
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 13/39/01. The contractual start date was in September 2013. The draft report began editorial review in January 2014 and was accepted for publication in April 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
David Baldwin has received honoraria for educational presentations from H. Lundbeck A/S; has acted as a paid consultant to Eli Lilly, GlaxoSmithKline, Grunenthal, H. Lundbeck A/S, Pfizer, Pierre Fabre and Servier; currently holds research grants (on behalf of his employer) from H. Lundbeck A/S and Pfizer; and has accepted paid speaking engagements in industry-supported satellite symposia or other meetings hosted by Eli Lilly, GlaxoSmithKline, Lundbeck, Pfizer, Pierre Fabre and Servier.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Barton et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Description of health problem
Anxiety disorders can affect people of all ages. In contrast to the appearance of anxiety that might be experienced during a stressful event, for example when taking a driving test, an anxiety disorder persists for a longer period and symptoms can progressively worsen if not treated. Anxiety disorders can develop at any age, but onset typically occurs between childhood and young adulthood, with few people (< 1%) developing an anxiety disorder for the first time after the age of 65 years. 1 –A US-based study (9282 English-speaking respondents aged ≥ 18 years) reported the median age at onset of anxiety disorders to be 11 years. 2 Although anxiety disorders among older people (≥ 65 years) are less common than in younger adults, it is acknowledged that the frequency in older adults is considerably higher than previously thought. Recognition of the difficulties in differentiating symptoms of anxiety from physiological and physical changes (e.g. changes in sleep pattern) arising from the ageing process, together with a common reluctance of older people to acknowledge psychological difficulties, has led to the realisation that anxiety in older people has been under-detected and under-treated. 1,3
Many people with an anxiety disorder also have other medical conditions, both physical and psychological, that can further complicate diagnosis and worsen the long-term outcomes of the anxiety disorder. Of other anxiety and psychological disorders, depression is the most common comorbidity among younger and older adults. 1 Studies suggest that between 13%4 and 23%5 of people aged 55 years and older with a diagnosis of an anxiety disorder will also meet the criteria for a diagnosis of a major depressive disorder. One study in adults aged > 70 years found that 29.4% of those with an anxiety disorder had a comorbid depressive disorder. 6 In comparison, 20% of younger adults (aged 18–54 years) with a diagnosis of any anxiety disorder in the previous 6 months are likely to receive a simultaneous diagnosis of some type of mood disorder. Disorders affecting physical health are common in older adults, and older adults are more likely to attribute their symptoms of anxiety to their physical illness, which could result in non-diagnosis of their anxiety disorder. 1 Development of an anxiety disorder has been linked with thyroid problems (e.g. hypothyroidism or hyperthyroidism), respiratory and gastrointestinal conditions, arthritis, migraine headaches and allergic conditions. 7
Treatments offered for an anxiety disorder are determined by the underlying cause of anxiety, though initial treatment might involve education and active monitoring. People whose symptoms of anxiety do not improve might subsequently be recommended to undergo psychological therapy or be prescribed a pharmacological treatment. Despite treatment, some people will continue to have symptoms of anxiety. With the exception of obsessive–compulsive disorder (OCD), there is no common definition as to what constitutes treatment resistance or treatment refractoriness in anxiety disorders. 8 People are generally considered to be resistant or refractory if they have an inadequate response (resistant) or do not respond (refractory) to first-line treatment, irrespective of whether the first-line treatment was a psychological or pharmacological intervention.
Diagnosis of an anxiety disorder
The term ‘anxiety disorder’ encompasses a broad range of conditions that manifest with symptoms of anxiety. Two major classification systems that can be used as a basis for differentiation between the different types of anxiety disorders are the Diagnostic and Statistical Manual of Mental Disorders (DSM)9,10 and the World Health Organization’s International Classification of Diseases (ICD). 11 Until 2013, the DSM identified 12 distinct anxiety disorders that could be captured within seven headings:9
-
generalised anxiety disorder (GAD)
-
OCD
-
phobias, encompassing specific (simple) phobias and social phobia (also known as social anxiety disorder)
-
stress disorders, including post-traumatic stress disorder (PTSD) and acute stress disorders
-
panic disorder (with or without agoraphobia)
-
anxiety disorders owing to known physical causes (e.g. medical conditions and symptoms caused by drug misuse)
-
anxiety disorder not otherwise specified (covers symptoms not meeting the criteria for other anxiety disorders).
In 2013, the latest version of the DSM (version 5) was released. 10 Within the updated DSM, OCD is separated from the other anxiety disorders and is presented in a discrete chapter alongside related disorders. In addition, the stress disorders (PTSD and acute stress disorder) now lie within the chapter covering trauma- and stressor-related disorders. Separation anxiety disorder and selective mutism, which had previously been classified as ‘Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence’, were added to the anxiety disorders. 12 An accompanying comment on the revisions highlights that the changes underscore the discrete nature of the individual anxiety disorders, but that the sequential presentation of the chapters in the manual reflects the interconnectedness of the conditions.
The ICD-10 lists anxiety disorders under the general heading ‘Neurotic, stress-related and somatoform disorders’, which comprises the subgroups of:11
-
phobic anxiety disorders (e.g. agoraphobia with or without panic disorder, social phobia and specific phobias)
-
other anxiety disorders (e.g. panic disorder, GAD, and mixed anxiety and depressive disorder)
-
OCD
-
reaction to severe stress and adjustment disorders (acute stress reaction, PTSD and adjustment disorders)
-
dissociative (conversion) disorders (e.g. dissociative amnesia and dissociative stupor)
-
somatoform disorders (e.g. somatisation disorder and hypochondriacal disorders)
-
other neurotic disorders (e.g. neurasthenia).
Diagnosis of an anxiety disorder can be challenging, particularly in older people. Symptoms of anxiety can be similar to those of other psychological conditions, such as depression, and the frequent presence of comorbid mental disorders further complicates diagnosis across all age groups. 13 Differentiating excessive anxiety from concerns around a recent distressing experience in older people, for example after a fall, can also prove difficult. 14 Anxiety in such scenarios might be expected by both the patient and the clinician and, therefore, the diagnosis of an anxiety disorder might not be considered. Additionally, some older people might have beliefs about emotional problems that make them reluctant to raise concerns about anxiety and it has also been recognised that older adults from ethnic minority groups often have different manifestations of anxiety. Both of these factors increase the difficulty in recognising anxiety in this age group. 13,15
Compared with younger adults, older people often present to their clinician with non-specific symptoms, such as tiredness, or symptoms that are frequently related to the ageing process, such as a changing sleep pattern. 16 A common symptom of anxiety is deterioration in memory, which could be interpreted as signs of cognitive decline or onset of dementia. 17 Across all age groups anxiety disorders are often associated with pain and physical symptoms that could be a sign of heart disease or another physical illness7 and, in these cases, identifying a presumed physiological cause is likely to be the focus of initial clinical investigations. Moreover, older people frequently require multiple concomitant treatments to manage comorbid psychological and chronic medical conditions, and symptoms of anxiety could be thought to be associated with pharmacological treatment.
If an anxiety disorder is suspected, standardised screening questionnaires can initially be used to evaluate the presence and severity of anxiety. Validated screening tests include the Beck Anxiety Inventory, Spielberger State–Trait Anxiety Inventory, the Generalised Anxiety Disorder 7 (GAD-7) assessment and the Hospital Anxiety and Depression Scale. 18 The individual scales evaluate a set number of items to determine the severity of a patient’s anxiety, with the number of items varying across the rating scales. The rating scales differ in that they were designed to assess anxiety in different patient groups; for example, the Beck Anxiety Inventory focuses on somatic symptoms of anxiety and was developed to differentiate between anxiety and depression. By contrast, the Hospital Anxiety and Depression Scale evaluates the presence of symptoms of anxiety and depression in physically ill people. 18 The effects of variation in language, education and culture across ethnic groups can lead to variation in judging the severity of patients’ symptoms. 15 Although useful for initial evaluation and assessing treatment response, the generalised questionnaires are inadequate for determining which specific anxiety disorder is present. A formal clinical diagnostic assessment by an experienced clinician is required to categorise the disorder (based on criteria in the DSM-V or ICD-10).
Psychological and physical symptoms of anxiety are common across all anxiety disorders. 19 Some of the common psychological manifestations of anxiety include difficulty concentrating, feelings of trepidation, stress and restlessness, whereas common physical symptoms include fatigue, heart palpitations and trembling. In addition to the general symptoms, each anxiety disorder is associated with characteristic symptoms. Symptoms or triggers that can distinguish one disorder from another are listed in Table 1. 20 DSM-IV and ICD-10 criteria for the individual anxiety disorders are presented in Appendix 1.
| Anxiety disorder | Disorder-specific symptoms |
|---|---|
| GAD | Constant worries and fears |
| OCD | Unwanted persistent or repetitive thoughts or behaviours that seem impossible to stop or control |
| Social phobia | A debilitating fear of being seen negatively by others and humiliated in public |
| Specific phobia | Excessive or irrational fear of a specific object or situation |
| PTSD | Extreme anxiety disorder that can occur in the aftermath of a traumatic or life-threatening event |
| Panic disorder | Repeated, unexpected panic attacks as well as fear of experiencing another episode |
Aetiology, pathology and prognosis
The specific cause of symptoms in each anxiety disorder is not well established and the underlying pathology of the disorders has yet to be fully elucidated. It is thought that a complex combination of genetic, environmental, psychological and developmental factors contribute to the development of an anxiety disorder. 21 Various factors have been found to increase the risk of developing an anxiety disorder, with some identified as specifically increasing this risk in older adults (summarised in Box 1). 1,19 Evidence indicates that susceptibility to anxiety disorders can be determined early in life. Early-life trauma has long been thought to increase the subsequent risk of developing a mental health illness. 21
-
Being female.
-
Traumatic experience in either childhood or adulthood.
-
Physical illness (e.g. thyroid problems and chronic medical conditions).
-
Stress over a prolonged period of time (e.g. ongoing concern about finances).
-
Genetic predisposition.
-
Drug or alcohol abuse.
-
Being female.
-
Having multiple chronic medical conditions (particularly chronic obstructive pulmonary disease, cardiovascular disease, thyroid disease and diabetes).
-
Being single, divorced or separated.
-
Lower level of education.
-
Perceived (self-reported) poor health.
-
Sleep disturbance.
-
Effects of medications (e.g. corticosteroids, antidepressants, stimulants and bronchodilators).
-
Alcohol or prescription medication misuse or abuse.
-
Physical limitations in daily activities.
-
Stressful life events.
-
Adverse events in childhood.
-
Neuroticism or preoccupation with somatic (physical) symptoms.
When a threat is perceived, various neurotransmitters and other chemical messengers, including circulating hormones, are released to modulate the neural circuitry involved in the generation of feelings of fear and anxiety. 22 The chief hormone involved in the autonomic nervous system is the catecholamine ‘adrenaline’ (also known as epinephrine), produced by the adrenal glands. Adrenaline triggers a physical response to stress, including increased heart rate and breathing rate. 22 At the same time another hormonal system, the hypothalamo–pituitary–adrenal axis, initiates a pathway involving several hormones and other messengers. The culmination of the various signalling interactions is the release of adrenal hormones, called glucocorticoids, of which cortisol is the most important. 22,23 Cortisol causes a rapid release of the body’s energy stores to maintain blood sugar levels and also suppresses any immune response. Dysregulation of the hypothalamo–pituitary–adrenal axis is known to be associated with an increased risk of development of major depression. 24 Furthermore, the ageing brain is less able to downregulate the hypothalamo–pituitary–adrenal axis and is more susceptible to physiological stressors. 25 Thus, in older adults chronic anxiety can cause hyperactivity of this system, which can detrimentally affect memory and executive function.
The main neurotransmitters implicated in anxiety disorders are noradrenaline, serotonin, dopamine and gamma-aminobutyric acid (GABA). 26 The discovery that anxiolytic (anti-anxiety) drugs interact with neurotransmitters led to the proposal that abnormal activity in the brain is a physiological characteristic of anxiety. 21
Imaging of brain activity during exposure to triggers of anxiety has suggested that the amygdala and the hippocampus have an integral role in eliciting feelings of fear and anxiety. 21,26 The amygdala is located deep in the anterior medial section of each temporal lobe and is thought to be involved in memory storage and communication. 27 It is thought that the amygdala facilitates signal transfer between the components of the brain that process incoming sensory signals and those that interpret the signals. An imbalance of the signalling pathway, possibly resulting from overactivity of the amygdala, is thought to contribute to excessive anxiety. 27 The amygdala functions as a warning system, alerting for potential impending threat and activating the nervous system to generate feelings of fear or anxiety. The central part of the amygdala is thought to store emotional memories and, thus, could have a role in the development of a specific phobia.
Located in the forebrain and forming part of the limbic system, which is the area of the brain that responds to stress, the hippocampus is important in spatial navigation and the formation of memories. 21 The hippocampus is involved in consolidating a life-threatening or traumatic event into a memory. Some studies suggested that the hippocampus is smaller in some people who have PTSD, with the change in size28–31 thought to be induced by sustained exposure to cortisol, which is known to damage the hippocampus23 during a prolonged period of stress. 32 However, recent research involving identical (monozygotic) twins suggests that reduced hippocampal volume is predetermined and volume is linked with susceptibility to PTSD. 33 Other studies in identical or non-identical (dizygotic) twins have found that all the anxiety disorders have a moderately strong genetic basis, accounting for 30–40% of the probability of a person developing an anxiety disorder. 34,35
The extent to which environmental factors determine the risk of developing an anxiety disorder is not established. However, one environmental factor known to be linked with the risk of a person developing an anxiety disorder is the childhood relationship with parents. 36,37 Positive parenting experiences are important to provide children with a feeling of security. Family conflict, lack of structure and discipline, and overprotection, amongst others, have been identified as parental experiences that predispose a person to developing an anxiety disorder, either during childhood or in later life. 37
Categorisation of treatment resistance in anxiety disorders is complex. It has been recommended that the assessment of remission and recovery in anxiety disorders includes an assessment of functional status. 38 Recognition of treatment resistance is further complicated by the frequent presence of symptoms of more than one anxiety disorder and the presence of a comorbid disorder that potentially disrupts treatment. Response to treatment or, conversely, non-response to treatment in anxiety disorders has been investigated in various studies. 38 Factors thought to contribute to poor response to treatment have been divided into four categories (outlined in Box 2): pathology, environment, patient and clinician. Difficulty in diagnosing treatment resistance is affected by the same problems encountered when diagnosing an anxiety disorder, including changes in, and variation across, criteria used to categorise anxiety disorders, under-recognition of the disorder and use of clinically inadequate doses of pharmacological agents in initial treatment.
-
Exact underlying pathophysiology is unknown.
-
Multiple neurotransmitters participation and interaction.
-
Complex receptor and feedback structure of every single transmitter system.
-
Diagnosis – dimension approach.
-
Genetics of the disorders overlap and unclear what is inherited.
-
Current biological treatments are empirical and have limitations.
-
Cognitive–behavioural theory is disconnected from biological substrate.
-
Severe stressors.
-
Childhood stressors.
-
Long-term persistent stressors.
-
Life cycles.
-
Severity.
-
Medical comorbidity.
-
Psychiatric comorbidity.
-
Non-compliance.
-
Cultural factors.
-
Lack of knowledge in primary care.
-
Cognitive–behavioural theory is disconnected from biological substrate.
-
Cost leading to limited doctor–patient relationship.
As with younger adults, the course of established anxiety disorders in older people is typically chronic or episodic in nature, and most disorders are unlikely to remit completely, even with long-term treatment. 39 One US-based study evaluating people with GAD (164 people) reported a mean age at onset of an anxiety disorder of 21 years and an average duration of illness of about 20 years. 40 Studies suggest that anxiety disorders are more chronic than other common mental disorders and that comorbid depression and anxiety has a worse prognosis. 41 The presence of an anxiety disorder has been identified as an independent risk factor for subsequent onset of suicidal ideation and attempts. 42 In all age groups, the frequent comorbidity of anxiety disorders, depression, and alcohol and drug misuse complicates the evaluation of long-term prognosis. In clinical trials involving a mixed-age population and different anxiety disorders, remission rates of 20–47% have been reported. 43 The study evaluating people with GAD found that, despite treatment, only 25% of patients achieved symptomatic remission from GAD at 3 years,40 with a risk of relapse over the subsequent year of about 15%; risk of relapse for those achieving partial symptomatic remission increased to 30%. 40
Incidence and prevalence
Data reported on prevalence and incidence vary across studies. This disparity can be attributed to different methodological procedures used, including sampling, with some studies using nationally representative samples and others using convenience samples; differences in the tools used to diagnose an anxiety disorder; and differences in the anxiety disorders included in the evaluation. 1
The prevalence of anxiety disorders in older people exceeds that of late-life depression and cognitive dysfunction,44 with estimated rates of anxiety disorders ranging from 3.2% to 14.2% in people aged over 65 years. 1 In England during 2007, 2.28 million people were estimated to have an anxiety disorder, with 13% of those being aged over 65 years. 45 The prevalence of anxiety disorders is even higher among older people who are housebound and require home care, those who live in residential care facilities (e.g. a nursing home or assisted living) and those who have a chronic medical illness. In addition, 15–20% of older people experience symptoms of anxiety that, although debilitating, do not meet criteria for a psychiatric diagnosis. 3 Most people with a primary anxiety disorder experienced the onset of the condition before the age of 41 years (90%), with 75% of people diagnosed with an anxiety disorder before the age of 21 years. 46
A UK-based epidemiological survey of common mental disorders [including depression, GAD, panic disorder, phobias (in general) and OCD] reported GAD to be the most common anxiety disorder affecting people in the UK, with a prevalence of 4.4%. The prevalence of PTSD was 3.0%, and only a small proportion of people (< 1.5%) met diagnostic criteria for the remaining disorders. 47 A review of the literature on prevalence of anxiety disorders in older people identified considerable variation in prevalence of the individual disorders (summarised in Table 2). 1 The results reported in the review suggest that estimates of prevalence are highest for social phobia (with or without agoraphobia) and GAD. However, elsewhere, it has been reported that GAD is the most common anxiety disorder affecting older adults, with a prevalence of 3.1–11.2%. 3 The authors of this comprehensive review note that, because of methodological issues identified earlier, it is not possible to draw definitive conclusions on prevalence. 3 Data on prevalence of treatment-resistant anxiety in older people were not identified.
| Anxiety disorder | Prevalence in older people |
|---|---|
| GAD | 1.2–7.3% |
| OCD | 0.1–0.8% |
| Social phobia | 3.1–10.2% |
| Specific phobia | Not reported |
| PTSD | 0.4–1.0% |
| Panic disorder | 0.1–1.0% |
Impact of health problem
When comparing older people with an anxiety disorder with people of the same age with what would be categorised as ‘normal’ worries, older people with an anxiety disorder frequently experience greater difficulty in managing their day-to-day lives and are at an increased risk of comorbid depressive disorders, falls, physical and functional disability, and loneliness. 1,3 Furthermore, the presence of an anxiety disorder is associated with reduced compliance with medical treatment and potential exacerbation of chronic conditions, which can result in loss of independence and increased reliance on family or carers. Anxiety has a considerable detrimental effect on the quality of life (QoL) of both the older person with an anxiety disorder and their carers.
Significance for the NHS
As a result of changing demographics, it is estimated that the number of people with an anxiety disorder in England will grow to 2.56 million by 2026, with the largest increases observed in older age groups. 45 Compared with data from 2007, it has been predicted that the number of people aged 85 years and older with an anxiety disorder in England will increase by 66% by 2026. 45 Anxiety disorders in older adults will become a source of increasing personal and societal cost.
Current service provision
The National Institute for Health and Care Excellence (NICE) has produced clinical guidelines (CGs) on the management of GAD and panic disorder [with or without agoraphobia; (CG113)],48 PTSD (CG26),49 OCD (CG31)50 and social anxiety disorder (CG159). 51 Of the guidelines available, CG113 addresses interventions for treatment-resistant GAD and CG31 outlines management of OCD that is not responding to treatment, but neither guideline outlines management of inadequate response to treatment specifically in older adults. Guidance from NICE advocates a stepped care pathway for GAD,52 panic disorder53 and OCD,54 as depicted in NICE clinical pathways. By contrast, the pathways for PTSD55 and social anxiety disorder56 are not based on a series of set treatment phases.
Although treatment strategies are tailored to treat the particular symptoms associated with the needs of the patient with an anxiety disorder, fundamentally the core principles of the clinical pathways for recognition and treatment of panic disorders are similar,52–56 with initial steps involving the identification and assessment of severity of the anxiety disorder. Providing patients with information to understand their disorder, and the treatment options available, are proposed as an important components of treatment across anxiety disorders. Evidence from a systematic review indicates that self-help is more effective than waiting list control in the treatment of anxiety, with a significant reduction in symptoms of anxiety [standardised mean difference (SMD) −0.86, 95% confidence interval (CI) −1.03 to −0.69 (20 studies, n = 1121)]. 57 It should be noted that the evidence in this review is based on a synthesis of data from trials in various anxiety disorders and moderate statistical heterogeneity (44%) was present. 57 Considered separately, the evidence base for the effectiveness of self-help in the individual anxiety disorders is limited. Self-help, either guided or non-guided, is described in CG113 as a low-intensity psychological treatment for GAD – these low-intensity psychological interventions listed in CG113 are summarised in Table 3. 48 Definition of what constitutes low-intensity psychological therapies varies across studies, but such interventions are generally those with little or no involvement of a therapist. 58 Examples include bibliotherapy and computer-guided interventions. As contact with a health-care professional is minimal, low-intensity psychological interventions increase access to psychological treatments for people experiencing mild to moderate anxiety and depressive disorders. 48 Increasing access to psychological interventions for the treatment of anxiety disorders and depression is a key tenet of the Improving Access to Psychological Therapies programme, which was launched in the UK in October 2007. 59
| Intervention | Description |
|---|---|
| Non-facilitated self-help | Self-administered intervention intended involving a self-help resource (usually a book or workbook) |
| Similar to guided self-help, but with minimal therapist contact (infrequent telephone call lasting no longer than 5 minutes) | |
| Guided self-help | Self-administered intervention intended to treat symptoms of anxiety |
| Typically involves a CBT-based self-help resource (e.g. leaflets, books, self-help workbook or multimedia) | |
| Limited support from a health-care professional: contact between the person and the health-care professional ranges from 3 to 10 sessions, totalling 3–6 hours of therapy delivered either face to face or by telephone | |
| Psychoeducational group | Psychoeducation delivered to a large group (typically 20–24 people) |
| Focuses on educating people about the nature of anxiety and ways of managing anxiety using cognitive–behavioural techniques | |
| Weekly sessions led by appropriately trained practitioners (one therapist to 12 group members) and involving presentations and self-help materials | |
| Sessions typically last for 2 hours and take place over a 6-week period |
In GAD, if symptoms of anxiety persist after low-intensity psychological interventions NICE recommends offering high-intensity psychological interventions as a treatment option. 48 People with anxiety disorders and depression frequently prefer to try psychological interventions before pharmacological agents. Compared with low-intensity therapies, high-intensity interventions are typically more resource intensive, involving more contact with appropriately trained health-care professionals; examples of high-intensity psychological interventions include cognitive–behavioural therapy (CBT) and applied relaxation (see Table 4). Alternatively, people may be offered a pharmacological treatment if they prefer, with a selective serotonin reuptake inhibitor (SSRI) typically the first choice for treatment. 48 For OCD that is associated with moderate functional impairment, NICE recommends offering a choice between higher-intensity CBT or a course of a SSRI as initial treatment. 50 Other pharmacological options for anxiety disorders include a serotonin–noradrenaline reuptake inhibitor (SNRI), pregabalin or a benzodiazepine. Benzodiazepines have been associated with toxicity, dependence, abuse and cognitive impairment, and are not recommended for the long-term treatment of anxiety. 60
| Intervention | Description |
|---|---|
| CBT | Psychotherapeutic approach encompassing various techniques based on cognitive–behavioural models of disorders. Working with the person with the disorder, the therapist designs specific techniques that target dysfunctional emotions and cognitive processes. Treatment goals might include recognising the impact of behavioural and/or thinking patterns on feeling states and encouraging alternative cognitive and/or behavioural coping skills |
| Applied relaxation | Focuses on applying muscular relaxation at times of anxiety and facilitates early response to feelings of anxiety. Applied relaxation is carried out by practitioners of CBT and sessions are typically weekly, lasting for 12–15 weeks. Components of applied relaxation include: |
|
|
|
|
|
|
|
|
|
|
| Psychodynamic therapy | Focuses on unconscious processes as manifested in a person’s present behaviour |
|
|
|
|
| Non-directive therapies | Psychotherapeutic approach in the person is helped to identify conflicts and to clarify and understand feelings and values, during which the practitioner does not proffer advice or interpretation |
| Trauma-focused CBT | Focuses memories, thoughts and feelings that a person has about the traumatic event |
| Eye movement desensitisation and reprocessing | Focuses on memories of the traumatic event (including negative thoughts, feelings and sensations experienced at the time of the event) with the goal of generating more positive emotions, thoughts and behaviour: |
|
|
|
|
|
|
| Exposure and response prevention | Goal is habituation and extinction of responses |
|
|
|
|
|
Patients who do not respond to initial psychological or pharmacological treatment, those who are at high risk of self-harm or neglect, and those suffering from substantial comorbidities might require complex drug and/or psychological treatment, crisis services, day hospitals or inpatient care. 48,50
Guidance on the treatment of anxiety and treatment-resistant anxiety in older adults is lacking. It is well recognised that anxiety in older people manifests differently from anxiety in younger people. Older people are more likely to consult their doctor because of somatic (i.e. physical) or general symptoms (e.g. change in sleep pattern) rather than concerns about their anxiety. 16 As a result, in primary care, older adults are more likely to be prescribed a benzodiazepine than a SSRI; benzodiazepines are most frequently used to manage insomnia, particularly in older adults in whom insomnia is caused by anxiety or depression. The main adverse effects associated with benzodiazepines are sleepiness, unsteadiness and difficulty with memory and concentration; all of which are more severe in older adults. Benzodiazepines are also associated with a considerable increase in the risk of falls for an older person. 61
Optimising treatment to manage anxiety disorders in older people is complex, and treatment typically involves a combination of psychotherapy, pharmacotherapy and complementary therapies. Older people frequently require multiple concomitant treatments to manage comorbid psychological and chronic medical conditions,1 and are at risk of under-treatment as physicians take care to restrict the number of medications prescribed. Physiological changes that occur during ageing lead to decreased metabolism and reduced clearance of pharmacological agents. As a result, older people are at an increased risk of adverse effects from treatment, a risk that is compounded by increasing the number of drugs administered. 62 Additionally, it is well recognised that adherence to treatment among older people can be lower than among younger adults. 1 Lower tolerability for treatment and decline in cognitive function, which is a natural part of ageing, both contribute to the lower rate of compliance. 62 Poor compliance can exacerbate chronic medical conditions, lead to increased reliance on carers and, ultimately, result in admission to a residential facility.
Alternative treatment strategies with potential for use in treatment-resistant anxiety include switching medication and combining pharmacotherapy and psychotherapy, but there is limited evidence evaluating these treatments. One strategy for which there is a strong evidence base in treating resistant anxiety in a mixed-age population is augmentation of pharmacotherapy with a second agent. In a review of the literature, Ipser et al. 63 identified 28 randomised controlled trials (RCTs) evaluating the addition of primarily antipsychotic drugs (17 RCTs) to ongoing pharmacotherapy. Most RCTs evaluated short-term (average follow-up of 7 weeks) augmentation of a SSRI with an antipsychotic for the treatment of people not responding to first-line treatment for OCD. Although the findings suggest that this augmentation approach can be effective in the short term, methodological and clinical heterogeneity among trials preclude drawing definitive conclusions on effectiveness. Treatment of older people is typically complicated by issues such as polypharmacy and comorbidity. Physiological functions change with age; for example, the way in which the body metabolises a drug could differ greatly in older adults compared with younger adults and, for these reasons, it might be considered inappropriate to extrapolate results from trials involving a mixed-age sample to older adults. Moreover, because of the additional complexity of treatment, clinicians in the primary care setting are likely to be cautious about prescribing psychotropic treatments for older people.
Description of technology under assessment
The interventions under assessment are those that would be used to treat symptoms of anxiety that had not responded to prior treatment, which, based on NICE guideline CG113 for GAD, would comprise offering people the choice of either high-intensity psychological treatments or a drug treatment and, in refractory cases, a combination of psychological and pharmacological treatments;48 guidance on treatment of persistent anxiety in older people is not available. In the case of GAD that has not responded to low-intensity psychological interventions, NICE recommends basing choice of treatment on patient preference as there is no evidence that one mode of treatment (i.e. psychological vs. pharmacological) is clinically more effective than the other. Based on clinical expert opinion and recommendations for escalation of treatment in CG113,48 for the review reported here, treatment resistance/refractoriness was defined as no substantial improvement in symptoms of anxiety, despite treatment with an intervention for which there is evidence of clinical effectiveness in the treatment of an anxiety disorder.
High-intensity psychological treatments
High-intensity psychological treatments typically involve one-to-one therapy with a mental health professional and take place over multiple treatment sessions. High-intensity psychological techniques are complex and considerably more resource intensive than low-intensity psychological interventions, comprising multiple components that are typically adapted to an individual; an overview of components of some high-intensity psychological therapies is presented in Table 4.
Cognitive–behavioural therapy is widely employed in the treatment of anxiety and depression, either on a one-to-one basis or delivered as part of a group session (see Table 4). CBT has been found to be clinically beneficial in treating anxiety symptoms associated with GAD,64 panic disorder,65 PTSD,66 social anxiety disorder67 and OCD. 68 Other forms of psychological intervention have been found to offer more benefit in some disorders than in others. For example, applied relaxation is an alternative to CBT that has benefit in the treatment of GAD64 and panic disorder65 (see Table 4), and trauma-focused CBT as well as eye movement desensitisation and reprocessing are used in the treatment of anxiety associated with PTSD49,66 (Table 4). Exposure and response prevention techniques are used in OCD,68 panic disorder65 and social anxiety disorder. 67
Despite evidence that psychological interventions can be effective, older adults generally have reduced access to such services compared with younger adults. In 2007, it was estimated that 51% of people with an anxiety disorder in England were not in contact with health-care services and, of those who were in contact, 46% were not receiving pharmacological or psychological therapy. 45 Information focusing on older adults was not identified. A report from the Older People’s Psychological Therapies Working Group in Scotland identified that fewer than 10% of older people with depression are referred to specialist mental health services, compared with 50% of younger adults. 69 Moreover, the survey also identified that 80% of older people with depression were not receiving any treatment. A lack of available services was identified as the largest barrier to older adults receiving high-intensity psychological interventions. The effectiveness of psychological interventions in older adults with treatment-resistant anxiety is unknown.
Pharmacological treatments
For OCD, social anxiety disorder, GAD and panic disorder, NICE guidance recommends offering a SSRI, in particular sertraline, as the first pharmacological treatment. 48,50,51 Although sertraline is not licensed for the treatment of GAD, NICE acknowledges that sertraline is clinically effective in treating anxiety disorders and appears to be the most cost-effective of the SSRIs. 48 Alternative pharmacological agents used to treat symptoms of anxiety are SNRIs, tricyclic antidepressants (TCAs), benzodiazepines (e.g. diazepam), some anticonvulsants [e.g. pregabalin (Lyrica®, Pfizer)], beta-blockers and other agents with an anxiolytic effect (e.g. buspirone). 70 In addition, augmentation of ongoing pharmacotherapy with an antipsychotic agent has been found to be clinically effective at improving symptoms of anxiety in treatment-resistant anxiety disorders. 63 However, the effectiveness of these agents in treatment-resistant older adults has not been evaluated. First-line pharmacological treatment is most likely to be prescribed by a primary care physician.
Clinical trials frequently exclude older adults, and thus there is limited information available on treatment response in this population. 62 Polypharmacy, age-related changes in physiological processes and increased risk of adverse events, including falls, confusion and depression, present challenges to prescribing pharmacological agents for older adults. Determination of the appropriate dose for older adults can also be troublesome. Age-related changes in physiology could lead to increased volume of distribution of the drug or decreased drug clearance, both of which may result in increased plasma drug concentrations and adverse effects. 62
Selective reuptake inhibitors
Selective serotonin reuptake inhibitors act by selectively inhibiting the reuptake of serotonin (5-hydroxytryptamine) and SNRIs act by selectively inhibiting the reuptake of noradrenaline and serotonin, both of which are neurotransmitters. Serotonin is involved in the regulation of mood, sleep and appetite, and noradrenaline has a role in the body’s response to stress. Dysfunction of the biological pathways involving serotonin and noradrenaline has long been thought to have a role in the pathogenesis of anxiety and depression. 71 It is thought that SSRIs and SNRIs alleviate symptoms of anxiety and depression by blocking reuptake and, thus, increasing the levels of serotonin and noradrenaline available. Various SSRIs and SNRIs have been recommended for the treatment of individual different anxiety disorders;70 anxiety disorders listed by indication for SSRIs or SNRIs as specified in the British National Formulary (BNF) are presented in Table 5. Oral doses for the individual SSRIs and SNRIs reported in the BNF are presented in Appendix 2.
| Drug | Indication | |||||
|---|---|---|---|---|---|---|
| GAD | OCD | Social anxiety disorder | Specific phobia | PTSD | Panic disorder | |
| SSRIs | ||||||
| Escitalopram (Cipralex®, Lundbeck) | ✓ | ✓ | ✓ | – | – | ✓ |
| Sertraline (Lustral®, Pfizer) | – | ✓ | ✓ | – | ✓ | ✓ |
| Paroxetine (Seroxat®, GlaxoSmithKline) | ✓ | ✓ | ✓ | – | ✓ | ✓ |
| Citalopram (Cipramil®, Lundbeck) | – | – | – | – | – | ✓ |
| Fluoxetine (Prozac®, Eli Lilly) | – | ✓ | – | – | – | – |
| Fluvoxamine (Faverin®, Abbott Healthcare) | – | ✓ | – | – | – | – |
| SNRIs | ||||||
| Venlafaxine (Efexor® XL, Pfizer) | ✓ | – | ✓ | – | – | – |
| Duloxetine (Cymbalta®, Eli Lilly) | ✓ | – | – | – | – | – |
Selective serotonin reuptake inhibitors are the first choice of pharmacological treatment for anxiety disorders and major depression because they have a better tolerability and adverse effect profile than other classes of antidepressants. 72 In particular, compared with TCAs, the SSRIs do not cause cardiac conduction abnormalities in overdose and have a low propensity to cause seizures. There are differences in the adverse effect profiles of the SSRIs, but frequently reported adverse effects include gastrointestinal disturbances(nausea, vomiting, abdominal pain, diarrhoea and constipation), dry mouth, drowsiness, insomnia, weight gain and sexual dysfunction.
Caution when prescribing SSRIs is advised for people with epilepsy, cardiac disease, diabetes mellitus, acute angle-closure glaucoma or those with a history of mania. In addition, caution should be used when a person has active, or a history of, gastrointestinal bleeding, or is already taking a drug that is associated with an increased risk of bleeding. 60
Benzodiazepines
Benzodiazepines act by enhancing the effect of the neurotransmitter GABA at the GABAA receptor complex. By increasing the effects of GABA, benzodiazepines induce sedative, hypnotic (sleep-inducing), anxiolytic, anticonvulsant and muscle-relaxing effects. 60 Most benzodiazepines are given orally, but they can also be administered intravenously, intramuscularly or rectally. 60 Examples of benzodiazepines used as anxiolytics include diazepam, alprazolam, chlordiazepoxide hydrochloride, lorazepam (Ativan®, Valeant) and oxazepam.
Prescription of benzodiazepines is widespread, but evidence of dependence (physical and psychological) and tolerance has restricted their usability. 60 Benzodiazepines can be effective in alleviating the acute symptoms of severe anxiety in the short term (2–4 weeks), but their use for mild anxiety or chronic conditions is generally not recommended. In addition, because older adults are at an increased risk of ataxia and confusion (which in turn increases risk of falling), use of benzodiazepines in older adults is not recommended. Older adults with an anxiety disorder are most likely to consult their general practitioner and, in this setting, might be inappropriately prescribed a benzodiazepine as an initial treatment. 73 Analysis of patient records from 131 UK general practices (including approximately 162,000 registered patients annually aged ≥ 65 years) found that in 2003, benzodiazepines (52.4/1000 people) were one of the most frequently prescribed potentially inappropriate drugs. 73
Tricyclic antidepressants
Originally developed in the 1950s and 1960s, TCAs act by inhibiting the reuptake of serotonin, noradrenaline and dopamine72 and include drugs such as amitriptyline, clomipramine hydrochloride and dosulepin hydrochloride. 60 Some TCAs inhibit reuptake of serotonin to a greater extent, whereas others may predominantly block reuptake of noradrenaline. However, most TCAs inhibit reuptake of both serotonin and noradrenaline. Unlike the SSRIs, the TCAs are non-selective and also interact with additional receptors and channels, including histamine, cholinergic, adrenergic and dopamine receptors. 74 Although the TCAs are clinically effective in treating anxiety and depression, their interaction with receptors that are unrelated to depression can lead to the development of often intolerable adverse effects, the most severe of which involve the cardiovascular system. 74 The adverse effect profile of TCAs limits their clinical use. The BNF lists clomipramine for use in phobic and obsessional states at an initial dose of 25 mg daily for younger adults, and an initial dose of 10 mg daily in older adults. 60 The dose can be increased over 2 weeks to 100–150 mg daily to a maximum of 250 mg daily. Older adults are particularly susceptible to the adverse effects associated with TCAs. A systematic review on the risk of adverse effects associated with antidepressant use in older adults identified a statistically significant increase in the risk of falls and of fractures with use of TCAs. 75 Initially a low dose should be used and patients should be monitored closely, particularly checking for psychiatric and cardiac adverse effects. 60
Tricyclic antidepressants and related antidepressants should be used with caution in people with cardiovascular disease, epilepsy, diabetes, and, because of the increased risk of arrhythmias, in people with concomitant conditions such as hyperthyroidism and phaeochromocytoma. 60 The antagonistic action of TCAs at muscarinic acetylcholine receptors means that caution is also needed when treating people with prostatic hypertrophy, chronic constipation, increased intraocular pressure or urinary retention or those with a susceptibility to angle-closure glaucoma. TCAs should be used with caution in people at high risk of suicide or with a history of psychosis or bipolar disorder; for people with bipolar disorder, treatment with a TCA should be stopped if the person enters a manic phase.
Antipsychotics
Antipsychotics are used to treat disorders involving psychosis (with symptoms such as delusions and hallucinations), including schizophrenia and bipolar mania. 76 However, the effectiveness of antipsychotics is not limited to treating psychosis, with evidence of benefit in mood and anxiety disorders, particularly when used as an adjunctive therapy. Antipsychotics have historically been categorised as first-generation (also known as typical or conventional) or second-generation (also known as ‘atypical’) antipsychotics, based on when they were developed;76 examples from the classes listed in the BNF are given in Table 6. 60 It is recommended that use of antipsychotics should be limited to the treatment of severe anxiety symptoms and that they should be used only for short-term treatment.
| Antipsychotic | Usual daily dose for short-term use in management of severe anxiety |
|---|---|
| First-generation antipsychotics | |
| Chlorpromazine | 75–300 mg |
| Haloperidol | 500 μg twice daily |
| Pericyazine | 15–30 mg divided into two doses |
| Perphenazine | 12 mg |
| Prochlorperazine | 15–20 mg in divided doses |
| Trifluoperazine | 2–4 mg in divided doses |
| Second-generation antipsychoticsa | |
| Amisulpride | 50–800 mg |
| Aripiprazole (Abilify®, Otsuka and Bristol-Myers Squibb) | 10–30 mg |
| Clozapine (Clozaril® and FazaClo®, Novartis Pharmaceuticals) | 200–450 mg |
| Olanzapine | 10–20 mg |
| Paliperidone (Invenga®, Janssen Pharmaceuticals) | 3–12 mg |
| Quetiapine | 300–450 mg |
| Risperidone | 4–6 mg |
The first-generation antipsychotics were developed in the 1950s, with second-generation antipsychotics emerging in the 1980s. 76 First- and second-generation antipsychotics both act by blocking dopamine receptors, but second-generation antipsychotics do so to a lesser extent. Second-generation antipsychotics also interact with receptors for neurotransmitters other than dopamine, including serotonin and histamine, and the variation in targeted receptors results in markedly different clinical and adverse effect profiles within the group. 76,77 Choice of treatment is typically determined by medication history and individual risk of particular side effects, such as weight gain or impaired glucose tolerance. Antipsychotics can be given orally or as a depot injection (i.e. antipsychotic injected in a formulation that releases the drug slowly over a period of time, with injections typically repeated every 2–4 weeks).
When used as an adjunctive treatment for treatment-resistant anxiety or depression, antipsychotics have predominantly been added to a SSRI (typically fluoxetine). 63,78 A systematic review of augmentation of pharmacotherapy in treatment-resistant anxiety disorders found that augmentation of ongoing therapy with an antipsychotic significantly reduced symptoms of anxiety in OCD (seven RCTs involving 198 people; SMD of −0.68, 95% CI −1.13 to −0.24). 63
Common adverse effects associated with first-generation antipsychotics include extrapyramidal symptoms (which involve motor control). 76 Compared with second-generation antipsychotics, first-generation antipsychotics increase the risk of hyperprolactinaemia. By contrast, adverse effects occurring more frequently with second-generation antipsychotics are weight gain and metabolic abnormalities. 76 Among the second-generation antipsychotics, paliperidone (Invenga®, Janssen Pharmaceuticals) may cause restlessness and rapid heartbeat, whereas quetiapine is most commonly associated with constipation and dry mouth. Ziprasidone (Geodon®, Pfizer) and aripiprazole (Abilify®, Otsuka and Bristol-Myers Squibb) are more likely to be associated with headache, nausea and constipation, but only minor weight gain.
Antipsychotic drugs should be used with caution in people with cardiovascular disease, epilepsy (and conditions predisposing to seizures), depression, myasthenia gravis, prostatic hypertrophy or a susceptibility to angle-closure glaucoma. 60 Caution is also recommended in severe respiratory disease and in patients with a history of jaundice or who have blood dyscrasias (perform blood counts if unexplained infection or fever develops).
When prescribing antipsychotics to older adults, the balance of risks and benefits should be considered. 60 Antipsychotic drugs have been found to be associated with a small increased risk of mortality and an increased risk of stroke or transient ischaemic attack in older adults with dementia. When prescribed, it is recommended that initial doses of antipsychotic drugs for older adults be reduced to half the recommended adult dose or less (adult doses as listed in the BNF presented in Table 6), and that dosage could be adjusted further after accounting for individual factors such as weight, comorbidity and concomitant medication. 60
Other drugs used as an anxiolytic
Other drug treatments used to treat the symptoms of anxiety include propranolol (beta-blocker). pregabalin (anticonvulsant) and buspirone (anxiolytic).
Propranolol is a non-selective beta-blocker, acting by inhibiting the binding of adrenaline and other stress hormones to the beta adrenoreceptor. Propranolol is primarily used to treat tremor, angina, high blood pressure, heart rhythm disorders and other heart or circulatory conditions. 60 In anxiety disorders propranolol might be used (typical dose of 40 mg once daily) when symptoms such as palpitation, sweating and tremor are present. 60 Common adverse effects associated with propranolol are gastrointestinal disturbances, low energy, trouble sleeping and feeling weak.
Pregabalin is a structural analogue of GABA but, unlike benzodiazepines, it does not bind directly to GABA receptors. 79 It is thought to elicit an anxiolytic effect through binding to a subunit of voltage-gated calcium channels in ‘overexcited’ presynaptic neurones in a state-dependent manner, thereby reducing the release of neurotransmitters, including glutamate and noradrenaline. Pregabalin is licensed for the treatment of GAD at a starting dose of 150 mg in two or three divided doses. 60 As with benzodiazepines, there are concerns about the tolerance of pregabalin during long-term treatment of anxiety disorders and the risk of symptoms of withdrawal on cessation of treatment. 79 Findings from preclinical studies and studies in healthy volunteers are disparate, and uncertainty remains whether or not the long-term use of pregabalin might be associated with similar issues observed during prolonged treatment with benzodiazepines. 79 Dizziness, drowsiness, dry mouth and constipation are recognised adverse effects when taking pregabalin.
Buspirone is a partial agonist of certain serotonin receptors (i.e. it binds to, and activates, a specific serotonin receptor, but has only partial efficacy compared with a full agonist). 80 Primarily used to treat GAD, the pharmacological profile of buspirone is different from other anxiolytics in that it alleviates symptoms of anxiety without the associated effects of sedation or functional impairment. In addition, the unique profile of buspirone means that use is not associated with dependence or with the risk of symptoms of withdrawal when treatment is discontinued. The usual dose of buspirone is 15–30 mg daily in divided doses, with a maximum dose of 45 mg daily. Common adverse effects of buspirone include dizziness, headache, drowsiness and nervousness. 60
Chapter 2 Definition of the decision problem
Decision problem
The population of interest is older people (defined as aged ≥ 65 years) who have a primary diagnosis of an anxiety disorder without a known physical cause and whose symptoms of anxiety have not improved despite treatment with an intervention for which there is evidence of clinical effectiveness in the treatment of anxiety.
Pharmacological interventions used for the treatment of anxiety disorders were evaluated in the review and were not restricted to those licensed in Europe. Additionally, psychological and alternative therapies were also considered. Interventions were eligible when given as a monotherapy or in combination with another intervention for the treatment of anxiety. Interventions were compared with each other, both as a monotherapy and in combination with another intervention.
The primary outcome of interest is a reduction in symptoms of anxiety as determined by a validated disease-specific outcome measure: dichotomous and continuous measures of response to treatment were to be reported. A clinically meaningful improvement in response would be determined by the outcome measure used.
Secondary outcomes of interest are:
-
response (defined as proportion of people experiencing ≥ 50% reduction in symptom score from baseline)
-
remission (as defined in the individual studies)
-
functional disability (encompasses effect on work, social interaction and family life)
-
sleep quality
-
development of, or change in, symptoms of depression
-
adherence to treatment
-
QoL
-
carer outcomes (including carers’ well-being, experience of care-giving and carers’ needs for professional support)
-
adverse effects (all-cause for any identified intervention).
Key issues
Treatment-resistant anxiety disorders have been the focus of numerous RCTs. Despite the burgeoning research in this field, as in treatment-resistant depression, criteria for treatment resistance and response and remission vary across studies, with some studies not reporting clear criteria. RCTs have defined resistance as inadequate response to treatment, but with no further detail on what would be classed as an inadequate response. As in treatment-resistant depression, treatment resistance in anxiety disorders has also been determined by no response after treatment with at least two antidepressants at adequate doses. 81–85 Again, studies vary in the required duration and adequate dosage of standard treatment. As noted earlier, categorisation of treatment resistance in anxiety disorders is further complicated by the nature of the disorders. Reduction in severity of symptoms does not necessarily denote response to treatment, and continued anxiety after treatment could suggest inadequate initial treatment or a natural transient reaction to a supervening stress factor rather than non-response. Variation in the criteria used across studies, and the complexity associated with evaluating anxiety disorders, contribute to the difficulty in interpreting the comparative clinical effectiveness of treatments from the limited evidence available.
It has been noted that populations enrolled across clinical trials evaluating treatments for older adults with anxiety disorders have not been, in the main, representative of older adults in general, in terms of age, functional status, ethnicity or medical health. 3 People enrolled in clinical trials are relatively homogeneous, having a specific disorder and few or no comorbidities, which does not perhaps represent older adults in general who typically have several comorbid physical or mental health illnesses. 86 Also, most trials have been carried out in an academic setting, with set treatment guides and set follow-up, which is atypical of the setting in which most older adults would receive care for their anxiety disorder.
Overall aims and objectives of assessment
The aim of the report was to evaluate the clinical effectiveness of medical, psychological and alternative therapies for treatment-resistant anxiety in older people. The lack of data assessing interventions in older people with treatment-resistant anxiety precluded achievement of the aim of the report. Potential areas for further research in the clinical area are outlined in Chapter 3 (Assessment of clinical effectiveness).
Chapter 3 Assessment of clinical effectiveness
Methods for reviewing effectiveness
The aim of the systematic review was to evaluate the clinical effectiveness of any intervention (i.e. pharmacological, psychological or alternative) used to treat anxiety, in older adults with a focus on the treatment of anxiety that had not improved after treatment with an intervention for which there is evidence of clinical effectiveness in treating anxiety. Evidence was assessed by conducting a systematic review of the published research literature. The review was undertaken following the general principles published by the Centre for Reviews and Dissemination (CRD). 87 The protocol for the systematic review is registered on PROSPERO (registration number CRD42013005612). 88
Identification of studies
Search strategies were designed to include medical subject headings (MeSH) and text terms for anxiety disorders (both as a collective term and as individual anxiety disorders), treatment failure and older adults. To maximise the number of potentially relevant studies retrieved, no MeSH or text terms were included for interventions of interest. Based on the results of the initial scoping search, it was anticipated that few RCTs that focused on older adults would be identified, despite the large number of studies retrieved. Therefore, the decision was taken to search additionally for prospective observational studies (matched control studies, case series and case–control studies). Search filters based on study design were identified via the InterTASC Information Specialists’ Sub-Group search filter resource. 89 Filters developed and validated by the Scottish Intercollegiate Guidelines Network (SIGN) were used to identify RCTs in MEDLINE and EMBASE. 90 Filters devised by Clinical Evidence (a collection of systematic overviews covering various conditions) were chosen to retrieve potentially relevant observational studies from MEDLINE and EMBASE. 91 For the search of PsycINFO, filters implemented for study type were those designed by the University of Texas School of Public Health to retrieve RCTs and observational studies. 92 Search terms for anxiety, treatment resistance and older adults were tailored to the database searched. Bibliographies of previous reviews and retrieved articles were searched for additional studies. A clinical trial registry (ClinicalTrials.gov) was also searched to identify planned, on-going and finalised clinical trials of interest. In addition, clinical experts were contacted with a request for information on any additional studies of which they had knowledge. Conference abstracts that were reviewed and found not to report additional results to those presented in the relevant full publication were excluded.
The electronic databases searched were:
-
MEDLINE In-Process & Other Non-Indexed Citations and Ovid MEDLINE
-
EMBASE
-
The Cochrane Library [specifically Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), Database of Abstracts of Reviews and Effects, and Health Technology Assessment Database]
-
PsycINFO
-
Web of Science.
Databases were searched from inception to September 2013 with the exception of Web of Science, and the initial search was carried out on 9 September 2013. Search parameters for Web of Science were limited to a search period of 2000–present, with study type restricted to article, meeting abstract, proceedings paper and corrections. Search results were uploaded into Reference Manager Version 11.0 (Thomson ResearchSoft, San Francisco, CA, USA) and deduplicated. Full details of the strategies are presented in Appendix 3.
Titles and abstracts returned by the search strategy were examined independently by two researchers [Charlotta Karner (CK) and Fatima Salih (FS)] and screened for possible inclusion. In cases where consensus could not be achieved, the full text of potentially relevant studies was ordered. During abstract appraisal, to facilitate discussion regarding whether or not sufficient evidence had been identified to restrict inclusion of study type to RCTs, potentially relevant studies were categorised as RCT, observational study or systematic review. To ensure that all relevant data were evaluated for inclusion, studies were not differentiated during appraisal of titles and abstracts based on age of the population, to allow for potential reporting of analysis of subgroups by age within the full text.
Full publications were assessed independently by two reviewers [Samantha Barton (SB) and CK] for inclusion or exclusion against prespecified criteria, with studies classified as a RCT evaluated first. After appraisal of full-text publications, the lack of RCTs meeting the prespecified inclusion criteria led to the evaluation of prospective observational studies for inclusion in the review. Disagreements on inclusion of a study, and on which consensus could not be reached, were resolved by discussion or input from a third reviewer [Steven J Edwards (SJE)].
Inclusion and exclusion criteria
Inclusion criteria were based on the decision problem outlined in Chapter 2, Decision problem (presented in Table 7). No restrictions were imposed on language of publication. Reference lists of identified systematic reviews were used as a source of potential additional studies, as well as a resource to compare studies retrieved from the systematic literature search. For the purposes of this review, a systematic review was defined as review reporting:
-
a focused research question
-
details of the search strategy, including databases searched and terms used, that would enable replication of the search
-
inclusion/exclusion criteria, with clear definitions for population, intervention(s), comparator(s) and outcome(s) of interest
-
critical appraisal of included studies.
| PICO | Criteria |
|---|---|
| Population | People aged ≥ 65 years with a primary diagnosis of an anxiety disorder and who are resistant/refractory to treatment |
| Anxiety and related disorders | Anxiety disorders specified as:
|
| Treatment resistance | Defined as no evidence of substantial improvement after 4 weeks’ treatment with a treatment for which there is evidence of clinical effectiveness in the treatment of anxiety |
| Interventions | Any intervention (psychological, pharmacological or alternative) used to treat treatment-resistant anxiety. Interventions given alone or in combination (e.g. combination of psychological plus pharmacological interventions) would be included |
| Comparators | Any intervention versus placebo, no intervention (e.g. waiting list control) or another active intervention (including interventions given alone or in combination) |
| Outcomes | Primary outcomes:
|
Secondary outcomes:
|
|
| Study design | RCTs and comparative observational studies (prospective matched control studies, case series and case–control studies) |
| Other criteria | No restrictions on language or date of publication |
Studies not meeting the prespecified inclusion criteria (Table 7)were excluded and studies specifying an age range as an inclusion criterion, and in which the upper age limit was 65 years, were excluded. Studies were also excluded if they were:
-
trials reporting only post-crossover results and pre-crossover results could not be obtained
-
case reports, historical articles, narrative reviews, editorials and opinion pieces
-
reports published as only meeting abstracts and where insufficient methodological details were reported to allow critical appraisal of study quality.
Where it was not possible to determine the age of the included population (e.g. baseline characteristics not reported), authors were contacted with a request for additional information. No additional information was provided within the prespecified deadline for return of comments (1 month).
Planned data abstraction, critical appraisal, subgroup analyses and evidence synthesis procedures are documented in the review protocol.
Results of the review of clinical effectiveness evidence
No study, either RCT or observational, meeting the prespecified inclusion criteria (Table 7)was identified. The search of clinical trial registries identified no ongoing or planned RCTs in older adults with a treatment-resistant anxiety disorder. The emergence of systematic reviews evaluating the clinical effectiveness of pharmacological and psychological treatments for anxiety in older adults highlights the increasing awareness of the need to manage this condition. 3,93,94
Quantity and quality of research available
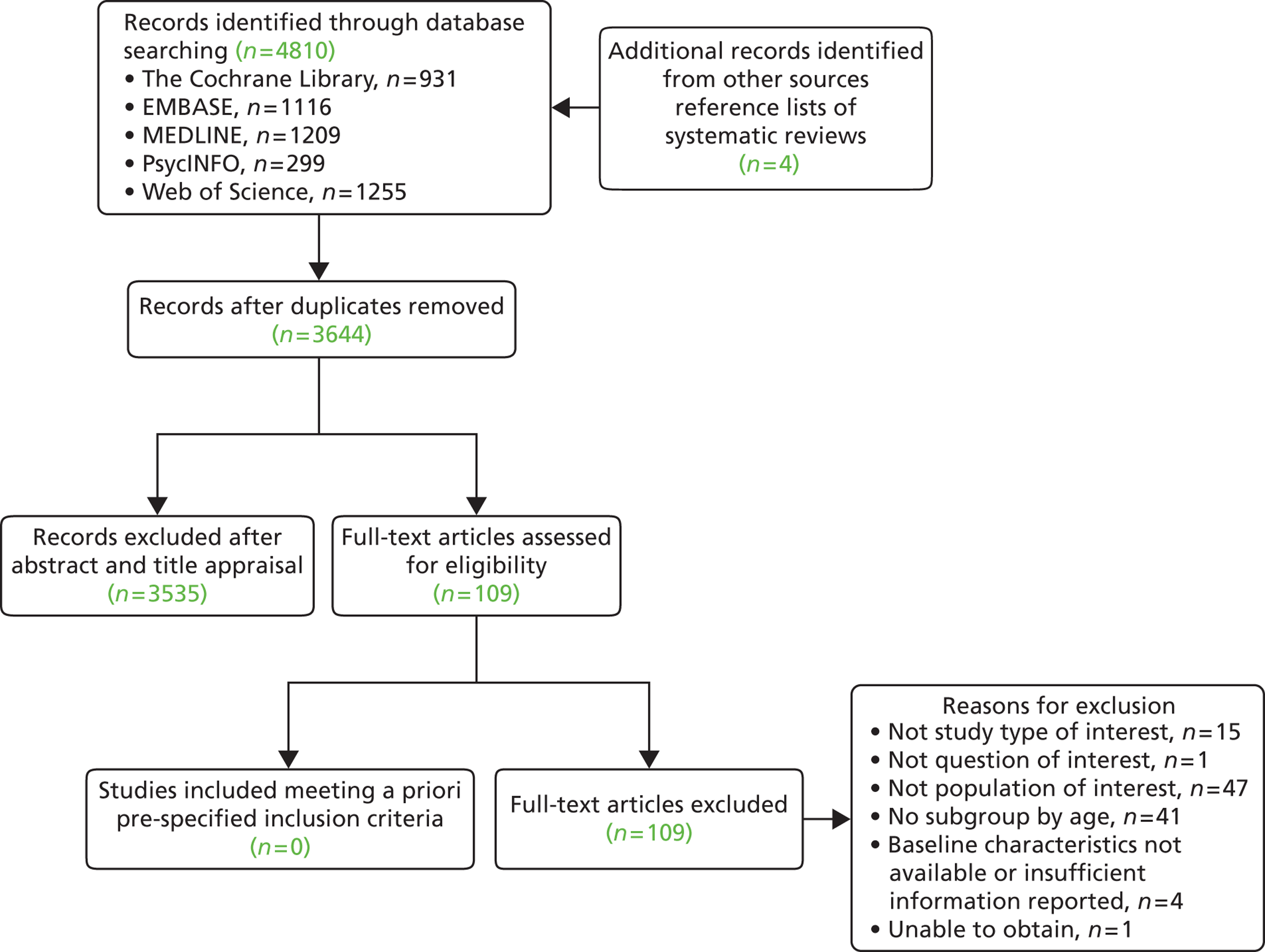
The searches retrieved a total of 3644 records (post deduplication) that were of possible relevance to the review (Figure 1). These were screened and 109 full references were ordered. Of the full references evaluated, the full publication of only one study was not obtained. 95 No study met the prespecified inclusion criteria outlined in Table 7.
FIGURE 1.
PRISMA flow diagram for studies included and excluded from the clinical effectiveness review.
The full list of studies screened and subsequently excluded (with reasons for exclusion) from the review is presented in Appendix 4.
Assessment of effectiveness
No study was identified that evaluated clinical effectiveness of interventions for treatment-resistant anxiety in older adults. Older adults present with manifestations of anxiety different from those of younger adults. Taken together with the finding that response to treatment is poorer in later life,96 it might be that results from studies in younger adults with anxiety disorders cannot be applied to older adults. Considering treatment of anxiety disorders in older adults, systematic reviews of interventions for the treatment of anxiety in later life have found that psychological93,97 and pharmacological94 treatments are effective in reducing symptoms of anxiety in this population, with the authors of one review commenting that evidence is strongest for the treatment of GAD. 3 However, it has been noted that the studies identified by the reviews were small, with an average of 16 people and 43 people in these studies evaluating psychological and pharmacological treatments, respectively. 98 Although there is an increasing awareness of the difficulties in treating anxiety in older adults, there is a lack of an evidence base in this population. 98
Chapter 4 Discussion
Statement of principal findings
This systematic review has highlighted the lack of an evidence base for the treatment of older adults with an anxiety disorder that have not responded, or has responded inadequately, to prior treatment. Although multiple RCTs were identified that evaluated clinical effectiveness of interventions for treatment-resistant anxiety disorders, many limited inclusion to adults aged 65 years and under. Of those studies that included people aged over 65 years, the mean ages reported at baseline suggest that most included people were younger than 65 years. The potentially small number of people likely to be aged 65 and over in the studies identified restricts the practicality and feasibility of carrying out a meta-analysis based on individual patient data. In addition, as the studies identified evaluated a range of treatments across various anxiety disorders, it is likely that the number of events for each treatment would be low, which would probably lead to considerable uncertainty in the results.
Strengths and limitations of the assessment
The review reported here is the first systematic review of interventions for treatment-resistant anxiety in older adults. The comprehensive methods implemented to carry out the review are a key strength of the research presented. However, the review highlights the lack of research in this area, identifying no comparative studies, which is a limitation.
Uncertainties
As no study was identified in older adults, there is considerable uncertainty as to which interventions might be clinically effective for older adults with an anxiety disorder that has not responded, or has responded inadequately, to prior treatment. Disparity between older and younger adults in the presentation of anxiety symptoms and in response to treatment could mean that results demonstrating the clinical effectiveness of interventions in treatment-resistant anxiety disorders in younger adults cannot necessarily be applied to older adults with comparable anxiety disorders.
Chapter 5 Conclusions
Implications for service provision
Identification and treatment of mental disorders is complex, and consideration of the needs and preferences of an individual is advocated when considering treatment choice. The review reported here supports conclusions from other studies that, at this time, the further management of treatment-resistant anxiety disorders in older adults cannot be guided by evidence from meta-analysis or RCTs. In older adults a common underlying reticence to discuss emotional symptoms, together with the misconception that anxiety is a natural part of the ageing process, means that older adults typically receive poorer mental health care than younger adults. The lack of high-level evidence in this area means that older adults are perhaps receiving inappropriate treatment or are not receiving a particular treatment because there is little evidence to support its use. At this time, there is scope to develop guidance on service provision and, as a consequence, to advance the standard of care received by older adults with an anxiety disorder in the primary and secondary settings.
Suggested research priorities
Studies evaluating interventions in older adults with an anxiety disorder that has not responded to first-line treatment are needed to address the lack of evidence in this clinical area. An important consideration would be the enrolment of older adults who would be representative of older adults in general, i.e. those with multiple comorbid physical and mental disorders that might require polypharmacy. In addition, it would be important to consider the setting in which the study was carried out to reflect the setting in which treatment is typically administered. In those taking multiple pharmacological agents, the properties of a particular drug could change considerably, leading to unexpected adverse effects as well as clinical effects. Therefore, assessment of adverse effects could be of equal importance to evaluation of clinical effectiveness.
Randomised controlled trials in anxiety disorders have often involved a heterogeneous population in terms of anxiety disorder, enrolling people with any form of anxiety disorder. As noted earlier, the different types of anxiety disorder respond to differing treatments and to varying degrees. Focusing on a particular anxiety disorder would be important to discern the most effective treatment for that disorder. However, acknowledged difficulties in defining and identifying treatment resistance in older adults could result in poor recruitment, both in terms of the low number of older adults likely to be categorised as treatment resistant and the heterogeneity in terms of prior treatment.
Anxiety disorders are typically chronic or episodic conditions, and maintaining an initial response is a key goal of treatment. Longitudinal studies that examine relapse or recurrence rates would provide an impression of the long-term effectiveness and acceptability of treatment interventions.
Given the often multiple drug treatment regimens taken by older adults, a focus on research into non-pharmacological treatments might be useful, building on currently implemented psychological therapies such as CBT. From the patient’s perspective, developing uncomplicated, undemanding interventions that can be delivered at home or in groups might be warranted. Physical frailty, which is common in older adults, might preclude older adults from accessing services that are some distance from their home.
Difficulties encountered when undertaking RCTs in older adults include the perceptions of health professionals and practical problems relating to attending for regular assessments. 99 From the patient perspective, older adults have expressed fear of trial treatment and a dislike of the randomisation process. 1,3,99 Issues with transport, time taken to be involved in the trial and concerns about compromising current care are also barriers, generally, to patient participation in a clinical trial. 99 To overcome these potential barriers, a prospective matched control observational study might be an appropriate study design.
In summary, studies focusing on a specific anxiety disorder in older adults who have not responded, or have made an inadequate response, to prior treatment are warranted, with a suggested initial focus on effectiveness of non-pharmacological treatments. Given the epidemiological evidence that GAD is the most common anxiety disorder affecting older adults, initial studies evaluating treatments for this disorder might give greatest clinical benefit to a wider population base. Furthermore, the typically chronic nature of anxiety disorders is such that longitudinal studies to monitor maintenance of treatment effect would be needed to provide an insight into the long-term effectiveness and acceptability of treatments.
Acknowledgements
We would like to thank Dr Bart Sheehan (Consultant in Psychological Medicine) and Dr Philip Wilkinson (Consultant Psychiatrist) for providing feedback on the report.
Contributions of authors
Samantha Barton Provided overall project management, designed and carried out literature searches for the systematic review, assessed full publications for inclusion, wrote and contributed to the editing of the report.
Charlotta Karner Assessed abstracts and titles for inclusion, assessed full publications for inclusion and contributed to the editing of the report.
Fatima Salih Assessed abstracts and titles for inclusion, and contributed to the editing of the report.
David S Baldwin Provided clinical input into the design of the literature search, advised on clinical matters and contributed to the editing of the report.
Steven J Edwards Contributed to the editing of the report and was overall director of the project and guarantor of the report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Wolitzky-Taylor KB, Castriotta N, Lenze EJ, Stanley MA, Craske MG. Anxiety disorders in older adults: a comprehensive review. Depress Anxiety 2010;27:190-211. http://dx.doi.org/10.1002/da.20653.
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62:593-602. http://dx.doi.org/10.1001/archpsyc.62.6.593.
- Wetherell JL, Lenze EJ, Stanley MA. Evidence-based treatment of geriatric anxiety disorders. Psychiatr Clin North Am 2005;28:871-96. http://dx.doi.org/10.1016/j.psc.2005.09.006.
- van Balkom AJ, Beekman AT, de Beurs E, Deeg DJ, van Dyck R, van Tilburg W. Comorbidity of the anxiety disorders in a community-based older population in The Netherlands. Acta Psychiatr Scand 2000;101:37-45. http://dx.doi.org/10.1034/j.1600-0447.2000.101001037.x.
- Cairney J, Corna LM, Veldhuizen S, Herrmann N, Streiner DL. Comorbid depression and anxiety in later life: patterns of association, subjective well-being, and impairment. Am J Geriatr Psychiatry 2008;16:201-8. http://dx.doi.org/10.1097/01.JGP.0000300627.93523.c8.
- Schaub RT, Linden M. Anxiety and anxiety disorders in the old and very old: results from the Berlin Aging Study (BASE). Compr Psychiatry 2000;41:48-54. http://dx.doi.org/10.1016/S0010-440X(00)80008-5.
- Sareen J, Jacobi F, Cox BJ, Belik SL, Clara I, Stein MB. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med 2006;166:2109-16. http://dx.doi.org/10.1001/archinte.166.19.2109.
- Lanouette N, Stein M. Advances in the Management of Treatment-Resistant Anxiety Disorders 2013. http://focus.psychiatryonline.org/article.aspx?articleID=53282 (accessed December 2013).
- Diagnostic and Statistical Manual of Mental Disorders. Arlington, VA: American Psychiatric Association; 2000.
- Diagnostic and Statistical Manual of Mental Disorders. Arlington, VA: American Psychiatric Association; 2013.
- World Health Organization . The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research 1993. www.who.int/classifications/icd/en/bluebook.pdf (accessed December 2013).
- Highlights of Changes from DSM-IV-TR to DSM-5. American Psychiatry Publishing; 2013.
- Gellis ZD, McCracken SG. Anxiety Disorders among Older Adults (literature review). Council for Social Work Education; 2007.
- Carmin CN, Wiegartz PS, Scher C. Anxiety disorders in the elderly. Curr Psychiatry Rep 2000;2:13-9. http://dx.doi.org/10.1007/s11920-000-0036-0.
- Lindesay J. Diagnosis of mental illness in elderly people from ethnic minorities. Adv Psychiatr Treat 1998;4:219-26. http://dx.doi.org/10.1192/apt.4.4.219.
- Hales RE, Hilty DA, Wise MG. A treatment algorithm for the management of anxiety in primary care practice. J Clin Psychiatry 1997;58:76-80.
- Meeks T, Lanouette N, Vahia I, Dawes S, Jeste DV, Lebowitz B. Psychiatric Assessment and Diagnosis in Older Adults 2009. http://focus.psychiatryonline.org/article.aspx?articleID=52781 (accessed December 2013).
- Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res 2011;63:S467-72. http://dx.doi.org/10.1002/acr.20561.
- Royal College of Psychiatrists . Anxiety, Panic and Phobias 2013. www.rcpsych.ac.uk/healthadvice/problemsdisorders/anxiety,panic,phobias.aspx (accessed December 2013).
- National Institute of Mental Health . Anxiety Disorders 2009. www.nimh.nih.gov/health/publications/anxiety-disorders/nimhanxiety.pdf (accessed December 2013).
- Gross C, Hen R. The developmental origins of anxiety. Nat Rev Neurosci 2004;5:545-52. http://dx.doi.org/10.1038/nrn1429.
- Ulrich-Lai YM, Herman JP. Neural regulation of endocrine and autonomic stress responses. Nat Rev Neurosci 2009;10:397-409. http://dx.doi.org/10.1038/nrn2647.
- Uno H, Tarara R, Else JG, Suleman MA, Sapolsky RM. Hippocampal damage associated with prolonged and fatal stress in primates. J Neurosci 1989;9:1705-11.
- Pariante CM, Lightman SL. The HPA axis in major depression: classical theories and new developments. Trends Neurosci 2008;31:464-8. http://dx.doi.org/10.1016/j.tins.2008.06.006.
- Lenze EJ, Wetherell JL. A lifespan view of anxiety disorders. Dialogues Clin Neurosci 2011;13:381-99.
- Freitas-Ferrari MC, Hallak JE, Trzesniak C, Filho AS, Machado-de-Sousa JP, Chagas MH, et al. Neuroimaging in social anxiety disorder: a systematic review of the literature. Prog Neuropsychopharmacol Biol Psychiatry 2010;34:565-80. http://dx.doi.org/10.1016/j.pnpbp.2010.02.028.
- Kim MJ, Loucks RA, Palmer AL, Brown AC, Solomon KM, Marchante AN, et al. The structural and functional connectivity of the amygdala: from normal emotion to pathological anxiety. Behav Brain Res 2011;223:403-10. http://dx.doi.org/10.1016/j.bbr.2011.04.025.
- Bremner JD. Neuroimaging studies in post-traumatic stress disorder. Curr Psychiatry Rep 2002;4:254-63. http://dx.doi.org/10.1007/s11920-996-0044-9.
- Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
- Gurvits TV, Shenton ME, Hokama H, Ohta H, Lasko NB, Gilbertson MW, et al. Magnetic resonance imaging study of hippocampal volume in chronic, combat-related posttraumatic stress disorder. Biol Psychiatry 1996;40:1091-9. http://dx.doi.org/10.1016/S0006-3223(96)00229-6.
- Stein MB, Koverola C, Hanna C, Torchia MG, McClarty B. Hippocampal volume in women victimized by childhood sexual abuse. Psychol Med 1997;27:951-9. http://dx.doi.org/10.1017/S0033291797005242.
- Bremner JD. Alterations in brain structure and function associated with post-traumatic stress disorder. Semin Clin Neuropsychiatry 1999;4:249-55.
- Gilbertson MW, Shenton ME, Ciszewski A, Kasai K, Lasko NB, Orr SP, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7. http://dx.doi.org/10.1038/nn958.
- Hettema JM, Neale MC, Kendler KS. A review and meta-analysis of the genetic epidemiology of anxiety disorders. Am J Psychiatry 2001;158:1568-78. http://dx.doi.org/10.1176/appi.ajp.158.10.1568.
- Pauls DL. The genetics of obsessive compulsive disorder: a review of the evidence. Am J Med Genet C Semin Med Genet 2008;148C:133-9. http://dx.doi.org/10.1002/ajmg.c.30168.
- Barlow DH. Unraveling the mysteries of anxiety and its disorders from the perspective of emotion theory. Am Psychol 2000;55:1247-63. http://dx.doi.org/10.1037/0003-066X.55.11.1247.
- Silove D, Parker G, Hadzi-Pavlovic D, Manicavasagar V, Blaszczynski A. Parental representations of patients with panic disorder and generalised anxiety disorder. Br J Psychiatry 1991;159:835-41. http://dx.doi.org/10.1192/bjp.159.6.835.
- Bystritsky A. Treatment-resistant anxiety disorders. Mol Psychiatry 2006;11:805-14. http://dx.doi.org/10.1038/sj.mp.4001852.
- Tyrer P, Baldwin D. Generalised anxiety disorder. Lancet 2006;368:2156-66. http://dx.doi.org/10.1016/S0140-6736(06)69865-6.
- Yonkers KA, Warshaw MG, Massion AO, Keller MB. Phenomenology and course of generalised anxiety disorder. Br J Psychiatry 1996;168:308-13. http://dx.doi.org/10.1192/bjp.168.3.308.
- Tyrer P, Seivewright H, Johnson T. The Nottingham Study of Neurotic Disorder: predictors of 12-year outcome of dysthymic, panic and generalized anxiety disorder. Psychol Med 2004;34:1385-94. http://dx.doi.org/10.1017/S0033291704002569.
- Sareen J, Cox BJ, Afifi TO, de Graaf R, Asmundson GJ, ten Have M, et al. Anxiety disorders and risk for suicidal ideation and suicide attempts: a population-based longitudinal study of adults. Arch Gen Psychiatry 2005;62:1249-57. http://dx.doi.org/10.1001/archpsyc.62.11.1249.
- Pollack MH, Otto MW, Roy-Byrne PP, Coplan JD, Rothbaum BO, Simon NM, et al. Novel treatment approaches for refractory anxiety disorders. Depress Anxiety 2008;25:467-76. http://dx.doi.org/10.1002/da.20329.
- Regier DA, Rae DS, Narrow WE, Kaelber CT, Schatzberg AF. Prevalence of anxiety disorders and their comorbidity with mood and addictive disorders. Br J Psychiatry Suppl 1998;34:24-8.
- McCrone P, Dhanasiri S, Patel A, Knapp M, Lawton-Smith S. Paying the Price. The Cost of Mental Health Care in England to 2026 2008. www.kingsfund.org.uk/sites/files/kf/Paying-the-Price-the-cost-of-mental-health-care-England-2026-McCrone-Dhanasiri-Patel-Knapp-Lawton-Smith-Kings-Fund-May-2008_0.pdf (accessed December 2013).
- Eaton WW, Kramer M, Anthony JC, Dryman A, Shapiro S, Locke BZ. The incidence of specific DIS/DSM-III mental disorders: data from the NIMH Epidemiologic Catchment Area Program. Acta Psychiatr Scand 1989;79:163-78. http://dx.doi.org/10.1111/j.1600-0447.1989.tb08584.x.
- McManus S, Meltzer H, Brugha T, Bebbington P, Jenkins R. Adult Psychiatric Morbidity in England, 2007. Results of a Household Survey. National Centre for Social Research and the Department of Health Sciences; 2007.
- Generalised Anxiety Disorder in Adults. The NICE Guideline on Management In Primary, Secondary and Community Care. NICE; 2011.
- Post-Traumatic Stress Disorder. The Management of PTSD in Adults and Children in Primary and Secondary Care. NICE; 2005.
- Obsessive–Compulsive Disorder: Core Interventions in the Treatment of Obsessive–Compulsive Disorder and Body Dysmorphic Disorder. NICE; 2005.
- Social Anxiety Disorder: Recognition, Assessment and Treatment. NICE; 2013.
- Pathway for Generalised Anxiety Disorder. NICE Pathways; 2013.
- Pathway for Panic Disorder. NICE Pathways; 2013.
- Pathway for Obsessive–Compulsive Disorder and Body Dysmorphic Disorder. NICE Pathways; 2013.
- Pathway for Post-Traumatic Stress Disorder. NICE Pathways; 2013.
- Pathway for Social Anxiety Disorder. NICE Pathways; 2013.
- Lewis C, Pearce J, Bisson JI. Efficacy, cost-effectiveness and acceptability of self-help interventions for anxiety disorders: systematic review. Br J Psychiatry 2012;200:15-21. http://dx.doi.org/10.1192/bjp.bp.110.084756.
- Rodgers M, Asaria M, Walker S, McMillan D, Lucock M, Harden M, et al. The clinical effectiveness and cost-effectiveness of low-intensity psychological interventions for the secondary prevention of relapse after depression: a systematic review. Health Technol Assess 2012;16. http://dx.doi.org/10.3310/hta16280.
- National Health Service . Improving Access to Psychological Therapies 2007. www.iapt.nhs.uk/ (accessed December 2013).
- British Medical Association and Royal Pharmaceutical Society of Great Britain . British National Formulary 2013. www.bnf.org/bnf/index.htm (accessed December 2013).
- Thorp SR, Ayers CR, Nuevo R, Stoddard JA, Sorrell JT, Wetherell JL. Meta-analysis comparing different behavioral treatments for late-life anxiety. Am J Geriatr Psychiatry 2009;17:105-15. http://dx.doi.org/10.1097/JGP.0b013e31818b3f7e.
- Rochon PA. Drug Prescribing for Older Adults 2013. www.uptodate.com/contents/drug-prescribing-for-older-adults (accessed December 2013).
- Ipser JC, Carey P, Dhansay Y, Fakier N, Seedat S, Stein DJ. Pharmacotherapy augmentation strategies in treatment-resistant anxiety disorders. Cochrane Database Syst Rev 2006;4.
- Gale C, Millichamp J. Generalised Anxiety Disorder 2011. http://clinicalevidence.bmj.com/x/systematic-review/1002/interventions.html (accessed December 2013).
- Kumar S, Malone D. Panic Disorder 2008. http://clinicalevidence.bmj.com/x/systematic-review/1010/interventions.html (accessed December 2013).
- Bisson JI. Post-Traumatic Stress Disorder 2009. http://clinicalevidence.bmj.com/x/systematic-review/1005/interventions.html (accessed December 2013).
- Canton J, Scott KM, Glue P. Optimal treatment of social phobia: systematic review and meta-analysis. Neuropsychiatr Dis Treat 2012;8:203-15. http://dx.doi.org/10.2147/NDT.S23317.
- Soomro GM. Obsessive Compulsive Disorder 2011. http://clinicalevidence.bmj.com/x/systematic-review/1004/interventions.html (accessed December 2013).
- Older People’s Psychological Therapies Working Group . The Challenge of Delivering Psychological Therapies for Older People in Scotland 2011. www.scotland.gov.uk/Resource/0039/00392671.pdf (accessed December 2013).
- Baldwin DS, Anderson IM, Nutt DJ, Bandelow B, Bond A, Davidson JR, et al. Evidence-based guidelines for the pharmacological treatment of anxiety disorders: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2005;19:567-96. http://dx.doi.org/10.1177/0269881105059253.
- Baldwin D, Rudge S. The role of serotonin in depression and anxiety. Int Clin Psychopharmacol 1995;9:41-5. http://dx.doi.org/10.1097/00004850-199501004-00006.
- Ferguson JM. SSRI antidepressant medications: adverse effects and tolerability. Prim Care Companion J Clin Psychiatry 2001;3:22-7. http://dx.doi.org/10.4088/PCC.v03n0105.
- De Wilde S, Carey IM, Harris T, Richards N, Victor C, Hilton SR, et al. Trends in potentially inappropriate prescribing amongst older UK primary care patients. Pharmacoepidemiol Drug Saf 2007;16:658-67. http://dx.doi.org/10.1002/pds.1306.
- Berger M, Roth B, Golan D, Tashjian A, Armstrong E, Armstrong A. Principles of Pharmacology: The Pathophysiologic Basis of Drug Therapy. Philadelphia, PA: Lippincott, Williams & Wilkins; 2011.
- Coupland C, Dhiman P, Morriss R, Arthur A, Barton G, Hippisley-Cox J. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ 2011;343. http://dx.doi.org/10.1136/bmj.d4551.
- Hartling L, Abou-Setta AM, Dursun S, Mousavi SS, Pasichnyk D, Newton AS. Antipsychotics in adults with schizophrenia: comparative effectiveness of first-generation versus second-generation medications: a systematic review and meta-analysis. Ann Intern Med 2012;157:498-511. http://dx.doi.org/10.7326/0003-4819-157-7-201210020-00525.
- Edwards SJ, Smith CJ. Tolerability of atypical antipsychotics in the treatment of adults with schizophrenia or bipolar disorder: a mixed treatment comparison of randomized controlled trials. Clin Ther 2009;31:1345-59. http://dx.doi.org/10.1016/j.clinthera.2009.07.004.
- Edwards S, Hamilton V, Nherera L, Trevor N. Lithium or an atypical antipsychotic drug in the management of treatment-resistant depression: a systematic review and economic evaluation. Health Technol Assess 2013;17. http://dx.doi.org/10.3310/hta17540.
- Baldwin DS, Ajel K. Role of pregabalin in the treatment of generalized anxiety disorder. Neuropsychiatr Dis Treat 2007;3:185-91. http://dx.doi.org/10.2147/nedt.2007.3.2.185.
- Eison AS, Temple DL. Buspirone: review of its pharmacology and current perspectives on its mechanism of action. Am J Med 1986;80:1-9. http://dx.doi.org/10.1016/0002-9343(86)90325-6.
- Koran LM, Aboujaoude E, Bullock KD, Franz B, Gamel N, Elliott M. Double-blind treatment with oral morphine in treatment-resistant obsessive–compulsive disorder. J Clin Psychiatry 2005;66:353-9. http://dx.doi.org/10.4088/JCP.v66n0312.
- Krystal JH, Rosenheck RA, Cramer JA, Vessicchio JC, Jones KM, Vertrees JE, et al. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: a randomized trial. JAMA 2011;306:493-502. http://dx.doi.org/10.1001/jama.2011.1080.
- Sachdev PS, Loo CK, Mitchell PB, McFarquhar TF, Malhi GS. Repetitive transcranial magnetic stimulation for the treatment of obsessive compulsive disorder: a double-blind controlled investigation. Psychol Med 2007;37:1645-9. http://dx.doi.org/10.1017/S0033291707001092.
- Storch EAG. Double-blind, placebo-controlled, pilot trial of paliperidone augmentation in serotonin reuptake inhibitor-resistant obsessive–compulsive disorder. J Clin Psychiatry 2013;74:e527-32. http://dx.doi.org/10.4088/JCP.12m08278.
- Zhang ZJ, Wang XY, Tan QR, Jin GX, Yao SM. Electroacupuncture for refractory obsessive–compulsive disorder: a pilot waitlist-controlled trial. J Nerv Ment Dis 2009;197:619-22. http://dx.doi.org/10.1097/NMD.0b013e3181b05fd1.
- Hoertel N, Le Strat Y, Blanco C, Lavaud P, Dubertret C. Generalizability of clinical trial results for generalized anxiety disorder to community samples. Depress Anxiety 2012;29:614-20. http://dx.doi.org/10.1002/da.21937.
- Centre for Reviews and Dissemination . CRD’s Guidance for Undertaking Reviews in Healthcare 2011. www.york.ac.uk/inst/crd/SysRev/!SSL!/WebHelp/SysRev3.htm (accessed December 2013).
- Clinical Effectiveness of Interventions for Treatment-Resistant Anxiety in Older People: a Systematic Review (PROSPERO record). University of York; 2013.
- Information Specialists’ Sub-Group . The InterTASC Information Specialists’ Sub-Group Search Filter Resource 2013. https://sites.google.com/a/york.ac.uk/issg-search-filters-resource/methods-of-developing-search-filters (accessed December 2013).
- Search Filters. SIGN; 2013.
- Clinical Evidence . Study Design Search Filters 2013. http://clinicalevidence.bmj.com/x/set/static/ebm/learn/665076.html (accessed December 2013).
- University of Texas (School of Public Health) . Search Filters for Ovid Medline, Ovid PsycINFO, PubMed, EBSCO CINAHL 2013. https://sph.uth.edu/charting/Ovid_PsycINFO_filters.htm (accessed December 2013).
- Nordhus IH, Pallesen S. Psychological treatment of late-life anxiety: an empirical review. J Consult Clin Psychol 2003;71:643-51. http://dx.doi.org/10.1037/0022-006X.71.4.643.
- Pinquart M, Duberstein PR. Treatment of anxiety disorders in older adults: a meta-analytic comparison of behavioral and pharmacological interventions. Am J Geriatr Psychiatry 2007;15:639-51. http://dx.doi.org/10.1097/JGP.0b013e31806841c8.
- Ginsberg DL. Ziprasidone for treatment-resistant generalized anxiety disorder. Prim Psychiatry 2005;12:28-9.
- Wetherell JL, Petkus AJ, Thorp SR, Stein MB, Chavira DA, Campbell-Sills L, et al. Age differences in treatment response to a collaborative care intervention for anxiety disorders. Br J Psychiatry 2013;203:65-72. http://dx.doi.org/10.1192/bjp.bp.112.118547.
- Gould RL, Coulson MC, Howard RJ. Efficacy of cognitive behavioral therapy for anxiety disorders in older people: a meta-analysis and meta-regression of randomized controlled trials. J Am Geriatr Soc 2012;60:218-29. http://dx.doi.org/10.1111/j.1532-5415.2011.03824.x.
- Voshaar RC. Lack of interventions for anxiety in older people. Br J Psychiatry 2013;203:8-9. http://dx.doi.org/10.1192/bjp.bp.113.127639.
- Bartlam B, Crome P, Lally F, Beswick AD, Cherubini A, Clarfield AM, et al. The views of older people and carers on participation in clinical trials: the PREDICT study. Clin Invest 2012;2:327-36. http://dx.doi.org/10.4155/cli.12.4.
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders 1994. http://justines2010blog.files.wordpress.com/2011/03/dsm-iv.pdf (accessed 6 June 2014).
- Abelson JL, Curtis GC, Sagher O, Albucher RC, Harrigan M, Taylor SF, et al. Deep brain stimulation for refractory obsessive–compulsive disorder. Biol Psychiatry 2005;57:510-16. http://dx.doi.org/10.1016/j.biopsych.2004.11.042.
- Aboujaoude E, Barry JJ, Gamel N. Memantine augmentation in treatment-resistant obsessive–compulsive disorder: an open-label trial. J Clin Psychopharmacol 2009;29:51-5. http://dx.doi.org/10.1097/JCP.0b013e318192e9a4.
- Allgulander C. Novel approaches to treatment of generalized anxiety disorder. Curr Opin Psychiatry 2010;23:37-42. http://dx.doi.org/10.1097/YCO.0b013e328333d574.
- Altamura AC, Serati M, Buoli M, Dell’Osso B. Augmentative quetiapine in partial/nonresponders with generalized anxiety disorder: a randomized, placebo-controlled study. Int Clin Psychopharmacol 2011;26:201-5. http://dx.doi.org/10.1097/YIC.0b013e3283457d73.
- Amiaz R, Fostick L, Gershon A, Zohar J. Naltrexone augmentation in OCD: a double-blind placebo–controlled cross-over study. Eur Neuropsychopharmacol 2008;18:455-61. http://dx.doi.org/10.1016/j.euroneuro.2008.01.006.
- Anderson SW, Booker MB. Cognitive behavioral therapy versus psychosurgery for refractory obsessive–compulsive disorder. J Neuropsychiatry Clin Neurosci 2006;18. http://dx.doi.org/10.1176/appi.neuropsych.18.1.129.
- Atmaca M, Kuloglu M, Tezcan E, Gecici O. Quetiapine augmentation in patients with treatment resistant obsessive–compulsive disorder: a single-blind, placebo-controlled study. Int Clin Psychopharmacol 2002;17:115-19. http://dx.doi.org/10.1097/00004850-200205000-00004.
- Barr LC, Goodman WK, Anand A, McDougle CJ, Price LH. Addition of desipramine to serotonin reuptake inhibitors in treatment-resistant obsessive–compulsive disorder. Am J Psychiatry 1997;154:1293-5.
- Bartzokis G, Lu PH, Turner J, Mintz J, Saunders CS. Adjunctive risperidone in the treatment of chronic combat-related posttraumatic stress disorder. Biol Psychiatry 2005;57:474-9. http://dx.doi.org/10.1016/j.biopsych.2004.11.039.
- Blank S, Lenze EJ, Mulsant BH, Dew MA, Karp JF, Shear MK, et al. Outcomes of late-life anxiety disorders during 32 weeks of citalopram treatment. J Clin Psychiatry 2006;67:468-72. http://dx.doi.org/10.4088/JCP.v67n0319.
- Blay SL, Marinho V, Blay SL, Marinho V. Anxiety disorders in old age. Curr Opin Psychiatry 2012;25:462-7. http://dx.doi.org/10.1097/YCO.0b013e3283578cdd.
- Brawman-Mintzer O, Knapp RG, Nietert PJ. Adjunctive risperidone in generalized anxiety disorder: a double-blind, placebo-controlled study. J Clin Psychiatry 2005;66:1321-5. http://dx.doi.org/10.4088/JCP.v66n1016.
- Bresolin N, Monza G, Scarpini E, Scarlato G, Straneo G, Martinazzoli A, et al. Treatment of anxiety with ketazolam in elderly patients. Clin Ther 1988;10:536-42.
- Bruno AM. Lamotrigine augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive–compulsive disorder: a double-blind, placebo-controlled study. J Psychopharmacol 2012;26:1456-62. http://dx.doi.org/10.1177/0269881111431751.
- Buchsbaum MS, Hollander E, Pallanti S, Baldini RN, Platholi J, Newmark R, et al. Positron emission tomography imaging of risperidone augmentation in serotonin reuptake inhibitor-refractory patients. Neuropsychobiology 2006;53:157-68. http://dx.doi.org/10.1159/000093342.
- Campanini RF, Schoedl AF, Pupo MC, Costa AC, Krupnick JL, Mello MF, et al. Efficacy of interpersonal therapy-group format adapted to post-traumatic stress disorder: an open-label add-on trial. Depress Anxiety 2010;27:72-7. http://dx.doi.org/10.1002/da.20610.
- Carey PD, Vythilingum B, Seedat S, Muller JE, Ameringen M, Stein DJ. Quetiapine augmentation of SRIs in treatment refractory obsessive–compulsive disorder: a double-blind, randomised, placebo-controlled study. BMC Psychiatry 2005;5. http://dx.doi.org/10.1186/1471-244X-5-5.
- Carr C, d’Ardenne P, Sloboda A, Scott C, Wang D, Priebe S. Group music therapy for patients with persistent post-traumatic stress disorder: an exploratory randomized controlled trial with mixed methods evaluation. Psychol Psychother 2012;85:179-202. http://dx.doi.org/10.1111/j.2044-8341.2011.02026.x.
- Crocq MA, Leclercq P, Guillon MS, Bailey PE, Crocq MA, Leclercq P, et al. Open-label olanzapine in obsessive–compulsive disorder refractory to antidepressant treatment. Eur Psychiatry 2002;17:296-7. http://dx.doi.org/10.1016/S0924-9338(02)00673-9.
- Csigo K, Harsanyi A, Demeter G, Rajkai C, Nemeth A, Racsmany M. Long-term follow-up of patients with obsessive–compulsive disorder treated by anterior capsulotomy: a neuropsychological study. J Affect Disord 2010;126:198-205. http://dx.doi.org/10.1016/j.jad.2010.02.127.
- Dannon PN, Sasson Y, Hirschmann S, Iancu I, Grunhaus LJ, Zohar J. Pindolol augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. Eur Neuropsychopharmacol 2000;10:165-9. http://dx.doi.org/10.1016/S0924-977X(00)00065-1.
- David D, De Faria L, Mellman TA. Adjunctive risperidone treatment and sleep symptoms in combat veterans with chronic PTSD. Depress Anxiety 2006;23:489-91. http://dx.doi.org/10.1002/da.20187.
- Denys D, van Megen HJ, van der Wee N, Westenberg HG. A double-blind switch study of paroxetine and venlafaxine in obsessive–compulsive disorder. J Clin Psychiatry 2004;65:37-43. http://dx.doi.org/10.4088/JCP.v65n0106.
- Depping AM, Komossa K, Kissling W, Leucht S. Second-generation antipsychotics for anxiety disorders. Cochrane Database Syst Rev 2010;12. http://dx.doi.org/10.1002/14651858.CD008120.pub2.
- Di NM, Tedeschi D, Martinotti G, De VO, Monetta M, Pozzi G, et al. Pregabalin augmentation in treatment-resistant obsessive–compulsive disorder: a 16-week case series. J Clin Psychopharmacol 2011;31:675-7. http://dx.doi.org/10.1097/JCP.0b013e31822c29a8.
- Dick PH, Sweeney ML, Crombie IK. Controlled comparison of day-patient and out-patient treatment for persistent anxiety and depression. Br J Psychiatry 1991;158:24-7. http://dx.doi.org/10.1192/bjp.158.1.24.
- Diniz JB, Shavitt RG, Pereira CA, Hounie AG, Pimentel I, Koran LM, et al. Quetiapine versus clomipramine in the augmentation of selective serotonin reuptake inhibitors for the treatment of obsessive–compulsive disorder: a randomized, open-label trial. J Psychopharmacol 2010;24:297-30. http://dx.doi.org/10.1177/0269881108099423.
- Diniz JB, Shavitt RG, Fossaluza V, Koran L, Pereira CA, Miguel EC. A double-blind, randomized, controlled trial of fluoxetine plus quetiapine or clomipramine versus fluoxetine plus placebo for obsessive–compulsive disorder. J Clin Psychopharmacol 2011;31:763-8. http://dx.doi.org/10.1097/JCP.0b013e3182367aee.
- Erzegovesi S, Guglielmo E, Siliprandi F, Bellodi L. Low-dose risperidone augmentation of fluvoxamine treatment in obsessive–compulsive disorder: a double-blind, placebo-controlled study. Eur Neuropsychopharmacol 2005;15:69-74. http://dx.doi.org/10.1016/j.euroneuro.2004.04.004.
- Fallon BA, Liebowitz MR, Campeas R, Schneier FR, Marshall R, Davies S, et al. Intravenous clomipramine for obsessive–compulsive disorder refractory to oral clomipramine: a placebo-controlled study. Arch Gen Psychiatry 1998;55:918-24. http://dx.doi.org/10.1001/archpsyc.55.10.918.
- Fava GA, Savron G, Zielezny M, Grandi S, Rafanelli C, Conti S. Overcoming resistance to exposure in panic disorder with agoraphobia. Acta Psychiatr Scand 1997;95:306-12. http://dx.doi.org/10.1111/j.1600-0447.1997.tb09636.x.
- Fineberg NA, Sivakumaran T, Roberts A, Gale T. Adding quetiapine to SRI in treatment-resistant obsessive–compulsive disorder: a randomized controlled treatment study. Int Clin Psychopharmacol 2005;20:223-6. http://dx.doi.org/10.1097/00004850-200507000-00005.
- Fineberg NA, Stein DJ, Premkumar P, Carey P, Sivakumaran T, Vythilingum B, et al. Adjunctive quetiapine for serotonin reuptake inhibitor-resistant obsessive–compulsive disorder: a meta-analysis of randomized controlled treatment trials. Int Clin Psychopharmacol 2006;21:337-43. http://dx.doi.org/10.1097/01.yic.0000215083.57801.11.
- Geus F, Denys D, Westenberg HG. Effects of quetiapine on cognitive functioning in obsessive–compulsive disorder. Int Clin Psychopharmacol 2007;22:77-84. http://dx.doi.org/10.1097/YIC.0b013e32801182f7.
- Goodman WK, Foote KD, Greenberg BD, Ricciuti N, Bauer R, Ward H, et al. Deep brain stimulation for intractable obsessive compulsive disorder: pilot study using a blinded, staggered-onset design. Biol Psychiatry 2010;67:535-42. http://dx.doi.org/10.1016/j.biopsych.2009.11.028.
- Haghighi M, Jahangard L, Mohammad-Beigi H, Bajoghli H, Hafezian H, Rahimi A, et al. In a double-blind, randomized and placebo-controlled trial, adjuvant memantine improved symptoms in inpatients suffering from refractory obsessive–compulsive disorders (OCD). Psychopharmacology 2013;228:633-40. http://dx.doi.org/10.1007/s00213-013-3067-z.
- Hinton DE, Pham T, Tran M, Safren SA, Otto MW, Pollack MH. CBT for Vietnamese refugees with treatment-resistant PTSD and panic attacks: a pilot study. J Traum Stress 2004;17:429-33. http://dx.doi.org/10.1023/B:JOTS.0000048956.03529.fa.
- Hinton DE, Chhean D, Pich V, Safren SA, Hofmann SG, Pollack MH. A randomized controlled trial of cognitive-behavior therapy for Cambodian refugees with treatment-resistant PTSD and panic attacks: a cross-over design. J Trauma Stress 2005;18:617-29. http://dx.doi.org/10.1002/jts.20070.
- Hinton DE, Hofmann SG, Pollack MH, Otto MW. Mechanisms of efficacy of CBT for Cambodian refugees with PTSD: improvement in emotion regulation and orthostatic blood pressure response. CNS Neurosci Ther 2009;15:255-63. http://dx.doi.org/10.1111/j.1755-5949.2009.00100.x.
- Hinton DE, Hofmann SG, Rivera E, Otto MW, Pollack MH. Culturally adapted CBT (CA-CBT) for Latino women with treatment-resistant PTSD: a pilot study comparing CA-CBT to applied muscle relaxation. Behav Res Ther 2011;49:275-80. http://dx.doi.org/10.1016/j.brat.2011.01.005.
- Hirschmann S, Dannon PN, Iancu I, Dolberg OT, Zohar J, Grunhaus L. Pindolol augmentation in patients with treatment-resistant panic disorder: A double-blind, placebo-controlled trial. J Clin Psychopharmacol 2000;20:556-9. http://dx.doi.org/10.1097/00004714-200010000-00011.
- Hoffart A, Due-Madsen J, Lande B, Gude T, Bille H, Torgersen S. Clomipramine in the treatment of agoraphobic inpatients resistant to behavioral therapy. J Clin Psychiatry 1993;54:481-7.
- Hofmann SG, Sawyer AT, Korte KJ, Smits JA. Is it beneficial to add pharmacotherapy to cognitive-behavioral therapy when treating anxiety disorders? A meta-analytic review. Int J Cogn Ther 2009;2:160-75. http://dx.doi.org/10.1521/ijct.2009.2.2.160.
- Hollander E, Baldini RN, Sood E, Pallanti S. Risperidone augmentation in treatment-resistant obsessive–compulsive disorder: a double-blind, placebo-controlled study. Int J Neuropsychopharmacol 2003;6:397-401. http://dx.doi.org/10.1017/S1461145703003730.
- Huff W, Lenartz D, Schormann M, Lee S-H, Kuhn J, Koulousakis A, et al. Unilateral deep brain stimulation of the nucleus accumbens in patients with treatment-resistant obsessive–compulsive disorder: outcomes after one year. Clin Neurol Neurosurg 2010;112:137-43. http://dx.doi.org/10.1016/j.clineuro.2009.11.006.
- Kampman MK. A randomized, double-blind, placebo-controlled study of the effects of adjunctive paroxetine in panic disorder patients unsuccessfully treated with cognitive-behavioral therapy alone. J Clin Psychiatry 2002;63:772-7. http://dx.doi.org/10.4088/JCP.v63n0904.
- Kang JI, Kim CH, Namkoong K, Lee CI, Kim SJ. A randomized controlled study of sequentially applied repetitive transcranial magnetic stimulation in obsessive–compulsive disorder. J Clin Psychiatry 2009;70:1645-51. http://dx.doi.org/10.4088/JCP.08m04500.
- Katz IRR. Venlafaxine ER as a treatment for generalized anxiety disorder in older adults: Pooled analysis of five randomized placebo-controlled clinical trials. J Am Geriatr Soc 2002;50:18-25. http://dx.doi.org/10.1046/j.1532-5415.2002.50003.x.
- Khan A, Atkinson S. Extended release quetiapine fumarate (Quetiapine XR) as adjunct therapy in patients with generalized anxiety disorder and a history of inadequate treatment response: a randomized, double-blind study. Psychopharmacol Bull 2011;44.
- Kolivakis TT, Margolese HC, Sookman D, Leahy RL. Treatment Resistant Anxiety Disorders. New York, NY: Taylor & Francis; 2010.
- Koran LM, Aboujaoude E, Ward H, Shapira NA, Sallee FR, Gamel N, et al. Pulse-loaded intravenous clomipramine in treatment-resistant obsessive–compulsive disorder. J Clin Psychopharmacol 2006;26:79-83. http://dx.doi.org/10.1097/01.jcp.0000195112.24769.b3.
- Koran LM, Aboujaoude E, Gamel NN. Double-blind study of dextroamphetamine versus caffeine augmentation for treatment-resistant obsessive–compulsive disorder. J Clin Psychiatry 2009;70:1530-5. http://dx.doi.org/10.4088/JCP.08m04605.
- Kordon A, Wahl K, Koch N, Zurowski B, Anlauf M, Vielhaber K, et al. Quetiapine addition to serotonin reuptake inhibitors in patients with severe obsessive–compulsive disorder: a double-blind, randomized, placebo-controlled study. J Clin Psychopharmacol 2008;28:550-4. http://dx.doi.org/10.1097/JCP.0b013e318185e735.
- Li X, May RS, Tolbert LC, Jackson WT, Flournoy JM, Baxter LR. Risperidone and haloperidol augmentation of serotonin reuptake inhibitors in refractory obsessive–compulsive disorder: a crossover study. J Clin Psychiatry 2005;66:736-43. http://dx.doi.org/10.4088/JCP.v66n0610.
- Lippitz BE, Mindus P, Meyerson BA, Kihlstrom L, Lindquist C, Lippitz BE, et al. Lesion topography and outcome after thermocapsulotomy or gamma knife capsulotomy for obsessive–compulsive disorder: relevance of the right hemisphere. Neurosurgery 1999;44:452-8. http://dx.doi.org/10.1097/00006123-199903000-00005.
- Lohoff FW, Etemad B, Mandos LA, Gallop R, Rickels K. Ziprasidone treatment of refractory generalized anxiety disorder: a placebo-controlled, double-blind study. J Clin Psychopharmacol 2010;30:185-9. http://dx.doi.org/10.1097/JCP.0b013e3181d21951.
- Macklin ML, Metzger LJ, Lasko NB, Berry NJ, Orr SP, Pitman RK. Five-year follow-up study of eye movement desensitization and reprocessing therapy for combat-related posttraumatic stress disorder. Compr Psychiatry 2000;41:24-7. http://dx.doi.org/10.1016/S0010-440X(00)90127-5.
- Maina G, Pessina E, Albert U, Bogetto F. 8-week, single-blind, randomized trial comparing risperidone versus olanzapine augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive–compulsive disorder. Eur Neuropsychopharmacol 2008;18:364-72. http://dx.doi.org/10.1016/j.euroneuro.2008.01.001.
- Mallet L, Polosan M, Jaafari N, Baup N, Welter ML, Fontaine D, et al. Subthalamic nucleus stimulation in severe obsessive–compulsive disorder. N Eng J Med 2008;359:2121-34. http://dx.doi.org/10.1056/NEJMoa0708514.
- Mansur CG, Myczkowki ML, de Barros CS, Sartorelli MC, Bellini BB, Dias AM, et al. Placebo effect after prefrontal magnetic stimulation in the treatment of resistant obsessive–compulsive disorder: a randomized controlled trial. Int J Neuropsychopharmacol 2011;14:1389-97. http://dx.doi.org/10.1017/S1461145711000575.
- Mantovani A, Simpson HB, Fallon BA, Rossi S, Lisanby SH. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessive–compulsive disorder. Int J Neuropsychopharmacol 2010;13:217-27. http://dx.doi.org/10.1017/S1461145709990435.
- Marshall RD, Beebe KL, Oldham M, Zaninelli R. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8. http://dx.doi.org/10.1176/appi.ajp.158.12.1982.
- Matsunaga H, Nagata T, Hayashida K, Ohya K, Kiriike N, Stein DJ. A long-term trial of the effectiveness and safety of atypical antipsychotic agents in augmenting SSRI-refractory obsessive–compulsive disorder. J Clin Psychiatry 2009;70:863-8. http://dx.doi.org/10.4088/JCP.08m04369.
- Mavissakalian MR. Sertraline in panic disorder: initial treatment versus switch strategy. J Clin Psychopharmacol 2003;23:646-51. http://dx.doi.org/10.1097/01.jcp.0000096248.95165.ac.
- McDougle CJ, Price LH, Goodman WK, Charney DS, Heninger GR. A controlled trial of lithium augmentation in fluvoxamine-refractory obsessive–compulsive disorder: lack of efficacy. J Clin Psychopharmacol 1991;11:175-84. http://dx.doi.org/10.1097/00004714-199106000-00005.
- McDougle CJ, Goodman WK, Leckman JF, Holzer JC, Barr LC, Cance-Katz E, et al. Limited therapeutic effect of addition of buspirone in fluvoxamine-refractory obsessive–compulsive disorder. Am J Psychiatry 1993;150:647-9.
- McDougle CJ, Goodman WK, Leckman JF, Lee NC, Heninger GR, Price LH. Haloperidol addition in fluvoxamine-refractory obsessive–compulsive disorder. A double-blind, placebo-controlled study in patients with and without tics. Arch General Psychiatry 1994;51:302-8. http://dx.doi.org/10.1001/archpsyc.1994.03950040046006.
- McDougle CJ, Epperson CN, Pelton GH, Wasylink S, Price LH. A double-blind, placebo-controlled study of risperidone addition in serotonin reuptake inhibitor-refractory obsessive–compulsive disorder. Arch Gen Psychiatry 2000;57:794-801. http://dx.doi.org/10.1001/archpsyc.57.8.794.
- Menza MA, Dobkin RD, Marin H. An open-label trial of aripiprazole augmentation for treatment-resistant generalized anxiety disorder. J Clin Psychopharmacol 2007;27:207-10. http://dx.doi.org/10.1097/01.jcp.0000248620.34541.bc.
- Mithoefer MC, Wagner MT, Mithoefer AT, Jerome L, Doblin R. The safety and efficacy of (±3,4-methylenedioxymethamphetamine)-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study. J Psychopharmacol 2011;25:439-52. http://dx.doi.org/10.1177/0269881110378371.
- Muscatello MR, Bruno A, Pandolfo G, Micò U, Scimeca G, Romeo VM, et al. Effect of aripiprazole augmentation of serotonin reuptake inhibitors or clomipramine in treatment-resistant obsessive–compulsive disorder: a double-blind, placebo-controlled study. J Clin Psychopharmacol 2011;31:174-9. http://dx.doi.org/10.1097/JCP.0b013e31820e3db6.
- Nakatani E, Nakagawa A. Outcome of additional behaviour therapy including treatment discontinuation for fluvoxamine non-responders with obsessive–compulsive disorder. Psychother Psychosom 2008;77:393-4. http://dx.doi.org/10.1159/000151521.
- Ninan PT, Koran LM, Kiev A, Davidson JR, Rasmussen SA, Zajecka JM, et al. High-dose sertraline strategy for nonresponders to acute treatment for obsessive–compulsive disorder: a multicenter double-blind trial. J Clin Psychiatry 2006;67:15-22. http://dx.doi.org/10.4088/JCP.v67n0103.
- Nuttin BJ, Gabriëls LA, Cosyns PR, Meyerson BA, Andréewitch S, Sunaert SG, et al. Long-term electrical capsular stimulation in patients with obsessive–compulsive disorder. Neurosurgery 2003;52:1263-72. http://dx.doi.org/10.1227/01.NEU.0000064565.49299.9A.
- Okun MS, Mann G, Foote KD, Shapira NA, Bowers D, Springer U, et al. Deep brain stimulation in the internal capsule and nucleus accumbens region: responses observed during active and sham programming. J Neurol Neurosurg Psychiatry 2007;78:310-14. http://dx.doi.org/10.1136/jnnp.2006.095315.
- Osuch EA, Benson BE, Luckenbaugh DA, Geraci M, Post RM, McCann U. Repetitive TMS combined with exposure therapy for PTSD: a preliminary study. J Anxiety Disord 2009;23:54-9. http://dx.doi.org/10.1016/j.janxdis.2008.03.015.
- Oude Voshaar RC, Hendriks GJ, Keijsers G, van Balkom AJ. Cognitive behavioural therapy for anxiety disorders in later life. Cochrane Database Syst Rev 2009;1.
- Peet M, Ali S. Propranolol and atenolol in the treatment of anxiety. Int Clin Psychopharmacol 1986;1:314-19. http://dx.doi.org/10.1097/00004850-198610000-00005.
- Pittenger CK. Riluzole augmentation in treatment-refractory obsessive–compulsive disorder: a series of 13 cases, with long-term follow-up. J Clin Psychopharmacol 2008;28:363-7. http://dx.doi.org/10.1097/JCP.0b013e3181727548.
- Pollack MH. Optimizing pharmacotherapy of generalized anxiety disorder to achieve remission. J Clin Psychiatry 2001;62:20-5.
- Pollack MH, Simon NM, Zalta AK, Worthington JJ, Hoge EA, Mick E, et al. Olanzapine augmentation of fluoxetine for refractory generalized anxiety disorder: a placebo controlled study. Biol Psychiatry 2006;59:211-15. http://dx.doi.org/10.1016/j.biopsych.2005.07.005.
- Prasko J, Pasková B, Záleský R, Novák T, Kopecek M, Bares M, et al. The effect of repetitive transcranial magnetic stimulation (rTMS) on symptoms in obsessive compulsive disorder. A randomized, double blind, sham controlled study. Neuro Endocrinol Lett 2006;27:327-32.
- Prasko J, Záleský R, Bares M, Horácek J, Kopecek M, Novák T, et al. The effect of repetitive transcranial magnetic stimulation (rTMS) add on serotonin reuptake inhibitors in patients with panic disorder: a randomized, double blind sham controlled study. Neuro Endocrinol Lett 2007;28:33-8.
- Raskind MA, Peskind ER, Kanter ED, Petrie EC, Radant A, Thompson CE, et al. Reduction of nightmares and other PTSD symptoms in combat veterans by prazosin: a placebo-controlled study. Am J Psychiatry 2003;160:371-3. http://dx.doi.org/10.1176/appi.ajp.160.2.371.
- Ravizza L, Barzega G, Bellino S, Bogetto F, Maina G. Therapeutic effect and safety of adjunctive risperidone in refractory obsessive–compulsive disorder (OCD). Psychopharmacol Bull 1996;32:677-82.
- Rickels K, Shiovitz TM, Ramey TS, Weaver JJ, Knapp LE, Miceli JJ. Adjunctive therapy with pregabalin in generalized anxiety disorder patients with partial response to SSRI or SNRI treatment. Int Clin Psychopharmacol 2012;27:142-50. http://dx.doi.org/10.1097/YIC.0b013e328350b133.
- Sachdev PS, McBride R, Loo CK, Mitchell PB, Malhi GS, Croker VM. Right versus left prefrontal transcranial magnetic stimulation for obsessive–compulsive disorder: a preliminary investigation. J Clin Psychiatry 2001;62:981-4. http://dx.doi.org/10.4088/JCP.v62n1211.
- Sayyah M, Sayyah M, Boostani H, Ghaffari SM, Hoseini A. Effects of aripiprazole augmentation in treatment-resistant obsessive–compulsive disorder (a double blind clinical trial). Depress Anxiety 2012;29:850-4. http://dx.doi.org/10.1002/da.21996.
- Schutters SI, van Megen HJ, Van Veen JF, Schruers KR, Westenberg HG, Schutters SIJ, et al. Paroxetine augmentation in patients with generalised social anxiety disorder, non-responsive to mirtazapine or placebo. Hum Psychopharmacol 2011;26:72-6. http://dx.doi.org/10.1002/hup.1165.
- Selvi Y, Atli A, Aydin A, Besiroglu L, Ozdemir P, Ozdemir O. The comparison of aripiprazole and risperidone augmentation in selective serotonin reuptake inhibitor-refractory obsessive–compulsive disorder: a single-blind, randomised study. Hum Psychopharmacol 2011;26:51-7. http://dx.doi.org/10.1002/hup.1169.
- Shapira NA, Ward HE, Mandoki M, Murphy TK, Yang MC, Blier P, et al. A double-blind, placebo-controlled trial of olanzapine addition in fluoxetine-refractory obsessive–compulsive disorder. Biol Psychiatry 2004;55:553-5. http://dx.doi.org/10.1016/j.biopsych.2003.11.010.
- Simon NM, Connor KM, Lang AJ, Rauch S, Krulewicz S, Lebeau RT, et al. Paroxetine CR augmentation for posttraumatic stress disorder refractory to prolonged exposure therapy. J Clin Psychiatry 2008;69:400-5. http://dx.doi.org/10.4088/JCP.v69n0309.
- Simon NM, Connor KM, Lebeau RT, Hoge EA, Worthington JJ, Zhang W, et al. Quetiapine augmentation of paroxetine CR for the treatment of refractory generalized anxiety disorder: preliminary findings. Psychopharmacology 2008;197:675-81. http://dx.doi.org/10.1007/s00213-008-1087-x.
- Simon NM, Otto MW, Worthington JJ, Hoge EA, Thompson EH, Lebeau RT, et al. Next-step strategies for panic disorder refractory to initial pharmacotherapy: a 3-phase randomized clinical trial. J Clin Psychiatry 2009;70:1563-70. http://dx.doi.org/10.4088/JCP.08m04485blu.
- Skapinakis P, Papatheodorou T, Mavreas V. Antipsychotic augmentation of serotonergic antidepressants in treatment-resistant obsessive–compulsive disorder: a meta-analysis of the randomized controlled trials. Eur Neuropsychopharmacol 2007;17:79-93. http://dx.doi.org/10.1016/j.euroneuro.2006.07.002.
- Stanley MA, Beck JG, Novy DM, Averill PM, Swann AC, Diefenbach GJ, et al. Cognitive-behavioral treatment of late-life generalized anxiety disorder. J Consult Clin Psychol 2003;71:309-12. http://dx.doi.org/10.1037/0022-006X.71.2.309.
- Stein MB, Sareen J, Hami S, Chao J. Pindolol potentiation of paroxetine for generalized social phobia: a double-blind, placebo-controlled, crossover study. Am J Psychiatry 2001;158:1725-7. http://dx.doi.org/10.1176/appi.ajp.158.10.1725.
- Stein MB, Kline NA, Matloff JL. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002;159:1777-9. http://dx.doi.org/10.1176/appi.ajp.159.10.1777.
- Tarrier N, Pilgrim H, Sommerfield C, Faragher B, Reynolds M, Graham E, et al. A randomized trial of cognitive therapy and imaginal exposure in the treatment of chronic posttraumatic stress disorder. J Consult Clin Psychol 1999;67:13-8. http://dx.doi.org/10.1037/0022-006X.67.1.13.
- Thorén P, Asberg M, Cronholm B, Jörnestedt L, Träskman L. Clomipramine treatment of obsessive–compulsive disorder. I. A controlled clinical trial. Arch Gen Psychiatry 1980;37:1281-5. http://dx.doi.org/10.1001/archpsyc.1980.01780240079009.
- van Balkom AJ, Emmelkamp PM, Eikelenboom M, Hoogendoorn AW, Smit JH, van OP, et al. Cognitive therapy versus fluvoxamine as a second-step treatment in obsessive–compulsive disorder nonresponsive to first-step behavior therapy. Psychother Psychosom 2012;81:366-74. http://dx.doi.org/10.1159/000339369.
- Wurthmann C, Klieser E, Lehmann E. Differential therapy in generalized anxiety disorders – 30 single-case experiments. Fortschr Neurol Psychiatr 1995;63:303-9. http://dx.doi.org/10.1055/s-2007-996631.
Appendix 1 Diagnostic criteria for anxiety disorders set out in DSM-IV and ICD-10 classification systems
| DSM-IV diagnostic criteria9,100 | ICD-10 diagnostic criteria11 |
|---|---|
| GAD | |
| A. Excessive anxiety and worry (apprehensive expectation), occurring on more days than not for at least 6 months, about a number of events or activities (such as work or school performance) | A. A period of at least six months with prominent tension, worry and feelings of apprehension, about every-day events and problems |
| B. The person finds it difficult to control the worry | B. At least four symptoms out of the following list of items must be present, of which at least one from items 1 to 4 Autonomic arousal symptoms
|
C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms present for more days than not for the past 6 months). Note that only one item is required in children
|
C. The disorder does not meet the criteria for panic disorder, phobic anxiety disorders, obsessive–compulsive disorder or hypochondriacal disorder |
| D. The focus of the anxiety and worry is not confined to features of an Axis I disorder, e.g. the anxiety or worry is not about having a panic attack (as in panic disorder), being embarrassed in public (as in social phobia), being contaminated (as in obsessive–compulsive disorder), being away from home or close relatives (as in separation anxiety disorder), gaining weight (as in anorexia nervosa), having multiple physical complaints (as in somatization disorder), or having a serious illness (as in hypochondriasis), and the anxiety and worry do not occur exclusively during PTSD | D. Most commonly used exclusion criteria: not sustained by a physical disorder, such as hyperthyroidism, an organic mental disorder or psychoactive substance-related disorder, such as excess consumption of amphetamine-like substances, or withdrawal from benzodiazepines |
| E. The anxiety, worry or physical symptoms cause clinically significant distress or impairment in social, occupational or other important areas of functioning | |
| F. The disturbance is not caused by the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition (e.g. hyperthyroidism) and does not occur exclusively during a mood disorder, a psychotic disorder, or a pervasive developmental disorder | |
| Obsessive–compulsive disorder | |
| A. Either obsessions or compulsions: Obsessions as defined by (1), (2), (3) and (4):
|
A. Either obsessions or compulsions (or both), present on most days for a period of at least 2 weeks |
| B. At some point during the course of the disorder the person has recognised that the obsessions or compulsions are excessive or unreasonable. Note that this does not apply to children | B. Obsessions (thoughts, ideas or images) and compulsions (acts) share the following features, all of which must be present:
|
| C. The obsessions or compulsions cause marked distress, are time-consuming (take more than 1 hour a day, or significantly interfere with the person’s normal routine, occupational (or academic) functioning or usual social activities or relationships | C. The obsessions or compulsions cause distress or interfere with the subject’s social or individual functioning, usually by wasting time. |
| D. If another Axis I disorder is present, the content of the obsessions or compulsions is not restricted to it (e.g. preoccupation with food in the presence of an eating disorder; hair pulling in the presence of trichotillomania; concern with appearance in the presence of body dysmorphic disorder; preoccupation with drugs in the presence of a substance use disorder; preoccupation with having a serious illness in the presence of hypochondriasis; preoccupation with sexual urges or fantasies in the presence of a paraphilia; or guilty ruminations in the presence of major depressive disorder) | D. Most commonly used exclusion criteria: not caused by other mental disorders, such as schizophrenia and related disorders, or mood (affective) disorders |
| E. The disturbance is not caused by the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition | |
| Panic disordera | |
A. Both (1) and (2):
|
A. Recurrent panic attacks that are not consistently associated with a specific situation or object and often occurring spontaneously (i.e. the episodes are unpredictable). The panic attacks are not associated with marked exertion or with exposure to dangerous or life-threatening situations |
| B. Absence of agoraphobia/presence of agoraphobia | B. A panic attack is characterised by all of the following:
|
| C. The panic attacks are not caused by the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition (e.g. hyperthyroidism) | C. Most commonly used exclusion criteria: not caused by a physical disorder, organic mental disorder, or other mental disorder such as schizophrenia and related disorders, affective disorders or somatoform disorders |
| D. The panic attacks are not better accounted for by another mental disorder, such as social phobia (e.g. occurring on exposure to feared social situations), specific phobia (e.g. exposure to a specific phobic situation), OCD (e.g. on exposure to dirt in someone with an obsession about contamination), PTSD (e.g. in response to stimuli associated with a severe stressor) or separation anxiety disorder (e.g. in response to being away from home or close relatives) | |
| PTSD | |
A. The person has been exposed to a traumatic event in which both of the following were present:
|
A. Exposure to a stressful event or situation (either short or long lasting) of exceptionally threatening or catastrophic nature, which is likely to cause pervasive distress in almost anyone |
B. The traumatic event is persistently re-experienced in one (or more) of the following ways:
|
B. Persistent remembering or ‘reliving’ the stressor by intrusive flash backs, vivid memories, recurring dreams or by experiencing distress when exposed to circumstances resembling or associated with the stressor |
C. Persistent avoidance of stimuli associated with the trauma and numbing of general responsiveness (not present before the trauma), as indicated by three (or more) of the following:
|
C. Actual or preferred avoidance of circumstances resembling, or associated with, the stressor (not present before exposure to the stressor) |
D. Persistent symptoms of increased arousal (not present before the trauma), as indicated by two (or more) of the following:
|
D. Either (1) or (2):
|
| E. Duration of the disturbance (symptoms in Criteria B, C and D) is more than 1 month | E. Criteria B, C and D all occurred within six months of the stressful event or the end of a period of stress (for some purposes, onset delayed more than six months may be included but this should be clearly specified separately) |
| F. The disturbance causes clinically significant distress or impairment in social, occupational or other important areas of functioning | |
| Social anxiety disorder | |
| A. A marked and persistent fear of one or more social or performance situations in which the person is exposed to unfamiliar people or to possible scrutiny by others. The individual fears that he or she will act in a way (or show anxiety symptoms) that will be humiliating or embarrassing. Note: in children, there must be evidence of the capacity for age-appropriate social relationships with familiar people and the anxiety must occur in peer settings, not just interactions with adults | A. Either (1) or (2):
|
| B. Exposure to the feared social situation almost invariably provokes anxiety, which may take the form of a situationally bound or situationally predisposed Panic attack. Note: in children, the anxiety may be expressed by crying, tantrums, freezing, or shrinking from social situations with unfamiliar people | B. At least two symptoms of anxiety in the feared situation at some time since the onset of the disorder, as defined in criterion B for agoraphobia and in addition one of the following symptoms:
|
| C. The person recognises that the fear is excessive or unreasonable. Note: in children, this feature may be absent | C. Significant emotional distress caused by the symptoms or by the avoidance |
| D. The feared social or performance situations are avoided or else are endured with intense anxiety or distress | D. Recognition that the symptoms or the avoidance are excessive or unreasonable |
| E. The avoidance, anxious anticipation, or distress in the feared social or performance situation(s) interferes significantly with the person’s normal routine, occupational (academic) functioning, or social activities or relationships, or there is marked distress about having the phobia | E. Symptoms are restricted to, or predominate in, the feared situation or when thinking about it |
| F. In individuals under age 18 years, the duration is at least 6 months | F. Most commonly used exclusion criteria: Criteria A and B are not caused by delusions, hallucinations or other symptoms of disorders such as organic mental disorders, schizophrenia and related disorders, affective disorders or OCD, and are not secondary to cultural beliefs |
| G. The fear or avoidance is not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication) or a general medical condition and is not better accounted for by another mental disorder (e.g., panic disorder with or without agoraphobia, separation anxiety, body dysmorphic disorder, a pervasive developmental disorder, or schizoid personality disorder) | |
| H. If a general medical condition or another mental disorder is present, the fear in Criterion A is unrelated to it, e.g. the fear is not of stuttering, trembling in Parkinson’s disease, or exhibiting abnormal eating behaviour in anorexia nervosa | |
Appendix 2 Doses of selective reuptake inhibitors for individual anxiety disorders as listed in the British National Formulary60
| Drug | Brand name | Manufacturer | Dose |
|---|---|---|---|
| SSRIs | |||
| Escitalopram | Cipralex® | H. Lundbeck A/S |
GAD and OCD
|
Panic disorder, with or without agoraphobia
|
|||
Social anxiety disorder
|
|||
| Sertraline (unlicensed) | Lustral® | Pfizer |
Panic disorder, with or without agoraphobia, social anxiety disorder and PTSD
|
OCD
|
|||
| Paroxetine | Seroxat® | GlaxoSmithKline |
Social anxiety disorder, PTSD and GAD
|
OCD
|
|||
Panic disorder
|
|||
| Citalopram | Cipramil® | Lundbeck |
Panic disorder
|
| Fluoxetine | Prozac® | Lilly |
OCD
|
| Fluvoxamine | Faverin® | Abbott Healthcare |
OCD
|
| SNRIs | |||
| Venlafaxine | Efexor® XL | Pfizer |
GAD
|
Social anxiety disorder
|
|||
| Duloxetine | Cymbalta® | Eli Lilly |
GAD
|
Appendix 3 Literature search strategies
| # | Term | Number of identified studies |
|---|---|---|
| 1 | exp Anxiety Disorders/ | 67,490 |
| 2 | ((anxi$ adj2 disorder) or (neuro$ adj2 worr$) or (neuro$ adj2 state$)).tw. | 12,999 |
| 3 | (obsess$ adj2 compuls$).tw. | 11,554 |
| 4 | ocd.ti,ab. | 5785 |
| 5 | (post adj2 trauma$).tw. | 20,194 |
| 6 | ptsd.ti,ab. | 12,360 |
| 7 | (social adj2 (phobi$ or anxi$)).tw. | 6584 |
| 8 | panic.ti,ab. | 11,765 |
| 9 | or/1-8 | 98,677 |
| 10 | exp Treatment Failure/ | 27,346 |
| 11 | (refract$ or resistan$ or nonrespon$ or non-respons$ or unrespon$ or fail$ or (incomplet$ adj respon$) or (no$ adj2 respon$)).tw. | 1,672,308 |
| 12 | (inadequat$ respon$ or (sub$ adj2 respon$) or (poor$ adj respon$)).tw. | 44,440 |
| 13 | or/10-12 | 1,713,541 |
| 14 | (adult$ or mature or full-grown or full grown or old$ or senior or elder or aged or geriatr$ or middleage$ or middle-age or late$ life or pension$ or late$ onset$).ti,ab. | 2,076,736 |
| 15 | exp Adult/ | 5,571,109 |
| 16 | exp Aged/ or exp Middle Aged/ or exp Retirement/ | 3,866,883 |
| 17 | or/14-16 | 6,602,926 |
| 18 | limit 17 to (“middle age (45 to 64 years)” or “middle aged (45 plus years)” or “all aged (65 and over)” or “aged (80 and over)”) | 3,863,723 |
| 19 | 9 and 13 and 18 | 2295 |
| 20 | exp cohort studies/ | 1,351,785 |
| 21 | cohort$.tw. | 276,045 |
| 22 | controlled clinical trial.pt. | 89,120 |
| 23 | epidemiologic methods/ | 30,831 |
| 24 | limit 23 to yr=1966-1989 | 11,289 |
| 25 | exp case-control studies/ | 655,023 |
| 26 | (case$ and control$).tw. | 331,389 |
| 27 | (case$ and series).tw. | 120,725 |
| 28 | or/20-22,24-27 | 1,960,600 |
| 29 | 19 and 28 | 821 |
| 30 | Randomized Controlled Trials as Topic/ | 101,374 |
| 31 | randomized controlled trial/ | 384,981 |
| 32 | Random Allocation/ | 81,084 |
| 33 | Double Blind Method/ | 130,411 |
| 34 | Single Blind Method/ | 19,282 |
| 35 | clinical trial/ | 501,321 |
| 36 | clinical trial, phase i.pt | 15,983 |
| 37 | clinical trial, phase ii.pt | 26,581 |
| 38 | clinical trial, phase iii.pt | 9981 |
| 39 | clinical trial, phase iv.pt | 963 |
| 40 | controlled clinical trial.pt | 89,120 |
| 41 | randomized controlled trial.pt | 384,981 |
| 42 | multicenter study.pt | 179,583 |
| 43 | clinical trial.pt | 501,321 |
| 44 | exp Clinical Trials as topic/ | 293,751 |
| 45 | (clinical adj trial$).tw | 222,887 |
| 46 | ((singl$ or doubl$ or treb$ or tripl$) adj (blind$3 or mask$3)).tw | 133,162 |
| 47 | PLACEBOS/ | 33,587 |
| 48 | placebo$.tw | 166,857 |
| 49 | randomly allocated.tw | 16,984 |
| 50 | (allocated adj2 random$).tw | 19,557 |
| 51 | or/30-50 | 1,209,986 |
| 52 | case report.tw | 200,646 |
| 53 | letter/ | 821,957 |
| 54 | historical article/ | 298,696 |
| 55 | or/52-54 | 1,309,918 |
| 56 | 51 not 55 | 1,179,947 |
| 57 | 19 and 56 | 599 |
| 58 | 29 or 57 | 1209 |
| # | Term | Number of identified studies |
|---|---|---|
| 1 | exp Anxiety Disorders/ | 140,768 |
| 2 | ((anxi$ adj2 disorder) or (neuro$ adj2 worr$) or (neuro$ adj2 state$)).tw. | 16,558 |
| 3 | (obsess$ adj2 compuls$).tw. | 15,206 |
| 4 | ocd.ti,ab. | 7611 |
| 5 | (post adj2 trauma$).tw. | 25,631 |
| 6 | ptsd.ti,ab. | 14,870 |
| 7 | (social adj2 (phobi$ or anxi$)).tw. | 8321 |
| 8 | panic.ti,ab. | 15,072 |
| 9 | or/1-8 | 171,198 |
| 10 | exp Treatment Failure/ | 79,790 |
| 11 | (refract$ or resistan$ or nonrespon$ or non-respons$ or unrespon$ or fail$ or (incomplet$ adj respon$) or (no$ adj2 respon$)).tw. | 1,980,617 |
| 12 | (inadequat$ respon$ or (sub$ adj2 respon$) or (poor$ adj respon$)).tw. | 53,340 |
| 13 | or/10-12 | 2,047,630 |
| 14 | (adult$ or mature or full-grown or full grown or old$ or senior or elder or aged or geriatr$ or middleage$ or middle-age or late$ life or pension$ or late$ onset$).ti,ab. | 2,527,084 |
| 15 | aged/ | 2,201,410 |
| 16 | exp middle aged/ | 1,154,678 |
| 17 | exp pensioner/ | 868 |
| 18 | exp retirement/ | 10,352 |
| 19 | or/14-18 | 4,748,715 |
| 20 | limit 19 to (adult < 18 to 64 years > or aged <65+ years>) | 3,181,884 |
| 21 | 9 and 13 and 20 | 2680 |
| 22 | exp cohort analysis/ | 157,783 |
| 23 | exp longitudinal study/ | 64,462 |
| 24 | exp prospective study/ | 249,085 |
| 25 | exp follow up/ | 743,046 |
| 26 | cohort$.tw. | 359,921 |
| 27 | exp case control study/ | 89,362 |
| 28 | (case$ and control$).tw. | 418,496 |
| 29 | exp case study/ | 21,169 |
| 30 | (case$ and series).tw. | 155,754 |
| 31 | or/22-30 | 1,769,502 |
| 32 | 21 and 31 | 772 |
| 33 | Clinical trial/ | 892,685 |
| 34 | Randomized controlled trial/ | 358,000 |
| 35 | Randomization/ | 63,374 |
| 36 | Single blind procedure/ | 18,220 |
| 37 | Double blind procedure/ | 119,966 |
| 38 | Crossover procedure/ | 38,383 |
| 39 | Placebo/ | 237,722 |
| 40 | Randomi?ed controlled trial$.tw. | 93,836 |
| 41 | Rct.tw. | 12,545 |
| 42 | Random allocation.tw. | 1335 |
| 43 | Randomly allocated.tw. | 19,845 |
| 44 | Allocated randomly.tw. | 1942 |
| 45 | (allocated adj2 random).tw. | 814 |
| 46 | Single blind$.tw. | 14,148 |
| 47 | Double blind$.tw. | 146,578 |
| 48 | (treble or triple) adj (blind$).tw. | 352 |
| 49 | Placebo$.tw. | 200,245 |
| 50 | Prospective study/ | 249,085 |
| 51 | or/33-50 | 1,392,985 |
| 52 | Case study/ | 21,169 |
| 53 | Case report.tw. | 261,442 |
| 54 | Abstract report/ or letter/ | 903,642 |
| 55 | or/52-54 | 1,180,920 |
| 56 | 51 not 55 | 1,355,531 |
| 57 | 21 and 56 | 576 |
| 58 | 32 or 57 | 1116 |
| # | Term | Number of identified studies |
|---|---|---|
| 1 | MeSH descriptor: [Anxiety Disorders] explode all trees | 4447 |
| 2 | ((anxi* near/2 disorder) or (neuro* near/2 worr*) or (neuro* near/2 state*)):ti,ab,kw | 3915 |
| 3 | (obsess* near/2 compuls*):ti,ab,kw | 1276 |
| 4 | ocd:ti,ab,kw | 594 |
| 5 | (post near/2 trauma*):ti,ab,kw | 1451 |
| 6 | ptsd:ti,ab,kw | 930 |
| 7 | (social near/2 (phobi$ or anxi*)):ti,ab,kw | 609 |
| 8 | panic:ti,ab,kw | 1885 |
| 9 | #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 | 8882 |
| 10 | MeSH descriptor: [Treatment Failure] explode all trees | 2537 |
| 11 | refract* or resistan* or nonrespon* or non-respons* or unrespon* or fail* or (incomplet* adj respon*) or (no* near/2 respon*):ti,ab,kw | 92,549 |
| 12 | (inadequat* near/1 respon* or (sub* near/2 respon*) or (poor* near/1 respon*)):ti,ab,kw | 4157 |
| 13 | #10 or #11 or #12 | 95,403 |
| 14 | MeSH descriptor: [Adult] explode all trees | 1133 |
| 15 | (adult* or mature or full-grown or full grown or old* or senior or elder or aged or geriatr* or middleage* or middle-age or late* life or pension* or late* onset*):ti,ab,kw | 432,233 |
| 16 | #14 or #15 | 432,233 |
| 17 | #9 and #13 and #16 | 931 |
| # | Term | Number of identified studies |
|---|---|---|
| 1 | exp Anxiety Disorders/ | 58,238 |
| 2 | ((anxi$ adj2 disorder) or (neuro$ adj2 worr$) or (neuro$ adj2 state$)).tw. | 12,854 |
| 3 | (obsess$ adj2 compuls$).tw. | 15,008 |
| 4 | ocd.ti,ab. | 6642 |
| 5 | (post adj2 trauma$).tw. | 8805 |
| 6 | ptsd.ti,ab. | 18,406 |
| 7 | (social adj2 (phobi$ or anxi$)).tw. | 10,397 |
| 8 | panic.ti,ab. | 13,143 |
| 9 | or/1-8 | 81,499 |
| 10 | (refract$ or resistan$ or nonrespon$ or non-respons$ or unrespon$ or fail$ or (incomplet$ adj respon$) or (no$ adj2 respon$)).tw. | 192,150 |
| 11 | (inadequat$ respon$ or (sub$ adj2 respon$) or (poor$ adj respon$)).tw. | 10,291 |
| 12 | 10 or 11 | 200,653 |
| 13 | (adult$ or mature or full-grown or full grown or old$ or senior or elder or aged or geriatr$ or middleage$ or middle-age or late$ life or pension$ or late$ onset$).ti,ab. | 678,919 |
| 14 | 9 and 12 and 13 | 1516 |
| 15 | ((case* adj5 control*) or (case adj3 comparison*) or case-comparison or control group*).ti,ab. not “Literature Review”.md. | 62,969 |
| 16 | (cohort or longitudinal or prospective or retrospective).ti,ab,id. or longitudinal study.md. or prospective study.md. or retrospective study.md. not “Literature Review”.md. | 169,825 |
| 17 | 15 or 16 | 226,508 |
| 18 | 14 and 17 | 145 |
| 19 | clinical trials/ or “treatment outcome clinical trial”.md. or ((randomi?ed adj7 trial*) or ((single or doubl* or tripl* or treb*) and (blind* or mask*)) or (controlled adj3 trial*) or (clinical adj2 trial*)).ti,ab,id. | 68,682 |
| 20 | 14 and 19 | 179 |
| 21 | 18 or 20 | 299 |
| # | Term | Number of identified studies |
|---|---|---|
| 1 | (anxiety disorder or neurotic or neurotic state or ocd or ptsd or post trauma or panic or phobia) | 73,338 |
| 2 | ((inadequate response or poor response or refract* or resistan* or nonrespon* or non-respon* or unrespon* or fail)) | 1,067,419 |
| 3 | (adult or old or senior or elder or aged or geriatr* or middleage* or middle-age* or late* life or pension* or late* onset) | 2,053,501 |
| 4 | #1 and #2 and #3 | 1422 |
| 5 | Limit 4 to article, meeting abstract, proceeding paper or correction | 1255 |
Appendix 4 Table of excluded studies with rationale
| Excluded study | Reason for exclusion |
|---|---|
| Abelson et al.101 | Not population of interest (all people aged < 65 years) |
| Aboujaoude et al.102 | Not study type of interest (single arm) |
| Allgulander103 | Not study type of interest (review) |
| Altamura et al.104 | No subgroup by age |
| Amiaz et al.105 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Anderson et al.106 | Not study type of interest (letter) |
| Atmaca et al.107 | Not population of interest (all people aged < 65 years) |
| Barr et al.108 | No subgroup by age |
| Bartzokis et al.109 | Not population of interest (all people aged < 65 years) |
| Blank et al.110 | Not population of interest (not treatment resistant) |
| Blay et al.111 | Not study type of interest (review) |
| Brawman-Mintzer et al.112 | No subgroup by age |
| Bresolin et al.113 | Not population of interest (not treatment resistant) |
| Bruno114 | No subgroup by age |
| Buchsbaum et al.115 | No subgroup by age |
| Campanini et al.116 | No subgroup by age |
| Carey et al.117 | Not population of interest (all people aged < 65 years) |
| Carr et al.118 | Not population of interest (all people aged < 65 years) |
| Crocq et al.119 | Not population of interest (all people aged < 65 years) |
| Csigo et al.120 | No subgroup by age |
| Dannon et al.121 | No subgroup by age |
| David et al.122 | No subgroup by age |
| Denys et al.123 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Depping et al.124 | Not study type of interest (review) |
| Di et al.125 | Not population of interest (all people aged < 65 years; inclusion criterion of age of 18–45 years) |
| Dick et al.126 | No subgroup by age |
| Diniz et al.127 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Diniz et al.128 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Erzegovesi et al.129 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Fallon et al.130 | Not population of interest (all people aged < 65 years) |
| Fava et al.131 | No subgroup by age |
| Fineberg et al.132 | No subgroup by age |
| Fineberg et al.133 | Not study type of interest (review) |
| Geus et al.134 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Ginsberg95 | Unable to obtain |
| Goodman et al.135 | Not population of interest (all people aged < 65 years) |
| Haghighi et al.136 | No subgroup by age |
| Hinton et al.137 | Baseline characteristics not reported |
| Hinton et al.138 | No subgroup by age |
| Hinton et al.139 | No subgroup by age |
| Hinton et al.140 | No subgroup by age |
| Hirschmann et al.141 | No subgroup by age |
| Hoffart et al.142 | No subgroup by age |
| Hofmann et al.143 | Not study type of interest (review) |
| Hollander et al.144 | No subgroup by age |
| Huff et al.145 | Not population of interest (inclusion criterion of age of 21–65 years) |
| Ipser et al.63 | Not study type of interest (review) |
| Kampman146 | Not population of interest (all people aged < 65 years) |
| Kang et al.147 | No subgroup by age |
| Katz148 | Not study type of interest (review) |
| Khan et al.149 | Abstract only; insufficient information to assess |
| Kolivakis et al.150 | Not study type of interest (book chapter) |
| Koran et al.81 | Not population of interest (all people aged < 65 years) |
| Koran et al.151 | Not population of interest (all people aged < 65 years; inclusion criterion of age of 18–55 years) |
| Koran et al.152 | Not population of interest (all people aged < 65 years) |
| Kordon et al.153 | Not population of interest (all people aged < 65 years) |
| Krystal et al.82 | No subgroup by age |
| Li et al.154 | Not population of interest (all people aged < 65 years) |
| Lippitz et al.155 | Not population of interest (not treatment resistant) |
| Lohoff et al.156 | Baseline characteristics not reported |
| Macklin et al.157 | No subgroup by age |
| Maina et al.158 | No subgroup by age |
| Mallet et al.159 | Not population of interest (all people aged < 65 years) |
| Mansur et al.160 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Mantovani et al.161 | No subgroup by age |
| Marshall et al.162 | Not population of interest (not treatment resistant) |
| Matsunaga et al.163 | No subgroup by age |
| Mavissakalian164 | Not population of interest (includes people who are not treatment resistant) |
| McDougle et al.165 | Not population of interest (all people aged < 65 years) |
| McDougle et al.166 | No subgroup by age |
| McDougle et al.167 | Not population of interest (most people aged < 65 years; only 2 people were aged ≥ 65 years) |
| McDougle et al.168 | Not population of interest (all people aged < 65 years) |
| Menza et al.169 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Mithoefer et al.170 | No subgroup by age |
| Muscatello et al.171 | No subgroup by age |
| Nakatani et al.172 | Not study type of interest (single arm study; no control group) |
| Ninan et al.173 | No subgroup by age |
| Nuttin et al.174 | Not population of interest (all people aged < 65 years) |
| Okun et al.175 | Not question of interest |
| Osuch et al.176 | Not population of interest (all people aged < 65 years) |
| Oude Voshaar et al.177 | Not study type of interest (review protocol) |
| Peet et al.178 | No subgroup by age |
| Pittenger179 | Not study type of interest (single arm study; no control group) |
| Pollack180 | Not study type of interest (single arm study; no control group) |
| Pollack et al.181 | No subgroup by age |
| Prasko et al.182 | Not population of interest (all people aged < 65 years; inclusion criterion of age of 18–45 years) |
| Prasko et al.183 | Not population of interest (all people aged < 65 years) |
| Raskind et al.184 | Not population of interest (not treatment resistant) |
| Ravizza et al.185 | No subgroup by age |
| Rickels et al.186 | No subgroup by age |
| Sachdev et al.187 | No subgroup by age |
| Sachdev et al.83 | No subgroup by age |
| Sayyah et al.188 | Not population of interest (all people aged < 65 years) |
| Schutters et al.189 | Not population of interest (includes people who are not treatment-resistant) |
| Selvi et al.190 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Shapira et al.191 | No subgroup by age |
| Simon et al.192 | No subgroup by age |
| Simon et al.193 | No subgroup by age |
| Simon et al.194 | Not population of interest (all people aged < 65 years) |
| Skapinakis et al.195 | Not study type of interest (review) |
| Stanley et al.196 | Not population of interest (not treatment resistant) |
| Stein et al.197 | Baseline characteristics not provided |
| Stein et al.198 | No subgroup by age |
| Storch84 | No subgroup by age |
| Tarrier et al.199 | Not population of interest (not treatment resistant) |
| Thorén et al.200 | Not population of interest (all people aged < 65 years) |
| van Balkom et al.201 | No subgroup by age |
| Wurthmann et al.202 | Not population of interest (inclusion criterion of age of 18–65 years) |
| Zhang et al.85 | Not population of interest (all people aged < 65 years) |
List of abbreviations
- BNF
- British National Formulary
- CBT
- cognitive–behavioural therapy
- CG
- clinical guideline
- CI
- confidence interval
- CRD
- Centre for Reviews and Dissemination
- DSM
- Diagnostic and Statistical Manual of Mental Disorders
- GABA
- gamma-aminobutyric acid
- GAD
- generalised anxiety disorder
- ICD
- International Classification of Diseases
- MeSH
- medical subject headings
- NICE
- National Institute for Health and Care Excellence
- OCD
- obsessive–compulsive disorder
- PTSD
- post-traumatic stress disorder
- QoL
- quality of life
- RCT
- randomised controlled trial
- SMD
- standardised mean difference
- SNRI
- serotonin–noradrenaline reuptake inhibitor
- SSRI
- selective serotonin reuptake inhibitor
- TCA
- tricyclic antidepressant
- WHO
- World Health Organization