
Notes
Article history
The research reported in this issue of the journal was commissioned by the HTA programme as project number 01/10/04. The contractual start date was in June 2003. The draft report began editorial review in October 2009 and was accepted for publication in February 2010. As the funder, by devising a commissioning brief, the HTA programme specified the research question and study design. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© 2010 Queen’s Printer and Controller of HMSO. This journal is a member of and subscribes to the principles of the Committee on Publication Ethics (COPE) (http://www.publicationethics.org/). This journal may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2010 Queen’s Printer and Controller of HMSO
Preface
In 2001, the Health Technology Assessment (HTA) programme produced the commissioning brief (HTA 01/10/04) for a trial on the use of a diet and lifestyle intervention versus laxatives to manage chronic constipation in older adults. The commissioning brief specified the key research question: ‘What is the comparative cost-effectiveness of laxatives compared with dietary and lifestyle changes in the treatment of elderly patients with chronic constipation?’ The brief was based on recommendations of a HTA-commissioned systematic review, which had found only weak evidence that laxatives can improve stool frequency and consistency, and related symptoms. Dietary and lifestyle interventions (increase in consumption of dietary fibre and fluid, moderate exercise, obeying the call to stool) had been shown to alleviate constipation. More generally, in studies aimed at the modification of dietary behaviour, brief interventions had been shown to have limited effect, while intensive, patient-tailored interventions had been more effective, though costly.
In response to the commissioning brief, the research team designed a pragmatic three-armed trial [diet and LIFEstyle versus LAXatives in the management of chronic constipation in older people (LIFELAX) – International Standard Randomised Controlled Trial Number (ISRCTN)73881345] to compare laxative treatment of chronic constipation in older people with both standardised, non-personalised dietary and lifestyle advice (delivered in a single, short consultation) and personalised dietary and lifestyle advice (delivered in a long consultation, with telephone reinforcement). Through this study design the trial team was able to address the following key questions, derived from the research brief:
-
What is the comparative clinical effectiveness and cost-effectiveness of laxatives versus a combination of dietary and lifestyle advice?
-
What is the comparative clinical effectiveness and cost-effectiveness of brief, standardised, non-personalised dietary and lifestyle advice versus personalised dietary and lifestyle advice, including reinforcement?
Running simultaneously with LIFELAX was another HTA-commissioned complex randomised controlled trial (RCT) investigating the cost-effectiveness of the stepped treatment of older adults on laxatives [Stepped Treatment Of Older adults on Laxatives (STOOL) – ISRCTN11557289]. The HTA Commissioning Board funded a small qualitative study alongside the STOOL and LIFELAX trials to investigate the definition and meaning of constipation among older people and health professionals. The results of this pilot work were used to inform a number of decisions made by the LIFELAX trial team while developing the interventions, the data collection tools and preparing patient information sheets.
Set-up and preparation for the LIFELAX trial (the development of the interventions, data collection tools – questionnaire and diaries, the production of the trial protocols, the production of practice training resources, and applications for regulatory, ethics and research governance approval) started in June 2003. Major changes to the Ethics and Research Governance structure and process during the life of the trial, challenges in practice recruitment and the lower than anticipated levels of patients’ participation meant that recruitment targets were not met in the time agreed with the HTA. Towards the end of the recruitment period available to LIFELAX, the infrastructure to support research activities in the primary care setting was in place [initiatives such as the UK Primary Care Research Networks (PCRNs), the UK Local Comprehensive Research Networks]. However, these networks were still very much in their infancy, and the LIFELAX Trial Steering Committee made the decision in September 2007 to close recruitment and follow up the small number of participants in the trial rather than recommend approaching the HTA for a further extension.
In conjunction with LIFELAX, the HTA programme funded an integrated qualitative process evaluation study. The aim of the process evaluation was to develop a critical understanding of the social processes and practices implicated in the development, implementation and dissemination of a RCT within the field of HTA. Because the process evaluation was ethnographic, qualitative research techniques were used, and it was therefore not appropriate to set out research questions in hypothetical form.
Methodologically, the approach taken by the process evaluation was a shift away from the conventional, with the relationship between the quantitative (LIFELAX) and qualitative (process evaluation) being integral rather than complementary. In this respect the process evaluation was concerned primarily with documenting HTA in action through implementation of an RCT, rather than the provision of supplementary qualitative data to support the key LIFELAX outcome measures.
Due to the lower than necessary levels of patient recruitment it has not been possible to conduct a full evaluation of the interventions, therefore this report has a slightly different emphasis to the model HTA monograph. We describe the background to, and rationale for, the study. We describe the development of the interventions and the various training resources. We present the design of the trial and detail the various strategies and techniques used in its implementation to optimise practice and patient participation. We examine the various barriers to successful implementation of LIFELAX at a practical level. We present the findings of the process evaluation and discuss the contribution it makes to our understanding of a complex intervention at work using the Normalisation Process Theory and the implications for future complex interventions in primary care.
Chapter 1 Background
Introduction
As a medical problem, constipation is often trivialised. 1 However, chronic constipation has a considerable impact upon the individual and all of the health-care resources associated with managing the condition. The effect of chronic constipation on quality of life (QoL) is considerable,2,3 and the burden on health-care resources, in terms of visits to health-care practitioners, and medications, is substantial. 4 In England and Wales, constipation generated some 450,000 general practitioner (GP) consultations per year in 1991–2,5 at an estimated cost of £4.5M per year. 6 The net ingredient cost in 2005 of prescriptions for laxatives was approximately £50M per year in England alone. 7
Defining constipation and ‘normal’ bowels
Constipation is ‘variably defined’8 by patients and medical professionals and is a common complaint of industrialised societies. 9 Patients perceive ‘regularity’ to be an important variable in determining good health. 10 In Scouting for Boys,11 Baden Powell declared that in order ‘to make yourself strong and healthy it is necessary to begin with your inside’, and recommendations for this included ‘making the stomach work to feed the blood’ with exercises such as the ‘cone’, or ‘body bending’, and ‘twisting’. In order to ‘make the bowels active to remove the remains of food and dirt from the body’ he suggested ‘body bending’ and ‘kneading the abdomen’, and suggested his scouts ‘drink plenty of good water’ and had, what he referred to as, a ‘regular daily rear’.
The frequency and consistency of stools are important in defining constipation and ‘normal bowels’, both in lay and clinical definitions. Regarding ‘frequency’, clinicians consider passing a stool anywhere from three times a day to three times a week as being ‘normal bowel function’. 12 Regarding ‘consistency’, as this is linked to transit time through the gut it is considered by clinicians to be a useful indicator of normal bowel function. 13–15 In everyday life, however, constipation means different things to different people. 16,17 Even to health-care professionals constipation remains a largely subjective diagnosis. 18 As the experiences of the STOOL (Stepped Treatment Of Older adults on Laxatives) trial and its associated qualitative study show, both constipation and normal bowel function are so difficult to define that it is entirely understandable that there is often a mismatch between what patients and health-care professionals mean when they use the term ‘constipation’ (p. 67). 19
Clinical definitions
It is not surprising that constipation is subjectively diagnosed when one considers the lack of an accepted definition of constipation in clinical practice. Attempts to define it have been made and the following working definition has been proposed:18 ‘straining at passing stools for more than 25% of bowel movements’. Others attempts at a definition have used the frequency of bowel movements: passing a stool ‘less than three times per week’ has been offered as an operational definition of constipation in clinical and epidemiological research. 20,21 According to the Rome II criteria for functional constipation,22 the ‘gold standard’ criteria at the time of designing the LIFELAX (diet and LIFEstyle versus LAXatives in the management of chronic constipation in older people) trial, for a diagnosis of constipation, individuals are required to have two or more of the following symptoms present for at least 12 consecutive weeks in the previous 12 months:
-
straining in more than one in four defecations
-
lumpy or hard stools in more than one in four defecations
-
sensation of incomplete evacuation in more than one in four defecations
-
manual procedures (e.g. digital evacuation or support of the pelvic floor) in more than one in four defecations
-
fewer than three defecations per week.
In the more recent Rome III criteria, a less restrictive time frame is introduced. Symptoms must have begun 6 months prior to diagnosis and be active for 3 months. Thus, onset of symptoms should begin at least 6 months before clinical presentation and the diagnostic criteria must be fulfilled for the last 3 months (rather than 1 year for Rome II). 23
Considering the complexity of the above, it is entirely understandable that there is so little agreement between a patient’s self-perceived constipation and assessments based on the Rome II criteria. 14,19 With the Rome II criteria for constipation being so far removed from the patient definition,19 underestimation of the prevalence of condition could be expected. In a systematic review of studies of the epidemiology of constipation in North America,24 the authors reported that the prevalence of self-reported constipation was consistently higher than that defined by the Rome II criteria. 22 Figures from a North American review paper estimate that, in addition to the 63 million people meeting the Rome II criteria for functional constipation, a further 50 million reported that they had constipation. The authors of the review suggest that these differences may reflect the lay perceptions and expectations of normal bowel function, in particular frequency. 24 In line with the STOOL report findings,19 it was the absence of a daily bowel movement that people described as ‘being constipated’. Evidence from the literature surrounding irritable bowel syndrome suggests that the Rome criteria are not used to any great extent within routine clinical practice in primary care, with estimates of between 12% and 20% of GPs knowing the criteria and only 3–4% using them. 25,26
Lay definitions
Frequency of bowel movements is an often-used lay criterion, with most people associating constipation with decreases in normal frequency of bowel movements. Within ‘frequency of bowel movements’ there are at least three distinctive experiences:
-
those who are unable to pass a stool despite having an urge to go (‘can’t go’)
-
those for whom there is an infrequent passing of stools (‘not going to the toilet’)
-
those who miss a day without a bowel movement (‘not going as often’). 19
In a UK-based study of hospital outpatients, almost one-half of the participants thought of constipation purely in terms of frequency of bowel action, without considering difficulty or pain on defecation. 27 The importance attached to the frequency of bowel movements is not just a UK finding, with both Japanese28 and Australian17 studies finding it to be of the highest importance28 to older people, and the most often cited description of constipation. 17
The STOOL report highlights the range of factors taken into account when people define constipation. 19 In addition to frequency, when defining constipation lay people place emphasis on a range of other symptoms, such as straining,29 bloating30 and unsatisfactory defecation. 31 To further add to the complexity of the lay definition of constipation, the importance, or implicit weighting, attached to different symptoms, or combinations of symptoms, varies from patient to patient. 17,19,28
Prevalence rates of constipation among older people
Given the lack of consensus on the definition of constipation in the clinical world, and the variation in definition and perceptions of constipation among lay people, it is not surprising that there is little agreement on the prevalence rates of the condition. UK estimates of prevalence rates of constipation in the general population range from 2% to 51.5%. 13,15,32–34 In the epidemiological study in North America mentioned earlier, prevalence rate estimates range from 1.9% to 27.2%. 24
Regardless of this lack of consensus over actual prevalence rates, there is agreement that the rates do increase with age5,35,36 (Table 1). In the HTA-commissioned systematic review of the effectiveness of laxatives in the elderly, the authors assert that approximately one-fifth of older people living in the community have symptoms of constipation. 1
| Consultation rates/10,000 | Age range of patients (years) |
|---|---|
| 75 | 45–64 |
| 200 | 65–74 |
| 400 | 77–84 |
| 600 | 85+ |
Impact of constipation on QoL in older people
Given the prevalence and burdensome nature of chronic constipation, the literature surrounding the impact it has upon QoL and standardised assessments to measure this is surprisingly sparse. 38 Many of the early studies attempting to investigate the overall burden of chronic constipation on QoL made use of general assessments such as the Gastrointestinal Symptom Rating Scale and the Psychological General Well-Being Index. 3 These assessments have been limited, however, to observational studies and cross-sectional comparisons.
Psychological General Well-Being Index scores (which assess anxiety and depression, perceived health, vitality, and overall well-being) were significantly lower (poorer) for people with constipation than the published scores for a general population sample. 3 In a cross-sectional, population-based survey of individuals of at least 65 years of age completing the Medical Outcomes Study Short Form General Health Survey, those with chronic constipation reported poorer role functioning and pain scores compared with those without constipation. 2 A similar pattern was shown in a mailed survey that assessed health-related QoL (HRQoL) (using the Short Form questionnaire-36 and Short Form questionnaire-12 items) among a Canadian population with self-reported functional constipation (Rome II criteria), when compared with Canadian norms. 39 In interviews with frail older people living at home, constipation was considered by 11% to be a major problem adversely affecting their QoL. 21 Although there is a paucity of them, studies that report the relationship between QoL and constipation show that people with constipation generally have impaired QoL compared with the general population.
Management of constipation in older people
The most common method to treat constipation in older people (> 50 years) is to use laxatives. However, there is little evidence to support either their clinical effectiveness or cost-effectiveness. 1 Readers interested in the evidence (or lack thereof) for the use of laxatives in the management of constipation in older people are encouraged to read the Health Technology Assessment (HTA)-commissioned review,1 Gallagher, O’Mahony and Quigley’s recent review40 and the STOOL trial report. 19
While there is little evidence supporting the use of laxatives in the treatment of constipation in older people, there is also little evidence-based guidance on what constitutes effective management of constipation in older people more generally. 1,41 The HTA review concludes that laxatives may not be an appropriate method for treating constipation for all people, and that change in general diet may be sufficient to treat and/or prevent the condition. However, the authors concede that there is a lack of good-quality evidence showing that dietary interventions are effective.
Petticrew et al. 1 proposed a stepped approach to the management of constipation, which first considered dietary and lifestyle changes then (if unsuccessful) considered dietary supplements, and then (if both of the previous interventions failed) considered the use of a prescribed cost-effective laxative treatment.
Taking into account the findings of the review, the advisory panel to the HTA proposed a further step in the constipation management strategy. This step involved prescribing a single class of laxative (bulk, stimulant or osmotic laxative) in the first instance and then, if this failed to resolve the constipation, adding in a second laxative from another class (e.g. stimulant plus bulk). In light of this, the HTA commissioned two independent randomised controlled trials (RCTs) – STOOL and LIFELAX.
The STOOL trial19 was commissioned to investigate the clinical effectiveness and cost-effectiveness of laxatives prescribed for older people from the three classes (bulk, stimulant or osmotic laxative) and for different management strategies of combining the classes.
LIFELAX was commissioned to compare the clinical effectiveness and cost-effectiveness of practice-based educational interventions to change the diets of older people who have constipation with traditional medical management using laxatives.
Impact of diet and lifestyle on constipation
Interest in the role of dietary fibre has existed from the Victorians, who believed that bran stimulated colonic movements. By the 1900s, fibre had received some attention for its role in relieving constipation, and in the 1930s dietary fibre was being investigated for its laxative properties. 42
Epidemiological evidence suggests that diseases of the large bowel, commonly seen in industrialised countries, are linked with decreasing fibre intake. 43 Findings from the recent European Prospective Investigation into Cancer and Nutrition study have suggested that where there is a low average fibre intake, doubling total fibre intake from foods could reduce the risk of colorectal cancer by 40%. 44
Intake of dietary fibre is just one of a number of factors that influence bowel frequency. 45 The most common causes of constipation in primary care are related to diet, fluid intake and psychological factors. 8 Although there is ‘no compelling medical evidence that inadequate fluid intake results in constipation’, it is generally agreed, both by the medical profession and the general public, that low levels of fluid intake are associated with constipation. 10
Constipation is more common in women than men and its prevalence increases with age. 46 In constipated older people, a lifetime of environmental risk factors, such as poor intake of dietary fibre, chronic use of laxatives and ignoring periods of high motility, rural living and colder temperatures are likely to have been causes of constipation. 45,47 Others have found evidence for gender (female), ageing, low energy intake, inactivity, number of medications taken, low income and low education level, as well as depression, physical and sexual abuse being factors associated with constipation. 48
Constipation is rarely seen in developing countries and it has been related to the low-fibre diet consumed in the typical industrialised society. 43 From this brief introduction it is apparent that the impact of diet and lifestyle on constipation is multifactorial. A more detailed consideration of the evidence of these factors and summary of the evidence, as was incorporated into the LIFELAX diet and lifestyle advice, follows.
Fibre and constipation
‘Fibre supplementation is generally the cornerstone of prophylaxis against constipation.’29 Increasing stool weight and improving bowel movement are two of the primary physiological functions of the large bowel49 in which dietary fibre has a role to play. Dietary fibre can be defined as a ‘plant-derived material’ that is ‘resistant to digestion by human alimentary enzymes’;50 it affects the large bowel more than any other dietary component. 51 Dietary fibre’s relationship with the gastrointestinal (GI) tract includes roles of being a substrate for bacterial fermentation, water holding, cation exchange and adsorptive functions. 50 These mechanisms cause an increase in stool output and dilute the colon’s contents. 51 The increase in faecal bulk depends upon the type of fibre ingested (e.g. wheat produces high faecal bulk compared with pectin). 52
Adding sources of insoluble fibre to the diet significantly increases stool weight. 49 Wheat bran and oat bran, which are composed of differing amounts of insoluble fibre (> 90% and 50–60%, respectively), have similar effects on daily stool output, although they work by a different mechanism. Oat bran, which consists of more soluble fibre, results in greater bacterial growth than wheat bran, whereas the insoluble fibre of wheat bran provides more slowly fermentable polysaccharides to maintain the microbial population during transit through the large intestine. Neither oat bran nor wheat bran should be thought of as the superior ‘treatment’ for constipation, as both have important (if different) roles to play.
Results from a double-blind controlled trial to measure the effects of wheat bran in the treatment of constipation suggest that bran was effective in improving bowel frequency and large bowel transit time, and that a daily dose of 20 g of bran in addition to a high-fibre diet is beneficial to patients with chronic non-organic constipation. 53 Gear et al. 54 also concluded that a high intake of dietary fibre is associated with more rapid transit times.
Non-starch polysaccharides (NSPs) refers to all fibre in the diet. Recommendations as to the amount of NSP the average adult diet should contain suggest at least 18 g per day. 55 The Dietary and Nutritional Survey of British Adults56 found that fibre intake was significantly greater in individuals from higher social classes, higher in men who did not smoke or drink and higher in older women. The National Diet and Nutrition Survey (NDNS)57 of people aged ≥ 65 years reported, nonetheless, that the mean NSP intakes for free-living men and women (13.5 g for men and 11.0 g for women) were significantly below the dietary reference value, with intake decreasing with age. There was a positive association between the number of bowel movements and NSP intake in free-living men and women in the NDNS;57 for women, this increased bowel movement with increased NSP intake was regardless of laxative use. Analysis from the Nurses’ Health Study58 found a higher dietary fibre intake to be associated with a decreased prevalence of constipation.
Though a systematic review concluded that neither strong nor consistent evidence existed regarding the effectiveness of using dietary fibre for constipation in older adults, this, the authors conceded, was due, in part, to weak study design. 59
Fluid and constipation
Whether or not fluid relieves constipation is a disputed fact. Health practitioners regularly recommend increased fluid intake to alleviate constipation, but the role of fluid has been challenged. Lindeman et al. 60 found no association between fluid intake and frequency of chronic constipation in the elderly, while Chung et al. 61 did not observe any significant increase in stool output by healthy volunteers when fluid intake was increased. There is, however, evidence which does suggest that increased fluid intake has a role in alleviating constipation. Klauser et al. 62 found that a relatively short period of fluid deprivation decreased stool frequency and stool weight in young healthy male volunteers. Positive associations between fluid intake and bowel movements were reported for women aged ≥ 65 years in the NDNS,57 while no relationship between fluid intake and bowel movement frequency was seen in men and women living in institutions. It is important that when individuals are advised to increase their fibre intake they are also advised to increase their fluid intake. 63
Probiotics, prebiotics and constipation
Probiotics and prebiotics both have a beneficial impact on gut microflora. 64 Prebiotics have an osmotic effect on the gut, as long as they are not fermented; when they are fermented by the endogenous flora they increase gas production. 64
Gut bacteria, of which 400–500 species exist in the human large intestine, carry out fermentation, which metabolises endogenously produced and dietary residues. 65 Dietary carbohydrates that have not been digested in the upper GI tract are the main substrates for gut bacterial growth, in addition to amino acids, bacterial secretions, lysis products, sloughed epithelial cells and mucins, which are metabolised to produce short-chain fatty acids (SCFAs). 65 In summary, the positive influences of gut microflora is that they prevent colonisation by harmful bacteria, have roles such as improving lactose tolerance, providing SCFAs as energy substrates, neutralising toxins, stimulating the intestinal immune system and having a role in reducing blood lipid levels.
Probiotics, defined as viable non-pathogenic microorganisms, which, on ingestion, exert a positive influence on host health or physiology,66 are either bacteria or yeast. 67 In a recent study,68 350 healthy elderly subjects consuming one, two and three 125-g servings per day of Bifidobacterium SP/DN-173010, had marked reduced transit time (22%, 40% and 47% reduction of initial values). This effect was still present for 2–6 weeks after the end of the product consumption.
Constipation was explored in a recent review of probiotics in human studies;69 the authors reported that few studies were of double-blind design and had adequate washout periods. Sample size was often limited and outcome markers were non-comparable, including both bowel frequency and transit time. They concluded, however, that probiotics do have a probable effect on gut transit time and on stool frequency, although this is species and strain specific rather than genus dependent.
Described as non-digestible food ingredients, prebiotics stimulate selectively the growth and activity of bifidobacteria and lactobacilli, which benefit health. 70 Non-digestible oligosaccharides are found in plant cells naturally and are also manufactured food components, they are non-digestible (in the upper GI tract) and are prebiotics; two well-studied and well-established prebiotics are inulin and oligofructose, which are fermented by the beneficial flora (bifidobacteria and also lactobacilli) The major food sources of both inulin and oligofructose in the typical Western diet are wheat (70%) and onions (25%). 71 Evidence indicates that these fructans are digested in the large intestine, increasing microbial mass and producing SCFAs,72 which also increases the stool mass, beneficial for bowel health. 51
The laxative effect of prebiotics was shown by Gibson et al. ,73 in whose study oligofructose and inulin significantly increased stool output, possibly due to an increase in biomass. In constipated patients, low-digestible carbohydrates, with a low molecular weight, had a positive effect on intestinal transit time in constipated patients. 74 An earlier study75 examined the effect of fructo-oligosaccharides – found naturally in onion, asparagus root, artichokes and wheat – on gut health. Increases in bifidobacteria – believed to be beneficial to the host – following fructo-oligosaccharide ingestion, were found to relieve both constipation and loose stools, as well as improving blood lipid profiles.
The definition of dietary fibre alludes to the fact that it consists of ‘remnants of edible plant cell polysaccharides and associated substances resistant to hydrolysis by human alimentary enzymes’. 76 Dietary fibre improves laxation by increasing stool weight from the fibre in the stools and also by bacterial cells (which have high water content). Higher faecal water content increases the ease of stool passing. Cherbut76 described how inulin and oligofructose, found in a number of vegetables, fruits and whole grains, both fit into the current concept of dietary fibre and contribute to a well-balanced diet.
Kleessen et al. 77 observed that inulin and lactose improved the clinical signs of constipation on elderly constipated individuals whose bowel movements increased from one or two per week to 7.5 times per week with a 40 g/day intake of lactose and eight to nine stools per week with either a 20 g/day or 40 g/day dose of inulin. The elderly tend to experience an increase in bifidobacteria and a decrease in enterococci and enterobacteria numbers with inulin, which had a better laxative effect than lactose. Use of prebiotics that change the elderly patient’s intestinal microflora, as seen in Kleessen et al. ’s77 elderly population, may be of benefit to the wider elderly population.
Exercise and constipation
There is perceived to be a lack of convincing data relating physical activity (or a lack thereof) to constipation. 29 Propulsive movements in the large intestine are increased by exercise. 78 Although it is thus assumed that increased activity stimulates bowel motility, an investigation on healthy young men failed to confirm this;79 however, mild exercise accelerated mouth–caecum transit time for a liquid-based meal by 20–25%. 80
In patients with chronic idiopathic constipation, 4 weeks of regular moderate physical activity did not alleviate slow transit constipation. 81 The authors of this study suggested that more vigorous activity, for a longer time period, might have shown more positive results, but compliance in an elderly population may have been reduced with a requirement for increased vigour.
In women aged 36–61 years, increased physical activity was related to a reduced prevalence of constipation;58 taking part in physical activity daily was independently associated with a 44% lower risk of constipation, while physical activity two to six times per week was associated with a 36% lower risk when compared with less than once daily. 58
A daily walking programme, within 30 minutes after a meal has been recommended, with stationary exercises for those who cannot walk. 29 The authors29 suggested that abdominal and pelvic floor strengthening exercises may be useful.
Position for defecation
In industrialised societies the preferred position for defecation is seated, while in Asia and Africa the main position is squatting. In a study carried out in individuals with normal bowel habits, the squatting position required less time and less straining for faeces depletion than any other sitting position. 82 In the squatting position the rectoanal junction is straightened, whereas in the seated position more straining is required to push the faeces through the right rectoanal junction. 82 The strain required to defecate in a seated position may lead to repeated Valsalva manoeuvres (forcibly exhaling against the closed airway) and may result in defecation syncope and death, while the squatting position is associated with reduced amounts of straining. 83
Summary of diet and lifestyle advice for the LIFELAX trial
-
Most people experience constipation at some point.
-
‘Normal’ bowel movement frequency is from three times/day to three times/week.
-
Signs of constipation include:
-
– hard stools that are difficult to pass
-
– frequency of stools decreasing
-
– cramp-like pains in lower abdomen.
-
-
Constipation may be caused by:
-
– not eating enough fibre (fruit, vegetables and cereals)
-
– not drinking enough fluid
-
– poor bowel habits (ignoring the ‘call to stool’)
-
– medicines (antacids, codeine, iron tablets, some antidepressants).
-
-
Constipation is made worse by:
-
– dehydration
-
– inactivity
-
– painful anal conditions (e.g. haemorrhoids).
-
-
Constipation can be eased by:
-
– eating regularly
-
– eating more fibre-rich foods (fruit, vegetables and cereals)
-
– drinking eight to ten cups of water/juice/soft drinks per day
-
– keeping active/regular exercise.
-
-
Toileting:
-
– sitting in a comfortable position
-
– spreading your legs slightly apart and leaning forward
-
– relaxing and taking your time.
-
Behaviour change
The nutritional evidence-based guidelines that underpinned both the standardised and personalised intervention arms were the same, and it was in the style and mode of delivery that the arms varied. Not all of the findings of the studies we used to inform the intervention were appropriate for both arms. Full discussion of the literature reviewed, and the theoretical approaches and models used to inform the behaviour change interventions used in LIFELAX, can be found in Chapter 3, which details the development of the intervention.
We were seeking to develop two notionally different interventions in LIFELAX. One of the arms (standardised) needed to sit firmly within the current nursing model in the UK84 and be suitable for delivery within a routine appointment time. The other arm (personalised) was informed by techniques that had been shown to be effective in interventions of behaviour change in similar topic areas with similar samples to ours.
In studies of individual behaviour change strategies, particularly those relating to dietary change and exercise,85–87 personalised interventions have been shown to be more effective than standard, non-customised approaches. Personalised interventions, however, are typically more resource intensive than non-individualised approaches. 88
Summary
Although it is often viewed as a trivial complaint, constipation is undoubtedly a major concern to both patients and the health-care system. For an intuitively simple condition, defining constipation continues to prove difficult. Among health professionals, there is little consensus on a formal definition of constipation. The Rome II (and more recently the Rome III) criteria were an attempt to formalise the assessment of constipation yet as we have seen, they are complex and few practitioners use them in practice. Rather, in clinical practice, constipation tends to be a subjective diagnosis. Frequency of bowel movement is an important factor in the assessment of constipation yet there is no consensus on how often the ‘normal’ bowel opens. Clinicians do agree, however, that there is a wide variation between individuals in the ‘normal’ frequency of bowel movements, ranging from three times per day to three times per week but many patients have expectations of a daily bowel movement.
Lay perceptions of constipation are far removed from the Rome II criteria though, as with health-care professionals, frequency of bowel movements is a key component of the definition of constipation for the majority of older people.
The Petticrew et al. 1 review found that there is little known about the clinical effectiveness and cost effectiveness of laxative treatment for constipation, although dietary and lifestyle changes may help in the prevention and treatment of constipation, there is also little clear evidence about the cost effectiveness of such management strategies.
Collectively the STOOL19 and LIFELAX trials were designed to provide such evidence. It is sad to report that given the recruitment difficulties in both trials, clinical trials to evaluate the clinical effectiveness and cost effectiveness of these treatments remain to be done in the UK.
Embedded qualitative process evaluation
Randomised controlled trials and process evaluation studies are complementary research methodologies. 89 Although the former excel in producing outcomes data, the latter provide procedural information, such as the fit between the study protocol and how the research is practically carried out. 89,90 Oakley90 describes the typical functions of embedded process evaluations in detail:90
Process evaluations within trials explore the implementation, receipt, and setting of an intervention and help in the interpretation of the outcome results. They may aim to examine the views of participants on the intervention; study how the intervention is implemented; distinguish between components of the intervention [and] investigate contextual factors that affect an intervention. Process evaluation can help to distinguish between interventions that are inherently faulty (failure of intervention concept or theory) and those that are badly delivered (implementation failure).
(p. 413)
Process evaluations are therefore particularly useful within RCTs of complex interventions, when it may be difficult to identify the active components of the interventions from contextual ‘noise’. 91 Examples of RCTs incorporating qualitative process evaluations include the Southampton Heart Integrated care Project (SHIP) in which the evaluation contributed towards interpretation of the research findings, and the Birmingham Rehabilitation Uptake Maximisation Study (BRUM), in which the evaluation provided insights regarding reasons for non-adherence. 92–94
Within the LIFELAX RCT, a qualitative process evaluation was used to collect data on the development and implementation of both the RCT and its interventions. Whereas in previous studies, process evaluations have largely functioned as auxiliary studies, supplementing the research findings of their host trials, in LIFELAX the process evaluation took a subtly, yet fundamentally broader, role by examining the process of HTA in action, through the medium of an RCT. In this respect the research questions were designed not to ask ‘how closely does implementation of the interventions fit the protocol?’ but ‘how is the protocol constructed and practically enacted, and what are the implications for the types of knowledge produced?’ The process evaluation was thus fully integrated into the RCT, rather than playing a complementary role; its results contributed information about the process of evaluation, the barriers faced by the trial team, the manner in which some of these barriers were circumvented, and the overarching structural problems that eventually prevented the trial’s completion.
Understanding the process of evaluation is important, for we actually know little about the practical conduct of HTA through RCTs, although there is a large and expanding body of literature that details either the RCT’s methods or the results of their application. In one specific field of HTA – the development and evaluation of ‘telehealthcare’ systems – May et al. have undertaken a series of studies95–98 that have examined the evaluation of a relatively unstable health technology using RCTs and other methods, and have developed a model of the social and technical process of HTA that defines the contingent points on the journey between ideation (i.e. the emergence of ideas about the value of a new technology) and normalisation (i.e. the point at which it becomes possible for it to be embedded in clinical practice). 99 Of specific interest here is the way that evaluation acts as a mediating set of practices between these two points on the ‘innovation journey’: specifically, the production of evidence supports – or hinders – the uptake of a new technology.
Evaluation is not a discrete asocial activity, nor is it self-evident. At the very outset, we place the kinds of evaluations that define the specific utility of health technologies within the frame of the larger ‘proto-discipline’ of HTA. HTA is one of the major research enterprises of our time. Broad in scope, and defined by its emphasis on formal – mainly quantitative – methods and its focus on clinical effectiveness and cost-effectiveness, HTA is directed at the production of evidence about the efficacy and utility of techniques and technologies of health-care delivery treatment modalities and ways of working. As a field of practice, HTA is orientated around the production of evidence that meets particular criteria of adequacy100,101 – its formal proof, as it were, is to be found in the outcomes of the RCT, systematic review and meta-analysis. The questions that inform it tend to arise directly from the thrust of health-care policy, and the outcomes of HTA practitioners’ work are specifically intended to mediate between policy and practice. So within the field of HTA, it is method that is prioritised either in the production of primary outcomes data or in the synthesis of existing knowledge. 102 The expository literature of HTA reflects the priority given to methods, not theories, by locating them in a rhetoric of political and social neutrality, and emphasising applied investigatory technique over broader political questions. None of this is intended to imply that practitioners of HTA are unaware of the political implications of their work or the wider social implications of their practice – the reverse is certainly the case. But HTA emulates the neutral rhetorical form of the wider field biomedical science, constructing apparently methodologically secure quantitative facts. So it has, at the outset, a first line of defence against wider political critique – it is given as quantitative science rather than politics.
In this broad context, HTA can be seen as the development of a field of research practice that accords well with contemporary notions of the place of ‘research’ in the complex political and social contexts of the advanced economies. For example, it fits well with the model of Gibbons et al. of ‘mode 2’ knowledge production through its connectedness with ‘user’ communities, its multidisciplinarity and because of the permeability of the institutional structures in which it is located. 103 Certainly the evaluation of new systems of working and of the delivery of treatments is not simply directed at establishing their fitness for specific tasks, but about adjudicating on their superiority over others. More than this, it is focused on evidence production: HTA is thus one of a number of regulatory systems of practice available to governments and others in the advanced economies to constrain the conduct of health professionals and health-care institutions. It can be understood as a form of institutional surveillance that governs the conduct of practice, defines the directions of innovation, and defines potential new fields of clinical organisation and practice. As Tanenbaum104 has observed, the thrust towards outcomes studies within the field of HTA (and across biomedicine more generally) can also be seen to represent a powerful and authoritative social movement.
Relevant work to conceptualise HTA to date has mainly been directed either at practical problems of recruitment into trials,105–111 or at macrolevel analyses of the relationship between policy formation and evidence production. 104,112 More localised critiques have investigated the assumptions that underpin outcomes themselves or the methods by which they are reached. 95 Much less work has investigated the specifics of HTA as a field of practice, the sociotechnical networks in which knowledge about efficacy is defined and generated, negotiations about criteria for its adequacy or the procedures through which these are enacted in concrete practices. The paucity of literature in this field is surprising, given the importance of the RCT as an HTA method. The process evaluation was necessary to provide a more detailed understanding of the organisation of RCTs, and to assist in the development of a robust theoretical model of HTA practice.
Chapter 2 Trial design
Overview
LIFELAX was designed as a pragmatic113 three-armed cluster (randomisation at the level of the individual general practice) RCT to compare laxative treatment (current practice) of chronic constipation in older people with both standardised, non-personalised dietary and lifestyle advice (delivered in a single, short consultation) and personalised dietary and lifestyle advice (delivered in one long consultation – or two shorter consultations – with telephone reinforcement) in the management of chronic constipation in older people. LIFELAX was to be conducted in north-east England and was to recruit patients aged ≥ 55 years, registered with practices participating in the trial, with a current diagnosis of functional constipation (operationalised as either having a recorded diagnosis of functional constipation or having received three or more prescriptions for laxatives in the preceding year). Due to poor levels of practice uptake and lower than expected levels of patient recruitment, it was necessary to approach the HTA for an extension to the LIFELAX trial and these eligibility criteria were revised in the subsequent protocol amendments. In Chapter 4, which details the implementation of the LIFELAX trial, we describe the protocol revisions in depth. Here we will describe the design of the trial as it was in the original protocol, agreed with the HTA and submitted to the Multi-Centre Research Ethics Committee (MREC). The original protocol (version 2, 4 October 2004) and the final version (version 5, 24 July 2006) can be found in Appendix 1.
Objectives
The primary objectives for the study were to investigate the clinical effectiveness and cost-effectiveness of:
-
laxatives versus dietary and lifestyle advice
-
standardised versus personalised dietary and lifestyle advice.
Health technologies being assessed
Treatment strategies at the patient level
LIFELAX was a cluster randomised trial. Practices were randomly assigned to one of the three treatment strategies, with all patients in the practice then getting their practice’s allocated strategy. Within the laxatives arm, free choice of class and dose of laxatives were allowed as there was insufficient evidence10,114 of the relative superiority of one class of laxatives over another or of combination therapies as opposed to single preparations. Free choice of laxative therapy more closely replicated the situation in routine clinical practice, therefore participant adherence to treatment protocol was expected to be better than should a change in drug have been required. For similar reasons, leeway in dosage was permitted within dose ranges commonly used in clinical practice. To minimise the risk of prescribing subtherapeutic doses, the practice training/initiation reminded participating health-care professionals of the therapeutic dose ranges for the available laxative preparations.
The dietary and lifestyle interventions were informed by findings from previous trials of diet and lifestyle interventions. 85,87,115,116 They drew upon theories of individual behaviour change, including the concept of self-efficacy117 and the stages-of-change model. 118
For the personalised intervention arm, a series of information leaflets on a range of topics were developed and tested. 119 These comprised eight patient information leaflets (PILs) on constipation, activity, bowel health, fruit and vegetables, fibre, fluid, alternative therapies and laxatives (see Appendix 3). In the standardised arm, participants were given a general constipation PIL. Copies of the materials produced can be obtained from the lead author.
In both of the diet and lifestyle intervention arms, the training package was designed to be delivered by practice nurses, community nurses or other appropriate health-care professionals (according to local custom). Appointments were generally offered at the surgery, although home visits were an option where appropriate. In the standardised, non-personalised arm, there was a single short (approximately 10 minutes) appointment, with delivery of a standard pack of information and brief and general explanation of the information leaflet. In the personalised arm, there was an initial long (30–45 minutes) appointment (though this could be undertaken in two shorter appointments should clinic time so dictate) and the technique of ‘motivational interviewing’ – ‘a directive client-centred counselling style for eliciting behaviour change by helping clients to explore and resolve ambivalence’88 – was undertaken. The personalised approach included a patient-specific assessment of barriers to and facilitators of change and delivery of a personalised pack of information with individual targets (tools were developed to assist nurses with setting personalised goals and plans). Patients in this arm received a follow-up motivational telephone call from the nurse at 1 week and 1 month after initial appointment.
A potential threat to patient recruitment and retention in this trial was patients’ unwillingness to forgo medication. For this reason, although diet and lifestyle was the first-line treatment for patients allocated to those arms, the option of continuing laxative use [either prescribed or over the counter (OTC)] was available if required; the need for and use of such medication was captured as part of the evaluation process.
Although a ‘washout period’ is recommended in trials in functional GI disorders120 the clinicians and dietitians involved in the design and management of LIFELAX took the decision not to implement this. There was a concern that patients would be reluctant to withdraw from any laxative regimen that was currently effective before embarking on any diet and lifestyle changes, and that this would have a negative impact upon recruitment. There was also a concern that even without a ‘washout’ period – as diet and lifestyle alterations typically take time to show change in bowel function – participants may see this as a failure of the intervention and not adhere to the protocol or withdraw. In light of this, participants in the diet and lifestyle intervention arms of the LIFELAX trial were able to continue to use laxatives (prescription or OTC) should they or their GP feel it appropriate, while those in the laxative arm continued to take their usual laxatives as prescribed.
Training strategies for health professionals
An orientation and training programme was developed for the practices recruited to the study. All practices had an on-site training visit to discuss aspects of the treatment protocol and how it was to be delivered in the practice. In addition, a dietitian with experience in health promotion delivered in-practice training on how to deliver the dietary and lifestyle intervention to patients, as follows:
-
Standardised dietary and lifestyle intervention All primary health-care professionals (GPs, practice and district nurses, and health visitors) in the practice were invited to a single 1-hour session to introduce the programme and the patient resource pack.
-
Personalised dietary and lifestyle intervention All primary health-care professionals in the practice were invited to an initial 1-hour session to introduce the programme and the patient pack. Practice staff involved in delivering the intervention to patients were invited to take part in two further 45-minute sessions on the delivery of a personalised pack and motivational interviewing techniques.
The choice of number and duration of training sessions was based on experience in other similar studies, and represented a balance between minimising the demands on busy health professionals’ resources, while having sufficient time to motivate doctors and nurses and to equip them with the knowledge and skills required to deliver the interventions to patients. Our personal experience, reinforced by the literature,121 suggested that in-practice delivery of training of this nature is more cost-effective than delivery at a single central location.
Study participants
Target population
The target population for the study was people aged ≥ 55 years (reduced to 50 years after protocol amendment) with chronic functional constipation, living at home. This ‘age’ choice was made after due consideration of the morbidity statistics from general practice,5 which indicated that GP consultation rates for constipation rise rapidly in the 45- to 64-year age group and continue to rise steadily with age. The exclusion of residents in long-term care reflected the different morbidity and the lack of autonomy over decisions pertaining to diet and lifestyle changes and lifestyle experience of long-term care residents. LIFELAX focused on a predominantly ambulant population able to attend independently a primary care clinic.
Inclusion criteria
The complexity of the Rome II criteria for functional constipation122 militates against their use in screening for chronic constipation. Moreover, newly incident cases of constipation, especially among older adults, should be investigated to determine the underlying cause of the constipation and to eliminate more serious problems123 before laxatives are prescribed. LIFELAX therefore identified and recruited only ‘prevalent’ cases, defined primarily in terms of those prescribed laxatives three or more times in the previous 12 months, or with a recorded diagnosis of functional constipation (although it was unusual to find such a diagnosis consistently recorded and coded). Participants meeting this criterion were identified from general practice computerised patient records using an electronic ‘query’ (the electronic query was designed to work with the EMIS practice computer system to interrogate repeat prescribing databases). It was recognised that the relapsing and remitting nature of constipation meant that not all patients thus identified would be constipated (by objective or subjective criteria) at any given time.
Patients who fitted one or more of the following criteria were therefore eligible for the trial:
-
a recorded diagnosis of chronic functional constipation
-
prescribed laxatives three or more times in the previous 12 months
-
prescribed a laxative (or combination thereof) continuously for the previous 12 months.
Exclusion criteria
-
Patients resident in long-term care.
-
Patients with inflammatory bowel disease, intestinal obstruction/bowel strictures, known colonic carcinoma, and conditions contraindicative to the prescription of laxative preparations. 124
-
Inability to read and understand written treatment plans and educational material.
-
Inability to complete outcome assessments, even with assistance (e.g. major cognitive impairment, lack of understanding of English).
-
Patients using opioid analgesics.
Consent
Favourable opinion from MREC was granted, although the request from the chief investigator (CI) for ‘no local investigator status’ was not approved. (For a full account of the trial’s status as ‘site-specific exempt’ see Chapter 4.) The implication of this was the need for a favourable opinion to a site-specific assessment (SSA) for each individual primary care practice (site) from appropriate Local Research Ethics Committees (LREC). Written informed consent was obtained for all participants recruited to the trial. All the patient recruitment materials followed Central Office of Research Ethics Committees (COREC) guidelines. The trial team used its experience from previous studies, where it had been felt that the COREC guidelines for information sheets led to a large, burdensome and often-intimidating document, and produced a short, succinct version to accompany the full version. A full patient information sheet (PIS) (version 6, 24 July 2006) (see Appendix 2) and a brief information leaflet (version 5, 26 May 2006) (see Appendix 2) were provided to send to patients via their GP. Patients were given time to consider the trial fully and ask any questions about the implications of the trial as part of the consent process.
Sampling design and implementation
Sample size
Participating practices were randomised to one of three arms. In calculating sample size for cluster randomised trials,125 it was necessary to take into account within-cluster variance, measured by an intraclass correlation (ICC). Our experience in previous studies suggested that ICCs of 0.05 for QoL outcomes were typical.
Preliminary analysis of data from the average-sized practices of one of the applicants suggested that there would be approximately 40 patients in such a practice meeting eligibility criteria. We recognised that patients in practices allocated to the diet and lifestyle arms of the trial might be reluctant to undertake a change to their diet or lifestyle and might therefore withhold consent to participate. It was in anticipation of this risk that we made the assumption that only 30 out of 40 patients identified (75%) would agree to participate and that only 25 would provide follow-up data for 12 months.
Our primary outcome was a continuous variable score on a QoL scale. In the absence of detailed data on the distribution of QoL scores in our population, we were able to specify, nonetheless, the effect size that we wished to detect. We arbitrarily set this at 0.3 standard deviations on the condition-specific QoL scale. 38 Within the literature on QoL assessment, there has been a growing consensus126 that an effect size (i.e. change over time divided by standard deviation at baseline) of < 0.2 represents a ‘negligible’ change, an effect size of 0.2–0.5 represents a ‘small’ effect, an effect size of 0.5–0.8 represents a ‘moderate’ change and an effect size of in excess of 0.8 represents a ‘large’ change. These criterion values, which have been shown to be stable across a range of settings, have been established by reference to what clinicians and patients consider to be an ‘important’ difference – the emphasis is therefore on clinical rather than statistical significance. Our proposed effect size of 0.3 therefore represented the difference between the threshold values for ‘small’, ‘moderate’ and ‘large’ changes (0.5 – 0.2; 0.8 – 0.5).
It is important to note that the LIFELAX trial was not a comparison of an intervention with placebo or with normal practice. Instead, there were three active treatment groups. It is not unreasonable to assume that we might have observed at least a small change over time in symptom-related and QoL outcomes in all of these treatment groups. What we were primarily interested in was whether one intervention offers a relative advantage over the others. For example, if the changes over time for the laxative and standardised diet and lifestyle interventions were ‘small’ by the established criteria set out above, but a ‘moderate’ improvement was observed in the individualised diet and lifestyle arms, we might reasonably conclude that this intervention offered a relative advantage.
For an effect size of 0.3, 90% power, a significance level of 5%, an ICC of 0.05, and the ability to recruit and retain 25 patients per practice, we therefore needed a total of 57 practices (19 per arm).
Recruitment
Practices
General practices in England and Scotland, UK, were invited by letter to participate. As the STOOL Trial19 was recruiting practices in the north-east of England at the same time as LIFELAX, we were careful to divide up the Primary Care Trusts (PCTs) so that the same practices were not approached by the two studies. When the STOOL Trial closed, personal approaches were made to the practices that had expressed interest in STOOL by the STOOL trial manager in a bid to ‘convert’ them to LIFELAX. The remaining (non-recruited) practices in the PCTs eligible for the STOOL trial were then approached by the LIFELAX team. It was felt that LIFELAX would be more appealing than STOOL to practices as there was a range of relevant training that accompanied the interventions, and therefore that practices which had not been willing to participate in STOOL might nonetheless be agreeable to take part in LIFELAX. All practices that wished to join LIFELAX were then randomised into one of the three trial arms. As each practice was recruited to the study it was allocated a study identification number by the research team. This together with a measure of the practice size (number of partners) was then passed to an independent statistician who then generated the treatment allocation using electronically generated random numbers. The research team were kept blind to the randomisation algorithm that was used (the probability that a practice was allocated to a particular treatment depended on the size and number of practices previously allocated to each of the treatment arms). We recognised that practices may have had preferences with respect to allocation of intervention arm. We made it clear to the practices approached to participate in LIFELAX that allocation to intervention arm was completely at random and that practice preferences could not be taken into account.
Note: details on rounds of recruitment and Trusts approached can be found in Chapter 4.
Participants
LIFELAX recruited only prevalent cases that were retrospectively identified through computerised records of laxative prescriptions, as described above. The electronic query was offered to all practices. However, many surgeries did not use the EMIS system and others preferred to run the searches manually. Patients were initially screened by practice staff to remove those identified as ineligible for the study by reference to exclusion criteria. Eligible participants were then invited to attend a practice nurse-led research clinic to discuss entry into the study. Following informed consent, a baseline assessment (a face-to-face interview and self-completion questionnaire) was completed. A copy of the signed consent form was posted back to the study team. The completed baseline assessments were posted back in a separate envelope. Following consent, the practice nurse contacted the study team and released the personal details of recruited patients. (This model of patient recruitment was the one used by the STOOL trial after several iterations of their approach to MREC to gain a favourable opinion. It proved to be rather time-consuming and burdensome to practices. As such, a different model was introduced after a major protocol amendment. This is covered in Chapter 4.)
Minimising bias and improving compliance
The commitment of GPs and practice staff was known to be crucial to the success of the study. Educational events were used to introduce the study protocol to health professionals from the participating practices. Regular updates on the study were included in Trust newsletters and also in the Northern Primary Care Research Network (NoReN)/Northern and Yorkshire Primary Care Research Network (NYReN) newsletter. Financial support was provided to practices to identify and recruit patients. Service support costs and excess treatment costs secured through the Support for Science (SfS) funding stream meant that there was be no financial ‘cost’ to practices for participating in the study. All study-related tasks were reimbursed at a generous level. Though a practice would not be able to look upon LIFELAX as a money-making activity, it would not be a drain on its resources.
The risk of recruitment bias (i.e. patients being unwilling to enter the trial because they may have to forgo their laxative treatment) was recognised. We believed that the availability of ‘rescue’ medication for patients randomised to the diet and lifestyle arms would reduce the risk of non-consent or loss to follow-up, due to anxieties about not being able to use medication. Likewise, the provision for continuing with an established and preferred laxative regimen in the laxatives arm was felt to increase the likelihood of participation and compliance.
Both at the point of recruitment and intervention initiation, the importance of adherence to the course of treatment, and of completion of questionnaires and diaries, was stressed to participants. Up to two written reminders were used for participants who failed to return postal questionnaires.
For LIFELAX, an intention-to-treat analysis was adopted, as it was important that we were able to estimate the extent of non-adherence by participants. We addressed this issue by collecting data about laxative use (both prescription and OTC) as part of the participants’ daily diary and in follow-up questionnaires.
Baseline and outcome measurement
Participants were followed up for 12 months from the date of intervention initiation. Follow-up data were captured through a daily self-completed structured diary (for 6 months), and telephone interviews and self-completed postal questionnaires at 3-, 6- and 12-month time points (Tables 2 and 3).
| Outcomes | Measurement method | When | Where |
|---|---|---|---|
| Primary outcome | |||
| HRQoL | Postal questionnaire | At 3 months post recruitment | Participant’s home |
| Secondary outcomes | |||
| HRQoL | Postal questionnaire | At 6 and 12 months post recruitment | Participant’s home |
| No. of bowel movements per week | Self-completed structured diary + postal questionnaire |
Daily for 6 months At 12 months |
|
| Other Rome criteria: straining at defecation, stool consistency, perceived incomplete evacuation | Self-completed structured diary + postal questionnaire |
Daily for 6 months and for 1 week at 12 months At 12 months |
|
| Subjective perception of whether constipated; satisfaction with bowel function | Telephone interview + postal questionnaire |
At 3 months At 6 months and 12 months |
|
| Adverse events: abdominal pain, nausea, bloating, flatulence, diarrhoea | Self-completed structured diary + postal questionnaire |
Daily for 6 months and for 1 week at 12 months At 12 months |
|
| Use of prescribed and OTC laxatives | Self-completed structured diary + postal questionnaire |
Daily for 6 months and for 1 week at 12 months At 12 months |
|
| Fluid and fibre intake | Self-completed structured diary + postal questionnaire |
1 day per month for 6 months At 12 months |
|
| Relapse rates, including repeat consultations | Self-completed structured diary, GP records | Daily for 6 months; 12 months post recruitment | Participant’s home (diary); general practices (GP records) |
| Personal measures of success with the management of constipation | Telephone interview | At 3 months and 6 months | Participant’s home |
| Impact | Measure | When | Where |
|---|---|---|---|
| Costs to participants of the condition and its management | Telephone interview | At 3 months | Participant’s home |
| At 6 and 12 months | |||
| Consultation rates and laxative prescriptions | GP records | End of 12-month follow-up period | General practices |
| Adherence to drug treatment | Health diary; telephone interview | Using different methods, at 3 months | Participant’s home |
| At 6 and 12 months | |||
| Patient satisfaction | Postal questionnaire | At 3 months | |
| At 6 and 12 months | |||
| HRQoL, including utility-based assessment of health state | Postal questionnaire | At 3 months | |
| At 6 and 12 months |
QoL and clinical outcomes
The primary outcome, and the criterion upon which the sample size calculations were based, was patient-reported condition-specific QoL at 3 months post recruitment. Our preferred measure of QoL was the constipation-specific Patient Assessment of Constipation-Symptoms (PAC-SYM)/ Patient Assessment of Constipation-Quality of Life (PAC-QOL),127 which had been demonstrated to have good validity and reliability. Permission to use this instrument was granted by the owners of the scale (Janssen Pharmaceuticals, Titusville, NJ, USA) after agreement that anonymised patient data (i.e. questionnaire responses) would be submitted to them for the purposes of further refinement of their scales and development of population norms. However, this measure is not utility based. For the purposes of the economic evaluation, a measure of the utility placed by patients on their health state was required. The condition-specific measure of QoL was therefore supplemented by the generic utility-based European Quality of Life-5 Dimensions (EQ-5D). 128,129 Secondary outcomes included bowel movement frequency, the presence/absence of the other Rome II criteria for constipation, patients’ own perceptions of whether or not they were constipated, patient satisfaction with bowel function, adverse effects of treatment; relapse/reconsultation rates, and fluid and fibre intake. In addition, the cost implications of the condition and its treatment (e.g. GP consultations, purchase of prescribed and OTC medication) was assessed, as part of the economic evaluation.
Methods of data collection
Table 4 shows participants’ pathways through the trial in the original recruitment protocol, the clinical assessments completed and data collection methods used at different points on the pathway.
| Activity |
|---|
| Potential participants identified from computerised practice databases using simple electronic query to flag individuals receiving prescriptions for constipation (three or more in previous 12 months) |
| Initial screen by practice to identify clear exclusions |
| Written invitation sent by practice; appointment date to give consent at practice set with patient |
| Consent given at practice; baseline assessments conducted. ‘Intervention start’ appointment made |
| Appointment at practice – laxative prescription issued or diet and lifestyle intervention initiated; all patient information and baseline data destroyed by research team if patient notifies practice of their wish to withdraw from study |
| 1-week reinforcement telephone call from nurse to patients randomised to personalised diet and lifestyle advice |
| Intervention fidelity measure – a small sample of patients in the standardised and personalised intervention arms of the trial receive a short postal questionnaire to ask about the diet and lifestyle advice |
| 1-month reinforcement telephone call from nurse to patients randomised to personalised diet and lifestyle advice |
| 3-month follow-up outcome assessment (postal questionnaire) and collection of cost data and personal levels of success (telephone interview) |
| 6-month follow-up outcome assessment (postal questionnaire) and collection of cost data and personal levels of success (telephone interview) |
| 12-month follow-up outcome assessment (postal questionnaire and 1-week symptom diary); review of practice notes to abstract data on consultation rates and prescription patterns |
Baseline assessment (T0)
Prior to any assessments being conducted, each participant was able to speak on the telephone with a member of the research team and was invited to discuss any aspect of participation in the study they wish. An appointment was made at the practice for patients to meet a practice nurse, who took informed consent and undertook the baseline assessment. This assessment included a short, structured face-to-face interview and a self- completion questionnaire. Current bowel function, fluid and fibre intake, patients’ self-perceptions of whether they were currently constipated, and levels of anxiety and depression130 were elicited, and data on activities of daily living,131 condition-specific QoL, laxative use (both prescribed and OTC) and personal criteria for successful outcomes (‘how would you define “successfully managed constipation” ’?) were collected. A weekly structured self-completed diary was left with the participant and details on how to complete it were given. After the consent and baseline assessment visit was complete, a second appointment was made for participants to start the intervention. Should patients decide to withdraw when they returned to collect either their laxative prescription or for their diet and lifestyle appointment, the practice notified the research team and all baseline assessment data and patient identification data were destroyed or deleted from the study database.
Daily diary
To minimise recall bias, data on bowel habits and symptoms based on the Rome II criteria122 were gathered by a structured diary (tick box format), completed daily and returned each month for 6 months. This diary was developed and piloted in parallel with the qualitative study that accompanied the STOOL study. It was designed to capture information on the number of bowel movements, other Rome II criteria, adverse events, relapse rates, use of laxative, costs of food purchased or activities undertaken as part of any diet or lifestyle changes made, and any out-of-pocket expenses associated with constipation and its management. Based on previous experiences of similar diaries in studies with older people, we expected that 90% of diaries would be returned completed. 132,133
Postal questionnaires
Follow-up self-completion questionnaires, with up to two reminders for initial non-respondents, were sent by post to arrive at T+3 months, T+6 months and T+12 months. These questionnaires contained the same items as the baseline self-completion questionnaire.
Follow-up telephone interviews
The follow-up telephone interviews were also administered at 3 months and at 6 months. They focused on (a) the participant’s perceptions of the outcome/success of treatment and (b) the use of health-care resources, and out-of-pocket expenses associated with the use of those resources, including purchase of OTC medication to manage constipation. The interviews were conducted by a trained member of the research team.
Medical records
Previous experience suggested that data on consultation rates and prescribed medication could be gathered most accurately and reliably from medical records. Our intention, therefore, was to collect such data about all study participants from practice-based medical records at the end of the follow-up period. Based on experiences in previous primary care trials,134,135 for efficiency in data capture, we proposed that this be done practice by practice at the end of the data-collection period. However this activity was not completed due to the premature closure of the trial.
Methods of data analysis
Analysis was to be on an intention-to-treat basis. No subgroup analyses were pre-planned. The data were to be analysed using mixed effects models, accepted practice for the analysis of data from cluster randomised trials. 125 Variation between practices and variation between patients nested within practices were to be fitted as random effects. The difference between treatment strategies (i.e. the three arms of the trial) was to be fitted as fixed effects. Most of the outcome variables [e.g. QoL scores, number of days with (or without) symptoms] were continuous and were to be analysed assuming a normal error structure. The dependent variable in each model was point of follow-up (3-, 6- and 12-month outcomes for QoL, symptoms and perceptions of bowel function, 12 months for consultation and prescription rates). For each patient, baseline data were to be included as covariates. The mixed models were to be used to generate interval estimates for the differences between alternative treatment strategies.
(Due to the poor recruitment rates, the planned analysis and economic evaluation described here did not take place. Chapter 5 describes the analyses agreed with the HTA after the decision was taken to close recruitment.)
Economic evaluation
Perspective of the evaluation
We planned to conduct a cost-effectiveness analysis, placing particular emphasis on the subset of costs and effects relevant to address the health service perspective at a macro level. We had hoped to supplement this by an individual participant perspective. Our selected outcome measures included condition- and treatment-specific QoL and a generic utility-based measure of health state, measured at the individual level. We also recorded the costs of the condition and its management, which were met directly by the patients themselves.
Measure of benefits used and type of study
Considering all of the measures of effectiveness estimated within the clinical trial, a cost-consequence analysis136 was outlined alongside the cost-effectiveness analysis. In the cost-consequence analysis, clinical and QoL profile scores, resources used for the implementation of the intervention strategies and related costs, were to be presented in a disaggregated way. For each arm of the trial, the breakdown of costs and outcomes was to be listed in a tabular format; no summary measures were to be presented. This type of evaluation and presentation provides readers with a more transparent interpretation of the results and allows them to make a more selective application of the findings to specific decision-making contexts.
Although QoL is an important indicator of benefit in the treatment of constipation, and was the primary outcome measure in this study, none of the currently available condition-specific measures yield a unique QoL score. A comparison/synthesis of costs and outcomes based on each of the separate QoL dimensions in our chosen profile measures would be methodologically invalid. For this reason, a utility-based, index measure – the EQ-5D128,129 – was also to be used, to facilitate calculation of quality-adjusted life-years (QALYs). We were, however, aware of the concerns about the use of QALYs in devising resource allocation strategies between different age cohorts. Therefore, we aimed to apply already existing ‘corrective’ measures to the results we obtained, so that our findings would not have unfavourable implications for the funding of health technologies for older people.
Furthermore, we anticipated that the EQ-5D might not be sensitive enough to detect differences in the population being studied. Therefore, alongside this utility-based measure, we aimed to calculate discomfort-free days (DFDs) as a new measure of outcome. This measure included the impact on patients’ well-being of unwanted symptoms due to both constipation and treatment side effects. It is a crude but meaningful measure of the patients’ perceived effectiveness of treatment. DFDs were to be derived through the self-completed structured diaries. Severity of impact was to be graded in levels, and the number of days spent in each level of discomfort was to be calculated. This information was to be used to assess correlation with DFDs responses. We believed that the comparison of DFDs with EQ-5D utilities would represent a useful addition to the body of knowledge on the assessment of cost-effectiveness in trials where the main impact is expected to be on palliation of symptoms and improvement of the QoL, rather than on extension of life.
Design of the integrated qualitative process evaluation
Introduction
The aim of the integrated qualitative process evaluation was to develop a critical understanding of the social processes and practices implicated in the development, implementation and dissemination of a RCT within the field of HTA. Because the study was ethnographic, qualitative research techniques were used, and it was therefore not appropriate to set out our research questions in hypothetical form. However, at the outset, we addressed the following specific questions:
-
Formation How are ideas about the appropriateness of health technologies and their clinical applications formed and mobilised in practice; how are the interests of consumers and other users defined and incorporated in the organisation of the trial?
-
Integration How are specific clinical and methodological problems within an RCT identified and resolved within professional groups and networks; how is the trial integrated into the existing organisation of clinical service provision, and what professional and organisational dynamics are involved in this integration; how is participation in the RCT negotiated and understood by subjects?
-
Implementation How are the production of results negotiated and organised within networks of researchers; how are its results mediated to the wider community and how is this negotiated and organised, both formally (through report writing and presentation), and informally; how are the mechanisms and results of the trial understood by subjects?
What lessons can be learned that will improve the organisation and conduct of HTA RCTs in the UK – and further afield? The study holds important implications for the organisation and conduct of HTA. It is important that its results can inform and develop both policy and practice.
Methods
The study design used the Normalisation Process Model (NPM), which had been developed through empirical work in the evaluation of telehealthcare systems in the UK. 137 The NPM is a useful means of identifying and explaining the socially-mediated factors that affect the implementation of new technologies in health-care settings.
Four primary groups of actors involved in the deployment of the RCT were targeted. These were (1) the trial team (n = 11), (2) senior clinical staff and practice managers at each site (n = 6), (3) the practice nurses enrolled in the trial to deliver the intervention (n = 9), and (4) recruited participants (n = 23). Collectively, we describe these groups as trial contributors.
Due to the concerns of the MREC that repeated multiple interviews of recruited participants or enrolled NHS staff might constitute harassment, we conducted multiple (follow-up) interviews with members of the trial team and single interviews with practice staff and participants. Data from the research team comprised transcriptions of project meetings and audio-recorded semistructured interviews, field notes written during periods of observation, internal and external correspondence, and formal and informal documentation. Audio-recorded semistructured interviews were used to provide data from primary care staff and trial participants. Table 5 presents the types of data collected through the process evaluation.
| Interviews with trial ‘contributors’ (trial team, enrolled NHS staff and trial participants) | Trial team | N = 11 |
| Practice nurses | N = 9: personalised (BCC), n = 6; brief intervention, n = 3; control, n = 0 | |
| GP/practice managers | N = 6: personalised (BCC), n = 1; brief intervention, n = 4; control, n = 1 | |
| Trial participants | N = 23: personalised (BCC), n = 6; brief intervention, n = 11; control n = 6 | |
| Steering group meetings | Each lasting approx. 80–100 min | N = 4 |
| Trial team meetings | Each lasting approx. 150 min | N = 16 |
| Working group meetings | Each lasting approx. 90 min | N = 8 |
| Field notes |
A B |
2003–4 2005–7) |
| Additional meetings | Press release | N = 1 |
| Additional materials | Numerous e-mails, protocol documents, letters, etc. | |
The data collected through the process evaluation were pooled and analysed as a complete data set. In this report we have drawn primarily on the interview data, as this facilitates a more concise account. However, in the analysis underpinning this report, all forms of data were utilised.
Recruitment strategy
Practices enrolled in LIFELAX were recruited to the process evaluation by a three-step process. Initially, information relating to the process evaluation was included in LIFELAX recruitment packs distributed by the trial team. When a practice had been identified as suitable for inclusion, a letter was sent to the practice manager or senior partner in accordance with previous methods of contact with that practice. The letter included a brief summary of the process evaluation and forewarned the staff that a researcher (BH) would contact the practice by telephone within several days. In addition, senior staff were asked to cascade the content of the letter to the practice nurses as per local custom. The final step in this recruitment strategy was to telephone the relevant member of senior staff and/or practice nurses to arrange an interview. In some instances it was not possible to speak to relevant members of staff on any given occasion, and repeated telephone calls were necessary. However, the availability of staff was hard to predict, and even when a time and date for a return telephone call had been made in advance, staff were not always available to speak on the telephone or asked to reschedule the call. Consequently, if staff had not expressed an interest in participating in the process evaluation after approximately four telephone calls to a practice, it was decided not to pursue the recruitment further at that site. The rationale for this decision was to both maximise the productive use of research time, and avoid undermining relationships between the practice and the trial team, and thus jeopardising the RCT.
During the opening phases of the RCT, the recruitment of practices ran behind intended targets. Consequently, at this point in the process evaluation, staff from all recruited practices were approached to take part in an interview. Towards the end of the trial, when recruited practices were distributed across the country, we purposively sampled practices according to their randomised allocation status and geographical location. Practices situated more than approximately 60 minutes drive from Newcastle, UK, were offered only a telephone interview rather than the option of a telephone or face-to-face encounter. Practices randomised to either of the two diet and lifestyle arms of the trial [behaviour change counselling (BCC) or brief intervention] were specifically targeted, as these conditions required the most input from practice staff. Unfortunately, relatively few practice staff were recruited to the process evaluation.
In following the research strategy outlined above it became apparent that in many practices the practice manager rather than a senior partner mediated between the trial team and the practice. While senior partners ultimately made the decision for their practice to participate in the RCT, their general involvement in the trial was limited, although possibly also included the screening of patients for contraindications and comorbidity. Only two senior clinicians were recruited to the process evaluation. With regard to senior practice staff, including practice managers, we observed that during interviews these staff usually struggled to discuss the research beyond the reason for the inclusion of their practice in the RCT. While these explanations were of interest to the research team, the senior staff viewed their lack of practical involvement in the trial as a limit for the scope and value of the interview. Therefore, we found it difficult to reach many senior staff and after a period of time questioned the value of pursuing interviews with this group. It would be inaccurate to claim therefore that saturation of data occurred within the sample, although meaningful data were nevertheless collected.
At their recruitment to the RCT, participants were informed about the purpose of the process evaluation, and the possibility that they might be asked to partake in an interview. All participants were given the opportunity to have their preferences recorded if they preferred not to be contacted. At the initial stages of the LIFELAX trial all participating patients who had not objected to being contacted were sent a recruitment pack for the process evaluation. This included an information sheet and a response slip. Once response slips had been obtained from the participants, those willing to be contacted by the research team were telephoned to arrange a time and place for an interview. In the latter stages of the trial, due to the over-representation of participants within the brief intervention arm, we approached all participants recruited to the trial with the exclusion of those randomised to this condition. As it was not possible to conduct repeat interviews with individual participants – due to concerns by the ethics committee of potential harassment – we recorded the stage of participation in the trial for each individual. The rationale for this approach was that different phases of the research might present new issues for participants, and that the meaning of the research might also vary along the continuum of involvement. Participants were interviewed from 5 weeks post recruitment to the trial, through to the time of completing a final 12-month questionnaire. Nevertheless, retrospective analysis of the data set did not reveal notable thematic differences across the participants’ stage of participation. Appendix 5 contains a consolidated standards of reporting trials (CONSORT) checklist for the process evaluation and an adapted flow chart of participant recruitment.
Role of the qualitative researcher in the trial team: ethnography
The ethnographer worked closely with the trial team on a daily basis. This proximity had clear advantages with regard to accessing materials, and attending/observing everyday events in the construction and deployment of the trial. All members of the trial team were accommodating of requests for interviews and recorded meetings; however, it took time for both parties to understand the role of the other. For the trial team it was initially disconcerting having their activities routinely observed and recorded, and for the ethnographer it was initially difficult to decide what was useful data from the vast quantity of information collected.
The status of the process evaluation as an integral component of the LIFELAX trial ensured that all team members gave their formal consent to participate in the ethnography, and, in this regard, access to some forms of data was assured. Formal consent was obtained from all individuals attending audio-recorded meetings, and additional consent was obtained for interview data. Formal and informal consent was obtained before reporting data contained in field notes.
The ethnographer was offered a significant level of disclosure and cooperation by the trial manager and the dietitian tasked with developing the training packages. In addition to offering personal friendship, the trial manager became a key informant and confidant during the conduct of the trial, facilitating the ethnographer’s understanding of the activities at hand. Both contacts facilitated initial attempts to understand and map the terminology of the RCT, the intricacies of its design, including the basis of the interventions, and, perhaps most usefully, the broader administrative and bureaucratic networks in which the RCT was embedded. Moreover, the ethnographer was occasionally given small tasks within the RCT. This role, however small, facilitated the ethnographer’s integration with other trial team members. Through observation, participation and personal contacts the ethnographer was therefore able to map interactions that would have been problematic topics within an interview setting.
Analysis
The process evaluation used a combination of qualitative research techniques. In broad terms, we followed the precepts of Glaser and Strauss’s model138 of constant comparison to develop first-order analyses of the data. The NPM137 was applied to emergent categories in a cyclical process, whereby the model’s constructs were partially redefined to fit the nature of the data. Because of the relatively large body of data collected we used nvivo 7 collation and management software. Analysis occurred through application of the model’s four constructs, as illustrated in Table 6.
| Interactional workability |
|---|
| How a complex intervention is practically enacted by the people using it |
| Q. How does the work get done? |
| (e.g. In LIFELAX, how did the trial team practically implement the trial? What did practice staff report regarding implementation of training materials and contact with participants?) |
| Skill-set workability |
| The distribution and conduct of work associated with a complex intervention in a division of labour |
| Q. How is the work distributed? |
| (e.g. In LIFELAX, which groups of NHS staff were targeted by the training interventions, and how did they configure the work alongside ongoing responsibilities?) |
| Relational integration |
| How knowledge and work about a complex intervention is mediated and understood within networks |
| Q. How is the work understood by the people doing it? |
| (e.g. In LIFELAX, how do the trial team reconcile differences in the implementation of RM&G guidance across PCT sites? How do practice nurses make sense of the training sessions based on BCC?) |
| Contextual integration |
| The incorporation of a complex intervention within an organisational domain |
| Q. How is the work supported? |
| (e.g. In LIFELAX, what work needs to be performed in order to implement an RCT in primary care practices?) |
Initial field work consisted of mapping both the stakeholders and structures of the system, from which a sample of both intervention situations and interviewees were chosen. It was particularly important to observe routine and problematic applications of each arm of the trial, especially the negotiations over treatment modalities and how the boundaries between these were agreed.
Local documentary materials (e.g. protocols, correspondence, minutes of meetings, notices, leaflets, entries in newsletters), in which the trial was explained to professionals and subjects, were analysed for comparison, with themes emergent in the interview data and with the wider literature concerning HTA as a discrete field.
Due to recruitment difficulties in both the LIFELAX trial and process evaluation, it is not possible to claim that we finished data collection at a point of ‘category saturation’ in thematic analysis (i.e. no new forms of data were emerging) for all of the categories of contributors (such as senior partners and practice managers). Nevertheless, data collected across the larger categories of ‘primary health-care staff’ and ‘participants’ was thematically consistent bar several ‘deviant cases’, as described in Chapter 7.
The nature of the process evaluation posed important ethical and practical problems. It was particularly important that the contributors at every level felt safe to report on difficulties and disagreements about the focus, design and implementation of the RCT. At the outset, therefore, we needed to be able to promise the contributors that ‘data’ would be treated in a way that was ‘non-attributable’, and that it would be protected in the same way that we would wish to protect, for example patients in a study using these techniques. To ensure that this was accomplished, we do not identify individuals or specific PCTs or practice sites in this report or in any other presentation or publication that was made as a result of this study. Our previous experience in such work has demonstrated to us that this is the only way to ensure openness and candour on the part of participants, and so effectively achieve the objectives of the study.
Chapter 3 Development of the interventions
In this chapter we will look at the evidence that supported the design of the two diet and lifestyle intervention arms in LIFELAX. In essence, the lifestyle and nutritional guidelines that underpinned both the standardised and personalised intervention arms were the same and it was in the style and mode of delivery that the arms varied.
In LIFELAX, the model we adopted was one in which health-care professionals (usually practice nurses) were trained to deliver the diet and lifestyle interventions. The models of delivery of both the standardised and personalised interventions were informed both by theories of behaviour change and by considerations of the practicalities of implementing these interventions in the primary care settings. We invested a great deal of time, effort and resources in the intervention development phase, working closely with practice staff and patients in two local surgeries to inform the design of interventions that health-care professionals could deliver and wanted to deliver. During this pilot phase, patients were consulted and this feedback was used to inform the content, language and layout of the information booklets we developed.
Not all of the findings of the studies on behaviour change that we used to inform the intervention were appropriate for both arms. We were seeking to develop two notionally different interventions. One of the arms (standardised diet and lifestyle advice) needed to sit firmly within the current nursing model in the UK84 and be suitable for delivery within a routine appointment time (10 minutes). The other arm (personalised diet and lifestyle advice) would be informed by techniques and skills that had been shown to be effective in interventions of behaviour change in similar topic areas and similar populations to ours. (The contents of both the standardised and personalised manuals, along with the information leaflets, can be found in Appendix 3. Copies of the manuals and patient literature are available for purchase from the LIFELAX team.)
Motivating patients and facilitating health behaviour change are key roles for health-care professionals; it was therefore important for the diet and lifestyle interventions to map on to these aspects of routine practice. The standardised intervention arm followed the Pendleton et al. 84 model. The Pendleton model has two main components. The first component is to do with the nature of the consultation – the aim is to produce an effective consultation between practitioner and patient in which they work together, both to define the problem and decide the solution. The second component of the model is to do with the teaching method used during the consultation – Pendleton et al. 84 describe a teaching method by which both the teacher and the learner enable the learner to build on his/her strengths and ability to be effective.
In the consultation there are a number of tasks:
-
Understanding the problem:
-
– the nature and history of the problem and its effects.
-
-
Understanding the patient:
-
– look at the problem from the patient’s perspective.
-
-
Sharing the understanding:
-
– consider other problems
-
– consider options and implications.
-
-
Sharing decision and responsibility:
-
– enable the patient to manage the problem
-
– choose the most appropriate course of action
-
– practitioner and patient both have responsibility
-
– agree goals.
-
Maintaining the relationship
It is by understanding the problem and the patient, and by sharing this understanding, that the health-care professional will be working towards fulfilling the aim of the first component one of the model: effective consultation. It is by using an educational style that allows the patient to build upon their existing abilities to manage the problem, rather than by telling the patient what to do, that the spirit of the Pendleton approach is upheld. The standardised intervention focused on enabling the practitioners to have the most up-to-date knowledge and information on constipation. One general PIL was developed for the standardised arm of the trial. The aim was to enable the practitioner to understand what constipation meant to their patient and to explore the options for management. The practitioner had 10 minutes in which to see patients and to set goals for changes to their diet and lifestyle.
The personalised intervention arm drew on a range of models of behaviour change. It is the development of the resources, training and materials for the personalised intervention arm that is the main focus of the remainder of this chapter.
Theories and models of behaviour change
There is a wide range of conceptual models of behaviour change, such as Bandura’s Social Cognitive Learning Theory, Becker’s Health Belief Model, Azjen and Fishbein’s Theory of Reasoned Action, Prochaska and DiClemente’s Stages of Change Theory (discussed in greater depth in the section entitled Motivational interviewing, below) that can be applied to the primary health-care setting. 139–141 When designing the interventions for LIFELAX we reviewed evidence from interventions, theories, techniques and counselling styles that had been used to encourage individual (patient) behaviour change. From the outset we were minded to produce interventions that would use techniques and skills already familiar to health-care professionals and that would be easily communicable to them so as to reduce any potential barriers and patient dissatisfaction that are documented to arise from poor communication. 142
Interventions for behaviour change in healthy eating
From a review of literature indexed in MEDLINE, Web of Science and CSA Illumina on the effectiveness of interventions to promote healthy eating in the general population, it was apparent that there was a number of specific characteristics common to the successful interventions. 140 According to the review, any intervention, whether the focus was on diet alone or on diet and exercise, should be based on a model of behaviour change (i.e. it should be theory and goal driven) rather than simply on the provision of information. Successful interventions tended to be the ones that emphasised personal contact and were related to specific behavioural change strategies. Tailoring the intervention to the patient by using individualised personalised materials or using trained personnel to deliver a case by case intervention was also shown to be beneficial. Opening a dialogue between the health-care professional and patient that allowed for feedback on changes in behaviour (i.e. multiple contacts over an extended time period) was also found to be advantageous.
Physical activity interventions in primary care
In a review of primary prevention and secondary prevention interventions (12 and 24 studies, respectively),143 the authors identified several components of an intervention to promote physical activity that are likely to improve success (some of which had also been identified as being associated with successful interventions for dietary change), these include:
-
using behavioural approaches (individualised goal setting and problem-solving, self-monitoring, feedback and reinforcement)
-
supervised exercise
-
provision of exercise equipment.
The concept of ‘self-efficacy’ was highlighted and shown to be closely linked to a stage of self-change in physical activity. Individuals at the different stages of preparedness to change have different ‘degrees of exercise specific self-efficacy’. 144 Individually tailored reports and self-help manuals matched to the patient’s stage of motivational readiness to start physical activity were found to increase physical activity significantly more than standard self-help materials. 145 A brief negotiation intervention, based on motivational interviewing, was found to be more effective than attempts to persuade or coerce. 146
Interventions for elderly people living in the community
The decision to exclude non-community dwelling older adults from the LIFELAX study had been taken at the design stage as it was felt in residential care people would have less control over what they ate, and therefore that there would be less opportunity for them to make lifestyle changes. As elderly people living alone in the community account for 80% of the lowest single household income groups147 it was important that the diet and lifestyle changes promoted by the interventions were not costly to the individual. There is a paucity of literature on interventions that are focused on community-based nutrition. From a review of 23 such studies, none of which was from the UK (21 from the USA, one in Australia and one in France), we concluded that there was limited evidence for the effectiveness of healthy eating interventions in the elderly. 147 However, the review did find that the strategies of individual feedback and goal-setting highlighted previously142 were beneficial and were associated with a positive intervention. 147 The review restated the fact that the elderly community dwelling population is a heterogeneous group and that more research is required to identify suitable approaches at different age groups, social class and health status. 147
Primary care as a setting
Promotion of behaviour change in general practice
General practitioners have very little time with a patient to embark upon any programme of individual behaviour change. In the UK, people see a GP on average five times a year for an average consultation time of 9.4 minutes, which equates to 47 minutes of contact time per year per patient. 148 This lack of contact time with the GP and the belief that the practice nurse was more likely to deal with patients with constipation added strength to the argument that it should be members of the nursing staff who were trained to deliver the intervention. Other studies149–151 have found that, although patients report high levels of satisfaction with both GP and nurse encounters, patients report greater levels of satisfaction with nurse consultation than with GP consultations. These studies found that there was no significant difference in other health outcomes and most found that consultations with nurses tended to be slightly longer than with GPs, that nurses gave more information to patients and that they offered more advice on self-care and disease self-management. These findings reinforced the choice of the practice nurse as the lead in delivering the diet and lifestyle interventions.
Based upon the knowledge that health-care professionals may not give advice during a consultation unless they understand and believe the information themselves,152 we decided to involve health-care professionals in the planning of the interventions and the production of the materials used.
There is good evidence for the use of counselling-style interventions in promoting dietary change in primary care. 153 Face-to-face dietary counselling either in small groups (two to three members) or individual sessions of 5 minutes (or less), which provided self-help material and interactive health communications, were viewed as being ‘promising’. 153 This review found that effective interventions are those that combine nutrition education with behaviour-orientated counselling to provide patients with the skills, motivation and support they require to make lifestyle adjustments. Examples include:
-
teaching self-monitoring
-
training individuals to overcome common barriers to eating a healthy diet
-
goal-setting
-
shopping and food preparation guidance
-
intratreatment social support.
The above recommendations were incorporated into the interventions.
A systematic review of 37 trials (10 dietary and six exercise behaviours) concluded that primary care-based health programmes do have a modest and variable effect on lifestyle change. 154 From this review, it was, however, difficult to draw any meaningful conclusions from the dietary trials as the interventions varied widely. Exercise interventions showed promising evidence of their effectiveness.
Though the importance of nutrition is not disputed by primary health-care professionals, there are a number of barriers that are known to restrict their provision of nutritional counselling. These include lack of time, lack of training in behaviour change,155 a belief that patients will not follow their advice, a lack of reimbursement for counselling and inadequate teaching materials. 156 As described in Chapter 4, despite our best efforts to address all of these in the interventions we designed and the support we provided, these barriers are highly resistant to change.
The practitioner, patient and concordance with regimens
Only about one-half of patients comply with long-term drug regimens and even fewer comply with changes in lifestyle, especially when an advice giving approach is used. 157 The dominant paternalistic style of a physician (or other health-care professional) giving their patient advice is often not a suitable model for chronic disease management or health promotion. The model of a ‘meeting between experts’, where both the patient and health-care professional are considered to be experts on the patient’s problem, and changes are negotiated to enhance the patient’s well-being, is a more successful approach. 157 Motivational interviewing is one such negotiation-based strategy; it is very much a ‘client’-centred approach (discussed below) and enables health-care professionals to share information and offer suggestions.
Delivery methods for behaviour change
With the absence of standardised definitions of the techniques included in behaviour change interventions, it is difficult to both replicate effective interventions and identify the techniques contributing to effectiveness across interventions. 158 At the outset we need to make it clear that the approaches or methods described below are not mutually exclusive. Many of the techniques and practitioner skills are common to several or all of the techniques, and are those shown to be effective in previous studies of interventions designed to promote individual behaviour change in diet, physical activity, etc. as described above. They also have a theoretical underpinning in models and theories of behaviour change. LIFELAX made use of a combination of the approaches outlined below to develop the most practical approach to the development and delivery of personalised diet and lifestyle advice by nurses in the primary care environment.
Tailored information
There are two main forms of health communication – targeted generic and tailored communications. 159 ‘Targeted generic’ information is defined as material intended to reach a specific subgroup of the general population, based on one or more demographic characteristics, while tailored information is designed to reach one individual, and is derived from individual assessment and is unique to that individual. Generic information is less costly to produce than tailored information, although there is evidence of the success of the use of tailored information disseminated using a variety of communication methods including the telephone, audio, video, internet or other electronic media. 159 A review of eight tailored/generic comparisons found evidence that tailored personalised communications were more effective than generic, non-tailored communications;160 therefore, in the personalised arm of LIFELAX all communications were suitably personalised (targeted to the individual).
Motivational interviewing
While motivational interviewing holds ‘substantial promise for health behaviour change’, is patient centred, can be tailored to the patients degree for readiness of change and is an effective means for working with patients who are ambivalent or not ready for change, it should be added as a note of caution that few controlled studies measuring the efficacy of motivational interviewing exist, and little is known about how to structure sessions. 161
Motivational interviewing is ‘a directive, client centred counselling style for eliciting behaviour change by helping clients to explore and resolve ambivalence’. 162 Motivational interviewing has four principles:163
-
expressing empathy
-
developing discrepancy
-
rolling with resistance
-
supporting self-efficacy.
Table 7 shows the characteristics of what is and what is not a characteristic of motivational interviewing.
| Motivational interviewing | Opposite to motivational interviewing |
|---|---|
|
Collaboration Partnership conducive to change |
Confrontation Ignoring patient’s perspective |
|
Evocation Intrinsic motivation to change is drawn from patient’s own goals |
Education Aim of the practitioner is to educate the patient for change to occur |
|
Autonomy Patient-led self-direction |
Authority Practitioner tells patient what to do |
Motivational interviewing is not defined as a technique per se but rather by ‘its spirit as a facilitative style for interpersonal relationship(s)’. 162 This ‘spirit’ involves collaboration between health-care professional and patient. The health-care professional elicits the motivation to change from the patient, through drawing on their patient’s own perceptions, goals and values, while the responsibility for change remains with the patient. 163 The focus of the motivational interview is to examine and resolve ambivalence, defined as a key obstacle to change, in a patient-centred and directive manner. 162
Although not explicitly based on any specific theory of behaviour change, motivational interviewing has been linked with the Transtheoretical Model of Change,164 which assists by ‘providing a framework for understanding the change process itself’, whereas motivational interviewing provides ‘a means of facilitating this change’. 161 The combination of motivational interviewing with the Transtheoretical Model has been described as an ‘optimal patient encounter’. 142
Because the notion of a readiness to change is important in all motivational interviewing approaches, including ‘brief motivational interviewing’, it is necessary to have a working understanding of the Transtheoretical Model (Figure 1). 165
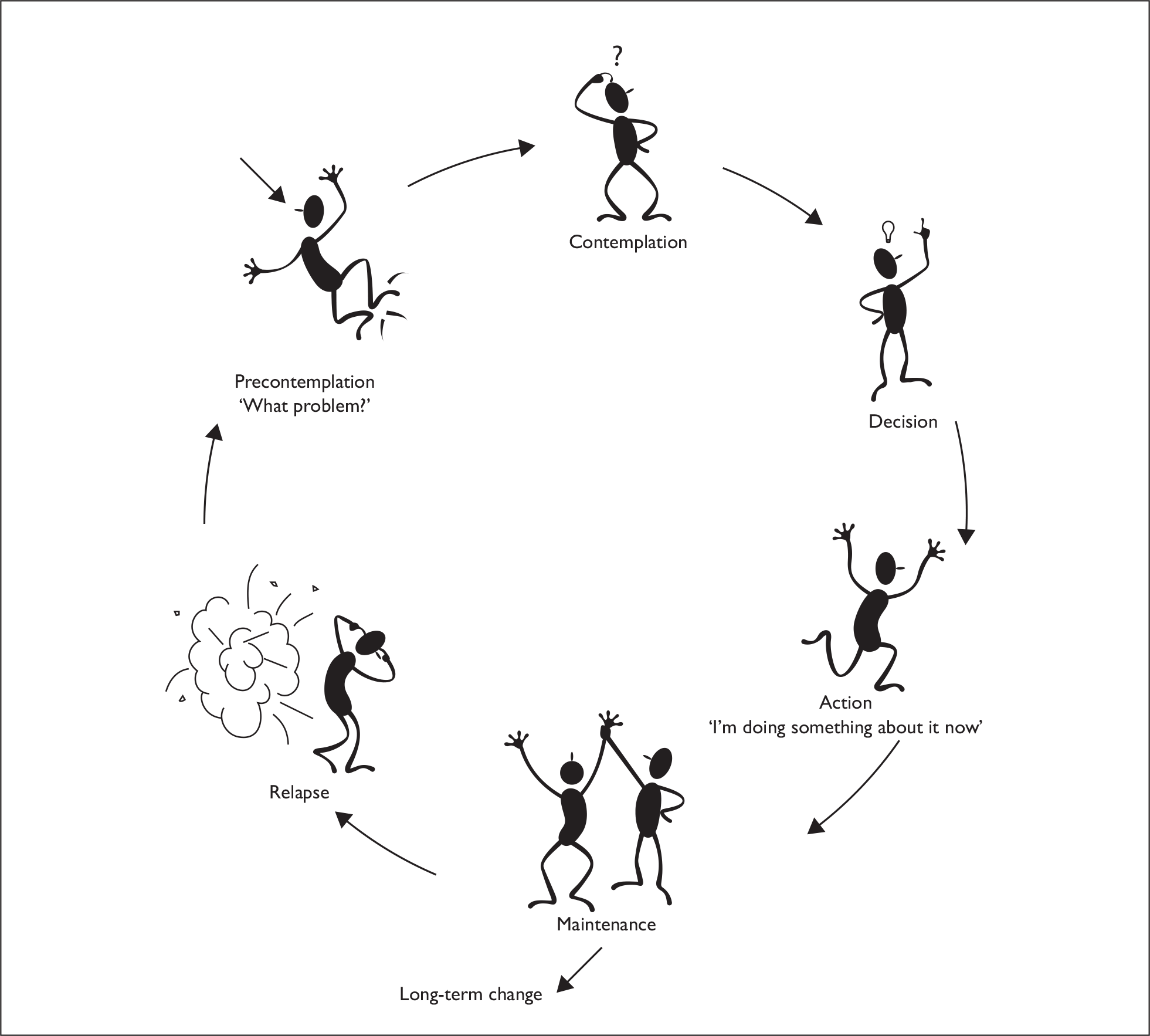
Debate as to the merits of the Transtheoretical Model as a predictive or descriptive model is beyond the scope of this report; suffice to say that this is a model with which health-care professionals are familiar, and it provides a useful lexicon to describe people as they undergo a behaviour change intervention. The rationale behind this model is that behaviour change does not happen in one step. People tend to progress through different stages on their way to successful behaviour change. People also progress through the stages at different rates. Expecting behaviour change from someone who is still in the ‘pre-contemplation’ stage is unlikely because, when in this stage, the individual is not ready to change. Decisions as to when to move through the stages (i.e. when a stage is complete) must be made by the patient, as opposed to being imposed by the health-care professional. In each of the stages there is a different set of issues and tasks that relate to changing behaviour. The health-care professional can use different tools and techniques at each stage.
The focus of traditional medical consultations regarding behaviour change is ‘advice giving’. As discussed above, this paternalistic approach is not always the most effective mechanism and may be met with resistance and disagreement between patient and practitioner. 166 In behaviour change interventions, ambivalence to change is an often encountered problem. Ambivalence to change can be characterised as a conflict between two courses of action (patient and counsellor). It is difficult to resolve as each party has benefits and costs associated with the behaviour change. 166 This is particularly true when a directional (e.g. advice giving) approach, with unequal partners, is adopted, rather than a negotiated strategy. Motivational interviewing, although it uses a non-directive counselling approach, is a negotiated approach and does focus explicitly on ambivalence and the resolution of it. 167 The practitioner can positively or negatively influence their patient’s resistance to change and the outcome of the consultation. Negotiations in which the patient expresses his/her perceptions of the costs and benefits of change have been shown to promote the patient’s motivation to change. 166 Behaviour change interventions that tailor advice to the patient’s readiness to change should ensure closer agreement between patient and practitioner, encounter less resistance and improve the effectiveness of the intervention. 166 The most successful use of motivational interviewing is when the patient is given individual, personalised feedback. 168
While we knew that some of the practice staff involved in the LIFELAX intervention delivery would have a specific interest or experience in constipation or GI conditions, there was good evidence to suggest that motivational interviewing could also be successfully used by health-care professionals that were non-specialist in a specific field. 169
Despite these theoretical benefits of motivational interviewing, we were aware that the most limiting factor in using motivational interviewing in a medical or public health setting is time,170 in particular the length of time available in the ‘normal’ appointment slot for either GPs or practice nurses. For LIFELAX, therefore, we recognised that a briefer format of motivational interviewing would be required. Within the time constraints of the normal encounter with a practice nurse, we felt that there might not be sufficient time to fully explore the patient’s ambivalence. We were also aware that asking health-care professionals to adopt the LIFELAX intervention protocols may require some adjustment from the traditional prescriptive methods of patient education (i.e. provision of advice) to becoming more facilitative and collaborative. 170 Health-care professionals delivering the interventions in the trial would be required to leave their traditional ‘expert’ role and allow the patient to become the expert. 167
Brief motivational interviewing
Brief motivational interviewing techniques have been used with success in brief interventions in primary care in a range of topics, for example perinatal drug use,171 to improve dietary adherence in adolescents172 and psychiatric patients’ attitudes to their care, motivation to change, compliance and outcome. 173 There are a number of key elements that characterise a successful brief intervention and these should be apparent to anyone observing such a consultation. These elements are represented by the acronym FRAMES. 174
-
Feedback Systematic assessment and feedback of individual findings.
-
Responsibility Emphasising the individual’s personal responsibility for change, that this change is a free choice and a personal decision
-
Advice Advice giving consists of two negative factors: first, it provides the patient with information (usually using tactics of fear induction), and, second, it uses persuasion (why a patient should do what you tell them).
-
Menu The variety of ways in which change could be accomplished.
-
Empathy Style of counselling.
-
Self-efficacy Intervention should contain elements to strengthen the individual’s self-efficacy.
Despite ‘advice’ being a key element, it is important to recognise that ‘brief motivational interviewing’ consultations are not in the traditional advice-giving mould; advice is not given without the patient’s permission, and when advice is given it needs to be accompanied by encouragement for patients to make their own decisions. 161
Brief motivational interviewing was developed for use in a medical setting, where most patients do not enter in a state of readiness to change. 175
An implication of the Transtheoretical Model is that, before attempting to give people the skills and resources needed to change their behaviour, it may be more effective to assess their readiness to change. A person’s preparedness to change can be assessed accurately by the use of a questionnaire;176 however, this is likely to prove to be impractical in a routine clinical setting. Other useful tools to assess readiness to change, including an agenda setting chart (Figure 2), a ‘pros and cons’ chart (Figure 3) and a readiness-to-change ruler (Figure 4), have also been developed. 177 In LIFELAX we produced an agenda-setting chart that allowed patients to address constipation-specific factors (known to impact on bowel health), such as exercise, diet and fluid, as well as three open options where the patient could identify their own priority areas. In the intervention, patients were encouraged to identify their own priority items and set achievable goals when they were ready (Figure 5). 178 We understood that patients might well have had a rigid mental picture as to the consultation that they should expect when they underwent the intervention. We were aware that changing the consultation process and associated behaviours might not be easy; however, we felt that the simplicity of the agenda-setting chart, and its ability to help patients express choice and take the lead in target-setting, would make it a useful instrument. 178
FIGURE 2.
LIFELAX agenda setting chart.

FIGURE 3.
LIFELAX pros and cons chart.
| Staying the same | Changing | |
|---|---|---|
| Pros | I wouldn’t have to change a thing | I could do without my laxatives |
| Cons | I’d still need my laxatives every day | I would have to change my diet |
FIGURE 4.
Scaling tools.
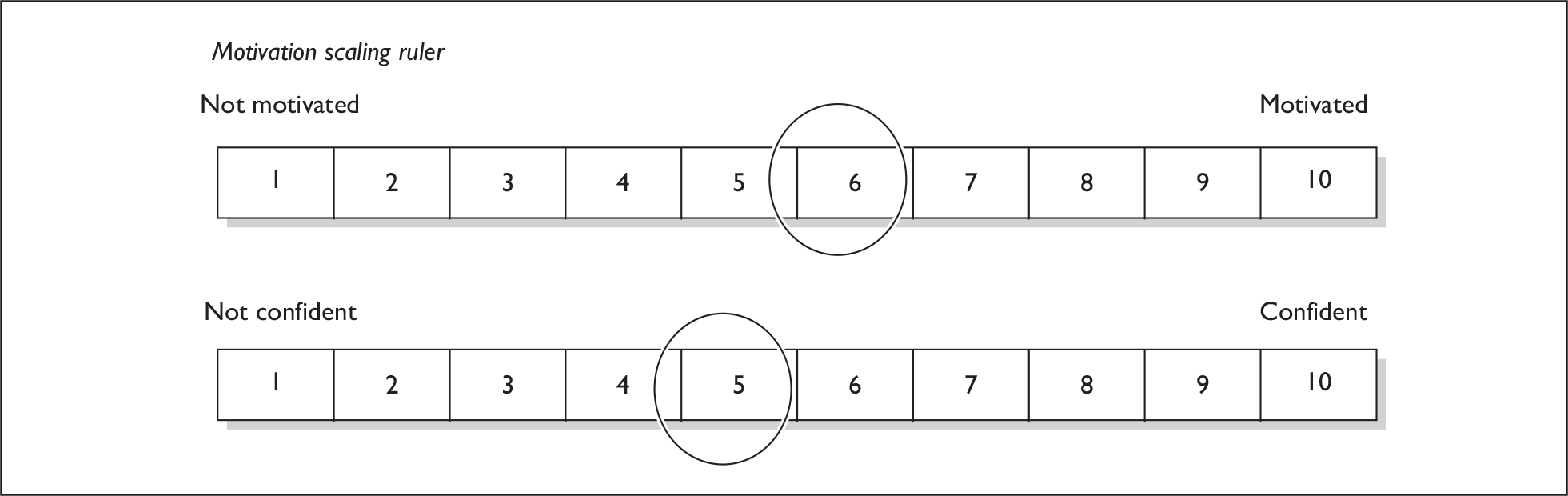
FIGURE 5.
Setting aims and plans.
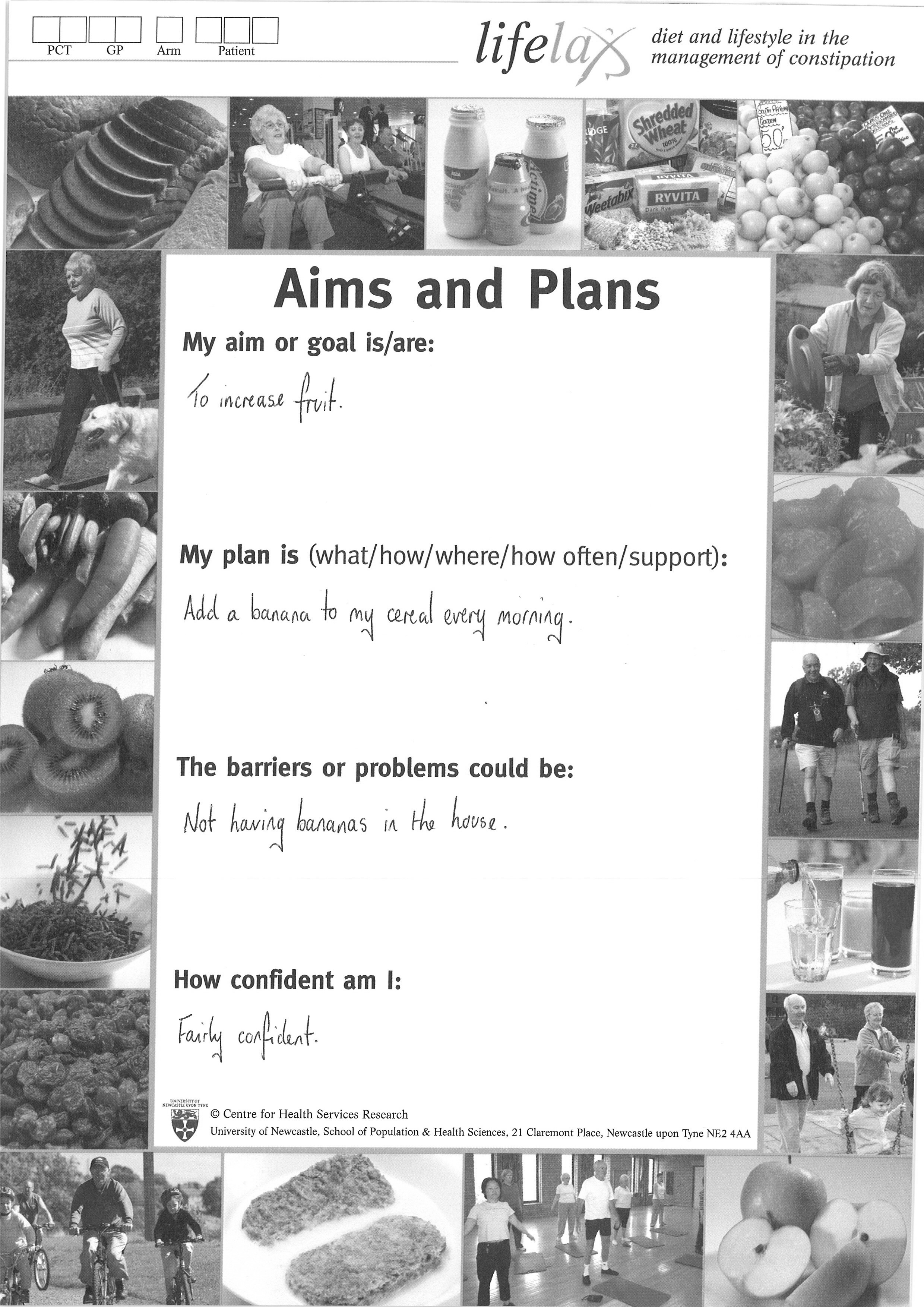
In order for behaviour to change, a person needs be motivated to change their behaviour and feel confident to do so. Motivation can be defined as the individual’s expectations of the costs and benefits of change, whereas confidence may be described as their ability to master the demands of assistance. Bandura’s Self-Efficacy Model and the distinction between outcome and efficacy expectation provide a theoretical framework to use motivation and confidence. 179 Exploring the importance of changing a behaviour with the patient is an important exercise. For this exploration, a ‘pros and cons’ chart was developed (see Figure 3). Using this chart it is possible to explore and record the positives of making a behaviour change and staying the same. Below is a worked example.
Confidence to change can be assessed simply by asking two questions:180
-
‘If on a scale of 1–10, where 1 is not at all motivated to eat more fruit and 10 is 100% motivated to eat more fruit, what number would you give yourself at the moment?’
-
‘If you were to decide to eat more fruit now, how confident are you that you would succeed? If, on a scale of 1–10, 1 means that you are not at all confident and 10 means you are totally confident that you could eat more fruit, what number would you give yourself now?’
After the topic (eating more fruit) had been raised, the aim of the next stage would be to identify arguments for change (motivation) and practical steps to make the change (confidence); this could be done through scaling questions
-
First, by asking the patient why they scored as they did rather than a lower number:
-
– ‘Why have you given yourself a score of 6 and not 1?’
-
-
Second, by asking the patient what would need to be in place for them to move to a higher number:
-
– ‘What would have to happen for your motivation score to move up from 6–9?’ ‘How could your confidence score move up from 5–8 or even 9?’
-
This information would then be incorporated into the ‘setting aims and plans’ sheet (Figure 5) as part of the ‘contract’ between the patient and health-care professional during the LIFELAX personalised intervention counter between the patient and health-care professional. Patients would take a copy of this away and a copy would also be retained in the practice for future reference in terms of follow-up telephone calls and follow-up visits.
Counselling
Counselling is defined as a ‘cooperative mode of interaction between the patient and primary care physician or related health-care staff members to assist patients in adopting behaviours associated with improved health outcomes’. 181 Improved behavioural outcomes in dietary counselling are thought to be associated with a number of factors, including the use of dietary assessment, enlisting family involvement, providing social support, using group counselling, emphasising food interaction (tasting, testing and cooking), encouraging goal setting and using advice appropriate to the patient group. 182
In a review of 21 studies, focusing on the counselling effect on changes in fat, fruit, vegetable and fibre intake, higher-intensity interventions, (more than one 30-minute contact) were found to be more effective than lower-intensity interventions. 181 Counselling interventions using self-help material and interactive communication alongside brief provider advice seemed to produce medium changes. Elsewhere, behavioural counselling to increase fruit and vegetables consumption have also been shown to be effective. 183 The PILs were designed to enable respondents to think about their current practice and to compare this with recommendations. For example, the PIL on ‘Fluid and constipation’ contained a fluid counter, the ‘Fibre and constipation’ PIL contained a fibre counter, and the ‘Activity and constipation’ PIL, an activity counter.
Behaviour change counselling
In addition to the principles of (brief) motivational interviewing, and the models and theories that underpin (brief) motivational interviewing (the Transtheoretical Model, and Bandura’s Self-Efficacy model), the personalised diet and lifestyle arm of LIFELAX also drew heavily on the BCC model. BCC184 is a set of consulting strategies derived from the patient-centred method,185 health behaviour change184 and motivational interviewing. 163 See Table 8 for a summary of the characteristics of BCC. As we described above, motivational interviewing is a directive, patient-centred counselling style for increasing intrinsic motivation by helping patients explore and resolve ambivalence. Being ‘patient-centred’ involves a number of factors:
-
It is an active process that involves both patient and practitioner.
-
There is a core partnership between patient and practitioner.
-
It is not directional advice giving.
-
Careful listening – listening to the patient to learn from them.
-
The patient has greater control in decision-making.
-
The practitioner and the patient reach joint decisions together.
| Goals |
Establish rapport, identify goals, exchange information Choose strategies/goals based on individual’s readiness Build on motivation for change |
| Style |
Practitioner – patient both active Seldom confrontational Use of an empathic style, information is exchanged |
| Skills |
Ask open-ended questions Summaries Ask permission Encourage patient choice and responsibility Provide advice Reflective listening |
Behaviour change counselling, like motivational interviewing and brief motivational interviewing, has been developed for brief health-care consultations to help the individual talk through the ‘why’ and ‘how’ of change. The practitioner’s main task is to understand how the person is feeling and his/her plans for change. 40
As in motivational interviewing and brief motivational interviewing, establishing rapport is an essential component of BCC consultations. Once rapport is established, two-way information exchange tends to occur more readily. Establishing the patient’s readiness for change and what behaviour to focus on are also parts of the BCC approach. Establishing and agreeing goals and strategies for behaviour change should involve the patient setting realistic aims and plans that can be achieved. The consultation is an active process that involves both the patient and the practitioner; it should be collaborative, rather than prescriptive, and should be non-confrontational. By the professional asking permission to discuss a topic during a consultation, the patient will not feel it has been forced upon them.
Empathy – which can be defined as: ‘the ability to share someone else’s feelings or experiences by imagining what it would be like to be in their situation’186 – is a further core skill of the BCC process. This includes empathic listening, an active listening process, and demonstration that the professional is indeed listening, by replying and reflecting to what the patient has just said. For example:
‘Being constipated makes me feel lethargic, I can’t be bothered doing anything and I am scared of leaving the house.’
‘Your constipation makes it difficult for you to be more active – that must be hard.’
The BCC interviewing style is one that ‘quiet and curious’ – allowing the patient to do more talking, using open-ended questions, rather than closed questions. 184 Empathic listening, reflection and summaries are useful in rapport building and also ensure that aims are understood by both patient and practitioner. The practitioner provides structure to the consultation but decision-making should be shared184 (Figure 6 – suggested BCC consultation ‘flow’) and should be the patient’s choice as well as their responsibility. In BCC, as in motivational interviewing, it is vital that practitioners avoid falling into a paternalistic, directional advice-giving trap. Evidence suggests that this generally does not induce behaviour change. 184 When advice needs to be given, a more positive form of advice giving is giving a number of options, with the patient choosing the most suitable one.
FIGURE 6.
The BCC consultation ‘flow’.
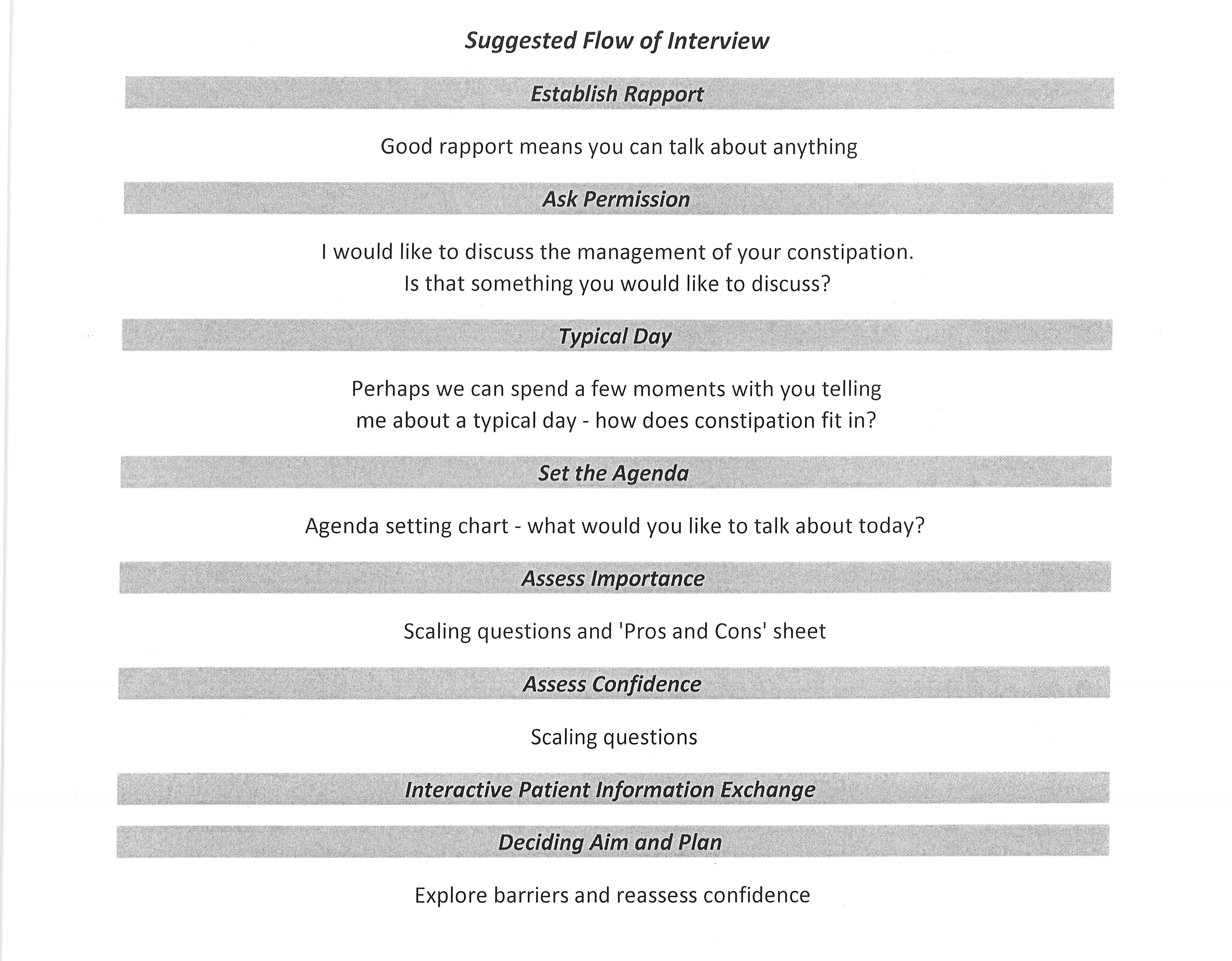
The key principles that underpinned the LIFELAX personalised intervention
-
Individualised goal identification.
-
Realistic goal setting.
-
Practitioner listening to the patient.
-
The intervention being directed by the patient.
-
Setting and following up the patient’s individual goals, using a range of novel tools: the agenda-setting chart, the scaling tools, the ‘pros and cons’ sheet and the goal-setting sheet.
-
Monitoring of patient’s progress using specifically developed PILs containing tools, such as a fluid counter, fibre counter, measures of physical activity.
-
A user-friendly and accessible practitioners’ manual that had all necessary trial information, and set out clearly and concisely what was required in the intervention.
-
Training materials and resources.
From visiting practices and speaking to practitioners, the study team established that there was a scarcity of independent constipation, diet and lifestyle PILs, with the majority being produced by drug companies and laxative producers. A comprehensive suite of materials and resources was developed to enhance the LIFELAX interventions. We worked closely with patients and health-care professionals to develop many of the tools and the information materials needed. For example, we used cognitive interviewing techniques to test the acceptability and comprehensibility of the PILs (from text to pictures) and thereby to ensure their relevance and acceptability to the target audience. 119
High-quality training and reference manuals for health-care professionals were produced for both the standardised and personalised diet and lifestyle intervention arms. These contained the entire set of information (see Chapter 1, Impact of diet and lifestyle on constipation) that health-care professionals would need about constipation and bowel health, as well as full details of the delivery style and techniques for the appropriate arm.
Training of practice staff was envisaged to take place over a number of visits (one to two) for the standardised arm and (two to three) for the personalised arm. The training sessions were conducted by the project dietitian and nutritionist. As we were aware that we might be asking practitioners to change their consulting behaviour, this training drew heavily on the behaviour change techniques we were passing on for LIFELAX. However, after much discussion within the team it was agreed that there would be no formal assessment of the any health-care professional’s preparedness to change their own consulting behaviour.
The time available to train health-care professionals in the intervention techniques was always an issue in this trial; however, the importance of training cannot be over emphasised. 167 We needed to be flexible and to tailor our training to fit in with the practice schedule. There is evidence that training based upon two or three 1- to 1.5-hour training sessions and role play demonstrations is successful. 177 We were told by the practices involved in developing the interventions that practice nurses would not readily enter into or enjoy role play, especially if senior colleagues were to be involved or observing. As a result of this, we elected to produce training DVDs in place of the role play. Evidence suggests, too, that outside of the training sessions few of the health-care professionals were willing to practice the training and techniques. 177 For this reason, we felt that the DVD would serve as a useful resource and aide-memoire.
Our experiences of practice training varied from practices that set aside the majority of a day for training to ones that required us to fit in with lunch breaks. Having project staff (a research dietitian) that were sympathetic to and understood the dynamics of working in a primary care environment was seen as an advantage.
We felt it important that staff should have a positive experience from the training, and worked to create sessions that were informative, interesting and with clear useable learning outcomes. We felt that our training DVD helped to avoid the embarrassment of role play and the unfeasibility of offering staff ‘refresher’ courses.
Novel ways for engaging practice staff and assessing their knowledge of the condition were used, for example we used the quiz show formats of ‘Who Wants to Be a Millionaire’ and ‘The Weakest Link’ rather than a more formal assessment or lecture. A lecture would imply they may not know how to deal with constipation, whereas the quiz format was a two-way process that facilitated discussions and information exchanges.
Summary
In designing both the standardised and personalised diet and lifestyle interventions for LIFELAX there were a number of theoretical models that we could have potentially chosen on which to base our materials, methods and resources. The standardised approach made use of the existing nursing model in use in primary care as the basis for those appointments. For the personalised intervention arm, we reviewed a number of trials that had successfully used a number of different models and techniques to deliver behaviour change with respect to diet, physical activity and other aspects of lifestyle. We drew on the recommendations from those papers and from other practising health-care professionals to produce training, training materials and literature, the likes of which were not otherwise available to practitioners in the UK.
Copies of the resource packs, PILs and training DVD are available for purchase from the central trial team.
Chapter 4 Implementation of the trial
Introduction
In this chapter we will describe the challenges encountered during the implementation of LIFELAX. These challenges arose both with the recruitment of practices and of patients. The planned recruitment model described in Chapter 2 (which formed the original study protocol) and the account of the reality presented here differ widely. Various reasons for the challenges will be documented in this chapter and the embedded Process Evaluation Study (see Chapter 6) offers a further interpretation on this account.
In summary, some 1114 practices in total were approached and invited to participate. Of these, 44 (just under 4% – 13 short of our target of 57) agreed to participate and were randomised. However, only 19 practices (43% of those randomised – 33% of the target of 57) recruited participants to the trial; 16 practices withdrew post randomisation and six practices were unable to recruit during the time frame available. Figure 7 presents the CONSORT diagram for the trial.
FIGURE 7.
LIFELAX CONSORT diagram. a, Although not all consented participants received the allocated intervention they were eligible for a baseline assessment; therefore n = 154 is used in the analyses of baseline data. b, Not all withdrawals were complete withdrawal from all follow-up assessments; consequently, some participants supplied questionnaire data and not diary data, and some participants agreed to telephone follow-up only.
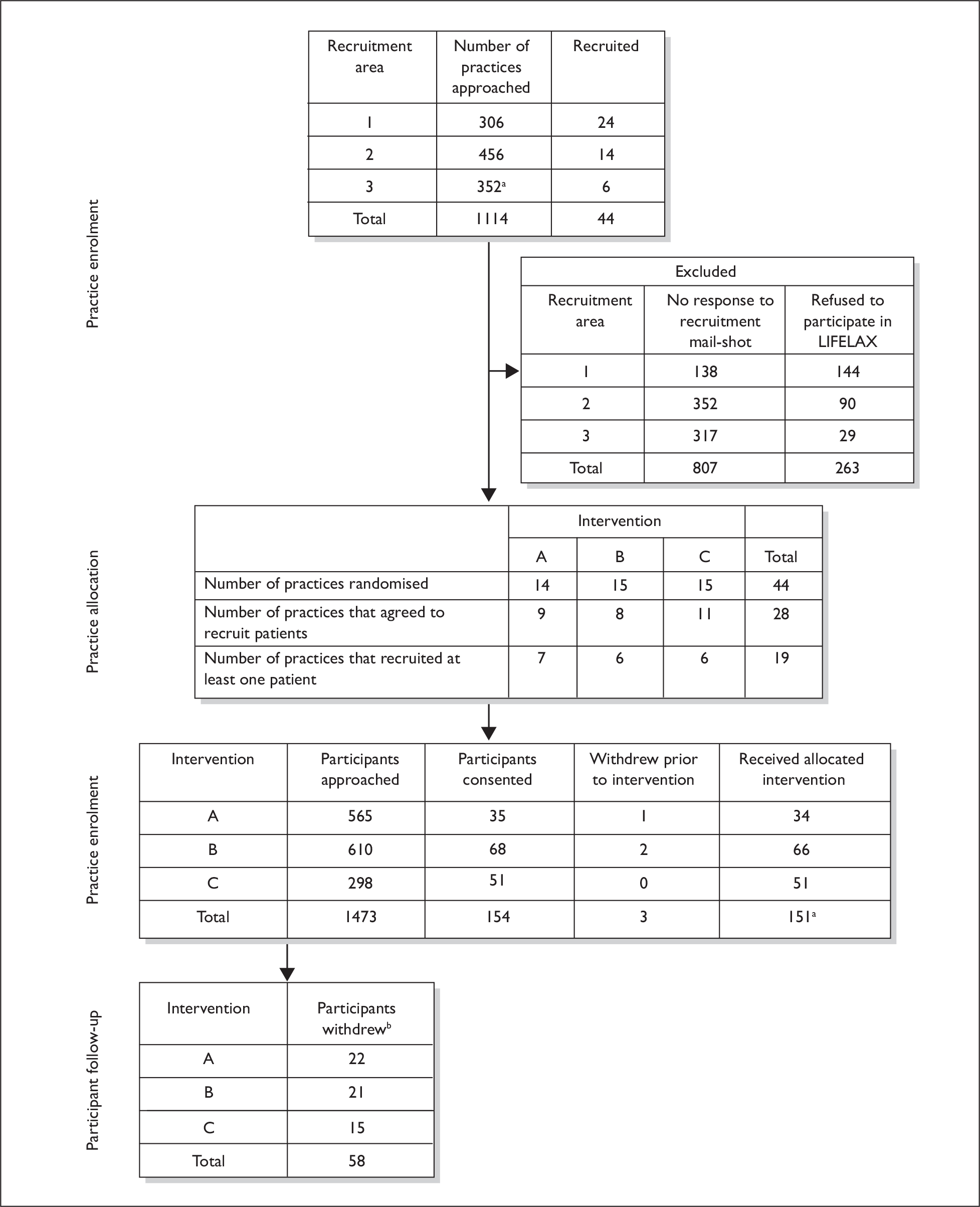
A total of 154 participants were recruited to LIFELAX. Initial calculations showed that in order to recruit the required number of participants (approximately 1800) for the trial we would need to recruit 57 GP practices (31 patients per practice on average). This would seem now to be a vast underestimate, given the poor levels of participant uptake we experienced.
Preparation and implementation of the trial protocol
For the findings of clinical trials such as LIFELAX to be generalisable across primary care (i.e. to have external validity), it is important for the amount of research and the proportion of research-active primary care staff, in particular GPs, to increase. 187 Increased participation in primary care trials is a priority in the UK,188 even although such trials have always been more challenging to researchers than trials in alternative environments, such as the more controlled and more research-orientated secondary care. Added to this ‘standard’ challenge of primary care research, LIFELAX also coincided with a period of considerable change within the NHS, both in terms of the emergence of a new research governance and ethics framework and the implementation of new GP contracts.
Regulatory approval
Although LIFELAX began after the publication of the EU Clinical Trials Directive, it was prior to the Directive’s enactment into UK law. This meant that although the LIFELAX trial appeared to meet the criteria for a clinical trial of an investigative medicinal product (ctIMP) we were able to apply for a Doctors’ and Dentists’ Exemption (DDX) certificate when obtaining regulatory approval from the Medicines and Healthcare products Regulatory Agency (MHRA). This meant that we did not need to submit a full application for a Clinical Trial Authorisation (CTA) to the MHRA. In common with all other trials at the time, the DDX was issued and was then ‘rolled over’ into a CTA on 1 May 2004. (With hindsight it would seem that the study could have made the case to the MHRA that the study was a trial of management strategies, rather than specific drugs. However, the general advice we received was that if there was any possibility of a study being a ctIMP the DDX/clinical trial exemption route should be followed to avoid the additional paperwork associated with obtaining a CTA.)
MREC approval
An overview of the time line for the trial is shown in Table 9. The initial ethics application was submitted to the allocated MREC in December 2003, at which time the subsequent approval of the LREC associated with each participating site was required, unless a ‘no local investigator’ (NLI) status was agreed by the MREC. To reduce the burden on the multiple GPs who were to be recruited to this study, we asked the MREC to consider NLI status for LIFELAX. Unfortunately, NLI status was not granted. The MREC reviewed the application on 22 January 2004. A number of minor changes were requested in the patient information sheets. The MREC delegated authority to their ‘lead reviewers’ for this application to approve these amendments once they had been received. The formal letter conferring the favourable opinion of the MREC was issued on 12 March 2004.
| Month (duration in months) | Activity or comment |
|---|---|
| June 2003 (1) |
Trial manager begins work on LIFELAX (tasks include securing LREC and Trust R&D approval for pilot, preparing the pilot study materials, training in pilot study research methods, and preparation of the documentation and materials needed for the MREC approval application) Dietitian appointed and begins work (full time) |
| July 2003 (2) | Dietitian reduces hours to part-time for personal reasons (work continued on developing the materials for the intervention and dietitian is trained in cognitive interview techniques) |
| October 2003 (4) | Dietitian returns to full time. Applications for NHS honorary contracts made |
| November 2003 (5) | LREC approval for pilot study, R&D approval given for pilot |
| December 2003 (6) | MREC application submitted |
| March 2004 (9) | Favourable opinion from MREC received; work begins on various LREC applications (i.e. SSAs); ad hoc funding is sought from the DH to ‘pay per patient’ recruited via the SfS funding stream |
| April 2004 (10) | Diet and lifestyle leaflets completed for the intervention |
| May 2004 (11) |
Pilot for nurse training begins; PCT/GP meetings attended by trial manager in order to promote LIFELAX and generate interest; ad hoc funding is secured Negotiations with COREC re. practices being ‘research consortia’ with one PI begin |
| July 2004 (13) | PCT/GP presentations continue; application made to LRECa and PCTs for R&D approval |
| August 2004 (14) | Pilot of nurse training completed; printing of ‘packs’ and associated intervention materials; training DVD produced |
| October 2004 (16) | COREC manager supports our attempt to gain SSA exemption |
| November 2004 (17) | Practice recruitment and staff training begins (area 1); the electronic query is run to identify patients |
| February 2005 (19) | Follow-up telephone calls begin to practices to discover why there was little interest in the study |
| March 2005 (20) | Work continues on promoting the trial and looking at ways of making it less burdensome to practices |
| May 2005 (23) | First training visits to practices arranged (area 1) |
| June 2005 (24) | Application to MREC made to revise recruitment protocol. Favourable opinion given (20 June 2006); application to revise the ad hoc funding in line with protocol revisions made |
| July 2005 (25) | Application made to HTA for 22-month extension; six participants consented |
| August 2005 (26) | 10 participants consented |
| September 2005 (27) | Five participants consented |
| October 2005 (28) | Three participants consented; SSA exemption given by MREC |
| November 2005 (29) |
Recruitment of practices begins (area 2) Four participants consented |
| December 2005 (30) | Eight participants consented |
| January 2005 (31) | Eight participants consented |
| March 2006 (33) | Three participants consented |
| April 2006 (34) | Eight participants consented |
| May 2006 (25) | Nine participants consented |
| June 2006 (36) |
Approach made to SPPIRe to recruit practices in Scotland; approach to MREC to change the face-to-face baseline assessment to a telephone assessment 10 participants consented |
| July 2006 (37) |
Favourable opinion from MREC received Seven participants consented |
| August 2006 (38) | Nine participants consented |
| September 2006 (39) | Three participants consented |
| October 2006 (40) | One participant consented |
| November 2006 (41) | Five participants consented |
| January 2007 (43) | Recruitment in area 3 begins |
| February 2007 (44) | Two participants consented |
| March 2007 (45) | Three participants consented |
| May 2007 (47) |
The TSC met and discussed whether there was a viable future for the trial; HTA briefed of the intention to reconvene in October 2007 to make the final decision over a further extension or close down Five participants consented |
| June 2007 (48) | Two participants consented |
| July 2007 (49) | 27 participants consented |
| August 2007 (50) | Five participants consented |
| October 2007 (52) | TSC make the close-down decision; recruitment is halted; participants already in the trial are to be followed up as per protocol |
The LIFELAX trial team had concerns over the burdensome nature of the recruitment protocol submitted to MREC as part of the approval process. This method had been approved by another MREC for the STOOL trial. 19 The approval process for STOOL had taken 15 months, and we were concerned that any deviation in LIFELAX from an already approved method might lead to unnecessary delay. [At this time there were many changes in the research ethics committee (REC) approval process. Many of the recruitment strategies that had been acceptable in earlier studies were deemed to be no longer so. It is in the context of this changing landscape and inconsistencies across RECs that LIFELAX operated.]
LREC approval
As LIFELAX was not able to operate as a NLI study, an extra level of approval was required before recruitment could begin. LRECs treated each general practice recruited into the study as a separate ‘site’ and required the submission of a separate SSA, accompanied by the CV of the GP taking on the role of principal investigator (PI) for that site, before they would consider that site for approval. The process was made additionally burdensome to GPs as it required that each local PI should apply for an LREC number, complete and sign the relevant form and send it to the appropriate LREC. These requirements created a number of difficulties: many GPs did not have readily available CVs of the type required; many GPs were unfamiliar with the new LREC forms and processes and did not have sufficient time to carry out these tasks; and others felt that they did not wish to be designated as responsible for a study that ‘wasn’t theirs’ and felt that responsibility for the study lay with the research team.
To facilitate this process we designed a short CV template that would allow GPs to provide us with the minimum amount of information required for LREC to carry out the SSA. Having heard anecdotal evidence/horror stories of trials that needed SSAs spending > 7 months on this part of the approval process alone, we made an approach to our MREC, the local COREC manager and the Director of NoReN (the local primary care research network) with an innovative solution.
The COREC guidelines at the time stated that if two or more GP practices had contracted to conduct research collaboratively, whether through a consortium or under the direct management of the PCT, they could be collectively identified as a single site and, in such cases, one of the investigators should be appointed as the PI for the site. Our solution to the local approvals dilemma proposed that NoReN (an inclusive organisation for all north-east general practices, not requiring any practice to ‘opt in’) should form the consortium with the other recruiting practices in the area, with the clinical director of NoReN (GR, already a coinvestigator on the study) acting as the PI for the purpose of the SSA. 189 This solution was accepted, and notification that the various LRECs had approved LIFELAX to run in the ‘Area 1’ PCTs came via MREC on 10 November 2004.
Although LIFELAX pioneered this approach, allowing us to speed up the SSA process in the areas covered by NoReN, we were not entirely happy with it as a model outside the NoReN area. Although successful in Cumbria with the CumbReN network (again with the CumbReN director acting as PI for the consortium), there was a concern that should the trial seek to recruit further afield the directors of other GP research networks might not agree to take responsibility as PI for the sites within their network’s geographical area. In light of this concern we again approached MREC and asked them to reconsider the ‘NLI’ status of LIFELAX. At the time of this final approach, the ‘NLI’ status for trials had ceased to exist. By this time, the LREC approval process required site-specific information (SSI) to be submitted to LREC as part of the local approval process or, in certain circumstances, an SSI exemption could be claimed. After consultation with the local COREC manager and the agreement of the COREC policy officer to support the MREC decision to support the SSI exemption, should it be granted, an approach to MREC for SSI exemption was made in October 2005. We argued that the LIFELAX was a ‘low-risk’ study, the prescribing of laxatives was in line with normal practice (with no stipulation on class or dosage) and that the behaviour change techniques were often used in routine practice.
After agreeing that LIFELAX was a ‘low-risk’ study, MREC considered that it could be an ‘SSI-exempt’ trial (favourable opinion 12 October 2005), which meant that sites no longer needed a GP to act as a PI and that no application to LREC for approval of sites (or consortia thereof) needed to be made.
PCT selection and R&D approval
Selection and recruitment of PCTs
Primary Care Trusts in north-east England, Yorkshire and Cumbria were initially allocated between the STOOL and the LIFELAX trials. STOOL was allocated some of the more geographically distant Trusts (Cumbria & Yorkshire) as we believed fewer visits were needed to practices to set up that study, as there was no requirement to train practices in the delivery of the stepped-drug-regimen intervention. Training for the diet and lifestyle interventions meant that LIFELAX practices would require many more visits so Trusts closer in proximity to Newcastle upon Tyne were prioritised for that study.
LIFELAX initially sought PCT research and development (R&D) approval from 11 local PCTs (area 1 recruitment) (all PCT names that follow refer to the PCTs in existence at the time of practice recruitment – since that time there have been a number of mergers and a reduction in the overall number of PCTs): Newcastle; Gateshead; South Tyneside; Northumberland; Durham & Chester-le-Street; North Tees; Derwentside; Sedgefield; Craven; Harrogate & Rural District; Scarborough; Whitby & Rydale, and Hambledon & Richmond. Across these 11 PCTs there was a total of 308 practices available to us. We were able to contact only 306 of them for the trial, as two of the practices had been involved in the both the development of the diet and lifestyle interventions and taken part in the STOOL trial qualitative study and we were keen not to overburden their staff and patients. Due to poor GP response rates (14 practices) from this first wave of recruitment, it became necessary for LIFELAX to expand its recruitment area.
In a bid to capitalise on the increased profile of constipation raised by the STOOL trial and to take advantage of the STOOL trial manager’s local knowledge, it was agreed that once it had closed down [the Trial Steering Committee (TSC) agreed the closure of the STOOL Trial in May 2005] LIFELAX would contact those PCTs originally selected for ‘STOOL’. Thus, in a second recruitment wave, we approached North Tyneside, Sunderland, Langbaurgh, Durham Dales, Easington, Hartlepool, Middlesbrough, Darlington, East Yorkshire, Yorkshire Wolds and Coast, West Cumbria, Eden Valley, Carlisle and District, Eastern Hull, West Hull, Selby and York, Doncaster Central, Doncaster East, Doncaster West, and Rotherham. This second wave of recruitment yielded a further 24 practices agreeing to participate and being randomised.
The total number of participating practices from these two waves of recruitment was still, at 38, short of our target of 57 practices. Therefore, in a third and final round of recruitment, we approached Birmingham East and North, Heart of Birmingham, South Birmingham, Central Manchester, North Manchester, and South Manchester. In addition to these Trusts we also worked in collaboration with the Scottish Practices and Professionals Involved in Research (SPPIRe) network [SPPIRe evolved into the Scottish Primary Care Research Network (SPCRN) during the time it was involved in the promotion of the LIFELAX trial]. In England, our method was to contact all practices within a particular PCT. In Scotland, SPPIRe operated a different system whereby the node coordinator (there was one coordinator for each of the four nodes – north, south, east and west) approached practices that they knew to be research active, or had expressed an interest in joining primary care trials. A further 14 practices (13 in England, 1 in Scotland) agreed to participate and were randomised following this third wave of recruitment.
With the advent of the National Institute of Health Research Clinical Research Network (NIHR CRN) and its development and support of a portfolio of ongoing trials, we also took the opportunity to promote the trial more widely in England. As a result, some UK PCRN managers contacted the study team asking for further information about the trial. (Many areas had existing PCRNs; in October 2008 the new PCRNs were officially launched.)
Although keen to help the study recruit, the decision of the TSC not to apply to the HTA for a further extension meant that these offers of assistance with recruitment were not taken up. With hindsight, it appears that this decision taken by the TSC was entirely appropriate, considering the number of insoluble barriers identified through the embedded process evaluation (see Chapter 6).
Obtaining PCT R&D approvals
The process of obtaining R&D approval from participating PCTs took varying lengths of time from 1 month up to a whole year. [For one PCT, approval proved impossible to secure, despite numerous unanswered approaches to them. On the advice of the neighbouring PCT’s R&D Manager (where we had secured approval) we waited until the two PCTs merged and we were given approval for the newly formed PCT.] In the majority of cases, approval was given within 1–2 months of our application. Most of the delays were caused by disagreements with respect to indemnity issues or honorary contracts. With respect to indemnity, the issue was concerned with where the responsibility for provision of indemnity for the study lay. The principle is that indemnity against negligent harm is available through the NHS indemnity scheme and/or through the GP’s own professional indemnity for practice staff. Members of the research team held honorary research contracts with the NHS, and this provided NHS indemnity for negligent harm in respect of their role in delivering the intervention (essentially in training practice staff in the intervention; members of the research team did not play any direct role in delivering the intervention to patients). Professional liability insurance carried by Newcastle University indemnified protocol authors (i.e. the research team) in respect of liabilities arising from negligence in study and protocol design. We made it clear to the Trusts that we did not anticipate there being any claims against either the NHS or the university in respect of negligent harm. The study design had been peer reviewed and the conduct of the study was monitored and reviewed on a regular basis by the funding body (NHS Health Technology Assessment programme) and by the TSC. However, we repeatedly needed to demonstrate to Trusts the professional liability insurance the University had in place to cover for negligent harm caused by the design of the study (as opposed to its execution, which was covered by NHS and GP professional indemnity, as indicated above).
The issue of non-negligent harm was a matter of concern for many PCTs. Our MREC deemed (as is usual for non-commercial studies, especially those where no novel drug was being used) that there was no requirement for us to have indemnity against non-negligent harm. However, not all Trusts accepted this. These issues were eventually resolved, but the process was burdensome, time consuming and frustrating. We soon learned that the best policy was to send, at the time of application, every document we had ever been asked for by other Trusts in support of our application, even though the standardised R&D approval form was all we were obliged to submit. Our experiences were common to other studies at the time. STOOL also reported a frustrating, burdensome and time-consuming account of the R&D approval process,19 but it was not just primary care trials of constipation that experienced the vagaries of the Trust approval process. 190
We were fortunate that all of the PCTs to which we applied were part of consortia. This meant that rather than an individual application for R&D approval being made to each individual PCT, one application could be made to the consortium to which the PCT belonged. LIFELAX did encounter one delay, as one of the PCTs in one of the Consortia would not approve the trial, despite the consortium’s lead PCT (which had reviewed the application) recommending that all member PCTs approve it. This issue was resolved after a discussion between the PCT responsible for the review and the non-approving PCT; although the delay was minimal, the frustration was not. Although the standardised NHS R&D form was a move towards a standardised approach by using a standardised application form, each of the consortia had their own application form. The detail required on the forms ranged from the minimal (akin to a study registration form – as LIFELAX was funded by the HTA and peer review was part of the funding process the R&D lead in this consortium required very little information about the methodology, sample size calculation and rationale for the trial, as this had been scrutinised previously) to the comprehensive (akin to the standardised R&D form).
All bar two consortia required that the trial be approved before approaches were made to any practices in their catchment area regarding their participation in the trial. One consortium (part of recruitment area 1) allowed us to approach practices while the governance issues (honorary contracts and individual PCT approval) were being resolved, on the proviso that no research activities were undertaken prior to approval being given. There was a further stipulation from this consortium that before a practice could actually ‘go live’, the R&D lead needed to decide on whether a practice was ‘suitable’. This was an interesting addition to the recruitment process, as this decision about a practice’s ‘suitability’ would have seemed to have been most appropriately made by the REC process; furthermore, the criteria to be applied by the R&D lead in assessing ‘suitability’ were not transparent. Nonetheless, with LIFELAX having circumvented the SSA process, we understood that there might be a concern from the R&D lead that a practice was not assessed for suitability and we therefore accepted this additional check. However, this check for suitability was also routinely carried out for practices that had already had an SSA by an LREC. The level and methods of checking for suitability are unclear and their effectiveness could perhaps be questioned.
After approving the practices for participation in LIFELAX, one senior partner in a practice deemed ‘suitable’ had a number of allegations made against him and was suspended, prior to resigning and the practice being taken over by the PCT. The allegations were initially made at the time we were asking for the practice to be approved. This calls into question the effectiveness of the process for assessing practice suitability that was in place locally. In another practice the computer system was replaced by the PCT and this change and subsequent delay meant there were considerable difficulties in searching for participants. This upgrade to practice prescribing systems was being carried out to all practices in the Trust, yet it was not identified by the R&D lead as a potential barrier to timely recruitment.
In another recruitment round (part of recruitment area 2), we were asked by the PCT to recruit practices before any approach for R&D approval from the PCT would be considered. Here the view was that unless there was interest from practices then it was not worth processing the application. This in itself was frustrating as all of the trial materials stipulated that we had PCT approval at the point of writing; we felt that having this approval would demonstrate to practices and patients alike that LIFELAX was a legitimate study and would lend it an air of importance. For reasons of cost and logistics (including the need to have revised patient information sheets reviewed and approved by the MREC, and old versions of the sheets withdrawn and replaced), we did not revise the information sheets. We did have practices wishing to join the trial in the area and so the PCT did eventually need to consider and approve the study. Fortunately, none of the practices joining the study from the PCT questioned the timing of this approval, and it was in place by the time patients were approached to participate.
Honorary contracts (both applying for them and having them issued) was another source of delay. There was lack of agreement between PCTs on which members of the research team required an honorary contract, what constituted a ‘current’ Criminal Records Bureau (CRB) check (and what level – standard or advanced – was required) and whether an occupational health check was needed. Some PCTs were prepared to issue a covering letter to act as a ‘mirror honorary contract’ once they had seen evidence of an honorary contract being issued by another PCT. In a number of other PCTs, a new honorary contract from the PCT concerned was required; in some of these, we were told that a new CRB check would need to be carried out, as those that had been carried out at the start of the trial were no longer ‘current’. The University HR department made it clear that it would only process one CRB check per person per study. We eventually managed to get Trusts to accept the initial ‘study’ CRB check, arguing that it was not a requirement for Trust substantive employees to have 6-monthly or annual renewals of CRB checks, and therefore that it would be inappropriate to apply more stringent criteria to those seeking honorary contracts.
As should be clear from Chapter 2, it was never intended that any members of the research team [with the exception of the researcher (BH) conducting the interviews in the embedded process evaluation study] should have face-to-face contact with patients. Although this changed over time in line with the revised recruitment protocol (described later in this chapter), initially all face-to-face contact for patients was to be with trained members of the GP practice staff. Most members of the research team were only ever to have access only to anonymised patient data, and in a few cases to practice premises and staff, and would not be materially affecting the quality of care received by patients, and so we felt that the stipulations in respect of honorary research contacts appeared overly cautious and added a level of unwarranted bureaucracy, delay and cost.
LIFELAX as a business
An RCT is a huge investment in time, money and people. For a long time it has been acknowledged that in order to succeed, trials need to be marketed and trial managers need to think like marketers. 191 Trial management involves lateral thinking, good communication, ethical marketing and common sense. 192 From the start of the trial, LIFELAX was looked upon as being very much a small business. We understood that we would need to find GPs and convince them to ‘buy into’ the study. However, when businesses market a product they are attempting to convince customers that they will gain benefits directly from their purchase of the product. In LIFELAX the marketing task was somewhat different in that we were seeking to gain a commitment from senior GPs to allow their practice to engage in the study, when they themselves would apparently make no direct material gain by doing so. Therefore, from the outset, it was vital for LIFELAX to identify the potential gains and benefits that would accrue from participation in the trial.
Although not specifically stated at the time that LIFELAX was being ‘marketed’, the subsequent publication of the Strategies for Trial Enrolment and Participation Study (STEPS) report193 and the influential ‘Marketing and clinical trials: a case study’194 allow us to retrospectively assess LIFELAX’s marketing strategies against these proposed models for success (Figure 8).
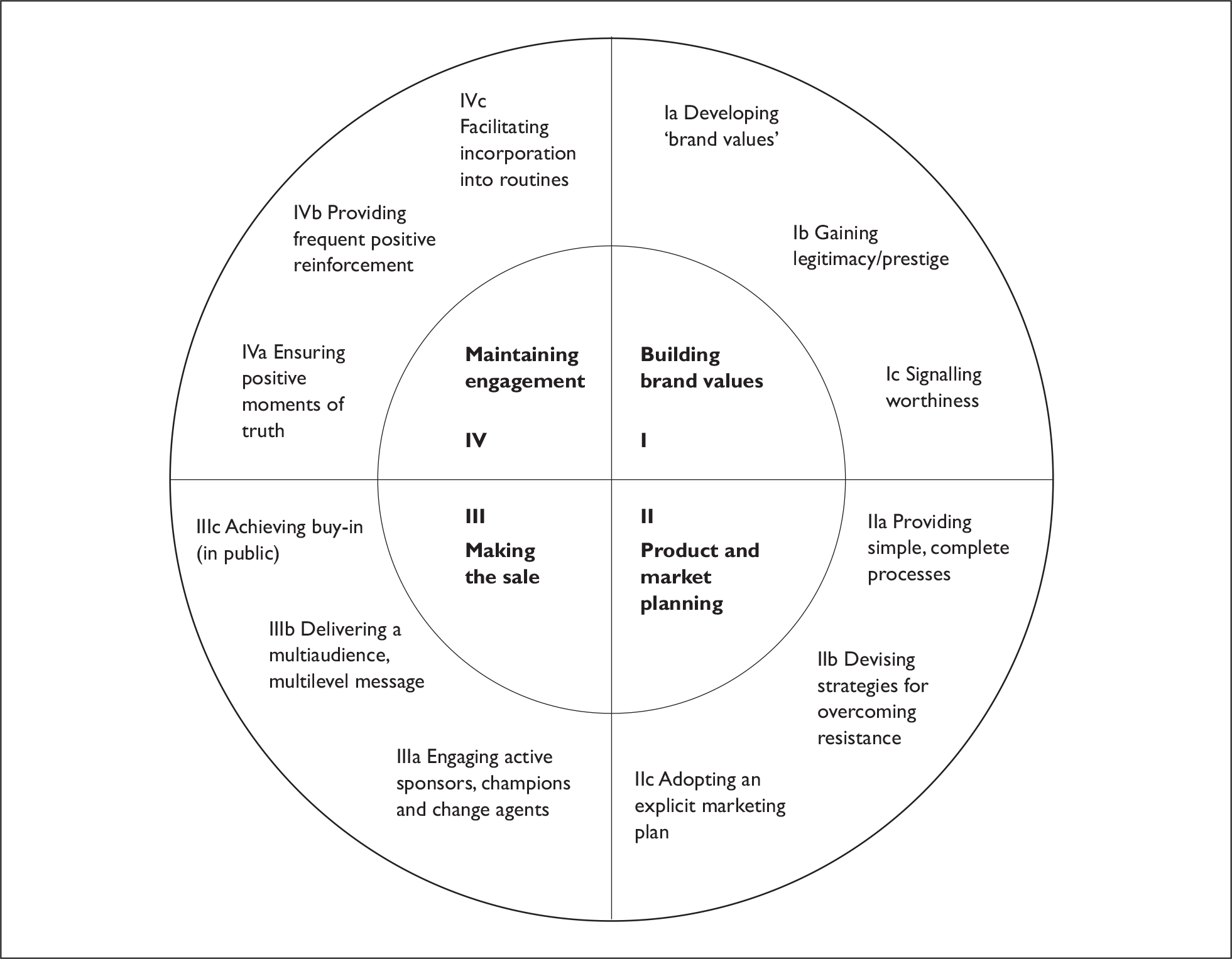
Developing ‘brand values’ (Ia)
Brand values define what a brand is and what it is not. Without this, it is impossible to communicate a coherent and persuasive perception of a trial’s ‘promise’ – i.e. what the trial intends to deliver to medicine, doctors, patients, etc. We worked closely with professional designers and graphic artists to develop the LIFELAX brand. We had our own distinct logo, font and colour scheme that featured on all of our trial related materials to render them easily identifiable. The ‘promise’ of our logo was life and vitality.
Gaining legitimacy/prestige (Ib)
Trials need legitimacy – they need to be positively’ tagged’ by association with prestigious individuals and institutions. LIFELAX was ‘tagged’ to the Newcastle University ‘brand’ (using the recognised crest) and to NoReN/NYReN (PCRN-NE) and its Clinical Director, Professor Greg Rubin. Legitimacy and prestige provide persuasive credibility, which is key to gaining access to decision-makers who decide whether a trial should be supported and maintain engagement. Practice senior partners and staff, particularly those in north-east England, would have been familiar with, and respectful of, both Newcastle University and NoReN/NYReN.
Signalling worthiness (Ic)
It is vital to signal to likely participants that ‘this trial will create greater value than the costs (time, effort or money) involved’. In LIFELAX we negated the ‘money’ cost by securing the SfS funding. This effectively meant that all LIFELAX-related ‘costs’ incurred by practices would be reimbursed. We were also able to present the training in the behaviour change techniques as a benefit to practice staff (training in such techniques is both costly and difficult to source) that would be generalisable and applicable beyond the LIFELAX study. By highlighting the benefits that changes to diet and lifestyle have on a range of conditions (not just constipation) we hoped to show the value of participation. The aim was to roll out the training in the behaviour change techniques to all participating practices at the end of the trial so this ‘value’ would be available to all.
Providing simple, complete processes (IIa)
Trials require participants to undertake work – for example, identifying, approaching and recruiting patients, delivering the intervention and completing study documentation – that is additional to their normal duties. Providing them with simple, complete processes reduces the opportunity and financial costs of participation and increases the chances that involvement will be affordable and manageable. We offered assistance with electronic queries to search for patients. We (following the protocol amendment) undertook the consent, recruitment and follow-up processes.
Devising strategies for overcoming resistance (IIb)
Potential participants frequently raise objections. Trials should have standard and persuasive answers to these. Having a persuasive answer for each objection increases the probability of ‘making a sale’. This is an interesting premise for LIFELAX. Due to the ‘opt in’ nature of the practice recruitment process, we intuitively felt that post-enrolment resistance would be low. We were not ‘cold calling’ practices and trying to convince them to join. However, as shall be seen later in this chapter, resistance to participation (barriers) were identified. The strategies we devised to overcome them are also discussed below.
Adopting an explicit marketing plan (IIc)
The marketing of a trial is too important and too complicated to be done informally. A formal marketing plan is required and should include a definition of target market segments (groups that need to buy in to the trial) and the trial’s unique selling points (USPs). LIFELAX may not score highly in this component as we did not as such. We were aware that the ‘way in’ and ‘sign up’ for practices usually has to be via the senior GPs, rather than the practice nurses, managers. We actually targeted all three in our approach, as we describe below. So in this respect it can be argued that we did adopt a marketing plan, We identified the trial’s USP for each of the categories to highlight the benefits of supporting the study.
Engaging active sponsors, champions and change agents (IIIa)
Selling a trial to prospective participants requires persuasion. This requires enrolling sponsors (public advocates), champions (activists) and change agents (facilitators). Trial managers need a network of supporters to spread the message. Persuasion is more likely to occur if the advocate is respected and known personally to the prospective participant. LIFELAX did have local champions (via NoReN/NYReN). However, we failed in our early attempts to recruit public advocates and our patient representatives’ activities were confined to TSC duties (though they were extremely supportive of the study).
Delivering a multiaudience, multilevel message (IIIb)
Trials need to convey sales messages through publicity, presentations, training materials, etc. These should be tuned to the distinctive needs of target groups – for example, surgeons are likely to be persuaded by different messages to administrators or nursing staff. Speaking in the language of the person being targeted and addressing their particular pattern of motivation is more likely to succeed than a ‘one size fits all’ approach. In LIFELAX we understood the importance of this. Our presentations (contents and style) were tailored to fit with our target audience (GPs, nurses or practice managers).
Achieving buy-in (in public) (IIIc)
Public buy-in requires that intended participants announce their commitment to join the trial in a setting where others hear them. This is important because when someone states, in public, that they are willing to undertake an action, then they are more likely to abide by their commitment than if they take a silent decision – that can be forgotten easily. This was not done in LIFELAX. With benefit of hindsight, we wonder whether techniques such as regular publication of lists of signed up practices might have acted as a signal of commitment. Anecdotal evidence of the lack of awareness in practices signed up to the study suggests that in some cases the senior partner did not even announce commitment to, and elicit support from, the rest of the practice team, leading to a lack of awareness of the study and them feeling that they were ‘pressed’ men and women.
Ensuring positive ‘moments of truth’ (IVa)
People evaluate organisations (including trial management teams) on the basis of their experiences at moments of truth. For example, if a doctor has a technical question about entering a patient into a trial, she will gain a strong impression of the trial management team’s competence by the way that the query is handled. In LIFELAX we had a clear and efficient way of handling queries so that accurate and timely responses were given. We set up a dedicated ‘LIFELAX.queries@…’ e-mail address so that practice staff could e-mail queries and questions to us directly. This account was checked routinely and the message passed to the most appropriate member of the trial team for response.
Providing frequent positive reinforcement (IVb)
Positive reinforcement for existing participants should be an important part of a trial’s participant retention strategy. It is more expensive to recruit new participants than to retain existing participants. We feel that we largely achieved this in LIFELAX. Those practices that underwent training and became active recruiting sites remained committed to the trial until the end.
Facilitating incorporation into routines (IVc)
Activities that become embedded as routines are more likely to be done than one-offs. Trial procedures should be incorporated into the routines of units undertaking the work. Due to the ‘stand alone’ nature of the patient search and mail out, it is difficult to see how this aspect of LIFELAX could be incorporated into practice routine. With regard to the intervention, we were concerned that nurses who saw participants on an infrequent basis might feel less confident in engaging with the techniques. Recognising this, we attempted to show how the principles and techniques of behaviour change taught in LIFELAX could be incorporated into routine practice, and so LIFELAX should not be seen as study-specific training.
With reference to the 12 components above, we are able to demonstrate that the LIFELAX marketing strategy used does fit closely to the proposed STEPS model for success, although we did not apply it explicitly in designing and conducting the study (the STEPS publications193,194 appeared in 2007).
Practice recruitment
Based upon knowledge from previous studies and from feedback from the practices involved in the development of the intervention, and in a bid to target the relevant information to key stakeholders, we sent three copies of all of the study paperwork to the practice. One copy was sent to the senior partner, one to the practice manager and one to the practice nurse. We felt that the trial would be most relevant to the practice nurse and in their letter they were encouraged to discuss participation in the trial with the senior partner or practice manager.
Recruitment of practices was managed in the following way:
-
Three copies of a promotional flyer, containing brief details about the study and alerting staff that more information was on its way were sent to staff at each practice as described above.
-
In the weeks following this, three personalised study packs (covering letter, information sheets, expression of interest form and SAE) were sent to staff at each practice as described above.
-
After 2 weeks, if the expression of interest form was not returned, duplicate reminder packs were sent to practices.
The expression of interest form allowed practices to indicate whether they would like to join the trial or would definitely not like to join the trial and therefore wanted no further information about it. If they required further information prior to reaching a decision, contact details for the trial team were included.
In addition to the mailshot to practices, the LIFELAX team undertook a number of other ‘profile-raising’ activities:
-
contacting relevant PCRNs and asking for their assistance in identifying research active/interested practices
-
writing articles for inclusion in PCT and research network newsletters.
-
attending PCT working groups, practice staff meetings and PCT nurse training events/meetings to discuss the trial.
-
attending PCRN research days and training events.
Recruitment of general practices to LIFELAX proved much more difficult and slow than originally anticipated. In the first round of recruitment (area 1) a total of 306 general practices (from 11 PCTs) were approached to join the study using the method described above (flyer, invitation letter, reminder letter). A total of 168 general practices (55%) responded to the invitation to join the study: 144 practices (47%) did not wish to join the study and did not wish for further contact about it, but 24 practices (8%) agreed to join and were randomised. Overall, 138 (45%) practices did not respond to either the initial recruitment letter or the reminder letter. Moreover, 10 of the practices that were randomised withdrew from the study before undertaking patient recruitment, leaving 14 (5%) practices as potential recruitment sites. Table 10 shows a breakdown of recruitment activity in each of the recruitment areas. Due to concerns over the low levels of expressed interest and practice recruitment rates, a decision was taken to telephone practices that had not returned a form to the trial team stating explicitly that they did not wish did to participate. Two members of the trial team rang 134 practices out of the 138 that did not respond and spoke to either the practice manager or the practice nurse. After this process we managed to recruit a further three practices to the trial. One of the practices became a recruiting site. The second had very low patient numbers (the search yielding single figures) and decided not to participate and the third withdrew prior to conducting any patient searches. This telephone follow-up of non-responding practices was a very resource-intensive process for the research team (often requiring multiple calls before being able to speak to the targeted individual), and due to its lack of success, it was not used in other recruitment areas.
| Recruitment area | Number of practices | Number of responses | Responded to say ‘no’ to LIFELAX | Recruited | Practices recruiting at least one patient in trial |
|---|---|---|---|---|---|
| 1 | 306 | 138 | 144 | 24 | 7 |
| 2 | 456 | 352 | 90 | 14 | 6 |
| 3 | 352 | 317 | 29 | 6 | 6 |
| Total | 1114 | 807 | 263 | 44 | 19 |
Barriers to recruitment of practices
Due to the concerns about practice recruitment levels in both STOOL and LIFELAX, we considered it was essential to identify the barriers to recruitment to the trials and, where possible, address these barriers. Feedback about LIFELAX and the perceived barriers to recruitment was collected in a number of different ways:
-
feedback from GPs, practice managers and practice nurses invited to take part in the study about what they thought were the difficulties of accommodating LIFELAX (this will be further explored in the embedded process evaluation – Chapter 6)
-
informal telephone interviews with GPs, practice managers and practice nurses from ‘non-responding’ practices as part of the recruitment drive described above
-
feedback from research-active GPs (colleagues of the members of the research team)
-
feedback from members of the extended research team and members of the TSC
-
feedback from PCT R&D managers and facilitators
-
feedback from the UK Trial Managers’ Network
-
literature that was being published at the time.
There was a wide range of issues that appeared to be barriers to participation in LIFELAX. Some of them were common to both LIFELAX and STOOL; others were common across all primary care research at the time. Some of the issues were specifically related to the topic and methods of LIFELAX, some to the Research Governance requirements, some to the practice resources. As shall be seen in the chapter detailing the embedded Process Evaluation Study, none of these issues exists in isolation; no matter how small any individual barrier appears to be, both alone, and in combination with others, it can have a major impact upon the successful implantation of a trial. The key issues identified were (no order of importance is implied):
The workload for practice staff
-
The burden to staff in identifying potentially eligible patients (i.e. running the searches).
-
The burden to staff in posting out study information to patients identified as being potentially eligible.
-
The burdensome nature of the LIFELAX recruitment process. There was a lack of nursing/staff time to carry out the informed consent process and baseline assessment.
-
The time taken to train staff to deliver the diet and lifestyle intervention arms.
-
The length of time needed to deliver the personalised intervention (45 minutes of clinic time + follow-up telephone calls).
-
The fear that taking part in a trial might make participants ‘constipation’ aware and thereby increase the number of appointments about a condition that had been managed successfully to that point with repeat laxative prescriptions.
Practice space
-
A lack of consulting space for the initial baseline assessment.
-
The space needed to train staff to deliver the diet and lifestyle intervention arms.
-
The clinic space needed to deliver the personalised intervention (rooms would be occupied for much longer).
Research and the research process
-
Lack of interest in research in general.
-
Lack of interest in the LIFELAX research question (as we shall see in the embedded process evaluation there is a very complex relationship in the perception of roles and responsibilities with reference to managing constipation; we were told that nurses were far more likely to deal with patients with constipation than were GPs, yet practice nurses felt that while they monitored drug regimes of patients with constipation the problem was essentially one that other staff dealt with – either GPs initially in prescribing laxatives or community nurses).
-
Changes in research governance regulations meant that many of the tasks that researchers routinely carried out to assist practices (e.g. approaching and recruiting patients directly) were no longer possible.
-
Paperwork and documentation required for research governance purposes (in particular the formal letter of agreement/contact) discouraged practitioners from taking part in research.
Changes in general practice
-
The introduction of the new General Medical Services (GMS) contracts.
-
Constipation did not form part of the Quality Outcomes Framework (QOF) and was therefore not as ‘valuable’ to practices as coronary heart disease, diabetes, etc.
-
Research activity was not recognised or rewarded under the QOF.
-
Lack of incentives (financial and staff provision) compared to commercially sponsored studies.
Reasons for practice withdrawal
As can be seen from Table 10, 16 of the recruited and randomised practices did not go on to become active recruiting sites. Feedback from these practices suggests a range of reasons for this. Being too busy (n = 9) was the most common cause cited. There was a concern among the research team that the perceived added workload for practices randomised to the personalised arm might make them more likely to withdraw post randomisation. In fact, we had three practices in each of the arms of the trial give this reason, suggesting that there was no one arm that appeared to be more burdensome than others to practices. Two practices gave staff shortages as the reason for withdrawal. In two further practices, too few patients were identified in the search for potentially eligible patients to make participation worthwhile. In another practice there was no one available to do the searches. In yet another, the senior partner had agreed to join the study without consulting the practice manager. The practice manager was not interested in the project and so the practice withdrew. The final practice that was recruited and then withdrew was the one discussed earlier regarding the complaint to the General Medical Council (GMC) in relation to a senior partner and was actually withdrawn at the behest of the PCT rather than the practice itself.
Protocol revisions and practice incentives to improve recruitment
After the decision was taken to close down STOOL, the LIFELAX research team approached the HTA in July 2005 with a request for an extension to the trial. The HTA was aware that the delays in the trial time line to that point were due in the main to bureaucratic issues outside the control of the research team. By taking an evidence-based approach, we were able to demonstrate to the HTA how we had identified barriers to participation in the study and to propose the measures we would put in place to overcome them. While we were only too aware of the difficulties for practices, we took the opportunity to investigate the recent literature on trial participation from the participant’s perspective and to incorporate this in our proposal to the HTA.
Evidence from trials to support the protocol amendment
There was good evidence to suggest that the amendments we proposed to make to the study protocol would allow LIFELAX to achieve the desired recruitment rate for the study. There was evidence from STOOL that the initial recruitment model was not effective. Consequently, this was the first aspect we addressed.
The practice and patient recruitment process in primary care research is much more difficult, more costly and takes far longer than expected. 195 Trial recruitment problems are common, with up to two-thirds falling short of their target, and one-third failing to enrol even 75% of their projected sample. Trials frequently over-run and 10% are abandoned with recruitment failure. 196
Burden of participating
Taking part in research places ‘additional demands’ on participants. 196 These additional demands included extra procedures, appointments, time, inconvenience and expense. The revision to the protocol we proposed minimised the number of additional demands taking part in LIFELAX made on participating practices and their staff. We no longer required patients to visit their GP practice to give informed consent and take part in the baseline assessment. Instead, we offered that a member of the research team would visit them at a time and place convenient to them, following ‘opt in’ by the patient. This change to the protocol meant that the burden and expense of the recruitment and consent procedure was borne by the research team and not the practice. This amendment had the additional bonus that patients could be visited on an evening or weekend should they wish, and therefore had the potential to increase patient participation rates.
From a practice perspective, this amendment immediately freed up clinic time and space for other activities and reduced the burden for them. For patients with transport or mobility problems, there was an additional benefit as there was no need for them to travel to the surgery for the baseline assessment.
Treatment preferences
Treatment preference and worries about treatment efficacy were also highlighted as potential barriers to participation. In LIFELAX, regardless of the intervention arm (we hoped that those in the diet and lifestyle arms would be able to reduce their laxative use), participants were able to request a laxative from their GP or self medicate using OTC products (the qualitative element of the STOOL study indicated that patients were reluctant to change or give up their laxatives, once an acceptable treatment regimen had been found). We felt that this would lessen these concerns.
Concerns about research
Distrust of, and unfamiliarity with, the research process and concerns about information and consent were also raised as points of concern by participants. We believed that by allowing patient participants to contact the study team anonymously or in confidence to discuss any aspect of the trial, we would be able to lessen this to an extent. At the face-to-face meeting with a member of the team we would be able to explain fully the research process, and clarify why we were doing what we were doing and to what ends. We were also able to explain fully just what data were being collected and why they were being collected. We were also able to explain fully how security and anonymity were achieved and maintained. The benefit of reallocating this task to the research team, as opposed to leaving practices to undertake it, was that there was no time constraint. A researcher was able take as much time as a patient participant needed and was better placed to answer questions regarding the study design and protocol.
The personal touch
It has been claimed that the most important aspect for researchers to control is the patient recruitment process and that during this phase of the study researchers needed to maximise their personal involvement. 196 Gabbay and Thomas196 believed that most of their recruitment was successful because they undertook it themselves. Working with other health professionals was, for them, helpful at times; however, they found that relying on others to conduct the recruitment was fraught with difficulties. Recruitment problems, they maintained, could be reduced if the research team carry it out. Foy et al. 197 recommend a range of ways in which patient recruitment to trials can be improved. Based on evidence from a systematic review of the literature and from seven RCTs, they concluded that the research team should conduct both the consent and recruitment aspects of trials, although current guidance on not releasing patient identifiable data to those outwith the clinical team without the patient’s consent, and on the need for ‘opt-in’ rather than ‘opt-out’ approaches presents a challenge in this respect.
Copies of the original protocol and the final protocol can be found in Appendix 1. The major changes between the protocols were in patient recruitment (including giving informed consent and the baseline assessment).
Original recruitment protocol (version 2, 18 February 2004)
-
Potentially eligible (by reference to inclusion criteria) patients were identified by practice staff from practice-held records.
-
GPs then screened these patients for contraindications and comorbid conditions that were exclusion criteria.
-
Patients meeting the study eligibility criteria were then written to by their practice and were sent the study information sheets. An appointment at the practice was also made for a future date and details of this appointment were included with the above paperwork.
-
Patients were asked to contact the practice to (1) confirm that they would attend the designated appointment or (2) rearrange a suitable appointment time. Non-attendance at the clinic was taken to imply that the patient did not wish to participate in the study. No reminders were sent to those who did not respond to the initial invitation.
-
Patients wishing to take part in the LIFELAX study were required to attend their GP practice, first, to give informed consent, and, second, to take part in a baseline assessment (on the same day, and subject to informed consent having been given). Practice staff were responsible both for taking the informed consent and conducting the baseline assessment.
-
After consent and the baseline assessment, participants in the control arm were able to collect their laxative prescription. Participants in the diet and lifestyle arms were required to make a further appointment for the intervention to be given.
Recruitment protocol, version 3+
-
Potentially eligible patients were identified by practice staff from practice-held records with assistance from the NoReN research nurse [the NoReN research nurse post was created to help practices take part in research; as the research nurse held a substantive NHS contract she was able (with permission from the practice) to help with patient identification]
-
GPs then screened these patients for contraindications and comorbid conditions.
-
Patients meeting the study eligibility criteria were then written to by their practice and were sent the study information sheets.
-
Patients also received a form on which they are asked to provide their contact details if they wish to join the study. Patients were asked to return this form to the study team in a prepaid envelope, i.e. an ‘opt-in’ approach. No reminders were sent to non-responders.
-
When a completed form was received by the study team, they arranged for an appropriately trained person (with an NHS honorary contract and CRB check) to arrange a suitable time and place to take informed consent and conduct the baseline assessment with a patient (as LIFELAX eventually recruited in Scotland and it was not possible to send staff there to take consent and carry out the baseline assessment, this was done over the telephone from protocol V4 onwards)
-
Once informed consent was given and the baseline assessment completed, a copy of the signed consent form was sent to the practice with instruction for them to contact the patient to arrange an appointment for the intervention to begin.
Support for Science funding
One of the barriers to practice participation was the ‘cost’ to practices in terms of staff time and practice resources. Feedback from research active GP colleagues and from the UK Trial Managers Network suggested that if we were able to demonstrate to practices that there would be no financial penalty to taking part in research that they would be more likely to get involved. To address this, an application was made to the Department of Health (DH) to secure funds to reimburse practices for their time spent on LIFELAX activities via the SfS (ad hoc) funding stream. We worked closely with NoReN (as a holder of Budget 1 funding, NoReN was eligible to receive and disburse SfS funding, unlike the majority of PCTs and general practices) during the application process. We agreed with the DH that all activities would be reimbursed at a Nurse, H-grade spine point 13a equivalent, including NI contributions, superannuation and increments. This equated to approximately £20.00/hour. We felt that this was a generous rate and most of the practice staff involved in LIFELAX would not be employed at as high a grade as this. The costing algorithm we agreed with the DH also took into account the hire of practice space, heating/lighting costs, postage costs and the cost of telephone calls during the trial.
We were able to access funding for both service support costs (in respect of practice activity in identifying, recruiting and consenting patients, and completing study assessments and documentation) and excess treatment costs (in respect of the additional time required to deliver the diet and lifestyle interventions). With the change in the recruitment protocol, informed consent and the baseline assessment were undertaken by the research team and the NoReN research nurse and so no reimbursement (in the form of service support costs) was due to practices for time spent on these activities. Practices were, however, asked to identify patients from records and send them a study pack. The rate of reimbursement for this was £7.31/patient. However, due to the way the SfS funding was allocated, this payment was dependent on a patient joining the study. This meant that if practices did write to all eligible patients and none decided to take part in LIFELAX, a claim could not be made. As a goodwill gesture, practices were paid a ‘site set-up’ fee of £50 from the project budget to cover the patient search and mail out, just in case no participants were recruited from a particular practice.
Excess treatment costs could also be reimbursed to practices. However, the DH was exacting on what constituted excess treatment. Only payments for genuine ‘excess treatment’ costs could be made. The DH was of the opinion that for the duration of LIFELAX each participant would be entitled to one appointment at their practice for their constipation and, as such, this appointment was not ‘excess treatment’. It was only trial activities in excess of this appointment that would qualify for reimbursement. As the control arm did not generate ‘excess treatments’ (it was standard care) no claim could be made. For practices randomised into either of the diet and lifestyle intervention arms, claims could be made as there was some excess treatment time for each patient (5 minutes per patient in the ‘standardised arm’ and 85 minutes per patient in the ‘personalised arm’); per-patient claims were agreed with DH at £2.73 and £46.35, respectively. While we recognised that these rates were vastly short of industry trial rates, and LIFELAX could not be considered to be a ‘cash cow’, we were confident that practices would not face any financial penalty by joining our trial.
Importance of research and constipation
One of the major frustrations we encountered when recruiting practices was the perceived lack of importance GPs attached to the research question posed by LIFELAX. We understood that it was most probably practice nurses who would deal with patients with constipation and attempted to target them with our trial literature (see Chapter 6 for a fuller discussion on practice nurses’ interests); however, in most cases it was a GP who would make the final decision about participation and unless they were convinced of the importance of the study there was little chance of the practice participating. Due to the new GMS contract and the QOF, there was less motivation for GPs to sacrifice staff and clinic time for an activity that was not part of the QOF (regardless of the SfS reimbursement). Hitting QOF targets was the priority in most practices.
It was ironic and frustrating that the majority of QOF target conditions (obesity, coronary heart disease, etc.) would benefit from changes in diet and lifestyle and so the training offered by LIFELAX on behaviour change in these areas would have been appropriate to the QOF topics as well as constipation (which was not part of the QOF). It was interesting that a number of the nurses who we worked with on the trial saw the skills they learned were generalisable and could form part of their routine clinical practice.
Patient recruitment
Identifying patients in practice
While it could be argued that LIFELAX had some success with the number of practices initially recruited into the trial (75% of the target) the number of patients from within the recruited practices to join the trial was far short of target. Patient recruitment was difficult right from the point of identification from practice records. What we had envisaged as being a routine first step in the process proved to be a hurdle for a number of practices.
We had commissioned a bespoke ‘electronic query’ that practices could use to help identify eligible patients from their databases. The query was designed to be used on the EMIS practice computer system, widely used in north-east general practices. Not all practices used EMIS. Even in EMIS practices, implementing the query was not always straightforward. The query was designed to be ‘read by’ the practice database, but it soon transpired that not all practices had staff with the IT skills needed to ‘run’ a query of this nature. The electronic query that we had hoped would reduce practice workloads actually proved to be more burdensome.
As all of the systems had search and query facilities with which practice managers and support staff were familiar, most practices preferred to conduct their own searches using their own search techniques. It soon became apparent that there was a great deal of variation between practices on the level of detail recorded on their databases and a lack of consistency in coding diagnoses. Using a diagnosis of ‘functional constipation’ often meant that no eligible patients were identified. Very few practices recorded this information. With this in mind, we asked for the searches to be ‘built up’ using either a diagnosis of functional constipation or three or more laxative prescriptions in the previous 12 months. With the introduction of the QOF we were aware that some practices in one area in particular (area 3) were prioritising (in terms of ensuring accurate and up-to-date coding) the patients and conditions that would form part of the QOF data submission process.
The account thus far may appear to present a very negative picture about the abilities of practices to carry out research. There was indeed a great deal of variability in the time and effort it took for us to recruit, train staff and for them to write out to patients (from 10 days up to 1 year). However, it must be stressed that, despite huge workloads and administrative and bureaucratic demands, those practices that did engage with LIFELAX did so fully and worked tirelessly to support the study.
Recruitment of participants
The first participants were recruited to the LIFELAX trial in July 2005. Poor response to the practice recruitment mail out to patients (as indicated above, only one letter of invitation, with no reminders, was allowed by MREC), and lack of attendance at scheduled baseline assessment clinics were experienced in all active sites recruited in the early days of the trial (using the burdensome V1 protocol). As soon as this became apparent, plans to amend the recruitment protocol began.
Barriers to recruitment of patients
As discussed above, it appears that the number of patients we expected to find and recruit in practices was lower than we had anticipated.
Conversations with nurses, and practice managers highlighted a number of reasons why they thought that people were not participating in the trial. It is interesting that some of the reasons mirror what patients said when they rang the LIFELAX trial team to discuss participation.
Because most of the practices in the trial were from deprived wards, with low socioeconomic status, practices thought that their patients probably would not be interested in research and would probably not read (or be able to comprehend) the information sheets sent to them (despite our efforts to write in a user-friendly and accessible manner). They also expressed concern at the questionnaires and daily diary as being particularly onerous and complex to complete. Based on experience, practice nurses also thought that their patients, in most cases, would not engage with any aspect of behaviour change.
Patients who rang the trial team often reported research as ‘not being for them’. They told us that they were not eligible as they did not have constipation and therefore could not take part. Their evidence for not having constipation was that they were able to ‘go’ every day (even though this required them to take laxatives which, by our definition, meant they had constipation). This perception of ‘not being constipated’ and therefore being ineligible reflects experience in the STOOL trial19 and is therefore a major threat to the ability to recruit prevalent cases. However, as discussed in Chapter 2, the option of opportunistic recruitment of incident cases (new presentations of constipation) was deemed inappropriate from the outset of the trial.
One potential participant went to great length to point out that they ‘knew all there was to know about healthy eating’ and that nothing their nurse could say would be new and therefore participation was ‘rather pointless’.
Due to comorbidity, a higher proportion of patients than that originally estimated by the research team were taking high-dosage codeine-based pain-killers and failed to meet the trial inclusion criteria.
Recruiting the required number of participants
From the 19 practices that recruited participants for LIFELAX, 1473 patients were identified as being eligible (an average of 77 per practice, higher than our anticipated number of 40 per average practice). The final number of patients recruited to the trial was 154, just under 10% of those eligible. In our initial power calculation for the trial we had expected that 75% of eligible patients would consent to be randomised to take part in the trial. Ultimately, the consent rate proved to be nearer to 10%. Using this figure, the size of the recruitment task becomes apparent. In order to recruit 1500 participants, LIFELAX would need to have identified 15,000 eligible patients. Based upon our experience, we would need to have recruited in the region of 200 practices.
Summary and implications
The implementation of the LIFELAX trial appears to have been unsuccessful for several reasons, related both to procedural issues (resulting from changes in ethical review and research governance processes) and to disappointingly low levels of interest and participation at both a practice and a patient level.
It was acknowledged by both the funding body for the trial (HTA) and the TSC that LIFELAX was operating at a time of considerable change and uncertainty around ethical and research governance issues. The process of seeking a favourable opinion from an ethics committee underwent several major changes during the duration of the trial. The initial approach LIFELAX made to MREC used the paper-based MS word form. The application system then underwent several electronic iterations, first using the ‘form filler’ program, and then the online COREC form, the National Research Ethics Service (NRES) form and the Integrated Research Application System.
Ethics committees reacted to a number of landmark documents and events, including the report of the Alder Hey inquiry,198 the European Human Rights Act199 (and its implementation) and preparation for the enactment of the EU Clinical Trials Directive. At this time the guidelines to which ethics committees adhered became more prescriptive, and committees became more risk aware and took measures to mitigate risk where possible. The guidance from COREC, at times, appeared to be inconsistent and inflexible, and anecdotal evidence from meetings with other trial managers at the UK Trial Managers Network annual meeting suggests that the differences between RECs were immense. Although LIFELAX had a good working relationship with its MREC, the process of ethical review was, and continued to be across the study’s lifetime, increasingly bureaucratic.
The publication of the Research Governance Framework200 created further challenges, with guidance and decisions taken at a local level appearing to be, at times, and at least, contradictory to national advice. The need for all members of the core research team deemed to be ‘hands on’ (including those such as the statistician and health economist, who were never expected to interact with practices, their staff or patients, or to have access to patient identifiable data) to undergo a full occupational health check (including, in some instances, throat swabbing) seemed to be time consuming, resource intensive, mildly unpleasant and a somewhat unnecessary procedure. Similarly the securing of honorary contracts was rather challenging. The information at a local level as to which members of the research team required an honorary contract was often contradictory, ranging from any person involved with the running of the trial to only those making visits to Trust premises, handling (identifiable) patient data or meeting patients. Although we welcomed the move by Trusts to implement the Research Governance Framework, the variability in interpretation of it and the lack of resources in some Trusts to implement it created a burdensome, often inefficient and slow process. These experiences are mirrored by others researchers undertaking studies in similar settings at a similar time. 201–203
In addition to the inevitable delays created by these developments, one of the major issues of concern to both the research team and the TSC was the necessity for participants to ‘opt in’ to LIFELAX and the apparent removal of contact with the research team until much later in the research process. This model has major implications for health services research in the future. 204 By implementing such a model, one immediately decreases the likelihood of participation and increases the risk of participation bias. 205 Communication between the trial team and the participant is crucial to the success of a trial. Opportunities for those most familiar with the study design and processes (i.e. the research team) to explain the trial or discuss any aspect of participation diminish once the GP practice becomes the primary contact point for information in the early stages of the trial and the ‘gate-keeper’ to trial participants. While practices in LIFELAX were happy to deal with medical queries arising from participation in the trial, they were reluctant and lacking in confidence to discuss general questions about the study, trial design and general participation, as they felt that this was the remit of the research team. Initial communication with potential participants was by covering letter from the GP, accompanied by the PIS. The information required by COREC/NRES to be included in the PIS is very detailed and complex. Our concern was that the PIS might appear so daunting that potential participants would simply ignore it rather than read it, and would either decide not to participate or would not be fully informed, as required for the consent process. Having successfully used a ‘brief’ and ‘full’ PIS system in another RCT concerning patients with ulcerative colitis,206 the same approach was used in LIFELAX. It was hoped that interested patients would be able to see from the brief PIS the essentials of what the study entailed and then, should they wish to participate, they would read the full PIS prior to giving consent.
The LIFELAX trial also coincided with the introduction of the new GP contract, including the QOF. Practices were heavily involved in setting up the necessary audit and IT systems required to meet the quality targets associated with this contract. As the new contract offered minimal incentives for research, any research activities were viewed by many GPs and their practice staff as a luxury and an unwelcome distraction from the other demands of practice life after the adoption of the new GMS contract.
The feedback that we gathered from both participating and non-participating practices suggests that there was a perception that the cost of taking part in LIFELAX was too great in terms of time, space and practice resources. For some, constipation was not a sufficiently interesting or important topic, a barrier also encountered in the STOOL trial. 19 The barriers to patient participation are less clear. Socioeconomic status may have been a factor – so too might the lack of understanding as to the pragmatic nature of the trial with regard to current and future laxative use. In STOOL, GP participants suggested that their patients would be unwilling to change from their preferred treatment regime, particularly if it were currently being successful. 19 It may be that in LIFELAX there was reluctance from potential participants to give up a strategy that worked for one in favour of another that may not. It may also be the case that constipation is not such an important or interesting topic for patients, as well as GPs and practice nurses, especially for those who are taking laxatives and are not currently constipated, at least by their own definition.
Chapter 5 Results
Following the recommendation of the TSC not to seek a further extension for the LIFELAX trial it was agreed with the funders that patient recruitment should cease, but follow-up should continue for already recruited participants. Due to the low number of patients in the trial, and therefore the lack of statistical power, it was agreed that we would not carry out a formal analysis of effectiveness, as anticipated in the original proposal. More specifically, we agreed that we would not conduct any hypothesis-driven statistical analyses. Rather, we agreed that our analysis of patterns of response to the patient-reported outcome measures would be largely descriptive.
As LIFELAX used a range of data collection tools (some previously validated, but in other populations, and others developed specifically for the trial) it was agreed to be beneficial to collect data on completion rates, item response rates, measures of validity and reliability, and marginal comments (indicative of acceptability and comprehensibility of the tools) to inform future trials that propose to use these tools in similar populations and conditions. This we do below for the self-completion questionnaire at baseline, 3, 6 and 12 months.
As psychometric properties of validity and reliability of existing scales (e.g. PAC-SYM and the PAC-QOL) may vary according to population and setting, we undertook these analyses on the baseline data in the belief that it would contribute to a general understanding of the performance of these measures in our sample and the general body of knowledge regarding the chosen instruments.
Due to the low number of participants it was not possible to conduct the formal comparative analysis of cost-effectiveness originally planned. A lesser level of comparative cost-effectiveness is presented, along with a descriptive analysis of the costs of living with, and managing, constipation.
Baseline characteristics of the LIFELAX participants
Here we report on the baseline data collected via the self-completion questionnaire and the face-to-face interview. Daily diaries were also completed for 6 months from the date of the start of the intervention. Diary data will be reported separately (below) from the two baseline measures. Further reporting on the effects on HRQoL at baseline can be found in the economic evaluation section below.
Baseline postal questionnaire
This questionnaire collected the following data:
Baseline face-to-face questionnaire
This questionnaire collected the following data:
-
general bowel health
-
use of prescription laxatives (length of time taking prescribed laxatives, use in previous 7 days, class of laxative)
-
use of OTC laxatives (length of time taking OTC laxatives, use in previous 7 days, class of laxative)
-
the main thing participants wanted to achieve by taking a laxative
-
participant-defined ‘successfully managed constipation’.
Baseline postal questionnaire
Demographics
The number of participants recruited by a practice ranged from 2 to 24; the average number of participants recruited by a practice was approximately eight. Patients came from 19 practices in 13 different areas. In total, 141 (92%) of the possible 154 self-completion postal questionnaires were returned, although not all data items were completed by all respondents.
Overall, 140 respondents provided details of gender (61 men and 79 women). Dates of birth were completed in 137 of the returned questionnaires. Based on age as calculated from date of birth and date of questionnaire completion, the youngest participant in the study was 51 years old, the oldest was 96 and the average age of participants was 71. On average, male participants were 3.5 years older than female participants. In the personalised arm the average age was 69, in the standardised arm the average age was 72, and in the control arm it was also 72. Of the 139 responses to the question asking about current situation in relation to paid work, 122 participants were retired, three were in full-time work, four in part-time work and two did not work as they were looking after their home and family. Eight participants were unable to work due to long-term sickness or disability.
Of the respondents 11% had remained in education beyond 17 years of age, whereas 44% of participants had no formal qualification. Only one respondent in the sample was not white, listing his/her ethnic group as ‘black’.
PAC-SYM
The PAC-SYM is a 12-item scale measuring stool, rectal and abdominal symptoms. Respondents report the severity of each symptom on a scale from 0 to 4, (with ‘4’ representing the greatest severity). An overall score (PAC-SYM global score) is computed by taking the average item response across the 12 symptoms. The three subscale scores are computed in the same manner, based on the symptom groupings (abdominal – four items; rectal – three items; stool – five items); algorithms for data imputation in the case of missing data mean that subscale scores can be calculated when one or two items in the subscale are missing. The mean scores and standard deviations for the PAC-SYM subscales and global score can be found in Table 11.
| PAC-SYM | n | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|
| Abdominal | 123 | 0.00 | 3.75 | 1.07 | 0.92 |
| Rectal | 119 | 0.00 | 4.00 | 0.74 | 0.92 |
| Stool | 122 | 0.00 | 3.25 | 1.38 | 0.94 |
| Global | 120 | 0.00 | 3.17 | 1.10 | 0.79 |
Figure 9 shows a histogram of the distribution of responses on the PAC-SYM global scale. This provides some evidence that there was a ceiling effect (patients scoring the lowest possible score at baseline, and therefore with no ‘capacity’ to capture improvement over time) in the study population.
FIGURE 9.
Distribution of patient assessment of constipation – symptoms (PAC-SYM) responses.
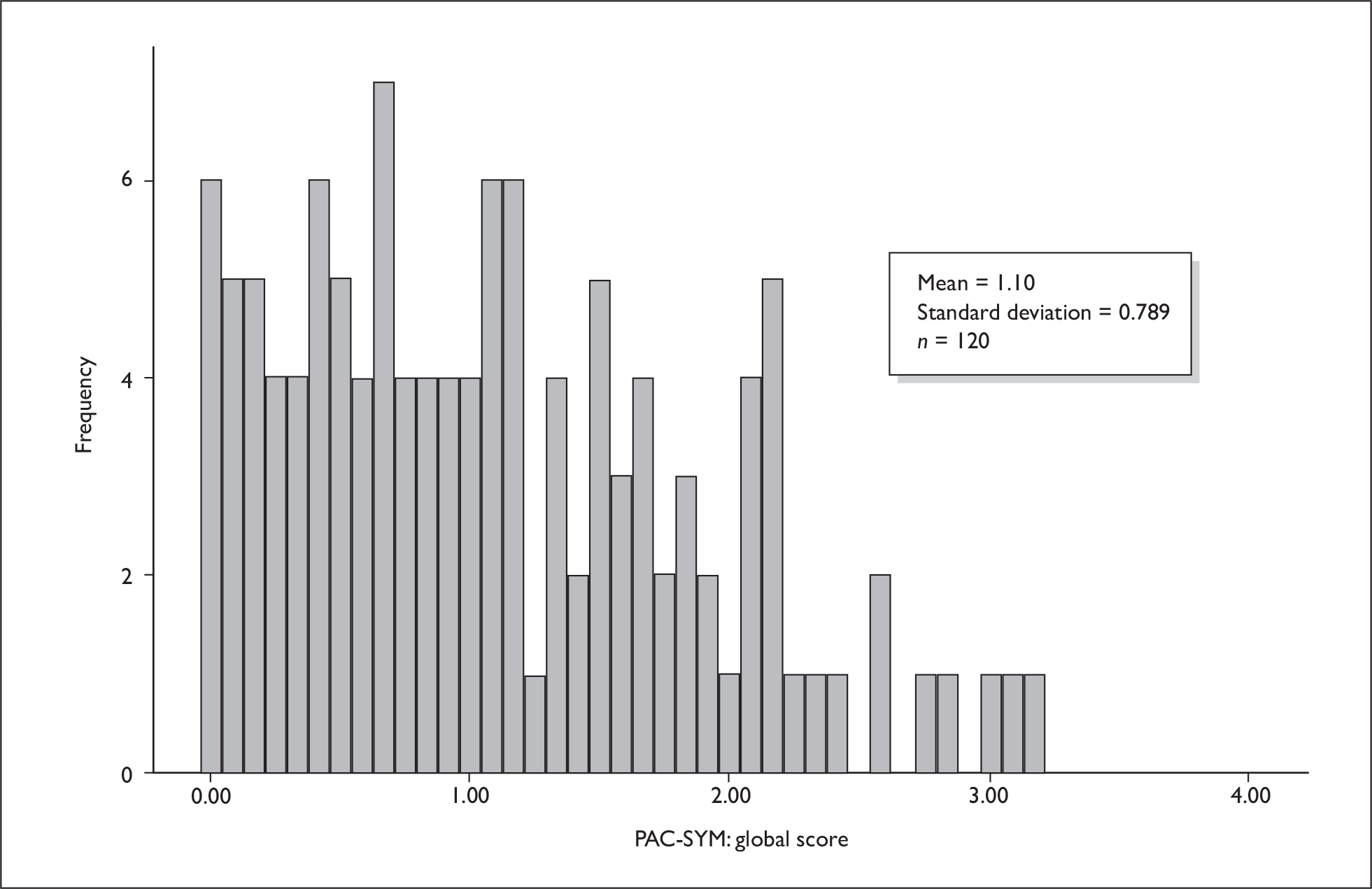
In the development of the PAC-SYM,127 Cronbach’s alpha for the total PAC-SYM score was reported as being 0.98. Subscale Cronbach’s alphas were 0.80 for stool symptoms, 0.84 for abdominal symptoms and 0.87 for rectal symptoms. Our findings were consistent with these figures with Cronbach’s alpha for the global score being 0.91 and the subscale alphas being 0.84 for stool symptoms, 0.87 for abdominal symptoms and 0.81 for rectal symptoms; all of these values exceed the criterion of 0.70, indicative of adequate internal consistency reliability at the group level. 208
The PAC-SYM mean scores suggest that the level of constipation symptoms experienced by our sample was low. This is supported by evidence from the objective measure of bowel movement frequency collected in the daily diary. The mean number of daily bowel movements was 1.5. This again supports the findings of the STOOL report19 that patients did not define themselves as having constipation, once a preferred pattern of bowel movements was established, regardless of whether it took the use of regular laxatives to achieve this.
PAC-QOL
The PAC-QOL questionnaire was developed as a patient-reported outcome measure to evaluate the impact of constipation on QoL over time. 38 In development work, the PAC-QOL scales have been established as being internally consistent (Cronbach’s alpha > 0.80 on each of them). Our findings were consistent with this. Cronbach’s alpha for the 28 items forming the global score was 0.93. For the subscales (dissatisfaction – five items; physical discomfort – four items; psychosocial discomfort – eight items; worries or concerns – 11 items) the Cronbach’s alphas were: dissatisfaction 0.86; physical discomfort 0.89; psychosocial discomfort 0.87; worries or concerns 0.93 – again, all in excess of the threshold level of 0.7 indicative of adequate internal consistency at the group level. 208
The correlations of the PAC-SYM and the PAC-QOL global scores at baseline were in line with what we would expect, with there being a greater impact upon QoL with increased symptoms (r = 0.76, p < 0.01).
The box plot shown in Figure 10 offers some suggestion that the groups were not evenly balanced with respect to constipation-related QoL at baseline.
FIGURE 10.
Box plot of the PAC-QOL overall scores.
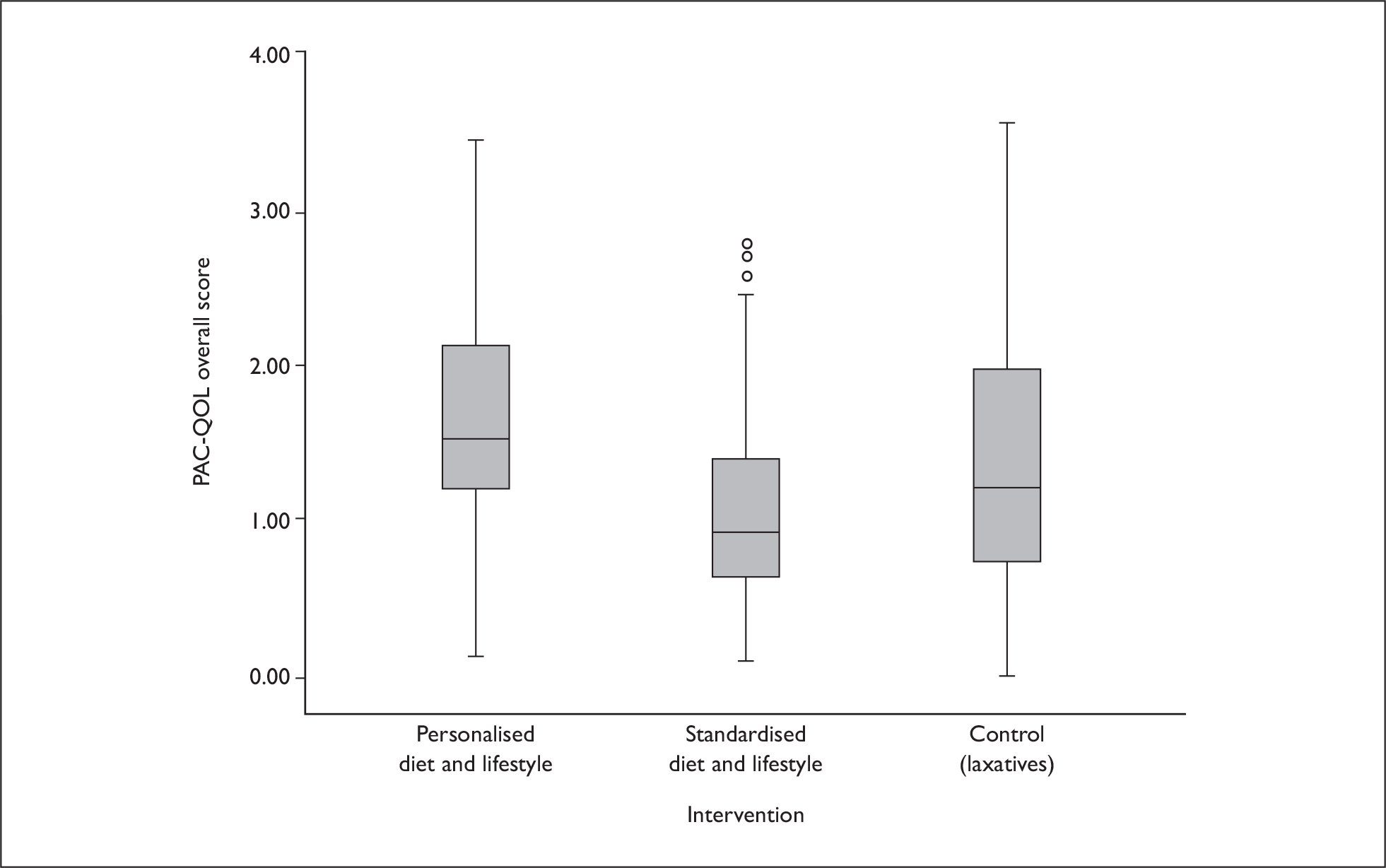
Longstanding disability and mobility
Overall, 73% of respondents reported having a longstanding disability or infirmity. The distribution across the intervention arms was not even, with 84% of respondents in the personalised intervention arm and 71% in the standardised intervention arm reporting this. In the control arm it was 67%. In total, 86% of respondents reported that their disability or infirmity limited their activities. As, due to small numbers of patients, we are not able to analyse formally the effectiveness of the intervention strategies, this baseline imbalance is not such an issue. However, any intervention that requires people to make changes to their lifestyle in terms of being more mobile and active would need to consider the level of disability or infirmity in its population.
None of our sample reported that they were either bedbound or chairbound at baseline. However, the groups were not well balanced in terms of the assistance they needed in order to carry out an activity such as getting up from their chair or bed and crossing the room: 76% of the control group reported they could do this without any assistance, whereas only 42% of the personalised intervention group and 63% of the standardised intervention group did not require assistance.
In terms of being able to undertake any vigorous activities, 59% reported that they would be unable to undertake these and 36% that they could but with difficulty. Again there was an imbalance in the groups with 74% of the personalised group reporting that they were unable to undertake any vigorous activity as opposed to 46% in the control group and 59% in the standardised group.
This finding that the control group was somewhat ‘fitter’ than the other intervention arms was consistent in all of the other questions that covered functions, such as bathing and dressing self, walking 100 yards and walking half a mile. As stated earlier, although not relevant to the analyses reported here, it may have had an impact on the intervention as not all arms were the same.
Diet
The data on the food and drink that we collected at baseline were intended to be used to explore changes in consumption over time, as each participant took part in the trial. As we are not able to provide such analyses, here we describe the baseline dietary data.
We collected data on the amount of bread (number of slices/rolls) consumed each day. Due to the range of bread types and their fibre content levels, and the contents of the other elements of each participant’s diet, it is difficult to fully assess the impact of bread consumption on bowel health and function. Nonetheless, it is possible to express some generalities. White bread is lower in fibre than a granary or wholemeal alternative. In our sample 47% did not consume any white bread at baseline; 44% ate at least one slice of wholemeal bread per day, but 55% reported that they did not eat any wholemeal bread. It is difficult to say whether these figures have a significant role to play in the bowel function of our sample, but it does suggest that there were a significant number of people who could have made a switch from white to granary or wholemeal bread and, depending on the remainder of their diet, this might have had an impact on their bowels.
With regard to breakfast cereal, we collected data on the frequency that different types of cereal were consumed. Sugary cereals tend to be lower in fibre than porridge/wheat/muesli or bran-type cereal. In our sample only 8% reported eating sugary breakfast cereals daily with > 70% never eating this type. Forty-two per cent of the respondents ate porridge/wheat/muesli cereal daily and a further 16% ate a bran type cereal daily. This would suggest that, in terms of the breakfast cereal of choice in our sample, those cereals that can benefit bowel health were being most frequently consumed. The scope for dietary improvement in this respect may therefore have been quite limited.
Approximately 41% of respondents said that they ate more than one serving of rice or pasta per week. Again we know little about the impact of this on bowel function; however, it does suggest that rice and pasta were not ‘alien’ foods to this population and that as wholemeal/brown varieties are available they could be incorporated into the diet without radical changes to current eating patterns.
Potatoes were eaten more frequently than rice and pasta, with 28% of the sample reporting that they had at least one serving of potatoes each day. We do not know from our data whether the skins of the potatoes were eaten too, so can draw no firm conclusion as to the fibre contribution potatoes made to the diet.
Vegetables were eaten by most people on most days with only 5% reporting eating less than one serving of vegetables per week. Pea and bean/lentil consumption were recorded as separate categories to ‘vegetables’. Approximately 70% of respondents reported eating at least one serving of peas per week and 54% reported eating at least one serving of beans/lentils a week.
Only six respondents (4%) said that they ate less than one serving of fruit in an average week. We were aware that eating fruit and vegetables is often difficult for older adults with dental issues; however, it would appear that the majority of respondents could eat these types of food and potentially increase consumption to the recommended five portions of fruit and vegetables per day.
Using the fibre calculator from the DINE questionnaire,139 upon which the fibre items in the baseline questionnaire were based gives us insight into the amount of fibre our sample was consuming at baseline. (Although the DINE was designed to be used in a consultation setting we found it to be an effective method for capturing data on the amount of fibre consumed, as it referred to ‘servings’ of particular food rather than requiring respondents to carry out any measuring or weighing prior to reporting.) The average score was 34, which falls into the ‘moderate’ consumption category. This does suggest that while fibre consumption was not low in our population, there was potential to increase consumption to the ‘high’ category recommended by the DINE authors.
With regard to fluid consumption, 85% of our sample reported that they drank less than the recommended eight glasses of water a day. This finding in itself is not unsurprising as we do know that the urge to drink decreases with age and often there is a worry that drinking more leads to more frequent visits to the toilet which can be inconvenient to people with mobility problems. However, hot drinks such as tea and coffee were consumed very frequently and although water may not be consumed to the level recommended, it appears that with the levels of consumption of fruit and vegetable juice, hot drinks and soft drinks (sugared and sugar free) the amount of fluid consumed is in keeping with the guidelines.
While we acknowledge that the baseline data may not tell us exact quantities of which foods make up the daily diet of our sample, they do provide a guide to the intake of our sample. It would seem that there were a number of areas in which changes to diet could be made and this may have an impact upon bowel health.
Satisfaction with prescription of laxatives
Evidence from the STOOL trial19 suggests that once someone has found a laxative regime that works satisfactorily then they would prefer to remain on it and not embark upon a new regime. When designing the LIFELAX intervention we were able to take this into account and rather than requiring people to give up on their laxatives (prescription or OTC) we made a decision to allow people to continue taking laxatives. We had hoped that, for those embarking on any diet and lifestyle changes, over time their reliance on laxatives would lessen as the changes began to improve bowel function.
From our sample, 60% of respondents indicated that they were satisfied with the ability of their prescription laxatives to treat or prevent constipation; 53% were satisfied with the way in which the prescribed laxatives relieved the symptoms of constipation; and 55% of respondents were satisfied with the amount of time it took for the prescription laxatives to start to work.
A total of 68% from our sample reported that they did not experience any side effects from taking their prescribed laxatives. Only 3% reported that they had any difficulty taking the laxative, as prescribed by their GP, in its prescribed form, and only 9% reported that they had any level of difficulty planning when to use their prescribed laxatives; 80% of the respondents said that it was convenient to take their laxatives as prescribed and only 9% felt that taking their laxatives was not a good thing; 70% of our sample reported that, taking everything into account, they were satisfied (satisfied, very satisfied or extremely satisfied) with their prescription laxatives. All of these data suggest that there was little reason or incentive for our population to give up their prescribed laxatives, a finding that is entirely in keeping with the findings in the STOOL report. 19
PAC-SYM, PAC-QOL and anxiety/depression
Studies investigating the link between psychological illness and disturbed defecation suggest that people with anxiety and depression often have bowel symptoms, with depression being positively associated with constipation209 and anxiety with increased bowel frequency. 210
On the HADS, each item is marked on a four-point (0–3) response category. Scores can range from 0 to 21 for anxiety and 0 to 21 for depression. These scales are independent. A score of 0–7 for either subscale could be regarded as being in the normal range, with a score of ≥ 11 indicating the probable presence of disorder and a score of 8–10 being just suggestive of the presence of anxiety and/or depression.
In our sample the mean scores on the HADS show there was no evidence of anxiety or depression either in the group as a whole or arm by arm (Table 12).
| Intervention arm | HADS | ||
|---|---|---|---|
| Anxiety | Depression | ||
| Personalised | Mean | 1.10 | 0.97 |
| n | 31 | 31 | |
| SD | 0.65 | 0.53 | |
| Standardised | Mean | 0.77 | 0.69 |
| n | 65 | 63 | |
| SD | 0.63 | 0.43 | |
| Control | Mean | 0.88 | 0.71 |
| n | 44 | 44 | |
| SD | 0.65 | 0.36 | |
| Total | Mean | 0.88 | 0.76 |
| n | 140 | 140 | |
| SD | 0.65 | 0.44 | |
Although there was no evidence of even ‘probable’ anxiety or depression in our sample, there was evidence that these scales did correlate with the global scales of the PAC-SYM and PAC-QOL (Table 13), providing further evidence of the construct validity of those measures. As stated earlier, the mean PAC-SYM and PAC-QOL scores suggest that although our sample did not experience extreme symptoms, as symptom scores rose so too did the impact upon QoL. These findings are entirely consistent with the view that people who experience greater symptoms of constipation experience both higher levels of depression and impact upon their QoL. Previous research210 indicates that anxiety is linked to increased gut transit time. Our results are at odds with this finding as our anxiety scores were also positively correlated with constipation symptoms. As our population’s mean anxiety score was not clinically significant, it would be both naive and erroneous to expect evidence of increased gut transit time in this case. It is understandable that people experiencing constipation may feel more anxious and perhaps this is one way to account for our findings.
| HADS | |||
|---|---|---|---|
| Anxiety | Depression | ||
| PAC-SYM: global score | Pearson correlation | 0.306 | 0.237 |
| n | 120 | 120 | |
| PAC-QOL: global score | Pearson correlation | 0.553 | 0.381 |
| n | 135 | 135 | |
Baseline face-to-face questionnaire
General bowel health
We began our face-to-face interviews with a very broad open question ‘Thinking back over the last month or so, how have your bowels been in general?’. On the advice of the clinicians attached to the study, a question such as this served a very important role. While it focused the interview on bowel health rather than general health, it also allowed interviewees to talk about themselves. There was a concern that often people did not have an avenue to talk about their bowels and a question such as this would be a welcome opportunity to talk about any aspect of their bowel health before moving to the more specific structured items. This was not designed to be an analysed question.
Over 45% of our sample had at least one bowel movement per day during the 7 days prior to interview. As normal frequency of bowel movement ranges from at least three in the previous 7 days, it is worthy of note that only 7% reported fewer than this number of motions per week. Over one-third of our sample passed a stool without straining in the 7 days prior to their assessment. However, two-thirds did strain and nearly 20% reported straining either on most days or daily.
In total, 36% of participants reported the absence of hard or lumpy stools, but about one-third of the sample experienced at least one or two per week; 88% of respondents experienced a feeling of incomplete emptying of their bowels, and half of them said that they felt that at least on one occasion in the previous 7 days when they were answering the call to stool, the stool could not be passed; and 30% of people had needed to press around their bottom to assist with the passing of a stool on at least one occasion in the week before interview.
Use of prescription laxatives
In our sample, over 30% of respondents had been taking a prescription laxative for 10 years or longer, and 90% had been taking a prescription laxative for more than a year. A breakdown of the duration for which respondents had been taking laxatives can be seen in Figure 11.
FIGURE 11.
Number of years taking prescribed laxatives.
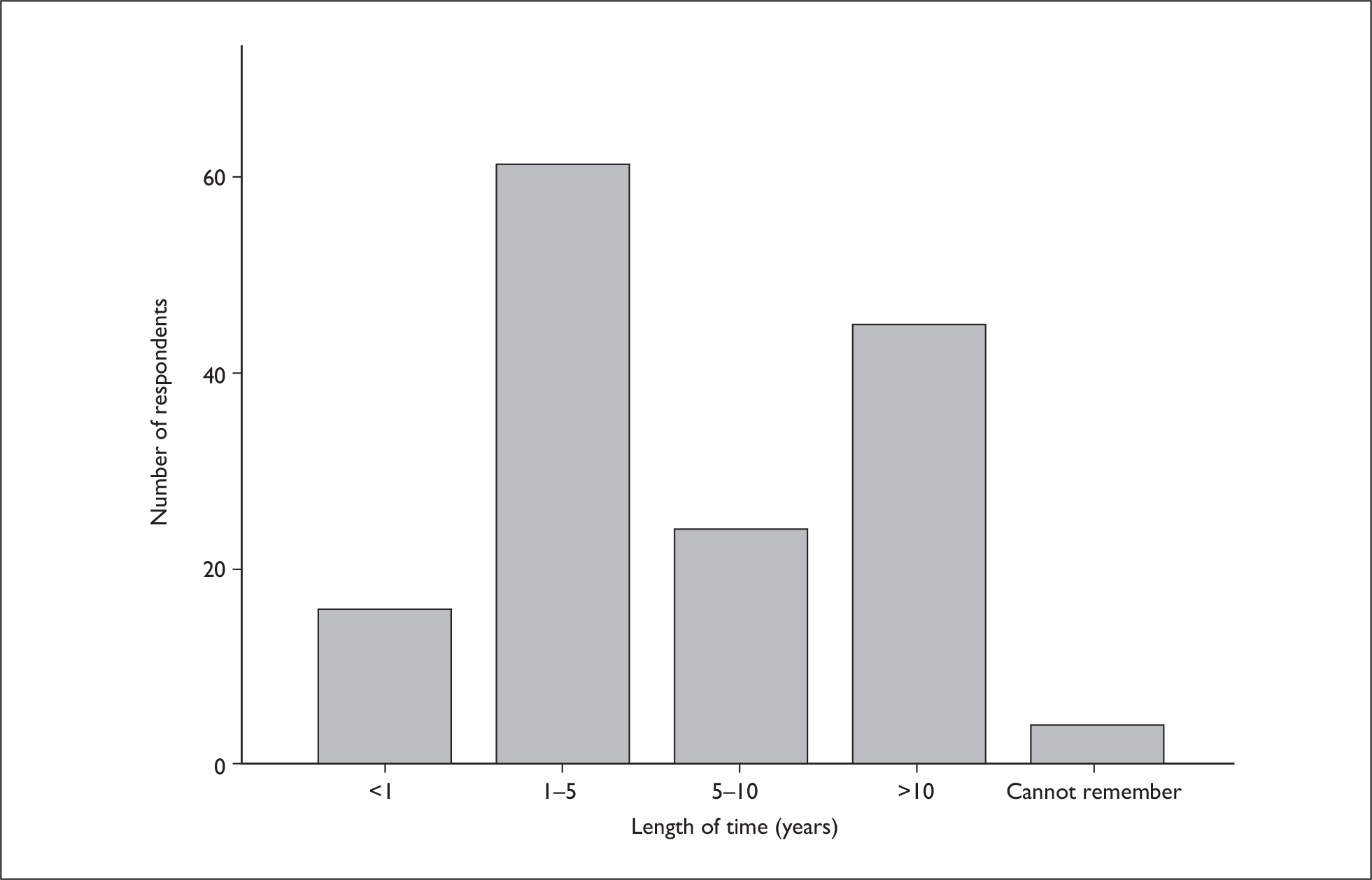
Nearly 90% of our participants had used a prescription laxative in the previous 7 days, with in excess of 41% of them being prescribed a stimulant laxative by their GP; 30% had been prescribed a second laxative and 5% of our sample was prescribed a third.
Half of the respondents had never taken an OTC laxative and approximately 15% had been taking them for 10 years or more.
Main thing participants wanted to achieve by taking laxatives
This was an open-ended question. The responses were varied, including references to an end to the feeling of lethargy associated with constipation and a belief that if the bowels were not completely emptied they could make you ill. The most common achievements that participants wished from their laxatives were ‘ease’ of stool; soft consistency for their stools; frequency and regularity in their visits to the toilet. As only 7% of our sample fell outside the ‘normal’ frequency for bowel movements, it suggests that the laxative regimes in our sample were working in terms of frequency and approximately one-third of our sample were achieving the wish not to strain at stool.
Participant-defined ‘successfully managed constipation’
The results of this question broadly reiterated what people wanted to achieve by taking a laxative, i.e. successfully managed constipation would mean ease, frequency, regularity and soft consistency of stools. However, only 10% of respondents to this question said that successfully managed constipation would mean ‘without the use of laxatives’. This finding again reiterates belief that managing constipation without a laxative is not a priority for many people.
Postal questionnaire follow-up response rates
The self-completion questionnaire was sent at three time points (3, 6 and 12 months). At 3 months the response rate was 80%; at both 6 and 12 months it was 85%. This suggests that, despite length of the questionnaire, the time taken to complete it and the added burden of the daily diary at the first two time points, respondent fatigue was not an issue.
Daily diary
The daily diary that we used in LIFELAX had been developed during the qualitative study that accompanied the set-up of the STOOL Trial. 19 The diary method was chosen in a bid to minimise recall bias. Data on bowel habits and symptoms based on the Rome II criteria122 were gathered in a structured way (tick box format), completed daily and returned each month for 6 months. In addition to these data, the diary collected information on adverse events, relapse rates, use of laxatives, costs of food purchased or activities undertaken as part of any diet or lifestyle changes made; and any out-of-pocket expenses associated with constipation and its management.
Although previous experiences of diaries in studies with older people suggested that 90% of diaries would be returned completed,132,133 we could find no evidence that a diary such as this had been used to collect data on bowel function/health and associated costs on a daily basis for such a length of time.
The greatest number of diaries was returned in round one, and the response rate was approximately 73%. In subsequent rounds there was a slight decrease in response rates (Table 14). The overall response rate to the diaries was 64%.
| Diary number | Number returned | Response ratea (%) |
|---|---|---|
| 1 | 112 | 73 |
| 2 | 109 | 70 |
| 3 | 103 | 66 |
| 4 | 93 | 60 |
| 5 | 90 | 58 |
| 6 | 84 | 55 |
| Total | 591 | 64 |
While these response rates were not of the magnitude of those in the previous studies cited above, we would not go as far as to say that as a data collection tool a daily diary of this sort for this population was inappropriate.
Anecdotal evidence from telephone conversations with participants suggests that there was sometimes a concern that they were just saying the same thing every day, or that nothing had changed, so there was nothing new to report and therefore a perception that it was not necessary to fill in the diary and send it back. Cognisant of this, we would recommend that any researchers contemplating using such a tool consider clearer instructions to participants regarding the importance of completing the diary even when they think that they have nothing of interest to report, and perhaps make use of regular reminders to encourage completion and return.
We also know from telephone calls to the LIFELAX office that some participants found the diary burdensome to complete. Given its physical size, the sensitivity of the subject area (a few respondents remarked that the diary was not something they wished to have on public view, so kept it in the bathroom or toilet), and the duration of the task, this sentiment was not entirely unexpected. As highlighted in the CONSORT diagram (see Chapter 4, Figure 7) we encountered a complex withdrawal pattern, with a number of participants partially withdrawing and selecting which assessment tools they would continue to complete. We had several participants electing to continue to receive the postal questionnaires and/or telephone interviews but not the diary.
Item response rates
Analyses of the item response rates suggest that the daily diary contents were not troublesome to participants.
Each day participants were asked to record the number of bowel movements during that day. This question was fully answered (i.e. a response on every day in the diary) in over 88% of diaries. In the remainder it was partially answered (i.e. a response was recorded, but not on every day). This suggests that the diary may be a useful way of collecting such data.
The items taken from the Rome II criteria (straining, hard/lumpy stool, incomplete evacuation, stool not passed and digital evacuation) were completed in full on 97% of occasions.
The item response completion rate was of a similarly high percentage for the items dealing with taking medication for constipation prescribed by the GP, bought OTC or any other measures taken to relieve constipation.
These data would suggest that the individual items within the diary used to collect information about bowel function and medication were not burdensome to complete, and that a diary is a satisfactory way of gathering them. However, the duration over which the diaries needed to be kept and the daily repetition may have led some participants to withdrawing from this aspect of the study.
Table 15 reports the estimated effects on our primary outcome measure (patient-reported QoL); however, we must stress that we feel that the interval estimates are too wide to be of very much use. In reporting them, if so desired, they can be entered into a meta-analysis. We do not believe the data collected would merit further analysis, but they will be banked. Should any future meta-analysis be undertaken we will share then with the investigator and they can decide whether to include them.
| Time (months) | Comparison of intervention | |||
|---|---|---|---|---|
| Personalised vs control | Standardised vs control | |||
| Mean | 95% CI | Mean | 95% CI | |
| PAC-QOL overall scorea | ||||
| 3 | 0.08 | –0.19 to 0.36 | 0.14 | –0.09 to 0.37 |
| 6 | –0.11 | –0.41 to 0.20 | 0.04 | –0.19 to 0.27 |
| 12 | –0.09 | –0.38 to 0.21 | –0.04 | –0.32 to 0.23 |
| PAC-SYM global scoreb | ||||
| 3 | 0.10 | –0.25 to 0.45 | –0.00 | –0.25 to 0.24 |
| 6 | –0.27 | –0.72 to 0.18 | –0.17 | –0.50 to 0.17 |
| 12 | –0.08 | –0.47 to 0.30 | 0.18 | –0.20 to 0.56 |
Economic evaluation
Resource usage and costs
Information was collected about visits to a general practice, visits to hospital and telephone consultations between the start of the intervention, and at 3 months post intervention. The total resource use across each arm is shown in Table 16.
| Arm | Control | Personalised | Standard |
|---|---|---|---|
| GP visit | 26 out of 27 | 12 out of 13 | 40 out of 42 |
| Outpatient | 2 out of 27 | 0 out of 13 | 1 out of 42 |
| Telephone GP | 0 out of 27 | 1 out of 13 | 2 out of 42 |
| Telehone practice nurse | 0 out of 27 | 1 out of 13 | 2 out of 42 |
The main comparison of interest was between the control arm and the two intervention arms, so common costs were ignored as they do not affect the choice between interventions. 211 Information collected on the use of health-care resources was strictly in connection with the condition being studied. Table 17 shows the unit cost data that were used to calculate results in Table 19.
| Item | Cost 2007–8 (£) | Source |
|---|---|---|
| Outpatient hospital visit | 193 | 2007–8 payment by result tariff for an outpatient gastroenterology, first visit (£95 if second visits)a |
| General practice visit | 34 | £31, 2006–7 PSSRU,b 3.5% inflator per annum |
| Telephone consultation: practice nurse | 9 | £8, 2006–7. PSSRU,b 3.5% inflator per annum |
| Telephone consultation: GP | 21 | £24, 2006–7. PSSRU,b 3.5% inflator per annum |
The mean per-case recorded costs for the intervention and control arms over 3 months were similar, and are shown in Table 18.
| Arm | Mean costs (£) |
|---|---|
| Control | 47.04 |
| Personalised | 33.69 |
| Standardised | 38.40 |
The amount of data collected about resource use was sparse due to the low number of respondents. In the 3 months of follow-up, there were two hospital visits for the control group, one telephone consultation with a GP, and one with a practice nurse for the personalised arm; and one hospital visit, one telephone consultation with a GP and one with a practice nurse for the standardised arm.
Table 19 shows that differences were found for the personalised arm in hospital visits and telephone consultations. For the standardised arm these differences were also found. These differences are based on resource use of a small numbers of cases in each arm and care should be taken if using these findings for predicting changes in service use.
| Arm | Difference (%) | |
|---|---|---|
| Hospital visits | Telephone consultations: GP and practice nurse | |
| Personalised | –0.074 | 0.077 |
| Standardised | –0.050 | 0.071 |
Across both intervention arms there had been a relative reduction in hospital visits at 3 months and a relative increase in the use of telephone consultations. For the personalised arm there was a 7.4% decrease in hospital visits and there was a 5% decrease for the standardised arm. For telephone consultations the personalised arm is associated with a 7.7% increase, compared to the control group, and the standardised arm is associated with a 7.1% increase. Table 20 shows that these differences translate to a small reduction in hospital costs for the intervention arms compared to the control arm and a smaller increase in telephone consultation costs.
| Mean difference (£) | |
|---|---|
| Personalised | |
| GP visit | 1.36 |
| Outpatient | 14.30 |
| Telephone GP | (1.62) |
| Telephone practice nurse | (0.69) |
| Total | 13.34 |
| Standardised | |
| GP visit | 0.36 |
| Outpatient | 9.70 |
| Telephone GP | (1.00) |
| Telephone practice nurse | (0.43) |
| Total | 8.63 |
The estimated savings in NHS costs are £13.34 for the personalised arm and £8.63 for the standardised arm.
Patient costs
Ideally, the above would be supplemented by costs incurred by patients while accessing NHS care. However, the participants supplied insufficient information for these to be computed.
Summary
In describing the participants in LIFELAX we are confident that the mean PAC-SYM and PAC-QOL scores at baseline suggest that our sample did not experience extreme symptoms or impact upon QoL. The mean scores on the HADS show there was no evidence of anxiety or depression either in the group as a whole or arm by arm.
Only a very small minority (7%) of participants fell outside the range for normal frequency of bowel movement. However, this frequency was not necessarily satisfactory to our participants.
In our sample over 30% of respondents had been taking a prescription laxative for 10 years or longer and 15% of the respondents had taken an OTC laxative for 10 years or more. This reinforces the chronic nature of the condition.
Item response rates suggest that the items within the diary used to collect information about bowel function and medication were not burdensome to complete and that a diary is a satisfactory way of gathering them. However, the number of diaries and the daily repetition may have led some participants to withdrawing from this aspect of the study.
Due to the quality and quantity of data collected we are reluctant to draw any firm conclusions as to the effectiveness of the intervention.
Regarding the economic evaluation, the recorded related health-care costs show a cost saving of £13.34 (£47.04 – £33.69) for those in the personalised arm compared with the control arm, and a smaller saving of £8.63 (£47.04 – £38.40) for the standardised arm. These savings occurred because of reduced hospital costs, offset by a smaller increase in costs incurred through additional telephone consultations. As there was no significant change measured in utility, cost minimisation would suggest that the personalised arm would be the preferred course, as it produced the greatest cost savings. This finding is qualified by the fact that the reduction in health-care costs was due to a relative small number of cases in a relatively small sample.
Effects on HRQoL
Baseline characteristics
Health-related quality-of-life data were collected from the trial participants at baseline (before the commencement of the arm appropriate intervention) and at 3 months (primary end point). HRQoL was measured using the EQ-5D,212 with 89 participants providing data at both time points. The EQ-5D is designed to be administered in the form of a self-completed questionnaire. Respondents are asked to define their own health state in terms of the five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) and their level (no problems, some/moderate problems/extreme problems) for each of the dimensions by ticking which statement applies for each dimension (see Appendix 4). EQ-5D is used to determine a utility value between 0 and 1, with ‘0’ representing death and ‘1’ perfect health.
The mean utility,213 at baseline, of the personalised intervention arm was lower than that of the control arm, as shown in Table 21.
| Arm | Mean utility | SD | n |
|---|---|---|---|
| Control | 0.714 | 0.231 | 29 |
| Personalised | 0.536 | 0.307 | 16 |
| Standardised | 0.711 | 0.269 | 44 |
Within-arm differences
Table 22, shows that all arms experienced a reduction over the a 3-month period. The largest reduction in utility scores was experienced by the control arm, the smallest reduction by the personalised arm.
| Arm | Baseline | 3 months | n | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Control | 0.714 | 0.232 | 0.680 | 0.305 | 29 |
| Personalised | 0.536 | 0.307 | 0.523 | 0.300 | 16 |
| Standardised | 0.711 | 0.268 | 0.686 | 0.288 | 44 |
Between-arm differences
Table 23 shows the change in mean utility of each of the treatment arms compared with the change in the control arm. The effect of both the personalised and standardised intervention arms was to relatively increase the utility or lessen the absolute reduction; the standardised arm having the greater effect and experiencing the smallest reduction in utility.
| Arm | Difference in mean | Variance pooled |
|---|---|---|
| Personalised | 0.02 | 0.04 |
| Standardised | 0.01 | 0.04 |
Summary
All of the trial arms experienced a reduction in utility, as measured by EQ-5D.
Chapter 6 Results: the process evaluation
Introduction
Within the LIFELAX trial the process evaluation provided a unique opportunity to investigate the stages of development and implementation of an RCT in ‘real time’ as events occurred. We observed that the trial team’s activities centred on two key ‘technologies’. The first was the development of the RCT itself, which – in common with other forms of research – required the investment of expertise, finance, clinical and bureaucratic support, and the sustained collaboration of a number of contributors. The second technology at stake was the development of training packages and materials for the diet and lifestyle interventions, and subsequent deployment of this training by the trial team, in particular the research dietitian and nutritionist, to an audience of practice nurses. The research dietitian and nutritionist delivered the training packages with the intention that the nurses would later deploy target skills and materials with patients in the practice. An important observation was that the underlying factors that supported each technology differed, such that while the trial team were able to overcome a number of barriers to the deployment of the RCT, many of the factors influencing the nurses’ reception of the training packages were beyond the trial team’s control.
In the first section of the chapter we discuss the key barriers that taxed the implementation of the RCT, and the trial team’s efforts to implement the trial in primary care practices. At the time of LIFELAX, the organisations on which the trial depended were in a stage of transition with regard to their interpretation of Research Management and Governance (RM&G) guidelines. Consequently, there was some ambiguity across these organisations about how the RM&G guidelines should be implemented and this had a number of effects on the trial team’s capacity to deploy the trial. In particular, the trial team received different instructions across PCTs regarding how the trial should be implemented. In most cases practices contemplating involvement in the trial were faced with the prospect of additional work on behalf of the trial team. In this regard, the LIFELAX RCT – in common with almost all forms of research – did not offer an immediate advantage to primary care practices. Indeed, quite the reverse was true. In this context, the trial team worked hard to find innovative solutions to potential barriers and reduce the amount of work required of NHS staff, while maximising the attractiveness of the research topic and experimental interventions. These issues, and the approach adopted by the trial team, have been described in more detail in Chapter 4, specifically with regard to assessing strategies against those proposed in the STEPS report,193 and other literature. 194 We draw primarily on interview data to describe the ‘technology of the RCT’, as transcripts of the trial team meetings provide a less concise and at times less explicit account of key issues. (In LIFELAX trial team meetings, many problems associated with RM&G guidelines or MREC decisions emerged over successive meetings. The trial team shared some understanding of the history of RM&G guidelines and MREC stipulations, and therefore the contexts underpinning particular problems were not always made explicit. In interviews, however, these issues were articulated overtly and unambiguously by the interviewees as they attempted to inform the ethnographer.)
In the latter half of the chapter we describe the ‘second technology’ of LIFELAX, namely the development and deployment of training packages for practice nurses. In the first instance, the trial team developed a training package in BCC techniques, and the production of diet and lifestyle materials (information sheets, a video and behaviour change manual). The second activity was the delivery of BCC training by the research dietitian and nutritionist to nurses in the BCC arm of the trial. The intention of the trial team was that the nurses receiving training in BCC would then deploy these skills with recruited participants in their own practice. Due to the pragmatic design of the trial, the interactions between the nurses and participants were unobserved by the trial team. In this chapter, we describe the perceived utility and reported use of the BCC materials and training through the accounts of practice nurses, GPs and practice managers enrolled in the trial. The reports from primary care staff suggested that the topic of the trial was not seen as a clinical priority when considered alongside targets identified in the GMS contract, and that diet and lifestyle approaches were informally considered part of the current skill set and training of practice nurses. In attempting to find meaning in the trial’s interventions, the practice nurses suggested that community nurses might benefit from the BCC techniques, as these staff were viewed as being more likely to work with patients suffering chronic constipation. Finally, we report how the interventions were perceived by participants through their interactions with enrolled nurses.
Technology of the RCT: bureaucratic work and the organisation of resources
The specific difficulties encountered by the trial team in meeting the requirements of the MREC and local governance bodies have been reported earlier in this report (primarily in Chapter 4). Consequently, we do not reiterate them in detail here. Nevertheless, we describe the overarching structural constraints that consumed much of the trial teams’ resources through the course of the research, and the key role of social networking in surmounting these barriers.
The LIFELAX RCT was set in primary care, where a number of organisations shaped the possibilities of the research. In particular, the trial protocol was required to be flexible enough to meet the requirements of various sites (general practices) and governing bodies (PCTs, the MREC, LRECs), while maintaining the scientific rigour of the RCT. In the opening phases of the RCT, the trial team’s activities were focused on the identification of relevant stakeholders, meeting the requests of regulatory bodies, negotiating the cooperation of organisational networks, procuring resources from these networks, and arranging access and integration in busy clinical environments. The sequence of work followed a trajectory set out by the RM&G framework for clinical trials in the UK. 214 However, some of these milestones proved to be difficult for the trial team to reach in practice. In particular, at the time of the trial, RM&G guidelines were under a process of continuous development, with a number of official documents being issued throughout the life of the trial and changes in policy, expectations and practice emerging over this period. This climate contributed to localised and sometimes stringent interpretation of the RM&G guidelines by different governance bodies. Consequently, both the LIFELAX and STOOL trial teams struggled to fit the design and conduct of their respective RCTs to RM&G requests across PCT sites. 19 As demonstrated by a growing number of reports in the literature (e.g. Wald215), the LIFELAX and STOOL trial teams were not alone in experiencing these difficulties. During the initial implementation of the LIFELAX RCT, the trial team encountered substantial difficulties in their attempt to meet the requirements of their MREC, and in particular, its request for SSAs. If the trial team had attempted to obtain SSAs at the level of individual general practice sites, recruitment may have been severely hampered. However, the trial team negotiated a workable solution by naming the head of a local PCRN as PI for the region. 216 SSAs for all practices within the domain of the research network were then obtained through the credentials of this one key individual. Although this strategy was effective in speeding administration for the trial and improving the possibility of successful practice recruitment, it required ad hoc problem-solving and negotiation on the part of the trial team. Responding to an article published in the British Medical Journal215 decrying the bureaucratic, seemingly obstructive process of seeking MREC/COREC approval, the trial manager explained how this strategy was developed for LIFELAX:216 ‘A casual remark from an LREC secretary, during another telephone conversation, about two or more sites “working together” opened up another possibility. I could try and find out whether practices would collaborate and therefore have one PI assuming responsibility for more than one site’.
The solution for the trial team was thus organised through informal networking and circumstantial conversation. Moreover, within the MREC there appeared – through access to several e-mails – to be a lack of agreement regarding what constituted ‘high risk’ to patients, and how workable solutions should be arranged, and a cautious approach was specified. In the execution of the LIFELAX trial, issues surrounding the interpretation of ethics and research governance placed a great deal of pressure on the trial team to continually develop creative and workable solutions. However, it is unclear to what extent these issues stemmed from the unsettled climate at the time of the LIFELAX trial, and what were more generic issues. Unfortunately, in the process evaluation we did not interview or otherwise investigate the perspective of the MREC or other governance bodies. Therefore, our report is based on the observed and reported experiences of the trial team, practice staff and participating patients.
The progression of the LIFELAX trial depended on cooperation between the trial team and key individuals from a number of external organisations. To facilitate the allocation of resources and other administrative tasks, the trial manager actively pursued external contacts and developed working relationships through a sequence of telephone calls, written communication, site visits and social gatherings, some of which occurred in ‘out of hours’ time. In this regard the trial relied heavily upon the social networks constructed and maintained by the trial manager to achieve various milestones. Social aptitude was a vital component of the trial manager’s repertoire, especially when teamed with skills more overtly recognised as desirable in the research context: such as those based on organisation, procedure and methodological rigour. Box 1 presents an abbreviated extract from a meeting in which the trial manager’s role in securing funding is explicitly recognised.
now the support for science funding and many, many, many thanks and congratulations in particular to [the trial manager], also to [trial manager 2] for filling in these forms and for [the trial manager] developing a super duper relationship with Jane [a science funding administrator] … erm but er, the bottom line is we have got the support for science funding so we will be able to offer practices a per patient recruited amount of approximately £60, … So [in summary] I think that’s going to be very attractive indeed to the practices erm, you and Jane and Claire [a second administrator] are still sorting out the nitty gritty for the administration
Indeed yes, the, Jane made some requests and we weren’t quite sure what the requests actually meant so I contacted Claire … Jane has been out until today and won’t be back until later this afternoon so [I’m] just working between the two of them
(Trial project meeting, 24 May 2004; authors’ emphasis, p. 6)
The extract in Box 1 provides some useful information regarding the imperative of social networking. Given the very slow rate of recruitment observed in a sister trial (STOOL19), NHS SfS funding was perceived as being crucial – ‘very attractive indeed’ – for the successful recruitment of practices into LIFELAX. Although the necessary step of ‘filling in … forms’ to secure this funding was mentioned by the CI, flexibility and responsiveness in the bureaucratic system was ascribed to personal interaction; in this case the ‘super duper relationship’ formed between the trial manager and ‘Jane’ (a DH Research and Development Manager).
The trial team worked within MREC guidelines regarding methods of recruitment. In particular, the trial’s design was shaped by an MREC ruling that the trial team could not directly access patient information or make direct contact with patients, but instead needed to work ‘through’ general practice staff. Consequently, much of the work of identifying, contacting and processing eligible patients was assigned to practice nurses. After experiencing a slow recruitment of practices, the trial manager reassessed the work asked of these staff, and proposed a new process. This was designed to simplify work by integrating it more fully into routine procedures, in accord with principles set out in the STEPS framework. 193 Essentially, the trial manager discovered, through discussion with practice representatives, that ‘normal’ (i.e. non-trial) invitations for patient appointments weren’t made on paper, but rather were initiated by a telephone call. This new means of patient contact was built into the amended recruitment process. The new process also fitted closely with the pragmatic design of the trial, which emphasised a ‘naturalistic’ application of trial procedures. Box 2 presents an extract of an interview in which the trial manager outlined the rationale for his plan.
… we haven’t been able to recruit the number of practices and that has implications for recruitment of patients … it’s this level of work that we are expecting [practices] to do for us that’s the sticking point and that’s what we have got to work around … [in particular] I have a concern about practices writing to patients with this appointment for a clinic, and I thought well it’s a pragmatic trial, and we need to really do things as they would happen in the real world, … if [the practices’] local custom is to ring patients to invite them [to talk] about their condition why are we insisting that they have to write to patients, that’s not what they would routinely do, and the whole point of this trial is that it maps onto routine practice life, as much as it possibly can. So I thought well we could always suggest an amendment to the protocol allowing GP’s and nurses and receptionists to ring patients …
(Interview II, trial manager, authors’ emphasis, pp. 1–4)
The trial manager’s account serves two purposes: demonstrating both personal enthusiasm and commitment to the trial, and an attempt to find a workable solution despite the limitation of having no direct access to patient details. In this instance the suggested course of action was to integrate trial work with existing patterns of activity in primary care settings. Nevertheless, the MREC reached the decision that the planned approach was unworkable on the basis that telephoning patients at home would constitute a form of harassment. The MREC decision also prevented recruited practices from telephoning patients to check if they had received an information letter or to see if the patient wanted to reschedule an appointment for the trial. This combination of barriers, in addition to those cited earlier in this chapter, contributed to a growing level of frustration within the trial team. Box 3 presents an extract from an interview with the trial’s CI in which she explained her assessment of the current climate of research governance.
Erm, I think initially there were very significant barriers … and also considerable delays in getting trust R&D approval sorted out for the [the trial], and I, you know, fully appreciate the need for … the research governance framework … but I think there has been overinterpretation of some of the stipulations and the requirements to the extent that it holds up research and I am thinking here not just of the experience with [the current trial] but with various other studies … since the research governance framework came into being erm, I think that its swung so far the other way now that people are being so ultracautious that there is a danger of research that is potentially beneficial to patients not actually being undertaken and in my opinion that’s as unethical as doing poor research and research that’s potentially detrimental to patients.
… I also think that some of the restrictions and the stipulations and the things that people in ethics committees and in trust R&D offices are asking for are probably symptoms of … [them being] primarily administrators and actually [they] have never done hands-on research themselves and don’t understand the realities of what its like doing research and the approaches that one needs to take to make things work so er, so for example the whole notion that in the interests of patient confidentiality, you know that we would all respect, that you have to have this kind of two stage approach to patients and that their names cannot possibly be released in any way to the research team until the patient has given their consent I think that shows perhaps a lack of understanding of barriers for busy practitioners, those very barriers that [the trial manager] has been talking about all along; that really practices don’t have the time and the resource to write out to patients, get them in, go through the whole process of explaining the study to them
(Interview, CI, authors’ emphasis, pp. 1–2)
The CI began her account by describing what she perceived as an ‘overinterpretation’ of RM&G and ethical principals by localised administrators and MRECs, respectively. Two effects of this bureaucratisation were identified: the process of research was stalled, ‘[held] up’, and more significantly an ‘unethical’ consequence was manifest through patients being denied the benefits of clinical research (either through participation in a research study or benefitting from evidence-based care). The CI also offered a description of the roles and responsibilities implicit in the deployment of clinical trials. In particular, she described fundamental differences between the work of three groups of actors: administrators, researchers and clinicians. Researchers, in the context of a pragmatic RCT, were described as having an understanding of the ‘grass roots’ issues of clinical practice with regards to research involvement. In particular, researchers were described as being aware that clinicians were unlikely to invest resources in purely research-based activities without significant incentives. Conversely, administrators were not ‘understand[ing] the realities’ of what was needed ‘to make things work’ in the context of primary care research. Thus the problem was identified as one of governance, and not the (mis)translation of research priorities to clinical practice. The CI’s account is underpinned by a powerful discourse of ethics and pragmatics: the trial team are identified as being qualified to deploy a sound clinical trial, while governance administrators risk generating ‘unethical’ practice through an overly cautious approach and seemingly arbitrary variations in judgement.
The issues affecting the successful deployment of LIFELAX and its sister trial STOOL were recounted by a senior member of the trial team (Senior Researcher 2 – SR2) in an interview, an excerpt of which is presented in Box 4.
… I think the real barriers are in primary care and this is where the situations have changed over the last 3–4 years with research governance framework so in the past doing the trial in primary care, you would make sure that having got agreement from the primary care team that they would allow their patients to participate in the trial, and the research team would do everything else … Er the consent form would be straight forward ‘I am willing to participate in the trial or I am not’, its … something which doesn’t have any major impacts on your life, you know, … its not a, a dangerous drug, its not a dangerous procedure, its nothing life threatening its just ‘will you participate in the research’. So the procedures were much more tailored to the severity of the risk is my view and … you know if I had been doing a study of heart transplants then clearly we would not have been using the same procedure then, then the procedure would be much closer to the way ethics committees and research governance need to operate, there would be a much fuller explanation by the consultants, exactly what it involved, etc., so it’s about matching risk to er bureaucracy
… you see it’s the enthusiasm of the researchers, … the focus of the research team that this is the only thing which is important to them, enables you to build a rapport with the participants, ensure they understand fully what’s going on, explain it to them, er and so that they are quite clear that it has no detrimental effect on their outcomes, etc. What you have got now though is a very very busy primary care and I no way am going to lambaste or criticise primary care, you’ve got very very busy primary care, these individuals have other priorities which are at the moment far worse than they probably were 5 years ago too, because of the new GP contract so primary care contracts have changed so that they are having to meet all these prevention targets making sure everybody, plenty of people have had flu vaccines with the number of kids out there who have been coughing all those things have to be met. So their work load is substantially more than it was say 5 years ago, life is far more complex, there is big business here, [a] division of labour, and none of the individuals involved have … anywhere near the same kind of commitment to the project as you or I do, as researchers, so no wonder the enthusiasm is not there for recruitment. So the barriers are not you know primary care, the barriers are about the way that research has to be done because of research governance so I think that’s the biggest barrier
(Interview: SR2, 22 April 2005, authors’ emphasis, pp. 2–3)
In Box 4, SR2 describes a problematic intersection between: (1) an evolving research governance framework; (2) the agenda of academic researchers; and (3) the concerns of primary care. In the first paragraph SR2 describes a change in the way ethics committees and research governance bodies have responded to research, citing escalating bureaucratic procedures that are not matched to the potential risks posed to participants. The quote contains a description of how research may have been conducted prior to changes in the research governance framework over ‘… the last 3–4 years’. Specifically, where studies posed little clinical risk to patients, researchers were able to deliver recruitment information that was tailored to this low level of risk and to the research design, keeping technical information to a minimum where appropriate, and thus making the process of consent ‘straightforward’ for both patients and researchers. However, SR2 explains that recent research governance stipulations universally require a more complex approach to consent, often involving the input of clinical staff. Therefore, although originally the research team ‘would do everything’ in the research process, the burden of patient recruitment in primary care has now passed to practice staff. SR2 adds a qualifying statement to his criticism of research governance, by identifying the ‘… need [of ethics/governance frameworks] to operate’ in matters where patient wellbeing is in question. Finally, SR2 summarises that the key concern is an increase in the undiscerning application of research governance stipulations in an uncritical and generally uniform manner across research studies. This approach requires, at times, unnecessarily complex recruitment procedures, greater input from clinicians, and correspondingly affords the trial team less control over the delicate recruitment process.
In the second paragraph of Box 4, SR2 explains why greater involvement of clinicians in the recruitment process is problematic. Specifically, the agenda of GPs and other primary care staff is shaped by the changing General Medical Services (GMS) contract. While researchers have the enthusiasm, resources and interest in implementing their own research projects, primary care staff are ‘… very very busy’ and have ‘… other priorities’. These priorities it is argued do not always overlap with those of research. Therefore the enforced transition of control over recruitment – from dedicated researchers to busy clinicians – is counterproductive. SR2 reiterates that the central problems to implementing research are not to be found in primary care, but in ‘… the way that research has to be done because of research governance’.
The LIFELAX RCT required bureaucratic approval and coordination across a range of organisations, including those concerned with ethics, administration, finance and human resources. Congruence between relevant networks was sustained by the social, largely hidden work of the trial manager in identifying, creating and maintaining relationships, with key individuals in relevant positions of authority in these organisations. Subsequently, in order for the trial to progress and meet milestones, the trial team had to rely on non-standardised and previously unreported methods. Although the trial team worked hard to promote the RCT and to enhance recruitment, the research was hampered by three key features of an ‘unstable research governance environment’, namely: (1) differences in interpretation and implementation of RM&G guidance across administering bodies; (2) an interpretation of RM&G guidance by PCTs, and ethical decisions by the MREC, that was viewed as ‘overcautious’ by senior research staff; and (3) by the trial team’s limited access to patient data and contact procedures as stipulated by the MREC. Reasons for particular interpretations of research governance and ethics, and disparities in interpretation, require further investigation. Notably the process evaluation did not include a detailed investigation of the perspectives of the MREC – other than via available e-mail correspondence and letters – or the views of PCT officials. However, an endemic fear of litigation in light of the incidents at Alder Hey, and more recently Northwick Park Hospital, may be a contributing factor to the ‘cautious’ approach of the MREC and PCTs, as perceived by the trial team.
A summary of the findings from observation of the trial team at work is presented in Table 24.
|
The trial team were primarily engaged in meeting administrative and practical objectives and completing ancillary paperwork. However, the RCT relies heavily on cooperative networks. Cooperation (congruence) between networks was sustained by the social – and largely ‘hidden’ – work of the trial manager in identifying, creating and maintaining relationships with key individuals in various organisations Due to differences in the application of RM&G guidelines across sites, and interpretations of the guidelines that were not ‘research friendly’, the trial team were under pressure to continually develop creative and workable solutions to emerging practical problems. This formed a barrier to the satisfactory and timely achievement (disposal) of essential milestones in the delivery of the trial The MREC ruled that the trial team could not directly access patient information. Consequently, much of the work of identifying, contacting and processing eligible patients was assigned to practice nurses. As practice staff were often busy, the recruitment process was initially very slow Additional barriers to the trial included a research topic that did not match the clinical priorities established through a new GMS contract and numerous problems in acquiring RM&G approval, such as a slow response from some PCTs, out-of-date application procedures and ‘broken’ or old web resources |
The ‘second technology’ of the LIFELAX trial: training packages for practice nurses
Studies investigating patients, their data or the work practices and systems implicated in their care often rely on the cooperation and commitment of medical staff. However, factors that affect the attractiveness of research participation for clinicians in various settings are multiple and poorly understood. 217–219 Moreover, given the level of commitment required of clinicians, it is perhaps not surprising that poor recruitment of this group to RCTs is an established subject within the literature. 220 Subsequently, in the LIFELAX trial, the research team attempted to maximise the attractiveness of the study by promoting its applicability for primary care medicine, following strategies set out in published research. 193,194 In particular, the introductory materials and presentations to practice staff emphasised the potential benefits of reducing laxative prescriptions, decreasing patient contacts and upskilling staff, by equipping them with transferable skills in patient education and delivery of lifestyle advice. Nevertheless, despite some initial expressions of interest, the trial team found it difficult to secure the commitment of practice managers and senior partners. While some of the barriers to practice recruitment have already been described in this report, additional – less readily apparent – concerns overlaid these practical obstacles. In particular, the nursing staff appeared to be unenthused by various aspects of the research. Nurses interviewed in the BCC arm of the trial described the counselling techniques as being familiar, or as one nurse commented; ‘… the information [was] … given to experienced health-care professionals; it wasn’t something we were unfamiliar with’ (Nurse 4, interview, 11 October 2004). Most of the nurses across all three arms of the trial described chronic constipation as a comparatively ‘uninteresting’ topic, and an issue that seldom arose in their routine encounters with patients. Consequently, interest in both the topic of the trial and the experimental interventions was low. In this section of the chapter we describe feedback from a range of practice staff regarding their perception of the research topic, and the role of practice nurses in implementing the LIFELAX RCT.
Barriers and facilitators to normalisation of the LIFELAX nurse training packages
Through the nurses’ accounts it is possible to identity two features of the training packages that were salient to them. The first was the central topic of the trial – chronic constipation, perceived by most respondents as a problem not routinely encountered by practice nurses in their interactions with patients. In this regard the LIFELAX trial was perceived by most of the nurses as presenting them with an additional clinical responsibility. In particular, chronic constipation was regarded as an issue that was typically managed fairly successfully by laxatives and that was typically within the remit of care delivered by other professionals (GPs, community nurses). The second issue for nurses in the personalised arm of the trial, were the BCC techniques. The nurses who received instruction in BCC described the training package as not offering new skills, but rather reinforcing current approaches. Nurses in both personalised and standardised advice arms of the trial reported the diet and lifestyle materials as having some relevance to their standard practice (for conditions such as obesity and healthy living). However, these comments were made in the context of a generally negative report of trial involvement, and it is not possible to determine how or if these materials would be used beyond the life of the research.
When presented with resource-intensive work that is poorly defined – such as the management of some chronic conditions – medical professions may attempt to divert responsibility for the condition to another closely aligned professional group (e.g. Viner221). Across the interviews with practice nurses, chronic constipation was described as falling outside the boundaries of their routine work, and as a responsibility distributed across community nursing teams and GPs. Box 5 presents a more detailed explanation through the independent accounts of two nurses.
… did you find [the research consultation] differed from how you would normally interact with those patients or –
Ah yes I would say so because I don’t, I mean unless we are doing a medication review with patients who are already on lactulose or the, whatever medication, then we probably wouldn’t; it’s not a question [chronic constipation] that ever comes up unless people are coming in, and I mean they wouldn’t come [in to see] the practice nurse anyway, to discuss that, if they had any problems they would come in to see the doctor or the nurse practitioner. So it’s not a subject that ever comes up really
(Interview: nurse 9, brief intervention, authors’ emphasis, p. 2)
Also:
I don’t specifically counsel people about the their bowel habits, erm it doesn’t tend to come into my role … I don’t get involved in it other than I give healthy eating advice, erm in the process of a lot of other consultations that are just a part of it, well-woman, well-man checks, we always give dietary advice we always give exercise advice … I think maybe the district nurses have a lot more to do with [chronic constipation in particular], because they get the other extreme – they are out in the community with elderly people who are really bunged up
(Interview: nurse 4, personalised intervention, authors’ emphasis, pp. 2–3)
Nurse 9 explained that the topic central to the trial’s interventions – chronic constipation – was not a key feature of practice nursing. Specifically, she identified the condition as a concern ‘for the doctor’ or ‘nurse practitioner’. In this regard, Nurse 9 viewed the topic of the research – and by extension the training packages – as having little direct relevance to her day-to-day work. In the second account, Nurse 4 echoed this interpretation. In particular, she explained clearly that the management of chronic constipation did not ‘come into [her] role’. Nevertheless she added that ‘healthy eating advice’ was part of a wider package of work including ‘well-woman’ and ‘well-man’ checks. Therefore, although the topic of chronic constipation was not considered a central area of work for practice nurses, they viewed the provision of diet and lifestyle information as part of their core skill set.
Regarding the second account in Box 5, an additional point is Nurse 4’s use of the term ‘dietary advice’. One concern among the trial team was that nurses in the personalised (BCC) arm of the trial would conflate directive advice giving with the counselling approach. However, while nurse 4 – who attended the BCC training – used the term ‘advice’ in her account, most of the nurses in the personalised arm described the techniques as being familiar, distinct from paternalistic approaches, and in routine use through their smoking cessation and obesity work.
Nurse 4 finished her response by emphasising that district nurses see ‘… the other extreme’ of chronic constipation with ‘… people who are really bunged up’. In this regard, Nurse 4 made a distinction between the preventative work of practice nurses through well-person initiatives, and the work of community nurses whose responsibilities include the ‘other extreme’ of chronic constipation: amelioration and treatment. In this example the aim of the trial – to train practice nurses to prevent rather than treat chronic constipation – is lost in the nurses’ explanation of why the trial’s topic is a low priority.
It is important to consider that while one interpretation of the nurses’ accounts is that they were attempting to pass responsibility for chronic constipation to community nurses, this glosses over a valuable message consistently delivered in the nurses’ interviews: that chronic constipation was not a problem that was pertinent to the nurses within their routine interactions with patients. Therefore, the trial team had to work within a set of parameters that were not conducive to the trial’s success; namely asking practice nurses to engage with a problem that was largely ‘invisible’ to them. Moreover, while some practice managers viewed chronic constipation as a financial burden to their practice, they reiterated the nurses’ position that it was a condition addressed more directly by a GP (through laxative prescription) or by nurses working in the community. One practice manager provided a ‘bird’s eye’ view of the distribution of work across the practice. An extract from this interview is presented in Box 6.
… I think we were talking about why this particular project could be tricky, you mentioned that it’s –
Right okay I think number one was the fact that this particular research project involves older people by default you tend you, it tends to be from the nursing side it tends to be our community nurses who are involved with our older group, erm, and they are the people who should be and would probably benefit from looking at a research project like this, unfortunately … we were unable to engage them to support us … So [it had to be] our practice nurses involved, and they felt that it really wasn’t erm their erm remit, you know chronic constipation and advice does very much tend to be outside the practice erm unfortunately it hasn’t worked!
(Interview, practice manager D, authors’ emphasis, p. 1)
Throughout her account, the practice manager made a series of important points regarding the division of labour within the practice, and the specified skill sets of various groups of nurses. While the age of patient populations was not used by the nurses as a means of demarcating professional boundaries, in the interview the practice manager alluded to a broad sector of work that was conducted between community nurses and ‘… our older group’. Following this perspective, the practice manager suggested that the community nurses ‘should be and would probably benefit from’ involvement in the research, but ultimately did not ‘support’ the practice in this instance. From this point onwards in the extract, the practice manager sets out the context for the ‘failure’ of the interventions in her practice. Specifically, the practice nurses were described as an inappropriate substitute to the community nursing team. In this regard the practice managers’ response is to assign responsibility for the problem of chronic constipation to health-care professionals beyond the control of the practice. As described earlier, the redirection of responsibility for particular patient populations from one professional group to another has been documented elsewhere in the NHS. 221 In the current account, the practice manager described the practice nurses as having responsibility for defining their own skill sets and spheres of activity. Specifically she explained that ‘…they felt that it really wasn’t erm [within their] remit’. Consequently, the extract suggests political tensions within the practice regarding the distribution of work implicated by LIFELAX. An investigation of the everyday running of practices enrolled into the RCT was beyond the scope of the process evaluation. However, task designation issues within each practice are likely to have contributed to how the trial was perceived in each site, particularly as the trial’s topic was comparatively ‘unglamorous’, involved a population of patients not prioritised in the QOF, and – like all research – included additional work for the clinical staff involved. In some instances practice nurses explained that there had been some direction by senior practice staff – ‘a little bit of pressure’ (Nurse 9, 16 April 2007) – to cooperate with the trial team, and consequently these nurses may have felt little ownership in the research. This situation arose in part due to the manner in which the trial team contacted and enrolled practices to the trial. Practice enrolment occurred via negotiations between the research team and GPs and practice managers, although most of the research tasks were targeted at nurses. Unfortunately, it was not possible to monitor the degree of consultation that occurred in each practice between senior and nursing staff.
A pertinent issue raised by primary health-care staff enrolled in the trial was the unsuitability of the interventions for practice nurses, and correspondingly their appropriateness for community nurses. However, while community nurses were initially included in the trial protocol, they were quickly identified as a potential confounding factor in the trial design. Box 7 includes an extract from an audio-recorded subgroup meeting in which the trial team explore reasons for excluding community nurses.
I don’t er, I just think it’s very hard to get hold of community nurses, they’re not employed by the practice, they’re employed by the PCT
PCT
Can I just put another little fly into that ointment?
The randomisation
The problem is that they do go from practice to practice so you will end up training a community nurse with the behaviour change who then goes into your standardised practice
That’s right, yes
Right
Who says ‘you should be doing this’?
Yes. And they also if they find something that they like, they are really very good at photocopying, and I have experience of this, and they distribute it to every practice that they go to, give it to nurses and say ‘do you like this?’. Em in [another study] we trained community nurses if the practices wanted them to be involved and we had our leaflets popping up in our control practices
(Subgroup meeting transcript, 16 March 2004, pp. 23–24)
Several interesting methodological points are raised through the extract in Box 7. The first is an observation that community nurses are employed by the PCT rather than the practice. This point links to the comments of the practice manager in Box 6, namely that the practice did not have absolute authority over the work of the community nurses, and therefore were unable to secure their cooperation in delivering the trial. Nevertheless, as described earlier, the practice manager capitalised on these differences to excuse practice staff from the tasks asked of them by the trial team. The practice manager suggested that in the context of chronic constipation, the research work was more appropriately suited to ‘outsiders’ in the community; in this example, PCT employed nurses. The second point is that the RCT design – specifically the rationale and practice of randomisation – precluded, or at least rendered very difficult, delivery of training to the most ‘appropriate’ group of staff: community nurses. As the senior dietitians explains ‘The problem is that [community nurses] go from practice to practice so you will end up training a community nurse with the behaviour change [approach] who then goes into your standardised practice [and contaminates the trial]’. In this regard, the methodological limitations of even a cluster RCT design undermined some aspects of the interventions’ assessment. Although in principle it would have been possible to use the community nurse as the unit of randomisation in this trial design, this would have required the trial team to identify the case load for each nurse, and to then recruit these patients to the trial. It is unlikely that this approach would have been feasible given the trial team’s limitations on access to patient data. Finally, the third related point is that the trial design, despite embracing a pragmatic agenda, conflicted with ‘real world’ practices regarding the dispersion of skills and materials. At the end of the extract the senior dietitian recounts an episode of normalisation-in-process, when she states ‘if [community nurses] find something that they like … they distribute it to every practice that they go to’. Ironically, the RCT disrupted the potential for normalisation by prohibiting the transfer of those techniques and materials that nurses found practically useful in their daily work. These limitations were unavoidable given the brief for a RCT.
Nurses in the personalised arm were sceptical that the training sessions they attended would furnish them with new skills, or improve their practice with patients. The BCC techniques were identified by the nurses as overlapping considerably with their current skill sets. Framing this feedback through the terminology of the NPM, the trial’s personalised intervention failed to dispose of clinical problems relevant for practice nurses, and did not enhance their confidence in working with chronically constipated patients. Neither the ‘problem’ of chronic constipation, nor the suggested ‘solution’ via BCC, were reported as valuable or significant for the nurses in their daily work. Given this context, the materials associated with the interventions (leaflets, BCC manual) were praised in their capacity to facilitate a sharing of ideas, or congruence, about diet and lifestyle issues between nurse and patient. Box 8 presents a summary of these points through the account of an additional nurse.
… [the leaflets could be] ideal because [patients] could look at the pictures and identify ‘well yeah I’m having so many of those a day or this amount of veg, this amount of fruit, or I’m not eating any at all’, I did find that one really good to use and I thought it would be good eventually if we could maybe have some to use in the clinic to use with our patients, or along those lines, because sometimes you speak to people and you ask them ‘which veg do you eat’, and they class two peas and things like that as veg, and they’re not really aware that there is not a lot of fibre, etc., you know and I found that was a good way of getting [the information] across to people
And later in the interview:
Do you think the techniques that [the dietitian] was demonstrating, do you think they differ much or at all from your usual practice? I mean … was there anything in the techniques themselves that’s different about how you interact with patients?
Well nothing really apart from those leaflets, … I think those information leaflets were really good … I think that was the best thing, [the dietitian] had obviously or whoever had thought a lot about what went into them, and making them easy to use [lowering voice] I think that was the best bit
(Nurse 3, personalised arm, authors’ emphasis, p. 2 and p. 5)
Importantly the quote from Nurse 3 demonstrates some perceived value in the behaviour change tools, particularly with regard to improving congruence between the nurse and patient. However, this positive assessment was made alongside Nurse 3 suggesting that the materials were ‘the best bit’ of participation in the trial. It is therefore not clear if Nurse 3’s praise of the materials was due to their practical merit in facilitating consultations or an attempt to find something positive to report to the interviewer. Nevertheless, Nurse 3 commented that she would value the use of the materials ‘in the clinic’ with patients outside a trial setting; conspicuously using the term ‘our patients’. Based on this particular account, the tools could be considered as a potential means of facilitating the disposal of some clinical problems relating to diet and lifestyle generally. However, none of the nurses described an intention of applying the tools post trial with patients suffering from chronic constipation specifically.
In a recent paper, Salmon et al. 219 identified factors affecting the relative attractiveness of research participation for practitioners in primary care in contrast with those in secondary care. The authors suggest that although a research portfolio might boost the careers of clinicians working in hospital settings, the same cannot be said for those established in primary care where research involvement may hold little or no incentive. Through the process evaluation we explored how practice-based staff viewed involvement in the LIFELAX trial specifically. Although we cannot comment on their experiences in other research settings, the feedback of our respondents suggests that they generally held little interest in the interventions or overall success of the research. Three out of the eight practice-based nurses countered this position by expressing interest in the RCT’s topic and success. However, two of the trio were employed as research nurses and the third held aspirations for a career as a nurse practitioner: a goal possibly facilitated by research involvement.
The topic of the trial – and, to some extent, the nature of the interventions – had been preset in the commissioning brief for the research. Consequently, the trial team attempted to meet the brief while also working to meet the realities and demands of clinical practice. With regard to the practice nurses, the trial team experienced frustration as their aspirations for the training packages were not realised. Likewise the nurses struggled to make sense of trial work within the context of their working practice. In attending the training sessions and applying relevant skills with participating patients, the practice nurses were frequently left perplexed by their participation. An analysis of their accounts suggest that they understood the trial as a request to tackle an already successfully managed ‘problem’ with an untested and time consuming ‘solution’. The nurses were therefore unconvinced that their time was being used appropriately, and for a worthwhile exercise. These findings lead us to reflect on the importance of programmes of work that use research methods in a timely and appropriate manner. In the case of the LIFELAX trial, an accumulation of evidence regarding the clinical effectiveness of BCC for chronic constipation, prior to a pragmatic trial of nurse training packages, may have been valuable. In particular, such evidence may have added weight to the argument that changing current patterns of work within primary care was worthwhile. More importantly, a feasibility study that identified problems with recruitment, low clinical interest, and RM&G issues may have precluded investment in LIFELAX. At the time of funding the HTA did not commission pilot or feasibility studies, although currently the HTA’s position on this issue has changed.
A summary of the findings from the practice nurses is presented in Table 25. In the third and final section of this chapter, we explore the views of the participating patients.
| Summary |
|---|
| The nurses reported that the topic of the trial was ill matched to the current work of practice nurses and the way in which chronic constipation was currently managed in primary care. Although the trial assessed the value of changing current practice from treatment of the condition to nurse-led preventative measures, the nurses generally focused on current patterns of work. Nevertheless some nurses argued that chronic constipation was a comparatively low-priority complaint, that it was successfully treated via laxatives in most cases, and that they were sceptical that motivation was instrumental in patients’ experiences of chronic constipation |
| Additional points |
|
The BCC techniques were identified by some nurses as overlapping with their current skill sets and therefore were not described as providing the nurses with new skills or tools The materials associated with the interventions (primarily pamphlets) may facilitate a sharing of ideas (congruence) about diet and lifestyle issues between nurse and patient, although praise of these materials was made in the context of a comparatively negative description of trial involvement Some of the nurses questioned the validity of attempting to motivate patients whose constipation was caused by lifestyle factors beyond their control. Consequently, rather than enhancing confidence in the conduct of their work, some nurses described the BCC approach as potentially undermining the interaction they had with patients Due the implementation of randomisation, the community nursing teams who may have found the techniques most applicable were excluded from the trial |
Making sense of participation in the context of chronic illness
Some of the barriers to the success of the LIFELAX trial, as explained earlier in the chapter, were due to a range of issues concerning RM&G guidelines and MREC rulings, and a notable lack of interest in the research across primary care sites. However, the participants’ accounts of their experience also offer a useful perspective regarding how the trial was deployed, and the significance of the interventions for patients suffering chronic constipation. The meaning of the trial for participants was shaped by their individual ‘illness trajectories’ or, specifically, the manner in which participation met ongoing, idiosyncratic priorities regarding their illness. 222 Specifically, although some participants had reached personally satisfying treatment decisions prior to the trial, others were actively seeking new solutions to the management of their chronic constipation. Participants in the two ‘active’ diet and lifestyle arms of the trial experienced an interaction with one of the practice nurses. Consequently, in these arms, the participants’ perception of the research was shaped by how the nurses conveyed – deliberately or subconsciously – their own views of the trial. It was difficult therefore to discern through a single interview with a given participant, sometimes a considerable time after the consultation with the nurse, how these factors independently affected the participants’ experiences. Nevertheless, three key topics were central to all accounts. These were: (1) reported motivations for participation; (2) experience of interacting with a nurse in the research consultation (in applicable arms); and (3) understanding of the outcomes of participation in the RCT.
Participation in the LIFELAX trial
The participants’ explanations regarding motivation for involvement in LIFELAX centred on the manner in which the trial met their priorities and expectations with regard to their illness. Participants who described having successfully established a means of coping with chronic constipation reported that the trial was a means of benefiting others. However, participants who were seeking solutions to their experience of symptoms identified the trial as an opportunity for adjunct therapy. In some interviews participants moved between these conceptualisations. Data for the process evaluation was collected from each participant through a single interview. Consequently, the motivations expressed by any one individual for participation may have changed over the course of their involvement with the trial. Box 9 presents the accounts of two participants when asked to describe what they hoped to achieve by participating in the trial.
… did you have any particular motivation in being part of this trial, other than you said you had experience of [being in other studies]?
I was suffering from a combination of [complaints] … we went through a variety of treatment options and we settled I think on [a medication] which seemed to do the trick … only just now unfortunately I’m having [side effects] … Er, in addition to having the [the side effects] I found that I’ve been [suffering constipation again], even though I was taking the [medication] …
… so do you think in terms of your motivation for being part of this trial, would you say then that you were looking for a solution? Do you think, would that be a fair summary, that you were –
(interjecting) – Yes, I have been looking for a solution for a long, long time
(Interview, participant ID 1315001, personalised consultation, pp. 1–2)
And:
I think to start with if we could just talk a little bit about how you first came to be involved in the trial, that would be really good
Right. Um, well first of all I think I had a letter from the [trial team] asking if I would like to take part … Now I didn’t think that I suffered from constipation at all so I was very surprised when I got this letter and I rang the [trial team] up and said ‘Well look I don’t suffer from constipation’. I do have [a related illness] so I think perhaps the doctor put my name forward because I’m on [a relevant medication] all the time … I think that’s why I was involved in it, but I’ve never had any history of constipation. But the people said well that was OK they would go ahead with it
Later in the interview:
Do you mind if I ask you if you had any particular motivations for taking part?
Er no, except, well, no I mean it was sort of they asked me, would I? And I said yes I would. It was just as simple as that really, I’d no objection to it … No, no, um as I say I was quite willing to take part in this, in the survey. Um and quite willing to leave it at that
(Interview, participant ID 1018009, standardised consultation, authors’ emphasis, pp. 1–3)
In the first extract the participant expressed his motivations as trying to find a satisfactory ‘solution’ to the problem of chronic constipation. Notably, he described a prolonged period of dissatisfaction with his current medication prior to the LIFELAX trial: ‘I have been looking for a solution for a long, long time’ (ID 1315001). In this respect the participant may be described as orientating towards the trial – at this particular instant – as a ‘patient seeking treatment’. 223,224 Conversely, the second participant describes themselves as ‘[not] suffer[ing] from constipation at all’ (ID 1018009), a theme also identified in the STOOL trial. 19 Throughout the extract the second participant explains their surprise at being asked to contribute to the LIFELAX trial, and offers an explanation as to why they might have been identified: ‘I think perhaps the doctor put my name forward because I’m on [a relevant medication] all the time’ (ID 1018009). In this regard, while the participant understood that they were taking laxative medication, the perceived effectiveness of the treatment was such that constipation (and the taking of laxatives) were not regarded as a problematic feature of daily life.
This perception (of laxatives being an effective solution to constipation) was so entrenched in the accounts of some respondents, that the purpose of the trial was put into question. Therefore, for this individual participation was a result of meeting a request from the trial team; ‘… I mean it was sort of they asked me, would I? And I said yes I would. It was just as simple as that really, I’d no objection to it’ (ID 1018009). The second respondent is an example of those participants who identified themselves primarily as ‘research subjects’ in an RCT, in much the same manner as participants described in a previous paper. 223 For these participants the trial was largely an altruistic exercise that might, potentially, benefit other patients in the future. These conceptualisations were helpful tools in understanding the trial’s significance for various participants. Those who were seeking treatment as patients may have benefited most from the personalised BCC consultation as they were by definition actively seeking intervention. However, we found that regardless of randomisation status or orientation to the trial as ‘patient’ or ‘research subject’, most participants struggled to make sense of their involvement in the LIFELAX trial. This finding does not reflect on the quality of the LIFELAX participant information materials, but is a common finding in qualitative research exploring the understandings of participants in RCTs. 225 In recent years researchers have focused on the importance of making sure participants understand RCT concepts, rather than simply being able to recall them by rote; however, to date there is no clear method of facilitating this process. 226,227 The practice nurses involved in the trial described the intervention techniques as ‘familiar’, and therefore the participants may have also struggled to understand the experimental components in the trial design. This is a point discussed in detail below.
The second topic central to the participants’ accounts was their understanding of the role of the practice nurse in the trial. The nurses were described both in regard to their perceived role and their performance. Participants tended to talk about these topics as they articulated what they perceived as poor or unexpected behaviour on the part of the practice nurse. Box 10 presents two accounts by participants disappointed by the perceived behaviour of the practice nurses.
… when I went to the practice nurse [for the trial consultation] … I think the attitude was, ‘eeh, oh yeah’ (rolling eyes) you know, ‘something else that we’ve got to do’. Er, well my own attitude was, em, if it’s going to be of benefit to others then I’m quite happy to go along with it
Later in the interview:
… it was at that time, that I gained the impression … oh this terrible, but I did gain the impression that she thought it was all going to be a waste of time. Right, now that is probably because they have an awful lot to do, and their time is, as you have just mentioned, a few minutes ago, it’s spent, dealing with patients who are ill and who need attention. Er, not filling in forms. You know what I mean?
(Interview, participant ID 1101003, standardised consultation, p. 3 and p. 6)
Another participant shared her perceptions:
… I know that we’ve already covered this slightly before, but when you went to see the nurse for this particular trial and she went through the information leaflets, did you get a sense that was different from the conversations that you’d had before, that there was a bit more time there to go through some of that information, or did you not really get that sense?
Well I got the sense really that ‘oh I’ve been asked to do this as a job, I’m handing out information’ erm, but it’s, it’s information; … you’ll already know it, but if you read it and it’s just common sense, you know – which okay things are common sense, – but when you’re troubled with constipation it’s, you know you would like other little bits of erm, any kind of snippets you can get really
(Interview, participant ID 1018001, standardised consultation, p. 7]
In the first interview presented in Box 10, the participant offered an evocative description of meeting with a practice nurse in the setting of a LIFELAX consultation. The nurse is described as having an attitude quite opposed to the trial, which the participant used in her account to contrast with her own position as a citizen ‘happy’ to ‘benefit … others’ (ID 1101003). Throughout the account the participant used a number of explanations for why the nurse may not have been enthused by the study such as having ‘an awful lot to do’ (ID 1101003) and ‘dealing with patients who are ill and who need attention’ (ID 1101003). Nevertheless, the participant was disappointed that the nurse ‘[gave] the impression that she thought it was all going to be a waste of time’ (ID 1101003). Finally, the participant contrasted this description of clinical activity with the work of the trial – ‘filling in forms’ (ID 1101003). In this instance the participant appeared to be disappointed and frustrated by the nurse’s attitude, although she demonstrated that she could understand some of the contextual reasons why the nurse might respond in this manner to the extra work involved. Both the nurses and participants shared similarities regarding their participation experience. Both struggled at times to make sense of their participation, and both were required to complete additional work. Consequently, we may interpret the participant’s account of the nurses’ behaviour as a means of expressing her own frustrations to the researcher. For this participant the trial was an exasperating experience, and the nursing staff served as ‘visible’ representatives of the trial, essentially the subjects of blame for an unsatisfactory participation experience. Some of these themes reoccur in the second participants’ account. However, here, the participant explained why receiving ‘common sense’ (ID1018001) advice was helpful when suffering from a condition such as chronic constipation. In this instance the nurse’s role was identified as being more than a neutral provider of information, but as a person interested in the participant’s complaint. The nurse therefore provides information that ‘… you’ll already know’ (ID 1018001), but the act of discussing the topic, face-to-face with another individual, was potentially helpful. Unfortunately, the participant’s perception was that the nurse was uninterested in the consultation and the trial as a whole.
It should be noted that the inner mechanisms of the trial – and therefore the work of the trial team – were almost entirely hidden from the participants. Consequently, within the participant interviews the most ‘visible’ components of the trial were the interactions with nurses and the diary exercises. The nurses were therefore expected to perform RCT work, and in this regard, the participants did not consider the nurses as independent agents with their own agenda and concerns. Consequently, the work of the practice nurses’ was commented upon in a manner that tended to draw criticism as and when problems arose.
The third topic central to the participants’ accounts was their attempts to make sense of the outcomes of participation. Regardless of their explanation for involvement or the randomised status of their practice, most participants’ accounts were marked by disappointment with respect to their experience in the trial. The participants described having difficulty understanding the manner in which the RCT might produce beneficial outcomes for themselves or others. This difficulty stemmed from the perceived ineffectiveness – or invisibility – of the trials’ interventions. For example, it was not clear to either the nurses or the participants how a BCC consultation might differ from a routine interaction – other than in topic and length of time available. Nevertheless, in some instances the participants attempted to positively frame the meaning of participation by emphasising the realised or expected benefits, even if the mechanisms by which these benefits might occur were not fully understood or articulated. One participant, who did not find remediation for her symptoms, expressed hope that others might benefit in some way from her participation (Box 11). The account, however, is marked by an overt desire for a personal solution.
I wait for something to happen, I am eating [a recommended diet] and what have you but it hasn’t changed anything
Later in the interview:
I would think that there [are] not many different avenues that you could go down with [the personalised consultation], it’s either different treatments, I don’t think you will change my [condition] with that at the minute er, no I think I will just go along … just follow the lead and hopefully in the end will get a little bit of feedback I’m quite happy with a little bit of feedback on what’s going on
Well I think that’s quite important isn’t it for people who are involved to get some –
(interjecting) Oh yes, I just want to know sort of, if you have helped somebody if you have helped somebody then it gives me hope for some reason
(Participant ID 0815005, personalised consultation, authors’ emphasis, p. 2 and p. 4)
In this example the participant was clear that after taking part in the personalised arm of the trial, they did not expect to be able to ‘change [their condition] … at the minute’ (ID 0815005). For this participant, ‘the value’ of participation hinged on having ‘helped somebody’ (ID 0815005) at some other point in time. Consequently, they asked for feedback from the trial team in order that they themselves might have some ‘hope’ (ID 0815005).
For most participants’ involvement in the trial consisted primarily of the daily diary exercise. Participants in both ‘active’ arms of the trial received information leaflets and advice or BCC that was reported as being unremarkable. Indeed, many participants struggled to recall having ‘an intervention’ at all. Box 12 presents an extract from two interviews in which participants explained their interpretation of the trial design, and for one participant, their hope for ‘an intervention’ at some point in the future.
… apart from obviously getting the diaries that you didn’t expect, has other aspects of [the trial] been what you thought it would be or has it been different?
Erm I thought initially this was what you would have to do before anything sort of concrete came out of it, … obviously you have got to take a wide survey of exactly what’s happening and then you obviously take it from there so expect something different after they have all sort of consulted all the diaries belonging to everyone that’s participated in the trial and then I think something might be gained from it
(Interview, participant ID 0223004, control arm, authors’ emphasis, pp. 2–3)
And:
… no [the trial] hasn’t been a hassle like I mean er, its just remembering to fill the book in every day like ya know just at the end of the week … I just put no no no all the way down and when I was bad I just wrote in that I was bad and when I was on holiday I just put in the book there that I was on holiday and had a bout of diarrhoea and what I took to stop it and er but I have never had any hassle or anything out of it no
Right well thank you very much
It has been worth er you know if it can help anybody else well that’s fair enough like so just that I would like to get rid of this problem what I have got this wind problem and I cannot at the moment its gone on for a long time
(Interview, participant ID 1105001, standardised consultation, authors’ emphasis, pp. 6–7)
In the first quote presented in Box 12, a participant in the control arm of the trial explained that the diary exercise was a precursor to an intervention: ‘… what you have to do before anything sort of concrete came out of it’ (ID 0223004). Specifically, the diary exercise was seen as a means of assessing ‘what’s happening’ (ID 0223004) for the participants before an intervention could be developed and implemented. Arguably, we might expect an explanation of this type from participants in the control arm of the trial, where an absence of any novel intervention by the trial team was an intentional design feature. However, in the second quote, a participant randomised to the personalised arm of the trial explained how their contribution primarily consisted of ‘… remembering to fill the book in every day’ (ID 0815005). In an attempt to attach some meaning to their experience in the trial, the participant explained that his participation had been valuable if it ‘help[ed] anybody else’ (ID 0815005); however, he was left seeking a solution to a ‘wind problem’ (ID 0815005) that had been troubling him long before his participation in the trial. In this respect the trials’ interventions were reported by most of the interviewed participants as having little potency with regard to helping them with their health problems. Interestingly, for both the nurses and the participants, the BCC interventions were not regarded as offering anything ‘new’. In the case of the participants it is not possible to ascertain if this finding was due to the way in which the nurses deployed the BCC, the inherent qualities of the interventions themselves or a combination of factors. A summary of the findings from interviews with participants is presented in Table 26.
|
Some participants reported a lack of understanding (congruence) between themselves and the practice nurse regarding the value of the research. For some participants, their encounter with the practice nurse was a demoralising experience. In particular, while some participants viewed their chronic constipation as an important problem they reported that the nurse did not appear to see the research as worthwhile For most of the participants seeking medical interventions, the BCC or standardised advice consultations failed to help them find solutions to problems related to health, diet or lifestyle issues. In contrast, three participants explicitly reported some benefits (either psychological and/or physiological) from a behaviour change consultation and described making a number of lifestyle changes as a result It is not possible, due to the pragmatic design of the trial, to separate the effects of BCC from its delivery by nurses The participants made sense of their participation largely through the daily diary exercise. Due to this exercise, some participants interpreted the trial as ‘survey’ research |
Discussion
The assessment of complex interventions can be a challenging process. 228 In the process evaluation, we observed two ‘complex interventions’: (1) diet and lifestyle training for practice nurses, but, more specifically, (2) the practical conduct of an HTA RCT. In light of the trial’s premature closure, data from the qualitative evaluation help to explain some of the processes that led to the trial’s closure, and how they might be avoided in future RCTs. Although we can comment on the structure and implementation of LIFELAX (and offer recommendations for future implementation of HTA research), the relative importance of clinical topics such as ‘chronic constipation’ and the merit of ‘BCC’ per se are less clear. Specifically through the process evaluation we observed the confluence of several ‘trajectories’ or processes:
-
The implementation of a pragmatic RCT in an ‘unsettled environment’ of research governance interpretation and ethical judgements.
-
The response of practice staff to involvement in an RCT concerning a condition not prioritised in GMS contracts.
-
The response of practice nurses to proposed changes in their work patterns.
-
The responses of practice staff to the problematisation of chronic constipation: practice nurses perceived chronic constipation to be a condition already successfully managed by laxatives.
-
The response of the nurses to BCC training as delivered by dietitians or nutritionists.
-
The response of participants to involvement in a pragmatic RCT (including management of expectations and research-related tasks, such as the daily diary).
-
The response of participants in the diet and lifestyle arms to the combined stimuli of the LIFELAX trial and an interaction with a practice nurse.
In this report we have attempted to describe the interaction of these processes on the success of the LIFELAX trial. Nevertheless, RM&G and ethics issues aside, it is not possible to isolate the factors from one another. For example, had the training been delivered to community nurses the response of these staff may have differed from that of the practice nurses in LIFELAX.
As the embedded process evaluation study was ethnographic, qualitative research techniques were employed, and it was therefore not appropriate to set out our research questions in hypothetical form. However, at the outset, we attempted to address the following specific questions:
-
Formation How are ideas about the appropriateness of health technologies and their clinical applications formed and mobilised in practice; how are the interests of consumers and other users defined and incorporated in the organisation of the trial?
The process evaluation explains some of the reasons for the early closure of LIFELAX and we draw a number of conclusions about the structural processes of HTA assessment from these data. However, it is not possible to make claims about specific public health topics, such as the significance of chronic constipation for primary care medicine. We did observe that practice nurses and managers perceive chronic constipation to be successfully managed by laxatives, and that roughly one-half our sample of participants also considered themselves either not to suffer from constipation or that they successfully managed their symptoms through the routine use of laxatives. However, the nurses also explained that they did not work with patients presenting primarily for chronic constipation. The ‘problem’ of chronic constipation may largely be one of economics for senior practice staff, or an issue of concern for community nurses, or an issue for some, but certainly not all, patients.
If we consider the ‘lessons learnt’ for future HTA trials, it is important to understand how and why the LIFELAX trial was commissioned considering the response of practices. A systematic review underpinning the commissioning of LIFELAX, identified both chronic constipation and diet/lifestyle interventions as pertinent topics in primary care. This finding, taken on face value, appears to be at odds with the outcome of the process evaluation. However, the cost of laxatives and the dependence of patients on medication were issues that concerned some practice staff in interviews. Nevertheless, the relative priority of this problem when compared with others in the practice was not high.
Most of the trial team’s efforts were invested in ensuring that the RCT was successfully embedded in individual practices and across PCT sites. However, the response of practice staff to the trial’s topic and interventions were identified only after the RCT had been deployed. These issues may have been identified through a prior feasibility study, if one had been funded. A small pilot study was conducted during the development of training materials. However, this work was focused on the development of BCC materials and not on the feasibility of a larger trial.
-
Integration How are specific clinical and methodological problems within an RCT identified and resolved within professional groups and networks; how is the trial integrated into the existing organisation of clinical service provision, and what professional and organisational dynamics are involved in this integration; how is participation in the RCT negotiated and understood by subjects?
This is a multifaceted question and, as such, we have addressed it in the current chapter via several different means. With regard to the clinical and methodological problems of the LIFELAX trial, the trial team engaged in a considerable amount of negotiation and bureaucratic work in order to integrate the trial in clinical environments, and to meet RM&G and MREC requests. We have discussed this process through the NPM constructs of interactional workability and contextual integration. Notably, we found that the RCT relied heavily on cooperative networks. Cooperation and a shared understanding of goals (congruence) were achieved through the social skills of the trial manager and his ability to negotiate access to resources with relevant personnel across NHS organisations at both a national, and local (PCT) level. This observation highlights the necessary (though potentially underacknowledged) skills required of trial managers in the current climate of primary care research.
Due to the decision of the MREC regarding SSAs and access to patient data, the evolving nature of RM&G guidelines, and various interpretations of these guidelines across PCT sites, the trial team were under pressure to continually develop creative and workable solutions to emerging problems. This formed a barrier to the satisfactory and timely achievement (disposal) of essential milestones – such as recruitment – in the delivery of the trial. A review of the practical implementation of MREC decisions and RM&G guidelines in primary care is also necessary in order to identify how to promote quality research while meeting ethical standards.
We addressed the research question ‘how is participation in the RCT negotiated and understood by subjects?’ through the NPM constructs of interactional workability and relational integration. Specifically, we found that some participants reported a lack of understanding or congruence between themselves and the practice nurse regarding the value of the research. For some participants, their encounter with the practice nurse was a demoralising experience as the nurse appeared to view the trial’s interventions as a poor use of time. Moreover, for most of the participants who sought medical interventions, the BCC or standardised advice consultations failed to help them dispose of problems related to health, diet or lifestyle issues. When describing their experiences in the RCT, the participants reported that the daily diary exercise was the most salient part. Most of the participants therefore struggled to make sense of the mechanics of the trial and how such a diary might usefully contribute to the amelioration of their, or others, chronic constipation. Therefore, whether participants viewed their constipation as problematic or not, both groups reported that they struggled to see how the trial would lead to results that would benefit suffers of chronic constipation. This finding may result from the intrinsically confusing experience of trial participation as reported in the literature,229–231 an issue more specific to the LIFELAX trial, such as the practice nurses’ perceptions of the research and their subsequent behaviour with participants, or a combination of factors.
-
Implementation How are the production of results negotiated and organised within networks of researchers; how are its results mediated to the wider community and how is this negotiated and organised, both formally (through report writing and presentation), and informally how are the mechanisms and results of the trial understood by subjects?
Following the premature closure of the LIFELAX RCT it was not possible to collect data relating to the development and publication of outputs from the trial. However, we have discussed the manner in which the participants attempted to understand the mechanisms and results of the trial through the context of their own illness trajectories and the NPM constructs of interactional workability and relational integration.
-
What lessons can be learned that will improve the organisation and conduct of HTA RCTs in the UK – and further afield? The study holds important implications for the organisation and conduct of HTA. It is important that its results can inform and develop both policy and practice?
A number of issues regarding the development and implementation of RCTs have been identified through the conduct of the process evaluation. The problem of the trial’s topic, setting and training packages may have been identified had a prior feasibility study been conducted. At the time of the LIFELAX trial the HTA did not fund pilot studies of this nature, although the HTA have now changed their policy in this regard. However numerous system wide problems – such as the changing RM&G guidelines and research briefs that did not match GMS contracts – also taxed the capacity of the trial to be successful. Following the results of the process evaluation, and the input of several of the reviewers of this report, we suggest the following:
-
Improved means and methods of communication are required between governance bodies, MRECs and researchers regarding the best way to conduct RCTs that are ethically, methodologically, and practically sound.
-
There is a need for a clear and consistent means of applying for RM&G approval across PCTs.
-
There is a clear need for pilot studies prior to the design and implementation of HTA RCTs. The pilot study should:
-
– Assess the feasibility of all aspects of the intended research but specifically ensure that the assumptions underpinning the study are correct. These assumptions may be multiple but should ensure that: (1) there is an identified need for a technological intervention; (2) the intended beneficiaries also perceive a need for intervention and are in equipoise regarding the proposed interventions and control; and (3) the definition of the need or problem is commensurate between researchers, users and beneficiaries.
-
– Pilot studies should assess whether the interventions will enable the intended users and/or beneficiaries to achieve relevant goals (such as disposal of symptoms).
-
– Pilot studies should assess whether the intended interventions fit within existing patterns of work, and where they do not, assess the likely disruption and acceptability to intended users.
-
– Pilot studies designed to assess the feasibility of the research should be conducted prior to any significant investment in the development of an RCT.
-
Conclusions
Through application of the NPM we were able to identify a number of factors that contributed to the premature closure of the LIFELAX RCT. Evaluation of the trial raises a number of important considerations for the deployment of other trials of complex interventions in primary care. In particular, the administrative difficulties encountered by the LIFELAX trial team, regarding the application of RM&G guidelines and research ethics, were indicative of the unsettled climate at the time of the trial, also experienced and reported by other researchers. 19,215 Nevertheless, research should be conducted to explore how the processes of implementing RCTs in primary care can be practically facilitated, and how procedures may be standardised and streamlined. In addition, it is important for funders such as the HTA to commission studies using appropriate forms of assessment. RCTs may not always be the most suitable method, particularly in the initial stages of development for new and complex technologies.
The trial team developed innovative solutions to practical problems of implementation. This work illustrated the importance of social, as well as technical, competence in the delivery of a multicentred RCT. However, there is a significant gap in the literature exploring how RCTs are practically accomplished. While the process evaluation contributed towards addressing this shortfall, further research is needed to explore the practical conduct of RCTs in different contexts in order to better understand the processes underpinning the formation of medical evidence.
Conventionally, when a large project fails, stakeholders attempt to identify the causal factors for this outcome. However, in the LIFELAX RCT, there was no central agent of blame for the trial’s failure. A number of significant problems accumulated across the life of the research to prevent the RCT from moving forwards. These structural problems included the contemporaneous climate of uncertainty regarding interpretation of ethical and RM&G governance, changing priorities in primary care expressed though the GMS contract, and a general lack of enthusiasm or commitment for research in primary care. Specifically, the clinical environment in which the LIFELAX trial was situated was largely indifferent to the research. Although the trial team worked hard to develop workable solutions to these problems, the numerous and unforeseeable issues encountered by the trial team exhausted the capacity of LIFELAX to be a workable trial.
Chapter 7 Conclusions
Due to the low number of participants in the trial, we are unable to draw any firm conclusions about the effectiveness of the interventions in LIFELAX. Nonetheless, at the conclusion of this study, there are a number of issues that we wish to highlight as they had a major impact upon the conduct and progress of the trial. We believe that they are relevant to anyone else conducting research on a similar topic or in a similar population.
Pilot studies
At the time of commissioning, the HTA did not fund pilot studies. If a rehearsal (external) pilot trial or feasibility study had been conducted first then it is likely that the full LIFELAX trial would either never have been commissioned or if it had, it would have had a major methodological overhaul. We are pleased that pilot and feasibility studies are now part of the HTA commissioning process.
Choice of data collection methods
Our findings suggest that the range of data collection methods we employed in LIFELAX were acceptable for use in a population of this age with constipation. The self-completion questionnaire response rates in excess of 80% suggests that despite the length of the questionnaire, the time taken to complete it and the added burden of the daily diary, at the first two time points at least respondent fatigue was not an issue.
Analyses of the response rates and item response rates suggest that the daily diary was not troublesome to participants. We would propose that a diary of this nature to collect information about bowel function and medication is not burdensome to complete and is a satisfactory way of gathering such information.
Defining ‘eligibility’ for studies of constipation
The experiences of both the STOOL Trial19 and LIFELAX would suggest that being able to define ‘constipation’ in a way that is both measurable and acceptable to all stakeholders is vital to future research in this field. When people do not think that they have a particular condition then it seems unlikely that they would be interested in or motivated to participate in research into that condition.
Though a common complaint of industrialised societies,9 there is much variability in definition of constipation, both within the medical literature and between patients and medical professionals. 8 Some attempts as at a definition have used the frequency of bowel movements. 20,21 Clinical definitions do exist within the Rome II22 and III23 criteria for functional constipation.
In the Rome II criteria for functional constipation,22 two or more of the following symptoms must have present for at least 12 consecutive weeks in the previous 12 months for a diagnosis of constipation:
-
straining in more than one in four defecations
-
lumpy or hard stools in more than one in four defecations
-
sensation of incomplete evacuation in more than one in four defecations
-
manual procedures (e.g. digital evacuation or support of the pelvic floor) in more than one in four defecations; and
-
fewer than three defecations per week.
In the Rome III criteria a somewhat less restrictive time frame has been introduced. 23
Practitioners, however, appear unlikely to apply the above criteria in their clinical practice and constipation is typically a subjective diagnosis. 18 Nonetheless, a level of consensus does exist among clinicians over the wide variation between individuals in the normal frequency of bowel movements (from three times per day to three times per week being normal). 12 The perceptions of older people reported by a small number of previous studies suggest that lay definitions of constipation differ from professional criteria. 14,16,17 From the STOOL report it is apparent that frequency and ‘ease’ of bowel movements, however, are key components of constipation for the majority of older people. 19
Our belief is that while there is such a lack of agreement – both within clinicians and patients, and between the two parties – as to what constipation is then recruiting to studies of ‘patients with chronic constipation’ will remain difficult. If objective criteria such as Rome II/III, or the number of laxatives prescribed in a given time frame are met with the circular argument from patients of ‘I take laxatives which produce my desired frequency of bowel movements, and therefore I am not constipated’ it would seem there is a hurdle that is particularly troublesome to overcome.
Difficulty implementing the LIFELAX trial
LIFELAX fulfilled all the criteria of a ‘marketable trial’. 232 LIFELAX was designed as a pragmatic113 three-armed cluster RCT to compare laxative treatment (current practice) of chronic constipation in older people with both standardised, non-personalised dietary and lifestyle advice (delivered in a single, short consultation) and personalised dietary and lifestyle advice (delivered in a long consultation, or two shorter consultations, with telephone reinforcement) in the management of chronic constipation in older people. LIFELAX was to be conducted in north-east England and was to recruit patients aged ≥ 55 years, registered with practices participating in the trial, with a current diagnosis of functional constipation.
Like the STOOL trial, LIFELAX was not successful in recruiting patients to the trial and experienced difficulty in encouraging general practices to fully engage with the research.
Though largely anecdotal and based upon the experiences and beliefs of the wider research team and collaborating GPs since the turn of the century, the climate of research has changed and there are now considerable barriers to complex trials of ‘routine’ interventions.
Ethics committees reacted (some would say over-reacted) to a number of landmark documents including the report of the Alder Hey enquiry,198 the European Human Rights Act199 (and its implementation) and preparation for the enactment of the EU Clinical Trials Directive. As a result, the guidelines to which ethics committees adhered became more prescriptive and committees became more risk aware and averse, and took measures to mitigate risk where possible. The publication of the Research Governance Framework for Health and Social Care200 created further challenges with guidance and decisions taken at a local level often appearing to be contradictory to national advice. Ethics committees and NHS Trusts, faced with the introduction of a more prescriptive and bureaucratic framework, were unable to respond to the increasing workload generated. Our experiences in these respects are echoed by other researchers conducting multicentre research involving primary care at a similar time. 201–203
In addition to the inevitable delays created by these developments, the necessity for participants to ‘opt in’ to LIFELAX and the apparent removal of direct contact with the research team until much later in the research process was one of the major issues of concern to both the research team and the TSC. This model has major implications for health services research in the future204 and by implementing such a model, one immediately decreases the likelihood of participation and increases the risk of participation bias. 205 Communication between a committed trial team and the participant is crucial to the success of a trial. Opportunities for those most familiar with the study design and processes (i.e. the research team) to explain the trial or discuss any aspect of participation diminish once the GP practice becomes the primary contact point for information in the early stages of the trial.
We are pleased that, since LIFELAX, many of the proposed measures to streamline the research process are slowly being implemented. The Integrated Research Application System is now running and continues to be revised. This will simplify the entire ethics and research governance approval process, especially for multicentre studies. The Research Passport (its imminent introduction was heralded during the set-up of LIFELAX), when available, will add to innovations such as the Central Sign-off Process for NHS R&D approval, and will hopefully further reduce the bureaucracy of the research process.
Insight from process evaluation
Through application of the NPM233 we were able to identify a number of factors that contributed to the premature closure of the LIFELAX RCT. However, it is important to note that within the constraints set by the commissioning brief – including the topic of the trial and nature of the interventions – the trial team could not have produced a successful outcome. Evaluation of this trial raises a number of important considerations for the deployment of other trials of complex interventions in primary care. In particular the bureaucratic difficulties encountered by the LIFELAX trial team, regarding the application of RM&G guidelines and research ethics, were indicative of the unsettled climate at the time of the trial, also experienced and reported by other researchers. 19,215 Nevertheless, research should be conducted to explore how the processes of implementing RCTs in primary care can be practically facilitated, and how procedures may be standardised and streamlined.
The trial team developed innovative solutions to practical problems of implementation. This work illustrated the centrality of socially-mediated processes across the lifespan of the RCT. There is a significant gap in the literature exploring how RCTs are practically accomplished. While the process evaluation contributed towards addressing this shortfall, further research is needed to explore the practical conduct of RCTs in different contexts in order to better understand the processes underpinning the formation of medical evidence.
Conventionally, when a large project fails, stakeholders attempt to identify the causal factors for this outcome. However, in the LIFELAX RCT, there was no central agent of blame for the trial’s failure. A number of significant problems accumulated across the life of the research to prevent the RCT from moving forward. These structural problems included the contemporaneous climate of uncertainty regarding ‘correct’ interpretation of ethical and RM&G governance, changing priorities in primary care expressed though the GMC contract, and a general lack of enthusiasm or commitment for research in primary care. Specifically, the clinical environment in which the LIFELAX trial was situated was largely indifferent to the research. Although the trial team worked hard to develop workable solutions to these problems, the numerous and unforeseeable issues encountered by the trial team exhausted the capacity of LIFELAX to be a workable trial.
Recommendations
The issues raised in this report are many and complex, some are condition and time bound (RM&G framework), and, as such, we are reluctant to make stringent recommendations as there may be little usefulness in doing so. However, there are a number of key learning points that we can highlight in the belief that these can be of use to researchers planning an RCT of a complex intervention in the future.
-
Our experience suggests that the topic under investigation needs to be relevant to both the people delivering the intervention and those receiving the intervention.
-
Rather than launching straight into conducting a full-scale intervention and trial, work needs to be undertaken to ascertain whether such a trial is feasible (we are pleased that pilot and feasibility studies are now part of the commissioning process for the HTA).
-
The inclusion criteria need to be clear and comprehensible to both the people identifying participants and the participants themselves.
-
If a ‘train-the-trainer’ approach is to be used for intervention delivery, there needs to be confidence that the trainees are fully supportive and motivated rather than participating because their institution has agreed to take part.
Although it is unclear whether ‘payment’ or financial incentives would make a future intervention a success, attention needs to be paid to the current funding arrangements and priority topic areas for the health-care practitioners with whom researchers will be working. Topics within the QOF have a much higher profile, interest and importance.
Acknowledgements
We are most grateful and extend our sincere thanks to all the patients and health professionals who took part in the study as participants and to those many health professionals and NHS employees who facilitated its process.
We would like to thank our trial steering committee who provided expert advice and support throughout the study and commented on earlier drafts of the report: Professor Ashley Adamson* (Nutritionist, Human Nutrition Research Centre and Institute of Health and Society, Newcastle University), Dr Sally Corbett* (Health Psychologist, Northumbria Healthcare NHS Trust), Dr Mary Dixon-Woods [Medical Sociologist (Chair from May 2004), Department of Health Sciences, University of Leicester], Professor Cam Donaldson [Health Economist (Chair until May 2004), Institute of Health and Society, Newcastle University], Professor Jenny Hewison (Health Psychologist, School of Medicine, University of Leeds), Dr Amelia Lake* (Dietitian and Public Health Nutritionist, Human Nutrition Research Centre and Institute of Health and Society, Newcastle University), Professor James Mason (Health Economist, School for Health, Durham University), Professor John Matthews (Medical Statistician, School of Mathematics, Newcastle University), Professor Carl May* (Medical Sociologist, Institute of Health and Society, Newcastle University), Professor Paula Moynihan* (Nutritionist, Human Nutrition Research Centre, Newcastle University; Institute for Ageing and Health, Newcastle University and Dental School, Newcastle University), Dr Julia Newton (Consultant in General Medicine, Newcastle upon Tyne Hospitals NHS Foundation Trust), Dr Pauline Pearson** (Community Nurse, School of Medical Education, Newcastle University), Mr Gavin Spencer (layperson), Mr Chris Storey (layperson) and Professor David Weller (General Practitioner, Division of Community Health Sciences, University of Edinburgh).
(*Members of the trial team who are also authors; **members of the trial team who are applicants, but not authors.)
Contribution of authors and other team members
Contribution to the study
Professor Roger Barton** (Professor of Clinical Medicine, Newcastle University and Director of Research, Northumbria Healthcare Trust) developed the protocol and provided clinical advice to the study. Professor Elaine McColl* (Director, Newcastle Clinical Trials Unit) was the CI. She was responsible for the overall management of the study, developed the protocol and edited the report for publication. Dr Richard Curless** (Consultant Physician) developed the protocol. Professor John Bond* (Professor of Social Gerontology and Health Services Research) developed the protocol, project managed the study and edited the report for publication. Professor Carl May* (Professor of the Sociology of Healthcare) developed the protocol of the Integrated Process Evaluation and edited the report for publication. Mr Chris Speed* (Research Associate) was the trial manager and main researcher on the project. He was responsible for the day-to-day management of the trial and recruitment of practices and patients to the trial. He contributed to the development of the behaviour change interventions. He was also responsible for preparing the report for publication. Mr Ben Heaven* (Junior Research Associate) was responsible for conducting the Integrated Process Evaluation and preparing the report for publication. Professor Greg Rubin* (Professor of General Practice and Clinical Director of NoReN) developed the protocol, provided clinical advice and managed the relationships between the study team and general practice. Professor Ashley Adamson* (Dietitian and Nutritionist), Professor Paula Moynihan* (Dietitian and Nutritionist) and Dr Sally Corbett* (Health Psychologist) contributed to the development of the behaviour change interventions. Dr Amelia Lake* (Dietitian and Public Health Nutritionist) contributed to the development of the behaviour change interventions and was jointly responsible for training practice nurses to deliver the intervention. Mrs Yolande Causebrook (Nutritionist) was jointly responsible for training practice nurses to deliver the intervention. Ms Anna Brookes (Nutrition Student) assisted with the development of the patient information and intervention materials. Dr Nick Steen* (Principal Research Associate – statistician) developed the protocol and provided statistical advice throughout the trial. Ms Alessandra Vanoli* (Senior Research Associate – health economist) developed the protocol for the economic evaluation. Mr Peter McMeekin* (Research Associate – health economist) conducted the economic analysis for the study.
We are extremely grateful to Mrs Linda Duckworth (project secretary), Mrs Erika Tandy (Project Secretary), Ms Lynne Oliver (Project Secretary) for their secretarial expertise and support throughout the study and Ms Joanne Dryburgh (NCTU Secretary) for her assistance with preparing the final report. We are very grateful to Ms Nicola Barnett (Research Nurse) for assisting with participant recruitment. We are especially grateful to NYReN staff for the support and expertise that they provided during the course of the study, in particular Ms Terri Harding (NYReN Administrator) for supporting the administration of the SfS funding and Ms Sarah Daniel (Research Nurse) for assisting with patient identification and participant recruitment.
Contribution to the report
Mr Chris Speed wrote the final report. Mr Ben Heaven wrote the sections of the final report which related to the integrated process evaluation. Professors Elaine McColl and John Bond edited the report. All members of the project team were responsible for critical review of the report and comments were also received from members of the Trial Steering Committee.
Publications
Lake A. Constipation in the older patient. Com Nutr 2004;4:23–5.
Lake A, Speed C, Brookes A, Heaven B, Adamson AJ, Moynihan P, et al. Development of a series of PILs for constipation using a range of cognitive interview techniques: LIFELAX. BMC Health Serv Res 2007;7:3.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- Petticrew M, Watt I, Sheldon T. Systematic review of the effectiveness of laxatives in the elderly. Health Technol Assess 1997;1.
- O’Keefe EA, Talley NJ, Zinsmeister AR, Jacobsen SJ. Bowel disorders impair functional status and quality of life in the elderly: a population-based study. J Gerontol 1995;50A:M184-9.
- Glia A, Lindberg G. Quality of life in patients with different types of functional constipation. Scand J Gastroenterol 1997;32:1083-9.
- Singh G, Kahler K, Bharathi V, Mithal A, Omar M, Triadafilopoulos G. Adults with chronic constipation have significant health care resource utilization costs of care. Am J Gastroenterol 2004;99.
- McCormick A, Fleming DF, Charlton J. Morbidity statistics from general practice: fourth national study. London: OPCS; 1995.
- Passmore AP. Economic aspects of pharmacotherapy for chronic constipation. Pharmacoeconomics 1995;7:14-2.
- NHS Health and Social Care Information Centre . Prescription Cost Analysis: England 2005 (prescription Items Dispensed in the Community in England and Listed Alphabetically Within Chemical Entity by Therapeutic Class) 2006.
- Camilleri M, Thompson WG, Fleshman JW, Pemberton JH. Clinical management of intractable constipation. Ann Int Med 1994;121:520-8.
- Gilliland R, Heymen S, Altomare DF, Park UC, Vickers D, Wexner SD. Outcome and predictors of success of biofeedback for constipation. Br J Surg 1997;84:1123-6.
- Prather CM, Ortiz-Camacho CP. Evaluation and treatment of constipation and fecal impaction in adults. Mayo Clin Proc 1998;73:881-6.
- Baden-Powell R. Scouting for boys. London: Horace Cox; 1908.
- Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, et al. US householder survey of functional gastrointestinal disorders: prevalence, sociodemography, health impact. Dig Dis Sci 1993;38:1569-80.
- Heaton KW, Radvan J, Cripps H, Mountford RA, Braddon FE, Hughes AO. Defecation frequency and timing, stool form in the general population: a prospective study. Gut 1992;33:818-24.
- Probert CS, Emmett PM, Heaton KW. Some determinants of whole-gut transit time: a population-based study. Q J Med 1995;88:311-15.
- Heaton KW, Cripps HA. Straining at stool and laxative taking in an English population. Dig Dis Sci 1993;38:1004-8.
- MacDonald L, Freeling P. Bowels: beliefs and behaviour. Fam Pract 1986;3:80-4.
- Annells M, Koch T. Older people seeking solutions to constipation: the laxative mire. J Clin Nurs 2002;11:603-12.
- Moriarty KJ, O’Donoghue N. Constipation, in ABC of colorectal diseases. London: BMJ Books; 1999.
- Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al. Stepped treatment of older adults on laxatives. The STOOL trial. Health Technol Assess 2008;12.
- Whitehead WE, Drinkwater D, Cheskin LJ, Heller BR, Schuster MM. Constipation in the elderly living at home: definition, prevalence, relationship to lifestyle and health status. J Am Geriatr Soc 1989;37:423-9.
- Wolfsen CR, Barker JC, Mitteness LS. Constipation in the daily lives of frail elderly people. Arch Fam Med 1993;2:853-8.
- Thompson WG, Longstreth GF, Drossman DA, Heaton KW, Irvine EJ, Müller-Lissner SA. Functional bowel disorders and functional abdominal pain. Gut 1999;45:43-7.
- Douglas AD. The Functional Gastrointestinal Disorders and the Rome III Process. Gastroenterology 2006;130:1377-90.
- Higgins PDR, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol 2004;99:750-9.
- Lea R, Hopkins V, Hastleton J, Houghton LA, Whorwell PJ. Diagnostic criteria for irritable bowel syndrome: utility and applicability in clinical practice. Digestion 2004;70:210-13.
- Gladman LM, Gorard DA. General practitioner and hospital specialist attitudes to functional gastrointestinal disorders. Aliment Pharmacol Ther 2003;17:651-4.
- Moore-Gillon V. Constipation: what does the patient mean?. J R Soc Med 1984;77:108-10.
- Nakaji S, Matsuzaka M, Umeda T, Shimoyama T, Sugawara K, Sakamoto J, et al. A population-based study on defecatory conditions in Japanese subjects: methods for self-evaluation. Tohoku J Exp Med 2004;203:97-104.
- Romero Y, Evans JM, Fleming KC, Phillips SF. Constipation and fecal incontinence in the elderly. Mayo Clin Proc 1996;71:81-92.
- Lennard-Jones JE. Clinical management of constipation. Pharmacology 47:216-23.
- Glia A, Lindberg G, Nilsson LH, Mihocsa L, Akerlund JE. Clinical value of symptom assessment in patients with constipation. Dis Colon Rectum 1999;42:1401-8.
- Connell AM, Hilton C, Irvine G, Lennard-Jones JE, Misiewicz JJ. Variation of bowel habit in two population samples. Br Med J 1965;i.
- Johanson JF, Sonnenberg A, Koch TA. Clinical epidemiology of chronic constipation. J Clin Gastroenterol 1989;11:525-36.
- Thompson WG, Heaton KW. Functional bowel disorders in apparently healthy people. Gastroenterology 1980;79:283-8.
- Talley NJ, Fleming KC, Evans JM, O’Keefe EA, Weaver AL, Zinsmeister AR, et al. Constipation in an elderly community: a study of prevalence and potential risk factors. Am J Gastroenterol 1996;91:19-25.
- Talley NJ, Weaver AL, Zinsmeister AR, Melton LJ. 3rd. Functional constipation and outlet delay: a population-based study. Gastroenterology 1993;105:781-90.
- McCormick A, Fleming D, Charlton J. Morbidity statistics from general practice: fourth national study. London: Office of Population Censuses and Surveys; 1995.
- Marquis P, De La Loge C, Dubois D, McDermott A, Chassany O. Development and validation of the patient assessment of constipation quality of life questionnaire. Scand J Gastroenterol 2005;40:540-51.
- Irvine EJ, Ferazzi S, Pare P, Thompson WG, Rance L. Health-related quality of life in functional GI disorders: focus on constipation and resource utilization. Am J Gastroenterol 2002;97:1986-93.
- Gallagher P, O’Mahony D, Quigley EMM. Management of chronic constipation in the elderly. Drugs Aging 2008;25:807-21.
- Petticrew M, Rodgers M, Booth A. Effectiveness of laxatives in adults. Qual Health Care 2001;10:268-73.
- Cummings JH, Spiller GA. CRC handbook of dietary fiber in human nutrition. Boca Raton, FL: CRC Press; 2001.
- Burkitt DP, Walker ARP, Painter NS. Effect of dietary fibre on stools and transit times and its role in the causation of disease. Lancet 1972:1408-11.
- Bingham SA, Day NE, Luben R, Ferrari P, Slimani N, Norat T, et al. Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC): an observational study. Lancet 2003;361:1496-501.
- Kamm MA. Constipation and its management. BMJ 2003;327:459-60.
- American Gastroenterological Association . American Gastroenterological Association Medical Position Statement: guidelines on constipation. Gastroenterology 2000;119:1761-78.
- Castle SC. Constipation: endemic in the elderly? Gerontopathophysiology, evaluation and management. Geriatr Med 1989;73:1497-509.
- Doughty DB. When fiber is not enough: current thinking on constipation management. Ostomy Wound Manage 2002;48:30-41.
- Chen HL, Haack VS, Janecky CW, Vollendorf NW, Marlett JA. Mechanism by which wheat bran and oat bran increase stool weight in humans. Am J Clin Nutr 1998;68:711-19.
- Kay RM. Dietary fiber. J Lipid Res 1982;23:221-42.
- Stephen AM, Cummings JH. Mechanism of action of dietary fibre in the human colon. Nature 1980;284:283-4.
- Hope AK, Down EC. Dietary fibre and fluid in the control of constipation in a nursing home population. Med J Aust 1986;144:306-7.
- Badiali D, Corazziari E, Habib FI, Tomei E, Bausano G, Magrini P, et al. Effect of wheat bran in treatment of chronic nonorganic constipation. A double blind controlled trial. Dig Dis Sci 1995;40:349-56.
- Gear JS, Brodribb AJ, Ware A, Mann JI. Fibre and bowel transit times. Br J Nutr 1981;45:77-82.
- Marlett JA, McBurney MI, Slavin JL. Position of the American Dietetic Association: health implications of dietary fiber. J Am Diet Assoc 2002;102:993-1000.
- Gregory J, Foster K, Tyler H, Wiseman M. The dietary and nutritional survey of British adults. London: Office of Population Censuses and Surveys; 1990.
- Finch S, Doyle W, Lowe C, Bates CJ, Prentice A, Smithers G, et al. National Diet and Nutrition Survey: people aged 65 years and over. London: The Stationery Office; 1998.
- Dukas L, Willett WC, Giovannucci EL. Association between physical activity, fiber intake, other lifestyle variables and constipation in a study of women. Am J Gastroenterol 2003;98:1790-6.
- Kenny KA, Skelly JM. Dietary fiber for constipation in older adults: a systematic review. Clin Effect Nurs 2001;5:120-8.
- Lindeman RD, Romero LJ, Liang HC, Baumgartner RN, Koehler KM, Garry PJ. Do elderly persons need to be encouraged to drink more fluids?. J Gerontol A Biol Sci Med Sci 2000;55:M361-5.
- Chung BD, Parekh U, Sellin JH. Effect of increased fluid intake on stool output in normal healthy volunteers. J Clin Gastroenterol 1999;28:29-32.
- Klauser AG, Beck A, Schindlbeck NE, Müller-Lissner SA. Low fluid intake lowers stool output in healthy male volunteers. Z Gastroenterol 1990;28:606-9.
- Rodrigues-Fisher LC, Bourguignon BV. Good, Dietary fiber nursing intervention: prevention of constipation in older adults. Clin Nurs Res 1993;2:464-77.
- Marteau P, Boutron-Ruault MC. Nutritional advantages of probiotics and prebiotics. Br J Nutr 2002;87:S153-7.
- Gibson GR. Dietary modulation of the human gut microflora using the prebiotics oligofructose and inulin. J Nutr 1999;129.
- Schrezenmeir J, de Verse M. Probiotics, prebiotics and synbiotics: approaching a definition. Am J Clin Nutr 2001;73:S361-4.
- Marteau P, Seksik P, Jian R. Probiotics and intestinal health effects: a clinical perspective. Br J Nutr 2002;88:S51-7.
- Meance S, Cayuela C, Turchet P, Raimondi A, Lucas C, Antoine JM. A fermented milk with a Bifidobacterium probiotic strain DN-173 010 shortened oro-fecal gut transit time in elderly. Microb Ecol Health Dis 2001;13:217-22.
- Pathmakanthan S, Meance S, Edwards CE. Probiotics: a review of human studies to date and methodological approaches. Micr Ecol Health Dis 2000;12:10-3.
- Cummings JH, Macfarlane GT. Gastrointestinal effects of prebiotics. Br J Nutr 2002;87:145-51.
- Moshfegh AJ, Friday JE, Goldman JP, Ahuja JK. Presence of inulin and oligofructose in the diets of Americans. J Nutr 1999;129:S1407-11.
- Schneeman BO. Fiber, inulin and oligofructoset: similarities and differences. J Nutr 1999;129:S1424-7.
- Gibson GR, Beatty ER, Wang X, Cummings JH. Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gastroenterology 1995;108:975-82.
- Clausen MR, Mortensen PB. Lactulose, disaccharides and colonic flora: clinical consequences. Drugs 1997;53:930-42.
- Hidaka H, Eida T, Takizawa T, Tokunaga T, Tashiro Y. Effects of fructooligosaccharides on intestinal flora and human health. Bifidobacteria Microflora 1986;5:37-50.
- Cherbut C. Inulin and oligofructose in the dietary fibre concept. Br J Nutr 2002;87:159-62.
- Kleessen B, Sykura B, Zunft HJ, Blaut M. Effects of inulin and lactose on fecal microflora, microbial activity, bowel habit in elderly constipated persons. Am J Clin Nutr 1997;65:1397-402.
- Holdstock DJ, Misiewicz JJ, Smith T. Propulsion (mass movement) in the human colon and its relationship to meals and somatic activity. Gut 1970;11:91-9.
- Coenen C, Wegener M, Wedmann B, Schmidt G, Hoffmann S. Does physical exercise influence bowel transit time in healthy young men?. Am J Gastroenterol 1992;87:292-5.
- Keeling W, Martin BJ. Gastrointestinal transit during mild exercise. J Appl Physiol 1987;63:978-81.
- Meshkinpour H, Selod S, Movahedi H, Nami N, James N, Wilson A. Effects of regular exercise in management of chronic idiopathic constipation. Dig Dis Sci 1998;43:2379-83.
- Sikirov D. Comparison of straining during defecation in three positions: results and implications for human health. Dig Dis Sci 2003;48:1201-5.
- Sirakov BA. Cardiovascular events at defecation: are they unavoidable?. Med Hypotheses 1990;32:231-3.
- Pendleton D, Schofield T, Tate P, Havelock P. The new consultation. Developing doctor–patient communication. Oxford: Oxford University Press; 2003.
- Glasgow RE, La Chance PA, Toobert DJ, Brown J, Hampson SE, Riddle MC. Long-term effects and costs of brief behavioural dietary intervention for patients with diabetes delivered from the medical office. Patient Educ Couns 1997;32:175-84.
- Eakin EG, Glasgow RE, Riley KM. Review of primary care-based physical activity intervention studies: effectiveness and implications for practice and future research. J Fam Pract 2000;49:158-68.
- Brug J, van Assema P. Differences in use and impact of computer-tailored dietary fat-feedback according to stage of change and education. Appetite 2000;34:285-93.
- Rollnick S, Miller WR. What is motivational interviewing?. Behav Cogn Psychother 1995;23:325-34.
- McGraw SA, Stone EJ, Osganian SK, Elder JP, Perry CL, Johnson CC, et al. Design of process evaluation within the Child and Adolescent Trial for Cardiovascular Health (CATCH). Health Educ Q 1994;21:5-26.
- Oakley A, Strange V, Bonell C, Allen E, Stephenson J. RIPPLE Study Team . Process evaluation in randomised controlled trials of complex interventions. BMJ 2006;332:413-16.
- May CR, Mair FS, Dowrick CF, Finch TL. Process evaluation for complex interventions in primary care: understanding trials using the normalization process model. BMC Fam Pract 2007;8.
- Jolly K, Bradley F, Sharp S, Smith H, Thompson S, Kinmonth AL, et al. Randomised controlled trial of follow up care in general practice of patients with myocardial infarction and angina: final results of the Southampton heart integrated care project (SHIP). BMJ 1999;318:706-11.
- Wiles R. Patients’ perceptions of their heart attack and recovery: the influence of epidemiological “evidence” and personal experience. Soc Sci Med 1998;46:1477-86.
- Jolly K, Lip GY, Sandercock J, Greenfield SM, Raftery JP, Mant J, et al. Home-based versus hospital-based cardiac rehabilitation after myocardial infarction or revascularisation: design and rationale of the Birmingham Rehabilitation Uptake Maximisation Study (BRUM): a randomised controlled trial [ISRCTN72884263]. BMC Cardiovasc Disord 2003;3.
- May C, Ellis NT. When protocols fail: technical evaluation, biomedical knowledge, the social production of ‘facts’ about a telemedicine clinic. Soc Sci Med 2001;53:989-1002.
- May C, Gask L, Atkinson T, Ellis N, Mair F, Esmail A. Resisting and promoting new technologies in clinical practice: the case of telepsychiatry. Soc Sci Med 2001;52:1889-901.
- May CR, Mort M, Williams T, Mair F, Shaw NT. Understanding the Evaluation of Telemedicine: The Play of the Social and the Technical, the Shifting Sands of Reliable Knowledge n.d.
- Mort M, May C, Williams T. Remote doctors and absent patients: acting at a distance in teledermatology. Sci Technol Hum Value 2003;28:274-95.
- May C, Mort M, Williams T, Mair F, Gask L. Health Technology Assessment in its local contexts: studies of telehealthcare. Soc Sci Med 2003;57:697-710.
- Woolf SH, Henshall C. Health technology assessment in the United Kingdom. Int J Technol Assess Health Care 2000;16:591-625.
- Goodman CS, Ahn R. Methodological approaches of health technology assessment. Int J Med Inform 1999;56:97-105.
- Pilgrim D, May C. Social scientists and the British National Health Service. Soc Sci Health 1998;4:42-54.
- Gibbons M, Limoges C, Nowotny H, Schwartzman S, Scott P, Trow M. The new production of knowledge. London: Sage; 1994.
- Tanenbaum SJ. Knowing and acting in medical research: the epistemological politics of outcomes research. J Health Polit Policy Law 1994;19:27-44.
- Taylor FC, Davidson O, King M, Haines A, Davidson O, Sharp D. Recruitment of general practitioners to a randomized trial. Br J Gen Pract 1998;48.
- Ward E, King M, Lloyd M, Bower P, Friedli K. Conducting randomized trials in general practice: methodological and practical issues. Br J Gen Pract 1999;49:919-22.
- Street A, Strong J, Karp S. Improving patient recruitment to multicentre clinical trials: the case for employing a data manager in a district general hospital-based oncology centre. Clin Oncol 2001;13:38-43.
- Haidich AB, Ioannidis JPA. Patterns of patient enrolment in randomized controlled trials. J Clin Epidemiol 2001;54:877-83.
- Sellors J, Cosby R, Trim K, Kaczorowski J, Howard M, Hardcastle L, et al. Recruiting family physicians and patients for a clinical trial: lessons learned. Fam Pract 2002;19:99-104.
- Allsup SJ, Gosney MA. Difficulties of recruitment for a randomized controlled trial involving influenza vaccination in healthy older people. Gerontology 2002;48:170-3.
- Shelton BJ, Wofford JL, Gosselink CA, McClatchey MW, Brekke K, Conry C, et al. Recruitment and retention of physicians for primary care research. J Community Health 2002;27:79-8.
- Lehoux P, Blume S. Technology assessment and the sociopolitics of health technologies. J Health Polit Policy Law 2000;25:1083-120.
- Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J Chronic Dis 1967;20:637-48.
- Tramonte SM, Brand MB, Mulrow CD, Amato MG, O’Keefe ME, Ramirez G. The treatment of chronic constipation in adults: a systematic review. J Gen Intern Med 1997;12:15-24.
- Kristal AR, Curry SJ, Shattuck AL, Feng Z, Li S. A randomized trial of a tailored, self-help dietary intervention: the Puget Sound Eating Patterns study. Prev Med 2000;31:380-9.
- Lutz SF, Ammerman AS, Atwood JR, Campbell MK, DeVellis RF, Rosamond WD, et al. Innovative newsletter interventions improve fruit and vegetable consumption in healthy adults. J Am Diet Assoc 1999;99:705-9.
- Bandura A. Self-efficacy: toward a unifying theory of behavioural change. Psychol Rev 1977;84:191-215.
- Prochaska JO, DiClemente CC, Miller W, Rollnick S. Toward a comprehensive model of change, in motivational interviewing. London: Gilford Press; 1991.
- Lake AA, Speed C, Brookes A, Heaven B, Adamson AJ, Moynihan P, et al. Development of a series of patient information leaflets for constipation using a range of cognitive interview techniques: LIFELAX. BMC Health Serv Res 2007;7.
- Veldhuyzen van Zanten SJ, Talley NJ, Bytzer P, Klein KB, Whorwell PJ, Zinsmeister AR. Design of treatment trials for functional gastrointestinal disorders. Gut 1999;45:1169-77.
- Cadman L. Bite-size training. Pract Nurse 1996;17:607-9.
- Thompson WG, Longstreth GF, Drossman DA, Heaton KW, Irvine EJ, Müller-Lissner SA. Functional bowel disorders and functional abdominal pain. Gut 1999;45:43-7.
- Schaefer DC, Cheskin LJ. Constipation in the elderly. Am Fam Physician 1998;58:907-14.
- British Medical Association and Royal Pharmaceutical Society of Great Britain . British National Formulary 2001.
- Donner AN, Klar N. Design and analysis of cluster randomization trials in health research. London: Arnold; 2000.
- Liang MH, Fossel AH, Larson MG. Comparisons of five health status instruments for orthopedic evaluation. Med Care 1990;28:632-42.
- Frank L, Kleinman L, Farup C, Taylor L, Miner P. Psychometric validation of a constipation symptom assessment questionnaire. Scand J Gastroenterol 1999;34:870-7.
- Brooks RG. EuroQol: the current state of play. Health Policy 1996;37:53-72.
- EuroQol Group . A new facility for the measurement of health related quality of life. Health Policy 1990;16:199-208.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70.
- MRC CFAS Medical Research Council Cognitive Function and Ageing Study Group . The description of activities of daily living in five centres in England and Wales. Age Ageing 1998;27:605-13.
- Davison J, Bond J, Dawson P, Steen IN, Kenny RA. Patients with recurrent falls attending Accident & Emergency benefit from multifactorial intervention: a randomised controlled trial. Age Ageing 2005;34:162-8.
- Shaw FE, Bond J, Richardson DA, Dawson P, Steen IN, McKeith IG, et al. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ 2003;326:73-5.
- Eccles M, Grimshaw J, Steen N, Parkin D, Purves I, McColl E, et al. The design and analysis of a randomized controlled trial to evaluate computerized decision support in primary care: the COGENT study. Fam Pract 2000;17:180-6.
- Eccles M, McColl E, Steen N, Rousseau N, Grimshaw J, Parkin D, et al. Effect of computerised evidence based guidelines on management of asthma and angina in adults in primary care: cluster randomised controlled trial. BMJ 2002;325:941-4.
- Mauskopf JA, Paul JE, Grant DM, Stergachis A. The role of cost-consequence analysis in healthcare decision-making. Pharmacoeconomics 1998;13:277-88.
- May C. A rational model for assessing and evaluating complex interventions in health care. BMC Health Serv Res 2006;6.
- Glaser BG, Strauss A. The discovery of grounded theory. Chicago, IL: Aldine; 1967.
- Roe L, Strong C, Whiteside C, Neil A, Mant D. Dietary intervention in primary care: validity of the DINE method for diet assessment. Fam Pract 1994;11:375-81.
- Roe L, Hunt P, Bradshaw H. Health promotion interventions to promote healthy eating in the general population: a review. London: Health Education Authority; 1997.
- Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al. A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change. Health Technol Assess 2002;6.
- Shinitzhy HE, Kub J. The art of motivating behaviour change: the use of motivational interviewing to promote health. Public Health Nurs 2001;18:178-85.
- Simons-Morton DG, Calfas KJ, Oldenburg B, Burton NW. Effects of interventions in health care settings on physical activity or cardiorespiratory fitness. Am J Prev Med 1998;15:413-30.
- Marcus BH, Banspach SW, Lefebvre RC, Rossi JS, Carleton RA, Abrams DB. Using the Stages of Change Model to increase the adoption of physical activity among community participants. Am J Health Promot 1992;6:424-9.
- Marcus BH, Bock BC, Pinto BM, Forsyth LH, Roberts MB, Traficante RM. Efficacy of an individualized, motivationally-tailored physical activity intervention. Ann Behav Med 1998;20:174-80.
- Hillsdon M, Thorogood M, White I, Foster C. Advising people to take more exercise is ineffective: a randomized controlled trial of physical activity promotion in primary care. Int J Epidemiol 2002;31:808-15.
- Fletcher A, Rake C. Effectiveness of interventions to promote healthy eating in elderly people living in the community: a review. London: Health Education Authority; 1998.
- Pereira Gray D. Forty-seven minutes a year for the patient. Br J Gen Pract 1998;48:1816-17.
- Horrocks S, Anderson E, Salisbury C. Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors. BMJ 2002;324:819-23.
- Shum C, Humphreys A, Wheeler D, Cochrane MA, Skoda S, Clement S. Nurse management of patients with minor illnesses in general practice: multicentre, randomised controlled trial. BMJ 2000;320:1038-43.
- Kinnersley P, Anderson E, Parry K, Clement J, Archard L, Turton P, et al. Randomised controlled trial of nurse practitioner versus general practitioner care for patients requesting ‘same day’ consultations in primary care. BMJ 2000;320:1043-8.
- Truswell AS. Family physicians and patients: is effective nutrition interaction possible?. Am J Clin Nutr 2000;71:6-12.
- US Preventive Services Task Force . Behavioral counseling in primary care to promote a healthy diet: recommendations and rationale. Am J Prev Med 2003;24:93-100.
- Ashenden RC, Silagy D, Weller A. systematic review of the effectiveness of promoting lifestyle change in general practice. Fam Pract 1997;14:160-76.
- Nicholas LG, Pond CD, Roberts DCK. Dietitian: general practitioner interface: a pilot study on what influences the provision of effective nutrition management. Am J Clin Nutr 2003;77:1039-42.
- Kushner RF. Barriers to providing nutrition counseling by physicians: a survey of primary care practitioners. Prev Med 1995;24:546-52.
- Butler C, Rollnick S, Stott N. The practitioner, the patient and resistance to change: recent ideas on compliance. CMAJ 1996;154:1357-62.
- Abraham C, Michie S. A taxonomy of behaviour change techniques used in interventions. Health Psychol 2008;27:379-87.
- Kreuter MW, Strecher VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Ann Behav Med 1999;21:276-83.
- Skinner CS, Campbell MK, Rimer BK, Curry S, Prochaska JO. How effective is tailored print communication?. Ann Behav Med 1999;21:290-8.
- Britt E, Hudson SM, Blampied NM. Motivational interviewing in health settings: a review. Patient Educ Couns 2003;53:147-55.
- Rollnick SW, Miller R. What is motivational interviewing?. Behav Cogn Psychother 1995;23:325-34.
- Miller WR, Rollnick S. Motivational interviewing. Preparing people for change. New York, NY: Gilford Press; 2002.
- Prochaska JO, DiClemente CC, Miller WR, Heather N. Treating addictive behaviours: processes of change. New York, NY: Plenum Press; 1986.
- Prochaska J, DiClemente C. Stages and processes of self change of smoking: toward an integrative model of change. J Consult Clin Psychol 1983;51:390-5.
- Rollnick S, Kinnersley P, Stott N. Methods of helping patients with behaviour change. BMJ 1993;307:188-90.
- Emmons KM, Rollnick S. Motivational interviewing in health care settings. Opportunities and limitations. Am J Prev Med 2001;20:68-74.
- Burke BL, Arkowitz H, Dunn C, Miller WR, Rollnick S. Motivational interviewing. Preparing people for change. New York, NY: Guilford Press; 2002.
- Dunn C, Deroo L, Rivara FP. The use of brief interventions adapted from motivational interviewing across behavioral domains: a systematic review. Addiction 2001;96:1725-42.
- Resnicow K, DiIorio C, Soet J, Miller WR, Rollnick S. Motivational interviewing. Preparing people for change. New York, NY: Guilford Press; 2002.
- Ondersma SJ, Chase SK, Svikis DS, Schuster CR. Computer-based brief motivational intervention for perinatal drug use. J Subst Abuse Treat 2005;28:305-12.
- Berg-Smith SM, Stevens VJ, Brown KM, Van Horn L, Gernhofer N, Peters E, et al. A brief motivational intervention to improve dietary adherence in adolescents. Health Educ Res 1999;14:399-410.
- Humfress H, Igel V, Lamont A, Tanner M, Morgan J, Schmidt U. The effect of a brief motivational intervention on community psychiatric patients’ attitudes to their care, motivation to change, compliance and outcome: A case control study. J Ment Health 2002;11:155-66.
- Miller WR. Motivational interviewing: research, practice and puzzles. Addict Behav 1996;21:835-42.
- Rollnick S, Heather N, Bell A. Negotiating behaviour change in medical settings: The development of brief motivational interviewing. J Ment Health 1992;1:25-37.
- Rollnick S, Heather N, Gold R, Hall W. Development of short ‘readiness to change’ questionnaire for use in brief, opportunistic interventions among excessive drinkers. Br J Addict 1992;87:743-54.
- Stott NC, Rollnick S, Rees MR, Pill RM. Innovation in clinical method: diabetes care and negotiating skills. Fam Pract 1995;12:413-18.
- Stott NC, Rees M, Rollnick S, Pill RM, Hackett P. Professional responses to innovation in clinical method: diabetes care and negotiating skills. Patient Educ Couns 1996;29:67-73.
- Bandura A. Self-efficacy: the exercise of control. New York, NY: Freeman; 1994.
- Rollnick S, Butler CC, Stott N. Helping smokers make decisions: enhancement of brief intervention for general medical practice. Patient Educ Couns 1997;31:191-203.
- Pignone MP, Ammerman A, Fernandez L, Orleans CT, Pender N, Woolf S, et al. Counseling to promote a healthy diet in adults. Am J Prev Med 2003;24:75-92.
- Ammerman A, Pignone MP, Fernandez L. Counselling to Promote a Healthy Diet. Systematic Evidence Review No. 18 2002. www.ahrq.gov/clinic/serfiles.htm (accessed 2003).
- Steptoe A, Doherty S, Rink E, Kerry S, Kendrick T, Hilton S. Behavioural counselling in general practise for the promotion of healthy behaviour among adults at increased risk of coronary heart disease: randomised trial. BMJ 1999;319:943-8.
- Rollnick S, Mason P, Butler C. Health behaviour change. A guide for practitioners. Edinburgh: Churchill Livingstone; 2002.
- Stewart M, Brown JB, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-centred medicine: transforming the clinical method. Thousand Oaks, CA: SAGE; 1995.
- Cambridge University Press . Cambridge Dictionaries Online n.d. http://dictionary.cambridge.org/ (accessed 16 April 2004).
- Salmon P, Peters S, Rogers A, Gask L, Clifford R, Iredale W, et al. Peering through the barriers in GPs’ explanations for declining to participate in research: the role of professional autonomy and the economy of time. Fam Pract 2007;24:269-75.
- Mant D. R&D in primary care: an NHS priority. Br J Gen Pract 1998;48.
- Speed C. Site-specific assessments: yet another barrier to research. BMJ 2004;329:282-4.
- Lecouturier J, Bamford C, Foy R, Eccles M. Did Changes in the NHS Guidance and Application Procedures Shorten Time Taken for Research Governance Approval? NoReN (Northern Primary Care Research Network) n.d.
- Rowe JC, Elling ME, Hazlewood JG, Zakhary R. A cure for clinical trials. McKinsey Quarterly 2002;2:134-41.
- Farrell B. Efficient management of randomised controlled trials: nature or nurture. BMJ 1998;317:1236-9.
- Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al. Recruitment to randomised trials: strategies for trial enrollment and participation study. The STEPS study. Health Technol Assess 2007;11.
- Francis D, Roberts I, Elbourne DR, Shakur H, Knight RC, Garcia J, et al. Marketing and clinical trials: a case study. Trials 2007;8.
- Nelson M. Recruitment in primary care research. Primary Care Alliance for Clinical Trials (PACT). Aust Fam Physician 2004;33:1039-40.
- Gabbay M, Thomas J. When free condoms and spermicide are not enough: barriers and solutions to participant recruitment to community-based trials. Control Clin Trials 2004;25:388-99.
- Foy R, Parry J, Duggan A, Delaney B, Wilson S, Lewin-Van Den Broek NT, et al. How evidence based are recruitment strategies to randomized controlled trials in primary care? Experience from seven studies. Fam Pract 2003;20:83-92.
- House of Commons Social Security Committee . The Royal Liverpool children’s Inquiry Report 2001.
- Human Rights Act. London: HMSO; 1998.
- Department of Health . Research Governance Framework for Health and Social Care 2001.
- Dumville JC, Watson J, Raynor P, Torgerson DJ. Research governance: a barrier to ethical research?. Q JM 2004;97:113-14.
- Ewing G, Rogers M, Barclay S, McCabe J, Martin A, Todd C. Recruiting patients into a primary care based study of palliative care: why is it so difficult?. Palliat Med 2004;18:452-9.
- Salisbury C, Leese B, McManus RJ. Ensuring that research governance supports rather than stifles research. Br J Gen Pract 2005;55:4-5.
- Hewison J, Haines A. Overcoming barriers to recruitment in health research. BMJ 2006;333:300-2.
- Angus VC, Entwistle VA, Emslie MJ, Walker KA, Andrew JE. The requirement for prior consent to participate on survey response rates: a population based survey in Grampian. BMC Health Serv Res 2003;3.
- McColl E, Lecoutrier J, Corbett S, Speed C, Vanoli A, Welfare M. Self-Management in Ulcerative Colitis: A Report of a Randomised Controlled Trial With Economic Evaluation and Qualitative Assessment 2003.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70.
- Cronbach L. Coefficient alpha and the internal structure of tests. Psychometrika 1951;16:287-334.
- Garvey M, Noyes R, Yates W. Frequency of constipation in major depression: relationship to other clinical variables. Psychosomatics 1990;31:204-6.
- Gorard DA, Gomborone JE, Libby GW, Farthing MJ. Intestinal transit in anxiety and depression. Gut 1996;39:551-5.
- Drummond M, Stoddard GL, Torrance GW. Methods for the economic analysis of health care programmes. Oxford: Oxford University Press; 1987.
- The EuroQol Group . EuroQol: a new facility for the measurement of health related quality of life. Health Policy 1990;16:199-208.
- Dolan P. Modeling Valuations for EuroQol Health States. Med Care 1997;35:1095-108.
- Department of Health . Research Governance Framework for Health and Social Care 2005.
- Wald DS. Bureaucracy of ethics applications. BMJ 2004;329:282-4.
- Speed C. Site-specific assessments: yet another barrier to research. Rapid response to: David S Wald, Bureaucracy of Ethics Applications. BMJ 2004;329:282-4.
- Levine RJ. Clinical trials and physicians as double agents. Yale J Biol Med 1992;65:65-74.
- Prout H, Butler C, Kinnersley P, Robling M, Hood K, Tudor-Jones R. A qualitative evaluation of implementing a randomised controlled trial in general practice. Fam Pract 2003;20:675-81.
- Salmon P, Peters S, Rogers A, Gask L, Clifford R, Iredale W, et al. Peering through the barriers in GPs’ explanations for declining to participate in research: the role of professional autonomy and the economy of time. Fam Pract 2007;24:269-75.
- Ross S, Grant A, Counsell C, Gillespie W, Russell I, Prescott R. Barriers to participation in randomised controlled trials: a systematic review. J Clin Epidemiol 1999;52:1143-56.
- Viner R. Transition from paediatric to adult care. Bridging the gaps or passing the buck?. Arch Dis Child 1999;81:271-5.
- Strauss AL. Social organization of medical work. Chicago, IL: University of Chicago Press; 1985.
- Heaven B, Murtagh M, Rapley T, May C, Graham R, Kaner E, et al. Patients or research subjects? A qualitative study of participation in a randomised controlled trial of a complex intervention. Patient Educ Couns 2006;62:260-70.
- Morris N, Bàlmer B. Volunteer human subjects’ understandings of their participation in a biomedical research experiment. Soc Sci Med 2006;62:998-1008.
- Wager E, Tooley PJ, Emanuel MB, Wood SF. How to do it: get patients’ consent to enter clinical trials. BMJ 1995;311:734-7.
- Snowdon C, Garcia J, Elbourne D. Making sense of randomization: responses of parents of critically ill babies to random allocation of treatment in a clinical trial. Soc Sci Med 1997;45:1337-55.
- Joffe S, Cook EF, Cleary PD, Clark JW, Weeks JC. Quality of informed consent: a new measure of understanding among research subjects. J Natl Cancer Inst 2001;93:139-47.
- Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, et al. Framework for design and evaluation of complex interventions to improve health. BMJ 2000;321:694-6.
- Featherstone K. The experience of trial participation. J Rheumatol 2003;30:646-7.
- Featherstone K, Donovan JL. Random allocation or allocation at random? Patients’ perspective of participation in a randomised controlled trial. BMJ 1998;317.
- Featherstone K, Donovan JL. ‘Why don’t they just tell me straight, why allocate it?’ The struggle to make sense of participating in a randomised controlled trial. Soc Sci Med 2002;55:709-19.
- McDonald AM, Knight RC, Campbell MK, Entwistle VA, Grant AM, Cook JA, et al. What influences recruitment to randomised controlled trials? A review of trials funded by two UK funding agencies. Trials 2006;7.
- May C. A rational model for assessing and evaluating complex interventions in health care. BMC Health Serv Res 2006;6.
Appendix 1 Protocols
LIFELAX protocol, version 2 (18 February 2004)
LIFELAX protocol, version 5 (24 July 2006)
Appendix 2 Patient information sheets
LIFELAX brief patient info sheet (PIS), version 5 (26 May 2006)
LIFELAX full PIS, version 6 (24 July 2006)
Appendix 3 Contents pages from the intervention manuals and patient information leaflets
Standardised intervention arm
Contents of the training manual
Standardised PIL
Personalised intervention arm
Contents of the training manual
Personalised PILs
Constipation
Activity
Bowel health
Fruit and vegetables
Fibre and constipation
Fibre
Fluids
Alternative therapies
Laxatives
Appendix 4 EQ-5D self-completion questionnaire
Appendix 5 Adapted CONSORT e-flowchart for process evaluation
FIGURE 12.
Adapted CONSORT e-flowchart for process evaluation. a, additional practice staff were approached, but refusal was only recorded if actually given. Contact with key practice staff was sometimes never established, the researcher stopped attempts after 3–4 repeat calls. b, iterative interview with one member.
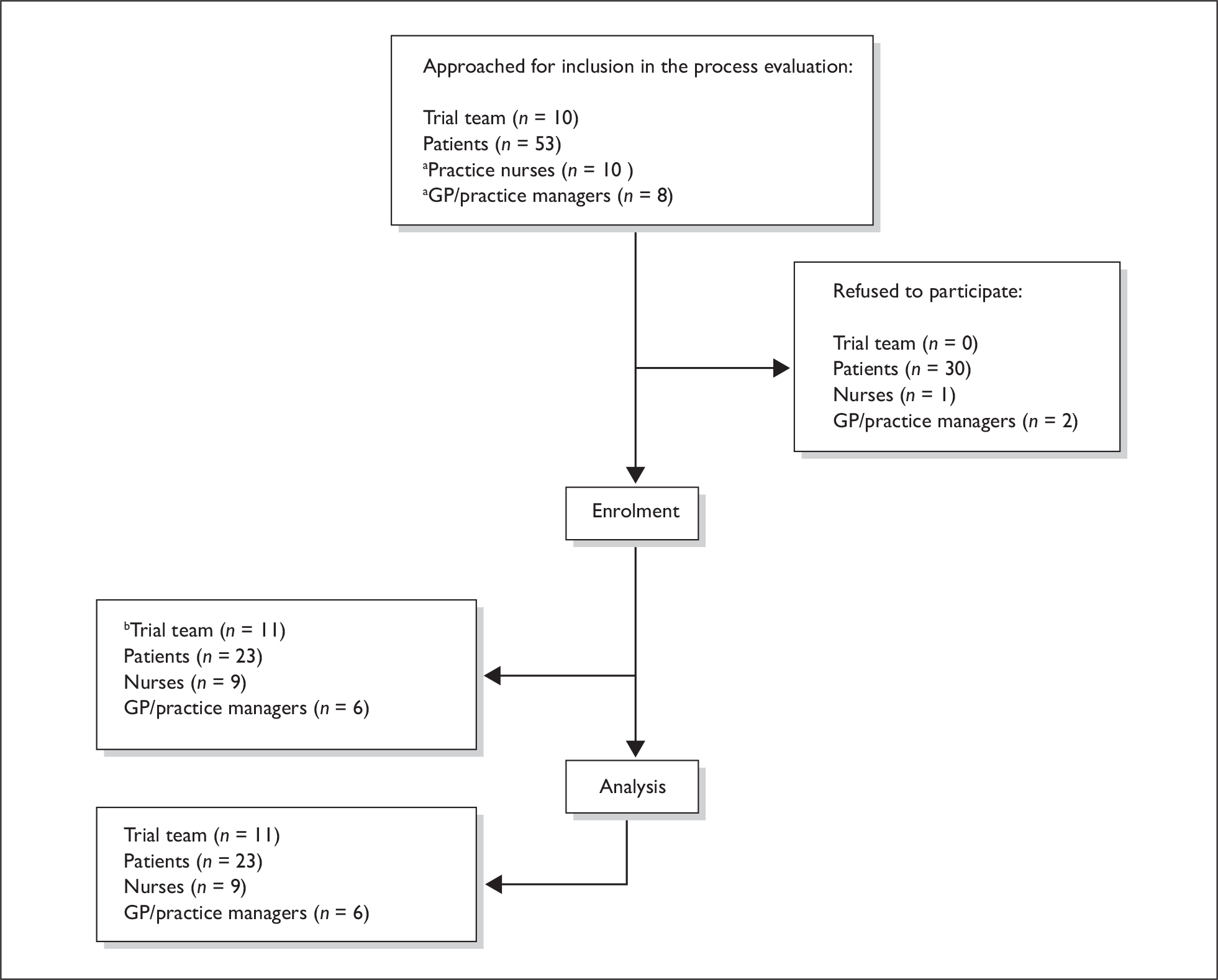
List of abbreviations
- BCC
- behaviour change counselling
- BNF
- British National Formulary
- CI
- chief investigator
- CONSORT
- consolidated standards of reporting trials
- COREC
- Central Office of Research Ethics Committees
- CRB
- Criminal Records Bureau
- CTA
- Clinical Trial Authorisation
- ctIMP
- clinical trial of an investigational medicinal product
- DDX
- Doctors’ and Dentists’ Exemption (certificate)
- DFD
- discomfort-free day
- DH
- Department of Health
- DINE
- Dietary Instrument for Nutrition Education
- EQ-5D
- European Quality of Life-5 Dimensions
- GI
- gastrointestinal
- GMC
- General Medical Council
- GMS
- General Medical Services
- GP
- general practitioner
- HADS
- Hospital Anxiety and Depression Scale
- HRQoL
- health-related quality of life
- HTA
- Health Technology Assessment (programme)
- ICC
- intraclass correlation
- LIFELAX
- diet and LIFEstyle versus LAXatives in the management of chronic constipation in older people
- LREC
- Local Research Ethics Committee
- MHRA
- Medicines and Healthcare products Regulatory Agency
- MREC
- Multi-Centre Research Ethics Committee
- NDNS
- National Diet and Nutrition Survey
- NIHR CRN
- National Institute of Health Research Clinical Research Network
- NLI
- no local investigator
- NoReN
- Northern Primary Care Research Network
- NPM
- Normalisation Process Model
- NRES
- National Research Ethics Service
- NSP
- non-starch polysaccharide
- NYReN
- Northern and Yorkshire Primary Care Research Network
- OTC
- over the counter (medication)
- PAC-QOL
- Patient Assessment of Constipation-Quality of Life
- PAC-SYM
- Patient Assessment of Constipation-Symptoms
- PCRN
- Primary Care Research Network
- PCT
- Primary Care Trust
- PI
- principal investigator
- PIL
- patient information leaflet
- PIS
- patient information sheet
- QALY
- quality-adjusted life-year
- QOF
- Quality Outcomes Framework
- QoL
- quality of life
- R&D
- research and development
- RCT
- randomised controlled trial
- REC
- Research Ethics Committee
- RM&G
- Research Management and Governance
- SCFAs
- short-chain fatty acids
- SfS
- Support for Science (funding)
- SPCRN
- Scottish Primary Care Research Network
- SPPIRe
- Scottish Practices and Professionals Involved in Research
- SSA
- site-specific assessment
- SSI
- site-specific information
- STEPS
- Strategies for Trial Enrolment and Participation Study
- STOOL
- Stepped Treatment Of Older adults on Laxatives
- TSC
- Trial Steering Committee
- USP
- unique selling point
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Riemsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA, Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant LD, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and cost-effectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
-
Randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of selective serotonin reuptake inhibitors plus supportive care, versus supportive care alone, for mild to moderate depression with somatic symptoms in primary care: the THREAD (THREshold for AntiDepressant response) study.
By Kendrick T, Chatwin J, Dowrick C, Tylee A, Morriss R, Peveler R, et al.
-
Diagnostic strategies using DNA testing for hereditary haemochromatosis in at-risk populations: a systematic review and economic evaluation.
By Bryant J, Cooper K, Picot J, Clegg A, Roderick P, Rosenberg W, et al.
-
Enhanced external counterpulsation for the treatment of stable angina and heart failure: a systematic review and economic analysis.
By McKenna C, McDaid C, Suekarran S, Hawkins N, Claxton K, Light K, et al.
-
Development of a decision support tool for primary care management of patients with abnormal liver function tests without clinically apparent liver disease: a record-linkage population cohort study and decision analysis (ALFIE).
By Donnan PT, McLernon D, Dillon JF, Ryder S, Roderick P, Sullivan F, et al.
-
A systematic review of presumed consent systems for deceased organ donation.
By Rithalia A, McDaid C, Suekarran S, Norman G, Myers L, Sowden A.
-
Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial.
By Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, et al.
-
A randomised controlled trial to compare minimally invasive glucose monitoring devices with conventional monitoring in the management of insulin-treated diabetes mellitus (MITRE).
By Newman SP, Cooke D, Casbard A, Walker S, Meredith S, Nunn A, et al.
-
Sensitivity analysis in economic evaluation: an audit of NICE current practice and a review of its use and value in decision-making.
By Andronis L, Barton P, Bryan S.
-
Trastuzumab for the treatment of primary breast cancer in HER2-positive women: a single technology appraisal.
By Ward S, Pilgrim H, Hind D.
-
Docetaxel for the adjuvant treatment of early node-positive breast cancer: a single technology appraisal.
By Chilcott J, Lloyd Jones M, Wilkinson A.
-
The use of paclitaxel in the management of early stage breast cancer.
By Griffin S, Dunn G, Palmer S, Macfarlane K, Brent S, Dyker A, et al.
-
Rituximab for the first-line treatment of stage III/IV follicular non-Hodgkin’s lymphoma.
By Dundar Y, Bagust A, Hounsome J, McLeod C, Boland A, Davis H, et al.
-
Bortezomib for the treatment of multiple myeloma patients.
By Green C, Bryant J, Takeda A, Cooper K, Clegg A, Smith A, et al.
-
Fludarabine phosphate for the firstline treatment of chronic lymphocytic leukaemia.
By Walker S, Palmer S, Erhorn S, Brent S, Dyker A, Ferrie L, et al.
-
Erlotinib for the treatment of relapsed non-small cell lung cancer.
By McLeod C, Bagust A, Boland A, Hockenhull J, Dundar Y, Proudlove C, et al.
-
Cetuximab plus radiotherapy for the treatment of locally advanced squamous cell carcinoma of the head and neck.
By Griffin S, Walker S, Sculpher M, White S, Erhorn S, Brent S, et al.
-
Infliximab for the treatment of adults with psoriasis.
By Loveman E, Turner D, Hartwell D, Cooper K, Clegg A
-
Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PoNDER trial.
By Morrell CJ, Warner R, Slade P, Dixon S, Walters S, Paley G, et al.
-
The effect of different treatment durations of clopidogrel in patients with non-ST-segment elevation acute coronary syndromes: a systematic review and value of information analysis.
By Rogowski R, Burch J, Palmer S, Craigs C, Golder S, Woolacott N.
-
Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
By Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, et al.
-
A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO trial.
By Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F, Dixon S, et al. , on behalf of the 3CPO study investigators.
-
Early high-dose lipid-lowering therapy to avoid cardiac events: a systematic review and economic evaluation.
By Ara R, Pandor A, Stevens J, Rees A, Rafia R.
-
Adefovir dipivoxil and pegylated interferon alpha for the treatment of chronic hepatitis B: an updated systematic review and economic evaluation.
By Jones J, Shepherd J, Baxter L, Gospodarevskaya E, Hartwell D, Harris P, et al.
-
Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis.
By Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al.
-
A double-blind randomised placebo-controlled trial of topical intranasal corticosteroids in 4- to 11-year-old children with persistent bilateral otitis media with effusion in primary care.
By Williamson I, Benge S, Barton S, Petrou S, Letley L, Fasey N, et al.
-
The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model.
By Bond M, Pitt M, Akoh J, Moxham T, Hoyle M, Anderson R.
-
Rehabilitation of older patients: day hospital compared with rehabilitation at home. A randomised controlled trial.
By Parker SG, Oliver P, Pennington M, Bond J, Jagger C, Enderby PM, et al.
-
Breastfeeding promotion for infants in neonatal units: a systematic review and economic analysis.
By Renfrew MJ, Craig D, Dyson L, McCormick F, Rice S, King SE, et al.
-
The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation.
By Picot J, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, et al.
-
Rapid testing for group B streptococcus during labour: a test accuracy study with evaluation of acceptability and cost-effectiveness.
By Daniels J, Gray J, Pattison H, Roberts T, Edwards E, Milner P, et al.
-
Screening to prevent spontaneous preterm birth: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Honest H, Forbes CA, Durée KH, Norman G, Duffy SB, Tsourapas A, et al.
-
The effectiveness and cost-effectiveness of cochlear implants for severe to profound deafness in children and adults: a systematic review and economic model.
By Bond M, Mealing S, Anderson R, Elston J, Weiner G, Taylor RS, et al.
-
Gemcitabine for the treatment of metastatic breast cancer.
By Jones J, Takeda A, Tan SC, Cooper K, Loveman E, Clegg A.
-
Varenicline in the management of smoking cessation: a single technology appraisal.
By Hind D, Tappenden P, Peters J, Kenjegalieva K.
-
Alteplase for the treatment of acute ischaemic stroke: a single technology appraisal.
By Lloyd Jones M, Holmes M.
-
Rituximab for the treatment of rheumatoid arthritis.
By Bagust A, Boland A, Hockenhull J, Fleeman N, Greenhalgh J, Dundar Y, et al.
-
Omalizumab for the treatment of severe persistent allergic asthma.
By Jones J, Shepherd J, Hartwell D, Harris P, Cooper K, Takeda A, et al.
-
Rituximab for the treatment of relapsed or refractory stage III or IV follicular non-Hodgkin’s lymphoma.
By Boland A, Bagust A, Hockenhull J, Davis H, Chu P, Dickson R.
-
Adalimumab for the treatment of psoriasis.
By Turner D, Picot J, Cooper K, Loveman E.
-
Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip and knee surgery: a single technology appraisal.
By Holmes M, C Carroll C, Papaioannou D.
-
Romiplostim for the treatment of chronic immune or idiopathic thrombocytopenic purpura: a single technology appraisal.
By Mowatt G, Boachie C, Crowther M, Fraser C, Hernández R, Jia X, et al.
-
Sunitinib for the treatment of gastrointestinal stromal tumours: a critique of the submission from Pfizer.
By Bond M, Hoyle M, Moxham T, Napier M, Anderson R.
-
Vitamin K to prevent fractures in older women: systematic review and economic evaluation.
By Stevenson M, Lloyd-Jones M, Papaioannou D.
-
The effects of biofeedback for the treatment of essential hypertension: a systematic review.
By Greenhalgh J, Dickson R, Dundar Y.
-
A randomised controlled trial of the use of aciclovir and/or prednisolone for the early treatment of Bell’s palsy: the BELLS study.
By Sullivan FM, Swan IRC, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al.
-
Lapatinib for the treatment of HER2-overexpressing breast cancer.
By Jones J, Takeda A, Picot J, von Keyserlingk C, Clegg A.
-
Infliximab for the treatment of ulcerative colitis.
By Hyde C, Bryan S, Juarez-Garcia A, Andronis L, Fry-Smith A.
-
Rimonabant for the treatment of overweight and obese people.
By Burch J, McKenna C, Palmer S, Norman G, Glanville J, Sculpher M, et al.
-
Telbivudine for the treatment of chronic hepatitis B infection.
By Hartwell D, Jones J, Harris P, Cooper K.
-
Entecavir for the treatment of chronic hepatitis B infection.
By Shepherd J, Gospodarevskaya E, Frampton G, Cooper K.
-
Febuxostat for the treatment of hyperuricaemia in people with gout: a single technology appraisal.
By Stevenson M, Pandor A.
-
Rivaroxaban for the prevention of venous thromboembolism: a single technology appraisal.
By Stevenson M, Scope A, Holmes M, Rees A, Kaltenthaler E.
-
Cetuximab for the treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck.
By Greenhalgh J, Bagust A, Boland A, Fleeman N, McLeod C, Dundar Y, et al.
-
Mifamurtide for the treatment of osteosarcoma: a single technology appraisal.
By Pandor A, Fitzgerald P, Stevenson M, Papaioannou D.
-
Ustekinumab for the treatment of moderate to severe psoriasis.
By Gospodarevskaya E, Picot J, Cooper K, Loveman E, Takeda A.
-
Endovascular stents for abdominal aortic aneurysms: a systematic review and economic model.
By Chambers D, Epstein D, Walker S, Fayter D, Paton F, Wright K, et al.
-
Clinical and cost-effectiveness of epoprostenol, iloprost, bosentan, sitaxentan and sildenafil for pulmonary arterial hypertension within their licensed indications: a systematic review and economic evaluation.
By Chen Y-F, Jowett S, Barton P, Malottki K, Hyde C, Gibbs JSR, et al.
-
Cessation of attention deficit hyperactivity disorder drugs in the young (CADDY) – a pharmacoepidemiological and qualitative study.
By Wong ICK, Asherson P, Bilbow A, Clifford S, Coghill D, R DeSoysa R, et al.
-
ARTISTIC: a randomised trial of human papillomavirus (HPV) testing in primary cervical screening.
By Kitchener HC, Almonte M, Gilham C, Dowie R, Stoykova B, Sargent A, et al.
-
The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation.
By Black C, Clar C, Henderson R, MacEachern C, McNamee P, Quayyum Z, et al.
-
Randomised preference trial of medical versus surgical termination of pregnancy less than 14 weeks’ gestation (TOPS).
By Robson SC, Kelly T, Howel D, Deverill M, Hewison J, Lie MLS, et al.
-
Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes.
By Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E, Davies S, et al.
-
VenUS II: a randomised controlled trial of larval therapy in the management of leg ulcers.
By Dumville JC, Worthy G, Soares MO, Bland JM, Cullum N, Dowson C, et al.
-
A prospective randomised controlled trial and economic modelling of antimicrobial silver dressings versus non-adherent control dressings for venous leg ulcers: the VULCAN trial.
By Michaels JA, Campbell WB, King BM, MacIntyre J, Palfreyman SJ, Shackley P, et al.
-
Communication of carrier status information following universal newborn screening for sickle cell disorders and cystic fibrosis: qualitative study of experience and practice.
By Kai J, Ulph F, Cullinan T, Qureshi N.
-
Antiviral drugs for the treatment of influenza: a systematic review and economic evaluation.
By Burch J, Paulden M, Conti S, Stock C, Corbett M, Welton NJ, et al.
-
Development of a toolkit and glossary to aid in the adaptation of health technology assessment (HTA) reports for use in different contexts.
By Chase D, Rosten C, Turner S, Hicks N, Milne R.
-
Colour vision testing for diabetic retinopathy: a systematic review of diagnostic accuracy and economic evaluation.
By Rodgers M, Hodges R, Hawkins J, Hollingworth W, Duffy S, McKibbin M, et al.
-
Systematic review of the effectiveness and cost-effectiveness of weight management schemes for the under fives: a short report.
By Bond M, Wyatt K, Lloyd J, Welch K, Taylor R.
-
Are adverse effects incorporated in economic models? An initial review of current practice.
By Craig D, McDaid C, Fonseca T, Stock C, Duffy S, Woolacott N.
-
Multicentre randomised controlled trial examining the cost-effectiveness of contrast-enhanced high field magnetic resonance imaging in women with primary breast cancer scheduled for wide local excision (COMICE).
By Turnbull LW, Brown SR, Olivier C, Harvey I, Brown J, Drew P, et al.
-
Bevacizumab, sorafenib tosylate, sunitinib and temsirolimus for renal cell carcinoma: a systematic review and economic evaluation.
By Thompson Coon J, Hoyle M, Green C, Liu Z, Welch K, Moxham T, et al.
-
The clinical effectiveness and cost-effectiveness of testing for cytochrome P450 polymorphisms in patients with schizophrenia treated with antipsychotics: a systematic review and economic evaluation.
By Fleeman N, McLeod C, Bagust A, Beale S, Boland A, Dundar Y, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer.
By Mowatt G, Zhu S, Kilonzo M, Boachie C, Fraser C, Griffiths TRL, et al.
-
Effectiveness and cost-effectiveness of arthroscopic lavage in the treatment of osteoarthritis of the knee: a mixed methods study of the feasibility of conducting a surgical placebo-controlled trial (the KORAL study).
By Campbell MK, Skea ZC, Sutherland AG, Cuthbertson BH, Entwistle VA, McDonald AM, et al.
-
A randomised 2 × 2 trial of community versus hospital pulmonary rehabilitation for chronic obstructive pulmonary disease followed by telephone or conventional follow-up.
By Waterhouse JC, Walters SJ, Oluboyede Y, Lawson RA.
-
The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation.
By Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al.
-
Dissemination and publication of research findings: an updated review of related biases.
By Song F, Parekh S, Hooper L, Loke YK, Ryder J, Sutton AJ, et al.
-
The effectiveness and cost-effectiveness of biomarkers for the prioritisation of patients awaiting coronary revascularisation: a systematic review and decision model.
By Hemingway H, Henriksson M, Chen R, Damant J, Fitzpatrick N, Abrams K, et al.
-
Comparison of case note review methods for evaluating quality and safety in health care.
By Hutchinson A, Coster JE, Cooper KL, McIntosh A, Walters SJ, Bath PA, et al.
-
Clinical effectiveness and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes: systematic review and economic evaluation.
By Cummins E, Royle P, Snaith A, Greene A, Robertson L, McIntyre L, et al.
-
Self-monitoring of blood glucose in type 2 diabetes: systematic review.
By Clar C, Barnard K, Cummins E, Royle P, Waugh N.
-
North of England and Scotland Study of Tonsillectomy and Adeno-tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non-randomised preference study.
By Lock C, Wilson J, Steen N, Eccles M, Mason H, Carrie S, et al.
-
Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial.
By Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FGR, Gillespie I, et al.
-
A randomised controlled multicentre trial of treatments for adolescent anorexia nervosa including assessment of cost-effectiveness and patient acceptability – the TOuCAN trial.
By Gowers SG, Clark AF, Roberts C, Byford S, Barrett B, Griffiths A, et al.
-
Randomised controlled trials for policy interventions: a review of reviews and meta-regression.
By Oliver S, Bagnall AM, Thomas J, Shepherd J, Sowden A, White I, et al.
-
Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review.
By McDaid C, Maund E, Rice S, Wright K, Jenkins B, Woolacott N.
-
A systematic review of outcome measures used in forensic mental health research with consensus panel opinion.
By Fitzpatrick R, Chambers J, Burns T, Doll H, Fazel S, Jenkinson C, et al.
-
The clinical effectiveness and cost-effectiveness of topotecan for small cell lung cancer: a systematic review and economic evaluation.
By Loveman E, Jones J, Hartwell D, Bird A, Harris P, Welch K, et al.
-
Antenatal screening for haemoglobinopathies in primary care: a cohort study and cluster randomised trial to inform a simulation model. The Screening for Haemoglobinopathies in First Trimester (SHIFT) trial.
By Dormandy E, Bryan S, Gulliford MC, Roberts T, Ades T, Calnan M, et al.
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.
By Black C, Sharma P, Scotland G, McCullough K, McGurn D, Robertson L, et al.
-
A randomised controlled trial of cognitive behaviour therapy and motivational interviewing for people with Type 1 diabetes mellitus with persistent sub-optimal glycaemic control: A Diabetes and Psychological Therapies (ADaPT) study.
By Ismail K, Maissi E, Thomas S, Chalder T, Schmidt U, Bartlett J, et al.
-
A randomised controlled equivalence trial to determine the effectiveness and cost–utility of manual chest physiotherapy techniques in the management of exacerbations of chronic obstructive pulmonary disease (MATREX).
By Cross J, Elender F, Barton G, Clark A, Shepstone L, Blyth A, et al.
-
A systematic review and economic evaluation of the clinical effectiveness and cost-effectiveness of aldosterone antagonists for postmyocardial infarction heart failure.
By McKenna C, Burch J, Suekarran S, Walker S, Bakhai A, Witte K, et al.
-
Avoiding and identifying errors in health technology assessment models: qualitative study and methodological review.
By Chilcott JB, Tappenden P, Rawdin A, Johnson M, Kaltenthaler E, Paisley S, et al.
-
BoTULS: a multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A.
By Shaw L, Rodgers H, Price C, van Wijck F, Shackley P, Steen N, et al. , on behalf of the BoTULS investigators.
-
Weighting and valuing quality-adjusted life-years using stated preference methods: preliminary results from the Social Value of a QALY Project.
By Baker R, Bateman I, Donaldson C, Jones-Lee M, Lancsar E, Loomes G, et al.
-
Cetuximab for the first-line treatment of metastatic colorectal cancer.
By Meads C, Round J, Tubeuf S, Moore D, Pennant M, Bayliss S.
-
Infliximab for the treatment of acute exacerbations of ulcerative colitis.
By Bryan S, Andronis L, Hyde C, Connock M, Fry-Smith A, Wang D.
-
Sorafenib for the treatment of advanced hepatocellular carcinoma.
By Connock M, Round J, Bayliss S, Tubeuf S, Greenheld W, Moore D.
-
Tenofovir disoproxil fumarate for the treatment of chronic hepatitis B infection.
By Jones J, Colquitt J, Shepherd J, Harris P, Cooper K.
-
Prasugrel for the treatment of acute coronary artery syndromes with percutaneous coronary intervention.
By Greenhalgh J, Bagust A, Boland A, Saborido CM, Fleeman N, McLeod C, et al.
-
Alitretinoin for the treatment of severe chronic hand eczema.
By Paulden M, Rodgers M, Griffin S, Slack R, Duffy S, Ingram JR, et al.
-
Pemetrexed for the first-line treatment of locally advanced or metastatic non-small cell lung cancer.
By Fleeman N, Bagust A, McLeod C, Greenhalgh J, Boland A, Dundar Y, et al.
-
Topotecan for the treatment of recurrent and stage IVB carcinoma of the cervix.
By Paton F, Paulden M, Saramago P, Manca A, Misso K, Palmer S, et al.
-
Trabectedin for the treatment of advanced metastatic soft tissue sarcoma.
By Simpson EL, Rafia R, Stevenson MD, Papaioannou D.
-
Azacitidine for the treatment of myelodysplastic syndrome, chronic myelomonocytic leukaemia and acute myeloid leukaemia.
By Edlin R, Connock M, Tubeuf S, Round J, Fry-Smith A, Hyde C, et al.
-
The safety and effectiveness of different methods of earwax removal: a systematic review and economic evaluation.
By Clegg AJ, Loveman E, Gospodarevskaya E, Harris P, Bird A, Bryant J, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of rapid point-of-care tests for the detection of genital chlamydia infection in women and men.
By Hislop J, Quayyum Z, Flett G, Boachie C, Fraser C, Mowatt G.
-
School-linked sexual health services for young people (SSHYP): a survey and systematic review concerning current models, effectiveness, cost-effectiveness and research opportunities.
By Owen J, Carroll C, Cooke J, Formby E, Hayter M, Hirst J, et al.
-
Systematic review and cost-effectiveness evaluation of ‘pill-in-the-pocket’ strategy for paroxysmal atrial fibrillation compared to episodic in-hospital treatment or continuous antiarrhythmic drug therapy.
By Martin Saborido C, Hockenhull J, Bagust A, Boland A, Dickson R, Todd D.
-
Chemoprevention of colorectal cancer: systematic review and economic evaluation.
By Cooper K, Squires H, Carroll C, Papaioannou D, Booth A, Logan RF, et al.
-
Cross-trimester repeated measures testing for Down’s syndrome screening: an assessment.
By Wright D, Bradbury I, Malone F, D’Alton M, Summers A, Huang T, et al.
-
Exploring the needs, concerns and behaviours of people with existing respiratory conditions in relation to the H1N1 ‘swine influenza’ pandemic: a multicentre survey and qualitative study.
By Caress A-L, Duxbury P, Woodcock A, Luker KA, Ward D, Campbell M, et al.
-
Influenza A/H1N1v in pregnancy: an investigation of the characteristics and management of affected women and the relationship to pregnancy outcomes for mother and infant.
By Yates L, Pierce M, Stephens S, Mill AC, Spark P, Kurinczuk JJ, et al.
-
The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK.
By Rubin GJ, Potts HWW, Michie S.
-
The impact of illness and the impact of school closure on social contact patterns.
By Eames KTD, Tilston NL, White PJ, Adams E, Edmunds WJ.
-
Vaccine effectiveness in pandemic influenza – primary care reporting (VIPER): an observational study to assess the effectiveness of the pandemic influenza A (H1N1)v vaccine.
By Simpson CR, Ritchie LD, Robertson C, Sheikh A, McMenamin J.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses: a Cochrane review.
By Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al.
-
Randomised controlled trial and parallel economic evaluation of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR).
By Peek GJ, Elbourne D, Mugford M, Tiruvoipati R, Wilson A, Allen E, et al.
-
Newer agents for blood glucose control in type 2 diabetes: systematic review and economic evaluation.
By Waugh N, Cummins E, Royle P, Clar C, Marien M, Richter B, et al.
-
Barrett’s oesophagus and cancers of the biliary tract, brain, head and neck, lung, oesophagus and skin.
By Fayter D, Corbett M, Heirs M, Fox D, Eastwood A.
-
Towards single embryo transfer? Modelling clinical outcomes of potential treatment choices using multiple data sources: predictive models and patient perspectives.
By Roberts SA, McGowan L, Hirst WM, Brison DR, Vail A, Lieberman BA.
-
Sugammadex for the reversal of muscle relaxation in general anaesthesia: a systematic review and economic assessment.
By Chambers D, Paulden M, Paton F, Heirs M, Duffy S, Craig D, et al.
-
Systematic review and economic modelling of the effectiveness and cost-effectiveness of non-surgical treatments for women with stress urinary incontinence.
By Imamura M, Abrams P, Bain C, Buckley B, Cardozo L, Cody J, et al.
-
A multicentred randomised controlled trial of a primary care-based cognitive behavioural programme for low back pain. The Back Skills Training (BeST) trial.
By Lamb SE, Lall R, Hansen Z, Castelnuovo E, Withers EJ, Nichols V, et al.
-
Recombinant human growth hormone for the treatment of growth disorders in children: a systematic review and economic evaluation.
By Takeda A, Cooper K, Bird A, Baxter L, Frampton GK, Gospodarevskaya E, et al.
-
A pragmatic randomised controlled trial to compare antidepressants with a community-based psychosocial intervention for the treatment of women with postnatal depression: the RESPOND trial.
By Sharp DJ, Chew-Graham C, Tylee A, Lewis G, Howard L, Anderson I, et al.
-
Group cognitive behavioural therapy for postnatal depression: a systematic review of clinical effectiveness, cost-effectiveness and value of information analyses.
By Stevenson MD, Scope A, Sutcliffe PA, Booth A, Slade P, Parry G, et al.
-
Screening for hyperglycaemia in pregnancy: a rapid update for the National Screening Committee.
By Waugh N, Royle P, Clar C, Henderson R, Cummins E, Hadden D, et al.
-
Open-label, randomised, parallel-group, multicentre study to evaluate the safety, tolerability and immunogenicity of an AS03B/oil-in-water emulsion-adjuvanted (AS03B) split-virion versus non-adjuvanted wholevirion H1N1 influenza vaccine in UK children 6 months to 12 years of age.
By Waddington CS, Andrews N, Hoschler K, Walker WT, Oeser C, Reiner A, et al.
-
Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections.
By Simonds AK, Hanak A, Chatwin M, Morrell MJ, Hall A, Parker KH, et al.
-
Evaluation of triage methods used to select patients with suspected pandemic influenza for hospital admission: cohort study.
By Goodacre S, Challen, K, Wilson R, Campbell M.
-
Virus shedding and environmental deposition of novel A (H1N1) pandemic influenza virus: interim findings.
By Killingley B, Greatorex J, Cauchemez S, Enstone JE, Curran M, Read R, et al.
-
Neuraminidase inhibitors for preventing and treating influenza in healthy adults: a Cochrane review.
By Jefferson T, Jones M, Doshi P, Del Mar C, Dooley L, Foxlee R.
-
Intensity-modulated radiotherapy for the treatment of prostate cancer: a systematic review and economic evaluation.
By Hummel S, Simpson EL, Hemingway P, Stevenson MD, Rees A.
-
Computerised decision support systems in order communication for diagnostic, screening or monitoring test ordering: systematic reviews of the effects and cost-effectiveness of systems.
By Main C, Moxham T, Wyatt JC, Kay J, Anderson R, Stein K.
-
Relapse prevention in UK Stop Smoking Services: current practice, systematic reviews of effectiveness and cost-effectiveness analysis.
By Coleman T, Agboola S, Leonardi-Bee J, Taylor M, McEwen A, McNeill A.
-
A systematic review of positron emission tomography (PET) and positron emission tomography/computed tomography (PET/CT) for the diagnosis of breast cancer recurrence.
By Pennant M, Takwoingi Y, Pennant L, Davenport C, Fry-Smith A, Eisinga A, et al.
-
Certolizumab pegol (CIMZIA®) for the treatment of rheumatoid arthritis.
By Connock M, Tubeuf S, Malottki K, Uthman A, Round J, Bayliss S, et al.
-
Capecitabine for the treatment of advanced gastric cancer.
By Norman G, Soares M, Peura P, Rice S, Suh D, Wright K, et al.
-
Rituximab for the treatment of relapsed/refractory chronic lymphocytic leukaemia.
By Dretzke J, Barton P, Kaambwa B, Connock M, Uthman O, Bayliss S, et al.
-
The clinical effectiveness and cost-effectiveness of rituximab for the first-line treatment of chronic lymphocytic leukaemia: an evidence review of the submission from Roche.
By Main C, Pitt M, Moxham T, Stein K.
-
Pemetrexed for the maintenance treatment of locally advanced or metastatic non-small cell lung cancer.
By Greenhalgh J, McLeod C, Bagust A, Boland A, Fleeman N, Dundar Y, et al.
-
Everolimus for the second-line treatment of advanced and/or metastatic renal cell cancer: a critique of the submission from Novartis.
By Pitt M, Crathorne L, Moxham T, Bond M, Hyde C.
-
Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line treatment of metastatic colorectal cancer.
By Whyte S, Pandor A, Stevenson M, Rees A.
-
Dronedarone for the treatment of atrial fibrillation and atrial flutter.
By Maund E, McKenna C, Sarowar M, Fox D, Stevenson M, Pepper C, et al.
-
Imatinib as adjuvant treatment following resection of KIT-positive gastrointestinal stromal tumours.
By Dretzke J, Round J, Connock M, Tubeuf S, Pennant M, Fry-Smith A, et al.
-
Gefitinib for the first-line treatment of locally advanced or metastatic non-small cell lung cancer.
By Brown T, Boland A, Bagust A, Oyee J, Hockenhull J, Dundar Y, et al.
-
Systematic review of the links between human resource management practices and performance.
By Patterson M, Rick J, Wood S, Carroll C, Balain S, Booth A.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of NETSCC, Health Technology Assessment
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Consultant Adviser, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Professor Ruairidh Milne, Director of NETSCC External Relations
-
Ms Kay Pattison, Senior NIHR Programme Manager, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Warwick Clinical Trials Unit
-
Director, Nottingham Clinical Trials Unit
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, University of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Ms Kay Pattison, NHS R&D Programme/DH, Leeds
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies and Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Mr A S Arunkalaivanan, Honorary Senior Lecturer, University of Birmingham and Consultant Urogynaecologist and Obstetrician, City Hospital
-
Dr Dianne Baralle, Consultant & Senior Lecturer in Clinical Genetics, Human Genetics Division & Wessex Clinical Genetics Service, Southampton, University of Southampton
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Dr Ron Gray, Consultant, National Perinatal Epidemiology Unit, Institute of Health Sciences, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, Academic Unit of Radiology, University of Sheffield
-
Mr Martin Hooper, Service User Representative
-
Professor Anthony Robert Kendrick, Professor of Primary Medical Care, University of Southampton
-
Dr Susanne M Ludgate, Director, Medical Devices Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr David Mathew Service User Representative
-
Dr Michael Millar, Lead Consultant in Microbiology, Department of Pathology & Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, University College London
-
Mrs Una Rennard, Service User Representative
-
Ms Jane Smith, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust, Leeds
-
Dr W Stuart A Smellie, Consultant, Bishop Auckland General Hospital
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Alan J Williams, Consultant in General Medicine, Department of Thoracic Medicine, The Royal Bournemouth Hospital
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist Commissioning Advisory Group (NSCAG), Department of Health
-
Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Dr Robert Cook Clinical Programmes Director, Bazian Ltd, London
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr Colin Greaves Senior Research Fellow, Peninsular Medical School (Primary Care)
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Dr Russell Jago, Senior Lecturer in Exercise, Nutrition and Health, Centre for Sport, Exercise and Health, University of Bristol
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Miss Nicky Mullany, Service User Representative
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Professor Irwin Nazareth, Professor of Primary Care and Director, Department of Primary Care and Population Sciences, University College London
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Mrs Jean Thurston, Service User Representative
-
Professor David Weller, Head, School of Clinical Science and Community Health, University of Edinburgh
-
Ms Christine McGuire, Research & Development, Department of Health
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
External Devices and Physical Therapies Panel
-
Consultant Physician North Bristol NHS Trust, Bristol
-
Reader in Wound Healing and Director of Research, University of Leeds, Leeds
-
Professor Bipin Bhakta Charterhouse Professor in Rehabilitation Medicine, University of Leeds, Leeds
-
Mrs Penny Calder Service User Representative
-
Professor Paul Carding, Professor of Voice Pathology, Newcastle Hospital NHS Trust, Newcastle
-
Dr Dawn Carnes, Senior Research Fellow, Barts and the London School of Medicine and Dentistry, London
-
Dr Emma Clark, Clinician Scientist Fellow & Cons. Rheumatologist, University of Bristol, Bristol
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and the London School of Medicine and Dentistry, London
-
Dr Shaheen Hamdy, Clinical Senior Lecturer and Consultant Physician, University of Manchester, Manchester
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Lorraine Pinnigton, Associate Professor in Rehabilitation, University of Nottingham, Nottingham
-
Dr Kate Radford, Division of Rehabilitation and Ageing, School of Community Health Sciences. University of Nottingham, Nottingham
-
Mr Jim Reece, Service User Representative
-
Professor Maria Stokes, Professor of Neuromusculoskeletal Rehabilitation, University of Southampton, Southampton
-
Dr Pippa Tyrrell, Stroke Medicine, Senior Lecturer/Consultant Stroke Physician, Salford Royal Foundation Hospitals’ Trust, Salford
-
Dr Sarah Tyson, Senior Research Fellow & Associate Head of School, University of Salford, Salford
-
Dr Nefyn Williams, Clinical Senior Lecturer, Cardiff University, Cardiff
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health , London
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Dr Ursula Wells PRP, DH, London
Interventional Procedures Panel
-
Consultant Surgeon & Honorary Clinical Lecturer, University of Sheffield
-
Mr David P Britt, Service User Representative, Cheshire
-
Mr Sankaran ChandraSekharan, Consultant Surgeon, Colchester Hospital University NHS Foundation Trust
-
Professor Nicholas Clarke, Consultant Orthopaedic Surgeon, Southampton University Hospitals NHS Trust
-
Mr Seamus Eckford, Consultant in Obstetrics & Gynaecology, North Devon District Hospital
-
Professor David Taggart, Consultant Cardiothoracic Surgeon, John Radcliffe Hospital
-
Dr Matthew Hatton, Consultant in Clinical Oncology, Sheffield Teaching Hospital Foundation Trust
-
Dr John Holden, General Practitioner, Garswood Surgery, Wigan
-
Dr Nadim Malik, Consultant Cardiologist/ Honorary Lecturer, University of Manchester
-
Mr Hisham Mehanna, Consultant & Honorary Associate Professor, University Hospitals Coventry & Warwickshire NHS Trust
-
Dr Jane Montgomery, Consultant in Anaesthetics and Critical Care, South Devon Healthcare NHS Foundation Trust
-
Dr Simon Padley, Consultant Radiologist, Chelsea & Westminster Hospital
-
Dr Ashish Paul, Medical Director, Bedfordshire PCT
-
Dr Sarah Purdy, Consultant Senior Lecturer, University of Bristol
-
Mr Michael Thomas, Consultant Colorectal Surgeon, Bristol Royal Infirmary
-
Professor Yit Chiun Yang, Consultant Ophthalmologist, Royal Wolverhampton Hospitals NHS Trust
-
Mrs Isabel Boyer, Service User Representative, London
Pharmaceuticals Panel
-
Professor in Child Health, University of Nottingham
-
Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Professor Robin Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Psychological and Community Therapies Panel
-
Professor of Psychiatry, University of Warwick
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School
-
Dr Sabyasachi Bhaumik, Consultant Psychiatrist, Leicestershire Partnership NHS Trust
-
Mrs Val Carlill, Service User Representative, Gloucestershire
-
Dr Steve Cunningham, Consultant Respiratory Paediatrician, Lothian Health Board
-
Dr Anne Hesketh, Senior Clinical Lecturer in Speech and Language Therapy, University of Manchester
-
Dr Yann Lefeuvre, GP Partner, Burrage Road Surgery, London
-
Dr Jeremy J Murphy, Consultant Physician & Cardiologist, County Durham & Darlington Foundation Trust
-
Mr John Needham, Service User, Buckingmashire
-
Ms Mary Nettle, Mental Health User Consultant, Gloucestershire
-
Professor John Potter, Professor of Ageing and Stroke Medicine, University of East Anglia
-
Dr Greta Rait, Senior Clinical Lecturer and General Practitioner, University College London
-
Dr Paul Ramchandani, Senior Research Fellow/Cons. Child Psychiatrist, University of Oxford
-
Dr Howard Ring, Consultant & University Lecturer in Psychiatry, University of Cambridge
-
Dr Karen Roberts, Nurse/Consultant, Dunston Hill Hospital, Tyne and Wear
-
Dr Karim Saad, Consultant in Old Age Psychiatry, Coventry & Warwickshire Partnership Trust
-
Dr Alastair Sutcliffe, Senior Lecturer, University College London
-
Dr Simon Wright, GP Partner, Walkden Medical Centre, Manchester
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Professor Tom Walley, HTA Programme Director, Liverpool
-
Dr Ursula Wells, Policy Research Programme, DH, London
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington