
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 10/140/02. The contractual start date was in May 2012. The draft report began editorial review in November 2013 and was accepted for publication in April 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Ken Stein is chair of the NIHR HTA Editorial Board and a member of the NIHR Journals Library Board.
Disclaimer
This report contains quotations from transcripts of interviews conducted in the course of research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2015. This work was produced by Richardson et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background
What is attention-deficit/hyperactivity disorder?
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by age-inappropriate levels of inattention, impulsivity and hyperactivity. 1 The current Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) categorises particular constellations of symptoms into three presentations of ADHD. These are (1) predominantly inattentive; (2) predominantly hyperactive/impulsive; and (3) combined, where symptoms of both inattention and hyperactivity/impulsivity criteria are present.
The DSM-5 diagnostic criteria for ADHD, published in May 2013, increased the age by which some symptoms must have been present from 7 to 12 years of age. 1 Another potentially key change in DSM-5 relates to the level of impairment; Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV)2 required clear evidence of clinically significant impairment for diagnosis, whereas DSM-5 requires only interference or a reduction in functioning. DSM-5 also requires clinicians to specify the severity level of a diagnosis: mild, moderate or severe. Given the recent publication of DSM-5 and the retrospective nature of evidence synthesis, the studies included in this review refer to diagnoses made according to Diagnostic and Statistical Manual of Mental Disorders-Third Edition (DSM-III) or DSM-IV criteria. 2,3
The International Classification of Diseases, Tenth Edition (ICD-10) classifies core ADHD symptoms as hyperkinetic disorder. 4 The diagnosis for hyperkinetic disorder is more restrictive, whereby inattention, hyperactivity and impulsivity must all be present. Thus, the ICD-10 diagnosis represents a subsample of the DSM-5 ‘combined presentation’ of severe ADHD. In Europe, ‘ADHD’ has become the diagnostic phrase most commonly used in practice, even when the narrower ICD-10 criteria are being used.
The aetiology of ADHD is complex and may be most clearly understood as involving the interplay of biological, psychological and social factors. 5 Several causal factors have been suggested to contribute to the onset and maintenance of ADHD. These include genetic factors, psychosocial factors, complications in pregnancy and delivery and environmental factors such as high lead exposure, head injury and diet. 6–9 Heritability is a major factor and appears to contribute approximately 75% of the aetiology of ADHD. 6 Although no large single gene effect has been isolated, the DRD2, DRD4 and DRD5 dopamine receptors appear to be involved. 10 Although the current DSM-5 diagnostic criteria continue to weigh heavily on core symptoms of inattention, hyperactivity and impulsivity, some research suggests that deficits in self-regulation and executive functioning could explain many of the problems of the condition and its impairments. 8 More recently, leading experts have argued for deficits in emotional self-regulation as a core feature of ADHD,9 but this has received relatively little research attention compared with the core symptoms of ADHD,11 and problems in emotional self-regulation are now the basis of a new category in DSM-5, ‘disruptive mood dysregulation disorder’, which may be associated with ADHD. 12
Prevalence
Attention-deficit/hyperactivity disorder is one of the most common disorders to present to child and adolescent mental health services; however, findings from studies that ascertain prevalence vary. The worldwide prevalence of ADHD is estimated at 2–5% for children aged < 18 years,13 with 3–16% of children displaying difficulties that do not reach the diagnostic threshold. Numerous studies have shown increases in the prevalence of clinical ADHD diagnoses and prescriptions for stimulant medication over recent decades, for instance, a 33% increase in prevalence of diagnosis from 5.69% in 1997–9 to 7.57% in 2006–8 according to US survey data. 14 Prevalence in the UK was found to be 3.62% for boys and 0.85% for girls, for a sample of over 10,000 children aged from 5 to 15 years in 1999. 15 Although a systematic review of research between 1978 and 2005 found no differences between European and US rates of ADHD,13 more recent studies sampling parent reports found that in the USA between 2008 and 2010, 6.3% of all children aged 5–9 years were reported by parents as having an ADHD diagnosis,16 whereas in the UK between 2007 and 2009, only 1.4% of children aged 6–8 years held ADHD diagnoses according to parent reports. 17
Although boys are more commonly diagnosed with ADHD than girls, the ratio varies between two and nine boys to one girl, depending on the category of ADHD presentation2 and whether prevalence is based on clinical or epidemiological populations. 18 Girls with ADHD may be less likely to be seen in clinics. 19 Younger childhood and low socioeconomic status have also been shown to be positively associated with prevalence. 20,21 Although prevalence appears to decline with age, a 2013 prospective study reported that ADHD persisted into adulthood for nearly a third of young people. 22 Despite the increasing clinical recognition in the UK, ADHD remains underdiagnosed in certain populations, including adults,23 children with intellectual difficulties24 and those with inattentive symptoms. 25 Differences in findings about prevalence are suggested to result from different study approaches to identification. 17 Differences in clinical practice,26 expression of symptoms and behaviour according to cultural, social and developmental contexts27,28 are argued to be additional contributing factors both within and between countries.
Co-existing issues
Attention-deficit/hyperactivity disorder frequently co-exists with other mental health disorders, particularly antisocial and oppositional behaviour, but also tic disorders, specific learning difficulties, autistic spectrum disorders (ASDs), anxiety and depression. 11,29–31 As many as two-thirds of all children with ADHD in the general population are reported to have at least one other co-existing condition. 32 Many children with ADHD also have difficulties with social interaction and low self-esteem that affect their relationships with their parents, relatives and friends, as well as practitioners at school. 33 Often, these problems are at least as important as ADHD in contributing to the longer-term outcome in the individual child. 34 In addition, ADHD has also been linked with lower than average intellectual potential and academic underachievement across the developmental spectrum, from preschoolers to adults. 14 Inattentive symptoms and their related executive functioning deficits have been particularly associated with learning difficulties. 7 In the longer term, those with ADHD are less likely to be employed full-time, and more likely to have a lower household income than age and gender matched controls. 18
Controversy
Despite the breadth of research relating to prevalence, the diagnosis of ADHD has stimulated considerable debate and sometimes strong and conflicting views. 35 ADHD remains a contested disorder; for instance, in 2009 O’Regan found that 50% of general practitioners and 20% of special educational needs (SEN) co-ordinators in the UK did not believe that ADHD was a ‘real neurological condition’ (p. 4). 36 Bailey discusses the contested aetiology of ADHD and the issues that acceptance of a biological basis for ADHD can raise,37 which include concern over the use of medication for long periods of time in young children38 and the belief that the core symptoms of ADHD, inattention, hyperactivity and impulsivity, are traits seen in many children, especially the very young. 39 It has been shown that higher percentages of diagnosis of ADHD may occur for the youngest children in school year groups, which has led some to suggest that behavioural differences attributed to ADHD may be due at least in part to immaturity. 40 The labelling of hyperactivity, impulsivity and inattention as ADHD when these behaviours interfere with expectations for correct classroom behaviour has been criticised by those who believe ADHD is a constructed response to the demands of modern academic education. 41 Timimi and Taylor argue that ADHD is best understood as a cultural construct, given the variability in prevalence internationally and rise in diagnosis rates in Western culture. 42
By contrast, other studies suggest that solely biological understandings of ADHD can be adopted by educational staff and/or parents and others as a means to transform ‘multifaceted problems into organic dysfunctions’ (p. 1). 43 The recently documented increase in diagnosis of, and medication for, ADHD has been linked to reduction in educational funding and restricted classroom discipline policies. 44 It has been suggested that pressures on health and educational institutions for higher attainment and rapid improvement mean that there is often a focus on short-term solutions provided by medication at the expense of more intensive, long-term educational support, such as that provided by non-pharmacological interventions. 45 Thus, polarised views of either cultural or biological origins continue to be reported in the literature, despite repeated research findings that suggest ADHD is a transaction between biological, environmental and psychosocial factors. 6,8–10
Interventions for children with or at risk of attention-deficit/hyperactivity disorder
The National Institute for Health and Care Excellence (NICE) clinical practice guidelines recommend that for school-age children and young people with severe ADHD, medication should be offered as the first-line treatment. 46 Parents should also be offered a group-based parent training/education programme. If the child or young person with ADHD has moderate levels of impairment, the parents or carers should first be offered referral to a group parent training/education programme, either on its own or together with a group treatment programme [such as cognitive–behavioural therapy (CBT) or social skills training] for the child or young person. Pharmacological treatment may then be added to the management plan if symptoms do not sufficiently respond to this approach. Teachers who have received training about ADHD and its management should provide behavioural interventions in the classroom to help children and young people with ADHD. Medication for children and young people with ADHD should always form part of a comprehensive treatment plan that includes psychological, behavioural and educational advice and interventions. Use of both medication and psychosocial treatment for ADHD varies widely within and across nations. 47 At present, the most common approaches to the treatment of ADHD are medication and/or psychological or behavioural interventions.
Pharmacological interventions
The most frequently used pharmacological treatments, and those with the largest evidence base, are the stimulant medications, methylphenidate and dexamfetamine,48 but their use remains controversial among some people who work with children. 49,50 The Care Quality Commission revealed in 2013 that the prescribing of methylphenidate for ADHD in the UK had risen by 56% in primary care from 420,421 in 2007 to 657,358 in 2012. 51 Meta-analyses of stimulant medications have shown them to be effective at decreasing the symptoms of hyperactivity, impulsivity and inattention, although their effectiveness on cognition and achievement are more modest. 52 However, any positive effects do not appear to persist once stimulants are no longer used53 and as many as 30% of children do not respond to stimulants. 54 The potential adverse effects of treatment with stimulants include decreased appetite, weight loss, insomnia, stomach ache, headache and irritability. 55
Several studies of the cost-effectiveness of pharmacological ADHD interventions have been undertaken. In 2001 in the UK, Gilmore and Milne examined the cost-effectiveness of different medications from the perspective of the NHS, finding methylphenidate to offer the best value for money. 56 NICE estimated the cost per quality-adjusted life-year gained by methylphenidate at £9200 to £14,600. 57 Cost-effectiveness studies have compared medication to behavioural treatment and combined treatments, often finding in favour of medication alone. 58
Non-pharmacological intervention
Non-pharmacological interventions target behaviour directly or indirectly through cognitive and affective processes and typically target children, teachers and parents. Interventions that target teachers and parents usually involve training for delivery of interventions that target the children. An early meta-analysis compared a range of treatments for ADHD including both pharmacological and non-pharmacological interventions and found larger effects from all interventions on behavioural (d = 0.56) rather than educational outcomes (d = 0.28). 59 These overall effects were larger for medical interventions (d = 0.45) than for educational (d = 0.39), psychosocial (d = 0.39), or parent training interventions (d = 0.31). However, the effects on educational outcomes were greater for educational interventions (d = 0.58) than for other types of psychosocial intervention. There was little support for the influence of any reduction in behavioural problems on educational outcomes across studies. Although it is widely accepted that intervention in ADHD should be based on multimodal treatment,55 some research has suggested that adding psychosocial interventions to medication does not improve outcomes significantly. 60,61
Several reviews point to the effectiveness of behavioural interventions, particularly behavioural parent training (BPT) and behavioural classroom management. 62–64 For example, Pelham and Fabiano examined three types of interventions, including behavioural modification in classroom settings (BMC) that consisted of ‘contingency management’ based on ‘social learning theory’, BPT and behavioural peer intervention (BPI). 64 Results were synthesised across a range of constructs related to ADHD (including behavioural observations, family functioning, academic productivity, peer relationships and cognitive functioning), informants (e.g. parents, teachers, children and clinicians), and intervention type. Average effects by study design indicated that methodologically weaker single- and within-subject (treatment group received multiple treatments over time in a crossover fashion) designs generally reported larger effects than controlled trials. For the comparison of treatment with waitlist/no treatment Cohen’s d ranged from –0.03 to 0.44 for BMC; –0.02 to 0.70 for BPT; and 0.29 to 0.63 for BPI. Cohen’s classification for interpreting effect sizes distinguished between ‘small’ (d = 0.20), ‘medium’ (d = 0.50) and ‘large’ (d = 0.80) sizes, with very small findings < 0.20 having the least clinical impact. 65 Although these findings include evidence for the effectiveness of these interventions, the wide range of reported effects does not clarify their size and consistency. Pelham and Fabiano suggested a range of potential moderating variables that could have influenced the treatment outcomes, which included recipient gender, age, comorbidity, socioeconomic status, therapist characteristics and treatment characteristics such as intensity and adherence. 64
Fabiano et al. conducted meta-analyses to evaluate the effectiveness of behavioural interventions that included parent training, child training and classroom-based behavioural interventions. 63 Effects were synthesised across intervention type; constructs related to ADHD (including two observational behavioural measures; ADHD symptoms, externalising symptoms, impairment productivity and achievement); intervention context (school and clinic); and informant types. As was found by Pelham et al. ,66 average effects by study design indicated that methodologically weaker single-subject, within-subject (treatment group received multiple treatments over time in a crossover fashion) and pre–post (treatment groups assessed pre and post intervention) designs reported larger effects than controlled trials. For the 20 controlled trials, the average weighted effect size was 0.67 with 95% confidence intervals (CIs) from 0.54 to 0.80. Significant reported heterogeneity across studies was perhaps due in part to the collapsing of data across different settings, outcomes and informants. 63
There is less evidence for the effectiveness of neurofeedback on ADHD. For example, Willis et al. conducted a systematic review of 14 empirical reports of neurofeedback treatment for children with ADHD and reported that neurofeedback is not well supported as an intervention for this disorder. 67 Furthermore, the cost-effectiveness of neurofeedback has been called into question. 68 Social skills training, summer treatment programmes and academic modifications have some support in the treatment of a range of ADHD symptoms and related impairments. 69 However, Barkley reports that social skills training shows less benefit for teenagers with ADHD compared with younger children, which suggests that age may be an important moderator of the effectiveness of social skills interventions. 70
In 2013 Sonuga-Barke et al. published a systematic review of peer-reviewed randomised controlled trials (RCTs) investigating the efficacy of non-pharmacological interventions delivered in various contexts (including home, school and clinic settings). 62 Statistically significant treatment effects were found for all the non-pharmacological interventions when the person rating the outcome used was the closest to the intervention setting (e.g. teacher ratings for interventions in school settings). 62 This was the case for all dietary [standardised mean difference (SMD) ranged from 0.21 to 0.48] and psychological treatments (SMD ranged from 0.40 to 0.64) that included cognitive training, neurofeedback and behavioural interventions. However, these treatment effects were not statistically significant for all psychological interventions when raters were blinded to the treatment participants were receiving. 62
School-based interventions
The education system has a front-line role in the management of ADHD. Results from the 2004 British Child Mental Health Survey showed that more families of children with ADHD had sought support from education in the past year than from professionals in specialist health services (74% vs. 51%). 71 Few systematic reviews and meta-syntheses have examined the effectiveness of non-drug interventions in school settings independently of those delivered entirely in home and clinical contexts. One exception is DuPaul et al. who updated a previous meta-analysis to provide a quantitative review of school-based ADHD intervention research that had been conducted between 1996 and 2010. 72 The authors examined the effects of three intervention types labelled as ‘academic’, ‘contingency management’ and ‘cognitive–behavioural’. ‘Academic’ involved study skills training and modification of academic instruction; ‘contingency management’ involved the application of techniques grounded in operant conditioning (such as rewards and punishments) and ‘cognitive–behavioural’ encompassed the development of self-control skills including self-instruction and problem-solving strategies. For the behavioural outcome comprising symptoms related to ADHD, statistically significant positive effects were identified for the within-subjects group (treatment groups assessed pre and post intervention) and single-subject designs but not for the controlled trials (d+ = 0.18, 95% CI –0.62 to 0.98). Similarly, all mean effect sizes were positive for the academic outcome and statistically significant results were reported for single-subject designs but not for controlled trials (d+ = 0.43, 95% CI –0.36 to 1.21) and within-subjects designs. However, analyses for the controlled trials were severely limited by the small number of studies included (n = 3).
Although stimulant medication and behaviour modification typically target and have proven to be effective interventions to increase on task, and reduce disruptive behaviour among children with ADHD within the classroom, a literature review conducted in 2006 which focused on academic interventions for ADHD concluded that the manipulation of antecedent conditions, such as academic instruction or materials, often improved both behavioural and academic outcomes. 73 However, in 2007 Trout et al. 74 systematically reviewed non-pharmacological interventions that targeted academic outcomes using single-subject and within-group (treatment groups assessed pre and post intervention) study designs. They categorised interventions as ‘antecedent’ (interventions that target children prior to an academic task); ‘consequence’ [interventions that targeted children post performance of the target behaviour(s)]; ‘peer-mediated’ (intervention that were delivered in part by peers); ‘parent-mediated’ (interventions that were delivered in part by parents); ‘self-regulation’ (interventions that targeted self-regulation of cognition and behaviours); and other interventions that used a combination of treatments. The authors suggested that peer tutoring and self-regulation show some evidence of effectiveness. Nonetheless, the authors reported that there were few systematic lines of research and reached few firm conclusions regarding the effectiveness of behavioural interventions that target children with ADHD. In an earlier review conducted in 2005, Reid et al. 75 reported beneficial effects for interventions based on ‘self-monitoring’ related to ‘self-regulation’ in their review of symptom and scholastic outcomes, providing further support of the beneficial effect of self-monitoring. However, as single-subject and within-group designs were the focus of this review, it is yet to be established if these effects are observed in controlled trials.
A 2010 questionnaire study of first-grade teachers76 points to the fact that interventions of the type reviewed in the studies cited above may not always match the interventions that teachers report using for children with ADHD difficulties. Teachers reported using environmental modifications, assignment modifications and behaviour modification strategies more frequently with inattentive students than with other students. Although some of the interventions mentioned by teachers, such as reward systems and time out, are considered evidence-based treatments for children with ADHD,64 other strategies the teachers reported using, such as preferential seating and additional time, are less often researched.
Reported effectiveness of school-based interventions may vary depending on the outcome of interest. In their 2005 review, Pelham et al. 66 compared a contingency management intervention to methylphenidate or the use of both treatments and reported effect sizes that were four to five times greater for the effectiveness of the educational intervention for classroom rule violations than for teacher ratings of ADHD behaviours. Although school-based behavioural interventions can improve targeted behaviours in the short term, they have been found less useful in reducing the core symptoms of ADHD. 60
Because of its prevalence and at times refractory course, childhood ADHD results in considerable costs for society, particularly to the educational system. In 2013, Telford et al. 77 considered the wider education, health and social care costs of adolescents with ADHD in the UK. The mean cost per adolescent for NHS, social care and education resources used in a 12-month period related to ADHD was £5493 in 2010 prices and the median was £2327. Education resources accounted for approximately three times the cost of health-care costs. The total annual cost of adolescents with ADHD in the UK is estimated to be £670M. 77
Methodological considerations
Reviews of quantitative research in school settings have frequently evaluated the preponderance of within-subject group and single-subject designs, which, although valuable, are more prone to bias than RCTs, which are the scientific ‘gold standard’ for evaluating treatment effects. 78 Many of the findings are difficult to interpret, as they combine results across different contexts (e.g. school, clinical and home), interventions, outcomes and informants. Tests of statistical significance and CIs are often not reported, which makes the findings difficult to interpret, and there are no standardised guidelines for interpreting effect sizes for within-subject group and single-subject designs and comparing these effects with those found in other study designs such as between-group designs where Cohen’s d is often reported. There are differences in the types of outcome measures used across study designs with most single-subject design studies employing proximal outcome measures such as curriculum-based measurements or direct observations of classroom behaviour. 72 In contrast, most controlled trials and within-subject group design studies used more distal measures such as teacher ratings or report card grades. 72
Sociopolitical aspects of educational research in the UK may contribute to a lack of research employing the most rigorous experimental designs. RCTs provide general information about interventions that are particularly useful to policy-makers. In contrast, educational researchers and/or practitioners may be more concerned about knowledge about the application of information to specific cases79,80 or be concerned about aspects of education that are not represented by straightforwardly measurable outcomes,81 for example those who suggest that education involves norms, values and processes of judgement that cannot be separated from extrinsic variables. 82 This may lead them to prefer approaches like case studies and action research. Educators may also be sensitive to moves towards a more central control of education, which some may associate with calls for evidence-based practice. 81
The measurement of attention-deficit/hyperactivity disorder symptoms and outcomes
A range of constructs have been used to evaluate the effectiveness of treatments that target children with or at risk of ADHD in school settings. These constructs can be categorised into three higher-order groups: (1) core ADHD diagnostic symptom categories (including inattention, hyperactivity/impulsivity, ADHD combined); (2) symptoms commonly associated with ADHD (including externalising symptoms, internalising symptoms, social skills); and (3) scholastic behaviours and achievement (including ‘perceptions of scholastic adjustment’, ‘standardised achievement’ and ‘curriculum’-based achievement). Core ADHD diagnostic symptom categories include the three diagnostic presentations of ADHD as specified in DSM-5: age-inappropriate ‘inattention’; ‘hyperactivity/impulsivity’; and ‘combined’ inattention and hyperactivity/impulsivity. The second category of ADHD-related symptoms encompass difficulties that frequently coexist with the core symptoms of ADHD and complicate its management, but are not relevant to diagnosis. Scholastic behaviours and achievement encompass perceived adjustment to school such as achievement, motivation, academic skills and abilities. These three higher-order constructs have been assessed by a range of behavioural measures, which include ratings and observations, as well as more relatively objective neurocognitive assessments and tests of scholastic achievement with objective performance criteria.
Assessments
When measuring the effectiveness of school-based interventions, the child’s core ADHD symptoms, ADHD-related symptoms and scholastic behaviours and outcomes are typically assessed by teacher and parent perception-based measures [e.g. Conners’ Rating Scale (CRS)],83 although independent observers (who have had no previous relationship with the study participant) are sometimes used (e.g. observer-based assessments of on-task behaviour). Neurocognitive assessments such as the test of variables of attention (TOVA)84 have also been employed to assess ‘inattention’ and ‘hyperactivity/impulsivity’ and a range of standardised achievement tests are used to measure academic outcomes (e.g. Wide Range Achievement Test). 85 Most studies include a range of outcomes assessed by a number of raters or informants.
Sonuga-Barke et al. ’s 2013 systematic review of non-pharmacological interventions found significant treatment effects for all of the non-pharmacological interventions when the person rating the outcome used was the closest to the intervention setting (e.g. teacher ratings for interventions in school settings). 62 However, these treatment effects were not statistically significant for all psychological interventions when using the most methodologically rigorous blinded assessments, which indicates the potential for bias in outcomes from raters who are involved in intervention delivery and/or expect the intervention to be successful. Blinding, however, was sometimes inferred from the study design rather than taken from the reported use of blinding. Moreover, findings were limited to a composite outcome combining core ADHD symptom measures and delivery settings, which may mask important effects and account for some of the significant heterogeneity in findings across the primary studies. 62 In addition, there may plausibly be limited generalisation of the impact of an intervention in one setting to perceptions of the child’s behaviour in another setting. Nonetheless, Sonuga-Barke et al. 62 highlight the importance of methodological evaluation alongside evidence synthesis of interventions that target children with or at risk of children with ADHD.
Triangulation of data in quantitative versus qualitative research
Mixed methods in primary studies are considered to enable additional grounds for inference owing to triangulation of data, methods and analysis. 86 The benefits of mixed-methods systematic review are similar. 87 However, triangulation of data, when defined as the additional confirmation of a finding through repetition from different studies, can be problematic in qualitative studies. Unlike experimental evaluations, where repetition increases finding strength, an interpretive approach does not seek a true answer; rather, it explores the meanings people make of their experiences. 88 In interpretive studies it is expected that different people will make sense of things in different ways. By contrast, similar sense of a topic made by different people is not taken as additional evidence of truth, but rather that the participants are drawing from a similar cultural ideology to make sense of their experiences. 89 Therefore, an isolated finding may be more important than repeated findings, for example because it illuminates a previously implicit and overlooked meaning. 88,90 In interpretive research, triangulation of data can be understood as the compilation of multiple perspectives, where the resulting representation of complexity of perspective and depth of meaning is a sign of study rigour. 91
Rationale
The research questions of a systematic review guide the criteria for included studies. 87,92 Our research questions ask about effectiveness of ADHD interventions in schools, factors that enhance or limit the delivery of school interventions for ADHD, and the experience of ADHD in schools. We were unable to locate any systematic reviews of either the experience of non-pharmacological interventions for ADHD, or the experience of ADHD more generally; therefore the synthesis of qualitative primary studies holds important potential to contribute new information on this topic. In this systematic review, we synthesise qualitative research in addition to experimental evaluation studies in order to explore attitudes, experiences and factors that may help explain how or why interventions for ADHD in school settings are or are not effective. Through the overarching synthesis of both quantitative and qualitative reviews, we will explore similarities, contradictions and gaps between these syntheses, further informing the research questions and implications for further research. 87
This review also holds the potential to contribute important new information about the effectiveness of non-pharmacological interventions for ADHD in schools. A range of non-pharmacological interventions have been developed and delivered in school settings by parents, teachers or other professionals. As outlined above, few published reviews have considered the effectiveness of non-pharmacological interventions in school settings independently of those delivered predominantly in other settings such as at home and in clinics. Therefore, a gap remains for a systematic review that considers the effectiveness and cost-effectiveness of such non-pharmacological interventions that are delivered primarily in school settings.
The reviews reported have typically taken a narrow focus in terms of the interventions and outcomes included and few have distinguished between different types of informants (see Fabiano et al. 63 for exception). Moreover, the focus has been on single-subject and within-group designs rather than on controlled trials, which compromises evidence synthesis as study design, intervention type, delivery context, outcomes and informant type may produce important differential effects. 62 Despite the current clinical recommendation for non-pharmacological ADHD interventions,46 there is a lack of clarity regarding their effectiveness and in particular their effectiveness in school settings. Moreover, their cost-effectiveness has not been systematically reviewed.
To build evidence-based guidelines for the treatment of ADHD in school settings, knowledge of the effectiveness of interventions is required. However, heterogeneity among findings across studies of intervention effectiveness is a common conclusion for many reviews that assess non-pharmacological interventions that target children with or at risk of ADHD. 62,63,72,74 Although average, weighted, effect sizes may help to establish the importance of non-pharmacological interventions in improving outcomes for children with or at risk of ADHD, it is critical that the components linked with the most successful interventions are identified so that the design, implementation and replication of future interventions can make the best use of scarce resources.
Repeated calls have been made for precise specification of what makes one behaviour change intervention more effective than another and how this can be understood theoretically (e.g. Rothman93). A range of programme features have been highlighted as potentially moderating the effectiveness of interventions that target children with or at risk of ADHD; these include characteristics of the child participant (e.g. age, medication status, sex), characteristics of the intervention (i.e. the change techniques constituting intervention content) and characteristics related to the delivery of the intervention (e.g. intensity of the intervention, fidelity of delivery). 64 The identification of programme features that are necessary for effective intervention implementation in school contexts will facilitate links between particular intervention components and effectiveness, and in turn could help resources to be used more efficiently and benefit children displaying ADHD symptoms, their carers and service providers.
Through the consideration of relevant qualitative research alongside the synthesis of quantitative studies this review has the potential to provide explanations of why particular interventions are effective and what factors operate as catalysts and barriers to effectiveness. The review will also identify any significant areas of uncertainty with regard to school-based interventions for ADHD and recommend any future research needed to address them.
Aim and research questions
The broad aim of this series of systematic reviews and their overarching synthesis is to evaluate the effectiveness and cost-effectiveness of non-pharmacological interventions delivered in school settings for children with, or at risk of, ADHD and to explore the factors that may enhance, or limit, the delivery of such interventions.
Four reviews were conducted. Review 1 (see Chapter 2) synthesises the effectiveness and the cost-effectiveness of non-pharmacological interventions delivered in school settings for children with or at risk of ADHD. Review 2 (see Chapter 3) considers quantitative studies that explore attitudes towards school-based non-pharmacological interventions for pupils with ADHD. Review 3 (see Chapter 5) synthesises the attitudes and experiences of children, teachers, parents and others using ADHD interventions in school settings. Review 4 (see Chapter 6) explores the experience of ADHD in school among children, their parents and teachers more generally. The four reviews are subsequently brought together in an overarching synthesis (see Chapter 7). Each review addresses particular research questions as outlined below.
Review 1
-
Are non-pharmacological interventions delivered in school settings for children with or at risk of ADHD effective in improving:
-
Core ADHD symptoms (inattention, hyperactivity/impulsivity, ADHD combined)?
-
ADHD-related symptoms (externalising symptoms, internalising symptoms, social skills)?
-
Scholastic behaviours and outcomes (perceptions of school adjustment, curriculum achievement, standardised achievement)?
-
-
Is effectiveness moderated by particular programme features?
-
Have such interventions been shown to be cost-effective?
Review 2
-
What attitudes do educators, children with or at risk of ADHD, their peers and their parents hold towards non-pharmacological interventions for ADHD used in school settings?
-
Which school-based non-pharmacological interventions for ADHD are preferred and how do attitudes towards these interventions compare to non-school interventions including pharmacological ones?
-
What factors affect attitudes held towards these non-pharmacological interventions (including children’s ADHD subtype and teacher experience)?
Review 3
-
What are the experiences of and attitudes towards ADHD interventions in school settings?
Review 4
-
What are the school-related experiences and perceptions of pupils diagnosed with or at risk of ADHD, their teachers, parents and peers?
Overarching synthesis
The aim of the overarching synthesis is to synthesise findings from reviews 1–4.
Chapter 2 Review 1: effectiveness of non-pharmacological interventions in school settings for children with or at risk of attention-deficit/hyperactivity disorder
Research questions
This chapter describes systematic review 1 and addresses the following three research questions:
-
Are non-pharmacological interventions delivered in school settings for children with, or at risk of, ADHD effective in improving:
-
Core ADHD symptoms (inattention, hyperactivity/impulsivity, ADHD combined)?
-
ADHD-related symptoms (externalising symptoms, internalising symptoms, social skills)?
-
Scholastic behaviours and outcomes (perceptions of school adjustment, curriculum achievement, standardised achievement)?
-
-
Is effectiveness moderated by particular programme features?
-
Have such interventions been shown to be cost-effective?
Methods
Search strategy
Electronic database search
A database search strategy was developed which combined three elements: ADHD plus synonyms and derivatives; terms related to a school context; and intervention terms. The database search strategies used a mixture of subject headings (controlled vocabulary) and free-text terms. Searches were restricted to years from 1980 onwards. Twenty electronic databases were searched {Applied Social Sciences Index and Abstracts (ASSIA)/ProQuest, MEDLINE/OvidSP, EMBASE/OvidSP, PsycINFO/OvidSP, British Education Index/ProQuest, Australian Education Index/ProQuest, Education Research Complete/EBSCOhost, Education Resources Information Center (ERIC)/ProQuest, The Cochrane Library [Cochrane Database of Systematic Reviews (CDSR), Database of Abstracts of Reviews of Effects (DARE), Cochrane Central Register of Controlled Trials (CENTRAL), Cochrane Methodology Register (CMR), Health Technology Assessment (HTA), NHS Economic Evaluation Database (NHS EED)], The Campbell Library, Health Management Information Consortium (HMIC)/OvidSP, Social Policy and Practice/OvidSP, Social Sciences Citation Index, Conference Proceedings Citation Index, Conference Proceedings Citation Index – Social Science & Humanities (via ISI Web of Science)}, from 16 to 28 May 2012. Searches were updated between 11 and 18 February 2013. An example search strategy used for the PsycINFO/OvidSP database is shown in Appendix 1. No language or geographical limitations were applied. Titles and abstracts returned by the search strategy were exported into EndNote v.X5 (Thomson Reuters, CA, USA) and independently screened by two of six researchers (MR, DM, TND, RW, MRo and RA) using the predefined criteria specified below. All disagreements were resolved by discussion between MR and DM. Where it was not possible to decide on exclusion of a paper based on the information in the title and abstract, the full text was retrieved. Two researchers (MR and DM) examined these independently for inclusion or exclusion using modified predefined criteria (specified below). Again, all disagreements were resolved through discussion. Where full-text papers were not easily retrievable (locally or from The British Library) authors were contacted. The same methods were applied to identify additional unique records from an updated search of the electronic databases conducted in February 2013.
Supplemental search strategies
Backward (searching the references of included articles) and forward (searching articles citing included articles using Web of Knowledge) searches were conducted by two researchers (MRo and DR) to locate further primary articles of potential relevance. In addition, DR searched websites (see Appendix 2 for a list of websites searched) and hand-searched five key journals published between 2008 and 2012: Journal of Child Psychology and Psychiatry; British Educational Research Journal; Journal of School Psychology; Journal of Attention Disorders; and Attention Deficit and Hyperactivity Disorders.
Inclusion and exclusion criteria
The screening of potentially relevant articles was carried out in two stages: at stage 1, predefined criteria were applied to titles and abstracts and at stage 2, these criteria were modified and applied to the screening of full-text articles. The criteria are detailed in Table 1 and parentheses indicate where they were applied at stage 2 only (for full-text screening).
| Criteria | Specification |
|---|---|
| Population | Inclusion:
|
| Intervention | Inclusion:
|
| Outcomes | Inclusion: Child outcomes including ADHD symptoms (i.e. inattention, hyperactivity/impulsivity); ADHD-related symptoms (i.e. externalising, internalising and social skills) and scholastic behaviours (i.e. perception of scholastic adjustment, standardised achievement and curriculum achievement)
|
| Study design | Inclusion:
|
| Comparators | Inclusion:
|
| Other | Exclusion:
|
Data extraction
Methodological information
A form was developed with reference to existing coding frames94,95 and modified after pilot testing to extract the relevant programme features of the included studies, which included bibliographic and study details, participant characteristics, outcome assessments, intervention package(s) and characteristics relating to the delivery of the intervention package(s). The typology of information extracted is reported in Table 2.
| Programme feature | Information extracted |
|---|---|
| Bibliographic and study details |
|
| Child participant characteristics |
|
| Outcome assessment(s) |
|
| Intervention package(s) |
|
| Characteristics relating to the delivery of the intervention package(s) |
|
Conceptual synthesis: mapping measures onto child-related constructs that assessed aspects of attention-deficit/hyperactivity disorder
Owing to the heterogeneity in assessment of child outcome measures, a classification system that mapped the measures reported in included studies onto nine commonly assessed child-related constructs assessing aspects of the condition was developed by MR and checked by DM. The classification system was developed by reading and rereading descriptions of the measures and items located in the primary papers and other online resources, and mapping them to definitions of the constructs. This tool was then used by MR to map outcome assessment instruments reported in the primary papers onto nine commonly assessed child-related constructs assessing aspects of ADHD. The labels and definitions of these constructs, as well as the measures and informants (parents, teachers, children and observers), are reported in Table 3.
| Construct label and definition | Measures (subscales italicised in parentheses where relevant) | Informant(s) |
|---|---|---|
| Construct label: inattention Construct definition: inability to focus and pay attention appropriate to task and context. For example, inattention, easy distractibility, disorganisation, procrastination and forgetfulness |
BASC-II (inattention)96 | Parent |
| SKAMP (cognitive impairment attention)97 | Teacher | |
| CRS;98 CRS-R (inattention/passivity, cognitive problems/inattention, daydream/attention problems, DSM-IV inattention)98 | Parent and teacher | |
| DBD (inattention)99 | Parent and teacher | |
| CBCL (attention)100 | Parent and teacher | |
| ADHD (inattention)2 | Parent and teacher | |
| VADTRS; VADPRS (inattention)101 | Parent and teacher | |
| d2 test of attention9 | Child | |
| BRIEF102 | Child | |
| MFFT (number of errors)103 | Child | |
| TOVA (visual and auditory omission)84 | Child | |
| Per cent on/off task104 | Observer | |
| Construct label: hyperactivity/impulsivity Construct definition: inability to manage activity levels appropriate to task and context. Fidgets, interrupts others, constantly in motion, inability to stay seated without excessive movement, restlessness, excessive talking, inability to engage in tasks quietly, impatience and inability to regulate emotions |
VADTRS; VADPRS (hyperactivity/impulsivity)101 | Parent |
| APRS (impulse control)105 | Teacher | |
| IOWA Conners’ Teacher Rating Scale (hyperactivity)106 | Teacher | |
| SCRS107 | Teacher | |
| ADHD (hyperactivity/impulsivity subtype)2 | Parent and teacher | |
| CRS;98 CRS-R (hyperactivity, DSM-IV hyperactivity/impulsivity)98 | Parent and teacher | |
| DBD (hyperactivity. impulsivity)99 | Parent and teacher | |
| Gordon’s Vigilance Task (impulsivity)108 | Child | |
| MFFT (commission)103 | Child | |
| TOVA (visual and auditory commission)84 | Child | |
| Construct label: ADHD combined type Construct definition: inability to focus and pay attention and to manage activity levels appropriate to task and context |
CSI-IV (ADHD)109 | Teacher |
| DBD (ADHD)99 | Teacher | |
| ADHD Rating Scale2 | Parent and teacher | |
| CBCL (ADHD)110 | Parent and teacher | |
| CRS;98 CRS-R (ADHD index, DSM-IV total)98 | Parent and teacher | |
| Construct label: externalising symptoms Construct definition: emotional and behavioural symptoms that are undercontrolled and externalised, for example fighting, bullying, defiance |
BASC-I (externalising composite score; aggression, conduct)111 | Parent |
| DBD (oppositional defiant, conduct disorder)99 | Teacher | |
| IOWA Conners’ Teacher Rating Scale (aggression)106 | Teacher | |
| SSQ112 | Teacher | |
| SSRS (problem behaviour subscale)113 | Teacher | |
| CBCL (delinquent, aggression, external)114,115 | Parent and teacher | |
| CRS;98 CRS-R (oppositional, conduct problems)98 | Parent and teacher | |
| ODD2 | Parent and teacher | |
| Pianta Conflict Scale116 | Parent and teacher | |
| Construct label: internalising symptoms Construct definition: emotional and behavioural symptoms that are overcontrolled and internalised, for example shyness, anxiety, withdrawal from social situations |
The Scale of Behavioural Problems (internalisation, anxiety)117 | Parent |
| CBCL (withdrawal, anxiety, depression, internalising)115,118 | Parent and teacher | |
| CRS;98 CRS-R98 (anxious/passive, emotional indulgent, perfectionism, anxiety)119 | Parent and teacher | |
| Piers-Harris Children’s Self-Concept Scale (anxiety)120 | Child | |
| Construct label: social skills Construct definition: capacity to communicate and interact with others effectively (including peers, siblings, teachers and parents) and appropriate to context |
Scale of Behavioural Problems (social adjustment)117 | Teacher |
| Merrell School Social Behaviour Scale (interpersonal skills)121 | Teacher | |
| Walker–McConnell Scale of Social Competence and School Adjustment122 | Teacher | |
| CBCL (social problems)110 | Parent and teacher | |
| CRS-R98 (asocial)98 | Parent and teacher | |
| IRS (social skills)123 | Parent and teacher | |
| SSRS (co-operation)113 | Parent and teacher | |
| Piers-Harris Children’s Self-Concept Scale (popularity)120 | Child | |
| Self-Esteem Inventory (social self subscale)124 | Child | |
| Construct label: school adjustment Construct definition: perceptions of scholastic behaviours encompassing adjustment to school. For example, achievement, motivation, productivity, and study skills (including time management and organisation) |
Homework Problem Checklist125 | Parent |
| Scale of Behavioural Problems (school problems)117 | Parent | |
| APRS (academic skills, productivity)105 | Teacher | |
| SSRS (academics)113 | Teacher | |
| IRS (classroom and academics)123 | Parent and teacher | |
| Children’s Organisational Skills (maladjustments)126 | Parent and teacher | |
| BASC-I (school maladjustment)111 | Child | |
| Piers-Harris Children’s Self-Concept Scale (intellectual, school status)120 | Child | |
| Self-Esteem Inventory (school, academics)124 | Child | |
| Dimensions of Self-Concept (academic interest, satisfaction)127 | Child | |
| Construct label: standardised achievement Construct definition: achievement in scholastic tasks as assessed by standardised intelligence and achievement tests |
CPM128 | Child |
| DIBELS (maths, reading)129 | Child | |
| Gates–MacGinitie Reading Tests (vocabulary, comprehension)130 | Child | |
| Gray Oral Reading Test (comprehension, fluency)131 | Child | |
| IOWA Test of Basic Skills (language)132 | Child | |
| Process Assessment of the Learner (reading, writing)133 | Child | |
| Wechsler Individual Achievement Test, Second Edition (numerical operations, maths fluency)134 | Child | |
| Wide Range Achievement Test, Third Edition (spelling, word reading)85 | Child | |
| Woodcock–Johnson Psychoeducational Test Battery135 | Child | |
| Construct label: curriculum achievement Construct definition: scholastic attainment on school-based curriculum tests and coursework |
School curriculum-based tests | Child |
| GPA | Child |
Conceptual synthesis: developing a classification system of interventions
As there was also a great deal of heterogeneity across interventions, MR developed a classification system of intervention content by reading and rereading descriptions of interventions (reported in the study papers and extracted as part of the data extraction phase) and identified (inductively) discrete ‘packages’ of interventions. Although some interventions target a combination of recipients including teacher, parents and children, we focused on the intervention packages that targeted the children alone. This process led to the identification of 15 ‘packages’ of techniques. The labels and definitions of these packages are reported in Table 4 and were developed using the descriptions of interventions in the included studies and reference to previous general classifications of behaviour change interventions. 136,137 These packages of interventions were categorised based on the similarity of active ingredients: (1) reward and punishment; (2) skills training and self-management; (3) creative-based therapies; and (4) physical treatments. Two packages (‘adaptations to learning environment’ and ‘information only’) could not be grouped into a higher-order category and were, therefore, categorised as ‘other’ packages. Packages in the ‘reward and punishment’ group are broadly based on the concepts of ‘rewards’ and ‘punishments’ originating from conditioning theories. 138 Self-management is more explicit in the ‘skills training and self-management’ group (as characterised by the skills training element) and can be broadly traced to self-regulation theories. 139 ‘Creative-based therapies’ include music and drama-based treatments, whereas ‘physical treatments’ target psychological processes indirectly via the physical body. ‘Information only’ refers to the provision of education only (independent of any further intervention), whereas ‘adaptations to learning environment’ refers to physical (e.g. change of seating arrangements in a classroom setting) and/or social adaptations (groups vs. one-to-one teaching format) implemented to enhance performance of the wanted behaviour(s) and/or a reduction in unwanted behaviour(s). The classification system was scrutinised conceptually by the other team members and subsequently used by MR (and checked by DM) to classify the text relating to the intervention(s) reported in the primary papers. The few disagreements were resolved through discussion between MR and DM. Teachers, parents and carers trained in managing children with ADHD were categorised as intervention providers and are detailed in Intervention delivery characteristics.
| Intervention | Definition |
|---|---|
| Reward and punishment | |
| 1. Contingency management | Systematic use of rewards and/or punishments to change, alter or redirect the child’s behaviour(s) |
| 2. DRC with contingency management | A method used in collaboration with a child to set goal(s) and monitor progress towards them. Rewards and/or punishments are then used in response to the child’s progress towards their goals in order to reinforce the wanted behaviour(s) or create barriers to the unwanted behaviour(s) |
| Skills training and self-management | |
| 3. Motivational beliefs | Encourage or facilitate the adoption of beliefs that facilitate self-motivation towards obtaining the focal behaviour(s) (e.g. the attribution of success at school to hard work and effort) |
| 4. Cognitive–behavioural self-regulation training | Establish methods for the child to self-monitor and record their behaviour(s). Includes analysing the factors that lead to problem behaviour(s) and identifying solutions to overcome them (‘problem solving’) and self-instruction on how to perform the behaviour(s) |
| 5. Cognitive retraining | Training and practice in the use of cognitive processes related to executive functioning (e.g. attention and working memory) |
| 6. Academic and study skills training | Training and practice in academic skills (e.g. reading and writing strategies) and general study strategies (e.g. note taking, test taking, organisation and time management) |
| 7. Social skills training | Training and practice in effective social interaction |
| 8. Emotional skills training | Training and practice in learning to recognise and control emotions (e.g. relaxation training and/or enhancing positive emotion) |
| 9. Biofeedback | Feedback about physiological or biochemical activity (e.g. heart rate and brain waves) using an external monitoring device to enhance self-control of wanted behaviour(s) |
| Creative-based therapy | |
| 10. Music therapy | Music used in a prescribed way to modify or alter thoughts, emotions and behaviours |
| 11. Play therapy | Play used in a prescribed way to modify or alter thoughts, emotions and behaviours |
| Physical treatment | |
| 12. Massage | Applying pressure to parts of the body (e.g. rubbing or kneading) in a prescribed way to modify or alter thoughts, emotions and behaviours |
| 13. Structured physical activity | Planned physical activity with the aim of increasing energy expenditure and improved physical fitness and health |
| Other packages | |
| 14. Adaptations to learning environment | Alteration to the environment (physical and social) where learning takes place and/or learning materials in order to facilitate performance of the wanted behaviour or create barriers to the unwanted behaviour (e.g. adapt teaching methods, tasks and classroom) |
| 15. Information | Provide information about focal behaviour(s) (e.g. information about positive peer relationships, communication skills) |
Statistical information
A data extraction form was developed to record the relevant statistical information for each trial meeting the inclusion criteria of review 1. For each relevant outcome/informant combination, post-test means, standard deviations (SDs) and sample sizes (or statistics that could be used to derive these) were extracted for the relevant treatment and control groups where available.
Effect size was calculated using the SMD, that is, the difference between the means in each of two groups divided by their pooled SD (Cohen’s d) with Hedges’ correction. 140 For continuous outcomes, the SMD and 95% CIs were calculated using the mean, SD and the sample size for intervention and control groups or, if these were not reported or were not available from the study authors, statistics that could be used to derive these (e.g. t statistic). For three studies that reported proportions rather than continuous data,141–143 the log-odds ratio was converted into a SMD [for formula see URL: www.campbellcollaboration.org/artman2/uploads/1/2_D_Wilson__Calculating_ES.pdf (accessed 16 December 2014)]. 144 For one study reporting change scores, the SMD was estimated by dividing the difference between the gain scores in each trial arm by the pooled SD while taking account of the pre–post correlations within each arm. The above calculations were performed using the online calculator at www.campbellcollaboration.org/escalc/html/EffectSizeCalculator-SMD1.php (accessed 16 December 2014). 144 For seven studies where the relevant empirical data were not reported or available from the study authors, only narrative synthesis was conducted. 141,162,180,186,191,192,198 All data were extracted by MR and checked by DM with all disagreements resolved successfully through discussion.
Quality appraisal was conducted simultaneously with data extraction using criteria adapted from the Cochrane risk of bias tool145 and an appraisal tool developed by Miller and Wilbourne. 146 The criteria assessed, reported in Table 5, consider selection bias (randomisation and allocation concealment for RCTs only); detection bias (blinding of outcome assessors); attrition bias [intention to treat (ITT) and response rate]; and use and length of follow-up(s). A trial was defined as meeting the ITT criteria when all participants remained in the intervention groups to which they were randomised and where data for all randomised participants were included in the analysis. 145 Quality appraisal decisions were made independently by two reviewers (DM and MR) and disagreements were resolved through discussion by these reviewers. The appraisals were used to evaluate study quality and were not used to exclude papers.
| Criteria | Coding |
|---|---|
| RCTs only | |
| What was the unit of randomisation? | Individual; cluster |
| Was the method used to generate randomisation specified? | Yes/no/partial |
| Was allocation concealment of randomisation reported? | Yes/no |
| Was ITT employed? | Yes/no |
| RCTs and non-RCTs | |
| Was blinding of assessor reported for one or more outcomes? | Yes/no |
| Was the response rate adequate? | 85–100%; 70–84%; < 70%; NR146 |
| Were follow-ups assessed? | Yes/no |
| Was the longest follow-up ≥ 6 months? | Yes/no |
Analytic strategy
Characteristics of the studies were summarised using means and SDs for continuous variables and percentages for categorical variables. Separate meta-analyses were conducted for each construct/informant combination (where data permitted). Tests of interaction using meta-regression were carried out to investigate whether or not study characteristics modified the effect of the interventions.
Meta-analysis
Random-effects meta-analysis models were fitted based on the assumption that the studies are estimating different effects. We are therefore estimating the average of multiple effects but, for simplicity, we generally refer to a singular pooled effect. To avoid underestimation of the standard error of the pooled estimate, when two or more measures assessing the same construct were reported in a given study, the estimated effects were combined into a summary effect for that study, applying a method that uses the correlations among the conceptually similar measures to calculate the 95% standard error for the study-specific estimate. 140 The correlations were obtained from the study report itself or unrelated papers that administered the outcomes and reported the correlations. In studies with two relevant active intervention groups, the outcome was combined across intervention groups based on the group-specific means, SDs and sample sizes using the ttesti command in Stata v.12.1 (StataCorp, College Station, TX, USA) prior to calculation of the SMD. Combining results across multiple treatment groups within studies before pooling avoids double counting participants in the control group and underestimating the standard error of the pooled effect size. 140
Final score means (adjusted for baseline where reported) were compared between groups; in three studies that reported comparisons at several time points over the duration of the intervention, effect sizes were calculated for each time point after the baseline observation and then averaged before entry into the meta-analyses. 159,160,197
Separate meta-analyses were conducted for RCTs and non-RCTs. Cohen’s65 guidelines were used to interpret effect sizes. Classifications for what are considered to be ‘small’, ‘medium’ and ‘large’ effect sizes are d+ = 0.20, d+ = 0.50 and d+ = 0.80, respectively.
Cochran’s (1954)147 test was used to assess evidence for heterogeneity, with a p-value < 0.05 taken to indicate evidence of heterogeneity. The I2 statistic (possible range 0–100%) was used to quantify the amount of between-study heterogeneity. 148 Values < 25% have been suggested to indicate low heterogeneity; values between 25% and 50% moderate heterogeneity; and values > 50% high heterogeneity. 148 Given that the Q test is sensitive to the number of included studies, the I2 statistic is our main method for identifying marked heterogeneity. 148
Publication bias was planned to be assessed by examining funnel plots for asymmetry using the metafunnel command in Stata v.12.1. 149 However, we were unable to assess funnel plots properly or use more advanced regression-based assessments to assess publication bias owing to the inadequate numbers of included trials and the substantial heterogeneity identified across studies. 150
Meta-regression analyses
Tests of interaction were performed using meta-regression to examine whether or not there was evidence that the pooled intervention effects differed across defined programme features. Planned analyses were conducted where there was evidence of heterogeneity (i.e. I2 values > 0%). 62 A range of programme features, including study details, participant characteristics, intervention package and intervention delivery elements were assessed.
Table 6 describes the potential moderators. Although a minimum of 10 studies is often cited as sufficient, there are no hard and fast rules, and, in light of the data collated, we adopted a lower threshold of eight studies. 140 For the dichotomised constructs, at least three studies were required to provide intervention effect data in each category of the potential moderator. Meta-regression models were fitted using the metareg command in Stata v.12.1. The Knapp and Hartung adjustment for multiple testing was adopted. 151 Adjusted R2, the proportion of between-cluster variability accounted for by the moderator variable, and I2, the proportion of residual between-study variation attributable to heterogeneity, were reported.
| Programme feature | Moderator |
|---|---|
| Study characteristic |
|
| Participant characteristics |
|
|
|
|
|
| Intervention packages |
|
|
|
| Delivery characteristics |
|
|
|
|
|
|
|
|
|
|
Empirical findings synthesised narratively
The findings from studies where meta-analysis was not appropriate or possible were summarised narratively.
Results
Number of studies included
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram152 in Figure 1 summarises the search process.
FIGURE 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram showing search process and study selection for review 1.

After the removal of duplicates, a total of 15,481 records were screened at title and abstract stage and a total of 655 potentially relevant articles were identified for which full texts were required. Of these, 567 (87%) were successfully retrieved, and of those that were not obtainable, 24 were foreign-language papers.
Research questions 1 and 2: evaluations that assess child outcomes
Fifty-four English-language papers met our full-text screening criteria and were included in the synthesis. Of the seven foreign-language papers retrieved and translated by BG, AJ, AV, SI, HK, none met our inclusion criteria.
Research question 3: evaluations that assess economic outcomes
Of the 54 studies that met the full-text screening criteria, there were no studies that included economic outcomes. Consequently, there are no further results in relation to research question 3 about the cost-effectiveness of interventions that target children with or at risk of ADHD in school settings.
Please refer to Appendix 3 for a complete list of reasons for the exclusion of 601 papers after full-text screening.
Descriptive statistics
Study and participant information: descriptive statistics
Fifty-four studies met the inclusion criteria, of which 39 were RCTs104,142,143,153–188 and 15 were non-RCTs. 141,189–202 Forty-seven contained data suitable for meta-analyses; seven studies141,162,180,186,191,192,198 included empirical data that could not be meta-analysed and that were, therefore, synthesised narratively. Three studies104,143,185 included some data that were meta-analysed and some data that were synthesised narratively. Tables 7 and 8 report on the study and participant characteristics for the RCTs (see Table 7) and non-RCTs (see Table 8). Ten studies155,153,163,169,178,184,186,192,198,202 were dissertations or theses (n = 10: 7 RCTs; 3 non-RCTs); the remaining were journal articles (n = 42:104,141–143,153,154,157–162,164–168,170,172–177,179–183,185,187–188,190,191,193–197,199–201 31 RCTs; 11 non-RCTs), a report (1 RCT)171 and a conference paper (1 non-RCT). 189 Studies were from North America (n = 44:104,141–143,153–169,171–176,178,179,181–184,188,189,191–194,197,198,200–202 33 RCTs; 11 non-RCTs); Europe (n = 6: 2 RCTs including one each from the Netherlands185 and Sweden;177 4 non-RCTs including 1 from Italy199 and 3 from Spain190,195,196); Asia (2 RCTs including 1 each from Iran170 and Jordan187); Africa (1 RCT)186 and New Zealand (1 RCT). 180 Forty-two studies104,141–143,153,155,156,159–168,170–173,177,180,182–187,189,190,192–202 included a treatment-as-usual or waitlist control (n = 42: 28 RCTs; 14 non-RCTs). Treatment as usual refers to a usual school routine and/or treatment obtained in the community relative to the participants in the study’s treatment arm. Eight RCTs154,157,158,174,175,176,181,188 and 1 non-RCT191 included comparators that were matched to the treatment group (i.e. irrelevant content, matched for time/contact). In the three studies169,178,179 where the control group included some but not all elements of the intervention, the unique components received by the treatment group were identified. Sample sizes were, on average, small and comprised fewer female than male students.
| First study author and year | Country | Publication status | Target(s) | Relevant treatment groups (n) | Type of control | Sample size | School level | Percentage of female participants | Percentage on medication for ADHD |
|---|---|---|---|---|---|---|---|---|---|
| aBarkley 2000104 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 2 | TAU | 119 | Elementary/primary | 36 | 0 |
| bBloomquist 1991153 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 2 | WLC | 52 | Elementary/primary | 31 | 0 |
| bCassar 2010154 | North America (Canada) | Journal article | Core symptoms and related symptoms | 1 | EXP | 6 | Elementary/primary | 50 | NR |
| bChacona 2008155 | North America (USA) | Thesis | Core symptoms | 1 | TAU | 60 | Elementary/primary | 30 | NR |
| bCloward 2003156 | North America (USA) | Thesis | Core symptoms | 1 | TAU | 8 | Elementary/primary | 38 | NR |
| bDenkowski 1984157 | North America (USA) | Journal article | Related symptoms and academic/study skills | 2 | EXP | 45 | Elementary/primary | NR | NR |
| bDenkowski 1983158 | North America (USA) | Journal article | Academic/study skills | 1 | EXP | 48 | Middle school | 0 | 0 |
| aDunson 1994143 | North America (USA) | Journal article | Core and related symptoms | 1 | TAU | 20 | Elementary/primary | 35 | Yes (% NR) |
| bEvans 2011159 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 49 | Middle school | 29 | 31 |
| bEvans 2007160 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 79 | Middle school | 23 | Yes (% NR) |
| bFabiano 2010161 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 63 | Elementary/primary | 14 | 52 |
| cFrame 2003162 | North America (USA) | Journal article | Related symptoms and academic/study skills | 1 | TAU | 65 | Elementary/primary | 30 | 83 |
| bHoover 1986163 | North America (USA) | Thesis | Core symptoms and academic/study skills | 1 | TAU | 70 | Elementary/primary | 43 | NR |
| bIseman 2011164 | North America (USA) | Journal article | Core symptoms and academic/study skills | 1 | TAU | 29 | Combination of school levels | 28 | 66 |
| bJurbergs 2010165 | North America (USA) | Journal article | Core symptoms and academic/study skills | 2 | TAU | 45 | Elementary/primary | 26% (of 43) | 23% (of 43) |
| bKhilnani 2003166 | North America (USA) | Journal article | Core and related symptoms | 1 | WLC | 30 | Combination of school levels | 20 | NR |
| bLangberg 2012167 | North America (USA) | Journal article | Core symptoms and academic/study skills | 1 | WLC | 47 | Middle school | 23 | 66 |
| bLangberg 2008168 | North America (USA) | Journal article | Academic/study skills | 1 | WLC | 37 | Elementary/primary | 16 | 43 |
| bLomas 2002169 | North America (USA) | Thesis | Core and related symptoms | 1 | ADD | 33 | Elementary/primary | 18 | 67 |
| bLooyeh 2012170 | Asia (Iran) | Journal article | Core symptoms | 1 | WLC | 14 | Elementary/primary | 100 | 0 |
| bMcGraw 2004171 | North America (USA) | Report | Academic/study skills | 1 | WLC | 53 | Middle school | 30 | NR |
| bMolina 2008172 | North America (USA) | Journal article | Related symptoms and academic/study skills | 1 | TAU | 23 | Middle school | 25 | 30 |
| bMurray 2008173 | North America (USA) | Journal article | Core symptoms and academic/study skills | 1 | TAU | 24 | Elementary/primary | 29 | 88 |
| bOmizo 1980174 | North America (USA) | Journal article | Core and academic/study skills | 1 | EXP | 56 | Middle school | 0 | 0 |
| bOmizo 1980175 | North America (USA) | Journal article | Related symptoms and academic/study skills | 1 | EXP | 52 | Elementary/primary | 0 | 0 |
| bOmizo 1982176 | North America (USA) | Journal article | Core symptoms | 1 | EXP | 32 | Elementary/primary | 0 | NR |
| bOstberg 2012177 | Europe (Sweden) | Journal article | Core and related symptoms | 1 | TAU | 70 | Elementary/primary | 16% (of 61) | 82% (of 61) |
| bPoley 1996178 | North America (USA) | Thesis | Core symptoms | 1 | ADD | 26 | Elementary/primary | 12 | 85 |
| bRabiner 2010142 | North America (USA) | Journal article | Core symptoms and academic/study skills | 2 | TAU | 77 | Elementary/primary | 31 | 7 |
| bReid 1987179 | North America (USA) | Journal article | Core symptoms and academic/study skills | 1 | ADD | 77 | Elementary/primary | NR | 0 |
| cRickson 2003180 | Australasia (New Zealand) | Journal article | Related symptoms | 2 | WLC | 18 | High school/secondary | 0 | 50 |
| bRivera 1980181 | North America (USA) | Journal article | Core symptoms | 1 | EXP | 36 | Elementary/primary | 0 | 0 |
| bSeeley 2009182 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 42 | Elementary/primary | 7 | 10 |
| bSteiner 2011183 | North America (USA) | Journal article | Core symptoms | 2 | WLC | 41 | Elementary/primary | 48 | 60 |
| bStorer 1994184 | North America (USA) | Thesis | Core and related symptoms | 2 | TAU | 24 | High school/secondary | 25 | NR |
| avan Lier 2004185 | Europe (the Netherlands) | Journal article | Core and related symptoms | 1 | TAU | 92 (class I) | Elementary/primary | 22 | NR |
| cVan der Westhuizen 2007186 | Africa (South Africa) | Thesis | Core symptoms and academic/study skills | 1 | WLC | 12 | Elementary/primary | 17 | 8 |
| bZaghlawan 2007187 | Asia (Jordan) | Journal article | Core symptoms | 1 | TAU | 60 | Elementary/primary | 45 | 0 |
| bZentall 2012188 | North America (USA) | Journal article | Academic/study skills | 1 | EXP | 17(ADHD) | Elementary/primary | 71 | NR |
| First study author and year | Country | Publication status | Target(s) | Relevant treatment groups (n) | Type of control | Sample size | Grade level | Percentage of female participants | Percentage on medication for ADHD |
|---|---|---|---|---|---|---|---|---|---|
| aAbikoff 1983189 | North America (USA) | Conference paper | Academic/study skills | 1 | TAU | 20 | Elementary/primary | 0 | 100 |
| aBornas 1992190 | Europe (Spain) | Journal article | Core symptoms and academic/study skills | 1 | TAU | 21 | Elementary/primary | 48 | NR |
| bEastman 1981191 | North America (USA) | Journal article | Core symptoms and academic/study skills | 1 | EXP | 11 | Elementary/primary | NR | NR |
| bEvans 2005141 | North America (USA) | Journal article | Related symptoms and academic/study skills | 1 | TAU | 27 | Middle school | 22 | 81 |
| bHarper 1996192 | North America (USA) | Thesis | Core and related symptoms | 2 | WLC | 33 | Elementary/primary | NR | 100 |
| aKapalka 2005193 | North America (USA) | Journal article | Core symptoms | 1 | TAU | 86 | Elementary/primary | 0% | Yes (% NR) |
| aKendrick 1995194 | North America (USA) | Journal article | Related symptoms and academic/study skills | 1 | TAU | 54 | Elementary/primary | 15 | Yes (% NR) |
| aMiranda 2006195 | Europe (Spain) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 33 | Elementary/primary | 12 | 0 |
| aMiranda 2002196 | Europe (Spain) | Journal article | Core and related symptoms and academic/study skills | 1 | TAU | 50 | Elementary/primary | 16 | 0 |
| aOwens 2005197 | North America (USA) | Journal article | Core and related symptoms and academic/study skills | 1 | WLC | 42 | Elementary/primary | 29 | 40 |
| bPoillion 1993198 | North America (USA) | Thesis | Core symptoms and academic/study skills | 1 | TAU | 106 | Elementary/primary | 39 | NR |
| aRe 2007199 | Europe (Italy) | Journal article | Core symptoms | 1 | TAU | 10 | Nursery/preschool | 50 | NR |
| aSemrud-Clikeman 1999200 | North America (USA) | Journal article | Core symptoms | 1 | TAU | 33 | Middle school | 16 | Yes (% NR) |
| aVerret 2012201 | North America (Canada) | Journal article | Core and related symptoms | 1 | TAU | 21 | Elementary/primary | 10 | 67 |
| aWebber 2012202 | North America (USA) | Thesis | Core symptoms and academic/study skills | 1 | TAU | 24 | Elementary/primary | 42 | Yes (% NR) |
The mean (SD) sample size was 44.9 (24.81) children or young people for the RCTs and comprised, on average, a mean (SD) of 26% (0.21) females. For the non-RCTs, the mean (SD) sample size was 38.1 (26.0) and comprised, on average, a mean (SD) of 23% (0.17) females. Some of the studies described participants as using medication for ADHD (n = 28: 19 RCTs;142,143,159–162,164,165,167–169,172,173,177,178,180,182,183,186 9 non-RCTs141,189,192–194,197,200–202) whereas some reported that no medication for ADHD was used (n = 11: 9 RCTs;104,153,158,170,174,175,179,181,187 two non-RCTs195,196). The reports for the remaining 15 studies did not clarify whether or not medication for ADHD was used (n = 15: 11 RCTs;154–157,163,166,171,176,184,185,188 4 non-RCTs190,191,198,199). The majority of intervention programmes targeted children at elementary/primary school level (n = 40: 28 RCTs;104,142,143,153–157,161–163,165,168–170,173,175–179,181–183,185–188 12 non RCTs189–198,201,202); with some that targeted children at middle school (n = 9: 7 RCTs;158–160,167,171,172,174 2 non-RCT141,200); high school (n = 2: 2 RCTs180,184) and preschool (n = 1: 1 non-RCT199). Only two studies included children at more than one school level (n = 2: 2 RCTs164,166).
Interventions
Of the 54 studies, 10 included two relevant treatment groups (n = 10: 8 RCTs;104,142,153,157,165,180,183,184 2 non-RCTs190,192); the remaining studies included one relevant treatment group each. Thus, there were a total of 64 relevant intervention groups across the 54 studies (n = 64: 47 RCTs; 17 non-RCTs). Frequency of intervention packages across the treatment groups for the studies that were RCTs and non-RCTs are presented in Tables 9 and 10, respectively, where the frequency and types of packages in each treatment group are reported and identified. With the exception of ‘structured physical activity’, all intervention packages were identified among the 47 treatment groups specified in the 39 RCTs with contingency management (n = 19104,142,143,153,159–161,165,167,168,172,173,177,182,185,187) being identified most frequently, followed by academic skills training (n = 12104,142,159,160,163,164,167,168,172,178,188); emotional skills training (n = 11104,153,157,158,162,174–176,181); self-regulation (n = 10104,153,156,163,164,172,178,184); biofeedback (n = 8157,158,174–176,181,183,186); daily report card (DRC) (n = 7104,143,161,165,173); social skills training (n = 6104,159,160,172,182); cognitive skills retraining (n = 4142,169,171,182); adaptation to the learning environment (n = 3143,154,187); music therapy (n = 3155,180); motivational beliefs (n = 2179,188); information only (n = 1184); play therapy (n = 1170); and massage (n = 1166). At the level of the higher-order group, using the total number of intervention packages identified within and across the RCTs (n = 88) as the denominator, packages within the ‘skills training and self-management’ group were most frequently identified (n = 53104,142,153,156–160,162–164,167–169,171,172,174–176,178–184,186,188) followed by packages within ‘reward and punishment’ (n = 26104,142,143,153,159–161,165,167,168,172,173,177,182,185,187); ‘adaptations to the environment’ (n = 3143,154,187); ‘creative-based therapies’ (n = 4155,170,180); ‘physical treatments’ (n = 1166); and ‘information only’ (n = 1184) subgroups. Within each treatment group, the number of intervention packages ranged from one to six. Using the total number of RCT treatment groups as the denominator (n = 47), 45% (n = 21154–157,162,165,166,169–171,177,179,180,183–186) included one package; 38% (n = 18142,153,157,158,161,163–165,167,168,173–177,178,181,182,187,188) two treatment packages; 11% (n = 5143,153,159,160) three treatment packages; 2% (n = 1172) four treatment packages; and 4% (n = 2104) six treatment packages.
| First study author and year | Reward and punishment | Skills training and self-management | Creative therapies | Physical treatment | Other packages | n packages per treatment group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Contingency management | DRC with behaviour modification | Motivational beliefs | Cognitive–behavioural self-regulation | Cognitive skills retraining | Academic and study skills training | Social skills training | Emotional skills training | Biofeedback | Music therapy | Play therapy | Massage | Structured physical activity | Adaptations to learning environment | Information only | ||
| aBarkley 2000104 (tg2) | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||||||
| aBarkley 2000104 (tg3) | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||||||
| bBloomquist 1991153 (tg2) | 1 | 1 | 1 | 3 | ||||||||||||
| bBloomquist 1991153 (tg3) | 1 | 1 | 2 | |||||||||||||
| bCassar 2010154 | 1 | 1 | ||||||||||||||
| bChacona 2008155 | 1 | 1 | ||||||||||||||
| bCloward 2003156 | 1 | 1 | ||||||||||||||
| bDenkowski 1984157 (tg1) | 1 | 1 | ||||||||||||||
| bDenkowski 1984157 (tg2) | 1 | 1 | 2 | |||||||||||||
| bDenkowski 1983158 | 1 | 1 | 2 | |||||||||||||
| aDunson 1994143 | 1 | 1 | 1 | 3 | ||||||||||||
| bEvans 2011159 | 1 | 1 | 1 | 3 | ||||||||||||
| bEvans 2007160 | 1 | 1 | 1 | 3 | ||||||||||||
| bFabiano 2010161 | 1 | 1 | 2 | |||||||||||||
| cFrame 2003162 | 1 | 1 | ||||||||||||||
| bHoover 1986163 | 1 | 1 | 2 | |||||||||||||
| bIseman 2011164 | 1 | 1 | 2 | |||||||||||||
| bJurbergs 2010165 (tg1) | 1 | 1 | ||||||||||||||
| bJurbergs 2010165 (tg2) | 1 | 1 | 2 | |||||||||||||
| bKhilnani 2003166 | 1 | 1 | ||||||||||||||
| bLangberg 2012167 | 1 | 1 | 2 | |||||||||||||
| bLangberg 2008168 | 1 | 1 | 2 | |||||||||||||
| bLomas 2002169 | 1 | 1 | ||||||||||||||
| bLooyeh 2012170 | 1 | 1 | ||||||||||||||
| bMcGraw 2004171 | 1 | 1 | ||||||||||||||
| bMolina 2008172 | 1 | 1 | 1 | 1 | 4 | |||||||||||
| bMurray 2008173 | 1 | 1 | 2 | |||||||||||||
| bOmizo 1980174 | 1 | 1 | 2 | |||||||||||||
| bOmizo 1980175 | 1 | 1 | 2 | |||||||||||||
| bOmizo 1982176 | 1 | 1 | 2 | |||||||||||||
| bOstberg 2012177 | 1 | 1 | ||||||||||||||
| bPoley 1996178 | 1 | 1 | 2 | |||||||||||||
| bRabiner 2010142 (tg1) | 1 | 1 | 2 | |||||||||||||
| bRabiner 2010142 (tg2) | 1 | 1 | 2 | |||||||||||||
| cRickson 2003180 (tg1) | 1 | 1 | ||||||||||||||
| cRickson 2003180 (tg2) | 1 | 1 | ||||||||||||||
| bRivera 1980181 | 1 | 1 | 2 | |||||||||||||
| bReid 1987179 (tg1) | 1 | 1 | ||||||||||||||
| bSeeley 2009182 | 1 | 1 | 2 | |||||||||||||
| bSteiner 2011183 (tg1) | 1 | 1 | ||||||||||||||
| bSteiner 2011183 (tg2) | 1 | 1 | ||||||||||||||
| bStorer 1994184 (tg1) | 1 | 1 | ||||||||||||||
| bStorer 1994184 (tg2) | 1 | 1 | ||||||||||||||
| cVan der Westhuizen 2007186 | 1 | 1 | ||||||||||||||
| avan Lier 2004185 | 1 | 1 | ||||||||||||||
| bZaghlawan 2007187 | 1 | 1 | 2 | |||||||||||||
| Zentall 2012188 | 1 | 1 | 2 | |||||||||||||
| Frequency of treatment package (n) across studies and treatment groups | 19 | 7 | 2 | 10 | 4 | 12 | 6 | 11 | 8 | 3 | 1 | 1 | 0 | 3 | 1 | |
| Frequency of treatment package (%) across studies and treatment groups (denominator = 47 treatment groups) | 40 | 15 | 4 | 21 | 9 | 26 | 13 | 23 | 17 | 6 | 2 | 2 | 0 | 6 | 2 | |
| First study author and year | Reward and punishment | Skills training and self-management | Creative therapies | Physical treatment | Other packages | n packages per treatment group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Contingency management | DRC with behaviour modification | Motivational beliefs | Cognitive–behavioural self-regulation | Cognitive skills retraining | Academic and study skills training | Social skills training | Emotional skills training | Biofeedback | Music therapy | Play therapy | Massage | Structured physical activity | Adaptations to learning environment | Information only | ||
| aAbikoff 1983189 | 1 | 1 | 2 | |||||||||||||
| aBornas 1992190 (tg1) | 1 | 1 | 2 | |||||||||||||
| aBornas 1992190 (tg2) | 1 | 1 | 2 | |||||||||||||
| bEastman 1981191 | 1 | 1 | ||||||||||||||
| bEvans 2005141 | 1 | 1 | 1 | 3 | ||||||||||||
| bHarper 1996192 (tg1) | 1 | 1 | ||||||||||||||
| bHarper 1996192 (tg2) | 1 | 1 | ||||||||||||||
| aKapalka 2005193 | 1 | 1 | ||||||||||||||
| aKendrick 1995194 | 1 | 1 | 2 | |||||||||||||
| aMiranda 2006195 (tg1) | 1 | 1 | 1 | 3 | ||||||||||||
| aMiranda 2002196 | 1 | 1 | 1 | 1 | 4 | |||||||||||
| aOwens 2005197 | 1 | 1 | 2 | |||||||||||||
| bPoillion 1993198 (tg2) | 1 | 1 | ||||||||||||||
| aRe 2007199 | 1 | 1 | ||||||||||||||
| aSemrud-Clikeman 1999200 | 1 | 1 | 2 | |||||||||||||
| aVerret 2012201 | 1 | 1 | ||||||||||||||
| aWebber 2012202 | 1 | 1 | 1 | 3 | ||||||||||||
| Frequency of treatment package (n) across studies and treatment groups | 7 | 2 | 0 | 7 | 3 | 5 | 3 | 0 | 1 | 0 | 0 | 0 | 1 | 3 | 0 | |
| Frequency of treatment package (%) across studies and treatment groups (denominator = 17 treatment groups) | 41 | 12 | 0 | 41 | 18 | 29 | 18 | 0 | 6 | 0 | 0 | 0 | 6 | 18 | 0 | |
Nine of the 15 types of intervention packages were reported for the 17 treatment groups specified in the 15 non-RCTs. The most frequently identified package was again contingency management (n = 7141,193–197,202) followed by cognitive–behavioural self-regulation (n = 7189–191,195,196,200); academic skills training (n = 5141,189,190,196); cognitive skills retraining (n = 3199,200,202); social skills training (n = 3141,192); adaptation to the environment (n = 3195,196,198); DRC (n = 2194,197); biofeedback (n = 1202); and physical activity (n = 1201). When analysed at the level of the higher-order group, using the total number of intervention packages within and across the non-RCTs (n = 32) as the denominator, packages most frequently identified were in ‘skills training and self-management’ (n = 19141,189–192,196,199,200,202), followed by ‘reward and punishment’ (n = 9141,193–197,202), ‘adaptations to learning environment’ (n = 3195,196,198) and ‘physical treatments’ (n = 1201). The number of intervention packages reported per treatment group ranged from one to four. Using the total number of non-RCT interventions as the denominator (n = 17) the percentage of treatment conditions including one treatment package was 41% (n = 7191–193,198,199,201); two treatment packages, 35% (n = 6189,190,194,197,200); three treatment packages ,18% (n = 3141,195,202); and four treatment packages, 6% (n = 1).
Intervention delivery characteristics
Tables 11 and 12 report on the intervention delivery characteristics for each treatment group among the RCTs (see Table 11) and non-RCTs (see Table 12).
| First study author and year | Multicontext? | School location | Time | Format | Provider | Training provided? | Duration (weeks) | Intensity (hours) | Fidelity assessed? |
|---|---|---|---|---|---|---|---|---|---|
| aBarkley 2000104 | School (tg2); school and home (tg3) | Classroom (tg2 and tg3) | Usual school hours (tg2 and tg3) | Classroom, group; individual (tg2 and tg3) | Teacher (tg2 and tg3) | Yes (tg2 and tg3) | 36 (tg2 and tg3) | NR (tg2 and tg3) | Yes (tg2 and tg3) |
| bBloomquist 1991153 | School and home (tg1); school (tg2) | Classroom/NR (tg1); classroom (tg2) | Usual school hours (tg2 and tg3) | Group (tg1); classroom (tg2) | SMH; teacher; student/researcher (tg1); teacher (tg2) | Yes (tg1 and tg2) | 10 (tg1 and tg2) | 20 (tg1 and tg2) | Yes (tg1 and tg2) |
| bCassar 2010154 | School | NR | Usual school hours | Group | Student/researcher | NR | 6 | 12 | No/NR |
| bChacona 2008155 | School | Other school room | Usual school hours | Group | Teacher | NR | 7 | 7 | No/NR |
| bCloward 2003156 | School | Classroom | Usual school hours | Classroom | Teacher | Yes | NR | NR | No/NR |
| bDenkowski 1984157 | School (tg1 and tg2) | NR (tg1 and tg2) | Usual school hours (tg1 and tg2) | Group (tg1); individual (tg2) | Student/researcher (tg1 and tg2) | NR (tg1 and tg2) | 8 (tg1 and tg2) | 3.3 (tg1 and tg2) | No/NR (tg1 and tg2) |
| bDenkowski 1983158 | School | NR | Usual school hours | Individual | SMH | NR | 12 | 2.5 | No/NR |
| aDunson 1994143 | School | Classroom | Usual school hours | Individual | Teacher | Yes | 2 | NR | Yes |
| bEvans 2011159 | School and home | NR | Before and after usual school hours | Individual; group | Student/researcher | Yes | 20 | 86 | Yes |
| bEvans 2007160 | School and home | NR | Usual school hours | Individual; group | Variable | Yes | 156 | NR | Yes |
| bFabiano 2010161 | School and home | Classroom | Usual school hours | Individual | Teacher | Yes | 28 | NR | Yes |
| cFrame 2003162 | School | NR | NR | Group | SMH | NR | 4 | NR | No/NR |
| bHoover 1986163 | School | Classroom | Usual school hours | Individual; group | Teacher | Yes | 8 | 6.66 | No/NR |
| bIseman 2011164 | School | Classroom | Usual school hours | Classroom | Teacher | Yes | 1.4 | 1.66 | Yes |
| bJurbergs 2010165 | School (tg1); school and home (tg2) | Classroom (tg1 and tg2) | Usual school hours (tg1 and tg2) | Individual (tg1 and tg2) | Teacher (tg1 and tg2) | Yes (tg1 and tg2) | 5 (tg1 and tg2) | NR (tg1 and tg2) | Yes (tg1 and tg2) |
| bKhilnani 2003166 | School | Other school room | Usual school hours | Individual | Other practitioner | NR | 4 | 2.66 | No/NR |
| bLangberg 2012167 | School and home | NR | Usual school hours | Individual | SMH | Yes | 13.8 | 5.18 | Yes |
| bLangberg 2008168 | School and home | NR | Before and after usual school hours | Individual; group | Student/researcher | Yes | 8 | 20 | Yes |
| bLomas 2002169 | School | NR | Usual school hours | NR | NR | Yes | 14 | 42 | No/NR |
| bLooyeh 2012170 | School | NR | Before and after usual school hours | Group | SMH | NR | 6 | 12 | No/NR |
| bMcGraw 2004171 | School | NR | Usual school hours | Group | Student/researcher | NR | Variable | Variable | No/NR |
| bMolina 2008172 | School and home | NR | Before and after usual school hours | Individual; group | Student/researcher | Yes | 10 | 40 | No/NR |
| bMurray 2008173 | School and home | Classroom | Usual school hours | Individual | Teacher | Yes | 13.6 | NR | Yes |
| bOmizo 1980174 | School | Other school room | NR | Individual | SMH | NR | 9 | 0.85 | No/NR |
| bOmizo 1980175 | School | Other school room | Usual school hours | Individual | NR | NR | NR | NR | No/NR |
| bOmizo 1982176 | School | Other school room | Usual school hours | Individual | SMH | NR | 8 | 1.66 | No/NR |
| bOstberg 2012177 | School and home | Classroom | Before and after usual school hours | Classroom | Teacher | Yes | 10 | NR | No/NR |
| bPoley 1996178 | School | Classroom | Usual school hours | Classroom | Student/researcher; teacher | Yes | 4 | 6 | No/NR |
| bRabiner 2010142 | School (tg1 and tg2) | NR (tg1 and tg2) | Before and after usual school hours (tg1 and tg2) | Group (tg1 and tg2) | Student/researcher; school staff (unspecified) (tg1 and tg2) | Yes (tg1 and tg2) | 14 (tg1 and tg2) | 35 (tg1 and tg2) | Yes (tg1 and tg2) |
| bReid 1987179 | School | Other school room | Usual school hours | NR | Other practitioner | Yes | NR | NR | No/NR |
| cRickson 2003180 | School (tg1 and tg2) | NR (tg1 and tg2) | NR (tg1 and tg2) | Group (tg1 and tg2) | Other practitioner (tg1 and tg2) | NR (tg1 and tg2) | 8 (tg1 and tg2) | 10 (tg1 and tg2) | No/NR (tg1 and tg2) |
| bRivera 1980181 | School | Other school room | Usual school hours | Individual | NR | NR | 1.2 | 0.4 | No/NR |
| bSeeley 2009182 | School and home | Classroom | Usual school hours | Classroom | Teacher; other practitioner | Yes | 12 | Variable | Yes |
| bSteiner 2011183 | School (tg1 and tg2) | NR (tg1 and tg2) | Usual school hours (tg1 and tg2) | Group (tg1 and tg2) | Student/researcher (tg1 and tg2) | Yes (tg1 and tg2) | 16 (tg1 and tg2) | 24 (tg1 and tg2) | Yes (tg1 and tg2) |
| bStorer 1994184 | School (tg1 and tg2) | Other school room (tg1 and tg2) | Usual school hours (tg1 and tg2) | Group (tg1 and tg2) | Student/researcher (tg1 and tg2) | NR (tg1 and tg2) | 4 (tg1 and tg2) | 6 (tg1 and tg2) | No/NR |
| cVan der Westhuizen 2007186 | School | NR | NR | Individual | Other practitioner | Yes | 11 | NR | No/NR |
| avan Lier 2004185 | School | Classroom | Usual school hours | Group/classroom | Teacher | Yes | 72 | NR | Yes |
| bZaghlawan 2007187 | School | Classroom | Usual school hours | Classroom | Teacher | Yes | 6 | Variable | Yes |
| bZentall 2012188 | School | Other school room | Usual school hours | Individual | NR | NR | NR | NR | No/NR |
| First study author and year | Multicontext? | School location | Time | Format | Provider | Training provided? | Duration (weeks) | Intensity (hours) | Fidelity assessed? |
|---|---|---|---|---|---|---|---|---|---|
| aAbikoff 1983189 | School | Other school room | Unusual school hours | Individual | NR | NR | 10 | NR | No/NR |
| aBornas 1992190 | School (tg1 and tg2) | Classroom and other school room (tg1 and tg2) | Unusual school hours (tg1 and tg2) | NR (tg1 and tg2) | NR (tg1 and tg2) | Yes (tg1 and tg2) | NR (tg1 and tg2) | 22 | No/NR (tg1 and tg2) |
| bEastman 1981191 | School | Classroom and other school room | Unusual school hours | Individual | Teacher | NR | 16 | NR | No/NR |
| bEvans 2005141 | School and home | NR | Before and after unusual school hours | Individual; group | NR | NR | 36 | 243 | No/NR |
| bHarper 1996192 | School (tg1 and tg2) | Classroom (tg1 and tg2) | Unusual school hours (tg1 and tg2) | Classroom (tg1 and tg2) | Student/researcher (tg1 and tg2) | Yes (tg1 and tg2) | 8 (tg1 and tg2) | 16 (tg1 and tg2) | No/NR (tg1 and tg2) |
| aKapalka 2005193 | School | Classroom | Unusual school hours | Individual | Teacher | Yes | NR | NR | No/NR |
| aKendrick 1995194 | School | Classroom | Unusual school hours | Individual | Teacher | NR | 6 | NR | No/NR |
| aMiranda 2006195 | School | Classroom | Unusual school hours | Classroom | Teacher | Yes | 16 | NR | No/NR |
| aMiranda 2002196 | School | Classroom | Unusual school hours | Classroom | Teacher | Yes | NR | NR | No/NR |
| aOwens 2005197 | School and home | Classroom | Unusual school hours | Individual; classroom; group | Teacher and other practitioner | Yes | 36 | NR | Yes |
| bPoillion 1993198 | School | NR | Unusual school hours | NR | Teacher | Yes | NR | NR | No/NR |
| aRe 2007199 | School | Classroom | Unusual school hours | Classroom/group | Teacher and other practitioner | NR | 9 | 18 | No/NR |
| aSemrud 1999200 | School | NR | Before and after unusual school hours | Group | Student/researcher | NR | 18 | 36 | No/NR |
| aVerret 2012201 | School | Other school room | Unusual school hours | Group | Other practitioner | NR | 10 | 22.5 | No/NR |
| aWebber 2012202 | School | Other school room | Unusual school hours | Group | Student/researcher | NR | NR | NR | No/NR |
Intervention location, format and time
Of the 64 treatment groups identified across all 54 included studies, 14 included elements delivered in both school and home settings (n = 14: 12 RCTs;104,153,159–161,165,167,168,172,173,177,182 2 non-RCT141,197) whereas the rest were based at school only (n = 50: 35 RCTs;104,142,143,153–158,162–166,169–171,174–176,178–181,183–188 15 non-RCTs189–196,198–202). Twenty-eight interventions were delivered in the classroom either entirely (n = 24: 16 RCTs;104,143,153,156,161,163–165,173,177,178,182,185,187 8 non-RCTs192–197,199) or partially (n = 4: 1 RCT,153 3 non-RCTs190,191). Of these, some interventions targeted children individually (n = 8: 5 RCTs;104,143,161,173 3 non-RCTs191,193,194); some in groups or class-wide (n = 13: 8 RCTs;153,156,164,177,178,182,185,187 5 non-RCTs192,195,196,199) and some a combination of individual, group and class-wide formats (n = 4: 3 RCTs;104,163 1 non-RCT197). The precise format was unclear for two non-RCTs.
Some of the interventions that were not delivered in a classroom were delivered in school rooms other than classrooms, such as gymnasiums and music rooms (n = 13: 10 RCTs;155,174–176,179,181,184,188 3 non-RCTs189,201,202); contextual information about delivery was not reported for the remaining interventions (n = 23: 20 RCTs;142,153,154,157–160,162,167–172,180,183,186 3 non-RCTs141,198,200). Of the interventions delivered in settings other than classrooms, some were delivered in group format (n = 17: 14 RCTs;142,153–155,157,162,170,171,180,183,184 3 non-RCTs200–202); some individually (n = 11: 10 RCTs;158,166,167,174–176,181,186,188 1 non-RCT189); some a combination of individual and group formats (n = 5: 4 RCTs;159,160,168,172 1 non-RCT141); and for the rest the format of the intervention was unclear or not reported (n = 3: 2 RCTs;169,179 1 non-RCT198).
Interventions took place primarily during normal school hours (n = 51: 36 RCTs;104,143,153–158,160,161,163–167,169,171,173,175–179,181–185,187,188 15 non-RCTs189–199,201,202). Some, however, were conducted before or after usual school hours (n = 8: 6 RCTs;142,159,168,170,172 2 non-RCTs141,200). Information on intervention timing was not reported for the remaining interventions (n = 5: 5 RCTs162,174,180,186).
Intervention provider(s)
Interventions were delivered by a range of providers including teachers (n = 21: 15 RCT;104,143,155,156,161,163–165,173,177,185,187 6 non-RCTs191,193–196,198); university students/researchers (n = 15: 11 RCTs;154,157,159,168,171,172,183,184 4 non-RCTs192,200,202); school mental health providers (n = 6: 6 RCTs158,162,167,170,174,176); other practitioners (n = 6: 5 RCTs;166,179,180,186 1 non-RCT201); a combination of student/researchers and teachers (n = 1: 1 RCT178); a combination of student/researchers and other school staff (n = 2: 2 RCTs142); a combination of teachers and other practitioners (n = 3: 1 RCT;182 2 non-RCTs197,199) and a combination of school mental health providers, teachers and student/researchers (n = 1: 1 RCT153). Provider information for eight interventions was not reported (n = 9: five RCTs;169,175,181,188 4 non-RCTs141,189,190).
Training
Training for intervention providers was reported in 38 treatment groups (n = 38: 29 RCTs;104,142,143,153,156,159–161,163–165,167–169,172,173,177–179,182,183,185–187 9 non-RCTs190,192,193,195–198). The remaining 26 treatment groups did not mention any training requirements or recommendations (n = 26: 18 RCTs;154,155,157,158,162,166,170,171,174–176,180,181,184,188 8 non-RCTs141,189,191,194,199–202), although providers in nine of these interventions included school mental health providers and/or independent clinicians who were presumably skilled in relation to the therapeutic intervention (n = 9: 7 RCTs;158,162,166,170,174,176,180 2 non-RCTs199,201).
Intervention length and dosage
The average length of interventions among RCTs was reported for 42 out of 47 interventions104,142,143,153–155,157–174,176–178,180–187 and ranged from 1.2 to 156 weeks (mean = 15.5; SD = 25.4 weeks), whereas 11 out of 17 non-RCTs141,189,191,192,196,195,197,199–201 reported intervention length that ranged from 6 to 36 weeks (mean = 16.7; SD = 10.5 weeks). The total dosage of interventions was reported in 28 out of 47 of the RCTs142,153–155,157–159,163,164,166–172,174,176,178,180–184,187 and 7 out of 17 of the non-RCTs. 141,190,192,199–201 For RCTs, reported duration ranged from 0.4 to 86 hours (mean = 15.8; SD = 18.6 hours) and for non-RCTs, from 22 to 243 hours (mean = 59.6; SD = 90.1 hours).
Quality of trials
Table 13 reports on the quality of trials for the RCTs and non-RCTs.
Unit of randomisation and description of randomisation process
Nine of the 39 RCTs were randomised at the cluster level (seven at the class level;143,156,162,164,178,182,185 two at the school level153,160); the remaining 30 studies were randomised at the level of the individual. Twelve studies104,154,157,158,167,172,174–177,181,188 randomised at the individual level used matched or stratified allocation. Ten of the 39 RCTs155,158,169,171,174–176,181,183,184 provided a description of the randomisation process. Only one trial155 was identified as having made a good attempt at allocation concealment and the prevention of inadvertent disclosure of assignment. The remaining 38 studies stated that they had used random allocation without providing adequate description of the randomisation procedures.
| First study author and year | Unit of randomisation | Method used to generate randomisation specified? | Allocation concealment? | ITT? | Blinding of outcome assessor? | Response rate at longest follow-up | Included follow-up(s)? | Longest follow-up 6 months or longer? | RCT or non-RCT? | Included in meta-analysis? |
|---|---|---|---|---|---|---|---|---|---|---|
| Abikoff 1983189 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Bornas 1992190 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✓ | ✓ | Non-RCT | Meta-analysed |
| Barkley 2000104 | Individual (stratification within gender) | ✗ | ✗ | ✗ | ✓ | 85–100% | ✓ | ✓ | RCT | Meta-analysed |
| Bloomquist 1991153 | Group: school | ✗ | ✗ | ✗ | ✓ | < 70% | ✓ | ✗ | RCT | Meta-analysed |
| Cassar 2010154 | Individual (matched) | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Chacona 2008155 | Individual | ✓ | ✓ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Cloward 2003156 | Group: class | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Denkowski 1984157 | Individual (matched) | ✗ | ✗ | ✗ | ✓ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Denkowski 1983158 | Individual (matched) | ✓ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Dunson 1994143 | Group: class | ✗ | ✗ | ✗ | ✓ | 85–100% | ✗ | ✗ | RCT | Meta-analysed and narrative |
| Eastman 1981191 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Narrative |
| Evans 2005141 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Evans 2011159 | Individual | ✗ | ✗ | ✗ | ✗ | NR | ✗ | ✗ | RCT | Meta-analysed |
| Evans 2007160 | Group: school | ✗ | ✗ | ✗ | ✗ | < 70% | ✗ | ✗ | RCT | Meta-analysed |
| Fabiano 2010161 | Individual | ✗ | ✗ | ✗ | ✓ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Frame 2003162 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Narrative |
| Harper 1996192 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Narrative |
| Hoover 1986163 | Group: class | ✗ | ✗ | ✗ | ✓ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Iseman 2011164 | Group: class | ✗ | ✗ | ✗ | ✗ | < 70% | ✓ | ✓ | RCT | Meta-analysed |
| Jurbergs 2010165 | Individual | ✗ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Kapalka 2005193 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Kendrick 1995194 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✓ | ✗ | Non-RCT | Meta-analysed |
| Khilnani 2003166 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Langberg 2012167 | Individual (matched) | ✗ | ✗ | ✓ | ✗ | NR | ✓ | ✗ | RCT | Meta-analysed |
| Langberg 2008168 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✓ | ✗ | RCT | Meta-analysed |
| Lomas 2002169 | Individual | ✓ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Looyeh 2012170 | Individual | ✗ | ✗ | ✓ | ✓ | 85–100% | ✓ | ✗ | RCT | Meta-analysed |
| McGraw 2004171 | Individual | ✓ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Miranda 2006195 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Miranda 2002196 | N/A | N/A | N/A | N/A | ✓ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Molina 2008172 | Individual (stratified by gender and grade level) | ✗ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Murray 2008173 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Omizo 1980174 | Individual (matched) | ✓ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Omizo 1980175 | Individual (matched) | ✓ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Omizo 1982176 | Individual (matched) | ✓ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Ostberg 2012177 | Individual (matched) | ✗ | ✗ | ✗ | ✗ | 85–100% | ✓ | ✗ | RCT | Meta-analysed |
| Owens 2005197 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Poillion 1993198 | N/A | N/A | N/A | N/A | ✗ | < 70% | ✓ | ✗ | Non-RCT | Meta-analysed |
| Poley 1996178 | Group: class | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Rabiner 2010142 | Individual | ✗ | ✗ | ✓ | ✓ | 85–100% | ✓ | ✓ | RCT | Meta-analysed |
| Re 2007199 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Reid 1987179 | Individual | ✗ | ✗ | ✗ | ✓ | 85–100% | ✓ | ✓ | RCT | Meta-analysed |
| Rickson 2003180 | Individual | ✗ | ✗ | ✗ | ✗ | 85–100% | ✓ | ✗ | RCT | Narrative |
| Rivera 1980181 | Individual (matched) | ✓ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Seeley 2009182 | Group: class | ✗ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Semrud 1999200 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Steiner 2011183 | Individual | ✓ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Storer 1994184 | Individual | ✓ | ✗ | ✗ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Van der Westhuizen 2007186 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Narrative |
| van Lier 2004185 | Group: class | ✗ | ✗ | ✓ | ✗ | 70–84% | ✗ | ✗ | RCT | Meta-analysed and narrative |
| Verret 2012201 | N/A | N/A | N/A | N/A | ✗ | 85–100% | ✗ | ✗ | Non-RCT | Meta-analysed |
| Webber 2012202 | N/A | N/A | N/A | N/A | ✗ | NR | ✗ | ✗ | Non-RCT | Meta-analysed |
| Zaghlawan 2007187 | Individual | ✗ | ✗ | ✓ | ✗ | 85–100% | ✓ | ✗ | RCT | Meta-analysed |
| Zentall 2012188 | Individual (stratified by gender and population) | ✗ | ✗ | ✓ | ✗ | 85–100% | ✗ | ✗ | RCT | Meta-analysed |
| Total frequencies across studies (n = 54) | Individual: 30 Group: 9 N/A: 15 |
✓: 10 ✗: 29 N/A: 15 |
✓: 1 ✗: 38 N/A: 15 |
✓: 19 ✗: 20 N/A: 15 |
✓: 10 ✗: 44 |
< 70%: 4 70–84%: 1 85–100%: 46 NR: 3 |
✓: 14 ✗: 40 |
✓: 5 ✗: 49 |
Intention to treat
Intention to treat was assumed when there were no reported changes to protocol. Based on this criterion, 19 of the 39 RCTs142,154–156,158,162,166–168,170,173–176,178,185–188 could be assumed to employ an ITT procedure, with only one study104 stating use of ITT explicitly. The remaining studies did not meet our criteria for ITT.
Blinding of outcome assessors
Nine RCTs104,142,143,153,157,161,163,170,179 reported blinding for at least one of the study measures, whereas the majority of RCTs (n = 30) did not implement or report on the blinding of outcome assessors. Only 1 of the 15 non-RCTs196 reported blinding of outcome assessors; the rest either did not report on or did not implement blinding of outcome assessors. Although completion rates were not always explicitly reported, they could be estimated based on the reported number of participants that consented to take part and the number of participants for whom there were data. Thirty-three of the 39 RCTs104,142,143,154–158,161–163,165,166,168–184,186–188 had a completion rate between 85% and 100% at final follow-up; one study between 70% and 84% and three studies < 70%;153,160,164 for two RCTs the completion rate was unclear. 159,167 Of the 15 non-RCTs, 13 had a completion rate of 85–100%;141,189–197,199–201 one study < 70%;198 and in one study the completion rate was unclear. 202 Across all 54 studies, only 10 reported blinding of assessor for at least one of the study measures and 46 had a completion rate between 85% and 100%.
Follow-ups
Eleven of the 39 RCTs104,142,153,164,166,167,170,177,179,180,187 reported included a follow-up after post-test. Follow-ups ranged from 2 weeks to 2 years post-randomisation (mean = 7.6 months, SD = 7.48) in the 10 studies that reported length of follow-up. 104,142,153,164,167,168,170,177,179,187 Three studies159,160,185 assessed outcomes at several time points throughout the duration of the intervention (in some instances over a relatively long intervention period) but did not continue to apply repeated measures once the intervention had ceased. Of the non-RCTs, three included one follow-up (at 2, 4 and 24 weeks),190,194,198 and one study197 assessed outcomes at several time points throughout the duration of the intervention, but did not continue to apply repeated measures once the intervention had ceased. Across all 54 studies, 14 studies employed follow-ups after post-test.
Analysis
Data description for the meta-analysed randomised controlled trials: constructs and informants
Data for 22 construct/informant combinations were reported and analyses were based on 2–16 independent studies. Ten of the 36 studies104,155,161,173,178,179,181,182,184,185 reported mean differences adjusted for baseline or data that could be used to derive these, with unadjusted mean differences reported (or data that could be used to derived these) in the remaining studies. Seven studies155,163,169,176,178,179,181 reported the use of neurocognitive assessments for child ‘inattention’ and eight reported neurocognitive assessments for child ‘hyperactivity/impulsivity’. 155,163,169,176,178,179,181 With the exception of assessments of ‘curriculum achievement’ (five studies154,164,165,172,179), ‘standardised achievement’ (10 studies104,142,154,157,158,161,163,164,171,188) and observer rated ‘inattention’ (four studies104,153,156,165), the remaining assessments comprised perception-based measures rated by key stakeholders. Of these, parent and teacher data were reported for all seven relevant constructs (‘inattention’; ‘hyperactivity/impulsivity’; ‘ADHD combined’; ‘externalising’ symptoms; ‘internalising’ symptoms; ‘social skills’ and ‘perceptions of school adjustment’) and for child informants three constructs only: ‘internalising’ symptoms, ‘social skills’ and ‘perceptions of school adjustment’ (data for child-informed ‘ADHD combined’ and ‘externalising’ symptoms were not identified in the literature and child-informed ‘inattention’ and ‘hyperactivity/impulsivity’ were based on neurocognitive assessments).
Data for perception-based measures were most frequently reported for teacher-assessed outcomes: ‘inattention’ (n = 12104,142,153,156,159,166,169,170,173,177,183,187); ‘hyperactivity/impulsivity’ (n = 16104,143,153,159,163,166,167,169,170,173,177–179,182–184); ADHD combined (n = 6156,161,169,170,177,183); ‘externalising’ symptoms (n = 9104,153,157,161,166,169,177,182,185), ‘internalising’ symptoms (n = 4104,166,169,177); ‘social skills’ (n = 6104,153,159,166,169,182) and ‘perceptions of school adjustment’ (n = 9104,142,153,159,161,167,168,173,182). Parent-informed outcomes were the next most frequently reported among the information: ‘inattention’ (n = 7104,159,160,167,169,177,183); ‘hyperactivity/impulsivity’ (n = 7159,160,167,169,177,178); ‘ADHD combined’ (n = 3169,177,183); ‘externalising’ symptoms (n = 4104,172,177,182); ‘internalising’ symptoms (n = 3104,172,177); ‘social skills’ (n = 4104,159,160,182); and ‘perceptions of school adjustment’ (n = 3104,159,182). Child self-perception-based measures were identified least frequently: ‘internalising’ symptoms (n = 3153,174,175); ‘social skills’ (n = 2153,184); and ‘perceptions of school adjustment’ (n = 5153,172,174,175,184).
Meta-analyses of the randomised controlled trials
Table 14 presents the meta-analysis results for the RCTs. Results are presented for each construct/informant combination where data permitted analysis and includes details of the number of independent studies on which each pooled effect size is based and the total sample size across included studies. For each construct, we report the pooled effect size using Cohen’s d (d+) with Hedges’ correction and corresponding 95% CIs, p-value, I2, and the p-value for Cochran’s Q test for between-study heterogeneity. Positive effect sizes indicate that, on average, the treatment group had a better outcome than the control group.
| Measure | Informant | Number of studies | Sample size (total) | aCohen’s d+ | 95% CI | p-value | I 2 (%)b | p-value for Q test of heterogeneityc |
|---|---|---|---|---|---|---|---|---|
| Core ADHD symptoms | ||||||||
| Inattention | Parent | 7 | 384 | 0.13 | –0.14 to 0.40 | 0.33 | 36 | 0.15 |
| Teacher | 12 | 548 | 0.60 | 0.14 to 1.06 | 0.01 | 83 | < 0.001 | |
| Child | 7 | 292 | 0.44 | 0.18 to 0.70 | 0.001 | 14 | 0.32 | |
| Observer | 4 | 203 | 1.30 | –0.17 to 2.77 | 0.08 | 93 | < 0.001 | |
| Hyperactivity/impulsivity | Parent | 7 | 285 | 0.16 | –0.07 to 0.39 | 0.17 | 0 | 0.63 |
| Teacher | 16 | 700 | 0.23 | –0.03 to 0.49 | 0.08 | 63 | 0.001 | |
| Child | 8 | 411 | 0.33 | 0.13 to 0.53 | 0.001 | 0 | 0.70 | |
| ADHD combined | Parent | 3 | 110 | 0.14 | –0.46 to 0.75 | 0.65 | 57 | 0.10 |
| Teacher | 6 | 218 | 0.16 | –0.22 to 0.54 | 0.42 | 40 | 0.14 | |
| ADHD-related symptoms | ||||||||
| Externalising symptoms | Parent | 4 | 232 | 0.21 | –0.04 to 0.45 | 0.10 | 0 | 0.55 |
| Teacher | 9 | 548 | 0.28 | 0.04 to 0.53 | 0.03 | 49 | 0.03 | |
| Internalising symptoms | Parent | 3 | 193 | 0.02 | –0.27 to 0.31 | 0.88 | 0 | 0.41 |
| Teacher | 4 | 252 | 0.14 | –0.46 to 0.73 | 0.65 | 83 | 0.001 | |
| Child | 3 | 167 | –1.16 | –1.15 to 3.47 | 0.32 | 97 | < 0.001 | |
| Social skills | Parent | 4 | 260 | –0.04 | –0.28 to 0.21 | 0.78 | 0 | 0.42 |
| Teacher | 6 | 304 | 0.32 | –0.09 to 0.73 | 0.13 | 63 | 0.02 | |
| Child | 2 | 59 | –0.27 | –0.81 to 0.27 | 0.33 | 0 | 0.43 | |
| Scholastic behaviours and outcomes | ||||||||
| Perceptions of school adjustment | Parent | 3 | 133 | 0.46 | –0.17 to 1.09 | 0.15 | 70 | 0.04 |
| Teacher | 9 | 497 | 0.26 | 0.05 to 0.47 | 0.02 | 23 | 0.23 | |
| Child | 5 | 190 | 0.05 | –0.24 to 0.34 | 0.72 | 4 | 0.38 | |
| Curriculum achievement | Child | 5 | 154 | 0.50 | –0.06 to 1.05 | 0.08 | 59 | 0.04 |
| Standardised achievement | Child | 10 | 502 | 0.19 | 0.04 to 0.35 | 0.02 | 0 | 0.65 |
Core attention-deficit/hyperactivity disorder symptoms
There was strong evidence of an average beneficial effect on ‘inattention’ assessed by neurocognitive assessment (d+ = 0.44, 95% CI 0.18 to 0.70; p = 0.001). Beneficial effects on ’hyperactivity/impulsivity’ assessed by neurocognitive assessment (d+ = 0.33, 95% CI 0.13 to 0.53; p = 0.001) and teacher-rated ‘inattention’ (d+ = 0.60, 95% CI 0.14 to 1.06; p = 0.01) were also observed. Applying Cohen’s (1992) guidelines65 (Box 1), the corresponding CIs indicate the impact could range between a very small effect (i.e. < 0.20) and ‘medium’ for neurocognitive assessments of child-informed ‘inattention’ and ‘hyperactivity/impulsivity’ and anywhere between very small (i.e. < 0.20) and ‘large’ for teacher-rated ‘inattention’. There was weak evidence of an effect for ‘inattention’ reported by independent observers (p = 0.08) and ‘hyperactivity/impulsivity’ rated by teachers (p = 0.08); the corresponding wide CIs indicate insufficient data to be certain that these are true effects and, if it were a true effect, about the likely effect size. There was little evidence of effects for the remaining construct/informant combinations for core ADHD symptoms.
‘Small’ d+ = 0.20.
‘Medium’ d+ = 0.50.
‘Large’ d+ = 0.80.
Attention-deficit/hyperactivity disorder-related symptoms
There was evidence of a beneficial effect on ‘externalising’ symptoms reported by teachers (d+ = 0.28, 95% CI 0.04 to 0.53; p = 0.03). Applying Cohen’s guidelines65 (see Box 1), the corresponding CIs indicate that the effect could range from very small (i.e. < 0.20) to ‘medium’. There was little evidence of any effects for the remaining construct/informant combinations for ADHD-related symptoms.
Scholastic behaviours and outcomes
There was evidence of a beneficial effect on ‘perceptions of scholastic adjustment’ as assessed by teachers (d+ = 0.26, 95% CI 0.05 to 0.47; p = 0.02) and ‘standardised achievement’ (d+ = 0.19, 95% CI 0.04 to 0.35; p = 0.02). Applying Cohen’s guidelines,65 the corresponding CIs indicate that the effects could be anywhere between very small (i.e. < 0.20) and ‘small’. There was only weak evidence for any effect on ‘curriculum achievement’ (p = 0.08); the corresponding wide CIs indicate insufficient data to be certain about the presence of an effect or, if present, the likely effect size. There was little evidence of effects for parent- and child-rated perception-based measures of ‘scholastic adjustment’.
Data description for the meta-analysed non-randomised controlled trials: constructs and informants
Data for 17 construct/informant combinations were reported and only 1 of 12 studies reported mean differences adjusted for baseline score or data that could be used to derive these;201 unadjusted mean differences were calculated for the rest of the studies. Four of the 12 studies included a neurocognitive assessment of ‘inattention’. 190,196,200,201 Three studies assessed ‘curriculum achievement’197,198,202 and two studies assessed ‘standardised achievement’. 189,190 The remaining assessments comprised perception-based measures. With the exception of parent-rated ‘ADHD combined’, data were reported for teachers and parents across all seven relevant constructs (‘inattention’; ‘hyperactivity/impulsivity’; ‘ADHD combined’; ‘externalising’ symptoms; ‘internalising’ symptoms; ‘social skills’; and ‘perceptions of school adjustment’). There were no data for child-informed perception-based measures. All analyses were based on between two and four independent studies. Table 15 reports the results of meta-analyses for the non-RCTs.
| Measure | Informant | Number of studies | Sample size (total) | aCohen’s d+ | 95% CI | p-value | I 2 (%)b | p-value for Q test of heterogeneityc |
|---|---|---|---|---|---|---|---|---|
| ADHD-related symptoms | ||||||||
| Inattention | 119 | Parent | 4 | 0.74 | –0.36 to 1.80 | 0.19 | 86 | < 0.001 |
| 123 | Teacher | 3 | 0.36 | 0.00 to 0.72 | 0.05 | 0 | 0.56 | |
| 125 | Child | 4 | 0.75 | 0.09 to 1.40 | 0.03 | 73 | 0.01 | |
| Hyperactivity/impulsivity | 101 | Parent | 3 | 0.57 | –0.18 to 1.32 | 0.13 | 65 | 0.06 |
| 123 | Teacher | 3 | 0.16 | –0.93 to 1.22 | 0.78 | 87 | < 0.001 | |
| 71 | Child | 2 | 0.06 | –0.87 to 0.99 | 0.90 | 67 | 0.82 | |
| ADHD combined | 133 | Teacher | 4 | 0.37 | 0.02 to 0.72 | 0.04 | 0 | 0.63 |
| ADHD-related symptoms | ||||||||
| Externalising symptoms | 36 | Parent | 2 | 0.20 | –0.50 to 0.90 | 0.22 | 34 | 0.22 |
| 213 | Teacher | 4 | 0.37 | –0.24 to 0.98 | 0.23 | 67 | 0.05 | |
| Internalising symptoms | 86 | Parent | 3 | 0.06 | –0.36 to 0.48 | 0.78 | 0 | 0.98 |
| 123 | Teacher | 3 | –0.29 | –0.66 to 0.09 | 0.13 | 17 | 0.30 | |
| Social skills | 68 | Parent | 2 | –0.15 | –0.64 to 0.35 | 0.57 | 69 | 0.69 |
| 94 | Teacher | 2 | –0.06 | –0.80 to 0.69 | 0.88 | 77 | 0.04 | |
| Scholastic behaviours and outcomes | ||||||||
| Perceptions of school adjustment | 68 | Parent | 2 | 0.29 | –0.60 to 1.17 | 0.53 | 67 | 0.08 |
| 105 | Teacher | 3 | 0.24 | –0.15 to 0.64 | 0.23 | 0 | 0.39 | |
| Curriculum achievement | 114 | Child | 3 | 0.28 | –0.46 to 1.03 | 0.46 | 77 | 0.14 |
| Standardised achievement | 41 | Child | 2 | 1.15 | –0.25 to 2.55 | 0.11 | 81 | 0.19 |
Core attention-deficit/hyperactivity disorder symptoms
There was some evidence of a beneficial effect on ‘inattention’ (d+ = 0.75, 95% CI 0.09 to 1.40; p = 0.03) assessed by neurocognitive assessment and ‘ADHD combined’ assessed by teachers (d+ = 0.37, 95% CI 0.02 to 0.72; p = 0.04). Applying Cohen’s guidelines,65 the corresponding CIs indicate the effect on ‘inattention’ could be anywhere between very small (i.e. < 0.20) and ‘large’ (see Box 1), and on ‘ADHD combined’ anywhere between very small (i.e. < 0.20) and ‘medium’. There was weak evidence of an effect for ‘inattention’ reported by teachers (p = 0.05); the corresponding wide CIs indicate insufficient data to be certain that these are true effects and about the likely effect size. There was little evidence of effects for the remaining construct/informant combinations for core ADHD symptoms.
Attention-deficit/hyperactivity disorder-related outcomes
There was little evidence of beneficial effects of interventions on ADHD-related outcomes among non-RCTs.
Scholastic behaviours and outcomes
There was little evidence of beneficial effects of intervention on scholastic behaviours and outcomes among the non-RCTs.
Comparison of meta-analysed randomised controlled trials and non-randomised controlled trials
With the exception of ‘inattention’ assessed by neurocognitive assessment and teachers, there was no overlap in the constructs that demonstrated a beneficial effect of non-pharmacological interventions between the meta-analysed RCTs and non-RCTs. Nonetheless, there were too few meta-analysed non-RCTs to enable a reliable comparison with the meta-analysed RCTs.
Publication bias
We were unable to assess funnel plots properly or use more advanced regression-based assessments to assess publication bias owing to the inadequate numbers of included trials and the substantial heterogeneity identified across studies. 150
Heterogeneity
Heterogeneity was explored and meta-regression models run for the meta-analyses RCTs only as there were too few non-RCTs to support this kind of analysis for these studies. Table 16 reports the level of heterogeneity by outcome as ‘high’, ‘moderate’ or ‘low’ based on the I2 values reported in Table 14. Among the RCTs, 9 of the 22 construct/informant combinations had I2 values ≥ 50%, which indicates a large amount of heterogeneity. With the exception of parent-informed ‘ADHD combined’ corresponding Q statistics were significant at the 5% level, providing further evidence of heterogeneity. Three construct/informant combinations had I2 values between 25% and 50%, which indicates moderate heterogeneity (parent-informed ‘inattention’; teacher-informed ‘ADHD combined’; teacher-informed ‘externalising’ symptoms), although the corresponding Q statistics were only significant for ‘externalising’ symptoms. The remaining 10 informant/construct combinations had non-significant Q statistics and I2 values < 25%, which indicated lower levels of heterogeneity. Of the nine construct/information combinations showing some beneficial evidence of effectiveness (reported in Table 14), with the exception of neurocognitive assessment of ‘inattention’ and ‘hyperactivity/impulsivity’, teacher ‘perceptions of school adjustment’ and ‘standardised achievement’ identified as having low heterogeneity all were shown to have high levels of heterogeneity across studies.
| High heterogeneity (I 2 values ≥ 50%) | Moderate heterogeneity (I 2 values 25–50%) | Low heterogeneity (I 2 < 25%) |
|---|---|---|
|
|
|
Moderator analyses among the randomised controlled trials
We used meta-regression, where data permitted, to examine whether or not the programme features described in Table 17 modified intervention effectiveness using the potential modifying variables in separate models (i.e. one predictor variable only).
| Moderator | Outcome(s) assessed | Operationalisation of moderator variable |
|---|---|---|
| Study characteristics | ||
|
|
N/A |
| Participant characteristics | ||
|
|
Dichotomous: high vs. low |
|
|
N/A |
|
|
N/A |
| Intervention packages | ||
|
|
Dichotomous: single vs. multiple |
|
Dichotomous: two vs. three or more | |
|
|
Dichotomous: present vs. absent |
|
|
Dichotomous: present vs. absent |
|
|
Dichotomous: present vs. absent |
|
|
Dichotomous: present vs. absent |
|
|
Dichotomous: present vs. absent |
|
|
Dichotomous: present vs. absent |
| Delivery characteristics | ||
|
|
Dichotomous: school and home vs. school only |
|
|
Dichotomous: teacher vs. any other provider |
|
|
Dichotomous: normal school hours vs. before/after school |
|
|
Dichotomous: classroom vs. all other settings |
|
|
Continuous weeks |
|
|
Continuous hours |
Moderator analyses were conducted for four construct/information combinations with eight or more studies including, teacher-informed ‘inattention’, ‘hyperactivity/impulsivity’, ‘externalising’ symptoms and ‘perceptions of school adjustment’. ‘Standardised achievement’ was not included as the corresponding I2 statistic was zero. There were too few studies to explore moderators for the remaining construct/informant combinations. Table 17 illustrates how each moderator was operationalised and for which potential moderators data were available. The distribution of moderator scores was assessed for each outcome. Potential moderators measured on a continuous scale were sometimes categorised into two groups to form a dichotomous variable. Cut-off values for categorisation were chosen on a case-by-case basis, informed by the distribution of scores.
The results of the meta-regression are reported in four tables. None of the heterogeneity in effect sizes for teacher-rated ‘inattention’ (Table 18), ‘hyperactivity/impulsivity’ (Table 19) and ‘externalising’ symptoms (Table 20) was explained by participant characteristics (medication status), intervention packages (contingency management; DRC, cognitive–behavioural self-regulation; cognitive skills retraining; academic study skills; and emotional skills training) and intervention delivery characteristics (context, provider, time, setting, duration and intensity). These results suggest that none of the characteristics assessed had an impact on intervention effectiveness for ‘inattention’, ‘hyperactivity/impulsivity’ and ‘externalising’ symptoms. For the ‘perceptions of school adjustment’ outcome (Table 21), there was weak evidence (p = 0.06) of a negative effect for the social skills intervention package, suggesting that inclusion of social skills training may have a negative impact on effectiveness. For the same outcome, there was also weak evidence for the negative effect of intervention length (p = 0.04) assessed on a continuous scale, suggesting that shorter interventions are more effective.
| Potential modifier | Number of studies (n) | Meta-regression results | I 2 (%)b | Adjusted R2 (%)c | ||
|---|---|---|---|---|---|---|
| Coefficienta | 95 CI% | p-value | ||||
| Study and participant characteristics | ||||||
| Medication status: high vs. low (reference)d | 10 | –0.74 | –2.10 to 0.63 | 0.25 | 85 | 6.0 |
| Intervention package | ||||||
| Frequency: multiple vs. single (reference)e | 12 | 0.20 | –1.11 to 1.52 | 0.74 | 84 | 0.0 |
| Contingency management: present vs. absent (reference)f | 12 | 0.09 | –1.27 to 1.46 | 0.88 | 84 | 0.0 |
| Cognitive–behavioural self-regulation: present vs. absent (reference)g | 12 | 0.06 | –1.52 to 1.64 | 0.94 | 84 | 0.0 |
| Cognitive skills/retraining: present vs. absent (reference)h | 14 | –0.44 | –1.71 to 0.84 | 0.47 | 82 | 0.0 |
| Delivery characteristics | ||||||
| Context: school and home vs. school only (reference)i | 14 | –0.65 | –1.69 to 0.39 | 0.20 | 79 | 6.1 |
| Provider: teacher vs. other (reference)j | 11 | 0.42 | –0.94 to 1.78 | 0.50 | 85 | 0.0 |
| Time: normal school hours vs. before/after school (reference)k | 12 | 0.09 | –1.42 to 1.61 | 0.90 | 84 | 0.0 |
| Setting: classroom vs. other (reference)l | 11 | 0.42 | –0.79 to 0.94 | 0.50 | 85 | 0.0 |
| Duration: weeks | 11 | –0.01 | –0.05 to 0.04 | 0.79 | 83 | 0.0 |
| Intensity: hours | 8 | –0.02 | –0.05 to 0.02 | 0.23 | 86 | 10.9 |
| Potential modifier | Number of studies (n) | Meta-regression results | I 2 (%)b | Adjusted R2 (%)c | ||
|---|---|---|---|---|---|---|
| Coefficienta | 95 CI% | p-value | ||||
| Study and participant characteristics | ||||||
| Medication status: high vs. low (reference)d | 11 | –0.61 | –1.35 to 0.13 | 0.09 | 66 | 21.30 |
| Intervention package | ||||||
| Frequency: multiple vs. single (reference)e | 16 | 0.40 | –0.17 to 0.96 | 0.15 | 60 | 9.63 |
| Contingency management: present vs. absent (reference)f | 16 | 0.37 | –0.19 to 0.93 | 0.18 | 61 | 4.5 |
| DRC: present vs. absent (reference)g | 16 | –0.04 | –0.81 to 0.73 | 0.92 | 61 | 0.00 |
| Cognitive–behavioural self-regulation: present vs. absent (reference)h | 16 | –0.19 | –0.81 to 0.42 | 0.51 | 61 | 0.00 |
| Cognitive skills/retraining: present vs. absent (reference)i | 18 | 0.08 | –0.68 to 0.52 | 0.78 | 67 | 0.00 |
| Delivery characteristics | ||||||
| Context: school and home vs. school only (reference)j | 18 | 0.10 | –0.45 to 0.65 | 0.71 | 59 | 0.00 |
| Provider: teacher vs. other (reference)k | 15 | 0.19 | –0.40 to 0.77 | 0.50 | 60 | 0.00 |
| Duration: weeks | 15 | –0.02 | –0.05 to 0.01 | 0.21 | 58 | 8.00 |
| Intensity: hours | 10 | –0.01 | –0.02 to 0.01 | 0.41 | 59 | 0.00 |
| Potential modifier | Number of studies (n) | Meta-regression results | I 2 (%)b | Adjusted R2 (%)c | ||
|---|---|---|---|---|---|---|
| Coefficienta | 95 CI% | p-value | ||||
| Intervention package | ||||||
| Frequency: multiple vs. single (reference)d | 9 | 0.26 | –0.42 to 0.95 | 0.40 | 53 | 0 |
| Emotional skills training: present vs. absent (reference)e | 10 | 0.10 | –0.60 to 0.81 | 0.74 | 54 | 0 |
| Delivery characteristics | ||||||
| Context: school and home vs. school only (reference)f | 11 | 0.10 | –0.41 to 0.62 | 0.67 | 44 | 0 |
| Duration: weeks | 9 | 0.01 | –0.01 to 0.02 | 0.47 | 51 | 0 |
| Potential modifier | Number of studies (n) | Meta-regression results | I 2 (%)b | Adjusted R2 (%)c | ||
|---|---|---|---|---|---|---|
| Coefficienta | 95 CI% | p-value | ||||
| Intervention package | ||||||
| Frequency: more than two vs. single (reference)d | 9 | 0.36 | –0.12 to 0.84 | 0.12 | 0 | 62.4 |
| DRC: present vs. absent (reference)e | 9 | –0.26 | –0.78 to 0.26 | 0.28 | 11 | 32.7 |
| Academic study skills: present vs. absent (reference)f | 10 | –0.24 | –0.71 to 0.23 | 0.27 | 9 | 20.9 |
| Social skills: present vs. absent (reference)g | 9 | –0.42 | –0.86 to 0.02 | 0.06 | 0 | 100.0 |
| Delivery characteristics | ||||||
| Duration: weeks | 9 | –0.02 | –0.04 to 0.00 | 0.04 | 0 | 100.0 |
Narrative synthesis
Findings for outcomes reported in 10 papers104,141,143,162,180,185,186,191,192,198 (13 treatment groups) are summarised narratively in this section as data suitable for inclusion in the meta-analyses were neither reported nor obtainable from the study authors.
Data description for the outcomes synthesised narratively: constructs and informants
Data were available for 13 construct/informant combinations. Assessments of ‘curriculum achievement’ were identified in five studies;141,185,186,191,198 assessments of observer-rated ‘inattention’,143,191 teacher-rated ‘hyperactivity/impulsivity’,143,192 teacher-informed ‘externalising’ symptoms,180,185 child-informed ‘internalising’ symptoms162,192 and ‘perceptions of school adjustment’162,198 were identified in two studies each; the remaining combinations were reported in one study only including neurocognitive assessments of ‘inattention’,186 neurocognitive186 and observer104 assessments of ‘hyperactivity/impulsivity’,180 parent-180 and observer-rated143 ‘externalising’ symptoms, teacher-rated ‘ADHD combined’185 and observer-rated ‘social skills’. 143 With the exception of neurocognitive and observer assessments of ‘inattention’, ‘hyperactivity/impulsivity’, observer assessments of ‘externalising’ symptoms and ‘social skills’, and assessments of curriculum achievement, all outcomes were teacher, parent or children perception-based measures. Table 22 reports the results of the findings synthesised narratively. The majority of effects reported showed no statistically significant improvement for treatment group participants compared with controls on the nine commonly assessed outcomes. Among the RCTs, Dunson et al. 143 reported a statistically significant effect for teacher-rated ‘hyperactivity/impulsivity’ (p = 0.005) but not for observer ratings of ‘inattention’, ‘externalising’ symptoms and ‘social skills’ (p-values ranged from 0.08 to 0.67). Frame et al. 162 reported statistically significant effects for child-rated ‘internalising’ symptoms (p-values range from p < 0.001 to p = 0.025). Van der Westhuizen186 reported a positive effect of neurofeedback on one of seven assessments of ‘curriculum achievement’ (‘addition in maths’) relative to the control group (p = 0.04). Finally, among the non-RCTs, Harper192 reported evidence for the beneficial effects of social skills training on teacher-rated ‘hyperactivity/impulsivity’ among treatment group 2 but not for treatment group 1. Treatment group 1 received their training alongside non-ADHD peers, whereas those in treatment group 2 received their training separate to non-ADHD peers. In the absence of effect sizes, it is difficult to compare these findings with those from the meta-analyses especially in light of the small sample sizes in all but two of the studies. 104,198
| First study author and year | Study design | Core | Related | School | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Inattention | Hyperactivity/impulsivity | ADHD combined type | Externalising symptoms | Internalising symptoms | Social Skills | School adjustment | Standardised achievement | Curriculum achievement | ||
| Barkley 2000104 (tg2) | RCT | → observer (6) | ||||||||
| Barkley 2000104 (tg3) | RCT | → observer (6) | ||||||||
| Dunson 1994143 | RCT | → observer (1) | ↑ teacher (1) | → observer (1) | → observer (1) | |||||
| Eastman 1981191 | Non-RCT | → observer (1) | → child (1) | |||||||
| Evans 2005141 | Non-RCT | → child (1) | ||||||||
| Frame 2003162 | RCT | ↑ child (4); → child (1) | → child (1) | |||||||
| Harper 1996192 (tg1) | Non-RCT | → teacher (1) | → child (1) | |||||||
| Harper 1996192 (tg2) | RCT | ↑ teacher (1) | → child (1) | |||||||
| Poillion 1993198 (tg2) | Non-RCT | → child (4) | → child (2) | |||||||
| Rickson 2003180 (tg1) | RCT | → parent (2); → teacher (2) | ||||||||
| Rickson 2003180 (tg2) | RCT | → parent (2); → teacher (2) | ||||||||
| Van der Westhuizen 2007186 | RCT | → child (3) | → child (1) | ↑ child (1); → child (6) | ||||||
| van Lier 2004185 | RCT | → teacher (1) | → teacher (1) | |||||||
Effectiveness findings for the data synthesised narratively
Results of the narrative synthesis are summarised in Table 22.
Discussion
This review synthesised studies that spanned 32 years of research about the effectiveness of non-pharmacological interventions that target children with, or at risk of, ADHD in school settings. Fifty-four evaluations that reported on one or more of nine commonly measured child-related constructs assessing aspects of the condition were synthesised. Informant types (i.e. parent, teacher, child and observer) were also distinguished. In addition to the investigation of whether or not non-pharmacological interventions are effective (research question 1), the review identified and tested a wide range of programme features that could impact on effectiveness, including the study design, participant characteristics, intervention package(s) and delivery elements of non-pharmacological interventions that target children with, or at risk of, ADHD in school settings (research question 2). The cost-effectiveness of non-pharmacological interventions could not be assessed as no studies were identified (research question 3).
Overall, the results provide support for the beneficial effects of non-pharmacological interventions on outcomes related to ADHD. Positive effects were observed for relatively objective assessments (including neurocognitive assessments and tests with objective performance criteria) and for some teacher perception-based measures but not for parental and child perception-based measures. The results indicate that interventions in this field are complex; they are typically composed of multiple features and few interventions consist of common sets of intervention elements. The heterogeneity of the interventions studied was compounded by the generally low methodological quality of included studies and the absence of an agreed set of outcome measures for assessing aspects related to ADHD. Applying Cohen’s guidelines for interpreting effect sizes, mean weighted effect sizes across outcomes ranged from very small (d+ < 0.20) to large (d+ ≥ 0.80), but 95% CIs were wide and substantial heterogeneity in effect size estimates across studies was reported. Moderator analyses did not clarify which of the particular programme features are linked with effectiveness (research question 2). The meta-analysed RCTs (n = 36) offer the highest level of evidence and therefore provide the most methodologically robust basis for the following discussion. We will, therefore, (1) review the magnitude of effect sizes across constructs and informants; (2) review the meta-regression results and the effect of various programme features on the success of interventions; (3) compare our findings with those of previous reviews; (4) identify limitations of this review; (5) reflect on the design and evaluation of interventions to optimise outcomes for children with, or at risk of, ADHD; and (6) highlight key conclusions for research and possible implications for practice.
Pooled effect sizes across constructs
Beneficial effects were observed for constructs within all three broad domains of ‘core ADHD’ symptoms, ‘ADHD-related’ symptoms and ‘scholastic behaviours and outcomes’. These included relatively objective measures of neurocognitive assessments, academic achievement (‘curriculum achievement’ and ‘standardised achievement’) and outcomes rated by independent observers. Evidence of effectiveness was also reported for five perception-rated outcomes reported by teachers, which provides support for the beneficial effect of non-pharmacological interventions that target children with or at risk of ADHD in school settings.
Specifically, statistically significant effects were reported for six construct/informant combinations including: neurocognitive assessments of ‘inattention’ (p = 0.001) and ‘hyperactivity’ (p = 0.001), teacher-rated ‘inattention’ (p = 0.01), teacher-rated ‘externalising’ symptoms (p = 0.03), as well as teacher-rated ‘scholastic adjustment’ (p = 0.02) and ‘standardised achievement’ (p = 0.02). Nonetheless, corresponding CIs were wide, which indicates considerable uncertainty about the true value of the pooled effect. There was weak evidence for the effect of interventions on observer-rated ‘inattention’ (p = 0.08), teacher-rated ‘hyperactivity/impulsivity’ (p = 0.08) and ‘curriculum achievement’ (p = 0.08). Small effects and statistically non-significant findings should not, however, necessarily be overlooked as the meta-analyses were not large enough to estimate the true effect size with precision and the 95% CIs were often so wide as to include both null and substantial effects. 145 This is especially relevant here as there is heterogeneity in the characteristics of the interventions evaluated.
There was no evidence of effectiveness on the child and parent perception-based measures. The lack of evidence for parent-rated outcomes could be due to few studies that included both home and school elements. Interventions that target children primarily in school settings do not necessarily ensure that behavioural changes transfer to the settings outside of the school such as the home, on which most parental ratings would be based. Parents are not usually present in classrooms and therefore would be dependent on reports from teachers and children on whether or not interventions influenced their child’s function at school. The lack of evidence for child perception-based measures is also unsurprising given that the majority of included studies targeted fairly young children at elementary/primary school who, understandably, may not be particular skilled or experienced in evaluating their own behaviours. Empirical studies suggest that self-report measures about mental health are rarely reliable among children under the age of 9 years,203 and frequently demonstrated surprisingly low levels of agreement across informants. 204
Moderator analyses
Analyses were restricted to four perception-based outcomes rated by teachers (‘inattention’, ‘hyperactivity/impulsivity’, ‘external’ symptoms, ‘perceptions of school achievement’) for which sufficient data were available. The potential moderators tested spanned a range of programme features including information on participant characteristics, intervention package(s) and intervention delivery characteristics. There was weak evidence (p = 0.06) for possible harmful effect of social skills training and longer (vs. shorter) interventions (p = 0.04) on teachers’ ‘perceptions of school adjustment’. Nonetheless, these analyses were based on nine studies only;104,142,153,159,161,167,168,173,182 with only three studies104,159,182 identified as including social skills training. The potential moderators tested do not explain the large proportion of unaccounted variance in effect size heterogeneity. It is possible that combinations of programme features may interact to account for this heterogeneity. However, the number of studies in the available literature does not allow us to reliably explore these potential interaction effects.
Comparison with previous reviews
Our classification of interventions led to the identification of 15 packages of techniques. Comparisons with previous classifications suggest moderate overlap. For example, our packages of ‘cognitive–behavioural self-regulation’ and ‘contingency management’ overlap with the ‘self-regulation’ interventions reviewed by Reid et al. 75 and with the ‘behavioural modification’ interventions reviewed by Fabiano et al. 63 In their review, DuPaul et al. 72 evaluated ‘contingency management’, ‘cognitive–behavioural’ and ‘academic’ interventions which overlap with our ‘contingency management’, ‘cognitive–behavioural self-regulation’ and ‘study skills’ packages. Three of our packages also overlap with Trout et al. ’s74 classification in a previous review, that is our packages of ‘adaptations to environment’, ‘contingency management’ and ‘cognitive–behavioural self-regulation’ correspond with their ‘antecedents-based interventions’, ‘consequence-based interventions’ and ‘self-regulation-based interventions’. Two of their remaining categorisations reflect modes of delivery, that is peer- and parent-mediated interventions rather than change techniques and the final one is a catch-all group comprising all other interventions.
The results of our review replicate and build on the conclusions of previous reviews72,74,75 and benefit from the inclusion of a larger set of controlled trials. For example, the results confirm DuPaul et al. ’s72 conclusions that non-pharmacological interventions delivered in school settings lead to improvement in both core ADHD symptoms and academic outcomes. Building on DuPaul et al. ,72 the results indicate that the effects of non-drug intervention in school settings vary by rater type. We assessed a more refined range of outcomes for children with or at risk of ADHD, classifying ‘symptoms’ and ‘scholastic behaviours and outcomes’ into relatively discrete constructs that have distinct theoretical bases and potentially differential implications for key stakeholders. For example, teachers and parents may be more concerned about academic outcomes than children, who in turn may be more concerned about making good friends (see Chapters 5 and 6 for a fuller discussion of this issue). In line with previous reviews, there was substantial heterogeneity in effect sizes across studies and, consistent with Trout et al. ,74 our results indicate that interventions in this field are composed of multiple features and few interventions consist of common sets of intervention elements.
The design and evaluation of interventions to optimise outcomes for children with or at risk of attention-deficit/hyperactivity disorder
The results offer support for the effectiveness of non-drug interventions that target children with or at risk of ADHD. The range of pooled effects across studies suggest that the success of non-pharmacological interventions in school settings are comparable to those in other contexts that target children with ADHD (e.g. in clinic settings) and interventions that target child mental health more generally. 205,206 Nonetheless, study quality of the included trials was generally low (see below) and, therefore, a key conclusion of this review is for the development and testing of better conducted RCTs in the future. Few interventions consist of common sets of intervention elements. For example, of the 43 intervention groups among the meta-analysed RCTs, 26 unique intervention packages or combinations thereof were identified, even before the consideration of other potentially active ingredients such as delivery characteristics. The current literature does not allow us to assess accurately which intervention elements are linked to effectiveness. To develop more effective interventions it is necessary to investigate the combinations of components that are most effective in changing a particular behaviour. There is evidence to suggest that having a theoretical basis to an intervention enhances its effectiveness. 94 Therefore, in the design of interventions that target children with ADHD, the methods used to change behaviour should be matched explicitly to the relevant theoretical constructs. Theoretical specification would facilitate the accumulation of knowledge and evidence synthesis. There is a growing evidence base about which techniques are useful in changing particular theoretical constructs that can enhance the design of interventions. 207 The adoption of these methods would not only help isolate the active ingredients of the interventions but would also help researchers and practitioners to replicate, implement and synthesise evidence on interventions that target children with ADHD. 208 Change targets should be considered not only at the child level but at professional (e.g. teacher) and organisational (e.g. school) levels too. Key stakeholders should be involved in the design of interventions at an early stage to ensure acceptability and relevance to local context209 (see Chapter 7 for a fuller discussion of this issue). Intervention mapping, a formal systematic method for the design and implementation of interventions, could usefully be applied. 209
Limitations
We set a broad net through our inclusion criteria, which was necessary to bring together different literatures, to provide an overview of the research to date and to outline the future research agenda in this field. However, the breadth of the range of both intervention and outcomes presents a challenge for analysis and interpretation. The absence of standardised tools to synthesise across measures and interventions meant that we had to develop our own systems. Several separate measures have been developed to assess the same constructs (see Table 3), with only a few derived from a rigorous psychometric development process. Overall, the current range of assessments reported in this review reflects the proliferation of measures that represent a limited number of underlying mechanistic constructs. This lack of standardised methods and measures makes theoretical integration difficult. Although we were satisfied with the level of categorisation of most constructs (e.g. the core ADHD symptoms were consistent with DSM-IV criteria for ADHD subtypes), in some cases decisions made were based on practical decisions such as the availability of data rather than being grounded in theory. For example, assessments of scholastic attainment could have been refined further into literacy and numerical skills, which, although correlated, may lead to differential outcomes and implications for key stakeholders. Other outcomes not included here may also be of interest but were too few to synthesise across the included controlled trials. These include assessments of executive functions, self-esteem, attributions and goal outcomes (see Table 65). Goal outcomes may be particularly useful given the recent trend in the use of idiographic assessments. This preliminary work provides a sound prototype of measures and ADHD-related constructs but further development is essential.
The range of interventions was similarly challenging to synthesise across descriptions that often implied the same content using different labels. For example, ‘contingency management’ may be labelled as ‘behaviour modification’ and ‘reinforcement’; ‘cognitive–behavioural self-regulation’ as ‘self-monitoring’ and ‘self-control’; and ‘attention training’ as ‘cognitive training’. These differences are reflected in the classification systems of the reviews that have looked at interventions that target ADHD. 72,74,75 For example, ‘consequence-based interventions’74 and ‘behavioural modification’63 reflect methods related to conditioning processes. 138 Similarly, ‘cognitive–behavioural’ and ‘self-regulation’ include a range methods that tap self-regulatory processes. 210 In the absence of a shared, reliable tool for characterising intervention content, it is difficult to establish the precise contents of interventions, isolate the potentially active ingredients and compare results reliably across reviews. This is reflected in the poor descriptions of interventions, for example in journals that can make the retrospective decoding of intervention content especially challenging.
Although the system that we developed was more refined than those that precede it, coding decisions necessarily involved some inference, owing to both poor descriptions of interventions and the absence of a reliable, consensually agreed coding framework for ADHD interventions. The 15 intervention packages identified in this current review were relatively broad and could be refined further to characterise more discrete theoretically-based change techniques. For example, specific techniques such as ‘punishment’, ‘reward’, ‘behaviour cost’ and ‘token economy’ were grouped within the package of ‘contingency management’. Each technique may be more or less effective for children with ADHD. Moreover, our classification system was restricted to child-based interventions, yet, many interventions that target children with or at risk of ADHD are complex and include teacher and parental targets in addition to children. Classification of teacher training interventions is therefore also warranted.
Abraham and Michie136 developed a reliable method for the characterisation intervention descriptions in terms of commonly used behaviour change techniques (BCTs). 136 Since then, this work has been extended211 and researchers have developed various domain-specific taxonomies of BCTs (e.g. for smoking), but such a classification remains to be undertaken for BCTs applied to children with ADHD. Methods for the characterisation of other potentially active ingredients such as change targets (e.g. behaviours and populations), delivery format (e.g. one to one or group based), the duration of intervention and the delivery context (e.g. in school/home/clinic) are also beginning to emerge in health psychology;208 the development and testing of similar tools to allow the specification of ADHD-related constructs and interventions is essential. This method can guide the design and implementation of interventions by clarifying what works for whom in what circumstance and would facilitate the efficient use of scarce resources. Although our classification systems were carefully developed, we anticipate development and empirical validation before they can be offered as reliable tools for other researchers.
In addition to the categorisations of interventions and measures, several other issues need to be considered in order to interpret the findings of the current review. Most of the synthesised studies included multiple and potentially interacting factors. Therefore, the pooled effects in meta-analysis only yield associative findings without controlling for potential confounders or moderators. Although foreign-language papers were specified in our inclusion criteria, we were unable to obtain 24 potentially relevant texts, and those that we were able to retrieve and translate (n = 7) did not meet our inclusion criteria. Thus, by default, we excluded non-English-language articles, which may limit the generalisation of the study findings beyond the geographical locations in which the studies were conducted, mainly in North America (44/54 studies). We were not able to locate 15% (88) of all potentially relevant articles (both foreign-language and English-language papers combined) at the stage of full-text screening. Of those we could access, 11% were identified as relevant. Applying this same proportion to those that we were not able to obtain, perhaps nine additional papers would have met the inclusion criteria had we been able to locate them. Although such exclusion is unlikely to alter our conclusions substantially, our inability to access these papers highlights that improved methods for retrieving papers for reviews are needed. This is a common problem across most topic areas and therefore warrants attention. Finally, although steps were taken to reduce the possibility of publication bias (e.g. hand-searching of relevant websites) we cannot be certain if and to what extent publication bias is a problem for these data, and were unable to conduct an analysis to look for evidence for this.
The remaining limitations are attributable to the shortcomings of the available evidence.
Although the inclusion of more controlled trials indicates that the methodological quality of reviewed studies in the current meta-analysis was superior to those that precede it,72,74,75 many included studies were judged to have a high potential for bias in one or more of the critical domains of allocation concealment and blinding of outcome assessors. Of the 39 RCTs, only one155 was identified as having made a good attempt at concealment of random allocation and only 10 of all 54 studies104,142,143,153,157,161,163,170,179,196 included at least one assessor blinded outcome assessment. No studies included both. Only two of the four RCTs assessing observer-rated ‘inattention’104,153 reported blinding of the outcomes assessor(s) leading to some uncertainty of the current finding of positive effects for the beneficial effects of non-drug interventions on observer-rated ‘inattention’. These quality appraisals were not conducted in the previous three reviews on non-drug interventions in school settings and therefore cannot be compared. Surprisingly, only 17 of 54 studies (31%)104,142,143,153,159–161,164,165,167,168,173,182,183,185,187,197 assessed some element of intervention fidelity. This is lower than the 55% (denominator = 60) reported by DuPaul et al. 72 and comparable to the 34% reported by Trout et al. 74 (denominator = 41). Fourteen of 54 studies (26%)104,142,153,164,166,167,170,177,179,180,187,190,194,198 included a follow-up. This is comparable with the 20% reported by DuPaul et al. 72 Although some of these shortcomings may be due to issues of reporting rather than actual methodological performance, the conclusions of our review must necessarily be tentative given the number of potentially biased studies on which it is based.
In general, it seems that greatly increased methodological rigour is required in this area. The practical and methodological challenges involved in the implementation of RCTs that target children with or at risk of ADHD in the school setting are undoubtedly a key factor in the poor quality of the current evidence base. Increased collaboration between schools, teachers, mental health practitioners and academics should enhance the successful design and implementation of interventions that target children with or at risk of ADHD in school settings.
In light of the small sample sizes in the included studies, it is difficult to establish if biased randomisation occurred, as imbalance is quite possible in a small sample with a perfectly executed randomised design. Few studies adjusted for baseline imbalance using appropriate methods and even fewer reported the corresponding adjusted mean differences and standard errors (or the statistics needed to reproduce these) for inclusion in the meta-analyses. Nonetheless, the adoption of a randomised design is very different qualitatively to non-RCTs which have not used randomisation. Concurrent pharmacological treatments need to be measured and adjusted in order to disentangle the effects of non-pharmacological interventions from drug treatments.
No studies included economic outcomes, thus the cost-effectiveness of non-drug interventions targeting children with or at risk of ADHD cannot be established and compared with other available treatments. Moreover, the value of information in relation to such interventions remains unclear in the absence of any indication of potential cost-effectiveness and associated uncertainty. However, such research would be ambitious at the current time – it is surprising that there have been no descriptions of even the cost associated with delivering interventions. Given the wide public health impact of ADHD, better understanding of the value of interventions and the way it might be realised across different sectors (e.g. health and education) is important.
Recommendations for research
In light of the potential health and economic benefits, we make the following four recommendations for future research:
-
Standardised tools should be used to describe intervention programme features to assess aspects of ADHD. These need to be developed so that the design, reporting, replication, implementation and synthesis of interventions that target children with or at risk of ADHD can be enhanced. Such work would facilitate examination of which particular behavioural change techniques or combinations thereof are most effective for ADHD.
-
There needs to be a better agreed set of outcomes in this area to facilitate understanding across studies and interventions. Given the wide range of outcome measures reported, identification of gold-standard outcome measures assessing aspects related to ADHD is essential.
-
Non-drug interventions that target children with or at risk of ADHD should be supported and rigorously evaluated using randomised controlled designs that conceal allocation, blind outcome assessors, use objective measures, control for baseline scores, have long-term follow-up, include economic evaluation and ensure tests intervention fidelity. Concurrent pharmacological interventions need to be measured and controlled for. Interventions in the UK and for older students at primary and secondary levels are under-represented and therefore should be especially supported.
-
Examination of what works and for whom should be the focus of intervention research and, therefore, interventions should be theory-based with BCTs explicitly matched to the relevant theoretical change targets in addition to the examination of theory-based potential moderators including intervention delivery (e.g. provider, context and length) and participant (e.g. sex, age and medication status) characteristics (see Chapter 7, Findings, Deductive synthesis: sources of heterogeneity – potential moderators identified in review 1, for a more detailed discussion of potential moderators identified in the overarching synthesis of reviews 1–4).
Implications for practice
Implications for research and practice are expanded on in subsequent chapters (see Chapter 7, Discussion, Implications, and Chapter 8, Implications for policy and practice, for a summary). Studies have employed a range of strategies that are available for school staff to test and evaluate. Given the tentative nature of the findings of this review, the impact of any interventions on the outcomes selected as targets should be evaluated carefully by the practitioners applying it.
Chapter 3 Review 2: a systematic review of quantitative research investigating attitudes towards non-pharmacological interventions for attention-deficit/hyperactivity disorder used in school settings
This chapter describes a systematic review of quantitative studies about the attitudes towards school-based non-pharmacological interventions for pupils with ADHD. This is the second of four reviews reported in this monograph. This review represents additional work not described in the study protocol. Our searches for quantitative effectiveness literature for review 1 (see Chapter 2) revealed a small but significant quantitative literature on attitudes towards ADHD interventions that to this point has not been considered within the research project as a whole. The attitudes of those involved in school-based interventions and the education more generally of children displaying ADHD symptoms is shown to be a key factor in the experience of ADHD in schools across numerous studies in reviews 3 and 4 (see Chapters 5 and 6). The methods used to identify and select evidence for this review followed the methodological approach published by the Centre for Reviews and Dissemination (University of York). 212
Aims
The aim of the overall research project is to evaluate non-pharmacological interventions delivered in school settings for children with, or at risk of, ADHD and, crucially, to explore the factors that may enhance, or limit, the delivery of such interventions.
This systematic review aims to include literature that is relevant to the following research questions:
-
What attitudes do educators, children with, or at risk, of ADHD, their peers and their parents hold towards non-pharmacological interventions for ADHD used in school settings?
-
Which school-based non-pharmacological interventions for ADHD are preferred and how do attitudes towards these interventions compare to non-school interventions, including pharmacological ones?
-
What factors affect attitudes held towards these non-pharmacological interventions (including children’s ADHD subtype and teacher experience)?
Identification of evidence
Inclusion/exclusion criteria
Population
Those with experience of non-pharmacological interventions in school settings, including educators, schoolchildren with, or at risk of, ADHD, aged between 4 and 18 years, their parents and their peers. Educators could include student teachers and psychologists where they are likely to have school-based experience.
Methods
Any study design (not necessarily comparative) that reported quantitative data and analysis typically using scale- or questionnaire-type measures to report participant attitudes.
Interventions
The interventions included were non-pharmacological interventions specific to, or most often used in, an educational setting. Participants indicated their attitude towards the intervention being used with children with, or at risk of, ADHD. Studies were included that measured attitudes to medication where there was also a comparison with attitudes towards at least one non-pharmacological intervention that is typically school-based. Given the breadth of research and the limitations of acceptability measures relating to interventions experienced by participants during primary research,213 attitudes towards specific interventions experienced during primary research are excluded.
Outcomes
Perceptions (including attitudes, perceived effectiveness and acceptability) of interventions measured using existing questionnaires and scales or measures designed for the purpose of the study.
Location and language
Given the importance of context for the formation and influence of attitudes, studies from societies and educational systems markedly different from the UK will be less informative. We therefore included only studies from Organisation for Economic Co-operation and Development (OECD) countries (see Appendix 6) in the review and carefully considered the applicability of findings to the UK setting during synthesis. Foreign-language papers were excluded.
Date
Only studies published or conducted (where unpublished) from 1980 onwards were included, reflecting significant changes to the diagnosis of ADHD that year. 3
The inclusion and exclusion criteria are summarised in Table 23.
| Criteria | Specification |
|---|---|
| Population | Include:
|
| Methods | Include:
|
| Intervention | Include:
|
| Outcome | Include:
|
Search strategy
The search strategy involved the following elements:
-
search of electronic databases
-
relevant papers screened for review 1
-
forward and backward citation chasing
-
hand-searching of journals
-
expert recommendations.
A database search strategy was developed which consisted of four elements: terms related to ADHD; terms related to non-pharmacological interventions; terms related to quantitative research or attitude scales; and attitude terms. The database search strategies used a mixture of subject headings (controlled vocabulary) and free-text terms. Searches were restricted to 1980 onwards. Twenty electronic databases were searched: ASSIA/ProQuest, MEDLINE/OvidSP, EMBASE/OvidSP, PsycINFO/OvidSP, British Education Index/ProQuest, Australian Education Index/ProQuest, Education Research Complete/EBSCOhost, ERIC/ProQuest, The Cochrane Library (CDSR, DARE, CENTRAL, CMR, HTA, NHS EED), The Campbell Library, HMIC/OvidSP, Social Sciences Citation Index, Conference Proceedings Citation Index, Conference Proceedings Citation Index – Social Science & Humanities (via ISI Web of Science). These searches were undertaken in August 2013. An example search strategy used for the MEDLINE/OvidSP database is shown in Appendix 4. Forward citation chasing of included papers, backward chasing of included papers’ reference lists, asking expert advisors from the project team for relevant research and hand-searching of papers published in key journals (Journal of Child Psychology and Psychiatry, British Educational Research Journal, Journal of School Psychology, Journal of Attention Disorders, Attention Deficit and Hyperactivity Disorders) from January 2008 to September 2013 were completed to identify additional relevant work. EndNote v.X5 reference management software was used to organise the search results, screening and full-text retrieval processes.
Study selection
Relevant studies were identified in two stages based on the inclusion/exclusion criteria given above. First, two reviewers conducted title/abstract screening independently for each record (six researchers shared this screening: DM, JR, TND, DR, RA, MRo) and disagreements were resolved through discussion (DM, TND, RA) according to the inclusion criteria reported above. Full texts of records that might potentially meet the inclusion criteria were then obtained wherever possible. Full texts were screened independently by two reviewers (five researchers shared this screening: DM, JR, TND, DR, RK) for inclusion and exclusion. Disagreements were resolved through discussion (DM, JR). A list of reasons for the exclusion of each paper screened at full text is located in Appendix 5.
Methods of analysis/synthesis
Data extraction
A data extraction form was adapted from that used for review 1 and piloted. Data on the study design, participants, attitude measure, interventions, outcomes and risk of bias were extracted by DM, JR or RK and checked by another reviewer (DM or JR). Data were extracted into Microsoft Office Excel v.2007 (Microsoft Corporation, Redmond, WA). Where data were missing that would allow reviewers to convert reported attitude statistics into percentages for each intervention studied, or there was a lack of detail regarding measures used, authors were contacted. 214–217 Only Kos replied with a copy of the scale used in that study. 216
Quality assessment
Quality assessment was conducted simultaneously with data extraction. Risk of bias and study quality appraisal was assessed using a checklist partially based on guidelines from the Centre for Reviews and Dissemination. 212 Quality assessment in systematic reviews is often focused on issues of randomisation, blinding and attrition. However, given the nature of this review, more appropriate checklist items were developed in response to the type of papers reviewed (Box 2). Questions were typically assigned a response of ‘yes’, ‘no’, ‘partial’ or not applicable (‘N/A’) as appropriate for each paper. Quality appraisal decisions were made by one of three reviewers (DM, JR or RK) and checked by another reviewer (DM or JR). Any discrepancies were discussed and resolved. The appraisals were not used to exclude papers.
Were demographic details about participants reported?
Have the intervention/s been defined by the author?
Have the interventions been defined for participants?
Details of group allocation and/or randomisation.
Is the relevant sample size small (< 20), medium (20–99), or large (100 +)?
Detail of dropouts, response rate and/or missing data provided?
Are vignettes piloted and/or assessed?
Psychometric detail reported regarding attitude measure.
Piloting of attitude measure reported if developed by author?
Data analysis and synthesis
As the majority of studies were anticipated to include attitude measures taken at one point in time and the review was not concerned with changes in attitude, meta-analysis would be inappropriate as a method of synthesis. A narrative synthesis was employed, following existing systematic reviews of attitudinal research. 218–221 In order to compare across studies that used different scales, mean scores on attitude scales, which may incorporate different numbers of points or different semantic points, were converted into percentages wherever possible so that the whole potential attitude score ranged from 0% to 100%, with 100% indicating the most positive attitude as measured by the scale. Given that 6-point Likert scales were the most frequently used approach (nine included studies214,222–229), attitude percentages were categorised as ‘positive’ when percentages were ≥ 60%, ‘negative’ when percentages were < 40% and ‘neutral’ when percentages were between 40% and 59%. These arbitrary cut-offs of 60% and 40% would equate to a mean score of the first positive attitude and first negative attitude point on a 6-point Likert scale. This categorisation was also used by Liu et al. 218 Despite this justification it is accepted that this categorisation is arbitrary and ignores the dispersion of attitude scores within samples. One must be tentative when comparing converted percentage attitude scores from different measures and research contexts.
Findings
The studies
Figure 2 shows how research was selected from the initial pool of studies located through searches of the literature. Searches identified a total of 4114 records which were screened at the title and abstract level. Of these, 3917 records were excluded because they did not meet inclusion criteria, and the full text of 197 potentially eligible papers was retrieved. After scanning the full text, 169 of these papers were not considered eligible or were unavailable after further efforts to locate full-text records. A list of reasons for exclusion of each paper screened at full text can be seen in Appendix 5. The most frequent reasons for exclusion after perusal of full text were studies that either focused on a specific intervention experienced by participants or did not consider any school-based interventions. Three papers230–232 were additional reports of research already included, which would not have added any additional relevant findings above the included paper. The final synthesis involved the remaining 28 papers that met the inclusion criteria outlined above.
FIGURE 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram152 showing search process and study selection for review 2.

Summary details of the 28 included study reports, which were published between 1993 and 2013, are provided in Table 24. The included studies represented the attitudes of a variety of educators, namely teachers, school psychologists, school social workers, school counsellors and student teachers. Only Dryer et al. ’s paper238 included relevant non-educator participants (parents of children with ADHD diagnoses) and, as such, only educators’ attitudes were analysed. Twelve 216,223,226,227,229,233,234,236,240,241,244,246 of the included papers were dissertations, whereas the remainder were journal articles in peer-reviewed publications. The aims of the studies were often broader than a focus on attitudes towards school-based interventions for children with ADHD, although Table 24 only provides the design relevant to attitudes towards interventions. Additional study content not extracted for this review included attitudes towards interventions for other disorders, measures of ADHD knowledge and measures of educators’ experience of interventions. Nineteen214–217,222,223,225–229,233,236,239,240,242,243,246 of the studies used vignettes, meaning that participants read a case description of a child displaying ADHD symptoms and then indicated their beliefs regarding intervention(s) to be used for that case.
| First study author and year | Country | Publication status | Design relevant to attitudes | Vignette study? | Participants | Sample size | Percentage female | Detail about participants’ school and grades |
|---|---|---|---|---|---|---|---|---|
| Alongi 2005233 | USA | Thesis/dissertation | School psychologists rated the effectiveness of social skills training for ADHD, autistic and learning disabled vignettes | Yes | School psychologists | 212 | 85.4 | 57 preschool, 149 elementary, 89 middle school, 81 high school, 9 clinic, 1 outpatient unit (101 participants practised in more than one setting) |
| Askew 1993234 | USA | Thesis/dissertation | Special educators rated the effectiveness of antecedent interventions, contingency management, cognitive–behavioural management and social skills interventions | No | Special education teachers | 183 | NR | NR |
| Bain 2009235 | USA | Journal article | Upper-level educational psychology students and teaching interns rated the effectiveness of guided imagery, Feingold diet, sugar, metacognitive, biofeedback and play therapy interventions | No | Upper-level educational psychology students, teaching interns | 99 | 89.9 | NR |
| Coles 2012215 | USA | Journal article | Teachers’ treatment preferences for behaviour modification, tutoring, learning assistance and other non-school interventions according to gender and ADHD subtype (including ODD comorbidity) | Yes | Teachers | 50 | 90.0 | Elementary and middle schools, kindergarten to fifth grade |
| Conforti 2012236 | USA | Thesis/dissertation | Teachers’ perceived efficacy of three categories of intervention (antecedent, consequent, academic) for four vignettes (each vignette displays one ADHD symptom: inattentiveness, wandering, poor peer interaction, speaking out of turn) | Yes | Teachers | 97 | 74.2 | Elementary and middle school |
| Cornell-Swanson 2005237 | USA | Journal article | School social workers rated the effectiveness of medication, psychotherapy, family therapy, parenting classes, special education services and applied behavioural intervention in the classroom | No | School social workers | 189 | 85.9 | 14.5% worked with birth–3 years; 40.3% worked with preschool students; 76.9% worked with elementary school students; 57% worked with middle/junior high school students; 43% worked with high school students |
| Curtis 2006222 | USA and New Zealand | Journal article | Teachers rated acceptability of DRC, response cost technique, Ritalin and classroom lottery according to gender, ADHD subtype and teachers’ nationalities (USA and New Zealand) | Yes | Teachers | 420 | 86.9 | Mix of urban and suburban schools: 12 USA, 17 New Zealand. Mix of regular and special education teachers |
| Dryer 2012238 | Australia | Journal article | Teachers and parents of children with ADHD rated the effectiveness of non-traditional interventions; parent interventions; school-based interventions (changing the education system; providing additional teacher input; training for teachers; developing individualised school programmes); and medical and allied health interventions | No | Teachers and parents of children with ADHD | 224 | NR | Primary schools. Mix of general and special education teachers |
| Eng 2008223 | USA | Thesis/dissertation | Teachers rated acceptability of response cost intervention according to their ADHD intervention knowledge | Yes | Teachers | 47 | 85.0 | Elementary school teachers, grades pre-kindergarten to sixth grade |
| Fairbanks 1997214 | USA | Journal article | Teachers, school psychologists and school social workers rated acceptability of positive contingency management intervention (verbal praise and token economy) and negative contingency management interventions (timeout from the positive intervention) | Yes | Teachers, school psychologists, school social workers | 97 | NR | Teachers from three schools. School social workers were selected from the Illinois Association of School Social Workers state directory |
| Girio 2009224 | USA | Journal article | Teachers rated the acceptability of three evidence-based ADHD interventions (medication, DRC, timeout) and three ‘promising’ interventions (self-reinforcement, social skills, peer tutoring | Yes | Teachers | 156 | 94.2 | 11 elementary schools |
| Graczyk 2005217 | USA | Journal article | PPS professionals and classroom teachers rated effectiveness of classroom interventions; mental health services; medication; ineffective interventions according to subtype of ADHD and gender | Yes | PPS professionals (school psychologists, social workers, and counsellors); classroom teachers | 428 | 85.0 | Elementary schools |
| Groenewald 2009239 | UK | Journal article | Teachers’ treatment preference of medication, learning support, working with parents and behaviour therapy for female students with ADHD according to ADHD subtype (combined subtype ADHD and inattentive subtype ADHD) | Yes | Teachers | 212 | 89.0 | 40 primary schools |
| Higgins 1999240 | USA | Thesis/dissertation | Teachers rated the acceptability of school–home notes, students self-monitoring and contingency contracting interventions according to the inattentive and combined subtypes of ADHD | Yes | Teachers | 101 | 69.0 | High schools and middle schools. Grades 6–12 |
| Kos 2004216 | Australia | Thesis/dissertation | Teachers rated effectiveness and benefits of classroom management interventions according to gender and ADHD subtype (ADHD combined type; ADHD predominantly hyperactive/impulsive type; predominantly inattentive type; no diagnosis) | Yes | Teachers | 120 | 75.8 | 10 Catholic and six private primary schools. Prep-grade 6 teachers |
| Krowski 2009241 | USA | Thesis/dissertation | Teachers rated effectiveness of instructional accommodations; behavioural interventions; environmental accommodations; mental health services; support services for teachers; and medication treatment according to their factual and perceived knowledge of ADHD, and the support available to them in their school | No | Teachers | 119 | 92.4 | Three large elementary schools |
| Nietfield 2005242 | USA | Journal article | Teachers and pre-service teachers rated appropriateness and effectiveness of behavioural and clinical interventions | Yes | Teachers, pre-service teachers | 171 | 87.1 | Three elementary schools. All regular education. Kindergarten to fifth grade |
| Ohan 2008243 | Australia | Journal article | Teachers rated perceived effectiveness of medication; learning assistance/educational support; changes within classroom; and changes at home according to pre-tested ADHD knowledge | Yes | Teachers | 140 | 85.0 | Elementary schools. Kindergarten through to sixth grade |
| Pisecco 2001225 | USA | Journal article | Teachers rated acceptability of DRC; response cost; classroom lottery; and medication according to gender and ADHD subtype | Yes | Teachers | 159 | 92.0 | Elementary schools |
| Rowan 2000226 | USA | Thesis/dissertation | Teachers rated acceptability of positive reinforcement, timeout and medication interventions according to child mental health diagnosis: ADHD, ODD, depression and no diagnosis | Yes | Teachers | 190 | 88.0 | Elementary schools. Grades 1 to 6 and kindergarten |
| Saddler 2007244 | USA | Thesis/dissertation | Teachers ranked perceived effectiveness of token reinforcement; response cost; behaviour contract; home–school communication; home–school contingencies; modelling; self-management | No | Teachers | 141 | NR | Elementary school. Grades kindergarten to fifth grade |
| Schmalzer 2006229 | USA | Thesis/dissertation | Teachers rated acceptability, effectiveness and timeliness of self-management interventions for ADHD according to years of teaching experience and self-perceived experience working with children with ADHD | Yes | Teachers | 25 | NR | Elementary and middle schools |
| Stinnett 2001228 | USA | Journal article | Students on undergraduate teacher education course rated acceptability of Ritalin and special education according to the diagnostic label (no label vs. ADHD) and urban vs. rural settings | Yes | Teacher education students (undergraduate teacher education courses) | 144 | 81.0 | Most were elementary education majors (n = 64, 44.4%) |
| Stinson 2009229 | USA | Thesis/dissertation | Teachers rated acceptability of stimulant medication, work completion and combined intervention according to the diagnostic label (no label vs. ADHD) and age of child (6 years vs. 11 years) | Yes | Teachers | 213 | NR | Elementary schools |
| Stormont 2001245 | USA | Journal article | Preschool teachers rated comfort level and importance of implementing behavioural management, instructional management and outside support intervention | No | Teachers (preschool) | 138 | 95.0 | 30 preschools |
| Subramony 2006246 | USA | Thesis/dissertation | Teachers rated acceptability of nine school-based ADHD interventions | Yes | Teachers | 109 | 94.0 | Elementary schools. Teachers of kindergarten (44%), third (36%) and fifth grade (20%) |
| Vereb 2004247 | USA | Journal article | Teachers’ acceptability ratings of medication and behaviour management and its relationship with knowledge of ADHD, knowledge of treatment, experience of ADHD and training | No | Teachers | 48 | 94.0 | Elementary schools. Teachers in grades kindergarten through to sixth grade |
| Whitworth 1998248 | USA | Journal article | Teachers ranked the effectiveness of a list of school-based interventions for students with ADD | No | Teachers | 100 | NR | 10 elementary schools. Teachers in first grade through to sixth grade |
Sample sizes ranged from 25 to 428, with the majority of samples (23 out of 28) deemed large (≥ 100 participants). Where reported, the majority of participants were female in all studies. The majority of educators were teaching younger (5–12 years-of-age) children in kindergarten and elementary/primary schools. The majority of studies were located in the USA (n = 24214,217,222–229,233–237,240–242,244–248). Australia is the only other country represented by more than one study (n = 3216,238,243). Although one study was located in the UK,239 this study did not use a Likert scale, and, therefore, no UK studies impacted on the synthesis of attitude scores. This limits the potential applicability of the findings to the UK educational context. Data relating to teachers’ ethnicity, age and teaching experience, and details of the children with ADHD they taught, were rarely reported.
Interventions studied
During data extraction, interventions were initially categorised according to the 15 categories used in review 1. However, only five of these categories were represented by more than one study. Special education was not one of these categories, but appeared in seven studies in this review. 215,228,237,239,242,243,246 Special education refers to additional learning support or alternative class settings and/or curriculum where children with ADHD may be taught. Definitions for other school-based interventions may be found in Chapter 2 (see Table 4). As this review was also interested in comparisons with non-school interventions, a category for medication and other non-school interventions was included. Sometimes studies asked participants about a large number of interventions that were then categorised into intervention types (e.g. Kos216 asks participants about 33 interventions categorised into the following five groups: reinforcement; negative consequences; planned ignoring; organising the classroom and curriculum; emotional support). Where this categorisation maps onto the categories used in this review, we have reported at this level, rather than for numerous individual interventions. Table 25 illustrates the frequencies of the types of intervention about which attitudes were measured for each paper. The most frequently appearing specific school-based categories were contingency management (18 studies214–217,224–226,229,234,236,239,240,242,244,246,248), adaptations to the learning environment (eight studies216,217,234,241–243,246,248) and DRCs (eight studies217,222,224,225,240,242,244,246).
| First study author and year | Contingency management | DRC | Cognitive–behavioural self-regulation | Social skills training | Adaptations to learning environment or materials | Special education | Other school-based | Medication | Other non-school | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Alongi 2005233 | 1 | 1 | ||||||||
| Askew 1993234 | 1a | 1 | 3 | 5 | ||||||
| Bain 2009235 | 3 | 3 | 6 | |||||||
| Coles 2012215 | 1 | 1 | 1 | 1 | 1 | 2 | 7 | |||
| Conforti 2012236 | 1 | 2 | 3 | |||||||
| Cornell-Swanson 2005237 | 1 | 1 | 1 | 3 | 6 | |||||
| Curtis 2006222 | 2 | 1 | 1 | 4 | ||||||
| Dryer 2012238 | 1 | 3 | 4 | |||||||
| Eng 2008223 | 1 | 1 | ||||||||
| Fairbanks 1997214 | 2 | 2 | ||||||||
| Girio 2009224 | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||
| Graczyk 2005217 | 3 | 1 | 5 | 1 | 1 | 5 | 16 | |||
| Groenewald 2009239 | 1 | 1 | 1 | 1 | 4 | |||||
| Higgins 1999240 | 1 | 1 | 1 | 3 | ||||||
| Kos 2004216 | 2 | 1 | 2 | 5 | ||||||
| Krowski 2009241 | 1 | 3 | 1 | 5 | ||||||
| Nietfield 2005242 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 | ||
| Ohan 2008243 | 1 | 1 | 1 | 1 | 4 | |||||
| Pisecco 2001225 | 2 | 1 | 1 | 4 | ||||||
| Rowan 2000226 | 2 | 1 | 3 | |||||||
| Saddler 2007244 | 3 | 1 | 1 | 2 | 7 | |||||
| Schmalzer 2006227 | 1 | 1 | ||||||||
| Stinnett 2001228 | 1 | 1 | 2 | |||||||
| Stinson 2009229 | 1 | 1 | 1 | 3 | ||||||
| Stormont 2001245 | 3 | 3 | ||||||||
| Subramony 2006246 | 3 | 1 | 1 | 1 | 2 | 1 | 9 | |||
| Vereb 2004247 | 1 | 1 | 2 | |||||||
| Whitworth 1998248 | 1 | 1 | 15 | 17 |
Measures
Details about the questionnaires and scales used to measure attitudes in the 28 included studies are provided in Table 26. The majority of the studies (n = 17215–217,233–237,239,241–248) used bespoke attitude measures that had been designed for the study in question. Most studies (n = 21214,216,217,222–229,234–241,247) also provided some detail about the psychometric properties of the scale used and/or piloting of the scale developed. Scales ranged in the constructs that they measured, and were most often categorised as either both acceptability and perceived effectiveness (n = 8222–227,240,242) or acceptability (n = 4214,228,229,247) and perceived effectiveness (n = 12217,233–239,241,243,244,248) separately. The Likert scales used ranged from 4-point scales to 9-point scales. Most often Likert scales used 6 points. Eight studies215,216,234,235,239,242,244,248 did not use Likert scales and, instead, either asked participants to make a dichotomous yes/no type measure or to rank interventions. Scores from these ranking and forced choice measures were not converted to percentage scores.
| First study author and year | Name of scale | Scale author | Psychometric detail and piloting | Construct/s | Measure detail | Any issues with questionnaire items |
|---|---|---|---|---|---|---|
| Alongi 2005233 | Attention-Deficit/Hyperactivity Disorder Vignette | Current study | NR | Perceived effectiveness | Measures effectiveness of social skills training in facilitating the acquisition and performance of social skills: two 4-point Likert scales (acquisition and performance), 1 (not at all effective); 2 (mildly effective); 3 (moderately effective); 4 (very effective) | Only answered if participants believe vignette shows social skill deficits. No definition of social skills training |
| Askew 1993234 | Questionnaire | Current study | Piloted | Perceived effectiveness | 26 (relevant questions), ticked if a preferred method/intervention | Ticking an intervention may not necessarily indicate preference |
| Bain 2009235 | ISS | Current study assumed | Internal consistency was measured using Cronbach’s alpha for 18 intervention items (α = 0.76) | Perceived effectiveness | Six questions (one per intervention) related to ADHD. Four points: 1, have heard, will work; 2, have not heard, will work; 3, have heard, will not work; 4, have not heard, will not work | Only whether will/will not work |
| Coles 2012215 | Treatment preferences | Current study | NR | Preference (likelihood of referral) | Ranked how likely they were to refer the child to each of nine intervention conditions on a 10-point Likert scale, 1 = least likely, 10 = most likely | |
| Conforti 2012236 | Teacher Interventions for ADHD Students | Current study | Low Cronbach’s alpha reliability coefficients were found for all three scales: academic (α = 0.30), antecedent (α = 0.18) and consequent (α = –0.42) | Perceived effectiveness | 24 items, six questions per vignette, 5-point scale (1 = very poor, 2 = poor, 3 = unsure, 4 = good, 5 = very good) | |
| Cornell-Swanson 2005237 | Questionnaire | Current study | Piloted | Perceived effectiveness | 49 questions overall, six 5-point Likert questions asking about perceived effectiveness of treatments (1 = strongly disagree, 3 = neutral, do not know, 5 = strongly agree) | |
| Curtis 2006222 | BIRS | Elliot 1991249 | Coefficient alphas for each construct demonstrated high reliability: acceptability (α = 0.97), effectiveness (α = 0.92) and timeliness (α = 0.87). Internal consistency was measured in this study using Cronbach’s alpha for BIRS for New Zealand teachers: acceptability (α = 0.90), effectiveness (α = 0.88) and timeliness of effect (α = 0.59) | Acceptability, perceived effectiveness and timeliness of effect | 24 items using a 6-point Likert scale, ranging from strongly agree to strongly disagree. Acceptability scale consists of 15 questions, seven effectiveness questions, and two timeliness questions. Lower scores indicate greater acceptability | |
| Dryer 2012238 | Questionnaire – Beliefs About ADHD | Dryer 2006250 | Internal consistency was measured using Cronbach’s alpha for each intervention factor: non-traditional (α = 0.88), parent intervention (α = 077), school based (α = 0.78) and medical/allied health (α = 0.57). Piloted | Perceived effectiveness | 23 items relevant 5-point rating scale (0 = not at all effective, 4 = extremely effective; intervening rating categories were not labelled) | |
| Eng 2008223 | BIRS | Elliot 1991249 | Coefficient alphas for each construct demonstrated high reliability estimation: acceptability (α = 0.97), effectiveness (α = 0.92) and timeliness (α = 0.87). The BIRS has been reported to correlate significantly with other measures of treatment acceptability (α = 0.97)249 | Acceptability, perceived effectiveness and timeliness of effect | 24 items using a 6-point Likert scale, ranging from strongly agree to strongly disagree. Acceptability scale consists of 15 questions, including seven effectiveness questions and two timeliness questions. Lower scores indicate greater acceptability | |
| Fairbanks 1997214 | IRP-15 | Martens 1985251 | The internal consistency of the IRP-15 has been assessed by Martens 1985251 (α = 0.98). The IRP-15 has been shown to be highly correlated with the evaluative component of the semantic differential252 | Acceptability | 15 items, 6-point Likert format (1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, and 6 = strongly agree). Scores range from 15 to 90 | |
| Girio 2009224 | IRP-10 | Power 1995253 | The internal consistency of IRP-10 has been demonstrated to be adequate253 (ranging from α = 0.95 to α = 0.97) | Acceptability (includes perceived effectiveness) | 10 items are rated on a 6-point scale that ranges from 1 (‘strongly disagree’) to 6 (‘strongly agree’) | |
| Graczyk 2005217 | Intervention Effectiveness Scale | Current study assumed | Internal consistency was measured using Cronbach’s alpha for CI, mental health services and ineffective intervention categories in PPS professionals and teachers. (PPS professionals: α = 0.83, α = 0.73 and α = 0.53, respectively; teachers: α = 0.79, α = 0.86 and α = 0.72, respectively) | Perceived effectiveness | 16 items. Participants rated the effectiveness of a list of frequently recommended interventions for students with ADHD using the following 5-point scale: 0 = cannot rate, unfamiliar strategy; 1 = never effective; 2 = sometimes effective; 3 = usually effective; and 4 = always effective | 0 point not included in study’s analysis |
| Groenewald 2009239 | Questionnaire | Current study | Piloted | Perceived effectiveness | Participants views (yes/no) on whether or not the child might benefit from interventions | Dichotomous yes/no |
| Higgins 1999240 | Modified TEI-SF | Kelley 1989254 | Internal consistency was measured using Cronbach’s alpha for TEI-SF. All items scored α > 0.9, except item 8 which was excluded from composite scores | Acceptability (includes perceived effectiveness) | Nine items (eight Likert), 5-point Likert scale (1 = strongly disagree, 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree) | Question 8 does not seem to fit the others in terms of agree = positive acceptability |
| Kos 2004216 | ADHD Questionnaire | Current study | Piloted | Willingness to use intervention | Respondents were asked to place a tick beside the strategies they would use in their classroom to manage the child depicted in the vignette they had just read. Responses to these items were coded as either yes (‘1’) or no (‘2’) | Dichotomous yes/no measure |
| Krowski 2009241 | Interventions and teacher support services | Current study | Internal consistency was measured using Cronbach’s alpha for all 12 categories (α > 0.5). Piloted | Perceived effectiveness | Participants rate effectiveness (U = unfamiliar, cannot rate; 1 = never; 2 = sometimes; 3 = often; 4 = always) | Items rated as U = unfamiliar were coded as ‘missing data’ |
| Nietfield 2005242 | Survey (attitude measure) | Current study | NR | Teachers: acceptance; pre-service teachers: perceived effectiveness | Participants asked to rank eight interventions for either acceptance or perceived effectiveness | Rankings only |
| Ohan 2008243 | Treatment ratings | Current study | NR | Perceived effectiveness | Four questions related to treatments, 9-point Likert scales. No benefit–definite benefit | One question asks about two interventions (behavioural therapy and changes at home) |
| Pisecco 2001225 | BIRS | Elliot 1991249 | Coefficient alphas for each construct demonstrated high reliability estimation: acceptability (α = 0.97), effectiveness (α = 0.92) and timeliness (α = 0.87) The BIRS has been reported to correlate significantly with other measures of treatment acceptability249 |
Acceptability, perceived effectiveness and timeliness of effect | 24 items using a 6-point Likert scale, ranging from strongly agree to strongly disagree. Acceptability scale consists of 15 questions, including seven effectiveness questions, and two timeliness questions. Lower scores indicate greater acceptability | |
| Rowan 2000226 | AARP | Tarnowski 1992255 | All items loaded on a single factor (acceptability) that accounted for 84.9% of the variance. Internal consistency yielded split-half and Cronbach’s alpha coefficients of 0.95 and 0.97, respectively | Acceptability (includes perceived effectiveness) | Eight-item questionnaire rated on a 6-point Likert scale (1 = strongly disagree, 6 = strongly agree). Scores range from 8 to 48 | |
| Saddler 2007244 | Teacher Knowledge and Use of Classroom Interventions for Students with ADHD | Current study | None for effectiveness questions | Perceived effectiveness | Rank seven interventions from 1 to 7, with 1 being most effective and 7 being least effective | Rankings only |
| Schmalzer 2006227 | BIRS | Elliot 1991249 | Coefficient alphas for each construct demonstrated high reliability estimation: acceptability (α = 0.97), effectiveness (α = 0.92) and timeliness (α = 0.87). The acceptability factor of the BIRS had a correlation of 0.78 with the semantic differential, a measure previously used in acceptability studies249 | Acceptability, perceived effectiveness and timeliness of effect | 24 items using a 6-point Likert scale, ranging from strongly agree to strongly disagree. Acceptability scale consists of 15 questions, including seven effectiveness questions, and two timeliness questions. Lower scores indicate greater acceptability | |
| Stinnett 2001228 | IRP-15 | Martens 1985251 | The internal consistency of IRP-15 has been assessed by Martens 1985251 with high reliability (α = 0.98) and validity; the scale has been shown to be highly correlated with the evaluative component of the semantic differential (Osgood 1957252) | Acceptability | 15 items, 6-point Likert format (1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, and 6 = strongly agree). Scores range from 15 to 90 | |
| Stinson 2009229 | IRP-15 | Martens 1985251 | Internal consistency was measured using Cronbach’s alpha. Alpha coefficient α = 0.98251 | Acceptability | 15 items, 6-point Likert format (1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = slightly agree, 5 = agree, and 6 = strongly agree). Scores range from 15 to 90 | |
| Stormont 2001245 | Intervention Preferences Questionnaire | Modified from the SMAC, (Zentall 1995256) | NR | Importance and comfort using interventions | 43 interventions, 7-point Likert scale. Interventions were rated on a 1–7 scale, where 1 = not at all important, 7 = extremely important. 1 = not at all comfortable, 7 = totally comfortable | |
| Subramony 2006246 | Treatment Preference Questionnaire | Current study | Internal consistency was measured using Cronbach’s alpha for each questions (range from α = 0.76 to α = 0.99) | Acceptability and decision to use | Nine interventions listed, six statements concerning each strategy were listed, accompanied by a 5-point scale: strongly agree, agree, undecided, disagree, strongly disagree | Asking whether or not strategy is appropriate for students may be biased by age teaching: kindergarten, third grade or fifth grade. More kindergarten teachers |
| Vereb 2004247 | KARE | Current study | Internal consistency was measured using Cronbach’s alpha for KARE, ranged from α = 0.58 (knowledge of treatments scale) to α = 0.81 (behavioural management acceptability). Test–retest stability (n = 24, 4-week interval) ranged from 0.76 (behaviour management acceptability scale) to 0.80 (medication acceptability) | Acceptability | 10 questions (five on medication, five on behaviour management), 4-point Likert format (1 = not at all likely to 4 = very likely) | |
| Whitworth 1998248 | Effectiveness Survey | Current study | NR | Perceived effectiveness | List of interventions to be ranked according to top five, number of items and further scale details N/R | No detail on scale or items. Ranking only |
Two established reliable and valid scales were used by more than one study. Four studies222,223,225,227 used Elliot and von Brock Treuting’s Behavioural intervention Rating Scale (BIRS)249 and three studies214,228,229 used Martens et al. ’s Intervention Rating Profile-15 (IRP-15). 251
The BIRS is a measure that consists of three distinct factors: intervention acceptability; perceived effectiveness; and perceived timeliness of effect. The measure consists of 24 items, follows a 6-point Likert-type format, and is divided into two general categories of acceptability and effectiveness. The acceptability scale consists of 15 items and is actually a revision of the IRP-15. Seven items measure perceived effectiveness and two items measure perceived timeliness. A lower overall score indicates more positive attitudes. The BIRS is designed to be used to measure attitudes towards any intervention. Coefficient alpha for the overall scale is high (α = 0.97), whereas each construct also demonstrates high reliability, with estimates of α = 0.97 (acceptability), α = 0.92 (effectiveness) and α = 0.87 (timeliness) provided by the scale developers. 249 The acceptability factor of the BIRS had a correlation of 0.78 with the semantic differential, a measure previously used in acceptability studies. 249
The IRP-15 is an instrument that can be used to evaluate the acceptability of behavioural interventions. The 15 items reflect one empirically derived general acceptability factor and the scale has excellent internal consistency (α = 0.98). 251 Martens et al. 251 also demonstrated validity for the IRP-15; the scale has been shown to be highly correlated with the evaluative component of the semantic differential, a scale that measures people’s reactions to stimulus concepts on bipolar scales with contrasting adjectives at each end. 252 Items on the IRP-15 are answered on a 6-point Likert format. Raw scores for each item are summed to yield an overall acceptability score. The IRP-15 has been used to evaluate school-based interventions in a number of studies. 257 At least two questions of the IRP-15 appear to measure perceived effectiveness: ‘Q3: This intervention should prove effective in changing the child’s behaviour’ and ‘Q14: This intervention is a good way to handle this child’s behaviour’. Therefore, in this review the IRP-15 is considered to measure both acceptability and perceived effectiveness.
Quality appraisal
A summary of results of the quality appraisal of included papers is displayed in Table 27. Quality appraisal was used as a means to raise awareness about a range of relevant factors for each paper, rather than as a basis for exclusion. Positive, negative and neutral appraisal scores are collated for each question and each paper. Most often responses were of the yes/no/partial kind; for group allocation and randomisation, details of whether or not groups were randomised are given. For sample size, large is considered positive, medium considered neutral and small considered negative. For the question regarding whether or not vignettes had been piloted, a neutral appraisal score was made when researchers had not piloted their vignettes but had detailed their use of DSM-III criteria within the vignettes. Using diagnostic criteria as part of vignettes was considered more robust than no piloting or associated detail of the rigour of vignette contents.
| First study author and year | Demographic details regarding participants reported? | Have the intervention/s been defined by the author? | Have the intervention/s been defined for participants? | Details of group allocation and/or randomisation? | Is the relevant sample size small (< 20), medium (20–99), or large (100 +)? | Detail of dropouts, response rate and/or missing data? | Are vignettes piloted and/or assessed? | Psychometric detail reported regarding attitude measure? | Piloting of attitude measure reported if developed by author? | Totals (yes/positive, no/negative, partial/neutral) |
|---|---|---|---|---|---|---|---|---|---|---|
| Alongi 2005233 | Yes | No | No | Random allocation | Large | Yes | DSM-IV | No | No | 4, 4, 1 |
| Askew 1993234 | Yes | Partial | No | No group allocation | Large | Yes | N/A | No | Yes | 4, 2, 1 |
| Bain 2009235 | Yes | No | No | No group allocation | Large | No | N/A | Yes | No | 3, 4, 0 |
| Coles 2012215 | Yes | No | No | No group allocation | Medium | Yes | Yes | No | No | 3, 4, 1 |
| Conforti 2012236 | Yes | Partial | Partial | No group allocation | Medium | Yes | DSM-IV | Yes | Yes | 4, 0, 4 |
| Cornell-Swanson 2005237 | Yes | No | No | No group allocation | Large | Yes | N/A | No | Yes | 4, 3, 0 |
| Curtis 2006222 | Yes | Yes | Yes | Random allocation | Large | Yes | DSM-IV | Yes | N/A | 7, 0, 1 |
| Dryer 2012238 | No | No | No | No group allocation | Large | Yes | N/A | Yes | Yes | 4, 3, 0 |
| Eng 2008223 | Yes | No | Partial | Teachers self-selected | Medium | Yes | Yes | Yes | N/A | 4, 2, 2 |
| Fairbanks 1997214 | No | Yes | Yes | No | Medium | No | No | Yes | N/A | 3, 4, 1 |
| Girio 2009224 | Yes | Yes | Yes | No group allocation | Large | Yes | Partial | Yes | N/A | 6, 0, 1 |
| Graczyk 2005217 | Yes | No | No | Random allocation | Large | Yes | DSM-IV | Yes | No | 5, 3, 1 |
| Groenewald 2009239 | Yes | No | No | Not random | Large | Yes | Yes | No | Yes | 5, 4, 0 |
| Higgins 1999240 | Yes | Yes | Yes | No group allocation | Large | Yes | Yes | Yes | N/A | 7, 0, 2 |
| Kos 2004216 | Yes | No | No | No | Large | Yes | Yes | No | Yes | 5, 4, 0 |
| Krowski 2009241 | Yes | No | No | No group allocation | Large | Yes | N/A | Yes | Yes | 5, 2, 2 |
| Nietfield 2005242 | Yes | No | No | No group allocation | Large | Yes | DSM-IV-TR | No | No | 3, 4, 1 |
| Ohan 2008243 | Yes | No | No | No group allocation | Large | Yes | Yes | No | No | 4, 4, 0 |
| Pisecco 2001225 | Yes | Yes | Yes | Random allocation | Large | No | DSM-IV | Yes | N/A | 6, 1, 1 |
| Rowan 2000226 | Yes | Yes | Yes | Random allocation | Large | Yes | No | Yes | N/A | 7, 1, 0 |
| Saddler 2007244 | No | Yes | Yes | No group allocation | Large | Yes | N/A | No | No | 4, 3, 0 |
| Schmalzer 2006227 | Yes | Yes | Yes | No group allocation | Medium | Yes | No | Yes | N/A | 5, 1, 1 |
| Stinnett 2001228 | Yes | No | No | No | Large | No | No | Yes | N/A | 3, 5, 0 |
| Stinson 2009229 | Yes | Yes | Yes | Random allocation | Large | No | No | Yes | N/A | 6, 2, 0 |
| Stormont 2001245 | Yes | Yes | Partial | No group allocation | Large | Yes | N/A | No | N/A | 4, 1, 1 |
| Subramony 2006246 | Yes | Yes | Yes | No group allocation | Large | Yes | Yes | Yes | No | 7, 1, 0 |
| Vereb 2004247 | Yes | No | No | No group allocation | Medium | Yes | N/A | Yes | Yes | 4, 2, 1 |
| Whitworth 1998248 | No | No | No | No group allocation | Large | No | N/A | No | No | 1, 6, 0 |
| Totals (yes/positive, no/negative, partial/neutral) | 24, 4, 0 | 11, 15, 2 | 10, 15, 3 | 6, 5, 0 | 23, 5, 0 | 22, 6, 0 | 7, 7, 5 | 17, 11, 0 | 8, 9, 0 |
Only two studies222,240 recorded no negative appraisal scores. Six studies214,215,228,235,242,248 recorded more negative than positive scores, in particular Whitworth248 had a large sample size (a positive response) but received a negative response for all other relevant questions. As a whole the papers were of low quality and prone to bias. Particular issues indicated by more frequent negative appraisal scores across a number of the studies were a lack of definitions of interventions, both within the papers and the measures used; and failure to pilot vignettes and attitude measures developed by authors. Psychometric detail about attitude measurement was often missing and this was more likely for scales developed specifically for an individual study.
Synthesis of attitudes findings
Nineteen papers were included in a quantitative synthesis of attitude findings. The remaining nine papers215,216,234,235,239,242,244,247,248 were not included because either they did not use Likert scales to measure attitudes (see Table 26) or, as in the case of Vereb and DiPerna,247 there was no detail regarding how the mean scores reported were calculated. Although the forced choice measures could have been used to calculate percentages, the range of percentages would have typically been higher than the Likert scale findings because of the difference between the construction of the scores, hence these were also omitted. The findings of these nine studies will be described briefly before moving onto a synthesis of the remaining studies.
Narrative synthesis
Whitworth248 and Nietfield and Hunt242 asked teachers to rank interventions according to their perceived effectiveness (Whitworth248) and both acceptability and effectiveness (Nietfield and Hunt242). Teachers ranked contingency management or adaptations to learning environment interventions as more effective than other school-based interventions in Whitworth’s paper. 248 Nietfield and Hunt242 found that teachers ranked contingency management and DRCs as the most acceptable and effective interventions; medication and special education received the lowest ranks. Teachers rated behaviour management as slightly more acceptable than medication in Vereb and DiPerna’s paper. 247
Askew234 reported that teachers most often indicated that special education, contingency management and self-monitoring were effective interventions for use with children with ADHD. Participants in Bain et al. ’s study235 most often believed that meta-cognitive skills training, guided imagery and play therapy would work for children with ADHD. UK-based teachers in Groenewald et al. ’s study239 nearly always believed a child with ADHD would benefit from learning support and school-based behaviour therapy, but rarely considered that medication would benefit such children. Kos216 found that teachers would choose to use positive reinforcement, emotional support or adaptations to learning environment or materials with children described in vignettes more often than negative reinforcement and punishment techniques. Teachers considered modelling, token reinforcement and home–school communication the most effective interventions in Saddler’s study. 244 Finally, results regarding treatment preferences for behaviour modification and medication reported by Coles et al. 215 are unclear.
Quantitative synthesis
For the remaining 19 papers that used Likert scales, percentages were calculated wherever possible to indicate the positivity of attitude towards each intervention measured. As mentioned above, an arbitrary cut off was set, which classified percentages of ≥ 60% as indicating a ‘positive attitude’ towards the interventions in question, 40–59% indicating a ‘neutral attitude’ and < 40% as a ‘negative attitude’. This allowed for a quantitative synthesis of these 19 studies. Table 28 provides the findings for all the school-based interventions across studies. Positive attitudes towards DRC-type interventions (includes school–home note/book) were found in all five studies for which a percentage was calculable for this intervention. 222,224,225,240,246 Two studies compare praise and punishment,226,246 and both reported positive attitudes towards praise as a strategy, whereas ‘lose points’ and ‘time out’ held percentages below 60%. Often attitudes towards particular interventions are mixed. Many interventions, including contingency management, self-monitoring, special education, social skills training and a range of classroom accommodations appear in both the positive column as well as the neutral/negative columns depending on the study. Finally, there appears to be variability in educators’ attitude scores across studies. For instance, all percentages are very low in Krowski’s paper,241 but very high in Stormont and Stebbins’ paper. 245 This may indicate differences in study context or the measures used.
| First study author and year | Name of scale | Positive attitude (≥ 60%) | Neutral attitude (40–59%) | Negative attitude (< 40%) |
|---|---|---|---|---|
| Alongi 2005233 | Attention-Deficit/Hyperactivity Disorder Vignette | Social skills training (49.7%) | ||
| Conforti 2012236 | Teacher Interventions for ADHD Students | Contingency (51.2%) Antecedent (58.3%) Academic (55.06%) |
||
| Cornell-Swanson 2005237 | Questionnaire | Applied behavioural intervention (75.3%) | Special education services (54.8%) | |
| Curtis 2006222 | BIRS | DRC (70.0%) | Response cost technique (57.0%) Classroom lottery (46.6%) |
|
| Dryer 2012238 | Questionnaire – Beliefs About ADHD | School-based interventions (72.5%) | ||
| Eng 2008223 | BIRS | Response cost technique (56.5%) | ||
| Fairbanks 1997214 | IRP-15 | Contingency management (58.4%) | ||
| Girio 2009224 | IRP-10 | DRC (71.4%) Self-reinforcement (69.1%) Social skills (67.1%) |
Peer tutoring (58.2%) Time out (50.1%) |
|
| Graczyk 2005217 | Intervention Effectiveness Scale | Classroom Interventions (57.5%) | ||
| Higgins 1999240 | Modified TEI-SF | Contingency contracting (61.3%) School–home notes (63.0%) |
Self-monitoring (55.9%) | |
| Krowski 2009241 | Interventions and teacher support services | Instructional accommodations (47.1%) | Behavioural interventions (33.7%) Environmental accommodations (35.0%) Support services for teachers (24.4%) |
|
| Ohan 2008243 | Treatment ratings | Learning assistance/educational support (62.7%) Changes within classroom (80.0%) |
||
| Pisecco 2001225 | BIRS | DRC (62.1–83.6%) Response cost technique acceptability and timeliness for female vignette (60.9–73.7%) |
Classroom lottery (40.8–53.1%) Response cost technique perceived effectiveness and timeliness for male vignette (48.5–59.7%) |
|
| Rowan 2000226 | AARP | Praise (72.3%) | Time out (46.7%) | |
| Schmalzer 2006227 | BIRS | Self-management intervention (68.6%) | ||
| Stinnett 2001228 | IRP-15 | Special education for rural teachers (46.7%) | Special education for urban teachers (31.7%) | |
| Stinson 2009229 | IRP-15 | Work completion (includes contingency management) (64.2%) | ||
| Stormont 2001245 | Intervention Preferences Questionnaire | Behavioural management (84.8%) Instructional management (81.7%) Outside support (84.9%) |
||
| Subramony 2006246 | Treatment Preference Questionnaire | Home–school notebook (80.1%) Visual schedule (66.3%) Praise (88.1%) Resource room (74.0%) |
Earn points (59.3%) Timer (55.3%) Lose points (57.9%) Extended time (57.9%) |
Table 29 displays the attitude percentages by study and intervention category and includes medication and other non-school interventions as measured. Again, DRC is the only intervention with a consistently positive attitude across studies. Although this preference for DRCs may be an artefact of the five studies that report attitudes towards them,222,224,225,240,246 each of these studies do include neutral attitudes towards other interventions, therefore we can assume that participants rating DRCs were not necessarily positive regardless of the intervention(s) that they were asked to rate. Attitudes towards medication span a very wide range of percentages from 16.2% reported by Ohan et al. 243 to 74.2% in Pisecco et al. ’s paper. 225 This does not appear to be impacted by the other interventions that teachers are rating. Where individual studies compare various school-based interventions to medication and/or other non-school interventions, there do not appear to be any trends in terms of whether school or medication and/or other non-school interventions receive more positive attitude ratings.
| First study author and year | Vignette? | Construct/s | Contingency management | DRC with behaviour modification | Cognitive–behavioural self-regulation | Social skills training | Adaptations to learning environment or materials | Special education | Other school based | Medication | Other non-school |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alongi 2005233 | Yes | Perceived effectiveness | O (49.7%) | ||||||||
| Conforti 2012236 | Yes | Perceived effectiveness | O (51.2%) | O (58.3%, 55.06%) | |||||||
| Cornell-Swanson 2005237 | No | Perceived effectiveness | O (54.8%) | + (75.3%) | + (73.5%) | (57.5–72.5%) | |||||
| Curtis 2006222 | Yes | BothBIRS | O (57.0%, 46.6%) | + (70.0%) | O (48.0%) | ||||||
| Dryer 2012238 | No | Perceived effectiveness | + (72.5%) | (47.5–70.0%) | |||||||
| Eng 2008223 | Yes | BothBIRS | O (56.5%) | ||||||||
| Fairbanks 1997214 | Yes | AcceptabilityIRP | O (58.4%) | ||||||||
| Girio 2009224 | Yes | Both | O (50.1%) | + (71.4%) | + (69.1%) | + (67.1%) | O (58.2%) | O (59.6%) | |||
| Graczyk 2005217 | Yes | Perceived effectiveness | O (57.5%) | + (63.9%) | O (55.9%) | ||||||
| Higgins 1999240 | Yes | Both | + (61.3%) | + (63.0%) | O (55.9%) | ||||||
| Krowski 2009241 | No | Perceived effectiveness | – (35.0%) | (24.4–47.1%) | + (63.8%) | ||||||
| Ohan 2008243 | Yes | Perceived effectiveness | + (78.0%) | + (62.7%) | – (16.2%) | + (77.4%) | |||||
| Pisecco 2001225 | Yes | BothBIRS | (40.8–73.7%) | + (62.1–83.6%) | (53.4–74.2%) | ||||||
| Rowan 2000226 | Yes | Both | (46.7–72.3%) | + (65.4%) | |||||||
| Schmalzer 2006227 | Yes | BothBIRS | + (68.6%) | ||||||||
| Stinnett 2001228 | Yes | AcceptabilityIRP | (31.6–46.7%) | O (40.5–47.9%) | |||||||
| Stinson 2009229 | Yes | AcceptabilityIRP | + (64.2%) | + (60.6%) | + (62.5%) | ||||||
| Stormont 2001245 | No | Both | + (81.7–84.9%) | ||||||||
| Subramony 2006246 | Yes | Both | (57.9–88.1%) | + (80.1%) | + (66.3%) | + (74.0%) | O (55.3–57.9%) | + (82.4%) |
Table 29 also indicates the studies in which vignettes were used and the attitude construct measured. It does not appear that the use of vignettes makes a clear difference to attitudes, given that the few studies that did not use vignettes include some of the highest (Stormont and Stebbins245) and lowest (Krowski241) attitude ratings. Likewise, there do not appear to be any clear trends regarding attitudes on account of whether acceptability, perceived effectiveness, or both are measured. Where different studies used the same measures and intervention categories, there does not appear to be close agreement for scores on either the IRP-15 or BIRS, although there is some consistency between findings reported by Curtis et al. 222 and Pisecco et al. 225 who used identical instruments including the BIRS. Overall, though, educators’ attitudes do not appear to be consistent across studies regardless of the similarity of measures used.
Variables related to attitudes to interventions
Table 30 summarises the findings from included studies related to variables regarding the educators who participated and the children with ADHD potentially receiving the interventions. Findings were included where papers reported a test of significance relating to attitude outcomes. Few of these variables were considered by more than one study and when they were, different interventions were often considered. We can tentatively suggest that teachers’ level of education may not affect intervention attitudes. However, teaching experience was significantly related to intervention attitudes in three studies. 224,236,246 There were conflicting findings regarding ADHD subtype of vignettes. Two of four studies found significant effects,239,240 but Higgins240 found greater treatment acceptance for inattentive subtypes, whereas Groenewald et al. 239 found medication less endorsed for inattention. Vignette studies suggested no difference in attitudes to intervention according to gender of vignette.
| Category | Variable | Significant difference/correlation | Non-significant difference/correlation | Total studies |
|---|---|---|---|---|
| Teacher demographics | General vs. special education teachers | General teachers more accepting of DRCs – Higgins 1999240 | 1 | |
| Teacher level of education | Conforti 2012236 Stormont 2001245 | 2 | ||
| Teacher ADHD knowledge | High knowledge more favourable perception of special education, classroom modification and changes at home – Ohan 2008243 Higher ADHD knowledge associated with higher medication acceptability – Vereb 2004247 |
Krowski 2009241 | 3 | |
| Teacher treatment knowledge | More treatment knowledge associated with higher behaviour management acceptability and lower medication acceptability – Vereb 2004247 | 1 | ||
| Teacher ADHD training | More ADHD training associated with higher medication and behaviour management acceptability – Vereb 2004247 | 1 | ||
| ADHD books read | Significant correlations between the number of books teachers read about ADHD and the effectiveness of instructional interventions and seating a child alone – Krowski 2009241 | 1 | ||
| Teacher experience | Teachers with more experience less likely to use two consequence interventions – Conforti 2012236 More experienced teachers are predictive of a greater preference for time-out over peer tutoring – Girio 2009224 Teachers with more years teaching more willing to use losing points strategy – Subramony 2006246 |
Nietfield 2005242 | 4 | |
| USA vs. New Zealand | New Zealand teachers rate medication as more effective and acceptable – Curtis 2006222 | 1 | ||
| Teacher age | Girio 2009224 | 1 | ||
| Experience teaching children with ADHD | More experience associated with higher medication acceptability – Vereb 2004247 | Girio 2009224 Stormont 2001245 | 3 | |
| Familiarity with ADHD | Number of friends and family members with ADHD significantly related to the effectiveness ratings of feedback from physicians, seating a child alone and instructional interventions – Krowski 2009241 | 1 | ||
| Confidence teaching ADHD | Teachers with more confidence in their ability to teach a student with ADHD provided greater effectiveness ratings for Instructional Interventions – Krowski 2009241 | 1 | ||
| Teacher self-efficacy | Girio 2009224 | 1 | ||
| Grade taught | Positive correlation with teachers’ acceptability rating of DRC and losing points contingency management – Subramony 2006246 | Girio 2009224 | 2 | |
| Use of teacher support services | Positive correlation with effectiveness of behavioural interventions, environmental accommodations – Krowski 2009241 | 1 | ||
| Perceived effectiveness of teacher support services | Positive relationships with effectiveness of behavioural interventions, environmental accommodations, instructional accommodations and mental health services – Krowski 2009241 | 1 | ||
| Intelligence | More intelligent teachers rate acceptability of clinical intervention lower and behavioural higher – Nietfield 2005242 | 1 | ||
| Teacher role | Teachers vs. school psychologists vs. school social workers | Fairbanks 1997214 | 1 | |
| Teachers vs. school support roles | Graczyk 2005217 | 1 | ||
| Disorder | ADHD vs. autism vs. LDs | Alongi 2005233 | 1 | |
| ADHD vs. LDs vs. behaviour disorder | Fairbanks 1997214 | 1 | ||
| ADHD vs. ODD vs. depression | Rowan 2000226 | 1 | ||
| Vignette | Vignette ADHD subtype | Treatments as a whole rated more acceptable for inattentive – Higgins 1999.240 Medication endorsed more for combined subtype than inattentive – Groenewald 2009239 | Coles 2012215 Kos 2004216 | 4 |
| Vignette gender | Coles 2012215 Curtis 2006222 | 2 | ||
| School level | Urban/rural high schools | Participants who reported that they had attended high school in an urban setting found the treatments significantly less acceptable than did participants from rural high schools – Stinnett 2001228 | 1 |
Discussion
This review of quantitative attitude research relating to school-based interventions for ADHD found 28 relevant studies that measured educators’ attitudes in terms of their beliefs regarding perceived effectiveness and/or acceptability of a range of school-based interventions for ADHD as well as comparison to some non-school interventions, particularly medication. There was a paucity of quantitative research considering children’s or parents’ views towards non-pharmacological interventions for ADHD in school settings. Therefore, this review focused only on educator attitudes.
Across these studies, educators held a variety of attitudes ranging from negative to positive. The most striking finding is the lack of consistency about attitudes towards particular interventions or types of interventions, with most rated positively or neutrally/negatively across different studies. The only intervention that consistently recorded positive attitudes from educators was DRCs, an intervention where behaviour is monitored and recorded at school on a card or in a book that the pupil then takes home to share with their parent or carer. Often the pupil will receive behavioural reinforcement at home and school on account of the report card contents. No variables were consistently identified across reviewed studies that affected attitudes towards interventions.
The majority of studies used vignettes to provide ADHD case descriptions to participants. Vignettes potentially offer a level of consistency as they aim to elicit beliefs in response to a consistent target with age, gender and symptoms often clearly specified. However, often these vignettes were not adequately piloted, so consistency across the vignettes used within studies may be questioned.
It is perhaps surprising that the majority of the studies developed attitude measures for the purpose of their research, rather than using an established reliable and valid scale for measuring attitudes towards interventions. Seven included studies used either the BIRS or IRP-15, which have both been shown to reliably and validly measure attitudes towards interventions. The BIRS holds the advantage that it explicitly measures both acceptability and effectiveness, whereas many of the studies only measured one of these aspects of intervention attitude. Indeed, there may be an intervention that teachers believe is effective but that they do not think is acceptable to use, and vice versa. Therefore, future research would benefit from taking advantage of existing measures and measure both acceptability and perceived effectiveness. For systematic reviews of attitude research, agreed standardised measures would avoid the need to convert varying Likert scores to a comparable format and arbitrarily decide what constitutes a positive attitude.
There was wide variation in the number of interventions that each study captured attitudes towards. Although these interventions could often be categorised in the manner that we applied in review 1 (see Chapter 2), few studies measured attitudes towards the same interventions and, therefore, direct comparison was rarely possible. Nevertheless, it appears that educators hold wide-ranging attitudes towards interventions for ADHD. Future research might attempt to investigate the reasons for the diversity in attitudes towards interventions for ADHD in school settings both within and between studies.
The reviewed studies varied in their quality appraisals. Some studies appeared to show little risk of bias, whereas others scored very low on the quality appraisal criteria developed for this study. If research wishes to measure attitudes to interventions more accurately then it is critical that the interventions are clearly defined and that the measures used are both piloted and assessed for reliability and validity. Too often this was not the case in studies reviewed.
Understanding the attitudes of those responsible for accepting and potentially delivering interventions, as is the case with educators and interventions for ADHD in school settings, is critical given that the attitudes of educators can operate as barriers or facilitators to the implementation and effectiveness of these interventions (see reviews 3 and 4). The lack of consistency across the studies reviewed may point to the different methods used, which could be addressed in future research. It is also likely to be indicative of the complexity regarding attitudes and beliefs that educators may hold. Future research that attempts to untangle this web should be welcomed.
Chapter 4 Methods for qualitative reviews 3 and 4
This chapter describes the methods used to undertake the qualitative reviews whose findings are described in Chapters 5 and 6. The methods used to identify and select evidence followed the methodological approach published by the Centre for Reviews and Dissemination (University of York). 212 A meta-ethnographic approach88 was used to synthesise findings across included studies in both reviews.
Aims
The aim of the overall research project is to evaluate non-pharmacological interventions delivered in school settings for children with, or at risk of, ADHD and to explore the factors that may enhance, or limit, the delivery of such interventions.
The foci of the qualitative reviews are:
-
review 3: the experiences of and attitudes held by parents, children, peers, teachers and others involved in ADHD interventions in schools
-
review 4: the school-related experiences and perceptions of pupils diagnosed with, or at risk of, ADHD, their teachers, parents and peers.
Identification of evidence
Inclusion/exclusion criteria
Population and setting
Studies whose populations of interest were schoolchildren with, or at risk of, ADHD, aged between 4 and 18 years, their parents, peers and/or those who work with these children in school settings were included. School settings could include mainstream schools, special schools, residential schools, preschools and pupil referral units. Types of school considered ranged from preschool to high school. Although experience at university level was excluded, retrospective accounts from adults with ADHD, including higher education college students who reported about their attitudes to and prior experiences of ADHD in school, were included. Populations described as having intellectual disabilities [i.e. intelligence quotient (IQ) of < 70] or brain injuries were excluded, whereas comorbidities and populations where only some of the sample had ADHD and/or experience of ADHD were included. Papers were excluded if the settings described were outside of ordinary school experience, such as summer-school settings, residential treatment centres, laboratory schools (schools that operate in association with researchers in order to facilitate educational research), clinics, hospitals and homes.
Location and language
Given the importance of context for the formation and influence of attitudes, studies from societies and educational systems markedly different from the UK will be less informative for this research. We therefore included only studies from countries belonging to the OECD (see Appendix 6) in the review and carefully considered the applicability of findings to the UK setting during synthesis. Only papers written in English were included given the focus on experiences and attitudes, which might be lost or distorted by translation from studies written in another language.
Study design
Papers were included when they reported primary research using methods for qualitative data collection and analysis. Therefore, research was excluded if qualitative data were presented but methods of analysis were not described or evident, and where there was quantitative analysis of qualitative data or quantitative measures of attitudes. The latter was explored as a separate focus of analysis and is reported in Chapter 3.
Intervention
Review 3 included non-pharmacological interventions with at least some unique elements delivered in an educational setting. Interventions could target children directly (such as study skills training) or indirectly (e.g. teacher training). Research was also included that focused on the teaching strategies used with pupils with ADHD, given that such practice includes components of interventions seen elsewhere (e.g. behaviour modification and special education classes). Interventions and experiences in settings that could not be generalised to mainstream school settings were excluded, for instance summer treatment programmes or laboratory schools.
Review 4, which focused on experiences of ADHD in schools, did not require inclusion criteria related to interventions.
Date
Only studies published or conducted (where unpublished) from 1980 onwards were included, reflecting significant changes to the diagnosis of ADHD that year3 that would mean earlier studies may sample different, albeit overlapping, populations of children.
The inclusion and exclusion criteria for reviews 3 and 4 are summarised in Table 31. Papers could be included in both reviews 3 and 4, given that some studies considered both relevant interventions and the wider experience of people with ADHD in school settings.
| Review(s) | Criteria | Specification |
|---|---|---|
| 3 and 4 | Population | Include:
|
| 3 and 4 | Methods | Include:
|
| 3 | Intervention | Include:
|
| 4 | Experience | Include:
|
Search strategy
The search strategy involved the following elements:
-
search of electronic databases
-
relevant papers located during searches for review 1
-
forward and backward citation chasing
-
web searches
-
hand-searching of key journals
-
contact with experts in the field.
A database search strategy was developed which combined three elements: terms related to ADHD; terms related to a school context; and a bespoke qualitative research filter. The database search strategies used a mixture of subject headings (controlled vocabulary) and free-text terms. Searches were restricted to years from 1980 onwards. Twenty electronic databases were searched [ASSIA/ProQuest, MEDLINE/OvidSP, EMBASE/OvidSP, PsycINFO/OvidSP, British Education Index/ProQuest, Australian Education Index/ProQuest, Education Research Complete/EBSCOhost, ERIC/ProQuest, The Cochrane Library (CDSR, DARE, CENTRAL, CMR, HTA, NHS EED), The Campbell Library, HMIC/OvidSP, Social Sciences Citation Index, Conference Proceedings Citation Index, Conference Proceedings Citation Index – Social Science & Humanities (via ISI Web of Science)], during July 2012. Searches were updated in March 2013. An example search strategy used for the PsycINFO/OvidSP database is shown in Appendix 7. Forward citation chasing of included papers, backward chasing of included papers’ reference lists, asking expert advisors from the project team for relevant papers, hand-searching of key journals and web searches were completed to identify additional relevant work (see Chapter 2 for list of hand-searched journals and websites examined for additional research). EndNote v.X5 management software was used to organise the search results, screening and full-text retrieval processes.
Study selection
Relevant studies were identified in two stages based on the inclusion/exclusion criteria given above (see Figure 4 for a study selection flow diagram for review 3, and Figure 6 for a study selection flow diagram for review 4). First, two reviewers conducted title/abstract screening independently for each record (six researchers shared this screening: DM, RGJ, TND, RW, RA, MR) and disagreements were resolved through discussion (DM, RGJ). A predefined checklist (see Appendix 8) was used to assess adherence to the inclusion criteria. Full texts of records that might potentially meet the inclusion criteria were then obtained. Full texts were screened independently by two reviewers (DM, RGJ) for inclusion and exclusion, with each included text allocated to a review (papers could be included in review 3, review 4, or both reviews). Disagreements were resolved through discussion (DM, RGJ).
Methods of analysis/synthesis
Data extraction
For both reviews 3 and 4, a data extraction form was adapted from a previous Cochrane mixed-methods systematic review. 258 The form was piloted by two reviewers (RGJ and DM) who extracted data from four studies initially, developing the form in response to identified gaps (please see Appendix 9 for an example of a completed data extraction form for review 4). For review 3 (about experience of interventions), in addition to the categories of data extracted for review 4, descriptive details about interventions were extracted using the relevant portions of the data extraction form used in review 1 (the quantitative review about intervention efficacy) (please see Appendix 10 for an example of a completed data extraction form for review 3). Data were extracted into the qualitative software package NVivo v.9.2 (QSR International, Warrington, UK) or extracted to Microsoft Office Word v.2007 (Microsoft Corporation, Redmond, WA, USA) and imported to NVivo when searchable portable document format (PDF) versions of included papers were not available. Data for reviews 3 and 4 were extracted by one reviewer and checked by another reviewer (shared between RGJ and DM). Where papers acknowledged qualitative analysis but did not provide sufficient detail, and contact details were available, authors were emailed to request further information. 28,259–265 Five authors replied with further details. 259–261,263,266
Quality assessment
During screening two questions were asked:
-
Does the paper report on findings from research that involved both qualitative methods of data collection and analysis?
-
Is the research relevant to the synthesis topic?
If one of the answers to these questions was ‘no’, the paper was excluded. The first question effectively excluded those papers that could be regarded as ‘fatally flawed’; if both answers were ‘yes’, the paper could be included and appraisal could proceed.
Study appraisal was conducted simultaneously with data extraction using criteria adapted from the Wallace Checklist. 267 This included 15 questions meant to act as sensitising ‘prompts’268 as follows: probing research questions; underpinning theory; study design; context; the sample; data collection and analysis; relationships between data and findings; limitations; generalisability; ethics; and reflexivity (Box 3). One question, ‘are the interventions of interest clearly described?’ was relevant to review 3 only. Questions were assigned a response of ‘yes’, ‘no’ or ‘cannot tell’ for each paper. Quality appraisal decisions were made independently by two reviewers (DM and RGJ), and disagreements were resolved through discussion by these reviewers.
Is the research question clear?
Is the theoretical or ideological perspective of the author explicit?
Has the theoretical or ideological perspective influenced the study design, methods or research findings?
Is the study design appropriate to answer the question?
Is the context or setting adequately described?
Is the sample adequate to explore the range of subjects and settings and has it been drawn from an appropriate population?
Was the data collection adequately described?
Was data collection rigorously conducted to ensure confidence in the findings?
Was there evidence that the data analysis was rigorously conducted to ensure confidence in the findings?
Are the findings substantiated by the data?
Has consideration been given to any limitations of the methods or data that may have affected the results?
Do any claims to generalisability follow logically and theoretically from the data?
Have ethical issues been addressed and confidentiality respected?
Is the author reflexive?
Are the interventions of interest clearly described? [Review 3 only.]
The appraisals were not used to exclude papers. Experience in previous qualitative reviews suggests that higher quality papers often contribute more to a synthesis,88 creating an integral, organic process of weighting the findings of better quality studies. 269 In addition, ‘poorer’ quality papers may support concepts and theories developed in the stronger papers270 and, therefore, make useful contributions to the review. Quality appraisal may relate to quality of reporting as much as to quality of the study. 271,272 Finally, there is a lack of consensus among qualitative researchers about how to measure quality in qualitative research. 273 These factors support the use of quality appraisal as a means to raise awareness about a range of relevant factors for each paper, rather than using it as a basis for exclusion.
The transferability of reviews 3 and 4 was explored in two workshops that took place during the time period in which data analysis occurred. One workshop was with behavioural advisory support teachers and one was with a support group for parents of children with ASDs and/or ADHD. Transferability in qualitative research refers to the judgements made by stakeholders about how relevant research findings are to their own experience, and has similarities to external validity in quantitative research. Stakeholders stated during both workshops that many of the themes discussed in reviews 3 and 4 were familiar to them, demonstrating that findings from the reviews were considered to be transferable to these populations (for more details see Appendix 11).
Data analysis and synthesis
Data analysis and synthesis broadly followed the principles of meta-ethnography, as developed by Noblit and Hare88 in order to synthesise qualitative studies. This approach has proved to be a useful method to interpret findings across multiple studies in health research. 271 Meta-ethnography aims to create new interpretations through a process of translation and refutation between studies. Translation involves ‘analogy between and/or amongst the studies’ (p. 10),88 and refutation involves the explanation of contradictory findings. Where possible, a ‘line-of-argument’ is created that synthesises translational and refutational relationships into a coherent whole. Noblit and Hare88 suggest that ‘meta-ethnography is best thought of as a series of phases that overlap and repeat as the synthesis proceeds’ (p. 26). 88 We found this to be the case; although we have described the analysis process in a primarily linear fashion below, syntheses for reviews 3 and 4 proceeded in a cyclical and iterative manner (Figure 3).
FIGURE 3.
Process of meta-ethnography for reviews 3 and 4. Subprocesses differed between reviews in response to differences in the content of studies.
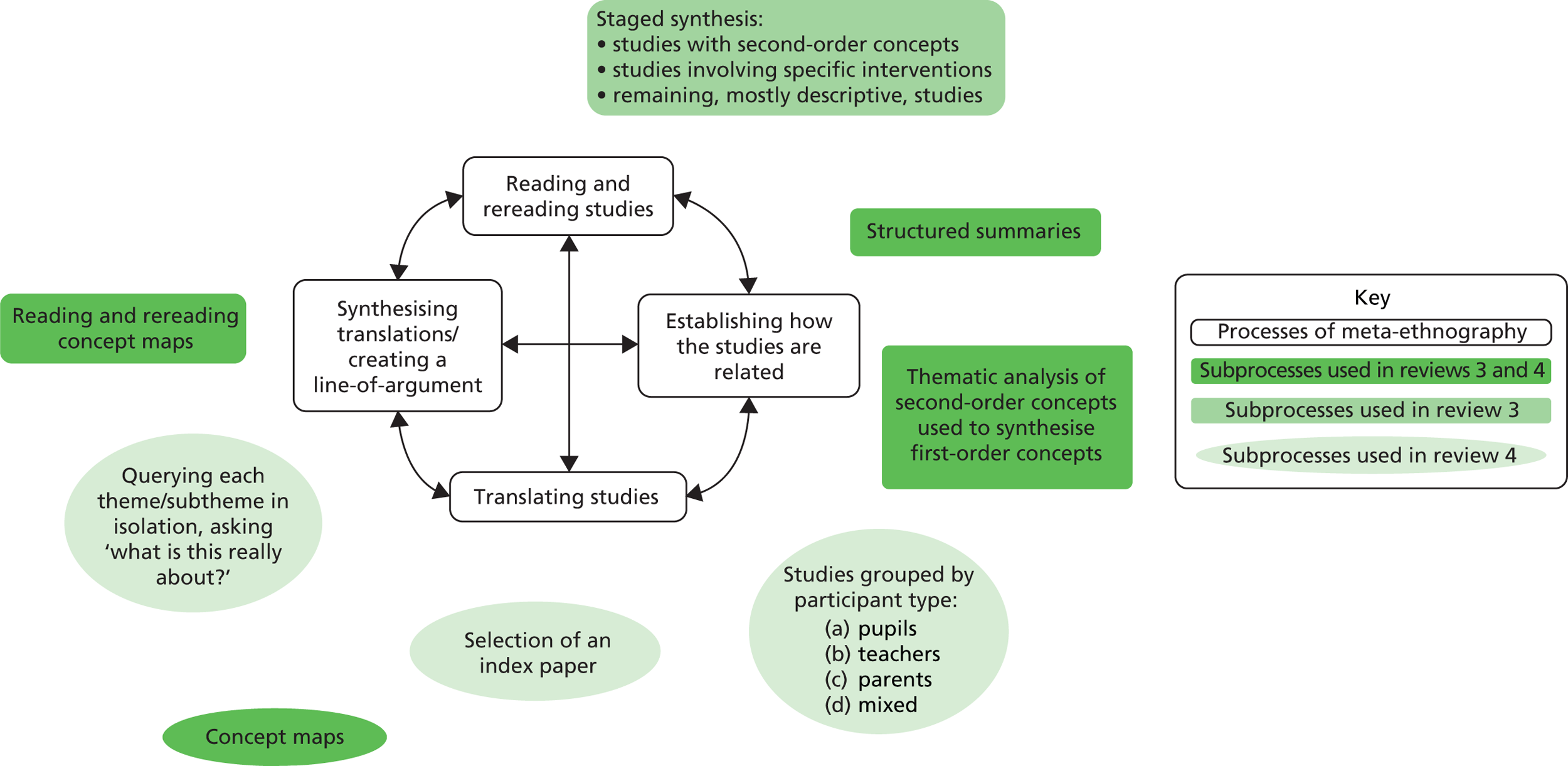
A useful distinction in the description of a synthesis of qualitative studies is the separation of first-, second- and third-order concepts, as first described by Schutz. 274 First-order concepts represent the perspectives of study participants, often communicated in studies by quoting transcript excerpts. Second-order concepts represent the theorisation of researchers about first-order concepts within their study, for example through the identification of themes and/or by applying social science theory to first-order concepts. Third-order concepts represent the theorisation of reviewers across the studies being reviewed, for example the development of themes synthesised across papers in the review. However, it is also worth noting that the distinctions between concept levels are not completely discrete; for example, researchers choose which parts of participant information to include and exclude, thus which first-order concepts are reported originate in decisions made by researchers.
In meta-ethnography, ‘the focus needs to be on the concepts, themes, organizers, and/or metaphors that the authors employ to explain what is taking place. These are the things to translate across studies’ (p. 39);88 so, according to Noblit and Hare, translation relies on second-order concepts. This complicates the application of meta-ethnography because many qualitative studies, including some of those reviewed in reviews 3 and 4, describe first-order concepts without developing them thematically and/or theoretically, therefore offering little in the way of second-order concepts to translate. We responded to this difficulty in two ways identified from other qualitative syntheses: (1) by the selection of an index paper to act as an organising thematic reference against which other studies can be compared;272 and (2) by thematic analysis of second-order concepts, which were then used to translate first-order concepts. 270
An additional challenge faced was the large quantity and breadth/diversity of content of papers. This was dealt with by grouping papers on the basis of similarities to create a staged process of synthesis, with smaller syntheses preceding the combination of these into an overall synthesis. For example, in review 3, papers containing interpretive analysis and second-order concepts were synthesised before more descriptive papers that reported mostly first-order concepts. In review 4, where content across studies was very broad, papers were synthesised in groups by participant type (pupils, teachers, parents, mixed) before combining these into a final overarching synthesis. Thus, details of analytical processes differed between reviews, not only according to differences in review aims, but also because of differences between the characteristics of the papers being synthesised. Processes common to both reviews are outlined below, followed by discussion of processes particular to each review.
Reading and rereading the included studies
This initial stage involved the careful reading of the included papers in order for reviewers to familiarise themselves with the studies and their findings. This process began in the screening phase and continued through data extraction and analysis.
Determining how the studies are related
Following data extraction, structured summaries275 were created in order to juxtapose the same type of information across papers for consideration of similarities and differences. Information tabulated included samples, methods, themes, first- and second-order concepts, metaphors, implications and/or developing third-order concepts created for each interpretive paper (see Appendix 12 for an example). The similarities and differences demonstrated through this process acted as a foundation for decisions about the structure and process of each synthesis. In the process of comparing the studies against each other, we looked for explicit differences between the studies in relation to a range of factors, including their participant group perspective, the age of relevant children with ADHD, intervention focus (review 3) and geographical location.
Reciprocal translation of studies
This stage involved the development of concept maps showing concepts and related subthemes, and narratives to explain how each concept was evidenced by the included studies and developing synthesis (for an example, see the concept maps for review 4’s synthesis of pupil views in Appendix 13).
Review 3
Although the previous stage had identified some similarities across studies, their diverse foci and the relatively descriptive themes meant that additional work was needed ahead of translating studies. Thematic analysis was used to inductively develop concepts from papers with second-order themes. 8 The resulting six themes were then compared with findings from more descriptive studies that considered specific interventions to assess their fit; two themes were adapted in light of this. Finally, the findings of the remaining, more descriptive, studies were compared with the themes. As a result of this an additional theme that had appeared to a lesser extent in the other papers was added, giving seven themes in total.
Next, concepts and themes in one article were compared with the concepts and themes in others. This translation involved the comparison of themes across papers and an attempt to ‘match’ themes from one paper with themes from another. We began with the themes identified in the thematic analysis process described above, considering how paper A’s findings related to these themes and then comparing paper B’s findings to this and so on using concept maps. It became clear that the studies were not refutations of one another, even though tensions amid categories were identified.
Review 4
Once subgroups of papers were established by participant type [(1) pupil, (2) teacher, (3) parent, (4) mixed views], the four subgroups were synthesised separately. For pupil and parent syntheses, an index paper, as defined above, was chosen. 261,276 Thus, for the pupil and parent syntheses the relationships of themes between studies were analysed deductively from the index paper themes. In addition, inductive thematic analysis was carried out for both first- and second-order concepts not represented by index paper themes. For the teacher and mixed views syntheses, there was not a paper that both included second-order concepts and broadly represented the other papers. Therefore, translation was conducted using inductive thematic analysis of first- and second-order concepts across papers. As can happen in meta-ethnography,277 seven papers were excluded during the data analysis stage for the following reasons: three papers included in both reviews 3 and 4 were found to have insufficient amounts of non-intervention related experience of ADHD;278–280 two studies did not contain sufficient school-related experience;281,282 and two papers did not contribute to the synthesis. 283,284
Synthesising translations/creating a line-of-argument
Review 3
To develop a line of argument88 (a third-order interpretation of the included studies as a whole), the concept maps for each theme developed during the reciprocal translation process were organised, read and reread. By reading the concepts and interpretations within the synthesis, a line of argument was developed from the reciprocally translated themes. This line of argument consisted of a model that captured how the themes related to one another and captured the experience of using non-pharmacological interventions for ADHD in school settings.
Review 4
The line of argument,88 as defined above, for each of the included studies in review 4 was a culmination of:
-
the processes described above
-
conceptual development gained through discussion with the wider research team in the process of critical review and comment (RG, DM, TF); and
-
a process of querying themes from each concept map.
The process of querying each concept map involved printing out the map for one of the four syntheses (see Appendix 13) and cutting out each box representing a theme or subtheme, which included descriptive text. Text from each theme was then read in isolation and the query, ‘what is this really about?’ was asked, with answers written as categories on the back. Themes were developed from these categories and then combined in a table showing relationships between first- and second-order concepts and third-order themes (see Chapter 6, Table 48 for review 4a, Table 52 for review 4b, Table 55 for review 4c and Table 59 for review 4d). This process established the structure of third-order lines of argument for the four subreviews, reviews 4a–d. For the overarching synthesis of review 4, third-order themes from reviews 4a–d were combined and refined into overarching third-order themes (see Chapter 6, Table 63).
It is commonly accepted within interpretive research that themes are developed through interpretations by researchers and that they may be developed in more than one way. 285 We grouped themes following decisions about how to highlight clearly important issues identified in included studies and their relative importance to the implementation of interventions for ADHD within schools. For example, in synthesis 4a (pupil views) we discuss stigma within ‘sociological aspects of ADHD symptoms’ rather than with spoiled identity under ‘psychological aspects of ADHD symptoms’, although the issues are evidently closely linked. This decision was made because the mechanisms of stigma work to make sociological aspects implicit and individual aspects explicit (for a further discussion of stigma see Chapter 6, Review 4a: the school experiences and perceptions of pupils diagnosed with attention-deficit/hyperactivity disorder, Overarching theme for review 4a: attention-deficit/hyperactivity disorder symptoms as an interaction between biological, sociological and psychological factors, Sociological factors, Stigma and Box 33). In addition, the sociological aspects are important to understanding the school context with reference to implementation of non-pharmacological interventions (for further discussion see Chapter 6, Review 4a: the school experiences and perceptions of pupils diagnosed with attention-deficit/hyperactivity disorder, Overarching theme for review 4a: attention-deficit/hyperactivity disorder symptoms as an interaction between biological, sociological and psychological factors, Sociological factors).
The findings of both qualitative reviews are presented and discussed in the subsequent two chapters, along with methodological issues that relate to each individual review. Review 3 in Chapter 5 examines ‘the experiences of and attitudes held by parents, children, peers, teachers and others involved in ADHD interventions in schools’, whereas review 4 in Chapter 6 reports ‘the school-related experiences and perceptions of pupils diagnosed with or at risk of ADHD, their teachers, parents and peers’.
Chapter 5 Review 3: a synthesis of qualitative studies about the use of non-pharmacological interventions and strategies for attention-deficit/hyperactivity disorder in school settings
Introduction
This chapter presents the findings of the systematic review of qualitative research addressing the research question ‘what are the experiences of and attitudes towards ADHD interventions in school settings?’ The method for this review was outlined in the previous chapter. This chapter describes the included studies and then presents the findings of the review. Although data analysis and synthesis followed the principles of meta-ethnography (see Chapter 4, Methods of analysis/synthesis, Data analysis and synthesis), the synthesis is presented thematically. A ‘line of argument’ was produced during the analysis of the included papers, which captures how the themes relate to one another and provides a model of the experience of using non-pharmacological interventions for ADHD in school settings. The chapter ends with conclusions, including implications for the education of pupils who display symptoms of ADHD and the development of interventions.
Included studies
Figure 4 gives the PRISMA flow chart showing study selection. 152 A total of 10,753 records were screened at the title and abstract level, excluding 10,361 papers. The full text of 392 potentially eligible papers was retrieved. After scanning the full text, 359 of these articles were either not considered eligible (n = 309) or unavailable after further efforts to locate full-text records (n = 50). A list of reasons for the exclusion of each paper screened at full text can be seen in Appendix 14. The most frequent reasons for exclusion after perusal of full text were studies lacking qualitative data and/or analysis (n = 94) or research that was not focused on the school setting (n = 83). The remaining 33 papers met the inclusion criteria outlined in the previous chapter.
FIGURE 4.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram showing search process and study selection for review 3.
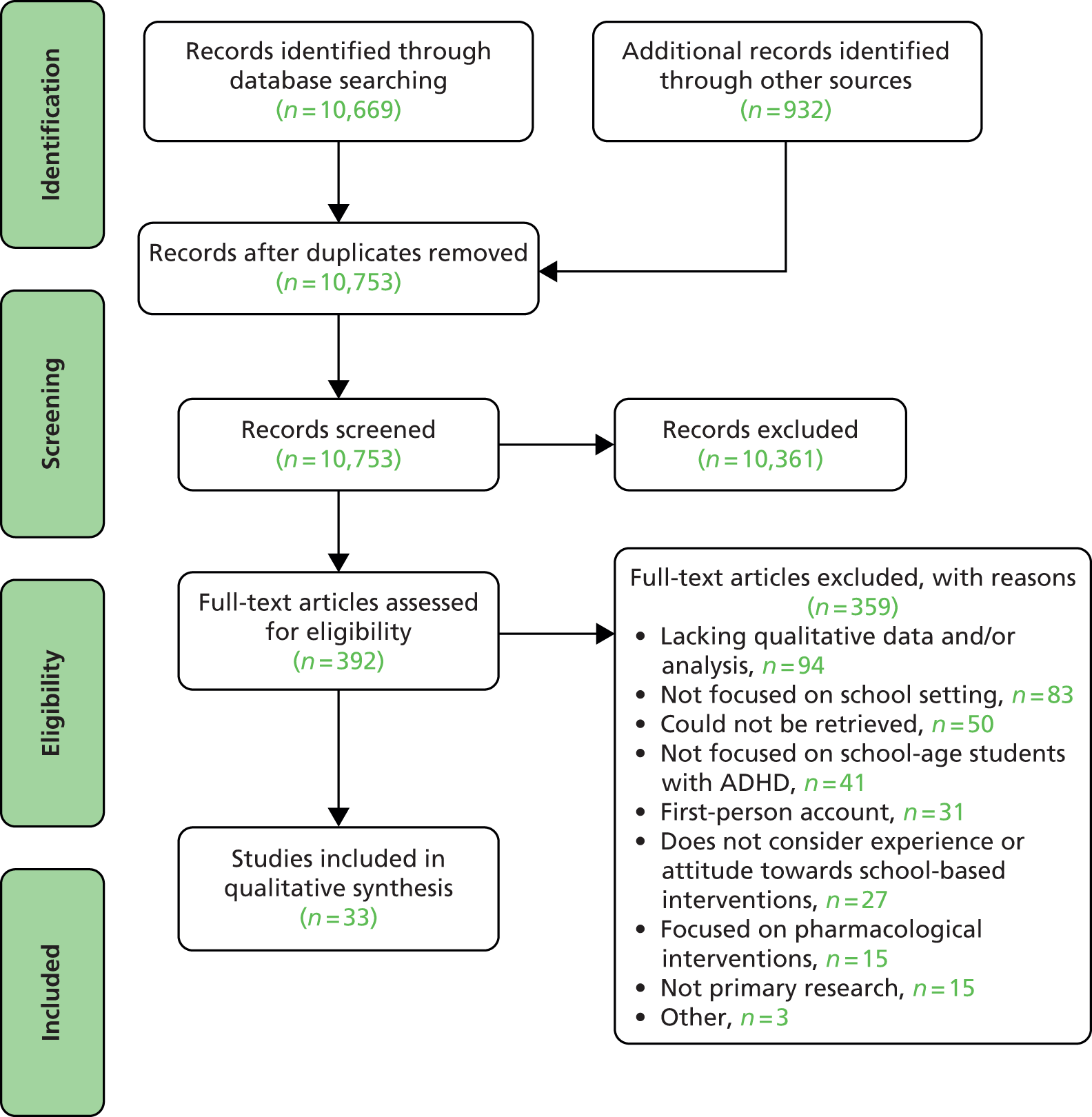
Study characteristics
Summary details of the 33 included study reports which were published between 1996 and 2011 are provided in Table 32. There were no studies that contributed more than one paper to the review; all included papers referred to distinct research and samples. However, one journal article307 used data and analysis that the author had previously published in a book. 314 Only the journal article was included as it focused on pedagogical practices experienced by secondary school pupils diagnosed with ADHD, whereas the book covered this plus broader content more relevant to review 4. The included studies represented the perspectives of a variety of relevant participant groups, namely education practitioners (most often teachers), children with ADHD or related symptoms, their parents, their mainstream peers without a diagnosis of ADHD and their peers attending the same interventions, who often held other SEN.
| First study author and year | Country of participants | Aim | Sample perspective | Agea | Particular intervention |
|---|---|---|---|---|---|
| Arcia 2000286 | USA | Describe teacher understanding of, attitudes about, and strategies towards disruptive behaviours | Teachers (n = 21) | 5–12 | No |
| Bartlett 2010287 | USA | Explore persons and strategies that college-enrolled young adults with a history of ADHD perceived were most and least helpful to their management of ADHD during childhood | College students (n = 16) | 18–25. Participants reflected on childhood | No |
| Bos 1997288 | USA | Explore the use of a workshop course on educating students with ADHD that incorporated features of interactive professional development. Describing the effects of such workshops not only on educators’ knowledge attitudes and perceived competence, but also on what aspects they deemed as valuable for their professional growth | Educators (n = 89) | 5–22 | ADHD Teacher Training Workshop |
| Ducharme 1996289 | USA | Focus on parents’ perceptions about four aspects of raising a child with ADHD: (1) parents’ feelings regarding their children and the school experience; (2) parents’ perceptions about their interactions with medical practitioners; (3) parents’ views regarding family and social issues, and (4) parents’ perceptions about their own experiences | Parents of children with ADHD (n = 7) | 12–19 | No |
| Edwards 2008290 | New Zealand | Identify some effective educational strategies that help the children in this study learn. To identify ineffective strategies and consider how social experiences with other children impacts learning | Mixed: children with gifted/ADHD (n = 6), their parents (n = 7) and one teacher who had worked with gifted children with ADHD | 6–10 | No |
| Einarsdottir 2008291 | Iceland | Investigate the experiences that the teachers have in working with children who have behavioural problems and ADHD-associated behaviour and the support and conditions they feel these children need given changes in the Icelandic context | Teachers (n = 16) | 2–7 | No |
| Furtick 2010292 | USA | Determine whether or not the use of constructivist practices are more appropriate/successful than traditional practices when used with elementary-aged students diagnosed with ADHD | Mixed: children with ADHD (n = 6); teachers (n = 6); parents (n = 6) | 9–11 | Constructivist teaching |
| Hands 2009293 | USA | Give voice to an underachieving gifted student with ADHD and a mild non-verbal LD about how his educational experience could better address his individual needs | Mixed: ADHD teenager (n = 1), his English and Science teachers (n = 2) and his mother | 16 | No |
| Hillman 2011294 | USA, UK, Canada | Examine teachers’ ability to identify ADHD and the qualitative content of their referral recommendations. This is intended to help determine if identification and recommendations for parents differ based on ethnicity and/or gender of the child | Teachers (n = 30) | 5–14 | No |
| Hjörne 2006295 | Sweden | Explore the pedagogical practices developed in a Swedish school in response to the diagnosis ADHD/DAMP. Focus on what educational strategies practitioners consider relevant when organising teaching and learning activities for children diagnosed with ADHD/DAMP | Mixed: ADHD boys (n = 6) and school staff (n = 5) | 7–12 | ADHD classroom (a special education classroom for pupils with ADHD) |
| Hong 2008265 | Korea | Understand and present the perspectives of teachers who struggled with and strived to perform their duties as teachers as they taught children with ADHD | Teachers (n = 23) | Up to 12 | No |
| Houghton 2006296 | Australia | Investigate how teachers deal with students diagnosed with ADHD | Teachers (n = 36) | NR | No |
| Isaksson 2010297 | Sweden | Examine how pupils with SEN and their parents experience the special support measures they receive from school | Children with ADHD among larger SEN sample (n = 8) | 13–15 | No |
| Jones 2008298 | USA | Explore how 20 currently practising pre-kindergarten teachers handle children identified with conduct disorder, ODD and ADHD in order to illuminate, from the perspective of teachers, the strategies that are working | Pre-kindergarten teachers (n = 20) | 2–5 | No |
| Kendall 2003299 | USA | Listen to the voices of children and adolescents diagnosed with ADHD, from diverse ethnic and socioeconomic backgrounds, and ask them what they felt was true for them and how they viewed ADHD and its treatments | Children with ADHD (n = 39) | 6–17 | No |
| Kreiss 2003300 | USA | Case studies documenting the varied experiences of adolescents attending an alternate high school; to identify factors in this school’s programme that appear to promote positive growth in students and to identify ways in which the programme might be improved | Adolescents attending alternate high school (n = 4) | NR | Alternative high school for emotionally and/or behaviourally disturbed adolescents |
| Langberg 2011301 | USA | Adapt and refine the HOPS intervention protocol to create a product that is highly acceptable to parents and schools and is feasible for schools to implement during the school day | School mental health providers – counsellors and psychologists (n = 10); teachers (n = 8) | 11–14 | Organisation and study skills training |
| Ljusberg 2011265 | Sweden | Highlight the physical and mental environment in the remedial classroom. Investigation through teacher interviews of how the classrooms are organised and structured and how do teachers report that the teaching is organised and structured | Remedial teachers (n = 10) | 9–12 | Remedial classroom |
| Ljusberg 2011302 | Sweden | Examine how pupils describe why they attend a remedial class and what it means to be a pupil in that setting | ADHD and concentration difficulties students (n = 10) | 10–12 | Remedial classroom |
| McNeil 2005303 | USA | Explore what the experience of growing up with ADHD means. To consider the extent to which ADHD interacts with schooling and the quality of education received | Female students with ADHD and emotional and behavioural problems (n = 3) | 15–16 | Self-contained Just Achieving Greatness programme |
| Mulligan 2001304 | USA | Identify which of the potentially useful classroom strategies for students with ADHD are being implemented by general education teachers and which strategies they perceive as being the most effective | General education teachers (n = 151) | 5–18 | No |
| Nowacek 2007305 | USA | Investigate what teachers understood about the characteristics associated with ADHD and what modifications and interventions they used with these students | Teachers (n = 8) | 6–14 | No |
| Ozdemir 2006306 | Turkey | Explore the perceptions of Turkish teachers and parents in regard to the First Steps to Success programme they experienced | Mixed: teachers (n = 4) and parents (n = 8) of children with ADHD | 6–7 | First Step to Success programme (school and home intervention) |
| Partridge 2009279 | Australia | Explore how adolescent boys diagnosed with ADHD respond to the efforts of their teachers to moderate their actions | Adolescents diagnosed with ADHD (n = 5) | 12–14 | No |
| Prosser 2008307 | Australia and USA | Investigate what student perspectives tell us about the relationship between ADHD and pedagogy | Adolescents diagnosed with ADHD (n = 12) | 14–16 | No |
| Rafalovich 2004308 | USA and Canada | Focus on the pedagogical responses that teachers employ in dealing with ADHD, describe the steps by which they modify assignment structure and the academic and social expectations of children with ADHD | Teachers (n = 25) | 2–16 | No |
| Santamaria 2009309 | USA | Study school counsellors’ perceptions of English-language learning students with ADHD in second grade and the strategies used to manage their behaviour | School counsellors (n = 10) | 7–8 | No |
| Smagorinsky 2007278 | USA | Given open-ended exploration and interpretation of literature investigates the factors appearing to contribute to Rita’s (adolescent with ADHD) efforts to attend to the text and task assigned by her teacher | Adolescents diagnosed with ADHD (n = 2) | 17–18 | Creative learning in English |
| Taylor Wilcoxson 2005310 | USA | Investigate the creative potential of children diagnosed with ADHD | Mixed: children with or at risk of ADHD (one diagnosed) (n = 4), their mothers (n = 4) and teachers (n = 5) | 9–10 | No |
| Wiebe 2007311 | Canada | Explore the experience of listening to music during individual seat work in the classroom and during homework, experienced by an adolescent boy | Mixed: adolescent diagnosed with ADHD (n = 1), his teachers (n = 2) and parents (n = 2) | 14 | Listening to music through headphones while working |
| Wong 2004280 | Canada | Investigate, describe and enhance the metacognitive processes of high school students with ADHD/LDs who were studying for and taking an examination | Teenagers with ADHD (n = 5) | 15–16 | Metacognitive skills training |
| Young 2009312 | UK | Explore what developmental experience is important among young offenders with ADHD | Young offenders with ADHD symptoms (n = 6) | 14–16 | No |
| Zimmerman 1998313 | USA | Investigate the perception of students about the influence of teachers and school counsellors on their academic success. Consider common characteristics among staff identified by the students as being supportive | Mixed: students with ADHD in high school or college (n = 6), their parents, high school teachers (n = 6) and counsellors | 16–21 | No |
The most frequent participant groups were educators (n = 13264,265,286,288,291,294,296,298,301,304,305,308,309), children and young people with ADHD (n = 10278–280,297,299,300,302,303,307,312) or multiple perspectives (n = 8290,292,293,295,306,310,311,313). This meant that over half of the studies included the perspectives of educators of children with ADHD (n = 21264,265,286,288,290–296,298,301,304–306,308–311,313) or the perspectives of children and young people with ADHD (n = 17278–280,290,292,293,295,297,299,300,302,303,307,310–313).
The aims of the studies were typically broader than a focus on attitudes and experiences of school-based interventions for children with ADHD on which this qualitative review focuses. Often only a small section of a study’s analysis was relevant, with the remaining analysis considering wider experiences of learning and teaching related to children with ADHD, growing up with an ADHD diagnosis or teaching SEN pupils (these other issues are considered by review 4, see Chapter 6).
The majority of studies were located in the USA (n = 19278,287–289,292–294,298–301,303–305,307–311,313). Sweden is the only other country represented by more than three studies (n = 4265,295,297,302). Only two studies were located in the UK,294,312 but one study294 also included participants from the USA and Canada. The age of relevant schoolchildren with ADHD was more often within adolescence or a range of ages across childhood than younger children. Ethnicity, deprivation, teaching experience and comorbid issues for participants with ADHD diagnoses were rarely reported by the included studies.
Interventions studied
Only 12 of the studies were focused on a particular intervention (Table 33),265,278,280,288,292,295,300–303,306,311 with the majority of included studies instead considering the range of interventions or strategies used in participants’ school settings (i.e. the practice routinely used by teachers working with pupils who display ADHD symptoms). Of the 12 studies focused on a particular intervention, the majority (n = 8265,278,292,295,300,302,303,311) could be classified according to the category ‘adaptations to learning environment’ used in the review of effectiveness reported in Chapter 2. The remaining interventions fit the categories academic and study skills training (n = 2280,301) or contingency management. 306 Bos et al. ’s study288 focused on a teacher training intervention, a category outside the scope of the review of effectiveness reported in Chapter 2. Only four studies reported interventions that were considered specific enough and contained enough procedural detail within the paper to allow for replication. 288,301,306,311 However, these four studies range from a manualised intervention evaluated by Langberg et al. 301 to the limited procedural detail given by Wiebe311 where the use of the intervention was left to teacher discretion. The broad, non-replicable interventions in the remaining eight studies often comprised attendance in special education classrooms and, as such, their content was varied as a result of the influence of local curriculum needs and the needs of the particular pupils in the classroom.
| First study author and year | Intervention | Intervention categorya | Focusb |
|---|---|---|---|
| Bos 1997288 | ADHD teacher training workshop | Information (teacher training) | Specific |
| Furtick 2010292 | Constructivist teaching | Adaptations to learning environment | Broad |
| Hjörne 2006295 | ADHD classroom | Adaptations to learning environment | Broad |
| Kreiss 2003300 | Alternative high school for emotionally and/or behaviourally disturbed adolescents | Adaptations to learning environment | Broad |
| Langberg 2011301 | Organisation and study skills training | Academic and study skills training | Specific |
| Ljusberg 2011265 | Remedial classroom | Adaptations to learning environment | Broad |
| Ljusberg 2011302 | Remedial classroom | Adaptations to learning environment | Broad |
| McNeil 2005303 | Self-contained Just Achieving Greatness programme | Adaptations to learning environment | Broad |
| Ozdemir 2006306 | First Step to Success programme (school and home intervention) | Contingency management | Specific |
| Smagorinsky 2007278 | Creative learning in English | Adaptations to learning environment | Broad |
| Wiebe 2007311 | Listening to music through headphones while working | Adaptations to learning environment | Specific |
| Wong 2004280 | Metacognitive skills training | Academic and study skills training | Broad |
Methods and analysis
Further details about the methods and analyses employed by the 33 included studies are given in Table 34. Sample sizes tended to be larger when the participant group were educators. Educators represented a range of teaching age groups, whereas samples of pupils with ADHD were more often adolescents. 278–280,293,297,303,307,312,313 Participants displaying ADHD symptoms were often clinically diagnosed and, where reported, the majority were taking medication for their ADHD. However, sample characteristics for teacher and parent participants were often not reported.
| First study author and year | Sample size, n | Sample characteristics | Data collection method | Sampling | School setting | Data analysis | Analysisa |
|---|---|---|---|---|---|---|---|
| Arcia 2000286 | 21 | 21 kindergarten to sixth grade teachers (one SEN), 81% female | Telephone interview (two per participant; second after initial analysis) | Purposive | Elementary | Qualitative analysis after Miles and Huberman 1994315 | Mainly descriptive |
| Bartlett 2010287 | 16 | 16 college students diagnosed with ADHD, aged 18–25 years, 81% female, 94% taking medication | Semistructured interviews | Opportunity sample | University (retrospective) | Content analysis | Mainly descriptive |
| Bos 1997288 | 89 | 89 kindergarten to post-secondary educators, 96% female | Open-ended evaluation questionnaire questions, journal and semistructured interviews | Self-selecting | NR | Category and theme analysis; constant comparative used to aggregate themes | Mainly descriptive |
| Ducharme 1996289 | 7 | Seven parents of children with ADHD, 71% female, aged 38–52 years | Life history and in-depth interviewing (three per participant) | NR | High school assumed (children aged 12–19 years) | Thematic perspective | Mainly descriptive |
| Edwards 2008290 | 14 (6 children, 1 teacher, 4 mothers, 3 fathers) | Six children with diagnosed ADHD and classified gifted (6–10 years old, 33% female), their parents and one teacher who had worked with gifted/children with ADHD | Semistructured interviews (two per child, second interview based on first interview findings) | Reputational | School for gifted children and mainstream schools | Narrative and thematic | Mainly descriptive |
| Einarsdottir 2008291 | 16 | 16 female preschool or grade 1 teachers | Interviews (semistructured assumed, 40–90 minutes) | NR | Preschool or primary | Phenomenological approach | Some interpretive analysis |
| Furtick 2010292 | 18 | Six boys aged 9–11 years with diagnosed ADHD, all on medication; six female teachers; six parents (unreported whether or not one parent per child) | Observations and interviews | Purposive | Elementary | Thematic, then categorised responses into positive/negative | Mainly descriptive |
| Hands 2009293 | 4 | One male with ADHD (also gifted and mild non-verbal LD), diagnosed at 16 years old, on medication, his English and Science teachers and his mother | Classroom observation, semistructured interviews (approximately 90–120 minutes), analysis of school documents | Reputational | Public high school and math and science magnet school | Constant comparative method | Mainly descriptive |
| Hillman 2011294 | 30 | 30 kindergarten to eighth grade teachers (25–34 years of age, 80% female) | Internet survey including open-ended questions | Self-selecting | Primary and secondary | Thematic analysis | Mainly descriptive |
| Hjörne 2006295 | 11 | Six ADHD/DAMP diagnosed boys aged 7–12 years and five school staff | Microethnography | NR | Primary | NR | Mainly descriptive |
| Hong 2008264 | 23 | 23 early years teachers | Open-ended questionnaire (23 participants), interview (seven participants, 30–60 minutes) and focus groups (six participants, 30–60 minutes) | Purposive | Day care, kindergarten and elementary | NR | Some interpretive analysis |
| Houghton 2006296 | 36 | 36 teachers | Semistructured interviews (approximately 1 hour) | Purposive | NR | Grounded theory | Some interpretive analysis |
| Isaksson 2010297 | 8 | Eight special educational needs children (two boys diagnosed with ADHD; aged 13–15 years) | Interview (semistructured assumed, 45–90 minutes) | Opportunity sample | Primary | Grounded theory | Mainly descriptive |
| Jones 2008298 | 20 | 20 female pre-kindergarten teachers aged 23–49 years | Semistructured interviews (50–90 minutes) then telephone calls and e-mails | Purposive and opportunity | Elementary | Phenomenological processes | Mainly descriptive |
| Kendall 2003299 | 39 | 39 children diagnosed with ADHD (33% female, aged 6–17 years) | Semistructured interviews (15–45 minutes) | Purposive | NR | Constant comparative method | Mainly descriptive |
| Kreiss 2003300 | 4 | Four adolescents attending alternative high school, 50% female, one boy and one girl with ADHD) | Semistructured interviews | Purposive | Special school for emotionally and behaviourally disturbed adolescents | Thematic | Mainly descriptive |
| Langberg 2011301 | 18 | 10 female school mental health providers – counsellors and psychologists, mean age 35 years; eight teachers (for final hour of focus group) | Focus groups (2.5 hours) plus intervention transcripts | NR | Middle school | Open coding, frames of analysis | Mainly descriptive |
| Ljusberg 2011265 | 10 | 10 remedial class teachers | Semistructured interviews | Opportunity/purposive | Primary | Thematic | Some interpretive analysis |
| Ljusberg 2011302 | 10 | 10 ADHD and concentration difficulties students, aged 10–12 years, 20% female, five diagnosed, five concentration difficulties | Semistructured interviews | Random sample from 45 who met inclusion criteria | Primary | Thematic | Some interpretive analysis |
| McNeil 2005303 | 3 | Three female ADHD-diagnosed students with emotional and behavioural problems, 15–16 years of age, 68% on medication | Heuristic enquiry and case study: ‘long interview’ (60 minutes approximately) and observation, cumulative and special education files, psychological evaluations and test results | Opportunity sample | Junior high school | Heuristic data analysis after Moustakas 1990316 | Mainly descriptive |
| Mulligan 2001304 | 151 | 151 general education teachers, 82% of 149 completing survey were female | Survey including two open-ended questions | Random sampling of all but two districts included | Kindergarten to high school | Content analysis | Mainly descriptive |
| Nowacek 2007305 | 8 | Eight teachers of grades 2–8, 63% female | Open-ended question, semistructured interview, classroom observation | Purposive | Elementary and middle schools | Constant comparative method | Some interpretive analysis |
| Ozdemir 2006306 | 12 | Four female grade 1 teachers (24–32 years of age) and eight parents of children with ADHD (50% female, 27–44 years old) | Semistructured interviews | Purposive | Elementary (kindergarten to grade 8) | Qualitative analysis (detail unspecified) | Mainly descriptive |
| Partridge 2009279 | 5 | Five ADHD-diagnosed male adolescents aged 12–14 years, 80% on medication; 24 non-diagnosed adolescents also sampled but analysis focuses on ADHD experience | Focus groups and semistructured interviews (two per participant; 45–60 minutes) | Purposive | Junior and senior (years 4–12, Australia) | Grounded theory | Some interpretive analysis |
| Prosser 2008307 | 12 | 12 male adolescents diagnosed with ADHD | ‘Critical narrative’ research strategies including interviews | Purposive | NR | Coded thematically and synthesised | Mainly descriptive |
| Rafalovich 2004308 | 25 | 25 teachers of preschool to 10th grade, 44% female, aged 28–64 years | Semistructured interviews (20–90 minutes) | Snowball | NR | Grounded theory | Some interpretive analysis |
| Santamaria 2009309 | 10 | 10 female school counsellors aged ≥ 41 years | Individual in-depth interviews | Purposive | Elementary | Within and across case analyses. Within general and ESOL counsellors and across the two types | Mainly descriptive |
| Smagorinsky 2007278 | 2 | Two adolescents 17–18 years of age, one female diagnosed with ADHD and medicated, other male attention difficulties | Classroom observation, retrospective protocol | Opportunity sample | 2 years at senior high school | Inductive and deductive thematic coding | Some interpretive analysis |
| Taylor Wilcoxson 2005310 | 13 | Four diagnosed ADHD boys, 9–10 years of age, 25% on medication, their mothers (aged 34–40 years) and five female teachers (aged 29–49 years) | Multiple case studies, qualitative component of semistructured interviews | Purposive | Elementary | Qualitative data analysis after Kvale 1996317 | Mainly descriptive |
| Wiebe 2007311 | 5 | One male aged 14 years, diagnosed with ADHD and on medication, his two teachers and parents | Semistructured interviews (three per participant) and observations | Purposive | NR | Case study and some thematic analysis after Stake 1995318 | Mainly descriptive |
| Wong 2004280 | 5 | Five male teenagers (aged 15–16 years) diagnosed with ADHD | Interviews (semistructured assumed) with students and teachers, ‘think-aloud’ with pupils, observation of tutorial sessions, field notes | Purposive | High school | Constant comparative method | Some interpretive analysis |
| Young 2009312 | 6 | Six male young offenders with ADHD symptoms, one diagnosed, aged 14–16 years old | Semistructured interviews (35–50 minutes) | Purposive | School at secure residential unit for adolescents aged 10–17 years who display difficult/challenging behaviours | Interpretive phenomenological analysis | Mainly descriptive |
| Zimmerman 1998313 | 5 students, 5 teachers, 3 counsellors, parents unreported | Five students with ADHD in high school or college (40% female, aged 16–21 years, 60% on medication at time of study), their parents, high school teachers and counsellors | Semistructured interviews (one or two per participant) | Purposive | High school focus | Situational analysis | Some interpretive analysis |
Five studies used mixed-method designs that also included quantitative data. 286,288,294,301,304 Langberg et al. ’s study301 focused on the evaluation of an intervention for which effectiveness results have been reported in a separate paper167 that was included in the review of effectiveness presented in Chapter 2. However, the paper included in the current review was focused on educators’ evaluations of the Homework, Organization, and Planning Skills (HOPS) intervention only. The majority of studies used purposive sampling (n = 17264,279,280,286,292,296,298–300,305–307,309–313). These studies typically made use of key informants who could provide access to the target population, for instance teachers who could identify their pupils with ADHD310 or headteachers who could recommend certain teachers and pupils. 305
Twenty-eight studies involved the use of interviews for data collection. 264,265,279,280,286–293,296–300,302,303,305–313 Most often the interviews were semistructured. Six studies included more than one interview with participants279,286,289,290,311,313 and 13 studies included more than one method of data collection. 264,278–280,288,292,293,295,298,301,303,305,311 Where reported, the school setting was most often primary or elementary settings and mainstream schools. The data analysis methods reported varied across the studies with some elements of thematic analysis (n = 11265,278,288–290,292,294,300,302,307,311) and grounded theory or constant comparative method (n = 9279,280,288,293,296,297,299,305,308) being the most frequently cited analytical frameworks employed. In several studies the analytical process was either unclear or unreported, although for the study to be included some qualitative analysis was clearly evident. Despite many studies claiming to use interpretive analytic frameworks, the majority of studies were judged as containing mainly descriptive analysis (n = 22286–290,292–295,297–301,303,304,306,307,309–312).
Quality appraisal
A summary of results of the quality appraisal of included papers is displayed in Table 35. As discussed in the previous chapter (see Chapter 4, Methods of analysis/synthesis, Quality assessment), and as is typical for systematic reviews of qualitative research,269,270,319 quality appraisal was used as a means to raise awareness about a range of relevant factors for each paper, rather than as a basis for exclusion. Two studies298,309 did not record a ‘no’ response against any of the questions. Both were PhD theses so it is arguable that these authors had more space to satisfactorily address issues of study quality and would be more likely to consider theoretical perspectives and reflexivity than authors of short journal articles. That said, the ‘lowest’ quality study as appraised here was also a PhD thesis,292 which scored eight ‘yes’ and seven ‘no’ responses, thus indicating that all studies received more positive than negative quality appraisals. Where previous qualitative reviews have excluded papers on the basis of quality appraisal, this has been attributable to negative answers to the majority of questions. 319
| First study author and year | 1. Is the research question clear? | 2. Is the theoretical or ideological perspective of the author explicit? | 3. Has the theoretical or ideological perspective influenced the study design, methods or research findings? | 4. Is the study design appropriate to answer the question? | 5. Is the context or setting adequately described? | 6. Is the sample adequate to explore the range of subjects and settings, and has it been drawn from an appropriate population? | 7. Was the data collection adequately described? | 8. Was data collection rigorously conducted to ensure confidence in the findings? | 9. Was there evidence that the data analysis was rigorously conducted to ensure confidence in the findings? | 10. Are the findings substantiated by the data? | 11. Has consideration been given to any limitations of the methods or data that may have affected the results? | 12. Do any claims to generalisability follow logically and theoretically from the data? | 13. Have ethical issues been addressed and confidentiality respected? | 14. Are the authors reflexive? | 15. Are interventions of interest clearly described? | Totals (Y, N, CT) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arcia 2000286 | Y | N | CT | Y | Y | Y | Y | Y | Y | CT | Y | Y | Y | N | N/A | 10, 2, 2 |
| Bartlett 2010287 | Y | N | CT | Y | Y | Y | Y | CT | Y | Y | Y | N | Y | N | N/A | 9, 3, 2 |
| Bos 1997288 | Y | N | CT | Y | N | Y | Y | Y | Y | Y | N | Y | CT | N | Y | 9, 4, 2 |
| Ducharme 1996289 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | Y | Y | N/A | 12, 2, 0 |
| Edwards 2008290 | Y | N | CT | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | N/A | 10, 3, 1 |
| Einarsdottir 2008291 | Y | Y | Y | Y | Y | CT | Y | CT | Y | Y | N | Y | CT | N | N/A | 9, 2, 3 |
| Furtick 2010292 | Y | N | N | N | Y | N | Y | Y | N | Y | Y | N | Y | Y | N | 8, 7, 0 |
| Hands 2009293 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | N | Y | Y | N/A | 11, 3, 0 |
| Hillman 2011294 | Y | Y | Y | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | N | N/A | 11, 2, 1 |
| Hjörne 2006295 | Y | N | CT | Y | Y | CT | Y | Y | N | Y | N | Y | Y | N | Y | 9, 4, 2 |
| Hong 2008264 | Y | N | CT | Y | Y | CT | Y | Y | N | Y | N | CT | CT | Y | N/A | 7, 3, 4 |
| Houghton 2006296 | Y | Y | Y | Y | N | Y | Y | CT | Y | Y | N | Y | CT | N | N/A | 9, 3, 2 |
| Isaksson 2010297 | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | Y | Y | Y | N | N/A | 11, 2, 1 |
| Jones 2008298 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | Y | N/A | 13, 0, 1 |
| Kendall 2003299 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | N/A | 12, 1, 1 |
| Kreiss 2003300 | Y | N | CT | Y | Y | Y | Y | CT | N | Y | Y | Y | Y | Y | Y | 11, 2, 2 |
| Langberg 2011301 | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | N | Y | 11, 2, 2 |
| Ljusberg 2011265 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | Y | 13, 2, 0 |
| Ljusberg 2011302 | Y | Y | Y | Y | Y | Y | Y | CT | Y | Y | N | Y | Y | N | N | 11, 3, 1 |
| McNeil 2005303 | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | 12, 2, 1 |
| Mulligan 2001304 | Y | N | CT | N | Y | Y | Y | Y | Y | Y | Y | Y | CT | N | N/A | 9, 3, 2 |
| Nowacek 2007305 | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | N | Y | N | N/A | 11, 2, 1 |
| Ozdemir 2006306 | Y | N | CT | Y | Y | Y | Y | CT | N | Y | Y | Y | CT | N | Y | 9, 3, 3 |
| Partridge 2009279 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N | 13, 2, 0 |
| Prosser 2008307 | Y | Y | Y | Y | N | Y | N | CT | CT | Y | N | Y | CT | Y | N/A | 8, 3, 3 |
| Rafalovich 2004308 | N | Y | Y | Y | N | Y | N | CT | Y | Y | N | Y | Y | CT | N/A | 8, 4, 2 |
| Santamaria 2009309 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N/A | 14, 0, 0 |
| Smagorinsky 2007278 | Y | Y | Y | Y | Y | CT | Y | N | Y | Y | N | CT | CT | N | Y | 9, 3, 3 |
| Taylor Wilcoxson 2005310 | Y | Y | Y | Y | N | N | Y | CT | N | Y | Y | Y | CT | N | N/A | 8, 4, 2 |
| Wiebe 2007311 | Y | N | CT | Y | N | N | Y | Y | Y | Y | Y | N | Y | N | N | 8, 6, 1 |
| Wong 2004280 | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | N | Y | 11, 2, 2 |
| Young 2009312 | N | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | N | N | 10, 5, 0 |
| Zimmerman 1998313 | Y | N | CT | Y | N | Y | Y | N | N | Y | Y | Y | Y | N | N/A | 8, 5, 1 |
| Totals (Y, N, CT) | 31, 2, 0 | 18, 15, 0 | 18, 1, 14 | 31, 2, 0 | 23, 10, 0 | 24, 4, 5 | 30, 3, 0 | 21, 2, 10 | 24, 8, 1 | 31, 0, 2 | 18, 15, 0 | 22, 6, 5 | 23, 0, 10 | 11, 21, 1 | 9, 5, 0 |
The majority of studies recorded a ‘yes’ in response to questions about the clarity of the research question, appropriate study design, data collection description and findings substantiated by data. Most studies were lacking in the reporting of study limitations and the author showing reflexivity. Thirteen responses to the question about whether or not the theoretical perspective influenced the study were ‘cannot tell’, simply because the theoretical perspective was often not reported. Few studies reported the context or setting, evidence that the data analysis was rigorously conducted or the author’s theoretical perspective. Finally, although data collection was often adequately described, reviewers frequently could not tell whether the data collection had been rigorously conducted.
Studies that contributed greatly to the synthesis development such as Ljusberg,265,302 Partridge,279 Wong280 and Hands293 tended to score higher than studies that contributed little like Zimmerman313 and Bartlett et al. 287 This pattern is often found in quality appraisal for qualitative reviews. 320
One other marker of study quality that we have attempted to remain cognisant of during the synthesis was the credibility of included papers. Some of the studies included data from multiple perspectives or used multiple methods of data collection in an attempt to provide a more holistic picture of the research focus (see Table 34). For instance, Partridge’s study,279 which compared findings from interviews with adolescents diagnosed with ADHD with their school reports, teacher interviews and parent interviews, might be considered higher quality owing to the potentially increased credibility of considering different participant perspectives. 203 Despite the lack of a related quality appraisal question, in the findings section we take care to indicate where the credibility of evidence reviewed may be stronger or weaker.
On a related note, several papers included quantitative measures that are not the focus of this review (see Methods and analysis). As such, although a study like Bos et al. ’s288 may seem prone to bias given that teacher participants were interviewed about the training course they had recently completed, this study included quantitative measures that demonstrated gains in teacher ADHD knowledge, attitudes and perceived competence, which supports the positive interview data. This review did not attempt to weight the contribution of papers to the synthesis on the quality appraisal markers in Table 35, rather the relevance to the review and conceptual richness of findings determined the impact on the synthesis presented in this chapter.
Findings
Overview
As outlined in the previous chapter and above, the 33 included studies were diverse in their focus and often descriptive in their analysis, which indicates that no one paper appeared suitable as an index paper to guide the meta-ethnography. Thematic analysis focused initially on the 11 more interpretive papers (see Table 34),264,265,278–280,291,296,302,305,308,313 which provided seven main themes that were used to organise and guide the synthesis of all 33 papers. These themes are:
-
individualising interventions
-
structure
-
time
-
impact of interventions
-
problem situated within the child
-
relationships
-
expectations.
The process of reciprocal translation compared each paper’s contribution to each theme. The included studies were not refutations of one another, hence the reciprocal translation, although tensions relating to themes were identified both between and within included papers. During this reciprocal translation a number of subthemes developed, which represent the key components of each of the main themes.
The seven themes that guided the reciprocal translation are also depicted in Figure 5, which outlines the line of argument that stemmed from the reciprocal translation of the studies reviewed. Part of the meta-ethnographic process, a line of argument aims to discover a whole among a set of parts, attempting to explain the elements of prior synthesis together in one model or tentative theory. 88 The line of argument incorporates the themes that organised the reciprocal translation and relationships between them. This line of argument offers an explanatory model of the experience of interventions and teaching strategies for ADHD in school settings according to the papers reviewed.
FIGURE 5.
Model of line of argument.

Table 36 provides a recap of some of the key terms relating to the meta-ethnographic process used to synthesise the reviewed studies.
| Key term | Definition |
|---|---|
| Meta-ethnography | An interpretive approach originally developed by Noblit and Hare88 for synthesising findings of research to create higher-order interpretations of reviewed studies |
| Thematic analysis | Coding of themes and concepts across papers to develop a set of key themes to guide the synthesis |
| Reciprocal translation | The comparison of themes and concepts across papers and an attempt to ‘match’ themes from one paper with themes from another, ensuring that a key construct captures similar themes from different papers |
| Refutational translation | Where the comparison of themes and constructs across papers reveals conflict between accounts, examining the implied relationship between competing explanations |
| Line-of-argument synthesis | The development of a new model, theory or understanding by synthesising and interpreting the reciprocal translation into a coherent whole |
The line of argument shows three categories, which incorporated the seven themes. The model suggests a cyclical process, whereby issues relating to the intervention or strategy response to ADHD in schools influences the action and reaction to such interventions. The reaction to interventions used has the potential to impact on issues of socialisation that involve children with ADHD, their teachers, peers and parents. Finally, the process continues as the socialisation of those people involved in the school lives of children with ADHD effects future intervention responses to ADHD.
Three themes on the right-hand side of the model relate to issues in responding to ADHD in schools. The amount of structure inherent in interventions is a key element that needs consideration when planning interventions. The extent to which an intervention will be tailored to the individuals receiving it is also an area for consideration. Time is a tension; interventions need time in order to make an impact, and teachers report time pressures in administering interventions. Other facilitators and challenges also influence the intervention response to ADHD taken. Three themes on the left-hand side of the model represent aspects of socialisation that act as a context within which interventions or teaching strategies for ADHD are implemented. Relationships, expectations and views on whether or not ADHD is a problem situated in the child as opposed to the school context will be held by all involved in attempting to use or introduce an intervention in school settings and, therefore, these important factors frame users’ expectations of interventions.
At the top centre of the model is the final theme related to the impact of interventions, which fits the category action and reaction. In this review the impact considered will be the perceptions of users of interventions and teaching strategies for ADHD. Importantly, the model shows that this impact may not simply be in terms of how users viewed the success of the intervention, but that interventions can impact aspects of socialisation.
The line of argument will be used to structure the presentation of the synthesis. In the next sections of this chapter, each of the seven themes shown in the line of argument model is considered in turn. For each theme a number of subthemes are discussed. These subthemes arose during the reciprocal translation process.
Table 37 shows the themes and subthemes, along with the line-of-argument category under which they fit and the papers contributing to each subtheme. The themes related to responding to ADHD in schools are considered first.
| Category | Theme | Subthemes | Contributing papers |
|---|---|---|---|
| Responding to ADHD in schools | Individualising interventions | Tailoring to the individual with ADHD | 264,265,279,286,287,290–293,297,304,308–310,313 |
| Making interventions meaningful to pupils | 278–280,290,292,293,300,301,308,311 | ||
| Child with ADHD vs. whole class orientation | 264,279,291–293,296,298,300,305,308,309,311 | ||
| Withdrawal | 264,265,280,286,289,291,295,297–299,303,305,308,309,312,313 | ||
| Just good teaching | 264,279,288,295,308 | ||
| Structure | Prescribed learning vs. choice | 265,278,286,288,290,291,293–296,300,301,304,305,308–312 | |
| Routine vs. flexibility | 265,278,279,287,290–292,295,301,304,310 | ||
| Control vs. responsibility | 264,265,280,291,293,295,296,302,304,312 | ||
| Supervision | 265,291,295,302,304,306,308,312 | ||
| Structural constraints | 265,291,300,302,304,306,308 | ||
| Time | Needing more time | 265,280,286,289,296,301,303,305,306,308,309 | |
| Need for immediate reinforcement | 279,286,300,301,310 | ||
| Action and reaction | Impact of interventions | Perceptions of effectiveness depend on goals | 265,278,280,288,292,294–296,298,300,303,310,311 |
| Mixed views of effectiveness | 279,292–295,298,300,301,306–308,310 | ||
| Lack of application beyond interventions | 265,280,300,306 | ||
| Need for study skills | 280,287,289,293,300 | ||
| Socialisation | Problem situated within the child | ADHD as a problem | 265,279,288,295,296,302,307,308 |
| Compensatory perspective | 265,290–292,295,302,307–309 | ||
| Self-concept | 280,286,295,296,303,306,311 | ||
| Stigmatisation | 287,293,295,297,300,302,303,308,309,313 | ||
| Relationships | Pupil–teacher relationships | 264,265,279,280,287,288,290,292,293,295,296,300–303,306 | |
| Relationships with peers | 264,265,278,280,286,290–293,295,296,300,302,305,306,308,310,311 | ||
| School–home relationship | 265,286,288,289,294,298,300,301,304,306,309,310,313 | ||
| Teachers’ relationships with colleagues | 288,291,294,298,304,305 | ||
| Expectations | Attitude to school and learning | 279,280,287,290,300,302,303,306,308,311 | |
| Attitude to ADHD | 287,288,293,295,296,303,304,306,308,309,313 | ||
| Resistance and indifference | 279,280,307,289,290,293,297,300,302,305,306,308,311 | ||
| Lack of guidance and knowledge | 264,265,286,288,296,298,304,305,308–310,313 |
Responding to attention-deficit/hyperactivity disorder in schools
Individualising interventions
The first theme under the category of responding to ADHD in schools concerns views from the full range of participants about whether or not interventions and teaching strategies used for schoolchildren with ADHD should be individualised, as well as the perceived impact of this. Teachers acknowledge an important tension between the need to individualise interventions for students with ADHD while fulfilling their responsibility to other learners. There are also issues in how pupils who display ADHD symptoms perceive their placement on various types of individualised interventions. Table 38 provides definitions of key terms relevant to this theme.
| Key term | Definition |
|---|---|
| Individualised intervention | An intervention that is tailored to the individual(s) receiving it |
| Differentiation | A term referring to the adaptation of teaching and learning in order to allow access to different pupils |
| Constructivist classrooms | Intervention classrooms studied by Furtick 2001292 selected when their teachers used constructivist teaching approaches, in which the active involvement of the learner in the generation of meaning and knowledge is seen as essential to the learning process |
| Withdrawal | An intervention that involves removing the pupil with ADHD from their regular class setting |
Tailoring to the individual with attention-deficit/hyperactivity disorder
Participants representing a variety of perspectives in many studies shared the view that interventions need to be tailored to individuals with ADHD. 287,291,293,304,308–310,313 Indeed, one teacher in Mulligan’s study304 captured this view: ‘Be sure the child fits the program . . . we need to service each child as an individual’ (general education teacher, p. 37). 304 Teachers report making individualised adjustments for children with ADHD including differentiating assignments,308 using individual education plans (IEPs),290 using visual information,290,293,306,309 using computers,290 working one-to-one with a special educator291 and tailoring discussions with these children. 293 Furthermore, some studies reported that such individualisation needed to be used on an ad hoc basis288,293,295,309 and that revising accommodations was considered to be critical. 287 This is not to say that teachers across all studies were carefully planning tailored responses. Arcia et al. 286 suggest that techniques referred to by teachers tended to be ‘reactive rather than proactive and did not represent a comprehensive plan of action that can be characterized as a strategy’ (author quote, p. 98). 286
Tailoring interventions to particular individuals is seemingly critical given that some studies note the heterogeneity between children with ADHD. 308 Indeed, as Partridge279 notes ‘[a] diversity of complex dilemmas faces the teacher of ADHD students since they present in a number of different and demanding ways in the classroom’ (p. 103). 279 Unsurprisingly, several studies report views that using generic and mainstream strategies do not work. 279,292,293 In the traditional classrooms described in Furtick’s study,292 all pupils were expected to complete the same assignments at the same pace, often resulting in observations of high levels of frustration among the pupils diagnosed with ADHD. Several studies mention strategies to tailor learning to the strengths of pupils with ADHD,291,313 although Ljusberg265 recognises that this cannot be at the expense of skills that need development.
There is also a tension reported between the needs of children with ADHD in terms of accessing learning and developing skills as opposed to following the school curriculum:291,308
It’s a question of do you force the student or do you adapt the curriculum, and I don’t think we have that sorted out yet.
North American seventh grade teacher, p. 116308
Moreover, there is evidence suggesting that children with ADHD are oppositional towards (see Resistance and indifference) and easily ignored by an academic curriculum. 291,308
Despite some sound arguments for tailoring interventions to individuals with ADHD, views on the effects of this type of strategy were mixed. 264,265,293,308 Although a teacher in Hands’ study293 reported that tailoring teaching strategies for the adolescent with ADHD seemed to improve his behaviour in class, a criticism of differentiation of the curriculum was the possibility of separation of children with ADHD from their peers even when they remain in the classroom308 (see Relationships with peers, below). Another reported argument for not individualising interventions is the claim from some teachers that ADHD symptoms are experienced by all children308 (see Problem situated within the child, below).
Making interventions meaningful to pupils
Many studies reported that pupils with ADHD believed that it was particularly important that interventions are meaningful. 278–280,290,292,300,301,311 Grouping children in terms of their interests was seen as successful by the pupils diagnosed with ADHD in Furtick’s study. 292 Teachers echo the importance of meaningful interventions:293,308
Teachers contend that the single most important professional response to ADHD children is to take whatever steps are necessary to make them feel a sense of connection with their academic pursuits, consequently making the classroom a less threatening environment.
Author quote, p. 109308
A lack of meaning and purpose were barriers to intervention success. This shaped the adolescents’ reported views of what they are learning in Partridge’s study:279
I just don’t like things that I think are pointless, like some things that we learn . . . we learn some stuff that I kind of find really hard to believe and I just think I could be doing something better now, like, in a different class.
Australian young person diagnosed with ADHD, p. 189279
It seems that there is a need for teachers to know pupils and their interests, although other research would suggest that this applies to all young people, not just those diagnosed with ADHD (e.g. Hooper and Rieber321).
Several studies noted a view from teachers and pupils who display ADHD symptoms themselves that allowing achievement while offering some challenge could make learning meaningful. 265,279,293,308 Challenge was an integral aspect of the preferred activities reported by adolescents with ADHD in Partridge’s study. 279 However, in order to make challenge meaningful, teaching has to be carefully pitched. Indeed, Edwards290 and Hands293 report that their participants with ADHD ‘like the challenge, but sometimes it’s too much challenge’ (aged 16 years, p. 145293). Some of these ideas are considered further in the synthesis of review 4 (see Chapter 6, Review 4a: the school experiences and perceptions of pupils diagnosed with attention-deficit/hyperactivity disorder, Overarching theme for review 4a: attention-deficit/hyperactivity disorder symptoms as an interaction between biological, sociological and psychological factors, Sociological factors, The role of context in attention-deficit/hyperactivity disorder symptoms).
Child with attention-deficit/hyperactivity disorder versus whole class orientation
Many studies highlight a tension for regular class teachers between the implementation of individualised strategies for children with ADHD and the management of a whole class of pupils. 264,279,292,300,306,308,309 Indeed, an elementary teacher stated:
The teacher can’t put the other children’s education aside and only help the children with ADHD.
Korean teacher, p. 405264
Not all teachers referred to struggling with this tension; the elementary school teachers in Nowacek and Mamlin’s study305 were observed as remaining oriented to the class as a whole, while wishing to make modifications for their pupils with ADHD that maintained the integrity of planned subjects and required little individualisation. Although Nowacek and Mamlin305 question the success of this viewpoint, it does relate to evidence from Ozdemir306 and Houghton et al. 296 concerning teacher beliefs about how this tension can be overcome by involving the whole class in an intervention:
Rewarding my whole class was the part that I liked most about the FSS [First Steps to Success] program. This system fostered each of my student’s care for the success of the target child and motivated meaningful group cooperation. I mean, not only the target child, but also my entire class became motivated to behave appropriately.
Turkish grade 1 teacher, p. 123306
Teachers in Houghton et al. ’s study296 present their structuring strategies as if designed for the whole class. They say that they take care not to identify the pupils with ADHD to whom the strategy was targeted. Meanwhile, teachers in Wiebe’s study311 question how beneficial an intervention primarily designed for a child with ADHD (here listening to music) may be for the whole class.
There is an allied tension relating to the perception of equity for pupils with and without ADHD. 264,279,293,296,298,300,306,309 Teachers in Houghton et al. ’s study296 noted this tension:
ADHD presents tremendous difficulties within the classroom as it not only affects the learning of the ADHD student but it also has a negative impact on all the other students in the class because the ADHD student demands more attention and needs more positive feedback than the other kids. This creates difficulties for the teacher and school to ensure that all students have a fair and equitable education.
Australian teacher, p. 122296
Korean teachers in Hong264 reported that treating the child like other normal children was considered critical. Furthermore, Partridge279 notes an injustice felt by all pupils when rewards and punishments vary according to the young person. So, individualising interventions may cause resentment from peers (see Relationships with peers). Although some teachers shared the view of a mainstream teacher in Hands’ study,293 ‘I just try to treat everybody equally . . . I don’t care if he has a “D” average or whatever. I treat him just like I will the others’ (high school teacher, p. 140293), such practice is considered ineffective elsewhere. 291,304,308–310 Although this tension remains unresolved, Hong264 concludes that a successful, individualised, and therefore seemingly inequitable intervention, may be of benefit to all in the classroom if it improves classroom dynamics and reduces disruptive behaviour. This subtheme is considered further in the synthesis of review 4 [see Chapter 6, Review 4b: the experiences and perspectives of teachers of pupils diagnosed with or at risk of attention-deficit/hyperactivity disorder, Findings for review 4b (teacher views), Orientation to the class as a whole and orientation to the individual child and Review 4d: the school experiences and perceptions of pupils diagnosed with, or at risk of, attention-deficit/hyperactivity disorder, their teachers, parents and peers, Findings for review 4d (mixed views), Orientation to the class versus the individual].
Withdrawal
Educators across many studies believed that withdrawing children from their regular classroom to allow for specialised learning is beneficial. 264,265,280,286,291,298,308,309 Reasons for this view, from a range of educators, include the needs of children with ADHD being better met in learning assistance centres,265,308 to benefit the child and their peers by offering a break from a tense classroom atmosphere264,291 and to help mainstream teachers who may not be able to handle children with ADHD. 309 Sometimes withdrawal was seen as beneficial by pupils with ADHD. 280,303,312 One young person said:
I like this class [. . .] I have three teachers and less than 15 kids, and I know that if I need help I know that I will get at least one of those teachers to help me if not more. I know that there are the other two teachers who are watching the other kids so that the teacher that is helping me is focused on me and on what they are helping me with.
American young person diagnosed with ADHD (aged 15 years), reviewer edit in parentheses, p. 155303
These comments about lower teacher–pupil ratios relate to concerns highlighted below in Structural constraints and Time.
Where interventions involve withdrawal from the classroom, the goal of such programmes is often a return to regular schooling. 265,295 Still, mainstream and special education teachers often noted dilemmas about withdrawal from mainstream classrooms to special classrooms. 264,291,295,305 Reasons for this included a belief that the separation of pupils from their mainstream peers was negative in terms of social relations and acceptance291,305 and a perception that teachers are responsible for all their pupils’ learning. 264 Parents and pupils studied also echoed these issues. Parents referred to concern about what their child with ADHD might miss in the regular classroom and how they would feel about withdrawal. 289,297 Young people with ADHD also noted the tension:
I feel that it is good as well as bad. I miss so much [. . .] but it’s also too hard within the ordinary class. I should be somewhere in between, so I don’t know.
Swedish young person diagnosed with ADHD (aged 13–15 years), reviewer edits in parentheses, p. 8297
Some effects of withdrawal can, therefore, be experienced negatively by children. Ljusberg302 reports that pupils wish that they were in the regular classroom. There is an effect of withdrawal on relationships suggested by participants across studies. On the basis of interviews with children, Ljusberg302 concludes:
Most of the pupils felt lonely after attending the remedial class and some even had to change schools. One of the most important things when the pupils talked about difficulties was about missing friends.
Author quote, p. 443302
Other problems were recognised by participants in Isaksson et al. ’s study. 297 A SEN group still contains a diverse range of pupils and may not be pitched at the right level for children with ADHD, who often do not share the cognitive issues of other children with SEN.
Just good teaching
Some studies report a belief held by teacher participants that, rather than individualising interventions or strategies for pupils with ADHD, their reported practice does not differ from their general effective teaching. 264,279,288,295,308 Teachers in Rafalovichis’ study308 consider that the model of the ideal ‘ADHD teacher’ presented at professional development workshops does not really address the specifics of ADHD, but instead describes an overall pedagogical competence. Likewise, several teachers completing the training workshop intervention in Bos et al. ’s study288 perceived that the strategies they learned as part of the workshop were ‘just good teaching strategies that help all learners in my class’ (American teacher, p. 141288).
Relying on regular teaching practice is not a considered choice for teachers, rather they report that it is a necessary resort given the lack of guidance available about teaching children with ADHD (see Lack of guidance and knowledge, below). The lack of specified school protocols for pupils with ADHD leaves many teachers the option of ‘doing what they do best’ (North American seventh grade teacher, p. 115308).
Implications relating to the theme of individualising interventions are given in Box 4.
Interventions need to be meaningful and flexible given the individual differences among children with ADHD.
Mainstream teachers who use interventions for children with ADHD face tensions about their responsibility to other learners and challenges in maintaining equity for learners.
Withdrawal programmes need to consider both the effects of withdrawal on children with ADHD, as well as provide applicable skills for their reintegration into mainstream settings where this is the goal.
Teachers need access to material that can increase their knowledge about ADHD and give practical recommendations for strategies that can be used.
Structure
The majority of the studies reviewed contributed to the theme of ‘structure’. This focuses on a tension explicitly mentioned in several studies between the structure, routine and control associated with interventions and strategy use for children with ADHD on the one hand and choice, flexibility and responsibility on the other hand. 265,278,293,308,311 However, several studies recognise that structure and choice are not mutually exclusive and therefore not necessarily in tension. The issues of structure to which the reviewed studies refer are typically decisions about the descriptive nature of teaching and interventions for children with ADHD. However, a range of terms relating to structure and choice are used across studies which often lack definition or consideration of participants’ potentially differing viewpoints. Table 39 provides definitions of key terms relevant to this theme. There appear to be a range of differing viewpoints as to the extent to which successful interventions for ADHD should be structured. Subthemes considering these viewpoints are discussed below.
| Key term | Definition |
|---|---|
| Structure | As used here, ‘structure’ typically captures the prescribed learning, routine, control and organisation often cited as used when teaching children with ADHD |
| Routine | Learning is clearly planned, timetables are articulated and followed |
| Control | Relates to the amount of control children with ADHD have over their learning or an intervention. Controlled learning suggesting the control is with the educator |
| Choice | Schoolchildren with ADHD are allowed to contribute to decisions about their learning or intervention use |
| Agency | The capacity of those involved in educating children with ADHD to act intentionally and make their own choices |
| Flexibility | The timetable or intervention procedure allows for change or deviation |
| Responsibility | Relates to the amount of responsibility children with ADHD have over their learning or intervention experience |
| ESOL counsellor | Counsellor focused on teaching ESOL |
| DAMP | Disorder of attention, motor control, and perception; predominantly co-existing ADHD and developmental co-ordination disorder |
| Structural constraint | The level of restriction placed on options, here referring to matters that constrain educators’ choices about interventions and strategies for pupils displaying ADHD symptoms |
Prescribed learning versus choice
The majority of studies reviewed consider issues of prescribed learning and choice and their place in interventions for children with ADHD in school settings. 265,278,307,286,288,290,291,293–297,300,301,304,305,308–312 Often the studies reviewed referred to the importance of ‘structure’, without adequately defining the term. In most papers it appears that this ‘structure’ relates to a prescriptive experience of learning or interventions for the pupil displaying ADHD symptoms, with little opportunity for the pupil to choose elements of their learning.
Many of the studies revealed that teachers and pupils claimed highly prescribed learning was necessary for children with ADHD. 291,293–297,305,310–312 Teachers in Einarsdottir’s study291 were typical of those in other studies in suggesting that children with ADHD need a clear framework and rules to follow. Several of these studies referred to teachers’ beliefs that such ‘structure’ is necessary given the symptoms displayed by children with ADHD. 291,295,296,310 Other reasons for prescribing learning for pupils with ADHD were given by parents in Edwards’ study,290 who suggested that boundaries for their children diagnosed with ADHD were important because clarity is essential and ‘makes them feel safe’ (father of 9-year-old, p. 105290). Adolescents in Young et al. ’s study312 spoke positively about the closed unit that they attended in that it provided structure, clear expectations of behaviour, and rules and sanctions. However, it was far more often that teachers, rather than young people, spoke about the virtues of prescribed learning for pupils with ADHD. Although structure was used as a guiding metaphor for practice in several studies, Hjörne295 suggests it might be applied too rigidly in the ADHD classroom: ‘The teachers consistently enforce the “structure” by limiting the possibilities for the pupils to choose’ (author quote, p. 185295).
Some studies noted that consistency in intervention and teaching strategy delivery is particularly important for children with ADHD. 291,304,305,309,311 For one school counsellor in Santamaria’s study,309 consistency was seen as critical to intervention success:
I think they’re effective [interventions] as long as you or the teacher, whoever is involved, is consistent.
American English for speakers of other languages school counsellor, reviewer edits in parentheses, p. 59309
However, these counsellors referred to teachers lacking consistency:
It is difficult for a regular classroom teacher to be consistent with the strategies because of the sheer numbers, the body of students that they deal with.
American general school counsellor, p. 106309
The idiosyncratic and non-systematic use of interventions for ADHD by teachers is another barrier to consistency of intervention delivery. 305
Many studies did recognise the tension between prescribed learning and choice, with pupils and teachers feeling that both must play a part in pedagogy for children with ADHD. 265,278,293,308,311 Special education teachers’ narratives in Ljusberg’s study265 are characterised by structure, clearness and limits when talking about the remedial classrooms that they teach in. However, the ‘structured classroom’ as is characterised by Ljusberg265 still is seen to retain flexibility and individualisation. Many participant reports concur with a teacher of biology in Hands’ study293 that boundaries need to be in place, but this is not necessarily directed at the core symptoms of ADHD or to exert power over pupils, but rather to offer these children direction, support and a sense of safety.
Some studies considered that highly prescribed learning environments may not be appropriate for all pupils with ADHD. 286,295 Special education teachers in Hjörne’s study295 report that a highly structured approach does not work with every pupil and provide the example of a child with ADHD difficulties described as ‘stressed by structure’ (p. 193). 295 Other studies suggest a lack of agency experienced by pupils who display ADHD symptoms during interventions and learning more generally. 288,300,301,307 For example, young people in Prosser’s study307 reported that they were not consulted about the strategies teachers used and it seemed to be assumed they would be passive receptors of interventions.
It is reported that teachers sometimes offer pupils what appears to be a choice in their learning, but, in the end, they expect the young people to conform to their expectations, even when those parameters were not made clear. 293 Other teachers claim that pupils ought to have choice, but there is a concern that children with ADHD may not make suitable choices. For instance, a teacher in Wiebe’s study311 using the music listening intervention was concerned that ‘even the kids that it does help, I’m not always convinced that they are making the right choices to use the kind of music that would help them’ (p. 66). 311
Teachers who had attended a training workshop in Bos et al. ’s study288 appeared to recognise the importance of giving their pupils with ADHD choice while learning:
Now I give students choices when they work on a given task. I used to think that was giving too much slack. It’s new for me this year to realise the importance of just offering them a different color [pen or pencil]. . . I don’t think I realised how for some kids that might be really helpful.
American special education teacher, p. 141288
Although offering a choice in pen or pencil use is not assumed to be an effective intervention, this teacher suggests the importance of allowing schoolchildren with ADHD some choice in their learning, as opposed to the highly prescribed learning seen elsewhere. As for the issue around the terminology of ‘structure’, the term ‘choice’ is used without critical consideration from the reviewed studies. When teachers, parents and pupils who display ADHD symptoms refer to ‘choice’, it is not clear what level of choice they are referring to or if the perceptions of these different participant groups about ‘choice’ are shared.
Routine versus flexibility
Many studies also considered the tension between routine and flexibility. 265,278,287,290–292,295,301,304,310 For both mainstream and special education teachers, routine and predictability were seen as important for pupils with ADHD:
[deficits in attention, motor control and perception (DAMP) pedagogy] is when everything looks the same all the time . . . in order, one thing following the next.
Swedish special education teacher, reviewer edits in parentheses, p. 192295
As for Prescribed learning versus choice above, teachers report that routine will help pupils feel secure and respond to issues of inattention.
Often teachers reported that their practice needed to include both routine and flexibility in order to successfully work with children with ADHD. For instance, although remedial class teachers’ narratives in Ljusberg’s study265 are characterised by structure, clearness and limits as noted above, they are also characterised by individuality and flexibility. These teachers appeared to feel it was ‘important to have variety so that the pupils can motivate themselves’ (Swedish remedial class teacher, p. 206). 265
Other studies more clearly stress the need for variety and flexibility in interventions used with children with ADHD. 279,287,291,292,301,310 Reasons for the perceived importance of flexibility for young people displaying ADHD symptoms included them getting bored easily279 and so teachers can spend time with pupils with ADHD in smaller groups. 291 Finally, the flexibility observed in the constructivist classrooms in Furtick’s study292 afforded pupils multiple opportunities to search for appropriate methods when solving problems. Children with ADHD here could experiment with learning, rather than focus on outcomes, which was interpreted positively by a range of participants.
Control versus responsibility
Mirroring the discussions in the previous two sections, several studies also reveal a tension between control and responsibility, with teachers recognising a decision about the amount of control applied:
The most difficult task in the beginning of the semester was to decide what level of control would be appropriate for children with ADHD because excessive control might cause them to lose their interest in kindergarten or make them avoid the teacher, who they recognise as the person who always says ‘no’. Yet, I can’t approve or allow all the things they want.
Korean kindergarten teacher, p. 403264
Teachers generally reported that they exerted high levels of control when working with children with ADHD. Teachers in Houghton et al. ’s study296 claimed to use disciplining strategies to maintain an authoritative control over the whole class. Teachers may feel that control is necessary given the widely reported difficulties in self-regulation faced by children with ADHD. 280,290 As for structure and routine, remedial class teachers’ narratives in Ljusberg’s study265 suggest a need for control in their remedial classrooms. However, Ljusberg265 acknowledges that a pitfall of maintaining control is that pupils could attribute success to the teacher and not themselves. Teachers therefore feel that they must rule but in dialogue with their pupils, ‘it is important that the pupils feel that they are involved in controlling’ (p. 205). 265 A range of teachers appear to believe that pupils who display ADHD symptoms need responsibility and agency, but in a structured and controlled setting. The teachers in Mulligan’s study304 expressed a need for a balance between the efforts they make to accommodate children with ADHD, while still holding the pupils accountable for their behaviour and the classroom demands placed on them.
Papers reviewed revealed barriers to pupils with ADHD taking responsibility. Only one of four 15- to 16-year-old pupils in a study by Wong280 acknowledged taking responsibility for his learning (or lack of it). Although the young person studied in Hands’ case study293 stated ‘I want to be held accountable’ (aged 16 years, p. 143),293 he appeared to feel disempowered to do anything about the lack of responsibility he held and ineffective accommodations he perceived.
Supervision
A related issue surrounds the supervision of pupils with ADHD. Studies generally consider that these children need close supervision and greater teacher attention than that typically required for other children. 265,291,302,304,306,308,312 For instance, teachers in a study by Einarsdottir291 reported that children with ADHD function better in small groups and with adults close to them. Moreover, the consensus is that pupils who display ADHD symptoms need support when working with others, as this quote illustrates:
I find they especially need support in the group. Just to have someone by their side, keep them near you
Icelandic playschool teacher, p. 386291
Teachers in Jones’ study298 share the view that close observation helps to prevent or limit disruption. Smaller staff–pupil ratios were the reason that young people with ADHD in Young et al. ’s study312 gave for receiving greater support and attention: ‘You get more attention. It’s a lot better [than mainstream school] ‘cos its [sic] three of you, four of you in a class and one teacher’ (aged 14–16 years, p. 60). 312 Increased support and attention appeared to enhance both the ability and sense of achievement for the males with ADHD studied.
In some studies focused on the use of special education classes, pupils responded negatively to such high levels of supervision. 295,302 Ljusberg302 found differences in the views of children in remedial classes, with some pupils stating that they did not need that much help and that the teachers disturbed and interrupted them at times. Hjörne295 shows that individual support of the kind seen in the ADHD classroom can lead to clashes; the pupil observed was reported to reject the assistance of his teacher and attempted to assert control. It cannot be assumed that one-to-one support will necessarily mean a better relationship with school staff or will be preferred by pupils who display ADHD symptoms; indeed, issues about control (see Control versus responsibility, above) may impact this. Educators in studies by Hong264 and Einarsdottir291 mentioned that giving their pupils with ADHD space to themselves when they needed it was effective.
Structural constraints
Finally, it is worth considering a related concern about perception of structural constraints imposed on those working in classrooms with pupils who display ADHD symptoms. The most frequently mentioned structural constraint was class size. 291,304,306,308 For instance, grade 1 teachers in Ozdemir’s306 research in Turkey report class sizes of over 40 pupils. Understandably then it is a challenge to provide the individualised intervention tested in this study in these circumstances. Indeed, the small class sizes seen in several of the interventions reported are considered to be advantageous, allowing pupils more one-to-one time. 265,300,302 For instance, small class sizes were reported to allow more one-to-one time in the alternative high school evaluated in a study by Kreiss300 as indicated by one young person:
I also thought the small class size, I think it was like around six to eight in a class or something. That was great for me. I could get more attention and stuff.
American young person diagnosed with ADHD, p. 220300
However, as noted above, increased supervision and one-to-one time with teachers is not always well received by pupils. Other structural constraints mentioned included funding and school accommodation,265 as well as the curriculum demands that may not suit pupils who display ADHD symptoms as discussed above (see Tailoring to the individual with attention-deficit/hyperactivity disorder, above).
Implications relating to the theme structure are given in Box 5.
Decisions about the level of prescribed learning, routine and control on the one hand and choice, flexibility and responsibility on the other hand are not dichotomies. Interventions and strategies perceived to be effective often incorporate structure and choice for the pupil with ADHD.
Consistency rather than control may be important.
Pupils with ADHD may respond negatively to the high levels of supervision that teachers assume they need.
Researchers need to explore the use of terms such as ‘structure’ and ‘choice’, which may hold multiple meanings for educators.
Class size appears to be an important factor, with lower teacher-to-pupil ratios said to be appreciated by pupils with ADHD.
Time
The pressure on teachers who feel a tension between the time spent working with a child with ADHD versus working with the rest of a mainstream class (e.g. Hong264) has been considered above (see Child with attention-deficit/hyperactivity disorder versus whole class orientation, above). It became clear as this synthesis progressed that time was a critical issue concerning the use of interventions for children with ADHD, often for the teacher under pressure, but also for the pupils themselves. In this section time is considered further in relation to two subthemes. Table 40 provides definitions of key terms relevant to this theme.
| Key term | Definition |
|---|---|
| Token economy | Reward system based on secondary reinforcement where tokens such as merit points are collected and later exchanged for a desirable reward |
Needing more time
Many teachers emphasise the time pressure involved in accommodating children with ADHD, both in regular and special education classes. 265,286,305,306,308 The studies focused on interventions often reported that teachers felt pressure to deliver the intervention to schedule. 265,280,301,303,306 Teachers in a study by Ozdemir306 stated that they found it difficult to find the time necessary for each child in order to fully implement the programme:
I really wanted to be part of the FSS [First Steps to Success] program and your study. However, I am not sure whether other teachers would be willing to be a part of the program. I think that they would be sceptical about the heavy time commitment required in the program.
Turkish grade 1 teacher, p. 126306
Remedial class teachers in Ljusberg’s study265 talk about the need to be highly prepared and know the stage at which every child is when planning lessons.
There is evidence that, to be successful, interventions often require more time than they are given. 280,303,309 In Wong et al. ’s study,280 the confidence of the children with ADHD and their use of the strategies learned during the intervention appeared to diminish over time. Duration is seen as a key moderator for the intervention studied by McNeil. 303 The young people for whom this intervention programme was considered a success were on the programme for a year. It was reported that students who attended the programme on a regular basis experienced more significant emotional and behavioural changes than those who did not. Impatience on the part of teachers was also evident. Likewise, counsellors in a study by Santamaria309 commented that teachers ‘do not follow protocol . . . they try for a week or two, adults get tired, they want a quick fix, and they tell us [counsellors] this is not working, and they stop, they quit’ (American English for speakers of other languages counsellor, p. 67). 309
However, it is not just the length of interventions that presents a challenge to educators. Regardless of the techniques used, teachers suggested a strong preference for interventions that do not demand a great deal of their time, frequently mentioning strategies such as preferential seating, writing children’s names on the board and using peer tutors (e.g. Arcia et al. 286). As noted above, individualisation was considered too time-consuming by some teachers, who therefore reported a preference for whole-class strategies. 305
Pupils with ADHD also need time to embed what they are learning during an intervention. 280,301 School mental health providers in Langberg et al. ’s study301 considered the pace of skills introduction to be too fast in the HOPS intervention. Pupils with ADHD may also need more time than their mainstream peers to complete tasks. 303 Furthermore, children in primary and elementary schools are often with their teacher only for a year. This presents a challenge in terms of what can be achieved in this time and is perceived as affecting some teachers’ willingness to invest effort in a pupil:
I believe ADHD kids are a bother to some teachers and they believe if they can get through that school year, they will not have to worry about that kid again.
American parent of a young person diagnosed with ADHD, p. 356289
Some teachers did state that they made extra time for children with ADHD. 264,286,293 College students with ADHD in a study by Bartlett et al. ,287 reflecting on what helped them at school, reported particularly appreciating teachers’ willingness to spend extra time with them. Notwithstanding the time pressure on teachers considered above, pupils with SEN including ADHD in Isaksson et al. ’s study,297 reported that support scheduled during their ‘free time’ meant they would have to sacrifice some time during their lunch when all the other pupils had a break. Other studies consider the opportunity for movement and socialising at break time as critical for pupils with ADHD. 289
Need for immediate reinforcement
A range of studies with participants across all perspectives highlight that one of the reasons for indifference towards behaviour modification (see Resistance and indifference, below) may be that children with ADHD need more rapid reinforcement than other children. 279,286,289,300,301,310 Equally, Arcia et al. 286 and Langberg et al. 301 both found that educators considered that token economies, where tokens could later be exchanged for a tangible reward, were unsuccessful for pupils with ADHD. This led to an amendment to Langberg et al. ’s301 HOPS intervention to allow for a more flexible use of the incentive system.
Implications relating to the theme time are given in Box 6.
Mainstream teachers attempting to use interventions for children with ADHD in their classes report that they are often under significant time pressure.
When contingency management is used with children with ADHD, immediate reinforcement is important.
Action and reaction
Impact of interventions
One theme regarding the impact of interventions and strategies for children with ADHD is included under the category of action and reaction (see Figure 5). Although the impact of non-pharmacological interventions for ADHD in school settings was considered quantitatively in Chapter 2, the studies in this review of qualitative evidence often revealed what participants thought about the effectiveness of interventions and strategies used with pupils who display ADHD symptoms. Participants’ views on the impact often revealed factors about their experiences that have not been captured quantitatively and may influence effectiveness in practice. Table 41 shows the subthemes relating to ‘impact of interventions’ that resulted from the reciprocal translation of included papers.
| Category | Theme | Subthemes | Contributing papers |
|---|---|---|---|
| Action and reaction | Impact of interventions | Perceptions of effectiveness depend on goals | 265,278,280,288,292,294–296,298,300,303,310,311 |
| Mixed views of effectiveness | 279,292–295,298,300,301,306–308,310 | ||
| Lack of application beyond interventions | 265,280,300,306 | ||
| Need for study skills | 280,287,289,293,300 |
Perceptions of effectiveness depend on goals
The majority of studies reported positive comments from users about the effectiveness of interventions. 280,288,292,294,296,310,311 The workshop for teachers that appeared in Bos et al. 288 was claimed to change teacher attitudes and increase their knowledge:
[I]t’s been a real eye opening experience. I can now deal with kids that I suspect have some attention deficit problems a lot more successfully than I had in the past.
American classroom teacher, p. 141288
Self-report information from the interviews conducted near the end of the following school year suggested that teachers believed that they had retained their knowledge and positive attitudes towards the education of pupils with ADHD. 288 The young person with ADHD who experienced listening to music during work in Wiebe’s study311 also reported improved mood, and attitude and motivation, which was endorsed by his parent’s views. So in some studies, interventions were considered to have a positive impact on the attitudes and motivation of those involved.
However, some interventions were seen to be effective for specific targeted skills, yet did not appear to impact on achievement (e.g. Furtick292). Educators in Langberg et al. ’s study301 saw the HOPS intervention as effective given quantitative data which showed that it improved the organisational behaviour it targeted. However, teachers noted that ‘better organizational skills did not necessarily translate into “getting more work done” and turned into [handed in to] the teacher’ (author quote, reviewer edits in parentheses, p. 151). 301 In a study by McNeil,303 pupils also claimed that they measure intervention success in terms of achievement and, therefore, one participant did not think special education classes help her:
Like, I learn it in a day but then I can’t remember it. Like I really don’t understand special ed classes. How they’re going to help me make it.
American young person diagnosed with ADHD, p. 162303
Hjörne295 questions whether or not the procedures applied in the ADHD classroom and the practising of social and pedagogic skills will give the child the necessary skills to function in the regular classroom. Little progress was seen in observations of the ADHD classroom. This and other withdrawal programmes (e.g. Ljusberg;265 Kreiss300) seem to indicate that such programmes are unsuccessful in supporting pupils to adapt to the regular classroom; instead, children are considered to be on a ‘road to nowhere’ (author quote, p. 195). 295 It seems, then, that participants perceive less intervention success when the goals are general, like achievement and return to mainstream education, rather than focused on the specific behaviours of children with ADHD.
Mixed views of effectiveness
Several studies clearly noted individual differences in how effective the interventions considered were perceived to be for different pupils with ADHD. School mental health providers in a study by Langberg et al. 301 noted that some young people seemed to get more out of the intervention than others. These practitioners suggested that this might be due to some pupils understanding the purpose of the intervention and wanting to improve. This suggestion relates to Making interventions meaningful to pupils. There was a suggestion from Kreiss300 that the alternative high school studied could work as a stepping stone, preparing young people to make better use of programmes in the future. This suggests both the importance of preparation for using any particular intervention for ADHD and that an intervention may produce longer term gains without necessarily demonstrating any tangible outcomes at the time. 300
Negative comments about interventions could often be traced to the challenges considered elsewhere in this chapter, for example mainstream class sizes,265 time pressure,305 inflexibility of interventions304 and pupils understanding the purpose of interventions. 301 Participant explanations for the ineffectiveness of interventions and strategies included pupil’s lack of motivation, passivity towards learning, anxiety,295 classroom management issues interfering with learning,298 a lack of consistency from teachers293 and a belief that some interventions work against the pupil; for instance, in Hands’ study293 both the young person with ADHD and his teacher believed that giving him extra time to complete work was ineffective as he tended to procrastinate further.
Although it was discussed above (see Just good teaching) that teachers reported relying on effective practice to teach children with ADHD, several studies reported that regular teaching strategies were ineffective when applied to children with ADHD. 279,292,293,307,308 Interviews with young people with ADHD reported by Prosser307 considered that mainstream strategies including traditional pedagogies, negative behavioural sanctions, verbal instruction and note-taking were deemed unsuccessful. Partridge279 generated a substantive theory about how adolescent boys diagnosed with ADHD respond to the efforts of their mainstream teachers to modify their actions. The teachers’ efforts were concluded to be largely ineffectual. Partridge279 finds that the adolescent boys diagnosed with ADHD claimed that they would prefer teachers to explain concepts well so they can work better, rather than focus on reward systems.
Lack of application beyond interventions
A lack of application of content beyond the specific intervention period is criticised by various participants. 265,280,306 Parents in a study by Ozdemir306 worried about what would happen post intervention, reporting a belief that once the intervention ended so would the improvement some of them had seen. Key for Wong280 are issues of applicability. Pupils were considered to understand when to implement their metacognitive skills they learned, but not how. Analysis also noted that motivation and anxiety would operate as barriers to children with ADHD applying intervention concepts in relevant learning situations. 280 The implication raised in these studies is the need for support beyond a period of intervention to ensure what is learned is applied.
Sometimes what is learned in an intervention is not necessarily applicable to other concepts, as discussed earlier (see Making interventions meaningful to pupils). For instance, special education teachers in Ljusberg’s study believe that ‘what pupils in remedial classes learn primarily is to be pupils in remedial classes’ (p. 208). 265 Although the teachers report that the children are meant to be adapted for return to regular schooling, the context is referred to as very different and the accommodations used may not be made or even be feasible in the regular classroom.
Need for study skills
Several studies noted that pupils with ADHD need support with study skills and that these skills are perceived to have a marked effect on the learning of these children. 280,287,289,293,300 Wong’s analysis280 across methods shows that without skills for study, adolescents with ADHD remain dependent on their teacher. Parents report that their children with ADHD need particular assistance with homework and organisational skills. 289,293 In a study by Bartlett et al. ,287 college students with ADHD reflecting on what helped them at school noted that working on study skills for one session a week was beneficial. Given the issues with withdrawal programmes to support pupils who display ADHD symptoms (see Withdrawal) and compensatory perspectives (see Compensatory perspective, below) considered elsewhere in this chapter, there is a need to include more study skills and processes of learning as a basis for ADHD pedagogy. However, Wong280 notes that teaching that is entirely focused on content or skills is insufficient, which implies that skills ought to be taught in relation to the curriculum content followed.
Implications relating to the theme impact of interventions are given in Box 7.
Interventions appear to hold different perceived levels of effectiveness for different individuals.
Interventions ought to teach skills that are applicable across contexts. There is a need for support beyond a period of intervention to ensure what is learned is applied.
Children with ADHD often need support with study skills as well as their symptoms of ADHD.
Socialisation
Problem situated within the child
Three themes fit the category ‘socialisation’ (see Figure 5). These themes will be discussed in turn, starting with views regarding ADHD as a ‘problem’. Many participants across studies and perspectives considered ADHD to be a problem located within the child, but out of the child’s control. 265,288,295,296,302,308 This seemed to impact on how the problem was seen to be addressed in the school setting, where the focus was typically on the child, rather than the school context. The view of ADHD held by those involved with these children’s education appears at times to lead to labelling and stigmatisation, particularly where it is clear the pupil is receiving an intervention for their ‘problem’. Table 42 shows the subthemes relating to the socialisation themes that resulted from the reciprocal translation of included papers.
| Category | Theme | Subthemes | Contributing papers |
|---|---|---|---|
| Socialisation | Problem situated within the child | ADHD as a problem | 265,279,288,295,296,302,307,308 |
| Compensatory perspective | 265,290–292,295,302,307–309 | ||
| Self-concept | 280,286,295,296,303,306,311 | ||
| Stigmatisation | 287,293,295,297,300,302,303,308,309,313 | ||
| Relationships | Pupil–teacher relationships | 264,265,279,280,287,288,290,292,293,295,296,300–303,306 | |
| Relationships with peers | 264,265,278,280,286,290–293,295,296,300,302,305,306,308,310,311 | ||
| School–home relationship | 265,286,288,289,294,298,300,301,304,306,309,310,313 | ||
| Teachers’ relationships with colleagues | 288,291,294,298,304,305 | ||
| Expectations | Attitude to school and learning | 279,280,287,290,300,302,303,306,308,311 | |
| Attitude to ADHD | 287,288,293,295,296,303,304,306,308,309,313 | ||
| Resistance and indifference | 279,280,289,290,293,297,300,302,305–308,311 | ||
| Lack of guidance and knowledge | 264,265,286,288,296,298,304,305,308–310,313 |
Table 43 provides definitions of key terms relevant to this theme.
| Key term | Definition |
|---|---|
| Compensatory perspective | From Ljusberg,265 this term indicates the view that ADHD difficulties are seen as situated within the child and therefore action is taken to compensate for these difficulties. It ignores the impact of context on said difficulties |
| Self-efficacy | Belief in one’s capabilities to achieve particular goals |
| Self-esteem | Refers to how much we value ourselves |
| Labelling | The process by which a label like ‘ADHD’ or ‘stupid’ is applied to a person rather than the problem. This label may then lead to stigmatisation from others and changes in behaviour regardless of the accuracy of the label |
| Stigma | Negative beliefs regarding those who are categorised with attributes outside what is considered to be ordinary and natural |
Attention-deficit/hyperactivity disorder as a problem
The attitudes reflected by participants across several of the studies cast ADHD as a problem. 265,288,295,296,302,308 Remedial class teachers in a study by Ljusberg265 consider the problem to relate to both the school and the pupils: ‘the pupils have the problem and the school cannot handle it’ (author quote, p. 200). 265 Pupils in Ljusberg’s study302 appear to recognise that they are regarded as difficult, with problematic behaviour, and that they are seen to be deviating from other pupils. Perceived reasons for attending a remedial class were all related to difficulties originating in themselves. Partridge’s279 participants reported that they were embarrassed about being diagnosed with ADHD, and did not want to disclose it for fear of it being used against them by peers.
Some studies reported that teachers held a biological understanding of ADHD, believing ADHD behaviours to be outside the child’s control. 288,308 This assumption was reported to lead to curricular adaptations; teachers in Bos et al. ’s study288 said that they redesigned classrooms, daily schedules and methods of instruction. However, this was not always the case, as teachers in a study by Houghton et al. 296 believed that ADHD behaviour was under the child’s control. They saw ADHD behaviour as attention-seeking, with inattention and disruption considered to be a response from pupils to finding tasks difficult, therefore masking their inability, a more psychological perspective. Such diverse attitudes affect the types of interventions that teachers may be willing to adopt.
Where interventions involve withdrawal from the classroom, the reported goal of such programmes is often to learn how to better fit the regular school classrooms295 (see Withdrawal, above). This relates to issues around ADHD being seen as a problem situated within the child, who therefore has to adapt to the classroom. Special education teachers in Ljusberg’s study265 note an expectation that their remedial classroom interventions prepare children with concentration difficulties for their return to their regular classrooms. Special education teachers in Hjörne’s study295 reinforce that the high level of structure in the ADHD classroom exists with the goal of joining the regular classroom in mind:
Pontus has to finish his story first . . . you tell it one at a time, that’s how you do it in school [the regular classroom].
Swedish special education teacher, reviewer edits in parentheses, p. 187295
Hjörne295 questions whether or not practising social and pedagogic skills will give the child the necessary skills to function in the regular classroom and suggests that the children with ADHD ‘are learning how to be handicapped in the normal setting’ (special education teacher, p. 195). 295
Compensatory perspective
Interventions and teaching strategies evident across a range of the studies reviewed indicate what Ljusberg describes as a ‘compensatory perspective’ (p. 441),302 meaning that action is taken to compensate for the problem, which is seen to be within the child, rather than seeing the context as potentially creating the problem. This is revealed in practice described by the studies. The social and material design of remedial classrooms in Ljusberg’s study265 is seen to indicate low expectations for the pupils in light of their difficulties. The pupils appear to see themselves as not fully adapted to school, something that is unlikely to change with the practice in the remedial classroom (see Mixed views of effectiveness, above). Ljusberg302 believes that this focus brings a restriction of options and hence a lack of agency for both the children and the remedial class teachers, while the school’s responsibility is rendered invisible. 302 Ljusberg265 concludes that there ought to be more focus on situated learning and acknowledges the role of context in the difficulties experienced by children displaying ADHD symptoms.
Hjörne295 reports that teachers in the ADHD classroom compensate for the symptoms of ADHD in the activities that they choose, including motor activities to give an outlet for hyperactivity and choosing subject matter that is likely to gain attention, ‘otherwise we won’t grab their attention’ (special education teacher, p. 188). 295 Likewise, several other papers mention giving motion and movement as beneficial for pupils displaying ADHD symptoms. 290,304,305,308 However, some studies report that non-mainstream educators believe too much movement between tasks290 and frequent activity changes309 are challenges for pupils with ADHD.
Teachers in a study by Einarsdottir291 report strategies that they used and found successful for teaching children with ADHD. However, these strategies are always focused on the child rather than the classroom; for instance, avoiding seating the child where they are easily disturbed. The compensatory perspective was not just held by teachers, but was also recognised in the experiences of young people in Prosser’s study307 and those pupils attending traditional classrooms in Furtick’s study. 292
Self-concept
Low self-esteem is seen as a barrier for children with ADHD. 280,286,295,296,311 For instance, teachers in a study by Houghton et al. 296 note the propensity for poor self-esteem in pupils with ADHD, which they attribute to triggers such as stigma, large classes, difficult subject matter, bullying and peer rejection. Often children with ADHD appeared to be embarrassed about their difficulties. 293,303,308 For example, one participant ‘felt humiliated when teachers treated him differently because of his ADD’ (author quote, p. 114):293 ‘No, no, no. I don’t expect any more time. I want to be treated like the other students’ (16-year-old diagnosed with ADHD, p.114). 293
Wong280 reported that pupils with ADHD held low self-efficacy, attributing learning outcomes to circumstances beyond their control. Despite such barriers in terms of self-concept seen across a range of studies, several papers reported that pupils felt their confidence increased as a result of interventions used (e.g. Wiebe311). Young people in McNeil’s study303 seemed to improve their view of themselves after attending the programme. Teachers and parents in Ozdemir’s study306 reported improved self-confidence related to social skills in the children with ADHD attending the intervention.
Stigmatisation
This view of ADHD as a problem situated within the diagnosed child leads to frequent stigmatisation, as evidenced across studies. In particular, attendance of an overt intervention appears to encourage this. Indeed, Ljusberg302 reported that attendance at an intervention can reinforce a deficit label: ‘Many think that we have got DAMP [deficits in attention, motor control and perception] or some other deficits just because we are attending the class’ (aged 10–12 years, p. 443). 302 Attendance at the remedial class is seen to have ‘a stigmatizing effect with the individual identified as one who cannot be in an ordinary class’ (author quote, p. 443). 302 Teachers in Zimmerman’s313 study believed that the separation of issues with learning from the individual in question was an important quality when working with children with ADHD.
A participant with ADHD in a study by Bartlett et al. 287 had this advice for teachers:
All in all – teach, but don’t make them [children] feel bad about it. Because it’s so easy for ADHD children to feel bad about themselves and who they are.
American college student, p. 229287
It appeared important to child participants that they were not negatively labelled and that their ADHD-type behaviours were not interpreted as character flaws. Sometimes pupils in Isaksson et al. ’s study297 said that they refused to leave the regular class because attendance at the resource room was stigmatising. The stigmatisation experienced is not necessarily perceived as being in relation to ADHD; in a study by McNeil303 the adolescents with ADHD initially felt like they were put on the programme because they were stupid and felt like others were judging them. One young person felt they were treated ‘Like an idiot . . . who would not be good at anything. I didn’t understand anything and everyone else thought I was stupid’ (aged 17 years, p. 172). 303
Interestingly, it seems that the children with ADHD themselves can participate in the labelling of their disorder. The children with ADHD in Hjörne’s study295 were observed to stigmatise their condition by calling their peers names like ‘DAMP kid’ (aged 8 years, p. 189). Theory suggests that individuals who carry stigmatised markers may ‘internalise’ the negative representations of their status as may be the case here. 322 This may impact self-esteem, reducing the likelihood that children with ADHD will challenge their devalued status. Indeed, there is no evidence from the included papers that children with ADHD reclaim and empower their label. 323
Labelling is not necessarily seen as a negative thing in all of the studies, with teachers and parents apparently considering the merits of labelling children with ADHD. Rafalovich308 shows that teachers are consciously aware of issues of labelling children diagnosed with ADHD and, indeed, that they have varied opinions on the effectiveness of labelling, ranging from damaging to the child’s self-esteem to a necessary precursor for effective school-based treatment. However, a parent in Zimmerman’s study313 stated ‘Schools are good at labelling but not so good at follow-through. At the high school level the counsellors are too busy to offer any real help to the child or parent’ (p. 186). 313 In these studies, formal labelling (or acquiring a diagnosis) is presumably considered necessary in order to acquire resources for ADHD. 324
The importance of being able to overcome stigma was seen in Kreiss’ study. 300 Part of the success for some pupils was considered to be due to young people having a new start and the chance to forge a new reputation. Yet, elsewhere, interventions are often reported to be experienced by children with ADHD as reinforcing difference. Rafalovich308 points out that curriculum modification may create further separation of children with ADHD from their peers even when they remain in the classroom, although this is seen by the teachers as an acceptable trade-off. A young person in McNeil’s303 intervention programme described the compromise between self-concept and need:
[I] felt like I [was] put in this program because I am stupid. But then I realised that I am being put in this program so I can help grasp what I am supposed to do in all my subjects [. . .] Occasionally I hate being in special ed because it makes me feel so stupid . . . like I am stupid and everyone is judging me. But in other times I know that it is just helping.
American young person diagnosed with ADHD (aged 17), reviewer edits in parentheses, p. 175303
As well as the ‘fresh start’ it offered, teenagers in Kreiss’s study300 liked the familiarity of the alternative high school. Even though it catered for emotionally and/or behaviourally disturbed adolescents, it did not reinforce their difference as it aimed to be run like high school, so not all interventions are liable to reinforce that children with ADHD are different. Stigmatisation is considered in further detail in the synthesis of review 4 [see Chapter 6, Discussion, Findings from the synthesis of reviews 4a–d, School expectations and structures establish boundaries for the identification of attention-deficit/hyperactivity disorder symptoms and can aggravate attention-deficit/hyperactivity disorder symptoms, Constituting deviance and invoking stigma and Implications of stigma for non-pharmacological interventions for attention-deficit/hyperactivity disorder in schools].
Implications relating to the theme of problem situated within the child are given in Box 8.
The role of context in the difficulties experienced by children with ADHD needs to be considered when designing interventions.
Children with ADHD’s low self-concept may be a barrier to engaging in interventions and needs to be considered in decisions about interventions.
Children with ADHD may be the victims of stigmatisation from others, particularly peers, as a result of both their diagnosis and the interventions they experience. This may impact effectiveness.
Relationships
The second theme under the category of socialisation refers to the relationships of those involved in interventions for children with ADHD in school settings. The relationships of pupils who display ADHD symptoms are a contextual factor that frames how certain interventions might be perceived by those pupils. Studies in this review also show that using interventions has an impact on these same relationships. This theme is considered further in the synthesis of review 4 [see Chapter 6, Review 4c: the experiences and perspectives of parents of pupils diagnosed with attention-deficit/hyperactivity disorder, Findings for review 4c (parent views), Relationships, Parent–teacher conflict is the norm, Fit between pupils diagnosed with attention-deficit/hyperactivity disorder and school and Relationships: attention-deficit/hyperactivity disorder symptoms as a threat to educational and parental identities].
Pupil–teacher relationships
All types of participants reported the importance of positive relationships between teachers and their pupils with ADHD. For instance, good pupil–teacher relationships are at the heart of the strategy that teachers report as most effective in Houghton et al. ’s study:296
I try to approach it in the calmest manner I can . . . I try to make them feel that I’m there to look after them and that I’m their friend.
Australian teacher, p. 126296
Both teachers and parents in a study by Hands293 claimed that the relationship between teacher and pupil was pivotal to the children’s ability to achieve. Multiple studies recognise a relationship between pupil–teacher rapport and the performance shown by pupils who display ADHD symptoms in the classroom. 279,280,287,292,293,300,303 It is therefore of little surprise that these relationships are perceived to predict intervention success. Studies mention the need for teachers to be caring, approachable and engaging when working with pupils displaying ADHD symptoms. 287,302,313
Conversely, poor relationships with teachers had a negative effect on intervention experience. Ljusberg302 found that some pupils believed that they were in remedial classrooms because their teacher in the ordinary class disliked them; pupils’ negative perception of this intervention is considered elsewhere (see Withdrawal, above). One young person’s view in Kreiss’ study300 demonstrated how the relationship could impact an intervention:
I had a bad attitude. I didn’t think I had a problem. I thought everyone else was the problem. I saw teachers and stuff as stupid and I didn’t listen to what they had to say. I wasn’t looking for anyone to help me because I didn’t think I needed help.
Young person diagnosed with ADHD, p. 228300
One other concern about the relationship between teachers and pupils with ADHD is the potential for pupils to over-rely on their teacher. This was reported in a study by Wong,280 where pupils appeared to depend on teacher instruction: ‘The teacher tells me what to study. Like what chapter and in which course, and they even make us underline sometimes’ (Canadian young person diagnosed with ADHD, aged 15–16 years, p. 151). 280 This was linked to pupils’ abdication of responsibility for their own learning (see Control versus responsibility, above).
Understanding appears to be critical to the relationship between teacher and pupil with ADHD:
Knowing one’s pupils, having contact with their parents, knowing how the pupils get on with their friends and how they get on outside the school are seen as important by the interviewed teachers.
Author quote, p. 206265
Several other studies suggest that teachers need to learn about their individual pupil’s needs279,290,303 (see Making interventions meaningful to pupils, above). However, a young person in McNeil303 stressed the importance of teachers being understood:
Yeah I got some help but I just didn’t understand what the teachers were saying. Every time I didn’t understand what they were trying to explain they tried to explain it in a different way. But every time they tried to explain it differently, I didn’t understand it.
American young person diagnosed with ADHD (aged 17 years), p. 171303
Understanding here is related to communication, although it was shown to impact the pupil–teacher relationship. 303
Sometimes specific interventions show teachers the importance of good relationships as a foundation for working with children with ADHD. Teachers claimed to recognise the importance of understanding ADHD from the pupil’s perspective and working collaboratively with them in Bos et al. ’s study,288 reporting that a deeper understanding of ADHD led to better working relationships and increased empathy. Likewise, teachers in a study by Ozdemir306 described prior negative relationships with their pupil with ADHD. The switch to focusing on positive behaviour was deemed by one teacher to be the major impact of the programme.
Several studies highlight the importance of the teacher as an intervention in themselves. 279,280,292 Both pupils and teachers report that the teacher can have a dramatic effect on the success of pupils who display ADHD symptoms in the classroom. Teachers need to be aware of the attitude that they are projecting as this informs the relationship they may hold with their pupils. For instance, Partridge279 suggests that the ambivalence that adolescents with ADHD show towards rewards used by teachers (see Resistance and ambivalence) reflects their belief that teachers’ motives are self-centred: ‘they want kids to listen to them’, ‘to get control of kids’, ‘to get kids to like them’, ‘students [to] behave better so it’s easier to teach them’ (young people diagnosed with ADHD, aged 12–14 years, p. 112). 279
Relationships with peers
Children with ADHD often have poor relationships with their peers. Peers may react to the different treatment that children with ADHD receive,264,265,296,302,308,311 regardless of the intervention in place. Teachers in a study by Rafalovich308 note that peers may form an exclusionary group as they notice children with ADHD receiving different treatment, such as attending learning assistance centres. Teachers in Houghton et al. ’s study296 expressed little sympathy for pupils with ADHD’s experience of peer rejection. They seem to consider the young people to be largely to blame for the rifts. Therefore, it fits that remedial class teachers in Ljusberg’s study265 consider the children with concentration difficulties in their classes as rejected; ‘the ones no one else likes or wants to have to do with in any way’ (remedial class teacher, p. 202). 265 Perhaps pupils’ views expressed in the other Ljusberg paper,302 that they attended remedial classes because their regular class teachers do not like them (see Pupil–teacher relationships, above), may hold some veracity.
In spite of the lack of friendships and reported experience of stigmatisation and sometimes bullying (e.g. Wiebe311), teachers often consider that it is important for children with ADHD to work with their peers to develop their interpersonal skills. 278,286,289–293,296,305,308,310 There were varying experiences of this in practice. Furtick292 notes that in traditional classrooms, children with ADHD are often not engaged when they are supposed to be working with their peers, whereas the intervention observed (constructivist classroom) was perceived to encourage productive group work, where pupils with ADHD valued the experience and contribution of peers and reported that they made friends more easily. Children with ADHD in a study by Edwards290 had contrasting preferences about working alone versus working in a group. However, they generally like working with friends. Having this friendship with a peer appeared to assist children with ADHD and enabled them to enjoy working with others.
The importance of social skills is recognised across a number of studies where such skills are actively incorporated into interventions and teaching strategies with perceived effectiveness. Special education teachers in a study by Ljusberg265 state that one of their primary goals in their work with children in remedial classrooms is to improve social skills. The intervention used in Ozdemir’s study306 was considered to improve social skills in some of the children. Special education teachers in Hjörne’s study295 had pupils ‘practice’ social skills. However, Hjörne295 notes that there was no evidence children used this social practice of their own volition as they were not given the opportunity to negotiate more complex social situations or be without supervision. Two studies264,296 reported that teachers perceived that they had limited ability to help children with ADHD get along with other children in the general classroom.
Peer pressure influences the actions of young people with ADHD and was evidenced in two studies. A potential reason for the lack of application of skills gained in the intervention studied by Wong280 was peer pressure to finish an exam quickly so a pupil would not be left by his friends:
I saw Ryan leaving and everybody was leaving and I didn’t want to stay so I just packed it in. Yeah because we were supposed to be going somewhere right after the test, so I had to go.
Canadian young person with ADHD diagnosis, p. 158280
When pupils’ friends were ‘discharged’ from the alternative high school studied by Kreiss300 they were less likely to attend. Such issues of the influence of peer pressure on engagement are not peculiar to ADHD. 325
Finally, several studies provided evidence that interventions can impact relationships with peers. Hong’s264 teacher participants reported that pairing children with ADHD with other children, however mature and understanding, was not successful as peers were reluctant to continue being paired with children who demonstrate hyperactivity, carelessness and dangerous or disruptive behaviours. In addition, as previously mentioned, withdrawal from the classroom is perceived to have a negative effect on relationships with peers, including loneliness and broken friendships302 (see Withdrawal, above).
School–home relationship
Educators across multiple studies voice the importance of effective relationships with parents and their impact on the success of interventions. 286,288,298,301,304,306,309,310,313 For instance, teachers in a study by Ozdemir306 report the necessity of active parent involvement in children’s education. The parent education module of the intervention was reportedly liked most by teachers as it facilitated active parent involvement. The involvement of parents seemed to be a key facilitator in quantitatively measured academic and social skill outcomes on the programme:
When you try to help a student and the parents refuse all sources of help, it’s frustrating, demanding and exhausting. But if you know that parents also invest their time and energy to help their child, then it becomes worth the effort, the worry, the frustration, and the stress to be here.
Turkish grade 1 teacher: pp. 124–5306
Teachers in Ozdemir’s study306 stated that they learned from a greater appreciation of the home life of children with ADHD. The intervention meant that teachers became aware of the impact of issues at home and appreciated that children struggle to learn while dealing with problems at home. However, teachers in a study by Jones298 recognised a lack of support from home; teachers in this study felt parental involvement was the key to success, but the teachers said they were frequently unsuccessful at making contact with parents.
Parents also reported benefits from working more closely with the school as part of the intervention used in Ozdemir’s study. 306 Parents recognised that the programme helped them support their child with school work. It also increased their understanding of school:
Before the program, I strongly believed that my son’s teacher failed to make an effort to help my son be successful at school. But now with the help of the FSS [First Steps to Success] program, we understand our part in our son’s problem behaviours.
Turkish parent of child diagnosed with ADHD, p. 133306
Parents stated that they appreciated being kept informed of issues by teachers in a study by Taylor Wilcoxson. 310 However, parent involvement is not always positive. One child’s teacher in Ozdemir’s study306 reported that parents can be overinvolved, with the result that children lacked self-sufficiency. There was also pressure from parents reported by young people for them to attend the alternative high school reported in Kreiss’s study. 300
Teachers and parents sometimes recognise that much of the communication occurring between school and home about children with ADHD is negative. 265,288,294 For instance, remedial class teachers in Ljusberg265 report that mainstream school teachers often contact parents only when their children have done something wrong. Parents also referred to experiencing mainly negative communication with teachers. 289 There was some reluctance to get in touch with parents expressed by teachers in a study by Hillman;294 instead they wanted to help children on their own before involving parents or other professionals. The implication is that both teachers and parents need to increase communication and deliberately focus on positive collaboration.
Teachers’ relationships with colleagues
Teachers have preconceptions about working with colleagues and other practitioners. Hong264 suggests that collaborations with professionals in special education are important for the successful education of children with ADHD, especially in the light of the comorbidities that are frequently held by pupils who display ADHD symptoms. 32 Teachers in Einarsdottir’s291 study reported that relationships with colleagues varied according to the age group they taught. Preschool teachers find additional staff very important, whereas primary school teachers see assistants as a burden and would prefer children with ADHD to be removed from the classroom, rather than have the additional responsibility of the assistant. As Jones298 suggests, support staff need an understanding of classroom issues if they are going to assist in educating children with ADHD in the mainstream classroom.
Teachers in a study by Bos et al. 288 said that they shared their intervention knowledge with colleagues, with their increased confidence seen as being a catalyst for this. This type of collaboration where teachers assist or seek assistance from colleagues was seen in other studies. 294,298,304,305 Teachers in Jones’ study298 said they sought out other teachers with experience of working with children with ADHD, yet there was a recognition that time was not always available for this important matter. Peer support (colleagues) was seen as more consistently helpful than outside experts, with teachers creating their own informal learning communities.
Implications relating to the theme of relationships are given in Box 9.
Pupil–teacher relationships appear critical to the success of classroom-based interventions.
Social skills are considered an important deficit for children with ADHD that interventions ought to consider.
Although positive school–home relationships are considered to be important, teachers and parents recognise that much of the communication about children with ADHD is frequently negative. This needs to be considered when interventions involve a home component.
Seeking advice from colleagues is reported to be invaluable for some teachers, but can be threatened by time pressures.
Expectations
This is a very broad theme, basically capturing the prior experiences and attitudes that individuals involved in the use of interventions for pupils with ADHD might hold. In particular attitudes towards education, ADHD and interventions are shown to be important in providing a context in which any future intervention must operate. The analysis implies that interventions for ADHD do not occur in a vacuum, while the experience of interventions can also affect these expectations going forward.
Attitude to school and learning
There are negative attitudes towards school and learning seen from children with ADHD. 279,280,290,293,306 Often this is equated to a lack of motivation, as indicated by this pupil with ADHD:
What do I do if I don’t understand something in class? I don’t know. I won’t ask the teacher. Oh, no I won’t ask questions because I am lazy.
Young person with ADHD diagnosis (aged 15–16 years), p. 133280
This lack of motivation was perceived to be due to lack of interest, difficulties learning and lack of perceived relevance (see Making interventions meaningful to pupils). Young people in a study by Edwards290 were described as having goal-oriented performance, wanting to appear competent, but not choosing challenging tasks. Sometimes children with ADHD did report positive attitudes towards their schooling, which would understandably impact their preconception about any different interventions put in place. 300,302 This finding is not peculiar to children with ADHD (e.g. see Hardré et al. 326 regarding rural high school pupils).
Some interventions and strategies did appear to positively affect attitudes to school and learning held by pupils with ADHD. 287,303,306,308,311 One young person diagnosed with ADHD in McNeil’s study303 who had reported motivational issues before special education placement said that she started liking school a little more because they started to understand what was being taught. ‘It was so good I thought I have never understood any of this stuff before and now I am getting it’ (aged 17 years, p. 175). 303 So interventions can affect attitudes held towards school.
Attitude to attention-deficit/hyperactivity disorder
One attitude towards ADHD held by teachers is that ADHD is not qualitatively different from other difficulties and that the behaviours are normal for all pupils. 308,313 Teachers in a study by Rafalovich308 claimed to believe that the distinction between when it is appropriate to use a normal strategy for a troubled pupil versus using strategies for a disordered pupil is hard to make. Some disbelief about the existence of ADHD or the severity of the disorder was seen from mainstream teachers and this was recognised by pupils. 296,303,304,308,309 One teacher stated:
[T]he condition has been used as an excuse by some students, who, although clearly capable of high quality work, see their disorder as an excuse for not putting in the effort.
Australian teacher, p. 120296
There was also some resistance to working with children with ADHD reported by teachers288,296,309 (see Resistance and indifference, below).
Children with ADHD referred to embarrassment about their diagnosis (see Stigmatisation, above). 293,303,308 However, the college-aged students in Bartlett et al. ’s study287 recognised that their childhood behaviours were challenging. They reported that they knew that they were taxing for others and that they valued the teachers who had persevered with them.
Interventions that targeted attitude towards ADHD were generally received positively by teachers and were perceived to improve attitudes. 288,296,306 After the workshop intervention, teachers in Bos et al. ’s288 study claimed to hold more positive attitudes towards children with ADHD, as well as greater tolerance and empathy:
Before class [workshop], having students with ADHD meant trouble, but the class has increased my understanding, changed my attitude, and improved my tolerance and patience.
American teacher, p. 141288
Knowledge gained seemed to improve attitudes for teachers in this study, and there appeared to be an interactive relationship among attitudes, perceived competence, and practice for these teachers. Teachers also said that they saw positive change in themselves as a result of the programme in Ozdemir’s study. 306 ‘My approach is changed forever’ (p. 129)306 stated a Turkish grade 1 teacher.
Resistance and indifference
Many studies noted that pupils are often resistant or indifferent towards the interventions and strategies put in place to support them at school. They are often indifferent towards rewards that they do not see as attainable and towards punishments whose severity is discounted. 279,280,290,297,300 For instance, teenagers attending the alternative high school in Kreiss’ study300 were ambivalent to rewards:
I think there could have been more positive stuff and privileges for students . . . Yeah, they give out these merits, but that was it. They would say you got a merit. I would think, great now what are you going to give me? But we never got anything. I think if you want to encourage students to behave, you gotta give them a reward or something for it.
American young person with ADHD diagnosis, p. 224300
This fits with the need among children with ADHD for immediate reinforcement discussed earlier (see Need for immediate reinforcement).
Pupils may resist the interventions put in place,280,302,306,307 which can be related to their attitude towards school and learning in general or focused on the particular intervention that they reject. For instance, a teacher in a study by Ozdemir306 described a child with ADHD: ‘He spends most of his energy avoiding anything and everything that may pose a challenge’ (Turkish grade 1 teacher, p. 122). 306 Wong282 reported that resistance varied across the components of the intervention in question. Young people in Prosser’s study307 appeared to resent conventional class-based interventions, seeing them as condescending:
Me and four other students are being made to sit down the front so the teacher can keep a watch on us . . . and we had to earn these little blocks for being good so we can go out for recess and lunch, and I just thought ‘this is bullshit’
Young person with ADHD diagnosis, p. 88307
Given the age of participants in this study (14–16 years), part of the resentment may be due to a feeling that the participants had outgrown interventions used for younger pupils.
Teachers themselves may be resistant to unfamiliar or unproven interventions. For instance, there was some reported resistance to the music listening intervention from teachers in a study by Wiebe. 311 Teachers said that MP3 players could be a nuisance. Parents in DuCharme’s study289 also indicated resistance about withdrawal to a resource room: ‘I was sort of resistive to it at first, kind of tentative about if it was a good idea’ (mother, p. 309). 289 This related to fears that her son might miss regular classroom activities and how he would feel about withdrawal, issues considered previously (see Withdrawal, above).
Given the resistance to mainstream interventions reported above, children with ADHD may be less resistant to interventions that they do not think they have previously encountered. For instance, teenagers with ADHD referred to their new start at an alternative high school (Kreiss300). Sometimes the context that determines the intervention(s) applied appears to influence the attitude towards them, as is clearly seen in this adolescent’s reaction to an IEP meeting:
The first time I went to that meeting for my 504 plan in school, it was horrible. I sat down and everybody was talking about me and how these aren’t working, the accommodations are bad for me and we’ve got to start over, and they asked my opinion maybe twice before I left. And I didn’t want any of the accommodations anymore because I didn’t want to go back in that room anymore. I didn’t want to have to talk to any of those people who were sitting down and saying, ‘Oh well, he can’t do this so let’s make it easier.’ And I always hated that.
Young person with ADHD diagnosis (aged 16 years), p. 143293
Lack of guidance and knowledge
Teachers’ lack of guidance and knowledge is perceived as a barrier by them across a large number of studies reviewed. 264,265,286,288,298,304,308–310,313 Teachers from many countries report that they are working in schools that do not have ADHD-specific guidance. There is a lack of knowledge at the individual level, coupled with a lack of guidance from schools or educational boards. 264 This lack of guidance and knowledge appears to be well known. A parent in Zimmerman’s313 study reported that a principal at her child’s high school had told her ‘we don’t have a clue what to do with or for these kids’ (parent, p. 173). 313 This lack of knowledge of course impacts the interventions received by pupils with ADHD. One special educational teacher declared that a lot of pupils have had a ‘rotten schooling’ (p. 202)265 because the teachers in the regular school do not have the right expertise.
Improved knowledge seemed to make a stark difference for teachers in their confidence and practice. A teacher in Bos et al. ’s study288 stated:
Just knowing about ADD and knowing that this child can’t necessarily control his behavior made all the difference in the way I see and interact with him in class.
American teacher, p. 140288
However, although teachers in Bos et al. ’s study288 perceived that their practice improved, it was highlighted earlier that there may be issues with the assumption that children with ADHD cannot control their behaviour (see Compensatory perspective, above). Yet this knowledge was claimed to improve attitudes and confidence: ‘the workshop changed my attitude towards kids with ADHD and gave me confidence to help my colleagues’ (American resource teacher, p. 141). 288 Likewise, the negative perceptions of pupils with ADHD reported by teachers in a study by Houghton et al. 296 altered only when the teachers were provided with substantive research information, professional training and in-house support.
Several studies noted the importance of reflection for teachers’ development. 288,296,298 Indeed, teachers in Houghton et al. ’s study296 asserted that they came to an acceptance of ADHD only after a period of personal reflection. This reflection was seen to be a positive step that helps them to re-evaluate and change their teaching styles. Even when teachers attend workshops this may not necessarily affect practice. For instance, teachers in a study by Nowacek and Mamlin305 often attended workshops, but still reported barriers to the implementation of what they had learned. Sometimes these barriers were considered to be insufficient information gained during training, but also a lack of support in school settings to implement changes and refine practice.
A key implication from McNeil303 was that, the more knowledge teachers have about ADHD, the more successful interventions will be, but this held for the pupils too: ‘Knowledge of the disorder also allows the individual to advocate for herself because she has the knowledge to inform others’ (author quote, p. 183). 303 Likewise, Zimmerman313 reported that pupils were often unaware of the frequency or intensity of their own behaviour and its effects: ‘I never knew I was doing that kind of stuff’ (American young person with ADHD diagnosis, p. 197). 313 Making pupils aware of the frequency and, particularly, the impact of their negative behaviour was considered to be important. Finally, teachers in a study by Hong264 stated that it was important to explain ADHD to children’s peers to attempt to increase their understanding and acceptance.
Implications relating to the theme of expectations are given in Box 10.
Interventions may need to address any negative attitudes held about school or ADHD which operate as a barrier to success.
Interventions need to be implemented with consideration to previous treatment as children with ADHD may be resistant or indifferent to interventions that are similar to those previously experienced negatively.
Although children may be more accepting of novel interventions, teachers may be resistant to unfamiliar or unproven interventions.
Interventions ought to address the lack of knowledge about ADHD both for teachers and children with ADHD themselves.
Facilitators, challenges and moderators
Many facilitators and challenges to effective intervention and strategies for pupils with ADHD have been revealed in the synthesis above. Facilitators include positive relationships;306 teacher consistency;264 teaching necessary study and social skills;300 relevant and purposeful interventions;279 appropriate levels of supervision;302 application beyond intervention period;280 working with peers;308 and low teacher–pupil ratios. 313 Challenges include mainstream class sizes;265 attitudes towards and stigmatisation about ADHD and interventions;287 time pressure;305 inflexibility of interventions;304 resistance to some interventions;307 knowledge regarding ADHD and appropriate teaching strategies;288 low self-concept;280 and pupils understanding the purpose of interventions. 301
Several moderators were mentioned by studies reviewed as influences on the effects of interventions used. For instance, the effect of the Just Achieving Greatness programme researched by McNeil303 was seen to be influenced by the success of medication for participants. The age of pupils with ADHD was frequently mentioned as something that may moderate the effect of interventions. 291,298,305,306,308,309 For example, middle grade teachers in a study by Nowacek and Mamlin305 were less likely to be observed using academic modifications; they believed interventions were used in earlier grades and part of their goal was to prepare pupils with ADHD for high school where they believed fewer modifications would be made, given the focus on academics rather than behaviour. Einarsdottir291 reports differences between the intervention practices of preschool and primary aged teachers in response to children with ADHD symptoms. This is considered indicative of the differences in the structure and expectations between these settings. On a related note, there were differences seen in the type of interventions used and viewed as successful according to the age of schoolchildren with ADHD. For instance, behaviour modification seemed to be resisted by older pupils,279 whereas social skills were used across a number of studies only with younger pupils. 265,295,306 Older pupils were more often positive about the study skills that they developed to support their school work. 280,301
Discussion
We identified 33 studies that included qualitative research related to interventions or strategies used with children with ADHD in school settings. The analysis identified seven themes, which were represented to some degree in all included studies. The relationship between the seven themes was demonstrated by a line of argument (see Figure 5), which shows the experience of intervention use captured by this synthesis.
Summary of findings
The synthesis revealed three main tensions related to responding to ADHD in schools. The first is whether interventions ought to be structured and controlled or whether they should offer choice and flexibility, although several studies recognise that structure and choice are not mutually exclusive. A second tension relates to the extent to which interventions ought to be individualised. The third concerns considerable time pressure reported by teachers in reviewed studies. Implementing an intervention can be time-consuming, and there is evidence that interventions are not always given sufficient time to take effect.
There are mixed views about the impact of interventions, although where participants feel that interventions are not effective, this can be traced to barriers recognised within the synthesis. There are some concerns that interventions may be effective for specific targeted skills and behaviours, but may not impact the academic achievement of children with ADHD, which is considered an important outcome by young people, parents and teachers. There are also issues concerning how well skills and knowledge learned during interventions are applied beyond the intervention period. Given that ADHD is often conceived as a deficit of self-regulation,327 barriers to the application of skills once learned ought to receive as much attention as initially learning the skills. It is clear that the interventions impact relationships, attitudes and participants’ conceptions of ADHD, but the reported positivity of this impact was mixed both across and within the different interventions. Of course, the heterogeneity of pupils diagnosed with ADHD may explain differences in perceived intervention effectiveness.
Finally, the importance of issues of socialisation and their impact on interventions was considered. The review indicates that those developing interventions used in a school setting ought to consider the relationships that the pupil displaying ADHD symptoms holds with teachers and peers, as well as home–school collaboration. Intervention implementation may also be challenged by the conception of ADHD as a ‘problem’ held by those involved in the intervention and children’s reported experience of stigmatisation as a result of having a diagnosis of ADHD or attending interventions. Attitudes regarding school, ADHD and interventions, as well as knowledge of ADHD, also appear to impact the use of interventions. 223 Issues related to the themes of relationships and expectations often complemented the discussion about individualising interventions. In particular, the degree to which interventions are tailored to individuals appears to affect the relationships pupils who display symptoms of ADHD have with their peers. Also some resistance was seen towards certain tailored interventions.
Strengths and limitations
Strengths of the review include the comprehensive search strategies employed and efforts to locate unpublished research where they were found. This review represents the first systematic review of qualitative research of which we are aware on the experience of school-based interventions for ADHD. The review took a broad focus on the strategies used in school settings with pupils displaying ADHD symptoms. This relatively wide scope allowed for a synthesis that captured the experience of school-based interventions, rather than only perceptions of effectiveness of specific intervention packages.
Few studies focused solely on the attitudes and experiences of those using specific intervention packages in school settings, and only one paper considered an intervention whose effectiveness has been quantitatively measured and reviewed in Chapter 2. 301 As discussed below, very few studies were conducted in the UK, thus the applicability of findings to UK education must be considered. Although included studies were of reasonable to very good quality according to quality appraisal criteria, the majority of studies contained mostly descriptive qualitative analysis, despite claims to use interpretive analytical tools. Review 4 included more papers with interpretive analysis and therefore some issues considered in this chapter, for example stigma and relationships, are considered in more explanatory detail in the next chapter.
Quality appraisal
Quality appraisal of qualitative research is widely debated (see Barbour328). Some researchers have argued that the value of each study should be judged through its contribution to the synthesis,88 as well as by scores on quality appraisal criteria. Given the ongoing debate regarding quality appraisal in qualitative synthesis,273 it made little sense to weight or exclude papers on the basis of a contested endeavour. There were certain questions from the checklist that was used to appraise the quality of research in this review that we considered less useful. Answering two questions about author theoretical perspective could be considered unnecessary when many studies did not report a clear theoretical perspective. The question regarding adequacy of the sample was considered to be subjective (see Table 35), particularly as qualitative research attempts to illuminate phenomena rather than represent populations. 329 Several case studies focused on only one participant with ADHD and this was often deemed an inadequate sample according to the quality appraisal question, in spite of these case studies considering child, teacher and parent perspectives (e.g. Wiebe311).
We found, as others undertaking qualitative evidence synthesis have, that the basic details of how participants were identified and recruited, and how study data were collected and analysed, were often sparsely reported. 273 Where we could not say that studies collected and analysed data with rigour, it did not make sense to exclude these papers, as often this was a result of poor or constrained reporting, rather than necessarily being indicative of poor research. 271 We considered that claims to generalisability followed logically from the data when authors were careful to not generalise from their small samples and made the lack of generalisability explicit. Therefore, many of the ‘yes’ quality appraisal ratings were for a considered lack of generalising.
Applicability
Only two of the 33 studies reviewed included participants from the UK; these were teachers in Hillman’s paper294 and adolescents in Young et al. ’s paper. 312 Neither study focused on a specific intervention or included highly interpretive findings and, therefore, did not contribute greatly to the development of the synthesis. However, the findings from these studies were congruent with other studies reviewed. Hillman’s294 study also included American and Canadian teachers, thus allowing the potential for comparison between different nationalities, although this is not considered in the paper. Young et al. ’s312 participants attended a young offenders’ secure unit, thus potentially limiting the applicability of these young people’s experiences to other pupils with ADHD in mainstream settings.
Two studies290,293 focused their case studies on young people with diagnoses of ADHD who were also recognised as gifted. There is a growing literature focused on the dual diagnosis of giftedness and ADHD (see Hartnett et al. 330). The educational content studied by such pupils may differ from their non-gifted peers with ADHD diagnoses; however, the issues faced by these young people echoed those seen for participants without the giftedness label in other studies.
Where participant groups were only educators the age of relevant children with ADHD tended to be younger than samples including pupils who display ADHD symptoms. This may affect the comparability of teachers’ and children’s perspectives. However, seven studies included both child and teacher participants and, thus, provide perspectives on the same experience. 290,292,293,295,310,311,313 Four studies only sampled educators who were not mainstream teachers. 265,290,295,309 These educators were either special education teachers or school counsellors. Often these educator’s views were particular to their role or the intervention used, yet sometimes these participants made more general comments that could be compared with other studies in mainstream settings.
As is true generally for qualitative studies, this qualitative review does not claim to represent the experiences and perceptions of all participants or assume the analysis can be generalised to individual experiences of ADHD and intervention use in schools. We claim credibility on the basis of clear review methodology and process of synthesis drawing on meta-ethnography. We also consulted with the project steering group to check our synthesis against specialist knowledge and experience; we can claim the potential for transferability based on consultation with parents and educators during stakeholder involvement activity, who endorsed the themes as resonating with their own experiences (see Appendix 11).
Implications for practice and recommendations for research
There appears to be a difference between the conception of ‘intervention’ held by researchers and teachers. In the studies reviewed teachers often referred to the ad hoc strategies that they implemented with their pupils with ADHD as ‘interventions’. 264,291,293,298,305,310 This differs from the view of intervention apparent in some papers where researchers were interested in experiences of particular intervention packages. 280,301,306,311 An exploration of this difference in understanding appears to be a gap in the wider research literature. This is potentially important if teachers hold the view that effective intervention for children with ADHD would constitute selecting from a range of strategies whose use may be flexible and contextual, while researchers continue to design and test intervention packages aiming for effectiveness across children with ADHD measured by specific outcomes.
Implications of this synthesis include the need to take into account contextual factors, prior experiences and attitudes of teachers, young people and parents during the design, evaluation and implementation of interventions for ADHD in school settings. Interventions that target specific ADHD behaviour must take into account the socialisation issues raised in the synthesis, as well as the consideration of how the intervention will itself impact such contextual factors. As some of the studies reviewed suggest, interventions that focus on relationships, attitudes, self-concept and understanding can have an impact on these aspects of the ADHD experience. 288,303,306 Thus, holistic interventions that consider the context, as well as focus on the individual child’s difficulties, ought to be considered. Still, such intervention design needs to remain aware of potential opposition to interventions, which may include children’s resistance to learning and educators’ resistance to working with children with ADHD, and which may have to be tackled in advance.
Some of the studies reviewed acknowledged the extended trajectories through school experienced by pupils displaying ADHD symptoms. Teachers, particularly those teaching younger year groups, may only work with a child who displays ADHD symptoms for a year and therefore it is questionable whether a short-term intervention implemented in one classroom in a single school year would be sufficient to improve pupils’ odds of long-term success. 72 Therefore schools need a co-ordinated approach to intervention, so that strategies learned are internalised and positive intervention outcomes are built on. 280
Many of the studies reviewed present a rigid view that ADHD in the school setting is a problem that resides in the child and that any issues relating to the classroom and curriculum are ignored. 265,302 The findings suggest that this attribution may compound the stigmatisation experienced by children with ADHD and affect their self-concept negatively. Several interventions aim to train pupils with ADHD to fit the regular classroom as if this is the preferred goal. What is missing from the studies reviewed is an explicit consideration of how the school setting contributes to the issues facing an individual with ADHD, even though the role of the school is considered critical to the construction, diagnosis and treatment of ADHD. 307 An implication then is for those designing interventions to consider the setting both in terms of implementing the intervention, but also as a moderating factor in the expression of symptoms of ADHD, particularly given the individual differences and changes with age highlighted by the research reviewed. 306
This synthesis emphasises that regular class teachers have a very challenging task in teaching and implementing interventions for their pupils with ADHD while maintaining their orientation to the class as a whole. 305 The synthesis suggests the importance of teachers’ relationships with their pupils with ADHD, as well as their families’. There are tensions for the teacher to resolve in relation to the structure of teaching and intervention use. Often it seems that these decisions are made with a lack of knowledge and insight about ADHD. Time pressure and structural constraints are reported to limit what can be achieved in regular class settings.
Given the above, it would seem that the withdrawal of children with ADHD from the classroom to tailored interventions ought to be preferable. However, the synthesis revealed that there are often issues with such special education. The problems reported by those involved primarily concern the impact of withdrawal on social relationships, stigmatisation and the lack of progress made in special education classes if the goal is to return to regular class. For those children who display ADHD symptoms and attend withdrawal programmes for part of their school day, the lack of co-ordination between special classes and their regular classes is an issue. Therefore, withdrawal programmes that are more co-ordinated with the regular classroom and actively combat issues of stigmatisation ought to hold potential.
A clear implication about the expectations held by those involved in interventions for children who have ADHD is to tackle the lack of knowledge about ADHD at an individual level and the lack of guidance regarding practice at a school and policy level. Greater knowledge of ADHD might assist with some of the apparent tensions concerning the structure and individualisation of interventions for pupils displaying ADHD symptoms, as some of the studies reviewed reveal that these tensions can be based on misconceptions or a particular attitude about ADHD. Teachers in the studies reviewed typically considered that discussion with more experienced colleagues was the most helpful method to provide guidance and increase confidence. However, any efforts to educate those involved in the implementation of interventions need to stay cognisant of the findings from this synthesis about the varying presentation of ADHD, as well as the similarities seen between these children and their non-diagnosed peers in several regards, including motivation, meaningfulness of teaching and the importance of relationships.
Finally, the heterogeneity of both pupils with ADHD themselves and their responses to interventions seen across the studies reviewed suggests that prescriptive interventions implemented in the same manner for all pupils with ADHD are unlikely to remain effective across different children. Findings from this synthesis of qualitative research suggest that a multitude of factors relate to the experience of non-pharmacological interventions for ADHD used in school settings, and suggest that interventions ought to be tailored to the individual and the wider context in which they experience their education.
Chapter 6 Review 4: a synthesis of qualitative studies about the school-related experiences and perceptions of pupils diagnosed with, or at risk of, attention-deficit/hyperactivity disorder, their teachers, parents and peers
Aims
The aim of review 4 was to explore the school-related experiences and perceptions of pupils diagnosed with, or at risk of, ADHD, their teachers, parents and peers.
Included studies
The process of study identification is shown in Figure 6. 152 A table giving papers excluded at full text with reasons may be found in Appendix 15.
FIGURE 6.
The PRISMA diagram showing search process and study selection for review 4. One study contributed to both syntheses 4a and 4b. Thirty-seven papers were included. One study in review 4a was reported in three papers; one study in review 4c was reported in two papers.

Structure of review 4
As described in Chapter 4 (see Methods of analysis/synthesis, Data analysis and synthesis, Synthesising translations/creating a line-of-argument), review 4 was divided into four initial syntheses by participant type: (4a) pupils, (4b) teachers, (4c) parents and (4d) mixed views. Table 44 shows the number of studies included in reviews 4a–d. Once completed these were synthesised in a further final step to create a synthesis of reviews 4a–d (see Findings from the synthesis of reviews 4a–d). Study characteristics and findings of included papers will be described separately for reviews 4a–d. As the nature of qualitative research is inherently interpretive and the structure of the findings is organised around third-order (reviewer) interpretations (see Chapter 4, Methods of analysis and synthesis, Data analysis and synthesis), findings will be discussed as they are reported to prevent the false distinction that could be created by their separation. Quality appraisal and applicability of studies will be discussed across papers in the discussion section with the synthesis of reviews 4a–d (see Discussion), followed by implications for policy and practice and recommendations for future research.
| Syntheses in review 4 | Number of included studies |
|---|---|
| 4a. The school experiences and perceptions of pupils diagnosed with ADHD (pupil views) | 11a |
| 4b. The school experiences and perceptions of teachers of pupils diagnosed with, or at risk of, ADHD (teacher views) | 11a |
| 4c. The school experience and perceptions of parents of pupils diagnosed with, or at risk of, ADHD (parent views) | 6 |
| 4d. The school experiences and perceptions of pupils diagnosed with, or at risk of, ADHD, their teachers, parents and peers (mixed views) | 7 |
| Total | 34a |
Review 4a: the school experiences and perceptions of pupils diagnosed with attention-deficit/hyperactivity disorder
Study characteristics for review 4a
A total of 11 studies reported in 13 papers were included in review 4a (pupil views). Summaries of included papers for review 4a are shown in Table 45. One study by Exley332,337,338 was reported in a journal article, a conference paper and a practitioner article; when citing this study only the journal article332 will be referenced to signify the singular nature of the study. Five studies involved participants from the USA,27,299,331,334,336 four studies involved participants from Australia,296,314,332,335 two studies involved participants from the UK27,261 and one study involved participants from Canada. 333 The UK study by Singh27 included participants from the UK and the USA. All the studies explored the experiences and perceptions of children and young people diagnosed with ADHD; however, it is possible to group the papers by their foci:
-
four studies explored experiences of pupils framed by the concept of ADHD, including their experience of symptoms, diagnosis, treatment and beliefs about the cause of ADHD (attributional beliefs)261,299,314,333
-
five studies explored social aspects of the experience of ADHD, including peer cultures and the role of anger and impulsivity in relationships;27,296,332,335,336 and
-
two studies focused on the experience of ADHD and learning/school. 331,334
| First study author and year (n = 11) | Country of participants | Aim | Number | Age (years) | Gender (% female) | ADHD status (diagnosed or at risk) |
|---|---|---|---|---|---|---|
| Brice 1998331 | USA | To understand the perspectives of young people diagnosed with ADHD regarding what allowed them to and prevented them from learning successfully | 10 | 13–18 | 10 | Diagnosed with ADHD |
| Cooper 1998261 | UK | To explore perceptions of pupils diagnosed with ADHD about the effects of ADHD symptoms, the diagnostic label and treatment for ADHD on their lives | 16 | 11–16 | 37 | Diagnosed with ADHD |
| Exley 2008332 | Australia | To understand the lived experience of children diagnosed with ADHD of social relations in informal play environments | 2 | 8–9 | 0 | Diagnosed with ADHD |
| Friio 1999333 | Canada | To explore the personal experiences of young people diagnosed with ADHD | 5 | 14–18 | 0 | Diagnosed with ADHD |
| Houghton 2006296 | Australia | To explore how students deal with the anger arising from the stress of living with ADHD | 20 | 6–17 | 30 | Diagnosed with ADHD |
| Kendall 2003299 | USA | To explore perceptions of children and adolescents with ADHD regarding their perceptions, meanings and experiences of living with this disorder in a context of controversy about the nature of ADHD | 39 | 6–17 | 33 | Diagnosed with ADHD |
| McDannel 2005334 | USA | To investigate student occupations within the classroom for young people diagnosed with ADHD | 3 | 17 | 0 | Diagnosed with ADHD |
| Prosser 2006314 | Australia and USA | To explore critically the impact of understanding ADHD as an individual biological deficit on the perceptions of young people diagnosed with ADH | 11 | 14–16 | 0 | Diagnosed with ADHD |
| Singh 201127 | UK and USA | To uncover the social and moral dimensions of ADHD diagnosis as manifested in the interplay of self-control, stigma and agency | 150 | 9–14 | NR | Comprised by three groups (numbers in each NR): those diagnosed with ADHD who are medicated; those diagnosed with ADHD who are not medicated; those without ADHD diagnosis or symptoms |
| Taylor 2008335 | Australia | To explore the perspectives of students diagnosed with ADHD about how they deal with the issue of initiating and sustaining peer friendships | 15 | 9–17 | 13 | Diagnosed with ADHD |
| Wolfberg 1999336 | USA | To explore how children with disabilities experience peer culture in inclusive preschool programmes | 10a | 4–5 | 0 | One diagnosed with ADHD (male aged 5 years)a |
Pupils attended a range of private, mainstream and special preschools, primary (or elementary) and secondary (or middle/high) schools. Pupils in the participant samples ranged in age from 4 to 18 years (Table 46). However, the large majority (82% of those for whom these data are available) were aged 11–18 years, so the synthesis represents older pupils’ perspectives more than those of younger children. The gender ratio of children and young people in the samples was approximately 3 to 1 (76% boys: 24% girls of those for whom these data are available); this ratio is broadly in line with current information about gender prevalence. 19 Although review selection criteria included studies that explore the experiences of pupils diagnosed with, or at risk of, ADHD, in fact, the selected studies explore the experiences of pupils, all of whom had been clinically diagnosed with ADHD.
| Type of participant | Paper | Number and gender of pupils diagnosed with ADHD | Preschool–primary | Secondary–college | ||
|---|---|---|---|---|---|---|
| Number | Male | Female | ||||
| Papers with participants in either primary or secondary school levels | Brice 1998331 USA |
10 | 9 | 1 | 10 (aged 13–18 years) | |
| Cooper 1998261 UK |
16 | 10 | 6 | 16 (aged 11–16 years) | ||
| Exley 2008332 Australia |
2 | 2 | 2 (aged 8–9 years) | |||
| Friio 1999333 Canada |
5 | 5 | 5 (aged 14–18 years) | |||
| McDannel 2005334 USA |
3 | 3 | 3 (aged 17 years) | |||
| Prosser 2006314 Australia |
11 | 11 | 11 (aged 14–16 years) | |||
| Wolfberg 1999336 USA |
1 | 1 | 1 (aged 4–5 years) | |||
| Houghton 2006296 Australia |
20 | 14 | 6 | 9 (aged 6–11 years) | 11 (aged 11–17 years) | |
| Taylor 2008335 Australia |
15 | 13 | 2 | 5 (mean age 9 years) | 10 (mean age 14 years) | |
| Totals | 83 | 68 | 15 | 17 | 66 | |
| Paper with participants across primary and secondary levels reporting gender | Kendall 2003299 USA |
39 | 26 | 13 | 39 (aged 6–17 years; mean 11.2 years) (numbers by school year NR) | |
| Totals | 122 | 94 | 28 | |||
| Paper with participants across primary and secondary levels not reporting gender | Singh 201127 UK and USA |
150a | NR | 150 (aged 9–14 years) (numbers by school year NR) | ||
Two studies296,299 are included in both review 3 and review 4a (pupil views), because they contain analysis of perceptions of school strategies and/or interventions as well as experience of ADHD more generally. Therefore, only part of the findings from these studies is reported here. Review 4a reports the findings about the school-related experiences and perceptions of pupils diagnosed with ADHD generally; for findings about the experiences of strategies and/or interventions from these studies, please see review 3 (see Chapter 5).
Study methodology for review 4a (pupil views)
Details of the study methodology are given in Table 47. Ten of the 11 studies collected data through semistructured interviews. 27,261,296,299,314,331–335 In addition to interviews, two used observation (classroom, playground),332,334 one used focus groups and the creation of group narratives,314 and one used a range of activities and a questionnaire. 27 The remaining study collected data through participant observation. 336
| First study author, year and location | Sample size | Sample characteristics | Data collection | Sampling | Theoretical approach/ADHD attributions | Data analysis |
|---|---|---|---|---|---|---|
| Brice 1998331 USA |
10 | Nine males and one female aged 13–18 years | Ten interviews | Convenience, purposive | Transcendental phenomenological analysis; concern over learning style Though not explicitly stated, the author demonstrates biopsychosocial beliefs about ADHD |
Line-by-line categorisation of transcript data according to research questions; separate descriptive accounts and a structural analysis were created for each participant; these were integrated to create an overall analysis |
| Cooper 1998261 UK |
16 | 10 males and six females aged 11–16 years | Thirty-two semistructured interviews | Convenience, purposive | The authors explored the impact of biopsychosocial vs. individual/medical views of ADHD | An inductive, iterative process of content analysis involved:
|
| Exley 2008332 Australia |
2 | Two males aged 8–9 years | Two semistructured interviews; playground observation | NR | Critical ethnography; use of Fairclough’s critical discourse analysis339 and exploration of the social construction of identity. Analysis is conducted from a sociological standpoint, but the author does not completely discount the potential for contribution of biological factors to ADHD symptoms | NR |
| Friio 1999333 Canada |
5 | Five males aged 14–18 years | Fifteen semistructured interviews | Convenience, purposive | Hermeneutic phenomenology; the author defines ADHD according to biological deficit, but in the conclusion he problematises medical/individual assumptions because of his findings that personal and contextual factors are also implicated in ADHD symptoms | Listening to and reading/rereading transcripts, initial coding following research questions, extracting significant statements, developing these into first-order thematic abstractions, second-order thematic clusters, then a between-person analysis. Member checks were conducted |
| Houghton 2006296 Australia |
20 | 14 males and six females aged 6–17 years | Twenty semistructured interviews | Purposive | Ecological validity; symbolic interactionism and grounded theory. These are substudies from a larger mixed-methods project, where a central aim was to explore not only biological aspects of ADHD, but the way these interact with psychological and sociological factors in natural settings | Constant comparative method; coding for patterns and salient features; codes constantly compared and interrogated by asking such questions as ‘What is this piece of data an example of? What property does this piece of data represent?’ until saturation. This process developed codes into categories and relationships between them were established. A second researcher independently coded 10% of transcripts to establish reliability |
| Kendall 2003299 USA |
39 | 26 males; and 13 females aged 6–17 years | Thirty-nine semistructured interviews | Purposive | Discuss ADHD as a postmodern illness because of its controversial nature; authors are seeking to establish whether or not ADHD is ‘truly a bonafide biological disease’ (p. 115) rather than exploring interactions between biological and social factors. They conclude with discussion of biological, social and psychological factors, but suggest ADHD ‘exists’ on the basis that there are biological contributors to symptoms; thus foregrounding the biological | Constant comparative method; open coding; phenomena were labelled and described in terms of properties, characteristics, attributes and dimensions until saturation. Codes were clustered to create categories; integration and inter-relationships of the categories formed the basis of the theoretical understanding of the data. NUDIST qualitative software (QSR International, Burlington, MA) was used; credibility supported through peer debriefing |
| McDannel 2005334 USA |
3 | Three males aged 17 years | 24 hours semistructured interviews; 64 hours classroom observation | Convenience, self-selecting, purposive | Ethnography; theories from occupational therapy, including Gallimore’s synactive theory | Constant comparative method; a recursive process in which the thick descriptions of classroom occupations, interview narratives and member checking narratives were coded in broad categories, then subsequently reprocessed several times into core themes. The open coding process included initially identifying unrestricted free nodes, blocking into coded categories, collapsing, revising and distilling these categories into the final analysis and study’s findings |
| Prosser 2006314 Australia |
11 | 11 males aged 14–16 years | Semistructured interviews and focus groups | Purposive; self-selecting | Narrative research following Clandinin 1994;340 the author follows Wakefield 1992341 in understanding ADHD as equally biological and social | Critical cover narratives were created. These involve the way private narratives and ‘official’ narratives are negotiated. The author developed relationships with young people during group meetings and semistructured interviews, then the group together wrote a narrative about a fictional character with ADHD. The author also constructed his own narratives that explored the dominant discourses about ADHD that he heard from the young people, and their effect on them. The author also carried out analysis of the macro-contexts of the participants and used these to make sense of the use of discourses by young people |
| Singh 201127 UK and USA |
Over 150a | Males and females aged 9–14 years | Semistructured interviews plus a range of activities and a questionnaire | Self-selecting; purposive | Use of Haimes’ 2002342 empirical bioethics to explore social and ethical impacts of biomedical styles of thought and biomedical technologies in context; Bronfenbrenner’s 1979343 model of the ecological niche. Singh explores the ‘ongoing and mutual process of shaping’ between individuals and their social and physical spaces and argues against sociological models that ‘locate disorder either in the child or in the environment’ and suggests diagnosis is part of the interplay between the two | Transcripts were read/reread then coded thematically by the primary investigator. Themes were further broken down into categories, and the relationships among categories were specified. Both a ground-up coding frame and a deductive ‘organising framework’ were developed. A coding frame had been drawn up earlier, and discussed in a team of three other coders to establish agreement and transparency |
| Taylor 2008335 Australia |
15 | Nine males and one female aged 11–18 years; four males and one female aged 6–11 years | 20 semistructured telephone interviews | Self-selecting; snowball | Symbolic Interactionism | Grounded theory was followed including simultaneous data collection, coding and analysis until saturation was achieved; the constant comparative method was used to analyse data. Reliability of coding was established using an independent rater |
| Wolfberg 1999336 USA |
10b | One male aged 5 years | Participant observation | Purposive | Bronfenbrenner’s 1979343 theory of ecological systems. The authors focus on social aspects of ADHD | Constant comparative method was employed involving quantitative and qualitative data; following coding, conceptual categories were classified and compared, then an educational ethnographer was consulted and the concept of peer culture was chosen as a focus for the further development of themes. Triangulation through multiple data forms and member checks contributed to credibility |
Most authors were not explicit about their chosen research methodologies. Those discussed involved ethnography,332,334,336–338 critical discourse analysis,332,337,338 grounded theory296,335 and phenomenology. 331,333 Most authors explicitly discussed conceptual frameworks used to structure studies and/or analysis, including theories of learning style 331 symbolic interactionism,296,335 postmodern illnesses,299 synactive theory,334 narrative research approaches,314 empirical bioethics27 and ecological systems. 27,296,335,336 Some studies were explicitly framed to explore attributional beliefs about ADHD261,314 and many others addressed and/or came to conclusions about the contribution of psychological and/or sociological and/or biological factors to ADHD symptoms. 27,299,332–334,337,338
Findings for review 4a (pupil views)
For review 4a (pupil views) Cooper and Shea’s study261 was chosen as an index paper272 because of its breadth of themes which represented the content of other papers well. It is also appropriate as an index paper because it was one of the first studies to be conducted from the perspective of pupils diagnosed with ADHD, and its authors are known for expertise in the field of ADHD. That the study was conducted in the UK also adds to its pertinence. Data analysis followed the process described in Chapter 4 (see Methods of analysis/synthesis, Data analysis and synthesis).
Overarching theme for review 4a: attention-deficit/hyperactivity disorder symptoms as an interaction between biological, sociological and psychological factors
The overarching theme identified was that ADHD symptoms are an interaction between biological, sociological and psychological factors. In the following sections, findings from papers that studied pupils diagnosed with ADHD are synthesised following the structure of the overarching theme by discussion of the experience of ADHD symptoms, sociological and psychological factors, and the impact of attributional beliefs about ADHD on the expression of symptoms. We chose to categorise sociological factors as the experience of relationships, stigma and classroom context and their relationship to symptoms of ADHD. There are arbitrary elements in both the reasons for ADHD stigma (see Stigma) and the context of classrooms [see Findings for review 4b (teacher views), Overarching theme for review 4b: factors that influence a teacher’s willingness to adapt their response to attention-deficit/hyperactivity disorder symptoms, Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms and Findings for review 4d (mixed views), Fit between pupils diagnosed with attention-deficit/hyperactivity disorder and school], that can be implicitly perceived as normal and right owing to sociological tradition. Therefore, stigma and the classroom context have been categorised as sociological factors, although stigma is also closely related to psychological aspects of ADHD (see Psychological factors) and the classroom context could be categorised as ecological. This has been done in order to highlight the sociological aspects, because these are important in understanding changes that could be made to support the implementation of non-pharmacological interventions for ADHD in schools. Psychological factors were more straightforwardly identified as experiences related to agency, identity and the desire for approval. We acknowledge the contribution of biological factors to ADHD symptoms, but as there are no clear boundaries for discerning biological aspects in pupil experience, we only mention them here (see Chapter 1, What is attention-deficit/ hyperactivity disorder?). We acknowledge that grouping factors in this way may create false distinctions; however, the intent is to discuss the role of particular factors related to ADHD symptoms where possible, while understanding that origins and expression of behaviour result from interactions between them. It is impossible to specify or adequately represent the relationships between biological, psychological and sociological factors, as potential combinations are multiple, reciprocal and complex; instead we will depict relationships broadly based on the findings from included papers in review 4a (for a schema of these see Figure 7).
Table 48 shows the relationships between first- (participant) and second-order (author) concepts from included papers, and third-order (reviewer) concepts. In review 4a (pupil views), the overarching theme identified was the ‘Expression of ADHD symptoms as an interaction between biological, sociological and psychological factors’. Four subthemes were identified:
-
the experience of ADHD symptoms
-
sociological factors that impact the expression of ADHD symptoms
-
psychological factors that impact the expression of ADHD symptoms
-
impacts of different attributional beliefs on ADHD symptoms.
Each will be discussed in turn below.
| First- and second-order concepts (index paper Cooper 1998261) | Third-order concepts (overarching theme: Expression of ADHD symptoms as an interaction between biological, sociological and psychological factors), themes and subthemes | |||||||
|---|---|---|---|---|---|---|---|---|
| Subtheme | Experience of ADHD symptoms | Sociological factors that impact the expression of ADHD symptoms | Psychological factors that impact the expression of ADHD symptoms | Impact of different attributions about ADHD | ||||
| Relationships | Classroom context | Stigma | Identity | Agency | Desire for approval | |||
| Behaviours: being disruptive, impulsive oppositionality, dangerousness: | ||||||||
| Sense of lack of control | ✗ | ✗ | ✗ | ✗ | ✗ | |||
| Spoiled identity | ✗ | ✗ | ||||||
| Role of context in determining problematic behaviour | ✗ | ✗ | ✗ | ✗ | ||||
| Concentration problems | ✗ | ✗ | ||||||
| Academic issues | ✗ | ✗ | ✗ | ✗ | ||||
| Diagnosis: acceptability and stigma | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ||
| Attitudes to treatment | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ |
| Contributing papers | 27,261,296,299,314,331,333,334 | 27,296,299,314,332–336 | 27,261,299,314,331–334 | 261,296,299,314,332,333 | 261,299,314,332–334 | 27,261,296,314,332,333,335 | 261,299,314,333,334 | 27,261,299,314,332 |
Confusion about ADHD was also demonstrated to be an important issue in review 4 in understanding barriers to the implementation of non-pharmacological interventions. Research suggests that ADHD symptoms are related to a difference in pupils’ genes and/or cognitive processing (for more discussion see Chapter 1). However, similar symptoms may also result from other phenomena such as trauma,45 lack of sleep344 and/or giftedness. 345,346 The behaviours that comprise the syndrome of ADHD are normally distributed in the general population and, thus, are present at times in most children to some degree. The lack of a direct link to biological explanatory factors contributes to the controversy surrounding ADHD. Although NICE clinical guidelines46 suggest the interaction of biological/sociological/psychological factors in relation to ADHD symptoms through their recommendation for multimodal treatment, the medicalisation of Western cultures can mean that lay people understand diagnosed conditions in particular ideological terms (Box 11). Pupils diagnosed with ADHD in review 4a made predominantly medicalised attributions about ADHD despite describing their experiences of ADHD symptoms in relation to sociological and psychological factors. For example, pupils describe the increased expression of ADHD symptoms as following stress brought about by relationships with others (see discussion below), including parents, teachers and peers (sociological factors); the specific demands of paying attention in the classroom (sociological factors); and disappointment in themselves for not meeting expectations (psychological factors).
Rafalovich347 defines medicalisation as the process by which deviant acts
-
become understood to originate from a medical cause and are therefore perceived to be beyond an individual’s control; and
-
are believed to be treatable through medical knowledge and the application of techniques by medical experts.
Experience of attention-deficit/hyperactivity disorder
Experience of ADHD symptoms described by pupils diagnosed with ADHD centre round the symptoms specified in clinical diagnostic guidelines: hyperactivity/impulsivity and inattention. Although all pupils might be expected to have had similar experiences to those described below at some point, it is the pervasiveness and intensity of these experiences that differentiates those diagnosed with ADHD, and suggests a biological difference. For example, Kendall et al. 299 found it common for pupils to experience a loss of emotional self-control daily, and a young person in Brice’s study said the following about difficulty in maintaining emotional control:
It’s not a one-time thing. It’s a constant struggle.
American young person diagnosed with ADHD (aged 13–18 years), p. 74331
Thus, despite shared experience of hyperactivity/impulsivity and inattention for all pupils, pupils with ADHD describe experiences that are qualitatively different from their peers because the severity and/or persistence of these symptoms interfere with their relationships and attainment at school.
Pupils diagnosed with ADHD talked primarily about aspects of impulsivity related to a lack of emotional self-control and problems of inattention. There was relatively little description of the experience of hyperactivity; only one researcher identified a theme that focused on experiences of hyperactivity (‘I gotta move’;333 for further discussion see Hyperactivity). This may be related to the age of most of the participants in these studies; Prosser found that by secondary school the hyperactive behaviour of most pupils had declined since leaving primary school. 314
Impulsivity/lack of emotional self-control
Although pupils sometimes refer to impulsive dangerous behaviour, for example jumping onto railway tracks,261 most describe impulsive behaviour in terms of a lack of emotional self-control. Young people in Brice’s study attributed many of their behaviours to the influence of mood, with good mood influencing positive behaviour as much as bad mood fostering negative behaviour. 331 The young people in Brice’s study were mostly unaware of the origins of good and bad moods. 331 Pupils in Houghton et al. ’s study referred to the origins of bad mood as ‘stress’. 296 Stressors described by pupils in the studies include:
-
home events such as arguments with siblings and parents296,299,331
-
distractions in the classroom296
-
the need to sit in the classroom without being able to move about or go outside333,334
-
frustration with the difficulties of schoolwork261,296,299,331
-
confused, swiftly moving thoughts that make it difficult to communicate with others. 261
Pupils describe a loss of control that can occur suddenly and unexpectedly or result from a slow buildup of many small stressors over time. 296,299 They sometimes describe experiences of these intense emotions, especially anger, through physical sensations:27,261,296
Red balls of fire that come up my chest and into my head.
Australian pupil diagnosed with ADHD (aged 6–17 years), p. 137296
Many of the pupils in these studies understood themselves to be unable to control these emotions:261,296,299,314
Things build up in you until you can’t take it anymore. It is then that you start yelling, screaming and carrying on. You just can’t stop yourself.
Australian pupil diagnosed with ADHD (aged 6–17 years), p. 131296
The intensity of emotion, inability to control it and the consequent negative impact on relationships that pupils describe is striking because of its prominence across studies. 27,261,296,299,314,331,334 This suggests that emotional self-regulation deserves further attention, whether with reference to its role as part of the constellation of symptoms of ADHD or as a discrete issue (see Chapter 1, What is attention-deficit/hyperactivity disorder?).
Inattention
A number of pupils described stimuli in the classroom as a barrier to learning. 261,299,331,333,334 Sounds and sights were difficult for them to filter out:
One minute I’m working and the next I’m in the middle of somebody’s conversation.
American young person diagnosed with ADHD (aged 13–18 years), p. 50331
The way some pupils described the intrusion of sound was unusual, so much so that Friio333 identified the theme, ‘what am I hearing?’ For some children and young people, sounds mix together and become something unrecognisable:
If my friend starts talking I’ll turn around and talk to him and try to divide my attention between what the teacher is saying and what the friend is saying and of course it ends up a jumble, and I get two voices talking at once . . . and they kinda blend into one and I can’t separate one from the other.
Canadian young person diagnosed with ADHD (aged 14–18 years), p.119333
Other sources of distraction mentioned were being touched;331 being interrupted by teachers or teaching assistants who, in an attempt to support, actually broke the pupils’ ability to concentrate;331 being unable to prioritise and/or make sense of large amounts of verbal or written information, including expectations for work:296,299,331
When I ask them for help . . . they go through the stuff I already understood, and I’ll pay attention to that and by the time they’ve gone through that stuff, I’m not paying attention to what I’m supposed to learn and it goes right over my head.
American young person diagnosed with ADHD (aged 13–18 years), p. 80331
Pupils also described becoming distracted by their own numerous, simultaneous thoughts:261,333,334
At school I’ll be asked something and I’ll be thinking about it and I’ll totally lose track of it. It will get lost in an ocean of other thoughts. It’s just I really have to concentrate to keep that one thing in my head [. . .] so you just lose your place in what you’re thinking.
Canadian young person diagnosed with ADHD (aged 14–18 years) [reviewer’s edits], p. 78333
Hyperactivity
Young people express a need to move, through activities like fidgeting, drawing or gross body movement:333,334
I’ll like start going like this [rubbing his hands] and twiddling my thumbs. I move my feet a lot and look at other stuff and move my head a lot . . . if I stop . . . I feel really funny so I keep on going. If I stop, well like I just start again. I don’t know why . . . I feel more comfortable when I start fidgeting again
Canadian young person diagnosed with ADHD (aged 14–18 years) [reviewer’s edits], p. 111333
McDannel334 found that young people in her study responded emotionally to context and that these emotions trigger ADHD symptoms; she concluded that such behaviour is unconsciously self-regulatory and an attempt to manage internal emotional states. She found that young people with ADHD in the classroom are often involved in a dynamic balancing act in response to stress as a result of classroom structures and expectations. They unconsciously self-regulate in an attempt to achieve stability of neurobehavioural states brought about by needs for alertness, arousal, selectivity or sustained attention. Examples of unconscious self-regulatory behaviour include posture; kinetic energy displays such as fidgeting, drawing, shaking a leg; pressured speech; irritability; increased arousal including loss of temper and changes in alertness (e.g. hyperfocusing or daydreaming). Unconscious self-regulation can help or hinder the schoolwork done by pupils; for example, by supporting sustained focus or, on becoming overwhelmed, the pupil may be unable to work (and go to sleep, or become disruptive enough to be expelled from the classroom). Young people in Friio’s333 study shared numerous stories of being overly active, in terms of physical activity, talking and repetitive motion in class such as drawing and fidgeting. As was true for participants in McDannel’s334 study above, they described a sense of relief that they experienced in response to movement.
Implications of young people’s experiences of ADHD for non-pharmacological interventions are given in Box 12.
Pupils diagnosed with ADHD describe impulsive emotional outbursts to be triggered by stress in relationships, by negative self-concepts and by their physical surroundings. This suggests non-pharmacological interventions designed to improve social and emotional well-being for pupils with ADHD are likely to decrease ADHD symptoms. In addition, the inclusion of adaptation to the physical environment (relevant to the individual pupil’s needs) holds the potential to decrease ADHD symptoms.
Pupils diagnosed with ADHD are likely to benefit from strategies for maintaining emotional self-control. Raising awareness in pupils of links between experiences and resulting mood might be necessary for them to understand when to apply these strategies.
Although they cause difficulty to teachers and parents, ADHD behaviours may not be ‘naughty’ but rather an unconscious attempt by pupils to regulate their emotions. Thus, punitive strategies may be inappropriate; a more constructive response would be to view excessive movement as a signal giving information to teachers and/or parents about a pupil’s emotional state.
Sociological factors
Cultural attitudes towards the origins of ADHD symptoms in pupils often involve the perception that they are a result of sociological factors, particularly relating to family dynamics,286,291,294,296 including poor parenting. However, sociological factors described by pupils diagnosed with ADHD in included studies involved relationships and the context of the classroom. An additional factor implicated in relationships was the dynamics of stigma. These themes are described in more detail below.
Relationships
A main finding from Prosser314 was that, unlike teachers and parents, the symptoms and label of ADHD were not a focus of concern for young people diagnosed with ADHD. Rather, the pupils’ focus for concern was on their relationships with peers, parents and teachers, and the ways in which ADHD symptoms made these relationships difficult. In particular, difficulties pupils report experiencing with emotional self-control seem to impact relationships negatively.
Young people in some studies314,333,334 commented that, in their experience, the most important means to academic success was an understanding, approachable teacher. Unfortunately, pupils also commonly described punitive teachers27,296,314,333,335 who left them feeling hurt, angry and/or disappointed. Pupils described teachers who put them ‘under the spotlight’, being excessively punitive while ignoring similar behaviour from other pupils,296,299,333 and teachers who could not spend more time explaining work to and supporting ADHD pupils because of large class sizes. 333 By contrast, pupils also described a few teachers whose approach supported them personally to learn,314,333 linking this to school years where they did all right:
I started school off well, like I had a good teacher, but then in year two I had a teacher who didn’t like me so I took a real dislike to her and so that didn’t work well at all.
Australian young person diagnosed with ADHD (aged 14–16 years), p. 102314
Pupils admitted to challenging purposely teachers who they thought treated them unfairly,296,314,333 suggesting that difficult behaviour may be ameliorated or exacerbated according to the quality of pupil–teacher relationships.
Young people in Friio’s333 study expressed the feeling that they were not listened to by most adults in their lives (parents, teachers, counsellors, doctors), describing a lack of communication about ADHD and medication, where they felt that they were not consulted about the ADHD issues that mattered to them. This was particularly poignantly expressed in relation to the counsellors or psychiatrists because of the expectation that they were meant to help them;
[the psychiatrist] wouldn’t really listen to what I had to say . . . she didn’t really see me as a person who had a problem . . . she just saw me as the problem . . . just diagnosing the problem, giving you medication, and letting you go away . . . She didn’t listen to me . . . that would have been a lot better for me because I think I did need that sort of thing.
Canadian young person diagnosed with ADHD (aged 14–18 years) [reviewer’s edits], p. 150333
Pupils in Kendall et al. ’s299 study also reported confusion over the meaning of ADHD, suggesting a lack of communication from adults. However, in contrast to Friio’s333 study where young people felt unsupported by their parents, pupils in Kendall et al. ’s299 study cited their mothers as the person who helped and supported them the most with their ADHD-related problems.
Pupils commonly expressed concern over the difficulties that they experienced in peer relationships,296,314,332,335 including emotional distress at feeling ‘left out’335 and/or bullied. 332 Taylor and Houghton335 found differences in perceptions about peer relationships by subtype of ADHD diagnosis. Pupils diagnosed with the inattentive type of ADHD believed that they were able to decide consciously whether or not to engage with peers. Pupils with hyperactive/impulsive type believed their ability to engage with peers were dependent on the actions of others, for example by blaming difficulty in relationships with peers on where they are seated by teachers in the classroom. In Wolfberg et al. ’s336 study of preschool peer interactions, young pupils with disabilities (one with ADHD, aged 5 years) experienced exclusion from peer culture because they misinterpreted and overlooked social cues, with peers eventually showing apathy and indifference to them. Children with disabilities were included in play when they established common ground with their peers (e.g. by finding other peers who were loners). They were also included when peers normalised their unconventional behaviour, for example when peers agreed to be involved in fantasy character rituals.
The role of context in attention-deficit/hyperactivity disorder symptoms
Most studies included in review 4a (pupil views) discussed ways that the expression of ADHD symptoms differed according to context. Cooper and Shea261 discuss the role that the attitudes of parents and teachers play in framing pupil’s interpretation of their behaviour as problematic; Kendall et al. 299 describe the dissonance pupils experience because they understand the expectation for them to ‘be good’ but that they are not meeting it. Thus, in both studies, the problems of ADHD are defined by the expectations of the adults in the contexts pupils find themselves in.
Singh27 identified differences in expression of ADHD symptoms according to ecological niche (Box 13) and cultural values. Her study explored a number of different settings in the USA and UK, and in the ecological niche of UK state schools in small, working-class communities with low social mobility, ADHD was understood by pupils to be an inability to control ones’ emotions, rather than a difficulty with hyperactivity and/or attention. The extent of punishment levied by teachers on pupils diagnosed with ADHD for poor behaviour led them to understand behaviour to be more important than learning. In other communities (in the USA and the UK) where attainment was more highly valued, impact on attainment caused by hyperactivity/inattention was given higher priority, although lack of control over anger and aggression was still perceived to be an important aspect of ADHD symptoms. Singh27 argues that the value placed on self-control in UK culture also contributed to an understanding of ADHD as lack of emotional control in this particular ecological niche.
Two studies (by Singh27 and Wolfberg et al. 336) in review 4a (pupil views) framed the design and analysis of their studies using Bronfenbrenner’s ecological theory. 343 This theory emphasises the fundamental importance of exploring reciprocal transactions between an individual, their social relationships and physical spaces in understanding child development.
Implications of young people’s experience of relationships for non-pharmacological interventions are given in Box 14.
Unlike parents and teachers, pupils diagnosed with ADHD may not be particularly concerned with symptoms of ADHD; rather, they may hold as a central concern the negative impact ADHD symptoms can have on their relationships with others. Therefore, non-pharmacological interventions that focus on supporting relationships between pupils diagnosed with ADHD and their parents, teachers and peers may be particularly welcomed and relevant to these pupils.
Pupils diagnosed with ADHD with poor friendships found this greatly troubling. Non-pharmacological interventions that teach social skills may improve these children’s well-being, as well as reducing expression of ADHD symptoms.
Many pupils diagnosed with ADHD in these studies describe the quality of their relationship with their teacher to be fundamentally important to their academic success, with good relationships ameliorating ADHD symptoms and poor relationships exacerbating them. The power of this relationship to act as a barrier or facilitator to improved behaviour and learning is an important topic for inclusion in teacher education about ADHD.
Some pupils diagnosed with ADHD in these studies expressed the feeling that their ADHD-related concerns were not listened to; many were confused about the meaning of ADHD. Non-pharmacological interventions that involve reciprocal interactions between those who administer them and the targeted pupils – where the views of ADHD pupils are sought and taken into account and/or that explain ADHD (see Explaining attention-deficit/hyperactivity disorder as an interaction between biological, sociological and psychological factors, below, for discussion of the benefits of describing ADHD as an interaction between biological, sociological and psychological factors) – may support these pupils’ well-being and decrease the expression of ADHD symptoms.
Other authors speak more specifically about the role of schools and classrooms in the expression of ADHD symptoms. Prosser314 discusses the way ADHD symptoms are expressed differently according to the different contexts of primary and secondary school. Young people in his study described a decrease in the effectiveness of medication as they aged (despite increased doses with growth). Prosser attributes this to lower levels of social difficulties in primary school years, with ADHD symptoms becoming more evident in response to the greater academic and social demands of high school.
Exley332 focuses on the way social groups in school create and/or perpetuate ADHD behaviour. School rules normalise what is good and bad, with ADHD behaviour identified as bad. Children respond to this by excluding children in the ‘bad’ category. This can exacerbate ADHD symptoms:
[when at home] he starts getting hyper and starts breaking things, [because] he imagines that someone is teasing him.
Child describing what a puppet diagnosed with ADHD might do [reviewer’s edits], p. 76332
Exley332 argues that, through a process of policing social boundaries, once a child is labelled bad, even when other children display similarly bad behaviour, the ADHD child is perceived as bad and the other children are perceived as good. This can lock pupils diagnosed with ADHD out of social groups.
McDannel334 identified two classroom genres that influence pupil behaviour. Pupils demonstrated greater ability to remain on task and to complete assigned schoolwork in ‘formal order classrooms’, whereas unconscious self-regulatory occupations (see Hyperactivity for a list of examples) were more pronounced in ‘Dada’ classrooms (see Box 15 for a description of formal order and Dada classrooms). However, pupils diagnosed with ADHD learned in both genres of classrooms, although in Dada classrooms the learning tended to be more social than academic. In the Dada classrooms, participants had greater difficulty with sustained attention and persistence. One of the pupils who completed little work in Dada classrooms exercised persistence with schoolwork when working in isolation, which suggests the important role such aspects of the classroom may have in the ability for pupils diagnosed with ADHD to access the curriculum.
In a formal order classroom there is a sense of order and the sense that the teacher is in control; desks are set up in rows and columns; teachers interact more formally in style with pupils, although are not impersonal. The environment is relatively quiet; rules such as raising one’s hand to speak are enforced.
Classroom genres: Dada classroomsDada classrooms negate ‘some traditional social canons and values for deportment’ (p. 135). Dada classrooms involve teachers who interact more informally with pupils and are less likely to establish consistent boundaries. Interactions in Dada classrooms are characterised by teachers who mediate resistance, hostility, alienation and stubbornness and pupils who take ‘an unremitting delight in employing the use of self in acts of creative freedom’ (p. 136). 334
Friio,333 although defining ADHD in his thesis through medical constructs of cognitive deficit, concluded on the basis of pupil accounts that much of the expression of ADHD symptoms is situational, and that the environment of school particularly contributes to, or triggers, these behaviours. Similarly, young people in Prosser’s314 study reported that it was the context of school where they experienced the greatest problems; they could negotiate other areas of life with some success. Young people in Brice’s331 study spoke of:
-
feeling frustrated, angry, drained and/or imprisoned by school
-
finding that the distraction of peer relationships, noise and movement in classrooms prevented them from learning (for related findings see Impulsivity/lack of emotional self-control).
In contrast to the above examples of contexts that exacerbate ADHD symptoms, Brice,331 in his doctoral thesis exploring the experience of learning for young people diagnosed with ADHD, described contexts in which these pupils learned despite their ADHD. These young people describe the experience of learning as:
-
feeling still, calm, confident (‘I know I can get the work done’), excited and happy (‘I just wanted to keep learning’)
-
learning via observation, trial and error and repetition, and preferred visual/kinaesthetic, active learning to static/rote learning
-
mostly learning alone, in some situations learning with others (teachers, parents and peers)
-
being self-motivated, where they determined how much effort to put into learning and the content, extent and depth of what they learned.
There were echoes of these findings in other studies. 261,299,333 Cooper and Shea261 note that pupils who struggle academically may also claim to do exceptionally well in other areas, such as art; one of the participants in their study described great difficulty writing an essay on The Merchant of Venice for a lesson, but had written a number of short stories and part of a novel outside of school. This pupil found it difficult to engage in the classroom, often mentally creating storylines during lessons instead of listening. Pupils in Kendall et al. ’s299 study commented on the difficulty they had sustaining attention when the lesson content was not intrinsically interesting to them. The statement by the young person below suggests that unless these pupils understand the purpose of their school activities they perceive them to be a waste of time:
[when I learn] I’m out on my own and not just sitting there doing nothing.
American young person diagnosed with ADHD (aged 13–18 years) [reviewer’s edits], p. 80331
Brice331 describes the difference between school learning and self-learning to be that school learning involves criteria that have to be performed on demand to authorities. School learning involves external time pressures, external expectations and relationships with authorities and these are all things that can be problematic for young people with ADHD.
Overall, the findings about context and ADHD symptoms suggest that the context of the classroom often creates barriers to learning for these pupils.
Implications of the role of the classroom context for non-pharmacological interventions are given in Box 16.
Included studies demonstrated that macro- and micro-cultural expectations can play a part in what are interpreted as being ADHD symptoms; non-pharmacological interventions could improve their relevancy by incorporating flexibility in structure so they could be adapted according to context.
Included studies found that pupils diagnosed with ADHD often experience peer relationships, noise and movement in classrooms as barriers to learning; this could be explored further in developing approaches to support these pupils.
Included studies found that pupils diagnosed with ADHD could experience learning as rewarding when it involved observation, trial and error and repetition, visual/kinaesthetic approaches, active/meaningful learning and self-motivation; this could be explored further in developing approaches to support such pupils. Although findings suggest that pupils may learn more easily while working alone, this neglects the social needs of these pupils. Developing constructive ways to work with others may, therefore, be more worthwhile.
Stigma
Stigma is a concept developed within the field of social psychology and is particularly well expressed by Goffman. 322 Goffman describes stigma as the disgrace incurred on those categorised with attributes outside what is considered to be ordinary and natural; ‘an undesired differentness’ that leads us to ‘believe the person with a stigma is not quite human’, justifying us to ‘exercise varieties of discrimination, through which we effectively, if often unthinkingly, reduce his [sic] life chances’ (p. 15). 322 Such disgrace can result in the ‘spoiled identity’ of the person on whom the stigma is visited, as they internalise these understandings as accurate. Thornicroft348 further discusses stigma in relation to mental illness by distinguishing aspects of ignorance (lack of knowledge about a mental illness), prejudice (negative stereotypical beliefs about people with a mental illness) and discrimination (actions that result in marginalising people with a mental illness through differential treatment). Importantly, the attributes that provoke stigma are not discrediting in and of themselves, but only according to the value systems of those allocating the stigma, who Goffman calls ‘normals’. 322 Labelling involves the assignment of the category name invoking the stigma onto a person, and can be informal or formal. An example of informal labelling of ADHD symptoms is ‘naughty boy’; formal labelling of ADHD symptoms would involve clinical diagnosis of ADHD.
The papers included in review 4a report varying amounts of stigma related to the symptoms of ADHD and/or the label of ADHD. Cooper and Shea261 found hyperactive/impulsive and/or combined types of ADHD to be more highly stigmatised than ADHD inattentive type, with school peers expressing irritation over ‘extreme and erratic’ behaviour. In contrast, ADHD inattentive type involves ‘a failure to meet expectations’ and, as it does not elicit negative reactions from others, it involves less stigma. Outside of school the authors characterise the label of ADHD, and medical treatment for it, to be stigmatising. Prosser314 found that the young people in his study were stigmatised on the basis of their ADHD symptoms rather than for the label of ADHD. They did not experience diagnosis of ADHD or taking medication for ADHD as stigmatising. Pupils in both Kendall et al. ’299 and Exley’s338 studies describe feeling stigmatised by teachers and/or peers for taking medication for ADHD at school. These findings suggest patterns of stigma vary according to micro culture.
Although the above findings referred to stigma explicitly, other findings seem to link to Goffman’s322 description of the workings of stigma (Box 17) without researchers’ explicit discussion of this concept. For example, descriptions by pupils of teachers who punish them excessively while ignoring similar behaviour by peers296,299,333 link to aspects of stigma described in Box 17c. Exley’s338 finding that ADHD children were labelled ‘bad’ and the resulting social exclusion is another example of similar behaviour (see The role of context in attention-deficit/hyperactivity disorder symptoms, above). In one of the quotes above from Friio’s333 study (see Relationships, above) a young person describes feeling that he is not treated as a human being; this links to the discussion of Goffman322 about stigma. In addition, symptoms of ADHD are problematic specifically to the requirements of a classroom (e.g. see Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms, below) rather than being problematic in and of themselves. Again, this fits with Goffman’s322 description of stigma. This demonstrates the stigmatised nature of ADHD symptoms and the term ‘ADHD’ itself, although differences in the experiences of stigma between pupils suggest the intensity of this stigma varies according to micro culture.
Goffman322 describes a number of potential ways that a stigmatising label may affect a normal’s perceptions or actions toward a stigmatised person:
-
generalising the particular faulty attribute to a wider gestalt of disability (e.g. assuming a child with ADHD is not capable of learning)
-
assuming the person exhibits the range of attributes by which the label is understood rather than seeking to understand the person
-
the person’s behaviour will be understood as an expression of the stigmatised attribute, whereas the same behaviour from a normal would not be regarded in the same way.
Implications of stigma for non-pharmacological interventions are given in Box 18.
The role of stigma in influencing ADHD symptoms relates to the barriers that it creates for teachers who support pupils with ADHD, in focusing attention on stereotypical beliefs about ADHD (whatever those might be) rather than directing focus to the child or young person. This can result in negative relationships between teachers and pupils, may result in choice of inappropriate strategies or interventions for ADHD, may act as an example for stigmatisation by peers, may negatively impact a pupil’s self-perceptions (see Identity) and, ultimately, further marginalises the pupil. All these factors can exacerbate the pupil’s expression of ADHD symptoms. The implication for non-pharmacological interventions involves the need for teachers to be educated about stigma. As stigmatising attitudes often involve implicitly held beliefs, reflective practice is likely to be needed in addition to information about ADHD and about the dangers of stigma in education for teachers.
Psychological factors
The included studies suggest that psychological factors are implicated in the expression of ADHD symptoms and that pupils diagnosed with ADHD can be personally impacted in important and powerful ways. In the following sections, the desire for approval that pupils diagnosed with ADHD express, their perceptions of agency (or lack thereof) and issues of identity are discussed.
Desire for approval
A number of authors note the desire expressed by pupils diagnosed with ADHD to meet expectations for behaviour and schoolwork:261,299,333
I have wanted to get over it . . . I have wanted to get better marks . . . and it just doesn’t work.
Canadian young person diagnosed with ADHD (aged 14–18 years), p. 137333
Similarly, the young people in Prosser’s314 study express frustration at not being able to meet social expectations, and remorse and regret following incidents of problematic behaviour. Young people in McDannel’s334 study said that they valued school as a means to gain qualifications that would help them get jobs.
Cooper and Shea261 note that, in light of the ill effects described by pupils in relation to medication (see Impact of polarised views, below), the benefits of medication for ADHD can be understood as more relevant to those other than pupils, such as teachers and parents, because it makes the pupil easier to control, or makes them more socially acceptable, rather than supporting the pupil personally, and is therefore a form of social control:
[The pills] calm me down, to help me work. They help me calm down, so I don’t embarrass my mother.
British pupil diagnosed with ADHD (aged 11–16 years) [author’s edits], p. 44261
The authors further note that many of the participants felt that this was a legitimate use of medication, indicating that it helped them to control their behaviour in order to please others, which they perceive themselves as incapable of doing otherwise. Some pupils do not want to take medication even if they perceive that this will bring them social acceptance, refusing to take it or complying only reluctantly. 261
Implications for non-pharmacological interventions of pupils with ADHD desire for approval are given in Box 19.
Teacher and parent education would benefit from emphasising that pupils diagnosed with ADHD in included papers often desired to please teachers, peers and parents. As ADHD symptoms prove so problematic to adults, it is possible for them to be interpreted as purposefully destructive and/or personal. These accounts from pupils diagnosed with ADHD suggest that pupils desire approval from adults and peers, and try to act in ways to secure it, but do not know how to do so.
Agency
Agency refers to the sense that one is capable of acting intentionally (i.e. is able to bring about an outcome of choice). 349 Authors of included papers often analyse the dynamics that result in either a lack of agency or a sense of agency for the pupils in these studies.
Exley332 explores the perception that children diagnosed with ADHD have of their capacity to control their behaviour by introducing participants to a puppet who is described as exhibiting hyperactive/impulsive behaviour, then asking questions about the puppet:
What are some of the things that [Puppy’s] teacher can do to help remind [Puppy] to control himself?
Maybe, um, ask his Mum and Dad to give him four tablets.
[Reviewer’s edits], p.72332
In this study, two boys diagnosed with ADHD, both on medication, understood medication as the way to control ADHD symptoms, rather than the puppet controlling himself. Exley332 and others261,333 conclude that medication supports a decreased sense of agency for pupils as they come to understand that they are medicated to control their behaviour because they are incapable of doing so themselves.
As described above, Exley332 also explored stigma and the role of peer social groups in excluding children diagnosed with ADHD. Once labelled ‘bad’, the child is excluded on the basis of the label as much as because of specific behaviour. Exley argues that this further reduces agency, because a change in the pupil’s behaviour does not necessarily result in a change to peer responses.
Singh27 describes the response teachers have to pupils diagnosed with ADHD according to their beliefs about the concept. Either they reject the concept of ADHD (seeing it as solely sociological) and, therefore, make no allowances for the behaviour of pupils identified with ADHD, or accept the concept of ADHD (seeing it as solely biological) and, therefore, excuse ADHD pupils’ aggressive behaviour. Singh argues that both approaches reduce the agency available to pupils.
Studies also identified ways that pupils diagnosed with ADHD demonstrate agency. Singh27 documents the agency ADHD pupils display in either curbing or releasing their feelings of anger and aggression. This suggests that these feelings are not entirely outside pupils’ control, unlike the perceptions they express. Pupils with ADHD rely on their friends to help them avoid fights with peers, either through friends standing up for them or talking them down. There are some insults, however, that once made, require a fight (e.g. insult to a boy’s mother). ADHD pupils, therefore, apply self-control in these situations as a moral obligation, either stopping themselves from fighting for their friends’ sakes, or deciding to fight for their mother’s sake. Peers can find loss of control of emotion frightening, and pupils use their label of ADHD purposefully in order to support their friends:
If they’re really bothering me, or bothering one of my mates, I’ll just go into my ADHD. I’ll flip on them and get really scary.
British pupil diagnosed with ADHD (aged 9–14 years), p. 89427
Singh27 argues this is a productive use of the stigma related to ADHD, as it is used to protect friends threatened by aggression. Singh27 also identifies exploitation of an ADHD diagnosis by pupils; they admit to using it to abdicate responsibility for poor behaviour. Pupils in Prosser’s314 and Taylor and Houghton’s335 study also confessed to defiant behaviours as a means to redress perceived injustices, and use of the ADHD label as an excuse to avoid consequences.
Houghton et al. 296 identify a process that pupils undergo, whereby they initially perceive themselves incapable of controlling their emotions and behaviour; they blame others for creating a hostile environment. However, they found that some older pupils show agency in taking action against ‘living up to a “bad”, “lazy” and/or hyperactive label’ (p. 140). 296 Short-term approaches include ‘armoring’, which is defined as switching off, avoiding issues that bring up anger, and is most often employed with peers. Other strategies include ‘feigning compliance’ (avoiding interaction with teachers, pretending to know what one is doing in the classroom); and ‘deflecting’ (attempts to redirect attention away from educational shortcomings by creating classroom drama). Longer-term solutions include ‘assessing self’, or the analysis of past emotional outbursts, and trying to understand why they vent.
If I am hyper then my friends are hyper and laugh with me but if I’m normal then they are normal. When I’m upset people just let me be. I think that the other students that aren’t my friends might be a little scared [. . .] sometimes they back away. Most of the time though they don’t do anything as I can feel it coming on and I just leave the classroom to cool down.
Australian pupil diagnosed with ADHD (aged 6–17 years) [reviewer’s edits], p. 143296
‘Feeling remorse’ involves reflection on the impact that past deeds may have had on themselves and others; ‘changing perspective’ involves a shift from perceiving themselves to lack control over their emotions and behaviour to understanding the dynamics of their emotions and behaviour and realising that they can control certain aspects of it:
I think ADD is like your level of tolerance which changes depending on the situation and how you are feeling. If you are feeling down or sore, then you will let things get to you easier and you will explode quicker. It is like you have a low level of resistance. On the one hand, when you are feeling good and happy with life, then people can pick on you all day and you won’t get angry. It is then like you have a high level of resistance.
Australian pupil diagnosed with ADHD (aged 6–17 years), p. 144296
‘Being proactive’ is the final stage identified, and this involves trying to influence their parents’ management of the home environment and teachers’ management of the classroom. Young people comment that there are no straightforward answers to their problems, and that adults do not always respond well to their suggestions. However, they act through communication with parents and teachers about the contexts of home and school, and suggest strategies that they consider would work better for them.
Prosser314 identifies action taken by young people to reframe the concept of ADHD more positively; however, he also concludes that pupils diagnosed with ADHD are the ‘big losers’:
Caught between condemnation from the sociological skeptics, and the neglect of their social needs in the medical model, they are attempting to forge their own path. These young people, showing an awareness to the sociological side of ADHD rarely shown by those who would speak on their behalf, are recreating the label, reforming identity, and resisting inequalities in school, with varying success.
Researcher, p. 273314
Thus, the way ADHD is understood and acted on by adults can decrease the agency of pupils diagnosed with ADHD. When they perceive themselves to be incapable of controlling their own emotions and behaviour, pupils are less likely to employ whatever control they have. This is likely to increase expression of ADHD symptoms. Some studies identified that pupils do have agency available to them,27,296,314 and that understanding and harnessing this appears to be a constructive way forward. Even when they act with agency, however, adults still hold the balance of power over the contextual factors that greatly impact pupils.
Implications related to agency for non-pharmacological interventions are given in Box 20.
Findings related to pupil agency would be relevant content for teacher and parent education about ADHD. Accounts from pupils diagnosed with ADHD in included studies suggest that, although they do not have the levels of emotional self-control that their peers have, they do have some self-control. Actions by teachers based on polarised conceptions of ADHD –
-
biological determinist (e.g. the child’s behavioural difficulties are due to brain deficit; therefore, they cannot control their own behaviour)
-
sociological (e.g. the child’s behavioural difficulties are due to poor parenting, not to any neurological difference; therefore, the child should be treated the same as any other child)
-
psychological (e.g. the child is naughty and additional discipline is needed)
– can undermine pupil agency. This suggests that supporting pupils diagnosed with ADHD to understand how to harness and develop the self-control that they do have is a constructive approach to reducing ADHD symptoms and fostering these pupils’ well-being by establishing in them a greater sense of agency.
Identity
Late childhood and adolescence are recognised as particularly important time periods for the development of identity,350,351 so the experiences of pupils diagnosed with ADHD during school years may be important to their developing identity. The development of identity is described by Bruner as a process that ‘proceeds from the outside in as well as from the inside out’ (p. 99). 349 We come to understand who we are through our interactions with others, as well as through our personal understanding and experiences, so teachers’, parents’ and peers’ perceptions of and responses to ADHD symptoms are likely to contribute to the identity of pupils diagnosed with ADHD.
Pupils in Cooper and Shea’s261 study perceived ADHD symptoms as ‘a serious flaw in their personal make up that pervades all aspects of their lives’ (p. 46). Pupils in both Cooper and Shea’s study261 and in Kendall et al. ’s299 study defined ADHD using the same words:
Pupils expressed a sense of failure and sometimes bewilderment because of their low levels of attainment. Low attainment and ADHD symptoms can link to low self-esteem261,299 and a sense of spoiled identity. For example, a participant in Cooper and Shea’s study,261 described above for his novel-writing ability, described this ability as a problem because figuring out storylines distracted him during lessons. The authors use this as an example of the potentially harmful effects of individual deficit explanations for learning and behavioural problems.
Cooper and Shea261 and Prosser314 note that most of the pupils in their studies expressed biological determinist beliefs – they described ADHD as ‘something wrong’ within them, rather than understanding ADHD symptoms to be the result of interactions between biological, sociological and psychological factors. Prosser314 notes that this can lead them to struggle with social issues in private because they perceive that the problem is theirs alone. Young people in Prosser’s314 study describe an initial reluctance about accepting their ADHD diagnosis, but response to medication was often dramatic and this led them to accept the diagnosis. There was a common misperception by them that medication ‘fixed’ neurological ADHD deficits, so improvement in response to medication confirmed diagnosis, whereas, in fact, studies show a response of increased concentration and calm behaviour is common across children with and without ADHD diagnosis and/or symptoms. 352,353
Attention-deficit/hyperactivity disorder pupils in Exley’s332 study (aged 6–8 years) perceived that their peers would understand ADHD as an illness that can be ‘caught’. This led them to want to hide their diagnosis and medication. Pupils in upper primary and secondary schools from Cooper and Shea’s261 and Kendall et al. ’s299 studies also demonstrated confusion about ADHD. Although some pupils understood ADHD in terms of its symptoms, others, although they described behaving in ways commensurate with ADHD symptoms, did not connect these with ADHD (they did not know what it meant). Such misunderstandings prompted Exley332 to emphasise the importance of explaining the biopsychosocial nature of ADHD, not only to pupils identified with ADHD but also their peers. This is particularly important for pupils diagnosed with ADHD because of the process of identity development that occurs in late childhood and teenage years.
Some pupils expressed discomfort or ambivalence about medication because its calming effect was experienced as changing their personality. 261 Sometimes this was valued, for example in the classroom, whereas other times this was resented, for example during free time:
If I do take [Ritalin] when we didn’t have school, I wouldn’t want to go outside and play with my friends.
British pupil diagnosed with ADHD (aged 11–16 years) [reviewer’s edits], p. 44261
Some pupils expressed that they were their true selves when unmedicated and they felt like someone else when medicated:
I like being myself instead of like calm.
British pupil diagnosed with ADHD (aged 11–16 years), p. 44261
Some pupils expressed enjoyment of their experiences more without medication:
I felt so dead when I was on it. I felt kinda like I was blinded . . . like there was a filter put in front of me. So I felt like colors [sic] stopped being so vivid and I stopped hearing so much.
Canadian pupil diagnosed with ADHD (aged 14–18 years), [reviewer’s edits], p. 145333
This suggests that some pupils may risk losing positive aspects of their identity by taking medication. Some pupils also reported stomach aches, headaches, bad taste and fear of addiction from taking medication. 299 However, many pupils took medication anyway, because it improved their classroom behaviour by helping them concentrate, think before acting, be calmer and work harder,261,299 which enabled them to please others (see the discussion above).
In contrast to the aspects of ADHD found to be potentially harmful to pupils, some pupils describe positive aspects of ADHD. Two of McDannel’s334 participants perceived ADHD as valuable; they felt people with ADHD were more interesting and more social, more ‘real’ about who they are than ‘normal’ people. However, they expressed their liking of ADHD alongside the perception that people with ADHD were not normal, and this demonstrates the complexity of their attitudes. Some participants in Kendall et al. ’s299 study also cited an outgoing personality or sense of humour as benefits of ADHD.
Implications related to identity for non-pharmacological interventions are given in Box 21.
Pupils can develop a spoiled identity in response to stigma related to ADHD symptoms and formal diagnosis of ADHD. Such negative self-perceptions can exacerbate ADHD symptoms (see Impulsivity/lack of emotional self-control) and be internalised in a pupil’s process of developing identity, with the potential to impact them negatively over their lifespan. Explaining ADHD to pupils as an interaction between biological, social and psychological factors, at the time of diagnosis and/or within non-pharmacological interventions, may support them to be able to understand themselves more constructively (see Explaining attention-deficit/hyperactivity disorder as an interaction between biological, sociological and psychological factors for further discussion).
Impact of polarised views
Findings from included studies resulted in the identification of the overarching theme that ADHD symptoms involve an interaction between biological, sociological and psychological factors. The accounts in included studies by pupils diagnosed with ADHD describe real difficulties in terms different to peers, suggesting biological influences. The accounts also demonstrate that ADHD symptoms are influenced by relationships, classroom context, stigma and resulting psychological responses from the pupil. However, commonly, pupils express understanding of ADHD as only biological; whereas it is common for teachers to describe it as only sociological (see Sociological factors: perceptions that attention-deficit/hyperactivity disorder symptoms result from difficulties in the home, below). The adoption of such polarised biological views by pupils diagnosed with ADHD may be related to the processes of diagnosis and medication. Singh27 argues that diagnosis and medication for ADHD are situated in an interaction between biological and social factors. There is no physical test that determines the presence of ADHD; rather, diagnosis is based on observation checklists completed by parents and teachers combined with observation of the child or young person by a clinician. The checklists are founded on normative ideas of classroom behaviour and these behaviours are evaluated on the basis of subjective perceptions, so diagnosis clearly involves sociological factors. However, there is an implicit link between ADHD symptoms and concepts of illness because diagnosis is carried out by medical doctors (because of the possible need to prescribe medication); therefore, diagnosis and pharmacological treatment of ADHD may prompt medicalised ideologies about ADHD for lay people,260 and this was common for pupils diagnosed with ADHD in included papers for review 4a. The following discussion explores pupils’ experiences of diagnosis and medication and its implicit links to polarised biological attributions for ADHD.
A number of papers identified positive factors that pupils described about diagnosis, linked to diagnosis functioning to alleviate rifts between expectations and behaviour. These included:
-
an explanation for difficulties299,314 including relief from guilt299
-
a way to explain behaviour objected to by others, for example, diagnosis resulted in the replacement of ‘blame and criticism with understanding and support’. 261,299 (This suggests that children and young people perceived that others held them accountable for their behaviour before diagnosis, and afterward made allowances for their behaviour.)
Kendall et al. 299 conclude that such positive factors mean that diagnosis of ADHD stabilises family life, preventing further compounding of problem behaviours and familial stress. However, a number of other papers discussed other factors related to diagnosis that proved problematic. Polarised biological attributions can render invisible the sociological and psychological factors that also play an important role in ADHD symptoms, which is likely to compound pupils’ ADHD symptoms on two fronts: by potentially diminishing pupils’ agency and self-perceptions27,261,314 (see Agency and Identity), and by removing focus away from sociological and psychological factors as sources for adaptation and amelioration of ADHD symptoms.
The consensus from pupils is that methylphenidate helps improves classroom behaviour;261 young people in Prosser’s314 study all reported that medication allowed them to think before acting. However, it did not predetermine better behavioural and learning outcomes, because sometimes pupils still chose to behave poorly or not to work. A central argument by Prosser314 is that the real problems of ADHD for young people are the social barriers to learning that it creates, and that medication is inadequate to deal with social difficulties. Prosser further notes the rift between young people in his study, and their conceptualisation versus experiences of ADHD. Participants all understood ADHD as biological in origin; however, the experiences of difficulties they described were social or psychological, for example difficulties in motivation, poor self-esteem, suicidal and violent thoughts, difficulties with relationships and depression.
A number of studies found that children and young people conceptualise treatment of ADHD as solely medical; when asked about what helped them deal with ADHD symptoms, they talked exclusively about medication,261,299,314,332 despite a number being involved in non-pharmacological interventions at school. Biological determinist understandings of ADHD may be a barrier to motivation for pupils to engage fully with non-pharmacological interventions; if they understand their difficulties to be solely biological in origin, they may see non-pharmacological interventions as a waste of time, they may also be more inclined to dismiss any benefits they experience from these interventions.
Such arguments against medication, alongside the evidence that, to some extent at least, ADHD symptoms are triggered by the context of the classroom, might be taken to imply adaptation to education is preferable to medication. However, the current state of structures within education suggest that medication is a prudent means to support pupils to cope with the mandatory demands of education while structures develop and change to become more inclusive, and to give pupils support while they mature and develop coping strategies themselves.
Explaining attention-deficit/hyperactivity disorder as an interaction between biological, sociological and psychological factors
The included studies in this synthesis have demonstrated that pupils diagnosed with ADHD describe the experience of ADHD symptoms in terms of an interaction between biological, sociological and psychological factors (for a schema of these see Figure 7). The pupils described in these studies demonstrate the value they often place in understanding why they are learning what they are asked to learn in school, a lack of engagement in subjects that have low perceived relevance, and deep engagement when there is motivation to learn. Explaining ADHD as an interaction between biological, social and psychological factors to children and young people gives them the conceptual framework from which to address a number of issues highlighted as important in these studies:
-
It gives them an explanation for the differences from their peers, in that they are experiencing heightened reactions to environmental stimuli, and this can be explained through differences in genes and cognitive processing. Understanding themselves to be different biologically offers a less personally negative, and therefore more constructive, basis for developing identity. It may also prevent the compounding of ADHD symptoms owing to decreased self-esteem.
-
It locates their behavioural and emotional self-control in an interaction between this biology, their environment including classroom structures and relationships, and their own perceptions and decisions. Self-control is not binary; something they do or do not have. Rather they are likely to have lower levels of self-control than their peers in some situations and not others. In all situations they have some self-control, and by learning when and how they lose control they can develop strategies to develop more control. This offers a foundation from which to foster a sense of agency and from which to take action.
-
It places the role of context on an equal footing with biological differences and pupil decisions in explaining the expression of ADHD symptoms. This encourages awareness and exploration of these kinds of factors by the pupil diagnosed with ADHD, and could lead to the development of self-understanding of trigger issues, which can be communicated with teachers, parents and/or peers and could form the basis for personalised strategies to improve function. Similar strategies are adopted in the management of other long-term conditions, such as asthma, migraine, stress and affective disorders.
-
Finally, it provides a conceptual foundation that explains why it is worth engaging with non-pharmacological interventions. Understanding ADHD symptoms as an interaction that includes not only pupils’ biology but also their decision-making processes and sociological context mean they can develop and improve their ability to function in these contexts. The findings suggest that pupils are often willing to take medicine which they experience as sometimes compromising physical well-being and/or personal identity in order to ‘fit in’ because they understand medication as the only way to treat their biologically caused behaviour. Should they understand processes of psychological and social development to be equally important, they may be highly motivated to engage with interventions developing other coping strategies which, if effective, may allow reductions in the dose of medication required.
FIGURE 7.
Schema of the experience of symptoms for pupils diagnosed with ADHD based on review 4a studies. Biological factors mean the pupil has less behavioural control than peers; interaction of these factors with sociological and psychological factors results in the expression of ADHD symptoms. Sociological and psychological factors can increase and decrease the expression of ADHD symptoms; factors that may increase symptoms are described in boxes. Thin black lines represent close relationship between sociological and psychological concepts.

Review 4b: the experiences and perspectives of teachers of pupils diagnosed with or at risk of attention-deficit/hyperactivity disorder
Study characteristics for review 4b (teacher views)
A total of eleven studies were included in synthesis 4b (teacher views). 41,263–265,286,291,294,296,298,305,324 Summaries of included papers for review 4b are shown in Table 49.
| First study author and year (n = 11) | Country of participants | Aim | n | Gender | Age of pupils taught (years) | ADHD status of pupils taught |
|---|---|---|---|---|---|---|
| Arcia 2000286 | USA | To describe teacher understanding and strategies towards disruptive behaviours | 21 | 17 females and four males | 5–12 | Diagnosed or at risk |
| Bailey 200941 | UK | To analyse some of the everyday micro-processes of the classroom in order to deconstruct assumed ideas of misbehaviour as symptomatic of ADHD, and rather explore the classroom structures and discourses which articulate it | 4 | Three females and one male | 5–7 | Diagnosed or at risk |
| Einarsdottir 2008291 | Iceland | To understand Icelandic early childhood teachers’ experiences and perspectives of children with behavioural problems and ADHD-associated behaviour given the ongoing enormous changes in the Icelandic way of life, the recent changes in the educational system and the increasing rates of diagnosis and medication for ADHD | 16 | 16 females | 2–7 | Diagnosed or at risk |
| Hillman 2011294 | USA, UK, Canada | To examine teachers’ ability to identify ADHD and the qualitative content of their referral recommendations with a focus on differences according to ethnicity and gender | 30 | 24 females and six males | 5–14 | NR |
| Houghton 2006296 | Australia | To explore how teachers deal with the frustration that arises from chaotic or near chaotic classroom conditions triggered by some students diagnosed with ADHD | 36 | Ratio: three females to two males | NR | Diagnosed or at risk |
| Hong 2008264 | The Republic of Korea | To investigate Korean early childhood teachers’ beliefs about child development by focusing on their perceptions of children with ADHD | 23 | Gender NR | 0–15 | Diagnosed or at risk (20), no (3) |
| Jones 2008298 | USA | To explore how 20 currently practising pre-kindergarten teachers handle children identified with conduct disorder, ODD and ADHD to illuminate the strategies that are working | 20 | 20 females | 3–5 | Diagnosed or at risk |
| Lee 2008324 | USA | To understand US teachers’ perceptions of problem behaviour, ADHD, diagnosis and medication treatment for children with ADHD and how this reflects local and larger cultural beliefs | 10 | Nine females and one male | 5–9 | Diagnosed or at risk |
| Ljusberg 2011265 | Sweden | To highlight the physical and mental environment in the remedial classroom | 10 | Not reported | 9–12 | Diagnosed or at risk |
| McMahon 2012263 | Australia | To better understand pre-service teachers’ response to and participation in discourses of ADHD in contemporary schooling cultures | 150 | Questionnaire: 85% female Interviews: six females Focus group: three females, one male |
NR | NR |
| Nowacek 2007305 | USA | To explore teacher understandings of the characteristics associated with ADHD and what modifications and interventions are used with students | 8 | Five females and three males | 7–14 | Diagnosed or at risk |
Five studies involved participants from the USA,286,294,298,305,324 two studies involved participants from Australia,263,296 two studies involved participants from the UK,41,294 one study involved participants from Canada,294 one study involved participants from Iceland,291 one study involved participants from the Republic of Korea (Hong264) and finally one study involved participants from Sweden. 265 One study294 involved participants from three countries: USA, Canada and the UK.
All the studies explored the school experiences and perceptions of teachers of pupils diagnosed with, or at risk of, ADHD; however, it is possible to group the papers by their foci. Five of the studies explore teacher school-based experiences and perceptions without discussion of sociological influence,264,286,296,298,305 whereas six studies explored teacher school experiences and perceptions in terms of sociological influences on ADHD (Bailey and Thompson:41 the role of classroom structure; Einarsdottir:291 changing society in Iceland; Hillman:294 gender and ethnicity; Lee:324 cultural expectations; Ljusberg:265 the environment of the remedial classroom; and McMahon:263 discourses and labelling). Teachers taught in a range of settings including private and mainstream preschools, primary (or elementary) and secondary (or middle/high) schools. Teachers taught pupils ranging in age from 3 to 18 years (Table 50), with approximately two-thirds of participants involved with preschool or primary education (30% teaching ages 3–6 years; 33% teaching ages 6–11 years; 29% teaching ages 11–18 years). The female to male ratio of teachers in the samples (where reported) was approximately 4 : 1, demonstrating a predominance of female teachers. Most studies41,265,286,291,296,298,305 involved teachers with experience of teaching pupils who were diagnosed with, at risk of, or demonstrating core symptoms of ADHD. Hillman294 does not report this information, whereas 3 of 23 teachers in Hong’s264 study did not have experience of teaching children diagnosed with, or at risk of, ADHD. Lee324 does not report this information; however, she states that 9% of pupils in the school district in which the study took place are diagnosed with ADHD. Finally, the pre-service teachers in McMahon’s263 study were completing their final year of a Bachelor’s degree in primary education, and the study did not report the extent of participants’ experience of teaching pupils diagnosed with, or at risk of, ADHD.
| First study author, year and location | Number of teachers and school years taught | Number of teachers teaching children aged 3–6 years | Number of teachers teaching children aged 6–11 years | Number of teachers teaching pupils aged 11–18 years | Number of SEN teachers |
|---|---|---|---|---|---|
| Papers reporting age ranges of children taught | |||||
| Arcia 2000286 USA |
21 kindergarten/primary school teachers Kindergarten (n = 3), grades 1 (n = 3), 2 (n = 2), 3 (n = 6), 4 (n = 5), 6 (n = 1), SEN (n = 1) |
3 | 16 | 1 | 1 |
| Bailey 200941 UK |
Four infant school teachers Year 1 (n = 4) |
4 | 0 | 0 | 0 |
| Einarsdottir 2008291 Iceland |
16 preschool and grade 1 teachers | 8 | 8 | 0 | 0 |
| Hong 2008264 The Republic of Korea |
23 preschool, kindergarten and elementary school teachers Preschool (n = 2), kindergarten (n = 8), elementary (n = 12), SEN (n = 1) |
10 | 12 | 0 | 1 |
| Houghton 2006296 Australia |
36 high school teachers School year taught NR |
0 | 0 | 36 | 0 |
| Jones 2008298 USA |
20 preschool teachers | 20 | 0 | 0 | 0 |
| Lee 2008324 USA |
Eight kindergarten/elementary school teachers Two teachers each for kindergarten to grade 3 |
2 | 6 | 0 | 0 |
| Ljusberg 2011265 Sweden |
10 remedial teachers Remedial class years 3–5 |
0 | 0 | 0 | 10 |
| Nowacek 2007305 USA |
Eight elementary/middle school teachers Grades 2, 3, 4, 6: two teachers taught grades 6–8 and two teachers taught grade 8 only |
0 | 3 | 5 | 0 |
| Totals | 146 | 47 | 45 | 42 | 12 |
| Papers that do not report age ranges of children taught | |||||
| Hillman 2011294 USA |
30 teachers kindergarten to grade 8 School year taught NR |
NR | |||
| McMahon 2012263 Australia |
150 pre-service teachers | N/A | |||
| Total | 322 | ||||
Seven studies264,265,286,291,294,296,298,305 are included in both review 3 and review 4b (teacher views) because they contain analysis of perceptions of school-based strategies and/or interventions as well as experience of ADHD more generally. Therefore, only relevant findings from these studies are reported here. Review 4b reports the findings about the school-based experiences and perceptions of teachers regarding ADHD; for findings about the experiences of strategies and/or interventions from these studies please see review 3 (see Chapter 5).
Study methodologies for review 4b (teacher views)
Details of study methods for included papers in review 4b are given in Table 51. Nine of the eleven studies collected data through semistructured interviews. 47,263,265,286,291,296,298,305,324 In addition to interviews, two used open-ended questions,263,305 one used classroom observation,305 and one used focus groups. 263 The remaining two papers collected data through participant observation41 and an online open-ended questionnaire. 294
| First study author, year and location | Sample size | Sample characteristics | Data collection | Sampling | Theoretical approach/ADHD attributions | Data analysis |
|---|---|---|---|---|---|---|
| Arcia 2000286 USA |
21 | Three kindergarten 18 elementary school teachers Grades 1 (n = 3); 2 (n = 2); 3 (n = 6); 4 (n = 5); 6 (n = 1); SEN (n = 1) |
Forty-two semistructured interviews Two telephone interviews with each participant completing rating scales |
Purposive | The authors are not explicit about theoretical underpinnings. They implicitly refer to ADHD as a cognitive deficit and do not acknowledge complexities/uncertainties | Analysis followed Miles 1994.315 Passages in the transcripts were coded according to interview topic areas with use of qualitative software (Folio Views; Folio Corporation, Provo, Utah) to manage data. The first author extracted all segments that addressed the interview topics. All authors, who independently reported their preliminary conclusions and interpretations, reviewed the subsequent text. These observations were compared with the extracted segments, and the database was queried again for emergent themes. The first and second authors then conducted further confirmatory analyses using matrices. Member checking was conducted |
| Bailey 200941 UK |
4 | Infant school teachers Year 1 (Two teachers, two teaching assistants) |
Participant observation; data was field notes consisting of descriptions, recorded speech, maps and reflections written over 10 weeks | NR | Ethnography; post-structuralism, the authors adopt a primarily sociological stance about ADHD | Although the authors describe the theoretical underpinnings of their approach, they do not provide detail about their process of analysis beyond stating they applied Foucault’s concepts of discourse and power to understand the data |
| Einarsdottir 2008291 Iceland |
16 | Eight preschool teachers and eight grade 1 teachers | 16 semistructured interviews | NR | Phenomenology with a sociological lens, discusses biopsychosocial vs. individual/medical views of ADHD | Following a phenomenological approach, interviews were read and reread then coded using NVivo. Interview questions were used as an initial coding framework, then themes were identified. Analysis was done first within-person then across playschool teachers and across primary school teachers |
| Hillman 2011294 USA, UK, Canada |
30 | 30 teachers, kindergarten to grade 8 (School year taught NR) |
Online open-ended questions followed one of four vignettes (half male, half female, half Caucasian, half African American) describing a child with ADHD symptoms | Self-selecting | Essentialist epistemological stance, theorising that language used is an accurate reflection of the participant’s thought and ideas. The author implicitly treats ADHD as a cognitive deficit | Thematic analysis following Braun 2006.354 An inductive approach of reading and rereading, coding and organising by content using qualitative software. Coded data and their inter-relationships were considered to generate higher-level themes. Themes were determined by relevance to the research questions and by prevalence |
| Houghton 2006296 Australia |
36 | High school teachers (School year taught NR) |
Thirty-six semistructured interviews | Purposive | Ecological validity; symbolic interactions and grounded theory. These are substudies from a larger mixed-methods project, where a central aim was to explore not only biological aspects of ADHD, but the way these interact with psychological and sociological factors in natural settings | Constant comparative method: coding for patterns and salient features; codes constantly compared and interrogated by asking such questions as: ‘What is this piece of data an example of? What property does this piece of data represent?’ until saturation. This process developed codes into categories and relationships between them were established. A second researcher independently coded 10% of transcripts to establish reliability |
| Hong 2008264 The Republic of Korea |
23 | Interviews: kindergarten, n = 4; elementary, n = 2; occupational therapist, n = 1 Focus group: kindergarten, n = 4; preschool, n = 2 Survey: 13 participants from the interviews and focus group, plus 10 elementary school teachers |
Seven semistructured interviews; one focus group; open-ended survey | Purposive | The author does not discuss theoretical underpinnings. The author appears to hold views of ADHD as individual, within-child deficit. Background section indicates that the Korean government does not acknowledge ADHD as a disability | The process of data analysis was not reported, beyond the author stating she focused mainly on issues identified in the semistructured interviews in the journal article |
| Jones 2008298 USA |
20 | 20 preschool teachers | Twenty semistructured interviews, follow-up telephone calls and e-mails | Convenience, purposive | Principles of phenomenology; constructionism. The author defines ADHD according to difficulties in the home and neurological deficit. Although discussing teacher strategies to ameliorate ADHD symptoms, she does not discuss the classroom environment as potentially exacerbating ADHD | Phenomenological processes following Moustakas’ 1994 study355 were conducted. The interviews were transcribed verbatim and significant statements identified by more than one participant were highlighted and extracted. Categories were listed in the margins of the interviews and later placed under subthemes. Subthemes were translated and organised into overall themes. The author created textural and structural descriptions, combining them in the final synthesis. The author conducted member checking |
| Lee 2008324 USA |
10 | 10 pre-kindergarten/kindergarten/elementary school teachers Two teachers each for pre-kindergarten to grade 3 |
Ten semistructured interviews | NR | Sociocultural theory; cultural psychology focusing on the cocreation of a person through interaction between the social and individual | Thematic analysis. Interview transcripts were searched for ‘culturally learned and taken-for-granted assumptions’ that teachers made about children in general and ADHD in particular, through reading and rereading. The author does not give further details about the analytic process |
| Ljusberg 2011265 Sweden |
10 | 10 remedial teachers Remedial class years 3–5 |
Ten semistructured interviews | Convenience and purposive | Sociocultural theory; discourse analysis The author focuses on a sociological perspective, exploring the way children acquire problems with attention through relationships with others and the classroom environment |
Thematic analysis involving looking for patterns, categorising text, identifying themes, reapplying themes systematically to interviews, evaluating the ability of themes to represent similarities and differences between teachers |
| McMahon 2012263 Australia |
150 | Pre-service teachers | One hundred and fifty open-ended questionnaires; six semistructured interviews; one focus group (four participants) | NR | Constructionism; critical approach; sociocultural theory; Foucauldian discourse analysis The author seeks to represent fairly biomedical, biopsychosocial and sociocultural perspectives |
Thematic analysis was conducted on questionnaires, interview and focus group transcripts. Five themes were identified but the journal article focused on only one of these, that of labelling, because of its unexpected nature (was not probed by questionnaires or interview schedules). The author carried out Foucauldian discourse analysis, comparing transcript discourses with known ADHD discourses in ADHD literature, using Foucault’s rules of discursive formation. The author carried out member checking of her findings |
| Nowacek 2007305 USA |
8 | Four elementary teachers: grades 2, 3, 4 and 6 Four middle school teachers: grades 6–8 (n = 2); grade 8 (n = 2) |
Open-ended question asking for definition of ADHD Eight semistructured interviews Classroom observations |
Purposive | Grounded theory; the authors introduce ADHD through discussion of psychological literature The authors focus on the practical issue of knowledge and implementation of non-pharmacological interventions |
Constant comparative method was employed; data were coded independently; codes were compared and differences negotiated between authors; categories were refined to be mutually exclusive. Categories were then applied to the transcripts to establish frequency and saliency to each participant |
Most authors explicitly described their research methodologies, which included discourse analysis,41,263,265 phenomenology,291,298 grounded theory296,305 and ethnography. 41 Some authors also explicitly discussed the conceptual frameworks that were used to structure studies and/or analysis, including theories from Foucault,41 essentialist epistemology,294 symbolic interactionism and ecological validity,296 and sociocultural theory. 263,265 Two authors were not explicit about their chosen research methodologies or conceptual frameworks. 264,286
Findings review 4b (teacher views)
For review 4b (teacher views), there was no single study appropriate for use as an index paper (for further discussion see Chapter 4, Methods of analysis/synthesis, Data analysis and synthesis, Synthesising translations/creating a line-of-argument). Instead, included study findings were coded inductively and relationships between codes were analysed and refined using concept maps and discussion with RG and DM. Following the data analysis process (for further discussion see Chapter 4, Methods of analysis/synthesis, Data analysis and synthesis), an overarching theme was identified, ‘Factors that influence a teachers’ willingness to adapt response to ADHD symptoms’ with two subthemes: (1) orientation to the class or child; and (2) perceptions of ADHD behaviour (sociological, biological, psychological and maturity). Relationships between first-/second-order concepts and third-order concepts are shown in Table 52.
| First- and second-order themes (inductive/deductive thematic analysis) | Third-order themes (overarching theme: factors that influence a teachers’ willingness to adapt response to ADHD symptoms) | |||||
|---|---|---|---|---|---|---|
| Orientation | Perceptions of ADHD behaviour | |||||
| Class | Child | Sociological | Biological | Psychological | Maturity | |
| Attributions for ADHD symptoms | ✗ | ✗ | ✗ | ✗ | ||
| Child agency | ✗ | ✗ | ✗ | ✗ | ||
| Conceptions of how to handle ADHD symptoms | ✗ | ✗ | ✗ | ✗ | ✗ | |
| Interactions with parents | ✗ | ✗ | ||||
| Knowledge of ADHD | ✗ | ✗ | ✗ | ✗ | ✗ | |
| Role of context in determining problematic behaviour | ✗ | ✗ | ✗ | |||
| Feelings | ✗ | |||||
| Orientation to the class as a whole | ✗ | |||||
| Contributing papers | 263,264,286,291,294,296,298,305,324 | 263–265,286,291,305,324 | 41,264,265,286,291,294,296,298,324 | 263,265,286,291,294 | 263,286,291,296 | 286,291,305,324 |
Overarching theme for review 4b: factors that influence a teacher’s willingness to adapt their response to attention-deficit/hyperactivity disorder symptoms
The overarching theme identified for review 4b was factors that influence a teacher’s willingness to adapt response to ADHD symptoms. The studies suggest that teachers are not always willing to adapt their teaching in response to ADHD symptoms, and through this theme we explore the situations when teachers are willing, when they are not willing and, where possible, why. The first main influence identified was the orientation of the teacher, which was usually to the classroom as a whole but also was occasionally towards the individual child. The second main influence identified was the teachers’ perceptions of the origins of ADHD symptoms, which tended to be sociological, with some teachers expressing biological beliefs. Most teachers did not explicitly discuss psychological origins for ADHD symptoms; however, they implicitly inferred this type of understanding through discussion of the concept of ‘naughtiness’. Finally, some teachers referred to the child’s maturity in explaining ADHD symptoms, and as the discussions of maturity involve sociological, biological and psychological aspects it is discussed separately.
Orientation to the class as a whole and orientation to the individual child
Elementary school teachers in Nowacek and Mamlin’s305 study demonstrated an ‘orientation to the class as a whole’, making decisions about strategies and modifications based on whether or not they impacted curricular content and how much individualisation in planning, pedagogy and resources were involved, with resistance to decisions that benefited one or two children to the cost of the group. Though this theme was only identified for teachers in this particular study, it is relevant to the studies with teachers across papers, with many examples of the perceptions of teachers being guided by this kind of consideration. Teachers also sometimes made classroom adaptations in response to consideration of the individual pupil. They also sometimes described themselves as experiencing dilemma, where an orientation to the pupil would result in negative impact to the classroom, and an orientation to the classroom would result in negative impact to the pupil. Those not responsible for a whole class, such as the study researchers, remedial teachers and pre-service teachers, were often oriented towards the needs of the individual child.
Importantly, one study author, Hong,264 reframed the concern that many teachers expressed over the disruption caused by ADHD symptoms to learning for the whole class as an argument for prioritising effective intervention for such behaviour, as such intervention not only supports learning for children displaying ADHD behaviours, but the learning of the whole class. Conversely, ignoring such behaviour neglects the rights to an education not only of the ADHD child, but the education of all the children in the class. Some of the teachers in Jones’298 study shared similar sentiments:
I know that I am doing an injustice to the other children in the room when I can’t handle these students.
American preschool teacher (pupils aged 3–5 years), p.75298
However, teachers cannot implement effective strategies and interventions for ADHD if they are not aware of them. These findings emphasise the importance of training and support for teachers on approaches to ameliorating ADHD symptoms.
Aspects that linked teachers’ orientation to decisions about support for ADHD were found to involve:
-
greater concern over hyperactive/impulsive than inattentive symptoms
-
stress caused to teachers by hyperactive/impulsive symptoms, and the need for teacher education
-
dilemmas between the whole class and individual child
-
orientation towards the whole class as justification for use of medication
-
orientation towards the individual child.
These will be discussed in sequence below.
Greater concern over hyperactive/impulsive versus inattentive symptoms
Many teachers demonstrated more awareness and/or concern over hyperactive/impulsive type ADHD than inattentive type ADHD, suggesting an orientation to the classroom as a whole rather than orientation towards the individual child. Teachers in Arcia et al. ’s286 study associated ADHD more with disruptive (hyperactive/impulsive) behaviours than inattentive ones, with two different teachers of the opinion that diagnoses of ADHD for two children were inaccurate because the children did not display disruptive behaviour. Kindergarten teachers in Hong’s264 study said that they would not consult with parents about a child’s inattentive behaviour even if it interfered with the child’s learning; they would contact parents only if it interfered with other children’s learning. Most of the teachers in Lee’s study324 took a similar view, explained by one teacher as:
listless children . . . are often overlooked because they’re so quiet.
American elementary school teacher (pupils aged 3–9 years), p. 421324
This demonstrates the priority teachers often express over dynamics and learning at the classroom rather than individual level.
Teachers in Lee’s324 study expressed a sense of pressure owing to accountability for all their pupil’s attainment, where display of ADHD symptoms was experienced as particularly problematic:
Especially in third grade, their learning is so vital because there’s so much pressure with the testing that we have to take. There’s not a lot of time to deal with severe problems. You want everything to flow smoothly so everyone can learn the best that they can and get ready for everything that they need to.
American primary school teacher (pupils aged 3–9 years), 421325
This finding provides another example of the way teachers’ concerns tend to be on learning taking place for the whole classroom, rather than on consideration of the individual child.
Concern over the emotional equilibrium and learning of the whole class
Teachers in a study by Houghton et al. 296 describe feeling stressed by the imposed inclusion of a pupil diagnosed with ADHD in their classrooms because they anticipate behaviour from ADHD pupils that may disrupt the emotional equilibrium of the class, so much so that the authors used the words of the teachers in naming the category of chaos to describe teachers’ experiences with ADHD pupils in the classroom:
They shout or yell in class, scream out the windows, slam their books on their tables, throw pencils and erasers around the room, kick the furniture, turn the chairs or desks over and lash out and hit their classmates.
Australian secondary school teacher (pupils aged 6–17 years), p. 112296
Houghton et al. 296 identified further themes describing teacher responses to the frustrations imposed by having an ADHD child in their classroom, one of which is ‘objecting’ (the vocalisation of a sense of unfairness in being required to teach ADHD pupils, when this was perceived as an unreasonable burden):
Looking after an AD/HD child requires vigilance and a constant monitoring which can be tiring for the teacher . . . [such inclusion] requires modification of work programs which can be difficult in a class of over thirty children.
Australian secondary school teacher (pupils aged 6–17 years) [reviewer’s edits], p. 113296
When teachers perceived the inclusion of an ADHD child in their classroom to be unfair, and their concerns not to be acknowledged and/or addressed by wider school support systems, the teachers not only failed to implement strategies and interventions, but their resentment had the potential to exacerbate the ADHD symptoms of the pupil:
I have had enough of this student. I despise him. He is so demanding and so disruptive that I cannot deal positively with him anymore. I find it really difficult to be nice to him and it has got to the stage where my feelings about him probably contribute to the situation and probably escalate his outbursts.
Australian secondary school teacher, pp. 113–14296
In addition to disrupting the emotional equilibrium of the class, teachers said that ADHD symptoms affected other children in the class, with some imitating inappropriate behaviour and generally reducing respect for teacher control. 264,296 Teachers reported in studies by both Hong264 and Lee324 that ADHD symptoms prevented them from carrying out their main responsibility as teachers by preventing learning for the whole class, whereas the lack of any means to counteract such behaviour left teachers feeling frustrated, helpless and ashamed. Hong264 concluded that teachers employed strategies to deal with ADHD symptoms that worked for typically developing pupils, but did not work for pupils with ADHD because of lack of training, and so were left frustrated in their attempts to respond to ADHD symptoms. This frustration explains the stance many teachers in Hong’s study take, that children with ADHD should be withdrawn from mainstream classrooms and supported by specialist teachers. Until teachers know approaches that are effective in dealing with disruptive behaviour from children with ADHD, it makes sense that they would turn to specialist intervention as a solution to the difficulty.
Authors of a number of included studies concluded that teacher participants lacked knowledge about ADHD and/or strategies to ameliorate ADHD symptoms. 264,286,294,296,305,324 Arcia et al. found that ‘teachers’ understanding of the condition, and of classroom management options, is very limited’ (p. 98). 286 In this study, teachers rarely discussed ADHD symptoms in terms of ADHD partly because they did not feel knowledgeable enough about ADHD as a condition. Instead, they reported numerous strategies that they administered according to their judgement developed through teaching experience. Nowacek and Mamlin305 found that, although teachers understood key symptoms of ADHD, their behaviour management strategies were idiosyncratic sets of modifications developed over years of teaching experience. Lee324 found that, although teachers knew core symptoms of ADHD, they often demonstrated a lack of knowledge about the need for ADHD symptoms to be persistent and pervasive before indicating ADHD. When teachers were asked to make hypothetical attributions for ADHD symptoms described in a vignette,294 a number of teachers refused to make any judgements. Some participants directly refused, whereas others qualified their judgements based on their lack of expertise. The authors suggest that this represents a desire to be accurate and to avoid making judgements about the child that may turn out to be incorrect. Such lack of knowledge may also mean that teachers are unable to distinguish between symptoms of ADHD and those of co-existing conditions such as conduct disorder.
Houghton et al. 296 identified the turning point from teachers who object to the presence of pupils diagnosed with ADHD in their classrooms to acceptance of these pupils in their classrooms, to a change in their understanding of ADHD and knowledge about approaches to managing ADHD symptoms in the classroom. Teachers in this study attributed such gain in knowledge to reading research and continuing professional development. Preschool teachers in Jones’298 study reported that their teacher education had prepared them for typical child development issues, and that they continually drew from this knowledge in their teaching. However, they had not been given information about atypical development, and did not know how to handle pupils displaying disruptive behaviour. Although the teachers sought advice by taking postgraduate degrees and/or consulting experts in the field, they often found such advice removed from the actual experience of teaching large numbers of preschool children while a few of these children disrupted the lesson. Instead, they reported learning most from colleagues working in similar contexts:
They come in. They don’t help. When you are not in the classroom you can’t imagine what it is like to deal with these students.
American preschool teacher (pupils aged 3–5 years), p. 138298
Arcia et al. 286 identified a lack of school-level support for teachers’ management of ADHD symptoms, and teachers’ sense of isolation as a result. Many preschool teachers in Jones’298 study also expressed a sense of isolation, which they attributed to a number of school-level factors which included (1) remote location of preschool classrooms in relation to administrators, which diminished shared management of behavioural problems; (2) lack of support from senior management; (3) perceptions of low status related to preschool compared with grade school; and (4) lack of knowledge by senior management about effective strategies for managing problematic behaviour.
By contrast, all nine schools in Jones’298 study provided teachers with a scheduled time to meet and plan together. The teachers described these interactions as their most effective source of ideas and strategies for dealing with ADHD symptoms. Teachers said that learning from past experiences through reflection and planned, regular discussion with colleagues was the only thing they had to help them deal with children displaying disruptive conduct disorder, oppositional defiant disorder and ADHD symptoms. The middle school teachers in Nowacek and Mamlin’s305 study also described the importance of working as a team in dealing with disruptive behaviours (ADHD-related or unrelated). They regularly (whether scheduled or impromptu) planned and discussed how to deal with specific pupils. They also reported the helpfulness of drawing on expertise from the ‘school wide assistance team’, a group of educational staff created to provide support and information to teachers:
I think that’s been one of the best things that I’ve had a chance to work on . . . You’re dealing with things that teachers have brought to this committee that there’s no simple solution.
American middle school teacher (pupils aged 11–14 years), p. 33305
Teachers in Nowacek and Mamlin’s305 study also discussed issues with pupils’ former teachers or new teachers. One teacher mentioned parents as a helpful resource, and two mentioned the value of workshops and in-service programmes.
A number of authors of included papers recommended that teachers be given additional information about ADHD during teacher education and through continuing professional development, and/or access to specialist teachers. 263,264,296,298,305 The findings from Jones298 and Houghton et al. 296 suggest that structured teacher collaboration that includes reflection and research findings may provide an effective approach to disseminating information about effective use of non-pharmacological interventions.
As well as lacking support from the wider school, teachers also report a lack of support from parents. 264,298,324 Teachers describe parents who blame their teaching for ADHD symptoms,324 who do not care about whether or not their child attains academically at school,264 perceive problem behaviour at school to be the responsibility of the teacher298,324 and dismiss problem behaviour as unimportant.
Dilemmas between the whole class and individual child
Some of the teachers in Hong’s264 study described experiencing a sense of dilemma over a conflict between the needs of the child and the needs of the classroom. They thought that in order to be fair they must treat all the children in the classroom the same; however, because of the repeatedly difficult behaviour of the ADHD pupils, they perceived discipline for every infraction to be counter-productive:
Consistently telling them about what they [shouldn’t] do might lead them not to do anything at all.
Korean primary school teacher (pupils aged 6–12 years) [reviewer’s edits], p. 408264
Different teachers responded differently to this dilemma. One teacher taught classroom peers how to respond to ADHD symptoms so that together they could respond consistently. This demonstrates that it is possible to take the needs of both the individual and the whole class into consideration, as the peers learned strategies for dealing with difficult ADHD behaviours and the pupils diagnosed with or at risk of ADHD were supported more constructively. Other teachers who thought punishing children diagnosed with ADHD in the same manner as peers was inappropriate were perplexed about how to proceed, as these children’s excessive behaviour still required control. A teacher who prioritised the classroom as a whole had the child stay after school so he could give additional support.
Teachers described an additional dilemma over the issue of inclusion or withdrawal. Some teachers in Hong’s264 study reported that children diagnosed with, or at risk of, ADHD often lacked friends, and this was the outcome that was of greatest concern to them. As a result of their concerns about the social isolation of these children, they felt inclusion rather than withdrawal for support was important, so that pupils diagnosed with ADHD had the greatest opportunity to develop social skills. By contrast, preschool teachers in Jones’298 study described the extent to which children diagnosed with ADHD disrupted their classes, requiring teachers to abandon lesson plans, including field trips and the use of some toys. The extent to which peers were prevented from learning and issues of safety meant they suggested that the removal of children displaying ADHD symptoms from the classroom was sometimes preferable.
In Einarsdottir’s291 study, teachers of children of different ages held different perspectives. Playschool teachers argued for the importance of working with the child in context, within their peer group, because this approach enabled the child with ADHD to experience peer interaction, which was what they most needed. First grade teachers thought that children with ADHD symptoms needed to be removed from the classroom for their own learning and the learning of their peers, because learning for both the individual child and their peers was disrupted by their presence. Einarsdottir291 makes sense of this according to responsibilities that first grade teachers had for delivering a more structured, academic curriculum.
Some teachers in Hong’s264 study also expressed a conundrum in their attitudes towards children with ADHD being medicated to treat their behaviour; they said that, when taking medication, they thought children looked depressed, but without it, the child interfered within the classroom, disrupting other children’s learning.
Justification for use of medication
Considerations for the classroom as a whole were implicated in attitudes towards whether or not medicating pupils for ADHD as a means to reduce ADHD symptoms was justified. Teachers in studies by Lee324 and Einarsdottir291 supported use of medication under certain conditions (in pupils over a certain age; depending on severity of symptoms; as a last resort; with careful monitoring) because it meant children can ‘function in a classroom much more effectively [. . .] by not interfering with their own and/or other children’s learning’ (p. 429; reviewer’s edits in parentheses). 324 Similarly, some teachers in Hong’s study264 cited the negative impact of ADHD symptoms on the academic attainment of peers as justifying any perceived risks of medication to pupils with ADHD. However, some of the teachers in Lee’s study324 said pupils’ improved behaviour was reason for opposing medication, dismissing it as an ‘easy way out’.
Orientation towards the individual child
Some classroom teachers described means to support individual children balanced with responsibility to the whole class, but mostly those who discussed the need to prioritise the needs of the individual child were the remedial teachers and authors.
Ljusberg265 argues that children’s agency is reduced when they are diagnosed with ADHD and/or the strategy of placing them in separate classrooms is employed because withdrawal from peers officially establishes a pupil’s deficits; when teachers take additional responsibility for pupils’ learning the children lose this measure of control; the ADHD label and remedial classrooms create low expectations of co-operation from pupils and high expectations of incompetence; and pupils tend to become what is expected of them.
Mid-grade teachers in Nowacek and Mamlin’s305 study understood that both self-acceptance and peer acceptance of ADHD pupils were highly important. Therefore, a concern for the individual child led them to be reluctant to apply strategies within the classroom that singled ADHD pupils out.
Teachers in Lee’s324 study reversed their orientation from the classroom to the individual child when speaking to the child’s parents in order to create a shared goal. These teachers perceived parents to be concerned about their child’s attainment but not their child’s behaviour in the classroom. In an attempt to establish shared goals, the teachers discussed the negative impact the child’s ADHD symptoms had on his or her academic attainment when talking to parents, rather than focusing on problem behaviour and its impact on the learning of the whole class.
Teachers in remedial classrooms seem to orient themselves to the individual needs of the child; for example, unlike classroom teachers who usually only contacted parents when a pupil disrupted their classroom264,265 (suggesting orientation towards the learning of the class as a whole), remedial teachers routinely established relationships of cooperation with parents. 265
Pre-service teachers in McMahon’s263 study expressed concern over assumptions teachers might make once a child has been diagnosed with ADHD:
Many teachers just label them ‘difficult’ and don’t appear to understand the condition – they don’t realise that these kids are not ‘trying to be naughty’ they just can’t help themselves.
Australian pre-service teacher (pupils’ ages unknown), p. 255263
Although this concern for the individual child comes from a pre-service teacher who does not yet have responsibility for a whole class, teachers in Arcia et al. ’s286 study also mentioned a similar concern.
Classroom teachers sometimes expressed concern over the lethargy shown by pupils on medication for ADHD:264,324
[a child who] was usually happy when causing havoc in the class . . . sat feebly dozing off [when on medication].
Korean elementary school teacher (pupils aged 6–12 years) [reviewer’s edits], p. 406264
Additional concerns expressed about medication included:
-
loss of appetite and growth324
-
filling children’s bodies with chemicals324
-
ADHD symptoms caused by other things such as diet, stress, lack of time with parents and poor parenting meant that medication was prescribed inappropriately. 291
Implications of teachers’ orientation to the class as a whole for non-pharmacological interventions are given in Box 22.
Teachers in these studies perceived their primary responsibility to be for the learning of the class as a whole, and ADHD symptoms often interfered with their ability to achieve this goal, at times creating high levels of stress for teachers. Implications for non-pharmacological interventions include:
-
inclusion of information about benefits of any intervention in relation not only to the pupil with ADHD but also to the rest of the class may support teachers’ willingness to implement non-pharmacological interventions
-
effective implementation of non-pharmacological interventions in schools needs to include training for teachers
-
non-pharmacological interventions that are meant to be delivered in the classroom should be evaluated in the classroom; optimal dissemination about non-pharmacological interventions may result from continuing professional development involving teacher collaboration
-
a useful approach to be communicated during training for interventions may be that non-pharmacological interventions targeted at pupils diagnosed with ADHD also support better learning for the whole class because they reduce ADHD symptoms
-
implementation of non-pharmacological interventions is likely to be most effective at the school rather than class level.
Perceptions of attention-deficit/hyperactivity disorder symptoms
The way teachers understood and perceived ADHD symptoms had an impact on whether or not they thought it was appropriate to intervene, either by referring for assessment or by adapting the approaches to discipline and teaching they generally applied within the classroom to better support pupils displaying these symptoms. As was found in review 4a (pupil views) [see Findings for review 4a (pupil views)], factors understood to contribute to ADHD symptoms can be categorised as biological, sociological and psychological factors.
Teachers often held polarised views, where they perceived ADHD symptoms to originate from social or biological factors, rather than understanding the behaviour as an interaction of factors. Although many included studies in review 4 describe a contribution of school-related factors to ADHD symptoms,27,41,260–263,265,266,291,293,296,314,324,331–334,347,356 the sociological factor that teachers tended to refer to was poor parenting. Often, teachers who attributed ADHD symptoms to sociological factors were not willing to adapt their teaching approach to support pupils who displayed this behaviour, because they understood the behaviour to result from poor parenting rather than the school context. This belief could reduce teacher perceptions of their own agency because the teacher could not control the parenting of the pupil. Often, teachers who attributed ADHD symptoms to biological factors were motivated to adapt their teaching to support pupils diagnosed with ADHD, because they believed ADHD symptoms to be out of the pupils’ control, unlike the pupils’ peers, justifying the adaptation. However, some teachers showing biological attributional beliefs did not refer to classroom adaptation but discussed only medication as treatment.
Although there was little discussion of psychological origins for ADHD symptoms, implicitly teachers described such beliefs through the concept of ‘the naughty child’. ‘Naughtiness’ is often attributed to poor parenting, and is therefore conceptualised implicitly as a transaction between sociological and psychological factors.
The understanding that ADHD symptoms are a result of immaturity in relation to peers is usually conceptualised biologically, where maturity is understood to develop with age due to biological and neurological growth. However, sociological and psychological learning was also implicated by one author,324 who argued that use of medication or contingency management programmes prevented, rather than supported, the development of self-control in pupils diagnosed with ADHD. In this case, medication and contingency management are understood to prevent the development of self-control because the pupil is deprived of the opportunity of practising it. This suggests a belief that elements of sociological and psychological factors interact to foster maturity. Because attributions to maturity for ADHD symptoms implicate biological, sociological and psychological factors, it was identified as a separate subtheme. Teachers who attributed ADHD symptoms to immaturity were reluctant to refer a child for assessment of ADHD. The author who argued that emotional self-control had to be developed through practice argued against treatment of ADHD using medication or contingency management.
Sociological factors: perceptions that attention-deficit/hyperactivity disorder symptoms result from difficulties in the home
In Arcia et al. ’s286 study, teachers were asked why children exhibited ADHD symptoms. Most teachers attributed ADHD symptoms to problems in the child’s home, specifically a disruptive family environment; family neglect (e.g. children kept indoors, not having someone at home to talk to, not being read to, education not valued); lack of discipline; single parenthood; an overprotective mother.
In many cases, the reason for the child acting up is a result of bad parenting, not setting limits and allowing the child to get away with it.
Australian secondary school teacher (pupils aged 11–18 years), p. 115296
Many teachers attributed ADHD symptoms to problems in the child’s home life, with examples including:
Sociological factors: impact of belief that attention-deficit/hyperactivity disorder symptoms originate in the home
Teachers in Arcia et al. ’s286 study, despite speaking of children who were known to be diagnosed with ADHD or had ADHD symptoms identified by rating scales, seldom linked children’s behaviour to ADHD. Teachers explained this reluctance in a number of ways, the most common being that they understood ADHD to be a result of home factors. Teachers in Hong’s study264 also mentioned that it is common for people to refuse to understand ADHD symptoms as a disorder. This may also impact perceptions about non-pharmacological interventions; for example, Arcia et al. 286 asked teachers what might really help the child, and most teachers responded with descriptions of improved home life. Specific suggestions included a stable home environment, more reading and less television, a male role-model, family counselling, more discipline at home, extra attention and active parental involvement in teaching and homework, rather than the implementation of non-pharmacological interventions in school. Perceptions that ADHD symptoms originate in problems in the home may also act as a potential barrier to constructive relationships and reduce teacher agency.
The perception that parents were unwilling to support teachers was expressed by Hong. 264 She concludes that Korean families often do not take responsibility for their children’s behaviour in school, because they do not seem to care about whether or not the children achieve their educational goals, or because they understand ADHD symptoms to be typical of all children. Jones298 also reported that teachers felt unsupported by parents of pupils with ADHD who dismissed the behaviours as unimportant or refused to attempt to address the problems with the child at home because they thought the child’s behaviour at school was the teacher’s problem. Thus, not only was it common in included papers for teachers to attribute ADHD behaviour to problems in the home, but some teachers also anticipated that parents would be unwilling to work with them to address difficulties with behaviour in school.
One way that teachers tried to change parenting behaviour was through the distribution of information about ADHD. Teachers in a number of different studies thought that parents would benefit from education about dealing with ADHD symptoms. In response to vignettes given to teachers in Hillman’s294 study, 8 out of 30 teachers hypothesised that they would try to inform parents about various aspects of ADHD, including assessment processes and non-pharmacological interventions such as contingency management. Hong264 concluded that parents could be provided with books or other resources such as community programmes in order to raise awareness of the impact of ADHD symptoms on a pupil’s peer relationships, social adjustments and about how such behaviours disrupt the lives, learning activities and overall educational achievement of other children. It is interesting to consider whether this should be the role of education or health services. Other teachers expressed the need for community support for parenting:
The only thing that is offered to parents is how to work academically with their child. We need parenting classes on behavior [sic] issues.
American preschool teacher (pupils aged 3–5 years), p. 80298
Teachers who gave hypothetical descriptions of contacting parents in Hillman’s294 study using vignettes of children displaying ADHD symptoms sometimes varied according to ethnicity. The author identified that a collaborative style of communication was used more often when contacting parents of Caucasian parents, whereas teachers more often described an approach of ‘gathering information’ when contacting parents of African American children. The author regarded the latter approach as more likely to foster a sense that teachers and parents were in opposition. This finding highlights the potential additional barrier to collaboration that differences in ethnicity between teachers and parents can contribute. This finding also has wider implications in suggesting that, should teachers contact parents having already made negative assumptions about them, for whatever reason, the potential for constructive relationships may be undermined.
Teachers in Lee’s324 study said that usually they eventually developed working relationships with parents, some of which were positive and productive. They identified the times when parents worked co-operatively with them as a key to making progress. Some teachers described situations where their perceptions of a child’s behaviour were different to parents’ perceptions and the problems that this caused. Sometimes a working relationship was not achieved, and in extreme cases parents removed their child from the class:
Well, I can go just right back . . . to this child whose parents withdrew him from my classroom [. . .] he distracted me. And the parents of this child saw him as being more ‘all boy’, that my classroom is too structured. My classroom is not real structured . . . And they also have problems with school culture. These are very educated people. Very educated. And they seem to think that school culture really favours girls . . . They just felt like I was zeroing in on their son, and that I had some axe to grind with him . . . they thought that my expectations were out of line.
American preschool teacher (pupils aged 3–5 years) [reviewer’s edits], p. 428324
In this case, both the teacher and parents make sociological attributions for ADHD behaviour, but these are opposite in context and in beliefs about why the child shows symptoms, with the teacher understanding ADHD to originate in the home and the parents understanding the behaviour to be the result of excessive structure in the classroom. This example describes a situation of negative assumptions from both teacher and parents about each other, as well as the unlikely nature of collaboration when both teacher and parents hold the other responsible for changing the child’s behaviour, rather than seeking to change the behaviour of the child in the context over which they have control.
Perceptions that attention-deficit/hyperactivity disorder symptoms result from other social and cultural factors
Some teachers and/or the authors of included studies attributed ADHD symptoms to social factors other than problems in the home. Some teachers expressed the perception that boys displayed ADHD symptoms more commonly than girls,324 with some attributing this to socialisation but others to genetic influences. 324 Hillman294 asked teachers how they would respond to ADHD symptoms in vignettes that varied by gender and ethnicity. Teachers were more likely to link ADHD symptoms in girls to learning difficulties than ADHD, especially in Caucasian girls compared with African American girls, whereas the same behaviour was more often attributed to ADHD in boys. Hillman294 suggests that as these teacher responses were hypothetical, they are more likely to represent beliefs based on stereotypes than if teachers were interacting with real children and parents. Teachers in this study were more likely to interact with African American parents in a style suggesting opposition than with Caucasian parents (see above). Although this finding is not necessarily applicable to the UK because of cultural differences, a more general interpretation of this finding is likely to be applicable; responses by teachers to parents based on stereotypical assumptions may create additional barriers, for example on the basis of class.
Lee324 asked teachers specifically about their experience of prevalence of ADHD according to ethnicity and socioeconomic status. Some teachers noted differences according to ethnicity, which were often related to the ethnic makeup of schools; teachers noticed higher numbers of pupils diagnosed with ADHD from the ethnic group in the majority. Overall it would appear that teachers may sometimes make assumptions based on stereotypical beliefs about ADHD and issues like ethnicity, gender, poor parenting, and, potentially in a UK context, class. Such assumptions may influence teachers’ response to ADHD symptoms in pupils and/or their relationship with the pupil’s parents. However, this is not necessarily the case:
I think I’m sometimes more self-conscious about [socio-economic status] than other people might be because I’m always looking, ‘Don’t make this assumption just because you think, “They’re black and they’re poor” ‘. I do see a lot of attention problems in my lower income black males. Is that because they watch a lot of TV and they’re unsupervised? I don’t know . . . It’s really hard to know which of the factors are contributing to it.
American elementary school teacher (pupils aged 6–12 years) [reviewer’s edits], p. 426324
This teacher takes care not to make assumptions, as well as showing awareness of the potential complexities of origins for ADHD symptoms.
Some authors of included papers discussed the role that cultural attitudes played in shaping teachers’ perceptions of ADHD. Teachers in Hong’s264 study described a lack of emotional self-control to be the most notable characteristic of children diagnosed with ADHD, rather than hyperactive behaviour. Hong argues264 that this is the result of the high value Korean culture places on being sensitive to others’ emotions and the need to express ones’ own emotions appropriately in order to ‘fit in’; that Korean teachers may have higher levels of tolerance for ‘rambunctious’ behaviour; or that teachers simply lack knowledge about ADHD. Some of the teachers in Lee’s324 study expressed the opinion that differences in societal expectations were expressed in differential diagnoses of ADHD by gender. For example, they surmised that generally permissive attitudes towards boys’ behaviour (‘boys will be boys’) did not prepare boys to be able to meet school expectations for controlled behaviour. Lee324 discusses the teachers’ overall positive response to medication for ADHD – that it allows children to be ‘successful and effectively functioning in school by managing one’s emotion and behaviour, being focused, getting work done, not interfering with one’s own and/or other children’s learning, and becoming a competent student’ – in terms of Western culture which values individual efficiency, productivity, order and predictability. Einarsdottir291 focuses on the cultural contingency of the concept of ADHD to explain the rise in ADHD diagnosis and treatment within Iceland since the late 1990s. Culturally contingent factors include cultural proximity to North America, with many pursuing academic study there, bringing back cultural influences. The author also discusses recent social changes in attitudes to child rearing and education, as well as changes to children’s lives such as less time to play outside, more structure and monitoring by adults and less time spent with parents.
Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms
Although mainstream teachers discuss how they use classroom strategies to manage ADHD symptoms, they do not seem to conceptualise them as originating in classroom structures. Only one study286 specifically asked why children display ADHD symptoms, and teachers in other studies might have attributed this kind of behaviour to classroom structures had they been asked specifically about it. In some schools teachers attributed ADHD symptoms to a child’s lack of knowledge of English,286 which suggests a propensity towards seeing difficulty within individual children rather than seeing the impact of school structure. These teachers taught in schools with large minority populations without bilingual instruction and it could easily be argued that the difficulty was with the school.
Remedial teachers, however, were explicit in naming classroom structure as a contributor to ADHD symptoms, and also mainstream teachers’ lack of expertise, or inability to adapt the classroom:
It can be easier to move the pupil than to move the teacher.
Swedish remedial teacher (pupils aged 9–12 years), p. 202265
Remedial teachers cited obstacles in mainstream classrooms as:
-
insufficient funds
-
unadapted accommodations
-
classes that are too big
-
insufficient educational knowledge
-
negative views on children and inclusion. 265
A number of authors provide second-order concepts related to the contribution of classroom structure to ADHD symptoms. Teachers in Lee’s study324 expressed a sense of pressure owing to accountability for pupils’ attainment, where ADHD symptoms were experienced as particularly problematic. Teachers perceived that during school years when exams were administered they did not have time to deal with difficult behaviour. Lee frames teachers’ acceptance of diagnosis and treatment for ADHD on the basis that it enables a child to be able to function in school, as what Nourot357 calls ‘academic pushdown’, where children are expected not only to master academic skills, but to be capable of behaving in school from the start of their school lives. Lee describes the school context as one where being young (chronologically or behaving young) is ‘not only devalued but is also considered pathological’ (p. 433). 324 Einarsdottir291 draws a similar conclusion based on her finding that more children are diagnosed with ADHD in first grade than playschool. She attributes this to differing classroom expectations, where playschool ‘emphasises play and creative activities, has fewer children in a group, has more adults and possesses a more informal layout and structure, while the first-grade classrooms are more structured with larger groups and fewer adults and often whole-group instruction’. She notes further that changes in school expectations, including ‘school entrance at earlier ages, a longer school day, bigger classes and an earlier emphasis on academics’ may all contribute to greater numbers of children being diagnosed and treated for ADHD.
Bailey and Thomson’s41 study focuses on the contribution of school classroom routines to the identification of ADHD behaviour following Foucauldian theory (Box 23). 358 Bailey was a teaching assistant in the classroom studied and while he was there two children were diagnosed with ADHD. BOX 23 Classroom routines establish ‘correct’ behaviour, and in this study examples of routines included entering and exiting the classroom, ways in which to line up, wash hands, interact with other children, sit, listen, speak, cut with scissors and read a book. Deeply held understanding of the ‘good teacher’ role in the prevention of disruption within the classroom meant that teachers worked hard to enforce such routines through punishment and communication with headteachers, SEN co-ordinators, or parents in response to breaches in behavioural rules. Through these teacher-determined routines, children were taught how to behave in school, and through the performance of these routines children established whether they fell inside or outside the norm. The authors identified these routines as the overarching strategy used for classroom management, where following routine was considered normal and natural.
Description of Foucaldian theory about power, knowledge and surveillance
Two studies included in review 4b, by Bailey and Thompson41 and McMahon,263 follow Foucauldian theory in their data analysis. Foucault defined power not as a thing but as a relation that was exercised at every level of social interaction. Foucauldian theory posits a relationship between power and knowledge, where power impacts what knowledge is accepted or rejected, and relationships between power and knowledge often involve the aim of social control. Foucault analysed institutional power exercised through use of architectural space, timetables and routine in order to regulate people’s behaviour, including the use of multiple approaches to surveillance. Surveillance is a means to collect information through unequal gaze, where the person being surveyed knows they may be watched but do not know when they will be watched. This encourages self-regulation. The information, according to chosen systems of knowledge, is used to maintain power.
The authors categorised routines into eight groups according to their function:
-
surveillance – supervising, closely observing, watching, threatening to watch, avoiding being watched
-
distribution – dividing into parts, arranging, ranking bodies in space
-
segregation – setting up enclosures, partitioning, creating functional sites
-
differentiation – normative classification of ability and difference among individuals or groups (note this use of the word ‘differentiation’ by Bailey and Thompson41 differs from standard use of the word in education to signify the personalisation of learning to the individual learner)
-
self-regulation – regulative practices directed at the self
-
examination – checking, recoding, measuring and displaying ability or progress
-
docility – rendering bodies still and/or silent, invoking passivity
-
legitimating an individual’s authority, routinising an individual’s presence.
We will discuss five of these categories (1, 2–4, 7) because they have particular relevance in relation to other findings in the review.
The function of surveillance was to make visible exceptions to the norm. As an example of surveillance, on his arrival as a teaching assistant, Bailey was given a list of six children who were ‘ones to watch’. These children were often topics of conversation, where teachers and teaching assistants kept each other abreast of breaches in the children’s behaviour. The children were not the only topic of interest; the children’s parents were also discussed:
Christopher [a ‘one to watch’] is the youngest child in the class . . . [the classroom teacher] and I had a chat about him . . . Sarah described Rosa [Christopher’s mother] as ‘carrying a lot of emotional baggage’, saying that she had ‘broken down’ during the meeting. Sarah clearly didn’t think much of her as a parent and thought Christopher was probably spoilt.
English teaching assistant field notes (pupils aged 5–6 years) [reviewer’s edits], p. 21641
The authors note that discussion of poor behaviour by a child and family circumstance were frequently ‘tied together’; this repeats the frequent assumption teachers make in other studies about ADHD symptoms and ‘poor parenting’. The authors also comment that the magnitude of the scrutiny these children were under was likely to increase the amount of problematic behaviour identified regardless of the quality of their behaviour in comparison to peers who were not watched so closely. Thus, the routine of surveillance functions as a process of stigmatisation (see Box 17).
The function of routines of distribution, segregation and differentiation are described as enabling surveillance. Children are distributed according to age and then subject across their school careers, as are teachers. The authors noted that segregation, where a child or group of children were withdrawn from the main group, invoked implicit notions about the children’s ability levels. Differentiation is described as a necessary result of nationally prescribed, normative curricular achievement, where not only are children required to attain certain levels, but also teachers are held accountable for whether or not they get there.
The authors describe docility as the desired outcome of all the other routines. When children do not become docile, they are identified as being outside the norm. This is highly relevant to ADHD symptoms, which are not negative in essence; they are a problem in the classroom. As the authors write, ‘There certainly seems to be nothing inherently productive about the ability to sit still, it may seem an odd skill for teachers to reward for itself’ (p. 225; author italics). 41 Thus, the idea of normal and abnormal is as pertinently social as individual.
Bailey and Thomson41 do not argue that school classroom routines are solely negative, rather they acknowledge their productive, essential nature. However, they also demonstrate the ‘dangerous and damaging’ effect such routines may have for a minority of children. Although routines cannot be abolished, the authors suggest a reorientation of teacher gaze away from the individual child as the problem, to investigation of possibilities for classroom adaptation. This study suggests that the behaviour of teachers follows other socially constructed norms where they are held accountable for keeping order and producing particular levels of achievement in order to meet professional obligations. Psychosocial interventions need to acknowledge these expectations and norms in order to successfully engage teaching staff.
Biological factors
Some teachers in Arcia et al. ’s286 study attributed ADHD symptoms to within-child factors including, for example, brain imbalance, heredity, an innate behaviour pattern or chemical difference, for example lead poisoning. When ADHD symptoms were described in vignettes by Hillman,294 some teachers mentioned ADHD (or other medically orientated disorders, such as ASD) as a possible reason for this behaviour. Remedial classroom teachers in Ljusberg’s265 study, who taught small groups of children who had been withdrawn permanently from mainstream classrooms owing to inattentive behaviour, understood the children to have deficits but also saw the schools as potentially able to compensate for these, thus demonstrating an understanding of an interaction between factors. Pre-service teachers in McMahon’s263 study often described a medical diagnosis of ADHD as though it represented a biological ‘truth’. Similarly, teachers in Einarsdottir’s291 study distinguished ADHD symptoms originating in sociological factors from ADHD symptoms originating in biological factors, where ‘ADHD proper’ only originated from biological factors. As a result, these pre-service263 and mainstream291 teachers perceived a diagnosis of ADHD to mean the child could not control ADHD symptoms, and saw diagnosis as settling the question of whether or not the pupil was ‘just being naughty’. Diagnosis could be understood as a prompt to give a pupil increased amounts of understanding and support, and some linked it to a willingness to adapt their teaching to be appropriate to the child’s needs. Some pre-service teachers in McMahon’s263 study expressed the view that an accurate diagnosis, although it risked stigma for the pupil, was ultimately preferable to no diagnosis because it supported the child’s learning experience by justifying adaptation of teaching approaches.
Commonly, medical diagnosis of ADHD has been synonymous to ‘labelling’ (see Stigma). However, McMahon’s263 study found that pre-service teachers understood diagnosis and labelling as unequivocal; medical diagnosis was an uncontested, neutral, biological ‘truth’, whereas construing a child as having ADHD before medical diagnosis, or making stereotypical assumptions about the child after diagnosis, involved inaccurate or unjust behaviour by a teacher that may result in stigma for the child. The author concludes that pre-service teachers understand ADHD from a medical model and that this belief impacts practice by rendering classroom adaptation and strategies for addressing ADHD symptoms contingent on a medical diagnosis. The author263 recommends pre-service teachers be challenged to reflect on ‘taken-for-granted’ assumptions regarding behaviour disorders, diagnosis and intervention.
This kind of simplistic understanding of ADHD as biologically caused and straightforwardly diagnosed is problematic on a number of grounds discussed elsewhere (see Overarching theme for review 4a: attention-deficit/hyperactivity disorder symptoms as an interaction between biological, sociological and psychological factors) and the interaction between biological, sociological and/or psychological factors is relevant before as well as after diagnosis. The issue of the extent to which a pupil displaying ADHD symptoms is capable of controlling behaviour is not possible to ascertain with any certainty; rather teachers have to make judgements about this based on their knowledge of the pupil. Attribution of too much control may result in excessive and therefore counterproductive correction and/or punishment; attribution of too little control removes agency from the pupil and encourages the pupil to use ADHD as an excuse for poor behaviour. The findings from McMahon suggest that teachers would benefit from preparation for such complexity. 263
Psychological factors
Teachers and authors of included studies rarely specifically referred to psychological factors as contributing to ADHD symptoms, although teachers in Arcia et al. ’s286 study mentioned poor self-esteem as a potential cause. Informally, however, ADHD symptoms are often attributed to psychological factors through the idea of ‘the naughty child’,263,291,296 where the behaviour is understood to be the chosen act of a pupil to ignore behavioural rules, and teachers of preschool-aged children in Einarsdottir’s291 study understood it to be possible to discriminate between ADHD and naughty behaviour according to whether or not the child was able to adapt their behaviour to the expectations of the classroom environment:
Sometimes you suspect that something is wrong, but then it is a mistake. You may think that a child is hyperactive or with attention deficit or something like that, but if you give them time for a few weeks or months, then you see it is okay; they just have to learn and get used to being in school.
Icelandic preschool teacher (pupils aged 2–6 years), p. 388291
This teacher understood that it was possible for ADHD symptoms to be a result of the child not understanding yet what the boundaries for behaviour were; once they understood these boundaries they were able to control their behaviour and, therefore, they did not ‘have ADHD’.
Maturity
Teachers also attribute ADHD symptoms to a lack of maturity, and this acts as a reason not to pursue assessment for ADHD because it is assumed the behaviour is not attributable to ADHD. For example, teachers in Arcia et al. ’s286 study cited immaturity as a reason for such behaviour. Many of the preschool teachers in Einarsdottir’s291 study expressed reluctance to refer a child for assessment of ADHD because they thought it was easy to conflate immaturity with ADHD. In their experience, younger children normally exhibited ADHD symptoms, and some had taught children who outgrew ADHD symptoms. As a result of a similar understanding, teachers in Lee’s324 study working with children aged ≤ 6 years focused on inattentive behaviours when discussing ADHD, whereas teachers working with older children focused on hyperactive/impulsive behaviour. Lee324 concludes that this is because hyperactive/impulsive behaviour is perceived as normal for younger children.
Lee324 further argues, from a maturational perspective, that the use of medication and contingency management interventions to control ADHD symptoms deprives the child of the time and opportunity to develop self-control and self-discipline, making them reliant instead on medication and/or adults to control their behaviour. Lee324 describes the school context as one where being young (chronologically or behaving young) is devalued.
In a slightly different understanding about maturity and ADHD symptoms, middle school teachers in Nowacek and Mamlin’s305 study perceived that they did not need to provide behavioural support to young people diagnosed with ADHD. They understood that by this age (11–14 years) the young people would have learned to control their behaviour. By contrast, the researchers completing classroom observations in this study found that these pupils still displayed inattentive and hyperactive behaviour.
Implications of teacher attributions for ADHD symptoms for non-pharmacological interventions are given in Box 24.
When training teachers to implement non-pharmacological interventions, teachers’ ability to formulate a constructive response to ADHD symptoms would be supported by information about the interaction of biological, sociological and psychological factors.
Sociological Problems with polarised viewsAlthough studies suggest the pertinence of classroom issues to ADHD symptoms, teachers who made sociological attributions often focused on issues in the pupil’s home without discussion of classroom factors. Such beliefs may lead to the perception that behaviour change is contingent on changes in parenting over which a teacher has no control, and may lead a teacher to dismiss the potential for non-pharmacological interventions to ameliorate ADHD symptoms.
Benefits in understanding social contributorsKnowledge of factors in the classroom that contribute to ADHD symptoms may support a teacher’s willingness to engage more deeply with non-pharmacological interventions. Understanding that by changing the classroom they may be able to change ADHD symptoms supports their sense of agency in the face of difficult behaviour.
Biological Problems with polarised viewsTeachers who understand ADHD symptoms to originate in biological factors may refuse to adapt their teaching response to pupils without a diagnosis of ADHD, and may regard the pupil with a diagnosis of ADHD as unable to control his or her behaviour, removing accountability from the pupil. They may also understand medication to be the only relevant response, dismissing non-pharmacological interventions because such interventions do not address biological origins.
Benefits in understanding biological contributorsKnowledge of biological factors that contribute to ADHD symptoms may support a teacher’s willingness to adapt their response to pupils’ ADHD behaviour on the grounds that these pupils are different to peers in the extent to which they can control their behaviour.
Psychological Problems with polarised viewsTeachers who understand ADHD symptoms to be the result of a ‘naughty child’ hold the child accountable for emotional and behavioural control in a similar way to the child’s peers. However, such response holds the pupils accountable for things they may not have control over. This can result in the child developing a spoiled identity and experiencing frustration and anger, and may exacerbate rather than reduce ADHD symptoms.
Benefits in understanding psychological contributorsKnowledge of psychological factors that contribute to ADHD symptoms can clarify that pupils diagnosed with ADHD have self-control, but lose control more easily than peers. This can support teachers to learn triggers for loss of self-control in pupils, which can inform classroom practice. It also justifies teaching coping strategies to pupils in order to support the development of greater self-control. Teachers can make better-informed judgements about the extent to which to hold pupils accountable for their behaviour.
Review 4c: the experiences and perspectives of parents of pupils diagnosed with attention-deficit/hyperactivity disorder
Study characteristics for review 4c (parent views)
A total of six studies reported in seven papers were included in review 4c. 28,262,266,276,356,359,360 Summaries of included papers for review 4c are shown in Table 53. Two studies involved participants from the USA,359,360 two studies involved participants from Canada,266,276 one study involved participants from Australia262 and two studies involved participants from the UK. 266,356 Malacrida’s study included parent participants from both Canada and the UK and is reported in two journal articles. 28,266 When describing information from either study only the earlier publication266 will be cited in order to signify the singular nature of the study.
| First study author and year (n = 6) | Country of participants | Aim | n | Gender (mother/father) | ADHD status of child (diagnosed or at risk) |
|---|---|---|---|---|---|
| Carpenter 2008262 | Australia | To explore mothers’ perceptions of the role of schools in the decision-making process leading to diagnosis and medication | 15 | Mothers | Diagnosed |
| Hibbitts 2010276 | Canada | To explore the experience of a parent when interacting with her children’s schools | 1 | Mothers | Diagnosed |
| Malacrida 200128,266 | Canada and the UK | To investigate what it is like, within two different cultural contexts, to be a mother confronting multiple ‘helping’ professionals while dealing with ADHD; to examine maternal narratives in order to understand the different ways that these mothers perceive educators’ roles in the medicalisation of their children’s behaviour | 34 | Mothers | Diagnosed |
| Margalit 2010359 | USA | To identify stressors, needs, supports and perceptions expressed by mothers of children with LDs and ADHD through their messages on an internet discussion board | 168a | Mothers | Diagnosed |
| Reid 1996360 | USA | To explore the way parents perceive the process they have gone through in obtaining services for their children with ADHD | 20 | Eighteen mothers and two fathers | Diagnosed |
| Watson 2011356 | UK | To analyse the narrative of a mother concerning the events surrounding the diagnosis of ADHD in her son, in particular the part played by the school in this process | 1 | Mothers | Diagnosed |
All the studies explored the school experiences and perceptions of parents of pupils diagnosed with ADHD; because of the nature of the research question for this review, which specifies school experiences, studies that focus on parent experiences of ADHD at home were excluded. Most of the papers were relatively congruent in their findings about the experiences of parents and the relationships with schools that developed following their children’s display of ADHD symptoms, except for Malacrida’s study266 which differed in that it focused on strategies of resistance for mothers. All of the children of the parents in included studies have clinical diagnoses of ADHD.
With the exception of two fathers in Reid et al. ’s360 study, all the parents in included papers are mothers. A number of authors262,266,356 comment on deeply ingrained cultural beliefs that hold mothers accountable for the work of parental nurturing, and that ‘inextricably link’262 the well-being of children to their mothers. Perhaps for this reason research on parenting and ADHD often focuses on mothers, through both purposive sampling by researchers and self-selection by mothers. Although teachers in included studies from review 4b sometimes attributed display of ADHD symptoms to poor parenting by fathers, where fathers are accused of providing violent examples to their children (e.g. see Bailey and Thompson41 and Carpenter and Austin262), ‘parent-blame’ is often a euphemism for ‘mother-blame’. 361 Perhaps this accounts for higher levels of engagement by mothers; for fathers there is not as much at stake. This cultural belief, that mothers are to blame for poor behaviour in their children, is of key importance in the synthesis of findings from the included papers in review 4c. To be clearer in the discussion of findings, we refer to ‘mothers’ or ‘fathers’ rather than ‘parents’.
Study methodologies for review 4c (parent views)
Details of study methods for included papers for review 4c (parent views) are given in Table 54. Three of the six studies collected data through semistructured interviews. 262,266,360 In addition to interviews, one of these studies also conducted focus groups262 and one study administered a questionnaire to collect additional demographic information. 360 Two studies276,356 analysed narratives written by mothers of children diagnosed with ADHD. Hibbitts’ study276 was an auto-narrative and Watson’s study356 was based on a narrative written by a colleague. Finally, data for the study by Margalit et al. 359 were based on 1502 internet messages written by mothers of children diagnosed with ADHD, ADHD and learning disabilities (LDs) or LDs.
| First study author, year and location | Sample size | Sample characteristics | Data collection | Sampling | Theoretical approach/ADHD attributions | Data analysis |
|---|---|---|---|---|---|---|
| Carpenter 2008262 Australia |
15 | Mothers | 45 semistructured interviews One focus group |
Purposive, self-selecting, convenience | Post-structural work of Butler 1997,362 2004363 and Fraser 1997,364 2000,365 2003.366 The authors approach ADHD from a primarily sociological standpoint using educational theory developed by Graham 2006,367 2008368 | A process of narrative enquiry beginning with descriptive coding followed by development and refinement into themes. Use of moral language, metastatements and the logic of narrative were used as sensitising concepts while coding |
| Hibbitts 2010276 Canada |
1 | Mother | 48 vignettes about experiences with her children’s schools written by the author over a 3-month period 3 years later she analysed these for a doctoral thesis |
N/A | Constructionism; phenomenology. The author is not explicit about her beliefs about ADHD. Implicitly she seems to understand her son’s behaviour as internally driven, and not in his complete control; she follows the advice given to her by her son’s doctor, ‘accept him and make the best of your lives’ | Auto-narrative using hermeneutic phenomenology following van Manen 1990,369 2002.370 The process of analysis involved bracketing, selective reading and detailed reading in order to identify themes which were then compared to literature about the parent–school interface in order to validate or discard/develop them. She involved an outsider to provide critical feedback while writing the thesis |
| Malacrida 200128,266 Canada and UK |
34 | Mothers | 34 semistructured interviews | Self-selecting; snowball | Constructionist; Foucauldian; theories of medicalisation.371 The author discusses the contested nature of ADHD, and approaches it from a primarily sociological standpoint | Inductive and deductive analysis; initial coding involved inductive narrative analysis starting with reflexive immersion in the mothers’ narratives and the eventual crystallisation of themes.372 Data were also considered deductively against theories of medicalisation and social control |
| Margalit 2010359 USA |
316 | Mothers of children diagnosed with ADHD (n = 44); ADHD and learning difficulties (n = 124); learning difficulties (n = 148) | 1502 internet messages | Self-selecting | The authors are not explicit about their methodology or theoretical framework, nor do they discuss the nature of ADHD | Content analysis373 of data expressing stress was conducted. Authors independently coded messages from the same 30 participants then met and discussed then agreed the three overarching themes. Inter-rater reliability of initial coding using these overarching codes was 0.97. Subcodes were added and overarching themes refined as analysis proceeded. Qualitative software was used to organise data |
| Reid 1996360 USA |
20 | 18 females and two males | 20 semistructured interviews 20 demographic questionnaires |
Self-selecting then purposive | Grounded theory; the authors are not explicit about any other use of theory. Their approach to ADHD is that it is an accurately established medical condition; for example, teachers who do not accept it as a valid condition are coded as having misconceptions or lack of knowledge. However, they are interested in exploring non-pharmacological interventions so acknowledge environmental influences | Procedures of grounded theory were followed; three interviews were open coded, the coding framework was refined then these were reapplied to the three papers. As the next 12 interviews were coded they applied axial coding, relational and variational sampling. They adapted the interview schedule for the final interviews and purposively selected the participants in response to the findings from the first 15 interviews. Finally, a core category was developed with a tentative conceptual model. Member and professional checking was conducted |
| Watson 2011356 UK |
1 | Mother of a child who is diagnosed with ADHD | One narrative | Purposive | Theories of stigma,322,374 mother blame,374 use of satire to disrupt implicit assumptions.375–377 She approaches ADHD from a primarily sociological perspective | The author does not describe her process of analysis beyond stating that scenes from the narrative were selected concerned with the positioning of the family as deviant by various external agencies; these were then fictionalised using satire following Barone 2007378 and Clough 2002379 |
Most authors explicitly described their research methodology and/or the use of conceptual frameworks to structure their research. Hibbitts276 conducted hermeneutic phenomenology; Reid et al. 360 used a grounded theory approach. Three studies were framed by sociological theory such as feminist theory and the constitution of disorderly behaviour in schools;262 theories of medicalisation and social control28 and theories of stigma and mother blame. 356 Only Margalit et al. 359,380 did not explicate the methodology or theoretical framework employed in their study.
Findings for review 4c (parent views)
For review 4c (parent views), an index paper was chosen as an organising framework because the breadth of themes in the study represented the content of other papers well. The index paper for the parent synthesis is an auto-narrative,276 the doctoral thesis of a parent of an ADHD child describing her experiences of interacting with her children’s schools. She has three children; her middle child has been diagnosed with ADHD and her youngest has been diagnosed with SEN. Some researchers argue that marginalised groups can be further marginalised when represented by researchers ‘outside’ the group;381 the choice of this study as an index paper is an attempt to represent parents’ experiences faithfully. Others have argued that auto-narrative approaches lack objectivity owing to their personal nature. 382 However, we decided that the author had addressed this potential weakness of auto-narrative because the paper represented themes from other parent perspective papers, because the author consulted academic literature about parent–school relationships to validate her emergent themes, because the index paper included a ‘critical outsider’ to critique the author’s analysis as part of the method, and because the author demonstrated reflexive awareness of researcher subjectivity. The process of data analysis followed that described earlier (see Chapter 4, Methods of analysis/synthesis, Data analysis and synthesis). An overarching theme with three subthemes was identified. Relationships between first-/second-order concepts and third-order concepts are shown in Table 55.
| First- and second-order concepts (inductive/deductive thematic analysis) | Third-order concepts (overarching theme: mothers are silenced) | |||
|---|---|---|---|---|
| Dashed expectations | Parent–teacher conflict is the norm | Resistance | ||
| Deferential | Assertive | |||
| Teachers as professionals vs. amateur parents; teacher as critic of parenting skills | ✗ | |||
| Cultural dissonance | ✗ | ✗ | ||
| Weapons of the weak: refuting criticism | ✗ | ✗ | ||
| Silencing | ✗ | ✗ | ✗ | ✗ |
| Expectations | ✗ | |||
| Schools as sites of the origins of ADHD | ✗ | |||
| Contributing papers | 262,266,276 | 262,266,276,356,359,360 | 262,266,356,360 | 262,266,276,356,360 |
Overarching theme for review 4c: mothers are silenced
The overarching theme identified for review 4c (parent views) was mothers are silenced. The index paper276 identified ‘silencing’ – both by others and self-silencing – as a theme. Although the other included papers do not discuss experiences specifically in terms of silencing, the experiences described by mothers and conclusions drawn by researchers are congruent. Silencing is a process involving social and political judgements of what is acceptable and unacceptable. 276 Hibbitts276 analyses the content of the vignettes constituting her auto-narrative, characterising them as passive (silenced; ‘I was told’) or active (empowerment; ‘I told’). Of 64 vignettes, she characterised 41 as primarily passive and 17 as primarily active. Hibbitts describes communication with teachers as:
The schools did do a lot of talking to me and I did little talking back. Most often, I did as I was told.
Canadian mother of a son diagnosed with ADHD, p. 273276
One vignette was almost entirely passive; here, a narrative is described of a meeting which she thought would be with her child’s teacher and was in fact attended by seven other professionals, including the school principal, other teaching professionals and administrative staff. During the meeting she was not asked to share her thoughts while school staff negatively evaluated her child. Following this event she reports feeling ‘humiliated, embarrassed and ashamed’. In her analysis of passive/active vignettes she notes a lack of active vignettes for some time after the team meeting, which she describes as a period of self-silencing. Most of the active vignettes occurred near the end of her children’s school careers, when she reports feeling a ‘renewed strength’.
Silencing is related to societal expectations for mothers. Authors of all the included papers in review 4c (parent views) comment on the way the problem behaviour of their children encouraged judgements about mothers to be made by other adults in their process of making sense of those behaviours. Carpenter and Austin383 describe the historical growth of the myth of ‘ “patriarchal motherhood” . . . incubated in the late part of the 19th century, and hatching fully feathered in the postwar 20th century’; including, most relevantly for studies of ADHD, ‘the measure of a mother is her child’ (p. 660). 383 The authors remark that despite the inappropriateness of these beliefs to 21st century Western culture, their interviews with mothers suggest that these beliefs are still firmly entrenched in both men and women’s value systems. Thus, the stigma of ADHD is not only towards the child, but is also what Goffman322 calls ‘courtesy stigma’ – stigma for those affiliated with someone who is stigmatised. Singh,384 in a social–scientific history of ADHD, demonstrates the linking of boys’ problem behaviour and problem mothers during the development of the psychiatric category of ADHD. Singh361 describes the influence of ‘mother-blame’, where societal blame laid on mothers for their child’s (particularly son’s) poor behaviour means that the acceptance of medication for their children can be perceived as acting as ‘a good mother’ with the promise of alleviating some of this blame. However, Singh361 further argues that, actually, a biological determinist belief of ADHD ‘contains, supports and reconstitutes opportunities for mother-blame’ (p. 1204). 361 The ways that mothers felt stigma from professionals, peers and family for their child’s behaviours formed a focal point for all the parent perspective papers in this review.
Both the discussions of silencing and ‘mother-blame’ above touched on a finding that recurs across the included papers, that of the ‘Catch-22’ nature of the situation faced by mothers of children diagnosed with ADHD. In Joseph Heller’s novel385 of that name, a World War II US army captain named Yossarian grapples with the military rule ‘Catch-22’ specifying that if one is sane, one must engage in combat missions; if one is crazy one does not have to. However, expression of concern over one’s safety was considered sane, so if Yossarian engaged in attempts to avoid combat he was sane – and had to engage in combat. The experiences described by mothers in their relationships with schools were similar in the ‘lose–lose’ nature of the interactions. Regardless of the way that mothers sought support for their children, or the way they interacted with school staff, almost universally they describe experiences of frustration and dismissal.
Three subthemes to the overarching theme ‘Mothers are silenced’ were identified: (1) dashed expectations; (2) parent–teacher conflict is the norm; and (3) resistance. Each will be discussed in turn below.
Dashed expectations
In her auto-narrative, Hibbitts276 identifies expectations as a theme. As university graduates both she and her husband had hopeful but not ambitious expectations for their own children at school. She hoped they would learn to ‘fend for themselves as adults’ and that they would experience the same sort of school experiences she and her husband had. Her hopeful expectations become despair, not because of the nature of her children’s behaviour at school, but because of the schools’ performance in educating them.
Although teachers’ orientation is to the class as a whole (see Orientation to the class as a whole and orientation to the individual child, above), mothers’ orientation is to the well-being, education and socialisation of the individual child. Mothers’ expectations are for their child to be reasonably happy at school. Mothers cite their child’s unhappiness as a primary reason they attempt to intervene at school:
He was very pale, he was very, he was more emotional, he was starting to pull eyelashes, he developed a tick, and I thought he’s obviously stressed. He’s more stressed than he should be . . . and he was saying ‘I would rather be dead then go to school’.
Australian mother of a son diagnosed with ADHD [reviewer’s edits], p. 40262
Malacrida266 argues that the primary impetus for mothers’ work to support their ADHD children in schools was ‘a desire to protect and care for their children’:
I knew that Tom wasn’t a bad boy, because at home I had seen how loving and really how lovely he could be. And as time wore on, I could see that side of him quite simply fading away. It was that hope that I could salvage the good part of him that kept me going.
British mother of a son diagnosed with ADHD, p. 261266
Malacrida266 further argues that women acted to challenge medical, psychiatric and educational professionals because they perceive experiences in school to be important to children’s well-being, as well as considerations such as academic attainment and qualifications, and this motivates them to work hard to improve the situation in school for their children. Thus, mothers had expectations that their child should be happy in school and when this did not happen they worked to change the situation. Singh361 frames mothers’ efforts to support their children with ADHD as an attempt to meet social ideology of ‘the good mother’ characterised by idealised notions of being understanding, protective, wise, selfless and close and harmonious in the relationship with their child.
Implications of mothers’ dashed expectations for their children diagnosed with ADHD for non-pharmacological interventions are given in Box 25.
Education and interventions for parents and teachers to raise awareness about ADHD can include information about the inherent differences in perspectives between mothers and teachers. Mothers are held responsible for the needs of their individual child and teachers are held responsible for the needs of the class as a whole. By drawing attention to the differences in responsibilities between parents and teachers both may be better prepared to accept and respect the others’ views.
Parent–teacher conflict is the norm
In Hibbitts’276 auto-narrative she identifies five ‘lifelines’, teachers who, over the course of her son’s school career, were supportive and helpful to him. She attributes his ability to endure what she characterises as a deeply stressful experience of education (which in fact culminates with him feeling a sense of rage towards school) to these few teachers’ support. Several mothers in Margalit et al. ’s study359 described relationships of trust and a sense of satisfaction and confidence that teachers had supported their children appropriately. Reid et al. 360 describe an episode of constructive teamwork between parents, teachers and other health professionals over transition between schools for a child diagnosed with ADHD. These experiences suggest just how powerful constructive and effective collaboration between teachers, parents, pupils and/or other professionals can be. Constructive relationships, however, between both parents and teachers, and children diagnosed with ADHD and teachers, tend to be described as exceptions to the norm. Potential reasons for difficult relationships drawn from included papers are discussed below, and can be characterised as:
-
only being contacted in response to a problem
-
‘being told’ rather than collaborating
-
feeling criticised
-
cultural dissonance/otherness
-
different notions of disability
-
perceptions that the origin of the problem is in the school.
Only contacted in response to a problem
Hibbitts276 tallies the reasons for being contacted by the school in her auto-narrative; 48 contacts were prompted by problems, two contacts by ‘good news’. Reid et al. 360 characterise school-initiated conversation as being motivated by a child’s negative behaviour. A mother in Malacrida’s266 study said:
Oh, they were always calling from the school. You know: We’ve been having problems in class [. . .] And always it was, ‘Is there something wrong at home?’
Canadian mother of a child diagnosed with ADHD [reviewer’s edits], p. 148266
Therefore, the initiation of the relationship between a parent and teacher may be a result of the problem behaviour of the child, with implicit, explicit or perceived blame of parenting as the reason for the poor behaviour as a subtext.
‘Being told’ rather than collaborating
Hibbitts276 experienced communicating with teachers as ‘being told’ rather than as a two-way conversation. Most of the Canadian mothers in Malacrida’s266 study were advised by teachers to have their children assessed by professionals. Some mothers experienced this as pressure to medicate without a willingness to engage in alternatives:
When I would suggest some strategy to them, they always asked me if I’d thought about putting Mike on medication.
Canadian mother of a child diagnosed with ADHD, p. 68266
Malacrida266 concludes that, although teachers are not qualified to make diagnoses, they wield considerable power to influence assessment and diagnosis. Although British educators did not push for diagnosis of ADHD (as they were adverse to the label) they pushed for psychiatric evaluation of family issues as they perceived poor behaviour to be a sign of a troubled home life. Teachers in both countries exerted pressure for assessment through exclusion, parent–teacher/team meetings, disciplining children ‘unfairly’ or pressing for assessment via telephone calls, classroom visits and school meetings. Reid et al. 360 characterise school-initiated communication about problem behaviour as concluding with the ‘demand’ that parents correct the situation. Watson356 describes the negative home–school relationship in her case study as involving the school’s tendency to interpret any disagreement with teacher’s requests as ‘evidence of familial deviance’. Therefore, interactions between parents and teachers may be ‘one way’ rather than collaborative.
Feeling criticised
Hibbitts276 identified teachers’ constructions of themselves as professionals, and the way they communicated with her as a parent, as the origin of the problems that she and her children experienced with schools. She describes feeling criticised as a parent, including feelings of shame and humiliation in response to teachers’ criticism. In some cases, however, she experienced direct criticism of parenting:
[The headteacher] said that based on [her son’s] behaviour he wondered if there was any discipline in the home at all.
Canadian mother of a son diagnosed with ADHD [reviewer’s edits], p. 153276
At other times the criticism was more indirect, as when a teacher asked one of her other children to make sure she dressed her (ADHD) son in snow pants and gloves, rather than the teacher asking her herself. Thus, explaining that she dressed him that way repeatedly and that he removed snow pants and gloves repeatedly was more difficult. Feeling criticised by others was also described by the mothers in Malacrida’s266 study. Malacrida characterised this with the theme ‘bad children have bad mothers’:
Women who pressed too hard to achieve a diagnosis, or who insisted that there was something that their children needed in order to achieve their full potential, were named by teachers, psychiatrists, psychologists and physicians as over-protective, over-achieving, or simply in denial of their children’s true limits. Women who were reluctant to have yet another assessment or therapy session, or who were loath to medicate their children, were accused of being negligent or in denial of their children’s difficulties.
Researcher, pp. 146–7266
Watson et al. 386 write up a case study of a mother with an ADHD son as a satire because the demands made by the school on the mother ‘invert rationality’:
The paradox of the home–school partnership is apparent here. The school ascribes the label of ‘deviant’ to the mother/family and simultaneously expects the parent [as ‘partner’] to play a policing role. This creates a tension that is impossible to reconcile, producing further deviance: the more the parent protests or cannot fulfill this role . . . the deeper they become mired.
Researcher [reviewer’s edits], p.24386
Malacrida266 concludes that medical and educational professionals were judgemental towards mothers, dismissed their perceptions, and assumed some level of maternal blame, while mothers responded with suspicion and anger. Carpenter and Austin262 describe this relationship as ‘educational disablement’ involving inequitable power relationships where both mother and child are devalued and stigmatised.
Cultural dissonance/otherness
Hibbitts276 identified cultural dissonance as a theme in her self-narrative, in response to the lack of diversity in her children’s schools and the impact this had on them as a family representing a culturally diverse identity. As an itinerant family who repeatedly moved across Canada following her husband’s job in mining management, they experienced variation in local cultures between places in these insular, sometimes rural, communities, for example, in terms of school clothing expectations and knowledge of local songs. Hibbitts attributes a number of the misunderstandings and conflicts between her family and their schools to such cultural dissonance. She remarks that their experience paralleled experiences of marginalisation and other forms of cultural dissonance in the literature, for example, the disadvantage in schools caused to children from ethnic minorities and those who look different and/or are from cultures different from their teachers and peers. Although the reasons for perceptions by school staff that a pupil is ‘different’ may vary according to local context, this can be a reason for misunderstanding between teachers and parents anywhere.
Hibbitts276 further identifies the theme of otherness as contributing to conflict between her family and schools. She distinguishes ‘otherness’ from cultural dissonance because it relates to more personal and private identity characteristics than the family’s differences owing to being newcomers to the area. Two of her three children had identified SEN (one with ADHD), and Hibbitts276 describes four of five of the family as ‘persons of size’. Thus, Hibbitts concludes negative, prejudicial assumptions about her children and family were made in response to these two factors, and exacerbated problems in communication between her and schools. As studies in some cultures link ADHD to obesity,387 this link is discussed in one included paper,27 and obese children are found to be particularly stigmatised at school, by both teachers and peers;388 being overweight may be a pertinent source of additional stigma for some children with ADHD, as may other sources of ‘difference’.
Different notions of disability
All the papers representing a mother’s perspective in this review noted the potential for conflict between mothers and schools owing to different notions of disability. Hibbitts,276 following her psychologist’s advice to ‘accept him as he is and get on with your lives’, understood ADHD as one position on a normal continuum of diversity. Despite school policy celebrating diversity and inclusion, Hibbitts experienced teachers’ approach to ADHD behaviour as ‘conversion to as normal as possible’ and ‘sickness, in need of healing’, suggesting a deficit model where the problem was understood to reside in the pupil. Carpenter and Austin262 conclude that many struggles between mothers and schools have a foundation in the uncertain nature of ADHD, and that despite inclusive policies, schools remain ambivalent about the nature of ADHD and their responsibilities in response to it. Reid et al. 360 echo this conclusion by emphasising the view of school staff to ADHD (‘problem recognition’) as a core theme, which they find to be the foundation for what action is taken following diagnosis, at both individual (teacher) and organisational (school) level. Reid et al. 360 conceptualise the understanding and acceptance of ADHD as a disorder to be the desired context for collaboration between parents and teachers/school, and identify that problems occur when teachers do not. However, Malacrida266 (Canadian mothers) and Watson356 (a UK mother) also document the potential for there to be conflict because the school desires ADHD diagnosis and treatment for a child when the mother does not. Finally, although initially reluctant to risk the stigma associated with a label like ADHD, Carpenter and Austin’s study262 found that mothers turned to diagnosis and medication as a last resort, in an attempt to adapt their child so they become ‘recognisable’ within schools. However, mothers reported that diagnosis did not ameliorate stigma. Such discussions across papers are interesting because of their focus on diagnosis and medication rather than on non-pharmacological strategies and/or interventions as treatment for ADHD.
Perceptions that the origin of the problem is in the school
It was common for mothers to perceive the attendance of their child at school to be the origin of the difficulties. Mothers in Carpenter and Austin’s262 study repeatedly noted the central role of schools in their narratives about ADHD, by describing the school context as the site where the ADHD behaviours first become apparent or where they are least manageable. This is echoed by Canadian mothers in Malacrida’s study,266 for whom their children’s teachers were responsible for initiating the process of diagnosis for most of the mothers. For these children, behaviour was not problematic enough to suggest pathology until they were in school, as is also the case in Watson’s356 case study of a UK family with a child diagnosed with ADHD. Mothers may resent being blamed for behaviour that in their experience originated in the classroom. Malacrida266 analyses interviews with mothers about their ADHD children in both the UK and Canada, with a focus on the power exerted over families by schools. Although the different cultures had quite different approaches to ADHD symptoms, Malacrida found that both exerted power over families, which she describes as a form of social control to secure amenable behaviour from children in schools.
Canadian mothers felt pressure from educational professionals to diagnose and medicate their children for ADHD. Malacrida266 reasons that as expulsion is difficult to bring about and the concept of ADHD was widely accepted and known in Canada, medication for problem behaviour was the obvious choice. In the UK, where concepts of ADHD were not so acceptable or integrated, educators pressured families to seek counselling and turned to exclusion. It was usual for the UK children to have previously been or currently be excluded from school during the study. In the UK, it was more common for mothers to pursue a diagnosis of ADHD, and for schools to refuse ADHD as an invalid syndrome.
Carpenter and Austin262 explore the way that the discourses and practices in schools might constitute the notion of ‘disorderly behaviour’ through use of the category of ADHD, where the school delineates what appropriate and inappropriate behaviour is. There are no consistent boundaries for behaviour that is appropriate; rather, this is decided according to local context and so may be different by classroom, school and area. Watson’s356 narrative analysis illustrates this:
. . . the appointments became routine to discuss and review his intolerable behaviour. Surprisingly we never discussed: violence, fighting, abuse, deceit, dishonesty or any other behaviour I consider unacceptable. We spoke about; not sitting still, walking around class, talking to other children, not finishing set work or homework and [coming to school without a tie].
British mother of a son (aged 9–11 years) diagnosed with ADHD [reviewer’s edits], p. 22356
Carpenter and Austin262 note that the child whose behaviour lies outside whatever the local boundaries might be, and his or her mother, tend to be stigmatised and devalued in the process of addressing the problem behaviours. Thus, parent–teacher conflicts may arise because mothers may perceive that they are receiving blame for issues that are the school’s responsibility.
Implications of information about the reasons for parent–teacher conflicts for non-pharmacological interventions are given in Box 26.
Information about the reasons for parent–teacher conflicts offer pertinent topics for teacher and parent education and training about ADHD. Main points include:
-
Constructive parent–teacher relationships are possible, and, where they occur, are powerful in improving educational experiences for pupils. However, constructive relationships may be the exception rather the norm, so an awareness of the possibility of conflict and strategies to optimise relationships are likely to be beneficial.
-
‘Mother-blame’ and stereotypical assumptions about cultural difference, otherness and disability all involve deeply held, although implicit, ideology, so education on these subjects would benefit from reflective practice.
-
Accounts from mothers emphasised the need for teachers to be educated about the interaction of biological, sociological and psychological aspects of ADHD symptoms to prevent implicit sole blame of parenting.
Resistance
Malacrida266 analyses the power that mothers of children with ADHD may exercise in their dealings with educators and psychiatrists to combat the stigma and surveillance associated with ADHD. Such resistance was shown to evolve over the trajectory of their ADHD ‘journey’, with initial responses characterised as non-confrontational ‘weapons of the weak’389 that are:
Tacit, informal and unwitting [. . .] Particularly in their early encounters with professionals, mothers’ efforts to restate the truth, to draw boundaries around intervention and judgement and to lay claim to services and information on their own terms occurred in an ad hoc way . . . These early resistance strategies typically occurred in an immediate response to breaches in women’s trust in professional knowledge and compassion, or in response to a dawning sense that they and their children were being judged inappropriately.
Researcher [reviewer’s edits], pp. 160–1266
In Hibbitts’ auto-narrative,276 she describes a similar initial phase which was followed by withdrawal as an expression of her hurt and anger. Later, near the end of her children’s school careers, she became more assertive in her resistance. This finding is repeated in Malacrida’s study,266 which found that following considerable conflict, mothers chose to take more public stances such as involving themselves in public advocacy or choosing to home school.
Malacrida266 emphasises the high risk involved with any form of resistance owing to the likelihood that they might be judged as poor mothers; however, mothers perceived a greater risk in inaction as they witnessed their children struggling at school and felt that they must act in order to protect and care for them. The form of resistance chosen was tempered by the fear that any non-compliance on their part might increase difficulties for their children at school by giving professionals more reason to view the family as troubled. Malacrida266 also points out resistance available to mothers was not equivalent; those who took the greatest action – home-schooled, volunteered for school boards or paid for private tuition – had greater levels of financial, intellectual and social capital available.
Ultimately, despite the creativity and resourcefulness shown by the mothers in Malacrida’s266 study in showing resistance, Malacrida266 concludes that the findings complicate post-structural theory which describes power as circulating and accessible to all subjects. Rather, these mothers were limited by the power ‘that is situated in institutions and practices that are able to withstand resistance and wield material power in ways that mothers cannot’. 266 She summarised that despite the great lengths to which mothers went on behalf of their children, professionals showed little appreciation for their efforts.
Following attempts to appear deferential and compliant, mothers in Malacrida’s266 study sometimes began to refuse to co-operate, although usually only after a number of negative parent–teacher interactions. A process of escalating action was also described by Watson,356 Margalit et al. ,359 and Hibbitts. 276
Approaches to resistance identified in included studies are:
-
compliant:
-
assertive
These will be discussed in turn in the following sections.
Compliant
Malacrida266 found that professional blame of mothers for their children’s problems at school was ‘almost universal’ in both sites of her study (Canada and the UK). Mothers combated this by presenting the family as normal, for example:
I just got to the point that I learned to smile and say, ‘No, home life is pretty good these days. Is there something wrong at school?’.
Canadian mother of a child diagnosed with ADHD, p. 148266
Another mother compiled a 50-page document that detailed other families’ difficulties with their children who had ADHD. Thus, she not only demonstrated her family to be numerically normal, she also chose to include other families based on ideas of normality (e.g. married, heterosexual, middle class – ‘respectable’). One approach identified by Carpenter and Austin262 that mothers took to making their child ‘fit’ for school was to frame the child’s behaviour as only slightly different from the norm, to claim ‘sameness’. Examples include suggesting ‘little’ adaptations to otherwise commonplace approaches and suggesting their child’s behaviour was improving even though they privately thought the child’s behaviour was getting worse. Mothers reported that these efforts were mostly ignored. Mothers in Carpenter and Austin’s262 study also attempted to demonstrate their family as normal through volunteering at the school, ‘As people got to know you in the school they gave your child that little bit of extra regard. They realise he comes from a nice family’. 262
‘Bearing witness’ involves the attempt to ‘return the gaze’ of professional scrutiny by keeping meticulous records (e.g. report cards, assessments, information sheets, letters) and by becoming involved in the school. All mothers in Malacrida’s266 study kept careful records to keep track of critical incidents, who said what and what promises were made, and to illuminate discrepancies. By volunteering in their child’s school they were able to understand better how their children were being treated; they were concerned that teachers’ frustrations might be vented on their children. In addition, involvement demonstrated their willingness to co-operate and that their child was supported. However, Malacrida266 found that, despite considerable contributions to the school, school staff did not always respond with consideration and respect.
A number of the mothers in Malacrida’s266 study were involved in ADHD advocacy work at levels beyond their child’s immediate school, with most of them claiming to have reduced their working hours in order to spend more time on advocacy. The mothers report trying to change policy at higher levels not only to support their own children, but to try to help ADHD children who will follow their own in the school system.
Mothers in Malacrida’s266 study took on professional workloads, saying they often spent 2–3 hours per night working with their children on homework owing to the fact that their children did not grasp the materials taught in the day (the average age of the children was 9 years). This commonly involved power struggles that had a negative impact on the mother, child and rest of the family. One mother, whose daughter was assessed to have extremely low IQ, found that when working with her one-to-one at home she seemed to read above what would be expected for her age, and that in fact she seemed to learn well. When she broached this with her daughter’s teacher, she was dismissed. She then spent hours in effect home schooling her daughter after school, to be told at school that she was a pushy mother and in denial about her daughter’s lack of ability. In Watson’s356 narrative analysis of a mother of a boy diagnosed with ADHD, the mother complies with his teacher’s request to police her son’s behaviour, leading to nagging and increased stress at home in what the mother had previously experienced as a ‘private, comparatively happy, family life’.
Following experiences where teachers rejected information about ADHD or their children, women in Malacrida’s266 study adopted the stance of ‘strategic diffidence’, where they learned to introduce information in a non-threatening way, for example by mentioning information already available in the school, like a previous teacher’s report. Parents in Reid et al. 360 also reported that teachers rejected information about ADHD from parents because they appeared to find it threatening.
Assertive
It was common for mothers (and this was also mentioned by one of the fathers in Reid et al. ’s study360) to provide information to teachers about ADHD. 262,266,360 Although parents in Reid et al. ’s360 study noted that teachers contacted them primarily with reference to behavioural problems, parents contacted teachers in order to provide information, either about ADHD or strategies to support the specific needs of their child. Mothers perceived a lack of knowledge and understanding about ADHD in teachers, and they attempted to ‘teach teachers’. Mothers perceived that they ‘educate every teacher every year’ and found this not only arduous but also frustrating, because teachers only rarely were receptive to such information. Reid et al. 360 comment on the lack of institutional-level structures to provide continuity of information as children move up a year, or a school (for linked findings see Processes of collaboration and Resources). Although Canadian teachers in Malacrida’s266 study more often initiated assessment and diagnosis than parents or clinicians, once a child was diagnosed they resisted parent-initiated discussion of implementing non-pharmacological school-based interventions, focusing on medication instead. Malacrida266 remarks on the misconception teachers can have of medication as an end to previous problems; rather, medication is the beginning of a process to support the child to catch up academically and socially on learning he or she missed out on during years of inappropriate behaviour. Some behaviour by teachers did demonstrate a lack of understanding; for example, a teacher wrote on a child’s report that a mother who was implementing a successful contingency management programme at home was spoiling her child by buying ‘him toys to make him behave’. 266 Reid et al. 360 comment that the strategies for ADHD that parents suggested to teachers were in line with those recommended by researchers and specialist practitioners, and suggest that teachers may not have acted on them because (1) lack of teacher education about ADHD; (2) lack of time to implement strategies because of overloading; (3) lack of organisation-level structures; and (4) lack of ownership of ADHD diagnosis and treatment because of its origins in medical diagnosis and treatment.
Malacrida266 suggests a further explanation, that educational professionals hold different perspectives than medical and psychological professionals. Some of the mothers in Malacrida’s266 study also paid outside professionals to come into their children’s schools to give information about ADHD to their child’s teacher, and dubbed this ‘Bringing in the Big Guns’. Malacrida draws a parallel between providing professional information to teachers and what Michel Foucault describes as ‘truth games’, where claims to legitimacy are made through language and general understandings of what is ‘true’. By drawing on professional advice and opinion, mothers were attempting to provide a ‘superior’ truth about ADHD. However, the teachers in the study, although polite to visiting professionals, did not seem to adopt the principles that they were told about. One mother said ‘It’s their choice not to be educated’ when she offered to pay for a visiting specialist and was told, ‘thanks but no thanks’.
When teachers rejected parents’ suggestions or information in Reid et al. ’s study,360 most endured the situation until the following year, hoping the next years’ teacher would be more receptive. However, some took issues to a higher authority by going to the school principal to insist that notice be taken of their input. Parents said this approach was useful in the short term but did not initiate any lasting changes in attitudes or behaviour.
Mothers in Malacrida’s266 study resorted to ‘refusing to play’ by changing to home schooling or moving their children from mainstream to private specialised settings. This action was the culmination of years of ‘efforts at conciliation, education and advocacy’ without rectifying what they perceived to be ‘inadequate and often punitive situations for their children’. One mother describes a change to her understanding of what education is, from being in a classroom learning a curriculum:
[to a] socialisation process that will hopefully keep [my daughter] intact in order for her to become an adult – where diversity is more acceptable.
Canadian mother of a daughter diagnosed with ADHD [author’s edits], p. 160266
Similarly, the mother in Watson’s356 narrative analysis removed her son from mainstream school following escalation of symptoms, where he experienced ‘nightmares, sleepwalking, hypochondria, fear of flying, depression’ and, finally, a serious cutting episode.
Mothers in Malacrida’s266 study described refusing to co-operate when they felt that the well-being of their child was in jeopardy. For example, one mother refused to include her child in parent–teacher meetings despite the school’s policy that children attend, because she anticipated that the meeting would involve negative messages about him. However, parents expressed concern about refusing to co-operate because it promoted lack of teamwork; also, parents expressed concern that refusal to co-operate could be used as confirmation of suspicions that the child’s behaviour originated in family problems. Mothers also were concerned that being branded a ‘bad mother’, an ‘overachieving mother’ or a ‘hostile mother’ would negatively impact treatment of their child at school. Another study that described lack of co-operation was the auto-narrative by Hibbitts,276 where she eventually refused to attend future parent–teacher conferences because they were too ‘demoralising’ and ‘depressing’ (p. 187),276 characterising the message she heard from teachers for all three of her children to be ‘Mrs. Hibbitts, your children are useless and no good’ (p. 156). 276 Watson356 describes a similar situation in her analysis of the parent–school paradox involved with homework and ADHD children, where the school judges the family to be deviant while also demanding them to play a policing role. When the tension created causes parents to protest, or find they cannot fulfil teachers’ expectations, they are simply further implicated in their role as deviant.
Overall, these findings about resistance suggest that ADHD can change the private family into a public space, justifying scrutiny and judgement of family life by schools.
Implications of mothers’ resistance for non-pharmacological interventions are given in Box 27.
The included papers suggest that knowledge about ADHD can be a contested area, with parents and teachers in conflict over its nature. Findings suggest the following might support collaboration between parents and teachers:
-
School policy for managing ADHD symptoms and developing teacher knowledge about ADHD, so that schools can lead the way in establishing common ground.
-
Mothers may start out with intentions to work in positive collaboration with teachers. By respecting mothers’ capacities, teachers could draw on their resources to support the work they both do for the pupil with ADHD.
-
The nature of escalation in resistance means that parent–teacher relationships will be influenced by the prior experiences of the parent.
Review 4d: the school experiences and perceptions of pupils diagnosed with, or at risk of, attention-deficit/hyperactivity disorder, their teachers, parents and peers
Study characteristics for review 4d (mixed views)
A total of seven studies were included in review 4d (mixed views). Summaries of included papers for review 4d are shown in Table 56. These studies analyse interactions between participant types (pupils diagnosed with ADHD, their teachers and/or parents and/or peers) rather than exploring perceptions of one participant type, as was the case for included papers in reviews 4a–c. Four of the included studies involved participants from the USA,293,347,390,391 two studies involved participants from Canada,347,392 one study involved participants from New Zealand290 and one study involved participants from the UK. 260 Rafalovich’s347 study included participants from both the USA and Canada. Each study is represented by a single publication.
| First study author and year (n = 7) | Country of participants | Aim | n | Participant type | Age of pupils (years) | ADHD status of pupils (diagnosed or at risk) |
|---|---|---|---|---|---|---|
| Edwards 2008290 | New Zealand | To identify some effective educational strategies that help the children diagnosed with ADHD in this study learn; to explore how their social experiences may impact their learning | 6 | Children | 6–10 | Diagnosed |
| 7 | Parents | |||||
| 1 | Teacher | |||||
| Guevara 2005390 | USA | To identify system-level problems in the communication and co-ordination of care provided to minority children with ADHD | Exact number not reported; between 42 and 130 participants (4–10 participants in 13 focus groups) | School staff (teaching kindergarten to eighth grade); parents of African American and Latino children; primary care providers,a mental health therapistsa | 5–14 | Diagnosed |
| Hands 2009293 | USA | To investigate what lessons can be learned from an underachieving gifted pupil with ADHD and a non-verbal LD about how education addresses his individual cognitive and affective needs | 1 | Young person | 16 | Diagnosed |
| 1 | Parent | |||||
| 2 | Teachers (English and science) | |||||
| Hughes 2007260 | UK | To identify the type of support required for pupils with ADHD | 14 | Pupils | 7–12 | Diagnosed |
| 14 | Parents | |||||
| 14 | Teachers | |||||
| 9 | Cliniciansa | |||||
| Koro-Ljungberg 2011391 | USA | To increase understanding of existing practices and preferences between parents of students with ADHD and their teachers by describing the shared meanings of effective desirable communication established during parent–teacher focus group interactions | 7 | Parents | 12–16 | At risk |
| 8 | Teacher | |||||
| Rafalovich 2005347 | USA and Canada | To detail how educators conceptualise the nature of ADHD children, including concepts of abilities/disabilities and organisation in response to pupils with ADHD, focusing on the school-based team and the way parents, teachers and clinicians account for their interactions with each other | 25 | Teachers | 6–17 | Diagnosed |
| 30 | Parents | |||||
| 26 | Cliniciansa | |||||
| Shea 2003392 | Canada | To gain insight into the experience of chronic peer victimisation for boys with ADHD | 4 | Young people | 11–13 | Diagnosed |
| 4 | Parents | |||||
| 4 | Teachers |
Four of the studies analyse the relationships between different participant types and what effect this has on support for pupils diagnosed with or at risk of ADHD. 260,347,390,391 Although three of these studies included views of clinicians,260,347,390 only the views of mothers, teachers and pupils will be discussed in full because the review is concerned with experiences of school. One of the studies integrates analysis between perceptions of a pupil diagnosed with ADHD and the perceptions of his teachers and mother with regards to meeting his learning needs in the classroom. 293 Two studies explore relationships between pupils diagnosed with ADHD and their peers from the perspective of pupils diagnosed with ADHD, their teachers and parents. As is common in most of the other included studies that incorporate pupil participants, the pupils have received clinical diagnoses of ADHD,260,290,293,347,390,392 with the exception of the pupils in one study391 where pupils had been scored as ‘high risk’ through school district-based screening. Four studies included multiple perspectives about the same pupil, which allowed a greater depth of analysis about the dynamics between participant types. 260,290,293,392
Numbers, gender and ages of pupils diagnosed with ADHD in review 4d are shown in Table 57. Four of the included studies in review 4d involve pupil participants. 260,290,293,392 Although the pupil participants were mostly of secondary school age in review 4a, the ages of pupils in review 4d were evenly distributed across preschool–primary school (aged 4–11 years) and secondary school (aged 11–18 years). There were more boys than girls among pupil participants in review 4d, as would be expected from the epidemiology of ADHD. Numbers and school year taught for teachers of pupils diagnosed with ADHD in review 4d (mixed views) are shown in Table 57. All of the included studies in review 4d (mixed views) involved teacher participants. The majority of the teachers in additional included studies for review 4d (mixed views) taught secondary school–college pupils (aged 11–18 years). The number and gender of parents of pupils diagnosed with ADHD in review 4d (mixed views) are shown in Table 57.
| First study author and year | Pupils diagnosed or at risk of ADHD | Teachers | Parents | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Sex | Age | n | Number of teachers teaching children aged 3–6 years | Number of teachers teaching children ages 6–11 years | Number of teachers teaching children and young people aged 11–18 years | Number of SEN teachers | n | Gender | ||||
| Female | Male | Preschool–primary (aged 4–11 years) | Secondary–college (aged 11–18 years) | Mother | Father | ||||||||
| Edwards 2008290 | 6 | 2 | 4 | 6 | 0 | 1 | 0 | 0 | 0 | 1 | 7 | 3 | 4 |
| Hands 2009293 | 1 | 0 | 1 | 0 | 1 | 2 | 0 | 0 | 2 | 0 | 1 | 1 | 0 |
| Shea 2003392 | 4 | 0 | 4 | 0 | 4 | 4 | 0 | 0 | 4 | 0 | 4 | 3 | 1 |
| Koro-Ljungberg 2011391 | N/A | 8 | 0 | 0 | 8 | 0 | 7 | 7 | 0 | ||||
| Totalsa | 11 | 2 | 9 | 6 | 5 | 15 | 0 | 0 | 14 | 1 | N/A | ||
| Rafalovich 2005347 | N/A | 25 | 16 teachers teaching pupils aged 6–17 years | 9 | 30 | 21 | 9 | ||||||
| Totalsa | N/A | 40 | 10 | 49 | 35 | 14 | |||||||
| Hughes 2007260 | 14 | 0 | 14 | 14 (aged 7–12 years) | 14 | 14 teachers teaching pupils aged 7–12 | 14 | NR | |||||
| Totalsa | 25 | 2 | 23 | N/A | 54 | 63 | N/A | ||||||
| Guevara 2005390 | N/A | Between 12 and 30 teachers teaching pupils aged 5–14 years | Between 16 and 40 parents of pupils diagnosed with ADHD | ||||||||||
All of the included studies for review 4d (mixed views) involved parent participants; however, one study did not report parent gender262 and one study did not report number or gender. 390 A greater proportion of the parent participants in the included studies for review 4d (mixed views) were fathers than when parent experience was studied alone (review 4c), although the majority were still mothers.
Two studies290,293 are included in both review 3 and review 4d (mixed views) because they contain analysis of perceptions of school strategies and/or interventions as well as experience of ADHD more generally. Therefore, only relevant findings from these studies are reported here. Review 4d reports only the findings about peer relationships290 and the interactions between a pupil diagnosed with ADHD and his teacher;293 for findings about the experiences of strategies and/or interventions from these studies see review 3 (see Chapter 5).
Study methodologies for review 4d (mixed views)
Details of study methods for included papers analysing mixed perspectives in review 4d are given in Table 58. Five of the seven studies collected data through semistructured interviews. 260,290,293,347,392 In addition to interviews, one study used picture cards to better engage pupils with ADHD with the interview questions and asked these pupils to create drawings,290 and one study included classroom observations which were used to prompt explanation for behaviour during semistructured interview with a pupil diagnosed with ADHD. 293 The other two studies collected data through focus groups, one involving only one type of participant in groups (e.g. parents, school staff or clinicians)390 and one mixing types of participants in groups (parents and teachers). 391
| First study author, year and location | Sample size | Sample characteristics | Data collection | Sampling | Theoretical approach/ADHD attributions | Data analysis |
|---|---|---|---|---|---|---|
| Edwards 2008290 New Zealand |
14 | Six children, seven parents and one teacher | 28 interviews (two with each participant) First interview with children: three picture cards used; this was more effective in keeping their attention than questions Second interview with children: picture cards were used alongside all questions. Children also drew pictures Parents: 14 semistructured interviews Teacher: two semistructured interviews |
Reputational | The author is not explicit about theoretical underpinnings of research design and/or analysis. In describing ADHD and giftedness the author draws on psychological literature and describes disability according to the New Zealand Minister of Health’s definition following social model of disability principles | The author conducted narrative and thematic analysis, applying her research questions deductively to the data (relating to effective strategies, ineffective strategies and social experiences). She also looked for unexpected findings. She conducted member checks |
| Guevara 2005390 USA |
NR | Regular and special education kindergarten to Grade 8 teachers Primary care staff (paediatricians and paediatric nurses)a Mental health staff (psychologists and social workers)a Parents of children with ADHD |
13 focus groups of 4–10 participants each were held Two groups with African Americans parents Two groups with Latino parents Three groups of primary care staffa Three groups of mental health therapistsa Three groups of educational staff |
Purposive and then self-selecting | The authors do not explicitly address their research methodology; however, they use RCA originating in patient safety literature as a conceptual framework to classify themes related to causality by technical factors, organisational factors and human factors. The authors do not discuss their orientation towards ADHD | Three researchers coded transcripts, meeting regularly to discuss codes and arrive at a consensus. The agreed themes were then applied to the transcripts by two researchers who used the constant comparative technique to support or refute themes for further development. They then applied RCA, attempting to categorise themes and subthemes within the three categories of technical factors, organisational factors and human factors |
| Hands 2009293 USA |
3 | Two teachers and one pupil | 5.5 hours of classroom observation (three 45-minute observations each for two classrooms) Teachers: two semistructured interviews Pupil: one semistructured interview including asking for explanations of events noted during classroom observation Parent: one semistructured interview |
Reputational | The author is not explicit about methodology, but structures data analysis using theory related to asynchrony393–395 and hope396,397 | The author applied the constant comparative method including immersion in the data, reconfiguration of categories, axial and selective coding. The author completed a matrix recording frequency and establishing triangulation between participants |
| Hughes 2007260 UK |
51 | 14 pupils; 14 parents; 14 teachers and nine cliniciansa | Pupils: 14 semistructured interviews Parents: 14 semistructured interviews Teachers: 14 semistructured interviews Clinicians: nine semistructured interviewsa |
Opportunistic then reputational | The author states a constructionist stance and frames the study with findings from a previous study where ‘despite the need for ADHD to be recognised as a biopsychosocial condition, medical and education domains continue to work in isolation to each other resulting in inconsistent support and professional dominance that undermines children’s individualism and need’ | The author completed case studies of each child by synthesising perceptions of child, teacher and parent. The author coded each transcript for key incidents and issues that impacted on the child, and used these to explore the issues in transcripts from the other participants, then followed the same procedure for teachers and parents. He explored similarities/differences, how issues were managed and the impact of this on each participant. The author chose to report five case studies because they represented dynamics found across the 14 |
| Koro-Ljungberg 2011391 USA |
15 | Seven mothers and eight teachers | Two focus groups: Three mothers/four teachers Four mothers/four teachers |
Purposive | The authors state a constructionist stance and they structure the study using theories and models of parent–teacher communication practice with consideration of structural, psychological and institutional barriers to communication. The authors are not explicit about their orientation towards ADHD, but their discussion focuses on sociological and psychological factors | Data analysis was triangulated and multilayered. The authors conducted domain analysis through open coding then to examine social symbols and social references.398–400 Terms related to communication were grouped into domains (interpersonal, situational, policy and political, purpose) and 26 subdomains. The authors also conducted discourse analysis to explore the communication that took place the focus groups89,339,401,402 |
| Rafalovich 2005347 Canada and USA |
81 | 25 teachers; 30 parents; 26 cliniciansa | Teachers: 25 semistructured interviews Parents: 30 semistructured interviews Clinicians: 26 semistructured interviewsa Face-to-face or by telephone |
Snowball | The study is underpinned by theories of symbolic interactionism and grounded theory and theory about the social construction of deviance403,404 and medicalisation405,406 | Analysis was conducted following grounded theory, with open coding (framed by types of trouble ADHD children encountered and the way adults accounted for the trouble) followed by selective coding (looking for social processes related to medicalisation) |
| Shea 2003392 Canada |
12 | Four pupils; four parents; four teachers | Pupils: four semistructured interviews Parents: four semistructured interviews Teachers: four semistructured interviews |
Purposive; drawn from a larger study | The study design follows grounded theory and defines bullying following Olweus 1993,407 2001.408 The authors are not explicit about their orientation towards ADHD | The authors applied the constant comparative method including open coding (using increasingly complex and inclusive categories), analytical notes (to keep track of conceptual decisions), axial coding (review of categories and notes to refine categories) and selective coding (integration of categories to create the story line). Ethnograph qualitative software was used to organise and manage the data |
Although most authors were not explicit about their research methodologies, most discussed the theory/theories that framed their study design and/or analysis. Methodologies included grounded theory347,392 and discourse analysis,391 with structuring theories including constructionism,260,391 root cause analysis,390 theories of asynchrony and hope,293 theory about the need for integrated attributions about ADHD,260 theories of parent–teacher communication,391 theories of the construction of deviance and medicalisation347 and theories of bullying. 392 One author was not explicit about methodology or theories structuring his study. 290
Findings for review 4d (mixed views)
The studies in review 4d (mixed views) focus on interactions between three groups:
-
parents and teachers347,390,391 (with integration of experiences of pupils diagnosed with ADHD)260
-
a pupil diagnosed with ADHD and his teachers (with integration of perceptions of his mother)293
-
pupils diagnosed with ADHD and their peers (from the perspective of pupils diagnosed with ADHD, their teachers and parents). 290,392
Data analysis followed the process described in Chapter 4 (see Methods of analysis/synthesis, Data analysis and synthesis). Because of differences in foci, there was not one paper that could act as an index paper. However, of the four papers focused on parent–teacher interactions,260,347,390,391 themes from Koro-Ljungberg et al. ’s study391 were used to organise findings from two of the other studies exploring teacher–parent interactions. 260,390 Rafalovich’s347 findings on the way deviance becomes formally constructed through interactions between teachers and parents was not represented by Koro-Ljungberg et al. ’s391 themes and so were framed using Rafalovich’s347 second-order concepts. First- and second-order concepts in the remaining papers were analysed thematically. Third-order concepts were then developed as described in Chapter 4 (see Methods of analysis/synthesis, Data analysis and synthesis, Synthesising translations/creating a line-of-argument), and the foundations for conflict was chosen as an overarching third-order construct. The relationships between first- and second-order concepts and third-order concepts are shown in Table 59.
| First- and second-order concepts (inductive/deductive thematic analysis) | Third-order concepts (overarching theme: foundations for conflict) | |||||
|---|---|---|---|---|---|---|
| Fit between pupils diagnosed with ADHD and school | Orientation to the class vs. the individual | Different funds of knowledge | Processes of collaboration | Accountability | Resources | |
| Interactions between teachers, parents and pupils diagnosed with ADHD | ||||||
| Role of interpersonal context | ✗ | ✗ | ✗ | ✗ | ||
| Role of policy and political context | ✗ | ✗ | ✗ | |||
| Role of situational context | ✗ | ✗ | ||||
| Creation of deviance | ✗ | ✗ | ||||
| Interactions between pupils diagnosed with ADHD and their peers | ||||||
| Factors that make relationships between pupils diagnosed with ADHD and peers difficult | ✗ | |||||
| ‘True’ peers | ✗ | |||||
| Bullying | ✗ | |||||
| Interactions between a pupil diagnosed with ADHD and their teachers | ||||||
| Factors that make relationships between the teachers and the pupil diagnosed with ADHD difficult | ✗ | ✗ | ✗ | ✗ | ||
| Teacher–pupil relationship is key to success | ✗ | ✗ | ||||
| Contributing papers | 290,293,347,392 | 293 | 260,347,391 | 390,391 | 390,391 | 293,390,391 |
Foundations for conflict
The overarching concept identified in review 4d (mixed views) was ‘foundations for conflict’. Six subthemes representing different foundations for conflict were identified:
-
the ‘fit’ between pupils diagnosed with ADHD and school
-
orientation to the class versus orientation to the individual
-
processes of collaboration
-
different funds of knowledge
-
accountability and
-
resources.
The foundations for conflict identified in review 4d (mixed views) represent cultural and structural aspects of the education system which can facilitate interpersonal conflict and the aggravation of ADHD symptoms through the sociological and psychological contributors discussed in review 4a (see Sociological factors and Psychological factors). The issues described by different participant types are similar to those expressed singly in reviews 4a–c; review 4d offers illustrative examples of the way difficulties between pupils diagnosed with ADHD, their teachers, parents and peers arise, with some studies allowing exploration of different viewpoints of the same pupil260,290,293,392 and how ADHD symptoms may be exacerbated. However, there are also illustrative examples of resolution, demonstrating the potential for the amelioration of ADHD symptoms.
Fit between pupils diagnosed with attention-deficit/hyperactivity disorder and school
The included studies in review 4d that explore interactions between pupils diagnosed with ADHD and their teachers and peers find differences between pupils and their peers in terms of learning needs and social skills. 290,293,392 These can be a foundation for conflict between pupils and their teachers and peers. In review 4d differences between classroom expectations and pupil behaviours are conceptualised as an issue of ‘fit’ between the pupils and their classroom and classroom relationships because it is not solely the behaviour of the pupil diagnosed with ADHD, but the interaction between the pupil and the classroom that proves problematic (for further discussion see Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms and Perceptions that the origin of the problem is in the school, above). 41,262,332 Findings from included papers in review 4d suggest that experiences of fit can be powerful in improving pupil behaviour, whereas experiences of disconnection can aggravate problem behaviour and may ultimately create barriers to future experiences of ‘fit’ for the pupil. When ADHD symptoms are perceived to arise solely from differences in the pupil, focus can be drawn away from the contribution made by classroom contexts and relationships. These papers illustrate the production of narrowed aims to create adaptation in the child while neglecting the powerful potential that adaptation to the classroom context and supportive relationships can have in the amelioration of ADHD symptoms.
This section will synthesise findings about the disconnection between pupils diagnosed with ADHD and their peers. Edwards290 and Shea and Wiener392 discuss findings from a case study that describes the potential for different classroom contexts to impact on learning behaviour,293 and then conclude with findings from a study exploring the role of teacher expectations and perceptions in the shift from understanding problematic behaviour as normal to formally identifying it as deviant. 347 These findings provide examples of both fit and disconnection, demonstrating that in certain classroom contexts pupils diagnosed with ADHD are able to cope in a manner acceptable to teachers and pupils. However, experiences of disconnection are prominent.
Shea and Wiener392 conducted a study that focused on peer victimisation of pupils diagnosed with ADHD that involved interviews the teachers and parents of bullied pupils as well as the bullied pupils. 392 They identified the theme of ‘being different’ as both an implicit and an explicit explanation for the common experience described by these boys of being bullied. The authors noted that study participants did not usually blame bullies or the school context for bullying, and specified that descriptions by teachers and parents of these pupils’ social skills deficits were not ‘blaming the victim’. For example, one teacher described a pupil diagnosed with ADHD thus:
Alan’s just different than them, you know, he has a great imagination, and, he, he’s a kind kid and he’s a good kid. He’s just a little bit more spontaneous, and [. . .] his personality is different than most kids, and kids don’t dislike him for being different but they don’t want to be friends with him because he’s just odd.
Canadian teacher of a pupil diagnosed with ADHD (aged 11–13 years) [reviewer’s edits], p. 65392
Studies of pupils with other disabilities have demonstrated that bullying can follow attitudes school staff display towards children. 409,410 Exley332,337,338 (see The role of context in attention-deficit/hyperactivity disorder symptoms, above) also describes bullying as a response by pupils to the way ADHD symptoms are identified as ‘bad’ by school staff, whereby peers then exclude them socially. Although the teacher in the extract above is understanding of Alan rather than accusing, it is still possible that responses to Alan by school staff contribute towards his peers’ response to him. Shea and Wiener392 posit that participants do not comment on bullies or contextual aspects of bullying, but describe it as a response to the nature of the pupil diagnosed with ADHD. However, exclusion based on stigmatised behaviour is implicitly sanctioned within the context in which it occurs, and those who enact it are not usually aware of the social aspects of the process but do ‘blame the victim’. That the four pupils in Shea and Wiener’s study392 are diagnosed with ADHD suggests that their behaviour is different enough from that of their peers to result in diagnosis; however, the stigmatisation of this different behaviour involves a social process in which the school culture is likely to play at least an implicit role.
Shea and Wiener392 identify four subcategories of being different:
-
Emotionally volatile: participants described the pupils as ‘explosive’; ‘volcanic’; ‘meltdown’. These descriptions, including those made by the pupils themselves, are similar to descriptions of a lack of emotional self-control found in other included studies (e.g. see Impulsivity/lack of emotional self-control).
-
Emotionally immature: mothers described their sons as emotionally immature, more interested in playing hide-and-seek, or with cars in the bath, than in the kinds of activities their peers are interested by, such as clothes and sex.
-
Lacking insight: teachers and parents describe the pupils as being unaware of the relationship between their different behaviour and the negative response of their peers:Pupil diagnosed with ADHD (aged 11–13 years), p. 67392
Like if they were kidding I might not yell at them and stuff but I don’t know that.
-
Social skills deficits: the inappropriate behaviour of pupils diagnosed with ADHD act as a barrier to social relationships, further preventing the pupils from developing social skills. They therefore became increasingly isolated with age.
The aspects of difference in pupils diagnosed with ADHD from their peers identified by Shea and Wiener392 are commensurate with descriptions of behaviour by pupils diagnosed with ADHD in other included studies (e.g. see Experience of attention-deficit/hyperactivity disorder, above). We have argued, however, that the bullying described by the authors as being in response to these behaviours is actually a response to the behaviours in the particular contexts of the boys’ schools (see Impact of a disconnect between pupils diagnosed with attention-deficit/hyperactivity disorder and peers: shunning and bullying, below). In other words, it is possible for other school contexts to include pupils displaying similar behaviour without bullying. This can be an important distinction, because without acknowledgement of the interaction between pupil and school, the pupil can be the focus for change rather than foregrounding both pupil and context in seeking resolution.
Hands293 describes the difference between the pupil in her case study and his peers as an ‘all or nothing personality’:
Everything is kicked up a notch, no matter what it is – it’s kicked up a notch. If he’s not going to pay attention, he’s not going to pay attention at all [. . .] or if something’s upsetting to him, to the degree that it would be upsetting to another child, it’s kicked up a notch. It’s just that much more upsetting.
Canadian mother of pupil (diagnosed with ADHD; aged 16 years) [reviewer’s edits], p. 91293
Hands293 does not position this behaviour as solely negative, but instead describes it as both a strength and weakness, where this intensity ‘breathes life’ into mundane situations, but also creates an extremity of emotion from which the pupil can suffer, as well as negatively impacting relationships. Both Hands293 and Edwards290 discuss differences between gifted pupils with ADHD and their peers in terms of the need for pupils diagnosed with ADHD to find ‘true peers’290 or ‘intellectual peers’293 where the pupils benefit from relationships with others who are like-minded. Both studies focus on gifted pupils with ADHD, and so this is in part a reference to the benefit these pupils can experience in interacting with other gifted pupils. The six gifted participants diagnosed with ADHD in Edwards’ study290 were friends with pupils younger than them and older than them, or friends with pupils of the same age who shared common interests (e.g. were gifted). An ‘intellectual peer’ is someone of similar intellect regardless of age, where this similarity provides a stronger basis for friendship than belonging to the same cohort. Edwards290 surmises that participants befriended older friends for reasons in addition to intellect, for example being attracted to boisterousness or the excitement of involvement in different pursuits from those of same-aged pupils. Both Edwards290 and Shea and Wiener392 noted that the pupils diagnosed with ADHD in their studies sometimes befriended younger pupils. The authors suggest that this is because:
-
the pupils diagnosed with ADHD are more emotionally immature (so younger children are true peers emotionally)392
-
they have no same-age friends392
-
they were less likely to be bullied by younger pupils. 392
True peer friendships are an example of an experience of fit for pupils diagnosed with ADHD, where the vicious cycle of social skills deficit compounded by social isolation is broken. Edwards290 linked experience of a true peer friendship to positive impact on both social and academic pursuits for pupils diagnosed with ADHD. The pupils in his study who had experience of a true peer were the ones who were happy to work with peers in groups, whereas those who did not have experience of a true peer were more likely to prefer to work alone. Edwards290 suggests that experience of a true peer friendship supports social interactions with others in general, although he also acknowledges that these may be pupils who already have better social skills, and it is these skills that enable friendship with true peers and positive working relationships with others.
Shea and Wiener392 attribute the peer victimisation of pupils diagnosed with ADHD to the differences between them and their peers identified above. The forms of victimisation identified by the authors include verbal abuse (e.g. name calling and insulting remarks about clothing) as the most common form of victimisation, but boys’ experiences also included physical abuse (pushing, shoving, hitting, having things thrown at them) and shunning (derisory looks and gestures). Much of the behaviour was subtle and covert and therefore difficult to punish. Daniel described his experiences:
[They’re] mean to you and just ‘cause you want to do something they leave you out. Like, I wanted to play a game and they say ‘Ew, Daniel’s here. We don’t want to play with him’.
Canadian young person diagnosed with ADHD (aged 11–13 years) [reviewer’s edits], p. 63392
This passage describes the social isolation the authors identified as a theme, demonstrating the purpose and outcome of bullying. The participants perceived that friends provided protection against bullying, but could not always be relied on:
They kind of stand-up for me . . . sometimes . . . like, ‘Leave him alone!’ Things like that. [But] sometimes he doesn’t . . . he doesn’t want to get bullied or hurt.
Canadian young person diagnosed with ADHD (aged 11–13 years) [author’s edits], p. 69392
This suggests that befriending bullied children may put the befriender at risk of being bullied too. One approach to coping with bullying was to withdraw from the peer group, for example by spending recess helping the teacher instead of being on the playground, where much of the bullying behaviour took place. Bullying, therefore, reinforced any social skills deficits by preventing positive interaction with peers.
The authors identified the theme ‘beaten down’ to represent the emotional and psychological distress that these boys experienced in response to bullying. Aspects of feeling beaten down included stigma, powerlessness and emotional and psychological distress. This study echoed studies in review 4a–c by finding that:
-
the development of a reputation for being disliked can legitimise future victimising behaviour by peers regardless of the future behaviour of the disliked child (see Agency)
-
the victimised boys described being punished for attempts to stand up for themselves
-
there can be a process where pupils diagnosed with ADHD begin by being bullied and then become bullies.
Hands’293 case study of one 16-year-old pupil diagnosed with ADHD, who was also gifted despite mild non-verbal LDs, provided an example of differences in pupil behaviour in response to a changed school context with a focus on difficulties related to learning, rather than the more common focus in included studies of difficulties with behaviour. Hands293 interviewed current teachers chosen by the pupil to represent a class in which he currently felt successful and one in which he currently struggled. He attended two schools: in the morning a ‘magnet’ school involving an accelerated curriculum, and in the afternoon a mainstream high school. The pupil chose his biology class at the ‘magnet’ school as the class in which he felt successful, and his mainstream high school honours English class as the class in which he felt he was struggling. Notably, his attainment was similar in both classes; he was failing the English class and nearly failing the biology class. However, Hands293 noted a marked difference in the pupil’s behaviour based on classroom observations in the two classes, where she characterised his behaviour as:
-
high-school English class: disengaged, rarely contributed to class discussion, isolated from peers and often left the classroom without reason
-
magnet school biology class: engaged with both peers and adults, laughed and made jokes, made valuable contributions to classroom discussion.
Hands293 described the pupils’ history of academic and behavioural difficulties established in elementary school, and suggests that the pupil had created barriers in response to previous punitive treatment that would take time to overcome in the magnet school, even though his biology teacher was committed to supporting his learning needs.
Rafalovich347 examined the process by which interactions between parents, teachers and clinicians transform children’s troubles into formalised types of deviance. He describes deviance according to sociological theory,403 which asserts that deviance is not recognised through intrinsic behavioural characteristics but through the way people respond to the behaviour. Rafalovich347 further explores the role of educational staff in medicalisation (see Box 11). He links Goffman’s322 discussion of informal and formal labelling (for further discussion see Stigma) to the process where behavioural trouble is normalised (Rafalovich347 calls this ‘personal trouble’), to a shift in social response where it is publicly acknowledged as deviant by experts (Rafalovich347 calls this ‘relational trouble’ because of the interaction between stakeholders that render this response). The author’s interest is focused on the key part that educational staff, as non-experts in medicine, play in this transformation, and the resistance that parents sometimes bring to the process. This study, therefore, focused on the role of schools in establishing when a pupil’s behaviour becomes a reason for clinical assessment.
Rafalovich347 notes that participants reported that concern over ADHD symptoms was often first expressed at a time when academic expectations increased, usually during or after second grade (aged 7–8 years) (for a similar discussion see findings from Einarsdottir, p. 312,291 although this referred to transition from playschool to first grade, when children were aged 6–7 years). Before this, poor performance is normalised, then if it persists general remedial efforts will be applied. If these do not succeed more formalised approaches ensue, including conferences with parents, additional academic assistance and lowered academic expectations. What is initially explained as a normal aspect of immaturity becomes a concern with time, as peers begin to perform in academically superior ways. Rafalovich347 gives as an example of the shift from informal to formal the characterisation of the behaviour as a ‘phase’, to the characterisation of the behaviour as a ‘symptom’. 347
Parents and teachers in Rafalovich’s347 study describe pupils diagnosed with ADHD as easily antagonised by others, and attribute this to difficulty in interpreting social cues. 347 This description of heightened irritability, often resulting in emotional outbursts, is in line with the experiences pupils describe themselves (e.g. see p. 260), as well as the findings from Shea and Wiener392 and Hands293 (see Impact of a disconnect between pupils diagnosed with attention-deficit/hyperactivity disorder and peers: shunning and bullying, above). Rafalovich347 finds that parents and teachers move from the evaluation of such responses as normal, to responding to them with heightened concern, when:
-
they are unprovoked
-
they are recurring, and
-
intervention by adults does not quickly resolve the behaviour. 347
The author suggests that medical explanations are invoked more quickly by displays of violence than by academic struggles, where parents and teachers perceive that behaving according to expectations is beyond the pupil’s capacity:
They get just plain crazy, but you take a step back and you can see something is wrong there. They don’t realize what they’re doing.
North American teacher of pupils diagnosed with ADHD (aged 7–8 years), p. 34347
However, as already discussed by other studies in the review,293,392 such aggravated behaviour is also linked to long-term experiences of frustration related to difficulties with relationships and learning in the classroom.
Unlike many of the teachers in review 4b (teacher views), who tended to attribute ADHD symptoms to poor parenting (see Sociological factors: perceptions that attention-deficit/hyperactivity disorder symptoms result from difficulties in the home), Rafalovich347 characterised attributions for ADHD symptoms by teachers in his study as polarised biological, where the symptoms are understood to result from neurological factors. Rafalovich347 identified a turning point to be the school-based team meeting, where current and previous teachers of the pupil, a school psychologist and/or the school principal might meet, in addition to parents, to discuss academic and behavioural difficulties of a pupil with inference about the cause of these difficulties. Rafalovich347 noted that such meetings often signalled a shift from educational staff in understanding difficulties as personal (normalised; a phase) to relational (formally identified as deviant), and, because of attributional beliefs, had the effect of narrowing treatment strategies to a focus on medication. One mother in his study described such a meeting:
I thought we would be able to have a conversation about what was going on, but there was none of that. The school had already made up their minds and it was this cut-and-dried thing. So, there I am trying to defend my daughter and they didn’t even want to listen. I felt very frustrated by the way they approached this . . . People were trying to put her into a nice neat box. But no one was acknowledging what a good kid she was. She gets along very well with other kids. She doesn’t have any of the social problems a lot of other kids have . . . Another thing that kept nagging at me was why they never gave her any other options for her school lessons. They try to cookie-cutter the kids all the same. She has lots of things that she is very capable of, but they never took the time to try and help her with some of those.
North American mother of a child diagnosed with ADHD (aged 6–17 years), p. 37347
Thus, the mother thought that the school had come to conclusions about her daughter before the meeting and she experienced her perceptions about her daughter, which included positive, normalising interpretations, as being dismissed (for other similar examples see Different notions of disability and Perceptions that the origin of the problem is in the school). Rather than understanding her child as having ADHD, she thought the school had not met her child’s educational needs adequately. Nonetheless, the child was referred to a clinician and diagnosed with ADHD, and prescribed a small dose of Ritalin.
Rafalovich’s347 study has similar findings to a number of other papers in review 4,27,41,293,332,356 that problematic behaviour associated with ADHD is not solely a result of neurological differences in the child, but a result of the interaction between the child and the perceptions of educational staff in a specific context.
In conclusion, differences in learning needs and social skills between pupils diagnosed with ADHD and their peers at school can be a foundation for conflict between these pupils and their teachers and peers. However, this is an interaction between pupil differences and the school context and experiences of fit can be powerful in improving pupil behaviour, whereas experiences of disconnection can aggravate problem behaviour. When ADHD symptoms are perceived to arise solely from differences in the pupil, focus can be drawn away from the contribution made by classroom contexts and relationships. This may result in narrowed aims to produce adaptation in the child while neglecting the powerful potential that the adaptation to the classroom context and supportive relationships can have in ameliorating ADHD symptoms. For a related discussion, see Sociological factors: perceptions that attention-deficit/hyperactivity disorder symptoms result from difficulties in the home and Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms.
Implications of the disconnection between pupils diagnosed with ADHD and school for non-pharmacological interventions are given in Box 28.
Included studies suggest that the relationship between a pupil with ADHD and the classroom, rather than the pupil only, create situations of ‘fit’ or ‘disconnect’, where ADHD symptoms are more problematic in situations of disconnect. Interventions that seek to adapt both classroom elements – for example the pupil–teacher relationship and classroom structure and ethos – as well as the pupil, therefore, all have the potential to improve behaviour.
Teacher education could include:
-
information about the contribution of the classroom and the pupil to ADHD symptoms
-
caution about the ease with which focus can rest with the pupil to the exclusion of classroom considerations, including the role of stigma in focusing blame on the pupil
-
information about the role of past experiences in contributing to behaviour, where pupils may become disillusioned through negative past experiences and so the establishment of constructive relationships can take time.
Orientation to the class versus the individual
Hands’ case study293 gives a detailed description of the manner in which teachers’ orientation to the class as a whole can act as a foundation for conflict between the teacher and the pupil diagnosed with ADHD. In this study, teachers’ unwillingness to meet the learning needs of a pupil who is academically gifted leads him initially to rage and aggravated behaviour and then eventually to passivity and internalised behaviour.
The pupil’s English teacher links his lack of concern over the pupil, ‘I don’t really worry about him too much. His behaviour is fine’ (p. 124),293 to the teacher’s orientation to the class as a whole:
. . . by him not handing in his work, it doesn’t really – believe me, I sleep very soundly at night. It’s no problem, you know what I mean? I have other things to deal with and I have other kids that I have responsibilities for – all these other kids too, so I’m worried about them getting their work in. But unless it just gets out of hand and he hasn’t handed anything in in a month or something, then we just can deal with it and I deal with it. We just go on to the next day.
American English teacher of young person (diagnosed with ADHD, aged 16 years), pp. 125–6293
Thus, the English teacher describes his level of concern over the pupil in relation to teaching the whole class, where concern over schoolwork is triggered at a certain point – ‘unless it just gets out of hand’ – and this point is determined by the balance of the pupil’s work in relationship to his classroom peers. The biology teacher expresses a related consideration when she talks about this pupil’s curiosity during lessons:
. . . the way in which he asks questions. There is a difference. He will go very quickly to a very high level place with his questions, which is excellent. Very good, you know. Sometimes I have to tell the young man that, ‘This is great, but we have to stop. It’s not part of the curriculum,’ and I did observe that he would get frustrated at times and it made me feel bad but I also have to think of the class as a whole.
American biology teacher of young person (diagnosed with ADHD, aged 16 years), p. 105293
Thus, his biology teacher respects his curiosity, even feels bad that she might stifle it; nonetheless, she has to meet her responsibility to the whole class first. However, for this pupil, who is academically gifted, the issue of whether or not he is learning something in class is deeply important to him. Hands293 attributes the pupil’s problem behaviour in late elementary and middle school years to rage over his frustrating inability to meet school expectations, where he lacked intellectual challenge but at the same time lacked the self-control to produce the work assigned to him. For example, in his fifth grade class weekly spelling words were learned by completing different daily tasks Monday to Thursday, with the spelling test on Friday. His mother describes how he knew the meanings and spellings of the words by Monday night and resisted the repetitive work that followed. As punishment for other problematic behaviour, he was asked to write his teacher an apology. He combined this task with his homework requiring him to use each spelling word in a sentence. His letter of apology read:
Dear Mrs. [teacher’s name], I’m so sorry to have protruded into your classroom. I should have camophlaged my carcass so as not to have been seen. It would have been much nicer to have basked in your glory than to have felt your wrath. Gratefully, not. Your student, [pupil’s name].
American child (diagnosed with ADHD, when in fifth grade, age 10–11 years) [reviewer’s edits], p. 120293
His mother reports that the school wanted to suspend her son in response to this letter, understanding it as insolence, whereas his mother understood it as a creative response to the tasks that faced him. His mother describes the destructive nature of this event, where the school perceived her to be supportive of her son’s misbehaviour, and she perceived school staff to be uncompromising and incapable of understanding her son. Hands293 characterises this time in this pupil’s school career as a point of rage, because he is actively expressing his frustration at not being able to succeed academically, whereas during the time of the study, approximately 6 years later, Hands293 characterises him as being in a phase of despair, where he is passively facing the sense that his goal of academic achievement is insurmountable. This is communicated by the pupil when he says about his underachievement:
I never tried to hold this kind of thing over a teacher and say that it’s his fault or her fault because a student is failing, and I think I hold this over myself. It’s never their fault that I’m not able to stay up to their curriculum and they shouldn’t have to make changes. The student who’s failing has to make the changes because he’s not doing what everybody else can.
American young person (diagnosed with ADHD, aged 16 years), p. 130293
This intimates the extent of his change from rage to internalisation and passivity. However, his mother does not express the same view:
It’s very frustrating to hear the teachers, and every one of them, at public high school and the [magnet school], has said to me, almost verbatim, ‘This child is brilliant. He is so much more knowledgeable and smarter than we can tell you . . .’ and I say . . . ‘but he’s getting an F in your class’. ‘Well that’s because he doesn’t do this, that and the other thing’. ‘But you have a report from a doctor who tells you he can’t do what you want him to do’. ‘Well, he still has an F’. And I want to say to these teachers, ‘You cannot say to a mother what you’re saying to me and then give my child an F, without you getting an F, because somewhere, somebody dropped the ball and I don’t think it’s him’.
Mother of son (diagnosed with ADHD, aged 16 years) [reviewer’s edits], pp. 185–6293
The author describes this exchange as a conflict between the needs of an individual pupil and the system-level expectations of the school. The pupil’s eventual acquiescence to the greater value of the curriculum over his own desire for learning and learning needs can be interpreted as the indication of a power imbalance between pupils (and their parents) and established educational systems. This analysis links the issue discussed first in review 4d, that of pupil fit and disconnection (see The potential for different classroom contexts to impact learning behaviour and The role of teacher expectations and perceptions in the shift from understanding problematic behaviour as normal to formally identifying it as deviant), to the responsibilities of teachers to the needs of most children in priority over the needs of an individual child.
Although the issue of the need for challenge may be particularly relevant to pupils who are academically gifted, this case study was valuable because it focused on difficulties with learning rather than behaviour. That it identified a number of issues identified in other studies, for example it found relationships with teachers as key (for other discussion see Relationships and Parent–teacher conflict is the norm), described a process of rage that developed over the time of his school career in response to stress (for related discussion see Relationships, Concern over the emotional equilibrium and learning of the whole class and Assertive) and discussed the importance of the content of what pupils are learning (for similar discussion see The role of context in attention-deficit/hyperactivity disorder symptoms), suggests that these experiences may be at least partly applicable to pupils diagnosed with ADHD who are not academically gifted.
Implications of teachers’ orientation to the class as a whole for non-pharmacological interventions are given in Box 29.
Teachers’ orientation to the class as a whole can prevent them from adequately addressing a single pupil’s learning needs. Particularly for more academically able children, this can exacerbate ADHD symptoms, and/or lead to internalisation of stigma.
Different funds of knowledge
Three studies refer to differences in understanding ADHD as a foundation for conflict between pupils diagnosed with ADHD, their teachers and parents. 260,347,391 Koro-Ljungberg et al. 391 link this to a concept called funds of knowledge (Box 30). Parents and teachers agreed that ‘stigma, disbelief and ignorance’ were common in relation to ADHD. 391 One mother commented:
You still have teachers who think [that attention-deficit disorder] and ADHD is some kind of made-up thing . . . They have to be transformed into believers that it is real and just like autism.
Mother of a young person diagnosed or at risk of ADHD (aged 12–16 years) [author edits], p. 56391
Funds of knowledge refer to historical and culturally situated forms of knowledge and/or skills used for functioning in social groups. Examples Koro-Ljungberg et al. 391 give related to ADHD include conceptions and misconceptions about ADHD, teacher experience and training, knowledge claims, and disagreements between parents and teachers. The potential for differences in professional knowledge between groups is discussed in a similar fashion by Malacrida266 (see Different notions of disability).
Rafalovich347 also notes the disputed nature of the ‘definition and solution for a relational trouble’; some clinicians in his study remarked that teachers could overstep professional boundaries by suggesting a child probably has ADHD to parents. Some clinicians suggested that teachers were avoiding professional responsibilities, because they ‘unjustifiably attribute children’s troubles to behaviour disorders rather than to the environment that causes or exacerbates them’. For further discussion see Biological factors, and also Concern over the emotional equilibrium and learning of the whole class for a discussion of the limited training and resources teachers may face. If options such as exclusion are not available, medication may be the most realistic choice for teachers in such a situation. This issue of the disputed nature of ADHD has occurred repeatedly across included papers (e.g. see Perceptions that attention-deficit/hyperactivity disorder symptoms result from other social and cultural factors and Different notions of disability). However, positions and attitudes can shift within and across participant type. In Rafalovich’s347 study with US and Canadian participants the teachers press for a diagnosis of ADHD, with reluctance to diagnosis and/or medication sometimes expressed by parents [for a similar example from review 4c involving UK participants, see Chapter 6, Review 4c: the experiences and perspectives of parents of pupils diagnosed with attention-deficit/hyperactivity disorder, Findings for review 4c (parent views), Different notions of disability]. For other UK participants,266 parents desire a diagnosis of ADHD whereas professionals resist (see ‘Being told’ rather than collaborating). Differences in attribution vary across and within participant types, with both teachers and parents tending to take polarised biological, psychological or sociological stances. As each stance results in differences in opinion about effective intervention, it is not surprising that conflict between stakeholders is the norm.
Hughes’ study260 involves 14 case studies that focus on the impact that different perceptions of ADHD (parent, teacher, pupil) can have on a child’s support in school. These can be understood as conflict between funds of knowledge. The following extracts that involve four young people and their teachers and parents illustrate four examples of conflicts in understanding.
Case study 1:
I get the impression that he can’t be bothered. It’s a lot of laziness. I think a lot of laziness. It’s, all, ‘I don’t want to do it. I can’t be bothered with it’.
Mother of child (diagnosed with ADHD, aged 7–11 years), p. 73260
The only reason he stands out from the others in the class is because he worries so much about what other people think of him.
Teacher of child (diagnosed with ADHD, aged 7–11 years), p. 73260
Some people beat me up. It’s been happening in school. A couple of days ago, every time I went outside all these boys jumped on me and started beating me up and said ‘We’ll be back to beat you up later’, and then they pretend to go, but they’re hiding behind the wall and I think, they’re gone, so I go outside and then they jump on me. I cry, sometimes on my own. My mum says that I sometimes act stupid and that’s why they tease me, but to me I’m not acting stupid, I don’t think it’s stupid.
British child (diagnosed with ADHD; aged 7–11 years), p. 73260
This pupil’s teacher and mother both believe that he is responsible for his own difficulties: his mother thinking he is lazy, and his teacher understanding his social insecurity to be the problem. They do not consider the influences of social factors on his behaviour. The author further describes that the pupil is anxious over his disability but afraid of being reprimanded, leaving him feeling isolated and let down. Without social and self-management skills to draw on, he is left open to bullying and academic difficulty. The author concludes that this case demonstrates the importance of support being available in a child’s school and home environment and the benefits that might be realised if social/emotional and/or self-management interventions were to be offered.
Case study 2:
My husband will not accept that he’s not just a naughty child and we have terrible weekends, because he believes he just needs a good smack and [my son] immediately picks up on this and reacts. His outbursts can last two hours, we have to restrain him, and when it’s over he slumps and he’ll say, ‘I’m sorry Mummy’, and he’ll put his arms round me and he’ll sob, he’ll sob his heart out.
Mother of child (diagnosed with ADHD, aged 7–11 years) [reviewer’s edits], p. 75260
You know, it is very much, ‘I have moods and tough, you’ve to put up with me’. I believe there is some element of reinforcement from home, that such things are accepted. Obviously at school you try and encourage the children to become part of the ‘norm’ system and to produce behaviour which is acceptable rather than accepting unacceptable behaviour. [The pupil] knows exactly what he is doing: he wants attention.
Teacher of child (diagnosed with ADHD, aged 7–11 years) [reviewer’s edits], p. 75260
I take my medication so I don’t get very hyper. So I don’t get to hit anyone in the class because if I do I get in bother. Medication makes it go away because it’s me temper – it just comes up. Don’t know why, sweeties and that.
British child (diagnosed with ADHD; aged 7–11 years), p. 76260
The author describes the inconsistency in response over the pupils’ home behaviour as reducing his confidence and emotional security. Because the pupil’s teacher believes his problematic behaviour is attributable to poor parenting and that he is seeking attention, she ignores the behaviour. The author concludes this is unfair punishment because the child does not understand why his teacher is ignoring him, and he may be incapable of controlling this behaviour. The inconsistency in response to his behaviour from his parents and teacher exacerbates his ADHD symptoms, and the child is left feeling that medication is the only form of support.
Case study 3:
I worried when he first took them. He has had chest pains last month, [and] the doctor gave him a scan. Now they didn’t think it was related to tablets, but he has pins and needles in his feet and that’s a problem, and he’s lost weight. Since he lost weight he’s got paranoid about his bones, I mean his bones seem to be like sticking out . . . I’ve explained and I’ve said that ‘these tablets will make you lose weight but they are to make you good, do you want to be good?’ and he said ‘Yeah’. . . He doesn’t like to be embarrassed. . . And this is what is happening at school, when his teacher was calling him out to take his medication, that would make him angry, the embarrassment.
Mother of child (diagnosed with ADHD, aged 11–12 years) [reviewer’s edits], pp. 76–7260
Sometimes the tablets work because sometimes they make me be good, but when they’re not working I don’t do any work.
British child (diagnosed with ADHD, aged 7–11 years), p. 77260
This pupil’s mother sets up medication to be the ‘answer’ to his problematic behaviour and academic difficulties. This puts the child in a pressured situation, where he has to choose between addressing the anxieties he feels over the negative effect he understands the medication to have on him and meeting parental and educational expectations. His agency is undermined by the way medication is positioned as the only way to control his behaviour, and he is undermined by the embarrassment he faces in the classroom over taking medication. His mother describes this latter situation as contributing to feelings of anger, which may exacerbate ADHD symptoms.
Case study 4:
I will be very, very good then, sitting quietly, sitting sensibly. I’m naughty, only when me tablets have wore off, I need me tablets to stop me from being naughty.
British child (diagnosed with ADHD; aged 7–11 years), p. 77260
He wasn’t getting an education because every other day I was being phoned up telling me that he was too bad and I had to come and get him, the Ritalin and school just didn’t seem to go together.
Mother of child, p. 77260
Even with Ritalin his concentration is still poor. He is less hyperactive though. But I believe that James has physical problems that are in his head, and his characteristics are too embedded for any changes to occur.
Teacher of child, p. 78260
This pupil understands medication as controlling his behaviour; the author makes the distinction that medication makes it easier for him to control his own behaviour. The pupil’s understanding of being good as ‘sitting quietly, sitting sensibly’, and of naughtiness as anything else is similar to findings in review 4b (see Biological factors). Despite the pupils’ understanding that medication has stopped him from being naughty, his mother and teacher suggest that his behaviour in school is still problematic. The school the pupil’s mother describes resorted to exclusion in response to his problematic behaviour (despite medication); she then moved him to a different school. However, the teacher in the new school has no expectation that James’ problematic behaviour can be addressed because medication has not worked. The author remarks that the child’s mother and teachers agree that he has no part to play in addressing his problem behaviours and that the case illustrates the way that faith in and focus on medication to treat ADHD symptoms can narrow or exclude strategies and options for other approaches.
The author concludes the study by emphasising that ‘parents and school staff sometimes only agree that the child is displaying problematic behaviour’;260 other included studies demonstrate that they do not always even agree about this. 276,298,356 Hughes260 summarises common differences in funds of knowledge between teachers and parents, and potential impacts, as:
-
they may disagree on why the child is displaying the behaviour, with disagreement orientated around the extent of the control the child has, and whether the behaviour results from biological or sociological influences
-
their response to the behaviour follows from the beliefs about ADHD that are held, or the belief that there is nothing that can be done which can result in abdication of responsibility
-
the failure to agree consistently on an approach to intervention between stakeholders is a ‘fundamental barrier to positive change’
-
the failure to agree consistently on an approach to intervention between stakeholders can exacerbate the problems, through patterns of blame or by ignoring wider factors
-
the failure to agree consistently on an approach to intervention between stakeholders can leave pupils diagnosed with ADHD feeling helpless and frustrated, and beliefs that medication is a powerful and effective intervention for ADHD without consideration of other strategies and intervention factors can encourage pupils to understand that they have no control over their behaviour. 260
The conclusions drawn here coincide with many from studies in reviews 4a–c (see Sociological factors: impact of belief that attention-deficit/hyperactivity disorder symptoms originate in the home; Perceptions that attention-deficit/hyperactivity disorder symptoms result from other social and cultural factors; Biological factors; Different notions of disability; Agency; and Impact of polarised view). This study was conducted in the UK, and the similarity of the issues highlighted here to papers from other countries supports the potential for applicability of studies across cultures. A range of views are expressed about ADHD behaviour, many of which are conflicting, but they are views also expressed by other participants in other countries. This study demonstrates clearly the way that confusion and disagreement about ADHD results in reduced effectiveness in dealing with ADHD symptoms and more difficult situations for pupils diagnosed with ADHD. That teachers respond to ADHD symptoms according to their understanding of ADHD supports the need for increased education about ADHD and strategies to address symptoms. The complexities of the case studies described in Hughes260 require sophisticated judgements in order to respond optimally to the pupils, and suggest that teachers need to have a relatively developed understanding of issues surrounding ADHD to be able respond in constructive ways.
Implications of findings of differences between funds of knowledge for non-pharmacological interventions are given in Box 31.
Differences in perceptions about ADHD between parents and school staff are identified as a fundamental barrier to consistent, effective intervention for ADHD symptoms.
ADHD interventions would benefit from designs that include support for relationships between parents and teachers of pupils displaying ADHD symptoms, particularly in relation to perceptions about ADHD.
Processes of collaboration
Two of the included studies specifically explored collaboration between teachers and parents of pupils diagnosed with ADHD. 390,391 Guevara et al. ,390 who separately interviewed clinicians, teachers and parents in focus groups, found that there was agreement over lack of collaboration across participant type. Koro-Ljungberg et al. ,391 who interviewed teachers and parents together in focus groups, found that, although on the surface the aims parents and teachers spoke of seemed similar, there was a lack of conceptualisation over what constructive collaboration between teachers and parents was. This prevented ‘these two roads from truly connecting’. 391 These findings suggest that processes of collaboration are a foundation for conflict between teachers and parents.
Koro-Ljungberg et al. 391 created a communication model that involved interpersonal, situational and policy/political contexts; all of these were found to be involved in the quality of collaboration. At the interpersonal level, communication involved a sender, receiver, message and feedback. Situational aspects such as ethnicity, gender, age and educational level influenced the message, its interpretation and its feedback. Finally, the method of communication (e.g. telephone, e-mail, letter) affected the interpretation of the message, as did perceptions of its purpose. This analysis is useful in providing a framework for understanding problems with communication between parents and teachers. For example, in other included studies mothers mention negative interpretations of situational aspects (e.g. ‘otherness’), method (e.g. a message to a mother sent through a pupil’s sibling) and perceptions of purpose (criticism of parenting skills) in communications from teachers, which then affected their feedback (see Parent–teacher conflict is the norm).
While discussing communication in focus groups for parents and teachers, a parent noted the need for a case manager for pupils diagnosed with ADHD. This person would be responsible for liaison between the stakeholders supporting the pupil and could keep records of correspondence and distribute important documents. She called them a ‘translator’:
[another participant] said, ‘relationships’; if you can’t get it with the teacher or teachers, then you have to find somebody in that school. ‘Why?’ Because you need that translation; I look at it as translations.
American mother of a young person (diagnosed with or at risk of ADHD, aged 12–16 years) [reviewer’s edits], p. 62391
The authors note that the parents’ use of the term ‘translation’ could refer to the sense that parents and school staff speak in different languages (see discussion of funds of knowledge in Different funds of knowledge). However, the mother does not then recommend that parents and teachers attempt to understand the others’ languages, rather she proposes that a third party is needed to enable constructive communication. This may signify the extent of the breach experienced by this parent.
Much of the discussion between parents and teachers in Koro-Ljungberg et al. ’s study391 involved descriptions of approaches that they had taken to communicate with each other that provided alternatives to the telephone or e-mail. These included:
-
attendance, behaviour and homework sheets
-
teacher notebooks (used in middle and high schools) which the pupil carried with them that acted as a source of information about pupil learning needs
-
the suggestion that teachers include information about ADHD in school newsletters to educate parents; and
-
that teachers propose ways for parents to support pupils and improve communication. 391
Despite similar content in things said by parents and teachers, the authors argue that parents and teachers did not necessarily share a commitment to particular action or improved communication. Rather, their statements reflected differences according to their identity. Teachers tended to position themselves as professionals, referring to communication with parents as a task requiring extra effort; parents were more inclined to refer to communication with teachers in terms of collaboration and relationship. One teacher explained their appreciation of advocacy by parents for their child:
As a teacher, I appreciate parents advocating for their child, because when you do teach 60 and 70 children, you can’t know and you can’t have those IEPs memorized and I appreciate a parent who stays in contact with me rather than expecting me to initiate.
American teacher of young people (diagnosed or at risk of ADHD, aged 12–16 years), p. 57391
This expression of appreciation by a teacher is also consistent with some of the experiences of parents in review 4c (parents’ views), who described positive or at least polite responses to their offers of information about their children. However, the action taken in response to the information was often inconsistent or lacking (see Assertive). Indeed, Koro-Ljungberg et al. 391 note that when parents and teachers communicate only with exchange of information, any response may be hypothetical. They conclude that communication related to activity, which implies commitment to specific responsibilities, is most likely to result in changed situations for the pupil in the classroom and improved parent–teacher relationships.
Although Koro-Ljungberg et al. 391 conclude that communication between parents and teachers involving the exchange of information without a focus on activity (where commitment to specific responsibilities are not made) are less likely to achieve constructive collaboration, they also acknowledge that resources may not be available for teachers to make such commitments (see Resources for further discussion). They also note that, despite higher stakes for parents and pupils, teachers hold the balance of power in influencing decisions and school action.
Koro-Ljungberg et al. 391 note that when effective collaboration occurred it was often the result of individual effort, or was accidental and/or inconsistent, rather than the result of a systemic model promoting equal access to effective collaboration. They further comment that a view of teacher–parent collaboration as solely personal could be a barrier to effective communication:
When communication is viewed merely as a reflection of relationship, it can result in less effective problem-solving efforts in response to conflicts, possibly further hindering effective communication. Instead, when communication is perceived as a complex process influenced by a variety of personal, interpersonal, contextual, and policy factors, communication problems can be attributed to diverse sources, and a more comprehensive problem-solving reply can be mounted in response.
Authors, p. 64391
This suggests the benefit of school-level education and/or guidelines about teacher–parent communication. Guevara et al. 390 have a similar finding. Participants in Guevara et al. ’s study390 rarely described constructive relationships and those that were described required ‘enormous effort to overcome obstacles’. 390 An exemplar of effective collaboration included a mandate to work together at the institutional level; however, such mandates were unusual. Institutional structures tended to create barriers to constructive interactions between stakeholders rather than facilitating them, in a way that the authors described as ‘system failure’. This study was conducted with minority inner-city schoolchildren and so collaboration might have been unusually complex. Nonetheless, the predominance of included studies that note problems in collaboration between teachers and parents suggested the need for system-level guidelines and structures that clarify expectations for constructive relationships and processes for building and maintaining them.
Guevara et al. 390 also identified discontinuity in care as a contributing factor to the fragmentation of support for minority pupils diagnosed with ADHD in inner cities in the USA. 390 This particularly occurred over transition periods between school years, through school moves or a change in teacher within the school year (as well as frequent clinical staff turnover). This resulted in a lack of continuity in educational support as each successive teacher or school was unfamiliar with the specifics of the child’s ADHD diagnosis and effective approaches for support, while new relationships between stakeholders had to be established. Transition points were perceived by the participants to require substantial levels of effort, but few institutional structures were in place to facilitate this.
The most frequent transition point was the beginning of a new school year. Teachers in Guevara et al. ’s study390 perceived that parents did not usually inform them about ADHD diagnosis before the start of the school year. Rather, teachers used their knowledge to identity pupils consistently displaying ADHD symptoms, and teachers perceived this to cause delay in implementing educational support:
When you have 30 kids in your class, you don’t get a list in September that says Juan is oppositional, Jose is ADD. We don’t get that information; you have to get that on your own.
American teacher of pupils (diagnosed with ADHD, aged 5–14 years), p. 514390
Thus, teachers can perceive that they lack the information needed from parents about pupils in order to support them. Parents in Guevara et al. 390 reported that work structures made daytime liaison with schools difficult and resulted in them scheduling school and clinical appointments on days off. One clinical participant remarked that what could look like ‘non-compliance’ could be related to work restrictions, where parents’ employment can become threatened because of the demands of caring for a child with ADHD. Thus, communication with teachers may prove difficult for parents. The experience described by the teacher above complements that described by a number of parents from review 4c (parent views), who described the need to educate their child’s teacher about ADHD every year, and that teachers were rarely engaging with the information given. How this may relate to differences in funds of knowledge between teachers and parents has been discussed earlier (see Box 31). However, institutional-level structures that encourage information-sharing between teachers, in addition to structures for information-sharing between teachers and parents, are one potential means to address this issue.
Processes of collaboration raise implications for non-pharmacological interventions which are given in Box 32.
Parent–teacher conflict over influences on and strategies to manage ADHD symptoms in pupils is the norm in included studies; collaborative relationships between parents and teachers occurred through great personal investment of time and overcoming structural barriers. Interventions might benefit from the systemic development of collaborative support, where schools structure constructive collaboration by defining and supporting processes (e.g. transfer of information between teachers at transition points and the purposes of parent–teacher communications) and/or by providing case workers to aid collaboration.
Accountability
Two included papers identified a lack of accountability as contributing to conflict between teachers and parents. 390,391 Participants in two other included papers within review 4d describe experiences of conflict related to a lack of accountability (see Different funds of knowledge and Resources). Teachers and parents in Koro-Ljungberg et al. ’s study391 identified two purposes of communication as important: (1) communication to exchange knowledge; and/or (2) to engage in activity. Parents and teachers agreed that it is appropriate for parents to:
-
communicate about medication changes
-
follow up on their children’s progress
-
be persistent regarding ongoing communication
-
be present and care, and
-
initiate contact with teachers.
Koro-Ljungberg et al. 391 note that, despite shared desire for effective communication, there was a ‘simultaneous displacement’ between teachers and parents about accountability relating to activity following on from communication. Any resulting lack of action could impair future communication. The authors conclude that there is no idea of what effective communication between parents and teachers in the context of ADHD would be – who holds responsibility for what, and what the form of interaction should be. They recommend that teachers and parents focus on ‘what’ and ‘how’ in their interactions.
Guevara et al. 390 identified a lack of accountability across participant type (clinicians, teachers and parents), with a lack of agreement about who was in the best position to take responsibility for overseeing care of pupils with ADHD. Those who took the view that other groups should lead often expressed unwillingness to take responsibility themselves owing to lack of knowledge or lack of time (see Resources). However, there was agreement between clinicians and teachers that most parents were not capable of taking responsibility, as they were perceived as ‘disorganised, misinformed, and inconsistent’:
You know it could be a whole laundry list of things. They could be on drugs, or they could be working. We really don’t always know. But there’s specific problems with certain kids, and they’re having difficulty succeeding here. And we’re trying to solicit parental help or to make suggestions, and we can’t get that message across. There’s no phone; there’s nobody home; or there’s no one willing or able to come here. And that’s one of the problems, probably the biggest.
American teacher of pupils (diagnosed with ADHD, aged 5–14 years), p. 514390
Such negative attitudes of parental capacity expressed by professionals in this study align with perceptions described by mothers in review 4c (parent views, for example see Feeling criticised), who felt dismissed and silenced by school staff. However, unlike the parents described here by the teacher, many of the mothers in review 4c were pursuing engagement with their child’s education. Parents in Guevara et al. ’s study390 describe some similar perceptions to mothers in review 4c, and reported that they felt dismissed by school staff when they shared concerns, that their perspectives were not appreciated and/or respected and so they sought help elsewhere.
Guevara et al. 390 identified the theme ‘finger pointing’ to describe the tendency for clinicians, teachers and parents to blame each other for inadequate levels of support for pupils diagnosed with ADHD. They also found that parents could be placed in the role of arbiter between different professionals who disagreed. Alongside perceptions of low-quality care professionals expressed distrust in the practice of others. By contrast, those who perceived they had good working relationships expressed appreciation for the work done by others and were more tolerant of others’ professional practice.
Resources
A lack of resources, in the form of knowledge, time and support structures, was identified as a foundation for conflict between a pupil diagnosed with ADHD and his teachers,293 and between teachers and parents. 390,391 Problems related to a lack of resources are found in other included studies in reviews 4a–c (see Relationships, Concern over the emotional equilibrium and learning of the whole class and Assertive).
The teachers interviewed in Hands’ case study293 of a young person diagnosed with ADHD acknowledged the pupil’s good conceptual ability, but expressed confusion about his inability to submit work on time, and to respond relevantly to assignment criteria. Their response to him is to attempt to be accepting on the basis that he has SEN rather than to attempt to communicate a strategy for him to learn how to turn in work on time, with the format and content needed to pass the assignment, and why it is worth learning how to do this. The pupil describes his difficulties to the researcher:
I have a problem with getting started. Sometimes I procrastinate a lot and just shove it off, shove off bigger projects for working on smaller things that I know I can get done [. . .] It’s just I use time in a way that I do everything. I procrastinate some work for other work that doesn’t need to be done. It’s really a dance.
American young person (diagnosed with ADHD, aged 16 years) [reviewer’s edits], p. 110293
This description suggests that the pupil is aware of the issue himself and would be capable of developing self-regulatory strategies, as well as benefiting from external support such as having large projects broken down into manageable chunks. Better education for the teachers might have provided a basis from which to understand and to act to support. The pupil’s mother comments:
We had a [Parent-teacher] meeting recently and they [the Magnet teachers] were at the last meeting. They don’t know what to do. They don’t. I don’t think they’ve dealt with his kind before. They really truly are at a loss. They’re like, ‘Well if he doesn’t do homework, then you know, what are we going to do?’ They have no idea and the problem is he’s the guinea pig.
Mother of young person (diagnosed with ADHD, aged 16 years) [reviewer’s edits], p. 97293
This suggests that the wider school, despite being a magnet school (see The potential for different classroom contexts to impact learning behaviour), did not have the knowledge themselves to provide support to the pupil’s teachers for developing strategies to help him. However, the biology teacher met with the pupil and a SEN consultant following this meeting:
I was just learning that there was a plan in place and I met with him and with the special ed. consultant and we talked about the accommodations just so it was clear to both of us at the same time and he’s made some efforts I think to get things in a little bit more often.
American biology teacher of young person (diagnosed with ADHD, aged 16 years), p. 98293
This comment suggests that even without a clear understanding of the pupil’s difficulties or a comprehensive strategy of support, collaboration between him, his mother and the teachers at the magnet school was at least partially productive. His biology teacher appears to have made a particular effort, by arranging the meeting with him and the SEN consultant. His English teacher was less proactive:
I haven’t called home, because I figure this is a long-standing problem, obviously, because [the pupil has] been through the evaluations and he’s probably been through a battery of tests by the Special Ed. Department and the psychologist . . . He’s been identified as a 504, so that means there’s a 504 team, so, you know, I think they’re looking after this.
American English teacher of pupil (diagnosed with ADHD, aged 16 years) [reviewer’s edits], pp. 98–9293
The English teacher seems to distance himself from the need to understand his pupil’s difficulties because he may perceive the team to be accountable for supporting the pupil rather than himself (see Accountability for further discussion). In both school contexts, to develop further knowledge about and strategies for the pupil, the teachers had to exert unusual effort. His biology teacher did this, whereas his English teacher did not; but, even with additional effort, the biology teacher did not seem to access adequate information about her pupil’s needs or strategies to support him. This situation illustrates the comment made by Koro-Ljungberg et al. 391 above, that, in collaboration with parents, teachers may share aims but not be willing to make commitments for action because they lack the resources to carry them through (see Processes of collaboration).
Other included papers address the issue of lack of resources. Guevara et al. 390 identified limited knowledge and resources as a barrier described by both teachers and parents in their study. Teachers and clinicians described the uncertainty they faced in understanding whether or not ADHD was the cause of the child’s symptoms, because it was difficult to untangle other issues such as chaotic home life and co-occurring difficulties. Teachers also described limited training about ADHD; those with adequate training said the field developed quickly and it was difficult to keep up with. Teachers were concerned by cutbacks in school support by specialists like educational psychologists and counsellors who might be able to give them information about behaviour management. Parents expressed the desire to attend support groups but did not know of any.
Koro-Ljungberg et al. 391 identify the situational context as a factor affecting parent–teacher interactions. Factors identified as being relevant to teachers included class size and grade level, with larger classes and/or multiple classes taught (as in secondary schools) adding additional barriers, and a difference in teacher attitude and tone for teachers teaching elementary (pupils aged 5–11 years), middle (pupils aged 11–14 years) and high (pupils aged 14–18 years) schools. The teachers described these factors as being relevant for all pupils, but that the additional complexities of ADHD symptoms act to increase barriers, including further hindering relationships with parents. One teacher described how difficult it was to prioritise the needs of pupils with ADHD over the needs of the rest of the pupils in a large classroom (see review 4b, Orientation to the class as a whole and orientation to the individual child and Orientation to the class versus the individual, for further discussion of orientation to the class as a whole). Although this issue results in teachers’ orientation to the class as a whole rather than individual pupils, the specific interest here is the reluctance for investment by teachers in understanding individual pupils because of limited time, and in the case of teachers of secondary aged pupils, a high number of pupils.
Several of the parents in Koro-Ljungberg et al. ’s391 study mentioned that they had found it easier to interact with teachers during their child’s elementary years (aged 5–11 years), when the child attended one class, but once their child transitioned to middle school where they had multiple teachers they experienced greater difficulties. Multiple teachers meant inconsistency in pedagogy and inconsistent knowledge about the nature of a child’s issues related to ADHD. Although meetings were held to discuss pupil IEPs, which were meant to act as information-sharing events, these were not attended by most of the child’s teachers.
Teachers in Guevara et al. ’s390 study perceived a lack of support by school management, where the focus was on attainment with a lack of support for behaviour management.
I think the teachers get a little disgusted because again with the time frame, it seems like all this paperwork [related to assessment procedures] they do, and then nothing ever happens. We also don’t have enough psychologists . . . So the school itself doesn’t have enough support to do what they are supposed to do and what they could do if they had the support.
American teacher of pupils (diagnosed with ADHD (aged 5–14 years) [author’s edits], p. 516390
This suggests that there is the potential for resentment when teachers spend limited time completing rating scales used for diagnosis and then do not receive additional behaviour management support owing to lack of resources. Teachers may become reluctant to invest limited time to understanding the learning and/or a behavioural need of individual pupils if, from past experience, they have learned that support is not available.
Discussion
Reviews 4a–d
As described in Structure of review 4, review 4 was conducted by grouping included studies by participant type into four subreviews (4a–d), and paper characteristics for each subreview were described in the relevant sections (4a pupil views; 4b teacher views; 4c parent views; 4d mixed views). Table 60 gives the number of included studies for reviews 4a–d.
| Syntheses in review 4 | Number of included studies |
|---|---|
| 4a. The school experiences and perceptions of pupils diagnosed with ADHD (pupil views) | 11a |
| 4b. The school experiences and perceptions of teachers of pupils diagnosed with or at risk of ADHD (teacher views) | 11a |
| 4c. The school experience and perceptions of parents of pupils diagnosed with ADHD (parent views) | 6 |
| 4d. The school experiences and perceptions of pupils diagnosed with or at risk of ADHD, their teachers, parents and peers (mixed views) | 7 |
| Total | 34a |
Across the 34 included papers, fewer children diagnosed with, or at risk of, ADHD (aged ≤ 11 years) were participants than young people (aged ≥ 12 years). By contrast, more teacher participants taught children diagnosed with, or at risk of, ADHD in preschool to primary years (ages 4–11 years) than taught young people in secondary to college years (ages 12–18 years). This suggests that there may be general mismatch in perspectives of the two groups owing to differences related to maturation of pupils and/or differences between educational context at preschool/primary school and secondary/college school levels, and identifies a research gap (see Recommendations for research).
Quality appraisal
Results of the quality appraisal (for discussion of methods, see Chapter 4, Methods of analysis/synthesis, Quality assessment) are shown in Table 61. All but one study260 showed clear research questions, all but two studies286,305 substantiated their findings by linking them to the data, all but one356 had study designs appropriate to answer their research questions, and all but three studies264,286,290 explicitly described research methodology and/or conceptual frameworks. The conceptual frameworks of the studies tended to influence design and/or findings; for example, when interest was shown in social aspects of ADHD symptoms,27,41,260–263,265,266,291,293,314,324,332,347,356,390,391 the findings were often centred round the dynamics of these. By contrast, studies that did not situate themselves in social theory264,286,294,296,298,299,305,335,359,360,392 often did not discuss findings in relation to the dynamics of social and/or cultural factors, or at least not in the same depth. Rather, they were more focused on categorising and describing content.
| First study author and year | 1. Is the research question clear? | 2. Is the theoretical or ideological perspective of the author explicit? | 3. Has the theoretical or ideological perspective influenced the study design, methods or research findings? | 4. Is the study design appropriate to answer the question? | 5. Is the context or setting adequately described? | 6. Is the sample adequate to explore the range of subjects and settings, and has it been drawn from an appropriate population? | 7. Was the data collection adequately described? | 8. Was data collection rigorously conducted to ensure confidence in the findings? | 9. Was there evidence that the data analysis was rigorously conducted to ensure confidence in the findings? | 10. Are the findings substantiated by the data? | 11. Has consideration been given to any limitations of the methods or data that may have affected the results? | 12. Do any claims to generalisability follow logically and theoretically from the data? | 13. Have ethical issues been addressed and confidentiality respected? | 14. Is/are the author/s reflexive? | Totals (Y, N, CN) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Papers from review 4a (pupil views; n = 11a) | |||||||||||||||
| Brice 1998331 | Y | Y | Y | Y | N | Y | N | CT | Y | Y | Y | Y | Y | Y | 11, 2, 1 |
| Cooper 1998261 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | CT | N | 11, 2, 1 |
| Exley 2005332,337,338 | Y | Y | Y | Y | Y | N | Y | Y | N | Y | N | CT | Y | N | 9, 4, 1 |
| Friio 1999333 | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 13, 1, 0 |
| Houghton 2006296 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | 12, 1, 1 |
| Kendall 2003299 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | 12, 1, 1 |
| McDannel 2005334 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | Y | 13, 0, 1 |
| Prosser 2006314 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 13, 1, 0 |
| Singh 201127 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | CT | N | 10, 3, 1 |
| Taylor 2008335 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | 12, 1, 1 |
| Wolfberg 1999336 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | N | 12, 1, 1 |
| Totals for review 4a (pupil views) (Y, N, CT) | 11, 0, 0 | 11, 0, 0 | 10, 1, 0 | 11, 0, 0 | 8, 3, 0 | 10, 1, 0 | 10, 1, 0 | 10, 0, 1 | 10, 1, 0 | 11, 0, 0 | 5, 6, 0 | 5, 0, 6 | 9, 0, 2 | 7, 4, 0 | 128, 17, 9 |
| Papers from review 4b (teacher views; n = 11a) | |||||||||||||||
| Arcia 2000286 | Y | N | CT | Y | Y | Y | Y | Y | Y | CT | Y | Y | Y | N | 10, 2, 2 |
| Bailey 200941 | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | CT | Y | Y | 11, 2, 1 |
| Einarsdottir 2008291 | Y | Y | Y | Y | Y | CT | Y | CT | Y | Y | N | Y | CT | N | 9, 3, 2 |
| Hillman 2011294 | Y | Y | Y | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | N | 11, 2, 1 |
| Houghton 2006296 | Y | Y | Y | Y | N | Y | CT | Y | Y | Y | N | Y | CT | N | 9, 3, 2 |
| Hong 2008264 | Y | N | CT | Y | Y | CT | Y | Y | N | Y | N | CT | CT | Y | 7, 3, 4 |
| Jones 2008298 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | Y | 13, 0, 1 |
| Lee 2008324 | Y | Y | Y | Y | Y | CT | Y | Y | Y | Y | N | Y | CT | Y | 11, 1, 2 |
| Ljusberg 2011265 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | 12, 2, 0 |
| McMahon 2012263 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | 13, 1, 0 |
| Nowacek 2007305 | Y | Y | Y | Y | Y | Y | Y | Y | Y | CT | Y | N | Y | N | 11, 3, 1 |
| Totals for review 4b (teachers views) (Y, N, CT) | 11, 0, 0 | 9, 2, 0 | 9, 0, 2 | 11, 0, 0 | 10, 1, 0 | 7, 0, 4 | 11, 0, 0 | 10, 0, 1 | 9, 2, 0 | 9, 0, 2 | 4, 7, 0 | 6, 1, 4 | 8, 0, 3 | 6, 5, 0 | 118, 20, 17 |
| Papers from review 4c (parent views; n = 6) | |||||||||||||||
| Carpenter 2008262 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Y | Y | Y | 12, 2, 0 |
| Hibbitts 2010276 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 14, 0, 0 |
| Malacrida 200128,266 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | 13, 1, 0 |
| Margalit 2010359 | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | 11, 2, 1 |
| Reid 1996360 | Y | N | CT | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | N | 10, 3, 1 |
| Watson 2011356 | Y | Y | Y | CT | Y | N | Y | Y | Y | Y | Y | CT | Y | Y | 11, 1, 2 |
| Totals for review 4c (parent views) (Y, N, CT) | 6, 0, 0 | 4, 2, 0 | 4, 0, 2 | 5, 0, 1 | 5, 1, 0 | 5, 1, 0 | 6, 0, 0 | 6, 0, 0 | 6, 0, 0 | 6, 0, 0 | 5, 1, 0 | 4, 1, 1 | 6, 0, 0 | 3, 3, 0 | 71, 9, 4 |
| Papers from review 4d (mixed views; n = 7) | |||||||||||||||
| Edwards 2008290 | Y | N | CT | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | 10, 3, 1 |
| Guevara 2005390 | Y | Y | Y | Y | Y | Y | N | CT | Y | Y | Y | Y | Y | N | 11, 2, 1 |
| Hands 2009293 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | N | N | Y | Y | 11, 3, 0 |
| Hughes 2007260 | N | Y | Y | Y | N | Y | Y | Y | Y | Y | N | CT | Y | N | 9, 4, 1 |
| Koro-Ljungberg 2011391 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | 13, 1, 0 |
| Rafalovich 2005347 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | N | 12, 2, 0 |
| Shea 2003392 | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | CT | Y | N | 10, 3, 1 |
| Totals from review 4d (mixed views) (Y, N, CT) | 6, 1, 0 | 6, 1, 0 | 6, 0, 1 | 7, 0, 0 | 4, 3, 0 | 6, 1, 0 | 6, 1, 0 | 7, 0, 0 | 6, 1, 0 | 7, 0, 0 | 3, 4, 0 | 4, 1, 2 | 7, 0, 0 | 2, 5, 0 | 77, 18, 4 |
| Totals for all papers in review 3 (n = 34a) (Y, N, C) | 33, 1, 0 | 29, 5, 0 | 28, 1, 5 | 32, 0, 2 | 26, 8, 0 | 26, 3, 5 | 31, 3, 0 | 29, 2, 3 | 29, 5, 0 | 32, 0, 2 | 17, 17, 0 | 18, 3, 13 | 28, 0, 6 | 17, 17, 0 | 374, 64, 39 |
A number of studies lacked sufficient reporting of methods, for example by failing to describe participant samples adequately,264,291,294,324 omitting contextual information27,260–262,290,294,296,331,392 such as description of schools, or by failing to describe the process of data analysis. 41,264,290,332 The areas in which studies were most often lacking involved the omission of discussion of study limitations,27,41,260,262–265,291,293,296,299,314,324,332,335,347,392 omission of discussion of aspects of generalisability,41,260,264,293,296,298,299,305,332,334–336,356,360,392 or the study authors were not reflexive in that they did not acknowledge the impact of their perspectives on the study designs and findings. 27,260,261,265,266,286,291,294,296,305,332,336,347,359,360,390–392 However, all but five studies260,264,291,296,332 met at least 10 out of the 14 criteria, suggesting a large majority were of good quality as assessed by these standards.
Issues of quality appraisal in qualitative systematic review are contested273 and the experience of conducting quality appraisal for review 4 suggested the criteria adopted were not as relevant as they could be; high appraisal scores did not necessarily predict the studies that contributed most to the synthesis. For example, the study by Margalit et al. 359 was descriptive in nature and, despite a relatively high rating for quality appraisal (11 of 14 possible ‘yes’ answers, see Table 61, review 4c), contributed the least out of the papers included in review 4c. This experience is supported by Garside’s conclusion273 that theoretical considerations such as reference to wider theory and the development of secondary, explanatory concepts in appraisal of quality are as important as more technical reporting aspects.
Applicability
Although inclusion criteria specified studies published or conducted from 1980 onwards, no included papers were published before 1996 (Figure 8) and a large majority (82%) were published in the past 10 years. Age of studies may be particularly relevant to judging applicability in this review because of societal changes, such as rapid increase in ADHD diagnosis, that mean that experiences of ADHD are likely to be dynamic. That all studies were conducted within the past 20 years, and most studies are relatively recent, supports greater applicability of the findings of these reviews.
FIGURE 8.
Total number of included studies in review 4 by year of publication.

Of the 34 included papers, seven involved participants from the UK (Table 62), and the majority were conducted with US participants. The low number of UK studies has potential relevance to applicability, for example because of cultural differences and differences in educational structure between countries. Although reviews 4a, c and d included only one or two UK studies each, these were all of high quality and contributed substantially to these subreviews. However, a lack of research on the experiences and perceptions of UK teachers of pupils diagnosed with ADHD is a particularly important gap in the included studies for review 4b. Although two studies involving UK teacher participants were included in review 4b (teacher views), one study294 was based on an online open-ended questionnaire for which the UK teacher participants were in the minority and was not a study that contributed substantially to review 4b. The other study,41 although contributing important information about the relationship between ADHD and UK classroom structures and processes, had more limited findings about teacher attitudes and experiences. Nonetheless, there are considerations that suggest findings from studies conducted in other countries are still applicable to the UK:
-
UK studies found differences within and/or between participant types with reference to experience of ADHD symptoms, diagnosis and medication,261 attributional beliefs about ADHD260,266,356 and within different UK contexts with reference to the expression of ADHD symptoms,27 suggesting that a range of beliefs and experiences are relevant within the UK.
-
The experiences and attitudes expressed by these UK participants had parallels in other countries, where the range of beliefs and experiences was similar, but with different aspects foregrounded or backgrounded (for an example, see ‘Being told’ rather than collaborating for the discussion of differences in the experiences of mothers in the UK and Canada regarding the kinds of pressure from schools that are felt by parents).
| Country | Number of studies |
|---|---|
| USA | 16a |
| UK | 7a |
| Australia | 6 |
| Canada | 6a |
| Iceland | 1 |
| The Republic of Korea | 1 |
| Sweden | 1 |
| New Zealand | 1 |
| Totals | 39a (34 studies) |
Some studies report experiences for participants related to subcategories of ADHD, for example ethnic minorities,294,390 pupils diagnosed with both ADHD and giftedness290,293 and experiences of peer victimisation. 392 Similarly, in these cases the findings had echoes in other included studies, which suggested differences of degree rather than kind. For example, in the study focused on peer victimisation, the participants were boys diagnosed with ADHD who had experience of bullying and who had been drawn from a larger study. Although pupils diagnosed with ADHD are not always victimised, some level of dislike and/or conflict between pupils diagnosed with ADHD and peers was a finding across many studies in review 4. 27,264,276,290,296,299,314,332,335,336 Thus, the findings from the study on peer victimisation hold the potential for transferability.
Overall, it was possible to make sense of findings from across countries using third-order concepts that encompassed the broader issues and allowed differences in expression within and between both participant groups and countries. At any rate, as is true for qualitative studies, review 4 does not claim to generally represent the school-based experiences and perceptions of pupils diagnosed with or at risk of ADHD, their teachers, parents and peers, even on the basis of UK studies. Rather, we claim credibility of the studies in representing participants on the basis of study designs incorporating approaches like member checks and consultation with the project Steering Group to check findings against specialist knowledge and experience; we also claim the potential for transferability based on consultation with the Steering Group and our experiences of stakeholder engagement during the project (for further discussion see Appendix 11). As there are a range of differences in perceptions and experience in different contexts, transferability is likely to be important, where the reader judges the relevance of findings according to knowledge of a particular context.
Limitations
The findings of review 4 are limited by the kinds of studies available for synthesis [e.g. issues of gender, pupil maturity and school level (primary/secondary) were noted to be relevant to the review]; however, there were no studies that focused on these issues. The study designs also limited the extent to which relationships could be established between factors; studies that involved multiple perspectives offered the chance to directly link different experiences and perspectives pertaining to a particular child, but were of limited number. The synthesis was also limited by the differences between studies, where underpinning theory and/or approaches to data collection were widely divergent (e.g. grounded theory vs. post-structural theories; semistructured interviews vs. entries to social networking websites). In such cases, assumptions were made about links between unrelated studies.
Findings from the synthesis of reviews 4a–d
An overarching synthesis was conducted for review 4, to combine findings from reviews 4a–d. Relationships between themes from reviews 4a–d were established by querying each theme (for further description, see Chapter 4, Review 4) in relation to the research questions (see Chapter 4, Aims).
Table 63 shows the relationships between third-order (reviewer) concepts identified in reviews 4a–d and the third-order concepts developed for the synthesis of reviews 4a–d. Many papers touched on the role that school expectations and/or structures could make towards ADHD-related behaviour in pupils. Owing to the rift between this finding and the way ADHD was conceptualised by participants, who rarely described ADHD in these terms, and because this finding is relevant to the implementation of non-pharmacological interventions for ADHD in schools, the overarching theme identified was ‘school expectations and structures can be one of the factors that compromise and/or aggravate ADHD symptoms’ with four subthemes:
-
constituting deviance and invoking stigma
-
school and the aggravation of ADHD symptoms
-
polarised attributions as an outcome of stigma; and
-
relationships: ADHD symptoms as a threat to educational and parental identities.
| Third-order concepts from reviews 4a–d | Overarching theme for review 3: school expectations and structures establish boundaries for the identification of ADHD symptoms and can aggravate ADHD symptoms | |||
|---|---|---|---|---|
| School and the aggravation of ADHD symptoms | Constituting deviance and invoking stigma | Relationships: ADHD symptoms as a threat to educational and parental identities | Polarised attributions as an outcome of stigma | |
| Synthesis 4a: expression of symptoms in pupils diagnosed with ADHD as an interaction of biological, sociological and psychological factors | ||||
| Experience of ADHD symptoms | ✗ | ✗ | ✗ | |
| Sociological factors that impact the expression of ADHD symptoms | ✗ | ✗ | ✗ | |
| Relationships | ✗ | ✗ | ||
| Classroom context | ✗ | ✗ | ||
| Stigma | ✗ | ✗ | ||
| Psychological factors that impact expression of ADHD symptoms | ✗ | ✗ | ✗ | |
| Relationships | ✗ | ✗ | ||
| Agency | ✗ | ✗ | ||
| Desire for approval | ✗ | |||
| Impact of polarised attributions about ADHD | ✗ | |||
| Synthesis 4b: factors that influence teachers’ willingness to adapt their response to ADHD symptoms | ||||
| Orientation | ✗ | ✗ | ||
| Class | ✗ | ✗ | ||
| Child | ✗ | |||
| Perceptions of ADHD behaviour | ✗ | |||
| Sociological | ✗ | |||
| Biological | ✗ | |||
| Psychological | ✗ | |||
| Maturity | ✗ | |||
| Synthesis 4c: mothers are silenced | ||||
| Dashed expectations | ✗ | |||
| Parent–teacher conflict | ✗ | ✗ | ||
| Resistance | ✗ | |||
| Deferential | ✗ | |||
| Assertive | ✗ | |||
| Synthesis 4d: relationships between participant types – conflict is the norm | ||||
| Foundations for conflict | ✗ | ✗ | ✗ | ✗ |
| Fit between pupils diagnosed with ADHD and school | ✗ | ✗ | ✗ | |
| Orientation to the class vs. the individual | ✗ | ✗ | ✗ | |
| Processes of collaboration | ✗ | ✗ | ||
| Different funds of knowledge | ✗ | ✗ | ✗ | |
| Accountability | ✗ | ✗ | ||
| Resources | ✗ | ✗ | ||
These will be discussed in turn below.
School expectations and structures establish boundaries for the identification of attention-deficit/hyperactivity disorder symptoms and can aggravate attention-deficit/hyperactivity disorder symptoms
In the following sections, findings that link ADHD symptoms to the school context will be explored. Our focus on the school context follows the directives of our research questions, but we emphasise the need to regard such issues in combination with other factors. We seek to redress a balance in understanding and response to complex issues surrounding ADHD that have been dominated by conceptions of within-pupil differences and/or contributions of home life, in order to contribute towards more holistic and effective design of non-pharmacological interventions and the evaluation of such interventions.
Constituting deviance and invoking stigma
Some papers in review 441,262,347,356 focused on the role of the school in constituting what acceptable and unacceptable behaviour was:
-
Bailey and Thompson41 by exploring school routines (see Classroom structure a contributor to attention-deficit/hyperactivity disorder symptoms)
-
Rafalovich347 by examining the process of a shift in perception of behaviours from being evaluated as ‘normal’ to ‘deviant’ (see The role of teacher expectations and perceptions in the shift from understanding problematic behaviour as normal to formally identifying it as deviant)
-
Carpenter and Austin262 by exploring the work mothers do either to reframe their child’s behaviour to establish it as normal by school standards or to seek diagnosis and medication for ADHD in order to change the child to fit school expectations (see Presentation of the family as normal and Different notions of disability) in response to the local schools’ boundaries for normal behaviour (see Perceptions that the origin of the problem is in the school)
-
Watson356 by analysis of a narrative written by the mother of a pupil diagnosed with ADHD about her dealings with her son’s school, where the author employed satire as a means to communicate the seemingly arbitrary nature of the school’s construction of deviant behaviour (see Perceptions that the origin of the problem is in the school and Feeling criticised).
These studies describe the way schools determine boundaries for acceptable behaviour, with differences at the local level. Processes that mark particular pupils as different from their peers hold the potential for stigma (Box 33 provides a recap of theories of stigma); however, stigma only results when the pupil becomes marginalised as a result of such decisions (for examples of mechanisms by which stigma operates, see Box 33a–c). Many studies find examples of stigma in relation to ADHD symptoms or the syndrome of ADHD;27,41,261–263,266,299,314,332,356,391,392 for example, Cooper and Shea261 found hyperactive/impulsive and/or combined types of ADHD to be more highly stigmatised than ADHD inattentive type (see Stigma). This hierarchy of stigma corresponds to the finding that classroom teachers tend to be orientated to the learning of the class as a whole (threatened by hyperactive/impulsive behaviour, see Concern over the emotional equilibrium and learning of the whole class) over the learning needs of individual pupils (threatened by symptoms of inattention). Therefore, the boundaries of stigma follow school priorities. Finally, other studies276,296,299,333,392 give findings where the mechanisms of stigma can be identified as being in operation even when study authors do not analyse the data with specific reference or full use of such theories. For example, pupils296,299,333,392 and parents/teachers392 describe situations where teachers punish pupils excessively while ignoring similar behaviour by peers. This links to aspects of stigma described in Box 33c. These findings suggest that the marginalisation associated with stigma is common in schools in relation to pupils diagnosed with or at risk of ADHD. As will be seen below, stigma can aggravate ADHD-related behaviour in pupils.
-
Goffman describes stigma as, ‘an undesired differentness’ that leads us to ‘believe that the person with a stigma is not quite human’ (p. 15). 322
-
The attributes that provoke stigma are not discrediting in and of themselves, but only according to the value systems of those allocating the stigma whom Goffman calls ‘normals’. 322
-
Often the attributes that provoke stigma threaten the effective functioning of social groups. 348
-
Labelling involves assigning the category name invoking the stigma onto a person, and can be informal (e.g. ‘naughty boy’) or formal (ADHD).
Goffman describes stigma as justification to ‘exercise varieties of discrimination, through which we effectively, if often unthinkingly, reduce his [sic] life chances’ (p. 15). 322 Examples of the mechanisms of discrimination include:
-
generalising the particular faulty attribute to a wider gestalt of disability (e.g. assuming a child with ADHD is not capable of learning)
-
assuming the pupil exhibits the range of attributes by which the label is understood rather than seeking to understand the pupil and/or the pupil’s specific circumstances
-
the pupil’s behaviour may be understood as an expression of the stigmatised attribute whereas the same behaviour from non-stigmatised peers would not be regarded in the same way.
School and the aggravation of attention-deficit/hyperactivity disorder symptoms
A number of study authors and parent and/or pupil participants commented that school was the context where their ADHD difficulties were most apparent. 262,266,314,331,333,334,356 Findings from included studies suggest the school context contributes to the aggravation of ADHD symptoms in at least two ways:
-
By triggering symptoms because of classroom structures, where pupils are expected to concentrate and/or remain still for long periods of time. Pupils describe an inability to learn in school, where peer relationships, noise and movement in classrooms were experienced as distractions. 261,296,299,331,333,334 One author334 found that pupils may unconsciously resort to the expression of ADHD symptoms like hyperactivity to cope with demands in the classroom (see Hyperactivity), so displays of such behaviour could be understood as clues about pupil needs. The same study identified that the pupil participants were more able to learn in quiet, ordered classrooms than in dynamic, less structured classrooms.
-
Through escalation of negative emotions and difficulties in relationships in pupils diagnosed with ADHD over the course of their school careers, where these can compound already-present ADHD-related difficulties with self-regulation and control. 296,299 Studies describe different aspects of this issue, for example as escalating ‘stress’296 or a sense of rage. 276,293,392 Some studies link this kind of pupil behaviour to pupil perception of injustice from teachers and peers,260,276,293,296,314,333 for example in response to overpunitive teachers who punish them for behaviour that peers are not punished for296,299,333,392 or in response to bullying. 332,392 Such findings suggest that this may be a pupil response to the marginalisation and/or social exclusion they face in response to stigma related to ADHD symptoms or diagnosis.
Polarised attributions as an outcome of stigma
One of the puzzling findings of review 4 was the mismatch between the experiences of ADHD described by pupils and teachers, and the attributional beliefs that they expressed about ADHD. During interviews, teachers described strategies they implemented to support pupils diagnosed with or at risk of ADHD in class,264,265,286,290,291,293,294,296,298,305 and pupils described how the classroom environment and their relationships could act as barriers to their learning. 261,293,296,299,331,333,334 These experiences provide the basis for understanding a link between the context of school and symptoms of ADHD. This is an important finding as it suggests that modification to the school context could contribute to managing pupils’ ADHD symptoms in school, and non-pharmacological interventions might benefit from classroom- and school-level change targets in addition to pupil-level targets.
However, interviews with teachers and pupils did not demonstrate this kind of understanding of ADHD. Pupils and teachers tended to focus on biological aspects of the pupil (pupils and teachers)27,260,261,263,286,291,294,299,314,332,347 when making attributions for ADHD symptoms, or on sociological aspects involving poor parenting (teachers). 260,286,291,294,296 The conclusion we draw in response to these findings is to suggest that this lack of conceptualisation about school factors is at least partly a result of the school’s role as the social group of ‘normals’ (see Box 33b) who determine the boundaries for the ‘undesired differentness’ (see Box 33a), which is the basis for stigma in response to either informal or formal aspects of ADHD. This would explain the ‘invisibility’ of school factors in teacher and pupil attributions for ADHD, because criteria for discrimination on the basis of stigma are implicit and appear normal and right to members of the group.
Relationships: attention-deficit/hyperactivity disorder symptoms as a threat to educational and parental identities
Studies in review 4 identify many reasons for conflict in school relationships associated with ADHD (see Disconnect between pupils and peers; Orientation to the class versus the individual; Different funds of knowledge; Processes of collaboration; Accountability; and Resources); this synthesis of reviews 4a–d adds to this by positing that the mechanisms of stigma establish a particularly emotive foundation from which this conflict plays out, by threatening important identities for teachers, pupils, peers and parents.
Thornicroft,348 in his discussion of stigma in relation to mental illness, describes reasons that human social groups invoke stigma:
Stigma originates in a universal human tendency to avoid danger. Stigmatisation is not therefore mainly directed against individuals, but against those who are understood to pose a threat. Such understandings are socially created, and individual ‘stigmatisers’ are essentially only repeating (and recreating) their society’s norms about what are appropriate feelings and behaviours to display to members of any threatening group.
p. 189348
Many teachers in included studies talk about the way that ADHD symptoms in the classroom prevent them from doing their jobs;264,286,296,298 Bailey and Thompson41 characterise the ‘good teacher’ role as centred round the prevention of disruption (see Classroom structure as a contributor to attention-deficit/hyperactivity disorder symptoms). Punitive responses of teachers to pupils who exhibit ADHD symptoms in the classroom can therefore be seen as the ‘appropriate feelings and behaviours to display to members of any threatening group’ as described by Thornicroft348 in the extract quoted above. The threat of ADHD symptoms to teacher identity may explain the determination with which some teachers approach the punishment of such pupils.
Many pupils diagnosed with ADHD in included studies describe the desire that they feel to meet expectations for behaviour and schoolwork,261,296,299,314,333,334,392 including acknowledgement of the value of educational qualifications334 and remorse at not meeting school expectations. 296,314 Therefore, ADHD symptoms also threaten an identity fundamentally important to children and young people in Western societies, that of the ‘good pupil’.
Although important identities for both teachers and pupils are threatened by ADHD, a power imbalance between the institution of schools and individual pupils and their families means, as Prosser314 puts it, that pupils diagnosed with ADHD are ‘the big losers’ (see Agency). Findings from review 4c would also suggest that mothers of pupils diagnosed with or at risk of ADHD also lose out in this power imbalance. 262,266,276,356 Although they have no educational identity under threat, the fundamentally important identity for women of ‘the good mother’ is threatened when their children display ADHD symptoms (see Overarching theme for review 4c: mothers are silenced and Dashed expectations). Some studies in review 4 also suggest that processes in school related to the informal and formal identification of deviance in pupils and a common teacher attribution of poor parenting in relation to ADHD symptoms justifies a breach in the privacy normally afforded to personal relationships in families. 41,356 Such loss of privacy may be experienced as an offence that acts in addition to threats to identity.
Implications of stigma for non-pharmacological interventions for attention-deficit/hyperactivity disorder in schools
Thornicroft348 argues that identification of stigma for mental illness may only perpetuate that stigma unless action is taken at individual, institutional and/or national levels, but that with action, change is possible. The findings of review 4 suggest that in order to address issues related to ADHD in schools, more than individual-level pupil interventions are needed; school-level issues, particularly the issue of stigma in relation to ADHD, need also to be addressed. Owing to the implicit nature of contravened norms in stigma, and because of the perceived threat to the effectiveness of existing educational practice that ADHD symptoms may pose, national-level intervention is implicated in establishing and upholding legislation and policies that support inclusion.
In response to Thornicroft’s distinction of different aspects of stigma as lack of knowledge, application of stereotypical assumptions and discrimination (see Stigma),348 review 4 suggests that the first of these, lack of knowledge, is an important aspect of the difficulties faced by all stakeholders in schools in response to ADHD symptoms, as well as an important candidate for potential change. Many included studies identify a lack of teacher knowledge about ADHD264–266,286,293,294,296,305,324,360 and a few included studies suggest increased knowledge reduces stigma not only through reduction of ignorance and response to stereotypical assumptions, but also because teachers feel less threatened by ADHD-related behaviour when they have strategies to alleviate it in the classroom (see Concern over the emotional equilibrium and learning of the whole class).
Conclusion
Implications for policy and practice
Review 4 findings suggested a need for school policies that:
-
provide guidelines for strategies that teachers can adopt to address disruptive behaviour related to ADHD
-
provide information and guidance related to the nature of ADHD (as differences in beliefs between parents and educational staff often acted as a barrier)
-
provide guidelines to structure collaboration between parents of children diagnosed with ADHD and their teachers
-
provide additional support strategies for pupil behaviour and learning during transitions between preschool and school, and then primary and secondary school, when academic demands change.
Review 4 findings suggested the following might be beneficial in educational practice.
Provision of education to teachers about ADHD, including:
-
information about ADHD symptoms that explores interactions between biological, sociological and psychological factors, including:
-
the nature of the differences between pupils with ADHD and peers
-
information about the potential for classroom factors either to aggravate or to relieve ADHD symptoms
-
the importance of relationships to school functioning for pupils diagnosed with ADHD, including the role of stigma in excluding pupils
-
potential impacts on pupil identity and agency
-
-
information about classroom strategies to support pupils
-
information about effective collaboration with parents.
Provision of resources such as:
-
structured regular time for collaboration between educational staff to discuss support of pupils experiencing difficulties
-
time for classroom teachers to spend in collaboration with parents of pupils diagnosed with ADHD, and/or for administering strategies or non-pharmacological interventions.
Recommendations for research
Gaps in content
There were gaps in research for studies exploring the following:
-
experiences of ADHD for UK teachers
-
experience of gender issues in ADHD in schools across countries (although this issue was repeatedly mentioned as relevant, it was not explored systematically)
-
the impact of increasing maturity for ADHD pupils and differences in school expectations between preschool and primary, and primary/secondary school (this was mentioned as important in different papers, but was not explored in depth). This might involve research exploring pupil and teacher experience, as well as exploration of the impact of additional behavioural and/or learning support for pupils diagnosed with or at risk of ADHD during these transitions.
There were only limited numbers of studies exploring:
-
the experiences of ADHD for secondary school teachers across countries
-
the experiences of children diagnosed with ADHD across countries
-
issues of learning in the classroom in relation to symptoms of inattention (the focus particularly in teacher studies tended to be on hyperactivity/impulsivity and/or disruptive behaviour)
-
teacher–pupil relationships (the key importance of this relationship was a repeated finding; however, only one case study293 explored such relationships in any depth).
Methodological gaps
Studies exploring the perception of more than one participant type in relation to a particular pupil diagnosed with ADHD were able to explore issues in more depth and complexity, but there were only a few studies that adopted this design. This design would be a particularly valuable means to explore:
-
experience of relationships between pupils diagnosed with ADHD and their teachers
-
teacher–parent collaboration for ADHD pupils.
Methodological and theoretical considerations will have influenced study findings; however, the approach to evidence synthesis applied in this review (meta-ethnography) synthesised study findings without reference to the impact of methods and author theoretical considerations on these findings. Considering the broad range of methods and theories that underpinned the studies synthesised, analyses such as meta-theory that evaluate relationships between methods, theory and findings might have allowed inferences to be established more securely. Analysis of such considerations in qualitative systematic review would also create knowledge about the productivity of methods and/or theory in relation to findings, and enable recommendations for the optimisation of useful findings through study design.
Chapter 7 Overarching synthesis
Aims
The aim of the overarching synthesis is to draw together the findings from reviews 1–4. The focus of each review is summarised below.
Review 1 (see Chapter 2) synthesises the evidence on the effectiveness and cost-effectiveness of non-pharmacological interventions delivered in school settings for children and young people with, or at risk of, ADHD.
Review 2 (see Chapter 3) considers quantitative studies that explore attitudes towards school-based non-pharmacological interventions for pupils with ADHD.
Review 3 (see Chapter 5) synthesises the attitudes and experiences of pupils, teachers, parents and others using ADHD interventions in school settings.
Review 4 (see Chapter 6) explores the experiences and perceptions of ADHD in school among pupils, their parents and teachers more generally.
Method
There are few established methods that integrate findings from quantitative and qualitative reviews. The Cochrane Collaboration Qualitative Methods Group argue that the integration of qualitative evidence with intervention reviews aims to inform, enhance, extend and/or supplement issues of interest in quantitative reviews of effectiveness. 411 In one of the few examples of quantitative and qualitative synthesis, Thomas et al. 412 use the findings from their qualitative review as a framework with which to combine these results with findings from their controlled trials. A matrix was used to juxtapose barriers, facilitators and implied recommendations from the qualitative reviews against the actual intervention evaluations reviewed quantitatively. The extent to which the interventions matched the implied qualitative recommendations was analysed, alongside an analysis of whether or not interventions meeting such recommendations proved to be more effective or explained heterogeneity. In another example, where quantitative and qualitative research questions were different, as is the case in the current project, a qualitative review was undertaken in order to explain a lack of evidence for or against the effectiveness of two different approaches to tuberculosis intervention. 413 The qualitative research questions focused on the meanings that people attached to their experiences of tuberculosis and its treatment, and how these shaped their treatment uptake behaviour. Findings in the qualitative review were used to explain quantitative findings by describing potential barriers to uptake and differences between user group needs. In our overarching synthesis, we have adopted similar approaches where they are relevant to our review. We take a dual approach of:
-
inductively working from the qualitative review findings (reviews 3 and 4) about the experience of ADHD interventions and of ADHD in schools more generally to create a model that identifies potential influences among contextual elements on the effectiveness of interventions
-
deductively working from the quantitative findings about the effectiveness of and moderators for interventions for ADHD in schools (review 1) to use findings from reviews 2, 3 and/or 4 to explore potential relationships between possible moderators and effectiveness.
Approach 1 draws from complexity theory414 that assumes any intervention needs to be understood in terms of larger environment and relationships. Approach 2 discusses potential variables and seeks to clarify and develop distinct ideas in relation to the experimental evaluation of interventions. In both cases we aim to identify qualitative findings that illuminate potential explanations for the findings of review 1.
While conducting this overarching synthesis, we had to be cognisant of challenges in the synthesis of different types of evidence, especially when drawing out the implications from this work. As discussed in the previous chapters, quantitative and qualitative research has different aims, methods and questions, and, therefore, different markers of study quality and potential sources of bias. For example, the aim of meta-analysis (conducted in review 1) is to test theory, and interpretation occurs largely before and after synthesis, whereas the aim of meta-ethnography (conducted in reviews 3 and 4) is to generate theory, and interpretation occurs during synthesis to develop meaning. 415 Therefore, although the reliability of the quantitative findings in reviews 1 and 2 may be strengthened through greater frequency of occurrence, qualitative findings in reviews 3 and 4 are strengthened by their ability to inform theory development and represent the complexity and depth of participant perceptions and meanings (for further discussion see Chapter 1, Triangulation of data in quantitative versus qualitative research). Each review has conducted quality appraisal and analysis of the applicability of studies according to its respective research questions, and identified methodological and/or analytical issues in the literature. In reviews 1 and 2, the poor methodological quality of some included studies was identified as a barrier to establishing effectiveness or comparing attitudes (see Table 13; Chapter 3, Discussion). In review 3 analysis used by the majority of studies was mainly at a descriptive level (see Chapter 5, Strengths and limitations). In review 4 important gaps in the literature were identified (see Limitations). Furthermore, in each separate synthesis, then here in this overarching synthesis, we make assumptions about relationships and shared meaning between unconnected studies. 416 In this overarching synthesis, therefore, we can only explore potential relationships between and explanations for review findings and any conclusions remain tentative. The following sections describe the procedure we undertook during this overarching synthesis.
We commenced the overarching synthesis by undertaking a collaborative question and answer exercise. This first stage occurred before the completion of review 2, so was conducted using findings from reviews 1, 3 and 4. Questions based on the findings of reviews 1, 3 and 4 were generated and used to interrogate the other two reviews for information that could potentially inform the findings or reveal gaps. Questions were framed systematically using the format ‘review 1 found X, can reviews 3 or 4 inform these findings?’. The lead reviewer of each review developed questions in the agreed format and the other lead reviewers responded to these questions from the perspectives of their reviews. The six resultant sets of questions and answers were analysed independently by the three reviewers (MR, DM, RGJ) and later discussed.
Analysis under the two approaches described above proceeded iteratively and in parallel, rather than sequentially. In approach 1, we started with the findings from reviews 3 and 4 in order to identify the contextual elements that might influence the effectiveness of interventions. DM and RGJ developed a coding framework derived from the question and answer exercise relating to reviews 3 and 4 (see first column of Table 64). DM and RGJ coded reviews 3 and 4 respectively in NVivo v.9.2 using this framework, and then short summaries of codes that appeared in each review were produced. These were reduced to short sentences and tabulated for the purpose of display in this chapter. These code summaries were further analysed and refined, leading to the identification of four levels of context, and identification of key categories linking to each level across reviews 3 and 4. A conceptual model (Figure 9) was created to represent a hierarchy of levels and key categories that might potentially influence the effectiveness of interventions for ADHD in schools. Finally, a narrative synthesis describing findings from reviews 3 and 4 about the relationships between levels, key categories and subthemes in the model and table was written.
| Level of context; key categories; subthemes | Findings from review 3: the attitudes and experiences of pupils, teachers, parents and others using ADHD interventions in school settings | Findings from review 4: the experiences and perceptions of ADHD in school among pupils, their parents and teachers more generally |
|---|---|---|
| Pupil-level factors: pupil knowledge about beliefs about ADHD | ||
| Lack of knowledge about ADHD | Awareness about their disorder was thought to help intervention success for pupils with ADHD | Pupils expressed confusion about the nature of ADHD, particularly a lack of knowledge about sociological and psychological aspects |
| Beliefs about ADHD including biological factors and medication | Pupils with ADHD often perceived reasons for attending interventions to relate to difficulties originating in themselves | Pupils most often expressed polarised biological attributions for ADHD, where they understood their symptoms as a problem in themselves, including a character flaw and/or biological deficit. It was common in studies for pupils to describe medication as the only potential treatment, and to express the belief that they were incapable of controlling their behaviour |
| Pupil-level factors: identity, agency, processes of stigma and marginalisation | ||
| Desire for approval | No relevant findings | Pupils wish to meet school expectations and are distressed and full of remorse that they cannot |
| Low self-esteem/issues of identity | Low self-esteem is seen as a problem for pupils with ADHD | ADHD is linked to negative impact on self-esteem and developing identity |
| Agency | Pupils with ADHD held low self-efficacy, attributing learning outcomes to circumstances beyond their control Studies noted the lack of agency seemingly experienced by pupils displaying ADHD symptoms during interventions and learning more generally |
Many factors related to ADHD have the tendency to decrease pupil agency |
| Negative attitudes towards school | There are negative attitudes towards school and learning seen from pupils with ADHD | Negative emotions about school can accumulate over the course of the school careers of pupils with ADHD |
| Pupil-level factors: prior experiences | ||
| The experience of ADHD symptoms | No relevant findings | Pupils often link their symptoms to issues in relationships, the classroom environment and self-perceptions. They express most concern over relationships |
| Lack of knowledge about ADHD | Awareness about their disorder was thought to help intervention success for pupils with ADHD | Pupils expressed confusion about the nature of ADHD, particularly a lack of knowledge about sociological and psychological aspects |
| Maturity important for intervention effectiveness | The age of pupils with ADHD was frequently mentioned as a moderator | No relevant findings |
| Classroom-level factors: fit of pupil to the class | ||
| Fit of pupil to the classroom | Teachers see ADHD as a problem situated within the child, meaning that action is taken to compensate for the child rather than address the context | A number of studies established that ADHD is a problem in the relationship between a pupil and a classroom as much as a problem with a pupil; for example, pupils with ADHD behaved differently in different classrooms according to relationships with teachers, teaching styles and classroom structure |
| Noise and movement barrier to learning | Some studies consider the opportunity for movement and socialising as critical for pupils with ADHD | Pupils with ADHD commonly describe the classroom as a difficult context in which to learn |
| Facilitators to learning | No relevant findings | Pupils described the enjoyment of learning; however, they usually experienced successful learning outside a school context |
| Teacher responsibility to the whole class | Many studies highlight a tension for regular class teachers between implementing individualised strategies for pupils with ADHD, while managing and remaining responsible to a whole class of pupils | Teachers’ primary responsibility was to the learning of the whole class and this could act as a barrier to responding to ADHD pupils in many ways |
| Teacher stress | No relevant findings | Without strategies to address ADHD behaviour in the classroom, teachers can experience high levels of stress |
| Withdrawal vs. inclusion | Educators across many studies believed that withdrawing pupils from their regular classroom to allow for specialised learning is beneficial. But there are dilemmas regarding withdrawal from mainstream classrooms | Classroom context and teacher knowledge influenced views on withdrawal/inclusion; classes (such as preschool) where academic attainment was not a priority were more likely to favour inclusion; classroom teachers of older pupils sometimes preferred withdrawal because of conflicts between inclusion and whole class learning |
| Classroom-level factors: teacher knowledge about ADHD | ||
| Lack of knowledge | Teachers’ lack of guidance and knowledge is perceived as a barrier by them across a large number of studies. One study found that a teacher training workshop successfully increased knowledge and attitude towards ADHD | Teachers described a lack of knowledge about ADHD in many papers Pupils described a lack of knowledge about ADHD in many papers Parents described a lack of teacher knowledge in many papers This seems to be an important barrier to the improvement of symptoms |
| Teacher collaboration | Peer support (colleagues) were seen as more consistently helpful than outside experts | Teachers describe learning through collaboration with colleagues as effective |
| Education changing attitudes and practice | Interventions that targeted attitude towards ADHD were generally received positively by teachers and were perceived to improve attitudes | Teachers describe changes in attitudes, practice and/or levels of stress in response to education about ADHD |
| Classroom-level factors: teacher pedagogy in response to ADHD | ||
| Curriculum/teaching style | Many studies recognised the tension between prescribed learning and choice, with pupils and teachers feeling that both must play a part in pedagogy for pupils with ADHD | Studies found that pupils with ADHD behaved differently in different classrooms according to relationships with teachers, teaching styles and classroom structure |
| Teacher strategies likened to good practice | Teachers report using existing mainstream teaching strategies with pupils with ADHD. Sometimes this is a necessary resort given the lack of guidance available regarding teaching pupils with ADHD | Teachers explained that knowledge gained in general teacher training that was effective with most pupils was often not effective with pupils diagnosed with ADHD |
| Structure and meaning | Tension was reported in several studies between the structure, routine and control associated with interventions and strategy use for pupils with ADHD on one hand and choice, flexibility and responsibility on the other hand. Several studies do recognise that structure and choice are not mutually exclusive | Pupils diagnosed with ADHD describe the added ease with which they engage with school topics that have personal relevance to them and/or that they are interested by. They also describe the desire to understand why they are learning what they are being taught |
| Supervision | Studies generally consider that these pupils need close supervision and greater teacher attention than that typically required for other children. Yet often pupils respond negatively to high levels of monitoring | Pupils describe how questions from teachers (asking how they are doing) can act to interrupt them from concentration which they then cannot return to |
| Perceived effectiveness of interventions | The majority of studies reported positive comments from users regarding the effectiveness of interventions | No relevant findings |
| Perceived need for study skills | Several studies noted that pupils with ADHD need support with study skills and that these skills are perceived to have a marked effect on learning | No relevant findings |
| Previous experiences of interventions impact future responses | Experience provides a context in which any future intervention must operate. Experience of prior interventions affects anticipation and experience of future interventions | Pupil’s negative attitudes and resistance from mothers are described as escalating across school careers |
| Classroom-level factors: teacher beliefs about ADHD | ||
| Beliefs about ADHD | Beliefs about ADHD often cast ADHD as a problem. There were mixed beliefs about how much control pupils with ADHD have over the expression of their symptoms. There was some resistance to working with pupils with ADHD reported by teachers. Knowledge gained about ADHD seemed to improve attitudes for teachers | Attributional beliefs were found to impact teacher response to ADHD behaviour, quality of relationships, pupil self-perceptions and expression of symptoms in both helpful and harmful ways Studies revealed that polarised attributions predominated, which could limit choice of strategies/interventions and often impacted pupils negatively. This included perceptions of pupil self-control, which was often perceived dichotomously |
| Polarised biological views of ADHD | Teachers see ADHD as a problem situated within the child, and action is taken to compensate for the child in preference to addressing the contextual factors that might have indicated alternative views | Potential benefit: explanation, basis for differential treatment (medication and sometimes classroom adaptation), relief of stress Potential limitation: can decrease teacher understandings of pupil accountability when linked to perceptions of no behavioural self-control, can narrow treatment to medication, can negatively impact identity and perceptions of agency in pupils |
| Polarised sociological views of ADHD | No relevant findings | Potential benefit (when understood as poor parenting): none identified Potential limitation: reason to dismiss concept of ADHD, to reject need for differential treatment and can act as a barrier to teacher–parent collaboration |
| Psychological views about ADHD | No relevant findings | Teachers: ‘naughty child’ = poor parenting (so same as sociological) Pupils: ‘naughty child’ = ‘something wrong with me’ (so same as biological) |
| Maturational views about ADHD | Teachers’ beliefs about or experience of which interventions would be effective differed according to the age of the pupil. For instance, some teachers reported that interventions were used less once children reached middle school years | Discussed by early years teachers Potential benefit: considers interactions between biological, sociological and psychological factors in ADHD behaviour so is a holistic response Potential limitation: reason to dismiss concept of ADHD, can prevent both drug and non-drug treatment |
| Differences in beliefs between stakeholders can be a barrier to interventions | No relevant findings | Differences in attributional beliefs about ADHD between parents and teachers were identified as a fundamental barrier to effective change |
| Classroom-level factors: relationships: processes of stigma and marginalisation | ||
| Teacher–pupil relationships | All types of participants across studies reported the importance of positive relationships between teachers and their pupils with ADHD | Conflict was the norm between teachers and pupils diagnosed with or at risk of ADHD |
| Teacher–parent relationships | Educators across multiple studies voice the importance of effective relationships with parents and its impact on the success of interventions Teachers and parents sometimes recognise that much of the communication occurring between school and home regarding pupils with ADHD is negative |
Conflict was the norm between teachers and mothers (who tended to be the parent involved with schools) of pupils diagnosed with or at risk of ADHD |
| Pupil–peer relationships | Pupils with ADHD often have poor relationships with their peers. Still teachers think pupils with ADHD should work with their peers | Studies commonly report difficulties with peer relationships, and greater numbers of pupils diagnosed or at risk of ADHD were bullied or were bullies Conflict was not necessarily the norm – with ‘shunning’ common, where the pupil was ignored |
| Stigma | The view of ADHD as a problem situated within the diagnosed child seen across research, leads to frequent stigmatisation as evidenced across studies | Studies suggested stigma could act as a mechanism that creates focus on ADHD pupils as ‘the problem’ to the exclusion of other factors |
| Stigma attributable to interventions | Stigmatisation experienced does not necessarily relate to ADHD, but attending interventions | No relevant findings |
| Stigma from teachers | Some disbelief regarding the existence of ADHD or the severity of the disorder was seen from mainstream teachers and this was recognised by pupils | Study data and/or findings from a number of papers suggested stigma for the ADHD label and/or ADHD symptoms was present |
| School-level factors: processes of stigma and marginalisation | ||
| Processes of stigma and marginalisation | No relevant findings | Schools may unintentionally support stigma when they perceive ADHD symptoms as a threat to existing educational practice; in such cases marginalisation may result |
| School-level factors: resources | ||
| Knowledge | Teachers from many countries report that they are working in schools that do not have ADHD specific guidance | Teachers explained that knowledge gained in training that was effective with most pupils was often not effective with pupils with ADHD, and many expressed the need for greater knowledge of ADHD. A shortage of capacity-building about ADHD and classroom strategies provided by teacher education and continuing professional development can be seen as a barrier to support for pupils diagnosed with ADHD |
| Class size | The most frequently mentioned structural constraint in review 3 was mainstream class size | Teachers, particularly those in secondary schools who teach multiple classes of different pupils, and who therefore find it harder to get to know their pupils and have less time to spend on addressing the needs of individual pupils, describe the need to relate to such a large number of pupils as a barrier to support for pupils diagnosed with ADHD |
| Time pressure | Many teachers across studies emphasise the time pressure involved in accommodating pupils with ADHD | Teachers talk about lack of time to address symptoms, give pupils individual attention, communicate with parents School culture dictates priorities, for example academic attainment over pastoral issues; preparation for national exams can act as a barrier |
| Lack of support | No relevant findings | Some teachers describe lack of support from senior management regarding behaviour management and provision for ADHD pupils |
| School-level factors: policy | ||
| Accountability | No relevant findings | Teachers and parents in some studies lacked understanding about what collaboration over a pupil diagnosed with or at risk of ADHD should be, including who was responsible for what. This finding was commensurate with other data from other studies that did not specifically identify that theme |
| ADHD policy | No relevant findings | Some studies identified that a lack of school-level guidance about ADHD acted as a barrier, in relation to classroom support of pupils diagnosed or at risk of ADHD and to collaboration between parents and teachers. School policies could lead with information about ADHD that could support resolution of differences in beliefs between parents and teachers |
| Sociopolitical-level factors | ||
| Medicalisation | No relevant findings | Some studies found pupils diagnosed with ADHD and/or some teachers and parents to hold medicalised beliefs about ADHD which could result in narrowed conceptualisation of effectiveness favouring medication over non-pharmacological intervention; authors concluded that trends towards more highly medicalised societies influence beliefs and actions with regard to ADHD |
| National educational policies and legislation | No relevant findings | National educational policy and legislation guide school expectations and constraints placed on teachers |
| Power imbalance | No relevant findings | Though the dynamics of ADHD tend to play out in the classroom, the drivers for these dynamics can be located in expectations established in the sociopolitical and then school level contexts. The interests expressed by pupils and parents were least often taken into account, despite outcomes having great impact on them |
FIGURE 9.
Contextual levels and key categories identified through synthesis of reviews 3 and 4, categorised at pupil, classroom, school and sociopolitical levels of context.

In approach 2, we started from the quantitative findings about the effectiveness of and moderators for interventions for ADHD in schools (review 1) in order to identify findings in reviews 2, 3 and/or 4 that offered hypotheses about the relationships between possible moderators and effectiveness. During this process three additional tables were created. In Table 65, the effectiveness findings from review 1 were tabulated, in Table 66 the potential moderators related to intervention packages from review 1 were tabulated, and in Table 67 the other potential moderators, including delivery characteristics, participant characteristics and study design, were tabulated. For each table reviewers then considered how the findings reported in reviews 2, 3 and 4 could inform, support or contradict what was reported in review 1 and generate potential hypotheses about the relationships between possible moderators and effectiveness.
| Outcome measure | Review 1 (95% CI)a | Review 3 | Review 4 |
|---|---|---|---|
| Core symptoms | |||
| Inattention (teacher) | d+ = 0.60 (0.14 to 1.06) | Teachers report that routine will help pupils feel secure and respond to issues of inattention | No relevant findings |
| Inattention (child) | d+ = 0.44 (0.18 to 0.70) | No relevant findings | No relevant findings |
| Inattention (observer) | d+ = 1.30 (–0.17 to 2.77) | No relevant findings | No relevant findings |
| Hyperactivity/impulsivity (teacher) | d+ = 0.23 (–0.03 to 0.49) | No relevant findings | Findings suggest that teachers often considered symptoms of hyperactivity and impulsivity to be of greater concern than symptoms of inattention |
| Hyperactivity/impulsivity (child) | d+ = 0.33 (0.13 to 0.53) | No relevant findings | Young people with ADHD report issues regarding emotional self-regulation more than hyperactivity and impulsivity |
| ADHD-related symptoms | |||
| Externalising symptoms (teacher) | d+ = 0.28 (0.04 to 0.53) | No relevant findings | Externalising behaviour such as anger and defiant behaviour were described as escalating over the school career in a number of papers exploring ADHD pupil experience; suggests these symptoms could be highest during secondary school years |
| Scholastic behaviours and outcomes | |||
| Perceptions of school adjustment (teacher) | d+ = 0.26 (0.05 to 0.47) | There are negative attitudes towards school and learning seen from pupils with ADHD | Negative attitudes to school |
| Curriculum achievement (child) | d+ = 0.50 (–0.06 to 1.05) | Some studies revealed that teachers and pupils with ADHD might be more interested in achievement than other outcomes | No relevant findings |
| Standardised achievement (child) | d+ = 0.19 (0.04 to 0.35) | Some interventions were seen to be effective for specific targeted skills, yet were not perceived to impact on achievement | No relevant findings |
| Other | Not applicable | Additional pupil outcome measures considered by studies: mood, attitude, motivation, organisational skills | Pupils’ emotional self-regulation, pupil and teacher attributional beliefs and pupil self-perceptions (e.g. agency/self-efficacy) suggested as relevant outcomes |
| Intervention package identified in review 1 | Definition of intervention package identified in review 1 | Frequency of intervention packages and summary of corresponding moderator analyses in review 1 | Review 3 relevant findings | Review 4 relevant findings | |
|---|---|---|---|---|---|
| Reward and punishment | |||||
| 1. | Contingency management | Systematic use of rewards and/or punishments to change, alter or redirect the child’s behaviour(s) | RCTs n = 19 Non-RCTs n = 7 Tested: no evidence from analysis that inclusion of contingency management may have an impact on effectiveness |
1/12306 studies that focused on interventions Pupils with ADHD, particularly adolescents, often indifferent to contingency management Negative behavioural sanctions deemed unsuccessful by pupils with ADHD Pupils with ADHD need immediate reinforcement |
No relevant findings |
| 2. | DRC with contingency managementa | A method used by teachers and/or parents in collaboration with a child to set goal(s), and monitor progress towards them. Rewards and/or punishments are then used in response to the child’s progress towards their goals in order to reinforce the wanted behaviour(s) or create barriers to the unwanted behaviour(s) | RCTs n = 7 Non-RCTs n = 2 Tested: no evidence from analysis that inclusion of DRCs may have an impact on effectiveness |
0/12 Parents reported benefits from working more closely with the school as part of the intervention used in Ozdemir’s 2006 study306 Teachers and parents sometimes recognise that much of the communication occurring between school and home regarding pupils with ADHD is negative. Collaboration can be challenging |
Collaboration found to be important but challenging for teachers and parents |
| Skills training and self-management | |||||
| 3. | Motivational beliefs | Encourage or facilitate the adoption of beliefs that facilitate self-motivation towards obtaining the focal behaviour(s) (e.g. the attribution of success at school to hard work and effort) | RCTs n = 2 Non-RCTs n = 0 Not tested: insufficient data for moderator analyses |
0/12 Participant explanations for the ineffectiveness of interventions and strategies included pupil’s lack of motivation and passivity towards learning Lack of motivation was perceived to be due to disinterest, difficulties learning and lack of perceived relevance |
A sense of lack of agency was found to be common in pupils diagnosed with ADHD for a number of reasons; also alienation from school and learning is highly likely to impact negatively on the motivation to learn |
| 4. | Cognitive–behavioural self-regulation training | Establish methods for the child to self-monitor and record their behaviour(s). Includes analysing the factors that lead to problem behaviour(s) and identifying solutions to overcome them (‘problem solving’) and self-instruction on how to perform the behaviour(s) | RCTs n = 10 Non-RCTs n = 7 Tested: (n.s.). No evidence from analysis that cognitive–behavioural self-regulation training has an impact on effectiveness |
0/12 studies Teachers recognised difficulties on self-regulation for pupils displaying ADHD symptoms |
Brice 1998331 found pupils diagnosed with ADHD are often unaware of situations that precede or trigger loss of behavioural control; Houghton 2006296 finds pupils who become aware of such triggers are better able to take control of their learning |
| 5. | Cognitive retraining | Training and practice in the use of cognitive processes related to executive functioning (e.g. attention and working memory) | RCTs n = 4 Non-RCTs n = 3 Not tested: insufficient data for moderator analyses |
1/12280 (metacognitive skills training) Issues of applicability for this study – students did not apply skills they had learned beyond intervention setting |
No relevant findings |
| 6. | Academic and study skills training | Training and practice in academic skills (e.g. reading and writing strategies) and general study strategies (e.g. note taking, test taking, organisation and time management) | RCTs n = 12 Non-RCTs n = 5 Tested (n.s.). No evidence from analysis that inclusion of academic and study skills training have an impact on effectiveness |
1/12301 Several studies280,287,289,293,300 noted that young people with ADHD need support with study skills and that these skills are perceived to have a marked effect on the learning of these pupils |
No relevant findings |
| 7. | Social skills training | Training and practice in effective social interaction | RCTs n = 6 Non-RCTs n = 3 Tested (p < 0.06). For the ‘perceptions of school adjustment’ outcome, there was weak evidence that inclusion of social skills training has a negative impact on effectiveness |
0/12 Part of skills taught in three special education classrooms to younger pupils (aged 6–12 years)295,302,303 Pupils with ADHD often have poor relationships with their peers The importance of social skills is recognised across a number of studies where such skills are actively incorporated into interventions and teaching strategies with perceived effectiveness |
Pupils of both primary and secondary age diagnosed with, or at risk, of ADHD express great concern over the difficulties they experience in relationships. Teachers and parents also remark on the importance of these difficulties. Authors of included studies remark on the greater social demands of secondary schools, and the greater social difficulties pupils face there |
| 8. | Emotional skills training | Training and practice in learning to recognise and control emotions (e.g. relaxation training and/or enhancing positive emotion) | RCTs n = 11 Non-RCTs n = 0 Tested (n.s.). No evidence from analysis that inclusion of emotional skills training has an impact on effectiveness |
0/12 In relation to emotional skills, low self-esteem is seen as a barrier to learning and intervention effectiveness for pupils with ADHD Several papers280,287,289,293,300 reported that pupils felt their self-confidence increased as a result of interventions used |
Lack of emotional self-control is an issue commonly described by pupils with ADHD; it is also commented on by teachers and parents. Authors link it to difficulty in relationships There is a predominance of poor self-perceptions in ADHD pupils |
| 9. | Biofeedback | Feedback about physiological or biochemical activity (e.g. heart rate and brain waves) using an external monitoring device to enhance self-control of behaviour(s) | RCTs n = 8 Non-RCTs n = 1 Not tested: insufficient data for moderator analyses |
0/12 | Same information relevant as for cognitive–behavioural regulation training; see above |
| Creative-based therapy | |||||
| 10. | Music therapy | Music used in a prescribed way to modify or alter thoughts, emotions and behaviours | RCTS n = 3 Non-RCTs n = 0 Not tested: insufficient data for moderator analyses |
0/12 Although not therapeutic, one intervention311 involved listening to music. Perceived to be effective by the pupil with ADHD, his parents and teacher |
Two studies331,334 describe pupils diagnosed with ADHD who choose to listen to music in the classroom because it enables them to concentrate |
| 11. | Play therapy | Play used in a prescribed way to modify or alter thoughts, emotions and behaviours (including narrative therapy) | RCTs n = 1 Non-RCTS n = 0 Not tested: insufficient data for moderator analyses |
0/12 | No relevant findings |
| Physical treatment | |||||
| 12. | Massage | Applying pressure to parts of the body (e.g. rubbing or kneading in a prescribed way to modify or alter thoughts, emotions and behaviours) | RCTs n = 1 Non-RCTs n = 0 Not tested: insufficient data for moderator analyses |
0/12 | No relevant findings |
| 13. | Structured physical activity | Planned physical activity with the aim of increasing energy expenditure and improved physical fitness and health | RCTs n = 0 Non-RCTs n = 1 Not tested: insufficient data for moderator analyses |
0/12 Studies consider the opportunity for movement and socialising at break time as critical for pupils with ADHD |
One study333 identified the theme ‘I gotta move’, where pupils described the way movement made them feel more comfortable; another study found similar334 |
| Other | |||||
| 14. | Adaptations to learning environment | Alteration to the environment (physical and social) where learning takes place and/or learning materials in order to facilitate performance of the wanted behaviour or create barriers to the unwanted behaviour (e.g. adapt teaching methods, tasks and classroom) | RCTs n = 3 Non-RCTs n = 3 Not tested: insufficient data for moderator analyses |
5/12 studies265,295,300,302,303 mainly focused on special educational programmes in alternative classrooms or schools Many adaptations to teaching made on ad hoc basis reported by teachers in other studies Many studies highlight a tension for regular class teachers between implementing individualised strategies for pupils with ADHD, while managing and remaining responsible to a whole class of pupils |
Expression of ADHD symptoms is more accurately conceptualised as an interaction between the pupil and their class rather than a problem in the pupil, suggesting interventions that target the learning environment for adaptation may be effective. Review 4 also found tension for regular class teachers between responsibilities for the whole class vs. one pupil |
| 15. | Information | Provide information about focal behaviour(s) (e.g. information about positive peer relationships, communication skills) | RCTs n = 1 Non-RCTs n = 0 Not tested: insufficient data for moderator analyses |
1/12288 (teacher training) Component of one programme for students with ADHD303 Regarding teachers’ psychoeducation, teachers’ lack of guidance and knowledge is perceived as a barrier by them across a large number of studies reviewed The workshop for teachers that appeared in Bos’ 1997 study288 was claimed to change teacher attitudes and increase their knowledge Helping pupils with ADHD understand their behaviour and its effects considered important |
Teachers and pupils (and some parents) expressed the need for information about ADHD. Review 4 findings suggest the way ADHD is understood can act as a barrier to addressing symptoms. Attributional beliefs that explain ADHD symptoms as an interaction between biological, psychological and sociological (including school relationships and school context) factors may provide a more beneficial approach to conceptualising ADHD than polarised biological or sociological explanations |
| Source of heterogeneity | Review 1 | Review 3 | Review 4 |
|---|---|---|---|
| Study characteristics | |||
| Comparator type: treatment as usual vs. Experiment | Not tested: insufficient number of studies | ||
| Participant characteristics | |||
| Medication status at start of treatment: high (≥ 60% using) medication vs. low (< 10% using) | Tested (n.s.) | Medication use improved the perceived effects of some interventions | Pupils, teachers and parents describe medication as helpful in improving attention and controlling behaviour; however, it can have a negative impact on pupil identity and agency; some pupils describe unpleasant side effects; some pupils do not want to take medication but do so to please parents and teachers |
| Gender: % female | Not tested: insufficient variance between studies | Lack of gender comparison | Differences were often identified between genders in relation to behavioural expectations and/or ADHD behaviours in review 4, but this issue was not addressed systematically in most studies that comment on it, and is sometimes discussed in confused terms. This seems to be an important gap |
| Grade level: elementary/primary vs. higher school levels | Not tested: insufficient variance between studies | The age of pupils with ADHD was frequently mentioned as a moderator More focus on academic interventions at secondary school. Differences between interventions used at preschool and primary school |
The finding that some symptoms decreased with age (hyperactivity) and some symptoms increased with age (difficulty with social skills; internalising and/or externalising behaviour) were represented in studies Differences between primary and secondary school structures were also suggested to contribute to pupil difficulties (e.g. added academic and social pressures of secondary schools alongside reduced teacher support) |
| Intervention delivery | |||
| Frequency of packages: single vs. multiple | Tested (n.s.) | No relevant findings | Different priorities for different stakeholders implies a need for multiple interventions (e.g. teachers value control of disruptive behaviour; pupils desire improved relationships) |
| Intervention context: school and home vs. school only | Tested (n.s.) | The inclusion of parents was considered a positive thing in one study306 | Parent–teacher collaboration suggested to be powerful in supporting behaviour change |
| Setting within school: classroom vs. all other settings | Tested (n.s.) | Mixed teacher perceptions regarding benefit of withdrawing pupils from their classroom | No relevant findings |
| Time of delivery: normal school hours vs. before/after school | Tested (n.s.) | No relevant findings | No relevant findings |
| Intervention provider: teachers vs. non-school staff | Tested (n.s.) | Teachers report time pressure and tension regarding responsibility to rest of class when they deliver interventions | Teachers describe importance of knowledge of classroom setting when implementing strategies in mainstream classes |
| Duration of intervention: weeks | Tested (p < 0.05) for ‘perceptions of school adjustment’, there was weak evidence for the negative effect of intervention length suggesting that shorter interventions are more effective | Of relevance when teachers provide the intervention, teachers emphasise the time pressure involved in accommodating pupils with ADHD. One study suggested teachers often do not see through interventions, hence shorter may be more likely to be implemented in full. However, several interventions experienced perceived to need more time | No relevant findings |
| Intensity of intervention: hours | Tested (n.s.) | Of relevance when teachers provide the intervention, teachers emphasise the time pressure involved in accommodating pupils with ADHD | No relevant findings |
| Frequency of packages: single vs. multiple | Tested (n.s.) | No relevant findings | Different priorities for different stakeholders implies a need for multiple interventions (e.g. teachers value control of disruptive behaviour; pupils desire improved relationships); the complexity of context suggests that interventions targeting isolated aspects of ADHD symptoms may be less effective |
Finally, in the discussion section we bring together the inductive and deductive approaches taken to highlight the key potential relationships between possible moderators and effectiveness of non-pharmacological school interventions and to consider the complexity of the context in which these interventions are used. Strengths and limitations of the approach that we used for this overarching synthesis are discussed and implications of the findings are considered. Implications for policy and practice, and recommendations for research, are drawn from the report as a whole and considered in Implications.
Findings
Inductive synthesis: complexity of context
In this section we summarise the findings from review 1 about the effectiveness of non-pharmacological interventions for ADHD in schools, and then report the inductively synthesised qualitative review findings (reviews 3 and 4) in the form of a model (see Figure 9) that identifies issues that are potentially relevant to the findings about the effectiveness and heterogeneity of interventions.
In summary, the results of review 1 indicate that interventions that target children with, or at risk of, ADHD are typically composed of multiple features and few interventions consist of common sets of intervention elements. Lack of consistently used outcome measures adds to the complexity, as several measures have been developed to assess the same constructs. Both these issues made synthesis difficult (see Table 3 in Chapter 2). Owing to the range of interventions reported in review 1 and the lack of overlap in intervention elements between studies, results were synthesised by outcome and rater across different types of intervention in the meta-analyses. The findings from review 1 provide overall support for the beneficial effects of non-pharmacological interventions on child outcomes related to ADHD. Focusing on the meta-analysed RCTs (n = 36), weak to strong evidence (p-values range from 0.08 to 0.001) of beneficial effects was observed for core ADHD symptoms (‘inattention’, ‘hyperactivity’), and ADHD-related symptoms (‘externalising’ symptoms) as well as scholastic behaviours and outcomes (‘perceptions of school adjustment’, ‘curriculum achievement’ and ‘standardised achievement’) (see Table 14 for the results of the meta-analyses of RCTs and Table 3 for definition of outcomes). Beneficial effects were reported for relatively objective assessments, which included neurocognitive assessments and tests with objective performance criteria (see Table 65). Beneficial effects were also observed for some teacher perception-based measures but not for parental- and child-reported perception-based measures. There was little evidence of beneficial effects of intervention for two ADHD-related symptoms (‘internalising’ symptoms, and ‘social skills’) and the core symptom ‘ADHD combined’, which includes both ‘hyperactivity’ and ‘inattention’.
Pooled effect sizes ranged from very small (d+ < 0.2) to large (d+ ≥ 0.8), and CIs were wide, which emphasises high levels of uncertainty about the true value of pooled effects. With the exception of neurocognitive assessment of ‘hyperactivity/impulsivity’, ‘standardised achievement’ and teacher ‘perceptions of school adjustment’, I2 values indicated substantial heterogeneity in effect sizes across studies. Meta-regressions showed weak evidence (p = 0.06) for possible harmful effect of social skills training on ‘perceptions of school adjustment’. For the same outcome, there was also weak evidence for harmful effect related to intervention length (p = 0.04), with longer interventions linked to negative outcomes. No effects were reported for the remaining potential moderators identified, which included a range of intervention packages, intervention delivery characteristics and participant characteristics. It is important to note that these meta-regressions were based on few studies of generally low methodological quality and, therefore, conclusions based on the findings must necessarily be tentative.
No studies included economic outcomes, thus the cost-effectiveness of non-pharmacological interventions targeting pupils with, or at risk of, ADHD cannot be established from the current evidence base.
In order to contextualise and illuminate potential explanations for the findings from review 1 regarding heterogeneity of effect sizes, the findings from reviews 3 and 4 were synthesised. This synthesis identified four levels of context: pupil, classroom, school and sociopolitical, within each of which we defined key categories, depicted in Figure 9. Such a categorisation by level of context is likely to be an overly simplistic distinction, in that many issues within key categories hold relevance for multiple levels, for example the operation of stigma for ADHD and time pressures on teachers relate to all levels of context from sociopolitical to the pupil concerned. In the narrative discussion in the remainder of this section, we give some examples of interactions across multiple contextual levels; however, in general we simply acknowledge this shortcoming in favour of the benefits of using this approach because of its ability to depict and help understanding of the complexity of interaction within and between levels.
Reviews 3 and 4 identify beliefs about ADHD to be an important potential moderator that can act at all contextual levels. A central finding from reviews 3 and 4 is the tendency by educational staff to focus either on biological or ‘within-child’ factors as an explanation for ADHD at the pupil level of context, or to reject the validity of the syndrome of ADHD and attribute ADHD symptoms to difficulties in the pupil’s home such as ‘poor parenting’. Either tendency may lead to the failure to consider other potentially important factors that may be present at the pupil, classroom, school and sociopolitical levels that could aggravate or ameliorate ADHD symptoms. This can confine the focus of interventions to those factors that target adaptation of the pupil, and exclude consideration of other potential targets for adaptation, such as teaching staff, classroom or school. Polarised beliefs can also negatively impact pupil self-perceptions and perceptions of agency, which may also aggravate ADHD symptoms (for further discussion, see Chapter 6, Impact of polarised views). Social trends such as increasing medicalisation (for a definition see Chapter 6, Box 11) were identified by studies as offering an ideology that supports the concept of ADHD as a within-child problem. Some studies linked polarised biological beliefs in educational staff to a focus on medication for ADHD to the exclusion of non-pharmacological intervention. However, teachers in other studies believed that ADHD diagnosis provided validation of these pupil’s different learning needs, and therefore justifies adaptation to pedagogy. Reviews 3 and 4 identified attitudes towards ADHD held by pupils with ADHD, their teachers, parents and peers to be important potential barriers and/or facilitators to non-pharmacological interventions in schools. Review 2 focused on attitudes towards school-based interventions for ADHD and found that educators had varying attitudes, and highlighted DRCs as the only intervention towards which educators showed positive attitudes across studies.
Reviews 3 and 4 demonstrated the significance of relationships, suggesting that they are potential moderators to intervention effectiveness, particularly relationships between the teacher and pupil, but also between pupils and peers. The relationships between pupils displaying ADHD symptoms and educators are a contextual factor that frames how interventions are perceived by both pupils and the intervention provider(s). For instance, review 3 suggests that pupil–teacher relationships are an active element of intervention and can impact the effectiveness of interventions. Stigma was identified as a potential reason for negatively impacted relationships at pupil, classroom and school levels that could further aggravate symptoms.
Findings from reviews 3 and 4 suggest that stigma for pupils who display symptoms of ADHD is common in schools and, therefore, that stigma is likely to influence how well interventions work. Stigma acts as a protective device for existing social practice (for further discussion see Chapter 6, Box 33) and, therefore, may act against the adaptation of current educational practice in addition to marginalising the pupil, and possibly the pupil’s family. Included studies suggest that ADHD symptoms result from an interaction between the pupil and the classroom structure and routine, for example where the need to sit still and concentrate for long periods of time can aggravate symptoms. Although educational structures and routines are broadly similar between schools, specific boundaries for accepted behaviour are established locally by school and even classroom. These are implicitly understood and accepted as normal; the pupil displaying ADHD symptoms contravenes these expectations and can first informally, then formally, be marginalised and excluded on the basis of such contraventions. Review 3 found that interventions and support intended to result in normalisation of the pupil can actually further aggravate stigma and marginalisation, because treating the pupil differently can make any perceived differences more explicit.
Studies in reviews 3 and 4 suggest that systemic issues at the national and school level may act to moderate the effectiveness of interventions. Power differences between the levels of context identified are evident; for instance, schools are required to follow national policy and legislation that can work against inclusive practice. For example, national targets for improved academic outcomes and school exam results published in league tables place pressure on schools, which, alongside financial constraints, can influence matters of resource at the school level. The purchase of interventions, education for teachers about ADHD and time allocated to teachers to implement classroom interventions and/or collaborate with colleagues and parents may receive lower priority than academic considerations for the majority of pupils. Policy moves towards more inclusive practice may mean reduced scope for specialist services; for example, pupils who would previously have attended pupil referral units or specialist schools might be placed in mainstream classes. Although the aim is towards inclusion, unless teachers receive adequate training and resources to meet additional demands for pedagogy and behaviour management, the result can be frustrated, stressed teachers and escalating behavioural difficulties from pupils.
Teachers are also required to teach within the constraints and priorities established at the school level. In reviews 3 and 4, teachers identify the time pressure involved in the accommodation of pupils with ADHD, particularly within mainstream classrooms. Lack of guidance and knowledge are perceived as barriers by teachers across a large number of studies reviewed; this lack of guidance often leads teachers to use general teaching methods, which may be ineffective for pupils with ADHD. Many teachers in reviews 3 and 4 describe their responsibility to the whole class rather than the individual pupil. Some review 4 studies found that, in order to meet the needs of pupils diagnosed with or at risk of ADHD, teachers had to expend additional personal effort to overcome school level barriers. Finally, studies suggested that pupils and parents often held the least amount of power, as their recommendations for school action were rarely taken into account. Although the dynamics of ADHD tend to play out in the classroom, the drivers for these dynamics can be located in expectations established at sociopolitical and school context levels.
In summary, the complexity of contextual issues related to ADHD in schools is demonstrated by multiple interactions within and between levels of context. This complexity is increased by the hidden nature of the role that the structures of education can have in aggravating symptoms of ADHD, through the local character of school expectations and through stigma. The role of these issues, although difficult to address, suggest that there are multiple ways to intervene to improve pupils’ ADHD symptoms, and that a range of diverse factors potentially moderate school-based interventions for ADHD.
Table 64 describes the findings contributed by reviews 3 and 4 for each level of context and key category. Subthemes under each key category that emerged during analysis are also considered here. Findings between reviews were complementary, and where there were gaps it most often seemed to be an artefact of differences between each review’s research questions. The table serves to provide more detailed information about the contextual levels and key categories, through the description of subthemes. A few highlights of this more detailed approach that were not evident in discussion of the model include:
-
The importance of pupil age for interventions and behaviour, which can be linked to differences in pupil maturity and differences in school’s expectations at preschool, primary and secondary school stages.
-
Differences in priority in relation to the perception of ADHD symptoms, where teachers in studies express most concern over disruptive classroom behaviour (e.g. core symptoms of hyperactivity and impulsivity, and secondary symptoms such as externalising behaviour), whereas pupils diagnosed with, or at risk of, ADHD most often express concern over their relationships.
-
Low self-esteem is seen as a problem for pupils with ADHD and therefore may act as a barrier to the effectiveness of interventions.
-
Participants across many studies recognised dilemmas regarding the withdrawal of pupils with ADHD from mainstream classrooms for interventions. Classroom context and teacher knowledge influenced views on withdrawal/inclusion.
-
There were varying beliefs from participants in the studies reviewed about how structured teaching should be for pupils with ADHD. For example, some teachers emphasised the need for pupils diagnosed with, or at risk of, ADHD to be closely supervised, whereas some pupils spoke about the negative effects of such close supervision. Participants more often agreed that meaningful educational content was important.
-
Although both reviews found that studies suggest the potential benefit to be gained from parent–teacher collaboration, teacher and parent differences in beliefs about ADHD, lack of structure and expectations regarding aims for collaboration, and lack of teacher time and knowledge acted as barriers to collaboration.
Deductive synthesis: effectiveness
Table 65 cross-references the findings from the meta-analyses reported in review 1 with relevant information identified in reviews 3 and 4. Column one reproduces the effect sizes reported in review 1 and corresponding CIs for child-related symptom and scholastic outcomes that showed weak to strong evidence of effectiveness (p-values range from 0.08 to 0.001) of non-pharmacological interventions (findings with p-values > 0.08 are not tabulated here), whereas columns 2 and 3 include qualitative information identified in reviews 3 and 4 as potentially relevant to the findings from review 1. The aim here is to consider how the other reviews may speak to review 1’s findings. Given that review 2 focused solely on attitudes towards particular types of interventions, these findings are not relevant to the synthesis of findings across different types of interventions (as synthesised and assessed in the meta-analyses in review 1) and are therefore not considered here. As highlighted above in Method, any associations between different reviews identified in this and Tables 66 and 67 are tentative given the different foci and evidence base in each review.
Reviews 3 and 4 support the identification of school adjustment as an important outcome and highlight that the negative attitude towards school held by many pupils who display ADHD symptoms may be an important factor in underachievement at school. Review 1 found a small beneficial effect of non-pharmacological interventions on ‘perceptions of scholastic adjustment’ assessed by teachers. Review 3 supports the identification of academic achievement as an important outcome in review 1, given that some teachers and pupils indicate that they prioritise achievement outcomes. There was weak evidence of effects for ‘curriculum achievement’ improvement according to child-based assessments but little evidence of effects for parent- and child-rated perception-based measures of ‘scholastic adjustment’ shown by review 1.
There are some differences in the perceived importance of outcomes indicated by review 3 and 4 compared with those used in review 1 studies. Review 4 noted that pupils reported deficits in emotional self-regulation more than hyperactivity, which may suggest that pupil emotional self-regulation outcomes ought to be considered when evaluating interventions. Pupils in review 4 described a lack of emotional self-regulation in response to stress which seemed to represent an absence of understanding about the process of emotional build-up and capacity to control venting of emotion. Thus, although failure to self-regulate is captured in some review 1 outcome measures, such as emotional distress (internalising) and loss of control (externalising and impulsivity), these constructs do not entirely represent emotional self-regulation, which may be conceptually distinct and warrants empirical investigation in the context of ADHD.
Review 4 suggests that teachers often considered symptoms of hyperactivity and impulsivity to be of greater concern than symptoms of inattention. Review 1 reported positive effectiveness of non-drug interventions on inattention across three raters, indicating that, despite being less of a priority or less problematic for teachers, interventions do improve inattentive symptoms.
Reviews 3 and 4 suggest that pupil outcomes rarely seen among the specific self-perceptions measured in review 1 are important for pupils with ADHD, including self-concept and a range of attitudes (e.g. perceptions of agency, attributions for ADHD and attitudes towards school and/or interventions). For example, although child perceptions of ‘school adjustment’, ‘social skills’ and ‘internalising’ symptoms were included in review 1, assessments of agency, attributions for ADHD and attitudes towards interventions were not. In addition, the majority of interventions in review 1 targeted children at elementary school (40/54 studies) aged typically ≤ 11 years. The ages of relevant children with ADHD in review 3 spanned across childhood and adolescence, whereas the age of pupils diagnosed with ADHD in review 4 was more often young people aged ≥ 11 years rather than children aged < 11 years. Older children are likely to be better at reporting on self-perceptions than younger children, and this is another potential contributor to differences between reviews. Given that these pupil outcomes were found to be important in both reviews 3 and 4 and could potentially act as a barrier to intervention implementation and effectiveness they should be considered as intervention targets in future interventions for pupils with ADHD.
Deductive synthesis: sources of heterogeneity – potential moderators identified in review 1
Intervention packages
Table 66 cross-references the intervention packages identified in review 1 with relevant findings across the other reviews. The frequencies with which interventions were identified across 54 studies in review 1 (including 39 RCTs and 15 non-RCTs) are reported alongside summary results of the relevant moderator analyses (conducted and reported in review 1, see Tables 18–21 for results). As noted earlier, where meta-regressions were conducted, we were constrained by the small number of studies and the generally low methodological quality. Therefore, conclusions based on these findings must necessarily be tentative. Attitudes of educators towards particular intervention packages synthesised in review 2 are highlighted where clear trends in the review were identified. Descriptions of relevant findings from reviews 3 and 4 are cross-referenced and information for review 3 includes the number of papers (out of a total of 12) that were focused on intervention packages identified in review 1.
Although contingency management was the intervention package that most frequently appeared in review 1 papers, its inclusion was not found to moderate effectiveness relative to a combination of other types of non-pharmacological interventions (review 1), and perceptions of its effectiveness (review 3) and educators attitudes (review 2) towards this type of intervention were varied. DRCs were the only intervention type towards which papers in review 2 consistently reported positive attitudes among educators. This is interesting as contingency management is usually an integral element of DRCs and therefore prompts the question of why contingency management without a DRC elicited mixed attitudes about effectiveness. Inclusion of a DRC was not found to moderate effectiveness relative to a combination of other types of non-pharmacological interventions in review 1. Review 3 suggests that a DRC may address some of the school–home relationship issues.
Reviews 3 and 4 suggest that self-regulation training is relevant to the needs of pupils diagnosed with or at risk of ADHD, for instance pupils sometimes describe a lack of awareness about the antecedents to loss of behavioural control, and one study296 suggested that by becoming aware of such antecedents pupils were more able to take control of their behaviour. However, review 1 did not find that inclusion of self-regulation training moderated effectiveness (relative to a combination of other non-pharmacological interventions). Reviews 3 and 4 suggest that emotional skills training could be valuable because of its potential ability to address issues of low self-esteem in pupils with ADHD, and review 4 suggests it could be valuable because of its potential to increase levels of emotional self-control. However, there were too few studies in review 1 to test these hypotheses.
Social skills training may have the potential to improve poor relationships with teachers and peers that are often reported by teachers and/or pupils displaying ADHD symptoms in reviews 3 and 4. However, for perceptions of school adjustment, review 1 reported weak evidence that inclusion of social skills training may have a negative impact on effectiveness relative to other types of interventions. This result has to be treated with caution as only three studies104,159,182 that included social skills training were included in the meta-regression analyses. Nevertheless, this finding would not be predicted by review 3 or 4, where relationships were considered to be critical to the experience of ADHD in school settings and, therefore, one might assume that effective social skills training would have indirect beneficial impact on perceptions of school adjustment through improved relationships with teachers and peers.
The specific social skills training used might suggest explanations for the discrepancy in findings across reviews. First, if social skills training makes pupils with ADHD more aware of their social difficulties and strained relationships, this may negatively affect school adjustment. Social skills training is often delivered to small groups, and, as discussed elsewhere, withdrawal from the regular classroom can be evaluated negatively and increase stigma, which may decrease school adjustment. Some studies in review 4 found that difficulties in relationships for pupils diagnosed with, or at risk of, ADHD are increased by stigma, and arise from teachers’ and peers’ behaviour in addition to the pupils’. This suggests that social skills interventions that target pupils, teachers and peers might be more effective than those that target pupils alone. Review 3 findings reported that social skills training was used as part of intervention packages for children aged 6–12 years, whereas review 4 found that social demands increased in secondary school, suggesting social skills training would be important across the school years.
Reviews 3 and 4 point to issues regarding adaptations to learning environments or materials, where both reviews found tensions between accommodation for one pupil and teacher responsibilities to the class as a whole, and both reviews found the need for greater consideration of adaptation at the classroom and school levels in addition to focus on pupil adaptation. A higher proportion of studies in review 3 compared with review 1 considered adaptations to learning environment, which may be indicative of differences between how schools and researchers typically view interventions (see Chapter 5, Implications for practice and recommendations for research). In review 3 special education was frequently seen by educators as a response to managing ADHD, whereas in review 1, the focus was on interventions specifically targeting children with ADHD, even among those studies conducted in special educational provision. Only six studies143,154,187,195,196,198 explicitly examined adaptations to the environment in review 1; a focus on the pupil without consideration of the environmental (physical and or social) could unwittingly reinforce perceptions of the pupil as the problem and hamper management of ADHD.
Reviews 3 and 4 found that psychoeducation for teachers and pupils with ADHD was desired and perceived to be helpful. Psychoeducation was not identified as an intervention package in review 1, thus the extent to which it is delivered alongside non-drug interventions remains to be clarified, and psychoeducation needs to be added to the next version of the classification system reported in review 1. Although the presence or absence of provider training was coded in review 1, the content of training was not coded; therefore, the extent to which psychoeducation has previously been included in complex interventions that involve training teachers to deliver interventions was not the focus of this report. In any case, the findings from reviews 3 and 4 suggest the need to include ADHD content in teacher training and that interventions ought to consider inclusion of psychoeducation for pupils and parents as well as teachers. Review 4 also suggests that the content of psychoeducation is important, for example that ADHD symptoms are explained as the result of an interaction of biological, psychological and social factors rather than as solely biological or solely sociological in their origin.
Study design, participant characteristics and intervention delivery characteristics
Table 67 considers the findings of each review about the remaining moderators specified in review 1 including study design, participant characteristics and intervention delivery characteristics (see Table 67, column one). For each potential moderator the second column summarises the findings from the moderator analysis conducted in review 1 (see Chapter 2, Heterogeneity for complete findings). Where reviews 3 and 4 have relevant findings this is tabulated in columns two and three, respectively. As noted above, conclusions regarding the results of the meta-regression must be interpreted in light of review 1’s limitations given the small number and therefore low power to detect effects and low quality of the studies on which they were based which compromises their reliability. Given these methodological provisos, a non-significant result does not necessarily indicate that a moderator has no effect, just as our conclusions about statistically significant moderators have to be similarly tentative.
The three participant characteristics included in review 1 were also considered by reviews 3 and 4. Reviews 3 and 4 suggest that medication for ADHD could potentially positively moderate the effectiveness of interventions, although this was not supported by the moderator analysis in review 1. Review 4 found a consensus for the beneficial effects of medication in the reduction of restlessness and improved concentration in the classroom. However, negative side effects, perceptions of reduced agency and reduced quality of pupil life experience were also reported. Control for medication status in intervention trials is essential. Intervention with trial arms that compare those on medication for ADHD with those who are not is critical to establish the importance of non-drug interventions over and above first-line drug treatment and informed treatment guidelines for ADHD. Although several studies294,324,391 in reviews 3 and 4 suggest that there are differences in experience for pupils diagnosed with or at risk of ADHD according to gender, there was a lack of analysis that focused on gender differences. There was insufficient heterogeneity with regards to the inclusion of female participants in review 1 to explore gender as a moderator of intervention effectiveness.
Review 3 points to differences in grade level that influence the response of participants to interventions. For instance, behaviour modification might be resisted by young people, whereas they could be more positive about study skills. Children, on the other hand, were considered to benefit from social skills training. Furthermore, review 4 findings suggested that social demands increased in secondary school, indicating continuing need for social skills training. There was insufficient variance in grade level (as a proxy for age) to assess this potential moderator in review 1. These findings suggest that the development (and associated understanding about issues relevant to delivery) needs to be highly age-sensitive. Review 4 also suggests that issues related to differences in the structures of primary and secondary school could be predicted to influence the school experience of ADHD; for example, greater academic and social demands in secondary schools with less pastoral support and more diffuse relationships with multiple teachers were cited as grounds for additional difficulties.
The weak evidence from review 1 suggests that shorter interventions were more effective for teacher ‘perceptions of school adjustment’ than longer interventions, which conflicts with review 3’s findings, where educators in two studies301,306 said that their pupils needed more time using the intervention they experienced. Length of intervention, however, does not provide information about the intensity of an intervention, the number of intervention packages employed or fidelity to intervention, which are all potential confounders of the relationship between intervention length and effectiveness. The effect of intervention length on effectiveness should, therefore, be explored controlling for intervention intensity and fidelity to intervention to help clarify these findings. In the light of review 3 and 4’s findings about stress and limited resources among teachers providing interventions, it seems plausible that longer interventions may be experienced by teachers as more stressful, which in turn could lead them to rate outcomes less favourably. This highlights the limitation of perception-based measures which are always prone to bias. Intervention context, related to whether interventions in review 1 were located at school only or involved some delivery at home, was not related to effectiveness. Delivery at home is assumed to support parent involvement and training in management of ADHD to aid consistency in the use of strategies across school and home settings. Reviews 3 and 4 highlight that parents’ involvement in interventions or collaboration with teachers is considered to be important, although challenging. Taken together, these findings suggest that methods to improve collaboration between parents and school staff in the management of ADHD warrant more detailed empirical study.
Findings of review 3 suggest that the setting within school might be predicted to moderate intervention effectiveness, although there were mixed perceptions in terms of whether or not withdrawing a pupil from their classroom for an intervention was preferable (see Chapter 5, Withdrawal). However, setting within school and time of delivery (i.e. during normal school hours vs. before/after school) was not found to moderate the effectiveness of interventions in review 1. Development and testing of interventions designed factorially to compare treatment in a pupil’s usual classroom and alternative school settings (e.g. playground or other school room) could, therefore, help to clarify if withdrawal from regular school classrooms compromises the effectiveness of interventions and adversely impacts self-perceptions and/or increases stigma. Similarly, class- and school-wide interventions could usefully be compared with pupil targeted treatments either within the classroom setting or elsewhere. The issue of time of delivery did not arise in either reviews 3 or 4, highlighting a potential gap for qualitative research. Before- or after-school interventions may address issues identified in review 3 about pupils missing work from mainstream classes if they are withdrawn for intervention during school hours. In North America, summer treatment programmes for pupils with ADHD are common and have been shown to be effective. 417 The design and testing of interventions outside of school hours in the UK could therefore usefully be tested. The findings from review 4 suggest that multiple intervention packages would be preferable given the range of needs that relate to ADHD in the classroom. There is a tension, however, between the need for highly complex intervention and the time and resource constraints also identified in reviews 3 and 4. The frequency of intervention packages was not found to moderate the effectiveness of interventions in review 1.
Discussion
In this chapter we have drawn together findings from the four reviews reported in previous chapters. We first took an inductive approach to explore the complexity of the context in which non-pharmacological school-based interventions for ADHD are used as revealed by qualitative reviews 3 and 4. Second, a deductive approach to synthesis was taken to consider potential relationships between possible moderators and effectiveness, starting from review 1 findings and examining how other review findings may provide potential explanations and relevant information in response to them.
The inductive approach 1 led to a model that indicated a range of contextual levels at play when school-based interventions are considered. Furthermore, factors like teachers’ time pressure operate across these contextual levels, making it hard to address particular issues in advance of implementing interventions. Key contextual issues that appear to impact the implementation and effectiveness of interventions are the relationships that pupils with ADHD have with their teachers and peers and the stigma that may be experienced because of ADHD symptoms, diagnosis or attendance of an intervention.
The deductive approach 2 revealed that outcomes that did not often feature in review 1 appeared to be important in reviews 3 and 4, such as attributions made by teachers and pupils about ADHD, attitudes towards school and/or interventions and pupils’ self-concept. Review 4 also suggests that emotional self-regulation is an important issue for pupils diagnosed with, or at risk of, ADHD and should be a measured outcome distinct from aspects of internalising, externalising and impulsivity measures. Regarding intervention packages, tests of heterogeneity in review 1 found weak evidence that social skills training corresponded to less beneficial effectiveness relative to other non-pharmacological interventions. This would not be predicted by reviews 3 and 4, where it could be concluded that social skills training would address the concerns with relationships that pupils with ADHD report are critical to them. There was some weak evidence in review 1 for the beneficial effect of shorter interventions on perceptions of school adjustment compared with longer interventions. Time was a concern for teachers revealed by reviews 3 and 4; however, teachers in review 3 also often wanted more time for interventions, suggesting some conflict in findings between reviews.
Strengths and limitations
There is a lack of examples of syntheses that bring together quantitative and qualitative reviews. Where such overarching reviews exist, they have typically been able to focus on explanations of the effectiveness findings and considered a quantitative and qualitative review focused on the same intervention. 412 In the current overarching synthesis we have drawn together findings from four reviews, with a focus at least as much on moderators of effectiveness as effectiveness itself. We developed an approach that allowed comparison across all reviews and, through adopting two approaches, captured a breadth of evidence of relevance to the use of ADHD interventions in school settings. Approach 1 (the inductive synthesis of findings from qualitative reviews 3 and 4) also provided a model that demonstrates the complexity of the context in which interventions in school settings are implemented, with a range of factors at different levels identified as potential influences on the use of non-pharmacological interventions for ADHD.
The main limitation of this overarching synthesis relates to the different research questions across the four reviews brought together in this chapter. Because of this, reviews 1–3 sometimes focused on different interventions, which presented a challenge to comparison. Review 1 identified a range of fairly discrete intervention packages targeted at children with ADHD, whereas the other reviews focused on attitudes and/or experiences of interventions or ADHD in school more generally, including a range of informants (parents, educators and pupils). The ages of pupils diagnosed with or at risk of ADHD differed across reviews, further contributing to difficulties in comparison. The majority of pupils in review 1 were children at elementary school level aged < 11 years. In review 2 the majority of educators were teaching younger children in kindergarten and elementary/primary schools (aged 5–12 years). The ages of relevant children with ADHD in review 3 spanned across childhood and adolescence and in review 4 more pupils were young people aged 11–18 years than children younger than 11 years. Of the child participants in review 4 most were aged 9–11 years. Although reviews 2 and 3 did adopt the intervention categories developed during review 1, there was little direct overlap between interventions studied across reviews. Interventions in review 1 were often composed of more than one intervention package with few interventions that consisted of common sets of intervention elements. Synthesis was, therefore, not only a challenge within review 1 but also across the reviews. A point of similarity between all four reviews was that most studies took place in the USA. Some interesting links between reviews were identified, but they remain tentative because of these identified limitations.
Implications
We have considered the implications for intervention design and research suggested by Tables 64–67. Here, we summarise implications in three groups: (1) context affecting interventions; (2) implications for development and evaluation of interventions; and (3) potential moderators of effectiveness. As reiterated throughout this chapter, any implications and recommendations remain tentative in light of the uncertainty in the evidence base.
Context affecting interventions
The inductive synthesis of review 3 and 4 identified a range of contextual levels that interact to provide a complex context in which interventions happen in school settings. The implication for implementation of interventions is that the particular context for a pupil with ADHD, their classroom, school and issues at the sociopolitical level need to be actively considered.
Despite review 1 findings of effectiveness across interventions, the qualitative reviews suggest that stigma and marginalisation may actually be increased through intervention. This is an important consideration for intervention development and implementation. Future interventions might involve an inclusive approach that does not single out pupils diagnosed with, or at risk of, ADHD, for example targeting the classroom rather than pupil level. Some studies suggested that educating teachers about ADHD and effective classroom strategies decreased stigma. Such approaches might be particularly helpful for milder levels of difficulties and may prevent the need for as many interventions targeted at specific pupils. The risk of additional stigma arising from the use of interventions that involve the withdrawal of individual pupils might be warranted for those who already demonstrate more severe levels of difficulty, but there is need to balance potential benefits against the potential harms. We believe that the role of stigmatisation deserves greater attention in intervention development and implementation.
The findings from reviews 3 and 4 about power imbalances between levels of context suggest that the development of inclusive strategies and interventions is not sufficient to address the issues of ADHD in the school context without policy and financial support at the sociopolitical level, and policy and support at the school level for teachers. Studies in reviews 3 and 4 suggest that systemic issues at the national and school level may act to moderate the effectiveness of interventions. The implication of these findings to intervention design is that adaptation at pupil and classroom contexts without support at school and sociopolitical levels is likely to be less effective. As teacher–parent collaboration was identified in reviews 3 and 4 as an important barrier and/or facilitator to intervention and the amelioration of ADHD symptoms, policy and support to guide these interactions may be particularly influential.
Educators and researchers may hold different conceptions of what an ‘intervention’ appropriate for a pupil with ADHD may look like. The examples of interventions that were evaluated for effectiveness in review 1 and appeared in qualitative papers synthesised in review 3 often differed, with special education classes more often considered in review 3, whereas general classroom teachers in several papers referred to the ad hoc teaching practice used with pupils with ADHD as interventions. 264,291,293,305 In which case, where teachers are involved in intervention delivery or support, the intervention’s purpose and design ought to be made explicit to them. For example, reviews 3 and 4 highlighted classroom teachers’ responsibility for the needs of the class as a whole. As ADHD symptoms are experienced to some extent by all pupils, interventions for ADHD that specify the potential to support all pupils may be more appealing to general classroom teachers. Findings suggest that if an intervention has salience it is more likely to be accepted and implemented.
Implications for development and evaluation of interventions
The findings from reviews 3 and 4 suggest that psychoeducation about ADHD could usefully be provided to staff and pupils as an adjunct to any intervention that targets pupils diagnosed with, or at risk of, ADHD. The importance of attributions about ADHD revealed by reviews 3 and 4 suggest that development of inclusive strategies and interventions should involve the provision of information about ADHD as an interaction of factors to combat tendencies towards polarised beliefs about ADHD, and that such education is important for staff, pupils with ADHD and their peers. Review 1 found inattention to improve across several raters for interventions reviewed, where the greatest effectiveness was demonstrated by observer ratings. Review 4 noted that teachers showed greater concern over symptoms of hyperactivity/impulsivity and may be less aware of changes in inattention. As such, psychoeducation regarding ADHD could stress the impact of inattention for pupils with ADHD on their academic work. Attitudes could be considered both in terms of beliefs regarding ADHD and attitudes towards particular interventions, as both may impact on effectiveness.
Given the importance of relationships highlighted by reviews 3 and 4 and the possible reduced effectiveness of social skills training for pupils with ADHD suggested by review 1, novel interventions that target the actual relationships with teachers and peers, as opposed to the social skills of pupils diagnosed with, or at risk of, ADHD only, would seem an important component for development. Interventions may need to target different behaviours for pupils with ADHD at different age levels. These different behaviours in turn require different interventions. For example, self-management and study skills may be more appropriate and might be more effective for older pupils, whereas social skills training may be appropriate across age ranges, but with content chosen to match the different social challenges faced by younger versus older pupils. 314
Reviews 3 and 4 highlight the relevance of pupil self-concept outcomes including self-esteem, perceived stigma related to ADHD and attributions about ADHD. Such outcomes could usefully be targeted by interventions directly but also assessed to explore whether or not attending non-pharmacological interventions impacts stigma experienced and self-esteem. Teacher and parental perceptions of stigma and attributions about ADHD were also identified as important as they may influence the implementation of interventions and management of ADHD. Pupil attitudes to school and learning and emotional self-regulation as a construct distinct from measures that focus on of self-regulation (e.g. internalising symptoms) were identified as relevant to pupils diagnosed with ADHD and, therefore, could be useful intervention targets. Although the child perception-based measures in review 1 were not linked to effectiveness, they sometimes involved different constructs to those identified in reviews 3 and 4, were infrequently measured and were based on perceptions of children mainly at elementary school level. Perception-based measures are more reliable for older children. 203
In line with current recommendations for intervention design and evaluation,209 the findings emphasise the importance of involving stakeholders in the design of interventions and in conducting a process evaluation alongside interventions to help understand why effectiveness and implementation are, or are not, realised. A combination of qualitative and quantitative evaluations holds the potential to isolate the most effective components and lead to the development and implementation of cost-effective interventions.
Moderators of effectiveness
Review 1 assessed the type of intervention provider; reviews 3 and 4 suggest that the quality of the relationship between pupils and providers (typically teachers) as potentially critical to effectiveness. This idea coincides with the finding that successful therapeutic outcomes are linked to alliance (e.g. between client and therapist) rather than the methods used to target behaviour change (e.g. CBT, psychoanalysis). 418 Thus, in addition to intervention content that specifically targets relationships for children with ADHD and their teachers and carers, the choice of intervention provider(s) may be critical to the effectiveness of any non-pharmacological intervention. Practical considerations aside, in the context of ADHD, teachers known to have a positive relationship with the target pupils could be more suitable for intervention delivery or particular elements thereof, than when there is no previous relationship or a negative relationship between the provider and pupil. This suggests that the provider–pupil relationship could be explored for ADHD interventions.
Findings suggest that a range of potential moderators could be researched, given their importance across reviews. These include age, whose effect as a potential moderator of effectiveness appears on several occasions in reviews 3 and 4; for instance, older pupils in review 3 were more likely to be resistant or indifferent to contingency management. Given the importance of home–school collaboration mentioned above and the positive attitudes towards DRCs reported by review 2, research teasing apart the influence of DRCs on parent–teacher collaboration, or comparing elements of home–school communication to elements of contingency management, is recommended. Research could consider the link between social skills training and its impact on relationships. As the moderator finding from review 1 focused on a comparison between social skills training and a combination of other non-pharmacological interventions, research could usefully investigate potential moderators comparing different elements of social skills training, for example age of pupil, intervention targets, intervention methods, quality of current relationships including presence of stigma and home–school collaboration, and intervention context. Intervention trials should control for medication status and report unadjusted means. In relation to issues of stigma and withdrawal from mainstream teaching, research could consider the impact of individual whole class interventions. Finally, intervention length could be explored more thoroughly; for instance, do time pressures on teachers imply that longer or shorter, and less or more intense interventions would be preferred?
Chapter 8 Discussion and conclusions
The aim of this research project was to evaluate the clinical effectiveness and cost-effectiveness of non-pharmacological interventions delivered in school settings for children and young people diagnosed with, or at risk of, ADHD and to explore the factors that may enhance, or limit, the delivery of such interventions. A series of four systematic reviews were conducted, and we have tried to relate these to each other in an overarching synthesis of the reviews. In this final chapter we summarise the findings of each review and the overarching synthesis, consider strengths and limitations, and present implications for practice and recommendations for research.
Summary of findings
Summary of review 1
In review 1 (see Chapter 2) a total of 54 controlled trials (39 RCTs; 15 non-RCTs) that assessed the effectiveness of non-pharmacological interventions were synthesised. Results indicate that few interventions consist of the same elements, which makes evidence synthesis and theoretical integration difficult. The absence of standardised tools to synthesise across interventions and outcome measures meant that we had to develop our own systems. Fifteen types of intervention packages were identified inductively and few studies included similar combinations of packages. Results from the primary studies were therefore synthesised across intervention packages to address whether or not non-pharmacological interventions in general lead to a reduction in symptoms and scholastic outcomes. As many different measures of the same underlying constructs were reported we had to map them onto the relevant outcomes prior to examination of effectiveness. Assessed outcomes included core ADHD symptoms (‘inattention’, ‘hyperactivity/impulsivity’ and ‘ADHD combined’); ADHD-related symptoms (‘externalising’ symptoms, ‘internalising’ symptoms and ‘social skills’) and scholastic behaviours and outcomes (‘perceptions of school adjustment’, ‘curriculum achievement’ and ‘standardised achievement’).
In line with previous work, we conclude that non-pharmacological interventions delivered in school settings lead to improvement in both symptom and academic outcomes. 72,74,75 Building on Dupaul et al. 72 our results indicate that the effects of non-drug interventions in school settings vary by particular symptom and scholastic outcomes, and assessments with beneficial effects were observed for relatively objective assessments including child-based neurocognitive assessments (d+ = 0.44; p = 0.001 for ‘inattention’ and d+ = 0.33; p = 0.001 for ‘hyperactivity/impulsivity’); observer-rated ‘inattention’ (d+ = 1.30; p = 0.08) and academic-related tests with objective performance criteria (d+ = 0.50; p = 0.08 for curriculum achievement and d+ = 0.19; p = 0.02 for standardised achievement). Of the tested perception-based measures, beneficial effects were reported for teacher-rated outcomes of ‘inattention’ (d+ = 0.60; p = 0.01), ‘hyperactivity/impulsivity’ (d+ = 0.23; p = 0.08); ‘externalising’ symptoms (d+ = 0.28; p = 0.03) and ‘perceptions of school adjustment’ (d+ = 0.26; p = 0.02), but not for children and parents. Applying Cohen’s guidelines for interpreting effect sizes,147 mean weighted effect sizes ranged from very small (d+ < 0.20) to large (d+ ≥ 0.80), but 95% CIs were generally very wide and substantial heterogeneity in effect size estimates across studies was reported. No studies included economic outcomes; thus, the cost-effectiveness of non-drug interventions targeting children with, or at risk of, ADHD cannot be established and compared with other available treatments.
With the exception of ‘standardised achievement’ and teacher ‘perceptions of school adjustment’, I2 values indicated substantial heterogeneity in effect sizes across studies. There was weak evidence (p = 0.06) for possible harmful effect of social skills training and longer (vs. shorter) interventions (p = 0.04) on teachers’ ‘perceptions of school adjustment’. The remaining potential moderators tested, including participant characteristics, intervention package(s) and intervention delivery characteristics, do not explain the large proportion of unaccounted variance in effect size heterogeneity.
Although the inclusion of more controlled trials indicates that the methodological quality of reviewed studies in the current meta-analysis was improved on those that precede it, only one of the 39 RCTs155 was identified as having made a good attempt at concealment of random allocation and only 10104,142,143,153,157,161,163,170,179,196 included at least one blinded outcome assessment. Few studies reported scores adjusted for baseline differences. Of all 54 included studies, only 17104,142,143,153,159,160,161,164,165,167,168,173,182,183,185,187,197 assessed some element of intervention fidelity and even fewer (14/54 studies104,142,153,164,166,167,170,177,179,180,187,190,194,198) included a follow-up. Conclusions, therefore, are necessarily tentative. The majority of included studies targeted children at elementary school (40/54 studies104,142,143,153–157,161–163,165,168–170,173,175–179,181–183,185–188,189–198,201,202) and none of the included studies were from the UK. Applicability of these findings to older students and students at schools in UK settings therefore warrants consideration.
The heterogeneity in effect sizes is unsurprising as the lack of standardised interventions and agreed outcome measures makes theoretical integration difficult. This leads us to echo Trout et al. ’s74 call for more systematic lines of research. Specifically, we call for the development and testing of a shared, reliable tool for characterising intervention content that could facilitate the identification of the precise contents of interventions, isolate the potentially active ingredients and compare results reliably within and across reviews. The current literature does not allow us to assess accurately which intervention elements are linked to effectiveness. The identification of an agreed set of outcomes with gold-standard measures would complement such work and facilitate evidence synthesis and the accumulation of knowledge in this field. Finally, more rigorously evaluated trials are needed. Theory-based interventions have been shown to be more effective and aid the systematic accumulation of knowledge. Intervention mapping,209 a formal systematic method for the design and implementation of interventions, could usefully be applied.
Summary of review 2
In review 2 (see Chapter 2) we reviewed quantitative research measuring attitudes towards school-based interventions for ADHD. The 28 included studies represented the attitudes of a variety of educators, namely teachers, school psychologists, school social workers, school counsellors and student teachers. Attitudes were measured in relation to nine types of intervention identified across studies. The majority of the studies used bespoke attitude measures rather than existing standardised assessment instruments. As a whole the included papers were of low quality and therefore prone to bias. Particular problems were lack of definitions of interventions and failure to pilot vignettes and attitude measures developed by authors. The psychometric detail of attitude measures was usually not tested, particularly for bespoke measures.
Likert scale scores were converted to percentages, allowing comparison across studies in 19 of the 28 included papers. 214,217,222–229,233,236–238,240,241,243,245,246 Across these studies educators held a variety of attitudes that ranged from negative to positive. The most striking finding is the lack of consistency among attitudes towards particular interventions or types of interventions. Most interventions were rated positively or neutrally across different studies. The only intervention that consistently recorded positive attitudes from educators were DRCs, an intervention where behaviour is monitored and recorded at school on a card or in a book that the pupil then takes home to share with their parent or carer. No variables were consistently identified across reviewed studies that affected attitudes towards interventions.
Summary of review 3
In review 3 (see Chapter 3) we have synthesised qualitative research on the experience of and attitude towards non-pharmacological interventions for ADHD delivered in school settings. Only 12 of the 33 included studies265,278,280,288,292,295,300–303,306,311 were focused on a particular intervention; the majority of included studies instead considered the range of interventions or strategies used in participants’ school settings. Seven main themes were used to organise and guide the synthesis. These themes are (1) individualising interventions; (2) structure; (3) time; (4) impact of interventions; (5) problem situated within the child; (6) relationships; and (7) expectations. A line of argument was developed that offers an explanatory model of the experience of interventions and teaching strategies for ADHD in school settings according to the papers reviewed (see Chapter 5, Figure 5). The model suggests a cyclical process, whereby issues relating to the intervention or strategy response to ADHD in schools influences the action and reaction to such interventions. The reaction to interventions used has the potential to impact on issues of socialisation that involve pupils with ADHD, their teachers, peers and parents. Finally, the process continues as the socialisation of those people involved in the school lives of pupils with ADHD affects future intervention responses to ADHD.
The synthesis revealed three main tensions related to responding to ADHD in schools. The first is if interventions ought to be structured and controlled or if they should offer choice and flexibility, although several studies recognise that structure and choice are not mutually exclusive. A second tension relates to the extent to which interventions ought to be individualised. The third concerns considerable time pressure reported by teachers in reviewed studies. There were some concerns reported by participants in reviewed studies that interventions may be effective for specific targeted skills and behaviours, but not impact the academic achievement, which is considered an important outcome by young people, parents and teachers. There are also issues concerning how well skills and knowledge learned during interventions are applied beyond the intervention period. It is clear that interventions may influence relationships, attitudes and participants’ conceptions of ADHD, but the reported positivity of this impact was mixed both across and within different interventions. The individual differences among participant pupils diagnosed with ADHD may explain differences in perceived intervention effectiveness.
The review indicated some potential challenges for the implementation of interventions for ADHD used in school settings. Contextual factors, including the relationships held by pupils displaying ADHD symptoms with their teachers and peers, may impact the experience of interventions. Attitudes regarding school, ADHD and interventions, as well as knowledge of ADHD, also appear to impact the use of interventions. Many of the studies reviewed present a rigid view that ADHD in the school setting is a problem that resides in the child and that any issues relating to the classroom and curriculum are ignored. This, along with pupils’ reported experience of stigmatisation owing to having a diagnosis of ADHD or attending interventions, implies that there are barriers to intervention use and that interventions also impact the context when they are used.
Summary of review 4
In review 4 (see Chapter 6) we explored the school-based experiences and perceptions of pupils diagnosed with, or at risk of, ADHD, their teachers, parents and peers. The 34 included studies were divided into four groups by participant types, then the subreviews were synthesised. The overarching themes identified for each subreview and the final synthesis were:
Review 4a, pupil views ‘Expression of ADHD symptoms as an interaction between biological, sociological and psychological factors’.
Review 4b, teacher views ‘Factors that influence teachers’ willingness to adapt their response to ADHD symptoms’.
Review 4c, parent views ‘Mothers are silenced’.
Review 4d, mixed views ‘Relationships between participant types: Conflict is the norm’.
Reviews 4a–d ‘School expectations and structures can be factors that compromise and/or aggravate ADHD symptoms’.
In review 4a, it was found that pupils diagnosed with ADHD described experiences commensurate with the core symptoms specified in diagnostic criteria for ADHD, including inattention, hyperactivity and impulsivity. However, they spoke most about impulsivity in relation to a lack of ability to self-regulate emotion. Pupils expressed great concern over the difficulties in relationships between themselves and their teachers, peers and parents that were a common feature of their experiences. They described the classroom as a place in which they found it difficult to learn, because of requirements to concentrate for long periods, remain still and remain silent. Studies identified differences in the expression of ADHD symptoms in pupils according to classroom features, with some authors concluding that the school context particularly triggered ADHD symptoms. Stigma for ADHD symptoms, diagnosis and/or medication was identified in a number of studies, and linked to poor self-perceptions by pupils. Pupils most commonly made polarised biological attributions for ADHD, where they understood the source of their behaviour to be biological without consideration of other potential contributors. Study authors linked such beliefs to poor self-perceptions, where pupils understood themselves to be flawed and incapable of controlling their behaviour.
In review 4b it was found that teachers of pupils diagnosed with or at risk of ADHD described their main professional responsibility to be to their classroom as a whole, and expressed reluctance to adapt their teaching to accommodate the individual needs of a pupil displaying ADHD symptoms if this might risk the reduction of learning for the whole class. Teachers commonly described time pressures and lack of knowledge about ADHD to be barriers to pupil accommodation. Many teachers attributed ADHD symptoms to problems in the home such as poor parenting, and this was linked to a reluctance to adapt teaching expectations and responses for such pupils. Other teachers understood symptoms to be a result of biological factors, leading to decisions that adaptation of classroom practice was justified on the basis of different need, or to conceptualisations of treatment that excluded all but medication.
In review 4c it was found that mothers of pupils diagnosed with or at risk of ADHD commonly characterised their experiences with school staff as ones of conflict, where they felt blamed for their child’s behaviour and dismissed when sharing information or making requests to school staff. Mothers described the nature of the conflict as escalating, where initially they expected to collaborate with teachers, they then began deferential resistance in response to breaches to trust, and sometimes eventually resorted to assertive resistance.
In review 4d studies exploring experiences of multiple participant types found a range of foundations for conflict between pupils diagnosed with ADHD and their teachers, pupils and peers, as well as parents and teachers. As might be expected, the conflict was linked to the interaction of many issues identified in reviews 4a–c, including lack of fit between pupil capacities and educational expectations, lack of pupil support owing to teacher responsibilities to the whole class, and difficulties in collaboration between teachers and parents. Some studies identified the barriers created by school structures, where in order to meet pupil needs and/or collaborate with parents, teachers were required to expend additional, personal, time and energy. The review suggests that existing educational provision did not always resource the necessary knowledge, time, or space for collaboration with parents and colleagues required to support pupils diagnosed with ADHD.
In drawing together reviews 4a–d, it was concluded that, although biological differences made pupils diagnosed with, or at risk of, ADHD prone to symptoms of inattention, hyperactivity and/or impulsivity, the context of schools can aggravate such behaviour through the nature of its expectations, and that local classroom contexts determined when such behaviour was or was not considered to be a problem. When behaviour was determined to threaten processes of learning in the school, mechanisms of stigma could operate in order to protect existing school practice. These could impact relationships negatively and might aggravate ADHD symptoms further, leading to escalating marginalisation. Polarised attributions, whether of poor parenting or for a biological basis, further drew attention away from the school contributions to the expression of ADHD symptoms. It was concluded that an important aspect of addressing ADHD symptoms in schools is to redress an imbalance by exploring the potential for adaptation to school practice to ameliorate symptoms in interaction with existing knowledge of approaches to pupil adaptation.
Summary of the overarching synthesis
The overarching synthesis (see Chapter 7) synthesised the findings from all four reviews. An inductive approach was used to explore the complexity of the context in which non-pharmacological school-based interventions for ADHD are used, drawing on findings from the two qualitative reviews (reviews 3 and 4). Second, a deductive approach to synthesis was taken to consider potential relationships between possible moderators and effectiveness, using review 1 findings and examining how other review findings may provide potential explanations and relevant information.
Despite the tension between the application of different research questions and methods of synthesis between the systematic reviews, the overarching synthesis led to a number of tentative implications. These implications were categorised as the context affecting interventions, the development and evaluation of interventions and moderators of intervention effectiveness. The highlights are summarised below.
The inductive approach revealed a range of contextual levels that influence the use of school-based interventions; these contextual levels form a hierarchy from the pupil diagnosed with ADHD through to the classroom, the school and the sociopolitical level. Key contextual issues that appear to impact the implementation and effectiveness of interventions operate across and within these levels and include the attributional beliefs that teachers and pupils hold about ADHD, the relationships that pupils with ADHD have with their teachers and peers and that their parents have with their teachers, and the stigma that may be experienced because of ADHD symptoms, diagnosis or attendance of an intervention. Differences in power between levels suggest that without school and sociopolitical level policy and support, non-pharmacological interventions for ADHD may be less effective. Differences in classroom context, for example between classes for pupils with SEN, mainstream classrooms and withdrawal settings, suggest the need for tailoring of interventions according to purpose, and the value for explicit intervention description that is accessible by teachers.
The deductive approach found some links across the systematic reviews, as well as some refutational evidence. With regards to the development and content of non-pharmacological interventions, the importance of psychoeducation for teachers, parents and pupils was acknowledged as a potentially useful adjunct to non-drug intervention to help overcome lack of knowledge and stigma around ADHD, both of which may have negative implications for implementation and effectiveness of non-pharmacological interventions for ADHD in schools. The relevance of building relationships between parents, teachers, pupils and peers was also highlighted in reviews 3 and 4 as critical to implementation and effectiveness of non-drug interventions. Although these conclusions conflict with the negative effect of social skills training for children in review 1, the latter evidence was weak and based on few studies of low methodological quality. Age of intervention target was commonly identified as a potentially important moderator of effectiveness; therefore, the content of interventions that target relationships may need to be highly age sensitive.
Several pupil outcomes were identified as important in reviews 3 and 4. These included pupil attitudes towards school, self-concept, perceived stigma and attributions about ADHD. These outcomes are therefore potentially useful intervention targets for pupils diagnosed with, or at risk of, ADHD and warrant empirical investigation. Such outcomes could also be assessed to explore if attending non-pharmacological interventions affect stigma experienced and self-esteem. Review 1 found no evidence of effectiveness on child perception-based outcomes among children typically at elementary school level. Nonetheless, perception-based measures in review 1 were infrequently measured and limited in range and may be more reliable among older children.
With regards to the moderators of effectiveness, the overarching synthesis suggested the potential importance of age; the quality of relationships of pupils diagnosed with, or at risk of, ADHD and their teachers, parents and peers; home–school collaboration; the presence of stigma; gender; length of intervention; medication status; and aspects of school context including type of classroom, school level and quality of school support to teachers.
Strengths and limitations
Strengths of the four reviews and overarching synthesis reported in previous chapters include the comprehensive search strategies employed and efforts to locate unpublished research where this was found. Review 1 included a wider range of non-pharmacological interventions and outcome measures, and benefited from a larger set of controlled trials than previous reviews that have investigated the effectiveness of non-pharmacological interventions that target children with or at risk of ADHD in school settings. Review 2 responded to a gap for quantitative synthesis of attitudes towards school-based interventions for ADHD. Although the main finding was varying attitudes from educators across papers reviewed, the review did allow for comparison to all other reviews in the overarching synthesis. Reviews 3 and 4 represent the first systematic reviews of qualitative research on the experience of school-based interventions for ADHD and the experience of ADHD in schools, respectively, of which we are aware. Both syntheses provide explanations of a range of relevant participants’ experiences relating to ADHD and school settings. As outlined in the overarching synthesis, these two reviews point to the complexity of the context within which non-pharmacological interventions for ADHD used in schools are expected to be implemented. They also shed light on some findings from review 1 related to effectiveness of interventions and moderators for this effectiveness.
The breadth of both interventions and outcomes in reviewed studies presented a challenge for categorisation, analysis and interpretation in review 1. The lack of common sets of intervention elements across studies meant that synthesis by intervention type was not feasible. The absence of standardised tools to synthesise across interventions and measures meant that we had to develop our own systems; this is an iterative, ongoing process and we anticipate further development. Many included studies were judged to have a high potential for bias in one or more of the critical domains of allocation concealment and blinding of outcome assessors; results therefore must be interpreted in light of the review’s limitations. None of the studies reviewed were conducted in the UK, and thus the applicability of findings to UK education must be considered.
There was a paucity of quantitative research considering children’s or parents’ views towards non-pharmacological interventions for ADHD in school settings. Therefore, review 2 focused only on educator attitudes. The majority of studies used vignettes to provide ADHD case descriptions to participants. However, often these vignettes were not adequately piloted, so consistency across the vignettes used within studies may be questioned. Many of the reviewed studies developed attitude measures for the purpose of their research, rather than using an established reliable and valid scale for measuring attitudes towards interventions. For systematic reviews of attitude research, agreed standardised measures would avoid the need to convert varying Likert scores to a comparable format and arbitrarily decide what constitutes a positive attitude.
Few review 3 studies focused solely on the attitudes and experiences of those using specific intervention packages in school settings and only one paper considered an intervention whose effectiveness had been quantitatively reviewed in review 1. This posed a challenge in terms of comparing qualitative and quantitative reviews of interventions, given that review 3 often focused on the strategies and teaching practice used in school settings for pupils with ADHD. Very few studies reviewed were conducted in the UK, and thus the applicability of findings to UK education must be considered. Although included studies were of reasonable to very good quality according to quality appraisal criteria, the majority of studies contained mostly descriptive qualitative analysis, despite claims to use interpretive analytical tools. This constrained the theoretical basis for discussion of themes and constructs seen across reviewed papers.
Findings related to non-pharmacological interventions for ADHD in schools were excluded from review 4 as these were covered by the other reviews; rather the focus was on experience of ADHD in schools more generally. Although offering a valuable overview that allowed the creation of hypotheses regarding implications to interventions, it was impossible to link findings specifically to interventions. Eleven studies264,265,286,290,291,293,294,296,298,299,305 were included in both reviews 3 and 4; however, data related to interventions were extracted to review 3 and data regarding more general issues unrelated to interventions were extracted to review 4. Some overlap in findings between reviews 3 and 4 may result from shared studies; however, other unshared studies in both reviews 3 and 4 also supported shared themes. Therefore, we do not see this as a limitation but as being generally supportive to the relevance of review 4 findings to interventions.
Quality appraisal found many review 4 studies to be of good methodological quality, and studies commonly employed theory in the design, framework for analysis and/or development of second-order (researcher) constructs. This supported the further application of theory in developing third-order (reviewer) themes, for example through the use of theory about stigma. The inclusion of seven studies27,41,260,261,266,294,356 involving UK participants allowed analysis of applicability, suggesting that findings from other countries seemed relevant to the UK educational context. Review 4 was limited by the content of studies available for synthesis. For example, issues of gender, pupil maturity and school level (primary/secondary) were noted to be relevant in included studies; however, there were no studies that focused on the experience and impact of these issues. The study designs also limited the extent to which relationships could be established between factors; studies that involved multiple perspectives offered the chance to directly link different experiences and perspectives pertaining to a particular pupil, but were of limited number. Disparate methodologies and underpinning theory provided a further challenge.
Implications for policy and practice
Here we consider the implications of the four reviews reported and their overarching synthesis. Given the nature of the review findings and challenges in synthesising across reviews considered in the previous chapters, recommendations for research and, in particular implications for policy and practice, can only be tentative. We discuss some implications for intervention design and implementation first.
The inductive synthesis of reviews 3 and 4 identified a range of contextual levels that interact to explain the complex situation in which interventions may be implemented in school settings. The implication for the design and implementation of interventions is that the particular context for a pupil with ADHD, their classroom, school and issues at the sociopolitical level need to be actively considered. This suggests a need to consider co-ordinated approaches to interventions where the response to an individual child with ADHD fits with policy and guidance at the class, school and wider contextual levels. An implication of review findings about intervention design is that intervention at pupil and classroom contexts without support at school and sociopolitical levels is likely to be less effective. Interventions that retain some flexibility such that they can be tailored to individual pupils with ADHD and the wider context in which the pupil experiences their education, would allow a response to individual contexts.
The qualitative reviews suggest that stigma and marginalisation may be increased through intervention. This is an important consideration for implementation. For instance, where children with ADHD are withdrawn from mainstream classes, such programmes can result in issues of stigmatisation. Alternatives might involve an inclusive approach that does not single out pupils diagnosed with, or at risk of, ADHD, for example that targets the classroom rather than pupil level. Some studies suggested that educating teachers about ADHD and effective classroom strategies decreased stigma.
The findings from reviews 3 and 4 suggest that psychoeducation about ADHD could usefully be provided to school staff, pupils with ADHD and their peers as an adjunct to any intervention that targets children with, or at risk of, ADHD. Provision of information about ADHD as an interaction of factors could combat tendencies towards polarised beliefs about ADHD. Findings also emphasise the importance of involving a range of stakeholders (e.g. parents, teachers, other school staff, mental health professionals, children, researchers) in the design of interventions. This may also help address different perceptions held by practitioners and researchers of what constitutes ‘an intervention’. Review 1 found inattention to improve across several raters for interventions reviewed. However, review 4 noted that teachers showed greater concern over symptoms of hyperactivity/impulsivity, and may be less aware of changes in inattention. As such, we believe that psychoeducation regarding ADHD could stress the impact of inattention for pupils with ADHD, and its potential to respond to intervention.
Different stakeholder priorities imply a need for interventions with multiple components that tackle different aspects of the difficulties that young people with ADHD face in coping with school. For example, teachers may prioritise behaviour management but pupils may prioritise social skills, and parents may prioritise self-concept. Interventions may need to target different behaviours for children with ADHD at different age levels. These different behaviours in turn require different interventions. For example, self-management and study skills may be more appropriate and possibly more effective for older pupils. We believe that ‘fine-tuning’ in the design of interventions may be valuable in matching therapy and need.
Given the importance of relationships highlighted by reviews 3 and 4 and the possible reduced effectiveness of social skills training for pupils with ADHD suggested by review 1, support for relationships with teachers and peers seems an important additional component of interventions. The choice of intervention provider(s) may be critical to the outcome of any intervention. Practical considerations aside, in the context of ADHD, teachers known to have a positive relationship with the target pupils could be more suitable for intervention delivery or particular elements thereof, than when there is no previous relationship or a negative relationship between the provider and child. Provider relationship is therefore important for future evaluation.
Implications for research practice identified by review 1 in particular suggest a benefit from raising the standards of the reporting of intervention content. In the absence of clear, detailed description of interventions and a shared, reliable tool for characterising intervention content, it is difficult to establish the precise content of interventions, isolate the potentially active ingredients and compare results reliably across papers.
Suggested research priorities
Methodological issues
-
Examination of what works and for whom should be the focus of intervention research and, therefore, interventions should be theory based with BCTs explicitly matched to the relevant outcomes (see review 1). A formal intervention mapping process could enhance the selection of appropriate change techniques and examination of potential moderators.
-
Non-pharmacological interventions that target children and young people diagnosed with or at risk of ADHD should be rigorously evaluated, conforming where feasible to Consolidated Standards of Reporting Trials (or other relevant) guidelines. In particular, cluster randomised controlled designs should be used and these trials should employ allocation concealment; blinding of outcome assessors; control for baseline characteristics, including pharmacological treatments for ADHD; the use of objective outcome measures; long-term follow-ups; collection of economic data alongside trials; and tests of intervention fidelity wherever possible.
-
Process evaluations should accompany evaluations of intervention trials in order to explore the experience and attitudes of those involved in interventions, which may profoundly influence the effectiveness and the experience of the intervention.
-
Some outcomes (e.g. self-concept of the child including perceptions of emotional self-control and child attitudes towards ADHD, school and learning) were identified as important in reviews 3 and 4 but were not commonly assessed in the RCTs identified in review 1; consideration should be given to the best way to measure and incorporate these into future trials. These issues are important to those who access services in terms of what they would like to improve.
-
Quantitative evaluations of intervention trials are needed to assess the acceptability and perceived effectiveness of interventions. For example, validated scales such as the BIRS and the IRP-15 are available and should be used in preference to bespoke measures with unproven validity to measure teacher attitudes.
Gaps in the current research literature
-
The development and testing of standardised tools to describe programme features relevant to ADHD, so that the design, reporting, replication, implementation and synthesis of interventions that target children with, or at risk of, ADHD can be enhanced. Such work would facilitate examination of which particular behavioural change techniques or combinations thereof are most effective for ADHD. It would also help encourage researchers and journal editors to raise standards on the reporting of intervention content.
-
Given the wide range of outcome measures reported in review 1, identification of gold-standard outcome measures assessing aspects related to ADHD is essential to facilitate comparison across studies and future meta-analysis.
-
No relevant cost-effectiveness studies were detected during review 1. Although this is an obvious gap in the literature, the tentative nature of the evidence of effectiveness, and the methodological complexities that surround the development, testing and implementation of school-based interventions for ADHD, suggest that there is a great deal of work needed to establish evidence of effectiveness before cost-effectiveness studies will provide meaningful results. However, there may be scope for modelling of potential cost-savings should effectiveness be demonstrated.
-
Findings suggest that a range of potential moderators could be researched alongside intervention trials given their importance across reviews. These include:
-
age
-
medication use
-
intensity and duration of intervention
-
individual versus group delivery
-
intervention packages that the overarching synthesis highlighted as being in need of further research to understand their effectiveness and moderators include DRCs and social skills training.
-
-
Reviews 3 and 4 identified important gaps in qualitative research related to the role of interventions in schools for the following:
-
UK teachers’ experiences of pupils with ADHD.
-
Experience of gender issues in ADHD in schools across countries, including exploration of any sociological contributions to differences by gender in perceptions of ADHD symptoms in the classroom and referral for clinical assessment.
-
The impact of increasing maturity for pupils diagnosed with, or at risk of, ADHD and differences in school expectations between primary and secondary school levels.
-
The experiences of ADHD for secondary school teachers across countries.
-
The experiences of children diagnosed with ADHD across countries.
-
Issues in relation to symptoms of inattention. The focus in review 4, particularly in teacher studies, tended to be on hyperactivity/impulsivity and/or disruptive behaviour; this mirrors wider literature in the field.
-
An exploration of the differing understandings of the term intervention held by teachers and researchers/evaluators.
-
-
Evaluations of interventions in the UK and for older students at primary and secondary levels are under-represented and therefore should be especially supported.
-
Given our findings regarding individual differences in the expression and experience of ADHD, it would be useful to explore the effectiveness of more flexible, individualised interventions for children with ADHD (e.g. functional behavioural assessment) in controlled trials.
-
Mixed-method research that draws on the complexity of the school context highlighted in Chapter 7, to investigate how factors influence the implementation of interventions. We need to understand what works best, for whom and how. Suggested foci for such studies include:
-
experience of relationships between pupils diagnosed with, or at risk of, ADHD and their teachers
-
teacher–parent collaboration for pupils diagnosed with, or at risk of, ADHD.
-
Acknowledgements
We would like to thank a range of parents and practitioners who either attended workshops during the design of the project, provided feedback on findings in later workshops, or replied to e-mails during the design of the project. In particular, we would like to the following for their essential contributions:
Catherine Shotton, a member of the Family Faculty at the University of Exeter Medical School’s Cerebra Research Unit, was involved in writing the project application, project design and commenting on Chapters 4–6.
Tracy Elliott, Head of Research and Education at the charity Cerebra, assisted with recruitment of parents for stakeholder involvement during the project. She, with her colleagues Jane Margetson and Melanie Dean, supported and promoted the well-attended dissemination event aimed at parents and practitioners held in Bristol, UK, 25 September 2013.
Will Pritchard, Professional Lead (Behaviour) at Babcock International Group, Exeter, supported the project application, project design and arranged a feedback workshop with advisory teachers (see Appendix 11).
This project was supported by a range of junior and senior academics who were generous with their time. In particular we would like to thank:
Rebecca Abbott for assistance with title and abstract screening for all reviews and comments on review 2.
Jeni Reeve for assistance in screening, data extraction, backward citation chasing and analysis for review 2.
Daniel Racey for assistance with backward citation chasing, hand-searching of journals and website searching for all reviews and screening for review 2.
Rosina Kyeremateng for assistance with full-text screening and data extraction for review 2.
Angelica Chan for assistance in proofreading the final report and preparing appendices.
Brahm Norwich, Professor of Education at the University of Exeter, was a member of our expert advisory group and provided expert advice on the design of the project, recommendations of relevant research and detailed comments on Chapters 4–6.
Carolyn Webster-Stratton, Professor of Psychology and Social Work at the University of Washington, was a member of our expert advisory group and provided expert advice on the design of the project and recommendations of relevant research.
Kapil Sayal provided feedback on the project workshop output and recommendations of relevant research.
Bogdan Grigore, Astrid Jannsens, Anni Vanhatalo, Sara Ingarfield and Hilary Kaube for translating foreign-language papers during full-text screening.
Kate Allen, Kate Grimes, Pamela Bowman, Emily Rhodes, Matt Allwood and Abigail Russell for assistance in proofreading draft chapters.
Chris Cooper for advice on literature searches.
We acknowledge funding from the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care for the South West Peninsula. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health in England.
Contributions of authors
Michelle Richardson, Research Fellow, led review 1, assisted with other reviews, developed the overarching synthesis, wrote and edited the final report, organised and conducted stakeholder involvement events.
Darren A Moore, Associate Research Fellow, led reviews 2 and 3, assisted with other reviews, developed the overarching synthesis, wrote and edited the final report, organised and conducted stakeholder involvement events.
Ruth Gwernan-Jones, Associate Research Fellow, led review 4, assisted with other reviews, developed the overarching synthesis, wrote and edited the final report, organised and conducted stakeholder involvement events.
Jo Thompson-Coon, Research Fellow in Health Services Research, was involved in study design, provided advice on systematic review methods and commented on draft chapters and the final report.
Obioha Ukoumunne, Senior Lecturer in Medical Statistics, advised on review 1 synthesis and commented on Chapter 2 drafts.
Morwenna Rogers, Information Specialist, designed and undertook literature searches, forward citation chasing for all reviews, title and abstract screening for reviews 1 and 2, and commented on draft chapters.
Rebecca Whear, Research Fellow, provided advice on systematic review methods, title and abstract screening for reviews 1, 3 and 4, and commented on final report.
Tamsin V Newlove-Delgado, Doctoral Research Fellow, was involved in screening across all reviews, data extraction for reviews 1 and 2, and commented on draft chapters.
Stuart Logan, Cerebra Professor of Paediatric Epidemiology, contributed to the initial application and commented on draft chapters.
Christopher Morris, Senior Research Fellow in Child Health, supported stakeholder involvement and commented on draft chapters.
Eric Taylor, Emeritus Professor of Child and Adolescent Psychiatry, was involved in study design, ADHD topic advice, recommendations of relevant research and commented on draft chapters.
Paul Cooper, Professor of Education, was involved in study design, ADHD topic advice, recommendations of relevant research and commented on the draft final report.
Ken Stein, Professor, Deputy Director, Peninsula Collaboration for Leadership in Applied Health Research and Care (PenCLAHRC), was involved in study design and commented on draft chapters and final report.
Ruth Garside, Senior Lecturer in Evidence Synthesis, was involved in study design, provided advice on qualitative review methods, assisted in qualitative synthesis and commented on draft chapters as well as the final report.
Tamsin J Ford, Professor of Child and Adolescent Psychiatry, supervised the project, was involved in study design, ADHD topic advice and commented on draft chapters and the final report.
Publications
Gwernan-Jones R, Moore DA, Garside R, Richardson M, Thompson-Coon J, Rogers M, et al. ADHD, parent perspectives and parent–teacher relationships: grounds for conflict [published online ahead of print]. Br J Special Educ 2015.
Moore DA, Richardson M, Gwernan-Jones R, Thompson-Coon J, Stein K, Rogers M, et al. Non-pharmacological interventions for ADHD in school settings: an overarching synthesis of systematic reviews [published online ahead of print 9 March 2015]. J Atten Disord 2015.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health.
References
- Diagnostic and Statistical Manual of Mental Disorders. Arlington, VA: American Psychiatric Publishing; 2013.
- Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 2000.
- Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 1980.
- The ICD-10 Classification of Mental and Behavioural Disorders. Geneva: WHO; 1992.
- Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press; 1990.
- Faraone SV, Perlis RH, Doyle AE, Smoller JW, Goralnick JJ, Holmgren MA, et al. Molecular genetics of attention-deficit/hyperactivity disorder. Biol Psychiatr 2005;57:1313-23. http://dx.doi.org/10.1016/j.biopsych.2004.11.024.
- Wu KK, Anderson V, Castiello U. Neuropsychological evaluation of deficits in executive functioning for ADHD children with or without learning disabilities. Dev Neuropsychol 2002;22:501-31. http://dx.doi.org/10.1207/S15326942DN2202_5.
- Barkley RA, Murphy KR. Attention-Deficit Hyperactivity Disorder: A Clinical Workbook. New York, NY: Guilford Publication; 2006.
- Barkley RA. Deficient emotional self-regulation is a core component of ADHD. J ADHD Relat Disord 2010;1:5-37.
- Wu J, Xiao H, Sun H, Zou L, Zhu LQ. Role of dopamine receptors in ADHD: a systematic meta-analysis. Mol Neurobiol 2012;45:605-20. http://dx.doi.org/10.1007/s12035-012-8278-5.
- Taylor E. Developing ADHD. J Child Psychol Psychiatr 2009;50:126-32. http://dx.doi.org/10.1111/j.1469-7610.2008.01999.x.
- Copeland WE, Angold A, Costello EJ, Egger H. Prevalence, comorbidity, and correlates of DSM-5 proposed disruptive mood dysregulation disorder. Am J Psychiatr 2013;170:173-9. http://dx.doi.org/10.1176/appi.ajp.2012.12010132.
- Polanczyk G, de Lima M, Horta B, Biederman J, Rohde L. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatr 2007;164:942-8. http://dx.doi.org/10.1176/ajp.2007.164.6.942.
- Boyle CA, Boulet S, Schieve LA, Cohen RA, Blumberg SJ, Yeargin-Allsopp M, et al. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics 2011;127:1034-42. http://dx.doi.org/10.1542/peds.2010-2989.
- Ford T, Goodman R, Meltzer H. The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Adolesc Psychiatr 2003;42:1203-11. http://dx.doi.org/10.1097/00004583-200310000-00011.
- Health, United States, 2011: With Special Feature on Socioeconomic Status and Health. Hyattsville, MD: Centers for Disease Control and Prevention; 2012.
- Russell G, Rodgers LR, Ukoumunne OC, Ford T. Prevalence of parent-reported ASD and ADHD in the UK: findings from the Millennium Cohort Study. J Autism Dev Disord 2014;44:31-40. http://dx.doi.org/10.1007/s10803-013-1849-0.
- Cantwell DP. Attention deficit disorder: a review of the past 10 years. J Am Acad Child Adolesc Psychiatr 1996;35:978-87. http://dx.doi.org/10.1097/00004583-199608000-00008.
- Ford T, Fowler T, Langley K, Whittinger N, Thapar A. Five years on: public sector service use related to mental health in young people with ADHD or hyperkinetic disorder five years after diagnosis. Child Adolesc Ment Health 2008;13:122-9. http://dx.doi.org/10.1111/j.1475-3588.2007.00466.x.
- Froehlich TE, Lanphear BP, Epstein JN, Barbaresi WJ, Katusic SK, Kahn RS. Prevalence, recognition, and treatment of attention-deficit/hyperactivity disorder in a national sample of US children. Arch Pediatr Adolesc Med 2007;161. http://dx.doi.org/10.1001/archpedi.161.9.857.
- Russell G, Ford T, Rosenberg R, Kelly S. The association of attention deficit hyperactivity disorder with socioeconomic disadvantage: alternative explanations and evidence. J Child Psychol Psychiatry 2014;55:436-45. http://dx.doi.org/10.1111/jcpp.12170.
- Barbaresi WJ, Colligan RC, Weaver AL, Voigt RG, Killian JM, Katusic SK. Mortality, ADHD, and psychosocial adversity in adults with childhood ADHD: a prospective study. Am Acad Pediatr 2013;131:637-44. http://dx.doi.org/10.1542/peds.2012-2354.
- Parker HC, Ellison AT, Sherman G, Frisch ME, Kay C, Burton BS, et al. Improving the diagnosis, treatment, and follow-up of adult attention deficit/hyperactivity disorder (ADHD) patients in primary care utilizing a performance improvement continuing medical education (PI CME) Activity. CE Meas 2012;6:3-12.
- Ahuja A, Martin J, Langley K, Thapar A. Intellectual disability in children with attention deficit hyperactivity disorder. J Pediatr 2013;163:890-5. http://dx.doi.org/10.1016/j.jpeds.2013.02.043.
- Mikami AY, DeWall CN. The Oxford Handbook of Social Exclusion. New York, NY: Oxford University Press; 2013.
- Reid R, Hakendorf P, Prosser B. Use of psychostimulant medication for ADHD in South Australia. J Am Acad Child Adolesc Psychiatr 2002;41:906-13. http://dx.doi.org/10.1097/00004583-200208000-00008.
- Singh I. A disorder of anger and aggression: children’s perspectives on attention deficit/hyperactivity disorder in the UK. Soc Sci Med 2011;73:889-96. http://dx.doi.org/10.1016/j.socscimed.2011.03.049.
- Malacrida C. Medicalization, ambivalence and social control: mothers’ descriptions of educators and ADD/ADHD. Health (Lond) 2004;8:61-80. http://dx.doi.org/10.1177/1363459304038795.
- Jarrett MA, Wolff JC, Davis TE, Cowart MJ, Ollendick TH. Characteristics of children with ADHD and comorbid anxiety [published online ahead of print 3 August 2012]. J Atten Disord 2012.
- Campbell Daley K. Update on attention-deficit/hyperactivity disorder. Curr Opin Pediatr 2004;16. http://dx.doi.org/10.1097/00008480-200404000-00020.
- Reiersen A, Constantino J, Volk H, Todd R. Autistic traits in a population-based ADHD twin sample. J Child Psychol Psychiatry 2007;48:464-72. http://dx.doi.org/10.1111/j.1469-7610.2006.01720.x.
- Larson K, Russ SA, Kahn RS, Halfon N. Patterns of comorbidity, functioning, and service use for US children with ADHD, 2007. Pediatrics 2011;127:462-70. http://dx.doi.org/10.1542/peds.2010-0165.
- Staikova E, Gomes H, Tartter V, McCabe A, Halperin JM. Pragmatic deficits and social impairment in children with ADHD. J Child Psychol Psychiatr 2013;54:1275-83. http://dx.doi.org/10.1111/jcpp.12082.
- Gillberg C, Gillberg IC, Rasmussen P, Kadesjö B, Söderström H, Råstam M, et al. Co-existing disorders in ADHD – implications for diagnosis and intervention. Eur Child Adolesc Psychiatr 2004;13:i80-92. http://dx.doi.org/10.1007/s00787-004-1008-4.
- Pajo B, Cohen D. The problem with ADHD: researchers’ constructions and parents’ accounts. IJEC 2012;45:11-33. http://dx.doi.org/10.1007/s13158-012-0064-z.
- O’Regan F. A review of SENCo and GP attitudes towards ADHD. ADHD in Practice 2009;1:4-7.
- Bailey S. Lost in Translation? Parental Agency and Specialist Therapeutics n.d.
- Mayes R, Bagwell C, Erkulwater J. ADHD and the rise in stimulant use among children. Harv Rev Psychiatr 2008;16:151-66. http://dx.doi.org/10.1080/10673220802167782.
- Scholtens S, Rydell A, Wallentin F. ADHD symptoms, academic achievement, self-perception of academic competence and future orientation: a longitudinal study. Scand J Psychol 2013;54:205-12. http://dx.doi.org/10.1111/sjop.12042.
- Elder T. The importance of relative standards in ADHD diagnoses: evidence based on exact birth dates. J Health Econ 2010;29:641-56. http://dx.doi.org/10.1016/j.jhealeco.2010.06.003.
- Bailey S, Thomson P. Routine (dis)order in an infant school. Ethnography Educ 2009;4:211-27. http://dx.doi.org/10.1080/17457820902972879.
- Timimi S, Taylor E. ADHD is best understood as a cultural construct. Br J Psychiatr 2004;184:8-9. http://dx.doi.org/10.1192/bjp.184.1.8.
- Hjörne E, Saljo R. ‘There Is Something About Julia’: symptoms, categories, and the process of invoking attention deficit hyperactivity disorder in the Swedish school: a case study. J Lang Ident Educ 2004;3:1-24. http://dx.doi.org/10.1207/s15327701jlie0301_1.
- Kiger G. Economic transformation and the processing of hyperactive school children. Mid Am Rev Sociol 2013;10:65-8.
- Karnik Niranjan S. Categories of control: foster children and ADHD. Child Youth Serv Rev 2001;23:761-80. http://dx.doi.org/10.1016/S0190-7409(01)00159-1.
- The NICE Guideline on Diagnosis and Management of ADHD in Children, Young People and Adults. London: NCCMH; 2011.
- Hinshaw SP, Scheffler RM, Fulton BD, Aase H, Banaschewski T, Cheng W, et al. International variation in treatment procedures for ADHD: social context and recent trends. Psychiatr Serv 2011;62:459-64. http://dx.doi.org/10.1176/ps.62.5.pss6205_0459.
- Coghill D. Use of stimulants for attention deficit hyperactivity disorder: FOR. BMJ 2004;329. http://dx.doi.org/10.1136/bmj.329.7471.907.
- Baldwin S, Cooper P. How should ADHD be treated?. Psychologist 2000;13:598-601.
- Timimi S. Inappropriate use of psychostimulants. Br J Psychiatr 2003;183. http://dx.doi.org/10.1192/bjp.183.2.173.
- The Safer Management of Controlled Drugs: Annual Report 2012. Newcastle: CQC; 2013.
- Prasad V, Brogan E, Mulvaney C, Grainge M, Stanton W, Sayal K. How effective are drug treatments for children with ADHD at improving on-task behaviour and academic achievement in the school classroom? A systematic review and meta-analysis. Eur Child Adolesc Psychiatr 2013;22:203-16. http://dx.doi.org/10.1007/s00787-012-0346-x.
- Swanson JM, McBurnett K, Wigal T, Pfiffner LJ, Lerner MA, Williams L, et al. Effect of stimulant medication on children with attention deficit disorder: a’ review of reviews’. Except Child 1993;60:154-61.
- Banaschewski T, Roessner V, Dittmann RW, Santosh PJ, Rothenberger A. Non–stimulant medications in the treatment of ADHD. Eur Child Adolesc Psychiatr 2004;13:i102-i116. http://dx.doi.org/10.1007/s00787-004-1010-x.
- Graham J, Banaschewski T, Buitelaar J, Coghill D, Danckaerts M, Dittmann RW, et al. European guidelines on managing adverse effects of medication for ADHD. Eur Child Adolesc Psychiatr 2011;20:17-3. http://dx.doi.org/10.1007/s00787-010-0140-6.
- Gilmore A, Milne R. Methylphenidate in children with hyperactivity: review and cost–utility analysis. Pharmacoepidemiol Drug Saf 2001;10:85-94. http://dx.doi.org/10.1002/pds.564.
- Lord J, Paisley S. The Clinical Effectiveness and Cost-Effectiveness of Methylphenidate for Hyperactivity in Childhood. London: National Institute for Health and Care Excellence; 2000.
- Foster EM, Jensen PS, Schlander M, Pelham WE, Hechtman L, Arnold LE, et al. Treatment for ADHD: is more complex treatment cost-effective for more complex cases?. Health Serv Res 2007;42:165-82. http://dx.doi.org/10.1111/j.1475-6773.2006.00599.x.
- Purdie N, Hattie J, Carroll A. A review of the research on interventions for attention deficit hyperactivity disorder: What works best?. Rev Educ Res 2002;72:61-99. http://dx.doi.org/10.3102/00346543072001061.
- Abikoff H, Hechtman L, Hibbs ED, Jensen PS. Psychosocial Treatments for Child and Adolescent Disorders: Empirically Based Strategies for Clinical Practice. Washington, DC: American Psychological Association; 1996.
- Jensen PS, Hinshaw SP, Swanson JM, Greenhill LL, Conners CK, Arnold LE, et al. Findings from the NIMH Multimodal Treatment Study of ADHD (MTA): implications and applications for primary care providers. J Dev Behav Pediatr 2001;22:60-73. http://dx.doi.org/10.1097/00004703-200102000-00008.
- Sonuga-Barke EJ, Brandeis D, Cortese S, Daley D, Ferrin M, Holtmann M, et al. Nonpharmacological interventions for ADHD: systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am J Psychiatr 2013;170:275-89. http://dx.doi.org/10.1176/appi.ajp.2012.12070991.
- Fabiano GA, Pelham WE, Coles EK, Gnagy EM, Chronis-Tuscano A, O’Connor BC. A meta-analysis of behavioral treatments for attention-deficit/hyperactivity disorder. Clin Psychol Rev 2009;29:129-40. http://dx.doi.org/10.1016/j.cpr.2008.11.001.
- Pelham WE, Fabiano GA. Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. J Clin Child Adolesc Psychol 2008;37:184-21. http://dx.doi.org/10.1080/15374410701818681.
- Cohen J. A power primer. Psychol Bull 1992;112. http://dx.doi.org/10.1037/0033-2909.112.1.155.
- Pelham WE, Burrows-MacLean L, Gnagy EM, Fabiano GA, Coles EK, Tresco KE, et al. Transdermal methylphenidate, behavioral, and combined treatment for children with ADHD. Exp Clin Psychopharmacol 2005;13:111-26. http://dx.doi.org/10.1037/1064-1297.13.2.111.
- Willis WG, Weyandt LL, Lubiner AG, Schubart CD. Neurofeedback as a treatment for attention-deficit/hyperactivity disorder: A systematic review of evidence for practice. J Appl Sch Psychol 2011;27:201-27. http://dx.doi.org/10.1080/15377903.2011.590746.
- Lofthouse N, Arnold LE, Hersch S, Hurt E, DeBeus R. A review of neurofeedback treatment for pediatric ADHD. J Atten Disord 2012;16:351-72. http://dx.doi.org/10.1177/1087054711427530.
- Chronis AM, Jones HA, Raggi VL. Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Clin Psychol Rev 2006;26. http://dx.doi.org/10.1016/j.cpr.2006.01.002.
- Barkley RA. Adolescents with attention-deficit/hyperactivity disorder: an overview of empirically based treatments. J Psychiatr Pract 2004;10:39-56. http://dx.doi.org/10.1097/00131746-200401000-00005.
- Sayal K, Ford T, Goodman R. Trends in recognition of and service use for attention-deficit hyperactivity disorder in Britain, 1999–2004. Psychiatr Serv 2010;61:803-10. http://dx.doi.org/10.1176/ps.2010.61.8.803.
- DuPaul GJ, Eckert TL, Vilardo B. The effects of school-based interventions for attention deficit hyperactivity disorder: a meta-analysis 1996–2010. SPR 2012;41:387-412.
- Raggi VL, Chronis AM. Interventions to address the academic impairment of children and adolescents with ADHD. Clin Child Fam Psychol Rev 2006;9:85-111. http://dx.doi.org/10.1007/s10567-006-0006-0.
- Trout AL, Lienemann TO, Reid R, Epstein MH. A review of non-medication interventions to improve the academic performance of children and youth with ADHD. Remedial and Special Education 2007;28:207-26. http://dx.doi.org/10.1177/07419325070280040201.
- Reid R, Trout AL, Schartz M. Self-regulation interventions for children with attention deficit/hyperactivity disorder. Except Child 2005;71:361-77.
- Murray DW, Rabiner DL, Hardy KK. Teacher management practices for first graders with attention problems. J Atten Disord 2011;15:638-45. http://dx.doi.org/10.1177/1087054710378234.
- Telford C, Green C, Logan S, Langley K, Thapar A, Ford T. Estimating the costs of ongoing care for adolescents with attention-deficit hyperactivity disorder. Soc Psychiatry Psychiatr Epidemiol 2013;48:337-44. http://dx.doi.org/10.1007/s00127-012-0530-9.
- Identifying and implementing educational practices supported by rigorous evidence: A user-friendly guide. Washington, DC: US Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance; 2003.
- Cartwright N, Kincaid H. The Oxford Handbook of Philosophy of Social Science. Oxford: Oxford University Press; 2012.
- Cartwright N. A philosophers view of the long road from RCTs to effectiveness. Lancet 2011;377:1400-1. http://dx.doi.org/10.1016/S0140-6736(11)60563-1.
- Hammersley M. On ‘systematic’ reviews of research literatures: a ‘narrative’ response to Evans & Benefield. Br Educ Res J 2013;27:553-4.
- Elliott J. Making evidence-based practice educational. Br Educ Res J 2013;27:555-74. http://dx.doi.org/10.1080/01411920120095735.
- Conners CK, Sitarenios G, Parker JD, Epstein JN. Revision and restandardization of the Conners Teacher Rating Scale (CTRS-R): factor structure, reliability, and criterion validity. J Abnorm Child Psychol 1998;26:279-91. http://dx.doi.org/10.1023/A:1022606501530.
- Greenberg LM, Waldmant ID. Developmental normative data on the test of variables of attention (TOVA). J Child Psychol Psychiatr 1993;34:1019-30. http://dx.doi.org/10.1111/j.1469-7610.1993.tb01105.x.
- Wilkinson GS, Robertson GJ. Wide Range Achievement Test (WRAT4). Lutz, FL: Psychological Assessment Resources; 2006.
- Teddlie C, Tashakkori A. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioural Sciences. London: Sage; 2009.
- Harden A, Thomas J. Methodological issues in combining diverse study types in systematic reviews. Int J Soc Res Methodol 2005;8:257-71. http://dx.doi.org/10.1080/13645570500155078.
- Noblit GW, Hare RD. Meta-Ethnography: Synthesising Qualitative Studies. Newbury Park, CA: Sage; 1988.
- Fairclough N. Language and Power. Harrow: Longman Publishers; 2001.
- Garside R. A Comparison of Methods for the Systematic Review of Qualitative Research: Two Examples Using Meta-Ethnography and Meta-Study. Exeter: University of Exeter; 2008.
- Gubrium J, Holstein J. The New Language of Qualitative Method. New York, NY: Oxford University Press; 1997.
- EPPI-Centre Methods for Conducting Systematic Reviews. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2010.
- Rothman AJ. ‘Is there nothing more practical than a good theory?’: why innovations and advances in health behavior change will arise if interventions are used to test and refine. Int J Behav Nutr Phys Activ 2004;1:1-7. http://dx.doi.org/10.1186/1479-5868-1-11.
- Dombrowski SU, Sniehotta FF, Avenell A, Johnston M, MacLennan G, Araujo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev 2012;6:7-32. http://dx.doi.org/10.1080/17437199.2010.513298.
- Taylor N, Conner M, Lawton R. The impact of theory on the effectiveness of worksite physical activity interventions: a meta-analysis and meta-regression. Health Psychol Rev 2012;6:33-7. http://dx.doi.org/10.1080/17437199.2010.533441.
- Kamphaus RW, Reynolds CR. Behavior Assessment System for Children Second Edition (BASC-2): Behavioral and Emotional Screening System (BESS). Bloomington, MN: Pearson; 2007.
- Swanson JM. School-Based Assessments and Interventions for ADD Students. Irvine, CA: KC Publishing; 1992.
- Conners CK. A teacher rating scale for use in drug studies with children. Am J Psychiatr 1969;126:884-8. http://dx.doi.org/10.1176/ajp.126.6.884.
- Pelham WE, Gnagy EM, Greenslade KE, Milich R. Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. J Am Acad Child Adolesc Psychiatr 1992;31:210-18. http://dx.doi.org/10.1097/00004583-199203000-00006.
- Achenbach TM. Child Behavior Checklist/4–18. Burlington, VT: University of Vermont; 1991.
- Wolraich ML, Feurer ID, Hannah JN, Baumgaertel A. Vanderbilt ADHD teacher rating scale (VADTRS) and the Vanderbilt ADHD parent rating scale (VADPRS). J Pediatr Psychol 2003;28:559-67. http://dx.doi.org/10.1093/jpepsy/jsg046.
- Cocciarella A, Wood R, Low KG. Brief behavioral treatment for attention-deficit hyperactivity disorder. Percept Mot Skills 1995;81:225-6. http://dx.doi.org/10.2466/pms.1995.81.1.225.
- Cairns ED, Cammock T. Development of a more reliable version of the matching familiar figures test. Dev Psychol 1978;14. http://dx.doi.org/10.1037/0012-1649.14.5.555.
- Barkley RA, Shelton TL, Crosswait C, Moorehouse M, Fletcher K, Barrett S, et al. Multi-method psycho-educational intervention for preschool children with disruptive behavior: preliminary results at post-treatment. J Child Psychol Psychiatry 2000;41:319-32. http://dx.doi.org/10.1111/1469-7610.00616.
- DuPaul GJ, Rapport MD, Perriello LM. Teacher ratings of academic skills: the development of the Academic Performance Rating Scale. Sch Psychol Rev 1991;20:284-300.
- Loney J, Wolraich M. Advances in Developmental and Behavioral Pediatrics. Greenwich: CT: JAI Press; 1982.
- Kendall PC, Wilcox LE. Self-control in children: development of a rating scale. J Consult Clin Psychol 1979;47. http://dx.doi.org/10.1037/0022-006X.47.6.1020.
- Gordon M. Tester For Measuring Impulsivity, Vigilance, and Distractibility 1988.
- Sprafkin J, Gadow KD, Salisbury H, Schneider J, Loney J. Further evidence of reliability and validity of the Child Symptom Inventory-4: parent checklist in clinically referred boys. J Clin Child Adolesc Psychol 2002;31:513-24. http://dx.doi.org/10.1207/S15374424JCCP3104_10.
- Achenbach TM. Integrative Guide for the 1991 CBCL/4–18, YSR, and TRF Profiles. Burlington, VT: Department of Psychiatry, University of Vermont Burlington; 1991.
- Reynolds CR. Behavior Assessment System for Children. Circle Pines, MN: American Guidance Service; 1992.
- Barkley RA, Edelbrock CS, Prinz R. Advances in Behavioural Assessment of Children and Families. Greenwich, CT: JAI Press; 1987.
- Gresham FM, Elliott SN. Social Skills Rating System (SSRS). Circle Pines, MN: American Guidance Service; 1990.
- Achenbach TM, Maruish ME. The Use of Psychological Testing for Treatment Planning and Outcomes Assessment. Hillsdale, NJ: Lawrence Erlbaum Associates Publishers; 1999.
- Achenbach TM, Edelbrock CS. Manual for the Teachers Report Form and Teacher Version of the Child Behavior Profile. Burlington, VT: University of Vermont; 1986.
- Pianta RC. Manual and Scoring Guide for the Student–Teacher Relationship Scale. Charlottesville, VA: University of Virginia; 1996.
- Navarro AM, Peiró R, Llácer MD, y Silva F, En Silva F, Martorell MC. Evaluacion Infanto Juvenil. Madrid: MEPSA; 1993.
- Achenbach TM, Edelbrock CS. Manual for the Child Behavior Checklist and Child Behavior Profile. Burlington, VT: University of Vermont; 1983.
- Goyette CH, Conners CK, Ulrich RF. Normative data on revised Conners parent and teachers rating scales. J Abnorm Child Psychol 1978;6:221-36. http://dx.doi.org/10.1007/BF00919127.
- Piers EV. Piers-Harris Children’s Self-Concept Scale: Revised Manual. Los Angeles: Western Psychological Services; 1984.
- Merrell KW. School Social Behavior Scales: Test Manual. Brandon, VT: Clinical Psychology Publishing Company; 1993.
- Walker HM, McConnell SR. The Walker-McConnell Scale of Social Competence and School Adjustment: A Social Skills Rating Scale for Teachers. Austin, TX: Pro-Ed; 1988.
- Fabiano GA, Pelham J, Waschbusch DA, Gnagy EM, Lahey BB, Chronis AM, et al. A practical measure of impairment: psychometric properties of the impairment rating scale in samples of children with attention deficit hyperactivity disorder and two school-based samples. J Clin Child Adolesc Psychol 2006;35:369-85. http://dx.doi.org/10.1207/s15374424jccp3503_3.
- Coopersmith S. Self-Esteem Inventories. Palo Alto, CA: Consulting Psychologists Press; 1987.
- Anesko KM, Schoiock G, Ramirez R, Levine FM. The homework problem checklist: assessing children’s homework difficulties. Behav Assess 1987;9:179-85.
- Abikoff HA, Gallagher R, McBurnett K, Pfiffner L. Attention Deficit Hyperactivity Disorder: Concepts, Controversies, New Directions. New York, NY: Information Healthcare USA; 2008.
- Michael WB, Smith RA. The development and preliminary validation of three forms of a self-concept measure emphasizing school-related activities. Educ Psychol Meas 1976;36:521-8. http://dx.doi.org/10.1177/001316447603600240.
- Raven JC, Raven JC, Court JH. Coloured Progressive Matrices. Oxford: Oxford Psychologists Press; 1962.
- Good RH, Kaminski RA. DIBELS Oral Reading Fluency Passages for First Through Third Grades. Technical report. Eugene, OR: University of Oregon; 2002.
- Gates AI, MacGinitie WH. Gates-MacGinitie Reading Tests. New York, NY: Columbia University Teachers’ College Press; 1965.
- Wiederholt JL, Bryant BR. GORT-4: Grey Oral Reading Tests. Austin, TX: Pro-Ed; 2001.
- Lindquist EF, Hieronymus AN. Manual For Administrators, Supervisors, and Counselors: Iowa Tests of Basic Skills. Iowa, IA: Iowa Testing Programs; 1964.
- Berninger VW. PAL: Process Assessment of the Learner, Test Battery for Reading and Writing. San Antonio, TX: Psychological Corporation; 2001.
- Wechsler D. Wechsler Individual Achievement Test (WIAT-II UK). London: Harcourt Assessment; 2005.
- Woodcock RW, McGrew KS, Mather N. Woodcock–Johnson Tests of Achievement. Itasca, IL: Riverside Publishing; 2001.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27. http://dx.doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Eccles M. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:81-95. http://dx.doi.org/10.1007/s12160-013-9486-6.
- Skinner BF. Operant behavior. Am Psychol 1963;18. http://dx.doi.org/10.1037/h0045185.
- Kanfer FH, Karoly P, Johnson RC, Dokecki PR, Mowrer OH. Conscience, Contract and Social Reality. New York, NY: Holt, Rinehart & Winston; 1972.
- Borenstein M, Harris MC, Ledges LV, Valentine JC. The Handbook of Research Synthesis and Meta-Analysis. New York, NY: Russell Sage Foundation; 2009.
- Evans SW, Langberg J, Raggi V, Allen J, Buvinger EC. Development of a school-based treatment program for middle school youth with ADHD. J Atten Disord 2005;9:343-53. http://dx.doi.org/10.1177/1087054705279305.
- Rabiner DL, Murray DW, Skinner AT, Malone PS. A randomized trial of two promising computer-based interventions for students with attention difficulties. J Abnorm Child Psychol 2010;38:131-42. http://dx.doi.org/10.1007/s10802-009-9353-x.
- Dunson RM, Hughes JN, Jackson TW. Effect of behavioral consultation on student and teacher-behavior. J Sch Psychol 1994;32:247-66. http://dx.doi.org/10.1016/0022-4405(94)90017-5.
- Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: Sage; 2001.
- Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: The Cochrane Collaboration and John Wiley and Sons Ltd; 2008.
- Miller WR, Wilbourne PL. Mesa Grande: a methodological analysis of clinical trials of treatments for alcohol use disorders. Addiction 2002;97:265-77. http://dx.doi.org/10.1046/j.1360-0443.2002.00019.x.
- Cochran WG. The combination of estimates from different experiments. Biometrics 1954;10:101-29. http://dx.doi.org/10.2307/3001666.
- Higgins J, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327. http://dx.doi.org/10.1136/bmj.327.7414.557.
- Higgins J, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539-58. http://dx.doi.org/10.1002/sim.1186.
- Ahmed I, Sutton AJ, Riley RD. Assessment of publication bias, selection bias, and unavailable data in meta-analyses using individual participant data: a database survey. BMJ 2012;344:1-10. http://dx.doi.org/10.1136/bmj.d7762.
- Knapp G, Hartung J. Improved tests for a random effects meta-regression with a single covariate. Stat Med 2003;22:2693-710. http://dx.doi.org/10.1002/sim.1482.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting items for Systematic Reviews and Meta-Analyses: the PRISMA statement. PLOS Med 2009;6:1-6. http://dx.doi.org/10.1371/journal.pmed.1000097.
- Bloomquist ML, August GJ, Ostrander R. Effects of a school-based cognitive–behavioural intervention for ADHD children. J Abnorm Child Psychol 1991;19:591-605. http://dx.doi.org/10.1007/BF00925822.
- Cassar AG, Jang EE. Investigating the effects of a game-based approach in teaching word recognition and spelling to students with reading disabilities and attention deficits. Aust J Learn Difficulties 2010;15:193-211. http://dx.doi.org/10.1080/19404151003796516.
- Chacona SM. Effect of world music drumming on auditory and visual attention skills of ADHD elementary students. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68.
- Cloward R. Self-monitoring increases time-on-task of attention deficit hyperactivity disordered students in the regular classroom. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64.
- Denkowski KM, Denkowski GC. Is group progressive relaxation training as effective with hyperactive children as individual EMG biofeedback treatment?. Biofeedback Self Regul 1984;9:353-64. http://dx.doi.org/10.1007/BF00998978.
- Denkowski KM, Denkowski GC, Omizo MM. The effects of EMG-assisted relaxation training on the academic performance, locus of control, and self-esteem of hyperactive boys. Biofeedback Self Regul 1983;8:363-75. http://dx.doi.org/10.1007/BF00998746.
- Evans SW, Schultz BK, Demars CE, Davis H. Effectiveness of the challenging horizons after-school program for young adolescents with ADHD. Behav Ther 2011;42:462-74. http://dx.doi.org/10.1016/j.beth.2010.11.008.
- Evans SW, Serpell ZN, Schultz BK, Pastor DA. Cumulative benefits of secondary school-based treatment of students with attention deficit hyperactivity disorder. Sch Psychol Rev 2007;36:256-73.
- Fabiano GA, Vujnovic RK, Pelham WE, Waschbusch DA, Massetti GM, Pariseau ME, et al. Enhancing the effectiveness of special education programming for children with attention deficit hyperactivity disorder using a daily report card. Sch Psychol Rev 2010;39:219-39.
- Frame K, Kelly L, Bayley E. Increasing perceptions of self-worth in preadolescents diagnosed with ADHD. J Nurs Scholarsh 2003;35:225-9. http://dx.doi.org/10.1111/j.1547-5069.2003.00225.x.
- Hoover VL. The effect of verbal self-instruction training on the cognitive styles of impulsive elementary school students. Dissertation Abstracts International, Section A: The Humanities and Social Sciences 1986;47.
- Iseman JS, Naglieri JA. A cognitive strategy instruction to improve math calculation for children with ADHD and LD: a randomized controlled study. J Learn Disabil 2011;44:184-95. http://dx.doi.org/10.1177/0022219410391190.
- Jurbergs N, Palcic JL, Kelley ML. Daily behavior report cards with and without home-based consequences: improving classroom behavior in low income, African American children with ADHD. Child Fam Behav Ther 2010;32:177-95. http://dx.doi.org/10.1080/07317107.2010.500501.
- Khilnani S, Field T, Hernandez-Reif M, Schanberg S. Massage therapy improves mood and behavior of students with attention-deficit/hyperactivity disorder. Adolescence 2003;38:623-38.
- Langberg JM, Epstein JN, Becker SP, Girio-Herrera E, Vaughn AJ. Evaluation of the homework, organization, and planning skills (HOPS) intervention for middle school students with attention deficit hyperactivity disorder as implemented by school mental health providers. Sch Psychol Rev 2012;41:342-64.
- Langberg JM, Epstein JN, Urbanowicz CM, Simon JO, Graham AJ. Efficacy of an organization skills intervention to improve the academic functioning of students with attention-deficit/hyperactivity disorder. Sch Psychol Q 2008;23:407-17. http://dx.doi.org/10.1037/1045-3830.23.3.407.
- Lomas KM. Computer-assisted cognitive training with elementary school-age children diagnosed with attention-deficit/hyperactivity disorder and mild/moderate comorbidity: a short-term prospective study on attention, planning and behavior. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63.
- Looyeh MY, Kamali K, Shafieian R. An exploratory study of the effectiveness of group narrative therapy on the school behavior of girls with attention-deficit/hyperactivity symptoms. Arch Psychiatr Nurs 2012;26:404-10. http://dx.doi.org/10.1016/j.apnu.2012.01.001.
- McGraw TM, Burdette K, Chadwick K. The Effects of a Consumer-Oriented Multimedia Game on the Reading Disorders of Children with ADHD. Charleston, WV: AEL; 2004.
- Molina BSG, Flory K, Bukstein OG, Greiner AR, Baker JL, Krug V, et al. Feasibility and preliminary efficacy of an after-school program for middle schoolers with ADHD: a randomised trial in a large public middle school. J Atten Disord 2008;12:207-17. http://dx.doi.org/10.1177/1087054707311666.
- Murray D, Rabiner D, Schulte A, Newitt K. Feasibility and integrity of a parent–teacher consultation intervention for ADHD students. Child Youth Care Forum 2008;37:111-26. http://dx.doi.org/10.1007/s10566-008-9054-6.
- Omizo MM. The effects of biofeedback-induced relaxation training in hyperactive adolescent boys. J Psychol 1980;105:131-8. http://dx.doi.org/10.1080/00223980.1980.9915141.
- Omizo MM. The effects of relaxation and biofeedback on dimensions of self concept (DOSC) among hyperactive male children. Educ Res Q 1980;5:22-30.
- Omizo MM, Michael WB. Biofeedback-induced relaxation training and impulsivity, attention to task, and locus of control among hyperactive boys. J Learn Disabil 1982;15:414-16. http://dx.doi.org/10.1177/002221948201500708.
- Ostberg M, Rydell AM. An efficacy study of a combined parent and teacher management training programme for children with ADHD. Nord J Psychiatr 2012;66:123-30. http://dx.doi.org/10.3109/08039488.2011.641587.
- Poley JA. Effects of classroom cognitive behavioral training with elementary school ADHD students: a pilot study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56.
- Reid MK, Borkowski JG. Causal attributions of hyperactive children: implications for teaching strategies and self-control. J Educ Psychol 1987;79. http://dx.doi.org/10.1037/0022-0663.79.3.296.
- Rickson DJ, Watkins WG. Music therapy to promote prosocial behaviors in aggressive adolescent boys – a pilot study. J Music Ther 2003;40:283-301. http://dx.doi.org/10.1093/jmt/40.4.283.
- Rivera E, Omizo MM. The effects of relaxation and biofeedback on attention to task and impulsivity among male hyperactive children. Exceptional Child 1980;27:41-5. http://dx.doi.org/10.1080/0156655800270104.
- Seeley JR, Small JW, Walker HM, Feil EG, Severson HH, Golly AM, et al. Efficacy of the first step to success intervention for students with attention-deficit/hyperactivity disorder. Sch Ment Health 2009;1:37-48. http://dx.doi.org/10.1007/s12310-008-9003-4.
- Steiner NJ, Sheldrick RC, Gotthelf D, Perrin EC. Computer-based attention training in the schools for children with attention deficit/hyperactivity disorder: a preliminary trial. Clin Pediatr 2011;50:615-22. http://dx.doi.org/10.1177/0009922810397887.
- Storer L. An evaluation of a cognitive–behavioural game therapy intervention on the self-efficacy of middle school students who exhibit behaviours associated with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1994;55.
- van Lier PA, Muthén BO, van der Sar RM, Crijnen AA. Preventing disruptive behavior in elementary schoolchildren: impact of a universal classroom-based intervention. J Consult Clin Psychol 2004;72. http://dx.doi.org/10.1037/0022-006X.72.3.467.
- Van der Westhuizen B. An Ecosystemic Approach to Addressing Attentional Difficulties and Heightened Motor Activity. Pretoria, Gauteng: University of South Africa; 2007.
- Zaghlawan HY, Ostrosky MM, Al-Khateeb JM. Decreasing the inattentive behavior of Jordanian children: a group experiment. Educ Treat Child 2007;30:49-64. http://dx.doi.org/10.1353/etc.2007.0018.
- Zentall SS, Lee J. A reading motivation intervention with differential outcomes for students at risk for reading disabilities, ADHD, and typical comparisons: ‘clever is and clever does’. Learn Disabil Q 2012;35:248-59. http://dx.doi.org/10.1177/0731948712438556.
- Abikoff H. Academic Cognitive Training and Stimulants in Hyperactivity: A Pilot Study n.d.
- Bornas X, Servera M. Cognitive training programs to reduce impulsivity-related achievement problems: The need of in-classroom interventions. Learn Instruct 1992;2:89-100. http://dx.doi.org/10.1016/0959-4752(92)90025-H.
- Eastman BG, Rasbury WC. Cognitive self-instruction for the control of impulsive classroom behavior: ensuring the treatment package. J Abnorm Child Psychol 1981;9:381-7. http://dx.doi.org/10.1007/BF00916842.
- Harper K. ADHD: Social Skills Effects on Impulsivity and Depression 1996.
- Kapalka GM. Avoiding repetitions reduces ADHD children’s management problems in the classroom. Emot Behav Difficulties 2005;10:269-79. http://dx.doi.org/10.1177/1363275205058999.
- Kendrick CP. A quasi-experimental study of the effect of feedback on the social behavior of school children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55.
- Miranda A, Jarque S, Rosel J. Treatment of children with ADHD: psychopedagogical program at school versus psychostimulant medication. Psicothema 2006;18:335-41.
- Miranda A, Presentacion MJ, Soriano M. Effectiveness of a school-based multicomponent program for the treatment of children with ADHD. J Learn Disabil 2002;35:546-62. http://dx.doi.org/10.1177/00222194020350060601.
- Owens JS, Richerson L, Beilstein EA, Crane A, Murphy CE, Vancouver JB. School-based mental health programming for children with inattentive and disruptive behavior problems: first-year treatment outcome. J Atten Disord 2005;9:261-74. http://dx.doi.org/10.1177/1087054705279299.
- Poillion MJ. Effects of teacher training on the alteration of teacher instructional style and the academic success of students identified with attention-deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1993;54.
- Re AM, Cornoldi C, Cook BG, Tankersley M, Landrum TJ. Advances in Learning and Behavioural Disabilities. Bradford: Emerald Group Publishing Limited; 2007.
- Semrud-Clikeman M, Nielsen KH, Clinton A, Sylvester L, Parle N, Connor RT. An intervention approach for children with teacher- and parent-identified attentional difficulties. J Learn Disabil 1999;32:581-90. http://dx.doi.org/10.1177/002221949903200609.
- Verret C, Guay MC, Berthiaume C, Gardiner P, Beliveau L. A physical activity program improves behavior and cognitive functions in children with ADHD: an exploratory study. J Atten Disord 2012;16:71-80. http://dx.doi.org/10.1177/1087054710379735.
- Webber JA. Is there a relationship between the play attention program and improved student achievement?. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2012;72.
- Schwandt TA, Lincoln YS, Guba EG. Judging interpretations: but is it rigorous? trustworthiness and authenticity in naturalistic evaluation. New Dir Eval 2007;114:11-25. http://dx.doi.org/10.1002/ev.223.
- Collishaw S, Goodman R, Ford T, Rabe-Hesketh S, Pickles A. How far are associations between child, family and community factors and child psychopathology informant-specific and informant-general?. J Child Psychol Psychiatr 2009;50:571-80. http://dx.doi.org/10.1111/j.1469-7610.2008.02026.x.
- Weisz JR, Jensen-Doss A, Hawley KM. Evidence-based youth psychotherapies versus usual clinical care: a meta-analysis of direct comparisons. Am Psychol 2006;61. http://dx.doi.org/10.1037/0003-066X.61.7.671.
- Kazdin AE. Evidence-based treatment and practice: new opportunities to bridge clinical research and practice, enhance the knowledge base, and improve patient care. Am Psychol 2008;63. http://dx.doi.org/10.1037/0003-066X.63.3.146.
- Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol 2008;57:660-80. http://dx.doi.org/10.1111/j.1464-0597.2008.00341.x.
- Abraham C, Abraham C, Kools M. Writing Health Communication: An Evidence-Based Guide. London: Sage; 2011.
- Bartholomew LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning Health Promotion Programs: An Intervention Mapping Approach. San Francisco, CA: Jossey-Bass; 2011.
- Bandura A. Social cognitive theory of self-regulation. Organ Behav Hum Decis Process 1991;50:248-87. http://dx.doi.org/10.1016/0749-5978(91)90022-L.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Eccles MP, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:1-15. http://dx.doi.org/10.1007/s12160-013-9486-6.
- Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. York: University of York; 2009.
- Eckert TL, Hintze JM. Behavioral conceptions and applications of acceptability: issues related to service delivery and research methodology. Sch Psychol Q 2000;15. http://dx.doi.org/10.1037/h0088782.
- Fairbanks LD, Stinnett TA. Effects of professional group membership, intervention type, and diagnostic label on treatment acceptability. Psychol Schools 1997;34:329-35. http://dx.doi.org/10.1002/(SICI)1520-6807(199710)34:4<329::AID-PITS4>3.0.CO;2-G.
- Coles EK, Slavec J, Bernstein M, Baroni E. Exploring the gender gap in referrals for children with ADHD and other disruptive behavior disorders. J Atten Disord 2012;16:101-8. http://dx.doi.org/10.1177/1087054710381481.
- Kos JM. Primary School Teachers’ Knowledge, Attitudes and Behaviours Toward Children With Attention-Deficit Hyperactivity Disorder 2004.
- Graczyk PA, Atkins MS, Jackson MM, Letendre JA, Kim-Cohen J, Baumann BL, et al. Urban educators’ perceptions of interventions for students with attention deficit hyperactivity disorder: a preliminary investigation. Behav Disord 2005;30:95-104.
- Liu Y, Norman IJ, While AE. Nurses attitudes towards older people: a systematic review. Int J Nurs Stud 2013;50:1271-82. http://dx.doi.org/10.1016/j.ijnurstu.2012.11.021.
- Walburn J, Gray R, Gournay K, Quraishi S, David AS. Systematic review of patient and nurse attitudes to depot antipsychotic medication. Br J Psychiatr 2001;179:300-7. http://dx.doi.org/10.1192/bjp.179.4.300.
- Saunders KE, Hawton K, Fortune S, Farrell S. Attitudes and knowledge of clinical staff regarding people who self-harm: a systematic review. J Affect Disord 2012;139:205-16. http://dx.doi.org/10.1016/j.jad.2011.08.024.
- Waddell L, Taylor M. Attitudes of patients and mental health staff to antipsychotic long-acting injections: systematic review. Br J Psychiatr 2009;195:S43-S50. http://dx.doi.org/10.1192/bjp.195.52.s43.
- Curtis DF, Pisecco S, Hamilton RJ, Moore DW. Teacher perceptions of classroom interventions for children with ADHD: a cross-cultural comparison of teachers in the United States and New Zealand. Sch Psychol Q 2006;21:171-96. http://dx.doi.org/10.1521/scpq.2006.21.2.171.
- Eng RV. Improving treatment acceptability among teachers by increasing knowledge of ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68.
- Girio EL, Owens JS. Teacher acceptability of evidence-based and promising treatments for children with attention-deficit/hyperactivity disorder. School Ment Health 2009;1:16-25. http://dx.doi.org/10.1007/s12310-008-9001-6.
- Pisecco S, Huzinec C, Curtis D. The effect of child characteristics on teachers’ acceptability of classroom-based behavioral strategies and psychostimulant medication for the treatment of ADHD. J Clin Child Psychol 2001;30:413-21. http://dx.doi.org/10.1207/S15374424JCCP3003_12.
- Rowan LA. The Effects of Child Diagnosis on teachers’ Judgements of Treatment Acceptability of Classroom Interventions 2000.
- Schmalzer SN. Teachers’ Perceptions of Self-Management Interventions for ADHD: An Initial Investigation 2006.
- Stinnett TA, Crawford SA, Gillespie MD, Cruce MK, Langford C. Factors affecting treatment acceptability for psychostimulant medication versus psychoeducational intervention. Psychol Schools 2001;38:585-91. http://dx.doi.org/10.1002/pits.1045.
- Stinson AM. Teacher Beliefs About Children With Attention and Behavioral Difficulties 2009.
- Doak JS. The effect of teachers’ beliefs, perceived stress, and student characteristics on teachers’ acceptance of treatment interventions for attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64.
- Whitworth JE, Fossler T, Harbin G. Teachers’ perceptions regarding educational services to students with attention deficit disorder. Rural Educat 1997;19:1-5.
- Curtis DF. A cross-cultural comparison between United States and New Zealand teacher acceptability of interventions for children with attention deficit hyperactive disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64.
- Alongi LM. School psychologists’ perceived effectiveness of social skills training: a comparison across diagnosed populations. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66.
- Askew BL. Practices of Special Education Teachers for Dealing With Students With ADD ADHD 1993.
- Bain SK, Brown KS, Jordan KR. Teacher candidates’ accuracy of beliefs regarding childhood interventions. Teach Educat 2009;44:71-89. http://dx.doi.org/10.1080/08878730902755523.
- Conforti D. Perceived Effectiveness of Classroom Management Interventions With Attention Deficit Hyperactivity Disorder (ADHD) Students 2012.
- Cornell-Swanson LV, Irwin M, Johnson K, Bowman K, Frankenberger W. The use of stimulant medication for treatment of attention-deficit/hyperactivity disorder: A survey of school social workers’ knowledge, opinions/attitudes, and experience. Sch Soc Work J 2005;29:62-8.
- Dryer R, Kiernan MJ, Tyson GA. Parental and professional beliefs on the treatment and management of ADHD. J Atten Disord 2012;16:398-405. http://dx.doi.org/10.1177/1087054710392540.
- Groenewald C, Emond A, Sayal K. Recognition and referral of girls with attention deficit hyperactivity disorder: case vignette study. Child Care Health Dev 2009;35:767-72. http://dx.doi.org/10.1111/j.1365-2214.2009.00984.x.
- Higgins MM. Perceptions of ‘Reasonable’ Accommodations in General Education for Secondary School Students With ADHD: Treatment Acceptability Ratings of Teachers 1999.
- Krowski KF. ADHD: Urban teachers’ knowledge, beliefs and classroom practice. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70.
- Nietfeld JL, Hunt AA. Elementary and pre-service teachers’ strategies for working with students with hyperactivity. Curr Issues Educ 2005;8.
- Ohan JL, Cormier N, Hepp SL, Visser TA, Strain MC. Does knowledge about attention-deficit/hyperactivity disorder impact teachers’ reported behaviors and perceptions?. Sch Psychol Q 2008;23:436-49. http://dx.doi.org/10.1037/1045-3830.23.3.436.
- Saddler ML. Teacher Knowledge and Use of Effective Classroom Interventions For Managing Students with Educational Manifestations of Attention Deficit Hyperactivity Disorder. Saint Louis, MO: Saint Louis University; 2007.
- Stormont M, Stebbins MS. Teachers’ comfort and importance ratings for interventions for preschoolers with AD/HD. Psychol Schools 2001;38:259-67. http://dx.doi.org/10.1002/pits.1016.
- Subramony R. Acceptability of treatment strategies for hyperactivity and attention problems of elementary grade students: a study of kindergarten, third, and fifth grade teachers. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;67.
- Vereb RL, DiPerna JC. Research brief: teachers’ knowledge of ADHD, treatments for ADHD, and treatment acceptability: an initial investigation. Sch Psychol Rev 2004;33:421-8.
- Whitworth JE. Classroom teachers’ perceptions regarding educational services to students with attention deficit disorders. Spec Serv Schools 1998;14:41-50. http://dx.doi.org/10.1300/J008v14n01_03.
- Elliott SN, von Brock Treuting M. The behavior intervention rating scale: development and validation of a pretreatment acceptability and effectiveness measure. J Sch Psychol 1991;29:43-51. http://dx.doi.org/10.1016/0022-4405(91)90014-I.
- Dryer R, Kiernan MJ, Tyson GA. Implicit theories of the characteristics and causes of attention-deficit hyperactivity disorder held by parents and professionals in the psychological, educational, medical and allied health fields. Aust J Psychol 2006;58:79-92. http://dx.doi.org/10.1080/00049530600730443.
- Martens BK, Witt JC, Elliott SN, Darveaux DX. Teacher judgments concerning the acceptability of school-based interventions. Prof Psychol Res Pract 1985;16. http://dx.doi.org/10.1037/0735-7028.16.2.191.
- Osgood CE. The Measurement of Meaning. Champaign, IL: University of Illinois Press; 1957.
- Power TJ, Hess LE, Bennett DS. The acceptability of interventions for attention-deficit hyperactivity disorder among elementary and middle school teachers. J Dev Behav Pediatr 1995;16:238-43. http://dx.doi.org/10.1097/00004703-199508000-00005.
- Kelley ML, Heffer RW, Gresham FM, Elliott SN. Development of a modified treatment evaluation inventory. J Psychopathol Behav Assess 1989;11:235-47. http://dx.doi.org/10.1007/BF00960495.
- Tarnowski KJ, Simonian SJ. Assessing treatment acceptance: the abbreviated acceptability rating profile. J Behav Ther Exp Psychiatr 1992;23:101-6. http://dx.doi.org/10.1016/0005-7916(92)90007-6.
- Zentall SS, Stormont-Spurgin M. Educator preferences of accommodations for students with attention deficit hyperactivity disorder. Teach Educ Spec Educ 1995;18:115-23. http://dx.doi.org/10.1177/088840649501800205.
- Miltenberger RG. Assessment of treatment acceptability a review of the literature. Top Early Child Spec Educ 1990;10:24-38. http://dx.doi.org/10.1177/027112149001000304.
- Husk K, Lovell R, Cooper C, Garside R. Participation in environmental enhancement and conservation activities for health and well-being in adults (protocol). Cochrane Database Syst Rev 2013;2:1-30.
- Wiebe J, Nicol JJ. Juxtaposition: ADHD and music at school. Can J Music Ther 2007;13:171-3.
- Hughes LA. The reality of living with AD/HD: children’s concern about educational and medical support. Emot Behav Difficult 2007;12:69-80. http://dx.doi.org/10.1080/13632750601135915.
- Cooper P, Shea T. Pupils’ perceptions of AD/HD. Emot Behav Difficult 1998;3:36-48. http://dx.doi.org/10.1080/1363275980030306.
- Carpenter L, Austin H. How to be recognized enough to be included?. Int J Inclusive Educ 2008;12:35-48. http://dx.doi.org/10.1080/13603110701683170.
- McMahon SE. Doctors diagnose, teachers label: the unexpected in pre-service teachers’ talk about labelling children with ADHD.?. Int J Inclusive Educ 2012;16:249-64. http://dx.doi.org/10.1080/13603116.2010.481799.
- Hong Y. Teachers’ perceptions of young children with ADHD in Korea. Early Child Dev Care 2008;178:399-414. http://dx.doi.org/10.1080/03004430701321829.
- Ljusberg AL. The structured classroom. Int J Inclusive Educ 2011;15:195-210. http://dx.doi.org/10.1080/13603110902763433.
- Malacrida C. Motherhood, resistance and attention deficit disorder: strategies and limits. Can Rev Sociol Anthropol 2001;38:141-65. http://dx.doi.org/10.1111/j.1755-618X.2001.tb00968.x.
- Wallace A, Croucher K, Quilgars D, Baldwin S. Meeting the challenge: developing systematic reviewing in social policy. Pol Polit 2004;32:455-70. http://dx.doi.org/10.1332/0305573042009444.
- Dixon-Woods M, Shaw RL, Agarwal S, Smith JA. The problem of appraising qualitative research. Qual Safe Health Care 2004;13:223-5. http://dx.doi.org/10.1136/qshc.2003.008714.
- Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Vomink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLOS Med 2007;4:1230-45. http://dx.doi.org/10.1371/journal.pmed.0040238.
- Smithson J, Garside R, Pearson M. Barriers to, and facilitators of, the prevention of unintentional injury in children in the home: a systematic review and synthesis of qualitative research. Inj Prev 2011;17:119-26. http://dx.doi.org/10.1136/ip.2010.026989.
- Atkins S, Lewin S, Smith H, Engel ME, Fretheim A, Vomink J. Conducting a meta-ethnography of qualitative literature: lessons learnt. BMC Med Res Methodol 2008;8:1-10. http://dx.doi.org/10.1186/1471-2288-8-21.
- Campbell R, Pound P, Morgan M, Daker-White G, Britten N, Pill R, et al. Evaluating meta-ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess 2011;15. http://dx.doi.org/10.3310/hta15430.
- Garside R. Should we appraise the quality of qualitative research reports for systematic reviews, and if so, how?. Innovat Eur J Soc Sci Res 2014;27:67-79. http://dx.doi.org/10.1080/13511610.2013.777270.
- Schutz A. Collected Papers. The Hague: Martinus Nijhoff; 1971.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. Lancaster: Institute for Health Research, Lancaster University; 2006.
- Hibbitts P. We do this for the next child: s mother’s phenomenological auto narrative inquiry into experiencing her children’s schools. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;71.
- Pound P, Britten N, Morgan M, Yardley L, Pope C, Daker-White G, et al. Resisting medicines: a synthesis of qualitative studies of medicine taking. Soc Sci Med 2005;61:133-55. http://dx.doi.org/10.1016/j.socscimed.2004.11.063.
- Smagorinsky P, Cameron T, O’Donnell-Allen C. ‘Achtung’ maybe: a case study of the role of personal connection and art in the literary engagement of students with attentional difficulties. Read Writ Q 2007;23:333-58. http://dx.doi.org/10.1080/10573560701501552.
- Partridge L. Teaching Adolescent AD/HD Boys Through ‘Self-Sufficient Reward Control’: A Sociological Investigation. Lewiston, NY: Edwin Mellen Press; 2009.
- Wong W. An Investigation to Describe and Enhance the Metacognitive Processes of High School Students With Attention Deficit Hyperactivity Disorder and Learning Disability Who Were Studying for an Examination 2004.
- Koro-Ljungberg M, Bussing R, Williamson P, Wilder J, Mills T. African-American teenagers’ stories of attention deficit/hyperactivity disorder. J Child Fam Stud 2008;17:467-85. http://dx.doi.org/10.1007/s10826-007-9168-8.
- Williamson P, Koro-Ljungberg M, Bussing R. Analysis of critical incidents and shifting perspectives: transitions in illness careers among adolescents with ADHD. Qual Health Res 2009;19. http://dx.doi.org/10.1177/1049732308329683.
- Davison JC, Ford DY. Perceptions of attention deficit hyperactivity disorder in one African American community. J Negro Educ 2001;70:264-74. http://dx.doi.org/10.2307/3211279.
- Taylor M, Houghton S. Examination-related anxiety in students diagnosed with AD/HD and the case for an allocation of extra time: perspectives of teachers, mothers and students. Emot Behav Difficult 2008;13:111-25. http://dx.doi.org/10.1080/13632750802027663.
- Saldana J. The Coding Manual for Qualitative Researchers. London: Sage; 2009.
- Arcia E, Frank R, Sanchez-LaCay A, Fernandez MC. Teacher understanding of ADHD as reflected in attributions and classroom strategies. J Atten Disord 2000;4:91-101. http://dx.doi.org/10.1177/108705470000400203.
- Bartlett TR, Rowe T, Shattell M. Perspectives of college students with childhood AD/HD. MCN Am J Matern Child Nurs 2010;35:226-31. http://dx.doi.org/10.1097/NMC.0b013e3181de3bb3.
- Bos CS, Nahmias ML, Urban MA. Implementing interactive professional development in a workshop course on educating students with AD/HD. Teach Educ Spec Educ 1997;20:132-45. http://dx.doi.org/10.1177/088840649702000207.
- Ducharme S. Parents’ Perceptions of Raising a Child With Attention Deficit Hyperactivity Disorder 1996.
- Edwards K. The learning experiences and preferred educational strategies of children who have been identified as gifted with ADHD. Australas J Gifted Educ 2008;17:15-22.
- Einarsdottir J. Teaching children with ADHD: Icelandic early childhood teachers’ perspectives. Early Child Dev Care 2008;178:375-97. http://dx.doi.org/10.1080/03004430701321696.
- Furtick KC. Successful Strategies Used With ADHD Students: Is an ADHD Classroom a Possibility? 2010.
- Hands RE. The phenomenon of underachievement: listening to the voice of a twice exceptional adolescent. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70.
- Hillman MK. An examination of teachers’ recommendations for children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;72.
- Hjörne E, Lloyd G, Stead J, Cohen D. Critical New Perspectives on ADHD. London: Routledge; 2006.
- Houghton S, Carroll A, Taylor M, O’Donoghue T. From Traditional to Ecological: Understanding Attention Deficit Disorders Through Quantitative and Qualitative Research. New York, NY: Nova Science Publishers; 2006.
- Isaksson J, Lindqvist R, Bergstrom E. Struggling for recognition and inclusion-parents’ and pupils’ experiences of special support measures in school. Int J Qual Stud Health Well-Being 2010;5. http://dx.doi.org/10.3402/qhw.v5i1.4646.
- Jones DB. Phenomenological study: what are pre-kindergarten teachers’ lived experiences with children identified with conduct disorder, oppositional defiance disorder, and attention-deficit hyperactivity disorder in the southeastern United States?. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;69.
- Kendall J, Hatton D, Beckett A, Leo M. Children’s accounts of attention-deficit/hyperactivity disorder. Adv Nurs Sci 2003;26:114-30. http://dx.doi.org/10.1097/00012272-200304000-00004.
- Kreiss DS. Case Studies of the Experiences of Students Referred for Problems of Disruptive and Or Aggressive Behavior to an Alternative High School Program 2003.
- Langberg JM, Vaughn AJ, Williamson P, Epstein JN, Girio-Herrera E, Becker SP. Refinement of an organizational skills intervention for adolescents with ADHD for implementation by school mental health providers. School Ment Health 2011;3:143-55. http://dx.doi.org/10.1007/s12310-011-9055-8.
- Ljusberg A. Children’s views on attending a remedial class – because of concentration difficulties. Child Care Health Dev 2011;37:440-5. http://dx.doi.org/10.1111/j.1365-2214.2010.01178.x.
- McNeil KN. Through our eyes: the shared lived experiences of growing up attention deficit hyperactive disordered. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66.
- Mulligan S. Classroom strategies used by teachers of students with attention deficit hyperactivity disorder. Phys Occup Ther Pediatr 2001;20:25-44. http://dx.doi.org/10.1080/J006v20n04_03.
- Nowacek EJ, Mamlin N. General Education Teachers and Students with ADHD: What Modifications Are Made?. Prev Sch Fail 2007;51:28-35. http://dx.doi.org/10.3200/PSFL.51.3.28-35.
- Ozdemir S. The first step to success program: implementation effectiveness with Turkish children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;67.
- Prosser BJ. Beyond ADHD: A consideration of attention deficit hyperactivity disorder and pedagogy in Australian schools. Int J Inclusive Educ 2008;12:81-97. http://dx.doi.org/10.1080/13603110701683147.
- Rafalovich A. Framing ADHD Children: A Critical Examination of the History, Discourse, and Everyday Experience of Attention Deficit. Lanhamm, MD: Lexington Books; 2004.
- Santamaria M. School counselors’ strategies supporting Vygotsky’s theory and affecting behavior of Hispanic English Language Learners (ELL) with ADHD in second grade. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70.
- Taylor Wilcoxson JL. Attention Deficit Hyperactivity Disorder and Creative Potential of Children: A Multiple Case Study 2005.
- Wiebe JE. ADHD, The Classroom and Music: A Case Study. Saskatchewan: University of Saskatchewan; 2007.
- Young S, Chesney S, Sperlinger D, Misch P, Collins P. A qualitative study exploring the life-course experiences of young offenders with symptoms and signs of ADHD who were detained in a residential care setting. Crim Behav Ment Health 2009;19:54-63. http://dx.doi.org/10.1002/cbm.721.
- Zimmermann SH. Portrait of Success: A Situational Analysis Case Study of Students Challenged by Attention-Deficit Hyperactivity Disorder 1998.
- Prosser BJ. Seeing Red: A Case of Critical Narrative in ADHD Research. Teneriffe, QLD: Post Pressed; 2006.
- Miles MB, Huberman AM. Qualitative Data Analysis: An Expanded Sourcebook. Thousand Oaks, CA: Sage; 1994.
- Moustakas C. Heuristic Research: Design, Methodology, and Applications. Newbury Park, CA: Sage; 1990.
- Kvale S. Interviews: An Introduction to Qualitative Research Interviewing. Thousand Oaks, CA: Sage; 1996.
- Stake RE. The Art of Case Study Research. Thousand Oaks, CA: Sage Publications; 1995.
- Campbell R, Pound P, Pope C, Britten N, Pill R, Morgan M, et al. Evaluating meta-ethnography: a synthesis of qualitative research on lay experiences of diabetes and diabetes care. Soc Sci Med 2003;56:671-84. http://dx.doi.org/10.1016/S0277-9536(02)00064-3.
- Smith LK, Pope C, Botha JL. Patients’ help-seeking experiences and delay in cancer presentation: a qualitative synthesis. Lancet 2005;366:825-31. http://dx.doi.org/10.1016/S0140-6736(05)67030-4.
- Hooper S, Rieber LP, Ornstein AC. Teaching: Theory into Practice. Needham Heights, MA: Allyn and Bacon; 1995.
- Goffman E. Stigma: Notes on the Management of Spoiled Identity. Englewood Cliffs, NJ: Prentice-Hall Inc.; 1963.
- Galinsky AD, Hugenberg K, Groom C, Bodenhausen GV. The reappropriation of stigmatizing labels: Implications for social identity. Res Manag Group Team 2003;5:221-56. http://dx.doi.org/10.1016/S1534-0856(02)05009-0.
- Lee K. ADHD in American early schooling: from a cultural psychological perspective. Early Child Dev Care 2008;178:415-39. http://dx.doi.org/10.1080/03004430701321852.
- Malcolm H, Wilson V, Davidson J, Kirk S. Absence From Schools: A Study of its Causes and Effects in Seven LEAs. Nottingham: Department for Education and Skills; 2003.
- Hardre PL, Sullivan DW, Crowson HM. Student characteristics and motivation in rural high schools. J Res Rural Educ 2009;24:1-19.
- Goldstein S, Naglieri JA. The school neuropsychology of ADHD: theory, assessment, and intervention. Psychol School 2008;45:859-74. http://dx.doi.org/10.1002/pits.20331.
- Barbour RS. Checklists for improving rigour in qualitative research: a case of the tail wagging the dog?. BMJ 2001;322. http://dx.doi.org/10.1136/bmj.322.7294.1115.
- Patton MQ. Qualitative Research. Chichester: Wiley Online Library; 2005.
- Hartnett DN, Nelson JM, Rinn AN. Gifted or ADHD? The possibilities of misdiagnosis. Roeper Review 2004;26:73-6. http://dx.doi.org/10.1080/02783190409554245.
- Brice PJ. The experience of learning for youth diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 1998;58.
- Exley B. ‘Staying in class so no one can get to him’: a case for the institutional reproduction of ADHD categories and behaviours. Int J Inclusive Educ 2008;12:65-80. http://dx.doi.org/10.1080/13603110701683196.
- Friio SS. The experiences of adolescents with ADHD: a phenomenological study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;59.
- McDannel RP. Classroom occupations from the perspectives of three high school students with attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65.
- Taylor M, Houghton SJ. Difficulties in initiating and sustaining peer friendships: perspectives on students diagnosed with AD/HD. Br J Spec Educ 2008;35:209-19. http://dx.doi.org/10.1111/j.1467-8578.2008.00398.x.
- Wolfberg PJ, Zercher C, Lieber J, Capell K, Matias S, Hanson M, et al. ‘Can I play with you?’ Peer culture in inclusive preschool programs. J Assoc Pers Sev Handicaps 1999;24:69-84. http://dx.doi.org/10.2511/rpsd.24.2.69.
- Exley B. The Behaviour ‘Crisis’: Young Children’s Mis Understandings of the Identities of ADHD n.d.
- Exley B. Young children’s mis/understandings of the ADHD label. Educ Young Child 2007;13:38-40.
- Fairclough N. Analysing Discourse: Textual Analysis for Social Research. London: Routledge; 2003.
- Clandinin D, Connelly F, Denzin N, Lincoln Y. Handbook of Qualitative Research. Newbury Park, CA: Sage; 1994.
- Wakefield J. The concept of mental disorder: on the boundary between biological facts and social values. Am Psychol 1992;47:373-88. http://dx.doi.org/10.1037/0003-066X.47.3.373.
- Haimes E. What can the social sciences contribute to the study of ethics? Theoretical, empirical and substantive considerations. Bioethics 2002;16:89-113. http://dx.doi.org/10.1111/1467-8519.00273.
- Bronfenbrenner U. The Ecology of Human Development. Cambridge, MA: Harvard University Press; 1979.
- Kidd AC. Sleep Disorders in Children: A Qualitative Research Study on the Comparison of Behavioral Symptoms Associated With Poor Quality Sleep and ADHD. San Diego, CA: Alliant International University; 2009.
- Gross C, Rinn AN, Jamieson KM. Gifted adolescents’ overexcitabilities and self-concepts: an analysis of gender and grade level. Roeper Review 2007;29:240-8. http://dx.doi.org/10.1080/02783190709554418.
- Nelson JM, Rinn AN, Hartnett DN. The possibility of misdiagnosis of giftedness and ADHD still exists: a response to Mika. Roeper Review 2006;28:243-8. http://dx.doi.org/10.1080/02783190609554371.
- Rafalovich A. Relational troubles and semiofficial suspicion: educators and the medicalization of ‘unruly’ children. Symbolic Interact 2005;28:25-46. http://dx.doi.org/10.1525/si.2005.28.1.25.
- Thornicroft G. Shunned: Discrimination Against People with Mental Illness. Oxford: Oxford University Press; 2006.
- Bruner JL. Acts of Meaning. Cambridge, MA: University of Harvard Press; 1990.
- Erikson E. Identity and the Life Cycle. New York, NY: InterVarsity Press; 1959.
- Rogers C. Client-Centred Therapy. Boston, MA: Houghton Mifflin; 1951.
- Rapaport J, Buschbaum M. Dextroamphetamine: its cognitive and behavioural effects in normal and hyperactive boys and normal men. Arch Gen Psychiatr 1980;37:933-43. http://dx.doi.org/10.1001/archpsyc.1980.01780210091010.
- Elia J, Rapaport J, Kirby J. Pharmacological treatment of attention deficit hyperactivity disorder. Psychiatr Res 1991;36:141-55. http://dx.doi.org/10.1016/0165-1781(91)90126-A.
- Braun V, Clarke V. Using thematic analysis in psychology. Res Psychol 2006;3:77-101. http://dx.doi.org/10.1191/1478088706qp063oa.
- Moustakas C. Phenomenological Research Methods. Thousand Oaks, CA: Sage; 1994.
- Watson C. Home–school partnership and the construction of deviance: being and becoming the Goldfish family. J Res Spec Educ Needs 2011;11:20-9. http://dx.doi.org/10.1111/j.1471-3802.2010.01183.x.
- Nourot PM, Roopnarine JL, Johnson JE. Approaches to Early Childhood Education. Upper Saddle River, NJ: Prentice Hall; 2003.
- Michel Foucault. London: Sage; 2005.
- Margalit M, Raskind MH, Higgins EL, Russo-Netzer P. Mothers’ voices on the internet: stress, support and perceptions of mothers of children with learning disabilities and attention deficit/hyperactivity disorder. J Learn Disabil 2010;16:3-14.
- Reid R, Hertzog M, Snyder M. Educating every teacher, every year: the public schools and parents of children with ADHD. Semin Speech Lang 1996;17:73-90. http://dx.doi.org/10.1055/s-2008-1064089.
- Singh I. Doing their jobs: mothering with Ritalin in a culture of mother-blame. Soc Sci Med 2004;59:1193-205. http://dx.doi.org/10.1016/j.socscimed.2004.01.011.
- Butler J. Excitable Speech: A Politics of the Performative. New York, NY: Routledge; 1997.
- Butler J. Precarious Life: The Powers of Mourning and Violence. London: Verso; 2004.
- Fraser N. Justice Interruptus: Critical Reflections on the ‘Postsocialist Condition’. New York, NY: Routledge; 1997.
- Fraser N. Rethinking recognition. NLR 2000;3:107-20.
- Fraser N, Fraser N, Honneth A. Redistribution or Recognition? A Political–Philosophical Exchange. New York, NY: Verso; 2003.
- Graham L. Caught in the net: a Foucaultian interrogation of the incidental effects of limited notions of inclusion. Int J Inclusive Educ 2006;10:3-25. http://dx.doi.org/10.1080/13603110500173217.
- Graham L. From ABCs to ADHD: the role of schooling in the construction of behaviour disorder and production of disorderly updates. Int J Inclusive Educ 2008;12:7-33. http://dx.doi.org/10.1080/13603110701683311.
- van Manen M. Researching Lived Experience. London, ON: The Althouse Press; 1990.
- van Manen M. Writing in the Dark: Phenomenological Studies Interpretive Inquiry. London, ON: Althouse Press; 2002.
- Porter R. A Social History of Madness: Stories of the Insane. London: Phoenix; 1987.
- Miller WL, Crabtree BL, Denzin NK, Lincoln YS. Strategies of Qualitative Research. Thousand Oaks, CA: Sage; 1998.
- Fleischmann A. Narratives published on the internet by parents of children with autism: what do they reveal and why is it important?. Focus Autism Other Dev Disabil 2004;19:35-43. http://dx.doi.org/10.1177/10883576040190010501.
- Hinshaw SP. The stigmatization of mental illness in children and parents: developmental issues, family concerns, and research needs. J Child Psychol Psychiatr 2005;46. http://dx.doi.org/10.1111/j.1469-7610.2005.01456.x.
- Bronowski J, Mazlish B. The Western Intellectual Tradition from Leonardo to Hegel. London: Hutchinson; 1960.
- MacLure M. A demented form of the familiar: postmodernism and educational research. J Philos Educ 2006;40:223-39. http://dx.doi.org/10.1111/j.1467-9752.2006.00505.x.
- Eisner EW. The promise and perils of alternative forms of data representation. Educ Res 2013;26:4-10. http://dx.doi.org/10.3102/0013189X026006004.
- Barone T. A return to the gold standard? Questioning the future of narrative construction as educational research. Qual Inq 2007;13:454-70. http://dx.doi.org/10.1177/1077800406297667.
- Clough P. Narratives and Fictions in Educational Research. Buckinghamshire: Open University Press; 2002.
- Margalit M, Raskind MH. Mothers of Children with LD and ADHD: empowerment through online communication. J Sepc Educ Tech 2009;24.
- Yearning: Race, Gender, and Cultural Politics. Boston, MA: South End Press; 1990.
- Maréchal G, Mills AJ, Durepos G, Wiebe E. Encyclopedia of Case Study Research. Thousand Oaks, CA: Sage; 2010.
- Carpenter L, Austin H. Silenced, silence, silent: motherhood in the margins. Qual Inq 2007;13:660-74. http://dx.doi.org/10.1177/1077800407301179.
- Singh I. ADHD, culture and education. Early Child Dev Care 2008;178:347-61. http://dx.doi.org/10.1080/03004430701321555.
- Heller J. Catch-22. London: Corgi Books; 1955.
- Watson SMR, Richels C, Michalek AP, Raymer A. Psychosocial treatments for ADHD: a systematic appraisal of the evidence. J Atten Disord n.d.;19:3-10. http://dx.doi.org/10.1177/1087054712447857.
- Fuemmeler BF, Østbye T, Yang C, McClernon FJ, Kollins SH. Association between attention-deficit/hyperactivity disorder symptoms and obesity and hypertension in in early adulthood: a population-based study. Int J Obes 2011;35:852-62. http://dx.doi.org/10.1038/ijo.2010.214.
- Blaine B. Understanding the Psychology of Diversity. Thousand Oaks, CA: Sage; 2007.
- Scott JC. Weapons of the Weak: Everyday Forms of Peasant Resistance. New Haven, CT: Yale University Press; 1985.
- Guevara JP, Feudtner C, Romer D, Power T, Eiraldi R, Nihtianova S, et al. Fragmented care for inner-city minority children with attention-deficit/hyperactivity disorder. Pediatrics 2005;116:e512-e517. http://dx.doi.org/10.1542/peds.2005-0243.
- Koro-Ljungberg M, Bussing R, Wilder J, Gary F. Role of communication in the context of educating children with attention-deficit/hyperactivity disorder: parents’ and teachers’ perspectives. J Sch Publ Relat 2011;32:41-75.
- Shea B, Wiener J. Social exile: the cycle of peer victimization for boys with ADHD. Can J Sch Psychol 2003;18:55-90. http://dx.doi.org/10.1177/082957350301800104.
- Silverman LK. Counseling the Gifted & Talented. Denver, CO: LOVE Publishing; 1993.
- Tolan S. Special problems of young highly gifted children. Understanding Our Gifted 1989;1:7-10.
- Lovecky DV. Different Minds: Gifted Children with AD/HD, Asperger’s Syndrome, and Other Learning Deficits. Philadelphia, PA: Jessica Kingsley Publishers; 2004.
- Snyder CR. The Psychology of Hope: You Can There From Here. New York, NY: Free Press; 1994.
- Snyder CR, Shorey HS, Cheavens J, Pulvers KM, Adams VH, Wiklund C. Hope and academic success in college. J Educ Psychol 2002;94:820-33. http://dx.doi.org/10.1037/0022-0663.94.4.820.
- LeCompte M, Schensul J. Analyzing and Interpreting Ethnographic Data. Walnut Creek, CA: AltaMira Press; 1999.
- Spradley J. You Owe Yourself A Drunk: An Ethnography of Urban Nomads. Boston, MA: Little, Brown; 1970.
- Spradley J. The Ethnographic Interview. New York, NY: Hold, Rinehart and Winston; 1979.
- Blommaert J, Bulcaen C. Critical discourse analysis. Annu Rev Anthropol 2000;29:447-66. http://dx.doi.org/10.1146/annurev.anthro.29.1.447.
- Wodak R, Gunnarsson BL, Linell P, Nordberg B. The Construction of Professional Discourse. London: Longman; 1997.
- Becker HS. Outsiders: Studies in the Sociology of Deviance. New York, NY: Free Press; 1963.
- Emerson RM, Messinger SL. The micro-politics of trouble. Soc Probl 1977;38:198-212. http://dx.doi.org/10.2307/800529.
- Conrad P. Identifying Hyperactive Children: The Medicalization of Deviant Behavior. Lexington, MA: Lexington Books; 1976.
- Conrad P, Schneider JW. Deviance and Medicalization: From Badness to Sickness. Philadelphia, PA: Temple University Press; 1992.
- Olweus D. Bullying At School: What We Know and What We Can Do. Oxford: Blackwell; 1993.
- Olweus D, Juvonen J, Graham S. Peer Harassment in School: The Plight of the Vulnerable and Victimized. New York, NY: The Guildford Press; 2001.
- Swann W. ‘Dyslexia’, Unit 25 Block 4 E206 of Personality, Development and Learning. Milton Keynes: Open University Press; 1985.
- Singer E. The strategies adopted by Dutch children with dyslexia to maintain their self-esteem when teased at school. J Learn Disabil 2005;38:411-23. http://dx.doi.org/10.1177/00222194050380050401.
- Noyes J, Lewin S, Hannes K, Harden A, Harris J, Lewin S, et al. Supplementary Guidance for Inclusion of Qualitative Research in Cochrane Systematic Reviews of Interventions. Cochrane Collaboration Qualitative Methods Group; 2011.
- Thomas J, Harden A, Oakley A, Oliver S, Sutcliffe K, Rees R, et al. Integrating qualitative research with trials in systematic reviews. BMJ 2004;328. http://dx.doi.org/10.1136/bmj.328.7446.1010.
- Noyes J, Popay J. Directly observed therapy and tuberculosis: how can a systematic review of qualitative research contribute to improving services? A qualitative meta-synthesis. J Adv Nurs 2007;57:227-43. http://dx.doi.org/10.1111/j.1365-2648.2006.04092.x.
- Montuori A. The complexity of transdisciplinary literature reviews. Complicity: Int J Complex Educ 2013;10:45-5.
- Anderson LM, Oliver SR, Michie S, Rehfuess E, Noyes J, Shemilt I. Investigating complexity in systematic reviews of interventions by using a spectrum of methods. J Clin Epidemiol 2013;66:1223-9. http://dx.doi.org/10.1016/j.jclinepi.2013.06.014.
- Pigott T, Shepperd S. Identifying, documenting, and examining heterogeneity in systematic reviews of complex interventions. J Clin Epidemiol 2013;66:1244-50. http://dx.doi.org/10.1016/j.jclinepi.2013.06.013.
- Chronis AM, Fabiano GA, Gnagy EM, Onyango AN, Pelham WE, Lopez-Williams A, et al. An evaluation of the summer treatment program for children with attention-deficit/hyperactivity disorder using a treatment withdrawal design. Behav Ther 2004;35:561-85. http://dx.doi.org/10.1016/S0005-7894(04)80032-7.
- Wampold BE. The Great Psychotherapy Debate: Models, Methods and Findings. Mahway, NJ: Lawrence Erlbaum Associates; 2001.
- Arcia E, Fernandez MC. Cuban mothers’ schemas of ADHD: development, characteristics and help seeking behavior. J Child Fam Stud 1998;7:333-7. http://dx.doi.org/10.1023/A:1022945628866.
- Conners CK. Conners’ Rating Scales. Toronto, ON: Multi-Health Systems; 1989.
- Danckaerts M, Sonuga-Barke EJS, Banaschewski T, Buitelaar J, Döpfner M, Hollis C, et al. The quality of life of children with attention deficit/hyperactivity disorder: a systematic review. Eur Child Adolesc Psychiatr 2009;19:83-105. http://dx.doi.org/10.1007/s00787-009-0046-3.
- Conrad P, Schneider J. Deviance and Medicalization: From Badness to Sickness. St. Louis, MO: The CV Mosby Company; 1980.
- Armstrong D. Political Anatomy of the Body: Medical Knowledge in Britain in the Twentieth Century. Cambridge: Cambridge University Press; 1983.
- Castel R, Castel F, Lovell A. The Psychiatric Society. New York, NY: Columbia University Press; 1982.
- Slee R. Finding a student voice in school reform: student disaffection, pathologies of disruption and educational control. Int Stud Sociol Educ 1994;4:147-72. http://dx.doi.org/10.1080/0962021940040202.
- It’s a Neurobiological Thing. Calgary, Alberta: CHADD; 1995.
- Chisholm P. The ADD dilemma: is ritalin the best way to treat attention deficit disorder?. MacLean’s Magazine n.d.:46-7.
- Singh I. Bad boys, good mothers, and the miracle of Ritalin. Sci Context 2002;15:577-603. http://dx.doi.org/10.1017/S0269889702000650.
- Strauss A, Corbin J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. Newbury Park, CA: Sage; 1990.
- Knight CA. The Literature of Satire. Cambridge: Cambridge University Press; 2004.
Appendix 1 Search strategy used for review 1
PsycINFO (via OvidSP)
URL: http://0-ovidsp.tx.ovid.com.lib.exeter.ac.uk/sp-3.14.0b/ovidweb.cgi.
Searched: 1967 to May Week 2 2012.
Search strategy
-
exp attention deficit disorder with hyperactivity/ (11,098)
-
ADHD.ti,ab. (14,279)
-
ADHS.ti,ab. (46)
-
ADDH.ti,ab. (129)
-
attention deficit.ti,ab. (16,587)
-
hyperactiv*.ti,ab. (23,610)
-
(hyper adj1 activ*).ti,ab. (69)
-
(Conduct adj3 (problem* or difficult* or disorder* or issue*)).ti,ab. (7625)
-
(Attention adj3 (problem* or difficult* or disorder* or issue*)).ti,ab. (20,840)
-
hyperk*.ti,ab. (1471)
-
minimal brain.ti,ab. (686)
-
inattenti*.ti,ab. (4334)
-
impulsiv*.ti,ab. (13,115)
-
restless*.ti,ab. (2497)
-
overactiv*.ti,ab. (1461)
-
or/1-15 (54,049)
-
school*.ti,ab. (220,799)
-
college*.ti,ab. (85,771)
-
nurser*.ti,ab. (2859)
-
preschool*.ti,ab. (26,400)
-
kindergarten*.ti,ab. (10,621)
-
classroom*.ti,ab. (50,276)
-
elementary.ti,ab. (29,135)
-
education* setting*.ti,ab. (3690)
-
((education* or behavio?r*) adj unit*).ti,ab. (311)
-
education* establishment*.ti,ab. (112)
-
education* system*.ti,ab. (4486)
-
learning environment*.ti,ab. (7200)
-
learning establishment*.ti,ab. (4)
-
teaching environment*.ti,ab. (210)
-
teaching establishment*.ti,ab. (6)
-
teacher*.ti,ab. (105288)
-
early years.ti,ab. (2190)
-
foundation stage.ti,ab. (67)
-
summer treatment program*.ti,ab. (48)
-
breakfast club*.ti,ab. (13)
-
holiday club*.ti,ab. (2)
-
pupil*.ti,ab. (13,914)
-
student*.ti,ab. (306,201)
-
or/17-39 (519,640)
-
intervention*.ti,ab. (187,941)
-
strateg*.ti,ab. (185,305)
-
program*.ti,ab. (234,366)
-
project*.ti,ab. (82,197)
-
train*.ti,ab. (185,259)
-
support*.ti,ab. (360,119)
-
therap*.ti,ab. (235,922)
-
(Behavio?r* adj2 (management or modification* or medicine or treatment*)).ti,ab. (19,574)
-
(education* adj2 (management or modification* or treatment*)).ti,ab. (2943)
-
(classroom adj2 (management or modification* or treatment*)).ti,ab. (1537)
-
(playground adj2 (management or modification*)).ti,ab. (1)
-
(psychosocial adj2 (management or modification* or treatment*)).ti,ab. (2405)
-
(cognitive adj2 (management or modification* or treatment*)).ti,ab. (5790)
-
behavio?r change technique*.ti,ab. (75)
-
bct*.ti,ab. (195)
-
exercise*.ti,ab. (34,126)
-
(social adj2 play).ti,ab. (1451)
-
(free adj2 play).ti,ab. (2026)
-
(physical adj2 (education or activit*)).ti,ab. (16,433)
-
meditat*.ti,ab. (4434)
-
class* size*.ti,ab. (854)
-
seating.ti,ab. (596)
-
incredible years.ti,ab. (106)
-
Triple P.ti,ab. (141)
-
good behavio?r game.ti,ab. (62)
-
123 magic.ti,ab. (0)
-
place2be.ti,ab. (3)
-
reinforcement.ti,ab. (27,920)
-
punishment*.ti,ab. (10,232)
-
response cost.ti,ab. (449)
-
time out.ti,ab. (1242)
-
reward*.ti,ab. (30,548)
-
prize*.ti,ab. (1481)
-
privilege*.ti,ab. (6354)
-
teacher pupil relationship*.ti,ab. (66)
-
teacher student relationship*.ti,ab. (445)
-
(Family adj2 school adj (partnership* or relationship* or involvement)).ti,ab. (221)
-
(Parent adj2 school adj (partnership* or relationship* or involvement)).ti,ab. (118)
-
(school adj2 parent adj (partnership* or relationship* or involvement)).ti,ab. (118)
-
(home adj2 school adj (partnership* or relationship* or involvement)).ti,ab. (201)
-
rule*.ti,ab. (36,823)
-
(routine or routines).ti,ab. (18,697)
-
contingent attention.ti,ab. (34)
-
daily report*.ti,ab. (248)
-
think* time.ti,ab. (44)
-
extra time.ti,ab. (201)
-
quiet.ti,ab. (3201)
-
indoor pass.ti,ab. (0)
-
verbal correction*.ti,ab. (14)
-
instruct*.ti,ab. (82,292)
-
clear commands.ti,ab. (3)
-
social stor*.ti,ab. (142)
-
(weigh* adj2 (jacket* or vest* or belt*)).ti,ab. (31)
-
(lesson adj2 structure*).ti,ab. (50)
-
(goal* adj3 setting).ti,ab. (4304)
-
(target* adj3 setting).ti,ab. (231)
-
behavio?r book.ti,ab. (2)
-
(peer adj2 (support or tutor*)).ti,ab. (2862)
-
champion*.ti,ab. (1581)
-
mentor*.ti,ab. (8142)
-
counsell*.ti,ab. (8376)
-
coach*.ti,ab. (7875)
-
cwpt.ti,ab. (47)
-
computer*.ti,ab. (59,337)
-
ICT.ti,ab. (1444)
-
(information adj2 technology).ti,ab. (3789)
-
social skills.ti,ab. (8876)
-
social problem solving.ti,ab. (1149)
-
life skills.ti,ab. (1179)
-
(anger adj2 (strateg* or manag* or modification*)).ti,ab. (1099)
-
CBT.ti,ab. (5834)
-
cognitive behavio?r*.ti,ab. (23,399)
-
worksheet*.ti,ab. (815)
-
timer*.ti,ab. (499)
-
break*.ti,ab. (20,036)
-
headphone*.ti,ab. (453)
-
music.ti,ab. (15,813)
-
timetable*.ti,ab. (425)
-
((individual or screen*) adj3 (desk* or table*)).ti,ab. (60)
-
traffic light*.ti,ab. (119)
-
whole class.ti,ab. (512)
-
breakfast club*.ti,ab. (13)
-
holiday club*.ti,ab. (2)
-
workshop*.ti,ab. (9658)
-
((self or personal) adj2 organis*).ti,ab. (309)
-
selfmanage.ti,ab. (0)
-
self manage.ti,ab. (141)
-
role play.ti,ab. (1841)
-
roleplay.ti,ab. (39)
-
multimodal.ti,ab. (4515)
-
multi agency.ti,ab. (394)
-
(chunk* or chunking).ti,ab. (1068)
-
brain gym.ti,ab. (15)
-
(stress adj2 (toy* or ball*)).ti,ab. (4)
-
circle time.ti,ab. (69)
-
transition.ti,ab. (26,001)
-
cube box.ti,ab. (1)
-
curriculum.ti,ab. (26,474)
-
remedial teaching.ti,ab. (89)
-
or/41-139 (1,296,528)
-
16 and 40 and 140 (6584)
-
limit 141 to yr=“1980 –Current” (6235)
Appendix 2 Websites and supplemental electronic resources
ADHD in Practice. URL: www.haywardpublishing.co.uk/adhd.aspx (accessed 27 November 2013).
The Association for Child and Adolescent Mental Health. URL: www.acamh.org.uk/ (accessed 27 November 2013).
The British Library. URL: www.bl.uk/ (accessed 27 November 2013).
ClinicalTrial.gov. URL: www.clinicaltrials.gov/ (accessed 27 November 2013).
CERUK Plus. URL: www.ceruk.ac.uk/ (accessed 27 November 2013).
Educational Evidence Portal. URL: www.eep.ac.uk/DNN2/ (accessed 27 November 2013).
Eppi-Centre. URL: http://eppi.ioe.ac.uk/cms/Default.aspx?tabid=185 (accessed 27 November 2013).
US National Library of Medicine. Health Services Research Projects in Progress. URL: www.nlm.nih.gov/pubs/factsheets/hsrproj.html (accessed 27 November 2013).
University College London. Institute of Education. URL: www.ioe.ac.uk/research.html (accessed 27 November 2013).
ISRCTN Registry. metaRegister of Controlled Trials (mRCT). URL: www.controlled-trials.com/mrct/ (accessed 27 November 2013).
National Foundation for Educational Research. URL: www.nfer.ac.uk/ (accessed 27 November 2013).
National Institute for Health Research. URL: www.nihr.ac.uk/Pages/default.aspx (accessed 27 November 2013).
National Institute for Health and Care Excellence. URL: www.nice.org.uk/ (accessed 27 November 2013).
Teaching and Learning Research Programme. URL: www.tlrp.org/ (accessed 27 November 2013).
ADDISS: ADHD Information Services. URL: www.addiss.co.uk/index.html (accessed 27 November 2013).
ADHD Foundation. ULR: www.adhdfoundation.org.uk/index.php (accessed 27 November 2013).
American Psychological Association. ADHD. URL: www.apa.org/topics/adhd/index.aspx (accessed 27 November 2013).
Centers for Disease Control and Prevention. Attention-Deficit/Hyperactivity Disorder (ADHD). URL: www.cdc.gov/ncbddd/adhd/ (accessed 27 November 2013).
Centre for Excellence and Outcomes in Children and Young People’s Services (C4EO). URL: www.c4eo.org.uk/library.aspx (accessed 27 November 2013).
National Child and Maternal Health Intelligence Network. Mental Health and Psychological Wellbeing. URL: www.chimat.org.uk/camhs (accessed 27 November 2013).
Centre for the Use of Research & Evidence in Education. URL: www.curee-paccts.com/ (accessed 27 November 2013).
Department for Education. URL: www.education.gov.uk/ (accessed 27 November 2013).
Economic and Social Research Council. URL: www.esrc.ac.uk/ (accessed 27 November 2013).
George Still Forum National Paediatric ADHD Network Group. URL: www.georgestillforum.co.uk/ (accessed 27 November 2013).
The Hyperactive Children’s Support Group. URL: www.hacsg.org.uk/ (accessed 27 November 2013).
Learning Assessment & Neurocare Centre Ltd. URL: www.lanc.uk.com/ (accessed 27 November 2013).
National Children’s Bureau. URL: www.ncb.org.uk/default.aspx (accessed 27 November 2013).
University of York, Centre for Reviews and Dissemination. PROSPERO, An International Database of Prospectively Registered Systematic Reviews. URL: www.crd.york.ac.uk/PROSPERO (accessed 27 November 2013).
Royal College of Paediatrics and Child Health. URL: www.rcpch.ac.uk/ (accessed 27 November 2013).
Social Care Institute for Excellence. URL: www.scie.org.uk/ (accessed 27 November 2013).
The British Psychological Society. URL: www.bps.org.uk/home-page.cfm (accessed 27 November 2013).
ADHD World Federation. URL: www.adhd-federation.org/ (accessed 27 November 2013).
YoungMinds. URL: www.youngminds.org.uk/ (accessed 27 November 2013).
Appendix 3 Studies excluded at full text from review 1, with reasons
| Reference | Reason for exclusion |
|---|---|
| Abel R. The relationship between academic achievement and social skill development in students with attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences. 2005;66:1631 | Not a controlled trial/design not reported |
| Aberson BD. An intervention for improving executive functioning and social/emotional adjustment of ADHD children: three single case design studies. Dissertation Abstracts International: Section B: The Sciences and Engineering. 1997;57:6553 | Not a controlled trial/design not reported |
| Abikoff H, Courtney ME, Szeibel PJ, Koplewicz HS. The effects of auditory stimulation on the arithmetic performance of children with ADHD and nondisabled children. J Learn Disabil 1996;29:238–46 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abikoff H, Ganeles D, Reiter G, Blum C, Foley C, Klein RG. Cognitive training in academically deficient ADDH boys receiving stimulant medication. J Abnorm Child Psychol 1988;16:411–32 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abikoff H, Gittelman R. Hyperactive children treated with stimulants: is cognitive training a useful adjunct? Arch Gen Psychiatr 1985;42:953–61 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abikoff H, Gittelman R. Does behavior therapy normalize the classroom behavior of hyperactive children? Arch Gen Psychiatr 1984;41:449–54 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abikoff H, Hechtman L, Klein RG, Gallagher R, Fleiss K, Etcovitch J, et al. Social functioning in children with ADHD treated with long-term methylphenidate and multimodal psychosocial treatment. J Am Acad Child Adolesc Psychiatr 2004;43:820–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abikoff H, Hechtman L, Klein RG, Weiss G, Fleiss K, Etcovitch J, et al. Symptomatic improvement in children with ADHD treated with long-term methylphenidate and multimodal psychosocial treatment. J Am Acad Child Adolesc Psychiatr 2004;43:802–11 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abramowitz AJ, Eckstrand D, O'Leary SG, Dulcan MK. ADHD children's responses to stimulant medication and two intensities of a behavioral intervention. Behav Modif 1992;16:193–203 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Abramowitz AJ, O'Leary SG. Effectiveness of delayed punishment in an applied setting. Behav Ther 1990;21:231–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ahonen T. Multimodal intervention in children with attention-deficit hyperactivity disorder. Eur J Spec Needs Educ 1994;9:168–81 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ajibola O, Clement PW. Differential effects of methylphenidate and self-reinforcement on attention-deficit hyperactivity disorder. Behav Modif 1995;19:211–23 | Not a controlled trial/design not reported |
| Almeraisi MJ. Effectiveness of cognitive-behavioral play therapy with children who have symptoms of attention deficit hyperactivity disorder (ADHD). Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;71:3926 | Not a controlled trial/design not reported |
| Alvarez L, Gonzalez-Castro P, Nunez JC, Gonzalez-Pienda JA, Alvarez D, Bernardo AB. Multimodel intervention programme for the improvement of attention deficits. Psychology in Spain 2008;12:81–7 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ammer JJ. Self-management strategies to increase the performance of hyperactive, underachieving, sixth, seventh and eighth grade students on selective attention tasks. Diss Abstr Int 1980;41:2548–9 | Not retrievable |
| Anastopoulos AD, Shelton TL, Barkley RA. Family-Based Psychosocial Treatments for Children and Adolescents With Attention-Deficit/ Hyperactivity Disorder. In Hibbs ED, Jensen PS, editors. Psychosocial Treatments for Child and Adolescent Disorders: Empirically Based Strategies for Clinical Practice. 2nd edn. Washington, DC: American Psychological Association; 2005. pp. 327–50 | Not retrievable |
| Anhalt K, McNeil CB, Bahl AB. The ADHD classroom kit: a whole-classroom approach for managing disruptive behavior. Psychol Schools 1998;35:67–79 | Not a controlled trial/design not reported |
| Aro T, Ahonen T, Tolvanen A, Lyytinen H, de Barra HT. Contribution of ADHD characteristics to the academic treatment outcome of children with learning difficulties. Dev Neuropsychol 1999;15:291–305 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Artesani AJ, Mallar L. Positive behavior supports in general education settings: combining person-centered planning and functional analysis. Intervention Sch Clin 1998;34:33–8 | Not a controlled trial/deign not reported |
| Asher MJ. Self-instructional training for teachers and other professionals working with attention deficit-hyperactive disorder children. Diss Abstr Int 1991;51:3552 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Atamanoff Gambert T. The effect of comorbid anxiety and comorbid oppositional defiant disorder on behavioral group training outcomes for children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;68:4808 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Atkinson B. Learning disabled students and LOGO. J Learn Disabil 1984;17:500–1 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Austin HM. Use of self-management techniques for the treatment of students diagnosed with ADHD: An empirical investigation of the self-regulation of behavior. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;64:2904 | Not a controlled trial/design not reported |
| Azrin NH, Vinas V, Ehle CT. Physical activity as reinforcement for classroom calmness of ADHD children: a preliminary study. Child Fam Behav Ther 2007;29:1–8 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Baeza Hernandez MC, Martinez Selva J. Intrasubject designs and school behavior changes: an application to two hyperactive subjects. Analisis y Modificacion de Conducta 1984;10:535–50 | Not retrievable |
| Baker K. Compensating for the Impact of Attention Deficit Hyperactivity Disorder on Reading Achievement: Michael's Story. Conference proceedings, AATE/ALEA National Conference 1–4 July 2005 Broadbeach, Queensland | Not retrievable |
| Baker K. Managing the Impact of Attention Deficit Hyperactivity Disorder on Reading Achievement: Initial Findings on the Efficacy of a New Reading Intervention. Paper presented at the AARE Annual Conference, Brisbane, 2002 | Not a controlled trial/design not reported |
| Baker K. Results of a Study into the Efficacy of a Reading Intervention for Students with Attention Deficit Hyperactivity Disorder. In Knight BA, Walker-Gibbs B, Harrison AG, editors. Researching Educational Capital in a Technological Age. Teneriffe, QLD: Post Pressed; 2002. pp. 75–100 | Not retrievable |
| Baker KB. Compensating for Cognitive Deficits in Students with Attention Deficit Hyperactivity Disorder. PhD thesis. North Rockhampton, QLD: Central Queensland University; 2003 | Not a controlled trial/design not reported |
| Baker TC. The use of mini-exercise breaks in the classroom management of ADHD-type behaviors. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66:2098 | Not retrievable |
| Barkley RA, Copeland AP, Sivage C. A self-control classroom for hyperactive children. J Autism Dev Disord 1980;10:75–89 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Barkley RA, Shelton TL, Crosswait C, Moorehouse M, Fletcher K, Barrett S, et al. Preliminary Findings of an Early Intervention Program with Aggressive Hyperactive Children. Understanding Aggressive Behavior in Children. New York, NY: New York Academy of Sciences; 1996. pp. 277–89 | Not retrievable |
| Barry LM, Messer JJ. A practical application of self-management for students diagnosed with attention- deficit/hyperactivity disorder. J Posit Behav Interv 2003;5:238–48 | Not a controlled trial/design not reported |
| Beaumont M. Making good the deficit: a therapeutic approach to ADHD. Educ Ther Teach 2001;7–20 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Beck SJ, Hanson CA, Puffenberger SS, Benninger KL, Benninger WB. A controlled trial of working memory training for children and adolescents with ADHD. J Clin Child Adolesc Psychol 2010;39:825–36 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bennett DE, Zentall SS, French BF, Giorgetti-Borucki K. The effects of computer-administered choice on students with and without characteristics of attention-deficit/hyperactivity disorder. Behav Disord 2006;31:189–203 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bensted EA, Bachor DG. The academic effects of low-achieving or inattentive students providing peer support to students with moderate to severe disabilities in general education classrooms. Exceptionality Educ Can 2002;12:51–73 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Berger M. Remediating hyperkinetic behavior with impulse control procedures. Sch Psychol Rev 1981;10:405–7 | Not a controlled trial/design not reported |
| Bicard DF, Neef NA. Effects of strategic versus tactical instructions on adaptation to changing contingencies in children with ADHD. J Appl Behav Anal 2002;35:375–89 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bice JE. Instructional Software and Attention Disorders: A Tool for Teachers. Oakland, MI: Oakland Schools; 1995 | Not retrievable |
| Billings DC, Wasik BH. Self-instructional training with preschoolers: an attempt to replicate. J Appl Behav Anal 1985;18:61–7 | Not a controlled trial/design not reported |
| Blanton J, Johnson LJ. Using computer assisted biofeedback to help children with attention-deficit hyperactivity disorder to gain self-control. J Spec Educ Tech 1991;11:49–56 | Not a controlled trial/design not reported |
| Bogle KE. Evaluation of a brief group parent training intervention in the context of an after-school program for middle-school students. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;69:665 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bolich B, Kavon N, McLaughlin TF, Williams RL, Urlacher S. The effects of a copy, cover, compare procedure and a token economy on the retention of basic multiplication facts by two middle school students with ADD and ADHD. BC J Spec Educ 1995;19:1–10 | Not a controlled trial/design not reported |
| Book RM. Management of the Child with an Attention Disorder in the School Setting. Paper presented at the Annual Convention of the American Psychological Association, Anaheim, CA, 26–30 August 1983 | Not retrievable |
| Bowers AJ. An educational management approach to hyperactive behaviour in the classroom. Remedial Educ 1980;15:28–31 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bowers DS, Clement PW, Fantuzzo JW, Sorensen DA. Effects of teacher-administered and self-administered reinforcers on learning disabled children. Behav Ther 1985;16:357–69 | Not a controlled trial/design not reported |
| Boyajian AE, DuPaul GJ, Handler MW, Eckert TL, McGoey KE. The use of classroom-based brief functional analyses with preschoolers at-risk for attention deficit hyperactivity disorder. Sch Psychol Rev 2001;30:278–93 | Not a controlled trial/design not reported |
| Boyd WD, Campbell SE. EEG biofeedback in the schools: the use of EEG biofeedback to treat ADHD in a school setting. J Neurotherapy 1998;2:65–71 | Not a controlled trial/design not reported |
| Boyer B, Kuin M, Prins P, Geurts HM, Van Der Oord S. A cognitive behavioral planning and organization treatment for adolescents with ADHD: a pilot study investigating short-term effects. Eur Child Adolesc Psychiatr 2010;19:S69 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bradley-Klug KL. The effects of a self-management intervention on the classroom behavior of young adolescents with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;58:1576 | Not a controlled trial/design not reported |
| Brasch TL, Williams RL, McLaughlin TF. The effects of a direct instruction flashcard system on multiplication fact mastery by two high school students with ADHD and ODD. Child Fam Behav Ther 2008;30:51–9 | Not a controlled trial/design not reported |
| Bright R. Kids who can't sit still. NEA Today. 2011:32–3 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Brown C-SE. The aftermath of Hurricane Iniki: development of a school-based intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 1997;57:6564 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Brown LL. Using a computer cognitive rehabilitation program with typical and ADHD junior high students to improve learning skills. Dissertation Abstracts International: Section B: The Sciences and Engineering 1995;56:3434 | Not retrievable |
| Brown RT, Conrad KJ. Remediation Efforts for Hyperactivity: Training in Attention or Inhibitory Control. Paper presented at the Annual Convention of the American Psychological Association, Los Angeles, CA, August 1981 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Brown RT, Conrad KJ. Remediation Efforts for Hyperactivity: Training in Attention or Inhibitory Control. Paper presented at the Annual Convention of the American Psychological Association, Los Angeles, CA, August 1981 | Duplicate |
| Brown RT, Wynne ME, Borden KA, Clingerman SR, Geniesse R, Spunt AL. Methylphenidate and cognitive therapy in children with attention deficit disorder: a double-blind trial. J Dev Behav Pediatr 1986;7:163–70 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Brown RT, Wynne ME, Medenis R. Methylphenidate and cognitive therapy: a comparison of treatment approaches with hyperactive boys. J Abnorm Child Psychol 1985;13:69–87 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Brown University. Integrated home-school behavioral treatment for ADHD, inattentive subtype. Brown Univ Child Adolesc Behav Lett 2007;23:3–4 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Bryant LE, Budd KS. Self-instructional training to increase independent work performance in preschoolers. J Appl Behav Anal 1982;15:259–71 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bullock GR. Cognitive rehabilitation: a method for improving sustained and selective attention in adolescents with attentional deficits. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1597 | Not a controlled trial/design not reported |
| Burns MK, Dean VJ. Effect of drill ratios on recall and on-task behavior for children with learning and attention difficulties. J Instr Psychol 2005;32:118–26 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Bussing R. Early school-based screening and intervention programmes for ADHD did not improve children's outcomes at age 10. Evid Based Ment Health 2010;13:118 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Cameron MI, Robinson VM. Effects of cognitive training on academic and on-task behavior of hyperactive children. J Abnorm Child Psychol 1980;8:405–19 | Not a controlled trial/design not reported |
| Campbell DS. Adolescent Impulsivity and Self-Instruction Training: A Pilot Study. Toronto, ON: Ministry of Colleges and Universities; 1983 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Campbell DS, Neill J, Dudley P. Computer-aided self-instruction training with hearing-impaired impulsive students. Am Annals of the Deaf 1989;134:227–31 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Campbell DS. Television feedback in self-instruction training for the impulsive student. BC J Spec Educ 1985;9:163–8 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Carlson CL, Mann M, Alexander DK. Effects of reward and response cost on the performance and motivation of children with ADHD. Cogn Ther Res 2000;24:87–98 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Carlson CL, Pelham WE Jr, Milich R, Dixon J. Single and combined effects of methylphenidate and behavior therapy on the classroom performance of children with attention-deficit hyperactivity disorder. J Abnorm Child Psychol 1992;20:213–32 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Carmody DP, Radvanski DC, Wadhwani S, Sabo MJ, Vergara L. EEG biofeedback training and attention-deficit/hyperactivity disorder in an elementary school setting. J Neurotherapy 2001;4:5–27 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Carpenter T. Teaching High School Students with Attention Deficit Hyperactivity Disorder Self Advocacy Skills and Strategies for Coping with their Disability in School. Ed.D thesis. Fort Lauderdale, FL: Nova Southeastern University; 1995 | Not a controlled trial/design not reported |
| Carrol A, Bain A, Houghton S. The effects of interactive versus linear video on the levels of attention and comprehension of social-behavior by children with attention disorders. Sch Psychol Rev 1994;23:29–43 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Caudle SE. Efficacy study of the Brief Evaluation and Intervention Program (BEIP) with four treatment groups. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;62:5956 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Chaban P. ADHD: from intervention to implementation. Educ Can 2010;50:32–5 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Chang H-H, Chang C-S, Shih Y-L. The process of assisting behavior modification in a child with attention-deficit hyperactivity disorder. J Nurs Res 2007;15:147–55 | Irrelevant study population(s), intervention context(s) and outcome(s) |
| Chang JJ, Cheon SM, Kim BK. The effects of free token response cost on disruptive behavior of hyperactive children. Kor J Counsel Psychother 1998;10:121–41 | Not retrievable |
| Chase SN, Clement PW. Effects of self-reinforcement and stimulants on academic performance in children with attention deficit disorder. J Clin Child Psychol 1985;14:323–33 | Not a controlled trial/design not reported |
| Chevalier N, Poissant H, Bergeron H, Girard-Lajoie A. The effect of visual-motor imagery training on CPT performance in children with attention deficit hyperactivity disorder. J Cognit Educ Psychol 2003;3:120–36 | Not a controlled trial/design not reported |
| Christie DJ, Dewitt RA, Kaltenbach P, Reed D. Using EMG biofeedback to signal hyperactive children when to relax. Except Child 1984;50:547–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Christie DJ, Hiss M, Lozanoff B. Modification of inattentive classroom behavior. Hyperactive children's use of self-recording with teacher guidance. Behav Modif 1984;8:391–406 | Not a controlled trial/design not reported |
| Chronis AM, Fabiano GA, Gnagy EM, Onyango AN, Pelham WE Jr, Lopez-Williams A, et al. An evaluation of the summer treatment program for children with attention deficit/hyperactivity disorder using a treatment withdrawal design. Behav Ther 2004;35:561–85 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Chudimov VF, Kulikov VP, Kuropiatnik NI, Boiko EA, Shadrina EN, Voronkova EI. [The use of hypoxically hypercapnic training for children with the attention deficit syndrome and hyperactivity for the correction of school disadaptation problems.] Vopr Kurortol Fizioter Lech Fiz Kult 2011;36–9 | Not retrievable |
| Cihak DF, Kirk ER, Boon RT. Effects of classwide positive peer ‘tootling’ to reduce the disruptive classroom behaviors of elementary students with and without disabilities. J Behav Educ 2009;18:267–78 | Not a controlled trial/design not reported |
| Clarfield J, Stoner G. Research brief: the effects of computerized reading instruction on the academic performance of students identified with ADHD. Sch Psychol Rev 2005;34:246–54 | Not a controlled trial/design not reported |
| Clark BJ. ‘The fun kids club’: developing an effective school-based program for children at risk. J Psychologist 1997;24:361–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Cocciarella A, Wood R, Low KG. Brief behavioral treatment for attention-deficit hyperactivity disorder. Percept Mot Skills 1995;81:225–6 | Not retrievable |
| Codding RS, Lewandowski L, Eckert T. Examining the efficacy of performance feedback and goal-setting interventions in children with ADHD: a comparison of two methods of goal setting. J Evid Base Pract Sch 2005;6:42–58 | Not a controlled trial/design not reported |
| Cohen NJ, Sullivan J, Minde K, Novak C, Helwig C. Evaluation of the relative effectiveness of methylphenidate and cognitive behavior modification in the treatment of kindergarten-aged hyperactive children. J Abnorm Child Psychol 1981;9:43–54 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Cohen SY. The effect of school based cognitive behavioral group therapy with a specific component of socialization, and self esteem, on the self esteem of ADHD children. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;59:4052 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Cole PL. The effects of taped relaxation training on physiological events and home and classroom behavior of hyperactive children. Diss Abstr Int 1981;42:1583 | Not retrievable |
| Coles EK, Pelham WE, Gnagy EM, Burrows-MacLean L, Fabiano GA, Chacko A, et al. A controlled evaluation of behavioral treatment with children with ADHD attending a summer treatment program. J Emot Behav Disord 2005;13:99–112 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Colton DL, Sheridan SM. Conjoint behavioral consultation and social skills training: enhancing the play behaviors of boys with attention deficit hyperactivity disorder. J Educ Psychol Consult 1998;9:3–28 | Not a controlled trial/design not reported |
| Corkum P, Corbin N, Pike M. Evaluation of a school-based social skills program for children with attention-deficit/hyperactivity disorder. Child Fam Behav Ther 2010;32:139–51 | Not a controlled trial/design not reported |
| Corkum PV, McKinnon M, Mullane JC. The effect of involving classroom teachers in a parent training program for families of children with ADHD. Child Fam Behav Ther 2005;27:29–49 | Not a controlled trial/design not reported |
| Cornish C, Carroll A. A cognitive-behavioural treatment for a child with attention-deficit disorder/without hyperactivity and comorbid anxiety. Aust Educ Dev Psychol 1998;15:6–22 | Not retrievable |
| Crabtree T, Alber-Morgan SR, Konrad M. The effects of self-monitoring of story elements on the reading comprehension of high school seniors with learning disabilities. Educ Treat Child 2010;33:187–203 | Not a controlled trial/design not reported |
| Creel C, Fore C, Boon RT, Bender WN. Effects of self-monitoring on classroom preparedness skills of middle school students with attention deficit hyperactivity disorder. Learn Disabil 2006;14:105–13 | Not a controlled trial/design not reported |
| Csilla S. Monitoring the effects of cognitive intervention on children with attention deficit and hyperactivity. Erdelyi Pszichologiai Szemle 2004;5:163–84 | Not retrievable |
| Cucu-Ciuhan G, Vasile AS. Efficiency of experiential psychotherapy in the treatment of children with attention deficit hyperactivity disorder. Procedia Soc Behav Sci 2010;5:920–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Cunningham CE, Clark M, Heaven RK, Durrant J, Cunningham LJ. The effects of coping-modelling problem solving and contingency management procedures on the positive and negative interactions of learning disabled and attention deficit disordered children with an autistic peer. Child Fam Behav Ther 1989;11:89–106 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Curtis K, Gladman P, Hampton K, Chambers J. Report on a Pilot Program: Strategies for Managing Students with Attentional Difficulties and/or Attention Deficit (Hyperactivity) Disorder. In International School Psychology Colloquium, Australian Guidance & Counselling Association, International School Psychology Association, editors. International School Psychology 20th Annual Colloquium. Melbourne, Australia: Australian Guidance and Counselling Association Ltd; 1997 | Not retrievable |
| Dansinger S. Academic Coaching for the Gifted Learner. In Walker B, Kutrumbus B, Hafenstein N, Rainey F, editors. Perspectives in Gifted Education: Twice-Exceptional Children. Denver, CO: University of Denver; 2001. pp. 108–13 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Davies S, Witte R. Self-management and peer-monitoring within a group contingency to decrease uncontrolled verbalizations of children with attention-deficit/hyperactivity disorder. Psychol Schools 2000;37:135–47 | Not a controlled trial/design not reported |
| Davis R, Hajicek JO. Effects of self-instructional training and strategy training on a mathematics task with severely behaviorally disordered students. Behav Disord 1985;10:275–82 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| De La Paz S. Teaching writing to students with attention deficit disorders and specific language impairment. J Educ Res 2001;95:37–47 | Not a controlled trial/design not reported |
| DiCesare EJ. An evaluation of live relaxation training as a treatment for primary aged school children described as hyperactive impulsive. Diss Abstr Int 1982;42:4927 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Diliberto JA, Beattie JR, Flowers CP, Algozzine RF. Effects of teaching syllable skills instruction on reading achievement in struggling middle school readers. Literacy Res Instruct 2009;48:14–27 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Dolyniuk CA. Using narrative to promote the conceptual development of adolescents with learning disability and attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;59:3346 | Not a controlled trial/design not reported |
| Dopfner M, Breuer D, Schurmann S, Metternich TW, Rademacher C, Lehmkuhl G. Effectiveness of an adaptive multimodal treatment in children with attention-deficit hyperactivity disorder – global outcome. Eur Child Adolesc Psychiatr 2004;13:I/117–I/29 | Active comparator |
| Drechsler R, Straub M, Doehnert M, Heinrich H, Steinhausen H-C, Brandeis D. Controlled evaluation of a neurofeedback training of slow cortical potentials in children with attention deficit/hyperactivity disorder (ADHD). Behav Brain Funct 2007;3:35 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Duckham-Shoor LA. Behavioral Alternatives to Stimulant Medication in Treating Childhood Hyperactivity: Effects on School and Home Behavior. Stanford, CA: Center for Educational Research at Stanford University; 1980 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Dunn FM, Howell RJ. Relaxation training and its relationship to hyperactivity in boys. J Clin Psychol 1982;38:92–100 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| DuPaul GJ, Eckert TL. The effects of school-based interventions for attention deficit hyperactivity disorder: a meta-analysis. Sch Psychol Rev 1997;26:5–27 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| DuPaul GJ, Ervin RA, Hook CL, McGoey KE. Peer tutoring for children with attention deficit hyperactivity disorder: effects on classroom behavior and academic performance. J Appl Behav Anal 1998;31:579–92 | Not a controlled trial/design not reported |
| DuPaul GJ, Guevremont DC, Barkley RA. Behavioral treatment of attention-deficit hyperactivity disorder in the classroom. The use of the attention training system. Behav Modif 1992;16:204–25 | Not a controlled trial/design not reported |
| DuPaul GJ, Helwig JR, Slay PM. Classroom Interventions for Attention and Hyperactivity. In Bray MA, Kehle TJ, editors. The Oxford Handbook of School Psychology. New York, NY: Oxford University Press; 2011. pp. 428–41 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| DuPaul GJ, Henningson PN. Peer tutoring effects on the classroom performance of children with attention deficit hyperactivity disorder. Sch Psychol Rev 1993;22:134–43 | Not a controlled trial/design not reported |
| DuPaul GJ, Jitendra AK, Volpe RJ, Tresco KE, Lutz JG, Vile Junod RE, et al. Consultation-based academic interventions for children with ADHD: effects on reading and mathematics achievement. J Abnorm Child Psychol 2006;34:635–48 | Duplicate |
| DuPaul GJ, Kern L, Gormley MJ, Volpe RJ. Early intervention for young children with ADHD: academic outcomes for responders to behavioral treatment. Sch Ment Health 2011;3:117–26 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Eber L, Rolf K, Sullivan MP. School-Based Systems of Care: Early Intervention and Day Treatment Examples from Illinois. Proceedings of the Annual Research Conference, A System of Care for Children's Mental Health: Expanding the Research Base, Tampa, FL, 8–11 March 1998 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Edleston C. A Program of Games and Activities to Increase Listening and Attentional Skills in Kindergarten Children. Ed.D thesis. Fort Lauderdale, FL: Nova Southeastern University; 1987 | Not retrievable |
| Edwards L, Salant V, Howard VF, Brougher J, McLaughlin TF. Effectiveness of self-management on attentional behavior and reading comprehension for children with attention deficit disorder. Child Fam Behav Ther 1995;17:1–17 | Not a controlled trial/design not reported |
| Egeland B, Rutner M. Modifying Response Latency and Error Rate of Impulsive Children. Paper presented at the annual meeting at the American Educational Research Association, New York, NY, 4–7 February 1971 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Eisenhower AS. Improving student-teacher relationships and school adjustment for children with disruptive behavior problems during the transition to kindergarten. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:6409 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Eisert HG, Eisert M, Schmidt MH. [Stimulant drug treatment and cognitive behavioral intervention in hyperactive children.] Z Kinder Jugenpsychiatr Psychother 1982;10:196–215 | Not retrievable |
| Elias MJ, Tobias SE, Friedlander BS. Enhancing skills for everyday problem solving, decision making, and conflict resolution in special needs students with the support of computer-based technology. Spec Serv Schools 1994;8:33–52 | Not retrievable |
| Elliot J, Prior M, Merrigan C, Ballinger K. Evaluation of a community intervention programme for preschool behavior problems. J Paediatr Child Health 2002;38:41–50 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Epstein JN, Willis MG, Conners CK, Johnson DE. Use of a technological prompting device to aid a student with attention deficit hyperactivity disorder to initiate and complete daily tasks: an exploratory study. J Spec Educ Tech 2001;16:19–28 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Erbey R, McLaughlin TF, Derby KM, Everson M. The effects of using flashcards with reading racetrack to teach letter sounds, sight words, and math facts to elementary students with learning disabilities. Int Electron J Elementary Educ 2011;3:213–26 | Not a controlled trial/design not reported |
| Eresund P. Psychodynamic psychotherapy for children with disruptive disorders. Int J Child Psychother 2007;33:161–80 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ervin RA, DuPaul GJ, Kern L, Friman PC. Classroom-based functional and adjunctive assessments: proactive approaches to intervention selection for adolescents with attention deficit hyperactivity disorder. J Appl Behav Anal 1998;31:65–78 | Not a controlled trial/design not reported |
| Ervin RA, Kern L, Clarke S, DuPaul GJ, Dunlap G, Friman PC. Evaluating assessment-based intervention strategies for students with ADHD and comorbid disorders within the natural classroom context. Behav Disord 2000;25:344–58 | Not a controlled trial/design not reported |
| Ervin RA. A functional assessment of the variables related to the occurrence and nonoccurrence of classroom problem behaviors for students with ADHD and comorbid ODD: toward a proactive approach to classroom management. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;57:1958 | Not retrievable |
| Evans JH, Ferre L, Ford LA, Green JL. Decreasing attention deficit hyperactivity disorder symptoms utilizing an automated classroom reinforcement device. Psychol Schools 1995;32:210–19 | Not a controlled trial/design not reported |
| Evans S. An investigation of the effects of behavioral and pharmacological interventions on the academic performance of students with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;68:8384 | Not a controlled trial/design not reported |
| Evans SW, Axelrod J, Langberg JM. Efficacy of a school-based treatment program for middle school youth with ADHD: pilot data. Behav Modif 2004;28:528–47 | Not a controlled trial/design not reported |
| Evans SW, Pelham W, Grudberg MV. The efficacy of note taking to improve behavior and comprehension of adolescents with attention deficit hyperactivity disorder. Exceptionality 1994;5:1 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Fabiano GA, Pelham WE Jr, Manos MJ, Gnagy EM, Chronis AM, Onyango AN, et al. An evaluation of three time-out procedures for children with attention-deficit/hyperactivity disorder. Behav Ther 2004;35:449–69 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Fabiano GA, Pelham WE Jr. Improving the effectiveness of behavioral classroom interventions for attention-deficit/hyperactivity disorder: a case study. J Emot Behav Disord 2003;11:124–30 | Not a controlled trial/design not reported |
| Fabiano GA, Pelham WE Jr, Gnagy EM, Burrows-MacLean L, Coles EK, Chacko A, et al. The single and combined effects of multiple intensities of behavior modification and methylphenidate for children with attention deficit hyperactivity disorder in a classroom setting. Sch Psychol Rev 2007;36:195–216 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Farmery V. Attention deficit disorder, anxiety disorder, and learning disabilities: preliminary results of an object-relational/psychoeducational treatment approach with an eight-year-old girl. Psychoanal Soc Work 2001;8:169–92 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Fasko SN, Leach R. A Math Fact Fluency Intervention with Scaffolding. Paper presented at the annual meeting of the Association for Behavior Analysis, Atlanta, GA, May 2006 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Fedewa AL, Erwin HE. Stability balls and students with attention and hyperactivity concerns: implications for on-task and in-seat behavior. Am J Occup Ther 2011;65:393–9 | Not a controlled trial/design not reported |
| Fenstermacher K, Olympia D, Sheridan SM. Effectiveness of a computer-facilitated, interactive social skills training program for boys with attention deficit hyperactivity disorder. Sch Psychol Q 2006;21:197–224 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Field TM, Quintino O, Hernandez-Reif M, Koslovsky G. Adolescents with attention deficit hyperactivity disorder benefit from massage therapy. Adolescence 1998;33:103–8 | Not a controlled trial/design not reported |
| Figarola PM, Gunter PL, Reffel JM, Worth SR, Hummel J, Gerber BL. Effects of self-graphing and goal setting on the math fact fluency of students with disabilities. Behav Anal Pract 2008;1:36–41 | Not a controlled trial/design not reported |
| Fine CT. Training children with attentional deficits to recruit reinforcement from teachers. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;57:1013 | Not retrievable |
| Fisher K, Haufe T. Developing Social Skills in Children Who Have Disabilities through the Use of Social Stories and Visual Supports. Chicago, IL: St Xavier University; 2009 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Fitzgerald G, Fick L, Milich R. Computer-assisted instruction for students with attentional difficulties. J Learn Disabil 1986;19:376–9 | Not a controlled trial/design not reported |
| Flem A, Moen T, Gudmundsdottir S. Towards Inclusive Schools: A Study of How a Teacher Facilitates Differentiated Instruction. Paper presented at the ECER Conference, Edinburgh, 2000 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Flood WA, Wilder DA, Flood AL, Masuda A. Peer-mediated reinforcement plus prompting as treatment for off-task behavior in children with attention deficit hyperactivity disorder. J Appl Behav Anal 2002;35:199–204 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Flood WA, Wilder DA. Antecedent assessment and assessment-based treatment of off-task behavior in a child diagnosed with attention deficit-hyperactivity disorder (ADHD). Educ Treat Child 2002;25:331–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Foks M. Neurofeedback training as an educational intervention in a school setting: how the regulation of arousal states can lead to improved attention and behaviour in children with special needs. Educ Child Psychol 2005;22:67–77 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Folk DK. Stress management and attention-deficit disorder intervention by teachers in the classroom for ADHD and non-ADHD children. Dissertation Abstracts International: Section B: The Sciences and Engineering 1994;55:1996 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ford MJ, Poe V, Cox J. Attending behaviors of ADHD children in math and reading using various types of software. J Comput Child Educ 1993;4:183–96 | Not a controlled trial/design not reported |
| Forness SR, Freeman SF, Paparella T. Recent randomized clinical trials comparing behavioral interventions and psychopharmacologic treatments for students with EBD. Behav Disord 2006;31:284–96 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Forster P, Doyle BA. Teaching listening skills to students with attention deficit disorders. Teach Except Child 1989;21:20–2 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Foster EM, Jensen PS, Schlander M, Pelham WE, Hechtman L, Arnold LE, et al. Treatment for ADHD: is more complex treatment cost-effective for more complex cases? Health Serv Res 2007;42:165–82 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Frame K. The STARS program: social empowerment training for preadolescents with attention deficit hyperactivity disorder (ADHD). J Sch Nurs 2004;20:257–61 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Frame KR. The effect of a support group on perceptions of scholastic competence, social acceptance and behavioral conduct in preadolescents diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63:737 | Duplicate |
| Fraser C, Belzner R, Conte R. Attention deficit hyperactivity disorder and self-control: a single case study of the use of a timing device in the development of self-monitoring. Sch Psychol Int 1992;13:339–45 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Friedman F. An Evaluation of the Integrated Cognitive-Behavioral Model for Improving Mathematics Performance and Attentional Behavior of Adolescents with Learning Disabilities and Attention-Deficit Hyperactivity Disorders. New York, NY: Columbia University Teachers College; 1992 | Not retrievable |
| Frost P. ‘Like Switching the Light On’ – The Raviv Method and its Contribution to Overcoming Learning Difficulties. Paper presented at the British Educational Research Association Annual Conference. Institute of Education, University of London, London, 5–8 September 2007 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Furtick KC. Successful Strategies Used with ADHD Students: Is an ADHD Classroom a Possibility? Minnesota, MN: Capella University; 2010 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Galen GC. The emotional and behavioral effects of hatha yoga used as an adjunct to traditional mental health treatment for adolescents with a range of psychiatric disorders. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:4419 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Gannon P. Is There a Functional Relationship Between Neurofeedback Training and the Behaviours Associated with ADHD? Paper Presented at Making Meaning: Creating Connections that Value Diversity: 30 Annual Conference of the Australian Association of Special Education, Brisbane, Australia, 23–25 September 2005 | Not retrievable |
| Garagouni-Areou F, Solomonidou C. Towards the Design of Educational Environments Suitable to the Needs of Pupils with Attention Deficit Hyperactivity Disorder (ADHD) Symptoms. In Cantoni L, McLoughlin C, editors. Proceedings of World Conference on Educational Media and Technology 2004. Norfolk: Assoc Advancement Computing Education; 2004. pp. 4446–51 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Garcia JA. The cost-effectiveness of treatments for attention-deficit/hyperactivity disorder in children. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;65:436 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Garcia Medina P. Treatment of hyperkinetic behaviors in a child through an experimental design of incompatible responses. Analisis y Modificacion de Conducta 1987;13:97–109 | Not retrievable |
| Garcia Soto XR, Munoz Garcia JJ, Navas Collado E. [Importance of the educational context in the diagnosis and treatment of hyperactivity disorder.] Anales de Psiquiatria 2004;20:236–45 | Not retrievable |
| Germer KA, Kaplan LM, Giroux LN, Markham EH, Ferris GJ, Oakes WP, et al. A function-based intervention to increase a second-grade student's on-task behavior in a general education classroom. Beyond Behav 2011;20:19–30 | Not a controlled trial/design not reported |
| Gevensleben H, Holl B, Albrecht B, Vogel C, Schlamp D, Kratz O, et al. Is neurofeedback an efficacious treatment for ADHD? A randomised controlled clinical trial. J Child Psychol Psychiatr 2009;50:780–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ghasabi S, Tajrishi MP, Zamani SMM. The effect of verbal self-instruction training on decreasing impulsivity symptoms in ADHD children. J Iranian Psychol 2009;5:209–20 | Not retrievable |
| Gittelman RH, Abikoff E, Pollack DF, Klein S, Katz S, Mattes J. A Controlled Trial of Behavior Modification and Methylphenidate in Hyperactive Children. In Walen CK, Henket B, editors Hyperactive Children: The Social Ecology of Identification and Treatment. New York, NY: Academic Press; 1980. pp. 221–43 | Duplicate |
| Glaaser DJ. The effects of improved classroom acoustics on the educational performance of students with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;69:1326 | Not a controlled trial/design not reported |
| Gooding LF. The effect of a music therapy-based social skills training program on social competence in children and adolescents with social skills deficits. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:2818 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Goodison-Farnsworth E. A Multimodal and Systemic Intervention for Children with Attention Deficit Hyperactivity Disorder. Wollongong, NSW: University of Wollongong; 2001 | Not retrievable |
| Gordon M, Thomason D, Cooper S, Ivers CL. Nonmedical treatment of ADHD/hyperactivity: the attention training system. J Sch Psychol 1991;29:151–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Graff RB, Green G, Libby ME. Effects of two levels of treatment intensity on a young child with severe disabilities. Behav Interv 1998;13:21–41 | Not a controlled trial/design not reported |
| Graham-Day KJ, Gardner R III, Hsin Y-W. Increasing on-task behaviors of high school students with attention deficit hyperactivity disorder: is it enough? Educ Treat Child 2010;33:205–21 | Not a controlled trial/design not reported |
| Granger DA, Whalen CK, Henker B, Cantwell C. ADHD boys' behavior during structured classroom social activities: effects of social demands, teacher proximity, and methylphenidate. J Attention Disord 1996;1:16–30 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Grauvogel-MacAleese AN, Wallace MD. Use of peer-mediated intervention in children with attention deficit hyperactivity disorder. J Appl Behav Anal 2010;43:547–51 | Not a controlled trial/design not reported |
| Gray SA, Chaban P, Martinussen R, Goldberg R, Gotlieb H, Kronitz R, et al. Effects of a computerized working memory training program on working memory, attention, and academics in adolescents with severe LD and comorbid ADHD; a randomized controlled trial. J Child Psychol Psychiatry 2012;53:1277–84 | Active comparator |
| Graybill D, Jamison M, Swerdlik ME. Remediation of impulsivity in learning disabled children by special education resource teachers using verbal self-instruction. Psychol Schools 1984;21:252–4 | Not a controlled trial/design not reported |
| Greenberg L. A multi-informant evaluation of a summer therapeutic camp for children with special needs: Parent and counselor ratings and child self-report. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:5123 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Greenewald MJ, Walsh C. The Effect of Environmental Accommodations on Attending Behavior of an ADHD Chapter I Student: An Action Research Study. Paper presented at the Annual Meeting of the American Educational Research Association, New York, NY, 8–12 April 1996 | Not a controlled trial/design not reported |
| Grin-Yatsenko V, Kropotov Y, Ponomarev V, Chutko L, Yakovenko E. Effect of biofeedback training of sensorimotor and beta 1EEG rhythms on attention parameters. Hum Physiol 2001;27:259–66 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Grisanzio WR. Evaluation of the effectiveness of an attention enhancement program for children diagnosed with ADHD administered in the school setting. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:5043 | Not a controlled trial/design not reported |
| Grizenko N, Zappitelli M, Langevin J-P, Hrychko S, El-Messidi A, Kaminester D, et al. Effectiveness of a social skills training program using self/other perspective-taking: a nine-month follow-up. Am J Orthopsychiatry 2000;70:501–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Grossman AC. Facilitating appropriate classroom behaviours through physical exercise. Melbourne, VIC: Monash University; 1987 | Not retrievable |
| Grosswald SJ, Stixrud WR, Travis F, Bateh MA. Use of the transcendental meditation technique to reduce symptoms of attention deficit hyperactivity disorder (ADHD) by reducing stress and anxiety: an exploratory study. Curr Issues Educ 2008;10:14 | Not a controlled trial/design not reported |
| Guderjahn L, Gold A, Stadler G, Gawrilow C. Self-regulation strategies support children with ADHD to overcome symptom-related behavior in the classroom. Atten Defic Hyperact Disord 2013;5:397–407 | Active comparator |
| Guli LA. The effects of creative drama-based intervention for children with deficits in social perception. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:3690 | Not a controlled trial/design not reported |
| Gulley V, Northup J, Hupp S, Spera S, LeVelle J, Ridgway A. Sequential evaluation of behavioral treatments and methylphenidate dosage for children with attention deficit hyperactivity disorder. J Appl Behav Anal 2003;36:375–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Gulley VS. A brief method for evaluating the effects of stimulant medication and behavioral interventions on the classroom performance of children with attention deficit hyperactivity disorder (ADHD). Dissertation Abstracts International: Section B: The Sciences and Engineering 1999;60:1290 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Gureasko-Moore S, Dupaul GJ, White GP. The effects of self-management in general education classrooms on the organizational skills of adolescents with ADHD. Behav Modif 2006;30:159–83 | Not a controlled trial/design not reported |
| Gureasko-Moore S, DuPaul GJ, White GP. Self-management of classroom preparedness and homework: effects on school functioning of adolescents with attention deficit hyperactivity disorder. Sch Psychol Rev 2007;36:647–64 | Not a controlled trial/design not reported |
| Gureasko-Moore SP. The effects of self-management on organizational skills of adolescents with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;65:1534 | Not a controlled trial/design not reported |
| Habboushe DF, Daniel-Crotty S, Karustis JL, Leff SS, Costigan TE, Goldstein SG, et al. A family-school homework intervention program for children with attention-deficit/hyperactivity disorder. Cogn Behav Pract 2001;8:123–36 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hall TF. Early intervention multimodal treatment program for children with attention deficit hyperactivity disorder: an outcome study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3474 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hamre BK, Pianta RC. Can instructional and emotional support in the first-grade classroom make a difference for children at risk of school failure? Child Dev 2005;76:949–67 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Harbeitner MH. The effects of social skills and peer/parent facilitation generalization training on the impulsive, aggressive, and noncompliant behavior of peer-rejected students diagnosed with attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;57:4647 | Not a controlled trial/design not reported |
| Harris KR, Friedlander BD, Saddler B, Frizzelle R, Graham S. Self-monitoring of attention versus self-monitoring of academic performance: effects among students with ADHD in the general education classroom. J Spec Educ 2005;39:145–56 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Harris KR. Self-monitoring of attentional behavior versus self-monitoring of productivity: effects on on-task behavior and academic response rate among learning disabled children. J Appl Behav Anal 1986;19:417–23 | Not a controlled trial/design not reported |
| Hauch Y. A multimodal treatment program for children with ADHD: A 16-month follow-up. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:1719 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hechtman L, Abikoff H, Klein RG, Weiss G, Respitz C, Kouri J, et al. Academic achievement and emotional status of children with ADHD treated with long-term methylphenidate and multimodal psychosocial treatment. J Am Acad Child Adolesc Psychiatr 2004;43:812–19 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hedin LR, Mason LH, Gaffney JS. Comprehension strategy instruction for two students with attention-related disabilities. Prev Sch Fail 2011;55:148–57 | Not a controlled trial/design not reported |
| Helms KS. A study of the impact of sensory integration strategies for reducing negative behaviors of ADHD students. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:4276 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Herman B. Treating Cognitively Impulsive Children Using Academic Materials and Peer Models. Indianna, IN: Indianna State University; 1982 | Not retrievable |
| Heuchert CM. Can teachers change behavior? Acad Ther 1983;18:321–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hill LJB, Williams JHG, Aucott L, Thomson J, Mon-Williams M. How does exercise benefit performance on cognitive tests in primary-school pupils? Dev Med Child Neurol 2011;53:630–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hilton-Prillhart AN, Hopkins MB, Skinner CH, McCane-Bowling S. Enhancing sight word reading in second-grade students using a computer-based sight word reading system. J Evid Base Pract Sch 2011;12:205–18 | Not retrievable |
| Hinshaw SP, Henker B, Whalen CK. Cognitive-behavioral and pharmacological interventions for hyperactive boys: comparative and combined effects. J Consult Clin Psychol 1984;52:739–49 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hoff KE, DuPaul GJ. Reducing disruptive behavior in general education classrooms: the use of self-management strategies. Sch Psychol Rev 1998;27:290–303 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hoff KE, Ervin RA, Friman PC. Refining functional behavioral assessment: analyzing the separate and combined effects of hypothesized controlling variables during ongoing classroom routines. Sch Psychol Rev 2005;34:45–57 | Not a controlled trial/design not reported |
| Hogg C, Callias M, Pellegrini D. Treatment of a 7-year-old hyperactive boy with educational problems. Behav Psychother 1986;14:145–61 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Holly PM, Trower TL, Chance DR. Wall-to-wall hugging and counseling. Elementary Sch Guid Counsel 1984;19:147–51 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Houck GM, King MC, Tomlinson B, Vrabel A, Wecks K. Small group intervention for children with attention disorders. J Sch Nurs 2002;18:196–200 | Not a controlled trial/design not reported |
| Hovik, Kjell Tore. Can PC-Based Training Boost Working Memory in ADHD Preadolescents on Medication? A Clinical Intervention Study. Oslo: University of Oslo; 2010 | Active comparator |
| Hovik KT, Aarlien AK, Saunes BK, Egeland J. Effects of working memory training on medicated ADHD preadolescents (10–12 years). Eur Child Adolesc Psychiatr 2010;19:S73 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hoza B, Mrug S, Pelham WE Jr, Greiner AR, Gnagy EM. A friendship intervention for children with attention-deficit/hyperactivity disorder: preliminary findings. J Attention Disord 2003;6:87–98 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hoza B, Pelham WE Jr, Sams SE, Carlson C. An examination of the ‘dosage’ effects of both behavior therapy and methylphenidate on the classroom performance of two ADHD children. Behav Modif 1992;16:164–92 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hubler SF. An instructional strategy designed to improve the problem solving abilities of students having an impulsive cognitive style. Diss Abstr Int 1990;50:3477–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hughes JN. Parents and cotherapists in think aloud. Psychol Schools 1985;22:436–43 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Hutchinson SW, Murdock JY, Williamson RD, Cronin ME. Self-recording PLUS encouragement equals improved behavior. Teach Except Child 2000;32:54–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Imhof M. Effects of color stimulation on handwriting performance of children with ADHD without and with additional learning disabilities. Eur Child Adolesc Psychiatr 2004;13:191–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Iovino I, Fletcher JM, Breitmeyer BG, Foorman BR. Colored oerlays for visual perceptual deficits in children with reading disability and attention deficit/hyperactivity disorder: are they differentially effective? J Clin Exp Neuropsychol 1998;20:791–806 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Iseman JS. A cognitive instructional approach to improving math calculation of children with ADHD: application of the pass theory. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:6274 | Duplicate |
| Isler L. Effects of gender on treatment outcome in young children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;69:659 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jacklyn HQ, Ravichandran S. Motivating Children with Attention Deficiency Disorder Using Certain Behavior Modification Strategies. In Lim CT, Goh JCH, editors. 13th International Conference on Biomedical Engineering, Vols 1–3. New York, NY: Springer; 2009. pp. 1057–60 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jacobson LT, Reid R. Improving the persuasive essay writing of high school students with ADHD. Except Child 2010;76:157–74 | Not a controlled trial/design not reported |
| Jacobson LT. Improving the writing performance of high school students with attention deficit/hyperactivity disorder and writing difficulties. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2954 | Not a controlled trial/design not reported |
| Jafarova O, Grebneva O, Lazareva O, Mazhirina K, Shtark M. The Use of the Neurofeedback Technology in the Correction of Attention Disorders in AD/HD Risk Groups. Liverpool: World Academic Union/World Academic Press; 2010 | Not a controlled trial/design not reported |
| Jarrett OS, Maxwell DM, Dickerson C, Hoge P, Davies G, Yetley A. Impact of recess on classroom behavior: group effects and individual differences. J Educ Res 1998;92:121–6 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jensen PS. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Arch Gen Psychiatr 1999;56:1073–86 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jensen PS, Arnold LE, Swanson JM, Vitiello B, Abikoff HB, Greenhill LL, et al. 3-year follow-up of the NIMH MTA study. J Am Acad Child Adolesc Psychiatr 2007;46:989–1002 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jensen PS, Garcia JA, Glied S, Crowe M, Foster M, Schlander M, et al. Cost-effectiveness of ADHD treatments: findings from the multimodal treatment study of children with ADHD. Am J Psychiatr 2005;162:1628–36 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jensen PS, Kenny DT. The effects of yoga on the attention and behavior of boys with attention-deficit/hyperactivity disorder (ADHD). J Attention Disord 2004;7:205–16 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jitendra AK, DuPaul GJ, Volpe RJ, Tresco KE, Junod RE, Lutz J, et al. Consultation-based academic intervention for children with attention deficit hyperactivity disorder: school functioning outcomes. Sch Psychol Rev 2007;36:217–36 | Duplicate |
| Jitendra AK, DuPaul GJ. Enhancing academic performance in children with ADHD. ADHD Report 2007;15:1–5 | Duplicate |
| Jitendra AK, Edwards LL, Starosta K, Sacks G, Jacobson LA, Choutka CM. Early reading instruction for children with reading difficulties: meeting the needs of diverse learners. J Learn Disabil 2004;37:421–39 | Not a controlled trial/design not reported |
| Johnson JW. The effect of strategy instruction on the reading comprehension of high school students with ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:1958 | Not a controlled trial/design not reported |
| Johnson K. Morningside academy. Behav Soc Issues 1997;7:31–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Johnson L, Sinnott J. The Effect of Acupressure for Moderating Behavior of Attention-Deficit/Hyperactivity Disorder Adolescents. Self-published 1998 | Not a controlled trial/design not reported |
| Johnson NP. The effect of the corrective reading program on junior high students with learning disabilities and attention deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70:1234 | Not a controlled trial/design not reported |
| Johnson SE. The effects of a silent signaling device on math performance for children rated as inattentive by teacher or parent. Dissertation Abstracts International: Section B: The Sciences and Engineering 2007;68:1914 | Not a controlled trial/design not reported |
| Johnson TL. Using Conjoint Behavioral Consultation To Enhance the Generalization of Behavioral Parent Training Effects to School Settings for Children with ADHD. Paper presented at the Annual Meeting of the National Association of School Psychologists, Seattle, WA, 4–5 March 1994 | Not a controlled trial/design not reported |
| Johnson WF. Working memory and ADHD: Can students with ADHD benefit from being taught strategies? Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:3847 | Not retrievable |
| Johnson-Glenberg MC. Web-Based Reading Comprehension Instruction: Three Studies of 3D-Readers. Reading Comprehension Strategies: Theories, Interventions, and Technologies. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 2007 | Not retrievable |
| Jolivette K, Lingo AS, Houchins DE, Barton-Arwood SM, Shippen ME. Building math fluency for students with developmental disabilities and attentional difficulties using ‘great leaps math’. Educ Train Dev Disabil 2006;41:392–400 | Not a controlled trial/design not reported |
| Jones KM, Drew HA, Weber NL. Noncontingent peer attention as treatment for disruptive classroom behavior. J Appl Behav Anal 2000;33:343–6 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Jones M, Boon RT, Fore C, Bender WN. ‘Our mystery hero!’ A group contingency intervention for reducing verbally disrespectful behaviors. Learn Disabil 2008;15:61–9 | Not a controlled trial/design not reported |
| Jones TS, Bodtker AM. Conflict education in a special needs population. Mediation Q 1999;17:109–24 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Joyce M, Siever D. Audio-visual entrainment program as a treatment for behavior disorders in a school setting. J Neurother 2000;4:9–25 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Juiliano F. The effects of goal-setting and self-charting on the academic performance of students with attention problems. Diss Abstr Int 1991;51:3698 | Not retrievable |
| Jurbergs AN. Relative efficacy of school-home notes and teacher feedback in minority elementary students with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:6276 | Duplicate |
| Jurbergs N, Palcic J, Kelley ML. School-home notes with and without response cost: Increasing attention and academic performance in low-income children with attention-deficit/hyperactivity disorder. Sch Psychol Q 2007;22:358–79 | Not a controlled trial/design not reported |
| Jurecska DE, Hamilton EB, Peterson MA. Effectiveness of the coping power program in middle-school children with disruptive behaviours and hyperactivity difficulties. Support Learn 2011;26:16–72 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kahraman H, Akgun S. The effects of empathy training on preschoolers empathic skills and conduct problems. Cocuk ve Genclik Ruh Sagligi Dergisi 2008;15:15–23 | Not retrievable |
| Kaiser M. Effect of behavior modification in the classroom on academic functioning and self-esteem in hyperactive children. Diss Abstr Int 1993;53:6534 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kang HW. The effectiveness of spatial visualization training for children with and without attention deficit hyperactivity disorder (ADHD). Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:3108 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kantavong P, Sivabaedya S. A professional learning program for enhancing the competency of students with special needs. Int J Whole Sch 2010;6:53–62 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kantner R, Tocco AM. Comparison of vestibular stimulation effects on classroom-behavior of 2 hyperactive-children with different hyperactive characteristics. Percept Mot Skills 1980;50:766 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kapalka GM. Managing students with ADHD in out-of-class settings. Emot Behav Difficult 2008;13:22–30 | Active comparator |
| Karper WB. Effects of gross motor training on attention-deficit behavior in one learning-disabled child. Percept Mot Skills 1986;63:219–25 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Katcher A, Teumer S. A 4-year Trial of Animal-Assisted Therapy With Public School Special Education Students. In Fine AH, editor. Handbook on Animal-Assisted Therapy: Theoretical Foundations and Guidelines for Practice. San Diego, CA: Academic Press; 2006. pp. 227–42 | Not retrievable |
| Katcher AH, Wilkins GG. The Centaur's Lessons: Therapeutic Education Through Care of Animals and Nature Study. In Fine AH, editor. Handbook on Animal-Assisted Therapy: Theoretical Foundations and Guidelines for Practice. San Diego, CA: Academic Press; 2000. pp. 153–77 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kaufman L, McLaughlin TF, Derby KM, Waco T. Employing reading racetracks and DI flashcards with and without cover, copy, and compare and rewards to teach of sight words to three students with learning disabilities in reading. Educ Res Q 2011;34:27–50 | Not a controlled trial/design not reported |
| Kayser KH, Wacker DP, Derby KM, Andelman MS, Golonka Z, Stoner EA. A rapid method for evaluating the necessity for both a behavioral intervention and methylphenidate. J Appl Behav Anal 1997;30:177–80 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Keeler KM. Fresh start: treatment effectiveness in a collaborative setting for behavioral-disordered children. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:6368 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kehle TJ, Clark E, Jenson WR, Wampold BE. Effectiveness of self-observation with behavior disordered elementary school children. Sch Psychol Rev 1986;15:289–95 | Not a controlled trial/design not reported |
| Kelley ML, McCain AP. Promoting academic performance in inattentive children. The relative efficacy of school-home notes with and without response cost. Behav Modif 1995;19:357–75 | Not a controlled trial/design not reported |
| Kercood S, Grskovic JA, Lee DL, Emmert S. The effects of fine motor movement and tactile stimulation on the math problem solving of students with attention problems. J Behav Educ 2007;16:303–10 | Not controlled trial/design not reported |
| Kercood S, Grskovic JA. The effects of highlighting on the math computation performance and off-task behavior of students with attention problems. Educ Treat Child 2009;32:231–41 | Not a controlled trial/design not reported |
| Kercood S, Zentall SS, Vinh M, Tom-Wright K. Attentional cuing in math word problems for girls at-risk for ADHD and their peers in general education settings. Contemp Educ Psychol 2012;37:106–12 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kern L, Delaney B, Clarke S, Dunlap G, Childs K. Improving the classroom behavior of students with emotional and behavioral disorders using individualized curricular modifications. J Emot Behav Disord 2001;9:239–47 | Not a controlled trial/design not reported |
| Kern L, DuPaul GJ, Volpe RJ, Sokol NG, Lutz J, Arbolino LA, et al. Multisetting assessment-based intervention for young children at risk for attention deficit hyperactivity disorder: Initial effects on academic and behavioral functioning. Sch Psychol Rev 2007;36:237–55 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kerns KA, Eso K, Thomson J. Investigation of a direct intervention for improving attention in young children with ADHD. Dev Neuropsychol 1999;16:273–95 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Khachapuridze N, Bakhtadze S, Geladze N, Kapanadze N. Impact of pharmacological versus non-pharmacological treatment on cognitive shift in attention deficit hyperactivity disorder. Eur Neuropsychopharmacol 2011;21:S600 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kim NS. The behavioral-cognitive treatment for modification of children's impulsivity. Kor J Counsel Psychother 1997;9:19–34 | Not retrievable |
| Kirby EA, Horne AM. Cognitive-Behavioral Modification with Hyperactive/Attention Deficit Disorder Children. Washington, DC: ERIC Clearinghouse; 1981 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kirby EA. Durable and Generalized Effects of Cognitive-Behavior Modification with Attention Deficit Disorder Children. Washington, DC: ERIC Clearinghouse; 1984 | Not retrievable |
| Kleiman G, Linday P. Microcomputers and hyperactive children. Creativ Comput 1981;7:93–4 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Klein RG, Abikoff H. Behavior therapy and methylphenidate in the treatment of children with ADHD. J Attention Disord 1997;2:89–114 | Active comparator |
| Koscinski ST, Gast DL. Computer-assisted instruction with constant time delay to teach multiplication facts to students with learning disabilities. Learn Disabil Res Pract 1993;8:157–68 | Not retrievable |
| Kotkin R. The Irvine Paraprofessional Program: promising practice for serving students with ADHD. J Learn Disabil 1998;31:556–64 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kraemer ES. Effectiveness of a home-school note procedure for increasing appropriate classroom behaviors exhibited by children diagnosed with attention-deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:3454 | Not retrievable |
| Kratter J, Hogan JD. The Use of Meditation in the Treatment of Attention Deficit Disorder with Hyperactivity. Jamaica, NY: St Johns University; 1982 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Krout R, Burnham A, Moorman S. Computer and electronic music applications with students in special education: from program proposal to progress evaluation. Music Ther Perspect 1993;11:28–31 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kuester DA, Zentall SS. Social interaction rules in cooperative learning groups for students at risk for ADHD. J Exp Educ 2012;80:69–95 | Not a controlled trial/design not reported |
| Kurtz BE, Borkowski JG. Development of strategic skills in impulsive and reflective children: a longitudinal study of metacognition. J Exp Child Psychol 1987;43:129–48 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kurtz BE, Borkowski JG. Metacognition and the Development of Strategic Skills in Impulsive and Reflective Children. Munich: Max Plank Institute for Psychological Research; 1985 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Kwako R. Relaxation as therapy for hyperactive children. Occup Ther Ment Health 1980;1:29–45 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lane KL, O'Shaughnessy TE, Lambros KM, Gresham FM, Beebe-Frankenberger ME. The efficacy of phonological awareness training with first-grade students who have behavior problems and reading difficulties. J Emot Behav Disord 2001;9:219–31 | Not a controlled trial/design not reported |
| Langberg JM, Arnold LE, Flowers AM, Epstein JN, Altaye M, Hinshaw SP, et al. Parent-reported homework problems in the MTA study: evidence for sustained improvement with behavioral treatment. J Clin Child Adolesc Psychol 2010;39:220–33 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Langberg JM, Vaughn AJ, Williamson P, Epstein JN, Girio-Herrera E, Becker SP. Refinement of an organizational skills intervention for adolescents with ADHD for implementation by school mental health providers. Sch Ment Health 2011;3:143–55 | Not a controlled trial/design not reported |
| Lantieri L. Teaching conflict resolution as an intervention for AD/HD. Reaching Today‘s Youth 1998;2:56–9 | Not retrievable |
| Lauth GW, Fellner C. Course of therapy and long-term effects of a multimodal therapy program in ADHD. Single case studies. Kindheit und Entwicklung 2004;13:167–79 | Not retrievable |
| Lee DL, Zentall SS. The effects of visual stimulation on the mathematics performance of children with attention deficit/hyperactivity disorder. Behav Disord 2002;27:272–88 | Not a controlled trial/design not reported |
| Lee DL. The effects of stimulation on the operant responses of children with attention/deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:0703 | Not a controlled trial/design not reported |
| Leigh L, Gersch I, Dix A, Haythorne D. Dramatherapy with Children, Young People and Schools: Enabling Creativity, Sociability, Communication and Learning. Oxford: Routledge, Taylor & Francis Group; 2012 | Not retrievable |
| Leisman G, Melillo R, Thum S, Ransom MA, Orlando M, Tice C, et al. The effect of hemisphere specific remediation strategies on the academic performance outcome of children with ADD/ADHD. Int J Adolesc Med Health 2010;22:275–83 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lena G, Andreas G, Caterina G. Self-regulation in the schools: a teacher training to reduce ADHD symptoms in the classroom. Psychol Health 2011;26:261–2 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lerew CD. The use of a cognitive strategy as an academic and behavioral intervention for children with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;64:3553 | Not a controlled trial/design not reported |
| LeVan RR. Development and assessment of a teacher-implemented self-instructional program for management of hyperactivity and associated behavior in the classroom. Dissertation Abstracts International 1981;41:3896 | Not retrievable |
| Levine ES, Anshel DJ. ‘Nothing works!’ A case study using cognitive-behavioral interventions to engage parents, educators, and children in the management of attention-deficit/hyperactivity disorder. Psychol Schools 2011;48:297–306 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lewandowski LJ, Lovett BJ, Parolin R, Gordon M, Codding RS. Extended time accommodations and the mathematics performance of students with and without ADHD. J Psychoeduc Assess 2007;25:17–28 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lienemann TO, Reid R. Using self-regulated strategy development to improve expository writing with students with attention deficit hyperactivity disorder. Except Child 2008;74:471–86 | Not a controlled trial/design not reported |
| Little AM. Perceptions of Baldrige criteria implementation in middle school inclusive language arts classrooms. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:887 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Liu J. Is electro-acupuncture, in combination with behaviour therapy, effective in preschool children with attention deficit hyperactivity disorder? Focus Alternative Compl Ther 2011;16:227–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lloyd A, Brett D, Wesnes K. Coherence training in children with attention-deficit hyperactivity disorder: cognitive functions and behavioral changes. Altern Ther Health Med 2010;16:34–42 | Active comparator |
| Loper AB, Hallahan DP, McKinney JD. The effect of reinforcement for global or analytic strategies on the performance of reflective and impulsive children. J Exp Child Psychol 1982;33:55–62 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Lorah KS. Effects of peer tutoring on the reading performance and classroom behavior of students with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1208 | Not a controlled trial/design not reported |
| Lorch EP, O'Neil K, Berthiaume KS, Milich R, Eastham D, Brooks T. Story comprehension and the impact of studying on recall in children with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol 2004;33:506–15 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Luckey AJ. Cognitive and academic gains as a result of cognitive training. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;71:84 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Luiselli JK, Steinman DL, Marholin D, Steinman WM. Evaluation of progressive muscle relaxation with conduct-problem, learning-disabled children. Child Behav Ther 1981;3:41–55 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Maag JW, Anderson JM. Sound-field amplification to increase compliance to directions in students with ADHD. Behav Disord 2007;32:238–53 | Not a controlled trial/design not reported |
| Macklem GL. No one wants to play with me. Acad Ther 1987;22:477–84 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mager WM. Effects of intervention group composition on young adolescents at-risk for externalizing behavior problems. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;64:4049 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Majeika CE, Walder JP, Hubbard JP, Steeb KM, Ferris GJ, Oakes WP, et al. Improving on-task behavior using a functional assessment-based intervention in an inclusive high school setting. Beyond Behav 2011;20:55–66 | Not a controlled trial/design not reported |
| Marley D. Meditation helps to calm hyperactive pupils in US. Times Educ Suppl 2009:15 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Martin AJ. The role of personal best (PB) goals in the achievement and behavioral engagement of students with ADHD and students without ADHD. Contemp Educ Psychol. 2012;37:91–105 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Martinez E. Neurotherapy as a treatment for attention deficit/hyperactivity disorder: a program design. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:6428 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mathes MY, Bender WN. The effects of self-monitoring on children with attention-deficit/hyperactivity disorder who are receiving pharmacological interventions. Remedial Spec Educ 1997;18:121 | Not a controlled trial/design not reported |
| Mathes MY. Effects of self-monitoring on male children with attention deficit hyperactivity disorder who are receiving psychostimulant medication. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;58:0423 | Not a controlled trial/design not reported |
| Matheson C. The effects of classwide peer tutoring on the academic achievement and classroom deportment of children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1998;58:2533 | Not a controlled trial/design not reported |
| Matson GD. Modifying the impulsive cognitive learning style by instructional materials and teacher modeling. Diss Abstr Int 1980;41:1872 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Matthews DB. Biofeedback: Its Uses in Education. Washington, DC: ERIC Clearinghouse; 1981 | Not retrievable |
| Mautone JA, DuPaul GJ, Jitendra AK. The effects of computer-assisted instruction on the mathematics performance and classroom behavior of children with ADHD. J Attention Disord 2005;9:301–12 | Not a controlled trial/design not reported |
| Maxwell V. Diagnosis and treatment of the gifted student with attention deficit disorder: a structure of intellect (SOI) approach. J Read Writ Learn Disabil Int 1989;5:247–52 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mazius MA. The educational impact of teacher-delivered self-instructional training on attention deficit hyperactivity disordered children. Diss Abstr Int 1991;51:4060 | Not retrievable |
| McAllister DA, Cutcher CL. Culminating Experience Action Research Projects. Chattanooga, TN: The University of Tennessee at Chattanooga; 2008 | Not a controlled trial/design not reported |
| McCain AP, Kelley ML. Managing the classroom behavior of an ADHD preschooler: the efficacy of a school-home note intervention. Child Fam Behav Ther 1993;15:33–44 | Not a controlled trial/design not reported |
| McClanahan B, Williams K, Kennedy E, Tate S. A breakthrough for Josh: how use of an iPad facilitated reading improvement. Tech Trends 2012;56:20–8 | Not a controlled trial/design not reported |
| McCord D. The effects of choice options on the reading performance of students with disabilities. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:139 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| McDaid JL. K-6 Early Intervention Project: Evaluation of the First Year of Implementation. San Diego, CA: San Diego City School; 1987 | Not retrievable |
| McGoey KE, DuPaul GJ, Eckert TL, Volpe RJ, Van Brakle J. Outcomes of a multi-component intervention for preschool children at-risk for attention-deficit/hyperactivity disorder. Child Fam Behav Ther 2005;27:33–56 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| McGoey KE, DuPaul GJ. Token reinforcement and response cost procedures: Reducing the disruptive behavior of preschool children with attention-deficit/hyperactivity disorder. Sch Psychol Q 2000;15:330–43 | Not a controlled trial/design not reported |
| McGoey KE. Positive reinforcement and response cost procedures: reducing the disruptive behavior of preschool children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 1998;58:6222 | Not a controlled trial/design not reported |
| Meftagh SD, Mohammadi N, Ghanizadeh A, Rahimi C, Najimi A. Comparison of the effectiveness of different treatment methods in children's attention deficit-hyperactivity disorders. J Isfahan Med Sch 2011;29:965–76 | Not retrievable |
| Mehta S, Mehta V, Mehta S, Shah D, Motiwala A, Vardhan J, et al. Multimodal behavior program for ADHD incorporating yoga and implemented by high school volunteers: a pilot study. ISRN Pediatr 2011;780745 | Not a controlled trial/design not reported |
| Meisel V, Garcia-Banda G, Servera M, Cardo E, Amengual L, Arroyo A, et al. Is neurofeedback able to improve behaviour and academic performance in children with attention deficit/hyperactivity disorder? A comparison with pharmacological intervention. Neurosci Lett 2011;500:e46 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Merrill MA. Captain's log: Effectiveness of computerized cognitive training on ADHD symptoms. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;68:5584 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Merriman DE, Codding RS. The effects of coaching on mathematics homework completion and accuracy of high school students with attention-deficit/hyperactivity disorder. J Behav Educ 2008;17:339–55 | Not a controlled trial/design not reported |
| Meyer K, Kelley ML. Improving homework in adolescents with attention-deficit/hyperactivity disorder: Self vs. parent monitoring of homework behavior and study skills. Child Fam Behav Ther 2007;29:25–42 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mezzacappa E, Buckner JC. Working memory training for children with attention problems or hyperactivity: a school-based pilot study. Sch Ment Health 2010;2:202–8 | Not a controlled trial/design not reported |
| Millard JL. Evaluation of an adolescent moral development, self-esteem, and conflict resolution skills program. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:3094 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Miranda A, Llácer MD, García C. Increasing the effectiveness of self-control training for hyperactive children by involving parents and teachers. Revista de Psicologia de la Educacion 1989;1:3–18 | Not retrievable |
| Miranda A, Llácer MD, García C. Does increase the efficacy of a training in auto-control for hyperactive children with the collaboration of parents and teachers? Revista de Psicologia de la Educacion 1989;1:3–18 | Not retrievable |
| Miranda A, Presentación MJ. Effects of cognitive-behavioural treatment in aggressive and nonaggressive children with attention deficit hyperactivity disorder: significant clinical change. Infancia y Aprendizaje 2000;92:51–70 | Not retrievable |
| Miranda A, Presentación MJ, Siegenthaler R, Jara P. Effects of a psychosocial intervention on the executive functioning in children With ADHD. J Learn Disabil 2013;46:363–76 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Molina BSG, Hinshaw SP, Swanson JM, Arnold LE, Vitiello B, Jensen PS, et al. The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study. J Am Acad Child Adolesc Psychiatr 2009;48:484–500 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Molloy GN. Chemicals, exercise and hyperactivity: a short report. Int J Disabil Dev Educ 1989;36:57–61 | Not a controlled trial/design not reported |
| Morand MK. The effects of mixed martial arts and exercise on behavior of boys with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;65:2609 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mosse LK, Hinojosa B. The use of EEG biofeedback in the treatment of ADD/ADHD in the school setting. Wheat Ridge, CO: The Association Applied Psychophysiology & Biofeedback; 1998 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Mozo DAL. Effects of a brief family and school-centered program on children's psychological and academic behaviors. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63:1261 | Not retrievable |
| Munoz JAL, Garcia IM. Multi-modal intervention in a case of child's hyperactivity: content, results and troubles with treatment. Clinica y Salud 2001;12:405–27 | Not retrievable |
| Muro J, Ray D, Schottelkorb A, Smith MR, Blanco PJ. Quantitative analysis of long-term child-centered play therapy. Int J Play Ther 2006;15:35–58 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Murray LK. Self-control training in young children. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63:3017 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Najafi M, Mohammadi MR, Assari S, Basirnia A, Tehranidoost M, Alaghband-rad J. Improving the dictation in attention deficit hyperactivity disorder by using computer based interventions: a clinical trial. Iran J Psychiatr 2006;1:123–7 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Najafi M. Improving the dictation in attention deficit hyperactivity disorder by using computer based interventions: A clinical trial. Eur Psychiatr 2010;25 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Narhi V. The effects of a short in-service training on teaching students with ADHD-symptoms: teacher's experiences and the behavior management techniques used. A pilot study. Eur Child Adolesc Psychiatr 2010;19:S74 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Neef NA, Bicard DF, Endo S. Assessment of impulsivity and the development of self-control in students with attention deficit hyperactivity disorder. J Appl Behav Anal 2001;34:397–408 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Neef NA, Lutz MN. Assessment of variables affecting choice and application to classroom interventions. Sch Psychol Q 2001;16:239–52 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Nguyen MT. A program design for ADHD students: assessment and classroom intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63:2597 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Noell GH, Gansle KA, Witt JC, Whitmarsh EL, Freeland JT, LaFleur LH, et al. Effects of contingent reward and instruction on oral reading performance at differing levels of passage difficulty. J Appl Behav Anal 1998;31:659–63 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Northup J, Fusilier I, Swanson V, Huete J, Bruce T, Freeland J, et al. Further analysis of the separate and interactive effects of methylphenidate and common classroom contingencies. J Appl Behav Anal 1999;32:35–50 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Nyden A, Myren K-J, Gillberg C. Long-term psychosocial and health economy consequences of ADHD, autism, and reading-writing disorder: a prospective service evaluation project. J Attention Disord 2008;12:141–8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Omizo MM. Relaxation training and biofeedback with hyperactive elementary school children. Elementary Sch Guid Counsel 1981;15:329–32 | Duplicate |
| Omizo MM, Cubberly WE, Semands SG, Omizo SA. The effects of biofeedback and relaxation training on memory tasks among hyperactive boys. Exceptional Child 1986;33:56–64 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Onghai JG. The use of metacognition to increase the attention, problem-solving skills, and learning performance of school-age children with attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2000;60:4320 | Not a controlled trial/design not reported |
| Orlando PC, Rivera RO. Neurofeedback for elementary students with identified learning problems. J Neurother 2004;8:5–19 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| O'Shea B, Hodes M, Down G, Bramley J. A school-based mental health service for refugee children. Clin Child Psychol Psychiatr 2000;5:189–201 | Not a controlled trial/design not reported |
| Ota KR, DuPaul GJ. Task engagement and mathematics performance in children with attention-deficit hyperactivity disorder: effects of supplemental computer instruction. Sch Psychol Q 2002;17:242–57 | Not a controlled trial/design not reported |
| Owens JS, Holdaway AS, Zoromski AK, Evans SW, Himawan LK, Girio-Herrera E, et al. Incremental benefits of a daily report card intervention over time for youth with disruptive behavior. Behav Ther 2012;43:848–61 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Owens JS, Johannes LM, Karpenko V. The relation between change in symptoms and functioning in children with ADHD receiving school-based mental health services. Sch Ment Health 2009;1:183–95 | Not a controlled trial/design not reported |
| Ozdemir S. The effects of the First Step to Success program on academic engagement behaviors of Turkish students with attention-deficit/hyperactivity disorder. J Posit Behav Interv 2011;13:168–77 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ozdemir S. The first step to success program: Implementation effectiveness with Turkish children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;67:2115 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ozmen SK, Lauth GW. The effects of a combined training program on children with attention deficit hyperactivity disorder in the classroom activity. Int J Psychol 2008;43:760 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Palcic JL, Jurbergs N, Kelley ML. A comparison of teacher and parent delivered consequences: improving classroom behavior in low-income children with ADHD. Child Fam Behav Ther 2009;31:117–33 | Not a controlled trial/design not reported |
| Pang WC, Zhang KC. Reading intervention for secondary students with hyperactive behaviours in Hong Kong. Emot Behav Difficult 2011;16:69–85 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Paniagua FA, Black SA. Correspondence training and observational-learning in the management of hyperactive-children – a preliminary-study. Child Fam Behav Ther 1992;14:1–19 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Paoni MF. The synthesis of a social information processing model of attention-deficit/hyperactivity disorder and social competence intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:6144 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pariseau ME, Fabiano GA, Massetti GM, Hart KC, Pelham WE Jr. Extended time on academic assignments: Does increased time lead to improved performance for children with attention-deficit/hyperactivity disorder? Sch Psychol Q 2010;25:236–48 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Parolin R. The effects of extended time on the mathematics performance of students with and without attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2007;67:6725 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Peck HL, Kehle TJ, Bray MA, Theodore LA. Yoga as an intervention for children with attention problems. Sch Psychol Rev 2005;34:415–24 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham Jr WE, Carlson C. Separate and combined effects of methylphenidate and behavior modification on boys with attention. J Consult Clin Psychol 1993;61:506 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham JWE, Gnagy EM. Summer sports: a recreationally based program for building peer relations. Reaching Today's Youth 1998;2:52–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham WE, Burrows-Maclean L, Gnagy EM, Fabiano GA, Coles EK, Tresco KE, et al. Transdermal methylphenidate, behavioral, and combined treatment for children with ADHD. Exp Clin Psychopharmacol 2005;13:111–26 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham WE, Gnagy EM, Greiner AR, Hoza B, Hinshaw SP, Swanson JM, et al. Behavioral versus behavioral and pharmacological treatment in ADHD children attending a summer treatment program. J Abnorm Child Psychol 2000;28:507–25 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham WE Jr, Waschbusch DA, Hoza B, Gnagy EM, Greiner AR, Sams SE, et al. Music and video as distractors for boys with ADHD in the classroom: comparison with controls, individual differences, and medication effects. J Abnorm Child Psychol 2011;39:1085–98 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pelham WE, Schnedler RW, Bologna NC, Contreras JA. Behavioral and stimulant treatment of hyperactive children: a therapy study with methylphenidate probes in a within-subject design. J Appl Behav Anal 1980;13:221–36 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Perry HW. A Perceptual Training Program For Children With Learning Disorders. Memphis, TN: Memphis Tennessee Public Schools; 1993 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pester J. An investigative assessment of the need for a Y9 pupil with learning difficulties and ADHD. Emot Behav Difficult 2002;7:215–27 | Not retrievable |
| Pettai R. Multidisciplinary Teamwork with Pre-School Children with Speech and Language Problems, Activity and Attention Problems. Bologna: Medimond S R L; 2005 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pfeiffer B, Henry A, Miller S, Witherell S. Effectiveness of Disc 'O' Sit cushions on attention to task in second-grade students with attention difficulties. Am J Occup Ther 2008;62:274–81 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pfeiffer LJ. Promoting Social Competency in Attention Deficit Hyperactivity Disordered Elementary-Aged Children. Florida, FL: Nova Southeastern University; 1994 | Not a controlled trial/design not reported |
| Pfiffner LJ, Kaiser NM, Burner C, Zalecki C, Rooney M, Setty P, et al. From clinic to school: translating a collaborative school-home behavioral intervention for ADHD. Sch Ment Health 2011;3:127–42 | Not a controlled trial/design not reported |
| Piana M. A multi-dimensional intervention for students with attention-deficit/hyperactivity symptomatology and low math performance: Targeting motivation and math skill development. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:1542 | Not a controlled trial/design not reported |
| Piscalkiene V. Experimental training of children with attention deficit/hyperactivity disorder. US-China Educ Rev 2009;6:17–30 | Not a controlled trial/design not reported |
| Plumer PJ, Stoner G. The relative effects of classwide peer tutoring and peer coaching on the positive social behaviors of children with ADHD. J Attention Disord 2005;9:290–300 | Not a controlled trial/design not reported |
| Plumer PJ. Using peers as intervention agents to improve the social behaviors of elementary-aged children with attention deficit hyperactivity disorder: Effects of a peer coaching package. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68:2813 | Not a controlled trial/design not reported |
| Poland A. The effects of cognitive behavior modification on the math achievement of reflective and impulsive second grade students. Diss Abstr Int 1982;42:3403 | Not retrievable |
| Polirstok SR. Training handicapped students in the mainstream to use self-evaluation techniques. Techniques 1987;3:9–18 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pop-Jordanova N, Markovska-Simoska S, Zorcec T. Neurofeedback treatment of children with attention deficit hyperactivity disorder. Prilozi 2005;26:71–80 | Not retrievable |
| Posavac HD, Sheridan SM, Posavac SS. A cueing procedure to control impulsivity in children with attention deficit hyperactivity disorder. Behav Modif 1999;23:234–53 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Poushaneh K, Bonab BG, Namin FH. Effect of training impulse control on increase attention of children with attention deficit/hyperactivity disorder. Procedia Soc Behav Sci 2010;5:983–7 | Not a controlled trial/design not reported |
| Powell LA, Potter L. Report on an intervention involving massage and yoga for male adolescents attending a school for disadvantaged male adolescents in the UK. Int J Spec Educ 2010;25:47–54 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Powell S, Nelson B. Effects of choosing academic assignments on a student with attention deficit hyperactivity disorder. J Appl Behav Anal 1997;30:181–3 | Not a controlled trial/design not reported |
| Power TJ, Karustis JL, Habboushe DF. Homework success for children with ADHD: a family-school intervention program. New York, NY: Guilford Press; 2001 | Not retrievable |
| Power TJ, Mautone JA, Soffer SL, Clarke AT, Marshall SA, Sharman J, et al. A family-school intervention for children with ADHD: results of a randomized clinical trial. J Consult Clin Psychol 2012;80:611–23 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Price AT, Martella RC, Marchand-Martella NE, Cleanthous CC. A comparison of immediate feedback delivered via an FM headset versus delayed feedback on the Inappropriate verbalization of a student with ADHD. Educ Treat Child 2002;25:159 | Not a controlled trial/design not reported |
| Prince KC, Ho EA, Hansen SB. Effects of a school based program to improve adaptive school behavior and social competencies among elementary school youth: the living skills program. J Res Character Educ 2010;8:39–59 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Prosser B. Beyond Deficit Views: Redesigning Pedagogies To Engage Students Identified With Attention Deficit Hyperactivity Disorder. Paper presented at the Culture, Knowledge and Understanding Conference, Singapore, May 2007 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Pumpuang W, Phuphaibul R, Orathai P, Putdivarnichapong W. The effects of a collaborative management programme on managing parents and teachers for children with attention deficit hyperactivity disorder (ADHD). Int J Nurs Pract 2012;18:27 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rabiner DL, Malone PS, Conduct Problems Prevention Research Group. The impact of tutoring on early reading achievement for children with and without attention problems. J Abnorm Child Psychol 2004;32:273–84 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rabone H. 'Space for acupuncture' at Stanchester Community School. Chin Med J 2006;41–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Radford PM, Ervin RA. Employing descriptive functional assessment methods to assess low-rate, high-intensity behaviors: a case example. J Posit Behav Interv 2002;4:146–55 | Not a controlled trial/design not reported |
| Rafferty LA, Arroyo J, Ginnane S, Wilczynski K. Self-monitoring during spelling practice: effects on spelling accuracy and on-task behavior of three students diagnosed with attention deficit hyperactivity disorder. Behav Anal Pract 2011;4:37–45 | Not a controlled trial/design not reported |
| Raggi VL, Chronis-Tuscano A, Fishbein H, Groomes A. Development of a brief, behavioral homework intervention for middle school students with attention-deficit/hyperactivity disorder. Sch Ment Health 2009;1:61–77 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Raggi VL. Development and preliminary testing of a brief, behavioral intervention to address the homework-related problems of middle school students with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:5789 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rappaport GC, Ornoy A, Tenenbaum A. Is early intervention effective in preventing ADHD? Isr J Psychiatry Relat Sci 1998;35:271–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rapport MD, Murphy HA, Bailey JS. Ritalin vs. response cost in the control of hyperactive children: a within-subject comparison. J Appl Behav Anal 1982;15:205–16 | Not a controlled trial/design not reported |
| Rapport MD, Murphy A, Bailey JS. The effects of a response cost treatment tactic on hyperactive children. J Sch Psychol 1980;18:98–111 | Not a controlled trial/design not reported |
| Rapport MD. A comparison of attentional training utilizing a response cost procedure and methylphenidate (ritalin) on the classroom behaviors of hyperactive children. Diss Abstr Int 1981;42:389 | Not a controlled trial/design not reported |
| Ray DC. Play Therapy With Children Exhibiting ADHD. In Baggerly JN, Ray DC, Bratton SC, editors. Child-Centered Play Therapy Research: The Evidence Base for Effective Practice. Hoboken, NJ: John Wiley & Sons Inc.; 2010. pp. 145–62 | Not a controlled trial/design not reported |
| Ray DC, Schottelkorb A, Tsai M-H. Play therapy with children exhibiting symptoms of attention deficit hyperactivity disorder. Int J Play Ther 2007;16:95–111 | Active comparator |
| Re AM, Cornoldi C. A treatment programme for preschool children with ADHD characteristics. Eur Child Adolesc Psychiatr 2010;19:S74–S5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Reddy L, Braunstein D, Springer C, Bartik C, Hauch Y, Hall T, et al. Randomized Trial of Three Child/Parent Training Groups for ADHD Children. Paper presented at the Annual Conference of the American Psychological Association, Chicago, IL, 22–25 August 2002 | Not retrievable |
| Reid R, Lienemann TO. Self-regulated strategy development for written expression with students with attention deficit/hyperactivity disorder. Except Child 2006;73:53–68 | Not a controlled trial/design not reported |
| Rerkjaree S. Home and School Based Intervention Model for Thai Children with Attention Deficit Hyperactivity Disorder. Paper Presented at the Proceedings of 2010 International Conference on Behavioral, Cognitive and Psychological Sciences, Singapore, 26–28 February 2010 | Not retrievable |
| Resnick A, Reitman D. The use of homework success for a child with attention-deficit/hyperactivity disorder, predominantly inattentive type. Clin Case Stud 2011;10:23–36 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rich LP. Prompting self-monitoring with assistive technology to increase academic engagement in students with attention-deficit/hyperactivity disorder symptoms. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:3158 | Not a controlled trial/design not reported |
| Richardson E, Kupietz S, Maitinsky S. What is the role of academic intervention in the treatment of hyperactive children with reading disorders. J Child Contemp Soc 1986;19:153–67 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Richter NC. Relaxation training with impulsive first grade students. Diss Abstr Int 1986;46:4413 | Not retrievable |
| Rickman D, Motzenbecker T. The Effects of a Response-Cost Program on the Classroom Behavior of Two Children with Attention Deficit/Hyperactivity Disorder. Warren, MI: Van Dyke Public Schools; 1996 | Not a controlled trial/design not reported |
| Rickson DJ. Instructional and improvisational models of music therapy with adolescents who have attention deficit hyperactivity disorder (ADHD): a comparison of the effects on motor impulsivity. J Music Ther 2006;43:39–62 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Ridgway A, Northup J, Pellegrin A, LaRue R, Hightshoe A. Effects of recess on the classroom behavior of children with and without attention-deficit hyperactivity disorder. Sch Psychol Q 2003;18:253–68 | Not a controlled trial/design not reported |
| Ridgway A. The effects of a recess or break and stimulant medication on the classroom behavior of children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;65:3693 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Riquelme Miralles MR, Baeza Hernandez MC, Martinez Selva J. Token economy application in a preschool classroom. Analisis y Modificacion de Conducta 1985;11:633–43 | Not retrievable |
| Robinson PW, Newby TJ, Ganzell SL. A token system for a class of underachieving hyperactive children. J Appl Behav Anal 1981;14:307–15 | Not a controlled trial/design not reported |
| Rogevich ME, Perin D. Effects on Science Summarization of a Reading Comprehension Intervention for Adolescents with Behavior and Attention Disorders. Except Child 2008;74:135–54 | Not a controlled trial/design not reported |
| Rooney KJ, Hallahan DP, Lloyd JW. Self-recording of attention by learning disabled students in the regular classroom. J Learn Disabil 1984;17:360–4 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rooney KJ. Independent strategies for efficient study: a core approach. Acad Ther 1989;24:383–90 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rosen LA, O'Leary SG, Joyce SA, Conway G, Pfiffner LJ. The importance of prudent negative consequences for maintaining the appropriate behavior of hyperactive students. J Abnorm Child Psychol 1984;12:581–604 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rosenberg MS. Maximizing the effectiveness of structured classroom management programs: implementing rule-review procedures with disruptive and distractible students. Behav Disord 1986;11:239–48 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rudolph TC. The effects of a school-based social skills training program on children with ADHD: generalization to the school setting. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66:894 | Not a controlled trial/design not reported |
| Rumain B. Efficacy of behavior management versus methylphenidate in a hyperactive child: the role of dynamics. Am J Orthopsychiatry 1988;58:466–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Rutherford LE, DuPaul GJ, Jitendra AK. Examining the relationship between treatment outcomes for academic achievement and social skills in school-age children with attention-deficit hyperactivity disorder. Psychol Schools 2008;45:145–57 | Not a controlled trial/design not reported |
| Saheban F, Amiri S, Kajbaf MB, Abedi A. The efficacy of short-term executive functions training on the reduction of symptoms of attention deficit and hyperactivity of elementary boy students in Esfahan metropolitan area. Adv Cognit Sci 2010;12:52–8 | Not retrievable |
| Sakelaris TL. Effects of a self-managed study skills intervention on homework and academic performance of middle school students with attention deficit hyperactivity disorder (ADHD). Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:0337 | Not a controlled trial/design not reported |
| Sams SE. The effects of functional intervention on the behavior of four students labeled ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:1081 | Not a controlled trial/design not reported |
| Sante AD, McLaughlin T, Weber KP. The use and evaluation of a direct instruction flash card strategy on multiplication math facts mastery with two students with developmental disabilities and attention deficit hyperactivity disorder. J Precis Teach Celeration 2001;17:68–75 | Not retrievable |
| Sayal K, Owen V, White K, Merrell C, Tymms P, Taylor E. Impact of early school-based screening and intervention programs for ADHD on children's outcomes and access to services: follow-up of a school-based trial at age 10 years. Arch Pediatr Adolesc Med 2010;164:462–9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Schilling DL, Washington K, Billingsley FF, Deitz J. Classroom seating for children with attention deficit hyperactivity disorder: therapy balls versus chairs. Am J Occup Ther 2003;57:534–41 | Not a controlled trial/design not reported |
| Schirduan V, Case KI. Mindful curriculum leadership for students with attention deficit hyperactivity disorder (ADHD): leading in elementary schools by using multiple intelligences theory (SUMIT). Teachers Coll Rec 2004;106:87–95 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Schleser R, Armstrong KJ, Allen JS Jr. Attention Deficit Hyperactive Disorder: New Directions. In Morgan SB, Okwumabua TM, Morgan S, editors. Child and Adolescent Disorders: Developmental and Health Psychology Perspectives. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.; 1990. pp. 105–33 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Schmitt RCO. The effects of a self-monitoring and video self-modeling intervention to increase on-task behavior for children with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:3758 | Not a controlled trial/design not reported |
| Schnoes CJA. Conjoint behavioral consultation, ADHD, and homework: a combined intervention package for middle school youth with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3461 | Not a controlled trial/design not reported |
| Schottelkorb A. Effectiveness of Child-Centered Play Therapy and Person-Centered Teacher Consultation on ADHD: A Single-Case Study Design. In Baggerly JN, Ray DC, Bratton SC, editors. Child-Centered Play Therapy Research: The Evidence Base for Effective Practice. Hoboken, NJ: John Wiley & Sons Inc.; 2010. pp. 209–30 | Not a controlled trial/design not reported |
| Schottelkorb AA, Ray DC. ADHD symptom reduction in elementary students: a single-case effectiveness design. Prof Sch Counsel 2009;13:11–22 | Not a controlled trial/design not reported |
| Schultz BK. Behavioral consultation for adolescents with ADHD: lessons learned in the Challenging Horizons Program. Emot Behav Disord Youth 2005;5:91 | Not retrievable |
| Schultz BK, Evans SW, Serpell ZN. Preventing failure among middle school students with attention deficit hyperactivity disorder: a survival analysis. Sch Psychol Rev 2009;38:14–27 | Duplicate |
| Schweitzer JB, Sulzer-Azaroff B. Self-control: teaching tolerance for delay in impulsive children. J Exp Anal Behav 1988;50:173–86 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Scope CR. The efficacy of conjoint behavioral consultation to reduce the off-task behavior of elementary school children diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1975 | Not a controlled trial/design not reported |
| Sealover IE. Counselor intervention using visual learning strategies for adolescent attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2002;62:4076 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Serpell ZN, Evans SW, Schultz BK, Pastor, Dena A. Incremental benefits of school-based treatment for adolescents with ADHD. ADHD Report 2008;16:1–7 | Duplicate |
| Seth-Smith F, Levi N, Pratt R, Fonagy P, Jaffey D. Do nurture groups improve the social, emotional and behavioural functioning of at risk children? Educ Child Psychol 2010;27:21–34 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Shapiro ES, DuPaul GJ, Bradley-Klug KL. Self-management as a strategy to improve the classroom behavior of adolescents with ADHD. J Learn Disabil 1998;31:545–55 | Not a controlled trial/design not reported |
| Shapiro ES. A Regional Consulting Center To Assist School Personnel in Working with Early Adolescents with Attention Deficit Disorders. Bethlehem, PA: Lehigh University; 1997 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Shaw R, Lewis V. The impact of computer-mediated and traditional academic task presentation on the performance and behaviour of children with ADHD. J Res Spec Educ Needs 2005;5:47–54 | Not a controlled trial/design not reported |
| Shechtman Z, Katz E. Therapeutic bonding in group as an explanatory variable of progress in the social competence of students with learning disabilities. Group Dynam 2007;11:117–28 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Shelton TL, Barkley RA, Crosswait C, Moorehouse M, Fletcher K, Barrett S, et al. Multimethod psychoeducational intervention for preschool children with disruptive behavior: two-year post-treatment follow-up. J Abnorm Child Psychol 2000;28:253–66 | Duplicate |
| Shepp MS, Jensen BF. A comparison of the treatment effects of an operant strategy, a cognitive strategy, and a combined approach with a hyperactive boy. Sch Psychol Rev 1983;12:199–204 | Not a controlled trial/design not reported |
| Sheridan SM, Eagle JW, Cowan RJ, Mickelson W. The effects of conjoint behavioral consultation results of a 4-year investigation. J Sch Psychol 2001;39:361–85 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Sheridan SM. Efficacy of conjoint behavioral consultation as a vehicle for inclusion. Am Psychol 1997;52:813–68 | Not retrievable |
| Shillingford MA, Lambie GW, Walter SM. An integrative, cognitive-behavioral, systemic approach to working with students diagnosed with attention deficit hyperactive disorder. Prof Sch Counsel 2007;11:105–12 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Shimabukuro SM, Prater MA, Jenkins A, Edelen-Smith P. The effects of self-monitoring of academic performance on students with learning disabilities and ADD/ADHD. Educ Treat Child 1999;22:397–414 | Not a controlled trial/design not reported |
| Sibley MH, Pelham WE, Evans SW, Gnagy EM, Ross JM, Greiner AR. An evaluation of a summer treatment program for adolescents with ADHD. Cogn Behav Pract 2011;18:530–44 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Silver AA. Children in classes for the severely emotionally handicapped. J Dev Behav Pediatr 1984;5:49–54 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Silverstein LL. The role of ability and attention deficit-hyperactivity disorder in learning-disabled students’ responses to verbal self-instruction training. Diss Abstr Int 1991;51:2687 | Not retrievable |
| Simpkins LL. Effects of adjusted teaching strategies on reading achievement of impulsive third grade students. Diss Abstr Int 1981;42:2594 | Not retrievable |
| Sims EL, McLaughlin TF. Classroom management for the hyperactive-child – an analysis. Correct Soc Psych J Behav Tech Methods Ther 1985;31:142–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Skinner JN, Veerkamp MB, Kamps DM, Andra PR. Teacher and peer participation in functional analysis and intervention for a first grade student with attention deficit hyperactivity disorder. Educ Treat Child 2009;32:243–66 | Not a controlled trial/design not reported |
| Slate SE, Meyer TL, Burns WJ, Montgomery DD. Computerized cognitive training for severely emotionally disturbed children with ADHD. Behav Modif 1998;22:415–37 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Smitheman-Brown V, Church RP. Mandala drawing: facilitating creative growth in children with A.D.D. or A.D.H.D. Art Ther J Am Art Ther Assoc 1996;13:252–60 | Not a controlled trial/design not reported |
| Smyth WD, Bebensee EL. The ‘success’ program and the A.D.D. child. Read Improv 1983;20:274–7 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Solomonidou C, Garagouni-Areou F, Zafiropoulou M. Information and communication technologies (ICT) and pupils with attention deficit hyperactivity disorder (ADHD) symptoms: do the software and the instruction method affect their behavior? J Educ Multimed Hypermed 2004;13:109–28 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Solomonidou C, Garagouni-Areou F. A Research Method to Study the Behavior of Pupils with Attention Deficit Hyperactivity Disorder (ADHD) Symptoms Working on the Computer. Paper presented at World Conference on Educational Multimedia, Hypermedia and Telecommunications, Lugano, Switzerland, 21–26 June 2004 | Not retrievable |
| Solovieva Y, Quintanar L. Methods of neuropsychological correction in Mexican preschoolers with attention deficit disorder. Cult Hist Psychol 2006;3:60–7 | Not retrievable |
| Soyoung P. Self-monitoring for students with ADHD: a look at self-monitoring strategies and their effects on improving attention and behavior for children with ADHD. Insight Learn Disabil 2011;8:51–68 | Not a controlled trial/design not reported |
| Sproull C. The impact of a digital role playing game on the executive functioning skills of students with ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2012;73:1381 | Active comparator |
| Stahr B, Cushing D, Lane K, Fox J. Efficacy of a function-based intervention in decreasing off-task behavior exhibited by a student with ADHD. J Posit Behav Interv 2006;8:201–11 | Not a controlled trial/design not reported |
| Stanutz AG. The effects of group relaxation training sessions utilizing the turtle technique upon the observed overactive behavior in preschool children. Diss Abstr Int 1983;43:3261 | Not retrievable |
| Stein LEC, Goldman J. Beginning reading instruction for children with minimal brain dysfunction. J Learn Disabil 1980;13:219–22 | Active comparator |
| Stein MT, Shafer M-A, Elliott GR, Levine S. An adolescent who abruptly stops his medication for attention-deficit hyperactivity disorder. J Dev Behav Pediatr 1999;20:106–10 | Not a controlled trial/design not reported |
| Steiner N, Sidhu TK, Frenette EC, Mitchell K, Perrin EC. Preliminary Analysis of a Randomized Trial of Computer Attention Training in Children with Attention-Deficit/Hyperactivity Disorder: Society for Research on Educational Effectiveness. Paper presented at the Society for Research on Educational Effectiveness 2011 Spring Conference, Washington, DC, 3–6 March 2011 | Duplicate |
| Steinhoff KW, Lerner M, Kapilinsky A, Kotkin R, Wigal S, Steinberg-Epstein R, et al. Attention-Deficit/Hyperactivity Disorder. In Luby JL editor. Handbook of Preschool Mental Health: Development, Disorders, and Treatment. New York, NY: Guilford Press; 2006. pp. 63–79 | Not retrievable |
| Steinmann E, Gerber-von Muller G, Siniatchkin M, Stephani U, Petermann F, Gerber WD. Neuropsychological and clinical effects of a multimodal behavioral ADHD summer camp training. Eur Child Adolesc Psychiatr 2011;20:S128–S9 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Sterling LA. An investigation of the effectiveness of an assessment-linked study skills intervention on homework completion and accuracy. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;66:2494 | Not a controlled trial/design not reported |
| Stevens L, Van Werkhoven W, Stokking K, Castelijns J, Jager A. Interactive instruction to prevent attention problems in class. Learn Environ Res 2000;3:265–86 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Stevens ML. Effects of classwide peer tutoring on the classroom behavior and academic performance of students with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 1999;59:4487 | Not a controlled trial/design not reported |
| Stewart KG, McLaughlin T. ‘Self-recording: effects of reducing off-task behavior with a high school student with an attention deficit hyperactivity disorder’: erratum. Child Fam Behav Ther 1993;15:106 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Stewart KG, McLaughlin TF. Self-recording – effects on reducing off-task behavior with a high-school student with an attention-deficit hyperactivity disorder. Child Fam Behav Ther 1992;14:53–9 | Not a controlled trial/design not reported |
| Strayhorn JM Jr, Bickel DD. Reduction in children’s symptoms of attention deficit hyperactivity disorder and oppositional defiant disorder during individual tutoring as compared with classroom instruction. Psychol Rep 2002;91:69–80 | Not a controlled trial/design not reported |
| Strehl U, Leins U, Goth G, Klinger C, Hinterberger T, Birbaumer N. Self-regulation of slow cortical potentials: a new treatment for children with attention-deficit/hyperactivity disorder. Pediatrics 2006;118:e1530–40 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Studer P, Gevensleben H, Wangler S, Rothenberger A, Moll GH, Heinrich H. Neurofeedback for children with attention-deficit/hyperactivity disorder: clinical and neurophysiological results of a randomised controlled trial. Eur Child Adolesc Psychiatr 2010;19:S15–S6 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Sullivan MA, O’Leary SG. Maintenance following reward and cost token programs. Behav Ther 1990;21:139–49 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Suzovic V, Marusic R, Simovic T. Voluntary work with ADHD children as psychosocial and psychoeducational intervention. Eur Child Adolesc Psychiatr 2011;20:S132 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Swanson J, Simpson S, Agler D, Kotkin R, Pfiffner L, Bender M, et al. UCI-OCDE School-Based Treatment Program for Children with ADHD/ODD. In Stefanis CN, Rabavilas AD, Soldatos CR, editors. Psychiatry: A World Perspective. Vol. 1. Amsterdam: Elsevier Science Publishers B. V.; 1990. pp. 1107–12 | Not retrievable |
| Swenson N, Lolich E, Williams RL, McLaughlin T. The effects of structured free-time on request compliance and on-task behavior of a preadolescent with ADHD. Child Fam Behav Ther 2000;22:51–9 | Not a controlled trial/design not reported |
| Tabaeian SR, Amiri S, Kalantari M, Neshatdoost HT, Karahmadi M. The effect of social skills training (SST) on improving peer relationships in primary school boys with attention deficit/hyperactivity disorder (ADHD). Int J Psychol 2008;43:605 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Tabassam W, Grainger J. Evaluation of effectiveness of a self-concept enhancement intervention for students with LD and LD/ADHD. Paper presented at the inaugral Self-concept Enhancement and Learning Facilitation (SELF) Research Centre International Conference, Sydney, Australia, 5–6 October 2000 | Not retrievable |
| Tabassam W, Grainger J. Self-Concept Enhancement for Students With Learning Difficulties With and Without Attention Deficit Hyperactivity Disorder. In Marsh HW, Craven RG, McInerney DM, editors. International Advances in Self Research. Greenwich: Information Age Publishing; 2003. pp. 231–60 | Not retrievable |
| Tabassam W. Exploring and Enhancing the Self-Concept of Students With Learning Difficulties, With and Without Attention Deficit Hyperactivity Disorder. Wollongong, NSW: University of Wollongong; 2001 | Not a controlled trial/design not reported |
| Tate DRW. Modification of Impulsivity in Young Children. Texas: Texas Woman’s University; 1975 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Teeter PA, Rumsey R, Natoli L, Naylor D, Smith R. Therapeutic interventions to increase social competence in teens with impulse control deficits. J Psychother Indepen Pract 2000;1:49–70 | Not retrievable |
| Terenzi CM, Ervin RA, Hoff KE. Classwide self-management of rule following. J Evid Base Pract Sch 2010;11:117–22 | Not a controlled trial/design not reported |
| Teta AR. Increasing homework completion in children with ADHD using the mystery motivator intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:3190 | Not a controlled trial/design not reported |
| Theodore LA, Kehle TJ, Bray MA. Homework success for children with ADHD: a family-school intervention program. Psychol Schools 2004;41:274 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Thompson L, Thompson M. Neurofeedback combined with training in metacognitive strategies: effectiveness in students with ADD. Appl Psychophysiol Biofeed 1998;23:243–63 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Tolor B, Tolor A. An Attempted Modification of Impulsivity and Self-Esteem in Kindergartners. Psychol Schools 1982;19:526–31 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Tormanen MR, Takala M, Sajaniemi N. Learning disabilities and the auditory and visual matching computer program. Support Learn 2008;23:80–8 | Not a controlled trial/design not reported |
| Totland K. Children and youth with attention disorders. Psykologisk Paedagogisk Radgivning 1998;35:146–52 | Not retrievable |
| Trahant DM. Behavioral improvement in children with ADHD: Independent and combined effects of behavioral treatment and medication. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;65:5384 | Not a controlled trial/design not reported |
| Trianes Torres MV, Rivas Moya T, Munoz A. Differential efficiency of a psychoeducational intervention on social abilities of inhibited and impulsive preschool children. Analisis y Modificacion de Conducta 1991;17:895–916 | Not retrievable |
| Trice AD, Parker FC, Furrow F, Iwata MM. An analysis of home contingencies to improve school behavior with disruptive adolescents. Educ Treat Child 1983;6:389–99 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Tryon WW, Tryon GS, Kazlausky T, Gruen W, Swanson JM. Reducing hyperactivity with a feedback actigraph: initial findings. Clin Child Psychol Psychiatry 2006;11:607–17 | Not a controlled trial/design not reported |
| Turner BLB. Effects of response cost, bibliotherapy and academic tutoring on attentional behavior, achievement, work productivity, accuracy, and self-esteem in children with Attention Deficit Hyperactivity Disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;57:1973 | Not a controlled trial/design not reported |
| Tymms P, Merrell C. The impact of screening and advice on inattentive, hyperactive and impulsive children. Eur J Spec Needs Educ 2006;21:321–37 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Umbreit J. Functional assessment and intervention in a regular classroom setting for the disruptive behavior of a student with attention deficit hyperactivity disorder. Behav Disord 1995;20:267–78 | Not a controlled trial/design not reported |
| Vahali HO, Kapur M. Group intervention with hyperkinetic boys in the school setting. Nimhans J 1995;13:1230–1 | Not a controlled trial/design not reported |
| van der Oord S, Bogels SM, Peijnenburg D. The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J Child Fam Stud 2012;21:139–47 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| van der Oord S, Prins PJM, Oosterlaan J, Emmelkamp PMG. Treatment of attention deficit hyperactivity disorder in children. Predictors of treatment outcome. Eur Child Adolesc Psychiatr 2008;17:73–81 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| VandenBerg NL. The use of a weighted vest to increase on-task behavior in children with attention difficulties. Am J Occup Ther 2001;55:621–8 | Not a controlled trial/design not reported |
| Veenstra B, van Geert PL, van der Meulen BF. Computer versus human-based support: effect on computer game performances in (in)effectively learning pre-schoolers. Educ Child Psychol 2010;27:56–72 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Vega LC, Dickey-Kurdziolek M, Shupp L, Perez-Quinones MA, Booker J, Congleton B. Taking Notes Together: Augmenting Note Taking. Paper presented at International Symposium on Collaborative Technologies and Systems, Orlando, FL, 21–25 May 2007 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Viadero D. Computer training found to help those with ADHD. Educ Week 2007;26:8 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Vio C, Offredi F, Marzocchi GM. Attention deficit hyperactivity disorder: experimentation with metacognitive training. Psicologia Clinica dello Sviluppo 1999;3:241–62 | Not retrievable |
| Vitaro F, Tremblay RE. Impact of a prevention program on aggressive children’s friendships and social adjustment. J Abnorm Child Psychol 1994;22:457–75 | Not a controlled trial/design not reported |
| Vogel MK. The effects of motor and cognitive training and ADHD students in the physical education environment. Diss Abstr Int 1992;52:2461 | Not retrievable |
| Vogelmann-Peper M. Teaching Elementary School Teachers Cognitive-Behavioral Techniques To Address ADDH Behaviors in the Classroom Setting. Ed.D thesis. Fort Lauderdale, FL: Nova Southeastern University; 1989 | Not retrievable |
| Voll CB. The effects of yoga on attention and self-concept in special education preschoolers. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:719 | Not a controlled trial/design not reported |
| Volpe RJ. Effects of two academic intervention protocols on the disruptive classroom behavior of children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;64:1890 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Volpe RJ, DuPaul GJ, Jitendra AK, Tresco KE. Consultation-based academic interventions for children with attention deficit hyperactivity disorder: effects on reading and mathematics outcomes at 1-year follow-up. Sch Psychol Rev 2009;38:5–13 | Active comparator |
| Vujnovic RK. Examining the influence of treatment integrity: accuracy of daily report card intervention implementation and student outcome. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:2420 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Wadhwani S, Radvanski DC, Carmody DP. Neurofeedback training in a case of attention deficit hyperactivity disorder. J Neurother 1998;3:42–9 | Not a controlled trial/design not reported |
| Wagner I. Attention training with individuals, groups and classes. Sch Psychol Int 1988;9:277–83 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Walker BC. The relative effects of painting and gross-motor activities on the intrinsic locus-of-control of hyperactivity in learning disabled elementary school pupils. Stud Art Educ 1980;21:13–21 | Not a controlled trial/design not reported |
| Walker P Jr. The effects of Ritalin and cognitive behavioral therapy on the academic functioning of African American children diagnosed with attention deficit hyperactivity disorder: a longitudinal study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;72:561 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Waller RJ, Albertini CL, Waller KS. Self-monitoring of performance to promote accurate work completion: a functional based intervention for a 4th grade student presenting challenging behavior. Adv Sch Ment Health Promot 2011;4:52–60 | Not retrievable |
| Wang X-L, Bernas R, Eberhard P. Engaging ADHD students in tasks with hand gestures: a pedagogical possibility for teachers. Educ Stud 2004;30:217–29 | Not a controlled trial/design not reported |
| Warnke MG. Self-monitoring procedures with elementary aged children of color with disruptive behaviors in an urban setting. Dissertation Abstracts International: Section A: Humanities and Social Sciences. 2004;64:3958 | Not retrievable |
| Waschbusch DA, Pelham WE Jr, Massetti G. The behavior education support and treatment (BEST) school intervention program: pilot project data examining schoolwide, targeted-school, and targeted-home approaches. J Attention Disord 2005;9:313–22 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Watkins DE, Wentzel KR. Training boys with ADHD to work collaboratively: social and learning outcomes. Contemp Educ Psychol 2008;33:625–46 | Not a controlled trial/design not reported |
| Watkins DE. Processes of social interaction and learning outcomes for attention deficit hyperactivity disordered males when collaborating with female peer partners trained to facilitate social interaction and strategic planning. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2001;62:81 | Not a controlled trial/design not reported |
| Watson CM. A breakfast club for children with emotional and behavioural difficulties. Education 2003;31:15–18 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Webb AD, McLaughlin TF. School intervention stressing positive classroom strategies with hyperactive students – some practical suggestions. Correct Soc Psych J Behav Tech Methods Ther 1985;31:77–82 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Webb LD, Myrick RD. A group counseling intervention for children with attention deficit hyperactivity disorder. Prof Sch Counsel 2003;7:108–15 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Webster-Stratton CM, Reid J, Beauchaine TP. One-year follow-up of combined parent and child intervention for young children with ADHD. J Clin Child Adolesc Psychol 2013;42:251–61 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Werry JS, Scaletti R, Mills F. Sensory integration and teacher-judged learning problems: a controlled intervention trial. J Paediatr Child Health 1990;26:31–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Wigal T, Swanson JM, Douglas VI, Wigal SB, Wippler CM, Cavoto KF. Effect of reinforcement on facial responsivity and persistence in children with attention-deficit hyperactivity disorder. Behav Modif 1998;22:143–66 | Not retrievable |
| Williams DC. The effects of structured exercise on the attention and mathematics achievement of hyperactive students. Diss Abstr Int 1991;52:431 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Williams RA, Horn S, Daley SP, Nader PR. Evaluation of access to care and medical and behavioral outcomes in a school-based intervention program for attention-deficit hyperactivity disorder. J Sch Health 1993;63:294–7 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Williamson BD, Campbell-Whatley GD, Lo YY. Using a random dependent group contingency to increase on-task behaviors of high school students with high incidence disabilities. Psychol Schools 2009;46:1074–83 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Williamson DA, Calpin JP, DiLorenzo TM. Treating hyperactivity with dexedrine and activity feedback. Behav Modif 1981;5:399–416 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Williford AP, Shelton TL. Using mental health consultation to decrease disruptive behaviors in preschoolers: adapting an empirically-supported intervention. J Child Psychol Psychiatr 2008;49:191–200 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Windwer CM. An ascending music stimulus program and hyperactive children. J Res Music Educ 1981;29:173–81 | Not a controlled trial/design not reported |
| Winklemolen D. Neurofeedback treatment in a patient with ADHD and ODD. Neurosci Lett 2011;500:e5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Woeppel P. Facilitating Social Skills Development in Learning Disabled and/or Attention Deficit Disordered Second to Fifth Grade Children and Parents. Fort Lauderdale, FL: Nova Southeastern University; 1990 | Not retrievable |
| Wolfe DE. The effect of interrupted and continuous music on bodily movement and task performance of third grade students. J Music Ther 1982;19:74–85 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Woods JM. The effects of cognitive-behavioral therapy on reduction of symptoms of attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 1995;55:5053 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Work PHL, Choi HS. Developing Classroom and Group Interventions Based on a Neuropsychological Paradigm. In D’Amato RC, Fletcher-Janze E, Reynolds CR, editors. Handbook of School Neuropsychology. Hoboken, NJ: John Wiley & Sons Inc.; 2005. pp. 663–83 | Not retrievable |
| Wragg J. Disruption in Schools: Options for Change: the Talk Sense to Yourself Programs: Self Management Skills for Children and Adolescents in Schools and Clinics. Paper presented at Queensland Guidance and Counselling Association fifth guidance conference, Brisbane, Australia, September 1988 | Not retrievable |
| Wyman PA, Cross W, Brown CH, Qin Y, Xin T, Eberly S. Intervention to strengthen emotional self-regulation in children with emerging mental health problems: proximal impact on school behavior. J Abnorm Child Psychol 2010;38:707–20 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Yellin AM, Kendall PC, Greenberg LM. Cognitive-behavioral therapy and methylphenidate with hyperactive children: preliminary comparisons. Res Comm Psychol Psychiatr Behav 1981;6:213–27 | Not a controlled trial/design not reported |
| Young LM. An analysis of the effect of the LOGO computer programming environment upon the reflective and impulsive cognitive styles of second-grade students. Diss Abstr Int 1983;44:64 | Not retrievable |
| Zakay D, Kreitler S, Bar-El Z. Cognitive orientation and changing impulsivity of children. Br J Educ Psychol 1984;54:40–50 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zanni CA. Attention and music: understanding young children’s attention and the potential of music to increase attention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:5128 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zentall SSL. Structured tasks: effects on activity and performance of hyperactive and comparison children. J Educ Res 1985;79:91–5 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zentall SS, Hall AM, Lee DL. Attentional focus of students with hyperactivity during a word-search task. J Abnorm Child Psychol 1998;26:335–43 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zentall SS, Javorsky J. Professional development for teachers of students with ADHD and characteristics of ADHD. Behav Disord 2007;32:78–93 | Not a controlled trial/design not reported |
| Zentall SS, Kuester DA, Craig BA. Social behavior in cooperative groups: students at risk for ADHD and their peers. J Educ Res 2011;104:28–41 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zentall SS, Shaw JH. Effects of classroom noise on performance and activity of 2nd-grade hyperactive and control children. J Educ Psychol 1980;72:830–40 | Irrelevant study population(s), intervention context(s) or outcome(s) |
| Zitomer EA. Decreasing impulsivity in grade school children: self instructional training and imagery. Diss Abstr Int 1981;42:2093 | Not retrievable |
Appendix 4 Search strategy used for review 2
Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations and Ovid MEDLINE(R)
(Also used for PsycINFO, EMBASE, Social Policy and Practice and HMIC.)
Searched 1946 to present.
Search strategy
-
exp attention deficit disorder with hyperactivity/ (19,987)
-
ADHD.ti,ab. (13,883)
-
ADHS.ti,ab. (408)
-
ADDH.ti,ab. (113)
-
(attention adj2 deficit*).ti,ab. (18,424)
-
hyperactiv*.ti,ab. (38,287)
-
(hyper adj1 activ*).ti,ab. (468)
-
(Attention adj3 (problem* or difficult* or disorder* or issue*)).ti,ab. (21,921)
-
hyperk*.ti,ab. (15,911)
-
minimal brain.ti,ab. (738)
-
damp.ti,ab. (2915)
-
or/1-11 (71,954)
-
intervention*.ti,ab. (547,560)
-
strateg*.ti,ab. (592,883)
-
program*.ti,ab. (569,124)
-
training.ti,ab. (238,506)
-
support*.ti,ab. (985,516)
-
therap*.ti,ab. (1,835,744)
-
treatment*.ti,ab. (3,043,703)
-
technique*.ti,ab. (1,061,597)
-
or/13-20 (6,545,507)
-
tool*.ti,ab. (395,415)
-
instrument*.ti,ab. (184,891)
-
scale*.ti,ab. (448,191)
-
questionnaire*.ti,ab. (297,807)
-
measure*.ti,ab. (2,243,280)
-
survey*.ti,ab. (396,075)
-
quantitative.ti,ab. (396,204)
-
(examine or examined).ti,ab. (1,409,286)
-
(assess or assessed).ti,ab. (1,200,125)
-
or/22-30 (5,217,344)
-
attitude*.ti,ab. (95,227)
-
belief*.ti,ab. (50,663)
-
stigma*.ti,ab. (17,884)
-
(perception or perceive*).ti,ab. (201,692)
-
(conception or conceive*).ti,ab. (32,338)
-
accept*.ti,ab. (296,395)
-
willing*.ti,ab. (22,934)
-
prefer*.ti,ab. (307,213)
-
or/32-39 (931,203)
-
12 and 21 and 31 and 40 (1256)
-
limit 41 to yr=“1980 – 2014” (1244)
Appendix 5 Studies excluded at full text from review 2, with reasons
| Reference | Reason for exclusion |
|---|---|
| Anhalt K, McNeil CB, Bahl AB. The ADHD classroom kit: a whole-classroom approach for managing disruptive behavior. Psychol Schools 1998;35:67–79 | Specific intervention only |
| Arcia E, Fernandez MC, Jaquez M. Latina mothers’ stances on stimulant medication: complexity, conflict, and compromise. J Dev Behav Pediatr 2004;25:311–17 | No school-based intervention |
| Atamanoff Gambert T. The effect of comorbid anxiety and comorbid oppositional defiant disorder on behavioral group training outcomes for children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;68:4808 | No school-based intervention |
| Bennett DS, Power TJ, Rostain AL, Carr DE. Parent acceptability and feasibility of ADHD interventions: assessment, correlates, and predictive validity. J Pediatr Psychol 1996;21:643–57 | No school-based intervention |
| Bogle KE. Evaluation of a brief group parent training intervention in the context of an after-school program for middle-school students. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;69:665 | Specific intervention only |
| Bradley-Klug KL. The effects of a self-management intervention on the classroom behavior of young adolescents with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;58:1576 | Specific intervention only |
| Breteler R, Pesch W, Nadorp M, Best N, Tomasoa X. Neurofeedback in residential children and adolescents with mild mental retardation and ADHD behavior. J Neurother 2012;16:172–82 | No school-based intervention |
| Brown University. Integrated home-school behavioral treatment for ADHD, inattentive subtype. Child Adol Behav Lett 2007;23:1–8 | No school-based intervention |
| Bussing R, Gary FA, Mills TL, Garvan CW. Parental explanatory models of ADHD – gender and cultural variations. Soc Psychiatry Psychiatr Epidemiol 2003;38:563–75 | Qualitative measure |
| Bussing R, Koro-Ljungberg M, Noguchi K, Mason D, Mayerson G, Garvan CW. Willingness to use ADHD treatments: a mixed methods study of perceptions by adolescents, parents, health professionals and teachers. Soc Sci Med 2012;74:92–100 | No school-based intervention |
| Bussing R, Schoenberg NE, Rogers KM, Zima BT, Angus S. Explanatory models of ADHD: do they differ by ethnicity, child gender, or treatment status? J Emot Behav Disord 1998;6:233–42 | Qualitative measure |
| Bussing R, Zima BT, Mason DM, Porter PC, Garvan CW. Receiving treatment for attention-deficit hyperactivity disorder: do the perspectives of adolescents matter? J Adolesc Health 2011;49:7–14 | No school-based intervention |
| Chaban P. ADHD: from intervention to implementation. Educ Can 2010;50:32–5 | Attitude not measured or not reported for intervention |
| Chen M, Seipp CM, Johnston C. Mothers’ and fathers’ attributions and beliefs in families of girls and boys with attention-deficit/hyperactivity disorder. Child Psychiatr Hum Dev 2008;39:85–99 | No school-based intervention |
| Cihak DF, Kirk ER, Boon RT. Effects of classwide positive peer ‘tootling’ to reduce the disruptive classroom behaviors of elementary students with and without disabilities. J Behav Educ 2009;18:267–78 | Not ADHD focus |
| Colton DL, Sheridan SM. Conjoint behavioral consultation and social skills training: enhancing the play behaviors of boys with attention deficit hyperactivity disorder. J Educ Psychol Consult 1998;9:3–28 | Specific intervention only |
| Concannon PE, Tang YP. Management of attention deficit hyperactivity disorder: a parental perspective. J Paediatr Child Health 2005;41:625–30 | Attitude not measured or not reported for intervention |
| Conners C, March JS, Frances A, Wells KC, Ross R. Treatment of attention-deficit/hyperactivity disorder: expert consensus guidelines. J Attention Disord 2001;4:S1–S128 | Could not retrieve full text |
| Corkum P, Rimer P, Schachar R. Parental knowledge of attention-deficit hyperactivity disorder and opinions of treatment options: impact on enrolment and adherence to a 12-month treatment trial. Can J Psychiatr 1999;44:1043–8 | No school-based intervention |
| Corkum PV, McKinnon M, Mullane JC. The effect of involving classroom teachers in a parent training program for families of children with ADHD. Child Fam Behav Ther 2005;27:29–49 | No school-based intervention |
| Crabtree T, Alber-Morgan SR, Konrad M. The effects of self-monitoring of story elements on the reading comprehension of high school seniors with learning disabilities. Educ Treat Child 2010;33:187–203 | Attitude not measured or not reported for intervention |
| Creel C, Fore C, Boon RT, Bender WN. Effects of self-monitoring on classroom preparedness skills of middle school students with attention deficit hyperactivity disorder. Learn Disabil 2006;14:105–13 | Qualitative measure |
| Curtis DF. A cross-cultural comparison between United States and New Zealand teacher acceptability of interventions for children with attention deficit hyperactive disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:394 | Additional papers from included studies |
| Cushman T, LeBlanc M, Porter G. ADHD: results of a national survey of school psychologists. Ethical Hum Psychol Psychiatry 2004;6:183–91 | Attitude not measured or not reported for intervention |
| DeOrio SJ. Factors associated with parental involvement in child’s preschool day treatment program and treatment outcome. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70:700 | Not ADHD focus |
| Dielmann KB. Treatment acceptability and perceived time to implement interventions for children with ADHD moderated by general education teachers’ training in ADHD and disability law, and eligibility for disabling conditions. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:5709 | Specific intervention only |
| Doak JS. The effect of teachers’ beliefs, perceived stress, and student characteristics on teachers’ acceptance of treatment interventions for attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:395 | Additional papers from included studies |
| DosReis S, Butz A, Lipkin PH, Anixt JS, Weiner CL, Chernoff R. Attitudes about stimulant medication for attention-deficit/hyperactivity disorder among African American families in an inner city community. J Behav Health Serv Res 2006;33:423–30 | No school-based intervention |
| DosReis SC. Patterns of psychopharmacologic treatment for attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:3880 | No school-based intervention |
| Dryer R, Kiernan MJ, Tyson GA. The effects of diagnostic labelling on the implicit theories of attention-deficit/hyperactivity disorder held by health professionals. Behav Change 2006;23:177–85 | Participants not school-related |
| Dunne RP. The need for training teachers about childhood psychiatric disorders in rural Pennsylvania. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;69:2226 | Attitude not measured or not reported for intervention |
| Dunson RM, Hughes JN, Jackson TW. Effect of behavioural consultation on student and teacher-behavior. J Sch Psychol 1994;32:247–66 | Attitude not measured or not reported for intervention |
| DuPaul GJ, Kern L, Volpe R, Caskie GI, Sokol N, Arbolino L, et al. Comparison of parent education and functional assessment-based intervention across 24 months for young children with attention deficit hyperactivity disorder. Sch Psychol Rev 2013;42:56–75 | No school-based intervention |
| DuPaul GJ, Ervin RA, Hook CL, McGoey KE. Peer tutoring for children with attention deficit hyperactivity disorder: effects on classroom behavior and academic performance. J Appl Behav Anal 1998;31:579–92 | Specific intervention only |
| DuPaul GJ, Jitendra AK, Volpe RJ, Tresco KE, Lutz JG, Vile Junod RE, et al. Consultation-based academic interventions for children with ADHD: effects on reading and mathematics achievement. J Abnorm Child Psychol 2006; 34:635–48 | Specific intervention only |
| Epstein JN, Willis MG, Conners CK, Johnson DE. Use of a technological prompting device to aid a student with attention deficit hyperactivity disorder to initiate and complete daily tasks: an exploratory study. J Spec Educ Tech 2001;16:19–28 | No school-based intervention |
| Erchul WP, DuPaul GJ, Bennett MS, Grissom PF, Jitendra AK, Tresco KE, et al. A follow-up study of relational processes and consultation outcomes for students with attention deficit hyperactivity disorder. Sch Psychol Rev 2009;38:28–37 | Specific intervention only |
| Ervin RA, DuPaul GJ, Kern L, Friman PC. Classroom-based functional and adjunctive assessments: proactive approaches to intervention selection for adolescents with attention deficit hyperactivity disorder. J Appl Behav Anal 1998;31:65–78 | Specific intervention only |
| Fabiano GA, Pelham WE Jr. Improving the effectiveness of behavioral classroom interventions for attention-deficit/hyperactivity disorder: a case study. J Emot Behav Disord 2003;11:124–30 | Specific intervention only |
| Fabiano GA, Vujnovic RK, Pelham WE, Waschbusch DA, Massetti GM, Pariseau ME, et al. Enhancing the effectiveness of special education programming for children with attention deficit hyperactivity disorder using a daily report card. Sch Psychol Rev 2010;39:219–39 | Specific intervention only |
| Fedewa AL, Erwin HE. Stability balls and students with attention and hyperactivity concerns: implications for on-task and in-seat behavior. Am J Occup Ther 2011;65:393–9 | Specific intervention only |
| Fegert JM, Slawik L, Nubling M, Muhlbacher A. Applying discrete choice experiments in mental health-an example on parents’ preferences in attention deficit hyperactivity disorder (ADHD) treatment. J Child Adolesc Psychopharmacol 2010;20:528 | Could not retrieve full text |
| Fegert JM, Slawik L, Wermelskirchen D, Nubling M, Muhlbacher A. Assessment of parents’ preferences for the treatment of school-age children with ADHD: a discrete choice experiment. Expert Rev 2011;11:245–52 | No school-based intervention |
| Fenstermacher K, Olympia D, Sheridan SM. Effectiveness of a computer-facilitated, interactive social skills training program for boys with attention deficit hyperactivity disorder. Sch Psychol Q 2006;21:197–224 | No school-based intervention |
| Ferrin M, Ruiz-Veguilla M, Blanc-Betes M, Abd SE, Lax-Pericall T, Sinclair M, et al. Evaluation of attitudes towards treatment in adolescents with attention deficit hyperactivity disorder (ADHD). Eur Child Adolesc Psychiatr 2012;21:387–401 | No school-based intervention |
| Fiks AG, Mayne S, Hughes CC, Debartolo E, Behrens C, Guevara JP, et al. Development of an instrument to measure parents’ preferences and goals for the treatment of attention deficit-hyperactivity disorder. Acad Pediatr 2012;12:445–55 | No school-based intervention |
| Fritz GK. Keep your eye on. Brown Univ Child Adolesc Behav Lett 2005;21: 2 | No school-based intervention |
| Fuchs T, Birbaumer N, Lutzenberger W, Gruzelier JH, Kaiser J. Neurofeedback treatment for attention-deficit/hyperactivity disorder in children: a comparison with methylphenidate. Appl Psychophysiol Biofeedback 2003;28 | Attitude not measured or not reported for intervention |
| Furnham A, Sarwar T. Beliefs about attention-deficit hyperactivity disorder. Counsell Psychol Q 2011;24:301–11 | Not ADHD focus |
| Furukawa E, Tripp G, Caparelli-Daquer E, Mattos P. Cross-cultural considerations in conducting research on reinforcement sensitivity and ADHD. Eur Child Adolesc Psychiatr 2010;19:S51 | Not primary research |
| Gage JD, Wilson LJ. Acceptability of attention-deficit/hyperactivity disorder interventions: a comparison of parents. J Attention Disord 2000;4:174–82 | No school-based intervention |
| Gal E, Schreur N, Engel-Yeger B. Inclusion of children with disabilities: teacher’s attitudes and requirements for environmental accommodations. Int J Spec Educ 2010;25:89–99 | No school-based intervention |
| Garrett TE. Psychiatrists’ and psychologists’ attitudes toward the psychosocial and medical models of attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;61:2758 | Participants not school related |
| Germer KA, Kaplan LM, Giroux LN, Markham EH, Ferris GJ, Oakes WP, et al. A function-based intervention to increase a second-grade student’s on-task behavior in a general education classroom. Beyond Behav 2011;20:19–30 | Not ADHD focus |
| Gevensleben H, Holl B, Albrecht B, Vogel C, Schlamp D, Kratz O, et al. Is neurofeedback an efficacious treatment for ADHD? A randomised controlled clinical trial. J Child Psychol Psychiatry 2009;50:780–9 | No school-based intervention |
| Glass CS, Wegar K. Teacher perceptions of the incidence and management of attention deficit hyperactivity disorder. Education 2000;121:412 | No school-based intervention |
| Gomes M, Palmini A, Barbirato F, Rohde LA, Mattos P. Knowledge about attention-deficit hyperactivity disorder in Brazil. J Brasileiro de Psiquiatria 2007;56:94–101 | Foreign Language |
| Graeper KD. ADHD in-service training: an examination of knowledge, efficacy, stress, teaching behavior, and irrational thoughts. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;72:1815 | Attitude not measured or not reported for intervention |
| Graham-Day KJ, Gardner R, III, Hsin Y-W. Increasing on-task behaviors of high school students with attention deficit hyperactivity disorder: Is it enough? Educ Treat Child 2010;33:205–21 | Specific intervention only |
| Grauvogel-MacAleese AN, Wallace MD. Use of peer-mediated intervention in children with attention deficit hyperactivity disorder. J Appl Behav Anal 2010;43:547–51 | Specific intervention only |
| Gude RBS. Effects of collaborative-consultation-training on selected teacher opinions and perceptions regarding referral, intervention and teaching of at-risk students. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56:4324 | Could not retrieve full text |
| Gulley VS. A brief method for evaluating the effects of stimulant medication and behavioral interventions on the classroom performance of children with attention deficit hyperactivity disorder (ADHD). Dissertation Abstracts International: Section B: The Sciences and Engineering 1999;60:1290 | No school-based intervention |
| Gureasko-Moore S, Dupaul GJ, White GP. The effects of self-management in general education classrooms on the organizational skills of adolescents with ADHD. Behav Modif 2006;30:159–83 | Specific intervention only |
| Gureasko-Moore S, DuPaul GJ, White GP. Self-management of classroom preparedness and homework: effects on school functioning of adolescents with attention deficit hyperactivity disorder. Sch Psychol Rev 2007;36:647–64 | Specific intervention only |
| Gureasko-Moore SP. The effects of self-management on organizational skills of adolescents with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;65:1534 | Specific intervention only |
| Habboushe DF, Daniel-Crotty S, Karustis JL, Leff SS, Costigan TE, Goldstein SG, et al. A family-school homework intervention program for children with attention-deficit/hyperactivity disorder. Cogn Behav Pract 2001;8:123–36 | No school-based intervention |
| Hall TF. Early intervention multimodal treatment program for children with attention deficit hyperactivity disorder: an outcome study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3474 | No school-based intervention |
| Hauch Y. A multimodal treatment program for children with ADHD: a 16-month follow-up. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2005;66:1719 | No school-based intervention |
| Havey J, Olson JM, McCormick C, Cates GL. Teachers’ perceptions of the incidence and management of attention-deficit hyperactivity disorder. Appl Neuropsychol 2005;12:120–7 | No school-based intervention |
| Hawkins J. Teacher perceptions, beliefs, and interventions regarding children with attention deficit disorders. Action Teach Educ 1991;13:52–9 | Could not retrieve full text |
| Hill RD, Olympia D, Angelbuer K. A comparison of preference for familial, social and material rewards between hyperactive and non-hyperactive boys. Sch Psychol Int 1991;12:225–9 | No school-based intervention |
| Hoff KE, DuPaul GJ. Reducing disruptive behavior in general education classrooms: the use of self-management strategies. Sch Psychol Rev 1998;27:290–303 | Not ADHD focus |
| Hoff KE, Ervin RA, Friman PC. Refining functional behavioral assessment: analyzing the separate and combined effects of hypothesized controlling variables during ongoing classroom routines. Sch Psychol Rev 2005;34:45–57 | Specific intervention only |
| Hoff KE, Ervin RA. Extending self-management strategies: the use of a classwide approach. Psychol Schools 2013;50:151–64 | Specific intervention only |
| Hukriede J, Miernicki SL. Intervention Types and the Perceptions of Academic Success of Students with Attention Deficit Hyperactivity Disorder (ADHD). Minnesota, MN: University of Wisconsin-River Falls; 2006 | No school-based intervention |
| Isberg E, Kjellman B. Multidisciplinary assessment of children with deficits relating to attention, motor activity and perception: evaluation of the ANSER model. Child Care Health Dev 1999;25:359–76 | Specific intervention only |
| Isler L. Effects of gender on treatment outcome in young children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2008;69:659 | No school-based intervention |
| Jakobsen AN. Using implicit theories about ADHD to understand teacher participation in classroom-based intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2007;68:3398 | Attitude not measured or not reported for intervention |
| Jitendra AK, Edwards LL, Starosta K, Sacks G, Jacobson LA, Choutka CM. Early reading instruction for children with reading difficulties: meeting the needs of diverse learners. J Learn Disabil 2004;37:421–39 | Specific intervention only |
| Johnson WF. Working memory and ADHD: can students with ADHD benefit from being taught strategies? Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:3847 | Specific intervention only |
| Jones KM, Lungaro CJ. Teacher acceptability of functional assessment-derived treatments. J Educ Psychol Consult 2000;11:323–32 | Not ADHD focus |
| Jurbergs N, Palcic J, Kelley ML. School-home notes with and without response cost: increasing attention and academic performance in low-income children with attention-deficit/hyperactivity disorder. Sch Psychol Q 2007;22:358–79 | Qualitative measure |
| Jurbergs N, Palcic JL, Kelley ML. Daily behavior report cards with and without home-based consequences: improving classroom behavior in low income, African American children with ADHD. Child Fam Behav Ther 2010;32:177–95 | Specific intervention only |
| Jurbergs AN. Relative efficacy of school-home notes and teacher feedback in minority elementary students with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:6276 | Specific intervention only |
| Kelley ML, McCain AP. Promoting academic performance in inattentive children. The relative efficacy of school-home notes with and without response cost. Behav Modif 1995;19:357–75 | No school-based intervention |
| Kendrick CP. A quasi-experimental study of the effect of feedback on the social behavior of school children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:2275 | Specific intervention only |
| Kothari J, Morgan S. Multi-agency training programmes for professionals and parents of children with ADHD. Arch Dis Child 2010;95:A97 | Could not retrieve full text |
| Kraemer EE, Davies SC, Arndt KJ, Hunley S. A comparison of the mystery motivator and the get’em on task interventions for off-task behaviors. Psychol Schools 2012;49:163–75 | Not ADHD focus |
| Kraemer ES. Effectiveness of a home-school note procedure for increasing appropriate classroom behaviors exhibited by children diagnosed with attention-deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:3454 | Could not retrieve full text |
| Krain AL, Kendall PC, Power TJ. The role of treatment acceptability in the initiation of treatment for ADHD. J Attention Disord 2005;9:425–34 | No school-based intervention |
| Krain AL. The role of parent and child perceptions of readiness for change, problem severity, and treatment acceptability in the pursuit of treatment for attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;64:3530 | No school-based intervention |
| Lane KL, O’Shaughnessy TE, Lambros KM, Gresham FM, Beebe-Frankenberger ME. The efficacy of phonological awareness training with first-grade students who have behavior problems and reading difficulties. J Emot Behav Disord 2001;9:219–31 | Specific intervention only |
| Langberg JM, Vaughn AJ, Williamson P, Epstein JN, Girio-Herrera E, Becker SP. Refinement of an organizational skills intervention for adolescents with ADHD for implementation by school mental health providers. Sch Ment Health 2011;3:143–55 | Specific intervention only |
| Layne AE. Factors affecting treatment acceptability in the classroom. Dissertation Abstracts International: Section B: The Sciences and Engineering 2002;63:533 | Attitude not measured or not reported for intervention |
| Lorah KS. Effects of peer tutoring on the reading performance and classroom behavior of students with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1208 | Specific intervention only |
| Losapio G. Children with attention-deficit/hyperactivity disorder: treatment methods and parental perceptions. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:7709 | No school-based intervention |
| Mathes MY, Bender WN. The effects of self-monitoring on children with attention-deficit/hyperactivity disorder who are. Remedial Spec Educ 1997;18:121 | Qualitative measure |
| Mathes MY. Effects of self-monitoring on male children with attention deficit hyperactivity disorder who are receiving psychostimulant medication. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;58:0423 | Qualitative measure |
| Mautone JA, DuPaul GJ, Jitendra AK. The effects of computer-assisted instruction on the mathematics performance and classroom behavior of children with ADHD. J Attention Disord 2005;9:301–12 | Specific intervention only |
| Mautone JA, Marshall SA, Sharman J, Eiraldi RB, Jawad AF, Power TJ. Development of a family-school intervention for young children with attention deficit hyperactivity disorder. Sch Psychol Rev 2012;41:447–66 | Attitude not measured or not reported for intervention |
| Mautone JA. The relationship between treatment integrity and treatment acceptability across two consultation models. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:1704 | Specific intervention only |
| McGoey KE, DuPaul GJ. Token reinforcement and response cost procedures: reducing the disruptive behavior of preschool children with attention-deficit/hyperactivity disorder. Sch Psychol Q 2000;15:330–43 | Specific intervention only |
| McGoey KE. Positive reinforcement and response cost procedures: reducing the disruptive behavior of preschool children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 1998;58:6222 | Specific intervention only |
| Merriman DE, Codding RS. The effects of coaching on mathematics homework completion and accuracy of high school students with attention-deficit/hyperactivity disorder. J Behav Educ 2008;17:339–55 | Specific intervention only |
| Meyer K, Kelley ML. Improving homework in adolescents with attention-deficit/hyperactivity disorder: Self vs. parent monitoring of homework behavior and study skills. Child Fam Behav Ther 2007;29:25–42 | No school-based intervention |
| Micou LL. Social evaluations of children with ADHD participating in peer pairing interventions: disconfirming behavior versus peer association. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;64:2419 | Attitude not measured or not reported for intervention |
| Molina BSG, Flory K, Bukstein OG, Greiner AR, Baker JL, Krug V, et al. Feasibility and preliminary efficacy of an after-school program for middle schoolers with ADHD: a randomized trial in a large public middle school. J Attention Disord 2008;12:207–17 | Specific intervention only |
| Morris GE. A survey study of drug and non-drug managements for the hyperactive child: treatment preferences of parents, teachers, special education personnel and physicians. Diss Abstr Int 1986;46:2266 | No school-based intervention |
| Murray DW, Rabiner D, Schulte A, Newitt K. Feasibility and integrity of a parent-teacher consultation intervention for ADHD students. Child Youth Care Forum 2008;37:111–12 | Specific intervention only |
| Niznik ME. An exploratory study of the implementation and teacher outcomes of a program to train elementary educators about ADHD in the schools. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:2899 | Attitude not measured or not reported for intervention |
| Oberthur AP. A Study of Parents’ Perceptions of the Behaviour and Learning of their Children with Attention Deficit Disorder. Brisbane, QLD: University of Queensland; 1996 | Could not retrieve full text |
| Ota KR, DuPaul GJ. Task engagement and mathematics performance in children with attention-deficit hyperactivity disorder: effects of supplemental computer instruction. Sch Psychol Q 2002;17:242–57 | Specific intervention only |
| Owens JS, Richerson L, Beilstein EA, Crane A, Murphy CE, Vancouver JB. School-based mental health programming for children with inattentive and disruptive behavior problems: first-year treatment outcome. J Attention Disord 2005;9:261–74 | Specific intervention only |
| Ozdemir S. The first step to success program: Implementation effectiveness with Turkish children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;67:2115 | Specific intervention only |
| Palacios-Cruz L, de la Pena F, Valderrama A, Patino R, Calle Portugal SP, Ulloa RE. Knowledge and beliefs in Mexican parents about attention deficit hyperactivity disorder (ADHD). Salud Ment 2011;34:149–55 | Foreign Language |
| Peck HL, Kehle TJ, Bray MA, Theodore LA. Yoga as an intervention for children with attention problems. Sch Psychol Rev 2005;34:415–24 | Specific intervention only |
| Pelham Jr WE, Carlson C. Separate and combined effects of methylphenidate and behavior modification on boys with attention. J Consult Clin Psychol 1993;61:506 | No school-based intervention |
| Pelham WE, Gnagy EM, Greiner AR, Hoza B, Hinshaw SP, Swanson JM, et al. Behavioral versus behavioral and pharmacological treatment in ADHD children attending a summer treatment program. J Abnorm Child Psychol 2000;28:507–25 | No school-based intervention |
| Pfiffner LJ, Kaiser NM, Burner C, Zalecki C, Rooney M, Setty P, et al. From clinic to school: translating a collaborative school-home behavioral intervention for ADHD. Sch Ment Health 2011;3:127–42 | Specific intervention only |
| Pfiffner LJ, Mikami AY, Huang-Pollock C, Easterlin B, Zalecki C, McBurnett K. A randomized, controlled trial of integrated home-school behavioral treatment for ADHD, predominantly inattentive type. J Am Acad Child Adolesc Psychiatr 2007;46:1041–50 | Attitude not measured or not reported for intervention |
| Pham AV, Carlson JS, Kosciulek JF. Ethnic differences in parental beliefs of attention-deficit/hyperactivity disorder and treatment. J Attention Disord 2010;13:584–91 | No school-based intervention |
| Piana M. A multi-dimensional intervention for students with attention-deficit/hyperactivity symptomatology and low math performance: targeting motivation and math skill development. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:1542 | Specific intervention only |
| Plumer PJ, Stoner G. The relative effects of classwide peer tutoring and peer coaching on the positive social behaviors of children with ADHD. J Attention Disord 2005;9:290–300 | Qualitative measure |
| Posavac HD, Sheridan SM, Posavac SS. A cueing procedure to control impulsivity in children with attention deficit hyperactivity disorder. Behav Modif 1999;23:234–53 | No school-based intervention |
| Power TJ, Mautone JA, Soffer SL, Clarke AT, Marshall SA, Sharman J, et al. A family-school intervention for children with ADHD: results of a randomized clinical trial. J Consult Clin Psychol 2012;8:611–23 | Specific intervention only |
| Rafferty LA, Arroyo J, Ginnane S, Wilczynski K. Self-monitoring during spelling practice: effects on spelling accuracy and on-task behavior of three students diagnosed with attention deficit hyperactivity disorder. Behav Anal Pract 2011;4:37–45 | Qualitative measure |
| Raggi VL, Chronis-Tuscano A, Fishbein H, Groomes A. Development of a brief, behavioral homework intervention for middle school students with attention-deficit/hyperactivity disorder. Sch Ment Health 2009;1:61–77 | No school-based intervention |
| Raggi VL. Development and preliminary testing of a brief, behavioral intervention to address the homework-related problems of middle school students with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:5789 | No school-based intervention |
| Rapport MD, Murphy A, Bailey JS. The effects of a response cost treatment tactic on hyperactive children. J Sch Psychol 1980;18:98–111 | Attitude not measured or not reported for intervention |
| Rapport MD. A comparison of attentional training utilizing a response cost procedure and methylphenidate (ritalin) on the classroom behaviors of hyperactive children. Diss Abstr Int 1981;42:389 | Attitude not measured or not reported for intervention |
| Resnick A, Reitman D. The use of homework success for a child with attention-deficit/ hyperactivity disorder, predominantly inattentive type. Clin Case Stud 2011;10:23–36 | Specific intervention only |
| Resnick A. How successful is homework success for children with ADHD? Dissertation Abstracts International: Section B: The Sciences and Engineering 2013;74 | No school-based intervention |
| Rich LP. Prompting self-monitoring with assistive technology to increase academic engagement in students with attention-deficit/hyperactivity disorder symptoms. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:3158 | Specific intervention only |
| Ridgway A, Northup J, Pellegrin A, LaRue R, Hightshoe A. Effects of recess on the classroom behavior of children with and without attention-deficit hyperactivity disorder. Sch Psychol Q 2003;18:253–68 | Attitude not measured or not reported for intervention |
| Ridgway A. The effects of a recess or break and stimulant medication on the classroom behavior of children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;65:3693 | No school-based intervention |
| Rodrigo MD, Perera D, Eranga VP, Williams SS, Kuruppuarachchi KA. The knowledge and attitude of primary school teachers in Sri Lanka towards childhood attention deficit hyperactivity disorder. Ceylon Med J 2011;56:51–4 | Attitude not measured or not reported for intervention |
| Rosenberg RP, Beck S. Preferred assessment methods and treatment modalities for hyperactive children among clinical child and school psychologists. J Clin Child Psychol 1986;15:142–7 | No school-based intervention |
| Sams SE. The effects of functional intervention on the behavior of four students labeled ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:1081 | Specific intervention only |
| Schilling DL, Washington K, Billingsley FF, Deitz J. Classroom seating for children with attention deficit hyperactivity disorder: therapy balls versus chairs. Am J Occup Ther 2003;57:534–41 | Qualitative measure |
| Schmitt RCO. The effects of a self-monitoring and video self-modeling intervention to increase on-task behavior for children with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:3758 | Specific intervention only |
| Schnoes CJA. Conjoint behavioral consultation, ADHD, and homework: a combined intervention package for middle school youth with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3461 | Specific intervention only |
| Scope CR. The efficacy of conjoint behavioral consultation to reduce the off-task behavior of elementary school children diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1975 | Specific intervention only |
| Seeley JR, Small JW, Walker HM, Feil EG, Severson HH, Golly AM, et al. Efficacy of the first step to success intervention for students with attention-deficit/hyperactivity disorder. Sch Ment Health 2009;1:37–48 | Specific intervention only |
| Shapiro ES. A Regional Consulting Center To Assist School Personnel in Working with Early Adolescents with Attention Deficit Disorders. Bethlehem, PA: Lehigh University; 1997 | Specific intervention only |
| Sheridan SM, Colton DL, Fenstermacher K, Lasecki K, Wilson K. Efficacy of Conjoint Behavioral Consultation as a Vehicle for Inclusion. Poster presented at the annual meeting of the American Psychological Association. Toronto, August 1996 | Could not retrieve full text |
| Sheridan SM, Eagle JW, Cowan RJ, Mickelson W. The effects of conjoint behavioral consultation results of a 4-year investigation. J Sch Psychol 2001;39:361–85 | Not ADHD focus |
| Sibley MH, Pelham WE, Evans SW, Gnagy EM, Ross JM, Greiner AR. An evaluation of a summer treatment program for adolescents with ADHD. Cogn Behav Pract 2011;18:530–44 | No school-based intervention |
| Sigelman CK, Shorokey JJ. Effects of treatments and their outcomes on peer perceptions of a hyperactive child. J Abnorm Child Psychol 1986;14:397–410 | No school-based intervention |
| Skinner JN, Veerkamp MB, Kamps DM, Andra PR. Teacher and peer participation in functional analysis and intervention for a first grade student with attention deficit hyperactivity disorder. Educ Treat Child 2009;32:243–66 | Specific intervention only |
| Stagg AM. Barriers to Attention-Deficit/Hyperactivity Disorder intervention implementation in the public school setting. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:6467 | Attitude not measured or not reported for intervention |
| Stahr B, Cushing D, Lane K, Fox J. Efficacy of a function-based intervention in decreasing off-task behavior exhibited by a student with ADHD. J Posit Behav Interv 2006;8:201–11 | Specific intervention only |
| Steiner NJ, Sheldrick RC, Gotthelf D, Perrin EC. Computer-based attention training in the schools for children with attention deficit/hyperactivity disorder: a preliminary trial. Clin Pediatr 2011;50:615–22 | Qualitative measure |
| Sterling LA. An investigation of the effectiveness of an assessment-linked study skills intervention on homework completion and accuracy. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;66:2494 | Specific intervention only |
| Stevens L, Van Werkhoven W, Stokking K, Castelijns J, Jager A. Interactive instruction to prevent attention problems in class. Learn Environ Res 2000;3:265–86 | Attitude not measured or not reported for intervention |
| Stevens ML. Effects of classwide peer tutoring on the classroom behavior and academic performance of students with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 1999;59:4487 | Not ADHD focus |
| Stief EA. Parental perceptions of attention-deficit/hyperactivity disorder: etiology, diagnosis, and treatment. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;64:5236 | Attitude not measured or not reported for intervention |
| Stroh J, Frankenberger W, Cornell-Swanson L, Wood C, Pahl S. The use of stimulant medication and behavioral interventions for the treatment of attention deficit hyperactivity disorder: a survey of parents’ knowledge, attitudes, and experiences. J Child Fam Stud 2008;17:385–401 | No school-based intervention |
| Stubbs JH. ADHD in young boys: a correlational study among early childhood educators in Louisiana. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2013;73 | Attitude not measured or not reported for intervention |
| Terenzi CM, Ervin RA, Hoff KE. Classwide self-management of rule following. J Evid Base Pract Sch 2010;11:117–22 | Specific intervention only |
| Teta AR. Increasing homework completion in children with ADHD using the mystery motivator intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:3190 | Specific intervention only |
| Trahant DM. Behavioral improvement in children with ADHD: Independent and combined effects of behavioral treatment and medication. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;65:5384 | Specific intervention only |
| Umbreit J. Functional assessment and intervention in a regular classroom setting for the disruptive behavior of a student with attention deficit hyperactivity disorder. Behav Disord 1995;20:267–78 | Specific intervention only |
| Vilardo BA, DuPaul GJ, Kern L, Hojnoski RL. Cross-age peer coaching: enhancing the peer interactions of children exhibiting symptoms of ADHD. Child Fam Behav Ther 2013;35:63–81 | Specific intervention only |
| Voll CB. The effects of yoga on attention and self-concept in special education preschoolers. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;70:719 | Specific intervention only |
| Walker HM, Seeley JR, Small J, Severson HH, Graham BA, Feil EG, et al. A randomized controlled trail of the first step to success early intervention–demonstration of program efficacy outcomes in a diverse, urban school district. J Emot Behav Disord 2009;17:197–212 | Specific intervention only |
| Warnke MG. Self-monitoring procedures with elementary aged children of color with disruptive behaviors in an urban setting. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2004;64:3958 | Not ADHD focus |
| Whitworth JE, Fossler T, Harbin G. Teachers’ perceptions regarding educational services to students with attention deficit disorder. Rural Educat 1997;19:1–5 | Additional papers from included studies |
| Zentall SS, Javorsky J. Professional development for teachers of students with ADHD and characteristics of ADHD. Behav Disord 2007;32:78–93 | Specific intervention only |
| Zentall SS, Stormont-Spurgin M. Educator preferences of accommodations for students with attention deficit hyperactivity disorder. Teach Educ Spec Educ 1995;18:115–23 | Attitude not measured or not reported for intervention |
Appendix 6 List of Organisation for Economic Co-operation and Development countries
Australia.
Austria.
Belgium.
Canada.
Czech Republic.
Denmark.
Finland.
France.
Germany.
Greece.
Hungary.
Iceland.
Ireland.
Italy.
Japan.
Luxembourg.
Mexico.
Netherlands.
New Zealand.
Norway.
Poland.
Portugal.
Slovak Republic.
Spain.
Sweden.
Switzerland.
The Republic of Korea.
Turkey.
UK.
Appendix 7 Search strategy used for reviews 3 and 4
PsycINFO
Searched 1987 to July week 3 2012.
Search strategy
-
exp attention deficit disorder with hyperactivity/ (10,891)
-
ADHD.ti,ab. (14,541)
-
ADHS.ti,ab. (46)
-
ADDH.ti,ab. (112)
-
attention deficit.ti,ab. (16,407)
-
hyperactiv*.ti,ab. (21,221)
-
(hyper adj1 activ*).ti,ab. (69)
-
(Attention adj3 (problem* or difficult* or disorder* or issue*)).ti,ab. (20,290)
-
hyperk*.ti,ab. (770)
-
minimal brain.ti,ab. (139)
-
inattenti*.ti,ab. (4054)
-
impulsiv*.ti,ab. (11,381)
-
restless*.ti,ab. (2096)
-
overactiv*.ti,ab. (1258)
-
1or/1-14 (42,945)
-
school*.ti,ab. (177,132)
-
college*.ti,ab. (63,398)
-
nurser*.ti,ab. (1623)
-
preschool*.ti,ab. (19,836)
-
kindergarten*.ti,ab. (7536)
-
classroom*.ti,ab. (41,078)
-
elementary.ti,ab. (21,900)
-
education* setting*.ti,ab. (3338)
-
((education* or behavio?r*) adj unit*).ti,ab. (230)
-
education* establishment*.ti,ab. (104)
-
education* system*.ti,ab. (3942)
-
learning environment*.ti,ab. (6879)
-
learning establishment*.ti,ab. (4)
-
teaching environment*.ti,ab. (197)
-
teaching establishment*.ti,ab. (5)
-
teacher*.ti,ab. (82,798)
-
early years.ti,ab. (2037)
-
foundation stage.ti,ab. (68)
-
breakfast club*.ti,ab. (13)
-
holiday club*.ti,ab. (2)
-
pupil*.ti,ab. (8449)
-
student*.ti,ab. (243,861)
-
homework.ti,ab. (2538)
-
learning.ti,ab. (166,980)
-
(learning adj (problem* or difficult* or disab* or disorder*)).ti,ab. (16,675)
-
39 not 40 (150,305)
-
reading.ti,ab. (53,010)
-
writing.ti,ab. (25,424)
-
literacy.ti,ab. (14,165)
-
math*.ti,ab. (28,008)
-
numeracy.ti,ab. (634)
-
or/16-46 (545,332)
-
exp qualitative research/ (3244)
-
recount.ti,ab. (453)
-
recounts.ti,ab. (798)
-
experience.ti,ab. (173,514)
-
experiences.ti,ab. (109,687)
-
understanding.ti,ab. (178,890)
-
interview*.ti,ab. (163,162)
-
narrative*.ti,ab. (30,926)
-
qualitative.ti,ab. (68,320)
-
perceive*.ti,ab. (115,365)
-
perception*.ti,ab. (139,748)
-
(views or view or viewpoint*).ti,ab. (112,964)
-
focus group.ti,ab. (7757)
-
attitude*.ti,ab. (94,221)
-
beliefs.ti,ab. (49,178)
-
feelings.ti,ab. (33,776)
-
(meaning or meanings).ti,ab. (55,922)
-
phenomenon*.ti,ab. (33,877)
-
ethnograph*.ti,ab. (13,739)
-
grounded theory.ti,ab. (7322)
-
hermeneutic*.ti,ab. (3856)
-
(constant adj (comparative or comparison)).ti,ab. (2172)
-
interpret.ti,ab. (10,533)
-
theme*.ti,ab. (52,711)
-
thematic.ti,ab. (7855)
-
discourse.ti,ab. (23,715)
-
((open or unstructured) adj questionnaire*).ti,ab. (94)
-
observation*.ti,ab. (71,090)
-
or/48-75 (940,245)
-
15 and 47 and 76 (4389)
-
limit 77 to animal (68)
-
77 not 78 (4321)
-
limit 79 to yr=“1980 – Current” (4321)
Appendix 8 Qualitative title/abstract screening checklist
| Q1 |
|
Yes or unsure | Go to Q2 |
| No | Exclude Custom 3/5: 0 |
||
| Q2 | Are the population described as having intellectual disabilities/mental retardation (IQ < 70) or brain damage? | No or unsure | Go to Q3 |
| Yes | Exclude Custom 3/5: 0 |
||
| Q3 | Were pupils identified as being with, or at risk of, ADHD by a measured scale, and/or are they described as having core symptoms of ADHD (hyperactivity, impulsivity and/or inattention)? | Yes or unsure | Go to Q4 |
| No | Exclude Custom 3/5: 0 |
||
| Q4 | Are methods:
|
Yes or unsure | Go to Q5 |
| No | Exclude Custom 3/5: 0 |
||
| Q5 | Is the paper written in English? | Yes | Go to Q6 |
| No | Exclude Custom 3/5: 0 |
||
| Q6 | Does the study include primary qualitative data about aspects of non-pharmacological interventions with at least some unique elements delivered in an educational setting? | Yes or unsure | Include as a treatment Custom 3/5: 1 Custom 4/6: treatment |
| NO | Go to Q7 | ||
| Q7 | Does the study include primary qualitative data about the school-related experience of ADHD, and/or school-related attitudes, beliefs and/or meanings about ADHD? | Yes or Unsure | Include Custom 3/5: 1 |
| No | Exclude Custom 3/5: 0 |
Appendix 9 Example of a completed qualitative data extraction form for review 4
Study details286
Authors
Arcia E, Frank R, Sánchez-LaCay A, Fernández MC.
Year published
2000.
Year of research
Pre-1998.
Title
Teacher understanding of ADHD as reflected in attributions and classroom strategies.
Aims
Larger study: to describe maternal understanding of, attitudes about and strategies towards disruptive behaviours (Arcia and Fernandez419). This study: to describe teacher understanding and strategies towards the same disruptive behaviours.
Funders
National Institute of Mental Health (U01 MH 50447) and the Leon Lowenstein Centre for the Study, Prevention and Treatment of Disruptive Behavior Disorders.
Research participant details
-
Participant group: primary teachers.
-
Original sample size: 21 teachers.
-
Dropouts: 0.
-
Range of ages: not reported.
-
% female: 81%.
-
Ethnicity: 14 Anglo-American; 7 Latino.
-
Years’ experience teaching (if teachers): not reported.
-
SEN education/experience (if teachers): all teachers had at least one pupil with ADHD symptoms.
-
Year taught during study (if teachers): kindergarten (n = 3), first grade (n = 3), second grade (n = 2), third grade (n = 6), fourth grade (n = 5), sixth grade (n = 1), SEN teacher (n = 1).
-
Comorbidities (if ADHD youth): not applicable.
-
% of ADHD youth on medication (if ADHD youth): not applicable.
-
Diagnosis (if ADHD youth): not applicable.
-
Measure/s of diagnoses (ADHD and at risk of ADHD): not applicable.
-
Diagnosis rated by: not applicable.
School information
-
Region: central North Carolina; Miami, Florida, New York.
-
Type of region (urban/rural): not reported.
-
Country: USA.
-
Type of school: primary.
-
Number of schools: not reported.
-
Deprivation index/% receiving free school meals: not reported.
-
Range of ages of children with ADHD: 5–11 years.
-
Number of children with ADHD: 21.
-
% female of children with ADHD: not reported.
-
Ethnicity of children with ADHD: not reported – Latina mothers.
-
Comorbidities: 2 also LD.
-
% of ADHD children on medication: 14% (3 of 21).
-
Diagnosis (diagnosed, at risk, core symptoms): nine pupils were formally diagnosed with ADHD; four were being assessed and were diagnosed by the end of the study; eight had ADHD symptoms but were not diagnosed by the end of the study. Of these eight, six received t-scores above 64 on the Hyperactivity Index or on the Daydreaming scale of the Conners’ Teacher Rating Scales.
Other population notes
-
Intervention description: not applicable.
Study design details
Data collection method
-
Completed Conners’ Teacher’s Rating Scale (CTRS-39; Conners420) on the target child in their classroom.
-
Telephone interview following a semistructured protocol. General questions were asked first with specific questions asked in a conversational style where necessary.
The interview questions covered:
-
class/grade taught
-
description of target child’s behaviour and assessment of the way and extent to which the behaviour interfered with learning, completion of schoolwork, and classroom functioning
-
description of any support services received by the child
-
attributions regarding the child’s behaviour
-
strategies used by the teacher to manage the child
-
nature and frequency of, and satisfaction with, parent–teacher communications
-
identification of other school or community resources that had been used to support the child
-
teacher’s opinion of strategies and resources that would help the child
-
any particular need with regard to working with Latino children exhibiting behaviour problems.
Description of recruitment
Teachers were mailed a letter describing the study, what was being asked of them to do, and that the child’s parents had given consent.
Sampling
All 24 teachers who taught the children of the Latino mothers in the Arcia and Fernandez419 study were invited to take part.
Analytic approach
Transcribed narratives were coded and analysed according with standard practice for qualitative data (Miles and Huberman315).
Researcher/reflexivity
None.
Ethical procedures
Permission for recording of telephone interview, anonymity of teacher gender.
Description of analysis process
Transcribed narratives were coded and analysed in accordance with standard practice for qualitative data (Miles and Huberman315). Passages in the transcripts were coded according to the topic areas listed above and according to subtopics such as references to medication.
Folio Views (1994; Folio Corporation, Provo, UT) was used to create and manage a database of transcribed interviews. This software program indexes all text and allows for multiple coding and labelling of data.
The first author extracted all segments that addressed the interview topics. The subsequent 49 pages of single-spaced, small-font text were reviewed by all authors, who independently reported their preliminary conclusions and interpretations. These observations were compared with the extracted segments, and the database was queried again for emergent themes. For instance, one of the observations from the first round of analysis was that teachers seldom characterised the children as having ADHD. This finding was confirmed by searching the database for the term ADHD and for other similar terms to determine whether or not the terms were used as label or characterisations. The first and second authors then conducted further confirmatory analyses using matrices to identify patterns and to count the frequency of specific responses.
Theoretical underpinning (of research) identified by the authors
None.
How is this used?
Notes.
Limitations of study as identified by authors
Small number of participants makes it difficult to establish applicability to elementary school teachers in general; teachers did not describe strategies exhaustively; the validity of the strategy implementation and effectiveness could not be verified.
Limitations of study as identified by review team
Little reflexivity. Theoretical/ideological stance and impact on study not addressed by authors.
Few quotes so difficult to evaluate data–findings relationship.
Findings
Key themes
The teachers’ report of things that might ‘really help the child’ was consistent with the environmental (poor parenting) attributions. According to teachers, the children would benefit most from a stable home environment; more reading and less television; a male role-model; family counselling; more discipline at home; extra attention; and active parental involvement in teaching and homework. School-related suggestions were much less frequent and consisted of (more) English classes; small group instruction; one-to-one instruction; and boosting the child’s self-esteem by ensuring success with easy academic tasks. Three teachers, who had initially associated the children’s behaviour with ADHD or with hyperactivity, suggested medication. One of these was the special education teacher. Two teachers suggested vision and/or speech and hearing tests. Strikingly, only the special education teacher suggested the continuation of a structured, behaviourally-based, educational setting such as the one in which the child was currently placed.
Reported techniques for classroom management
The teachers had numerous techniques for managing their students’ behaviour. These could be grouped loosely into the following four categories: behavioural, instructional, environmental, and interpersonal. Techniques were classified as behavioural if they appeared to be aimed at increasing the occurrence of a behaviour (i.e. rewards – happy faces, stickers, praise, ‘telling him when he is doing well’), if they appeared to be intended to decrease a behaviour (i.e. punishment – name on board, ignoring, sending a note home, sending the child to the office or home, losing a privilege such as recess, staying after school, and demonstrating disapproval), or if a management strategy such as a token economy was employed. Sixteen teachers described using at least one behavioural technique. However, it was evident that teacher did not have a clear understanding of the principles on which these techniques were based. With the exception of the special education teacher, who had a token economy with class-wide and individual behavioural targets, none of the other teachers had a fully coherent or systematic strategy. Regular education teachers did not appear cognisant of the feasibility of using a token economy to target-specific behaviours of children with ADHD.
Five teachers reported using token economies. These were generally referred to as ‘point systems’ possibly because, as one teacher pointed out, she did not use tokens. The economies tended to have long or random intervals and to reinforce behaviours that were not clearly specified. In these and other ways, economies were often implemented in manners that could be expected to diminish their effectiveness. For example, one teacher collected all individually-earned points at the end of the week and redistributed them evenly across all the children in the classroom. Another teacher, in an attempt to boost the child’s self-esteem, provided rewards even when the criterion level of behaviour was approached but not achieved. Still, another teacher became unable to deliver a child’s reward because of a change in schedule. In reporting the events, this teacher was puzzled as to why the child’s behavior had deteriorated. Thus, the general lack of mention of token economies, the lack of individualised target behaviours, and the often faulty implementation indicated that teachers did not have a sufficiently in-depth understanding of behavioural principles that would allow them to use token economies most effectively for the typical child with ADHD.
Ten teachers mentioned use of rewards outside the context of token economy and eight teachers mentioned techniques that clearly fell under the subcategory of punishment. However, none of the teachers used the term ‘punishment’. Teachers used techniques to reduce the frequency of undesirable behaviours but were unaware of these as punishment. Indeed, one teacher was careful to point out that punishment was unwarranted for non-volitional rule breaking. Perhaps owing to a lack of understanding of behavioural principles or stemming from a desire not to appear to use punishments, rewards and punishments were sometimes confused. For example, one teacher kept the target child after school as a consequence for failing to complete his schoolwork, but hastened to add that the student enjoyed the individiualised attention that this provided. Other opportunities for behavioural management were overlooked. For example, many parents were informed of the children’s behaviours in parent–teacher conferences or in notes sent home with the child, but these were not tied to an integral school–home plan of rewards and punishment designed to improve the child’s behaviour.
Instructional techniques were reported by 12 teachers as strategies for managing the target student’s classroom functioning. These strategies included one-to-one instruction, peer tutoring, a decrease in workload to accommodate the child’s ability and extra instruction after school or during the teacher’s free periods.
Environmental techniques were similarly popular. Of these, preferential seating was the technique most frequently cited (n = 8). Children with behaviour problems were seated close to the teacher or with a well-behaved, high-achieving child (often a girl). This latter technique had the advantage of also increasing one-to-one instruction because the high-achieving child sometimes served as a peer tutor. However, structure, like punishment, was perceived negatively. One teacher, who by all accounts had made great strides with her student, hastened to add, ‘I’m really not like a drill sergeant, kind of thing, but I feel like you have to have . . . [structure] . . . with so many kids in that room . . . We have a great time in my room, but my thing is too that there is a time and place for everything’. This teacher’s tone was very apologetic.
Five teachers used techniques that, for lack of a better label, were designated as ‘interpersonal’. These teachers talked with the children to convince them or pressure them into behaving appropriately. Also, one teacher included information on ADHD and a child-oriented film about it in her curriculum.
Generally, teachers described using multiple techniques across several categories. Regardless of the category of the techniques used, teachers did seem to have a strong preference for those techniques which do not demand a great deal of their time – thus, the frequent mention of interventions such as preferential seating, writing children’s names on the board and using peer tutors. However, it was obvious that teachers did not have a plan of action for students with disruptive and/or inattentive behaviour. As one teacher said in response to the feedback letter that commented on the numerous techniques used by teachers, ‘We do have numerous strategies, but not because all of us are very well-informed sometimes, you know. There’s just things that you see and you make your own judgment and you say, well, this child needs this, they need that, that type of thing’. Other teachers echoed the sentiment that they approach problems in a case-by-case, trial-and-error approach. It is unfortunate that the provision of a label or diagnosis of ADHD did not seem to suggest to teachers a comprehensive strategy.
Salient by their absence were school- or community-based resources for teacher support. Aside from sending a disruptive child to another classroom or to the office, only a couple of teachers reported management strategies that involved other school personnel. In one case, a teacher rewarded the target child by allowing him to clean cafeteria tables with the school custodian. Whether or not teachers are as unsupported as their reports suggest, teachers felt notably isolated in meeting challenges:
But you know, you’re also caught between a rock and a hard place, because you can’t say to a mother – although you can try to start channelling it by having an evaluation – that ‘I think your child has to be tested or evaluated, because his or her behaviour is not regular’. I mean, how do you say to a mother ‘Something’s wrong with your kid?’
Key concepts
Techniques adopted for behaviour management: behavioural, instructional, environmental and interpersonal approaches (only three teachers suggested medication).
Strong preference for techniques that did not demand a great deal of their time.
No comprehensive strategies.
From ‘Conclusions and Implications’:
Teachers’ understanding of the condition, and of classroom management options, is very limited.
p. 98286
. . . the teachers in this study used a wide range of techniques . . . However, the techniques they employed . . . did not represent a comprehensive plan of action . . . Thus, teachers were not well prepared to meet the demands they faced – demands that they met frequently with little institutional support.
p. 98286
Teachers are not sufficiently well versed in the behavioural principles needed to design and implement an effective behavioural intervention. This ability, although it cannot guarantee normalisation of the behaviour of children with ADHD, is critical to successful classroom functioning and to maximise student achievement irrespective of children’s diagnostic status or teachers’ causal attributions.
Interventions to increase the rate of appropriate behaviour require identifying and quantifying target behaviours, determining appropriate reinforcers, and delivering these reinforcers at sufficiently brief intervals for them to be effective. Given typical class sizes and the diverse types of need common in most classrooms, teachers need support to design and implement such interventions in a reliable and consistent manner.
The teachers demonstrated a negative attitude towards structure, punishment and labelling.
The teachers’ negative attitude towards punishment was not a deterrent to this use, because according to teacher reports, they employed numerous techniques intended to decrease the rate of inappropriate behaviour. These techniques appeared to have been compromised in effectiveness by the teachers’ lack of information about their appropriate use.
Relevant quotes
Most quotes in the paper are short and express category names rather than revealing information about the attitudes of the speaker, for example ‘point systems’ given as the term teachers use for token economies, ‘telling him when he is doing well’ categorised as a behaviour technique. Longer quotes include:
I’m really not like a drill sergeant, kind of thing, but I feel like you have to have . . . [structure] . . . with so many kids in that room . . . We have a great time in my room, but my thing is too that there is a time and place for everything.
We do have numerous strategies, but not because all of us are very well-informed sometimes, you know. There’s just things that you see and you make your own judgment and you say, well, this child needs this, they need that, that type of thing.
You’re also caught between a rock and a hard place, because you can’t say to a mother . . . that ‘I think your child has to be tested or evaluated . . . ’ I mean, how do you say to a mother ‘Something’s wrong with your kid’?
This last quote was not discussed by the authors but quoted in isolation at the end of the findings section.
Quality appraisal (adapted from Wallace et al.267)
-
Is the research question clear? Y N CT
-
Is the theoretical or ideological perspective of the author (or funder) explicit? Y N CT
-
Has this influenced the study design, methods or research findings? Y N CT
-
Is the study design appropriate to answer the question? Y N CT
-
Is the context or setting adequately described? Y N CT
-
Is the sample adequate to explore the range of subjects and settings, and has it been drawn from an appropriate population? Y N CT
-
Was the data collection adequately described? Y N CT
-
Was data collection rigorously conducted to ensure confidence in the findings? Y N CT
-
Was there evidence that the data analysis was rigorously conducted to ensure confidence in the findings? Y N CT
-
Are the findings substantiated by the data? Y N CT
-
Has consideration been given to any limitations of the methods or data that may have affected the results? Y N CT
-
Do any claims to generalisability follow logically and theoretically from the data? Y N CT
-
Have ethical issues been addressed and confidentiality respected? Y N CT
-
Is/are the author/s reflexive? Y N CT
-
Are the interventions of interest clearly described? Y N N/A
Appendix 10 Example of a completed qualitative data extraction form for review 3
Study details288
Authors
Bos CS, Nahmias ML, Urban MA.
Year published
1997.
Title
Implementing interactive professional development in a workshop course on educating students with AD/HD.
Year of research
1993–4.
Aims
Explored the use of a workshop course on educating students with AD/HD that incorporated features of interactive professional development. Describing the effects of such workshops not only on educators’ knowledge attitudes and perceived competence, but also on what aspects they deemed as valuable for their professional growth.
Funders
US Department of Education, Office of Special Education Programs to University of Arizona.
Research participant details
-
Participant group: educators: teachers, teaching assistants, principals, counsellors, university students.
-
Focus perspective: teacher evaluation of teacher training intervention.
-
Original sample size: 89.
-
Dropouts: 0.
-
Range of ages: 18 aged 21–30 years; 34 aged 31–40 years; 31 aged 41–50 years; 6 aged ≥ 50 years.
-
% female: 95.5%.
-
Ethnicity: not reported.
-
Years’ experience teaching (if teachers): not reported.
-
SEN education/experience (if teachers): students taught with ADHD, teacher training on ADHD, in-services and TV programmes figures reported, table 2. 288
-
Year taught during study (if teachers): 71, kindergarten to fifth grade; 12, sixth grade to eighth grade; 1, ninth grade to twelfth grade; 5, postsecondary.
-
Comorbidities (if ADHD youth): not applicable.
-
% of ADHD youth on medication (if ADHD youth): not applicable.
-
Diagnosis (if ADHD youth): not applicable.
-
Measure/s of diagnoses (ADHD and at risk of ADHD): not applicable.
-
Diagnosis rated by: not applicable.
School information
-
Region: not reported.
-
Type of region (urban/rural): not reported.
-
Country: USA (assumed).
-
Type of school: not reported.
-
Number of schools: not reported.
-
Deprivation index/% receiving free school meals: not reported.
Intervention description
Recruitment
Number of participants approached for intervention: 89.
Number of participants meeting eligibility criteria: not applicable, voluntary.
Number of participants who consented to participate: 89.
Number of participants there is qualitative data for: 89 + 19 interviewed.
Number of dropouts: 0.
Reason for dropout: 0.
Setting
Location of intervention (school, home, multi): not reported.
Type of setting (school): not reported.
Type of setting (class): general and special education.
Type of school (public, etc.): not reported.
Treatment
Active ingredients intervention described (yes/no): yes.
Control group active ingredients described (yes/no): not applicable.
Number of treatment conditions: 1.
Treatment group 1 label: interactive professional development workshop course.
Intervention treatment group 1 description
The workshop course was developed and implemented using interactive professional development. Topics for the workshop were developed to include those identified by national organisations and respected experts, and by participants in a needs survey conducted prior to the workshop.
The workshop was designed with an interactive format and incorporated presentations, discussions, videotapes and group activities. To interweave personal knowledge including attitudes and perceived competence with external knowledge, special emphasis was placed on interactive discussions and activities based on authentic learning experiences. Group activities, such as creating posters of classroom accommodations and teaching strategies for students at various grade levels, provided opportunities for participants to interact, collaborate and construct knowledge. The workshop also incorporated guest presenters followed by interactive discussions to provide ways for teachers to explore their beliefs and construct knowledge. Guest presenters included a behavioural paediatrician on the medical and neurobiological aspects of AD/HD and the use of medication, a psychologist/psychiatrist on multidisciplinary assessment, a parent of a school-age student with AD/HD, an individual with AD/HD or a videotape of a student with AD/HD and a behaviour and educational specialist who taught students with AD/HD. During the workshop, participants wrote reflective journals and after the workshop completed action plans and other assignments, allowing time to reflect on and integrate new knowledge into their teaching plans.
The workshop course included 20 hours of instruction over 5 days with participants completing assignments for the course 1–3 weeks after completion of the workshop. The instructor was available during this time as requested. The participants had the option of taking the workshop course for one university credit.
Content outline for workshop course with time allocations
1 hour: overview of AD/HD.
1 hour: definition of AD/HD.
2 hours: characteristics of students with AD/HD.
30 minutes: historical trends and background of AD/HD.
2 hours: aetiology/medical aspects of AD/HD.
1.5 hours: laws and legal aspects of AD/HD, public laws, roles and responsibilities of school personnel.
2 hours: multidisciplinary assessment and identification.
8 hours: multimodal interventions for students with AD/HD:
3 hours educational
1 hours behavioural
2 hours medical
1 hours: psychological.
2 hours: communication and collaboration:
1 hour: parents
30 minutes: professionals
30 minutes: students.
Intervention treatment: theoretical underpinning intervention
Need for professional dialogues that allow for the examination of external knowledge and personal knowledge, and the interaction and synthesis of both knowledge bases. Interactive professional development allows both opportunities to discuss personal experiences and learning new knowledge and strategies for teaching.
Teachers’ attitudes and knowledge both influence classroom practices, which in turn influence students’ successes at school. The perceived relationship between beliefs and actions is interactive in that beliefs are thought to drive actions; however, experiences and reflection on actions may lead to changes in and additions to beliefs (reciprocal relationship between beliefs and actions).
Treatment
Type of intervention (categorical): teacher training.
Delivery
Intervention target group: teachers and other educators.
Was training to deliver intervention received: not reported.
Where school components delivered: not applicable.
When delivered: summer.
Who delivered: instructor, not specified.
Recipient population: educators: teachers, teaching assistants, principals, counsellors, university students.
Grouping: one group of 47 in 1993, 42 in 1994.
Number facilitators: not reported.
Intervention period: 20 hours of instruction over 5 days.
Contacts spaced: daily.
Number of sessions: 5.
Total dosage: 20 hours.
Intervention attendance: not reported.
Incentives: one university credit.
Intervention manual used: not reported.
Fidelity measured: no.
Tailored: no.
Study design details
-
Data collection method: qualitative measures – reflective journal, workshop course evaluation questionnaires (open-ended questions), semistructured interview.
-
Description of recruitment: voluntarily participated.
-
Sampling: self-selected.
-
Analytic approach: category and theme analysis.
Researcher/reflexivity
Not reported.
Ethical procedures
Not reported.
Description of analysis process
For the open-ended evaluation questions and journals, a sample of entries were read by two reviewers, who developed categories. Next, the text of the journals and the responses to the evaluation questions were coded for categories by two independent reviewers and inconsistencies in coding were resolved. The data in the categories of ‘attitudes and beliefs about AD/HD’ and ‘attitudes and beliefs about the workshop course’ were used in this study.
The interviews were analysed using category and theme analysis. First, a sample of interviews were read by three independent reviewers and categories were developed. Next, each interview was coded for categories by two independent reviewers and a reliability level for categories of 0.85 was established. Interview summaries by categories were generated to facilitate macro-analysis and the emergence of themes. Themes were aggregated across participants using constant comparative procedures. Data from the workshop evaluations, reflective journals and interviews were triangulated for emerging themes or trends across the data sources.
Theoretical underpinning (of research) identified by the authors
Not reported, see above for intervention theory.
How is this used?
Not applicable.
Notes
Limitations of study as identified by authors
The current study is limited in that it did not directly address the question of change in classroom practice.
Limitations of study as identified by review team
Positivist description of analytical processing, with independent raters. No mention of ethics.
Findings
Key themes
-
Importance of knowledge related to the neurobiological/medical aspects of ADHD including presumed aetiology, role of medications as part of therapeutic interventions, and teachers’ roles in monitoring medication effects in school.
-
Importance of understanding ADHD from parents’ and students’ perspectives and importance of working collaboratively with parents’ and students’.
-
Relevance of knowledge about educational and behavioural strategies for accommodating students in the classroom.
-
More positive attitudes and perceived competence in working with students with ADHD because of increased knowledge.
-
Value of interactive format including the balance of presentations with discussions, group activities and opportunities for reflection and application.
Some of the most valuable information discussed during the workshops was practical, neurobiological and medical knowledge about ADHD: ‘Just knowing about ADD and knowing that this child can’t necessarily control his behaviour has made all the difference in the way I see and interact with him in class. I’m more compassionate and have more ways to help this child since the class [intervention]’.
About the second theme, participants consistently expressed the importance of their new knowledge and understanding of school and home challenges for parents and students with ADHD and the importance of home–school collaboration. One of the classroom teachers recounted:
The workshop reminded me that I do need to communicate with parents. But it seems like a lot of the interactions I have seen [with a student with ADHD whom the teacher will have next year] are kind of negative or nonexistent. I want to make sure that when I talk to her parents, it’s in a way that is not that she’s in trouble and then they’ll go home and take it out on her. I’ve learned we need to do a very delicate job and some education.
Similarly, another teacher reported on her greater appreciation of home-school collaboration.
The third theme that emerged was the relevance of the information on effective teaching strategies. Participants consistently reported on the value of acquiring new knowledge about strategies for educational and behavioural accommodations for students with ADHD. One teacher stated that, ‘I think that my knowledge is 20 times better than in the past’ and that ‘it is very useful to have a bigger bag of tricks’. Several teachers noted that the strategies were in many cases ‘just good teaching strategies that would help all learners in my class’. In the interviews, teachers consistently reported incorporating the strategies into their teaching practices. For example, a classroom teacher noted, ‘I now break things down into segments, use colour-coding, and make things visual’. Another teacher noted, ‘Not only did I learn a lot of new strategies, I have integrated them into my teaching’.
The fourth theme that emerged from the data was increased perceived competence and more positive attitudes because of new knowledge. These outcomes were often coupled with a greater tolerance and empathy for students with ADHD. Another classroom teacher noted that ‘it’s been a real eye opening experience. I can now deal with the kids that I suspect have some attention deficit problems a lot more successfully than I did in the past’. Another teacher indicated, ‘Before class [intervention], having students with ADHD meant trouble, but the class has increased my understanding, changed my attitude, and improved my tolerance and patience’. Both general and special education teachers spoke of how they redesigned their classrooms, daily schedules and methods of instruction based on what they learned. For example, one teacher commented during the interview, ‘I learned that I need to be more clear in my instructions and expectations. This is something that I’ve improved on this year and continue to work on’. The same teacher also spoke of how she had changed the classroom environment for one student with ADHD, ‘I’ve seated him in a place relatively free from distractions and away from traffic. I reduced what was up on the walls.’ One special education teacher noted, ‘this year I am more creative and patient because I have a better handle on what to do with ADD students with or without hyperactivity’.
The same teacher noted:
I have changed my approach toward tasks. Now I give students choices when they work on a given task. I used to think that was giving too much slack. It’s new for me this year to realise the importance of just offering them a different colour [pen or pencil] . . . I don’t think I realised how for some kids that might be really helpful.
One difference in the perceived competence for classroom teachers and special education teachers was the role that some of the special education teachers envisioned for this new competence and knowledge. Although classroom teachers generally spoke of their competence in relation to change in classroom practice and student outcomes, several special education teachers also envisioned sharing this competence and knowledge with others. For example, during her interview, one resource teacher stated that ‘the workshop change my attitude towards kids with ADHD and gave me confidence to help my colleagues’. Similarly, another special education teacher indicated, ‘I went to the workshop and it encouraged me . . . a couple of times at lunch when teachers have been expressing distress over a student, I’d say, “Do you know what might be going on here?” It’s a time to teach’.
The fifth theme focused on the interactive nature of the workshop course with its balance among presentation of knowledge, interactive discussions and activities, and opportunities for teacher integration of personal knowledge and external knowledge. With regard to external knowledge, a number of educators spoke or wrote about the style of the medical presentation. For example, one counsellor commented on the ‘clarity of the explanation for the neurobiological basis for ADHD and the visuals that stand out in my mind’. They also commented on the importance of the discussions, knowledge sharing, collaboration and reflection for their learning. For example, one classroom teacher commented, ‘the workshop was most helpful because of the variety of experiences: brainstorming ideas, videos, and all the information that was shared’. Another teacher noted, ‘I appreciated the opportunities to discuss ideas with other teachers about kids and strategies’.
These interactive activities were intended to provide participants with opportunities to integrate their personal experiences with new knowledge. For example, after a presentation on characteristics and symptoms followed by an activity where participants developed large charts of ADHD characteristics and their affects on various aspects of a student’s life, a classroom teacher wrote in her journal, ‘it’s amazing how diverse the symptoms are. I keep thinking of kids I’ve had who fit the mould perfectly in one way or another’.
Key concepts
Self-report information from the interviews conducted near the end of the following school year suggest that teachers retained their knowledge and positive attitudes towards educating students with ADHD.
The interview data would suggest that teachers perceived themselves as more knowledgeable and competent in assisting ADHD students in the classroom.
Participants valued the information on the neurobiological and medical aspects of ADHD. In contrast to information on teaching strategies, this content focused on the underlying bases for ADHD. Participants’ comments indicated that this information assisted them in dealing with their misconceptions about the nature, existence and impact of ADHD on students. Teachers’ regard for this information suggests one explanation for their increased positive attitudes toward educating students with ADHD. It also addresses the importance of including information about the underlying bases of a disability, particularly when the disability has a controversial history as in the case of ADHD. 5
Relevant quotes
Just knowing about ADD and knowing that this child can’t necessarily control his behavior made all the difference in the way I see and interact with him in class.
p. 140288
The workshop changed my attitude towards kids with ADHD and gave me confidence to help my colleagues.
p. 141288
Before class [workshop], having students with ADHD meant trouble, but the class has increased my understanding, changed my attitude, and improved my tolerance and patience.
p. 141288
I appreciated the opportunities to discuss ideas with other teachers about kids and strategies.
p. 142288
I think that my knowledge is 20 times better than in the past . . . it is very useful to have a bigger bag of tricks.
p. 141288
It’s amazing how diverse the symptoms are.
p. 142288
Quality appraisal (adapted from Wallace et al.267)
-
Is the research question clear? Y N CT
-
Is the theoretical or ideological perspective of the author (or funder) explicit? Y N CT
-
Has this influenced the study design, methods or research findings? Y N CT
-
Is the study design appropriate to answer the question? Y N CT
-
Is the context or setting adequately described? Y N CT
-
Is the sample adequate to explore the range of subjects and settings, and has it been drawn from an appropriate population? Y N CT
-
Was the data collection adequately described? Y N CT
-
Was data collection rigorously conducted to ensure confidence in the findings? Y N CT
-
Was there evidence that the data analysis was rigorously conducted to ensure confidence in the findings? Y N CT
-
Are the findings substantiated by the data? Y N CT
-
Has consideration been given to any limitations of the methods or data that may have affected the results? Y N CT
-
Do any claims to generalisability follow logically and theoretically from the data? Y N CT
-
Have ethical issues been addressed and confidentiality respected? Y N CT
-
Is/are the author/s reflexive? Y N CT
-
Are the interventions of interest clearly described? Y N CT
Appendix 11 Stakeholder involvement activities
Stakeholder involvement has been an important aspect of this project, from planning stages through to analysis stages and dissemination, with examples including:
-
parent and teacher views were sought at the outset of this project to assist in refining the project aims in order to make them salient to the families of children with ADHD
-
co-applicants and expert advisory board members included parents and teachers
-
the mother of four children diagnosed with ADHD commented on the monograph at draft stage
-
we conducted three events involving parents, practitioners and researchers
-
we disseminated study findings to parents and practitioners through collaboration with a third-sector organisation
-
we have plans for further dissemination to student teachers
-
we have plans for writing lay literature in order to disseminate research findings to parents and practitioners through collaboration with a third-sector organisation.
The aim of stakeholder involvement is to work in collaboration with stakeholders in order to tailor the relevance of the reviews and their dissemination to parents, teachers, schools and policy-makers. In addition to the co-applicants and expert advisory board members, we recruited several other regional parents and practitioners with whom we engaged (including 10 parents and five practitioners). Over the course of the project we conducted a number of stakeholder involvement events that included not only dissemination but also feedback from those who attended, which informed the research process. These included:
June 2012: event 1 – a workshop for parents, practitioners and researchers; this included exploration of views for stakeholders who were unable to attend.
May 2013: event 2 – a seminar for behavioural support advisory teachers.
May 2013: event 3 – a seminar for parents of children or young people diagnosed with ASDs and/or ADHD.
We also attended or will attend events with the purpose to disseminate research findings to parents and practitioners. The following are events that have been completed or are planned; however, we are likely to take up additional opportunities that arise for dissemination:
September 2013: day-long seminar held by a third-sector organisation; a mother of a son diagnosed with ADHD began the day by describing her experiences, and then DM and RGJ disseminated project findings; the day ended with a discussion session. This seminar was oversubscribed, and attended by parents and practitioners and policy-makers in psychology and education.
February 2014: two workshops involving 60 student teachers held by a local university. An hour-long session to be given about the experiences of ADHD in schools for pupils, parents and teachers, where findings from the project will be disseminated.
Following submission: in collaboration with a third-sector organisation, leaflets in lay language describing findings from the review will be written for distribution to parents and practitioners.
The events described above, where stakeholders contributed knowledge and experience, are detailed further to describe stakeholder contributions. During event 1 we explored the experiences of stakeholders to inform our knowledge of interventions for ADHD in schools and the kinds of outcomes that stakeholders thought were important. This contributed to the conceptual framework regarding interventions and outcomes developed in review 1 (for more information see the next section). During event 2 we disseminated interim results from reviews 1, 3 and 4 to behavioural support advisory teachers (for more detailed information see Event 2). During event 3, we disseminated interim results about parent experiences and perceptions from review 4 to parents of children and young people diagnosed with ASDs and/or ADHD. We asked them to comment on the relevancy of our findings. Overall, stakeholders recognised and supported these findings (for more information see Event 3).
Event 1
A central part of our planned patient/public involvement included a workshop involving members of the wider project group, school practitioners and parents of children with ADHD. This workshop was held on 11 June 2012 with 16 attendees. The purpose of event 1 was to share information about the aims of the project and to explore stakeholder knowledge and experience about non-pharmacological interventions and child outcomes in schools.
The agenda for this meeting included a presentation giving a broad overview of the project and two small group-based discussions. Discussion one sought to identify and discuss psychosocial (non-drug) interventions that are used to treat children with ADHD in school settings, whereas discussion two sought to identify and discuss outcomes that may be used to assess the effectiveness of such interventions. Notes were made during each discussion and fed back to the wider group. Feedback sessions were minuted and a summary of the workshop content was sent to attendees (including those unable to attend) asking for additional feedback. The group discussions and additional feedback led to the identification of over 40 named interventions and over 40 outcomes that could be used to evaluate the effectiveness of interventions. These intervention and outcome categories provided a starting point from which to begin the synthesis of outcomes and interventions in reviews 1 and 3. Other important issues were raised that warranted attention in the discussion of our study findings (including the role of context and the usefulness/relevance of outcomes used to assess effectiveness; liaison between home and school; and tension between managing behaviour and attainment, with different stakeholders perhaps having different priorities).
Summary of feedback from event 1
MR and DM presented on the background to the project and methods, then two discussions were held (a summary of their content is detailed below, together with e-mail feedback from those unable to attend the workshop in person).
Discussion 1
Groups were organised by participants’ backgrounds: academics, practitioners and parents.
Participants identified and discussed (non-drug) interventions that have been used to treat children with ADHD in school settings.
Feedback
Over 40 interventions were named and have been categorised into nine groups:
1. Whole school initiatives:
-
Nurture groups.
-
Forest School.
-
Social and emotional aspects of learning.
-
Sherborne movement.
-
Thrive.
-
Incredible Years.
-
Waves 1–3 intervention (provision mapping).
-
Stepping Stones (inclusion).
2. Additional support:
-
Private tutor.
-
One-to-one support, teaching assistant.
-
Extra time for exams, exams in separate room.
-
Summer schools.
-
Breakfast club, after-school club.
-
ADHD champion.
3. Accommodations:
-
Place 2 be.
-
Smaller classes.
-
Indoor pass.
-
Weighted jacket.
-
Stress toy.
-
Vibration pads.
-
Voice recognition software.
-
Break time activities.
4. Behaviour management:
-
Time out.
-
Behavioural book.
-
Praise, rewards, reward charts, token economies.
5. Parent support applied to classroom:
-
123 Magic.
6. Social interventions:
-
Social skills groups.
-
Social stories.
-
The Incredible 5-Point Scale.
-
Peer tutoring, coaching.
-
Circle of friends.
7. Self-regulation:
-
Computerised attention training.
-
Neurofeedback.
-
Biofeedback.
8. Alternative treatments:
-
Massage.
-
Meditation.
9. Miscellaneous:
-
Training for teachers.
-
Physical activity.
Other points raised
-
Home–school liaison was considered very important to intervention effectiveness (e.g. what is done at school should complement what is done at home and vice versa).
-
Training for teachers is often a prerequisite for many interventions, although some participants noted that psychoeducational interventions aimed at teachers can also be effective (e.g. improving awareness leads to better classroom management and child outcomes).
-
It was highlighted that interventions that are used in schools locally rarely focus on ADHD; often universal interventions that target the whole school or class are preferred.
-
It was noted that interventions are rarely used in isolation. Multimodal, that is, combination of interventions (e.g. parental + specific classroom strategies are usually implemented).
-
A potential tension between managing behaviour and attainment was highlighted, with different stakeholders perhaps having different priorities.
Discussion 2
Two mixed groups identified and discussed outcomes that may be used to assess the effectiveness of interventions that are used to treat children with ADHD in school settings.
Feedback
Over 40 outcomes, primarily related to children with ADHD, were named and have been categorised into 10 groups:
1. Symptoms:
-
Attention.
-
Impulsivity.
-
Hyperactivity.
2. School outcomes:
-
Attainment, learning.
-
Attitude, engagement.
-
Exam preparedness.
-
Exclusion.
-
Detentions.
-
Attendance.
3. Scholastic behaviours:
-
Focus.
-
Disruptiveness.
-
On-taskness, concentration.
-
Task completion.
-
Reduction in ‘out of seat’ behaviour.
4. Social functioning/relationships:
-
Social relationships, friends, intimate relationships.
-
Relationships with adults and peers.
-
Effect on peers, parents, siblings.
-
Family functioning.
-
Reduced stigmatism.
-
Increased communication with and between teacher and families.
-
Co-operation.
5. Intrapersonal:
-
Self-efficacy.
-
Self-esteem.
-
Self-awareness (especially of how ADHD affects others).
-
Confidence.
6. Emotional functioning:
-
Enjoyment/happiness at school.
-
Depression.
-
Patience.
-
Empathy.
7. Behavioural issues:
-
Risk.
-
Antisocial.
-
Crime.
-
Bullying: bully and victim.
-
Aggression.
8. General functioning:
-
Quality of life (Danckaerts et al. 421).
-
Personal and life skills.
-
Activities, hobbies.
-
Creativeness.
9. Health behaviours:
-
Smoking.
-
Alcohol.
-
Drug use.
10. Miscellaneous:
-
Driving (less school related).
Other issues raised
-
It was suggested that differences between cultures, schools, classes, teachers and students (e.g. age) means that context plays a key role in the effectiveness of interventions and the usefulness/relevance of outcomes used to assess effectiveness (e.g. many European countries have children start school later than the UK). Practitioners mentioned how exclusion rates vary considerably in local schools. We need to assess variables that may impact the effectiveness of interventions.
-
It was suggested that it would be useful to report how frequently different types of outcomes are reported, for example are some outcomes reported more often than others?
-
It was suggested to consider the potential conflict regarding the importance of various outcomes to different stakeholders (e.g. parents, practitioners and students).
-
The difficulty of using RCTs in schools was discussed.
-
It was suggested that the qualitative reviews could consider the difficulty in overcoming labels (e.g. ‘naughty boy’).
-
The following sources of potentially useful information were identified: The Sutton Trust, Children and Adults with Attention-Deficit/Hyperactivity Disorder and Attention Deficit Disorder Information and Support Service (grey literature here).
-
It was suggested that we make contact with the Chief Inspector of Schools and Department of Education early to discuss dissemination activities.
-
The following key authors were mentioned: Dopfner, Merrell, Tymms, Spence, Pelham, Meichenbaum and Coghill.
E-mail response by members of the expert advisory panel about the workshop summary of discussions included the following comments:
A wide range of sound interventions are mentioned, but as is often the case (in my view), there is not enough emphasis on pedagogy, and perhaps too much emphasis on pupil management. This is a pity, given that the school is a major site for the expression of ADHD, and one of the most useful ways of thinking about ADHD, from an educational viewpoint, is as reflecting psychological and behavioural differences, rather than a disorder to be in some way corrected. One of the striking things about ADHD is the way in which the diagnostic criteria (both APA [American Psychiatric Association] and WHO [World Health Organization]) can be seen to carry a subtext which depicts the classroom as a place where teachers lecture to passive students. However, when schools and teachers adopt approaches to teaching and learning which are flexible and student centered many of the problems associated with ADHD are rendered far less problematic than they are in the rigid teacher-centered approaches which are still too prevalent. In some cases, ADHD-type symptoms may even prove an educational asset (e.g. the tendency non sequential thinking can be reframed as a tendency to lateral thinking – cf Edward DeBono’s ideas about creative thinking).
It is good to see nurture groups in the list, because nurture groups (at their best) reflect many key features of an ADHD-friendly pedagogy, including:
-
an emphasis on the emotional underpinnings of learning and the need for emotional security as a prerequisite for effective educational engagement (this involves the explicit application of insights from attachment theory in many nurture groups)
-
a holistic curriculum, taking in social–emotional aspects of learning alongside the formal curriculum (e.g. National Curriculum) (i.e. staff and students often spend all of their time together during the nurture group day, including mealtimes, with minimal distinctions being drawn between ‘work’ and ‘play’, the view being that all experiences are learning experiences)
-
a constructivist approach to learning which takes as its starting point the student’s developmental characteristics and then scaffolds an individualised learning programme from this
-
provision of a wide range of opportunities for different forms of educational engagement (e.g. active/kinesthetic as well as reflective/abstract approaches) and encouragement for students to employ their preferred learning modes
-
small group setting (usually 10-12 students) with two adults who are able to engage with individuals, as well model positive interpersonal behaviours through their interactions with one another
-
regular and detailed consultation between nurture group staff and parents, enabling careful monitoring of progress and the sharing of information pertinent to the child’s functioning at home and school; sharing of strategies for supporting the child at home and school.
The reason why this is worth highlighting is the fact that there is a small but growing evidence base to support the efficacy of nurture groups for children and young people with a wide range of emotional and behavioural disorders, including those with ADHD-type symptoms. Furthermore, there is a growing interest in the so-called ‘nurturing school’, which adopts nurture group approaches and strategies and employs them throughout the school. In fact, one of the interesting findings from research has been the whole-school effect of nurture groups, whereby significant improvements in social–emotional and behavioural functioning have been detected in not only students attending the nurture groups but also students not attending nurture groups.
A related issue is strategies adopted by schools to address ‘recess deprivation’. AD Pellegrini has been a major figure in research in this area. His work has shown that behaviours associated with ADHD can be exacerbated and even induced by an overemphasis on sedentary behaviour in classrooms. There is strong evidence to show that the use of frequent short breaks for physical activity significantly reduce hyperactivity and increase productive educational engagement.
These examples highlight an important educational maxim: sometimes we have to change the child to fit the school, but more often we need to change the school to accommodate the child. The important thing is that we need to be aware of which one of these things we are doing and why. Management strategies of the type listed tend to be of the former type, whereas approaches such as nurture groups and recess deprivation strategies are more of the latter type. Of course, in practice it is often the case that we want to combine the two. Unfortunately, there is a tendency to neglect the latter and concentrate on the former.
__________________________________________________________________________________________
Thanks for this. It was good to meet you when I came down and to have the opportunity to discuss this project. We are keen to support dissemination activity. Look forward to hearing from you in September.
__________________________________________________________________________________________
Thanks for this very interesting summary and the outcomes from it about interventions and outcomes. This is a very broad approach to interventions and you note some of the important points about the complexity involved. I have little to add at this point except one point. I am not sure why you put.
Exclusion:
Detentions:
Attendance:
Under academic outcomes. They seem to be school behaviours (amended above).
Event 2
On 21 May 2013, MR, DM and RGJ gave a seminar to a group of approximately 20 behavioural support advisory teachers organised through one of the project’s practitioner co-applicants. The seminar was structured so that each researcher disseminated interim findings from the review they had led, and then, following the presentation, practitioners worked in small groups to contribute information about their experiences relevant to that review. The worksheet given to teachers is shown in Figure 10. In this way the researchers spoke in turn about reviews 1, 3 and 4. In relation to review 1, we asked teachers what moderators they considered to be important in the implementation of interventions. In relation to review 3 we explored teachers’ perceptions of the model representing experience of interventions for ADHD in schools, the relative importance of pupil engagement and achievement, issues related to withdrawing pupils for interventions from the classroom, and barriers to interventions that address relationships and attitudes. In relation to review 4 we asked stakeholders about their experiences of teacher attributions for ADHD, relationships with parents, and teacher knowledge of ADHD. With reference to the two qualitative reviews, reviews 3 and 4, we explored the extent to which our findings were recognisable by practitioners in order to establish levels of transferability. Transferability refers to the judgements made by those outside research about how relevant findings are to their own practice (see Chapter 5, Applicability and Chapter 6, Applicability). The practitioners confirmed the relevance of the interim themes of the reviews, in recognising the issues, confirming many as important, and being able to offer commentary and critique. This supported the transferability of the interim findings of reviews 3 and 4 with that group of teachers.
FIGURE 10.
Discussion worksheet for event 2.


Feedback from teachers
Review 1
What affects the success or failure of an intervention?
-
Environmental factors (more than one mention): sleep; food; water (basic needs); time of day; class size.
-
Individual factors: other issues – emotional human needs; child’s understanding of intervention; mood; differing behaviours from children with ADHD; differences over time; hundreds of differences.
-
Relationships (adult and child): family break-up; bullying; change; bereavement loss; separation, etc.
-
Context: gender; norms in classroom; socioeconomic; attitude/belief everyone needs to be on board; perception regarding intervention; transfer back to classroom; transition after; teacher involvement; ownership and understanding key (if feel cut off don’t deliver).
-
Consistency of intervention delivery, is it being implemented as planned?
-
Wording regarding success/failure: look for good things and you find them; look for the bad and you find them.
Review 3
(1) Does the model capture the experience of intervention use?
Yes.
(2) Tension between perceived impact on outcomes like engagement and lack of impact on achievement:
-
Agreed, teachers may favour achievement.
-
Differences between enjoyment and achievement, may need more time to measure achievement (× 2).
-
Difficulty measuring attainment.
-
Parents more interested if child is happy, included gets on with others, communicates, not so much about what level at.
-
Attainment as measured can miss things that are important: social, behavioural. These might impact academic attainment.
-
Teachers responsible for attainment, blight on their record if child doesn’t meet requirements.
(3) Are issues with withdrawal programmes presented fair?
Yes.
-
Social and emotional impact of withdrawal recognised. Low expectations for SEN group, ADHD may be high achievers.
-
Conflict between when children are out and back in classroom context.
-
Transferable skills needed.
-
Transferable context needed small group to large group (need to scaffold return).
-
Primary National Strategy (UK) Waves model all (whole school) > small group > 1 : 1 less issues with withdrawal.
-
Problem with withdrawal: teacher has no responsibility, despite any improvements, nothing changes in the classroom.
(4) What are some barriers to recommendations of targeting relationships and attitudes as well as specific skills and symptoms?
-
Lack understanding ADHD.
-
Teachers have perception that ADHD children are low achievement – not necessarily accurate.
-
Differing practice – consistency.
-
Age, choice of intervention differs with age.
-
The only person we can change is ourselves – suggests increased responsibility needed.
Review 4
(1) Do you recognise these issues?
Attributions for ADHD symptoms: themes mentioned as being recognised –classroom, family, environmental, individual/medical/within-child.
Comments: in response to attributions to the classroom – get everybody out of the classroom more often. More time outside (forest school, beach school).
Interactions with parents
-
Blame teachers–parents recognised, school and home views often differ.
-
Teachers resistant to admitting it is hard. Protecting selves.
-
Belief that problem with the child, not with the teacher.
-
Family members with ADHD has an impact attitude, preconceptions, view of school.
-
Parents used to Child and Adolescent Mental Health Services so often have more knowledge.
Knowledge of attention-deficit/hyperactivity disorder
-
Networks and peer support for teachers, reflecting on experience important, teachers supported by mentoring and coaching.
-
Teachers valuing learning communities rather than inset – less about knowledge of ADHD, more about the individual child, confidence, hear other experience.
-
Knowledge of individual critical, as well as general knowledge gap.
-
Need whole school inclusive approach, not in isolation.
-
Issues regarding wrong diagnosis, lack understanding. Overdiagnosed, looking for a label.
-
Cross-cultural differences.
Lack awareness of child development, treat as if ADHD child can choose, can talk about feelings.
Are there any issues related to these themes that are not addressed and if so what are they?
-
Resources placed early years, preventive, parenting issues.
-
Need more emphasis on being outside – forest school, etc.
-
Increased testing gives stress for children with ADHD.
Event 3
On 23 May 2013, RGJ gave a seminar during a parent support group coffee morning to a group of approximately 25 parents of children and young people diagnosed with ASDs and/or ADHD. From responses during the talk, it was determined that parents of children diagnosed with ADHD were in the minority. The researcher asked parents to comment freely, but to specify the diagnosis of their child on their response sheets. Only comments related specifically to ADHD are detailed below.
The seminar was structured so that interim findings from review 4 relevant to parent experiences were disseminated, and then, following the presentation, parents working in small groups contributed responses about their own experiences in relation to these findings. We described the theme ‘mothers are silenced’, and deferential and assertive forms of resistance from reviewed studies. Parents did not necessarily use the conceptual terminology of researcher second-order concepts, but the experiences they described were mostly commensurate with those from review 4. Overall, this event supported the transferability of findings from review 4 to this group of parents.
| Theme/quote | Comments from seven parents, denoted A–F |
|---|---|
| Attempts to refute criticism through assertive action | [F]tick Assertiveness was misinterpreted by overly defensive staff as ‘aggression’ |
| Lack of co-operation | [F]tick The expression of concerns often causes an unwarranted over-reaction by school and over-defensiveness and as a result energies used attacking the compliant, RATHER than listening and using constructive criticism to adapt/change current practice ☹ |
| Bringing in the big guns | |
| Taking issues to a higher authority | [B]tick Questioning official letters etc and passing details up the system to get action [F]tick Just experienced ‘closing ranks’ within LEA and Dept of Education and a Head now INTENT on defaming my character as a result of my legitimate concerns being expressed ☹ Has lead to my emotional mental health being affected (depression diagnosis) and treatment ongoing after original complaint nearly 2 yrs ago [F] Also let down by school Governors who acknowledged Head’s inappropriate behaviour, but failed to anything to improve things (ie policy). Head=control freak and Governors unsure of their ‘power’ to bring change ☹ (closing ranks) |
| Refusing to play | [A] WARNING: home education offers no county support (written by LA practitioner) [E] I wanted to remove my children, THEY REFUSED to be home educated |
| Attempts to refute criticism while remaining deferential/compliant to teachers | [F] can still be respectful of staff, even though may not necessarily agree with every decision |
| Strategic diffidence | |
| Presentation of the family as normal | |
| Bearing witness | |
| Taking on professional workloads | [F] When school lacks understanding, you end up keyworking your own child literally |
| Policy work and advocacy | [D] I know I am my child’s strongest advocate and I am constantly texting my [social?] and keyworkers information. Get very frustrated at meetings at lack of help and services. Meetings do not solve things [F] Frustrating when schools don’t acknowledge their legislated responsibilities and often don’t make any effort to accept parents’ pointing out schools’ legal responsibilities |
| Issues not addressed | [A] Key worker co-ordination to help to facilitate all the help that is available and how it can be disseminated and/or collated and then used usefully for the child with needs |
| [A] Communication is key to all of it | |
| [D] I have asked for extra help/medication intervention but not offered in this area or too expensive | |
| [E] Lack of available services & waiting lists | |
| [D] School was a main trigger for my child | |
| Additional quotes | [B] ADHD traits ignored and considered irrelevant by some teachers |
| [B] my child was diagnosed with Asperger’s and ADHD. Positive experience with SENCO @ school – open relationship and clear communication line – been able to copy him in for all communications and has backed up our arguments if things not happening | |
| [C] My daughter is undiagnosed but suspected ADHD. She has had 2 teachers that have taken extra time and effort to inform her educational and behaviours in early years (Yrs 1/2/3) that gave my daughter a good foundation on behaviour and attainment in class. The school uses a “thermometer” system for behaviour where the child’s name is moved up the thermometer if behaviour is challenging – the child then loses time off “discover time” at the end of the week if they have been up the thermometer. This was effective for my daughter as she disliked the fact her name was moved up this and also that her peers could see this. However when my daughter moved into YR4 the teacher did not “person centre” her education to get my daughter to perform in class. Now she is in YR5 and due to the teaching style she received in YR4 is really struggling in all aspects of education | |
| [D] ADHD/AS child. After diagnosis the only option is medication. There doesn’t seem to be any alternative help alongside like social skills, behaviour/anger management Star Charts DO NOT WORK! Late diagnosis. ADHD behaviour becomes learnt behaviour by that time. Ends up with diagnosis around same time as puberty Media needs educating |
|
| [F] Aspergers and diagnosis as ADD traits (not hyperactive). 13.5 yr old boy, now YR8 (may 2013) Because my son generally conformed with the school routine and we had the ‘volcano effect’ the minute he walked out of school, a Headteacher (at statutory annual review) said “What I’m wondering is, why you are getting this behaviour at home, but it’s not evident at school” . . . a CLEAR criticism of my parenting and implication of parenting issues. Luckily the TA and YR 5 teacher (YR 5 teacher was amazing, Y2&6 was the problem) butted in and spoke in my defence about this behaviour being ‘normal’ in ASD kids In YR6 I spoke with the (very knowledgeable) TA about my son not being fully engaged by the teacher and asked would it be helpful to offer the teacher a book that includes “tips for teachers”. She said yes, a good idea . . . I was labelled as undermining and pushy and it was taken as an insult and NOT an attempt to help and share information for the benefit of the child. Still feel bullied 2 yrs on by the Head for my criticism of management for not enough training opportunities for staff. Even the (relatively young and inexperienced) SENCo became overly defensive and was critical of my attempts to share good practice ideas, for my son’s benefit |
|
| Quotes ‘ticked’ | |
| ‘You brief the teacher. Boom, boom, boom. Nothing happens’ | [B] tick [F]tick Worse than that . . . you get labelled as “pushy” and “undermining staff” (by YR6 staff) |
| ‘The teacher we had was excellent... She has continued to have interest in attention deficit...’ | [B]tick (note: ‘Good Senco!’) |
| ‘... dashed expectations... not as a result of the children’s performance but as a result of the school’s performance’ | [D]tick (note: ‘schools need more training’) [F]tick And Heads understanding and apparent lack of importance put on ASD staff training, even SENCOs (Primary not Secondary, they are VERY impressive) |
| ‘I went to the school and said, ‘You have a professional development day coming up ... I will pay the fee of having Dr P come to your school ... they refused...’ | [D]tick (note: ‘more specialised help for ADHD kids in school – not colouring & chart management. Always put on parenting courses as a treatment) |
| ‘Even when a child’s diagnosed with ADD ... you’re always told then ‘Oh well it’s bad parenting’... | [D]tick (note: ‘still seen as bad parenting incl. by teachers) |
Conclusion
Service user/public involvement has been an important aspect of this project, with input from parents and teachers providing direction for research practice in event 1, assessment of interim research findings in events 2 and 3, and feedback about findings through draft manuscript comments from a parent of children diagnosed with ADHD in the final stages of the project. These activities supported the relevance of the research project to stakeholders, and parents and teachers contributed to the robustness of qualitative reviews through assessment of transferability of interim findings, when they endorsed the findings to be in keeping with their experiences. These inputs have provided a valuable ‘reality check’ which has demonstrated the pertinence and quality of the project.
Appendix 12 Example of a structured summary for review 4c
Structured summaries of papers that explore parent perspectives: seven papers, six studies.
| Information | Papers | |||
|---|---|---|---|---|
| Carpenter and Austin262 | Hibbitts276 | Malacrida266 | Malacrida28 | |
| Authors, date, country, participants and setting (ages, how ADHD is identified, medication, school context, any other relevant information) | This is an Australian study with mothers of children diagnosed or with core symptoms of ADHD (number of participants not reported; 12 women quoted) Most of the children attended schools in Queensland, QLD |
Hibbitts276 is a Canadian EdD thesis. It is an auto-narrative of the experience of mothering three children with SEN, one of whom is diagnosed with ADHD at 26 months and receives medication which does not help, so is discontinued. The son with ADHD is followed from ages 5–18 years, over which time he attends six schools in Northern Ontario, Newfoundland, Northern BC and Lower Mainland Canada | Malacrida266 reports part of a Canadian PhD thesis (same study as Malacrida28). The study is cross-cultural, carried out in Alberta, Canada and south-east England with 34 (17 from each country) mothers of children aged 5–18 years who had been diagnosed with ADHD. Some children were medicated but numbers were not reported | Malacrida28 reports part of a Canadian PhD thesis (same study as Malacrida266). The study is cross-cultural, carried out in Alberta, Canada and south-east England with 34 (17 from each country) mothers of children aged 5–18 years who had been diagnosed with ADHD. Some children were medicated but numbers were not reported |
| Study aims/research questions | The authors examine mother’s perceptions of the role of schools in the decision-making process leading to diagnosis and medication | The over-riding research question of this thesis is ‘what is the experience of a parent when interacting with her children’s schools?’ | The author describes the aim of the study, ‘I sought to understand what it is like, within two different cultural contexts, to be a mother confronting multiple “helping” professionals while dealing with this highly controversial diagnosis’ | The author described the aim of the study, ‘this essay examines maternal narratives in order to understand the different ways that these mothers perceive educators’ roles in the medicalisation of their children’s behavior’ |
| Theoretical underpinnings and relevance to the study | Epistemology: constructionist; post structural Theory used to structure the study: Butler’s362 and Fraser’s364,366 work on the concept of recognition ADHD beliefs: the authors approach ADHD primarily from a sociological standpoint, where disorderly behaviour is constructed and recognised through structures of education following Graham368 |
Epistemology: constructionist ADHD beliefs: the author’s focus in the thesis is on her relationship with the school; the focus is not on ADHD per se, rather her middle child is diagnosed with it. She describes ADHD medically, as something he ‘has’, and not something influenced by relationships or his environment. They try medication but do not find any that is useful, so they take him off it Though she does not explicitly state this, she seems to see his behaviour as internally driven and that he doesn’t have clear control over it. She describes a doctor’s advice of ‘accept him and make the best of your lives’ and this seems to be her approach |
Epistemology: constructionist; post structural Theory used to structure the study: the author uses Foucauldian notions of knowledge, power and resistance to inform the study ADHD beliefs: the author’s stance on ADHD is about its contested nature – she cites authors who question the diagnosis (Conrad and Schneider;422 Kiger;44 Armstrong;423 Castel et al.;424 Porter;371 Slee425) rather than describing its definition and theories of cognitive deficit as is common. Her focus seems to be on sociological construction |
Epistemology: constructionist; post structural Theory used to structure the study: the author draws on theory about medicalisation (Porter371) where trends for less tolerance of difference and greater psychiatric surveillance with medicalisation of society; where increasingly narrow ideas of normality mean behaviours that encompass most children one way or another, when extreme, are seen as abnormal ADHD beliefs: Malacrida28 applies the above theory to ADHD. She again discusses its contested nature – she cites the same authors who question the diagnosis (Conrad and Schneider;422 Kiger;44 Armstrong;423 Castel et al.;424 Porter;371 Slee425) and also those who champion it (CHADD;426 Chisholm427) |
| Data collection process | The authors draw on transcripts of interviews and focus groups with mothers | The author made a list of 48 incidences (vignettes) in which she could remember interacting with her children’s schools. She then wrote on vignette per free evening from October 2005 to January 2006. These were complete for almost 3 years before the author wrote the rest of the thesis | The author conducted semistructured interviews with each participant, lasting ≥ 45 minutes. She ‘asked mothers to tell me not only about how they felt their lives to be scrutinized and constrained by professional discursive practice, but also to tell me of the ways they struggled to be heard, to effect change, and to resist stigmatization’. Thus, the author’s stance about ADHD structured her research questions | The author conducted semistructured interviews with each participant, lasting ≥ 45 minutes. ‘ . . . mothers were asked to describe interactions with educators, with medical or psy sector professionals, with family and social networks and their encounters with ADD/ADHD-related discourse, as a way to examine the intersections of the personal and the social when dealing with disability’ |
| Data analysis process | The authors do not describe their process of analysis beyond citing the theoretical underpinnings of their approach (as described above) | The author carried out hermeneutic phenomenology following van Manen.369 Her process of analysis involved phenomenological bracketing, selective reading and detailed reading in order to identify themes. These she compared with literature about the parent–school interface in order to validate or discard/develop them. She involved outsiders in the autonarrative to provide feedback | Analysis of the data was both inductive and deductive. In the initial data coding, inductive narrative analysis was used, starting with reflexive immersion in the mothers’ narratives and the eventual crystallisation of themes emerging from the data (Miller and Crabtree372). In addition to this approach, the data were considered deductively against theoretical insights on medicalisation and social control | Analysis of the data was both inductive and deductive. In the initial data coding, inductive narrative analysis was used, starting with reflexive immersion in the mothers’ narratives and the eventual crystallisation of themes emerging from the data (Miller and Crabtree372). In addition to this approach, the data were considered deductively against theoretical insights on medicalisation and social control |
| Findings (key themes/concepts) | The authors discuss findings but not structured through themes; they discuss:
|
Themes identified:
|
Themes identified:
|
Themes identified:
|
| Margalit et al.359 | Reid et al.360 | Watson356 | ||
| Authors, date, country, participants and setting (ages, how ADHD is identified, medication, school context, any other relevant information) | Margalit et al.359 is a study using data collected from a US internet site; its participants, 316 mothers of children diagnosed with LD (n = 148), LD and ADHD (n = 124) and ADHD (n = 44) (mean age of children 10.99 years; SD 3.32 years) therefore come from a range of States, localities (urban, suburban, rural) and ethnicities. The sample was drawn from a population of 1308 people posting 42,811 messages on the website during a 12-month period (June 2005–6). Participants were those identified to have professionally diagnosed children | Reid et al.360 is a US study with 20 parents (18 mothers, 2 fathers; 17 white, 2 Native American, 1 African American) of 22 children (males aged 5–18 years; 90% on medication; six also with LD and/or behavioural disorders) diagnosed with ADHD. The children attended schools in urban, suburban and rural areas of Mid-Western States | Watson356 is a UK narrative case study from a mother’s perspective, following a boy eventually diagnosed with ADHD from upper primary school to secondary school. He tries medication but it is withdrawn | |
| Study aims/research questions | The authors write, ‘The current study aimed at identifying stressors, needs, supports and perceptions expressed by mothers of children with learning disabilities and ADHD through their messages on an Internet discussion board’ | Research question: ‘how do parents perceive the process they have gone through in obtaining services for their children with ADHD?’ | The author writes, ‘This paper concerns the experiences of Jenny, a parent with a son diagnosed as having attention-deficit/hyperactivity disorder (ADHD). It explores Jenny’s narrative concerning the events surrounding the diagnosis, in particular the part played by the school in this process’ | |
| Theoretical underpinnings and relevance to the study | Epistemology: the authors do not explicitly address the theoretical underpinnings of the study. From the literature review, discussion of a ‘true self’, reporting of inter-rater reliability and lack of reflexivity their beliefs are likely to be objectivist Theory used to structure the study: the authors draw on psychological and sociological literature on well-being and social support The authors do not problematise the construct of ADHD; presumably they hold medical/individual beliefs of cognitive impairment, or biopsychosocial beliefs |
Epistemology: the authors do not explicitly address theoretical underpinnings. Their aims are pragmatic; they wanted to explore and describe the perceptions of parents of children with ADHD about their experiences with the school system, particularly in order to establish what kind of treatment, if any, ADHD children were receiving in schools. They chose an interpretive approach in order to establish contextual information and to consider process as well as outcomes. The lead author has conducted surveys with teachers to explore practice with ADHD children. These factors suggest objectivist views ADHD beliefs: the authors treat ADHD as an established phenomenon as shown by their discussion of teachers’ responses to it, so if teachers do not ‘believe’ in it, they are coded as having misconceptions or lack of knowledge. This suggests views of ADHD as individual/medical cognitive deficit, or biopsychosocial views |
Epistemology: constructionism; post structuralism Theory used to structure the study: theories related to stigma, including Hinshaw374 (stereotyping, prejudice and discrimination; internalisation of degradation). Goffman’s322 ‘courtesy stigma’ – stigma acquired by virtue of a connection with the stigmatised person Theory related to ‘mother blame’, where mental disturbances in a child are directly linked to faulty parenting [read mothering] (Hinshaw374) View of ADHD: the author cites Singh’s428 comment ‘The important question . . . is not about the reality of ADHD; rather it has to do with the desire for ADHD diagnosis’, thus the author sidesteps this issue. However, the case study is couched in terms of the construction of ADHD by the school, which suggests sociological beliefs |
|
| Data collection process | Participants wrote 1502 messages; between 1 and 69 each. The messages were copied and pasted into Word for analysis | The authors carried out one semistructured interview lasting 20–40 minutes with each participant. Two semistructured protocols were used; the first was used with 15 participants; after preliminary analysis the protocol was then revised to focus more narrowly on school services, and five more interviews were completed. Each participant also completed a short questionnaire gathering demographic data and information on the child, diagnosis, school and SEN services | A former colleague shared with the author that she was so troubled by her son’s experiences at school that she had written about them. This manuscript acted as the data for this study | |
| Data analysis process | The authors describe their process of analysis as, ‘ . . . content analysis was conducted to search for expressions of stress in the online messages. Using qualitative approaches that have previously been used to study the narratives on the internet (Fleischmann373) three of the researchers read all messages from the first 30 (alphabetically) participants. In a case analysis meeting (Miles and Huberman315) among three of the researchers, lengthy discussions yielded three codes/themes, content domains: specific content/subject matter contained in messages; communication styles/structures: general structure–kind of information contained in messages; and parent perceptions–understandings: perceptions/views/understanding of self, child, and school. Several subcodes were added as discussions continued, and general themes were refined. In order to determine inter-rater reliability, the three researchers read and coded the first 30 participants’ messages as to the presence of one or more of the above three master codes. Inter-rater reliability was 0.97’ | The authors followed grounded theory analysis procedures (Strauss and Corbin429). They completed open coding for three interviews; codes were grouped in 17 preliminary categories, then these were reapplied to the three interviews. They then began axial coding. Existing and additional codes were developed with the next 12 interviews, with use of relational and variational sampling in choice of participant to broaden understanding. The second interview protocol was based on analysis to this point. It was designed to gain insight on major transition points (i.e. diagnosis). Finally, a core category was developed with a tentative conceptual model about that category. The authors carried out member and professional checking | The author analysed the manuscript, ‘selecting scenes that were concerned with the positioning of the Goldfish family by various external agencies, since it is in and through this material positioning that deviance is constructed’. She fictionalised parts using satire (Bronowski and Mazlish;375 Knight430), following Barone378 and Clough379 as a means to ‘raise significant questions’ and ‘speak to the heart of social consciousness’ | |
| Findings (key themes/concepts) | Themes identified:
|
Themes identified:
|
Headings within the narrative:
|
|
Appendix 13 Example of concept map (review 4a)
Appendix 14 Studies excluded at full text from review 3, with reasons
| Aberson BD. An intervention for improving executive functioning and social/emotional adjustment of ADHD children: three single case design studies. Dissertation Abstracts International: Section B: The Sciences and Engineering 1997;57:6553 | Lacking qualitative data and/or analysis |
| Allen T. Attention deficit hyperactive disorder . . . a teacher’s perspective. Educ Today 2005;2:12–13 | First person account |
| Al-Sharbati M, Al-Sharbati Z, Al-Lawatiya S, Al-Jahwari S. Teachers’ awareness about attention deficit hyperactivity disorder (ADHD) in Oman. Asian J Psychiatr 2012;5:277–8 | Lacking qualitative data and/or analysis |
| Anonymous. AD/AD: two parents tell their personal stories. Emot Behav Difficult 1997;2:25–9 | First person account |
| Artesani AJ, Mallar L. Positive behavior supports in general education settings: combining person-centered planning and functional analysis. Interv Sch Clin 1998;34:33–8 | Lacking qualitative data and/or analysis |
| Askew BL. Practices of Special Education Teachers for Dealing with Students with ADD/ADHD. Chicago, IL: St Xavier University; 1993 | Could not retrieve |
| Baba C, Tanaka-Matsumi J. Positive behavior support for a child with inattentive behavior in a Japanese regular classroom. J Posit Behav Interv 2011;13:250–3 | Not primary research |
| Bailey S, Thomson P. Routine (dis)order in an infant school. Ethnography Educ 2009;4:211–27 | Lacking qualitative data and/or analysis |
| Bailey S. Disordered experiences – beyond myth/reality. Br Educ Res J 2008;34:135–41 | Not focused on school-age students with ADHD |
| Bain SK, Brown KS, Jordan KR. Teacher candidates’ accuracy of beliefs regarding childhood interventions. Teach Educ 2009;44:71–89 | Lacking qualitative data and/or analysis |
| Baker K. Compensating for the Impact of Attention Deficit Hyperactivity Disorder on Reading Achievement: Michael’s Story. Adelaide, SA: Australian Literacy Educators’ Association; 2005 | Could not retrieve |
| Baker KB. Compensating for cognitive deficits in students with attention deficit hyperactivity disorder. North Rockhampton, QLD: Central Queensland University; 2003 | Does not consider experience or attitude toward school-based interventions |
| Barbin-Daniels CM. Mainstreaming. Learning 1992;20:49 | First person account |
| Bekle B. Review of research on teachers’ knowledge and attitudes about attention-deficit hyperactivity disorder (ADHD). Australas J Spec Educ 2001;25:67–85 | Not primary research |
| Bell PS. Jamaican teachers’ attitudes toward children with oppositional defiant disorder, conduct disorder, and attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;67:2214 | Does not consider experience or attitude toward school-based interventions |
| Berger M. Remediating hyperkinetic behavior with impulse control procedures. Sch Psychol Rev 1981;10:405–7 | Could not retrieve |
| Blahy TL. Understanding ADHD: our personal journey. Reclaim Child Youth 2004;13:56 | Lacking qualitative data and/or analysis |
| Book RM. Management of the Child with an Attention Disorder in the School Setting. Paper presented at the Annual Convention of the American Psychological Association, Anaheim, CA, 26–30 August 1983 | Could not retrieve |
| Bosco JJ, Robin SS. Parent, Teacher and Physician in the Life of the Hyperactive Child: The Coherence of the Social Environment. Springfield, IL: Charles C Thomas Pub Ltd; 1980 | Could not retrieve |
| Brennan EM, Ama SM, Gordon LJ. Inclusion of Children with Emotional or Behavioral Challenges in Child Care Settings: An Observational Study. Paper presented at Head Start’s Sixth National Research Conference: The First Eight Years – Pathways to the Future, Washington, DC, June 2002 | Not focused on school-age students with ADHD |
| Breusch S. ’More a Lifestyle Than a Disorder’: A Review of Attention-Deficit-Disorder and Social Relationships. Conference paper, 1992 | Could not retrieve |
| Brice PJ. The experience of learning for youth diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 1998;58:6801 | Does not consider experience or attitude toward school-based interventions |
| Brinkman WB, Sherman SN, Zmitrovich AR, Visscher MO, Crosby LE, Phelan KJ, et al. In their own words: adolescent views on ADHD and their evolving role managing medication. Acad Pediatr Assoc 2012;12:53–61 | Focused on pharmacological interventions |
| Brodin J, Ljusberg AL. Teaching children with attention deficit hyperactivity disorder in remedial classes. Int J Rehabil Res 2008;31:351–5 | Lacking qualitative data and/or analysis |
| Brook U, Boaz M. Attention deficit and hyperactivity disorder (ADHD) and learning disabilities (LD): adolescents perspective. Patient Educ Counsel 2005;58:187–91 | Lacking qualitative data and/or analysis |
| Brook U, Boaz M. Attention deficit and hyperactivity disorder/learning disabilities (ADHD/LD): parental characterization and perception. Patient Educ Counsel 2005;57:96–100 | Lacking qualitative data and/or analysis |
| Brook U, Geva D. Knowledge and attitudes of high school pupils towards peers’ attention deficit and learning disabilities. Patient Educ Counsel 2001;43:31–6 | Lacking qualitative data and/or analysis |
| Brook U, Watemberg N, Geva D. Attitude and knowledge of attention deficit hyperactivity disorder and learning disability among high school teachers. Patient Educ Counsel 2000;40:247–52 | Lacking qualitative data and/or analysis |
| Brophy JE, Rohrkemper MM. Motivational Factors in Teachers’ Handling of Problem Students. East Lansing, MI: Michigan State University; 1982 | Could not retrieve |
| Brown D. Recollections. Acad Ther 1980;15:351–6 | First person account |
| Brown PJ. Parents’ perceptions and children’s functioning: a combined scientific and phenomenological perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;64:409 | Not focused on school setting |
| Buck GH. Smoothing the rough edges of classroom transitions. Interv Sch Clin 1999;34:224–27,35 | Lacking qualitative data and/or analysis |
| Bullard JA. Parent perceptions of the effect of ADHD child behavior on the family: the impact and coping strategies. Dissertation Abstracts International: Section B: The Sciences and Engineering 1996;57:7755 | Not focused on school setting |
| Burcham B, Carlson L, Milich R. Promising school-based practices for students with attention deficit disorder. Except Child 1993;60:174–80 | Lacking qualitative data and/or analysis |
| Burcham B, Carlson L. Promising Practices in Identifying and Educating Children with Attention Deficit Disorder. Education of Children with Attention Deficit Disorder. Lexington, KY: Federal Resource Center for Special Education; 1993 | Could not retrieve |
| Burchfield CM. Exploring the meanings related to ADHD: a qualitative investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;67:532 | Not focused on school setting |
| Burgess J. The impact of teaching thinking skills as habits of mind to young children with challenging behaviours. Emot Behav Difficult 2012;17:47–63 | Not focused on school-age students with ADHD |
| Bussing R, Koro-Ljungberg M, Noguchi K, Mason D, Mayerson G, Garvan CW. Willingness to use ADHD treatments: a mixed methods study of perceptions by adolescents, parents, health professionals and teachers. Soc Sci Med 2012;74:92–100 | Not focused on school setting |
| Bussing R, Koro-Ljungberg ME, Gary F, Mason DM, Garvan CW. Exploring help-seeking for ADHD symptoms: a mixed-methods approach. Harv Rev Psychiatr 2005;13:85–101 | Not focused on school setting |
| Bussing R, Schoenberg NE, Rogers KM, Zima BT, Angus S. Explanatory models of ADHD: do they differ by ethnicity, child gender, or treatment status? J Emot Behav Disord 1998;6:233–42 | Lacking qualitative data and/or analysis |
| Callwood-Brathwaite DJ. Co-occurrence of attention deficit/hyperactivity disorder in a school-identified sample of students with emotional and behavioral disorders: Implications for educational programming. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1998;59:0415 | Lacking qualitative data and/or analysis |
| Canfield SK. The lonely journey: parental decision-making regarding stimulant therapy for ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:4647 | Not focused on school setting |
| Carpenter L, Austin H. Silenced, silence, silent: motherhood in the margins. Qual Inq 2007;13:660–74 | Not focused on school setting |
| Carpenter L, Austin H. How to be recognized enough to be included? Int J Inclusive Educ 2008;12:35–48 | Does not consider experience or attitude toward school-based interventions |
| Carpenter L, Emerald E. Stories From the Margin: Mothering A Child With ADHD or ASD. Teneriffe, QLD: Post Pressed; 2009 | Not focused on school setting |
| Carpenter LR. The Effect of a Child’s Attention Deficit Hyperactivity Disorder on a Mother: The Hidden Disability of Motherhood. Nathan, QLD: Griffith University; 1999 | Not focused on school setting |
| Carpenter T. Teaching High School Students with Attention Deficit Hyperactivity Disorder Self Advocacy Skills and Strategies for Coping with Their Disability in School. Florida, FL: Nova Southeastern University; 1995 | Could not retrieve |
| Carpenter-Song E. Caught in the psychiatric net: meanings and experiences of ADHD, pediatric bipolar disorder and mental health treatment among a diverse group of families in the United States. Cult Med Psychiatr 2009;33:61–85 | Not focused on school setting |
| Carragher G, Campbell-Evans G, Forlin C. The Voice of the Adolescent with Attention-Deficit/Hyperactivity Disorder (AD/HD) in Individual Case Conferences: How Adolescents with AD/HD Manage the Symptoms of their Disorder and the Treatment Strategies. Paper presented to the Australian Association for Research in Education Conference, University of Notre Dame, Western Australia, 2–6 December 2001 | Not primary research |
| Carragher GL. Life After Diagnosis: The Social Experience of Adolescents Diagnosed with Attention-Deficit/Hyperactivity Disorder and How They Manage their Lives. Perth, WA: Edith Cowan University; 2003 | Could not retrieve |
| Carragher GL. Teachers’ Conceptualisations Of, and Resistance To, The Inclusion of ADHD Students in Mainstream Classrooms. Crawley, WA: University of Western Australia; 1999 | Could not retrieve |
| Cassar AG, Jang EE. Investigating the effects of a game-based approach in teaching word recognition and spelling to students with reading disabilities and attention deficits. Aust J Learn Disabil 2010;15:193–211 | Lacking qualitative data and/or analysis |
| Chang H-H, Chang C-S, Shih Y-L. The process of assisting behavior modification in a child with attention-deficit hyperactivity disorder. J Nurs Res 2007;15:147–55 | Focused on pharmacological interventions |
| Chevreau LP. Neurofeedback and childhood ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:2870 | Not focused on school setting |
| Cline B. Raising Alan alone. Except Parent 1985;15:44–6 | First person account |
| Coker K. School and family based treatment of children with attention-deficit hyperactivity disorder. Fam Soc 1990;71:276–82 | Lacking qualitative data and/or analysis |
| Cook M. Attention deficit disorder: a teacher perspective. Melbourne, VIC: La Trobe University; 2000 | Could not retrieve |
| Cooper P, Shea T. Pupils’ perceptions of AD/HD. Emot Behav Difficult 1998;3:36–48 | Does not consider experience or attitude toward school-based interventions |
| Cooper P. The Inner Life of Children With Emotional and Behavioural Difficulties. In Varma VP, editor. The Inner Life of Children With Special Needs. Philadelphia, PA: Whurr Publishers; 1996. pp. 95–111 | Not focused on school-age students with ADHD |
| Copeland LA. Adaptive processes and the development of executive functions in preschoolers with ADHD in a head start early childhood program. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;63:2452 | Could not retrieve |
| Cosser CP. Raising a child with attention deficit hyperactivity disorder: a parents’ perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;68:3391 | Not focused on school setting |
| Couture C, Royer E, Dupuis FA, Potvin P. Comparison of Quebec and British teachers’ beliefs about, training in and experience with attention deficit hyperactivity disorder. Emot Behav Difficult 2003;8:284–302 | Lacking qualitative data and/or analysis |
| Currie D, Lee DL, Scheeler MC. Using PDAs to increase the homework completion of students with ADHD. J Evid Base Pract Sch 2005;6:151–62 | Lacking qualitative data and/or analysis |
| Davis-Berman JL, Pestello FG. Medicating for ADD/ADHD: personal and social issues. Int J Ment Health Addict 2010;8:482–92 | Not focused on school setting |
| Davison JC, Ford DY. Perceptions of attention deficit hyperactivity disorder in one African American community. J Negro Educ 2001;70:264–74 | Focused on pharmacological interventions |
| Debonis DA. An evaluation of an executive function-based intervention program for adolescents with ADHD and their parents. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1998;59:1902 | Lacking qualitative data and/or analysis |
| Diaz Y. Latino parents’ perceptions of, and response to, child attention-deficit/hyperactivity disorder and oppositional defiant disorder: an ecological perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;71:1339 | Not focused on school setting |
| DiCesare EJ. An evaluation of live relaxation training as a treatment for primary aged school children described as hyperactive impulsive. Diss Abstr Int 1982;42:4927 | Lacking qualitative data and/or analysis |
| Dielman MB, Franklin C. Brief solution-focused therapy with parent and adolescents with attention-deficit hyperactivity disorder. Soc Work Educ 1998;20:261–8 | Lacking qualitative data and/or analysis |
| dosReis S, Barksdale CL, Sherman A, Maloney K, Charach A. Stigmatizing experiences of parents of children with a new diagnosis of ADHD. Psychiatr Serv 2010;61:811–16 | Not focused on school setting |
| dosReis S, Mychailyszyn MP, Myers M, Riley AW. Coming to terms with ADHD: how urban African-American families come to seek care for their children. Psychiatr Serv 2007;58:636–41 | Not focused on school setting |
| Duke University, NC Medical Center. Symposium on Literacy and Disabilities. Durham, NC: Duke University, Durham, NC Medical Center; 1997 | Could not retrieve |
| Dunaway C. Attention deficit hyperactivity disorder: an authentic story in the schools and its implications. Semin Speech Lang 2004;25:271–5 | First person account |
| Dunne L, Moore A. From boy to man: a personal story of ADHD. Emot Behav Difficult 2011;16:351–64 | Not focused on school setting |
| Dyer-Wiley CM. Dealing with a disruptive child. Principal 1999;78:30–1 | First person account |
| Edwards L, Salant V, Howard VF, Brougher J, McLaughlin TF. Effectiveness of self-management on attentional behavior and reading comprehension for children with attention deficit disorder. Child Fam Behav Ther 1995;17:1–17 | Lacking qualitative data and/or analysis |
| Epstein JN, Willis MG, Conners CK, Johnson DE. Use of a technological prompting device to aid a student with attention deficit hyperactivity disorder to initiate and complete daily tasks: an exploratory study. J Spec Educ Tech 2001;16:19–28 | Not focused on school setting |
| Exley B. ‘Staying in class so no one can get to him’: a case for the institutional reproduction of ADHD categories and behaviours. Int J Inclusive Educ 2008;12:65–8 | Does not consider experience or attitude toward school-based interventions |
| Exley B. The Behaviour ’Crisis’: Young Children’s Mis/Understandings of the Identities of ADHD. Conference paper presented at the Australian Association for Research in Education 2005 International Education Research Conference, Parramatta, Australia, 28 November–1 December | Focused on pharmacological interventions |
| Exley B. Young children’s misunderstandings of the ADHD label. Educ Young Child 2007;13:38–40 | Focused on pharmacological interventions |
| Fachin K. Teaching Tommy: a second-grader with attention deficit hyperactivity disorder. Phi Delta Kappan 1996;77:437–41 | Lacking qualitative data and/or analysis |
| Farmer JL. The development of the personal strengths intervention (PSI) to improve self-determination and social-emotional levels in postsecondary students with learning disabilities and/or ADHD: a multiple baseline study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2012;72:3710 | Not focused on school-age students with ADHD |
| Fiks AG, Gafen A, Hughes CC, Hunter KF, Barg FK. Using freelisting to understand shared decision making in ADHD: parents’ and pediatricians’ perspectives. Patient Educ Counsel 2011;84:236–44 | Not focused on school setting |
| Filmer R. When Giftedness, Dyslexia and Attention Deficit Hyperactivity Disorder (ADHD) Meet: Two Case Studies of Educational Management. In Wormald C and Vialle W, editors. Dual Exceptionality. Sydney, NSW: Australian Association for the Education of the Gifted and Talented Ltd; 2011. pp. 127–31 | Lacking qualitative data and/or analysis |
| Fiore TA, Becker EA. Promising Classroom Interventions for Students with Attention Deficit Disorders. Research Triangle Park, NC: Research Triangle Institution; 1994 | Lacking qualitative data and/or analysis |
| Firmin MW, Phillips A. A qualitative study of families and children possessing diagnoses of ADHD. J Fam Issues 2009;30:1155–74 | Not focused on school setting |
| Folk DK. Stress management and attention-deficit disorder intervention by teachers in the classroom for ADHD and non-ADHD children. Dissertation Abstracts International: Section B: The Sciences and Engineering 1994;55:1996 | Not focused on school-age students with ADHD |
| Fournier CJ. Teacher perceptions of impact of hyperactivity on classroom situations and on ratings of intervention acceptability. Diss Abstr Int 1988;48:2832–3 | Could not retrieve |
| Francis A. Stigma in an era of medicalisation and anxious parenting: how proximity and culpability shape middle-class parents’ experiences of disgrace. Sociol Health Illness 2012;34:927–42 | Not focused on school-age students with ADHD |
| Fraser C, Belzner R, Conte R. Attention deficit hyperactivity disorder and self-control: a single case study of the use of a timing device in the development of self-monitoring. Sch Psychol Int 1992;13:339–45 | Lacking qualitative data and/or analysis |
| Fraser KM. Too young for attention deficit disorder? Views from preschool. J Dev Behav Pediatr 2002;23:S46–50 | Lacking qualitative data and/or analysis |
| Friio SS. The experiences of adolescents with ADHD: a phenomenological study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;59:4357 | Does not consider experience or attitude toward school-based interventions |
| Frost P. ‘Like Switching the Light On’ – The Raviv Method and its Contribution to Overcoming Learning Difficulties. Presented at the British Educational Research Association Annual Conference. Institute of Education, University of London, London, 5–8 September 2007 | Lacking qualitative data and/or analysis |
| Fuller PC. Stabilizing attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:4725 | Not focused on school setting |
| Furtick J Jr. The impact of labeling on African American males diagnosed with attention deficit disorder (ADD) and attention deficit hyperactive disorder (ADHD): a social work perspective. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66:759 | Could not retrieve |
| Gajaria A, Yeung E, Goodale T, Charach A. Beliefs about attention-deficit/hyperactivity disorder and response to stereotypes: youth postings in Facebook groups. J Adolesc Health 2011;49:15–20 | Not focused on school setting |
| Gallo MP. College students diagnosed with ADHD: insights into their experiences. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68:4999 | Could not retrieve |
| Garro LC, Yarris KE. ‘A massive long way’: interconnecting histories, a ‘special child’, ADHD, and everyday family life. Cult Med Psychiatr 2009;33:559–607 | Does not consider experience or attitude toward school-based interventions |
| Gharibi H, Gholizadeh Z. Phenomenology of Mothers’ Experiences in Living with Children with AD/HD Disorder. Conference paper presented at 2nd World Conference on Psychology, Counselling and Guidance, Antalya, Turkey, 25–29 May 2011 | Not focused on school setting |
| Ghiora WL. Investigation of information offered parents of ADD or ADHD elementary school students in San Diego county schools (California). Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:34 | Not focused on school setting |
| Gillies V. Review of parenting and inclusive education: discovering difference, experiencing difficulty. Sociology 2009;43:1205–6 | Does not consider experience or attitude toward school-based interventions |
| Gleeson G. Experiences, Problems and ’Felt Needs’ of Teachers Educating Students with Attentional Deficits. Paper presented at the National Conference on the Behaviour management and behavior Change of Children and Youth with emotional and/or behaviour problems, Melbourne, 1996 | Could not retrieve |
| Golda Meir Mount Carmel International Centre. Course on the Education of the Young Child with Special Needs. Israel: Golda Meir Mount Carmel International Centre; 1993 | Could not retrieve |
| Goldstein S. Bye bye Brady Bunch. Fam Ther Network 1986;10:31–2, 76–8 | Not focused on school setting |
| Graham LG. Traditional martial arts and children with ADHD: self-perceptions of competence. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:1407 | Not focused on school setting |
| Graham-Day KJ, Gardner R, III, Hsin Y-W. Increasing on-task behaviors of high school students with attention deficit hyperactivity disorder: Is it enough? Educ Treat Child 2010;33:205–21 | Lacking qualitative data and/or analysis |
| Grant WS, Flynn B. The hyperactive child: a pediatrician’s program. A mother’s point of view. Except Parent 1980;10:5–10 | First person account |
| Gray GB. Career decision making for male students with attention deficit hyperactivity disorder: a model of critical factors aiding in transitional efforts. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2396 | Not focused on school setting |
| Griffin E, Pollak D. Student experiences of neurodiversity in higher education: insights from the BRAINHE project. Dyslexia 2009;15:23–41 | Not focused on school-age students with ADHD |
| Griswold DS. Perceptions of elementary educators concerning ADDH in children. Diss Abstr Int 1991;52:472 | Could not retrieve |
| Guevara JP, Feudtner C, Romer D, Power T, Eiraldi R, Nihtianova S, et al. Fragmented care for inner-city minority children with attention-deficit/hyperactivity disorder. Pediatrics 2005;116:e512–17 | Not focused on school setting |
| Guli LA, Semrud-Clikeman M, Lerner MD, Britton N. Social competence intervention program (SCIP): a pilot study of a creative drama program for youth with social difficulties. Arts Psychother 2013;40:37–44 | Not focused on school setting |
| Guli LA. The effects of creative drama-based intervention for children with deficits in social perception. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:3690 | Not focused on school-age students with ADHD |
| Hansen DL, Hansen EH. Caught in a balancing act: parents’ dilemmas regarding their ADHD child’s treatment with stimulant medication. Qual Health Res 2006;16:1267–85 | Focused on pharmacological interventions |
| Harris KR, Friedlander BD, Saddler B, Frizzelle R, Graham S. Self-monitoring of attention versus self-monitoring of academic performance: effects among students with ADHD in the general education classroom. J Spec Educ 2005;39:145–56 | Lacking qualitative data and/or analysis |
| Harris KR. Self-monitoring of attentional behavior versus self-monitoring of productivity: effects on on-task behavior and academic response rate among learning disabled children. J Appl Behav Anal 1986;19:417–23 | Lacking qualitative data and/or analysis |
| Harvey WJ, Reid G, Bloom GA, Staples K, Grizenko N, Mbekou V, et al. Physical activity experiences of boys with and without ADHD. Adapt Phys Activ Q 2009;26:131–50 | Not focused on school setting |
| Hervey-Jumper H, Douyon K, Falcone T, Franco KN. Identifying, evaluating, diagnosing, and treating ADHD in minority youth. J Attention Disord 2008;11:522–8 | Not primary research |
| Hibbitts P. We do this for the next child: a mother’s phenomenological auto narrative inquiry into experiencing her children’s schools. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;71:1152 | Does not consider experience or attitude toward school-based interventions |
| Hjörne E, Säljö R. ‘There is something about Julia’: symptoms, categories, and the process of invoking attention deficit hyperactivity disorder in the Swedish school: a case study. J Lang Ident Educ 2004;3:1–24 | Lacking qualitative data and/or analysis |
| Hogg CM. Hyperactive Children and Their Social Relationships. Cambridge: University of Cambridge; 1986 | Could not retrieve |
| Hollwey S. A demon in the nursery. Montessori Courier 1991;2:18–19 | Could not retrieve |
| Holmes KD. An exploration of attention deficit hyperactivity disorder in adults. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:3968 | Not focused on school-age students with ADHD |
| Holst J. Danish teachers’ conception of challenging behaviour and DAMP/ADHD. Early Child Dev Care 2008;178:363–74 | Not focused on school-age students with ADHD |
| Holthouse D. Speak out for understanding. Teach Tolerance 2009:30–3 | Not focused on school-age students with ADHD |
| Huber JS. The mediating effect of sibling warmth on parental stress in families with children who have attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:3053 | Not focused on school setting |
| Hudyma SAM. Teacher’s Knowledge of Attention Deficit Hyperactivity Disorder (ADHD) and How Students with ADHD are Supported in Western Australian schools. Crawley, WA: University of Western Australia; 2007 | Could not retrieve |
| Hughes LA. The reality of living with AD/HD: children’s concern about educational and medical support. Emot Behav Difficult 2007;12:69–80 | Lacking qualitative data and/or analysis |
| Innes C. Integration or separation? Catering for students with special needs. Christ Teach J 2008;16:22–5 | Not focused on school-age students with ADHD |
| Jamieson H. Social Outcomes: A Whole School Approach. Paper presented at National Educators Conference, Perth, Australia, 2004 | Could not retrieve |
| Jennings RG. Parental Aspirations for Children and Children’s Aspirations: A Longitudinal Study of Educational and Career Aspirations among Hyperactive and Non-Hyperactive Children. Macomb, IL: Western Illinois University; 1992 | Could not retrieve |
| Jefferson County School District R-1. Kids Explore the Gifts of Children with Special Needs. Westridge Young Writers Workshops. Sante Fe, NM: John Muir Publications; 1994 | Lacking qualitative data and/or analysis |
| Jerome L. Teaching Children to Ignore Teasing: A Cognitive Behavioural Family Strategy for Dealing with Teasing and Reactive Bullying. J Can Acad Child Adolesc Psychiatry 2006;15:91 | Lacking qualitative data and/or analysis |
| Johnsen SK, Kendrick J. Teaching Gifted Students with Disabilities. Waco, TX: Prufrock Press; 2005 | First person account |
| Johnson KK. Teaching Shakespeare to learning disabled students. Engl J 1998;87:45 | Not focused on school-age students with ADHD |
| Jones E. A parent’s experience of schooling for a child with ADHD. Reach 2006;20:55–9 | First person account |
| Jones MM. Chapter Four: Two Sides of Isis. In Jones MM, editor. Whisper Writing: Teenage Girls Talk about Ableism and Sexism in School. Oxford: Peter Lang Publishing Inc.; 2004. pp. 59–79 | First person account |
| Kaidar I, Wiener J, Tannock R. The attributions of children with attention-deficit/hyperactivity disorder for their problem behaviors. J Attention Disord 2003;6:99–109 | Lacking qualitative data and/or analysis |
| Kakouros E, Maniadaki K, Papaeliou C. How Greek teachers perceive school functioning of pupils with ADHD. Emot Behav Difficult 2004;9:41–53 | Lacking qualitative data and/or analysis |
| Kamras J. A trip to the rose garden. Education Next 2006;6:88 | Not focused on school-age students with ADHD |
| Kaplan M. Review of framing ADHD children: a critical examination of the history, discourse, and everyday experience of attention deficit/hyperactivity disorder. Psychiatr Serv 2006;57:586–7 | Not focused on school setting |
| Kaplan ME. Improving reading performance in inattentive children through mediated learning experience. Diss Abstr Int 1991;51:3018 | Could not retrieve |
| Karnik NS. Categories of control: foster children and ADHD. Child Youth Serv Rev 2001;23:761–80 | Not focused on school setting |
| Kean B. The Risk Society and attention deficit hyperactivity disorder (ADHD): a critical social research analysis concerning the development and social impact of the ADHD diagnosis. Ethical Hum Psychol Psychiatry 2005;7:131–42 | Focused on pharmacological interventions |
| Kellner RN. Attention-deficit/hyperactivity disordered children’s social self-perceptions of their peer-related personal and interpersonal problems. Crawley: University of Western Australia; 2000 | Could not retrieve |
| Kennedy TK. A case of an UGLDS: unidentified gifted/learning disabled student. Australas J Gift Educ 2004;13:24–34 | Could not retrieve |
| Khan UU. Emotional Reactivity of Children and Adolescents Diagnosed with an Attention-Deficit Disorder: Teachers’ Perspectives. Crawley, WA: University of Western Australia; 2003 | Could not retrieve |
| Kidd AC. Sleep disorders in children: A qualitative research study on the comparison of behavioral symptoms associated with poor quality sleep and ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70:1555 | Not focused on school-age students with ADHD |
| Kidder RM. When don’t you tell the teacher? Educ Can 2009;49:35 | First person account |
| Kildea S, Wright J, Davies J. Making sense of ADHD in practice: a stakeholder review. Clin Child Psychol Psychiatr 2011;16:599–619 | Not focused on school setting |
| King GA, Brown EG, Smith LK. Resilience: Learning from People with Disabilities and the Turning Points in their Lives. Westport, CT: Praeger Publishers/Greenwood Publishing Group; 2003 | First person account |
| King JL. Adults’ descriptions of their lived experience taking methylphenidate in their school-aged years: a phenomenological investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;70:5827 | Not focused on school setting |
| Kingston AK. Mothering Special Needs: A Different Maternal Journey. London, England: Jessica Kingsley Publishers; England; 2007 | Not focused on school setting |
| Knezevic-Floric O, Zukovic S, Ninkovic S. Case study: school experience of children with attention deficit hyperactivity disorder. Health Med 2012;6:3482–7 | Other |
| Knipp DK. Teens’ perceptions about attention deficit/hyperactivity disorder and medications. J Sch Nurs 2006;22:120–5 | Focused on pharmacological interventions |
| Knippenberg CA, Ernewein P. The feeling de jour: a therapist’s and teacher’s perspective on the emotional impairments of exceptional children. Educ Psychol J2010;47:22–6 | First person account |
| Knowles T. The Kids behind the Label: Understanding ADHD. Educ Digest 2010;76:59–61 | First person account |
| Konza D. An Effective Teaching Model Based on Classroom Observations of Students with Attention Deficit Hyperactivity Disorder. Wollongong, NSW: University of Wollongong; 1999 | Could not retrieve |
| Konza D. Gifted? ADHD? Or Both? In Embracing Diversity. Proceeding of the 21st National Conference of the Australia Association of Special Education Inc., 20–28 September. Brisbane, QLD: Australian Association of Special Education; 1997 | Could not retrieve |
| Koro-Ljungberg M, Bussing R, Wilder J, Gary F. Role of communication in the context of educating children with attention-deficit/hyperactivity disorder: parents’ and teachers’ perspectives. J Sch Publ Relat 2011;32:41–75 | Does not consider experience or attitude toward school-based interventions |
| Koro-Ljungberg M, Bussing R, Williamson P, Wilder J, Mills T. African-American teenagers’ stories of attention deficit/hyperactivity disorder. J Child Fam Stud 2008;17:467–85 | Does not consider experience or attitude toward school-based interventions |
| Koro-Ljungberg M, Bussing R. The management of courtesy stigma in the lives of families with teenagers with ADHD. J Fam Issues 2009;30:1175–200 | Not focused on school setting |
| Kos JM, Richdale AL, Hay DA. Children with attention deficit hyperactivity disorder and their teachers: a review of the literature. Int J Disabil Dev Educ 2006;53:147–60 | Not primary research |
| Kostelnik MJ, Onaga E, Rohde B, Whiren A. Children with Special Needs: Lessons for Early Childhood Professionals. In Kostelnik MJ, editor. Early Childhood Education Series. Williston, VT: Teachers College Press; 2002. pp. 100–19 | First person account |
| Kothari J, Morgan S. Multi-agency training programmes for professionals and parents of children with ADHD. Arch Dis Child 2010;95:A97 | Lacking qualitative data and/or analysis |
| Krout R, Burnham A, Moorman S. Computer and electronic music applications with students in special education: From program proposal to progress evaluation. Music Ther Perspect 1993;11:28–31 | Lacking qualitative data and/or analysis |
| Landwehr JM. Understanding youth with ADHD in the context of mother-child and father-child relationships: a mixed methods study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2012;73:1294 | Not focused on school setting |
| Laughlin C, Hall SB. When is ritalin the answer? Learning 1995;24:56–8 | Lacking qualitative data and/or analysis |
| Laurell GC. ADHD and other stories from the forsaken garden. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:412 | Does not consider experience or attitude toward school-based interventions |
| Lavorata CM. Attention deficit hyperactivity disorder: families choosing alternate management approaches. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2001;62:1706 | Focused on pharmacological interventions |
| Law J, Plunkett C, Taylor J, Gunning M. Developing policy in the provision of parenting programmes: integrating a review of reviews with the perspectives of both parents and professionals. Child Care Health Dev 2009;35:302–12 | Not focused on school setting |
| Lee K. ADHD in American early schooling: from a cultural psychological perspective. Early Child Dev Care 2008;178:415–39 | Does not consider experience or attitude toward school-based interventions |
| Lensch CR. Making sense of attention deficit/hyperactivity disorder. Westport, CT: Bergin & Garvey; 2000 | Not primary research |
| Leslie LK, Plemmons D, Monn AR, Palinkas LA. Investigating ADHD treatment trajectories: listening to families’ stories about medication use. J Dev Behav Pediatr 2007;28:179–88 | Focused on pharmacological interventions |
| Levine ES, Anshel DJ. ‘Nothing works!’ A case study using cognitive-behavioral interventions to engage parents, educators, and children in the management of attention-deficit/hyperactivity disorder. Psychol Schools 2011;48:297–306 | Lacking qualitative data and/or analysis |
| Levine JE. Learning from Behavior: How to Understand and Help ‘Challenging’ Children in School. Westport, CT: Praeger Publishers/Greenwood Publishing Group; 2007 | Lacking qualitative data and/or analysis |
| Litt J. Women’s carework in low-income households – the special case of children with attention deficit hyperactivity disorder. Gend Soc 2004;18:625–44 | Not focused on school setting |
| Little AM. Perceptions of Baldrige criteria implementation in middle school inclusive language arts classrooms. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:887 | Lacking qualitative data and/or analysis |
| Ljusberg A-L, Brodin J. Self-concept in children with attention deficits. Int J Rehabil Res 2007;30:195–201 | Lacking qualitative data and/or analysis |
| Lovey J. Dealing with AD/HD in the classroom: one teacher’s experience. Emot Behav Difficult 1998;3:30–6 | Lacking qualitative data and/or analysis |
| Maddern L, Franey J, McLaughlina V, Cox S. An evaluation of the impact of an inter-agency intervention programme to promote social skills in primary school children. Educ Psychol Pract 2004;20:135–55 | Not focused on school-age students with ADHD |
| Magiati I, Dockrell JE, Logotheti AE. Young children’s understanding of disabilities: the influence of development, context, and cognition. J Appl Dev Psychol 2002;23:409–30 | Lacking qualitative data and/or analysis |
| Malacrida C. Medicalization, ambivalence and social control: mothers’ descriptions of educators and ADD/ADHD. Health (Lond) 2004;8:61–80 | Does not consider experience or attitude toward school-based interventions |
| Malacrida C. Motherhood, resistance and attention deficit disorder: strategies and limits. Can Rev Sociol Anthropol 2001;38:141–65 | Not focused on school setting |
| Margalit M, Raskind MH, Higgins EL, Russo-Netzer P. Mothers’ Voices on the internet: stress, support and perceptions of mothers of children with learning disabilities and attention deficit/hyperactivity disorder. Learn Disabil 2010;16:3–14 | Does not consider experience or attitude toward school-based interventions |
| Margalit M, Raskind MH. Mothers of children with LD and ADHD: empowerment through online communication. J Spec Educ Tech 2009;24:2 | Not focused on school setting |
| Marks SU, Schrader C, Levine M. Paraeducator experiences in inclusive settings: helping, hovering, or holding their own? Except Child 1999;65:315–28 | Not focused on school-age students with ADHD |
| Mattingly G, Surman CB, Mao AR, Eagan CA, Onofrey M, Lerner M. Improving communication in ADHD care: results from in-office linguistic research. CNS Spectrums 2011;16 | Not focused on school setting |
| Mattison RE. Consultation interactions between special education teachers and child psychiatrists. Child Adolesc Psychiatr Clin N Am 2001;10:67–82 | Lacking qualitative data and/or analysis |
| McDannel RP. Classroom occupations from the perspectives of three high school students with attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:2550 | Does not consider experience or attitude toward school-based interventions |
| McFerran K. Quenching a desire for power: the role of music therapy for adolescents with ADHD. Australas J Spec Educ 2009;33:72–83 | Other |
| McHoul A, Rapley M. A case of attention-deficit/hyperactivity disorder diagnosis: Sir Karl and Francis B. slug it out on the consulting room. Discourse Soc 2005;16:419–49 | Not focused on school setting |
| McIntyre R, Hennessy E. ‘He’s just enthusiastic. Is that such a bad thing?’ Experiences of parents of children with attention deficit hyperactivity disorder. Emot Behav Difficult 2012;17:65–82 | Not primary research |
| McKinney JD, Feagans L. Adaptive classroom behavior of learning disabled students. J Learn Disabil 1983;16:360–7 | Not primary research |
| McMahon SE. Doctors diagnose, teachers label: the unexpected in pre-service teachers’ talk about labelling children with ADHD. Int J Inclusive Educ 2012;16:249–64 | Does not consider experience or attitude toward school-based interventions |
| McMenamy JM, Perrin EC, Wiser M. Age-related differences in how children with ADHD understand their condition: biological or psychological causality? J Appl Dev Psychol 2005;26:111–31 | Not focused on school setting |
| McMenamy JM, Perrin EC. The impact of experience on children’s understanding of ADHD. J Dev Behav Pediatr 2008;29:483–92 | Not focused on school setting |
| McMenamy JM. Children’s understanding of psychological and physical conditions: an investigation of domain-specificity. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:5029 | Not focused on school setting |
| McNeil KN. The Guardian of the Dream: A Journey through Attention Deficit Hyperactive Disorder to the Other Side of Me. In Pena RA, Guest K, Matsuda L, editors. Community and Difference: Stories about Social Justice and Teaching. New York, NY: Peter Lang Publishing Inc.; 2007. pp. 123–43 | First person account |
| Meadows NB. Meeting the challenges of responsible inclusion. Prev Sch Fail 1996;40:139–42 | First person account |
| Meaux JB, Hester C, Smith B, Shoptaw A. Stimulant medications: a trade-off? The lived experience of adolescents with ADHD. J Spec Pediatr Nurs 2006;11:214–26 | Not focused on school setting |
| Mickelson J-R. Our sons were labeled behavior disordered: here are the stories of our lives. Troy, NY: Educator’s International Press; 2000 | Not focused on school-age students with ADHD |
| Miller AR, Condin CJ, McKellin WH, Shaw N, Klassen AF, Sheps S. Continuity of care for children with complex chronic health conditions: parents’ perspectives. BMC Health Serv Res 2009;9:242 | Not focused on school-age students with ADHD |
| Miller TW, Nigg JT, Miller RL. Attention deficit hyperactivity disorder in African American children: what can be concluded from the past ten years? Clin Psychol Rev 2009;29:77–86 | Not primary research |
| Mills I. Understanding parent decision making for treatment of ADHD. Sch Soc Work J 2011;36:41–60 | Focused on pharmacological interventions |
| Mintz J. Understanding of special educational needs terms by student teachers and student paediatric nurses. Eur J Spec Needs Educ 2010;25:225–38 | Lacking qualitative data and/or analysis |
| Model SLF. Bear up early childhood teachers . . . accommodate attention deficit disorder children. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:3407 | Not primary research |
| Moen OL, Hall-Lord ML, Hedelin B. Contending and adapting every day: Norwegian parents’ lived experience of having a child with ADHD. J Fam Nurs 2011;17:441–62 | Not focused on school setting |
| Monaco T, Eichenold D, Kasper V, Gonzales CV, Jackson S, Earle M, et al. Teachers identify and support at-risk gifted students. Acad Leader 2010;8:1–9 | Lacking qualitative data and/or analysis |
| Montgomery CM. Discipline and love in African-Americans parenting children with attention deficit hyperactivity disorder: cultural dilemmas in becoming a ’good’ parent. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:1532 | Not focused on school setting |
| Montgomery JK. Characteristics and development of male adolescent students who are gifted, gifted twice-exceptional, or attention deficit: a mixed-methods study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:2407 | Lacking qualitative data and/or analysis |
| Moon SM, Zentall SS, Grskovic JA, Hall A, Stormont M. Emotional and social characteristics of boys with AD/HD and giftedness: a comparative case study. J Educ Gift 2001;24:207–47 | Does not consider experience or attitude toward school-based interventions |
| Morrison R, Burgman I. Friendship experiences among children with disabilities who attend mainstream Australian schools. Can J Occup Ther 2009;76:145–52 | Not focused on school-age students with ADHD |
| Morse E. Caretakers of children with ADHD: issues and experiences. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3930 | Could not retrieve |
| Morthel RD. A gender based comparative study of attention deficit hyperactivity disorder on behavior and achievement of elementary students. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2387 | Lacking qualitative data and/or analysis |
| Moses T. Being treated differently: stigma experiences with family, peers, and school staff among adolescents with mental health disorders. Soc Sci Med 2010;70:985–93 | Not focused on school-age students with ADHD |
| Moss JJ. Biomedicalizing schoolroom performances. Constructions of attention deficit disorder and reading disability in the first grade. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2756 | Lacking qualitative data and/or analysis |
| Mueller TG. IEP facilitation: a promising approach to resolving conflicts between families and schools. Teach Except Child 2009;41:60–7 | Lacking qualitative data and/or analysis |
| Murray E. ’Don’t Give Up On Them’: Managing Attention Deficit Hyperactivity Disorder in Schools: What Teachers and Parents Believe and Know. Perth, WA: Murdoch University; 2009 | Lacking qualitative data and/or analysis |
| Naughton J. Disabilities from an insider’s perspective. Res Teach Dev Educ 2011;28:43–9 | First person account |
| Navarro V, Danforth S. A case study of ADHD diagnosis in middle school: perspectives and discourses. Ethical Hum Psychol Psychiatry 2004;6:111–24 | Focused on pharmacological interventions |
| Neophytou K, Webber R. Attention deficit hyperactivity disorder: the family and social context. Aust Soc Work 2005;58:313–25 | Not focused on school setting |
| Neophytou K. ADHD, a Social Construct? The Experience of Families Who Have a Child Diagnosed with Attention Deficit Hyperactivity Disorder. Melbourne: Australian Catholic University; 2004 | Focused on pharmacological interventions |
| Nicholls CJ. Lessons learned in living with attention-deficit hyperactivity disorder. J Child Neurol 2004;19:828–30 | First person account |
| Nielsen JA. Increasing awareness of learning disabilities. Alberta J Educ Res 1997;43:169–72 | Not focused on school setting |
| Nilholm C, Alm B. An inclusive classroom? A case study of inclusiveness, teacher strategies, and children’s experiences. Eur J Spec Needs Educ 2010;25:239–52 | Not focused on school-age students with ADHD |
| Norgard L. A strength-based behavioral approach to reduce stimulant medication referrals in elementary schools. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;67:3165 | Not focused on school-age students with ADHD |
| Norris JA, Hoffman PR. Attaining, sustaining, and focusing attention: intervention for children with ADHD. Semin Speech Lang 1996;17:59–71 | Not focused on school setting |
| Oberthur AP. A Study of Parents’ Perceptions of the Behaviour and Learning of their Children With Attention Deficit Disorder. Brisbane, QLD: University of Queensland; 1996 | Could not retrieve |
| Okafor MN. Narrating realities of Latino mothers of children with attention deficit hyperactivity disorder {ADHD} using ecological and cultural approach. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;67:4595 | Not focused on school setting |
| Olaniyan O, dosReis S, Garriett V, Mychailyszyn MP, Anixt J, Rowe PC, et al. Community perspectives of childhood behavioral problems and ADHD among African American parents. Ambul Pediatr 2007;7:226–31 | Not focused on school setting |
| Olmeda RE, Thomas AR, Davis CP. An analysis of sociocultural factors in social skills training studies with students with attention deficit/hyperactivity disorder. Multiple Voices 2003;6:58–72 | Could not retrieve |
| O’Regan F, Cooper P. Ruby Tuesday: a student with ADHD and learning difficulties. Emot Behav Difficult 2001;6:265–9 | First person account |
| Oslington G. Our family’s experience with the ’DORE’ program. Gifted 2008:6–8 | Could not retrieve |
| Pang WC, Zhang KC. Reading intervention for secondary students with hyperactive behaviours in Hong Kong. Emot Behav Difficult 2011;16:69–85 | Lacking qualitative data and/or analysis |
| Paoni MF. The synthesis of a social information processing model of attention-deficit/hyperactivity disorder and social competence intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:6144 | Not focused on school setting |
| Papadopoulos TC, Mulcahy RF. Pedagogy of integration: interactions between children with and without special needs in early childhood and elementary integrated settings. Can J Spec Educ 1995;10:136–58 | Lacking qualitative data and/or analysis |
| Partridge L, Williams N. What’s In It For Me? New Perspectives on Motivating Students With AD/HD. In PL Jeffery, editor. Proceedings of AARE 2007 International Education Research Conference. 2007 November 26-29; Fremantle, Australia. Melbourne, VIC: Australian Association for Research in Education; 2008 | Not primary research |
| Partridge RK. Listening to the AD/HD-Diagnosed Schoolboy as ‘Insider’: A Grounded Theory Study. Perth, WA: University of Western Australia; 2006 | Could not retrieve |
| Pelham WE, Milich R. Peer relations in children with hyperactivity/attention deficit disorder. J Learn Disabil 1984;17:560–7 | Not primary research |
| Pellegrini AD, Landers-Pott M. Children, classroom context and activity and attention to tasks. Emot Behav Difficult 1996;1:29–35 | Not primary research |
| Perry SN, Franklin KK. An Analysis of College Students with AD/HD at a Private and Public Institution in Arkansas Using a Grounded Theory Approach. Paper presented at the Annual Meeting of the Mid-South Educational Research Association, Chattanooga, TN, 6–8 November 2002 | Could not retrieve |
| Pester J. An investigative assessment of the need for a Y9 pupil with learning difficulties and ADHD. Emot Behav Difficult 2002;7:215–27 | Lacking qualitative data and/or analysis |
| Peters K, Jackson D. Mothers’ experiences of parenting a child with attention deficit hyperactivity disorder. J Adv Nurs 2009;65:62–71 | Not focused on school setting |
| Peterson D, Maddux CD. Rural regular and special education teachers’ perceptions of teaching hyperactive students. Rural Spec Educ Q 1988;9:10–15 | Lacking qualitative data and/or analysis |
| Petruzzi L. Attention deficit disorder: family physicians’ perspective on diagnosis and treatment. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:2806 | Not focused on school setting |
| Plumer PJ. Using peers as intervention agents to improve the social behaviors of elementary-aged children with attention deficit hyperactivity disorder: effects of a peer coaching package. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68:2813 | Lacking qualitative data and/or analysis |
| Poillion MJ. Effects of teacher training on the alteration of teacher instructional style and the academic success of students identified with attention-deficit hyperactivity disorder. Diss Abstr Int 1993;54:2121 | Lacking qualitative data and/or analysis |
| Poley JA. Effects of classroom cognitive behavioral training with elementary school ADHD students: a pilot study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56:2616 | Lacking qualitative data and/or analysis |
| Porter L. Collaboration with parents. Teach Learn Netw 2009;16:23–5 | Not focused on school-age students with ADHD |
| Pretorius D. How Parents of Children Diagnosed with Attention-Deficit/Hyperactivity Disorder Manage their Children: Scaffolding in Chaos. Perth, WA: University of Western Australia; 2005 | Could not retrieve |
| Prigg A. Experiences and perceived roles of occupational therapists working with children with special learning needs during transition to school: a pilot study. Aust Occup Ther J 2002;49:100–11 | Not focused on school-age students with ADHD |
| Prosser B. Behaviour Management or Management Behaviour? A Sociological Study of Attention Deficit Hyperactivity Disorder (ADHA) in Australian and American Secondary Schools. Perth, WA: Murdoch University; 2001 | Not focused on school setting |
| Prosser B. Beyond Deficit Views: Redesigning Pedagogies To Engage Students Identified With Attention Deficit Hyperactivity Disorder. Paper presented at the Culture, Knowledge and Understanding Conference, Singapore, May 2007 | Lacking qualitative data and/or analysis |
| Prosser B. Hearing silenced voices: using narrative research with marginalised youth. Crit Pedagog Netw 1998;11:1–11 | Could not retrieve |
| Prosser B. Media and Pedagogical Exchange: Taking ADHD to Radio 2GB. In Jeffery PL, editor. Proceedings of the AARE 2009 International Education Research Conference; 2009 December 2; Canberra, Australia. Melbourne, VIC: Australian Association for Research in Education; 2010 | Not focused on school setting |
| Prosser B. Weaving a Whole Cloth: Metaphor as a Response to Representational Challenges in Critical Narrative Research. In Jeffery PL, editor. Proceedings of the AARE 2007 International Education Research Conference; 2007 November 28; Fremantle, Australia. Melbourne, VIC: Australian Association For Research in Education; 2008 | Lacking qualitative data and/or analysis |
| Prosser BJ. Seeing Red: A Case of Critical Narrative in ADHD Research. Teneriffe, QLD: Post Pressed; 2006 | Does not consider experience or attitude toward school-based interventions |
| Anonymous. Pupils I’ll never forget. Times Educ Suppl 2004:7 | Not focused on school-age students with ADHD |
| Quinn PO. Adolescents and ADD: Gaining the Advantage. Washington, DC: Magination Press/American Psychological Association; 1995 | First person account |
| Radford PM, Ervin RA. Employing descriptive functional assessment methods to assess low-rate, high-intensity behaviors: a case example. J Posit Behav Interv 2002;4:146–55 | Lacking qualitative data and/or analysis |
| Rafalovich A. Relational troubles and semiofficial suspicion: educators and the medicalization of ‘unruly’ children. Symbolic Interact 2005;28:25–46 | Not focused on school-age students with ADHD |
| Rapport MD. A comparison of attentional training utilizing a response cost procedure and methylphenidate (ritalin) on the classroom behaviors of hyperactive children. Diss Abstr Int 1981;42:389 | Lacking qualitative data and/or analysis |
| Raskind MH, Margalit M, Higgins EL. ‘My LD’: children’s voices on the internet. Learn Disabil Q 2006;29:25–68 | Not focused on school-age students with ADHD |
| Reiber C, McLaughlin TF. Classroom interventions: methods to improve academic performance and classroom behavior for students with attention-deficit/hyperactivity disorder. Int J Spec Educ 2004;19:1–13 | Lacking qualitative data and/or analysis |
| Reid R, Hertzog M, Snyder M. Educating every teacher, every year: the public schools and parents of children with ADHD. Semin Speech Lang 1996;17:73–90 | Not focused on school-age students with ADHD |
| Reis EM. Attention deficit hyperactivity disorder: implications for the classroom teacher. J Instr Psychol 2002;29:175–8 | Not primary research |
| Risley J. Her grades fell. It was hard to watch. Working Mother 2003:50 | Could not retrieve |
| Robbins KS. The social construction of attention deficit disorder: an ethnography and archaeology (Michel Foucault). Dissertation Abstracts International: Section A: Humanities and Social Sciences 2000;60:3534 | Not focused on school setting |
| Robin SS, Bosco JJ. Creating an Approach for Understanding the Diagnosis and Treatment of Hyperkinetic Children. Paper presented at the Annual Meeting of the American Educational Research Association. Boston, MA, April 1980 | Could not retrieve |
| Robins M, Gilbert RN. Welcome to Our World: Realities of High School Students. Thousand Oaks, CA: Corwin Press, Inc.; 1998 | Not focused on school-age students with ADHD |
| Robinson K. Reflections on parenting a child with ADHD: exploring professional–client relationships. J Fem Fam Ther 2003;15:75–90 | Not focused on school setting |
| Rosenzweig JM, Brennan EM, Ogilvie A. Work-family fit: voices of parents of children with emotional and behavioral disorders. Soc Work 2002;47:415–24 | Not focused on school-age students with ADHD |
| Ross E, Ross EC. The identification of ADHD. Infants Young Child 2006;19:164–7 | First person account |
| Rudnick P. My Billy. New Yorker 2006;82:40 | First person account |
| Ruenzel D. Addicted. Teach Mag 1996;8:28–9,32,4–5 | First person account |
| Rush C, Harrison P. Ascertaining teachers’ perceptions of working with adolescents diagnosed with attention-deficit/hyperactivity disorder. Educ Psychol Pract 2008;24:207–23 | Lacking qualitative data and/or analysis |
| Rush S, Wheeler J. Ascertaining disabling perceptions using perceptual mapping: applications to teachers’ perceptions of adolescents with attention-deficit/hyperactivity disorder. Disabil Soc 2011;26:743–56 | Lacking qualitative data and/or analysis |
| Rush S. Teachers’ perceptions of working with adolescents with attention-deficit/hyperactivity disorder: a concept-mapping approach. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:1223 | Could not retrieve |
| Ryan S. ‘I used to worry about what other people thought but now I just think . . . well I don’t care’: shifting accounts of learning difficulties in public places. Health Place 2008;14:730–9 | Not focused on school setting |
| Salt N, Parkes E, Scammell A. GPs’ perceptions of the management of ADHD in primary care: a study of Wandsworth GPs. Prim Health Care Res Dev 2005;6:162–71 | Not focused on school setting |
| Sams SE. The effects of functional intervention on the behavior of four students labeled ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:1081 | Lacking qualitative data and/or analysis |
| Schaedler JS. A phenomenological study of the developmental course and adult outcome of women with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:4908 | Could not retrieve |
| Schirduan V, Case K. Mindful curriculum leadership for students with attention deficit hyperactivity disorder: leading in elementary schools by using multiple intelligences theory (SUMIT). Teachers Coll Rec 2004;106:87–95 | Lacking qualitative data and/or analysis |
| Schirduan V, Case KI. Mindful Curriculum Leadership for Students with Attention Deficit Hyperactivity Disorder (ADHD): Leading in Elementary Schools by Using Multiple Intelligences Theory (SUMIT[C]). Paper presented at the Annual Meeting of the American Education Research Association, Seattle, WA, 10–14 April 2001 | Lacking qualitative data and/or analysis |
| Schirduan VM. Elementary students with attention deficit hyperactivity disorder (ADHD) in schools using multiple intelligences theory: Intelligences, self-concept, and achievement. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2000;61:891 | Lacking qualitative data and/or analysis |
| Schmalzer SN. Teachers’ perceptions of self-management interventions for ADHD: an initial investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:6435 | Lacking qualitative data and/or analysis |
| Scope CR. The efficacy of conjoint behavioral consultation to reduce the off-task behavior of elementary school children diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1975 | Lacking qualitative data and/or analysis |
| Seabi J. Foundation phase educators’ perceptions of attention deficit hyperactivity disorder at a mainstream primary school. S Afr J High Educ 2010;24:616–29 | Does not consider experience or attitude toward school-based interventions |
| Segal E. Mothering a child with attention-deficit hyperactivity disorder: learned mothering. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56:4950 | Not focused on school setting |
| Segal R, Frank G. The extraordinary construction of ordinary experience: scheduling daily life in families with children with attention deficit hyperactivity disorder. Scand J Occup Ther 1998;5:141–7 | Not focused on school setting |
| Segal R, Hinojosa J. The activity setting of homework: an analysis of three cases and implications for occupational therapy. Am J Occup Ther 2006;60:50–9 | Not focused on school setting |
| Segal R. The construction of family occupations: a study of families with children who have attention deficit/hyperactivity disorder. Can J Occup Ther 1998;65:286–92 | Not focused on school setting |
| Shattell MM, Bartlett R, Rowe T. ‘I have always felt different’: the experience of attention-deficit/hyperactivity disorder in childhood. J Pediatr Nurs 2008;23:49–57 | Not focused on school setting |
| Shaw K, Wagner I, Eastwood H, Mitchell G. A qualitative study of Australian GPs’ attitudes and practices in the diagnosis and management of attention-deficit/hyperactivity disorder (ADHD). J Fam Pract 2003;20:129–34 | Not focused on school setting |
| Shea B, Wiener J. Social exile: the cycle of peer victimization for boys with ADHD. Can J Sch Psychol 2003;18:55–90 | Not focused on school setting |
| Sheehan AD, Sheehan CM. Lost in a sea of ink: how I survived the storm. J Adolesc Adult Literacy 2000;44:20 | Lacking qualitative data and/or analysis |
| Singer B. The psychological experience of siblings of children with ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 1997;58:2700 | Could not retrieve |
| Singh I. A disorder of anger and aggression: children’s perspectives on attention deficit/hyperactivity disorder in the UK. Soc Sci Med 2011;73:889–96 | Does not consider experience or attitude toward school-based interventions |
| Singh I. Boys will be boys: fathers’ perspectives on ADHD symptoms, diagnosis, and drug treatment. Harv Rev Psychiatr 2003;11:308–16 | Not focused on school setting |
| Singh I. Doing their jobs: mothering with Ritalin in a culture of mother-blame. Soc Sci Med 2004;59:1193–205 | Not focused on school setting |
| Slee R. Finding a student voice in school reform: student disaffection, pathologies of disruption and educational control. Int Stud Sociol Educ 1994;4:147–72 | Lacking qualitative data and/or analysis |
| Smith M, Tett L. New community schools and pupils with social, emotional and behavioural difficulties. Scot Educ Rev 2002;34:151–62 | Not focused on school-age students with ADHD |
| Spicer CD. The Emotional Toll of Being a Twice Exceptional Adult : A Case Study. In Wormald C and Vialle W, editors. Dual Exceptionality. Sydney, NSW: Australian Association for the Education of the Gifted and Talented Ltd; 2011. pp. 33–6 | Not focused on school setting |
| St James O’Connor T, Meakes E, Pickering M, Schuman M. On the right track: client experience of narrative therapy. Contemp Fam Ther 1997;19:479–95 | Not focused on school-age students with ADHD |
| Stagg AM. Barriers to attention-deficit/hyperactivity disorder intervention implementation in the public school setting. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:6467 | Lacking qualitative data and/or analysis |
| Stinnett TA, Crawford SA, Gillespie MD, Cruce MK, Langford CA. Factors affecting treatment acceptability for psychostimulant medication versus psychoeducational intervention. Psychol Schools 2001;38:585 | Lacking qualitative data and/or analysis |
| Stolowitz MA. How to achieve academic and creative success in spite of the inflexible, unresponsive higher education system. J Learn Disabil 1995;28:4–7 | First person account |
| Stone KL. An investigation of sibling relationships of children with AD/HD and their older siblings. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:4255 | Lacking qualitative data and/or analysis |
| Stultz CH, Flannagan D. Talk about school between mothers and children with or without ADHD. J Child Fam Stud 1999;8:425–35 | Lacking qualitative data and/or analysis |
| Tan TS, Cheung WS. Effects of computer collaborative group work on peer acceptance of a junior pupil with attention deficit hyperactivity disorder (ADHD). Comput Educ 2008;50:725–41 | Lacking qualitative data and/or analysis |
| Taylor M, Houghton S, Durkin K. Getting children with attention deficit hyperactivity disorder to school on time. J Fam Issues 2008;29:918–43 | Not focused on school setting |
| Taylor M, Houghton S. Examination-related anxiety in students diagnosed with AD/HD and the case for an allocation of extra time: perspectives of teachers, mothers and students. Emot Behav Difficult 2008;13:111–25 | Does not consider experience or attitude toward school-based interventions |
| Taylor M, Houghton SJ. Difficulties in initiating and sustaining peer friendships: perspectives on students diagnosed with AD/HD. Br J Spec Educ 2008;35:209–19 | Does not consider experience or attitude toward school-based interventions |
| Taylor M, O’Donoghue T, Houghton S. To medicate or not to medicate? The decision-making process of Western Australian parents following their child’s diagnosis with an attention deficit hyperactivity disorder. Int J Disabil Dev Educ 2006;53:111–28 | Not focused on school setting |
| Teasley M. Effective Interventions for Students with ADHD. In Franklin C, Harris MB, Allen-Meares P, editors. The School Practitioner’s Concise Companion to Mental Health. New York, NY: Oxford University Press; US; 2008. pp. 19–34 | Not primary research |
| Terenzi N. In my own words. Reaching Today’s Youth 1999;4:4–7 | Could not retrieve |
| Terry J. Coping with ADHD. Child Educ 1998;75:48–9 | Could not retrieve |
| TES. Friday hero. Times Educ Suppl 2005:3 | Not focused on school-age students with ADHD |
| Thompson D, Emira M. ‘They say every child matters, but they don’t’: an investigation into parental and carer perceptions of access to leisure facilities and respite care for children and young people with autistic spectrum disorder (ASD) or attention deficit, hyperactivity disorder (ADHD). Disabil Soc 2011;26:65–78 | Not focused on school setting |
| Thorlakson CE. The experiences that enhance and inhibit learning for post-secondary students diagnosed with ADHD: a qualitative study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:77 | Not focused on school-age students with ADHD |
| Tidefors I, Strand J. Life history interviews with 11 boys diagnosed with attention-deficit/hyperactivity disorder who had sexually offended: a sad storyline. J Trauma Dissociation 2012;13:421–34 | Not focused on school setting |
| Timmer DF. Group support for teenagers with attention deficit hyperactivity disorder. Soc Work Educ 1995;17:194–8 | Not focused on school setting |
| Tracey DK, Gleeson G. Sense of coherence, loneliness and interpersonal concerns in adolescents with AD/HD: a comparison of adolescents’ and mothers’ perceptions. Aust J Guid Counsell 1998;8:49–58 | Lacking qualitative data and/or analysis |
| Travell C, Visser J. ‘ADHD does bad stuff to you’: young people’s and parents’ experiences and perceptions of attention deficit hyperactivity disorder (ADHD). Emot Behav Difficult 2006;11:205–16 | Focused on pharmacological interventions |
| Tsurumaki M. Self-esteem enhancement in children with attention-deficit/hyperactivity disorder. Tohoku Psychol Folia 2007;66:105–11 | Lacking qualitative data and/or analysis |
| Turk TN, Campbell DA. What’s wrong with Doug: the academic struggles of a gifted student with ADHD from preschool to college. Gift Child Today 2002;25:48 | First person account |
| Tyler Junior College. Tutor Training for Occupational Students with Learning Disabilities. PY95 Final Detailed Report. Texas, TX: Tyler Junior College; 1995 | Lacking qualitative data and/or analysis |
| Tyson K. Using the teacher-student relationship to help children diagnosed as hyperactive: an application of intrapsychic humanism. Child Youth Care Forum 2000;29:265–89 | Lacking qualitative data and/or analysis |
| Underwood DJ, Kopels S. Complaints filed against schools by parents of children with AD/HD: implications for school social work practice. Child Schools 2004;26:221–33 | Lacking qualitative data and/or analysis |
| Vail A, Mandiloff V. Cultivating Our Garden: Serving Students with Learning Disabilities in Family and Consumer Sciences. In Vail A, editor. Family & Consumer Sciences Education Association. Ellensburgh, WA: Central Washington University; 1996 | Could not retrieve |
| Van Der Westhuizen B. An ecosystemic approach to addressing attentional difficulties and heightened motor activity. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;69:4248 | Lacking qualitative data and/or analysis |
| Vogl TA. Navigating the glass maze: towards a phenomenology-derived learning model of graduate students with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:438 | Not focused on school-age students with ADHD |
| Volpe RJ, Anastasio RJ, DuPaul GJ. Classroom and Instructional Strategies. In Goldstein S, Nagliere JA, DeVries M, editors. Learning and Attention Disorders in Adolescence and Adulthood: Assessment and Treatment. 2nd edn. Hoboken, NJ: John Wiley & Sons Inc.; 2011. pp. 467–87 | Could not retrieve |
| Waite R, Tran M. Explanatory models and help-seeking behavior for attention-deficit/hyperactivity disorder among a cohort of postsecondary students. Arch Psychiatr Nurs 2010;24:247–59 | Not focused on school setting |
| Wallace N. The perceptions of mothers of sons with ADHD. Aust New Zeal J Fam Ther 2005;26:193–9 | Not focused on school setting |
| Ware JN, Ohrt JH, Swank JM. A phenomenological exploration of children’s experiences in a social skills group. J Spec Group Work 2012;37:133–51 | Not focused on school-age students with ADHD |
| Watson C, Marr C. A breakfast club for children with emotional and behavioural difficulties. Education 2003;31:150–8 | Not focused on school-age students with ADHD |
| Watson C. Home-school partnership and the construction of deviance: being and becoming the Goldfish family. J Res Spec Educ Needs 2011;11:20–9 | Not focused on school setting |
| Weiss M, Hechtman L, Weiss G. ADHD in parents. J Am Acad Child Adolesc Psychiatr 2000;39:1059–61 | Lacking qualitative data and/or analysis |
| Wheeler L, Pumfrey P, Wakefield P. Variability of ADHD symptoms across primary school contexts: an in-depth case study. Emot Behav Difficult 2009;14:69–84 | Lacking qualitative data and/or analysis |
| Wheeler L. Mixed Method Research into the Variability of ADHD Symptoms in Educational Settings. Paper presented at the BERA conference 2011. London; Institution of Education; 2011 | Lacking qualitative data and/or analysis |
| White-McMahon M. What you see is not what you get. Reclaim Child Youth 2010;19:58–61 | First person account |
| Wiebe J, Nicol JJ. Juxtaposition: ADHD and music at school. Can J Music Ther 2007;13:171–3 | Lacking qualitative data and/or analysis |
| Williams MA. Exploration of effect of diagnosis of high school girls with attention deficit disorder on their mothers and the mother-daughter relationship. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;72:1786 | Not focused on school setting |
| Williams NJ. Gaining Control: Perspectives Of Parents Of Children With AD/HD. Perth, WA; University of Western Australia; 2009 | Does not consider experience or attitude toward school-based interventions |
| Williams Orlando C. Parental explanatory models of children’s attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;71:2277 | Does not consider experience or attitude toward school-based interventions |
| Williamson P, Koro-Ljungberg ME, Bussing R. Analysis of critical incidents and shifting perspectives: transitions in illness careers among adolescents with ADHD. Qual Health Res 2009;19:352–65 | Does not consider experience or attitude toward school-based interventions |
| Willis J. Using my neuroscience to treat the sickness in our classrooms. Catalyst for Change 2010;36:46–55 | First person account |
| Wolfberg PJ, Zercher C, Lieber J, Capell K, Matias S, Hanson M, et al. ‘Can I play with you?’ Peer culture in inclusive preschool programs. J Assoc Pers Sev Handicaps 1999;24:69–84 | Not focused on school-age students with ADHD |
| Woods C. My brave hyperactive son. Times Educ Suppl 2007;23 | First person account |
| Wright MS. The Readiness of Adults with Attention Deficit Hyperactivity Disorder for Self-Directed Learning. Mississippi, MS: University of Southern Mississippi; 2001 | Could not retrieve |
| Wright SF. ‘A little understood solution to a vaguely defined problem’: parental perceptions of Ritalin. Educ Child Psychol 1997;14:50–9 | Focused on pharmacological interventions |
| Yehle AK, Wambold C. An ADHD success story: strategies for teachers and students. Teach Except Child 1998;30:8–13 | Lacking qualitative data and/or analysis |
| Yoon ML. An evaluation of the application of the suggestive-accelerative model of learning and teaching on high school students. Melbourne, VIC: RMIT University; 2005 | Could not retrieve |
| Young-Loveridge J. A personal perspective on challenging behaviour: ADHD? Aust J Early Child 1997;22:1–6 | First person account |
| Zentall SS, Moon SM, Hall AM, Grskovic JA. Learning Characteristics of Boys with Attention Deficit/Hyperactivity Disorder and/or Giftedness. Paper presented at the Annual Meeting of the American Educational Research Association, Chicago, IL, March 1997 | Other |
| Zentall SS, Moon SM, Hall AM, Grskovic JA. Learning and motivational characteristics of boys with AD/HD and/or giftedness. Except Child 2001;67:499–519 | Not focused on school-age students with ADHD |
| Ziesing-Clark S. Confusion, heartache and tears : some mother’s experiences of children diagnosed with attention deficit hyperactive disorder. Aust J Early Child 1998;23:31–5 | Lacking qualitative data and/or analysis |
Appendix 15 Studies excluded during full-text screening for review 4, with reasons
| Reference | Reason for exclusion |
|---|---|
| Aberson BD. An intervention for improving executive functioning and social/emotional adjustment of ADHD children: three single case design studies. Dissertation Abstracts International: Section B: The Sciences and Engineering 1997;57:6553 | Lacking qualitative data and/or analysis |
| Allen T. Attention deficit hyperactive disorder . . . a teacher’s perspective. Educ Today 2005;2:12–13 | Lacking qualitative data and/or analysis |
| Al-Sharbati M, Al-Sharbati Z, Al-Lawatiya S, Al-Jahwari S. Teachers’ awareness about attention deficit hyperactivity disorder (ADHD) in Oman. Asian J Psychiatr 2012;5:277–8 | Lacking qualitative data and/or analysis |
| Anonymous. AH/AD: two parents tell their personal stories. Emot Behav Difficult 1997;2:25–9 | Lacking qualitative data and/or analysis |
| Anonymous. Pupils I’ll never forget. Times Educ Suppl 2004:7 | Lacking qualitative data and/or analysis |
| Artesani AJ, Mallar L. Positive behavior supports in general education settings: combining person-centered planning and functional analysis. Interv Sch Clin 1998;34:33–8 | Lacking qualitative data and/or analysis |
| Askew BL. Practices of special education teachers for dealing with students with ADD/ADHD. Chicago, IL: St Xavier University; 1993 | Could not retrieve |
| Baba C, Tanaka-Matsumi J. Positive behavior support for a child with inattentive behavior in a Japanese regular classroom. J Posit Behav Interv 2011;13:250–3 | Lacking qualitative data and/or analysis |
| Bailey S. Disordered experiences – beyond myth/reality. Br Educ Res J 2008;34:135–41 | Not primary research |
| Bain SK, Brown KS, Jordan KR. Teacher candidates’ accuracy of beliefs regarding childhood interventions. Teach Educat 2009;44:71–89 | Lacking qualitative data and/or analysis |
| Baker K. Compensating for the Impact of Attention Deficit Hyperactivity Disorder on Reading Achievement: Michael’s Story. Adelaide, SA: Australian Literacy Educators’ Association; 2005 | Could not retrieve |
| Baker KB. Compensating for Cognitive Deficits in Students with Attention Deficit Hyperactivity Disorder. North Rockhampton, QLD: Central Queensland University; 2003 | Lacking qualitative data and/or analysis |
| Barbin-Daniels CM. Mainstreaming. Learning 1992;20:49 | Lacking qualitative data and/or analysis |
| Bartlett R, Rowe TS, Shattell MM. Perspectives of college students on their childhood ADHD. MCN Am J Matern Child Nurs 2010;35:226–31 | Focused on school-based interventions |
| Bekle B. Review of research on teachers’ knowledge and attitudes about attention-deficit hyperactivity disorder (ADHD). Australas J Spec Educ 2001;25:67–85 | Not primary research |
| Bell PS. Jamaican teachers’ attitudes toward children with oppositional defiant disorder, conduct disorder, and attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;67:2214 | Not focused on school-age students with ADHD |
| Berger M. Remediating hyperkinetic behavior with impulse control procedures. Sch Psychol Rev 1981;10:405–7 | Could not retrieve |
| Blahy TL. Understanding ADHD: our personal journey. Reclaim Child Youth 2004;13:56 | Lacking qualitative data and/or analysis |
| Book RM. Management of the Child with an Attention Disorder in the School Setting. Paper presented at the Annual Convention of the American Psychological Association, Anaheim, CA, 26–30 August 1983 | Could not retrieve |
| Bos CS, Nahmias ML, Urban MA. Implementing interactive professional development in a workshop course on educating students with AD/HD. Teach Educ Spec Educ 1997;20:132–45 | Focused on school-based interventions |
| Bosco JJ, Robin SS. Parent, Teacher and Physician in the Life of the Hyperactive Child: The Coherence of the Social Environment. Springfield, IL: Charles C Thomas Pub Ltd; 1980 | Could not retrieve |
| Brennan EM, Ama SM, Gordon LJ. Inclusion of Children with Emotional or Behavioral Challenges in Child Care Settings: An Observational Study. Paper presented at Head Start’s Sixth National Research Conference: The First Eight Years – Pathways to the Future, Washington, DC, June 2002 | Not focused on school-age students with ADHD |
| Breusch S. ’More a Lifestyle Than a Disorder’: A Review of Attention-Deficit-Disorder and Social Relationships. Conference paper, 1992 | Could not retrieve |
| Brinkman WB, Sherman SN, Zmitrovich AR, Visscher MO, Crosby LE, Phelan KJ, et al. In their own words: adolescent views on ADHD and their evolving role managing medication. Acad Pediatr Assoc 2012;12:53–61 | Focused on pharmacological interventions |
| Brodin J, Ljusberg AL. Teaching children with attention deficit hyperactivity disorder in remedial classes. Int J Rehabil Res 2008; 31:351–5 | Lacking qualitative data and/or analysis |
| Brook U, Boaz M. Attention deficit and hyperactivity disorder (ADHD) and learning disabilities (LD): adolescents perspective. Patient Educ Counsel 2005;58:187–91 | Lacking qualitative data and/or analysis |
| Brook U, Boaz M. Attention deficit and hyperactivity disorder/learning disabilities (ADHD/LD): parental characterization and perception. Patient Educ Counsel 2005;57:96–100 | Lacking qualitative data and/or analysis |
| Brook U, Geva D. Knowledge and attitudes of high school pupils towards peers’ attention deficit and learning disabilities. Patient Educ Counsel 2001;43:31–6 | Lacking qualitative data and/or analysis |
| Brook U, Watemberg N, Geva D. Attitude and knowledge of attention deficit hyperactivity disorder and learning disability among high school teachers. Patient Educ Counsel 2000;40:247–52 | Lacking qualitative data and/or analysis |
| Brophy JE, Rohrkemper MM. Motivational Factors in Teachers’ Handling of Problem Students. Institute for Research on Teaching. East Lansing, MI: Michigan State University; 1982 | Could not retrieve |
| Brown D. Recollections. Acad Ther 1980;15:351–6 | Lacking qualitative data and/or analysis |
| Brown PJ. Parents’ perceptions and children’s functioning: a combined scientific and phenomenological perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;64:409 | Not focused on school setting |
| Buck GH. Smoothing the rough edges of classroom transitions. Interv Sch Clin 1999;34:224–35 | Lacking qualitative data and/or analysis |
| Bullard JA. Parent perceptions of the effect of ADHD child behavior on the family: the impact and coping strategies. Dissertation Abstracts International: Section B: The Sciences and Engineering 1996;57:7755 | Not focused on school setting |
| Burcham B, Carlson L, Milich R. Promising school-based practices for students with attention deficit disorder. Except Child 1993;60:174–80 | Lacking qualitative data and/or analysis |
| Burcham B, Carlson L. Promising Practices in Identifying and Educating Children with Attention Deficit Disorder. Education of Children with Attention Deficit Disorder. Lexington, KY: Federal Resource Center for Special Education; 1993 | Could not retrieve |
| Burchfield CM. Exploring the meanings related to ADHD: a qualitative investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;67:532 | Not focused on school setting |
| Burgess J. The impact of teaching thinking skills as habits of mind to young children with challenging behaviours. Emot Behav Difficult 2012;17:47–63 | Not focused on school-age students with ADHD |
| Bussing R, Koro-Ljungberg M, Noguchi K, Mason D, Mayerson G, Garvan CW. Willingness to use ADHD treatments: a mixed methods study of perceptions by adolescents, parents, health professionals and teachers. Soc Sci Med 2012;74:92–100 | Other |
| Bussing R, Koro-Ljungberg ME, Gary F, Mason DM, Garvan CW. Exploring help-seeking for ADHD symptoms: a mixed-methods approach. Harv Rev Psychiatr 2005;13:85–101 | Not focused on school setting |
| Bussing R, Schoenberg NE, Rogers KM, Zima BT, Angus S. Explanatory models of ADHD: Do they differ by ethnicity, child gender, or treatment status? J Emot Behav Disord 1998;6:233–42 | Not focused on school setting |
| Callwood-Brathwaite DJ. Co-occurrence of attention deficit/hyperactivity disorder in a school-identified sample of students with emotional and behavioral disorders: Implications for educational programming. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1998;59:0415 | Other |
| Canfield SK. The lonely journey: parental decision-making regarding stimulant therapy for ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:4647 | Lacking qualitative data and/or analysis |
| Carpenter L, Austin H. Silenced, silence, silent: motherhood in the margins. Qual Inq 2007;13:660–74 | Not focused on school setting |
| Carpenter L, Emerald E. Stories From the Margin: Mothering A Child With ADHD or ASD. Teneriffe, QLD: Post Pressed; 2009 | Lacking qualitative data and/or analysis |
| Carpenter LR. The Effect of a Child’s Attention Deficit Hyperactivity Disorder on a Mother: The Hidden Disability of Motherhood. Nathan, QLD: Griffith University; 1999 | Lacking qualitative data and/or analysis |
| Carpenter T. Teaching High School Students with Attention Deficit Hyperactivity Disorder Self Advocacy Skills and Strategies for Coping with Their Disability in School. Florida, FL: Nova Southeastern University; 1995 | Could not retrieve |
| Carpenter-Song E. Caught in the psychiatric net: meanings and experiences of ADHD, pediatric bipolar disorder and mental health treatment among a diverse group of families in the United States. Cult Med Psychiatr 2009;33:61–85 | Not focused on school setting |
| Carragher G, Campbell-Evans G, Forlin C. The Voice of the Adolescent with Attention-Deficit/Hyperactivity Disorder (AD/HD) in Individual Case Conferences: How Adolescents with AD/HD Manage the Symptoms of their Disorder and the Treatment Strategies. Paper presented to the Australian Association for Research in Education Conference, University of Notre Dame, Western Australia, 2–6 December 2001 | Lacking qualitative data and/or analysis |
| Carragher GL. Life After Diagnosis: The Social Experience of Adolescents Diagnosed with Attention-Deficit/Hyperactivity Disorder and How They Manage their Lives. Perth, WA: Edith Cowan University; 2003 | Could not retrieve |
| Carragher GL. Teachers’ Conceptualisations Of, and Resistance To, The Inclusion of ADHD Students in Mainstream Classrooms. Crawley, WA: University of Western Australia; 1999 | Could not retrieve |
| Cassar AG, Jang EE. Investigating the effects of a game-based approach in teaching word recognition and spelling to students with reading disabilities and attention deficits. Aust J Learn Disabil 2010;15:193–211 | Lacking qualitative data and/or analysis |
| Chang H-H, Chang C-S, Shih Y-L. The process of assisting behavior modification in a child with attention-deficit hyperactivity disorder. J Nurs Res 2007;15:147–55 | Focused on pharmacological interventions |
| Chevreau LP. Neurofeedback and childhood ADHD. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:2870 | Lacking qualitative data and/or analysis |
| Cline B. Raising Alan alone. Except Parent 1985;15:44–6 | Lacking qualitative data and/or analysis |
| Coker K. School and family based treatment of children with attention-deficit hyperactivity disorder. Fam Soc 1990;71:276–82 | Lacking qualitative data and/or analysis |
| Cook M. Attention deficit disorder: a teacher perspective. Victoria, VIC: La Trobe University; 2000 | Could not retrieve |
| Cooper P. The Inner Life of Children With Emotional and Behavioural Difficulties. In Varma VP, editor. The Inner Life of Children With Special Needs. Philadelphia, PA: Whurr Publishers; 1996. pp. 95–111 | Lacking qualitative data and/or analysis |
| Copeland LA. Adaptive processes and the development of executive functions in preschoolers with ADHD in a head start early childhood program. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;63:2452 | Could not retrieve |
| Cosser CP. Raising a child with attention deficit hyperactivity disorder: a parents’ perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;68:3391 | Not focused on school setting |
| Couture C, Royer E, Dupuis FA, Potvin P. Comparison of Quebec and British teachers’ beliefs about, training in and experience with attention deficit hyperactivity disorder. Emot Behav Difficult 2003;8:284–302 | Lacking qualitative data and/or analysis |
| Currie D, Lee DL, Scheeler MC. Using PDAs to increase the homework completion of students with ADHD. J Evid Base Pract Sch 2005;6:151–62 | Other |
| Davis-Berman JL, Pestello FG. Medicating for ADD/ADHD: personal and social issues. Int J Ment Health Addict 2010;8:482–92 | Not focused on school setting |
| Davison JC, Ford DY. Perceptions of attention deficit hyperactivity disorder in one African American community. J Negro Educ 2001;70:264–74 | Other |
| Debonis DA. An evaluation of an executive function-based intervention program for adolescents with ADHD and their parents. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1998;59:1902 | Not focused on school setting |
| Diaz Y. Latino parents’ perceptions of, and response to, child attention-deficit/hyperactivity disorder and oppositional defiant disorder: an ecological perspective. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;71:1339 | Not focused on school setting |
| DiCesare EJ. An evaluation of live relaxation training as a treatment for primary aged school children described as hyperactive impulsive. Diss Abstr Int 1982;42:4927 | Lacking qualitative data and/or analysis |
| Dielman MB, Franklin C. Brief solution-focused therapy with parent and adolescents with attention-deficit hyperactivity disorder. Soc Work Educ 1998;20:261–8 | Lacking qualitative data and/or analysis |
| DosReis S, Barksdale CL, Sherman A, Maloney K, Charach A. Stigmatizing experiences of parents of children with a new diagnosis of ADHD. Psychiatr Serv 2010;61:811–16 | Not focused on school setting |
| Dosreis S, Mychailyszyn MP, Myers M, Riley AW. Coming to terms with ADHD: how urban African-American families come to seek care for their children. Psychiatr Serv 2007;58:636–41 | Not focused on school setting |
| Ducharme S. Parents’ perceptions of raising a child with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1997;57:3887 | Focused on school-based interventions |
| Duke University, NC Medical Center. Symposium on Literacy and Disabilities. Durham, NC: Duke University, Durham, NC Medical Center; 1997 | Could not retrieve |
| Dunaway C. Attention deficit hyperactivity disorder: an authentic story in the schools and its implications. Semin Speech Lang 2004;25:271–5 | Lacking qualitative data and/or analysis |
| Dunne L, Moore A. From boy to man: a personal story of ADHD. Emot Behav Difficult 2011;16:351–64 | Lacking qualitative data and/or analysis |
| Dyer-Wiley CM. Dealing with a disruptive child. Principal 1999;78:30–1 | Lacking qualitative data and/or analysis |
| Edwards L, Salant V, Howard VF, Brougher J, McLaughlin TF. Effectiveness of self-management on attentional behavior and reading comprehension for children with attention deficit disorder. Child Fam Behav Ther 1995;17:1–17 | Lacking qualitative data and/or analysis |
| Epstein JN, Willis MG, Conners CK, Johnson DE. Use of a technological prompting device to aid a student with attention deficit hyperactivity disorder to initiate and complete daily tasks: an exploratory study. J Spec Educ Tech 2001;16:19–28 | Lacking qualitative data and/or analysis |
| Fachin K. Teaching Tommy: a second-grader with attention deficit hyperactivity disorder. Phi Delta Kappan 1996;77:437–41 | Lacking qualitative data and/or analysis |
| Farmer JL. The development of the personal strengths intervention (PSI) to improve self- determination and social-emotional levels in postsecondary students with learning disabilities and/or ADHD: a multiple baseline study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2012;72:3710 | Lacking qualitative data and/or analysis |
| Fiks AG, Gafen A, Hughes CC, Hunter KF, Barg FK. Using freelisting to understand shared decision making in ADHD: parents’ and pediatricians’ perspectives. Patient Educ Counsel 2011;84:236–44 | Not focused on school setting |
| Filmer R. When Giftedness, Dyslexia and Attention Deficit Hyperactivity Disorder (ADHD) Meet: Two Case Studies of Educational Management. In Wormald C and Vialle W, editors. Dual Exceptionality. Sydney, NSW: Australian Association for the Education of the Gifted and Talented Ltd; 2011. pp. 127–31 | Lacking qualitative data and/or analysis |
| Fiore TA, Becker EA. Promising Classroom Interventions for Students with Attention Deficit Disorders. Research Triangle Park, NC: Research Triangle Institution; 1994 | Lacking qualitative data and/or analysis |
| Firmin MW, Phillips A. A qualitative study of families and children possessing diagnoses of ADHD. J Fam Issues 2009;30:1155–74 | Not focused on school setting |
| Folk DK. Stress management and attention-deficit disorder intervention by teachers in the classroom for ADHD and non-ADHD children. Dissertation Abstracts International: Section B: The Sciences and Engineering 1994;55:1996 | Not focused on school-age students with ADHD |
| Fournier CJ. Teacher perceptions of impact of hyperactivity on classroom situations and on ratings of intervention acceptability. Diss Abstr Int 1988;48:2832–3 | Could not retrieve |
| Francis A. Stigma in an era of medicalisation and anxious parenting: how proximity and culpability shape middle-class parents’ experiences of disgrace. Sociol Health Illness 2012;34:927–42 | Not focused on school setting |
| Fraser C, Belzner R, Conte R. Attention deficit hyperactivity disorder and self-control: a single case study of the use of a timing device in the development of self-monitoring. Sch Psychol Int 1992;13:339–45 | Lacking qualitative data and/or analysis |
| Fraser KM. Too young for attention deficit disorder? Views from preschool. J Dev Behav Pediatr 2002;23:S46–50 | Lacking qualitative data and/or analysis |
| Frost P. ‘Like Switching the Light On’ – The Raviv Method and its Contribution to Overcoming Learning Difficulties. Presented at the British Educational Research Association Annual Conference. Institute of Education, University of London, London, 5–8 September 2007 | Other |
| Fuller PC. Stabilizing attention deficit disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:4725 | Not focused on school setting |
| Furtick J Jr. The impact of labeling on African American males diagnosed with attention deficit disorder (ADD) and attention deficit hyperactive disorder (ADHD): a social work perspective. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66:759 | Could not retrieve |
| Furtick KC. Successful Strategies Used with ADHD Students: Is an ADHD Classroom a Possibility? Minnesota, MN: Capella University; 2010 | Focused on school-based interventions |
| Gajaria A, Yeung E, Goodale T, Charach A. Beliefs about attention-deficit/hyperactivity disorder and response to stereotypes: youth postings in Facebook groups. J Adolesc Health 2011;49:15–20 | Not focused on school setting |
| Gallo MP. College students diagnosed with ADHD: insights into their experiences. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68:4999 | Could not retrieve |
| Garro LC, Yarris KE. ‘A massive long way’: interconnecting histories, a ‘special child’, ADHD, and everyday family life. Cult Med Psychiatr 2009;33:559–607 | Not focused on school setting |
| Gharibi H, Gholizadeh Z. Phenomenology of Mothers’ Experiences in Living with Children with AD/HD Disorder. Conference paper presented at 2nd World Conference on Psychology, Counselling and Guidance, Antalya, Turkey, 25–29 May 2011 | Other |
| Ghiora WL. Investigation of information offered parents of ADD or ADHD elementary school students in San Diego county schools (California). Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:34 | Other |
| Gillies V. Review of parenting and inclusive education: discovering difference, experiencing difficulty. Sociology 2009;43:1205–6 | Other |
| Gleeson G. Experiences, Problems and ’Felt Needs’ of Teachers Educating Students with Attentional Deficits. Paper presented at the National Conference on the Behaviour management and behavior Change of Children and Youth with emotional and/or behaviour problems, Melbourne, 1996 | Could not retrieve |
| Golda Meir Mount Carmel International Centre. Course on the Education of the Young Child with Special Needs. Israel: Golda Meir Mount Carmel International Centre; 1993 | Could not retrieve |
| Goldstein S. Bye bye Brady Bunch. Fam Ther Network 1986;10:31–2,76–8 | Lacking qualitative data and/or analysis |
| Graham LG. Traditional martial arts and children with ADHD: self-perceptions of competence. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:1407 | Lacking qualitative data and/or analysis |
| Graham-Day KJ, Gardner R, III, Hsin Y-W. Increasing on-task behaviors of high school students with attention deficit hyperactivity disorder: is it enough? Educ Treat Child 2010;33:205–21 | Lacking qualitative data and/or analysis |
| Grant WS, Flynn B. The hyperactive child: a pediatrician’s program. A mother’s point of view. Except Parent 1980;10:5–10 | Lacking qualitative data and/or analysis |
| Gray GB. Career decision making for male students with attention deficit hyperactivity disorder: a model of critical factors aiding in transitional efforts. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2396 | Not focused on school setting |
| Griffin E, Pollak D. Student experiences of neurodiversity in higher education: insights from the BRAINHE project. Dyslexia 2009;15:23–41 | Lacking qualitative data and/or analysis |
| Griswold DS. Perceptions of elementary educators concerning ADDH in children. Diss Abstr Int 1991;52:472 | Could not retrieve |
| Guli LA, Semrud-Clikeman M, Lerner MD, Britton N. Social competence intervention program (SCIP): a pilot study of a creative drama program for youth with social difficulties. Arts Psychother 2013;40:37–44 | Lacking qualitative data and/or analysis |
| Guli LA. The effects of creative drama-based intervention for children with deficits in social perception. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:3690 | Lacking qualitative data and/or analysis |
| Hansen DL, Hansen EH. Caught in a balancing act: parents’ dilemmas regarding their ADHD child’s treatment with stimulant medication. Qual Health Res 2006;16:1267–85 | Focused on pharmacological interventions |
| Harris KR, Friedlander BD, Saddler B, Frizzelle R, Graham S. Self-monitoring of attention versus self-monitoring of academic performance: effects among students with ADHD in the general education classroom. J Spec Educ 2005;39:145–56 | Lacking qualitative data and/or analysis |
| Harris KR. Self-monitoring of attentional behavior versus self-monitoring of productivity: effects on on-task behavior and academic response rate among learning disabled children. J Appl Behav Anal 1986;19:417–23 | Lacking qualitative data and/or analysis |
| Harvey WJ, Reid G, Bloom GA, Staples K, Grizenko N, Mbekou V, et al. Physical activity experiences of boys with and without ADHD. Adapt Phys Activ Q 2009;26:131–50 | Other |
| Hervey-Jumper H, Douyon K, Falcone T, Franco KN. Identifying, evaluating, diagnosing, and treating ADHD in minority youth. J Attention Disord 2008;11:522–8 | Not primary research |
| Hjörne E, Säljö R. There is something about Julia: symptoms, categories, and the process of invoking attention deficit hyperactivity disorder in the Swedish school: a case study. J Lang Ident Educ 2004;3:1–24 | Lacking qualitative data and/or analysis |
| Hjörne E. Pedagogy in the ‘ADHD Classroom’: An exploration of ‘The Little group’. In Lloyd G, Stead J and Cohen D editors. Critical New Perspectives on Attention Deficit/Hyperactivity Disorder. London: Routledge; 2006 | Focused on school-based interventions |
| Hogg CM. Hyperactive Children and their Social Relationships. Cambridge: University of Cambridge; 1986 | Could not retrieve |
| Hollwey S. A demon in the nursery. Montessori Courier 1991;2:18–19 | Could not retrieve |
| Holmes KD. An exploration of attention deficit hyperactivity disorder in adults. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:3968 | Not focused on school setting |
| Holst J. Danish teachers’ conception of challenging behaviour and DAMP/ADHD. Early Child Dev Care 2008;178:363–74 | Not focused on school-age students with ADHD |
| Holthouse D. Speak out for understanding. Teach Tolerance 2009:30–3 | Lacking qualitative data and/or analysis |
| Huber JS. The mediating effect of sibling warmth on parental stress in families with children who have attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;71:3053 | Other |
| Hudyma SAM. Teacher’s Knowledge of Attention Deficit Hyperactivity Disorder (ADHD) and How Students with ADHD are Supported in Western Australian schools. Crawley, WA: University of Western Australia; 2007 | Could not retrieve |
| Innes C. Integration or separation? Catering for students with special needs. Christ Teach J 2008;16:22–5 | Lacking qualitative data and/or analysis |
| Isaksson J, Lindqvist R, Bergstrom E. Struggling for recognition and inclusion-parents’ and pupils’ experiences of special support measures in school. Int J Qual Stud Health Well-Being 2010;5:10 | Focused on school-based interventions |
| Jamieson H. Social Outcomes: A Whole School Approach. Paper presented at National Educators Conference, Perth, Australia, 2004 | Could not retrieve |
| Jefferson County School District R-1. Kids Explore the Gifts of Children with Special Needs. Westridge Young Writers Workshops. Sante Fe, NM: John Muir Publications; 1994 | Lacking qualitative data and/or analysis |
| Jennings RG. Parental Aspirations for Children and Children’s Aspirations: A Longitudinal Study of Educational and Career Aspirations among Hyperactive and Non-Hyperactive Children. Macomb, IL: Western Illinois University; 1992 | Could not retrieve |
| Jerome L. Teaching Children to Ignore Teasing: A Cognitive Behavioural Family Strategy for Dealing with Teasing and Reactive Bullying. J Can Acad Child Adolesc Psychiatry. 2006;15:91 | Lacking qualitative data and/or analysis |
| Johnsen SK, Kendrick J. Teaching Gifted Students with Disabilities. Waco, TX: Prufrock Press; 2005 | Lacking qualitative data and/or analysis |
| Johnson KK. Teaching Shakespeare to learning disabled students. Engl J 1998;87:45 | Lacking qualitative data and/or analysis |
| Jones E. A parent’s experience of schooling for a child with ADHD. Reach 2006;20:55–9 | Lacking qualitative data and/or analysis |
| Jones MM. Chapter Four: Two Sides of Isis. In Jones MM, editor. Whisper Writing: Teenage Girls Talk about Ableism and Sexism in School. Oxford: Peter Lang Publishing Inc.; 2004. pp. 59–79 | Lacking qualitative data and/or analysis |
| Kaidar I, Wiener J, Tannock R. The attributions of children with attention-deficit/hyperactivity disorder for their problem behaviors. J Attention Disord 2003;6:99–109 | Lacking qualitative data and/or analysis |
| Kakouros E, Maniadaki K, Papaeliou C. How Greek teachers perceive school functioning of pupils with ADHD. Emot Behav Difficult 2004;9:41–53 | Lacking qualitative data and/or analysis |
| Kamras J. A trip to the rose garden. Education Next 2006;6:88 | Lacking qualitative data and/or analysis |
| Kaplan M. Review of framing ADHD children: a critical examination of the history, discourse, and everyday experience of attention deficit/hyperactivity disorder. Psychiatr Serv 2006;57:586–7 | Lacking qualitative data and/or analysis |
| Kaplan ME. Improving reading performance in inattentive children through mediated learning experience. Diss Abstr Int 1991;51:3018 | Could not retrieve |
| Karnik NS. Categories of control: foster children and ADHD. Child Youth Serv Rev 2001;23:761–80 | Other |
| Kean B. The Risk Society and attention deficit hyperactivity disorder (ADHD): a critical social research analysis concerning the development and social impact of the ADHD diagnosis. Ethical Hum Psychol Psychiatry 2005;7:131–42 | Focused on pharmacological interventions |
| Kellner RN. Attention-deficit/hyperactivity disordered children’s social self-perceptions of their peer-related personal and interpersonal problems. Crawley, WA: University of Western Australia; 2000 | Could not retrieve |
| Kennedy TK. A case of an UGLDS: unidentified gifted/learning disabled student. Australas J Gift Educ 2004;13:24–34 | Could not retrieve |
| Khan UU. Emotional Reactivity of Children and Adolescents Diagnosed with an Attention-Deficit Disorder: Teachers’ Perspectives. Crawley, WA: University of Western Australia; 2003 | Could not retrieve |
| Kidd AC. Sleep disorders in children: a qualitative research study on the comparison of behavioral symptoms associated with poor quality sleep and ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70:1555 | Lacking qualitative data and/or analysis |
| Kidder RM. When don’t you tell the teacher? Educ Can 2009;49:35 | Lacking qualitative data and/or analysis |
| Kildea S, Wright J, Davies J. Making sense of ADHD in practice: a stakeholder review. Clin Child Psychol Psychiatr 2011;16:599–619 | Not focused on school setting |
| King GA, Brown EG, Smith LK. Resilience: Learning from People with Disabilities and the Turning Points in their Lives. Westport, CT: Praeger Publishers/Greenwood Publishing Group; 2003 | Not focused on school setting |
| King JL. Adults’ descriptions of their lived experience taking methylphenidate in their school-aged years: a phenomenological investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;70:5827 | Not focused on school setting |
| Kingston AK. Mothering Special Needs: A Different Maternal Journey. London, England: Jessica Kingsley Publishers; England; 2007 | Lacking qualitative data and/or analysis |
| Knezevic-Floric O, Zukovic S, Ninkovic S. Case study: school experience of children with attention deficit hyperactivity disorder. Health Med 2012;6:3482–7 | Other |
| Knipp DK. Teens’ perceptions about attention deficit/hyperactivity disorder and medications. J Sch Nurs 2006;22:120–5 | Focused on pharmacological interventions |
| Knippenberg CA, Ernewein P. The feeling de jour: a therapist’s and teacher’s perspective on the emotional impairments of exceptional children. Educ Psychol J2010;47:22–6 | Lacking qualitative data and/or analysis |
| Knowles T. The Kids behind the Label: Understanding ADHD. Educ Digest 2010;76:59–61 | Lacking qualitative data and/or analysis |
| Konza D. An Effective Teaching Model Based on Classroom Observations of Students with Attention Deficit Hyperactivity Disorder. Wollongong, NSW: University of Wollongong; 1999 | Could not retrieve |
| Konza D. Gifted? ADHD? Or Both? In Embracing Diversity. Proceeding of the 21st National Conference of the Australia Association of Special Education Inc., 20–28 September. Brisbane, QLD: Australian Association of Special Education; 1997 | Could not retrieve |
| Koro-Ljungberg M, Bussing R, Williamson P, Wilder J, Mills T. African-American teenagers’ stories of attention deficit/hyperactivity disorder. J Child Fam Stud 2008;17:467–85 | Not focused on school setting |
| Koro-Ljungberg M, Bussing R. The management of courtesy stigma in the lives of families with teenagers with ADHD. J Fam Issues 2009;30:1175–200 | Not focused on school setting |
| Kos JM, Richdale AL, Hay DA. Children with attention deficit hyperactivity disorder and their teachers: a review of the literature. Int J Disabil Dev Educ 2006;53:147–60 | Not primary research |
| Kostelnik MJ, Onaga E, Rohde B, Whiren A. Children with Special Needs: Lessons for Early Childhood Professionals. In Kostelnik MJ, editor. Early Childhood Education Series. Williston, VT: Teachers College Press; 2002. pp. 100–19 | Lacking qualitative data and/or analysis |
| Kothari J, Morgan S. Multi-agency training programmes for professionals and parents of children with ADHD. Arch Dis Child 2010;95:A97 | Not focused on school setting |
| Kreiss DS. Case studies of the experiences of students referred for problems of disruptive and/or aggressive behavior to an alternative high school program. Dissertation Abstracts International: Section B: The Sciences and Engineering 2004;65:3137 | Focused on school-based interventions |
| Krout R, Burnham A, Moorman S. Computer and electronic music applications with students in special education: from program proposal to progress evaluation. Music Ther Perspect 1993;11:28–31 | Lacking qualitative data and/or analysis |
| Landwehr JM. Understanding youth with ADHD in the context of mother-child and father-child relationships: a mixed methods study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2012;73:1294 | Not focused on school setting |
| Langberg JM, Vaughn AJ, Williamson P, Epstein JN, Girio-Herrera E, Becker SP. Refinement of an organizational skills intervention for adolescents with ADHD for implementation by school mental health providers. Sch Ment Health;3:143–55 | Focused on school-based interventions |
| Laughlin C, Hall SB. When is ritalin the answer? Learning 1995;24:56–8 | Lacking qualitative data and/or analysis |
| Laurell GC. ADHD and other stories from the forsaken garden. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:412 | Not focused on school setting |
| Lavorata CM. Attention deficit hyperactivity disorder: families choosing alternate management approaches. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2001;62:1706 | Lacking qualitative data and/or analysis |
| Law J, Plunkett C, Taylor J, Gunning M. Developing policy in the provision of parenting programmes: integrating a review of reviews with the perspectives of both parents and professionals. Child Care Health Dev 2009;35:302–12 | Not focused on school setting |
| Lensch CR. Making Sense of Attention Deficit/Hyperactivity Disorder. Westport, CT: Bergin & Garvey; 2000 | Not primary research |
| Leslie LK, Plemmons D, Monn AR, Palinkas LA. Investigating ADHD treatment trajectories: listening to families’ stories about medication use. J Dev Behav Pediatr 2007;28:179–88 | Other |
| Levine ES, Anshel DJ. ‘Nothing works!’ A case study using cognitive-behavioral interventions to engage parents, educators, and children in the management of attention-deficit/hyperactivity disorder. Psychol Schools 2011;48:297–306 | Lacking qualitative data and/or analysis |
| Levine JE. Learning from Behavior: How to Understand and Help ‘Challenging’ Children in School. Westport, CT: Praeger Publishers/Greenwood Publishing Group; 2007 | Lacking qualitative data and/or analysis |
| Litt J. Women’s carework in low-income households – the special case of children with attention deficit hyperactivity disorder. Gend Soc 2004;18:625–44 | Not focused on school setting |
| Little AM. Perceptions of Baldrige criteria implementation in middle school inclusive language arts classrooms. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:887 | Lacking qualitative data and/or analysis |
| Ljusberg A. Children’s views on attending a remedial class – because of concentration difficulties. Child Care Health Dev 2011;37:440–5 | Focused on school-based interventions |
| Ljusberg A-L, Brodin J. Self-concept in children with attention deficits. Int J Rehabil Res. 2007;30:195–201 | Lacking qualitative data and/or analysis |
| Lovey J. Dealing with AD/HD in the classroom: one teacher’s experience. Emot Behav Difficult 1998;3:30–6 | Lacking qualitative data and/or analysis |
| Maddern L, Franey J, McLaughlina V, Cox S. An evaluation of the impact of an inter-agency intervention programme to promote social skills in primary school children. Educ Psychol Pract 2004;20:135–55 | Not focused on school-age students with ADHD |
| Magiati I, Dockrell JE, Logotheti AE. Young children’s understanding of disabilities: the influence of development, context, and cognition. J Appl Dev Psychol 2002;23:409–30 | Lacking qualitative data and/or analysis |
| Margalit M, Raskind MH. Mothers of children with LD and ADHD: empowerment through online communication. J Spec Educ Tech 2009;24:2 | Lacking qualitative data and/or analysis |
| Marks SU, Schrader C, Levine M. Paraeducator experiences in inclusive settings: helping, hovering, or holding their own? Except Child 1999;65:315–28 | Not focused on school-age students with ADHD |
| Mattingly G, Surman CB, Mao AR, Eagan CA, Onofrey M, Lerner M. Improving communication in ADHD care: results from in-office linguistic research. CNS Spectrums 2011;16 | Not focused on school setting |
| Mattison RE. Consultation interactions between special education teachers and child psychiatrists. Child Adolesc Psychiatr Clin N Am 2001;10:67–82 | Lacking qualitative data and/or analysis |
| McFerran K. Quenching a desire for power: the role of music therapy for adolescents with ADHD. Australas J Spec Educ 2009;33:72–83 | Not focused on school setting |
| McHoul A, Rapley M. A case of attention-deficit/hyperactivity disorder diagnosis: Sir Karl and Francis B. slug it out on the consulting room. Discourse Soc 2005;16:419–49 | Not focused on school setting |
| McIntyre R, Hennessy E. ‘He’s just enthusiastic. Is that such a bad thing?’ Experiences of parents of children with attention deficit hyperactivity disorder. Emot Behav Difficult 2012;17:65–82 | Not focused on school setting |
| McKinney JD, Feagans L. Adaptive classroom behavior of learning disabled students. J Learn Disabil 1983;16:360–7 | Not primary research |
| McMenamy JM, Perrin EC, Wiser M. Age-related differences in how children with ADHD understand their condition: biological or psychological causality? J Appl Dev Psychol 2005;26:111–31 | Lacking qualitative data and/or analysis |
| McMenamy JM, Perrin EC. The impact of experience on children’s understanding of ADHD. J Dev Behav Pediatr 2008;29:483–92 | Lacking qualitative data and/or analysis |
| McMenamy JM. Children’s understanding of psychological and physical conditions: an investigation of domain-specificity. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:5029 | Lacking qualitative data and/or analysis |
| McNeil KN. The Guardian of the Dream: A Journey through Attention Deficit Hyperactive Disorder to the Other Side of Me. In Pena RA, Guest K, Matsuda L, editors. Community and Difference: Stories about Social Justice and Teaching. New York, NY: Peter Lang Publishing Inc.; 2007. pp. 123–43 | Lacking qualitative data and/or analysis |
| McNeil KN. Through our eyes: the shared lived experiences of growing up attention deficit hyperactive disordered. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;66:2049 | Focused on school-based interventions |
| Meadows NB. Meeting the challenges of responsible inclusion. Prev Sch Fail 1996;40:139–42 | Lacking qualitative data and/or analysis |
| Meaux JB, Hester C, Smith B, Shoptaw A. Stimulant medications: a trade-off? The lived experience of adolescents with ADHD. J Spec Pediatr Nurs 2006;11:214–26 | Not focused on school setting |
| Mickelson J-R. Our Sons were Labeled Behavior Disordered: Here are the Stories of our Lives. Troy, NY: Educator’s International Press; 2000 | Lacking qualitative data and/or analysis |
| Miller AR, Condin CJ, McKellin WH, Shaw N, Klassen AF, Sheps S. Continuity of care for children with complex chronic health conditions: parents’ perspectives. BMC Health Serv Res 2009;9:242 | Not focused on school setting |
| Miller TW, Nigg JT, Miller RL. Attention deficit hyperactivity disorder in African American children: what can be concluded from the past ten years? Clin Psychol Rev 2009;29:77–86 | Not primary research |
| Mills I. Understanding parent decision making for treatment of ADHD. Sch Soc Work J. 2011;36:41–60 | Lacking qualitative data and/or analysis |
| Mintz J. Understanding of special educational needs terms by student teachers and student paediatric nurses. Eur J Spec Needs Educ 2010;25:225–38 | Lacking qualitative data and/or analysis |
| Model SLF. Bear up early childhood teachers . . . accommodate attention deficit disorder children. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1995;55:3407 | Lacking qualitative data and/or analysis |
| Moen OL, Hall-Lord ML, Hedelin B. Contending and adapting every day: Norwegian parents’ lived experience of having a child with ADHD. J Fam Nurs 2011;17:441–62 | Not focused on school setting |
| Monaco T, Eichenold D, Kasper V, Gonzales CV, Jackson S, Earle M, et al. Teachers identify and support at-risk gifted students. Acad Leader 2010;8:1–9 | Lacking qualitative data and/or analysis |
| Montgomery CM. Discipline and love in African-Americans parenting children with attention deficit hyperactivity disorder: cultural dilemmas in becoming a ’good’ parent. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:1532 | Not focused on school setting |
| Montgomery JK. Characteristics and development of male adolescent students who are gifted, gifted twice-exceptional, or attention deficit: a mixed-methods study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:2407 | Lacking qualitative data and/or analysis |
| Moon SM, Zentall SS, Grskovic JA, Hall A, Stormont M. Emotional and social characteristics of boys with AD/HD and giftedness: a comparative case study. J Educ Gift 2001;24:207–47 | Not focused on school setting |
| Morrison R, Burgman I. Friendship experiences among children with disabilities who attend mainstream Australian schools. Can J Occup Ther 2009;76:145–52 | Not focused on school-age students with ADHD |
| Morse E. Caretakers of children with ADHD: issues and experiences. Dissertation Abstracts International: Section B: The Sciences and Engineering 2003;63:3930 | Could not retrieve |
| Morthel RD. A gender based comparative study of attention deficit hyperactivity disorder on behavior and achievement of elementary students. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2387 | Lacking qualitative data and/or analysis |
| Moses T. Being treated differently: stigma experiences with family, peers, and school staff among adolescents with mental health disorders. Soc Sci Med 2010;70:985–93 | Lacking qualitative data and/or analysis |
| Moss JJ. Biomedicalizing schoolroom performances. Constructions of attention deficit disorder and reading disability in the first grade. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2010;70:2756 | Lacking qualitative data and/or analysis |
| Mueller TG. IEP facilitation: a promising approach to resolving conflicts between families and schools. Teach Except Child 2009;41:60–7 | Lacking qualitative data and/or analysis |
| Mulligan S. Classroom strategies used by teachers of students with attention deficit hyperactivity disorder. Phys Occup Ther Pediatr 2001;20:25–44 | Focused on school-based interventions |
| Murray E. ’Don’t Give Up On Them’: Managing Attention Deficit Hyperactivity Disorder in Schools: What Teachers and Parents Believe and Know. Perth, WA: Murdoch University; 2009 | Lacking qualitative data and/or analysis |
| Naughton J. Disabilities from an insider’s perspective. Res Teach Dev Educ 2011;28:43–9 | Lacking qualitative data and/or analysis |
| Navarro V, Danforth S. A case study of ADHD diagnosis in middle school: perspectives and discourses. Ethical Hum Psychol Psychiatry 2004;6:111–24 | Focused on pharmacological interventions |
| Neophytou K, Webber R. Attention deficit hyperactivity disorder: the family and social context. Aust Soc Work 2005;58:313–25 | Not focused on school setting |
| Neophytou K. ADHD, a Social Construct? The Experience of Families who Have a Child Diagnosed with Attention Deficit Hyperactivity Disorder. Melbourne, VIC: Australian Catholic University; 2004 | Not focused on school setting |
| Nicholls CJ. Lessons learned in living with attention-deficit hyperactivity disorder. J Child Neurol 2004;19:828–30 | Lacking qualitative data and/or analysis |
| Nielsen JA. Increasing awareness of learning disabilities. AlbertaJ Educ Res 1997;43:169–72 | Not focused on school setting |
| Nilholm C, Alm B. An inclusive classroom? A case study of inclusiveness, teacher strategies, and children’s experiences. Eur J Spec Needs Educ 2010;25:239–52 | Not focused on school-age students with ADHD |
| Norgard L. A strength-based behavioral approach to reduce stimulant medication referrals in elementary schools. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;67:3165 | Lacking qualitative data and/or analysis |
| Norris JA, Hoffman PR. Attaining, sustaining, and focusing attention: intervention for children with ADHD. Semin Speech Lang 1996;17:59–71 | Lacking qualitative data and/or analysis |
| Oberthur AP. A Study of Parents’ Perceptions of the Behaviour and Learning of their Children with Attention Deficit Disorder. Brisbane, QLD: University of Queensland; 1996 | Could not retrieve |
| Okafor MN. Narrating realities of Latino mothers of children with attention deficit hyperactivity disorder {ADHD} using ecological and cultural approach. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;67:4595 | Not focused on school setting |
| Olaniyan O, dosReis S, Garriett V, Mychailyszyn MP, Anixt J, Rowe PC, et al. Community perspectives of childhood behavioral problems and ADHD among African American parents. Ambul Pediatr 2007;7:226–31 | Not focused on school setting |
| Olmeda RE, Thomas AR, Davis CP. An analysis of sociocultural factors in social skills training studies with students with attention deficit/hyperactivity disorder. Multiple Voices 2003;6:58–72 | Could not retrieve |
| O’Regan F, Cooper P. Ruby Tuesday: a student with ADHD and learning difficulties. Emot Behav Difficult. 2001;6:265–9 | Lacking qualitative data and/or analysis |
| Oslington G. Our family’s experience with the ’DORE’ program. Gifted 2008:6–8 | Could not retrieve |
| Ozdemir S. The first step to success program: Implementation effectiveness with Turkish children with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2006;67:2115 | Focused on school-based interventions |
| Pang WC, Zhang KC. Reading intervention for secondary students with hyperactive behaviours in Hong Kong. Emot Behav Difficult 2011;16:69–85 | Lacking qualitative data and/or analysis |
| Paoni MF. The synthesis of a social information processing model of attention-deficit/hyperactivity disorder and social competence intervention. Dissertation Abstracts International: Section B: The Sciences and Engineering 2001;61:6144 | Not focused on school setting |
| Papadopoulos TC, Mulcahy RF. Pedagogy of integration: interactions between children with and without special needs in early childhood and elementary integrated settings. Can J Spec Educ 1995;10:136–58 | Lacking qualitative data and/or analysis |
| Partridge L, Williams N. What’s In It For Me? New Perspectives on Motivating Students With AD/HD. In PL Jeffery, editor. Proceedings of AARE 2007 International Education Research Conference. 2007 November 26–29; Fremantle, Australia. Melbourne, VIC: Australian Association for Research in Education; 2008 | Not primary research |
| Partridge L. Teaching Adolescent AD/HD Boys Through ‘Self-Sufficient Reward Control’: A Sociological Investigation. Lewiston, NY: Edwin Mellen Press; 2009 | Focused on school-based interventions |
| Partridge RK. Listening to the AD/HD-diagnosed schoolboy as ’insider’: a grounded theory study. Crawley, WA: University of Western Australia; 2006 | Could not retrieve |
| Pelham WE, Milich R. Peer relations in children with hyperactivity/attention deficit disorder. J Learn Disabil 1984;17:560–7 | Not primary research |
| Pellegrini AD, Landers-Pott M. Children, classroom context and activity and attention to tasks. Emot Behav Difficult. 1996;1:29–35 | Not primary research |
| Perry SN, Franklin KK. An Analysis of College Students with AD/HD at a Private and Public Institution in Arkansas Using a Grounded Theory Approach. Paper presented at the Annual Meeting of the Mid-South Educational Research Association, Chattanooga, TN, 6–8 November 2002 | Could not retrieve |
| Pester J. An investigative assessment of the need for a Y9 pupil with learning difficulties and ADHD. Emot Behav Difficult 2002;7:215–27 | Other |
| Peters K, Jackson D. Mothers’ experiences of parenting a child with attention deficit hyperactivity disorder. J Adv Nurs 2009;65:62–71 | Not focused on school setting |
| Peterson D, Maddux CD. Rural regular and special education teachers’ perceptions of teaching hyperactive students. Rural Spec Educ Q 1988;9:10–15 | Lacking qualitative data and/or analysis |
| Petruzzi L. Attention deficit disorder: family physicians’ perspective on diagnosis and treatment. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:2806 | Not focused on school setting |
| Plumer PJ. Using peers as intervention agents to improve the social behaviors of elementary-aged children with attention deficit hyperactivity disorder: effects of a peer coaching package. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2008;68:2813 | Lacking qualitative data and/or analysis |
| Poillion MJ. Effects of teacher training on the alteration of teacher instructional style and the academic success of students identified with attention-deficit hyperactivity disorder. Diss Abstr Int 1993;54:2121 | Lacking qualitative data and/or analysis |
| Poley JA. Effects of classroom cognitive behavioral training with elementary school ADHD students: a pilot study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56:2616 | Lacking qualitative data and/or analysis |
| Porter L. Collaboration with parents. Teach Learn Netw 2009;16:23–5 | Lacking qualitative data and/or analysis |
| Pretorius D. How parents of children diagnosed with attention-deficit/hyperactivity disorder manage their children: scaffolding in chaos. Crawley, WA: University of Western Australia; 2005 | Could not retrieve |
| Prigg A. Experiences and perceived roles of occupational therapists working with children with special learning needs during transition to school: a pilot study. Aust Occup Ther J 2002;49:100–11 | Lacking qualitative data and/or analysis |
| Prosser B. Behaviour Management or Management Behaviour? A Sociological Study of Attention Deficit Hyperactivity Disorder (ADHA) in Australian and American Secondary Schools. Perth, WA: Murdoch University; 2001 | Not focused on school setting |
| Prosser B. Beyond Deficit Views: Redesigning Pedagogies To Engage Students Identified With Attention Deficit Hyperactivity Disorder. Paper presented at the Culture, Knowledge and Understanding Conference, Singapore, May 2007 | Lacking qualitative data and/or analysis |
| Prosser B. Hearing silenced voices: using narrative research with marginalised youth. Crit Pedagog Netw 1998;11:1–11 | Could not retrieve |
| Prosser B. Media and Pedagogical Exchange: Taking ADHD to Radio 2GB. In Jeffery PL, editor. Proceedings of the AARE 2009 International Education Research Conference; 2009 December 2; Canberra, Australia. Melbourne, VIC: Australian Association for Research in Education; 2010 | Lacking qualitative data and/or analysis |
| Prosser B. Weaving a Whole Cloth: Metaphor as a Response to Representational Challenges in Critical Narrative Research. In Jeffery PL, editor. Proceedings of the AARE 2007 International Education Research Conference; 2007 November 28; Fremantle, Australia. Melbourne, VIC: Australian Association For Research in Education; 2008 | Not focused on school setting |
| Prosser BJ. Beyond ADHD: a consideration of attention deficit hyperactivity disorder and pedagogy in Australian schools. Int J Inclusive Educ 2008;12:81–97 | Lacking qualitative data and/or analysis |
| Quinn PO. Adolescents and ADD: Gaining the Advantage. Washington, DC: Magination Press/American Psychological Association; 1995 | Lacking qualitative data and/or analysis |
| Radford PM, Ervin RA. Employing descriptive functional assessment methods to assess low-rate, high-intensity behaviors: a case example. J Posit Behav Interv 2002;4:146–55 | Lacking qualitative data and/or analysis |
| Rafalovich A. Framing ADHD Children: A Critical Examination of the History, Discourse, and Everyday Experience of Attention Deficit. Maryland, MD: Lexington Books; 2004 | Focused on school-based interventions |
| Rapport MD. A comparison of attentional training utilizing a response cost procedure and methylphenidate (Ritalin) on the classroom behaviors of hyperactive children. Diss Abstr Int 1981;42:389 | Lacking qualitative data and/or analysis |
| Raskind MH, Margalit M, Higgins EL. ’My LD’: children’s voices on the internet. Learn Disabil Q 2006;29:253–68 | Not focused on school-age students with ADHD |
| Reiber C, McLaughlin TF. Classroom interventions: methods to improve academic performance and classroom behavior for students with attention-deficit/hyperactivity disorder. Int J Spec Educ 2004;19:1–13 | Lacking qualitative data and/or analysis |
| Reis EM. Attention deficit hyperactivity disorder: Implications for the classroom teacher. J Instr Psychol 2002;29:175–8 | Not primary research |
| Risley J. Her grades fell. It was hard to watch. Working Mother 2003:50 | Could not retrieve |
| Robbins KS. The social construction of attention deficit disorder: An ethnography and archaeology (Michel Foucault). Dissertation Abstracts International: Section A: Humanities and Social Sciences 2000;60:3534 | Lacking qualitative data and/or analysis |
| Robin SS, Bosco JJ. Creating an Approach for Understanding the Diagnosis and Treatment of Hyperkinetic Children. Paper presented at the Annual Meeting of the American Educational Research Association, Boston, MA, April 1980 | Could not retrieve |
| Robins M, Gilbert RN. Welcome to Our World: Realities of High School Students. Thousand Oaks, CA: Corwin Press, Inc.; 1998 | Lacking qualitative data and/or analysis |
| Robinson K. Reflections on parenting a child with ADHD: exploring professional–client relationships. J Fem Fam Ther 2003;15:75–90 | Lacking qualitative data and/or analysis |
| Rosenzweig JM, Brennan EM, Ogilvie A. Work-family fit: voices of parents of children with emotional and behavioral disorders. Soc Work 2002;47:415–24 | Not focused on school setting |
| Ross E, Ross EC. The identification of ADHD. Infants Young Child 2006;19:164–7 | Lacking qualitative data and/or analysis |
| Rudnick P. My Billy. New Yorker 2006;82:40 | Lacking qualitative data and/or analysis |
| Ruenzel D. Addicted. Teach Mag 1996;8:28–9,32,4–5 | Lacking qualitative data and/or analysis |
| Rush C, Harrison P. Ascertaining teachers’ perceptions of working with adolescents diagnosed with attention-deficit/hyperactivity disorder. Educ Psychol Pract 2008;24:207–23 | Lacking qualitative data and/or analysis |
| Rush S, Wheeler J. Ascertaining disabling perceptions using perceptual mapping: applications to teachers’ perceptions of adolescents with attention-deficit/hyperactivity disorder. Disabil Soc 2011;26:743–56 | Lacking qualitative data and/or analysis |
| Rush S. Teachers’ perceptions of working with adolescents with Attention-Deficit/Hyperactivity Disorder: a concept-mapping approach. Dissertation Abstracts International: Section B: The Sciences and Engineering 2005;66:1223 | Could not retrieve |
| Ryan S. ‘I used to worry about what other people thought but now I just think . . . well I don’t care’: shifting accounts of learning difficulties in public places. Health Place 2008;14:730–9 | Not focused on school setting |
| Salt N, Parkes E, Scammell A. GPs’ perceptions of the management of ADHD in primary care: a study of Wandsworth GPs. Prim Health Care Res Dev 2005;6:162–71 | Not focused on school setting |
| Sams SE. The effects of functional intervention on the behavior of four students labeled ADHD. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;60:1081 | Lacking qualitative data and/or analysis |
| Santamaria M. School counselors’ strategies supporting Vygotsky’s theory and affecting behavior of Hispanic English language learners (ELL) with ADHD in second grade. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;70:448 | Focused on school-based interventions |
| Schaedler JS. A phenomenological study of the developmental course and adult outcome of women with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:4908 | Could not retrieve |
| Schirduan V, Case K. Mindful curriculum leadership for students with attention deficit hyperactivity disorder: leading in elementary schools by using multiple intelligences theory (SUMIT). Teachers Coll Rec 2004;106:87–95 | Lacking qualitative data and/or analysis |
| Schirduan V, Case KI. Mindful Curriculum Leadership for Students with Attention Deficit Hyperactivity Disorder (ADHD): Leading in Elementary Schools by Using Multiple Intelligences Theory (SUMIT[C]). Paper presented at the Annual Meeting of the American Education Research Association, Seattle, WA, 10–14 April 2001 | Lacking qualitative data and/or analysis |
| Schirduan VM. Elementary students with attention deficit hyperactivity disorder (ADHD) in schools using multiple intelligences theory: Intelligences, self-concept, and achievement. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2000;61:891 | Other |
| Schmalzer SN. Teachers’ perceptions of self-management interventions for ADHD: an initial investigation. Dissertation Abstracts International: Section B: The Sciences and Engineering 2009;69:6435 | Lacking qualitative data and/or analysis |
| Scope CR. The efficacy of conjoint behavioral consultation to reduce the off-task behavior of elementary school children diagnosed with attention deficit hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2003;64:1975 | Lacking qualitative data and/or analysis |
| Seabi J. Foundation phase educators’ perceptions of attention deficit hyperactivity disorder at a mainstream primary school. S Afr J High Educ 2010;24:616–29 | Lacking qualitative data and/or analysis |
| Segal E. Mothering a child with attention-deficit hyperactivity disorder: learned mothering. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1996;56:4950 | Not focused on school setting |
| Segal R, Frank G. The extraordinary construction of ordinary experience: scheduling daily life in families with children with attention deficit hyperactivity disorder. Scand J Occup Ther 1998;5:141–7 | Lacking qualitative data and/or analysis |
| Segal R, Hinojosa J. The activity setting of homework: an analysis of three cases and implications for occupational therapy. Am J Occup Ther 2006;60:50–9 | Not focused on school setting |
| Segal R. The construction of family occupations: a study of families with children who have attention deficit/hyperactivity disorder. Can J Occup Ther 1998;65:286–92 | Not focused on school setting |
| Shattell MM, Bartlett R, Rowe T. ‘I have always felt different’: the experience of attention-deficit/hyperactivity disorder in childhood. J Pediatr Nurs 2008;23:49–57 | Not focused on school setting |
| Shaw K, Wagner I, Eastwood H, Mitchell G. A qualitative study of Australian GPs’ attitudes and practices in the diagnosis and management of attention-deficit/hyperactivity disorder (ADHD). J Fam Pract 2003;20:129–34 | Not focused on school setting |
| Sheehan AD, Sheehan CM. Lost in a sea of ink: how I survived the storm. J Adolesc Adult Literacy 2000;44:20 | Lacking qualitative data and/or analysis |
| Singer B. The psychological experience of siblings of children with ADHD (attention deficit hyperactivity disorder, learning disabilities. Dissertation Abstracts International: Section B: The Sciences and Engineering 1997;58:2700 | Could not retrieve |
| Singh I. Boys will be boys: fathers’ perspectives on ADHD symptoms, diagnosis, and drug treatment. Harv Rev Psychiatr 2003;11:308–16 | Not focused on school setting |
| Singh I. Doing their jobs: mothering with ritalin in a culture of mother-blame. Soc Sci Med 2004;59:1193–205 | Not focused on school setting |
| Slee R. Finding a student voice in school reform: student disaffection, pathologies of disruption and educational control. Int Stud Sociol Educ 1994;4:147–72 | Lacking qualitative data and/or analysis |
| Smagorinsky P, Cameron T, O’Donnell-Allen C. ‘Achtung’ maybe: a case study of the role of personal connection and art in the literary engagement of students with attentional difficulties. Read Writ Q 2007;23:333–58 | Focused on school-based interventions |
| Smith M, Tett L. New community schools and pupils with social, emotional and behavioural difficulties. Scot Educ Rev 2002;34:151–62 | Not focused on school-age students with ADHD |
| Spicer CD. The Emotional Toll of Being a Twice Exceptional Adult : A Case Study. In Wormald C and Vialle W, editors. Dual Exceptionality. Sydney, NSW: Australian Association for the Education of the Gifted and Talented Ltd; 2011. pp. 33–6 | Lacking qualitative data and/or analysis |
| St James O’Connor T, Meakes E, Pickering M, Schuman M. On the right track: client experience of narrative therapy. Contemp Fam Ther 1997;19:479–95 | Not focused on school setting |
| Stagg AM. Barriers to attention-deficit/hyperactivity disorder intervention implementation in the public school setting. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;71:6467 | Lacking qualitative data and/or analysis |
| Stinnett TA, Crawford SA, Gillespie MD, Cruce MK, Langford CA. Factors affecting treatment acceptability for psychostimulant medication versus psychoeducational intervention. Psychol Schools 2001;38:585 | Lacking qualitative data and/or analysis |
| Stolowitz MA. How to achieve academic and creative success in spite of the inflexible, unresponsive higher education system. J Learn Disabil 1995;28:4–7 | Lacking qualitative data and/or analysis |
| Stone KL. An investigation of sibling relationships of children with AD/HD and their older siblings. Dissertation Abstracts International: Section B: The Sciences and Engineering 2000;60:4255 | Lacking qualitative data and/or analysis |
| Stultz CH, Flannagan D. Talk about school between mothers and children with or without ADHD. J Child Fam Stud 1999;8:425–35 | Lacking qualitative data and/or analysis |
| Tan TS, Cheung WS. Effects of computer collaborative group work on peer acceptance of a junior pupil with attention deficit hyperactivity disorder (ADHD). Comput Educ 2008;50:725–41 | Lacking qualitative data and/or analysis |
| Taylor M, Houghton S, Durkin K. Getting children with attention deficit hyperactivity disorder to school on time. J Fam Issues 2008;29:918–43 | Not focused on school-age students with ADHD |
| Taylor M, Houghton S. Examination-related anxiety in students diagnosed with AD/HD and the case for an allocation of extra time: perspectives of teachers, mothers and students. Emot Behav Difficult 2008;13:111–25 | Other |
| Taylor M, O’Donoghue T, Houghton S. To medicate or not to medicate? The decision-making process of Western Australian parents following their child’s diagnosis with an attention deficit hyperactivity disorder. Int J Disabil Dev Educ 2006;53:111–28 | Not focused on school setting |
| Taylor Wilcoxson JL. Attention deficit hyperactivity disorder and creative potential of children: a multiple case study. Dissertation Abstracts International: Section B: The Sciences and Engineering 2006;66:4502 | Focused on school-based interventions |
| Teasley M. Effective Interventions for Students with ADHD. In Franklin C, Harris MB, Allen-Meares P, editors. The School Practitioner’s Concise Companion to Mental Health. New York, NY: Oxford University Press; 2008. pp. 19–34 | Lacking qualitative data and/or analysis |
| Terenzi N. In my own words. Reaching Today’s Youth 1999;4:4–7 | Could not retrieve |
| Terry J. Coping with ADHD. Child Educ 1998;75:48–9 | Could not retrieve |
| TES. Friday hero. Times Educ Suppl 2005:3 | Lacking qualitative data and/or analysis |
| Thompson D, Emira M. ‘They say every child matters, but they don’t’: an investigation into parental and carer perceptions of access to leisure facilities and respite care for children and young people with autistic spectrum disorder (ASD) or attention deficit, hyperactivity disorder (ADHD). Disabil Soc 2011;26:65–78 | Not focused on school setting |
| Thorlakson CE. The experiences that enhance and inhibit learning for post-secondary students diagnosed with ADHD: a qualitative study. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2011;72:77 | Not focused on school setting |
| Tidefors I, Strand J. Life history interviews with 11 boys diagnosed with attention-deficit/hyperactivity disorder who had sexually offended: a sad storyline. J Trauma Dissociation 2012;13:421–34 | Not focused on school setting |
| Timmer DF. Group support for teenagers with attention deficit hyperactivity disorder. Soc Work Educ 1995;17:194–8 | Lacking qualitative data and/or analysis |
| Tracey DK, Gleeson G. Sense of coherence, loneliness and interpersonal concerns in adolescents with AD/HD: a comparison of adolescents’ and mothers’ perceptions. Aust J Guid Counsell 1998;8:49–58 | Lacking qualitative data and/or analysis |
| Travell C, Visser J. ‘ADHD does bad stuff to you’: young people’s and parents’ experiences and perceptions of attention deficit hyperactivity disorder (ADHD). Emot Behav Difficult 2006;11:205–16 | Lacking qualitative data and/or analysis |
| Tsurumaki M. Self-esteem enhancement in children with attention-deficit/hyperactivity disorder. Tohoku Psychologica Folia 2007;66:105–11 | Lacking qualitative data and/or analysis |
| Turk TN, Campbell DA. What’s wrong with Doug: the academic struggles of a gifted student with ADHD from preschool to college. Gift Child Today 2002;25:48 | Lacking qualitative data and/or analysis |
| Tyler Junior College. Tutor Training for Occupational Students with Learning Disabilities. PY95 Final Detailed Report. Texas, TX: Tyler Junior College; 1995 | Lacking qualitative data and/or analysis |
| Tyson K. Using the teacher-student relationship to help children diagnosed as hyperactive: an application of intrapsychic humanism. Child Youth Care Forum 2000;29:265–89 | Lacking qualitative data and/or analysis |
| Underwood DJ, Kopels S. Complaints filed against schools by parents of children with AD/HD: implications for school social work practice. Child Schools 2004;26:221–33 | Lacking qualitative data and/or analysis |
| Vail A, Mandiloff V. Cultivating Our Garden: Serving Students with Learning Disabilities in Family and Consumer Sciences. In Vail A, editor: Family & Consumer Sciences Education Association. Ellensburgh, WA: Central Washington University; 1996 | Could not retrieve |
| Van Der Westhuizen B. An ecosystemic approach to addressing attentional difficulties and heightened motor activity. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2009;69:4248 | Lacking qualitative data and/or analysis |
| Vogl TA. Navigating the glass maze: towards a phenomenology-derived learning model of graduate students with attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2007;68:438 | Not focused on school setting |
| Volpe RJ, Anastasio RJ, DuPaul GJ. Classroom and Instructional Strategies. In Goldstein S, Nagliere JA, DeVries M, editors. Learning and Attention Disorders in Adolescence and Adulthood: Assessment and Treatment. 2nd edn. Hoboken, NJ: John Wiley & Sons Inc.; 2011. pp. 467–87 | Could not retrieve |
| Waite R, Tran M. Explanatory models and help-seeking behavior for attention-deficit/hyperactivity disorder among a cohort of postsecondary students. Arch Psychiatr Nurs 2010;24:247–59 | Not focused on school setting |
| Wallace N. The perceptions of mothers of sons with ADHD. Aust New Zeal J Fam Ther 2005;26:193–9 | Lacking qualitative data and/or analysis |
| Ware JN, Ohrt JH, Swank JM. A phenomenological exploration of children’s experiences in a social skills group. J Spec Group Work 2012;37:133–51 | Not focused on school-age students with ADHD |
| Watson C, Marr C. A breakfast club for children with emotional and behavioural difficulties. Education 2003;31:15–18 | Lacking qualitative data and/or analysis |
| Weiss M, Hechtman L, Weiss G. ADHD in parents. J Am Acad Child Adolesc Psychiatr 2000;39:1059–61 | Lacking qualitative data and/or analysis |
| Wheeler L, Pumfrey P, Wakefield P. Variability of ADHD symptoms across primary school contexts: an in-depth case study. Emot Behav Difficult 2009;14:69–84 | Other |
| Wheeler L. Mixed Method Research into the Variability of ADHD Symptoms in Educational Settings. Paper presented at the BERA conference 2011. London; Institution of Education; 2011 | Lacking qualitative data and/or analysis |
| White-McMahon M. What you see is not what you get. Reclaim Child Youth 2010;19:58–61 | Lacking qualitative data and/or analysis |
| Wiebe J, Nicol JJ. Juxtaposition: ADHD and music at school. Can J Music Ther 2007;13:171–3 | Lacking qualitative data and/or analysis |
| Wiebe JE. ADHD, the classroom and music: a case study. Saskatchewan, SK: University of Saskatchewan; 2007 | Focused on school-based interventions |
| Williams MA. Exploration of effect of diagnosis of high school girls with attention deficit disorder on their mothers and the mother-daughter relationship. Dissertation Abstracts International: Section B: The Sciences and Engineering 2011;72:1786 | Not focused on school setting |
| Williams NJ. Gaining control: perspectives of parents of children with AD/HD. Crawley, WA: The University of Western Australia; 2009 | Not focused on school setting |
| Williams Orlando C. Parental explanatory models of children’s attention deficit hyperactivity disorder. Dissertation Abstracts International: Section B: The Sciences and Engineering 2010;71:2277 | Not focused on school setting |
| Williamson P, Koro-Ljungberg ME, Bussing R. Analysis of critical incidents and shifting perspectives: transitions in illness careers among adolescents with ADHD. Qual Health Res 2009;19:352–65 | Not focused on school setting |
| Willis J. Using my neuroscience to treat the sickness in our classrooms. Catalyst for Change 2010;36:46–55 | Not focused on school-age students with ADHD |
| Wong W. An investigation to describe and enhance the metacognitive processes of high school students with attention deficit hyperactivity disorder and learning disability who were studying for an examination. Dissertation Abstracts International: Section A: Humanities and Social Sciences 2005;65:4455 | Focused on school-based interventions |
| Woods C. My brave hyperactive son. Times Educ Suppl 2007;23 | Lacking qualitative data and/or analysis |
| Wright MS. The Readiness of Adults with Attention Deficit Hyperactivity Disorder for Self-Directed Learning. Mississippi, MS: University of Southern Mississippi; 2001 | Could not retrieve |
| Wright SF. ’A little understood solution to a vaguely defined problem’: parental perceptions of Ritalin. Educ Child Psychol 1997;14:50–9 | Lacking qualitative data and/or analysis |
| Yehle AK, Wambold C. An ADHD success story: strategies for teachers and students. Teach Except Child. 1998;30:8–13 | Lacking qualitative data and/or analysis |
| Yoon ML. An Evaluation Of The Application Of The Suggestive-Accelerative Model Of Learning And Teaching On High School Students. Melbourne, VIC: RMIT University; 2005 | Could not retrieve |
| Young S, Chesney S, Sperlinger D, Misch P, Collins P. A qualitative study exploring the life-course experiences of young offenders with symptoms and signs of ADHD who were detained in a residential care setting. Crim Behav Ment Health 2009;19:54–63 | Could not retrieve |
| Young-Loveridge J. A personal perspective on challenging behaviour: ADHD? Aust J Early Child 1997;22:1–6 | Lacking qualitative data and/or analysis |
| Zentall SS, Moon SM, Hall AM, Grskovic JA. Learning Characteristics of Boys with Attention Deficit/Hyperactivity Disorder and/or Giftedness. Paper presented at the Annual Meeting of the American Educational Research Association, Chicago, IL, March 1997 | Lacking qualitative data and/or analysis |
| Zentall SS, Moon SM, Hall AM, Grskovic JA. Learning and motivational characteristics of boys with AD/HD and/or giftedness. Except Child 2001;67:499–519 | Lacking qualitative data and/or analysis |
| Ziesing-Clark S. Confusion, heartache and tears: some mother’s experiences of children diagnosed with attention deficit hyperactive disorder. Aust J Early Child 1998;23:31–5 | Not focused on school setting |
| Zimmermann SH. Portrait of success: a situational analysis case study of students challenged by attention-deficit/hyperactivity disorder. Dissertation Abstracts International: Section A: Humanities and Social Sciences 1999;59:2368 | Focused on school-based interventions |
List of abbreviations
- ADHD
- attention-deficit/hyperactivity disorder
- ASD
- autistic spectrum disorder
- ASSIA
- Applied Social Sciences Index and Abstracts
- BCT
- behaviour change technique
- BIRS
- Behavioural Intervention Rating Scale
- BMC
- behavioural modification in classroom settings
- BPI
- behavioural peer intervention
- BPT
- behavioural parent training
- CBT
- cognitive–behavioural therapy
- CDSR
- Cochrane Database of Systematic Reviews
- CENTRAL
- Cochrane Central Register of Controlled Trials
- CI
- confidence interval
- CMR
- Cochrane Methodology Register
- CRS
- Conners’ Rating Scale
- DARE
- Database of Abstracts of Reviews of Effects
- DRC
- daily report card
- DSM-III
- Diagnostic and Statistical Manual of Mental Disorders-Third Edition
- DSM-IV
- Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition
- DSM-5
- Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition
- ERIC
- Education Resources Information Center
- HMIC
- Health Management Information Consortium
- HOPS
- Homework, Organization, and Planning Skills
- HTA
- Health Technology Assessment
- ICD-10
- International Classification of Diseases, Tenth Edition
- IEP
- individual education plan
- IQ
- intelligence quotient
- IRP-15
- Intervention Rating Profile-15
- ITT
- intention to treat
- LD
- learning disability
- NHS EED
- NHS Economic Evaluation Database
- NICE
- National Institute for Health and Care Excellence
- OECD
- Organisation for Economic Co-operation and Development
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
- randomised controlled trial
- SD
- standard deviation
- SEN
- special educational needs
- SMD
- standardised mean difference
- TOVA
- test of variables of attention