PWLE) of loneliness. Some participants thought local authority adult social care staff less likely to understand loneliness owing to having fewer opportunities for ongoing, community-based contact with PWLE. Learning from PWLE was discussed as key for understanding how people negotiated loneliness and discovering what people valued from loneliness support. This greater understanding could lead to the co-design and development of new activities or adaptations to existing support.
Local staff talked in terms of population groups or characteristics. Most commented that the focus of loneliness support was on older people, echoing the research literature and our interview study findings, with older people’s loneliness prompted by situations common in their life stage, such as bereavement, living alone and loss of independence. Participants were aware of other population groups experiencing loneliness, including younger people, people with poor physical health, people with mental health issues, people from minority ethnic groups and people living in poverty. Staff recognised that younger people experiencing loneliness received less attention and were often less visible owing to the associated stigma of being ‘a bit of a loser’ or being pitied for having no friends. Staff also spoke about people from minority ethnic communities feeling disconnected from their local community, for example due to language barriers, or feeling undervalued because of their cultural identity.
Participants commented on how loneliness could be interwoven with changes in life circumstances such as loss of employment, marital breakdown, retirement or taking on a new role such as that of an unpaid carer. Also highlighted were situations such as domestic abuse, which might necessitate people moving away from their local area, and substance misuse resulting in family members breaking off ties.
There was acknowledgement that anyone could experience loneliness. Some staff talked about their own experiences, or those of people close to them, as available to draw upon when crafting and delivering support. COVID-19 was highlighted as having increased awareness of loneliness and what it can feel like. However, staff also spoke about loneliness as nuanced. For example, some people may not be aware that they were experiencing loneliness because they had lived that way for so long that it had become the norm. Similarly, people who may appear to be sociable, with many connections with family or friends, could also feel lonely if lacking the special relationships they want.
‘Hallmarks’ of good loneliness support
For the purposes of prompting discussion in the co-design workshop, ‘hallmarks’ of good support were identified from the analysis.
A key hallmark was identifying people in the community who are lonely. Doncaster participants discussed including attention to loneliness as part of their Making Every Contact Count (MECC) approach. MECC encourages staff who have routine interactions with people in the community to initiate conversations related to how they might improve their health or well-being. 107
Related to MECC, participants stressed the importance of looking at a person’s situation holistically when they presented to staff for something other than loneliness, and finding out whether and what they wanted to change. Key to this work was having time to develop trusted relationships that could support people to help themselves.
A further hallmark of good support was the personalised matching of support with the person’s needs. Local staff said they felt inspired by the range and volume of loneliness support on offer in Doncaster; however, it could be challenging to be aware of everything and to keep information up to date, despite a locality model in which staff had strong contacts with communities.
Physical accessibility of activities or groups was another hallmark. The affordability of public transport, and for some people their willingness or ease of using it, could act as a key barrier.
Accessibility was also considered in terms of the lack of confidence people had to access groups and the support needed to improve this. Participants were proud of their in-depth knowledge of the activities available, sometimes attending new activities themselves to offer people a good match with their interests. Having first-hand experience of an activity/group meant they could answer people’s questions, so they could feel more confident about trying something out. A related issue was the value of offering graduated support, more intense initially (e.g. accompanying someone to their first session of a new activity) then tapering as the person gained confidence. Staff felt that better connections between different providers of loneliness support would enable their different offers to be used in a joined-up, stepwise manner as people’s confidence grew.
In turn, staff felt a further hallmark of good support was its function as a conduit to help people make their own meaningful and authentic relationships. Local staff were pleased with the way support services and activities actively engineered these initial opportunities for social contact which facilitated people to find and grow their own meaningful connections. In carrying out this work, staff pointed out the importance of recognising that some people might only want limited contact with others.
Findings from the national staff interviews
The national interviews contained considerable overlap with the local interviews, and here we present the additional insights offered. Participants mentioned:
-
The challenges around balancing the right to privacy with the identification of people as potentially lonely so that interventions might be offered to improve their well-being.
-
The importance of shared goals across multidisciplinary teams. There were examples of common goals and evaluation methods across geographical areas, encompassing statutory and non-statutory sectors working towards a common measurement and understanding of successful loneliness support.
-
Having a local champion to keep loneliness support at the top of the local agenda.
-
Considerations around loneliness support group size and longevity, and the importance of having suitable exit plans.
-
Stigma was raised in two ways: association with attending groups badged as addressing loneliness; and association with some of the areas/venues where activities took place. This raised questions about how best to describe and promote uptake of these local activities if not as loneliness support.
Conclusion
This part of the study was effective in generating knowledge about the local loneliness offer in Doncaster and in raising the profile of the co-design work. The national interview data demonstrated considerable overlap with the local interviews, suggesting that the findings of the co-design phase will have relevance beyond Doncaster.
Chapter 5 Co-design phase methods
Introduction
Accelerated experience-based co-design is an accelerated version of EBCD, an approach to co-designing healthcare quality improvements, which draws on both co-production and design science. The EBCD process has two sequential phases: discovery and co-design. The discovery phase (see Chapters 2–4) created two key outputs for use in the co-design phase: a catalyst film of themed excerpts from interviews with PWLE of loneliness support; and a themed summary of interviews with staff who offer support. While in this report we use the shorthand ‘PWLE’ to refer to people drawing on loneliness support, we also acknowledge that staff who offer such support may also have lived experience of loneliness.
Aim and objective
Aim
To assess whether an effective and efficient co-design approach, AEBCD, can be translated from health to social care.
Objective
To explore, with one local authority, whether an approach to service improvement, known to be effective in health care, could be adapted for use in social care.
Methods
The co-design phase comprised a local intervention (adapted AEBCD) with a parallel process evaluation led by the University of York research team, using loneliness support as an exemplar for how AEBCD could be adapted and transferred to a social care setting. The intervention and evaluation components are described separately below. The research study funded intervention costs of venue hire, refreshments, travel expenses for all participants and vouchers (£20) for PWLE/unpaid staff participants for each co-design event/meeting and an evaluation interview. Not funded by the research study was the time of the local staff who led and supported the intervention, principally the Project Lead and Co-design Supporter (more on these roles below).
The intervention: adapted accelerated experience-based co-design
The adapted AEBCD intervention was carried out in Doncaster, where the local authority had identified loneliness support as a priority and commissioned the creation of the Alliance of VCF support providers. Doncaster Council’s Public Health Lead for Working Age and Healthy Lives was the designated ‘Project Lead’ responsible overall for delivery of the intervention. She worked closely with the Alliance’s Programme Manager, who provided a range of day-to-day support for the local co-design process, including initial recruitment of staff and PWLE, a role described in this report as ‘Co-design Supporter’.
Preparatory work
Preparation for the co-design began during the discovery phase. The Project Lead and Co-design Supporter met regularly to develop and progress a local plan for the co-design intervention, supported by the evaluator (Maddison). The work initially focused on familiarisation with the EBCD approach and how its accelerated version had been used in the NHS, along with any limits on adaptations. Two main sources were used: first, the online EBCD Toolkit108 hosted by the Point of Care Foundation, which provided practical information and advice from people involved in using the approach; and second, co-investigator Locock and a healthcare professional experienced in using AEBCD hosted an open question-and-answer session for the Project Lead, Co-design Supporter, and evaluator.
Two features of the AEBCD process were identified as distinctive and essential for replication of the approach: use of a catalyst film and of the co-design small group work. Other aspects, for example the number and content of workshops, were open to local adaptation.
The next stage involved agreeing the respective roles of Project Lead, Co-design Supporter, and evaluator, and planning the practical elements and sequencing of the intervention to fit within the timescale for completing the evaluation and overall research study. During this period, the Project Lead and Co-design Supporter also raised awareness about the co-design intervention within their respective council and VCF local networks.
Recruitment
A total of 26 people took part in one or more elements of the intervention: 20 staff (15 paid; 5 volunteers) and 6 PWLE.
PWLE were recruited via participating staff. This strategy had two key benefits. First, staff already had some knowledge about the co-design intervention, which was helpful when approaching people they supported. Second, staff represented a wide range of participating organisations with potential for recruiting people with experience drawn from different loneliness support. During the co-design work, we learnt that the six PWLE recruited varied in age from 18 to 84 years. Five were female, one male, and all were white. Three people described themselves as disabled. Two people mentioned having current caring responsibilities; another person had cared for their spouse for several years before their death and lost their own social network during this time. One person talked about feeling anxious in social situations; another said they were sometimes affected by social phobia. At the time of the study, types of loneliness support PWLE participants were accessing included community arts activities, theatre projects, membership of a carer group, membership of an Age UK project, and Chair of the Board of Trustees for a small VCF organisation. One person interested in accessing more support spoke about barriers to accessing information posed by having dyslexia and not using computers.
Staff were recruited from two main routes: first, as in previous AEBCD studies, via taking part in a local discovery phase interview; and second, the Co-design Supporter approached member organisations of the Alliance that supported people in communities not yet represented, for example LGBTQ+ and asylum seekers. An attempt by the Project Lead to recruit Doncaster Council social services staff was unsuccessful, owing to severe COVID-19-related workload pressures. The council’s well-being team was represented initially by a manager who later moved to another council and was replaced in the co-design by a team leader colleague.
Volunteers were initially recruited as PWLE. This recruitment strategy was suggested by organisations helping with recruitment who knew that some people’s experiences of loneliness had prompted them to become volunteers. Therefore, in the first, workshop stage of the co-design (see Steps in the co-design intervention), volunteers attended the workshop for PWLE, sharing their experiences of loneliness and the personal value gained from volunteering, including how it helped counter feelings of loneliness. However, in the later co-design group work, in which staff and PWLE worked together, volunteers tended to contribute from their perspective as unpaid staff who offered loneliness support, rather than as PWLE. While lived experience of loneliness and support is potentially universal, to avoid the study overstating the number of people participating primarily from a PWLE perspective, volunteers were recategorised as staff participants.
The Doncaster team did not formally collect participant characteristics as part of the co-design work. However, during events and meetings, considerable diversity among staff characteristics was revealed (as outlined above), including gender, ethnicity, disability, mental health and asylum-seeker status.
Steps in the co-design intervention
Overview
The intervention in Doncaster followed the two-stage AEBCD process of a series of workshops followed by small group co-design work. The first stage involved three workshops: one workshop for staff and one for PWLE; and a third, joint workshop that brought staff and PWLE together to agree priority areas for improving local loneliness support to be worked on in the second stage of the process. In this stage, smaller co-design groups (comprising both staff and PWLE) focused on one priority area each to co-design suggestions for improvements. A celebration event was held at the end of the intervention phase.
Figure 2 shows a flow chart of the AEBCD process in Doncaster with the timings of events.
FIGURE 2.
Flow chart of the AEBCD process in Doncaster.

An external, professional facilitator, expert in social care co-design approaches, facilitated the workshops. The facilitator worked closely with the Project Lead and Co-design Supporter, assisted by the evaluator, to plan the content and format of the three half-day workshops. While there was uncertainty about whether COVID-19 rules would permit in-person workshops (and a REC amendment was secured to permit remote workshops), in the end, all three workshops took place as in-person events. See Report Supplementary Material 3 for an example agenda (joint workshop).
Staff workshop
The staff workshop was held in November 2021. Nine people took part: seven from VCF organisations, one from a housing association, and one from a private sector home care provider. Seven participants were interviewed in the discovery phase. Following the AEBCD process, the catalyst film was not shown in this workshop, to give the opportunity for staff to first consider their understanding of loneliness and share related support issues from their provider perspective. To help prepare participants to build a broad coalition around improving loneliness support and generate a list of priority areas for improvement, the Project Lead spoke at the workshop about the history of local loneliness support in Doncaster and how it became a local priority. The evaluator presented a thematic summary of the findings from the local discovery phase staff interviews, which prompted discussion around staff understanding of loneliness, hallmarks of good local support and potential areas for improvement. The remainder of the workshop involved staff thinking individually about ideas for improving support, then sharing these ideas in small groups and finally agreeing between groups an overall ‘top five’ improvement list (not ranked):
-
Information – to improve information about loneliness support and services available and connect partner organisations
-
Group activities – to develop more tailored activities to better reflect diversity in the local population, for example specific groups for people from ethnic minority communities
-
One-to-one support – to improve this offer for people needing support to access group activities
-
Transport – to improve this and other practical barriers to accessing loneliness support, especially for people on low incomes
-
Extending the ‘Circles’ model of support – currently in place locally for older people but seen as having potential to expand to other people experiencing loneliness (a circle of support is a group of family, friends and supportive workers who come together to give support and friendship to a person)
People with lived experience workshop
The PWLE workshop was held in January 2022. Seven people took part, two of whom were also volunteer providers of support. The aim was to bring together PWLE to generate and prioritise ideas for improving loneliness support to share with staff in the third, joint workshop. The Co-design Supporter also shared information about Doncaster’s Alliance of 50+ VCF organisations offering loneliness support.
The workshop began with participants sharing their experiences and feelings around loneliness. They then viewed the catalyst film developed during the discovery phase (see Chapter 2). The film was used to prompt discussion around what constituted good and less good practice in loneliness support. Then, mirroring the staff workshop, participants spent time thinking individually about their ideas for improving support, then sharing these ideas with other participants, finally agreeing an overall ‘top five’ of improvement priorities. A live scribe created a visual representation of the workshop discussions (Figure 3).
FIGURE 3.
Live scribe representation of the PWLE workshop discussion. Reproduced with permission from Stephen Lee Hodgkins.

The top five improvement priorities were summarised by the facilitator (not ranked):
-
Information – better information about ‘what’s out there’ in Doncaster for people experiencing loneliness.
-
Groups – providing more groups for people to attend where they can meet other people, share experiences, support each other, and get involved in fun and meaningful activities such as cooking, walking, drama, sports, singing and being with animals.
-
One-to-one help and support – it can be difficult to come to a group for the first time, so people may need support to do so. Everyone needs help of some kind. People want a chance to receive help and help others.
-
Transport – the costs of transport and the need for assistance because of disability, mental health issues or long-term health conditions can create obstacles around public transport.
-
Attention to other barriers – it is important that people are treated fairly and not excluded from getting involved in groups or activities. This means paying attention to the various aspects which can make it hard for people to get involved, such as disability, mental health issues, age, race, gender, sexuality and not having English as their first language.
Members of the group volunteered to recap the main points on each topic in the third workshop. To help members prepare, the facilitator circulated a summary of the conversation on each topic.
Joint workshop
The joint workshop was held in February 2022, bringing together staff and PWLE for the first time. Thirteen people took part: six staff and seven PWLE (three of whom were also volunteer providers of support). Eight people had attended a previous workshop: four staff and four PWLE (including one person who was also a volunteer provider). The workshop aims were for staff and PWLE to build a coalition around improving loneliness support, to agree joint improvement priorities and to form smaller co-design groups to take these priorities forward to develop more practical steps.
Participants first shared their reasons for wanting to come together and carried out a practical group task designed to prompt discussion around co-production principles. The catalyst film was then shown – the first time staff had seen it – followed by an open discussion on issues raised by its content. Staff felt the themes in the film resonated with their own work, the main area they discussed being differing views on the extent to which it was appropriate for staff to share aspects of their personal selves to people drawing on their support. This discussion was prompted by a clip in the film in which a person cited this sharing from staff as a valued aspect of support.
Staff and PWLE then shared the five improvement priorities identified at their respective workshops, four of which were revealed as common to both: information, transport, groups and one-to-one support. The fifth priority identified by staff – to extend the Circles model of support – was left aside, since it was known that work was already under way on this topic. The fifth priority identified in the PWLE workshop – attention to other barriers – was also left aside after the agreement that attention to diversity and inclusivity should underpin all improvement suggestions.
With the focus on the four common priorities, participants first decided that they had capacity to create two co-design groups. After a facilitated process involving general discussion and a ranking exercise, it was decided to leave aside the ‘information’ priority. Although information is crucial to finding support, Doncaster Council was known to be repopulating its website information on all local activities post COVID-19 and it was thought more appropriate to review information once that initial work had been completed. The ‘transport’ improvement priority was selected for one co-design group and ‘support’ for the other (covering both group activities and one-to-one support to engage in groups). Before leaving the workshop, participants volunteered to take part in one or other of these co-design groups. A live scribe attended virtually and created a visual representation of the workshop discussions (Figure 4).
FIGURE 4.
Live scribe representation of the joint workshop discussion. Reproduced with permission from Stephen Lee Hodgkins.
Co-design groups
Both the Transport and Support groups held seven 2-hour monthly meetings between March and October 2022, working up improvement ideas for practical implementation. Seventeen people took part in this stage. A few participants withdrew during the 7 months, for personal reasons. Thirteen people remained in the groups throughout (six in one group, seven in the other). Both groups had two PWLE members; other participants were paid and unpaid staff.
Each group had a ‘coordinator’, a role volunteered for by a group member and which was designed to facilitate group discussions, note key meeting points and actions (in a meeting log) and maintain the group’s momentum. The Co-design Supporter role in this part of the process was to support the groups, primarily by carrying out associated practical tasks (agreeing meeting dates, arranging venues, booking refreshments, and administering travel expenses and vouchers for eligible participants) but also being open to supporting the groups in other ways that might emerge as needed during the process (including nurturing individual involvement), given this new and different way of working.
Celebration event
At the end of the period set aside for the co-design small group work, an in-person half-day celebration event was held in October 2022. Although common in previous AEBCD work, this event was not included in the original study proposal. The Project Lead, Co-design Supporter and evaluator discussed the potential value of a celebration event. Three areas were identified: (1) to bring participants back together to share and celebrate their work; (2) to consider what might happen locally to take forward and build on what the process had achieved; and (3) to reflect on the experience of using the AEBCD process.
The workshop facilitator collaborated with the Project Lead, Co-Design Supporter and evaluator on the planning and agenda. Seven participants attended: three PWLE and four staff (of whom two were in paid roles and two unpaid). Other attendees were from Doncaster Council, the Project Lead and two public health colleagues; the Co-design Supporter; the Alliance lead; principal investigator (PI) and evaluator.
A live scribe created a visual representation of the event discussions (Figure 5).
FIGURE 5.
Live scribe representation of the celebration event discussion. (Image drawn by Cara Holland of Graphic Change). Reproduced with permission.

Evaluation
Design
The process evaluation was guided by the following study research questions:
-
What kinds of improvements did the co-design groups complete?
-
Was the process acceptable to staff and PWLE?
-
What suggestions might they have for improving the process?
-
What adaptations might be needed for future use in social care?
A range of data sources was used: ethnographic observation; questionnaires; individual and group interviews; evaluator notes of in-person meetings; and e-mail conversations with the Doncaster Project Lead and Co-design Supporter throughout the intervention.
Evaluation participants, ethics and consent
Research ethics approval for the co-design evaluation was obtained as part of the approval for the wider project (see Chapter 2). Staff who had consented to an earlier discovery phase interview were consented separately for the co-design evaluation. All staff and PWLE were given a participant information sheet explaining the steps of the intervention and the accompanying evaluation. All participants gave consent to be observed and interviewed.
Data collection
Data collection took place between November 2021 and November 2022. Table 4 shows the evaluation data collection methods and participants involved in each.
| Evaluator observation | Questionnaire | Interview | |
|---|---|---|---|
| PWLE | PWLE workshop Joint workshop Co-design meetings Celebration event |
PWLE workshop evaluation form Joint workshop evaluation form Whole process evaluation form (completed on or after celebration event) |
Exit interview (group) |
| Staff (paid and unpaid) | Staff workshop Joint workshop Co-design meetings Celebration event |
Staff workshop evaluation form Joint workshop evaluation form Whole process evaluation form (completed on or after celebration event) |
Exit interview (individual) |
| Doncaster project team: (Project Lead and Co-design Supporter) |
Co-design meetings (Co-design Supporter) | N/A | Interim interview (joint) after workshop stage Exit interview (group – joined by colleague of Project Lead) |
| Workshop facilitator | All three workshops | N/A | Individual |
Observations of workshops, co-design group meetings and the celebration event totalled 46 hours. These events were not audio-recorded in case recording inhibited participants from speaking freely. The evaluator made field notes.
An evaluation form was completed at the end of each workshop. A total of 24 forms were completed from 29 participants (6 people needed to leave the workshop early). Whole-process evaluation forms were completed by 9 of 14 participants (all 13 participants who remained in the co-design groups at the end of the study were asked to complete a form, along with another participant who had attended only early meetings but had not formally withdrawn).
Template questionnaires are in Report Supplementary Materials 4 and 5.
A total of 11 exit evaluation interviews were carried out with 14 people. Eight of these interviews were with study participants: seven individual staff interviews and one group interview with three PWLE. A template topic guide for participant interviews can be found in Report Supplementary Material 6. The remaining three interviews comprised one with the workshop facilitator and two joint interviews (one interim, one exit) with the Project Lead and Co-design Supporter. In the latter’s exit interview, they were joined by a colleague in the Project Lead’s public health team, who had attended several co-design group meetings to identify potential links into local public health work.
Interviews were audio-recorded and either transcribed in full or, for shorter interviews, summarised from the recordings. Questionnaire feedback was entered verbatim into a spreadsheet. Observations and brief conversations were recorded as field notes. The evaluator kept an ongoing note of issues arising throughout the intervention relevant to the transfer of AEBCD from health care to this new social care setting.
Notes of meetings with the Doncaster project team were taken by the evaluator and shared with the Project Lead and Co-design Supporter. All team e-mail correspondence was saved for the evaluation. Other data supporting the evaluation included photographs of flipcharts from the workshop priority-setting activities and co-design group work and the live scribe drawings capturing discussion in two workshops and the celebration event.
The evaluator also kept a reflective diary on maintaining the boundaries of their role, which covered reasons for occasional active involvement in the management intervention itself and their impact. Locock was on hand throughout for general advice on how the role had been handled in previous AEBCD studies.
Analysis
The data were analysed thematically, drawing on a framework approach,109 a widely used iterative approach to qualitative data analysis, particularly suited to applied research. Analysis was guided by the four overarching evaluation questions.
The first stage of analysis involved familiarisation with the data in Table 4. Each item was read to identify relevant issues and concepts, enabling a framework to be built of potential themes for interpreting the findings under each question. Relevant data were then summarised for visual display in a (spreadsheet) chart. The chart column headings related to each evaluation question with its themes. Each row was a data source item (e.g. an interview transcript), with summarised material entered into cells under the appropriate evaluation question columns. Cell entries included notation for easy reference back to the fuller source material. Reading down the chart columns therefore displayed visually a summary of the data under each evaluation question. Reading across the rows displayed the full summarised account for a data source item such as an interview transcript. Observation field notes and other material available to the evaluator (e.g. notes of Doncaster team meetings) were included for data triangulation and further interpretation of the data. Having the chart enabled the evaluator to view an initial full summary of the data and then move back and forth between the summary and its source material to develop and refine themes. The analysis process was supported by ongoing sense-checking dialogue with the Doncaster project team and research team members, and discussions with the project advisory panel and SSC.
Chapter 6 Co-design phase findings
Results
The co-design work in Doncaster sought to explore whether the AEBCD approach to service improvement could be adapted for use in a social care setting, using loneliness support as an exemplar.
This section presents implications of the change in setting from the NHS to social care loneliness support for the set-up and operation of the co-design groups, followed by additional sections covering findings for each of the four questions that guided the evaluation.
Implications of the change in setting for the set-up and operation of co-design groups
Unlike the use of AEBCD in NHS organisations, where staff and patients are drawn from a single ‘host’ service/organisation, the Doncaster co-design work was undertaken by staff and PWLE involved in varied types of loneliness support offered by a range of (predominantly VCF) organisations in the local community. This had implications for the set-up and operation of the co-design group work.
The main implication was that the co-design groups had a broad remit to work across as many or as few organisations and/or areas of support as necessary.
A second implication of working across multiple services and organisations was anticipation that routes to implementation of co-designed solutions would be longer and more complex than for comparable work within single organisations. The timescale for the small group work (7 months: March–September 2022) was defined by the evaluation period. Groups were free to decide on area(s) of focus, asked only to be in a position at the end of the evaluation period to describe their proposals or make recommendations in sufficient detail to be taken forward locally.
Third, the appointment of co-design group facilitators was also complicated by the number of organisations involved. In NHS AEBCD work, there is the option to draw on in-house staff from the ‘host’ organisation to facilitate the groups. In the current study, without a single ‘host’, the model of seeking a volunteer from each group as its Co-ordinator was used.
For both groups, a staff member volunteered for this role. In one group (Transport), the Co-ordinator ran a voluntary organisation, a role which brought valuable experience and skills, including consensus-seeking and ensuring all voices were heard. In the Support group, settling on a Co-ordinator proved more difficult. The role was initially taken by a staff member skilled in one-to-one listening and sourcing support. At the end of the first meeting, another staff member, experienced in PAR methods, offered to work alongside the Co-ordinator in a support role, for example recording key points as discussions flowed. However, for personal reasons, the original Co-ordinator withdrew from the group, after which two other staff members agreed to rotate the Co-ordinator function flexibly, according to who was able to attend. The member who had taken on the support role continued throughout, although was unable to attend all sessions. When present, their support in helping to facilitate and noting key discussion points on a flipchart to retain for subsequent meetings proved invaluable, both for giving members visual recall and for encouraging momentum to move on from discussion to identifying action points.
Asking the Co-ordinators to complete meeting logs proved unsuccessful owing to capacity pressures and no protected time being available for this task. As a result, co-design group meetings began to lose efficiency, each needing to begin with recall/recap of the previous meeting, and actions promised between meetings being forgotten. In response to this problem, the Co-design Supporter gradually extended her role. She took notes in each meeting, e-mailing participants a summary of key points discussed and any actions agreed. She reshared the e-mail with members before the next meeting as a reminder and contacted Co-ordinators to help shape a plan for the session. This liaison proved more challenging for the Co-design Supporter in the case of the Support group, given their arrangement for two rotating Co-ordinators. The evaluator, who attended all co-design meetings, took meeting notes as a safety net for the Co-design Supporter.
Question 1: what kinds of improvements did the co-design groups make?
This section describes how each co-design group decided on the main support improvements they wanted to influence and what they did.
Transport group
Main focus of improvement activities
At meeting 1, the Co-ordinator acknowledged the breadth of the chosen topic and potential limits of the co-design group to directly influence transport services. Members shared their reasons for interest in this topic, the ensuing discussions scoping three potential areas for improvement: buses, community transport and taxi travel.
The group decided to focus on taxi travel because both PWLE and staff felt that although taxis were the preferred form of transport for some people (such as people who used a wheelchair or people with dementia), taxi travel could be a potentially unsafe experience, for example when drivers appeared reluctant to take wheelchairs or refused a certified assistance dog. People were unsure which drivers would be reliable and responsive to their needs. During the meeting, the idea was suggested of developing a recognised ‘gold standard’ for taxi drivers regarding customers made vulnerable in this way. Group members were keen to take this forward.
At the second meeting, the group started to scope how a gold standard for taxi drivers might work. They envisaged it as an optional scheme, with the gold standard awarded when a taxi driver completed additional training around working with ‘vulnerable’ customers. On completion, drivers would display a ‘gold standard’ badge in their taxi which would serve as a marker of reliability. When booking taxis, the group envisaged customers being able to enquire about the availability of drivers with the gold standard. Before developing the idea in more detail, the group decided to explore their proposal with Doncaster Council’s taxi licensing officer, who was invited to their next meeting.
The Co-design Supporter sent the taxi licensing officer a summary of the outline idea. He attended the meeting virtually and responded positively. He envisaged the gold standard as a potentially valuable counterpoint to his own role, seeing it as a positive/aspirational ‘carrot’ to encourage good driver practice rather than relying solely on the regulatory licensing role of a ‘stick’ to address poor driver practices. Should the group wish to seek views from drivers at any point, the licensing officer volunteered to circulate requests, and/or set up ‘Survey Monkey’ feedback via a regular newsletter he sent to all drivers. He envisaged potential spread of a gold standard beyond Doncaster to neighbouring local authorities through his membership of a South Yorkshire network of licensing officers. The network sought to maintain consistent policies and practices across the county and was a forum for sharing ideas. The positive reception from the licensing officer encouraged the group, and members committed to working up more detailed content for a draft gold standard.
To help understand the scope of relevant existing taxi driver training, the group Co-ordinator and Co-design Supporter attended a routine taxi driver safeguarding training day. This helped them to understand and report back to the group, the drivers’ perspective, and to gain an appreciation of the wide range of issues around which drivers were expected to be aware in relation to safeguarding. Group members continued to flesh out details in their meetings, becoming increasingly aware that operating such a scheme would require a host organisation and funding. They acknowledged that both were unlikely to be achieved within the evaluation time frame.
At the final meeting, the group agreed the Co-ordinator and Co-design Supporter would make an application for Motability funding to continue developing the initiative. A follow-up meeting was arranged with the taxi licensing officer for December 2022, after the formal end of the intervention and evaluation period. At that meeting it was agreed that a wider group would be set up (potentially involving members of the Transport co-design group) to develop a funding bid for submission in March 2023.
Short-term legacies
In addition to the main work developing the gold standard, the Transport co-design group initiated other improvement actions regarding taxi transport:
-
Improving information about new statutory guidance on access to taxis and private hire vehicles for disabled users – group members were initially unaware of this new guidance (issued June 2022) which dovetailed with their work. They thought many disabled people who used taxis might be unaware of this strengthening of their rights, which might help people feel more confident about challenging unsafe practices, for example insufficient securing of wheelchairs. The Co-ordinator approached the local Citizens Advice Bureau who agreed to run an information campaign about this new guidance.
-
Improving information about taxi complaints procedure – at the group meeting attended by the taxi licensing officer, he commented that while people complained about poor taxi services on social media, there were few formal complaints to the licensing team, meaning action could not be taken. He explained that, had a formal complaint been made about the group’s example of a taxi driver refusing a certified assistance dog, the driver’s licence would have been revoked since no taxi driver in Doncaster currently had the medical exemption required for such a refusal. Group members were surprised to learn that the formal taxi complaints process route was via the local authority, having assumed a customer would need to make a complaint to the taxi company. The taxi licensing officer agreed to investigate making the complaints process clear on Doncaster Council’s website, along with the taxi licensing e-mail address for complaints which was at that time (unintentionally) ‘buried’ within the site.
-
Participation in related research – when exploring potential funding opportunities for the gold standard, the Co-ordinator noticed that a national organisation supporting independent living (Leonard Cheshire) was researching disabled people’s experiences of using taxis. The Co-design Supporter contacted the study team, who invited her and the Co-ordinator to take part in a joint interview for their study, findings from which were launched in the House of Commons in January 2023. 110
Longer-term legacies
The Transport co-design group’s work included the following potential for longer-term legacies:
-
The Alliance has included the group’s work in its draft strategy to be taken forward with its members and Doncaster Council.
-
The Doncaster Project Lead is taking forward work on potential connections with other Doncaster Council agendas, in particular, the Disability-friendly and Age-friendly agendas. Transport is already a named domain in the Age-friendly agenda. Group members hoped Doncaster’s acquisition of city status during the co-design period might help push forward the take-up of transport issues within these agendas, owing to some local cities having done more sustained work on loneliness and transport.
-
Group members expressed interest in continuing their contribution in some form, whether as a standing Transport group member, or as part of a wider group of interest on this topic. In making this suggestion, members were mindful that in focusing on taxi provision, they had left aside community transport and bus travel issues which would also likely benefit from co-designed improvements.
-
The group’s Co-ordinator was approached about taking part in a further transport-related research project.
Support group
Main focus of improvement activities
The group’s initial sphere of interest spanned two priorities for improvement: (1) group activities for loneliness support; and (2) one-to-one support to help people access groups or otherwise become involved in their community.
After discussion in the first meeting, the strongest concern to emerge was that some people who formerly used loneliness support had become more socially isolated during the pandemic and appeared reluctant to re-engage. This issue was initially raised by staff in the group, but PWLE members concurred, being aware of people in this situation. Staff members explained that although they were offering face-to-face loneliness support activities again, they had limited capacity to work in depth with people who were not re-engaging.
The group agreed to focus, at least initially, on how to fill this perceived gap in one-to-one outreach to help people re-engage with loneliness support. Some members expressed their desire to also leave time for the second priority, the provision of group activities, thought particularly important for underserved groups.
The group drafted a pilot one-to-one outreach support model which comprised six chronological steps: (1) identifying the person’s barriers to taking up support; (2) identifying their interests; (3) identifying appropriate provision; (4) connecting to transport if needed; (5) initial accompanied support to attend; and (6) follow-up to identify with the person what worked or did not work (for the person and for the pilot). The sixth step meant that the model could be used as a cycle, moving on to repeat steps if necessary. The model was represented in diagram form on a flipchart which the group referred to in later meetings.
The group then became uncertain about how to proceed, for three reasons: they lacked the capacity or funds to trial the model; they had no obvious route to recommend its uptake for trialling by others; and they felt unsure about the extent to which the model might overlap with existing ways of one-to-one working by other community-based staff such as social prescribers and community connectors.
Similar to the breakthrough the Transport group had when they met the taxi licensing officer, the Support group had a breakthrough when a Doncaster Council staff member was replaced by a colleague who led a community-based team supporting people to find ways to improve their well-being, including tackling loneliness. This new member saw immediate potential for working with the group’s ideas, which helped members situate their model more firmly in the VCF sector, distinguishing it from council-led work and from social prescribing. The latter also had the disadvantage of being accessible only via general practitioners, when not everyone who was lonely would necessarily disclose this.
In the final meeting, members decided to target the model for use with ‘trusted organisations’, meaning VCF organisations (such as those represented in the group) which people struggling to re-engage with loneliness support had previously used. The well-being team leader was not able to attend this final meeting, but since their own team focused on well-being support, the group’s proposal was that members of the well-being team could pilot spending time in VCF ‘trusted organisations’ using the model. Staff from these organisations could identify people at risk of disengaging from, or struggling to re-engage with, their support. Crucially, being already known to these people, staff felt they would respond to their personal request to visit the organisation’s familiar surroundings for a conversation with a well-being team member. The team member would then assist the person to re-engage with the original support or access other loneliness support offers.
The Co-design Supporter volunteered to discuss this proposal with the well-being team leader. If well-being teams could not help, the group agreed that VCF trusted organisations would apply for funding, supported by the Alliance, for a shared post to create capacity for someone to spend dedicated time in several organisations using the model to encourage known individuals back into loneliness support. In December 2022, after the close of the study, the Co-Design Supporter met with the new lead of the Alliance, who agreed the Alliance would take forward/oversee the next work stage, focusing on the group’s suggestions and identifying any feasible alternatives.
Short-term legacies
In addition to the main work developing the one-to-one outreach model, members of the support co-design group initiated individual action points:
-
One staff member began using co-design principles and experiences from the group to inform their humanitarian work around well-being.
-
One staff member planned to use the one-to-one outreach model with individuals they supported.
-
Members of the group spoke about being better informed about local loneliness support as a result of their discussions, and one PWLE member felt ready to take part in more community activities.
-
The Co-design Supporter helped this PWLE to complete an online well-being team referral form and the person was visited soon after by a well-being team member.
Longer-term legacies
Longer-term legacies focused on staff potential for building on the discussions and contacts forged in the group around members’ shared interests in loneliness support. For example:
-
The Doncaster Council staff member was keen to strengthen links with the Alliance to improve the two-way flow of information and potential for collaboration.
-
Staff members identified others in the group for potential collaboration around further topics. For example, the Support group’s second priority is to consider group activities in the community, particularly with regard to diversity. This work had not been tackled owing to the time constraint of the evaluation.
-
The Alliance has included the group’s work in its draft strategy, to be taken forward with its members and Doncaster Council.
Question 2: was the accelerated experience-based co-design process acceptable to staff and people with experience of loneliness support?
A key focus of the evaluation was whether the AEBCD approach was acceptable in social care, in this case to the community setting of loneliness support. Overall, the AEBCD process as evaluated in the community setting of loneliness support in Doncaster was experienced positively and considered by participants as worthwhile.
Acceptability to staff
Staff workshop
Staff involved in providing loneliness support in Doncaster first came together in the staff workshop. When asked for feedback on the event, the participants, workshop facilitator and Doncaster project team commented on the lively atmosphere. Owing to COVID-19 restrictions, the workshop was the first in-person work event people had attended for some time, which attendees said added to their sense of energy and enthusiasm.
Overall, staff feedback was positive and focused on three areas: the opportunity to connect with others whose work included loneliness support; the useful ideas generated by the discussion; and the prospect of carrying ideas forward into co-design group work.
Staff attended from a range of organisations and clearly valued the workshop to ‘connect’ around their shared interest in improving loneliness support. Attendees also commented on the workshop being an opportunity to have ‘an important conversation’ and saw the project as an early, tangible piece of work for members of the Alliance to collaborate on:
. . . it felt good to be able to meet colleagues from other organisations who have shared goals.
. . . like-minded people coming together all understanding each other’s issues – feels really positive.
. . . seeing the passion everyone has.
Staff talked about learning about other loneliness support offered locally. One person noted the workshop’s value for front-line staff like herself, since usually only managers were members of networks for exchanging information and ideas. The same person commented on the value of the facilitator, who created an atmosphere of openness in which attendees felt safe from the start to say what they really thought, rather than feeling wary of what staff in other organisations might think of their views.
Discussions at the staff workshop were reported as ‘focused’ and ‘positive’, yielding useful improvement ideas:
. . . some really good ideas and priorities . . .
. . . lots of ideas for moving forward.
Staff also valued the workshop because it was the start of a process. Staff said they were looking forward to co-design group work with people who used loneliness support; they were ‘interested to hear their thoughts and ideas’ and expected the process would help staff ‘to understand more about loneliness’. One person reported feeling nervous about the prospect, saying, ‘I don’t want to offend or seem “top down”’.
Despite the positive atmosphere, one attendee was cautious about whether and how any proposed improvements would be taken forward, given that VCF organisations were the main providers:
It’s early days . . . We think the issues are important but need recognition of it from funders/public sector – not individual funding bids that don’t join up collectively!
Nonetheless, staff thought a co-design process might be a way ‘to move forward in partnership working’ and felt the process ‘may yield some long-term results’.
Joint workshop
After this workshop, in which staff and PWLE worked together, staff noted in their feedback how enjoyable the event had been, appreciating it for giving them ‘a real insight’ into different experiences and perspectives among staff and people with experience of loneliness and support. They reported ‘recognising so many shared experiences and priorities’ and feeling ‘energised’ about the prospect of taking forward priorities into the co-design group work:
It was nice to hear about similar themes from different communities.
I hope that what we share can make some changes in meeting needs of those who are lonely. Would like to talk more, so meetings for future groups are a good idea.
One staff member also identified opportunities at the workshop to collaborate with staff from other organisations.
Staff viewed the catalyst film for the first time in this workshop. They commented that the film had been valuable in three main ways: for hearing about further lived experiences of loneliness and related support; for resonance with their own work; and for its relevance to the improvement priorities under local consideration for the co-design groups:
I found it engaging, thought-provoking and valuable to hear people’s unique experiences.
As mentioned in Chapter 5, the film prompted discussion about where staff draw professional/personal boundaries in terms of sharing personal experiences. For one staff attendee, any sharing risked leading to ‘client dependency’, whereas other staff saw decisions around sharing as more nuanced, part of their professional judgement, since some sharing could be valuable for rapport and authenticity in supporting people. The person who had focused on ‘dependency’ later commented that they could see the validity of this alternative view.
Staff reported being surprised at the joint workshop to discover the strong overlap in improvement priorities identified by staff and PWLE in the two earlier workshops. However, reflecting on working as a whole group to select final joint priorities, two people reported tensions between the group approach and their own perspective:
[The process was] good, but as there are so many organisations we all come from a very different angle . . . [for me] the outcomes are really what we already have, ‘groups’ all over – I run four a week already.
I felt it difficult to separate the priorities between those I knew we could support as an organisation and the priorities identified by the group. I was sceptical at first about our capacity to tackle some of the priority objectives chosen. However, I acknowledged the [choice of priorities] and recognise the importance of the group. I can see now how we could work to a better understanding of the issues and how we might be able to have some influence [to make change].
Co-design small group work
Staff in both groups reported positive attributes to the process. Across the groups, staff members commented on the passion and motivation inherent in group conversations:
Everyone was passionate about the topic and open to looking at ways of making improvements.
Staff member, Transport group
I think the group of people who came together were all really motivated to make change and discuss ideas, and this is key in any project.
Staff member, Support group
They discussed the importance of the ‘power’ of bringing together people with different perspectives so that they could share experiences, listen to and learn from each other:
I’m passionate about making a change to how individuals are supported across the borough . . . I can take some of the information/concerns passed to me back to my team, and we can hopefully start to address some of these.
Staff member, Support group
Some staff members in the Transport group wanted to continue the group’s work or take part in other projects they hoped might lead to ‘something similar’:
I started a little sceptical and was pleasantly surprised.
Very satisfying, we had a wide remit and were able to land on a topic we could focus on.
I feel amazed – it exceeded my expectations.
In both groups, staff commented on the importance of listening to people’s experiences and using these to steer the work of the group. In the Support group, staff members talked about long, rich and satisfying discussions which raised awareness about how loneliness was experienced and supported in different communities. However, at times the sheer diversity of what was being shared could feel overwhelming:
There were so many different voices and ways of self-expression in the group, different languages and worlds, the width of the tangents sometimes blew my mind.
Staff member, Support group
A Transport group staff member commented that, although they previously thought themselves sufficiently aware of transport problems, hearing stories of transport user experiences strengthened their own, and the group’s, determination to find solutions:
A really great group. First-hand experience was key, it helped identify the areas to explore.
Staff member, Transport group
Staff from both groups were satisfied with the service improvements they developed. Support group staff members commented on their one-to-one outreach model’s applicability across Doncaster’s diverse range of communities. Its proposed use with trusted organisations was also seen as a new and important step for loneliness support:
. . . it’s a proper gap. [Senior managers] expect people to take individual responsibility and [simply take up the local loneliness support available], but marginalised people can’t necessarily do that.
Staff member, Support group
While the co-design process was reported to be generally acceptable, staff from both groups reported common challenges:
-
Unfamiliarity with co-design processes – although staff had experience of collaborating with external organisations and drawing on the views of people using the support they provided, they reported finding it unusual to bring these perspectives together over time with a sustained focus on local support improvement.
-
Openness of expectations – working with a ‘blank canvas’ was reported to be unusual. In staff experience, collaborative work was usually directed towards a specific outcome from the start. One person who felt happier as the process moved on to developing more ‘concrete’ recommendations, reflected how ‘[i]t was tricky at the start, wondering what the group could deliver – where are we going? I found that frustrating' (Staff member, Transport group).
-
Openness of the process – staff found the ambiguity of the process challenging, given the breadth of the priority areas, the fixed timescale for the work and the range of perspectives among group members. However, for staff more comfortable with ambiguity, being non-directed offered a freer way of working which they felt could bring benefits: ‘Sometimes you don’t know what will happen and being organic is good, as it allows for getting differing ideas’ (Staff member, Support group).
-
The scope of the priority area – staff in both groups reported that managing the wide-ranging scope of the chosen priority areas was difficult, with Support group members in particular describing boundaries as ‘loose’. One staff member expressed concern that some of the group’s wide-ranging discussions had drifted into a focus on aspects more immediately relevant to staff, which risked sidelining the voices of PWLE.
-
Lack of capacity – staff reported that they lacked time to attend all meetings and were unable to carry out tasks between the sessions.
-
A sense of unfinished business – at the end of the 7-month co-design period, staff commented some work felt unfinished. This came from concerns that their priority areas had been tackled only in part, and uncertainty about whether and how the groups’ work would be taken forward after the project ended:
Providing the recommendations to the council licensing team are taken forward by them, I think we moved things forward relating to helping improve transport services.
Staff member, Transport group
Despite these challenges, staff reflections on the co-design work were positive, summed up by one person as ‘a valuable tool for connecting on a human level’. In their exit interviews, several staff said they had found it a ‘privilege’ to have been involved.
Acceptability to people with experience of loneliness support
People with lived experience workshop
People with lived experience first came together in this workshop. In their feedback, some members reported feeling apprehensive beforehand because they were not sure what to expect. However, as one person stated, they had wanted to come along ‘to see what the project meant to me as I had no idea what it was until I took part’.
Attendees commented on the relaxed and open atmosphere at the workshop. They described how this put them at ease and made them able to share emotionally painful experiences around loneliness and ideas for improving support:
It felt just right, apprehensive at first but being with like-minded people made me feel at ease.
I feel great and [now] know there’s more [lonely] people out there of any age.
I really enjoyed it, it’s a lovely open group and I felt relaxed. It also helped to formulate thoughts as to the best way to move forward.
When asked what they saw as the most important outcomes from the workshop, participants’ responses focused on two areas. People spoke about the revelation, through talking together as a group, that feelings about loneliness, including stigma, were remarkably common, despite differences in age and personal situations. The other outcome was motivation; attendees wanted to carry on with the priorities work they had started to make improvements to local support:
We all agreed that we all have the same feeling about loneliness.
Knowing that there are things [we can] ‘do’ something about.
The catalyst film contributed to both outcomes. After viewing the film, attendees commented on how it had brought more diverse voices to the workshop and underlined their sense of shared feelings about loneliness. An extract from an interview with a man with human immunodeficiency virus was cited as particularly hard-hitting in its messages about the need to consider diversity and sustainability in loneliness support. This crystallised attendees’ commitment to pay attention to both aspects in any co-design work.
Joint workshop
People with lived experience reported that the joint workshop with staff was a positive experience. They felt the sharing of perspectives with a wider group created a sense of all contributions being valuable:
It was interesting, nice to hear from the professionals’ viewpoint.
I enjoyed taking part. I made some kind of difference.
One person also commented the group was ‘starting to gel’ because there was a sense of staff and PWLE coming together as a group with shared interests around loneliness.
At this workshop, PWLE viewed the catalyst film for a second time. They reported that this second viewing helped them notice more content and confirmed their commitment to wanting to help other people who were lonely. The process of working with staff to agree priorities to take forward cemented for PWLE the value of the workshop stage:
By the end of the afternoon it seemed like it could be a productive and interesting piece of work. It was interesting to determine individuals’ viewpoints on loneliness and the effects it can have throughout life no matter who you are, before we continued in more depth.
I found the meeting very encouraging . . . and [felt] privileged to be part of a group trying to find ways of incorporating lonely and isolated people into social groups.
A big responsibility, but the chance to make a difference will make it worthwhile.
Co-design small group work
Overall, PWLE said they enjoyed taking part in the co-design groups, particularly because they felt able to contribute to the process and be listened to:
I felt like I had a lot of experience in this [transport] subject, both positive and negative, that may add value to the group as a whole . . . I always had the opportunity to share my experiences and views . . . it seemed productive and it was good to get my experiences out there to new people. I feel like it is important for as many people to know and understand as possible.
PWLE member, Transport group
I enjoyed having my voice out there making a difference . . . having input into something.
PWLE member, Transport group
They reported learning about and from others’ (PWLE and staff) experiences and perspectives:
Listening to other people’s life stories and experiences . . . learning from different cultures, things that had been tried and failed, the effect of COVID . . . seeing things from the [staff] . . . point of view and difficulties they face.
PWLE member, Support group
Similarly, PWLE appreciated learning new information, including about local support and how to access it, and about the taxi complaints process and new legislation. Participation was appreciated by PWLE as an intervention; being a co-design group member helped ease feelings of loneliness and/or the sense of being alone in associated struggles:
I have enjoyed having a little input and loved being with so many lovely and dedicated people . . . it made me feel much better about things . . . I have been very lonely.
PWLE member, Support group
I feel much happier within myself.
PWLE member, Transport group
It was nice to be reminded that I am not the only one that struggles to get transport, having the sympathetic ear of the group was an extra comfort . . . [and] a sounding-board for feeling less alone when bad taxi experiences happen.
PWLE member, Transport group
People with lived experience also reported experiencing some challenges in the process:
-
Uncertainty about roles – at the start of the process, PWLE reported feeling unsure about the part they could play and what their experiences could bring to the group: ‘At first I didn’t think I had anything to give, I just wondered what I was doing there, but the group seemed to think it was OK’ (PWLE member, Support group).
-
Group size – in both groups, there were more staff members than PWLE. This meant that in some meetings only one PWLE member was present, which for some people made it a challenge to feel confident sharing their views: ‘I felt listened to, everyone was kind and patient [but] I found it difficult when I was the only non-professional there and I was asked to share my thoughts as the only one from our side’ (PWLE member, Support group).
-
A sense of unfinished business – PWLE said that coming to the end of the work felt difficult, owing to a sense of unfinished business and because people had enjoyed being part of the group and needed to adjust to the process ending: ‘It took a lot of talk, time and commitment, a rollercoaster, but all enjoyable . . . It’s the longest time I’ve been involved in a single group, it feels a bit difficult to be ending’ (PWLE member, Transport group).
People with lived experience expressed interest in being part of further work, but the opportunities for that were (at the close of the evaluation period) unclear: ‘Thank you for the opportunity to be involved. I am looking forward to seeing if there are any strands of work that arise from this, so I can continue to be involved somehow’ (PWLE member, Transport group).
Workshop facilitator view on acceptability
The workshop facilitator was an expert in co-design approaches used in community settings but new to AEBCD. In his reflections, he saw the workshops as a valuable preliminary stage to small co-design work, particularly for enabling staff and PWLE to have time to work separately before coming together to develop joint priorities:
I think the staff need their sort of safe group to start thinking about what it’s gonna be like involving people who use services, you need to address their anxieties around that and sort of think it through with them so they’re comfortable with it before you bring in service users into that equation. And in the same way, I think it’s really important for the people who use services to have their own kind of safe group as well, almost like . . . sort of working out their identity and that sort of thing, that’s kind of an ongoing process. So in the service user group, trying to help them do that . . . and sort of empower them to see what they had in common and what they really thought and give them the sense that their views are really valued.
Workshop facilitator
Question 3: what suggestions might participants have for improving the process?
This section builds on challenges outlined in the findings reported above. In addition to data from participants, suggestions from the Doncaster project team and the workshop facilitator are included. It is important to preface these suggestions by noting that this type of feedback from any local use of a process such as AEBCD will necessarily reflect and blend components of the process itself with how (and how well) these were adapted for local use (for the current study, described in Chapter 5, Methods), along with contextual factors such as, in the Doncaster study, recruitment being lower than planned owing to COVID-19.
Overall, there was strong support for the AEBCD process. Improvements were suggested in the following areas: clarifying and reinforcing the process and expectations; ground rules; co-design group facilitation and support; co-design group membership; routes to implementing co-designed improvements; and dealing with endings.
Clarifying and reinforcing accelerated experience-based co-design process and expectations
The co-design process was new to all participants. With some people struggling initially to understand what was involved, suggestions for improving the process in this regard focused on making it as transparent as possible from the outset:
-
Explain the co-design group work in more detail – participants felt that more time could have been spent during the workshops outlining the following co-design group stage. This would add depth to information shared by the Doncaster project team and evaluator in writing and verbally, in advance of the process and at the start of each workshop:
I knew that the work was going to narrow down to key priorities and would be taken forward, but not really what the co-design groups meant. Maybe more could have been said at the staff workshop to help prepare mentally before [signing up to a group at] the joint workshop?
Staff member
-
Clarify the time commitment involved – each group could set their pattern of meetings within the co-design work period. However, it became clear in the joint workshop that members wanted guidance on their expected time commitment, especially staff who struggled with capacity. It was agreed each group would hold a monthly 2-hour meeting, a decision that was helpful to group members and which gave the Doncaster project team more certainty around budget management for venue hire and other costs.
-
Offer guidance to help co-design groups navigate their priority area – the issue here was the openness of the work; there were no predefined limits to the scale or scope of what each group might tackle within their designated priority area. While this freedom was seen as having advantages for the groups’ self-determination, participants felt more guidance would have been helpful. The following suggestions were made for future co-design group work:
-
Clarify expectations – clarify that groups are not expected to tackle all aspects of a large priority area and outputs can vary. For example, a group might make recommendations, develop detailed proposals, or trial improvement ideas. It is helpful to think in terms of distinguishing shorter-term practical ‘wins’ and potential longer-term ‘legacies’ from the work.
-
Start group work with a thorough discussion of the priority area – consider the priority and how best to tackle it by sharing experiences and thoughts. Divide the priority into subtopics for improvement, discuss each subtopic and agree a realistic focus to work on given the group’s capacity. Make sure the experiences of PWLE are heard fully at the start to help identify a suitable focus and unite the group around it.
-
Agree an outcome and milestones – once the group focus is established, agree outcomes that can help the group stay action-focused, and if possible, milestones to maintain momentum. Bear in mind outcomes and milestones might need to be set out in very general terms, at least initially, to allow the co-design work to flow in unforeseen directions.
-
-
Clarify that groups can bring in external knowledge and expertise – co-design groups were not able to predict at the start the topic knowledge and expertise which might be helpful. This was due to the breadth of the priority areas of Transport and Support, coupled with the openness of the co-design process which meant the work focus developed over time. Gaps in relevant knowledge or expertise within both groups became apparent. Contacting Doncaster’s taxi licensing officer resulted in a positive and informative response which helped steer the Transport group’s main work, opening further areas for their influence. The Support group’s work slowed in part owing to uncertainty about whether their proposal overlapped with existing support models. A new member bringing a fresh route to collaboration allowed the group’s model to be targeted more precisely. Reflecting on the impacts of seeking or not seeking external views, the Co-design Supporter felt it important to clarify for co-design groups that they can seek external involvement in their work, and the role of a Co-design Supporter should include this liaison (see Co-design group leadership, facilitation and support).
Ground rules for co-design groups
Ground rules were agreed at the start of the three workshops but were not set in the co-design groups. On reflection, the Doncaster project team felt this would have been valuable, not least since some co-design group members had not attended the workshops. A recap of co-design group ground rules would have been helpful as a reminder to involve all members and, for staff, avoid jargon.
Similarly, the workshop facilitator stressed the importance of using learning from the workshops in the co-design group work, particularly learning about working in equal partnership. He was aware that in any group-based work there can be ‘schisms in the groups or personality stuff, or conflicts of interest between organisations, or whatever’ and so during the joint workshop he facilitated a practical exercise to help raise participants’ awareness of these issues. He suggested notes could be taken of workshop discussions of this type and built into co-design group ground rules, to remind members of previous learning.
Open conflict within the groups was experienced only once in an early meeting of one group when, as one staff member described, the ‘parental tone’ of another staff member’s perspective jarred with the otherwise ‘respectful’ nature of the conversations. Group members discussed their concerns with the Co-design Supporter outside the meeting to resolve the issue. Any ground rules agreed by the group about free speech and resolving conflict may have helped here.
Co-design group leadership, facilitation and support
Capacity pressures meant the tasks assigned to the Co-ordinator role were difficult to fulfil in both groups. Very few meeting logs were completed, resulting in some loss of group memory and promised actions between meetings. The Co-design Supporter’s role expanded to take on tasks of note-taking and circulating key points and actions, freeing the Co-ordinator to focus on facilitating the meetings.
Members of both groups drew attention to the importance of good facilitation for ensuring everyone was heard, maintaining the agreed focus, and ensuring momentum. While all members in one group felt this was achieved, some members in the other group felt their work would have benefited from stronger facilitation. Both groups saw the expanded role of the Co-design Supporter as crucial to the group’s achievements. They viewed that person’s own interest in, and knowledge around, loneliness support as important, for example in nurturing individual members’ participation and in liaison with external experts.
Reflecting on the approach taken to facilitation and support, group members and the Doncaster project team recommended each co-design group should have the clearly defined roles of meetings facilitator and process supporter.
-
Meetings facilitator:
-
This role requires skills essential for co-design work, such as ensuring members are equal partners and helping the group achieve and maintain focus and momentum.
-
The facilitator can be internal to the group, which brings valued characteristics of interest and experience around the co-design priority. Time between the joint workshop and the first co-design group meeting could be used by the process supporter to clarify the role in more detail with group members, agree the best person for the role and identify any preparation they require.
-
-
Process supporter:
-
The process supporter should take on all tasks not covered by the facilitator, including:
-
- administrative tasks: agreeing meeting dates, booking venues/refreshments, participant travel expenses and vouchers
-
- meeting note-taking, circulating summary notes and action points to members
-
- liaison with individual members, including encouraging/nurturing continued involvement
-
- liaison with people external to the group who might input to the work.
-
-
The process supporter tasks could be split between more than one person, but an interest/knowledge in the co-design priority is valued by group members.
-
Group membership
Participants suggested careful consideration of the size and composition of groups. Owing to COVID-19, recruitment to the current study had been affected, meaning groups were smaller and less diverse than planned (see Chapter 5, Methods).
Group size
There were mixed feelings around the group size. Some participants said they preferred the groups being small to make progress, while others felt larger groups would have offered benefits of protection against some people dropping out of the process and enabled more opinions and experiences to be heard.
Suggestions for helping recruitment to the process included:
-
Payments for staff workload to be covered – staff spoke about how severe pressures on their capacity affected their ability to maintain participation. Backfill payments were suggested to alleviate this problem; some staff knew a similar scheme was under consideration for staff involved in work for local Integrated Care Systems.
-
Provide alternative means of involvement – the Co-design Supporter contacted a local Deaf community group about taking part in the project, and it became evident the workshop format was a barrier to inclusivity even with multiple British Sign Language interpreters. A separate meeting was scheduled, with workshop themes shared with members of the Deaf community group for comments. It was suggested by the Co-design Supporter that consideration be given to alternative forms of involvement in future use of the process.
Group composition
In both groups, the number of PWLE was small relative to the number of staff. Participants felt that increasing the number of PWLE in groups would be advantageous.
People felt that staff represented and brought perspectives from a variety of loneliness support providers. This brought ‘dynamism’ to the group work and a willingness to share and listen to others’ views. While Doncaster Council staff participation was low, they made a pivotal contribution to both groups. In the Transport group, this was in terms of external support from the taxi licensing officer.
Participants suggested widening staff involvement to include other organisations with roles in identifying, referring or supporting people experiencing loneliness and social isolation, such as Doncaster Council staff and representation from NHS mental health teams.
Routes to implementation and dealing with endings
Although the end of the co-design work was imposed by the evaluation and research funding, participants said a defined timescale had been helpful when deciding whether to commit to taking part. The evaluator observed that as the end date approached, co-design groups focused more intently on what they could achieve by the deadline. Nevertheless, having tackled such broad priorities with limited capacity, there was understandably a sense of unfinished business.
A connected issue was sadness around the work ending after a period during which people enjoyed working together. For some staff this was their longest group collaboration on a single issue, and PWLE described feeling sad to be ending what had been a positive experience in distinct ways: having their voice heard; feeling they could make a difference; and, in relation to experiencing loneliness, the benefit of being part of a meaningful group activity.
Both issues led to suggestions for ensuring attention is paid to the end of the co-design period and what might happen next.
-
Routes to implementation – participants were uncertain what would happen to their work after their involvement ended because this depended on funding and/or commitment from others to take it forward. Attention focused on what the council might do. However, the Doncaster Project Lead was not able to make firm commitments, in part due to the groups’ freedom to navigate their priority areas rather than having a predetermined focus with outcomes that the council could have planned for or already included in other agendas. For some staff participants, this underlined the importance of having more council staff as active members of co-design groups:
To be really effective you need someone from the local authority as part of the group because making improvements is either dependent on funding or setting something up which they need to be involved in. It’s common that the local authority sets something up itself and then doesn’t fully participate because it can’t get people to attend. Having everyone in the co-design room is important for impact.
Staff member, Transport group
-
Dealing with endings – participants were motivated by unfinished business and for personal reasons to carry on with the work. They suggested that thought should be given earlier to ways of continuing the work, even if further work did not follow the co-design process. For example, the Transport group might form the nucleus of a longer-term standing group, given transport was an existing priority in local public health agendas.
Participants saw the celebration event as important for acknowledging the end of the co-design period and recognising what had been achieved. As such, they felt a celebration event should always be a component part of the process.
Question 4: what adaptations might be needed for future use of accelerated experience-based co-design in social care?
Experience-based co-design and its accelerated form AEBCD, used in this study, were originally developed as an approach for co-designing improvements in patient healthcare experiences. Transferring the approach to community-based social care identified adaptations to consider in three key areas: the characteristics of the setting; the scope of the co-design work; and how staff and PWLE experiences are framed. These areas are considered below.
Some participants felt using AEBCD in a more analogous single social care service/organisation setting (e.g. a needs assessment process or a care home) may have proved more straightforward than in community-based loneliness support, where provision is delivered by multiple providers. This is not to say that the approach was seen as inappropriate in this context, and indeed a good deal of the evaluation evidence suggests the contrary, but rather it was a stiffer exploration of the approach.
Furthermore, reflecting on the experience of running the workshops, the external facilitator summed up some benefits of loneliness support as an exemplar in not being attached to a single organisation:
I think the nice thing about this was it was almost quite a pure form of co-production [and] it’s very unusual that you are in that situation really, you know, [more often] . . . you’re kind of trying to work out a strategy of how you can introduce co-production into an organisation or into a project or something that’s already got its sort of own momentum, whereas what was nice about this was that the starting point was you had this topic but you were just sort of saying ‘Well what would help, you know, to improve people’s isolation and loneliness?’ in a really open way . . . and so I think that was a really genuine place to start.
Workshop facilitator
Setting for the co-design work
Establishing boundaries
Community-based loneliness support is offered in different ways by a range of (predominantly VCF sector) providers. This less defined setting means decisions need to be made about which organisations/staff should take part and how to draw a sample to reflect the support offered. Similarly, as there is no equivalent of the ‘patient list’, the method for identifying and sampling PWLE who have used loneliness support is equally challenging. While defining and mapping support over a geographical area is a logical step, this is far from straightforward. At the time of the current study, Doncaster Council was attempting to update its online information resource on loneliness support. Identifying relevant providers and activities was difficult, in part owing to the frequent reshaping of support on offer due to short-term funding.
A practical adaptation to AEBCD is to ensure recruitment focuses on variations in the characteristics of provider organisations and personal characteristics of PWLE to make sure that as many types of support and people as possible are represented. In this study, Doncaster’s local Alliance of (now over 50) self-selected VCF providers proved a good starting point for initial recruitment. Other geographical areas might have different networks to support recruitment.
Building coalitions
The absence of an existing ‘staff team’ (as in the NHS) means that using AEBCD in multiprovider settings such as loneliness support requires additional work to build a sense of staff coalition. This is in addition to the partnership between staff and PWLE required for the co-design work.
In Doncaster, staff experiences in the co-design groups suggest extra time may be needed at the start of the process to build a coalition through sharing and understanding their different perspectives on and contributions to local loneliness support. The Doncaster project team felt the local Alliance was helpful in providing a degree of synergy as a starting point for the staff coalition. The workshop facilitator, however, saw the multiplicity of providers, and therefore initial lack of coalition, as an advantage; he felt it gave an element of purity to the co-design work, lowering the risk of ‘contamination’ from an organisation’s internal politics, bureaucracy, or culture which, in his experience, could impact the co-design process in single services or organisations.
In relation to the coalition between staff and PWLE, the Co-design Supporter raised the issue of PWLE being less likely to know participating staff than patients taking part in an AEBCD approach in the NHS, because staff represented different organisations. She felt this reinforced the need for time at the start of the co-design phase for groups to find common ground and feel comfortable working together.
Additional expertise
A corollary of the loose boundaries around both the topic and recruitment is the need to stay alert during the process for times when direction might benefit from additional local expertise. An example here is Doncaster Council’s taxi licensing officer. His input could not have been envisaged in advance, but the Transport group’s decision to approach him resulted in them receiving not only useful information but also external validation which encouraged members to pursue their ideas and his commitment to stay in touch with developments. In this example, seeking external expertise also served to find potential linchpins connecting the developing co-design work with existing relevant provision and so potential routes to effecting concrete change.
Implementing improvements
Without a ‘host’ organisation, clarifying responsibilities for implementing loneliness support improvements was tricky, and co-design group members expressed uncertainty about what would happen to the results of their work. These feelings were more pronounced in the Support group, who were proposing to fill a gap in support, than in the Transport group, who were seeking to improve the quality of existing provision and had identified a funding opportunity. More generally, VCF providers saw themselves as influencing change in Doncaster, but with limited capacity or power to secure implementation. The local authority was seen as the most appropriate organisation to lead on the implementation of improvement suggestions, and both groups felt the focus of their suggested improvements connected in a tangible way to the council’s work to taxi licensing and the work of council well-being teams.
The local project team lead was a public health manager for Doncaster Council and as such was well placed to consider how the longer-term legacies of the groups’ work fitted with wider local agendas. However, with the co-design group briefs deliberately left open to group members, at the start she was able to commit only in very general terms to seeing how suggested improvements could dovetail with existing agendas.
Separating co-designed improvement suggestions into shorter-term ‘wins’ (with easier/quicker routes to implementation) and longer-term ‘legacies’ proved helpful, for example in the Transport group for identifying the Citizens Advice Bureau as a route for making disabled people more aware of their rights when travelling by taxi. When members collated what had come out of their group’s work for the celebration event, making this short-/long-term separation allowed them to appreciate some of their wider, unintended outcomes of their work, such as forging new collaborations among members.
While overall responsibility and oversight for embedding co-designed improvements remained unclear at the end of the formal evaluation period, the Project Lead (on behalf of the council) and the Co-design Supporter (on behalf of the Alliance) committed to using the evaluation report to help prepare their own joint internal report. This report will identify how the group work will be taken forward. From the council perspective, this is likely to include embedding the work in local Age-friendly and Disability-friendly agendas. During the intervention, the Alliance also emerged as a valuable ‘home’ for the groups’ outputs, which will help to steer the Alliance’s emerging strategy and search for funding opportunities.
Scope of co-design work
Co-design in healthcare AEBCD is about identifying gaps and opportunities to improve patient experience along a clinical pathway. By contrast, the social care equivalents of clinical pathways, especially in areas such as loneliness support, are less well defined, meaning questions about ‘what works best for whom’ are more open to debate. A corollary of this difference between health and social care is that the scope of AEBCD service improvement in social care might legitimately extend beyond the experience of a service or support to addressing perceived gaps in provision itself.
In turn, where this is the case, and a support opportunity is co-designed, it is likely this will need funding. By comparison, implementing NHS AEBCD co-design improvements does not always cost – and sometimes may save – money. In the current study, a member of staff interviewed in the discovery phase declined to take part in the co-design work owing to scepticism about the likelihood of obtaining funding for any improvements suggested.
In the co-design work, the Support group sought to fill the gap identified to help people to re-engage with loneliness support post COVID. The Transport group’s focus on developing a taxi driver gold standard, although closer to service improvement, also required implementation funding. Extending the scope of AEBCD to fill gaps in support or services, rather than focusing more narrowly on experiences of a predetermined pathway, makes questions around responsibility and funding for the outputs of co-design work more pertinent. Two participants suggested an adaptation for AEBCD use in social care to include funds for an additional phase to trial co-design ideas. An alternative would be to identify external funding opportunities as the work of co-design groups progresses.
Framing ‘patient’ and staff experience
There were differences around the use of the catalyst film compared with NHS AEBCD, where it is used to map patient ‘touch points’ of experiences along the pathway or setting. In the current study, staff struggled with the concept of ‘touch points’, preferring the more general notion of ‘hallmarks’ of success (see Chapter 4). However, although the catalyst film was not used in the same way as in NHS studies, the evaluation found it was a valuable tool for resonance-checking, widening the diversity of voices being heard and prompting discussion.
In the design of healthcare AEBCD, staff and patient experiences are framed as distinct and unlikely to overlap, though some may have illness/care experiences which influence their views. In the current study, staff may have had experience of loneliness, and some staff shared these. Since most staff were from VCF organisations, their work involved day-to-day contact with people experiencing loneliness and seeking support. This commonality of experience was highlighted by staff, particularly how loneliness had been heightened during COVID-19 restrictions. The impact of this potential for shared experiences and understanding could be useful when thinking about future use of AEBCD in social care. Staff readily relating to aspects of loneliness was a helpful start to the co-design work; the workshop facilitator commented that it gave discussions more immediate shared meaning and allowed staff and PWLE to connect quickly on a human level. However, these shared experiences may also account in part for the lack of emotional impact reported by staff on viewing the catalyst film. This compares with the film’s more powerful emotional impact reported in healthcare use, particularly on NHS staff previously unaware of negative touch points, or hallmarks, in patient experiences along their clinical pathway.
The end-of-project event
A half-day event was held in Manchester Metropolitan University in January 2023. Just under 50 people attended either online or in person, including 9 members of the Doncaster co-design team, self-advocates, social care and health professionals, commissioners, third-sector organisations and Care Quality Commission representatives, academics, the project team, and members of the project advisory panel and SSC.
The project design and findings were presented, and members of the co-design working groups reflected on their involvement in the project.
Discussion
Transferring accelerated experience-based co-design to social care, using the exemplar of loneliness support
The evaluation demonstrated the potential for transferring a co-design service improvement approach called AEBCD from its original healthcare setting to social care, using the exemplar of loneliness support. The process generated co-designed recommendations for improving local support for people experiencing loneliness. Participants reported broad acceptability of the approach. Some challenges, such as the quality of group facilitation, capacity constraints on staff to taking part, and complexity around implementation of co-designed improvements, feature in previous studies (e.g. Adams et al. ,27 Locock et al. ,6 Tanay et al. 111).
Donetto et al. 39 note considerable variation in how the concept of co-design is understood and practised in the UK; it can often include limited, one-off feedback or consultation. They use the four dimensions in Bradwell and Marr’s40 definition of co-design to set out how EBCD is operationalised. These four dimensions are summarised as:
-
Participation – co-design is a collaborative process in which as many stakeholders as possible have input.
-
Development – co-design evolves as a process, maturing and adapting as it takes place: ‘[I]t involves the exchange of information and expertise relating to both the subject of the design process and the process itself. In this sense, co-design teaches co-design.’40
-
Ownership and power – co-design shifts power to the process, seeking to transform usual hierarchical power relations between staff and ‘client’ stakeholders and generate collective ownership.
-
Outcomes and intent – co-design has a practical focus, although unplanned processes and transformations are likely to occur as side effects of the process.
Bradwell and Marr40 acknowledge, as have others offering frameworks for co-design (e.g. Leach38), that these principles represent ideals which can be difficult to achieve fully in practice. Nevertheless, they serve as a guide to key aspects of co-design that deserve attention.
In relation to the current study, the evaluation found evidence of both achievement and challenges across all four domains. Study recruitment was affected by COVID-19, with capacity issues and competing pressures on local authority social care and public health staff particularly severe. This in turn affected staff recruitment of PWLE. Nevertheless, a sufficiently diverse range of participants, including external stakeholders, provided input to the process. The co-design groups evolved and matured over time as participants built positive relationships and learnt more about the process and how to work as a group. While ownership and power relations differed between the co-design groups, factors in this social care setting suggest a less hierarchical starting point than assumed in health care. This is discussed in more detail below. Finally, the co-design group focus was practical, but with the brief being open to outcomes and intent, the process was exposed to more unplanned developments than anticipated in the fourth dimension of co-design.
When considering how to adapt AEBCD for social care, evaluation findings suggest it is important to reflect on its original healthcare context. Writing about the scope and challenges of co-production in health care, McMullin and Needham14 draw on Bransden and Honingh’s112 differentiation between co-production in ‘core services’ and in ‘complementary tasks’ surrounding core services. For McMullin and Needham,14 this is a useful distinction in health care, where patients cannot co-produce clinical practice or treatments due to the medical expertise required, but their lived experience can help shape its delivery. This recognition of the limits of co-design is reflected in the AEBCD approach, developed for co-designing improvements in the quality of patient experiences along their journey following a defined clinical pathway or setting.
The social care context is different to health, as discussed in Chapter 1. Social care can happen in a range of different settings across a community, with a diverse set of activities and tasks. The evidence base around many interventions is also less developed, and what constitutes best practice is less bounded by professional expertise. This difference widens the potential scope of co-design in social care to include improvements to provision itself. In the current study, this is indeed what happened; one co-design group chose to focus on filling a gap in one-to-one support to help people re-engage with group activities to tackle loneliness post COVID-19. For social care, the potential scope for co-design work to include gaps in existing provision raises issues around how and by whom the scope of the co-design work should be narrowed or, if not, improvement suggestions taken forward and funded.
McMullin and Needham14 identified the hierarchical nature of expertise and knowledge in the healthcare field – fostered by the highly professionalised character of the workforce, which typically requires many years of training – as a particular challenge for co-production. This hierarchy can lead to personal and cultural resistance to the value of patient expertise and a reluctance to engage fully in co-design. 113 By contrast, in community-based preventative social care, such as loneliness support, provision is dominated by VCF sector staff, paid and unpaid. In common with many areas of social care, the relationship between practitioner and client is different to that between doctor and patient; decisions about social care support are often shaped by strengths, or asset-based approaches, which, as McMullin and Needham14 point out, focus on people’s capabilities, rather than a deficit or impairment focus which can prevail in healthcare contexts.
It follows that AEBCD was developed with awareness of aspects of health care which can run counter to co-design principles. This context helps explain why a hallmark of the approach is the catalyst film of patient experiences along their clinical journey. This generates often emotionally charged ‘touch points’ for potential quality improvements. When used in health care, the use of the catalyst film has been reported as having an eye-opening, positive impact on professionals’ commitment to the co-design process. 114
By comparison, in the current study, staff’s emotional reactions to the catalyst film were low key. Several reasons may account for this difference. First, loneliness as a universal experience was observed as enabling staff and PWLE to connect on a human level. This is less likely when co-designing improvements in, say, the patient experience of intensive care, or a hospital cancer pathway, where few, if any, participating staff may have had a corresponding patient experience. Secondly, with multiple providers involved in loneliness support and no single pathway or journey, the current study did not use the film to identify or elaborate on emotional touch points along a journey but instead served to prompt discussion more generally around support. These differences in the use and impact of the catalyst film call into question whether it is always needed, especially given the effort required to produce it. However, its prime aim to prompt discussion was successful, and retention of the film has been urged as a distinctive feature by Donetto et al. following an international survey of EBCD studies:
The film is an important catalyst in the co-design process as the visualisation of patient experiences helps (re)connect people with similar experiences and stories, whether users or providers of a service, and offers an emotionally and cognitively powerful starting point for the co-design process. 20
The authors further suggest that using film makes the process distinct ‘from other consultative formats in which anonymity and circumspection can hinder rather than enable quality improvement’. 20 Publishing the catalyst film on Socialcaretalk.org will make it available for use in similar co-design work elsewhere. For future use of AEBCD in other areas of social care, questions arise around how similar resources might best be created, given that healthcare AEBCD benefits from a longer-standing and more extensive web video archive of patient experiences (https://healthtalk.org) which can be drawn upon for developing films on new AEBCD topics.
When considering the adaptations suggested for using AEBCD in social care, it is important to remember that the study exemplar of loneliness support falls under prevention in social care, in a community setting with multiple providers who draw on a variety of funding sources. This setting is noteworthy for two reasons. First, it does not reflect all of social care, some of which – for instance, the work of local authority social work teams – may have more similarities with healthcare teams, reducing the need for some adaptations when using the AEBCD approach. For example, such single-service/-organisation social care teams may be more comparable to those in health care, in terms of having clearer lines of authority and accountability for taking forward co-designed improvement suggestions. Second, despite differences between the new setting of loneliness support and healthcare settings where AEBCD has been used, the approach produced positive results. Therefore, some adaptations suggested by the evaluation are more a question of degree or nuance than departure from the original model. For example, regardless of setting, time will be needed to build staff rapport, but more time may be needed in a multiprovider setting to build a staff coalition/consensus at the start than in a single-provider setting where staff will have some common understandings.
Transferring AEBCD to a social care setting does nevertheless throw up new challenges. Challenges stem from extending the scope of co-design work into gaps in provision and, in community settings, the lack of a clear host organisation for routes to, and funding for, implementation of co-designed improvements.
It is, however, important to acknowledge that previous studies demonstrate that implementing AEBCD in health care is not necessarily straightforward. Barriers include staff culture being resistant to change and uncertainties around how to take forward improvement suggestions which require commitment from other services or organisations. 6
The commentary at the end-of-project event was striking in terms of how people described the impact on them. For example, one staff member said, ‘we learned from ourselves too’, and she was able to use this learning in her voluntary work with a Chinese Elders group. A PWLE member joined a church-related group due to finding the co-design experience rewarding. Group members underlined the importance of listening to people’s stories and how empowering this could be, not least by learning that they were not alone in experiencing loneliness. It was clear from contributions that the two groups were supportive and encouraging and that people felt a strong sense of achievement and commitment.
The discussion about the project findings more broadly involved robust challenge about the process, its component parts and how it might fit within social care. Ryan received e-mails from attendees following the event which added additional points for consideration. These included that AEBCD could be conceived of as a project to tackle the loneliness of project members regardless of the project’s focus. Concern was raised about the tension between creating a supportive group environment and that group being necessarily short-lived, potentially leaving members with a sense of loss.
The event ended with one attendee reiterating the point that the exemplar of loneliness was a challenging focus for exploring the use of AEBCD in social care. One attendee added that the findings of this project should make it easier for people to use the approach in future since we had, in effect, tested AEBCD ‘to the max’.
Conclusion
The evaluation found that AEBCD has considerable potential for transfer from the healthcare improvement field to social care. The adapted process used in Doncaster was acceptable to co-design participants, who reported a range of benefits and enjoyed the work. The co-design groups identified a range of loneliness support improvements, some of which had more easily defined routes to implementation than others.
Learning from the evaluation pointed to common aspects of using AEBCD in health care and in loneliness support and differences requiring attention to improve the fit of AEBCD for use in social care settings. We present our recommendations in Chapter 8.
Chapter 7 Public involvement
In this chapter, we describe how members of the public contributed to proposal development, project oversight and management, and dissemination. The study was advised throughout by patient and public involvement (PPI) co-applicants Bebbington and Lambat.
Proposal development
As part of proposal development, PI Ryan spoke to older carers of people with learning disabilities about their experiences of loneliness via the Embolden project, a small National Lottery-funded project led by Oxfordshire Family Support Network. Vaid (a family carer and member of the SSC) provided continuity between the Embolden project and this study. These individual discussions highlighted how loneliness is a complex and debilitating experience.
Development of the proposal also involved input from co-applicants Bebbington and Lambat. Bebbington has a learning disability and works for an Oxfordshire-based self-advocacy organisation, My Life My Choice. She discussed the experience of loneliness with Ryan during monthly walks Bebbington initiated to support people with learning disabilities to enjoy the outdoors and come together socially. Loneliness was an important issue for several of the people who came on these walks. Funding for support for Bebbington was incorporated into the proposal design to enable her to be meaningfully involved.
Lambat is the manager of LMCP Care Link, a small registered charity based in Moss Side, Manchester, supporting development and health improvements within the South Asian communities. Lambat has extensive expertise in advocating on behalf of those at risk of social exclusion, and specifically to ensure that equality and diversity are reflected in service development. Lambat provided feedback about the plain English summary in the proposal, suggesting certain words that might be challenging for people for whom English is not their first language, and the summary was rewritten with Lambat’s input.
Advisory Panel and Study Steering Committee
The Advisory Panel comprised professionals, the two PPI co-applicants (Bebbington and Lambat) and two other members of the public: Monks (founder of a social enterprise) and Menan Mirza (expert by experience).
Recruitment of PPI members to the advisory panel was discussed in initial full research team meetings. The research team agreed to recruit two people who experienced loneliness and had eligible care needs; however, it was not possible to find someone within the latter criteria, which proved to be a consistent finding across the project. Monks was recruited via colleagues at Doncaster Council as a person who has lived experience of social isolation/loneliness. Menan Mirza was a participant in the discovery phase interviews conducted by Malli. Malli invited Menan Mirza to be part of the advisory panel following his interview as he shared his insightful experience with loneliness and brought his experience of being part of a minority ethnic group.
The advisory panel met for the first time in November 2020. At the start of the meeting, the chair, Ryan, covered the role of public involvement, and an overview of the project was provided in a presentation.
The PPI member Monks contributed during the first meeting by instigating a useful discussion around the COVID-19 pandemic and loneliness, highlighting how awareness of loneliness has been raised by the pandemic and the impact of loneliness is profound and often forgotten alongside other issues such as well-being. Menan Mirza contributed separately during an initial conversation with Ryan and Malli and raised issues pertinent to young people. He underlined how loneliness is typically characterised as a problem experienced by older people, a point which is borne out by our research findings and in the wider literature. These contributions highlighted how anyone can experience, or be susceptible to, loneliness.
Ryan met with people individually or as a smaller group, if PPI members of the advisory panel were unable to attend meetings or if separate follow-up meetings were necessary to discuss pertinent issues and/or ensure people felt confident to contribute. On some occasions, Vaid also joined these meetings to maintain their engagement.
The separate SSC included two PPI representatives, Bostock (experienced PPI representative for NIHR) and Vaid. Vaid reported on PPI activity at SSC meetings.
Training and support
The support needs of lay contributors were overseen by project managers, Martin (University of Oxford) and Morrissey (Manchester Metropolitan University); this included providing minutes as an audio file and in traditional written format. Training in how to participate in research and research ethics was provided to Bebbington and Vaid. Training was provided by Bostock and was arranged jointly for PPI representatives from other NIHR projects on which Ryan is PI [both based on learning disability: HSDR-funded NIHR129491 and School for Social Care Research (SSCR)-funded ‘Bridging the translation gap between learning disability policy and practice in search of flourishing lives’].
Patient and public involvement: activities and influence during the study
As the project involved interviews and workshops with participants in the discovery and co-design phases, the research design ensured we were working with the public during the study. This approach ensured PPI was interwoven throughout the study rather than being a stand-alone activity, and this approach was strongly encouraged by our two SSC PPI representatives.
Both PPI co-applicants either participated in full research team meetings and advisory panel meetings when they were available or met with Ryan separately. For example, Ryan and Lambat met online early in the project with co-applicant Wilberforce to discuss the recruitment of a diverse sample, and Ryan and Lambat met in Manchester in November 2022 to discuss Lambat’s contribution to the final stages of the project. Meetings were predominantly via videoconference due to COVID-19. Mindful that it is not always easy for PPI members to contribute effectively via this route, we invited our PPI representatives to separate, additional meetings with the project PI where they were able to elaborate their thoughts further.
Vaid sat on the interview panel for the appointment of researcher Malli. PPI representation on the panel provided the team with different insights into candidates and helped candidates to consider questions from a different perspective.
In the discovery phase of the project, PPI co-applicants Bebbington and Lambat suggested groups of people and periods in one’s life where one might be lonely as well as keywords around loneliness and social isolation. Bebbington and Lambat also helped to shape the questions for the interviews with PWLE, and feedback on the interview topic guide was also sought from three participants after the first few interviews. Feedback helped to shorten questions and order them in a logical sequence, and ensured academic jargon was not used.
Patient and public involvement: role in developing outputs and dissemination
Patient and public involvement members have been consulted throughout the project about the development of the loneliness resource on Socialcaretalk, including the list of summaries that were written by Malli and Ryan and the content of the catalyst film co-produced from the interview data (used in the co-design workshops and published on Socialcaretalk). We also connected with relevant people and organisations on a regular basis, such as advisory panel members from Supported Loving, the Campaign to End Loneliness and Doncaster Social Isolation and Loneliness Alliance. They will cascade the project outputs via their networks.
Throughout the project, Monks underlined the importance of the outputs clearly presenting loneliness as a condition we can all experience. Monks and Menan Mirza both cautioned against the mediums (and language) we use in our outputs not becoming exclusionary in themselves, a point also raised by a member of the Doncaster co-design team during the end-of-project event (see Chapter 8).
Lambat voiced concerns about the lack of culturally and religiously appropriate health and social care resources more widely. This led to a strong focus in recruiting a diverse sample of participants for the discovery phase public interviews, which was successful (see Chapter 2, Table 2).
Socialcaretalk resource
Ryan held meetings with Monks, Menan Mirza and Vaid to obtain their views on what should be included in the Socialcaretalk resource as it was in development. Monks and Vaid provided useful suggestions for ways of presenting users’ stories on Socialcaretalk, such as including poignant extracts from a diversity of participants to highlight the fact that loneliness is a global problem and to ensure there is a greater chance that people will connect with the resource. Malli also held meetings with five participants from the discovery phase interviews to discuss how their experiences are presented on Socialcaretalk to ensure the resource is accessible. This group felt the example resources shown from Healthtalk.org (sister site of Socialcaretalk) were written for an audience with too high an educational attainment; considerable effort was taken to ensure the new Socialcaretalk resource was written in very plain English.
The resource consists of 21 summaries covering different aspects of participants’ experiences of loneliness illustrated with video, audio and text extracts from the interviews. Individual summaries were shared with our PPI and advisory panel members to make sure that they were accessible, resonated with readers and had no glaring omissions. The feedback was positive, with people reporting that the summaries were powerful, accessible and wide-ranging.
The various meetings have fed into a revised, less text-heavy and more accessible output for publication on Socialcaretalk.org. Furthermore, a recent formative evaluation of Socialcaretalk led by co-applicant Ziebland with Ryan, Martin and SSC PPI member for this study Bostock engaged with potential users of the platform to develop recommendations for how material is best presented, and these were followed in development of the loneliness resource.
Catalyst film for service improvement
Bebbington (supported by Davidson) was involved in the development of the catalyst film during its production. Bebbington and Davidson highlighted areas that were too fast-paced, and requested an easy-read version of the film. Feedback led to the addition of subtitles, a voiceover for the title of each section of the film and an easy-read summary to explain the main points of the film.
Lambat reviewed the catalyst film and felt social care commissioners could learn from it as participants made their points extremely well.
Academic papers
Advisory panel member Kalpa Kharicha, who was the Chief Executive Officer of the Campaign to End Loneliness, was a co-author on the first project paper. 56
End-of-project stakeholder event
All PPI members attended the end-of-project stakeholder event, which was held in Manchester in January 2023. Bebbington introduced the event and briefly talked about her involvement in the project.
Relationship with the study team: lay panel view
Reflecting on his relationship with the study team, PPI co-applicant Lambat said:
As this was the first time I worked with Ryan, the Principal Investigator, I greatly appreciated her meeting with me personally, face to face. This provided a valuable opportunity to learn more about the research project and to share how I could contribute given my experience. There were ongoing opportunities to learn about the progress and to provide feedback. The research administrators were very helpful in providing guidance on paperwork completion.
Practicalities of patient and public involvement: challenges faced and lessons learnt
In the last SSC meeting, Vaid reflected on the importance of the careful ending of PPI in a research project to ensure people are not just ‘dropped’ when the funding ends after being heavily invested in the process, sometimes for a considerable time. This is an important point which is reflected in our co-design phase. We will ensure that accessible project findings are shared with our public contributors at the end of the project, and people will be individually thanked for the contributions they have made. Furthermore, relationships developed during the project will continue in different ways. For example:
-
Lambat and LMCP Care Link have invited Ryan to become a trustee, which will enable the continuation of a working relationship and the potential for expertise and experience to be shared reciprocally.
-
Following their positive experience of involvement in the project, three PWLE co-design participants have been recruited to Curious Minds, the PPI group attached to the University of York’s research/practice initiative, The Curiosity Partnership.
We faced challenges finding members of the public to join the advisory panel despite the team having strong networks on social media and in real life. This was in part due to the impact of the COVID-19 pandemic and the associated disruption it caused.
The nature of the project, examining a co-production approach, meant that PPI was embedded through the research design. However, we feel that we could have shared more regular updates, particularly during periods of time when there were few involvement opportunities.
Chapter 8 Conclusions and recommendations
In this concluding chapter, we summarise equality, diversity and inclusion and public involvement across the project and draw out concluding comments about the research. We finish by presenting our recommendations for the future use of AEBCD in social care settings.
Equality, diversity and inclusion
The participant representation in both parts of the project was diverse (see Chapter 2, Table 2 for participant identities in the discovery phase public interviews). Active steps were taken in the discovery phase to achieve this, as a diverse range of different support groups were contacted to ensure that the sample included different views and experiences. The sample of six people with experience of loneliness support in the co-design phase included different characteristics (see Chapter 5, Recruitment). This sample was recruited via participating staff.
The project aimed to be accessible, with easy-read versions of project documents produced for the discovery phase interviews; time was spent making sure people understood what taking part in the project involved, and we circulated audio as well as text versions of project meetings. The evaluation suggested that people were not as well informed as we expected given the steps taken, and we suggest that producing a clear, one-page graphic that presents the stages of the research and what will be expected of participants would be useful in future research. This could be reshared at the start of each meeting to highlight what stage the project is at and what is left to do.
As discussed in Chapter 6, the format of the AEBCD approach we used was not suitable for D/deaf people, and the Co-design Supporter met separately with this group to discuss the project and share themes from the workshop held for PWLE. While the workshop format was felt to be an important part of the process, thinking of ways of increasing the accessibility of this format, or alternative ways of bringing in people’s views for whom the format is a barrier, is important going forward.
While the academic research team members were white, the wider team including advisory panel, SSC and PPI groups included members from groups that are under-represented in the field of social care research. There was a range of experience and expertise across the team, and developmental opportunities were offered to the researchers and project co-ordinator to attend training courses, for example being involved in research and the use of Photosymbols (Photosymbols Ltd, Bristol, UK).
Public involvement
As outlined in Chapter 7, our ‘formal’ public contributors were involved with the project from the design stage, across the discovery and co-design phases and the end-of-project event. We took a flexible approach to involvement, which meant thinking about how people were able to contribute and how we could improve our communications and engagement by offering to meet people outside of formal project meetings and producing audio versions of minutes. Loneliness as a topic is something we could all relate to, which enabled the development of good working relationships across the team that will continue beyond the end of the project. It was apparent by the end of the project that people had grown in confidence in relation to working on a research project.
In summary, the project was immeasurably enhanced by our PPI contributors in many ways, including keeping us in check and asking critical questions, providing feedback and sense-checking outputs and resources, offering ideas and thoughts based on individual experiences of loneliness, and helping us to learn how better to involve members of the public in research. The importance of endings was a consideration in the final months, and we will produce an accessible and engaging findings document to share with our contributors and wider public.
Study limitations
Both phases of the project were affected by the pandemic and associated lockdown conditions. Fieldwork for the discovery phase was moved online or conducted by telephone, which may have affected who could participate. The capacity of the Doncaster Project Lead to set up the intervention in the co-design phase was affected because priority had to be given to urgent tasks in her council role as a public health lead. Pandemic work pressures also led to smaller than hoped-for numbers and types of participating staff, which had a knock-on impact on recruiting PWLE, since they were recruited primarily via staff. COVID-19 also led to a delayed start to the co-design workshops to enable these to be run in person rather than online, a decision taken in part owing to the topic of loneliness support and a belief that in-person encounters may better support the development of human connectedness for a genuine collaboration.
Turnover in the Doncaster project team during the planning stage created temporary challenges for capacity in setting up the intervention. Towards the end of the co-design phase, the decision to add the celebration event further extended the period required for evaluation data collection.
Future research
Discovery phase
The experience of loneliness and lack of emotional support experienced by people who are unexpectedly bereaved is a neglected topic, including the social needs of bereaved people who do not fit commonly held stereotypes. The findings further highlight loneliness in childhood, relating to specific exclusionary contexts, an area identified by Mansfield et al. 47 Research should identify government mechanisms and social infrastructures that isolate people, rather than viewing loneliness as a deficit located within the person. Our findings support other work that indicates loneliness is socially stigmatised, and it is important to explore factors that contribute to this and ensure interventions do not unintentionally further perpetuate shame and misconceptions around it.
Co-design phase
Areas for future research are: the costs and opportunity costs of the approach compared to more ‘top-down’ initiatives; exploring the purpose and focus of the catalyst film; the impact of AEBCD as an intervention for people who use social care services – what this might mean to participants, and the potential of the approach to generate service improvements; the adaptation of the approach to enable greater inclusion and accessibility; and exploring whether using AEBCD in a more clearly defined area avoids some of the challenges identified in this study.
The availability of the catalyst film based on a national sample of interviews and learning from the current study might help encourage the replication of co-designing improvements in loneliness support in other geographical areas. Such work could lead to refinements and/or additional suggested adaptations of AEBCD.
Socialcaretalk.org includes new sections about social care topics with video and audio extracts of people talking about their experiences. Recent and planned topics include self-funding social care for older people115 [funded by NIHR Research for Social Care (RfSC)], the experiences of social care leavers (funded by NIHR RfSC), and the experiences of carers of people with dementia and people with early-stage dementia (funded by NIHR SSCR). Catalyst films for service improvement are a potential output of these projects.
Concluding thoughts and recommendations
A strength of AEBCD is the opportunities it generates for developing or enhancing active citizenship and democratic research practices. Co-production approaches have been linked to the creation of public value, of satisfying a collective need jointly defined by government and the public. 1 Loneliness as a UK government priority increased in importance as an outcome of COVID-19, which acted as an unexpected backdrop to the project, and it remains a key strategic priority for Doncaster Council. Public participants in both stages of the research presented compelling accounts of the importance of trying to ameliorate or ease loneliness and of the complexity underpinning it, not least the importance of exploring loneliness beyond ‘deficit’ and ‘personal failings’ lenses to broader societal and government mechanisms and social infrastructures that generate or contribute to it.
There was consistent constructive collaboration across the stages of the project, and across existing literature and the project findings. The analysis of public and staff discovery phase data sets underlined how: loneliness is a stigmatised condition; there is a lack of focus on young people; and certain groups are marginalised or disproportionately impacted by it. The field review, including pandemic-related research, highlighted consensus around the importance of future research focusing across the life course rather than on older people, with consideration of inequalities and the differential experiences and impact of loneliness on diverse groups (see, e.g. Mansfield et al. 47).
We discussed criticisms of co-production approaches more generally in Chapter 1, and we return to consider these briefly here. Criticisms include costs associated with AEBCD, the administrative burden, the professionalisation of the process and tendency towards the over-involvement of middle-class people, and risks of ‘co-destruction’ rather than co-production. 33 Oliver et al. 35 tabled a set of challenges and associated costs, which include different priorities and values among stakeholders raising the possibility of damage to relationships, reputation and credibility, challenges around analysis, framing the findings, formulating recommendations, dissemination and implementing change.
In this project, these potential challenges did not materialise, and we suggest several factors that may account for this:
-
The recruitment in the discovery phase of people from groups that are under-represented in research led to the production of a catalyst film that placed diversity firmly at the table for the co-design phase.
-
The co-design phase recruited a small and similarly diverse group of PWLE who brought a set of experiences that widened the potential scope of what the co-design groups chose to focus on, enhancing the robustness and relevance of the project findings.
-
This was a funded research project with Maddison carefully encouraging ownership of the process by the Doncaster co-design team while working behind the scenes to ensure that the stages of the co-design process happened. The research funding covered the costs of venue hire, travel expenses and an external facilitator for the workshops and the celebration event. It also gave the project an identity, time-bound momentum and external accountability.
-
Loneliness is a condition that everybody is likely to experience to a degree at some point, as evidenced by the similarities in the priority lists generated in workshops 1 and 2. This sharing of priorities helped to develop relationships and trust between group members early on.
We suggest this project contributes to the public values mentioned in Chapter 1. 17 These contributions are demonstrated by the strong articulation by working group members of feelings of empowerment and the importance of being listened to. The development of active citizenship and political value is apparent in the way working group members discussed how they would take learning from the project to other settings, and their determination to continue with the work. As one member said at the end-of-project event: ‘It’s an open book for me now to realise what none of us knew before, the information we found out.’
The project as a form of loneliness intervention was something discussed at the proposal development stage and across the project. The strength of feeling and sadness expressed by working group members at the project ending was unexpected, however, and raised ethical considerations. While the Doncaster celebration event was not part of the original project design, it created a space for the co-design team to come together in Doncaster to share and celebrate their work. The end-of-project event in Manchester enabled Bebbington (supported by Davidson) and Lambat to end, in person, their formal involvement in a project that had been conducted online for over 2 years although, as discussed in Chapter 7, new opportunities have been created for ongoing partnership and collaboration.
It was apparent from the start of the project, in discussions about the meaning of social care in relation to loneliness, that social care is a different context to health care for the use of co-design approaches. The fuzziness of boundaries between social care, voluntary sector activities and health care at times means pathways are not well defined, and it may be that some services that get funding from social care resources do not outwardly market themselves as such, partly due to the stigma associated with using council-funded services for some people. Our focus on loneliness, for which there is no clear definition, amplified this lack of a clear pathway, which offered benefits as well as challenges. The co-design groups had more freedom to take the work in any direction, which could be unsettling, and it was not initially clear how the work of the groups would fit with the council agendas. However, it also led to the development of unexpectedly creative and innovative ideas, the future development of which has been taken up by Doncaster Council and the local Social Isolation and Loneliness Alliance. We finish with a summary quote from a staff participant, who experienced AEBCD as ‘a valuable tool for connecting on a human level’.
Recommendations
In designing this project, our focus was on whether AEBCD can be used effectively in a social care setting, and we looked to its use in health care as a benchmark throughout. The evaluation findings and end-of-project event discussions suggest that comparing the use of AEBCD in social care to its use in health is less useful because of the myriad differences between the two settings. This may be because our focus was on broad community-based provision of loneliness support rather than a narrower social care service pathway such as needs assessment, which may have had more parallels with healthcare use of AEBCD.
The strengths of the approach within social care are very apparent, and future research and practice could explore the following areas: the costs and opportunity costs of the approach compared to more ‘top-down’ initiatives; the purpose and focus of the catalyst film; the impact of AEBCD as an intervention for people who use social care services and what this might mean to participants and the potential of the approach to generate service improvements; the adaptation of the approach to enable greater inclusion and accessibility; whether using AEBCD in a more clearly defined area avoids some of the challenges identified in this study; and finally, using AEBCD in multisector improvement efforts, for example in mental health care, learning disabilities and frailty in old age.
We end with a set of recommendations to start this process, many of which echo wider research on the conditions for successful organisational change.
Recommendations specific to using accelerated experience-based co-design in social care
-
Identify people or organisations who potentially could have responsibility for implementing improvements, including finding relevant funding.
-
Identify an appropriate sample of staff and PWLE, taking time to fill gaps in representation of provision, knowledge and people’s characteristics, and consider whether staff and PWLE have distinct or shared experiences and how to build on these.
-
Allow the necessary time for coalition-building, developing trusted relationships and understanding different perspectives.
-
Ensure information about the research and co-design phase is clear and accessible and reshare this at the start of each meeting to highlight what stage the project is at and what is left to do.
-
Consider whether PWLE and staff participants have pre-existing relationships or should be selected on account of these, and the impact of having or not having such relationships.
-
Consider opportunities for co-design group members to continue contributing their expertise.
General recommendations
-
Ensure good facilitation of the workshops and the co-design group work. Facilitation is especially important for agreeing ground rules and creating the right atmosphere for the honest sharing, open discussion and mutual respect required for the process.
-
Ensure that paid staff involved in the co-design – whether as participants or supporting the process itself – have protected time for the work involved.
-
Be clear about processes, aims and roles from the outset. This includes taking time to explain the EBCD process of small groups working over an extended period and being clear about the time commitment involved. In small group work, ensure expectations, goals and roles are discussed and agreed. Remember to discuss how and when the co-design process will end.
-
Ensure that groups are large enough to represent all relevant parties. Not all members will be able to attend all meetings, so an over-representation of PWLE can help ensure individuals do not become a lone voice for PWLE in some meetings.
-
Keep the first two workshops separate – one for staff and one for PWLE. This helps to create safe spaces where participants can build trust and think about issues from their perspective.
-
Consider aspects of the process which may exclude some people, such as the workshop format, and any adaptations to accommodate these, for example to enable deaf people to participate.
-
Ensure co-design group participants know that they can seek outside views and bring in external experts, as necessary.
Additional information
Acknowledgements
The authors would like to thank:
The participants in the discovery and co-design phases of the study.
Doncaster Council for being the site for the AEBCD approach and exhibiting a strong commitment to the project despite the pandemic-related pressures they were under at the time.
Doncaster Social Isolation and Loneliness Alliance who worked with Doncaster Council in supporting this project and will take forward some of the legacies from the co-design work.
Kate Bell, the Alliance’s Programme Manager, for her role as Co-design Supporter, which was instrumental in the recruitment to and day-to-day support for the co-design process.
Nikki Greenfield, Doncaster Council, for working closely with Kate Bell to support the co-design groups.
Susan Hampshaw, Doncaster Council, for her ongoing support of the Doncaster Project Lead during the delivery of the intervention in the co-design phase.
Melina Malli, a researcher who conducted and analysed the discovery phase public interviews.
Pete Fleischmann, an expert in social care co-design approaches used in community settings, for planning and facilitating all three co-design workshops.
Melanie Gager, a healthcare professional experienced in using AEBCD (Royal Berkshire NHS Trust), for leading a workshop to prepare Doncaster Council and the University of York for the co-design work.
Stephen Lee Hodgkins, a live scribe, for creating visual representations of the PWLE co-design workshop and joint co-design workshop discussions. Stephen also produced a graphic representation of the themes identified which captured participants’ experiences of loneliness (public discovery phase interviews).
Cara Holland, a live scribe, for creating a visual representation of the co-design celebration event discussions.
Vanessa Eade, Research Operations Assistant (University of Oxford), who was responsible for gaining the necessary ethics and research governance approvals.
Namrata Dhillon, Monitoring Programme Manager at NIHR, for providing support and sound advice.
The members of the advisory panel who engaged with the project and acted as ‘critical friends’ throughout: Dr Claire Bates, Elaine James, Kalpa Karicha, Rob Mitchell, Glenn Monks, Georgia Pavlopoulou, John Whiteley.
The external members of the SSC: Glenn Robert (Kings College London, and chairperson of the SSC), Victoria Hart (South London and Maudsley NHS Foundation Trust), Andrew Power (University of Southampton), Janet Heaton (University of the Highlands and Islands) and Angeli Vaid and Jennifer Bostock (lay representatives).
Arne Mueller (Manchester Metropolitan University) for supporting the referencing in this report.
Adam Barnett from the DIPEx Charity, who published the online resource.
Contributions of authors
Sara Ryan (https://orcid.org/0000-0002-7406-1610) Professor, Social Care. Was the PI for the study; led the overall design, provided academic leadership for the study, supervised the discovery phase public interviews, led the development of the online resource, sat on the SSC, led the writing of the final report, and gave final approval of the manuscript.
Jane Maddison (https://orcid.org/0000-0002-7963-211X) Research Associate, Applied Social Care. Was a researcher for the study; conducted and analysed the discovery phase staff interviews, conducted the evaluation of the AEBCD process during the co-design phase and analysed the data to inform recommendations for use of AEBCD in social care, was lead author of Chapters 5 and 6, contributed to other chapters of the final report and gave final approval of the manuscript.
Kate Baxter (https://orcid.org/0000-0002-3094-9546) Senior Research Fellow, Applied Social Care Research. Was a co-investigator for the study; contributed to the overall study design, supervised the discovery phase staff interviews and evaluation of the AEBCD process, co-authored Chapter 1, was lead author of Chapter 4, contributed to other chapters of the final report, and gave final approval of the manuscript.
Mark Wilberforce (https://orcid.org/0000-0001-6977-4483) Senior Research Fellow, Applied Social Care Research. Was a co-investigator for the study; contributed to the overall study design, contributed to the final report, and gave final approval of the manuscript.
Yvonne Birks (https://orcid.org/0000-0002-4235-5307) Professor, Applied Social Care Research. Was a co-investigator for the study; contributed to the overall study design, contributed to the final report, and gave final approval of the manuscript.
Emmie Morrissey (https://orcid.org/0000-0003-0801-8128) Research Project Manager, Project Management. Was a co-ordinator for the study; managed the conduct of the study, co-authored Chapter 7, co-ordinated and contributed to the final report and gave final approval of the manuscript.
Angela Martin (https://orcid.org/0000-0001-6196-0409) Research Operations Manager, Project Management. Was a co-investigator for the study; contributed to aspects of the study design and managed the conduct of the study, co-authored Chapter 7, contributed to the final report and gave final approval of the manuscript.
Ahmed Lambat (https://orcid.org/0000-0002-8866-5837) PPI Representative. Was a co-investigator for the study; advised on PPI throughout the project, contributed to Chapter 7, contributed to the final report, and gave final approval of the manuscript.
Pam Bebbington (https://orcid.org/0000-0002-4274-9883) PPI Representative. Was a co-investigator for the study; advised on PPI throughout the project, reviewed and commented on the plain English summary, contributed to the final report, and gave final approval of the manuscript.
Sue Ziebland (https://orcid.org/0000-0002-6496-4859) Professor, Medical Sociology. Was a co-investigator for the study; contributed to the overall study design, contributed to discovery phase analysis and dissemination, contributed to the final report, and gave final approval of the manuscript.
Louise Robson (https://orcid.org/0000-0001-7905-0972) Public Health Lead; Working Age and Healthy Lives; Public Health, Leisure and Strategic Commissioning. Was a co-investigator for the study; provided local advisory support to the AEBCD stage in Doncaster, contributed to Chapters 5 and 6, contributed to the final report, and gave final approval of the manuscript.
Louise Locock (https://orcid.org/0000-0002-8109-1930) Professor, Health Services Research. Was a co-investigator for the study; contributed to the overall study design, led the co-design phase, contributed to the final report, and gave final approval of the manuscript.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/MYHT8970.
Primary conflicts of interest: Each named author has completed the ICMJE Uniform Disclosure Form for Potential Conflicts of Interest. Sara Ryan declares membership of the National Institute for Health and Care Research (NIHR) RfSC Funding Committee and is a Trustee of LMCP Care Link. Kate Baxter declares membership of the NIHR RfSC Funding Committee and HSDR Funding Committee Members 16 June 2012–30 June 2018. Mark Wilberforce declares membership of the NIHR RfSC Funding Committee and NIHR Policy Research Programme. Yvonne Birks is the lead in York for the NIHR SSCR Phase III (PD-SSC-117-20010). Yvonne Birks is Chair of the SSC for a NIHR Health and Social Care Delivery Research (HSDR) programme-funded project (NIHR131322: Witness to Harm), Chair of the Steering Committee for NIHR Consortium bid 21/54 Palliative and End of Life Care (PEoLC): Implementing research partnerships, networks and collaborations across Suffolk and North-East Excess ICS, Suffolk, County Council and Waveney, and a member of the NIHR Health Technology Assessment (HTA) Prioritisation Committee: Social Care. She was a COVID-19 reviewer 1 June 2020–1 September 2020. She is the Chief Investigator on NIHR13158; and co-investigator on NIHR134029, NIHR200702 and NIHR153779. She is co-investigator on the Economic and Social Research Council (ESRC) funded projects: Supporting Adult Social Care Innovation (ES/T001364/1) and DETERMinants of quality of life, care and costs IN people with Dementia and their careers after diagnosis (ES/S010351/1) and a NIHR 153779 £3,114,971.29 York Evidence Synthesis Centre Co-Applicant (awarded, not yet commenced). Sue Ziebland declares her work as Programme Director of the NIHR Research for Patient Benefit programme (2017–22). Sue Ziebland is a NIHR Senior Investigator emerita and NIHR Senior Investigator, until April 2022. She is a trustee of the Foundation for the Sociology of Health and Illness. She is a trustee of Green Templeton College, University of Oxford, and member of the Governing Body. She was also a COVID-19 reviewer 1 June 2020–1 September 2020. Louise Locock received a personal honorarium for teaching on the Foundations for Patients Experience course for the Point of Care Foundation. She was also a HSDR Funding Committee Member 16 June 2014–30 June 2019.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to all anonymised data may be granted following review.
Ethics statement
The study was reviewed and given favourable opinion by West Midlands – Coventry and Warwickshire REC on 2 October 2020. Ethics reference: 20/WM/0223.
Information governance statement
Manchester Metropolitan University and University of Oxford are committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, University of Oxford and Manchester Metropolitan University are joint Data Controllers for the social care user interview data collected in the discovery phase. Manchester Metropolitan University is the Data Controller for the discovery phase interviews with staff, and the co-design phase of the study. You can find out more about how Manchester Metropolitan University and University of Oxford handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officers, here www.mmu.ac.uk/data-protection and data.security@phc.ox.ac.uk.
Department of Health and Social Care disclaimer
This report presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the HSDR programme or the Department of Health and Social Care.
This monograph was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Publication
Malli MA, Ryan S, Maddison J, Kharicha K. Experiences and meaning of loneliness beyond age and group identity. Sociol Health Illn 2023;45:70–89. https://doi.org/10.1111%2F1467-9566.13539
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care.
References
- McMullin C. Individual, group, and collective co-production: the role of public value conceptions in shaping co-production practices. Adm Soc 2023;55:239-63. https://doi.org/10.1177/00953997221131790.
- Coulter A, Locock L, Ziebland S, Calabrese J. Collecting data on patient experience is not enough: they must be used to improve care. BMJ 2014;348. https://doi.org/10.1136/bmj.g2225.
- Robert G, Cornwell J, Locock L, Purushotham A, Sturmey G, Gager M. Patients and staff as codesigners of healthcare services. BMJ 2015;350. https://doi.org/10.1136/bmj.g7714.
- Blackwell RW, Lowton K, Robert G, Grudzen C, Grocott P. Using experience-based co-design with older patients, their families and staff to improve palliative care experiences in the emergency department: a reflective critique on the process and outcomes. Int J Nurs Stud 2017;68:83-94. https://doi.org/10.1016/j.ijnurstu.2017.01.002.
- Robert G. Understanding and Using Health Experiences: Improving Patient Care. Oxford; 2013.
- Locock L, Robert G, Boaz A, Vougioukalou S, Shuldham C, Fielden J, et al. Testing accelerated experience-based co-design: a qualitative study of using a national archive of patient experience narrative interviews to promote rapid patient-centred service improvement. Health Serv Delivery Res 2014;2. https://doi.org/10.3310/hsdr02040.
- NHS Digital . Latest Key Statistics on Adult Social Care Include Council Spending in 2021–22: Statistical Press Release 2022. https://digital.nhs.uk/news/2022/adult-social-care-stats-2021-22 (accessed 26 January 2023).
- Skills for Care . The State of the Adult Social Care Sector and Workforce in England, 2022 (Leeds, 2022) 2022. www.skillsforcare.org.uk/Adult-Social-Care-Workforce-Data/Workforce-intelligence/documents/State-of-the-adult-social-care-sector/The-state-of-the-adult-social-care-sector-and-workforce-2022.pdf (accessed 26 January 2023).
- NHS Digital . Adult Social Care Activity and Finance Report, England 2021–22. n.d. https://digital.nhs.uk/news/2022/adult-social-care-stats-2021-22 (accessed 10 February 2022).
- Baxter K, Glendinning C. People Who Fund Their Own Social Care. A Scoping Review. London: School for Social Care Research; 2014.
- Baxter K, Heavey E, Birks Y. Choice and control in social care: experiences of older self-funders in England. Soc Policy Adm 2020;54:460-74. https://doi.org/10.1111/spol.12534.
- Masterson D, Areskoug Josefsson K, Robert G, Nylander E, Kjellström S. Mapping definitions of co-production and co-design in health and social care: a systematic scoping review providing lessons for the future. Health Expect 2022;25:902-13. https://doi.org/10.1111/hex.13470.
- Bovaird T. Beyond engagement and participation: user and community coproduction of public services. Public Adm Rev 2007;67:846-60. https://doi.org/10.1111/j.1540-6210.2007.00773.x.
- McMullin C, Needham C. Co-Production and Co-Creation. Engaging Citizens in Public Services. New York: Routledge; 2018.
- Dunston R, Lee A, Boud D, Brodie P, Chiarella M. Co-production and health system reform – from re-imagining to re-making. Aust J Public Adm 2009;68:39-52. https://doi.org/10.1111/j.1467-8500.2008.00608.x.
- Bevir M, Needham C, Waring J. Inside co-production: ruling, resistance, and practice. Soc Policy Adm 2019;53:197-202. https://doi.org/10.1111/spol.12483.
- Bovaird T, Loeffler E. From engagement to co-production: the contribution of users and communities to outcomes and public value. Voluntas 2012;23:1119-38. https://doi.org/10.1007/s11266-012-9309-6.
- Vennik FD, Van de Bovenkamp HM, Putters K, Grit KJ. Co-production in healthcare: rhetoric and practice. Int Rev Adm Sci 2016;82:150-68.
- Osborne SP, Radnor Z, Strokosch K. Co-production and the co-creation of value in public services: a suitable case for treatment?. Public Manag Rev 2016;18:639-53. https://doi.org/10.1080/14719037.2015.1111927.
- Donetto S, Tsianakas V, Robert G. Using Experience-Based Co-Design (EBCD) to Improve the Quality of Healthcare: Mapping Where We Are Now and Establishing Future Directions. London: King’s College London; 2014.
- McIntyre A. Participatory Action Research. London: SAGE Publications Ltd; 2007.
- Bate P, Robert G. Bringing User Experience to Healthcare Improvement: The Concepts, Methods and Practices of Experience-Based Design. London: Radcliffe Publishing; 2007.
- Woods A, Springham N. On learning from being the in-patient. Int J Art Ther 2011;16:60-8. https://doi.org/10.1080/17454832.2011.603697.
- Springham N, Robert G. Experience based co-design reduces formal complaints on an acute mental health ward. BMJ Qual Improv Rep 2015;4. https://doi.org/10.1136/bmjquality.u209153.w3970.
- Mulvale G, Moll S, Miatello A, Murray-Leung L, Rogerson K, Sassi RB. Co-designing services for youth with mental health issues: novel elicitation approaches. Int J Qual Methods 2019;18. https://doi.org/10.1177/1609406918816244.
- Dimopoulos-Bick TL, O’Connor C, Montgomery J, Szanto T, Fisher M, Sutherland V, et al. ‘Anyone can co-design?’: a case study synthesis of six experience-based co-design (EBCD) projects for healthcare systems improvement in New South Wales, Australia. Patient Exp J 2019;6:93-104. https://doi.org/10.35680/2372-0247.1365.
- Adams M, Maben J, Robert G. Improving Patient-Centred Care Through Experience-Based Co-Design (EBCD): An Evaluation of the Sustainability and Spread of EBCD in a Cancer Centre. London: King’s College London; 2013.
- Ramos M, Bowen S, Wright PC, Ferreira MGG, Forcellini FA. Experience based co-design in healthcare services: an analysis of projects barriers and enablers. Des Health 2020;4:276-95. https://doi.org/10.1080/24735132.2020.1837508.
- Girling M, Le Couteur A, Finch T. Experience-based co-design (EBCD) with young people who offend: innovating methodology to reach marginalised groups. PLOS ONE 2022;17. https://doi.org/10.1371/journal.pone.0270782.
- Gander-Zaucker S, Unwin GL, Larkin M. The feasibility and acceptability of an experience-based co-design approach to reducing domestic abuse. Societies 2022;12. https://doi.org/10.3390/soc12030093.
- Barker RE, Brighton LJ, Maddocks M, Nolan CM, Patel S, Walsh JA, et al. Integrating home-based exercise training with a hospital at home service for patients hospitalised with acute exacerbations of COPD: developing the model using accelerated experience-based co-design. Int J Chron Obstruct Pulmon Dis 2021;16:1035-49. https://doi.org/10.2147/COPD.S293048.
- Bielinska AM, Archer S, Darzi A, Urch C. Co-designing an intervention to increase uptake of advance care planning in later life following emergency hospitalisation: a research protocol using accelerated experience-based co-design (AEBCD) and the behaviour change wheel (BCW). BMJ Open 2022;12. https://doi.org/10.1136/bmjopen-2021-055347.
- Steen T, Brandsen T, Verschuere B. Co-Production and Co-Creation. Engaging Citizens in Public Services. New York: Routledge; 2018.
- Brandsen T, Helderman JK. The trade-off between capital and community: the conditions for successful co-production in housing. Voluntas 2012;23:1139-55. https://doi.org/10.1007/s11266-012-9310-0.
- Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research?. Health Res Policy Syst 2019;17. https://doi.org/10.1186/s12961-019-0432-3.
- Dodge J. Addressing democratic and citizenship deficits: lessons from civil society?. Public Adm Rev 2013;73:203-6. https://doi.org/10.1111/puar.12009.
- Williams O, Sarre S, Papoulias SC, Knowles S, Robert G, Beresford P, et al. Lost in the shadows: reflections on the dark side of co-production. Health Res Policy Syst 2020;18. https://doi.org/10.1186/s12961-020-00558-0.
- Leach WD. Collaborative public management and democracy: evidence from western watershed partnerships. Public Adm Rev 2006;66:100-10. https://doi.org/10.1111/j.1540-6210.2006.00670.x.
- Donetto S, Pierri P, Tsianakas V, Robert G. Experience-based co-design and healthcare improvement: realizing participatory design in the public sector. Des J 2015;18:227-48. https://doi.org/10.2752/175630615X14212498964312.
- Bradwell P, Marr S. Making the Most of Collaboration. An International Survey of Public Service Co-Design. London: Demos; 2008.
- Verhaeghe P. What About Me?: The Struggle for Identity in a Market-based Society. London: Scribe Publications; 2014.
- Cacioppo JT, Cacioppo S. The growing problem of loneliness. Lancet 2018;391. https://doi.org/10.1016/S0140-6736(18)30142-9.
- Vincent D. A History of Solitude. Oxford: John Wiley & Sons; 2020.
- Local Government Association . Combating Loneliness. A Guide for Local Authorities 2016. www.local.gov.uk/sites/default/files/documents/combating-loneliness-guid-24e_march_2018.pdf (accessed 1 January 2023).
- Local Government Association . Loneliness. How Do You Know Your Council Is Actively Tackling Loneliness? 2018. https://local.gov.uk/sites/default/documents/22.28%20-%20Loneliness%20Must%20Know_02.pdf (accessed 3 February 2023).
- Fried L, Prohaska T, Burholt V, Burns A, Golden J, Hawkley L, et al. A unified approach to loneliness. Lancet 2020;395. https://doi.org/10.1016/S0140-6736(19)32533-4.
- Mansfield L, Victor C, Meads C, Daykin N, Tomlinson A, Lane J, et al. A conceptual review of loneliness in adults: qualitative evidence synthesis. Int J Environ Res Public Health 2021;18. https://doi.org/10.3390/ijerph182111522.
- Moustakas CE. Loneliness. Maryland, USA: Pickle Partners Publishing; 2016.
- Bolmsjö I, Tengland PA, Rämgård M. Existential loneliness: an attempt at an analysis of the concept and the phenomenon. Nurs Ethics 2019;26:1310-25. https://doi.org/10.1177/0969733017748480.
- Mikulincer M, Shaver PR. The Handbook of Solitude: Psychological Perspectives on Social Isolation, Social Withdrawal, and Being Alone. Oxford: Wiley-Blackwell; 2013.
- Perlman D, Peplau LA. Loneliness: A Sourcebook of Current Theory, Research and Therapy. New Jersey, USA: Wiley; 1982.
- Young JE. Loneliness: A Sourcebook of Current Theory, Research and Therapy. New Jersey, USA: Wiley; 1982.
- Victor C, Mansfield L, Kay T, Daykin N, Lane J, Duffy LG, et al. An Overview of Reviews: The Effectiveness of Interventions to Address Loneliness at All Stages of the Life-Course. 2018.
- Campaign to End Loneliness . Promising Approaches Revisited: Effective Action on Loneliness in Later Life 2021. www.campaigntoendloneliness.org/wp-content/uploads/Promising_Approaches_Revisited_FULL_REPORT.pdf (accessed 1 February 2023).
- Barreto M, Victor C, Hammond C, Eccles A, Richins MT, Qualter P. Loneliness around the world: age, gender, and cultural differences in loneliness. Pers Individ Dif 2021;169. https://doi.org/10.1016/j.paid.2020.110066.
- Malli MA, Ryan S, Maddison J, Kharicha K. Experiences and meaning of loneliness beyond age and group identity. Sociol Health Illn 2023;45:70-89. https://doi.org/10.1111/1467-9566.13539.
- Wong A, Chau AKC, Fang Y, Woo J. Illuminating the psychological experience of elderly loneliness from a societal perspective: a qualitative study of alienation between older people and society. Int J Environ Res Public Health 2017;14. https://doi.org/10.3390/ijerph14070824.
- Tanskanen J, Anttila T. A prospective study of social isolation, loneliness, and mortality in Finland. Am J Public Health 2016;106:2042-8. https://doi.org/10.2105/AJPH.2016.303431.
- Galanaki EP, Mylonas K, Vogiatzoglou PS. Evaluating voluntary aloneness in childhood: initial validation of the Children’s Solitude Scale. Eur J Dev Psychol 2015;12:688-700. https://doi.org/10.1080/17405629.2015.1071253.
- Victor CR, Rippon I, Barreto M, Hammond C, Qualter P. Older adults’ experiences of loneliness over the lifecourse: an exploratory study using the BBC loneliness experiment. Arch Gerontol Geriatr 2022;102. https://doi.org/10.1016/j.archger.2022.104740.
- Karhe L, Kaunonen M. Patient experiences of loneliness: an evolutionary concept analysis. ANS Adv Nurs Sci 2015;38:E21-34. https://doi.org/10.1097/ANS.0000000000000096.
- Lindgren BM, Sundbaum J, Eriksson M, Graneheim UH. Looking at the world through a frosted window: experiences of loneliness among persons with mental ill‐health. J Psychiatr Ment Health Nurs 2014;21:114-20. https://doi.org/10.1111/jpm.12053.
- Gardiner C, Geldenhuys G, Gott M. Interventions to reduce social isolation and loneliness among older people: an integrative review. Health Soc Care Community 2018;26:147-57. https://doi.org/10.1111/hsc.12367.
- Foot J, Hopkins T. A Glass Half-full: How an Asset Approach Can Improve Community Health and Well-being. Improvement and Development Agency (IDeA); 2010.
- Galvez-Hernandez P, González-de Paz L, Muntaner C. Primary care-based interventions addressing social isolation and loneliness in older people: a scoping review. BMJ Open 2022;12. https://doi.org/10.1136/bmjopen-2021-057729.
- Noone C, Yang K. Community-based responses to loneliness in older people: a systematic review of qualitative studies. Health Soc Care Community 2022;30:e859-73. https://doi.org/10.1111/hsc.13682.
- Gorenko JA, Moran C, Flynn M, Dobson K, Konnert C. Social isolation and psychological distress among older adults related to COVID-19: a narrative review of remotely-delivered interventions and recommendations. J Appl Gerontol 2021;40:3-13. https://doi.org/10.1177/0733464820958550.
- Fakoya OA, McCorry NK, Donnelly M. Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Health 2020;20. https://doi.org/10.1186/s12889-020-8251-6.
- Lee C, Kuhn I, McGrath M, Remes O, Cowan A, Duncan F, et al. NIHR SPHR Public Mental Health Programme . A systematic scoping review of community-based interventions for the prevention of mental ill-health and the promotion of mental health in older adults in the UK. Health Soc Care Community 2022;30:27-5. https://doi.org/10.1111/hsc.13413.
- Williams T, Lakhani A, Spelten E. Interventions to reduce loneliness and social isolation in rural settings: a mixed-methods review. J Rural Stud 2022;90:76-92. https://doi.org/10.1016/j.jrurstud.2022.02.001.
- Rodrigues NG, Han CQY, Su Y, Klainin-Yobas P, Wu XV. Psychological impacts and online interventions of social isolation amongst older adults during COVID-19 pandemic: a scoping review. J Adv Nurs 2022;78:609-44. https://doi.org/10.1111/jan.15063.
- Williams CYK, Townson AT, Kapur M, Ferreira AF, Nunn R, Galante J, et al. Interventions to reduce social isolation and loneliness during COVID-19 physical distancing measures: a rapid systematic review. PLOS ONE 2021;16. https://doi.org/10.1371/journal.pone.0247139.
- Bourne P, Camic PM, Crutch SJ. Psychosocial outcomes of dyadic arts interventions for people with a dementia and their informal caregivers: a systematic review. Health Soc Care Community 2021;29:1632-49. https://doi.org/10.1111/hsc.13267.
- Luchetti M, Lee JH, Aschwanden D, Sesker A, Strickhouser JE, Terracciano A, et al. The trajectory of loneliness in response to COVID-19. Am Psychol 2020;75:897-908. https://doi.org/10.1037/amp0000690.
- Killgore WDS, Cloonan SA, Taylor EC, Miller MA, Dailey NS. Three months of loneliness during the COVID-19 lockdown. Psychiatry Res 2020;293. https://doi.org/10.1016/j.psychres.2020.113392.
- Palgi Y, Shrira A, Ring L, Bodner E, Avidor S, Bergman Y, et al. The loneliness pandemic: loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J Affect Disord 2020;275:109-11. https://doi.org/10.1016/j.jad.2020.06.036.
- Campaign to End Loneliness . Loneliness Beyond COVID-19. Learning the Lessons of the Pandemic for a Less Lonely Future 2021. www.campaigntoendloneliness.org/wp-content/uploads/Loneliness-beyond-Covid-19-July-2021.pdf (accessed 6 February 2023).
- Dahlberg L. Loneliness during the COVID-19 pandemic. Aging Ment Health 2021;25:1161-4. https://doi.org/10.1080/13607863.2021.1875195.
- Saltzman LY, Hansel TC, Bordnick PS. Loneliness, isolation, and social support factors in post-COVID-19 mental health. Psychol Trauma 2020;12:S55-7. https://doi.org/10.1037/tra0000703.
- Groarke JM, Berry E, Graham-Wisener L, McKenna-Plumley PE, McGlinchey E, Armour C. Loneliness in the UK during the COVID-19 pandemic: cross-sectional results from the COVID-19 psychological wellbeing study. PLOS ONE 2020;15. https://doi.org/10.1371/journal.pone.0239698.
- Bu F, Steptoe A, Fancourt D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health 2020;186:31-4. https://doi.org/10.1016/j.puhe.2020.06.036.
- Loades ME, Chatburn E, Higson-Sweeney N, Reynolds S, Shafran R, Brigden A, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry 2020;59:1218-39.e3. https://doi.org/10.1016/j.jaac.2020.05.009.
- Wickens CM, McDonald AJ, Elton-Marshall T, Wells S, Nigatu YT, Jankowicz D, et al. Loneliness in the COVID-19 pandemic: associations with age, gender and their interaction. J Psychiatr Res 2021;136:103-8. https://doi.org/10.1016/j.jpsychires.2021.01.047.
- Mortimer J. No One Should Have No One. Working to End Loneliness Among Older People n.d. www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/reports-and-briefings/health--wellbeing/rb_dec16_no_one_should_have_no_one.pdf (accessed 23 March 2021).
- Herxheimer A, Ziebland S. Narrative Research in Health and Illness. Massachusetts, Oxford, Victoria: Blackwell Publishing; 2004.
- Ziebland S, Locock L, Fitzpatrick R, Stokes T, Robert G, O’Flynn N, et al. Informing the development of NICE (National Institute for Health and Care Excellence) quality standards through secondary analysis of qualitative narrative interviews on patients’ experiences. Health Serv Deliv Res 2014;2. https://doi.org/10.3310/hsdr02450.
- Anderson C, Kirkpatrick S. Narrative interviewing. Int J Clin Pharm 2016;38:631-4. https://doi.org/10.1007/s11096-015-0222-0.
- Kidd J, Ziebland S. Narratives of experience of mental health and illness on healthtalk.org. BJPsych Bull 2016;40:273-6. https://doi.org/10.1192/pb.bp.115.052217.
- Hinton L, Locock L, Ziebland S. Illness Narratives in Practice: Potentials and Challenges of Using Narratives in Health-related Contexts. Oxford: Oxford University Press; 2018.
- Bate P, Robert G. Experience-based design: from redesigning the system around the patient to co-designing services with the patient. Qual Saf Health Care 2006;15:307-10. https://doi.org/10.1136/qshc.2005.016527.
- Mattingly C, Garro LC. Narrative and the Cultural Construction of Illness and Healing. Oakland, CA: University of California Press; 2000.
- Blumer H. Symbolic Interactionism: Perspective and Method. Oakland, CA: University of California Press; 1986.
- Coyne IT. Sampling in qualitative research. Purposeful and theoretical sampling; merging or clear boundaries?. J Adv Nurs 1997;26:623-30. https://doi.org/10.1046/j.1365-2648.1997.t01-25-00999.x.
- Parkinson S, Bromfield L. Recruiting young adults to child maltreatment research through Facebook: a feasibility study. Child Abuse Negl 2013;37:716-20. https://doi.org/10.1016/j.chiabu.2013.04.009.
- Brickman Bhutta C. Not by the book: Facebook as a sampling frame. Sociol Methods Res 2012;41:57-88. https://doi.org/10.1177/0049124112440795.
- Victor C, Scambler S, Bond J, Bowling A. Being alone in later life: loneliness, social isolation and living alone. Rev Clin Gerontol 2000;10:407-17. https://doi.org/10.1017/S0959259800104101.
- Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med 2022;292. https://doi.org/10.1016/j.socscimed.2021.114523.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Stein JY, Solomon Z. Narratives of Loneliness. London: Routledge; 2017.
- Killeen C. Loneliness: an epidemic in modern society. J Adv Nurs 1998;28:762-70. https://doi.org/10.1046/j.1365-2648.1998.00703.x.
- de Jong Gierveld J. A review of loneliness: concept and definitions, determinants and consequences. Rev Clin Gerontol 1998;8:73-80. https://doi.org/10.1017/S0959259898008090.
- Franklin A, Barbosa Neves B, Hookway N, Patulny R, Tranter B, Jaworski K. Towards an understanding of loneliness among Australian men: gender cultures, embodied expression and the social bases of belonging. J Sociol 2019;55:124-43. https://doi.org/10.1177/1440783318777309.
- Pinquart M, Sorensen S. Influences on loneliness in older adults: a meta-analysis. Basic Appl Soc Psych 2001;23:245-66. https://doi.org/10.1207/S15324834BASP2304_2.
- McGraw JG. Loneliness, its nature and forms: an existential perspective. Man World 1995;28:43-64. https://doi.org/10.1007/BF01278458.
- Cacioppo JT, Hawkley LC, Ernst JM, Burleson M, Berntson GG, Nouriani B, et al. Loneliness within a nomological net: an evolutionary perspective. J Res Pers 2006;40:1054-85. https://doi.org/10.1016/j.jrp.2005.11.007.
- Cacioppo JT, Patrick W. Loneliness: Human Nature and the Need for Social Connection. New York, USA: WW Norton & Company; 2008.
- Public Health England . Making Every Contact Count (MECC): Consensus Statement 2016. www.england.nhs.uk/wp-content/uploads/2016/04/making-every-contact-count.pdf (accessed 26 January 2023).
- Point of Care Foundation . EBCD: Experience-Based Co-Design Toolkit n.d. www.pointofcarefoundation.org.uk/resource/experience-based-co-design-ebcd-toolkit/ (accessed 26 January 2023).
- Spencer L, Ritchie J, Ormston R, O’Connor W, Barnard M. Qualitative Research Practice. A Guide for Social Science Students and Researchers. London: Sage; 2013.
- Cheshire Leonard. Driving Change: Improving the Accessibility of Taxis and Private Hire Vehicles for Disabled People 2023. www.leonardcheshire.org/sites/default/files/2023-01/Driving-Change.pdf (accessed 4 October 2022).
- Tanay MAL, Armes J, Oakley C, Sage L, Tanner D, Roca J, et al. Co-designing a cancer care intervention: reflections of participants and a doctoral researcher on roles and contributions. Res Involv Engagem 2022;8. https://doi.org/10.1186/s40900-022-00373-7.
- Brandsen T, Honingh M. Co-Production and Co-Creation. Engaging Citizens in Public Services. New York: Routledge; 2018.
- Sharma S, Conduit J, Rao Hill S. Organisational capabilities for customer participation in health care service innovation. Australas Mark J 2014;22:179-88. https://doi.org/10.1016/j.ausmj.2014.08.002.
- Clarke D, Gombert-Waldron K, Honey S, Cloud G, Harris R, Macdonald A, et al. Co-designing organisational improvements and interventions to increase inpatient activity in four stroke units in England: a mixed-methods process evaluation using normalisation process theory. BMJ Open 2021;11. https://doi.org/10.1136/bmjopen-2020-042723.
- Baxter K. You’ve Got a Friend in Social Care Talk 2022. https://socialcare.blog.gov.uk/2022/01/17/youve-got-a-friend-in-social-care-talk/ (accessed 26 January 2023).
List of abbreviations
- AEBCD
- accelerated experience-based co-design
- EBCD
- experience-based co-design
- HSDR
- Health and Social Care Delivery Research
- LGBTQ
- lesbian, gay, bisexual, transgender and queer
- MECC
- Making Every Contact Count
- NIHR
- National Institute for Health and Care Research
- PAR
- participatory action research
- PI
- principal investigator
- PPI
- patient and public involvement
- PWLE
- people with lived experience
- REC
- Research Ethics Committee
- SSC
- Study Steering Committee
- SSCR
- School for Social Care Research
- VCF
- voluntary, community and faith
Notes
Supplementary material can be found on the NIHR Journals Library report page (https://doi.org/10.3310/MYHT8970).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.