
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 12/27/16. The contractual start date was in April 2013. The draft report began editorial review in April 2014 and was accepted for publication in July 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Elizabeth Taylor Buck and Chris Wood are registered art therapists with the Health Care Professions Council. Kim Dent-Brown is a registered arts therapist with the Health Care Professions Council.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Uttley et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background to the underlying health problem
Definition and prevalence of non-psychotic mental disorders
Among people under 65 years, nearly half of all ill health is mental illness, which accounts for 38% of all morbidity in the UK burden of disease. 1 Mental ill health is the largest single cause of disability in our society. 2 Mental disorders can be broadly categorised as either psychotic or non-psychotic, with non-psychotic disorders accounting for most (94%) mental health morbidity in adults. 1,3 Non-psychotic mental disorders include anxiety disorders such as phobias and obsessive–compulsive disorder, mood disorders such as depression and major depressive disorder, and other conditions such as eating disorders and personality disorders. Depression alone accounts for the greatest burden of disease among all mental health problems. 4,5 In addition, nearly one-third of all people with long-term physical conditions have a comorbid mental health problem such as depression or anxiety disorders, indicating an interaction between physical and mental illness. 6–8 Figures for mental illness quoted in the London School of Economics and Political Science report do not include dementia and alcohol and substance misuse, which are also important issues in their own right, and account for part of the outlay in mental health services in the UK NHS. 1
Costs to the NHS
Mental health receives a 13% share of the NHS expenditure despite mental health accounting for 23% in the burden of disease. 1 The largest part of this expenditure is on psychotic disorders, but these disorders account for less than 6% of people suffering with mental illness. One-quarter of all those with mental health problems are in treatment, compared with the vast majority of those with physical illnesses. 1 Research indicates that the costs of psychological therapy are low compared with general care admissions,9,10 and recovery rates are high. 11 Unlike most long-term physical conditions, much mental illness is curable. 11 For depression and anxiety the number needed to treat is estimated to be under 3. 1 Moreover, the same research used data from relevant National Institute for Health and Care Excellence (NICE) guidance compiled by the National Collaborating Centre for Mental Health and posits that ‘more expenditure on the most common mental disorders would almost certainly cost the NHS nothing’ because ‘when people with physical symptoms receive psychological therapy, the average improvement in physical symptoms is so great that the resulting savings on NHS physical care outweigh the cost of the psychological therapy’. 1
The NHS is under increasing pressure to provide cost-effective treatments to service users in a timely manner. The UK government initiative for Improving Access to Psychological Therapies (IAPT) for depression and anxiety disorders within the NHS offers evidence-based psychological therapies that are recommended by NICE. However, IAPT is facing increasing criticism that it is too limited to handle the mental health problems of people with long-term physical conditions or medically unexplained symptoms. 1 Recent evidence also suggests that only one-quarter of people with a mental illness receive treatment for it and that mental health is seriously undervalued, under-recognised and underfunded in the NHS. 1 It may be that more mental health treatment options are needed, which vary according to the type and severity of mental disorder, rather than a one-size-fits-all approach across professions. In addition, recent evidence suggests that psychological treatment may be a preferred treatment option over pharmacological treatment for many who are undergoing treatment for a psychiatric disorder. 12,13 Moreover, patient preference for treatment may impact on adherence and treatment outcome. 14,15 Therefore, evaluation of forms of psychological therapy other than cognitive–behavioural therapy (CBT) need to be conducted in addition to the evaluation of specific pathways within those psychological therapies, in order to create a strategic framework of pathways for managing the burden of mental health morbidity.
Evaluation of psychological therapies such as art therapy is therefore critical in order to inform future recommendations for its use. There is a small body of evidence to support the claim that art therapy is effective in treating a variety of symptoms and disorders in patients of different ages. 16 However, to date a full systematic review of the clinical effectiveness and cost-effectiveness of art therapy for non-psychotic mental disorders has not been undertaken. This project aimed to evaluate the current evidence for art therapy for people with non-psychotic mental disorders in order to inform researchers and commissioners about the value of future use of art therapy in the NHS.
Art therapy
Description of intervention
The intervention of interest is art therapy as might be delivered in the NHS. Art therapy involves using painting, clay work and other creative visual art-making (including creative digital media) as a form of non-verbal expression, in conjunction with other modes of communication within a therapeutic relationship in an appropriate therapeutic setting. Art therapy is a specific branch of treatment under the umbrella term ‘arts therapies’ used by the Health and Care Professions Council (HCPC) which includes drama therapy and music therapy. Dance movement therapy is also described as one of the arts therapies but is not yet regulated. For the purpose of this technology assessment these other forms of arts therapies, which do not centre on the creation of a sustainable physical piece of visual art, are excluded.
Despite art therapy being an established and practised form of psychological therapy for decades, only more recently have researchers in the field of art therapy addressed the need to integrate art therapy into a model of evidence-based practice. Therefore, an abundance of literature exists consisting of single case studies or theoretical concepts in art therapy. Proponents of art therapy17–19 and of the arts therapies20,21 only relatively recently have come to realise that randomised controlled studies of art therapy are needed in order to create a pluralistic body of evidence. As a consequence there has been limited formal synthesis of evidence16,22 for the clinical effectiveness and cost-effectiveness of art therapy in order to assess its relevance as a treatment for the most common mental disorders in the NHS.
Current use of art therapy in NHS
Currently, CBT is the most widely recommended psychological therapy for most mental health problems. However, NICE has identified that the arts therapies (including art therapy) may have specific benefits for people with psychosis and schizophrenia and, therefore, recommends art therapy to be considered for these patients, above counselling and supportive psychological therapy. 23 There are a number of non-psychotic mental health problems that are typified by service users’ reluctance or inability to communicate their feelings verbally. Art therapy is currently being used in the NHS for many non-psychotic mental disorders. For example, arts therapies are included in the autistic spectrum disorder (ASD) Strategic Plan for Wales20 as an accessible and appropriate form of psychotherapy for those with ASD. For these and other service users, it may be that art therapy is a more appropriate treatment than standard talking therapies, but the evidence base for the use and acceptability of art therapy in non-psychotic mental disorders has yet to be formally evaluated. There are clinical guidelines by art therapists for working with elderly people,24 working with prisoners,25 working with children, adolescents and families,26 and working with people with a diagnosis of personality disorder,27 indicating movement in the profession towards more specific systematic practice and research. There are currently no national guidelines in the UK specifically for the use of art therapy for non-psychotic mental disorders.
Art therapy is a widely used psychological therapy which has HCPC approval, higher education Quality Assurance Agency for Higher Education subject benchmarks and a professional organisation for its practitioners – the British Association of Art Therapists (BAAT). While testimonials and case studies occupied much of the evidence for art therapy in the past, there has been less focus on producing rigorous randomised controlled trials (RCTs) of art therapy. The purpose of this review is to assess systematically the evidence that is relevant to whether or not art therapy is effective, how it may be clinically effective and whether or not it is cost-effective in people with non-psychotic mental health disorders.
The results of the 2014 BAAT Workforce Survey represented one-third of members from the professional association; with 70 responses from Scotland and 567 responses from England, Wales and Northern Ireland. The survey results suggested that:
-
In England, Wales and Northern Ireland, the NHS employs around half of art therapists who responded. Other large employers are third-sector organisations (charities, voluntary and independent organisations), educational institutions, private practices and local authorities.
-
Over half of art therapists who responded use generic skills in their work, such as assessments and key working, possibly reflecting a change towards delivering other services in addition to providing art therapy.
-
The majority of client groups served are adults, children and young people. Elderly people and families account for smaller proportions.
-
The range of mental health difficulties dealt with by art therapists who responded includes complex trauma and abuse, learning disabilities, alcohol and substance use, forensic mental health, criminal justice, elderly people and palliative care.
There are likely to be regional variations in the availability and practice of art therapy in the UK not captured by this survey.
There is no definitive criterion for who is routinely referred for art therapy, and at what point in their care pathway. 28 The only standardised guidelines for its use are in relation to schizophrenia. 29 However, discernible clusters of people undergo art therapy according to published literature, including people who have been abused and traumatised, who are on the autistic spectrum, who have addictions, dementia, eating disorders or learning difficulties, who are offenders, who are in palliative care, who have depression or personality disorders or who were displaced as a result of political violence. Therefore, adults are referred from a broad range of diagnostic categories, but they tend not to be referred on the basis of diagnosis alone. They may be referred on the basis of behavioural problems, including problems with engaging with services or problems with putting distress into words, for which talking therapies would not be the preferred option. Other clinicians making referrals to art therapy are often looking to widen the range of treatment options for people who, in addition to having complex, severe and enduring mental health problems, face emotional and socioeconomic deprivation. As seen in the use of art therapy for service users in palliative care, people facing the emotional consequences of serious physical health may also be referred.
Defining the use of art therapy for children and adolescents is also problematic. This is because children’s problems tend to be grouped as ‘emotional’ or ‘behavioural’ in the absence of diagnosed disorders. 30 Published outcome data are scarcer for children and adolescents, with more qualitative descriptions of art therapy occurring in the literature. However, BAAT reports that, in November 2010, of the approximately 1800 full members of BAAT, 878 described themselves as working with children, young people and/or families. Seemingly, therefore, art therapy is currently being widely practised with children and young people and should be duly considered in this review.
The art therapist’s role in the mental health service pathway
In service contexts where art therapists are working more briefly with service users, they may also refer on to other services. This is particularly important for clients who have long-term conditions, as it leaves the way open for clients to return for more art therapy at a later stage. Accordingly, art therapists have a professional responsibility to consider carefully referrals that they receive and that they make. Figure 1 indicates the mental health service pathway open to art therapists who are working in a multiagency context. This diagram is adapted from a presentation at the BAAT annual general meeting in 2010,31 in which a two-way bridge was highlighted as a potentially important relationship for art therapists who are working, clinically, with service users for relatively short periods of time.
FIGURE 1.
Mental health service pathway for art therapists working in a multiagency context.

Adapting the research to the research question
The protocol for this research project was designed by the research team in consultation with a project steering group consisting of external health professionals and service users (see Appendix 1). The steering group was made up of consultant psychiatrists with experience of referring to art therapy and service users who had been referred to art therapy. The purpose of the steering group was to ensure that the research team’s proposed research design was open to the views of stakeholders. In addition, the protocol was also publicly available online and the project was registered on the PROSPERO database of systematic reviews (registration no. CRD4201300395732).
One of the major challenges in delivering the research lay in tailoring the research methodology to fit with the research question. The research question can be regarded as non-standard in that it centres on the intervention rather than the population. This health technology assessment can therefore be regarded as an evidence portfolio for art therapy. The population under review is patients with non-psychotic mental disorders. Psychosis is not a precise mental health condition but is a symptom that can feature in several mental health disorders; for example, conditions such as bipolar disorder and depression can occur with or without psychotic symptoms. Conversely, schizophrenia is perhaps one of the few mental health conditions that is characterised by psychosis, along with delusional disorder, acute and transient psychotic disorder, schizoaffective disorder, non-organic psychotic disorder and organic psychotic disorder. These are, therefore, some of the few mental health conditions that can be regarded as falling outside the population for this research.
Art therapy as a clinical intervention: definition
Although art therapy is a HCPC-approved form of psychological therapy in the UK, there is currently a lack of a clear single definition of art therapy. The BAAT describes art therapy as a form of psychological therapy that uses the art-making process as its primary mode of communication and can therefore be particularly helpful to people who find it hard to express their thoughts and feelings verbally. Clients who are referred to an art therapist do not need to have previous experience or skill in art, and the overall aim of its practitioners is to enable the client to explore and express their feelings in a safe and facilitating environment. Art therapy can be regarded as a three-way process between the client, the therapist and the image or artefact. 33
The concept of art therapy may sometimes be confused with creative arts movements or strategies designed to improve well-being through art (often called ‘arts in health’ approaches) which, although potentially beneficial, are not specific formal therapeutic interventions to target mental health conditions in individual service users. In order to distinguish the psychotherapeutic use of art therapy as is under investigation in this research question, a criterion to define art therapy as a form of psychological therapy has been formulated. This pragmatic definition was developed as a screening tool and a guide for assessing papers for inclusion into the systematic review. It is not intended to be an exhaustive definition and needed to be sufficiently flexible to include practices in the UK and abroad.
Definition of art therapy in this review:
-
The procedure includes establishing therapeutic boundaries appropriate for art therapy interventions (such as clarity about the start and finish of therapy and the frequency and length of sessions).
-
The intervention takes places in the presence of a therapist with whom there is an appropriate therapeutic relationship.
-
The intervention includes the therapeutic use of art materials.
-
The description of art therapy is appropriate to the cultural and service context.
Art therapy as a complex intervention
Non-pharmacological treatments such as psychotherapies are often considered to be complex interventions. The key features of complex interventions have been described (Craig et al. 200834) as:
-
having a number of interacting components
-
having a number and difficulty of behaviours required by those delivering or receiving the intervention
-
having a number of groups or organisational levels targeted by the intervention
-
having a number and variability of outcomes
-
requiring a degree of flexibility or tailoring of the intervention permitted (non-standardisation/reproducibility).
Art therapy can be regarded as a complex intervention according to each of these features for the following reasons:
-
Art therapy may often be used in service users with complex clinical presentations who may or may not have responded to several other treatments in mental health services. It is frequently delivered as part of a wider package of treatment and sometimes as a last resort when other treatments have failed.
-
Art therapy is not delivered for any one specific health condition or symptom. It is used in a variety of patient populations. In addition, art therapy is not alone in lacking a clear single definition; psychological therapy more generally is open to heterogeneity through its delivery by different individuals.
-
Art therapy is frequently used in service users with comorbid physical long-term conditions which may actually be their primary health diagnosis. There is no set clinical pathway for who should receive art therapy and at what stage of treatment. Therefore, it is difficult to define or exhaustively list comparators for art therapy.
-
There is currently no standard outcome measure for defining ‘successful’ treatment through art therapy in clinical practice.
-
Art therapists do not offer a set package but tend to tailor the course of treatment, as well as each individual session, to the client.
Thus, confidence in building a coherent network of evidence for a mixed treatment comparison that would contain all possible comparators, comparable study designs and homogeneous participants was low. The use of substantial resources to construct a comparison with potentially low internal validity, in terms of the relative dearth of relevant art therapy evidence, was not deemed appropriate.
Non-psychotic mental health population: definition
The population under consideration is people undergoing treatment for mental health symptoms that do not include psychosis. However, one of the complexities of this population is that not everyone who is being treated for mental health symptoms has a mental health diagnosis. The target population can be described as:
-
Mainstream mental health clinical samples with or without formal diagnoses.
The primary health diagnosis for many people who are service users in mental health may be for a long-term physical health condition or illness that impacts on their mental health. A second group who are also relevant to the research question can be defined as the study population:
-
b(i) Reversible or fluctuating physical conditions where the treatment goals of art therapy include reduction of mental health symptoms (such as depression, anxiety or trauma) as demonstrated by the outcome measures used.
In addition, service users may be in receipt of mental health services for conditions where the primary goal of treatment cannot be considered solely as ‘recovery’ from symptoms, but may be to cope with the symptoms of chronic conditions such as dementia. Therefore, a third group which can also be regarded as relevant to the research question can be defined as the study population:
-
b(ii) Irreversible AND/OR deteriorating physical conditions for which mental health outcomes (such as reduction in depression, anxiety or trauma symptoms) were explicitly targeted and measured.
The use of a more flexible definition for the population, while unconventional in the majority of health technology assessments, is employed here in order to ensure that, while adhering to the research question, the review is also providing a complete picture of the literature relevant to the research question.
Positive outcomes and ‘success’ in mental health treatment
In the field of mental health there is a movement to accept the term ‘recovery’ rather than ‘cure’. This is because recovery can be seen as an ongoing experience which may not be comparable to end points in pharmacological trials. The term ‘recovery’ accommodates the concept that the journey of transitioning from a negative mental health state may be non-linear and may include setbacks as well as progress. 21,35 Essential elements of the recovery approach are reported to be those that facilitate the rebuilding of a meaningful life despite the continuing presence of mental health problems. 36
In addition, the measurement of recovery from a mental health disorder requires the use of a user-validated outcome measure. 37,38 In this sense, the majority of service users would need to agree that the measure makes sense and evaluates human factors that are important to them. Crucially, the outcome measure selected to evaluate treatment needs to be valid, reliable and sensitive to change over time. Mental health disorders can be chronic, recurring and multistage, and it is important that formal evaluation of mental health states is able to capture these complexities.
Time points for measuring recovery should also receive consideration. Individual differences may account for some variation in response to treatment but programmes of psychological treatment themselves vary in duration and frequency. Interventions may or may not be tailored to the individual service user according to service provision. Measurement of patient response to treatment using long-term follow-up, as well as within the time period of the intervention, are essential to determine sustained benefit of psychological interventions.
Research questions addressed in this review
-
What is the evidence that art therapy is clinically effective in people with non-psychotic mental health disorders?
-
What are the user and service provider perspectives on the acceptability and relative benefits and potential harms of art therapy for people with non-psychotic mental disorders?
-
What is the evidence that art therapy is cost-effective in people with non-psychotic mental health disorders?
Chapter 2 Clinical effectiveness of art therapy: quantitative systematic review
This chapter aims to provide an overview of the evidence examining the clinical effectiveness of art therapy in people with non-psychotic mental health disorders.
Literature search methods
Bibliographic database searching
Comprehensive literature searches were used to inform the quantitative, qualitative and cost-effectiveness reviews. A search strategy was developed to identify reviews, RCTs, economic evaluations, qualitative research and all other study types relating to art therapy. Methodological search filters were applied where appropriate. No other search limitations were used and all databases were searched from inception to present. Searches were conducted from May to July 2013. The full search strategies can be found in Appendix 2.
To ensure that the full breadth of literature for the non-psychotic population was included, it was pragmatic to search for all art therapy studies and then subsequently exclude studies manually (through the sifting process) that were conducted in people with a psychotic disorder or a disorder in which symptoms of psychosis were reported. It is therefore possible for the reviewer to view all potentially relevant records available and manually exclude studies of samples with psychotic disorders. This method of searching through the literature is in contrast to an approach that uses a search strategy listing all possible mental health disorders that are considered to be ‘non-psychotic’ in the search terms. The latter method may not retrieve all relevant studies from populations that are not indexed under the named mental health disorders.
In addition to the range of conditions covered by the population, the evidence from the studies being generated was frequently not a clear-cut diagnosed ‘mental health disorder’ and the populations retrieved were not the clinical populations of common mental health problems that were first anticipated. At this point in the study identification process it would have been easy to exclude any study that did not include patients with a clinically diagnosed mental health disorder. If this approach had been taken, there would have been three studies in the quantitative review. Instead a pragmatic approach was taken by identifying, including and describing the populations that art therapy is being studied in, with reference to targeting mental health symptoms (see Chapter 1, Non-psychotic mental health population: definition).
Databases searched
-
MEDLINE and MEDLINE In-Process & Other Non-Indexed citations (OvidSP).
-
EMBASE (OvidSP).
-
Cochrane Database of Systematic Reviews (The Cochrane Library).
-
Cochrane Central Register of Controlled Trials (The Cochrane Library).
-
Database of Abstracts of Review of Effects (The Cochrane Library).
-
NHS Economic Evaluation Database (The Cochrane Library).
-
Health Technology Assessment Database (The Cochrane Library).
-
Science Citation Index (Web of Science via Web of Knowledge).
-
Social Sciences Citation Index (Web of Science via Web of Knowledge).
-
CINAHL: Cumulative Index to Nursing and Allied Health Literature (EBSCOhost).
-
PsycINFO (OvidSP).
-
AMED: Allied and Complementary Medicine Database (OvidSP).
-
ASSIA: Applied Social Sciences Index and Abstracts (ProQuest).
Sensitive keyword strategies using free-text and, where available, thesaurus terms using Boolean operators and database-specific syntax were developed to search the electronic databases. Date limits or language restrictions were not used on any database. All resources were searched from inception to May 2013.
Grey literature searching
A number of sources were searched to identify any relevant grey literature. Relevant grey literature or unpublished evidence would include reports and dissertations that report sufficient details of the methods and results of the study to permit quality assessment. Conference proceedings without a corresponding final report (published or unpublished) would not qualify for inclusion, as they are unlikely to contain sufficient information to permit quality assessment and can often be different to results published in the final report. 39,40
Sources searched
-
NHS Evidence (Guidelines): www.evidence.nhs.uk/.
-
The BAAT: www.baat.org/index.html.
-
UK Clinical Research Network Portfolio Database: public.ukcrn.org.uk/Search/Portfolio.aspx.
-
National Research Register Archive: www.nihr.ac.uk/Pages/NRRArchive.aspx.
-
Current Controlled Trials: www.controlled-trials.com/.
-
OpenGrey: www.opengrey.eu/.
-
Google Scholar: scholar.google.co.uk/.
-
Mind: www.mind.org.uk/.
-
International Art Therapy Organisation: www.internationalarttherapy.org/.
-
National Coalition of Arts Therapies Associations: www.nccata.org/.
Additional search methods
A hand search of the International Journal of Art Therapy (formerly Inscape) was conducted. The additional search methods of reference list checking and citation searching of the included studies were utilised. Other complementary search methods were considered such as pearl growing; however, because the search method employed was considered to be very inclusive, such additional methods were unlikely to generate additional relevant records.
Review methods
Screening and eligibility
The operational sifting criteria (eligibility criteria) were defined and verified by two reviewers (LU and AS). Titles and abstracts of all records generated from the searches were scrutinised by one assessor and checked by a second assessor to identify studies for possible inclusion into the quantitative review. All studies identified for inclusion at abstract stage were obtained in full text for more detailed appraisal. Non-English studies were translated and included if relevant. For conference abstracts or clinical trial records without study data, authors were contacted via e-mail; however, no additional data were retrieved by contacting study authors. There was no exclusion on the basis of quality. If closer assessment of studies at full text indicated that eligible studies were not RCTs, then the studies were excluded. Agreement on inclusion, for 20% of the total search results (n = 2015), was calculated at title/abstract sift demonstrating 0.93 agreement using the kappa statistic. If there was uncertainty regarding the inclusion of a study, the reviewers sought the opinion of the team members with the relevant clinical, methodological or subject expertise to guide the decision.
Accumulation of results
All references were accumulated in a database using Reference Manager Version 12 (Thomson Reuters, Philadelphia, PA, USA), enabling studies to be retrieved in categories by keyword searches and duplicates to be removed.
Study appraisal
Two reviewers (LU and AS) performed data extraction independently for all included papers and discrepancies were resolved by discussion between reviewers. When necessary, authors of the studies were contacted for further information. Data were input into a data extraction template using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA), which was designed for the purpose of this review and verified by two reviewers. Information related to study population, sample size, intervention, comparators, potential biases in the conduct of the trial, outcomes including adverse events, follow-up and methods of statistical analysis was abstracted from the published papers directly into the electronic data extraction spreadsheet.
The evidence generated from the comprehensive searches highlighted that the majority of research in art therapy is conducted by or with art therapists. This indicates potential researcher allegiance towards the intervention in that art therapists are likely to have a vested interest in the output of the study. For this reason it was deemed important to focus on the highest quality evidence available from the study literature. Trials that were non-randomised (i.e. in which the researcher was able to select and allocate participants to treatment arms) were considered to be too low in methodological rigour to be included in this review. The consequence of including data from non-randomised studies into the review is that the resulting data are biased and therefore not robust or sufficient to inform and contribute to the evidence base. 41,42 The inclusion and exclusion criteria for the quantitative review are shown in Figure 2.
FIGURE 2.
Eligibility criteria for the quantitative review.

Setting
Studies could be conducted in any setting, including primary, secondary, community based or inpatient.
Sessions
Study selection was not limited by the number of sessions, and studies that provided the intervention in a single session were included.
Timing of outcome assessment
Post-treatment outcomes and outcomes at reported follow-up points were extracted and summarised when reported.
Quality assessment strategy
Quality assessment of included RCTs was performed for all studies independently by two reviewers using quality assessment criteria adapted from the Cochrane risk of bias,44 Centre for Reviews and Dissemination (CRD) guidance45 and Critical Appraisal Skills Programme (CASP)46 checklists to develop a modified tool for the purpose of this review. The modified tool was developed to incorporate relevant elements across several tools to allow comprehensive and relevant quality assessment for the included trials. Judgements and corresponding reasons for judgements for each quality criterion for all studies were stated explicitly and recorded. Risk of bias was assessed to be low, high or unclear. Where insufficient details were reported to make a judgement, risk of bias was stated to be unclear and authors were not contacted for further details. Discrepancies in judgements were resolved by discussion between the two reviewers.
Results of the quantitative review
The total number of published articles yielded from electronic database searches after duplicates were removed was 10,073 (see Figure 3). An additional 197 records were identified from supplementary searches, resulting in a total of 10,270 records for screening. Of these, 10,221 records were excluded at title/abstract screening. Common reasons for exclusion from the review can be seen in Table 1. A full list of the studies excluded from the quantitative review at full text stage (with reasons for exclusion) can be found in Appendix 3.
FIGURE 3.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of studies included in the quantitative review.

| Common reasons for exclusion | Examples |
|---|---|
| Not art therapy | Arts-based initiatives not adhering to art therapy definition (see Art therapy as a clinical intervention: definition), antiretroviral therapy |
| Not a RCT | Before-and-after study, no control group, no randomisation |
| Psychotic disorder | Patients with schizophrenia or psychosis |
| Arts therapies | Combination of therapies without individual results for art therapy |
| No study data | Abstract without data and no response from author contact, studies which focused on the artwork itself and did not measure health outcomes |
The grey literature searches yielded very few potentially relevant records that were not generated by the electronic searches. One record appeared highly relevant to the research question and related to a clinical trial record of and RCT of art therapy in personality disorder (CREATe) for which the status was ‘ongoing’. However, e-mail contact with the primary investigator of this trial confirmed that the trial had been terminated because of poor recruitment.
Included studies: quantitative review
Fifteen RCTs were identified for inclusion into the review which were reported in 18 sources (see Table 2). For clarity in this comparison, where a study with multiple sources is discussed only one of the sources has been noted.
| Study author and year | Journal/publication | Country | n | Patients |
|---|---|---|---|---|
| Target population | ||||
| Chapman et al. 200149 | Art therapy | USA | 85a | Children with PTSD |
| Lyshak-Stelzer et al. 200748 | Art therapy | USA | 29 | Adolescents with PTSD |
| Thyme et al. 200747 | Psychoanalytic Psychotherapy | Sweden | 39 | Depressed female adults |
| Study population | ||||
| Beebe et al. 201058 | Journal of Allergy and Clinical Immunology | USA | 22 | Children with asthma |
| Broome et al. 200150 | Journal of National Black Nurses’ Association | USA | 97a | Children (n = 65) and adolescents (n = 32) with sickle cell disease |
| Gussak 200759 | International Journal of Offender Therapy and Comparative Criminology | USA | 44a | Incarcerated males |
| Hattori et al. 201151 | Geriatrics and Gerontology International | Japan | 39 | Patients with Alzheimer’s disease |
| Kim 201352 | The Arts in Psychotherapy | Korea | 50 | Non-clinical older adults (no formal mental health diagnosis) |
| McCaffrey et al. 201153 | Research in Gerontological Nursing | USA | 39 | Older adults |
| Monti and Peterson 200460 | Psychiatric Times | USA | 111a | Women with cancer |
| Monti et al. 200661 | Psycho-Oncology | |||
| Monti et al. 201254 | Stress and Health | USA | 18 | Women with breast cancer (no clinical mental health problem) |
| Puig et al. 200655 | The Arts in Psychotherapy | USA | 39 | Women with breast cancer |
| Rao et al. 200956 | AIDS Care | USA | 79a | Adults with HIV/AIDS |
| Rusted et al. 200657 | Group Analysis | UK | 45a | Patients with dementia |
| Thyme et al. 200962 | Palliative and Supportive Care | Sweden | 41 | Women with breast cancer |
| Svensk et al. 200963 | European Journal of Cancer Care | |||
| Oster et al. 200664 | Palliative and Supportive Care | |||
Ten out of the 15 included studies were conducted in the USA, while only one study was conducted in the UK (see Tables 2 and 3). Eleven of the studies were conducted in adults (who are the primary focus of this review) and four were conducted in children. All trials had small final sample sizes with the number of participants reported to be included in each study ranging between 18 and 111. The mean sample size was 52.
| Study type | Comparator | Study | Control group description |
|---|---|---|---|
| Non-active control | Treatment as usual | Chapman et al. 200149 | Standard hospital careb |
| Gussak 200759 | No treatment | ||
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | No art therapy | ||
| Wait-list | Beebe et al. 201058 | Crossover not reported | |
| Monti and Peterson 2004;60 Monti et al. 200661 | Control offered crossover at 9 weeks | ||
| Puig et al. 200655 | Control offered crossover at 4 weeks | ||
| Active control | Attention placebo | aBroome et al. 200150 | Fun activities |
| Hattori et al. 201151 | Simple calculations | ||
| Kim 201352 | Regular programme activities | ||
| Lyshak-Stelzer et al. 200748 | Arts and craft activities | ||
| McCaffrey et al. 201153 | Guided garden walking | ||
| Monti et al. 201254 | Educational support group | ||
| Rao et al. 200956 | Video tape on use of art therapy | ||
| Rusted et al. 200657 | Activity group | ||
| Psychological therapy | aBroome et al. 200150 | CBT relation for pain | |
| Thyme et al. 200947 | Verbal dynamic psychotherapy |
Three studies are of patients from the target population of people with non-psychotic mental disorders. 47–49 Of these three studies, only one was conducted in adults. 47
In the remaining 12 studies, the study population comprised individuals without a formal mental health diagnosis. 49–59,61,62 The populations in these studies are, therefore, mainly people with long-term medical conditions which are not reported to be accompanied by a mental health diagnosis; however, outcomes targeted in these studies were mental health symptoms.
The total number of patients in the included studies is 777. Nine studies compared art therapy with an active control group and six studies compared art therapy with a wait-list control or treatment as usual.
Two studies were reported to be conducted in an inpatient setting48,49 and one study was conducted in prison. 59 The majority of studies were conducted in community/outpatient setting, although the precise setting for conducting the intervention was not reported in six studies. 50,52,54–56,61
Brief descriptions of the art therapy interventions are provided in Tables 4 and 5.
| Study | Age (years), range (mean) | Duration and type | Art therapy description | Control description |
|---|---|---|---|---|
| Broome et al. 200150 | 6–18 (child, 9.2; adolescent, 15.3) | 4 weeks; group | Opportunity to express feelings about pain and develop social skills through interactions with others using art as a focal point | CBT relaxation for pain; or attention control (fun activities e.g. picnic, museum) for children group only |
| Hattori et al. 201151 | 73–83 (74) | 12 weeks; group (approximately n = 5) session | Primary task to colour abstract patterns, which are unclear before colouring. Encouraged to draw familiar objects based on memories or favourite seasons | Simple calculations (additions and multiplications of one- or two-digit numbers). No preset target; patients completed as many as they could in session |
| Kim 201352 | 69–87 (78) | 4 weeks; group | Introductory 10–15 minutes ‘unfreezing’ phase, followed by 35–40 minutes for individual art-making, 15–20 minutes for group discussion | Regular programme activities such as reading books, playing board games and watching television |
| Lyshak-Stelzer et al. 200748 | 13–17 (15) | 16 weeks; group (approximately n = 2 to 5) session | Completion of 13 > collages or drawings to express a ‘life story’ narrative. Encouraged but not required to discuss dreams, memories and feelings related to their trauma | ‘Treatment as usual’ – arts and craft making activity group |
| McCaffrey et al. 201153 | 65–NR (74) | 6 weeks; NR | Drawing self-portraits; presented to group; create new drawings; display and discuss (art therapy was reported as the control) | The two intervention groups were individual (n = 13) or guided (n = 13) garden walking in the Morikami Museum and Japanese Gardens in Delray Beach |
| Monti et al. 201254 | 52–77 (54) | 8 weeks; group | Mindfulness-based art therapy. Art-making paired with meditation and ways of expressing emotional information in a personally meaningful manner | Educational support group: control given equal time and provided with support and resources to maximise quality of life including expert speakers on topics and time for sharing and supportive exchanges |
| Rao et al. 200956 | 18–NR (42) | Brief (1 session); individual | Art therapist learns about patient and then offers art materials and assures patient they can use them in any way. Therapist helped participant process the meaning of the work and then discussed thoughts and feelings elicited | Viewed a video tape on the uses of art therapy |
| Rusted et al. 200657 | 67–92 (82) | 40 weeks; group (approximately n = 6) | Group-interactive psychodynamic approach | Activity groups: a selection of recreational activities from different centres in the locality |
| Thyme et al. 200947 | 19–35 (34) | 10 weeks; NR | Psychodynamic art therapy. Painting and reflective dialogue between the participant and the therapist | Verbal psychodynamic psychotherapy |
| Study | Age (years), range (mean) | Duration and type | Art therapy description |
|---|---|---|---|
| Beebe et al. 201058 | 7–14 (NR) | 7 weeks; group | Included an opening activity; discussion of the weekly topic and art intervention; art-making; opportunity for the parents to share their feelings related to the art they created; and the closing activity |
| Chapman et al. 200149 | 7–17 (10.7) | NR; individual | Chapman Art Therapy Treatment Intervention including drawing; verbal narrative and encouragement to express trauma-specific fears |
| Gussak 200759 | 21–59 (NR) | 8 weeks; group | Asked to draw person picking an apple from a tree and other similar art therapy tasks |
| Monti and Peterson 200460 Monti et al. 200661 |
26–82 (54) | 8 weeks; group | Mindfulness-based art therapy multimodal programme including a standardised mindfulness-based stress reduction curriculum; art therapy tasks and supportive group therapy |
| Puig et al. 200655 | 18-NR (51) | 4 weeks; individual | Semistructured creative experiences using art creation. Creative freedom encouraged in order to facilitate and explore emotional expression, spirituality and psychological well-being state |
| Thyme et al. 200962 Svensk et al. 200963 Oster et al. 200664 |
37–69 (median: 59 and 55) | 5 weeks; individual | Art-making with an art therapist including reflection and expression using verbal and non-verbal methods. Aimed at triggering a chain of feelings and thoughts an important object for communication. Basic idea was to use the participant’s picture as the new mode of expression, followed by a reflective dialogue |
Study duration ranged between the 15 studies from 1 session to 40 sessions, with a mean number of nine sessions (see Tables 4 and 5). Most studies with an active control group were of ‘group’ art therapy. One study which was a ‘brief’ intervention consisting of one individual session per participant. 56 Two studies did not state explicitly if sessions were in a group or individual. 47,53 Three studies with no active control were group art therapy58,59,61 and three studies were individual art therapy. 49,55,62
The symptoms or outcome domains under investigation and associated outcome measures are reported in Table 6.
| Study author and year | Outcome domains investigated | Outcome measures | Time points |
|---|---|---|---|
| Adults | |||
| Gussak 200759 | Depression | BDI-II | Exact time point post test NR |
| Hattori et al. 201151 | Mood; vitality; behavioural impairment; QoL; ADL; cognitive function | MMSE, WMS-R, GDS; Apathy Scale (Japanese version) SF-8 – Physical and Mental components; Barthel Index; DBD; Zarit Caregiver Burden Interview | 12 weeks |
| Kim et al. 201352 | Positive/negative affect; state-trait anxiety; self-esteem | PANAS; STAI; RSES | NR: assume 4 weeks |
| McCaffrey et al. 201153 | Depression | GDS | 6 weeks |
| Monti 200660,61 | Symptoms of distress including depression, anxiety and quality of life | SCL-90-R, GSI; SF-36 | 8 and 16 weeks |
| Monti et al. 201254 | Correlation of CBF on fMRI with experimental condition | fMRI; CBF; correlation with anxiety using SCL-90-R | Within 2 weeks of end of 8-week programme |
| Puig et al. 200655 | Mood symptoms including depression and anxiety | POMS; EACS | 4 weeks |
| Rao et al. 200956 | Physical symptoms including pain etc.; anxiety | ESAS; STAI | Immediately following session |
| Rusted et al. 200657 | Depression; mood; sociability and physical involvement | CSDD; MOSES; MMSE; RBMIT; TEA; Benton Fluency Task | 10, 20 and 40 weeks during trial then 44-week and 56-week follow-up |
| Thyme et al. 200747 | Stress reactions after a range of traumatic events; mental health symptoms; depression | IES; SCL-90; BDI; HRSD | 10 weeks and 3 month follow-up |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | Depression; anxiety; somatic and general symptoms; QoL Coping methods | SASB; GSI; SCL-90; WHOQOL-BREF; EORTC QoL Questionnaire-BR23; CRI | 2 and 6 months |
| Children and adolescents | |||
| Beebe et al. 201058 | QoL; behavioural and emotional adaptation | PedsQL; Asthma module Beck Youth Inventories – Second Edition | 7 weeks and 6 months |
| Broome et al. 200150 | Coping and health care utilisation | SCSI; A-COPE; ER visits; clinic visits; hospital admissions | 4 weeks and 12 months |
| Chapman et al. 200149 | PTSD symptoms | Children’s PTSD-I | 1 week, 1 month and 6 months after discharge |
| Lyshak-Stelzer et al. 200748 | PTSD symptoms | University of California, Los Angeles PTSD Reaction Index for DSM-IV Child Version; Milieu behavioural measures, e.g. use of restraints | NR: reports (n) for 2 years. Study is ongoing in a further 15 patients |
Data synthesis
Heterogeneity of the included studies
The study populations are heterogeneous (Figure 4), highlighting the wide application of art therapy in this small number of included RCTs but also demonstrating the difficulty in obtaining a pooled estimate of treatment effect. In this respect the clinical profile of patients can be regarded as a potential treatment effect modifier.
FIGURE 4.
Patient clinical profiles in the 15 included RCTs.

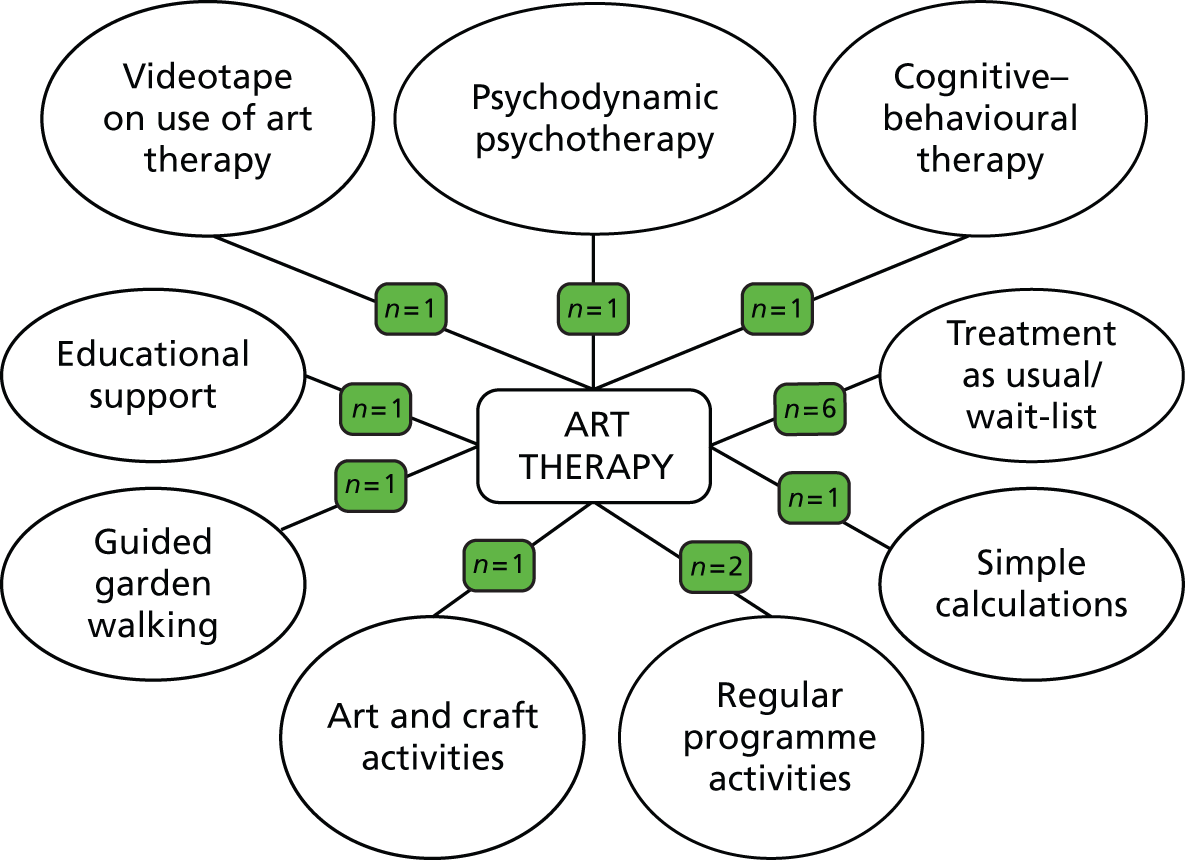
The control groups across the included studies are heterogeneous (Figure 5); therefore, there may be different estimates of treatment effects depending on what art therapy is compared against. Creating a network meta-analysis, which would incorporate all relevant evidence for all the comparators, for all non-psychotic mental health disorders, would be beyond the remit for this research project.
FIGURE 5.
Comparator arms in the 15 included RCTs.
In addition, despite common mental health symptoms being investigated across the included RCTs, the majority of studies were using different measurement scales to assess these outcomes (Table 7). Therefore, as there are insufficient comparable data on outcome measure across studies, it is not possible to perform a formal pooled analysis.
| Outcome measure | n studies | Study names |
|---|---|---|
| SCL-90-R | 4 | Monti and Peterson 2004;60 Monti et al. 200661 |
| Monti et al. 201254 | ||
| Thyme et al. 200747 | ||
| Thyme et al. 200962 | ||
| GDS | 2 | Hattori et al. 201151 |
| McCaffrey et al. 53 | ||
| GSI | 2 | Monti and Peterson 2004;60 Monti et al. 2006;61 aThyme et al. 200962 |
| STAI | 2 | Rao et al. 201156 |
| Kim 201352 | ||
| A-COPE | 1 | Broome et al. 200150 |
| Apathy Scale (Japanese version) | 1 | Hattori et al. 201151 |
| Barthel Index | 1 | Hattori et al. 201151 |
| BDI | 1 | Thyme et al. 200747 |
| BDI-II | 1 | Gussak 200759 |
| Beck Youth Inventories – Second Edition | 1 | Beebe et al. 201058 |
| Benton Fluency Task | 1 | Rusted et al. 200657 |
| Children’s PTSD-I | 1 | Chapman et al. 200149 |
| CRI | 1 | aOster et al. 200664 |
| CSDD | 1 | Rusted et al. 200657 |
| DBD | 1 | Hattori et al. 201151 |
| ESAS | 1 | Rao et al. 200956 |
| EORTC QoL Questionnaire-BR23 | 1 | aSvensk et al. 200963 |
| ER visits; clinic visits; hospital admissions | 1 | Broome et al. 50 |
| HRSD | 1 | Thyme et al. 200747 |
| IES | 1 | Thyme et al. 200747 |
| Medical Outcomes Study SF-36 | 1 | Monti and Peterson 2004;60 Monti et al. 200661 |
| MMSE | 1 | Hattori et al. 201151 |
| MOSES | 1 | Rusted et al. 200657 |
| PedsQL Asthma module | 1 | Beebe et al. 201058 |
| PANAS | 1 | Kim 201352 |
| POMS | 1 | Puig et al. 200655 |
| RBMIT | 1 | Rusted et al. 200657 |
| RSES | 1 | Kim 201352 |
| SCSI | 1 | Broome et al. 200150 |
| SF-8 – Physical (PCS-8) and Mental (MCS-8) | 1 | Hattori et al. 201151 |
| SASB | 1 | aThyme et al. 200962 |
| TEA | 1 | Rusted et al. 200657 |
| University of California, Los Angeles PTSD Reaction Index for DSM-IV Child Version | 1 | Lyshak-Stelzer et al. 200748 |
| WMS-R | 1 | Hattori et al. 201151 |
| WHOQOL-BREF | 1 | aSvensk et al. 200963 |
Potential treatment effect modifiers in the included studies
As well as the patient’s clinical profile, several other treatment effect modifiers can be identified from the included studies.
Experience/qualification of the art therapist
Twelve of the 15 included studies stated that the art therapy was delivered by one or more art therapists. One study was reported in three sources to use a ‘trained’ art therapist. 62–64 One study reported the art therapist as ‘licensed’. 56 Two studies reported using a ‘qualified’ art therapist. 48,57 Two studies reported using a ‘certified’ art therapist. 50,53 One study was reported in two sources as using a ‘registered’ art therapist. 60,61 One study reported using ‘experienced art psychotherapists’. 47 Four studies simply stated ‘art therapist’ without reference to accreditation. 49,52,58,59 One study stated that the sessions were run by one artist and two speech therapists. 51 One study stated that the sessions were run by two mental health counsellors. 55 One study did not state whether or not an art therapist was involved. 54 While there was considerable variability in the reporting of the accreditation of the therapist, most studies were conducted by a person who was considered to be qualified as an art therapist.
Individual versus group art therapy
The majority of RCTs are of group art therapy with only 4 of the 15 RCTs examining individual art therapy. 49,55,56,62
Gender
Five RCTs involved only women,47,54,55,61,62 and one RCT only men. 59 In the remaining nine RCTs the subjects were of mixed gender.
Pre-existing physical condition
In nine studies patients had pre-existing physical conditions. 50,51,54–58,61,62 The remaining six studies involved people who were depressed,47,59 people with post-traumatic stress disorder (PTSD)48,49 or older people. 52,53
Other
Other potential treatment effect modifiers which are not fully explored in the included RCTs include duration of disease (mental or physical), underlying reason for mental health disorder and patient preference for art therapy.
Owing to the degree of clinical heterogeneity across the studies and the lack of comparable data on outcome measures, meta-analysis was not appropriate. Therefore, the synthesis of data is limited to a narrative review to analyse the robustness of the data, which includes trial summaries as well as tabulation of results.
Study summaries
This section provides short overviews of each study with reference to statistically significant differences between groups that were reported in each of the studies.
Beebe et al. 201058
This was a RCT in children (n = 22) with asthma of art therapy versus wait-list control. Sessions lasting 60 minutes were provided once a week for seven weeks. Outcomes were measured at baseline, immediately following completion of therapy and 6 months after the final session. Targeted variables were quality of life (QoL) and behavioural and emotional adaptation. Outcome measurement tools were the Paediatric QoL asthma module and Beck Youth Inventories. Pre- and post-test scores were compared between groups using analysis of variance (ANOVA) and Dunnett’s test. Compared with baseline scores, the intervention group showed a significant reduction in 4 out of 10 QoL items at 7 weeks and in 2 out of 10 QoL items at 6 months. Significant improvement relative to the control group was found in two out of five items of the Beck Youth Inventory at 7 weeks and in one out of five items at 6 months.
Broome et al. 200150
This was a three-arm RCT in children and adolescents (n = 97) with sickle cell disease of art therapy versus CBT (relaxation for pain) or attention control (fun activities). Group sessions were provided over 4 weeks. Outcomes were measured at baseline and at 4 weeks and 12 months. The targeted variable was coping and the authors hypothesised that coping strategies would increase after attending a self-care intervention. Outcome measures were the Schoolagers’ Coping Strategies Inventory and Adolescent Coping Orientation for Problem Experiences scores and numbers of emergency room visits, clinic visits and hospital admissions. The number of coping strategies used was analysed at three time points using Pearson’s correlations, independent t-tests and ANOVA. Coping strategies increased in children and adolescents in all three groups, but data regarding the difference between the intervention and control groups were not reported.
Chapman et al. 200149
This RCT of brief art therapy versus treatment as usual was carried out in children (n = 85) hospitalised with PTSD. A 1-hour individual session was provided but the number of sessions was not reported. Outcomes were measured at baseline and at 1 week, 1 month, and 6 and 12 months (in children who were still symptomatic). The targeted symptom was PTSD. The outcome measurement tool was Children’s Post Traumatic Stress Disorder Index (PTSD-I). The method of statistical analysis was not described. No significant differences were found between groups, but a non-significant trend towards greater reduction in PTSD-I scores was observed in the intervention group relative to the control group.
Gussak 200759
This was a RCT in incarcerated adult males (n = 44) of art therapy versus no treatment. Eight weekly group sessions were provided. Outcomes were measured pre- and post-test (exact time points not reported). The targeted symptom was depression. The outcome measure was the Beck Depression Inventory-Short Form (BDI-II). The change in BDI-II scores from pre-test to post test was calculated and differences between groups analysed using independent-samples t-tests. Depression was significantly lower in the intervention group than in the control group post test.
Hattori et al. 201151
This was a RCT in Alzheimer disease (n = 39) of art therapy versus a ‘simple calculation’ control group. Twelve 45-minute weekly sessions were provided (individual/group not reported). Outcomes were measured at baseline and at 12 weeks. Targeted variables were mood, vitality, behavioural impairment, QoL, activities of daily living and cognitive function. Outcome measures were the Mini Mental State Examination Score (MMSE), the Wechsler Memory Scale revised; the Geriatric Depression Scale (GDS); the Apathy Scale (Japanese version); Short Form questionnaire-8 items (SF-8) – Physical (PCS-8) and Mental (MCS-8) components; the Barthel Index; the Dementia Behaviour Disturbance Scale; and the Zarit Caregiver Burden Interview. Outcomes were measured at baseline and 12 weeks. The percentage of responders who showed a 10% or greater improvement relative to baseline score before the intervention was compared between groups using a chi-squared test. A significant improvement in the intervention group was seen in MCS-8 subscale of the SF-8 and the Apathy Scale. The control group showed a significant improvement in MMSE relative to the intervention group. No significant differences between groups in other items were reported.
Kim 201352
This RCT in older adults (n = 50) compared art therapy with regular programme activities. Between 8 and 12 sessions lasting 60–75 minutes were provided over 4 weeks. Targeted variables were positive/negative affect, state–trait anxiety and self-esteem. Outcomes were measured using the Positive & Negative Affect Schedule, the State–Trait Anxiety Inventory (STAI) and the Rosenberg Self-Esteem Scale. Time points for measurement were not reported (assumed 4 weeks). Independent group t-tests were performed to compare pre- and post-test scores between groups. Significant improvements in the intervention were seen in all three outcomes compared with the control group.
Lyshak-Stelzer et al. 200748
This RCT in adolescents (n = 29) with PTSD compared art therapy with arts and crafts activities. Sixteen weekly group sessions were provided. The targeted symptom was PTSD. Outcome measurement tools were the University of California, Los Angeles (UCLA) PTSD Reaction Index (Diagnostic and Statistical Manual of Mental Disorders – Fourth Edition, Child Version) (primary measure) and milieu behavioural measures (e.g. use of restraints). Measurement time points were not reported, but data at two years were provided. Pre- and post-test scores were compared between groups using repeated-measures ANOVA. The intervention was significantly better than control at reducing PTSD symptoms, according to the UCLA PTSD Reaction Index.
McCaffrey et al. 201153
This was a RCT in older adults (n = 39) of art therapy versus garden walking (individual and group). Twelve 60-minute sessions (group/individual not reported) were provided over 6 weeks. The targeted symptom was depression. The outcome measurement tool was the GDS. Pre- and post-test scores were compared between groups using repeated-measures ANOVA. Measurement was at baseline and 6 weeks. Depression significantly improved from baseline in all three groups with no significant differences between groups.
Monti and Peterson 2004;60 Monti et al. 200661
This RCT in women with cancer (n = 111) compared mindfulness-based art therapy with wait-list control. The trial was sized to have 80% power to detect a standardised effect size of 0.62. Eight 150-minute group sessions were provided over 8 weeks. Targeted variables were distress, depression, anxiety and QoL. Outcome measurement tools were the Symptom Checklist-90-Revised (SCL-90-R), the Global Severity Index (GSI) and the Short Form questionnaire-36 items (SF-36). Measurement was at baseline and at 8 weeks and 16 weeks. Pre-and post-test measures were compared between groups using mixed-effects repeated-measures ANOVA. A significant decrease in symptoms of distress and highly significant improvements in some areas of the QoL scale were observed in the intervention group compared with the control group.
Monti et al. 201254
This RCT of women with breast cancer (n = 18) compared mindfulness-based art therapy with educational support (control group). Eight 150-minute weekly group sessions were provided. The targeted symptom was anxiety but the authors were interested in whether or not cerebral blood flow (CBF) correlated with experimental condition. The primary outcome measurement was functional magnetic resonance imaging (fMRI) CBF and the correlation with anxiety using SCL-90-R. Measurement was at baseline and within 2 weeks of the end of the 8-week programme. The method of statistical analysis was not described and the effectiveness of the intervention was not the primary outcome. Anxiety was reduced in the intervention group but not in the control group. CBF on fMRI changed in certain brain areas in the art therapy group only. It should be noted that patients with a confirmed diagnosis of a psychiatric disorder were excluded from this study.
Puig et al. 200655
This was a RCT in women with breast cancer (n = 39) of art therapy versus delayed treatment. Four 60-minute weekly sessions were provided. Targeted symptoms were anger, confusion, depression, fatigue, anxiety, activity and coping. The outcomes, the Profile of Mood States and the Emotional Approach Coping Scale (EACS) scores, were measured before and 2 weeks after the intervention. Pre- and post-test scores were compared between groups using ANOVA. The intervention group showed significant improvements in the anger, confusion, depression and anxiety mood states but fatigue and activity were not significantly different between the groups. In the intervention group, EACS coping scores increased, but were not significantly different from those in the delayed treatment control group.
Rao et al. 200956
In this RCT in adults with HIV/AIDS (n = 79), the intervention group received brief art therapy while the controls watched a video tape on the uses of art therapy. Only one 60-minute session of individual art therapy was provided. Targeted symptoms were anxiety and physical symptoms, including pain. The outcome measures used were Edmonton Symptom Assessment Scale (ESAS) scores (primary outcome) and STAI scores. Pre-and post-test scores were compared between groups using analysis of covariance (ANCOVA) and adjusted for age, gender and ethnicity. Measurements were recorded before and immediately after the intervention or control session. The intervention group experienced significant improvements in physical symptoms (ESAS) compared with the control group, but anxiety was not significantly different between the groups.
Rusted et al. 200657
In this RCT in adults with dementia (n = 45), art therapy was compared with an activity group control. Forty 60-minute weekly group sessions were provided. Targeted symptoms were depression, mood, sociability and physical involvement. Outcome measures were the Cornell Scale for Depression in Dementia the Multi Observational Scale for the Elderly, MMSE, The Rivermead Behavioural Memory Test, Tests of Everyday Attention and the Benton Fluency Task. Measurements were recorded at baseline, 10 weeks, 20 weeks, 40 weeks and at follow-up at 44 and 56 weeks. Pre- and post-test scores were compared between groups using ANOVA with time of assessment as repeated measures. At 40 weeks, the intervention group was significantly more depressed than the control group, but this effect was reduced at follow-up. However, groups were not comparable at baseline, as the art therapy group were more depressed at the beginning of the study than the control group.
Thyme et al. 200747
This was a RCT in depressed female adults (n = 39) of psychodynamic art therapy versus verbal dynamic psychotherapy. Ten 60-minute weekly sessions (individual/group not reported) were provided. Targeted symptoms were stress reactions after a range of traumatic events, mental health symptoms and depression. Outcome measurements were Impact of Event Scale, Symptom-Checklist-90 (SCL-90), Beck Depression Inventory (BDI) and Hamilton Rating Scale of Depression scores. Measurements were recorded at baseline, at 10 weeks and at a 3-month follow-up. All patients improved from baseline on all scales (p < 0.001). There were no significant differences between groups so art therapy was not significantly different to the comparator at either time point.
Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664
This RCT in women with breast cancer (n = 41) compared art therapy with treatment as usual as a control. Five 60-minute weekly individual session were provided. Targeted symptoms were depression, anxiety, somatic, general symptoms, QoL and coping methods. Outcome measure tools were the Structural Analysis of Social Behavior, the GSI, the SCL-90, the World Health Organization (WHO) QoL instrument – Swedish version, the European Organization for Research and Treatment of Cancer (EORTC) QoL Questionnaire-BR23 and the Coping Resources Inventory (CRI). Measurements were recorded at baseline and at 2 months and 6 months. The intervention significantly improved depressive, anxiety, somatic and general symptoms compared with the control. Pre- and post-test scores were compared between groups using t-tests, ANOVA and linear regression. On the WHOQoL, scores on the overall, general health and environmental domains at 6 months were significantly higher in the intervention group than in the control group. There were no significant differences between groups on the EORTC. In the intervention group, the score on only the ‘social’ dimension of the CRI was increased relative to the control group.
Results
Findings of the included studies
The directions of statistically significant results from the 15 included RCTs are summarised in Table 8.
| Direction of significant findings | n | Studies |
|---|---|---|
| Significant positive effects in all outcome measurements investigated in the art therapy group compared with the control group | 1 | Kim 201352 |
| Significant positive effects in some, but not all, outcome measurements investigated in the art therapy group compared with the control group | 9 | Beebe et al. 201058 |
| Gussak 200759 | ||
| aHattori et al. 201151 | ||
| Lyshak-Stelzer et al. 200748 | ||
| Monti and Peterson 2004;60 Monti et al. 200661 | ||
| Monti et al. 201254 | ||
| Puig et al. 200655 | ||
| Rao et al. 200956 | ||
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | ||
| Improvement from baseline but no significant difference between groups | 4 | Broome et al. 200150 |
| Chapman et al. 200149 | ||
| McCaffrey et al. 201153 | ||
| Thyme et al. 200747 | ||
| Art therapy worse than comparator at baseline and follow-up | 1 | Rusted et al. 200657 |
As can be seen in Table 8, in 14 of the 15 included studies there were improvements from baseline in some outcomes in the art therapy groups. However, both the intervention and the control groups improved from baseline in four studies, with no significant difference between the groups. 47,49,50,53 The control groups across these four studies were verbal psychodynamic psychotherapy,47 treatment as usual,49 CBT50 and garden walking,53 and verbal psychodynamic psychotherapy, respectively.
In eight studies, art therapy was significantly better than the control group for some but not all outcome measures. Table 9 shows the results according to the mean change from baseline between groups in these eight studies.
| Study and control description | Outcome measures | Mean CFB and ps |
|---|---|---|
| Beebe et al. 201058 Wait-list |
PedsQL Asthma module | Intervention positive reduction in 4 out of 10 QoL items at 7 weeks Between-group means at 7 weeks: QoL – parent total (6.167 vs. –13.091), p = 0.025; QoL – child total (9.727 vs. –13.364), p = 0.0123; QoL – parent worry (47.917 vs. –13.182), p = 0.0144; QoL – child worry (54.545 vs. –45.909), p = 0.0142 Intervention positive reduction in 2 out of 10 at 6 months Between-group means at 6 months: QoL – Parent worry (58.333 vs. –40.909), p = 0.024; QoL – child worry (79.545 vs. –25.000), p = 0.0279 |
| Beck Youth Inventories – Second Edition | Intervention significant reduction in 2 out of 5 items at 7 weeks compared with control Beck – Anxiety (–15.6 vs. 5.3), p = 0.0388, Beck – Self-concept (12.091 vs. –3.545), p = 0.0222 Intervention significant reduction 1/5 at 6 months: Beck – Anxiety (–14 vs. 0.545), p = 0.03 No significant differences for depression component of Beck youth inventory at 7 weeks (p = 0.21) or 6 months (p = 0.29) Baseline means NR |
|
| Gussak 200759 Treatment as usual |
BDI-II | Statistically significantly greater decrease in intervention compared with control: BDI Intervention mean CFB (–7.81) vs. control (+ 1.0), p < 0.05 |
| Hattori et al. 201151 Simple calculations |
SF-8 – PCS-8 and MCS-8 | Intervention significant improvement from baseline in MCS-8 subscale of SF-8 components: percentage of patients showing a ≥10% improvement was compared between groups by chi-squared test. MCS-8 (p = 0.038; odds ratio 5.54) |
| Apathy Scale (Japanese version) | Statistically significant improvement from baseline (p = 0.0014) in Apathy Scale but not significantly different to control: CFB Intervention (–3.2) vs. control (–1.1), p = 0.09 | |
| MMSE | Control group significant improvement in MMSE compared with art therapy intervention: CFB Intervention (–0.02) vs. control (+ 1.1), p < 0.01 | |
| WMS-R; GDS; Barthel Index; DBD; Zarit Caregiver Burden Interview | No significant differences in other items | |
| Lyshak-Stelzer et al. 200748 Arts and craft |
University of California, Los Angeles PTSD Reaction Index (DSM-IV Child Version) | Intervention significantly better at reducing trauma symptoms than control: CFB intervention (–20.8) vs. control (–2.5) p < 0.01 |
| Milieu behavioural measures (e.g. use of restraints) | No significant differences for behavioural milieu | |
| Monti and Peterson 2004;60 Monti et al. 200661 Wait-list |
GSI | Intervention significantly decreased symptoms of distress and resulted in highly significant improvements in some QoL areas compared with control: intervention (–0.20) vs. control (–0.04), p < 0.001 |
| SCL-90-R | Anxiety, intervention (–0.26) vs. control (–0.10), p = 0.02; depression, intervention (–0.27) vs. control (–0.08), p = 0.01 | |
| Medical Outcomes Study SF-36 | SF-36: general health intervention (7.97) vs. control (–0.59), p = 0.008; mental health intervention (13.05) vs. control (2.16), p < 0.001 | |
| Monti et al. 201254 Educational support group |
SCL-90-R | Anxiety reduced in intervention but not control group: SCL-90-R decrease in intervention (p = 0.03) but not in control (p = 0.09) |
| fMRI CBF and correlation with anxiety using CBF | fMRI changed in certain brain areas in art therapy group only. No changes in control group | |
| Puig et al. 200655 Wait-list |
POMS | ANCOVA showed intervention had significantly decreased symptoms of:
|
| EACS | No significant differences for coping | |
| Rao et al. 200956 Video-tape on the uses of art therapy |
ESAS | Intervention significantly better for physical symptoms (ESAS) than control: adjusted ESAS total score (21.1 vs. 26.2), p < 0.05 |
| STAI | Not significantly different for anxiety | |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 Treatment as usual |
General | Intervention significantly improved depressive, anxiety, somatic and general symptoms compared with no significant improvements in control |
| SCL-90 | Depression, intervention (–0.37) vs. control (–0.15), p = 0.002; anxiety, intervention (–0.26) vs. control (–0.09), p = 0.009 | |
| SASB | Intervention (–0.14) vs. control (–0.03), p = 0.049 | |
| GSI | Intervention (–0.16) vs. control (–0.05), p =0.005 | |
| WHOQOL-BREF | Intervention significantly improved WHOQoL overall and on the general health and environmental domains vs. control at 6 months WHOQoL CFB: overall Intervention (+10) vs. control (–5.12), p = 0.003; general health intervention (+ 13.75) vs. control (–4.52), p = 0.024; environment intervention (–0.35) vs. control (–2.1), p = 0.034 |
|
| CRI | Intervention significantly improved only the ‘social’ domain, out of five possible domains, for coping resources compared with control (p < 0.05 at 2 and 6 months) | |
| EORTC QoL Questionnaire-BR23 | No significant differences between groups |
In one study,52 all outcomes were significantly better in the art therapy intervention group than in the control group. Table 10 shows the results from the Kim52 study.
| Study and control description | Outcome measures | Results |
|---|---|---|
| Kim 201352 Regular programme activities |
General | Significant improvements in all three outcomes in the intervention group compared with control |
| PANAS | CFB: intervention (19.88) vs. control (–5.64), p < 0.01 | |
| STAI | CFB State: intervention (–13.17) vs. control (+3.08), p < 0.01 CFB Trait: intervention (–7.84) vs. control (+2.96), p < 0.01 |
|
| RSES | CFB: intervention (4.24) vs. control (–0.48), p < 0.01 |
In one study57 of a sample of people with dementia, outcomes were worse for the art therapy group than for the control group, which was an activity control group. An unusual pattern of results is presented, including a significant increase in anxious/depressed mood (p < 0.01) at 40 weeks which was not present at the 10- or 20-week time points and dissipated by 44 and 56 weeks. The authors discuss several reasons for this result including the high level of attrition; the reliance on observer ratings in the frail and elderly sample (and subsequent potential impact of observer bias); the increased depression as a response to the sessions ending; and the possibility that art therapy was contraindicated in this sample.
Narrative subgroup analysis of studies by mental health outcome domains
Table 11 presents the results for effectiveness of art therapy across relevant mental health outcome domains.
| Symptom/variable | Art therapy significantly better than control group | Improvement from baseline but no difference between groups | No improvement from baseline/control group better |
|---|---|---|---|
| Depression (n = 9 studies) | Gussak59 | aBeebe et al.58 | Rusted et al.57 |
| Monti and Peterson 2004;60 Monti et al. 200661 | Hattori et al.51 | ||
| Puig et al.55 | McCaffrey53 | ||
| Thyme et al. 200747 | Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | ||
| Anxiety (n = 7 studies) | aBeebe et al.58 | Rao et al.56 | |
| Kim52 | |||
| Monti and Peterson 2004;60 Monti et al. 200661 | |||
| Monti et al. 201254 | |||
| Puig et al.55 | |||
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | |||
| Mood (n = 4 studies) | Hattori et al.;51 Kim 2013;52 Puig et al.55 | Rusted et al.57 | |
| Trauma (n = 3 studies) | aChapman et al. 2001;49 aLyshak-Stelzer et al.;48 Thyme et al. 200747 | ||
| Distress (n = 3 studies) | Monti and Peterson 2004;60 Monti et al. 200661 | Thyme et al. 200747 | |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | |||
| Quality of life (n = 4 studies) | aBeebe et al.58 | ||
| Hattori et al.51 | |||
| Monti and Peterson 2004;60 Monti et al. 200661 | |||
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | |||
| Coping (n = 3 studies) | Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | aBroome et al.;50 Puig et al.55 | |
| Cognition (n = 1 study) | Hattori et al.51 | ||
| Self-esteem (n = 1 study) | Kim 201352 |
Depression
Among the nine studies examining depression,47,51,53,55,57–59,61,62 art therapy resulted in significant reduction in depression in six studies. 47,53,55,59,61,62 In four of these six studies,55,59,61,62 art therapy was significantly more effective than the control. Data relating to significant differences are reported in Table 9.
Anxiety
Among the seven studies examining anxiety,52,54–56,58,61,62 art therapy resulted in significant reduction of anxiety in six studies. 52,54,55,58,61,62 In these six studies, art therapy was significantly more effective than the control. Data relating to significant differences are reported in Tables 8 and 9.
Mood
Among the four studies examining mood or affect,51,52,55,57 art therapy resulted in significant positive improvements to mood in three studies. 51,52,55 In these three studies, art therapy was significantly more effective than the control. Data relating to significant differences are reported in Tables 8 and 9.
Trauma
Among the three studies examining trauma,47–49 art therapy resulted in significant reduction of symptoms of trauma in all studies. While trauma improved from baseline, there was no significant difference between the art therapy and control groups in any of the three studies.
Distress
Among the three studies examining distress,47,61,62 art therapy resulted in significant reduction of distress in all studies. In two studies,61,62 art therapy was significantly more effective than the control group. Data relating to significant differences are reported in Table 9.
Quality of life
In the four studies examining QoL,51,58,61,62 art therapy resulted in significant improvements to some but not all components of the QoL measures in all studies. In all studies, art therapy was significantly more effective than the control. Data relating to significant differences are reported in Table 9.
Coping
Among the three studies examining coping,50,55,62 art therapy resulted in significant improvements to coping resources in all studies. In one study,62 art therapy was significantly more effective than the control. In another study, there was no difference between groups. 55 In the third study, significant differences between the art therapy and control groups were not reported. 50 Data relating to significant differences are reported in Table 9.
Adverse events
Adverse events were not reported in any of the included RCTs. However, three studies reported outcomes that may be indirectly related to the safety of art therapy. The Lyshak-Stelzer et al. 48 study reported no significant differences between groups in the number of incidents, seclusions, restraints or ‘PRN [pro re nata, as needed] orders’. The Broome et al. 50 study reported a decrease in emergency room visits, clinic visits and hospital admissions over time in both the art therapy and control groups. In addition, the Beebe et al. 58 study reported equal asthma exacerbation numbers in each group but these occurred after the trial has finished.
The lack of adverse event data in the majority of included studies is not necessarily evidence that there were no adverse events in the included trials. It may indicate only that adverse events were not recorded. Potential harms and negative effects of art therapy are further explored in the qualitative review (see Chapter 3).
Quality assessment: strength of the evidence
Table 12 illustrates the types of study designs and the number of studies included into the quantitative and qualitative reviews.
| Evidence | Study design | Quantitative review | Qualitative review |
|---|---|---|---|
| Experimental | RCT: active comparator | n = 9 | – |
| RCTs with no active comparator | n = 6 | – | |
| Quasi-experimental (non-randomised studies) | – | ||
| Single-arm studies | – | ||
| Observational | Cohort studies | n = 12 | |
| Case–control studies | – | ||
| Cross-sectional studies | – | ||
| Before-and-after studies | – | ||
| Case series | – | ||
| Case studies |
Critical appraisal of the potential sources of bias in the included studies
Method of recruitment
Participants were typically convenience samples from existing clinical patient groups. Few details were provided on the inclusion/exclusion criteria of the patients in the studies, as can be seen from Table 13.
| Study | Method recruitment | Inclusion/exclusion criteria |
|---|---|---|
| Beebe et al. 201058 | Recruited students from a particular school | NR |
| Broome et al. 200150 | Invited if eligible from two comprehensive sickle cell centres | Criteria relating to vaso-occlusive episodes |
| Chapman et al. 200149 | Screened for eligibility if admitted for injury | Inclusion criteria: admitted to a level 1 trauma centre for traumatic injuries; injury severe enough to warrant hospital admission > 24 hours. Exclusion criteria: admitted for injuries resulting from burns, child abuse or severe head injury; non-English speakers |
| Gussak 200759 | Call for volunteers made on all units | NR |
| Hattori et al. 201151 | Hospital outpatients | Inclusion criteria: 65–85 years; mild impairment; MMSE score > 20; exhibiting neurological signs of dementia on magnetic resonance imaging or single-photon emission computed tomography (SPECT); recent memory impairment; < 6 months since donepezil hydrochloride. Exclusion criteria: MMSE score > 25; primary symptoms of speech and executive function impairments |
| Kim 201352 | All attendees at two day centres were assessed for eligibility using the MMSE | Inclusion criteria: no previous experience of art therapy; MMSE score > 25 out of 30 within 6 months prior to study |
| Lyshak-Stelzer et al. 200748 | 142 referred and then assessed for inclusion | Inclusion criteria: age 13–18 years; able to sustain school programme for 2 weeks running and expected to stay in hospital for at least 16 weeks from date of parental consent. Exclusion criteria: treatment court mandated or contraindicated |
| McCaffrey et al. 201153 | Purposive sampling to enrol first 48 people who volunteered and met inclusion criteria. Fliers placed at local senior centres and an information session held at the gardens | Inclusion criteria: age > 65 years; self-diagnosed of health-care provider diagnosed depression; able to walk approximately 1 mile; could get to the gardens twice per week for 6 weeks |
| Monti and Peterson 2004;60 Monti et al. 200661 | Females recruited through the Jefferson Cancer Network | Inclusion criteria: between 4 months and 2 years after diagnosis (original or recurrence). Exclusion criteria: terminal cancer; diagnosis of major mood disorder or psychotic disorder; significant cognitive defects |
| Monti et al. 201254 | Recruited through Thomas Jefferson University as a supplement to a parent study RO1 CA111832 | Inclusion: received breast cancer diagnosis between 6 months and 3 years prior to enrolment. Exclusion criteria: psychiatric disorder; not expected to live for more than 6 months; diagnosis of thought disorder, mood disorder or psychotic disorder; significant cognitive defects; use of psychotropic medication |
| Puig et al. 200655 | Referred by private physician, hospital or the American Cancer Society support network | Inclusion criteria: > 18 years; diagnosed with stage I or stage II breast cancer within 12 months prior to entering study |
| Rao et al. 200956 | Recruitment fliers and advanced practice nurse recruited over 6 months | Inclusion criteria: age > 18 years; cognitively intact; able to participate for 1 hour; English speaking |
| Rusted et al. 200657 | Volunteers invited to participate | Inclusion criteria: diagnosis of dementia; attendance at day care or residential facility; previous diagnosis by consultant psychogeriatrician; confirmatory diagnosis from medical records. Exclusion criterion: additional psychiatric disorders |
| Thyme et al. 200747 | Women who agreed to take part from a psychiatric clinic | Inclusion criteria: diagnosed with dysthymic disorder according to DSM-IV or had depressive symptoms and difficulties. Exclusion criterion: psychopharmacological treatment |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | Consecutive selection ‘convenience sample’: 143 answered written invitation to participate for 6 months in a study related to the start of radiotherapy | Exclusion criteria: pre-existing physical or psychiatric illness; dementia or severe psychiatric illness |
Allocation bias: Method of randomisation
Table 14 shows the descriptions of randomisation from the included RCTs. Randomisation usually refers to the random assignment of participants to two or more groups. Randomisation was not described in seven studies. 48–50,54,55,58,59 This information could simply be missing from the published journal paper and, if benefit of the doubt were applied, it could be assumed that proper randomisation may have been done but not reported. This would represent an unclear risk of bias. However, it could also be assumed that proper randomisation did not take place and the method of selecting participants into the studies was flawed. This would represent a high risk of bias. Therefore, there is an unclear/high risk that randomisation was not adequately performed in these six studies.
| Study | Method of randomisation as described in the paper |
|---|---|
| Beebe et al. 201058 | NR |
| Broome et al. 200150 | NR |
| Chapman et al. 200149 | NR |
| Gussak 200759 | NR |
| Hattori et al. 201151 | Stratified by age (≤ 75 and ≥ 76 years), sex and MMSE score and then minimisation method |
| Kim 201352 | Randomly assigned either to the intervention or to the control group based on programme days first, and then assigning them to each group (intervention or control) alternately |
| Lyshak-Stelzer et al. 200748 | NR |
| McCaffrey et al. 201153 | Sealed envelope technique |
| Monti and Peterson 200460 Monti et al. 200661 |
Paired by age with one subject of each pair randomised to either intervention or control |
| Monti et al. 201254 | NR |
| Puig et al. 200655 | NR |
| Rao et al. 200956 | Stratified randomisation |
| Rusted et al. 200657 | Random allocation was based on participant ID numbers being drawn by chance |
| Thyme et al. 200747 | A randomisation procedure was implemented between the collection of the self-rated data and the first interview before therapy. The research leader administered the box with 50 pieces of paper, half of them were given one sign and the others were given a different sign. An impartial individual performed the randomisation using this box. When the impartial individual in charge had picked one piece of paper and the group assignment was documented, the piece of paper was put back into the box |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al.64 | Computer generated and stratified according to receipt of chemotherapy to ensure equal numbers treated with cytostatics between groups |
Allocation bias: allocation concealment
In order to ensure that the sequence of treatment allocation was concealed, a robust method of allocation to the study arms should be undertaken and documented. Allocation concealment was not reported in any of the included studies. Lack of allocation concealment can destroy the purpose of randomisation, as it can permit selective assignment to the study arms.
Appropriate randomisation for allocation to study arms includes undertaking ‘simple’ randomisation (e.g. tossing a coin), which avoids introducing excessive stratification to prevent imbalanced groups, and ‘distance’ randomisation so that researchers are unable to influence allocation (e.g. a central randomisation service which notes basic patient details and issues a treatment allocation). Several of the eight randomisation methods described are likely to be open to allocation bias either because they did not use distance randomisation or because the reports do not provide enough details about what measures were taken to ensure that allocation was truly concealed to the investigators. For example, the Hattori et al. 51 study describes stratification by three variables. Stratifying by more than one variable can be problematic, and stratifying by more than two variables is not advisable. 65 In addition, the Kim52 study does not clearly describe how randomisation was undertaken. The sealed envelope technique employed in the McCaffrey et al. 53 study is intended to ensure that equal numbers receive the intervention and the control but is vulnerable to subterfuge. Few of the included RCTs reported adequate details of methods of randomisation and, consequently, these studies, as reported, had an unclear risk of allocation bias.
Performance bias: blinding
Blinding of participants was not conducted in any of the included RCTs. Blinding of participants to their experimental condition is understandably unfeasible in trials of psychological therapy as opposed to pharmacological interventions. Therefore, while lack of blinding across the included trials means that the trials are at risk of performance bias, the trials cannot be deemed to be of poor quality on this basis.
Performance bias: baseline comparability
Groups were reported to be comparable at baseline in 7 out of the 15 studies (Table 15). 48,51–54,56,62 (Baseline comparability was unclear or not reported and therefore was unable to be assessed in five studies. 47,49,50,55,58) In three studies,57,59,61 patients in the art therapy group appeared to have more severe illness at baseline. These differences could reflect a potential allocation bias resulting from flawed randomisation procedures in the studies.
| Study | Baseline comparability |
|---|---|
| Beebe et al. 201058 | Unclear (NR and baseline demographics not provided) |
| Broome et al. 200150 | Unclear (NR and baseline demographics not provided) |
| Chapman et al. 200149 | Unclear (NR and baseline demographics not provided) |
| Gussak 200759 | No. More were in receipt of medication in the art therapy group; different numbers allocated to groups (27 versus 17); baseline BDI scores were not provided but were reported to be ‘slightly higher’ in the art therapy group |
| Hattori et al. 201151 | Yes |
| Kim 201352 | Yes |
| Lyshak-Stelzer et al. 200748 | Yes |
| McCaffrey et al. 201153 | Yes |
| Monti and Peterson 2004;60 Monti et al. 200661 | No. Levels of depression and anxiety at baseline were higher in the art therapy group |
| Monti et al. 201254 | Yes |
| Rao et al. 200956 | Yes |
| Rusted et al. 200657 | No. Art therapy group had a significantly higher mean depression score (p < 0.01) than the control group |
| Thyme et al. 200747 | Unclear (NR and baseline demographics not provided) |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | Yes |
Performance bias: groups treated equally
As blinding was not possible, all studies are at risk of performance bias. In the case of the six studies49,55,58,59,61,62 that had wait-list/treatment as usual controls rather than an active comparator group, it can be argued that the groups were not treated equally, as the control groups were not given the time and attention that an active control group would receive. Therefore, the risk of performance bias in the art therapy group is higher in these six studies.
Reporting bias: selective outcome reporting
No studies appeared to have collected data on outcomes that were not reported in the results.
Reporting bias: incomplete outcome data
In three studies,48,54,57 outcome data were incomplete, indicating a high risk of reporting bias. The reasons for this were: data on 20% completers only (80% of participants withdrew or were excluded);48 actual data not provided (only p-values reported);54 and group numbers not provided at any time point. 57 In four studies the risk of reporting bias was unclear because incomplete outcome data were reported. 49,50,58,59
Detection bias
Blinding of clinical outcome assessment was reported to be conducted in only one study. 58 Therefore, 14 out of the 15 included RCTs are at unclear to high risk of detection bias, as assessors may have influenced the recording of clinical outcomes.
Researcher allegiance
In the Kim52 study there was only one author, and the two researchers are reported to be art therapists. The author is also a senior art therapist. The Gussak 200759 study also has only one author, who is a professor of art therapy. Trials that are published by one author are unlikely to have been conducted as collaborative projects adhering to standards of good clinical practice. The risk of researcher allegiance in these studies is, therefore, high.
The McCaffrey et al. 201153 study was funded by the owners of the gardens that were the basis of the comparator. The gardens are profit-making, and participants who completed the study were given 1 year’s free membership. The risk of researcher allegiance for the control group in this study, can, therefore, be considered to be high.
As can be seen from Table 16, all studies were prone to many instances of unclear risk of bias. Some studies were prone to several instances of high risk of bias. In the context of this review, with the exception of blinding participants, all the risk of bias domains are important to be able to establish internal validity of these trials. Currently the only domain that is at low risk of bias is selective outcome reporting. Owing to the risks of bias highlighted by the critical appraisal of these studies, it can be concluded that the included RCTs are generally of low quality.
| Study | Sequence generation | Treatment allocation concealment | Performance bias (participant blind) | Detection bias (outcome assessment blind) | Baseline comparability | Groups treated equally | Selective outcome reporting | Incomplete outcome data | Researcher allegiance |
|---|---|---|---|---|---|---|---|---|---|
| Beebe et al. 201058 | Unclear | Unclear | High | Low | Unclear | High | Low | Unclear | Low |
| Broome et al. 200150 | Unclear | Unclear | High | Unclear | Unclear | Low | Low | Unclear | Low |
| Chapman et al. 200149 | Unclear | Unclear | High | Unclear | Unclear | High | Low | Unclear | Low |
| Gussak 200759 | Unclear | Unclear | High | Unclear | High | High | Low | Unclear | High |
| Hattori et al. 201151 | Unclear | Unclear | High | Unclear | Low | Low | Low | Low | Low |
| Kim 201352 | Unclear | Unclear | High | High | Low | Low | Low | Low | High |
| Lyshak-Stelzer et al. 200748 | Unclear | Unclear | High | Unclear | Low | Low | Low | High | Low |
| McCaffrey et al. 201153 | Low | Unclear | High | Unclear | Low | Low | Low | Low | High |
| Monti and Peterson 2004;60 Monti et al. 200661 | Unclear | Unclear | High | Unclear | High | High | Low | Low | Low |
| Monti et al. 201254 | Unclear | Unclear | High | Unclear | Low | Low | Low | High | Low |
| Puig et al. 200655 | Unclear | Unclear | High | Unclear | Unclear | High | Low | Low | Low |
| Rao et al. 200956 | Unclear | Unclear | High | Unclear | Low | Low | Low | Low | Low |
| Rusted et al. 200657 | Unclear | Unclear | High | Unclear | High | Low | Low | High | Low |
| Thyme et al. 200747 | Low | Low | High | Unclear | Unclear | Low | Low | Low | Low |
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al.64 | Low | Unclear | High | Unclear | Low | High | Low | Low | Low |
Critical appraisal of other potential sources of confounding
Attrition
Withdrawals and exclusions are reported in Table 17.
| Study | Randomised | Completed, % (n/N) | Between-group withdrawals | Reasons for withdrawal |
|---|---|---|---|---|
| Beebe et al. 201058 | 22 | 100% (22/22) | N/A | N/A |
| Broome et al. 200150 | 97 | 51% (49/97) | ‘No significant differences’ | NR |
| Chapman et al. 200149 | 85 | 68% (58/85) | NR | No PTSD symptoms (n = 27) |
| Gussak 200759 | 44 | 66% (29/44) | Art therapy (n = 11) | NR |
| Control (n = 4) | ||||
| Hattori et al. 201151 | 43 | 91% (39/43) | Art therapy (n = 2) | Owing to physical diseases (n = 4) |
| Control (n = 2) | ||||
| Kim 201352 | 50 | 100% (50/50) | N/A | N/A |
| Lyshak-Stelzer et al. 200748 | 77 | 38% (29/77) | NR | Discharged prior to completion (n = 23) |
| Withdrew (n = 5) | ||||
| Withdrawn by clinical team (n = 3) | ||||
| Ongoing, no data yet (n = 15) | ||||
| NR (n = 2) | ||||
| McCaffrey et al. 201153 | 48 | 81% (39/48) | Art therapy (n = 3) | Surgery (n = 2) |
| Control (n = 6) | Respiratory infection (n = 5) | |||
| Family issues (n = 2) | ||||
| Monti and Peterson 2004;60 Monti et al. 200661 | 111 | 84% (93/111) | NR | ‘The majority of dropouts were due to progression of illness and/or cancer treatment complications’ |
| Monti et al. 201254 | 18 | 100% (18/18) | N/A | N/A |
| Puig et al. 200655 | 39 | 100% (39/39) | N/A | N/A |
| Rao et al. 200956 | 79 | 96% (76/79) | NR | Drowsiness (n = 2) |
| Consulting with physician (n = 1) | ||||
| Rusted et al. 200657 | 45 | 46% (21/45) | NR | Died (n = 10) |
| Moved away (n = 5) | ||||
| Incomplete data (n = 9) | ||||
| Thyme et al. 200747 | 43 | 91% (39/43) | Art therapy (n = 3) | Dropped out (n = 3) |
| Control (n = 1) | Referred to long-time art therapy (n = 1) | |||
| Thyme et al. 2009;62 Svensk et al. 2009;63 Oster et al. 200664 | 55 | 75% (41/55) | Art therapy (n = 5) | Too much strain (n = 7) |
| Disease complication (n = 2) | ||||
| Control (n = 8) | Dissatisfaction with randomisation outcome (n = 4) | |||
| Data incomplete and discarded (n = 1) |
As can be seen from Table 17, there were only four studies in which all participants completed the trial. 52,54,55,58 While several studies reported substantial numbers of dropouts, only one study reported to be sized with reference to effect size. 61 Considering that the sample sizes in the remaining 14 RCTs are small and not sufficiently powered to account for attrition, these dropouts have a significant impact on the reliability of these RCTs. For example, in the Rusted et al. 57 study, attrition was 53.3%, meaning that the final data are reported for 9 versus 12 people in the art therapy and activity control groups, respectively. This small number of completers calls into question the reliability of this study’s results.
Only 5 of the 11 studies in which dropouts occurred reported the breakdown of withdrawal between groups. Two studies50,59 do not report the reasons for withdrawal in the dropouts that occurred. In addition, attrition was not handled appropriately in the included RCTs as imputation for missing data were generally not reported or were reported to be not conducted except in one study. 62 The risk of attrition bias in the 11 studies where dropouts occurred is, therefore, unclear.
Concomitant treatment
Co-therapy or concomitant medication was not reported in eight trials. 49–52,55–58 In a further two studies,53,61 participants were eligible to take part if in receipt of mental health treatment but the actual data for concomitant therapy (overall or between groups) are not reported.
In the Gussak59 study, 93% (n = 25/27) of participants in the intervention group were taking medication for a mental illness, compared with 27% (n = NR) in the control group. In the Thyme et al. 47 study, it was reported that psychopharmacological treatment was an exclusion criterion. It is subsequently stated that ‘in the [art therapy] group, one participant were [sic] prescribed antidepressants during therapy (n = 1) and one between termination of therapy and the 3-month follow-up (n = 1), and in the [verbal therapy] group three during therapy (n = 1) [sic] and two after (n = 2). Two participants in VT accepted Body Awareness as an additional treatment during psychotherapy.’47
In the Thyme et al. 200962 study the usage of antidepressants was self-reported, and therefore this information may be incomplete. In the Chapman et al. 49 study, ‘treatment as usual’ hospital care was defined as the normal and usual course of paediatric care including Child Life services, art therapy, and social work and psychiatric consultations. While only the Monti et al. 201254 study reports that use of psychotropic medication was an exclusion criterion, there is generally an unclear/high risk of confounding as a result permitted additional treatment across the included studies.
Treatment fidelity
Sufficient measures to ensure treatment fidelity would include monitoring the therapy sessions through audio or video tapes to allow independent checking. No such measures to ensure that the intervention was being delivered consistently were reported in any of the studies. However, one study58 does provide an appendix of the content of each session. In addition, one study61 provides the art therapy programme details in the first of the two resulting publications. 60 Most studies provided brief synopses of the intervention programme and content of the sessions. 48,50,52,54–56,62 However, some studies provided scant details of what took place in the sessions. 47,49,51,53,57,66 Moreover, Chapman et al. 49 do not even state how many sessions were provided. Therefore, the included RCTs have unclear risk of poor treatment fidelity.
The risk of bias assessment and the potential areas of confounding including attrition, concomitant treatment and treatment fidelity illustrate that the included trials are generally of low quality and, therefore, the results of the 15 RCTs that are included in the quantitative review should be interpreted with caution. Three studies47,51,56 can be considered as being of slightly better quality because there are no instances of high risk of bias (other than blinding, which is a common hurdle in trials of psychological therapy) and at low risk of bias on at least four domains.
Discussion
Discussion of the quantitative review
The aim of the quantitative systematic review was to assess the evidence of clinical effectiveness of art therapy compared with control for treating non-psychotic mental health disorders. The limited available evidence showed that patients receiving art therapy had significant positive improvements in 14 out of 15 RCTs. In 10 of these studies, art therapy resulted in significantly more improved outcomes than the control, while in four studies art therapy resulted in an improvement from baseline but the improvement in the intervention group was not significantly greater than in the control group. In one study, outcomes were better in the control group than in the art therapy group. Relevant mental health outcome domains that were targeted in the included studies were depression, anxiety, mood, trauma, distress, QoL, coping, cognition and self-esteem. Improvements were frequently reported in each of these symptoms except for cognition.
Limitations of the quantitative evidence
Despite every possible effort to identify all relevant trials, the number of studies that qualified for inclusion was small. Despite a large number of records on art therapy yielded from the searches, very few studies were RCTs, demonstrating a slow uptake of the evidence-based medicine model in this field. The study samples are heterogeneous and few samples can be regarded strictly as the target population for this review – people diagnosed with a mental health condition. The limited selection of mental health disorders in the included study samples means that the external validity to the population with non-psychotic mental health disorders is limited. In addition, the sample sizes are small, and as yet there are no large-scale RCTs of art therapy in non-psychotic mental health disorders. The paucity of RCT evidence means that it is not possible to make generalisations about specific disorders or population characteristics.
The risk assessment of bias highlighted that, although all studies were reported to be RCTs, few studies reported how patients were randomised, and in the majority of studies there were several instances of high risk of bias. Areas of potential confounding frequently associated with the studies included attrition, concomitant treatment and treatment fidelity. Consequently, the internal validity of the included studies is threatened. Owing to the low quality of the 15 RCTs, the results included in the quantitative review should be interpreted with caution. As this systematic review did not search for and include direct evidence about other interventions for non-psychotic mental health disorders, it has not been possible to identify indirect evidence for the effect of art therapy in a mixed treatment comparison within the scope of this research. Therefore, the effectiveness of art therapy compared with other commonly used treatments that have been shown to be effective is unknown. In addition, the underlying mechanisms of action in art therapy remain unclear from this evidence. The qualitative systematic review that is presented in the next chapters will explore the factors that may contribute to the therapeutic action in art therapy.
Conclusions
From the limited number of studies identified, in patients with different clinical profiles, art therapy was reported to have statistically significant positive effects compared with control in a number of studies. The symptoms most relevant to the review question which were effectively targeted in these studies were depression, anxiety, low mood, trauma, distress, poor QoL, inability to cope and low self-esteem. The small evidence base, consisting of low-quality RCTs, indicated that art therapy was associated with an improvement from baseline in all but one study and was a more effective treatment for at least one outcome than the control groups in the majority of studies.
Chapter 3 The acceptability and relative benefits and potential harms of art therapy: qualitative systematic review
This chapter aims to provide an overview of the evidence for service user and service provider perspectives on the acceptability, relative benefits and potential harms of art therapy for people with non-psychotic mental health disorders.
Review methods
Bibliographic database searching
As the searches for the clinical effectiveness were comprehensive for art therapy literature, the same database was used for both the quantitative and qualitative reviews (see Chapter 2, Literature search methods).
Screening and eligibility
All abstracts, and then full papers, were read by two reviewers (AS and LU) who made independent decisions regarding inclusion or exclusion, and consensus, where possible, was obtained by meeting to compare decisions. In the event of disagreement, a third reviewer (EK) read the paper and made the decision. Study types included were:
-
qualitative research reporting the perspectives and attitudes of people with non-psychotic mental health disorders who have received art therapy in order to examine issues of acceptability
-
qualitative data embedded in trial reports or in accompanying process evaluations, to inform an understanding of how issues of acceptability are likely to affect the clinical effectiveness of art therapy
-
qualitative data either from separately conceived research or embedded within quantitative study reports, reporting the acceptability of art therapy to health care practitioners.
The inclusion and exclusion criteria for the qualitative review are reported in Figure 6. Studies in all settings were included, although the community was the main setting of interest.
FIGURE 6.
Eligibility criteria for the qualitative review.

Quality assessment strategy
Studies meeting the inclusion criteria were evaluated by two reviewers using the CerQual approach. CerQual (certainty of the qualitative evidence67) aims to assess how much certainty can be placed in the qualitative evidence for the review finding, or, in other words, how reliable the review finding is. This approach relies on assessing both the methodological quality of the individual included studies and the coherence of the review finding as defined by the extent to which a clear pattern across the individual study data is identifiable.
To assess methodological quality individual studies were appraised using an abbreviated version of the CASP quality assessment tool for qualitative studies. 68
Two reviewers (AS and LU) independently applied the set of quality criteria to each included study. In the event of a disagreement, a third reviewer (EK) was consulted. Studies were included in the review regardless of study quality.
Whereas study quality applies to each individual included study, ‘coherence’ relates to the review finding which is subsequently developed through the synthesis of the individual studies. Therefore, the coherence of each review finding was then assessed by looking at the extent to which a clear pattern across the data was identified and was contributed by each individual study. This was assessed by looking to see if the review finding was consistent across multiple contexts and if the review finding incorporated explanations for any variation across individual studies. Coherence was further strengthened when the individual studies contributing to the finding were drawn from a wide range of settings. Using the assessment of methodological quality and assessment of coherence together, the certainty of each review finding was rated as high, moderate or low.
Data extraction strategy
Data extraction from included qualitative studies was undertaken independently by AS using a data extraction tool adapted and tailored for the precise purpose of the qualitative review. All data extractions were checked by LU, with any discrepancies being discussed by both data extractors. Where data for included studies were missing, reviewers attempted to contact the authors at their last known e-mail addresses.
For the purpose of data extraction, two principal approaches to decide what counts as qualitative evidence have been proposed. 69 In the first, only data from primary studies which are illustrated by a direct quotation from the respondent are extracted, whereas in the second all qualitative data identified in the primary studies and relevant to the review question are extracted. Given the anticipated paucity of evidence, the latter, more inclusive, approach to data type was adopted, together with a selective approach to extract data relevant to the specific research question. A framework for extraction was developed which focused specifically on data relating to the review question, including how art therapy helped (relative benefits); how art therapy was unhelpful (potential harms); neutral effects (neither benefits or harms); barriers to participation [acceptability (a)]; and recommendations for service delivery [acceptability (b)] from patients and health practitioners. Table 18 illustrates the data extraction elements.
| Elements of the research question | Evidence from patients/health professionals | To inform intervention – elements of the intervention | Service delivery |
|---|---|---|---|
| Relative benefits | How art therapy helped | What to do | How to do it |
| Potential harms | How art therapy was unhelpful | What not to do | How not to do it |
| Neither benefits nor harms | Neutral effects of art therapy | Contribute to understanding of suitable potential patients | Specify suitable potential patients |
| Acceptability (a) | Barriers to participation | Are the barriers real? Can they be addressed? | Address barriers/specify any unsuitable groups (if any) |
| Acceptability (b) | Recommendations for service delivery | Assess feasibility | Direct recommendations to be considered for incorporation into the service |
Data synthesis strategy
Qualitative meta-synthesis was undertaken to provide added value to the quantitative analysis by indicating patient issues around the acceptability of art therapy as a treatment for non-psychotic mental health disorders. Specifically, thematic synthesis was used to aggregate the findings. 70 The framework developed for data extraction was used to shape the synthesis of the findings.
Combining the quantitative and qualitative data
Methodological work to date has been unable to establish the superiority of conducting the qualitative and quantitative synthesis in parallel or of conducting quantitative followed by qualitative, qualitative followed by quantitative or some more iterative approach. Our choice of method of combining data was determined by the needs of this particular review, in which the quantitative data were the main focus and the qualitative data were used for their explanatory potential. We, therefore, employ methods similar to those described by Noyes et al. 71 to explore the effectiveness review in the light of supporting qualitative research data.
Results of the qualitative review
Included studies: qualitative review
From the 10,270 citations identified from the initial searches (see Chapter 2), 290 were considered following abstract sift and 42 papers were considered at full paper sift for the qualitative review. Figure 7 shows the flow chart of studies included in the qualitative review. The sifting process resulted in the inclusion of 12 studies (13 sources) at full paper sift. All included full papers were published between 2002 and 2013 (although one study was an unpublished manuscript linked to a published abstract within this time scale72). Two were theses,73,74 and one of these had an associated peer-reviewed paper75 which reported the same study.
FIGURE 7.
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart of studies included in the qualitative review.

Study respondents
Eleven studies assessed patients’ attitudes and two studies assessed health practitioner attitudes to the intervention [general practitioners (GPs) = 1; art therapists = 1]. The studies contained qualitative data from 188 patients and 16 health practitioners. The primary diagnoses of the patient populations studied included cancer (n = 6), depression/anxiety/stress (n = 3), PTSD (n = 1) and obesity (n = 1). The symptoms being treated by art therapy included depression, stress, anxiety, psychological distress, low self-esteem, fatigue and fear.
Six studies did not report the age of the participants. Where age range was reported,73,76–78 ages ranged from 26 to 82 years. Five studies77,81–84 did not report the gender of the participants. In four studies,72,73,76,78 all participants were female, while one study79 included 69 men and 88 women and a final study80 included four women and one man.
Study setting
Three studies80–82 were conducted in the UK. One of these studies82 provided data from patients and the other from GPs who referred patients to art therapy. 81 Four studies73,74,78,83 were conducted in the USA, with one of these studies73 also including participants from Canada. Three of these studies73,78,83 provided data from patients and the final study74 provided data from art therapists. The remaining five studies were conducted in European countries, Sweden,76 Germany,77 France,72 Italy79 and Switzerland,84 and provided data from patients.
In seven studies,72,74,76,77,79,82,84 the art therapy took place in secondary care; one study81 took place in primary care and one study78 took place in a state correctional facility (USA). In another study73 participants had taken part in art therapy in varied settings including secondary care and private sessions. The setting was not reported in two studies. 80,83
Intervention description
The reporting of the art therapy intervention was limited in a number of cases. One study81 did not report any details of the intervention, and two studies73,80 reported on perceptions of patients who had taken part in a variety of different interventions, although details of each were not reported. Of the remaining eight studies assessing patient views of art therapy, in four studies77,82,83,84 the art therapy had been conducted in a group, with group sizes ranging from four to nine participants, while three studies76,78,79 reported on individual sessions; in one study,72 the format was not reported. In six studies72,76,79,82–4 it was reported that the intervention had been delivered by an art therapist. This was reported to be a professional or qualified art therapist in three of these studies72,79,82 and an art therapy psychotherapist in a further study. 84 The service provider was not reported in the remaining two studies. 77,78 Sessions were 1 hour in length in three studies72,78,79 and 2 hours in length in two studies;82,84 duration was not reported in three studies. 76,77,83 The number of sessions delivered ranged from 1 to 22. Sessions were reported as occurring weekly in four studies; the frequency was not reported in three studies. One study82 reported perceptions of patients who had taken part in art therapy as part of a rolling programme. Table 19 shows the study characteristics of qualitative studies with data from patients.
| Author, Year | Country | Population details | n (contributing qualitative evidence) | Study methods (yielding qualitative data) | Intervention details | ||||
|---|---|---|---|---|---|---|---|---|---|
| Primary diagnosis/population | Symptoms being treated (by AT) | Age (years) | Gender | Duration, numbers in group, etc. | Intervention/facilitator | ||||
| Collie et al. 2004;73 Collie et al. 200675 | Canada and USA | Breast cancer | Stress | 37–82 (mean 56.5) | All female | 17 | In-depth interviews | NR | Varied |
| Oster et al. 200976 | Sweden | Breast cancer | Stress, depression, fatigue | 37–69 (median = 59 years) | All female | 20 | Interviews, women’s diaries, art therapist’s field notes | Five sessions, frequency or duration NR | Individual sessions delivered by an art therapist |
| Geue et al. 201177 | Germany | Cancer (majority breast cancer) | Psychological distress – depression, fear and fatigue | 26–62 | NR | 27 | Semistructured interview | 22 weekly sessions, duration NR, 4–8 patients per group | Group sessions, facilitator not reported |
| Forzoni et al. 201079 | Italy | Cancer | Stress | NR | Female (n = 88) Male (n = 69) |
54 | Semistructured questionnaire (one open-ended question; one forced choice question) | Up to 10 sessions, frequency NR, duration up to an hour | Individual sessions delivered by a qualified art therapist |
| Rhondali et al. 201072 | France | Cancer | Psychological distress – depression and anxiety | Median = 58 (Q1–Q3 = 55–64) | Female (n = 12) | 12 | Semistructured interview | One session, 1 hour in duration | Format not reported, delivered by a professional art therapist |
| McCaffrey 200783 | USA | Depression | Depression | Mean = 75 | NR | 20 | Focus groups | Six weekly sessions, duration NR, 6–9 patients per group | Group sessions delivered by an art therapist |
| Turnbull et al. 200281 | UK | Anxiety, depression, stress | Anxiety, depression, stress | NR | NR | 5 | Semistructured interview | NR | NR |
| Lobban 201282 | UK | PTSD (veterans) | PTSD | NR | NR | 5 | Media group discussion during AT session (transcribed) | Rolling programme of art therapy, each session 2 hours in duration, numbers of patients per group not reported | Group sessions delivered by a qualified art therapist |
| Anzules et al. 200784 | Switzerland | Obesity | Self-esteem | NR | NR | Unclear (intervention n = 15) | Semistructured interview | Six weekly 2-hour sessions with a minimum of five patients per group | Group sessions delivered by an art therapy psychotherapist |
| Ferszt et al. 200478 | USA | Incarcerated women | Anxiety, depression, stress | 29–42 | All female | 8 | Semistructured interview | Eight weekly 1-hour sessions | Individual sessions, facilitator not reported |
| Wood et al. 201380 | UK | Cancer (breast, ovarian, uterus, bowel) | Psychological distress | NR | Female (n = 4) Male (n = 1) |
5 | Semistructured interview | NR | NR |
Table 20 shows the study characteristics of qualitative studies with data from service providers.
| Author, Year | Country | Population | n (contributing qualitative evidence) | Study methods (yielding qualitative data) |
|---|---|---|---|---|
| Turnbull et al. 200281 | UK | GPs on art therapy for anxiety, depression and stress | 4 | Semistructured interview |
| Sharf 200474 | USA | Art therapists on art therapy for substance abuse | 12 | Semistructured interview |
Quality of the included studies
Table 21 shows the methodological quality assessment of the included studies (adaptation of the critical appraisal skills programme checklist for qualitative studies.
| Question | Yes/somewhat | |
|---|---|---|
| N = 12 studies, % (n) | ||
| 1 | Is the study qualitative research or does it provide qualitative data? | 100 (12) |
| 2 | Is the study context and aims clearly described? | 75 (9) |
| 3 | Is there evidence of researcher reflexivity? | 42 (5) |
| 4 | Are the sampling methods clearly described and appropriate for the research question? | 66 (8) |
| 5 | Are the methods of data collection clearly described and appropriate to the research question? | 66 (8) |
| 6 | Is the method of analysis clearly described and appropriate to the research question? | 58 (7) |
| 7 | Are the claims made supported by sufficient evidence (i.e. did the data provide sufficient depth, detail and richness)? | 42 (5) |
Our inclusion criteria specified that qualitative research or qualitative data within mixed methods studies were acceptable for inclusion; however, only three studies could be described as qualitative research. 74–76 Researcher reflexivity can be described as awareness of the researcher’s contribution to the construction of meanings throughout the research process and an acknowledgement of the impossibility of remaining ‘outside of’ one’s subject matter while conducting research. Few studies made reference to researcher reflexivity, and in those that did these descriptions were often brief. Most studies provided descriptions of the context and aims of the study, recruitment methods and data collection methods, although these tended to be brief. The study methods used were interview methods in most studies (n = 10) [semistructured interviews (n = 7), in-depth interview (n = 1), interview (n = 2)]. One study used the focus group method, one used patient diaries, one used field notes, and one used the transcription of a video-recorded group discussion which had been used for a television programme. Only around half of the included studies provided an adequate description of data analysis methods, and in only a few studies were in-depth, detailed and rich data presented. It should be noted that this may have been, in part, a result of limitations imposed by journals. Furthermore, the level of evidence that was included was extended to include data identified in both the results section and the discussion and will include author comments and interpretation. If data were limited only to participants, it was feared that important data would be missed.
Certainty of the review findings
As described in the Quality assessment strategy section, the CerQual approach to assess the certainty of the review findings was applied. The CASP quality assessment finding, together with the number of studies contributing to the finding, and an assessment of the consistency of study setting and population, was assessed. Each finding could potentially be graded as being of high, moderate or low certainty. For the evidence from patients, there were a total of 38 findings: 20 were assessed to be of moderate certainty and 18 were assessed to be of low certainty. For the evidence from service providers, as only two studies contributed to the evidence, there were a total of 25 findings: 19 were assessed to be of moderate certainty and six were assessed to be of low certainty. Owing to the limited number of studies contributing to each finding, together with the fact that the majority of the individual studies included in the review were of low to moderate quality, no findings were assessed as being of high certainty.
Qualitative synthesis: evidence from patients
Table 22 shows the patient views regarding how art therapy helped (relative benefits).
| Theme | Synthesised finding – art therapy is effective when: | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment | Subtheme(s) and explanation of certainty in the evidence assessment (subtheme) |
|---|---|---|---|---|---|
| Relationships | A relationship with the art therapist is established | McCaffrey (2007)83 [low] | Moderate certainty | The studies overall were of moderate quality. The finding was seen across several studies, settings and populations | |
| Forzoni (2010)79 [moderate] | |||||
| Wood (2013)80 [moderate] | |||||
| Relationships with other group members can be established | McCaffrey (2007)83 [low] | Moderate certainty | The studies ranged in quality from low to high. The finding was seen across several studies, in different settings and populations (cancer and PTSD) | It provides support from other group members73 This subtheme was seen in only one study, which was high quality, in a breast cancer population |
|
| Collie (2004);73 Collie (2006)75 [high] | It allows a shared experience with other group members77,82 This subtheme was seen in two studies of low to moderate quality, and in different settings and populations |
||||
| Geue (2011)77 [low/moderate] | |||||
| Lobban (2012)82 [low/moderate] | |||||
| Wood (2013)80 [moderate] | |||||
| It facilitates an improved relationship with family, friends and caregivers | Rhondali (2010)72 [high] | Moderate certainty | The finding was seen in only one study of high quality, specific to the cancer population | ||
| It counters isolation | Turnbull (2002)81 [low] | Low certainty | The finding was seen in only one study, which was of low quality | ||
| Understanding | It facilitates increased understanding of self | McCaffrey (2007)83 [low] | Moderate | In general the studies were of moderate quality. The finding was seen across several studies, settings and populations | |
| Forzoni (2010)79 [moderate] | |||||
| Anzules (2007)84 [low] | |||||
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Geue (2011)77 [low/moderate] | |||||
| Lobban (2012)82 [low/moderate] | |||||
| It facilitates understanding of illness | Anzules (2007)84 [low] | Low certainty | This finding was observed in only two studies: one of high quality and one of low quality, and in different populations | ||
| Collie (2004);73 Collie (2006)75 [high] | |||||
| It promotes future thinking | McCaffrey (2007)83 [low] | Moderate certainty | In general, the studies were of moderate quality, and the finding was seen across several studies, settings and populations | ||
| Rhondali (2010)72 [high] | |||||
| Oster (2009)76 [moderate] | |||||
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Geue (2011)77 [low/moderate] | |||||
| Turnbull (2002)81 [low] | |||||
| Perspective | It give strength/provides perspective | McCaffrey (2007)83 [low] | Low certainty | The studies were of moderate quality, but the finding was seen in only a small number of studies although across different settings, and populations (cancer vs. depression) | |
| Oster (2009)76 [moderate] | |||||
| Distraction | It provides distraction from pain | Rhondali (2010)72 [high] | Low certainty | The finding was seen in only one high quality study | |
| It provides distraction from the illness/escapism | Rhondali (2010)72 [high] | Moderate certainty | In general, the studies were of moderate quality, although the finding was seen over a relatively small number of studies they had similar populations and settings (e.g. cancer, obesity) | ||
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Anzules (2007)84 [low] | |||||
| Personal achievement | It provides pleasure/satisfaction/accomplishment/pride | Rhondali (2010)72 [high] | Moderate certainty | In general, the studies were of moderate quality. The finding was seen across several studies, settings and populations | |
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Anzules (2007)84 [low] | |||||
| Ferszt (2004)78 [low] | |||||
| Forzoni (2010)79 [moderate] | |||||
| It provides the opportunity for legacy | Rhondali (2010)72 [high] | Low certainty | The finding was seen in only one study, although this was of high quality | ||
| Expression | It allows participants to express their feelings | Ferszt (2004)78 [low] | Moderate certainty | In general, the studies were of moderate quality and the finding was seen across several studies, settings and populations | It provides a safe place/to express fear In general, the studies were of moderate quality and the subtheme was seen across several studies, settings and populations |
| It provides an opportunity to express anger73,75 The subtheme was seen in only one study, although this was high quality |
|||||
| Oster (2009)76 [moderate] | |||||
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Geue (2011)77 [low/moderate] | |||||
| Lobban (2012)82 [low/moderate] | |||||
| Turnbull (2002)81 [low] | |||||
| Wood (2013)80 [moderate] | |||||
| Relaxation | It provides a healing experience/comfort encouragement and support/relaxation | Ferszt (2004)78 [low] | Moderate certainty | In general, the studies were of moderate quality, and the finding was seen across several studies, settings and populations | |
| Collie (2004);73 Collie (2006)75 [high] | |||||
| Geue (2011)77 [low/moderate] | |||||
| Turnbull (2002)81 [low] | |||||
| Wood (2013)80 [moderate] | |||||
| Empowerment | It promotes empowerment | Oster (2009)76 [moderate] | Moderate certainty | In general, the studies were of moderate quality. Although the finding was seen across only a relatively small number of studies, these were in different settings and populations | It promotes control over emotions In general, the studies were of moderate quality. Although the subtheme was seen across only a relatively small number of studies, these were in different settings and populations |
| Collie (2004);73 Collie (2006)75 [high] | It promotes control over real-life situations76 The subtheme was seen in only one moderate quality study |
||||
| Turnbull (2002)81 [low] | |||||
| Wood (2013)80 [moderate] | |||||
| It raises self-esteem | Ferszt (2004)78 [low] | Low certainty | The finding was seen in only one study, and this was rated as low quality |
Table 23 shows the patient views regarding how art therapy was unhelpful (relative harms).
Table 24 shows the patient views regarding the neutral effects of art therapy (neither nor benefits)/acceptability.
| Patients reported that art therapy was unhelpful when: | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment | Change to service delivery implicated? |
|---|---|---|---|---|
| It caused anxiety | Rhondali (2010)72 [high] | Moderate certainty | Although each of these findings was seen in a study of high quality, it was reported in only one study and, therefore, cannot be generalised to other settings or populations | Analysis of suitable patients for art therapy |
| It increased pain | Rhondali (2010)72 [high] | Moderate certainty | Analysis of assistance needed or assessment of suitability for patients who are physically very ill | |
| It resulted in the activation of emotions which were not resolved | Collie (2004);73 Collie (2006)75 [high] | Moderate certainty | Debriefing required or ensuring competence of the deliverer | |
| The art therapist was not skilled | Collie (2004);73 Collie (2006)75 [high] | Moderate certainty | Ensuring competence of the deliverer | |
| Art therapy was suddenly terminated | Collie (2004);73 Collie (2006)75 [high] | Moderate certainty | Ensuring other support is available if required |
| Neutral effects of art therapy – themes | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment | Change to service delivery implicated? |
|---|---|---|---|---|
| Superficial | Forzoni (2003)79 [moderate] | Low certainty | The finding was seen in only one study of moderate quality | Analysis of suitable patients for art therapy |
| Childish | Forzoni (2003)79 [moderate] | Low certainty | ||
| Preference for other therapies | Ferszt (2004)78 [low] | Low certainty | The finding was seen in only one study of low quality | |
| Self-indulgent | Turnbull (2002)81 [low] | Low certainty |
Table 25 shows the service delivery recommendations from patients.
| Patient views identified | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment |
|---|---|---|---|
| Important considerations for art therapy. Patients wanted: | |||
| Their privacy to be respected | Oster (2009)76 [moderate] | Low | The finding was seen in only one study of moderate quality |
| Emotional support | Collie (2004);73 Collie (2006)75 [high] | Moderate | The finding was seen in only one study of high quality |
| A good relationship with the art therapist | Collie (2004);73 Collie (2006)75 [high] | Moderate | The finding was seen in only two studies, of which one was high quality |
| Turnbull (200281) [low] | |||
| The art therapist as a guide | Collie (2004);73 Collie (2006)75 [high] | Moderate | The finding was seen in only one study of high quality |
| Barriers to participation in art therapy. Patients felt they could not participate in art therapy: | |||
| When they thought they were too ill to do so | Rhondali (2010)72 [high] | Moderate | The finding was seen in only one study of high quality |
| When art therapy was restricted to certain medical conditions. | Wood (2013)80 [moderate] | Low | The finding was seen in only one study of moderate quality. |
| When they lacked an understanding of art therapy | Forzoni (2003)79 [moderate] | Low | The finding was seen in only two studies of moderate quality |
| Wood (2013)80 [moderate] | |||
| When they feared not being ‘good at art’ | Wood (2013)80 [moderate] | Low | The finding was seen in only one study of moderate quality |
| Suggested improvements. Patients felt: | |||
| They needed further sessions of art therapy | Ferszt (2004)78 [low] | Low | The finding was seen in only one study of low quality |
| They need additional input from other therapies (e.g. individual counselling) | Ferszt (2004)78 [low] | Low | The finding was seen in only one study of low quality |
Benefits of art therapy
Relationships
A number of respondents across several studies72,73,77,79–83 talked about relationships as important in art therapy. They suggested that art therapy was effective when a relationship with the art therapist was established. 79,80,83 One patient commented ‘I felt she [the art therapist] really understood what I am going through’. 79 A good relationship with the art therapist was seen as a requirement for an optimal art therapy programme,73,81 and that the art therapist should act as a guide. 73 However, it was also noted that art therapy could be unhelpful if the art therapist was not skilled. 73 One patient recounted, ‘I was getting very, sort of out there in terms of the anxiety and that kind of thing, and it seemed to become evident she couldn’t go there with me . . . She couldn’t deal with it, which was quite upsetting’. 73
Respondents also discussed relationships with other group members and felt that art therapy was beneficial when these relationships could be established. 73,77,80,82,83 These findings were observed in studies across a range of settings and in a range of populations.
Respondents also felt that art therapy had the effect of facilitating improved relationships with family members, friends and caregivers. 72 This finding was observed in only one study, in which respondents had cancer, and therefore this finding may not be generalisable to other populations. In one study,81 respondents with anxiety, depression and stress suggested that art therapy could serve to reduce isolation.
Understanding
Several studies included data concerning the importance of increased understanding as a beneficial result of art therapy. 72,73,76,77,79,81–84 More specifically, respondents talked about an increased understanding of self73,77,79,81–84 and that art therapy promoted thinking about the future. 72,73,76,77,81,83 These findings appeared to be consistent across different populations. In two studies, one in patients with obesity84 and the other in people with breast cancer,73 art therapy was felt to facilitate understanding of these illnesses; thus, this finding may be specific to people with a diagnosis of a physical illness.
Perspective
A further beneficial effect of art therapy was the provision of strength and perspective. 76,83 This was illustrated by a participant in the McCaffrey et al. study:
These classes have put some perspective on my feelings and even though I am still sad and would give the whole world to have my husband back, I realize I can go on and I can have a good life.
McCaffrey et al. 83 (p. 83)
However, it should be noted that this finding was judged to be of low certainty because it occurred in only two studies of overall low quality.
Distraction
Respondents highlighted distraction as a beneficial aspect of art therapy. 72,73,84 More specifically, respondents pointed to distraction from pain72 and distraction from the illness, or escapism. 72,73,84 As might be expected, these findings were restricted to cancer and obesity populations, and were, therefore, rated as low to moderate certainty.
Personal achievement
Several studies included data reflecting that the provision of art therapy gave participants a sense of personal achievement. In a number of studies,72,73,78,79,84 respondents commented that art therapy provided pleasure, satisfaction, accomplishment and a sense of pride. A patient reported, ‘I underestimate myself and didn’t think I was capable of doing what I did and of having any ideas. I am proud and I’ve rarely been that in my life’. 84 In one study of women with cancer,72 it was reported that art therapy provided an opportunity to leave a legacy for loved ones.
Expression
Freedom of expression emerged as important across a range of studies. 73,76,77,78,80–82 A patient commented, ‘It can touch the feelings that are buried . . . the art frees you up to touch deeper down that [sic] you would verbally’. 81 Specifically, art therapy was thought of as a safe place to express emotions, such as fear73,76–78,81,82 and anger. 73
Relaxation
A number of studies reported data suggesting art therapy provided a healing experience, comfort, encouragement, support and relaxation. 73,77,78,80,81 One participant reported, ‘it was really relaxing and afterwards I felt good and encouraged’. 77
Empowerment
Recipients of art therapy expressed that it gave them a sense of empowerment. This came in the form of control over emotions. 73,76,80,81 In the Collie study,73 the author reports:
[The art therapist stated] ‘What art can do is it gives you . . . access to a larger part of who you are.’ She said art can take people away from their pain and show them that they are more than pain, and therefore can give a sense of control.
Collie73 (p. 77)
Art therapy also promoted control over real-life situations76 and it was also cited as raising self-esteem. 78
Acceptability and potential harms of art therapy
Although recipients in most of the studies indicated a high level of acceptability of art therapy, some studies also described less positive attitudes. 72,73,78,79,81 Some respondents made comments that indicated that, although they did not feel art therapy would be harmful, they did not feel it would be beneficial. In one study,79 a participant commented that art therapy was superficial; ‘I did not find anything particularly useful in it: afterwards I felt as before [she makes a gesture of opening her hands]. It is a little chat with a person who maybe can understand you, but in the end . . .’. Another patient felt it was childish. In another study,81 a participant felt it was self-indulgent, and, in a final study,78 a participant simply had a preference for other therapies. These findings were seen across only three studies of low to moderate quality.
More serious concerns included art therapy causing anxiety,72 increasing pain,72 and resulting in the activation of emotions that were not resolved. 73 In one study,73 a participant was also concerned that art therapy may be harmful if the art therapist was not skilled. A final concern was that it may be harmful if art therapy is suddenly terminated. 73 These findings were seen across only two studies, both in patients with cancer.
The provision of art therapy
Across several studies73,76,78,81 recommendations for art therapy were made. A participant in one study76 said that it was important that privacy be respected during art therapy. In addition, emotional support,73 a good relationship with the art therapist73,81 and that the art therapist should act as a guide73 were suggested to be important aspects of art therapy. Suggested improvements for art therapy were made in one study,78 including the need for further sessions of art therapy and for additional input from other therapies, such as individual counselling.
Barriers to participation
Barriers to participation in art therapy were reported in three studies. 72,79,80 Respondents commented that they thought they were too ill to take part in the therapy,72 and in a further study respondents reported that art therapy was restricted to people with certain medical conditions. 80 Other barriers included a fear of not being ‘good at art’80 and in two studies79,80 participants commented that a lack of understanding of art therapy could be a barrier to participation. Figure 8 shows the overall synthesis of patients’ views regarding the relative benefits, harm and acceptability of art therapy.
FIGURE 8.
Overall synthesis of patients’ views regarding the relative benefits, harms and acceptability of art therapy.
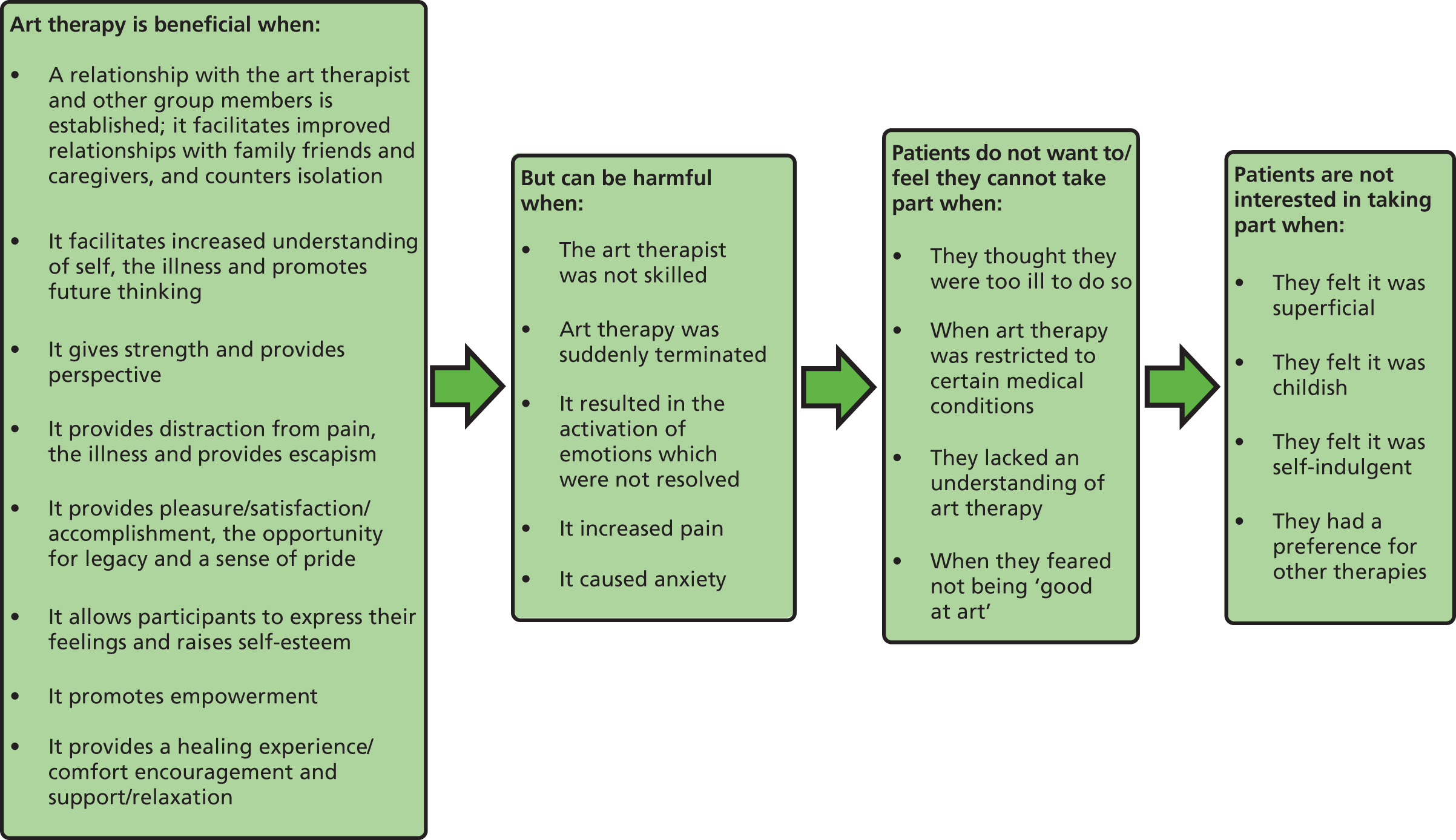
Qualitative synthesis: evidence from service providers
Table 26 shows the service providers’ views regarding how art therapy was helpful (relative benefits).
| Synthesised finding – art therapy is effective when: | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment |
|---|---|---|---|
| Patients have time invested in them | Turnbull (2002)81 [low] | Low | The finding was seen in only one low-quality study |
| Patients like it/felt they benefited | Turnbull (2002)81 [low] | Moderate | The finding was seen in only two studies, of which one was high quality |
| Sharf (2004)74 [high] | |||
| The therapist examines the effect of art-making process on clients | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Clients can communicate through artwork | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Art therapists help clients improve their ability to manage anger | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| It increases pride and self-esteem | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Thoughts and feelings are expressed more effectively | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Provides an opportunity for clients to do something better with their time | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
Table 27 shows the service providers’ views regarding how art therapy was unhelpful (relative harms).
| Service providers reported that art therapy was unhelpful when: | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment |
|---|---|---|---|
| Administrative decisions led to poor treatment outcomes | Sharf (2004)74 [high] | Moderate | These findings were seen in only one high-quality study |
| The client lacks commitment or is non-compliant | Sharf (2004)74 [high] | Moderate | |
| The client is resistant to art therapy | Sharf (2004)74 [high] | Moderate |
Table 28 shows the service providers’ views regarding the neutral effects of art therapy (neither harms nor benefits)/acceptability.
| Neutral effects of art therapy – themes: | Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment |
|---|---|---|---|
| Lack of understanding of art therapy | Turnbull (2002)81 [low] | Low | These findings were seen in only one low-quality study |
| The art bit is irrelevant | Turnbull (2002)81 [low] | Low | |
| Does not help everyone | Turnbull (2002)81 [low] | Low | |
| Time back/pressure off | Turnbull (2002)81 [low] | Low |
Table 29 shows the service delivery recommendations from service providers.
| Evidence source(s) [CASP assessment of quality] | Certainty in the evidence | Explanation of certainty in the evidence assessment | |
|---|---|---|---|
| Important considerations for art therapy: | |||
| A good relationship with the art therapist/strong therapeutic relationship | Turnbull (2002)81 [low] | Moderate | The finding was seen in only two studies, of which one was high quality |
| Sharf (2004)74 [high] | |||
| One-to-one contact | Turnbull (2002)81 [low] | Low | The finding was seen in only one low-quality study |
| Client commitment to recovery | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Client to enjoy art therapy | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Safe environment to express thoughts, feelings and experiences | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Match techniques and materials to clients | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| To display artwork | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Create art along with clients | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Barriers to participation in art therapy. Service providers felt patients were not able to participate in art therapy when: | |||
| Art therapists were not respected as professionals by members of other professional groups | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
| Suggested improvements. Service providers wanted: | |||
| Art therapist and other professionals working together | Sharf (2004)74 [high] | Moderate | The finding was seen in only one high-quality study |
Benefits of art therapy
In many ways the data from the two studies examining service provider views of art therapy mirrored those of the patients. Service providers felt that art therapy was beneficial when patients have time invested in them. 81 One GP stated that ‘simply having the time to have somebody interested in them is therapeutic in itself’. 81 Service providers also felt that a good indicator of the benefit of art therapy was when the patients say they like it or they felt they benefited. 74,81 Art therapists felt that art therapy was most helpful when the therapist examines the effect of art-making process with clients. 74 Furthermore, it was seen as beneficial when clients can communicate through artwork,74 when art therapists help clients improve their ability to manage anger,74 when it increases pride and self-esteem,74 and when thoughts and feelings are expressed more effectively. 74 Finally, on a more practical level, art therapists felt that art therapy could be beneficial when it provides an opportunity for clients to do something better with their time. 74
Acceptability and potential harms of art therapy
Service providers made a number of observations about the acceptability and potential harms of art therapy. According to the study that examined the perspectives of GPs referring patients to art therapy81 GPs, while not believing that art therapy could be harmful, do not regard it as beneficial either. In that study, GPs referring patients to art therapy commented on a lack of understanding of art therapy, reporting, ‘I don’t think I understood what the art bit was about’. 81 They also suggested that the art part of the therapy was irrelevant, stating ‘[I] thought it was about offering people an opportunity to discuss things in therapy. If you or I went to a group we’d get something out of it’. 81 They felt it was unlikely to help everyone,81 and on a more practical note they felt that art therapy gave them with an opportunity to take time back: ‘leaves me free for more medical care’. 81 It should be noted that all of these neutral findings were generated from only one study of low quality, which looked at the opinions of GPs referring patients to art therapy and, therefore, cannot be generalised across other groups.
In terms of more serious detrimental effects of art therapy, Sharf74 reported findings from art therapists. These potential harms included when administrative decisions lead to poor treatment outcomes, for example when a client is not allowed to continue with art therapy; when the client lacks commitment or is non-compliant; and when the client is resistant to art therapy.
The provision of art therapy (service delivery)
Both types of service providers (GPs and art therapists), like patients, felt that a good relationship with the art therapist was important. 74,81 GPs also reported that they felt the one-to-one contact was an important aspect of the therapy. 81 Art therapists also felt that client commitment to recover, the client’s enjoyment of art therapy, providing a safe environment to express thoughts, feelings and experiences, matching techniques and materials to clients, displaying artwork, and creating art along with clients were important aspects of effective art therapy. 74
Barriers to the provision of art therapy
Art therapists felt that their profession was not respected by members of other professional groups,74 and that this created a barrier to patients being referred to art therapy. Art therapists went on to suggest that, in situations where art therapists and other professionals were able to work together, improvements to the service, patient outcomes and accessibility of art therapy were made. Figure 9 shows the overall synthesis of service providers’ views regarding the relative benefits, harms and acceptability of art theraphy.
FIGURE 9.
Overall synthesis of service providers’ views regarding the relative benefits, harms and acceptability of art therapy.
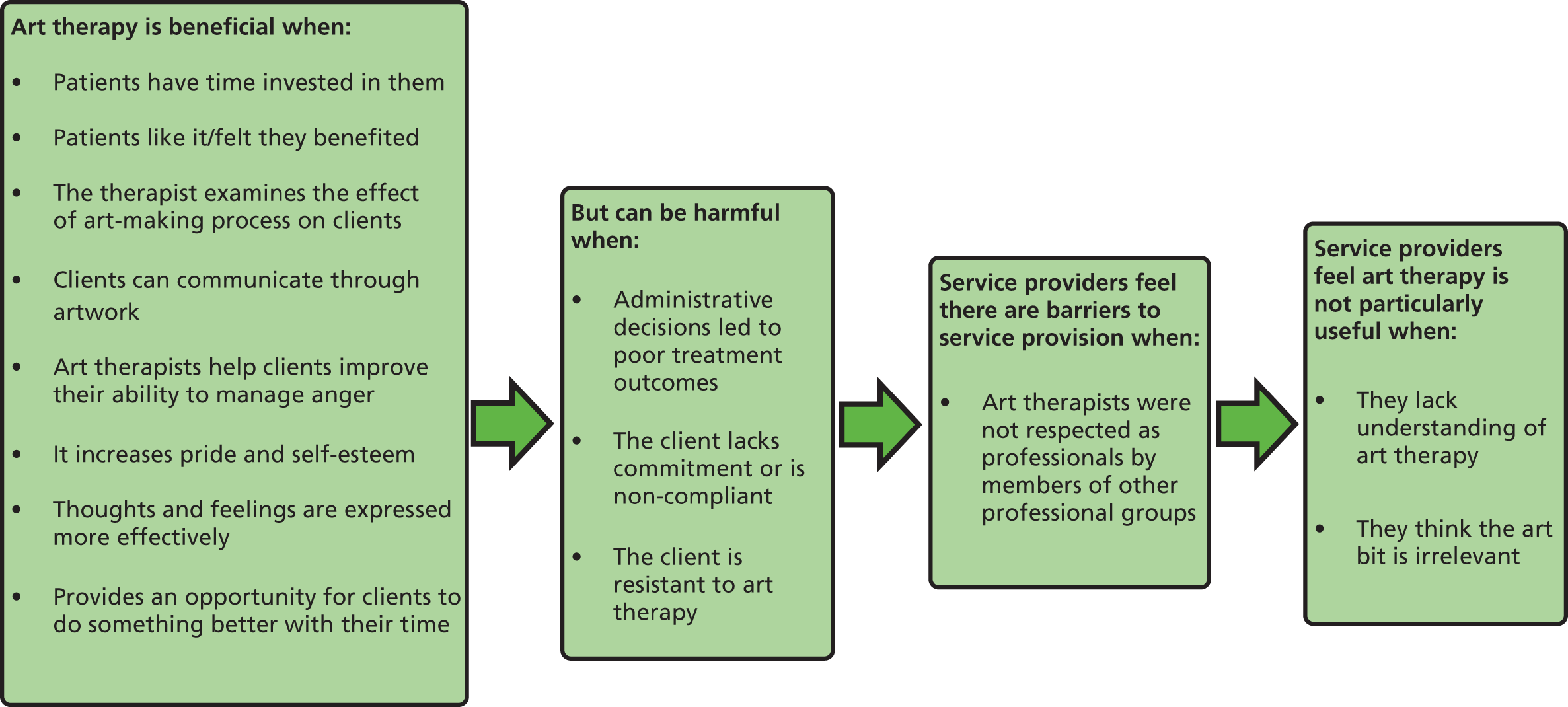
Combining the quantitative and qualitative findings
Qualitative meta-synthesis was undertaken to provide added value to the quantitative analysis by indicating patient issues around the acceptability of art therapy as a treatment for non-psychotic mental health disorders. This section aims to synthesise the findings from the two reviews.
The findings from the quantitative review demonstrated that depression, anxiety, low mood, distress and self-esteem were significantly reduced, and QoL and coping were significantly increased, relative to the control group in one to six studies. 48,52,58,59,61,62 Trauma was not significantly improved relative to the control group despite an improvement from baseline in three studies. 47–49 Cognition was not significantly improved in the one study it was reported in. 51 The findings of the qualitative review demonstrated that, overall, art therapy was viewed as an acceptable treatment by patients and service providers, with relatively few reports describing art therapy as unhelpful or unacceptable.
Some of the outcomes reported in the quantitative studies appear to map on to the qualitative findings around the beneficial and, in a smaller number of cases, the harmful outcomes of taking part in art therapy. Table 30 illustrates this mapping of outcomes from each review.
| Qualitative themes | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Relationships | Understanding | Perspective | Distraction | Personal achievement | Expression vs. unresolved emotion increased | Relaxation improved vs. anxiety increased | Empowerment | Pain increased | ||
| Quantitative outcome domains significant improvement relative to control (n/total N) | Depression (n = 4/9) | |||||||||
| Anxiety (n = 6/7) | ✗ | |||||||||
| Mood (n = 3/4) | ✓ | |||||||||
| Trauma (n = 0/3) | ||||||||||
| Distress (n = 2/3) | ✓ | |||||||||
| Quality of life (n = 4/4) | ✓ | |||||||||
| Coping (n = 1/3) | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ | ✓ | ✗ | ||
| Cognition (n = 0/1) | ||||||||||
| Self-esteem (n = 1/1) | ✓ | ✓ | ||||||||
Findings from the qualitative review that appear to map on to the quantitative coping outcome include both helpful and unhelpful qualitative findings. Self-esteem also mapped on to qualitative findings. Quantitative outcome domains that mapped to a lesser extent to the qualitative findings were QoL, distress, mood and anxiety (although in opposite directions). There was no qualitative evidence that mapped specifically to the quantitative outcome domains of depression, trauma or cognition.
More in-depth synthesis of the findings of the two reviews was particularly challenging given that, despite art therapy being defined as a complex intervention, the quantitative primary studies did not explore the mechanisms of art therapy that may modify its effectiveness, such as therapist skill. However, the qualitative review findings can help to elucidate the potential treatment effect modifiers identified in the quantitative review, despite the fact that in most cases it was not possible to assess their effect on outcomes. The potential treatment effect modifiers identified in the studies included, in the quantitative review included, experience/qualification of the art therapist, individual versus group art therapy, age, gender and pre-existing physical conditions.
Experience/qualification of the art therapist
The review of the quantitative evidence demonstrated that there was considerable variability in the reporting of the accreditation of the therapist, although most studies were conducted by a person who was seen be qualified as an art therapist. The findings of the qualitative review demonstrated that a good relationship with the art therapist was reported as an important for art therapy to be helpful. Therefore, it appears that the experience and skill of the art therapist may be an important mechanism of art therapy.
Individual versus group art therapy
The quantitative review reported that the majority of RCTs are of group art therapy, with only four of the 15 RCTs examining individual art therapy. 49,55,56,62 Of the studies of individual art therapy, two49,62 did not demonstrate an improvement on quantitative measures compared with the control group. Given that the qualitative findings also pointed to the importance of relationships with other group members as a particularly beneficial aspect of art therapy, with this finding seen in across several studies, an important mechanism in art therapy may be the group setting.
Pre-existing physical condition
The quantitative review highlighted that in nine studies patients had pre-existing physical conditions. 50,51,54–58,61,62 The remaining six studies were in people who were depressed,47,59 people with PTSD,48,49 or older people. 52,53 Neither the qualitative review nor the quantitative review found evidence that the effectiveness or helpfulness of art therapy differed across patients with or without pre-existing physical conditions. However, the qualitative review showed that a small number of themes appeared to apply mainly to people with pre-existing physical conditions. These themes included the facilitation of an improved relationship with family, friends and caregivers; facilitation of an understanding of the illness in two studies,72,84 one of obesity and one of palliative care impatients; distraction from pain; distraction from the illness/escapism; and providing the opportunity for legacy. These findings may have implications for how art therapy is delivered to different populations to maximise beneficial effects.
Although age and gender were identified as potential treatment modifiers in the quantitative review, neither review was able to demonstrate any evidence that these variables had an effect on quantitative outcomes or patients’ perspectives and attitudes towards art therapy.
Discussion
Discussion of the qualitative review
The aim of the qualitative systematic review was to provide a detailed user perspective on the acceptability and relative benefits and potential harms of art therapy. Overall, art therapy was viewed as an acceptable treatment across the populations of participants studied.
A number of beneficial aspects of art therapy emerged, together with a relatively smaller number of harmful aspects of art therapy, with relative harms being reported in only two studies. 72,73 An important theme emerging from the data was the relationship with the art therapist. This was raised as a positive and beneficial aspect of art therapy but also as potentially harmful, and further as a recommendation for service provision. A good relationship between the patient and art therapist was viewed as essential for successful, effective art therapy. However, harm could be caused in situations in which a positive relationship was not achieved, the therapist was viewed as unskilled, when emotions activated through therapy could not be resolved or the therapist was suddenly unavailable through sudden termination of the service. This finding was seen in evidence reported by patients and by service providers,74,81 who also stressed the importance of a good therapeutic relationship.
Some themes, such as the importance of expression, the relationship with the art therapist and with other group members and the facilitation of an increased understanding of self, were consistent across populations, while a small number of themes appeared to apply to populations in which a diagnosis of a pre-existing physical condition was present. These themes included the facilitation of an improved relationship with family, friends and caregivers, identified in one study of a cancer population,72 facilitation of an understanding of the illness in two studies (one of obesity84 and one of cancer73), distraction from pain in one study of cancer,72 distraction from the illness/escapism in two studies of cancer populations72,73 and one of an obesity population84 and providing the opportunity for legacy in a study of a cancer population. 72
Understanding and personal achievement were other important themes emerging from the evidence. In addition, some barriers to participation were reported. A small number of participants also reported that they did not want to take part in art therapy, which reiterates the importance of considering patient preference in choice of treatment. 14,15
The combination of the findings from the quantitative and qualitative reviews examined how outcomes from the quantitative review mapped on to themes emerging from the qualitative review. This demonstrated that a number of themes from the qualitative review appear to map on to the quantitative coping outcome. This included both helpful and unhelpful qualitative themes. Self-esteem also mapped on to qualitative findings. Furthermore, the combining of the two reviews identified a number of mechanisms within art therapy that may modify the effectiveness and acceptability of the treatment and should be considered in further research and in the implementation of art therapy.
Limitations
Overall the evidence base was small (n = 12), with only two studies examining service provider views74,81 and, furthermore, only one of these74 examined art therapists’ views. The majority of the included studies were of low or moderate quality. Limitations on word limits imposed by journals may have contributed to this, as theses and grey literature provided better-quality evidence. Lack of rich data was the main limiting factor relating to the qualitative evidence base.
Other significant limitations in the evidence base include the fact that the vast majority of studies reported only positive findings. This may have been because of researcher bias, in that most of the authors of the reports were art therapists,85 and the method of investigation in a number of studies appears to be biased towards the reporting of positive findings.
There was a lack of evidence comparing art therapy with other treatment options; therefore, we are unable to make comparisons regarding the acceptability of art therapy compared with other potential treatments participants might be offered.
Combining the qualitative and quantitative data proved difficult because of the paucity of the evidence base as a whole and the fact that meta-analysis was not possible. However, coping emerged as an important factor across both reviews, and this is an outcome domain that is likely to be pertinent to people with long-term health conditions. The small evidence base means it is not currently possible to make any generalisations around age, gender or setting.
Conclusions
From the small number of qualitative studies identified, art therapy was reported to be an acceptable treatment. The benefits associated with art therapy included the development of relationships with the therapist and other group members, understanding the self/own illness/the future, gaining perspective, distraction, personal achievement, expression, relaxation and empowerment. Small numbers of patients reported varying reasons for not wanting to take part and therefore art therapy may not be a preferred treatment option for everyone. A small number of cases highlighted potentially negative effects of art therapy, which included the evoking of feelings that could not be resolved. Overall, there was low to moderate certainty in the review findings.
Chapter 4 Economic evaluation
This chapter addresses what the likely cost-effectiveness of art therapy in the treatment of non-psychotic mental health disorders is and will draw on the clinical effectiveness data presented in Chapter 3.
Review methods
A systematic review was undertaken to identify existing economic analyses of the use of art therapy in the treatment of non-psychotic mental health disorders specifically from the perspective of the NHS and Personal Social Services. The purpose of this review was to identify, appraise and summarise published models of cost-effectiveness and other evidence concerning the cost-effectiveness of art therapy in order to inform our own modelling methodology.
Form of evaluation
The evaluation to be undertaken is that of a cost–utility analysis in order that the results presented can be compared with interventions in other disease areas and be framed within the cost-effectiveness thresholds [of £20,000–30,000 per quality-adjusted life-year (QALY)] reported by NICE. 86 Ideally, RCTs would report utility measures directly, but where this was not the case mappings from outcome measures reported to a preference-based utility [such as the European Quality of Life-5-dimensions (EQ-5D) health instrument] would be considered, as would using intermediate metrics to arrive at a utility value, such as mapping from outcome A to outcome B, which could be mapped into a preference-based utility.
Comparators
The comparators are limited to those that have been included in a RCT and compared directly with art therapy. This represents a limited selection of possible comparators, as any potential comparators that have been trialled only against a control strategy would not be included. This decision has been taken for three principal reasons: (1) the clinical profile of patients considered for art therapy is heterogeneous and thus any estimated comparisons of effectiveness made indirectly through a common intervention could be highly uncertain; (2) the position of art therapy may vary within packages of care which may affect the observed efficacy; and, most importantly, (3) there are myriad treatments that could be considered which would have resulted in a very large number of records identified in a literature search. The approach taken was supported by the project steering group and resulted in the following potential set of comparators: treatment as usual, wait-list control, CBT, verbal therapy, educational support, guided garden walking, art and craft activities, regular programme activities, simple calculations and video tape on use of art therapy.
Search methods
The comprehensive searches from the quantitative and qualitative reviews of art therapy were designed to capture relevant economic studies. Within these searches, synonyms relating to the condition were combined with a search filter aimed at restricting results to economic and cost-related studies (used in the searches of MEDLINE, CINAHL, EMBASE, and PsycINFO, with an amended version used for Web of Science; see Appendix 2).
Screening and eligibility
All citations generated from the comprehensive searches (see Chapter 2) were reviewed by at least one reviewer (LU or AS) and any studies reporting on costs or economics were flagged as potentially relevant to the project health economic modellers. UK-specific citations were identified and the abstracts of these were sifted to identify any potentially relevant economic evaluations for inclusion in the review. One health economic modeller (AR) independently screened the relevant titles and abstracts. When there was uncertainty in the decision, a second health economic modeller (MS) was consulted and a consensus was obtained through discussion. Owing to the small number of papers identified from the title/abstract sift, a conservative strategy was employed that included papers for appraisal at full text if there were even a small possibility that relevant data could be reported. Full papers of potentially relevant studies were obtained and assessed by one modeller (AR), with discussion with a second modeller (MS) where appropriate. In addition, the studies included in the review of clinical effectiveness were also appraised to identify any potentially relevant economic information. A modified preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram for the selection process is provided in Figure 10.
FIGURE 10.
Modified PRISMA flow diagram for the systematic review of cost-effectiveness.
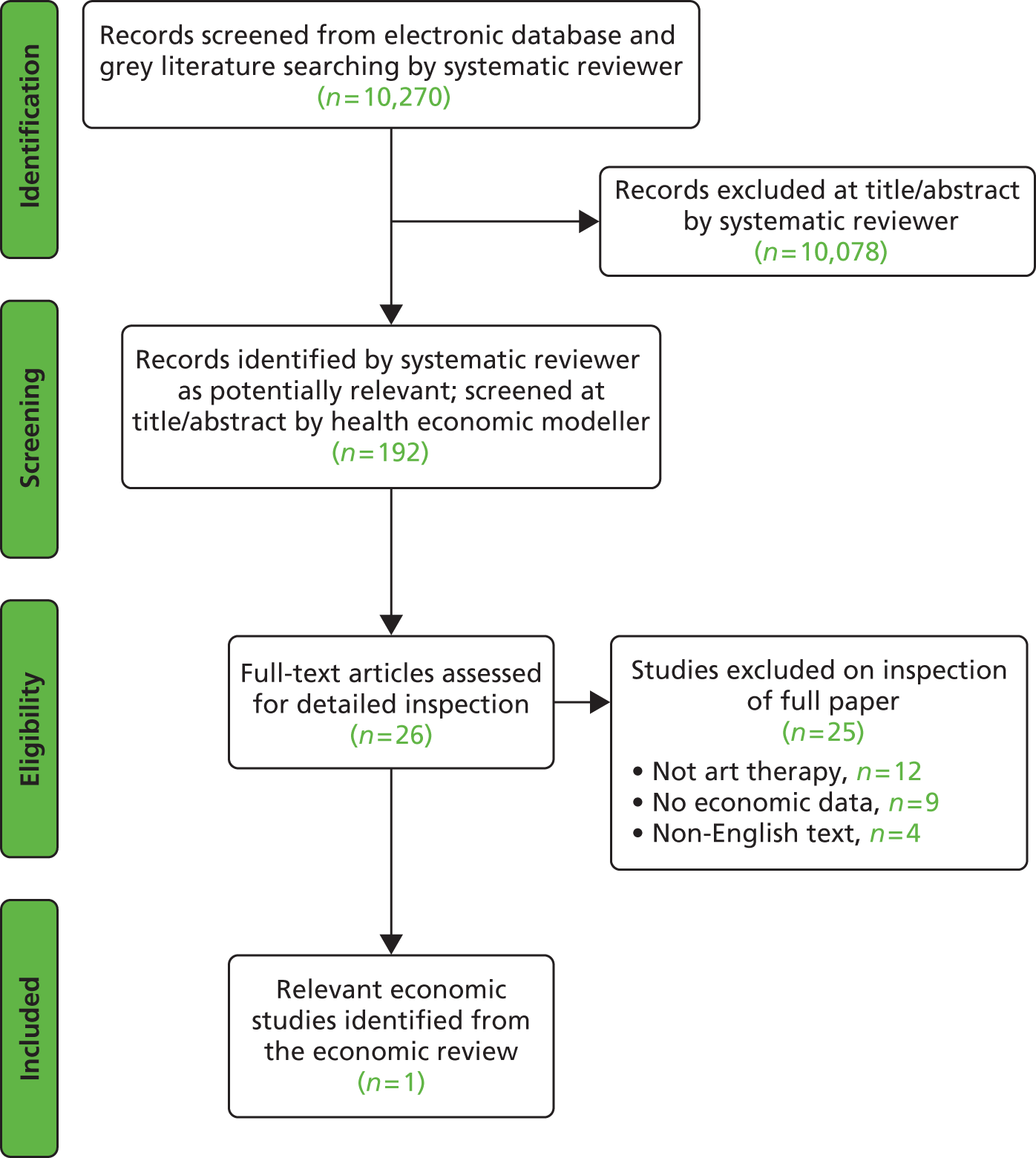
Inclusion and exclusion criteria
Studies were selected for inclusion according to predetermined eligibility criteria. Studies were included if they reported the cost-effectiveness of art therapy using the definitions outlined in Chapter 1 of this report. Owing to the dearth of evidence surrounding the cost-effectiveness of art therapy, studies were also included if they investigated the costs incurred and health-related benefits accrued by the use of the art therapy to treat patients with a diagnosed non-psychotic mental health illness and delivered by the NHS.
Studies that evaluated the cost-effectiveness of art therapy combined with any other therapy were excluded, as were studies not published in the English language.
Results of the economic systematic review
Included studies: economic evaluation
Of the 10,270 total records, 192 records were identified by a systematic reviewer as potentially relevant to the review of cost-effectiveness. Following a further title/abstract sift and subsequent full paper sift by health economic modellers, only one study was considered as relevant that had not been included in the clinical evidence base because it was not a RCT. A table of studies excluded at full text level is provided in Appendix 5 along with the reason for exclusion. Although the identified study is not an economic appraisal, it does investigate the costs incurred and health-related benefits accrued by the use of the art therapy. 87
Applying an economic checklist, such as that by Drummond et al. ,88 was deemed inappropriate. A considerable limitation of this case study is that it reports costs and outcomes over a 6-year period for only a single patient, who had been receiving ‘other forms of psychological treatment for many years’. Six years would be considered an extreme time period for receiving art therapy and it is unlikely that patients in the NHS would receive treatment for this length of time. In addition, although 357 patients were recruited to the full research study, the results for only one participant were reported, with no discussion of the impact of selection bias on the results presented.
In total, the patient received 233 sessions of art therapy, each lasting 1.25 hours, over the 6-year period. It was commented that the patient was receiving additional psychological therapy together with pharmacological treatments at the time she started art therapy, but after 2 years of art therapy these treatments were discontinued. Effectiveness was measured through two metrics, the Clinical Outcomes in Routine Evaluation Outcome Measure89 and the BDI,90 both of which improved throughout the art therapy and were maintained at 3 years’ follow-up.
The total cost of providing art therapy to this patient over the 6-year period was £7915 including salary and trust overheads (assumed to be 2004 figures), which equates to approximately £34 per session or £27 per hour. At the time of the study the authors state that the adult mental health cost per day was £300 for an inpatient and thus the total cost of art therapy was equivalent to approximately 26 days’ hospital admission, although hospital admission data were not reported. In addition, the patient was discharged from psychiatric outpatient therapy and stopped taking antidepressant medication, reducing costs to the health service.
The conceptual model
As no existing models of art therapy were identified, a de novo model was constructed instead. The model could be populated with data that had been identified in the clinical efficacy review but did not meet the inclusion criteria for the cost-effectiveness review. Owing to the nature of the study question, it was deemed that a complex model was not required and that a simple model would be sufficient and could more clearly demonstrate the impact of key drivers within the cost-effectiveness ratio. As such, an area under the curve model was developed to estimate the gain in utility with the following assumptions in the base case:
-
the maximum treatment effect would be associated with the time at which treatment ended
-
there would be a linear increase in treatment effect, from zero at baseline to the maximum at the time at which treatment ended
-
there would be a residual effect of treatment with a linear decline in benefit until there was zero benefit at 52 weeks
-
given the short assumed duration of benefit, discounting was not necessary.
The rationale for choosing 52 weeks as the base case duration of residual benefit was based on a number of relevant references. Discussing data in Nicholson and Berman91 and in Lambert and Ogles,92 Cooper wrote that ‘findings from the empirical research are fairly clear: clients, on average, do not tend to improve once their therapy is over . . ., but equally they do not tend to deteriorate rapidly’. 93 More recent data provided in Sportel et al. 94 (table 3) indicate that when Cognitive Bias Modification and Cognitive Behavioural Group Training provided larger decreases in an outcome measure (the Spielberger Test Anxiety Inventory95), the effect had not entirely waned at 12-month follow-up. This may be generalisable to other forms of successful psychological therapy, and conservatively we elected to assume that all benefit had dissipated at 52 weeks post treatment, although a longer period of 104 weeks was used in sensitivity analyses.
The conceptual model used to calculate the utility gain across time is shown in graphical form in Figure 11. In this figure it is assumed that there is a gain in utility of 0.0780 at week 8. The area under the curve was then translated into QALYs assuming 52.18 weeks per year.
FIGURE 11.
An illustration of the conceptual model of utility.
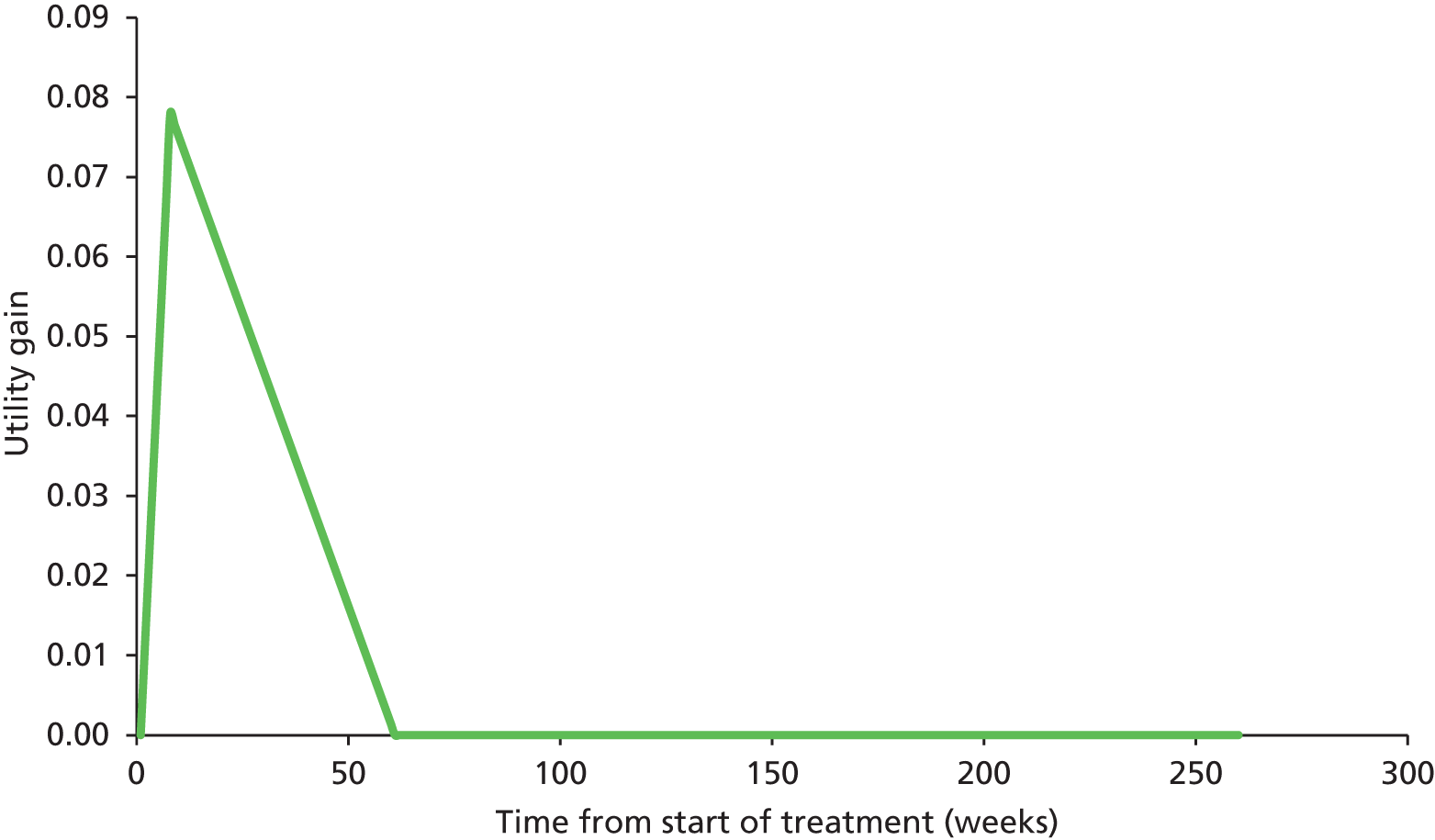
The estimate incremental costs of an intervention would be divided by the estimated incremental QALYs to form a cost per QALY gained ratio.
Effectiveness data
The number of outcomes reported in the included RCTs was large but, given the aim of performing a cost–utility analysis, few were deemed relevant. None of the RCTs identified included a preference-based utility measure. To assess the applicability of the outcome measures, an online database (Health Economics Research Centre database of mapping studies, Version 2, Health Economics Research Centre, Oxford. Available at: www.herc.ox.ac.uk/downloads/mappingdatabase) reported by Dakin96 was used to identify previously published mappings to the EQ-5D. Two outcome measures reported in the RCTs were shown to be mapped on to EQ-5D: the SF-36, an outcome reported in Monti et al. ,61 and the Barthel Index, an outcome reported in Hattori et al. 51 There were two published mappings from the SF-36: one by Ara and Brazier97 and one by Rowen et al. 98 Three mappings were found for the Barthel Index. 99–101
However, in the Hattori et al. 51 study, which was conducted in Japan, the Barthel index is reported for the overall score only, and mapping to the EQ-5D would require the individual component scores. The authors were contacted to enquire if the individual component data could be shared. However, the authors declined owing to their intention to publish the data in a forthcoming publication (see Appendix 6).
The study that reported changes in SF-3661 was conducted in the USA and recruited 111 women. Included patients had a breast cancer diagnosis (various stages) and were paired by age and randomised to either an 8-week mindfulness-based art therapy group (n = 56) or a wait-list control group (n = 55). All participants had a diagnosis of breast cancer and were recruited between 4 months and 2 years post diagnosis. Women with a terminal diagnosis, or who had a current diagnosis of a major mood disorder, psychotic disorder or significant cognitive deficit, were excluded. Those receiving any type of mental health care could be included but had to obtain written permission from their treating health professional to enter the study.
These data could be used to estimate a change in EQ-5D, albeit with the caveat that the patient group may not be representative of those who are treated with art therapy in England and Wales. The changes in the SF-36 scores are provided in Table 31. Only those variables that have been used in the mapping algorithms have been reported. It is noted that the data for physical role and emotional roles at week 8 are medians (and change in the median) as a result of the non-normality of the data. However, there appears to be a discrepancy in the results for the physical role scale, as the values reported at weeks 0 and 8 indicate a change of 25 across the 8-week period [(50 – 0) – (25 – 0)]. For this report we have assumed that the values of zero reported in change between art therapy and wait-list are correct, which would appear unfavourable to art therapy. A further caveat regarding the reliability of these efficacy data is that only women with values at baseline (week 0) and at end of treatment (week 8) were included in the analysis, with no imputation for missing data. There were 11 dropouts in the art therapy arm and seven dropouts in the control arm. If these reported dropouts were not random but related to lack of (perceived) efficacy, then it is possible that the reported results favour art therapy.
| SF-36 scale | Wait-list control arm | Art therapy arm | Change over the 8-week period | Difference in change (art therapy – wait-list control) over an 8-week period (95% confidence interval) | |||
|---|---|---|---|---|---|---|---|
| Week 0 | Week 8 | Week 0 | Week 8 | Wait-list control | Art therapy | ||
| Physical functioning | 64.37 | 64.42 | 58.23 | 65.01 | 0.05 | 6.78 | 6.73 (–13.8 to 0.37) |
| Social functioning | 60.04 | 64.91 | 51.22 | 66.60 | 4.87 | 15.38 | 10.51 (–20.9 to –0.10) |
| Physical rolea | 0.00 | 25.00 | 0.00 | 50.00 | 25.00 | 50.00 | 0.00 |
| Emotional role | 33.33 | 66.67 | 33.33 | 66.67 | 33.34 | 33.34 | 0.00 |
| Mental health | 64.91 | 67.07 | 56.90 | 69.95 | 2.16 | 13.05 | 10.89 (–16.8 to –4.96) |
| Vitality | 42.63 | 42.91 | 40.26 | 50.06 | 0.28 | 9.80 | 9.52 (–16.7 to –2.37) |
| Bodily pain | 58.14 | 58.74 | 54.23 | 60.14 | 0.60 | 5.91 | 5.31 (–14.1 to 3.50) |
| General health | 55.78 | 55.19 | 47.13 | 55.09 | –0.59 | 7.96 | 8.56 (–14.8 to –2.29) |
Table 32 provides estimates of the utility gain associated with art therapy compared with control in the Monti et al. 61 study, assuming the deterministic values of change in each SF-36 scale provided in Table 31. In the Ara and Brazier97 paper, the authors state that ‘we advocate model EQ(1) as the first choice for predicting mean EQ-5D scores from mean dimension SF-36 scores when patient level data are not available. Nevertheless, when comparing incremental differences between study arms or changes over time, model EQ(4) is the preferred choice’. Ideally, we would therefore use EQ(4) from Ara and Brazier,97 which is a linear regression, with the independent variables being the eight scales of the SF-36 (as shown in Table 31) and the following additional variables: age, physical functioning,2 social function,2 mental health2 and bodily pain. 2
| SF-36 scale | Source of mapping equation and selected model | |
|---|---|---|
| Ara and Brazier97 – EQ(1) | Rowen et al.98 – GLS 1 | |
| Physical functioning | 0.00370 | 0.00332 |
| Social functioning | 0.00110 | 0.00115 |
| Physical rolea | 0.00024 | –0.00060 |
| Emotional role | 0.00024 | 0.00010 |
| Mental health | 0.00256 | 0.00237 |
| Vitality | –0.00063 | –0.00039 |
| Bodily pain | 0.00286 | 0.00303 |
| General health | 0.00052 | 0.00169 |
However, Monti et al. 61 provide confidence intervals (CIs) only for the relative changes between art therapy and wait-list control and not for individual components at 8 weeks, which meant that evaluation of the uncertainty in the reported results could be undertaken only where the absolute values did not affect the estimation. EQ(1) does not rely on the absolute values and was, therefore, chosen for use in this report. The same logic was used to select generalised least squares model 1 from the Rowen et al. 98 paper, which was marginally inferior to models 2 and 3, in terms of R2, but did not rely on absolute values. An additional reason for selecting a model with a parsimonious number of variables is because of the uncertainty in the physical and emotional role data presented by Monti et al.,61 which could have a greater influence on the estimated values when variables interact or have polynomial forms.
The coefficients associated with changes in SF-36 scores in Ara and Brazier97 and Rowen et al. 98 are shown in Table 32. To allow a comparison to be made more easily, the coefficients from Rowen et al. ,98 which were based on SF-36 scores that ranged from 0 to 100, have been divided by 100 to be concordant with the results of Ara and Brazier, which were based on SF-36 scores ranging from 0 to 1.
The estimated gain in EQ-5D within the Monti et al. 61 RCT is shown in Table 33. The Monti et al. paper also reported change in the SCL-90-R and its summary score, the GSI. 102 This was associated with a positive effect on the GSI with a decrease of 0.16 (95% CI 0.08 to 0.24). Thus, an inference regarding the impact of a changed GSI on utility can be calculated, which is also shown in Table 33.
| Estimated utility gain | Source of mapping equation and selected model | |
|---|---|---|
| Ara and Brazier97 – EQ(1) | Rowen et al.98 – GLS 1 | |
| Associated with art therapy compared with wait-list | 0.0780 | 0.0871 |
| Associated with a unit decrease in GSI | 0.4873 | 0.5422 |
Making such an inference allows RCTs that report the GSI from the SCL-90-R as an outcome measure to be considered within the evidence base; however, this will increase the uncertainty within the results. The only RCTs in which GSI data from the SCL-90-R were presented in an appropriate form were by Thyme et al. 47,62 The outcome measures recorded in these studies were also used to try and broaden the evidence base, as inferences on the change in EQ-5D could be made for changes in the BDI-II, the Hamilton Rating Scale of Depression, the Impact of Event scale and the Structural Analysis of Social Behaviour. However, no further RCTs could be linked into the evidence network. This meant that a cost per QALY estimate could be estimated only for art therapy compared with wait-list control and the comparators in the Thyme et al. 47 and Thyme et al. 62 RCTs, which were psychodynamic art therapy and control respectively.
The Thyme et al. 47 study compared short-term psychodynamic art therapy and short-term psychodynamic verbal therapy, henceforth shortened to art therapy and verbal therapy. The RCT was conducted in Sweden and recruited 44 women. At recruitment, 28 (63.6%) study participants were diagnosed with dysthymic disorder and 16 (36.4%) study participants had depressive symptoms and difficulties. One participant withdrew before randomisation, resulting in a final study population at randomisation of 43 women (n = 21, art therapy; n = 22, verbal therapy). Of these, 39 women completed the study (n = 18, art therapy; n = 21, verbal therapy).
The reported results are potentially confounded by concomitant treatment. Two participants in the verbal therapy group ‘accepted body awareness as an additional treatment during psychotherapy’,47 compared with none in the art therapy arm, and the mechanism by which these women were to be offered body awareness is unclear. In addition, the use of antidepressants may differ between arms, as the text is unclear: ‘In the [art therapy] group, one participant were [sic] prescribed antidepressants during therapy (n = 1) and one between termination of therapy and the 3-month follow-up (n = 1), and in the [verbal therapy] group three during therapy (n = 1) [sic] and two after (n = 2).’47 Data from women who dropped out of the study (n = 2, art therapy; n = 1, verbal therapy) or who were referred to long-term art psychotherapy (n = 1, art therapy; n = 0, verbal therapy) were not included in the analysis, which may add uncertainty to the results. It is noted that as two active interventions were trialled no inference could be made with respect to the relative efficacy compared with no treatment.
The Thyme et al. 62 RCT comparing individual art therapy with control was conducted in Sweden and recruited women with breast cancer (n = 20 in the art therapy group; n = 22 in the control group). Candidates were excluded if they had a pre-existing physical or psychiatric illness. Additional treatments were permitted and this, again, may confound the results. At baseline, four participants in the art therapy arm and three participants in the control arm were using antidepressants. Two months later, only two participants in the art therapy arm were using antidepressants, and at 4-month follow-up (6 months after baseline) only one participant was taking antidepressants; in contrast, all three participants in the control arm remained on antidepressants. The results presented were based on a total of 41 women, 20 from the art therapy group and 21 from the control group. Data for one participant in the control arm were incomplete and were discarded; this may bias the results against art therapy if the reason for the data being incomplete was related to a worsening of the underlying condition.
The GSI data from Thyme et al. 47 and Thyme et al. 62 are provided in Table 34. It is noted that these will have increased uncertainty owing to an assumed relationship between GSI and the utility mapped from the SF-36 and may also be confounded by the use of adjunct treatments. It is seen that verbal therapy appears better than art therapy, as the difference in GSI increased by 0.23, with a decline of 0.07 at 4-month follow-up. Such a pattern was not replicated in the Thyme et al. 62 RCT where the gain (a reduction in GSI) was slight, being an additional 0.04 at the end of therapy; however, this benefit had increased 3 months later by an additional 0.07.
| Baseline | At completion of treatment | At follow-upa | |
|---|---|---|---|
| Reported difference in GSI score associated with art therapy compared with verbal therapy (Thyme et al.47) | 0.10 | 0.33 | 0.26 |
| Reported difference in GSI score associated with art therapy compared with control (Thyme et al.62) | –0.04 | –0.08 | –0.15 |
Thyme et al. 47 provided standard deviations for the GSI scores, which allow the CIs to be calculated for the change in GSI score between verbal therapy and art therapy. These calculations are undertaken in Table 34, with the conclusion being that there is significant uncertainty regarding which therapy is more effective.
Using the assumed relationship between GSI and utility detailed in Table 34, and using data from Thyme et al.,62 it can be estimated that, at the end of treatment, art therapy compared with control was associated with a utility gain of 0.019, using the Ara and Brazier97 mapping, or 0.022, using the Rowen et al. 98 mapping. These values are considerably lower than those calculated from Monti et al. 61 A discussion of the possible reasons for this is provided later. The estimated utility gain of verbal therapy over art therapy in Thyme et al. 47 was larger: 0.112 using the Ara and Brazier97 mapping and 0.125 using the Rowen et al. 98 mapping.
The process described has allowed evidence from three RCTs to be considered, although there are caveats regarding the mappings, the study population and the small sample sizes, all of which increase the uncertainty in our results. At the project outset it was envisaged that there would be sufficient evidence to be able to undertake a network meta-analysis; however, this was not facilitated by the evidence because of the lack of comparable data from outcome measures used in the RCTs. A possible solution to the problem of not all studies reporting the same outcome measure would be to perform a multivariate network meta-analysis. This would allow strength to be borrowed about the effect on each outcome measure, allowing for correlation within and between studies. Such an analysis would require each outcome measure to have been reported alongside at least one other outcome measure and external evidence with which to estimate the within study correlation. In the event, this was not possible because the outcome measures were not collected as required. Nevertheless, such an analysis would still have been beyond the scope of the project.
The three RCTs will be modelled distinctly rather than meta-analysed, with scenario analyses undertaken where appropriate.
Given the modelling of the three RCTs individually, it is important that the costs accrued within the RCTs are established, as these must be linked to the observed benefits. Assuming that the benefits would be maintained with a different ratio of therapists to patients, different numbers or duration of sessions or a different grade of therapist would be naive. Therefore, the anticipated costs assuming each regimen in the RCT is delivered in the NHS needs to be estimated. These costs are detailed for each of the three RCTs.
Costs associated with the Monti et al.,61 Thyme et al.47 and Thyme et al.62 randomised controlled trials
Only the costs of art therapy have been included in the analyses. Any effect on other costs, for example that of prescription medication hospitalisations or specialist care, has been excluded, owing to the lack of robust data.
The costs presented are estimated on the assumption that those receiving group art therapy remain in the group until the end of the sessions, even were there to be regular non-attendance. It was assumed that those receiving individual treatment who did not attend still incurred the cost of attendance, as the art therapist would be required to be present. If these assumptions were relaxed, it is anticipated that the cost per patient could decrease, although the impact on effectiveness in group therapy because of a higher ratio of participants to therapists would be unknown.
Monti et al.61
The RCT ran for 16 months and resulted in seven intervention groups and seven control groups: those allocated to wait-list control were offered art therapy 8 weeks later than those randomised to the art therapy arm. This RCT design meant that comparative data were valid only for the period of 8 weeks before the control group received art therapy.
As 56 patients received art therapy and there were seven groups, it can be calculated that the group size was eight, although not all patients attended all eight sessions (median number of sessions attended was six). The groups were led by a single study investigator who was a registered art therapist and each lasted for 2.5 hours, resulting in 20 hours per treatment course.
Two estimates were made regarding the costs of replicating the Monti et al. 61 art therapy treatment in England and Wales. In addition to standard unit costs reported in Curtis,103 it was deemed worthwhile exploring if any art therapy-specific costs were available. Our clinical advisors sought information from the BAAT, which provided estimated figures which were used in addition to those reported by Curtis. The first estimate from BAAT was £72 per hour (Val Huet, BAAT, 2014, personal communication), whereas the second estimate used a cost of £99 reported by Curtis. 103 The latter estimate is a cost for delivering CBT and is likely to be an overestimate, as it assumes a clinical psychologist at band 8, at which grade few art therapists are employed. However, the costs from Curtis103 were used in a sensitivity analysis. The estimated costs of the art therapy course conducted in Monti et al. 61 were £1440 using the BAAT estimate and £1980 using the Curtis103 estimate. Assuming eight women per course, this would equate to cost per woman of £180 (BAAT) or £247.50 (Curtis103).
Thyme et al.47
The art therapy intervention consisted of 10 sessions each lasting 60 minutes; these sessions were delivered by two experienced art psychotherapists. The verbal therapy intervention consisted of 10 sessions each lasting 45 minutes; these sessions were delivered by three experienced verbal psychotherapists, although one withdrew from the study as a result of illness and was not replaced (the time at which this occurred was not reported within the paper). For calculation of the costs of verbal therapy we have assumed that the illness occurred midway through the intervention and have assumed 2.5 therapists.
Assuming a cost of £72 per hour per art therapist, it is estimated that the cost of the art therapy intervention was £1440 (£72 × 2 × 10 × 1); if a value of £99 per hour was used instead, this cost rose to £1980. Assuming that there were 18 women within the art therapy group, to align with the outcome data, these would equate to costs of £80 or £110 per participant.
Assuming a cost of £72 per hour per verbal therapist, it is estimated that the cost of the verbal therapy intervention was £1350 (£72 × 2.5 × 10 × 0.75); if a value of £99 per hour was used instead, this cost rose to £1856. Assuming that there were 21 women within the verbal therapy group, to align with the outcome data, these costs would equate to £64 or £88 per participant.
Thyme et al.62
The Thyme et al. 62 RCT assessed the effectiveness of an individual brief (5-week) art therapy intervention compared with a control group in women with breast cancer. The duration of the session was not reported; therefore, a clear estimate of the cost could not be provided. As a lower bound, if the session was assumed to be 1 hour in duration, this would result in the participant receiving 5 hours of an art therapist’s time and would be costed at £360 per participant (assuming £72 per hour) or at £495 per participant (assuming £99 per hour).
Evaluation of the robustness of results reported in Monti et al.,61 Thyme et al.47 and Thyme et al.62
An assessment of the clinical methodology used within each of the three RCTs that provide an estimate of utility differences has been undertaken in order to evaluate the robustness of the reported results. All of the three studies had limitations, but the Thyme et al. 47,62 RCTs were shown to have the most potential confounding and uncertainty in the true effect size.
The report by Monti et al. 61 does not offer a discursive description of the working art therapy definition used for the trial, but it contains a table showing the linking of the mindfulness aspects with the art therapy which provides a clear indication of what was being tested.
The comparison between verbal therapies and art therapy reported in Thyme et al. 47 may be problematic. The verbal psychotherapy treatment follows the long-established ideas of Mann104 on brief structured psychotherapy. Mann is clear about structure and about significant aspects of brief therapy. In contrast, the range of art therapy literature cited (Cane,105 Waller and Gilroy,106 Betensky107 and Schaverien108) represent very different approaches to art therapy. One chapter in one of these four books contains some speculative ideas about brief work,106 but brief work is not mentioned in the rest. The differences between the art therapy approaches cited are evident in the apparently unconnected, somewhat prescriptive, tasks the women in the group are asked to undertake. This is in contrast to the relative coherence of Mann’s ideas for brief work,104 which are sometimes used, incidentally, by art therapists. In addition, the results may be confounded by the imbalances between the trial arms in the numbers of patients with borderline personality organisation (BPO), receiving adjunct antidepressants and receiving adjunct body awareness treatment. It was seen that four (22%) participants receiving art therapy had BPO compared with three (14%) receiving verbal therapy. A smaller proportion of participants were using antidepressants in the art therapy group [11% (n = 2)] than in the verbal therapy group [14% (n = 3)]. Potentially of more importance was the fact that 10% (n = 2) of participants in the verbal therapy group also received body awareness treatment, compared with no participants in the art therapy group. These factors raise concerns regarding whether or not the results are confounded, particularly as the sample size in the study is small. However, the authors do state that ‘the results indicated that the variables did not distort the main results of the study. Neither did the interviews that were performed after the psychotherapy and at 3-month follow-up disclose any major changes in the participants’ life that could explain our results.’104
The art therapy intervention in the Thyme et al. 62 RCT appeared more clearly structured and described than the Thyme et al. 47 RCT. It is believed that the structure of the treatment programme (individual and for only five sessions) was because of logistical reasons; however, this may present limitations in the generalisability of the results. It was observed, in contrast to Monti et al. 61 and Thyme et al. ,47 that benefits increased after cessation of treatment. It is unclear whether or not this benefit is related to the shorter duration of treatment. While the Thyme et al. 47 RCT does provide data that can be used in the cost-effectiveness analyses, it is believed that conclusions produced from these should be interpreted with caution.
Methodology for producing results
Results were produced deterministically using the mean value for each parameter, with a number of scenario analyses undertaken. These included use of the Rowen et al. 98 and the Ara and Brazier97 mapping functions, extending the duration of response to 2 years and using cost estimates from BAAT and from Curtis. 103
Probabilistic results were generated by sampling from appropriate distributions. These included the relative effects reported by Monti et al. 61 in the SF-36 dimensions used in the mapping, and the relative effect of art therapy compared with verbal therapy in the Thyme et al. 47 RCT. Scenario analyses were also conducted for the probabilistic results.
As no correlation parameters were reported in the RCTs, it was assumed that all parameters were independent. This would not be the case between the measures of SF-36 and GSI recorded in Monti et al. ,61 which are, it was assumed, likely to be highly correlated. However, for simplicity, we assumed that the GSI effect was constant and recalculated the relationship of GSI and utility when the effects of art therapy on the SF-36 dimensions were sampled.
To estimate the uncertainty in the Thyme et al. 47 results, the width of the CI of the mean effect was estimated using the number of participants and the reported standard deviations before therapy and on completion of therapy through a t-test. There were an estimated 34 degrees of freedom for the art therapy arm and 38 degrees of freedom for the verbal therapy arm. The CI of the mean was used to estimate a standard error of the mean.
Probabilistic results were not undertaken for the Thyme et al. 62 scenario, as there were no data to quantify uncertainty about parameters.
Conducting probabilistic sensitivity analyses (PSAs) allows a quantification of uncertainty in the output: 1000 PSA samples were evaluated. This has been displayed in a number of ways. Initially, the range in the mean cost per QALY gained was estimated using a percentile method. Then a cost-effectiveness acceptability curve (CEAC) was generated. 109 The CEAC provides the probability of each intervention being optimal at different cost per QALY thresholds. Furthermore, a jackknifed estimate was performed to assess whether sufficient probabilistic samples had been run to determine the mean cost per QALY. 110 Finally, a histogram of the estimated utility gain was constructed.
Table 35 provides summary statistics for the distributions within the model. For all parameters, a normal distribution has been assumed, although it is acknowledged that at extreme samples, non-credible utility gains greater than 1 could be generated. This limitation was deemed to have minimal impact on the results given the predicted changes in utility provided in Table 34.
| Parameter | Mean value | 2.5th percentile | 97.5th percentile |
|---|---|---|---|
| Utility gain in the Monti et al.61 RCT of art therapy compared with wait-list controla | 0.078 | 0.034 | 0.119 |
| Utility gain in the Monti et al.61 RCT of art therapy compared with wait-list controlb | 0.087 | 0.043 | 0.126 |
| Relationship between one unit decrease in GSI and utility gain (using Ara and Brazier97) | 0.485 | 0.212 | 0.744 |
| Relationship between one unit decrease in GSI and utility gain (using Rowen et al.98) | 0.542 | 0.271 | 0.790 |
| GSI decrease of verbal therapy compared with art therapy in the Thyme et al.47 RCT | 0.235 (verbal therapy more effective) | –0.270 (art therapy more effective) | 0.721 (verbal therapy more effective) |
| Derived utility gain in the Thyme et al.47 RCT of verbal therapy compared with art therapy (using Ara and Brazier97) | 0.114 | –0.145 | 0.386 |
| Derived utility gain in the Thyme et al.47 RCT of verbal therapy compared with art therapy (using Rowen et al.98) | 0.127 | –0.160 | 0.426 |
In addition, a threshold analysis has been conducted to ascertain the likely level of gain in utility that would be required for art therapy, as typically used in England and Wales, to be deemed cost-effective using thresholds of £20,000 and £30,000 per QALY gained. To undertake this analysis, assumptions regarding the likely cost, and likely durations of treatment and residual benefit were required. While it is acknowledged that there is a spectrum of needs and treatments, it was believed that the majority of patients would be treated in either an art therapy outpatient group or a community recovery setting, with only a small proportion needing more expensive treatment. Using data from the BAAT, it was assumed that typical treatment would be of 42 sessions over a 52-week period and with a cost per patient of £750. Analyses were run using an assumed residual benefit of either 52 or 104 weeks.
Results
The focus of this section is on the results generated using the data reported in the Monti et al. 61 RCT. Exploratory analyses using the data reported in Thyme et al. 47 and Thyme et al. 62 are reported, but these should be viewed with caution given the limitations within these trials.
Primary results
The deterministic results from Monti et al. 61 are shown in Table 36. It is seen that in all cases art therapy had a cost per QALY gained of less than £6000, providing an indication that art therapy is highly cost-effective compared with wait-list control using thresholds of either £20,000 or £30,000 per QALY gained.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) | ||
| 52 weeks | BAAT | 180 | 0.0448 | 4015 | 180 | 0.0501 | 3595 |
| 52 weeks | Curtis | 248 | 0.0448 | 5520 | 248 | 0.0501 | 4943 |
| 104 weeks | BAAT | 180 | 0.0837 | 2151 | 180 | 0.0935 | 1926 |
| 104 weeks | Curtis | 248 | 0.0837 | 2957 | 248 | 0.0935 | 2648 |
Probabilistic results are provided in Table 37. These are very similar to the deterministic results, with the discrepancy caused by Monte Carlo sampling error. The jackknifed mean costs per QALY values had small CIs, indicating that 1000 PSA samples were sufficient. The CEAC for the scenario least favourable to art therapy is provided in Figure 12, with a histogram of the utility gain in this scenario provided in Figure 13.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) (95% CI) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) (95% CI) | ||
| 52 weeks | BAAT | 180 | 0.0447 | 4031 (2628–9202) | 180 | 0.0499 | 3610 (2477 to 7229) |
| 52 weeks | Curtis | 248 | 0.0447 | 5542 (3613–12,653) | 248 | 0.0499 | 4963 (3405 to 9940) |
| 104 weeks | BAAT | 180 | 0.0834 | 2159 (1408–4930) | 180 | 0.0931 | 1934 (1327 to 3873) |
| 104 weeks | Curtis | 248 | 0.0834 | 2969 (1936–6779) | 248 | 0.0931 | 2659 (1824 to 5325) |

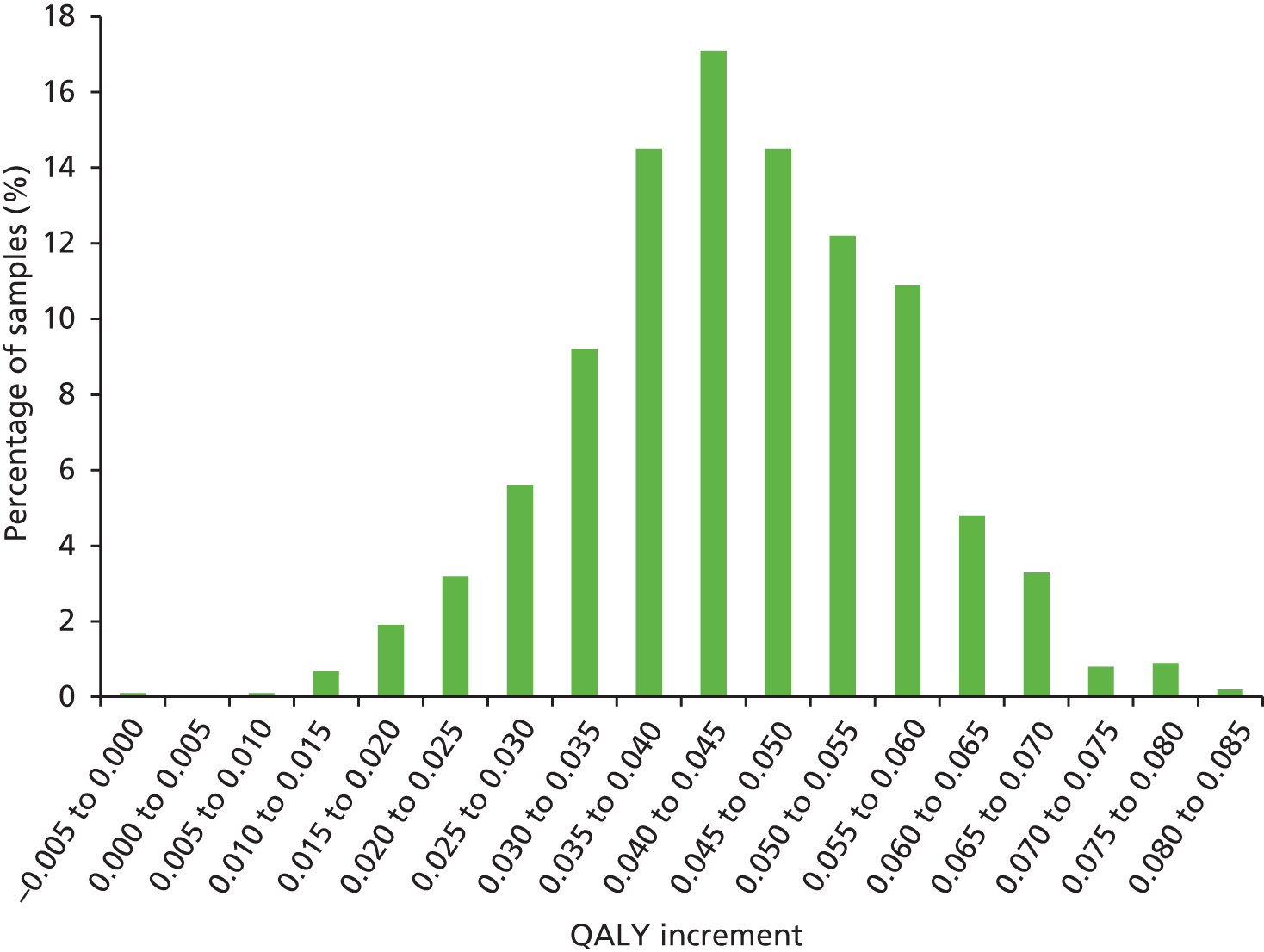
It is seen that even with the scenario least favourable to art therapy there is a high probability of art therapy being optimal assuming a cost per QALY threshold of £10,000.
It is seen that, in the vast majority of cases, art therapy resulted in a QALY increase, although in one sample (0.1% of all samples) it was estimated that art therapy could have a detrimental effect. This is shown on the far left of the graph and is coloured black. Typically the gain in QALYs was between 0.035 and 0.050.
Estimating the utility gain required at 52 weeks in order for art therapy, as employed in England and Wales, to be deemed cost-effective
The estimated utility gain required at 52 weeks in order for art therapy to be cost-effective is given in Table 38.
| Duration of residual benefit | Assumed cost per QALY threshold | |
|---|---|---|
| £20,000 | £30,000 | |
| 52 weeks | 0.038 | 0.026 |
| 104 weeks | 0.026 | 0.017 |
It is estimated that the largest utility gain required would be below 0.04. This compares favourably with the values reported in the Monti et al. 61 RCT (reported in Table 33), which are estimated to be in excess of 0.075, although this value was generated in a group of women with breast cancer and the generalisability to a population with non-psychotic mental health disorders is not known. Thus, it is plausible that art therapy, as used in England and Wales, is a cost-effective use of resources compared with no treatment.
Exploratory results
Thyme et al.47
The deterministic results from Thyme et al. 47 are shown in Table 39. It is seen that in all cases verbal therapy was estimated to dominate art therapy, in that it is cheaper and more efficacious. However, as will be detailed, there is considerable uncertainty in these results.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) | ||
| 52 weeks | BAAT | –16 | 0.0666 | Dominated | –16 | 0.0744 | Dominated |
| 52 weeks | Curtis | –22 | 0.0666 | Dominated | –22 | 0.0744 | Dominated |
| 104 weeks | BAAT | –16 | 0.1224 | Dominated | –16 | 0.1367 | Dominated |
| 104 weeks | Curtis | –22 | 0.1224 | Dominated | –22 | 0.1367 | Dominated |
Probabilistic results are provided in Table 40. These are very similar to the deterministic results. The jackknifed mean costs per QALY values had small CIs indicating 1000 PSA samples were sufficient. Although the mean cost per QALY value looks considerably favourable to verbal therapy in all scenarios the 95% CIs indicate that art therapy may have a cost per QALY gained compared with verbal therapy of less than £300.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) | ||
| 52 weeks | BAAT | –16 | 0.0675 | Dominating (dominating – 183a) | –16 | 0.0757 | Dominating (Dominating – 99a) |
| 52 weeks | Curtis | –22 | 0.0675 | Dominating (dominating – 251a) | –22 | 0.0757 | Dominating (Dominating – 136a) |
| 104 weeks | BAAT | –16 | 0.1241 | Dominating (dominating – 168a) | –16 | 0.1391 | Dominating (Dominating – 91a) |
| 104 weeks | Curtis | –22 | 0.1241 | Dominating (dominating – 230a) | –22 | 0.1391 | Dominating (Dominating – 125a) |
The CEAC for the scenario least favourable to verbal therapy is provided in Figure 14, with a histogram of the utility gain in this scenario provided in Figure 15.


It is seen that there is considerable uncertainty in the optimal decision, with art therapy being optimal in 20% of the PSA evaluations. As there is little difference in the cost of these interventions, this uncertainty is caused solely by uncertainty in which treatment is the most efficacious, as shown in Figure 14. In addition, limitations within the Thyme et al. 62 RCT would increase the uncertainty of the results.
It is seen that there is considerable uncertainty in the results regarding whether art therapy or verbal therapy is more efficacious. The bars coloured black and white indicate where art therapy is estimated to be more efficacious, with those in green indicating where verbal therapy is estimated to be more efficacious. The analyses of uncertainty indicate that further research is required before a definitive statement could be made, and it is commented that the data presented may be confounded (see Chapter 2).
Thyme et al.62
The deterministic results from Thyme et al. 62 are shown in Table 41. It is seen that the cost per QALY is much higher than in the Monti et al. 61 RCT, reflecting both an increased cost (as would be expected in individual therapy) and a reduced effectiveness. Only where the cost per patient was low and residual benefit high was the cost per QALY below £20,000.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) | ||
| 52 weeks | BAAT | 360 | 0.0106 | 33,811 | 360 | 0.0119 | 30,275 |
| 52 weeks | Curtis | 495 | 0.0106 | 46,490 | 495 | 0.0119 | 41,628 |
| 104 weeks | BAAT | 360 | 0.0204 | 17,681 | 360 | 0.0227 | 15,832 |
| 104 weeks | Curtis | 495 | 0.0204 | 24,311 | 495 | 0.0227 | 21,769 |
A further exploratory analysis was undertaken assessing the change in the cost per QALY should the increased benefits shown at 4 months’ follow-up be included. In this scenario, a linear gain to 21 weeks was assumed before the residual benefit was assumed. These results are shown in Table 42. In this analysis, the cost per QALY values are markedly reduced and never rise above £15,000.
| Duration of residual benefit | Costing source | Using the Ara and Brazier97 mapping | Using the Rowen et al.98 mapping | ||||
|---|---|---|---|---|---|---|---|
| Incremental costs (£) | Incremental QALY | Cost per QALY (£) | Incremental costs (£) | Incremental QALY | Cost per QALY (£) | ||
| 52 weeks | BAAT | 360 | 0.0375 | 9600 | 360 | 0.0419 | 8596 |
| 52 weeks | Curtis | 495 | 0.0375 | 13,200 | 495 | 0.0419 | 11,820 |
| 104 weeks | BAAT | 360 | 0.0642 | 5606 | 360 | 0.0717 | 5020 |
| 104 weeks | Curtis | 495 | 0.0642 | 7709 | 495 | 0.0717 | 6893 |
Owing to the method of data reporting, PSA was not performed on the analyses relating to the Thyme et al. 62 RCT.
Value of information analyses
Value of information analyses were not undertaken as these would be specific to the RCT being evaluated and could easily be misleading. For example, in the analysis of the Monti et al. 61 RCT there is little uncertainty that art therapy appears more cost-effective than wait-list control. Undertaking expected value of perfect information analysis111 would indicate that further research would not represent cost-effective use of resources. However, there are significant differences, particularly in terms of duration between the art therapy undertaken in the Monti et al. 61 RCT and that which is employed in England and Wales. The same is true of the art therapy techniques used in Thyme et al. 47 and Thyme et al. 62 Currently, there are very few data, if any, on the cost-effectiveness of art therapy as used in England and Wales, and a well-conducted RCT is required to establish the likely cost-effectiveness of art therapy in this setting. While it may be possible to elicit values from experts, this is subject to limitations and was outside the scope of the project.
Discussion
Discussion of the economic evaluation
The primary analyses indicate that art therapy as delivered in the Monti et al. 61 RCT may be highly cost-effective compared with wait-list but the generalisability of this study to patients in England and Wales is unknown, as the population consisted of women with breast cancer and the percentage with a non-psychotic mental health disorder was unknown. Confirmatory studies would be required to establish this definitively. An analysis of the effectiveness, in terms of utility gain that would need to be produced for art therapy as used in England and Wales, to be cost-effective was undertaken. This indicated that the values reported in the 8-week Monti et al. 61 RCT would be associated as a cost-effective intervention even with the costs associated with a year of treatment.
Exploratory analyses using data from Thyme et al. 47 indicate that, when using midpoint values, verbal therapy appears more efficacious than art therapy. However, there is considerable uncertainty in this estimation and a possibility that the results are confounded by concomitant treatments. Further research is required before definitive conclusions can be made on the cost-effectiveness of art therapy against verbal therapy.
The results produced using the data from Thyme et al. 62 change markedly based on the assumptions used. Given this and the potential for the results to be confounded by concomitant treatment, further research is required before any definitive conclusion can be made on the cost-effectiveness of individual art therapy against control.
Limitations
The analyses undertaken have been simplistic, a decision necessitated by the dearth of RCT evidence available; as such any conclusions reached should be treated with a degree of caution. The key RCT on which our conclusions are based recruited women with breast cancer and the generalisability of data from this group to those with non-psychotic mental health disorders is unclear. In addition, results generated from Thyme et al. 47 and Thyme et al. 62 may be confounded. The Thyme et al. RCTs47,62 also required mapping from GSI data from the SCL-90-R to the SF-36, and then from these data to the EQ-5D, compared with a mapping of SF-36 to EQ-5D for Monti et al. 61 The simplistic model did, however, allow key variables that affect the cost-effectiveness ratio to be determined, and it is seen that the assumed length of residual benefit, on which very few data are available, significantly impacts on the estimated QALYs gained.
Conclusions
From the limited available evidence used to perform the economic evaluation it appears plausible that art therapy is cost-effective compared with wait-list, although further research would be required to support this conclusion and to establish if shorter durations of treatment are more cost-effective than the current duration.
Exploratory analyses indicate that verbal therapy appears more efficacious than art therapy, but there is considerable uncertainty in this estimation and further research is required before definitive conclusions can be made on the cost-effectiveness of art therapy against verbal therapy. The results produced change markedly, based on the assumptions used. Given this and the potential for the results to be confounded, further research is required before any definitive conclusion can be made on the cost-effectiveness of individual art therapy compared with control.
Chapter 5 General discussion
Discussion of findings from the quantitative, qualitative and cost-effectiveness reviews
On the basis of the evidence retrieved from the quantitative review, art therapy appears to have a beneficial effect in improving mental health symptoms in a number of different clinical profiles and against a variety of comparators. However, the data from the studies are of low quality, with small sample sizes, and have substantial risk of bias; therefore, the results from the studies cannot be regarded as reliable. With regards to the review question, there are insufficient data from RCTs which use the same outcome measure to inform a robust analysis relating to the target population of people with non-psychotic mental health disorders. There are limited data to be able to conclude about specific populations including mental health disorders, age, gender or setting.
In estimating treatment effects, psychotherapies can be considered at greater risk of confounding variables than pharmacological interventions. Art therapy is a complex intervention and, as such, it may be difficult to attribute changes in mental health outcomes to be a direct result of the intervention unless more high-quality RCTs are implemented. Figure 16 depicts the potential errors that can result at the various stages of conducting a RCT of psychotherapy which can threaten the quality and validity of the trial if good conduct is not implemented. Future research should ensure that trials have both internal and external validity and should adhere to Consolidated Standards of Reporting Trials (CONSORT)40 guidelines in conducting and reporting trials.
FIGURE 16.
Potential error associated with RCTs of psychological therapy.

The qualitative review helped to elucidate some of the beneficial components from the small quantity of evidence conducted in service users and service providers. The patient–therapist relationship appears to be an important determinant in successful treatment. In addition, harm could be caused if the therapist was viewed as unskilled and when they would be unable to help resolve emotions activated by the therapy. The importance, therefore, of regulating and monitoring therapist competence is highlighted. In addition, the importance of access to art therapy was emphasised as a concern should art therapy services suddenly be terminated, and this was mirrored in the data from service providers. A small, low-quality study of service providers also highlighted that some GPs may not understand the specific benefits of art therapy per se but see it as a treatment option that alleviates their own time/capacity.
The cost-effectiveness review found that using the limited available data, art therapy may be cost-effective compared with wait-list. There is a dearth of relevant economic evidence to inform whether or not recommending art therapy versus an alternative psychological therapy or a pharmacological treatment would be cost saving to the NHS. In addition, as art therapy is used in complex cases there is the potential for its effects to impact on other health resources. As a consequence the full range of opportunity costs may be difficult to identify, measure and value. There are likely to be regional variations in art therapy service delivery and subsequently variations in relevant resource costs. As such it is important to identify the broad range of costs and benefits of other interventions for non-psychotic mental health disorders.
Definitions of relevant comparators for evaluations may be subject to geographical heterogeneity as a result of local provision and access to art therapy services and, moreover, this may differ according to the particular clinical population under evaluation. Future research should ensure the interventions and comparators assessed in trials are relevant from a policy perspective. Preference-based health-related QoL instruments (e.g. the EQ-5D) should be used as a matter of course.
Limitations of this health technology assessment
Owing to the experience of the research team in systematic review methodology, the potential for bias in the selection of evidence for this review is low. While two of the authors for this health technology assessment are art therapists (ETB and CW) and one is an arts therapist (KDB), they were not responsible for selection of studies into the quantitative, qualitative or economic reviews and therefore did not influence the evidence selected for inclusion into the review. A project steering group consisting of consultant psychiatrists and service users who were not directly affiliated with art therapy attended two meetings to review and comment on the research design and main findings. In addition, the research protocol has been available online via the NIHR and PROSPERO websites since commencement of the project to facilitate public scrutiny of the proposed research methods.
The research design for this review could be considered as being led by the evidence as well as the research question. The inclusion criteria were shaped to fit the research question and were influenced, to a degree, by the initial scoping searches prior to project commencement. This resulted in the broadened inclusion criteria for the study population. While this review can be considered as an evidence portfolio for art therapy across several non-psychotic mental health disorder, it suffers from substantial heterogeneity in the patient clinical profiles included, which is likely to be a treatment effect modifier. Focusing the population of interest to specific health conditions or outcome domains in future systematic reviews will increase the precision of any resulting pooled treatment effects.
Chapter 6 Final report conclusions
Conclusions of the research
From the limited available evidence, the following conclusions can be drawn from this health technology assessment:
-
Art therapy appears to have statistically significant positive effects compared with controls in a number of studies in patients with different clinical profiles. The most relevant symptoms which were effectively targeted in these studies were depression, anxiety, low mood, trauma, distress, reduced QoL, low coping skills and self-esteem. The small RCT evidence base indicated that art therapy was associated with an improvement from baseline in all but one study and was a more effective treatment than control groups in the majority of studies.
-
Art therapy was reported to be an acceptable treatment and was associated with a number of benefits from a small number of studies including the development of relationships with the therapist and other group members, understanding the self/own illness/the future, gaining perspective, distraction, personal achievement, expression, relaxation and empowerment. Small numbers of patients reported varying reasons for not wanting to take part and, therefore, art therapy may not be a preferred treatment option for everyone.
-
Art therapy appears to be cost-effective versus wait-list but confirmatory studies are needed to confirm this finding as well as evidence to inform future cost-effective analyses of art therapy versus other treatments.
Recommendations for future research
-
More multiarm controlled trials. Future art therapy trials should consider the value of a non-active treatment as usual/wait-list control arm, an attentional control (art and craft activities) and an active psychological comparator to art therapy (e.g. CBT). The following need to be examined in future trials:
-
Whether or not simply doing anything works: the non-active arm is necessary to demonstrate whether or not patients with non-psychotic mental health symptoms experience regression to the mean even without receiving treatment. Within this category no treatment may be compared with wait-list in the event that expectation of receiving the intervention is better than never being offered it.
-
Whether or not doing art therapy works: to mitigate potential performance bias through being allocated to the active treatment group and assess the relative efficacy of art therapy, an attention art-based placebo control will ensure that groups are treated equally. In turn this may inform on the value of the qualified art therapist.
-
Whether or not art therapy works better than anything else: using a gold standard active psychological therapy comparator or proven effective treatment will inform on the benefits of art therapy relative to other available packages of care. Consideration to geographical heterogeneity and policy perspective should be given when selecting relevant comparators.
-
-
Pre-specified populations. Currently the evidence is sporadic across clinical profiles. Consideration should be given to what the mental health symptoms of interest are and in which patient populations these symptoms can be studied. Patients rarely occur in distinct clinical groups in practice such as ‘depressed’, and therefore studying patients with complex comorbid conditions for symptoms of depression may be a more feasible approach to recruiting future research populations.
-
Randomised selection of patients for recruitment as well as random allocation: undeniably psychiatrists and other referrers select patients for art therapy who they believe may be likely to benefit from it. But does this mean that we can generalise the results from people who are referred to those who are not referred? Trials should adhere to CONSORT40 guidelines to ensure quality in the conduct and reporting of future RCTs of art therapy.
-
Allocation concealment as well as randomisation: not only does proper randomisation need to be conducted and reported but allocation to groups should be concealed. This is discrete from blinding and refers to how patients are allocated to either the art therapy or the control group once recruited into the study.
-
User-validated outcomes. Do the selected outcome measurements reflect a clinically meaningful improvement to patients’ mental health? Do the patients being studied agree that the outcome measures are externally valid? Preference-based health-related QoL instruments should be used, such as the EQ-5D. Trials employing several outcome measures should state the primary outcome measure a priori, as opposed to using several measurements, focusing on those with significant results.
-
Follow-up: measuring success at the end of the trial only is not adequate to capture residual benefits of treatment. Long-term follow-up is required to establish the duration of effect and whether or not re-treatment is an option for those who relapse. The duration of follow-up should also be sufficient to capture all costs.
-
Considering the influence of the therapist: unlike pills in pharmacotherapy, no two therapists are alike and subsequently the possibility of ‘therapist effects’112 should be considered. Art therapists may take an approach informed by a particular therapeutic model (mindfulness, brief work; psychodynamic); a service user-led recovery or collaborative approach; an approach based in guidelines about principles of practice,24,25,27 or use evidence of what works for whom. Such differences should be documented and explored in future trials. In addition, art therapists who are involved in research should be experienced practitioners in the clinical area of interest to facilitate consensus on practice as usual.
-
Quantifying good practice: it is important to elucidate the beneficial factors in art therapy to inform good practice protocols. Measures to ensure treatment fidelity should be employed by researchers in future trials of art therapy. Moreover, instruments designed to describe the ideal regimen of psychotherapy sessions should be explored for art therapy interventions. 113,114 Standardisation of good practice for specific patient clinical profiles rather than a ‘one-size-fits all’ approach will facilitate quantitative comparison and analysis of interventions.
-
Robust qualitative evidence: qualitative evidence gathered using robust methods to provide rich data should be nested in future RCTs of art therapy. This would facilitate further assessment of preference, acceptability and harms and may help to identify treatment mechanisms which influence and modify treatment outcomes with art therapy.
Acknowledgements
The authors wish to thank the psychiatrists and service users who contributed to the project steering group meetings for their time and opinions on the design of the research. In addition, many thanks to Andrea Shippam, who provided administrative support throughout the project and formatted the report.
The contents of the report remain the responsibility of the authors.
Contributions of authors
Lesley Uttley was the primary investigator and project lead for this assessment.
Lesley Uttley and Alison Scope carried out the quantitative and qualitative systematic reviews and wrote the report.
Matt Stevenson and Andrew Rawdin carried out the economic evaluation and wrote the report.
Elizabeth Taylor Buck and Chris Wood acted as clinical advisors, advised on the definition and use of art therapy, contributed to the writing and reviewed the report.
Anthea Sutton carried out the literature searches and reviewed the report.
John Stevens provided statistical input and reviewed the report.
Eva Kaltenthaler and Kim Dent-Brown contributed to the design of the research and revised the manuscript.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Layard R. How Mental Illness Loses Out in the NHS: A Report by the Centre for Economic Performance’s Mental Health Policy Group. London: Centre for Economic Performance, The London School of Economics and Political Science; 2012.
- World Health Organization . Global Burden of Disease Report 2004. www.who.int/healthinfo/global_burden_disease/2004_report_update/en/ (accessed 11 December 2014).
- Mind The Mental Health Charity . Mind 2014. www.mind.org.uk/information-support/types-of-mental-health-problems/statistics-and-facts-about-mental-health/how-common-are-mental-health-problems/ (accessed 11 December 2014).
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression chronic diseases and decrements in health: results from the World Health Surveys. Lancet 2007;370:851-8. http://dx.doi.org/10.1016/S0140-6736(07)61415-9.
- Murray C, Lopez A. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases Injuries and Risk Factors in 1990 and Projected to 2020. Cambridge, MA: Harvard School of Public Health on Behalf of the World Health Organization and the World Bank; 1996.
- Naylor C, Parsonage M, McDaid D, Knapp M, Fossey M, Galea A. Long-term Conditions and Mental Health. The Cost of Co-Morbidities. London: The King’s Fund; 2012.
- Unutzer J, Schoenbaum M, Katon W, Fan M, Pincus H, Hogan D, et al. Healthcare costs associated with depression in medically ill fee-for-service medicare participants. J Am Geriatr Soc 2009;57:506-10. http://dx.doi.org/10.1111/j.1532-5415.2008.02134.x.
- Vamos EP, Mucsi I, Keszei A, Kopp M, Novak M. Comorbid depression is associated with increased healthcare utilization and lost productivity in persons with diabetes: a large nationally representative Hungarian population survey. Psychosom Med 2009;71:501-7. http://dx.doi.org/10.1097/PSY.0b013e3181a5a7ad.
- National Health Service . Commissioning Talking Therapies for 2011 12: Improving Access to Psychological Therapies. IAPT 2011. www.iapt.nhs.uk/silo/files/commissioning-talking-therapies-for-201112.pdf (accessed 11 December 2014).
- Kmietowicz Z. Increasing access to psychological therapies will cost NHS nothing says report. BMJ 2012;344. http://dx.doi.org/10.1136/bmj.e4250.
- Layard R, Clark D, Knapp M, Mayraz G. Cost-benefit Analysis of Psychological Therapy. London: Centre for Economic Performance, The London School of Economics and Political Science; 2007.
- McHugh RK, Whitton SW, Peckham AD, Welge JA, Otto MW. Patient preference for psychological vs pharmacologic treatment of psychiatric disorders: a meta-analytic review. J Clin Psychiatry 2013;74:595-602. http://dx.doi.org/10.4088/JCP.12r07757.
- van Schaik DJ, Klijn AF, van Hout HP, van Marwijk HW, Beekman AT, de Haan M, et al. Patients’ preferences in the treatment of depressive disorder in primary care. Genl Hosp Psychiatry 2004;26:184-9. http://dx.doi.org/10.1016/j.genhosppsych.2003.12.001.
- Van HL, Dekker J, Koelen J, Kool S, van Aalst G, Hendriksen M, et al. Patient preference compared with random allocation in short-term psychodynamic supportive psychotherapy with indicated addition of pharmacotherapy for depression. Psychother Res 2009;19:205-12. http://dx.doi.org/10.1080/10503300802702097.
- Lin P, Campbell D, Chaney E, Liu CF, Heagerty P, Felker B, et al. The influence of patient preference on depression treatment in primary care. Ann Behav Med 2005;30:164-73. http://dx.doi.org/10.1207/s15324796abm3002_9.
- Slayton SC. Outcome studies on the efficacy of art therapy: a review of findings. Art Ther 2010;27:108-18. http://dx.doi.org/10.1080/07421656.2010.10129660.
- Wood C. Gathering evidence: expansion of art therapy research strategy. Inscape 1999;4:51-6. http://dx.doi.org/10.1080/17454839908413077.
- Gilroy A. Art Therapy Research and Evidence-Based Practice. London: Sage Publications Ltd; 2006.
- Kapitan L. Introduction to Art Therapy Research. Oxford: Taylor & Francis Ltd; 2010.
- Vink A, Bruinsma M. Evidence based music therapy. Music Therapy Today 2003;4. www.wfmt.info/Musictherapyworld/modules/mmmagazine/issues/20031103132043/20031103134548/Vink.pdf (accessed 11 December 2014).
- Edwards J. Using the Evidence Based Medicine Framework to support music therapy posts in healthcare settings. Br J Music Ther 2002;16.
- Wood MJ, Molassiotis A, Payne S. What research evidence is there for the use of art therapy in the management of symptoms in adults with cancer? A systematic review. Psycho-Oncology 2011;20:135-45. http://dx.doi.org/10.1002/pon.1722.
- CG178 Psychosis and Schizophrenia in Adults: Treatment and Management. London: NICE; 2014.
- Sheppard L, Waller D. Guidelines for Art Therapists Working with Older People with Dementia. London: Goldsmiths University of London; 2006.
- Teasdale C. Guidelines for Arts Therapists Working in Prisons. London: Home Office, HM prison sevice for England & Wales, Crown Publications; 2002.
- Developing Best Practice Guidelines for Art Therapists working with Children Adolescents and Families. Principles of Best Practice. London: BAAT; 2012.
- Springham N, Dunne K, Noyse S, Swearingen K. Art therapy for personality disorder: 2012 UK professional consensus guidelines development process and outcome. Int J Art Ther 2012;17:130-4. http://dx.doi.org/10.1080/17454832.2012.734834.
- Wilson C. A Time-limited model of art therapy in general practice. Inscape 2002;7:16-2. http://dx.doi.org/10.1080/17454830208414038.
- Schizophrenia: Core Interventions in the Treatment and Management of Schizophrenia in Adults in Primary and Secondary Care. Clinical Guideline 82. London: NICE; 2009.
- Gilroy A. Art Therapy Research and Evidence-Based Practice. London: SAGE Publications Ltd; 2006.
- British Association of Art Therapists (BAAT) . Working in Multi-Agency Contexts n.d.
- Uttley L, Kaltenthaler E, Scope A, Dent-Brown K, Taylor Buck L, Wood C, et al. Systematic Review and Cost Effectiveness Modelling of the ClINIcal and Cost-Effectiveness of Art Therapy Among People With Non-Psychotic Mental Health Disorders 2013. www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013003957 (accessed March 2014).
- British Association of Art Therapists (BAAT) . What Is Art Therapy? 2014. www.baat.org/About-Art-Therapy (accessed 11 December 2014).
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337.
- Anthony W. Recovery from mental illness: The guiding vision of the mental health service system in the 1990s. Psychosoc Rehab J 1993;16:11-23. http://dx.doi.org/10.1037/h0095655.
- Repper J, Perkins R. Social Inclusion and Recovery. A Model for Mental Health Practice. London: Balliere Tindall; 2003.
- Gould D. A Checklist of Good Practice from Service Users. The Care Programme Approach and Recovery 2012. www.mentalhealth.org.uk/content/assets/PDF/publications/checklist-good-practice-approaches-recovery.pdf (accessed 11 December 2014).
- Thornicroft G, Tansella M. Mental Health Outcome Measures. London: RCPsych Publications; 2010.
- Chokkalingam A, Scherer R, Dickersin K. Agreement of data in abstracts compared to full publications. Control Clin Trials 1998;19:S61-2. http://dx.doi.org/10.1016/S0197-2456(98)80159-1.
- Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG, et al. CONSORT for reporting randomized controlled trials in journal and conference abstracts: explanation and elaboration. PLOS Med 2008;5. http://dx.doi.org/10.1371/journal.pmed.0050020.
- Deeks J, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al. Evaluating non-randomised intervention studies. Health Technol Assess 2003;7. http://dx.doi.org/10.3310/hta7270.
- Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, et al. Design and Endpoints of Clinical Trials in Hepatocellular Carcinoma. J Natl Cancer Inst 2008;100:698-711. http://dx.doi.org/10.1093/jnci/djn134.
- Merlin T, Weston A, Tooher R. Extending an evidence hierarchy to include topics other than treatment: revising the Australian ‘levels of evidence’. BMC Med Res Methodol 2009;9. http://dx.doi.org/10.1186/1471-2288-9-34.
- Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions 2011. www.cochrane-handbook.org (accessed 11 December 2014).
- Undertaking Systematic Reviews of Research on Effectiveness. York: University of York; 2001.
- Public Health Resource Unit . Critical Appraisal Skills Programme (CASP) 2009. www.phru.nhs.uk/Pages/PHD/CASP.htm (accessed March 2014).
- Thyme K, Sundin EC, Stahlberg G, Lindstrom B, Eklof H, Wiberg B. The outcome of short-term psychodynamic art therapy compared to short-term psychodynamic verbal therapy for depressed women. Psychoanal Psychother 2007;3:250-64. http://dx.doi.org/10.1080/02668730701535610.
- Lyshak-Stelzer F, Singer P, St. John P, Chemtob CM. Art therapy for adolescents with posttraumatic stress disorder symptoms: a pilot study. Art Ther 2007;24:163-9. http://dx.doi.org/10.1080/07421656.2007.10129474.
- Chapman L, Morabito D, Ladakakos C, Schreier H, Knudson M. The effectiveness of art therapy interventions in reducing post traumatic stress disorder (PTSD) symptoms in pediatric trauma patients. Art Ther 2001;18:100-4. http://dx.doi.org/10.1080/07421656.2001.10129750.
- Broome ME, Maikler V, Kelber S, Bailey P, Lea G. An intervention to increase coping and reduce health care utilization for school-age children and adolescents with sickle cell disease. J Natl Black Nurses Assoc 2001;12:6-14.
- Hattori H, Hattori C, Hokao C, Mizushima K, Mase T. Controlled study on the cognitive and psychological effect of coloring and drawing in mild Alzheimer’s disease patients. Geriatr Gerontol Int 2011;11:431-7. http://dx.doi.org/10.1111/j.1447-0594.2011.00698.x.
- Kim SK. A randomized controlled study of the effects of art therapy on older Korean-Americans’ healthy aging. Arts Psychother 2013;40:158-64. http://dx.doi.org/10.1016/j.aip.2012.11.002.
- McCaffrey R, Liehr P, Gregersen T, Nishioka R. Garden walking and art therapy for depression in older adults: a pilot study. Res Gerontol Nurs 2011;4:237-42. http://dx.doi.org/10.3928/19404921-20110201-01.
- Monti DA, Kash KM, Kunkel EJ, Brainard G, Wintering N, Moss AS, et al. Changes in cerebral blood flow and anxiety associated with an 8-week mindfulness programme in women with breast cancer. Stress Health 2012;28:397-40. http://dx.doi.org/10.1002/smi.2470.
- Puig A, Lee SM, Goodwin L, Sherrard PAD. The efficacy of creative arts therapies to enhance emotional expression spirituality and psychological well-being of newly diagnosed Stage I and Stage II breast cancer patients: A preliminary study. Arts Psychother 2006;3:218-28. http://dx.doi.org/10.1016/j.aip.2006.02.004.
- Rao D, Nainis N, Williams L, Langner D, Eisin A, Paice J. Art therapy for relief of symptoms associated with HIV/AIDS. AIDS Care 2009;21:64-9. http://dx.doi.org/10.1080/09540120802068795.
- Rusted J, Sheppard L, Waller D. A multi-centre randomized control group trial on the use of art therapy for older people with dementia. Group Analysis 2006;4:517-36. http://dx.doi.org/10.1177/0533316406071447.
- Beebe A, Gelfand EW, Bender B. A randomized trial to test the effectiveness of art therapy for children with asthma. J Allergy Clinl Immunol 2010;126:263-6. http://dx.doi.org/10.1016/j.jaci.2010.03.019.
- Gussak D. The effectiveness of art therapy in reducing depression in prison populations. Int J Offender Ther Comp Criminol 2007;51:444-60. http://dx.doi.org/10.1177/0306624X06294137.
- Monti DA, Peterson C. Mindfulness-based art therapy: results from a two-year study. Psychiatr Times 2004;21:63-5.
- Monti DA, Peterson C, Kunkel EJ, Hauck WW, Pequignot E, Rhodes, et al. A randomized controlled trial of mindfulness-based art therapy (MBAT) for women with cancer. Psycho-Oncology 2006;15:363-73. http://dx.doi.org/10.1002/pon.988.
- Thyme KE, Sundin EC, Wiberg B, Oster I, Astrom S, Lindh J. Individual brief art therapy can be helpful for women with breast cancer: a randomized controlled clinical study. Palliat Support Care 2009;7:87-95. http://dx.doi.org/10.1017/S147895150900011X.
- Svensk AC, Oster I, Thyme KE, Magnusson E, Sjodin M, Eisemann M, et al. Art therapy improves experienced quality of life among women undergoing treatment for breast cancer: a randomized controlled study. Eur J Cancer Care 2009;18:69-77. http://dx.doi.org/10.1111/j.1365-2354.2008.00952.x.
- Oster I, Svensk AC, Magnusson E, Thyme KE, Sjodin M, Astrom S, et al. Art therapy improves coping resources: a randomized controlled study among women with breast cancer. Palliat Support Care 2006;4:57-64. http://dx.doi.org/10.1017/S147895150606007X.
- Torgerson DJ, Torgerson CJ. Designing Randomised Trials in Health Education and the Social Sciences. Basingstoke: Palgrave Macmillan; 2008.
- Gussak D. The effectiveness of art therapy in reducing depression in prison populations. Int J Offender Ther Comp Criminol 2007;51:444-60. http://dx.doi.org/10.1177/0306624X06294137.
- Glenton C, Colvin C, Carlsen B, Swartz A, Lewin S, Noyes J, et al. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: qualitative evidence synthesis. Cochrane Database Syst Rev 2013;10.
- Critical Appraisal Skills Programme (CASP) . 10 Questions to Help You Make Sense of Qualitative Research 2011. www.caspinternational.org/mod_product/uploads/CASP%20Qualitative%20Research%20Checklist%2031.05.13.pdf (accessed 11 December 2014).
- Noyes J, Lewin S, Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-45.
- Noyes J, Popay J, Pearson A, Hannes K, Higgings JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2008.
- Rhondali W, Filbet M. Art Therapy Effectiveness on Pain and Other Symptoms for Palliative Care Inpatients: A Pilot Qualitative Study 2010;19:S52-3.
- Collie K. A Narrative View of Visual Creative Expression as Psychosocial Support for Women with Breast Cancer. Vancouver, BC: University of British Columbia; 2004.
- Sharf K. Art Therapists’ Perceptions of Their Work with Patients in Treatment for Substance Abuse: A Qualitative Investigation. New York, NY: New York University; 2004.
- Collie K, Bottorff JL, Long BC. A narrative view of art therapy and art making by women with breast cancer. J Health Psychol 2006;11:761-75. http://dx.doi.org/10.1177/1359105306066632.
- Oster I, Astrom S, Lindh J, Magnusson E. Women with breast cancer and gendered limits and boundaries: Art therapy as a ‘safe space’ for enacting alternative subject positions. Arts Psychother 2009;1:29-38. http://dx.doi.org/10.1016/j.aip.2008.10.001.
- Geue K, Gotze H, Buttstadt M, Kleinert E, Singer S. ‘About me and my disease’ – the making of an individual book within an art therapy course for cancer patients. Rehabilitation 2011;50:57-62. http://dx.doi.org/10.1055/s-0030-1265141.
- Ferszt GG, Hayes PM, DeFedele S, Horn L. Art therapy with incarcerated women who have experienced the death of a loved one. Art Ther 2004;4:191-9. http://dx.doi.org/10.1080/07421656.2004.10129695.
- Forzoni S, Perez M, Martignetti A, Crispino S. Art therapy with cancer patients during chemotherapy sessions: an analysis of the patients’ perception of helpfulness. Palliat Support Care 2010;8:41-8. http://dx.doi.org/10.1017/S1478951509990691.
- Wood MJM, Low J, Molassiotis A, Tookman A. Art therapy’s contribution to the psychological care of adults with cancer: A survey of therapists and service users in the UK. Int J Art Ther 2013;18:42-53. http://dx.doi.org/10.1080/17454832.2013.781657.
- Turnbull J, Omay F. GPs’ and clients’ views of art therapy in an Edinburgh practice. Inscape 2002;7:26-9. http://dx.doi.org/10.1080/17454830208414039.
- Lobban J. The invisible wound: Veterans’ art therapy. Int J Art Ther 2012;19:1-16.
- McCaffrey R. The effect of healing gardens and art therapy on older adults with mild to moderate depression. Holist Nurs Pract 2007;21:79-84. http://dx.doi.org/10.1097/01.HNP.0000262022.80044.06.
- Anzules C, Haennl C, Golay A. An experience of art therapy for patients suffering from obesity. Eur Diabetes Nurs 2007;2:72-6. http://dx.doi.org/10.1002/edn.81.
- Cohen DJ, Crabtree BF. Evaluative criteria for qualitative research in health care: controversies and recommendations. Ann Fam Med 2008;6:331-9. http://dx.doi.org/10.1370/afm.818.
- Guide to the Methods of Technology Appraisals. London: NICE; 2013.
- Greenwood H, Leach C, Lucock M, Noble R. The process of long-term art therapy: a case study combining artwork and clinical outcome. Psychother Res 2007;17:588-99. http://dx.doi.org/10.1080/10503300701227550.
- Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. BMJ 1996;313:275-83. http://dx.doi.org/10.1136/bmj.313.7052.275.
- Barkham M, Margison F, Leach C, Lucock M, Benson E, Mellor-Clark J, et al. Service profiling and outcomes benchmarking using the CORE-OM: towards practice-based evidence in the psychological therapies. J Consult Clin Psychol 2001;69:184-96. http://dx.doi.org/10.1037/0022-006X.69.2.184.
- Beck A, Ward C, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561-71. http://dx.doi.org/10.1001/archpsyc.1961.01710120031004.
- Nicholson R, Berman J. Is follow-up necessary in evaluating psychotherapy. Psycholog Bull 1983;93:261-78. http://dx.doi.org/10.1037/0033-2909.93.2.261.
- Lambert M, Ogles B, Lambert M. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change. New York, NY: John Wiley & Sons; 2004.
- Cooper M. Essential Research Findings in Counselling and Psychotherapy: The Facts are Friendly. London: Sage Publications; 2008.
- Sportel B, de Hullu E, de Jong P, Nauta M. Cognitive bias modification versus CBT in reducing adolescent social anxiety: a randomized controlled trial. PLOS ONE 2013;8. http://dx.doi.org/10.1371/journal.pone.0064355.
- Van der Ploeg H. Handleiding bij de Examen/Toets attitude vragenlijst ETAV: Een nederlandstalige bewerking van de spielberger test anxiety inventory. Lisse: Swets en Zeitlinger; 1988.
- Dakin H. Review of studies mapping from quality of life or clinical measures to EQ-5D: an online database. Health Qual Life Outcomes 2013;11. http://dx.doi.org/10.1186/1477-7525-11-151.
- Ara R, Brazier J. Deriving an Algorthm to convert the eight mean SF-36 Dimension scores into a mean EQ-5D preference-based score from published studies (where patient level data are not available). Value Health 2008;11:1131-43. http://dx.doi.org/10.1111/j.1524-4733.2008.00352.x.
- Rowen D, Brazier J, Roberts R. Mapping SF-36 onto the EQ-5D index: how reliable is the relationship. Health Qual Life Outcomes 2009;7. http://dx.doi.org/10.1186/1477-7525-7-27.
- Kaambwa B, Billingham L, Bryan S. Mapping utility scores from the Barthel index. Eur J Health Econ 2013;14:231-41. http://dx.doi.org/10.1007/s10198-011-0364-5.
- van Exel N, Scholte op Reimer W, Koopmanschap M. Assessment of post-stroke quality of life in cost-effectiveness studies: the usefulness of the Barthel Index and the EuroQoL-5D. Qual Life Res 2004;13:427-33. http://dx.doi.org/10.1023/B:QURE.0000018496.02968.50.
- Whynes D, Sprigg N, Selby J, Berge E, Bath P. Testing for differential item functioning within the EQ-5D. Med Decis Making 2013;33:252-60. http://dx.doi.org/10.1177/0272989X12465016.
- Derogatis L. SCL-90-R: Administration Scoring and Procedures Manual. Minneapolis, MN: National Computer Systems Inc; 1994.
- Curtis L. Unit Costs of Health and Social Care. Cantebury: Personal Social Services Research Unit, University of Kent; 2013.
- Mann J. Handbook of Short-Term Dynamic Psychotherapy. New York, NY: Basic Books; 1991.
- Cane F. The Artist in Each of Us. Washington, DC: Baker-Webster Printing Co.; 1983.
- Waller D, Gilroy A. Art Therapy: A Handbook. Buckingham: Open University Press; 1992.
- Betensky MG. What Do You See? Phenomenology of Therapeutic Art Expression. Ringwood: Reader’s Digest; 1995.
- Schaverien J. The Revealing Image: Analytical Art Psychotherapy in Theory and Practice. London: Routledge; 1995.
- Fenwick E, Claxton K, Sculpher M. Representing uncertainty: the role of cost-effectiveness acceptability curves. Health Econ 2001;10:779-87. http://dx.doi.org/10.1002/hec.635.
- Iglehart D. Simulating stable stochastic systems, V: comparison of ratio estimators. Naval Res Logist Quart 1975;22:553-65. http://dx.doi.org/10.1002/nav.3800220311.
- Claxton K, Posnett J. An economic approach to clinical trial design and research priority-setting. Health Econ 1996;5:513-24. http://dx.doi.org/10.1002/(SICI)1099-1050(199611)5:6<513::AID-HEC237>3.0.CO;2-9.
- Okiishi JC, Lambert MJ, Eggett D, Nielsen L, Dayton DD, Vermeersch DA. An analysis of therapist treatment effects: Toward providing feedback to individual therapists on their clients’ psychotherapy outcome. J Clin Psychol 2006;62:1157-72. http://dx.doi.org/10.1002/jclp.20272.
- Ablon JS, Jones EE. Psychotherapy process in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. J Consult Clin Psychol 1999;67. http://dx.doi.org/10.1037/0022-006X.67.1.64.
- Ablon JS, Levy RA, Smith-Hansen L. The contributions of the Psychotherapy Process Q-set to psychotherapy research. Res Psychother 2011;14:14-48.
Appendix 1 Patient and public involvement for project 12/27/16
The project steering group
The NICE HTA programme has developed an evidence-based approach to involving service users in research and development agenda-setting. In accordance with this, this research project developed a project steering group for the purpose of allowing scrutiny of the research team’s proposed methods of investigation and also to present main findings of the research.
The research team for this project, who are the listed co-authors for the manuscript, worked with two service users and five external clinical experts in the project steering group to discuss the proposed research design and preliminary findings. The patient representatives were people with non-psychotic mental health disorders who had experience of taking part in art therapy and were recruited through online advertisement on the ‘People in Research’ website upon advice from a patient and public involvement (PPI) representative at the School of Health and Related Research (ScHARR), University of Sheffield. The external clinical experts were consultant psychiatrists and were selected as key professionals with an interest in treatment for non-psychotic mental health disorders.
Setting and context
The steering group met on two occasions for 2 hours over the 12-month research contract period. Communications including meeting agendas, notes and directions were provided via e-mail prior to and following meetings. The purpose of the first meeting was to describe and discuss the research team’s proposed investigation for this health technology assessment. The protocol for the project was also provided and lay summaries were presented by members of the research team to describe the intentions and methods of the research.
The purpose of the second meeting was to present a lay summary of the preliminary findings from the three systematic reviews and gather any further views on the research methodology used.
How the contributions of the steering group influenced the project
Service users highlighted important considerations for patients in the provision of art therapy including the element of patient choice, the potential adverse effects of art therapy when delivered by an untrained individual and the potential appeal of art therapy compared with other treatments. These views aided the project team in understanding the issues to service users and were reflected in the assessment report.
Clinical experts highlighted the complexities of assessing psychological therapies compared with pharmacological interventions, the difficulties in defining the appropriate comparators to art therapy and the complex nature of the populations that art therapy may be used in. These issues helped the project team to frame the background context for art therapy usage and highlighted the relevant issues in assessment of psychological therapies more generally.
Reflections on the process
Travelling to an academic institution as a patient representative can be an intimidating experience and requires confidence and trust in the research project. The patient representatives are a minority and so only a few people could potentially fill the role. As the service users are people diagnosed with non-psychotic mental health disorder, they could also be considered as vulnerable people. Accordingly, only a limited number (four people) who were eligible to fill the role responded to the advert despite the offer of expenses paid and an incentive reward.
Regardless of the amount recommended and granted by the funding body for reward payments for PPI, the amount that can be paid to incentivise participation needs to be in line with the institution’s (University of Sheffield) policy. This may result in PPI representatives being out of pocket for attending and potentially creates an impression that contributions are not rewarded in line with other institutes’ patient committees (e.g. NICE). Furthermore, if expenses are paid and an incentive reward is issued, PPI representatives are required to enrol on the institution’s bank worker system to ensure that National Insurance contributions are made. This enrolment in itself can be perceived as a barrier to participation to service users, who may be the relevant vulnerable population at the focus of the research.
The contributions of the service users and clinical experts in the steering group were valuable to the project. The views were helpful and informative to the project team. However, there is theoretical incongruence in the concept of integrating the views of a small number of individuals into a large scale project that is endeavouring to be evidence based. Future projects should consider what input from the project steering group should be fairly considered and incorporated by the research team in the absence of more comprehensive and accessible public consultation on these issues that may be relevant to stakeholders.
Appendix 2 Search strategies for quantitative, qualitative and economic reviews
MEDLINE
-
Art Therapy/
-
art therap$.ti,ab.
-
art psychotherap$.ti,ab.
-
or/1–3
-
meta analysis.sh.
-
meta-anal$.tw.
-
metaanal$.tw.
-
meta analysis.id.
-
(systematic and (review or overview)).tw.
-
(critical and apprais$).tw.
-
(critical and review$).tw.
-
or/5–11
-
literature review.sh.
-
literature review.id.
-
13 or 14
-
12 or 15
-
case report.sh.
-
16 not 17
-
limit 18 to human
-
4 and 19 [to identify reviews]
-
treatment effectiveness evaluation.sh.
-
(random$ and trial$).tw.
-
(random$ and allocat$).tw.
-
double blind.tw.
-
single blind.tw.
-
clinical trial.id.
-
clinical trial$.tw.
-
((singl$ or doubl$ or trebl$ or tripl$) adj5 blind).tw.
-
(clin$ adj25 trial$).ti,ab.
-
placebo$.tw.
-
placebo$.id.
-
placebo$.ti,ab.
-
random$.ti,ab.
-
methodology.sh.
-
experimental design.sh.
-
experimentation.sh.
-
experimental methods.sh.
-
or/21–37
-
limit 38 to human
-
4 and 39 [to identify clinical trials]
-
‘costs and cost analysis’/
-
‘Cost Containment’/
-
(economic adj2 evaluation$).ti,ab.
-
(economic adj2 analy$).ti,ab.
-
(economic adj2 (study or studies)).ti,ab.
-
(cost adj2 evaluation$).ti,ab.
-
(cost adj2 analy$).ti,ab.
-
(cost adj2 (study or studies)).ti,ab.
-
(cost adj2 effective$).ti,ab.
-
(cost adj2 benefit$).ti,ab.
-
(cost adj2 utili$).ti,ab.
-
(cost adj2 minimi$).ti,ab.
-
(cost adj2 consequence$).ti,ab.
-
(cost adj2 comparison$).ti,ab.
-
(cost adj2 identificat$).ti,ab.
-
(pharmacoeconomic$ or pharmaco-economic$).ti,ab.
-
or/41–56
-
(task adj2 cost$).ti,ab,id.
-
(switch$ adj2 cost$).ti,ab,id.
-
((energy or oxygen) adj cost).ti,ab,id.
-
((energy or oxygen) adj expenditure).ti,ab,id.
-
or/58–61
-
(animal or animals or rat or rats or mouse or mice or hamster or hamsters or dog or dogs or cat or cats or bovine or sheep or ovine or pig or pigs).ab,ti,id,de.
-
editorial.dt.
-
letter.dt.
-
dissertation abstract.pt.
-
or/63–66
-
57 not (62 or 67)
-
4 and 68 [to identify economic evaluations]
-
experiences.tw.
-
interview$.tw.
-
qualitative.tw.
-
or/70–72
-
4 and 73 [to identify qualitative research]
-
20 or 40 or 69 or 74
-
4 not 75 [to identify other study types]
EMBASE
-
art therapy/
-
art therap$.ti,ab.
-
art psychotherap$.ti,ab.
-
or/1–3
-
Meta analysis/
-
Metaanaly$.tw.
-
exp Literature review/
-
(systematic adj (review or overview)).tw.
-
Meta analys$.tw.
-
or/5–9
-
(letter or commentary or editorial).pt.
-
animals/
-
11 or 12
-
10 not 13
-
14 and 14 [to identify reviews]
-
exp clinical trials/
-
Clinical trial.pt.
-
(clinic$ adj trial$1).tw.
-
((singl$ or doubl$ or trebl$ or tripl$) adj (blind$3 or mask$3)).tw.
-
Randomi?ed control$ trial$.tw.
-
Random assignment/
-
Random$ allocat$.tw.
-
Placebo$.tw.
-
Placebos/
-
Quantitative studies/
-
Allocat$ random$.tw.
-
or/16–26
-
4 and 27 [to identify clinical trials]
-
exp Financial Management/
-
exp *economics/
-
exp financial support/
-
exp financing organized/
-
exp business/
-
(cost or costs or economic$ or pharmacoeconomic$ or price$ or pricing$).tw.
-
Health resource allocation.sh.
-
Health resource utilization.sh.
-
(editorial or letter or news).pt.
-
(or/29–32 or/34–36) not (33 or 37)
-
4 and 38 [to identify economic evaluations]
-
findings.tw.
-
interview.tw.
-
qualitative.tw.
-
or/40–42
-
4 and 43 [to identify qualitative research]
-
15 or 28 or 39 or 44
-
44 not 45 [to identify other study types]
The Cochrane Library
#1. MeSH descriptor: [Art Therapy] explode all trees
#2. ‘art therap*’
#3. ‘art psychotherap*’
#4. #1 or #2 or #3
Citation Indexes (Web of Science)
| #1 | TI = (art therap* or art psychotherap*) DocType = All document types; Language = All languages; |
| #2 | Topic = (meta-anal* or metaanal* or quantitativ* review* or quantitativ* overview or systematic* review* or systematic* overview* or methodologic* review* or methodologic* overview* or integrative research review* or research integration* or quantitativ* synthes*) DocType = All document types; Language = All languages; |
| #3 | #2 AND #1 – to identify reviews DocType = All document types; Language = All languages; |
| #4 | Topic = (random* or placebo* or single blind* or double blind* or triple blind*) DocType = All document types; Language = All languages; |
| #5 | Topic = (randomized or randomly) DocType = All document types; Language = All languages; |
| #6 | Topic = (clin* trial*) DocType = All document types; Language = All languages; |
| #7 | #6 OR #5 OR #4 DocType = All document types; Language = All languages; |
| #8 | #7 AND #1 – to identify clinical trials DocType = All document types; Language = All languages; |
| #9 | Topic = (economic* or cost* or fiscal or funding or financial or finance or pharmacoeconomic* or price* or pricing) DocType = All document types; Language = All languages; |
| #10 | #9 AND #1 – to identify economic evaluations DocType = All document types; Language = All languages; |
| #11 | Topic = (findings or interview or qualitative) DocType = All document types; Language = All languages; |
| #12 | #11 AND #1 – to identify qualitative research DocType = All document types; Language = All languages; |
| #13 | #12 OR #10 OR #8 OR #3 – to identify other study types (these results were imported into Reference Manager and duplicates were removed) DocType = All document types; Language = All languages; |
Cumulative Index to Nursing and Allied Health Literature (CINAHL)
| S1 | (MH ‘Art Therapy’) |
| S2 | TI art therap* OR AB art therap* |
| S3 | TI art psychotherap* OR AB art psychotherap* |
| S4 | or/S1–S3 |
| S5 | (MH ‘Meta Analysis’) |
| S6 | TI meta analys* OR AB meta analys* |
| S7 | TI metaanaly* OR AB metaanaly* |
| S8 | (MH ‘Literature Review+’) |
| S9 | TI ( (systematic n1 review) or (systematic n1 overview) ) OR AB ( (systematic n1 review) or (systematic n1 overview) ) |
| S10 | S5 OR S6 OR S7 OR S8 OR S9 |
| S11 | PT commentary |
| S12 | PT letter |
| S13 | PT editorial |
| S14 | (MH ‘Animals’) |
| S15 | S11 OR S12 OR S13 OR S14 |
| S16 | S10 NOT S15 |
| S17 | S4 AND S16 [to identify reviews] |
| S18 | (MH ‘Economics+’) |
| S19 | (MH ‘Financial Management+’) |
| S20 | (MH ‘Financial Support+’) |
| S21 | (MH ‘Financing, Organized+’) |
| S22 | (MH ‘Business+’) |
| S23 | S19 OR S20 OR S21 OR S22 |
| S24 | S18 NOT S23 |
| S25 | (MH ‘Health Resource Allocation’) |
| S26 | (MH ‘Health Resource Utilization’) |
| S27 | S25 OR S26 |
| S28 | S24 OR S27 |
| S29 | TI ( (cost or costs or economic* or pharmacoeconomic* or price* or pricing*) ) OR AB ( (cost or costs or economic* or pharmacoeconomic* or price* or pricing*) ) |
| S30 | S28 OR S29 |
| S31 | PT editorial |
| S32 | PT letter |
| S33 | S31 OR S32 |
| S34 | S30 NOT S33 |
| S35 | (MH ‘Animal Studies’) |
| S36 | S34 NOT S35 |
| S37 | AU anonymous |
| S38 | S36 NOT S37 |
| S39 | S4 AND S38 [to identify economic evaluations] |
| S40 | TI findings OR AB findings |
| S41 | TI interview OR AB interview |
| S42 | TI qualitative OR AB qualitative |
| S43 | S40 OR S41 OR S42 |
| S44 | S4 AND S43 [to identify qualitative research] |
| S45 | (MH ‘Clinical Trials+’) |
| S46 | PT Clinical trial |
| S47 | TX clinic* n1 trial* |
| S48 | TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) |
| S49 | TX randomi* control* trial* |
| S50 | (MH ‘Random Assignment’) |
| S51 | TX random* allocat* |
| S52 | TX placebo* |
| S53 | (MH ‘Placebos’) |
| S54 | (MH ‘Quantitative Studies’) |
| S55 | TX allocat* random* |
| S56 | S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 |
| S57 | S4 AND S56 [to identify clinical trials] |
| S58 | S17 OR S39 OR S44 OR S57 |
| S59 | S4 NOT S58 [to identify other study types] |
PsycINFO
-
Art Therapy/
-
art therap$.ti,ab.
-
art psychotherap$.ti,ab.
-
or/1–3
-
meta analysis.sh.
-
meta-anal$.tw.
-
metaanal$.tw.
-
meta analysis.id.
-
(systematic and (review or overview)).tw.
-
(critical and apprais$).tw.
-
(critical and review$).tw.
-
or/5–11
-
literature review.sh.
-
literature review.id.
-
13 or 14
-
12 or 15
-
17. case report.sh.
-
16 not 17
-
limit 18 to human
-
4 and 19 [to identify reviews]
-
treatment effectiveness evaluation.sh.
-
(random$ and trial$).tw.
-
(random$ and allocat$).tw.
-
double blind.tw.
-
single blind.tw.
-
clinical trial.id.
-
clinical trial$.tw.
-
((singl$ or doubl$ or trebl$ or tripl$) adj5 blind).tw.
-
(clin$ adj25 trial$).ti,ab.
-
placebo$.tw.
-
placebo$.id.
-
placebo$.ti,ab.
-
random$.ti,ab.
-
methodology.sh.
-
experimental design.sh.
-
experimentation.sh.
-
experimental methods.sh.
-
or/21–37
-
limit 38 to human
-
4 and 39 [to identify clinical trials]
-
‘costs and cost analysis’/
-
‘Cost Containment’/
-
(economic adj2 evaluation$).ti,ab.
-
(economic adj2 analy$).ti,ab.
-
(economic adj2 (study or studies)).ti,ab.
-
(cost adj2 evaluation$).ti,ab.
-
(cost adj2 analy$).ti,ab.
-
(cost adj2 (study or studies)).ti,ab.
-
(cost adj2 effective$).ti,ab.
-
(cost adj2 benefit$).ti,ab.
-
(cost adj2 utili$).ti,ab.
-
(cost adj2 minimi$).ti,ab.
-
(cost adj2 consequence$).ti,ab.
-
(cost adj2 comparison$).ti,ab.
-
(cost adj2 identificat$).ti,ab.
-
(pharmacoeconomic$ or pharmaco-economic$).ti,ab.
-
or/41–56
-
(task adj2 cost$).ti,ab,id.
-
(switch$ adj2 cost$).ti,ab,id.
-
((energy or oxygen) adj cost).ti,ab,id.
-
((energy or oxygen) adj expenditure).ti,ab,id.
-
or/58–61
-
(animal or animals or rat or rats or mouse or mice or hamster or hamsters or dog or dogs or cat or cats or bovine or sheep or ovine or pig or pigs).ab,ti,id,de.
-
editorial.dt.
-
letter.dt.
-
dissertation abstract.pt.
-
or/63–66
-
57 not (62 or 67)
-
4 and 68 – to identify economic evaluations
-
experiences.tw.
-
interview$.tw.
-
qualitative.tw.
-
or/70–72
-
4 and 73 – to identify qualitative research
-
20 or 40 or 69 or 74
-
4 not 75 – to identify other study types
Allied and Complementary Medicine Database (AMED)
-
art therapy/
-
art therap$.ti,ab.
-
art psychotherap$.ti,ab.
-
or/1–3
-
Meta analysis/
-
Metaanaly$.tw.
-
exp Literature review/
-
(systematic adj (review or overview)).tw.
-
Meta analys$.tw.
-
or/5–9
-
(letter or commentary or editorial).pt.
-
animals/
-
11 or 12
-
10 not 13
-
4 and 14 [to identify reviews]
-
exp clinical trials/
-
Clinical trial.pt.
-
(clinic$ adj trial$1).tw.
-
((singl$ or doubl$ or trebl$ or tripl$) adj (blind$3 or mask$3)).tw.
-
Randomi?ed control$ trial$.tw.
-
Random assignment/
-
Random$ allocat$.tw.
-
Placebo$.tw.
-
Placebos/
-
Quantitative studies/
-
Allocat$ random$.tw.
-
or/16–26
-
4 and 27 – to identify clinical trials
-
exp Financial Management/
-
exp *economics/
-
exp financial support/
-
exp financing organized/
-
exp business/
-
(cost or costs or economic$ or pharmacoeconomic$ or price$ or pricing$).tw.
-
Health resource allocation.sh.
-
Health resource utilization.sh.
-
(editorial or letter or news).pt.
-
(or/29–32 or/34–36) not (33 or 37)
-
4 and 38 [to identify economic evaluations]
-
findings.tw.
-
interview.tw.
-
qualitative.tw.
-
or/40–42
-
4 and 43 [to identify qualitative research]
-
15 or 28 or 39 or 44
-
44 not 45 [to identify other study types]
Applied Social Sciences Index and Abstracts (ASSIA)
Search strategy
-
SU.EXACT(‘Art therapy’) OR (ti(art therap* OR art psychotherap*) OR ab(art therap* OR art psychotherap*))
-
ti((meta-anal* OR metaanal* OR quantitativ* review* OR quantitativ* overview OR systematic* review* OR systematic* overview* OR methodologic* review* OR methodologic* overview* OR integrative research review* OR research integration* OR quantitativ* synthes*)) OR ab((meta-anal* OR metaanal* OR quantitativ* review* OR quantitativ* overview OR systematic* review* OR systematic* overview* OR methodologic* review* OR methodologic* overview* OR integrative research review* OR research integration* OR quantitativ* synthes*))
-
1 AND 2 [to identify reviews]
-
ti(random* OR placebo* OR single blind* OR double blind* OR triple blind* OR randomized OR randomly OR clin* trial*) OR ab(random* OR placebo* OR single blind* OR double blind* OR triple blind* OR randomized OR randomly OR clin* trial*)
-
1 AND 4 [to identify clinical trials]
-
ti(economic* OR cost* OR fiscal OR funding OR financial OR finance OR pharmacoeconomic* OR price* OR pricing) OR ab(economic* OR cost* OR fiscal OR funding OR financial OR finance OR pharmacoeconomic* OR price* OR pricing)
-
1 AND 6 [to identify economic evaluations]
-
ti(findings OR interview OR qualitative) OR ab(findings OR interview OR qualitative)
-
1 AND 8 [to identify qualitative research]
-
3 OR 5 OR 7 OR 9
-
1 NOT 10 [to identify other study types]
Appendix 3 Studies excluded at full text from the quantitative review
| No. | Reference | Reason for exclusion |
|---|---|---|
| 1 | Ando M, Imamura Y, Kira H, Nagasaka T. Feasibility and efficacy of art therapy for Japanese cancer patients: A pilot study. Arts Psychother 2013;40:130–3 | No control group |
| 2 | Ash-Lee S, Simoneau T, Talucci L. The use of an art therapy group in women with cancer: A pilot study. Psycho-oncology Conference: 7th Annual Conference of the American Psychosocial Oncology Society, 18–21 February 2010, New Orleans, LA, USA. Conference Publication. 2010;19:S43 | No control group |
| 3 | Baptista AS, Jones A, Cardoso FP, Schaffir BC, Coelho ERW, Orlandi A, et al. Assessment of art therapy program for women with fibromyalgia: randomized controlled blinded study. Arthritis and Rheumatism Conference: 12th Annual Scientific Meeting of the American College of Rheumatology and Association of Rheumatology Health Professionals, Washington, DC, USA, 9–14 November 2012. Conference Publication. 2012;64:S794 | Conference proceeding. No study data – contacted author (andreia.baptista@unifesp.br) but no response |
| 4 | Bar-Sela G, Atid L, Danos S, Gabay N, Epelbaum R. Art therapy improved depression and influenced fatigue levels in cancer patients on chemotherapy. Psycho-Oncology 2007;16:980–4 | No randomisation |
| 5 | Bell CE, Robbins SJ. Effect of art production on negative mood: a randomized controlled trial. Art Ther 2007;24:71–5 | Not art therapy intervention |
| 6 | Elbing U, Schulze C, Zillmann H, Raak CK, Ostermann T. Arthedata-An online database of scientific references on art therapy. Eur J Integr Med 2009;1:39–42. URL: http://cambase.dmz.uni-wh.de/CiXbase/kunthera/ (accessed 11 December 2014) | Not a reference, but a link to a German art therapy database |
| 7 | Elkis-Abuhoff DL, Goldblatt RB, Gaydos M, Corrato S. Effects of clay manipulation on somatic dysfunction and emotional distress in patients with Parkinson’s disease. Art Therapy 2008;25:122–8 | Not a RCT; parkinsons vs. non-parkinsons groups |
| 8 | Freilich R, Shechtman Z. The contribution of art therapy to the social emotional and academic adjustment of children with learning disabilities. The Arts in Psychotherapy 2010;2:97–105 | No randomisation |
| 9 | Gabriel B, Bromberg E, Vandenbovenkamp J, Walka P, Kornblith AB, Luzzato P. Art therapy with adult bone marrow transplant patients in isolation: A pilot study. Psycho-Oncology 2001;10:114–23 | No control group |
| 10 | Goetze H, Geue K, Buttstaedt M, Braehler E. Art therapy for patients with haematological cancer in the ambulatory aftercare. Psycho-oncology Conference: 11th World Congress of Psycho-Oncology of the International Psycho-Oncology Society IPOS, Vienna, Austria, 2009. Conference Publication. 21–25 June 2009;18:S238–9 | Not a RCT; no randomisation to groups |
| 11 | Jones G. An art therapy group in palliative cancer care. Nurs Times 2000;96:42–3 | Editorial; no study data |
| 12 | Madden J, Mowry-Rutter P, Foreman N. Results of randomized study of creative arts therapy for pediatric brain tumor patients during outpatient chemotherapy. Neurooncology 2008;10:459–60 | Arts therapies combined |
| 13 | McCabe C, Roche D, Hegarty F, McCann S. ‘Open window’: A randomized trial of the effect of new media art using a virtual window on quality of life in patients’ experiencing stem cell transplantation. Psycho-oncology 2013;2:330–7 | Not art therapy intervention |
| 14 | Odell-Miller H, Hughes P, Westacott M. An investigation into the effectiveness of the arts therapies for adults with continuing mental health problems. Psychother Res 2006;1:122–39 | Mostly psychotic with outcome data not broken down by condition |
| 15 | Oster I. Art therapy with women with breast cancer-results from a randomized study. Psycho-Oncology Conference: 11th World Congress of Psycho-Oncology of the International Psycho-Oncology Society IPOS, Vienna, Austria, 21–25 June 2009. Conference Publication. 2009;18:S22–3 | Conference proceeding of the Oster Thyme Svensk study – no data |
| 16 | Plecity DM, Danner-Weinberger A, Szkura L, von Wietersheim J. The effects of art therapy on the somatic and emotional situation of the patients – A quantitative and qualitative analysis. Psychothere Psychosomat Med Psychol 2008;59:364–9 | Not a RCT; qualitative study abstract no data |
| 17 | Richardson P, Jone K, Evans C, Stevens P, Rowe A. An exploratory randomised trial of group based art therapy as an adjunctive treatment in severe mental illness. Unpublished Report. 1994 | Trial records of schizophrenia study published 2007 |
| 18 | Richardson P. Art therapy as an adjunctive treatment in severe mental illness: a randomised controlled evaluation. Curr Control Trials 2004 | Trial records of schizophrenia study published 2007 |
| 19 | Richardson P. Randomised controlled trial of group interactive art therapy as an adjunctive treatment in severe mental illness. National Research Register 2001;1 | Trial records of schizophrenia study published 2007 |
| 20 | Rodriguez J, Troll G. [Experiments in art therapy]. Soins – Psychiatrie 1990;34:118–19 | Not a RCT |
| 21 | Rosal ML. Comparative group art therapy research to evaluate changes in locus of control in behavior disordered children. Arts Psychother 1993;3:231–41 | Pre-test/post-test design |
| 22 | Ryan BR. Effects of two group approaches on life satisfaction and mood of older females in nursing homes. Dissertation Abstracts International: Section B: The Sciences and Engineering 4347;72(7-B) | Dissertation ordered (not a RCT) |
| 23 | Sela N, Baruch N, Assali A, Vaturi M, Battler A, Ben GT. [The influence of medical art therapy on quality of life and compliance of medical treatment of patients with advanced heart failure]. Harefuah 2009;150:79–83 | Cannot locate corresponding reference to citation |
| 24 | Sela N, Baruch N, Stein R, Yaari V, Pinchas A, Battler A, et al. Long term medical art therapy: influence on quality of life functional capacity and compliance in advanced heart failure patients. Supplement Conference Heart Failure 2010 Congress Berlin, Germany. 29 May–1 June 2010. Eur J Heart Fail 2010;9:S173 | Not a RCT; no control group |
| 25 | Szawarski Z. Placebo and art therapy. Med Dypl 2003;12:21–6 | Cannot locate corresponding reference to citation |
| 26 | Valladares AC, Carvalho AM. [Art therapy and behavior development in the context of hospitalization]. Revista Da Escola De Enfermagem Da Usp 2006;40:350–5 | Not a RCT; no randomisation to groups |
| 27 | van den Broek E, Keulen-de VM, Bernstein DP. Arts therapies and Schema Focused therapy: A pilot study. Arts Psychother 2011;38 | Arts not art therapy; does not define art therapy intervention |
| 28 | Volker CA. Treatment of sexual assault survivors utilizing cognitive therapy and art therapy. (self-esteem posttraumatic stress disorder victimization). San Francisco, CA: California Institute of Integral Studies; 1999 | Dissertation-insufficient data reported and final sample (n = 6) |
| 29 | Wallace J. Psychosocial changes associated with participation in art therapy interventions for siblings of pediatric hematopoietic stem cell transplant patient. Palo Alto, CA: Palo Alto University; 2012 | Dissertation – not randomised |
| 30 | Zeltzer BB, Stanley S, Melo L, LaPorte KM. Arts therapies promote wellness in elders. Behavioural Healthcare Tomorrow 2003;12:7–12 | Not a RCT; no randomisation to groups |
| 31 | Zimmerman ML, Wolbert WA, Burgess AW, Hartman CR. Art and group work: interventions for multiple victims of child molestation (Part II). Arch Psychiatr Nurs 1987;1:40–6 | Not a RCT; no randomisation to groups |
Appendix 4 Studies excluded at full text from the qualitative review
| No. | Reference | Reason for exclusion |
|---|---|---|
| 1 | Agnese A, Lamparelli T, Bacigalupo A, Luzzatto P. Supportive care with art therapy for patients in isolation during stem cell transplant. Palliat Support Care 2012;10:91–8 | Case study |
| 2 | Allen KN, Wozniak DF. The language of healing: women’s voices in healing and recovering from domestic violence. [References]. Soc Work Ment Health 2011;1:37–55 | Not art therapy |
| 3 | Baumann M, Peck S, Collins C, Eades G. The meaning and value of taking part in a person-centred arts programme to hospital-based stroke patients: findings from a qualitative study. Disabil Rehabil 2013;35:244–56 | Not art therapy |
| 4 | Beesley K, White JH, Alston MK, Sweetapple AL, Pollack M. Art after stroke: the qualitative experience of community dwelling stroke survivors in a group art programme. Disabil Rehabil 2011;33:2346–55 | Not art therapy |
| 5 | Crone DM, O’Connell EE, Tyson PJ, Clark-Stone F, Opher S, James DVB. ‘It helps me make sense of the world’: The role of an art intervention for promoting health and wellbeing in primary care - Perspectives of patients health professionals and artists. [References]. J Public Health 2012;5:519–24 | Not art therapy |
| 6 | Dickson C. An evaluation study of art therapy provision in a residential Addiction Treatment Programme (ATP). Int J Art Ther 2007;12:17–27 | No qualitative data |
| 7 | Fulton J. Art therapy and chronic illness: An enquiry into aspects of service provision for patients with atopic skin disease. Inscape 2002;7:2–15 | No qualitative data |
| 8 | Geue K, Buttstadt M, Singer S, Kleinert E, Richter R, Gotze H, et al. (2011) [The impact of an art therapy programme for cancer patients – an analysis from different points of view]. Forschende Komplementarmedizin 18:127–33 | No qualitative data |
| 9 | Gussak D. Comparing the effectiveness of art therapy on depression and locus of control of male and female inmates. [References]. Arts Psychother 2009;4:202–7 | No qualitative data |
| 10 | Kwiatkowska G. [Reception and evaluation of art therapy by patients with neuroses.] Psychiatria Polska 1990;24:136–40 | No qualitative data |
| 11 | Makin S, Gask L. ‘Getting back to normal’: the added value of an art-based programme in promoting ‘recovery’ for common but chronic mental health problems. Chronic Illn 2012;8:64–75 | Not art therapy |
| 12 | Murphy J, Paisley D, Pardoe L. An art therapy group for impulsive children. Inscape 2004;9:59–68 | Unobtainable |
| 13 | Oster I. Art therapy with women with breast cancer-results from a randomized study. Psycho-Oncology Conference: 11th World Congress of Psycho-Oncology of the International Psycho-oncology Society, IPOS Vienna, Austria, 21–25 June 2009. [Conference Publication]. 2009;18:S22–3 | Abstract superseded by full paper |
| 14 | Pizarro JE-MA, Pizarro JJE. The efficacy of art and writing therapy: increasing positive mental health outcomes and participant retention after exposure to traumatic experience. [References]. Art Ther 2004;21 | No qualitative data |
| 15 | Plecity D, Danner-Weinberger A, Szkura L, von Wietersheim J. Effects of art therapy on the physical and emotional state of health of patients – a quantitative and qualitative analysis. Psychother Psychosomat Med Psychol 2007;57:100 | No qualitative data |
| 16 | Plecity DM, Danner-Weinberger A, Szkura L, von Wietersheim J. The effects of art therapy on the somatic and emotional situation of the patients - A quantitative and qualitative analysis. [German]. [References]. Psychother Psychosomat Med Psychol 2009;59:364–9 | No qualitative data |
| 17 | Reynolds F, Lim KH. Contribution of visual art-making to the subjective well-being of women living with cancer: a qualitative study. Arts Psychother 2007;34:1–10 | Not art therapy |
| 18 | Reynolds F, Prior S. Creative adventures and flow in art-making: a qualitative study of women living with cancer. Br J Occup Ther 2006;69:255–62 | Not art therapy |
| 19 | Rusted J, Sheppard L, Waller D. A Multi-centre randomized control group trial on the use of art therapy for older people with dementia. Group Analysis 2006;4:517–36 | Case study |
| 20 | Sainsbury S, Lee K. Art as therapeutic recreation following acquired brain injury (ABI) to enhance emotional regulation. Brain Impairment Conference: 9th Annual Conference of the Special Interest Group in Neuropsychological Rehabilitation of the World Federation for NeuroRehabilitation WFNR. 2–3 July 2012, Bergen, Norway. Conference 13. http://dx.doi.org/10.1017/BrImp.2012.11 | Only abstract available |
| 21 | Sainsbury SA, Lee K. Art therapy in cases of acquired brain injury: helping participants find social context through creative self-expression. Brain Impairment Conference: 2011 International Neuropsychological Society Mid-Year Meeting/ASSBI 4th Pacific Rim Conference. 6–9 July 2011, Auckland, New Zealand. Conference Publication. 2011;12:33 | Abstract only available |
| 22 | Singh BE-MA, Singh BBC. The therapeutic effects of art making in patients with cancer. [References]. Arts Psychother 2011;38 | Not art therapy |
| 23 | Smeijsters H, Cleven G. The treatment of aggression using arts therapies in forensic psychiatry: results of a qualitative inquiry. [References]. The Arts in Psychotherapy 2006;1:37–58 | Not about attitudes to art therapy |
| 24 | Steward Aron. Art therapy intervention with “at-risk” adolescent boys: Effects on self-image and perceptions of loss. [Database]. Dissertation Abstracts International: Section B: The Sciences and Engineering [5-B]. 2007. US, State University New York At Buffalo. Ref Type: Thesis/Dissertation | Not about attitudes to art therapy |
| 25 | ter Maat MB. A group art therapy experience for immigrant adolescents. Am J Art Ther 1997;36:11–19 | Case study |
| 26 | Webb-Ferebee Kelly Lea. Expressive arts therapy with bereaved families. [Database]. Dissertation Abstracts International: Section A: Humanities and Social Sciences [9-A], 3119. 2003. US, U North Texas. Ref Type: Thesis/Dissertation | Not art therapy |
| 27 | Wilson C. A time-limited model of art therapy in general practice. Inscape 2002;7:16–26 | Case study |
| 28 | Wolf Bordonaro Gaelynn P. Art therapy with hospitalized pediatric patients. [Database]. Dissertation Abstracts International: Section A: Humanities and Social Sciences [5-A]. 2005. US, The Florida State University. Ref Type: Thesis/Dissertation | Case study |
| 29 | Woolhiser J. Collage as a therapeutic modality for reminiscence in patients with dementia. Art Therapy 2010;27:136–40 | Not about attitudes to art therapy |
Appendix 5 Studies excluded at full text from the economic review
| No. | Reference | Reason for exclusion |
|---|---|---|
| 1 | Karapostoli N, Polyzos N, Tsegos I. The cost of therapy services provided by a day psychotherapy unit. Group Analysis 2012;45:515–35 | Does not investigate art therapy |
| 2 | Abbass A. Intensive short-term dynamic psychotherapy in a private psychiatric office: clinical and cost effectiveness. Am J Psychother 2002;56:225–32 | Does not investigate art therapy |
| 3 | Berg M, Smit F, Vos T, Baal PH. Cost-effectiveness of opportunistic screening and minimal contact psychotherapy to prevent depression in primary care patients. PLOS ONE 2011;6 | Does not investigate art therapy |
| 4 | Berghout CC, Zevalkink J, Hakkaart-van RL. A cost–utility analysis of psychoanalysis versus psychoanalytic psychotherapy. Int J Technol Assess Health Care 2010;26:3–10 | Does not investigate art therapy |
| 5 | Bosmans JE, Schaik DJ, Heymans MW, Marwijk HW, Hout HP, Bruijne MC. Cost-effectiveness of interpersonal psychotherapy for elderly primary care patients with major depression. Int J Technol Assess Health Care 2007;23:480–7 | Does not investigate art therapy |
| 6 | Browne G, Steiner M, Roberts J, Gafni A, Byrne C, Dunn E, et al. Sertraline and/or interpersonal psychotherapy for patients with dysthymic disorder in primary care: 6-month comparison with longitudinal 2-year follow-up of effectiveness and costs. J Affect Disord 2002;68:317–30 | Does not investigate art therapy |
| 7 | Frank B. The economics of preference change: The case of arts therapy – response. J Econ Psychol 1997;18:465–8 | Descriptive/qualitative paper no economic data |
| 8 | Goldman W, McCulloch J, Cuffel B. A four-year study of enhancing outpatient psychotherapy in managed care. Psychiatr Serv 2003;54:41–4 | Does not investigate art therapy |
| 9 | Marchand A, Germain V, Reinharz D, Mainguy N, Landry P. Analysis of the cost and the effectiveness of a psychotherapy for panic disorder with agoraphobia (PDA) versus a treatment combining pharmacotherapy and psychotherapy. Sante Mentale Au Quebec 2004;29:201–20 | Full paper in French |
| 10 | McCrone P, Weeramanthri T, Knapp M, Rushton A, Trowell J, Miles G, et al. Cost-effectiveness of individual versus group psychotherapy for sexually abused girls. Child Adolesc Ment Health 2005;10:26–31 | Does not investigate art therapy |
| 11 | Poinsier B, Laurin A.S. Economic evaluation of a simulated program of brief psychotherapy for children with mild problems. Sante Mentale Au Quebec 1995;20:203–18 | Full paper in French |
| 12 | Pulliam JC, Somerville P, Prebluda J, Warja-Danielsson M. Three heads are better than one: the expressive arts group assessment. Arts Psychother 1988;1:71–7 | Descriptive/qualitative paper no economic data |
| 13 | Soeteman DI, Busschbach JJ, Verheul R, Hoomans T, Kim JJ. Cost-effective psychotherapy for personality disorders in the Netherlands: the value of further research and active implementation. Valuen Health 2011;14:229–39 | Does not investigate art therapy |
| 14 | Soeteman DI, Verheul R, Delimon J, Meerman AM, Eijnden E, Rossum BV, et al. Cost-effectiveness of psychotherapy for cluster B personality disorders. Br J Psychiatry 2010;196:396–403 | Does not investigate art therapy |
| 15 | Soeteman DI, Verheul R, Meerman AM, Ziegler U, Rossum BV, Delimon J, et al. Cost-effectiveness of psychotherapy for cluster C personality disorders: a decision-analytic model in the Netherlands. J Clin Psychiatry 2011;72:51–9 | Does not investigate art therapy |
| 16 | Teneycke T, Hoshino J, Sharpe D. The bridge drawing: an exploration of psychosis. Arts Psychother 2009;5:297–303 | Descriptive/qualitative paper no economic data |
| 17 | White M. Establishing common ground in community-based arts in health. J R Soc Promot Health 2006;126 | Descriptive/qualitative paper no economic data |
| 18 | West C. Art therapy. Nurs Older People 2008;20:18–19 | Overview no economic data |
| 19 | Asselt A.D, Dirksen C.D, Arntz A, Giesen-Bloo J.H, Dyck R, Spinhoven P, et al. Out-patient psychotherapy for borderline personality disorder: cost-effectiveness of schema-focused therapy v transference-focused psychotherapy. Br J Psychiatry 2008;192:450–7 | Does not investigate art therapy |
| 20 | Siskind D, Baingana F, Kim J. Cost-effectiveness of group psychotherapy for depression in Uganda. J Ment Health Policy Econ 2008;11:127–33 | Descriptive/qualitative paper no economic data |
| 21 | Abbass A, Sheldon A, Gyra J, Kalpin A. Intensive short-term dynamic psychotherapy for DSM-IV personality disorders: a randomized controlled trial. J Nerv Ment Dis 2008;196:211–16 | Descriptive/qualitative paper no economic data |
| 22 | Maljanan T, Paltta P, Harkanen T, Virtala E, Lindfors O, Laaksonen M, et al. The cost-effectiveness of short-term psychodynamic psychotherapy and solution-focused therapy in the treatment of depressive and anxiety disorder during a one-year follow-up. J Ment Health Policy Econ 2012;15:13–23 | Descriptive/qualitative paper no economic data |
| 23 | Park A, McDaid D, Wahlbeck K, Forsman A. What do we know about economic evaluations of psychosocial interventions to promote mental health and wellness in older people? Psychiatrische Praxis Conference: 9th International Conference of the European Network for Mental Health Service Evaluation ENMESH, 23–25 June 2011, Ulm, Germany. [Conference Publication]. 2011;38 | Full paper in German |
| 24 | Frisch M.J, Herzog D.B, Franko D.L. Residential treatment for eating disorders. Int J Eat Disord 2006;39 | Descriptive/qualitative paper no economic data |
| 25 | Albrecht M, Krauth C, Rieger J, Lamprecht F, Kersting A, Schwartz FW. [Extended psychosomatic rehabilitation programme for outpatients: Concept for health economy evaluation of short-term and long-term cost and efficiency parameters.] Gesundheitswesen 2000;62:2000 | Full paper in German |
Appendix 6 Contact with authors
From: Lesley Uttley [mailto:l.uttley@sheffield.ac.uk]
Sent: Thursday, 19 December 2013 16:09 PM
To: hideyuki@ncgg.go.jp
Subject: Your study published in Geriatric Gerontology International 2010
Dear Hideyuki Hattori,
I would be very grateful for your help. Your study “Controlled study on the cognitive and psychological effect of coloring and drawing in mild Alzheimer’s disease patients” has been included in a systematic review of art therapy that I am conducting for the National Institute for Health Research, UK (http://www.nets.nihr.ac.uk/projects/hta/122716). The review also includes a cost effectiveness analysis for which we can map data from the Barthel index which is used in your study. You report the overall score for the Barthel index but it would be very helpful if you could also provide us with the scores for the following individual components:
1) Grooming;
2) Toilet;
3) Feeding;
4) Transfer;
5) Mobility;
6) Dressing;
7) Stairs;
8) Bathing;
9) Bladder;
10) Bowels.
Please let me know if it would be possible to provide us with this data? Many thanks in advance for your help with this.
Best wishes
Lesley
--
Dr Lesley Uttley
Systematic Reviewer
Health Economics and Decision Science (HEDS)
School of Health and Related Research (ScHARR)
On 19 December 2013 22:58, Hideyuki Hattori <hideyuki@ncgg.go.jp> wrote:
Dear Dr Lesley Attley
Thank you for emailing me. But I am afraid that I cannot disclose the data because we are going to research more about art therapy for dementia patient and the data in the paper will be used or refered in the future study.
I am sorry.
Dr Hideyuki Hattori
TEL:0562-46-2311
FAX:0562-44-8518
Email: hideyuki@ncgg.go.jp
On Friday, 20 December 2013 1:10, Lesley Uttley [l.uttley@sheffield.ac.uk] wrote:
Dear Hideyuki Hattori
Many thanks for your swift reply.
For your information we are able to include information that can remain “academic in confidence” in the health technology assessment report so can guarantee that this information would be blacked out and not published.
In any case, I thank you for your help so far and good luck with your forthcoming study and publication.
Best wishes
Lesley
--
Dr Lesley Uttley
Systematic Reviewer
Health Economics and Decision Science (HEDS)
School of Health and Related Research (ScHARR)
On 29/07/2013 16:48, Mail Delivery System [MAILER-DAEMON@saira.epm.br] wrote:
This is the mail system at host saira.epm.br.
I’m sorry to have to inform you that your message could not be delivered to one or more recipients. It’s attached below.
For further assistance, please send mail to postmaster.
If you do so, please include this problem report. You can delete your own text from the attached returned message.
The mail system
<andreia.baptista@unifesp.br>: host harpia.epm.br[172.22.29.24] said: 550 5.1.1 <andreia.baptista@unifesp.br>: Recipient address rejected: User unknown in local recipient table (in reply to RCPT TO command)
Final-Recipient: rfc822; andreia.baptista@unifesp.br
Original-Recipient: rfc822;andreia.baptista@unifesp.br
Action: failed
Status: 5.1.1
Remote-MTA: dns; harpia.epm.br
Diagnostic-Code: smtp; 550 5.1.1 <andreia.baptista@unifesp.br>: Recipient address rejected: User unknown in local recipient table
From: Lesley Uttley <l.uttley@sheffield.ac.uk>
To: andreia.baptista@unifesp.br
Cc: Alison Scope <a.scope@sheffield.ac.uk>
Date: Mon, 29 Jul 2013 16:20:45 +0100
Subject: Art therapy for fibromyalgia study for inclusion in a systematic review
Dear Andreia Baptista
I am a systematic reviewer at the University of Sheffield, United Kingdom. We are undertaking a research project for the UK National Institute for Health Research (NIHR) to examine the clinical and cost effectiveness of art therapy.
Your abstract in Arthritis and Rheumatism (2012) Vol 64, has come up in our searches and I am assessing the study for inclusion into our review. We would be interested to know when you will be publishing any further results from this study? Currently we would need more data on the methods and results to be included in the review.
More details about this project can be found here <http://www.hta.ac.uk/project/3030.asp>. Many thanks in anticipation of your response.
Best wishes
Lesley Uttley
--
Dr Lesley Uttley
Systematic Reviewer
Health Economics and Decision Science (HEDS)
School of Health and Related Research (ScHARR)
From: Lesley Uttley [l.uttley@sheffield.ac.uk]
Sent: 22 July 2013 15:39
To: Crawford, Mike J
Subject: CREATe trial status
Dear Mike Crawford
I’m currently conducting a systematic review of art therapy for the National Institute for Health Research HTA programme. The CREATe trial (ISRCTN74217860) has come up in our searches and I wondered if you’d be able to let me know the status of this trial and a rough idea of when you hope the data will be published.
Many thanks in advance.
Best wishes
Lesley Uttley
--
Dr Lesley Uttley
Systematic Reviewer
Health Economics and Decision Science (HEDS)
School of Health and Related Research (ScHARR)
On 22/07/2013 16:09PM, Crawford, Mike J [m.crawford@imperial.ac.uk] wrote:
The study was abandoned due to poor recruitment – good luck with your review – mike
List of abbreviations
- ANCOVA
- analysis of covariance
- ANOVA
- analysis of variance
- ASD
- autistic spectrum disorder
- BAAT
- British Association of Art Therapists
- BDI
- Beck Depression Inventory
- BPO
- borderline personality organisation
- CASP
- Critical Appraisal Skills Programme
- CBF
- cerebral blood flow
- CBT
- cognitive–behavioural therapy
- CEAC
- cost-effectiveness acceptability curve
- CONSORT
- Consolidated Standards of Reporting Trials
- CRD
- Centre for Reviews and Dissemination
- CRI
- Coping Resources Inventory
- EQ-5D
- European Quality of Life-5 Dimensions
- ESAS
- Edmonton Symptom Assessment Scale
- fMRI
- functional magnetic resonance imaging
- GDS
- Geriatric Depression Scale
- GP
- general practitioner
- GSI
- Global Severity Index
- HCPC
- Health and Care Professions Council
- IAPT
- Improving Access to Psychological Therapies
- MMSE
- Mini Mental State Examination Score
- NICE
- National Institute for Health and Care Excellence
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSA
- probabilistic sensitivity analysis
- PTSD
- post-traumatic stress disorder
- QALY
- quality-adjusted life-year
- QoL
- quality of life
- RCT
- randomised controlled trial
- SCL-90
- Symptom-Checklist-90
- SCL-90-R
- Symptom-Checklist-90-Revised
- SF-36
- Short Form questionnaire-36 items
- SF-8
- Short Form questionnaire-8 items
- STAI
- State–Trait Anxiety Inventory