

Notes
Article history
The research reported in this issue of the journal was funded by the HSDR programme or one of its preceding programmes as project number NIHR127281. The contractual start date was in July 2019. The final report began editorial review in October 2020 and was accepted for publication in June 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HSDR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2022 Baker et al. This work was produced by Baker et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2022 Baker et al.
Chapter 1 Background
This chapter sets out the study context, explaining why it is important to enhance knowledge about restrictive practices in children and young people’s (CYP’s) institutional settings, and how the behavior change technique (BCT) taxonomy can contribute to the development and understanding of interventions.
Restrictive practices in children and young people’s institutional settings
There are approximately 80,000 CYP living in state and privately run institutions in England alone;1 such institutions include residential children’s homes, residential schools, young offender institutions, secure training centres, secure children’s homes and immigration detention centres, in addition to NHS inpatient settings through Child and Adolescent Mental Health Services (approximately 1140 beds). 2 The CYP in these disparate institutional settings share some characteristics: many have experienced trauma, abuse and loss;3–8 some present serious risks of harm to themselves and/or others;9,10 and some exhibit behavioural and/or psychological difficulties. The health and safety of these CYP and the staff who work with them hinges on the safe and effective avoidance and management of incidents involving violence, aggression and self-harm.
Definition of restrictive practices, rates of use
Staff responses to incidents involving violence, aggression or self-harm may involve the use of potentially harmful restrictive practices (defined by the Department of Health and Social Care as ‘deliberate acts on the part of other person(s) that restrict an individual’s movement, liberty and/or freedom to act independently in order to: take immediate control of a dangerous situation where there is a real possibility of harm to the person or others if no action is undertaken’11,12). Restrictive practices, such as restraint, seclusion and (in health settings) the use of forced medication, are a common occurrence. Rates of use are similar in psychiatric and criminal justice settings. One study calculated that one-quarter of CYP treated in psychiatric settings have had at least one seclusion episode and 29% have had at least one restraint episode,13 whereas the level is estimated at 28% (in 2014) in custodial settings. The rate is estimated to be higher in learning disability services, with more than half of CYP experiencing seclusion, restraint or a harmful incident. 14
Prevalence data are not available from other settings, although individual cases have attracted media attention. 15 Some studies have found that approximately 60–70% of all reported seclusions or restraints in CAMHS can be accounted for by a small minority (7–15%) of all hospitalised CYP. 16,17 Recent UK figures revealed that 17% of girls in CAMHS facilities had been physically restrained, compared with 13% of boys. 18 Face-down restraint was more commonly used on individuals < 18 years old, with > 2500 occurrences in 2014/15, and, again, in particular with girls (> 2300 occurrences), often repeatedly with the same girls. 18
Risks and costs: physical, psychological, financial
Restrictive practices carry high risks of physical and psychological harm. In the UK, 45 CYP died in restraint-related circumstances in inpatient psychiatric facilities in the period 1993–200313,19,20 and two have died in youth custody in the past 15 years. 21,22 In 2015 alone, there were 429 injuries to children resulting from restraint in youth custody. 23
Research has described the negative impact of experiencing restrictive practices in adult service users but little is known about CYP’s experiences. 21,22 It is thought that, as with adults, such practices can have a profoundly detrimental effect on therapeutic relationships between care staff and CYP24 and they are particularly counter-therapeutic for CYP with an abuse history. 25 The subsequent costs of restrictive practices to the NHS are substantial [estimated by the National Institute for Health and Care Excellence (NICE) at £20.5M per year for damage and injury, £88M per year for observations and £6.1M for restraint]. 26 Evidence-based interventions to reduce the use of restrictive practices clearly have the potential to result in significant cost savings.
Concerns regarding overuse
The problem of overuse of restrictive practices within UK state-provided children’s services has become a matter for serious concern. The United Nations raised specific concerns regarding the use of restrictive practices with CYP who have psychosocial disorders, and at the end of 2017 called again for the UK to end all use of restraint in the context of disability, segregation and isolation practices, and any practices that might be considered to be torture or degrading treatment (Section 73a). 27 Voluntary organisations such as Mind (London, UK),24 Article 39 (Nottingham, UK)1 and Agenda (London, UK)18 have ongoing campaigns on the issue.
Legislative frameworks for the use of restrictive practices
Legal provision for restrictive practices varies across these settings. For example, in the UK, pain-inducing restraint techniques remain lawful in Ministry of Justice settings but have been made unlawful by the Departments of Education and Health. Nevertheless, the UK government has sought to reduce restrictive practices across all settings. The Ministry of Justice implemented the Minimising and Managing Physical Restraint (MMPR) programme, although this has been criticised on the grounds that the restraint techniques it authorises are life-threatening. 28 In 2014, the Department of Health and Social Care launched the Positive and Pro-active Care guidance,12 aimed at phasing out face-down restraint and deeming restrictive interventions a ‘last resort’ across health and social care provider organisations. Since then, services’ use of restraint has been subject to inspection by the Care Quality Commission. 29
More recently, in its publication Reducing the Need for Restraint and Restrictive Intervention with Children and Young People with Learning Disabilities, Autistic Spectrum Disorder and Mental Health Difficulties,30 the Department of Health and Social Care and Department for Education has set out core principles for the use of restraint: it should be used only where necessary to prevent risk of serious harm, and not as punishment; with the minimum force necessary; by appropriately trained staff; and should be documented, monitored and reviewed. 30 In 2018, The Mental Health Units (Use of Force) Bill31 – which sought to manage the use of force in mental health services in England and Wales, requiring commitment to a reduction in the use of force and reporting on its use – became law.
Strategies to address reduction of restrictive practices
There is a growing body of research into the reduction of restrictive practices. In the UK, initiatives to reduce restrictive practices in mental health care such as ‘Safewards’,32 ‘Six Core Strategies’33 (6CS) and ‘No Force First’34 have been promoted and adopted by some mental health trusts, including in CAMHS; some of these initiatives have been evaluated and reported in the literature. 32,35 There has been similar research carried out seeking to reduce the use of restraint with people with learning disabilities. 36,37 These have typically aimed to reduce violent and aggressive behaviour by changing staff behaviour to encourage use of de-escalation techniques, supported by various policy and procedural changes.
There is some evidence of interventions that are effective in reducing the use of restrictive measures specifically with CYP in mental health services; however, empirical data are limited13,19,38–41 and often primarily use case studies of single-facility initiatives. 19,42 Although the outcomes of some of these interventions have been the subject of systematic reviews,32 their specific content has not been examined in detail and the causal mechanisms through which they might change behaviour are not fully understood. It remains unclear which components of these interventions have contributed to their effectiveness. Furthermore, it is not known to what extent those interventions that have resulted in reductions in the use of restrictive practices (or other outcomes such as increased staff confidence) have features in common.
The research context for the current study
The existing literature on restrictive practices repeatedly calls for guidance to be based on robust, transparent studies,43,44 and for interventions to be better described and better evaluated. Livingston et al. 45 reviewed training interventions to reduce restrictive practices and highlighted the difficulty of reaching conclusions, as the evaluated interventions comprised ‘different types of aggression management programs, which contain a variety of approaches’ and ‘the focus, curriculum, and duration of the training vary substantially from one program to another’. 45 The NICE guideline on violence and aggression46 calls for research to be carried out into the content and nature of effective de-escalation techniques, together with the most effective and efficient approaches to training professionals in their use. 46 According to the guideline, research is needed that will apply a systematic approach to the description and reporting of de-escalation techniques currently in use. 46 With specific reference to CYP, it notes the ‘lack of research on the nature and efficacy of verbal and non-verbal de-escalation of seriously agitated children and young people with mental health problems’ and recommends research to ‘systematically describe expert practice in adults, develop and test those techniques in aroused children and young people with mental health problems, and develop and test different methods of training staff’46 (NICE. Violence and Aggression: Short-term Management in Mental Health, Health and Community Settings. London: NICE; 2015. © NICE 2015 Violence and Aggression: Short-term Management in Mental Health, Health and Community Settings. Available from www.nice.org.uk/guidance/ng10. All rights reserved. Subject to Notice of Rights. NICE guidance is prepared for the National Health Service in England. All NICE guidance is subject to regular review and may be updated or withdrawn. NICE accepts no responsibility for the use of its content in this product/publication).
The current study is one of a pair addressing NICE’s recommendation to systematically describe restrictive practices with adults and children. The research team’s original study, COMPARE (HSDR 16/53/17),47 fulfilled the first part of NICE’s recommendation by systematically describing practice with adults in mental health inpatient settings. The current review, CONTRAST, is a companion study that took the same approach but reviewed the evidence for interventions to reduce staff use of restrictive practices in child and adolescent institutional settings, including, but not limited to, mental health contexts. It was anticipated that the features of an intervention (its content and delivery) were likely to interact with the delivery context (the target population and setting) and with the features of the target behaviour. 48 Although the target behaviour (use of restrictive practices) was the same as the original study, the context shifted to a range of institutions caring for children and adolescents with different physical, psychological and developmental abilities, employing a wide range of professions, and in which the legality and guidelines for the use of restrictive practices vary. The intention was to compare interventions across these settings to permit exploration of the relationship between intervention features (content and delivery) and context (target population and setting), together with the identification of differences in content, influences on delivery and potential implications for effectiveness.
Addressing the limitations of the evidence base using the behavior change technique taxonomy
The reporting of non-pharmacological trials is challenging because of the absence of a common language with which to describe their components. 49,50 A review51 found that only 39% of interventions were ‘adequately’ described when published. In response to this lack of consensus, the Medical Research Council (MRC) supported the development of a taxonomy of BCTs that can be used across all theory-based interventions aimed at patients or professionals,52 both prospectively in their design and/or to synthesise evidence restrospectively. 52,53 A BCT is defined as ‘an observable, replicable, and irreducible component of a programme designed to alter or redirect causal processes that regulate behaviour’. 52 All interventions to reduce restrictive practices use BCTs. For example, role-playing verbal de-escalation strategies could be coded as rehearsal of relevant skills involving social comparison (BCT 6.2), monitoring of emotional consequences (BCT 5.4) and feedback on behaviour (BCT 2.2). Delivery of information by an expert about risks of restraint could involve information about health consequences delivered by a credible source (BCT 5.1). The taxonomy therefore enables reliable, precise and transparent reporting, replication and comparison of interventions,54 along with more successful implementation with proven effectiveness. 52 It is increasingly used internationally to report interventions,55 synthesise evidence56,57 and reanalyse existing interventions to explore their components. 58 It is also influencing intervention design48 and contributing to the identification of potentially effective BCTs. 52
Chapter 2 Aim and objectives
Aim
The study aim was to identify, standardise and report the effectiveness of components of interventions that seek to reduce restrictive practices in CYP’s institutional settings using the behaviour change taxonomy.
Objectives
The study objectives were to:
-
provide an overview of interventions aimed at reducing restrictive practices with CYP
-
classify components of those interventions in terms of BCTs and determine their frequency of use
-
identify the role of process elements in intervention delivery
-
explore the evidence of effectiveness by examining BCTs and intervention outcomes, where possible
-
compare the components of interventions in CYP’s settings with those in adult psychiatric inpatient settings47 and identify potential explanations for any differences
-
identify and prioritise BCTs that show the most promise of effectiveness and that require testing in future high-quality evaluations.
Chapter 3 Methods
This chapter describes the study design, including approaches to the literature search, data extraction and analysis.
Design overview
Design and conceptual framework
The study approach was a systematic mapping review. An ‘intervention’ was any documented approach that sought to reduce the use of restrictive practices through BCTs. The literature review focused on ascertaining the range and characteristics of interventions, irrespective of evidence of effectiveness, which involved systematically searching and reviewing all reports of interventions seeking to reduce the use of restrictive practices (Figure 1).
FIGURE 1.
Design of systematic mapping review.
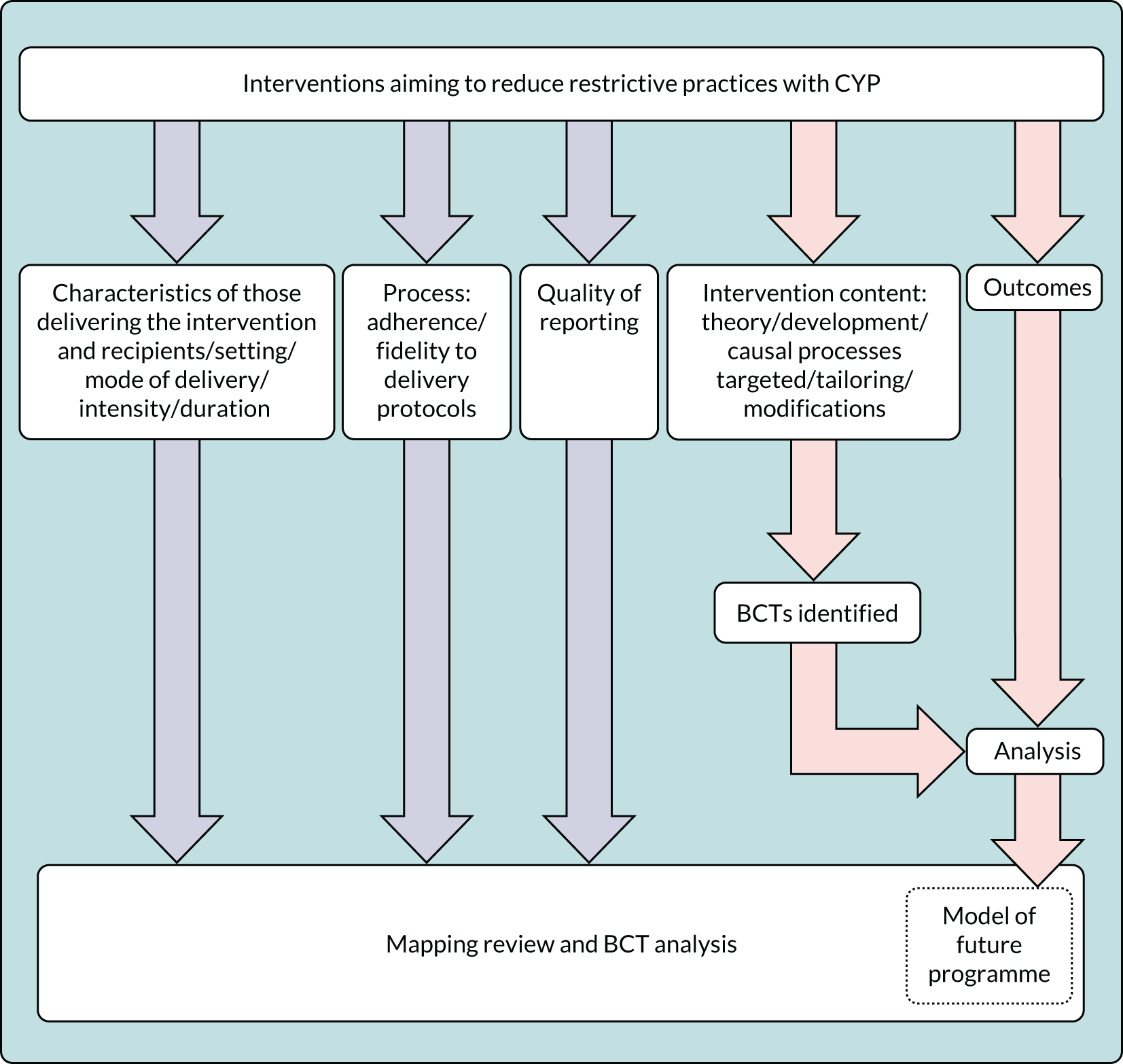
The study design comprised the following six objectives.
Environmental scan involving a systematic search of all English-language reports of interventions to reduce restrictive practices in children and young people’s institutional settings (objective 1)
The search strategy approach drew on the increasingly used method of mapping59–64 to inform the purpose and output of the review, but differed from the method described by Bradbury-Jones et al. 59 with respect to the broad scope of the search and inclusion of interventions in the current study. It was known that, in addition to a small number of well-known interventions reported in the academic literature, there were numerous small-scale, stand-alone initiatives available for implementation in services. Not all of these would appear in a search restricted to the published research literature, as they could be reported in unpublished literature or relevant sources that are not reporting research. Furthermore, the current study required the documentation from the interventions (e.g. training programmes) themselves, offering full descriptions of the interventions in addition to research studies evaluating the intervention.
Therefore, an environmental scanning approach was applied. Environmental scanning methods were developed to identify broader information about an area than that which is retrievable solely from published literature. They allow flexibility in the approach to obtaining materials. Environmental scans have been used for identifying and evaluating online resources or training and for reviews of training programmes. 65–67 In health-care settings, this method has been used to inform future-planning, to document evidence of current practice and to raise awareness of an issue. 68
Application of the method can take a ‘passive’ approach in which existing data, both published and unpublished, are collected and analysed, or an ‘active’ approach in which additional knowledge is generated through primary data collection. 68 This study used passive environmental scanning methods to collect available descriptive or evaluative information about interventions that aim to reduce staff use of restrictive practices.
This approach fitted well with the need to search using internet search engines and social media, plus a large number and wide variety of websites, to identify training programme materials. Hence, it was an appropriate choice for expanding the scope of the search strategy.
Synthesis of the features of interventions, alongside a critical appraisal of all retrieved records (objectives 2, 4 and 6)
The study design is illustrated in Figure 1.
Examples included delivery to groups or individuals, the person delivering the intervention, and the setting, timing and frequency of the interventions. 49 These were recorded using WIDER (Workgroup for Intervention Development and Evaluation Research),69 a checklist that prompts detailed recording of interventions based on the questions ‘why, what, who, how, where, when and how much?’. WIDER serves as an extension to both CONSORT (Consolidated Standards of Reporting Trials) and SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials). 51
Critical appraisal was informed by the Mixed Methods Appraisal Tool (MMAT), which is an appraisal tool specifically designed for mixed-methods reviews. 70,71
The Behaviour Change Wheel
To support the synthesis of the context of the interventions, the Behaviour Change Wheel was used. This was produced from a synthesis of frameworks of behaviour change research literature. 72 It is based on a model of behaviour called the COM-B, which attempts to describe how Capability, Opportunity and Motivation can change Behaviour. The Behaviour Change Wheel contains the higher-order categories of BCTs at its hub (e.g. ‘social’ or ‘reflective’). The next level includes intervention functions such as ‘training’ or ‘incentivisation’, and the third, outer, level contains policy categories such as ‘legislation’ or ‘regulation’.
The initial data extraction included the categories from the Behaviour Change Wheel. The subsequent, more detailed, BCT coding of interventions was therefore an extension to this process, focusing on the detail of the study in which it was reported, and relating it back to intervention function in the Behaviour Change Wheel. For example, providing information on consequences of restrictive practices would relate to the intervention functions of ‘education’ and ‘persuasion’. Use of the Behaviour Change Wheel in this way facilitated reporting of all interventions in different levels of detail.
Extraction of intervention content for analysis using a validated, structured taxonomy (the behavior change technique taxonomy) to identify the content of the interventions, when possible (objective 2)
The behavior change technique taxonomy
When possible, content of the interventions was extracted using the BCT taxonomy, which is supported by the MRC. 73 The MRC BCT taxonomy consists of 93 items, each one an individual BCT, for example BCT 6.2 (social comparison) or BCT 1.2 (problem-solving). Individual BCTs are also grouped into clusters, for example cluster 1 (goals and planning). The taxonomy provides examples of these items, often related to patient behaviour, although recent studies have provided examples of health-care professionals’ behaviour to inform studies such as this that seek to code health-care professionals’ behaviours. 73
The BCT taxonomy is a reliable method for extracting data regarding the content of interventions. 52 All materials available for each intervention (e.g. manuals, evaluation reports) were coded by trained coders using the taxonomy. This process identified the individual BCTs detected in each intervention and their frequency of use.
Where possible, extraction of the outcomes of coded interventions and relating of them to the behavior change technique taxonomy (objectives 3 and 4)
When an intervention was coded for BCTs, available outcome data were then extracted.
Comparison of components of interventions in children and young people’s settings with those in adult psychiatric inpatient settings (objective 5)
The two settings were compared to address questions about the comparability and transferability of interventions to reduce restrictive practices and their specific BCT components, such as:
-
Do interventions aimed at staff of different professions working in children’s services take account of the significant differences in population?
-
Are the BCT components of interventions aimed at staff in children’s settings different from those in adult settings, and should they be?
It was possible that interventions in adult settings might comprise particular BCTs that were not found in interventions in children’s settings. If identified as effective, these BCTs could be considered to be worth testing in children’s settings (and vice versa).
Analysis of potential relationships between reduction of restrictive practices and behaviour change techniques (objective 6)
Analysis of potential relationships between reduction of restrictive practices and BCTs was carried out with the aim of generating hypotheses for future testing and developing potential causal models for future trials.
Literature search strategy
Search strategy
The approach to searching and screening was guided by the mapping and scoping literature59–64 and provided an initial draft search. This draft search went through several iterations before a final search was conducted. The reviewers screened some sample search results to consider the relevance of the studies. Research literature, policies and grey literature, including training manuals, were identified using comprehensive search strategies developed in collaboration with the information specialist and from consulting the known literature and database thesauri (e.g. medical subject heading).
Searches were developed for the following concepts: child or child behaviours; restraint practices or named programmes; and a variety of institutional, health-care and educational settings. The search was limited to material after 1989 because of changes in attitudes to children’s rights, as reflected in the United Nations Convention on the Rights of the Child (UNCRC) 198974 and, in the UK, the 1989 Children Act,75 which introduced comprehensive reforms to the law in terms of the care and protection of children.
Restraint studies relating to road safety or traffic incidents were excluded. Subject headings and free-text words were identified for use in the search concepts by the information specialist and project team members. Further terms were identified and tested from known relevant papers.
All searches were peer reviewed by an information specialist. Search strategies were adapted with the aim of producing fewer and more relevant results without missing relevant studies. Additional studies were identified via bibliographies of reviews and retrieved articles, targeted author searches, contacting international experts and forward citation searching. The project management group was asked for details of any known interventions, and authors of current and recently completed research projects were contacted directly.
In June 2019, academic databases were searched for studies looking at child restraint in a variety of settings. The searches were updated in January 2020 in all but the Education Abstracts and Scopus databases. Analysis of the studies selected for inclusion from the 2019 searches showed that none had come exclusively from these two databases. Table 1 indicates the databases that were searched within the stated dates.
| Database | Date range searched |
|---|---|
| ASSIA (ProQuest) | 1987 to 24 January 2020 |
| British Nursing Index (HDAS) | 1992 to 24 January 2020 |
| CINAHL (EBSCOhost) | 1981 to 30 January 2020 |
| Child Development and Adolescent Studies (EBSCOhost) | 1927 to 24 January 2020 |
| Criminal Justice Abstracts (EBSCOhost) | 1830 to 30 January 2020 |
| Education Abstracts (H. W. Wilson) (EBSCOhost) | 1983 to present, updated 14 June 2019 |
| EMBASE Classic and EMBASE (Ovid) | 1947 to 21 January 2020 |
| ERIC (EBSCOhost) | 1966 to 30 January 2020 |
| Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily | 1946 to 20 January 2020 |
| PsycInfo (Ovid) | 1806 to week 2 January 2020 |
| Scopus (Elsevier B. V.) | 1823 to 13 June 2019 |
Grey literature searches were conducted in August 2019 and updated in January 2020 in the websites and databases in Box 1. See Appendix 1 for full details of all searches.
Agency for Healthcare Research and Quality.
AGENDA: Alliance for Women & Girls At Risk.
Article 39.
Barnardo’s.
British Association of Social Workers.
British Institute of Learning Disabilities.
British Society of Criminology.
Challenging Behaviour Foundation.
Children Society.
Crisis Prevention Institute.
Foundation for Professionals in Services to Adolescents.
Google (Google Inc., Mountain View, CA, USA).
HM Inspector of Constabulary and HM Inspector of Fire & Rescue Services.
HM Inspectorate of Prisons for England and Wales.
HM Inspectorate of Probation.
Howard League.
INQUEST.
MENCAP.
National Children’s Bureau.
National Police Library.
National Society for the Prevention of Cruelty to Children.
National Youth Work.
Prison Reform Trust.
Prisons and Probation Ombudsman.
ProQuest Dissertations & Theses A&I (ProQuest) 1743 to 24 January 2020.
Restraint Reduction Network.
SAFE Crisis Management.
SCIE.
Secure Children’s Homes/Secure Accommodation Network.
Social Care Online (SCIE) 1980 to 28 January 2020.
Twitter (www.twitter.com; Twitter, Inc., San Francisco, CA, USA).
Young Minds.
Youth Justice Board for England and Wales.
Eligibility
In keeping with objective 1 (to provide an overview of interventions aimed at reducing restrictive practices in children’s settings), the search criteria targeted diverse reports of non-pharmacological interventions aimed at changing the behaviour of service staff to reduce restrictive practices. The scope of the searches was necessarily broad to include all records of an intervention, whether it was an evaluation or a descriptive report. To include as many interventions as possible within the scope of the search, no quality threshold was imposed either indirectly (by restricting the search to high-impact journals) or directly via the search criteria or by screening. Inclusion was not restricted by study design. Interventions that solely involved policy change and those that aimed to reduce the use of one type of restrictive practice by replacing it with another were not eligible for inclusion. 59–64,68,70,71
In addition to interventions intended to reduce or eliminate restrictive practices, reports of interventions designed to improve quality or reduce or manage violence were included if their procedures and/or outcome measures addressed restrictive practices. The search for relevant interventions records was informed by the ‘environmental scanning’ approach68 described above. Eligibility criteria are shown in Table 2. See Appendix 1 for full details of all searches.
| Criterion | Include | Exclude |
|---|---|---|
| Population | Staff working in state and privately operated CYP’s institutional settings [including children’s homes; residential schools; boarding schools; young offender institutions; secure training centres; immigration detention centres; and inpatient child and adolescent mental health, child and adolescent hospitals (non-mental health) and learning disability services] | Interventions to reduce staff use of restrictive practices with adults (only > 18 years) |
| Date | Dated 1989 to date | Pre-1989 |
| Interventions | Intervention: documented interventions aimed at reducing staff use of restrictive practices with CYP in institutional settings |
Pharmacological only intervention Non-English-language interventions |
| Outcomes | Outcomes: reduction of restrictive practices | |
| Language | English |
Data management and review
All potentially eligible records were stored and managed in the reference management software EndNote™ version X9 (Clarivate Analytics, Philadelphia, PA, USA). Two reviewers screened titles. When both reviewers agreed to exclude an article, the reason for exclusion was recorded. When there was disagreement, the full text of the articles was reviewed and any unresolved disagreement was subject to third-party review. When there was agreement between the two reviewers on inclusion, the full-text article was retrieved and independently assessed against the inclusion criteria by the two reviewers and, again, any disagreement was subject to third-party review.
Quality appraisal using the Mixed Methods Appraisal Tool
Because the inclusive search criteria identified very diverse record formats, quality appraisals were used not to exclude papers but to inform the synthesis by identifying study designs and, hence, evaluations. Study quality was assessed using the MMAT. This tool is suitable for appraising studies with diverse designs. 70,71 The characteristics of the MMAT70,71 make it the most suitable tool with which to judge study quality in the context of wide-ranging research methods.
The MMAT was developed for use in complex systematic literature reviews that include quantitative, qualitative and mixed-methods studies (Figure 2). It was developed from theory and a literature review and has been found to have good validity. 76 The MMAT algorithm for selecting study categories is illustrated in Figure 3. Using the MMAT algorithm, reports of milieu change and case studies were categorised as qualitative studies if reporting suggested a primarily qualitative approach.
FIGURE 2.
Mixed Methods Appraisal Tool, version 2018. Adapted from Hong Qn, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT), version 2018. 70 Registration of Copyright (#1148552) Canadian Intellectual Property Office, Industry Canada.
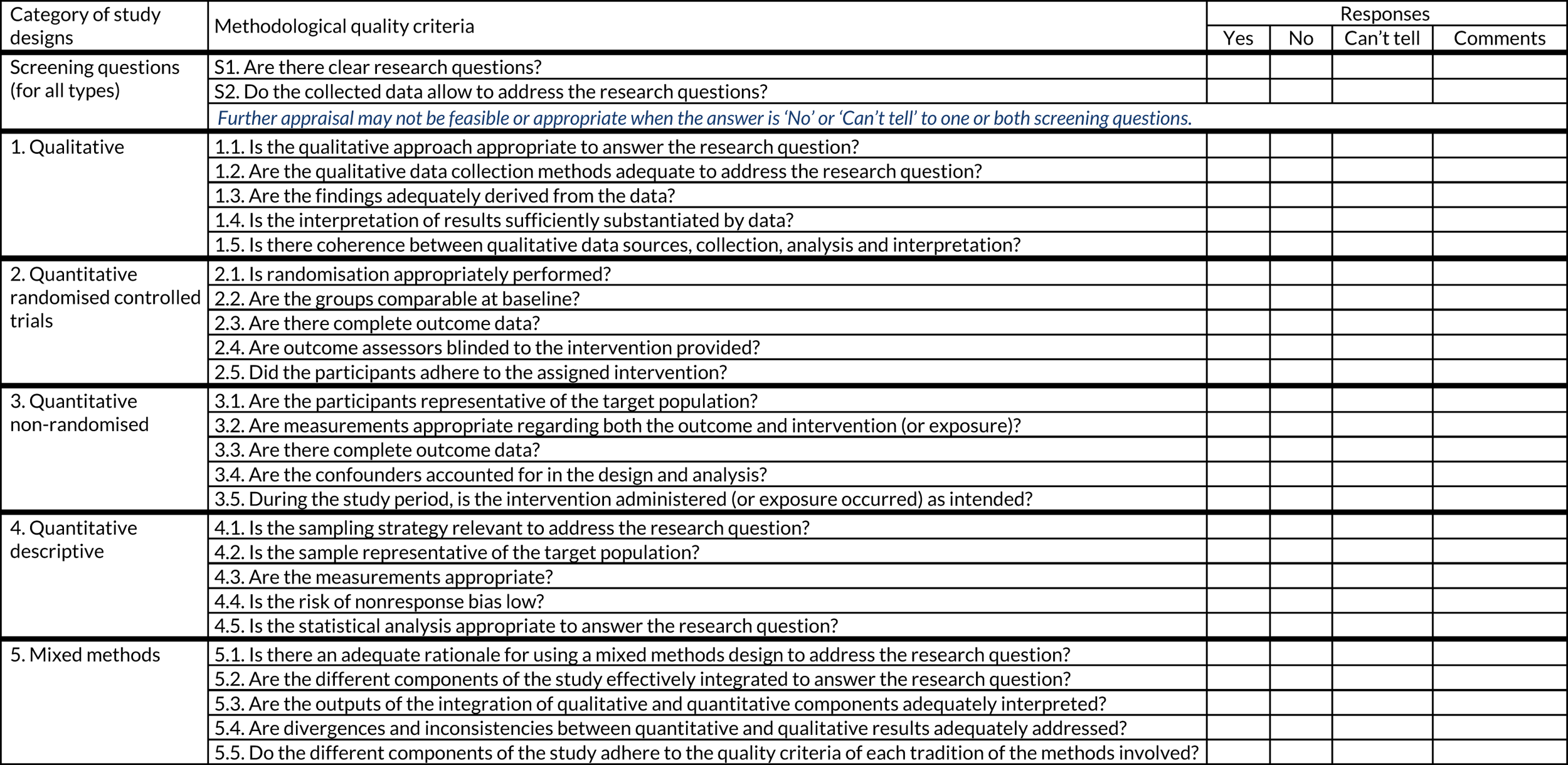
FIGURE 3.
Mixed Methods Appraisal Tool algorithm for selecting study categories. Adapted with permission from Hong Qn, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT), version 2018. 70 Registration of Copyright (#1148552) Canadian Intellectual Property Office, Industry Canada.

Using the MMAT, quantitative and qualitative studies are judged against four criteria and mixed-methods studies are judged against three. The quantitative domain is split into three subdomains: randomised controlled, non-randomised and descriptive. As applied in the current study, surveys, case reports, descriptive cross-sectional studies and ecological studies were categorised as ‘quantitative descriptive’ if reporting suggested a primarily quantitative approach. The mixed-methods category included reports of milieu change with substantial quantitative analysis.
Therefore, the tool was used at two levels: (1) to identify records of interventions that had been evaluated to get a sense of the quality of the evidence using the two initial screening questions, and (2) to assess the quality of the evaluation reports. The application of the MMAT to screen and categorise all the records informed the narrative accounts provided in Chapters 4 and 5.
Documented interventions were identified. Data extraction was governed by a pro forma that allowed systematic collection of data relating to the interventions. Analysis of the features of interventions revealed the context of how interventions were delivered (e.g. delivery to groups or individuals; the person delivering the intervention; and the setting, timing and frequency of the interventions). 49 When available, these details were recorded using the WIDER69 checklist. WIDER is a tool for assessing reporting quality. It contains a number of relevant categories that facilitated this process.
Content extraction
The content of interventions was extracted to allow their components to be coded using the BCT taxonomy. Extraction was carried out by two reviewers and any discrepancies were subject to third-party review. Extraction categories were developed from the WIDER69 checklist. Data were extracted about the characteristics of each intervention, including participants, setting, intervention type, outcome measures, fidelity, acceptability, recommendations and quality. When information was available, associated costs were described in terms of training materials, delivery and staff time.
Intervention coding
The researchers were fully trained in the application of the BCT taxonomy. Using the taxonomy and supporting examples, the researchers independently coded the selected interventions. Interventions that were coded for BCT components had information about their outcomes extracted to examine the efficacy of these techniques.
Coding was carried out by importing all intervention materials (published papers, manuals, slides, handbooks) into NVivo 12 (QSR International, Warrington, UK), a flexible qualitative software package that facilitates the coding of multimedia materials for analysis. Each of the 93 items of the BCT taxonomy was turned into a code within NVivo and considered for each intervention. The codes were applied when there was evidence of the BCT being used; for example, when a professional received information about the potentially harmful effects of restraint during a training session, this was coded as BCT 5.1 (information about health consequences). Any assumptions made by the coder were recorded, also within NVivo, in order that discrepancies could be discussed. Once the coding was complete, NVivo was used to generate individual study reports that revealed discrepancies between coders. Each discrepancy was discussed and resolved by the coders and, if necessary, further discussion took place with other expert members of the team to achieve resolution. This discussion consisted of the coder explaining their reasoning as to why they had assigned the code. The individual study reports were compiled to produce a summary of how many of the possible 93 BCTs were found in interventions, how often they occurred and whether or not they were from particular clusters. Study outcome data were extracted and used to explore whether or not there were potential relationships between study outcomes and particular BCTs.
Data synthesis
The approach to data synthesis was designed to suit the diverse set of included records. It was not relevant to apply stringent academic appraisal techniques in a conventional way because the data set included some records that were neither academic publications nor formal reports. For example, a key source of information about the 6CS intervention was a set of workshop slides. 77
Meeting the objectives set out in this chapter involved exploring and categorising the records, identifying intervention evaluations and then conducting a detailed analysis of the available information about the interventions. The purpose of this was to identify BCTs to produce a synthesis of intervention characteristics, components in terms of BCTs, process elements, effectiveness evidence in terms of BCTs and intervention outcomes, and also to compare the results with the results of the companion COMPARE study47 focusing on adult acute mental health settings.
Therefore, data were synthesised by a process of close scrutiny of the included records, and tailored application of the MMAT and WIDER recommendations to understand the scope and quality of the materials and meet the study objectives.
Following extraction, the records were organised into groups according to the intervention or interventions they described. This allowed for a primary focus on the evidence for each intervention, rather than the overall evidence (objectives 4 and 6) in parallel with the classification and analysis of intervention components (objective 2).
Narrative synthesis
Interventions were placed in subgroups according to the setting and type of restrictive practice that they seek to reduce [e.g. p.r.n. (pro re nata) medication, physical and seclusion]. A narrative synthesis across and within each subgroup was carried out exploring and describing the features of the interventions including their theoretical basis, population, outcomes and conclusions. The content of the types of intervention was described in terms of the types and frequency of BCTs that could be identified [e.g. social support, skills practice and modelling (Table 3)]. The outcome data from the interventions were presented in relation to the BCTs present, and hypotheses were formulated around whether specific types of BCTs appeared more frequently, or not at all, in studies reporting certain outcomes.
| Type of BCT | Example of how this BCT has been used in a model reducing restrictive practices |
|---|---|
| Health consequences | Information given about the potential risks of asphyxiation or cardiac events during restraint33 |
Chapter 4 Results of literature search
Introduction
The chapter provides an overview of the literature search results, including a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) figure to indicate the extraction process. The included records are listed in Appendix 2. In this chapter, the results are described in detail and key characteristics of the data set are highlighted. As per objective 1 and in keeping with the mapping approach, a narrative overview of interventions aimed at reducing restrictive practices with CYP is then provided. It describes the characteristics of the interventions identified within the data set of records, including their scope and common features. The description of the evaluations is informed by WIDER reporting recommendations. Figure 4 summarises the study processes.
FIGURE 4.
Summary of study processes.
Search results
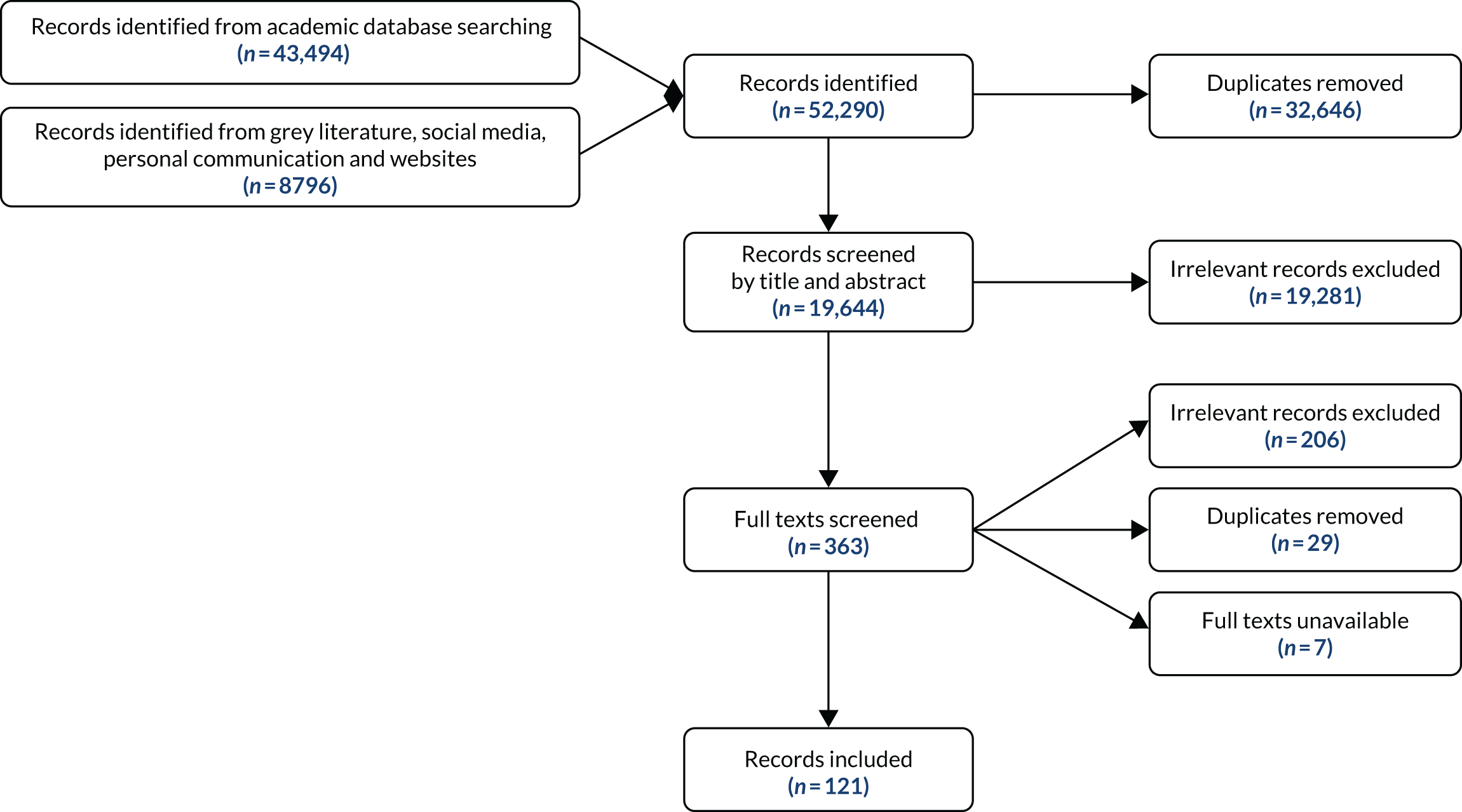
As illustrated in the PRISMA figure (Figure 5), the search of academic databases identified 43,494 records and these, as well as 8796 records found in the grey literature (including social media), were entered into Covidence (Melbourne, VIC, Australia) for further analysis. After the removal of duplicates, and accounting for records that were not available, 19,644 records were subjected to title and abstract screening. The final data set consisted of 121 records for extraction. Further details of the search strategy and results are available in Appendices 1 and 2.
FIGURE 5.
The PRISMA figure. Grey literature: non-academic databases and websites, social media and ‘other’ records. ‘Other’ records: discovered using forward citation searches and contact with authors. Excluded because not relevant: records excluded because they report not an intervention but, for instance, a generic policy change or replacement of one restrictive practice with another.
Responses to requests for intervention materials
In addition to the processes described above, attempts were made to request further information about interventions to supplement information found in the 121 included records. This involved sending e-mails to authors and co-authors, and, when appropriate, to organisations, using contact details provided in or otherwise gleaned from the records. Seventy-one e-mail requests were sent (see Appendix 3), resulting in new information about six of the interventions: Six Core Strategies for Reducing Seclusion and Restraint Use,33 Trauma Affect Regulation,78 Neurosequential Model of Therapeutics,79 Milieu Nurse Shift Assignments,80 Crisis Intervention81 and Checklist for Assessing Your Organisation’s Readiness. 82
Study screening
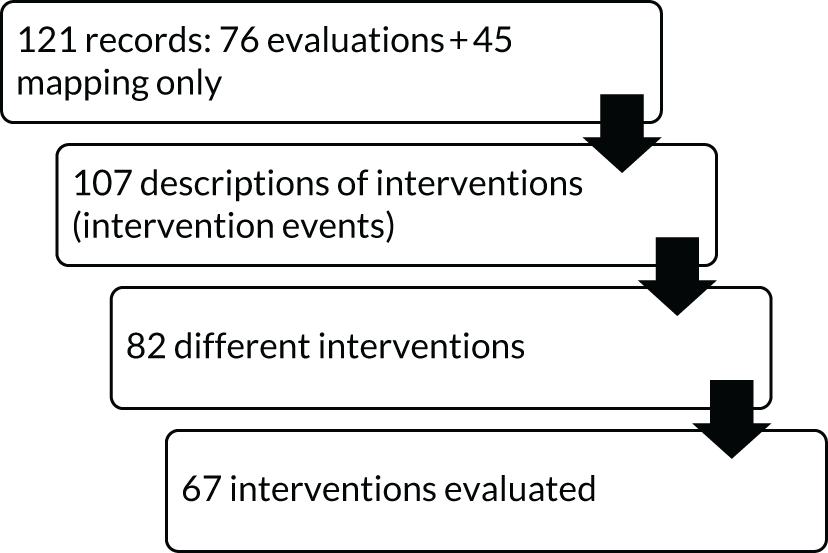
The records were diverse in terms of format and reporting quality. The first two questions of the MMAT70 were applied to screen the 121 records to identify those that were evaluations. In all, there were 76 records that were evaluations and 45 records that were descriptive only and did not contain evaluations. These 45 were used for mapping only and consisted of training resources, blogs, websites and almost all of the reports (e.g. reports to organisations).
Categorising the studies
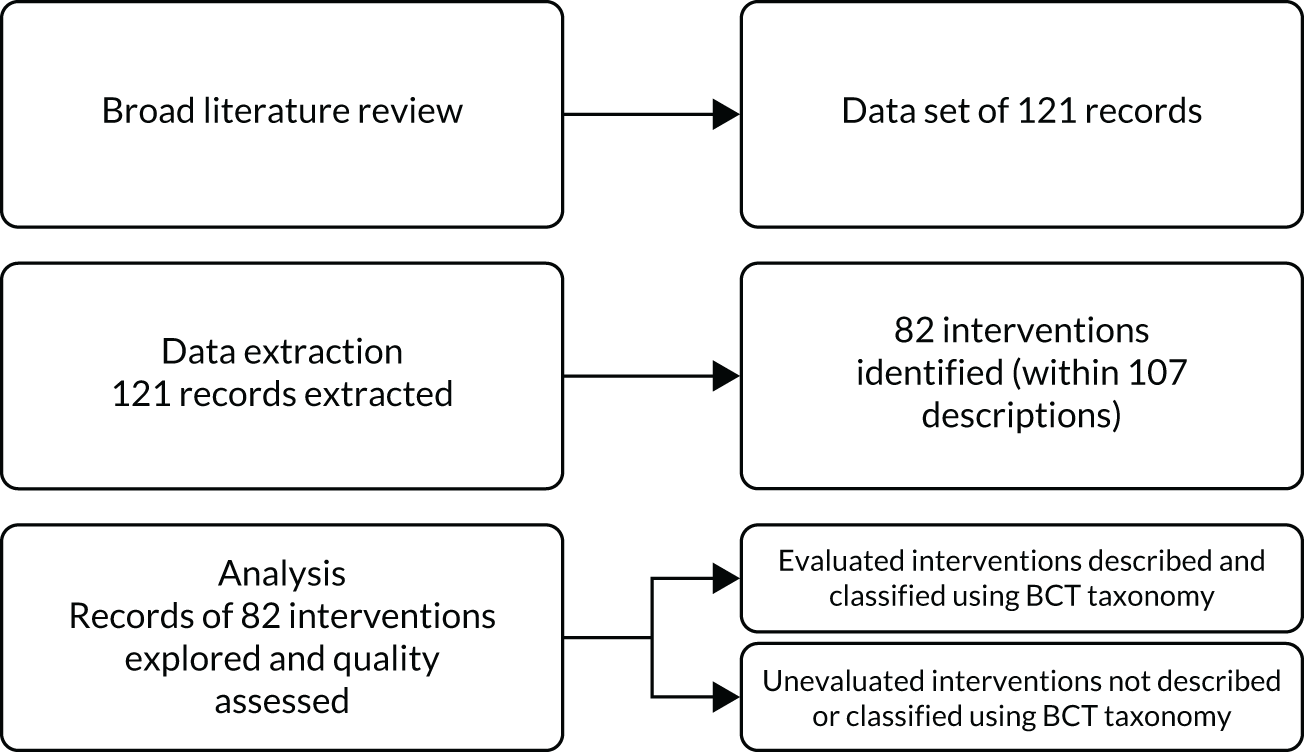
Some interventions occurred in more than one record, some records reported more than one intervention and some reports were mentioned in more than one record. Overall, the data set contained 107 descriptions of interventions, referring to 82 interventions in total, of which 67 interventions had been evaluated. The data set is summarised in Figure 6.
FIGURE 6.
Summary of the data set.
Categorisation of study (evaluation) design
In view of the widely ranging literature retrieved from the searches, the MMAT was used to categorise all 121 records by study design. As reported above, 76 records were classified as evaluations; the remainder were descriptive only. The 76 evaluations were allocated, where possible, to one of the five MMAT categories:70 qualitative description, randomised controlled trial (RCT), non-randomised trial, quantitative description or mixed-methods study. As summarised in Table 4, the majority of the 76 records of evaluations reported non-randomised designs. Thirty-two evaluation records lacked sufficient detail for categorisation by study design with the MMAT. None was categorised as a RCT. Only 15 of the 45 mapping records provided detail of study design; however, as indicated above, not all mapping records were research reports. Based on the MMAT screening questions, intervention study design was as follows: non randomised, n = 41; quantitative, n = 21; mixed methods, n = 5; qualitative, n = 5; no study design reported, n = 2.
| Study design | Evaluation records (n = 76) | Mapping records (n = 45) | Total |
|---|---|---|---|
| RCT | 0 | 0 | 0 |
| Non-randomised trial | 41 | 3 | 44 |
| Quantitative description | 23 | 7 | 30 |
| Qualitative description | 5 | 3 | 8 |
| Mixed-methods study | 5 | 2 | 7 |
| Insufficient detail | 2 | 30 | 32 |
| Total | 76 | 45 | 121 |
Consistency and comprehensiveness of intervention reporting
Overall, reporting about interventions lacked consistency and comprehensiveness. The WIDER tool69 that was used to develop the data extraction strategy also informed the appraisal of reporting quality and identified a great deal of missing information about key aspects of interventions. Within the evaluation records, intervention recipient and setting were well reported, but intervention aims and by whom the intervention was delivered were not consistently reported. Most evaluation records did not report on intervention dose, fidelity to the intervention protocol, whether or not modifications were made to the intervention, whether or not intervention protocols were used and whether or not service users were involved in the development of the intervention. Within the mapping records, reporting was weak across the WIDER categories. The detail is presented in Table 5. Evaluation and mapping records are reported separately because of the differing overall characteristics of each subset. The detail provided in Table 5 reflects information as reported directly in the records, rather than inferred or extrapolated.
| Reporting | WIDER recommendation | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Detailed description of interventions | Assumed change process and design principles | Access to manuals/protocols | |||||||||||
| By whom delivered | Recipient | Setting | Mode of delivery in implementationa | Dose | Modification | Fidelity | Theory informedb | Developmentc | Materials | ||||
| Duration | Intensity | ||||||||||||
| Evaluation records (N = 76) | |||||||||||||
| R | n | 42 | 72 | 76 | 22 | 22 | 15 | 3 | 12 | 43 | 10 | 10 | |
| % | 55.26 | 94.73 | 100 | 28.95 | 28.95 | 19.74 | 3.95 | 15.79 | 56.58 | 13.16 | 13.16 | ||
| NR | n | 34 | 4 | 0 | 54 | 54 | 60 | 64 | 64 | 33 | 66 | 66 | |
| % | 44.74 | 5.26 | 0 | 71.05 | 71.05 | 78.95 | 84.21 | 84.21 | 43.42 | 86.84 | 86.84 | ||
| N/A | n | 0 | 0 | 0 | 0 | 0 | 1 | 9 | 0 | 0 | 0 | 0 | |
| % | 0 | 0 | 0 | 0 | 0 | 1.32 | 11.84 | 0 | 0 | 0 | 0 | ||
| Mapping records (N = 45) | |||||||||||||
| R | n | 8 | 11 | 15 | 4 | 0 | 2 | 2 | 2 | 1 | 4 | ||
| % | 17.78 | 24.44 | 13.33 | 8.89 | 0 | 4.44 | 4.44 | 4.44 | 2.22 | 8.89 | |||
| NR | n | 7 | 4 | 0 | 11 | 15 | 13 | 13 | 13 | 14 | 11 | ||
| % | 15.56 | 8.89 | 0 | 24.44 | 33.33 | 28.89 | 28.89 | 28.89 | 31.1 | 24.44 | |||
| N/A | n | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | ||
| % | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | 66.67 | |||
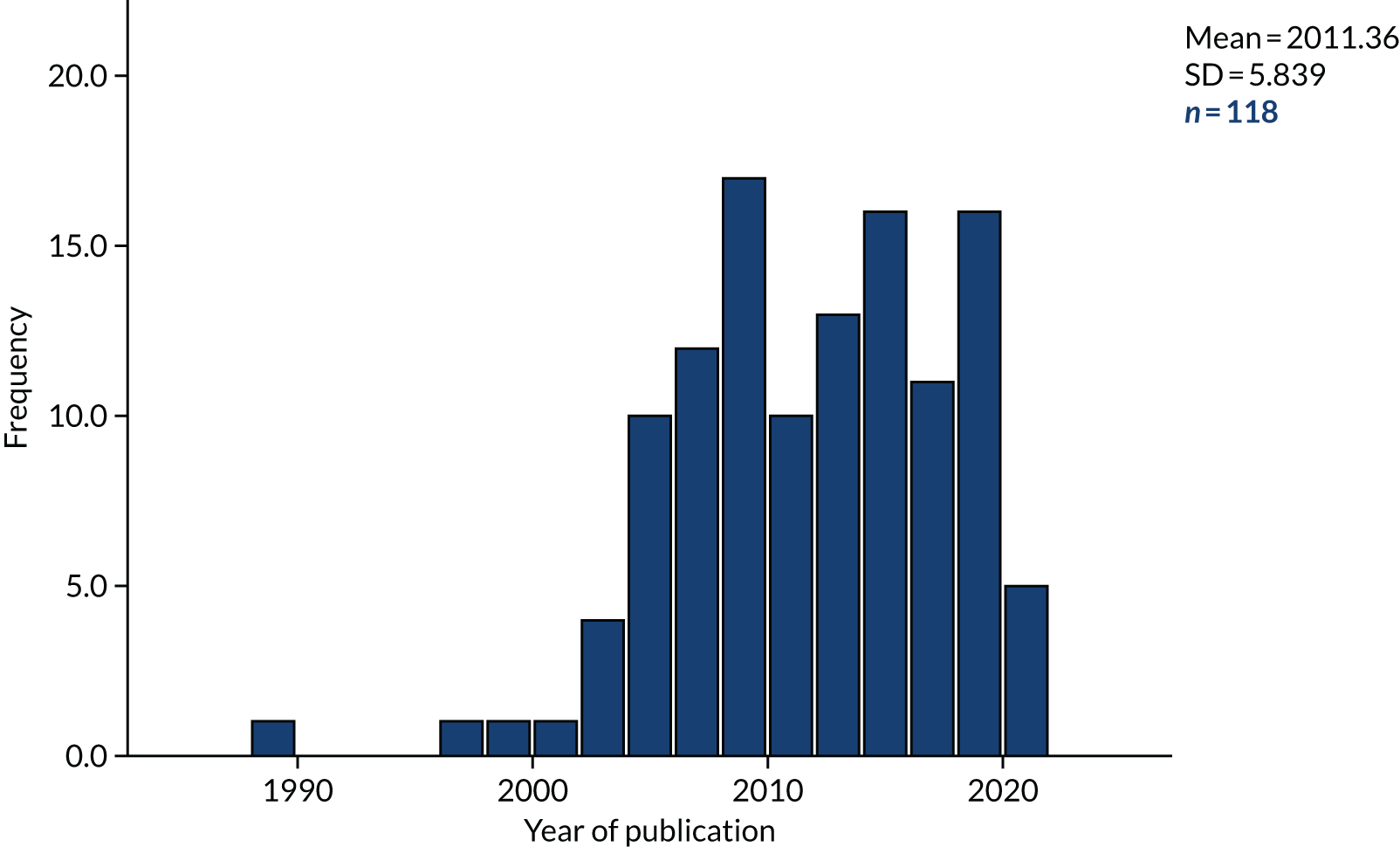
Publication date and format
Figure 7 illustrates the pattern of publication dates of 118 of the records. Three records were undated training resources in which the context and content indicated that they fell within the inclusion criteria. The figure shows that there was a brief increase in publications in the late 1980s and a sharp increase from the mid-2000s. The latter increase coincides with a US-wide policy response83,84 to a series of newspaper reports published in 1998 in the Hartford Courant newspaper, highlighting deaths related to the use of restraint in mental health and learning disability facilities across the USA. 33,83,84
FIGURE 7.
Publication dates.
Characteristics of records
The 121 records were organised by format type. Study designs of evaluations and mapping records are summarised in Table 6. Over half of the records were published in academic journals (n = 61). Eighty (66.1%) of the 121 records were peer reviewed. The additional peer-reviewed sources included book chapters (n = 3),85–87 dissertations (n = 11)88–98 and conference proceedings (n = 5). 99–103 The other records comprised training resources (n = 12); newsletters (n = 6); professional magazines (n = 4); presentation slides (n = 4); websites (n = 3) and blogs (n = 2); and reports (n = 10), of which seven were for government departments (UK, Wales, USA), two were for training organisations and one was for a US health-care service provider. 104
| Record type | Number of records (N = 121), n | Percentage |
|---|---|---|
| Peer reviewed | ||
| Academic journals | 61 | 50.4 |
| Book chapters | 3 | 2.5 |
| Dissertations | 11 | 9.1 |
| Conference proceedings | 5 | 4.1 |
| Other | ||
| Training resources | 12 | 9.9 |
| Newsletters | 6 | 5.0 |
| Professional magazines | 4 | 3.3 |
| Presentation slides | 4 | 3.3 |
| Websites | 3 | 2.5 |
| Blogs | 2 | 1.7 |
| Reports | 10 | 8.3 |
| Total | 121 | 100.0 |
Peer-reviewed sources
The 11 peer-reviewed sources that featured more than once appear in Table 7. The most frequently occurring single source was the Journal of Child and Adolescent Psychiatric Nursing.
| Peer-reviewed source | Frequency |
|---|---|
| Journal of Child and Adolescent Psychiatric Nursing | 9 |
| Psychiatric Services | 7 |
| Residential Group Care Quarterly | 6 |
| Residential Treatment for Children & Youth | 6 |
| Dissertation Abstracts International | 5 |
| Journal of the American Academy of Child and Adolescent Psychiatry | 4 |
| Chapters from same book | 3 |
| Dissertation unpublished/other | 3 |
| Journal of Family Violence | 2 |
| Journal of Psychiatric Practice | 2 |
| Research on Social Work Practice | 2 |
Service setting
Just under half of the records (60/121) came from mental health settings. The other service settings were health and social care, criminal justice and education. Three evaluation records and 14 mapping records reported more than one setting within a single service and were categorised as ‘generic’ (Table 8).
| Setting | Frequency | Percentage |
|---|---|---|
| Mental health | 60 | 49.6 |
| Health and social care | 23 | 19.0 |
| Generica | 17 | 14.0 |
| Criminal justice | 11 | 9.1 |
| Education | 10 | 8.3 |
| Total | 121 | 100.0 |
Records and interventions by geographical setting
Records by geographical setting
The majority of records (87/121) reported evaluations or projects conducted in the USA. A further 21 were conducted in Europe and the remainder were conducted in Canada, Australia, Singapore or in more than one country. Three records did not report a location. The spread of geographical settings by record is detailed in Table 9.
| Country | Frequency | Percentage |
|---|---|---|
| USA | 87 | 71.9 |
| UK | 18 | 14.9 |
| Canada | 4 | 3.3 |
| New Zealand | 1 | 0.8 |
| Australia | 3 | 2.5 |
| Finland | 1 | 0.8 |
| Netherlands | 1 | 0.8 |
| France | 1 | 0.8 |
| Singapore | 1 | 0.8 |
| International | 1 | 0.8 |
| Total | 118 | 97.5 |
| Missing | 3 | 2.5 |
| Total | 121 | 100.0 |
Interventions by geographical setting
Only 2 of the 82 interventions had been applied in more than one country: Therapeutic Crisis Intervention (TCI) [UK, USA and one other intervention event (i.e. separate occurrences of the specific intervention) with an unreported location] and Modified Positive Behavioral Interventions and Supports (M-PBIS) (UK, Wales and USA). All other interventions that were applied more than once were implemented in the USA. These were the 6CS (n = 11 events), Collaborative Problem-Solving (CPS) (n = 7 events), comfort versus control (n = 2 events), the Grafton program (n = 2 events), Trauma Affect Regulation: Guide for Education and Therapy (TARGET) (n = 2 events), and Devereux’s Safe and Positive Approach (SPA) (n = 2 events).
There were 74 ‘stand-alone’ interventions (i.e. were applied in a single event). They were often developed within and for a specific setting and were not necessarily given a name. Of these, 51 were delivered in the USA, seven in the UK, three in Canada, three in Wales (UK), three in Australia, two in international projects and one each in Finland, New Zealand, Singapore, the Netherlands and France. Therefore, in both range and quantity, the vast majority of interventions were applied in the USA.
Reporting of interventions
An ‘intervention event’ indicates an occasion on which an intervention was implemented. For example, an intervention implemented on two separate occasions generated two ‘intervention events’. The same intervention implemented on a single occasion generated one ‘intervention event’, regardless of the number of records reporting it.
Two records seemed to pertain to an ongoing programme,38,105 but there were no other follow-up or replication studies. Several interventions were reported in more than one record, for example Craig88 and Canady,106 including some instances in which the same intervention evaluation was reported in different formats, such as a dissertation and a published paper (e.g. CPS89,107 and the Grafton program88,108).
The intervention for which the most records were identified was the 6CS [n = 12 records, including five evaluations (journal articles) and seven mapping records, comprising one journal article, one magazine, one training resource, one set of presentation slides, two blogs and one implementation tool]. The next largest group of records (n = 9) pertained to CPS. This group consisted of evaluations only, and comprised four dissertations,90–93 one publication from a dissertation107 and four journal articles. 109–112
The eight remaining interventions were comfort versus control (two events), TCI (three events), the Grafton program (two events), CPS (seven events), M-PBIS (three events), TARGET (two events) and SPA (two events). Those interventions that featured more than once are shown in Table 10. All records of interventions in evaluation studies and mapping studies are listed by author in Appendix 4, and further details are given in Appendix 5.
| Intervention | Intervention events (n) | Where delivered | Evaluation records (n) | Mapping records (n) | Number of records |
|---|---|---|---|---|---|
| 6CS | 12 | USA | 538,77,104,113,114 | 733,105,115–119 | 12 |
| CPS | 9 | USA | 989,91–93,107,109–112 | 0 | 9 |
| Comfort vs. control | 2 | USA | 288,120 | 0 | 2 |
| TCI | 3 | UK, USA | 181 | 4121–124 | 5 |
| Grafton program | 2 | USA | 288,108 | 0 | 2 |
| M-PBIS | 3 | UK, USA | 2100,125 | 2126,127 | 4 |
| TARGET | 2 | USA | 2128,129 | 1130 | 3 |
| SPA | 2 | USA | 1131 | 1132 | 2 |
| Total | 32 |
Intervention aims
All interventions aimed to reduce restrictive practices, and most focused on achieving that by changing staff behaviour.
Intervention recipient
When the recipient was reported, all interventions were delivered to staff, with some also aimed at service users and/or introduced within a wider organisation or as milieu change. Seventy-nine intervention events targeted staff only, 13 targeted staff and service users, and two included staff and/or service users in the context of change in milieu (Table 11).
| Delivered to | Frequency | Percentage |
|---|---|---|
| Staff | 79 | 73.8 |
| Staff and service users | 13 | 12.1 |
| Staff, service users and milieu | 1 | 0.9 |
| Staff and milieu | 1 | 0.9 |
| Total (excluding missing data) | 94 | 87.9 |
| Missing data (i.e. not reported) | 13 | 12.1 |
| Total | 107 | 100.0 |
Outcomes reporting
The 82 interventions described in the records reported a total of 228 outcome measures, with the number of measures described per record ranging from 0 to 11. The number of occasions when restraint was used was reported in 63 of the records, and the number of times seclusion was used was reported in 36 of the records. Other outcomes were reported in ≤ 11 records. Outcome measures are listed in Table 12.
| Outcome category | Outcome |
|---|---|
| Staff development and activity | Number of interventions |
| Intervention duration | |
| Number of behaviour plans in place | |
| Staff trained | |
| Staff knowledge/perceptions/attitude | |
| Use of restrictive methods | Mechanical restraint |
| Documentation of restraint | |
| Use of force | |
| Resource implications (financial and human) | Worker compensation |
| Injuries to all | |
| Patient progression and satisfaction | Patient satisfaction |
| Recidivism | |
| Number of elopements | |
| Client goal mastery | |
| Frequency of rule violation |
Outcomes categories
Outcomes reported were in four broad categories: staff development and activity, use of restrictive methods, resource implications, and patient progression and satisfaction (see Table 12).
Use of standardised outcomes measures
The reporting of standardised measures is shown in Tables 13 and 14. The range of measures reported per record was 0 to 7. In 106 of the records, no standardised measures were reported. One record129 reported the use of seven standardised measures to evaluate an intervention. In total, 22 different standardised outcome measures were reported across the 121 records.
| Number of standardised measures reported per record | Number of records |
|---|---|
| 0 | 106 |
| 1 | 7 |
| 2 | 6 |
| 3 | 1 |
| 7 | 1 |
| Measure | Number of times used in 121 records |
|---|---|
| CAFAS133 | 3 |
| CBCL134 | 2 |
| Global Assessment of Functioning135 | 2 |
| ADR92 | 1 |
| BASC-2136 | 1 |
| UCLA PTSD Reaction Index137 | 2 |
| CECI138 | 1 |
| Children’s Global Assessment Scale139 | 1 |
| CAPE140 | 1 |
| Devereux Scales of Mental Disorder Manual141 | 1 |
| Freemantle Acute Arousal Scale142 | 1 |
| MAYSI-2143 | 1 |
| MFQ143,144 | 1 |
| Perceived Stress Scale145 | 1 |
| QOC measure146 | 1 |
| Self-report BDI147 | 1 |
| Self-report for Childhood Anxiety Related Disorders148 | 1 |
| Suicidal Ideation Questionnaire149 | 1 |
| The Generalised Expectancies for Negative Mood Regulation150 | 1 |
| The Ohio Scales151 | 1 |
| Toronto Mindfulness Scale152 | 1 |
| Trauma Events Screening Inventory153 | 1 |
Assumed change process and design principles
Fifty-two records reported mandatory participation in the interventions, including 31 records that described interventions involving a whole system, either across a whole organisation (e.g. a hospital) or in a self-contained unit (e.g. a section of a residential school). Nine records reported voluntary engagement in interventions, and in the remaining 60 records it was unclear whether engagement in the intervention was mandatory or voluntary.
Many studies lacked internal congruence, in that the relationships between the aims, intervention, mechanisms of change and reported outcomes were not necessarily clear. For example, reductions in restraint data occurring after a staff education intervention might be interpreted as an effect of the intervention, with little attention to potential confounding factors or fidelity. This point is noted in the literature. 40,112
Mandatory changes
Mandatory changes to services were reported in 50 out of 107 (47%) records of interventions, and a permanent change was described in 40 out of 107 (38%) (e.g. revised policies or protocols, changes to the care approach or changes to the physical environment). This was consistent with the tendency for records to report on changes to practice that were made and evaluated within a particular organisation, in contrast to introducing an intervention specifically to test it.
Reference to theory
There was some indication of the theory informing the intervention in 44 out of 107 records of interventions (41%), but without further details about what the intervention was, how it had been developed and how it was tested and refined. Many of the ‘quality improvement’ interventions used a ‘plan, do, study, act’ cycle, a mechanism to repeat and adjust interventions until they achieve the desired effect.
Some interventions made explicit reference to programme-level theories that had informed their intervention procedures, such as sensory modulation or trauma-informed care. Other programme-level theories cited sought to explain staff behaviour, service user behaviour, therapeutic relationships and organisational change. These studies often sought to test or modify not the actual theory, but rather the impact of using interventions based on the theories in relation to the reduction of restrictive practices.
The most frequently cited theory related to staff behaviour was social learning theory, used to support training interventions that sought to improve the self-efficacy of individual staff and staff teams.
Mode of delivery: intervention procedures
The intervention procedures are set out by theme in Table 15. The most common procedures focused on staff training. Other procedures related to guideline or policy change, risk assessment tools, data review, milieu changes and changes to therapeutic approach (e.g. introducing trauma-informed care, and staff involvement in intervention development).
| Theme | n | Percentage |
|---|---|---|
| Staff training | 16 | 57.1 |
| Guidelines or policy change | 3 | 10.7 |
| Risk assessment tools | 3 | 10.7 |
| Data review | 3 | 10.7 |
| Milieu changes | 1 | 3.6 |
| Changed approach (TCI) | 1 | 3.6 |
| Staff involvement | 1 | 3.6 |
| Total | 28 | 100.0 |
Staff-focused procedures
Staff-focused procedures were those that were aimed at and undertaken solely by staff, with a view to influencing staff use of restrictive practices. One dominant procedure was training, which could cover, among other topics, the use of a newly introduced resource (e.g. the ‘feelings thermometer’,154 aromatherapy155 or a sensory modulation room156); a strategy or therapy such as ‘restraint reduction meetings’,157 ‘deactivation therapy’158 or ‘milieu therapy’;159 or skills such as verbal communication. 160 Another staff-focused procedure was role modelling, which could involve supervision or mentoring (e.g. Health Sciences Centre Winnipeg104), and was seen in complex interventions that were encouraging changes to the culture, structure and/or values of a setting (e.g. Verret et al. ,161 Eblin162 and Dean et al. 163).
Alternative approaches
Compared with the companion review focused on adult mental health settings,47 there were more interventions involving non-medical or psychological approaches to reducing restrictive practices. These included sensory modulation via the installation of sensory or comfort rooms,156,164,165 aromatherapy155 and activities. 166,167
Incident-focused procedures
Other procedures were incident-focused, that is they were responses to incidents of restrictive practices. 89,105 These included incident review procedures, in which organisations (staff and managers) collected and monitored their incident data to establish baseline and progress rates to identify patterns for targeted intervention or to conduct retrospective audits. 23,115,117,168,169 In contrast to this whole-system review, debriefing was conducted immediately or soon after an incident (e.g. Magnowski and Cleveland80 and Leitch94).
Organisation-focused procedures
In addition, several organisation-focused procedures were identified. These were system-wide structural and cultural changes including making changes to staffing levels85,109,132,170 or the way staffing was organised. 80 Another procedure involved changing therapeutic approaches (e.g. to a trauma-informed approach78,171,172). This theme also included improvements to communication (e.g. Ercole-Fricke et al. 89 and Kalogjera et al. 173), community meetings102 and de-escalation. 161 Further procedures focused on policy change115,174 and leadership, in which senior management tended to be directly involved in meetings and made statements of commitment. 38,78,175
The extraction process highlighted the procedures used by each intervention to address restrictive practices. The maximum number of procedures found in a single intervention was 15. A total of 16 unique procedures were identified from the analyses (Figure 8). The average number of unique procedures reported per record was 4.28 (mean) and 3 (median).
FIGURE 8.
Count of unique procedures per intervention. Unique procedures across interventions, n = 16. Maximum number of unique procedures per intervention, n = 15.
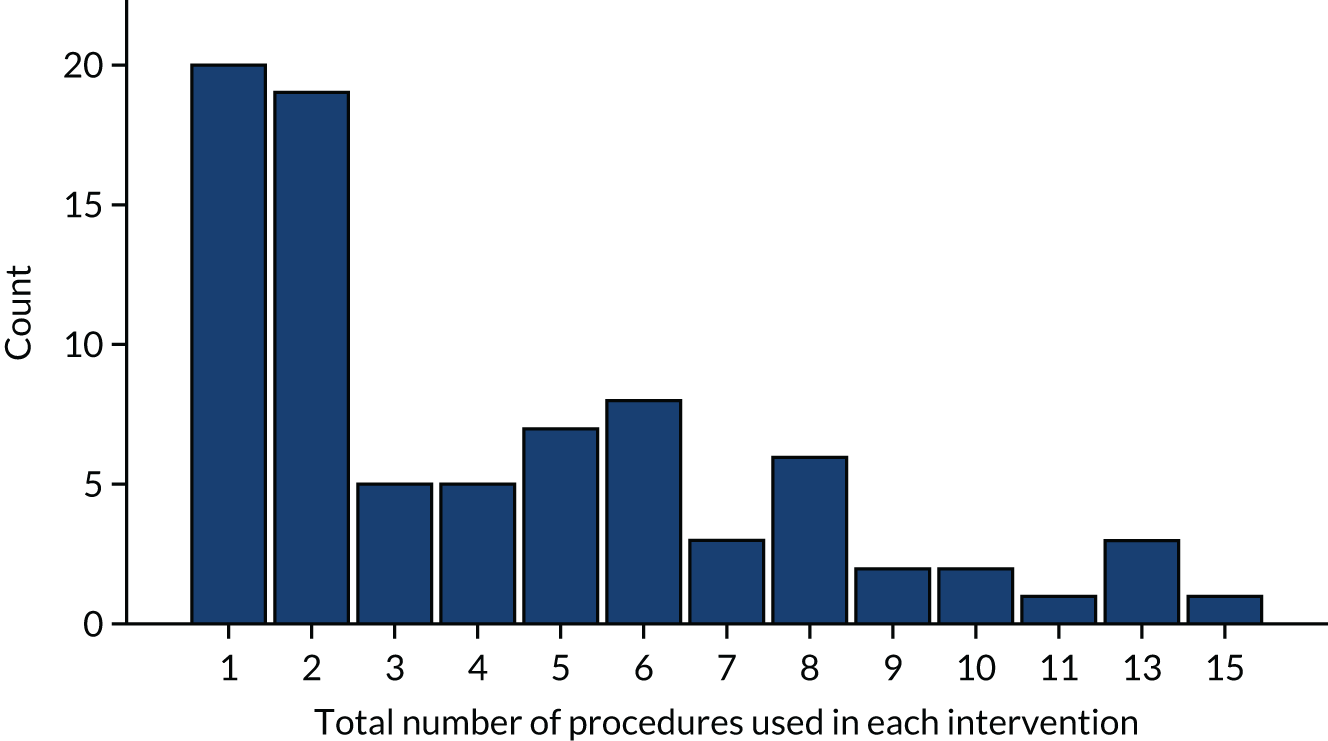
Twenty interventions (24%) used a single procedure only, and the most common single procedure was staff training (Table 16). However, many interventions (n = 62) used more than one procedure.
| Procedure | n | Percentage |
|---|---|---|
| Training | 88 | 19.3 |
| Changed approach (e.g. TIC) | 58 | 12.7 |
| Guidelines or policy change | 44 | 9.6 |
| Data review | 36 | 7.9 |
| Care planning changes | 33 | 7.2 |
| Debriefing | 33 | 7.2 |
| Enhanced leadership | 30 | 6.6 |
| Risk assessment tools | 21 | 4.6 |
| Milieu changes | 20 | 4.4 |
| Environmental changes | 17 | 3.7 |
| Staff involvement | 17 | 3.7 |
| CYP involvement | 15 | 3.3 |
| Family involvement | 14 | 3.1 |
| Enhanced staffing | 13 | 2.9 |
| Activities | 9 | 2.0 |
| Sensory approaches | 8 | 1.8 |
| Total procedures reported | 456 | 100.0 |
Procedures used in interventions
The reporting on the procedures used in interventions was inconsistent and at times limited.
Reporting on procedures
Staff training was the most widely reported procedure, although reporting of details could be brief. In 84 out of 107 records of interventions, the total hours of training were not reported. Few reported the content, mode of delivery or training provider in any detail.
Staff training occurred in 88 procedures, making it the most frequently used intervention procedure across all interventions (including those using a single procedure and those using multiple procedures). The least often used procedures were activities (n = 9) and sensory approaches (n = 8). One intervention incorporated visits to other units. 94
Delivery of training
Where training was used it was delivered in house in 40 interventions (37%). Training providers were not reported in 58 of the records. Although 23 records reported that it was delivered by an external provider, there was little further detail. It appeared that where an intervention was a commercially available or copyrighted product, such as the 6CS, training was likely to be brought in as part of the package.
Table 17 illustrates the total number of hours of training provided. This varied widely, from 1 to 35 hours.
| Hours of training reported | Number of records reporting training time | Percentage |
|---|---|---|
| 1.0 | 1 | 0.9 |
| 1.5 | 1 | 0.9 |
| 2.0 | 2 | 1.9 |
| 3.0 | 4 | 3.7 |
| 4.0 | 1 | 0.9 |
| 7.0 | 1 | 0.9 |
| 8.0 | 1 | 0.9 |
| 15.0 | 2 | 1.9 |
| 16.0 | 1 | 0.9 |
| 19.0 | 1 | 0.9 |
| 21.0 | 2 | 1.9 |
| 24.0 | 1 | 0.9 |
| 28.0 | 1 | 0.9 |
| 30.0 | 1 | 0.9 |
| 35.0 | 3 | 2.8 |
| Total reported | 23 | 21.5 |
| Not reported | 84 | 78.5 |
| Total | 107 | 100.0 |
Service user involvement in interventions
Service user involvement in interventions development is recommended in the literature, but involvement was reported in only 16 records, and CYP’s involvement was reported in only 15 records. Service user involvement in interventions development was reported in only 9 of the 107 evaluation records. Across the records, this aspect of the intervention reporting lacked detail and so it was unclear as to the type and extent of the involvement (Table 18).
| Involvement | Number of records | Percentage |
|---|---|---|
| Involvement reported | 9 | 8.4 |
| Involvement not reported | 98 | 91.6 |
| Total | 107 | 100.0 |
Service user or family involvement was reported as an intervention component in the 6CS,38,105 and several stand-alone interventions, for example HM Government,30 Fralick176 and Nunno et al. 177
Intervention dose, duration and intensity
Many evaluations did not report details about the duration and intensity of the intervention. Partial details (e.g. overall duration of the intervention or of an individual component, usually training) were sometimes, but not always, provided. Often, the evaluation period and the duration of intervention implementation were not distinguishable. Similarly, the duration of individual intervention components was often not reported. With this proviso, interventions ranged in length from 3 months98,129 to 13 years. 120 Some interventions described providing stand-alone training sessions, whereas others were conducted over a short period of time (e.g. 1 week) or longer (e.g. several months). Some evaluations, for example that by Fralick,176 described ongoing training including refresher sessions or supervision.
Intervention materials
Interventions reported using various materials in the implementation of the intervention, including training materials, guidelines, multimedia resources, tools, posters, slides, and policies. Some referred to materials that are publicly available on the internet, such as:
-
Collaborative Problem Solving (CPS)
-
Cognitive milieu therapy
-
Modified Positive Behavioral Intervention Support (M-PBIS)
-
Six Core Strategies © (6Cs)
-
Therapeutic Crisis Intervention (TCI)
-
Trauma Affect Regulation: Guide for Education and Therapy (TARGET)
-
Trauma Systems Therapy (TST).
Intervention evaluation
Evaluations were identified by scrutinising each report using the screening questions of the MMAT to ascertain whether or not a research question was described and whether or not the data required to answer the question had been collected. Those reports that passed the screening were then appraised, again using the MMAT. The MMAT prompts an appraisal of if qualitative methods are appropriate; if the data collection methods are adequate, and the findings and their subsequent interpretations are sufficiently reported; and if the study has overall coherence. Evaluations are detailed in Appendix 5.
As seen in Appendix 5, there are more evaluation data about the 6CS and CPS than about any of the other interventions reported or described in the 121 retrieved records. Although the 6CS is more frequently reported, only 5 of the 12 6CS records are evaluations, as defined by the WIDER criteria. In comparison, there are nine separate implementations of CPS, all evaluated. The 6CS evaluations span 10 years, from 2007 to 2017, and the CPS evaluations span 8 years, from 2008 to 2016. Therefore, over a similar timespan, 6CS has been used more but evaluated less than CPS. This suggests that intervention use is not routinely generating evaluation data, and that intervention choice may not be informed by evaluation data.
Reporting on the design of evaluation studies
Evaluation design was often not described, and when it was reported a variety of terms were used. Accordingly, design had to be inferred from other study details in some cases. When study design was described, no RCTs were identified, and only around one-third of the records (36/121) reported quantitative data. Details of evaluation study design are provided in Appendix 6.
As reported in Table 7 and Appendix 6, most evaluations were non-randomised studies. Only eight were controlled. Twenty-two generated quantitative data only, and five generated both quantitative and qualitative data. The great majority of the quantitative studies compared counts or rates of restrictive practices before and after a period of intervention implementation.
All evaluations were considered to have recruited participants who were representative of the target population and used suitable outcome measures. Several were not considered to have reported complete outcome data and few discussed confounders, with some exceptions that were principally reflections on the challenges of evaluating complex interventions, for example the evaluation by LeBel et al. 40 There was very little reporting of modifications and fidelity to the intervention protocol, with only 12 evaluations reporting this.
Twenty-one quantitative studies were identified. There were several evaluations of cultural or organisational change that took a systems approach and presented qualitative data. Some of these focused on process (e.g. Fralick176 and Elwyn et al. 178) and others focused on outcomes (e.g. Eblin162). A number of stand-alone interventions incorporating system change were presented as case studies (e.g. Thompson et al. 87 and Fralick176).
A common approach to evaluation was to compare counts or rates of restrictive practices before and after an intervention (e.g. Huckshorn77). However, causal links were rarely explored in the reports despite the prevalence of multicomponent interventions.
Reporting on setting size and sample size
There were two main approaches to describing the size of the setting in which the intervention was conducted. Some reported setting size in terms of the number of beds (n = 25) and others in terms of the size of the service user population (n = 15). The size of the setting varied greatly in both cases, from 7 to 925 beds (mean 65.32) and from 27 to 5600 service users (mean 475.53).
Likewise, sample size was reported in diverse ways, including numbers of service users, patient-days, admissions, beds and staff. Number of service users was the most common (n = 30) way to report sample size, and service user-days (n = 2) and beds (for health settings) (n = 2) were the least common (Table 19).
| Basis of sample size calculation | Number of studies | Sample size | ||
|---|---|---|---|---|
| Minimum | Maximum | Mean | ||
| Patient-days | 2 | 279 | 1000 | 639.50 |
| Admissions | 5 | 65 | 1485 | 621.20 |
| Beds | 2 | 23 | 52 | 37.50 |
| Staff | 10 | 13 | 340 | 93.20 |
| Service user-days | 30 | 3 | 6361 | 486.97 |
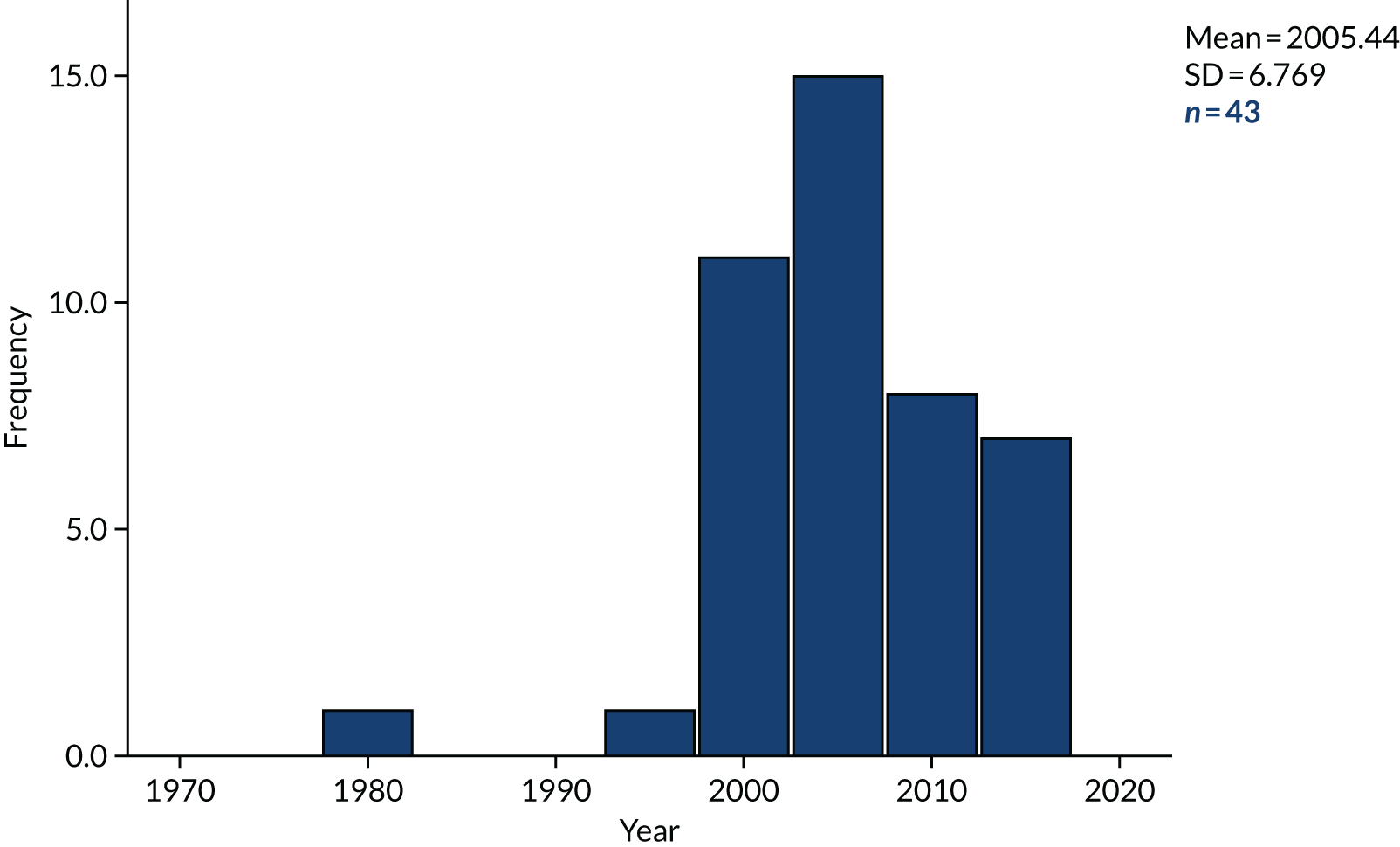
Year of evaluation
As seen in Figure 9, starting in the mid-1990s, the number of evaluations that were commenced suddenly increased compared with the previous decade. Evaluations published prior to 1989 were not eligible for inclusion in the review. The commencement of evaluations appeared to then decrease steadily from the mid-2000s.
FIGURE 9.
Year evaluation commenced.
Outcome measures in evaluations
Seventy-one outcome measures were reported (mean 3, range 0–9 outcome measures). The most common outcome measure was the number of restraints, followed by duration of restraint, number and duration of seclusions, number of injuries, number of incidents and length of stay. Injuries to staff was an outcome measure in three evaluations and injuries to all was an outcome measure in eight. No evaluation specifically used injuries to service users as an outcome measure, although two counted the service users involved in an incident (Table 20). For standardised outcome measures identified in the evaluation, see Table 14.
| Outcome measure | Number of studies | Percentage | Percentage of studies |
|---|---|---|---|
| Number of staff trained | 1 | 0.6 | 1.6 |
| Patient satisfaction | 1 | 0.6 | 1.6 |
| Number of care plans in place | 1 | 0.6 | 1.6 |
| Service user goal mastery | 1 | 0.6 | 1.6 |
| Staff compensation | 1 | 0.6 | 1.6 |
| Rule violation | 1 | 0.6 | 1.6 |
| Use of force | 1 | 0.6 | 1.6 |
| Number of observations | 1 | 0.6 | 1.6 |
| Use of sensory room | 1 | 0.6 | 1.6 |
| Discharge of placement | 1 | 0.6 | 1.6 |
| Quality of restraint | 1 | 0.6 | 1.6 |
| Number of accidents | 1 | 0.6 | 1.6 |
| Number of errors | 1 | 0.6 | 1.6 |
| Staff sick leave | 1 | 0.6 | 1.6 |
| Security use | 1 | 0.6 | 1.6 |
| Service user mood | 1 | 0.6 | 1.6 |
| Staff knowledge | 2 | 1.2 | 3.1 |
| Use of mechanical restraint | 2 | 1.2 | 3.1 |
| Duration of interventions | 2 | 1.2 | 3.1 |
| Number of service users involved in incident | 2 | 1.2 | 3.1 |
| Staff turnover | 2 | 1.2 | 3.1 |
| Number of interventions | 3 | 1.8 | 4.7 |
| Staff injury | 3 | 1.8 | 4.7 |
| Culture change | 3 | 1.8 | 4.7 |
| p.r.n. | 4 | 2.5 | 6.3 |
| Length of stay | 6 | 3.7 | 9.4 |
| Duration of seclusion | 7 | 4.3 | 10.9 |
| Injuries all | 8 | 4.9 | 12.5 |
| Incidents | 9 | 5.5 | 14.1 |
| Duration of restraints | 10 | 6.1 | 15.6 |
| Number of seclusions | 30 | 18.4 | 46.9 |
| Number of restraints | 53 | 32.5 | 82.8 |
| Total | 163 | 100.0 | 254.7 |
Several interventions used existing routinely collected data for their evaluations, such as archived data and incident reports. Some evaluations developed measures for the purposes of their evaluation, whereas others developed or adapted tools to collect data.
Reporting on use of measures in interventions
Standardised outcome measures were reported to have been used in 14 interventions, with a minimum of one and maximum of seven per evaluation (details are provided in Table 15). The measures used more than once were the Child and Adolescent Functional Assessment Scale133 and Global Assessment of Functioning. 135
Reporting on evaluation findings
Ninety-six per cent of evaluations reported findings; however, there was very wide variation between the 82 interventions, as described above. This presented considerable challenges for the assessment of intervention effectiveness.
The finding that most of the studies reported some positive outcomes in relation to reducing restrictive practices may be related to publication bias, especially in the grey literature. Many of the studies that reported evaluations contained anecdotal findings (i.e. did not present full figures), and these were excluded from this assessment. Evaluations published in journals or via academic conferences were examined in more detail. Some evaluations104,120,179 were not considered to have reported findings that could be used as evidence of effectiveness related to the reduction of restrictive practices.
At least one positive finding in relation to reducing restrictive practices was reported in all of the evaluations; however, 42 did not report statistical significance. All findings reported that the intervention successfully addressed the use of restrictive practices, directly (e.g. reducing frequency, intensity or duration of seclusion and/or restraint) or indirectly (e.g. improvements to the social milieu), although this could be qualified with additional information. Qualifiers varied, such as reporting that the effect of the intervention on the use of restrictive practices could appear deleterious initially but prove beneficial after a period of settling in (e.g. Kalogjera et al. 173). A more frequently reported qualifier was identifying specific areas that were affected positively or otherwise (e.g. reduction in seclusion and restraint within a juvenile justice setting but less clear evidence of whether or not the intervention had an impact on recidivism rates,128 reductions in seclusion but not restraint171 or differential impact between sites within a study, e.g. Glew92).
The majority of these evaluations reported interventions using more than one procedure (e.g. training with data review and policy changes). As these procedure categories are themselves broad, there is little to be learnt from relating positive or negative outcomes back to their use. Interventions using a single procedure may be more useful in determining what type of procedures might reduce the use of restrictive practices. Twenty-two evaluations reported interventions using a single procedure. Of these, 14 also reported significant results (Table 21), although the numbers are too modest to suggest a pattern here. The remainder used a variety of strategies, and all reported positive findings.
| Results | Procedure evaluation detail | |||||
|---|---|---|---|---|---|---|
| Training | Data review | Milieu change | Policy or guidelines change | New therapeutic approach | Risk assessment | |
| Single procedure reported (number of evaluations) | 12 | 3 | 2 | 3 | 1 | 1 |
| Significant results reported (number of evaluations) | 8 | 1 | 2 | 2 | 1 | 0 |
Significant findings were also reported in four of the mapping records, which were a discussion paper,175 conference paper,127 training consultancy website126 and a Welsh government document. 180
Controlled trials
Although there were no RCTs, 10 evaluation studies used a control for comparison purposes. As seen in Table 22, nine reported significant findings in relation to the decrease in use of a restrictive practice. 89,95,107,128,129,164,171,181,182 However, as illustrated in Table 22, they did not all use the same definition for the restrictive practices. Table 22 also shows whether or not fidelity was reported and the number of outcome measures used in these nine evaluations.
| Evaluation study | Procedure introduced | Definition of restrictive practice | Fidelity reported | Outcome measures (n) |
|---|---|---|---|---|
| Boel-Studt171 | Trauma-informed approach | Restraint and seclusion | Reported informally | 6 |
| Borckardt et al.181 | Engagement model | Restraint and seclusion | No | 4 |
| Ercole-Fricke89 | CPS | Restraint and seclusion | No | 1 |
| Ercole-Fricke et al.107 | CPS | Seclusion and loss of privilege | No | 5 |
| Ford and Hawke128 | TARGET | Various punitive sanctions | Yes | 2 |
| Magnowski95 | Milieu nurse | Restraint | No | 4 |
| Marrow et al.129 | TARGET | Restraint and seclusion | No | 8 |
| Miller et al.182 | Organisational intervention | Restraint | No | 3 |
| West et al.164 | Sensory room | N/A: focus on distress reduction | No | 3 |
Costs reported
Twelve evaluations reported financial costs, eight of which provided some detail. This differed considerably between studies in terms of the cost unit, time period and accounting period. For instance, Craig88 reported savings to the organisation of between US$12,236,934 and US$1,538,027. LeBel and Goldstein39 reported a 92% reduction in restraint costs, with some detail regarding how this figure was calculated, and Nunno et al. 81 reported that the intervention was provided free of charge in return for evaluation period by a university. Sanders108 compared ‘salary and replacement costs for employee lost time pre- and post-intervention and described this as a 93% reduction in expenses from client induced employee injuries’. Paccione-Dyszlewski et al. 170 compared the costs of initial staff training, US$340,000, with savings, calculated to be ‘approximately $470,000 across the 2-year post-project period (or approximately $130,000 when cost of implementation is considered)’.
Modification of and fidelity to intervention protocols
Twelve of the evaluations reported whether or not they tailored or modified the intervention protocol. One referred to possible unintended ‘drift’ from the model,79 and three reported modifying a tool. 109,129,170 Others reported tailoring the intervention to meet service user needs, making modifications as the intervention proceeded and allowing wards to choose the intervention.
Fifteen evaluations81,86,92,94,100,128,170,172,183–185 reported fidelity, but in contrast with this study’s companion review focusing on adult mental health settings, it was not possible to identify trends in fidelity reporting. The dates of publications reporting fidelity ranged from 2003 to 2019.
Chapter 5 Results of the behaviour change technique synthesis: the presence and frequency of behaviour change techniques in interventions
This chapter provides a narrative account of the presence and frequency of BCTs identified in interventions.
Individual behaviour change techniques identified across all interventions
The result of the search strategy was a data set of 121 records, which on analysis was found to report a total of 82 interventions. All 121 records were examined for BCT content. Descriptions of intervention content were usually found within the methods sections of studies, although additional details were occasionally provided in the results or discussion sections.
Thirty-six out of a possible 93 BCTs (39%) were identified across the 121 records. At least one BCT was detected in 78 of the interventions (95%). BCTs were not detected in four interventions because of a lack of content to code: two from mental health settings,103,158 one from a generic setting186 and one from the criminal justice system. 187
Behaviour change techniques found at least once across the interventions are shown in Figure 10. Figure 10 indicates the proportion of interventions in which each BCT was detected. For example, BCT 4.1 (instruction on how to perform the behaviour) was detected in the majority (71%) of interventions, whereas BCT 10.10 [reward (outcome) of the behaviour] was detected in only 1% of interventions. Figure 10 also illustrates which BCTs were the most and the least often detected across interventions. Seven were identified in > 20% of interventions (range 28–71%) and 11 were identified in ≤ 2% of interventions (range 1–2%).
FIGURE 10.
Individual BCTs identified in 82 interventions (% of interventions).
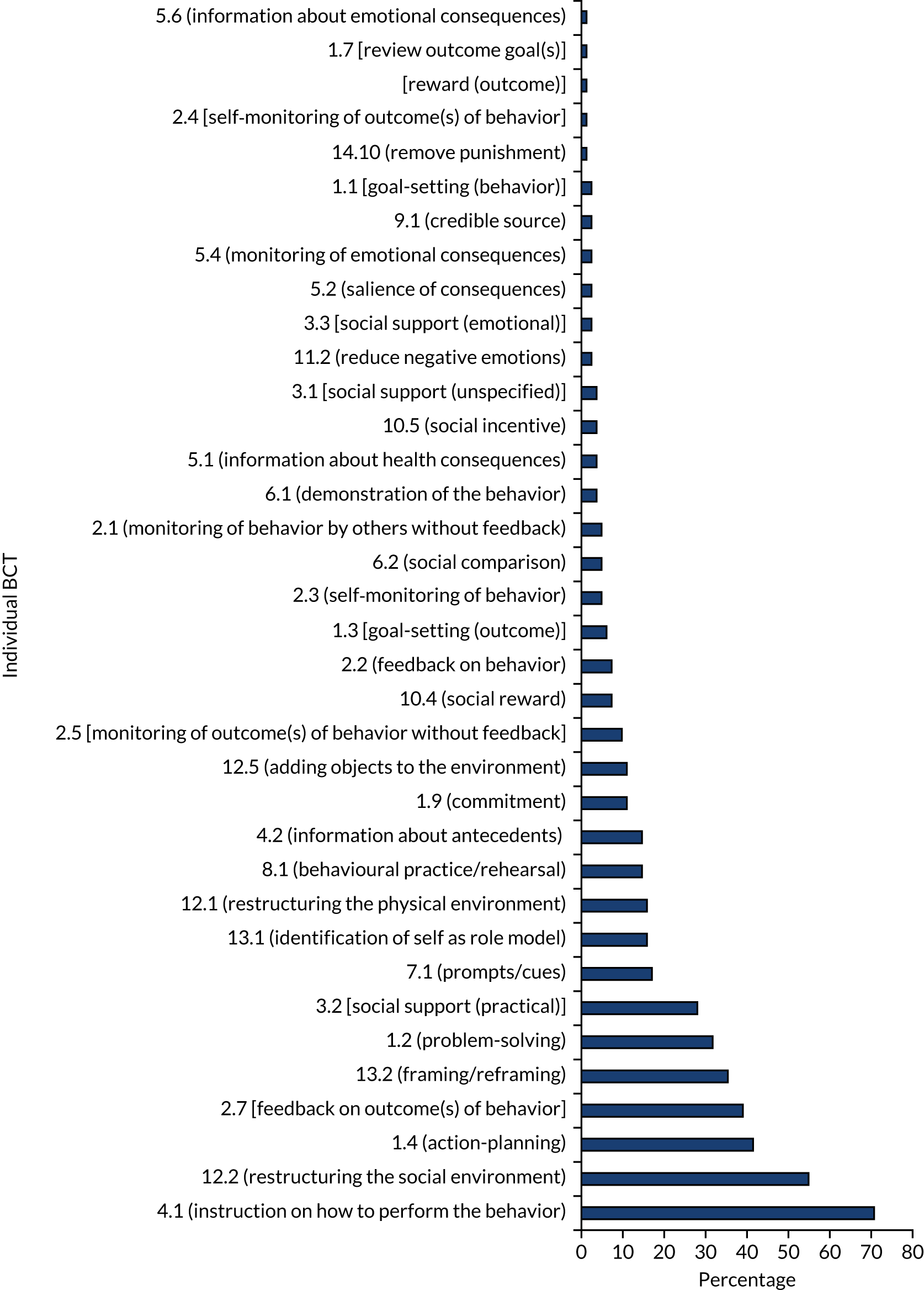
Identification of individual behaviour change techniques by setting
Table 23 illustrates the distribution of individual BCTs across interventions in different children’s settings in the order of frequency identified. Six BCTs (17% of BCTs detected) were detected in interventions from only one setting: four in mental health settings {BCT 14.10 [remove punishment], BCT 2.4 [self-monitoring of outcome(s) of behaviour], BCT 10.10 [reward (outcome)] and BCT 1.1 [goal setting (behaviour)]} and two in health and social care {BCT 1.7 [review outcome goal(s)] and BCT 5.1 [information about emotional consequences]}. These BCTs came from five clusters in total (36% of clusters detected).
| Individual BCTs identified, ranked by number of settings in which they were detected | Mental health | Health and social care | Education | Criminal justice | Generic | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| Identified in one setting (N = 6, 17%)a | ||||||||||
| 14.10 Remove punishment | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2.4 Self-monitoring of outcome(s) of behaviour | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 10.10 Reward (outcome) | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1.7 Review outcome goal(s) | 0 | 0 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5.6 Information about emotional consequences | 0 | 0 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1.1 Goal setting (behaviour) | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Identified in two settings (N = 14, 39%) | ||||||||||
| 9.1 Credible source | 1 | 2 | 0 | 0 | 0 | 0 | 1 | 11 | 0 | 0 |
| 2.1 Monitoring of behaviour by others without feedback | 2 | 5 | 0 | 0 | 0 | 0 | 2 | 22 | 0 | 0 |
| 11.2 Reduce negative emotions | 1 | 2 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3.3 Social support (emotional) | 1 | 2 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5.2 Salience of consequences | 1 | 2 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5.4 Monitoring of emotional consequences | 1 | 2 | 0 | 0 | 0 | 0 | 1 | 11 | 0 | 0 |
| 6.1 Demonstration of the behaviour | 2 | 5 | 0 | 0 | 0 | 0 | 1 | 11 | 0 | 0 |
| 5.1 Information about health consequences | 1 | 2 | 2 | 14 | 0 | 0 | 0 | 0 | 0 | 0 |
| 10.5 Social incentive | 0 | 0 | 2 | 14 | 0 | 0 | 1 | 11 | 0 | 0 |
| 3.1 Social support (unspecified) | 0 | 0 | 2 | 14 | 0 | 0 | 1 | 11 | 0 | 0 |
| 6.2 Social comparison | 3 | 7 | 1 | 7 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2.2 Feedback on behaviour | 3 | 7 | 3 | 21 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12.5 Adding objects to the environment | 8 | 20 | 0 | 0 | 0 | 0 | 1 | 11 | 0 | 0 |
| 4.2 Information about antecedents | 8 | 20 | 4 | 29 | 0 | 0 | 0 | 0 | 0 | 0 |
| Identified in three settings (N = 5, 14%) | ||||||||||
| 2.3 Self-monitoring of behaviour | 1 | 2 | 1 | 7 | 2 | 29 | 0 | 0 | 0 | 0 |
| 1.3 Goal setting (outcome) | 3 | 7 | 1 | 7 | 0 | 0 | 0 | 0 | 1 | 9 |
| 10.4 Social reward | 2 | 5 | 3 | 21 | 0 | 0 | 1 | 11 | 0 | 0 |
| 1.9 Commitment | 4 | 10 | 4 | 29 | 1 | 14 | 0 | 0 | 0 | 0 |
| 7.1 Prompts or cues | 9 | 22 | 2 | 14 | 0 | 0 | 3 | 33 | 0 | 0 |
| Identified in four settings (N = 4, 11%) | ||||||||||
| 2.5 Monitoring of outcome(s) of behaviour without feedback | 4 | 10 | 1 | 7 | 2 | 29 | 0 | 0 | 1 | 9 |
| 8.1 Behavioural practice or rehearsal | 4 | 10 | 2 | 14 | 4 | 57 | 2 | 22 | 0 | 0 |
| 12.1 Restructuring the physical environment | 8 | 20 | 3 | 21 | 0 | 0 | 1 | 11 | 1 | 9 |
| 3.2 Social support (practical) | 12 | 29 | 4 | 29 | 4 | 57 | 3 | 33 | 0 | 0 |
| Identified in five settings (N = 7, 19%) | ||||||||||
| 13.1 Identification of self as role model | 6 | 15 | 3 | 21 | 1 | 14 | 1 | 11 | 2 | 18 |
| 1.2 Problem-solving (identify triggers, influences, strategies) | 18 | 44 | 5 | 36 | 1 | 14 | 1 | 11 | 1 | 9 |
| 13.2 Framing or reframing perspective | 16 | 39 | 6 | 43 | 2 | 29 | 2 | 22 | 3 | 27 |
| 2.7 Feedback on outcome(s) of behaviour | 20 | 49 | 8 | 57 | 1 | 14 | 1 | 11 | 2 | 18 |
| 1.4 Action-planning | 21 | 51 | 6 | 43 | 4 | 57 | 1 | 11 | 2 | 18 |
| 12.2 Restructuring the social environment | 26 | 63 | 12 | 86 | 3 | 43 | 2 | 22 | 2 | 18 |
| 4.1 Instruction on how to perform the behaviour | 32 | 78 | 12 | 86 | 7 | 100 | 4 | 44 | 3 | 27 |
Seven BCTs (19% of BCTs detected) were identified in interventions from all five settings. As seen in Figure 11, these BCTs came from five clusters in total (36% of clusters detected). Of these, BCT 4.1 (instruction on how to perform the behaviour) was the most often detected, although at lower rates in criminal justice and generic settings. This BCT was the only one to be detected in all interventions from a single setting (education). BCT 12.2 (restructuring the social environment) and BCT 1.4 (action-planning) were among the most often detected BCTs in all settings except the criminal justice system; both were detected in smaller percentage of interventions from generic settings. Similarly, BCT 13.2 (framing/reframing) was among the most often detected BCTs in all settings except education. BCT 2.7 [feedback on outcome(s) of behaviour] was among the most often detected BCT in three settings and BCT 1.2 (problem-solving) in two settings. BCT 13.1 (identification of self as role model) was among the most often detected BCTs in generic settings only.
FIGURE 11.
Percentage of BCTs detected in multiple settings (n = 36).
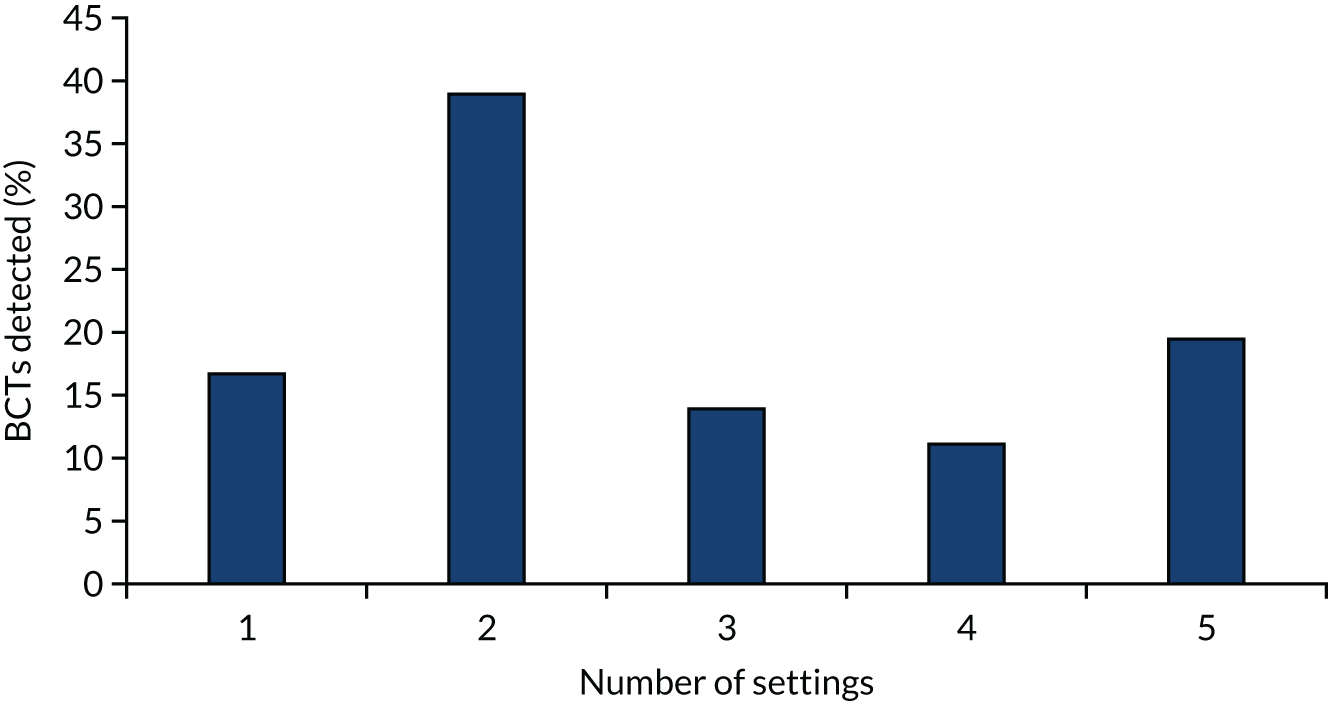
Although BCT 2.1 (monitoring of behaviour by others without feedback) was detected in interventions from four settings, it was among the top detected BCTs in criminal justice settings only. Similarly, BCT 7.1 (prompts or cues) was detected in interventions from three settings but was among the top detected BCTs in criminal justice settings only. BCT 2.3 (self-monitoring of behaviour) was another outlier, identified in three settings but among the top detected BCTs in education settings only (Figure 12).
FIGURE 12.
Individual BCTS by setting (% of interventions in that setting).
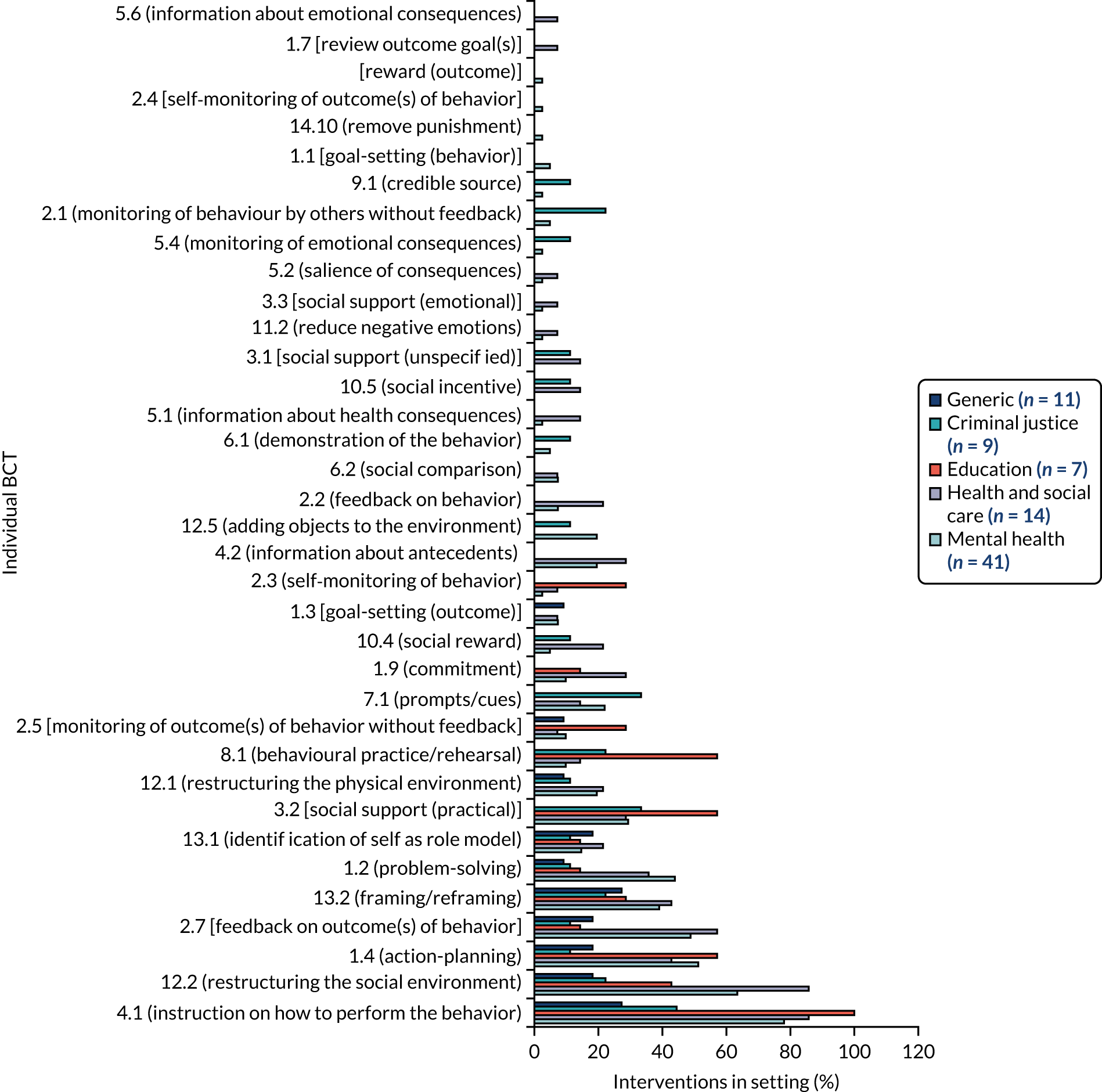
Individual BCTs detected in one or more settings were not necessarily detected in all settings, as detailed in Appendix 7. Four (11%) BCTs detected elsewhere were not identified in mental health settings, nine (25%) were undetected in health and social care, 24 (67%) in education, 17 (47%) in criminal justice and 26 (72%) in generic settings.
Clusters of behaviour change techniques identified in interventions
The BCT taxonomy52 organises BCTs into 16 clusters; for example, BCT 4.1 (instruction on how to perform the behaviour) belongs to cluster 4 (shaping knowledge). The BCT number preceding the name indicates the cluster. The 36 BCTs identified in the interventions came from 14 of the possible 16 clusters within the BCT taxonomy. The 14 clusters, the content that was coded to BCTs within them and the BCTs that were not identified are described below.
Figure 13 shows BCTs identified in interventions by cluster (%). The majority of the BCTs identified belonged to four clusters and were detected in over half of all interventions: cluster 1 (goals and planning), cluster 12 (antecedents), cluster 4 (shaping knowledge) and cluster 2 (feedback and monitoring). Less than 1% of identified BCTs came from two clusters and were detected in less than 2% of interventions [cluster 9 (comparison of outcomes) and cluster 14 (scheduled consequences)].
FIGURE 13.
Behavior change technique clusters identified (% of interventions).
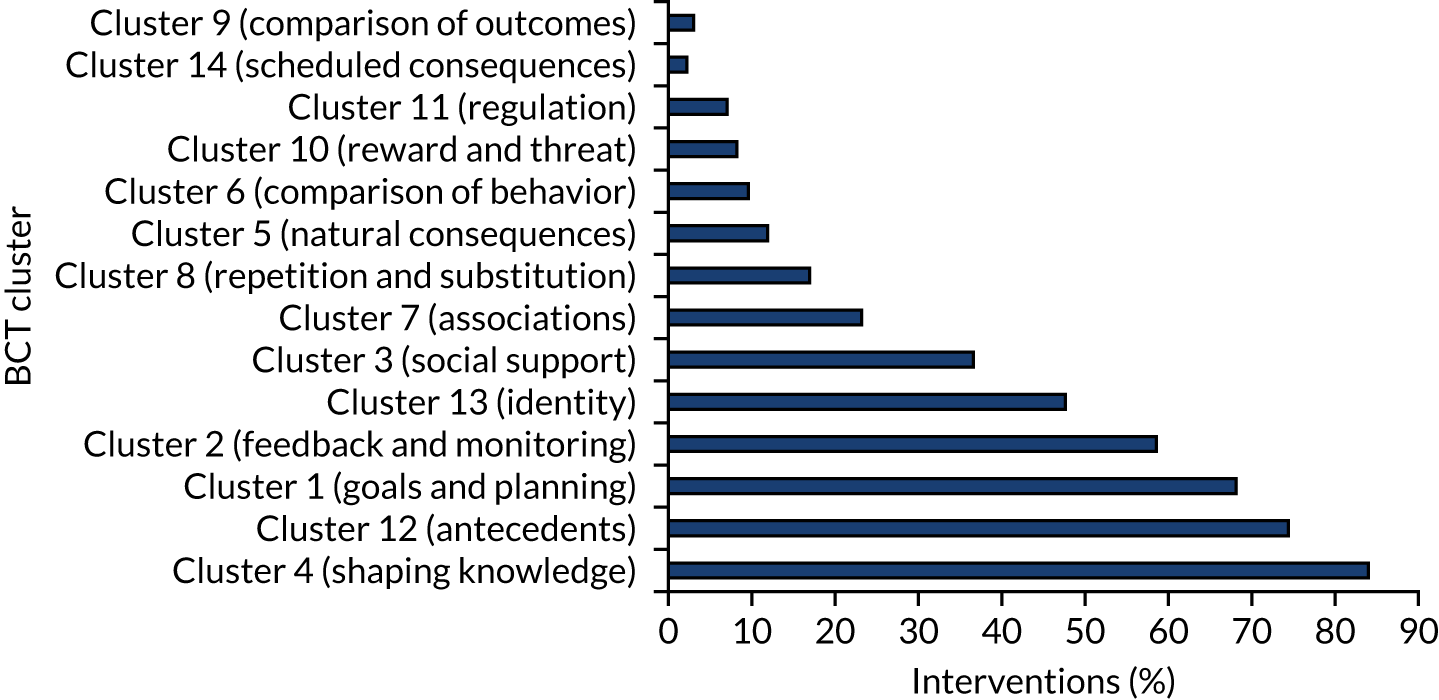
Five clusters featured only by virtue of one BCT being coded:
-
cluster 7 (associations) – BCT 7.1 (prompts/cues)
-
cluster 8 (repetition and substitution) – BCT 8.1 (behavioural practice/rehearsal)
-
cluster 9 (comparison of outcomes) – BCT 9.1 (credible source)
-
cluster 11 (regulation) – BCT 11.2 (reduce negative emotions)
-
cluster 14 (scheduled consequences) – BCT 14.1 (remove punishment).
Clusters of behaviour change techniques by setting
Figure 14 shows the distribution of BCT clusters across interventions in different children’s settings. Eleven out of the 14 clusters detected were identified in four or five settings. Only one cluster was detected in a single setting [cluster 9 (comparison of outcomes) in the criminal justice setting], one in two settings [cluster 8 (repetition and substitution) in mental health and health and social care settings] and one in three settings [cluster 3 (social support) in mental health, health and social care, and criminal justice settings].
FIGURE 14.
Behavior change technique clusters as percentages of settings and interventions.
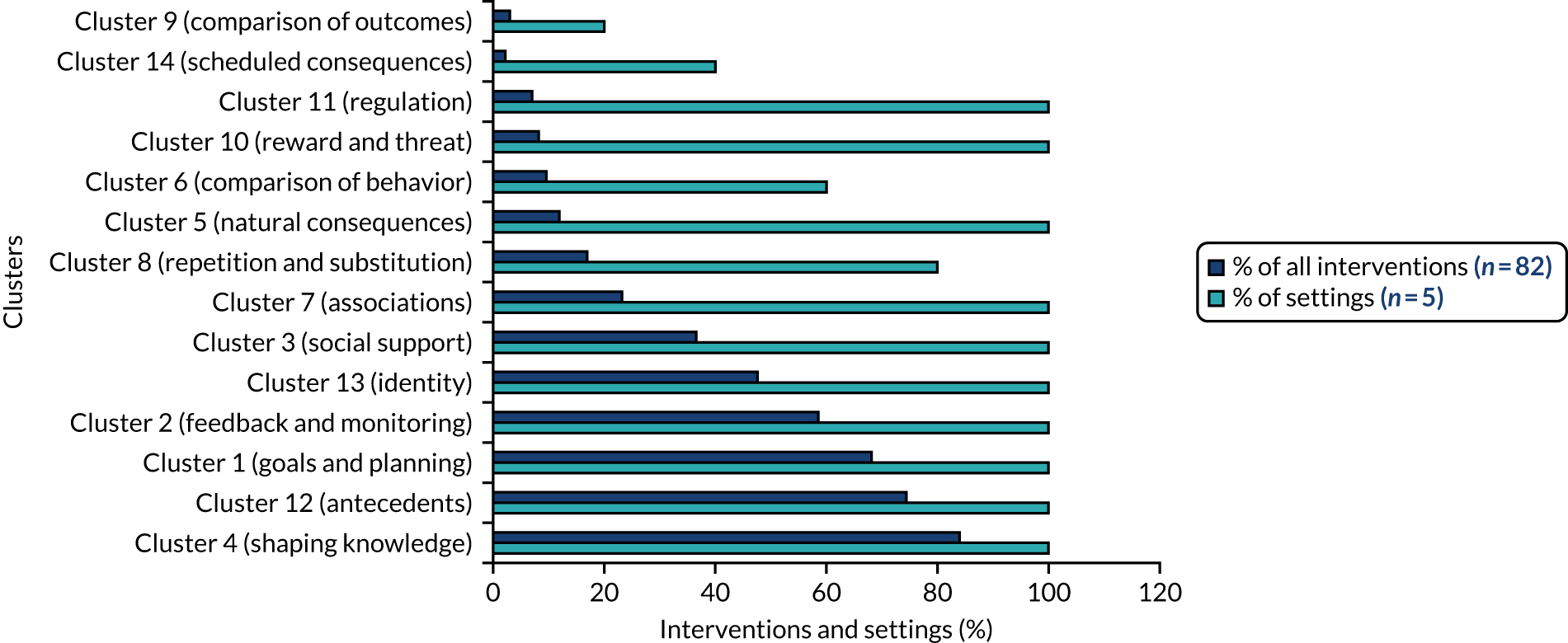
Interventions from mental health settings were coded with BCTs from all clusters except cluster 9 (comparison of outcomes). Interventions from health and social care settings were coded with BCTs from all clusters except cluster 9 (comparison of outcomes) and cluster 14 (scheduled consequences). Interventions from criminal justice settings were coded with BCTs from all clusters except cluster 11 (regulation) and cluster 14 (scheduled consequences). Interventions from educational settings were identified in seven clusters, and interventions from generic settings from nine clusters (Figure 15).
FIGURE 15.
Behaviour change technique cluster by settings (percentages of interventions in each setting, containing BCTs from each cluster).
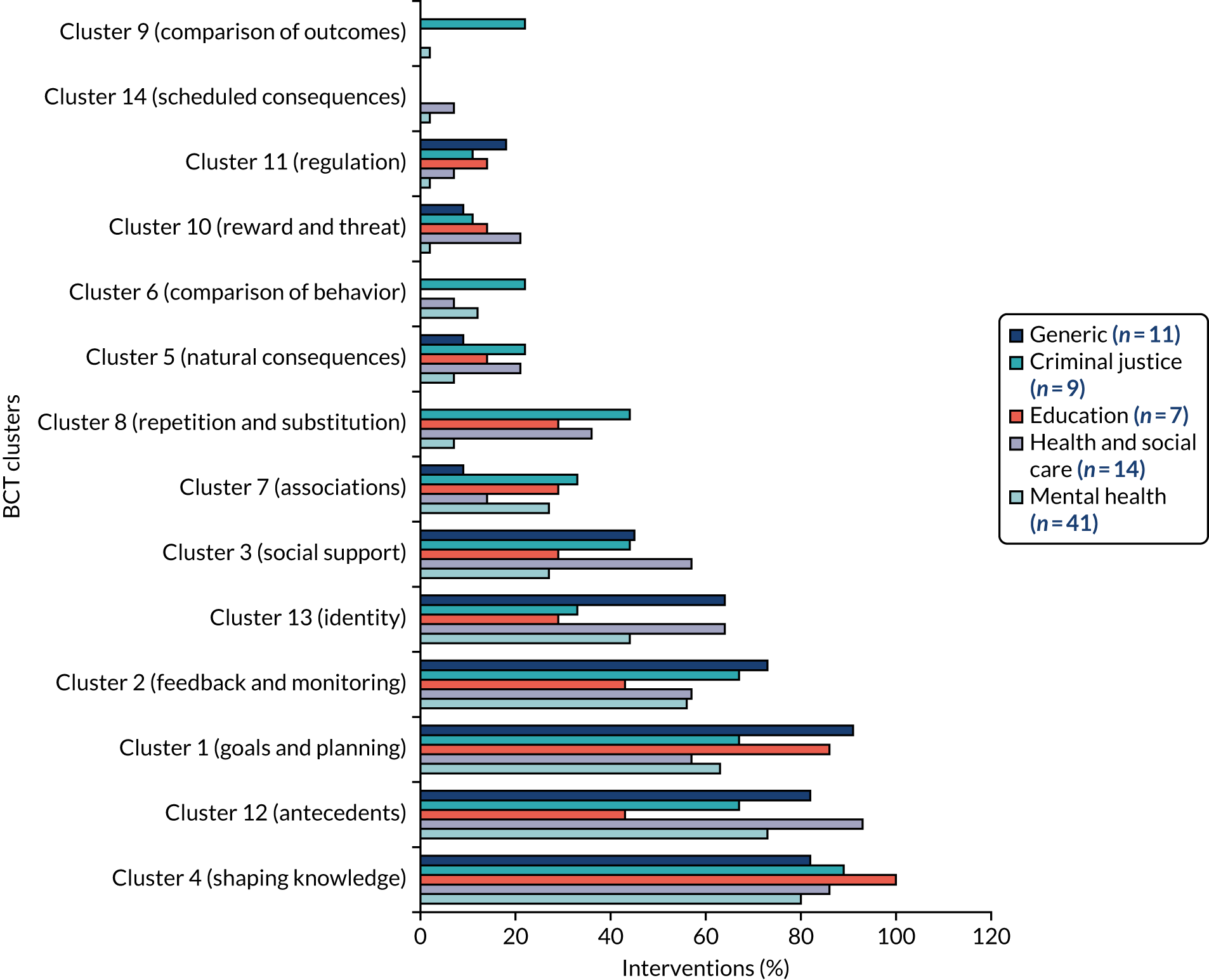
Description of behavior change techniques and behavior change technique clusters identified
The BCTs and BCT clusters identified in the interventions are summarised in Figure 16.
FIGURE 16.
Detected BCTs by cluster (percentage of interventions).
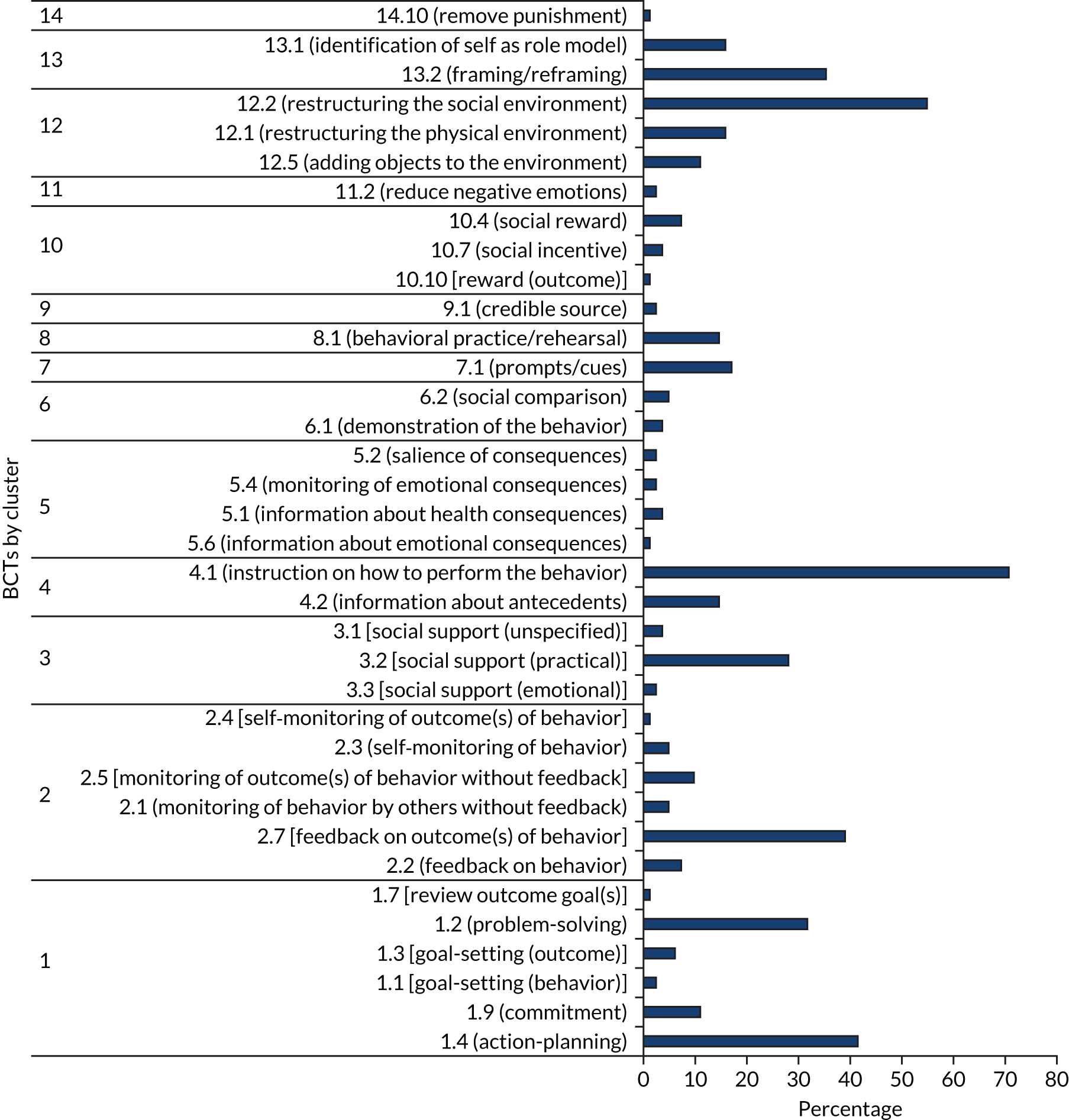
Cluster 1 (goals and planning)
Six out of the nine BCTs in cluster 1 (goals and planning) were identified: BCT 1.4 (action-planning), BCT 1.2 (problem-solving), BCT 1.9 (commitment), BCT 1.1 [goal setting (behaviour)], BCT 1.3 [goal setting (outcome)] and BCT 1.7 [review outcome goal(s)]. These six BCTs accounted for 17% of all identified BCTs (n = 36). BCTs from this cluster were identified in 68% of interventions overall (n = 82) from all five settings. Almost all interventions (91%) from generic settings were coded with BCTs from this cluster, compared with around half (57%) from health and social care settings (Figure 17).
FIGURE 17.
Cluster 1 (goals and planning) by setting (% of interventions in each setting containing BCTs from this cluster).
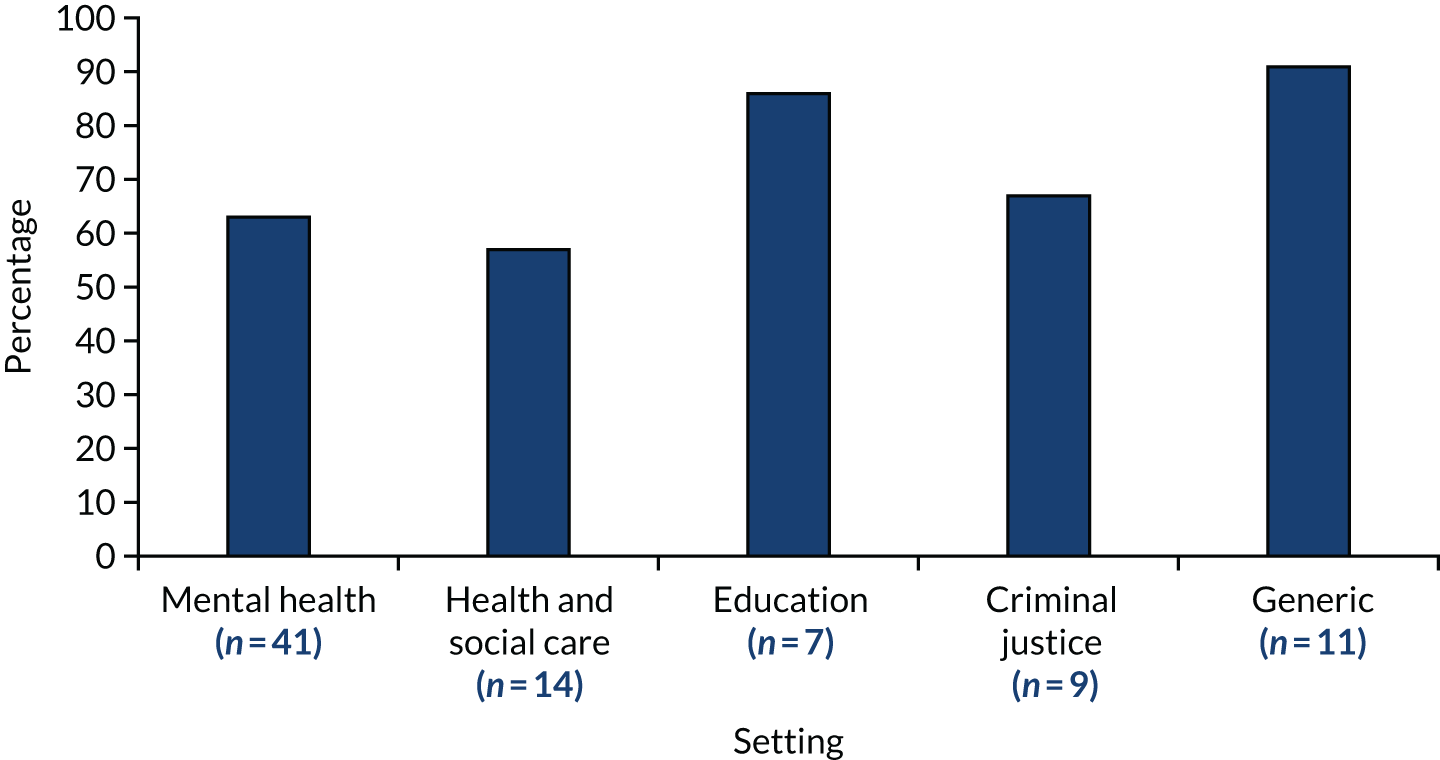
Action-planning (behavior change technique 1.4)
Prompt, detailed planning of performance of the behavior (must include at least one of context, frequency, duration and intensity). Context may be environmental (physical or social) or internal (physical, emotional or cognitive) (includes ‘Implementation Intentions’).
Michie et al. 52
Behavior change technique 1.4 (action-planning) was one of the most often identified BCTs, found in 41% of interventions and in all five settings. Written action plans were produced for a variety of purposes, including setting out how to support or modify the behaviour of children or staff,30,97,100,102,180,185,188 how to support recovery33 plans for follow-up33,77,113,189 and how to prevent or respond to crises,85,122 as illustrated in Lebel et al. :40
Using the tool, a patient, family member (as appropriate), and staff person collaboratively develop a plan . . . that identifies preferred strategies for de-escalation . . . and restraint preferences to consider if restraint becomes necessary.
Lebel et al. 40
In some interventions such planning formed, or was incorporated into, individuals’ treatment plans:82,95,105,160,162,172,188,190,191
The interdisciplinary treatment team (IDT) met to review the treatment plan, conduct additional assessments (e.g., antecedent analyses and functional analyses), and determine possible etiological factors associated with the patient’s frequent crises. Behavioral and pharmacological treatments were then re-evaluated for possible modification.
Schreiner et al. 41
Plans could be aimed at individuals, but could also require teams or organisations to perform incident reviews or implement restraint reduction plans. 33,77,182,188,193 Foci included crises, behaviour, treatment, restraint reduction,179 incidents requiring the use of restrictive practices23,86,192 and safety:
The action plan was developed by the Executive Director of the region taking into account the feedback gathered by employees with particular focus on providing employees support and reassurance that safety would be the top priority. The action plan was reviewed with employees by the Executive Director.
Sanders108
Plans were often proactive, detailing actions or strategies to prevent scenarios with the potential to lead to restrictive practices162,193 to ‘proactively respond in stressful situations’171 and to ‘proactively identify and address problems in a more productive manner’78 before the situation escalates. 194 Action plans could also detail the steps required in specific situations, for example ‘situations in which the youth is likely to exhibit disruptive or oppositional behaviors’,112 or during crisis and emergency situations, as described by Schreiner et al. :41
Staff members were trained . . . to provide patients with concrete de-escalation steps. Rather than telling a patient to calm down . . . staff might tell a patient to go to his room, sit on his bed, take five deep breaths, and think about a pleasant event.
Schreiner et al. 41
Other situations might include single incidents of violence and/or restrictive practices,101,115,122,174,194,195 children exhibiting particular characteristics or patterns of behaviour156,196 or a pattern of restrictive practice use. 197 A checklist from the National Association of State Mental Health Program Directors (NASMHPD)33 suggests that the S/R reduction team could develop a policy to clarify how this level of review would be triggered, for example a child who receives more than three holds in a single week, an event resulting in an injury or an unusual pattern of use of S/R.
Some action plans were developed with the involvement of children. 171,181,188,192 For example, Finnie91 refers to working collaboratively with children to find mutually satisfactory solutions by ‘articulating the problem to be solved . . . associated concerns, the possible solutions and likely outcomes, and whether outcomes are feasible and will be mutually satisfying’.
Problem-solving (behavior change technique 1.2)
Analyse, or prompt the person to analyse, factors influencing the behavior and generate or select strategies that include overcoming barriers and/or increasing facilitators (includes ‘Relapse Prevention’ and ‘Coping Planning’).
Michie et al. 52
Behavior change technique 1.2 (problem-solving) was another commonly identified BCT and was identified in 32% of interventions from all five settings. As illustrated in Greene et al. ,110 some interventions93,111,125,132,161,162,178,193 explicitly referred to ‘problem-solving’:
In its focus on facilitating adult–child problem-solving . . . the CPS approach differs from models typically employed in many restrictive facilities. [. . .] The manner in which the CPS model teaches adults to solve problems collaboratively with patients also has important implications for staff interactions with each other.
Greene et al. 110
The process of ‘problem-solving’ involved identifying problems and solutions41,174,188 (e.g. Thomann98 and Kaltiala-Heino et al. 198) and identifying barriers to these plans. 115,193 Analyses were conducted in clinical reviews,182,193 debriefings or incident reviews,122,162,192 regular meetings and risk assessments. 77 The purpose was to identify factors that influenced the behaviour of staff and children, including existing plans, strategies and values. 116,190 Just one intervention178 referred to organisational ‘problem-solving’. Often organisational problem-solving involved the analysis of triggers, for example for challenging behaviour:33,77,89,105,110,115,154,165,174,189,193,199
. . . using CPS with a youth . . . generates a list of specific unmet expectations and triggers . . . in which the youth is likely to exhibit disruptive or oppositional behaviors. [For example] . . . unmet academic expectations (e.g., turning in homework), . . . safety expectations (e.g., staying sober), or social triggers (e.g., exclusion during playground games).
Pollastri et al. 112
Behavior change technique 1.2 (problem-solving) was mostly concerned with the individual behaviour (of children), but there were examples that were concerned with broader influences. For instance, the Youth Justice Board for England and Wales stated that assessment should not be limited to describing facts but should aim to understand the situation and behaviour of a young person, including factors relating to diversity. 199
Other examples included risk assessment,77 strategies for ‘stressful situations’ and ‘red flags’,171 ‘warning signs’30 and redesigning environmental conditions:
[A functional behavioral assessment] is used to analyze environmental factors, including any history of trauma (e.g., physical abuse), that contribute to a child’s inappropriate (e.g., disrespect, noncompliance, insubordination, out-of-seat) behaviors.
[These data inform] positive behavioral strategies that emphasize redesigning environmental conditions, which may include changes in staff approaches.
Problem-solving activities resulted in the generation of ‘lessons learned’199 that inform future strategies,88,174,194 the development of (potential) solutions78,120 and improvements in practice. 168,192
Commitment (behavior change technique 1.9)
Ask the person to affirm or reaffirm statements indicating commitment to change the behavior.
Michie et al. 52
As shown in Figure 17, 18% of interventions described organisational-level ‘commitment’ (BCT 1.9) to reduce restrictive practices. For example, Caldwell et al. 115 emphasised the role of leadership in prioritising the reduction of restraint and seclusion within the organisation, with a focus on assessing its use.
This took various forms including a mandate issued by the Chief Executive Officer,108 a ‘statement of beliefs’182 or a declaration as a ‘unit priority’. 41 Reynolds et al. 100 described requiring individual staff to make a commitment to reducing restrictive practices:
Tier 1 strategies included establishing commitment from the staff (of note, 100% of the unit staff voted to implement the program), defined set of positively worded expectations (i.e. be safe, be responsible, be respectful).
Reynolds et al. 100
Goal setting for behaviour (behavior change technique 1.1) and outcome (behavior change technique 1.3)
Set or agree on a goal defined in terms of the behavior to be achieved.
Michie et al. 52
Set or agree on a goal defined in terms of a positive outcome of wanted behavior.
Michie et al. 52
Seven per cent of interventions described ‘goal setting for outcome’ and 2% described ‘goal setting for behaviour’ (see Figure 17). BCT 1.1 [goal setting (behaviour)] was identified in mental health settings only. Considerably fewer interventions described setting goals (BCT 1.1)33,40,81,179,190,191,193 than BCT 1.4 (action-planning). BCT 1.4 (action-planning) requires mention of context, frequency, duration or intensity within the plan. In the case of those that specified the goal,179,191 the goal was a reduction in or the prevention of the use of restrictive practices:
Specific patterns of restraint use were reviewed by the team each meeting, and goals for restraint prevention/reduction were set.
Holstead et al. 191
There was some variation in whether these goals were set for teams, individual staff or children. In Plant179 the goals were set for teams, and in Azeem et al. 193 the goals were set for teams and individual staff, whereas in Holstead et al. 191 the goals were set for staff and children. Both interventions describing goal setting in relation to behaviour (BCTs 1.1 and 1.3) referred to the joint goal setting between staff and youth171 and by staff in collaboration with children and families. 163
Review outcome goal(s) (behavior change technique 1.7)
Review outcome goal(s) jointly with the person and consider modifying goal(s) in light of achievement. This may lead to resetting the same goal, a small change in that goal or setting a new goal instead of, or in addition to the first.
Michie et al. 52
Behaviour change technique 1.7 [review outcome goal(s)] was detected in health and social care settings only. Just 5% of interventions (see Figure 17) described reviewing or evaluating outcome goals:
Progress towards the goals was evaluated monthly and ideas to further reduce restraints were discussed.
Holstead et al. 191
As described, the aim of review was to ensure that goals remained ‘fit for purpose’180 and were revised when necessary. 33
Cluster 2 (feedback and monitoring)
Behaviour change techniques from cluster 2 (feedback and monitoring) accounted for 17% of all identified BCTs. All but one BCT [BCT 2.6 (biofeedback)] from this cluster were identified: BCT 2.1 (monitoring of behavior by others without feedback), BCT 2.5 [monitoring of outcome(s) of behavior without feedback], BCT 2.3 (self-monitoring of behavior), BCT 2.2 (feedback on behavior) and BCT 2.4 [self-monitoring of outcome(s) of behavior]. Feedback and monitoring were detected in relation to both outcomes and behaviour. Monitoring was either self-monitoring or monitoring by others, for example at an organisational level. BCTs from cluster 2 were identified in 52% of interventions overall and at similar proportions across settings, except for generic settings where they were detected in 71% of interventions (Figure 18).
FIGURE 18.
Cluster 2 (feedback and monitoring) by setting (% of interventions in each setting containing BCTs from this cluster).
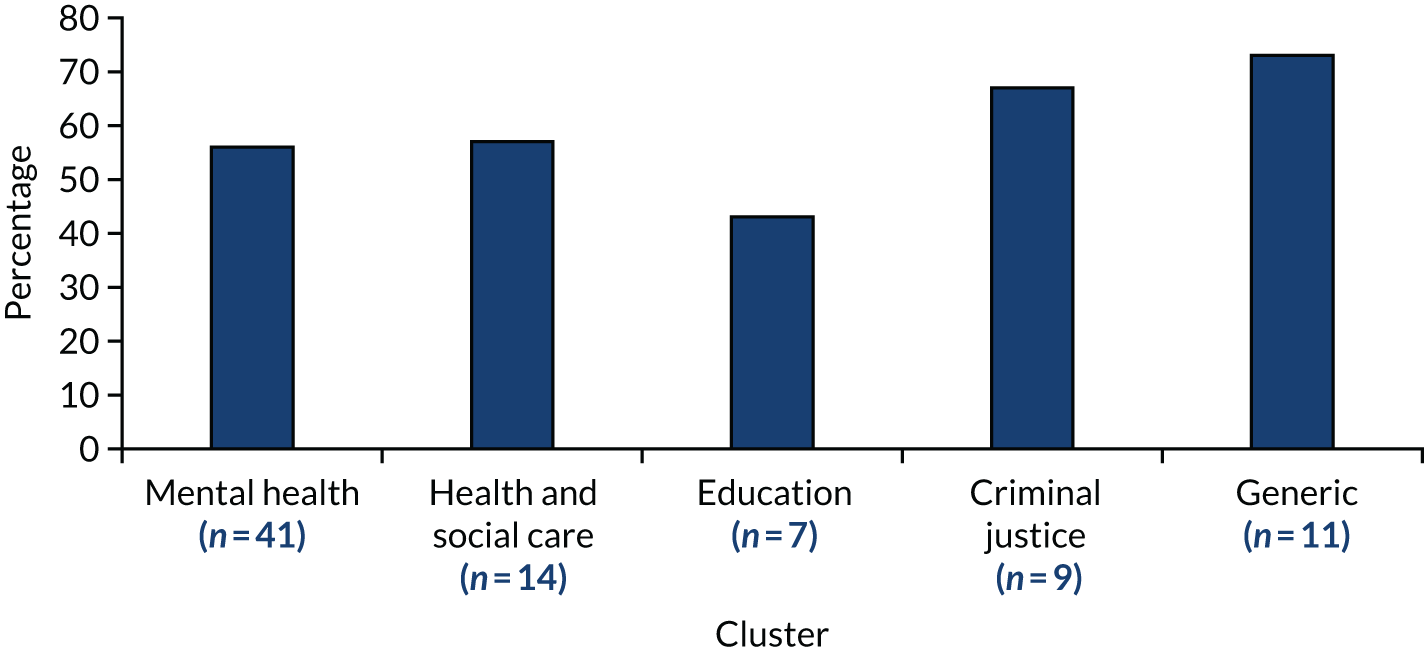
Self-monitoring of outcome(s) of behaviour (behavior change technique 2.4)
Establish a method for the person to monitor and record the outcome(s) of their behavior as part of a behavior change strategy.
Michie et al. 52
Behavior change technique 2.4 [self-monitoring of outcome(s) of behavior] was identified in 1% of interventions, and all identifications came from mental health settings (see Figure 18). Here, ‘self’ refers to the staff-monitoring incidents that occurred in their area {distinct from the centralised system described under BCT 2.5 [monitoring of outcome(s) of behaviour]}. Facilities can be encouraged to participate in setting goals and monitoring changes. 33
Monitoring could also take the form of supervision174 or debriefing23,82,174,192 but both of these were aimed at generating reflection following incidents. A positive staff debrief would involve active discussion about what happened, what went well, what might be done better, the possible effect on the child and how to avoid restraining the child in the future. 200
Self-monitoring of behaviour (behavior change technique 2.3)
Establish a method for the person to monitor and record their behavior(s) as part of a behavior change strategy.
Michie et al. 52
Behavior change technique 2.3 (self-monitoring of behaviour) (rather than outcomes) was identified in five interventions from three settings. BCT 2.3 (self-monitoring of behaviour) was coded when staff monitored and reflected on ‘near misses’174,193 and ‘what worked’193 when restrictive practices were successfully avoided:
These sessions were expected to provide staff with an opportunity to reflect on practices and offer peer support through encouragement and critical feedback [. . .] while also affording an opportunity for trainers to assess the efficiency of the process and make adjustments as necessary.
Glew92
Holstead et al. 191 actively trained staff ‘to recognize and be more aware of their own internal experiences during these critical moments.’191 Sanders108 emphasised that the purpose of debriefs was to be supportive of staff and not critical.
Feedback on behaviour (behavior change technique 2.2)
Monitor and provide informative or evaluative feedback on performance of the behavior (e.g. form, frequency, duration, intensity).
Michie et al. 52
Behavior change technique 2.2 (feedback on behaviour) was identified in 7% of interventions from two settings. BCT 2.2 (feedback on behaviour) was provided in the same ways as self-monitoring, such as debriefing and supervision, but specifically involved providing feedback to staff. Feedback had a number of functions including helping staff to develop awareness of ‘common precipitants’ and how effective they have been in the past190 and ‘to role model how to identify reactive behaviors’. 128 Jones and Timbers201 described the involvement of children in contributing to evaluations of staff performance.
Feedback on outcome(s) of behaviour (behavior change technique 2.7)
Monitor and provide feedback on the outcome of performance of the behavior.
Michie et al. 52
Behavior change technique 2.7 (feedback on outcomes of behaviour) was one of the most frequently identified BCTs, detectable in 39% of interventions across from all five settings. Interventions monitored data and incidents and gave feedback with a view to understanding what could have been done differently108,114,180,192,193 as well as identifying ‘critical success factors’. 202
Sanders108 described how every restraint incident was carefully scrutinised by an executive team that established whether or not the restraint had been necessary, offered feedback such as recommendations for changes to the environment and reported to a regional body.
Some interventions described having data monitoring systems in place through which rates of restrictive practices could be fed back to staff41,125,127,185 to help identify trends and inform change,180 including ‘when staff members had high rates of using restraint and seclusion’. 114
Feedback could also involve children:101,188,194
Following each hands-on incident, the patient is asked his or her interpretation of the incident. . . . Recommendations or individual preferences offered by the patient at this or any other time are communicated to the treatment team . . . The treatment plan then is reviewed and/or updated.
Visalli et al. 188
Monitoring of behavior by others without feedback (behavior change technique 2.1)
Observe or record behavior with the person’s knowledge as part of a behavior change strategy.
Michie et al. 52
Feedback was not always provided following monitoring. BCT 2.1 (monitoring of behaviour by others without feedback) was detected in 5% of interventions. These interventions, which came from mental health and criminal justice settings, described monitoring behaviour using, for example, ward-based registers,163 video- and audio-recorded footage and information from the debriefing of young people and staff. 192 They also described the collection of a variety of data, as in Finnie,91 in which it was reported that data were collected on an ongoing basis for each variable that had been identified [i.e. counts of episodes of four-point restraint, locked seclusion, staff and patient injuries, involvement of security staff to assist with managing a child’s ‘explosive’ episode’ and the use of p.r.n. medication for agitation].
The behaviours being monitored included aggressive incidents, security support and restraint;163 individual incidents;199 and the use of force. 192 Rather than for providing feedback, the purpose of monitoring was described by the Youth Justice Board for England and Wales as providing a ‘total picture’ of restrictive interventions over a period of time199 and acting as an ‘accurate record’: a way of verifying whether or not correct restraint techniques have been used and to permit investigation of antecedents. 192
Monitoring of outcome(s) of behavior without feedback (behavior change technique 2.5)
Observe or record outcomes of behavior with the person’s knowledge as part of a behaviour change strategy.
Michie et al. 52
Similarly, where monitoring of outcomes of behavior was described, feedback was not always provided as the end point. Indeed, BCT 2.5 (monitoring of outcomes of behaviour without feedback) was more common. It was detected in 10% of interventions (see Figure 18) and in all settings except criminal justice. This type of monitoring was usually undertaken at an organisational level with the systems in place to ensure the central collection and analysis of data:
All seclusion and restraint events were chart audited through the hospital’s EMR [electronic medical record] system. The documented nursing note on each patient placed in seclusion and restraint was reviewed to determine if staff followed the decision making algorithm.
Eblin162
. . . establishments should collect the following information about incidents involving the use of restraint and analyse this information at least monthly: reason for restraint . . . emerging patterns of restraint; restraint ‘hotspots’, for example . . . locations; time restraint incidents occur; which staff . . . were involved; risks in restraint techniques; training gaps identified.
Youth Justice Board for England and Wales199
The Youth Justice Board for England and Wales199 stated that institutions should, at least monthly, collect and analyse restraint data concerning why restraint had been used and any patterns of restraint use, such as locations, timing, staff involved, risks arising from restraint techniques and implications for training needs.
These data might be reviewed internally by medical, nursing or operational directors or others at an executive level105,120 or the data may be made available outside the individual institution to an overarching governing body such as the Youth Justice Board for England and Wales199 or the National Offender Management System. 23
In some interventions, all incidents were recorded161,192 but not necessarily reviewed. Elsewhere, reviews occurred either as the incidents happened87,105 or on a regular basis. 90,120 Two interventions described specific features, such as an individual experiencing multiple incidents in a given period that triggered notification for review by the medical director. 105,203
Cluster 3 (social support)
There was evidence for all three BCTs – that is emotional, practical and unspecified social support – from cluster 3 (social support). These three BCTs amounted to 8% of all BCTs identified (n = 36) and were detected in 37% of interventions overall, but slightly more often in health and social care settings (57%) (Figure 19).
FIGURE 19.
Cluster 3 (social support) by setting (% of interventions in each setting containing BCTs from this cluster).
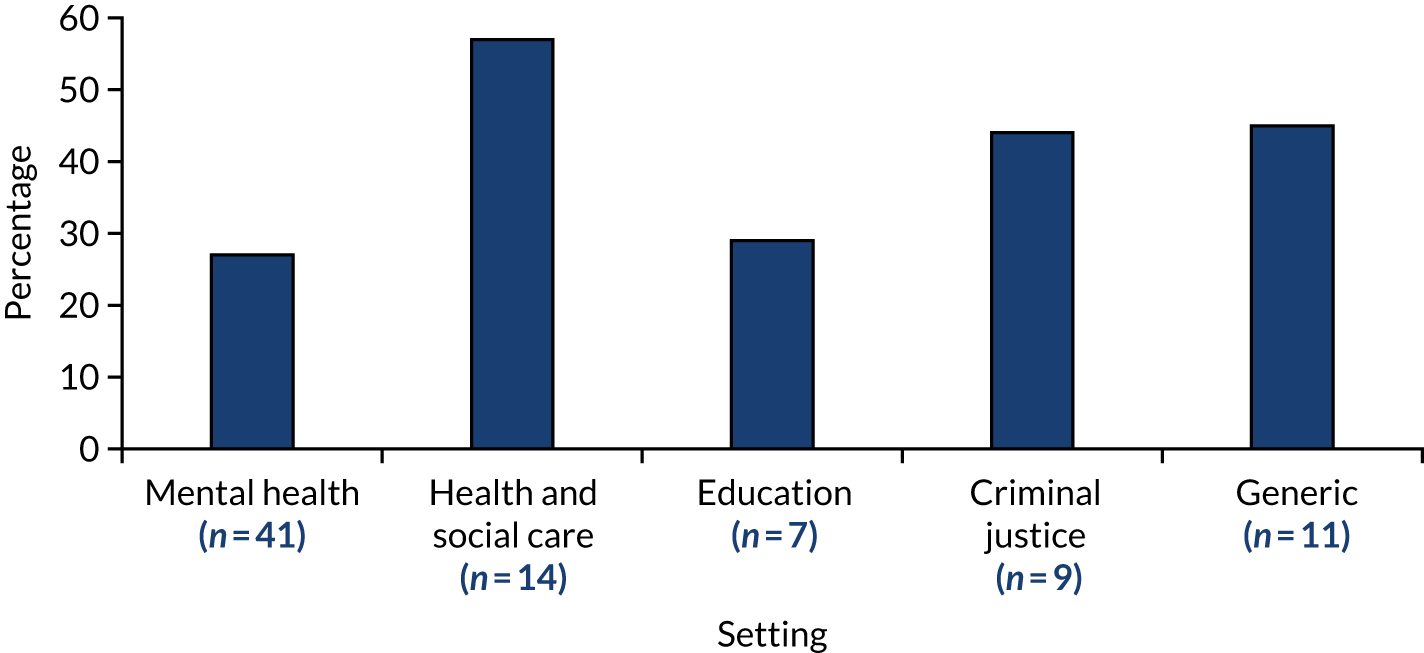
Social support (practical) (behavior change technique 3.2)
Advise on, arrange, or provide practical help (e.g. from friends, relatives, colleagues, ‘buddies’ or staff) for performance of the behavior.
Michie et al. 52
Behavior change technique 3.2 [social support (practical)] was detected in 28% of interventions from all settings except those that were ‘generic’. It was also one of the most often detected BCTs in education and criminal justice settings. Various forms of practical (as opposed to emotional or unspecified) support were described. Several interventions deployed response teams to provide additional support following incidents115 or during incidents to assist with, for example, conflict resolution or de-escalation to prevent escalation of an incident. 99,105,194,198 This support might be provided via coaching191 or modelling. 108 Another approach evolved organically:
Staff began briefly consulting with each other prior to approaching a patient in crisis. This practice enabled staff to focus on the individual’s treatment plan, brainstorm creative alternatives in the choices offered to patients in crisis, and provide consistent, professional interactions with an individual in crisis.
Witte160
Other types of practical support were also identified, including coaching,108,114,119,174,180,204 staff forums and meetings,40,122,175 peer support and the use of peers and buddies,92,160,174,205 mentoring and modelling,114,180 and supervision. 178,182,183,206
Some interventions set up a committee specifically to perform these functions. 41,125 These functions could also be provided by an external party, such as the intervention developer or trainer:40,111,128,129,178
Each facility was assigned a trainer-mentor to provide on-going consultation, modeling, and coaching in PARS concepts, techniques, and methods.
Wisdom et al. 114
Social support (emotional) (behavior change technique 3.3)
Advise on, arrange, or provide emotional social support (e.g. from friends, relatives, colleagues, ‘buddies’ or staff) for performance of the behavior.
Michie et al. 52
Less often, BCT 3.3 [social support (emotional)] was detected (in 2% of interventions from two settings). These interventions described offering emotional (as distinct from practical) social support193 via events for the purpose of reinforcing staff ‘well-being through self-care’,105 culture change183 and debriefing. 30,122,180 Advice from Holden et al. 122 was to ensure a positive outcome from a crisis. This could be facilitated by recognising its emotional impact on staff, and allowing them to process that by conducting an incident review once the urgent safety concerns had been dealt with.
Provision of emotional support was also an item in two intervention checklists. 33,207
Social support unspecified (behavior change technique 3.1)
Advise on, arrange or provide social support (e.g. from friends, relatives, colleagues,’ buddies’ or staff) or noncontingent praise or reward for performance of the behavior. It includes encouragement and counselling, but only when it is directed at the behavior.
Michie et al. 52
Behavior change technique 3.1 [social support (unspecified)] was also identified, but in just 4% of interventions from two settings. 201,204,208,209
Cluster 4 (shaping knowledge)
Two out of four possible BCTs were identified from cluster 4 (shaping knowledge). These were BCT 4.2 (information about antecedents) and BCT 4.1 (instruction on how to perform the behaviour). These two BCTs amounted to 6% of all BCTs identified (n = 36). This cluster was detected in 84% of interventions overall, but was present in all interventions from the education setting (Figure 20).
FIGURE 20.
Cluster 4 (shaping knowledge) by setting (% of interventions in each setting containing BCTs from this cluster).
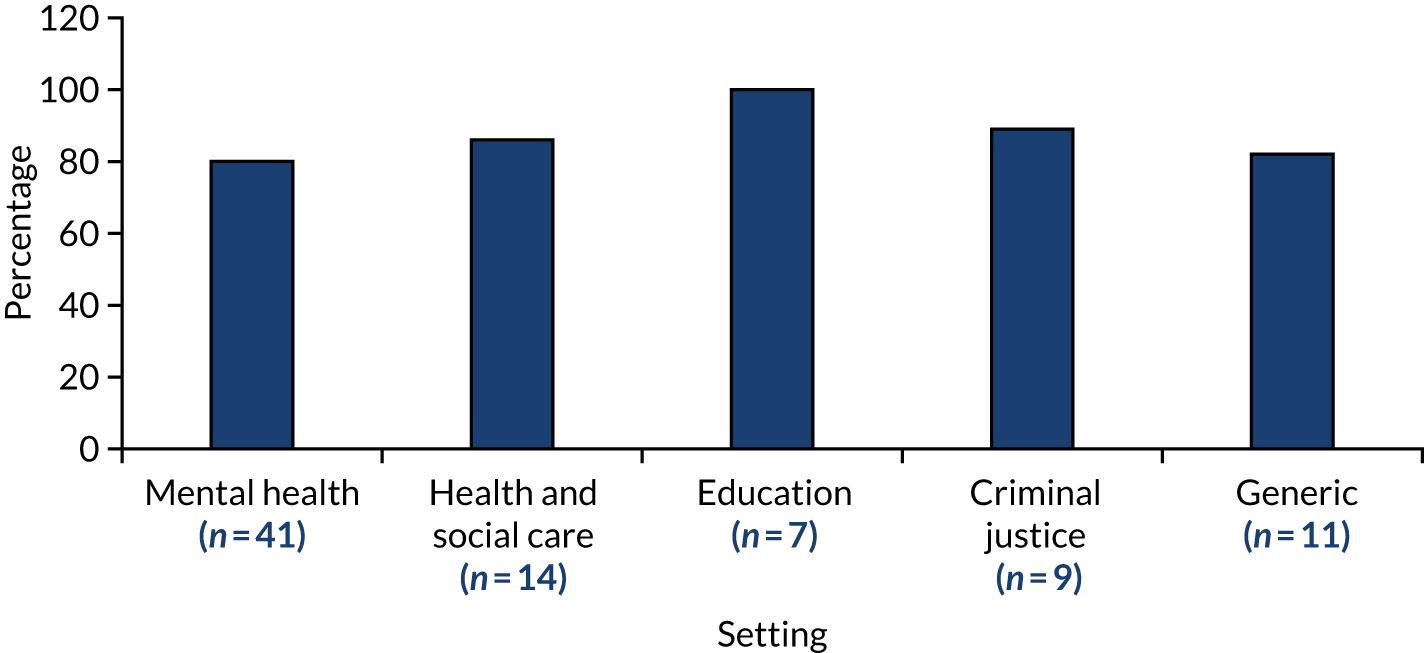
Instruction on how to perform the behaviour (behavior change technique 4.1)
Advise or agree on how to perform the behaviour (includes ‘Skills training’).
Michie et al. 52
Behavior change technique 4.1 (instruction on how to perform the behaviour) was the most common BCT, detectable in 71% of interventions. This BCT was usually evident when interventions described training of some sort. The type and duration of training varied widely, as did descriptions of its content and delivery. Some interventions described a training curriculum, whereby training was ongoing, substantial and multifaceted. 30,33,82,92,100,107,113,114,125,175,178–180,191,207,210 In one children’s centre, a training department was set up with two professional staff trainers who were employed full time. 211
The RRCs [Restraint Reduction Committee] implemented staff training that was centered on less restrictive interventions (LRIs) for aggressiveness and covered assessment of the client and situation, behavior management, and verbal de-escalation strategies. Although training included quarterly refresher courses, training was not limited to single, discrete sessions.
Miller et al. 182
These were in contrast to one-off or time-limited training sessions (which also ranged in depth and duration) described by others. 93,161,172,177 Several referred to training resulting in accreditation. 169,170,174 Some interventions specified that training was aimed at all staff in the setting:128,159,183
All detention center personnel (including food service, clerical, maintenance and janitorial, educator, administrator, and clinician staff) received an introductory training and periodic refresher trainings from one of two TARGET consultants.
Ford et al. 128
This BCT was also coded when instructions were provided in a manual89,165,209 or multimedia sources:79,89
A comprehensive training manual was supplied to all participants. The training manual . . . mirrored the training.
Bobier et al. 165
Training content included how to implement the intervention,91,125,193,204 how to use a tool,154,165 how to perform a specific skill such as de-escalation,23,92,101,105,115,119,159,202 and models and theories underpinning interventions such as trauma-informed care105,115,120,129,183 or sensory modulation. 155,156,164 In a Crisis Prevention Institute blog, Rettmann119 explained that Nonviolent Crisis training was delivered to staff involved in direct care and supervisors. Although, in most cases, the staff had received the training previously, on this occasion there was greater emphasis on the importance of developing professional relationships with the young people, and proper use of the Nonviolent Crisis Intervention de-escalation techniques.
Information about antecedents (behavior change technique 4.2)
Provide information about antecedents (e.g. social and environmental situations and events, emotions, cognitions) that reliably predict performance of the behaviour.
Michie et al. 52
Evidence of BCT 4.2 (information about antecedents) could be found in 15% of interventions from two settings. Several interventions made specific reference to antecedents:85,111,182,191,194,197,199,202,207
CPS seeks to identify pertinent social and cognitive pathway impairments and precipitating antecedent events.
Martin et al. 111
Antecedents were also referred to as ‘warning signs’. 30,114,174,194 Familiarity with an individual’s early warning signs, for example pacing, avoiding eye contact or going silent, was identified as important knowledge that would help practitioners in preventing service users from becoming over-agitated. 174
This BCT was also detected when interventions provide information about triggers in debriefings, on admission (from children and families), risk assessment or in training:85,98,114,115,122,132,163,164,189,191,194,198,202,203
All staff, including a number of non-agency temporary staff during the first two years, received skills-oriented, criteria-based training in the GBT [Girls and Boys Town] Psychoeducational Treatment Model, including teaching youth behavioral and cognitive techniques for recognizing antecedents and triggers.
O’Brien202
Cluster 5 (natural consequences)
The four BCTs [i.e. BCT 5.6 (information about emotional consequences), BCT 5.1 (information about health consequences), BCT 5.4 (monitoring of emotional consequences) and BCT 5.2 (salience of consequences)] from cluster 5 (natural consequences) accounted for just 8% of identified BCTs. BCTs from this cluster were identified in 12% of interventions overall. As illustrated in Figure 21, BCTs from this cluster were detected at varying rates in each setting.
FIGURE 21.
Cluster 5 (natural consequences) by setting (% of interventions in each setting containing BCTs from this cluster).
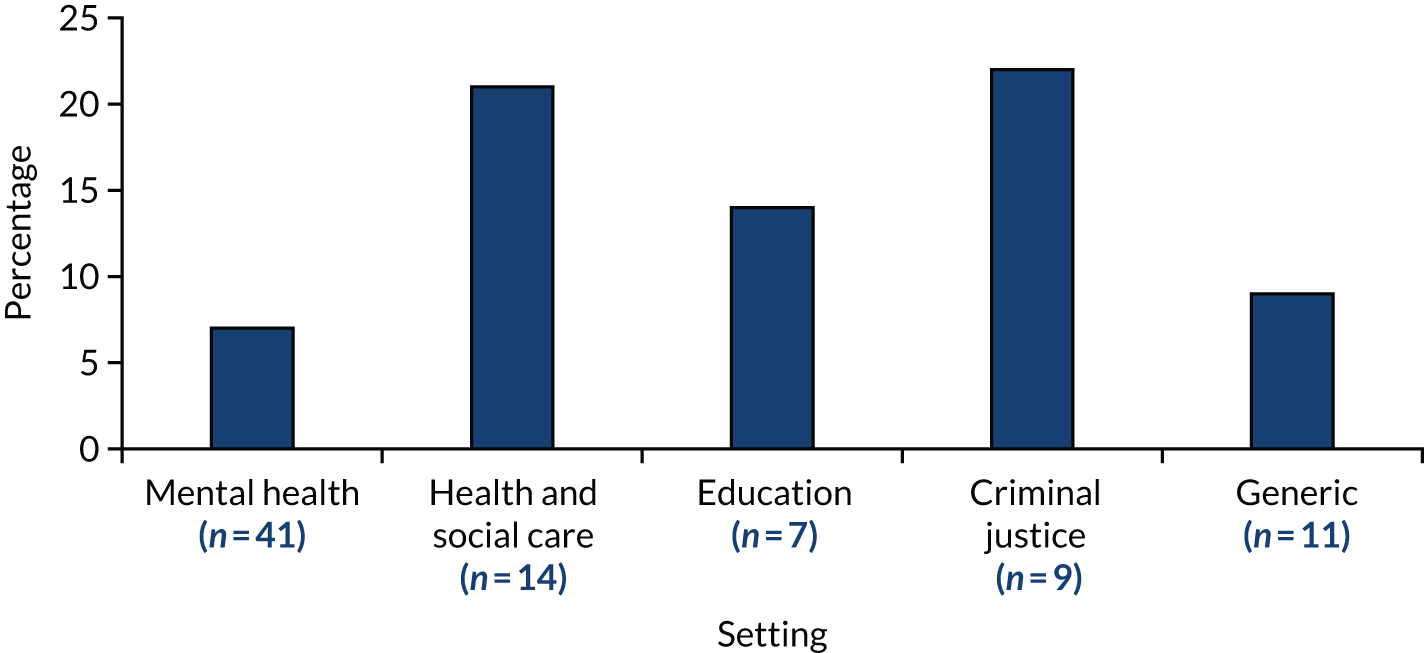
Information about health consequences (behavior change technique 5.1)
Provide information (e.g. written, verbal, visual) about health consequences of performing the behavior.
Michie et al. 52
Behavior change technique 5.1 (information about health consequences) was detected in 4% of interventions from two settings. Interventions provided staff with information about the high-risk nature of restrictive practices as well as the negative impact on the physical health of staff and children, which may include injury and death:33,122,170,194
Investigations have shown that the causes of restraint- or seclusion-related death include suffocation, heart complications, drug overdoses or interactions, blunt trauma, strangulation or choking, fire or smoke inhalation, and aspiration.
World Health Organization (WHO). 194
Staff are taught and acknowledge that emergency physical interventions are risky for both the child and the staff and that such techniques should be used only when the risk of intervening is outweighed by the risk of not intervening.
Paccione-Dyszleski et al. 170
Salience of consequences (behavior change technique 5.2)
Use methods specifically designed to emphasise the consequences of performing the behaviour with the aim of making them more memorable (goes beyond informing about consequences).
Michie et al. 52
Behavior change technique 5.2 (salience of consequences) was detected in 2% of interventions from two settings in the representation of the seriousness of restrictive practices as ‘human rights violations’ and ‘violent adverse events’,194 and in the form of testimonies of staff and children who had experienced the consequences of restrictive practices:115,174,191,211
Training content should include contributions from people with lived experience of having restraint or other restrictive practices used on them. It is important that practitioners who apply restraint have an understanding of the personal and often traumatic impact it can have.
Welsh Government. 180
Monitoring of emotional consequences (behavior change technique 5.4)
Prompt assessment of feelings after attempts at performing the behavior.
Michie et al. 52
This BCT was detected in recommendations for immediate post-incident review,33,199 apparent in just 2% of interventions from two settings.
Information about emotional consequences (behavior change technique 5.6)
Provide information (e.g. written, verbal, visual) about emotional consequences of performing the behaviour. Note: consequences can be related to emotional health disorders (e.g. depression, anxiety) and/or states of mind (e.g. low mood, stress).
Michie et al. 52
Just 1% of interventions provided information about the emotional consequences (BCT 5.6) of restrictive practices, which may include trauma. 122,180,194 This BCT was detected in health and social care settings only.
Cluster 6 (comparison of behavior)
Two BCTs [i.e. BCT 6.1 (demonstration of the behaviour) and BCT 6.2 (social comparison)] out of the three BCTs in cluster 6 (comparison of behavior) were identified. This constituted just 6% of all identified BCTs. Cluster 6 was identified in 10% of all interventions but at varying rates (range 7–22%) in the different settings. It was not identified at all in education or generic settings (Figure 22).
FIGURE 22.
Behavior change techniques in cluster 6 (comparison of behavior) by setting (% of interventions in each setting containing BCTs from this cluster).
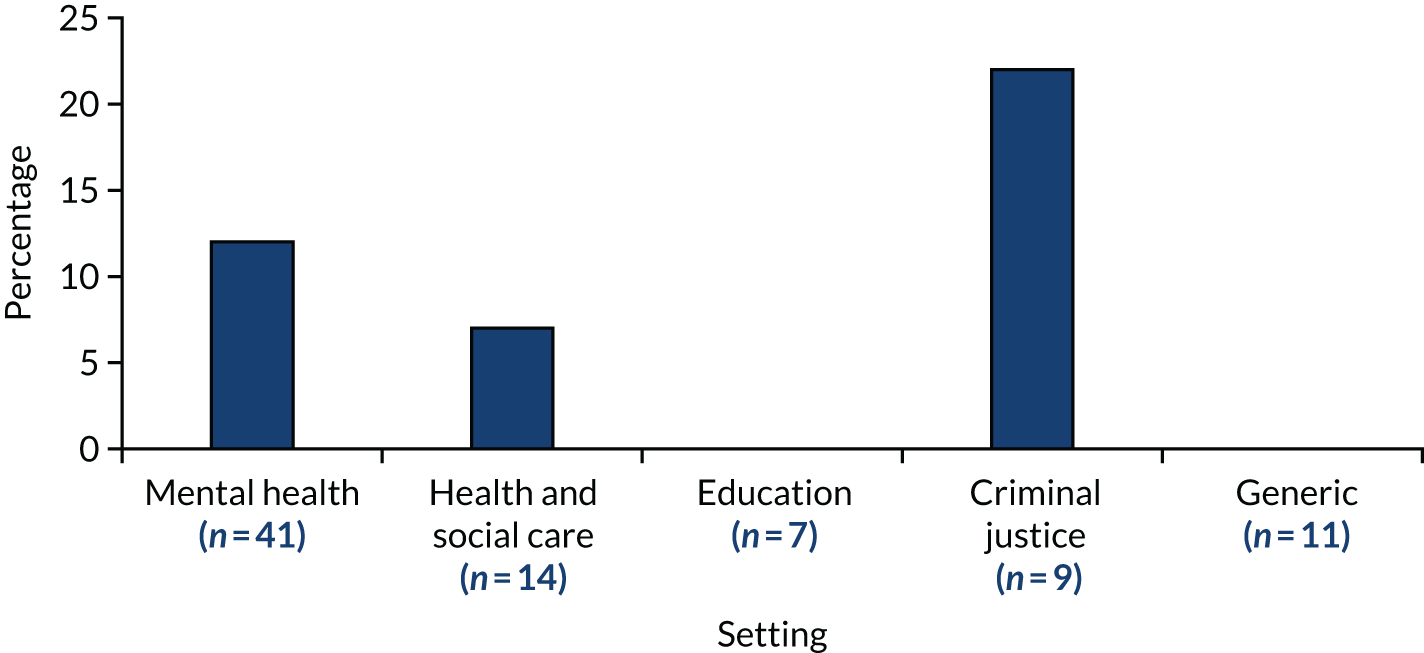
Demonstration of the behavior (behavior change technique 6.1)
Provide an observable sample of the performance of the behaviour, directly in person or indirectly e.g. via film, pictures, for the person to aspire to or imitate (includes ‘Modelling’).
Michie et al. 52
The BCT demonstration of the behavior (BCT 6.1) was identified in 4% of interventions from two settings. Examples included interventions demonstrating the desired skills or a tool to staff204 or providing example scripts of interactions. 91 For example, one training programme explained that a skill should be modelled in a way that illustrates the behavioral steps clearly and unambiguously, and, furthermore, than the skill will be viewed as important and effective where the trainer is viewed as having high-level skills, competence and relatable experience, and as friendly, helpful and successful in their career. 122
Social comparison (behavior change technique 6.2)
Draw attention to others’ performance to allow comparison with the person’s own performance.
Michie et al. 52
Social comparison (BCT 6.2) was identified in 6% of interventions (see Figure 22), for example where they recommended or implemented visits or contact with other organisations,105,116 attending presentations,40 field trips or conferences. 102 The purpose of these was to make comparisons,175 foster healthy competition33,193 and to learn from the successful implementation of an intervention. 116 BCT 6.2 (social comparison) could be identified within183 or across organisations105,116 or both. 33
Cluster 7 (associations)
Behavior change technique 7.1 (prompts or cues) was the only BCT from a possible eight to be identified from cluster 7 (associations). This amounted to 3% of total BCTs identified. Nevertheless, this BCT (and, therefore, the cluster) was identified in 23% of interventions overall. Rates of detection varied across settings, from 9% in generic settings to 33% in criminal justice (Figure 23).
FIGURE 23.
Cluster 7 (associations) by setting (% of interventions in each setting containing BCTs from this cluster).
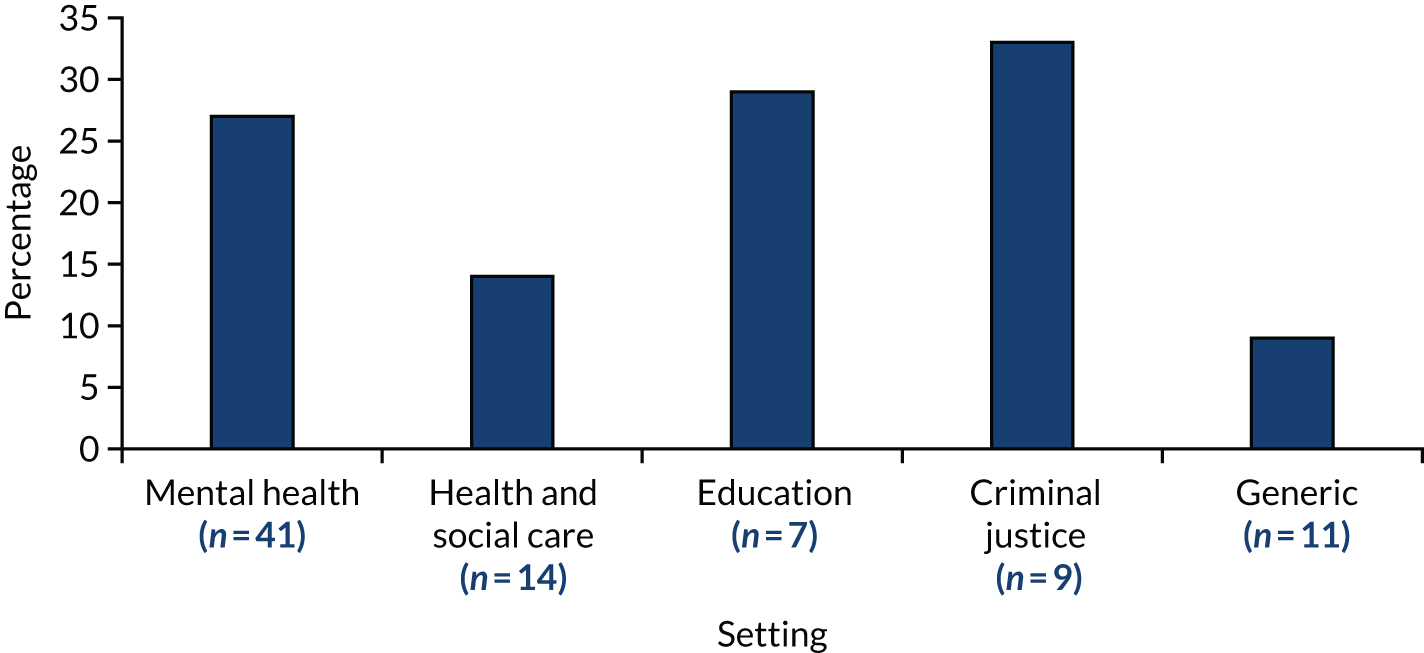
Prompts or cues (behavior change technique 7.1)
Introduce or define environmental or social stimulus with the purpose of prompting or cueing the behavior. The prompt or cue would normally occur at the time or place of performance.
Michie et al. 52
The BCT prompts or cues (BCT 7.1) was identified in 23% of interventions from all settings except generic (see Figure 23). It was also one of the most often detected BCTs in education and criminal justice settings. A prompt or cue could take the form of a tool (i.e. a safety planning tool, a risk assessment tool, prevention tools or a risk management tool33,77,114,156). Examples of such tools included the personal safety assessment tool165 and the ‘moment by moment assessment’ tool. 78 Tools could be used to prompt preventative behaviour (i.e. through assessment and planning) to assist advanced decision-making and advance directives30,33,77 or to aid responsive decision-making:
The decision-making algorithm with an agitated patient was to be used before the initiation of seclusion and restraints and included the following steps: verbal de-escalation, assessing effectiveness, notifying the physician for emergency medication, then assessing again for effectiveness.
Eblin162
Moments in time were also coded as prompts or cues. For example, in several interventions a specific process, such as carrying out risk assessments30,77,162,169,176 or person-centred assessments180 or the formulation of crisis management strategies,189,198 would be prompted by preadmission, admission or an incident. Prompts or cues also appeared in visual displays (i.e. signs, posters and displays):183,184
One program created an ‘On Track Action’ wall . . . to reinforce positive steps that each client could take . . . The goal of the wall was to provide clients with weekly and monthly incentives for positive behaviors and to provide staff members with a systematic tool for consistently giving praise.
Hodgdon et al. 183
In some interventions, prompts or cues occurred in the form of cards to be carried or t-shirts displaying the curriculum logo to be worn:183,184
They also had all staff and residents make safety plan cards (written plans of how to handle triggers and other safety measures) and made sure that everyone wore them.
Elwyn et al. 178
Staff members were also instructed to carry a pocket-sized tool step guide (i.e., that listed all of the steps for each tool) at all times.
Crosland et al. 204
Cluster 8 (repetition and substitution)
Just one BCT, behavioral practice/rehearsal (BCT 8.1), was identified from the seven available BCTs in cluster 8 (repetition and substitution), representing 3% of all identified BCTs; however, this BCT was detected in 17% of all interventions. It was not detected in generic settings, and rates of detection ranged from 7% in mental health settings to 44% in criminal justice settings (Figure 24).
FIGURE 24.
Cluster 8 (repetition and substitution) by setting (% of interventions in each setting containing BCTs from this cluster).

Behavioral practice/rehearsal (behavior change technique 8.1)
Prompt practice or rehearsal of the performance of the behavior one or more times in a context or at a time when the performance may not be necessary, in order to increase habit and skill.
Michie et al. 52
From cluster 8 (repetition and substitution), the single BCT behavioral practice/rehearsal (BCT 8.1) was identified. This BCT was detected in 17% of interventions from all settings except generic (see Figure 24). It was also one of the most often detected BCTs in education and criminal justice settings. This BCT involved practising various techniques,92,93,108,122,128,183,204 sometimes with supervision. For example, a resource document from the US Department of Education197 specified that, with regard to the prevention of restrictive practices, staff should practise and review their approaches regularly and frequently, under supervision, as they would a fire drill.
Techniques reported included role-play40,85,107,174 and other exercises:184
All staff members practiced and rehearsed the procedures in the training sessions. The program concluded with the staff members applying the material learned in situational role plays and discussing post intervention techniques.
Ryan and Rigby212
Skill practice exercises for monitoring and enhancing appropriate staff-to-youth communication in areas such as body language, voice tone, facial expressions.
O’Brien202
Cluster 9 (comparison of outcomes)
The single BCT credible source (BCT 9.1) was identified from cluster 9 (comparison of outcomes) and constituted < 3% of all identified BCTs. This cluster was one of the least often detected, appearing in only 3% of interventions. This BCT was detected in 22% of criminal justice setting interventions but only 2% of mental health settings (Figure 25).
FIGURE 25.
Cluster 9 (comparison of outcomes) by setting (% of interventions in each setting containing BCTs from this cluster).
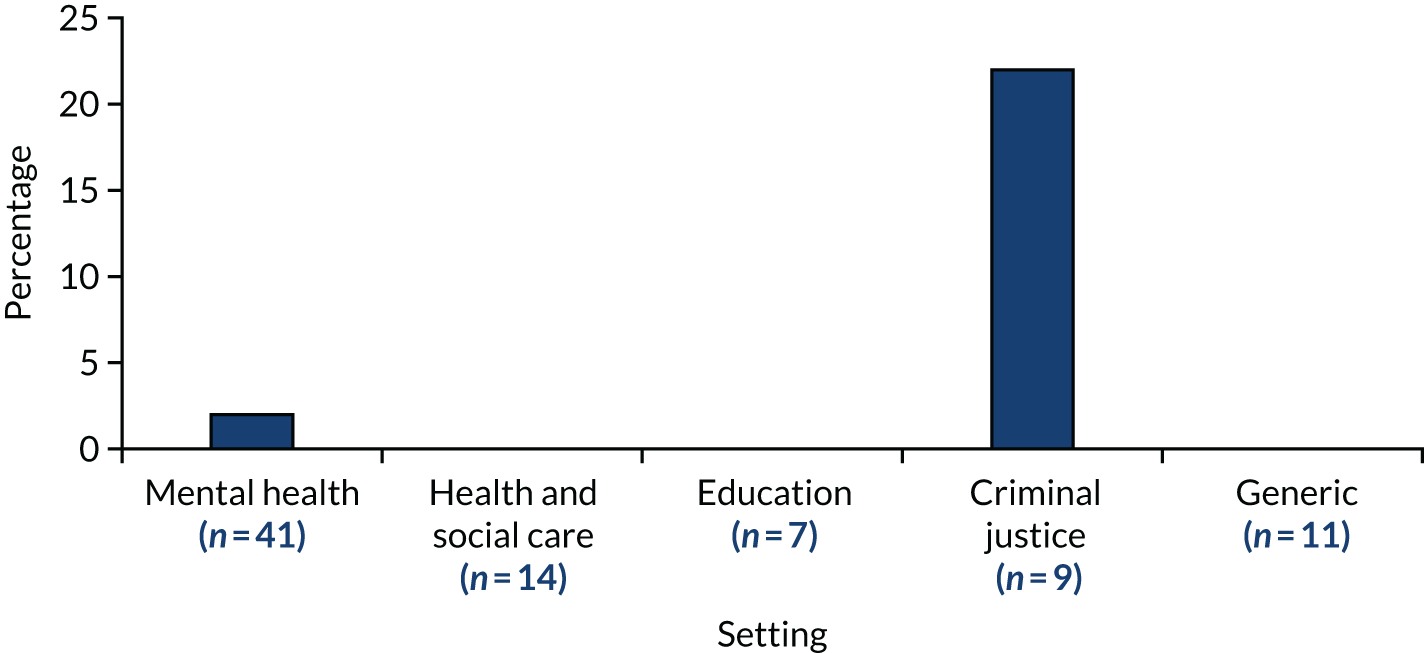
Credible source (behavior change technique 9.1)
Present verbal or visual communication from a credible source in favour of or against the behavior.
Michie et al. 52
Behavior change technique 9.1 (credible source) was identified in criminal justice settings204 and mental health settings. 122 Crosland et al. 204 described training being given by certified behaviour analysts, whereas in Holden et al. ’s study122 staff were asked to provide credibility by describing their experience of working with CYP.
Cluster 10 (reward and threat)
Three BCTs out of a possible 11 from cluster 10 (reward and threat) were identified {BCT 10.10 [reward (outcome)], BCT 10.5 [social incentive] and BCT 10.4 [social reward]}. These three BCTs accounted for 8% of all identified BCTs and were detected in 8% of all interventions, but at a rate of only 2% in mental health settings, compared with 22% in health and social care settings (Figure 26).
FIGURE 26.
Cluster 10 (reward and threat) by setting (% of interventions in each setting containing BCTs from this cluster).

Social incentive (behavior change technique 10.5)
Inform that a verbal or non-verbal reward will be delivered if and only if there has been effort and/or progress in performing the behavior (includes ‘Positive reinforcement’).
Michie et al. 52
The BCT social incentive (BCT 10.5) was identified in 4% of interventions (see Figure 26). Although social incentive for staff could take the form of individual recognition,178 for Schreiner et al. 41 the incentive was the potential improvement to the workplace:
Staff were enticed to participate in the project through potential benefits (e.g., a more pleasant patient living environment, a more pleasant work environment for staff, and decreased risk of patient and staff injuries).
Schreiner et al. 41
Social reward (behavior change technique 10.4)
Arrange verbal or non-verbal reward if and only if there has been effort and/or progress in performing the behavior (includes ‘Positive reinforcement’).
Michie et al. 52
The BCT social reward (BCT 10.4) was detected in all settings except generic, amounting to 8% of interventions (see Figure 26). Examples included recognition of best practices, celebration of successes,180,193 awards,119 weekly peer nominations100,125 and praise. 41,185 The example below from Hodgdon et al. 183 illustrates how social incentives and rewards could be identified in conjunction:
[Staff] encouraged each other . . . by providing reinforcement (giving a fellow staff member a chip) when they observed a skill being used with a client. At the end of a 2-week period, the staff with the most chips was recognized in staff meeting and also earned an incentive.
Hodgdon et al. 183
Reward (outcome) (behavior change technique 10.10)
Arrange for the delivery of a reward if and only if there has been effort and/or progress in achieving the behavioral outcome (includes ‘Positive reinforcement’).
Michie et al. 52
Similarly, reward (outcome) (BCT 10.10) was manifested as staff recognition164 in just 1% of interventions (see Figure 26). This BCT was detected in mental health settings only.
Cluster 11 (regulation)
The only BCT (of four possible) identified from cluster 11 (regulation) was BCT 11.2 (reduce negative emotions). This amounted to 3% of all BCTs identified. This BCT (and, therefore, cluster) was detected in 7% of interventions, but rates varied from 2% in mental health settings to 18% in generic settings (Figure 27).
FIGURE 27.
Cluster 11 (regulation) by setting (% of interventions in each setting containing BCTs from this cluster).
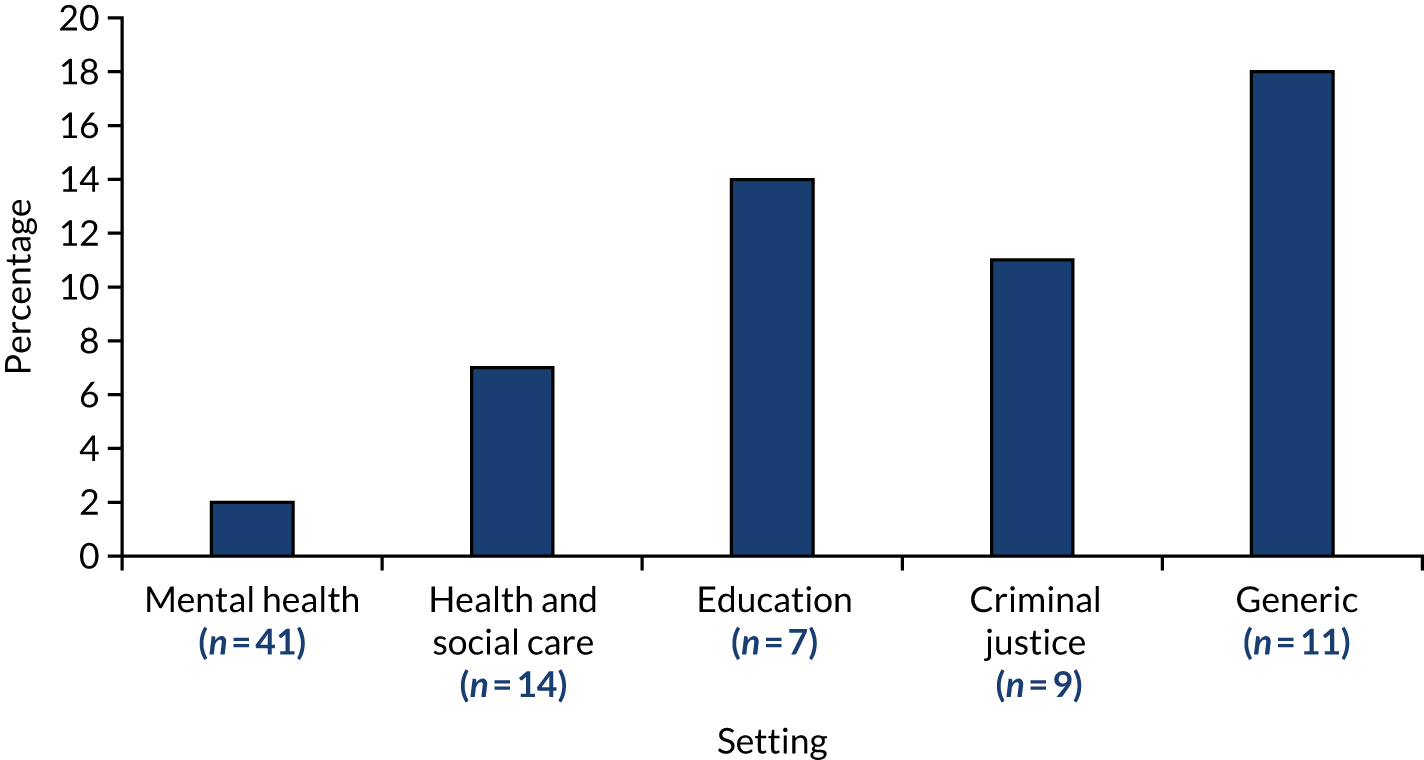
Reduce negative emotions (behavior change technique 11.2)
Advise on ways of reducing negative emotions to facilitate performance of the behavior (includes ‘Stress Management’).
Michie et al. 52
The BCT reduce negative emotions (BCT 11.2) was detected in 7% of interventions (Figure 27). Interventions offering post-incident support to involved staff and witnesses to reduce trauma and other negative outcomes were coded with this BCT:105,122,180,207
Organisations should have a person-centred policy for providing both immediate and longer-term support after any use of restrictive practices. The policy should indicate future options for accessing longer term support or counselling if needed. This may include individual and/or group supervision/debriefing and individual psychological therapy delivered by trained professionals.
Welsh Government. 180
This BCT was identified where interventions encouraged reflection30,122 and self-regulation. 122,183 A secondary purpose of reducing negative emotions was preventing ‘workplace stress’ from adversely affecting practice. 180
Cluster 12 (antecedents)
Behaviour change techniques identified from cluster 12 (antecedents) accounted for 16% of all BCTs identified. Three BCTs were identified from this cluster: BCT 12.5 (adding objects to the environment), BCT 12.1 (restructuring the physical environment) and BCT 12.2 (restructuring the social environment). This cluster was the second most commonly detected across all settings, at a rate of 74%. BCTs from this cluster were identified in almost all interventions (93%) from the health and social care setting but in less than half (43%) in the education settings (Figure 28).
FIGURE 28.
Cluster 12 (antecedents) by setting (% of interventions in each setting containing BCTs from this cluster).
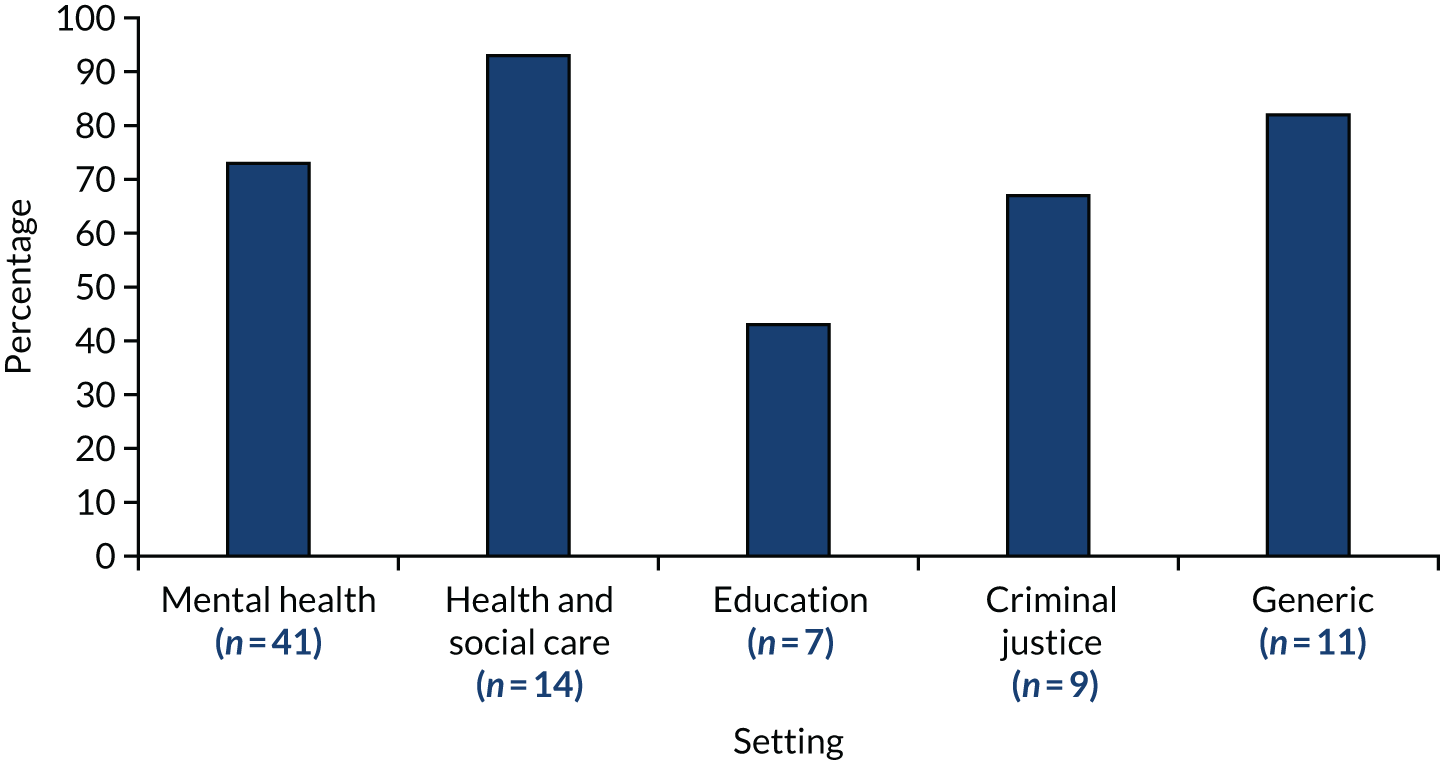
Restructuring the physical environment (behavior change technique 12.1)
Change, or advise to change the physical environment in order to facilitate performance of the wanted behavior or create barriers to the unwanted behavior (other than prompts/cues, rewards and punishments).
Michie et al. 52
Examples of restructuring the physical environment were found in 23% of interventions (see Figure 28). Multiple examples of changes to the physical environment were detected, many of which involved the installation of a sensory or comfort room or zone:33,77,114,129,156,164,165,183,194
The Unit’s sensory room contained a variety of sensory equipment, including a rocking chair, weighted blankets, fidget toys, scented oils, candy and teas, pictograph cards (i.e. flashcards depicting pleasant or calming images), music and projected images (e.g. bubbles floating or rivers running).
West et al. 164
The introduction or improvement of recreational spaces, such as playgrounds, was another physical change. 114,166 Some interventions also reported making physical changes to create a low-stimulation environment (i.e. with low noise and lighting)85,122 and decorative changes to improve the appearance and maintenance of the setting82,102,122,168,181,202 and personal spaces, such as bedrooms:122,172
The therapeutic environment intervention involved making inexpensive physical changes, including repainting walls with warm colors, placement of decorative throw rugs and plants, and rearrangement of furniture [. . .] The second intervention included replacing worn-out furniture.
Borckardt et al. 181
Others removed locks and improved free access to outdoor spaces to facilitate independence. 168,174,180
Restructuring the social environment (behavior change technique 12.2)
Change, or advise to change the social environment in order to facilitate performance of the wanted behaviour or create barriers to the unwanted behaviour (other than prompts/cues, rewards and punishments).
Michie et al. 52
Restructuring the social environment (BCT 12.2) was the second most common BCT detected, appearing in 69% of interventions (see Figure 28) and in three out of the five settings. The frequency with which this BCT was detected is partly attributable to its broad definition and how it was operationalised. The social environment was conceptualised in three ways: (1) milieu and culture, (2) communication and social interaction and (3) staffing and peer support.
Various interventions referred to changing the culture,89,120,174 for example ‘creating a culture of caring’,116 organisational culture change82,116 and creating a supportive and therapeutic milieu:82,110,183
Assessing for distress or threat within the therapeutic milieu of residential programs is [an important innovation]. Residential-based TST teams now have a system and format for regularly discussing [team functioning] and ascertaining whether individual team members (or the team as a whole) are effecting a distressed or threatening environment.
Brown et al. 78
These broad changes often included revising rules,82,178,181 clarifying expected behaviours,163,168,199 increasing freedoms33,89,176,203 and introducing restrictive practice reduction policies:210
The rules and language intervention included the establishment of a team for each unit that was tasked with reviewing and modifying unit rules and policies to be less restrictive to patients or eliminating unit rules that were too restrictive.
Borckardt et al. 181
This BCT was also coded where interventions described making changes to improve communication or social interaction. Some changes involved opportunities for children to socialise with each other89 or with their families:105,115
Youth and family commitment was a key to [. . .] success [. . .] The hospital has implemented many youth and family activities, which have enhanced their participation together at the facility. Many families were reimbursed for . . . travel to family meetings, or medical cabs were accessed. Visitation by families has been encouraged.
Azeem et al. 105
Others involved opportunities for staff to socialise with children, such as at mealtimes. 89,105,115,168 Often in conjunction with such social opportunities were improvements to communications with children and their families, such as via meetings or information-sharing:82,89,105,168,174,178,181
Other Sanctuary Model tools such as community meetings, where the ‘community’ of staff and girls would gather regularly, and red-flag meetings, arranged to defuse a potentially serious incident, were held consistently. Sanctuary was also incorporated into after-care planning and in work with the girls’ families.
Elwyn et al. 178
Azeem et al. 105 also mentioned providing access to interpreters.
A key aspect of improved communication as a form of restructuring of the social environment was the active involvement of children and their families in planning and setting goals in meetings,82,85,115,168,176,193,207 training sessions and evaluations. 89,116 Similarly, the involvement of front-line staff by management in planning and achieving change was coded to this BCT:89,116,178,211
Involve staff. Staff asked to make this change must be part of the process; otherwise early buy-in and support for the new direction will be compromised. Staff often know far better where the operational obstacles lie and have pragmatic ideas about how to address them.
Caldwell and LeBel116
Staffing changes, such as increased staffing during critical periods, and task-sharing were also coded as restructuring the social environment. 82,85,168,178,207 Colton82 reported that it was possible for organisations to influence the implementation of seclusion and restraint measures, provided that staffing levels were adequate at critical points in the day such as transitions, shift changes and evenings.
Changes to staffing and organisational culture were reinforced by managerial support and leadership,30,82,88,105,115,116,178,207 peer support,105,178 team building115 and the establishment of working groups, task forces and implementation teams:85,168,183
Development of strategies to improve interdisciplinary communication. A subcommittee of the task force set up multidisciplinary mini-meetings, where the work of the aggression-free task was discussed and feedback was encouraged.
Goren et al. 168
Adding objects to the environment (behavior change technique 12.5)
Add objects to the environment in order to facilitate performance of the behavior.
Michie et al. 52
Adding objects to the environment (BCT 12.5) was detected in 11% of interventions (see Figure 28), such as where sensory equipment33,39,105,114,129,156,164,165,194 and recreational/occupational equipment105,114,115 were provided as part of the intervention. Kaltiala-Heino et al. 198 also described the requirement for staff to carry an alarm device.
Cluster 13 (identity)
Two out of the five BCTs in cluster 13 (identity) were identified, accounting for 6% of all BCTs identified. These BCTs were BCT 13.1 (framing or reframing) and BCT 13.2 (identification of self as role model) and they were identified in 48% of interventions overall (although the rate ranged from 29% to 64%) (Figure 29).
FIGURE 29.
Cluster 13: Identity by setting (% of interventions in each setting containing BCTs from this cluster).
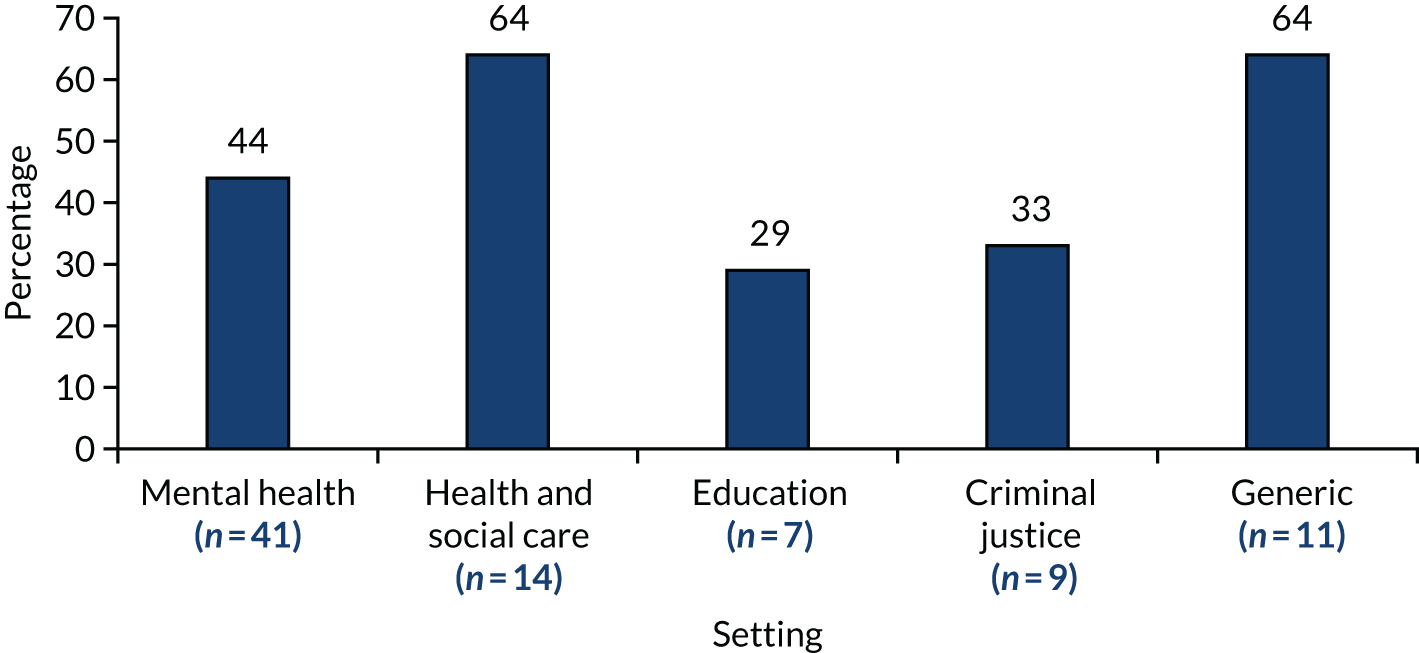
Identification of self as role model (behavior change technique 13.1)
Inform that one’s own behavior may be an example to others.
Michie et al. 52
The BCT identification of self as role model (BCT 13.1) was detected in 24% of the interventions (see Figure 29). Several interventions used the concept of a role model or role modelling by managers,108,160,178 team leaders174 and other key staff:41,183
Managers modelled responses to challenging situations in ways that did not include the use of physical restraints.
Sanders108
In some interventions, trained staff took on the role of internal expert, trainer or champion:115,168–170,178,194
Develop a cadre of staff who can share their expertise by providing training to their colleagues, thus expanding our still-limited training resources.
Girelli210
Often this drew on a train-the-trainer model79,118,172,176,183 or mentoring. 128,180,213
Framing/reframing (behavior change technique 13.2)
Suggest the deliberate adoption of a perspective or new perspective on behavior (e.g. its purpose) in order to change cognitions or emotions about performing the behavior (includes ‘Cognitive structuring’).
Michie et al. 52
Framing/reframing (BCT 13.2) was another commonly identified BCT, detectable in 42% of interventions (see Figure 29). Many interventions sought to encourage staff using framing/reframing and often this was informed by a specified model or approach, such as strengths-based care,40,105,116,214 trauma-informed care,78,85,105,114,116,120,122,171,172,177,178,181,183,190,193,207 recovery-oriented care,77,99,188,193 CPS92,112 and positive behavioural support:100,126
For trauma-informed care, all unit staff attended a half-day standardized training seminar on the nature of trauma and its effects on patients’ experiences, physiology, and psychological processes, along with instructions on how to minimize engaging in behaviors that could exacerbate trauma related reactions from patients.
Borckardt et al. 181
Within or in addition to these approaches, staff were encouraged to reframe their views of the children they worked with, such as the origins of their challenging behaviour174 or their expectations of their abilities:
Through debriefings, case processing, and team meetings, we found that staff interventions were based on the patient’s chronological and/or physical age rather than on the patient’s cognitive/social/emotional age. [. . .] We educated staff . . . for assessing and reassessing a patient’s developmental ages and discussed appropriate developmental age expectations and interventions.
Fralick176
Similarly, interventions encouraged framing/reframing of staff views of children’s behaviour and its meaning. 110,168,180 Finally, staff were encouraged to reframe their beliefs about restraint, for example as a ‘last resort’33 and as harmful and not therapeutic. 194 They were also encouraged to view their relationships with the children as a therapeutic tool. 170,210 Framing/reframing was usually initiated through training. 33,39,111 At the organisational level, framing/reframing could be detected in descriptions of culture change89,108,193 and paradigm shifts. 91,115
Cluster 14 (scheduled consequences)
The single BCT identified from the 10 in cluster 14 (scheduled consequences) accounted for < 3% of all BCTs identified. Cluster 14 was the least often detected (2% of interventions). It was not detected at all in education, criminal justice or generic settings, and at very low rates in mental health and health and social care settings (Figure 30).
FIGURE 30.
Cluster 14 (scheduled consequences) by setting (% of interventions in each setting containing BCTs from this cluster).
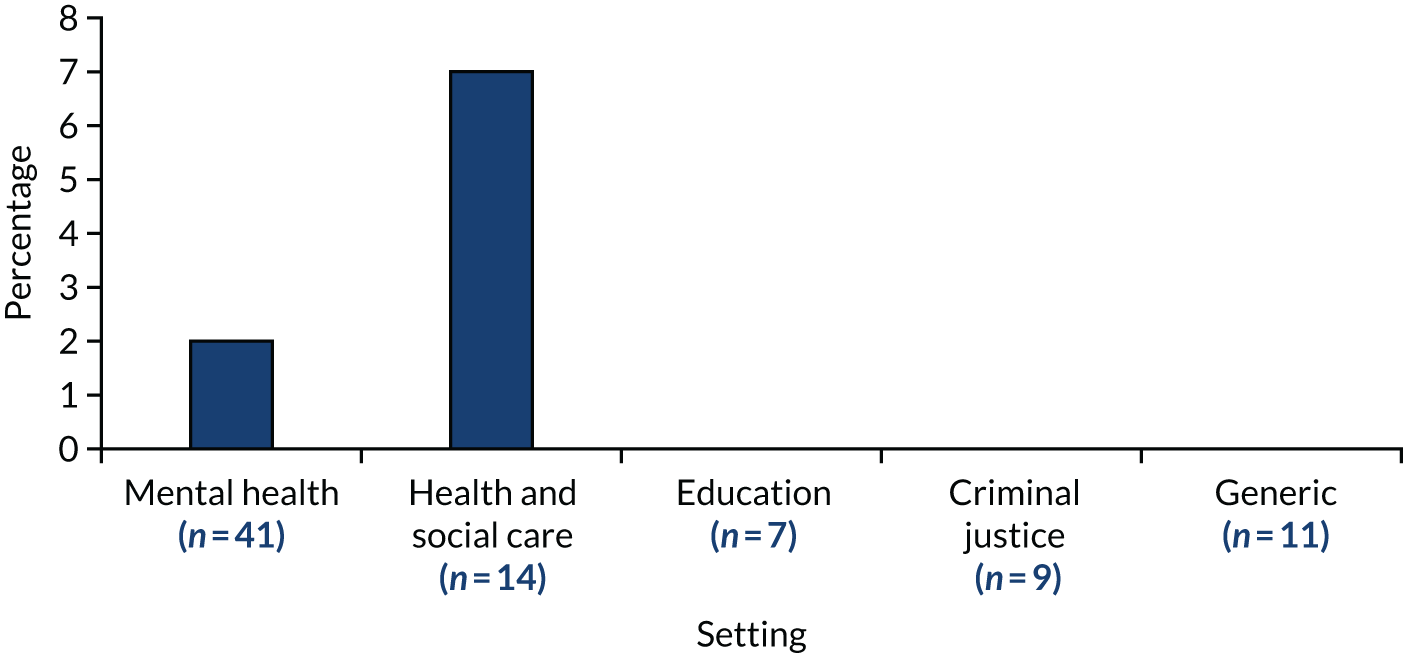
Remove punishment (behavior change technique 14.10)
Arrange for removal of an unpleasant consequence contingent on performance of the wanted behavior (includes ‘Negative reinforcement’).
Michie et al. 52
Only one BCT from cluster 14 (scheduled consequences) was identified: remove punishment (BCT 14.10). This BCT was detected in interventions from mental health settings only, amounting to 2% of all interventions (see Figure 30). This BCT captures the avoidance of undesirable consequences if the desired behaviour is performed. Three interventions described creating a non-punitive environment and debriefing sessions being conducted in a non-punitive and supportive manner, without attributing blame. 33,174,193
Undetected behavior change techniques and behavior change technique clusters in interventions
Behavior change techniques from cluster 15 (self-belief) and cluster 16 (covert learning) were not detected in any of the interventions.
A total of 56 (60%) individual BCTs were not identified in any of the interventions (see Appendix 7). It should be noted that for a BCT to be identified in an intervention, evidence of its presence needed to be documented in the intervention materials. Therefore, there may be instances in which a BCT remained unidentified because of a lack of evidence.
Conclusion
Application of the BCT taxonomy to 82 interventions that sought to reduce restrictive practices in children’s settings identified 36 out of a possible 93 BCTs. The most frequently BCT identified was BCT 4.1 (instruction on how to perform the behaviour), reflecting the high use of training within interventions.
Chapter 6 Results of the behaviour change technique synthesis: behaviour change techniques related to intervention procedures, outcomes and mechanisms of action
This chapter presents further detail about how the BCTs identified related to the different intervention procedures, intervention outcomes and the mechanisms of action theorised to be at work.
Intervention procedures
The majority of the interventions used more than one procedure (e.g. staff training and data review), and, as such, it was not possible to identify which BCTs were found within individual procedures. However, 20 of the interventions used only one procedure (six different procedures were used only once); therefore, it was possible to look at what BCTs were used in relation to these six procedures. The six different procedures and the number of interventions they were used in are shown in Table 24.
| Intervention procedure | Responses | |
|---|---|---|
| Number | Percentage | |
| Training | 9 | 45 |
| Data review | 3 | 15 |
| Risk assessment tools | 3 | 15 |
| Guidelines or policy change | 3 | 15 |
| Staff involvement | 1 | 5 |
| Milieu changes | 1 | 5 |
| Total | 20 | 100 |
Training was the most frequently used single procedure and was used in nine interventions. The most frequently identified BCTs were BCT 4.1 (instruction on how to perform the behaviour), BCT 12.2 (restructuring the social environment), BCT 1.1 (problem-solving), BCT 1.4 (action-planning), BCT 2.7 (feedback on outcomes of behaviour) and BCT 13.2 framing/reframing.
The rest of the procedures were used in only a small number of interventions. Data review, risk assessment and guidelines or policy change were all identified as lone procedures in three interventions each. The most frequently identified BCTs in data review studies were BCT 4.1 (instruction on how to perform the behavior), BCT 12.2 (restructuring the social environment), BCT 2.7 [feedback on outcome(s) of behavior], BCT 1.4 (action-planning) and BCT 1.2 (problem-solving). The BCTs associated with the introduction of risk assessment were BCT 4.1 (instruction on how to perform the behavior), BCT 12.2 (restructuring the social environment), BCT 2.7 [feedback on outcome(s) of behavior], BCT 1.4 (action-planning), BCT 1.2 (problem-solving) and BCT 13.2 (framing/reframing). Three studies used guidelines and policy change as a lone procedure. The BCTs most frequently identified in these three studies were BCT 2.7 [feedback on outcome(s) of behaviour], BCT 1.4 (action-planning), BCT 1.2 (problem-solving) and BCT 13.2 (framing/reframing).
Milieu changes and staff involvement alone were used in one study each. Apart from the restructuring and instruction, the most frequent BCT related to milieu change was BCT 13.2 (framing/reframing). The BCTs related to staff involvement were BCT 13.1 (identification of self as role model), BCT 3.2 [social support (practical)], BCT 1.4 (action-planning), BCT 2.7 [feedback on outcome(s)] and BCT 13.2 (framing/reframing).
When BCTs used in all interventions, regardless of the number of procedures, were collected, all had BCT 4.1 (instruction on how to perform the behavior) and BCT 12.2 (restructuring the social environment) as the two most commonly identified. When the remainder of the interventions are looked at by the procedures, some differences can be seen. (It was not possible to disaggregate any of these procedures from the others used simultaneously, so these BCTs must be viewed in that context.)
Figure 31 shows the BCTs identified in ≥ 50% of the interventions according to the procedures they contained. The only other BCT used in > 50% of interventions using sensory approaches was BCT 7.1 (prompts/cues). Similarly, only BCT 13.2 (framing/reframing) was commonly used in interventions using milieu changes. Over half of interventions using staffing changes used BCT 13.2 (framing/reframing) and BCT 13.1 (identification of self as role model). BCT 1.4 (action-planning) was found across all the interventions except these three. The interventions that used environmental changes and promoted involvement of CYP and their families used a higher number of BCTs than those that did not.
FIGURE 31.
Different BCTs identified in interventions using specific procedures.

Behaviour change techniques and outcomes
One objective of the study was to identify and prioritise BCTs that show promise of effectiveness for testing in future interventions. Sixty-seven of the interventions had been subject to evaluation and, of these, 29 had reported statistically significant positive findings and 38 had not. Table 25 shows the different BCT content of interventions that had reported positive findings and those that did not.
| BCT | Percentage of interventions with positive findings in which BCT was detected | Percentage of interventions without positive findings in which BCT was detected | Difference (%) |
|---|---|---|---|
| 4.1 (instruction on how to perform the behavior) | 87 (rank 1) | 71 (rank 1) | 16 |
| 12.2 (restructuring the social environment) | 63 (rank 2) | 68 (rank 2) | –5 |
| 2.7 [feedback on outcome(s) of behavior] | 40 (rank 4) | 58 (rank 4) | –18 |
| 1.2 (problem-solving) | 40 (rank 4) | 42 (rank 5) | –2 |
| 13.2 (framing/reframing) | 37 (rank 5) | 37 (rank 7) | 0 |
| 1.4 (action-planning) | 33 (rank 6) | 66 (rank 3) | –32 |
| 4.2 (information about antecedents) | 30 (rank 7) | 16 | 14 |
| 13.2 [social support (practical)] | 20 (rank 10) | 39 (rank 6) | –19 |
| 12.1 (restructuring the physical environment) | 20 (rank 10) | 24 (rank 8) | –4 |
| 13.1 (identification of self as role model) | 20 (rank 10) | 21 (rank 9) | –1 |
| 7.1 (prompts/cues) | 21 | 20 (rank 10) | –1 |
| 8.1 (behavioral practice or rehearsal) | 16 | 17 | 1 |
| 1.9 (commitment) | 21 | 13 | –8 |
| 2.5 [monitoring of outcome(s) of behavior without feedback] | 13 | 13 | 0 |
| 12.5 (adding objects to the environment) | 11 | 10 | –1 |
| 10.4 (social reward) | 8 | 10 | 2 |
| 2.2 (feedback on behavior) | 8 | 10 | 2 |
| 6.2 (social comparison) | 5 | 10 | 5 |
| 3.1 [social support (unspecified)] | 3 | 10 | 7 |
| 3.3 [social support (emotional)] | 3 | 10 | 7 |
| 2.3 (self-monitoring of behavior) | 13 | 7 | –6 |
| 1.3 [goal setting (outcome)] | 11 | 7 | –4 |
| 5.1 (information about health consequences) | 8 | 7 | –1 |
| 11.2 (reduce negative emotions) | 3 | 7 | 4 |
| 1.1 [goal setting (behavior)] | 0 | 7 | 7 |
| 2.1 (monitoring of behavior by others without feedback) | 0 | 7 | 7 |
| 2.4 [self-monitoring of outcome(s) of behavior] | 8 | 3 | –5 |
| 10.5 (social incentive) | 5 | 3 | –2 |
| 5.2 (salience of consequences) | 5 | 3 | –2 |
| 6.1 (demonstration of the behavior) | 5 | 3 | –2 |
| 1.7 [review outcome goal(s)] | 3 | 3 | 1 |
| 10.10 [reward (outcome)] | 0 | 3 | 3 |
| 14.10 (remove punishment) | 0 | 3 | 3 |
| 5.4 (monitoring of emotional consequences) | 0 | 3 | 3 |
| 5.6 (information about emotional consequences) | 5 | 0 | –5 |
| 9.1 (credible source) | 5 | 0 | –5 |
The ranking of the BCTs is very similar. The two most frequent are the same, although the percentage of interventions with positive outcomes is higher for BCT 4.1 (instruction on how to perform the behavior) than for BCT 12.2 (restructuring the social environment), both found in > 60% of all interventions. Those interventions without positive findings featured BCT 1.4 (action-planning) third most frequently, used in 66% of those without positive findings compared with only 33% of those with positive findings. In those interventions with positive findings, the most frequent BCTs were BCT 2.7 [feedback on outcome(s) of behavior] and BCT 1.2 (problem-solving). Eighteen per cent more of the unsuccessful interventions used BCT 2.7 than those reporting positive outcomes.
The evaluations used a broad range of outcome measures, as described in Chapter 4. This makes it difficult to compare interventions on their specific outcomes. However, the two most frequently reported outcomes were (1) a reduction in the number of incidents of restraint (used by 30% of interventions; n = 20) and (2) a reduction in the number of incidents of seclusion (used by 14% of interventions, n = 9). Eighteen evaluated interventions reported a significant reduction in incidents of restraint and six reported a significant reduction in incidents seclusion. The BCTs identified in > 20% of these interventions are shown in Figure 32.
FIGURE 32.
The BCTs identified in > 20% of interventions that successfully reduced incidents of restraint and seclusion.
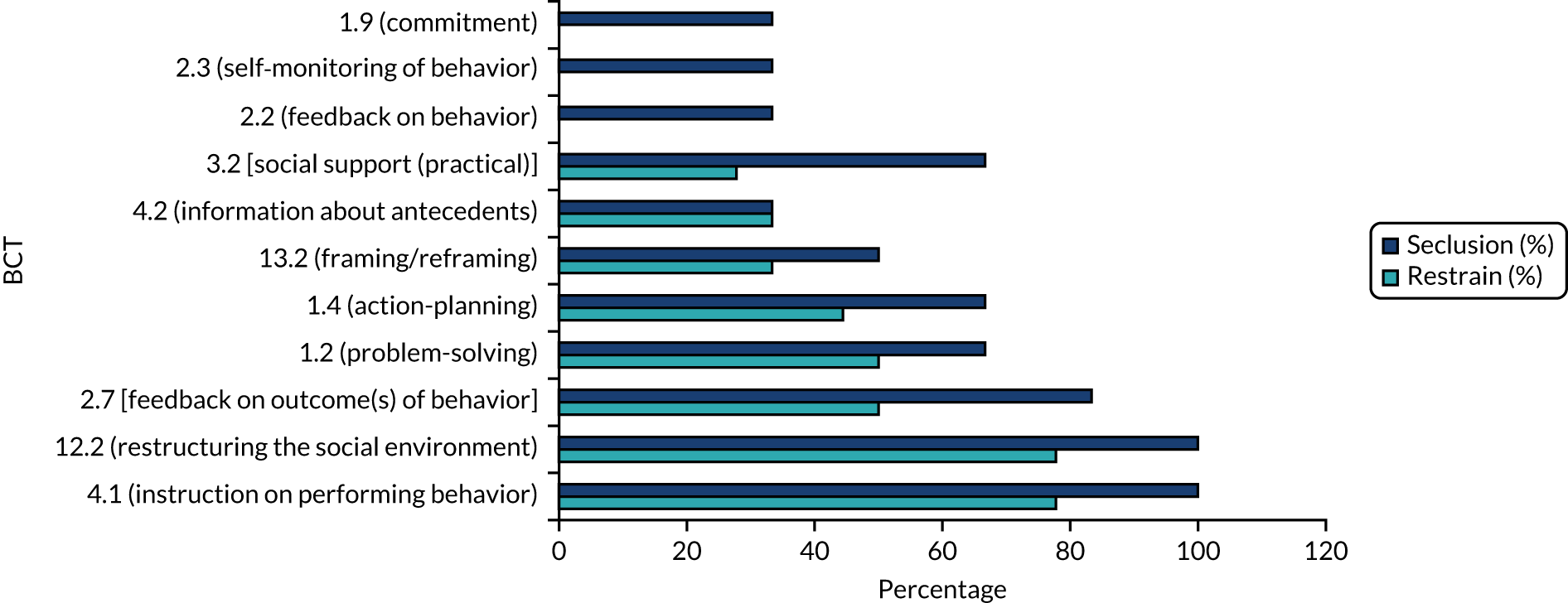
As seen in Table 26, the two most frequently identified BCTs are again BCT 4.1 (instruction on how to perform the behavior) and BCT 12.2 (restructuring the social environment), with BCT 2.7 [feedback on outcome(s) of behavior] ranking third for both outcomes. BCT 13.2 (framing/reframing), BCT 13.2 [social support (practical)], BCT 1.4 (action-planning) and BCT 1.2 (problem-solving) were identified in higher percentages of interventions that reduced incidents of seclusion, as well as BCT 2.2 (feedback on behavior), BCT 2.3 (self-monitoring of behavior) and BCT 1.9 (commitment), which were absent from > 20% of the interventions that reduced incidents of restraint.
| All interventions | Interventions that significantly reduced restraint | Interventions that significantly reduced seclusion |
|---|---|---|
| 4.1 (instruction on how to perform the behavior) | 4.1 (instruction on how to perform the behavior) | 4.1 (instruction on how to perform the behavior) |
| 12.2 (restructuring the social environment) | 12.2 (restructuring the social environment) | 12.2 (restructuring the social environment) |
| 1.4 (action-planning) | 2.7 [feedback on outcome(s) of behavior] | 2.7 [feedback on outcome(s) of behavior] |
| 2.7 [feedback on outcome(s) of behavior] | 1.2 (problem-solving) | 1.2 (problem-solving) |
| 1.2 (problem-solving) | 1.4 (action-planning) | 1.4 (action-planning) |
| 13.2 (framing/reframing) | 13.2 (framing/reframing) | 3.2 [social support (practical)] |
| 3.2 [social support (practical)] | 4.2 (information about antecedents) | 13.2 (framing/reframing) |
| 4.2 (information about antecedents) | 3.2 [social support (practical)] | 4.2 (information about antecedents) |
The list of identified BCTs does not account for the multiple procedures within these interventions, nor does it account for the small number of studies that reported significant reduction in incidents of seclusion (n = 6). When these are compared with all interventions, BCT 1.4 (action-planning) drops rank from third to fifth with both groups of interventions that reduced restraint and seclusion and BCT 2.7 [feedback on outcome(s) of behavior] and BCT 1.2 (problem-solving) are ranked third and fourth. The ranking of the two most frequent BCTs remains unchanged.
The intervention evaluations were implemented in different settings. Those that reported significant positive findings were separated by setting and the BCTs were examined (criminal justice was excluded from this analysis as there was only one case). Mental health and social care settings were both dominated by BCTs 4.1 (instruction on how to perform the behaviours) and 12.2 (restructuring the social environment).
The interventions designed for use in generic settings used the most BCTs. Notably, all used BCT 2.7 [feedback on outcome(s) of behavior]. Educational settings were the only setting where over half of the interventions used BCT 7.1 (prompts/cues) to change staff behaviour (Figure 33).
FIGURE 33.
The BCTs identified in > 50% of interventions reporting significant positive findings by setting.

Mechanisms of action
Mechanisms of action are theoretical constructs that explain how BCTs affect behaviour. Twenty-six mechanisms of action, derived from both the theoretical domains framework and a systematic review of 83 behaviour change theories, have been specified. Understanding how specific BCTs change behaviour can support intervention theory development and testing and inform increasingly effective and efficient interventions. The Theory and Technique tool215 was used to identify the mechanisms of action for which there were identified links with the BCTs most frequently identified in studies reporting positive findings. These are summarised in Table 27 in addition to the mechanisms of actions through which they are theorised to work.
| BCT | Kn | Sk | SPRI | BaCa | Op | BaCo | Re | In | Go | MADP | ECR | Si | Em | BR | No | SN | Attb | Mo | SI | Ne | Va | FP | SLI | BC | GAB | Psv |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Problem-solving | ||||||||||||||||||||||||||
| Action-planning | ||||||||||||||||||||||||||
| Feedback on outcomes of behaviour | ||||||||||||||||||||||||||
| Social support (practical) | ||||||||||||||||||||||||||
| Instruction on how to perform behaviour | ||||||||||||||||||||||||||
| Information about antecedents | ||||||||||||||||||||||||||
| Prompts/cues | ||||||||||||||||||||||||||
| Restructuring the physical environment | ||||||||||||||||||||||||||
| Restructuring the social environment | ||||||||||||||||||||||||||
| Identification of self as role model | ||||||||||||||||||||||||||
| Framing/reframing perspective |
The most common mechanisms of action related to BCTs used in studies with positive significant findings was environmental control and resources. This is defined as changes to ‘aspects of a person’s situation or environment that discourage or encourage the behaviour’. 216 BCTs linked with this were 3.2 [social support (practical)], 7.1 (prompts/cues), 12.1 (restructuring the physical environment) and 12.2 (restructuring the social environment).
The second most frequently occurring mechanism of action was behavioural cueing, defined as the process by which a behaviour is triggered from the external environment, the emergence of ideas or the performance of another behaviour. The BCTs that were related to this mechanism were 1.4 (action-planning), 7.1 (prompts/cues) and 12.1 (restructuring the physical environment).
The third most common mechanisms of action were knowledge, behavioural regulations and belief about capabilities. Knowledge was targeted by two BCTs: BCT 4.1 (instruction on how to perform the behavior) and BCT 4.2 (information about antecedents). Behavioural regulation was targeted by BCT 4.2 (information about antecedents) and BCT 1.2 (problem-solving). Belief about capabilities included BCT 1.2 (problem-solving) and BCT 4.1 (instruction on how to perform the behavior).
This more detailed look at where different BCTs were used has shown that where procedures had been used on their own interventions they showed little variation in the two most popular BCTs, 4.1 (instruction on how to perform the behavior) and 12.2 (restructuring of the social environment). After these two there was some variation by procedure. Exploration of outcomes was also hampered by the use of many different outcome measures used in interventions. When studies reporting positive findings in the two most frequently used outcomes (incidents of restraint and incidents of seclusion) were explored, these showed that the same BCTs were in most frequent use in interventions that successfully reduced incidents. The mechanisms of action related to the most frequently identified BCTs were those relating to changes to a person’s broad social and physical environment to encourage desired behaviours. These relationships are summarised in Table 27.
Chapter 7 Discussion
Introduction
In March 2020, the UK press217 reported that the Ministry of Justice was being challenged by Article 39, a children’s charity, to release details of child restraint in prisons. The Ministry of Justice was asked to release records giving the reasons for the use of pain-inducing restraint [i.e. ‘managing and minimising physical restraint’ (MMPR)] had been used, on 260 occasions during 2017–18, in young offender institutions and secure training centres. 217
The use of restrictive practices with children remains a pertinent, ongoing issue. Children who are already vulnerable may be at higher risk of being restrained. Wisdom et al. 114 reported that, according to the New York Office of Mental Health, children were five times more likely than adults to be put in restraint or seclusion. Restraints seem to be performed more frequently on elementary/primary students (aged 5–11 years) than their older peers. 113,218
Overall, the literature on interventions to reduce restrictive practices in CYP’s settings presents a complex picture. There is a lack of consistency and comprehensiveness in reporting. This results in an evidence base that is of limited value for informing decisions about the development, implementation and evaluation of interventions. There is a strong tendency for interventions to have multiple components, and this, combined with the poor reporting, further limits the potential of the evidence base to inform practice. The study results therefore suggest an urgent need to simplify and streamline interventions and intervention reporting.
Criminal justice
The review included records addressing the use of restrictive practices in youth justice settings.
In 2004, 14-year-old Adam Rickwood died in custody in the UK, having taken his own life after being struck by a member of staff using an approved restraint technique. 23 Concerns surrounding this event led to an independent review of restraint in juvenile secure settings,219 which concluded that, in secure settings (secure training centres, young offender institutions and secure children’s homes), if a child’s behavior constitutes a high risk to themselves or others, it might on occasion be necessary to use force to restrain children.
The report219 recommended that, when physical restraint is used, the focus should be on preventing the risk of physical or psychological harm and risk of harm to a safe environment; moreover, consistent criteria for using restraint should be introduced and adhered to, alongside other mechanisms to enhance and audit standards of care.
Subsequent UK government publications from the Youth Justice Board for England and Wales concerned guidance for secure establishments on the development of restraint minimisation strategies199 and governance and safeguarding processes associated with MMPR. 192 In 2011, a follow-up report187 on implementing the independent review of restraint in juvenile secure settings concluded that there had been progress towards changing the culture around the restraint used in CYP’s secure settings. At the same time, the authors highlighted a concern around pain compliance (using pain to achieve compliance).
That cultural change was taking place in tandem with the continuation of potentially harmful practices raises a familiar question of whether to prioritise systemic issues or day-to-day practice in the setting. However, the current review has found that many interventions to reduce restrictive practices take a whole-systems approach intended to address problematic issues at different points within the organisation.
There is more recent government guidance on reducing the need for restraint and restrictive interventions with CYP in health, education and some residential settings (e.g. Department for Education and Department of Health and Social Care30). MMPR23 is an example of the separate guidance that pertains to the youth criminal justice sector.
Minimising and managing physical restraint/pain compliance
The use of MMPR in youth justice settings was reviewed in 2015. 23 At this point in the roll-out of MMPR, the reviewers raised specific concerns about restraining children on the floor, head holds and pain-inducing techniques, but found sufficient indicators of progress to support a cautious recommendation that the programme should continue. 23 Nevertheless, concerns about MMPR techniques, including pain compliance, were acknowledged by the government,187 the voluntary sector220 and elsewhere. 217
In 2018, the Ministry of Justice commissioned an independent review of the use of pain-inducing techniques in the youth secure estate. 221 The report’s recommendations, including a ban on pain-inducing restraint in youth custodial settings, were all accepted by the government. 222,223 Hence, in the period since Adam Rickwood’s death,217,222,223 progress has been reported in cultural and structural dimensions. The ending of pain compliance may represent some movement away from punitive value systems.
Beyond the UK
The developments in the UK are not dissimilar to those in the USA. After the press exposé in 1998 of abuses in the US children’s sector,83 there was a rapid growth in the development of interventions to reduce restrictive practices, as this review has shown. Among these, TARGET was adopted by the Juvenile Justice System128 and the 6CS enjoyed the support of SAMSHA (Substance Abuse and Mental Health Services Administration) and NASMHPD and was suggested as suitable for juvenile justice settings. 116 As the current review has highlighted, the strategies that emerged tended to share, first, a philosophy of trauma-informed care and, second, a preference for multifaceted interventions.
This review found evidence of a trauma-informed approach in many of the interventions, including those applied or applicable in justice settings. 105,116,119,121,128–130,178 Greene et al. 110 reported that CPS was effective in juvenile detention settings, and the TARGET intervention, which arguably has more complexity, demonstrated a positive correlation between trauma-informed approaches and good outcomes in justice settings. 128 When the intention was to achieve improvements via system change, this might also be trauma informed. For instance, Elwyn et al. 178 reported a trauma-informed organisational change model in a girls’ juvenile justice setting. The 6CS also targets system change, as do many of the stand-alone interventions found in this review.
This highlights what Elwyn et al. 178 described as an essential contradiction between organisational goals of care and rehabilitation versus punishment and control. 178 Lipsey224 pointed out that the evidence does not favour punitive regimens, even (or especially) in the justice system, where there is a particularly high proportion of children who have experienced trauma. WHO’s position194 is that seclusion and restraint should not be considered to be interventions of last resort, and Kaltiala-Heino et al. ,198 advocating for a therapeutic environment in justice settings, argued that physical restraint per se does not have therapeutic merit.
Overview of interventions
This review has generated an overview of interventions aimed at reducing restrictive practices with CYP in institutional settings, and thus meets objective 1. The environmental scanning method68 identified useful grey literature and social media sources, including training organisation websites and videos, showing that many service providers are developing their own interventions, adapting existing ones without reporting fidelity or applying existing ones without reporting useful levels of detail about intervention or study procedures. Therefore, an important advantage of the environmental scanning approach is that it can capture interventions that may not have been evaluated, reported or published, but which are nevertheless used in real-world settings, with real children.
The most common procedures focused on staff training. Other procedures related to guideline or policy change, risk assessment tools, data review, milieu changes and changes to therapeutic approach (e.g. introducing trauma-informed care). This contrasted slightly with the most common procedures in the earlier companion review47 of interventions to reduce restrictive practices in adult mental health inpatient services, which found that the most commonly used procedures in those settings were training, audit and feedback, and nursing changes. This may in part be attributable to the wider variety of settings explored in the current review.
These observations should be viewed with caution. The value of a review of the literature is that it can collate and synthesise evidence to inform policy and practice decisions. In the present case, such decisions are likely to have a direct effect on the experiences of vulnerable CYP in institutional settings. It has been noted throughout the review that the reporting found in the literature is poorly aligned with the WIDER recommendations for reporting. 69 Evidence-informed decision-making relies on a sufficiently robust evidence base, yet despite the importance of the topic focused on in this review, the evidence appears to be weak.
Service user perspectives
The review found very few reported examples of service user involvement in the development of interventions, or even in their evaluation, despite the United Nations’ principle of children’s participation27,225,226 Service users interviewed in a Canadian study227 explained that restraint made them feel sad and angry; in contrast, staff interviewed for the same study described feelings of anxiety in relation to restraining service users. This suggests important differences with potentially great relevance for strategies to reduce the use of restrictive practices. The current review has identified what may be a lack of children’s participation in this field. Empirical research from Norway and other countries has identified barriers to children’s involvement including structural constraints,228 lack of understanding of why children’s perspectives are relevant229 and reluctance on the child’s part. 229
Classification of intervention components
Intervention components were classified in terms of BCTs and their frequency of use was determined, thus meeting objective 2.
Multicomponent interventions
A number of records (e.g. Girelli210) made the argument that complex problems require multidimensional solutions but, although the components appear to work better together than in isolation, the approach defies attempts to evaluate individual strands. Multicomponent interventions may involve many process elements that cannot be evaluated separately (e.g. Ubana et al. 102).
Despite a lack of effectiveness evidence, there appears to be more investment in complex interventions that use a number of mechanisms (e.g. at both individual and setting levels) than with simple interventions. It may be the case that an intervention with a single component, such as educating staff about trauma or installing a sensory room, would be sufficient to address issues with restrictive practices.
A tendency for multicomponent interventions was previously noted in the literature. Wilson et al. 230 observed that methodological inconsistencies in the literature limit the relevance of reported reductions in restraint, but also made the point that interventions are not necessarily designed with a view to producing evidence. To enhance the potential success of interventions development, it may be beneficial to consider participatory or collaborative approaches that are developed in partnership with both children and staff. 29
Identification of process elements
Process elements in intervention delivery were identified to some extent and, therefore, objective 3 was partially met.
It was not necessarily clear whether or not process elements had been considered, and to what extent they may have affected outcomes. For instance, gender may affect intervention delivery: Shadili et al. 101 suggested that the gender of the staff may have influenced how violence was managed. The way in which interventions were introduced could also confound attempts to clarify cause and effect. 111,112,125 It is clear that this is not easily resolved. LeBel et al. 40 (2009), whose work routinely incorporates costing calculations, explained that it had not yet been possible to quantify the interventions that help to reduce restraint and seclusion, and thus firm conclusions could not be made.
It is unclear whether or not multicomponent interventions that combine, for example, training, a new nursing model, management changes and the introduction of a service user forum would increase benefits.
The records included a number of reports of milieu interventions that incorporated, as well as staff training, enhancements to staffing and leadership; generally, this is not clearly reflected in outcomes reporting and, therefore, it is not possible to conclude how individuals may be influencing the use of restrictive practices. It appears likely that staff are highly influential on the process of intervention delivery, yet the tendency to pool staff data masks the impact of individual staff roles. Staff were often treated as an homogeneous group for data collection, without acknowledgement of the impact of individuals and individual roles. Studies exploring differences between staff in the health and social sectors have identified that factors such as training, experience, skill mix, age, gender, job satisfaction and expectations can all have an impact on how an individual approaches their professional duties. 231,232
Costs
Some records reported costs (e.g. LeBel and Goldstein,39 Health Sciences Center Winnipeg104 and Forrest et al. 172), but, again, with widely varying units of calculation that prevented comparison. Arguably, it would be advisable to avoid investing financial and other resources in interventions that have not been rigorously evaluated, or else have not demonstrated effectiveness.
Restraint and seclusion as measurable outcomes
The review also identified a lack of clarity about how to achieve aims. The broad aim of all the interventions was to reduce restrictive practices: restraints, seclusions or the use of as required medication. However, there was a range of strategies to achieve the aim, reflected in outcomes reporting that was inconsistent across the records.
One study178 reported that the introduction of a new social culture and trauma-informed practice ultimately led to the departure of individuals who did not want the change, which helped the new regime to thrive. This level of detail about individual staff was unusual in the retrieved literature, but suggests that it may be relevant to consider staff retention as an outcome measure or even a change mechanism.
Comparisons across the data set were made difficult by differences in the outcomes measured between studies, even with respect to using the same intervention. For example, although the most common measurables by far were numbers of restraint and seclusion incidents, the numbers were calculated in different ways, such as simple counts or rates (e.g. per number of service users over a time period).
A count or a rate of restrictive practices does not portray specifics: potentially, a brief, low-intensity restriction without need for a physical intervention could be included for counting alongside a lengthy, complex and high-intensity incident. Restraint and seclusion incident numbers were by far the most common measured outcomes, and there was little reporting of other relevant factors, such as the duration of a restrictive practice, whether or not mechanical restraints were used, how many patients were involved in the incident or how many people sustained injuries as a result. It can be argued that broad, collapsed data of this type may not easily portray the realities of practice and, therefore, have limited value for informing decision-making.
Comparison of intervention components between settings
Components of interventions in CYP’s settings across target populations (i.e. different professions) and policy area (i.e. health, welfare, criminal justice) were compared with those in adult acute psychiatric inpatient settings47 (see Comparison with the results of the COMPARE study). Potential explanations for any differences were considered and discussed, meeting objective 5.
Effectiveness
Evidence of effectiveness was explored through the examination of BCTs and intervention outcomes, although, again, the limitations of the evidence restricted the potential of the review to meet objective 4.
There was a lack of consistency in the approaches taken to evaluation. When the study design was described, no RCTs were identified, and only around one-third of the records reported quantitative data. Hence, there is a dearth of effectiveness evidence within and across interventions. This has been highlighted in the literature; for instance, Wilson et al. 230 identified a need for the use of robust methodologies, such as RCTs, to evaluate effectiveness.
Such difficulties add to study-specific issues that can confound attempts to evaluate cause and effect. Although in general confounders were rarely discussed, one report96 highlighted the possibility that the observed reduction in restraint use might be associated with a change in prescribing practice during the course of the study.
Identification of potentially effective behaviour change techniques
As discussed, the review did not find robust evidence to support the identification and prioritisation of BCTs showing most promise of effectiveness; hence, objective 6 was only partially met.
For example, staff training was a consistent component of the identified interventions, yet reporting was at best inconsistent, with limited information about how many were trained, how the training was delivered and other relevant details. This made meaningful comparisons across studies impossible. For instance, nearly half of the records did not report whether training was delivered in-house or by an external provider, and only around one-fifth reported the number of training hours involved, with even fewer reporting how it was delivered, or detailing which staff groups received it. In addition, there appeared to be a widespread assumption that staff training would lead directly to staff behaviour change. Budlong169 pointedly summarised some of the issues with training, describing a review of training vendors that:
[L]ed us to realize that trainers in the area of restraint claim an expertise and display an arrogance about their programs that prevent any meaningful dialogue about the inherent risks in their methods. All claim to be safe, effective [and widely applicable] with little or no risk of injury.
Buldong169
This discussion further identified a ‘guru’ mentality169 in many of the larger training programmes that impeded objective analysis of inherent risks to young people, and appeared to be associated with a lack of scrutiny from accrediting bodies. Budlong169 further argued that training should be perceived by organisational administrators and leaders as their responsibility, rather than something that can be bought in, delivered and forgotten about, and warned against a ‘separation of training from organizational goals and everyday operations’. 169
Budlong’s article appeared in a practitioner-oriented publication,233 alongside others that showcased how children’s service providers had used federal funding to address restrictive practices following the Hartford Courant exposé. 83,84 In the same publication, O’Brien202 cautioned against over-reliance on training:
Interestingly, training data revealed that [a sub group of staff], on average, had the highest ratings on written and skill practice assessments, suggesting that training alone – independent of ongoing, consistent staff support and development – is a fairly weak intervention.
O’Brien202
This example of staff training highlights the need to avoid conflating prevalence of intervention components with effectiveness. The effectiveness evidence should be viewed with caution. Nonetheless, the BCT analysis identified BCTs that showed most promise of effectiveness and would be suitable for further exploration and testing. In ranked order, these were:
-
instruction on how to perform the behavior (BCT 4.1 – frequently found in mental health and social care settings)
-
restructuring the social environment (BCT 12.2)
-
feedback on outcome(s) of behavior (BCT 2.7 – frequently found in generic settings)
-
problem-solving (BCT 1.2).
Lack of detail in restrictive practices data
In addition to the need for consistency in outcome reporting, the evidence base would be enhanced by greater detail about the specifics of the restrictive practices. The number of staff involved in an incident was not reported at all, and neither was psychological harm. Furthermore, the fact that four records reported the number of injuries to staff and eight reported injuries to all, but no record reported both, suggests a lack of focus on injuries, especially to service users.
Recommendations from Wilson et al. ’s230 review remain relevant, and include a greater focus on assessing the effect of restraint and more detail about the type of restraint, including how it is defined.
It is widely accepted that some children in some settings are subjected to poor, potentially harmful, practices,194 and that there can be difficulties with the accuracy and quality of incident reporting. The lack of service user perspectives in the evidence is therefore a concern and arguably an urgent matter for practice and research.
Comparison with the results of the COMPARE study47
As set out at the beginning of this report, this study is one of a pair addressing NICE’s recommendation to systematically describe restrictive practices with adults and children, and is therefore linked with the research team’s original study,47 which fulfilled the first part of NICE’s recommendation by systematically describing practice with adults. The current study reviewed the evidence for interventions to reduce staff use of restrictive practices in child/adolescent institutional settings. As anticipated, the results showed that the features of an intervention (its content and delivery) are likely to interact with the delivery context and with the features of the target behaviour. The intention was to compare interventions across these settings to permit exploration of the relationship between intervention features (content and delivery) and context (target population and setting), together with the identification of differences in content, influences on delivery and potential implications for effectiveness.
| CONTRAST: children’s institutional settings | COMPARE: adult mental health inpatient settings |
|---|---|
| Multiple interventions, mostly stand alone | Multiple interventions, mostly stand alone |
| BCT credible source was detected in 2% of interventions from all children’s settings | BCT credible source was detected in 18% of interventions |
| The (potential) contribution of the behaviour of individual staff was acknowledged in the interventions examined in CONTRAST | The (potential) contribution of the behaviour of individual staff was not addressed in the interventions examined in CONTRAST |
| Aspects of interventions coded with the BCTs action-planning (BCT 1.4), goal setting (BCT 1.1), monitoring of outcome(s) of behavior without feedback (BCT 2.5) and feedback on outcomes of behavior (BCT 2.7) included examples of interventions seeking, monitoring and planning for individual staff with high or unusual rates of restrictive practice use, or with training needs identified following involvement in an incident33,114,162,193,199 | No such examples of targeting individual staff were found |
| Very little evidence of service user perspectives | Little evidence of service user perspectives |
| Interest in interventions involving non-medical or psychological approaches to reducing restrictive practices | Relatively little evidence of interest in non-medical or psychological approaches |
| Interest in trauma-informed approaches | Little evidence of interest in trauma-informed approaches |
Analysis of the robustness of the results
As discussed (see Effectiveness), the review was unable to identify robust evidence of effectiveness and could only draw tentative conclusions regarding four promising BCTs. Robust conclusions may be drawn concerning the frequency of use of specific intervention components, notably staff training and programmes that restructure the social or physical environment. Furthermore, the BCT analysis found that the most frequently occurring BCTs tended to occur in the same interventions that showed promising outcomes. Interventions are listed by study design in Appendix 8.
Strengths
To our knowledge, no previous reviews have looked at both the outcomes and components of interventions that aim to reduce restrictive practices in CYP’s institutional settings. This study aimed to identify the most promising intervention components and recommend them to be tested within a trial setting, with a view to seeking future funding to develop and test an intervention based on the results of the review. The recommendations generated by this review are transferable, and this is one of its strengths: institutions that have children in their care could benefit from interventions that are better defined, more acceptable to children and staff, more completely and accurately implemented, and more cost-effective.
Table 28 compares and contrasts key findings from the current review of the use of restrictive practices in children’s institutions settings, with key findings from the companion review of the use of restrictive practices in adult mental health settings. 46
Limitations
The search strategy combined traditional search techniques for retrieving research and grey literature, with a scanning approach to identify potential alternative sources of relevant material. This had the advantage of enabling the retrieval of diverse records that reported intervention content and was useful for mapping the number and range of interventions; however, the diverse quality of reporting in some records retrieved in this way presented a challenge for the meaningful assimilation of findings. For example, a lack of detailed description of interventions may have masked the presence of BCTs, that consequently were not detected.
The adoption of a broad approach to searching and inclusion criteria led to the inclusion of a wide range of interventions in diverse formats. No criteria for exclusion on the basis of quality were developed. This is substantially different from normal systematic reviews of evidence. However, current practice in this area is of adopted interventions without a clear evidence base. There may remain some institutional settings/interventions which were not captured in our search as a result of databases searched.
The literature search was restricted to English-language records and there was limited evidence from countries outside the USA, so the findings may have limited international transferability. As noted in one of the included studies, there was a:
[C]lear divide between the numbers of published studies coming out of America compared to the rest of the world [which was] likely to change in the coming years.
Wilson et al. 230
The scope of the study did not allow for detailed analysis of effectiveness by setting, population group, culture, national context, or institutional ethos. Contextual factors, for example criminal justice settings or service users with intellectual disability, are likely to be highly relevant to decision-making regarding interventions. In addition, the finding that the evidence was weak restricted the scope of the study to examine the effectiveness of BCTs used in interventions. In these terms, transferability of the tentative conclusions about effectiveness has yet to be demonstrated. These are relevant areas for future research.
Implications for policy and practice and future research
The need to reduce restrictive practices in CYP’s institutional settings is ongoing: this should be considered a priority for policy-makers. However, without clarity about current use of restrictive practices in CYP’s institutional settings, evaluation of interventions could remain problematic.
It is clear that some groups may experience more severe restrictive practices than others; therefore, better understanding of the influence of gender, ethnicity, disability, and institutional setting and its governance is required. Exploration of how interventions can be adapted to reduce restrictive practice for different contexts is urgently needed.
Accessible guidelines for a core outcomes set that is feasible for researchers and practitioners to use in real-world settings could be a valuable step towards improving practice in CYP’s settings.
With regard to both the more widely used interventions and the stand-alone interventions, there appears to be little appetite for simplicity. Simple interventions would facilitate like-for-like comparison so that it would be more possible to identify key ingredients and understand what works and what does not work. However, practice experts may be aware of factors that suggest complex interventions are suitable; therefore, interventions developers could consider all relevant factors (i.e. theoretical, practical, contextual) to ensure optimum conditions for delivery and evaluation of effective interventions. Alternatively, if complex interventions are inevitable, recent guidance suggests better reporting of complexity considerations,234 and better reporting of intervention development generally. 235
Those interventions that are developed to reduce staff use of restrictive practices need to be better defined, with clear links to theory, and contain more robust and rigorous approaches to evaluation. Specifically, it may be worthwhile to address the question of why so much training is directed at staff, many of whom are likely to have been previously trained to work in the setting. It may also be worthwhile to address data-monitoring, which is a component of many of the interventions; it has the potential to activate powerful psychological mechanisms such as shame and social norms when combined with feedback, and could be a quick and straightforward means of generating useful data. Key practice, policy and research recommendations are presented in Table 29.
| Policy | Practice | Future research |
|---|---|---|
| Support for research to develop the evidence base could be prioritised over commissioning of interventions for practice | Selection or development of interventions based on available evidence | Testing of promising BCTs, using robust designs to establish effectiveness such as RCTs |
|
Investigation of the most promising BCTs by type, potentially within the type of institutional settings where they are often found {e.g. BCT 4.1 [instruction on how to perform the behavior] mental health and social care settings; BCT 12.2 [restructuring the social environment]/BCT 2.7 (feedback on outcome(s) of behavior] generic settings} Problem-solving |
||
| On-site interventions development, delivery, evaluation and reporting could utilise incorporation validated outcomes measures, consider potential impact of confounding factors | Focus on development of the evidence base for different settings (e.g. criminal justice, populations with intellectual disability) | |
| Research/practice collaborations should be encouraged and facilitated to ensure (1) relevance and (2) robustness of studies | Research/practice collaborations would support the above | Researchers should work with practitioners to develop feasible, acceptable interventions that are underpinned by appropriate theory and can be evaluated using robust methods |
| Adherence to reporting guidelines (e.g. WIDER recommendations) | ||
| Research funding could be directed to understand how different interventions work in different settings | Development of a core outcomes set incorporating validated outcomes measures | |
| Better understanding of how the effect of an intervention may vary depending on institutional setting, institutional ethos, staffing mix, service user needs and/or behaviours, political context, funding context, cultural context | ||
| Evaluation of interventions outside the USA |
Conclusion
Despite numerous enquiries, policy initiatives and recommendations, there remains ongoing concern about the use of restrictive practices in CYP’s institutional settings. The impact of restrictive practices on the psychological and physical welfare of both CYP and staff should not be underestimated. The care of CYP will remain suboptimal unless there is a sustained focus on reducing these practices. Without a sustained effort, these practices will continue to occur in institutional settings worldwide.
This study has generated, to our knowledge, the first known synthesis of the evidence on the content and effectiveness of interventions to reduce restrictive practices in CYP’s institutional settings. This synthesis provides a useful resource for practitioners, policy-makers and researchers aiming to implement or develop a restraint reduction intervention.
The new information generated adds to the research evidence base in the form of a comprehensive description of interventions, their components, context and outcomes, as far as can be ascertained from the limited evidence. The limitations are important because they suggest a need for caution in the use of interventions assumed to be effective.
Taken as a whole, these suggestions from our research for practice, policy and research can inform the development and testing of different models to reduce restrictive practices across a range of CYP’s institutional settings. They have the potential to affect the everyday practice of professionals working with children by supporting management decision-making in children’s services with regard to staff training and other interventions. The new insights generated from this study could lead to improved therapeutic outcomes, organisational efficiencies arising from reduced staff sickness and litigation costs, and better subjective experiences of children and staff. These could contribute towards improving the health and safety of vulnerable children and the staff who work with them in institutional care by protecting them from trauma, injury and death, and could thus benefit wider society.
Acknowledgements
We are grateful to NIHR and the colleagues who have supported this study.
Contributions of authors
John Baker (https://orcid.org/0000-0001-9985-9875) was responsible for leading the study and the protocol development, and contributed to literature searches, data extraction and analysis, and writing and editing the report.
Kathryn Berzins (https://orcid.org/0000-0001-5002-5212) was responsible for co-ordinating the study and contributed to literature searches, data extraction and analysis, BCT mapping, and writing and editing the report.
Krysia Canvin (https://orcid.org/0000-0001-6571-6411) contributed to literature searches, data extraction and analysis, BCT mapping, and writing and editing the report.
Sarah Kendal (https://orcid.org/0000-0001-8557-5716) contributed to literature searches, data extraction and analysis, BCT mapping, and writing and editing the report.
Stella Branthonne-Foster (https://orcid.org/0000-0002-5545-9199) was our PPI representative throughout the project, and contributed to the public involvement, the Plain English summary and the dissemination strategy.
Judy Wright (https://orcid.org/0000-0002-5239-0173) developed and advised on the search strategies and contributed to the final report.
Tim McDougall (https://orcid.org/0000-0002-9843-9315) provided expertise and contributed to writing and editing the final report.
Barry Goldson (https://orcid.org/0000-0002-9714-868X) developed and advised on the search strategies and contributed to the final report.
Ian Kellar (https://orcid.org/0000-0003-1608-5216) provided expertise in regards to BCT mapping, writing and editing the report.
Joy Duxbury (https://orcid.org/0000-0002-1772-6874) developed and advised on the search strategies and contributed to the final report.
Data-sharing statement
All available data can be obtained from the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HSDR programme or the Department of Health and Social Care.
References
- Article 39 . What We Do 2018. https://article39.org.uk/what-we-do/ (accessed 27 March 2021).
- Frith E. Inpatient Provision for Children and Young People with Mental Health Problems. London: Education Policy Institute; 2017.
- Baglivio MT, Wolff KT, Piquero AR, Epps N. The relationship between adverse childhood experiences (ACE) and juvenile offending trajectories in a juvenile offender sample. J Crim Justice 2015;43:229-41. https://doi.org/10.1016/j.jcrimjus.2015.04.012.
- Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Psychiatry 2007;190:319-25. https://doi.org/10.1192/bjp.bp.106.025023.
- Jacobson J, Bhardwa B, Gyateng T, Hunter G, Hough M. Punishing Disadvantage: A Profile of Children in Custody. London: The Prison Reform Trust; 2010.
- Jensen TK, Fjermestad KW, Granly L, Wilhelmsen NH. Stressful life experiences and mental health problems among unaccompanied asylum-seeking children. Clin Child Psychol Psychiatry 2015;20:106-16. https://doi.org/10.1177/1359104513499356.
- McDougall T, Nolan T, McDougall T. Children and Young People’s Mental Health: Essentials for Nurses and Other Professionals. London: Routledge; 2016.
- Schilling EA, Aseltine RH, Gore S. Adverse childhood experiences and mental health in young adults: a longitudinal survey. BMC Public Health 2007;7. https://doi.org/10.1186/1471-2458-7-30.
- Lüdtke J, In-Albon T, Schmeck K, Plener PL, Fegert JM, Schmid M. Nonsuicidal self-injury in adolescents placed in youth welfare and juvenile justice group homes: associations with mental disorders and suicidality. J Abnorm Child Psychol 2018;46:343-54. https://doi.org/10.1007/s10802-017-0291-8.
- Ruddick L, Davies L, Bacarese-Hamilton M, Oliver C. Self-injurious, aggressive and destructive behaviour in children with severe intellectual disability: prevalence, service need and service receipt in the UK. Res Dev Disabil 2015;45:307-15. https://doi.org/10.1016/j.ridd.2015.07.019.
- NHS Security Management Service . Cost of Violence Against NHS Staff. A Report Summarising the Economic Cost to the NHS of Violence Against Staff. 2007 2008. 2010.
- Department of Health and Social Care . Positive and Proactive Care: Reducing the Need for Restrictive Interventions 2014.
- De Hert M, Dirix N, Demunter H, Correll CU. Prevalence and correlates of seclusion and restraint use in children and adolescents: a systematic review. Eur Child Adolesc Psychiatry 2011;20:221-30. https://doi.org/10.1007/s00787-011-0160-x.
- Health and Social Care Information Centre . Learning Disability Census Report – England, 30th of September 2013 2013.
- Allison E, Hattenstone S. Head of scandal-hit immigration centre ran jail where children were abused. The Guardian 2017.
- Day DM. A Review of the Literature on Restraints and Seclusion with Children and Youth: Toward the Development of a Perspective in Practice. Toronto, ON: The Intersectoral/Interministerial Steering Committee on Behaviour Management Interventions for Children and Youth in Residential and Hospital Settings; 2000.
- Delaney KR, Fogg L. Patient characteristics and setting variables related to use of restraint on four inpatient psychiatric units for youths. Psychiatr Serv 2005;56:186-92. https://doi.org/10.1176/appi.ps.56.2.186.
- Agenda: Alliance for Women and Girls at Risk . Agenda Briefing on the Use of Restraint Against Women and Girls 2017.
- LeBel J, Huckshorn KA, Caldwell B. Restraint use in residential programs: why are best practices ignored?. Child Welfare 2010;89:169-87.
- Nunno MA, Holden MJ, Tollar A. Learning from tragedy: a survey of child and adolescent restraint fatalities. Child Abuse Negl 2006;30:1333-42. https://doi.org/10.1016/j.chiabu.2006.02.015.
- Fish R, Culshaw E. The last resort? Staff and client perspectives on physical intervention. J Intellect Disabil 2005;9:93-107. https://doi.org/10.1177/1744629505049726.
- Steckley L, Kendrick A, Nunno MA, Day DM, Bullard L. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. Arlington, VA: Child Welfare League of America; 2008.
- HM Inspectorate of Prisons . Behaviour Management and Restraint of Children in Custody: A Review of the Early Implementation of MMPR by HM Inspectorate of Prisons 2015.
- MIND . Mental Health Crisis Care: Physical Restraint in Crisis. A Report on Physical Restraint in Hospital Settings in England 2013.
- Goldson B. Vulnerable Inside: Children in Secure and Penal Settings. London: The Children’s Society; 2003.
- National Institute for Health and Care Excellence (NICE) . Costing Statement: Violence and Aggression. Implementing the NICE Guideline on Violence and Aggression 2015.
- United Nations Committee on the Rights of Persons with Disabilities . Convention on the Rights of Persons With Disabilities: Concluding Observations on the Initial Report of the United Kingdom of Great Britain and Northern Ireland United Nations 2017.
- Allison E, Hattenstone S. Approved restraint techniques can kill children, MoJ found. The Guardian 2016.
- Care Quality Commission . Care Quality Commission n.d. www.cqc.org.uk/ (accessed 4 May 2021).
- Department of Health and Social Care . Reducing the Need for Restraint and Restrictive Intervention: Children and Young People With Learning Disabilities, Autistic Spectrum Conditions and Mental Health Difficulties in Health and Social Care Services and Special Education Settings 2019.
- Great Britain . Mental Health Units (Use of Force) Act 2018 2018.
- Bowers L, James K, Quirk A, Simpson A, Stewart D, Hodsoll J. SUGAR . Reducing conflict and containment rates on acute psychiatric wards: the Safewards cluster randomised controlled trial. Int J Nurs Stud 2015;52:1412-22. https://doi.org/10.1016/j.ijnurstu.2015.05.001.
- National Association of State Mental Health Program Directors (NASMHPD) . Six Core Strategies for Reducing Seclusion and Restraint Use 2006.
- Riley D, Benson I. No Force First: eliminating restraint in a mental health trust. Nurs Times 2018;114:38-9.
- Putkonen A, Kuivalainen S, Louheranta O, Repo-Tiihonen E, Ryynänen OP, Kautiainen H, et al. Cluster-randomized controlled trial of reducing seclusion and restraint in secured care of men with schizophrenia. Psychiatr Serv 2013;64:850-5. https://doi.org/10.1176/appi.ps.201200393.
- Deveau R, McDonnell A. As the last resort: reducing the use of restrictive physical interventions using organisational approaches. Br J Learn Disabil 2009;37:172-7. https://doi.org/10.1111/j.1468-3156.2008.00536.x.
- Luiselli JK, Treml T, Kane A, Young N. Physical restraint intervention: case report evaluation of an implementation-reduction strategy and long term outcome. Ment Health Aspect Dev Disabil 2004;7:91-6.
- Azeem M, Aujla A, Rammerth M, Binsfeld G, Jones RB. Effectiveness of six core strategies based on trauma informed care in reducing seclusions and restraints at a child and adolescent psychiatric hospital. J Child Adolesc Psychiatr Nurs 2017;30:170-4. https://doi.org/10.1111/jcap.12190.
- Lebel J, Goldstein R. The economic cost of using restraint and the value added by restraint reduction or elimination. Psychiatr Serv 2005;56:1109-14. https://doi.org/10.1176/appi.ps.56.9.1109.
- LeBel J, Stromberg N, Duckworth K, Kerzner J, Goldstein R, Weeks M, et al. Child and adolescent inpatient restraint reduction: a state initiative to promote strength-based care. J Am Acad Child Adolesc Psychiatry 2004;43:37-45. https://doi.org/10.1097/00004583-200401000-00013.
- Schreiner GM, Crafton CG, Sevin JA. Decreasing the use of mechanical restraints and locked seclusion. Adm Policy Ment Health 2004;31:449-63. https://doi.org/10.1023/b:apih.0000036413.87440.83.
- Delaney KR. Evidence base for practice: reduction of restraint and seclusion use during child and adolescent psychiatric inpatient treatment. Worldviews Evid Based Nurs 2006;3:19-30. https://doi.org/10.1111/j.1741-6787.2006.00043.x.
- Möhler R, Meyer G. Development methods of guidelines and documents with recommendations on physical restraint reduction in nursing homes: a systematic review. BMC Geriatr 2015;15. https://doi.org/10.1186/s12877-015-0150-9.
- Wynn R. The use of physical restraint in Norwegian adult psychiatric hospitals. Psychiatry J 2015;2015. https://doi.org/10.1155/2015/347246.
- Livingston JD, Verdun-Jones S, Brink J, Lussier P, Nicholls T. A narrative review of the effectiveness of aggression management training programs for psychiatric hospital staff. J Forensic Nurs 2010;6:15-28. https://doi.org/10.1111/j.1939-3938.2009.01061.x.
- National Institute for Health and Care Excellence (NICE) . Violence and Aggression: Short-Term Management in Mental Health, Health and Community Settings 2015.
- Baker J, Berzins K, Canvin K, Benson I, Keller I, Wright J, et al. Non-pharmacological interventions to reduce restrictive practices in adult mental health inpatient settings: the COMPARE systematic mapping review. Health Serv Deliv Res 2021;9. https://doi.org/10.3310/hsdr09050.
- Michie S, Churchill S, West R. Identifying evidence-based competences required to deliver behavioural support for smoking cessation. Ann Behav Med 2011;41:59-70. https://doi.org/10.1007/s12160-010-9235-z.
- Davidson KW, Goldstein M, Kaplan RM, Kaufmann PG, Knatterud GL, Orleans CT, et al. Evidence-based behavioral medicine: what is it and how do we achieve it?. Ann Behav Med 2003;26:161-71. https://doi.org/10.1207/S15324796ABM2603_01.
- Michie S, Fixsen D, Grimshaw JM, Eccles MP. Specifying and reporting complex behaviour change interventions: the need for a scientific method. Implement Sci 2009;4. https://doi.org/10.1186/1748-5908-4-40.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:1-31. https://doi.org/10.1007/s12160-013-9486-6.
- Berzins KM, Gray TA, Waterman H, Francis JJ. Specifying active components of educational interventions to promote adherence to treatment in glaucoma patients: application of a taxonomy of behavior change techniques. Psychol Res Behav Manag 2015;8:201-9. https://doi.org/10.2147/PRBM.S74664.
- Michie S, Hyder N, Walia A, West R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict Behav 2011;36:315-19. https://doi.org/10.1016/j.addbeh.2010.11.016.
- Michie S, Whittington C, Hamoudi Z, Zarnani F, Tober G, West R. Identification of behaviour change techniques to reduce excessive alcohol consumption. Addiction 2012;107:1431-40. https://doi.org/10.1111/j.1360-0443.2012.03845.x.
- Abraham C, Good A, Warren MR, Huedo-Medina T, Johnson B. Developing and testing a SHARP taxonomy of behavior change techniques included in condom promotion interventions. Psychol Health 2011;26.
- Centre for Reviews and Dissemination . Undertaking Systematic Reviews of Research on Effectiveness: CRD’s Guidance for Those Carrying Out or Commissioning Reviews 2001. www.york.ac.uk/inst/crd/crdreports.htm (accessed 27 April 2021).
- Araújo-Soares V, McIntyre T, MacLennan G, Sniehotta FF. Development and exploratory cluster-randomised opportunistic trial of a theory-based intervention to enhance physical activity among adolescents. Psychol Health 2009;24:805-22. https://doi.org/10.1080/08870440802040707.
- Bradbury-Jones C, Breckenridge JP, Clark MT, Herber OR, Jones C, Taylor J. Advancing the science of literature reviewing in social research: the focused mapping review and synthesis. Int J Soc Res Methodol 2019;22:451-62. https://doi.org/10.1080/13645579.2019.1576328.
- Carter EW, Lane KL, Crnobori M, Bruhn AL, Oakes WP. Self-determination interventions for students with and at risk for emotional and behavioral disorders: mapping the knowledge base. Behav Disord 2011;36:100-16. https://doi.org/10.1177/019874291103600202.
- Clapton J, Rutter D, Sharif N. SCIE Research Resource 03: SCIE Systematic Mapping Guidance. London: Social Care Institute for Excellence; 2009.
- Cooper ID. What is a ‘mapping study?’. J Med Libr Assoc 2016;104:76-8. https://doi.org/10.3163/1536-5050.104.1.013.
- Perryman CL. Mapping studies. J Med Libr Assoc 2016;104:79-82. https://doi.org/10.3163/1536-5050.104.1.014.
- Pham MT, Rajić A, Greig JD, Sargeant JM, Papadopoulos A, McEwen SA. A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods 2014;5:371-85. https://doi.org/10.1002/jrsm.1123.
- Fajardo MA, Weir KR, Bonner C, Gnjidic D, Jansen J. Availability and readability of patient education materials for deprescribing: an environmental scan. Br J Clin Pharmacol 2019;85:1396-406. https://doi.org/10.1111/bcp.13912.
- Parker RMN, Boulos LM, Visintini S, Ritchie K, Hayden J. Environmental scan and evaluation of best practices for online systematic review resources. J Med Libr Assoc 2018;106:208-18. https://doi.org/10.5195/jmla.2018.241.
- Agency for Healthcare Research and Quality . Environmental Scan of Patient Safety Education and Training Programs 2020. www.ahrq.gov/research/findings/final-reports/environmental-scan-programs/index.html (accessed 27 April 2021).
- Graham P, Evitts T, Thomas-MacLean R. Environmental scans: how useful are they for primary care research?. Can Fam Physician 2008;54:1022-3.
- Albrecht L, Archibald M, Arseneau D, Scott SD. Development of a checklist to assess the quality of reporting of knowledge translation interventions using the Workgroup for Intervention Development and Evaluation Research (WIDER) recommendations. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-52.
- Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf 2018;34:285-91. https://doi.org/10.3233/EFI-180221.
- Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud 2012;49:47-53. https://doi.org/10.1016/j.ijnurstu.2011.07.002.
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci 2011;6. https://doi.org/10.1186/1748-5908-6-42.
- Presseau J, Ivers NM, Newham JJ, Knittle K, Danko KJ, Grimshaw JM. Using a behaviour change techniques taxonomy to identify active ingredients within trials of implementation interventions for diabetes care. Implement Sci 2015;10. https://doi.org/10.1186/s13012-015-0248-7.
- United Nations General Assembly . United Nations Convention on the Rights of the Child 1989.
- Great Britain . Children Act 1989 1989.
- Pluye P, Gagnon MP, Griffiths F, Johnson-Lafleur J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int J Nurs Stud 2009;46:529-46. https://doi.org/10.1016/j.ijnurstu.2009.01.009.
- Huckshorn KA. Preventing Violence, Trauma, and The Use of Seclusion and Restraints In Mental Health Settings: Preventing Conflict, Violence and the Use of Seclusion Restraint. Workshop Slides, IACC Meetings 2010.
- Brown AD, McCauley K, Navalta CP, Saxe GN. Trauma systems therapy in residential settings: improving emotion regulation and the social environment of traumatized children and youth in congregate care. J Fam Violence 2013;28:693-70. https://doi.org/10.1007/s10896-013-9542-9.
- Hambrick EP, Brawner TW, Perry BD, Wang EY, Griffin G, DeMarco T, et al. Restraint and critical incident reduction following introduction of the Neurosequential Model of Therapeutics (NMT). Resid Treat Child Youth 2018;35:2-23. https://doi.org/10.1080/0886571X.2018.1425651.
- Magnowski SR, Cleveland S. The impact of milieu nurse-client shift assignments on monthly restraint rates on an inpatient child/adolescent psychiatric unit. J Am Psychiatr Nurses Assoc 2020;26:86-91. https://doi.org/10.1177/1078390319834358.
- Nunno MA, Holden MJ, Leidy B. Evaluating and monitoring the impact of a crisis intervention system on a residential child care facility. Child Youth Serv Rev 2003;25:295-31. https://doi.org/10.1016/S0190-7409(03)00013-6.
- Colton D. Checklist for Assessing Your Organization’s Readiness for Reducing Seclusion and Restraint. Staunton, VA: Commonwealth Center for Children and Adolescence; 2004.
- Weiss EM. Deadly restraint: a Hartford Courant investigative report. Hartford Courant 1998.
- Busch AB, Shore MF. Seclusion and restraint: a review of recent literature. Harv Rev Psychiatry 2000;8:261-70. https://doi.org/10.3109/hrp.8.5.261.
- Carter J, Jones J, Stevens K, Nunno MA, Day DM, Bullard LB. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. Arlington, VA: Child Welfare League of America; 2008.
- Ryan JB, Peterson RL, Tetreault G, van der Hagen E, Nunno MA, Day DM, et al. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. Arlington, VA: Child Welfare League of America; 2008.
- Thompson RW, Huefner JC, Vollmer DG, Davis JL, Daly DL, Nunno MA, et al. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. Arlington, VA: Child Welfare League of America; 2008.
- Craig JH. Evaluation of a program model for minimizing restraint and seclusion. Diss Abstr B Sci Eng 2015;77.
- Ercole-Fricke E. Effects of a collaborative problem solving approach on an inpatient adolescent psychiatric unit. Diss Abstr B Sci Eng 2014;76.
- Farina MV. Toward Reducing the Utilization of Seclusion and Restraint: Exploring a Paradigm Shift and Its Success 2006.
- Finnie HM. The Collaborative Problem-Solving Approach With Traumatized Children: Its Effectiveness in the Reduction of Locked Seclusion in an Inpatient Psychiatric Setting 2013.
- Glew B-A. Reducing the Use of Seclusion and Restraint in Segregated Special Education School Settings through Implementation of the Collaborative Problem Solving Model 2012.
- Kilgore A. Effectiveness of Collaborative Problem Solving Model in Reducing Seclusion and Restraint in a Child Psychiatric Unit. 2018.
- Leitch S. The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions (RPI) in Residential Services for Children and Young People. Canterbury: University of Kent; 2009.
- Magnowski S. The Impact of Milieu Nurse-Patient Shift Assignments on Monthly Restraint Rates on an Inpatient Child and Adolescent Psychiatric Unit 2018.
- McGlinn CJ. The effect of federal regulations on the physical restraint of children and adolescents in residential treatment with an analysis of client, staff, and environmental variables. Diss Abstr B Sci Eng 2006;67.
- Miguel ES. The Dynamics and Ramifications of Severe Challenging Behaviors: Daring to Reduce Challenging Behavior in Schools Without Physical Restraint and Seclusion 2016.
- Thomann J. Factors in Restraint Reduction in Residential Treatment Facilities for Adolescents. Diss Abstr B Sci Eng 2010;70.
- Padhi A, Norcott J, Yoo E, Vakili A. Eliminating seclusion and reducing restraint: hope on an acute adolescent psychiatric ward. Aust N Z J Psychiatry 2019;53:119-20.
- Reynolds EK, Grados MA, Praglowski N, Hankinson JC, Parrish C, Ostrander R. Implementation of Modified Positive Behavioral Interventions and Supports in a youth psychiatric partial hospital program. J Patient Saf Risk Manag 2019;24:64-70. https://doi.org/10.1177/2516043518811758.
- Shadili G, Brocco C, De Vieille I, Piot MA, Lavergne P. Violence in an adolescent psychiatric inpatient unit: a behavioural management plan. Eur Neuropsychopharmacol 2012;22:S417-18. https://doi.org/10.1016/S0924-977X(12)70654-5.
- Ubana RL, Ng JWL, Tan CSM, Raj HP, Ong EY, Ang LK, et al. Continued implementation of an advanced practice nurse-led multidisciplinary programme to reduce disruptive incidences in young patients with mental health conditions. Ann Acad Med Singapore 2015;1.
- Valenkamp M, Verheij F, Van De Ende J, Verhulst F. Development and evaluation of the individual proactive aggression management method for residential child psychiatry and child care. Eur Child Adolesc Psychiatry 2011;20:S7-223.
- Health Sciences Centre Winnipeg . Workplace Innovation Project: Enhancing Seclusion and Restraint-Free Mental Health Services: Promoting Employee Safety through Cultural Change, Trauma-Informed Care, and the Use of Innovative Strategies for Violence Prevention and Management 2015.
- Azeem MW, Reddy B, Wudarsky M, Carabetta L, Gregory F, Sarofin M. Restraint reduction at a pediatric psychiatric hospital: a ten-year journey. J Child Adolesc Psychiatr Nurs 2015;28:180-4. https://doi.org/10.1111/jcap.12127.
- Canady VA. Model of care effort reduces need for restraint, seclusion at BH facility. Ment Health Wkly 2018;28:1-3. https://doi.org/10.1002/mhw.31580.
- Ercole-Fricke E, Fritz P, Hill LE, Snelders J. Effects of a collaborative problem-solving approach on an inpatient adolescent psychiatric unit. J Child Adolesc Psychiatr Nurs 2016;29:127-34. https://doi.org/10.1111/jcap.12149.
- Sanders K. The effects of an action plan, staff training, management support and monitoring on restraint use and costs of work-related injuries. J Appl Res Intellect Disabil 2009;22:216-20. https://doi.org/10.1111/j.1468-3148.2008.00491.x.
- Bonnell W, Alatishe YA, Hofner A. The effects of a changing culture on a child and adolescent psychiatric inpatient unit. J Can Acad Child Adolesc Psychiatry 2014;23:65-9.
- Greene RW, Ablon JS, Hassuk B, Regan KM, Martin A. Innovations: child & adolescent psychiatry: use of collaborative problem solving to reduce seclusion and restraint in child and adolescent inpatient units. Psychiatr Serv 2006;57:610-12. https://doi.org/10.1176/ps.2006.57.5.610.
- Martin A, Krieg H, Esposito F, Stubbe D, Cardona L. Reduction of restraint and seclusion through collaborative problem solving: a five-year prospective inpatient study. Psychiatr Serv 2008;59:1406-12. https://doi.org/10.1176/appi.ps.59.12.1406.
- Pollastri AR, Lieberman RE, Boldt SL, Ablon J. Minimizing seclusion and restraint in youth residential and day treatment through site-wide implementation of Collaborative Problem Solving. Resid Treat Child Youth 2016;33:186-205. https://doi.org/10.1080/0886571X.2016.1188340.
- Ryan JB, Peterson R, Tetreault G, van der Hagen E. Reducing seclusion timeout and restraint procedures with at-risk youth. J At-Risk Issues 2007;13:7-12.
- Wisdom JP, Wenger D, Robertson D, Van Bramer J, Sederer LI. The New York State Office of Mental Health Positive Alternatives to Restraint and Seclusion (PARS) project. Psychiatr Serv 2015;66:851-6. https://doi.org/10.1176/appi.ps.201400279.
- Caldwell B, Albert C, Azeem MW, Beck S, Cocoros D, Cocoros T, et al. Successful seclusion and restraint prevention efforts in child and adolescent programs. J Psychosoc Nurs Ment Health Serv 2014;52:30-8. https://doi.org/10.3928/02793695-20140922-01.
- Caldwell B, LeBel J. Reducing restraint and seclusion: how to implement organizational change. Children’s Voice 2010;19:10-4.
- Crisis Prevention Institute . The Nonviolent Crisis Intervention® Training Program and the National Association of State Mental Health Program Directors: Six Core Strategies for the Reduction of Restraint and Seclusion 2013.
- Lietzke A. Restraint Reduction and CPI Training 2014. www.crisisprevention.com/en-CA/Blog/Restraint-Reduction-and-CPI-Training (accessed 13 October 2021).
- Rettmann R. Changes in Attitudes, Changes in Outcomes 2019. www.crisisprevention.com/Library/Changes-in-Attitudes-Changes-in-Outcomes (accessed 13 October 2021).
- Craig JH, Sanders KL. Evaluation of a program model for minimizing restraint and seclusion. Adv Neurodev Disabil 2018;2:344-52. https://doi.org/10.1007/s41252-018-0076-2.
- Cooper S. Use of Restraint Reduced by Therapeutic Intervention 2008. www.cypnow.co.uk/other/article/use-of-restraint-reduced-by-therapeutic-intervention (accessed 20 September 2021).
- Holden MJT, Andrea J, Heresniak R, Ruberti M, Holden JC, Saville E. Therapeutic Crisis Intervention Activity Guide. TCI Training of Trainers Program. Ithaca, NY: The Residential Child Care Project, Bronfenbrenner Center for Translational Research, College of Human Ecology, Cornell University; 2020.
- Holden MJ, Turnbull AJ, Holden JC, Heresniak R, Ruberti M, Saville E. Therapeutic Crisis Intervention Reference Guide. Ithaca, NY: The Residential Child Care Project, Bronfenbrenner Center for Translational Research, College of Human Ecology, Cornell University; 2020.
- Holden MJ, Turnbull AJ, Holden JC, Heresniak R, Ruberti M, Saville E. Therapeutic Crisis Intervention Student Workbook. TCI Training of Trainers Program. Ithaca, NY: The Residential Child Care Project, Bronfenbrenner Center for Translational Research, College of Human Ecology, Cornell University; 2020.
- Reynolds EK, Grados MA, Praglowski N, Hankinson JC, Deboard-Lucas R, Goldstein L, et al. Use of Modified Positive Behavioral Interventions and Supports in a psychiatric inpatient unit for high-risk youths. Psychiatr Serv 2016;67:570-3. https://doi.org/10.1176/appi.ps.201500039.
- PRICE Training . Price Training UK n.d. www.pricetraining.co.uk (accessed 27 April 2021).
- Reynolds EK, Praglowski N, Parrish C, Ostrander R, Grados MA. 5.68 Implementation of Modified Positive Behavioral Interventions and Supports (M-Pbis) in acute psychiatric care inpatient and day hospital settings: immediate and long-term gains. J Am Acad Child Adolesc Psychiatry 2019;58:S267-8. https://doi.org/10.1016/j.jaac.2019.08.382.
- Ford JD, Hawke J. Trauma affect regulation psychoeducation group and milieu intervention outcomes in juvenile detention facilities. J Aggress Maltreat Trauma 2012;21:365-84. https://doi.org/10.1080/10926771.2012.673538.
- Marrow MT, Knudsen KJ, Olafson E, Bucher SE. The value of implementing TARGET within a trauma-informed juvenile justice setting. J Child Adolesc Trauma 2012;5:257-70. https://doi.org/10.1080/19361521.2012.697105.
- Ford J. Adolescent Individual Manual Facilitator Guide Twelve – Session. Trauma Affect Regulation: Guide for Education & Therapy. Mansfield, CT: University of Connecticut; 2013.
- Russell M, Maher C, Dorrell M, Pitcher C, Henderson L. A comparison between users and non-users of Devereux’s Safe and Positive Approaches training curricula in the reduction of injury and restraint. Resid Treat Child Youth 2009;26:209-20. https://doi.org/10.1080/08865710903130301.
- Guilfoile M. The Devereux Glenholme School. Resid Group Care Q 2004;5:6-7.
- Hodges K, Wong MM, Latessa M. Use of the Child and Adolescent Functional Assessment Scale (CAFAS) as an outcome measure in clinical settings. J Behav Health Serv Res 1998;25:325-36. https://doi.org/10.1007/BF02287471.
- Achenbach TM, Verhulst FC, Baron GD, Althaus M. A comparison of syndromes derived from the Child Behavior Checklist for American and Dutch boys aged 6-11 and 12-16. J Child Psychol Psychiatry 1987;28:437-53. https://doi.org/10.1111/j.1469-7610.1987.tb01765.x.
- Hall RC. Global assessment of functioning. A modified scale. Psychosomatics 1995;36:267-75. https://doi.org/10.1016/S0033-3182(95)71666-8.
- Reynolds CR, Kamphaus RW. Behavior Assessment System for Children, Second Edition: Manual. Circle Pines, MN: AGS Publishing; 2004.
- Steinberg AM, Brymer MJ, Kim S, Briggs EC, Ippen CG, Ostrowski SA, et al. Psychometric properties of the UCLA PTSD reaction index: part I. J Trauma Stress 2013;26:1-9. https://doi.org/10.1002/jts.21780.
- Murphy K, Moore KA, Redd Z, Malm K. Trauma-informed child welfare systems and children’s well-being: a longitudinal evaluation of KVC’s bridging the way home initiative. Child Youth Serv Rev 2017;75:23-34. https://doi.org/10.1016/j.childyouth.2017.02.008.
- Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, et al. A children’s global assessment scale (CGAS). Arch Gen Psychiatry 1983;40:1228-31. https://doi.org/10.1001/archpsyc.1983.01790100074010.
- Delaney KR, Johnson ME, Fogg L. Development and testing of the combined assessment of psychiatric environments: a patient-centered quality measure for inpatient psychiatric treatment. J Am Psychiatr Nurses Assoc 2015;21:134-47. https://doi.org/10.1177/1078390315581338.
- Naglieri JA, Goldstein S, LeBuffe P. Resilience and impairment: an exploratory study of resilience factors and situational impairment. J Psychoeduc Assess 2010;28:349-56. https://doi.org/10.1177/0734282910366845.
- Castle D, Alderton D, Castle DJ, Copolov DL, Wykes T. Pharmacological and Psychosocial Treatment in Schizophrenia. London: Martin Dunitz; 2003.
- Costello EJ, Angold A. Scales to assess child and adolescent depression: checklists, screens, and nets. J Am Acad Child Adolesc Psychiatry 1988;27:726-37. https://doi.org/10.1097/00004583-198811000-00011.
- Grisso T, Barnum R, Fletcher KE, Cauffman E, Peuschold D. Massachusetts Youth Screening Instrument for mental health needs of juvenile justice youths. J Am Acad Child Adolesc Psychiatry 2001;40:541-8. https://doi.org/10.1097/00004583-200105000-00013.
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav 1983;24:385-96. https://doi.org/10.2307/2136404.
- Donabedian A. The quality of care. How can it be assessed?. Arch Pathol Lab Med 1997;121:1145-50.
- Beck AT, Steer RA, Ball R, Ranieri WF. Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. J Pers Assess 1996;67:588-97. https://doi.org/10.1207/s15327752jpa6703_13.
- Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry 1997;36:545-53. https://doi.org/10.1097/00004583-199704000-00018.
- Gutierrez PM, Osman A. Getting the best return on your screening investment: an analysis of the Suicidal Ideation Questionnaire and Reynolds Adolescent Depression Scale. School Psychol Rev 2009;38:200-17. https://doi.org/10.1080/02796015.2009.12087832.
- Catanzaro SJ, Mearns J. Measuring generalized expectancies for negative mood regulation: initial scale development and implications. J Pers Assess 1990;54:546-63. https://doi.org/10.1080/00223891.1990.9674019.
- Ogles BM, Melendez G, Davis DC, Lunnen KM. The Ohio Scales: practical outcome assessment. J Child Fam Stud 2001;10:199-212. https://doi.org/10.1023/A:1016651508801.
- Lau MA, Bishop SR, Segal ZV, Buis T, Anderson ND, Carlson L, et al. The Toronto Mindfulness Scale: development and validation. J Clin Psychol 2006;62:1445-67. https://doi.org/10.1002/jclp.20326.
- Ford JD, Racusin R, Ellis CG, Daviss WB, Reiser J, Fleischer A, et al. Child maltreatment, other trauma exposure, and posttraumatic symptomatology among children with oppositional defiant and attention deficit hyperactivity disorders. Child Maltreat 2000;5:205-17. https://doi.org/10.1177/1077559500005003001.
- Andrassy BM. Feelings thermometer: an early intervention scale for seclusion/restraint reduction among children and adolescents in residential psychiatric care. J Child Adolesc Psychiatr Nurs 2016;29:145-7. https://doi.org/10.1111/jcap.12151.
- Fowler NA. Aromatherapy, used as an integrative tool for crisis management by adolescents in a residential treatment center. J Child Adolesc Psychiatr Nurs 2006;19:69-76. https://doi.org/10.1111/j.1744-6171.2006.00048.x.
- Seckman A, Paun O, Heipp B, Van Stee M, Keels-Lowe V, Beel F, et al. Evaluation of the use of a sensory room on an adolescent inpatient unit and its impact on restraint and seclusion prevention. J Child Adolesc Psychiatr Nurs 2017;30:90-7. https://doi.org/10.1111/jcap.12174.
- Deveau R, Leitch S. The impact of restraint reduction meetings on the use of restrictive physical interventions in English residential services for children and young people. Child Care Health Dev 2014;41:587-92.
- Murphy CJ, Siv AM. A one year study of mode deactivation therapy: adolescent residential patients with conduct and personality disorders. Int J Behav Consult Ther 2011;7. https://doi.org/10.1037/h0100924.
- Jani S, Knight S, Jani S. The implementation of milieu therapy training to reduce the frequency of restraints in residential treatment centers. Adolesc Psychiatry 2011;1:251-4. https://doi.org/10.2174/2210677411101030251.
- Witte L. Using training in verbal skills to reduce the use of seclusion and restraint. J Safe Manag Disruptive Assaultive Behav 2007:13-7.
- Verret C ML, Lagacé-Leblanc J, Delisle G, Doyon J. The impact of a schoolwide de-escalation intervention plan on the use of seclusion and restraint in a special education school. Emot Behav Diffic 2019;24:357-73. https://doi.org/10.1080/13632752.2019.1628375.
- Eblin A. Reducing seclusion and restraints on the inpatient child and adolescent behavioral health unit: a quality improvement study. J Child Adolesc Psychiatr Nurs 2019;32:122-8. https://doi.org/10.1111/jcap.12248.
- Dean AJ, Duke SG, George M, Scott J. Behavioral management leads to reduction in aggression in a child and adolescent psychiatric inpatient unit. J Am Acad Child Adolesc Psychiatry 2007;46:711-20. https://doi.org/10.1097/chi.0b013e3180465a1a.
- West M, Melvin G, McNamara F, Gordon M. An evaluation of the use and efficacy of a sensory room within an adolescent psychiatric inpatient unit. Aust Occup Ther J 2017;64:253-63. https://doi.org/10.1111/1440-1630.12358.
- Bobier C, Boon T, Downward M, Loomes B, Mountford H, Swadi H. Pilot investigation of the use and usefulness of a sensory modulation room in a child and adolescent psychiatric inpatient unit. Occup Ther Mental Health 2015;31:385-401. https://doi.org/10.1080/0164212X.2015.1076367.
- Rowan C. Schools Operating Safely (SOS) – Child Behavior Management Policy 2013. www.zoneinworkshops.com/pdf/Schools%20Operating%20Safely%20(SOS).pdf (accessed 27 April 2021).
- Witte L. Reducing the use of seclusion and restraint. A Michigan provider reduced its use of seclusion and restraint by 93% in one year on its child and adolescent unit. Behav Healthc 2008;28:54-7.
- Goren S, Abraham I, Doyle N. Reducing violence in a child psychiatric hospital through planned organizational change. J Child Adolesc Psychiatr Nurs 1996;9:27-8. https://doi.org/10.1111/j.1744-6171.1996.tb00255.x.
- Budlong MJ. Lessons learned and organizational changes implemented as a result of the SAMHSA restraint and seclusion grant. Resid Group Care Q 2004;5:10-1.
- Paccione-Dyszlewski MR, Conelea CA, Heisler WC, Vilardi JC, Sachs HT. A crisis management quality improvement initiative in a children’s psychiatric hospital: design, implementation, and outcome. J Psychiatr Pract 2012;18:304-11. https://doi.org/10.1097/01.pra.0000416022.76085.9e.
- Boel-Studt SM. A quasi-experimental study of trauma-informed psychiatric residential treatment for children and adolescents. Res Soc Work Pract 2017;27:273-82. https://doi.org/10.1177/1049731515614401.
- Forrest S, Gervais R, Lord KA, Sposato A, Martin L, Beserra K, et al. Building communities of care: a comprehensive model for trauma-informed youth capacity building and behavior management in residential services. Resid Treat Child Youth 2018;35:265-85. https://doi.org/10.1080/0886571X.2018.1497930.
- Kalogjera IJ, Bedi A, Watson WN, Meyer AD. Impact of therapeutic management on use of seclusion and restraint with disruptive adolescent inpatients. Hosp Community Psychiatry 1989;40:280-5. https://doi.org/10.1176/ps.40.3.280.
- Care Council For Wales . Positive Approaches: Reducing Restrictive Practices in Social Care 2016.
- Donovan A, Siegel L, Zera G, Plant R, Martin A. Child & adolescent psychiatry: seclusion and restraint reform: an initiative by a child and adolescent psychiatric hospital. Psychiatr Serv 2003;54:958-9. https://doi.org/10.1176/appi.ps.54.7.958.
- Fralick SL. A restraint utilization project. Nurs Adm Q 2007;31:219-25. https://doi.org/10.1097/01.NAQ.0000278935.11374.b0.
- Nunno MA, Smith EG, Martin WR, Butcher S. Benefits of embedding research into practice: an agency–university collaboration. Child Welfare 2015;94:113-33.
- Elwyn LJ, Esaki N, Smith CA. Importance of leadership and employee engagement in trauma-informed organizational change at a girls’ juvenile justice facility. Hum Serv Organ Manag Lead Gov 2017;41:106-18. https://doi.org/10.1080/23303131.2016.1200506.
- Plant R. Courageous patience part II: lessons learned from a five-year program to reduce/eliminate restraint and seclusion. Resid Group Care Q 2004;5:12-3.
- Welsh Government . Guidance on Reducing Restrictive Practices Framework: A Framework to Promote Measures and Practice That Will Lead to the Reduction of Restrictive Practices in Childcare, Education, Health and Social Care Settings. Welsh Government Consultation Document. WG38962 2019.
- Borckardt JJ, Madan A, Grubaugh AL, Danielson CK, Pelic CG, Hardesty SJ, et al. Systematic investigation of initiatives to reduce seclusion and restraint in a state psychiatric hospital. Psychiatr Serv 2011;62:477-83. https://doi.org/10.1176/ps.62.5.pss6205_0477.
- Miller JA, Hunt DP, Georges MA. Reduction of physical restraints in residential treatment facilities. J Disabil Policy Stud 2006;16:202-8. https://doi.org/10.1177/10442073060160040101.
- Hodgdon HB, Kinniburgh K, Gabowitz D, Blaustein ME, Spinazzola J. Development and implementation of trauma-informed programming in youth residential treatment centers using the ARC framework. J Fam Violence 2013;28:679-92. https://doi.org/10.1007/s10896-013-9531-z.
- van Loan CL, Gage NA, Cullen JP. Reducing use of physical restraint: a pilot study investigating a relationship-based crisis prevention curriculum. Resid Treat Child Youth 2015;32:113-33. https://doi.org/10.1080/0886571X.2015.1043787.
- Williams DE, Grossett DL. Reduction of restraint of people with intellectual disabilities: an organizational behavior management (OBM) approach. Res Dev Disabil 2011;32:2336-9. https://doi.org/10.1016/j.ridd.2011.07.032.
- Partnership Projects . Neuro De-Escalation 2020. www.partnershipprojectsuk.com/project/neuro-de-escalation/ (accessed 27 April 2021).
- Smallridge P, Williamson A. Report on Implementing the Independent Review of Restraint in Juvenile Secure Settings 2011.
- Visalli H, McNasser G. Reducing seclusion and restraint: meeting the organizational challenge. J Nurs Care Qual 2000;14:35-44. https://doi.org/10.1097/00001786-200007000-00007.
- Jonikas JA, Cook JA, Rosen C, Laris A, Kim JB. A program to reduce use of physical restraint in psychiatric inpatient facilities. Psychiatr Serv 2004;55:818-20. https://doi.org/10.1176/appi.ps.55.7.818.
- Barnett SR, dosReis S, Riddle MA. Maryland Youth Practice Improvement Committee for Mental Health . Improving the management of acute aggression in state residential and inpatient psychiatric facilities for youths. J Am Acad Child Adolesc Psychiatry 2002;41:897-905. https://doi.org/10.1097/00004583-200208000-00007.
- Holstead J, Lamond D, Dalton J, Horne A, Crick R. Restraint reduction in children’s residential facilities: implementation at Damar Services. Resid Treat Child Youth 2010;27:1-13. https://doi.org/10.1080/08865710903507961.
- Youth Justice Board . Minimising and Managing Physical Restraint: Safeguarding Processes, Governance Arrangements, and Roles and Responsibilities 2012.
- Azeem MW, Aujla A, Rammerth M, Binsfeld G, Jones RB. Effectiveness of six core strategies based on trauma informed care in reducing seclusions and restraints at a child and adolescent psychiatric hospital. J Child Adolesc Psychiatr Nurs 2011;24:11-5. https://doi.org/10.1111/j.1744-6171.2010.00262.x.
- World Health Organization (WHO) . Strategies to End Seclusion and Restraint. WHO QualityRights Specialized Training. Course Guide 2019.
- Leitch S. ‘Hands Off’ The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions in Services for Children and Young People. Canterbury: Tizard Centre, University of Kent; 2009.
- Reynolds EK, Silver A, Morris A, Hankinson J, Perry-Parish C, Specht MW, et al. Factors related to length of stay on a child and adolescent inpatient psychiatric unit. J Am Acad Child Adolesc Psychiatry 2016;55. https://doi.org/10.1016/j.jaac.2016.09.324.
- U.S. Department of Education . Restraint and Seclusion: Resource Document 2012.
- Kaltiala-Heino R, Berg J, Selander M, Työläjärvi M, Kahila K. Aggression management in an adolescent forensic unit. Int J Forens Ment Health 2007;6:185-96. https://doi.org/10.1080/14999013.2007.10471262.
- Youth Justice Board . Developing a Restraint Minimisation Strategy: Guidance for Secure Establishments on the Development of Restraint Minimisation Strategies 2009.
- British Association of Social Workers (BASW) . Behaviour Management and Restraint of Children in Custody: A Review of the Early Implementation of MMPR by HM Inspectorate of Prisons 2015. www.basw.co.uk/resources/behaviour-management-and-restraint-children-custody (accessed 27 April 2021).
- Jones RJ, Timbers GD. Minimizing the need for physical restraint and seclusion in residential youth care through skill-based treatment programming. Fam Soc 2003;84:21-9. https://doi.org/10.1606/1044-3894.81.
- O’Brien C. Best practices in behavior support: preventing and reducing the use of restraint and seclusion. Resid Group Care Q 2004;5:14-6.
- Hellerstein DJ, Staub AB, Lequesne E. Decreasing the use of restraint and seclusion among psychiatric inpatients. J Psychiatr Pract 2007;13:308-17. https://doi.org/10.1097/01.pra.0000290669.10107.ba.
- Crosland KA, Cigales M, Dunlap G, Neff B, Clark HB, Giddings T, et al. Using staff training to decrease the use of restrictive procedures at two facilities for foster care children. Res Soc Work Pract 2008;18:401-9. https://doi.org/10.1177/1049731507314006.
- Nunno MA, Day DM, Bullard LB. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. Arlington, VA: Child Welfare League of America; 2008.
- Bensimhon P, Villablanca JG, Sender LS, Matthay KK, Park JR, Seeger R, et al. Peripheral blood stem cell support for multiple cycles of dose intensive induction therapy is feasible with little risk of tumor contamination in advanced stage neuroblastoma: a report from the Children’s Oncology Group. Pediatr Blood Cancer 2010;54:596-602. https://doi.org/10.1002/pbc.22344.
- Colton D, Xiong H. Reducing seclusion and restraint: questionnaire for organizational assessment. J Psychiatric Pract 2010;16:358-62. https://doi.org/10.1097/01.pra.0000388632.74899.86.
- Rasimas JJ, Sachdeva K, Salama AM, Helmick TJ, Donovan JW. A review of bedside toxicologic experience with physostigmine and flumazenil. Clin Toxicol 2010;48.
- Deveau R, Leitch S. The impact of restraint reduction meetings on the use of restrictive physical interventions in English residential services for children and young people. Child Care Health Dev 2015;41:587-92. https://doi.org/10.1111/cch.12193.
- Girelli S. Lessons learned in the reduction of restraint and seclusion: a three-year (plus) retrospective. Resid Group Care Q 2004;5:8-9.
- Campbell N. STAR project outcomes. Resid Group Care Q 2004;5:3-5.
- Ryan S, Rigby P. Toward development of effective custom child restraint systems in motor vehicles. Assist Technol 2007;19:239-48. https://doi.org/10.1080/10400435.2007.10131880.
- Ali S, Bokharey IZ. Maladaptive cognitions and physical health of the caregivers of dementia: an interpretative phenomenological analysis. Int J Qual Stud Health Well-Being 2015;10. https://doi.org/10.3402/qhw.v10.28980.
- Singh NN, Singh SD, Davis CM, Latham LL, Ayers JG. Reconsidering the use of seclusion and restraints in inpatient child and adult psychiatry. Child Fam Stud 1999;8:243-53. https://doi.org/10.1023/A:1022039711096.
- Human Behaviour Change Project . Theory and Technique Tool 2021. https://theoryandtechniquetool.humanbehaviourchange.org/ (accessed 27 April 2021).
- Connell LE, Carey RN, de Bruin M, Rothman AJ, Johnston M, Kelly MP, et al. Links between behavior change techniques and mechanisms of action: an expert consensus study. Ann Behav Med 2018;53:708-20. https://doi.org/10.1093/abm/kay082.
- Allison E. MoJ challenged to release details of child restraint in prisons. The Guardian 2020.
- Villani VS, Parsons AE, Church RP, Beetar JT. A descriptive study of the use of restraint and seclusion in a special education school. Child Youth Care Forum 2012;41:295-309. https://doi.org/10.1007/s10566-011-9165-3.
- Smallridge P, Williamson A. Independent Review of Restraint in Juvenile Secure Settings. London: Ministry of Justice and Department for Children, Schools and Families, HM Government; 2008.
- Willow C. Child Prison Restraint Manual FOI Appeal 2015. https://article39.org.uk/2015/10/09/child-prison-restraint-manual-foi-appeal/ (accessed 27 April 2021).
- Taylor C. Independent Review of the Use of Pain-inducing Techniques in the Youth Secure Estate. London: Ministry of Justice and HM Prison and Probation Service; 2020.
- Willow C. Review Calls for Ban of Pain-Inducing Restraint 2020. https://article39.org.uk/2020/06/18/review-calls-for-ban-of-pain-inducing-restraint/ (accessed 27 April 2021).
- Ministry of Justice . Independent Review of Pain-Inducing Techniques – Government Response 2020.
- Lipsey MW. The primary factors that characterize effective interventions with juvenile offenders: a meta-analytic overview. Victims Offenders 2009;4:124-47. https://doi.org/10.1080/15564880802612573.
- Archard D, Skivenes M. Hearing the child. Child Fam Soc Work 2009;14:391-9. https://doi.org/10.1111/j.1365-2206.2008.00606.x.
- McLaughlin H. Service-user Research in Health and Social Care. London: SAGE Publications Ltd; 2009.
- Mérineau-Côté J, Morin D. Restraint and seclusion: the perspective of service users and staff members. J Appl Res Intellect Disabil 2014;27:447-57. https://doi.org/10.1111/jar.12069.
- Bruheim Jensen I. What are the perspectives of children in child protection work among social workers in Norway and Chile?. Child Youth Serv Rev 2020;118. https://doi.org/10.1016/j.childyouth.2020.105410.
- Diaz C, Pert H, Thomas NP. Independent Reviewing Officers’ and social workers’ perceptions of children’s participation in Children in Care Reviews. J Child Serv 2019;14:162-73. https://doi.org/10.1108/JCS-01-2019-0003.
- Wilson C, Rouse L, Rae S, Jones P, Kar Ray M. Restraint Reduction in Mental Healthcare: A Systematic Review. Fulbourn: Cambridgeshire and Peterborough NHS Foundation Trust; 2015.
- Chambers M, Guise V, Välimäki M, Botelho MA, Scott A, Staniuliené V, et al. Nurses’ attitudes to mental illness: a comparison of a sample of nurses from five European countries. Int J Nurs Stud 2010;47:350-62. https://doi.org/10.1016/j.ijnurstu.2009.08.008.
- Munro S, Baker J. Outcomes associated with skill mix interventions in acute mental health wards: a synthesis of evidence. J Ment Health Train Educ Pract 2007;2:25-33. https://doi.org/10.1108/17556228200700018.
- Kirkwood S. Child welfare league of America IWDC. Resid Group Care Q 2004;5.
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ 2021;374. https://doi.org/10.1136/bmj.n2061.
- Duncan E, Cathain A, Rousseau N, Croot L, Sworn K, Turner KM, et al. Guidance for reporting intervention development studies in health research (GUIDED): an evidence-based consensus study. BMJ Open 2020;10. https://doi.org/10.1136/bmjopen-2019-033516.
- Hallman IS, O’Connor N, Hasenau S, Brady S. Improving the culture of safety on a high-acuity inpatient child/adolescent psychiatric unit by mindfulness-based stress reduction training of staff. J Child Adolesc Psychiatr Nurs 2014;27:183-9. https://doi.org/10.1111/jcap.12091.
- Leitch S. The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions in Services for Children and Young People. Canterbury: Tizard Centre, University of Kent; 2009.
- Leitch S. Together Trust. Canterbury: Tizard Centre, University of Kent; 2008.
- Leitch S. Training Plan. Canterbury: Tizard Centre, University of Kent; n.d.
- Leitch S. Training Plan. Canterbury: Tizard Centre, University of Kent; 2008.
- Magnowski S. Restraint Implications 2008.
- Studio III. Training Systems and Psychological Services. Low Arousal Training 2021. www.studio3.org/low-arousal-training (accessed 27 April 2021).
- Ponge L, Harris J. Reduction of seclusion and restraint in a children’s psychiatric center. Commun Nurs Res 2006;39.
Appendix 1 Search strategies
Includes all 2020 update search strategies and those from 2019 if they were not included in the update or where 2020 and 2019 searches used different strategies.
Academic database searches
| Academic database searched | Date range searched |
|---|---|
| ASSIA ProQuest | 1987 to 24 January 2020 |
| British Nursing Index (HDAS) | 1992 to 24 January 2020 |
| CINAHL (EBSCOhost) | 1981 to 30 January 2020 |
| Child Development and Adolescent Studies (EBSCOhost) | 1927 to 24 January 2020 |
| Criminal Justice Abstracts (EBSCOhost) | 1830 to 30 January 2020 |
| Education Abstracts (H.W. Wilson) (EBSCOhost) | 1983 to 14 June 2019 |
| Embase Classic+Embase (Ovid) 1947 to 2020 January 21 | 1947 to 21 January 2020 |
| ERIC | 1966 to 30 January 2020 |
| Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily | 1946 to 20 January 2020 |
| PsycInfo (Ovid) 1806 to January Week 2 2020 | 1806 to January Week 2 2020 |
| Scopus (Elsevier B.V.) 1823 to 13/06/19 | 1823 to 13 June 2019 |
Search terms
| Search terms | Number of hits |
|---|---|
| ASSIA (ProQuest) 1987 to 24 January 2020 | |
| S16 (S8 AND S15)AND pd(19890101-20201231) | 1520 |
| S15 S9 OR S10 OR S11 OR S12 OR S13 OR S14 | 403,037 |
| S14 ti,ab(asylum OR refugee OR refugees OR migrant or migrants OR immigrant OR immigrants OR immigration) | 21,003 |
| S13 ti,ab((“Health Services” or hospital or hospitals or ward or ward or inpatient or patient or forensic OR forensics OR CAMHS OR “pediatric intensive care unit” OR “paediatric intensive care unit” OR PICI OR PICU OR “Care Facility” OR “Care Facilities” OR “Rehabilitation Center” OR “rehabilitation centers” OR “Rehabilitation Centre” OR “Rehabilitation Centres”)) | 232,866 |
| S12 ti,ab(((health OR medical OR medicine OR psychiatry OR psychiatric OR mental) near/1(service OR services OR centres OR centre OR Center OR centers OR department OR departments OR facility OR facilities OR ward OR wards OR units OR unit)) OR ((child OR children or young or pediatric or paediatric or adolescent or adolescents) near/2 (service OR services))) | 60,895 |
| S11 ti,ab(((pupil OR pupils OR school OR schools OR schoolchildren OR child OR children OR education) near/2 (referral OR referrals)) OR ((education OR educational) near/1 (service OR services OR facility OR facilities OR institution OR institutions)) OR (Kindergarten OR Kindergartens OR Nursery OR pre-school OR pre-schools OR classroom OR classrooms OR school OR schools)) | 86,446 |
| S10 ti,ab((“juvenile justice” OR incarcerate OR incarcerated OR incarceration OR detention OR Custody OR Prison OR prisons OR prisoner OR prisoners OR jail OR jails OR detain OR detained OR inmate OR inmates OR Delinquent OR delinquents OR Delinquency) OR (secure near/2 (home OR homes OR accommodation OR unit OR units OR centre OR centres OR center OR centers OR service OR services OR facility Or facilities))) | 26,323 |
| S9 ti,ab(((youth or young or juvenile) near/1 (offending OR offender OR offenders)) OR ((foster OR residential) near/2 (care OR home OR homes)) OR ((children OR childrens) near/1 (home OR homes)) OR ((foster OR fostered OR fostering OR “looked after”) AND (child OR children)) OR (“Foster Care” OR “Assisted Living” OR Orphanage OR Ophanages OR “Residential Care” OR “social worker” OR “social workers” OR “Social Work” OR “social care” OR orphan OR orphans)) | 43,759 |
| S8 S1 AND (S2 OR S3 OR S4 OR S5 OR S6 OR S7) | 3843 |
| S7 ti,ab(((prn OR “pro re nata”) NEAR/1 (medicate OR medicated OR medication OR medications)) OR ((rapid OR rapidly) AND (tranquillise OR tranquillize OR tranquilliser OR tranquillizer OR tranquillisers OR tranquillizers)) OR (safety NEAR/1 (huddle OR huddles OR plan OR plans OR planning)) OR ((weight OR weighted OR comfort) NEAR/1 (blanket OR blankets)) OR ((comfort OR safe OR sensory) NEAR/2 (room OR rooms)) OR ((restrict OR restricts OR restrictive OR restriction OR restrictions) NEAR/2 (practice OR practices OR intervention OR interventions OR liberty))) | 555 |
| S6 ti,ab(((lock OR locked or locking) NEAR/1 (door OR doors OR ward OR wards OR room OR rooms)) OR (forced NEAR/1 (medicate OR medication OR medications OR medicated OR sedate OR sedation OR sedated OR drug OR drugs OR treatment OR treatments)) OR (involuntary NEAR/1 (medicate OR medication OR medications OR medicated OR sedate OR sedation OR sedated OR drug OR drugs OR treatment OR treatments))) | 288 |
| S5 ti,ab((violence NEAR/4 (prevent OR prevents OR prevention OR prevented OR manage OR managed OR management OR managing) NEAR/4 training) OR ((patient or patients) NEAR/1 (isolation OR segregation)) OR ((physical or physically) NEAR/1 (immobilise OR immobilize OR immobilised OR immobilized OR control))) | 297 |
| S4 ti,ab((Aggression OR Aggressive OR Aggressively) NEAR/4 (prevent OR prevents OR prevention OR prevented OR manage OR managed OR management OR managing) NEAR/4 training) | 45 |
| S3 ti,ab(holding NEAR/2 (therapeutic OR parent OR parents OR procedure OR procedures OR clinical OR physical OR treatment OR safe OR supportive)) OR (one-to-one NEAR/1 (nursing OR nurse OR nurses)) | 185 |
| S2 ti,ab(pain-compliance OR “solitary confinement” OR isolation OR compulsion OR compulsivity OR “calm down” OR “soft word” OR “soft words” OR “talk down” OR de-escalat* OR deescalat* OR seclusion OR seclude OR secluded OR restrain OR restraining OR restraint OR restraints OR restrains OR coercive OR coercion OR coerced) | 12,214 |
| S1 su,ti,ab((infant OR infants OR young OR schoolchild OR schoolchildren OR childhood OR children OR child OR adolescen* OR teen OR teens OR teenager OR teenagers OR youth OR youths OR girl OR girls OR boy OR boys OR pediatric OR pediatrics OR paediatric OR paediatrics OR juvenile OR juveniles)) | |
| British Nursing Index (HDAS) 1992 to 24 January 2020 | |
| 1 (infant OR infants OR young OR schoolchild* OR childhood OR children OR child OR adolescen* OR teen OR teens OR teenager* OR youth OR youths OR girl OR girls OR boy OR boys OR paediatric* OR pediatric* OR juvenil*).ti,ab | 112,671 |
| 2 (one-to-one ADJ1 nurs*).ti,ab | 35 |
| 3 (Aggress* ADJ3 (prevent* OR manag*)).ti,ab | 540 |
| 4 (violence ADJ3 (prevent* OR manag*)).ti,ab | 844 |
| 5 (patient* ADJ3 (isolation OR segregation)).ti,ab | 269 |
| 6 (physical* ADJ2 (immobili* OR control)).ti,ab | 134 |
| 7 ((lock OR locked OR locking) ADJ1 (door* OR ward* OR room*)).ti,ab | 79 |
| 8 (forced ADJ1 (medic* OR sedat* OR drug* OR treatment*)).ti,ab | 50 |
| 9 (involuntary ADJ1 (medic* OR sedat* OR drug* OR treatment*)).ti,ab | 29 |
| 10 ((prn OR “pro re nata”) ADJ1 medicat*).ti,ab | 62 |
| 12 (rapid* AND tranq*).ti,ab | 2 |
| 13 (safety ADJ1 (huddle* OR plan*)).ti,ab | 186 |
| 14 ((weight* OR comfort) ADJ1 blanket*).ti,ab | 7 |
| 15 ((comfort OR safe OR sensory) ADJ2 room*).ti,ab | 58 |
| 16 (restric* ADJ2 (practice* OR intervention* OR liberty)).ti,ab | 293 |
| 17 (pain-compliance).ti,ab | 4 |
| 18 (solitary confinement).ti,ab | 20 |
| 19 isolation OR compulsion OR compulsivity OR “calm down” OR “soft word*” OR “talk down” OR de-escalat* OR deescalat* OR seclusion OR seclude* OR restrain* OR coercive OR coercion OR coerced | 6416 |
| 20 (2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 12 OR 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19) | 8567 |
| 21 ((youth OR young OR juvenile) ADJ1 offend*).ti,ab | 204 |
| 22 (juvenile justice OR incarcerat* OR detention OR Custody OR Prison* OR Delinquen* OR jail* OR detain* OR inmate*).ti,ab | 4670 |
| 23 (secure ADJ2 (home* OR accommodation OR unit* OR centre* OR center* OR service* OR facilit*)).ti,ab | 535 |
| 24 ((foster OR residential) ADJ2 (care OR home*)).ti,ab | 2919 |
| 25 (“Foster Care” OR Assisted Living OR Orphanage* OR “Residential Care” OR social worker* OR Social Work OR social care OR orphan*).ti,ab | 25,822 |
| 26 ((pupil* OR school* OR child* OR education) ADJ2 referral).ti,ab | 202 |
| 27 (education* ADJ1 (service* OR facilit* OR institution*)).ti,ab | 2011 |
| 28 (Kindergarten* OR Nursery OR pre-school* OR classroom* OR school*).ti,ab | 27650 |
| 29 ((health OR medic* OR psychiatr* OR mental) ADJ1 (service* OR centre* OR center* OR department* OR facilit* OR Unit OR Units OR ward*)).ti,ab | 46,408 |
| 30 ((child* OR young OR pediatric OR paediatric OR adolescent*) ADJ2 services).ti,ab | 2635 |
| 31 (Health Services OR hospital* OR ward* OR inpatient OR patient OR forensic* OR CAMHS OR “pediatric intensive care unit” OR “paediatric intensive care unit” OR PICI OR PICU OR Care Facilities OR Hospital Units OR Hospital* OR Rehabilitation Center* OR Rehabilitation Centre*).ti,ab | 211,252 |
| 48 ((foster* OR “looked after”) AND child*).ti,ab | 619 |
| 49 (children* ADJ1 home*).ti,ab | 400 |
| 50 (asylum OR refugee* OR migrant* OR immigrant* OR immigration).ti,ab | 6210 |
| 53 (1 AND 20) | 1381 |
| 54 (21 OR 22 OR 23 OR 24 OR 25) | 33,084 |
| 65 (53 AND 54) | 206 |
| 66 (26 OR 27 OR 28) | 29,558 |
| 67 (53 AND 66) | 167 |
| 68 (29 OR 30) | 47,920 |
| 70 (29 AND 53) | 134 |
| 71 (30 OR 31 OR 48 OR 49 OR 50) | 223,261 |
| 72 (53 AND 71) | 483 |
| 73 (72 or 70 or 67 or 65) | 709 |
| CINAHL (EBSCOhost) 1981 to 30 January 2020 | |
| S99 s91 NOT s97 (Limiters – Published Date: 19890101-present) | 4058 |
| S98 s91 NOT s97 | 4081 |
| S97 S92 OR S93 OR S94 OR S95 OR S96 | 28,045 |
| S96 TX ((car or vehicle) N1 (restraint* or safety or crash*)) | 4323 |
| S95 TX ((Road or Traffic) N1 (injur* or trauma or accident*)) | 16,825 |
| S94 TX “motor vehicle*” | 9321 |
| S93 TX (seat or seats or seatbelt* or “road safety” or “passenger safety”) | 7252 |
| S92 (MH “Car Safety Devices”) | 2199 |
| S91 S6 AND S50 AND S90 | 4528 |
| S90 S58 OR S68 OR S74 OR S86 OR S89 | 3,849,499 |
| S89 S87 OR S88 | 25,505 |
| S88 (MH “Emigration and Immigration”) OR (MH “Immigrants+”) OR (MH “Refugees”) | 24,180 |
| S87 TX ((asylum OR refugee* OR migrant* OR immigrant* OR immigration) N4 (service* OR center* OR center* OR department* OR facilit* OR unit* OR reception OR accommodation)) | |
| S86 S75 OR S76 OR S77 OR S78 OR S79 OR S80 OR S81 OR S82 OR S83 OR S84 OR S85 | 3,721,859 |
| S85 TX (“pediatric intensive care unit”) | 3570 |
| S84 TX ((health or medic* or psychiat* or mental) N2 (service? or center? or centre? or department? or facilit* or unit? or ward?)) | 1,751,717 |
| S83 TI forensic* OR AB forensic* | 8602 |
| S82 TX CAMHS | 1144 |
| S81 TX PICU OR PICI | 3210 |
| S80 (MH “Intensive Care Units, Pediatric”) | 5469 |
| S79 TX (inpatient or patient) | 1,916,873 |
| S78 TX (hospital? or ward?) | 1,436,813 |
| S77 (MH “Health Services+”) | 919,549 |
| S76 TX ((child* or young or pediatric or paediatric or adolescent*) N2 services) | 30,761 |
| S75 MH “Ambulatory Care Facilities”) OR ((MH “Facility Design and Construction+”)) OR (MH “Hospital Units+”) OR (MH “Hospitals+”) OR (MH “Rehabilitation Centers+”) | 202,905 |
| S74 S69 OR S70 OR S71 OR S72 OR S73 | 204,058 |
| S73 TX (Kindergarten* or Nursery or pre-school*) | 8278 |
| S72 TX ((pupil* or school* or child or children* or education) and (referral N1 (unit* or centre* or center* or facilit* or service*)) | 3870 |
| S71 TX classroom* or school* | 165,640 |
| S70 TX (education* N1 (service* or facilit* or institution*)) | 13,625 |
| S69 (MH “Schools+”) | 66,167 |
| S68 S59 OR S60 OR S61 OR S62 OR S63 OR S64 OR S65 OR S66 OR S67 | 72,499 |
| S67 TX “social worker*” | 17,419 |
| S66 (MH “Social Work+”) | 11,905 |
| S65 TX “social care” | 19,152 |
| S64 TX orphan* | 5977 |
| S63 TX ((foster* or “looked after”) and child*) | 13,637 |
| S62 TX (children* N1 home*) | 2035 |
| S61 TX ((foster or residential) N (care or home*)) | 147 |
| S60 TX (secure N3 (home* or accommodation or unit* or centre* or center* or service* or facilit*)) | 1353 |
| S59 (MH “Foster Home Care”) OR (MH “Assisted Living”) OR ((MH “Orphans and Orphanages”)) OR (MH “Residential Care”) | 13,437 |
| S58 S51 OR S52 OR S53 OR S54 OR S55 OR S56 OR S57 | 28,060 |
| S57 TX “juvenile justice” | 1460 |
| S56 TX (incarcerat* or detention or custody or prison* or jail* or detain* or inmate*) | 20,875 |
| S55 (MH “Involuntary Commitment”) | 1846 |
| S54 (MH “Child Custody”) | 1326 |
| S53 (MH “Prisoners”) | 8319 |
| S52 (MH “Juvenile Offenders”) OR (MH “Juvenile Delinquency”) OR (MH “Correctional Facilities”) | 9821 |
| S51 TX ((youth or young or juvenile*) N2 offend*) | 2610 |
| S50 S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 | 24,840 |
| S49 “Br#set Violence Checklist*” | 19 |
| S48 TX “Proactive Management of Integrated Service* and Environment*” | 303 |
| S47 TX (“Positive and Safe” N1 (team? or plan?)) | 1 |
| S46 TX “ReSTRAIN YOURSELF” | 2 |
| S45 TX “manag* of actual or potential aggress*” | 3 |
| S44 TX (MAPA N5 (aggress* or cris#s)) | 7 |
| S43 TX (MAPA N1 (training or intervention or program*)) | 1 |
| S42 TX (CALM N1 (training or intervention or program*)) | 37 |
| S41 TX (CALM and (cris#s N6 manag*)) | 10 |
| S40 TX “crisis and aggression limitation and management” | 1 |
| S39 TX (“Creating Safety” N5 training) | 460 |
| S38 TX “People are and feel safe” | 3 |
| S37 TX “Roadmap to seclusion” | 1 |
| S36 TX “no force first” | 3 |
| S35 TX safewards | 23 |
| S34 S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 | 24,764 |
| S33 (isolation n3 (booth* or room*) | 268 |
| S32 TX pain-compliance | 12 |
| S31 TX (holding N3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive)) | 278 |
| S30 TX (one-to-one N2 nurs*) | 371 |
| S29 TX (Aggress* N5 (prevent* or manag*) N5 training) | 98 |
| S28 TX (Violence N5 (prevent* or manag*) N5 training) | 195 |
| S27 TX (patient? N3 (isolation or segregation)) | 3541 |
| S26 TX (physical* N1 (immobili* or control)) | 668 |
| S25 (lock or locked or locking) N3 (door* or ward? or room?) | 200 |
| S24 TX “solitary confinement” | 56 |
| S23 TX forced N3 (medic* OR sedat* or drug? or treatment?) | 839 |
| S22 TX (involuntary N3 (medic* OR sedat* or drug? or treatment?) | 331 |
| S21 TX compulsion or compulsivity | 991 |
| S20 TX ((prn or “pro re nata”) N1 medicat*) | 190 |
| S19 TX (rapid* N2 tranq*) | 63 |
| S18 TX safety N2 (huddle? OR plan?) | 513 |
| S17 TX ((weight* or comfort) N1 blanket*) | 30 |
| S16 TX ((comfort or safe or sensory) N2 room?) | 145 |
| S15 TX “calm down” or “soft word?” or “talk down” | 92 |
| S14 TX (de-escalat* or deescalat*) | 1156 |
| S13 TX restric* N2 (practice* or intervention* or liberty) | 1456 |
| S12 TX seclusion or seclude* | 1178 |
| S11 TX restrain* | 10,414 |
| S10 TX coercive or coercion or coerced | 3697 |
| S9 (MH “Coercion”) or (MH “Involuntary Treatment”) | 1965 |
| S8 (MH “Patient Seclusion”) | 596 |
| S7 (MH “Restraint, Physical”) | 3975 |
| S6 S1 OR S2 OR S3 OR S4 OR S5 | 1,181,600 |
| S5 TX (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”) | 527,514 |
| S4 (MH “Adolescent Health”) OR (MH “Child Health”) | 18,820 |
| S3 (MH “Adolescence+”) OR (MH “Child+”) | 876,348 |
| S2 (MH “Adolescent Behavior”) OR (MH “Child Behavior”) OR (MH “Infant Behavior”) | 25,822 |
| S1 TI ((child or childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or paediatric or pediatric or juvenil*)) OR AB ((child or childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or paediatric or pediatric or juvenil*)) (580,951) | 580,951 |
| Child Development and Adolescent Studies (EBSCOhost) 1927 to 24 January 2020 | |
| Same strategy as Criminal Justice Abstracts | |
| Criminal Justice Abstracts (EBSCOhost) 1830 to 30 January 2020 | |
| S65 S58 NOT S63 (Limiters – Published Date: 19890101-present) | 863 |
| S64 S58 NOT S63 | 900 |
| S63 S59 OR S60 OR S61 OR S62 | 8401 |
| S62 TX ((car or vehicle) N1 (restraint* or safety or crash*)) | 2999 |
| S61 TX ((Road or Traffic) N1 (injur* or trauma or accident*)) | 5235 |
| S60 TX “motor vehicle*” | 5765 |
| S59 TX (seat or seats or seatbelt* or “road safety” or “passenger safety”) | 1956 |
| S58 S3 and s31 and s57 | 1030 |
| S57 S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 OR S56 | 237,211 |
| S56 TX ((asylum OR refugee* OR migrant* OR immigrant* OR immigration) N4 (service* OR center* OR center* OR department* OR facilit* OR unit* OR reception OR accommodation)) | 2393 |
| S55 TX (“pediatric intensive care unit” or “paediatric intensive care unit” or PICI or PICU) | 20 |
| S54 TX ((health or medic* or psychiat* or mental) N2 (service? or center? or centre? or department? or facilit* or unit? or ward?)) | 63,333 |
| S53 TI forensic* OR AB forensic* | 20,560 |
| S52 TX CAMHS | 152 |
| S51 TX hospital? or ward? or inpatient? or patient? | 53,547 |
| S50 TX “Health Services” | 17,612 |
| S49 TX ((child* or young or pediatric or paediatric or adolescent*) N2 services) | 7573 |
| S48 TX “Care Facilit*” OR “Hospital Unit*” OR Hospital? OR “Rehabilitation Center?” or “Rehabilitation Centre?” | 38,956 |
| S47 TX (Kindergarten* or Nursery or pre-school*) | 1336 |
| S46 TX ((pupil* or school* or child* or education) and (referral N1 (unit* or centre* or center* or facilit* or service*))) | 125 |
| S45 TX classroom* or school* | 108,421 |
| S44 TX (education* N1 (service* or facilit* or institution*)) | 8177 |
| S43 TX “social work” OR “social worker*” | 27,435 |
| S42 TX “social care” | 856 |
| S41 TX orphan* | 290 |
| S40 TX (((foster* or “looked after”) and child*)) | 3299 |
| S39 TX (children* N1 home*) | 939 |
| S38 TX (((foster or residential) N1 (care or home*))) | 9340 |
| S37 TX ((secure N3 (home* or accommodation or unit* or centre* or center* or service* or facilit*))) | 1157 |
| S36 TX (“Foster Care” OR “Assisted Living” OR Orphanage? OR “Residential Care”) | 9276 |
| S35 TX (Involuntary N1 (Commitment or hospitali*)) | 206 |
| S34 TX (prison* or custody or incarcerat* or detention or jail* or detain* or inmate*) | 48,786 |
| S33 TX (“Juvenile Delinquen*” or “juvenile justice”) | 11,230 |
| S32 TX (((youth or young or juvenile) N2 offend*)) | 5701 |
| S31 S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 | 7631 |
| S30 TX (isolation n3 (booth* or room*) | 4 |
| S29 TX (((violence or aggression) N5 (prevent* or manag*) N5 training)) | 52 |
| S28 TX (patient? N3 (isolation or segregat*)) | 11 |
| S27 TX (“Br#set Violence Checklist*”) | 4 |
| S26 TX “ReSTRAIN YOURSELF” | 4 |
| S25 TX “manag* of actual or potential aggress*” | 0 |
| S24 TX (MAPA N5 (aggress* or cris#s)) | 0 |
| S23 TX (MAPA N1 (training or intervention or program*)) | 2 |
| S22 TX (CALM N1 (training or intervention or program*)) | 2 |
| S21 TX (CALM and (cris#s N6 manag*)) | 5 |
| S20 TX “crisis and aggression limitation and management” | 554 |
| S19 TX (“Creating Safety” N5 training) | 1005 |
| S18 TX (pain-compliance or safewards or “six core strategies” or “Roadmap to seclusion” or “People are and feel safe”) | 6 |
| S17 TX ((holding N3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive))) | 41 |
| S16 TX (one-to-one N2 nurs*) | 1 |
| S15 TX ((physical* N1 (immobili* or control))) | 90 |
| S14 TX ((lock or locked or locking) N3 (door* or ward? or room?)) | 116 |
| S13 TX “solitary confinement” | 484 |
| S12 TX ((involuntary or forced) N3 (medic* OR sedat* or drug? or treatment?)) | 368 |
| S11 TX ((prn or “pro re nata”) N1 medicat*) | 3 |
| S10 TX (rapid* N2 tranq*) | 2 |
| S9 TX (safety N1 (huddle? OR plan?)) | 87 |
| S8 TX ((weight* or comfort) N1 blanket*) | 569 |
| S7 TX (((comfort or safe or sensory) N2 room?)) | 19 |
| S6 TX (“calm down” or “soft word?” or “talk down”) | 8 |
| S5 TX (restric* N2 (practice* or intervention* or liberty)) | 196 |
| S4 TX ((coercive or coercion or coerced or restrain* or seclude* or seclusion or de-escalat* or deescalat*))) | 6417 |
| S3 S1 OR S2 | 93,170 |
| S2 TX (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”) | 12,547 |
| S1 TI (child OR childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric? or juvenil*) OR AB (child OR childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric? or juvenil*) | 87,778 |
| Education Abstracts (H.W. Wilson) (EBSCOhost) 1983 to 14 June 2019 | |
| # Query Results | |
| S97 S94 OR S95 (Limiters – Published Date: 19890101-present) | |
| Limiters - Published Date: 19890101 | 968 |
| S96 S94 OR S95 | 991 |
| S95 DE “Physical restraint & seclusion of students” | 25 |
| S94 S88 NOT S93 | 975 |
| S93 S89 OR S90 OR S91 OR S92 | 7997 |
| S92 TX ((car or vehicle) N1 (restraint* or safety or crash*)) | 834 |
| S91 TX ((Road or Traffic) N1 (injur* or trauma or accident*)) | 1108 |
| S90 TX “motor vehicle*” | 3177 |
| S89 TX (seat or seats or seatbelt* or “road safety” or “passenger safety”) | 4429 |
| S88 S5 AND S48 AND S87 | 1003 |
| S87 S56 OR S67 OR S72 OR S83 OR S86 | 778,463 |
| S86 S84 OR S85 | 7512 |
| S85 DE “Alien detention centers” OR DE “Immigrants” | 2450 |
| S84 TX ((asylum OR refugee* OR migrant* OR immigrant* OR immigration) N4 (service* OR center* OR center* OR department* OR facilit* OR unit* OR reception OR accommodation)) | 5525 |
| S83 S73 OR S74 OR S75 OR S76 OR S77 OR S78 OR S79 OR S80 OR S81 OR S82 | 113,796 |
| S82 DE “Mental health services” OR DE “Crisis intervention (Mental health services)” OR DE “Psychotherapy” OR DE “School mental health services” | 3727 |
| S81 TX (“pediatric intensive care unit”) | 8 |
| S80 TX ((health or medic* or psychiat* or mental) N2 (service? or center? or centre? or department? or facilit* or unit? or ward?)) | 53,279 |
| S79 TI forensic* OR AB forensic* | 1228 |
| S78 TX PICU OR PICI | 56 |
| S77 TX CAMHS | 71 |
| S76 TX (inpatient or patient) | 42,895 |
| S75 TX (hospital? or ward?) | 24,996 |
| S74 TX ((child* or young or pediatric or paediatric or adolescent*) N2 services) | 18,435 |
| S73 TX “Care Facilit*” OR Hospital? OR “Rehabilitation Center?” or “Rehabilitation Centre?” | 23,519 |
| S72 S68 OR S69 OR S70 OR S71 | 680,566 |
| S71 TX (Kindergarten* or Nursery or pre-school*) | 21,503 |
| S70 TX ((pupil* or school* or child or children* or education) and (referral N1 (unit* or centre* or center* or facilit* or service*)) | 287 |
| S69 DE “Schools” OR DE “Adult education facilities” OR DE “Alternative schools” OR DE “American schools abroad” OR DE “Art schools” OR DE “Bilingual schools” OR DE “Boarding schools” OR DE “British schools” OR DE “Business schools” OR DE “Cathedral schools” OR DE “Charity-schools” OR DE “Charter schools” OR DE “Coeducational schools” OR DE “Commercialism in schools” OR DE “Community & school” OR DE “Computer programming schools” OR DE “Cooking schools” OR DE “Cooperative schools” OR DE “Correspondence schools & courses” OR DE “Cosmetology schools” OR DE “Court reporting schools” OR DE “Dance schools” OR DE “Day schools” OR DE “Disadvantaged schools” OR DE “Effective schools” OR DE “Elementary schools” OR DE “Ethnic schools” OR DE “European schools” OR DE “Evening & continuation schools” OR DE “Failing schools” OR DE “Film schools” OR DE “Fishery schools” OR DE “Flight schools” OR DE “Forestry schools” OR DE “Grant-maintained schools” OR DE “Gymnasiums (Educational institutions)” OR DE “Gülen movement schools” OR DE “Harassment in schools” OR DE “Health occupations schools” OR DE “Heterosexism in schools” OR DE “Homophobia in schools” OR DE “Hospital schools” OR DE “Institutional schools” OR DE “Instructional materials centers” OR DE “International schools” OR DE “Irish Gaelic language schools” OR DE “Jewish religious schools” OR DE “Laboratory schools” OR DE “Landscape architecture schools” OR DE “Language schools” OR DE “Libraries & schools” OR DE “Library schools” OR DE “Manual training” OR DE “Military post schools” OR DE “Mining schools” OR DE “Mission schools” OR DE “Mobile schools” OR DE “Montessori schools” OR DE “Museums & schools” OR DE “Music conservatories” OR DE “Naturopathic schools” OR DE “Open-air schools” OR DE “Platoon schools” OR DE “Preschools” OR DE “Primary schools” OR DE “Private schools” OR DE “Professional schools” OR DE “Public schools” OR DE “Refugee camp schools” OR DE “Religious schools” OR DE “Rural schools” OR DE “School bullying” OR DE “School closings” OR DE “School districts” OR DE “School enrollment” OR DE “Schools of architecture” OR DE “Secondary schools” OR DE “Secretary schools” OR DE “Singing schools” OR DE “Single sex schools” OR DE “Small schools” OR DE “Special education schools” OR DE “Suburban schools” OR DE “Summer schools” OR DE “Sunday schools” OR DE “Textile schools” OR DE “Theater schools” OR DE “Traditional schools” OR DE “Universities & colleges” OR DE “Urban schools” OR DE “Vacation schools” OR DE “Virtual schools” OR DE “Vocational schools” OR DE “Year-round schools” | 65,275 |
| S68 TX classroom* or school* | 670,431 |
| S67 S57 OR S58 OR S59 OR S60 OR S61 OR S62 OR S63 OR S64 OR S65 OR S66 | 17,537 |
| S66 DE “Social workers” OR DE “Child welfare workers” OR DE “Psychiatric social workers” OR DE “Social workers as teachers” OR DE “Social workers in education” | 1744 |
| S65 TX “social worker*” | 4758 |
| S64 TX orphan* | 1382 |
| S63 DE “Foster home care” OR DE “Adoption” OR DE “Foster children” | 2531 |
| S62 TX ((foster* or “looked after”) and child*) | 8307 |
| S61 TX (children* N1 home*) | 1683 |
| S60 TX ((foster or residential) N (care or home*)) | 78 |
| S59 TX (secure N3 (home* or accommodation or unit* or centre* or center* or service* or facilit*)) | 237 |
| S58 DE “Group homes” OR DE “Foster home care” OR DE “Institutional care” | 1792 |
| S57 TX “Foster Care” OR “Assisted Living” OR Orphanage? OR “Residential Care” | 4574 |
| S56 S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 | 20,032 |
| S55 TX incarcerat* or detention | 5259 |
| S54 TX (prison* OR custody OR jail* OR detain* OR inmate*) | 14,019 |
| S53 TX “Juvenile Delinquen*” | 3663 |
| S52 TX “juvenile justice” | 1096 |
| S51 ((ZU “juvenile prisoners”)) or ((ZU “prisoners”)) | 852 |
| S50 DE “Problem youth” OR DE “Juvenile delinquents” OR DE “Gangs” OR DE “Juvenile detention homes” OR DE “Detention facilities” | 1645 |
| S49 ((youth or young or juvenile) N2 offend*) | 1648 |
| S48 S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 OR S34 OR S35 OR S36 OR S37 OR S38 OR S39 OR S40 OR S41 OR S42 OR S43 OR S44 OR S45 OR S46 OR S47 | 6440 |
| S47 DE “Timeout method” | 85 |
| S46 TX (isolation n3 (booth* or room*) | 12 |
| S45 TX “Br#set Violence Checklist*” | 2 |
| S44 TX “Proactive Management of Integrated Service* and Environment*” | 1166 |
| S43 TX (“Positive and Safe” N1 (team? or plan?)) | 1108 |
| S42 TX “manag* of actual or potential aggress*” | 5 |
| S41 TX (MAPA N5 (aggress* or cris#s)) | 2 |
| S40 TX (MAPA N1 (training or intervention or program*)) | 7 |
| S39 TX (CALM N1 (training or intervention or program*)) | 5 |
| S38 TX (CALM and (cris#s N6 manag*)) | 3 |
| S37 TX “crisis and aggression limitation and management” | 634 |
| S36 TX (“Creating Safety” N5 training) | 1231 |
| S35 TX “People are and feel safe” | 498 |
| S34 TX “Roadmap to seclusion” | 2 |
| S33 TX “no force first” | 855 |
| S32 TX “six core strategies” | 570 |
| S31 TX safewards | 0 |
| S30 TX pain-compliance | 55 |
| S29 TX (holding N3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive)) | 99 |
| S28 TX (one-to-one N2 nurs*) | 8 |
| S27 TX (Aggress* N5 (prevent* or manag*) N5 training) | 14 |
| S26 TX (Violence N5 (prevent* or manag*) N5 training) | 24 |
| S25 TX (patient? N3 (isolation or segregation)) | 10 |
| S24 TX (physical* N1 (immobili* or control)) | 72 |
| S23 (lock or locked or locking) N3 (door* or ward? or room?) | 93 |
| S22 TX “solitary confinement” | 112 |
| S21 TX forced N3 (medic* OR sedat* or drug? or treatment?) | 30 |
| S20 TX (involuntary N3 (medic* OR sedat* or drug? or treatment?) | 25 |
| S19 TX compulsion or compulsivity | 778 |
| S18 TX ((prn or “pro re nata”) N1 medicat*) | 3 |
| S17 TX (rapid* N2 tranq*) | 726 |
| S16 TX (rapid* N2 tranq*) | 726 |
| S15 TX safety N2 (huddle? OR plan?) | 123 |
| S14 TX ((weight* or comfort) N1 blanket*) | 7 |
| S13 TX ((comfort or safe or sensory) N2 room?) | 31 |
| S12 TX “calm down” or “soft word?” or “talk down” | 59 |
| S11 TX (de-escalat* or deescalat*) | 71 |
| S10 TX restric* N2 (practice* or intervention* or liberty) | 177 |
| S9 ((ZU “restraint of patients”)) or ((ZU “seclusion of psychiatric hospital patients”)) | 122 |
| S8 TX seclusion or seclude* | 276 |
| S7 TX restrain* | 3059 |
| S6 TX coercive or coercion or coerced | 1582 |
| S5 S1 OR S2 OR S3 OR S4 | 279,420 |
| S4 TX (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”) | 48,659 |
| S3 DE “Youth” OR DE “At-risk youth” OR DE “Bisexual youth” OR DE “Black youth” OR DE “Juvenile delinquents” OR DE “LGBT youth” OR DE “Mentally ill youth” OR DE “Minority youth” OR DE “Problem youth” OR DE “Religious education of young people” OR DE “School dropouts” OR DE “Teenagers” OR DE “Urban youth” OR DE “Young adults” OR DE “Youth with disabilities” OR DE “Adolescence” OR DE “Children” | 27,931 |
| S2 (((ZU “children”)) or ((ZU “adolescence”))) or ((ZU “teenagers”)) | 15,456 |
| S1 TI (child or childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric? or juvenil*) OR AB (child or childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric? or juvenil*) | 246,211 |
| Embase Classic+Embase (Ovid) 1947 to 21 January 2020 | |
| 1 child Restraint system/ | 556 |
| 2 Patient Isolation/ | 634 |
| 3 aggression/pc | 10 |
| 4 (coercive or coercion or coerced).tw,kw. | 6984 |
| 5 restrain*.tw,kw. | 53,917 |
| 6 (seclusion or seclude*).tw,kw. | 2135 |
| 7 (restric* adj2 (practice* or intervention* or liberty)).tw,kw. | 1743 |
| 8 (de-escalat* or deescalat*).tw,kw. | 4838 |
| 9 (“calm down” or “soft word?” or “talk down”).tw,kw. | 148 |
| 10 ((comfort or safe or sensory) adj2 room?).tw,kw. | 170 |
| 11 ((weight* or comfort) adj1 blanket*).tw,kw. | 19 |
| 12 safety huddle?.tw,kw. | 93 |
| 13 safety plan?.tw,kw. | 468 |
| 14 (rapid* adj2 tranq*).tw,kw. | 205 |
| 15 ((prn or “pro re nata”) adj1 medicat*).tw,kw. | 339 |
| 16 (compulsion or compulsivity).tw,kw. | 3426 |
| 17 (involuntary adj3 medic*).tw,kw. | 209 |
| 18 (involuntary adj3 sedat*).tw,kw. | 13 |
| 19 (involuntary adj3 drug?).tw,kw. | 82 |
| 20 (forced adj3 medic?).tw,kw. | 1 |
| 21 (forced adj3 drug?).tw,kw. | 283 |
| 22 (forced adj3 treatment?).tw,kw. | 760 |
| 23 (forced adj3 sedat*).tw,kw. | 15 |
| 24 solitary confinement.tw. | 122 |
| 25 (lock* adj3 door*).tw,kw. | 267 |
| 26 (lock* adj3 ward?).tw,kw. | 184 |
| 27 ((lock* or locked or locks or locking) adj3 room?).tw,kw. | 170 |
| 28 (physical* adj (immobili* or control)).tw,kw. | 476 |
| 29 (patient? adj3 (isolation or segregation)).tw,kw. | 5393 |
| 30 (Violence adj5 (prevent* or manag*) adj5 training).tw,kw. | 144 |
| 31 (Aggress* adj5 (prevent* or manag*) adj5 training).tw,kw. | 114 |
| 32 (one-to-one adj2 nurs*).tw,kw. | 223 |
| 33 (holding adj3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive)).tw,kw. | 687 |
| 34 pain-compliance.tw,kw. | 28 |
| 35 (isolation adj3 (booth* or room*)).tw,kw. | 878 |
| 36 or/1-35 [Restraint Coercion or de escalation Practices] | 82,615 |
| 37 safewards.tw. | 22 |
| 38 “no force first”.tw. | 2 |
| 39 “six core strategies”.tw. | 20 |
| 40 “Roadmap to seclusion”.tw. | 0 |
| 41 “People are and feel safe”.tw. | 0 |
| 42 (“Creating Safety” adj5 training).tw. | 1 |
| 43 “crisis and aggression limitation and management”.tw. | 0 |
| 44 (CALM and (cris#s adj6 manag*)).tw. | 10 |
| 45 (CALM adj (training or intervention or program*)).tw. | 29 |
| 46 (MAPA adj (training or intervention or program*)).tw. | 0 |
| 47 (MAPA adj5 (aggress* or cris#s)).tw. | 0 |
| 48 “manag* of actual or potential aggress*”.tw,kw. | 0 |
| 49 “ReSTRAIN YOURSELF”.tw. | 6 |
| 50 (“Positive and Safe” adj (team? or plan?)).tw. | 0 |
| 51 “Proactive Management of Integrated Service* and Environment*”.tw. | 1 |
| 52 “Br#set Violence Checklist*”.tw. | 36 |
| 53 or/37-52 [Restraint reduction programmes] | 124 |
| 54 36 or 53 [Restraint practices or programmes] | 82,690 |
| 55 (childhood or children or child or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric? or juvenil*).tw. | 2,453,890 |
| 56 (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”).tw. | 630,354 |
| 57 adolescent behavior/ | 9381 |
| 58 Infant Behavio?r.tw. | 870 |
| 59 child behavior/ | 44,482 |
| 60 exp child/ | 2,957,728 |
| 61 infant/ | 689,598 |
| 62 child, preschool/ | 432,377 |
| 63 adolescent health/or child health/ | 33,875 |
| 64 Adolescent/or juvenile/ | 1,652,678 |
| 65 or/55-64 [Children] | 4,540,974 |
| 66 ((youth or young) adj2 offend*).tw,kw. | 971 |
| 67 ((child or childhood or children or adolescen* or teen* or girl? or boy? or p?ediatric* or juvenil*) adj offend*).tw,kw. | 1259 |
| 68 Juvenile Delinquency/ | 9010 |
| 69 prison/or detention/ | 18,606 |
| 70 prisoner/or criminal/ | 31,240 |
| 71 (police* or custody or prison* or jail* or detain* or inmate*).tw,kw. | 50,266 |
| 72 incarcerat*.tw,kw. | 14,559 |
| 73 detention.tw,kw. | 4321 |
| 74 juvenile justice.tw,kw. | 1352 |
| 75 or/66-74 [Criminal Justice Setting] | 91,676 |
| 76 foster care/ | 4889 |
| 77 residential home/or assisted living facility/or orphanage/(10630) | 10,630 |
| 78 (secure adj3 (home* or accommodation or unit* or centre* or center* or service* or facilit*)).tw,kw. | 1579 |
| 79 ((foster or residential) adj (care or home*)).tw,kw. | 8408 |
| 80 (Children* adj home*).tw,kw. | 1244 |
| 81 ((foster* or “looked after”) and child*).tw,kw. | 7840 |
| 82 orphan*.tw,kw. | 23,197 |
| 83 social care.tw,kw. | 7842 |
| 84 exp Social Work/ | 26,382 |
| 85 social worker*.tw,kw. | 16,739 |
| 86 or/76-85 [Social or residential care] | 94,533 |
| 87 exp School/ | 380,991 |
| 88 (education* adj (service* or facilit* or institution*)).tw,kw. | 6817 |
| 89 classroom*.tw,kw. | 20,247 |
| 90 school*.tw,kw. | 362,284 |
| 91 ((pupil* or school* or child* or education) and (referral adj1 (unit* or centre* or center* or facilit* or service*))).tw,kw. | 5796 |
| 92 (Kindergarten* or Nursery or pre-school*).tw,kw. | 25,560 |
| 93 or/87-92 [Educational institutions] | 650,724 |
| 94 ((exp ambulatory care/or exp healthcare facility/or exp hospital subdivisions/) and components/) or exp hospital/or exp rehabilitation center/ | 1,205,943 |
| 95 ((child* or young or p?ediatric or adolescent*) adj2 services).tw. (13648) | 13,648 |
| 96 exp health service/ | 5,458,744 |
| 97 (hospital? or ward?).tw,kw. | 1,764,428 |
| 98 (inpatient or patient).tw,kw. | 3,534,702 |
| 99 Intensive Care/ | 123,003 |
| 100 CAMHS.tw,kw. | 773 |
| 101 forensic*.tw,kw. | 65,695 |
| 102 ((health or medic* or psychiat* or mental) adj2 (service? or center? or centre? or department? or facilit*or ward? or unit?)).tw,kw. | 467,131 |
| 103 (“pediatric intensive care unit” or PICI or PICU).tw,kw. | 14,371 |
| 104 or/94-103 [Health care setting] | 8,790,988 |
| 105 immigrant/or exp refugee/ | 28,528 |
| 106 migration/or immigration/ | 45,846 |
| 107 ((asylum or refugee* or migrant* or immigrant* or immigration) adj4 (service* or center* or center* or department* or facilit* or unit* or reception or accommodation)).tw,kw. | 4551 |
| 108 or/105-107 [refugee settings] | 71,154 |
| 109 75 or 86 or 93 or 104 or 108 [Settings] | 9,264,068 |
| 110 54 and 65 and 109 | 6269 |
| 111 (seat or seats or seatbelt* or “road safety” or “passenger safety”).tw,kw. | 16,071 |
| 112 motor vehicle*.tw,kw. | 19,048 |
| 113 ((Road or Traffic) adj (injur* or trauma or accident*)).tw,kw. | 19,582 |
| 114 ((car or vehicle) adj (restraint* or safety or crash*)).tw,kw. | 5532 |
| 115 or/111-114 [seat belts] | 51,659 |
| 116 110 not 115 | 5684 |
| 117 exp animals/not exp human/ | 5,366,155 |
| 118 exp nonhuman/not exp human/ | 4,544,080 |
| 119 exp experimental animal/ | 689,337 |
| 120 exp veterinary medicine/ | 46,916 |
| 121 animal experiment/ | 2,478,525 |
| 122 or/117-121 [animal studies] | 7,591,696 |
| 123 116 not 122 | 5584 |
| 124 limit 123 to yr = “1989 -Current” (5120) | 5120 |
| ERIC 1966 to 30 January 2020 | |
| Same strategy as Criminal Justice Abstracts | |
| Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily 1946 to 20 January 2020 | |
| 1 Restraint, Physical/ | 11,724 |
| 2 Patient Isolation/or involuntary treatment/or involuntary treatment, psychiatric/ | 3880 |
| 3 coercion/ | 4528 |
| 4 (coercive or coercion or coerced).tw,kw. | 6212 |
| 5 restrain*.tw,kw. | 43,001 |
| 6 (seclusion or seclude*).tw,kw. | 1707 |
| 7 (restric* adj2 (practice* or intervention* or liberty)).tw,kw. | 1309 |
| 8 (de-escalat* or deescalat*).tw,kw. | 2309 |
| 9 (“calm down” or “soft word?” or “talk down”).tw,kw. | 91 |
| 10 ((comfort or safe or sensory) adj2 room?).tw,kw. | 116 |
| 11 ((weight* or comfort) adj1 blanket*).tw,kw. | 14 |
| 12 safety huddle?.tw,kw. | 32 |
| 13 safety plan?.tw,kw. | 339 |
| 14 (rapid* adj2 tranq*).tw,kw. | 132 |
| 15 ((prn or “pro re nata”) adj1 medicat*).tw,kw. | 201 |
| 16 (compulsion or compulsivity).tw,kw. | 1957 |
| 17 (involuntary adj3 medic*).tw,kw. | 154 |
| 18 (involuntary adj3 sedat*).tw,kw. | 12 |
| 19 (involuntary adj3 drug?).tw,kw. | 62 |
| 20 (forced adj3 medic?).tw,kw. | 2 |
| 21 (forced adj3 drug?).tw,kw. | 176 |
| 22 (forced adj3 treatment?).tw,kw. | 520 |
| 23 (forced adj3 sedat*).tw,kw. | 11 |
| 24 solitary confinement.tw. | 110 |
| 25 (lock* adj3 door*).tw,kw. | 187 |
| 26 (lock* adj3 ward?).tw,kw. | 136 |
| 27 ((lock* or locked or locks or locking) adj3 room?).tw,kw. | 122 |
| 28 (physical* adj (immobili* or control)).tw,kw. | 375 |
| 29 (patient? adj3 (isolation or segregation)).tw,kw. | 3120 |
| 30 (Violence adj5 (prevent* or manag*) adj5 training).tw,kw. | 122 |
| 31 (Aggress* adj5 (prevent* or manag*) adj5 training).tw,kw. | 91 |
| 32 (one-to-one adj2 nurs*).tw,kw. | 153 |
| 33 (holding adj3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive)).tw,kf. | 473 |
| 34 pain-compliance.tw,kw. | 13 |
| 35 (isolation adj3 (booth* or room*)).tw,kw. | 518 |
| 36 or/1-35 [Restraint Coercion or de escalation Practices] | 72,310 |
| 37 safewards.tw. | 23 |
| 38 “no force first”.tw. | 2 |
| 39 “six core strategies”.tw. | 19 |
| 40 “Roadmap to seclusion”.tw. | 0 |
| 41 “People are and feel safe”.tw. | 0 |
| 42 (“Creating Safety” adj5 training).tw. | 1 |
| 43 “crisis and aggression limitation and management”.tw. | 1 |
| 44 (CALM and (cris#s adj6 manag*)).tw. | 6 |
| 45 (CALM adj (training or intervention or program*)).tw. | 25 |
| 46 (MAPA adj (training or intervention or program*)).tw. | 0 |
| 47 (MAPA adj5 (aggress* or cris#s)).tw. | 0 |
| 48 “manag* of actual or potential aggress*”.tw,kw. | 0 |
| 49 “ReSTRAIN YOURSELF”.tw. | 6 |
| 50 (“Positive and Safe” adj (team? or plan?)).tw. | 0 |
| 51 “Proactive Management of Integrated Service* and Environment*”.tw. | 2 |
| 52 “Br#set Violence Checklist*”.tw. | 31 |
| 53 or/37-52 [Restraint reduction programmes] | 111 |
| 54 36 or 53 [Restraint practices or programmes] | 72,376 |
| 55 (child* or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric* or juvenil*).tw. | 1,824,786 |
| 56 (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”).tw. | 473,184 |
| 57 adolescent behavior/ | 29,867 |
| 58 Infant Behavior/ | 3395 |
| 59 child behavior/ | 18,044 |
| 60 child/ | 1,655,935 |
| 61 infant/ | 777,831 |
| 62 child, preschool/ | 901,017 |
| 63 adolescent health/or child health/or infant health/ | 3654 |
| 64 Adolescent/ | 1,985,884 |
| 65 or/55-64 [Children] | 3,905,593 |
| 66 ((youth or young) adj2 offend*).tw,kf. | 717 |
| 67 ((child or childhood or children or adolescen* or teen* or girl? or boy? or p?ediatric* or juvenil*) adj offend*).tw,kf. | 1020 |
| 68 Juvenile Delinquency/ | 8479 |
| 69 prisons/ | 9404 |
| 70 prisoners/or criminals/ | 20,252 |
| 71 (police* or custody or prison* or jail* or detain* or inmate*).tw,kf. | 38,215 |
| 72 incarcerat*.tw,kw. | 11,201 |
| 73 detention.tw,kw. | 2897 |
| 74 juvenile justice.tw,kw. | 1074 |
| 75 or/66-74 [Criminal Justice Setting] | 66,001 |
| 76 foster home care/ | 3568 |
| 77 residential facilities/or assisted living facilities/or group homes/or orphanages/ | 7995 |
| 78 (secure adj3 (home* or accommodation or unit* or centre* or center* or service* or facilit*)).tw,kw. | 996 |
| 79 ((foster or residential) adj (care or home*)).tw,kf. | 6673 |
| 80 (Children* adj home*).tw,kw. | 984 |
| 81 orphan*.tw,kf. | 16,689 |
| 82 ((foster* or “looked after”) and child*).tw,kw. | 6054 |
| 83 social care.tw,kf. | 5965 |
| 84 exp Social Work/ | 17,378 |
| 85 social worker*.tw,kf. | 9541 |
| 86 or/76-85 [Social or residential care] | 64,880 |
| 87 exp Schools/ | 115,264 |
| 88 (education* adj (service* or facilit* or institution*)).tw,kf. | 5194 |
| 89 classroom*.tw,kf. | 16,539 |
| 90 school*.tw,kf. | 276,091 |
| 91 ((pupil* or school* or child* or education) and (referral adj1 (unit* or centre* or center* or facilit* or service*))).tw,kf. | 3537 |
| 92 (Kindergarten* or Nursery or pre-school*).tw,kf. | 19,781 |
| 93 or/87-92 [Educational institutions] | 362,644 |
| 94 exp ambulatory care facilities/or exp “facility design and construction”/or exp hospital units/or exp hospitals/or exp rehabilitation centers/ | 437,574 |
| 95 ((child* or young or p?ediatric or adolescent*) adj2 services).tw. | 9902 |
| 96 exp health services/ | 2,083,410 |
| 97 (hospital? or ward?).tw,kf. | 1,130,394 |
| 98 (inpatient or patient).tw,kf. | 2,215,426 |
| 99 Intensive Care Units, Pediatric/ | 7380 |
| 100 CAMHS.tw,kf. | 361 |
| 101 forensic*.tw,kf. | 44,153 |
| 102 ((health or medic* or psychiat* or mental) adj2 (service? or center? or centre? or department? or facilit*or ward? or unit?)).tw,kf. | 337,422 |
| 103 (“pediatric intensive care unit” or PICI or PICU).tw,kw. | 7535 |
| 104 or/94-103 [Health care setting] | 4,846,730 |
| 105 Refugees/or “Emigration and Immigration”/or exp “Emigrants and Immigrants”/ | 43,513 |
| 106 ((asylum or refugee* or migrant* or immigrant* or immigration) adj4 (service* or center* or center* or department* or facilit* or unit* or reception or accommodation)).tw,kw. | 4607 |
| 107 or/105-106 [refugee setting] | 45,132 |
| 108 75 or 86 or 93 or 104 or 107 [Settings] | 5,190,254 |
| 109 54 and 65 and 108 | 5376 |
| 110 Seat Belts/ | 3789 |
| 111 (seat or seats or seatbelt* or “road safety” or “passenger safety”).tw,kw. | 12,177 |
| 112 motor vehicle*.tw,kw. | 14,164 |
| 113 ((Road or Traffic) adj (injur* or trauma or accident*)).tw,kw. | 14,192 |
| 114 ((car or vehicle) adj (restraint* or safety or crash*)).tw,kw. | 4600 |
| 115 or/110-114 [seatbelts] | 39,265 |
| 116 109 not 115 | 4855 |
| 117 exp Animals/not exp Humans/ | 4,665,657 |
| 118 116 not 117 | 4846 |
| 119 limit 118 to yr = “1989 -Current” | 4290 |
| PsycInfo (Ovid) 1806 to January Week 2 2020 | |
| 22-0 1 Physical Restraint | 2080 |
| 2 Patient seclusion | 500 |
| 3 coercion/or exp Involuntary Treatment/ | 3369 |
| 4 (coercive or coercion or coerced).tw,id. | 9212 |
| 5 restrain*.tw,id. | 14,924 |
| 6 (seclusion or seclude*).tw,id. | 1619 |
| 7 (restric* adj2 (practice* or intervention* or liberty)).tw,id. | 603 |
| 8 (de-escalat* or deescalat*).tw,id. (629) | 629 |
| 9 (“calm down” or “soft word?” or “talk down”).tw,id. | 122 |
| 10 ((comfort or safe or sensory) adj2 room?).tw,id. | 67 |
| 11 ((weight* or comfort) adj1 blanket*).tw,id. | 11 |
| 12 safety huddle?.tw,id. | 2 |
| 13 safety plan?.tw,id. | 226 |
| 14 (rapid* adj2 tranq*).tw,id. | 123 |
| 15 ((prn or “pro re nata”) adj1 medicat*).tw,id. | 142 |
| 16 (compulsion or compulsivity).tw,id. | 4013 |
| 17 (involuntary adj3 medic*).tw,id. | 194 |
| 18 (involuntary adj3 sedat*).tw,id. | 6 |
| 19 (involuntary adj3 drug?).tw,id. | 44 |
| 20 (forced adj3 medic?).tw,id. | 0 |
| 21 (forced adj3 drug?).tw,id. | 73 |
| 22 (forced adj3 treatment?).tw,id. | 206 |
| 23 (forced adj3 sedat*).tw,id. | 5 |
| 24 “solitary confinement”.tw. | 203 |
| 25 ((lock or locked) adj3 door*).tw,id. | 170 |
| 26 ((lock or locked) adj3 ward*).tw,id. | 183 |
| 27 ((lock* or locked or locks or locking) adj3 room?).tw,id. | 119 |
| 28 (physical* adj (immobili* or control)).tw,id. | 140 |
| 29 (patient? adj3 (isolation or segregation)).tw,id. | 290 |
| 30 (Violence adj5 (prevent* or manag*) adj5 training).tw,id. | 160 |
| 31 (Aggress* adj5 (prevent* or manag*) adj5 training).tw,id. | 131 |
| 32 (one-to-one adj2 nurs*).tw,id. | 36 |
| 33 (holding adj3 (therapeutic or parent* or procedure* or clinical or physical or treatment or safe or supportive)).tw,id. | 378 |
| 34 pain-compliance.tw,id. | 6 |
| 35 (isolation adj3 (booth* or room*)).tw,id. | 53 |
| 36 or/1-35 [Restraint Coercion or de escalation Practices] | 33,345 |
| 37 safewards.tw. | 15 |
| 38 “no force first”.tw. | 1 |
| 39 “six core strategies”.tw. | 19 |
| 40 “Roadmap to seclusion”.tw. | 0 |
| 41 “People are and feel safe”.tw. | 0 |
| 42 (“Creating Safety” adj5 training).tw. | 1 |
| 43 “crisis and aggression limitation and management”.tw. | 0 |
| 44 (CALM and (cris#s adj6 manag*)).tw. | 6 |
| 45 (CALM adj (training or intervention or program*)).tw. | 23 |
| 46 (MAPA adj (training or intervention or program*)).tw. | 0 |
| 47 (MAPA adj5 (aggress* or cris#s)).tw. | 0 |
| 48 “manag* of actual or potential aggress*”.tw,id. | 0 |
| 49 “ReSTRAIN YOURSELF”.tw. | 4 |
| 50 (“Positive and Safe” adj (team? or plan?)).tw. | 0 |
| 51 “Proactive Management of Integrated Service* and Environment*”.tw. | 1 |
| 52 “Br#set Violence Checklist*”.tw. | 32 |
| 53 or/37-52 [Restraint reduction programmes] | 100 |
| 54 36 or 53 [Restraint practices or programmes] | 33,403 |
| 55 (child* or adolescen*).ag. | 773,653 |
| 56 (child or childhood or children or adolescen* or teen or teens or teenager* or youth or youths or girl or girls or boy or boys or p?ediatric* or juvenil*).tw. | 901,563 |
| 57 (infant or infants or “young people” or “young person” or “young adult” or “ young m?n” or “young wom?n” or “schoolchild*”).tw. | 132,121 |
| 58 adolescent attitudes/ | 19,619 |
| 59 child attitudes/ | 7212 |
| 60 preschool students/ | 10,874 |
| 61 or/55-60 [Children] | 1,169,277 |
| 62 ((youth or young) adj2 offend*).tw,id. | 2216 |
| 63 ((child or childhood or children or adolescen* or teen* or girl? or boy? or p?ediatric* or juvenil*) adj offend*).tw,id. | 3636 |
| 64 Juvenile Delinquency/or juvenile justice/ | 18,531 |
| 65 prisons/or exp correctional institutions/or incarceration/ | 13,537 |
| 66 prisoners/or criminal behavior/or legal detention/ | 19,679 |
| 67 (police* or custody or prison* or jail* or inmate* or detain*).tw,id. | 56,775 |
| 68 incarcerat*.tw,id. | 12,556 |
| 69 detention.tw,id. | 3511 |
| 70 juvenile justice.tw,id. | 3756 |
| 71 or/62-70 [Criminal Justice Setting] | 88,635 |
| 72 foster care/ | 5842 |
| 73 residential care institutions/or assisted living/or group homes/or orphanages/ | 12,198 |
| 74 (secure adj3 (home* or accommodation or unit* or centre* or center* or service* or facilit*)).tw. | 1435 |
| 75 ((foster or residential) adj (care or home*)).tw,id. | 11,091 |
| 76 (Children* adj home*).tw,id. | 1040 |
| 77 ((foster* or “looked after”) and child*).tw,id. | 15,649 |
| 78 orphan*.tw,id. | 3314 |
| 79 social care.tw,id. | 4166 |
| 80 exp Social Work/ | 17,911 |
| 81 social worker*.tw,id. | 24,405 |
| 82 or/72-81 [Social or residential care] | 72,388 |
| 83 exp Schools/ | 67,633 |
| 84 (education* adj (service* or facilit* or institution*)).tw,id. | 10,781 |
| 85 classroom*.tw,id. | 89,044 |
| 86 school*.tw,id. | 398,015 |
| 87 ((pupil* or children or child or education) and (referral adj1 (unit* or centre* or center* or facilit* or service*))).tw,id. | 354 |
| 88 (Kindergarten* or Nursery or pre-school*).tw,id. | 25,141 |
| 89 or/83-88 [Educational institutions] | 470,238 |
| 90 exp healthcare facilities/or exp hospital environment/or exp hospitals/or exp rehabilitation centers/ | 26,176 |
| 91 ((child* or young or p?ediatric or adolescent*) adj2 services).tw. | 10,093 |
| 92 exp health services/ | 0 |
| 93 (hospital? or ward?).tw,id. | 131,559 |
| 94 (inpatient or patient).tw,id. | 264,410 |
| 95 Intensive Care/ | 4132 |
| 96 CAMHS.tw,id. | 590 |
| 97 forensic*.tw,id. | 19,051 |
| 98 ((health or medic* or psychiat* or mental) adj2 (service? or center? or centre? or department? or facilit* or ward? or unit?)).tw,id. | 117,231 |
| 99 (“pediatric intensive care unit” or PICI or PICU).tw,id. | 506 |
| 100 or/90-99 [Health care setting] | 458,342 |
| 101 refugees/or immigration/or Asylum Seeking/ | 26,542 |
| 102 ((asylum or refugee* or migrant* or immigrant* or immigration) adj4 (service* or center* or center* or department* or facilit* or unit* or reception or accommodation)).tw,id. | 4247 |
| 103 or/101-102 [refugee settings] | 27,552 |
| 104 71 or 82 or 89 or 100 or 103 [Settings] | 1,041,327 |
| 105 54 and 61 and 104 | 3126 |
| 106 (seat or seats or seatbelt* or “road safety” or “passenger safety”).tw,id. | 5169 |
| 107 exp Safety Belts/ | 581 |
| 108 motor vehicle*.tw,id. | 3785 |
| 109 ((Road or Traffic) adj (injur* or trauma or accident*)).tw,id. | 2904 |
| 110 ((car or vehicle) adj (restraint* or safety or crash*)).tw,id. | 1460 |
| 111 or/106-110 [seatbelts] | 11,495 |
| 112 105 not 111 | 3056 |
| 113 limit 112 to yr = “1989 -Current” | 2624 |
| Scopus (Elsevier B.V.) 1823 to 13 June 2019 | |
| ((TITLE-ABS ((infant OR infants OR young OR schoolchild* OR child OR childhood OR children OR adolescen* OR teen OR teens OR teenager* OR youth OR youths OR girl OR girls OR boy OR boys OR pediatric* OR paediatric* OR juvenil*))) AND ((TITLE-ABS ((holding W/2 (therapeutic OR parent* OR procedure* OR clinical OR physical OR treatment OR safe OR supportive)))) OR (TITLE-ABS ((aggress* W/4 (prevent* OR manag*) W/4 training))) OR (TITLE-ABS ((violence W/4 (prevent* OR manag*) W/4 training))) OR (TITLE-ABS (one-to-one W/1 nurs*)) OR (TITLE-ABS ((patient* W/1 (isolation OR segregation)))) OR (TITLE-ABS ((physical* W/1 (immobili* OR control)))) OR (TITLE-ABS ((lock OR locked OR locking) W/1 (door* OR ward* OR room*))) OR (TITLE-ABS (forced W/1 (medic* OR sedat* OR drug* OR treatment*))) OR (TITLE-ABS (involuntary W/1 (medic* OR sedat* OR drug* OR treatment*))) OR (TITLE-ABS ((prn OR “pro re nata”) W/1 medicat*)) OR (TITLE-ABS ((rapid* AND tranq*))) OR (TITLE-ABS (safety W/1 (huddle* OR plan*))) OR (TITLE-ABS (((weight* OR comfort) W/1 blanket*))) OR (TITLE-ABS (((comfort OR safe OR sensory) W/2 room*))) OR (TITLE-ABS (restric* W/2 (practice* OR intervention* OR liberty))) OR (TITLE-ABS (isolation OR “calm down” OR “soft word*” OR “talk down” OR de-escalat* OR deescalat* OR seclusion OR seclude* OR restrain*))) AND ((TITLE-ABS ((youth OR young OR juvenile) W/1 offend*)) OR (TITLE-ABS (“juvenile justice” OR incarcerat* OR detention OR custody OR prison* OR jail* OR inmate* OR detain* OR “juvenile delinquen*”)) OR (TITLE-ABS ((secure W/2 (home* OR accommodation OR unit* OR centre* OR center* OR service* OR facilit*))) OR (TITLE-ABS (((foster OR residential) W/2 (care OR home*)))) OR (TITLE-ABS ((children* W/1 home*))) OR (TITLE-ABS (((foster OR “looked after”) W/2 child*)))) OR (TITLE-ABS (“Foster Care” OR “assisted living” OR orphanage* OR “Residential Care” OR “social worker*” OR “social work” OR “social care” OR orphan*)) OR (TITLE-ABS ((pupil* OR school* OR child* OR education) W/2 referral)) OR (TITLE-ABS ((education* W/1 (service* OR facilit* OR institution*)))) OR (TITLE-ABS (kindergarten* OR nursery OR pre-school* OR classroom* OR school*)) OR (TITLE-ABS ((asylum OR refugee* OR migrant* OR immigrant* OR immigration) W/4 (service* OR center* OR center* OR department* OR facilit* OR unit*))) OR (TITLE-ABS (((health OR medic* OR psychiatr* OR mental) W/1 (service* OR center* OR center* OR department* OR facilit* OR unit* OR Ward*)))) OR (TITLE-ABS ((child* OR young OR pediatric OR paediatric OR Adolescent*) W/2 services)))) AND NOT ((seat or seats or seatbelt* or “road safety” or “passenger safety”) or (((Road or Traffic) W/1 (injur* or trauma or accident*))) or (((car or vehicle) W/1 (restraint* or safety or crash*)))) AND (EXCLUDE (SUBJAREA,”IMMU”) OR EXCLUDE (SUBJAREA,”BIOC”) OR EXCLUDE (SUBJAREA,”AGRI”) OR EXCLUDE (SUBJAREA,”ENGI”) OR EXCLUDE (SUBJAREA,”VETE”) OR EXCLUDE (SUBJAREA,”MATE”) OR EXCLUDE (SUBJAREA,”PHYS”) OR EXCLUDE (SUBJAREA,”CHEM”) OR EXCLUDE (SUBJAREA,”CENG”)) AND (LIMIT-TO (PUBYEAR,2019) OR LIMIT-TO (PUBYEAR,2018) OR LIMIT-TO (PUBYEAR,2017) OR LIMIT-TO (PUBYEAR,2016) OR LIMIT-TO (PUBYEAR,2015) OR LIMIT-TO (PUBYEAR,2014) OR LIMIT-TO (PUBYEAR,2013) OR LIMIT-TO (PUBYEAR,2012) OR LIMIT-TO (PUBYEAR,2011) OR LIMIT-TO (PUBYEAR,2010) OR LIMIT-TO (PUBYEAR,2009) OR LIMIT-TO (PUBYEAR,2008) OR LIMIT-TO (PUBYEAR,2007) OR LIMIT-TO (PUBYEAR,2006) OR LIMIT-TO (PUBYEAR,2005) OR LIMIT-TO (PUBYEAR,2004) OR LIMIT-TO (PUBYEAR,2003) OR LIMIT-TO (PUBYEAR,2002) OR LIMIT-TO (PUBYEAR,2001) OR LIMIT-TO (PUBYEAR,2000) OR LIMIT-TO (PUBYEAR,1999) OR LIMIT-TO (PUBYEAR,1998) OR LIMIT-TO (PUBYEAR,1997) OR LIMIT-TO (PUBYEAR,1996) OR LIMIT-TO (PUBYEAR,1995) OR LIMIT-TO (PUBYEAR,1994) OR LIMIT-TO (PUBYEAR,1993) OR LIMIT-TO (PUBYEAR,1992) OR LIMIT-TO (PUBYEAR,1991) OR LIMIT-TO (PUBYEAR,1990) OR LIMIT-TO (PUBYEAR,1989)) | 3292 |
Grey literature sources including social media
Agency for Healthcare Research and Quality.
AGENDA: Alliance for Women & Girls At Risk.
Article 39.
Barnardo’s.
British Association of Social Workers.
British Institute of Learning Disabilities.
British Society of Criminology.
Challenging Behaviour Foundation.
Children’s Society.
Crisis Prevention Institute (CPI).
Foundation for Professionals in Services to Adolescents.
Google.
HM Inspector of Constabulary and HM Inspector of Fire & Rescue Services.
HM Inspectorate of Prisons for England and Wales.
HM Inspectorate of Probation.
Howard League.
INQUEST.
MENCAP.
National Children’s Bureau.
National Police Library.
National Society for the Prevention of Cruelty to Children.
National Youth Work.
Prison Reform Trust.
Prisons and Probation Ombudsman.
ProQuest Dissertations & Theses A&I (Proquest) 1743 to 24 January 2020.
Restraint reduction network.
SAFE crisis management.
SCIE.
Secure Children’s Homes/Secure accommodation network.
Social Care Online (SCIE) 1980 – 28 January 2020.
Twitter.
Young Minds.
Youth Justice Board for England and Wales.
Note that the number of records listed for the website searches include duplicates found during the update search.
| Source | Website | Date searched | Searches | Total number of records |
|---|---|---|---|---|
| Agency for Healthcare Research and Quality | www.ahrq.gov/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 21 |
| 28 January 2020 | Used advanced search field ‘Results with a least one of the words’. Searched for string: restraint coercive coercion restrict de-escalate de-escalation restrictive restraints restrained coerced restricted. In TI only | |||
| Agenda, the alliance for women & girls at risk | https://weareagenda.org/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications | 17 |
| 28 January 2020 | Browsed all research articles. Also searched for term ‘Restraint’ | |||
| Article 39 | https://article39.org.uk | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications | 20 |
| 28 January 2020 | Browed all publications in publications library | |||
| Barnardo’s | www.barnardos.org.uk/ | 31 July 2019 | No search function. All sections browsed | 26 |
| 28 January 2020 | Browsed all reports in publications www.barnardos.org.uk/get-involved/campaign-with-us/publications | |||
| The British Association of Social Workers (BASW) | www.basw.co.uk/ | 31 July 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour (in resources section) | 85 |
| 28 January 2020 | Searched as a string in Resources section: restraint coerce de-escalate de-escalation restrained seclusion restrictive coercion coercive. Refined to Specialism Children and Families | |||
| British Institute of Learning Disabilities | www.bild.org.uk/ | 6 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 96 |
| 28 January 2020 | In webpage search box searched as one string: restraint restraints restrain restrict coercive coerce coercion de-escalate de-escalation restrictive | |||
| British Society of Criminology (BSC) | www.britsoccrim.org/ | 1 August 2019 | No search function. Browsed publications, and conference sections | 1 |
| 28 January 2020 | Browsed publications and conference sections | |||
| The Challenging Behaviour Foundation | www.challengingbehaviour.org.uk/ | 6 August 2019 | No search functionally. Browsed website | 33 |
| 28 January 2020 | Searched ‘restraint’ and ‘child’ in webpage search box | |||
| The Children’s Society | www.childrenssociety.org.uk/ |
1 August 2019 28 January 2020 |
Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 5 |
| Navigated website from What we do > Publications library then searched above terms | ||||
| Crisis Prevention Institute (CPI) | www.crisisprevention.com/ | 6 August 2019 | No search functionally. Browsed website | 20 |
| 28 January 2020 | Browsed Resources > Topic = restraint reduction | |||
| Foundation for Professionals in Services to Adolescents | www.foundationpsa.org.uk/ | 31 July 2019 | No search function. Browsed Resources, Reports and News sections | 2 |
| 28 January 2020 | Browsed Resources, Reports and News sections | |||
| 8 August 2019 |
Searched the 1st 25 countries in the Legatum Prosperity Index (ranked for Health) www.prosperity.com/rankings Norway, Netherlands, USA, New Zealand, Ireland, Slovenia, Finland, Iceland, Malta, Switzerland, Luxembourg, France, Denmark, Australia, Singapore, Sweden, Germany, Hong Kong, UK, Austria, Japan, Canada, Belgium, Portugal, Spain Google Advanced Search interface For each country searched allintitle: restraint site:.no filetype:pdf allintitle: seclusion site:.no filetype:pdf allintitle: coercion site:.no filetype:pdf Note, in this example the site:.no refers to the country domain.no for Norway |
1825 | ||
| 29 January 2020 |
Searched the 25 country domains as above but limited to content added to Google in last 12 months. Also, used a search string for seclusion restraint coercion For each country searched: any of the words: restraint seclusion coercion last update: upto a year ago site or domain:.no terms appearing: allintitle file type: pdf |
124 | ||
| HM Inspector of Constabulary and HM Inspector of Fire & Rescue Services | www.justiceinspectorates.gov.uk/hmicfrs/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 38 |
| 28 January 2020 | Entered into webpage search box: (restraint restraints restrictive coercive coerce coercion de-escalate de-escalation) AND (child adolescent juvenille youth). Then limited to 2020 or dates since July 2019 using date filters | |||
| HM Inspectorate of Prisons for England and Wales | www.justiceinspectorates.gov.uk/hmiprisons | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 16 |
| 28 January 2020 | Used search string: Search string: restraint restraints coercion coerce coercive de-escalation de-escalate behaviour restrictive. Then limited to 2020 or dates since July 2019 using date filters | |||
| HM Inspectorate of Probation | www.justiceinspectorates.gov.uk/hmiprobation/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 31 |
| 28 January 2020 | Used search string: Search string: restraint restraints coercion coerce coercive de-escalation de-escalate behaviour restrictive. Then limited to 2020 or dates since July 2019 using date filters | |||
| The Howard League for Penal Reform | https://howardleague.org/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications and research | 33 |
| 28 January 2020 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications and research | |||
| INQUEST | www.inquest.org.uk/ | 1 August 2019 | No search function. Browsed research and policy section | 4 |
| 28 January 2020 | Browsed research and policy section | |||
| MENCAP | www.mencap.org.uk/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 123 |
| 28 January 2020 | Used search string restraint restrict coerce coercive coercion de-escalate de-escalation behaviour | |||
| National Children’s Bureau | www.ncb.org.uk/ | 31 July 2019 | No search function. All sections browsed | 0 |
| 28 January 2020 | All sections browsed | |||
| National Police Library | https://library.college.police.uk/HeritageScripts/Hapi.dll/search1 | 30 July 2019 | Separate searches for restrain* or restrain* or coercive or coercion or coerced or seclude or seclusion or seclusive or de-escalat* | 413 |
| 28 January 2020 | Searched in ‘All Fields’ for (restrict* OR restrain* OR coercive OR coercion OR coerced OR seclude OR seclusion OR seclusive OR de-escalat* OR immobili*) AND (child* OR teen* OR adolescen* OR youth* OR young* OR infant* OR juvenil*) | 128 | ||
| National Youth Work | https://nya.org.uk/ | 31 July 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 17 |
| 28 January 2020 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | |||
| NSPCC | www.nspcc.org.uk/? | 31 July 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour and all sections browsed | 3 |
| 28 January 2020 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, and all sections browsed | |||
| Prisons and Probation Ombudsman | www.ppo.gov.uk/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 18 |
| 28 January 2020 | As above but combined with child youth young | |||
| Prison Reform Trust | www.prisonreformtrust.org.uk/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications | 8 |
| 28 January 2020 | Browsed 2019–20 publications | |||
| ProQuest Dissertations & Theses A&I (Proquest) 1743 to 24-01-2020 | Date range searched: 1743 to 24 January 2020 Same search strategy as ASSIA | 2473 | ||
| Restraint Reduction Network | www.restraintreductionnetwork.org | 6 August 2019 | No search functionally. Browsed website | 42 |
| 29 January 2020 | https://restraintreductionnetwork.org/toolsandresources/Tools and Resources screened | |||
| Safe Crisis Management | www.safecrisismanagement.org/ | 6 August 2019 | No search functionally. Browsed website | 0 |
| 28 January 2020 | Browsed website | |||
| Secure Children’s Homes/Secure Accommodation Network |
www.securechildrenshomes.org.uk/ www.securechildrenshomes.org.uk/secure-accommodation-network/ |
31 July 2019 | No search function. All sections browsed | 0 |
| 28 January 2020 | All sections browsed | |||
| Social Care Institute for Excellence (SCIE) | www.scie.org.uk/ | 30 July 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation (auto truncates) | 18 |
| 28 January 2020 | Browsed SCIE Resources and services within the SCIE websites | |||
| Social Care Online (SCIE) 1980 to 28-01-2020 | 28 January 2020 |
Used Advanced search interface (1) - SubjectTerms:’”children” ‘including narrower terms – OR SubjectTerms:’ ”young people” ‘including narrower terms – OR AllFields:’child*’ – OR AllFields:’teen*’ – OR AllFields:’paediatric’ – OR AllFields:’paediatric’ – OR AllFields:’adolescent’ – OR AllFields:’juvenile’ – OR AllFields:’youth’ – OR AllFieldsExact:’young person’ – OR AllFieldsExact:’young people’] |
64,325 | |
| (2) – SubjectTerms:’”restraint” ‘including this term only – OR SubjectTerms:’”physical restraint” ‘including this term only – OR SubjectTerms:’”compulsory treatment” ‘including this term only – OR AllFields:’restrain’ – OR AllFields:’”restraint” ‘– OR AllFieldsExact:’restrictive’ *this reduced count significantly a got rid of a lot of unrelated papers – OR AllFields:’coercive’ – OR AllFields:’coercion’ – OR AllFields:’coerced’ – OR AllFields:’seclude’ – OR AllFields:’seclusive’ – OR AllFields:’seclusion’ – OR AllFields:’de-escalate’ – OR AllFields:’de-escalation’ – OR AllFields:’isolation booth’ – OR AllFields:’clinical holding’ – OR AllFields:’physical holding’ – OR AllFields:’immobilisation’ – OR AllFields:’immobilisation’ | 1842 | |||
| Child (1) AND Restraint (2) search combined | 270 | |||
| 8 August 2019 |
#restraintReduction #training #restraint #training #seclusion |
5 | ||
| 28 January 2020 |
#restraintReduction #training #restraint #training #seclusion |
11 | ||
| YoungMinds | https://youngminds.org.uk/ | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour. Browsed publications | 58 |
| 28 January 2020 | Used search string: restraint restrict restraints restrictive coercive coerce coercion de-escalate de-escalation | |||
| Youth Justice Board for England and Wales | www.gov.uk/government/organisations/youth-justice-board-for-england-and-wales | 1 August 2019 | Separate searches for restraint, restrict, coercive, coerce, coercion, de-escalate, de-escalation, behaviour | 31 |
| 28 January 2020 | Browsed policies, research and guidance sections |
Appendix 2 Included records
| Author(s) | Title | Journal/source | F | Year | Intervention name |
|---|---|---|---|---|---|
| Evaluations | |||||
| Azeem M, Aujla A, Rammerth M, Binsfeld G, Jones RB | Effectiveness of six core strategies based on trauma informed care in reducing seclusions and restraints at a child and adolescent psychiatric hospital | JCAPN | 1 | 2017 | ‘six core strategies based on trauma informed care’ |
| Bobier C, Boon T, Downward M, Loomes B, Mountford H, Swadi H | Pilot investigation of the use and usefulness of a sensory modulation room in a child and adolescent psychiatric inpatient unit | Occup Ther Ment Health | 1 | 2015 | ‘sensory modulation room’ |
| Boel-Studt SM | A quasi-experimental study of trauma-informed psychiatric residential treatment for children and adolescents | Res Soc Work Pract | 1 | 2017 | TI-PRC |
| Bonnell W, Alatishe YA, Hofner A | The effects of a changing culture on a child and adolescent psychiatric inpatient unit | J Can Acad Child Adolesc Psychiatry | 1 | 2014 | CPS |
| Borckardt JJ, Madan A, Grubaugh AL, Danielson CK, Pelic CG, Hardesty SJ, et al. | Systematic investigation of initiatives to reduce seclusion and restraint in a state psychiatric hospital | Psychiatr Serv | 1 | 2011 | engagement model (adaptation from the work of Bloom) |
| Campbell N | STAR project outcomes | Resid Group Care Q | 2 | 2004 | STAR |
| Craig JH, Sanders KL | Evaluation of a program model for minimizing restraint and seclusion | Adv Neurodev Disord | 1 | 2018 | Trauma informed approach (TIA). Comfort vs. control. ‘program model for minimizing restraint and seclusion’ |
| Craig JH | Evaluation of a program model for minimizing restraint and seclusion | Diss Abstr B Sci Eng | 7 | 2015 | ‘program model for minimizing restraint and seclusion’ (Grafton model) |
| Crosland KA, Cigales M, Dunlap G, Neff B, Clark HB, Giddings T, et al. | Using staff training to decrease the use of restrictive procedures at two facilities for foster care children | Res Soc Work Pract | 1 | 2008 | BASP |
| Dean AJ, Duke SG, George M, Scott J | Behavioral management leads to reduction in aggression in a child and adolescent psychiatric inpatient unit | JAACAP | 1 | 2007 | ‘milieu-based behavioral management program’ |
| Deveau R, Leitch S | The impact of restraint reduction meetings on the use of restrictive physical interventions in English residential services for children and young people | Child Care Health Dev | 1 | 2015 | RRM |
| Eblin A | Reducing seclusion and restraints on the inpatient child and adolescent behavioral health unit: a quality improvement study | JCAPN | 1 | 2019 | ‘quality improvement’ |
| Elwyn L, Esaki N, Smith C | Importance of leadership and employee engagement in trauma-informed organizational change at a girls’ juvenile justice facility | Hum Serv Organ Manag Lead Gov | 1 | 2017 | The Sanctuary Model |
| Ercole-Fricke E, Fritz P, Hill LE, Snelders J | Effects of a collaborative problem-solving approach on an inpatient adolescent psychiatric unit | JCAPN | 1 | 2016 | CPS |
| Ercole-Fricke E | Effects of a collaborative problem solving approach on an inpatient adolescent psychiatric unit | Diss Abstr B Sci Eng | 7 | 2014 | CPS |
| Farina MV | Toward reducing the utilization of seclusion and restraint: Exploring a paradigm shift and its success | Diss Abstr B Sci Eng | 7 | 2007 | evaluation of impact of new seclusion and restraint policy |
| Finnie HM | The collaborative problem-solving approach with traumatized children: Its effectiveness in the reduction of locked seclusion in an inpatient psychiatric setting | Thesis | 7 | 2013 | CPS |
| Ford JD, Hawke J | Trauma affect regulation psychoeducation group and milieu intervention outcomes in juvenile detention facilities | J Aggress Maltreat Trauma | 1 | 2012 | TARGET |
| Forrest S, Gervais R, Lord KA, Sposato A, Martin L, Beserra K, Spinazzola J | Building Communities of Care: a comprehensive model for trauma informed youth capacity building and behavior management in residential services | Resid Treat Child Youth | 1 | 2018 | BCC |
| Fowler NA | Aromatherapy, used as an integrative tool for crisis management by adolescents in a residential treatment center | JCAPN | 1 | 2006 | ‘aromatherapy for crisis management’ |
| Fralick SL | A restraint utilization project | Nurs Adm Q | 1 | 2007 | Rapid Cycle Model for Improvement |
| Glew B-A | Reducing the Use of Seclusion and Restraint in Segregated Special Education School Settings Through Implementation of the Collaborative Problem Solving Model | Thesis | 7 | 2012 | CPS |
| Greene RW, Ablon JS, Hassuk B, Regan KM, Martin A. | Innovations: child & adolescent psychiatry: use of collaborative problem solving to reduce seclusion and restraint in child and adolescent inpatient units | Psychiatr Serv | 1 | 2006 | CPS |
| Hallman IS, O’Connor N, Hasenau S, Brady S | Improving the culture of safety on a high-acuity inpatient child/adolescent psychiatric unit by mindfulness-based stress reduction training of staff | JCAPN | 1 | 2014 | Mindfulness-based Stress Reduction training program |
| Hambrick EP, Brawner TW, Perry BD, Wang EY, Griffin G, DeMarco T, et al. | Restraint and critical incident reduction following introduction of the neurosequential model of therapeutics (NMT) | Resid Treat Child Youth | 1 | 2018 | NMT |
| Health Sciences Center Winnipeg | WCB Workplace Innovation Project | Report | 4 | 2015 | 6CS |
| Hellerstein DJ, Staub AB, Lequesne E | Decreasing the use of restraint and seclusion among psychiatric inpatients | J Psychiatric Pract | 1 | 2007 | ‘hospital-wide effort’ |
| Hodgdon HB, Kinniburgh K, Gabowitz D, Blaustein ME, Spinazzola J | Development and implementation of trauma-informed programming in youth residential treatment centers using the ARC framework | J Fam Violence | 1 | 2013 | ARC framework |
| Holstead J, Lamond D, Dalton J, Horne A, Crick R | Restraint reduction in children’s residential facilities: implementation at Damar Services | Resid Treat Child Youth | 1 | 2010 | ‘restraint reduction initiative‘ |
| Huckshorn KA | Preventing Violence, Trauma, and the Use of Seclusion and Restraint in Mental Health Settings: Preventing Conflict, Violence and the use of Seclusion/Restraint | Workshop slides (unpublished) | 10 | 2010 | 6CS |
| Jani, Knight S, Jani S | The implementation of milieu therapy training to reduce the frequency of restraints in residential treatment centers | Adolesc Psychiatry | 1 | 2011 | milieu therapy training and CPS |
| Jones RJ, Timbers GD | Minimizing the need for physical restraint and seclusion in residential youth care through skill-based treatment programming | Fam Soc | 1 | 2003 | Teaching-Family Model |
| Jonikas JA, Cook JA, Rosen C, Laris A, Kim JB | A program to reduce use of physical restraint in psychiatric inpatient facilities | Psychiatr Serv | 1 | 2004 | ‘a program to reduce the use of physical restraint’ |
| Kalogjera IJ, Bedi A, Watson WN, Meyer AD | Impact of therapeutic management on use of seclusion and restraint with disruptive adolescent inpatients | Hosp Community Psychiatry | 1 | 1989 | ‘therapeutic management’ |
| Kaltiala-Heino R, Berg J, Selander M, Työläjärvi M, Kahila K | Aggression management in an adolescent forensic unit | Int J Forens Ment Health | 1 | 2007 | ‘a systematic and comprehensive aggression management program’ |
| Kilgore A | Effectiveness of collaborative problem solving model in reducing seclusion and restraint in a child psychiatric unit | Diss Abstr B Sci Eng | 7 | 2012 | CPS |
| Lebel J, Goldstein R | The economic cost of using restraint and the value added by restraint reduction or elimination | Psychiatr Serv | 1 | 2005 | ‘statewide initiative to reduce or eliminate the use of seclusion and restraint among children and adolescents’ |
| LeBel J, Stromberg N, Duckworth K, Kerzner J, Goldstein R, Weeks M, Harper G, LaFlair L, Sudders M | Child and adolescent inpatient restraint reduction: a state initiative to promote strength-based care | J Am Acad Child Adolesc Psychiatry | 1 | 2004 | ‘systems approach’ |
| Leitch S. | The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions (RPI) in Residential Services for Children and Young People | Dissertation | 7 | 2009 | RPI |
| Magnowski S | The Impact of Milieu Nurse Patient Shift Assignments on Monthly Restraint Rates on an Inpatient Child and Adolescent Psychiatric Unit | Supplied intervention material | 7 | 2018 | ‘milieu nurse’ |
| Magnowski S, Cleveland S | The impact of milieu nurse-client shift assignments on monthly restraint rates | J Am Psychiatr Nurses Assoc | 1 | 2019 | ‘cognitive milieu therapy’ |
| Marrow MT, Knudsen KJ, Olafson E, Bucher SE | The value of implementing TARGET within a trauma-informed juvenile justice setting | J Child Adolesc Trauma | 1 | 2012 | ‘multifaceted trauma-focused intervention’ including TARGET |
| Martin A, Krieg H, Esposito F, Stubbe D, Cardona L | Reduction of restraint and seclusion through collaborative problem solving: a five-year prospective inpatient study | Psychiatr Serv | 1 | 2008 | CPS |
| McGlinn CJ. | The effect of federal regulations on the physical restraint of children and adolescents in residential treatment with an analysis of client, staff, and environmental variables | Diss Abstr B Sci Eng | 7 | 2006 | federal regulations |
| Miguel ES | The Dynamics and Ramifications of Severe Challenging Behaviors: Daring to Reduce Severe Challenging Behavior in Schools Without Physical Restraint and Seclusion | Thesis | 7 | 2016 | Functional Communications Training and Systema Breathing |
| Miller JA, Hunt DP, Georges MA | Reduction of physical restraints in residential treatment facilities | J Disabil Policy Stud | 1 | 2006 | ‘2-phase (organizational and milieu) physical restraint reduction intervention’ |
| Murphy CJ, Siv AM | A one year study of mode deactivation therapy: adolescent residential patients with conduct and personality disorders | Int J Behav Consult Ther | 1 | 2011 | (MDT |
| Nunno MA, Smith EG, Martin WR, Butcher S | Benefits of embedding research into practice: an agency-university collaboration | Child Welfare | 1 | 2015 | the CARE model |
| Nunno MA, Holden MJ, Leidy B | Evaluating and monitoring the impact of a crisis intervention system on a residential child care facility | Child Youth Serv Rev | 1 | 2003 | TCI |
| O’Brien C | Best practices in behavior support: preventing and reducing the use of restraint and seclusion | Resid Group Care Q | 2 | 2004 | ‘psychoeducational treatment model’ |
| Paccione-Dyszlewski MR, Conelea CA, Heisler WC, Vilardi JC, Sachs HT | A crisis management quality improvement initiative in a children’s psychiatric hospital: design, implementation, and outcome | J Psychiatr Pract | 1 | 2012 | QBS, Inc. SafetyCare Behavioral Safety Management program |
| Padhi A, Norcott J, Yoo E, Vakili A | Eliminating seclusion and reducing restraint: hope on an acute adolescent psychiatric ward | Aust N Z J Psychiatry | 9 | 2019 | ‘cultural transformation’ |
| Plant R. | Courageous patience part II: lessons learned from a five-year program to reduce/eliminate restraint and seclusion | Resid Group Care Q | 2 | 2004 | The ABCD program including TACE staff training |
| Pollastri AR, Lieberman RE, Boldt SL, Ablon J | Minimizing seclusion and restraint in youth residential and day treatment through site-wide implementation of Collaborative Problem Solving | Resid Treat Child Youth | 1 | 2016 | CPS |
| Ponge L, Harris J | Reduction of seclusion and restraint in a children’s psychiatric center | Commun Nurs Res | 1 | 2006 | multidisciplinary, multimodal approach |
| Reynolds EK, Grados MA, Praglowski N, Hankinson JC, Deboard-Lucas R, Goldstein L, Perry-Parrish C, Specht M, Ostrander R | Use of modified positive behavioral interventions and supports in a psychiatric inpatient unit for high-risk youths | Psychiatr Serv | 1 | 2016 | M-PBIS |
| Reynolds EK, Grados MA, Praglowski N, Hankinson JC, Parrish C, Ostrander R | Implementation of Modified Positive Behavioral Interventions and Supports in a youth psychiatric partial hospital program | J Patient Saf Risk Manag | 1 | 2019b | M-PBIS |
| Russell M, Maher C, Dorrell M, Pitcher C, Henderson L | A comparison between users and non-users of Devereux’s Safe and Positive Approaches training curricula in the reduction of injury and restraint | Resid Treat Child Youth | 1 | 2009 | SPA |
| Ryan JB, Peterson R, Tetreault G, Hagen EV | Reducing seclusion timeout and restraint procedures with at-risk youth | J At-Risk Issues | 1 | 2007 | CPI’s Nonviolent Crisis Intervention Training |
| Ryan JB, Peterson RL, Tetreault G, van der Hagen E | Reducing the Use of Seclusion and Restraint in a Day School Program | Chapter in Nunno M, Day D, Bullard L. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. New York: Child Welfare League of America; 2008 | 3 | 2008 | therapeutic Intervention |
| Sanders K | The effects of an action plan, staff training, management support and monitoring on restraint use and costs of work-related injuries | J Appl Res Intellect Disabil | 1 | 2009 | Grafton program |
| Schreiner GM, Crafton CG, Sevin JA | Decreasing the use of mechanical restraints and locked seclusion | Adm Policy Ment Health | 1 | 2004 | ‘restraint reduction process’ |
| Seckman A, Paun O, Heipp B, Van Stee M, Keels-Lowe V, Beel F, et al. | Evaluation of the use of a sensory room on an adolescent inpatient unit and its impact on restraint and seclusion prevention | JCAPN | 1 | 2017 | sensory room |
| Shadili G, Brocco C, De Vieille I, Piot MA, Lavergne P | Violence in an adolescent psychiatric inpatient unit: a behavioural management plan | Eur Neuropsychopharmacol | 9 | 2012 | behavioural management planning |
| Singh NN, Singh SD, Davis CM, Latham LL, Ayers JG | Reconsidering the use of seclusion and restraints in inpatient child and adult psychiatry | J Child Fam Stud | 1 | 1999 | unnamed |
| Thomann J | Factors in Restraint Reduction in Residential Treatment Facilities for Adolescents | Thesis | 7 | 2009 | unnamed |
| Thompson RW, Huefner JC, Vollmer DG, Davis JL, Daly DL | A Case Study of an Organizational Intervention to Reduce Physical Interventions: Creating Effective, Harm-free Environments | Chapter in Nunno M, Day D, Bullard L. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. New York: Child Welfare League of America; 2008 | 3 | 2008 | Components of a Harm-Free Environment |
| Ubana RL, Ng JWL, Tan CSM, Raj HP, Ong EY, Ang LK, et al. | Continued implementation of an advanced practice nurse-led multidisciplinary programme to reduce disruptive incidences in young patients with mental health conditions | Ann Acad Med Singapore | 9 | 2015 | ‘multidisciplinary programme’ |
| Valenkamp M, Verheij F, Van De Ende J, Verhulst F | Development and evaluation of the individual proactive aggression management method for residential child psychiatry and child care | Eur Child Adolesc Psychiatry | 9 | 2011 | Pro-ACT |
| van Loan CL, Gage NA, Cullen JP | Reducing use of physical restraint: a pilot study investigating a relationship-based crisis prevention curriculum | Resid Treat Child Youth | 1 | 2015 | Shifting Gears |
| Verret C, Massé L, Lagacé-Leblanc J, Delisle G, Doyon J | The impact of a schoolwide de-escalation intervention plan on the use of seclusion and restraint in a special education school | Emot Behav Diffic | 1 | 2019 | schoolwide de-escalation intervention plan |
| West M, Melvin G, McNamara F, Gordon M | An evaluation of the use and efficacy of a sensory room within an adolescent psychiatric inpatient unit | Aust Occup Ther J | 1 | 2017 | guided sensory room use |
| Williams DE, Grossett DL | Reduction of restraint of people with intellectual disabilities: an organizational behavior management (OBM) approach | Res Dev Disabil | 1 | 2011 | OBM |
| Wisdom JP, Wenger D, Robertson D, Van Bramer J, Sederer LI | The New York State Office of Mental Health Positive Alternatives to Restraint and Seclusion (PARS) project | Psychiatr Serv | 1 | 2015 | 6CS |
| Witte L. | Reducing the use of seclusion and restraint. A Michigan provider reduced its use of seclusion and restraint by 93% in one year on its child and adolescent unit | Behav Healthc | 1 | 2008 | Six Steps to Success |
| Witte L. | Using training in verbal skills to reduce the use of seclusion and restraint | J Safe Manag Disruptive Assaultive Behav | 6 | 2007 | CPI’s Enhancing Verbal Skills: Applications of Life Space Crisis InterventionSM |
| Mapping records | |||||
| Andrassy BM | Feelings thermometer: an early intervention scale for seclusion/restraint reduction among children and adolescents in residential psychiatric care | JCAPN | 1 | 2016 | Feelings Thermometer Scale |
| Azeem MW, Reddy B, Wudarsky M, Carabetta L, Gregory F, Sarofin M | Restraint Reduction at a pediatric psychiatric hospital: a ten-year journey | JCAPN | 1 | 2015 | ‘six core strategies based on trauma informed care’ |
| Barnett SR, dosReis S, Riddle MA, Maryland Youth Practice Improvement Committee for Mental Health | Improving the management of acute aggression in state residential and inpatient psychiatric facilities for youths | J Am Acad Child Adolesc Psychiatry | 1 | 2002 | ‘guide to improve management of client acute aggressive behaviour’ |
| Brown AD, McCauley K, Navalta CP, Saxe GN | Trauma systems therapy in residential settings: improving emotion regulation and the social environment of traumatized children and youth in congregate care | J Fam Violence | 1 | 2013 | Trauma Systems Therapy (TST) |
| Budlong M | Lessons learned and organizational changes implemented as a result of the SAMHSA restraint and seclusion grant | Resid Group Care Q | 2 | 2004 | unnamed |
| Caldwell B, Albert C, Azeem MW, Beck S, Cocoros D, Cocoros T, et al. | Successful seclusion and restraint prevention effort in child and adolescent programs | J Psychosoc Nurs Ment Health Serv | 1 | 2014 | 6CS |
| Caldwell B, LeBel J | Reducing restraint and seclusion: how to implement whole system change | Children’s Voice | 6 | 2010 | 6CS |
| Canady V. | Model-of-care effort reduces need for restraint, seclusion at BH facility | Ment Health Wkly | 6 | 2018 | Comfort vs. control |
| Care Council for Wales | Positive Approaches – Reducing Restrictive Practices in Social Care (Version 1) | Learning resource | 5 | 2016 | Positive Behaviour Support, Active Support and Restorative Approaches |
| Carter J, Jones J, Stevens K | Beyond a Crisis Management Program: How we Reduced our Restraints by Half in One Year | Chapter in Nunno M, Day D, Bullard L. For Our Own Safety: Examining the Safety of High-risk Interventions for Children and Young People. New York: Child Welfare League of America; 2008 | 3 | 2008 | PMAB |
| Colton D | Checklist for Assessing Your Organization’s Readiness for Reducing Seclusion and Restraint | Report (unpublished) | 4 | 2014 | Checklist for Assessing Your Organization’s Readiness for Reducing Seclusion and Restraint |
| Colton D, Xiong H | Reducing Seclusion and Restraint – Organizational Questionnaire | Supplied intervention material | 5 | 2009 | unnamed |
| Cooper S | Use of restraint reduced by therapeutic intervention | Children & Young People Now | 6 | 2008 | TCI |
| CPI | The Nonviolent Crisis Intervention ® Training Program and the National Association of State Mental Health Program Directors: Six Core Strategies for the Reduction of Restraint and Seclusion | CPI publication | 5 | 2013 | CPI’s Nonviolent Crisis Intervention®: Six Core Strategies |
| Donovan A, Siegel L, Zera G, Plant R, Martin A | Seclusion and restraint reform: an initiative by a child and adolescent psychiatric hospital | Child Adolesc Psychiatry | 1 | 2003 | Riverview program |
| Ford J | TARGET Adolescent Individual Manual Facilitator Guide Twelve-Session | Supplied intervention material | 5 | 2013 | TARGET (FREEDOM Steps) |
| Girelli S | Lessons learned in the reduction of restraint and seclusion: a three-year (plus) retrospective | Resid Group Care Q | 2 | 2004 | unnamed |
| Goren S, Abraham I, Doyle N | Reducing violence in a child psychiatric hospital through planned organizational change | JCAPN | 1 | 1996 | unnamed |
| Guilfoile M | The Devereux Glenholme School | Resid Group Care Q | 2 | 2004 | Devereux Glenholme internal quality improvement process |
| Department for Education and Department for Health and Social Care | Reducing the Need for Restraint and Restrictive Intervention: Children and Young People with Learning Disabilities, Autistic Spectrum Conditions and Mental Health Difficulties in Health and Social Care Services and Special Education Settings | Government report | 4 | 2019 | ‘a positive and proactive approach to behaviour’ |
| HM Inspectorate of Prisons | Behaviour Management and Restraint of Children in Custody | Report | 4 | 2015 | MMPR |
| Holden MJ, Turnbull AJ, Heresniak R, Ruberti M, Holden JC, Saville E | Therapeutic Crisis Intervention Activity Guide, 7th Edition | Supplied intervention material | 5 | 2020 | TCI |
| Holden MJ, Turnbull AJ, Holden JC, Heresniak R, Ruberti M, Saville E | Therapeutic Crisis Intervention Reference Guide, 7th Edition | Supplied intervention material | 5 | 2020 | TCI |
| Holden MJ, Turnbull AJ, Holden JC, Heresniak R, Ruberti M, Saville E | Therapeutic Crisis Intervention Student Workbook, 7th Edition | Supplied intervention material | 5 | 2020 | TCI |
| Leitch S | The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions in Services for Children and Young People | Supplied intervention material | 10 | 2009 | unnamed |
| Leitch S | ‘Hands off’ The Impact of Restraint Reduction Meetings on the Use of Restrictive Physical Interventions in Services for Children and Young People | Supplied intervention material | 10 | 2009 | Hands Off |
| Leitch S | Together Trust 6th June 2008 | Supplied intervention material | 10 | 2008 | unnamed |
| Leitch S | Training | Supplied intervention material | 5 | undated | unnamed |
| Leitch S | Training Plan 6th June 2008 | supplied intervention material | 5 | 2008 | unnamed |
| Lietzke A | Restraint Reduction and CPI Training | CPI blog | 8 | 2014 | CPI’s Nonviolent Crisis Intervention |
| Magnowski S | Restraint Implications | Supplied intervention material | 5 | undated | unnamed |
| NASMHPD | Six Core Strategies for Reducing Seclusion and Restraint Use | NASMHPD | 5 | 2006 | 6CS |
| Partnership Projects | Neuro De-escalation | www.partnershipprojectsuk.com/project/neuro-de-escalation/ | 11 | 2020 | Neuro De-escalation |
| PRICE Training | Price Training | www.pricetraining.co.uk | 11 | 2020 | Positive Behaviour Support |
| Rettmann R | Changes in Attitudes, Changes in Outcomes | CPI blog | 8 | 2019 | CPI’s Nonviolent Crisis Intervention |
| Reynolds EK, Praglowski N, Parrish C, Ostrander R, Grados MA | Implementation of modified positive behavioral interventions and supports (M-PBIS) in acute psychiatric care inpatient and day hospital settings: immediate and long-term gains | J Am Acad Child Adolesc Psychiatry | 9 | 2019a | M-PBIS |
| Rowan C | Schools Operating Safely: Ten Alternatives to Medication, Seclusion and Restraints | www.zonein.ca | 4 | 2010 | Schools Operating Safely |
| Smallridge P, Williamson A. | Report on Implementing the Independent Review of Restraint in Juvenile Secure Settings | Report | 4 | 2011 | CRT |
| Studio III Training Systems and Psychological Services | Low Arousal Training | www.studio3.org/low-arousal-training | 11 | 2019 | LASER |
| US Department of Education | Restraint and Seclusion: Resource Document | US Department of Education | 4 | 2012 | unnamed |
| Visalli H, McNasser G | Reducing seclusion and restraint: meeting the organizational challenge | J Nurs Care Qual | 1 | 2000 | ‘changing criterion design’ |
| Welsh Government | Guidance on Reducing Restrictive Practices in Childcare, Education, Health and Social Care Settings | Consultation document | 4 | 2019 | Reducing Restrictive Practices Framework |
| WHO | Strategies to end seclusion and restraint. WHO Quality Rights Specialized training | WHO | 5 | 2019 | Strategies to end seclusion and restraint |
| Youth Justice Board for England and Wales | Developing a Restraint Minimisation Strategy: Guidance for Secure Establishments on the Development of Restraint Minimisation Strategies | Welsh Youth Justice Board report | 4 | 2009 | ‘restraint minimisation’ |
| Youth Justice Board for England and Wales | Minimising and Managing Physical Restraint Safeguarding Processes, Governance Arrangements, and Roles and Responsibilities | Welsh Youth Justice Board report | 4 | 2012 | MMPR |
Appendix 3 Request for intervention materials
Text of e-mail request for intervention materials for CONTRAST mapping review:
Dear
Re: Request for intervention materials for CONTRAST mapping review
I am contacting you on behalf of the CONTRAST research team at the University of Leeds, UK. We are conducting a review of interventions designed to reduce the use of restrictive practices in children’s settings. We identified the following publication:
xxxxxxxxxxxxxxx
We would like to request copies of any materials (see examples below) that were used in this intervention. You can supply these in hard or electronic copy or via a weblink. We would be very grateful for your assistance as we are extremely keen to include your work with as much detail as possible. Any references to materials that you supply will be fully credited to their source. We would greatly appreciate any response by 28th February 2020. This project is led by Professor John Baker at the University of Leeds and is funded by the National Institute for Health Research, Health Services & Delivery Research ID NIHR127281. Further information is available at: www.crd.york.ac.uk/prospero/display_record.php?RecordID%20=%20124730.
The study is also registered with PROSPERO (ID CRD42019124730) and you can follow updates on Twitter: #BCTContrast.
Many thanks and best wishes,
MATERIALS (examples – not an exhaustive list)
-
Training, education or instruction materials or resources, such as:
-
booklets
-
leaflets/handouts
-
powerpoint slides
-
DVDs, videos, YouTube
-
vignettes
-
exercises
-
workshop materials and activities
-
course objectives/curriculum/plans
-
annual training plan/requirements
-
instructions/manuals
-
posters/display items.
-
-
Any tool or proforma (including validated tools or tools developed for the intervention/study), such as:
-
data collection/recording tools
-
safety/violence assessment tool
-
planning tools/templates
-
debriefing/feedback proformas
-
review procedure proforma
-
checklist
-
sensory room log
-
tracking spreadsheet proforma.
-
Appendix 4 All records of interventions in evaluation studies and mapping studies, by author
Interventions occurring more than once across the included records
| Intervention | Evaluation and mapping (n) | Intervention reported in evaluation records (n) | Intervention reported in mapping records (n) |
|---|---|---|---|
| 6CS | 12 | 5 | 7 |
| CPS | 7 | 7 | 0 |
| Comfort vs. control | 2 | 2 | 0 |
| TCI | 3 | 1 | 2 |
| The Grafton program | 2 | 1 | 1 |
| M-PBIS | 3 | 2 | 1 |
| TARGET | 2 | 1 | 1 |
| SPA | 2 | 1 | 1 |
Interventions evaluated in the evaluation records
| Author(s) and year | INTa | Name/description of interventionb |
|---|---|---|
| Azeem et al.38 2017 | 2 | six core strategies based on trauma informed care |
| Bobier et al.165 2015 | 4 | sensory modulation room |
| Boel-Studt171 2017 | 5 | TI-PRC |
| Bonnell et al.109 2014 | 6 | CPS |
| Borckardt et al.181 2011 | 7 | engagement model |
| Campbell211 2004 | 10 | STAR |
| Craig and Sanders120 2018 | 11 | TIA. Comfort vs. control. ‘program model for minimizing restraint and seclusion’ |
| Craig88 2015 | 17 | ‘program model for minimizing restraint and seclusion’ (Grafton model) |
| Crosland et al.204 2008 | 18 | Behavior Analysis Services Program |
| Dean et al.163 2007 | 19 | ‘milieu-based behavioral management program’ |
| Deveau and Leitch209 2015 | 20 | RRM |
| Eblin162 2019 | 22 | ‘quality improvement’ |
| Elwyn et al.178 2017 | 23 | The Sanctuary Model |
| Ercole-Fricke et al.107 2016 | 24 | CPS |
| Ercole89 2014 | 24 | CPS |
| Farina90 2006 | 25 | evaluation of impact of new seclusion and restraint policy |
| Finnie91 2013 | 24 | CPS |
| Ford and Hawke128 2012 | 26 | TARGET |
| Forrest et al.172 2018 | 27 | BCC |
| Fowler155 2006 | 28 | ‘aromatherapy for crisis management’ |
| Fralick176 2007 | 29 | Rapid Cycle Model for Improvement |
| Glew92 2012 | 24 | CPS |
| Greene et al.110 2006 | 24 | CPS |
| Hallman et al.236 2014 | 33 | Mindfulness-based Stress Reduction training program |
| Hambrick et al.79 2018 | 34 | NMT |
| Health Sciences Center Winnipeg104 2015 | 2 | 6CS |
| Hellerstein et al.203 2007 | 35 | ‘a hospital-wide effort to decrease restraint and seclusion of psychiatric inpatients’ |
| Hodgdon et al.183 2013 | 38 | ARC Framework |
| Holstead et al.191 2010 | 39 | ‘a restraint reduction initiative’ |
| Huckshorn77 2010 | 2 | 6CS |
| Jani et al.159 2011 | 44 | milieu therapy training and collaborative problem solving |
| Jones and Timbers201 2003 | 40 | Teaching-Family Model |
| Jonikas et al.189 2004 | 41 | ‘a program to reduce the use of physical restraint’ |
| Kalogjera et al.173 1989 | 42 | ‘therapeutic management’ |
| Kaltiala-Heino et al.198 2007 | 43 | ‘a systematic and comprehensive aggression management program’ |
| Kilgore93 2018 | 24 | CPS |
| Lebel and Goldstein39 2005 | 45 | ‘statewide initiative to reduce or eliminate the use of seclusion and restraint among children and adolescents‘ |
| LeBel et al.40 2004 | 46 | ‘a systems approach’ |
| Leitch94 2009 | 47 | RPI |
| Magnowski95 2018 | 48 | ‘the milieu nurse’ |
| Magnowski and Cleveland80 2019 | 48 | ‘cognitive milieu therapy’ |
| Marrow et al.129 2012 | 26 |
Incorporated TARGET plus other elements ‘a multifaceted trauma-focused intervention’ |
| Martin et al.111 2008 | 24 | CPS |
| McGlinn96 2006 | 49 | described (in title) as ‘The effect of federal regulations on the physical restraint of children and adolescents in residential treatment’ |
| Miguel97 2016 | 50 | ‘Functional Communications Training’ and ‘Systema Breathing’ |
| Miller et al.182 2006 | 51 | ‘2-phase (organizational and milieu) physical restraint reduction intervention’ |
| Murphy and Siv158 2011 | 52 | MDT |
| Nunno et al.177 2015 | 53 | the CARE model |
| Nunno et al.81 2003 | 16 | TCI |
| O’Brien202 2004 | 54 | key interventions including ‘GBT Psychoeducational Treatment Model’ |
| Paccione-Dyszlewski et al.170 2012 | 55 | QBS, Inc. SafetyCare Behavioral Safety Management program |
| Padhi et al.99 2019 | 56 | unnamed, described as a ‘cultural transformation’ |
| Plant 2004 | 58 | The ABCD program (Autonomy, Belonging, Competence, and Doing for Others) including TACE staff training |
| Pollastri et al.217 2016 | 24 | collaborative problem-solving |
| Ponge and Harris 2006 | 59 | multidisciplinary, multimodal approach |
| Reynolds et al.125 2016 | 60 | M-PBIS |
| Reynolds et al.127 2019 | 60 | M-PBIS |
| Russell et al.131 2009 | 32 | SPA |
| Ryan et al.113 2007 | 2 | CPI’s Nonviolent Crisis Intervention Training |
| Ryan et al.86 2008 | 62 | Therapeutic Intervention |
| Sanders108 2009 | 17 | Grafton program |
| Schreiner et al.41 2004 | 63 | ‘restraint reduction process’ |
| Seckman et al.156 2017 | 88 | sensory room |
| Shadili et al.101 2012 | 65 | ‘behavioural management plan’ |
| Singh et al.214 1999 | 66 | ‘reducing the use of seclusion and restraints’ |
| Thomann98 2009 | 69 | ‘restraint reduction’ |
| Thompson et al.87 2008 | 70 | Components of a Harm-Free Environment |
| Ubana et al.102 2015 | 71 | ‘multidisciplinary programme’ |
| Valenkamp et al.103 2011 | 73 | Pro-ACT |
| van Loan et al.184 2015 | 74 | Shifting Gears |
| Verret et al.161 2019 | 75 | schoolwide de-escalation intervention plan |
| West et al.164 2017 | 77 | guided sensory room use |
| Williams et al.185 2011 | 78 | OBM |
| Wisdom et al.114 2015 | 2 | 6CS |
| Witte167 2008 | 79 | Six Steps to Success |
| Witte160 2007 | 80 | CPI’s Enhancing Verbal Skills: Applications of Life Space Crisis InterventionSM |
Interventions described in mapping records
| Author(s) and year | INTa | Intervention name/descriptionb |
|---|---|---|
| Andrassy154 2016 | 1 | ‘Feelings Thermometer Scale’ |
| Azeem et al.105 2015 | 2 | ‘six core strategies based on trauma informed care’ |
| Barnett et al.190 2002 | 3 | guide to improve management of client acute aggressive behaviour |
| Brown et al.78 2013 | 8 | Trauma Systems Therapy (TST) |
| Budlong169 2004 | 9 | ‘model training approaches designed to reduce the use of restraint and seclusion in residential services for youth’ |
| Caldwell et al.115 2014 | 2 | 6CS |
| Caldwell and LeBel116 2010 | 2 | 6CS |
| Canady106 2018 | 11 | Comfort vs. control |
| Care Council for Wales174 2016 | 12 | Positive Behaviour Support, Active Support and Restorative Approaches |
| Carter et al.85 2008 | 13 | PMAB |
| Colton82 2004 | 14 | Checklist for Assessing Your Organization’s Readiness for Reducing Seclusion and Restraint |
| Colton and Xiong207 2009 | 15 | unnamed |
| Cooper121 2008 | 16 | TCI |
| CPI117 2013 | 2 | Nonviolent Crisis Intervention®: Six Core Strategies |
| Donovan et al.175 2003 | 21 | Riverview program, based on ABCD (Brendtro and Ryan and associates) |
| Ford130 2013 | 26 | TARGET (FREEDOM Steps) |
| Girelli210 2004 | 30 | reflects on a three year period of trying to reduce S/R |
| Goren et al.168 1996 | 31 | ‘a project to reduce violence within a public child psychiatric hospital’ |
| Guilfoile132 2004 | 32 | ‘Devereux Glenholme internal quality improvement process’ |
| HM Government 201929 | 36 | ‘a positive and proactive approach to behaviour’ |
| HM Inspectorate of Prisons23 2015 | 37 | MMPR |
| Holden et al.122 2020 | 16 | TCI |
| Holden et al.123 2020 | 16 | TCI |
| Holden et al.124 2020 | 16 | TCI |
| Leitch237 2009 | 47 | unnamed |
| Leitch195 2009 | 47 | Hands Off |
| Leitch238 2008 | 47 | unnamed |
| Leitch239 (no date) | 47 | unnamed |
| Leitch240 2008 | 47 | unnamed |
| Lietzke118 2014 | 2 | Nonviolent Crisis Intervention |
| Magnowski241 (no date) | 48 | unnamed |
| NASMHPD33 2006 | 2 | 6CS |
| Partnership Projects186 2020 | 57 | Neuro De-escalation |
| PRICE Training 2020 | 60 | Pragmatic approach to programmes |
| Rettmann119 2019 | 2 | Nonviolent Crisis Intervention |
| Reynolds et al.127 2019 | 60 | M-PBIS |
| Rowan166 2010 | 61 | Schools Operating Safely |
| Smallridge and Williamson187 2011 | 67 | CRT |
| Studio III Training Systems and Psychological Services242 2019 | 68 | most relevant = LASERof educ |
| US Department of Education197 2012 | 72 | unnamed |
| Visalli and McNasser188 2000 | 76 | ‘behavior mapping, the Anger Management Assessment and the Triangle of Choices’ |
| Welsh Government180 | 60 | PBS |
| World Health Organization194 2019 | 81 | strategies to end seclusion and restraint |
| Youth Justice Board for England and Wales199 2009 | 82 | ‘restraint minimisation strategies’ |
| Youth Justice Board for England and Wales192 2012 | 83 | MMPR |
Appendix 5 Records of interventions in evaluation studies and mapping studies
Comparative numbers of intervention events, evaluation records and mapping records
| Intervention | Intervention events (n) | Mapping records by author (year) | n | Evaluation records by author (year) | n | All records (n) |
|---|---|---|---|---|---|---|
| 6CS | 11 |
Azeem et al. 105 2015 Caldwell et al. 115 2014 Caldwell and LeBel116 2010 CPI117 2013 Lietzke118 2014 NASMHPD33 2006 Rettmann119 2019 |
7 |
Azeem et al. 38 2017 Health Sciences Center Winnipeg104 2015 Huckshorn77 2010 Ryan et al. 113 2007 Wisdom et al. 114 2015 |
5 | 12 |
| CPS | 9 | 0 |
Bonnell et al. 109 2014 Ercole-Fricke et al. 107 2016 Ercole-Fricke89 2014 Finnie91 2013 Glew92 2012 Greene et al. 110 2006 Kilgore93 2018 Martin et al. 111 2008 Pollastri et al. 112 2016 |
9 | 9 | |
| CvC | 2 | Canady106 2018 | 1 | Craig and Sanders120 2018 | 1 | 2 |
| GRAFTON | 2 | 0 |
Craig88 2015 Sanders108 2009 |
2 | 2 | |
| M-PBIS | 3 |
PRICE Training126 2020 Reynolds et al. 127 2019a Welsh Government180 2019 |
3 |
Reynolds et al. 125 2016 Reynolds et al. 100 2019b |
2 | 5 |
| SPA | 2 | Guilfoile132 2004 | 1 | Russell et al.131 2009 | 1 | 2 |
| TARGET | 2 | Ford130 2013 | 1 |
Ford and Hawke128 2012 Marrow et al. 129 2012 |
2 | 3 |
| TCI | 3 |
Cooper121 2008 Holden et al. 122 2020a Holden et al. 123 2020b Holden et al. 124 2020c |
4 | Nunno et al.81 2003 | 1 | 5 |
| Stand alone |
Andrassy124 2016 Barnett et al. 190 2002 Brown et al. 78 2013 Budlong169 2004 Care Council for Wales174 2016 Carter et al. 85 2008 Colton82 2004 Colton and Xiong207 2009 Donovan et al. 175 2003 Girelli210 2004 Goren et al. 168 1996 HM Government30 2019 HM Inspectorate of Prisons23 2015 Leitch 2008 (unpublished) Leitch 2008 (unpublished) Leitch 2009 (unpublished) Leitch 2009 (unpublished) Leitch (no date; unpublished) Magnowski241 nd Partnership Projects186 2020 Rowan166 2010 Smallridge and Williamson187 2011 Studio III Training Systems and Psychological Services242 2019 US Department of Education197 2012 Visalli and McNasser188 2000 WHO194 2019 Youth Justice Board for England and Wales199 2009 Youth Justice Board for England and Wales192 2012 |
28 |
Boel-Studt171 2017 Bobier et al. 167 2015 Borckardt et al. 181 2011 Campbell211 2004 Crosland et al. 204 2008 Dean et al. 163 2007 Deveau and Leitch209 2015 Eblin162 2019 Elwyn et al. 178 2017 Farina90 2007 Forrest et al. 172 2018 Fowler155 2006 Fralick176 2007 Hallman et al. 236 2014 Hambrick et al. 79 2018 Hellerstein et al. 203 2007 Hodgdon et al. 183 2013 Holstead et al. 191 2010 Jani et al. 159 2011 Jones and Timbers201 2003 Jonikas et al. 189 2004 Kalogjera et al. 173 1989 Kaltiala-Heino et al. 198 2007 Lebel and Goldstein39 2005 LeBel et al. 40 2004 Leitch94 2009 Magnowski95 2018 Magnowski and Cleveland80 2019 McGlinn96 2006 Miguel97 2016 Miller et al. 182 2006 Murphy and Siv158 2011 Nunno et al. 177 2015 O’Brien202 2004 Paccione-Dyszlewski et al. 170 2012 Padhi et al. 99 2019 Plant179 2004 Ponge and Harris209 2006 Ryan et al. 86 2008 Schreiner et al. 41 2004 Seckman et al. 156 2017 Shadili et al. 101 2012 Singh et al. 214 1999 Thomann98 2009 Thompson et al. 87 2008 Ubana et al. 102 2015 Valenkamp et al. 193 2011 van Loan184 2015 Verret et al. 161 2019 West et al. 164 2017 Williams et al. 193 2011 Witte160 2007 Witte167 2008 |
53 | ||
| Mapping records | 45 | Evaluation records | 76 | 121 |
Evaluation records: interventions by author
| Author(s) (n = 76) | Intervention numbera | Name/descriptionb |
|---|---|---|
| Azeem et al.38 2017 | 2 | 6CS |
| Bobier et al.165 2015 | 4 | sensory modulation room |
| Boel-Studt171 2017 | 5 | TI-PRC |
| Bonnell et al.109 2014 | 6 | CPS |
| Borckardt et al.181 2011 | 7 | engagement model |
| Campbell211 2004 | 10 | STAR |
| Craig and Sanders120 2018 | 11 | TIA. Comfort vs. control. ‘program model for minimizing restraint and seclusion’ |
| Craig88 2015 | 17 | ‘program model for minimizing restraint and seclusion’ (Grafton model) |
| Crosland et al.204 2008 | 18 | Behavior Analysis Services Program |
| Dean et al.163 2007 | 19 | ‘milieu-based behavioral management program’ |
| Deveau and Leitch209 2015 | 20 | RRM |
| Eblin162 2019 | 22 | ‘quality improvement’ |
| Elwyn et al.178 2017 | 23 | The Sanctuary Model |
| Ercole-Fricke et al.107 2016 | 24 | CPS |
| Ercole89 2014 | 24 | CPS |
| Farina90 2007 | 25 | evaluation of impact of new seclusion and restraint policy |
| Finnie91 2013 | 24 | CPS |
| Ford and Hawke128 2012 | 26 | TARGET |
| Forrest et al.172 2018 | 27 | BCC |
| Fowler155 2006 | 28 | ‘aromatherapy for crisis management’ |
| Fralick176 2007 | 29 | Rapid Cycle Model for Improvement |
| Glew92 2012 | 24 | CPS |
| Greene et al.110 2006 | 24 | CPS |
| Hallman et al.236 2014 | 33 | Mindfulness-based Stress Reduction training program |
| Hambrick et al.79 2018 | 34 | NMT |
| Health Sciences Center Winnipeg104 2015 | 2 | 6CS |
| Hellerstein et al.203 2007 | 35 | ‘a hospital-wide effort to decrease restraint and seclusion of psychiatric inpatients’ |
| Hodgdon et al.183 2013 | 38 | ARC Framework |
| Holstead et al.191 2010 | 39 | ‘a restraint reduction initiative‘ |
| Huckshorn77 2010 | 2 | 6CS |
| Jani et al.159 2011 | 44 | milieu therapy training and collaborative problem solving |
| Jones and Timbers201 2003 | 40 | Teaching-Family Model |
| Jonikas et al.189 2004 | 41 | ‘a program to reduce the use of physical restraint’ |
| Kalogjera et al.173 1989 | 42 | ‘therapeutic management’ |
| Kaltiala-Heino et al.198 2007 | 43 | ‘a systematic and comprehensive aggression management program’ |
| Kilgore93 2018 | 24 | CPS |
| Lebel and Goldstein39 2005 | 45 | ‘statewide initiative to reduce or eliminate the use of seclusion and restraint among children and adolescents‘ |
| LeBel et al.40 2004 | 46 | ‘a systems approach’ |
| Leitch195 2009 | 47 | RPI |
| Magnowski95 2018 | 48 | ‘the milieu nurse’ |
| Magnowski and Cleveland80 2019 | 48 | ‘cognitive milieu therapy’ |
| Marrow et al.129 2012 | 26 | Incorporated TARGET plus other elements. ‘a multifaceted trauma-focused intervention’ |
| Martin et al.111 2008 | 24 | CPS |
| McGlinn96 2006 | 49 | described (in title) as ‘The effect of federal regulations on the physical restraint of children and adolescents in residential treatment’ |
| Miguel97 2016 | 50 | ‘Functional Communications Training’ and ‘Systema Breathing’ |
| Miller et al.182 2006 | 51 | ‘2-phase (organizational and milieu) physical restraint reduction intervention’ |
| Murphy and Siv158 2011 | 52 | MDT |
| Nunno et al.177 2015 | 53 | the CARE model |
| Nunno et al.81 2003 | 16 | TCI |
| O’Brien202 2004 | 54 | key interventions including ‘GBT Psychoeducational Treatment Model’ |
| Paccione-Dyszlewski et al.170 2012 | 55 | QBS, Inc. SafetyCare Behavioral Safety Management program |
| Padhi et al.99 2019 | 56 | unnamed, described as a ‘cultural transformation’ |
| Plant179 2004 | 58 | The ABCD program including TACE staff training |
| Pollastri et al.112 2016 | 24 | collaborative problem-solving |
| Ponge and Harris243 2006 | 59 | multidisciplinary, multimodal approach |
| Reynolds et al.125 2016 | 60 | M-PBIS |
| Reynolds et al.100 2019 | 60 | M-PBIS |
| Russell et al.131 2009 | 32 | SPA |
| Ryan et al.113 2007 | 2 | CPI’s Nonviolent Crisis Intervention Training |
| Ryan et al.86 2008 | 62 | Therapeutic Intervention |
| Sanders108 2009 | 17 | Grafton program |
| Schreiner et al.41 2004 | 63 | ‘restraint reduction process’ |
| Seckman et al.156 2017 | 88 | sensory room |
| Shadili et al.101 2012 | 65 | ‘behavioural management plan’ |
| Singh et al.214 1999 | 66 | ‘reducing the use of seclusion and restraints’ |
| Thomann98 2010 | 69 | ‘restraint reduction’ |
| Thompson et al.87 2008 | 70 | Components of a Harm-Free Environment |
| Ubana et al.102 2015 | 71 | ‘multidisciplinary programme’ |
| Valenkamp et al.103 2011 | 73 | Pro-ACT |
| van Loan et al.184 2015 | 74 | Shifting Gears |
| Verret et al.161 2019 | 75 | schoolwide de-escalation intervention plan |
| West et al.164 2017 | 77 | guided sensory room use |
| Williams et al.185 2011 | 78 | OBM |
| Wisdom et al.164 2015 | 2 | 6CS |
| Witte167 2008 | 79 | Six Steps to Success |
| Witte160 2007 | 80 | CPI’s Enhancing Verbal Skills: Applications of Life Space Crisis InterventionSM |
Mapping records: interventions by author
| Author(s) | INTa | Name/descriptionb |
|---|---|---|
| Andrassy154 2016 | 1 | ‘Feelings Thermometer Scale’ |
| Azeem et al.105 2015 | 2 | ‘six core strategies based on trauma informed care’ |
| Barnett et al.190 2002 | 3 | Guide to improve management of client acute aggressive behaviour |
| Brown et al.78 2013 | 8 | TST |
| Budlong169 2004 | 9 | ‘training approaches designed to reduce the use of restraint and seclusion in residential services for youth’ |
| Caldwell et al.115 2014 | 2 | 6CS |
| Caldwell and LeBel116 2010 | 2 | 6CS |
| Canady106 2018 | 11 | Comfort vs. control |
| Care Council for Wales174 2016 | 12 | Positive Behaviour Support, Active Support and Restorative Approaches |
| Carter et al.85 2008 | 13 | PMAB |
| Colton78 2014 | 14 | Checklist for Assessing Your Organization’s Readiness for Reducing Seclusion and Restraint |
| Colton and Xiong 2009 | 15 | unnamed |
| Cooper121 2008 | 16 | TCI |
| CPI117 2013 | 2 | Nonviolent Crisis Intervention®: Six Core Strategies |
| Donovan et al.175 2003 | 21 | Riverview program, based on ABCD (Brendtro and Ryan and associates) |
| Ford128 2013 | 26 | TARGET (FREEDOM Steps) |
| Girelli210 2004 | 30 | ‘comprehensive, multidimensional approach’ |
| Goren et al.168 1996 | 31 | ‘a project to reduce violence within a public child psychiatric hospital’ |
| Guilfoile132 2004 | 32 | ‘Devereux Glenholme internal quality improvement process’ |
| HM Government30 2019 | 36 | ‘a positive and proactive approach to behaviour’ |
| HM Inspectorate of Prisons23 2015 | 37 | MMPR |
| Holden et al.122 2020 | 16 | TCI |
| Holden et al.123 2020 | 16 | TCI |
| Holden et al.124 2020 | 16 | TCI |
| Leitch238 2008 | 47 | Hands Off |
| Leitch240 2008 | 47 | Hands Off |
| Leitch237 2009 | 47 | Hands Off |
| Leitch195 2009 | 47 | Hands Off |
| Leitch239 (no date) | 47 | Hands Off |
| Lietzke118 2014 | 2 | Nonviolent Crisis Intervention |
| Magnowski241 (no date) | 48 | unnamed |
| NASMHPD33 2006 | 2 | 6CS |
| Partnership Projects186 2020 | 57 | Neuro De-escalation |
| PRICE Training126 2020 | 60 | PRICE Training |
| Rettmann119 2019 | 2 | Nonviolent Crisis Intervention |
| Reynolds et al.127 2019 | 60 | M-PBIS |
| Rowan166 2010 | 61 | Schools Operating Safely |
| Smallridge and Williamson187 2011 | 67 | CRT |
| Studio III Training Systems and Psychological Services242 2019 | 68 | Various interventions, including LASER |
| US Department of Education197 2012 | 72 | unnamed |
| Visalli and McNasser188 2000 | 76 | ‘behavior mapping, the Anger Management Assessment and the Triangle of Choices’ |
| Welsh Government180 | 60 | PBS |
| World Health Organization194 2019 | 81 | strategies to end seclusion and restraint |
| Youth Justice Board for England and Wales199 2009 | 82 | ‘restraint minimisation strategies’ |
| Youth Justice Board for England and Wales192 2012 | 83 | MMPR |
Appendix 6 Evaluation study design by author
| Author(s) | Intervention name/brief descriptiona | Intervention number | Intervention eventb | Des | Eval? | Rand? | Contr? | Finds? | Sig? (p ≤ 0.05) |
|---|---|---|---|---|---|---|---|---|---|
| Azeem et al.38 2017 | 6CS | 2 | 2 | NR | 1 | 0 | 0 | 1 | 0 |
| Bobier et al.165 2015 | SM | 4 | 14 | QTD | 1 | 0 | 0 | 1 | 1 |
| Boel-Studt171 2017 | TIC | 5 | 15 | NR | 1 | 0 | 1 | 1 | 1 |
| Bonnell et al.109 2014 | CPS | 6 | 16 | NR | 1 | 0 | 0 | 1 | 1 |
| Borckardt et al.181 2011 | engagement model | 7 | 17 | NR | 1 | 0 | 1 | 1 | 1 |
| Campbell211 2004 | STAR | 10 | 20 | QTD | 1 | 0 | 0 | 1 | 0 |
| Craig and Sanders120 2018 | TIA | 11 | 22 | QTD | 1 | 0 | 0 | 0 | 0 |
| Craig88 2015 | Grafton program | 17 | 30 | NR | 1 | 0 | 0 | 1 | 0 |
| Crosland et al.204 2008 | Behavior Analysis Services Program | 18 | 32 | NR | 1 | 0 | 0 | 1 | 0 |
| Dean e et al.163 2007 | milieu-based program | 19 | 33 | QTD | 1 | 0 | 0 | 1 | 1 |
| Deveau and Leitch209 2015 | RRM | 20 | 34 | NR | 1 | 0 | 0 | 1 | 1 |
| Eblin162 2019 | quality improvement | 22 | 36 | QTD | 1 | 0 | 0 | 1 | 0 |
| Elwyn et al.178 2017 | Sanctuary Model | 23 | 37 | QL | 1 | 0 | 0 | 1 | 0 |
| Ercole-Fricke et al.107 2016 | CPS | 24 | 38 | NR | 1 | 0 | 1 | 1 | 1 |
| Ercole89 2014 | CPS | 24 | 38 | NR | 1 | 0 | 1 | 1 | 1 |
| Farina90 2007 | evaluation of impact | 25 | 45 | NR | 1 | 0 | 0 | 1 | 1 |
| Finnie91 2013 | evaluation of process | 24 | 39 | MM | 1 | 0 | 0 | 1 | 1 |
| Ford and Hawke128 2012 | TARGET | 26 | 46 | NR | 1 | 0 | 1 | 1 | 1 |
| Forrest et al.172 2018 | BCC | 27 | 48 | QTD | 1 | 0 | 0 | 1 | 0 |
| Fowler155 2006 | aromatherapy | 28 | 49 | QTD | 1 | 0 | 0 | 1 | 1 |
| Fralick176 2007 | Rapid Cycle Model | 29 | 50 | QL | 1 | 0 | 0 | 1 | 0 |
| Glew92 2012 | CPS | 24 | 40 | QTD | 1 | 0 | 0 | 1 | 1 |
| Greene110 2006 | CPS | 24 | 41 | NR | 1 | 0 | 0 | 1 | 1 |
| Hallman et al.236 2014 | Mindfulness | 33 | 55 | NR | 1 | 0 | 0 | 1 | 1 |
| Hambrick et al.79 2018 | NMT | 34 | 56 | NR | 1 | 0 | 0 | 1 | 1 |
| Health Sciences Center Winnipeg104 2015 | 6CS | 2 | 6 | NR | 1 | 0 | 0 | 0 | 0 |
| Hellerstein et al.203 2007 | hospital-wide initiative | 35 | 57 | NR | 1 | 0 | 0 | 1 | 0 |
| Hodgdon et al.183 2013 | ARC Framework | 38 | 60 | MM | 1 | 0 | 0 | 1 | 1 |
| Holstead et al.191 2010 | restraint reduction initiative | 39 | 61 | QTD | 1 | 0 | 0 | 1 | 0 |
| Huckshorn77 2010 | 6CS | 2 | 7 | NR | 1 | 0 | 0 | 1 | 0 |
| Jani et al.159 2011 | milieu therapy training and CPS | 44 | 66 | QTD | 1 | 0 | 0 | 1 | 1 |
| Jones and Timbers201 2003 | Teaching-Family Model | 40 | 62 | NR | 1 | 0 | 0 | 1 | 1 |
| Jonikas et al.189 2004 | improvement programme | 41 | 63 | QTD | 1 | 0 | 0 | 1 | 1 |
| Kalogjera et al.173 1989 | therapeutic management | 42 | 64 | NR | 1 | 0 | 0 | 1 | 1 |
| Kaltiala-Heino et al.198 2007 | aggression management | 43 | 65 | NR | 1 | 0 | 0 | 1 | 0 |
| Kilgore93 2018 | CPS | 24 | 42 | NR | 1 | 0 | 0 | 1 | 1 |
| Lebel and Goldstein39 2005 | state-wide initiative | 45 | 67 | QTD | 1 | 0 | 0 | 1 | 0 |
| LeBel et al.40 2004 | systems approach | 46 | 68 | NR | 1 | 0 | 0 | 1 | 0 |
| Leitch195 2009 | RPI | 47 | 69 | QTD | 1 | 0 | 0 | 1 | 1 |
| Magnowski95 2018 | milieu nurse | 48 | 70 | QTD | 1 | 0 | y | 1 | 1 |
| Magnowski and Cleveland80 2019 | cognitive milieu therapy | 48 | 70 | QL | 1 | 0 | 0 | 1 | 1 |
| Marrow et al.129 2012 | TARGET | 26 | 47 | QTD | 1 | 0 | y | 1 | 1 |
| Martin et al.111 2008 | CPS | 24 | 43 | QTD | 1 | 0 | 0 | 1 | 1 |
| McGlinn96 2006 | evaluation of federal regulations | 49 | 71 | MM | 1 | 0 | 0 | 1 | 1 |
| Miguel97 2016 | ‘Functional Communications Training’ and ‘Systema Breathing’ | 50 | 72 | QL | 1 | 0 | 0 | 1 | 0 |
| Miller et al.182 2006 | organizational and milieu intervention | 51 | 73 | NR | 1 | 0 | 1 | 1 | 1 |
| Murphy and Siv158 2011 | MDT | 52 | 74 | NR | 1 | 0 | y | 1 | 0 |
| Nunno et al.177 2015 | CARE model | 53 | 75 | MM | 1 | 0 | 0 | 1 | 1 |
| Nunno et al.81 2003 | TCI | 16 | 29 | NR | 1 | 0 | 0 | 1 | 1 |
| O’Brien202 2004 | psychoeducation | 54 | 76 | QTD | 1 | 0 | 0 | 1 | 1 |
| Paccione-Dyszlewski et al.170 2012 | safety management program | 55 | 77 | NR | 1 | 0 | 0 | 1 | 1 |
| Padhi et al.99 2019 | cultural transformation | 56 | 78 | NR | 1 | 0 | 0 | 1 | 0 |
| Plant179 2004 | ABCD program | 58 | 80 | QTD | 1 | 0 | 0 | 0 | 0 |
| Pollastri et al.112 2016 | CPS | 24 | 44 | MM | 1 | 0 | 0 | 1 | 1 |
| Ponge and Harris243 2006 | multidisciplinary, multimodal approach | 59 | 81 | NR | 1 | 0 | 0 | 1 | 0 |
| Reynolds et al.125 2016 | M-PBIS | 60 | 83 | NR | 1 | 0 | 0 | 1 | 1 |
| Reynolds et al.100 2019 | M-PBIS | 60 | 83 | 0 | 1 | 0 | 0 | 1 | 1 |
| Russell et al.131 2009 | SPA | 32 | 54 | NR | 1 | 0 | 0 | 1 | 1 |
| Ryan et al.113 2007 | Nonviolent Crisis Intervention Training | 2 | 11 | NR | 1 | 0 | 0 | 1 | 0 |
| Ryan et al.86 2008 | Therapeutic Intervention | 62 | 86 | NR | 1 | 0 | 0 | 1 | 0 |
| Sanders108 2009 | Grafton program | 17 | 31 | NR | 1 | 0 | 0 | 1 | 0 |
| Schreiner et al.41 2004 | restraint reduction process | 63 | 87 | NR | 1 | 0 | 0 | 1 | 0 |
| Seckman et al.156 2017 | sensory room | 88 | 88 | NR | 1 | 0 | 0 | 1 | 0 |
| Shadili et al.101 2012 | behavioural management | 65 | 89 | NR | 1 | 0 | 0 | 1 | 0 |
| Singh et al.214 1999 | organisational programme | 66 | 90 | NR | 1 | 0 | 0 | 1 | 0 |
| Thomann98 2009 | restraint reduction | 69 | 93 | QD | 1 | 0 | 0 | 1 | 1 |
| Thompson et al.87 2008 | Components of a Harm-Free Environment | 70 | 94 | QD | 1 | 0 | 0 | 1 | 1 |
| Ubana et al.102 2015 | multidisciplinary programme” | 71 | 95 | NR | 1 | 0 | 0 | 1 | 0 |
| Valenkamp et al.103 2011 | Pro-ACT | 73 | 97 | NR | 1 | 0 | 0 | 1 | 0 |
| van Loan184 2015 | Shifting Gears | 74 | 98 | NR | 1 | 0 | 0 | 1 | 0 |
| Verret et al.161 2019 | schoolwide intervention | 75 | 99 | QTD | 1 | 0 | 0 | 1 | 1 |
| West et al.164 2017 | sensory room | 77 | 101 | QTD | 1 | 0 | 1 | 1 | 1 |
| Williams et al.185 2011 | OBM | 78 | 102 | NR | 1 | 0 | 0 | 1 | 0 |
| Wisdom et al.114 2015 | 6CS | 2 | 12 | NR | 1 | 0 | 0 | 1 | 1 |
| Witte167 2008 | ‘Six Steps to Success’ | 79 | 103 | QL | 1 | 0 | 0 | 1 | 0 |
| Witte160 2007 | Verbal Skills | 80 | 104 | QTD | 1 | 0 | 0 | 1 | 0 |
Appendix 7 Behavior change techniques not detected, or rarely detected, by setting
| MH (n = 4) | HSC (n = 9) | EDU (n = 24) | CJS (n = 17) | GEN (n = 26) |
|---|---|---|---|---|
| 5.6 (information about emotional consequences) | 12.5 (adding objects to the environment) | 12.5 (adding objects to the environment) | 1.9 (commitment) | 12.5 (adding objects to the environment) |
| 1.7 [review outcome goal(s)] | 9.1 (credible source) | 9.1 (credible source) | 2.2 (feedback on behavior) | 8.1 (behavioral practice/rehearsal) |
| 10.5 (social incentive) | 6.1 (demonstration of the behavior) | 6.1 (demonstration of the behavior) | 1.1 [goal setting (behavior)] | 1.9 (commitment) |
| 3.1 [social support (unspecified)] | 1.1 [goal setting (behavior)] | 2.2 (feedback on behavior) | 1.3 [goal setting (outcome)] | 9.1 (credible source) |
| 2.1 (monitoring of behaviour by others without feedback) | 1.1 [goal setting (behavior)] | 4.2 (information about antecedents) | 6.1 (demonstration of the behavior) | |
| 5.1 (monitoring of emotional consequences) | 1.3 [goal setting (outcome)] | 5.6 (information about emotional consequences) | 2.2 (feedback on behavior) | |
| 14.10 (remove punishment) | 4.2 (information about antecedents) | 5.1 (information about health consequences) | 1.1 [goal setting (behavior)] | |
| 10.10 [reward (outcome)] | 5.6 (information about emotional consequences) | 2.1 (monitoring of behaviour by others without feedback) | 4.2 (information about antecedents) | |
| 2.4 [self-monitoring of outcome(s) of behaviour] | 5.1 (information about health consequences) | 11.2 (reduce negative emotions) | 5.1 (information about health consequences) | |
| 2.1 (monitoring of behaviour by others without feedback) | 14.10 (remove punishment) | 2.1 (monitoring of behaviour by others without feedback) | ||
| 5.1 (monitoring of emotional consequences) | 1.7 [review outcome goal(s)] | 5.1 (monitoring of emotional consequences) | ||
| 5.7 (prompts/cues) | 10.10 [reward (outcome)] | 5.7 (prompts/cues) | ||
| 11.2 (reduce negative emotions) | 5.2 (salience of consequences) | 11.2 (reduce negative emotions) | ||
| 14.10 (remove punishment) | 2.3 (self-monitoring of behaviour) | 14.10 (remove punishment) | ||
| 12.1 (restructuring the physical environment) | 2.4 [self-monitoring of outcome(s) of behaviour] | 5.2 (salience of consequences) | ||
| 1.7 [review outcome goal(s)] | 6.2 (social comparison) | 2.3 (self-monitoring of behaviour) | ||
| 10.10 [reward (outcome)] | 3.3 [social support (emotional)] | 2.4 [self-monitoring of outcome(s) of behaviour] | ||
| 5.2 (salience of consequences) | 6.2 (social comparison) | |||
| 2.4 [self-monitoring of outcome(s) of behaviour] | 10.5 (social incentive) | |||
| 6.2 (social comparison) | 10.4 (social reward) | |||
| 10.5 (social incentive) | 3.3 [social support (emotional)] | |||
| 10.4 (social reward) | [social support (practical)] | |||
| 3.3 [social support (emotional)] | 3.1 [social support (unspecified)] | |||
| 3.1 [social support (unspecified)] | 10.10 [reward (outcome)] | |||
| 1.7 [review outcome goal(s)] | ||||
| 5.6 (information about emotional consequences) |
Clusters with one behavior change technique coded
| Cluster | BCT |
|---|---|
| 7 (associations) | 7.1 (prompts/cues) |
| 8 (repetition and substitution) | 8.1 (behavioral practice/rehearsal) |
| 9 (comparison of outcomes) | 9.1 (credible source) |
| 11 (regulation) | 11.2 (reduce negative emotions) |
| 14 (scheduled consequences) | 14.1 (remove punishment) |
Behavior change techniques not detected, by cluster
| Cluster | BCT |
|---|---|
| 1 (goals and planning) | 1.5 [review behavior goal(s)] |
| 1.6 (discrepancy between current behavior and goal) | |
| 1.8 (behavioral contract) | |
| 2 (feedback and monitoring) | 2.6 (biofeedback) |
| 4 (shaping knowledge) | 4.3 (re-attribution) |
| 4.4 (behavioral experiments) | |
| 5 (natural consequences) | 5.3 (information about social and environmental consequences) |
| 5.5 (anticipated regret) | |
| 6 (comparison of behavior) | 6.3 (information about others’ approval) |
| 7 (associations) | 7.2 (cue signalling reward) |
| 7.3 (reduce prompts/cues) | |
| 7.4 (remove access to the reward) | |
| 7.5 (remove aversive stimulus) | |
| 7.6 (satiation) | |
| 7.7 (exposure) | |
| 7.8 (associative learning) | |
| 8 (repetition and substitution) | 8.2 (behavior substitution) |
| 8.3 (habit formation) | |
| 8.4 (habit reversal) | |
| 8.5 (overcorrection) | |
| 8.6 (generalisation of target behavior) | |
| 8.7 (graded tasks) | |
| 9 (comparison of outcomes) | 9.2 (pros and cons) |
| 9.3 (comparative imagining of future outcomes) | |
| 10 (reward and threat) | 10.1 [material incentive (behavior)] |
| 10.2 [material reward (behavior)] | |
| 10.3 (non-specific reward) | |
| 10.6 (non-specific incentive) | |
| 10.7 (self-incentive) | |
| 10.8 [incentive (outcome)] | |
| 10.9 (self-reward) | |
| 10.10 [reward (outcome)] | |
| 10.11 (future punishment) | |
| 11 (regulation) | 11.1 (pharmacological support) |
| 11.3 (conserving mental resources) | |
| 11.4 (paradoxical instructions) | |
| 12 (antecedents) | 12.3 (avoidance/reducing exposure to cues for the behavior) |
| 12.4 (distraction) | |
| 12.6 (body changes) | |
| 13 (identity) | 13.3 (incompatible beliefs) |
| 13.4 (valued self-identity) | |
| 13.5 (identity associated with changed behavior) | |
| 14 (scheduled consequences) | 14.1 (behavior cost) |
| 14.2 (punishment) | |
| 14.3 (remove reward) | |
| 14.4 (reward approximation) | |
| 14.5 (rewarding completion) | |
| 14.6 (situation-specific reward) | |
| 14.7 (reward incompatible behavior) | |
| 14.8 (reward alternative behavior) | |
| 14.9 (reduce reward frequency) | |
| 15 (self-belief) | 15.1 (verbal persuasion about capability) |
| 15.2 (mental rehearsal of successful performance) | |
| 15.3 (focus on past success) | |
| 15.4 (self-talk) | |
| 16 (covert learning) | 16.1 (imaginary punishment) |
| 16.2 (imaginary reward) | |
| 16.3 (vicarious consequences) |
Appendix 8 Interventions by study design
| Author | Name of interventiona | Intervention numberb | Intervention event | Des? | Eval? | Rand? | Contr? | Finds? | Sig? |
|---|---|---|---|---|---|---|---|---|---|
| Azeem et al.38 2017 | 6CS (based on trauma informed care) | 2 | 2 | NR | 1 | 0 | 0 | 1 | 0 |
| Bobier et al.165 2015 | ‘a sensory modulation room’ | 4 | 14 | QTD | 1 | 0 | 0 | 1 | 1 |
| Boel-Studt171 2017 | TI-PRC | 5 | 15 | NR | 1 | 0 | 1 | 1 | 1 |
| Bonnell et al.109 2014 | (CPS) | 6 | 16 | NR | 1 | 0 | 0 | 1 | 1 |
| Borckardt et al.181 2011 | the engagement model (an adaptation from the work of Bloom) | 7 | 17 | NR | 1 | 0 | 1 | 1 | 1 |
| Campbell211 2004 | STAR | 10 | 20 | QTD | 1 | 0 | 0 | 1 | 0 |
| Craig and Sanders120 2018 | TIA. Comfort vs. control. ‘program model for minimizing restraint and seclusion’ | 11 | 22 | QTD | 1 | 0 | 0 | 0 | 0 |
| Craig88 2015 | Minimisation of restraint and seclusion model (Grafton 2010) | 17 | 30 | NR | 1 | 0 | 0 | 1 | 0 |
| Crosland et al.204 2008 | Behavior Analysis Services Program | 18 | 32 | NR | 1 | 0 | 0 | 1 | 0 |
| Dean et al.163 2007 | ‘a milieu-based behavioral management program’ | 19 | 33 | QTD | 1 | 0 | 0 | 1 | 1 |
| Deveau and Leitch209 2015 | RRM | 20 | 34 | NR | 1 | 0 | 0 | 1 | 1 |
| Eblin162 2019 | ‘quality improvement’ (title) | 22 | 36 | QTD | 1 | 0 | 0 | 1 | 0 |
| Elwyn et al.178 2017 | The Sanctuary Model | 23 | 37 | QL | 1 | 0 | 0 | 1 | 0 |
| Ercole-Fricke et al.107 2016 | CPS | 24 | 38 | NR | 1 | 0 | 1 | 1 | 1 |
| Ercole89 2014 | CPS | 24 | 38 | NR | 1 | 0 | 1 | 1 | 1 |
| Farina90 2007 | evaluation of impact of new S/R policy | 25 | 45 | NR | 1 | 0 | 0 | 1 | 1 |
| Finnie91 2013 | N/A. CPS recently introduced but impact not measured in this study | 24 | 39 | MM | 1 | 0 | 0 | 1 | 1 |
| Ford and Hawke128 2012 | TARGET | 26 | 46 | NR | 1 | 0 | 1 | 1 | 1 |
| Forrest et al.172 2018 | BCC | 27 | 48 | QTD | 1 | 0 | 0 | 1 | 0 |
| Fowler155 2006 | ‘aromatherapy for crisis management’ | 28 | 49 | QTD | 1 | 0 | 0 | 1 | 1 |
| Fralick176 2007 | Rapid Cycle Model for Improvement | 29 | 50 | QL | 1 | 0 | 0 | 1 | 0 |
| Glew92 2012 | CPS | 24 | 40 | QTD | 1 | 0 | 0 | 1 | 1 |
| Greene et al.110 2006 | collaborative problem-solving | 24 | 41 | NR | 1 | 0 | 0 | 1 | 1 |
| Hallman et al.236 2014 | Mindfulness-based Stress Reduction training program | 33 | 55 | NR | 1 | 0 | 0 | 1 | 1 |
| Hambrick et al.79 2018 | NMT | 34 | 56 | NR | 1 | 0 | 0 | 1 | 1 |
| Health Sciences Center Winnipeg104 2015 | 6CS (based on trauma informed care) | 2 | 6 | NR | 1 | 0 | 0 | 0 | 0 |
| Hellerstein et al.203 2007 | ‘a hospital-wide effort to decrease restraint and seclusion of psychiatric inpatients.’ | 35 | 57 | NR | 1 | 0 | 0 | 1 | 0 |
| Hodgdon et al.183 2013 | ARC Framework | 38 | 60 | mm | 1 | 0 | 0 | 1 | 1 |
| Holstead et al.191 2010 | ‘a restraint reduction initiative’ | 39 | 61 | QTD | 1 | 0 | 0 | 1 | 0 |
| Huckshorn77 2010 | 6CS (based on trauma informed care) | 2 | 7 | 0 | 1 | 0 | 0 | 1 | 0 |
| Jani et al.159 2011 | milieu therapy training and collaborative problem-solving | 44 | 66 | QTD | 1 | 0 | 0 | 1 | 1 |
| Jones and Timbers201 2003 | Teaching-Family Model | 40 | 62 | NR | 1 | 0 | 0 | 1 | 1 |
| Jonikas et al.189 2004 | ‘a program to reduce the use of physical restraint’ | 41 | 63 | QTD | 1 | 0 | 0 | 1 | 1 |
| Kalogjera et al.173 1989 | ‘therapeutic management’ | 42 | 64 | NR | 1 | 0 | 0 | 1 | 1 |
| Kaltiala-Heino et al.198 2007 | ‘a systematic and comprehensive aggression management program’ | 43 | 65 | NR | 1 | 0 | 0 | 1 | 0 |
| Kilgore93 2018 | CPS | 24 | 42 | NR | 1 | 0 | 0 | 1 | 1 |
| Lebel and Goldstein39 2005 | ‘statewide initiative to reduce or eliminate the use of seclusion and restraint among children and adolescents’ | 45 | 67 | QTD | 1 | 0 | 0 | 1 | 0 |
| LeBel et al.40 2004 | ‘a systems approach’ | 46 | 68 | NR | 1 | 0 | 0 | 1 | 0 |
| Leitch195 2009 | RPI | 47 | 69 | QTD | 1 | 0 | 0 | 1 | 1 |
| Magnowski95 2018 | ‘the milieu nurse’ | 48 | 70 | QTD | 1 | 0 | y | 1 | 1 |
| Magnowski and Cleveland80 2019 | ‘cognitive milieu therapy’ | 48 | 70 | QL | 1 | 0 | 0 | 1 | 1 |
| Marrow et al.129 2012 | Incorporated TARGET plus other elements“a multifaceted trauma-focused intervention’ | 26 | 47 | QTD | 1 | 0 | y | 1 | 1 |
| Martin et al.111 2008 | CPS | 24 | 43 | QTD | 1 | 0 | 0 | 1 | 1 |
| McGlinn96 2006 | described (in title) as ‘The effect of federal regulations on the physical restraint of children and adolescents in residential treatment’ | 49 | 71 | MM | 1 | 0 | 0 | 1 | 1 |
| Miguel97 2016 | ‘Functional Communications Training’ and ‘Systema Breathing’ | 50 | 72 | QL | 1 | 0 | 0 | 1 | 0 |
| Miller et al.182 2006 | ‘2-phase (organizational and milieu) physical restraint reduction intervention’ | 51 | 73 | NR | 1 | 0 | yes, phased design | 1 | 1 |
| Murphy and Siv158 2011 | MDT | 52 | 74 | NR | 1 | 0 | y | 1 | 0 |
| Nunno et al.177 2015 | the CARE model | 53 | 75 | MM | 1 | 0 | 0 | 1 | 1 |
| Nunno et al.81 2003 | TCI | 16 | 29 | NR | 1 | 0 | 0 | 1 | 1 |
| O’Brien202 2004 | key interventions including ‘GBT Psychoeducational Treatment Model’ | 54 | 76 | QTD | 1 | 0 | 0 | 1 | 1 |
| Paccione-Dyszlewski et al.170 2012 | QBS, Inc. SafetyCare Behavioral Safety Management program | 55 | 77 | NR | 1 | 0 | 0 | 1 | 1 |
| Padhi et al.99 2019 | unnamed, described as a ‘cultural transformation’ | 56 | 78 | NR | 1 | 0 | 0 | 1 | 0 |
| Plant179 2004 | The ABCD program including TACE staff training | 58 | 80 | QTD | 1 | 0 | 0 | 0 | 0 |
| Pollastri et al.112 2016 | collaborative problem-solving | 24 | 44 | MM | 1 | 0 | 0 | 1 | 1 |
| Ponge and Harris243 2006 | multidisciplinary, multimodal approach | 59 | 81 | NR | 1 | 0 | 0 | 1 | 0 |
| Reynolds et al.125 2016 | M-PBIS | 60 | 83 | NR | 1 | 0 | 0 | 1 | 1 |
| Reynolds et al.100 2019 | M-PBIS | 60 | 83 | 0 | 1 | 0 | 0 | 1 | 1 |
| Russell et al.131 2009 | SPA | 32 | 54 | NR | 1 | 0 | 0 | 1 | 1 |
| Ryan et al.113 2007 | CPI’s Nonviolent Crisis Intervention Training | 2 | 11 | NR | 1 | 0 | 0 | 1 | 0 |
| Ryan et al.86 2008 | Therapeutic Intervention | 62 | 86 | NR | 1 | 0 | 0 | 1 | 0 |
| Sanders108 2009 | Grafton program | 17 | 31 | NR | 1 | 0 | 0 | 1 | 0 |
| Schreiner et al.41 2004 | ‘restraint reduction process’ | 63 | 87 | NR | 1 | 0 | 0 | 1 | 0 |
| Seckman et al.156 2017 | ‘a sensory room and its impact on R/S use, staff–patient relationships, and patients’ ‘aggressive behaviors.’ | 88 | 88 | NR | 1 | 0 | 0 | 1 | 0 |
| Shadili et al.101 2012 | ‘a behavioural management plan’ (title) | 65 | 89 | NR | 1 | 0 | 0 | 1 | 0 |
| Singh et al.214 1999 | ‘reducing the use of seclusion and restraints’ | 66 | 90 | NR | 1 | 0 | 0 | 1 | 0 |
| Thomann98 2010 | ‘restraint reduction’ (abstract) | 69 | 93 | QD | 1 | 0 | 0 | 1 | 1 |
| Thompson et al.87 2008 | Components of a Harm-Free Environment | 70 | 94 | QD | 1 | 0 | 0 | 1 | 1 |
| Ubana et al.102 2015 | ‘nurse-led multidisciplinary programme’ | 71 | 95 | NR | 1 | 0 | 0 | 1 | 0 |
| Valenkamp et al.103 2011 | Pro-ACT | 73 | 97 | NR | 1 | 0 | 0 | 1 | 0 |
| van Loan et al.184 2015 | Shifting Gears | 74 | 98 | NR | 1 | 0 | 0 | 1 | 0 |
| Verret et al.161 2019 | ‘schoolwide de-escalation intervention plan’ | 75 | 99 | QTD | 1 | 0 | 0 | 1 | 1 |
| West et al.164 2017 | ‘guided sensory room use’ | 77 | 101 | QTD | 1 | 0 | 1 | 1 | 1 |
| Williams et al.185 2011 | OBM | 78 | 102 | NR | 1 | 0 | 0 | 1 | 0 |
| Wisdom et al.164 2015 | 6CS (based on trauma informed care) | 2 | 12 | NR | 1 | 0 | 0 | 1 | 1 |
| Witte167 2008 | ‘Six Steps to Success’ | 79 | 103 | QL | 1 | 0 | 0 | 1 | 0 |
| Witte160 2007 | CPI’s Enhancing Verbal Skills: Applications of Life Space Crisis Intervention | 80 | 104 | QTD | 1 | 0 | 0 | 1 | 0 |
Glossary
- Behaviour change technique
- A specific, irreducible, active component of an intervention designed to change behaviour, for example providing ‘information about health consequences’.
- Behavior change technique taxonomy
- A list of 93 behaviour change techniques organised into 16 clusters for standardised reporting of behaviour change interventions. Note that the taxonomy was published in US English and, therefore, US spelling is used here when referring to behavior change technique taxonomy terms.
- Behaviour Change Wheel
- A model produced from a synthesis of frameworks of behaviour change research literature. It is based on a model of behaviour called the COM-B, which attempts to describe how Capability, Opportunity and Motivation can change Behaviour. For comparison, the theoretical domains framework, which is used to explore changing clinical practice, can be viewed as a variant of the COM-B model; the components of COM-B have similar domains. The behaviour change wheel contains the higher-order categories of behaviour change techniques at its hub, for example social or reflective. The next level includes intervention functions, such as training or incentivisation, and the third, outer, level contains policy categories, such as legislation or regulation.
- Chemical restraint
- The use of medication that is intended to prevent, restrict or subdue movement of any part of the service user’s body.
- Children
- In this report, the term is used to mean children and/or young people.
- Evaluations
- Evaluations of interventions are reported in research articles and anecdotal reports. Replication studies and follow-up studies are counted as separate evaluations, and reports of different analyses from the same study are counted as a single evaluation.
- Instructions
- Instructions for the performance of an intervention.
- Intervention
- Any documented approach that seeks to reduce the use of restrictive practices through behaviour change techniques. They are action or actions intended to address restrictive practices in adult mental health acute settings, for example a staff training initiative with or without organisational change. Some interventions are developed within and for an individual setting. Others may be well-known interventions that have been developed previously and are applied across several time periods or settings.
- Isolation
- Any seclusion or segregation that is imposed on a service user.
- Manual restraint
- A hands-on method of physical restraint.
- Mechanical restraint
- A method of physical intervention involving the use of equipment.
- Mixed Methods Appraisal Tool
- A tool suitable for appraising studies with diverse designs.
- Pro re nata medication
- Medication given when needed, rather than at regular times.
- Procedures
- Actions taken as part of intervention, for example a training session.
- Restrictive practices
- Deliberate actions undertaken with the aim of restricting an individual’s movement, liberty and/or freedom to act independently. The intervention is intended to take rapid control of a dangerous situation in which there is a real possibility of harm to the person or others.
- Seclusion
- The confinement of a service user in a room, which may be locked.
List of abbreviations
- 6CS
- Six Core Strategies
- BCT
- behaviour change technique
- CPS
- Collaborative Problem-Solving
- CYP
- children and young people
- MMAT
- Mixed Methods Appraisal Tool
- MMPR
- Managing and Minimising Physical Restraint
- M-PBIS
- Modified Positive Behavioral Interventions and Supports
- MRC
- Medical Research Council
- NICE
- National Institute for Health and Care Excellence
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- p.r.n.
- pro re nata
- RCT
- randomised controlled trial
- SPA
- Devereux’s Safe and Positive Approach
- TARGET
- Trauma Affect Regulation: Guide for Education and Therapy
- TCI
- Therapeutic Crisis Intervention
- WIDER
- Workgroup for Intervention Development and Evaluation Research