
Notes
Article history
This themed issue of the Health Technology Assessment journal series contains a collection of research commissioned by the NIHR as part of the Department of Health’s (DH) response to the H1N1 swine flu pandemic. The NIHR through the NIHR Evaluation Trials and Studies Coordinating Centre (NETSCC) commissioned a number of research projects looking into the treatment and management of H1N1 influenza. NETSCC managed the pandemic flu research over a very short timescale in two ways. Firstly, it responded to urgent national research priority areas identified by the Scientific Advisory Group in Emergencies (SAGE). Secondly, a call for research proposals to inform policy and patient care in the current influenza pandemic was issued in June 2009. All research proposals went through a process of academic peer review by clinicians and methodologists as well as being reviewed by a specially convened NIHR Flu Commissioning Board.
Declared competing interests of authors
none
Permissions
Copyright statement
© 2010 Queen’s Printer and Controller of HMSO. This journal is a member of and subscribes to the principles of the Committee on Publication Ethics (COPE) (http://www.publicationethics.org/). This journal may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2010 Queen’s Printer and Controller of HMSO
Chapter 1 General introduction
How members of the public react when informed about the outbreak of a novel infectious disease can play a large role in determining the outbreak’s health,1 social2 and economic3 impact. Depending on the disease and the cultural context, governments often recommend that members of the public adopt protective behaviours, such as wearing masks,1 avoiding social events,4 washing their hands more frequently,1 taking prophylactic medication5 or receiving a vaccination. 6 Other actions that members of the public sometimes take, such as avoiding economically important activities that are perceived to be risky,3 shunning particular social groups2 or unnecessarily seeking medical care,7 are often discouraged by governments as causing more harm than good.
Levels of compliance with these official recommendations are rarely perfect. 5,8,9 As well as information received from public health campaigns, information from social contacts or the media and previous experiences with similar incidents can influence how people react during an outbreak, or if they will react at all. One important task that public health bodies can perform during any major incident is to assess how the public responds to the novel threat and what factors are important in influencing those responses. 10,11 Armed with this information, communication campaigns can be designed or fine-tuned to target those factors, with the aim of improving uptake of recommended behaviours and reducing the rates of other, less helpful, actions. Measuring and analysing public responses using theoretical frameworks of behaviour change strengthens this process; it provides greater understanding of the psychological mechanisms through which communication campaigns translate into behaviour and it informs us about the behaviour change techniques that are likely to be effective. 12
The influenza A H1N1v pandemic of 2009–10, commonly referred to in the UK as the ‘swine flu’ outbreak, saw the UK government make several behaviour recommendations to the public using an extensive multimedia campaign. After the first cases of swine flu were confirmed in the UK on 27 April 2009, the government’s messages focused on the importance of hygiene behaviours, such as hand-washing and tissue use, as ways to reduce the spread of the virus, and the appropriate use of NHS health services by people who were concerned that they might have caught swine flu. Later in the outbreak, the government also recommended that those who were believed to be at heightened risk from swine flu should receive the newly available vaccination against it. Consideration was also given to offering this vaccine to the UK population more generally. However, although this policy was widely discussed, it was never put into practice.
In order to assess the impact of the government’s communications campaigns, the Department of Health, England commissioned a series of 40 telephone surveys in which randomly selected members of the public were asked about the information they had heard regarding swine flu and about a range of cognitive, emotional and behavioural responses to the outbreak. As well as providing data that were of immediate relevance in informing policy, the surveys also provided an opportunity to gather data to improve communication strategies in future influenza pandemics or in outbreaks of other forms of infectious disease.
In this report, we present three studies that used unweighted data drawn from the first 36 of these surveys, which took place between 1 May 2009 and 10 January 2010. Data for the final four surveys were still being checked and finalised at the time of our analyses. In the first study we assessed how public perceptions relating to the swine flu outbreak changed over time, with a particular focus on levels of self-reported worry about the possibility of catching swine flu. Because media reporting is an area that official agencies may be able to influence during an outbreak, we also assessed the association between changes in the volume of media attention devoted to swine flu and changes in public perceptions.
In the second study, we used data from 20 of the surveys that were conducted before, during and after the UK’s summer wave of swine flu in order to assess how many people would have accepted the swine flu vaccine, had it been offered to them. Using cross-sectional analyses of the survey data, we also assessed whether the amount of information people had heard about the outbreak or their level of satisfaction with that information was associated with likely acceptance of the vaccine, and whether other factors that could be targeted by future communications campaigns were associated with likely acceptance, such as worry about the possibility of catching swine flu.
In the third study, we analysed data from the first five surveys that were conducted during May 2009, prior to any large-scale community spread of swine flu occurring in the UK. We assessed the percentage of people who had complied with official recommendations to carry tissues, had bought sanitising gel in order to clean their hands, avoided public transport (a behaviour that was not recommended by the UK government) and unnecessarily used NHS resources for a flu-related reason. We also assessed whether exposure to advertising or media coverage about swine flu influenced whether or not people had engaged in these behaviours, and whether this influence was because exposure altered the amount of knowledge they had regarding swine flu, their perceptions about the information available to them about swine flu, their perceptions about the efficacy of different protective actions or their level of worry about the possibility of catching swine flu.
These studies therefore assessed changes in the survey data over time (study 1) and the cross-sectional associations within the survey data at specific points during the outbreak (studies 2 and 3). Our approach to these analyses was informed by existing psychological models suggesting that worry about a health risk and perceptions about the efficacy of protective behaviours are important factors determining whether an individual will perform a given behaviour in response to a health threat. 13
Our research arose from collaborative work between the Department of Health’s Communications Directorate and the Behaviour and Communications subgroup of the UK’s Scientific Pandemic Influenza Committee, which reported to the Scientific Advisory Group in Emergencies during the outbreak (see Appendix 1 for our initial protocol). Analyses were led by the research team of psychologists and a statistician, with regular consultations with colleagues in the Department of Health’s Communications Directorate.
Chapter 2 Study 1: The influence of the media on levels of worry in the community
Key points
-
Members of the public get much of their information about health risks from the mass media. How the media report a given health risk therefore has the potential to affect how the public perceive it.
-
Using aggregate data from 36 UK national telephone surveys, this study demonstrated a correlation between the volume of media reporting about swine flu at any given time point and the number of people worried about the possibility of catching it. However, this association was only observable during the first wave of the outbreak during the summer of 2009. No such associations existed before swine flu had become established in the UK or during the second (winter) wave of the outbreak.
-
In future outbreaks involving a prolonged risk to the public’s health, attempting to keep the media’s attention focused on the outbreak is unlikely to maintain public concern about the risk over the medium to long term and hence their motivation to adhere to recommended protective behaviours. Other strategies may need to be used to maintain the public’s motivation.
Introduction
Members of the public are regularly exposed to health-related information from multiple sources, including friends and family, the internet, commercial advertising and health-care professionals. Most of the health-related information that people receive, however, is obtained from television, radio and the print media. 14,15 Reporting by these news sources has long been recognised as a key factor that can affect people’s health-related behaviours and have both positive and negative consequences for the public’s health. 16–22
One way in which the media exert these effects is by ‘setting the agenda’. The theory of agenda setting suggests that the more coverage an issue receives, regardless of the nature of that coverage, the more important it becomes to members of the public. 23,24 Where the issue is a health risk, an extension to the theory suggests that the more coverage the risk receives then the more concerned about it the public will become, regardless of the nature of the coverage. 25 Numerous studies have demonstrated a link between greater exposure to media reports about a health issue and concern, worry or anxiety about it: examples include anxiety about breast cancer,26 disquiet about genetically modified foods,27 fear of avian influenza28 or worry about a cryptosporidiosis outbreak. 29 Whether such effects persist during a sustained period of reporting is less certain. Two previous studies have assessed the impact of media coverage about severe acute respiratory syndrome (SARS) or the 2001 US anthrax attacks on distress or behaviour change. 9,30 In both studies, while media coverage in the early stages of the incident strongly predicted emotional or behavioural responses, media coverage in the later stages had little impact.
The content of media reporting about a risk may also affect how the public reacts to it. The theories of ‘second-level agenda setting’ and the closely related concept of ‘framing’31 suggest that those attributes of an issue that are made particularly salient by the media, or which are used to place an issue in context, can affect how people perceive it. 24 For health risks, there is a tendency for the media to make salient those attributes that are known to cause greater concern among the public or to reduce the perceived credibility or competence of the government. Examples of such attributes are a hazard’s adverse effects on children, its fatal consequences, and disagreement or uncertainty among scientific experts about the nature of the risk. 32–34 Conversely, portrayal of a risk as having been deliberately exaggerated by politicians, scientists or the media may increase scepticism among the public as to the true importance of the issue and result in decreased levels of concern. 35,36
The 2009 outbreak of swine flu was accompanied by extensive reporting by the UK news media. 36,37 In this study, we assessed whether the quantity of media reporting over the period of the outbreak was associated with changes in the number of people who reported being worried about the possibility of catching swine flu. We also sought to assess whether the amount of media reporting that specifically related to children, deaths, scientific uncertainty or disagreement, or which portrayed swine flu as an overexaggerated risk, was associated with levels of worry. Because swine flu was portrayed as a particular risk to children, we also conducted subgroup analyses to examine the relationship between media reporting and worry for survey respondents who had children in their households. As secondary outcomes, we assessed whether media reporting was associated with being satisfied with the amount of information available about swine flu, having heard a lot recently about swine flu, believing that too much fuss had been made about the risk of swine flu or believing that the government was well prepared for a swine flu pandemic.
Methods
The telephone surveys
Thirty-six telephone surveys were conducted between 1 May 2009 and 10 January 2010 by the Ipsos MORI Social Research Institute on behalf of the Department of Health, England. Each collected data over a 3-day period. The first five surveys were run with less than 2 days between them. Subsequent surveys were run weekly and then fortnightly. Random digit dialling and proportional quota sampling were used to ensure that each sample was demographically representative of the UK population, as determined by the most recent census data, with quotas based on age, gender, geographical region and social grade. 38 To be eligible for a survey, respondents had to be 16 years or over and speak English. Each survey was introduced to respondents as being ‘a national survey covering a variety of subjects’. Any other subjects were covered after the flu-related questions had been asked. The questions included in the surveys changed as the pandemic progressed, with time for completion ranging from 8 to 15 minutes.
The first survey (1–3 May 2009) had a sample size of 1173. All others had sample sizes of between 1047 and 1070. These sample sizes provided a sampling error of about plus or minus 3% for each survey. The total sample size for all 36 surveys was 38,182. Response rates for each survey, calculated as the number of completed interviews divided by the total number of people spoken to regardless of eligibility, were in the region of 8–11%. This is typical for surveys of this nature. 35,39,40
Survey questions
Participants in all surveys were told that ‘Swine flu is a form of influenza that originated in pigs but can be caught by, and spread among, people’ and were then asked ‘How worried, if at all, would you say you are now about the possibility of personally catching swine flu?’ Possible answers were ‘very worried’, ‘fairly worried’, ‘not very worried’ and ‘not at all worried’.
Participants were also asked ‘How satisfied or dissatisfied are you with the amount of information available to you about swine flu, from any source?’ Responses of ‘very satisfied’, ‘fairly satisfied’, ‘neither satisfied nor dissatisfied’, ‘fairly dissatisfied’ or ‘very dissatisfied’ were recorded.
Participants were asked ‘Please tell me whether you agree or disagree with the following statement: too much fuss is being made about the risk of swine flu.’ Responses of ‘strongly agree’, ‘tend to agree’, ‘neither agree nor disagree’, ‘tend to disagree’ and ‘strongly disagree’ were allowed.
Perceptions of governmental preparedness were assessed by asking ‘How well prepared do you think the government is for a swine flu pandemic?’ Possible responses were ‘very well prepared’, ‘fairly well prepared’, ‘not very well prepared’ and ‘not at all well prepared’.
In five surveys conducted between 1 May and 17 May 2009, participants were asked ‘How much have you heard about swine flu?’, with possible responses being ‘a lot’, ‘a moderate amount’, ‘a little’ or ‘nothing at all’. A similar question was then introduced in 22 surveys between 24 July 2009 and 10 January 2010, in which participants were asked ‘How much have you heard about swine flu in the past week?’, with responses of ‘a great deal’, ‘a fair amount’, ‘not very much’ or ‘nothing at all’ being allowed. For these later surveys, participants who reported having heard anything about swine flu in the past week were asked where they had heard this information. Responses were coded as relating to advertising (in newspapers or on television), news coverage (in local or national newspapers, on television or on radio), via a general practitioner (through a GP’s surgery or a letter from the GP), on the internet, from friends/family or at work.
In addition to a range of other personal and demographic questions, all participants were asked to state how many, if any, children under the age of 16 years were in their household.
All questions allowed participants to give a response of ‘don’t know’. ‘Don’t know’ responses accounted for no more than 1% of responses to the ‘worry’ and ‘how much have you heard’ items in any given survey, and no more than 3% for the ‘too much fuss’ and ‘satisfaction with the amount of information available’ items. The item relating to government preparedness was the hardest for participants to answer, with between 4% and 13% of respondents replying ‘don’t know’ in each survey. We excluded ‘don’t know’ responses from all analyses.
Media coverage
We assessed media coverage using software supplied by Meltwater News (http://meltwaternews.com). All searches were restricted to the internet sites of 11,132 UK-based news sources. These sources included a mix of national and regional newspapers, magazines, trade journals, television and radio stations and internet news providers. Searches were performed for the start dates of the 36 surveys.
As an indicator of the total amount of coverage devoted to swine flu we searched for any stories that contained the words swine flu, ‘pandemic’ or ‘H1N1’ in their opening paragraph. To assess the number of stories in which children were specifically linked to swine flu, we added a requirement that stories must include a word such as ‘child’, ‘baby’, ‘pupil’ or ‘school’ in the title. Similarly, to identify stories that discussed deaths relating to swine flu we added a requirement that the story must include a word such as ‘death’, ‘dies’ or ‘dead’ in its title. Stories relating to uncertainty or disagreement were identified as those which included the following terms, or common variations, in their title: ‘contradiction’, ‘muddle’, ‘disagree’, ‘uncertain’, ‘controversy’, ‘debate’, ‘doubt’, ‘argument’, ‘confusion’, ‘inconsistent’ or ‘critic’. Stories relating to the exaggeration of swine flu were identified as those that included variations on the following terms in the title: ‘alarmist’, ‘hype’, ‘hysteria’, ‘exaggerated’, ‘overplayed’, ‘overreacting’, ‘over the top’, ‘overstated’, ‘overblown’, ‘embellished’, ‘inflated’ or ‘sensationalised’. The exact searches used are given in Appendix 2.
In order to describe the type of reporting occurring on the start date for each survey, we also conducted a separate search using the Nexis database (www.lexisnexis.com/uk/nexis) to identify all UK-based national or regional newspaper stories with the terms swine flu, ‘H1N1’ or ‘pandemic’ in their title. A random sample of 30 stories was selected for each day to generate a short synopsis of the main aspects of media reporting.
Potential confounders
Because any association between public concern about swine flu and media reporting of it might simply reflect the changing severity of the outbreak, we obtained data on hospitalisations from swine flu in England as an objective marker of outbreak severity. These data were obtained from the Health Protection Agency41 and reflected the number of new patients admitted to hospital with suspected swine flu over a 7-day period.
Analyses
All media variables had a large positive skew, because of a small number of dates on which there was an unusually high level of media reporting. For our analyses, we transformed these data by adding 1 and taking the natural log. For the survey data we grouped together participant responses of ‘very worried’ and ‘fairly worried’ about the possibility of catching swine flu, ‘strongly agree’ and ‘tend to agree’ about too much fuss having been made, answers that the government was ‘very well prepared’ or ‘fairly well prepared’, and answers that the participant was ‘very satisfied’ or ‘fairly satisfied’ with the amount of information available about swine flu. For worry, although responses of ‘very worried’ might have reflected qualitatively different underlying mechanisms than responses of ‘fairy worried’, in practice the data for these two responses showed similar changes over time.
A consistent time interval between the data was required for our analyses. We therefore excluded results from the second and fourth surveys, and from the last three surveys to ensure that those surveys that were included had a gap of roughly 1 week between them. Most analyses were therefore based on data from 31 surveys. We excluded all of the May results for the question relating to the amount heard about swine flu, because excluding the second and fourth surveys left only three results for May followed by a lengthy gap until the question was reintroduced in July. This variable was therefore analysed for 19 surveys. Results from all surveys were plotted on the figures given below.
For the associations between survey data and hospitalisation or media data, we used regression models with autoregressive moving average disturbances. Here the dependent variable is regressed on the independent variable(s) as in a normal regression model but an autoregressive integrated moving average (ARIMA) model is fitted to the residuals to take into account the time series nature of the data. Although some of the variables are non-stationary, the residuals broadly meet the required assumptions, allowing this approach. For each dependent variable, diagnostic plots were examined and suggested low-order autoregressive modes with either one or two terms. The final model was selected based on the lowest Akaike’s information criterion: a first order autoregressive [AR(1)] model was the best fitting for all of the variables. Associations between the survey variables were then assessed using a likelihood ratio test comparing an AR(1) model with no independent variable and an AR(1) model with a survey variable as the independent variable. Associations between the media variables were tested using Kendall’s non-parametric correlation.
Subgroup analyses were conducted for worry data obtained from people who had children aged under 16 years of age in the household (between 21.7% and 27.9% of respondents in each survey).
Results
Changes in outcome measures over the course of the outbreak
Figure 1 shows the percentages of people within each survey who reported being worried about the possibility of catching swine flu, agreed that too much fuss had been made about the risk of swine flu, felt that the government was well prepared for a pandemic, were satisfied with the amount of information available about swine flu and reported having heard a lot or a moderate amount about swine flu.
FIGURE 1.
Changes over time in survey data. WHO, World Health Organization.
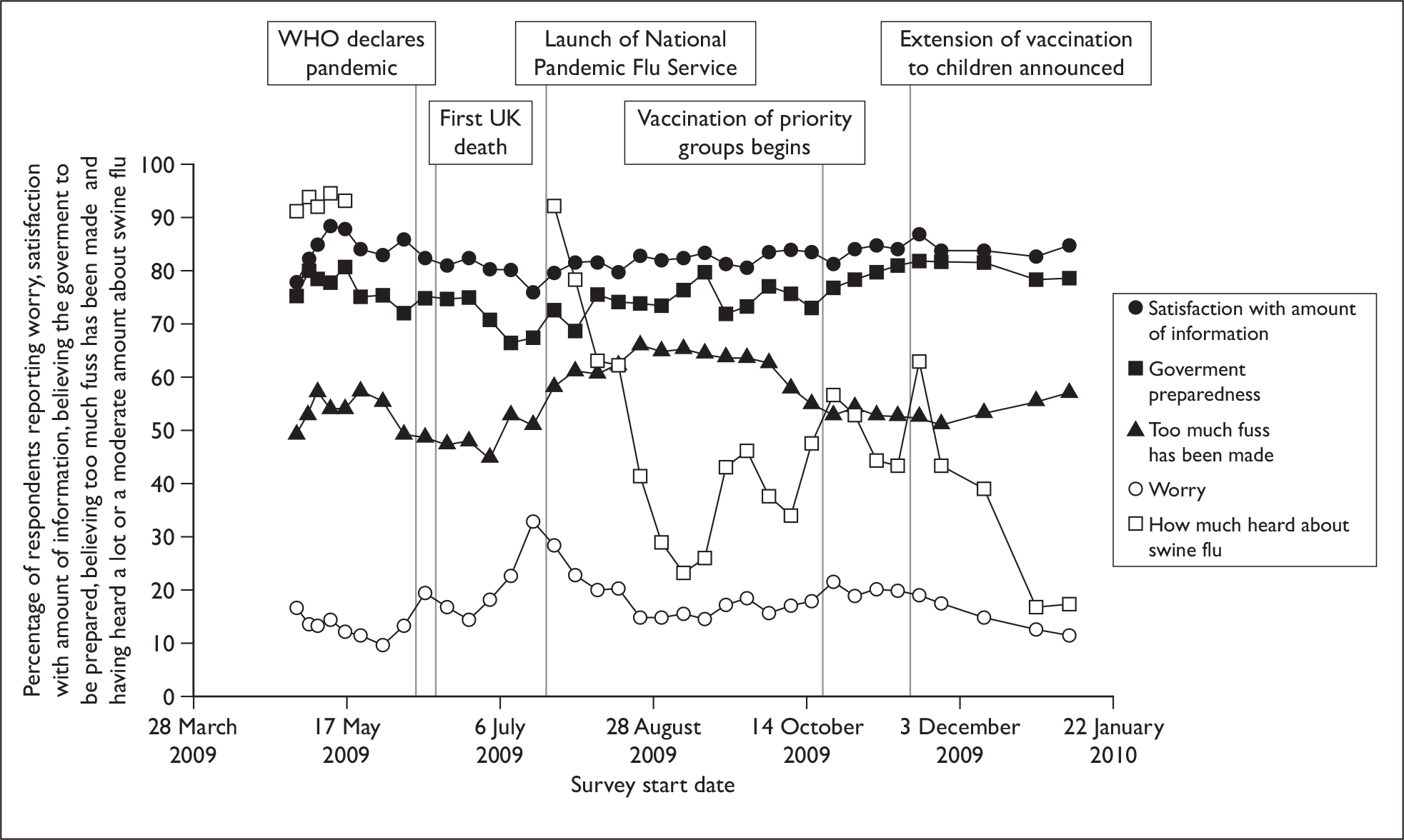
The percentage of people who were satisfied with the amount of information available or who felt that the government was well prepared for a pandemic ranged from 77.6% to 88.4% and from 66.4% to 81.7% respectively. Levels of worry showed larger fluctuations in the first half of the data collection period, rising from initially low levels (9.6–16.6% during May) to a peak of 19.3% in mid-June immediately following the declaration of a full pandemic by the World Health Organization, and a second peak of 32.9% in mid-July at the height of the summer wave of the outbreak. Following the summer wave, levels of worry then remained more stable from the end of August onwards, although smaller increases coinciding with the start of the winter wave of the outbreak and the start of the vaccination campaign were observed. Reports of the amount heard about swine flu showed the most dramatic changes, from initially high levels with over 90% of respondents reporting that they had heard ‘a lot’ or a ‘a moderate amount’ dropping to 11.4% having heard ‘a great deal’ or ‘a fair amount’ by early January 2010. Three noticeable peaks in ‘how much heard’ were observed in late September, late October and late November. These appeared to coincide with the winter wave of swine flu, the start of the swine flu vaccination campaign and the extension of the vaccination campaign to young children, respectively.
Table 1 shows the associations between the aggregate survey data. Overall, a higher level of worry about the possibility of catching swine flu tended to occur at the same time as lower satisfaction with the amount of information available about swine flu and having heard more about swine flu. Higher levels of belief that the government was very or fairly well prepared for a pandemic were associated with greater satisfaction with the amount of information available.
| Predictor variable | Dependent variable | |||
|---|---|---|---|---|
| Very or fairly worried about the possibility of catching swine flu | Strongly agree or agree that too much fuss has been made about swine flu | Believe that the government is very well prepared or fairly well prepared for a pandemic | Very satisfied or fairly satisfied with the amount of information available about swine flu | |
| Too much fuss | χ2(1) = 3.2, p = 0.074, coeff. = –0.3 | |||
| Government preparedness | χ2(1) = 2.0, p = 0.2, coeff. = –0.3 | χ2(1) = 0.1, p = 0.8, coeff. = 0.1 | ||
| Satisfaction with amount of information available | χ2(1) = 12.1, p < 0.001, coeff. = –0.8 | χ2(1) = 3.6, p = 0.058, coeff. = 0.4 | χ2(1) = 5.1, p = 0.024, coeff. = 0.6 | |
| Heard a lot about swine flu | χ2(1) = 22.5, p < 0.001, coeff. = 0.2 | χ2(1) = 1.1, p = 0.3, coeff. = 0.0 | χ2(1) = 2.1, p = 0.1, coeff. = –0.1 | χ2(1) = 1.9, p = 0.2, coeff. = 0.0 |
Participants who had heard something about swine flu had mostly received their information from the mainstream news media (n = 13,581, 74.7%), followed by friends, family or work (n = 3579, 19.7%), advertisements (n = 1959, 10.8%), the internet (n = 1426, 7.8%) and GPs (n = 846, 4.7%).
Changes in media reporting and hospitalisations
The general themes in media reporting on the start dates of each survey are summarised in Appendix 3. Overall, the media were consistent in characterising swine flu as a mild illness for most people. More specific themes changed over time. Throughout most of May, media reports about UK cases of swine flu typically described their connection to Mexico or the USA, either as a result of travel or through contact with a returned traveller. This trend was no longer apparent by early June, as the number of tertiary cases or cases with no known history of travel or contact with a traveller increased. Initial reports focused on ‘firsts’, such as the first cases occurring in local areas or the first instance of person-to-person transmission in the UK. As cases increased during the summer wave of the outbreak, media reporting started to focus on issues relating to government strategy, the capacity of the NHS, the suitability of the newly set up National Pandemic Flu Service, and the safety and efficacy of antiviral medications. From the start of August, the issue of swine flu vaccination became more prominent, with concerns raised about the vaccine’s safety, efficacy and availability, the information given about the order in which it would be provided to different sections of the population, and the apparently low uptake of the vaccine.
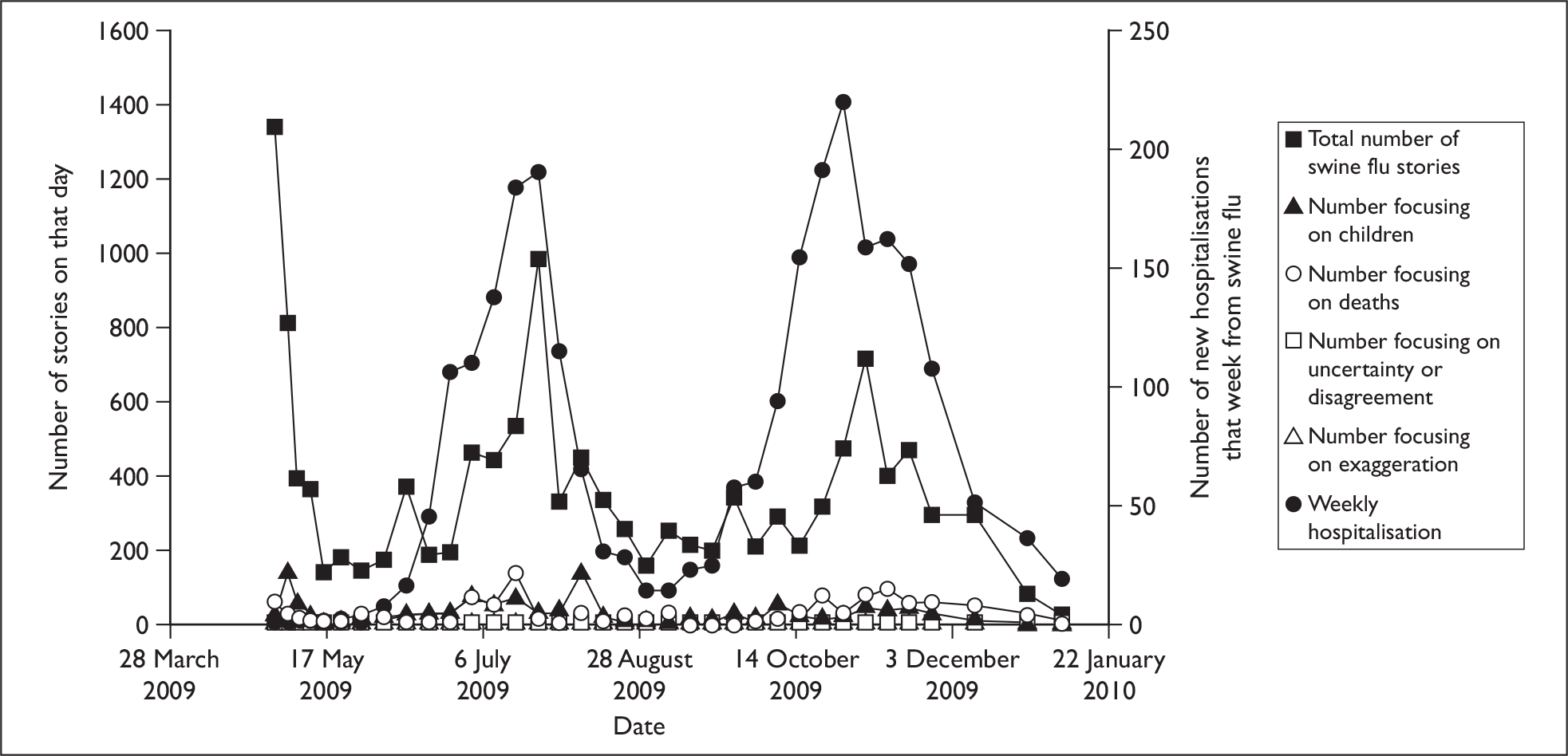
Figure 2 shows the changes in media reporting over time in terms of the total number of stories relating to swine flu and the number relating to children, death, uncertainty or exaggeration. Figure 2 also shows the changes in the number of new hospitalisations from swine flu reported to the Health Protection Agency. The total volume of media reporting started at a high level on 1 May, but decreased rapidly. After a small spike in reporting, which related to the World Health Organization’s declaration of a full pandemic on 11 June, two main peaks in reporting were observed, which largely coincided with the increased prevalence of swine flu during the summer and winter months. There was relatively little reporting that specifically focused on children or deaths. Those reports mentioning death showed a similar pattern to the total volume of coverage, with increases coinciding with the peaks of the outbreak. Articles mentioning children showed two main peaks: on 5 May 2009 following the reporting of the closure of two schools in London and on 7 August 2009 during discussions on whether or not to vaccinate school children. Levels of reporting relating to uncertainty or exaggeration were too low to be analysed and were dropped from all further analyses.
FIGURE 2.
Media reporting and number of new hospitalisations from swine flu.
The association between survey outcomes and media reporting
Table 2 shows the associations between the survey and hospitalisation data, and between the survey and media data adjusting for hospitalisations. Across the whole epidemic, the percentage of people reporting worry about the possibility of catching swine flu correlated with the number of hospitalisations recorded that week [χ2(1) = 8.2, p = 0.004, coefficient = 0.04], the total volume of reporting relating to swine flu after adjusting for hospitalisations [χ2(1) = 6.6, p = 0.010, coefficient = 2.6] and the total number of stories relating to death after adjusting for hospitalisations [χ2(1) = 4.3, p = 0.038, coefficient = 1.0]. Restricting the worry data to that obtained from participants with children in the house did not affect the pattern of results. There was no effect of the volume of reporting relating to children adjusting for hospitalisations [χ2(1) = 0.9, p = 0.3, coefficient = 0.8].
| No. of new hospitalisations that week from swine flu | Total no. of storiesa | No. of stories relating to childrena | No. of stories relating to deatha | |
|---|---|---|---|---|
| Worry about the possibility of catching swine flu | χ2(1) = 8.2, p = 0.004, coeff. = 0.04 | χ2(1) = 6.6, p = 0.010, coeff. = 2.6 | χ2(1) = 0.6, p = 0.4, coeff. = 0.0 | χ2(1) = 4.3, p = 0.038, coeff. = 1.0 |
| Too much fuss is being made about the risk of swine flu | χ2(1) = 0.3, p = 0.6, coeff. = –0.01 | χ2(1) = 0.8, p = 0.4, coeff. = –1.1 | χ2(1) < 0.1, p = 0.8, coeff. = 0.1 | χ2(1) = 4.7, p = 0.030, coeff. = –1.0 |
| Perceptions of government preparedness | χ2(1) < 0.1, p = 0.9, coeff. = 0.00 | χ2(1) = 0.1, p = 0.8, coeff. = 0.3 | 2(1) < 0.1, p = 0.9, coeff. = 0.1 | χ2(1) < 0.1, p = 0.9, coeff. = 0.0 |
| Satisfaction with amount of information available | χ2(1) = 0.2, p = 0.6, coeff. = 0.00 | χ2(1) = 6.0, p = 0.014, coeff. = –2.0 | χ2(1) = 1.4, p = 0.2, coeff. = –0.7 | χ2(1) = 1.0, p = 0.3, coeff. = –0.4 |
| How much have you heard about swine flu in the past week? | χ2(1) = 7.7, p = 0.006, coeff. = 0.19 | χ2(1) = 0.7, p = 0.4, coeff. = 4.9 | χ2(1) = 0.2, p = 0.7, coeff. = –1.1 | χ2(1) = 3.0, p = 0.083, coeff. = –4.5 |
Adjusting for hospitalisations, lower volume of reporting about swine flu was associated with greater satisfaction with the amount of information available [χ2(1) = 6.0, p = 0.014, coefficient = –2.0], and fewer stories relating to death was associated with more frequent perceptions that too much fuss had been made about the risk of swine flu [χ2(1) = 4.7, p = 0.030, coefficient = –1.0]. How much someone had heard about swine flu in the past week was associated with the number of hospitalisations for swine flu [χ2(1) = 7.7, p = 0.006, coefficient = 0.19].
The significant associations we identified between the survey data and reporting relating to children or death might have reflected the fact that both reporting relating to children (τb = 0.53, p < 0.001) and to death (τb = 0.51, p < 0.001) were correlated with the total volume of reporting. We investigated this by calculating additional models to test whether adjusting for the total volume of reporting affected the relevant associations shown in Table 2. With worry about the possibility of catching swine flu as the dependent variable, adding the number of stories relating to death to a model that already included the total number of stories did not significantly add to the effect [χ2(1) = 1.6, p = 0.2]. Similarly, with perceptions of too much fuss as the dependent variable, adding the number of stories relating to death to a model that already included the total volume of reporting as an independent variable did not significantly improve the model [χ2(1) = 3.8, p = 0.053].
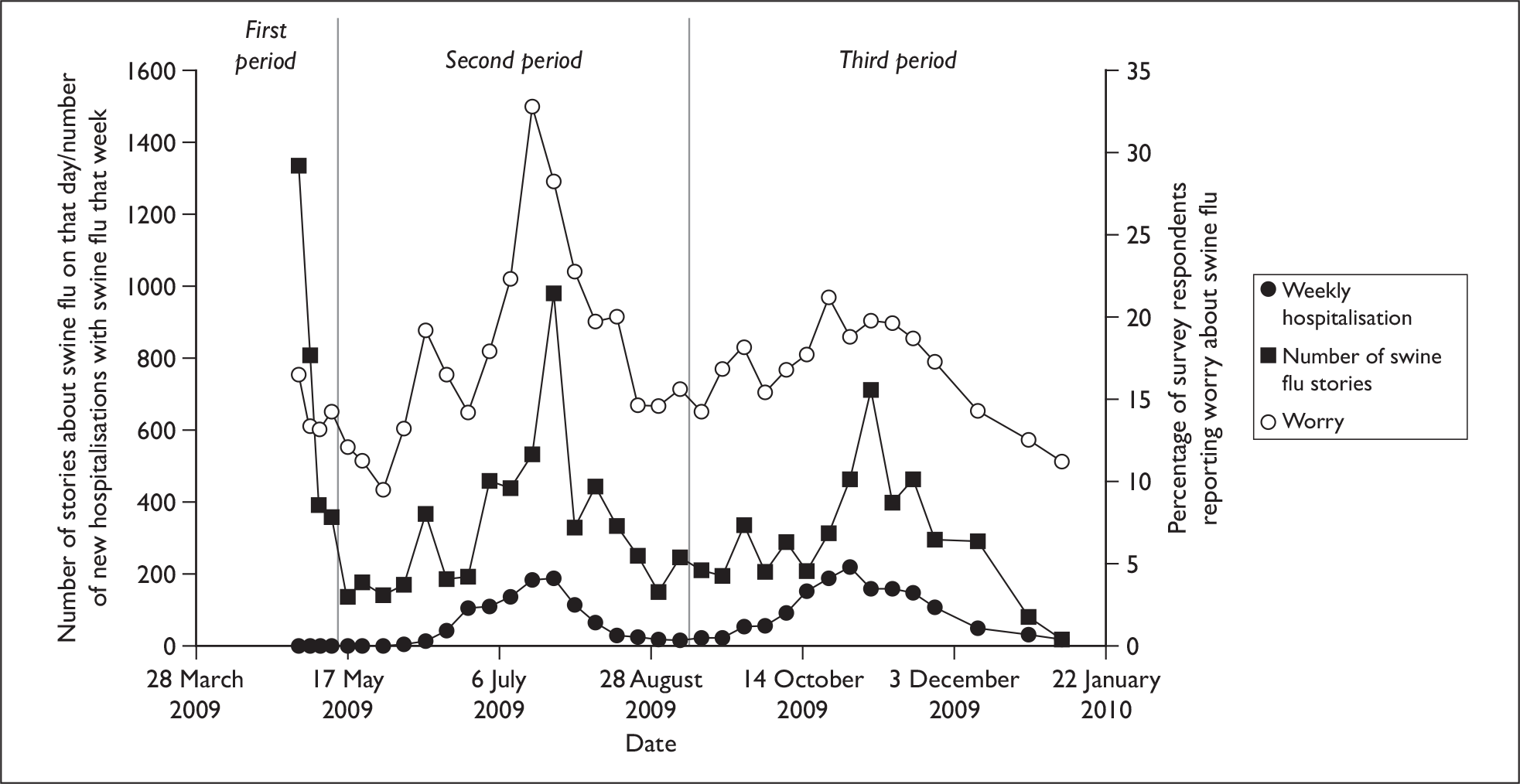
Figure 3 shows changes over time in worry about the possibility of catching swine flu, hospitalisation and the total amount of reporting. On the basis of visual inspection, we split the data into three periods: a first period in which a large volume of media reporting existed but without any substantial spread of swine flu in the community and two further periods reflecting the two peaks of the outbreak (see Figure 3). Although there were insufficient data to assess the relevant associations in the first period, the total volume of media reporting was positively associated with worry about the possibility of catching swine flu in the second and third periods (Table 3). After adjusting for the number of hospitalisations, however, this association remained only in the second period [χ2(1) = 6.8, p = 0.009, coefficient = 6.9].
FIGURE 3.
Changes over time for hospitalisations, media reporting and worry.
| Total no. of stories | Total no. of storiesa | |
|---|---|---|
| Worry about the possibility of catching swine flu (period 2) | χ2(1) = 13.1, p < 0.001, coefficient = 11.0 | χ2(1) = 6.8, p = 0.009, coefficient = 6.9 |
| Worry about the possibility of catching swine flu (period 3) | χ2(1) = 5.2, p = 0.023, coefficient = 3.2 | χ2(1) = 1.4, p = 0.2, coefficient = 1.1 |
Discussion
Our results show that public worry about the possibility of catching swine flu remained at relatively low levels throughout the outbreak. These levels showed some fluctuation, however, and were generally associated with the amount of media reporting about swine flu even after controlling for the potentially confounding influence of the changing nature of the outbreak.
The influence of total volume of reporting
The data relating to the outbreak’s summer wave were largely consistent with a theory suggesting that the total volume of reporting plays an important role in predicting levels of public concern. 25 Indeed, across the outbreak as a whole, quantitative changes in more specific aspects of media reporting, such as coverage relating to children or to deaths, were not associated with changes in worry about the possibility of catching swine flu after we adjusted for the severity of the outbreak and for the total volume of reporting. Although previous research has suggested that the personal relevance of a news story is a key factor in determining whether someone will pay attention to it,42 this lack of effect for specific aspects of reporting held true even for the effects of child-related reporting on participants who had children in their household.
This support for the quantity of coverage theory did not hold for every stage of the outbreak, however. In particular, it was notable that the earliest stage of the outbreak had the highest levels of media reporting yet relatively low levels of worry about the possibility of catching swine flu. One possible explanation for the apparent lack of association during this period is that at the time media reporting did not contain many examples of people in the UK being affected by swine flu unless they had some form of contact with the outbreak in Mexico. 43 This may have led many members of the public to conclude that swine flu was unlikely to be a risk to them. Previous research has suggested that a degree of geographical proximity may be required before people feel that a risk applies to them. 44 This may be particularly true for media coverage relating to infectious disease outbreaks, as the UK press has a history of reporting emerging infectious diseases, such as avian influenza, SARS and Ebola fever, which subsequently failed to become a risk to most people in the UK.
Levels of worry about the possibility of catching swine flu during the winter wave of the swine flu outbreak also failed to show any robust association with the total volume of media reporting. In part, this may reflect the fact that by the time the winter wave had arrived, members of the public had already built up a coherent understanding of the illness and of the outbreak, something that additional reporting did little to change. The decreased level of worry during the second wave suggests that the public had become habituated to flu-related messages and/or that their experience had demonstrated that worst-case scenarios had not occurred. It may also be that changes in the nature of the media reporting were responsible for this lack of an association, with a large proportion of the swine flu-related coverage during the winter period discussing the risks, benefits and roll-out of the swine flu vaccination rather than the impact of the disease itself.
The influence of key events
Although the total volume of media reporting did not show any clear association with worry about the possibility of catching swine flu during the winter period, examination of where changes in survey data occurred suggested that specific developments in the pandemic, such as the start of the winter wave of infections, the start of the vaccination campaign and discussions about the vaccination of children, did appear to be associated with an increase in the proportions of people who had recently heard information about swine flu and who were worried about the possibility of catching it. Even several months into the pandemic, key events were still able to generate increased concern.
One event that did not seem to trigger an increase in worry about the possibility of catching swine flu was the first death in the UK. This is inconsistent with reports from other countries. 45 It is possible than any genuine effect of this event was masked by a greater effect produced by the World Health Organization’s statement that a full pandemic had begun 4 days previously. Alternatively, any effect of the first death may have subsided over the 4-day interval which occurred before data collection began for the next survey wave. Other notable events that might be expected to trigger increased worry, such as the UK’s first case of swine flu, the move by the World Health Organization to phase 5 of its pandemic alert system, and the first case of swine flu in the UK resulting from transmission within the community, occurred either before or on the start date of the first survey, preventing us from examining their effects.
Changes in non-worry variables
Aside from worry about the possibility of catching swine flu and the amount of information heard about swine flu, the other survey data were notable for their relative stability. Satisfaction with the amount of information available about swine flu and belief that the government was well prepared for a pandemic showed little fluctuation and remained at relatively high levels throughout. It may be that this stability reflected the general lack of worry about the outbreak, which restricted any fluctuation in these variables to the minority of people who were worried. With little motivation to actively seek out information, it makes sense that most people were satisfied with the amount of information available to them. It is also understandable that most people were not overtly critical of governmental preparedness for a swine flu pandemic, given that they themselves did not believe swine flu to be particularly concerning. Perceptions that too much fuss had been made were also relatively stable, although some reductions that coincided with the summer and winter waves of the outbreak were observed. The relative stability of this variable suggests that this perception was determined by factors that were not readily amenable to change, for example an already established scepticism regarding the credibility of health warnings issued by the media or the government. 46
Methodological limitations
Several methodological limitations should be borne in mind when considering these results:
-
First, and most importantly, because they were based on aggregate data, our analyses ran the risk of falling prey to the ecological fallacy. 47 While our results indicate that periods of high reporting tended to coincide with high levels of worry about the possibility of catching swine flu among the community, this does not necessarily imply that the same correlations existed on an individual level.
-
Second, our measures of the quantity of media reporting were not ideal. It is likely that we missed some coverage, particularly for news stories that were broadcast on television or radio. Many of these stories will not have been catalogued by the database we used for our searches. Given that television and radio are widely used, this will have reduced the accuracy of our media measures. We were also unable to produce a metric to represent the amount that each story had been viewed, listened to or read. This would have resulted in a more accurate estimate of the effect of media coverage than simply calculating the total number of stories present on any given day. A more detailed content analysis of reporting by specific UK newspapers, coupled with individual-level data on the newspaper-reading habits of the survey participants, will allow a more fine-grained analysis to be conducted at a later date.
-
Third, our use of hospitalisation data as an objective marker of outbreak severity was limited. As well as being influenced by the number of people with swine flu, this measure may also have been affected by changes in doctor and patient behaviour as a result of changing information, perceptions or concerns about the illness. 48 However, alternative measures, such as the volume of calls to a telephone helpline or the number of GP consultations relating to influenza-like illness, were even more likely to be affected by levels of worry in the community,7,45 whereas the number of deaths from swine flu were too low to be a useful marker.
-
Fourth, the power of our analyses was restricted by the number of surveys that we were able to include. In particular, this may have had implications for those analyses that were restricted to data collected during the winter period of the outbreak. These analyses were based on only 12 surveys.
-
Fifth, the generalisability of our findings to other countries or other, more severe, outbreaks cannot be assumed. It is conceivable, for example, that at higher levels of threat and worry, the association between media coverage and worry might disappear, or even reverse. Similarly, in situations where media reporting diverges more dramatically from the official government position, it is possible that media reporting will have a larger impact on levels of uncertainty or worry among the public. Cross-cultural difference in terms of patterns of media use or perceptions of the trustworthiness of the media may also limit the generalisability of our findings.
Conclusions
Despite these methodological caveats, our results suggest that once a new risk has arrived in a country, the volume of media reporting about it will help to determine changes in the level of concern among members of the public. Once the risk has become more familiar, however, this association may be weakened. Given that worry about a risk is an important factor that motivates people to take protective actions13 and that the use of recommended protective actions can fade over time during an infectious disease outbreak,49 maintaining a degree of public concern about a new risk might be an important medium-term strategy for public health bodies that wish to promote the use of particular protective behaviours. Our results imply that attempting to influence the volume of media reporting about a new risk may become a less productive way of achieving this as public familiarity with the risk grows. Nonetheless, the occurrence of key events may continue to trigger increased levels of worry and, potentially, uptake of protective behaviours, even several months after a new risk has emerged.
In terms of the aspects of media reporting that might be the most important to engage with or monitor in any future infectious disease outbreak, our results suggest that the traditional news media remain the source most used by the public in obtaining information about public health incidents. About 75% of survey respondents who had heard anything about swine flu reported having heard this information via local or national newspapers, television or radio. In comparison, despite a growing interest in the use of the internet to convey information to the public,50 only 8% of the public reported having seen information on the internet. While 70% of UK households have internet access,51 there is clearly some way to go before this can become the main route of information transmission between the government and the public during a public health emergency.
Chapter 3 Study 2: Factors predicting likely acceptance of vaccination against swine or seasonal flu
Key points
-
Within the UK, vaccination against swine flu was restricted to specific priority groups. Although wider vaccination of the general public was discussed, it was never implemented.
-
Analysis of survey data collected prior to the start of the swine flu vaccination campaign suggested that only 56.1% of the general population were likely to have accepted the vaccine if offered it. Strong predictors for being likely to accept it were being worried about the possibility of personally catching swine flu, or being worried about the possibility of one’s children catching it, and disagreeing that too much fuss had been made about the risk of swine flu. Predictors for being more likely to accept the seasonal flu vaccine as a result of swine flu were similar, but also included the misperception that the seasonal flu vaccine would protect against swine flu.
-
If a vaccine needs to be given to the general public during a future infectious disease outbreak, messages that highlight people’s concerns or worries about the outbreak may be effective in improving uptake. Communications that emphasise the effectiveness of the vaccine in protecting against the disease are also likely to be effective.
Introduction
Within the UK, vaccination against swine flu began to be provided to priority groups from 21 October 2009. These groups consisted of frontline health and social care staff, people in clinical at-risk groups for seasonal influenza, pregnant women and household contacts of people with compromised immune systems. Other members of the public were also considered for vaccination at a later date,52 although this policy was never put into practice. At the time, efforts to increase the uptake of the seasonal flu vaccine were also renewed. 53
Maximising the uptake of either vaccine would have reduced the health and economic impact of influenza during the pandemic,54 but it is unclear what uptake rates would have been possible. In the UK, uptake of the seasonal flu vaccine for people aged 65 or over was 74.1% in 2008, close to World Health Organization targets;55 whether the focus on swine flu during 2009 increased this rate is currently uncertain. Given that swine flu was a relatively mild illness for most people, it is possible that had the swine flu vaccine been offered to the general public, its uptake would have been relatively low. 56,57 Furthermore, while confidence in the government’s handling of the outbreak appears to have been high35 and might be expected to have improved compliance with official recommendations concerning vaccination,58 the perception by some members of the public that journalists, scientists and other commentators had overexaggerated the risks of swine flu may have partly counteracted this effect. 35,59
Specific perceptions concerning the nature of the swine flu outbreak may also have affected desire for vaccination. For example, research conducted during the SARS outbreak of 2003 suggested that changes in media reporting relating to the incidence, prevalence and location of cases had an effect on levels of anxiety and other health-related behaviours. 9,19,60 Although the impact of mass media campaigns on vaccine uptake has previously been documented,20,61 few studies have assessed whether the way in which an infectious disease outbreak is reported or perceived affects desire for vaccination. 21
In this study, we analysed data from the telephone surveys commissioned by the Department of Health, England to identify variables associated with the 2009 swine flu outbreak that might encourage people to receive vaccination. We assessed the extent to which worry about the possibility of catching swine flu, perceptions of government preparedness for swine flu and perceiving that too much fuss had been made about the risk of swine flu predicted self-reported likelihood of accepting an offer of vaccination against swine flu. We also assessed whether the amount and type of information heard about swine flu, and satisfaction with the amount of information available predicted likely uptake. Because we were also interested in whether the 2009 outbreak might encourage people to receive the seasonal flu vaccine, we assessed whether any of these variables were associated with a self-reported increase in the likelihood of accepting the offer of vaccination against seasonal flu as a result of swine flu.
Methods
The surveys
Twenty of the telephone surveys contained relevant data for these analyses. These surveys were conducted between 8 May 2009 and 13 September 2009. Their sample sizes varied between 1047 and 1070.
Likely vaccine uptake
Likely uptake of the swine flu vaccine was measured in five surveys conducted between 14 August and 13 September 2009. Participants were asked: ‘The government announced recently that a swine flu vaccination programme will be rolled out across the UK starting this autumn. How likely, if at all, are you to take up a swine flu vaccination if offered it?’ Possible answers were ‘very likely’, ‘fairly likely’, ‘not very likely’ and ‘not at all likely’. These were divided into ‘likely’ and ‘not likely’ for our analyses.
Likely uptake of the seasonal flu vaccine was measured in all 20 surveys from 8 May to 13 September. Participants were asked whether they agreed or disagreed that ‘as a result of swine flu, I am now more likely to get the regular winter flu jab’. Possible answers were ‘strongly agree’, ‘tend to agree’, ‘neither agree nor disagree’, ‘tend to disagree’ and ‘strongly disagree’. For our analyses, responses were dichotomised into ‘agree’ versus ‘disagree’. Because the question would have been hypothetical for some respondents, particularly those who would not usually expect to be offered the seasonal flu vaccine, we felt that responses of ‘neither agree nor disagree’ might have indicated either a participant’s uncertainty about being vaccinated or the fact that they did not feel the question was applicable to them. Rather than conflate these two groups, we chose to exclude responses of ‘neither agree nor disagree’.
Worry and perceptions
All participants were asked ‘How worried, if at all, would you say you are now about the possibility of personally catching swine flu?’ Possible answers were ‘very worried’, ‘fairly worried’, ‘not very worried’ or ‘not at all worried’. In four surveys (conducted from 21 August to 13 September), parents of children aged under 16 years were also asked how worried they were about the possibility of their child or children catching swine flu. Participants in all surveys were asked ‘How well prepared do you think the government is for a swine flu pandemic? Would you say very well, fairly well, not very well, or not at all well prepared?’ They were also asked whether they agreed or disagreed that ‘Too much fuss is being made about the risk of swine flu.’ Finally, in six surveys (7 August to 13 September), participants were asked whether they, or anyone they knew, had caught swine flu.
Information heard about swine flu
Participants in eight surveys (24 July–13 September) were asked ‘How much have you heard about swine flu in the past week?’, with possible responses being ‘a great deal’, ‘a fair amount’, ‘not very much’ and ‘nothing at all’. Those who had heard anything were asked to describe what they had heard. We categorised responses to this open-ended item as relating to: increased number of deaths; increased number of new cases; decreased number of new cases; information about vaccines or priority groups for vaccination; information about antiviral drugs or hygiene measures; and suggestions that the number of cases would rise later in the year. Three true or false items were included relating to vaccines or immunity: ‘Currently, there is no vaccine to protect against swine flu’ (true: 14 surveys, 8 May–2 August), ‘If swine flu breaks out, most people will have some natural immunity to it’ (false: three surveys, 8–17 May) and ‘The ordinary flu vaccine will protect me from swine flu’ (false: 14 surveys, 8 May–2 August). All participants were asked about their satisfaction with the amount of information available to them about swine flu (‘very satisfied’, ‘fairly satisfied’, ‘neither satisfied nor dissatisfied’, ‘fairly dissatisfied’, ‘very dissatisfied’).
Personal and health-related variables
Personal data collected included: gender, age, social grade,38 working status, ethnicity, parental status and household size (the number of adults or children living at home, including self). For ethnicity, although 16 categories were included, the sample sizes for many of our analyses prevented us from comparing between these categories. We therefore separated the 16 categories into ‘white’ and ‘ethnic minority’ groups. All participants were asked whether their health in general was very good or good, fair, or poor or very poor, and whether they had any ‘long-standing illness, disability or infirmity’. Participants were also asked in which region of the UK they lived.
Analyses
We used binary logistic regressions to calculate the univariate associations between personal and health-related variables and likely uptake of vaccination. We calculated a second set of regressions for each personal or health-related variable, which adjusted for the effects of all other personal or health-related variables. In order to assess whether coming from a region that had been heavily affected by the outbreak affected these associations, we recalculated these regressions using data from participants who lived only in England and adjusting for whether a participant lived in one of the two regions of England with the highest prevalence rates of swine flu (London and the West Midlands). 41 This did not noticeably alter any of the aORs and is not discussed further.
We used two sets of binary logistic regressions to assess the univariate associations between other variables and likely uptake of vaccination, and to assess the multivariate associations adjusting for those personal or health-related variables that were found to have significant univariate associations with the outcome measure.
Finally, in order to assess the potential role of worry in mediating any of the effects that we identified, we calculated another set of logistic regressions for any variable that showed a significant multivariate association with vaccination uptake, including worry about the possibility of personally catching swine flu as one of the variables for which we adjusted.
We maximised the statistical power for these analyses by combining data from all surveys that included the relevant questions. As different questions were used in different weeks, the sample sizes for each analysis differed. While the frequencies for individual variables obtained for these surveys changed over time, we assumed that the associations between variables would remain constant. In order to check this, we identified three periods during the data collection period that, we judged, might be qualitatively different in terms of public perceptions relating to swine flu. Two periods (May to July and August to mid-September) reflected relatively low levels of activity in media reporting, internet searches in the UK for the phrase swine flu62 and GP consultations for influenza like-illnesses. 41 The other period (July to August) reflected higher activity in all three parameters. For any univariate analysis that drew on data from two or more of these periods, we calculated the equivalent odds ratios (ORs) for that analysis using only the individual surveys closest to the midpoints of the respective periods. Wald tests were used to compare the regression coefficients obtained for these individual surveys. Six associations were found to differ significantly over time (data not shown). In all cases but one, these differences reflected relatively small changes in the strength of the association. An association between ethnicity and being more likely to accept the seasonal flu vaccine as a result of swine flu appeared to display larger changes over time. Plotting the relevant OR from each individual survey over time showed no readily interpretable pattern.
In all analyses, we counted responses of ‘don’t know’, ‘unsure’ or ‘neither agree nor disagree’ as missing data: such responses typically had low frequencies for the predictor variables. For six surveys in which the relevant question was asked (7 August 2009 to 13 September 2009), we excluded participants who reported that they had already had swine flu (2–3% of participants in each survey).
Results
Likely vaccine uptake
Out of 5175 eligible respondents questioned between 14 August 2009 and 13 September 2009, 1642 (31.7%) reported being very likely to accept the swine flu vaccine if offered it, 1263 (24.4%) were fairly likely, 1005 (19.4%) were not very likely and 1074 (20.8%) were very unlikely; 191 (3.7%) said they did not know. Out of 20,999 eligible participants interviewed between 8 May and 13 September, 3506 (16.7%) strongly agreed that as a result of swine flu they were now more likely to get the seasonal flu vaccine, 2700 (12.9%) tended to agree, 3219 (15.3%) neither agreed nor disagreed, 5865 (27.9%) tended to disagree and 5475 (26.1%) strongly disagreed; 234 respondents (1.1%) did not know.
Association with personal and health-related variables
Tables 4 and 5 show the association between personal or health-related variables and vaccine-related outcomes. After adjusting for all other personal or health-related variables, the following groups reported being most likely to accept the swine flu vaccine if offered it: participants aged 16–24 (aOR versus those aged 65 or more: 1.6, 95% CI 1.1 to 2.4); people from ethnic minority groups (aOR 1.9, 95% CI 1.4 to 2.5); people from households of six individuals or more (aOR versus those who lived alone: 2.1, 95% CI 1.2 to 3.6); people who rated their health as fair (aOR versus those with good or very good health: 1.4, 95% CI 1.1 to 1.7); and people with long-standing illnesses or disabilities (aOR 1.5, 95% CI 1.3 to 1.7). The same groups also reported being more likely to accept the seasonal flu vaccine as a result of swine flu. In addition, participants aged 65 or more, people from social groups C2DE (that is, manual or unskilled workers, or those dependent on state welfare),38 and participants who rated their health as poor or very poor were also more likely to accept the seasonal flu vaccine (see Table 5 for ORs).
| Variable levels | n (%) | n (%) likely to accept vaccine | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|
| Sex | ||||
| Female | 2957 (59.3) | 1747 (59.1) | 1.1 (1.0 to 1.2) | 1.1 (1.0 to 1.3) |
| Male | 2027 (40.7) | 1158 (57.1) | Reference | Reference |
| Age – years | ||||
| 16–24 | 435 (8.7) | 308 (70.8) | 1.5 (1.2 to 1.9) | 1.6 (1.1 to 2.4) |
| 25–34 | 578 (11.6) | 360 (62.3) | 1.0 (0.8 to 1.3) | 1.2 (0.8 to 1.6) |
| 35–54 | 11,677 (33.6) | 884 (52.7) | 0.7 (0.6 to 0.8) | 0.7 (0.5 to 1.0) |
| 55–64 | 927 (18.6) | 511 (55.1) | 0.8 (0.6 to 0.9) | 0.8 (0.7 to 1.1) |
| ≥ 65 | 1367 (27.4) | 842 (61.6) | Reference | Reference |
| Social grade | ||||
| C2DE | 2225 (44.6) | 1334 (60.0) | 1.1 (1.0 to 1.3) | 1.0 (0.9 to 1.1) |
| ABC1 | 2759 (55.4) | 1571 (56.9) | Reference | Reference |
| Working status | ||||
| Housewife | 241 (4.8) | 143 (59.3) | 1.2 (0.9 to 1.5) | 1.0 (0.7 to 1.4) |
| Unemployed | 173 (3.5) | 106 (61.3) | 1.3 (0.9 to 1.7) | 1.0 (0.7 to 1.5) |
| Retired | 1633 (32.8) | 985 (60.3) | 1.2 (1.1 to 1.4) | 1.0 (0.8 to 1.3) |
| Student | 242 (4.9) | 162 (66.9) | 1.6 (1.2 to 2.1) | 0.9 (0.6 to 1.3) |
| Other (including disabled) | 167 (3.4) | 102 (61.1) | 1.3 (0.9 to 1.7) | 1.0 (0.7 to 1.5) |
| Working full or part-time | 2528 (50.7) | 1407 (55.7) | Reference | Reference |
| Ethnicity | ||||
| Other ethnicity | 357 (7.2) | 260 (72.8) | 2.0 (1.6 to 2.6) | 1.9 (1.4 to 2.5) |
| White | 4627 (92.8) | 2645 (57.2) | Reference | Reference |
| Parental status | ||||
| Has child 16 years or under | 947 (23.9) | 529 (55.9) | 0.9 (0.8 to 1.1) | 1.0 (0.8 to 1.2) |
| Has older child or no children | 3022 (76.1) | 1730 (57.2) | Reference | Reference |
| Household size | ||||
| Six people or more | 97 (2.0) | 73 (75.3) | 2.1 (1.3 to 3.4) | 2.1 (1.2 to 3.6) |
| Three to five people | 1660 (33.5) | 978 (58.9) | 1.0 (0.9 to 1.2) | 1.1 (0.9 to 1.4) |
| Two people | 1802 (36.4) | 1017 (56.4) | 0.9 (0.8 to 1.0) | 0.9 (0.8 to 1.1) |
| One person | 1395 (28.2) | 823 (59.0) | Reference | Reference |
| General health status | ||||
| Poor or very poor | 350 (7.0) | 231 (66.0) | 1.5 (1.3 to 1.8) | 1.1 (0.9 to 1.5) |
| Fair | 766 (15.4) | 507 (66.2) | 1.5 (1.2 to 1.9) | 1.4 (1.1 to 1.7) |
| Very good or good | 3855 (77.5) | 2159 (56.0) | Reference | Reference |
| Does participant have any long-standing infirmity or illness? | ||||
| Yes | 1477 (29.7) | 960 (65.0) | 1.5 (1.3 to 1.7) | 1.5 (1.3 to 1.7) |
| No | 3496 (70.3) | 1938 (55.4) | Reference | Reference |
| Variable levels | n (%) | n (%) more likely to accept vaccine | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|
| Sex | ||||
| Female | 10,283 (58.6) | 3720 (36.2) | 1.1 (1.0 to 1.2) | 1.0 (0.9 to 1.2) |
| Male | 7263 (41.4) | 2486 (34.2) | Reference | Reference |
| Age – years | ||||
| 16–24 | 1584 (9.0) | 649 (41.0) | 0.5 (0.5 to 0.6) | 0.7 (0.5 to 1.1) |
| 25–34 | 2082 (11.9) | 517 (24.8) | 0.3 (0.2 to 0.3) | 0.4 (0.3 to 0.6) |
| 35–54 | 5982 (34.1) | 1269 (21.2) | 0.2 (0.2 to 0.2) | 0.3 (0.2 to 0.4) |
| 55–64 | 3219 (18.3) | 1109 (34.5) | 0.4 (0.4 to 0.4) | 0.5 (0.4 to 0.7) |
| ≥ 65 | 4679 (26.7) | 2662 (56.9) | Reference | Reference |
| Social grade | ||||
| C2DE | 7773 (44.3) | 3497 (45.0) | 2.1 (2.0 to 2.3) | 1.5 (1.3 to 1.7) |
| ABC1 | 9773 (55.7) | 2709 (27.7) | Reference | Reference |
| Working status | ||||
| Housewife | 773 (4.4) | 269 (34.8) | 1.8 (1.5 to 2.1) | 1.1 (0.7 to 1.6) |
| Unemployed | 701 (4.0) | 247 (35.2) | 1.8 (1.6 to 2.2) | 1.2 (0.8 to 1.8) |
| Retired | 5547 (31.6) | 2989 (53.9) | 4.0 (3.7 to 4.2) | 1.1 (0.9 to 1.5) |
| Student | 837 (4.8) | 359 (42.9) | 2.5 (2.2 to 2.9) | 1.2 (0.8 to 1.9) |
| Other (including disabled) | 636 (3.6) | 277 (43.6) | 2.6 (2.2 to 3.1) | 1.2 (0.8 to 1.9) |
| Working full or part-time | 9052 (516) | 2065 (22.8) | Reference | Reference |
| Ethnicity | ||||
| Other ethnicity | 1277 (7.3) | 585 (45.8) | 1.6 (1.4 to 1.8) | 2.5 (1.9 to 3.4) |
| White | 16,269 (92.7) | 5621 (34.6) | Reference | Reference |
| Parental status | ||||
| Has child 16 years or under | 832 (24.7) | 216 (26.0) | 0.6 (0.5 to 0.7) | 1.0 (0.7 to 1.2) |
| Has older child or no children | 2542 (75.3) | 959 (37.7) | Reference | Reference |
| Household size | ||||
| Six people or more | 378 (2.2) | 169 (44.7) | 1.0 (0.8 to 1.3) | 2.2 (1.3 to 3.4) |
| Three to five people | 5801 (33.3) | 1565 (27.0) | 0.5 (0.4 to 0.5) | 1.0 (0.8 to 1.3) |
| Two people | 6295 (36.1) | 2266 (36.0) | 0.7 (0.7 to 0.8) | 0.9 (0.7 to 1.1) |
| One person | 4944 (28.4) | 2160 (43.7) | Reference | Reference |
| General health status | ||||
| Poor or very poor | 1338 (7.7) | 719 (53.7) | 2.6 (2.3 to 2.9) | 1.5 (1.2 to 1.9) |
| Fair | 2733 (15.6) | 1316 (48.2) | 2.1 (1.9 to 2.3) | 1.5 (1.2 to 1.9) |
| Very good or good | 13,422 (76.7) | 4145 (30.9) | Reference | Reference |
| Presence of any long-standing infirmity or illness | ||||
| Yes | 5264 (30.1) | 2428 (46.1) | 1.9 (1.8 to 2.1) | 1.3 (1.0 to 1.5) |
| No | 12,224 (69.9) | 3756 (30.7) | Reference | Reference |
Association with worry and perceptions
Controlling for personal and health-related factors, the following variables were associated with being more likely to accept the swine flu vaccine if offered it (Table 6): having higher levels of worry about the possibility of your child catching swine flu (aOR 8.0, 95% CI 4.6 to 13.9); having higher levels of worry about the possibility of personally catching swine flu (aOR 4.7, 95% CI 3.2 to 7.0); disagreeing that too much fuss had been made about the risk of swine flu (aOR 2.2, 95% CI 1.9 to 2.7); perceiving the government to be well prepared for swine flu (aOR 1.6, 95% CI 1.3 to 1.8); and knowing someone who had had swine flu (aOR 1.2, 95% CI 1.0 to 1.3). All of these variables except for perceptions about government preparedness and knowing someone who had had swine flu were associated with being more likely to accept the seasonal flu vaccine as a result of swine flu (Table 7).
| Variable levels | n (%)a | n (%) likely to accept vaccine | Unadjusted OR (95% CI) | aOR (95% CI)b |
|---|---|---|---|---|
| Worry about self catching swine flu | ||||
| Very worried | 177 (3.6) | 143 (80.8) | 5.1 (3.5 to 7.5) | 4.7 (3.2 to 7.0) |
| Fairly worried | 624 (12.6) | 498 (79.8) | 4.8 (3.9 to 5.9) | 4.9 (4.0 to 6.2) |
| Not very worried | 1916 (38.6) | 1233 (64.4) | 2.2 (1.9 to 2.5) | 2.3 (2.0 to 2.6) |
| Not at all worried | 2246 (45.3) | 1014 (45.1) | Reference | Reference |
| Worry about child catching swine flu | ||||
| Very worried | 180 (19.1) | 148 (82.2) | 9.7 (5.7 to 16.4) | 8.0 (4.6 to 13.9) |
| Fairly worried | 301 (32.0) | 187 (62.1) | 3.4 (2.2 to 5.3) | 3.3 (2.1 to 5.3) |
| Not very worried | 328 (34.8) | 149 (45.4) | 1.7 (1.1 to 2.7) | 1.7 (1.1 to 2.7) |
| Not at all worried | 133 (14.1) | 43 (32.3) | Reference | Reference |
| Too much fuss is being made about the risk of swine flu | ||||
| Disagree | 1351 (29.8) | 952 (70.5) | 2.1 (1.9 to 2.4) | 2.2 (1.9 to 2.5) |
| Agree | 3178 (70.2) | 1679 (52.8) | Reference | Reference |
| How well prepared is the government for swine flu? | ||||
| Well prepared | 3423 (75.4) | 2100 (61.3) | 1.4 (1.2 to 1.6) | 1.6 (1.3 to 1.8) |
| Not well prepared | 1118 (24.6) | 590 (52.8) | Reference | Reference |
| Has anyone you know been ill with swine flu? | ||||
| Yes | 1600 (32.1) | 976 (61.0) | 1.2 (1.0 to 1.3) | 1.2 (1.0 to 1.3) |
| No | 3384 (67.9) | 1929 (57.0) | Reference | Reference |
| Variable levels | n (%)a | n (%) more likely to accept vaccine | Unadjusted OR (95% CI) | aOR (95% CI)b |
|---|---|---|---|---|
| Worry about self catching swine flu | ||||
| Very worried | 714 (4.1) | 441 (61.8) | 4.0 (3.4 to 4.7) | 4.5 (3.0 to 6.9) |
| Fairly worried | 2372 (13.6) | 1203 (50.7) | 2.6 (2.3 to 2.8) | 3.2 (2.5 to 4.1) |
| Not very worried | 6835 (39.1) | 2359 (34.5) | 1.3 (1.2 to 1.4) | 1.8 (1.5 to 2.1) |
| Not at all worried | 7544 (43.2) | 2154 (28.6) | Reference | Reference |
| Worry about child catching swine flu | ||||
| Very worried | 164 (19.8) | 79 (48.2) | 5.3 (2.9 to 9.5) | 3.4 (1.8 to 6.4) |
| Fairly worried | 257 (31.0) | 67 (26.1) | 2.0 (1.1 to 3.5) | 1.7 (0.9 to 3.1) |
| Not very worried | 289 (34.8) | 51 (17.6) | 1.2 (0.7 to 2.2) | 1.1 (0.6 to 2.0) |
| Not at all worried | 120 (14.5) | 18 (15.0) | Reference | Reference |
| Too much fuss is being made about the risk of swine flu | ||||
| Disagree | 6398 (39.6) | 2479 (38.7) | 1.3 (1.2 to 1.4) | 1.5 (1.3 to 1.8) |
| Agree | 9776 (60.4) | 3255 (33.3) | Reference | Reference |
| How well prepared is the government for swine flu? | ||||
| Well prepared | 12,221 (73.9) | 4309 (35.3) | 1.0 (0.9 to 1.0) | 1.2 (1.0 to 1.4) |
| Not well prepared | 4308 (26.1) | 1554 (36.1) | Reference | Reference |
| Has anyone you know been ill with swine flu? | ||||
| Yes | 1583 (31.6) | 518 (32.7) | 0.8 (0.7 to 0.9) | 0.9 (0.8 to 1.1) |
| No | 3425 (68.4) | 1327 (38.7) | Reference | Reference |
Association with information heard about swine flu
Tables 8 and 9 show the associations between information heard about the outbreak and likely vaccine uptake. Adjusting for personal and health-related variables, only two variables were associated with being more likely to accept the swine flu vaccine if offered it: being satisfied with the amount of information available about swine flu (aOR 1.5, 95% CI 1.2 to 1.9) and having recently heard that the number of deaths from swine flu had increased (aOR 1.3, 95% CI 1.0 to 1.6). Once personal variables and health were controlled for, only satisfaction with the amount of information available about swine flu (aOR 1.5, 95% CI 1.1 to 2.0) and believing that the seasonal flu vaccine would protect against swine flu (aOR 2.4, 95% CI 2.1 to 2.7) were associated with being more likely to get the seasonal flu vaccine as a result of swine flu.
| Variable levels | n (%)a | n (%) likely to accept vaccine | Unadjusted OR (95% CI) | aOR (95% CI)b |
|---|---|---|---|---|
| How much have you heard about swine flu this week? | ||||
| A great deal | 684 (13.7) | 388 (56.7) | 1.0 (0.8 to 1.2) | 1.0 (0.8 to 1.2) |
| A fair amount | 1139 (22.9) | 695 (61.0) | 1.2 (1.0 to 1.4) | 1.2 (1.0 to 1.4) |
| Not very much | 1939 (39.0) | 1131 (58.3) | 1.1 (0.9 to 1.2) | 1.1 (0.9 to 1.3) |
| Nothing at all | 1215 (24.4) | 687 (56.5) | Reference | Reference |
| How satisfied are you with the amount of information available? | ||||
| Satisfied | 4024 (90.9) | 2437 (55.0) | 1.4 (1.1 to 1.7) | 1.5 (1.2 to 1.9) |
| Not satisfied | 403 (9.1) | 212 (52.6) | Reference | Reference |
| What have you heard? | ||||
| Number of cases increased | ||||
| Heard | 454 (12.3) | 290 (63.9) | 1.3 (1.0 to 1.6) | 1.2 (1.0 to 1.5) |
| Not heard | 3243 (87.7) | 1882 (50.9) | Reference | Reference |
| Number of cases decreased | ||||
| Heard | 740 (20.0) | 1767 (59.8) | 0.8 (0.7 to 1.0) | 0.9 (0.7 to 1.0) |
| Not heard | 2957 (80.0) | 405 (54.7) | Reference | Reference |
| Number of deaths increased | ||||
| Heard | 370 (10.0) | 238 (64.3) | 1.3 (1.0 to 1.6) | 1.3 (1.0 to 1.6) |
| Not heard | 3327 (90.0) | 1934 (58.1) | Reference | Reference |
| Anything about vaccination | ||||
| Heard | 375 (10.1) | 228 (60.8) | 1.1 (0.9 to 1.4) | 1.1 (0.9 to 1.4) |
| Not heard | 3322 (89.9) | 1944 (58.5) | Reference | Reference |
| Anything about antiviral agents or hygiene | ||||
| Heard | 433 (11.7) | 258 (59.6) | 1.0 (0.8 to 1.3) | 1.0 (0.8 to 1.3) |
| Not heard | 3264 (88.3) | 1914 (58.6) | Reference | Reference |
| Number of cases will rise later in year | ||||
| Heard | 153 (4.1) | 84 (54.9) | 0.8 (0.6 to 1.2) | 1.0 (0.7 to 1.4) |
| Not heard | 3544 (95.9) | 2088 (58.9) | Reference | Reference |
| Variable levels | n (%)a | n (%) more likely to accept vaccine | Unadjusted OR (95% CI) | aOR (95% CI)b |
|---|---|---|---|---|
| How much have you heard about swine flu this week? | ||||
| A great deal | 1665 (24.7) | 603 (36.2) | 1.0 (0.9 to 1.2) | 0.9 (0.7 to 1.2) |
| A fair amount | 1862 (27.6) | 791 (42.5) | 1.3 (1.1 to 1.5) | 1.0 (0.8 to 1.3) |
| Not very much | 2080 (30.8) | 743 (35.7) | 1.0 (0.9 to 1.2) | 0.9 (0.7 to 1.1) |
| Nothing at all | 1145 (17) | 410 (35.8) | Reference | Reference |
| How satisfied are you with the amount of information available? | ||||
| Satisfied | 14,337 (89.6) | 5154 (35.9) | 0.9 (0.8 to 1.0) | 1.5 (1.1 to 2.0) |
| Not satisfied | 1656 (10.4) | 644 (38.9) | Reference | Reference |
| There is no vaccine for swine flu | ||||
| True | 5873 (50.4) | 1963 (33.4) | 0.9 (0.9 to 1.0) | 0.9 (0.8 to 1.0) |
| False | 5774 (49.6) | 2013 (34.9) | Reference | Reference |
| Most people have some natural immunity to swine flu | ||||
| True | 1501 (62.8) | 451 (30.0) | 1.2 (1.0 to 1.5) | 1.2 (1.0 to 1.5) |
| False | 889 (37.2) | 231 (26.0) | Reference | Reference |
| The ordinary flu vaccine will protect me from swine flu | ||||
| True | 1787 (15.6) | 966 (54.1) | 2.7 (2.5 to 3.0) | 2.4 (2.1 to 2.7) |
| False | 9636 (84.4) | 2903 (30.1) | Reference | Reference |
| What have you heard? | ||||
| Number of cases increased | ||||
| Heard | 1215 (22.0) | 470 (38.7) | 1.0 (0.9 to 1.1) | 1.1 (0.8 to 1.5) |
| Not heard | 4297 (78.0) | 1631 (38.0) | Reference | Reference |
| Number of cases decreased | ||||
| Heard | 809 (14.7) | 282 (34.9) | 0.8 (0.7 to 1.0) | 0.9 (0.7 to 1.1) |
| Not heard | 4703 (85.3) | 1819 (38.7) | Reference | Reference |
| Number of deaths increased | ||||
| Heard | 765 (13.9) | 303 (39.6) | 1.1 (0.9 to 1.3) | 1.2 (0.9 to 1.6) |
| Not heard | 4747 (86.1) | 1798 (37.9) | Reference | Reference |
| Anything about vaccination | ||||
| Heard | 459 (8.3) | 164 (35.7) | 0.9 (0.7 to 1.1) | 1.0 (0.7 to 1.4) |
| Not heard | 5053 (91.7) | 1937 (35.1) | Reference | Reference |
| Anything about antiviral agents or hygiene | ||||
| Heard | 680 (12.3) | 244 (35.9) | 0.9 (0.8 to 1.1) | 1.0 (0.8 to 1.4) |
| Not heard | 4832 (87.7) | 1857 (33.7) | Reference | Reference |
| Number of cases will rise later | ||||
| Heard | 169 (3.1) | 49 (29.0) | 0.7 (0.5 to 0.9) | 1.0 (0.6 to 1.5) |
| Not heard | 5343 (96.9) | 2052 (38.4) | Reference | Reference |
Adjusting for worry about the possibility of catching swine flu
Controlling for worry about the possibility of personally catching swine flu did not substantially alter the strength of association for any of the significant non-worry-related predictor variables (results not shown), other than reducing to insignificance for the predictor ‘having heard that the number of deaths from swine flu had increased’ (aOR 1.0, 95% CI 0.6 to 1.6).
Discussion
The usefulness of vaccination as a means of reducing the overall impact of influenza depends on the willingness of members of the public to be vaccinated. 54 At the time of our data collection (14 August to 13 September 2009), only 56.1% of respondents reported being likely to accept the swine flu vaccination if offered it. While this figure may have altered following the start of the Department of Health’s vaccine-related communications campaign, this pre-campaign baseline suggests that ample scope existed for interventions to improve uptake. Our identification of demographic and psychological predictors for increased likelihood of accepting both swine and seasonal flu vaccines suggests possible ways of developing effective communication campaigns in future, and suggests that the same messages delivered as part of a single vaccine-related communications campaign may be effective in improving the uptake of both types of vaccine.
By far the strongest predictors were worry about the possibility of personally catching swine flu and, for parents, worry about a child catching swine flu. Similar associations between emotional and behavioural responses to an infectious disease outbreak have been observed before. 35,60,63 Focusing on the more worrying aspects of catching flu, be they financial, social or health, may be one way of increasing vaccination rates. However, it should be noted that this will depend on the baseline level of worry in any population and that there are individual differences, so that increasing worry may have negative consequences for some members of the population. At the levels of worry present during this pandemic outbreak, messages intended to reassure people about the risks from swine flu are unlikely to have a positive impact on vaccine uptake.
Conversely, perceiving that too much fuss had been made about the risk of swine flu was associated with decreased likelihood of accepting either form of vaccine. This corresponds well with earlier work showing that people who felt that the risks from swine flu were being exaggerated were less likely to adopt recommended behaviours such as increased hand-washing. 35 From a policy perspective, no easy short-term answer exists to this. Providing an appropriate level of warning and advice to members of the public while not being perceived as ‘making too much fuss’ is inevitably difficult. 64 At a minimum, giving sufficient assurances to the public that the necessary plans and resources are in place to deal with the situation does appear to be helpful, with respondents who expressed confidence in government preparedness being more likely to accept vaccination.
Consistent with studies that have previously examined how information provision that specifically relates to a particular vaccine can affect its uptake,20,61,65,66 this study identified the importance of vaccine-specific information. We found an association between believing, incorrectly, that the seasonal flu vaccine is effective against swine flu and being more likely to accept the seasonal flu vaccine as a result of swine flu. Less research has assessed the effects of information about the course of an infectious disease outbreak on desire for vaccination, although at least one study has suggested that media reporting about the unexpected severity of a flu outbreak played a larger role in driving uptake of the vaccine than vaccine-specific reporting. 21 Several studies have suggested that media reporting about features of an outbreak, such as the number of cases or deaths, might influence key health behaviours. 9,19,60,67 However, we found no evidence to suggest that how much people had heard about swine flu in the past week affected likely vaccine uptake or that specific aspects of what they had heard had any substantial impact. The only exception was a weak association between having heard that the number of deaths from swine flu had increased recently and greater likelihood of accepting the swine flu vaccine. Given the large number of statistical tests we calculated, it is possible that this solitary finding reflects a type 1 error rather than a genuine effect.
One explanation for this discrepancy between our findings concerning the role of receiving information about the outbreak and those of previous studies9,19,60,67 is that information may have a different effect on vaccine intentions depending on the stage of the outbreak. While the spread of information during the study period had no impact on likely vaccine uptake, stronger associations might have been observed earlier in the swine flu outbreak when members of the public were less certain about the transmission or nature of the illness. By the time of our study, it is possible that most members of the public had already formed a stable understanding of the severity and prevalence of swine flu and the most effective ways of preventing it, which additional information did little to alter.
The role of personal variables
Several personal variables were found to predict greater likelihood of vaccine uptake. Those people in groups prioritised to be offered the swine flu vaccine first or who are regularly offered the seasonal flu vaccine reported being more likely to accept either (e.g. those with long-standing illnesses, worse general health or aged 65 years and over). People from social groups C2DE (manual or unskilled workers, or those dependent on state welfare),38 ethnic minority groups or large households were also found to be more likely to be willing to accept vaccination. The explanation for higher likely uptake in these groups is unclear. While adjusting for worry about the possibility of catching swine flu did not alter the associations, other variables that we did not measure, such as a stronger tendency to follow health advice or less concern about potential side effects,68 may be relevant.
Methodological issues
Three methodological issues in particular should be borne in mind with this study. First, as is common in research of this type, the need for data to be collected quickly in order to inform policy meant that conventional epidemiological methods involving random probability sampling and attempts to recontact initial non-responders could not be used. 11 Instead, rapid-turnaround telephone surveys with quota sampling were used to ensure that the eventual samples were demographically representative of the UK population. Inevitably, this meant that the response rates for these surveys were low, although not unusually low. 35,39,40 Whether participants were psychologically representative of the general population is uncertain.
Second, while we have speculated about potential causal links between the predictor and outcome measures, the data that we have relied on are correlational. It is possible that some third variable, such as general civic-mindedness or trust in the government, could have been responsible for some of the associations that we identified. Experimental studies are required to confirm the causal nature of the associations that we found.
Third, given the number of statistical tests that we conducted it is possible that some of the significant associations that we identified were type 1 errors. However, given the correlated nature of our predictor variables, applying a Bonferroni correction to our results would have been too conservative. It is therefore appropriate to consider those results that achieved only marginal significance as exploratory.
Conclusions
If uptake of vaccines is to be encouraged during this or any future pandemic, communication campaigns should focus on factors shown to be associated with intended uptake. Our results suggest that, while providing information that relates to the outbreak is unlikely to increase uptake, messages that highlight people’s concerns and worries about the illness in question may be effective. In addition, highlighting the efficacy of vaccination may also be an effective way to increase uptake. In this study, people who incorrectly believed that the seasonal flu vaccine would be effective against swine flu were more likely to say that they would accept it.
Chapter 4 Study 3: The effects of advertising and media coverage on behavioural change during the early stages of the swine flu outbreak
Key points
-
During the early stages of the swine flu outbreak, government communications focused on encouraging people to adopt specific respiratory and hand hygiene behaviours in order to reduce the spread of swine flu. People were also encouraged to use remote facilities to access NHS advice if they were concerned that they might have swine flu. Other behaviours, such as avoiding public transport, were not encouraged.
-
Telephone surveys conducted between 1 and 17 May 2009 suggested that 33.1% of the public were carrying tissues with them as advised, 9.5% had bought sanitising hand gel to help clean their hands, 2.0% had avoided public transport and 1.6% had visited a GP or hospital or called NHS Direct for flu-related reasons.
-
Path analyses suggested that exposure to advertising and media coverage about swine flu was associated with performance of these four behaviours and that they had broadly similar effects. Exposure to either advertising or media coverage appeared to promote the carrying of tissues and purchasing of sanitising gel, and discourage avoidance of public transport or unnecessary use of NHS services. These effects partly occurred because exposure to both advertising and media coverage increased the perceived efficacy of hygiene-related behaviours and decreased the perceived efficacy of avoidance-related behaviours.
-
In future outbreaks, messages that emphasise the efficacy of recommended behaviours may help to promote their uptake, without promoting the uptake of other behaviours.
Introduction
Immediately after the emergence of swine flu, the UK government launched a major advertising campaign to encourage people to engage in a set of behaviours intended to reduce the effects of the outbreak. This campaign included a leaflet that was sent to every household in the country and extensive television, radio, internet, print and poster advertising. 69 The campaign conveyed basic facts about swine flu, provided information about the government’s level of preparedness, and stressed the importance of using and disposing of tissues for coughs and sneezes, and regularly cleaning hands with soap and water or sanitising gel. In order to reduce the spread of swine flu, people who had just returned from an affected country and who had developed flu-like symptoms were asked to stay at home, to check their symptoms using an internet site or an automated telephone system, and to telephone their GP or NHS Direct, a national telephone advice line ‘if [they had] taken these steps and [were] still concerned’. 69 These messages were reinforced by commercial advertising for tissues, hand sanitisers and other products, which regularly repeated the official hygiene slogan of ‘Catch it, Bin it, Kill it’.
At the time that this campaign began, traditional news media and internet sources devoted large amounts of coverage to the unfolding events. While some commentators accused the media of ‘scaremongering’,70 others36,37 noted that ‘the mass media coverage of the H1N1 outbreak has […] been balanced and rational’. 36
The extensive advertising and media coverage during this initial period of the pandemic might have influenced people’s behaviour through several mechanisms. For example, levels of worry about a disease outbreak, perceptions about how effective preventative measures are and perceptions about how well the government is coping can all affect how people behave in response to a disease outbreak. 35,56,58,63 Similarly, how much a person thinks they know about a given hazard, their satisfaction with how much they know and how well informed they actually are might also help to determine whether or not people feel at risk and what, if any, action they decide to take. These mechanisms are consistent with a literature review of the determinants of protective behaviours during a pandemic, and with several explanatory models of how people react to a health threat, for example the Protection Motivation Theory and the Health Belief Model. 71
In practice, what impact the advertising and media coverage actually had on behavioural change, and via what mechanism, is unknown. In this study we tested the association between exposure to advertisements or media coverage during the first 3 weeks of the swine flu outbreak and four self-reported behaviours. Two of these behaviours were encouraged by the government’s advertisements: namely carrying tissues and buying sanitising gel. A third behaviour, avoiding public transport, represented a preventative strategy known to be used by some members of the public35 but was not specifically recommended. The fourth behaviour, contacting the health services for a flu-related reason, was discouraged except for rare cases of flu-like illness among travellers returning from an affected country. However, GPs and NHS Direct both reported a sharp increase in consultation rates for influenza-like illness during May 2009. 41,72 We also assessed several potential mediators between exposure to advertising or media coverage and behaviour: knowledge about swine flu, the perceived efficacy of various preventative behaviours, perceptions about the government’s level of preparedness for a pandemic and levels of worry about the possibility of catching swine flu.
Methods
Design
The first five cross-sectional telephone surveys commissioned by the Department of Health, England contained data that were relevant to these analyses. These surveys began data collection on 1 May 2009 and ended on 17 May 2009. Sample sizes for each varied between 1058 and 1173.
Behavioural outcomes
Respondents were asked ‘Have you done any of the following since the beginning of the swine flu outbreak?’ Eleven behaviours were specified, of which three were analysed here. These were ‘carried tissues with me’, ‘bought antibacterial gel’ and ‘avoided using public transport’.
Respondents were also asked whether they had been to see a GP, visited a hospital, called NHS Direct or the Swine Flu Information Line or visited www.nhs.uk for flu-related issues in the last 2 weeks. Participants who reported having visited their GP or a hospital or having called NHS Direct (or a related telephone service for Northern Irish, Scottish or Welsh participants) because of flu-related issues were counted as health-care users.
Exposure to advertising and media coverage
Participants were asked whether they recalled having seen or heard any advertising or media coverage on the subject of swine flu and, if so, where. Responses were categorised as relating to media coverage or advertising.
Information-related variables
Participants were asked how much they had heard about swine flu, with responses dichotomised into ‘a lot or a moderate amount’ versus ‘a little or nothing at all’. Perceived knowledge was assessed by asking ‘how much do you think you know about swine flu’ with responses dichotomised as ‘a lot or a moderate amount’ versus ‘a little or nothing at all’. Participants were asked how satisfied or dissatisfied they were with the amount of information available to them about swine flu, from any source; responses to this item were dichotomised as ‘very satisfied or fairly satisfied’ versus ‘fairly or very dissatisfied’. A middle option (‘neither satisfied nor dissatisfied’) was excluded from our analyses. Participants were also asked what additional information they would like to receive about swine flu, with responses grouped thematically and categorised as ‘wanting additional information’ and ‘does not want additional information’. To assess actual knowledge, six true or false statements were presented, with responses summed to produce a knowledge score of 0–6. The statements were: ‘currently, there is no vaccine to protect against swine flu’ (true); ‘there are ways to help slow the spread of swine flu’ (true); ‘if swine flu breaks out, it is likely that most people will have some natural immunity to it’ (false); ‘the ordinary flu vaccine will protect me from swine flu’ (false); ‘it is possible to catch swine flu from eating pork’ (false); ‘thousands of people worldwide have died from swine flu’ (false). Finally, participants were asked to state how well prepared they thought the government was for a swine flu pandemic, with responses dichotomised as ‘very well prepared or fairly well prepared’ versus ‘not very well prepared or not at all well prepared’.
Worry about the possibility of catching swine flu
A single item asked participants to state how worried, if at all, they were about the possibility of personally catching swine flu. Responses were dichotomised into ‘very worried or fairly worried’ versus ‘not very or not at all worried’.
Efficacy of preventative actions
Participants were asked to rate eight actions on a scale from 1 (‘it will make no difference at all’) to 10 (‘it is vital’) in terms of how effective it would be in preventing the spread of swine flu. The eight actions were: ‘washing hands frequently with soap and water’, ‘covering nose and mouth with a tissue when sneezing and coughing’, ‘disposing of dirty tissues promptly and carefully in a bin or bag’, ‘avoiding non-essential travel whenever possible’, ‘avoiding large crowds whenever possible’, ‘cleaning hard surfaces such as kitchen worktops and door handles frequently’, ‘getting the yearly flu jab’ and ‘wearing a surgical/hygienic facemask’. Factor analysis using principal axis factoring and direct oblimin rotation suggested that two factors were present in the data, accounting for 57.8% of the variance. The first factor, which we labelled ‘hygiene efficacy’, was loaded on by hand-washing, use of tissues, disposal of tissues and cleaning hard surfaces. The second factor, ‘avoidance efficacy’, was loaded on by avoidance of crowds and avoidance of public transport. Scores on these factors were calculated by taking the mean score for the relevant items. Neither the yearly flu jab item nor the surgical facemask item loaded on either factor. These items were dropped from subsequent analyses. Because scores on the hygiene and avoidance efficacy scales were skewed, we dichotomised them, based around the median score for each scale.
Personal variables
Personal data collected included: gender, age, social grade,38 ethnicity and household size. Participants were asked whether their health in general was very good or good, fair, or poor or very poor, and whether they had any ‘long-standing illness, disability or infirmity’.
Analyses
We assessed univariate associations between the categorical predictor variables and the four behavioural outcomes using binary logistic regressions adjusting for all personal or health-related variables. In order to assess whether coming from a region that had been heavily affected by the outbreak affected the associations between exposure to advertising or media coverage and any of the four outcome variables, we recalculated these regressions using only data from participants who lived in England and adjusting for whether a participant lived in one of the two regions of England with the highest prevalence rates of swine flu (London and the West Midlands). 41 This did not noticeably alter any of the aORs and is not discussed further. We assessed univariate associations between the actual knowledge score and each outcome variable using t-tests.
We hypothesised pathways linking exposure to media coverage or advertising and behaviour (Figure 4). We hypothesised that personal variables would predict exposure to advertising or media coverage. We further hypothesised that exposure to advertising or media coverage would predict the information-related variables, which, in turn, would predict the worry- and efficacy-related variables. The behavioural outcomes were placed at the end of this causal chain. We assumed that any of the variables might be directly influenced by any other variable at the same level as it in Figure 4, or at any of the preceding levels. In order to test this path diagram, each information, worry, efficacy and behaviour variable was used as a dependent variable in a binary logistic regression or multiple regression, as applicable. These regressions used any variables at the same or preceding levels as predictor variables. Associations that were identified as significant at p < 0.05 were plotted on a revised path diagram.
FIGURE 4.
Input path diagram specifying the hypothesised pathways between exposure to advertising or media coverage and behaviour. Each variable may have been predicted by any other variable from the same level or from any preceding level of the diagram.
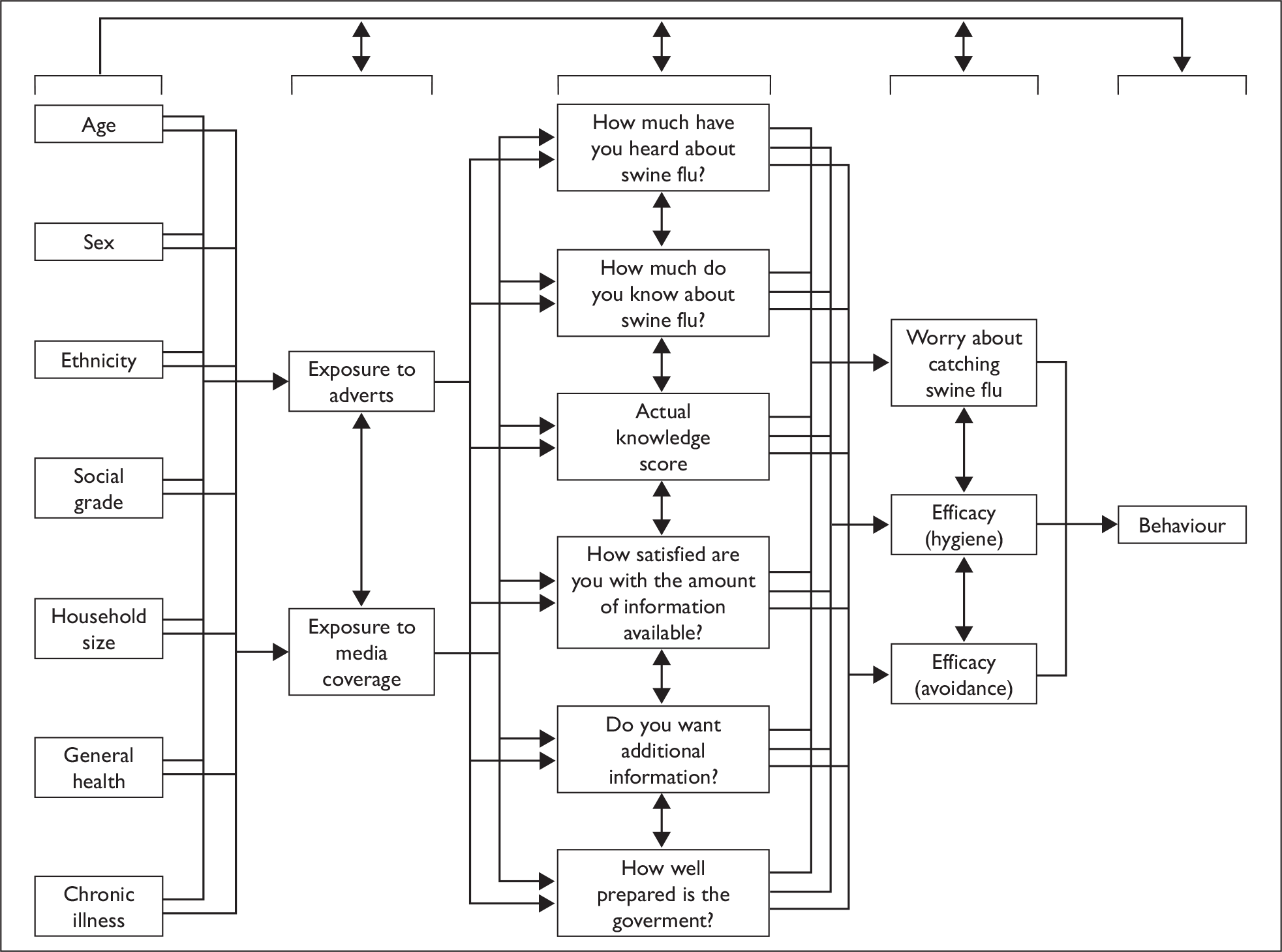
We chose not to use structural equation modelling to analyse the path diagrams. Structural equation modelling is appropriate as a confirmatory technique when one is able to specify a model. Here, we were limited by the variables available to us and did not expect to be able to specify a complete model. We thus took a more exploratory approach and the results should be interpreted in that context.
Results
In total, 5419 people took part in the surveys: 1793 (33.1%) reported carrying tissues with them, 513 (9.5%) reported having bought sanitising gel, 111 (2.0%) reported avoiding public transport and 88 (1.6%) reported having visited a GP or hospital or phoning NHS Direct for flu-related reasons.
Personal characteristics
Tables 11–14 in Appendix 4 show the association between each personal characteristic and the four behavioural outcomes. Adjusting for all other personal variables, women (aOR 2.1, 95% CI 1.8 to 2.3), ethnic minority participants (aOR 1.8, 95% CI 1.4 to 2.3) and participants with poor or very poor health compared with those with good or very good health (aOR 1.3, 95% CI 1.02 to 1.7) were more likely to carry tissues, whereas those aged 25–34 (aOR 0.7, 95% CI 0.6 to 0.9) or 35–54 (aOR 0.8, 95% CI 0.7 to 0.96) were less likely than those aged 65 or more to carry tissues.
Women (aOR 2.4, 95% CI 2.0 to 3.0), participants aged 16 to 54 (aOR 95% CIs for these three categories ranged from 1.2 to 3.4), ethnic minority participants (aOR 1.5, 95% CI 1.1 to 2.0), participants from households of two or more people (aOR 95% CIs for these three categories ranged from 1.02 to 3.5) and participants with poor or very poor health (aOR 1.6, 95% CI 1.1 to 2.4) were more likely have bought sanitising hand gel. Participants from ethnic minority groups (aOR 4.1, 95% CI 2.5 to 6.8) and those with poor or very poor health (aOR 2.6, 95% CI 1.3 to 5.1) were more likely to have avoided public transport. People from ethnic minority groups (aOR 2.2, 95% CI 1.2 to 4.2), those from households of six people or more (aOR 3.3, 95% CI 1.2 to 9.1) and people with poor or very poor health (aOR 2.6, 95% CI 1.3 to 5.5) were more likely to have visited a GP or hospital or to have telephoned NHS Direct for flu-related reasons.
Exposure to advertising and media coverage
Overall, 4167 participants (76.9%) reported having seen media coverage of swine flu, while 2735 (50.5%) reported having seen advertising relating to swine flu. Tables 15–18 in Appendix 4 show the associations between exposure to advertising or media coverage and each behavioural outcome. Adjusting for personal variables, participants who had been exposed to advertising were more likely to have carried tissues (aOR 1.2, 95% CI 1.05 to 1.3), to have bought sanitising hand gel (aOR 1.4, 95% CI 1.2 to 1.7) and were less likely to have avoided public transport (aOR 0.7, 95% CI 0.4 to 0.99). Participants exposed to media coverage were less likely to have contacted a GP, hospital or NHS Direct for flu-related reasons (aOR 0.6, 95% CI 0.4 to 0.9).
Information about swine flu
A total of 4817 people (92.9%) had heard a lot or a moderate amount about swine flu, 3808 (73.6%) felt they knew a lot or a moderate amount about swine flu, and 4462 (91.0%) were very or fairly satisfied with the amount of information available about swine flu, while 1998 (36.9%) still had one or more specific pieces of information that they wanted to know. Table 10 shows the specific types of information that they wanted. In total, 4014 participants (78.3%) felt that the government was very or fairly well prepared for a swine flu pandemic. The mean number of correct answers on the six knowledge questions was 4.2 (standard deviation 1.2).
| What additional information would you like to receive? | No. of participants (%) (n = 5415)a |
|---|---|
| None | 3138 (58.0) |
| Details on symptoms | 594 (11.0) |
| Advice on prevention | 440 (8.1 |
| Advice on treatment | 417 (7.7) |
| Wants to receive the Government leaflet | 212 (3.9) |
| Regular/up-to-date updates | 156 (2.9) |
| Outbreaks in local area | 124 (2.3) |
| Advice for people who might need more tailored information, such as those with pre-existing conditions | 112 (2.1) |
| Availability of medicine/vaccine | 69 (1.3) |
| How any affected/where | 69 (1.3) |
| Travel advice | 58 (1.1) |
| How it is spread | 50 (0.9) |
| What other countries are doing | 34 (0.6) |
| Other | 607 (11.2) |
| Don’t know | 281 (5.2) |
The association between the information-related variables and the behavioural outcomes are given in Tables 15–18 in Appendix 4. Adjusting for all personal variables, participants who thought that they knew a lot or a moderate amount about swine flu (aOR 1.2, 95% CI 1.03 to 1.4) and those who wanted more information about swine flu (aOR 1.4, 95% CI 1.3 to 1.6) were more likely to carry tissues. Those who wanted more information were also more likely to have bought sanitising hand gel (aOR 1.5, 95% CI 1.3 to 1.9). Participants were less likely to avoid public transport if they thought they had heard a lot or a moderate amount about swine flu (aOR 0.4, 95% CI 0.2 to 0.6), if they thought they knew a lot or a moderate amount about swine flu (aOR 0.6, 95% CI 0.4 to 0.99) or if they were very or fairly satisfied with the amount of information available to them (aOR 0.4, 95% CI 0.2 to 0.7). They were more likely to avoid public transport if they wanted more information (aOR 2.8, 95% CI 1.9 to 4.2).
There were no significant differences in knowledge between participants who had or had not contacted the health services, bought sanitising gel or carried tissues (all p values > 0.09). Avoiding public transport was associated with less knowledge (mean difference 0.4, t(5417) = 3.8, p < 0.001).
Worry about the possibility of catching swine flu
In total, 757 participants (14.0%) reported being very or fairly worried about the possibility of catching swine flu. Adjusting for personal variables, worry was significantly associated with carrying tissues (aOR 1.7, 95% CI 1.5 to 2.0), buying sanitising gel (aOR 2.3, 95% CI 1.9 to 2.9), avoiding public transport (aOR 4.1, 95% CI 2.7 to 6.2) and contacting health-care services for flu-related reasons (aOR 2.3, 95% CI 1.4 to 3.4).
Response efficacy
Median efficacy scores were 6 (interquartile range 4.0 to 8.0) for the avoidance efficacy scale and 9 (7.75 to 10.0) for the hygiene efficacy scale. Participants who perceived avoidance measures to be highly effective were more likely to have avoided public transport (aOR 4.1, 95% CI 2.5 to 6.8) and to have carried tissues (aOR 1.2, 95% CI 1.1 to 1.4). Those who perceived hygiene measures to be highly effective were more likely to have carried tissues (aOR 1.6, 95% CI 1.4 to 1.8) and to have bought sanitising gel (aOR 1.8, 95% CI 1.5 to 2.2).
Path analyses
Figures 5–8 show the significant associations identified within our path diagrams. These associations adjusted for all personal variables and for all predictor variables at the same or preceding levels as in Figure 4. The initial stages of each figure are identical. Overall, exposure to advertising or media coverage was associated with believing hygiene behaviours to be more effective. According to the path diagram, this was the result of higher perceived knowledge about swine flu and increased satisfaction with the amount of information available about swine flu, together with greater perceptions of government preparedness, and a direct effect of exposure to advertising. In contrast, exposure to advertising or media coverage was associated with believing avoidance behaviours to be less effective. For exposure to advertising, this was due to a direct effect, whereas for exposure to media coverage the effect was due to increased satisfaction with the amount of information available and thus reduced desire for more information. Exposure to either advertising or media coverage reduced worry about the possibility of catching swine flu, with exposure to advertising having this effect by increasing perceived and actual knowledge levels, whereas exposure to media coverage had an effect by increasing satisfaction with the amount of information available and therefore reducing desire for more information.
FIGURE 5.
Path diagram showing the significant paths (p < 0.05) between the information-related, efficacy and worry variables, and whether participants carried tissues. Unless stated otherwise, all numbers are ORs adjusting for all personal and health-related variables, for all other variables at the same level as the outcome variable and for all other variables at preceding levels. For clarity, significant associations with personal or health-related variables have been omitted.
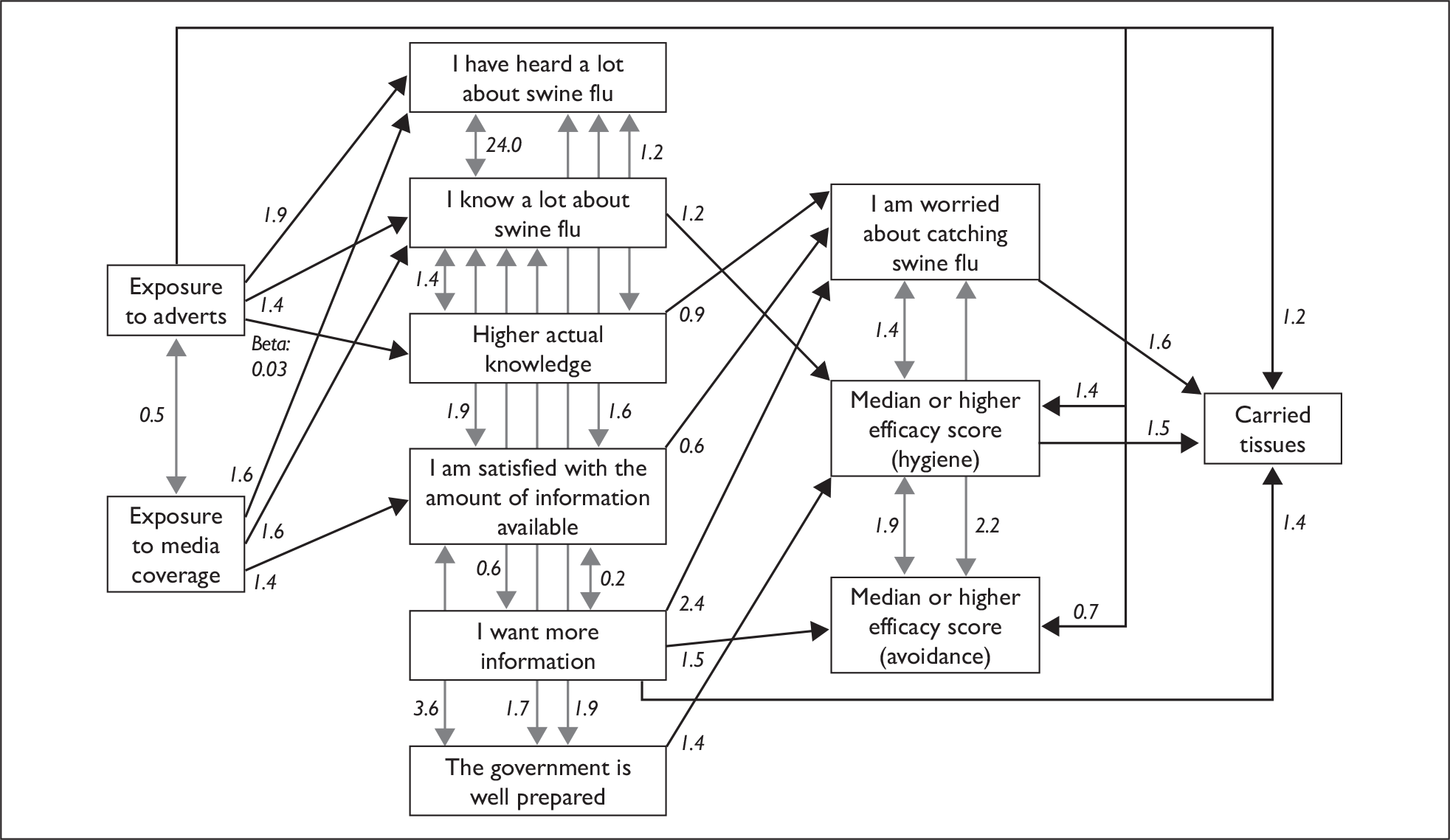
Extending the pathways to include carrying tissues (Figure 5) and buying sanitising gel (Figure 6) revealed identical patterns of results. By increasing the perceived efficacy of hygiene behaviours, both exposure to advertising and media coverage increased the likelihood of people engaging in these behaviours. A direct effect of advertising on carrying tissues or buying sanitising gel was also observed. These effects were partly offset by the fact that exposure to advertising or media coverage reduced worry about the possibility of catching swine flu and desire for more information, both of which had positive associations with the two behaviours.
FIGURE 6.
Path diagram showing the significant paths (p < 0.05) between the information-related, efficacy and worry variables, and whether participants had bought sanitising (‘antibacterial’) hand gel. Unless stated otherwise, all numbers are ORs adjusting for all personal and health-related variables, for all other variables at the same level as the outcome variable and for all other variables at preceding levels. For clarity, significant associations with personal or health-related variables have been omitted.
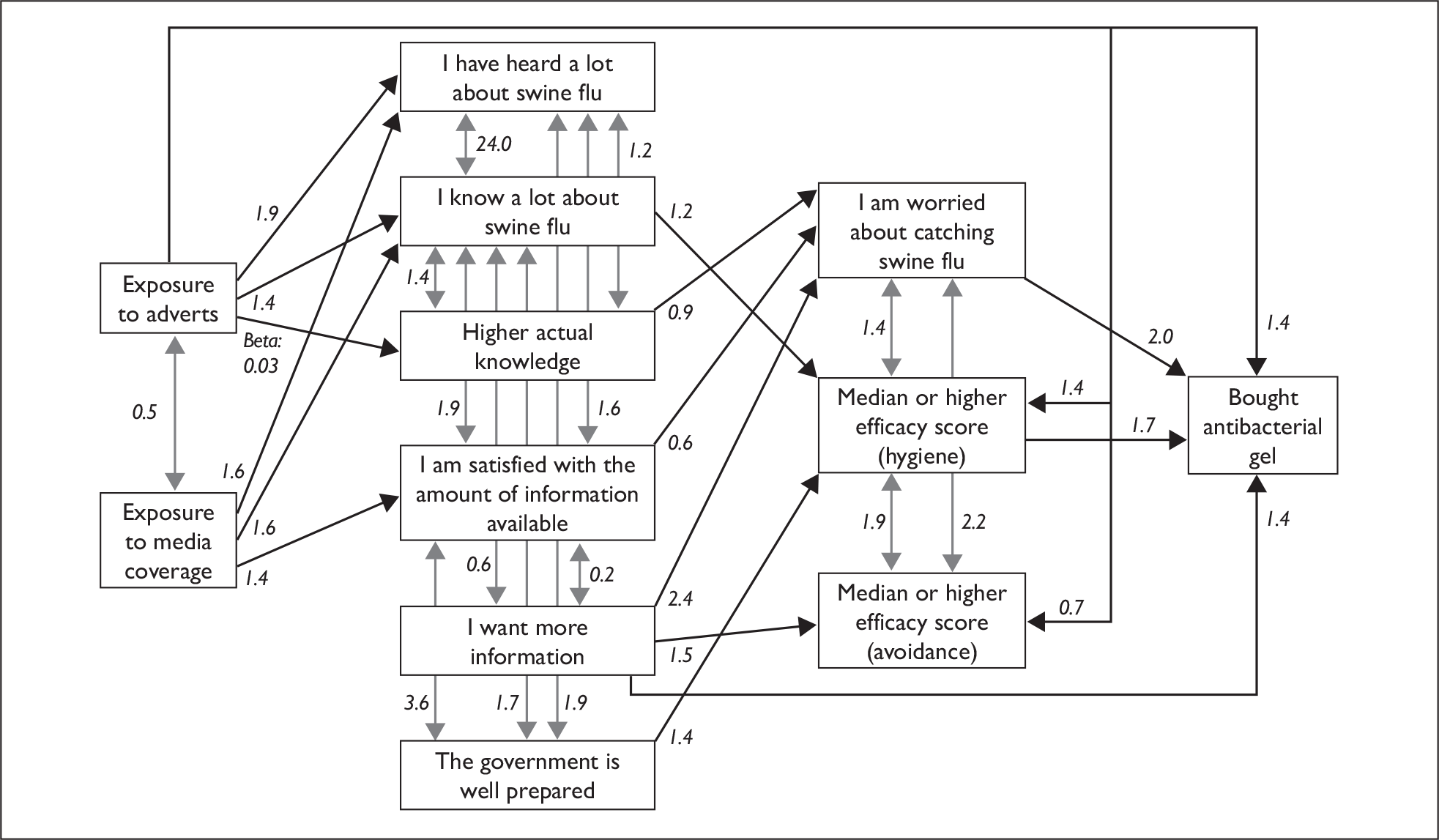
Every pathway leading from exposure to advertising or media coverage tended to reduce avoidance of public transport by reducing worry about the possibility of catching swine flu, increasing the amount heard about swine flu, reducing the perceived efficacy of avoidance measures and reducing the desire for more information (Figure 7).
FIGURE 7.
Path diagram showing the significant paths (p < 0.05) between the information-related, efficacy and worry variables, and whether participants had avoided public transport. Unless stated otherwise, all numbers are ORs adjusting for all personal and health-related variables, for all other variables at the same level as the outcome variable and for all other variables at preceding levels. For clarity, significant associations with personal or health-related variables have been omitted.
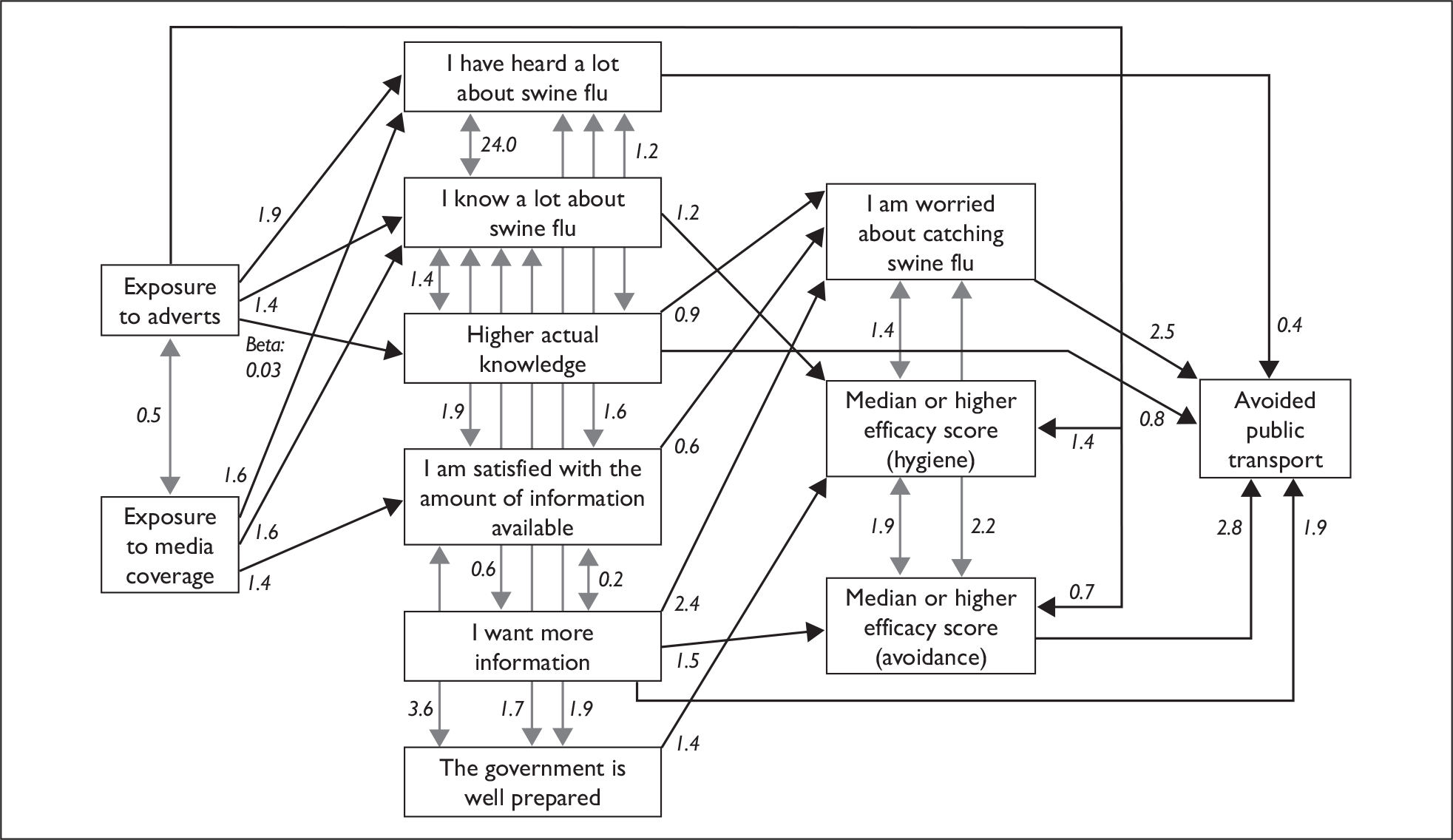
Exposure to advertising or media coverage decreased health-care service use by reducing worry about the possibility of catching swine flu and by a direct effect of exposure to media coverage (Figure 8).
FIGURE 8.
Path diagram showing the significant paths (p < 0.05) between the information-related, efficacy and worry variables, and whether participants had contacted the health services for a flu-related reason. Unless stated otherwise, all numbers are ORs adjusting for all personal and health-related variables, for all other variables at the same level as the outcome variable and for all other variables at preceding levels. For clarity, significant associations with personal or health-related variables have been omitted.
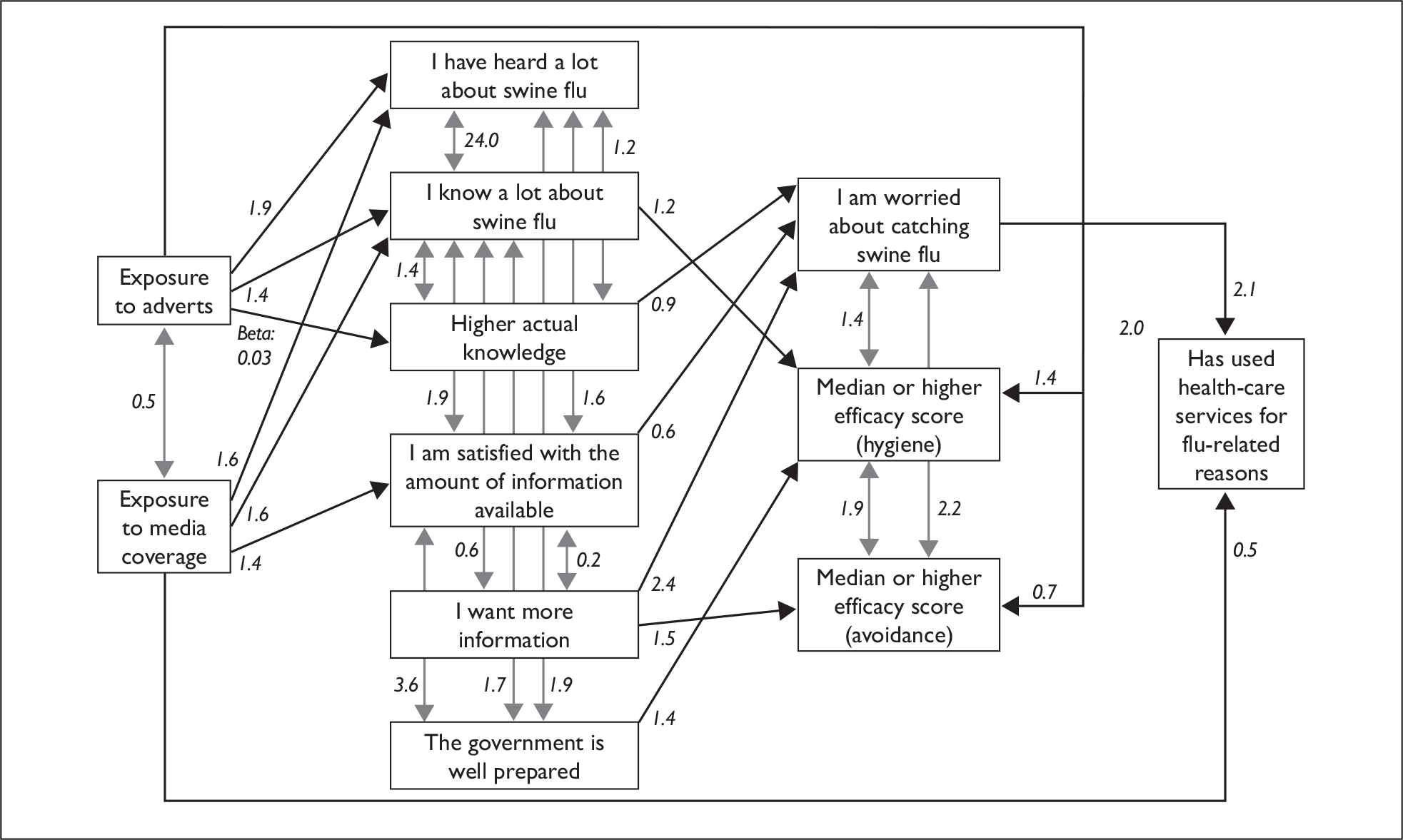
Discussion
In the early stages of the swine flu outbreak, the numbers of people in the UK who reported carrying tissues (33.1%) or having bought sanitising hand gel (9.5%) were low, despite both measures having been promoted by the government. 69 These low rates suggest that the government’s advertising campaign and the attendant media coverage failed to convince most people to make changes to their daily routine that were intended to reduce the spread of infection. This finding tallies with the results of other studies conducted during this period. 35
Rates of behaviours that had not been recommended by the government were lower. Only 2.0% of participants reported having avoided public transport, a proportion consistent with that identified by another survey. 35 Although previous outbreaks of an emerging infectious disease have occasionally been accompanied by a high level of avoidant behaviour among members of the public, this did not occur in the UK during the swine flu outbreak. Similarly, only 1.6% of participants reported having visited a GP or hospital or phoning NHS Direct for a flu-related reason. Although small, this proportion reflects a large volume of consultations for the health-care services and is therefore of more concern,72 particularly as the increase above seasonal norms for flu-related consultations during this period is unlikely to have reflected a genuine increase in rates of infection in the community,41 and is more likely to have been caused by social or psychological factors. 7
Our results also suggest that both advertising and media coverage had beneficial effects on people’s behaviours, both in terms of increasing recommended behaviours and reducing behaviours that were not recommended. As a result of the direct and indirect pathways identified in our path analyses, exposure to either form of information provision tended to result in increased rates of tissue carrying and purchasing of sanitising gel, and decreased rates of public transport avoidance or health-care use. Only 76.9% of respondents reported having been exposed to any media coverage relating to swine flu, while only 50.5% reported having seen any advertising. While maintaining media interest and increasing the visibility of an advertising campaign requires time and resources, our results suggest that this approach may have a beneficial effect on public behaviour during any future outbreak. 22
As well as increasing the quantity of advertising or media articles, ensuring that their content reflects factors shown to improve adherence to behavioural recommendations would also be beneficial. Our path analyses suggest two factors that may be particularly relevant. First, worry about the possibility of catching swine flu was an important variable that was associated with increased rates of all of the behaviours that we examined. A link between worry or anxiety and behaviour change has been observed before in the context of the swine flu outbreak. 35,63 According to some psychological models, a degree of fear is an important precondition if someone is to be encouraged to engage in a behaviour designed to protect them from a hazard. 13 However, while a certain amount of public concern may be helpful in any future outbreak, our results suggest that deliberately increasing worry may cause people to adopt both desirable behaviours (e.g. carrying tissues) and undesirable behaviours (e.g. avoiding public transport). Targeting variables that are more specifically associated with recommended behaviours is likely to be preferable.
A second factor suggested by our analyses may provide this more targeted way of encouraging behaviour change. Our path analyses demonstrated that the perceived efficacy of behaviours was associated with their uptake, and that this followed a logical pattern, with the perceived efficacy of hygiene behaviours being associated with tissue carrying and buying sanitising gel, while the perceived efficacy of avoidance behaviours was associated with avoidance of public transport. This finding, which has been observed before,71 fits with psychological theories of how behaviour change can be brought about in people faced with a potential threat. 13 Importantly, exposure to media coverage or advertising had the effect of increasing the perceived efficacy of hygiene behaviours while decreasing the perceived efficacy of avoidance behaviours. A useful strategy in future outbreaks will be to ensure that advertising and media coverage focus on the efficacy of recommended behaviours, while also highlighting, where relevant, the reasons why other behaviours are not effective.
In addition to effects that were mediated by worry about the possibility of catching swine flu and by perceived efficacy, exposure to advertising also had the direct, unmediated effect of increasing tissue carrying or purchasing of sanitising gel, while exposure to media coverage had a direct effect of reducing health-care use for flu-related reasons. It is likely that the influence of advertising reflects a ‘mere exposure’ effect, in which higher levels of familiarity with an advertised product result in more favourable attitudes towards it. 73 It is also possible that other variables we did not measure, such as perceptions of the capacity of health-care services, the severity of swine flu, or the mechanisms through which swine flu can be contracted, acted as mediators for these effects.
Our path analyses suggested that the mechanisms linking exposure to media coverage or advertising and behaviour were largely similar. Exposure to either form of information tended to increase knowledge, perceived knowledge and satisfaction with the amount of information available, which then affected levels of worry about the possibility of catching swine flu and perceptions of efficacy, and hence behaviour. The similarity between the effects of media and advertising exposure may reflect the fact that information from the government influenced not only its own advertising, but also the coverage given to swine flu by the media, with many media stories including information from government briefings or press releases. 36,37 Some differences between the effects of advertising and the effects of media coverage were observed, however. In particular, while the effects of media exposure were largely mediated by the information-related variables that we assessed, advertising had additional effects on perceptions of efficacy and on behaviour that were not mediated by knowledge or information-related perceptions. Additional research to explore the reason for these direct effects is warranted. In terms of practical implications for future outbreaks, it may be that in situations where knowledge or worry are difficult to alter, advertising can still play an important role in producing behaviour change via these other mechanisms.
Methodological issues
In addition to the caveats raised in study 2 concerning the sampling strategy and response rates for these surveys, six methodological issues should be considered with respect to the analyses presented in this study. First, although we specified causal pathways linking our variables, these pathways remain hypothetical. Given the correlational nature of our data, other interpretations are possible. For example, although we specified that exposure to advertising or media coverage would affect information-related variables and that these, in turn, would affect worry, alternative conceptualisations are possible, including a reversal of this pathway74 or the influence of some other factor that was not measured.
Second, we assumed that the behaviours we assessed were largely driven by the swine flu outbreak. In terms of buying sanitising hand gel and avoiding public transport, this seems a reasonable assumption as these are usually relatively uncommon behaviours. In contrast, it is likely that some of our respondents would have used health-care services for flu-related reasons or would have carried tissues even if the swine flu outbreak had not occurred. This would weaken any association we observed between these outcomes and our predictor variables and thus increase our confidence that the associations we observed for these variables are robust.
Third, the outcome variables that we could include in these analyses were restricted by the questions that were asked in the surveys. The absence of any questions relating to hand-washing presented difficulties. Not only was this one of the behaviours that was most heavily promoted by the government, but also it was also closely tied to communications relating to sanitising hand gel: washing hands or using gel were presented as equally effective alternatives. Had we been able to construct a variable that indicated whether a participant had used sanitising gel or had washed their hands more often than normal as a result of the outbreak, we might have observed a stronger link with media reporting or advertising.
Fourth, because of the need to collect data quickly in order to inform policy, the surveys relied on self-reported behaviour, rather than observed behaviour. The validity of the self-reports of the four outcome measures used in this study is uncertain. For clear-cut behaviours that an individual either has or has not exhibited, such as carrying tissues, having bought sanitising hand gel or speaking to NHS Direct, it is possible that self-reports are reasonably accurate. Avoidance of public transport may be harder for people to quantify, however, as the word ‘avoid’ may be open to interpretation. The role of social desirability in affecting how participants responded to each of these items is also unclear. Further research on the validity of such self-report measures may help to inform the design of future surveys.
Fifth, we assumed that recall for exposure to advertising and media coverage relating to swine flu was an accurate indicator of actual exposure. However, self-reports for such exposures may be poor, largely as a result of poor memory for exposure to news sources. 75,76 Given that our participants were categorised as having been exposed to media coverage and/or advertising based on their recall of where they had heard information about swine flu, it is likely that some misclassification may have occurred for this variable, potentially blurring any distinction between the effects of media coverage and the effects of advertising.
Finally, our analytical approach assumed that exposure to advertising might be expected to have qualitatively different effects from exposure to media reporting. In practice, during the swine flu outbreak the content of both types of information were largely driven by government communications, either directly, in the case of advertising, or through the influence of press releases, official announcements, quotes from official spokespeople or interviews with government experts in the case of media coverage. In future incidents, the impact of these two forms of information might differ more dramatically.
Conclusions
During the early stages of the swine flu outbreak, less than one-third of the public complied with official recommendations relating to hygiene behaviours, while the proportions that avoided public transport or approached the health-care services for flu-related advice were even lower. Exposure to media coverage or advertising relating to swine flu was associated with higher uptake of recommended behaviours and lower performance of non-recommended behaviours, largely as a result of changes in the perceived efficacy of these actions. Exposure was also associated with lower rates of worry about the possibility of catching swine flu, contradicting previous suggestions that media coverage during the early stages of the outbreak had been unnecessarily alarmist or scaremongering. 70,77 In future outbreaks, maximising the reach of any advertising campaigns and ensuring that they explicitly mention the efficacy of any recommended behaviours may help to improve public compliance with key recommendations.
Chapter 5 General discussion
Public reactions to the swine flu outbreak
Contrary to speculation that a new influenza pandemic would be accompanied by panic,43,78 the UK public displayed relatively little concern about swine flu throughout the 10 months covered by our data collection period. Even at the height of the first wave of the outbreak, less than one-third of survey respondents reported being worried about the possibility of catching the disease. For most of the outbreak, this figure fluctuated between 10% and 20%. Similarly, most people did not appear to have made any substantial changes to their daily lives as a result of the outbreak, even when we considered relatively cost-free activities that were being heavily promoted by the government – carrying tissues, for example. Prior to the start of the government’s vaccination campaign, willingness to be vaccinated against swine flu was also low, with only 56% of the public saying that they were likely to accept the vaccine if it was offered to them. Meanwhile, perceptions that too much fuss had been made about the risk of swine flu were high, with roughly one-half to two-thirds of respondents endorsing this statement in any given survey.
These results illustrate the challenges that can be faced by public health communicators during an infectious disease outbreak. It is inevitably difficult to improve rates of compliance with behaviours intended to reduce the impact of an outbreak in the face of general scepticism about the importance of the outbreak. In this regard, it is possible that the perception that too much fuss was made about the risk of swine flu will adversely affect how the public respond to government recommendations during the early stages of the next major infectious disease outbreak. If the credibility of official health warnings was eroded by people’s experiences during this flu pandemic, encouraging members of the public to adopt precautionary behaviour may prove even harder at the start of the next pandemic. This makes it all the more important that the impact of any future communications campaign is maximised by ensuring that it draws on scientific evidence concerning the factors that influence behaviour during an infectious disease outbreak; the three studies presented in this report provide lessons from the swine flu outbreak, which can assist with this. Key findings from this work relate to the central role of worry and response efficacy as variables that determine behaviour, and to the role of media reporting and information provision in affecting this process.
The role of worry
Worry about the possibility of catching swine flu was strongly associated with increased likelihood of performing each of the protective behaviours that we examined. This was true regardless of whether these behaviours were endorsed by the government (being vaccinated, carrying tissues, buying sanitising gel), were portrayed as unnecessary (avoiding public transport) or were explicitly discouraged (consulting NHS staff for flu-related reasons). That worry about the possibility of catching a disease should act as a non-specific motivator for people to take action is consistent with psychological models of behaviour change, such as the Extended Parallel Process Model. 13 This proposes that fear about a given health threat increases the likelihood of someone altering their behaviour in response to it, and that this effect is increased if paired with information about what can be done to reduce the threat.
In the context of communicating about a novel public health threat, the practical implications of this finding may be limited. During the early stages of a major incident, when there is pervasive uncertainty as to how severe the incident will prove to be, describing a reasonable worst-case scenario in order to encourage members of the public to take protective action might be acceptable. 64 However, if the worst-case scenario does not occur, this strategy risks damaging the credibility of future warnings and recommendations. 79 Once a reasonably clear picture has emerged as to the true nature of the risk, compliance with recommended behaviours will be increased by communicators being honest with the public about the nature of the health threat. 22 If this increases worry, this will not have a detrimental effect on compliance, unless the nature of the threat, and hence level of worry, is substantially higher than that previously studied. A corollary to this is that explicit attempts to reassure the public rather than to inform them about the level of risk that they face may also be ill advised. Not only can such attempts make the public distrustful as to why reassurance is being given out,40 but also our results suggest that successful reassurance will reduce uptake of behaviours that might protect against the risk. Providing clear information about the true level of risk faced by the public, based on the best available scientific evidence, is important if the public’s trust in official agencies is to be maintained. 71
The role of efficacy
While our research showed worry about the possibility of catching swine flu to be a motivator for taking action, perceptions about the efficacy of protective strategies were more specific in the way in which they predicted behaviour. Our path analyses in study 3 demonstrated that perceiving avoidance strategies to be effective ways of reducing the spread of swine flu was associated with avoiding public transport, but not with carrying tissues or buying sanitising hand gel, while the opposite was true for the perceived efficacy of hygiene strategies. Study 2 demonstrated that believing, incorrectly, that the seasonal flu vaccine was effective against swine flu was associated with greater likelihood of having the seasonal flu vaccine. Again, these findings fit with the Extended Parallel Process Model,13 which suggests that while worry or fear about a risk can increase a person’s motivation to take action, it is the perceived efficacy of protective actions that determines what action someone will take. Our results therefore suggest that communications campaigns during any future infectious disease outbreak should seek to emphasise the efficacy of any protective behaviours that are being recommended. This suggestion is also supported by previous research in this field. 71 How best to emphasise the efficacy of a protective action is an important question that requires further study.
The role of media reporting and information provision in influencing behaviours
Given that worry appears to act as a motivator for taking protective action, maintaining a degree of public concern throughout any future disease outbreak is likely to assist in promoting uptake of recommended behaviours. This may be particularly relevant during ‘slow burn’ incidents, in which levels of concern are liable to wane along with the rates of behaviours such as hand-washing,49 and in future pandemics when separate waves of infections may require the public to renew their protective activities after periods in which any threat appears to have died away. To a certain extent, it may be possible for communicators to keep an issue in the public eye by scheduling press events, briefing journalists, or putting forward experts or patients for interview. The results of study 1 suggest that once a new risk has become familiar to the public, slow and steady attempts to increase the volume of attention that the media devote to it may have limited, if any, effect on levels of worry in the community. Larger events, such as the introduction of a new vaccine or announcements concerning the beginning of a new wave of infection, may be required before elevations in worry are observed.
During the summer wave of swine flu, the total volume of media reporting was associated with higher levels of worry about the possibility of catching swine flu in the population. From this, it might be expected that at an individual level, increased exposure to information about swine flu during this period would be associated with greater uptake of protective behaviours. Yet in study 2, although likely uptake of vaccination between May and September was strongly predicted by greater worry about the possibility of catching swine flu, it showed no association with the amount of information that a person had heard recently about swine flu. Similarly, in study 3, although exposure to media coverage or advertising about swine flu was associated with increased uptake of recommended behaviours, these effects were largely mediated by the impact of exposure on perceptions of response efficacy. In fact, exposure to media coverage or advertising appeared to reduce, rather than increase, worry about the possibility of catching swine flu. In part, these seemingly contradictory results may reflect a methodological artefact. The surveys on which study 3 was based were conducted at the start of the outbreak, at a time when a high level of media reporting did not result in a high level of worry. A different relationship between exposure to media reporting and worry might have been observed in study 3 had these surveys been conducted later. A more fundamental difference between the studies also needs to be considered. While the cross-sectional studies assessed the impact of media exposure or amount of information heard on worry about the possibility of catching swine flu, behaviour or likely behaviour, the time series analysis used in study 1 assessed whether changes in the volume of media reporting were associated with changes in the number of people who were worried. It is possible that, for the majority of people in any given survey who were worried about the possibility of catching swine flu, their worry reflected reasons that were unrelated to media reporting. At the same time, media reporting may have played a large role in determining worry for a minority of people. Under such circumstances, changes in reporting would predict changes in the number of people who are worried over time, as seen in study 1, even although at any given point in time the amount of reporting that survey respondents had been exposed to would show a poor association with whether or not an individual respondent was worried. Extrapolating from the aggregate data used in the time series analysis to the individual-level data, as used in the cross-sectional analyses, may not be valid. 47
Methodological limitations
Although the specific methodological limitations relating to our three individual studies are discussed in the relevant chapters, one more general limitation that has not yet been raised affected the findings of all three. This relates to the questions included in the surveys we analysed. The surveys were primarily intended to track awareness of, and attitudes to, swine flu. Therefore, many variables that might have been of interest as predictors of behaviour were not included. For example, the surveys did not include items relating to perceived susceptibility to or severity of swine flu, the perceived self-efficacy of people in performing the various behaviours we assessed, perceptions about what other people would like the participant to do or absolute levels of trust in the government, all factors that might have been pertinent. 71 In addition, they did not include questions relating to some behaviours that were important from a public health perspective, such as hand-washing. Although our analyses have identified some factors that may be associated with behaviour change in a future outbreak, these are unlikely to be the only psychological variables that are relevant.
Chapter 6 Conclusions
The conclusions of each study are presented in Chapters 2–4. Overall, our results lead to several broad conclusions regarding recommendations that can be made for practice and for future research.
Implications for practice
-
Our results showed that uptake of recommended behaviours during the swine flu outbreak was low. Maximising the impact of communication campaigns during future pandemics is therefore important. Our studies demonstrated that psychological processes are important to consider when designing these campaigns. Although such campaigns often need to be designed quickly, seeking evidence-based advice from behavioural scientists as to how best to incorporate psychological principles into these campaigns is likely to strengthen them.
-
Our results also demonstrate that rapid-turnaround surveys can be used to improve communications campaigns by identifying factors that mediate between communication and behaviour. These surveys are often considered to be an integral part of the public health response to a major incident, given that they can help policy-makers to design and fine tune their communication strategies. Conducting informative analyses of this type of data requires that appropriate questions and response options for both rates and predictors of behaviour are used. Again, although such surveys often need to be commissioned very quickly, seeking timely advice from behavioural scientists as to what questions to ask, and how, is very worthwhile. We also suggest that efforts are made to design such surveys ahead of time.
-
More specifically, our results suggest that deliberately raising levels of worry about the possibility of catching a disease from low levels among the public is likely to increase uptake of behavioural recommendations during future infectious disease outbreaks. However, doing this without regard to the true nature of the risk faced by the public might erode levels of trust in public health communicators. In addition, our results showed that elevated worry may result in the uptake of behaviours that are not desirable. Caution should therefore be exercised in deciding how to implement this finding.
-
Conversely, given the importance of worry about the possibility of catching swine flu in motivating uptake of protective behaviours, it is likely that attempts to reassure the public about their chances of becoming ill during a future infectious disease outbreak will reduce rates of behaviour change. Reassuring the public on the one hand, while recommending protective behaviours on the other, may also give out mixed messages and affect the impact and credibility of these communications.
-
During any major public health incident certain events will inevitably occur which increase worry and motivation to take action. The time period surrounding these events may therefore be good times to provide the public with information encouraging the uptake of protective actions. We suggest that predicting, and planning responses to, these events should therefore be a focus for public health organisations.
-
The results of studies 2 and 3 suggest that emphasising the efficacy of recommended behaviours in any future campaign will help to maximise the campaign’s impact on those behaviours. Importantly, although increasing levels of worry might increase rates of all protective behaviours, regardless of whether they have been recommended or not, our results suggest that communicating the efficacy of a specific behaviour may have an impact on that behaviour alone.
Research recommendations
-
While our results suggest that successfully communicating information about the efficacy of protective behaviours will increase the uptake of these behaviours, we are unable to say what the best techniques are for providing information about efficacy. Additional research on this topic would help to guide future communications campaigns.
-
Across all the behavioural outcomes that we assessed, there was evidence that people from particular demographic groups were more inclined to engage in behavioural change. As with previous studies, our results showed that ethnicity, age, household size, health status, socioeconomic status and gender all played a role in determining whether someone engaged in a given behaviour or not. 71 The mechanisms underlying these effects are likely to be complex and may have important implications for the way in which messages for these subgroups should be framed. 80 Additional research to understand the reasons for and implications of these effects might help in the design of more effective communications campaigns in future pandemics. Exploring differences within each of these subgroups is also recommended. For example, differences are likely to exist in terms of the concerns of, and most appropriate messages for, people from different ethnic subgroups or with different underlying health conditions.
-
Since the cross-sectional analyses reported in studies 2 and 3 were completed, additional data from the surveys have become available. These include potential outcome variables, such as hand-washing data and actual, rather than intended, vaccine uptake. We recommend further analysis of this data set focusing on these variables. Similarly, the database would also allow a more detailed analysis of the content of media reporting to be used as a predictor of worry during the outbreak.
-
The perception that too much fuss was being made about the risk of swine flu was relatively high throughout the outbreak, but showed low levels of fluctuation as the outbreak developed. It may be that experience with previous health scares and outbreaks was the key factor influencing this perception. It is unclear how people’s experiences during the swine flu outbreak have affected their perception of health warnings produced by scientists, the media or the government, what impact this might have on their response to future warnings, or how best to ameliorate any scepticism. Additional research addressing these areas is warranted.
-
For the foreseeable future, telephone surveys are likely to remain the only pragmatic way to obtain rapid, quantitative data with which to inform policy decisions during public health incidents. Additional research to improve the validity of this technique is therefore warranted. As a first step, testing the validity of self-report measures of different types of behaviour would be of value.
Acknowledgements
The surveys were designed and funded by the Department of Health.
Contribution of authors
Susan Michie (Professor of Health Psychology) and Henry Potts (Lecturer, Health Informatics) had the original idea for the analysis and developed the analytical design with James Rubin (Research Fellow, Psychology as Applied to Medicine). The main statistical analyses were conducted by James Rubin, who also wrote the first draft of the report. All authors contributed to further drafts and had full access to all of the data.
We are grateful to Richard Amlôt, Elizabeth Bailey, Alison Bish, Richard Bowyer, Rachel Carter, Julia Clark, Michele Corrado, Eamonn Ferguson, George Margesson, Robert West and Oliver Wright for their helpful assistance in putting the data into context and commenting on drafts. We also grateful to Fiona Mowbray for her assistance with the analysis of the media data.
Disclaimers
The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health.
References
- Cowling BJ, Chan K-H, Fang VJ, Cheng CKY, Fung ROP, Wai W, et al. Facemasks and hand hygiene to prevent influenza transmission in households. A cluster randomized trial. Ann Intern Med 2009;151:437-46.
- De Jarlais DC, Galea S, Tracey M, Tross S, Vlahov D. Stigmatization of newly emerging infectious diseases: AIDS and SARS. Am J Public Health 2008;96:561-7.
- Brahmbhatt M, Dutta A. On SARS type economic effects during infectious disease outbreaks. Washington, DC: The World Bank; 2008.
- Smith R. Social measures may control pandemic flu. BMJ 2007;334.
- Shepard CW, Soriano-Gabarro M, Zell ER, Hayslett J, Lukacs S, Goldstein S, et al. Antimicrobial postexposure prophylaxis for anthrax: adverse events and adherence. Emerg Infect Dis 2002;8:1124-32.
- Osterholm MT. How to vaccinate 30,000 people in three days: realities of outbreak management. Public Health Rep 2001;116:74-8.
- Rubin GJ, Dickmann P. How to reduce the impact of ‘low risk patients’ following a bioterrorist incident: lessons from SARS, anthrax and pneumonic plague. Biosecur Bioterror 2010;8:37-43.
- Rubin GJ, Amlôt R, Rogers MB, Hall I, Leach S, Simpson J, et al. Perceptions and reactions with regard to pneumonic plague. Emerg Infect Dis 2010;16:120-2.
- Lau JTF, Yang X, Tsui H, Kim JH. Monitoring community responses to the SARS epidemic in Hong Kong: from day 10 to day 62. J Epidemiol Community Health 2003;57:864-70.
- Blendon RJ, Benson JM, DesRoches CM, Weldon KJ. Using opinion surveys to track the public’s response to a bioterrorist attack. J Health Communication 2003;8:83-92.
- Rubin GJ, Amlôt R, Page L, Wessely S. Methodological challenges in assessing general population reactions in the immediate aftermath of a terrorist attack. Int J Methods Psychiatr Res 2008;17:S29-35.
- Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Applied Psychol Int Rev 2008;57:660-80.
- Witte K. Putting the fear back into fear appraisals: The extended parallel process model. Commun Monogr 1992;59:329-49.
- Schwitzer G. Ten troublesome trends in TV health news. BMJ 2004;329.
- Eggener S. The power of the pen: medical journalism and public awareness. JAMA 1998;279.
- Begg N, Ramsay M, White J, Bozoky Z. Media dents confidence in MMR vaccine. BMJ 1998;316.
- Soumerai SB, Ross-Degnan D, Kahn JS. Effects of professional and media warnings about the association between aspirin use in children and Reye’s syndrome. Milbank Q 1992;70:155-82.
- Remuzzi G, Schieppati A. Lessons from the Di Bella affair. Lancet 1999;353:1289-90.
- Heiber M, Lou WYW. Effect of the SARS outbreak on visits to a community hospital emergency department. Can J Emerg Med 2006;8:323-8.
- Mason BW, Donnelly PD. Impact of a local newspaper campaign on the uptake of the measles, mumps and rubella vaccine. J Epidemiol Community Health 2000;54:473-4.
- Ma KK, Schaffner W, Colmenares C, Howser J, Jones J, Poehling KA. Influenza vaccinations of young children increased with media coverage in 2003. Pediatrics 2006;117:157-63.
- Hyer RH, Covello VT. Effective media communication during public health emergencies. Geneva: World Health Organization; 2005.
- McCombs ME, Shaw DL. The agenda setting function of the mass media. Public Opin Q 1972;36:176-87.
- McCombs M. A look at agenda-setting: past, present and future. Journalism Studies 2005;6:543-57.
- Mazur A, Lee J. Sounding the global alarm: environmental issues in the US national news. Soc Stud Sci 1993;23:681-720.
- Lemal M, Van den Bulck J. Television news exposure is related to fear of breast cancer. Prev Med 2009;482:189-92.
- Gaskell G, Bauer MW, Durant J, Allum NC. Worlds apart? The reception of genetically modified foods in Europe and the US. Science 1999;285:384-7.
- Van den Bulck J, Custers K. Television exposure is related to fear of avian flu, an ecological study across 23 member states of the European Union. Eur J Public Health 2009;19:370-4.
- Griffin RJ, Dunwoody S, Zabala F. Public reliance on risk communication channels in the wake of a cryptosporidium outbreak. Risk Anal 1998;18:367-75.
- Dougall AL, Hayward MC, Baum A. Media exposure to bioterrorism: stress and the anthrax attacks. Psychiatry 2005;68:28-42.
- Weaver DH. Thoughts on agenda setting, framing and priming. J Commun 2007;57:142-7.
- Hohenemser C, Kates RW, Slovic P. The nature of technological hazard. Science 1983;220:378-84.
- Cappella JN, Jamieson KH. News frames, political cynicism and media cynicism. Ann Am Acad Pol Soc Sci 1996;546:71-84.
- Forgette R, Morris JS. High conflict television news and public opinion. Polit Res Quart 2006;59:447-66.
- Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: a cross-sectional telephone survey. BMJ 2009;339.
- Anonymous . Putting influenza A H1N1 in its place. Lancet Infect Dis 2009;9.
- Duncan B. How the media reported the first days of the pandemic (H1N1) 2009: results of EU-wide media analysis. Eurosurveillance 2009;14:1-3.
- The Market Research Society . Occupation Groupings: A Job Dictionary 2006. www.mrs.org.uk/publications/downloads/occgroups6.pdf.
- Rubin GJ, Brewin CR, Greenberg N, Simpson J, Wessely S. Psychological and behavioural reactions to the bombings in London on 7 July 2005: cross-sectional survey of a representative sample of Londoners. BMJ 2005;331:606-11.
- Rubin GJ, Page LA, Morgan O, Pinder RJ, Riley P, Hatch S, et al. Public information needs after the poisoning of Alexander Litvinenko with polonium-210 in London: cross-sectional telephone survey and qualitative analysis. BMJ 2007;335:1143-6.
- Health Protection Agency . HPA Weekly National Influenza Report n.d. www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/SwineInfluenza/.
- Cooper CP, Roter DL. ‘If it bleeds it leads’? Attributes of TV health news stories that drive viewer attention. Public Health Rep 2000;115:331-8.
- Harding P. Pandemics, plagues and panic. Br Journalism Rev 2009;20:27-31.
- Blendon RJ, Benson JM, DesRoches CM, Pollard WE, Parvanta C, Hermann MJ. The impact of anthrax attacks on the American public. Med Gen Med 2002;4.
- Shapiro JS, Genes N, Kuperman G, Chason K. Health information exchange, biosurveillance efforts, and emergency department crowding during the spring 2009 H1N1 outbreak in New York City. Ann Emerg Med 2010;55:274-9.
- Wray R, Becker SM, Henderson N, Glik D, Jupka K, Middleton S, et al. Communicating with the public about emerging health threats: lessons from the pre-event message development project. Am J Public Health 2008;98:2214-22.
- Robinson WS. Ecological correlations and the behaviour of individuals. Int J Epidemiol 2009;38:337-41.
- Baxter R. Surveillance lessons from first-wave pandemic (H1N1) 2009, Northern California, USA. Emerg Infect Dis 2010;16:504-6.
- Manning S, Barry T, Wilson N, Baker MG. Update: follow-up study showing post-pandemic decline in hand sanitiser use, New Zealand, December 2009. Eurosurveillance 2010;15:1-2.
- Pandey A, Patni N, Singh M, Sood A, Singh G. YouTube as a source of information on the H1N1 influenza pandemic. Am J Prev Med 2010;38:e1-3.
- National Statistics Online . Internet Access: 70% of Households Had Internet Access in 2009 n.d. www.statistics.gov.uk/cci/nugget asp?ID = 8.
- Department of Health . Swine Flu Vaccines Start Today n.d. www.dh.gov.uk/en/Publichealth/Flu/Swineflu/DH_107340.
- Department of Health . Seasonal Flu: Why You Should Have the Vaccination n.d. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_105352.
- Brouwers L, Cakici B, Camitz M, Tegnell A, Boman M. Economic consequences to society of pandemic H1N1 influenza 2009 – preliminary results for Sweden. Eurosurveillance 2009;14:1-7.
- Begum F, Peabody R. Influenza vaccine uptake among 65 years and over/under 65 years at risk in England winter season 2008–9. Department of Health and Health Protection Agency; n.d.
- Quinn SC, Kumar S, Freimuth VS, Kidwell K, Musa D. Public willingness to take a vaccine of drug under emergency use authorization during the 2009 H1N1 pandemic. Biosecur Bioterror 2009;7:1-16.
- Brewer NT, Chapman GB, Gibbons FX, Gerrard KD, McCaul KD, Weinstein ND. Meta-analysis of the relationship between risk perception and health behavior: the example of vaccination. Health Psychol 2007;26:136-45.
- Tang CSK, Wong C-Y. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J Public Health 2003;93:1887-8.
- Seale H, McLaws M-L, Heywood AE, Ward KF, Lowbridge CP, Van D, et al. The community’s attitude towards swine flu and pandemic influenza. Med J Aust 2009;191:267-9.
- Leung GM, Ho L-M, Chen SKK, Ho S-Y, Bacon-Shone J, Choy RYL, et al. Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clin Infect Dis 2005;40:1713-20.
- Zimicki S, Hornik RC, Verzosa CC, Hernandez JR, de Guzman E, Davrit M, et al. Improving vaccination coverage in urban areas through a health communication campaign: the 1990 Philippine experience. Bull World Health Organ 1994;72:409-22.
- GoogleTrends n.d. www.google.co.uk/trends (accessed 8 June 2010).
- Jones JH, Salathe M. Early assessment of anxiety and behavioural response to novel swine-origin influenza A(H1N1). PLoS One 2009;4.
- Sandman PM. Pandemics: good hygiene is not enough. Nature 2009;459:322-3.
- Qureshi AM, Hughes NJM, Murphy E, Primrose WR. Factors influencing uptake of influenza vaccination among hospital-based health care workers. Occup Med 2004;54:197-201.
- Friederichs V, Cameron JC, Robertson C. Impact of adverse publicity on MMR vaccine uptake: a population based analysis of vaccine uptake records for one million children born 1987–2004. Arch Dis Child 2006;91:465-8.
- Young ME, Norman GR, Humphreys KR. Medicine in the popular press: the influence of the media on perceptions of disease. PLoS One 2008;3.
- Petrie KJ, Wessely S. Modern worries, new technology, and medicine: new technologies mean new health complaints. BMJ 2002;324:690-1.
- Department of Health . Important Information about Swine Flu 2009.
- Jenkins S. Swine flu? A panic stoked in order to posture and spend. The Guardian 2009. www.guardian.co.uk/commentisfree/2009/apr/29/swine-flu-mexico-uk-media1.
- Bish A, Michie S. Demographic and attitudinal determinants of protective behaviours during a pandemic: a review. Br J Health Psychol 2010.
- Chapman N, Wogan M. NHS Direct Chief Executive’s Report n.d. www.nhsdirect.nhs.uk/media.aspx?id = 1465.
- Zajonc RB. Mere exposure: a gateway to the subliminal. Curr Dir in Psychol Sci 2001;10:224-8.
- Griffin RJ, Yang Z, Huurne ET, Boerner F, Ortiz S, Dunwoody S. After the flood: anger, attribution and the seeking of information. Sci Commun 2008;29:285-31.
- Prior M. The immensely inflated news audience: assessing bias in self-reported news exposure. Public Opin Q 2009;1:1-14.
- Prior M. Improving media effects research through better measurement of news exposure. J Polit 2009;71:893-908.
- Allam MF. Influenza A (H1N1) pandemic: true or false alarm. J Epidemiol Community Health 2009.
- Gensheimer KF, Meltzer MI, Postema AS, Strikas RA. Influenza pandemic preparedness. Emerg Infect Dis 2003;9:1645-8.
- Wray R, Rivers J, Whitworth A, Jupka K, Clements B. Public perceptions about trust in emergency risk communication: qualitative research findings. Int J Mass Emerg Disaster 2006;24:45-7.
- Vaughan E, Tinker T. Effective heath risk communication about pandemic influenza for vulnerable populations. Am J Public Health 2009;99:S324-32.
Appendix 1 Protocol (original grant application)
Project title: Public responses to swine flu communications: a longitudinal analysis
Planned investigation
Research objectives
-
To analyse the Department of Health (DH) swine flu public attitudes and behaviour survey to examine how far behaviour can be understood in terms of specific beliefs and emotional responses.
-
To assess how far behaviour, beliefs and emotional responses vary with socioeconomic and other demographic variables, geographic area, and over time.
-
To assess the effect of NHS/DH communication initiatives and media/new media coverage on behaviour, beliefs and emotional responses.
Existing research
The influenza pandemic is an important ongoing health problem. The second most effective method of preventing the spread of flu, after provision of vaccines, involves behaviours, such as hand and respiratory hygiene behaviours, taking up vaccines and staying at home when ill. They are also key to limiting the severity of illness by, for example using the National Pandemic Flu Service or taking antivirals as prescribed. Data from the Health Protection Agency shows that about a third of schoolchildren given antivirals did not complete the course. Effective communication requires targeting specific behaviours central to preventing ill health and influencing attitudes and beliefs that are determinants of those behaviours. Moreover, we have an unprecedented opportunity in this pandemic to build up knowledge about public attitudes to pandemics and similar health threats more generally. This is important to prepare for the next pandemic, something that remains an ongoing threat, particularly in the context of avian flu and emerging zoonoses.
Existing research on preventative behaviours (e.g. hand-washing, respiratory hygiene, vaccine uptake), avoidant behaviours (e.g. staying at home) and management behaviours (e.g. uptake of antivirals) relevant to flu has been identified and summarised in consultation with the Behaviour & Communications (B&C) Group of the Scientific Pandemic Influenza Advisory Committee (SPI) in June 2009. This literature has been drawn from a range of countries, populations, infections (e.g. SARS, avian flu, swine flu, pandemics) and designs (e.g. hypothetical scenarios). The literature search focused on studies of associations between demographic characteristics, attitudes and behavioural measures, either reported, intended or actual behaviour.
The studies found are of variable quality, with some carried out in the middle of the outbreak, while others investigate intentions to behave in the event of an outbreak (see list of references). We can extract some broad principles from the current evidence. Perceptions about the diseases in question are more important predictors of behaviour than perceptions about the behaviours required. The research shows that perceived susceptibility to the disease and its perceived severity are important, as are issues of trust in authorities. There is also evidence that general levels of anxiety can influence the adoption of protective behaviours. As might be expected, belief in the effectiveness of recommended behaviours to protect against the disease can also predict behaviour. Generally, being older, female, non-white or more educated are associated with a higher chance of adopting the behaviours. Figure 1 shows an example of one of the conceptual maps of the predictors of preventative behaviour; we have also developed similar maps for avoidant and management behaviours.
Most research in this area lacks an explicit theoretical framework, partly as the studies were carried out in rapid response to the emerging pandemic threats of SARS and avian flu. Few use multivariate analyses, where the relative contribution of factors to the reported behaviour can be examined. Most are cross-sectional in design.
Only one study, Rubin et al. (2009), was carried out exclusively in the UK and focused on perceptions of swine flu at the very beginning of the outbreak. This cross-sectional study found that people were more likely to follow recommended behaviour if they perceived swine flu to be severe, that they are likely to catch it, that the outbreak will last a long time, that the authorities can be trusted, that good information has been provided and that people can control their risk of catching swine flu and that specific behaviours are effective in reducing the risk. Being uncertain about the outbreak and believing that the outbreak had been exaggerated were associated with a lower likelihood of change. Because of its cross-sectional design, it is difficult to have a clear idea of causality or to study the mediating effect of attitudes and beliefs on the association between media and government communication and behaviour.
What is currently needed is an investigation of the extent to which determinants identified in other situations are relevant to the current swine flu outbreak. We will draw on both the specific literature identified above, but also the more general health psychology literature to identify appropriate theoretical frameworks. Despite this substantial literature on public health attitudes and beliefs, little past research has been sufficiently resourced to track public attitudes longitudinally in such detail as the DH’s weekly tracking survey is currently doing, or has studied as significant a health event as this.
Public attitudes are influenced by multiple information sources, including but not limited to official advice from the DH/NHS or the Government more generally. The literature on risk perception (Adams 1995) has established that public concerns about risk are higher with novel threats and when individuals do not feel in control of the risk, both factors with the flu pandemic. How individuals interpret information depends on their prior knowledge and attitudes. A substantial literature has demonstrated how illness perceptions predict health behaviours (Hagger and Orbell 2003). Illness perceptions are the cognitive representations individuals have about an illness. These may be discordant with professional advice. Faced with a new threat, individuals build a mental model of the threat (Petrie and Weinman 1997, 2006), which, in turn, elicits an emotional reaction, which drives behaviours relating to that threat. The illness perception literature provides a theoretical model to understand attitudes. However, most illness perception research has been concerned with individuals with chronic diseases rather than large threats to public health.
Since the last influenza pandemic in 1968–9, there have been huge changes in media and communication technologies; in approaches to public health psychology; and in polling methodology and statistical analysis. Even since the near pandemic of SARS in 2002–3, there have been significant changes in media and communication technologies. The rise of internet technologies such as Twitter have already been recognised as having significant sociopolitical implications, while traditional media, like local newspapers, continue to decline. Such changes have impacted on health care too (Potts 2006). We have moved from a paternalistic model of health care, with patients being the target of education, to models of shared decision-making and patient choice. Our understanding of large-scale polls has matured, and the range of statistical tools to analyse the resulting data is larger. We have the expertise in our team to consider these changes in the proposed research.
Research methods
The DH’s Communications Directorate has commissioned MORI to conduct a weekly public attitudes tracking survey. Telephone interviews selected from a set of 40 questions are conducted with a representative sample of > 1000 members of the general public to monitor changes in awareness of swine flu communications, trust in information sources, perceptions of swine flu (e.g. severity, controllability), worry about swine flu, perceived efficacy of a variety of preventative behaviours (e.g. hand-washing) and avoidant behaviour (e.g. avoiding travel), and predicted engagement in flu management behaviours (e.g. telephoning Swine Flu Information, staying at home).
The survey started on May 1 and is planned to continue for the next 6 months. There is thus a wealth of data that can be analysed to influence policy and practice. Although DH is analysing these figures as they are produced, the B&C Sub-Group of the SPI Advisory Committee is keen to commission a broader piece of analysis looking at the associations between recalled government and other media communications, cognitive and emotional determinants of behaviours, and reported behaviours. Understanding these will enhance the B&C Group’s ability to make recommendations to DH on these issues.
This research will be shaped, supported and informed by the SPI B&C Sub-Group. The SPI Sub-Group is represented on the Government’s Scientific Advisory Group for Emergencies, and is working closely with the DH Communications Directorate who manage the public attitudes tracking survey. The academic partners will be UCL’s Health Psychology Unit (led by SM), Health Behaviour Research Centre (RW) and Centre for Health Informatics and Multiprofessional Education (HP). We will have a commercial media monitoring partner, such as Meltwater News, to be decided in consultation with the DH Communications Directorate.
Data analysis will be from May 1 and cover the period for which the SPI modelling group have estimated that peak infections of the current outbreak may occur (September 2009 to February 2010).
Work stream 1: Review of survey content and methods for event monitoring
The cumulative survey data will be reviewed and the literature review of behavioural determinants carried out by the B&C group will be updated and considered in the broader context of work on public attitudes. The results of these will be used to ascertain whether any items should be added and/or dropped from the survey. This will be fed back to the DH and MORI as soon as possible. The method for monitoring and identifying key government and DH communications will be finalised and the electronic media monitoring search strategy agreed.
Government/DH communications
Elizabeth Bailey, Head of Planning, Briefing & Messaging, will arrange for regular alerts of all significant DH communications or other noted events that may influence attitudes and behaviour. We will also seek to liaise with DH/NHS over web access statistics pertinent to swine flu (e.g. page hits, search terms). DH estimates of cases and deaths each week will also be collated.
Media monitoring: DH and electronic
An overnight update for swine flu is produced by the DH duty press officer and wider media monitoring services, daily media briefings and broadcast summaries are commissioned through the Central Office of Information Media Monitoring Unit. In addition, one-off specialist monitoring is commissioned as needed.
Electronic media monitoring will be provided, subject to consultation with DH Communications Directorate, by Meltwater News (http://meltwater.com/mnews), an established and highly regarded company serving academic research, government and ‘third sector’ organisations and companies. A bespoke search strategy will produce weekly reports of printed media, frontline websites and blog coverage tailored to the key cognitions (e.g. perceived risk and severity, trust in government sources), emotions (e.g. anxiety, anger) and behaviours (e.g. staying away from work, hand hygiene). Printed media and website coverage represent key channels through which government advice is transmitted to the public; blogs will assess the ways in which the public interpret and act (or not) on advice, information and misinformation. The search strategy can be tailored by time (e.g. the last 2 days), national versus geographical region, and type of media (e.g. tabloids versus quality). It also can be changed week by week to reflect new issues as they arise. Analysis can be qualitative (e.g. tonal quality) as well as quantitative. We will have an individual consultant assigned to the project to adapt the search strategy according to need. The monitoring output will be reported in chart formats and in spreadsheets for statistical analysis by the research team.
Work stream 2: data analysis
The weekly cross-sectional data sets will be analysed multivariately to investigate associations between communication events, behavioural determinants and reported behaviours and to identify any mediators of association between these. Methods will include time series and structural equation modelling. Variations across region (mapped against outbreaks), socioeconomic status and other demographic characteristics will be described and their effects in modifying relationships between communication events and attitudes, worry and reported behaviours will be investigated. Analyses will be conducted, reported and discussed with DH on a monthly basis (more frequently if required).
The goal will be to arrive at a parsimonious model that accounts for as much cross-sectional variance in key target behaviours as possible in terms of emotional responses and specific beliefs. Changes over time in key elements of the model will then be explored in relation to DH communications and media coverage of events. It is recognised that in a fast moving situation, even weekly surveys may not be sufficiently frequent to disentangle the effects of different events and also that some of the effects may be cumulative or lagged. Therefore, it is not possible to state at the outset what kinds of answer will emerge from the data.
Conceptual framework
Mass media campaigns are more likely to be effective if principles of campaign design are adhered to; one of the key principles is to use relevant theories of behaviour change as a conceptual framework, since it will suggest important determinants around which to develop messages (Noar 2006). Data analysis will be informed by two conceptual frameworks in order to identify determinants to inform DH communication and campaigns.
The first is a synthesis of empirical data about the determinants of three categories of behaviour relevant to protecting health within the context of outbreaks of infectious disease (SARS, avian flu and swine flu). This was carried out for the SPI B&C group to guide the DH in designing the survey so as to be maximally useful to policy and planning. This synthesis is summarised and illustrated as a series of ‘conceptual maps’ (see Figure 1), linking attitudinal determinants and other predictors with three key sets of behaviours: preventative (e.g. washing hands with soap), avoidant (e.g. staying at home when ill) and management (e.g. using the National Flu Service when symptoms are detected). A mapping exercise between MORI items and relevant evidence has been conducted by the B&C group to inform discussions with the DH about items to add to the current data set.
The second conceptual framework will be PRIME Theory of motivation (West 2006). This aims to provide an overarching model into which diverse aspects of motivation can be fitted. It pulls together decision-making theories, learning theory, theories of self-regulation and identity, and theories regarding the influence of drives and emotional responses to arrive at an account of the moment-to-moment control of behaviour. It proposes that deliberate actions arise from the strongest of competing feelings of ‘want’ (involving anticipated pleasure or satisfaction) and ‘need’ (involving anticipated relief from mental or physical discomfort or drive states). Beliefs about what is beneficial or harmful, and intentions concerning future actions will only influence behaviour if they generate sufficiently strong immediate wants or needs at the time. The model proposes that identity (self-descriptions including personal rules) are potentially powerful sources of want or need that need to be considered when predicting many behaviours. In relation to responses to the flu pandemic, anticipated relief from anxiety and extent to which identity involves following rules will prove important drivers of particular behaviours.
The study’s ability to inform policy will be shaped by the survey questions included within the DH attitudes survey. It will be limited by the timing of the results; whilst they will not be able to inform response to an autumn flu peak, they will be able to inform policy in relation to the pandemic in the New Year. This proposal will also constitute a dummy run from which we have the opportunity to learn lessons for the future and a possible more severe form of a pandemic flu outbreak.
Statistical analysis
Time series analyses will consider variation over time in key survey responses since May 1 and how these relate to key events (DH activity or media). Analyses will be repeated at both a regional and national level. Data on cases and deaths, key DH communication activity and media/new media activity will be investigated as predictors of public attitudes. Analyses will consider that such relationships may, in turn, vary by demographic factors (e.g. the effect of different media/communication sources may vary by age given known differences by age in use of traditional and online information channels).
Cross-sectional analyses using structural equation modelling will combine data over multiple weeks on a bimonthly basis. This will give a very large statistical power to investigate associations between demography, beliefs, knowledge, attitudes and behaviour. This analysis will be performed three times over the 6 months’ period to investigate whether the associations between variables also change over time.
Data interpretation
The results will be interpreted within the context of the literature review that the B&C group is currently conducting of effective communication and other interventions to change flu preventative and management behaviours.
Work stream 3: dissemination and advice on communication strategy
Dissemination will be guided by Richard Bowyer, Deputy Director of Strategy, Planning & Insight, DH Communications Directorate, and SM, who is a member of the Scientific Advisory Group in Emergencies (SAGE) and therefore is informed on a weekly basis of policy and planning needs. The survey analyses will be discussed on a regular basis by relevant members of the pandemic flu team within the DH Communications Directorate and by the B&C Group (of which SM is Chair) that reports to SAGE. The B&C group is charged with providing scientific advice to underpin policy in communication strategy and in behavioural management, a key aspect of reducing infection transmission and illness severity.
Ethical arrangements
Since the proposed study is to analyse anonymous survey data that is already being collected by the DH, no further ethics/governance permissions are required. The possibility of data being identifiable from demographic variables is very low, but all data will be securely stored.
We are conscious that merely asking a question on beliefs about flu has the potential to spread false information, and will thus carefully discuss survey wording with MORI.
Project timetable and milestones
In an emerging and unpredictable context, we offer an approach that is flexible enough to capture ongoing developments, and robust enough to produce valid conclusions. A detailed Gantt chart will be constructed outlining weekly targets for the duration of the project.
The applicants (SM and HP) will meet with the researcher employed on the study at least once a week to review past week’s work and plan the next week’s. We will plan for a fast turnaround for analysis to allow the research and the tracking surveys to respond to developments, but we will also reserve time for more detailed analysis. There will be fortnightly contact with the B&C Group of the SPI and the DH’s Communications Directorate to ensure that the findings are influencing policy and practice in a timely and effective manner. Both of these organisations are central to the management of the project. Meetings/teleconferences with our assigned advisor from the media monitoring organisation will be as and when needed.
The timeline for this research is:
-
October Review of survey content and methods for monitoring of DH communications and media and linking to data set; setting up working partnerships; begin analysis of past data.
-
November Data analysis and first report; dissemination and advice to DH on communication strategy.
-
December Refined and repeated data analysis and reports, dissemination and advice to DH on communication strategy.
-
December/January Final report for DH.
-
February & March Further analysis, dissemination and advice to DH on communication strategy; at least one and probably two journal articles (one addressing first two objectives and one addressing third). Timing of article submission for publication will be coordinated with the DH timetable for publishing the data.
Milestones
-
Oct 14
-
– Data analysis protocol developed for Objectives 1 and 2.
-
– Initial meeting with DH representatives to discuss DH’s needs re. monitoring communication events, desirability of adding items to survey and key questions to be addressed by analyses.
-
– Initial meeting with Meltwater News to agree search and reporting strategy.
-
-
Nov 1
-
– Initial data analyses run on past data.
-
– Summary of media and other event monitoring by DH.
-
– Data analysis protocol for Objective 3.
-
-
Nov 14
-
– First data analysis report addressing all three objectives.
-
– Presentation of report to DH communications team.
-
-
Dec 1
-
– Refined and repeated data analysis and reports.
-
-
Dec 14
-
– Final report for DH of analyses addressing three objectives.
-
-
Jan 14
-
– Meeting with DH to discuss future analyses that will inform work at this stage of the pandemic.
-
-
Feb 1
-
– Draft of Paper 1.
-
-
Feb 14
-
– Meeting with DH to present results of subsequent analyses. Data analysis plan for final 6 weeks.
-
-
Mar 1
-
– Draft of Paper 2.
-
– Discussion with DH Communications about possible future research to inform their communication design, output and evaluation.
-
-
Mar 14
-
– Submission of Paper 1, assuming DH publication of data.
-
-
Mar 31
-
– Final report to DH of findings from agreed subsequent analyses.
-
– Submission of Paper 2, assuming DH publication of data.
-
Expertise
Susan Michie is Professor of Health Psychology leading the Health Psychology Unit in UCL’s Division of Psychology and Language Sciences. She is known internationally for her work on understanding health-related behaviours and applying psychological theory to designing interventions to change behaviour. She works at the interface of science and policy, acting as part-time consultant to the DH’s Health Improvement Directorate to advise on several communication and behavioural intervention programmes. She is a member of the Government’s SPI Advisory Committee and SAGE, chairing its B&C group.
Henry Potts is a health informaticist and statistician in UCL Medical School. He brings to the team expertise in statistical analysis for a health psychology context. He is also a recognised expert on new information and communication technologies and their role in health care, including non-traditional media and social networking.
Robert West (collaborator) is Professor of Health Psychology leading a team of researchers within the Health Behaviour Research Centre in UCL’s Department of Epidemiology and Public Health. He brings to the team expertise in human motivation, having recently published a comprehensive theory that describes how beliefs and emotions interact with environmental events to generate behaviour. He also runs a longitudinal study of beliefs, emotional responses and behaviours relating to smoking (the Smoking Toolkit Study), which tracks responses on a monthly basis and involves similar kinds of analyses to those proposed here.
Meltwater News is a global specialist in online media monitoring, working with more than 15,000 companies and academic and other organisations to track critical information published online. They provide unlimited and filtered results for research purposes, and analysis is provided including topic, timeline, sources and geographical cross-section.
Service users
The analyses and their dissemination will be guided by SM in collaboration with Richard Bowyer, Deputy Director of Strategy, Planning & Insight, DH Communications Directorate. They will feed directly into the DH Communications Directorate and the B&C Group (of which SM is Chair) that reports to SAGE. The B&C group is charged with providing scientific advice to underpin policy in communication strategy and in behavioural management, a key aspect of reducing infection transmission and illness severity.
Justification of support required
We will require 5% of SM’s time to oversee the project and report writing, liaise with the DH and the B&C group and manage the researcher. We will require 10% of HP’s time to oversee the statistical analyses and write the statistical parts of the report.
We are asking for the cost of a postdoctoral researcher to conduct the analyses, draft reports and give administrative support to the project. SM, HP and the researcher will meet with the identified DH communications team members. The researcher will need a computer, statistical software and printer. We will require the cost of teleconferences and inner London travel. Finally, we are asking for a small budget to cover casual assistance, which will be provided, as needed, by Alison Bish, a health psychologist providing support to SPI’s B&C group.
| Evidence that predicts behaviour | No evidence that predicts behaviour | |
|---|---|---|
| Included in MORI poll |
Q3 Heard of swine flu (knowledge) Q4 How much heard Q5 How much do you know (4 and 5 possibly more perception than actual knowledge) Q7 Worry* Q10 No vaccine?* (sort of knowledge/sort of severity) Q11 There are ways to slow down spread (knowledge/severity) Q12 Natural immunity? (knowledge/severity) Q13 Flu vaccine will protect me (knowledge/severity) Q14 Catch from pork? (knowledge) Q15 Thousands died? (knowledge/severity) Q16 Washing hands with soap effectiveness* (effectiveness of behaviour) Q17 Covering nose and mouth effectiveness* (effectiveness of behaviour) Q18 Disposing of tissues effectiveness* (effectiveness of behaviour) Q19 Avoiding travel effectiveness (effectiveness of behaviour) Q20 Avoiding crowds effectiveness (effectiveness of behaviour) Q21 Cleaning surfaces effectiveness (effectiveness of behaviour) Q23 Wearing masks effectiveness (effectiveness of behaviour) Q27 Satisfied with amount of information* (communication) Q29 Government prepared?* (communication) Q33 Too much fuss being made* (communication) Q36 What is pandemic flu/How is it different from normal flu* (knowledge) Q37 Pandemic flu is more severe than swine flu* (severity/knowledge) Q38 Pandemic flu is the same as swine flu but more widespread* (severity/knowledge) Age* Ethnicity* Gender* Children under 16* Marital status* |
QA NHS number QB Where to find it (however, these 2 items are clearly important administratively) Q1 General health* Q2 Longstanding disability* Q8 Source of information Q9 Websites used Q26 Who trusted Q28 What extra information is required (although important to know this) Q30 How to get Tamiflu* Q31 (a) receipt of leaflet (b) TV advert awareness (c) radio advert awareness (d) radio advert awareness (e) newspaper advert awareness Q34 Where expect to receive information from: working status home ownership car ownership job status Which newspaper read Whether self, friends, family work for NHS (useful markers of social class) Geographical region (important as at the moment some areas are more affected than others) |
| Not included in MORI poll |
Perceived severity for the individual in various ways e.g. financially, medically – although some items touch on this Perceived susceptibility in terms of feeling at risk/feeling vulnerable/likelihood of catching it Perceived behavioural control and self-efficacy Level of trust (rather than just who is trusted) State anxiety Social pressure/social norms Educational level Income level Presence of symptoms/cues to action Illness perceptions, e.g. beliefs about pandemic flu – its time course (how long are you ill for?), severity (including likelihood of death), what causes it (a virus? a bacterium?), how is it spread (through the air? through food? through contact with another person? from surfaces?) Have you had swine flu? Do you know personally anyone who has had swine flu? |
|
| Behavioural responses included in MORI poll | Behavioural responses not included in MORI poll | |
|
Q6 Been to see GP/hospital/Called NHS Direct Q24/Q25 Intentions to seek help if symptomatic (Q25 unprompted) call doctor call helpline go to GP call swine flu information stay at home and self-treat visit NHS website go to A&E visit pharmacist speak to family and friends go to walk in centre take medication ask doctor to come to house keep away from people stay at home call A&E call pharmacy inform my employers Q32 Done any of the following since the outbreak carrying tissues bought antibacterial gel looked for information online avoided eating pork/ham/bacon avoided public transport visited GP telephoned GP rearranged travel visited A&E tried to buy Tamiflu telephoned NHS Direct |
Avoided crowds Avoided work Taken antiviral agents Used National Flu Line Washed hands more frequently Cleaned surfaces Coughed into tissues Worn mask Made flu friend plans Used antibacterial gel |
|
FIGURE 1.
Example of conceptual maps of predictors of preventative behaviours
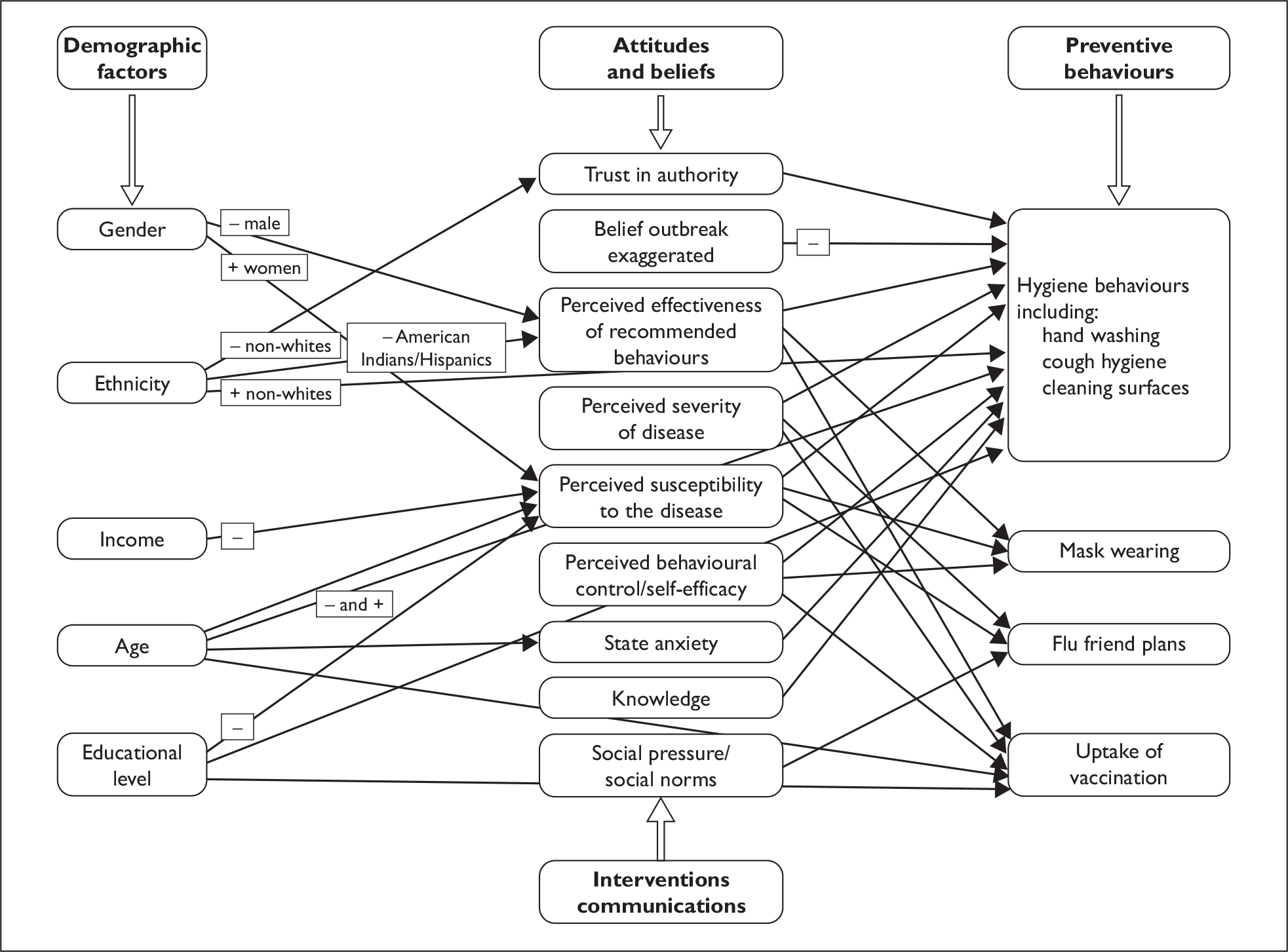
References
-
Adams J. Risk. UCL Press: London; 1995.
-
Hagger M, Orbell S. A meta analytic review of the common-sense model of illness representations. Psychol Health 2003;18:141–84.
-
Lau JTF, Yang X, Tsui H, Kim JH. Monitoring community responses to the SARS epidemic in Hong Kong: from day 10 to day 62. J Epidemiol Community Health 2003;57:864–70.
-
Noar SM. A 10-year retrospective of research in health mass media campaigns: where do we go from here? J Health Commun, 2006;11:21–42.
-
Petrie KJ, Weinman J. Perceptions of health and illness: current research and applications. Harwood: the Netherlands; 1997.
-
Petrie KJ, Weinman J. Why illness perceptions matter. Clin Med 2006;6:536–9.
-
Potts HWW. Is e-health progressing faster than e-health researchers? J Med Internet Res 2006;8:e24.
-
Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: a cross-sectional telephone survey. BMJ 2009;339:b2651.
-
Tang CSK, Wong C-Y. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J PublicHealth 2003;9:1887–8.
-
West R. Theory of addiction. Wiley Blackwell: Oxford; 2006.
Appendix 2 Searches used to identify media stories relating to specific aspects of swine flu
Children-related search
(ingress:“H1N1” or ingress:“swine flu” or ingress:“pandemic”) and (title:“children” or title:“child” or title:“kids” or title:“baby” or title:“babies” or title:“babe” or title:“tots” or title:“tot” or title:“toddler” or title:“toddlers” or title:“school” or title:“nursery” or title:“infant” or title:“infants” or title:“pupil” or title:“pupils” or title:“schools” or title:“nurseries”)
Death-related search
(ingress:“swine flu” or ingress:“H1N1” or ingress:“pandemic”) and (title:“death” or title:“deaths” or title:“dead” or title:“die” or title:“fatality” or title:“kill” or title:“kills” or title:“killed” or title:“killer” or title:“deadly” or title:“lethal” or title:“fatal”)
Exaggeration-related search
(ingress:“swine flu” or ingress:“H1N1” or ingress:“pandemic”) and (ingress:“alarmist” or ingress:“alarmism” or ingress:“overstate” or ingress:“overstated” or ingress:“over the top” or ingress:“hype” or ingress:“hyping” or ingress:“hyped” or ingress:“over hyped” or ingress:“overhyped” or ingress:“hysteria” or ingress:“hysterical” or ingress:“exaggerate” or ingress:“exaggerated” or ingress:“exaggerating” or ingress:“exaggerates” or ingress:“overplay” or ingress:“overplayed” or ingress:“over-react” or ingress:“overreact” or ingress:“over react” or ingress:“over reacts” or ingress:“over reacting” or ingress:“over reacted” or ingress:“over blown” or ingress:“sensationalised” or ingress:“sensationalism” or ingress:“embelished” or ingress:“embelish” or ingress:“inflated”)
Uncertainty or disagreement-related search
(ingress:“H1N1” or ingress:“swine flu” or ingress:“pandemic”) and (title:“uncertain” or title:“uncertainties” or title:“controversy” or title:“controversies” or title:“debate” or title:“debates” or title:“doubt” or title:“doubts” or title:“query” or title:“queries” or title:“argument” or title:“arguments” or title:“confusion” or title:“confusions” or title:“confusing” or title:“contradiction” or title:“contradictions” or title:“contradictory” or title:“muddle” or title:“muddles” or title:“disagree” or title:“disagrees” or title:“disagreement” or title:“disagreements” or title:“inconsistent” or title:“inconsistencies” or title:“critic” or title:“criticism” or title:“critics”)
Appendix 3 Key themes identified in media reporting for the start date of each survey
| Survey start date | Main themes in that day’s media reporting (key dates of other events recorded in parentheses) |
|---|---|
| 01/05/09 | Reporting focuses on news of a UK citizen who contracted swine flu in the UK, the first time community transmission has been recorded. Several local newspapers quote council or local NHS trust spokespeople as saying that local agencies are well prepared for a large-scale outbreak. Reports describe swine flu as still mild, but highlight concerns that it might mutate at some stage in the future. Official advice about respiratory and hand hygiene measures are repeated |
| 05/05/09 | Reports of local cases still predominate in the local press. The closure of two large private schools in London and distribution of Tamiflu to the pupils is reported. Official spokespeople are quoted giving advice about respiratory and hand hygiene measures. The illness is typically described as mild by most papers. Initial people who caught it are described as coming out of quarantine and returning to normal life |
| 08/05/09 | Although still reporting swine flu to be mild, concerns are voiced that the vaccine might mutate at some point in the future. Some stories report that the response to swine flu may have been an over-reaction. An MP is quoted as saying it is good for people to catch the virus now ‘whilst it’s still relatively weak’. Warnings about online scams involving fake medication are given |
| 12/05/09 | Local cases of swine flu continue to be reported. Some discussion over the use of ‘hyperbole’ by journalists and scientists occurs. While some new schools are closed, previously closed schools are reported as reopening. Comparisons are made with the 1957 pandemic, as a result of a newly recent study |
| 17/05/09 | Limited amount of reporting occurs, describing the impact of swine flu on tourism to Mexico now that the Foreign Office is no longer advising against travel to the region, and some new cases occurring among members of the public |
| 22/05/09 | Local newspapers report the first cases occurring in their area. Victims of swine flu are being treated with antiviral drugs. Local and national health officials and ministers are quoted as saying that it is right to prepare for a pandemic, that the health services are working well to contain the spread of disease, and that there is no cause for public alarm |
| 29/05/09 | Most articles focus on the closure of a famous private school and a breakthrough in the development of a vaccine. Several stories about swine flu spreading faster in UK than in the rest of EU and the first report of a life-threatening UK case |
| 05/06/09 | Reports focus on the geographical clustering of cases (particularly in Scotland and Birmingham). There are also stories about first cases in particular counties within the UK |
| 12/06/09 | The majority of stories cover the fact that the World Health Organization has now declared swine flu to be a global pandemic. Focus is also on the use of a containment strategy to control the spread and the provision of Tamiflu to at-risk groups as a prevention measure (World Health Organization declares a full pandemic – 11 June) |
| 19/06/09 | Stories focus on the possible overdiagnosis of swine flu by GPs and indicate that there will be greater reliance on lab testing now (first UK death occurs – 15 June) |
| 26/06/09 | A coming rise in cases during autumn and winter is suggested as well as reinforcement of advice about hand hygiene and who to contact if ill. Several stories about a surge in people calling NHS Direct worried they may have swine flu. The largest 1-day increase in cases since the outbreak began is reported. Tamiflu is now only being given to those who are ill, rather than contacts |
| 03/07/09 | The media suggest that cases cannot be contained. There is talk of 100,000 new cases a day by August. There has been a move to a treatment rather than containment phase. People are warned not to go to work if they’re feeling ill and to be cautious of counterfeit drugs. First mention of ‘swine flu parties’ (government announces a change in strategy from containment of swine flu to treatment – 2 July) |
| 10/07/09 | Some papers talk about a potential plan to let people stay off work for 14 days without needing a GP’s note in order to ease the burden on GPs and to help prevent the spread of the disease. Talk of business resilience plans. A leaked government memo is reported as saying that the country is ‘not ready’ to deal with an epidemic |
| 17/07/09 | Immunisation programme is set to begin in the autumn and the National Pandemic Flu Service (NPFS) helpline will soon be launched. Lots of stories about the death toll rising, but the spread slowing due to the end of the school year |
| 24/07/09 | Stories stress that pandemic plans have been in place for years and the country is prepared. There was huge demand as soon as the NPFS website was launched. Impossible to accurately calculate the number of cases since the beginning of the outbreak as swabbing and testing is no longer done (NPFS goes live – 23 July) |
| 31/07/09 | Cases may have plateaued for the moment. Reports of Tamiflu side effects in children taking it (nausea and nightmares). Pregnant women described as particularly at risk from swine flu and four times more likely to be admitted to hospital. Vaccine trials have begun |
| 07/08/09 | Concerns are raised about the safety of fast-tracking the vaccine. Reminders of hand hygiene and tissue use are issued. Decreasing number of cases for now but warnings of a second wave when schools go back. Worry that the NHS won’t get enough doses of the vaccine before the possible second wave of cases. No evidence the virus is mutating or getting stronger. Health workers and pregnant women to take priority for vaccination. Worry about ‘unqualified’ swine flu advisors on the NPFS helpline |
| 14/08/09 | Mass immunisation is to begin in the autumn. Clarifications in many articles in terms of at-risk groups and the order in which people will be vaccinated. Travel companies report losing business. Warnings are given to people who are ill that they should try to avoid public events |
| 21/08/09 | Launch of an awareness campaign about what to do if you have swine flu, as well as a leaflet (‘Worried about swine flu’). Focus on the difficulty of predicting when the second wave could hit. Only an estimated 1 in 10 people who sought treatment really have swine flu |
| 28/08/09 | Swine flu rates continue to fall even in ‘hotspots’. Reinforced messages of not panicking and that most deaths have had underlying complications. First batches of vaccine have been delivered to government but won’t be used until October. Businesses holding swine flu seminars to raise awareness and help stop spread |
| 04/09/09 | UK businesses told to prepare for staff absences of up to 50%. Deaths could actually be less than half those of the normal flu. Criticism that the government overexaggerated the severity of swine flu. Discussion of practicalities surrounding vaccine administration, such as how much GPs should be paid |
| 11/09/09 | Some experts say Tamiflu should not be given to children because of severe side effects. The next wave of swine flu predicted to peak between late August and late September |
| 18/09/09 | A Northern Irish pig farm has tested positive for swine flu. Cases have increased again over the past week – lots of talk of the ‘return of swine flu’ |
| 25/09/09 | Continued rise in cases. Regulators approve swine flu vaccine for use in UK. Vaccine tests to be done on young children. Alcohol-based hand gels banned in prisons after inmates drink it. Plans are under way to set up vaccination centres |
| 02/10/09 | Continues to be a steady increase in cases but is still mild in severity for most people. Reiteration of the symptoms and what to do if ill. Increase in number of people admitted to hospital with swine flu who have no underlying health conditions. Seasonal flu campaign begins |
| 09/10/09 | A drop in cases is happening again, but further increases said to be likely – other papers report increases in cases calling it the beginning of the second wave. Preliminary evidence showing there may be a link between obesity and swine flu complications. Reminder messages about good hygiene |
| 16/10/09 | UK death toll passes 100. Pregnant women urged to get vaccine after a pregnant woman and her baby die from swine flu. National vaccination programme to begin from 21 October. Postal strike could disrupt the sending out of letters by GPs to vaccine candidates |
| 23/10/09 | Four people in Scotland die within 24 hours. Children in special schools to be vaccinated as a priority. Vaccination programme is under way – US vaccination facing delays. Concern about the proportion of younger people dying. NHS may soon struggle to cope with the demand on hospital services. Invention of first ‘swine flu wipe’ (vaccination starts – 21 October) |
| 30/10/09 | Reminder of symptoms. Second wave appears to be slow moving, although a number of articles talk about 50% increase in cases. Encouragement to take up the vaccination offer. Pharmaceutical companies report increased profits. GP clinics still don’t have the vaccine so there is confusion about when people can get vaccinated. A celebrity duo may have swine flu. Launch of TV ad campaign to ‘catch it, bin it, kill it’ |
| 06/11/09 | Four people die in the West Midlands. Statement issued saying that all school children may potentially be vaccinated. Only a ‘small increase’ in cases overall this week. Poor school attendance rates in Ireland |
| 13/11/09 | Some Irish papers report that the worst of the outbreak has passed. All priority groups to be vaccinated by Christmas. Cases seem to be falling in England and Ireland but still slowly rising in Scotland. Death of another pregnant woman and urges for at-risk groups to get vaccinated |
| 20/11/09 | Healthy children under 5 are to be vaccinated against swine flu. Deaths from swine flu still increasing – 21% of deaths have been under-14-year-olds. Concern that parents will not allow their children to get the vaccination (extension of vaccination programme to children is announced – 19 November) |
| 27/11/09 | Decrease in cases, but an increase in number needing hospital treatment. More deaths in Scotland. Calls for parents to get children vaccinated. Review to come in terms of whether NPFS needs to continue. A drug-resistant strain of swine flu identified |
| 11/12/09 | Swine flu to be a ‘slow burn’ until spring rather than a huge outbreak. Only about one-quarter of people in risk groups have opted to get the vaccination. A medical study suggests there is no clear evidence that Tamiflu cuts risk of complications. Some GPs claim they are underpaid for administering the swine flu vaccine. Death rate lower than was originally feared |
| 28/12/09 | Another rise in Scottish cases. Vaccination for children under 5 has begun. Overall number of cases has been lower than expected |
| 08/01/10 | Diagnosis levels have fallen and the worst may be over but people are encouraged to remain vigilant. Vaccination in children under 5 continues. EU governments are scaling back their orders for vaccine |
Appendix 4 Tables relating to study 3
| Variable | Variable levels | n (%) | n (%) carrying tissues | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Sex | Female | 3101 (57.2) | 1229 (39.6) | 2.0 (1.8 to 2.3) | 2.1 (1.8 to 2.3) |
| Male | 2318 (42.8) | 564 (24.3) | Reference | Reference | |
| Age – years | 16–24 | 518 (9.6) | 173 (33.4) | 0.9 (0.7 to 1.1) | 0.9 (0.7 to 1.1) |
| 25–34 | 662 (12.2) | 206 (31.1) | 0.8 (0.7 to 0.97) | 0.7 (0.6 to 0.9) | |
| 35–54 | 1917 (35.4) | 608 (31.7) | 0.8 (0.7 to 0.9) | 0.8 (0.7 to 0.96) | |
| 55–64 | 979 (18.1) | 320 (32.7) | 0.9 (0.7 to 1.0) | 0.9 (0.7 to 1.04) | |
| ≥ 65 | 1343 (24.8) | 486 (36.2) | Reference | Reference | |
| Social grade | C2DE | 2268 (41.9) | 755 (33.3) | 1.0 (0.9 to 1.1) | 0.9 (0.8 to 1.1) |
| ABC1 | 3151 (58.1) | 1038 (32.9) | Reference | Reference | |
| Ethnicity | Other ethnicity | 361 (6.7) | 153 (42.4) | 1.5 (1.2 to 1.9) | 1.8 (1.4 to 2.3) |
| White | 5010 (93.3) | 1616 (32.3) | Reference | Reference | |
| Household size | Six people or more | 105 (2.0) | 36 (34.3) | 1.0 (0.7 to 1.6) | 1.1 (0.7 to 1.7) |
| Three to five people | 1806 (33.7) | 599 (33.2) | 1.0 (0.9 to 1.1) | 1.1 (0.9 to 1.3) | |
| Two people | 1943 (36.3) | 636 (32.7) | 1.0 (0.8 to 1.1) | 1.0 (0.9 to 1.2) | |
| One person | 1502 (28.0) | 501 (33.4) | Reference | Reference | |
| General health status | Poor or very poor | 407 (7.5) | 165 (40.5) | 1.4 (1.2 to 1.8) | 1.3 (1.02 to 1.7) |
| Fair | 841 (15.6) | 279 (33.2) | 1.0 (0.9 to 1.2) | 1.0 (0.8 to 1.1) | |
| Very good or good | 4153 (76.9) | 1346 (32.4) | Reference | Reference | |
| Does participant have any long-standing infirmity or illness? | Yes | 1522 (28.2) | 557 (36.6) | 1.2 (1.1 to 1.4) | 1.2 (0.995 to 1.4) |
| No | 3874 (71.8) | 1228 (31.7) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) buying sanitising gel | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Sex | Female | 3101 (57.2) | 383 (12.4) | 2.4 (1.9 to 2.9) | 2.4 (2.0 to 3.0) |
| Male | 2318 (42.8) | 130 (5.6) | Reference | Reference | |
| Age – years | 16–24 | 518 (9.6) | 77 (14.9) | 2.7 (2.0 to 3.8) | 2.3 (1.6 to 3.4) |
| 25–34 | 662 (12.2) | 83 (12.5) | 2.2 (1.6 to 3.1) | 1.9 (1.3 to 2.8) | |
| 35–54 | 1917 (35.4) | 203 (10.6) | 1.8 (1.4 to 2.4) | 1.7 (1.2 to 2.2) | |
| 55–64 | 979 (18.1) | 69 (7.0) | 1.2 (0.8 to 1.6) | 1.2 (0.8 to 1.6) | |
| ≥ 65 | 1343 (24.8) | 81 (6.0) | Reference | Reference | |
| Social grade | C2DE | 2268 (41.9) | 214 (9.4) | 1.0 (0.8 to 1.2) | 1.1 (0.9 to 1.3) |
| ABC1 | 3151 (58.1) | 299 (9.5) | Reference | Reference | |
| Ethnicity | Other ethnicity | 361 (6.7) | 53 (14.7) | 1.7 (1.3 to 2.3) | 1.5 (1.1 to 2.0) |
| White | 5010 (93.3) | 456 (9.1) | Reference | Reference | |
| Household size | Six people or more | 105 (2.0) | 17 (16.2) | 3.0 (1.7 to 5.2) | 1.9 (1.02 to 3.5) |
| Three to five people | 1806 (33.7) | 230 (12.7) | 2.3 (1.8 to 2.9) | 1.7 (1.3 to 2.3) | |
| Two people | 1943 (36.3) | 173 (8.9) | 1.5 (1.2 to 2.0) | 1.4 (1.1 to 1.9) | |
| One person | 1502 (28.0) | 91 (6.1) | Reference | Reference | |
| General health status | Poor or very poor | 407 (7.5) | 45 (11.1) | 1.2 (0.9 to 1.7) | 1.6 (1.1 to 2.4) |
| Fair | 841 (15.6) | 80 (9.5) | 1.0 (0.8 to 1.3) | 1.3 (0.97 to 1.7) | |
| Very good or good | 4153 (76.9) | 387 (9.3) | Reference | Reference | |
| Does participant have any long-standing infirmity or illness? | Yes | 1522 (28.2) | 137 (9.0) | 0.9 (0.8 to 1.1) | 1.0 (0.8 to 1.3) |
| No | 3874 (71.8) | 375 (9.7) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) avoiding public transport | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Sex | Female | 3101 (57.2) | 65 (2.1) | 1.1 (0.7 to 1.5) | 1.1 (0.7 to 1.6) |
| Male | 2318 (42.8) | 46 (2.0) | Reference | Reference | |
| Age – years | 16–24 | 518 (9.6) | 16 (3.1) | 1.4 (0.8 to 2.7) | 1.5 (0.7 to 3.2) |
| 25–34 | 662 (12.2) | 11 (1.7) | 0.8 (0.4 to 1.5) | 0.8 (0.4 to 1.8) | |
| 35–54 | 1917 (35.4) | 45 (2.3) | 1.1 (0.7 to 1.7) | 1.3 (0.7 to 2.2) | |
| 55–64 | 979 (18.1) | 10 (1.0) | 0.5 (0.2 to 0.96) | 0.5 (0.3 to 1.1) | |
| ≥ 65 | 1343 (24.8) | 29 (2.2) | Reference | Reference | |
| Social grade | C2DE | 2268 (41.9) | 51 (2.2) | 1.2 (0.8 to 1.7) | 1.0 (0.7 to 1.6) |
| ABC1 | 3151 (58.1) | 60 (1.9) | Reference | Reference | |
| Ethnicity | Other ethnicity | 361 (6.7) | 24 (6.6) | 4.1 (2.6 to 6.6) | 4.1 (2.5 to 6.8) |
| White | 5010 (93.3) | 85 (1.7) | Reference | Reference | |
| Household size | Six people or more | 105 (2.0) | 6 (5.7) | 2.6 (1.1 to 6.4) | 1.4 (0.5 to 3.8) |
| Three to five people | 1806 (33.7) | 36 (2.0) | 0.9 (0.5 to 1.4) | 0.8 (0.4 to 1.3) | |
| Two people | 1943 (36.3) | 34 (1.7) | 0.8 (0.5 to 1.2) | 0.8 (0.5 to 1.3) | |
| One person | 1502 (28.0) | 34 (2.3) | Reference | Reference | |
| General health status | Poor or very poor | 407 (7.5) | 16 (3.9) | 2.3 (1.3 to 4.0) | 2.6 (1.3 to 5.1) |
| Fair | 841 (15.6) | 23 (2.7) | 1.6 (0.99 to 2.6) | 1.6 (0.96 to 2.8) | |
| Very good or good | 4153 (76.9) | 72 (1.7) | Reference | Reference | |
| Does participant have any long-standing infirmity or illness? | Yes | 1522 (28.2) | 36 (2.4) | 1.2 (0.8 to 1.8) | 1.0 (0.6 to 1.6) |
| No | 3874 (71.8) | 75 (1.9) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) using health care services | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Sex | Female | 3101 (57.2) | 53 (1.7) | 1.1 (0.7 to 1.7) | 1.1 (0.7 to 1.8) |
| Male | 2318 (42.8) | 35 (1.5) | Reference | Reference | |
| Age – years | 16–24 | 518 (9.6) | 13 (2.5) | 1.7 (0.8 to 3.4) | 1.2 (0.5 to 2.9) |
| 25–34 | 662 (12.2) | 10 (1.5) | 1.0 (0.5 to 2.2) | 0.9 (0.4 to 2.2) | |
| 35–54 | 1917 (35.4) | 32 (1.7) | 1.1 (0.6 to 2.0) | 0.9 (0.5 to 1.8) | |
| 55–64 | 979 (18.1) | 13 (1.3) | 0.9 (0.4 to 1.8) | 0.9 (0.4 to 1.8) | |
| ≥ 65 | 1343 (24.8) | 20 (1.5) | Reference | Reference | |
| Social grade | C2DE | 2268 (41.9) | 43 (1.9) | 1.3 (0.9 to 2.0) | 1.1 (0.7 to 1.8) |
| ABC1 | 3151 (58.1) | 45 (1.4) | Reference | Reference | |
| Ethnicity | Other ethnicity | 361 (6.7) | 13 (3.6) | 2.5 (1.4 to 4.5) | 2.2 (1.2 to 4.2) |
| White | 5010 (93.3) | 74 (1.5) | Reference | Reference | |
| Household size | Six people or more | 105 (2.0) | 6 (5.7) | 3.7 (1.5 to 9.3) | 3.3 (1.2 to 9.1) |
| Three to five people | 1806 (33.7) | 39 (2.2) | 1.4 (0.8 to 2.3) | 1.6 (0.8 to 2.9) | |
| Two people | 1943 (36.3) | 18 (0.9) | 0.6 (0.3 to 1.1) | 0.6 (0.3 to 1.1) | |
| One person | 1502 (28.0) | 24 (1.6) | Reference | Reference | |
| General health status | Poor or very poor | 407 (7.5) | 13 (3.2) | 2.5 (1.3 to 4.5) | 2.6 (1.3 to 5.5) |
| Fair | 841 (15.6) | 20 (2.4) | 1.8 (1.1 to 3.0) | 1.7 (0.9 to 3.1) | |
| Very good or good | 4153 (76.9) | 55 (1.3) | Reference | Reference | |
| Does participant have any long-standing infirmity or illness? | Yes | 1522 (28.2) | 31 (2.0) | 1.4 (0.9 to 2.2) | 1.2 (0.6 to 2.0) |
| No | 3874 (71.8) | 56 (1.4) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) carrying tissues | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Exposure to media coverage | Exposed | 4167 (76.9) | 1387 (33.3) | 1.0 (0.9 to 1.2) | 1.0 (0.9 to 1.2) |
| Not exposed | 1251 (23.1) | 405 (32.4) | Reference | Reference | |
| Exposure to advertising | Exposed | 2735 (50.5) | 942 (34.4) | 1.1 (1.01 to 1.3) | 1.2 (1.05 to 1.3) |
| Not exposed | 2683 (49.5) | 850 (31.7) | Reference | Reference | |
| How much have you heard about swine flu? | A lot or a moderate amount | 4817 (92.9) | 1618 (33.6) | 1.2 (0.97 to 1.5) | 1.3 (0.99 to 1.6) |
| A little or nothing | 366 (7.1) | 107 (29.2) | Reference | Reference | |
| How much do you know about swine flu | A lot or a moderate amount | 3803 (73.6) | 1308 (34.4) | 1.2 (1.05 to 1.4) | 1.2 (1.03 to 1.4) |
| A little or nothing | 1365 (26.4) | 416 (30.5) | Reference | Reference | |
| How satisfied are you with amount of information? | Very or fairly satisfied | 4462 (91.0) | 1520 (34.1) | 1.0 (0.8 to 1.2) | 1.0 (0.8 to 1.2) |
| Very or fairly dissatisfied | 441 (9.0) | 155 (35.1) | Reference | Reference | |
| Do you want more information? | Yes | 1998 (36.9) | 775 (38.8) | 1.5 (1.3 to 1.7) | 1.4 (1.3 to 1.6) |
| No | 3417 (63.1) | 1016 (29.7) | Reference | Reference | |
| How well prepared is the government? | Very or fairly well prepared | 4014 (78.3) | 1347 (33.6) | 1.1 (0.95 to 1.3) | 1.1 (0.97 to 1.3) |
| Not very or not at all well prepared | 1113 (21.7) | 351 (31.5) | Reference | Reference | |
| How worried are you about swine flu? | Very or fairly worried | 757 (14.0) | 348 (46.0) | 1.9 (1.6 to 2.2) | 1.7 (1.5 to 2.0) |
| Not very or not at all worried | 4642 (86.0) | 1441 (31.0) | Reference | Reference | |
| Hygiene efficacy score | Median or higher | 2827 (52.2) | 1095 (38.7) | 1.7 (1.5 to 1.9) | 1.6 (1.4 to 1.8) |
| Lower than median | 2588 (47.8) | 698 (27.0) | Reference | Reference | |
| Avoidance efficacy score | Median or higher | 2728 (50.5) | 989 (36.3) | 1.3 (1.2 to 1.5) | 1.2 (1.1 to 1.4) |
| Lower than median | 2674 (49.5) | 801 (30.0) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) buying sanitising gel | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Exposure to media coverage | Exposed | 4167 (76.9) | 394 (9.5) | 1.0 (0.8 to 1.2) | 1.1 (0.8 to 1.3) |
| Not exposed | 1251 (23.1) | 118 (9.4) | Reference | Reference | |
| Exposure to advertising | Exposed | 2735 (50.5) | 308 (11.3) | 1.5 (1.3 to 1.9) | 1.4 (1.2 to 1.7) |
| Not exposed | 2683 (49.5) | 204 (7.6) | Reference | Reference | |
| How much have you heard about swine flu? | A lot or a moderate amount | 4817 (92.9) | 469 (9.7) | 1.3 (0.9 to 1.9) | 1.4 (0.9 to 2.1) |
| A little or nothing | 366 (7.1) | 28 (7.7) | Reference | Reference | |
| How much do you know about swine flu | A lot or a moderate amount | 3803 (73.6) | 380 (10.0) | 1.2 (0.95 to 1.5) | 1.2 (0.97 to 1.5) |
| A little or nothing | 1365 (26.4) | 117 (8.6) | Reference | Reference | |
| How satisfied are you with amount of information? | Very or fairly satisfied | 4462 (91.0) | 439 (9.8) | 1.0 (0.7 to 1.3) | 0.9 (0.7 to 1.3) |
| Very or fairly dissatisfied | 441 (9.0) | 45 (10.2) | Reference | Reference | |
| Do you want more information? | Yes | 1998 (36.9) | 249 (12.5) | 1.7 (1.4 to 2.0) | 1.5 (1.3 to 1.9) |
| No | 3417 (63.1) | 264 (7.7) | Reference | Reference | |
| How well prepared is the government? | Very or fairly well prepared | 4014 (78.3) | 372 (9.3) | 0.9 (0.7 to 1.1) | 0.9 (0.7 to 1.1) |
| Not very or not at all well prepared | 1113 (21.7) | 115 (10.3) | Reference | Reference | |
| How worried are you about swine flu? | Very or fairly worried | 757 (14.0) | 145 (19.2) | 2.8 (2.2 to 3.4) | 2.3 (1.9 to 2.9) |
| Not very or not at all worried | 4642 (86.0) | 366 (7.9) | Reference | Reference | |
| Hygiene efficacy score | Median or higher | 2827 (52.2) | 339 (12.0) | 1.9 (1.6 to 2.3) | 1.8 (1.5 to 2.2) |
| Lower than median | 2588 (47.8) | 174 (6.7) | Reference | Reference | |
| Avoidance efficacy score | Median or higher | 2728 (50.5) | 274 (10.0) | 1.1 (0.9 to 1.4) | 1.2 (0.99 to 1.5) |
| Lower than median | 2674 (49.5) | 239 (8.9) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) carrying tissues | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Exposure to media coverage | Exposed | 4167 (76.9) | 82 (2.0) | 0.8 (0.6 to 1.3) | 0.9 (0.6 to 1.4) |
| Not exposed | 1251 (23.1) | 29 (2.3) | Reference | Reference | |
| Exposure to advertising | Exposed | 2735 (50.5) | 44 (1.6) | 0.6 (0.4 to 0.9) | 0.7 (0.4 to 0.99) |
| Not exposed | 2683 (49.5) | 67 (2.5) | Reference | Reference | |
| How much have you heard about swine flu? | A lot or a moderate amount | 4817 (92.9) | 85 (1.8) | 0.3 (0.2 to 0.5) | 0.4 (0.2 to 0.6) |
| A little or nothing | 366 (7.1) | 20 (5.5) | Reference | Reference | |
| How much do you know about swine flu | A lot or a moderate amount | 3803 (73.6) | 65 (1.7) | 0.6 (0.4 to 0.9) | 0.6 (0.4 to 0.99) |
| A little or nothing | 1365 (26.4) | 40 (2.9) | Reference | Reference | |
| How satisfied are you with amount of information? | Very or fairly satisfied | 4462 (91.0) | 81 (1.8) | 0.4 (0.2 to 0.6) | 0.4 (0.2 to 0.7) |
| Very or fairly dissatisfied | 441 (9.0) | 21 (4.8) | Reference | Reference | |
| Do you want more information? | Yes | 1998 (36.9) | 72 (3.6) | 3.2 (2.2 to 4.8) | 2.8 (1.9 to 4.2) |
| No | 3417 (63.1) | 39 (1.1) | Reference | Reference | |
| How well prepared is the government? | Very or fairly well prepared | 4014 (78.3) | 73 (1.8) | 0.6 (0.4 to 0.9) | 0.7 (0.5 to 1.1) |
| Not very or not at all well prepared | 1113 (21.7) | 33 (3.0) | Reference | Reference | |
| How worried are you about swine flu? | Very or fairly worried | 757 (14.0) | 49 (6.5) | 5.1 (3.5 to 7.5) | 4.1 (2.7 to 6.2) |
| Not very or not at all worried | 4642 (86.0) | 62 (1.3) | Reference | Reference | |
| Hygiene efficacy score | Median or higher | 2827 (52.2) | 63 (2.2) | 1.2 (0.8 to 1.8) | 1.2 (0.8 to 1.9) |
| Lower than median | 2588 (47.8) | 47 (1.8) | Reference | Reference | |
| Avoidance efficacy score | Median or higher | 2728 (50.5) | 89 (3.3) | 4.3 (2.6 to 6.9) | 4.1 (2.5 to 6.8) |
| Lower than median | 2674 (49.5) | 21 (0.8) | Reference | Reference |
| Variable | Variable levels | n (%) | n (%) using health services | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|---|
| Exposure to media coverage | Exposed | 4167 (76.9) | 57 (1.4) | 0.5 (0.4 to 0.8) | 0.6 (0.4 to 0.9) |
| Not exposed | 1251 (23.1) | 31 (2.5) | Reference | Reference | |
| Exposure to advertising | Exposed | 2735 (50.5) | 43 (1.6) | 0.9 (0.6 to 1.4) | 0.9 (0.6 to 1.5) |
| Not exposed | 2683 (49.5) | 45 (1.7) | Reference | Reference | |
| How much have you heard about swine flu? | A lot or a moderate amount | 4817 (92.9) | 77 (1.6) | 3.0 (0.7 to 12.1) | 3.6 (0.9 to 14.9) |
| A little or nothing | 366 (7.1) | 2 (0.5) | Reference | Reference | |
| How much do you know about swine flu | A lot or a moderate amount | 3803 (73.6) | 63 (1.7) | 1.5 (0.9 to 2.7) | 1.8 (0.99 to 3.2) |
| A little or nothing | 1365 (26.4) | 15 (1.1) | Reference | Reference | |
| How satisfied are you with amount of information? | Very or fairly satisfied | 4462 (91.0) | 70 (1.6) | 0.6 (0.3 to 1.1) | 0.6 (0.3 to 1.2) |
| Very or fairly dissatisfied | 441 (9.0) | 12 (2.7) | Reference | Reference | |
| Do you want more information? | Yes | 1998 (36.9) | 45 (2.3) | 1.8 (1.2 to 2.8) | 1.5 (0.97 to 2.3) |
| No | 3417 (63.1) | 43 (1.3) | Reference | Reference | |
| How well prepared is the government? | Very or fairly well prepared | 4014 (78.3) | 65 (1.6) | 0.9 (0.6 to 1.6) | 1.3 (0.7 to 2.0) |
| Not very or not at all well prepared | 1113 (21.7) | 19 (1.7) | Reference | Reference | |
| How worried are you about swine flu? | Very or fairly worried | 757 (14.0) | 27 (3.6) | 2.8 (1.8 to 4.4) | 2.3 (1.4 to 3.4) |
| Not very or not at all worried | 4642 (86.0) | 61 (1.3) | Reference | Reference | |
| Hygiene efficacy score | Median or higher | 2827 (52.2) | 52 (1.8) | 1.4 (0.9 to 2.1) | 1.5 (0.9 to 2.4) |
| Lower than median | 2588 (47.8) | 35 (1.4) | Reference | Reference | |
| Avoidance efficacy score | Median or higher | 2728 (50.5) | 49 (1.8) | 1.3 (0.8 to 1.9) | 1.3 (0.8 to 2.0) |
| Lower than median | 2674 (49.5) | 38 (1.4) | Reference | Reference |
List of abbreviations
- aOR
- adjusted odds ratio
- ARIMA
- autoregressive integrated moving average
- CI
- confidence interval
- GP
- general practitioner
- OR
- odds ratio
- SARS
- severe acute respiratory syndrome
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.