
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 09/109/04. The contractual start date was in July 2011. The draft report began editorial review in October 2013 and was accepted for publication in January 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Linda Davies provided expert consultancy advice to the Home Office funded by grants to the University of Manchester (Drug Data Warehouse; planned evaluation of drug strategy).
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Hayhurst et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
Class A drugs
A range of drugs is included in the category of class A substances, which is a legal classification under the Misuse of Drugs Act 1971. 1 The Act identifies three classes of drugs (A, B and C). Those designated as class A carry the most severe legal penalties for possession or supply. Class A comprises a heterogeneous group of drugs, including (but not limited to):
-
powder cocaine
-
crack cocaine
-
ecstasy
-
LSD (lysergic acid diethylamide)
-
psilocybin
-
heroin
-
methadone.
Some of these (e.g. powder cocaine, ecstasy, LSD and psilocybin) are more commonly associated with a pattern of recreational use. Heroin, methadone and crack cocaine are more commonly associated with chronic and dependent use.
Prevalence of class A drug use
The Crime Survey for England and Wales (CSEW)2 provides estimates of the ‘past year’ prevalence of class A drug use. The CSEW is a survey of approximately 50,000 households in England and Wales. Estimates derived from the CSEW (2012/13) suggest that a total of 846,000 [95% confidence interval (CI) 763,000 to 930,000] individuals aged 16–59 years had consumed a class A drug in the previous year. Individuals who had used drugs such as powder cocaine (627,000 individuals, 95% CI 555,000 to 699,000 individuals); ecstasy (415,000 individuals, 95% CI 357,000 to 474,000 individuals); amphetamines (211,000 individuals, 95% CI 169,000 to 253,000 individuals) and hallucinogens (121,000 individuals 95% CI 90,000 to 153,000 individuals) accounted for the majority of drug use. The CSEW 2012/13 estimates the prevalence of opiate use as 38,000 individuals (95% CI 20,000 to 56,000 individuals) and crack use as 47,000 individuals (95% CI 27,000 to 67,000 individuals), in England and Wales. These estimates for use of opiates or crack cocaine are much lower than the 164,671 opiate and/or crack users known to have received treatment for substance misuse in England during 2011–12. 3 Surveys are unlikely to capture those marginal populations at high risk of dependent use of opiates/crack adequately, such as prisoners or the homeless. Estimates of the prevalence of opiate and/or crack cocaine use based on indirect estimation methods, not subject to the same biases as survey approaches, suggest that there were 298,752 (95% CI 294,858 to 307,225) opiate and/or crack cocaine users aged 15–64 years in England during 2010/11. 4 Combining the mid-point estimate with treatment figures suggests that around 58% of the opiate- and/or crack-using population were in receipt of drug treatment services during 2010–11. This proportion is higher than that estimated for most other European countries and comparable with that seen in Australia and the USA. 5 The use of crack or cocaine nationally increased from approximately 14% of treated drug users at the time of the National Treatment Outcome Research Study (NTORS) in 19966 to at least 40% in 2010/11. 7 The largest proportion were treated crack users (72,000 treated crack users, with < 10,000 treated cocaine users).
There is considerable debate concerning the precise nature of the relationship between drug use and criminal behaviour. Regular, recent use of opiate drugs and/or crack cocaine is very common among UK samples of arrestees. Use is at rates that are very much greater than prevalence rates in the general population. 8 The bulk of those arrestees consider that they are dependent on these drugs. 9 Experience of class A drug use is also considerably higher among the prison, than the general, population. Across European countries, prisoners have a lifetime prevalence of 6–53% for cocaine use and 15–39% for heroin use. This compares with 0.3–10% and < 1%, respectively, in the general population. 10
Although the prevalence of other types of class A drug misuse is much greater, it is estimated that opiate and/or crack users account for 99% of the social and economic costs associated with class A drug use. 11 Opiate and/or crack users are the group primarily served by substance misuse treatment services. In the UK, they are the main focus of criminal justice system (CJS) diversion initiatives for drug misusers. Hence, it is the primary focus of the work described in this report.
Class A drug use and crime
Criminal justice system referral is an increasingly important route through which drug users access the treatment system. In 2010/11, 30% of clients starting new treatment journeys did so via a CJS referral. The Drug Interventions Programme (DIP) referrals accounted for 14% of referrals overall. 7 Nevertheless, arrest referral services were argued by some to do little to introduce ‘hidden’ client groups to treatment opportunities. 12 Offenders who misuse drugs often have more serious drug problems than the general population of drug users and they are potentially less responsive to treatment. 12–15
The pattern of offending differs somewhat between drug users and non-drug users. Samples of arrestees in England and Wales indicate that, for example, assault accounts for 29% of arrests yet just 4% of these were individuals reporting at least weekly use of heroin and/or crack. Conversely, shoplifting accounted for 10% of arrests yet 45% of these were problem drug users. 16,17 Indeed it has been estimated that over half of all such recorded acquisitive crime in the UK is drug related, motivated by the need to obtain income for drugs, rather than violence associated with pharmacological effects or drug markets. 18,19 However, the literature suggests a more complex association between drug misuse and acquisitive offending than a simple causal relationship. 20–23 Not all drug users commit acquisitive offences. Acquisitive crime often pre-dates problem drug use. 15,24 Drug use and criminality may develop in parallel,25 perhaps via a third factor such as socioeconomic deprivation. 23 The Drug Treatment Outcomes Research Study (DTORS)26 evaluation found that behavioural and demographic factors were stronger predictors of involvement in acquisitive crime than drug use expenditure. This suggests that the need to finance drug use is not necessarily the main factor driving acquisitive offending by drug users. 27
Use of cocaine, in particular crack cocaine, has been linked to acquisitive crime. In the Research Outcome Study in Ireland (ROSIE),28 people using cocaine/crack were more likely to report criminal activity than those not taking cocaine or crack. 29 In NTORS, predictors of acquisitive offending included regular use of cocaine (powder and/or crack). 15 Age may also predict criminal involvement: two-thirds of a 2009 class A drug-using offender cohort were aged < 35 years and arrestee surveys highlight the likelihood of acquisitive crime declining with increasing age among drug users. 16,30 Polysubstance-using offenders commit twice as many offences as those not reporting multiple drug use. 31 High levels of polydrug use are recorded among drug-using arrestees. 16
Policy context
The UK policy focus on reducing drug-related crime first emerged during the 1990s, most visibly with the publication of a series of reports by the Advisory Council on the Misuse of Drugs (ACMD). These considered responses to drug misuse within the CJS and highlighted the prevalence of class A drug misuse, particularly opiate use, among acquisitive offenders. 32
The issue gained political prominence in 1994 with the Labour Party stating, while in opposition, that a half of the £4B cost of recorded theft was attributable to drug misuse. This contrasted with the government estimate of between £58M and £864M for the cost of heroin-related acquisitive crime in England and Wales. 33 A subsequent, and independent, estimate suggests that the wider social and economic costs of problematic class A drug use in England and Wales was £12B (range £10.1B–17.4B) during 2000. Drug-related crime accounted for approximately 88% of that total. 34
Notwithstanding the accuracy of the above estimates, there was concern about the social consequences of problem drug use, particularly drug-related crime. This culminated in a strong emphasis on the potential for effective treatment to contain or reduce these consequences. The ACMD highlighted that,
. . . there is now an onus on these [drug treatment] agencies to take a broader view and develop their focus to incorporate community safety as well as care of the individual drug misuser.
ACMD32
The contemporary government drug strategy included the objective to, ‘reduce the incidence of drug-related crime’. 35 Although focusing primarily on law enforcement, the strategy recommended diversion of arrested drug misusers into treatment. A later review of drug misuse services36 concluded that contact with the CJS provided opportunities to engage problem drug users with treatment. In addition, the need to safeguard communities was reaffirmed within the subsequent government strategy for tackling drug misuse, which included the aim ‘to protect our communities from drug-related antisocial and criminal behaviour’. 37
In the latest government drug strategy document,38 covering England and Wales, CJS diversionary schemes continue to be a focus of contact with drug users. The coalition government expresses its desire to ‘. . . ensure that offenders are encouraged to seek treatment and recovery at every opportunity in their contact with the CJS’. 38 The 2010 strategy identified the importance of early intervention for young people and families to help those who may be at risk of involvement in crime and antisocial behaviour.
Current service provision
Drug treatment and rehabilitation services are commissioned and provided in four tiers. Tier 1 relates to primary-care services. Tier 2 provides open-access and non-structured drug treatment services; information, advice and harm-reduction services; screening for drug misuse and referral to specialist drugs services. Tier 3 provides structured community-based drug treatment and rehabilitation services. Services in tier 4 provide residential drug treatment and rehabilitation, aimed at individuals with a high level of presenting need. Tier 3 and 4 services account for around 70% of total drug treatment costs.
Following the introduction of arrest referral schemes14 the national DIP was introduced in 2003. DIP aimed to identify and work with drug-misusing offenders at each stage of their contact with the CJS from the custody suite through to community The core remit of DIP is to address drug misuse and offending to help individuals ‘get out of crime and into treatment and other support’. 39 The programme includes both custodial and community components, with voluntary and coercive elements. The bulk of provision, in terms of its diversionary component, centres on identification and appropriate treatment referral of drug-misusing offenders at the point of arrest or charge. Although the programme has evolved at various stages, its key components include:
-
identification of drug-misusing offenders – including, in some areas, drug testing (for opiate and cocaine metabolites) at the point of arrest (initially charge) for specific, acquisitive, ‘trigger’ offences (see Appendix 1) or at the discretion of a senior police officer
-
comprehensive and standard assessment of treatment and other support needs – assessment by a referral worker who is ‘embedded’ in the custody setting, latterly (from 2007), with new police powers for adults who test positive for drugs to be required to attend an assessment
-
case management designed to help break the (presumed) cycle of drugs and offending.
Rationale for this study
The National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme’s call for research in this field concluded that:
The evidence bases on effectiveness of diversion and aftercare are limited, with methodological problems and inconsistent costing methodology. The ways these two interventions are delivered remain poorly understood, with particularly limited evidence on aftercare. High quality research is required to determine effectiveness and cost-effectiveness of such strategies.
NIHR HTA40
The DIP is the mainstay of CJS diversion for drug misusers in the UK. During 2012/13 central funding for DIP exceeded £91M. To set this figure in context, the economic and social costs of class A drug use for England and Wales in 2003/4 were estimated at £15B11 and the UK government’s Serious Organised Crime Agency currently estimates that drug trafficking to the UK costs £17.6B per year. 41
A number of previous studies suggest that drug treatment impacts favourably on reducing levels of offending. 34,42,43 Evaluation of DIP indicates that levels of offending are reduced following contact with the programme,44 although the evidence for this is weak.
The US Drug Abuse Treatment Outcome Study45 highlighted decreased crime costs following drug treatment in both residential and outpatient settings. 46 Drug treatment in ROSIE28 was associated with a significant decrease in acquisitive offending29 and 1-year follow-up in the UK NTORS observed a two-third reduction in the level of acquisitive offences compared with baseline. 47 A further UK analysis based on linking treatment data from the National Drug Treatment Monitoring System (NDTMS) with the Police National Computer (PNC) points to levels of recorded offending falling after the initiation of substitute prescribing. 48 Although this study is subject to some ascertainment bias, the reduction in recorded offending was greatest in those with the longest period of substitute prescribing treatment.
Interviews with service providers in DTORS identified possible positive and negative impacts from increases in referrals from the CJS. Concern was expressed about the effectiveness of treatment if CJS referred clients demonstrated lower levels of motivation. 49 However, the same study found that referral through the CJS did not seem to impact on levels of motivation. 49 This supported findings from the quantitative component of DTORS, that CJS referral was not negatively associated with levels of motivation. 50
A number of evaluations of diversion schemes in the US conclude that there may be cost savings from the identification, assessment and referral of offenders into drug treatment services. 51–53 However, none of these studies provides a full economic evaluation and are primarily cost analyses. A systematic review concluded that there was uncertainty about the costs and cost-effectiveness of interventions for drug-using offenders. 54,55 Furthermore, the effectiveness and cost-effectiveness of diversion schemes to identify and refer offenders who misuse drugs for treatment is unclear.
The use of the CJS as a means of referral into drug treatment has frequently been examined as a predictor of treatment success. Various studies have concluded that legal pressure either is, or is not, an effective means of achieving success in drug treatment. Within North America, several studies have concluded that legal pressure has a strong and positive impact on treatment entry and, subsequently, retention and positive outcomes. 56–59 Indeed, three of these studies suggest significantly improved performance for legally referred compared with voluntary clients However, it should be noted that they relate to either primary alcohol users,59 adolescents in specialist (CJS referral only) residential units58 or female offenders serving out alternatives to custody and/or child custody procedures. 56 Each of these represents a specific set of circumstances and motivational issues.
Other studies have concluded a negative impact of CJS compared with elective referral. 59–62 Again, the context of these studies varies and two of these59,60 were concerned with adolescents or primary alcohol users only. There is also literature that theorises the possible negative results of a policy of criminal justice referrals into treatment based on presumptions of need and non-empirical evidence bases. 63–65
The largest group of studies have found no statistically significant difference in the outcomes experienced by criminal justice referrals compared with referral through other routes. 57,65–75 Not all of these studies were designed specifically to examine the impact of legal pressure on outcomes. Even so, they generally show that clients sourced from the CJS experience outcomes that are not significantly different to other clients of treatment services. Indeed, both sets of clients (CJS and non-CJS) display statistically significant improvements after a set period of treatment. 66
Thus, the greater number of existing studies support the notion that CJS-referred clients can experience equal, or similar, advantages to treatment as non-CJS referrals but that these are not automatic. The majority of studies have focused on the effect of treatment provided as an alternative to sentencing, reflecting different practice and policy emphasis internationally. In England, CJS referral mechanisms are not homogenous and voluntary CJS initiated treatment engagement is much more common in the UK than in other settings such as North America.
The literature that concerns itself with treatment effectiveness reflects several permutations of formal and informal legal pressure, combined with different types of treatment intervention. The nature of the methods of diversion from CJS to treatment varies considerably. They include first, arrest referral schemes in England which provide a voluntary treatment referral system from within CJS settings to, in the main, community-based prescribing services; second, drug court referrals in the USA, dealing largely with individuals charged with drug-related offences and referring to abstinence-based residential programmes; and, finally, a host of European schemes that either provide, via a range of schemes, a choice of treatment or punishment or actually impose treatment-based sentences, such as in Austria, Germany or the Netherlands. 76
The current study systematically reviews the efficacy of diversion and aftercare programmes for offenders using class A drugs. In addition, it summarises and evaluates the economic evidence about the cost-effectiveness of diversion and aftercare for drug-using criminal offenders.
Chapter 2 Definition of the decision problem
Population
-
Offenders, with or without a mental health problem, who are aged 18 years or older; and
-
using class A drugs; and
-
offered diversion and/or aftercare programmes (or as part of a control group in a study examining this type of intervention); and
-
study participants diverted to an intervention that has at least an element of treatment, which is specifically designed to treat and/or reduce substance misuse.
Intervention
The effectiveness and economic reviews included studies that reported evaluation of diversion and/or aftercare programmes. For the purposes of the reviews, the following definitions of diversion and aftercare were used:
-
Diversion is a process whereby offenders who use class A drugs are identified as having a drug problem at any point in the CJS. This then results in subsequent criminal justice interventions comprising wholly, or partly, of specific treatment, rehabilitation or education requirements for drug abuse. These are either voluntary, mandated by the court, and/or monitored by probation, or drug, services.
-
Aftercare is the treatment or intervention activity following any relevant diversion event, as per review inclusion/exclusion criteria.
Evaluation of aftercare interventions comprised studies which examined care following the diversion process, not care following prison or another intervention. In addition, studies which sought to evaluate prison-based interventions were not included.
Control
For the purpose of this review the following definitions of control group were used:
-
matched to characteristics of experimental group, but receives nothing
-
matched to characteristics of experimental group and receives placebo/pseudo-intervention
-
matched to characteristics of experimental group and receives treatment as usual (TAU)
-
not matched to characteristics of experimental group and receives nothing
-
not matched to characteristics of experimental group and receives placebo/pseudo-intervention
-
not matched to characteristics of experimental group and receives TAU.
Outcomes
The review of effectiveness focused on studies that reported one or more of the following outcomes: reoffending/rearrest/recidivism/reincarceration; reduction or increase in drug use; health, risk and service variables, such as hospital admission; and mortality data.
Aims and objectives
-
To review systematically the efficacy of diversion and aftercare programmes for offenders using class A drugs.
-
Based on a systematic review of the data, to model the impact of diversion and aftercare programmes for offenders using class A drugs.
-
To summarise and evaluate the economic evidence about the cost-effectiveness of diversion and aftercare for drug-using criminal offenders.
-
To identify and explore the consequences of potential characteristics of diversion and aftercare interventions that may have most impact on the cost-effectiveness of the programmes.
-
To estimate probability, cost and outcome data, relevant to the UK setting, to populate an economic model.
-
To integrate the findings from the above objectives and make recommendations for the design of high-quality primary research studies to further inform future HTA research.
See commissioning brief in Appendix 2.
Chapter 3 Review of effectiveness
Methods
Advisory panel
The project team included clinicians, commissioners/service providers and experts in the field. The full project team had input into the methods and design of the reviews. The role of this panel was to inform the choice of population, interventions and outcomes to define the initial search strategy and inclusion criteria and to help identify the relevant databases to be searched. The group was also asked to comment on the draft report.
Search strategy
The design of the systematic effectiveness review followed guidelines set out in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 77 Sources included both medical and social science databases chosen in consultation with the project team and with systematic review experts. Sources were chosen to provide a balance between the health, social science and criminal justice literature and to include material derived from both mainstream and ‘grey’ literature sources.
The following databases provided a comprehensive search of the literature: MEDLINE; PsycINFO; Web of Science; Wiley Online Library; JSTOR; EMBASE; Ingenta; Cumulative Index to Nursing and Allied Health Literature; Criminal Justice Abstracts; Wilson Social Science Abstracts; Social Sciences Index; Campbell Collaboration Social, Psychological, Education, and Criminological Trials Registry; Informa Healthcare; Sage; Science Direct; HighWire; ProQuest; Applied Social Sciences Index and Abstracts; British Humanities Index; National Criminal Justice Reference Service; Social Services Abstracts, International Bibliography of the Social Sciences; Sociological Abstracts; ProQuest Dissertations and Theses; SciVerse; Metapress; Scopus; Taylor and Francis Online; System for Information on Grey Literature in Europe; Centre for Reviews and Dissemination Database; Allied and Complementary Medicine and TRIP (formerly known as Turning Research into Practice).
The project team developed a robust search string. The search strategy balanced sensitivity (to ensure that relevant material was identified) and specificity (to ensure that a reasonable proportion of the material was relevant). Medical subject heading terms and text words for inclusion in the search strategy were developed from terms relating to elements of the review question, namely: offenders, class A drugs, and diversion and aftercare programmes. Search strategy development was informed by the successive fractions approach. 78 This allows for objective testing of the productivity of main terms, restriction terms, and terms taken in combination, to optimise the balance between sensitivity and specificity.
Initial trials of the search strategy were carried out in MEDLINE and subsequently refined. Testing by proxy was used to select terms. A term was deemed sufficiently productive if at least 10% of citations were relevant to the review. Additional relevant search terms were identified by examining key papers and consulting experts. All new search terms were tested for retrieval of novel citations, i.e. those not previously identified by existing search terms. Sensitivity and specificity were tested by applying the search string to a ‘dummy database’, comprising known relevant and irrelevant citations. Subsequently, sensitivity was increased by the addition of further search terms. Specificity was improved by the addition of the Boolean term, ‘NOT’ which excluded irrelevant material. Final evaluation of the search string included testing against a control list of papers referenced by previous reviews and a cardinal list of key papers in the field. The final search strategy is listed in Appendix 3.
Databases were searched between 2 November 2011 and 6 January 2012. Electronic database searches were limited to papers published in English between January 1985 and January 2012. It was decided not to update the search prior to publication of this report. This was based on the paucity of evidence identified for the review from the original search. Given changes in the organisation and provision of the NHS and social care that also affect services for addiction it was felt that swift publication was of greater importance. Libraries of retrieved studies were exported into EndNote citation manager software (EndNote X6, Thomson Reuters, CA, USA) and deduplicated. The reference lists of all full-text articles retrieved, including grey literature, were hand-searched for additional material.
Inclusion criteria
Population criteria
-
Aged ≥ 18 years.
-
Class A drug users or reporting of class A drug user subsample.
-
Contact with any part of the CJS.
-
In any country.
Where eligibility for age or class A drug use was not specified or unclear the authors were contacted for additional information.
Diversion intervention criteria
Diversion was defined as a criminal sanction that is, or contains an element of, treatment which is specifically designed to treat and/or reduce drug. The intervention might, or might not, be accompanied by a reduction in disposal severity and/or sentence length for treatment compliance.
Diversion intervention included individuals who:
-
receive drug treatment and testing orders (DTTOs) as a community sentence, or have drug treatment requirements as a sentence alone or alongside other probation orders (e.g. specific programme or course)
-
were sent to prison initially but then released with a drug treatment requirement as a condition of parole
-
people who receive drug treatment via specialist court/probation programme in lieu of imprisonment
-
receive drug treatment via specialist court, or probation programme in lieu of reduced charges, or reduced sentence
-
were receiving treatment in any form of community-based treatment setting, for example specialist prescribing, residential detoxification, day centre attendees, counselling, cognitive–behavioural therapy and therapeutic communities.
Relevant outcomes
These included treatment completion; reduction or increase in drug use; health service contact; mental and, or physical illness; health risk behaviour, i.e. injecting; mortality; social functioning, i.e. employment, training, education, homelessness, family and/or social support; and CJS contact for any offence type, i.e. rearrest, recidivism and imprisonment. Studies reporting only predictors of drug treatment completion were not included.
Exclusion criteria
Exclusion criteria were:
-
participants were in prison at the time of the intervention
-
participants were not in contact with the CJS
-
participants were not diverted
-
participants were probationers and intervention or treatment was part of probation case management
-
participants were aged under 18 years
-
the sample contained mixed drug use with no class A drug primary or subanalysis
-
there were no relevant outcomes reported
-
there were no relevant outcomes for class A drug users only predictor analyses.
These inclusion/exclusion criteria were applied to the titles and/or abstracts of studies identified by the search strategy (see Appendix 4). A second reviewer independently screened 50% of identified studies following the establishment of an acceptable level of inter-rater reliability (κ = 0.7). References in the following formats, books, conference proceedings, dissertations, or theses, were excluded. Potentially relevant references were copied into a separate file and the full text of the article obtained. Two reviewers independently assessed each study for inclusion with any disagreement resolved by consensus and a third reviewer, if necessary. Reasons for exclusion of full-text references were documented (see Figure 1).
Quality assessment
There are a large number of available instruments for the objective evaluation of study quality. However, few of these have been adequately validated79 and the vast majority are directly applicable only to randomised controlled trials (RCTs). RCTs remain a rarity in the field of criminal justice research and none of the studies meeting our inclusion criteria followed this methodology, although one study80 derived its data from a previously conducted RCT.
Objective quality assessment scales that directly address the type of ‘real-world’ approach, which is the natural methodology of drug diversion research, are virtually non-existent. One exception to this general rule is the Maryland Scale of Scientific Methods81 summarised in Appendix 6. This scale was developed specifically to address the constraints of research in the criminal justice setting and is currently the most widely utilised quality evaluation scale in this context. The scale considers both broad aspects of research design (e.g. controls and randomisation) but, more importantly in this context, considers also in greater detail threats to internal validity.
Data extraction
Data extraction (see Appendix 5) was carried out independently by at least two reviewers. Data pertaining to study design, intervention, sample demographic characteristics, relevant outcomes and any relevant statistical analyses were extracted and inputted into Statistical Product and Service Solutions (SPSS), version 20 (IBM Corporation, Armonk, NY, USA; 2011). Any disagreements were resolved by consensus and a third reviewer, if necessary.
Data synthesis
An initial narrative synthesis of the available material was used to explore and outline the extent, nature and quality of the available evidence in this area. This qualitative assessment of the available data also explored observed heterogeneity in study and participant characteristics, study designs and study outcomes. It was used to inform the structure of subsequent quantitative synthesis of the data, including the choice of comparisons to be made and the outcome measures amenable to quantitative treatments. A bivariate analysis of outcomes explored the potential associations between study and participant characteristics and outcomes identified via narrative review. Outcomes suited to meta-analysis were then converted to odds ratios (ORs) and data from individual studies combined to provide a quantitative evaluation of heterogeneity. Where studies evaluating a particular outcome (e.g. reduction in primary drug use) were identified as both statistically and conceptually amenable to combined analysis, meta-analytic models were developed to identify a pooled effect size. Meta-analysis was also used to explore publication bias.
Results
Study flow
Database and bibliography searches identified 28,408 potentially relevant studies. Screening of titles and/or abstracts led to the exclusion of 27,110 studies, with 1328 articles proceeding to an examination of the full text. Full-text review led to the exclusion of a further 1284 articles and 14 papers, relating to 16 studies, were included in the quantitative synthesis. This process is summarised in Figure 1.
FIGURE 1.
Flow chart of included studies.

Selection of included studies
Data analysis for 15 of the 16 studies was based on secondary data drawn from available published reports; complete raw data were available for one study,82 with partial raw data available for one study in which a part of the sample met our inclusion criteria. 83 Reasons for exclusion of the studies not included in the review are listed in Figure 1 and a comparison between included and excluded studies is provided in Appendix 6.
Profile of included studies
Publication date
The review covered the period January 1985 to January 2012. However, the bulk of relevant studies identified (n = 14, 87.5%) were published post 2000. The focus of the relevant literature on drug courts, first established in 1989, accounts for this.
Publication type
All of the included studies were published studies. Over half were published in academic, peer-reviewed journals, with the majority of the remainder being publicly available government reports and one study52 was a university publication (see Table 1).
Country of origin
Included studies primarily (62.5%) provide information regarding the US situation. The small number of UK-based studies (n = 2, reports with a combined total of four studies; 25% of studies in total) focused on interventions which are, effectively, the UK equivalent of drug courts – DTTOs. The two remaining studies52,84 reported outcomes from a Toronto drug treatment court and an Australian early court intervention pilot, again both equivalents of the US drug court model (see Table 1).
Table 1 sets out descriptive summaries of each of the included studies. Note that Eley et al. 88 is an ‘umbrella’ study addressing the roll-out of a programme in two locations. The report of this study divides into three substudies, two outlining outcomes for each location and the third providing additional outcomes for a sample drawn from the combined data. In order to clarify which substudy is being discussed the individual substudies will be included in the citation [Eley et al. 88(Fife) for the Fife substudy, Eley et al. 88(Glasgow) for the Glasgow substudy and Eley et al. 88(combined) for the analysis of both the Fife and Glasgow substudies combined].
| Study | Country | Study description | Design |
|---|---|---|---|
| Anglin et al., 200785 | USA | Comparison of treatment outcomes (primarily recidivism) for SACPA-referred methamphetamine users and SACPA-referred users of other drugs. Journal article | Concurrent group comparison |
| Brecht and Urada, 201186 | USA | Evaluation of treatment performance and outcome indicators for Proposition 36 (SACPA)-referred methamphetamine users, comparing outcomes with similar groups either not referred via Proposition 36 or not using methamphetamine. Journal article | Concurrent group comparison |
| Brewster, 200187 | USA | Evaluation of the Chester County Drug Court Programme, comparing recidivism and drug use outcomes for clients on the programme, with outcomes for a group of clients on probation prior to the programme’s introduction who would have been eligible for inclusion had the programme existed previously. Journal article | Cross-sectional group comparison |
| Chun et al., 200782 | USA | Evaluates treatment outcomes (CJS involvement and drug use) for opioid dependent clients. Comparisons drawn between treated (therapeutic community plus methadone maintenance) and untreated (therapeutic community but no methadone maintenance) clients and between treated and untreated clients on probation and treated and untreated clients referred via Proposition 36 (SACPA). Journal article (raw data provided by author) | Concurrent group comparison |
| Eley et al., 200288(Fife) | UK (Scotland) | Programme and outcome evaluation of pilot DTTO programmes in Glasgow and Fife. Government report | Longitudinal follow-up |
| Eley et al., 200288(Glasgow) | UK (Scotland) | Programme and outcome evaluation of pilot DTTO programmes in Glasgow and Fife. Government report | Longitudinal follow-up |
| Eley et al., 200288(combined) | UK (Scotland) | Programme and outcome evaluation of pilot DTTO programmes in Glasgow and Fife. Government report | Case series |
| Hartley and Phillips, 200189 | USA | Analysis of drug court case files to evaluate factors potentially contributing to likelihood of successful ‘graduation’. Journal article | Correlational |
| Hevesi, 199990 | USA | Evaluation of probation case records for crack/cocaine users to determine if drug treatment programmes contributed to reduced recidivism based on arrests for misdemeanours, drug-related crime and violent and non-violent felony. Government report | Correlational |
| Longshore et al., 200791 | USA | Evaluation of treatment completion and outcome indicators for clients referred through Proposition 36 (SACPA) either via probation or while on parole, with outcomes for those referred either via the CJS but not through SACPA or referred through non-CJS routes. Government report | Cross-sectional group comparison |
| Marinelli-Casey et al., 200880 | USA | Evaluation of drug court treatment outcomes comparing methamphetamine users receiving outpatient treatment under drug court supervision with a similar group of methamphetamine users not under drug court supervision. Journal article | Concurrent group comparison |
| Newton-Taylor et al., 200984 | Canada | Evaluation of participant intake and treatment compliance as predictors of treatment completion in a Toronto drug treatment court focused on non-violent crack/cocaine and opiate users. Journal article | Concurrent group comparison |
| Passey et al., 200352 | Australia | Evaluation of the Lismore MERIT pilot programme, designed to promote early referral into treatment for drug-using offenders. Other (university publication) | Concurrent group comparison |
| Saum and Hiller, 200892 | USA | An evaluation of whether or not a history of violent offending is significantly related to the likelihood of recidivism following referral to treatment via a drug court. Journal article | Before-and-after comparison |
| Turnbull and Webster, 200793 | UK | Process and outcome evaluation of DTTOs for crack-using offenders in a London borough. Government report | Correlational |
| Van Stelle et al., 199483 | USA | Evaluation of recidivism following referral of substance-using offenders to the Wisconsin TAP, a treatment programme based on the TASC model. Journal article (raw data provided by author) | Longitudinal follow-up |
Quality assessment
The evaluation of study quality relates to each study taken as a whole. For a number of studies (see Appendix 6) only a subgroup of participants met our inclusion criteria and subsequent analyses of outcomes are therefore based only on outcomes for these individuals. However, to evaluate the extent to which outcomes can be relied on, it is the overall study design which provides the best indicator of research ‘quality’.
Table 2 sets out the design profiles of included studies, indicating study design, sample size, allocation of participants, length of follow-up and attrition and details in line with the Maryland Scale of Scientific Methods criteria. Table 2 highlights the fact that included studies were not of a rigorously high methodological standard. Designs were, in the main, retrospective and/or correlational; sample sizes tended to be modest and there was no, or limited, follow-up beyond the intervention end point. None of the studies used random selection or random allocation of participants or was able to blind raters, where more than one group was available for analysis.
| Study | Data collection | Power calculation | Sample size: N (n used in analyses) | Group allocation; comparison group (n) | Control variables; variable measurements | Attrition % lost; control for any attrition | Length of follow-up (days) | Statistical tests/effect sizes | Core level |
|---|---|---|---|---|---|---|---|---|---|
| Anglin et al., 200785 | Retrospective | No | 36,132 (29,757) | Post hoc; 3 | 5; 3 | 17.7%; 2 | 730–1095 (varied) | Yes | 4 |
| Brecht and Urada, 201186 | Prospective | No | 145,947 (73,805) | Post hoc; 3 | 5; 3 | 55.5%; 2 | 0 (main outcomes measured only at discharge) | Yes | 4 |
| Brewster, 200187 | Retrospective | No | 235 (235) | Post hoc; 3 | 1; 3 | 0.0% | 365 | Yes | 2 |
| Chun et al., 200782 | Prospective | No | 85 (18–85) | Post hoc; 4 | 5; 3 | 78.8%; 2 | Unclear | Yes | 4 |
| Eley et al., 200288(Fife) | Prospective | No | 49 (unclear) | NA (single group only) | NA (single group only); 4 | Unclear | Unclear | No | 2 |
| Eley et al., 200288(Glasgow) | Prospective | No | 47 (unclear) | NA (single group only) | NA (single group only); 4 | Unclear | Unclear | No | 2 |
| Eley et al., 200288(combined) | Prospective | No | 10 (10) | NA (single group only) | NA (single group only); 1 | 0.0% | 0 | No | 2 |
| Hartley and Phillips, 200189 | Retrospective | No | 196 (196) | NA (single group only) | NA (single group only); NA (focus on treatment completion) | 0.0% | Not stated | Yes | 1 |
| Hevesi, 199990 | Retrospective | No | 154 (147) | NA (single group only) | NA (single group only); 1 | 0.0% | 1460, but intervention length unclear | Yes | 2 |
| Longshore et al., 200791 | Mixed | No | 492,966 (unclear) | Post hoc; 3 | 3; 3 | 12.7%; 2 | 900 for year 1 intake; 365 for years 2 and 3, varied on participant | Yes | 2 |
| Marinelli-Casey et al., 200880 | Prospective | No | 287 (287) | Post hoc; 3 | 5; 4 | 0.0% | 365 | Yes | 4 |
| Newton-Taylor et al., 200984 | Prospective | No | 365 (365) | Post hoc; 3 | 1; 2 | 0.0% | 730 | Yes | 1 |
| Passey et al., 200352 | Prospective | No | 266 (262) | Post hoc; 3 | 5; NA (focus on treatment completion) | 1.5%; 2 | Varied (average 270) | Yes | 1 |
| Saum and Hiller, 200892 | Retrospective | No | 456 (452) | NA (single group only) | NA (single group only); 3 | 0.9%; 2 | 1095 for 70% of participants | Yes | 2 |
| Turnbull and Webster, 200793 | Mixed | No | 70 (70) | NA (single group only) | NA (single group only); 1 | 0.0% | 540 | No | 2 |
| Van Stelle et al., 199483 | Mixed | No | 259 (259) | NA (single group only) | NA (single group only); 1 | 0.0% | 540 (average) varied on participant | Yes | 2 |
Appendix 6 sets out additional characteristics that affect the plausibility and interpretability of studies. The likely reliability and validity of outcome measures was rarely addressed. The use of intention-to-treat (ITT) analyses was restricted to retrospectively collected data. Baseline differences between comparator groups were not always controlled for. More recent studies tended to be of a higher quality when the overall evaluation of study quality was taken into consideration (rho = 0.74; p < 0.001) but not when the more restricted set of Maryland criteria only were used to judge this (rho = 0.34; p = 0.20).
Studies were grouped into three broad categories based on quality. This is a relative measure of quality between the included studies only. As stated, all included studies were not of a high methodological standard.
Highest quality
-
Marinelli-Casey et al. :80 Maryland Scale level 4, concurrent group comparison, adequate sample size and follow-up, clear focus on choice of variables and control for effect modifiers.
-
Chun et al. :82 Maryland Scale level 4, prospective, concurrent group design with repeated measures, clear focus on choice of variables and control for effects modifiers, but small sample size.
-
Brecht and Urada:86 Maryland Scale level 4, prospective concurrent group design, control for effect modifiers, but high dropout and data collected via chart review.
-
Anglin et al. :85 Maryland Scale level 4, concurrent group design with a large sample size, long follow-up and good control for effect modifiers, but retrospective data collection.
Medium quality
-
Newton-Taylor et al. :84 prospective concurrent group design, adequate sample size with no attrition, longitudinal data, but Maryland Scale level 1.
-
Passey et al. :52 prospective concurrent group design, low attrition with adequate follow-up, control for modifier effects, but Maryland Scale level 1.
-
Saum and Hiller:92 before-and-after design with long follow-up, adequate sample size and low attrition, but retrospective data collection and Maryland Scale level 2.
Lower quality
-
Hevesi:90 retrospective correlational study, with data collected via chart review but long follow-up and Maryland Scale level 2.
-
Van Stelle et al. :83 longitudinal follow-up design with some prospective data collection and adequate sample size, Maryland Scale level 2, but authors make specific reference to difficulty of collecting reliable data.
-
Hartley and Phillips:89 retrospective correlational study, data collected via chart review, Maryland Scale level 1.
-
Brewster:87 cross-sectional group design, but with an historical control group, adequate sample size and length of follow-up, Maryland Scale level 2, but data collection retrospective and poor control for modifier effects.
-
Longshore et al. :91 cross-sectional group comparison, with some data collected prospectively, adequate follow-up and large sample size, Maryland Scale level 2 and some attention to controlling for effect modifiers, but authors note a lack of clarity regarding whether data collated from different sites referred to ‘episodes’ or ‘individuals’, hence sample size is estimated and may conflate people and treatment episodes.
-
Eley et al. :88 (three studies) longitudinal follow-up design, either single cohort or case series. Repeated measures and triangulation on main outcome measure, Maryland Scale level 2, but small sample size and length of follow-up and attrition not stated.
-
Turnbull and Webster:93 correlational study, with some prospectively collected data, but data collection primarily via chart review, Maryland Scale level 2, authors make specific reference to difficulty of collecting reliable data.
Study design
All 16 studies identified a potential cohort of participants, primarily via existing services (e.g. probation) or routine data sources, for example California Outcomes Measurement System (CalOMS) and California Alcohol and Drug Data System. These cohorts were used to compare outcomes for interventions. Where comparisons were drawn between experimental and (broadly defined) control groups (n = 8), allocation to groups was post hoc. Data collection in eight studies was either wholly or partly retrospective. None of the studies used either randomised selection or randomised allocation of participants. Although it was impossible to blind participants to the receipt of an active intervention, studies did not report any attempt to blind those analysing the data to participant allocation. Validation of key outcomes, such as continued drug use, via triangulation (e.g. use of self-report and other report), or via an evaluation of reliability (e.g. repeated assessment) or validity (e.g. comparison of self-report use with urine testing) was almost entirely lacking (Eley et al. 88 did compare self-report and urine screening).
Sample size
Sample size or power calculations were not reported in any of the included studies. It is unclear whether or not sample size or power calculations were used to estimate sample requirements for the analyses. Small sample size is likely to have impacted on the robustness of outcomes presented for a number of the studies. 82,88,93 Studies with large sample sizes85,86,91 and consequent statistical power, tended to be characterised by uncertainties about the reliability of data collected.
Length of follow-up
Ideally, length of follow-up would be measured to a point beyond the timescale occupied by the intervention itself. Length of follow-up, for a number of the studies reported here, referred either to time while in treatment,84,88(combined) or included an unspecified or individually variable length of time during which treatment was still taking place. 52,86,87,90,91,93 Some authors failed to clarify whether or not follow-up included time in treatment82,85 and three studies88(Fife),88(Glasgow),89 provided no information about length of follow-up. Only three studies80,83,92 explicitly set out a follow-up period which began at the point of treatment discharge. For these three studies, the mean length of post-discharge follow-up was 666 days, the shortest length of follow-up was 365 days. 80 These latter studies provide a strong indicator of the likely durability of the treatment modalities addressed.
Attrition
Dropout during the course of a study undermines faith in the reliability and generalisability of outcomes. Of those studies with some, or all, outcome data collected prospectively, five80,83,84,88(combined),93 reported no loss to follow-up. For the four studies with prospective or mixed data collection which reported some loss to follow-up, attrition ranged widely from 1.5%52 to 78.8%82 (the latter was subsequently excluded from analysis). Two studies had attrition at levels sufficient to substantially undermine outcomes. 82,86 Two further studies, both of which had substantive sample sizes, also suffered a significant loss to follow-up of 12.7%91 and 17.7%. 85
Analysis design
Intention to treat
In the absence of ITT analysis, it is unclear whether or not outcomes reflect treatment effectiveness on the sample who started treatment. Any observed positive impact could demonstrate efficacy only in those who fully engaged with, and completed, both the intervention and its evaluation. Four studies88(Fife),88(Glasgow),88(combined),93 report no statistical analysis of outcomes and are consequently excluded from an evaluation of whether or not analyses are ITT. Of the remainder, five80,84,87,89,90 (41.7%) reported, or were identified by the review team, as carrying out all analyses on an ITT basis. Of these, four studies80,84,87,89 had experienced no attrition from their sample. The remaining study90 had experienced minimal sample attrition. The two studies85,86 identified as failing to carry out any of their analyses on an ITT basis both had substantive attrition. Of the remaining studies which carried out statistical analyses, three52,82,83 used ITT analysis for at least some of the analyses presented. In all three cases, the analyses which did not use an ITT approach were those for which data for the outcome analysed were missing.
Baseline equivalence
Eight of the included studies drew comparisons between different groups of participants. With regard to outcome measures, four of the eight group comparison studies52,80,82,84 did evaluate baseline equivalence for all relevant variables, using statistical analyses. Of the remainder, one used statistical analysis, but only for a subset of the outcome measures86 and three, although commenting on baseline characteristics for some or all of the measures, failed to carry out statistical evaluations to establish equivalence between groups. 85,87,91
Outcome focus
Treatment completion was the most commonly reported measure overall, with all but one study88(combined) reporting outcomes for this variable (Table 3). All but two studies52,85 provided data on drug use during, or subsequent to, the intervention. Of those studies reporting drug use, the most common measure used was self-reported drug use (n = 7, 50%). Urine tests, or other forms of drug screening,80,88(Fife),88(Glasgow),87,93 and drug-related arrests83,87,91–93 were variously reported in a number of studies. None of the studies reported drug-related convictions as an outcome. Four studies80,82,88(Fife),88(Glasgow) used a scale-based measure of drug use [Addiction Severity Index (ASI)].
| Study | Outcome measure | |||||||
|---|---|---|---|---|---|---|---|---|
| Self-reported drug use | Drug screening | Treatment completion | Scale-based outcomes | Drug-related arrests | General arrests | Arrests for violent offending | Incarceration | |
| Anglin et al., 200785 | Methamphetamine users less likely to complete treatment than alcohol or marijuana users, more likely to complete than cocaine users or opiate users | |||||||
| Brecht and Urada, 201186 | No significant differences between SACPA methamphetamine users and SACPA other-drug users for treatment completion rate or 90-day treatment retention rates | |||||||
| Brewster, 200187 | No statistically significant difference, by type of drug | |||||||
| Chun et al., 200782 | Significant reductions in self-reported alcohol, heroin, cocaine, other sedative use in last 30 days, but no significant group differences except for heroin use where ‘untreated, referred from probation’ group showed a greater reduction | No significant group differences for days’ retention in treatment | Significant reduction in ASI-measured alcohol and drug scores, employment and psychiatric scores The ‘untreated referred from probation’ group showed significantly lower mean reductions in ASI employment score |
No differences in proportion of participants arrested in last 30 days | No significant differences in days incarcerated in last 30 days | |||
| Hartley and Phillips, 200189 | No statistically significant differences, by referral methods | |||||||
| Hevesi et al., 199990 | Treatment completers significantly less likely to reoffend than non-completers | |||||||
| Longshore et al., 200791 | Heroin/opiate users less likely to complete treatment than users of other drugs. Women more likely to complete than men, older people than younger people, people from ethnic minorities less likely to complete than white groups, longer continuous drug use likely to increase likelihood of completion, frequent use decreased likelihood of completion, referral from parole decreased likelihood of completion in contrast to referral from probation | |||||||
| Marinelli-Casey et al., 200880 | Significant group differences in mean methamphetamine use at discharge, 6- and 12-month follow-ups for drug court participants | Drug court participants significantly more likely to remain abstinent/have more methamphetamine-free urine tests than non-drug court participants | Drug court participants more likely to remain in treatment > 30 days, more weeks retained in treatment and higher % completed treatment than non-drug court participants | Drug court participants significant reductions in ASI drug scores at 6 and 12 months compared with non-drug court participants | ||||
| Newton-Taylor et al., 200984 | Significant group differences in self-reported substance abuse for graduated participants vs. expelled–engaged and expelled–non-engaged participants | Graduated and expelled–engaged participants significantly better treatment compliance than expelled–non-engaged participants | ||||||
| Passey et al., 200352 | Heroin users more likely to complete treatment vs. other drugs | |||||||
| Saum and Hiller, 200892 | Increasing age significantly decreased likelihood of rearrest | No significant differences except that time at risk and lifetime charges increased likelihood of rearrest | Primary cocaine users more likely to be rearrested for any violent offence than participants using other drugs as their primary drug Time at risk and lifetime charges were increased likelihood of rearrest, increasing age reduced likelihood of rearrest |
|||||
Seven studies reported outcomes for general offending82,83,86,87,90–92 and five reported outcomes relating to arrests for violent offending. 83,87,90–92 None of the studies reported outcomes in respect of convictions for violent offending, although one study83 did report outcomes relating to convictions for general offending behaviour. In addition, five studies reported outcomes relating to incarceration82,83,86,87,93 and one study82 reported offending behaviour evaluated using the ASI.
A small number of studies considered other potential outcomes of an intervention. Three82,86,87 reported outcomes for employment or training; one86 reported on family and social support outcomes; and one84 reported on compliance with treatment programme and court conditions.
A noticeable absence from the list of outcomes reported was any assessment of the impact of an intervention on the physical or mental health of participants. None of the studies reported outcomes for either hospital admissions or mortality. One study only82 reported medical and psychiatric status, with outcomes based on the ASI.
Intervention characteristics
The level of detail provided about the interventions evaluated varied substantially, but overall few specific details (e.g. proportion of participants diverted to a particular treatment modality) were provided. Interventions were largely pragmatic and ad hoc (e.g. utilising services available in the local area) rather than tailor-made for a particular programme. Details of the diversion process (e.g. how decisions were made about which intervention might be most appropriate for particular individuals) were also few and far between. The lack of information regarding these key issues is problematic. It leaves outcomes open to wide interpretation regarding what aspect of treatment has or has not worked in a given context. This is notable where treatment options are diverse in focus or delivery as is the case for the majority of the included studies.
Type and focus of intervention
One study90 provided no details of the intervention evaluated, other than that a number of participants received a ‘drug treatment programme’ while the remainder were on probation with no such programme. Of the remaining fifteen studies, seven (43.7%)80,83,88(Fife),88(Glasgow),88(combined),89,92 are best described as multifactorial day programmes, a further five (31.2%)52,85,86,91,93 as multifactorial day and residential programmes and one82 as a multifactorial residential programme. Details for the remaining two studies focus on expectations participants were required to satisfy, rather than on treatment received as such. In total, 80% of the interventions evaluated were multifactorial programmes, with the remaining 20% either not described at all or subject to broad interpretation.
Of the multifactorial interventions offering clients both day and residential options, three52,91,93 provide details of how the treatment options on offer were distributed between participants. Two studies,85,86 evaluating Substance Abuse and Crime Prevention Act (SACPA) interventions (SACPA-referred methamphetamine users compared with other groups given the same treatment options), set out a broad summary of treatment options. They gave no indication of the proportion of participants in experimental or comparator groups who were offered any given option. The options available to participants in both studies are broadly similar. Participants in Anglin et al. 85 were offered detoxification, methadone detoxification, methadone maintenance, outpatient non-methadone treatment and residential treatment/recovery. Participants in Brecht and Urada86 were offered outpatient treatment, residential treatment lasting either < 30 days or > 30 days, detoxification, Narcotic Treatment Programme (NTP) detoxification or NTP maintenance.
Of the seven studies80,83,88(Fife),88(Glasgow),88(combined),89,92 evaluating multifactorial programmes offering only day (non-residential) treatment, one80 provides a detailed outline of the intervention received by participants. This study evaluates the matrix model of intervention offered by the Methamphetamine Treatment Project (MTP). It compared outcomes of this programme for methamphetamine users either under, or not under, drug court supervision. The remaining six studies within this category, provide accounts of the intervention being evaluated which vary in their level of detail. None of the studies provide a clear indication of the proportion of participants receiving a specific treatment option.
Setting/diversion
The main focus of included studies was on drug courts; participants in just over half (56.2%)82,84,85(Fife),88(Glasgow),88(combined),87,89,92,93 of the studies were diverted to treatment ‘from court’. Participants in six other studies included participants diverted from a broader range of settings. 52,78,83,85,88,90,91 One study,86 fails to provide any details of the setting(s) from which participants were referred to treatment. In this study, for the SACPA group at least, this is likely to follow the ‘referred by court or recommended by probation or parole’ pattern identified for other studies evaluating the SACPA.
Level of intervention
The majority of studies (n = 9, 56.2%) indicated that components of the intervention(s) offered were based on both individual and group therapies. None of these studies, however, clarified the proportion of participants given either level of therapeutic intervention. Six studies82,84,85–87,90 are exceptions to this mixed pattern of intervention, which indicated that all interventions were given at the individual level only.
Prior treatment
Half of the included studies (n = 8, Table 4) failed to provide any details about the treatment history of their participants. These included prospective studies in which the researchers had at least some control over data collection. 84,88(Fife),88(combined) All studies providing details of treatment history52,80,82,85–88(Glasgow),91 identified that at least a proportion of participants had prior experience of drug treatment. This ranged from 2% (non-drug court comparator group)87 to 79% (SACPA participants). 82 Taking an average across the studies providing this information, just over half (50.4%) of the participants included had prior experience of drug treatment. Excluding figures for Brewster,87 which is a clear outlier in this context, 57.2%, on average, had prior experience.
| Study | Intervention(s) | Setting | Level | Treatment history | |
|---|---|---|---|---|---|
| Divert from | Divert to | ||||
| Anglin et al., 200785 | Multifactorial day and residential | Mixed settings | Mixed settings | Individual | Yes |
| Brecht et al., 201186 | Multifactorial day and residential | Not stated | Mixed settings | Individual | Yes |
| Brewster, 200187 | Drug court | Court | Community | Individual | Yes |
| Chun et al., 200782 | Multifactorial residential | Court | Residential therapeutic community | Individual | Yes |
| Eley et al., 200288(Fife) | Multifactorial day | Court | Community | Mixed | Not stated |
| Eley et al., 200288(Glasgow) | Multifactorial day | Court | Community | Mixed | Yes |
| Eley et al., 200288(combined) | Multifactorial day | Court | Community | Mixed | Not stated |
| Hartley and Phillips, 200189 | Multifactorial day | Court | Community | Mixed | Not stated |
| Hevesi, 199990 | Not stated | Mixed settings | Community | Individual | Not stated |
| Longshore et al., 200791 | Multifactorial day and residential | Mixed settings | Mixed settings | Unclear | Yes |
| Marinelli-Casey et al., 200880 | Multifactorial day | Mixed settings | Community | Mixed | Yes |
| Newton-Taylor et al., 200984 | Harm reduction | Court | Community | Individual | Not stated |
| Passey et al., 200352 | Multifactorial day and residential | Mixed settings | Mixed settings | Mixed | Yes |
| Saum and Hiller, 200892 | Multifactorial day | Court | Community | Mixed | Not stated |
| Turnbull and Webster, 200793 | Multifactorial day and residential | Court | Mixed Setting | Mixed | Not stated |
| Van Stelle et al., 199483 | Multifactorial day | Mixed settings | Community | Mixed | Not started |
The six group studies identifying prior treatment experience noted that both experimental and comparator group(s) included participants with experience of drug treatment. 80,82,85–87,91 Two of these studies80,82 carried out statistical analyses comparing the proportion of participants in each group previously engaged in treatment. Marinelli-Casey et al. 80 reports that drug court participants were significantly less likely to have had prior treatment than the comparator group of non-drug court participants (33.3% vs. 52.2%, χ2 = 6.49; p < 0.01). Details in Chun et al. 82 indicate that, while there were no statistically significant differences between SACPA and non-SACPA groups in respect of history of substance abuse treatment as measured by the Circumstances, Motivation and Readiness (CMR) scale, SACPA participants were more likely to already be in receipt of methadone treatment at baseline (p < 0.001).
Participant profile
Appendix 6 provides details of the participant profiles, which are summarised below.
Participant demographics
Details of participant demographics provided for a number of the studies do not map directly onto the samples used for study outcomes. Discrepancies are set out in Appendix 6. The extent of demographic information available (Table 5) varied substantially between studies. For studies where demographic data are presented separately for different groups,80,84,85–87,91 the values given are mean values taken from the individual values for all groups. Values for all demographic characteristics are baseline values and any statistically significant differences are detailed in the text.
| Study | Age (years), mean (range) | Gender, % male | Ethnicity, % white | Employment | Education |
|---|---|---|---|---|---|
| Anglin et al., 200785 | 33 (–) | 73.3 | 45.1 | Employed, 29.6% | Mean highest grade completed, 11.2 |
| aBrecht and Urada, 201186 | Not stated | 73.9 | 41.0 | Employed, 33.2% | High school or above, 60.9% |
| Brewster, 200187 | 28 (18–75) | 81.0 | 49.4 | Employed, 57.2% | High school graduate/GED or above, 33.5% |
| Chun et al., 200782 | 39 (20–62) | 63.5 | 54.1 | 70.6% lowest income category, further details not available | High school/GED, 47.1% |
| Eley et al., 200288(Fife) | 25 (19–34) | 93.9 | Not stated | Employment at DTTO, 0.0% | Not stated |
| Eley et al., 200288(Glasgow) | 30 (19–58) | 80.4 | Not stated | Not stated | Not stated |
| Eley et al., 200288(combined) | Not stated | 100.0 | Not stated | Not stated | Not stated |
| Hartley and Phillips, 200189 | 34 (21–60) | 66.3 | 55.6 | Employed prior to programme, 67.3% | High school/GED, 63.3% |
| Hevesi, 199990 | – (19–29) | 100.0 | Not stated | Employed at time of arrest, 18.4% | Not stated |
| Longshore et al., 200791 | 33 (–) | 67.7 | 45.7 | Not stated | Not stated |
| Marinelli-Casey et al., 200880 | 32 (18–57) | 62.7 | 56.7 | Employed, 71.5% | High school graduate, 52.8% |
| Newton-Taylor et al., 200984 | 35 (–) | 75.1 | Not stated | Employed, 22.0% | Secondary education or above, 90.5% |
| bPassey et al., 200352 | Not stated | 75.9 | Unclear | Employment, 7.1% | Tertiary, 6.6% |
| Saum and Hiller, 200892 | 30 (18–59) | 78.5 | 27.2 | Not stated | Not stated |
| Turnbull and Webster, 200793 | 31c (20–46) | 93.0 | 57.1 | Not stated | Not stated |
| Van Stelle, 199483 | Not stated | 100.0 | Not stated | Majority employed full time | Majority high school diploma or less |
| Total sample | 31.8 | 80.7 | 47.9 |
Age
Mean age did not vary substantively between the included studies. Our inclusion criteria were set to age 18 years and above, but no upper age boundary was set. Few studies (n = 3, 18.7%) indicated that they had included any participants in the 60+ years age bracket. Given the mean ages for these studies (28 years,87 39 years82 and 34 years89), it is unlikely that substantive numbers from this older age group were included.
Of the eight group comparison studies,52,80,82,84–87,91 four carried out statistical analysis evaluating the relative age profiles of comparison groups. 80,82,84,86 Of these, no significant differences were identified for two studies,80,82 whereas one study implied that there were significant differences86 (i.e. methamphetamine users were younger than non-methamphetamine users) but presented no further information and one identified a clear distinction between the experimental and control groups (graduates were older than either of the expelled groups; F = 5.62, p = 0.004). 84
Gender
All included studies provided details regarding participant gender. Statistical analyses comparing the proportion of men and women in comparator groups are available for only three (37.5%)80,82,84 of the eight group comparison studies. 52,80,82,84–87,91 No statistically significant differences were found. All but three studies83,88(combined),90 included female participants. The average proportion of women in studies with both male and female participants was close to one-quarter (24.2%).
Ethnicity
Further details on non-white ethnicity are available in Appendix 6. Nearly one-third of studies (n = 5, 31.2%) made no reference to ethnicity,84,88(Fife),88(Glasgow),88(combined),90 with a further three studies52,83,89 (18.7%) making reference only to the proportion of ethnic minority participants and providing either no further details,89 or providing a description of ethnicity which lacked clarity. 52,83 Statistical analyses of group differences in ethnicity are available for only two studies. 80,82 No statistically significant differences were identified for Chun et al. ,82 while in Marinelli-Casey et al. 80 there were statistically more Latino participants in the drug court experimental group than in the non-drug court comparator sample (chi-squared analysis, p < 0.05). Brecht and Urada86 reported that methamphetamine users were more likely to be white or Hispanic than non-methamphetamine users, but again no specific details of any statistical analysis are provided.
Employment status
Only two studies82,87 provided details of the proportion of participants in different income groups. The general profile set out is one of a largely unemployed group of participants on low or very low incomes. This having been said, there was substantial variation between studies reporting these data. For a minority of studies,80,89 full-time employment was the norm rather than the exception for participants. Statistical analyses to explore potential group differences in employment status were available for three studies. 80,82,84 None of the statistical analyses showed significant differences. Brecht and Urada86 reported that SACPA groups had higher rates of employment than non-SACPA groups, but no details of any statistical analysis are set out.
Educational level
Nine studies provided information about participants’ educational status (see Table 5). Overall, the profile presented is of a fairly poorly educated population of participants. However, as with the profile for employment status, there are notable exceptions to the rule. Nearly one-fifth of participants, for whom information is available, completed a comparatively high level of education. Three studies reporting statistical analysis of potential group differences80,82,84 found no evidence of a significant difference in educational status between their experimental and comparator groups. Brecht and Urada86 noted that ‘SACPA groups had a higher level of education than non-SACPA groups’, but again analyses specific to this distinction are not set out.
Mental and physical health
Participant mental and physical health status is summarised in Table 6. Fewer than half of the studies (43.7%)52,82,84,88(Fife),88(Glasgow),85,91 discussed participant mental health issues, and, of these, only five (31.2% of included studies)52,82,88(Fife),88(Glasgow),85 provided any figures for the proportion of participants with a mental health condition. No study provided any detailed breakdown of diagnoses. Details available in respect of participant physical health are even more limited. Slightly less than one-third of studies (31.2%)52,82,88(Fife),88(Glasgow),85 provided any information regarding the physical health of participants. The proportion of participants with a physical health problem was clearly set out in only three studies (18.7%). 52,82,85
| Study | Mental health | Physical health |
|---|---|---|
| Anglin et al., 200785 | 7.7% of methamphetamine users reported ever having chronic mental illness compared with average of 9.5% of other drug users | 10.0% of methamphetamine users reported a physical disability compared with an average of 11.7% of other drug users |
| Brecht and Urada, 201186 | Not stated | Not stated |
| Brewster, 200187 | Not stated | Not stated |
| Chun et al., 200782 | Mean ASI psychiatric score for the sample as a whole: 0.16, 41.2% of the participants had a score of 0 indicating no identified psychiatric problem | Mean ASI medical score for the sample as a whole: 0.31, 51.8% of the participants had a score of 0 indicating no identified medical problem |
| Eley et al., 200288(Fife) | Details from 55 initial assessments 15 (27.3%) referenced mental health concerns, including physical and emotional abuse, bereavement, memory impairment and blackouts | 48 of 55 assessments (87.3%) referenced physical health. Of these, health was reported as good in 11 cases (22.9%), problems reported related primarily to drug use, including hepatitis B and C, abscesses, deep-vein thrombosis and seizures |
| Eley et al., 200288(Glasgow) | ||
| Eley et al., 200288(combined) | Not stated | Not stated |
| Hartley, 200189 | Not stated | Not stated |
| Hevesi, 199990 | Not stated | Not stated |
| Longshore et al., 200791 | All three groups (both experimental and control) across all 3 years contained participants with diagnosed mental health disorders, these were described as mixed diagnoses, but no further details are givena | Not stated |
| Marinelli-Casey et al., 200880 | Not stated | Not stated |
| Newton-Taylor et al., 200984 | Participants not accepted onto the programme if they had mental health concerns that would interfere with their ability to participate fully | Not stated |
| Passey et al., 200352 | 39.1% of participants reported a mental health problem, 26.3% reported a previous suicide attempt | 74.8% of participants reported a chronic physical disease, 45.9% reported infection with hepatitis B or C |
| Saum and Hiller, 200892 | Not stated | Not stated |
| Turnbull and Webster, 200793 | Not stated | Not stated |
| Van Stelle et al., 199483 | Not stated | Not stated |
Drug use
Considering first a broad overview of the profiles set out (see Table 7), it is clear that the ‘bias’ of included studies towards US drug court evaluations and, particularly, evaluations of SACPA referral, has produced a parallel bias towards a focus on methamphetamine use. Three studies explicitly evaluate outcomes for methamphetamine users. 80,85,86 A further study,91 while not setting out to ‘recruit’ methamphetamine users, reports figures indicating that the single largest group of participants in the study are methamphetamine users. The four UK-based studies88(Fife),88(Glasgow),88(combined),93 show an equivalent bias resulting from the focus on evaluations of DTTO programmes, with all four studies evaluating outcomes for participants who are primary users of heroin or crack/cocaine.
Six studies80,84,88(Fife),88(Glasgow),88(combined),90 (37.5%) focused on users of a single type of class A drug only. Of these, three focused on heroin,88(Fife),88(Glasgow),88(combined) two on cocaine84,90 and one on methamphetamine. 80 Two studies focused on a single class A drug (both on methamphetamine) but included comparator groups with primary users of a range of different drugs. 85,86 Three studies focused solely on class A drug users, but participants included primary users of a number of different class A drugs. 82,89,93 Five studies drew their samples from users of a range of different drugs, but included participants who were primary class A drug users. 52,83,87,91,92 Six studies80,82,85,88(Glasgow),91,93 (37.5%) provide data which allows an evaluation of the extent and type of polydrug use in general and also additional, albeit more restricted, information regarding the profile of polydrug use for particular categories of class A drug user.
Six studies80,85,86,88(Fife),88(Glasgow),91 gave details of their participants’ past history of drug use. Figures presented in Table 7 indicate that, for the most part, participants, despite their comparatively young age, had been using drugs for substantive periods of time. For the three studies85,86,80 providing these data as mean years of drug use, figures range from 7.6 years (non-drug court methamphetamine users)80 to 17.6 years (SACPA-referred users of other drugs)86 depending on study and participant group. Taken as a mean across all participant groups, the number of years participants in these four studies had been using their drug of choice averaged 12.4 years, for participants whose average age is around 30 years.
| Study | Drug type (% use) | History/frequency of use | Severity/other details |
|---|---|---|---|
| Anglin et al., 200785 |
|
Methamphetamine users:
|
Methamphetamine users: 10.7% inject |
Other drug users:
|
Other drug users: 20.7% inject | ||
| aBrecht and Urada, 201186 | Methamphetamine users compared with users of other drugs (unspecified) | Methamphetamine users:
|
SACPA methamphetamine users: 12.2% inject |
Other drug users:
|
SACPA other drug users: 17.2% inject | ||
| Brewster, 200187 | Drug court sample, primary drug:
|
Frequency of use (primary drug) Drug court sample:
|
Not stated |
Comparison sample, primary drug:
|
Comparison sample:
|
||
| Chun et al., 200782 | Primary drug:
|
Used in the last 30 days (% yes):
|
Mean ASI alcohol use, 0.11; mean ASI drug use, 0.25 |
| Eley et al., 200288(Fife) | Heroin users | Age first used heroin ranged from 16 to 26 years | Not stated |
| Eley et al., 200288(Glasgow) | 33 used heroin only 13 used heroin and benzodiazepines 1 used heroin and cocaine |
Age first used heroin ranged from 14 to 20 years ASI-X 21 participants: age first used drug, mean years:
Used in 30 days prior to DTTO, n (%):
|
Not stated |
| Eley et al., 200288(combined) | Heroin users (no further details) | Not stated | Not stated |
| Hartley and Phillips, 200189 | Referred for:
|
Not stated | Not stated |
| Hevesi, 199990 | Cocaine/crack users (no further details) | Not stated | Not stated |
| Longshore et al., 200791 | Primary drug: SACPA:
|
Years of primary drug: SACPA:
|
Drug problem severity (mean ASI score, year 1 sample only):
|
| Marinelli-Casey et al., 200880 | Methamphetamine users | All used methamphetamine in month before treatment Drug court group:
|
Drug court group: methamphetamine use:
|
| Newton-Taylor et al., 200984 | Crack/cocaine users | Expelled–non-engaged group:
|
Not stated |
| Passey et al., 200352 | Primary drug (% of sample, n = 266):
|
Drugs regarded as ‘problem use’b (% of sample, n = 266):
|
Not stated |
| Saum and Hiller, 200892 | Primary drug (% of total sample):
|
Not stated | Not stated |
| Turnbull Webster, 200793 | Crack only (38.6% of total sample) Crack and heroin (61.4% of total sample) |
Not stated | Not stated |
| Van Stelle et al., 199483 | 52% of sample ‘alcohol dependent’ 40 participants (15.4%) class A drug users |
Not stated | Not stated |
Only half of the studies (n = 8) provided information regarding current frequency of drug use at baseline. 52,80,82,84–87,91 Of these, three52,82,86 (18.7% of all studies) indicated only whether or not participants had used a drug within the last 30 days. Five studies80,84,85,87,91 (31.2%) gave some indication of the actual frequency of use.
Details of offending behaviour
Only one study91 included a comparator group composed of non-offenders. Four studies52,90,92,93 provided specific details of the offences committed by participants and none provided details of offences committed by participants in comparator samples. Only seven studies (43.7%)52,82–84,86,87,90 provided information on the extent of CJS involvement (e.g. prior arrests, incarceration). Some additional details can be gleaned from information presented for subsamples of participants or by reference to the offender populations included. Table 8 sets out the details available.
| Study | Offences, % | Previous arrests | Previous convictions | Previous incarceration | |||
|---|---|---|---|---|---|---|---|
| Violent | Non-violent | Drug | Other | ||||
| Anglin et al., 200785 | Not stateda | Not stated | Not stated | Not stated | |||
| Brecht and Urada, 201186 | Not stateda | Any arrests, jail or prison days in past 30 days: SACPA methamphetamine users: 32.3% SACPA other primary drug users: 31.2% |
Not stated | Not stated | |||
| Brewster et al., 200187 | Not statedb | Not stated |
|
Not stated | |||
| Chun et al., 200782 | Not stateda | 98.8% arrested (life) 0% arrested last 30 days |
29.4% in last 30 days Days incarcerated in last 30 days: mean 4.66 days |
Not stated | |||
| Eley et al., 200288(Fife) | Unclear | Not stated | Not stated | Not stated | |||
| Eley et al., 200288(Glasgow) | 0% | 92% | 8% | 0% | Not stated | Not stated | Not stated |
| Eley et al., 200288(combined) | No details | Not stated | Not stated | Not stated | |||
| Hartley and Phillips, 200189 | Not stated | Most participants first time offenders | |||||
| Hevesi, 199990 | 6.1% | 65.3% | 67.3% | 28.6% |
|
||
| Longshore et al., 200791 | Not statedc | Not stated | Not stated | Not stated | |||
| Marinelli-Casey et al., 200880 | Not stated | Not stated | Not stated | Not stated | |||
| Newton-Taylor et al., 200984 | Programme focused on needs of non-violent criminal offenders | Not stated |
|
Not stated | |||
| Passey et al., 200352 | 14.3% |
|
45.9% | 12% | Not stated |
|
60.9% |
| Saum and Hiller, 200892 | 76% |
|
83% | 75% | Not stated | Not stated | Not stated |
| Turnbull and Webster, 200793 |
|
10% | 10% | Not stated | Not stated | Not stated | |
| Van Stelle et al., 199483 | Not stated | Lifetime average of 10 arrests | Lifetime average of six convictions | Average 526 days incarcerated over lifetime | |||
Offences
For three of the four studies providing specific information of offences committed by participants, non-violent offending predominated. Two of these studies52,90 reported a high proportion of drug-related offences. The fourth study92 explicitly set out to evaluate intervention outcomes for violent offenders, although the high proportion of violent offending reported (76%) is not a function solely of sample selection. This is because the sample was based on consecutive admissions to a drug court programme, albeit only drawn from those participating in the ‘probation violators’ track of the programme. All four studies present a picture of a participant group engaging in a mixed range of offences.
Criminal justice system involvement
The main focus for those studies providing CJS information was on contextualising possible differences between groups included in their studies. Overall, the information presented is partial and inconsistently recorded. This makes direct comparison between studies difficult. Levels of prior experience noted for experimental groups range from most participants being first time offenders89 to virtually all (98.8%)82 having been arrested at least once in their lifetime. Taking data from the three studies which provide unambiguous figures for number of prior convictions,52,87,90 around half of the experimental group participants (51.1%) can be expected to have had significant prior contact with the CJS.
Bivariate and meta-analyses
Not all outcomes presented by study authors are available in a format suited to further analysis. Table 9 sets out the outcome measures reported by each study which are relevant to the review parameters. These are contrasted with the outcomes which were available for bivariate and/or meta-analysis. Although no study has been entirely excluded from our statistical analyses, one or more outcomes had to be discarded for eight studies. 83,86,87,88(Fife),88(Glasgow),88(combined),91,93 Ten studies had a total of nine separate outcome measures for evaluation using bivariate and meta-analysis:
-
drug screening80
| Study | Outcome measures | Outcomes available for meta-analysis |
|---|---|---|
| Anglin et al., 200785 | Treatment completion | Treatment completion |
| Brecht and Urada, 201186 | Self-reported drug use, arrests for other offences, incarceration, treatment completion, other | Self-reported drug use, arrests for other offences, other (employment, living situation, family conflict, social support) All of the above for two participant groups only |
| Brewster, 200187 | Drug screening, drug-related arrests, arrests for violent offences, arrests for other offences, incarceration, treatment completion, other | Treatment completion |
| Chun et al., 200782 | Self-reported drug use, arrests for other offences, incarceration, treatment completion, scale-based outcomes, other | Self-reported drug use, arrests for other offences, incarceration, treatment completion, scale-based outcomes (ASI and CMR composite scores), other (employment and training) |
| Eley et al., 200288(Fife) | Self-reported drug use, drug screening, treatment completion, scale-based outcomes, other | Drug screening |
| Eley et al., 200288(Glasgow) | Self-reported drug use, drug screening, treatment completion, scale-based outcomes, other | Drug-screening |
| Eley et al., 200288(combined) | Self-reported drug use | Self-reported drug use, offending to support drug use, incarceration (the latter two measures were not outcome measures as such, but basic figures are available in the text) |
| Hartley and Phillips, 200189 | Treatment completion | Treatment completion |
| Hevesi, 199990 | Drug-related arrests, arrests for violent offences, arrests for other offences, treatment completion | Drug-related arrests, arrests for violent offences, arrests for other offences, treatment completion |
| Longshore et al., 200791 | Drug-related arrests, arrests for violent offences, arrests for other offences, treatment completion | Felony arrests, misdemeanour arrests, treatment completion |
| Marinelli-Casey et al., 200880 | Self-reported drug use, drug screening, treatment completion, scale-based outcomes | Self-reported drug use, drug screening, treatment completion, scale-based outcomes (ASI composite drug scores) |
| Newton-Taylor et al., 200984 | Self-reported drug use, treatment completion, other | Self-reported drug use, treatment completion, other (breaches of conditions, attendance at court sessions) |
| Passey et al., 200352 | Treatment completion | Treatment completion |
| Saum and Hiller, 200892 | Drug-related arrests, arrests for violent offences, arrests for other offences | Drug-related arrests, arrests for violent offences, arrests for other offences |
| Turnbull and Webster, 200793 | Drug screening, incarceration, treatment completion | Drug screening, incarceration, treatment completion |
| Van Stelle et al., 199483 | Drug-related arrests, arrests for violent offences, arrests for other offences, convictions for other offences, incarceration, treatment completion | Any arrests, treatment completion (for a subgroup of 40 participants only) |
Outcomes presented in papers but not available for our analyses were excluded either because relevant statistical data were not presented by the authors,83,88(Fife),88(Glasgow),88(combined),86,87,91,93 or, less commonly, because the data presented did not differentiate between participant groups meeting our inclusion criteria and those not doing so. 83,87
Bivariate associations
Four of the included studies carried out no statistical analyses at all. 88(Fife),88(Glasgow),88(combined),93 One additional study83 did not present any statistical analyses which were disaggregated by participant groups of relevance to this review. The remainder of the studies, which did evaluate one or more relevant outcomes on the basis of statistical tests, all reported at least one statistically significant outcome. As outcomes for the funnel plot (Figure 2) indicate, this may be suggestive of publication bias, rather than interventions which are in actuality shown to be particularly effective or ineffective.
Looking in greater detail at the direction of effect of the 106 analyses available, exactly half (n = 53 analyses, drawn from four studies82,86,89,92) found no statistically significant differences in outcomes.
Five studies52,80,82,84,90 reported a total of 21 analyses (19.8% of all available analyses) showing a statistically significant outcome in favour of expectations for the intervention evaluated. The bulk of these positive outcomes (11 analyses, 52.4%), however, stemmed from one study alone. 80
Of the remaining 31 relevant statistical analyses extracted from the included studies (29.2%, reported by six studies82,84,85,87,91,92), just under half (n = 14, 45.2%) identified a positive change (e.g. a change over time for all participants). However, there were no group differences for the comparisons of interest to this review (e.g. treated vs. untreated or class A vs. other drug users). A further three analyses reported by one study82 found similarly general outcomes evidencing change over time but with no group differences identified for either treated compared with untreated (non-methadone) or SACPA compared with non-SACPA participants. Taken overall then, although a substantive number of individual statistical analyses are available for consideration, outcomes which suggest an unambiguous reduction in key behaviours (drug use and offending) as a result of treatment intervention are few and far between.
Publication bias
The funnel plot in Figure 2 is a scatterplot of effect size against standard error (expected to closely associate with sample size). A distribution which is substantially uneven is generally seen as an indication that there is a publication bias, usually in favour of studies reporting statistically significant outcomes (which tend to be studies with larger sample size). 94 To avoid duplication, only one outcome measure from each study was used in producing the funnel plot, the choice of outcome measure was made on the basis that the measure represented the main focus of the study.
FIGURE 2.
Funnel plot to assess publication bias.
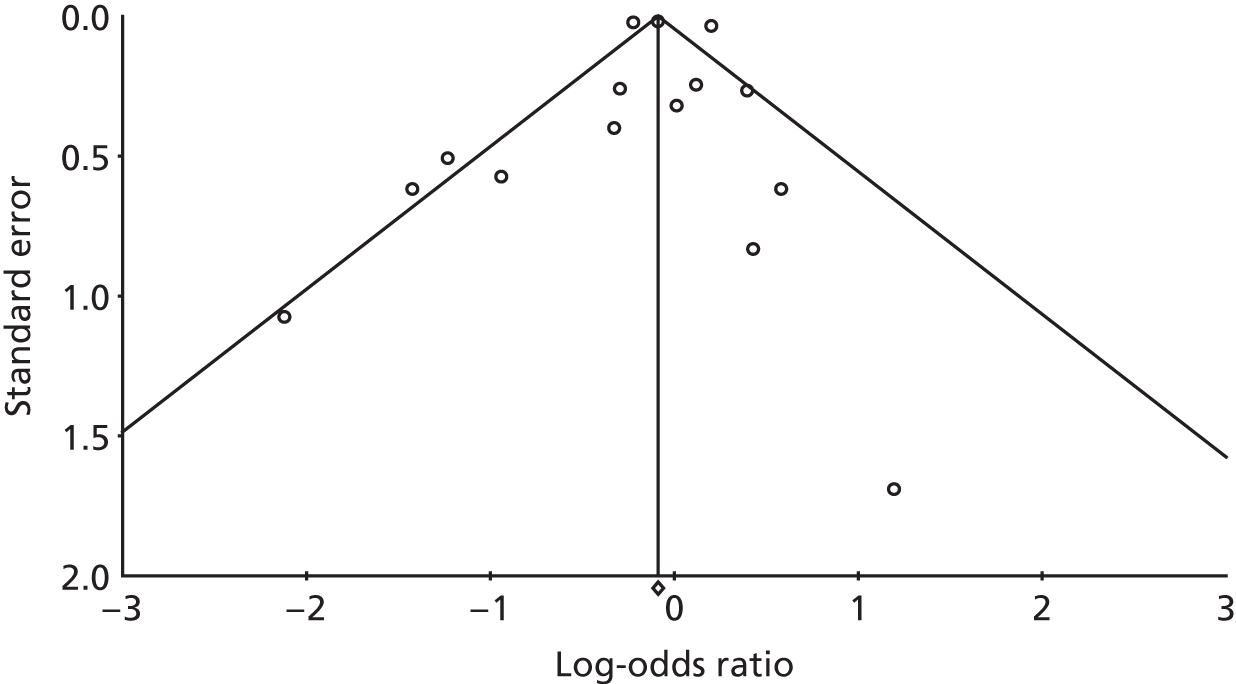
While the number of studies is small and there are clear outliers in the data, the uneven distribution shown in Figure 2 is broadly indicative of publication bias. This should be borne in mind in considering the outcome of the studies reported below and throughout the text.
Meta-analyses
All included studies provided one or more metrics suited to conversion to ORs, using equations provided by Lipsey and Wilson. 95 For each meta-analysis, we present combined ORs for both fixed- and random-effects models, rather than making a priori assumptions regarding the data. We also present two measures of heterogeneity. The Q-statistic is a reliable and commonly used measure of heterogeneity, but it does not provide an estimate of the likely extent of heterogeneity. The I2-statistic provides this information. To arrive at the final models set out below, we carried out a number of exploratory analyses, each of the models given here represent the most robust model we were able to identify for a given outcome measure.
Model 1: continued primary drug use
Six studies provided data for this key outcome. 80,82,86,88(Fife),88(Glasgow),88(combined) An initial exploratory meta-analysis found no significant heterogeneity, underlining the similarity in focus of included studies. We subsequently excluded data for two of the studies. Brecht and Urada86 was excluded since, in contrast with other studies it provided only a comparison between methamphetamine users and other drug users, rather than evaluating the impact of intervention per se. Eley et al. 88(combined) was excluded because of the exceptionally large CIs associated with this study’s very small sample size (n = 10). All four of the above models were equally valid from a statistical perspective, with no significant degree of heterogeneity identified. The direction of effect across the four models was consistently in favour of a slight reduction in primary drug use as a consequence of treatment.
Table 10 sets out model characteristics for the most substantive of the four models, which is also the model focusing on the most similar interventions (varying treatment approaches, but all effected via drug court diversion). Table 10 also provides details for this model in respect of heterogeneity. The forest plot given in Figure 3 provides a visual summary of the direction of effect for each outcome measure separately and for the random-effects model used to combine outcome.
| Model | Study | Comparison | Outcome | Statistics for each study | z-value | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | ||||||||||
| Chun et al., 200782 | SACPA vs. non-SACPA | Heroin in last 30 days (change from assessments 1 to 2) | 2.326 | 0.972 to 5.566 | 1.896 | 0.058 | |||||
| Eley et al., 200288(Glasgow) | DTTO participants | Positive tests for opiates at first test vs. at fifth test | 1.795 | 0.532 to 6.054 | 0.943 | 0.346 | |||||
| Eley et al., 200288(Fife) | DTTO participants | Positive tests for opiates at first test vs. at fifth test | 1.542 | 0.300 to 7.919 | 0.519 | 0.604 | |||||
| Marinelli-Casey et al., 200880 | Methamphetamine (MTP + drug court) vs. methamphetamine (MTP only) | Reduction in methamphetamine use – 6 months after treatment | 1.492 | 0.881 to 2.527 | 1.488 | 0.137 | |||||
| Fixed | 1.684 | 1.118 to 2.535 | 2.493 | 0.013 | |||||||
| Random | 1.684 | 1.118 to 2.535 | 2.493 | 0.013 | |||||||
| Effect size (95% CI) | Test of null hypothesis (two-tail) | Heterogeneity | τ2 | ||||||||
| z-value | p-value | Q-value | df (Q) | p-value | I 2 | τ2 | Standard error | Variance | τ | ||
| Fixed | 1.684 (1.118 to 2.535) | 2.493 | 0.013 | 0.751 | 3.000 | 0.861 | 0.000 | 0.000 | 0.187 | 0.035 | 0.000 |
| Random | 1.684 (1.118 to 2.535) | 2.493 | 0.013 | ||||||||
FIGURE 3.
Continued primary drug use: forest plot.
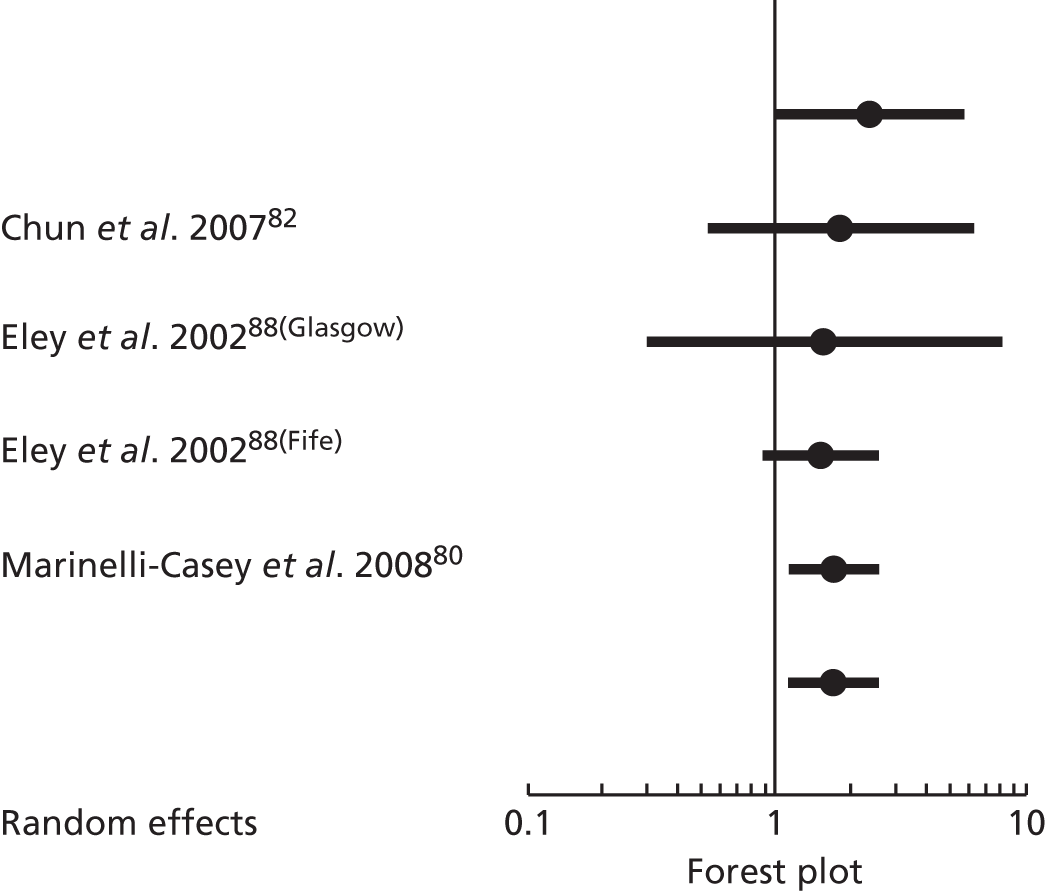
Model 2: continued use of other drugs
Three studies provided outcome measures suited to inclusion in a meta-analysis of the impact of treatment on reductions in use of drugs other than the participant’s primary drug of choice. One relevant outcome measure only was available for Marinelli-Casey et al. ,80 three for Newton-Taylor et al. 84 and a rather broader range for Chun et al. 82 (14 in total). Substantial heterogeneity was identified for this exploratory model (Q = 51.6, p = 0.0001, I2 = 67.1). To tailor outcomes more closely to the main focus of the review, we first removed comparisons which identified reductions in alcohol use only (four outcomes from Chun et al. 82). We then explored a number of alternative models incorporating in separate meta-analyses the remaining ten contrasts taken from Chun et al. 82 (outcomes for SACPA vs. non-SACPA and therapeutic community vs. therapeutic community plus methadone were evaluated for each of the following drugs: sedatives, cocaine, amphetamines, cannabis and drug use measured via ASI drug composite scores). Since the three outcomes taken from Newton-Taylor et al. 84 were paired comparisons for the three included participants against one another, we selected from these only the most salient comparison, as identified in the study details outlined previously (graduated vs. expelled–non-engaged).
Three of the models evaluated showed significant heterogeneity between the included study outcome measures. All three were models in which outcomes for Chun et al. 82 ran in a direction counter to the anticipated impact of treatment. Two outcome measures were involved here. The first, sedative use at 30 days (Q = 8.11, p < 0.02, I2 = 75.3) had increased slightly from baseline for both treated (therapeutic community plus methadone) and untreated (therapeutic community-only) groups, but more so for the latter. The second was cannabis use at 30 days, while cannabis use had decreased for all comparator groups, the decrease was less for both experimental groups compared with their comparators [SACPA vs. non-SACPA (Q = 7.33, p < 0.03, I2 = 72.3) and therapeutic community plus methadone vs. therapeutic community alone (Q = 10.45, p < 0.005, I2 = 80.9]. Running a comparable model with outcomes for Marinelli-Casey et al. 80 and Newton-Taylor et al. 84 no significant degree of heterogeneity was identified.
All remaining models, again favoured treatment with slightly greater combined decreases in other drug use following treatment compared to primary drug use. For Marinelli-Casey et al. ,80 this included ASI drug composite scores at 6 months subsequent to treatment. For Newton-Taylor et al. ,84 this included the proportion of court appearances during the first month at which self-reported drug use (any illicit substance) was recorded. The substances evaluated in separate analyses for Chun et al. 82 which showed slight decreases (all proportionately less than those reported by Marinelli-Casey et al. 80 and Newton-Taylor et al. 84) were cocaine use, amphetamine use and general drug use as measured by ASI drug composite scores. The relative impact of treatment on reductions in drug use was fairly similar across all models, ranging from a fixed OR of 2.14 to 2.97 (random OR 1.95 to 2.97).
Clearly, the outcome measures used in each of the three studies are, for the most part, not directly comparable, comprising a range of self-report outcomes for diverse drugs, scale-based outcomes and outcomes based on court records. To set out details for a model which incorporates measures which are as close as possible conceptually, Table 11 presents outcomes and heterogeneity statistics for three comparisons between drug court and non-drug court participants. Table 11 reports outcomes for SACPA compared with non-SACPA,82 and MTP plus drug court compared with MTP only. 80 Both of these are based on reductions in drug use measured by changes in ASI drug composite scores. Newton-Taylor et al. 84 differs from both other studies in that all participants are diverted via a drug court, but the comparators either successfully completed treatment (graduated group) or were expelled from the programme (expelled–non-engaged group). Although outcomes in this study are based on self-reported drug use, data were collected via court records not a purpose-designed scale. Nevertheless, study and outcome profiles are sufficiently similar statistically to be suited to inclusion in a combined analysis. Figure 4 provides the forest plot for this analysis.
| Model | Study | Comparison | Outcome | Statistics for each study | z-value | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | ||||||||||
| Chun et al., 200782 | SACPA vs. non-SACPA | ASI drug (change from assessment 1 to 2) | 1.633 | 0.687 to 3.884 | 1.110 | 0.267 | |||||
| Marinelli-Casey et al., 200880 | Methamphetamine (MTP + drug court) vs. methamphetamine (MTP only) | ASI drug – 6 months after treatment | 2.441 | 1.435 to 4.151 | 3.293 | 0.001 | |||||
| Newton-Taylor et al., 200984 | TDTC graduated vs. expelled–non-engaged | Court appearances – substance abuse reported | 3.859 | 1.966 to 7.574 | 3.925 | 0.000 | |||||
| Fixed | 2.609 | 1.792 to 3.799 | 5.001 | 0.000 | |||||||
| Random | 2.599 | 1.696 to 3.982 | 4.387 | 0.000 | |||||||
| Effect size (95% CI) | Test of null hypothesis (two-tail) | Heterogeneity | τ2 | ||||||||
| z-value | p-value | τ2 | df (Q) | p-value | I 2 | τ2 | Standard error | Variance | τ | ||
| Fixed | 2.609 (1.792 to 3.799) | 5.001 | 0.000 | 2.478 | 2.000 | 0.290 | 19.278 | 0.028 | 0.148 | 0.022 | 0.169 |
| Random | 2.599 (1.696 to 3.982) | 4.387 | 0.000 | ||||||||
FIGURE 4.
Continued other drug use: forest plot.

Model 3: continued offending behaviour
Nearly half of the included studies (n = 7, 43.7%)82–84,86,88(combined),90,92 provided outcome measures suited to inclusion in a meta-analysis of continued offending behaviour. Given the number of studies for which outcome measures were available and also the diversity of these measures (including incarceration and rearrest for a range of offences, or for any offence within or subsequent to the treatment programme), it is not surprising that an initial exploratory model including all relevant study outcomes highlighted significant heterogeneity (Q = 107.43, p < 0.0001, I2 = 61.8).
Identifying studies with a sufficient commonality of outcomes was not straightforward, as the outcome measures, even where focused on the same basic distinction (e.g. non-violent offending) tended to capture outcomes in slightly different ways (e.g. arrested for property offence vs. arrested for non-violent felony). Statistically, there was a greater degree of similarity between studies, with a number of potential models showing no significant heterogeneity between studies or study outcomes. Five models were chosen for further exploration, on the basis of broad similarities in the authors’ focus. Only one model included outcome measures for more than two studies. This model focused on offending during, or subsequent to, the programme, which included any offence without further specification. Offending behaviour in the context of this model was defined broadly as any arrest or identified reoffence occurring during, or subsequent to, treatment. Outcome measures for this model were drawn from four studies. 82,83,84,90 A further study88(combined) was initially also included, but, again due to small sample size, CIs were too wide to allow the model to benefit from the inclusion of this study. A further study92 was excluded as outcomes evaluated reductions in rearrest for comparisons drawn between drug types, rather than for the intervention per se. However, the ORs calculated for the five comparisons drawn here are of interest, since they indicate that cocaine users are more likely than users of alcohol, opioids or other drugs to reoffend following treatment (ORs of 0.90, 0.79 and 0.87, respectively); while opioid users are less likely to do so (ORs of 4.37 and 1.09 compared with alcohol and other drugs, respectively).
All studies included in the above model provided more than one relevant outcome measure. To select between these, we identified the main comparator for each study, where this was evident. So, the outcome measure chosen for Hevesi et al. 90 contrasted participants who had completed the drug court programme with those who had not been diverted via drug court. The outcome measure selected for Newton-Taylor et al. 84 again compared drug court graduates with participants classified as expelled–non-engaged and the outcome measure for Van Stelle et al. 83 compared Treatment Alternative Program (TAP) participants using class A drugs with TAP participants using other drugs. No such clear divide allowed an unbiased selection between outcome measures for Chun et al. ,82 which again contrasted outcomes for SACPA compared with non-SACPA and therapeutic community only compared with therapeutic community plus methadone. As previously, we ran preliminary models including the two Chun et al. 82 measures separately, to identify whether or not either combination of measures showed substantial heterogeneity.
A preliminary model including only outcome measures for three studies83,84,90 showed no significant heterogeneity and evidence of a fairly substantive decrease in general reoffending following treatment (fixed and random effects OR 4.06). The addition of Chun et al. ’s82 comparisons of treated (therapeutic community plus methadone maintenance) compared with untreated (therapeutic community alone) to this model resulted in significant heterogeneity (Q = 11.05, p < 0.01, I2 = 72.9), with the treated group more likely to reoffend than the untreated group. This was not the case for the SACPA compared with non-SACPA comparison, where outcomes broadly matched those of the three studies above. However, the apparently positive outcomes for the final model chosen were undermined by the large CIs of the outcome measures chosen for three of the four studies (Chun et al. ,82 OR 3.68, 95% CI 0.43 to 31.2; Newton-Taylor et al. ,84 OR 8.29, 95% CI 1.0 to 68.5; and Van Stelle et al. ,83 OR 4.13, 95% CI 1.22 to 13.9).
The two study model for incarceration, although statistically viable, was rejected on conceptual grounds, since, unlike Chun et al. ,82 Brecht and Urada et al. 86 included arrests which might have led to incarceration as well as actual incarceration. The focus of the latter study was on a comparison between methamphetamine users and users of other drugs, rather than on the impact of treatment as such, which was the main focus of Chun et al. 82
Three additional models, which all relied on combining outcomes for Hevesi90 with outcomes for Saum and Hiller92 (for drugs offending, non-violent and violent offending, respectively) were rejected on similar grounds. Hevesi90 focused either on a comparison between people who had completed a drug court programme and people who either had not completed or were not included in the programme (non-violent and violent offending) or on a comparison between a subgroup of offenders in either group who had recidivated (drugs offences), while Saum and Hiller92 focused on comparisons between users of different types of drug. With regard to the latter study, the relatively favourable outcomes for opioid users in comparison with cocaine users noted in respect of general offending were not replicated in respect of offences broken down by category.
Overall then, meta-analysis of the included studies was not able to add additional insight into the likely impact of treatment on offending behaviour beyond the analyses set out for individual studies taken as stand-alone data. Here, the problem was not so much with an inability to combine studies at the statistical level, but simply a lack of commonality in outcome measures and focus which would have rendered the combined analyses meaningless.
Model 4: treatment completion
As previously noted, treatment completion was a focus for the bulk of the included studies and 10 studies (62.5%),52,80,83–87,89,91,93 provided statistics suited to inclusion in meta-analysis. The primary focus for the majority of studies in this context was on the different completion rates achieved by users of different drug types. Three exceptions to this were:
-
An exploration of treatment completion for different modes of intervention (MTP programme under drug court supervision vs. MTP programme without). 80
-
A comparison of the number of treatment sessions attended during the first month of a programme (based on whether or not the participants subsequently graduated from the programme and, for those who failed to graduate, whether or not they were seen as engaging or not engaging with the programme). 84
-
A comparison of completion rates for day compared with residential therapy. 93 Outcomes for Longshore et al. ,91 drew comparisons between drug types, but only in separate comparisons, with each comparison primarily focused on contrasting completion rates for different referral sources (e.g. SACPA vs. CJS).
Outcomes for all of these studies were included in an initial exploratory meta-analysis, but were subsequently excluded because of a lack of comparable focus in all other outcome measures. The very high levels of heterogeneity identified in the exploratory analysis (Q = 391.05, p < 0.0001, I2 = 94.1) underlined the differences in approach to treatment completion adopted by the included studies.
Although the remaining studies52,83,85–87,89 all focused on comparing between drug types, the individual comparisons drawn were quite diverse (e.g. class A drugs vs. all other drugs; methamphetamine vs. other drugs; cocaine vs. heroin). A preliminary model including only the four studies which had a single outcome measure each was used to evaluate the extent of statistical heterogeneity these diverse outcome measures generated. These studies compared class A drugs with other drugs,83 heroin with other drugs,52 methamphetamine with other drugs86 and cocaine with cannabis. 87 Despite the difference in drug types included in the individual comparisons, no significant degree of heterogeneity was identified. Combining the study outcomes indicated a consistent pattern, with users of class A drugs showing lower completion rates overall than users of other drugs (fixed and random OR 0.918, CIs 0.881 to 0.957 and 0.853 to 0.987, respectively). The tight CIs are an indication that this fairly predictable outcome is robust.
We then explored the available outcomes for individual class A drugs. The first of these models compared treatment completion rates for heroin users with other drugs52,89 and heroin users with cannabis users. 85 Outcomes for this model were similar, with the combined OR for the studies (fixed and random OR 0.830, 95% CI 0.748 to 0.921) indicating a generally lower treatment completion rate for heroin users than for users of other drugs. The outcome for Passey et al. 52 was slightly more promising than for the other two studies, with heroin users (51%) and users of other drugs (48%) showing fairly similar completion rates.
A second model for individual types of drug compared treatment completion for cocaine users with completion rates for other drug users,89 cannabis users87 and alcohol users. 85 Again, the model showed no significant heterogeneity despite the different comparator drugs. Treatment completion for cocaine users was lower across the board than treatment completion rates for other drug users (fixed and random OR 0.731, 95% CI 0.663 to 0.806).
A final individual drug model with sufficient outcome measures for inclusion in meta-analysis focused on methamphetamine users, comparing treatment completion rates for these participants with users of other drugs86,89 and cannabis users. 85 This analysis trended in the same direction, with lower treatment completion rates identified in the two comparisons with unspecified other drugs, but slightly more positive outcomes for Anglin et al. 85 (treatment completion rates of 33% for methamphetamine users compared with 29% for cannabis users).
Given the overall lack of heterogeneity generated by combining between different drug type comparisons, we selected a single outcome measure from each study. The aim was to cover as diverse a range of class A drugs as possible within this set of studies. The choice of comparators was built up from the pragmatic base of four studies which had a single outcome measure available only – class A compared with other drugs,83 heroin compared with other drugs,52 methamphetamine compared with other drugs86 and cocaine compared with cannabis. 87 Hartley and Phillips89 provided an additional comparison between crack and other drug users. Anglin et al. 85 offered a number of outcome measures ranging across the class A drugs evaluated by the already included studies. The majority of these measures, included individually in a number of preliminary models, generated too much heterogeneity to allow valid combination. This left us with two choices of outcome measure for Anglin et al. ,85 contrasting treatment completion for cocaine users with cannabis users, the other contrasting treatment completion for heroin users with cannabis users. Of these, the OR for the heroin/cannabis comparison was more closely in line with ORs for the other included studies, so this gave us our final model. Outcomes from this model, which aimed to evaluate the strength of the evident trend for class A drug users to have lower rates of treatment completion are set out in Table 12 and Figure 5 provides a forest plot, to give a visual representation of the strength of effect. The details set out, suggest that the overall impact of primary drug type is to result in a slight but consistent reduction in treatment completion for class A drug users compared with users of other drugs.
| Model | Study | Comparison | Outcome | Statistics for each study | p-value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | z-value | |||||||||
| Anglin et al., 200785 | SACPA (heroin/opiate vs. marijuana/hashish) | Treatment completion | 0.821 | 0.736 to 0.915 | –3.575 | 0.000 | |||||
| Brecht and Urada, 201186 | SACPA (methamphetamine vs. other drugs) | Treatment completion | 0.919 | 0.881 to 0.958 | –3.978 | 0.000 | |||||
| Brewster, 200187 | Drug court (cocaine vs. marijuana) | Survival in programme | 0.931 | 0.512 to 1.691 | –0.236 | 0.813 | |||||
| Hartley and Phillips, 200189 | Drug court (referred for crack vs. not) | Treatment completion | 0.747 | 0.447 to 1.249 | –1.111 | 0.266 | |||||
| Passey et al., 200352 | MERIT + heroin vs. MERIT + other drugs | Treatment completion | 1.131 | 0.696 to 1.838 | 0.495 | 0.620 | |||||
| Van Stelle et al., 199483 | TAP (class A vs. other drug) | Treatment completion | 0.519 | 0.251 to 1.074 | –1.766 | 0.077 | |||||
| Fixed | 0.904 | 0.870 to 0.940 | –5.105 | 0.000 | |||||||
| Random | 0.878 | 0.801 to 0.961 | –2.810 | 0.005 | |||||||
| Effect size (95% CI) | Test of null (2-tail) | Heterogeneity | τ2 | ||||||||
| z-value | p-value | τ2 | df (Q) | p-value | I 2 | τ2 | Standard error | Variance | τ | ||
| Fixed | 0.904 (0.870 to 0.940) | –5.105 | 0.000 | 7.206 | 5.000 | 0.206 | 30.616 | 0.003 | 0.008 | 0.000 | 0.058 |
| Random | 0.878 (0.801 to 0.961) | –2.810 | 0.005 | ||||||||
FIGURE 5.
Treatment completion: forest plot.

Model 5: other outcomes
Only two studies provided statistics for outcomes other than the above suited to inclusion in meta-analysis. 82,86 Brecht and Urada86 provided details for employment and training, homelessness and social support or conflict, Chun et al. 82 provided details for paid work and training and ASI composite scores for the scales medical, employment, legal, family and psychiatric. This allowed three comparisons to be drawn combining the two studies: currently employed/days paid in last 30 days; currently employed or in training/training in last 30 days and family conflict in past 30 days/ASI family change. For each of these combined analyses, Chun et al. 82 provided two outcome measures, one comparing SACPA-diverted with non-SACPA diverted participants, one comparing participants treated with methadone plus inclusion in a therapeutic community with participants receiving treatment via inclusion in a therapeutic community only. These measures were run in separate analyses.
Although statistically compatible, with no evidence of significant heterogeneity for any of the exploratory models, the outcome measures were too conceptually distinct to combine meaningfully, other than for the purposes of identifying possible trends in the data. For all three comparisons, Brecht and Urada86 contrasted outcomes for methamphetamine users with users of other drugs, while Chun et al. 82 provided comparisons for the interventions themselves (diversion via SACPA vs. diversion via probation and therapeutic community alone vs. therapeutic community plus methadone maintenance).
The analyses also failed to identify a consistent trend for these other outcomes. With regard to employment and training, Brecht and Urada86 found marginally better outcomes for methamphetamine users than users of other drugs, while both Chun et al. ’s82 experimental groups (SACPA diverted and participants treated with both therapeutic community and methadone maintenance) fared either slightly worse or were closely similar to their comparators in terms of broadly the same outcomes. With regard to family conflict, Brecht and Urada’s86 methamphetamine users showed a substantially worse profile than their other drug-using comparators, while Chun et al. ’s82 SACPA and treated groups showed outcomes very similar to their non-SACPA and therapeutic community-only comparators. In summary, the limited range of outcome measures available in the included studies and, again, their diversity of focus, prevents any meaningful conclusions being drawn from meta-analysis, despite the statistical comparability of the data presented.
Meta-analyses: outcome modifiers
The potential impact of study characteristics which may account for the heterogeneity identified in the combinations of studies and outcome measures which failed to meet criteria for inclusion in meta-analysis was further explored. Details of outcome modifiers are available from the authors on request.
Chapter 4 Review of economic evaluations
Methods
Search strategy
The search strategy for the economic review combined the search terms used for the effectiveness review with economic search terms. As the economic review included those inclusion criteria used in the effectiveness review, economic search terms, plus a drug use limiter term were applied to the database of studies identified by the effectiveness review search strategy. The search strategy is listed in Appendix 7. The effectiveness review search string was also applied to further electronic databases; American Economic Association’s electronic bibliography (EconLit; via Ovid), and NHS Economic Evaluation Database (NHS EED; via Cochrane). Supplementary searches were performed on the following online sources: UK Home Office; Scottish Government; Northern Ireland Office; United Nations Office of Drugs and Crime; and a search for the author Christine Godfrey. Further efforts to identify additional studies included screening bibliographies of retrieved manuscripts, with a particular focus on review papers identified in the search.
Figure 6 sets out the process of identifying studies for inclusion in the economic review. Database searches took place from November 2011 to February 2012, retrieving studies published between January 1985 and January 2012. Libraries of retrieved studies were exported into Reference Manager (version 11; Thomson Reuters, San Francisco, CA, USA) software and duplicate entries removed.
FIGURE 6.
Flow diagram for identifying studies for the systematic review of economic evidence.
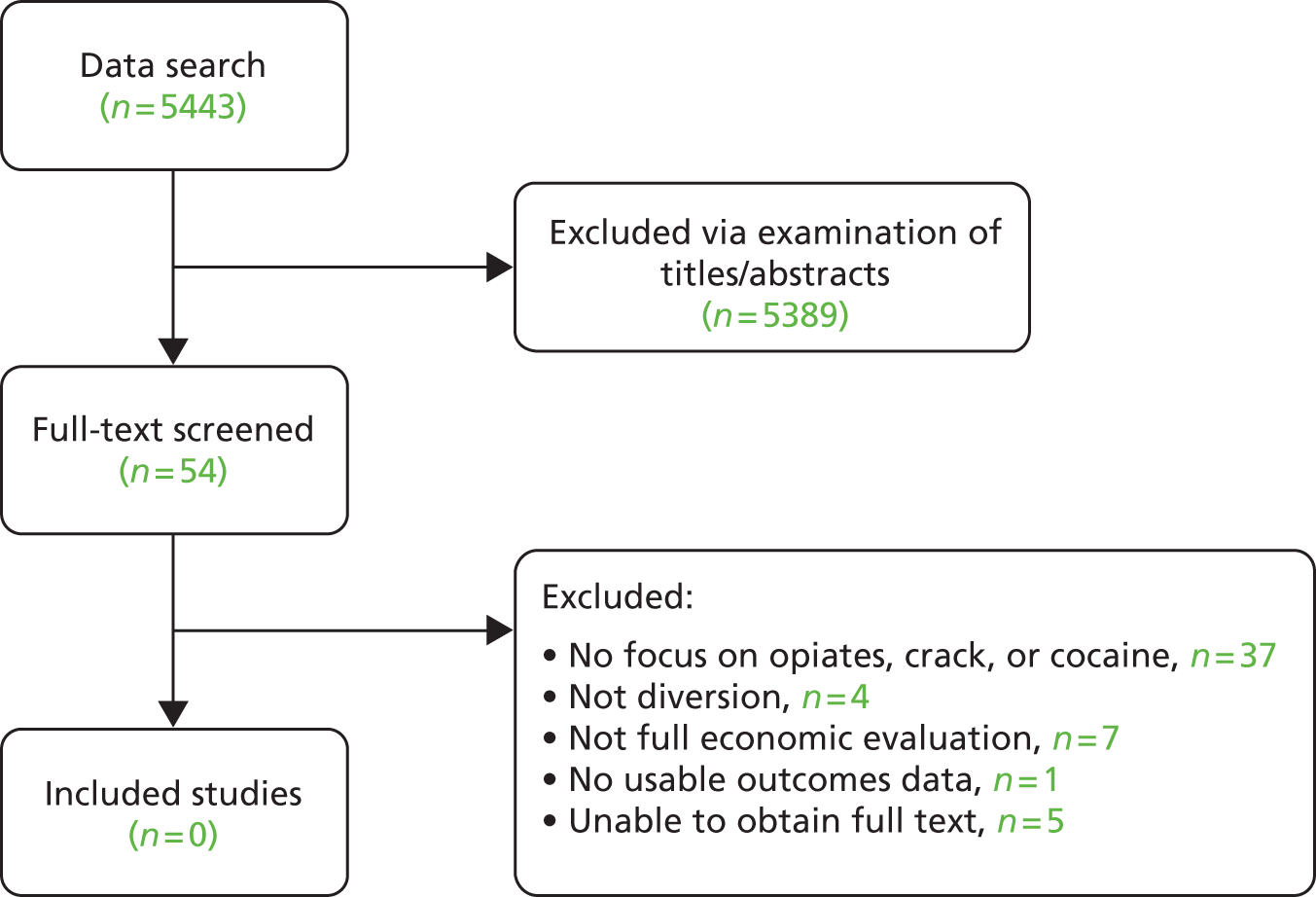
Inclusion criteria
The following inclusion criteria were applied to retrieved studies, in addition to criteria used to establish eligibility for the effectiveness review:
-
focus on use of any of the following drugs: opiates; crack cocaine; powder cocaine
-
inclusion of any of the following economic data: health economics analysis; details of patient costs; outcomes for inclusion in economic model
-
comparison group available for economic analysis
-
based on primary data collection or systematic review
-
resource use and costs reported separately
-
data other than charge data used
-
report resource use or costs generalisable to the UK setting
-
sufficient detail reported to extract costs and outcome data relevant to long-term comparisons of diversion and aftercare strategies for economic modelling.
An eligibility form, using these criteria (see Appendix 8), was applied to the titles and/or abstracts of studies identified by the search strategy. Inter-rater reliability was established with a second reviewer prior to screening. Random subsamples of those studies screened out as ineligible were subject to double-checking by a second reviewer at two further stages. Studies reported in books, conference proceedings, dissertations or theses were excluded.
Potentially relevant references were copied into a separate file and the full text of the article obtained. Two reviewers independently assessed studies, at this stage, for inclusion, with any differences resolved by discussion with a third reviewer. Only studies reporting a full economic evaluation were included in the review such as those:
-
that included direct costs/savings and a measure of benefit to the participants
-
where diversion/aftercare was compared with a comparison group not exposed to such an intervention
-
where the incremental cost-effectiveness or cost–benefit was estimated.
Reasons for exclusion of full-text references were documented (see Figure 6).
Data extraction
An economic data extraction form was developed and piloted on five randomly selected studies (see Appendix 9).
Results
Study flow
Database and bibliography searches identified 5443 potentially relevant studies. Screening of titles and/or abstracts led to the exclusion of 5389 studies, with 54 manuscripts proceeding to an examination of the full text. All of these studies were excluded from the review because of no focus on opiates, crack cocaine, or powder cocaine (37); no full economic evaluation (7); no usable outcomes data (1); not a study of diversion (4); or unable to obtain full text via library services (5). This process is summarised in Figure 6.
Partial economic evaluations
The partial economic evaluations51–55,83,88,96–101 were also reviewed to assess whether or not they included data to populate an economic model of the cost-effectiveness of diversion and aftercare. None of the studies included observed service use, unit cost or utility data to supplement the data sources identified for the economic model (see Chapter 5, Data sources). Reasons for this included:
-
primary or secondary resource use and costs not reported separately or in sufficient detail to extrapolate to current UK service context
-
observed resource use and costs related to services that are not relevant to the UK service context.
Chapter 5 Economic model: methods and data
Approach
An economic model was constructed to synthesise clinical and economic data to estimate the incremental cost per unit of outcome gained by diversion and aftercare interventions. The perspective taken was that of the CJS, NHS and social care providers and offenders. These comprise the key components of a societal perspective. The consequences of offending behaviour for victims are included indirectly by including the costs to victims in the cost estimates of offences.
Current practice varies in the diversion and aftercare packages and sequence of treatment and support interventions used. In the UK, the main approach is the DIP. However, this varies in the intensity and range of approaches used to identify, assess and refer substance using offenders to treatment and aftercare. For the primary analysis, the diversion and aftercare intervention was broadly defined to cover the variety of interventions provided in the UK. Sensitivity analyses were used to explore the impact of varying the intensity and scope of the DIP on the probability of reoffending, costs and outcomes.
The comparator for the primary analysis is no formal identification and assessment process to refer substance-using offenders into treatment and aftercare. The model includes the fact that a proportion of offenders will already be in contact with treatment services at the time of arrest or will engage with treatment and aftercare services. This may be by informal referral or advice from the CJS or by another route. This applies to both the intervention and comparator arms of the model.
The measures of health benefit for the economic analysis were the quality-adjusted life-year (QALY) for the primary analysis and life-years gained for the sensitivity analysis. In addition, proxy measures of outcome were used in the sensitivity analysis to estimate the incremental cost per person reoffending and incremental cost per person using class A drugs.
The time horizon for the primary analysis is the 12 months following the index contact with the CJS. The evidence about the relative long-term benefits (in terms of reoffending, drug use and health status) of diversion and aftercare is limited and uncertain. It is also confounded by the type and effectiveness of treatment and aftercare interventions used. In addition, the use of a time frame longer than 1 year for the analysis, with a high level of uncertainty about these outcomes of treatment, may mask the costs, outcomes and uncertainty resulting from the use of the alternative diversion and aftercare packages. The long-term impact (5 and 10 years) is explored in sensitivity analyses (see Sensitivity analysis and key assumptions) and discounted at 3.5% as recommended by the National Institute for Health and Care Excellence (NICE). 102
Data sources
The economic model was intended to synthesise clinical and economic data from the systematic reviews carried out as part of the project, together with that obtained from available databases of observed data. It was anticipated that insufficient data would be obtained from the existing published literature to fully populate the economic model with data on the probabilities of events, UK-specific cost data or with final health-related measures of outcome such as QALYs. Relevant data on outcomes, costs and events were therefore extracted from a range of sources (detailed below) to populate the economic model for the primary analyses. Data from the effectiveness review were used to estimate probabilities of reoffending for the sensitivity analyses to explore the impact of different types of diversion programme.
The Drug Data Warehouse (DDW)103 is a case-linked collection of national data sets relating to substance users in England and Wales between 1 April 2005 and 31 March 2009. It includes data from prison and probation services, criminal justice referral and/or drug testing on arrest schemes, and drug treatment services (England only), with additional linkage to criminal records data from the PNC. The DTORS26,50,104 was a longitudinal, observational, multisite cohort study, recruiting from 342 agencies within 94 Drug Action Teams in England during 2006/7. A cost-effectiveness analysis was carried out alongside DTORS. 42 Additional data sources included UK Home Office reports. 105–107 These were supplemented with unit costs of CJS estimated by the Home Office specifically for the DTORS analysis. 42 Cost data were adjusted to reflect 2012 prices using the annual percentage increase in the Retail Price Index, as recommended by The Green Book. Appraisal and Evaluation in Central Government,108 and accessed via the Office for National Statistics (ONS). 109
Economic model
Population
The population for the model is opiate- and/or crack-using offenders who come into contact with the CJS. Offenders who are already in contact with treatment and aftercare services are included in this population since a proportion will have a new referral via the diversion service. The model for the primary analysis focuses on people who will receive a community-based sentence. This implies that the type of sentence is known before the decision to refer a person via the DIP. The rationale for this is based on the following factors:
-
The majority of substance users report offences that would typically attract a community rather than custodial sentence, such as shoplifting, buying and selling stolen goods, other stealing. 26
-
In the UK, there is no formal link between involvement with DIP and those sentencing options determined by the court, although having sought treatment may impact on the court’s decision.
-
There is a paucity of data with which to estimate the proportions who would receive a community, custodial or no sentence with and without DIP.
However, the Drug Interventions Programme Operational Handbook39 is clear that the decision to use DIP should be made when a person is identified as a substance user at the point of arrest and before the sentence for the offences associated with the index arrest is known. In addition, for a proportion of people committing minor offences, the volume of repeat offending may lead to a custodial sentence. The relative cost-effectiveness of DIP for the broader population of substance user arrestees is explored in the sensitivity analysis. This broader population incorporates the possibility of a prison sentence or no sentence for the offences associated with the index arrest.
Model structure
The cost-effectiveness of diverting drug-misusing offenders into appropriate treatment at arrest, was compared with the usual pathway of such offenders through the CJS was assessed using a decision analytic model. The structure and design of the model was agreed with the wider project group which included experts in offending and drug use research and forensic practitioners.
The model for the primary analysis (community-based sentences) starts with a simple decision tree. This represents the sequence of possible events following an index arrest and decision to manage an offender suspected of substance use by DIP with or without a drug test over a 1-year time horizon. A simplified version of the decision tree is shown diagrammatically in Figures 7 (DIP and treatment pathways) and 8 (subsequent offending pathways) for the 1-year time horizon used in the primary analysis. Appendix 10 presents the full decision tree in tabular format. For the longer time horizons in the sensitivity analyses, subsequent cycles are included using a Markov approach.
FIGURE 7.
Decision tree, year 1. a, DIP and treatment pathways; and b, subsequent offending pathways.

FIGURE 8.
Decision tree, year 1 (continued): subsequent offending pathway.

The tree begins with a square decision node, where a choice is made between the alternative strategies of DIP with or without a drug test or no DIP with or without a drug test. Circular chance nodes indicate a point where a number of subsequent events are possible; these events are assigned a likelihood that they will occur (probability). The design of the tree sets out possible progression through a number of chance nodes from the starting point of an index arrest to the end point of further offence/no offence (within a 1-year time horizon). This design leads to 112 mutually exclusive sequences of events, or pathways (see Appendix 10). Each pathway probability reflects a joint probability, estimated by multiplying probabilities along the pathway. 110 The model does not explicitly include whether or not those entering treatment, or not, achieve abstinence or complete treatment, or not. This is because of a lack of clear indicators of what constitutes a completed treatment episode or what constitutes abstinence or a successful treatment outcome. However, there is evidence that longer times in treatment are associated with reduced substance use, lower levels of offending, lower overall costs and improved health status. Accordingly, the model explicitly includes the impact of treatment entry on new recorded offences. The model also includes time in treatment for the different branches of the pathway for those receiving treatment. The time in treatment is used to estimate the costs of treatment and the health status utilities associated with the different treatment pathways.
For the longer time horizons in the sensitivity analyses, at the start of the second and subsequent cycles, people can be in one of two states: alive or dead. Those alive will fall into one the following categories (Figure 9):
-
substance user
-
not dependent on class A drugs.
FIGURE 9.
Markov states in subsequent cycles for longer time horizons.
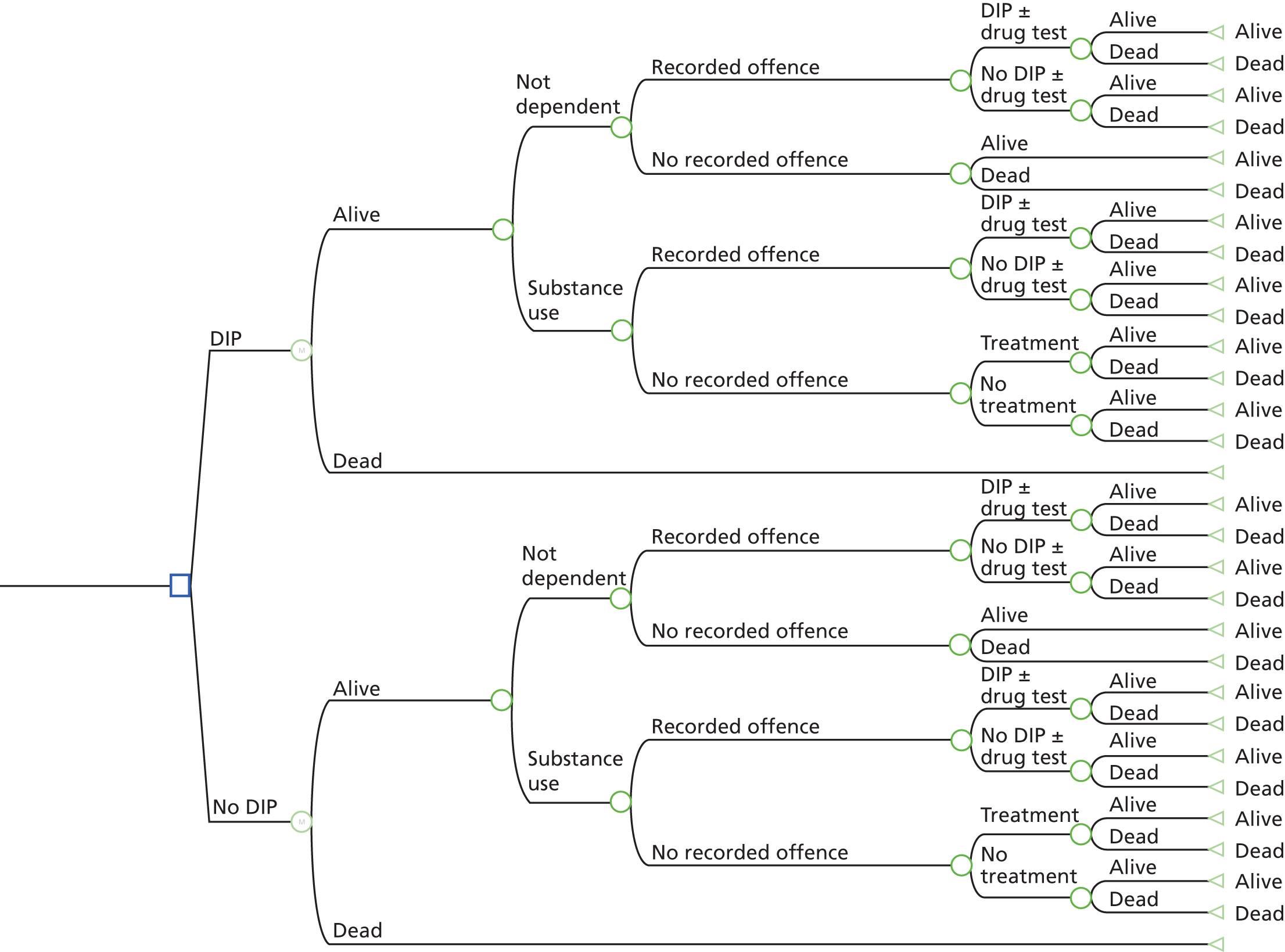
The series of events that occur within a cycle for people with a recorded offence include a chance that the person will be subject to DIP with or without a drug test, or not, and then incur the costs and QALYs associated with the treatment and reoffence pathways in the initial decision tree (see Figures 7 and 8).
Variable estimation
The following categories of data were required to populate the decision model: likelihood of events, resource use and costs, and outcomes. Overall, there were relatively few sources of data to populate the model. The limitations of these are explored in the sensitivity analyses and the implications discussed in Chapter 6.
Likelihood of events
Likelihood of treatment
The probability of treatment assigned to each pathway was estimated using primary data sourced from the DDW. The source sample comprised adult offenders (n = 81,082) who used opiates or crack cocaine on a weekly, or more frequent basis, provided they acknowledged such drug use at a prison and/or probation assessment. A subset of these (n = 35,611) were recorded by the PNC as being arrested for a criminal offence (index arrest), of any type, between 1 April 2005 and 31 March 2007. Participants who were imprisoned between their index arrest and subsequent arrest were excluded. This was to ensure a sample that were in the community, had the opportunity to enter treatment and were at risk of subsequent offending and arrest. The probability of treatment at a branch node is the equivalent of an absolute risk (n of event/n of relevant sample). The decision tree depicts four separate treatment chance nodes (see Figure 7):
-
treatment or no treatment
-
entry into treatment or already in treatment
-
subsequent treatment entry (considered unrelated to the DIP/no DIP decision) or no subsequent treatment entry
-
treatment ongoing or treatment ceased.
Likelihood of offending behaviour
The probability of further offending behaviour assigned to each pathway was also estimated using the prison/probation sample derived from the DDW (described above). Again, it was calculated as the absolute risk (n of event/n of relevant sample) of further recorded offending behaviour within a 1-year time horizon. The decision tree depicts these events as the following decision nodes (see Figure 7):
-
recorded offence or no recorded offence
-
arrest or no arrest
-
technical offence (breach of conditions) or new offence
-
prison or remain in community (probation or bail)
-
probation or no probation
-
new-recorded offence or no new-recorded offence.
Probability distributions
Treatment probabilities and offending probabilities were assigned beta distributions, with parameter approximation utilising estimates of the mean and standard deviation (SD). A series of logistic regressions were used to predict progress through the model based on available covariates in the probation/prison sample. Where low pathway numbers precluded distribution estimation, similar pathways were pooled to obtain probability distributions.
Resource use and costs
Pathway costs include the following:
-
cost of DIP with or without drug test
-
cost of drug test
-
cost of drug treatment
-
costs associated with arrest
-
costs associated with prison
-
costs associated with remaining in the community after arrest and conviction
-
costs associated with subsequent recorded offence.
The offences associated with the index arrest are assumed to be the same whether a person follows the DIP or no DIP pathway. This implies that there will be no difference in the type and costs of community sentences between DIP and no DIP. Accordingly, the costs of the initial sentences are excluded from the primary analysis. The impact of assuming that DIP also has an impact on the type and cost of community sentence at this stage is explored in sensitivity analysis. All unit costs were adjusted to 2012 values using the annual percentage increase in the Retail Price Index, accessed via the ONS. 109 The cost of DIP was derived from unit costs provided by the National Treatment Agency for Substance Misuse (now part of Public Health England). This analysis costed contact per treatment entry via DIP at a range of values from £85 to £213, at 2004/5 prices.
The cost of a drug test was derived from the Home Office report, Evaluation of Drug Testing in the Criminal Justice System. 106 Cost per on-charge drug test across nine UK sites ranged from £44 to £168, with a mean unit cost of £79 (2001 prices). Not all people who receive DIP have a drug test; the unit cost of the drug test was weighted by the probability of having the test, based on actual proportions receiving a drug test in the DDW prison/probation sample.
The average (mean) cost per day of drug treatment was derived from the DTORS cost-effectiveness analysis. 42 The total cost of treatment from triage to second follow-up was divided by the number of days of treatment received from triage to second follow-up, for the DTORS participants who received treatment. This cost per day was then multiplied by the number of days of treatment recorded for the DDW sample.
The costs associated with offending behaviour included:
-
cost of next arrest
-
cost of prison
-
cost of probation
-
cost of subsequent offending.
Unit costs of offending were derived from a Home Office report,107 supplemented by the costs of offences produced for the DTORS study. 42 The unit costs of prison and probation are the average costs per offender, rather than the cost per offender receiving a prison or probation sentence, which is the cost required for the economic model. Published statistics111 reporting the proportion of offenders in prison and serving community-based sentences (community orders and suspended sentences) were applied to estimate the cost per offender sentenced to prison and the cost per offender having probation.
These costs were used to estimate the costs for each individual in the DDW prison/probation sample with an arrest. The arrests were costed by type of offence(s) occurring within a 1-year time horizon of the index arrest. A proportion (27%) of individuals arrested in the DDW prison/probation sample were charged with committing more than one offence. For those people in the DDW prison/probation sample with only one offence, the cost of arrest included the CJS cost of proceedings for that offence. In addition, the wider non-CJS costs of offence were added to the costs of proceedings.
The costs associated with a number of crime types were not available (drugs offences – misuse; drugs offences – supply; fraud and forgery; other indictable offences; and other summary offences). Costs assigned to these categories were estimated using the average CJS unit costs associated with minor crime (theft; theft of vehicle; theft from vehicle; attempted vehicle theft; criminal damage).
For the primary analysis, the costs of subsequent offending were estimated from the model to take into account the uncertainty in the data. For the sensitivity analysis the costs associated with subsequent offending were estimated using the mean total offending costs of arrested individuals in the sample:
Costs associated with the model were assigned gamma (mean and SD) or triangular distributions (best estimate and range).
Outcomes, utility values and quality-adjusted life-years
Utilities assigned to each pathway were derived from the DTORS cost-effectiveness analysis. 42 DTORS participants completed a self-report measure of health (Short Form questionnaire-12 items). 112 This assesses physical function, limitations in role as a result of physical or emotional problems, the effect of pain on normal work and activities, general health, vitality, and the impact of physical or emotional problems on social activities and mental health. 42 Utility weights derived from a general population sample were used to aggregate question responses into a composite measure of health-related quality of life. 113
The data from DTORS were reanalysed to estimate the mean utilities of the index arrest and utility while in treatment. SDs were calculated to estimate distributions for the model.
The DTORS participants were referred from a variety of CJS and non-CJS, not all of which were formal DIP schemes. However, at baseline the reported health status and utility values did not vary between the different forms of CJS referral and referral from other sources (linear regression, p > 0.20). Accordingly, the full DTORS sample who reported offending in the 4 weeks prior to baseline was used to estimate the starting utilities for the DIP with or without drug test pathways. There were differences in the utility values at follow-up and by whether or not the person started treatment. For those who started treatment, utility increased as time in treatment increased. Accordingly, separate utility values were estimated for those who entered treatment and those who did not, which were applied to the treatment and no treatment events in the model. The utility values were multiplied by time spent in the treatment pathways to estimate QALYs for this section of the model.
The DTORS sample was characterised by differences in the utility values of those who reported offending in the 4 weeks prior to follow-up and those who did not. For pathways resulting in treatment and no recorded offence, the utility value was estimated from the DTORS sample completing a follow-up assessment, receiving treatment and not reporting an offence in the previous 4 weeks. QALYs for this section of the model were estimated as 365 days minus time in treatment.
For pathways resulting in treatment and a recorded offence, the utility value was estimated from the DTORS sample who completing a follow-up assessment, had treatment and reported an offence in the previous 4 weeks. It was not possible to estimate utility values from the DTORS data for arrest and subsequent imprisonment or community sentence. For the primary analysis, it was assumed that arrest and imprisonment would reduce health status and utilities to baseline values, but that arrest and community sentence would not. The DTORS sample who reported offending at follow-up were used to estimate the utility values to apply to the model pathways for community sentences. These utility values were applied to the time remaining following treatment, for those who received treatment and had a recorded offence.
Analysis of economic model
A probabilistic sensitivity analysis (PSA) was conducted for the primary analysis and each of the sensitivity analyses. This approach takes into account the uncertainty inherent in each of the estimates of the probability, cost and outcomes associated with the model events and pathways. Monte Carlo simulation with 10,000 iterations was used to estimate the (expected) costs and outcomes for the PSAs. The Monte Carlo simulation samples from the distribution of possible values for each parameter in the decision model. This means that mean costs and outcomes, and measures of variance (SD and 95% CI) can be estimated to assess the uncertainty inherent in the data used for the model.
These simulated data were used for a cost-effectiveness acceptability analysis (CEAA). The CEAA estimated the probability that DIP with or without drug test was cost-effective compared with no DIP with or without drug test. This is an approach recommended by NICE for health technology appraisals. 102 The approach revalues effects or outcomes in monetary terms. However, in the UK there is no universally agreed monetary value for the types of outcome measures used in cost-effectiveness analyses. An approach used in health care is to ask the question: what is the maximum amount decision-makers are willing to pay to gain one unit of outcome? An analysis of decisions made by NICE suggests a range of implicit values between £15,000 and £30,000 for the amount a decision-maker is prepared to pay to gain one QALY. 114
For this analysis, the outcomes were revalued using a range of maximum willingness-to-pay values from £1 to £30,000 to gain one unit of outcome. These reflect a range of hypothetical willingness-to-pay thresholds (WTPTs) from decision-makers being willing to pay £1 to gain a one unit increase in outcome to them being willing to pay £30,000 to gain a one unit increase in outcome. The unit of outcome for the primary analysis was the QALY, the measure used to define the range of hypothetical values implied by NICE decisions. However, some of the sensitivity analyses used alternative measures of outcome, such as reduction in offending. Decision-makers may not be willing to pay the same to gain these other types of outcome measured as they would to gain one QALY.
The data for the cost-effectiveness acceptability curve (CEAC) are derived by first revaluing each of the 10,000 net outcomes from the simulation by a single WTPT. This is repeated for each WTPT. A net benefit (NB) statistic for each pair of simulated net costs and net outcomes for each WTPT can then be calculated as:
where O = net outcome score and C = net cost.
This calculation was repeated for each WTPT. Cost-effectiveness acceptability curves plot the proportion of simulations where the NB of an intervention is greater than zero for each WTPT. 115–118
Sensitivity analysis and key assumptions
One- and multiple-way sensitivity analyses, varying elements of the model structure, time horizons, measures of health benefit, probabilities, cost and utility estimates were used to identify whether or not changes would affect the conclusions of the primary analysis. The costs, effects, incremental cost-effectiveness ratios (ICERs) and CEACs were re-estimated for each sensitivity analysis. PSA was used to assess parameter uncertainty for each of the sensitivity analyses.
A number of simplifying assumptions were used for the primary analysis and these were explored in the sensitivity analyses.
Key assumptions
-
The offences associated with the index arrest are assumed to be the same whether a person follows the DIP or no DIP pathway. This suggests that there will be no difference in the type and costs of community sentences between DIP and no DIP. Accordingly, the costs of the initial sentences are excluded from the primary analysis.
-
The primary analysis focuses on the population of offenders who will receive a community sentence for the offences associated with the index arrest.
-
The primary analysis includes people who are already attending treatment at the index arrest.
-
The primary analysis assigns all DIP and treatment costs at the start of the 1-year time horizon. This assumes that there will be no additional DIP or treatment costs following subsequent offences. The approach gives an accurate estimate of the total DIP costs and community-based treatment for the first year (estimated from the DDW). However, it may underestimate the costs of prison-based treatment services for those who reoffend and receive a prison sentence.
-
For the primary analysis, the probability and costs of recorded offences, arrests, type of offence and whether a person received a prison or community sentence was assumed to be the same for the DIP and no DIP arms of the model. This was based on the assumption that the main effect of a CJS treatment referral was on entry into treatment. A related assumption is that subsequent offending behaviour depended on engagement with treatment and the effectiveness of treatment services. It is also supported by the analysis of DDW data used to estimate parameter values. However, it is important to note that the DDW data may reflect selection biases because of differences in the characteristics of people who received CJS treatment referral via the DIP and those who did not. In addition, it is possible CJS treatment referral also affected the severity of offending behaviour and the CJS and non-CJS costs of offences.
-
Health status and utility was higher after treatment than before. It was also assumed that any gains in utility were maintained after treatment, for those people who did not reoffend. This implies either that there was no relapse or that relapse did not affect health status and utility.
-
People who entered treatment and had a recorded offence after the index arrest did so because treatment was less effective or ineffective at dealing with the drug use problem and, therefore, offending behaviour. Accordingly, the health status and utility of people with a recorded offence following the index arrest was assumed to be lower than during treatment, resulting in lower overall QALYs. In addition, it was assumed that health status after treatment remained higher than that at baseline, for people with a recorded offence.
Chapter 6 Economic model: data inputs and results
Data inputs
The probabilities of events are summarised in Tables 13–15, with the detailed data used to estimate these given in Appendix 10.
| Event | n | Mean (SD) | 95% CI |
|---|---|---|---|
| Treatment | |||
| DIP | 2911 | 0.533 (0.040) | 0.532 to 0.535 |
| No DIP | 32,700 | 0.363 (0.074) | 0.362 to 0.364 |
| Enter treatment | |||
| DIP → treatment | 1573 | 0.371 (0.022) | 0.369 to 0.372 |
| No DIP → treatment | 11,142 | 0.084 (0.008) | 0.0835 to 0.0840 |
| Subsequent treatment | |||
| DIP → no treatment | 1338 | 0.205 (0.076) | 0.199 to 0.210 |
| No DIP → no treatment | 21,558 | 0.115 (0.037) | 0.1146 to 0.1158 |
| Treatment ongoing | |||
| DIP → treatment (enter treatment) | 626 | 0.762 (0.060) | 0.755 to 0.768 |
| DIP → treatment (already in treatment) | 947 | 0.887 (0.024) | 0.885 to 0.889 |
| DIP → no treatment → subsequent treatment | 283 | 0.766 (0.145) | 0.743 to 0.789 |
| No DIP → treatment (enter treatment) | 1063 | 0.771 (0.045) | 0.768 to 0.775 |
| No DIP → treatment (already in treatment) | 10,079 | 0.859 (0.010) | 0.8587 to 0.8591 |
| No DIP → no treatment → subsequent treatment | 2666 | 0.785 (0.018) | 0.784 to 0.786 |
| Event | DIP: probability of recorded offences | No DIP: probability of recorded offences | ||||
|---|---|---|---|---|---|---|
| n | Mean (SD) | 95% CI | n | Mean (SD) | 95% CI | |
| New treatment, ongoing | 466 | 0.823 (0.086) | 0.812 to 0.834 | 807 | 0.848 (0.058) | 0.843 to 0.853 |
| New treatment, ceased | 160 | 0.776 (0.083) | 0.757 to 0.795 | 256 | 0.743 (0.112) | 0.725 to 0.761 |
| Already in treatment, ongoing | 844 | 0.808 (0.079) | 0.801 to 0.815 | 8664 | 0.816 (0.066) | 0.814 to 0.817 |
| Already in treatment, ceased | 103 | 0.672 (0.125) | 0.640 to 0.704 | 1415 | 0.711 (0.080) | 0.706 to 0.716 |
| Subsequent treatment, ongoing | 225 | 0.636 (0.132) | 0.612 to 0.659 | 2051 | 0.611 (0.062) | 0.608 to 0.615 |
| Subsequent treatment, ceased | 58 | 0.500 (0.096) | 0.467 to 0.533 | 615 | 0.487 (0.102) | 0.476 to 0.498 |
| No treatment | 1055 | 0.908 (0.031) | 0.906 to 0.911 | 18,892 | 0.851 (0.059) | 0.849 to 0.852 |
| Event | Range of mean probabilities (detailed data reported in Appendix 10) | |
|---|---|---|
| DIP | No DIP | |
| Arrest for recorded offence | 0.833–0.993 | 0.956–0.983 |
| Technical (breach) offences | 0.117–0.281 | 0.167–0.267 |
| New offences | 0.719–0.883 | 0.733–0.833 |
| Prison, technical offence | 0.036–0.222 | 0.052–0.222 |
| Prison, new offence | 0.231–0.457 | 0.271–0.381 |
| Subsequent offences | 0.400–0.833 | 0.533–0.816 |
The unit costs of DIP, drug test and treatment services are summarised in Table 16. The average time in treatment was estimated for each pathway of the model and is summarised in Appendix 10.
| Service | Average unit cost | Distribution type |
|---|---|---|
| Referral via DIP | 210 (range 108–269) | Triangular |
| Drug test | 111 (SD 54) | Gamma |
| Treatment (per day) | 36 (SD 42) | Gamma |
It was assumed that all people in the DIP arm incurred the cost of the drug intervention programme referral. Overall, the average proportion of people in the DDW sample who had a drug test was 69% of those with a DIP referral and 20% of those who did not have a DIP referral. Table 17 gives the probabilities of drug test used in the model.
| Treatment | DIP | No DIP | ||
|---|---|---|---|---|
| Mean | SD | Mean | Assumed range for triangular distribution | |
| Treatment entry following index arrest or treatment ongoing at time of index arrest | 0.65 | 0.23 | 0.24 | 0.00–0.50 |
| No treatment entry following index arrest or no treatment ongoing at time of index arrest | 0.62 | 0.26 | 0.18 | 0.00–0.40 |
Table 18 presents the unit costs of offences, by type of offence, updated to 2012 prices. The average costs of arrests, offences, prison- and community-based sentences used in the primary analysis are summarised in Table 19. Appendix 10 reports the detailed costs of offences, by model pathway, which were used in the sensitivity analysis. The average costs of subsequent offences for the primary analysis were estimated as £8807 (SD £8133, 95th percentiles £537 to £30,264) and £9902 (SD £6901, 95th percentiles £1445 to £27,240) for the DIP and no DIP arms of the model, respectively. The average costs of subsequent offences for the sensitivity analyses were estimated as £20,720 (SD £26,854) and £22,763 (SD £28,885) for the DIP and no DIP arms of the model, respectively.
| Type of offence | Cost of arrest (£) | Non-CJS cost (£) | Cost of prison (£) | Cost of probation (£) |
|---|---|---|---|---|
| Breach offencesa | 1013 | 51 | 12,182 | 2690 |
| Commercial burglary | 12,370 | 4216 | 19,885 | 9138 |
| Criminal damagea | 1013 | 51 | 12,182 | 2690 |
| Domestic burglary | 11,085 | 2742 | 65,114 | 13,427 |
| Drugs offences – misuse | 6653 | 0 | 66,237 | 5286 |
| Drugs offences – supply | 6653 | 0 | 66,237 | 5286 |
| Forgery | 2335 | 429 | 15,821 | 4787 |
| Fraud | 2335 | 429 | 15,821 | 4787 |
| Health and safetya | 1013 | 51 | 12,182 | 2690 |
| Motoring offencesa | 1013 | 51 | 12,182 | 2690 |
| Obstructing justicea | 1013 | 51 | 12,182 | 2690 |
| Other theft | 6207 | 429 | 42,127 | 3758 |
| Public ordera | 1013 | 51 | 12,182 | 2690 |
| Receiving stolen goods | 1906 | 0 | 15,821 | 4787 |
| Robbery | 29,666 | 6022 | 78,803 | 47,671 |
| Sexual offencesa | 962 | 0 | 12,182 | 2690 |
| Theft from shop | 1972 | 66 | 15,821 | 4787 |
| Theft from person | 6207 | 429 | 42,127 | 3758 |
| Theft from work | 6207 | 429 | 42,127 | 3758 |
| Theft from vehicle | 4157 | 1039 | 22,405 | 3931 |
| Theft of vehicle | 6317 | 5067 | 52,443 | 3494 |
| Violence – ABHb | 25,169 | 1525 | 78,803 | 47,671 |
| Violence – common assaultb | 25,169 | 1525 | 78,803 | 47,671 |
| Violence – GBHb | 25,169 | 1525 | 78,803 | 47,671 |
| Violence – harassmentb | 25,169 | 1525 | 78,803 | 47,671 |
| Violence – seriousb | 25,169 | 1525 | 78,803 | 47,671 |
| Weapons – firearmb | 25,169 | 1525 | 78,803 | 47,671 |
| Weapons – knife and otherb | 25,169 | 1525 | 78,803 | 47,671 |
| Event | Technical offence | New offence | ||||
|---|---|---|---|---|---|---|
| Mean (£) | SD (£) | 95% CI (£) | Mean (£) | SD (£) | 95% CI (£) | |
| Non-CJS cost of offences | ||||||
| Overall | 59 | 28 | 58 to 59 | 865 | 1616 | 843 to 886 |
| DIP | 56 | 28 | 52 to 58 | 791 | 1542 | 720 to 862 |
| No DIP | 59 | 28 | 58 to 60 | 871 | 1623 | 849 to 894 |
| Arrest plus non-CJS cost of offences | ||||||
| Overall | 1021 | 28 | 1020 to 1021 | 7196 | 8405 | 7085 to 7307 |
| DIP | 1018 | 28 | 1015 to 1020 | 6299 | 7362 | 5961 to 6636 |
| No DIP | 1021 | 28 | 1020 to 1022 | 7277 | 8489 | 7160 to 7394 |
| Prison | ||||||
| Overall | 12,182 | All same | All same | 12,239 | 23,430 | 11,930 to 12,549 |
| DIP | 12,182 | All same | All same | 12,362 | 23,186 | 11,298 to 13,425 |
| No DIP | 12,182 | All same | All same | 12,228 | 23,453 | 11,905 to 12,551 |
| Community-based sentence | ||||||
| Overall | 2690 | All same | All same | 7166 | 13,184 | 6992 to 7340 |
| DIP | 2690 | All same | All same | 5560 | 10,250 | 5090 to 6030 |
| No DIP | 2690 | All same | All same | 7311 | 13,409 | 7126 to 7496 |
The utility values used to estimate QALYs are reported in Table 20.
| Event | Mean | SD |
|---|---|---|
| Index arrest | 0.648 | 0.139 |
| Treatment | 0.698 | 0.142 |
| Offended | 0.683 | 0.141 |
| Not offended | 0.713 | 0.142 |
Results
Primary analysis
Table 21 shows the overall expected 1-year cost and QALYs for the DIP and no DIP options considered in the model and the incremental or net costs and QALYs associated with DIP. The cost-effectiveness plane is shown in Figure 10, and Figure 11 presents the CEAC.
| Analysis | DIP | No DIP | ||
|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | |
| Expected cost per person, UK, 2012 | £14,404 | £3116 to £37,559 | £14,551 | £4346 to £33,190 |
| Expected QALYs per person | 0.655 | 0.473 to 0.871 | 0.650 | 0.437 to 0.909 |
| Incremental cost, UK, 2012 | –£147 | –£17,573 to £16,317 | NA | NA |
| Incremental QALYs | 0.005 | –0.057 to 0.065 | NA | NA |
| Incremental cost per QALY gained | No significant differences in costs and QALY | NA | NA | |
FIGURE 10.
Cost-effectiveness plane, primary analysis.

FIGURE 11.
Cost-effectiveness acceptability curve of DIP, primary analysis.
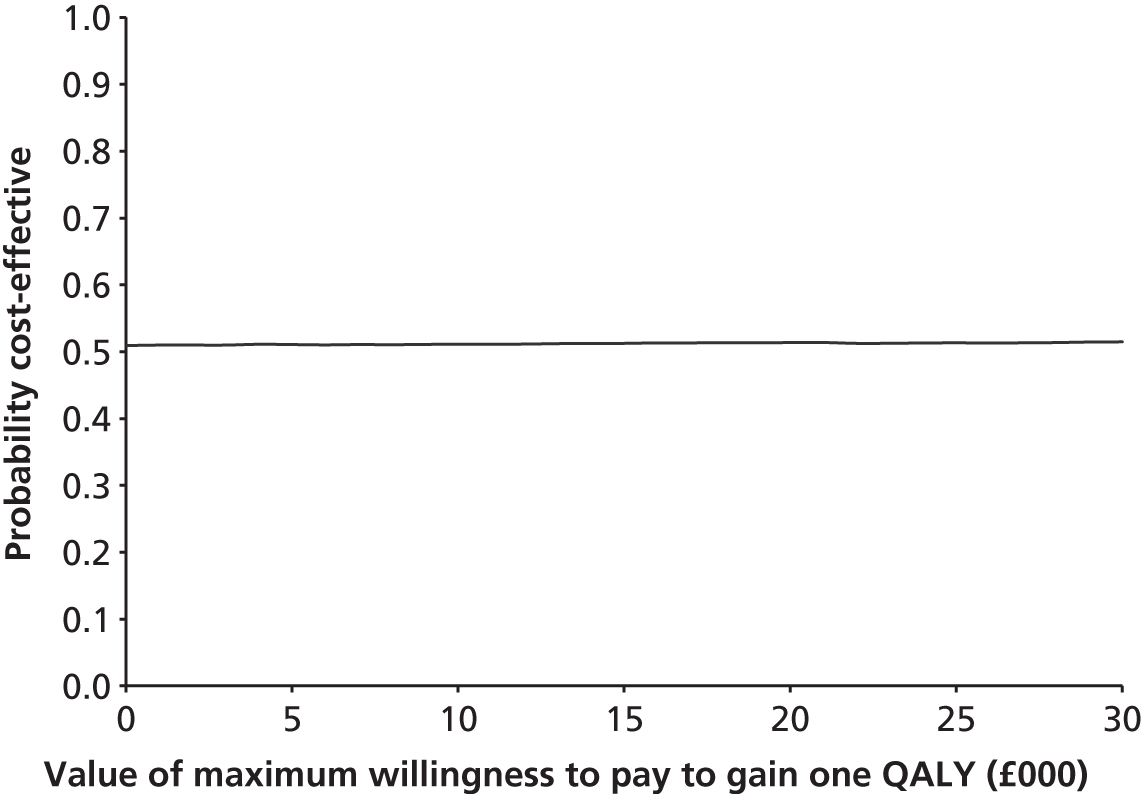
Overall, DIP is associated with net additional savings and a small net QALY. However, the CIs for each of these are wide and cross zero. This suggests that any differences are not statistically significant and could be due to chance. The cost-effectiveness plane shown in Figure 10 indicates that DIP is likely to be associated with similar costs and similar QALYs than no DIP in the majority of the 10,000 simulations run for the analysis.
The CEAC (see Figure 11) suggests that DIP may be cost-effective in around 50% of the simulations. This means that if decision-makers were willing to pay up to £30,000 to gain one additional QALY for arrested drug users to receive DIP, there may be a 50% chance that DIP would be cost-effective. However, this result needs to be treated with caution, as the primary analysis indicates that there is no evidence of a difference in costs or QALYs between DIP and no DIP. Furthermore, limitations with the data and uncertainty about structural aspects of the evaluation mean that it is not clear whether DIP has no impact compared with no DIP or whether or not the evidence is insufficient to identify a difference. The sensitivity analyses explore whether or not changes in key parameters, design choices or the model structure would change the conclusions of the analysis and whether or not there are specific parameters to focus on in further research.
Sensitivity analyses
Table 22 shows the results of key sensitivity analyses to address uncertainty in the sources and methods used to estimate data. Table 23 reports the results of key sensitivity analyses to assess the impact of changes in the model structure and design choices. Only the results where the probability that diversion is cost-effective is < 48% or > 52% are shown. The parameters that were changed for the sensitivity analyses are shown in Appendix 10 together with the results of the sensitivity analyses conducted.
| Analysis | Net cost of DIP, mean (95% CI) | Net QALY of DIP mean (95% CI) | ICER | Net monetary benefit mean (95% CI) | Probability DIP is cost-effective at a WTPT of £30K per QALY |
|---|---|---|---|---|---|
| Probability of treatment following diversion (DIP) is equal to no diversion | –£575 (–£18,206 to £16,526) | 0.002 (–0.028 to 0.033) | No differences | £583 (–£16,623 to £18,163) | 0.54 |
| Probability of treatment ceased is higher and equates to treatment completion, utility of treatment ceased is higher | –£444 (–£18,010 to £16,315) | 0.007 (–0.057 to 0.071) | No differences | £595 (–£15,246 to £18,446) | 0.54 |
| Probability of reoffending is zero following treatment | –£716 (–£14,785 to £12,765) | 0.013 (–0.055 to 0.090) | No differences | £1255 (–£11,828 to £14,612) | 0.57 |
| Probability of treatment following diversion is higher and reoffending is zero following treatment | –£1344 (–£17,886 to £18,817) | 0.035 (–0.133 to 0.221) | No differences | £2383 (–£19,711 to £19,578) | 0.65 |
| Probability of reoffending is lower following diversion (DIP) than no diversion | –£631 (–£18,036 to £15,082) | 0.009 (–0.054 to 0.075) | No differences | £958 (–£15,259 to £17,365) | 0.55 |
| Probability of treatment is higher and reoffending lower following diversion (DIP) | –£376 (–£18,548 to £17,904) | 0.021 (–0.136 to 0.182) | No differences | £1096 (–£16,757 to £20,301) | 0.56 |
| Probability of treatment is higher and reoffending lower following diversion (DIP), treatment leads to higher health status and utility | –£376 (–£18,548 to £17,904) | 0.027 (–0.128 to 0.190) | No differences | £1302 (–£16,121 to £20,434) | 0.57 |
| Cost per day of treatment is 2× higher | £936 (–£16,751 to 18,695) | 0.005 (–0.057 to 0.065) | No differences | –£698 (–£17,757 to £16,650) | 0.46 |
| Probability of treatment following diversion (DIP) is higher and cost per day of treatment is 2× higher | £3559 (–£16,070 to £28,858) | 0.012 (–0.146 to 0.164) | No differences | –£3213 (–£28,935 to £17,117) | 0.39 |
| Probability of treatment following diversion (DIP) is higher, treatment leads to higher health status and utility and cost per day of treatment is 2× higher | £3559 (–£16,070 to £28,858) | 0.016 (–0.141 to 0.169) | No differences | –£3077 (–£28,860 to £17,262) | 0.40 |
| Analysis | Net cost of DIP mean (95% CI) | Net QALY of DIP mean (95% CI) | ICER | Net monetary benefit mean (95% CI) | Probability DIP is cost-effective at a WTPT of £30K per QALY |
|---|---|---|---|---|---|
| Population eligible for diversion (DIP) excludes those already in treatment at index arrest | –£366 (–£17,761 to £16,210) | 0.003 (–0.058 to 0.062) | No differences | £540 (–£16,262 to £16,867) | 0.53 |
| Population eligible for diversion includes people with prison sentence for index arrest equal probability DIP and no DIP | £5974 (–£15,796 to £48,503) | 0.005 (–0.057 to 0.065) | No differences | –£5725 (–£45,636 to £14,256) | 0.38 |
| Population eligible for diversion includes people with prison sentence for index arrest lower probability of prison for DIP | £5100 (–£15,927 to £41,765) | 0.005 (–0.057 to 0.065) | No differences | –£4873 (–£39,613 to £14,260) | 0.39 |
| Population eligible for diversion includes people with prison sentence for index arrest, zero probability of prison for DIP | –£1590 (–£20,578 to £17,491) | 0.005 (–0.057 to 0.065) | No differences | £1676 (–£17,948 to £19,848) | 0.60 |
| Outcome is rate of treatment completers; probability of treatment ceased is higher and equals treatment completion | –£444 (–£18,010 to £16,315) | 0.109 (–0.004 to 0.211) | No differences | £3632 (–£12,298 to £20,389) | 0.70 |
| Outcome is rate of treatment completers; probability of treatment ceased is higher and equals treatment completion | –£444 (–£18,010 to £16,315) | 0.109 (–0.004 to 0.211) | No differences | WTPT = £0, £444 (–£18,010 to £16,315) | 0.52 |
| Outcome is rate of people free from dependency if treated; probability of treatment ceased is higher and equates to treatment completion, assumed free from dependency | –£444 (–£18,010 to £16,315) | 0.075 (–0.004 to 0.153) | No differences | £2739 (–£13,562 to £20,158) | 0.52 |
| Outcome is rate of people free from dependency if treated; probability of treatment ceased is higher and equates to treatment completion, assumed free from dependency | –£444 (–£18,010 to £16,315) | 0.075 (–0.004 to 0.153) | No differences | WTPT = £0, £444 (–£18,010 to £16,315) | 0.65 |
| Outcome is reoffenders averted | –£147 (–£17,573 to £16,317) | 0.03 (0.001 to 0.063) | No differences | £1036 (–£15,297 to £18,657) | 0.56 |
| Outcome is reoffenders averted | –£147 (–£17,573 to £16,317) | 0.03 (0.001 to 0.063) | No differences | WTPT = £0, –£147 (–£17,573 to £16,317) | 0.51 |
| Time horizon = 10 years | –£222 (–£22,232 to £24,635) | 0.005 (–0.311 to 0.314) | No differences | £422 (–£29,019 to £25,584) | 0.53 |
Overall, the sensitivity analysis indicates that there is substantial uncertainty. Although the probability that diversion is cost-effective is > 52% in some cases, the 95% CIs for the net costs, net outcomes and NB statistic are wide and all cross zero.
Summary of economic model analyses
The primary and sensitivity analyses indicate a high level of uncertainty with a high level of variance around the net costs, outcomes and NB statistics. All the analyses demonstrated wide 95th percentiles around the net costs, QALYs and NB statistics. This means that there is a lack of evidence with which to draw conclusions about the cost-effectiveness or otherwise of diversion. This is supported by the use of multiple-way sensitivity analyses to reflect changes in more than one parameter at a time.
Chapter 7 Discussion
Summary of key findings
The main finding is that the available evidence was of poor methodological quality and relevance to the objectives of this systematic review and economic evaluation. The review of the effectiveness literature identified a limited number of aspects where diversion may be effective in the US setting and population. In addition, the economic evaluation highlighted the lack of evidence and high levels of uncertainty about the costs, QALYs and potential value for money of diversion and aftercare in the UK setting.
Key aims of the commissioning brief (that identified the need for this review and economic evaluation) were, first, to achieve a clearer understanding of the elements of diversion and aftercare that contribute most to their effectiveness. Clearly the evidence available is not sufficient to address this aim. A second and closely related aim was to make recommendations for the design of high-quality primary research studies to inform further research and future practice. The process of identification, screening and analysis of studies and data for the effectiveness review and economic evaluation identified key gaps in the evidence. These suggest further research priorities and methods. The key limitations of the evidence are discussed below and form the basis for the research priorities discussed in Chapter 8.
Scope of available effectiveness evidence
The scope of the literature initially identified for inclusion in the review covered nearly 1300 studies that potentially met the inclusion criteria. However, only 16 provided data that were relevant to the population, intervention, control and outcomes specified for the review.
Nearly one-third of the studies identified for possible inclusion (n = 400, 30.8%) were excluded from analysis. This was because it was not possible to identify outcomes specifically for class A drug users, the population of interest for this review. The outcomes evaluated in the review indicated that the type of drug use prior to or at the start of a diversion intervention is important in determining the likely impact of an intervention. The analysis of studies included in the review also highlights the importance of tailoring interventions to the needs of particular user groups. These factors mean that the under-reporting of the characteristics of study participants found in the studies screened is particularly unfortunate. One of the key requirements of effective clinical practice is to be able to identify whether or not a given intervention is appropriate for a particular user group. The current research literature does not facilitate this.
In common with other similar literatures119 an additional problem is the lack of empirical evidence about the impact of the intervention on participants. Nearly half of the available, potentially relevant, studies (n = 627, 48.2%) presented little or no evidence at all of the outcomes of the interventions considered. These 627 studies focused instead on describing an intervention; a narrative evaluation of process, procedures or implementation; or prioritising a discussion of policy-related issues. All of these are, of course, valid contributions to the literature. However, in the absence of an evidence base, they achieve little in terms of the core goal of improving clinical practice and promoting a reduction in drug use and offending.
Evidence of effectiveness
Included studies were of poor methodological quality and characterised by modest sample size, high attrition rate, retrospective data collection, limited follow-up and no random allocation. The majority of studies comprised US methamphetamine users and there was evidence of publication bias in the available literature. Meta-analysis indicated a consistent but small impact of diversion interventions reducing drug use [an OR of 1.68 (95% CI 1.12 to 2.53) for reduced primary drug use and an OR of 2.60 (95% CI 1.70 to 3.98) for reduced use of other (secondary) drugs].
Evidence of cost-effectiveness
A systematic review of the cost-effectiveness of diversion and aftercare for opiate-, crack-, or cocaine-using adult offenders did not identify any relevant studies. The majority of studies identified by the search and screening of abstracts and titles were excluded because they did not meet the criteria for a full economic evaluation. These criteria included a comparison of the diversion intervention with an alternative and a formal comparison of the net costs and benefits (i.e. effectiveness, QALY or monetary measure of participant health and well-being) of diversion in a cost-effectiveness or cost–benefit ratio.
The analyses of the economic model highlighted a lack of evidence for the cost-effectiveness or otherwise of diversion in the UK setting. This was primarily because of high uncertainty in the data estimates. The primary analysis indicated the 95th percentiles for both net cost and net QALYs cross zero, suggesting no statistically significant differences in cost and outcome (net cost –£147, 95th percentiles –£17,573 to £16,317; net QALY 0.005, 95th percentiles –0.057 to 0.065). The wide 95th percentiles of net cost, net outcome and NB for the primary and sensitivity analyses indicate a high level of uncertainty about the parameter estimates used. Furthermore, limitations with the data and uncertainty about structural aspects of the evaluation mean that it is not clear whether or not DIP has no impact compared to no DIP or whether or not the evidence is insufficient to identify a difference.
Strengths and limitations of the assessment
Effectiveness
Methodological limitations
Inclusion of studies was limited to those published post 1985. The rationale for this was that drug courts were first established in 1989 (Miami-Dade County, FL, USA). We included the 4 years prior to this to capture any early pilot work. The bulk of relevant studies identified (n = 14, 87.5%) were published post 2000. The review was comprehensive, i.e. the search string was applied to a wide selection of databases and considerable efforts were made to identify additional relevant material, including checking the reference lists of both excluded and included studies.
The Maryland Scale81 was used to evaluate the quality of studies. Quality assessment is a problematic area, given that issues threatening internal validity can be qualitatively different, thus the standard practice of summing across scale criteria to give a total quality score lacks meaning. The Maryland Scale takes this issue at least partly into account, by assigning levels based primarily on whether or not the design can establish causal associations. Nevertheless, study quality is not appropriately captured by simple quantitative scoring, depending rather on context and, in particular, on the nature of the question being addressed. To address this, we also analysed outcomes by considering individual aspects of study design such as sample size and length of follow-up.
Evidence base limitations
Study design
Included studies were, on the whole, of poor methodological quality, with only four rated highest quality, and even these studies had design flaws such as small sample size,82 high attrition rates86 and retrospective data collection. 85 The main problems with study design were modest sample sizes, retrospective and/or correlational designs, no or limited follow-up beyond the end point of an intervention, no use of either random selection/random allocation of participants and no blinding of raters where more than one group was available for analysis. In addition, the reliability and validity of outcome measures were rarely addressed, i.e. triangulation of key outcome measures against corroborating data and use of ITT analysis were also underutilised. The majority of studies focused on ad-hoc evaluations of pragmatic real-world intervention programmes, it is perhaps not surprising that the design quality of the included studies was variable. None of the studies achieved the gold standard of a RCT and only four studies overall could be regarded as having a relatively strong methodological profile. These latter studies80,82,85,86 focused primarily on SACPA-diverted populations and/or on methamphetamine users, emphasising again the restricted nature of the evidence available.
However, included studies were not of particularly poor quality in comparison with other studies carried out within the CJS. Evidence-based research in the criminal justice context remains in its infancy and many studies commonly cite ethical and practical constraints on the use of RCTs in criminal justice settings. Others in the field have argued that the current lack of high-quality studies capable of providing robust evidence of effectiveness is no longer justifiable. 120 They cite drug courts (the main focus of this review) as a case in point in this context, ‘Internationally, RCTs on restorative justice are setting a new standard that special drugs courts . . . have sidestepped’. 120 Included studies also had an absence of qualitative data. This is particularly unfortunate in a field where the value of such data could perhaps substitute for the ‘gold standard’ requirements of an RCT design. 121 In addition, although the main focus of included studies was offending behaviour by class A drug users, the lack of engagement with participant-oriented outcomes represents a missed opportunity, notably in those studies with a prospective design. Three studies84,88(Fife),88(Glasgow) did provide brief discussion of participant perceptions of interventions, but solely for illustrative purposes. Participant insight into the ‘lived experience’ of interventions is an important aspect of programme evaluation, given the difficulty of achieving and maintaining active participation in this hard-to-engage population.
Generalisability
The 16 studies included serve to identify further gaps in our available evidence base. Although our focus was explicitly on the international literature, 10 of the included studies (62.5%) were US-based, with only four studies (all evaluating pilot DTTO programmes) based in the UK and only two in other locations. This is not an unusual profile for any current literature, but it does significantly restrict the likely generalisability of outcomes. There are different legal and related processes and practices, as well as differences in drug use profiles, between the USA, the UK and other locations internationally.
Although our inclusion criteria were not overly strict (interventions for class A drug-using offenders), the population from which participants were drawn was very limited in scope. Not only were participants primarily recruited in the USA, but experimental groups for nearly one-third of studies (31.2%) were drawn from California. The three UK studies drew their participants from two regions of Scotland (Fife and Glasgow), with one study recruiting from London. The membership of comparator groups is equally restricted, with participants drawn from the same location and either the same treatment programme (but a different referral source) or from offenders placed on probation and receiving no treatment. To put these limitations in context, the polarisation of sample sizes between the US studies and others, results in the fact that nearly all participants included in this review (99.6%) are drug-using offenders diverted to treatment via the California-specific SACPA or their comparators.
This has significant implications for the generalisability of findings.
Participant sociodemographic characteristics
The details presented about participants’ sociodemographic characteristics were limited. However, there was greater diversity in participants’ characteristics, within and between studies than there was in the geographical or treatment setting of the studies.
The age profile of individuals in included studies broadly matches that previously observed for US drug court participants, estimated for US programmes at around 30 years of age. 122 The age of participants was similar within and between studies. There was a maximum of 6 years average difference between groups of participants within any one study. The mean age ranged from 25 years to 39 years between studies. The age profile of the single largest group of participants (US drug court participants) was similar to that for studies focused on other participant groups. Older participants (60+ years) were under-represented in these studies and significant age differences between groups of participants for whom comparisons are drawn are clearly identified for only one study. 84 Since our inclusion criteria placed a lower age limit (18+ years) on participants, it is not possible to evaluate whether or not younger groups are similarly under-represented.
All of the included studies provided details of the gender of their participants. No study focused on women only and three studies did not include women. 83,88(Fife),88(Glasgow),88(combined),90 For those studies including both men and women, the percentage of female participants ranged from 6% to 37%. Averaging across these studies, nearly one-quarter of participants were female (24%).
The ethnicity profile of included studies is representative of drug court membership generally. 123 However, the included studies did not focus as closely on the ethnicity of their participants as on their gender or age. Nearly one-third of studies (n = 5, 31%) made no reference to ethnicity at all, with a further three studies making only passing reference to the inclusion of people from different ethnic backgrounds. For those studies providing at least basic details, the mean proportion of participants from ethnic minorities was slightly over half (51%), indicating an over-representation of ethnic minorities in the research setting in contrast to within the actual population of drug-using offenders. The most commonly represented ethnic groups were black/African-American and Hispanic groups.
Other demographic details available for the included studies are rather sparse. Sociodemographic status was not reported by any study. Economic status was referenced by the majority of studies (n = 11, 69%) in terms of employment status or source of income. Overall, the economic profile of participants was poorly reported in many of the included studies. This is unfortunate since employment is a known factor associated with recidivism in substance abusers. 124 For those studies with comparable information available, the economic profile of participants was overall not as impoverished as might be expected, with over one-third of participants, on average (36%), able to hold down full-time employment, despite their evident drug use and other problems. There is a wide range of employment rates, with studies reporting levels of full-time employment within their participant groups between 4% and 72%.
Education level was also poorly reported by the included studies. Additionally, education profiles were reported in a range of different ways. Overall, the profile presented is of a fairly poorly educated population of participants, although there are some notable exceptions to this in individual studies; Brecht and Urada86 and Chun et al. 82 both included participants with university- or college-level education.
Finally, although offenders125 and drug users126 have high rates of mental and physical problems, the health of participants was poorly described. This means it is not possible to provide an overview of the physical and mental health of participants overall, other than to note that the likelihood is that a substantial proportion of participants suffered, not unexpectedly, from mental and/or physical health difficulties. 125,126
Participant drug use and offending profiles
Profiles of drug use were set out in substantially greater detail for most of the included studies compared with other participant characteristics. The focus on Californian drug courts means there is a bias within the studies towards the evaluation of outcomes for interventions directed at methamphetamine users. Other studies that focused on single drug types evaluated outcomes for heroin and cocaine users. Other than these three primary drugs, participants within experimental groups tended to be described (by 63% of studies) as using either unspecified class A drugs, or as polydrug users with one or more class A drugs included in their drug use pattern. Comparator groups ranged from users of alcohol or cannabis only to other users of class A drugs. For the most part, participants, despite their comparatively young age, had been using drugs for substantive periods of time, with varying degrees of frequency.
In terms of drug use focus, UK-based studies concentrate primarily on heroin and crack use, whereas the vast majority of US studies focus on methamphetamine use. The prominence of methamphetamine use in the US literature may not translate to UK settings where, although prevalence data of methamphetamine use are lacking, use appears to be much less common.
Details about the offending behaviour of participants are surprisingly limited given the focus of all of the included studies on drug-using offenders and only one study91 includes a comparator group of non-offenders. Only four studies (25%) provide specific details of the offences committed by participants in their experimental groups and none provide details for their comparator groups. Partial information is available to give some insight into the profiles of participants in a number of additional studies (e.g. SACPA diversion is only available to non-violent offenders who have committed drugs offences).
Taken together, the available information suggests that non-violent and drug offences are the predominant offence categories overall. However, there is a very broad range of offence severity and frequency recorded both within and between studies. Although the available information does not allow detailed profiling, it is clear that a substantive proportion of participants have a long track record of experience within the CJS (around one-third or more). A greater proportion of participants had prior experience of treatment for their offence-related drug-using behaviour (estimates averaging around a half, dependent on study and group).
Interventions evaluated
The range of studies included was limited in terms of the interventions evaluated. Primarily, we are able to provide information on effectiveness for mainstream or local drug court programmes. The range of interventions evaluated was also surprisingly limited. In line with the US focus of the literature, over half of the included studies (n = 9, 56.2%) evaluated outcomes for programmes linked to drug court diversion. All four UK-based studies evaluated programmes which were the UK equivalent of drug court diversion (DTTOs). While, given our focus on diversion, this is not entirely unexpected, the general tendency for these studies was to focus on the diversion itself (e.g. one-quarter of the included studies evaluated outcomes by contrasting SACPA diverted vs. non-SACPA diverted participants) rather than on the intervention(s) carried out.
There are key differences between diversion in the USA, which is generally court mandated and diversion in the UK, which is primarily based on DIP. In the UK there is no formal link between involvement with DIP (at the point of arrest and before the sentence for the offences associated with the index arrest is known)39 and the sentencing options determined by the court.
The level of detail reported about the interventions was so limited that we were only able to base analyses on very broad characteristics such as whether an intervention provided only day or also residential treatment. The limited information reported confirmed that the interventions evaluated in most of the included studies (n = 13, 81.2%) were ad-hoc multifactorial programmes. These were typically based on existing treatment opportunities available in the local area. Interventions were largely pragmatic (utilising services available in the local area) rather than tailor-made for particular client needs. The remaining three studies either failed to describe the evaluated intervention at all90 or described the intervention(s) in a way which left the actual features of the programme open to broad interpretation,84,87 with the main focus on expectations that participants were asked to satisfy rather than on the treatment opportunities provided to them. Details of the diversion process (e.g. how decisions were made regarding which intervention might be most appropriate for particular individuals) were also few and far between. This lack of information is problematic, leaving outcomes open to wide interpretation about what aspect of treatment has, or has not, worked in a given context. This is particularly an issue where treatment options are diverse in focus or delivery as is the case for the majority of the included studies.
Outcomes measured
Choice of outcome measure, although better described, was also limited in scope and not entirely focused on providing a robust evaluation of core outcomes (reductions in drug use and offending). Treatment completion, for example, was the most commonly reported outcome measure overall (n = 15, 93.7%). While clearly a very important adjunct to any analysis of outcomes, this measure is not itself a direct indicator of the overall success of a programme in reducing drug use or offending, but it was the single outcome presented in greatest detail across the studies. Self-report and scale-based measures of drug use were the primary mechanism for establishing whether or not reductions in drug use had been achieved. Objective evaluation, via urine or other drug screening, was used only in a minority of studies (n = 4, 25%).
For offending behaviour, only half of the studies reported outcomes for offences other than drug offences. The recording of outcomes for offending was also inconsistent between studies (e.g. proportions for general offending not further specified or number with convictions for robbery). This makes a robust analysis of outcomes difficult for both bivariate comparisons and meta-analysis.
Few studies reported on other social, health and well-being outcomes. A noticeable absence from the studies was any assessment of the impact of an intervention on the physical or mental health of participants. None of the studies reported outcomes for longer-term impacts such as hospital admissions or mortality, with only one study82 reporting on changes in medical or psychiatric status and this was only via scale-based evaluation using ASI composite scores. In general, this literature is lacking a focus on participant-oriented outcomes. Future studies incorporating objective (e.g. drug screening), quantitative measures of reductions in drug use and offending, but also in-depth qualitative evaluations of participant perceptions of efficacy and the reasons for success or failure would be of particular benefit to practice.
In addition, an important factor to consider in the evaluation of outcomes is the prior treatment history of participants. A history of failed treatments may, for example, indicate a lack of motivation to change, reducing the likelihood of successful future intervention. 62 In over half of the included studies, no details of prior treatment was recorded.
Implications for bivariate analyses
Despite the small number of included studies and the limitations described above, the statistical data available for analysis were quite substantial, with a total of 106 comparisons available for bivariate analysis. Using additional figures presented in the text of papers describing the included studies, 148 comparisons were available for meta-analysis.
Outcomes for studies taken individually were not, however, overly promising. Few analyses suggested an unambiguous reduction in either drug use or offending as a result of intervention. Exceptions to this were outcomes from one high-quality study,80 which identified a clear reduction in methamphetamine use. This reduction was ratified via drug screening for participants receiving a multifactorial day treatment programme under drug court supervision (MTP matrix programme). Additionally, one lower-quality retrospective chart review study90 reported a reduction in arrests following completion of an unspecified treatment intervention. This was for probationers who used crack/cocaine.
Other statistically significant positive outcomes reported by individual studies were limited by the following:
-
The analyses related to treatment completion only.
-
The reported results were ambiguous about cause and effect. For example, post-hoc analyses of outcomes contrasted participants only on the basis of whether or not they had completed treatment rather than whether they achieved reductions in drug use or offending.
-
The analyses relied purely on self-report or scale-based measures without objective corroboration. To put the latter in context, exactly half of the analyses presented for these studies reported no statistically significant outcomes for the comparisons drawn.
We carried out bivariate comparisons to identify potential subgroups of analyses which might flag positive outcomes for particular groups of participants or indicate which study characteristics (whether in respect of design or other characteristics) might be associated with better outcomes. The bivariate analyses included assessment of the impact of the following on outcomes:
-
study design and quality profiles
-
publication date
-
type of outcome measure
-
data collection source
-
participant demographics, drug use and offending profiles
-
comparisons based on the very broad profile of interventions provided.
Of these characteristics, only one, the source of data collected, emerged as having any statistically significant association with outcome. None of the studies that only used higher-level, non-specific information from existing national or local data sources identified positive outcomes. This indicates that studies using data specific to the programme being evaluated, and in particular purpose-designed data collection methods are more likely to identify a statistically significant impact of the intervention on the outcome measured. It is important to note here that the association is not driven by the larger sample sizes available in the studies using existing, non-specific data sources.
Implications for meta-analyses
Given both the small number of studies and the large and diverse range of analyses presented for these, combining outcomes in meta-analyses to establish whether or not any firm patterns can be observed is of particular importance. We performed a number of initial exploratory meta-analyses to identify studies and outcome measures that were appropriate, conceptually as well as statistically, to include in the combined analyses.
The exploratory meta-analyses identified four robust models that gave further insight into the outcomes of drug use, offending and treatment completion. The first of these found a small but consistent reduction in primary drug use in the intervention group, in contrast to the results from the individual studies. Furthermore, the reductions were greatest for users of other opiates treated via methadone maintenance and for heroin users diverted via SACPA to a multifactorial treatment programme. A second model combined three studies to explore the outcomes of the reduced use of drugs other than the primary drug of choice. This model indicated a consistent and slightly greater impact, again, in favour of the treatment intervention.
The third model explored the impact of intervention on offending behaviour. However, the diverse range of measures used to assess this outcome meant that combining results on this outcome was conceptually meaningless, albeit statistically coherent. This meant that it was not possible to provide any greater insight than if the studies were considered individually. The analysis of the impact of diversion on offending highlights the need for researchers to develop a standardised approach to treatment evaluation. This is particularly important when treatment evaluations (e.g. evaluations of the UK DTTO programmes included in this review) continue to lack the sample sizes needed to identify unambiguous outcomes.
The fourth model to produce meta-analyses of treatment completion identified a clear trend for class A drug users to fail in treatment both more frequently and earlier than non-class A drug-using participants.
The number of studies with data suited to inclusion in individual meta-analyses was too small to allow any in-depth evaluation of potential outcome modifiers. Nonetheless, we were able to draw a more general picture of how participant and study characteristics might impact on outcomes, by combining data relating to the single very broad measure of whether or not an outcome favoured either the intervention itself or the outcomes for class A drug users versus others receiving the same intervention. On the basis of this, admittedly, very broad-brush measure, the study and participant characteristics which made a difference were:
-
Study outcomes focused on the key goals of reducing drug use and/or offending were less likely to result in success while outcomes such as treatment completion were more likely to do so.
-
Choice of outcome measure, with, perhaps surprisingly, studies using self-report measures less likely to report positive outcomes in contrast to studies using objective measures such as drug screening.
-
Study quality, with higher-quality studies more likely to have positive outcomes.
-
SACPA-diverted offenders were less likely to have positive outcomes than participants drawn from other diversion sources.
-
Studies including a higher proportion of females were more likely to report positive outcomes.
-
Studies reporting a higher proportion of participants from ethnic minorities were less likely to report positive outcomes.
These findings are broadly in line with the outcomes of previous evaluations of interventions for drug-using offenders, and argue both for a more careful targeting of interventions and for greater attention to the choice of methodology, outcomes and outcome measures and participants to improve the research evidence available to practice.
Cost-effectiveness
Evidence base limitations
No relevant studies were identified for the cost-effectiveness review. There was an absence of full economic evaluations of diversion/aftercare in the existing evidence base. As was the case with the published evidence screened for the effectiveness review, a proportion of studies were excluded from the review of economic evidence because of their non-reporting of key features, such as drug use details of participants.
Identified partial economic evaluations were screened to assess whether or not data were available to populate the economic model. Although no such data were found, this exercise indicated that US studies dominated the current, limited, economic evidence base. Differences in drug use characteristics and criminal justice policies mean that such economic findings, in the main, have limited generalisability to the UK setting.
Economic model
Strengths and limitations of data sources
The main data source used to populate the economic model for the primary analyses was the DDW. 102 This is a case-linked set of health and criminal justice data sets for around one million substance misusers identified via these sources between 1 April 2005 and 31 March 2009. Case linkage within the DDW was based on a pseudo-unique, minimal identifier. The identifier consisted of an encrypted, anonymised version of case initials, date of birth and gender and, for those cases with CJS contact, an encrypted, anonymised version of their unique PNC Identifier (ID). Pairing of multiple PNC IDs with a single minimal identifier (23% of 284,278 unique minimal identifiers) indicated that more than one individual might share the latter details and case linkage was not undertaken for these cases. Nevertheless, some misclassification may have occurred, although this is unlikely to exert any systematic influence on the analyses reported here.
It is important to emphasise that the DDW contains information about recorded offending, that is offending resulting in a caution, warning, reprimand or a guilty verdict at court rather than the totality of offending behaviour.
The cases identified for potential inclusion in the analyses described here were recorded at prison, or probation, assessment as being weekly, or more frequent, users of opiates or crack cocaine. No additional information about the severity of their drug dependence, or indication of the degree of their treatment need, was recorded. As an observational study, assignment of cases to DIP or non-DIP contact conditions was not random and there exists the possibility that event sequences subsequent to arrest reflect different patterns of severity and/or need.
Analyses are based on a subset of individuals arrested for a recorded offence after April 2005, with those imprisoned between the first such offence and the end of follow-up excluded. This was necessary, in order to ensure that the cohort remained at large in the community with the opportunity to offend again. However, exclusion of imprisoned cases may have introduced bias as those excluded because of imprisonment may exhibit the most serious offending patterns. However, the economic model was designed to examine diversion occurring in non-prison settings. Sensitivity analyses indicated that including those who receive a prison sentence for the index arrest in the model, may make diversion less cost-effective. This is as a result of the higher costs assigned to people in the diversion arm, on the assumption that those imprisoned would incur additional in-prison treatment costs, compared with those in the no diversion group.
Analyses examined the sequence of events following the first recorded offence for each case during the study period (index arrest). In the absence of definitive data, events were linked according to operational definitions based on their temporal proximity. Most (75%) DIP contacts occurred within ±7 days of the charge date for the index arrest. Where treatment contact was initiated within 28 days of a DIP contact linked to the index arrest it was assumed that treatment had arisen as a consequence of that DIP contact. Eighty-five per cent of such treatment contacts occurred within 14 days of the DIP contact. As the majority of events occurred in a shorter time frame than required by operational definitions, it is likely that the operational definitions were reasonably sensitive. This may have been at the expense of some degree of specificity, although the operational definition for treatment arising from DIP contact was much stricter than the 12-week period used in other UK studies. 44
It is important to note that the analysis of DDW data did not take account of cases censored due to death: ongoing analysis of the DDW opiate- and/or crack-using cohort suggests that we should expect that around 250 cases might have died during the 1-year follow-up. Death was not included in the 1-year time frame for the primary analysis, but was included in the sensitivity analyses and the analyses of longer time frames. These included alternative assumptions about whether the death rate in the diversion group was the same or lower than that in the non-DIP group.
The analysis of the DDW data to estimate model parameters indicated a high level of variance. There was little evidence of differences in the probabilities and costs of recorded offences and sentences following the index arrest. These may account for the high uncertainty in the model. However, the sensitivity analyses explored the impact of diversion having a greater impact on the costs and QALYs of drug-using offenders. Despite this, the analyses indicated high levels of uncertainty.
Overall, the sensitivity analyses that included PSA to explore the impact of data on the results suggested that the conclusions do not differ from those of the primary analyses. Key exceptions to this are for the level of reoffending and subsequent substance use. Deterministic analyses support this finding. However, the deterministic analyses found no clear evidence that changes in the value of other parameters substantially changed the net costs and QALYs of the primary analysis.
Methodological limitations
There are key methodological limitations associated with the economic model, in addition to the data issues discussed above. First, the model structure is a simplification of events which required a number of assumptions. These mean that there is inherent uncertainty in the pathways used for the model. The structure used for the analyses with a 1-year time horizon is restricted in terms of the population and sequence of events. The discussion below highlights the impact model structure and design choices have on the results found in the sensitivity analyses.
The model does not explicitly include whether or not those entering treatment achieve abstinence or complete treatment. This is because of a lack of clear indicators of what constitutes a completed treatment episode or what constitutes abstinence or a successful treatment outcome. However, there is evidence that longer times in treatment are associated with reduced substance use, lower levels of offending, lower overall costs and improved health status. Accordingly, the model explicitly includes the impact of treatment entry on new recorded offences. The model also includes time in treatment for the different branches of the pathway for those receiving treatment. The time in treatment is used to estimate the costs of treatment and the health status utilities associated with the different treatment pathways.
In addition, the sensitivity analyses indicate that the results are unlikely to change substantially if it is assumed that treatment cessation equates to treatment completion and higher rates of treatment completion are used. The longer-term analyses do include the probability that a person is not dependent on class A drugs. However, there were limited data to estimate the probabilities of this, with wide ranges used to estimate the distribution. Additionally, there is no evidence about the differences in offending between those who are no longer dependent on drugs and those who continue to be substance users.
The model structure is sequential and does not allow for multiple reoffending or relapse rates. Multiple reoffending is accounted for by the analysis of data from the DDW to estimate probabilities and costs of reoffending, which includes all recorded offences. The primary analysis focuses on the population of offenders who will receive a community sentence for the offences associated with the index arrest. The offences associated with the index arrest are assumed to be the same whether a person follows the diversion or no diversion pathway, suggesting that there will be no difference in the type and costs of community sentences between diversion and no diversion. The impact of relaxing this assumption indicated that the probability diversion is cost-effective is lower at around 40%. However, the 95% CIs indicate wide variation and uncertainty.
The primary analysis includes people who are already attending treatment at the index arrest. Excluding this group from the analysis does not appear to impact on the results.
The primary analysis assigns all DIP and treatment costs at the start of the 1-year time horizon. It is assumed that there will be no additional DIP or treatment costs following subsequent offences. This gives an accurate estimate of the total DIP costs and community-based treatment for the first year (estimated from the DDW). However, it may underestimate the costs of prison-based treatment services for those who reoffend and receive a prison sentence. Increasing the costs of prison sentences did not change the overall results of the analysis.
For the primary analysis, the probability and costs of recorded offences, arrests, type of offence and whether a person received a prison or community sentence was assumed to be the same for the DIP and no DIP arms of the model. This was based on the assumption that the main effect of a CJS treatment referral was on entry into treatment. A linked assumption is that subsequent offending behaviour depended on engagement with treatment and the effectiveness of treatment services. It is possible CJS treatment referral also affected the severity of offending behaviour and the CJS and non-CJS costs of offences. This was tested in sensitivity analysis using detailed data from the DDW. However, it is important to note that the DDW data may reflect selection biases. These biases could be due to differences in the characteristics of people who received CJS treatment referral via the DIP and those who did not. However, as with many of the sensitivity analyses, using estimates of the probability and costs of recorded offences, arrests, type of offence and whether a person received a prison or community sentence that favour diversion did not improve the likelihood that it is cost-effective or substantially reduce the uncertainty in the data.
Health status and utility were higher after treatment than before. It was also assumed that any gains in utility were maintained after treatment for those people who did not reoffend. This implies either that there was no relapse or that relapse did not affect health status and utility. The impact of lower utility values following treatment was explored in the sensitivity analysis. People who entered treatment and had a recorded offence after the index arrest did so because treatment was less effective or ineffective at dealing with the drug use problem and, therefore, offending behaviour. Accordingly, the health status and utility of people with a recorded offence following the index arrest was assumed to be lower than during treatment, resulting in lower overall QALYs. This assumption was tested by keeping health status and utility at the same level after a recorded offence. In addition, it was assumed that health status after treatment remained higher than that at baseline, for people with a recorded offence. This was tested by re-estimating the model with lower levels of utility attached to the pathways with a recorded offence after treatment. The estimates of the relative cost-effectiveness of diversion were not substantially altered by the sensitivity analyses of these variables.
Chapter 8 Conclusions
Research on offenders in the community, in general, is sparse as efforts tend to be focused on those in prison. Although it is possible, it is perceived to be difficult to conduct a RCT of offenders in the community. This has contributed to the lack of studies within the community and, therefore, the lack of studies found by this research.
Although diversionary schemes continue to be a strategic focus for policy in relation to tackling problems of drug misuse, the evidence base for the effectiveness of these schemes is not in place. The review reported here demonstrates the paucity of studies able to predict or reflect the likelihood of the effectiveness of diversionary schemes within the English drug treatment model and population. Indeed, no single study was identified that demonstrates sufficient quality for the English drug treatment population, neither for the offending drug-using population or the CJS diversionary schemes that target them. Three of the four higher-quality studies identified, concentrated on methamphetamine users who account for only 0.1 per cent of the English treatment population. 80,85,86
The search for economic evaluations also identified no relevant studies, further exemplifying the inability of existing research to inform the English situation. As a result, this evaluation relied solely on bespoke analysis of data sets pertinent to the study population. The primary economic analysis, supported by sensitivity models, indicated that even if £30k was spent to achieve one additional QALY, DIP would be cost-effective in no more than half of cases. Furthermore, it could also be argued that the model applied the minimal level of DIP costs, specifically the cost of referral into treatment only, thereby over-estimating the cost-effectiveness of DIP.
Currently, there is not sufficient evidence to demonstrate whether or not diversionary schemes within England provide robust levels of benefit for their clients in a cost-effective manner. It is important to note that similarly, there is no evidence that diversion interventions are not effective or cost-effective.
Implications for service provision
The findings from this body of work suggest that it is unclear whether or not diversion or aftercare will improve the outcomes for patients with class A drug use. This is because of a range of methodological limitations in the studies included in the systematic review. In particular, the majority of studies are of diversion services in the USA. The data are limited by heterogeneity and an absence of randomisation making firm conclusions more uncertain. There is some evidence from other sources that treatment for substance misuse and addiction to class A drugs may work in the community,103,127,128 and that treatment for opioid dependence in prison may also be effective,129 although the costs of treatment in prison, compared with the community, are substantially higher. Further research into drug treatment via diversionary programmes, such as DIP, using robust design and methodology is required.
The implementation of the government’s Transforming Rehabilitation (TR) agenda also emphasises the need to focus on providing evidence of effectiveness and cost-effectiveness of diversionary schemes. DIP involves multiagency inputs from organisations that are funded by contracts that will be affected by TR. As payment by results becomes the focus of these contracts, service providers will be likely to focus their resources only on schemes that have been shown to be effective and for which there is evidence that they could support the achievement of the results they are being paid for.
Suggestions for research priorities
The low quality and relevance of the existing evidence base identified by the effectiveness and economic reviews, coupled with the high level of uncertainty inherent in the economic evaluation represents an important outcome of this research programme. These clearly highlight the need for high-quality, UK-based studies. The review and economic evaluation identified a number of methodological limitations of the existing evidence, which are discussed in detail in Chapter 7. New research is needed to address these issues and evaluate diversion and aftercare programmes. There are different biological mechanisms associated with the range of drugs included in the class A category. There are also differences between the drugs in the reasons for, and patterns of, their use. The reasons for, and patterns of, non-drug-related offences may also differ. Future research would have more relevance to UK diversion populations if it were to focus on clients with problematic use of opiates and/or crack cocaine use rather than all drugs contained within the class A drug category. In the UK setting whether or not further differentiation is necessary will depend on the setting and intervention evaluated. For example, DIP and CJS drug testing on arrest does not distinguish crack from cocaine.
There is a need for further research in populations outside of the USA and, specifically, the UK population. The analyses presented in the review suggested two specific subpopulations of interest: women and older drug-using offenders (≥ 50 years of age). There is also a need for development and evaluation of interventions other than drug courts, particularly of purpose-designed, rather than ad-hoc, interventions.
Diversion and aftercare programmes display many of the characteristics of a complex intervention. The systematic review and economic evaluation have highlighted that they are multifactorial with the potential for each component to have an independent effect on outcome. In addition, there is the potential for one or more components to mediate or modify the impact of other components on outcome. There are a range of important and inter-related outcomes that are relevant to differing levels to participants, service providers and policy-makers. The Medical Research Council guidance for the development and evaluation of complex interventions suggests the following key elements are needed:130
-
Development of interventions using best evidence and theory.
-
Phased evaluation of the intervention starting with studies to test the acceptability and feasibility of implementing the interventions, the acceptability and feasibility of alternative evaluation designs and procedures, to develop and assess methods of recruitment and retention of participants, and to estimate sample size. These are required prior to exploratory and definitive trials of effectiveness and cost-effectiveness.
-
Implementation, monitoring and surveillance of the intervention.
Development and standardisation of interventions
The systematic review highlighted that there are a number of inter-related components in the way in which drug-using offenders are identified, diverted into treatment, as well as in the treatment provided. In particular, the effectiveness of any diversion scheme in reducing drug use and/or offending is reliant on the effectiveness of the treatment package a person is diverted into. Additionally, there is variation in drug-using offenders in terms of the level and duration of offending, type of drug use and reasons for drug use and offending that indicate potential differences in behaviour and the effectiveness of both diversion and subsequent treatment.
The studies included in the review were typically ad-hoc evaluations of existing interventions, which were inadequately described. While this has many benefits in terms of evaluating real-life practice, the rationale for the intervention (e.g. theoretical models of causation) and understanding of the mode of action is unclear.
Research is needed to identify and develop the theoretical basis for diversion as an intervention to reduce drug use and/or related offending and to identify whether or not there is likely to be a need for the diversion and treatment programme to be tailored for different groups of drug-using offenders. For example, is it likely that different approaches may be needed for people who had a history of offending prior to drug use compared to those who were drug users and offend as a result of drug use. Alternatively, different diversion strategies and treatment may depend on the profile of primary and secondary drug use. This information can be used to develop/refine standardised and manualised diversion interventions for prospective evaluation of effectiveness and cost-effectiveness.
An important finding of this review was that the included evaluations did not include assessment of the acceptability and feasibility of the interventions. In addition, it is not clear what proportion of drug-using offenders will receive a DIP assessment/drug test. The estimate used for the sensitivity analysis was 14%, but this was based on expert opinion. National statistics suggest that 57,000 people arrested had a formal DIP assessment in 2009. However, it is unclear how many people arrested were eligible for a DIP assessment, with or without drug testing. In addition, the proportion of treatment referrals from DIP is approximately 13% of all referrals and 30% of new referrals. There may be a number of reasons why DIP is, or is not, used and evidence about these issues is required.
Research is needed to assess the scale of use and acceptability of diversion interventions and identify barriers and facilitators of implementation in the CJS setting. This needs to consider the perspectives of the drug user and those responsible for implementing a diversion intervention. Insight into the lived experience of diversion interventions is an important aspect of programme evaluation, particularly given the difficulty of achieving and maintaining active participation in this hard to engage population.
Key methods to address research priorities 1 and 2 include best evidence reviews of the qualitative, quantitative and mixed-methods literature about the development and process of diversion (this systematic review excluded over 600 papers concerned with a narrative evaluation of process, procedures or implementation; or prioritising a discussion of policy-related issues). This may also need to include (1) elements of realist review methods to map relevant theories and models underlying diversion programmes to evidence of their effectiveness; (2) interviews and focus groups with stakeholders (e.g. drug-using offenders and staff in the CJS and drug treatment services as well as staff in related health and social care services); and (3) review and analysis of documentary evidence of local and national policies and procedures, existing diversion and national treatment databases to identify the processes and mechanisms which facilitate or hinder the implementation of diversion programmes. For example, the NDTMS now provides the capacity for long-term follow-up of treatment access and outcomes among those contacted by diversionary schemes.
Development of core outcome set
This review highlighted the diversity of outcomes and measurement methods used to evaluate the effectiveness of diversion and the difficulties this raises for meaningful meta-analysis of study outcomes. Another key finding is that existing studies typically focus on a limited range of outcomes of diversion programmes, mainly centred around treatment completion. The impact of diversion on offending (drug and non-drug offences), changes in drug-using behaviour or abstinence was not consistently evaluated, and the impact on participant health and well-being or broader social benefits was not included in the studies reviewed. The economic evaluation highlighted a lack of evaluation of health status and use of measures to estimate health-related utility and QALYs. The latter are currently the measure preferred by NICE for health technology assessments. However, whether or not they are appropriate measures of outcome for evaluations of the effectiveness and cost-effectiveness of diversion is an area where further research is required. 131
Work is needed to establish an agreed set of standardised outcomes that are relevant to study participants, those who provide diversion services and policy-makers. Instruments to measure these outcomes that are valid, reliable, acceptable and feasible to use also need to be identified/developed. Work is needed to assess whether or not the QALY is an appropriate outcome measure in this setting, and explore or develop alternatives for economic evaluation.
Key stages and methods include:
-
Qualitative research with stakeholders to identify the range of relevant outcomes. The stakeholders include drug-using offenders and family/carers; professionals in relevant CJS, treatment health and social care services; researchers/experts; and policy-makers.
-
Review of existing literature to identify any additional outcomes and supplement the list developed from the qualitative research.
-
Formal methods such as Delphi surveys and consensus meetings with stakeholders to agree and validate the content of the core outcome set.
-
A systematic literature review to identify outcome measures and assess the properties of those instruments for inclusion in the core outcome set.
-
Stated preference surveys to assess the preferences and priorities of key decision-makers (service users, carers, health care professionals and policy-makers) for the core outcomes identified in stages 1–3.
Evaluation of specific interventions
The systematic review and economic evaluation indicated that the evidence from published evaluations of effectiveness, cost-effectiveness and existing secondary data in the UK is uncertain. This is as a result of the low methodological quality of the studies included in the review. There were also differences between the US and UK settings, which means that the relevance of much of the evidence to the UK was unclear. The available data from secondary sources in the UK were collected for different purposes. This means that they do not include key measures to estimate the service use and outcomes of events related to diversion or to control for biases in the data. An implication is that further research may be needed to evaluate the effectiveness and cost-effectiveness of diversion programmes in the UK CJS and treatment settings, and in the UK drug-using population. Whether or not further evaluation is required, and what interventions are assessed, will depend to some extent on the outcomes of the research outlined above. This will also determine the extent of the feasibility and pilot work (described in research priorities 4 and 5 below) required. In general, it is important that the work below includes accurate recording of the drug-use profile of participants; the intervention(s) and its component parts and the characteristics of participants. Important aspects of the latter include ethnicity, sociodemographic profile, educational level, mental health status and prior and current offending behaviour.
If new interventions are defined or existing models of diversion are substantially changed from current practice, mixed-method evaluations are required to qualitatively and quantitatively assess the feasibility of implementing the diversion interventions; barriers and facilitators to implementation; likely compliance and the acceptability of these to drug-using offenders and staff.
The review highlighted the fact that evidence-based research in the criminal justice context remains in its infancy and many studies cited ethical and practical constraints on the use of RCTs in criminal justice settings. However, others in the field have argued that the current lack of high-quality studies capable of providing robust evidence of effectiveness is no longer justifiable. 120 The evidence considered in this review and economic evaluation suggests that a RCT is likely to be necessary to identify potentially small, but important and relevant, effects of the intervention that may take some time to occur following diversion. In addition, there are likely to be important effects of selection, allocation and unobservable biases.
Mixed-methods research is needed to qualitatively and quantitatively assess the feasibility and acceptability of a RCT of diversion interventions, to all stakeholders. The research should also identify key confounders, biases and barriers to evaluation and any barriers and facilitators to the recruitment and retention of study centres, staff and participants. A comparison of the specific strengths and weaknesses of alternative designs to evaluate diversion interventions in the UK setting is an important component of this stage. A major aim of this research would be to inform the design of the full RCT/controlled non-randomised evaluation of effectiveness and cost-effectiveness.
Research priority 5bPilot and/or small exploratory trials are required to test the study design for a full, definitive trial. The main objectives for these trials include assessment of methods to recruit and retain study centres, staff and participants; document likely dropout rates; explore reasons for non-compliance with the study protocol and/or interventions; the feasibility and acceptability of data collection methods and instruments to measure outcomes and service use.
Limitations of the existing evidence may in part be due to the fact that they were ad hoc evaluations of existing interventions, which in some cases made use of existing higher-level data. There was inadequate description of the following:
-
participant samples and the target population
-
recruitment and selection procedures
-
the components of the diversion interventions and any comparators and the rationale for their selection
-
whether or not there was sufficient sample size to give the power to detect statistically significant and important differences in effectiveness.
In addition, it was unclear whether or not there was adequate follow-up post intervention to identify the impact of diversion on subsequent treatment, reoffending and substance use. These factors were identified in the economic evaluation as potentially important influences on the costs and outcomes of DIP. Finally, triangulation of key outcome measures against corroborating data is needed to assess the reliability and validity of outcome measures and process evaluation to assess procedures and explore the experience of participants.
Full definitive RCTs/controlled, integrated effectiveness and cost-effectiveness evaluations are needed in the UK setting. The design of the trials should address the methodological limitations of the existing evidence base, identified in this review and economic evaluation. The target population and participant sample, the intervention and comparator, and the outcomes and measures need to be clearly described and analysed. The design of the evaluation needs to be evidence based. Unless there is sufficient information in the evidence excluded from this review, it is likely that the prior work identified in research priorities 1–5 will be needed to inform the design of the trial. The length of follow-up needs to be sufficient to identify the impact of the diversion intervention on the likelihood that the participant receives and completes treatment and whether or not they reoffend.
Acknowledgements
We would like to express our thanks to the following people who provided essential support to the project: Vanessa Haves, Naomi Humber, Heather Noga and Louise Robinson.
Contribution of authors
Karen P Hayhurst (Research Fellow) was responsible for developing and undertaking electronic literature searches for the economic systematic review, acquisition of data, analysis and interpretation of data for the economic analysis, economic model construction, and drafting and revision of the final report.
Maria Leitner (Research Director) co-ordinated the effectiveness systematic review, was responsible for the acquisition of data, analysis and interpretation of data for the effectiveness systematic review, including statistical analysis and meta-analysis, and drafting and revision of the final report.
Linda Davies (Professor of Health Economics) was responsible for the design and supervision of the economic review, supervision of economic model construction, economic analysis, and drafting and revision of the final report.
Rachel Flentje (Research Associate) and Carlene King (Research Associate) were responsible for the acquisition of data, analysis and interpretation of data for the clinical effectiveness systematic review, and drafting and revision of the final report.
Tim Millar (Senior Research Fellow) was responsible for the design and management of secondary data analysis, acquisition of data, analysis and interpretation of data for the economic analysis, and drafting and revision of the final report.
Andrew Jones (Research Fellow) was responsible for secondary data analysis, and drafting and revision of the final report.
Michael Donmall (Reader), Michael Farrell (Professor of Addiction Psychiatry) and Matthew Hickman (Professor of Public Health and Epidemiology) provided interpretation of the findings from the drug treatment perspective and in terms of the epidemiology of drug misuse.
Seena Fazel (Forensic Psychiatrist) and Soraya Mayet (Consultant Psychiatrist) provided systematic review expertise and interpretation of study findings from a clinical perspective.
Rochelle Harris (Research Manager of Probation Service) provided interpretation of study findings from the service provision perspective.
Charlotte Lennox (Research Associate) was responsible for drafting and revision of the final report.
Jane Senior (Research Manager) provided project management support to the study.
Jennifer Shaw (Professor of Forensic Psychiatry) was responsible for conception and scientific design, and drafting and revision of the final report.
All co-authors critically reviewed the study methods and draft versions of the report and took part in its production.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Misuse of Drugs Act 1971: Elizabeth II. Chapter 38. London: The Stationery Office; 1971.
- Drug Misuse. Findings from the 2012 to 2013 Crime Survey for England and Wales. London: Home Office; 2013.
- Statistics from the National Drug Treatment Monitoring System (NDTMS) 1 April 2011–31 March 2012. London: NTA; 2012.
- Hay G, Rael dos Santos A, Millar T. Estimates of the Prevalence of Opiate Use and/or Crack Cocaine Use, 2010/11: Sweep 7 Report. London: National Treatment Agency for Substance Misuse; 2013.
- European Drug Report. Trends and Development. Lisbon: EMCDDA; 2013.
- Drug Misuse Statistics for Six Months Ending September 1996. London: DH; 1998.
- Statistics from the National Drug Treatment Monitoring System (NDTMS) 1 April 2010–31 March 2011. London: NTA; 2012.
- Bennett T, Holloway K, Williams T. Drug Use and Offending: Summary Results from the First Year of the New-Adam Research Programme. London: Home Office Research, Development & Statistics Directorate; 2001.
- Holloway K, Bennett T. The Results of the First Two Years of the NEW-ADAM Programme. London: Home Office; 2004.
- Prisons and Drugs in Europe: the Problem and Responses. Selected Issue 2012. Lisbon: EMCDDA; 2012.
- Gordon L, Tinsley L, Godfrey C, Parrott S, Singleton N, Murray R, et al. Measuring Different Aspects of Problem Drug Use: Methodological Developments. London: Home Office; 2006.
- Oerton J, Hunter G, Hickman M, Morgan D, Turnbull P, Kothari G, et al. Arrest Referral in London police stations: characteristics of the first year. A key point of intervention for drug users?. Drugs: Educ Prev Policy 2003;10:73-85. http://dx.doi.org/10.1080/0968763021000040914.
- Millar T, Beatty S, Jones A, Donmall M. Outcome of Arrest Referral: Treatment Uptake, Treatment Retention and Behaviour Change Amongst Drug Misusing Offenders Referred for Drug Treatment. London: Research report for the Home Office Research, Development and Statistics Directorate; 2002.
- Sondhi A, O’Shea J, Williams T. Arrest Referral: Emerging Findings from The National Monitoring & Evaluation Programme. London: Home Office Drugs Prevention Advisory Service; 2002.
- Stewart D, Gossop M, Marsden J, Rolfe A. Drug misuse and acquisitive crime among clients recruited to the National Treatment Outcomes Research Study (NTORS). Crim Behav Ment Health 2000;10:10-2. http://dx.doi.org/10.1002/cbm.339.
- Boreham R, Cronberg A, Dollin L, Pudney S. The Arrestee Survey 2003–2006. London: Home Office; 2007.
- A Fresh Approach to Drugs. London: UKDPC; 2012.
- Boyum DA, Kleiman MAR, Wilson JQ, Petersilia J. Crime: Public Policies for Crime Control. Oakland, CA: Institute for Contemporary Studies Press; 2002.
- White HR, Gorman DM. Criminal Justice 2000 Volume 1. The Nature of Crime: Continuity and Change. Washington, DC: US Department of Justice; 2000.
- Best D, Sidwell C, Gossop M, Harris J, Strang J. Crime and expenditure amongst polydrug misusers seeking treatment. Br J Criminol 2001;41:119-26. http://dx.doi.org/10.1093/bjc/41.1.119.
- Buchanan J. Drug policy under New Labour 1997–2010: prolonging the war on drugs. Probation J 2010;57:250-62. http://dx.doi.org/10.1177/0264550510373809.
- Hammersley R. Drugs and Crime. Cambridge: Polity Press; 2008.
- Seddon T. Explaining the drug-crime link: theoretical, policy and research issues. J Soc Policy 2000;29:95-107. http://dx.doi.org/10.1017/S0047279400005833.
- Pudney S. The Road to Ruin? Sequences of Initiation into Drug Use and Offending by Young People in Britain. London: Home Office; 2002.
- Edmunds M, May T, Hearnden I, Hough M. Arrest Referral. Emerging Lessons from Research. London: Home Office; 1998.
- Donmall M, Jones A, Weston S, Davies L, Hayhurst KP, Millar T. The Drug Treatment Outcomes Research Study (DTORS): research design and baseline data. Open Addiction J 2012;5:1-11. http://dx.doi.org/10.2174/1874941001205010001.
- Hayhurst KP, Jones A, Millar T, Pierce M, Davies L, Weston S, et al. Drug spend and acquisitive offending by substance misusers. Drug Alcohol Depend 2013;130:24-9. http://dx.doi.org/10.1016/j.drugalcdep.2012.10.007.
- Comiskey CM, Kelly P, Leckey Y, McCulloch L, O’Duill B, Stapleton RD, et al. The ROSIE Study. Drug Treatment Outcomes in Ireland. Dublin: National Advisory Committee on Drugs; 2009.
- Cox GM, Comiskey CM. Does concurrent cocaine use compromise 1-year treatment outcomes for opiate users?. Subst Use Misuse 2011;46:1206-16. http://dx.doi.org/10.3109/10826084.2010.501649.
- Drug-Misusing Offenders: Results from the 2009 Cohort for England and Wales. London: Home Office; 2010.
- Bennett T, Holloway K. The association between multiple drug misuse and crime. Int J Offender Ther Comp Criminol 2005;49:63-81. http://dx.doi.org/10.1177/0306624X04269003.
- Drug Misusers and the Criminal Justice System Part 1: Community Resources and the Probation Service. London: HMSO; 1991.
- Newton T, Howard M, Bottomley V, Shephard G, Heathcoat-Armory D. Green Paper. Tackling Drugs Together: A Consultation Document On A Strategy For England 1995–8. London: Her Majesty’s Stationery Office; 1994.
- Godfrey C, Eaton G, McDougall C, Culyer A. The Economic and Social Costs of Class A Drug Use in England and Wales, 2000. Home Office Research Study 249. London: Home Office; 2002.
- Newton T, Howard M, Bottomley V, Shephard G, Heathcote-Armory D. White Paper. Tackling Drugs Together: A Strategy for England 1995–8. London: HMSO; 1995.
- Report of an Independent Review of Drug Treatment Services in England. London: Department of Health; 1996.
- Tackling Drugs to Build a Better Britain. London: HMSO; 1998.
- Drug Strategy 2010 Reducing Demand, Restricting Supply, Building Recovery: Supporting People to Live a Drug Free Life. London: Home Office; 2010.
- Drug Interventions Programme Operational Handbook. London: Home Office; 2010.
- NIHR HTA . HTA - 09 109 04: The Clinical and Cost Effectiveness of Diversion and Aftercare Programmes for Offenders Using Class A Drugs – a Systematic Review and Economic Model 2009. www.nets.nihr.ac.uk/projects/hta/0910904 (accessed 6 August 2014).
- Serious Organised Crime Agency . Drugs n.d. www.soca.gov.uk/threats/drugs (accessed 6 August 2014).
- Davies L, Jones A, Vamvakas G, Dubourg R, Donmall M. The Drug Treatment Outcomes Research Study (DTORS): Cost-effectiveness analysis. London: Home Office; 2009.
- Reuter P, Stevens A. Assessing UK drug policy from a crime control perspective. Criminol Criminal Justice 2008;8:461-82. http://dx.doi.org/10.1177/1748895808096473.
- Skodbo S, Brown G, Deacon S, Cooper A, Hall A, Millar T, et al. The Drug Interventions Programme (DIP): Addressing Drug Use and Offending Through ‘Tough Choices’. London: Home Office; 2007.
- Flynn PM, Craddock SG, Hubbard RL, Anderson J, Etheridge RM. Methodological overview and research design for the Drug Abuse Treatment Outcome Study (DATOS). Psychol Addict Behav 1997;11:230-43. http://dx.doi.org/10.1037/0893-164X.11.4.230.
- Flynn PM, Kristiansen PL, Porto JV, Hubbard RL. Costs and benefits of treatment for cocaine addiction in DATOS. Drug Alcohol Depend 1999;57:167-74. http://dx.doi.org/10.1016/S0376-8716(99)00083-6.
- Gossop M, Marsden J, Stewart D, Rolfe A. Reductions in acquisitive crime and drug use after treatment of addiction problems: 1-year follow-up outcomes. Drug Alcohol Depend 2000;58:165-72. http://dx.doi.org/10.1016/S0376-8716(99)00077-0.
- Millar T, Jones A, Donmall M, Roxburgh M. Changes in Offending Following Prescribing Treatment for Drug Misuse. London: National Treatment Agency for Substance Misuse; 2008.
- Barnard M, Webster S, O’Connor W, Jones A, Donmall M. The Drug Treatment Outcomes Research Study (DTORS): Qualitative Study. London: Home Office; 2009.
- Jones A, Weston S, Moody A, Millar T, Dollin L, Anderson T, et al. The Drug Treatment Outcomes Research Study (DTORS): Baseline Report. London: Home Office; 2007.
- Aos S, Phipps P, Barnoski R, Lieb R. The Comparative Costs and Benefits of Programs to Reduce Crime. Olympia, WA: Washington State Institute for Public Policy; 2001.
- Passey M, Patete S, Bird G, Bolt S, Brooks L, Lavender K, et al. Evaluation of the Lismore MERIT Pilot Program. Final report. Lismore, NSW, Australia: Northern Rivers University Department of Rural Health; 2003.
- Zarkin, GA, Dunlap LJ, Belenko S, Dynia PA. A benefit-cost analysis of the King’s County district attorney’s office Drug Treatment Alternative to Prison (DTAP) program. Justice Res Pol 2005;7:1-25. http://dx.doi.org/10.3818/JRP.7.1.2005.1.
- Perry A, Coulton S, Glanville J, Godfrey C, Lunn J, McDougall C, et al. Interventions for drug-using offenders in the courts, secure establishments and the community. Cochrane Database Syst Rev 2008;3.
- Perry AE, Darwin Z, Godfrey C, McDougall C, Lunn J, Glanville J, et al. The effectiveness of interventions for drug-using offenders in the courts, secure establishments and the community: a systematic review. Subst Use Misuse 2009;44:373-400. http://dx.doi.org/10.1080/10826080802347560.
- Berkowitz G, Brindis C, Clayson Z, Peterson S. Options for recovery: promoting success among women mandated to treatment. J Psychoactive Drugs 1996;28:31-8. http://dx.doi.org/10.1080/02791072.1996.10471712.
- Collins JJ, Allison M. Legal coercion and retention in drug-abuse treatment. Hosp Community Psychiatry 1983;34:1145-9.
- Pompi KF, Resnick J. Retention of court-referred adolescents and young-adults in the therapeutic-community. Am J Drug Alcohol Abuse 1987;13:309-25. http://dx.doi.org/10.3109/00952998709001516.
- Watson CG, Brown K, Tilleskjor C, Jacobs L, Pucel J. The comparative recidivism rates of voluntary-admission and coerced-admission male-alcoholics. J Clin Psychol 1988;44:573-81. http://dx.doi.org/10.1002/1097-4679(198807)44:4<573::AID-JCLP2270440414>3.0.CO;2-M.
- Harford RJ. Effects of legal pressure on prognosis for treatment of drug-dependence. Am J Psychiatry 1976;133:1399-404.
- Howard DL, McCaughrin WC. The treatment effectiveness of outpatient substance misuse treatment organizations between court-mandated and voluntary clients. Subst Use Misuse 1996;31:895-926. http://dx.doi.org/10.3109/10826089609063962.
- Simpson DD, Joe GW, Rowan-Szal GA. Drug abuse treatment retention and process effects on follow-up outcomes. Drug Alcohol Depend 1997;47:227-35. http://dx.doi.org/10.1016/S0376-8716(97)00099-9.
- Wild TC. Social control and coercion in addiction treatment: towards evidence-based policy and practice. Addiction 2006;101:40-9. http://dx.doi.org/10.1111/j.1360-0443.2005.01268.x.
- Wild TC, Newton-Taylor B, Ogborne AC, Mann R, Erickson P, MacDonald S. Attitudes toward compulsory substance abuse treatment: a comparison of the public, counselors, probationers and judges’ views. Drugs: Educ Prev Pol 2001;8:33-45. http://dx.doi.org/10.1080/09687630124249.
- Wild TC, Roberts AB, Cooper EL. Compulsory substance abuse treatment: An overview of recent findings and issues. Eur Addict Res 2002;8:84-93. http://dx.doi.org/10.1159/000052059.
- Anglin MD, Brecht ML, Maddahian E. Pretreatment characteristics and treatment performance of legally coerced versus voluntary methadone-maintenance admissions. Criminology 1989;27:537-57. http://dx.doi.org/10.1111/j.1745-9125.1989.tb01045.x.
- Brecht ML, Anglin MD, Wang JC. Treatment effectiveness for legally coerced versus voluntary methadone-maintenance clients. Am J Drug Alcohol Abuse 1993;19:89-106. http://dx.doi.org/10.3109/00952999309002668.
- DeLeon G. Legal pressure in therapeutic communities. J Drug Issues 1988;18:625-40.
- Farabee D, Prendergast M, Anglin MD. The effectiveness of coerced treatment for drug-abusing offenders. Federal Probation 1998;62:3-10.
- Gostin LO. Compulsory treatment for drug-dependent persons - justifications for a public-health approach to drug dependency. Milbank Q 1991;69:561-93. http://dx.doi.org/10.2307/3350228.
- Hall W. The role of legal coercion in the treatment of offenders with alcohol and heroin problems. Aust N Z J Criminol 1997;30:103-20. http://dx.doi.org/10.1177/000486589703000201.
- Hser YI, Anglin MD, Liu Y. A survival analysis of gender and ethnic-differences in responsiveness to methadone-maintenance treatment. Int J Addict 1991;25:1295-31.
- Kelly JF, Finney JW, Moos R. Substance use disorder patients who are mandated to treatment: Characteristics, treatment process, and 1-and 5-year outcomes. J Subst Abuse Treat 2005;28:213-23. http://dx.doi.org/10.1016/j.jsat.2004.10.014.
- Lurigio AJ. Drug treatment availability and effectiveness - studies of the general and criminal justice populations. Crim Justice Behav 2000;27:495-528. http://dx.doi.org/10.1177/0093854800027004005.
- Siddall JW, Conway GL. Interactional variables associated with retention and success in residential drug-treatment. Int J Addict 1988;23:1241-54.
- Stevens A, Berto D, Heckmann W, Kerschl V, Oeuvray K, Van Ooyen M, et al. Quasi-compulsory treatment of drug dependent offenders: an international literature review. Subst Use Misuse 2005;40:269-83. http://dx.doi.org/10.1081/JA-200049159.
- Moher D, Liberati A, Tetzlaff J, Altman D, Group TP. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. BMJ 2009;339:332-9. http://dx.doi.org/10.1136/bmj.b2535.
- Hartley RJ, Keen EM, Large JA, Tedd LA. On-line Searching: Principles and Practice. London: Butterworths; 1990.
- Moher D, Jadad AR, Nichol G, Penman M, Tugwell P, Walsh S. Assessing the quality of randomized controlled trials: an annotated bibliography of scales and checklists. Control Clin Trials 1995;16:62-73. http://dx.doi.org/10.1016/0197-2456(94)00031-W.
- Marinelli-Casey P, Gonzales R, Hillhouse M, Ang A, Zweben J, Cohen J, et al. Drug court treatment for metamphetamine dependence: treatment response and posttreatment outcomes. J Subst Abuse Treat 2008:34-8.
- Sherman LW, Gottfredson D, MacKenzie D, Eck J, Reuter P, Bushway S. Preventing Crime: What Works, What Doesn’t, What’s Promising: A report to the United States Congress, Prepared for the National Institute of Justice. Baltimore, MD: University of Maryland, Department of Criminology and Criminal Justice; 1998.
- Chun JS, Guydish JR, Sorensen JL, Haug NA, Andrews S, Nelson L. Outcomes in a sample of opioid-dependent clients treated under California’s Proposition 36. J Drug Issues 2007;37:699-715. http://dx.doi.org/10.1177/002204260703700310.
- Van Stelle KR, Mauser E, Moberg DP. Recidivism to the criminal justice system of substance-abusing offenders diverted into treatment. Crime Delinq 1994;40:175-96. http://dx.doi.org/10.1177/0011128794040002003.
- Newton-Taylor B, Patra J, Gliksman L. Toronto drug treatment court: participant intake characteristics as predictors of “successful” program completion. J Drug Issues 2009;39:965-87. http://dx.doi.org/10.1177/002204260903900410.
- Anglin DM, Urada D, Brecht M-L, Hawken A, Rawson R, Longshore D. Criminal justice treatment admissions for methamphetamine use in California: a focus on Proposition 36. J Psychoactive Drugs 2007;39:367-81. http://dx.doi.org/10.1080/02791072.2007.10399898.
- Brecht M-L, Urada D. Treatment outcomes for methamphetamine users: California Proposition 36 and comparison clients. J Psychoactive Drugs 2011;43:68-76. http://dx.doi.org/10.1080/02791072.2011.602279.
- Brewster MP. An evaluation of the Chester County (PA) drug court program. J Drug Issues 2001;31:177-206. http://dx.doi.org/10.1177/002204260103100110.
- Eley S, Gallop K, McIvor G, Morgan K, Yates R. Drug Treatment and Testing Orders: Evaluation of the Scottish Pilots. Edinburgh: Scottish Government; 2002.
- Hartley RE, Phillips RC. Who graduates from drug courts? Correlates of client success. Am J Crim Justice 2001;26:107-19. http://dx.doi.org/10.1007/BF02886860.
- Hevesi AG. Quitting Drugs, Quitting Crime: Reducing Probationers’ Recidivism Through Drug Treatment Programs. New York, NY: Office of Policy Management, Office of the Comptroller; 1999.
- Longshore D, Urada D, Conner BT, Hawken A, Hiromoto S, Du D, et al. Evaluation of the Substance Abuse and Crime Prevention Act Final Report. CA: California Health and Human Services Agency, Department of Alcohol and Drug Programs; 2007.
- Saum CA, Hiller ML. Should violent offenders be excluded from drug court participation? An examination of the recidivism of violent and nonviolent drug court participants. Criminal Justice Rev 2008;33:291-307. http://dx.doi.org/10.1177/0734016808322267.
- Turnbull PJ, Webster R. Supervising Crack-Using Offenders on Drug Treatment and Testing Orders. London: National Treatment Agency for Substance Misuse; 2007.
- Elvik R. Evaluating the statistical conclusion validity of weighted mean results in meta-analysis by analysing funnel graph diagrams. Accid Anal Prev 1998;30:255-66. http://dx.doi.org/10.1016/S0001-4575(97)00076-6.
- Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage Publications; 2001.
- Anglin MD, Longshore D, Turner S, McBride D, Inciardi J, Prendergast M. Studies of the Functioning and Effectiveness of Treatment Alternatives to Street Crime (TASC) Programs. UCLA Drug Abuse Research Center; 1996.
- Evaluation of the Substance Abuse and Crime Prevention Act. Final report. Los Angeles, CA: University of California Los Angeles; 2007.
- Evaluation of Drug Testing in the Criminal Justice System. Home Office Research Study 286. London: Home Office; 2004.
- Orr KS, McCoard S, McCartney P. Evaluation of the Mandatory Drug Testing of Arrestees Pilot. Edinburgh: Scottish Government Social Research; 2009.
- Roman J, Harrell A. Assessing the costs and benefits accruing to the public from a graduated sanctions program for drug-using defendants. Law Pol 2001;23:237-68. http://dx.doi.org/10.1111/1467-9930.00112.
- Rossman S, Sridharan S, Gouvis C, Buck J, Morley E. Impact of the Opportunity to Succeed (OPTS) Aftercare Program For Substance-Abusing Felons: Comprehensive Final Report. Washington, DC: The Urban Institute; 1999.
- Guide to the Methods of Technology Appraisal. London: NICE; 2008.
- Millar T, Ahmad M, Richardson A, Skodbo S, Donmall M, Jones A. The Drug Data Warehouse: Linking Data on Drug Misusers and Drug-Misusing Offenders. London: Home Office; 2012.
- Jones A, Donmall M, Millar T, Moody A, Weston S, Anderson T, et al. The Drug Treatment Outcomes Research Study (DTORS): Final Outcomes Report. London: Home Office; 2009.
- Brand S, Price R. The Economic and Social Costs of Crime. London: Home Office; 2000.
- Evaluation of Drug Testing in the Criminal Justice System. London: Home Office Research, development and statistics directorate; 2004.
- Dubourg R, Hamed J, Thorns J. The Economic and Social Costs of Crime Against Individuals and Households 2003/04. London: Home Office; 2005.
- The Green Book. Appraisal and Evaluation in Central Government. London: Treasury Stationery Office; 2003.
- Retail Price Indices 1987 to 2013. London: ONS; n.d.
- Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford: Oxford University Press; 2006.
- Ministry of Justice (MoJ) . Offender Management Caseload Statistics; 2012 Tables n.d. www.gov.uk/government/publications/offender-management-statistics-quarterly--2 (accessed 5 August 2014).
- Ware JE, Kosinski M, Keller SD. A 12-item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996;34:220-33. http://dx.doi.org/10.1097/00005650-199603000-00003.
- Brazier J, Roberts J. The estimation of a preference-based measure of health from the SF-12. Med Care 2004;42:851-9. http://dx.doi.org/10.1097/01.mlr.0000135827.18610.0d.
- Rawlins MD, Culyer AJ. National Institute for Clinical Excellence and its value judgments. BMJ 2004;329:224-7. http://dx.doi.org/10.1136/bmj.329.7459.224.
- Briggs AH, O’Brien BJ, Blackhouse G. Thinking outside the box: recent advances in the analysis and presentation of uncertainty in cost-effectiveness studies. Annu Rev Public Health 2002;23:377-401. http://dx.doi.org/10.1146/annurev.publhealth.23.100901.140534.
- Hoch JS, Briggs AH, Willan AR. Something old, something new, something borrowed, something blue: a framework for the marriage of health econometrics and cost-effectiveness analysis. Health Econ 2002;11:415-30. http://dx.doi.org/10.1002/hec.678.
- Fenwick E, Claxton K, Sculpher M. Representing uncertainty: the role of cost-effectiveness acceptability curves. Health Econ 2001;10:779-87. http://dx.doi.org/10.1002/hec.635.
- Sendi PP, Briggs AH. Affordability and cost-effectiveness: decision-making on the cost-effectiveness plane. Health Econ 2001;10:675-80. http://dx.doi.org/10.1002/hec.639.
- Hockenhull JC, Whittington R, Leitner M, Barr W, McGuire J, Cherry MG, et al. A systematic review of prevention and intervention strategies for populations at high risk of engaging in violent behaviour. Health Technol Assess 2012;16. http://dx.doi.org/10.3310/hta16030.
- Bird SM, Goldacre B, Strang J. We should push for evidence-based sentencing in criminal justice. BMJ 2011;342. http://dx.doi.org/10.1136/bmj.d612.
- Wilcox A, Hoyle C. Are randomised controlled trials really the ‘Gold Standard’ in restorative justice research. Br J Crim Justice 2005;3:39-4.
- Looking at a Decade of Drug Courts. Office of Justice Programs, US Department of Justice: Drug Courts Program Office; 1998.
- Huddleston W, Marlowe DB. Painting the Current Picture: a National Report on Drug Courts and other Problem-Solving Court Programs in the United States. Alexandria, VA: National Drug Court Institute; 2011.
- Peters RH, Haas A, Murrin MR. Predictors of retention and arrest in drug courts. Nat Drug Court Inst Rev 1999;2:33-60.
- Peay J, Maguire M, Morgan R, Reiner R. The Oxford Handbook of Criminology. 4th ed. Oxford: Oxford University Press; 2007.
- Gordon AJ. Physical Illness and Drugs of Abuse: a Review of the Evidence. Cambridge: Cambridge University Press; 2010.
- Gossop M, Marsden J, Stewart D, Edwards C, Lehmann P, Wilson W, et al. The National Treatment Outcome Research Study in the United Kingdom: Six-Month Follow-Up Outcomes. Psychol Addict Behav 1997;11:324-37. http://dx.doi.org/10.1037/0893-164X.11.4.324.
- Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev 2009;3.
- Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction 2012;107:501-17. http://dx.doi.org/10.1111/j.1360-0443.2011.03676.x.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and Evaluating Complex Interventions: New Guidance n.d. www.mrc.ac.uk/documents/pdf/complex-interventions-guidance/ (accessed 20 October 2014).
- Payne K, McAllister M, Davies L. Valuing the economic benefits of complex interventions: when maximising health is not sufficient. Health Econ 2013;22:258-71. http://dx.doi.org/10.1002/hec.2795.
- Operational Process Guidance for Implementation of Testing on Arrest, Required Assessment and Restriction on Bail. London: Home Office; 2010.
Appendix 1 List of trigger offences (with effect from 1 August 2007)
Text reproduced from Home Office. 132
-
Section 1 (theft).
-
Section 8 (robbery).
-
Section 9 (burglary).
-
Section 10 (aggravated burglary).
-
Section 12 (taking motor vehicle or other conveyance without authority).
-
Section 12A (aggravated vehicle-taking).
-
Section 22 (handling stolen goods). a
-
Section 25 (going equipped for stealing, etc.).
-
Section 4 (restriction on production and supply of controlled drugs).
-
Section 5(2) (possession of controlled drug).
-
Section 5(3) (possession of controlled drug with intent to supply).
-
Section 1 (fraud).
-
Section 6 (possession etc. of articles for use in frauds).
-
Section 7 (making or supplying articles for use in frauds).
-
Any of the following provisions of the Theft Act 1968a
-
Section 1 (theft).
-
Section 8 (robbery).
-
Section 9 (burglary).
-
Section 22 (handling stolen goods).
-
-
Section 1 of the Fraud Act 2006 (fraud). c
-
Section 3 (begging).
-
Section 4 (persistent begging).
a Offences added to the trigger offences in Schedule 6 to the Criminal Justice and Court services Act 2000 by The Criminal Justice and Court Services Act 2000 (Amendment) Order 2004, (S.I. 2004/1892), which came into force on 27 July 2004.
b Offences added by the Fraud Act 2006, which came into force on 15 January 2007.
c Offences added by the Criminal Justice and Court Services Act 2000 (Amendment) Order 2007 which came into force on 1 August 2007.
Appendix 2 Commissioning brief
National Institute for Health Research Health Technology Assessment Programme HTA no 09/109
Efficacy of diversion and aftercare programmes for offenders using class A drugs
Introduction
The aim of the HTA programme is to ensure that high-quality research information on the effectiveness, costs and broader impact of health technologies is produced in the most efficient way for those who use, manage, provide care in or develop policy for the NHS. Topics for research are identified and prioritised to meet the needs of the NHS. Health technology assessment forms a substantial portfolio of work within the National Institute for Health Research and each year about fifty new studies are commissioned to help answer questions of direct importance to the NHS. The studies include both primary research and evidence synthesis.
Question
What is the clinical and cost-effectiveness of diversion and aftercare programmes for offenders using class A drugs?
-
Technology: diversion and aftercare programmes.
-
Target group: offenders who are using class A drugs.
-
Setting: drug intervention programmes in England.
-
Control or comparator treatment: normal care (to be described).
-
Design: a wide systematic review of studies of the effectiveness of diversion and aftercare programmes with the development of a cost-effectiveness model. The aim is to achieve a clearer understanding of the elements of diversion and aftercare that contribute most to their effectiveness. Recommendations for design of high-quality primary research studies are required to inform further HTA research.
-
Outcomes of interest: cost-effectiveness, a description of the aspects and elements that increase effectiveness, quality of life; use of class A drugs, reoffending.
Background to commissioning brief
Approximately one-third of all problematic drug users in England and Wales are in the care of the correctional services at any one time. Cannabis is the drug used by the largest proportion (54%), followed by heroin (27%) and illicit use of tranquilisers (15%). Other drugs include crack (7%), cocaine (5%), ecstasy (4%) and amphetamines (2%). Daily use of cannabis drops from 59% pre-prison to 14% in prison with daily use of heroin dropping from 82% pre-prison to 3% in prison. Furthermore, 10% of all UK deaths from drug overdoses are recently released prisoners. There are high reoffending rates for drug users, highlighting the importance of breaking the cycle of substance misuse and crime supporting drug habits.
Diversion strategies aim to redirect drug-involved offenders away from the criminal justice system and into treatment. Aftercare is the term for what happens after offenders are released from custodial sentences, complete community sentences and/or leave treatment. The evidence bases on effectiveness of diversion and aftercare are limited, with methodological problems and inconsistent costing methodology. The way these two interventions are delivered remain poorly understood, with particularly limited evidence on aftercare. High quality research is required to determine effectiveness and cost-effectiveness of such strategies.
Making an application
The NIHR Health Technology Assessment programme is funded by the NIHR, with contributions from the CSO in Scotland and WORD in Wales. Researchers from Northern Ireland should contact NETSCC to discuss their eligibility to apply.
If you wish to submit a proposal on this topic, complete the on-line application form at http://www.hta.ac.uk/funding/standardcalls/index.shtml and submit it on line by 1pm on 8 January 2010. You need to send a copy of the application form with original signatures, along with a detailed project description, to the HTA Commissioning Manager at the National Coordinating Centre for Health Technology Assessment, Alpha House, Enterprise Road, Southampton Science Park, Chilworth, Southampton, SO16 7NS.
Your full proposal will be assessed by designated board members, alongside other applications submitted in the same topic area. A maximum of three proposals will be taken forward for peer review by external referees, and subsequent consideration by the HTA Commissioning Board at its meeting in March/April 2010.
Applications received electronically after 1300 hours on the due date will not be considered.
Please see GUIDANCE ON APPLICATIONS overleaf.
Guidance on applications
Methods
Applicants should demonstrate knowledge of current research in the field and of systematic review methods and state how these would apply to the question posed. Valid and reliable methods should be proposed for identifying and selecting relevant material, assessing its quality and synthesising the results. Guidance on choice of appropriate methods is contained in NHS CRD Report 4 Undertaking systematic reviews of research on effectiveness (www.york.ac.uk/inst/crd/report4.htm). Where policy implications are considered, the emphasis should be on assessing the likely effects of a range of policy options open to decision-makers rather than a judgement on any single strategy. Where epidemiological modelling or economic evaluation is required, the range of uncertainty associated with the results should be assessed. In the assessment of cost-effectiveness, further data collection may be required to estimate resource use and costs. If there is evidence that the ratio of costs and benefits may differ between readily identifiable groups, applicants are encouraged to state how they will identify these differences.
Cochrane
Applicants wishing to produce and maintain a Cochrane systematic review from this HTA commissioned systematic review should make the case in their proposal. This will need to include the approval of the relevant Cochrane Review Group (www.cochrane.org). Any additional costs associated with the initial preparation of a Cochrane review should be included in your project proposal. Maintenance costs cannot be met.
Public involvement in research
The HTA programme recognises the benefit of increasing active involvement of members of the public in research and would like to support research projects appropriately. The HTA programme encourages applicants to consider how the scientific quality, feasibility or practicality of their proposal could be improved by involving members of the public. Examples of how this has been done for health technology assessment projects can be found at http://www.hta.ac.uk/PPIguidance/. Research teams wishing to involve members of the public should include in their application: the aims of active involvement in this project; a description of the members of the public (to be) involved; a description of the methods of involvement; and an appropriate budget. Applications that involve members of the public will not, for that reason alone, be favoured over proposals that do not but it is hoped that the involvement of members of the public will improve the quality of the application.
Updating
It is the policy of NETSCC, HTA that all search strategies undertaken as part of evidence synthesis/secondary research projects must not be more than 12 months out of date when the draft final report is submitted. We expect that most projects will manage to bring their searches up to date prior to analysis and writing up. As research funders we are aware that exceptional circumstances can apply that would not allow this to be case but this must be the exception rather than the rule and will be assessed on a case-by-case basis. The expectation is that projects funded by the HTA programme will deliver information that is both relevant and timely.
In addition, in order to inform decisions on whether and when to update the review, researchers will be expected to give some indication of how fast the evidence base is changing in the field concerned, based on the nature and volume of on-going work known at the time the review is completed. Applicants should note that they will not be expected to carry out any future updating as part of the contract to complete the review.
Communication
Communication of the results of research to decision-makers in the NHS is central to the HTA Programme. Successful applicants will be required to submit a single final report for publication by the HTA programme. They are also required to communicate their work through peer-reviewed journals and may also be asked to support NETSCC, HTA in further efforts to ensure that results are readily available to all relevant parties in the NHS. Where findings demonstrate continuing uncertainty, these should be highlighted as areas for further research.
Appendix 3 Search strategy for the effectiveness review
Final search strategy for the effectiveness review
((drug court$) OR (diversion program$) OR DTTO$ OR (communit$ correction$) OR (mental health court$) OR (diversion scheme$) OR (arrest$ refer$) OR (magistrates early referral into treatment) OR (drug abuse resistance education) OR ((Interven$ AND drug$) AND (offend$ OR delinquen$ OR parole$ OR jail$ OR prison$ OR crim$ OR custod$ OR coerc$)) OR ((Interven$ AND offend$) AND (cocaine$ OR substance$ OR narcotic$)) OR ((control$ AND drug$) AND (offend$ OR parole$ OR jail$ OR penitentia$ OR prison$ OR probation$ OR remand$ OR detain$ OR custod$ OR coerc$ OR crim$ OR recidiv$)) OR ((reduc$ AND drug$) AND (offend$ OR convict$ OR parole$ OR jail$ OR prison$ OR incarcerat$ OR recidiv$)) OR (reduc$ AND offend$ AND substance$) OR ((program$ AND (drug$ OR substance$)) AND (offend$ OR probation$ OR coerc$ OR recidiv$ OR crim$ OR inmate$ OR prison$ OR correction$)) OR ((program$ AND offend$) AND (substance$ OR addict$)) OR ((mental$ AND drug$) AND (offend$ OR delinquen$ OR parole$ OR jail$ OR prison$ OR probation$ OR custod$ OR coerc$)) OR (mental$ AND offend$ AND substance$) OR (reduc$ AND offend$ AND (mental$ ill$)) OR (control$ AND offend$ AND (mental$ ill$)) OR (program$ AND offend$ AND (mental health$)) OR ((drug$ OR substance$) AND treat$ AND (court$ OR offend$ OR crim$ OR parole$ OR jail$ OR prison$)) OR ((therapeut$ AND communit$) AND (drug$ OR substance$ OR treat$)) OR ((criminal justice) AND (drug$ OR substance$ OR treat$)) OR ((case manag$) AND (drug$ OR substance$)) OR (aftercare AND (drug$ OR substance$)) OR ((juvenile justice) AND (drug$ OR substance$ OR treat$)) OR (drug$ AND diver$ AND court$) OR (treat$ AND (addict$ OR coerc$) AND (offend$ OR detain$)) NOT (HIV OR AIDS OR vascular OR cancer OR heart OR disease OR surgery OR surgical OR infection$))
Appendix 4 Inclusion/exclusion form for the clinical effectiveness review
Inclusion criteria
Primary research paper that includes at least one research sample which is:
-
Class A drug users or class A drug user subsample analysis.
-
In contact with the CJS (any part of the CJS except prison).
-
Diverted (CJS sanction changed due to drug use/getting a different criminal outcome that is or contains a treatment element for drugs/reduction in severity of disposal/reduction in length of sentence for treatment compliance)
-
people who were sent to prison initially but then released with a drug treatment requirement as a condition of parole
-
people who receive drug treatment via specialist court/probation programme in lieu of imprisonment
-
people who receive drug treatment via specialist court/probation programme in lieu of reduced charges/reduced sentence
-
people who receive DTTOs as a community sentence/or have drug treatment requirements as a sentence alone or alongside other probation orders (e.g. specific programme/course).
-
-
18+ years.
-
Relevant outcomes reported.
-
– CJS contact (reoffending, rearrest for any offence type).
-
– Imprisonment.
-
– Drug use (increase or decrease).
-
– Treatment completion.
-
– Health (including mental and physical health, hospital admission, health service contact, illness/disease).
-
– Risk-taking behaviour.
-
– Mortality.
-
– Social functioning (including employment/training/education/homelessness/family and/or social support).
-
Exclusion criteria
-
(f) Prisoners/imprisonment at time of treatment (e.g. drug wing, boot camps).
-
(g) Background paper which contains no primary data.
-
(h) No contact with the CJS (e.g. general population/community treatment sample).
-
(i) Sample includes people aged 17 years or younger and analysis is not separated from adults.
-
(j) Mixed drug use sample and no class A drug subanalysis.
-
(k) Meets all other criteria but no relevant outcomes for class A drug users.
-
(l) Meets all other criteria but no outcomes for class A drug users are predictors only.
-
(m) Drug user sample unclear or not specified.
-
(n) Sample not diverted.
-
– People who are in drug treatment and are arrested/convicted/charged, etc.
-
– Probationer and treatment is part of probation case management work.
-
– Non-relevant outcomes include: client satisfaction.
-
Appendix 5 Data extraction form for the effectiveness review
Appendix 6 Effectiveness review supplementary tables
Comparison of studies included and excluded
| Study characteristic | Excluded, n (%) | Included, n (%) | |
|---|---|---|---|
| Date of publication | 1985–9 | 33 (2.6) | 0 (0.0) |
| 1990–9 | 391 (30.5) | 2 (12.6) | |
| 2000–1 | 174 (13.6) | 2 (12.6) | |
| 2002–7 | 508 (39.5) | 8 (50.0) | |
| 2008–9 | 102 (8.0) | 3 (18.8) | |
| 2010 onwards | 75 (5.8) | 1 (6.3) | |
| Country study carried out in | UK | 152 (11.8) | 4 (25.0) |
| USA | 970 (75.5) | 10 (62.5) | |
| Other single country | 128 (10.0) | 2 (12.5) | |
| Multinational | 15 (1.9) | 0 (0.0) | |
| Unknown | 9 (0.7) | 0 (0.0) | |
| Publication type | Journal article | 825 (64.3) | 9 (56.2) |
| Government report | 221 (17.2) | 6 (37.5) | |
| Other | 238 (18.5) | 1 (6.2) | |
Quality assessment: Maryland Scale of Scientific Methods Coding Scheme
| Level | Comparison group(s) | Control variables | Variable measurement | Control for effects of attrition | Core level: study able to infer cause and effect |
|---|---|---|---|---|---|
| 1 | No comparison group(s) | No use of control variables to adjust for initial group differences | No systematic reproducible approach to variable measurement is employed | Attrition from treatment or control group is > 50% and no attempt is made to determine the effects of attrition on the outcome measures | Correlation between an intervention and an outcome at a single point in time |
| 2 | Separate comparison group(s) present, but non-randomly constituted and limited or no information on pretreatment equivalence of groups (e.g. only demographic variables) | No indication of how study variables were constructed or obtained | No accounting given of cases that dropped out of the study, or attrition from treatment or control group is moderate and no attempt is made to determine the effects of attrition on the outcome measures | Temporal sequence between an intervention and an outcome clearly observed, or the presence of a comparison group without demonstrated comparability to the treatment group | |
| 3 | Separate comparison group(s) present, but non-randomly constituted; extensive information provided on pretreatment equivalence of groups; obvious group differences on important variables | Control variables used, but many possible relevant differences uncontrolled | Some attention to constructing or obtaining high-quality measures, but reliability not demonstrated | Differences between study participants (both treatment and comparison) who were present at the pretest and absent at the post-test are identified and discussed | A comparison between two or more comparable units of analysis, one with and one without the intervention |
| 4 | Separate comparison group(s) present, but non-randomly constituted; extensive information provided on pre-treatment equivalence of groups; only minor (or no) group differences evident | Variables developed or selected with some consideration of use in prior studies and reliability of measurement; reliability reported; not all measures demonstrated to be reliable | Differences between study participants (both treatment and comparison) who were present at the pretest and absent at the post-test are identified and discussed; possible differential attrition between treatment and comparison group is discussed | Comparison between multiple units with and without the intervention, controlling for other factors, or using comparison units that evidence only minor differences | |
| 5 | Random assignment to comparison and treatment groups; differences between groups are not more than expected by chance; units for random assignment match units for analysis | Most relevant initial differences (e.g. differences on a pretreatment measure of the dependent variable or variables highly associated with the dependent variable) between groups controlled statistically OR random assignment to groups resulted in no initial differences | Careful selection of relevant variables considering their prior use and reliability demonstrated for all or most of the measures | Careful statistical controls for the effects of attrition are employed, or attrition is shown to be minimal; threat of differential attrition for treatment and comparison groups is addressed adequately | Random assignment and analysis of comparable units to treatment and comparison groups |
Profile of included studies: quality indicators for analyses presented
| Study | ITT analyses? | Baseline equivalence evaluated by authors (using statistical tests?) – experimental variables | Baseline equivalence evaluated by authors (using statistical tests?) – non-experimental variables | Experimental variables – equivalent baselines for all? | Non-experimental variables – equivalent baselines for all? | Validity of outcomes established? | Reliability of outcomes established? | Triangulation of outcomes? |
|---|---|---|---|---|---|---|---|---|
| Anglin et al., 200785 | No | Yes for all (no) | Yes for all (no) | No | No | NA | NA | NA |
| Brecht and Urada, 201186 | No | Yes for some (yes) | Yes for some (yes) | Unclear | Unclear | No | No | No |
| Brewster, 200187 | Yes for all | Yes for some (no) | Yes for some (no) | No | No | No | No | No |
| Chun et al., 200782 | Yes for some | Yes for all (yes) | Yes for all (yes) | No | Yes | No | No | No |
| Eley et al., 200288(Fife) | NA | NA | NA | NA | NA | No | No | Yes |
| Eley et al., 200288(Glasgow) | NA | NA | NA | NA | NA | No | No | Yes |
| Eley et al., 200288(combined) | NA | NA | NA | NA | NA | No | No | Yes |
| Hartley and Phillips, 200189 | Yes for all | NA | NA | NA | NA | NA | NA | NA |
| Hevesi, 199990 | Yes for all | NA | NA | NA | NA | No | No | No |
| Longshore et al., 200791 | Unclear | Yes for some (no) | Yes for some (no) | No | No | No | No | No |
| Marinelli-Casey et al., 200880 | Yes for all | Yes for all (yes) | Yes for all (yes) | No | No | No | No | Yes |
| Newton-Taylor et al., 200984 | Yes for all | Yes for all (yes) | Yes for all (yes) | No | No | No | No | No |
| Passey et al., 200352 | Yes for some | Yes for all (yes) | Yes for all (yes) | No | No | No | No | No |
| Saum and Hiller, 200892 | Unclear | NA | NA | NA | NA | No | No | No |
| Turnbull and Webster, 200793 | NA | NA | NA | NA | NA | No | No | No |
| Van Stelle et al., 199483 | Yes for some | NA | NA | NA | NA | No | No | No |
Participant demographics
Details of participant demographics provided for a number of the studies do not map directly onto the samples used for study outcomes. Discrepancies are set out here:
Brecht and Urada:86 participant characteristics are defined on the basis of data coded on the CalOMS system for ‘unduplicated admissions to treatment’. In contrast, outcomes are evaluated against a sample drawn from this system on the basis of ‘episodes of continuing care’, with the latter defined as a contiguous sequence of one or more ‘service sets’ and each service set delineated by an admission and discharge to a single type of service/modality.
Brewster:87 due to missing data regarding drug of primary use, analyses including participants meeting our inclusion criteria are restricted to a subsample of 144 individuals, while demographic data are available only for the sample as a whole.
Passey et al. :52 relevant data from this study are restricted to evaluations related to treatment completion. The sample was split post hoc into ‘completers’ and ‘non-completers’, with non-completers defined as those whose exit status was classified as breached, removed, withdrawn or other. Four participants for whom data were not available by the cut-off point were excluded by default. Demographic characteristics are, in contrast, set out for the sample as a whole (n = 266 ‘episodes of care’) rather than for completers compared with non-completers (n = 262). In addition, while the study uses a variety of data sources, some evaluations of client characteristics are based solely on a subset of interview data. Successful recruitment to interview was substantially lower than the total of 238 people making up the total sample of 266 episodes. Only 69 people were recruited for entry interviews (44% of those eligible) of which 50 were available for exit interviews and 55 for follow-up. This does not impact on the number available for the only relevant outcomes analysis (treatment completion), but does impact on the data available for profiling participant demographic characteristics.
Longshore et al. :91 Demographic data are derived from three prior annual reports, since the main report focused on in this review does not disaggregate data for SACPA years 1–3, but the earlier reports themselves do not present outcome data meeting our inclusion criteria. The demographic data presented are averaged across the three participant groups and across all 3 years of data collection. Relevant outcome analysis in the main report is based on comparatively small subsamples, while demographic and other participant details are given only for each group taken as a whole. An exception is where analyses refer to broad characteristics such as ‘includes women’ for which demographic data apply equally to the sample as a whole and to the subsamples used for our analyses.
Van Stelle et al. :83 data meeting our inclusion criteria were restricted to a subsample of 40 participants, for whom outcome details, but no information regarding demographics or other participant characteristics were provided by the author. Very few details of demographics are, in any case, provided for the study as a whole. The economic and educational status information applies to the sample as a whole. Since the proportion of men in the sample is 100%, this information applies equally to the subsample of 40 participants and is, therefore, used in our analyses.
Study profile: review inclusion criteria
| Study | Participant groups meeting review inclusion criteria |
|---|---|
| Anglin et al., 200785 | All participants |
| Brecht and Urada, 201186 | SACPA (Proposition 36) methamphetamine users (n = 20,870) and SACPA users of other primary drugs (n = 16,200). Two non-SACPA groups (also methamphetamine vs. users of other primary drugs) were excluded as they included participants too young to meet our inclusion criteria |
| Brewster, 200187 | All participants potentially met inclusion criteria as either experimental or comparison group, but there were substantial missing data regarding primary drug. As a result, the only relevant analysis is for a subgroup of the ‘drug court’ participants for which a comparison was drawn between those whose primary drug was cocaine (n = 63) and those whose primary drug was marijuana (n = 81) |
| Chun et al., 200782 | All participants |
| Eley et al., 200288(Fife) | All participants |
| Eley et al., 200288(Glasgow) | All participants |
| Eley et al., 200288(combined) | All participants |
| Hartley and Phillips, 200189 | All participants |
| Hevesi, 199990 | All participants |
| Longshore et al., 200791 | All participantsa |
| Marinelli-Casey et al., 200880 | All participants |
| Newton-Taylor et al., 200984 | All participants |
| Passey et al., 200352 | All participants (treatment completion sample only)b |
| Saum and Hiller, 200892 | All participants |
| Turnbull et al., 200793 | All participants |
| Van Stelle et al., 199483 | Subsample of class A drug users (n = 40) |
Included studies reporting on group comparisons
| Study | Groups (n) |
|---|---|
| Anglin et al., 200785 |
|
| Brecht and Urada, 201186 |
|
| Brewster, 200187 |
|
| Chun et al., 200782 |
|
| aLongshore et al., 200791 |
|
| Marinelli-Casey et al., 200880 |
|
| Newton-Taylor et al. 200984 |
|
| Passey et al. 200352 |
|
Details of ethnicity reported in included studies
| Study | Ethnicity |
|---|---|
| Anglin et al., 200785 | Black/African-American, Hispanic, Asian/Pacific Islander, Native American, other |
| Brecht and Urada, 201186 | Hispanic, black, other |
| Brewster, 200187 | African-American, Hispanic/Latino, Native American |
| Chun et al., 200782 | African American, Latino, other |
| Eley et al., 200288(Fife) | Not stated |
| Eley et al., 200288(Glasgow) | Not stated |
| Eley et al., 200288(combined) | Not stated |
| Hartley and Phillips, 200189 | Not stated |
| Hevesi, 199990 | Not stated |
| Longshore et al., 200791 | Black UK, black Caribbean, black African, Bangladeshi |
| Marinelli-Casey et al., 200880 | Latino, Asian |
| Newton-Taylor et al., 200984 | Not stated |
| Passey et al., 200352 | 16.1% Aboriginal, 83.9% not Aboriginal |
| Saum and Hiller, 200892 | Black, Hispanic, other |
| Turnbull et al., 200793 | Hispanic, African American, Asian/Pacific Islander, Native American, other |
| Van Stelle et al., 199483 | ‘Persons of colour’ |
Outcomes of statistical analyses by type of outcome measure and study
| Measure | Study | Outcome |
|---|---|---|
| Self-reported drug use (ASI scores) | Chun et al., 200782 | ANOVA of self-reported alcohol use in the last 30 days showed significant reductions between assessment 1 and assessment 2 (mean difference 4.46), no other pairwise comparisons were statistically significant ANOVA of self-reported alcohol use in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported alcohol use in the last 30 days showed no significant difference between treated and untreated groups Regression analysis of self-reported alcohol use in the last 30 days including demographic variables and CMR scores showed that controlling for other variables the only statistically significant difference related to assessment number with slight increases across time (mean at assessment 1, 3.94; mean at assessment 5, 4.22) but no significant differences shown for any other variable including treatment group ANOVA of self-reported alcohol intoxication in the last 30 days showed significant reductions between assessment 1 and assessment 2 (mean difference 3.19), no other pairwise comparisons were statistically significant ANOVA of self-reported alcohol intoxication in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported alcohol intoxication in the last 30 days showed no significant difference between treated and untreated groups Regression analysis of self-reported alcohol intoxication in the last 30 days including demographic variables and CMR scores showed that controlling for other variables the only statistically significant difference related to assessment number with decreases in mean reported intoxication across time (mean at assessment 1, 2.46; mean at assessment 5, 0.06) but no significant differences shown for any other variable including treatment group ANOVA of self-reported heroin use in the last 30 days showed significant reductions between assessment 1 and assessment 2 (mean difference 5.57), no other pairwise comparisons were statistically significant ANOVA of self-reported heroin use in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported heroin use in the last 30 days showed no significant difference between treated and untreated groups Regression analysis of self-reported heroin use in the last 30 days including demographic variables and CMR scores showed that controlling for other variables, there was a slight but significant increase across time, with a mean of 7.13 at assessment 1, compared with a mean of 7.22 at assessment 5. Participant group also showed significant differences controlling for other variables, with participants in the ‘untreated, referred from probation’ group showing a greater reduction is use from assessment 1 (mean 4.14) to assessment 5 (mean 0.00) compared with all three other groups which, on average, showed a slight increase in use (mean across groups at assessment 1, 10.64; mean at assessment 5, 12.15) ANOVA of self-reported other opiate use in the last 30 days showed no significant difference between assessments ANOVA of self-reported other opiate use in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported other opiate use in the last 30 days showed no significant difference between treated and untreated groups ANOVA of self-reported barbiturate use in the last 30 days showed no significant difference between assessments ANOVA of self-reported barbiturate use in last 30 days showed no significant group by assessment interaction ANOVA of self-reported barbiturate use in the last 30 days showed no significant difference between treated and untreated groups ANOVA of self-reported other sedative use in the last 30 days showed significant reductions overall, but no statistically significant pairwise differences between assessments ANOVA of self-reported other sedative use in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported other sedative use in the last 30 days showed no significant difference between treated and untreated groups ANOVA of self-reported cocaine use in the last 30 days showed significant reductions overall, but no statistically significant pairwise differences between assessments ANOVA of self-reported cocaine use in the last 30 days showed no significant group by assessment interaction ANOVA of self-reported cocaine use in the last 30 days showed no significant difference between treated and untreated groups ANOVA of self-reported amphetamine use in the last 30 days showed no significant difference between assessments ANOVA of self-report amphetamine use in last 30 days showed no significant group by assessment interaction ANOVA of self-report amphetamine use in last 30 days showed no significant difference between treated and untreated groups ANOVA of self-report cannabis use in last 30 days showed no significant difference between assessments ANOVA of self-report cannabis use in last 30 days showed no significant group by assessment interaction ANOVA of self-report cannabis use in last 30 days showed no significant difference between treated and untreated groups |
| Marinelli-Casey et al., 200880 | ANOVA of mean methamphetamine use based on a combination of self-report and urine testing (how the mean is calculated is not stated) at discharge favours drug court participants (average 2.73 methamphetamine-free days) over non-drug court participants (average 5.52 methamphetamine-free days) ANOVA of mean methamphetamine use based on a combination of self-report and urine testing (how the mean is calculated is not stated) 6 months post discharge favours drug court participants (average 3.18 methamphetamine-free days) over non-drug court participants (average 5.09 methamphetamine-free days) ANOVA of mean methamphetamine use based on a combination of self-report and urine testing (how the mean is calculated is not stated) 12 months post-discharge favours drug court participants (average 2.91 methamphetamine-free days) over non-drug court participants (average 3.96 methamphetamine-free days) |
|
| Newton-Taylor et al., 200984 | ANOVA analysis of percentage of court appearances in the first programme month at which substance abuse was self-reported favoured graduated participants (22.5%) over the combined group of expelled–engaged (46.1%) and expelled–non-engaged (53.8%) participants | |
| Drug screening | Marinelli-Casey et al., 200880 | Regression analysis of in-treatment abstinence (mean methamphetamine-free urine tests during entire course of treatment). Poorly described, independent variables only referred to by the phrase ‘controlling for baseline factors’. Drug court participants were significantly more likely to remain abstinent (97.3%) than non-drug court participants (90.5%) (β = –4.93); People using methamphetamine less frequently at baseline and assigned to the drug court programme were significantly more likely to stay abstinent (β = 0.28) ANOVA of mean methamphetamine-free urine tests across the whole course of treatment favoured drug court participants (average 8.51 methamphetamine-free days) over non-drug court participants (average 5.98 methamphetamine-free days) |
| Drug-related arrests | Saum and Hiller, 200892 | Chi-squared analysis of percentage rearrested for any drug offence shows no statistically significant difference between participants using cocaine as their primary drug and participants using other drugs as their primary drug Regression analysis of any drug rearrest (whether arrested or not), including demographic variables, primary drug, time at risk, programme discharge status (failed, graduated, ‘neutral’) and lifetime charges showed no significant impact on rearrest for cocaine use or opioid use, the only significant factor was increasing age, which decreased the likelihood of rearrest |
| General arrests | Chun et al., 200782 | Generalised estimating equation for proportion of participants arrested in the last 30 days (limited to participants still in the study at assessment 4 and evaluated between assessments 2 and 4 only) showed no significant differences between assessments, or between treated vs. untreated groups and no significant group by assessment interactions |
| Hevesi et al., 199990 | Regression analysis of general recidivism (recidivated/did not recidivate) included drug treatment, previous convictions and employment status. Participants who successfully completed treatment were significantly less likely (β = –1.34) to have recidivated, participants with previous convictions were significantly more likely (β = 1.03) to have recidivated, employment status was not independently predictive of outcome | |
| Saum and Hiller, 200892 | Chi-squared analysis of percentage rearrested for any offence shows no statistically significant difference between participants using cocaine as their primary drug and participants using other drugs as their primary drug Chi-squared analysis of percentage rearrested for a felony offence shows no statistically significant difference between participants using cocaine as their primary drug and participants using other drugs as their primary drug Chi-squared analysis of percentage rearrested for any property offence shows no statistically significant difference between participants using cocaine as their primary drug and participants using other drugs as their primary drug Regression analysis of any rearrest (whether arrested or not), including demographic variables, primary drug, time at risk, programme discharge status (failed, graduated, ‘neutral’) and lifetime charges showed no significant impact on rearrest for cocaine use or opioid use, time at risk and lifetime charges were both significant factors in increased likelihood of rearrest Regression analysis of any felony rearrest (whether arrested or not), including demographic variables, primary drug, time at risk, programme discharge status (failed, graduated, ‘neutral’) and lifetime charges showed no significant impact on rearrest for cocaine use or opioid use, time at risk and lifetime charges were both significant factors in increased likelihood of rearrest, increased age was a significant factor reducing the likelihood Regression analysis of any property rearrest (whether arrested or not), including demographic variables, primary drug, time at risk, programme discharge status (failed, graduated, ‘neutral’) and lifetime charges showed no significant impact on rearrest for cocaine use or opioid use, time at risk and lifetime charges were both significant factors in increased likelihood of rearrest |
|
| Arrests for violent offending | Saum and Hiller, 200892 | Chi-squared analysis of percentage rearrested for any violent offence favours participants using cocaine as their primary drug (19.2%) over participants using other drugs as their primary drug (26.8%). Users of alcohol were more likely to be rearrested for violent offences, creating the difference between the two groups Regression analysis of any violent rearrest (whether arrested or not), including demographic variables, primary drug, time at risk, programme discharge status (failed, graduated, ‘neutral’) and lifetime charges showed no significant impact on rearrest for cocaine use or opioid use, time at risk and lifetime charges were both significant factors in increased likelihood of rearrest, increasing age was a significant factor in reducing the likelihood of rearrest |
| Incarceration | Chun et al., 200782 | ANOVA of days incarcerated in the last 30 days showed no significant difference between assessments ANOVA of days incarcerated in the last 30 days showed no significant group by assessment interaction ANOVA of days incarcerated in the last 30 days showed no significant difference between treated and untreated groups Generalised estimating equation for proportion of participants incarcerated in the last 30 days (limited to participants still in the study at assessment 5 and evaluated between assessments 1 and 5 only) showed no significant differences between assessments, or between treated vs. untreated groups and no significant group by assessment interactions |
| Treatment completion | Anglin et al., 200785 | Regression analysis of treatment completion (completed/did not complete) including type of drug; type of drug use; demographic factors and prior treatment experience. Controlling for other variables, methamphetamine users were less likely to complete treatment than alcohol or marijuana users (20% and 14% lower likelihood, respectively), slightly more likely to complete than cocaine users (an 8% difference) and more likely to complete than opiate users (a 30% difference) |
| Brecht and Urada, 201186 | Regression analysis of treatment completion (% completed) including demographic factors, whether injected or not and years of drug use. Controlling for other variables, SACPA methamphetamine users had a slightly (but significantly) lower treatment completion rate (37.2%) than SACPA ‘other drug’ users (38.5%) Regression analysis of 90-day treatment retention rates (% retained at 90 days) including demographic factors, whether or not injected and years of drug use. Controlling for other variables, no significant differences were found between SACPA methamphetamine users (50.3%) and SACPA users of other drugs (48.9%) |
|
| Brewster, 200187 | Survival analysis (Wilcoxon Z, with survival defined as no revocation or ‘other unsuccessful closure’) controlling for gender, race, primary drug of choice and frequency of use of primary drug found no significant difference between cocaine users and marijuana users for length of time on programme (no figures are given, a graph of cumulative survival suggests that at 13 months around 70% of cocaine users were still in the programme, compared with around 80% of marijuana users) | |
| Chun et al., 200782 | ANOVA for days retention in treatment showed no significant difference, either between treated (methadone maintenance in addition to therapeutic community) and ‘untreated’ (therapeutic community only) groups or between these groups split by SACPA referral vs. probation. Mean days retention in treatment were: treated, 170.6 days; untreated, 215.6 days; SACPA, 200.7 days; non-SACPA 186.8 days | |
| Hartley and Phillips, 200189 | Zero-order correlations from a logistic regression are presented to infer that there are no statistically significant differences in the likelihood of programme completion for:
|
|
| Marinelli-Casey et al., 200880 | Regression analysis of the proportion of participants completing treatment, the analysis is poorly described, presentation of independent variables is limited to the phrase ‘controlling for baseline participant and drug use factors’, outcomes are limited to ‘being enrolled in the drug court programme was the most significant factor in treatment completion’ Chi-squared analysis of ‘percentage engagement’ (proportion remaining in treatment for longer than 30 days) favoured drug court participants (79.9%) over non-drug court participants (56.5%) ANOVA of mean number of weeks retained in treatment favoured drug court participants (11.2 weeks) over non-drug court participants (7.8 weeks) Chi-squared analysis of percentage-completed treatment (defined as not missing more than 2 consecutive weeks of treatment) favoured drug court participants (56.1%) over non-drug court participants (31.7%) |
|
| Newton-Taylor et al., 200984 | ANOVA analysis of treatment compliance (defined as mean number of treatment sessions attended in the first month of the programme) favoured the combined group of graduated and expelled–engaged participants (8.85 sessions) over expelled non-engaged participants (6.10 sessions) ANOVA analysis of treatment compliance (defined as mean number of treatment sessions missed in the first month of the programme) favoured the combined group of graduated and expelled–engaged participants (1.20 sessions) over expelled non-engaged participants (2.40 sessions) Discriminant function analysis identifying characteristics differentiating between expelled–non-engaged, expelled–engaged and graduated participants. A final model containing the following variables: age, number of days used crack/cocaine in last 90 days, age at first adult charge, total number of lifetime criminal convictions, total number of lifetime administrative justice convictions, per cent of first month court appearances at which reported substance use, per cent of first month court appearances at which breaches were reported, number of court sessions attended in first month of programme, number of court sessions missed in first month of programme, number of treatment sessions attended in first month of programme, number of treatment sessions missed in first month of programme correctly categorised 65.7% of participants into their group membership |
|
| Passey et al., 200352 | Chi-squared analysis of proportion successfully completing treatment favours heroin users (51.5%) over users of ‘amphetamines, cannabis or other drugs’ (48.5%). Note here that two participants using ‘other opiates’ were included in the comparator group | |
| Longshore et al., 200791 | Regression analysis of treatment completion, including demographic variables, primary drug, age since first use of primary drug, frequency of recent drug use, prior treatment (any vs. none) and referral source (SACPA, non-SACPA CJS, non-CJS) identified heroin/opiate users as less likely to complete (adjusted OR 0.73) treatment than users of other drugs [methamphetamine was the reference category (i.e. 1.0), marijuana (1.03), cocaine (0.94), alcohol (1.25)]. A large number of other factors in the model also had a significant impact on treatment completion (women were more likely to complete than men, older people were more likely to complete than younger people, people from ethnic minorities were less likely to complete than people from white groups, greater number of years of continuous drug use was likely to increase likelihood of completion, while frequent use decreased the likelihood of completion, referral from parole also decreased likelihood of completion in contrast with referral from probation. The analysis was carried out using data for the second tranche of data collection only | |
| Scale-based outcomes | Chun et al., 200782 | ANOVA of ASI alcohol composite scores showed a significant reduction in alcohol use between first and second assessments, for both treated (decline from score of 0.12 to 0.03) and untreated (0.12 to 0.04) groups, but no difference between groups ANOVA comparing ASI alcohol composite scores only for those participants ‘surviving’ in treatment until the third assessment showed no significant difference for either assessment number or group ANOVA comparing ASI alcohol composite scores only for those participants ‘surviving’ in treatment until the fourth assessment showed a significant reduction in alcohol use between first and second assessments for both treated (decline from a score of 0.15 to 0.01) and untreated (0.11 to 0.03) groups, but no difference between groups Regression analysis of ASI alcohol composite scores including demographic variables and CMR scores showed that controlling for other variables the only statistically significant difference related to assessment number with reductions across time (mean at assessment 1, 0.11; mean at assessment 5, 0.04) but no significant differences shown for any other variable including treatment group ANOVA of ASI drug composite scores showed a significant reduction in drug use between assessments 1 and 2 for the full sample of participants (mean reduction 0.13) also between assessments 1 and 3 (0.12) and between assessments 1 and 4 (0.10) there were no significant differences between other assessments ANOVA of ASI drug composite scores showed no interaction between time and group membership ANOVA of ASI drug composite scores showed an overall mean difference in drug use (0.07) with the ‘treated’ group achieving a lower score than the untreated group Regression analysis of ASI drug composite scores including demographic variables and CMR scores showed that controlling for other variables the only statistically significant difference related to assessment number with reductions across time (mean at assessment 1, 0.25; mean at assessment 5, 0.22) but no significant differences shown for any other variable including treatment group ANOVA of ASI medical composite scores showed no significant difference in scores between assessments ANOVA of ASI medical composite scores showed no significant group by time interaction ANOVA of ASI medical composite scores showed no significant differences between treated and untreated groups ANOVA of ASI employment composite scores showed significantly lower scores at assessment 3 than at assessment 1 (mean difference 0.12) and significantly lower scores at assessment 3 than at assessment 2 (mean difference 0.17), no other significant differences between assessments ANOVA of ASI employment composite scores showed no significant group by time interaction ANOVA of ASI employment composite scores showed no significant differences between treated and untreated groups Regression analysis of ASI employment composite scores including demographic variables and CMR scores showed significant differences between assessments (reduction from 0.92 at assessment 1 to 0.78 at assessment 2); but also between groups (the ‘untreated referred from probation’ group showed significantly lower mean reductions in score from assessment 1 to 5 (0.89 to 0.83) than all other groups (mean across groups: 0.94 at assessment 1, 0.77 at assessment 5). Differences between groups with different educational attainment were also significant. Participants who had not completed higher education showed a mean increase in score (0.06) between assessment 1 and assessment 5, while participants who had completed higher education showed a mean reduction of 0.16 points. No other variables showed any significant differences ANOVA of ASI legal composite scores showed no significant differences between assessments ANOVA of ASI legal composite scores showed no significant group by time interaction ANOVA of ASI legal composite scores showed no significant differences between treated and untreated groups ANOVA of ASI family composite scores showed no significant differences between assessments ANOVA of ASI family composite scores showed no significant group by time interaction ANOVA of ASI family composite scores showed no significant differences between treated and untreated groups ANOVA of ASI psychiatric composite scores showed a significant reduction from assessment 1 to assessment 2 (mean difference 0.10), from assessment 1 to assessment 3 (mean difference 0.11) and from assessment 1 to assessment 4 (mean difference 0.15); no other pairs of assessments showed any significant differences ANOVA of ASI psychiatric composite scores showed no significant group by time interaction ANOVA of ASI psychiatric composite scores showed no significant differences between treated and untreated groups Regression analysis of ASI psychiatric composite scores including demographic variables and CMR scores showed a significant increase between assessments (mean at assessment 1, 0.16; mean at assessment 5, 0.26) once other variables were controlled for. Significant differences were also shown between ethnic groups, with scores increasing from 0.19 at assessment 1 to 0.30 at assessment 5 for white participants, but only from 0.12 at assessment 1 to 0.20 at assessment 5 for participants from ethnic minorities. No other variables, including treatment group, showed any significant differences |
| Marinelli-Casey et al., 200880 | ANOVA of ASI drug composite scores showed significantly greater reduction in drug use at 6 months for drug court participants compared with non-drug court participants (no further details given) ANOVA of ASI drug composite scores showed significantly greater reduction in drug use at 12 months for drug court participants compared with non-drug court participants (no further details given) |
|
| Other outcomes | Chun et al., 200782 | ANOVA of days paid for working in last 30 days showed significant increases in the number of days paid between assessment 1 and assessment 2 (mean difference 4.5 days), between assessment 1 and assessment 3 (mean difference 6.8 days) and between assessment 1 and assessment 4 (mean difference 9.57 days ANOVA of days paid for working in last 30 days showed no significant group by time interaction ANOVA of days paid for working in last 30 days showed no significant differences between treated and untreated groups Regression analysis of days paid for working in last 30 days including demographic variables and CMR scores showed a significant increase between assessments, from a mean of 0.93 days at assessment 1 to a mean of 3.67 days at assessment 5. Differences between participants achieving different educational levels were also significant, with participants who had not completed higher education showing a reduction in mean days paid for working from 0.19 to 0.0 days between assessment 1 and assessment 5, while participants who had completed higher education showed an increase from a mean of 1.17 days at assessment 1 to a mean of 4.13 days at assessment 5. No other variables, including treatment group, showed any significant differences ANOVA of number of technical training days in last 30 days showed no significant change between assessments ANOVA of number of technical training days in last 30 days showed no significant group by time interaction ANOVA of number of technical training days in last 30 days showed no significant differences between treated and untreated groups Generalised estimating equation for proportion of participants in training in the last 30 days (limited to participants still in the study at assessment 3 and evaluated between assessments 1 to 3 only) showed a significant decline between assessment 1 (31.8% in training) and assessment 3 (7.0% in training), no significant differences were identified for treated vs. untreated groups and no significant group by assessment interactions were identified Regression analysis of proportion in training in last 30 days including demographic variables and CMR scores and restricted to participants remaining in the study at assessment 4, showed that controlling for other variables, the proportion in training decreased significantly across time (31.8% were in training at assessment 1, compared with 2.2% at assessment 4). Participants in the ‘untreated’ SACPA group had a statistically significant lower reduction in the proportion in training, but only due to a lower start point (60% in training reducing to zero, compared with an average of 68.7% reducing to 2.6%). No other variables showed significant differences |
| Newton-Taylor et al., 200984 | Chi-squared analysis of percentage of participants with further criminal charges obtained while on the programme favoured the combined group of expelled–engaged and graduated participants (15.8%) over expelled–non-engaged participants (50.3%) ANOVA analysis of percentage of first month’s court appearances at which breaches of TDTC conditions were reported Favoured graduated participants (25.7%) over expelled–engaged participants (46.6%) and both over expelled non-engaged participants (66.7%) ANOVA analysis of court compliance (defined as mean number of court sessions attended in the first month of the programme) favoured the combined group of graduated and expelled–engaged participants (6.85) over expelled–non-engaged participants (5.20) |
Appendix 7 Search strategy for the economic review
Search string
((economic) OR (economics) OR (economical) OR (cost) OR (costs) OR (costly) OR (costing) OR (price) OR (prices) OR (pricing) OR (pharmacoeconomic) OR (pharmacoeconomics) OR (budget) OR (budgets) OR (budgetary) OR (value) OR (valued) OR (valuing) OR (money) OR (business) OR (financial) OR (financing) OR (finance) OR (finances) OR (resource) OR (allocation) OR (utilization) OR (utilisation) OR (minimisation) OR (minimization) OR (containment) OR (expenditure) OR (spend) OR (efficient) OR (efficiency)) AND ((drug) OR (drugs) OR (opioid) OR (opioids) OR (opiate) OR (opiates) OR (heroin) OR (methadone) OR (cocaine) OR (crack) OR (substance) OR (substances))
Appendix 8 Eligibility form for the economic review
| Study (author, date) = | RefMan number = | ||
|---|---|---|---|
| Yes | No | Unclear | |
| 1. Meets inclusion/exclusion criteria for effectiveness review? (a) Population: offenders, with or without a mental health problem. Eighteen years and older (b) Intervention: must be diverted to an intervention that has at least an element of the treatment which is specifically designed to treat/reduce substance misuse (c) Setting: diversion itself can take place at any criminal justice setting; police station, court, probation, jail or prison (out of/away from). The treatment (aftercare) would take place in the community. Someone on parole may have been diverted if a condition of their parole is that they undertake this treatment (include). If treatment has already taken place in prison and they then continue this as a parolee then this would not be counted as diversion. (d) Study design: any (e) Outcomes: reoffending/rearrest/recidivism/reincarceration; drug use reduction/increase; health, risk and service variables such as hospital admission; mortality data |
|||
| 2. Focus on use of any of the following drugs? Opiates Crack cocaine Powder cocaine |
|||
| 3. Inclusion of any of the following economic data? Health economics analysis Details of patient costs Outcomes for inclusion in economic model |
|||
| 4. Comparison group available for economic analysis? | |||
| 5. Based on primary data collection or systematic review? | |||
| 6. Report resource use and costs separately? | |||
| 7. Data other than charge data used? | |||
| 8. Report resource use or costs generalisable to the UK setting? | |||
| 9. Report sufficient detail to extract costs and outcome data relevant to long-term comparisons of diversion and aftercare strategies for economic modelling? | |||
| 10. Conform to quality criteria used for critical appraisal of studies included in NHS EED database? | |||
Appendix 9 Data extraction form for the economic review
Appendix 10 Economic model supplementary tables
Time in treatment, by model pathway
| Model pathway | Time in treatment (days), mean (SD)a | ||
|---|---|---|---|
| DIP | No DIP | ||
| Mean (SD) | Mean (SD) | ||
| 1 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → breach → prison | 103 (141) | 80 (57) |
| 2 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → breach → no prison → arrest | 91 (66) | 92 (67) |
| 3 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → breach → no prison → no arrest | 154 (101) | 135 (86) |
| 4 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → new offence → prison | 70 (79) | 71 (78) |
| 5 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → new offence → no prison → arrest | 70 (73) | 72 (66) |
| 6 | Treatment (enter treatment) → treatment ongoing → recorded offence → arrest → new offence → no prison → no arrest | 121 (103) | 120 (85) |
| 7 | Treatment (enter treatment) → treatment ongoing → recorded offence → no arrest (within 1 year) | 195 (132) | 224 (109) |
| 8 | Treatment (enter treatment) → treatment ongoing → no recorded offence | 335 (50) | 333 (59) |
| 9 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → breach → prison | 85 (43) | 59 (36) |
| 10 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → breach → no prison → arrest | 75 (61) | 70 (62) |
| 11 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → breach → no prison → no arrest | 93 (93) | 103 (77) |
| 12 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → new offence → prison | 60 (55) | 50 (50) |
| 13 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → new offence → no prison → arrest | 52 (53) | 55 (52) |
| 14 | Treatment (enter treatment) → treatment ceased → recorded offence → arrest → new offence → no prison → no arrest | 100 (91) | 84 (82) |
| 15 | Treatment (enter treatment) → treatment ceased → recorded offence → no arrest (within 1 year) | 161 (108) | 104 (104) |
| 16 | Treatment (enter treatment) → treatment ceased → no recorded offence | 143 (103) | 145 (92) |
| 17 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → breach → prison | 102 (91) | 62 (61) |
| 18 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → breach → no prison → arrest | 106 (77) | 84 (67) |
| 19 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → breach → no prison → no arrest | 191 (98) | 158 (100) |
| 20 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → new offence → prison | 71 (76) | 70 (77) |
| 21 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → new offence → no prison → arrest | 75 (80) | 78 (75) |
| 22 | Treatment (already in treatment) → treatment ongoing → recorded offence → arrest → new offence → no prison → no arrest | 141 (110) | 154 (106) |
| 23 | Treatment (already in treatment) → treatment ongoing → recorded offence → no arrest (within 1 year) | 196 (124) | 234 (108) |
| 24 | Treatment (already in treatment) → treatment ongoing → no recorded offence | 348 (52) | 351 (48) |
| 25 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → breach → prison | 85 (43) | 59 (69) |
| 26 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → breach → no prison → arrest | n = 0 | 63 (64) |
| 27 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → breach → no prison → no arrest | 125 (121) | 92 (81) |
| 28 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → new offence → prison | 65 (61) | 59 (65) |
| 29 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → new offence → no prison → arrest | 66 (59) | 57 (59) |
| 30 | Treatment (already in treatment) → treatment ceased → recorded offence → arrest → new offence → no prison → no arrest | 100 (97) | 106 (85) |
| 31 | Treatment (already in treatment) → treatment ceased → recorded offence → no arrest (within 1 year) | 161 (108) | 126 (90) |
| 32 | Treatment (already in treatment) → treatment ceased → no recorded offence | 217 (97) | 166 (109) |
| 33 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → breach → prison | n = 0 | 86 (92) |
| 34 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → breach → no prison → arrest | 72 (45) | 72 (57) |
| 35 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → breach → no prison → no arrest | 96 (64) | 114 (80) |
| 36 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → new offence → prison | 73 (61) | 77 (71) |
| 37 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → new offence → no prison → arrest | 68 (64) | 68 (58) |
| 38 | No treatment → subsequent treatment → treatment ongoing → recorded offence → arrest → new offence → no prison → no arrest | 107 (78) | 100 (79) |
| 39 | No treatment → subsequent treatment → treatment ongoing → recorded offence → no arrest (within 1 year) | 154 (132) | 117 (85) |
| 40 | No treatment → subsequent treatment → treatment ongoing → no recorded offence | 215 (97) | 183 (101) |
| 41 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → breach → prison | n = 0 | 74 (67) |
| 42 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → breach → no prison → arrest | 79 (30) | 51 (33) |
| 43 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → breach → no prison → no arrest | 80 (24) | 85 (60) |
| 44 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → new offence → prison | 75 (62) | 53 (49) |
| 45 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → new offence → no prison → arrest | 67 (48) | 63 (50) |
| 46 | No treatment → subsequent treatment → treatment ceased → recorded offence → arrest → new offence → no prison → no arrest | 67 (46) | 71 (68) |
| 47 | No treatment → subsequent treatment → treatment ceased → recorded offence → no arrest (within 1 year) | 95 (96) | 98 (76) |
| 48 | No treatment → subsequent treatment → treatment ceased → no recorded offence | 117 (76) | 106 (79) |
| 49 | No treatment → no subsequent treatment → recorded offence → arrest → breach → prison | NA | NA |
| 50 | No treatment → no subsequent treatment → recorded offence → arrest → breach → no prison → arrest | NA | NA |
| 51 | No treatment → no subsequent treatment → recorded offence → arrest → breach → no prison → no arrest | NA | NA |
| 52 | No treatment → no subsequent treatment → recorded offence → arrest → new offence → prison | NA | NA |
| 53 | No treatment → no subsequent treatment → recorded offence → arrest → new offence → no prison → arrest | NA | NA |
| 54 | No treatment → no subsequent treatment → recorded offence → arrest → new offence → no prison → no arrest | NA | NA |
| 55 | No treatment → no subsequent treatment → recorded offence → no arrest (within 1 year) | NA | NA |
| 56 | No treatment → no subsequent treatment → no recorded offence | NA | NA |
Probability of treatment
| Event | n | Estimated probabilitya | |||
|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| Treatment | No treatment | ||||
| DIP | 2911 | 0.533 (0.040) | 0.532 to 0.535 | 0.467 (0.040) | 0.465 to 0.468 |
| No DIP | 32,700 | 0.363 (0.074) | 0.362 to 0.364 | 0.637 (0.074) | 0.636 to 0.638 |
| Enter treatment | Already in treatment | ||||
| DIP → treatment | 1573 | 0.371 (0.022) | 0.369 to 0.372 | 0.629 (0.022) | 0.628 to 0.631 |
| No DIP → treatment | 11,142 | 0.084 (0.008) | 0.0835 to 0.084 | 0.916 (0.008) | 0.916 to 0.9165 |
| Subsequent treatment | No subsequent treatment | ||||
| DIP → no treatment | 1338 | 0.205 (0.076) | 0.199 to 0.210 | 0.795 (0.076) | 0.790 to 0.801 |
| No DIP → no treatment | 21,558 | 0.115 (0.037) | 0.1146 to 0.1158 | 0.885 (0.037) | 0.8842 to 0.8854 |
| Treatment ongoing | Treatment ceased | ||||
| DIP → treatment (enter treatment) | 626 | 0.762 (0.060) | 0.755 to 0.768 | 0.238 (0.060) | 0.232 to 0.245 |
| DIP → treatment (already in treatment) | 947 | 0.887 (0.024) | 0.885 to 0.889 | 0.113 (0.024) | 0.111 to 0.115 |
| DIP → no treatment → subsequent treatment | 283 | 0.766 (0.145) | 0.743 to 0.789 | 0.234 (0.145) | 0.211 to 0.257 |
| No DIP → treatment (enter treatment) | 1063 | 0.771 (0.045) | 0.768 to 0.775 | 0.229 (0.045) | 0.225 to 0.232 |
| No DIP → treatment (already in treatment) | 10,079 | 0.859 (0.010) | 0.8587 to 0.8591 | 0.141 (0.010) | 0.1409 to 0.1413 |
| No DIP → no treatment → subsequent treatment | 2666 | 0.785 (0.018) | 0.784 to 0.786 | 0.215 (0.018) | 0.214 to 0.216 |
Probability of next recorded offence
| Event | Estimated probabilitya | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| DIP | No DIP | |||||||||
| DIP n | Recorded offence | No recorded offence | No DIP n | Recorded offence | No recorded offence | |||||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI | |||
| Treatment (enter treatment) → treatment ongoing | 466 | 0.823 (0.086) | 0.812 to 0.834 | 0.177 (0.086) | 0.166 to 0.188 | 807 | 0.848 (0.058) | 0.843 to 0.853 | 0.152 (0.058) | 0.147 to 0.157 |
| Treatment (enter treatment) → treatment ceased | 160 | 0.776 (0.083) | 0.757 to 0.795 | 0.224 (0.083) | 0.205 to 0.243 | 256 | 0.743 (0.112) | 0.725 to 0.761 | 0.257 (0.112) | 0.239 to 0.275 |
| Treatment (already in treatment) → treatment ongoing | 844 | 0.808 (0.079) | 0.801 to 0.815 | 0.192 (0.079) | 0.185 to 0.199 | 8664 | 0.816 (0.066) | 0.814 to 0.817 | 0.184 (0.066) | 0.183 to 0.186 |
| Treatment (already in treatment) → treatment ceased | 103 | 0.672 (0.125) | 0.640 to 0.704 | 0.328 (0.125) | 0.296 to 0.360 | 1415 | 0.711 (0.080) | 0.706 to 0.716 | 0.289 (0.080) | 0.284 to 0.294 |
| No treatment → subsequent treatment → treatment ongoing | 225 | 0.636 (0.132) | 0.612 to 0.659 | 0.364 (0.132) | 0.341 to 0.388 | 2051 | 0.611 (0.062) | 0.608 to 0.615 | 0.389 (0.062) | 0.385 to 0.392 |
| No treatment → subsequent treatment → treatment ceased | 58 | 0.500 (0.096) | 0.467 to 0.533 | 0.500 (0.096) | 0.467 to 0.533 | 615 | 0.487 (0.102) | 0.476 to 0.498 | 0.513 (0.102) | 0.502 to 0.524 |
| No treatment → no subsequent treatment | 1055 | 0.908 (0.031) | 0.906 to 0.911 | 0.092 (0.031) | 0.089 to 0.094 | 18,892 | 0.851 (0.059) | 0.849 to 0.852 | 0.149 (0.059) | 0.148 to 0.151 |
Probability of next arrest
| Event | n | Estimated probabilitya | |||
|---|---|---|---|---|---|
| Arrest | No arrest | ||||
| Mean (SD) | 95% CI | Mean (SD) | 95%CI | ||
| DIP → treatment (enter treatment) → treatment ongoing → offence | 349 | 0.980 (0.017) | 0.978 to 0.982 | 0.020 (0.017) | 0.018 to 0.022 |
| DIP → treatment (enter treatment) → treatment ceased → offence | 111 | 0.949 (0.023) | 0.943 to 0.955 | 0.051 (0.023) | 0.045 to 0.057 |
| DIP → treatment (already in treatment) → treatment ongoing → offence | 655 | 0.974 (0.005) | 0.9737 to 0.9747 | 0.026 (0.005) | 0.0253 to 0.0263 |
| DIP → treatment (already in treatment) → treatment ceased → offence | 63 | 0.976 (0.065) | 0.955 to 0.996 | 0.024 (0.065) | 0.004 to 0.045 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence | 142 | 0.947 (0.066) | 0.931 to 0.962 | 0.053 (0.066) | 0.038 to 0.069 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence | 27 | 0.833 (0.164) | 0.752 to 0.915 | 0.167 (0.164) | 0.085 to 0.248 |
| DIP → no treatment → no subsequent treatment → offence | 927 | 0.993 (0.008) | 0.9920 to 0.9933 | 0.007 (0.008) | 0.0067 to 0.0080 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence | 653 | 0.975 (0.006) | 0.9741 to 0.9753 | 0.025 (0.006) | 0.0247 to 0.0259 |
| No DIP → treatment (enter treatment) → treatment ceased → offence | 162 | 0.956 (0.053) | 0.946 to 0.966 | 0.044 (0.053) | 0.034 to 0.054 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence | 6826 | 0.9825 (0.007) | 0.9824 to 0.9827 | 0.0175 (0.007) | 0.0173 to 0.0176 |
| No DIP → treatment (already in treatment) → treatment ceased → offence | 964 | 0.9657 (0.004) | 0.965 to 0.966 | 0.0343 (0.004) | 0.034 to 0.035 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence | 1195 | 0.965 (0.016) | 0.964 to 0.966 | 0.035 (0.016) | 0.034 to 0.036 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence | 265 | 0.958 (0.033) | 0.953 to 0.963 | 0.042 (0.033) | 0.037 to 0.047 |
| No DIP → no treatment → no subsequent treatment → offence | 15,297 | 0.978 (0.004) | 0.9779 to 0.9781 | 0.022 (0.004) | 0.0219 to 0.0221 |
Next offence type (probability)
| Event | n | Estimated probabilitya | |||
|---|---|---|---|---|---|
| Technical offence (breach) only | New offence | ||||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| DIP → treatment (enter treatment) → treatment ongoing → offence → arrest | 341 | 0.281 (0.034) | 0.276 to 0.285 | 0.719 (0.034) | 0.715 to 0.724 |
| DIP → treatment (enter treatment) → treatment ceased → offence → arrest | 106 | 0.179 (0.072) | 0.159 to 0.198 | 0.821 (0.072) | 0.802 to 0.841 |
| DIP → treatment (already in treatment) → treatment ongoing → offence → arrest | 642 | 0.238 (0.032) | 0.235 to 0.241 | 0.762 (0.032) | 0.759 to 0.765 |
| DIP → treatment (already in treatment) → treatment ceased → offence → arrest | 62 | 0.150 (0.103) | 0.117 to 0.183 | 0.850 (0.103) | 0.817 to 0.883 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest | 136 | 0.268 (0.090) | 0.246 to 0.289 | 0.732 (0.090) | 0.711 to 0.754 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest | 23 | 0.133 (0.352) | –0.062 to 0.328 | 0.867 (0.352) | 0.672 to 1.062 |
| DIP → No treatment → no subsequent treatment → offence → arrest | 913 | 0.117 (0.015) | 0.116 to 0.118 | 0.883 (0.015) | 0.882 to 0.884 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence → arrest | 639 | 0.229 (0.049) | 0.224 to 0.233 | 0.771 (0.049) | 0.767 to 0.776 |
| No DIP → treatment (enter treatment) → treatment ceased → offence → arrest | 157 | 0.167 (0.074) | 0.152 to 0.181 | 0.833 (0.074) | 0.819 to 0.848 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence → arrest | 6695 | 0.237 (0.025) | 0.236 to 0.238 | 0.763 (0.025) | 0.762 to 0.764 |
| No DIP → treatment (already in treatment) → treatment ceased → offence → arrest | 930 | 0.247 (0.015) | 0.246 to 0.248 | 0.753 (0.015) | 0.752 to 0.754 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest | 1155 | 0.249 (0.061) | 0.245 to 0.253 | 0.751 (0.061) | 0.747 to 0.755 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest | 247 | 0.267 (0.027) | 0.263 to 0.271 | 0.733 (0.027) | 0.729 to 0.737 |
| No DIP → no treatment → no subsequent treatment → offence → arrest | 14,925 | 0.183 (0.021) | 0.1824 to 0.1832 | 0.817 (0.021) | 0.8168 to 0.8176 |
Probability of prison following next offence
| Event | n | Estimated probabilitya | |||
|---|---|---|---|---|---|
| Prison | No prison | ||||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → breach | 89 | 0.036 (0.116) | 0.005 to 0.068 | 0.964 (0.116) | 0.932 to 0.995 |
| DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → new offence | 252 | 0.348 (0.094) | 0.332 to 0.363 | 0.652 (0.094) | 0.637 to 0.668 |
| DIP → treatment (enter treatment) → treatment ceased → offence → arrest → breachb | 23 + 7 | 0.063 (0.250) | –0.071 to 0.196 | 0.937 (0.250) | 0.804 to 1.071 |
| DIP → treatment (enter treatment) → treatment ceased → offence → arrest → new offence | 83 | 0.457 (0.070) | 0.436 to 0.477 | 0.543 (0.070) | 0.523 to 0.564 |
| DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → breach | 137 | 0.056 (0.020) | 0.051 to 0.060 | 0.944 (0.020) | 0.940 to 0.949 |
| DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → new offence | 505 | 0.302 (0.095) | 0.291 to 0.313 | 0.698 (0.095) | 0.687 to 0.709 |
| DIP → treatment (already in treatment) → treatment ceased → offence → arrest → breachb | 23 + 7 | 0.063 (0.250) | –0.071 to 0.196 | 0.937 (0.250) | 0.804 to 1.071 |
| DIP → treatment (already in treatment) → treatment ceased → offence → arrest → new offence | 55 | 0.324 (0.174) | 0.263 to 0.384 | 0.676 (0.174) | 0.616 to 0.737 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → breacha | 36 + 300 | 0.078 (0.047) | 0.072 to 0.085 | 0.922 (0.047) | 0.915 to 0.928 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → new offence | 100 | 0.250 (0.059) | 0.233 to 0.267 | 0.750 (0.059) | 0.733 to 0.767 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → breachb | 5 + 59 | 0.222 (0.087) | 0.196 to 0.248 | 0.778 (0.087) | 0.752 to 0.804 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → new offence | 18 | 0.231 (0.243) | 0.084 to 0.378 | 0.769 (0.243) | 0.622 to 0.916 |
| DIP → no treatment → no subsequent treatment → offence → arrest → breach | 96 | 0.206 (0.117) | 0.177 to 0.236 | 0.794 (0.117) | 0.764 to 0.823 |
| DIP → no treatment → no subsequent treatment → offence → arrest → new offence | 817 | 0.410 (0.103) | 0.400 to 0.419 | 0.590 (0.103) | 0.581 to 0.600 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → breach | 140 | 0.052 (0.032) | 0.045 to 0.058 | 0.948 (0.032) | 0.942 to 0.955 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → new offence | 499 | 0.303 (0.077) | 0.294 to 0.311 | 0.697 (0.077) | 0.689 to 0.706 |
| No DIP → treatment (enter treatment) → treatment ceased → offence → arrest → breach | 29 | 0.167 (0.383) | –0.024 to 0.357 | 0.833 (0.383) | 0.643 to 1.024 |
| No DIP → treatment (enter treatment) → treatment ceased → offence → arrest → new offence | 128 | 0.389 (0.105) | 0.367 to 0.411 | 0.611 (0.105) | 0.589 to 0.633 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → breach | 1400 | 0.094 (0.031) | 0.093 to 0.096 | 0.906 (0.031) | 0.904 to 0.907 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → new offence | 5295 | 0.309 (0.069) | 0.306 to 0.311 | 0.691 (0.069) | 0.689 to 0.694 |
| No DIP → treatment (already in treatment) → treatment ceased → offence → arrest → breach | 212 | 0.144 (0.113) | 0.127 to 0.161 | 0.856 (0.113) | 0.839 to 0.873 |
| No DIP → treatment (already in treatment) → treatment ceased → offence → arrest → new offence | 718 | 0.377 (0.096) | 0.368 to 0.385 | 0.623 (0.096) | 0.615 to 0.632 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → breacha | 36 + 300 | 0.078 (0.047) | 0.072 to 0.085 | 0.922 (0.047) | 0.915 to 0.928 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → new offence | 855 | 0.271 (0.073) | 0.265 to 0.277 | 0.729 (0.073) | 0.723 to 0.735 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → breachb | 5 + 59 | 0.222 (0.087) | 0.196 to 0.248 | 0.778 (0.087) | 0.752 to 0.804 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → new offence | 188 | 0.381 (0.087) | 0.365 to 0.397 | 0.619 (0.087) | 0.603 to 0.635 |
| No DIP → no treatment → no subsequent treatment → offence → arrest → breach | 2393 | 0.123 (0.030) | 0.121 to 0.124 | 0.877 (0.030) | 0.876 to 0.879 |
| No DIP → no treatment → no subsequent treatment → offence → arrest → new offence | 12,532 | 0.381 (0.078) | 0.379 to 0.383 | 0.619 (0.078) | 0.617 to 0.621 |
Probability of subsequent offending following probation
| Event | n | Estimated probabilitya | |||
|---|---|---|---|---|---|
| Subsequent offence | No subsequent offence | ||||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → breach → no prison | 84 | 0.547 (0.132) | 0.511 to 0.584 | 0.453 (0.132) | 0.416 to 0.489 |
| DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → new offence → no prison | 177 | 0.772 (0.099) | 0.751 to 0.792 | 0.228 (0.099) | 0.208 to 0.249 |
| DIP → treatment (enter treatment) → treatment ceased → offence → arrest → breach → no prisonb | 22 + 6 | 0.400 (0.222) | 0.277 to 0.523 | 0.600 (0.222) | 0.477 to 0.723 |
| DIP → treatment (enter treatment) → treatment ceased → offence → arrest → new offence → no prison | 51 | 0.600 (0.201) | 0.517 to 0.683 | 0.400 (0.201) | 0.317 to 0.483 |
| DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → breach → no prison | 130 | 0.612 (0.083) | 0.594 to 0.630 | 0.388 (0.083) | 0.370 to 0.406 |
| DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → new offence → no prison | 372 | 0.746 (0.063) | 0.737 to 0.755 | 0.254 (0.063) | 0.245 to 0.263 |
| DIP → treatment (already in treatment) → treatment ceased → offence → arrest → breach → no prisonb | 22 + 6 | 0.400 (0.222) | 0.277 to 0.523 | 0.600 (0.222) | 0.477 to 0.723 |
| DIP → treatment (already in treatment) → treatment ceased → offence → arrest → new offence → no prison | 37 | 0.696 (0.231) | 0.596 to 0.796 | 0.304 (0.231) | 0.204 to 0.404 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → breach → no prison | 36 | 0.421 (0.206) | 0.322 to 0.520 | 0.579 (0.206) | 0.480 to 0.678 |
| DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → new offence → no prison | 72 | 0.641 (0.202) | 0.576 to 0.706 | 0.359 (0.202) | 0.294 to 0.424 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → breach → no prisonb | 5 + 48 | 0.600 (0.084) | 0.571 to 0.629 | 0.400 (0.084) | 0.371 to 0.429 |
| DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → new offence → no prison | 13 | 0.700 (0.088) | 0.637 to 0.763 | 0.300 (0.088) | 0.237 to 0.363 |
| DIP → no treatment → no subsequent treatment → offence → arrest → breach → no prison | 80 | 0.700 (0.149) | 0.658 to 0.742 | 0.300 (0.149) | 0.258 to 0.342 |
| DIP → no treatment → no subsequent treatment → offence → arrest → new offence → no prison | 511 | 0.833 (0.062) | 0.825 to 0.840 | 0.167 (0.062) | 0.160 to 0.175 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → breach → no prison | 133 | 0.728 (0.050) | 0.718 to 0.739 | 0.272 (0.050) | 0.261 to 0.282 |
| No DIP → treatment (enter treatment) → treatment ongoing → offence → arrest → new offence → no prison | 357 | 0.816 (0.039) | 0.811 to 0.821 | 0.184 (0.039) | 0.179 to 0.189 |
| No DIP → treatment (enter treatment) → treatment ceased → offence → arrest → breach → no prison | 25 | 0.533 (0.257) | 0.391 to 0.676 | 0.467 (0.257) | 0.324 to 0.609 |
| No DIP → treatment (enter treatment) → treatment ceased → offence → arrest → new offence → no prison | 86 | 0.727 (0.057) | 0.712 to 0.743 | 0.273 (0.057) | 0.257 to 0.288 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → breach → no prison | 1279 | 0.652 (0.108) | 0.646 to 0.659 | 0.348 (0.108) | 0.341 to 0.354 |
| No DIP → treatment (already in treatment) → treatment ongoing → offence → arrest → new offence → no prison | 3843 | 0.781 (0.064) | 0.779 to 0.783 | 0.219 (0.064) | 0.217 to 0.221 |
| No DIP → treatment (already in treatment) → treatment ceased → offence → arrest → breach → no prison | 182 | 0.564 (0.060) | 0.554 to 0.573 | 0.436 (0.060) | 0.427 to 0.446 |
| No DIP → treatment (already in treatment) → treatment ceased → offence → arrest → new offence → no prison | 465 | 0.737 (0.070) | 0.730 to 0.745 | 0.263 (0.070) | 0.255 to 0.270 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → breach → no prison | 279 | 0.568 (0.074) | 0.557 to 0.579 | 0.432 (0.074) | 0.421 to 0.443 |
| No DIP → no treatment → subsequent treatment → treatment ongoing → offence → arrest → new offence → no prison | 645 | 0.693 (0.037) | 0.689 to 0.696 | 0.307 (0.037) | 0.304 to 0.311 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → breach → no prisonb | 5 + 48 | 0.600 (0.084) | 0.571 to 0.629 | 0.400 (0.084) | 0.371 to 0.429 |
| No DIP → no treatment → subsequent treatment → treatment ceased → offence → arrest → new offence → no prison | 130 | 0.575 (0.096) | 0.553 to 0.598 | 0.425 (0.096) | 0.402 to 0.447 |
| No DIP → no treatment → no subsequent treatment → offence → arrest → breach → no prison | 2114 | 0.712 (0.065) | 0.709 to 0.715 | 0.288 (0.065) | 0.285 to 0.291 |
| No DIP → no treatment → no subsequent treatment → offence → arrest → new offence → no prison | 8282 | 0.783 (0.064) | 0.782 to 0.785 | 0.217 (0.064) | 0.215 to 0.218 |
Mean time to next arrest
| DIPa | n b | Mean (days)b | SD (days)b | 95% CIb | No DIPa | n b | Mean (days)b | SD (days)b | 95% CIb |
|---|---|---|---|---|---|---|---|---|---|
| A1 | 5 | 126 | 138.1 | –45 to 298 | B1 | 7 | 90 | 62.6 | 32 to 148 |
| A2 | 44 | 98 | 63.6 | 78 to 117 | B2 | 96 | 107 | 68.4 | 94 to 121 |
| A3 | 40 | 173 | 100.8 | 141 to 205 | B3 | 37 | 156 | 96.1 | 124 to 188 |
| A4 | 75 | 83 | 77.0 | 65 to 101 | B4 | 142 | 87 | 81.6 | 73 to 100 |
| A5 | 132 | 83 | 76.8 | 70 to 97 | B5 | 282 | 86 | 71.1 | 78 to 94 |
| A6 | 45 | 136 | 107.0 | 103 to 168 | B6 | 75 | 143 | 98.6 | 120 to 166 |
| A7 | 8 | NA | – | – | B7 | 14 | NA | – | – |
| A8 | 117 | NA | – | – | B8 | 154 | NA | – | – |
| A9 | 1 | 183 | n = 1 | n = 1 | B9 | 4 | 99 | 47.5 | 23 to 175 |
| A10 | 13 | 148 | 56.0 | 114 to 181 | B10 | 15 | 139 | 67.0 | 102 to 176 |
| A11 | 9 | 253 | 90.1 | 184 to 322 | B11 | 10 | 204 | 108.6 | 126 to 281 |
| A12 | 32 | 160 | 89.4 | 128 to 192 | B12 | 42 | 131 | 78.2 | 106 to 155 |
| A13 | 33 | 132 | 84.6 | 99 to 159 | B13 | 58 | 132 | 78.2 | 112 to 153 |
| A14 | 18 | 212 | 87.9 | 168 to 255 | B14 | 28 | 196 | 110.6 | 153 to 269 |
| A15 | 5 | NA | – | – | B15 | 5 | NA | – | – |
| A16 | 49 | NA | – | – | B16 | 94 | NA | – | – |
| A17 | 7 | 98 | 94.5 | 10 to 185 | B17 | 121 | 63 | 61.6 | 52 to 74 |
| A18 | 80 | 110 | 79.5 | 92 to 128 | B18 | 809 | 85 | 67.9 | 80 to 90 |
| A19 | 50 | 197 | 92.2 | 171 to 224 | B19 | 470 | 164 | 102.9 | 154 to 173 |
| A20 | 133 | 72 | 77.6 | 59 to 86 | B20 | 1452 | 72 | 80.1 | 68 to 76 |
| A21 | 275 | 76 | 80.4 | 67 to 86 | B21 | 2915 | 80 | 77.0 | 77 to 83 |
| A22 | 97 | 146 | 110.4 | 124 to 168 | B22 | 928 | 158 | 107.2 | 151 to 165 |
| A23 | 13 | NA | – | – | B23 | 131 | NA | – | – |
| A24 | 189 | NA | – | – | B24 | 1838 | NA | – | – |
| A25 | 1 | 302 | n = 1 | n = 1 | B25 | 30 | 117 | 89.6 | 84 to 151 |
| A26 | 0 | n = 0 | n = 0 | n = 0 | B26 | 99 | 112 | 78.5 | 96 to 128 |
| A27 | 6 | 180 | 107.3 | 67 to 292 | B27 | 83 | 188 | 94.4 | 167 to 209 |
| A28 | 18 | 139 | 66.2 | 106 to 172 | B28 | 253 | 126 | 93.3 | 114 to 138 |
| A29 | 26 | 131 | 84.8 | 96 to 165 | B29 | 329 | 126 | 84.4 | 117 to 135 |
| A30 | 11 | 183 | 100.6 | 116 to 251 | B30 | 136 | 227 | 96.4 | 211 to 244 |
| A31 | 1 | NA | – | – | B31 | 34 | NA | – | – |
| A32 | 40 | NA | – | – | B32 | 451 | NA | – | – |
| A33 | 0 | n = 0 | n = 0 | n = 0 | B33 | 21 | 170 | 100.7 | 124 to 216 |
| A34 | 17 | 157 | 78.8 | 116 to 197 | B34 | 145 | 159 | 71.2 | 148 to 171 |
| A35 | 19 | 222 | 80.0 | 183 to 261 | B35 | 134 | 233 | 88.8 | 218 to 248 |
| A36 | 28 | 158 | 84.0 | 125 to 190 | B36 | 210 | 169 | 89.3 | 157 to 181 |
| A37 | 47 | 162 | 85.8 | 136 to 187 | B37 | 425 | 155 | 75.9 | 148 to 162 |
| A38 | 25 | 209 | 75.9 | 178 to 241 | B38 | 220 | 228 | 89.7 | 216 to 240 |
| A39 | 6 | NA | – | – | B39 | 40 | NA | – | – |
| A40 | 83 | NA | – | – | B40 | 856 | NA | – | – |
| A41 | 0 | n = 0 | n = 0 | n = 0 | B41 | 11 | 215 | 87.4 | 156 to 273 |
| A42 | 3 | 196 | 34.4 | 111 to 281 | B42 | 22 | 177 | 65.7 | 147 to 206 |
| A43 | 2 | 216 | 6.4 | 158 to 273 | B43 | 26 | 268 | 69.0 | 240 to 296 |
| A44 | 5 | 257 | 83.7 | 153 to 361 | B44 | 58 | 212 | 85.7 | 189 to 234 |
| A45 | 9 | 230 | 71.1 | 176 to 285 | B45 | 70 | 195 | 68.7 | 179 to 212 |
| A46 | 4 | 286 | 70.1 | 174 to 397 | B46 | 60 | 254 | 75.3 | 234 to 273 |
| A47 | 4 | NA | – | – | B47 | 18 | NA | – | – |
| A48 | 31 | NA | – | – | B48 | 350 | NA | – | – |
| A49 | 16 | 61 | 67.7 | 25 to 97 | B49 | 279 | 66 | 71.0 | 58 to 75 |
| A50 | 59 | 102 | 83.1 | 80 to 124 | B50 | 1450 | 83 | 69.9 | 80 to 87 |
| A51 | 21 | 139 | 99.7 | 94 to 184 | B51 | 664 | 155 | 104.9 | 147 to 163 |
| A52 | 306 | 63 | 73.0 | 55 to 72 | B52 | 4250 | 79 | 81.0 | 76 to 81 |
| A53 | 420 | 64 | 66.3 | 57 to 70 | B53 | 6216 | 77 | 74.8 | 75 to 79 |
| A54 | 91 | 132 | 114.3 | 105 to 153 | B54 | 2066 | 156 | 106.2 | 152 to 161 |
| A55 | 14 | NA | – | – | B55 | 372 | NA | – | – |
| A56 | 128 | NA | – | – | B56 | 3595 | NA | – | – |
Costs (2012) associated with Drug Interventions Programme, drug test and drug treatment
| DIPa | DIP (£)b,c | Drug test (£)c,d,e | Treatment (£)c,e,f | No DIPa | Treatment (£)c,e,f |
|---|---|---|---|---|---|
| A1 | 195.63 | 44.48 | 2680.62 | B1 | 2066.83 |
| A2 | 195.63 | 85.62 | 2365.02 | B2 | 2389.18 |
| A3 | 195.63 | 61.16 | 3991.06 | B3 | 3495.46 |
| A4 | 195.63 | 80.06 | 1821.63 | B4 | 1853.84 |
| A5 | 195.63 | 82.29 | 1815.65 | B5 | 1873.58 |
| A6 | 195.63 | 84.51 | 3141.94 | B6 | 3125.05 |
| A7 | 195.63 | 55.60 | 5068.50 | B7 | 5822.04 |
| A8 | 195.63 | 68.94 | 8694.87 | B8 | 8639.80 |
| A9 | 195.63 | 111.20 | 2194.89 | B9 | 1539.02 |
| A10 | 195.63 | 94.52 | 1948.13 | B10 | 1809.68 |
| A11 | 195.63 | 74.50 | 2424.25 | B11 | 2672.83 |
| A12 | 195.63 | 80.06 | 1551.23 | B12 | 1328.23 |
| A13 | 195.63 | 57.82 | 1339.79 | B13 | 1426.29 |
| A14 | 195.63 | 80.06 | 2593.08 | B14 | 2186.58 |
| A15 | 195.63 | 111.20 | 4168.99 | B15 | 2711.79 |
| A16 | 195.63 | 78.95 | 3712.87 | B16 | 3755.73 |
| A17 | 195.63 | 78.95 | 2649.45 | B17 | 1619.02 |
| A18 | 195.63 | 75.62 | 2758.29 | B18 | 2184.50 |
| A19 | 195.63 | 82.29 | 4964.34 | B19 | 4114.70 |
| A20 | 195.63 | 75.62 | 1831.76 | B20 | 1806.04 |
| A21 | 195.63 | 81.18 | 1960.33 | B21 | 2023.45 |
| A22 | 195.63 | 85.62 | 3675.20 | B22 | 3996.51 |
| A23 | 195.63 | 76.73 | 5081.23 | B23 | 6080.49 |
| A24 | 195.63 | 75.62 | 9032.81 | B24 | 9110.73 |
| A25 | 195.63 | 111.20 | 2194.89 | B25 | 1520.32 |
| A26 | n = 0 | n = 0 | n = 0 | B26 | 1630.19 |
| A27 | 195.63 | 36.70 | 3233.89 | B27 | 2391.00 |
| A28 | 195.63 | 62.27 | 1695.65 | B28 | 1544.73 |
| A29 | 195.63 | 72.28 | 1708.38 | B29 | 1486.29 |
| A30 | 195.63 | 61.16 | 2604.51 | B30 | 2748.67 |
| A31 | 195.63 | Zero | 4168.99 | B31 | 3268.17 |
| A32 | 195.63 | 72.28 | 5628.26 | B32 | 4316.53 |
| A33 | n = 0 | n = 0 | n = 0 | B33 | 2246.32 |
| A34 | 195.63 | 91.18 | 1863.97 | B34 | 1877.21 |
| A35 | 195.63 | 64.50 | 2504.51 | B35 | 2967.38 |
| A36 | 195.63 | 60.05 | 1899.81 | B36 | 2004.75 |
| A37 | 195.63 | 85.62 | 1774.09 | B37 | 1770.46 |
| A38 | 195.63 | 80.06 | 2786.60 | B38 | 2602.70 |
| A39 | 195.63 | 55.60 | 3987.16 | B39 | 3047.65 |
| A40 | 195.63 | 72.28 | 5595.53 | B40 | 4756.80 |
| A41 | n = 0 | n = 0 | n = 0 | B41 | 1922.15 |
| A42 | 195.63 | 111.20 | 2060.60 | B42 | 1311.74 |
| A43 | 195.63 | 111.20 | 2078.00 | B43 | 2217.75 |
| A44 | 195.63 | 88.96 | 1937.74 | B44 | 1375.38 |
| A45 | 195.63 | 86.74 | 1748.90 | B45 | 1645.00 |
| A46 | 195.63 | 27.80 | 1740.33 | B46 | 1836.95 |
| A47 | 195.63 | 27.80 | 2474.12 | B47 | 2555.68 |
| A48 | 195.63 | 78.95 | 3045.83 | B48 | 2759.06 |
| A49 | 195.63 | 76.73 | NA | B49 | NA |
| A50 | 195.63 | 75.62 | NA | B50 | NA |
| A51 | 195.63 | 63.38 | NA | B51 | NA |
| A52 | 195.63 | 73.39 | NA | B52 | NA |
| A53 | 195.63 | 76.73 | NA | B53 | NA |
| A54 | 195.63 | 77.84 | NA | B54 | NA |
| A55 | 195.63 | 95.63 | NA | B55 | NA |
| A56 | 195.63 | 67.83 | NA | B56 | NA |
Costs (2012) associated with next arrest, prison and probation
| DIPa | Arrest (£)b,c,d | Prison (£)b,c,d | Probation (£)b,c,d | |||
|---|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI | |
| A1 | 1013.00 (all breach) | All breach | 12,182.00 (all breach) | All breach | NA | NA |
| A2 | 1019.95 (20.84) | 1013.62 to 1026.29 | NA | NA | 2690.00 (all breach) | All breach |
| A3 | 1013.00 (all breach) | All breach | NA | NA | 2690.00 (all breach) | All breach |
| A4 | 7867.59 (8930.34) | 5812.90 to 9922.27 | 36,764.59 (26,681.69) | 30,625.69 to 42,903.49 | NA | NA |
| A5 | 4483.38 (5502.72) | 3535.90 to 5430.86 | NA | NA | 6992.61 (9794.98) | 5306.07 to 8679.14 |
| A6 | 6941.58 (8252.61) | 4462.22 to 9420.94 | NA | NA | 10,604.58 (14,746.06) | 6174.37 to 15,034.78 |
| A7 | NA | NA | NA | NA | NA | NA |
| A8 | NA | NA | NA | NA | NA | NA |
| A9 | 1013.00 (all breach) | All breach | 12,182.00 (all breach) | All breach | NA | NA |
| A10 | 1013.00 (all breach) | All breach | NA | NA | 2690.00 (all breach) | All breach |
| A11 | 1024.33 (34.00) | 998.20 to 1050.47 | NA | NA | 2690.00 (all breach) | All breach |
| A12 | 8839.38 (8591.46) | 5741.82 to 11,936.93 | 44,865.38 (26,116.40) | 35,449.41 to 54,281.34 | NA | NA |
| A13 | 7030.42 (7716.96) | 4294.11 to 9766.74 | NA | NA | 10,328.94 (14,229.54) | 5283.36 to 15,374.52 |
| A14 | 7735.44 (8636.09) | 3440.82 to 12,030.07 | NA | NA | 12,361.17 (16,387.34) | 4211.93 to 20,510.40 |
| A15 | NA | NA | NA | NA | NA | NA |
| A16 | NA | NA | NA | NA | NA | NA |
| A17 | 1042.14 (57.83) | 988.66 to 1095.63 | 12,182.00 (all breach) | (All breach) | NA | NA |
| A18 | 1016.19 (14.84) | 1012.89 to 1019.49 | NA | NA | 2690.00 (all breach) | All breach |
| A19 | 1015.04 (10.10) | 1012.17 to 1017.91 | NA | NA | 2690.00 (all breach) | All breach |
| A20 | 7997.13 (8578.65) | 6525.69 to 9468.56 | 36,968.89 (26,178.00) | 32,478.76 to 41,459.01 | NA | NA |
| A21 | 5241.84 (6326.87) | 4489.36 to 5994.31 | NA | NA | 8066.11 (11,293.11) | 6751.23 to 9439.87 |
| A22 | 6556.45 (7426.81) | 5059.62 to 8053.29 | NA | NA | 9778.79 (13,747.76) | 7008.01 to 12,549.58 |
| A23 | NA | NA | NA | NA | NA | NA |
| A24 | NA | NA | NA | NA | NA | NA |
| A25 | 1013.00 (all breach) | (All breach) | 12,182.00 (all breach) | (All breach) | NA | NA |
| A26 | n = 0 | n = 0 | NA | NA | n = 0 | n = 0 |
| A27 | 1021.50 (20.82) | 999.65 to 1043.35 | NA | NA | 2690.00 (all breach) | (all breach) |
| A28 | 7139.50 (7444.13) | 3437.62 to 10,841.38 | 38,181.17 (25,334.12) | 25,582.80 to 50,779.53 | NA | NA |
| A29 | 4908.31 (6463.46) | 2297.66 to 7518.96 | NA | NA | 8019.69 (11,721.91) | 3285.11 to 12,754.27 |
| A30 | 7351.09 (7052.73) | 2613.00 to 12,089.18 | NA | NA | 9527.82 (13,023.02) | 778.84 to 18,276.80 |
| A31 | NA | NA | NA | NA | NA | NA |
| A32 | NA | NA | NA | NA | NA | NA |
| A33 | n = 0 | n = 0 | n = 0 | n = 0 | NA | NA |
| A34 | 1016.00 (12.37) | 1009.64 to 1022.36 | NA | NA | 2690.00 (all breach) | All breach |
| A35 | 1018.37 (16.08) | 1010.62 to 1026.12 | NA | NA | 2690.00 (all breach) | All breach |
| A36 | 11,493.11 (10,390.66) | 7464.03 to 15,522.19 | 48,033.14 (27,588.89) | 37,335.29 to 58,731.00 | NA | NA |
| A37 | 5565.98 (7148.66) | 3467.05 to 7664.90 | NA | NA | 8504.89 (12,228.68) | 4914.42 to 12,095.37 |
| A38 | 4480.32 (5244.89) | 2315.34 to 6645.30 | NA | NA | 6801.36 (8916.47) | 3120.82 to 10,481.90 |
| A39 | NA | NA | NA | NA | NA | NA |
| A40 | NA | NA | NA | NA | NA | NA |
| A41 | n = 0 | n = 0 | n = 0 | n = 0 | NA | NA |
| A42 | 1030.00 (29.44) | 956.85 to 1103.15 | NA | NA | 2690.00 (all breach) | All breach |
| A43 | 1013.00 (all breach) | All breach | NA | NA | 2690.00 (all breach) | All breach |
| A44 | 11,288.60 (8913.92) | 220.50 to 22,356.70 | 48,444.20 (30,193.95) | 10,953.46 to 85,934.94 | NA | NA |
| A45 | 7019.22 (7136.23) | 1533.83 to 12,504.61 | NA | NA | 9290.44 (14,408.31) | –1784.77 to 20,365.65 |
| A46 | 4629.50 (4611.10) | –2707.78 to 11,966.78 | NA | NA | 3791.50 (861.18) | 2421.17 to 5161.83 |
| A47 | NA | NA | NA | NA | NA | NA |
| A48 | NA | NA | NA | NA | NA | NA |
| A49 | 1019.38 (17.42) | 1010.09 to 1028.66 | 12,182.00 (all breach) | All breach | NA | NA |
| A50 | 1013.86 (6.64) | 1012.13 to 1015.59 | NA | NA | 2690.00 (all breach) | All breach |
| A51 | 1034.86 (100.16) | 989.26 to 1080.45 | NA | NA | 2690.00 (all breach) | All breach |
| A52 | 7665.06 (8549.92) | 6703.28 to 8626.84 | 36,683.82 (25,663.07) | 33,796.98 to 39,570.66 | NA | NA |
| A53 | 5126.55 (6081.91) | 4543.21 to 5709.88 | NA | NA | 7735.12 (10,690.94) | 6709.71 to 8760.52 |
| A54 | 6230.85 (6669.55) | 4841.85 to 7619.85 | NA | NA | 8876.32 (12,254.61) | 6324.17 to 11,428.46 |
| A55 | NA | NA | NA | NA | NA | NA |
| A56 | NA | NA | NA | NA | NA | NA |
| No DIPa | Arrest (£)b,c,d | Prison (£)b,c,d | Probation (£)b,c,d | |||
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | Mean (SD) | 95% CI | |
| B1 | 1020.29 (19.28) | 1002.46 to 1038.11 | 12,182.00 (all breach) | All breach | NA | NA |
| B2 | 1023.09 (39.59) | 1015.07 to 1031.11 | NA | NA | 2690.00 (all breach) | All breach |
| B3 | 1019.89 (21.38) | 1012.76 to 1027.02 | NA | NA | 2690.00 (all breach) | All breach |
| B4 | 8045.73 (8934.99) | 6563.41 to 9528.05 | 38,186.14 (26,383.40) | 33,809.12 to 42,563.16 | NA | NA |
| B5 | 5215.73 (7021.04) | 4392.73 to 6038.73 | NA | NA | 8545.45 (12,583.78) | 7070.39 to 10,020.51 |
| B6 | 6987.75 (7756.57) | 5203.12 to 8772.37 | NA | NA | 10,638.65 (14,788.28) | 7236.18 to 14,041.13 |
| B7 | NA | NA | NA | NA | NA | NA |
| B8 | NA | NA | NA | NA | NA | NA |
| B9 | 1025.75 (25.50) | 985.17 to 1066.33 | 12,182.00 (all breach) | (All breach) | NA | NA |
| B10 | 1013.00 (all breach) | (All breach) | NA | NA | 2690.00 (all breach) | All breach |
| B11 | 1028.30 (34.42) | 1003.68 to 1052.92 | NA | NA | 2690.00 (all breach) | All breach |
| B12 | 6492.93 (6655.06) | 4419.07 to 8566.79 | 39,393.43 (24,801.78) | 31,664.65 to 47,122.21 | NA | NA |
| B13 | 5965.48 (7815.50) | 3910.50 to 8020.46 | NA | NA | 9983.40 (14,233.90) | 6240.78 to 13,726.01 |
| B14 | 5965.39 (7173.02) | 3183.99 to 8746.80 | NA | NA | 8989.79 (13,679.47) | 3685.44 to 14,294.13 |
| B15 | NA | NA | NA | NA | NA | NA |
| B16 | NA | NA | NA | NA | NA | NA |
| B17 | 1026.91 (35.46) | 1020.53 to 1033.29 | 12,182.00 (all breach) | (All breach) | NA | NA |
| B18 | 1021.64 (31.88) | 1019.44 to 1023.84 | NA | NA | 2690.00 (all breach) | All breach |
| B19 | 1020.38 (32.30) | 1017.45 to 1023.31 | NA | NA | 2690.00 (all breach) | All breach |
| B20 | 7568.28 (8207.43) | 7145.34 to 7991.23 | 35,975.26 (25,555.85) | 34,658.31 to 37,292.20 | NA | NA |
| B21 | 5479.64 (7075.82) | 5222.67 to 5736.61 | NA | NA | 8866.86 (12,835.08) | 8400.73 to 9332.99 |
| B22 | 7633.50 (8698.99) | 7073.08 to 8193.91 | NA | NA | 12,268.46 (16,441.52) | 11,209.25 to 13,327.67 |
| B23 | NA | NA | NA | NA | NA | NA |
| B24 | NA | NA | NA | NA | NA | NA |
| B25 | 1033.40 (51.18) | 1014.29 to 1052.51 | 12,182.00 (all breach) | (All breach) | NA | NA |
| B26 | 1017.64 (16.44) | 1014.36 to 1020.92 | NA | NA | 2690.00 (all breach) | All breach |
| B27 | 1020.37 (22.71) | 1015.41 to 1025.33 | NA | NA | 2690.00 (all breach) | All breach |
| B28 | 8600.61 (9186.00) | 7463.23 to 9737.99 | 38,298.87 (26,580.04) | 35,007.83 to 41,589.92 | NA | NA |
| B29 | 5400.60 (6781.05) | 4665.15 to 6136.05 | NA | NA | 8485.92 (12,124.34) | 7170.96 to 9800.89 |
| B30 | 8579.74 (9577.30) | 6955.56 to 10,203.91 | NA | NA | 14,505.70 (18,504.31) | 11,367.63 to 17,643.76 |
| B31 | NA | NA | NA | NA | NA | NA |
| B32 | NA | NA | NA | NA | NA | NA |
| B33 | 1017.86 (22.26) | 1007.73 to 1027.99 | 12,182.00 (all breach) | All breach | NA | NA |
| B34 | 1019.33 (20.72) | 1015.93 to 1022.73 | NA | NA | 2690.00 (all breach) | All breach |
| B35 | 1015.28 (10.59) | 1013.47 to 1017.09 | NA | NA | 2690.00 (all breach) | All breach |
| B36 | 8721.10 (9235.12) | 7464.77 to 9977.43 | 39,472.67 (27,235.67) | 35,767.58 to 43,177.76 | NA | NA |
| B37 | 5137.67 (6356.17) | 4531.64 to 5743.69 | NA | NA | 7811.77 (11,170.37) | 6746.74 to 8876.80 |
| B38 | 7906.74 (8805.28) | 6736.74 to 9076.74 | NA | NA | 12,362.47 (16,509.87) | 10,168.72 to 14,556.22 |
| B39 | NA | NA | NA | NA | NA | NA |
| B40 | NA | NA | NA | NA | NA | NA |
| B41 | 1013.00 (all breach) | All breach | 12,182.00 (all breach) | All breach | NA | NA |
| B42 | 1019.95 (32.62) | 1005.49 to 1034.42 | NA | NA | 2690.00 (all breach) | All breach |
| B43 | 1018.88 (22.00) | 1010.00 to 1027.77 | NA | NA | 2690.00 (all breach) | All breach |
| B44 | 9406.93 (8704.70) | 7118.15 to 11,695.72 | 42,897.95 (25,510.42) | 36,190.33 to 49,605.57 | NA | NA |
| B45 | 4956.39 (6496.30) | 3407.40 to 6505.37 | NA | NA | 7465.06 (11,341.15) | 4760.86 to 10,169.26 |
| B46 | 7872.27 (8770.08) | 5606.71 to 10,137.82 | NA | NA | 12,539.25 (16,876.17) | 8179.67 to 16,898.83 |
| B47 | NA | NA | NA | NA | NA | NA |
| B48 | NA | NA | NA | NA | NA | NA |
| B49 | 1026.34 (32.64) | 1022.50 to 1030.19 | 12,182.00 (all breach) | All breach | NA | NA |
| B50 | 1019.93 (25.07) | 1018.64 to 1021.22 | NA | NA | 2690.00 (all breach) | All breach |
| B51 | 1019.84 (24.02) | 1018.01 to 1021.67 | NA | NA | 2690.00 (all breach) | All breach |
| B52 | 8944.71 (9395.00) | 8661.88 to 9227.55 | 39,447.50 (27,200.33) | 38,628.63 to 40,266.36 | NA | NA |
| B53 | 6576.99 (8092.02) | 6375.69 to 6778.29 | NA | NA | 10,564.13 (14,993.33) | 10,201.27 to 10,947.41 |
| B54 | 8720.27 (9259.67) | 8320.76 to 9119.79 | NA | NA | 13,867.08 (17,750.17) | 13,101.24 to 14,632.93 |
| B55 | NA | NA | NA | NA | NA | NA |
| B56 | NA | NA | NA | NA | NA | NA |
Costs (2012) associated with subsequent offending
| DIPa | Subsequent offence (£)b,c,d | No DIP | Subsequent offence (£)b,c,d | ||
|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| A1 | NA | NA | B1 | NA | NA |
| A2 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B2 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A3 | NA | NA | B3 | NA | NA |
| A4 | NA | NA | B4 | NA | NA |
| A5 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B5 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A6 | NA | NA | B6 | NA | NA |
| A7 | NA | NA | B7 | NA | NA |
| A8 | NA | NA | B8 | NA | NA |
| A9 | NA | NA | B9 | NA | NA |
| A10 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B10 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A11 | NA | NA | B11 | NA | NA |
| A12 | NA | NA | B12 | NA | NA |
| A13 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B13 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A14 | NA | NA | B14 | NA | NA |
| A15 | NA | NA | B15 | NA | NA |
| A16 | NA | NA | B16 | NA | NA |
| A17 | NA | NA | B17 | NA | NA |
| A18 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B18 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A19 | NA | NA | B19 | NA | NA |
| A20 | NA | NA | B20 | NA | NA |
| A21 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B21 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A22 | NA | NA | B22 | NA | NA |
| A23 | NA | NA | B23 | NA | NA |
| A24 | NA | NA | B24 | NA | NA |
| A25 | NA | NA | B25 | NA | NA |
| A26 | n = 0 | n = 0 | B26 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A27 | NA | NA | B27 | NA | NA |
| A28 | NA | NA | B28 | NA | NA |
| A29 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B29 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A30 | NA | NA | B30 | NA | NA |
| A31 | NA | NA | B31 | NA | NA |
| A32 | NA | NA | B32 | NA | NA |
| A33 | NA | NA | B33 | NA | NA |
| A34 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B34 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A35 | NA | NA | B35 | NA | NA |
| A36 | NA | NA | B36 | NA | NA |
| A37 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B37 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A38 | NA | NA | B38 | NA | NA |
| A39 | NA | NA | B39 | NA | NA |
| A40 | NA | NA | B40 | NA | NA |
| A41 | NA | NA | B41 | NA | NA |
| A42 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B42 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A43 | NA | NA | B43 | NA | NA |
| A44 | NA | NA | B44 | NA | NA |
| A45 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B45 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A46 | NA | NA | B46 | NA | NA |
| A47 | NA | NA | B47 | NA | NA |
| A48 | NA | NA | B48 | NA | NA |
| A49 | NA | NA | B49 | NA | NA |
| A50 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B50 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A51 | NA | NA | B51 | NA | NA |
| A52 | NA | NA | B52 | NA | NA |
| A53 | 20,720.30 (26,854.38) | 19,603.11 to 21,837.49 | B53 | 22,762.82 (28,885.43) | 22,402.80 to 23,122.85 |
| A54 | NA | NA | B54 | NA | NA |
| A55 | NA | NA | B55 | NA | NA |
| A56 | NA | NA | B56 | NA | NA |
Changes to parameter values for sensitivity analyses of data estimates
| Parameter | Value in primary analysis | Value in sensitivity analysis |
|---|---|---|
| Probability values | ||
| Probability of new or ongoing treatment following diversion (DIP) is higher than no diversion | Mean 0.533 (SD 0.040) |
0.75 (range 0.53–1.00) |
| Probability of new or ongoing treatment following diversion (DIP) is equal to no diversion (DIP) | Mean 0.533 (SD 0.040) |
0.363 (SD 0.074) |
| Probability of treatment ceased is higher and utility equals treatment completion | ||
| Probability treatment ceased | DIP: 0.11–0.24 No DIP: 0.14–0.23 |
DIP and no DIP: 0.52 (range 0.18–0.52) |
| Utility of completed treatment | 0.698 (SD 0.142) | 0.713 (SD 0.142) |
| Probability of reoffending is lower following diversion (DIP) than no diversion | DIP: 0.50–0.91 No DIP: 0.49–0.85 |
DIP: 0.50 (range 0.5–0.91) No DIP: 0.85 (range 0.5–0.91) |
| Probability of reoffending is zero following treatment | DIP: 0.50–0.82 No DIP: 0.49–0.85 |
0.00 |
| Utility values | ||
| Treatment leads to higher health status | ||
| Utility at end of treatment | Mean 0.698 (SD 0.142) |
Mean 0.713 (SD 0.142) |
| Utility non-offenders | Mean 0.713 (SD 0.142) |
Mean 0.752 (SD 0.134) |
| Health status and utility is lower at the end of 1 year due to relapse, non-offenders | ||
| Equal relapse DIP/no DIP 0.15, utility for relapse 0.648 (baseline value) | 0.713 (SD 0.142) | 0.658 (SD 0.142) |
| Lower relapse DIP 0.00, utility for relapse 0.648 (baseline value) | 0.713 (SD 0.142) | DIP: 0.713 No DIP: 0.703 |
| Utility value assigned to reoffenders is higher and equals that of non-offenders at end of 1st year | Mean 0.683 (SD 0.141) | 0.713 (SD 0.142) |
| Utility value assigned to reoffender is lower at end of first year and equal to baseline value | Mean 0.683 (SD 0.141) | 0.648 (SD 0.139) |
| Cost values | ||
| Cost of diversion (DIP) is 2× higher | Best estimate £195 (range £108–269) | £390 (range £108–390) |
| Cost of diversion (DIP) is 3× higher | Best estimate £195 (range £108–269) | £585 (range £108–585) |
| Cost of drug test is 2× higher | Mean £111 (range £57–165) | £222 (range £57–222) |
| Cost of drug test is 3× higher | Mean £111 (range £57–165) | £333 (range £57–333) |
| Cost per day of treatment is 2× higher | Mean = £36 (SD £42) | £72 (SD £42) |
Changes to parameter values for sensitivity analyses for model structure and design choices
| Parameter | Value in primary analysis | Value in sensitivity analysis |
|---|---|---|
| Population eligible for diversion (DIP) excludes those in treatment at index arrest, probability of new treatment for those having treatment | Mean 0.371 (SD 0.022) | 1.00 (no range) |
| Population eligible for diversion includes people with prison sentence for index arrest | ||
| Probability prison sentence DIP | 0 | 0.20 (range 0.18–0.22) |
| Probability prison sentence No DIP | 0 | 0.20 (range 0.18–0.22) |
| Cost prison sentence DIP includes treatment costs | 0 | £44,000 (range £12,000–44,000) |
| Cost prison sentence no DIP excludes treatment costs | 0 | £12,228 (SD £23,453) |
| Population eligible for diversion includes people with prison sentence for index arrest | ||
| Probability prison sentence DIP | 0 | 0.18 (range 0.18–0.22) |
| Probability prison sentence No DIP | 0 | 0.22 (range 0.18–0.22) |
| Probability reoffending is higher following prison sentence DIP and no DIP | ||
| Cost prison sentence DIP includes treatment costs | 0 | £44,000 (range £12,000–44,000) |
| Cost prison sentence no DIP excludes treatment costs | 0 | £12,228 (SD £23,453) |
| Outcome is rate of treatment completers; probability of treatment ceased is higher and equates to treatment completion | ||
| Probability treatment ceased | DIP: 0.11–0.24 No DIP: 0.14–0.23 |
DIP and no DIP: 0.52 (range 0.18–0.52) |
| Outcome is completed treatment | NA | 1 |
| Outcome is rate of people free from dependency if treated; probability of treatment ceased is higher and equates to treatment completion, assumed free from dependency | ||
| Probability treatment ceased | DIP: 0.11–0.24 No DIP: 0.14–0.23 |
DIP and no DIP: 0.52 (range 0.18–0.52) |
| Outcome is free from dependency if treated, p = 0.29 (range 0.15–0.47) | NA | 1 |
Results of sensitivity analyses for data estimates
| Analysis | Net cost of DIP, mean (95% CI) | Net QALY of DIP, mean (95% CI) | ICER | Net monetary benefit, mean (95% CI) | Probability DIP is cost-effective at WTPT of £30K per QALY |
|---|---|---|---|---|---|
| Primary analysis | –£147 (–£17,573 to £16,317) | 0.005 (–0.057 to 0.065) | No differences | £300 (–£15,927 to £16,719) | 0.51 |
| Probability of treatment following diversion (DIP) is higher | £566 (–£17,233 to £18,440) | 0.012 (–0.146 to 0.164) | No differences | –£109 (–£16,865 to £18,322) | 0.49 |
| Probability of treatment following diversion (DIP) is equal to no diversion | –£575 (–£18,206 to £16,526) | 0.002 (–0.028 to 0.033) | No differences | £583 (–£16,623 to £18,163) | 0.54 |
| Probability of treatment ceased is higher and equates to treatment completion, utility of treatment ceased is higher | –£444 (–£18,010 to £16,315) | 0.007 (–0.057 to 0.071) | No differences | £595 (–£15,246 to £18,446) | 0.54 |
| Probability of reoffending is zero following treatment | –£716 (–£14,785 to £12,765) | 0.013 (–0.055 to 0.090) | No differences | £1255 (–£11,828 to £14,612) | 0.57 |
| Probability of treatment following diversion is higher and reoffending is zero following treatment | –£1344 (–£17,886 to £18,817) | 0.035 (–0.133 to 0.221) | No differences | £2383 (–£19,711 to £19,578) | 0.65 |
| Probability of reoffending is lower following diversion (DIP) than no diversion | –£631 (–£18,036 to £15,082) | 0.009 (–0.054 to 0.075) | No differences | £958 (–£15,259 to £17,365) | 0.55 |
| Probability of treatment is higher and reoffending lower following diversion (DIP) | –£376 (–£18,548 to £17,904) | 0.021 (–0.136 to 0.182) | No differences | £1096 (–£16,757 to £20,301) | 0.56 |
| Probability of treatment is higher and reoffending lower following diversion (DIP), treatment leads to higher health status and utility | –£376 (–£18,548 to £17,904) | 0.027 (–0.128 to 0.190) | No differences | £1302 (–£16,121 to £20,434) | 0.57 |
| Treatment leads to higher health status and utility | –£147 (–£17,573 to £16,317) | 0.006 (–0.055 to 0.067) | No differences | £486 (–£15,880 to £16,486) | 0.52 |
| Relapse leads to lower utility, non-offenders | No differences | ||||
| Equal relapse DIP/no DIP | –£147 (–£17,573 to £16,317) | 0.004 (–0.530 to 0.060) | No differences | £265 (–£15,928 to £16,726) | 0.51 |
| Lower relapse DIP | –£147 (–£17,573 to £16,317) | 0.005 (–0.059 to 0.068) | No differences | £330 (–£15,926 to £16,718) | 0.52 |
| Probability of treatment following diversion (DIP) is higher and treatment leads to higher health status and utility | £561 (–£17,282 to £18,461) | 0.016 (–0.141 to 0.169) | No differences | £25 (–£16,736 to £18,472) | 0.50 |
| Utility value assigned to reoffenders is higher | –£147 (–£17,573 to £16,317) | 0.007 (–0.056 to 0.071) | No differences | £538 (–£16,162 to £16,957) | 0.52 |
| Utility value assigned to reoffenders is lower | –£147 (–£17,573 to £16,317) | 0.002 (–0.037 to 0.044) | No differences | £236 (–£15,911 to £17,035) | 0.51 |
| Utility value assigned to reoffender is lower and relapse reduces utility to baseline values, relapse is equal DIP and No DIP | –£147 (–£17,573 to £16,317) | 0.001 (–0.034 to 0.039) | No differences | £201 (–£16,067 to £17,043) | 0.51 |
| Cost of DIP and drug test is 2× higher | £97 (–£17,315 to £16,568) | 0.005 (–0.057 to 0.065) | No differences | £57 (–£16,149 to £16,451) | 0.50 |
| Cost of DIP and drug test is 3× higher | £341 (–£17,078 to £16,901) | 0.005 (–0.057 to 0.065) | No differences | –£187 (–£16,379 to £16,182) | 0.49 |
| Cost of DIP and drug test is 3× higher and utility of relapse and reoffenders is lower | £341 (–£17,078 to £16,901) | 0.001 (–0.034 to 0.039) | No differences | –£287 (–£16,585 to £16,511) | 0.48 |
| Cost of offences following diversion (DIP) is lower | No differences | ||||
| Cost per day of treatment is 2× higher | £936 (–£16,751 to £18,695) | 0.005 (–0.057 to 0.065) | No differences | –£698 (–£17,757 to £16,650) | 0.46 |
| Probability of treatment following diversion (DIP) is higher and cost per day of treatment is 2× higher | £3559 (–£16,070 to £28,858) | 0.012 (–0.146 to 0.164) | No differences | –£3213 (–£28,935 to £17,117) | 0.39 |
| Probability of treatment following diversion (DIP) is higher, treatment leads to higher health status and utility and cost per day of treatment is 2× higher | £3559 (–£16,070 to £28,858) | 0.016 (–0.141 to 0.169) | No differences | –£3077 (–£28,860 to £17,262) | 0.40 |
Results of sensitivity analyses for model structure and design choices
| Analysis | Net cost of DIP, mean (95% CI) | Net QALY of DIP, mean (95% CI) | ICER | Net monetary benefit, mean (95% CI) | Probability DIP is cost-effective at WTPT of £30K per QALY |
|---|---|---|---|---|---|
| Primary analysis | –£147 (–£17,573 to £16,317) | 0.005 (–0.057 to 0.065) | No differences | £300 (–£15,927 to £16,719) | 0.51 |
| Population eligible for diversion (DIP) excludes those already in treatment at index arrest | –£366 (–£17,761 to £16,210) | 0.003 (–0.058 to 0.062) | No differences | £540 (–£16,262 to £16,867) | 0.53 |
| Population eligible for diversion includes people with prison sentence for index arrest equal probability DIP and no DIP | £5974 (£15,796 to £48,503) | 0.005 (–0.057 to 0.065) | No differences | –£5725 (–£45,636 to £14,256) | 0.38 |
| Population eligible for diversion includes people with prison sentence for index arrest lower probability of prison for DIP | £5100 (£15,927 to £41,765) | 0.005 (–0.057 to 0.065) | No differences | –£4873 (–£39,613 to £14,260) | 0.39 |
| Population eligible for diversion includes people with prison sentence for index arrest, probability of prison for DIP = 0 | £5100 (£15,927 to £41,765) | 0.005 (–0.057 to 0.065) | No differences | –£4873 (–£39,613 to £14,260) | 0.39 |
| Outcome is rate of treatment completers; probability of treatment ceased is higher and equals treatment completion | –£444 (–£18,010 to £16,315) | 0.109 (–0.004 to 0.211) | No differences | £3632 (–£12,298 to £20,389) | 0.70 |
| Outcome is rate of treatment completers; probability of treatment ceased is higher and equals treatment completion | –£444 (–£18,010 to £16,315) | 0.109 (–0.004 to 0.211) | No differences | WTPT £0, £444 (–£18,010 to £16,315) | 0.52 |
| Outcome is rate of people free from dependency if treated; probability of treatment ceased is higher and equates to treatment completion, assumed free from dependency | –£444 (–£18,010 to £16,315) | 0.075 (–0.004 to 0.153) | No differences | £2739 (–£13,562 to £20,158) | 0.52 |
| Outcome is rate of people free from dependency if treated; probability of treatment ceased is higher and equates to treatment completion, assumed free from dependency | –£444 (–£18,010 to £16,315) | 0.075 (–0.004 to 0.153) | No differences | WTPT £0, £444 (–£18,010 to £16,315) | 0.65 |
| Outcome is reoffenders averted | –£147 (–£17,573 to £16,317) | 0.03 (0.001 to 0.063) | No differences | £1036 (–£15,297 to £18,657) | 0.56 |
| Outcome is reoffenders averted | –£147 (–£17,573 to £16,317) | 0.03 (0.001 to 0.063) | No differences | WTPT£0 –£147 (–£17,573 to £16,317) | 0.51 |
| Time horizon = 5 years | –£242 (–£22,911 to £24,635) | 0.005 (–0.311 to 0.314) | No differences | £1155 (–£25,428 to £24,822) | 0.52 |
| Time horizon = 10 years | –£222 (–£22,232 to £24,635) | 0.005 (–0.311 to 0.314) | No differences | £422 (–£29,019 to £25,584) | 0.53 |
List of abbreviations
- ACMD
- Advisory Council on the Misuse of Drugs
- ASI
- Addiction Severity Index
- CalOMS
- California Outcomes Measurement System
- CEAA
- cost-effectiveness acceptability analysis
- CEAC
- cost-effectiveness acceptability curve
- CI
- confidence interval
- CJS
- criminal justice system
- CMR
- Circumstances, Motivation and Readiness
- CSEW
- Crime Survey for England and Wales
- DDW
- Drug Data Warehouse
- DIP
- Drug Interventions Programme
- DTORS
- Drug Treatment Outcomes Research Study
- DTTO
- drug treatment and testing order
- HTA
- Health Technology Assessment
- ICER
- incremental cost-effectiveness ratio
- ID
- identifier
- ITT
- intention to treat
- LSD
- lysergic acid diethylamide
- MTP
- Methamphetamine Treatment Project
- NB
- net benefit
- NDTMS
- National Drug Treatment Monitoring System
- NHS EED
- NHS Economic Evaluation Database
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- NTORS
- National Treatment Outcome Research Study
- NTP
- Narcotic Treatment Programme
- ONS
- Office for National Statistics
- OR
- odds ratio
- PNC
- Police National Computer
- PSA
- probabilistic sensitivity analysis
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- ROSIE
- Research Outcome Study in Ireland
- SACPA
- Substance Abuse and Crime Prevention Act
- SD
- standard deviation
- TAP
- Treatment Alternative Program
- TAU
- treatment as usual
- TR
- Transforming Rehabilitation agenda
- WTPT
- willingness-to-pay threshold